User login
ALUR: Alectinib topped chemo in pretreated ALK-positive NSCLC
The second-generation anaplastic lymphoma kinase (ALK) inhibitor alectinib (Alcensa) topped chemotherapy in crizotinib-pretreated ALK+ non–small cell lung cancer (NSCLC), according to results from the phase 3 ALUR trial.
Median investigator-assessed progression-free survival was 9.6 months with alectinib and 1.4 months with chemotherapy (hazard ratio, 0.15; P less than .001), reported Silvia Novello, MD, PhD, of University of Turin (Italy) and her associates. Among patients with measurable central nervous system disease, the rate of CNS objective response was significantly higher for alectinib (54%) versus chemotherapy (0%; P less than .001), Dr. Novello and her associates reported in Annals of Oncology.
The multicenter, open-label ALUR trial was the first to directly compare alectinib with standard chemotherapy in patients with ALK-rearranged NSCLC that previously had been treated with both platinum-based chemotherapy and crizotinib. In all, 107 patients were randomly assigned on a 2:1 basis to receive either alectinib (600 mg twice daily) or chemotherapy (clinician’s choice of pemetrexed 500 mg/m2 or docetaxel 75 mg/m2 every 3 weeks).
A blinded independent review committee calculated median progression-free survival (PFS) times that were 2.5 months shorter for alectinib and 0.2 months longer for chemotherapy. Consequently, the hazard ratio for PFS was somewhat attenuated at 0.32 but remained highly significant (95% confidence interval, 0.17-0.59). “[Median] PFS with alectinib in ALUR has exceeded that observed with [second-line] ceritinib” during the ASCEND-5 study, the researchers wrote. In ASCEND-5, median independent review committee–assessed PFS time was 5.4 months, which is 1.7 months shorter than that for alectinib in ALUR. In each study, chemotherapy yielded a median PFS time of 1.6 months, which facilitated intertrial comparisons, they wrote.
Rates of all-grade and serious adverse events were similar between arms in ALUR. Alectinib therapy caused no fatal adverse events, while chemotherapy was associated with one fatality deemed unrelated to treatment. Alectinib was more likely to produce constipation, dyspnea, and hyperbilirubinemia, while chemotherapy was more likely to cause nausea, alopecia, neutropenia, diarrhea, pruritus, stomatitis, and bacterial pneumonia. Although patients stayed on alectinib a median of 14 weeks longer than on chemotherapy, they were less likely to stop alectinib (6%) than chemotherapy (9%) for adverse events.
Dr. Novello disclosed personal fees from Roche, which markets alectinib. Eleven coinvestigators also disclosed employment, stock ownership, or other financial ties to Roche.
SOURCE: Novello S et al. Ann Oncol. 2018 Apr 14. doi: 10.1093/annonc/mdy121.
Questions about which next-generation anaplastic lymphoma kinase (ALK) tyrosine kinase inhibitor is best for treatment-naive ALK+ NSCLC will incite “vigorous debate and the inevitable cross-trial comparison that everyone frowns upon but does anyway,” wrote Misako Nagasaka, MD; Viola W. Zhu, MD, PhD; and Sai-Hong Ignatius Ou, MD, PhD, in an editorial accompanying the study in Annals of Oncology.
Median progression-free survival time in ALUR was 7.1 months, versus 5.4 months in the similarly designed ASCEND-5 trial of second-line ceritinib in ALK+ NSCLC, they noted. “ALUR seems to confirm the superiority of alectinib [over ceritinib] in the post-crizotinib setting.”
Similarly, first-line alectinib produced a longer median progression-free survival time (25.7 months) in the ALEX trial than did first-line ceritinib (16.6 months) in the ASCEND-4 trial, the editorialists noted.
They called brigatinib “the one ALK TKI [anaplastic lymphoma kinase tyrosine kinase inhibitor] that can challenge alectinib.” The global phase 3 Brigatinib 3001 trial will directly compare brigatinib with alectinib in the post-chemotherapy and post-crizotinib setting.
Dr. Nagasaka is with Wayne State University, Detroit; she reported having no conflicts of interest. Dr. Zhu and Dr. Ou are with the University of California, Irvine; they disclosed ties to Roche/Genentech, Pfizer, and Takeda/Ariad. These comments summarize their editorial (Ann Oncol. 2018 Apr 14. doi: 10.1093/annonc/mdy144 )
Questions about which next-generation anaplastic lymphoma kinase (ALK) tyrosine kinase inhibitor is best for treatment-naive ALK+ NSCLC will incite “vigorous debate and the inevitable cross-trial comparison that everyone frowns upon but does anyway,” wrote Misako Nagasaka, MD; Viola W. Zhu, MD, PhD; and Sai-Hong Ignatius Ou, MD, PhD, in an editorial accompanying the study in Annals of Oncology.
Median progression-free survival time in ALUR was 7.1 months, versus 5.4 months in the similarly designed ASCEND-5 trial of second-line ceritinib in ALK+ NSCLC, they noted. “ALUR seems to confirm the superiority of alectinib [over ceritinib] in the post-crizotinib setting.”
Similarly, first-line alectinib produced a longer median progression-free survival time (25.7 months) in the ALEX trial than did first-line ceritinib (16.6 months) in the ASCEND-4 trial, the editorialists noted.
They called brigatinib “the one ALK TKI [anaplastic lymphoma kinase tyrosine kinase inhibitor] that can challenge alectinib.” The global phase 3 Brigatinib 3001 trial will directly compare brigatinib with alectinib in the post-chemotherapy and post-crizotinib setting.
Dr. Nagasaka is with Wayne State University, Detroit; she reported having no conflicts of interest. Dr. Zhu and Dr. Ou are with the University of California, Irvine; they disclosed ties to Roche/Genentech, Pfizer, and Takeda/Ariad. These comments summarize their editorial (Ann Oncol. 2018 Apr 14. doi: 10.1093/annonc/mdy144 )
Questions about which next-generation anaplastic lymphoma kinase (ALK) tyrosine kinase inhibitor is best for treatment-naive ALK+ NSCLC will incite “vigorous debate and the inevitable cross-trial comparison that everyone frowns upon but does anyway,” wrote Misako Nagasaka, MD; Viola W. Zhu, MD, PhD; and Sai-Hong Ignatius Ou, MD, PhD, in an editorial accompanying the study in Annals of Oncology.
Median progression-free survival time in ALUR was 7.1 months, versus 5.4 months in the similarly designed ASCEND-5 trial of second-line ceritinib in ALK+ NSCLC, they noted. “ALUR seems to confirm the superiority of alectinib [over ceritinib] in the post-crizotinib setting.”
Similarly, first-line alectinib produced a longer median progression-free survival time (25.7 months) in the ALEX trial than did first-line ceritinib (16.6 months) in the ASCEND-4 trial, the editorialists noted.
They called brigatinib “the one ALK TKI [anaplastic lymphoma kinase tyrosine kinase inhibitor] that can challenge alectinib.” The global phase 3 Brigatinib 3001 trial will directly compare brigatinib with alectinib in the post-chemotherapy and post-crizotinib setting.
Dr. Nagasaka is with Wayne State University, Detroit; she reported having no conflicts of interest. Dr. Zhu and Dr. Ou are with the University of California, Irvine; they disclosed ties to Roche/Genentech, Pfizer, and Takeda/Ariad. These comments summarize their editorial (Ann Oncol. 2018 Apr 14. doi: 10.1093/annonc/mdy144 )
The second-generation anaplastic lymphoma kinase (ALK) inhibitor alectinib (Alcensa) topped chemotherapy in crizotinib-pretreated ALK+ non–small cell lung cancer (NSCLC), according to results from the phase 3 ALUR trial.
Median investigator-assessed progression-free survival was 9.6 months with alectinib and 1.4 months with chemotherapy (hazard ratio, 0.15; P less than .001), reported Silvia Novello, MD, PhD, of University of Turin (Italy) and her associates. Among patients with measurable central nervous system disease, the rate of CNS objective response was significantly higher for alectinib (54%) versus chemotherapy (0%; P less than .001), Dr. Novello and her associates reported in Annals of Oncology.
The multicenter, open-label ALUR trial was the first to directly compare alectinib with standard chemotherapy in patients with ALK-rearranged NSCLC that previously had been treated with both platinum-based chemotherapy and crizotinib. In all, 107 patients were randomly assigned on a 2:1 basis to receive either alectinib (600 mg twice daily) or chemotherapy (clinician’s choice of pemetrexed 500 mg/m2 or docetaxel 75 mg/m2 every 3 weeks).
A blinded independent review committee calculated median progression-free survival (PFS) times that were 2.5 months shorter for alectinib and 0.2 months longer for chemotherapy. Consequently, the hazard ratio for PFS was somewhat attenuated at 0.32 but remained highly significant (95% confidence interval, 0.17-0.59). “[Median] PFS with alectinib in ALUR has exceeded that observed with [second-line] ceritinib” during the ASCEND-5 study, the researchers wrote. In ASCEND-5, median independent review committee–assessed PFS time was 5.4 months, which is 1.7 months shorter than that for alectinib in ALUR. In each study, chemotherapy yielded a median PFS time of 1.6 months, which facilitated intertrial comparisons, they wrote.
Rates of all-grade and serious adverse events were similar between arms in ALUR. Alectinib therapy caused no fatal adverse events, while chemotherapy was associated with one fatality deemed unrelated to treatment. Alectinib was more likely to produce constipation, dyspnea, and hyperbilirubinemia, while chemotherapy was more likely to cause nausea, alopecia, neutropenia, diarrhea, pruritus, stomatitis, and bacterial pneumonia. Although patients stayed on alectinib a median of 14 weeks longer than on chemotherapy, they were less likely to stop alectinib (6%) than chemotherapy (9%) for adverse events.
Dr. Novello disclosed personal fees from Roche, which markets alectinib. Eleven coinvestigators also disclosed employment, stock ownership, or other financial ties to Roche.
