User login
Mixin’ it up
What percentage of your office visits are a response to an acute complaint? What percentage are prescheduled well-child visits? And how many are follow-ups to manage chronic conditions and behavioral problems?
You probably have a sense of how you are spending your time in the office, but do you really have the numbers to support your guesstimate of the patient mix? Does anyone in your organization have that data? You probably could come up with some numbers in a few hours with a pencil and your office schedule for the last 2 months. However, learning how much of your income is generated by each category of visit would be more difficult.
Before you run out to the front desk and ask the receptionist to delete your same-day slots and replace them with a few preventive and chronic care visits, we should question a few of Mr. Hart’s assertions.
Of course, like you, I never spent the time to learn which categories of office visit were driving my income. However, I do know that I saw a stimulating mix of acute and chronic visits, and the most important number, the bottom line, was more than adequate for my needs. To achieve this profitable balance of visits meant that I needed to be as efficient as the patients’ complaints would allow. There is an often-repeated myth that there is a direct correlation between the length of time a physician spends with the patient and the quality of the visit. In my experience, patients are more impressed by the physician’s level of attention and concern than the amount of time he spends in the exam room.

You might argue that you just don’t have the time to fit in all those acute visits. But have you had the courage to open up your schedule, maybe hire more staff, and give it a try? It takes a bit of shift in mindset and the acknowledgment that a large part of what we call preventive care has not proved effective. Immunizations? Yes, but the rest, not so much.
I know this is a heretical proposition but I found that I knew my patients better after seeing them when they were in need rather than in the less frequent but longer encounters of a health maintenance visit. It takes work, but there is room for both kinds of visit.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Email him at [email protected].
What percentage of your office visits are a response to an acute complaint? What percentage are prescheduled well-child visits? And how many are follow-ups to manage chronic conditions and behavioral problems?
You probably have a sense of how you are spending your time in the office, but do you really have the numbers to support your guesstimate of the patient mix? Does anyone in your organization have that data? You probably could come up with some numbers in a few hours with a pencil and your office schedule for the last 2 months. However, learning how much of your income is generated by each category of visit would be more difficult.
Before you run out to the front desk and ask the receptionist to delete your same-day slots and replace them with a few preventive and chronic care visits, we should question a few of Mr. Hart’s assertions.
Of course, like you, I never spent the time to learn which categories of office visit were driving my income. However, I do know that I saw a stimulating mix of acute and chronic visits, and the most important number, the bottom line, was more than adequate for my needs. To achieve this profitable balance of visits meant that I needed to be as efficient as the patients’ complaints would allow. There is an often-repeated myth that there is a direct correlation between the length of time a physician spends with the patient and the quality of the visit. In my experience, patients are more impressed by the physician’s level of attention and concern than the amount of time he spends in the exam room.
You might argue that you just don’t have the time to fit in all those acute visits. But have you had the courage to open up your schedule, maybe hire more staff, and give it a try? It takes a bit of shift in mindset and the acknowledgment that a large part of what we call preventive care has not proved effective. Immunizations? Yes, but the rest, not so much.
I know this is a heretical proposition but I found that I knew my patients better after seeing them when they were in need rather than in the less frequent but longer encounters of a health maintenance visit. It takes work, but there is room for both kinds of visit.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Email him at [email protected].
What percentage of your office visits are a response to an acute complaint? What percentage are prescheduled well-child visits? And how many are follow-ups to manage chronic conditions and behavioral problems?
You probably have a sense of how you are spending your time in the office, but do you really have the numbers to support your guesstimate of the patient mix? Does anyone in your organization have that data? You probably could come up with some numbers in a few hours with a pencil and your office schedule for the last 2 months. However, learning how much of your income is generated by each category of visit would be more difficult.
Before you run out to the front desk and ask the receptionist to delete your same-day slots and replace them with a few preventive and chronic care visits, we should question a few of Mr. Hart’s assertions.
Of course, like you, I never spent the time to learn which categories of office visit were driving my income. However, I do know that I saw a stimulating mix of acute and chronic visits, and the most important number, the bottom line, was more than adequate for my needs. To achieve this profitable balance of visits meant that I needed to be as efficient as the patients’ complaints would allow. There is an often-repeated myth that there is a direct correlation between the length of time a physician spends with the patient and the quality of the visit. In my experience, patients are more impressed by the physician’s level of attention and concern than the amount of time he spends in the exam room.
You might argue that you just don’t have the time to fit in all those acute visits. But have you had the courage to open up your schedule, maybe hire more staff, and give it a try? It takes a bit of shift in mindset and the acknowledgment that a large part of what we call preventive care has not proved effective. Immunizations? Yes, but the rest, not so much.
I know this is a heretical proposition but I found that I knew my patients better after seeing them when they were in need rather than in the less frequent but longer encounters of a health maintenance visit. It takes work, but there is room for both kinds of visit.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Email him at [email protected].
Nickel allergy common in children, significantly higher in girls
said Erin M. Warshaw, MD, MS, of the University of Minnesota, Minneapolis, and her associates.
“Although nickel sensitivity is reported to be problematic in children, the pediatric population is often underrepresented in large-scale epidemiologic studies,” they added.
In this retrospective, cross-sectional study of 1,894 children aged 18 years or younger tested by the North American Contact Dermatitis Group (NACDG) between 1994 and 2014, 23.7% of those patch tested were found to be sensitive to nickel. This included 6.5% who were 5 years or younger, 34.2% who were 6-12 years, and 59.4% who were 13-18 years.
Among all three patient groups, jewelry was the most common source of nickel sensitivity (36.4%), and this sensitivity was found to increase with age (5 years and younger, 20.7%; 6-12 years, 28.3%; and 13-18 years, 42.9%; P = .0006).
More than two-thirds of positive patch test reactions to nickel were found to be extreme or strong, Dr. Warshaw and her colleagues reported in the Journal of the American Academy of Dermatology.
Notably, girls were significantly more likely to exhibit nickel sensitivity than boys, a result the authors credit to “trends and social norms. ”
Citing a separate study conducted recently by NACDG on the correlation between piercing and nickel sensitivity across all ages, researchers found that females were significantly more likely to have piercings than were males, and with age, they speculated, “girls may be more likely to encounter high nickel release through piercing jewelry, bracelets, necklaces, hair clips, etc., resulting in higher proportions of girls than boys with nickel allergy.”
Nickel release, not nickel content, is an important factor in cases of nickel allergic contact dermatitis, the authors added. For nickel release to occur, prolonged skin contact is required. According to the European Chemicals Agency, prolonged exposure is defined as more than 10 minutes over three or more occasions within a 2-week period or more than 30 minutes over one or more occasion within the same 2 weeks.
The research was funded by the Minneapolis Veterans Affairs Medical Center, and in part, by the Nickel Producers Environmental Research Association. Three of the researchers have ties to various pharmaceutical companies and other organizations. Dr. Warshaw and the remaining researchers had no relevant financial disclosures.
SOURCE: Warshaw EM et al. J Am Acad Dermatol. 2018 Apr 14. doi: 10.1016/j.jaad.2018.02.071.
said Erin M. Warshaw, MD, MS, of the University of Minnesota, Minneapolis, and her associates.
“Although nickel sensitivity is reported to be problematic in children, the pediatric population is often underrepresented in large-scale epidemiologic studies,” they added.
In this retrospective, cross-sectional study of 1,894 children aged 18 years or younger tested by the North American Contact Dermatitis Group (NACDG) between 1994 and 2014, 23.7% of those patch tested were found to be sensitive to nickel. This included 6.5% who were 5 years or younger, 34.2% who were 6-12 years, and 59.4% who were 13-18 years.
Among all three patient groups, jewelry was the most common source of nickel sensitivity (36.4%), and this sensitivity was found to increase with age (5 years and younger, 20.7%; 6-12 years, 28.3%; and 13-18 years, 42.9%; P = .0006).
More than two-thirds of positive patch test reactions to nickel were found to be extreme or strong, Dr. Warshaw and her colleagues reported in the Journal of the American Academy of Dermatology.
Notably, girls were significantly more likely to exhibit nickel sensitivity than boys, a result the authors credit to “trends and social norms. ”
Citing a separate study conducted recently by NACDG on the correlation between piercing and nickel sensitivity across all ages, researchers found that females were significantly more likely to have piercings than were males, and with age, they speculated, “girls may be more likely to encounter high nickel release through piercing jewelry, bracelets, necklaces, hair clips, etc., resulting in higher proportions of girls than boys with nickel allergy.”
Nickel release, not nickel content, is an important factor in cases of nickel allergic contact dermatitis, the authors added. For nickel release to occur, prolonged skin contact is required. According to the European Chemicals Agency, prolonged exposure is defined as more than 10 minutes over three or more occasions within a 2-week period or more than 30 minutes over one or more occasion within the same 2 weeks.
The research was funded by the Minneapolis Veterans Affairs Medical Center, and in part, by the Nickel Producers Environmental Research Association. Three of the researchers have ties to various pharmaceutical companies and other organizations. Dr. Warshaw and the remaining researchers had no relevant financial disclosures.
SOURCE: Warshaw EM et al. J Am Acad Dermatol. 2018 Apr 14. doi: 10.1016/j.jaad.2018.02.071.
said Erin M. Warshaw, MD, MS, of the University of Minnesota, Minneapolis, and her associates.
“Although nickel sensitivity is reported to be problematic in children, the pediatric population is often underrepresented in large-scale epidemiologic studies,” they added.
In this retrospective, cross-sectional study of 1,894 children aged 18 years or younger tested by the North American Contact Dermatitis Group (NACDG) between 1994 and 2014, 23.7% of those patch tested were found to be sensitive to nickel. This included 6.5% who were 5 years or younger, 34.2% who were 6-12 years, and 59.4% who were 13-18 years.
Among all three patient groups, jewelry was the most common source of nickel sensitivity (36.4%), and this sensitivity was found to increase with age (5 years and younger, 20.7%; 6-12 years, 28.3%; and 13-18 years, 42.9%; P = .0006).
More than two-thirds of positive patch test reactions to nickel were found to be extreme or strong, Dr. Warshaw and her colleagues reported in the Journal of the American Academy of Dermatology.
