User login
Substance use linked to conversion to schizophrenia
People with schizotypal disorder who use cannabis, amphetamines, and opioids might be more likely to convert to schizophrenia, according to a prospective cohort study.
The study, published online April 25 by JAMA Psychiatry, involved 2,539 Danish individuals with incident schizotypal disorder – but without a diagnosis of schizophrenia – who had been followed from birth.
After 20 years of follow-up, about one-third (33.1%) of the total cohort had converted to schizophrenia. Among individuals without any substance use disorder, the conversion rate was 30.6%, while among individuals with cannabis use disorders, the conversion rate was 58.2%. Meanwhile, those with alcohol use disorder had a conversion rate of 47%, reported Carsten Hjorthøj, PhD, of Copenhagen University Hospital, Mental Health Center Copenhagen, and coauthors.
Participants with any substance use disorder had a 34% higher risk of converting to schizophrenia, but the risk was more than twofold higher with opioid use disorder (hazard ratio, 2.74; 95% confidence interval, 1.38-5.45), 30% higher with cannabis use disorder, and 90% higher with amphetamine use disorder.
Patients who had been prescribed antipsychotics also showed a higher risk of converting to schizophrenia (HR, 1.42; 95% CI, 1.18-1.70), which the authors suggested might reflect the fact that these patients were likely to be the most severely ill.
These associations were found even after adjustment for factors such as sex, birth year, all other individual types of substance use disorders, and parental mental disorders.
Dr. Hjorthøj and coauthors said the association between cannabis use and conversion to schizophrenia might be causal. “First, the association appears to be dose-dependent; second, the association is stronger for more potent types of cannabis; third, cannabis use is associated with earlier onset of psychosis; and fourth, age at onset of cannabis use is associated with age at onset of schizophrenia,” they wrote.
However, they also acknowledged that schizophrenia itself might increase the risk of individuals starting to use cannabis and other substances – a theory supported by the wide range of substances associated with conversion to schizophrenia.
“In our study, the first registered date of substance use disorder came before the first registered date of schizophrenia, but delays in diagnoses may have caused schizophrenia or its preclinical symptoms to predate substance use.”
The association between alcohol use disorder and conversion to schizophrenia was seen only in sensitivity analyses that ignored the birth year of the cohort, which the authors suggested may have been the result of increased power in this analysis.
Among the limitations cited by the authors was their inability to validate the schizotypal disorder diagnoses. Also, they wrote, the participants’ diagnoses were based on ICD-8 and ICD-10 criteria, and it was unclear whether the study results are generalizable to DSM-5 diagnoses.
The Lundbeck Foundation supported the study. No conflicts of interest were declared.
SOURCE: Hjorthøj C et al. JAMA Psychiatry. 2018 Apr 25. doi: 10.1001/jamapsychiatry.2018.0568.
People with schizotypal disorder who use cannabis, amphetamines, and opioids might be more likely to convert to schizophrenia, according to a prospective cohort study.
The study, published online April 25 by JAMA Psychiatry, involved 2,539 Danish individuals with incident schizotypal disorder – but without a diagnosis of schizophrenia – who had been followed from birth.
After 20 years of follow-up, about one-third (33.1%) of the total cohort had converted to schizophrenia. Among individuals without any substance use disorder, the conversion rate was 30.6%, while among individuals with cannabis use disorders, the conversion rate was 58.2%. Meanwhile, those with alcohol use disorder had a conversion rate of 47%, reported Carsten Hjorthøj, PhD, of Copenhagen University Hospital, Mental Health Center Copenhagen, and coauthors.
Participants with any substance use disorder had a 34% higher risk of converting to schizophrenia, but the risk was more than twofold higher with opioid use disorder (hazard ratio, 2.74; 95% confidence interval, 1.38-5.45), 30% higher with cannabis use disorder, and 90% higher with amphetamine use disorder.
Patients who had been prescribed antipsychotics also showed a higher risk of converting to schizophrenia (HR, 1.42; 95% CI, 1.18-1.70), which the authors suggested might reflect the fact that these patients were likely to be the most severely ill.
These associations were found even after adjustment for factors such as sex, birth year, all other individual types of substance use disorders, and parental mental disorders.
Dr. Hjorthøj and coauthors said the association between cannabis use and conversion to schizophrenia might be causal. “First, the association appears to be dose-dependent; second, the association is stronger for more potent types of cannabis; third, cannabis use is associated with earlier onset of psychosis; and fourth, age at onset of cannabis use is associated with age at onset of schizophrenia,” they wrote.
However, they also acknowledged that schizophrenia itself might increase the risk of individuals starting to use cannabis and other substances – a theory supported by the wide range of substances associated with conversion to schizophrenia.
“In our study, the first registered date of substance use disorder came before the first registered date of schizophrenia, but delays in diagnoses may have caused schizophrenia or its preclinical symptoms to predate substance use.”
The association between alcohol use disorder and conversion to schizophrenia was seen only in sensitivity analyses that ignored the birth year of the cohort, which the authors suggested may have been the result of increased power in this analysis.
Among the limitations cited by the authors was their inability to validate the schizotypal disorder diagnoses. Also, they wrote, the participants’ diagnoses were based on ICD-8 and ICD-10 criteria, and it was unclear whether the study results are generalizable to DSM-5 diagnoses.