SOURCE: Novello S et al. Ann Oncol. 2018 Apr 14. doi: 10.1093/annonc/mdy121.
The second-generation anaplastic lymphoma kinase (ALK) inhibitor alectinib (Alcensa) topped chemotherapy in crizotinib-pretreated ALK+ non–small cell lung cancer (NSCLC), according to results from the phase 3 ALUR trial.
Median investigator-assessed progression-free survival was 9.6 months with alectinib and 1.4 months with chemotherapy (hazard ratio, 0.15; P less than .001), reported Silvia Novello, MD, PhD, of University of Turin (Italy) and her associates. Among patients with measurable central nervous system disease, the rate of CNS objective response was significantly higher for alectinib (54%) versus chemotherapy (0%; P less than .001), Dr. Novello and her associates reported in Annals of Oncology.
The multicenter, open-label ALUR trial was the first to directly compare alectinib with standard chemotherapy in patients with ALK-rearranged NSCLC that previously had been treated with both platinum-based chemotherapy and crizotinib. In all, 107 patients were randomly assigned on a 2:1 basis to receive either alectinib (600 mg twice daily) or chemotherapy (clinician’s choice of pemetrexed 500 mg/m2 or docetaxel 75 mg/m2 every 3 weeks).
A blinded independent review committee calculated median progression-free survival (PFS) times that were 2.5 months shorter for alectinib and 0.2 months longer for chemotherapy. Consequently, the hazard ratio for PFS was somewhat attenuated at 0.32 but remained highly significant (95% confidence interval, 0.17-0.59). “[Median] PFS with alectinib in ALUR has exceeded that observed with [second-line] ceritinib” during the ASCEND-5 study, the researchers wrote. In ASCEND-5, median independent review committee–assessed PFS time was 5.4 months, which is 1.7 months shorter than that for alectinib in ALUR. In each study, chemotherapy yielded a median PFS time of 1.6 months, which facilitated intertrial comparisons, they wrote.
Rates of all-grade and serious adverse events were similar between arms in ALUR. Alectinib therapy caused no fatal adverse events, while chemotherapy was associated with one fatality deemed unrelated to treatment. Alectinib was more likely to produce constipation, dyspnea, and hyperbilirubinemia, while chemotherapy was more likely to cause nausea, alopecia, neutropenia, diarrhea, pruritus, stomatitis, and bacterial pneumonia. Although patients stayed on alectinib a median of 14 weeks longer than on chemotherapy, they were less likely to stop alectinib (6%) than chemotherapy (9%) for adverse events.
Dr. Novello disclosed personal fees from Roche, which markets alectinib. Eleven coinvestigators also disclosed employment, stock ownership, or other financial ties to Roche.
SOURCE: Novello S et al. Ann Oncol. 2018 Apr 14. doi: 10.1093/annonc/mdy121.
FROM ANNALS OF ONCOLOGY
Key clinical point: Alectinib topped chemotherapy in patients with advanced/metastatic crizotinib-pretreated, ALK-positive NSCLC.
Major finding: Median investigator-assessed progression-free survival was 9.6 months with alectinib and 1.4 months with chemotherapy (hazard ratio, 0.15; P less than .001).
Study details: ALUR, which is a randomized, multicenter, open-label, phase 3 trial of 107 patients.
Disclosures: Dr. Novello disclosed personal fees from Roche, which markets alectinib. Eleven coinvestigators also disclosed employment, stock ownership, or other financial ties to Roche.
Source: Novello S et al. Ann Oncol. 2018 Apr 14. doi: 10.1093/annonc/mdy121
Suicidality assessment of people with autism needs better tools
WASHINGTON – People with autism spectrum disorder face a double whammy on suicide risk: They have cognitive, social, and emotional behaviors that increase their vulnerability to suicide, but they also often find it difficult to communicate their depression and suicidality and so may often go unrecognized as suicidal. Or if they are identified, conventional prevention interventions might be less effective.
To try to address this, clinicians are trying to develop a suicide screening questionnaire that is better geared for use on people with autism spectrum disorder (ASD), Jacqueline Wynn, PhD said at the annual conference of the American Association of Suicidology.

Many people with ASD “have impaired language capabilities” that make their expressions of depression and suicide ideation more complex, she observed.
“The point is that we need better measures in the ASQ,” said John P. Ackerman, PhD, a clinical psychologist and suicide prevention coordinator at the Center for Suicide Prevention and Research at Nationwide Children’s. “There is a misperception that because people with autism don’t express their emotions and can’t always access the words they don’t have suicide ideation. They do,” he declared in an interview.
People with ASD have high rates of depression and anxiety, decreased inhibitory control and emotional regulation, rigidity or thought, and difficulty asking for help or accepting help. Youth with ASD undergo psychiatric hospitalization more than 10-fold more often than similarly aged youth without a psychiatric diagnosis, Dr. Ackerman noted. In one recent study of 374 adults with Asperger’s syndrome, two-thirds reported having suicidal ideation and one-third self-reported a planned or attempted suicide (Lancet Psychiatry. 2014 Jul;1[2]:142-7).
The risks that people with ASD have for depression and suicide contrasts with the way clinicians currently address this issue. “There are many gaps” in suicide-risk assessment and prevention interventions aimed at people with ASD, he said. For example, a depression symptom checklist that asks whether someone is withdrawn or feeling disconnected focuses on commonplace characteristics among people with ASD.

The recognition that people with ASD need tailored methods for both identifying and intervening with suicidality appears to be part of an emerging appreciation by clinicians who work on suicide prevention of the “need to meet people where they are,” Dr. Ackerman said. Similar approaches might be needed for various ethnic and racial groups, gays, transgender people, those who are hearing impaired, and others who might respond better to novel approaches.
Dr. Wynn and Dr. Ackerman had no disclosures.
WASHINGTON – People with autism spectrum disorder face a double whammy on suicide risk: They have cognitive, social, and emotional behaviors that increase their vulnerability to suicide, but they also often find it difficult to communicate their depression and suicidality and so may often go unrecognized as suicidal. Or if they are identified, conventional prevention interventions might be less effective.
To try to address this, clinicians are trying to develop a suicide screening questionnaire that is better geared for use on people with autism spectrum disorder (ASD), Jacqueline Wynn, PhD said at the annual conference of the American Association of Suicidology.
Many people with ASD “have impaired language capabilities” that make their expressions of depression and suicide ideation more complex, she observed.
“The point is that we need better measures in the ASQ,” said John P. Ackerman, PhD, a clinical psychologist and suicide prevention coordinator at the Center for Suicide Prevention and Research at Nationwide Children’s. “There is a misperception that because people with autism don’t express their emotions and can’t always access the words they don’t have suicide ideation. They do,” he declared in an interview.
People with ASD have high rates of depression and anxiety, decreased inhibitory control and emotional regulation, rigidity or thought, and difficulty asking for help or accepting help. Youth with ASD undergo psychiatric hospitalization more than 10-fold more often than similarly aged youth without a psychiatric diagnosis, Dr. Ackerman noted. In one recent study of 374 adults with Asperger’s syndrome, two-thirds reported having suicidal ideation and one-third self-reported a planned or attempted suicide (Lancet Psychiatry. 2014 Jul;1[2]:142-7).
The risks that people with ASD have for depression and suicide contrasts with the way clinicians currently address this issue. “There are many gaps” in suicide-risk assessment and prevention interventions aimed at people with ASD, he said. For example, a depression symptom checklist that asks whether someone is withdrawn or feeling disconnected focuses on commonplace characteristics among people with ASD.
The recognition that people with ASD need tailored methods for both identifying and intervening with suicidality appears to be part of an emerging appreciation by clinicians who work on suicide prevention of the “need to meet people where they are,” Dr. Ackerman said. Similar approaches might be needed for various ethnic and racial groups, gays, transgender people, those who are hearing impaired, and others who might respond better to novel approaches.
Dr. Wynn and Dr. Ackerman had no disclosures.
WASHINGTON – People with autism spectrum disorder face a double whammy on suicide risk: They have cognitive, social, and emotional behaviors that increase their vulnerability to suicide, but they also often find it difficult to communicate their depression and suicidality and so may often go unrecognized as suicidal. Or if they are identified, conventional prevention interventions might be less effective.
To try to address this, clinicians are trying to develop a suicide screening questionnaire that is better geared for use on people with autism spectrum disorder (ASD), Jacqueline Wynn, PhD said at the annual conference of the American Association of Suicidology.
Many people with ASD “have impaired language capabilities” that make their expressions of depression and suicide ideation more complex, she observed.
“The point is that we need better measures in the ASQ,” said John P. Ackerman, PhD, a clinical psychologist and suicide prevention coordinator at the Center for Suicide Prevention and Research at Nationwide Children’s. “There is a misperception that because people with autism don’t express their emotions and can’t always access the words they don’t have suicide ideation. They do,” he declared in an interview.
People with ASD have high rates of depression and anxiety, decreased inhibitory control and emotional regulation, rigidity or thought, and difficulty asking for help or accepting help. Youth with ASD undergo psychiatric hospitalization more than 10-fold more often than similarly aged youth without a psychiatric diagnosis, Dr. Ackerman noted. In one recent study of 374 adults with Asperger’s syndrome, two-thirds reported having suicidal ideation and one-third self-reported a planned or attempted suicide (Lancet Psychiatry. 2014 Jul;1[2]:142-7).
The risks that people with ASD have for depression and suicide contrasts with the way clinicians currently address this issue. “There are many gaps” in suicide-risk assessment and prevention interventions aimed at people with ASD, he said. For example, a depression symptom checklist that asks whether someone is withdrawn or feeling disconnected focuses on commonplace characteristics among people with ASD.
The recognition that people with ASD need tailored methods for both identifying and intervening with suicidality appears to be part of an emerging appreciation by clinicians who work on suicide prevention of the “need to meet people where they are,” Dr. Ackerman said. Similar approaches might be needed for various ethnic and racial groups, gays, transgender people, those who are hearing impaired, and others who might respond better to novel approaches.