Notably, girls were significantly more likely to exhibit nickel sensitivity than boys, a result the authors credit to “trends and social norms. ”
Citing a separate study conducted recently by NACDG on the correlation between piercing and nickel sensitivity across all ages, researchers found that females were significantly more likely to have piercings than were males, and with age, they speculated, “girls may be more likely to encounter high nickel release through piercing jewelry, bracelets, necklaces, hair clips, etc., resulting in higher proportions of girls than boys with nickel allergy.”
Nickel release, not nickel content, is an important factor in cases of nickel allergic contact dermatitis, the authors added. For nickel release to occur, prolonged skin contact is required. According to the European Chemicals Agency, prolonged exposure is defined as more than 10 minutes over three or more occasions within a 2-week period or more than 30 minutes over one or more occasion within the same 2 weeks.
The research was funded by the Minneapolis Veterans Affairs Medical Center, and in part, by the Nickel Producers Environmental Research Association. Three of the researchers have ties to various pharmaceutical companies and other organizations. Dr. Warshaw and the remaining researchers had no relevant financial disclosures.
SOURCE: Warshaw EM et al. J Am Acad Dermatol. 2018 Apr 14. doi: 10.1016/j.jaad.2018.02.071.
FROM THE JOURNAL OF THE AMERICAN ACADEMY OF DERMATOLOGY
Key clinical point: This U.S. study reinforces other recent investigations citing high occurrence of pediatric nickel-associated allergic contact dermatitis.
Major finding: Almost one-quarter (23.7%) of almost 2,000 children patch tested were found to have nickel sensitivity.
Study details: Retrospective, cross-sectional study of 1,894 pediatric patients.
Disclosures: The research was funded by the Minneapolis Veterans Affairs Medical Center, and in part by the Nickel Producers Environmental Research Association. Three of the researchers have ties to various pharmaceutical companies and other organizations. Dr. Warshaw and the remaining researchers had no relevant financial disclosures.
Source: Warshaw EM et al. J Am Acad Dermatol. 2018 Apr 14. doi: 10.1016/j.jaad.2018.02.071.

Leg lymphedema after gynecologic lymphadenectomy exceeds expectations
NEW ORLEANS – Leg lymphedema occurred in 19%-40% of women with a gynecologic cancer who underwent surgery with lymphadenectomy in a prospective study of 821 U.S. patients.
The incidence of lymphedema of the lower extremity (LLE) during 2 years of follow-up was 18% among 672 endometrial cancer patients, 25% among 124 cervical cancer patients, and 40% among 24 vulvar cancer patients, Jay W. Carlson, DO, said at the annual meeting of the Society of Gynecologic Oncology.
Although the study followed patients for 2 years after surgery, 84% of the LLE events occurred within the first 6 months after surgery, and 95% within the first 12 months. The robust incidence rates documented in this study contrasted with a general perception that LLE is relatively uncommon, leading Dr. Carlson to note that the new data show “the incidence of LLE is under recognized.” The findings also bucked conventional wisdom by showing no link between the incidence of LLE and number of lymph nodes dissected or with use of radiation treatment, said Dr. Carlson, a gynecologic oncologist at Mercy Clinic Women’s Oncology in Springfield, Mo.
To better define the incidence of LLE after lymphadenectomy for gynecologic cancers, the Gynecologic Oncology Group organized the Lymphedema and Gynecologic Cancer (LEG) study, run at more than 70 U.S. centers during June 2012–November 2014. The study enrolled patients scheduled for surgery to treat endometrial, cervical, or vulvar cancer, and applied systematic leg measurement to patients just before and at several prespecified times following surgery through 2 years of follow-up.
The study began with a total of 1,054 patients, but the final analysis that Dr. Carlson presented excluded patients who did not actually undergo lymphadenectomy during their surgery, did not have leg volume data available both before and after their surgery, or had a comorbidity or change in body mass that could have caused the change in leg size. The researchers also required patients identified with LLE to have completed the Gynecologic Cancer Lymphedema Questionnaire (Gynecol Oncol. 2010 May;117[2]:317-23) and tallied a score of at least 4, and to have at least a 10% increase in leg volume at the time of diagnosis, compared with the presurgical volume.
The exclusions yielded a total of 672 patients with endometrial cancer, including 127 who developed LLE (19%); 124 patients with cervical cancer, including 31 who developed LLE (25%); and 25 patients with vulvar cancer, including 10 who developed LLE (40%), Dr. Carlson reported.
Analysis of the patients who developed LLE showed no significant association with type of surgery (open, robotic, or laparoscopic), and no significant associations with several patient-specific factors including age, race, cancer stage, surgical blood loss, or serum albumin, he said.
[email protected]
On Twitter @mitchelzoler
SOURCE: Carlson J et al. SGO 2018, Abstract 11.
NEW ORLEANS – Leg lymphedema occurred in 19%-40% of women with a gynecologic cancer who underwent surgery with lymphadenectomy in a prospective study of 821 U.S. patients.
The incidence of lymphedema of the lower extremity (LLE) during 2 years of follow-up was 18% among 672 endometrial cancer patients, 25% among 124 cervical cancer patients, and 40% among 24 vulvar cancer patients, Jay W. Carlson, DO, said at the annual meeting of the Society of Gynecologic Oncology.
Although the study followed patients for 2 years after surgery, 84% of the LLE events occurred within the first 6 months after surgery, and 95% within the first 12 months. The robust incidence rates documented in this study contrasted with a general perception that LLE is relatively uncommon, leading Dr. Carlson to note that the new data show “the incidence of LLE is under recognized.” The findings also bucked conventional wisdom by showing no link between the incidence of LLE and number of lymph nodes dissected or with use of radiation treatment, said Dr. Carlson, a gynecologic oncologist at Mercy Clinic Women’s Oncology in Springfield, Mo.
To better define the incidence of LLE after lymphadenectomy for gynecologic cancers, the Gynecologic Oncology Group organized the Lymphedema and Gynecologic Cancer (LEG) study, run at more than 70 U.S. centers during June 2012–November 2014. The study enrolled patients scheduled for surgery to treat endometrial, cervical, or vulvar cancer, and applied systematic leg measurement to patients just before and at several prespecified times following surgery through 2 years of follow-up.
The study began with a total of 1,054 patients, but the final analysis that Dr. Carlson presented excluded patients who did not actually undergo lymphadenectomy during their surgery, did not have leg volume data available both before and after their surgery, or had a comorbidity or change in body mass that could have caused the change in leg size. The researchers also required patients identified with LLE to have completed the Gynecologic Cancer Lymphedema Questionnaire (Gynecol Oncol. 2010 May;117[2]:317-23) and tallied a score of at least 4, and to have at least a 10% increase in leg volume at the time of diagnosis, compared with the presurgical volume.
The exclusions yielded a total of 672 patients with endometrial cancer, including 127 who developed LLE (19%); 124 patients with cervical cancer, including 31 who developed LLE (25%); and 25 patients with vulvar cancer, including 10 who developed LLE (40%), Dr. Carlson reported.
Analysis of the patients who developed LLE showed no significant association with type of surgery (open, robotic, or laparoscopic), and no significant associations with several patient-specific factors including age, race, cancer stage, surgical blood loss, or serum albumin, he said.
[email protected]
On Twitter @mitchelzoler
SOURCE: Carlson J et al. SGO 2018, Abstract 11.
NEW ORLEANS – Leg lymphedema occurred in 19%-40% of women with a gynecologic cancer who underwent surgery with lymphadenectomy in a prospective study of 821 U.S. patients.
The incidence of lymphedema of the lower extremity (LLE) during 2 years of follow-up was 18% among 672 endometrial cancer patients, 25% among 124 cervical cancer patients, and 40% among 24 vulvar cancer patients, Jay W. Carlson, DO, said at the annual meeting of the Society of Gynecologic Oncology.
Although the study followed patients for 2 years after surgery, 84% of the LLE events occurred within the first 6 months after surgery, and 95% within the first 12 months. The robust incidence rates documented in this study contrasted with a general perception that LLE is relatively uncommon, leading Dr. Carlson to note that the new data show “the incidence of LLE is under recognized.” The findings also bucked conventional wisdom by showing no link between the incidence of LLE and number of lymph nodes dissected or with use of radiation treatment, said Dr. Carlson, a gynecologic oncologist at Mercy Clinic Women’s Oncology in Springfield, Mo.
To better define the incidence of LLE after lymphadenectomy for gynecologic cancers, the Gynecologic Oncology Group organized the Lymphedema and Gynecologic Cancer (LEG) study, run at more than 70 U.S. centers during June 2012–November 2014. The study enrolled patients scheduled for surgery to treat endometrial, cervical, or vulvar cancer, and applied systematic leg measurement to patients just before and at several prespecified times following surgery through 2 years of follow-up.
The study began with a total of 1,054 patients, but the final analysis that Dr. Carlson presented excluded patients who did not actually undergo lymphadenectomy during their surgery, did not have leg volume data available both before and after their surgery, or had a comorbidity or change in body mass that could have caused the change in leg size. The researchers also required patients identified with LLE to have completed the Gynecologic Cancer Lymphedema Questionnaire (Gynecol Oncol. 2010 May;117[2]:317-23) and tallied a score of at least 4, and to have at least a 10% increase in leg volume at the time of diagnosis, compared with the presurgical volume.
The exclusions yielded a total of 672 patients with endometrial cancer, including 127 who developed LLE (19%); 124 patients with cervical cancer, including 31 who developed LLE (25%); and 25 patients with vulvar cancer, including 10 who developed LLE (40%), Dr. Carlson reported.
Analysis of the patients who developed LLE showed no significant association with type of surgery (open, robotic, or laparoscopic), and no significant associations with several patient-specific factors including age, race, cancer stage, surgical blood loss, or serum albumin, he said.
[email protected]
On Twitter @mitchelzoler
SOURCE: Carlson J et al. SGO 2018, Abstract 11.
REPORTING FROM SGO 2018
Key clinical point: Leg lymphedema is common following lymphadenectomy for a gynecologic cancer.
Major finding: Leg lymphedema incidence was 19%-40% during 2-year follow-up after lymphadenectomy during gynecologic cancer surgery.
Study details: LEG, a multicenter, U.S. prospective study with 821 gynecologic cancer patients in the final analysis.