The Lundbeck Foundation supported the study. No conflicts of interest were declared.
SOURCE: Hjorthøj C et al. JAMA Psychiatry. 2018 Apr 25. doi: 10.1001/jamapsychiatry.2018.0568.
People with schizotypal disorder who use cannabis, amphetamines, and opioids might be more likely to convert to schizophrenia, according to a prospective cohort study.
The study, published online April 25 by JAMA Psychiatry, involved 2,539 Danish individuals with incident schizotypal disorder – but without a diagnosis of schizophrenia – who had been followed from birth.
After 20 years of follow-up, about one-third (33.1%) of the total cohort had converted to schizophrenia. Among individuals without any substance use disorder, the conversion rate was 30.6%, while among individuals with cannabis use disorders, the conversion rate was 58.2%. Meanwhile, those with alcohol use disorder had a conversion rate of 47%, reported Carsten Hjorthøj, PhD, of Copenhagen University Hospital, Mental Health Center Copenhagen, and coauthors.
Participants with any substance use disorder had a 34% higher risk of converting to schizophrenia, but the risk was more than twofold higher with opioid use disorder (hazard ratio, 2.74; 95% confidence interval, 1.38-5.45), 30% higher with cannabis use disorder, and 90% higher with amphetamine use disorder.
Patients who had been prescribed antipsychotics also showed a higher risk of converting to schizophrenia (HR, 1.42; 95% CI, 1.18-1.70), which the authors suggested might reflect the fact that these patients were likely to be the most severely ill.
These associations were found even after adjustment for factors such as sex, birth year, all other individual types of substance use disorders, and parental mental disorders.
Dr. Hjorthøj and coauthors said the association between cannabis use and conversion to schizophrenia might be causal. “First, the association appears to be dose-dependent; second, the association is stronger for more potent types of cannabis; third, cannabis use is associated with earlier onset of psychosis; and fourth, age at onset of cannabis use is associated with age at onset of schizophrenia,” they wrote.
However, they also acknowledged that schizophrenia itself might increase the risk of individuals starting to use cannabis and other substances – a theory supported by the wide range of substances associated with conversion to schizophrenia.
“In our study, the first registered date of substance use disorder came before the first registered date of schizophrenia, but delays in diagnoses may have caused schizophrenia or its preclinical symptoms to predate substance use.”
The association between alcohol use disorder and conversion to schizophrenia was seen only in sensitivity analyses that ignored the birth year of the cohort, which the authors suggested may have been the result of increased power in this analysis.
Among the limitations cited by the authors was their inability to validate the schizotypal disorder diagnoses. Also, they wrote, the participants’ diagnoses were based on ICD-8 and ICD-10 criteria, and it was unclear whether the study results are generalizable to DSM-5 diagnoses.
The Lundbeck Foundation supported the study. No conflicts of interest were declared.
SOURCE: Hjorthøj C et al. JAMA Psychiatry. 2018 Apr 25. doi: 10.1001/jamapsychiatry.2018.0568.
FROM JAMA PSYCHIATRY
Key clinical point: Patients with schizotypal disorder who have substance use disorders are more likely to convert to schizophrenia.
Major finding: The conversion rate from schizotypal disorder to schizophrenia was 58.2% in individuals with substance use disorder.
Study details: Prospective cohort study in 2,539 individuals with schizotypal disorder.
Disclosures: The Lundbeck Foundation supported the study. No conflicts of interest were declared.
Source: Hjorthøj C et al. JAMA Psychiatry. 2018 Apr 25. doi: 10.1001/jamapsychiatry.2018.0568.
FDA advisory committee votes to recommend update to celecoxib safety labeling
SILVER SPRING, MD. – An FDA advisory committee voted (15 yes, 5 no, 1 abstention) to update the safety information in the label of celecoxib, a nonsteroidal anti-inflammatory drug (NSAID), for use in patients with osteoarthritis (OA) and rheumatoid arthritis, on the basis of results of the PRECISION trial.

A Joint Meeting ofthe Arthritis Advisory Committee and the Drug Safety and Risk Management Advisory Committee was convened April 24-25 to address two issues, the first being the consideration of Pfizer’s application for celecoxib and the second, to assess the safety of celecoxib and other common NSAIDs like ibuprofen and naproxen.
The randomized controlled PRECISION (Prospective Randomized Evaluation of Celecoxib Integrated Safety vs. Ibuprofen or Naproxen) trial compared celecoxib, naproxen, and ibuprofen and their cardiovascular outcomes. The PRECISION trial was undertaken after another selective COX-2 inhibitor, rofecoxib (Vioxx), was withdrawn from the market because of associated cardiovascular events. It compared the three drugs among more than 24,000 patients with painful arthritis and elevated cardiovascular risk.
Main results showed that the rates of cardiovascular events (cardiovascular death, myocardial infarction, or stroke) were 2.3% with celecoxib, 2.5% with naproxen, and 2.7% with ibuprofen during a follow-up approaching 3 years, showing noninferiority for celecoxib.
In a post hoc analysis presented by Steven Nissen, MD, patients taking ibuprofen and naproxen experienced adjudicated cardiovascular, GI, or renal events 28% and 15% more than did patients taking celecoxib.