Dr. Wynn and Dr. Ackerman had no disclosures.
REPORTING FROM THE AAS ANNUAL CONFERENCE
CMS floats Medicare direct provider contracting
Under a direct provider contracting (DPC) arrangement, Medicare could pay physicians or physician groups a monthly fee to deliver a specific set of services to beneficiaries, who would gain greater access to the physicians. The physicians would be accountable for those Medicare patients’ costs and care quality.

CMS is looking at how to incorporate this concept into the Medicare ranks. On April 23, CMS issued a request for information (RFI) seeking input across a wide range of topics, including provider/state participation, beneficiary participation, payment, general model design, program integrity and beneficiary protection, and how such models would fit within the existing accountable care organization framework.
The RFI offered one possible vision on how a direct provider contracting model could work.
“Under a primary care–focused DPC model, CMS could enter into arrangements with primary care practices under which CMS would pay these participating practices a fixed per beneficiary per month (PBPM) payment to cover the primary care services the practice would be expected to furnish under the model, which may include office visits, certain office-based procedures, and other non–visit-based services covered under the physician fee schedule, and flexibility in how otherwise billable services are delivered,” the RFI states.
Physicians could also earn performance bonuses, depending on how the DPC is structured, through “performance-based incentives for total cost of care and quality.”
CMS noted it also “could test ways to reduce administrative burden though innovative changes to claims submission processes for services included in the PBPM payment under these models.”
The direct provider contracting idea grew out of a previous RFI issued in 2017 by CMS’s Center for Medicare and Medicaid Innovation to collect ideas on new ways to deliver patient-centered care. The agency released the more than 1,000 comments received from that request on the same day it issued the RFI on direct provider contracting.
In those comments, a number of physician groups offered support for a direct-contracting approach.
For example, the American Academy of Family Physicians wrote that it “sees continued growth and interest in family physicians adopting this practice model in all settings types, including rural and underserved communities.” And the AAFP suggested that the innovation center should work with DPC organizations to learn more about them.
The American College of Physicians reiterated its previous position that it “supports physician and patient choice of practice and delivery models that are accessible, ethical, and viable and that strengthen the patient-physician relationship.” But the ACP raised a number of issues that could impede access to care or result in lower quality care.
The American Medical Association offered support for “testing of models in which physicians have the ability to deliver more or different services to patients who need them and to be paid more for doing so.”
The AMA suggested that some of the models to be tested include allowing patients to contract directly with physicians, with Medicare paying its fee schedule rates and patients paying the difference; allowing patients to receive their care from DPC practices and get reimbursed by Medicare; or allowing “physicians to define a team of providers who will provide all of the treatment needed for an acute condition or management of a chronic condition, and then allowing patients who select the team to receive all of the services related to their condition from the team in return for a single predefined cost-sharing amount.”
Comments on the RFI are due May 25.
Under a direct provider contracting (DPC) arrangement, Medicare could pay physicians or physician groups a monthly fee to deliver a specific set of services to beneficiaries, who would gain greater access to the physicians. The physicians would be accountable for those Medicare patients’ costs and care quality.
CMS is looking at how to incorporate this concept into the Medicare ranks. On April 23, CMS issued a request for information (RFI) seeking input across a wide range of topics, including provider/state participation, beneficiary participation, payment, general model design, program integrity and beneficiary protection, and how such models would fit within the existing accountable care organization framework.
The RFI offered one possible vision on how a direct provider contracting model could work.
“Under a primary care–focused DPC model, CMS could enter into arrangements with primary care practices under which CMS would pay these participating practices a fixed per beneficiary per month (PBPM) payment to cover the primary care services the practice would be expected to furnish under the model, which may include office visits, certain office-based procedures, and other non–visit-based services covered under the physician fee schedule, and flexibility in how otherwise billable services are delivered,” the RFI states.
Physicians could also earn performance bonuses, depending on how the DPC is structured, through “performance-based incentives for total cost of care and quality.”
CMS noted it also “could test ways to reduce administrative burden though innovative changes to claims submission processes for services included in the PBPM payment under these models.”
The direct provider contracting idea grew out of a previous RFI issued in 2017 by CMS’s Center for Medicare and Medicaid Innovation to collect ideas on new ways to deliver patient-centered care. The agency released the more than 1,000 comments received from that request on the same day it issued the RFI on direct provider contracting.
In those comments, a number of physician groups offered support for a direct-contracting approach.
For example, the American Academy of Family Physicians wrote that it “sees continued growth and interest in family physicians adopting this practice model in all settings types, including rural and underserved communities.” And the AAFP suggested that the innovation center should work with DPC organizations to learn more about them.
The American College of Physicians reiterated its previous position that it “supports physician and patient choice of practice and delivery models that are accessible, ethical, and viable and that strengthen the patient-physician relationship.” But the ACP raised a number of issues that could impede access to care or result in lower quality care.
The American Medical Association offered support for “testing of models in which physicians have the ability to deliver more or different services to patients who need them and to be paid more for doing so.”
The AMA suggested that some of the models to be tested include allowing patients to contract directly with physicians, with Medicare paying its fee schedule rates and patients paying the difference; allowing patients to receive their care from DPC practices and get reimbursed by Medicare; or allowing “physicians to define a team of providers who will provide all of the treatment needed for an acute condition or management of a chronic condition, and then allowing patients who select the team to receive all of the services related to their condition from the team in return for a single predefined cost-sharing amount.”
Comments on the RFI are due May 25.
Under a direct provider contracting (DPC) arrangement, Medicare could pay physicians or physician groups a monthly fee to deliver a specific set of services to beneficiaries, who would gain greater access to the physicians. The physicians would be accountable for those Medicare patients’ costs and care quality.
CMS is looking at how to incorporate this concept into the Medicare ranks. On April 23, CMS issued a request for information (RFI) seeking input across a wide range of topics, including provider/state participation, beneficiary participation, payment, general model design, program integrity and beneficiary protection, and how such models would fit within the existing accountable care organization framework.
The RFI offered one possible vision on how a direct provider contracting model could work.
“Under a primary care–focused DPC model, CMS could enter into arrangements with primary care practices under which CMS would pay these participating practices a fixed per beneficiary per month (PBPM) payment to cover the primary care services the practice would be expected to furnish under the model, which may include office visits, certain office-based procedures, and other non–visit-based services covered under the physician fee schedule, and flexibility in how otherwise billable services are delivered,” the RFI states.
Physicians could also earn performance bonuses, depending on how the DPC is structured, through “performance-based incentives for total cost of care and quality.”
CMS noted it also “could test ways to reduce administrative burden though innovative changes to claims submission processes for services included in the PBPM payment under these models.”
The direct provider contracting idea grew out of a previous RFI issued in 2017 by CMS’s Center for Medicare and Medicaid Innovation to collect ideas on new ways to deliver patient-centered care. The agency released the more than 1,000 comments received from that request on the same day it issued the RFI on direct provider contracting.
In those comments, a number of physician groups offered support for a direct-contracting approach.
For example, the American Academy of Family Physicians wrote that it “sees continued growth and interest in family physicians adopting this practice model in all settings types, including rural and underserved communities.” And the AAFP suggested that the innovation center should work with DPC organizations to learn more about them.
The American College of Physicians reiterated its previous position that it “supports physician and patient choice of practice and delivery models that are accessible, ethical, and viable and that strengthen the patient-physician relationship.” But the ACP raised a number of issues that could impede access to care or result in lower quality care.
The American Medical Association offered support for “testing of models in which physicians have the ability to deliver more or different services to patients who need them and to be paid more for doing so.”
The AMA suggested that some of the models to be tested include allowing patients to contract directly with physicians, with Medicare paying its fee schedule rates and patients paying the difference; allowing patients to receive their care from DPC practices and get reimbursed by Medicare; or allowing “physicians to define a team of providers who will provide all of the treatment needed for an acute condition or management of a chronic condition, and then allowing patients who select the team to receive all of the services related to their condition from the team in return for a single predefined cost-sharing amount.”
Comments on the RFI are due May 25.
Liquid nicotine for e-cigarettes may poison young children
said Preethi Govindarajan of the Research Institute at Nationwide Children’s Hospital in Columbus, Ohio, and his associates.
Since January 2015, pediatric exposures to liquid nicotine have decreased, which may be attributable to legislation requiring child-resistant packaging for liquid nicotine containers and also greater public awareness of the risks associated with e-cigarette products, they noted.
There was a significant increase in the monthly number of liquid nicotine exposures of 2,390% (P less than .001) from November 2012 through January 2015, and a significant decrease of 48% (P less than .001) from January 2015 through April 2017. “From August 2016 (175 exposures), the first month after the federal Child Nicotine Poisoning Prevention Act went into effect, to April 2017 (142 exposures), there was an 18.9% decrease in the number of monthly liquid nicotine exposures,” Mr. Govindarajan and his associates said.
“Child-resistant e-cigarette devices, use of flow restrictors on liquid nicotine containers, and regulations on e-cigarette liquid flavoring, labeling, and concentrations could further reduce the incidence of these exposures and the likelihood of serious medical outcomes when exposures do occur,” they concluded.
SOURCE: Govindarajan P et al. Pediatrics. 2018;141(5):e20173361.
said Preethi Govindarajan of the Research Institute at Nationwide Children’s Hospital in Columbus, Ohio, and his associates.
Since January 2015, pediatric exposures to liquid nicotine have decreased, which may be attributable to legislation requiring child-resistant packaging for liquid nicotine containers and also greater public awareness of the risks associated with e-cigarette products, they noted.