Disclosures: LEG had no commercial funding. Dr. Carlson had no disclosures.
Source: Carlson J et al. SGO 2018, Abstract 11.
Dasatinib activity prominent in subset of GIST patients
Dasatinib might have activity in some subsets of patients with imatinib-resistant gastrointestinal stromal tumors (GISTs), investigators have reported.
The tyrosine kinase inhibitor had a 29% rate of 6-month progression-free survival (PFS) in a nonrandomized, 50-patient study.
That PFS rate was well above the 10% threshold that would have constituted evidence of inactive treatment, but it “fell just short of our goal” of 30% that would have been considered evidence of drug activity, wrote Scott M. Schuetze, MD, PhD, of the department of internal medicine, University of Michigan, Ann Arbor, and his coauthors. The report was published in JAMA Oncology.
It was also higher than the 16% 6-month PFS rate reported in a randomized trial of sunitinib, which was approved for imatinib-resistant GIST treatment in 2006. However, it was lower than the 38% 6-month PFS rate reported for regorafenib, which was approved in 2013 for that indication, the researchers noted.
Exploratory analyses did identify a few biomarker-driven subsets that might particularly benefit from dasatinib therapy. Notably, the 6-month PFS rate was 50% for patients with tumors expressing phosphorylated SRC.
While intriguing, the results of the exploratory analyses are hampered by the small number of patients enrolled in the trial; only 14 patients in the study had phosphorylated SRC.
“Further studies should explore whether activated SRC is a prognostic biomarker of more indolent disease, or is a predictive biomarker of response to tyrosine kinase therapy,” the researchers wrote.
Patients in the study had imatinib refractory GIST. They received dasatinib 70 mg twice daily. They were enrolled in 2008-2009 and followed for at least 5 years.
In addition to previously receiving imatinib, most enrollees (80%) had already been treated with sunitinib as well. The study started before the approval of sunitinib in GIST, but after the approval of regorafenib, the investigators noted.
“Preclinical research suggested that dasatinib had higher potency against mutations in the activation domain of KIT and PDGFRA than imatinib and sunitinib,” the authors recounted.
This trial did provide some evidence in support of that preclinical data: One patient with a specific mutation in PDGFRA exhibited prolonged tumor control.
Bristol-Myers Squibb provided funding for the trial and dasatinib. Dr. Schuetze reported disclosures related to Novartis, Amgen, Janssen, Daiichi-Sankyo, Eli Lilly, and AB Science.
SOURCE: Schuetze SM et al. 2018 Apr 26. doi: 10.1001/jamaoncol.2018.0601.
Dasatinib might have activity in some subsets of patients with imatinib-resistant gastrointestinal stromal tumors (GISTs), investigators have reported.
The tyrosine kinase inhibitor had a 29% rate of 6-month progression-free survival (PFS) in a nonrandomized, 50-patient study.
That PFS rate was well above the 10% threshold that would have constituted evidence of inactive treatment, but it “fell just short of our goal” of 30% that would have been considered evidence of drug activity, wrote Scott M. Schuetze, MD, PhD, of the department of internal medicine, University of Michigan, Ann Arbor, and his coauthors. The report was published in JAMA Oncology.
It was also higher than the 16% 6-month PFS rate reported in a randomized trial of sunitinib, which was approved for imatinib-resistant GIST treatment in 2006. However, it was lower than the 38% 6-month PFS rate reported for regorafenib, which was approved in 2013 for that indication, the researchers noted.
Exploratory analyses did identify a few biomarker-driven subsets that might particularly benefit from dasatinib therapy. Notably, the 6-month PFS rate was 50% for patients with tumors expressing phosphorylated SRC.
While intriguing, the results of the exploratory analyses are hampered by the small number of patients enrolled in the trial; only 14 patients in the study had phosphorylated SRC.
“Further studies should explore whether activated SRC is a prognostic biomarker of more indolent disease, or is a predictive biomarker of response to tyrosine kinase therapy,” the researchers wrote.
Patients in the study had imatinib refractory GIST. They received dasatinib 70 mg twice daily. They were enrolled in 2008-2009 and followed for at least 5 years.
In addition to previously receiving imatinib, most enrollees (80%) had already been treated with sunitinib as well. The study started before the approval of sunitinib in GIST, but after the approval of regorafenib, the investigators noted.
“Preclinical research suggested that dasatinib had higher potency against mutations in the activation domain of KIT and PDGFRA than imatinib and sunitinib,” the authors recounted.
This trial did provide some evidence in support of that preclinical data: One patient with a specific mutation in PDGFRA exhibited prolonged tumor control.
Bristol-Myers Squibb provided funding for the trial and dasatinib. Dr. Schuetze reported disclosures related to Novartis, Amgen, Janssen, Daiichi-Sankyo, Eli Lilly, and AB Science.
SOURCE: Schuetze SM et al. 2018 Apr 26. doi: 10.1001/jamaoncol.2018.0601.
Dasatinib might have activity in some subsets of patients with imatinib-resistant gastrointestinal stromal tumors (GISTs), investigators have reported.
The tyrosine kinase inhibitor had a 29% rate of 6-month progression-free survival (PFS) in a nonrandomized, 50-patient study.
That PFS rate was well above the 10% threshold that would have constituted evidence of inactive treatment, but it “fell just short of our goal” of 30% that would have been considered evidence of drug activity, wrote Scott M. Schuetze, MD, PhD, of the department of internal medicine, University of Michigan, Ann Arbor, and his coauthors. The report was published in JAMA Oncology.
It was also higher than the 16% 6-month PFS rate reported in a randomized trial of sunitinib, which was approved for imatinib-resistant GIST treatment in 2006. However, it was lower than the 38% 6-month PFS rate reported for regorafenib, which was approved in 2013 for that indication, the researchers noted.
Exploratory analyses did identify a few biomarker-driven subsets that might particularly benefit from dasatinib therapy. Notably, the 6-month PFS rate was 50% for patients with tumors expressing phosphorylated SRC.
While intriguing, the results of the exploratory analyses are hampered by the small number of patients enrolled in the trial; only 14 patients in the study had phosphorylated SRC.
“Further studies should explore whether activated SRC is a prognostic biomarker of more indolent disease, or is a predictive biomarker of response to tyrosine kinase therapy,” the researchers wrote.
Patients in the study had imatinib refractory GIST. They received dasatinib 70 mg twice daily. They were enrolled in 2008-2009 and followed for at least 5 years.
In addition to previously receiving imatinib, most enrollees (80%) had already been treated with sunitinib as well. The study started before the approval of sunitinib in GIST, but after the approval of regorafenib, the investigators noted.
“Preclinical research suggested that dasatinib had higher potency against mutations in the activation domain of KIT and PDGFRA than imatinib and sunitinib,” the authors recounted.
This trial did provide some evidence in support of that preclinical data: One patient with a specific mutation in PDGFRA exhibited prolonged tumor control.
Bristol-Myers Squibb provided funding for the trial and dasatinib. Dr. Schuetze reported disclosures related to Novartis, Amgen, Janssen, Daiichi-Sankyo, Eli Lilly, and AB Science.
SOURCE: Schuetze SM et al. 2018 Apr 26. doi: 10.1001/jamaoncol.2018.0601.
FROM JAMA ONCOLOGY
Key clinical point: The efficacy of dasatinib in imatinib-resistant GIST was just short of what investigators considered evidence of an active drug.
Major finding: The estimated rate of 6-month progression-free survival was 29% overall, though it was 50% in one biomarker-defined patient subset.
Study details: A nonrandomized single-arm study of 50 patients with GIST treated with dasatinib 70 mg twice daily.
Disclosures: Bristol-Myers Squibb provided funding for the trial and dasatinib. Dr. Schuetze reported disclosures related to Novartis, Amgen, Janssen, Daiichi-Sankyo, Eli Lilly, and AB Science.
Source: Schuetze SM et al. JAMA Oncol. 2018 Apr 26. doi: 10.1001/jamaoncol.2018.0601.
MS drugs in Medicare Part D: Higher tiers, less coverage, more prior authorizations
LOS ANGELES – Under Medicare Part D, private prescription drug plans and those bundled with Medicare Advantage plans have steadily raised injectable and oral disease-modifying therapies for multiple sclerosis to higher tiers with higher cost sharing, reduced coverage of particular drugs, and increased prior authorizations during the 10-year period of 2007-2016, according to an analysis conducted by Oregon State University researchers.
At the annual meeting of the American Academy of Neurology, Daniel Hartung, PharmD, of Oregon Health and Science University, Portland, and his colleagues reported that the proportion of plans with disease-modifying therapies (DMTs) in the highest tiers, generally tier 5 and above, rose from 11% in 2007 to 95% in 2016.
The scope of drugs covered by the plans declined marginally. Over the 10-year period, plans covering at least three DMTs declined from 98% to 95%, but plans that covered interferon beta-1b, intramuscular or subcutaneous interferon beta-1a, or glatiramer acetate declined from 85%-100% of plans to 60%-81%.
Plans with prior authorizations for DMTs rose across the board. The percentage of plans with at least one DMT not needing prior authorization dropped from 40% to 27%, while plans that covered interferon beta-1b, intramuscular or subcutaneous interferon beta-1a, or glatiramer acetate rose from 62%-65% to 77%-80%.
Based on 2016 coverage characteristics, Dr. Hartung and his associates estimated that the expected annual out-of-pocket costs for patients in 2019 would be over $5,000 for all drugs in the analysis, after accounting for the Bipartisan Budget Act’s closing the Part D coverage gap in 2019.
Part D covers noninfusible DMTs, which in this analysis included glatiramer acetate 20 and 40 mg (Copaxone 20 and Copaxone 40), generic glatiramer acetate 20 mg (Glatopa), interferon beta-1a intramuscular (Avonex), interferon beta-1a subcutaneous (Rebif), interferon beta-1b (Extavia and Betaseron), peginterferon beta-1a (Plegridy), fingolimod (Gilenya), teriflunomide (Aubagio), and dimethyl fumarate (Tecfidera). The infusible drugs natalizumab (Tysabri), alemtuzumab (Lemtrada), and ocrelizumab (Ocrevus) fall under Medicare Part B.