The results of the study could inform clinical strategy, said Dr. Nissen, chair of cardiovascular medicine at the Cleveland Clinic in Ohio. “For arthritis patients who require NSAIDs to achieve an acceptable quality of life, particularly those at high cardiovascular, GI, or renal risk, the PRECISION trial suggests that a clinical strategy of starting patients on celecoxib 200 mg daily may be the safest approach, reserving full therapeutic doses of ibuprofen and naproxen for patients who do not respond to celecoxib."
SILVER SPRING, MD. – An FDA advisory committee voted (15 yes, 5 no, 1 abstention) to update the safety information in the label of celecoxib, a nonsteroidal anti-inflammatory drug (NSAID), for use in patients with osteoarthritis (OA) and rheumatoid arthritis, on the basis of results of the PRECISION trial.
A Joint Meeting ofthe Arthritis Advisory Committee and the Drug Safety and Risk Management Advisory Committee was convened April 24-25 to address two issues, the first being the consideration of Pfizer’s application for celecoxib and the second, to assess the safety of celecoxib and other common NSAIDs like ibuprofen and naproxen.
The randomized controlled PRECISION (Prospective Randomized Evaluation of Celecoxib Integrated Safety vs. Ibuprofen or Naproxen) trial compared celecoxib, naproxen, and ibuprofen and their cardiovascular outcomes. The PRECISION trial was undertaken after another selective COX-2 inhibitor, rofecoxib (Vioxx), was withdrawn from the market because of associated cardiovascular events. It compared the three drugs among more than 24,000 patients with painful arthritis and elevated cardiovascular risk.
Main results showed that the rates of cardiovascular events (cardiovascular death, myocardial infarction, or stroke) were 2.3% with celecoxib, 2.5% with naproxen, and 2.7% with ibuprofen during a follow-up approaching 3 years, showing noninferiority for celecoxib.
In a post hoc analysis presented by Steven Nissen, MD, patients taking ibuprofen and naproxen experienced adjudicated cardiovascular, GI, or renal events 28% and 15% more than did patients taking celecoxib.
The results of the study could inform clinical strategy, said Dr. Nissen, chair of cardiovascular medicine at the Cleveland Clinic in Ohio. “For arthritis patients who require NSAIDs to achieve an acceptable quality of life, particularly those at high cardiovascular, GI, or renal risk, the PRECISION trial suggests that a clinical strategy of starting patients on celecoxib 200 mg daily may be the safest approach, reserving full therapeutic doses of ibuprofen and naproxen for patients who do not respond to celecoxib."
SILVER SPRING, MD. – An FDA advisory committee voted (15 yes, 5 no, 1 abstention) to update the safety information in the label of celecoxib, a nonsteroidal anti-inflammatory drug (NSAID), for use in patients with osteoarthritis (OA) and rheumatoid arthritis, on the basis of results of the PRECISION trial.
A Joint Meeting ofthe Arthritis Advisory Committee and the Drug Safety and Risk Management Advisory Committee was convened April 24-25 to address two issues, the first being the consideration of Pfizer’s application for celecoxib and the second, to assess the safety of celecoxib and other common NSAIDs like ibuprofen and naproxen.
The randomized controlled PRECISION (Prospective Randomized Evaluation of Celecoxib Integrated Safety vs. Ibuprofen or Naproxen) trial compared celecoxib, naproxen, and ibuprofen and their cardiovascular outcomes. The PRECISION trial was undertaken after another selective COX-2 inhibitor, rofecoxib (Vioxx), was withdrawn from the market because of associated cardiovascular events. It compared the three drugs among more than 24,000 patients with painful arthritis and elevated cardiovascular risk.
Main results showed that the rates of cardiovascular events (cardiovascular death, myocardial infarction, or stroke) were 2.3% with celecoxib, 2.5% with naproxen, and 2.7% with ibuprofen during a follow-up approaching 3 years, showing noninferiority for celecoxib.
In a post hoc analysis presented by Steven Nissen, MD, patients taking ibuprofen and naproxen experienced adjudicated cardiovascular, GI, or renal events 28% and 15% more than did patients taking celecoxib.
The results of the study could inform clinical strategy, said Dr. Nissen, chair of cardiovascular medicine at the Cleveland Clinic in Ohio. “For arthritis patients who require NSAIDs to achieve an acceptable quality of life, particularly those at high cardiovascular, GI, or renal risk, the PRECISION trial suggests that a clinical strategy of starting patients on celecoxib 200 mg daily may be the safest approach, reserving full therapeutic doses of ibuprofen and naproxen for patients who do not respond to celecoxib."
REPORTING FROM AN FDA ADVISORY COMMITTEE MEETING
FDA places partial hold on trials after secondary lymphoma
The drugmaker after a pediatric patient developed a secondary T-cell lymphoma.
The Food and Drug Administration had issued a partial clinical hold in April on new enrollment of any patients with genetically defined solid tumors and hematologic malignancies. Patients already enrolled who have not had disease progression can continue to receive tazemetostat.
Tazemetostat is a first-in-class EZH2 inhibitor being studied as monotherapy in phase 1 and 2 trials for certain molecularly defined solid tumors, follicular lymphoma and diffuse large B-cell lymphoma, mesothelioma, and in combination studies of DLBCL and non–small cell lung cancer.
Epizyme is currently working to update informed consent, the investigator’s brochure, and study protocols, the company said in a statement.