There was a significant increase in the monthly number of liquid nicotine exposures of 2,390% (P less than .001) from November 2012 through January 2015, and a significant decrease of 48% (P less than .001) from January 2015 through April 2017. “From August 2016 (175 exposures), the first month after the federal Child Nicotine Poisoning Prevention Act went into effect, to April 2017 (142 exposures), there was an 18.9% decrease in the number of monthly liquid nicotine exposures,” Mr. Govindarajan and his associates said.
“Child-resistant e-cigarette devices, use of flow restrictors on liquid nicotine containers, and regulations on e-cigarette liquid flavoring, labeling, and concentrations could further reduce the incidence of these exposures and the likelihood of serious medical outcomes when exposures do occur,” they concluded.
SOURCE: Govindarajan P et al. Pediatrics. 2018;141(5):e20173361.
said Preethi Govindarajan of the Research Institute at Nationwide Children’s Hospital in Columbus, Ohio, and his associates.
Since January 2015, pediatric exposures to liquid nicotine have decreased, which may be attributable to legislation requiring child-resistant packaging for liquid nicotine containers and also greater public awareness of the risks associated with e-cigarette products, they noted.
There was a significant increase in the monthly number of liquid nicotine exposures of 2,390% (P less than .001) from November 2012 through January 2015, and a significant decrease of 48% (P less than .001) from January 2015 through April 2017. “From August 2016 (175 exposures), the first month after the federal Child Nicotine Poisoning Prevention Act went into effect, to April 2017 (142 exposures), there was an 18.9% decrease in the number of monthly liquid nicotine exposures,” Mr. Govindarajan and his associates said.
“Child-resistant e-cigarette devices, use of flow restrictors on liquid nicotine containers, and regulations on e-cigarette liquid flavoring, labeling, and concentrations could further reduce the incidence of these exposures and the likelihood of serious medical outcomes when exposures do occur,” they concluded.
SOURCE: Govindarajan P et al. Pediatrics. 2018;141(5):e20173361.
Targeting inactivity, mood, and cognition could be key to reducing OA mortality
LIVERPOOL, ENGLAND – Osteoarthritis is associated with an increased risk in mortality, but three factors – inactivity, low mood, and cognitive ability – could be important targets to reduce this risk, according to the results of a study presented at the World Congress on Osteoarthritis.
“There’s recently been increasing interest in whether osteoarthritis (OA) is associated with mortality as the literature has failed to find a consistent link,” said Simran Parmar, a third-year medical student at Keele University, Newcastle-Under-Lyme, U.K.

Three years later, data from another study (BMJ. 2011;342:d1165) suggested an increased risk, with standardized mortality ratios calculated to be 1.55 for all-cause mortality and 1.71 for cardiovascular-specific mortality when comparing those with OA to those without OA in the general population.
However, more recent meta-analyses, performed in 2016, have failed to show a relationship between mortality and OA (Semin Arthritis Rheum. 2016;46[2]:160–7; Sci Rep. 2016;6:24393).
“This could be because of heterogeneity among the studies,” Mr. Parmar reasoned, adding that there was still an unclear relationship between OA and mortality.
So the aim of the current study was not only to take another look at the association to determine its strength but also to see what factors might be mediating the association in order to perhaps explain why OA might be associated with an increased risk of death.
The analysis used data on more than 8,000 individuals participating in the NorStOP (North Staffordshire Osteoarthritis Project). This is a large, population-based, prospective cohort initiated in 2002 that includes adults aged 50 years or older who are registered at any of six general practices.
At baseline, the mean age of participants was 65 years, 51% were female, and just under 30% had OA. During 10 years of follow-up, 1,188 (14.7%) participants died.
Osteoarthritis was significantly associated with mortality in both unadjusted and adjusted analyses.
“For the average person presenting to general practice in North Staffordshire, there’s a 39.4% increased risk of mortality if they have osteoarthritis compared to if they don’t,” Mr. Parmar said.
After adjustment for potential confounding factors, such as age, NSAID use, and common comorbidities, the increased mortality risk remained, with around a 15% increased risk of death for those with OA versus those without.
“We proposed six different mediators of this relationship,” Mr. Parmar said. These were depression, anxiety, low walking frequency, cognitive impairment, insomnia, and obesity. “The reason we chose these is because they can be targets for therapy in primary care.”
Three mediators significantly affected the relationship: low walking frequency, depression, and cognitive impairment; the respective hazard ratios and 95% confidence intervals were 1.12 (1.09-1.15), 1.11 (1.08-1.15), and 1.06 (1.03-1.09).
“This tells us that these could possibly be on the pathway between osteoarthritis and mortality, and this could provide further evidence that they could be used for targeted therapy of osteoarthritis,” Mr. Parmar suggested.
“This type of mediation analysis has not been done in the osteoarthritis field before,” Mr. Parmar observed. He conceded that the mediators found might actually have contributed to the development of OA and that pain interference used in the definition of OA could have been caused by other factors.
Nevertheless, these data suggest that there may be actionable factors that could be used in primary care to reduce mortality in OA.
Mr. Parmar suggested that “encouraging physical activity and considering the impact of comorbidities can help reduce the risk of mortality in adults with osteoarthritis.”
The study was funded by Arthritis Research UK, the North Staffordshire Primary Care Consortium, and the Medical Research Council. Mr. Parmar had no conflicts of interest to disclose.
SOURCE: Parmar S et al. Osteoarthritis Cartilage. 2018;26(1):S14-15.
LIVERPOOL, ENGLAND – Osteoarthritis is associated with an increased risk in mortality, but three factors – inactivity, low mood, and cognitive ability – could be important targets to reduce this risk, according to the results of a study presented at the World Congress on Osteoarthritis.
“There’s recently been increasing interest in whether osteoarthritis (OA) is associated with mortality as the literature has failed to find a consistent link,” said Simran Parmar, a third-year medical student at Keele University, Newcastle-Under-Lyme, U.K.
Three years later, data from another study (BMJ. 2011;342:d1165) suggested an increased risk, with standardized mortality ratios calculated to be 1.55 for all-cause mortality and 1.71 for cardiovascular-specific mortality when comparing those with OA to those without OA in the general population.
However, more recent meta-analyses, performed in 2016, have failed to show a relationship between mortality and OA (Semin Arthritis Rheum. 2016;46[2]:160–7; Sci Rep. 2016;6:24393).
“This could be because of heterogeneity among the studies,” Mr. Parmar reasoned, adding that there was still an unclear relationship between OA and mortality.
So the aim of the current study was not only to take another look at the association to determine its strength but also to see what factors might be mediating the association in order to perhaps explain why OA might be associated with an increased risk of death.
The analysis used data on more than 8,000 individuals participating in the NorStOP (North Staffordshire Osteoarthritis Project). This is a large, population-based, prospective cohort initiated in 2002 that includes adults aged 50 years or older who are registered at any of six general practices.
At baseline, the mean age of participants was 65 years, 51% were female, and just under 30% had OA. During 10 years of follow-up, 1,188 (14.7%) participants died.
Osteoarthritis was significantly associated with mortality in both unadjusted and adjusted analyses.
“For the average person presenting to general practice in North Staffordshire, there’s a 39.4% increased risk of mortality if they have osteoarthritis compared to if they don’t,” Mr. Parmar said.
After adjustment for potential confounding factors, such as age, NSAID use, and common comorbidities, the increased mortality risk remained, with around a 15% increased risk of death for those with OA versus those without.
“We proposed six different mediators of this relationship,” Mr. Parmar said. These were depression, anxiety, low walking frequency, cognitive impairment, insomnia, and obesity. “The reason we chose these is because they can be targets for therapy in primary care.”
Three mediators significantly affected the relationship: low walking frequency, depression, and cognitive impairment; the respective hazard ratios and 95% confidence intervals were 1.12 (1.09-1.15), 1.11 (1.08-1.15), and 1.06 (1.03-1.09).
“This tells us that these could possibly be on the pathway between osteoarthritis and mortality, and this could provide further evidence that they could be used for targeted therapy of osteoarthritis,” Mr. Parmar suggested.
“This type of mediation analysis has not been done in the osteoarthritis field before,” Mr. Parmar observed. He conceded that the mediators found might actually have contributed to the development of OA and that pain interference used in the definition of OA could have been caused by other factors.
Nevertheless, these data suggest that there may be actionable factors that could be used in primary care to reduce mortality in OA.
Mr. Parmar suggested that “encouraging physical activity and considering the impact of comorbidities can help reduce the risk of mortality in adults with osteoarthritis.”
The study was funded by Arthritis Research UK, the North Staffordshire Primary Care Consortium, and the Medical Research Council. Mr. Parmar had no conflicts of interest to disclose.
SOURCE: Parmar S et al. Osteoarthritis Cartilage. 2018;26(1):S14-15.
LIVERPOOL, ENGLAND – Osteoarthritis is associated with an increased risk in mortality, but three factors – inactivity, low mood, and cognitive ability – could be important targets to reduce this risk, according to the results of a study presented at the World Congress on Osteoarthritis.
“There’s recently been increasing interest in whether osteoarthritis (OA) is associated with mortality as the literature has failed to find a consistent link,” said Simran Parmar, a third-year medical student at Keele University, Newcastle-Under-Lyme, U.K.
Three years later, data from another study (BMJ. 2011;342:d1165) suggested an increased risk, with standardized mortality ratios calculated to be 1.55 for all-cause mortality and 1.71 for cardiovascular-specific mortality when comparing those with OA to those without OA in the general population.
However, more recent meta-analyses, performed in 2016, have failed to show a relationship between mortality and OA (Semin Arthritis Rheum. 2016;46[2]:160–7; Sci Rep. 2016;6:24393).
“This could be because of heterogeneity among the studies,” Mr. Parmar reasoned, adding that there was still an unclear relationship between OA and mortality.
So the aim of the current study was not only to take another look at the association to determine its strength but also to see what factors might be mediating the association in order to perhaps explain why OA might be associated with an increased risk of death.