The study was supported by the National Multiple Sclerosis Society. None of the authors had anything to disclose.
SOURCE: Hartung D et al. AAN 2018. Abstract P3.161
LOS ANGELES – Under Medicare Part D, private prescription drug plans and those bundled with Medicare Advantage plans have steadily raised injectable and oral disease-modifying therapies for multiple sclerosis to higher tiers with higher cost sharing, reduced coverage of particular drugs, and increased prior authorizations during the 10-year period of 2007-2016, according to an analysis conducted by Oregon State University researchers.
At the annual meeting of the American Academy of Neurology, Daniel Hartung, PharmD, of Oregon Health and Science University, Portland, and his colleagues reported that the proportion of plans with disease-modifying therapies (DMTs) in the highest tiers, generally tier 5 and above, rose from 11% in 2007 to 95% in 2016.
The scope of drugs covered by the plans declined marginally. Over the 10-year period, plans covering at least three DMTs declined from 98% to 95%, but plans that covered interferon beta-1b, intramuscular or subcutaneous interferon beta-1a, or glatiramer acetate declined from 85%-100% of plans to 60%-81%.
Plans with prior authorizations for DMTs rose across the board. The percentage of plans with at least one DMT not needing prior authorization dropped from 40% to 27%, while plans that covered interferon beta-1b, intramuscular or subcutaneous interferon beta-1a, or glatiramer acetate rose from 62%-65% to 77%-80%.
Based on 2016 coverage characteristics, Dr. Hartung and his associates estimated that the expected annual out-of-pocket costs for patients in 2019 would be over $5,000 for all drugs in the analysis, after accounting for the Bipartisan Budget Act’s closing the Part D coverage gap in 2019.
Part D covers noninfusible DMTs, which in this analysis included glatiramer acetate 20 and 40 mg (Copaxone 20 and Copaxone 40), generic glatiramer acetate 20 mg (Glatopa), interferon beta-1a intramuscular (Avonex), interferon beta-1a subcutaneous (Rebif), interferon beta-1b (Extavia and Betaseron), peginterferon beta-1a (Plegridy), fingolimod (Gilenya), teriflunomide (Aubagio), and dimethyl fumarate (Tecfidera). The infusible drugs natalizumab (Tysabri), alemtuzumab (Lemtrada), and ocrelizumab (Ocrevus) fall under Medicare Part B.
The study was supported by the National Multiple Sclerosis Society. None of the authors had anything to disclose.
SOURCE: Hartung D et al. AAN 2018. Abstract P3.161
LOS ANGELES – Under Medicare Part D, private prescription drug plans and those bundled with Medicare Advantage plans have steadily raised injectable and oral disease-modifying therapies for multiple sclerosis to higher tiers with higher cost sharing, reduced coverage of particular drugs, and increased prior authorizations during the 10-year period of 2007-2016, according to an analysis conducted by Oregon State University researchers.
At the annual meeting of the American Academy of Neurology, Daniel Hartung, PharmD, of Oregon Health and Science University, Portland, and his colleagues reported that the proportion of plans with disease-modifying therapies (DMTs) in the highest tiers, generally tier 5 and above, rose from 11% in 2007 to 95% in 2016.
The scope of drugs covered by the plans declined marginally. Over the 10-year period, plans covering at least three DMTs declined from 98% to 95%, but plans that covered interferon beta-1b, intramuscular or subcutaneous interferon beta-1a, or glatiramer acetate declined from 85%-100% of plans to 60%-81%.
Plans with prior authorizations for DMTs rose across the board. The percentage of plans with at least one DMT not needing prior authorization dropped from 40% to 27%, while plans that covered interferon beta-1b, intramuscular or subcutaneous interferon beta-1a, or glatiramer acetate rose from 62%-65% to 77%-80%.
Based on 2016 coverage characteristics, Dr. Hartung and his associates estimated that the expected annual out-of-pocket costs for patients in 2019 would be over $5,000 for all drugs in the analysis, after accounting for the Bipartisan Budget Act’s closing the Part D coverage gap in 2019.
Part D covers noninfusible DMTs, which in this analysis included glatiramer acetate 20 and 40 mg (Copaxone 20 and Copaxone 40), generic glatiramer acetate 20 mg (Glatopa), interferon beta-1a intramuscular (Avonex), interferon beta-1a subcutaneous (Rebif), interferon beta-1b (Extavia and Betaseron), peginterferon beta-1a (Plegridy), fingolimod (Gilenya), teriflunomide (Aubagio), and dimethyl fumarate (Tecfidera). The infusible drugs natalizumab (Tysabri), alemtuzumab (Lemtrada), and ocrelizumab (Ocrevus) fall under Medicare Part B.
The study was supported by the National Multiple Sclerosis Society. None of the authors had anything to disclose.
SOURCE: Hartung D et al. AAN 2018. Abstract P3.161
REPORTING FROM AAN 2018

FDA approves epinephrine autoinjector for infants and toddlers
according to a press release from Kaléo, a privately-held pharmaceutical company.
“Anaphylactic reactions can be frightening and serious, and when experienced by the very young, some of whom can’t communicate about what’s happening, these episodes can be particularly alarming,” Vivian Hernandez-Trujillo, MD, a pediatric allergist and fellow of the American Academy of Allergy, Asthma and Immunology, said in a statement. “Now, caregivers can have the AUVI-Q 0.1 mg in hand to respond to an allergic emergency and safely administer epinephrine to infants and toddlers.”
The approval comes at a time when a higher percentage of children are being admitted to the hospital for food-related anaphylaxis: a 130% increase among children aged 0-4 years and a 196% increase in children aged 5-17 years.
The epinephrine autoinjector will be available for $0 out of pocket for commercially insured patients using the AUVI-Q AffordAbility Program and Direct Delivery Service starting May 1, 2018. More information concerning this EAI can be found here.
according to a press release from Kaléo, a privately-held pharmaceutical company.
“Anaphylactic reactions can be frightening and serious, and when experienced by the very young, some of whom can’t communicate about what’s happening, these episodes can be particularly alarming,” Vivian Hernandez-Trujillo, MD, a pediatric allergist and fellow of the American Academy of Allergy, Asthma and Immunology, said in a statement. “Now, caregivers can have the AUVI-Q 0.1 mg in hand to respond to an allergic emergency and safely administer epinephrine to infants and toddlers.”
The approval comes at a time when a higher percentage of children are being admitted to the hospital for food-related anaphylaxis: a 130% increase among children aged 0-4 years and a 196% increase in children aged 5-17 years.
The epinephrine autoinjector will be available for $0 out of pocket for commercially insured patients using the AUVI-Q AffordAbility Program and Direct Delivery Service starting May 1, 2018. More information concerning this EAI can be found here.
according to a press release from Kaléo, a privately-held pharmaceutical company.
“Anaphylactic reactions can be frightening and serious, and when experienced by the very young, some of whom can’t communicate about what’s happening, these episodes can be particularly alarming,” Vivian Hernandez-Trujillo, MD, a pediatric allergist and fellow of the American Academy of Allergy, Asthma and Immunology, said in a statement. “Now, caregivers can have the AUVI-Q 0.1 mg in hand to respond to an allergic emergency and safely administer epinephrine to infants and toddlers.”
The approval comes at a time when a higher percentage of children are being admitted to the hospital for food-related anaphylaxis: a 130% increase among children aged 0-4 years and a 196% increase in children aged 5-17 years.
The epinephrine autoinjector will be available for $0 out of pocket for commercially insured patients using the AUVI-Q AffordAbility Program and Direct Delivery Service starting May 1, 2018. More information concerning this EAI can be found here.
Key to MGUS and myeloma may lie in Iceland
NEW ORLEANS – Everyone aged 40 years and older on the island nation of Iceland is being screened for monoclonal gammopathy of undetermined significance, smoldering myeloma, and full-blown multiple myeloma in an unprecedented project to identify the malignancy’s genetic roots, Joseph Mikhael, MD, said at the annual meeting of the American College of Physicians.
This effort to decode the underlying genetics of multiple myeloma is enormously facilitated by the fact that the DNA sequencing of the entire Icelandic population is already known, and everyone’s blood samples are stored in the national health care system.
The International Myeloma Foundation is funding the Icelandic project, called iStopMM (Iceland Screens Treats or Prevents Multiple Myeloma).
The results of iStopMM could be far reaching, in part because the findings will show whether screening an asymptomatic general population for MGUS – as for example, all American adults – is worthwhile.
In the interim, it’s important for primary care physicians to recognize when it is and isn’t appropriate to order a serum protein electrophoresis (SPE) study, on which the diagnosis of MGUS hinges. It’s also essential to recognize the difference between smoldering and full-blown multiple myeloma, because the distinction has implications for patient monitoring and treatment, added Dr. Mikhael, a hematologist at the City of Hope Cancer Center in Duarte, Calif.
Multiple myeloma accounts for 1% of all cancers and 10% of hematologic malignancies. MGUS is an obligate precursor of multiple myeloma. But MGUS is common, and therein lies a challenge for physicians – as well as a major source of anxiety for many MGUS-positive patients.
In a 12-year-old study, MGUS had a 3% prevalence in the general U.S. population older than age 50 years, and a greater than 5% prevalence after age 70. However, Dr. Mikhael thinks that more refined testing will show the true figure to be close to 10%. Thus, the great majority of patients with MGUS will never develop multiple myeloma.
Pending the potentially practice-changing outcome of iStopMM, Dr. Mikhael said SPE shouldn’t be ordered routinely in an asymptomatic patient, even one with a positive family history for multiple myeloma. The annual cost of monitoring the roughly 540,000 U.S. patients who now carry a diagnosis of MGUS – typically established as an incidental finding by primary care physicians while doing a work-up for another reason – is at least $110 million. And there’s no point in adding to that burden until the benefit of mass screening has been established.
An SPE is appropriate, however, in an older patient with unexplained anemia, known low immunoglobulin levels, unexplained renal insufficiency or neuropathy, or osteopenia or osteoporosis inconsistent with the patient’s age or gender – provided the patient doesn’t have a coexisting plasma cell dyscrasia or B-cell lymphoproliferative disorder, which would throw off the prognostic value of the test results, he continued.