The drugmaker after a pediatric patient developed a secondary T-cell lymphoma.
The Food and Drug Administration had issued a partial clinical hold in April on new enrollment of any patients with genetically defined solid tumors and hematologic malignancies. Patients already enrolled who have not had disease progression can continue to receive tazemetostat.
Tazemetostat is a first-in-class EZH2 inhibitor being studied as monotherapy in phase 1 and 2 trials for certain molecularly defined solid tumors, follicular lymphoma and diffuse large B-cell lymphoma, mesothelioma, and in combination studies of DLBCL and non–small cell lung cancer.
Epizyme is currently working to update informed consent, the investigator’s brochure, and study protocols, the company said in a statement.
The drugmaker after a pediatric patient developed a secondary T-cell lymphoma.
The Food and Drug Administration had issued a partial clinical hold in April on new enrollment of any patients with genetically defined solid tumors and hematologic malignancies. Patients already enrolled who have not had disease progression can continue to receive tazemetostat.
Tazemetostat is a first-in-class EZH2 inhibitor being studied as monotherapy in phase 1 and 2 trials for certain molecularly defined solid tumors, follicular lymphoma and diffuse large B-cell lymphoma, mesothelioma, and in combination studies of DLBCL and non–small cell lung cancer.
Epizyme is currently working to update informed consent, the investigator’s brochure, and study protocols, the company said in a statement.
Hidradenitis suppurativa packs mighty QOL impact
KAUAI, HAWAII – Anyone who has treated patients with hidradenitis suppurativa (HS) recognizes that this can be a debilitating disease. Helping put that into fuller perspective, recent evidence has shown that the quality of life effects of moderate to severe HS are objectively worse than those of moderate to severe psoriasis, according to Iltefat H. Hamzavi, MD, president of the Hidradenitis Suppurativa Foundation and a dermatologist at Henry Ford Hospital in Detroit.
He was lead author of a study in which he and his coinvestigators compared weighted averages of a variety of quality of life measures in patients with moderate to severe HS or psoriasis who participated in five AbbVie-sponsored randomized clinical trials of biologic agents (J Am Acad Dermatol. 2017 Dec;77[6]:1038-46).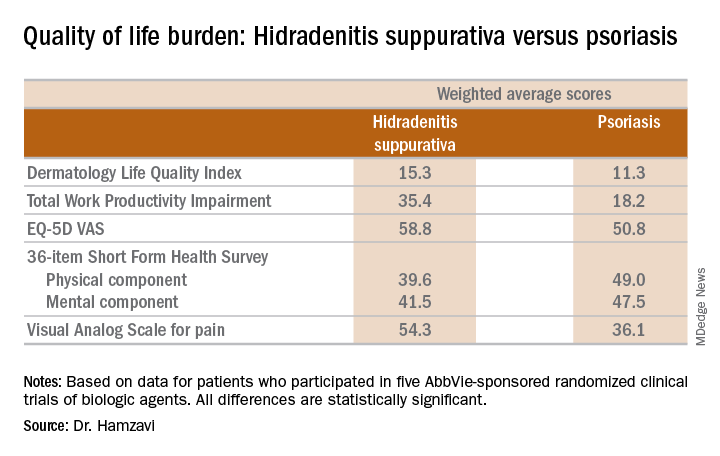
“The number of HS patients who experience downward drift – losing their job and their health insurance and ultimately being unable to move out of a lower socioeconomic group – is staggering,” the dermatologist said.
which underscores the importance of a psychiatric evaluation as part of routine care for patients with this dermatologic disease. “Suicide is much more common in the HS population than in almost any other dermatologic disease,” Dr. Hamzavi added.
He reported serving as a consultant for AbbVie, Incyte, and UCB.
SDEF/Global Academy for Medical Education and this news organization are owned by the same parent company.
KAUAI, HAWAII – Anyone who has treated patients with hidradenitis suppurativa (HS) recognizes that this can be a debilitating disease. Helping put that into fuller perspective, recent evidence has shown that the quality of life effects of moderate to severe HS are objectively worse than those of moderate to severe psoriasis, according to Iltefat H. Hamzavi, MD, president of the Hidradenitis Suppurativa Foundation and a dermatologist at Henry Ford Hospital in Detroit.
He was lead author of a study in which he and his coinvestigators compared weighted averages of a variety of quality of life measures in patients with moderate to severe HS or psoriasis who participated in five AbbVie-sponsored randomized clinical trials of biologic agents (J Am Acad Dermatol. 2017 Dec;77[6]:1038-46).
“The number of HS patients who experience downward drift – losing their job and their health insurance and ultimately being unable to move out of a lower socioeconomic group – is staggering,” the dermatologist said.
which underscores the importance of a psychiatric evaluation as part of routine care for patients with this dermatologic disease. “Suicide is much more common in the HS population than in almost any other dermatologic disease,” Dr. Hamzavi added.
He reported serving as a consultant for AbbVie, Incyte, and UCB.
SDEF/Global Academy for Medical Education and this news organization are owned by the same parent company.
KAUAI, HAWAII – Anyone who has treated patients with hidradenitis suppurativa (HS) recognizes that this can be a debilitating disease. Helping put that into fuller perspective, recent evidence has shown that the quality of life effects of moderate to severe HS are objectively worse than those of moderate to severe psoriasis, according to Iltefat H. Hamzavi, MD, president of the Hidradenitis Suppurativa Foundation and a dermatologist at Henry Ford Hospital in Detroit.