The analysis used data on more than 8,000 individuals participating in the NorStOP (North Staffordshire Osteoarthritis Project). This is a large, population-based, prospective cohort initiated in 2002 that includes adults aged 50 years or older who are registered at any of six general practices.
At baseline, the mean age of participants was 65 years, 51% were female, and just under 30% had OA. During 10 years of follow-up, 1,188 (14.7%) participants died.
Osteoarthritis was significantly associated with mortality in both unadjusted and adjusted analyses.
“For the average person presenting to general practice in North Staffordshire, there’s a 39.4% increased risk of mortality if they have osteoarthritis compared to if they don’t,” Mr. Parmar said.
After adjustment for potential confounding factors, such as age, NSAID use, and common comorbidities, the increased mortality risk remained, with around a 15% increased risk of death for those with OA versus those without.
“We proposed six different mediators of this relationship,” Mr. Parmar said. These were depression, anxiety, low walking frequency, cognitive impairment, insomnia, and obesity. “The reason we chose these is because they can be targets for therapy in primary care.”
Three mediators significantly affected the relationship: low walking frequency, depression, and cognitive impairment; the respective hazard ratios and 95% confidence intervals were 1.12 (1.09-1.15), 1.11 (1.08-1.15), and 1.06 (1.03-1.09).
“This tells us that these could possibly be on the pathway between osteoarthritis and mortality, and this could provide further evidence that they could be used for targeted therapy of osteoarthritis,” Mr. Parmar suggested.
“This type of mediation analysis has not been done in the osteoarthritis field before,” Mr. Parmar observed. He conceded that the mediators found might actually have contributed to the development of OA and that pain interference used in the definition of OA could have been caused by other factors.
Nevertheless, these data suggest that there may be actionable factors that could be used in primary care to reduce mortality in OA.
Mr. Parmar suggested that “encouraging physical activity and considering the impact of comorbidities can help reduce the risk of mortality in adults with osteoarthritis.”
The study was funded by Arthritis Research UK, the North Staffordshire Primary Care Consortium, and the Medical Research Council. Mr. Parmar had no conflicts of interest to disclose.
SOURCE: Parmar S et al. Osteoarthritis Cartilage. 2018;26(1):S14-15.
REPORTING FROM OARSI 2018
Key clinical point:
Major finding: OA is associated with a 15% increased risk of mortality in the general population.
Study details: A large, prospective cohort study that included more than 8,000 adults older than 50 years in the general population who participated.
Disclosures: The study was funded by Arthritis Research UK, the North Staffordshire Primary Care Consortium, and the Medical Research Council. Mr. Parmar had no conflicts of interest to disclose.
Source: Parmar S et al. Osteoarthritis Cartilage. 2018;26(1):S14-15.
May 2018 - What's your diagnosis?
By Umberto G. Rossi, MD, Paolo Rigamonti, MD, and Maurizio Cariati, MD
Intraluminal gallbladder arterial hemorrhage as a complication of arteriosclerosis and anticoagulant therapy
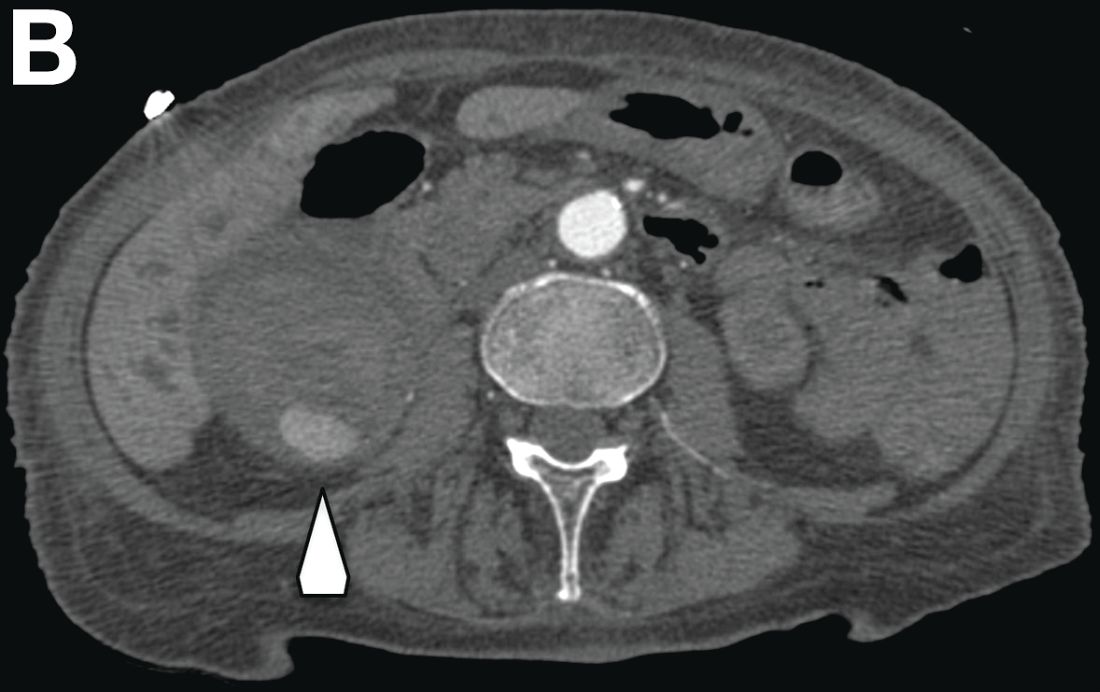
This radiologic sign on multiphasic contrast-enhanced multidetector computed tomography with axial images (Figure A-C), coronal multiplanar reconstruction (Figure D) and coronal volume rendering technique were indicative for active hemorrhage of gallbladder wall. During the urgent surgical treatment, there was confirmation of that distended gallbladder. Postoperatively, opening of the gallbladder revealed in its lumen the presence of bile mixed with dishomogeneous blood clots. Pathologic evaluation demonstrated arteriosclerosis of the cystic artery, with a pseudoaneurysmatic tear of one of its collateral branches with focal surround inflammatory tissue of gallbladder wall. The postoperative course was uneventful, and the patient was discharged on day 8.
Hemorrhage from the gallbladder is not a frequent event.1 The etiologies for hemorrhage of the gallbladder are trauma, neoplasms, inflammation of the wall with gallstones, aneurysms, varicose veins with portal hypertension, arteriosclerosis, and coagulopathy. However, isolated gallbladder arterial hemorrhage owing to anticoagulation therapy has been reported rarely. This pathologic state can be detected by contrast-enhanced ultrasound, contrast-enhanced computed tomography, and digital subtraction angiography.2,3
References
1. Hudson, P.B., Johnson, P.P. Hemorrhage from the gall bladder. N Engl J Med. 1946;234:438-41.
2. Krudy, A.G., Doppman, J.L., Bissonette, M.B., et al. Hemobilia: computed tomographic diagnosis. Radiology. 1983;148:785-9.
3. Pandya, R., O'Malley, C. Hemorrhagic cholecystitis as a complication of anticoagulant therapy: role of CT in its diagnosis. Abdom Imaging. 2008;33:652-3.
By Umberto G. Rossi, MD, Paolo Rigamonti, MD, and Maurizio Cariati, MD
Intraluminal gallbladder arterial hemorrhage as a complication of arteriosclerosis and anticoagulant therapy
This radiologic sign on multiphasic contrast-enhanced multidetector computed tomography with axial images (Figure A-C), coronal multiplanar reconstruction (Figure D) and coronal volume rendering technique were indicative for active hemorrhage of gallbladder wall. During the urgent surgical treatment, there was confirmation of that distended gallbladder. Postoperatively, opening of the gallbladder revealed in its lumen the presence of bile mixed with dishomogeneous blood clots. Pathologic evaluation demonstrated arteriosclerosis of the cystic artery, with a pseudoaneurysmatic tear of one of its collateral branches with focal surround inflammatory tissue of gallbladder wall. The postoperative course was uneventful, and the patient was discharged on day 8.
Hemorrhage from the gallbladder is not a frequent event.1 The etiologies for hemorrhage of the gallbladder are trauma, neoplasms, inflammation of the wall with gallstones, aneurysms, varicose veins with portal hypertension, arteriosclerosis, and coagulopathy. However, isolated gallbladder arterial hemorrhage owing to anticoagulation therapy has been reported rarely. This pathologic state can be detected by contrast-enhanced ultrasound, contrast-enhanced computed tomography, and digital subtraction angiography.2,3
References
1. Hudson, P.B., Johnson, P.P. Hemorrhage from the gall bladder. N Engl J Med. 1946;234:438-41.
2. Krudy, A.G., Doppman, J.L., Bissonette, M.B., et al. Hemobilia: computed tomographic diagnosis. Radiology. 1983;148:785-9.
3. Pandya, R., O'Malley, C. Hemorrhagic cholecystitis as a complication of anticoagulant therapy: role of CT in its diagnosis. Abdom Imaging. 2008;33:652-3.
By Umberto G. Rossi, MD, Paolo Rigamonti, MD, and Maurizio Cariati, MD
Intraluminal gallbladder arterial hemorrhage as a complication of arteriosclerosis and anticoagulant therapy
This radiologic sign on multiphasic contrast-enhanced multidetector computed tomography with axial images (Figure A-C), coronal multiplanar reconstruction (Figure D) and coronal volume rendering technique were indicative for active hemorrhage of gallbladder wall. During the urgent surgical treatment, there was confirmation of that distended gallbladder. Postoperatively, opening of the gallbladder revealed in its lumen the presence of bile mixed with dishomogeneous blood clots. Pathologic evaluation demonstrated arteriosclerosis of the cystic artery, with a pseudoaneurysmatic tear of one of its collateral branches with focal surround inflammatory tissue of gallbladder wall. The postoperative course was uneventful, and the patient was discharged on day 8.