When ordering an SPE to rule in/out MGUS, it’s essential to also order serum free light-chain testing, because it provides key prognostic information.
A landmark study led by investigators at the Mayo Clinic demonstrated that the risk of progression of MGUS to multiple myeloma or a related disorder is independently predicted by three key factors: a high serum M-protein spike of 15 g/L or more on the SPE; the presence of non-IgG MGUS; and an abnormal serum free light-chain ratio of less than 0.26 or more than 1.65. In this study, the 20-year risk of malignant transformation of MGUS ranged from 58% if all three risk factors were present, to just 5% if none were (Blood. 2005 Aug 1;106[3]:812-7).
CRAB vs. SLiM CRAB
Myeloma, smoldering myeloma, and MGUS were redefined a few years ago to reflect differences in prognosis. MGUS still requires the presence of a serum monoclonal protein in a concentration of 3 g/dL or less, less than 10% plasmacytosis in the bone marrow, asymptomatic status, and absence of end-organ damage as traditionally defined in the acronym CRAB (calcium elevation, renal insufficiency, anemia, or bony disease).
If CRAB is present in a patient with at least 10% plasma cells in bone marrow, that is by definition multiple myeloma warranting treatment. Smoldering myeloma requires at least 10% plasmacytosis in bone marrow and absence of the CRAB criteria. However, in a significant change, ultra–high-risk smoldering melanoma, defined by the acronym SLiM CRAB, is now considered active myeloma and should be treated (Lancet Oncol. 2014 Nov;15[12]:e538-48).
“Traditionally, we waited until CRAB [to define myeloma],” Dr. Mikhael explained. “But if you’re running toward a cliff, I don’t have to wait until you’re falling off to know you’re in trouble.”
The SLiM half of SLiM CRAB consists of 60% or more plasmacytosis in bone marrow, light chains in a kappa-to-lambda or lambda-to-kappa ratio of greater than 100, and MRI showing one or more focal lesions. If a patient is SLiM, with or without CRAB, that is now considered active myeloma warranting treatment.
Not all MGUS needs a bone marrow biopsy
A bone marrow biopsy and skeletal survey via whole-body CT or conventional radiographs can be deferred in patients with low-risk MGUS and no bony symptoms. Using the Mayo Clinic risk stratification model, low risk is defined as a serum M protein of 1.5 g/dL or less on SPE, an IgG isotype, and a normal free light-chain ratio.
The lifetime risk of progression in patients with MGUS who meet all three criteria is only about 2%. They can be followed at 6 months with an SPE, free light-chain testing, a CBC, and serum calcium and creatinine, then annually thereafter.
“For those who aren’t in this low-risk category, we actually do need to do a bone marrow test,” according to Dr. Mikhael. “Then, based on that, if they have malignancy, send them to a myeloma geek like me or to another hematologist. And if they don’t have a malignancy, they can be followed at 6 months and then subsequently at least every year.”
Dr. Mikhael has received research grants from AbbVie, Celgene, and Sanofi.
NEW ORLEANS – Everyone aged 40 years and older on the island nation of Iceland is being screened for monoclonal gammopathy of undetermined significance, smoldering myeloma, and full-blown multiple myeloma in an unprecedented project to identify the malignancy’s genetic roots, Joseph Mikhael, MD, said at the annual meeting of the American College of Physicians.
This effort to decode the underlying genetics of multiple myeloma is enormously facilitated by the fact that the DNA sequencing of the entire Icelandic population is already known, and everyone’s blood samples are stored in the national health care system.
The International Myeloma Foundation is funding the Icelandic project, called iStopMM (Iceland Screens Treats or Prevents Multiple Myeloma).
The results of iStopMM could be far reaching, in part because the findings will show whether screening an asymptomatic general population for MGUS – as for example, all American adults – is worthwhile.
In the interim, it’s important for primary care physicians to recognize when it is and isn’t appropriate to order a serum protein electrophoresis (SPE) study, on which the diagnosis of MGUS hinges. It’s also essential to recognize the difference between smoldering and full-blown multiple myeloma, because the distinction has implications for patient monitoring and treatment, added Dr. Mikhael, a hematologist at the City of Hope Cancer Center in Duarte, Calif.
Multiple myeloma accounts for 1% of all cancers and 10% of hematologic malignancies. MGUS is an obligate precursor of multiple myeloma. But MGUS is common, and therein lies a challenge for physicians – as well as a major source of anxiety for many MGUS-positive patients.
In a 12-year-old study, MGUS had a 3% prevalence in the general U.S. population older than age 50 years, and a greater than 5% prevalence after age 70. However, Dr. Mikhael thinks that more refined testing will show the true figure to be close to 10%. Thus, the great majority of patients with MGUS will never develop multiple myeloma.
Pending the potentially practice-changing outcome of iStopMM, Dr. Mikhael said SPE shouldn’t be ordered routinely in an asymptomatic patient, even one with a positive family history for multiple myeloma. The annual cost of monitoring the roughly 540,000 U.S. patients who now carry a diagnosis of MGUS – typically established as an incidental finding by primary care physicians while doing a work-up for another reason – is at least $110 million. And there’s no point in adding to that burden until the benefit of mass screening has been established.
An SPE is appropriate, however, in an older patient with unexplained anemia, known low immunoglobulin levels, unexplained renal insufficiency or neuropathy, or osteopenia or osteoporosis inconsistent with the patient’s age or gender – provided the patient doesn’t have a coexisting plasma cell dyscrasia or B-cell lymphoproliferative disorder, which would throw off the prognostic value of the test results, he continued.
When ordering an SPE to rule in/out MGUS, it’s essential to also order serum free light-chain testing, because it provides key prognostic information.
A landmark study led by investigators at the Mayo Clinic demonstrated that the risk of progression of MGUS to multiple myeloma or a related disorder is independently predicted by three key factors: a high serum M-protein spike of 15 g/L or more on the SPE; the presence of non-IgG MGUS; and an abnormal serum free light-chain ratio of less than 0.26 or more than 1.65. In this study, the 20-year risk of malignant transformation of MGUS ranged from 58% if all three risk factors were present, to just 5% if none were (Blood. 2005 Aug 1;106[3]:812-7).
CRAB vs. SLiM CRAB
Myeloma, smoldering myeloma, and MGUS were redefined a few years ago to reflect differences in prognosis. MGUS still requires the presence of a serum monoclonal protein in a concentration of 3 g/dL or less, less than 10% plasmacytosis in the bone marrow, asymptomatic status, and absence of end-organ damage as traditionally defined in the acronym CRAB (calcium elevation, renal insufficiency, anemia, or bony disease).
If CRAB is present in a patient with at least 10% plasma cells in bone marrow, that is by definition multiple myeloma warranting treatment. Smoldering myeloma requires at least 10% plasmacytosis in bone marrow and absence of the CRAB criteria. However, in a significant change, ultra–high-risk smoldering melanoma, defined by the acronym SLiM CRAB, is now considered active myeloma and should be treated (Lancet Oncol. 2014 Nov;15[12]:e538-48).
“Traditionally, we waited until CRAB [to define myeloma],” Dr. Mikhael explained. “But if you’re running toward a cliff, I don’t have to wait until you’re falling off to know you’re in trouble.”
The SLiM half of SLiM CRAB consists of 60% or more plasmacytosis in bone marrow, light chains in a kappa-to-lambda or lambda-to-kappa ratio of greater than 100, and MRI showing one or more focal lesions. If a patient is SLiM, with or without CRAB, that is now considered active myeloma warranting treatment.
Not all MGUS needs a bone marrow biopsy
A bone marrow biopsy and skeletal survey via whole-body CT or conventional radiographs can be deferred in patients with low-risk MGUS and no bony symptoms. Using the Mayo Clinic risk stratification model, low risk is defined as a serum M protein of 1.5 g/dL or less on SPE, an IgG isotype, and a normal free light-chain ratio.
The lifetime risk of progression in patients with MGUS who meet all three criteria is only about 2%. They can be followed at 6 months with an SPE, free light-chain testing, a CBC, and serum calcium and creatinine, then annually thereafter.
“For those who aren’t in this low-risk category, we actually do need to do a bone marrow test,” according to Dr. Mikhael. “Then, based on that, if they have malignancy, send them to a myeloma geek like me or to another hematologist. And if they don’t have a malignancy, they can be followed at 6 months and then subsequently at least every year.”
Dr. Mikhael has received research grants from AbbVie, Celgene, and Sanofi.
NEW ORLEANS – Everyone aged 40 years and older on the island nation of Iceland is being screened for monoclonal gammopathy of undetermined significance, smoldering myeloma, and full-blown multiple myeloma in an unprecedented project to identify the malignancy’s genetic roots, Joseph Mikhael, MD, said at the annual meeting of the American College of Physicians.
This effort to decode the underlying genetics of multiple myeloma is enormously facilitated by the fact that the DNA sequencing of the entire Icelandic population is already known, and everyone’s blood samples are stored in the national health care system.
The International Myeloma Foundation is funding the Icelandic project, called iStopMM (Iceland Screens Treats or Prevents Multiple Myeloma).
The results of iStopMM could be far reaching, in part because the findings will show whether screening an asymptomatic general population for MGUS – as for example, all American adults – is worthwhile.
In the interim, it’s important for primary care physicians to recognize when it is and isn’t appropriate to order a serum protein electrophoresis (SPE) study, on which the diagnosis of MGUS hinges. It’s also essential to recognize the difference between smoldering and full-blown multiple myeloma, because the distinction has implications for patient monitoring and treatment, added Dr. Mikhael, a hematologist at the City of Hope Cancer Center in Duarte, Calif.
Multiple myeloma accounts for 1% of all cancers and 10% of hematologic malignancies. MGUS is an obligate precursor of multiple myeloma. But MGUS is common, and therein lies a challenge for physicians – as well as a major source of anxiety for many MGUS-positive patients.
In a 12-year-old study, MGUS had a 3% prevalence in the general U.S. population older than age 50 years, and a greater than 5% prevalence after age 70. However, Dr. Mikhael thinks that more refined testing will show the true figure to be close to 10%. Thus, the great majority of patients with MGUS will never develop multiple myeloma.