He was lead author of a study in which he and his coinvestigators compared weighted averages of a variety of quality of life measures in patients with moderate to severe HS or psoriasis who participated in five AbbVie-sponsored randomized clinical trials of biologic agents (J Am Acad Dermatol. 2017 Dec;77[6]:1038-46).
“The number of HS patients who experience downward drift – losing their job and their health insurance and ultimately being unable to move out of a lower socioeconomic group – is staggering,” the dermatologist said.
which underscores the importance of a psychiatric evaluation as part of routine care for patients with this dermatologic disease. “Suicide is much more common in the HS population than in almost any other dermatologic disease,” Dr. Hamzavi added.
He reported serving as a consultant for AbbVie, Incyte, and UCB.
SDEF/Global Academy for Medical Education and this news organization are owned by the same parent company.
EXPERT ANALYSIS FROM SDEF HAWAII DERMATOLOGY SEMINAR
Gluten-Free Diet May Help Patients With Neuropathic Pain
LOS ANGELES—A strict gluten-free diet may help protect against the nerve pain that some patients with gluten sensitivity experience, according to a preliminary study presented at the American Academy of Neurology’s 70th Annual Meeting. “These findings are exciting because it might mean that a relatively simple change in diet could help alleviate painful symptoms tied to gluten neuropathy,” said lead author Panagiotis Zis, MD, PhD, Honorary Senior Lecturer at the University of Sheffield, United Kingdom. “While our study shows an association between a self-reported gluten-free diet and less pain, it does not show that one causes the other.”

Gluten neuropathy is the second most common neurologic manifestation of gluten sensitivity, after cerebellar ataxia. It is defined as an idiopathic neuropathy, in the absence of an alternative etiology despite extensive investigations, and in the presence of serologic evidence of gluten sensitivity (IgA and/or IgG antigliadin antibodies).
To establish the prevalence of pain in patients with gluten neuropathy and to describe any contributory factors, Dr. Zis and colleagues invited all consecutive patients with gluten neuropathy attending a specialist gluten/neurology clinic to participate in their study. Pain was assessed via the DN4 questionnaire and the visual analog scale. The Overall Neuropathy Limitations Scale (ONLS) was used to assess the severity of neuropathy. The Mental Health Index (MHI-5) was used to measure participants’ general mental health status.
In all, 60 patients (76.7% males, mean age 70) with gluten neuropathy were recruited. Pain was present in 33 patients (55.0%). Comparison between groups of painful and non-painful gluten neuropathy did not show significant differences regarding age, gender, neuropathy severity, or neuropathy type. Patients with painless gluten neuropathy were more likely to be on a strict gluten-free diet (55.6% vs 21.2%). Patients with painful gluten neuropathy presented with significantly worse MHI-5 score (75.9 vs 87.4). Multivariate analysis showed that, after adjusting for age, gender, and MHI-5 score, adherence to a strict gluten-free diet was associated with lowering the odds of peripheral neuropathic pain by 88.7%.
“This study is promising because it shows that a gluten-free diet may help lower the risk of pain for people with gluten neuropathy,” Dr. Zis said. “More research is needed to confirm these results and to determine whether the gluten-free diet led to the reduction in pain.”
LOS ANGELES—A strict gluten-free diet may help protect against the nerve pain that some patients with gluten sensitivity experience, according to a preliminary study presented at the American Academy of Neurology’s 70th Annual Meeting. “These findings are exciting because it might mean that a relatively simple change in diet could help alleviate painful symptoms tied to gluten neuropathy,” said lead author Panagiotis Zis, MD, PhD, Honorary Senior Lecturer at the University of Sheffield, United Kingdom. “While our study shows an association between a self-reported gluten-free diet and less pain, it does not show that one causes the other.”
Gluten neuropathy is the second most common neurologic manifestation of gluten sensitivity, after cerebellar ataxia. It is defined as an idiopathic neuropathy, in the absence of an alternative etiology despite extensive investigations, and in the presence of serologic evidence of gluten sensitivity (IgA and/or IgG antigliadin antibodies).
To establish the prevalence of pain in patients with gluten neuropathy and to describe any contributory factors, Dr. Zis and colleagues invited all consecutive patients with gluten neuropathy attending a specialist gluten/neurology clinic to participate in their study. Pain was assessed via the DN4 questionnaire and the visual analog scale. The Overall Neuropathy Limitations Scale (ONLS) was used to assess the severity of neuropathy. The Mental Health Index (MHI-5) was used to measure participants’ general mental health status.
In all, 60 patients (76.7% males, mean age 70) with gluten neuropathy were recruited. Pain was present in 33 patients (55.0%). Comparison between groups of painful and non-painful gluten neuropathy did not show significant differences regarding age, gender, neuropathy severity, or neuropathy type. Patients with painless gluten neuropathy were more likely to be on a strict gluten-free diet (55.6% vs 21.2%). Patients with painful gluten neuropathy presented with significantly worse MHI-5 score (75.9 vs 87.4). Multivariate analysis showed that, after adjusting for age, gender, and MHI-5 score, adherence to a strict gluten-free diet was associated with lowering the odds of peripheral neuropathic pain by 88.7%.