Hemorrhage from the gallbladder is not a frequent event.1 The etiologies for hemorrhage of the gallbladder are trauma, neoplasms, inflammation of the wall with gallstones, aneurysms, varicose veins with portal hypertension, arteriosclerosis, and coagulopathy. However, isolated gallbladder arterial hemorrhage owing to anticoagulation therapy has been reported rarely. This pathologic state can be detected by contrast-enhanced ultrasound, contrast-enhanced computed tomography, and digital subtraction angiography.2,3
References
1. Hudson, P.B., Johnson, P.P. Hemorrhage from the gall bladder. N Engl J Med. 1946;234:438-41.
2. Krudy, A.G., Doppman, J.L., Bissonette, M.B., et al. Hemobilia: computed tomographic diagnosis. Radiology. 1983;148:785-9.
3. Pandya, R., O'Malley, C. Hemorrhagic cholecystitis as a complication of anticoagulant therapy: role of CT in its diagnosis. Abdom Imaging. 2008;33:652-3.

She had a medical history of cardiac arrhythmia (atrial fibrillation) with pacemaker insertion and anticoagulant therapy (warfarin 2.5 mg/d).
There was no alteration in liver function tests.
She underwent abdominal multiphasic contrast-enhanced multidetector computed tomography.
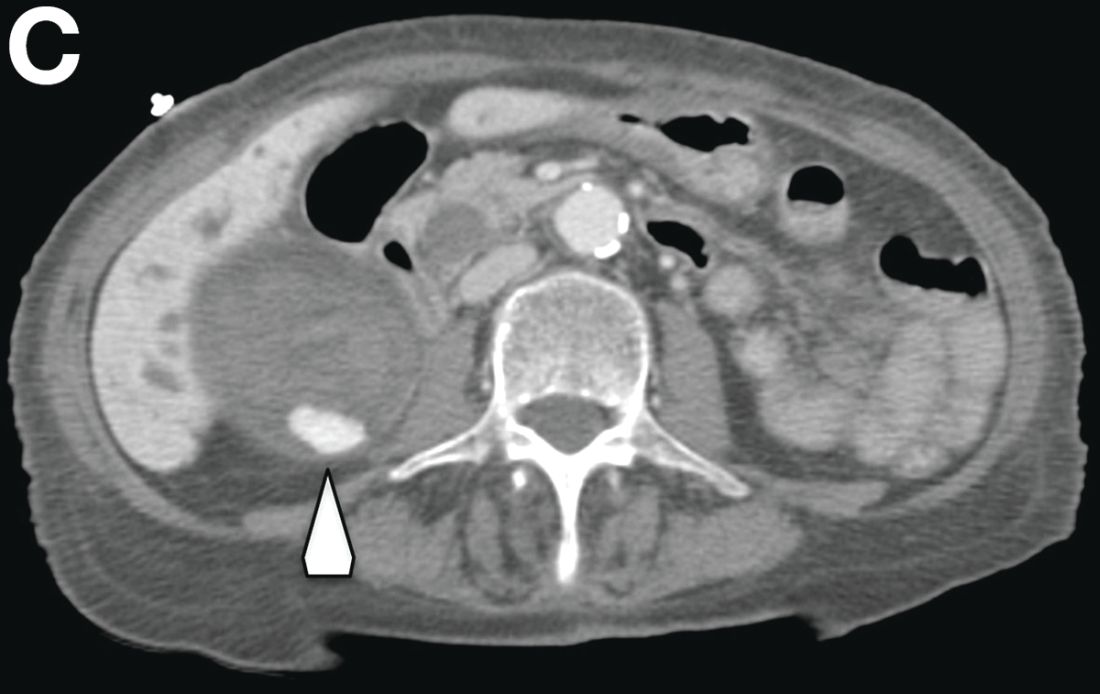
On the arterial phase (Figure B, arrowhead) it appeared inside the lumen of the gallbladder at the middle third of the inferior wall, a focal contrast media area, which become more evident on venous phase (Figure C, D, arrowhead).

CMS will release Medicare Advantage claims data to researchers
WASHINGTON – Centers for Medicare & Medicaid Services Administrator Seema Verma announced.

“We recognize that the Medicare Advantage data are not perfect, but we have determined that the quality of the available data is adequate enough to support research,” Ms. Verma told attendees April 26 at an annual conference on health data and innovation.
CMS is starting with the Medicare managed care plans’ encounter data from 2015, and Ms. Verma said the data will be updated annually.
In addition, she announced that in 2019 CMS will make Medicaid and Children’s Health Insurance Program data available. That will give researchers access to data from another 70 million patients.
Ms. Verma noted that the Medicaid population includes a range of people, including people with disabilities, pregnant women, children, and low-income adults. Those low-income adults “often experience multiple health issues and face challenges managing their care,” Ms. Verma noted. “Our hope is that these data will be used for critical research on this vulnerable population.”
CMS also will look to the health information technology developer community to create open application program interface tools “to modernize how we share data with our partners,” she said. That push is part of the overall MyHealthEData initiative to improve patient access to their health data and become more informed about their own health care.
“Who knows what knowledge, treatments, and cures are hidden in the reams of CMS data?” Ms. Verma said. “Help us use it securely. After all, this is knowledge that could change the life of a patient or the trajectory of a health care system.”
WASHINGTON – Centers for Medicare & Medicaid Services Administrator Seema Verma announced.
“We recognize that the Medicare Advantage data are not perfect, but we have determined that the quality of the available data is adequate enough to support research,” Ms. Verma told attendees April 26 at an annual conference on health data and innovation.
CMS is starting with the Medicare managed care plans’ encounter data from 2015, and Ms. Verma said the data will be updated annually.
In addition, she announced that in 2019 CMS will make Medicaid and Children’s Health Insurance Program data available. That will give researchers access to data from another 70 million patients.
Ms. Verma noted that the Medicaid population includes a range of people, including people with disabilities, pregnant women, children, and low-income adults. Those low-income adults “often experience multiple health issues and face challenges managing their care,” Ms. Verma noted. “Our hope is that these data will be used for critical research on this vulnerable population.”
CMS also will look to the health information technology developer community to create open application program interface tools “to modernize how we share data with our partners,” she said. That push is part of the overall MyHealthEData initiative to improve patient access to their health data and become more informed about their own health care.
“Who knows what knowledge, treatments, and cures are hidden in the reams of CMS data?” Ms. Verma said. “Help us use it securely. After all, this is knowledge that could change the life of a patient or the trajectory of a health care system.”
WASHINGTON – Centers for Medicare & Medicaid Services Administrator Seema Verma announced.
“We recognize that the Medicare Advantage data are not perfect, but we have determined that the quality of the available data is adequate enough to support research,” Ms. Verma told attendees April 26 at an annual conference on health data and innovation.
CMS is starting with the Medicare managed care plans’ encounter data from 2015, and Ms. Verma said the data will be updated annually.
In addition, she announced that in 2019 CMS will make Medicaid and Children’s Health Insurance Program data available. That will give researchers access to data from another 70 million patients.
Ms. Verma noted that the Medicaid population includes a range of people, including people with disabilities, pregnant women, children, and low-income adults. Those low-income adults “often experience multiple health issues and face challenges managing their care,” Ms. Verma noted. “Our hope is that these data will be used for critical research on this vulnerable population.”
CMS also will look to the health information technology developer community to create open application program interface tools “to modernize how we share data with our partners,” she said. That push is part of the overall MyHealthEData initiative to improve patient access to their health data and become more informed about their own health care.
“Who knows what knowledge, treatments, and cures are hidden in the reams of CMS data?” Ms. Verma said. “Help us use it securely. After all, this is knowledge that could change the life of a patient or the trajectory of a health care system.”
REPORTING FROM HEALTH DATAPALOOZA 2018
DDSEP8 Quick quiz May question 2
Correct Answer: B
Rationale
This patient has a neuroendocrine tumor (e.g., carcinoid). These tumors are derived from enterochromaffin-like cells and appear as nests or ribbons of endocrine cells. There are three types of carcinoids. Type 1 is the most common and has a benign course. Type 1 neuroendocrine tumors can be multifocal, well-differentiated and associated with type A chronic atrophic gastritis. Small tumors can be treated with endoscopic resection. Type 2 lesions tend to be multifocal and associated with Zollinger-Ellison syndrome (ZES) and multiple endocrine neoplasia 1 (MEN1). Up to 30% of type 2 tumors present with lymph node metastases. Type 3 gastric carcinoids are not associated with hypergastrinemia and have poor prognosis. Type 3 gastric carcinoids should be managed with surgery.
References
1. ASGE Standards of Practice Committee, Evans JA, Chandrasekhara V, et al. The role of endoscopy in the management of premalignant and malignant conditions of the stomach. Gastrointest Endosc. 2015;82(1):1-8.
2. Shaib YH, Rugge M, Graham DY, et al. Management of gastric polyps: an endoscopy-based approach. Clin Gastroenterol Hepatol. 2013;11(11):1374-84.
Correct Answer: B
Rationale
This patient has a neuroendocrine tumor (e.g., carcinoid). These tumors are derived from enterochromaffin-like cells and appear as nests or ribbons of endocrine cells. There are three types of carcinoids. Type 1 is the most common and has a benign course. Type 1 neuroendocrine tumors can be multifocal, well-differentiated and associated with type A chronic atrophic gastritis. Small tumors can be treated with endoscopic resection. Type 2 lesions tend to be multifocal and associated with Zollinger-Ellison syndrome (ZES) and multiple endocrine neoplasia 1 (MEN1). Up to 30% of type 2 tumors present with lymph node metastases. Type 3 gastric carcinoids are not associated with hypergastrinemia and have poor prognosis. Type 3 gastric carcinoids should be managed with surgery.
References
1. ASGE Standards of Practice Committee, Evans JA, Chandrasekhara V, et al. The role of endoscopy in the management of premalignant and malignant conditions of the stomach. Gastrointest Endosc. 2015;82(1):1-8.