Pending the potentially practice-changing outcome of iStopMM, Dr. Mikhael said SPE shouldn’t be ordered routinely in an asymptomatic patient, even one with a positive family history for multiple myeloma. The annual cost of monitoring the roughly 540,000 U.S. patients who now carry a diagnosis of MGUS – typically established as an incidental finding by primary care physicians while doing a work-up for another reason – is at least $110 million. And there’s no point in adding to that burden until the benefit of mass screening has been established.
An SPE is appropriate, however, in an older patient with unexplained anemia, known low immunoglobulin levels, unexplained renal insufficiency or neuropathy, or osteopenia or osteoporosis inconsistent with the patient’s age or gender – provided the patient doesn’t have a coexisting plasma cell dyscrasia or B-cell lymphoproliferative disorder, which would throw off the prognostic value of the test results, he continued.
When ordering an SPE to rule in/out MGUS, it’s essential to also order serum free light-chain testing, because it provides key prognostic information.
A landmark study led by investigators at the Mayo Clinic demonstrated that the risk of progression of MGUS to multiple myeloma or a related disorder is independently predicted by three key factors: a high serum M-protein spike of 15 g/L or more on the SPE; the presence of non-IgG MGUS; and an abnormal serum free light-chain ratio of less than 0.26 or more than 1.65. In this study, the 20-year risk of malignant transformation of MGUS ranged from 58% if all three risk factors were present, to just 5% if none were (Blood. 2005 Aug 1;106[3]:812-7).
CRAB vs. SLiM CRAB
Myeloma, smoldering myeloma, and MGUS were redefined a few years ago to reflect differences in prognosis. MGUS still requires the presence of a serum monoclonal protein in a concentration of 3 g/dL or less, less than 10% plasmacytosis in the bone marrow, asymptomatic status, and absence of end-organ damage as traditionally defined in the acronym CRAB (calcium elevation, renal insufficiency, anemia, or bony disease).
If CRAB is present in a patient with at least 10% plasma cells in bone marrow, that is by definition multiple myeloma warranting treatment. Smoldering myeloma requires at least 10% plasmacytosis in bone marrow and absence of the CRAB criteria. However, in a significant change, ultra–high-risk smoldering melanoma, defined by the acronym SLiM CRAB, is now considered active myeloma and should be treated (Lancet Oncol. 2014 Nov;15[12]:e538-48).
“Traditionally, we waited until CRAB [to define myeloma],” Dr. Mikhael explained. “But if you’re running toward a cliff, I don’t have to wait until you’re falling off to know you’re in trouble.”
The SLiM half of SLiM CRAB consists of 60% or more plasmacytosis in bone marrow, light chains in a kappa-to-lambda or lambda-to-kappa ratio of greater than 100, and MRI showing one or more focal lesions. If a patient is SLiM, with or without CRAB, that is now considered active myeloma warranting treatment.
Not all MGUS needs a bone marrow biopsy
A bone marrow biopsy and skeletal survey via whole-body CT or conventional radiographs can be deferred in patients with low-risk MGUS and no bony symptoms. Using the Mayo Clinic risk stratification model, low risk is defined as a serum M protein of 1.5 g/dL or less on SPE, an IgG isotype, and a normal free light-chain ratio.
The lifetime risk of progression in patients with MGUS who meet all three criteria is only about 2%. They can be followed at 6 months with an SPE, free light-chain testing, a CBC, and serum calcium and creatinine, then annually thereafter.
“For those who aren’t in this low-risk category, we actually do need to do a bone marrow test,” according to Dr. Mikhael. “Then, based on that, if they have malignancy, send them to a myeloma geek like me or to another hematologist. And if they don’t have a malignancy, they can be followed at 6 months and then subsequently at least every year.”
Dr. Mikhael has received research grants from AbbVie, Celgene, and Sanofi.
EXPERT ANALYSIS FROM ACP INTERNAL MEDICINE
Noninvasive cardiac testing to rule out acute coronary syndromes provides no benefit in low-risk chest pain patients
Background: The 2014 American College of Cardiology/American Heart Association clinical guideline includes a recommendation for noninvasive testing (exercise test or coronary commuted tomographic angiography [CCTA]) in patients with chest pain but no evidence of ischemia. The ROMICAT-II (Rule Out Myocardial Ischemia/Infarction by Computer Assisted Tomography) trial randomized 1,000 ED patients with chest pain to undergo CCTA or usual care with unknown benefits and risks of this testing recommendation. The question of whether this testing may be omitted is addressed in secondary analysis.
Study design: Retrospective analysis of the ROMICAT-II trial data.
Setting: Emergency department.
Synopsis: As compared with 882 patients who underwent noninvasive testing, 118 patients in the ROMICAT-II usual care group who did not undergo noninvasive testing had shorter lengths of stay (20.3 vs. 27.9 hours; P less than .001), lower rates of diagnostic testing (P less than .001), angiography (2% vs. 11%; P less than .001), and lower costs ($2,261.50 vs. $2,584.30). There was no difference in percutaneous coronary intervention (2% vs. 5%; P = .15), coronary artery bypass surgery (0% vs. 1%; P = .61), major adverse cardiac events (MACE; 2% vs. 1%; P = .24), or return ED visits (5.8% vs. 2.8%; P = .08) during the 28-day follow-up period. These findings suggest noninvasive cardiac testing may be omitted in low- to intermediate-risk patients presenting with chest pain. However, this study was not designed or powered to address this question and patients were not randomized. These data may support hospitalists who choose not to order noninvasive testing in ED patients with chest pain.
Bottom line: In this secondary analysis of ROMICAT-II clinical trial data, patients who underwent clinical evaluation without noninvasive testing had shorter length of stay, less diagnostic testing, lower radiation exposure, and reduced costs with no difference in missed diagnosis of acute coronary syndromes, development of MACE, or return ED visits.
Citation: Reinhardt SW et al. Noninvasive cardiac testing vs. clinical evaluation alone in acute chest pain: A secondary analysis of the ROMICAT-II randomized clinical trial. JAMA Intern Med. 2018 Feb 1;178(2):212-9.

Dr. Moulder is assistant professor, University of Virginia Health System.
Background: The 2014 American College of Cardiology/American Heart Association clinical guideline includes a recommendation for noninvasive testing (exercise test or coronary commuted tomographic angiography [CCTA]) in patients with chest pain but no evidence of ischemia. The ROMICAT-II (Rule Out Myocardial Ischemia/Infarction by Computer Assisted Tomography) trial randomized 1,000 ED patients with chest pain to undergo CCTA or usual care with unknown benefits and risks of this testing recommendation. The question of whether this testing may be omitted is addressed in secondary analysis.
Study design: Retrospective analysis of the ROMICAT-II trial data.
Setting: Emergency department.
Synopsis: As compared with 882 patients who underwent noninvasive testing, 118 patients in the ROMICAT-II usual care group who did not undergo noninvasive testing had shorter lengths of stay (20.3 vs. 27.9 hours; P less than .001), lower rates of diagnostic testing (P less than .001), angiography (2% vs. 11%; P less than .001), and lower costs ($2,261.50 vs. $2,584.30). There was no difference in percutaneous coronary intervention (2% vs. 5%; P = .15), coronary artery bypass surgery (0% vs. 1%; P = .61), major adverse cardiac events (MACE; 2% vs. 1%; P = .24), or return ED visits (5.8% vs. 2.8%; P = .08) during the 28-day follow-up period. These findings suggest noninvasive cardiac testing may be omitted in low- to intermediate-risk patients presenting with chest pain. However, this study was not designed or powered to address this question and patients were not randomized. These data may support hospitalists who choose not to order noninvasive testing in ED patients with chest pain.
Bottom line: In this secondary analysis of ROMICAT-II clinical trial data, patients who underwent clinical evaluation without noninvasive testing had shorter length of stay, less diagnostic testing, lower radiation exposure, and reduced costs with no difference in missed diagnosis of acute coronary syndromes, development of MACE, or return ED visits.
Citation: Reinhardt SW et al. Noninvasive cardiac testing vs. clinical evaluation alone in acute chest pain: A secondary analysis of the ROMICAT-II randomized clinical trial. JAMA Intern Med. 2018 Feb 1;178(2):212-9.
Dr. Moulder is assistant professor, University of Virginia Health System.
Background: The 2014 American College of Cardiology/American Heart Association clinical guideline includes a recommendation for noninvasive testing (exercise test or coronary commuted tomographic angiography [CCTA]) in patients with chest pain but no evidence of ischemia. The ROMICAT-II (Rule Out Myocardial Ischemia/Infarction by Computer Assisted Tomography) trial randomized 1,000 ED patients with chest pain to undergo CCTA or usual care with unknown benefits and risks of this testing recommendation. The question of whether this testing may be omitted is addressed in secondary analysis.
Study design: Retrospective analysis of the ROMICAT-II trial data.
Setting: Emergency department.
Synopsis: As compared with 882 patients who underwent noninvasive testing, 118 patients in the ROMICAT-II usual care group who did not undergo noninvasive testing had shorter lengths of stay (20.3 vs. 27.9 hours; P less than .001), lower rates of diagnostic testing (P less than .001), angiography (2% vs. 11%; P less than .001), and lower costs ($2,261.50 vs. $2,584.30). There was no difference in percutaneous coronary intervention (2% vs. 5%; P = .15), coronary artery bypass surgery (0% vs. 1%; P = .61), major adverse cardiac events (MACE; 2% vs. 1%; P = .24), or return ED visits (5.8% vs. 2.8%; P = .08) during the 28-day follow-up period. These findings suggest noninvasive cardiac testing may be omitted in low- to intermediate-risk patients presenting with chest pain. However, this study was not designed or powered to address this question and patients were not randomized. These data may support hospitalists who choose not to order noninvasive testing in ED patients with chest pain.
Bottom line: In this secondary analysis of ROMICAT-II clinical trial data, patients who underwent clinical evaluation without noninvasive testing had shorter length of stay, less diagnostic testing, lower radiation exposure, and reduced costs with no difference in missed diagnosis of acute coronary syndromes, development of MACE, or return ED visits.
Citation: Reinhardt SW et al. Noninvasive cardiac testing vs. clinical evaluation alone in acute chest pain: A secondary analysis of the ROMICAT-II randomized clinical trial. JAMA Intern Med. 2018 Feb 1;178(2):212-9.