“This study is promising because it shows that a gluten-free diet may help lower the risk of pain for people with gluten neuropathy,” Dr. Zis said. “More research is needed to confirm these results and to determine whether the gluten-free diet led to the reduction in pain.”
LOS ANGELES—A strict gluten-free diet may help protect against the nerve pain that some patients with gluten sensitivity experience, according to a preliminary study presented at the American Academy of Neurology’s 70th Annual Meeting. “These findings are exciting because it might mean that a relatively simple change in diet could help alleviate painful symptoms tied to gluten neuropathy,” said lead author Panagiotis Zis, MD, PhD, Honorary Senior Lecturer at the University of Sheffield, United Kingdom. “While our study shows an association between a self-reported gluten-free diet and less pain, it does not show that one causes the other.”
Gluten neuropathy is the second most common neurologic manifestation of gluten sensitivity, after cerebellar ataxia. It is defined as an idiopathic neuropathy, in the absence of an alternative etiology despite extensive investigations, and in the presence of serologic evidence of gluten sensitivity (IgA and/or IgG antigliadin antibodies).
To establish the prevalence of pain in patients with gluten neuropathy and to describe any contributory factors, Dr. Zis and colleagues invited all consecutive patients with gluten neuropathy attending a specialist gluten/neurology clinic to participate in their study. Pain was assessed via the DN4 questionnaire and the visual analog scale. The Overall Neuropathy Limitations Scale (ONLS) was used to assess the severity of neuropathy. The Mental Health Index (MHI-5) was used to measure participants’ general mental health status.
In all, 60 patients (76.7% males, mean age 70) with gluten neuropathy were recruited. Pain was present in 33 patients (55.0%). Comparison between groups of painful and non-painful gluten neuropathy did not show significant differences regarding age, gender, neuropathy severity, or neuropathy type. Patients with painless gluten neuropathy were more likely to be on a strict gluten-free diet (55.6% vs 21.2%). Patients with painful gluten neuropathy presented with significantly worse MHI-5 score (75.9 vs 87.4). Multivariate analysis showed that, after adjusting for age, gender, and MHI-5 score, adherence to a strict gluten-free diet was associated with lowering the odds of peripheral neuropathic pain by 88.7%.
“This study is promising because it shows that a gluten-free diet may help lower the risk of pain for people with gluten neuropathy,” Dr. Zis said. “More research is needed to confirm these results and to determine whether the gluten-free diet led to the reduction in pain.”
Is Sodium Oxybate Effective in Children With Narcolepsy?
LOS ANGELES—Sodium oxybate reduces cataplexy and excessive sleepiness in children with narcolepsy type 1, according to a study described at the 70th Annual Meeting of the American Academy of Neurology. The treatment’s safety profile in this population is similar to that in adults.
Although symptoms of narcolepsy often begin during childhood or adolescence, few studies have evaluated treatments for narcolepsy in pediatric patients. Sodium oxybate is approved for the treatment of cataplexy and excessive daytime sleepiness in adults with narcolepsy, but it had not previously been studied in a large pediatric narcolepsy trial. Chad Ruoff, MD, Clinical Assistant Professor of Psychiatry and Behavioral Sciences at the Stanford Center for Sleep Sciences and Medicine in California, and colleagues conducted a double-blind, placebo-controlled, randomized-withdrawal study to evaluate the efficacy and safety of sodium oxybate in pediatric patients with narcolepsy type 1.
A Randomized-Withdrawal Study
Eligible participants were children and adolescents between ages 7 and 16 who had been diagnosed with narcolepsy type 1 and had cataplexy. Patients who were on stable doses of sodium oxybate and patients who were sodium-oxybate-naïve were included. Patients with evidence of sleep-disordered breathing were excluded.
Sodium-oxybate-naïve participants were titrated to a stable dose. After a stable-dose period, all participants began a two-week, double-blind, placebo-controlled withdrawal period. The investigators randomized participants in equal groups to continue sodium oxybate or to be switched to placebo. At the end of the double-blind period, all participants received open-label sodium oxybate treatment. Efficacy assessments compared measurements during or at the end of the double-blind period with those taken the last two weeks of the stable-dose period. The study’s primary end point was change in weekly number of cataplexy attacks.
Study Was Terminated Early
Dr. Ruoff and colleagues randomized 63 participants. Approximately 41% of the population was between ages 7 and 11, 44% was female, and 38% was receiving sodium oxybate at baseline. A preplanned interim analysis of 35 participants indicated that sodium oxybate was effective, based on the primary end point result. The double-blind, randomized-withdrawal period thus was terminated early.
For the total group of 63 randomized participants, weekly cataplexy attacks were significantly increased in the placebo group (median, 12.7/week), compared with the sodium-oxybate-treated group (median, 0.3/week). Cataplexy severity, assessed using the Clinical Global Impression of Change (CGI-C), was worse in the placebo group than in the sodium-oxybate group. For 65% of participants in the placebo group, cataplexy was rated “much worse” or “very much worse,” compared with 17% of the sodium-oxybate group. Excessive sleepiness, assessed using the Epworth Sleepiness Scale for Children and Adolescents, also was worse in the placebo group (median increase, 3.0 points) than in the sodium-oxybate group (no change). In addition, the CGI-C for narcolepsy overall was worse in the placebo group.