2. Shaib YH, Rugge M, Graham DY, et al. Management of gastric polyps: an endoscopy-based approach. Clin Gastroenterol Hepatol. 2013;11(11):1374-84.
Correct Answer: B
Rationale
This patient has a neuroendocrine tumor (e.g., carcinoid). These tumors are derived from enterochromaffin-like cells and appear as nests or ribbons of endocrine cells. There are three types of carcinoids. Type 1 is the most common and has a benign course. Type 1 neuroendocrine tumors can be multifocal, well-differentiated and associated with type A chronic atrophic gastritis. Small tumors can be treated with endoscopic resection. Type 2 lesions tend to be multifocal and associated with Zollinger-Ellison syndrome (ZES) and multiple endocrine neoplasia 1 (MEN1). Up to 30% of type 2 tumors present with lymph node metastases. Type 3 gastric carcinoids are not associated with hypergastrinemia and have poor prognosis. Type 3 gastric carcinoids should be managed with surgery.
References
1. ASGE Standards of Practice Committee, Evans JA, Chandrasekhara V, et al. The role of endoscopy in the management of premalignant and malignant conditions of the stomach. Gastrointest Endosc. 2015;82(1):1-8.
2. Shaib YH, Rugge M, Graham DY, et al. Management of gastric polyps: an endoscopy-based approach. Clin Gastroenterol Hepatol. 2013;11(11):1374-84.
A 78-year-old woman presents with anemia and peripheral neuropathy. Laboratory evaluation reveals elevated MCV and vitamin B12 deficiency. Antiparietal and anti-intrinsic factor antibodies are positive. Endoscopy reveals atrophic-appearing mucosa and an 8-mm nodule in the gastric body. Complete endoscopic resection of the nodule is performed.
DDSEP8 Quick quiz May question 1
Correct Answer: C
Rationale
In a population study of U.S. veterans infected with hepatitis C (n = 110,484), a Cox proportional hazards model was used to determine risk of developing cirrhosis and hepatocellular carcinoma for genotypes 1-4, after adjusting for age, period of service, race, gender, human immunodeficiency virus (HIV) infection, alcohol use, diabetes, body mass index, and antiviral treatment. Despite genotype 3 patients being younger, their risk of developing cirrhosis was highest with hazard ratio = 1.30 (1.22, 1.39), compared to genotype 1 (reference, HR 1.0), genotype 2 with HR = 0.68 (0.64, 0.73), and genotype 4 with HR = 0.94 (0.78, 1.14). Likewise, the risk of development of hepatocellular carcinoma was highest for genotype 3 HCV with HR = 1.80 (1.60, 2.03), compared to a genotype 2 (HR = 0.55, 0.47, 0.63), and genotype 4 (0.99, 0.68, 1.45).
It is speculated that the hepatic steatosis that is a direct result of genotype 3 HCV may contribute to the accelerated progression to cirrhosis and HCC, but this has not been proven and was not evaluated in this Veteran Affairs study.
Reference
1. Kanwal F, Kramer JR, Ilyas J, et al. HCV genotype 3 is associated with an increased risk of cirrhosis and hepatocellular cancer in a national sample of U.S. veterans with HCV. Hepatology. 2014;60(1):98-105.
Correct Answer: C
Rationale
In a population study of U.S. veterans infected with hepatitis C (n = 110,484), a Cox proportional hazards model was used to determine risk of developing cirrhosis and hepatocellular carcinoma for genotypes 1-4, after adjusting for age, period of service, race, gender, human immunodeficiency virus (HIV) infection, alcohol use, diabetes, body mass index, and antiviral treatment. Despite genotype 3 patients being younger, their risk of developing cirrhosis was highest with hazard ratio = 1.30 (1.22, 1.39), compared to genotype 1 (reference, HR 1.0), genotype 2 with HR = 0.68 (0.64, 0.73), and genotype 4 with HR = 0.94 (0.78, 1.14). Likewise, the risk of development of hepatocellular carcinoma was highest for genotype 3 HCV with HR = 1.80 (1.60, 2.03), compared to a genotype 2 (HR = 0.55, 0.47, 0.63), and genotype 4 (0.99, 0.68, 1.45).
It is speculated that the hepatic steatosis that is a direct result of genotype 3 HCV may contribute to the accelerated progression to cirrhosis and HCC, but this has not been proven and was not evaluated in this Veteran Affairs study.
Reference
1. Kanwal F, Kramer JR, Ilyas J, et al. HCV genotype 3 is associated with an increased risk of cirrhosis and hepatocellular cancer in a national sample of U.S. veterans with HCV. Hepatology. 2014;60(1):98-105.
Correct Answer: C
Rationale
In a population study of U.S. veterans infected with hepatitis C (n = 110,484), a Cox proportional hazards model was used to determine risk of developing cirrhosis and hepatocellular carcinoma for genotypes 1-4, after adjusting for age, period of service, race, gender, human immunodeficiency virus (HIV) infection, alcohol use, diabetes, body mass index, and antiviral treatment. Despite genotype 3 patients being younger, their risk of developing cirrhosis was highest with hazard ratio = 1.30 (1.22, 1.39), compared to genotype 1 (reference, HR 1.0), genotype 2 with HR = 0.68 (0.64, 0.73), and genotype 4 with HR = 0.94 (0.78, 1.14). Likewise, the risk of development of hepatocellular carcinoma was highest for genotype 3 HCV with HR = 1.80 (1.60, 2.03), compared to a genotype 2 (HR = 0.55, 0.47, 0.63), and genotype 4 (0.99, 0.68, 1.45).
It is speculated that the hepatic steatosis that is a direct result of genotype 3 HCV may contribute to the accelerated progression to cirrhosis and HCC, but this has not been proven and was not evaluated in this Veteran Affairs study.
Reference
1. Kanwal F, Kramer JR, Ilyas J, et al. HCV genotype 3 is associated with an increased risk of cirrhosis and hepatocellular cancer in a national sample of U.S. veterans with HCV. Hepatology. 2014;60(1):98-105.
Which HCV genotype is associated with the highest risk of cirrhosis and hepatocellular carcinoma?
High Cajal cell count with gastric electrical stimulation improves symptoms for refractory gastroparesis patients
and researchers suggested patients with depleted Cajal cells who did not improve could have lost certain Cajal cells.
Thomas L. Abell, MD, from the department of medicine and division of gastroenterology, hepatology and nutrition at the University of Louisville (Ky.) and his colleagues recruited 23 patients with drug-refractory gastroparesis to undergo gastric electrical stimulation (GES) therapy for 12 months. Patients were white females with a mean age of 45.7 years. They performed a gastric-emptying test before therapy; the composite symptom scores were 23.89 plus or minus 34.10 for 4-hour gastric emptying in the group with interstitial cells of Cajal (ICC) less than 2.00 and a 22.62 plus or minus 25.51 in the group with ICC greater than or equal to 2.00.
“We believe neurostimulation might modify or augment the function of ICC cells. However, in patients with severe depletion, the ICC density might be too sparse to be augmented and hence contribute to suboptimal response to GES,” Dr. Abell and colleagues wrote in their study.
The GES system consisted of an “implanted pulse generator, two leads, and the stimulator programmer.” Patients used a trial GES system for 1-2 weeks, in which a “temporary lead is placed endoscopically through the nose and inserted into the gastric mucosa in the middle of the stomach.”
After the trial GES system, the researchers performed a gastric wall biopsy to determine ICC counts to divide the patients into two groups: those with less than 2 ICC and those with greater than or equal to 2 ICC (per high power field). Following the trial, a more permanent system was implanted and researchers analyzed results after 12 months with the Student t test, patient-reported symptom assessment, and Total Symptom Score (TSS) using a Likert scale.
After GES, 1-hour gastric emptying improved in the group with ICC greater than or equal to 2.00 from pretreatment (75.47 plus or minus 13.80) to posttreatment (57.97 plus or minus 21.34) with a mean between-group difference of 17.5% (95% confidence interval, 1.41-33.58; P = .035). Dr. Abell and colleagues noted a nonstatistically significant improvement in 2-hour (mean between-group difference, 8%) and 4-hour (4%) gastric emptying (P = .032). Compared with pretreatment, patients with an ICC count less that 2 showed no significant change at 1-hour (63.78 plus or minus 26.01 vs. 68.86 plus or minus 33.14; P = .646), 7% worsening at 2-hour (41.22 plus or minus 33.44 vs. 49.37 plus or minus 34.21; P = .343) and 7% worsening at 4-hour gastric emptying (23.89 plus or minus 34.10 vs. 30.82 plus or minus 30.82; P = .166).
Researchers found patients with “normal to moderate depletion of ICC counts” had a significantly higher change in serosal amplitude, with a mean amplitude change of 0.19 (P = .05). Patients with “severe depletion of ICC” showed no significant change in amplitude (mean amplitude change, 0.01; P = .79). Among patients with normal or moderate depletion of ICC, the pre-GES serosal frequency was 3.96 plus or minus 1.02 and the post-GES frequency was 3.83 plus or minus 1.36 (P = .79), while the patients with severe depletion of ICC had a pre-GES frequency of 4.67 plus or minus 1.57 and a post-GES frequency of 4.23 plus or minus 1.30 (P = .54).
Nausea and vomiting symptoms significantly improved in the group with ICC greater than or equal to 2.00 (vomiting change, –2.07; P less than .001 and bloating change, –1.80; P less than .001) with a weaker association with symptom improvement in the group with ICC less than 2.00 (vomiting change, –1.65; P =.035 and bloating change, –1.00; P = 0.86). TSS improved by 52% in the ICC group with greater than or equal to 2.00 (P = .002) and by 29.6% in the ICC less than 2.00 group (P = .047).
“The observation that some patients with severe depletion of ICC showed improvement in symptoms might indicate differential loss of specific type of ICC cells,” Dr. Abell and his colleagues wrote. “Better understanding of response to GES in patients with particular type of ICC loss might shed light on the mechanism of GES, as well as predicting and selecting patients who respond better. Future studies should focus on stratifying patients based on predominant type of ICC loss as it relates to severity of symptoms and response to GES.”