Dr. Moulder is assistant professor, University of Virginia Health System.
Medicare sets outpatient CAR T-cell therapy rates
Officials at the Centers for Medicare & Medicaid Services announced reimbursement rates for outpatient administration of two chimeric antigen receptor (CAR) T-cell therapies, settling on a fee that is roughly the wholesale acquisition cost plus 6%.
The agency will pay $395,380 to those who administer axicabtagene ciloleucel (Yescarta) on an outpatient basis and $500,839 for outpatient use of tisagenlecleucel (Kymriah), a similar CAR T-cell therapy for cancer patients. The two drugs have list prices of $373,000 and $475,000, respectively.

Although CMS set the Medicare Part B copayment for axicabtagene ciloleucel at $79,076, the agency later clarified that out-of-pocket expenses for Medicare patients are capped at around $1,340 in 2018 – the amount of the inpatient hospital deductible.
The Medicare rate is a first step to being able to use and get paid for CAR T-cell therapies, said Richard T. Maziarz, MD, a bone marrow transplantation and blood cancer specialist at the Oregon Health and Science University Knight Cancer Institute in Portland. However, the rate is not as straight forward as it sounds, he pointed out.
“This is big news,” Dr. Maziarz said in an interview. “This allows us to start to deliver these therapies, but there is a risk: If we give this in the outpatient setting and someone ends up needing hospitalization, we may end up not being reimbursed for the drug product.”
That’s because of CMS’s 3-day payment window rule, Dr. Maziarz explained: If medical treatment is provided in an outpatient setting and the patient needs inpatient care within 72 hours, all payments prior to that 72-hour window become part of the inpatient stay, according to the rule. Inpatient reimbursement varies depending on treatment, previous patient comorbidities, and complications during their stay. Analysts say that inpatient care is likely to occur with CAR T-cell therapies because some patients will need to be admitted so doctors can monitor them for serious side effects.
“If I have a drug that costs me $373,000, what happens if I admit the patient?” Dr. Maziarz said. “I don’t get $373,000; I get between $8,000 and $18,000. So if we give this and someone gets sick in 48 hours, then we may be at risk for losing.”
On the inpatient side, Medicare payment for CAR T-cell therapy is currently bundled into the payment for the inpatient stay, rather than being paid separately. The drug manufacturers – Gilead Sciences and Novartis AG – have requested that CMS set a separate “new technology add-on payment,” but the agency has not yet issued a decision.

Further advancements are expected for CAR T-cell therapies in 2018, said Cai Xuan, PhD, senior analyst in oncology and hematology for GlobalData, a data analytics and commercial intelligence firm.
For starters, pharmaceutical companies are now working toward next-generation CAR T-cell therapies that can be mass produced, Ms. Xuan noted. At a recent American Association for Cancer Research meeting, for example, the biopharmaceutical company Cellectis presented early clinical data in pediatric B-cell acute lymphoblastic leukemia for its off-the-shelf CAR T-cell candidate UCART19. Additionally, CRISPR Therapeutics presented preclinical data for one of its off-the-shelf CAR T-cell candidates for multiple myeloma, and the company announced it would apply for approval to start human trials by the end of 2018.
“The trend for 2018 is very much focusing on how to eliminate some of the profitability issues with first-generation CAR Ts because companies realize that manufacturing individualized treatments for each patient is not an ideal business model,” Dr. Xuan said in an interview.
More market competition is also in the forecast, particularly from smaller companies, Dr. Xuan said.
“What we are likely to see in the future is larger companies acquiring smaller ones once their CAR T technology has matured to a certain point,” she said. “We have seen it with the Gilead-Kite acquisition, as well as Celgene’s acquisition of Juno Therapeutics, and this trend will continue as long as smaller companies are able to develop proprietary next-generation CAR T technologies.”
Cost and accessibility remain key concerns with the therapies, especially for the Medicare population. Cost estimates have put the cost of CAR T-cell therapies as high as $1.5 million per patient.
“There remain unanswered questions about value and cost in older adults,” said Walid F. Gellad, MD, codirector for the Center for Pharmaceutical Policy and Prescribing at the University of Pittsburgh. “There are many life-saving treatments in the medical system that cost much less than this therapy. Presumably, its cost will go down as the indications expand and the experience with creating the CAR T cells improves. At least, one would hope.”

“In the longer term, there’s obviously a lot of people looking at how [the treatments] can be made more accessible,” she said in an interview. “These are the first generation CAR T [products], and I think there’ll be lots of refinements – both to make them more effective and safer, but also eventually with trying to use a third party product – to bring the cost of goods down.”
Other lingering unknowns about CAR T-cell therapies include how many patients in real-world clinical practice will have serious side effects, compared with those in trials, and the long-term recurrence rates after therapy use, Dr. Gellad noted. A recent paper by Dr. Gellad in the New England Journal of Medicine proposes that government payers reimburse only the cost of manufacturing and some predetermined mark-up for such therapies until confirmatory trials demonstrate clinical benefit (N Engl J Med. 2017;376[21]:2001-04).
Time will tell how reimbursement plays out during clinical practice, but one thing is for certain: The current CAR T-cell therapies are only the beginning, Dr. Maziarz said.
“Genetically-engineered cell products are going to explode over the next decade,” he said. “This is not the end of the line, this is the starting point.”
Dr. Maziarz has received consulting fees from Novartis, Juno Therapeutics, and Kite Pharma. Dr. Heslop has received consulting fees from Novartis, has conducted research for Cell Medica and holds intellectual property rights/patents from Cell Medica, and has ownership interest in ViraCyte and Marker Therapeutics. Dr. Gellad reports grants from Express Scripts.
Officials at the Centers for Medicare & Medicaid Services announced reimbursement rates for outpatient administration of two chimeric antigen receptor (CAR) T-cell therapies, settling on a fee that is roughly the wholesale acquisition cost plus 6%.
The agency will pay $395,380 to those who administer axicabtagene ciloleucel (Yescarta) on an outpatient basis and $500,839 for outpatient use of tisagenlecleucel (Kymriah), a similar CAR T-cell therapy for cancer patients. The two drugs have list prices of $373,000 and $475,000, respectively.
Although CMS set the Medicare Part B copayment for axicabtagene ciloleucel at $79,076, the agency later clarified that out-of-pocket expenses for Medicare patients are capped at around $1,340 in 2018 – the amount of the inpatient hospital deductible.
The Medicare rate is a first step to being able to use and get paid for CAR T-cell therapies, said Richard T. Maziarz, MD, a bone marrow transplantation and blood cancer specialist at the Oregon Health and Science University Knight Cancer Institute in Portland. However, the rate is not as straight forward as it sounds, he pointed out.
“This is big news,” Dr. Maziarz said in an interview. “This allows us to start to deliver these therapies, but there is a risk: If we give this in the outpatient setting and someone ends up needing hospitalization, we may end up not being reimbursed for the drug product.”
That’s because of CMS’s 3-day payment window rule, Dr. Maziarz explained: If medical treatment is provided in an outpatient setting and the patient needs inpatient care within 72 hours, all payments prior to that 72-hour window become part of the inpatient stay, according to the rule. Inpatient reimbursement varies depending on treatment, previous patient comorbidities, and complications during their stay. Analysts say that inpatient care is likely to occur with CAR T-cell therapies because some patients will need to be admitted so doctors can monitor them for serious side effects.
“If I have a drug that costs me $373,000, what happens if I admit the patient?” Dr. Maziarz said. “I don’t get $373,000; I get between $8,000 and $18,000. So if we give this and someone gets sick in 48 hours, then we may be at risk for losing.”
On the inpatient side, Medicare payment for CAR T-cell therapy is currently bundled into the payment for the inpatient stay, rather than being paid separately. The drug manufacturers – Gilead Sciences and Novartis AG – have requested that CMS set a separate “new technology add-on payment,” but the agency has not yet issued a decision.
Further advancements are expected for CAR T-cell therapies in 2018, said Cai Xuan, PhD, senior analyst in oncology and hematology for GlobalData, a data analytics and commercial intelligence firm.
For starters, pharmaceutical companies are now working toward next-generation CAR T-cell therapies that can be mass produced, Ms. Xuan noted. At a recent American Association for Cancer Research meeting, for example, the biopharmaceutical company Cellectis presented early clinical data in pediatric B-cell acute lymphoblastic leukemia for its off-the-shelf CAR T-cell candidate UCART19. Additionally, CRISPR Therapeutics presented preclinical data for one of its off-the-shelf CAR T-cell candidates for multiple myeloma, and the company announced it would apply for approval to start human trials by the end of 2018.
“The trend for 2018 is very much focusing on how to eliminate some of the profitability issues with first-generation CAR Ts because companies realize that manufacturing individualized treatments for each patient is not an ideal business model,” Dr. Xuan said in an interview.
More market competition is also in the forecast, particularly from smaller companies, Dr. Xuan said.
“What we are likely to see in the future is larger companies acquiring smaller ones once their CAR T technology has matured to a certain point,” she said. “We have seen it with the Gilead-Kite acquisition, as well as Celgene’s acquisition of Juno Therapeutics, and this trend will continue as long as smaller companies are able to develop proprietary next-generation CAR T technologies.”
Cost and accessibility remain key concerns with the therapies, especially for the Medicare population. Cost estimates have put the cost of CAR T-cell therapies as high as $1.5 million per patient.
“There remain unanswered questions about value and cost in older adults,” said Walid F. Gellad, MD, codirector for the Center for Pharmaceutical Policy and Prescribing at the University of Pittsburgh. “There are many life-saving treatments in the medical system that cost much less than this therapy. Presumably, its cost will go down as the indications expand and the experience with creating the CAR T cells improves. At least, one would hope.”
“In the longer term, there’s obviously a lot of people looking at how [the treatments] can be made more accessible,” she said in an interview. “These are the first generation CAR T [products], and I think there’ll be lots of refinements – both to make them more effective and safer, but also eventually with trying to use a third party product – to bring the cost of goods down.”