Treatment-emergent adverse events occurring in more than 10% of the overall sample were enuresis, nausea, vomiting, headache, and decreased weight. These adverse events had been reported in previous trials of sodium oxybate in adults with narcolepsy.
The study was sponsored by Jazz Pharmaceuticals.
LOS ANGELES—Sodium oxybate reduces cataplexy and excessive sleepiness in children with narcolepsy type 1, according to a study described at the 70th Annual Meeting of the American Academy of Neurology. The treatment’s safety profile in this population is similar to that in adults.
Although symptoms of narcolepsy often begin during childhood or adolescence, few studies have evaluated treatments for narcolepsy in pediatric patients. Sodium oxybate is approved for the treatment of cataplexy and excessive daytime sleepiness in adults with narcolepsy, but it had not previously been studied in a large pediatric narcolepsy trial. Chad Ruoff, MD, Clinical Assistant Professor of Psychiatry and Behavioral Sciences at the Stanford Center for Sleep Sciences and Medicine in California, and colleagues conducted a double-blind, placebo-controlled, randomized-withdrawal study to evaluate the efficacy and safety of sodium oxybate in pediatric patients with narcolepsy type 1.
A Randomized-Withdrawal Study
Eligible participants were children and adolescents between ages 7 and 16 who had been diagnosed with narcolepsy type 1 and had cataplexy. Patients who were on stable doses of sodium oxybate and patients who were sodium-oxybate-naïve were included. Patients with evidence of sleep-disordered breathing were excluded.
Sodium-oxybate-naïve participants were titrated to a stable dose. After a stable-dose period, all participants began a two-week, double-blind, placebo-controlled withdrawal period. The investigators randomized participants in equal groups to continue sodium oxybate or to be switched to placebo. At the end of the double-blind period, all participants received open-label sodium oxybate treatment. Efficacy assessments compared measurements during or at the end of the double-blind period with those taken the last two weeks of the stable-dose period. The study’s primary end point was change in weekly number of cataplexy attacks.
Study Was Terminated Early
Dr. Ruoff and colleagues randomized 63 participants. Approximately 41% of the population was between ages 7 and 11, 44% was female, and 38% was receiving sodium oxybate at baseline. A preplanned interim analysis of 35 participants indicated that sodium oxybate was effective, based on the primary end point result. The double-blind, randomized-withdrawal period thus was terminated early.
For the total group of 63 randomized participants, weekly cataplexy attacks were significantly increased in the placebo group (median, 12.7/week), compared with the sodium-oxybate-treated group (median, 0.3/week). Cataplexy severity, assessed using the Clinical Global Impression of Change (CGI-C), was worse in the placebo group than in the sodium-oxybate group. For 65% of participants in the placebo group, cataplexy was rated “much worse” or “very much worse,” compared with 17% of the sodium-oxybate group. Excessive sleepiness, assessed using the Epworth Sleepiness Scale for Children and Adolescents, also was worse in the placebo group (median increase, 3.0 points) than in the sodium-oxybate group (no change). In addition, the CGI-C for narcolepsy overall was worse in the placebo group.
Treatment-emergent adverse events occurring in more than 10% of the overall sample were enuresis, nausea, vomiting, headache, and decreased weight. These adverse events had been reported in previous trials of sodium oxybate in adults with narcolepsy.
The study was sponsored by Jazz Pharmaceuticals.
LOS ANGELES—Sodium oxybate reduces cataplexy and excessive sleepiness in children with narcolepsy type 1, according to a study described at the 70th Annual Meeting of the American Academy of Neurology. The treatment’s safety profile in this population is similar to that in adults.
Although symptoms of narcolepsy often begin during childhood or adolescence, few studies have evaluated treatments for narcolepsy in pediatric patients. Sodium oxybate is approved for the treatment of cataplexy and excessive daytime sleepiness in adults with narcolepsy, but it had not previously been studied in a large pediatric narcolepsy trial. Chad Ruoff, MD, Clinical Assistant Professor of Psychiatry and Behavioral Sciences at the Stanford Center for Sleep Sciences and Medicine in California, and colleagues conducted a double-blind, placebo-controlled, randomized-withdrawal study to evaluate the efficacy and safety of sodium oxybate in pediatric patients with narcolepsy type 1.
A Randomized-Withdrawal Study
Eligible participants were children and adolescents between ages 7 and 16 who had been diagnosed with narcolepsy type 1 and had cataplexy. Patients who were on stable doses of sodium oxybate and patients who were sodium-oxybate-naïve were included. Patients with evidence of sleep-disordered breathing were excluded.
Sodium-oxybate-naïve participants were titrated to a stable dose. After a stable-dose period, all participants began a two-week, double-blind, placebo-controlled withdrawal period. The investigators randomized participants in equal groups to continue sodium oxybate or to be switched to placebo. At the end of the double-blind period, all participants received open-label sodium oxybate treatment. Efficacy assessments compared measurements during or at the end of the double-blind period with those taken the last two weeks of the stable-dose period. The study’s primary end point was change in weekly number of cataplexy attacks.
Study Was Terminated Early
Dr. Ruoff and colleagues randomized 63 participants. Approximately 41% of the population was between ages 7 and 11, 44% was female, and 38% was receiving sodium oxybate at baseline. A preplanned interim analysis of 35 participants indicated that sodium oxybate was effective, based on the primary end point result. The double-blind, randomized-withdrawal period thus was terminated early.