Dr. Abell is the founder of ADEPT-GI and has intellectual property rights related to the technology in this study. The other authors declare no relevant financial disclosures.
SOURCE: Omer E et al. J Clin Gastroenterol. 2018 Apr 18. doi: 10.1097/MCG.0000000000001025.
*This story was updated on 4/30/2018.
and researchers suggested patients with depleted Cajal cells who did not improve could have lost certain Cajal cells.
Thomas L. Abell, MD, from the department of medicine and division of gastroenterology, hepatology and nutrition at the University of Louisville (Ky.) and his colleagues recruited 23 patients with drug-refractory gastroparesis to undergo gastric electrical stimulation (GES) therapy for 12 months. Patients were white females with a mean age of 45.7 years. They performed a gastric-emptying test before therapy; the composite symptom scores were 23.89 plus or minus 34.10 for 4-hour gastric emptying in the group with interstitial cells of Cajal (ICC) less than 2.00 and a 22.62 plus or minus 25.51 in the group with ICC greater than or equal to 2.00.
“We believe neurostimulation might modify or augment the function of ICC cells. However, in patients with severe depletion, the ICC density might be too sparse to be augmented and hence contribute to suboptimal response to GES,” Dr. Abell and colleagues wrote in their study.
The GES system consisted of an “implanted pulse generator, two leads, and the stimulator programmer.” Patients used a trial GES system for 1-2 weeks, in which a “temporary lead is placed endoscopically through the nose and inserted into the gastric mucosa in the middle of the stomach.”
After the trial GES system, the researchers performed a gastric wall biopsy to determine ICC counts to divide the patients into two groups: those with less than 2 ICC and those with greater than or equal to 2 ICC (per high power field). Following the trial, a more permanent system was implanted and researchers analyzed results after 12 months with the Student t test, patient-reported symptom assessment, and Total Symptom Score (TSS) using a Likert scale.
After GES, 1-hour gastric emptying improved in the group with ICC greater than or equal to 2.00 from pretreatment (75.47 plus or minus 13.80) to posttreatment (57.97 plus or minus 21.34) with a mean between-group difference of 17.5% (95% confidence interval, 1.41-33.58; P = .035). Dr. Abell and colleagues noted a nonstatistically significant improvement in 2-hour (mean between-group difference, 8%) and 4-hour (4%) gastric emptying (P = .032). Compared with pretreatment, patients with an ICC count less that 2 showed no significant change at 1-hour (63.78 plus or minus 26.01 vs. 68.86 plus or minus 33.14; P = .646), 7% worsening at 2-hour (41.22 plus or minus 33.44 vs. 49.37 plus or minus 34.21; P = .343) and 7% worsening at 4-hour gastric emptying (23.89 plus or minus 34.10 vs. 30.82 plus or minus 30.82; P = .166).
Researchers found patients with “normal to moderate depletion of ICC counts” had a significantly higher change in serosal amplitude, with a mean amplitude change of 0.19 (P = .05). Patients with “severe depletion of ICC” showed no significant change in amplitude (mean amplitude change, 0.01; P = .79). Among patients with normal or moderate depletion of ICC, the pre-GES serosal frequency was 3.96 plus or minus 1.02 and the post-GES frequency was 3.83 plus or minus 1.36 (P = .79), while the patients with severe depletion of ICC had a pre-GES frequency of 4.67 plus or minus 1.57 and a post-GES frequency of 4.23 plus or minus 1.30 (P = .54).
Nausea and vomiting symptoms significantly improved in the group with ICC greater than or equal to 2.00 (vomiting change, –2.07; P less than .001 and bloating change, –1.80; P less than .001) with a weaker association with symptom improvement in the group with ICC less than 2.00 (vomiting change, –1.65; P =.035 and bloating change, –1.00; P = 0.86). TSS improved by 52% in the ICC group with greater than or equal to 2.00 (P = .002) and by 29.6% in the ICC less than 2.00 group (P = .047).
“The observation that some patients with severe depletion of ICC showed improvement in symptoms might indicate differential loss of specific type of ICC cells,” Dr. Abell and his colleagues wrote. “Better understanding of response to GES in patients with particular type of ICC loss might shed light on the mechanism of GES, as well as predicting and selecting patients who respond better. Future studies should focus on stratifying patients based on predominant type of ICC loss as it relates to severity of symptoms and response to GES.”
Dr. Abell is the founder of ADEPT-GI and has intellectual property rights related to the technology in this study. The other authors declare no relevant financial disclosures.
SOURCE: Omer E et al. J Clin Gastroenterol. 2018 Apr 18. doi: 10.1097/MCG.0000000000001025.
*This story was updated on 4/30/2018.
and researchers suggested patients with depleted Cajal cells who did not improve could have lost certain Cajal cells.
Thomas L. Abell, MD, from the department of medicine and division of gastroenterology, hepatology and nutrition at the University of Louisville (Ky.) and his colleagues recruited 23 patients with drug-refractory gastroparesis to undergo gastric electrical stimulation (GES) therapy for 12 months. Patients were white females with a mean age of 45.7 years. They performed a gastric-emptying test before therapy; the composite symptom scores were 23.89 plus or minus 34.10 for 4-hour gastric emptying in the group with interstitial cells of Cajal (ICC) less than 2.00 and a 22.62 plus or minus 25.51 in the group with ICC greater than or equal to 2.00.
“We believe neurostimulation might modify or augment the function of ICC cells. However, in patients with severe depletion, the ICC density might be too sparse to be augmented and hence contribute to suboptimal response to GES,” Dr. Abell and colleagues wrote in their study.
The GES system consisted of an “implanted pulse generator, two leads, and the stimulator programmer.” Patients used a trial GES system for 1-2 weeks, in which a “temporary lead is placed endoscopically through the nose and inserted into the gastric mucosa in the middle of the stomach.”
After the trial GES system, the researchers performed a gastric wall biopsy to determine ICC counts to divide the patients into two groups: those with less than 2 ICC and those with greater than or equal to 2 ICC (per high power field). Following the trial, a more permanent system was implanted and researchers analyzed results after 12 months with the Student t test, patient-reported symptom assessment, and Total Symptom Score (TSS) using a Likert scale.
After GES, 1-hour gastric emptying improved in the group with ICC greater than or equal to 2.00 from pretreatment (75.47 plus or minus 13.80) to posttreatment (57.97 plus or minus 21.34) with a mean between-group difference of 17.5% (95% confidence interval, 1.41-33.58; P = .035). Dr. Abell and colleagues noted a nonstatistically significant improvement in 2-hour (mean between-group difference, 8%) and 4-hour (4%) gastric emptying (P = .032). Compared with pretreatment, patients with an ICC count less that 2 showed no significant change at 1-hour (63.78 plus or minus 26.01 vs. 68.86 plus or minus 33.14; P = .646), 7% worsening at 2-hour (41.22 plus or minus 33.44 vs. 49.37 plus or minus 34.21; P = .343) and 7% worsening at 4-hour gastric emptying (23.89 plus or minus 34.10 vs. 30.82 plus or minus 30.82; P = .166).
Researchers found patients with “normal to moderate depletion of ICC counts” had a significantly higher change in serosal amplitude, with a mean amplitude change of 0.19 (P = .05). Patients with “severe depletion of ICC” showed no significant change in amplitude (mean amplitude change, 0.01; P = .79). Among patients with normal or moderate depletion of ICC, the pre-GES serosal frequency was 3.96 plus or minus 1.02 and the post-GES frequency was 3.83 plus or minus 1.36 (P = .79), while the patients with severe depletion of ICC had a pre-GES frequency of 4.67 plus or minus 1.57 and a post-GES frequency of 4.23 plus or minus 1.30 (P = .54).
Nausea and vomiting symptoms significantly improved in the group with ICC greater than or equal to 2.00 (vomiting change, –2.07; P less than .001 and bloating change, –1.80; P less than .001) with a weaker association with symptom improvement in the group with ICC less than 2.00 (vomiting change, –1.65; P =.035 and bloating change, –1.00; P = 0.86). TSS improved by 52% in the ICC group with greater than or equal to 2.00 (P = .002) and by 29.6% in the ICC less than 2.00 group (P = .047).
“The observation that some patients with severe depletion of ICC showed improvement in symptoms might indicate differential loss of specific type of ICC cells,” Dr. Abell and his colleagues wrote. “Better understanding of response to GES in patients with particular type of ICC loss might shed light on the mechanism of GES, as well as predicting and selecting patients who respond better. Future studies should focus on stratifying patients based on predominant type of ICC loss as it relates to severity of symptoms and response to GES.”
Dr. Abell is the founder of ADEPT-GI and has intellectual property rights related to the technology in this study. The other authors declare no relevant financial disclosures.
SOURCE: Omer E et al. J Clin Gastroenterol. 2018 Apr 18. doi: 10.1097/MCG.0000000000001025.
*This story was updated on 4/30/2018.
FROM JOURNAL OF CLINICAL GASTROENTEROLOGY
Key clinical point: Higher Cajal cell counts were linked to improved symptoms and gastric electrical activity in patients with drug-refractory gastroparesis who underwent neurostimulation.
Major finding: The rate of 1-hour gastric emptying significantly improved in patients with interstitial cells of Cajal greater than or equal to two after gastric electrical stimulation with a mean group difference of 17.5%, as well as a mean serosal amplitude change of 0.19.
Study details: A single-center study of 23 women with drug-refractory gastroparesis recruited from the gastric motility clinic at the University of Mississippi.
Disclosures: Dr. Abell is the founder of ADEPT-GI and has intellectual property rights related to the technology in this study. The other authors declare no relevant financial disclosures.
Source: Omer E et al. J Clin Gastroenterol. 2018 Apr 18. doi: 10.1097/MCG.0000000000001025.