Other lingering unknowns about CAR T-cell therapies include how many patients in real-world clinical practice will have serious side effects, compared with those in trials, and the long-term recurrence rates after therapy use, Dr. Gellad noted. A recent paper by Dr. Gellad in the New England Journal of Medicine proposes that government payers reimburse only the cost of manufacturing and some predetermined mark-up for such therapies until confirmatory trials demonstrate clinical benefit (N Engl J Med. 2017;376[21]:2001-04).
Time will tell how reimbursement plays out during clinical practice, but one thing is for certain: The current CAR T-cell therapies are only the beginning, Dr. Maziarz said.
“Genetically-engineered cell products are going to explode over the next decade,” he said. “This is not the end of the line, this is the starting point.”
Dr. Maziarz has received consulting fees from Novartis, Juno Therapeutics, and Kite Pharma. Dr. Heslop has received consulting fees from Novartis, has conducted research for Cell Medica and holds intellectual property rights/patents from Cell Medica, and has ownership interest in ViraCyte and Marker Therapeutics. Dr. Gellad reports grants from Express Scripts.
Officials at the Centers for Medicare & Medicaid Services announced reimbursement rates for outpatient administration of two chimeric antigen receptor (CAR) T-cell therapies, settling on a fee that is roughly the wholesale acquisition cost plus 6%.
The agency will pay $395,380 to those who administer axicabtagene ciloleucel (Yescarta) on an outpatient basis and $500,839 for outpatient use of tisagenlecleucel (Kymriah), a similar CAR T-cell therapy for cancer patients. The two drugs have list prices of $373,000 and $475,000, respectively.
Although CMS set the Medicare Part B copayment for axicabtagene ciloleucel at $79,076, the agency later clarified that out-of-pocket expenses for Medicare patients are capped at around $1,340 in 2018 – the amount of the inpatient hospital deductible.
The Medicare rate is a first step to being able to use and get paid for CAR T-cell therapies, said Richard T. Maziarz, MD, a bone marrow transplantation and blood cancer specialist at the Oregon Health and Science University Knight Cancer Institute in Portland. However, the rate is not as straight forward as it sounds, he pointed out.
“This is big news,” Dr. Maziarz said in an interview. “This allows us to start to deliver these therapies, but there is a risk: If we give this in the outpatient setting and someone ends up needing hospitalization, we may end up not being reimbursed for the drug product.”
That’s because of CMS’s 3-day payment window rule, Dr. Maziarz explained: If medical treatment is provided in an outpatient setting and the patient needs inpatient care within 72 hours, all payments prior to that 72-hour window become part of the inpatient stay, according to the rule. Inpatient reimbursement varies depending on treatment, previous patient comorbidities, and complications during their stay. Analysts say that inpatient care is likely to occur with CAR T-cell therapies because some patients will need to be admitted so doctors can monitor them for serious side effects.
“If I have a drug that costs me $373,000, what happens if I admit the patient?” Dr. Maziarz said. “I don’t get $373,000; I get between $8,000 and $18,000. So if we give this and someone gets sick in 48 hours, then we may be at risk for losing.”
On the inpatient side, Medicare payment for CAR T-cell therapy is currently bundled into the payment for the inpatient stay, rather than being paid separately. The drug manufacturers – Gilead Sciences and Novartis AG – have requested that CMS set a separate “new technology add-on payment,” but the agency has not yet issued a decision.
Further advancements are expected for CAR T-cell therapies in 2018, said Cai Xuan, PhD, senior analyst in oncology and hematology for GlobalData, a data analytics and commercial intelligence firm.
For starters, pharmaceutical companies are now working toward next-generation CAR T-cell therapies that can be mass produced, Ms. Xuan noted. At a recent American Association for Cancer Research meeting, for example, the biopharmaceutical company Cellectis presented early clinical data in pediatric B-cell acute lymphoblastic leukemia for its off-the-shelf CAR T-cell candidate UCART19. Additionally, CRISPR Therapeutics presented preclinical data for one of its off-the-shelf CAR T-cell candidates for multiple myeloma, and the company announced it would apply for approval to start human trials by the end of 2018.
“The trend for 2018 is very much focusing on how to eliminate some of the profitability issues with first-generation CAR Ts because companies realize that manufacturing individualized treatments for each patient is not an ideal business model,” Dr. Xuan said in an interview.
More market competition is also in the forecast, particularly from smaller companies, Dr. Xuan said.
“What we are likely to see in the future is larger companies acquiring smaller ones once their CAR T technology has matured to a certain point,” she said. “We have seen it with the Gilead-Kite acquisition, as well as Celgene’s acquisition of Juno Therapeutics, and this trend will continue as long as smaller companies are able to develop proprietary next-generation CAR T technologies.”
Cost and accessibility remain key concerns with the therapies, especially for the Medicare population. Cost estimates have put the cost of CAR T-cell therapies as high as $1.5 million per patient.
“There remain unanswered questions about value and cost in older adults,” said Walid F. Gellad, MD, codirector for the Center for Pharmaceutical Policy and Prescribing at the University of Pittsburgh. “There are many life-saving treatments in the medical system that cost much less than this therapy. Presumably, its cost will go down as the indications expand and the experience with creating the CAR T cells improves. At least, one would hope.”
“In the longer term, there’s obviously a lot of people looking at how [the treatments] can be made more accessible,” she said in an interview. “These are the first generation CAR T [products], and I think there’ll be lots of refinements – both to make them more effective and safer, but also eventually with trying to use a third party product – to bring the cost of goods down.”
Other lingering unknowns about CAR T-cell therapies include how many patients in real-world clinical practice will have serious side effects, compared with those in trials, and the long-term recurrence rates after therapy use, Dr. Gellad noted. A recent paper by Dr. Gellad in the New England Journal of Medicine proposes that government payers reimburse only the cost of manufacturing and some predetermined mark-up for such therapies until confirmatory trials demonstrate clinical benefit (N Engl J Med. 2017;376[21]:2001-04).
Time will tell how reimbursement plays out during clinical practice, but one thing is for certain: The current CAR T-cell therapies are only the beginning, Dr. Maziarz said.
“Genetically-engineered cell products are going to explode over the next decade,” he said. “This is not the end of the line, this is the starting point.”
Dr. Maziarz has received consulting fees from Novartis, Juno Therapeutics, and Kite Pharma. Dr. Heslop has received consulting fees from Novartis, has conducted research for Cell Medica and holds intellectual property rights/patents from Cell Medica, and has ownership interest in ViraCyte and Marker Therapeutics. Dr. Gellad reports grants from Express Scripts.
Female physicians face enduring wage gap
Male physicians make more money than female physicians, and that seems to be a rule with few exceptions. Among the 50 largest metro areas, there were none where women earn as much as men, according to a new survey by the medical social network Doximity.
The metro area that comes the closest is Las Vegas, where female physicians earned 20% less – that works out to $73,654 – than their male counterparts in 2017. Rochester, N.Y., had the smallest gap in terms of dollars ($68,758) and the second-smallest percent difference (21%), Doximity said in its 2018 Physician Compensation Report.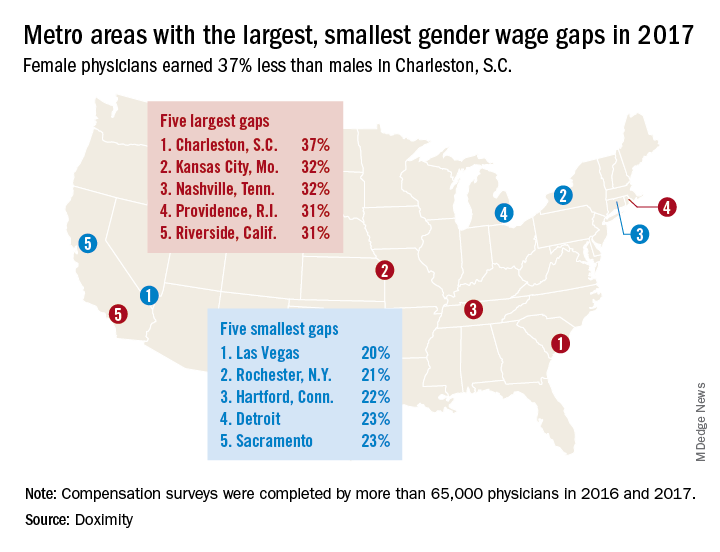
A quick look at the 2016 data shows that the wage gap between female and male physicians increased from 26.5% to 27.7% in 2017, going from more than $92,000 to $105,000. “Medicine is a highly trained field, and as such, one might expect the gender wage gap to be less prominent here than in other industries. However, the gap endures, despite the level of education required to practice medicine and market forces suggesting that this gap should shrink,” Doximity said.
Male physicians make more money than female physicians, and that seems to be a rule with few exceptions. Among the 50 largest metro areas, there were none where women earn as much as men, according to a new survey by the medical social network Doximity.
The metro area that comes the closest is Las Vegas, where female physicians earned 20% less – that works out to $73,654 – than their male counterparts in 2017. Rochester, N.Y., had the smallest gap in terms of dollars ($68,758) and the second-smallest percent difference (21%), Doximity said in its 2018 Physician Compensation Report.
A quick look at the 2016 data shows that the wage gap between female and male physicians increased from 26.5% to 27.7% in 2017, going from more than $92,000 to $105,000. “Medicine is a highly trained field, and as such, one might expect the gender wage gap to be less prominent here than in other industries. However, the gap endures, despite the level of education required to practice medicine and market forces suggesting that this gap should shrink,” Doximity said.
Male physicians make more money than female physicians, and that seems to be a rule with few exceptions. Among the 50 largest metro areas, there were none where women earn as much as men, according to a new survey by the medical social network Doximity.
The metro area that comes the closest is Las Vegas, where female physicians earned 20% less – that works out to $73,654 – than their male counterparts in 2017. Rochester, N.Y., had the smallest gap in terms of dollars ($68,758) and the second-smallest percent difference (21%), Doximity said in its 2018 Physician Compensation Report.
A quick look at the 2016 data shows that the wage gap between female and male physicians increased from 26.5% to 27.7% in 2017, going from more than $92,000 to $105,000. “Medicine is a highly trained field, and as such, one might expect the gender wage gap to be less prominent here than in other industries. However, the gap endures, despite the level of education required to practice medicine and market forces suggesting that this gap should shrink,” Doximity said.