For the total group of 63 randomized participants, weekly cataplexy attacks were significantly increased in the placebo group (median, 12.7/week), compared with the sodium-oxybate-treated group (median, 0.3/week). Cataplexy severity, assessed using the Clinical Global Impression of Change (CGI-C), was worse in the placebo group than in the sodium-oxybate group. For 65% of participants in the placebo group, cataplexy was rated “much worse” or “very much worse,” compared with 17% of the sodium-oxybate group. Excessive sleepiness, assessed using the Epworth Sleepiness Scale for Children and Adolescents, also was worse in the placebo group (median increase, 3.0 points) than in the sodium-oxybate group (no change). In addition, the CGI-C for narcolepsy overall was worse in the placebo group.
Treatment-emergent adverse events occurring in more than 10% of the overall sample were enuresis, nausea, vomiting, headache, and decreased weight. These adverse events had been reported in previous trials of sodium oxybate in adults with narcolepsy.
The study was sponsored by Jazz Pharmaceuticals.
Intraventricular enzyme replacement slows CLN2 disease progression
LOS ANGELES – Intraventricular administration of cerliponase alfa seemed to slow the rate of motor and language decline in an open-label trial of 23 children with neuronal ceroid lipofuscinosis type 2 disease.
Neuronal ceroid lipofuscinosis type 2 disease (CLN2), a form of Batten’s disease, is a rare lysosomal storage disorder that causes progressive dementia in children. Patients have pathogenic variants in the gene encoding lysosomal enzyme tripeptidyl peptidase 1 (TPP1). Without functioning enzyme, lysosomal storage material accumulates in neurons throughout the CNS and retina.
Symptoms start at 2-4 years with seizures and language delays, followed by rapid motor, language, and cognitive declines, and blindness. Children die in early adolescence. Treatment is symptomatic; there are no approved therapies.
The idea of the study was to replace the enzyme in the CNS with cerliponase alfa, a recombinant form of TPP1. Twenty-four children aged 3-16 years received 30 mg, 100 mg, or 300 mg intraventricular infusions every 2 weeks during the dose-finding phase of the open-label trial; they were then switched to 300 mg infused over 4 hours every 14 days for at least 96 weeks. One child dropped out after the first dose in the study, but the others continued.
The investigators used Ommaya or Rickham ventricular reservoirs to deliver the enzyme, which were more convenient than intrathecal administration, said investigator Emily de Los Reyes, MD, a pediatric neurologist at Nationwide Children’s Hospital, Columbus, Ohio.
The primary outcome was the time until a 2-point decline on the motor and language scores of the CLN2 Clinical Rating Scale, with 0 representing no function and 6 representing normal function in both domains. The mean unadjusted rate of decline in the motor-language score per 48-week period was 0.27 points in treated patients, versus 2.12 points in 42 historical controls (P less than .001). The treatment difference at 96 weeks was about 3.3 points. There was also a decrease in seizure severity and frequency.

All but one child experienced convulsions, over two-thirds pyrexia, and almost two-thirds vomiting and hypersensitivity. About half developed upper respiratory tract infections, and about half had increased CSF white-cell counts. There were also cases of device leakage, and two children developed infections detected by CSF monitoring, without symptoms of meningitis. Both continued treatment after removal of the intraventricular device, followed by antibiotics, and device replacement.
Fourteen patients (58%) had at least one grade 3 adverse event, and there was one grade 4 event: status epilepticus deemed unrelated to the study. Side effects resolved on their own or responded to medical management. There were no deaths, study discontinuations, or dose reductions.
The mean age in the study was 60 months, about two-thirds of the patients were girls, and CLN2 diagnosis was confirmed by genotyping. Almost all the children had seizure histories. The majority were moderately advanced at baseline, with motor-language scores of 3 out of 6 in 11 patients.
An audience member asked Dr. de Los Reyes if there would be even more benefit by starting treatment before children became symptomatic. “I think all the neurologists in this group, we know that the earlier the treatment for rare diseases, the better the response,” she said.
The results were published simultaneously in the New England Journal of Medicine.
BioMarin Pharmaceutical funded the work, along with grants from the German Federal Ministry of Education and Research, the European Union’s Horizon 2020 Research and Innovation Program, and the National Institute for Health Research. Several authors were BioMarin employees. Dr. de Los Reyes is a consultant and reported a grant from the company.
SOURCE: Schulz A et al. N Engl J Med. 2018 Apr 24. doi: 10.1056/NEJMoa1712649.
LOS ANGELES – Intraventricular administration of cerliponase alfa seemed to slow the rate of motor and language decline in an open-label trial of 23 children with neuronal ceroid lipofuscinosis type 2 disease.
Neuronal ceroid lipofuscinosis type 2 disease (CLN2), a form of Batten’s disease, is a rare lysosomal storage disorder that causes progressive dementia in children. Patients have pathogenic variants in the gene encoding lysosomal enzyme tripeptidyl peptidase 1 (TPP1). Without functioning enzyme, lysosomal storage material accumulates in neurons throughout the CNS and retina.
Symptoms start at 2-4 years with seizures and language delays, followed by rapid motor, language, and cognitive declines, and blindness. Children die in early adolescence. Treatment is symptomatic; there are no approved therapies.
The idea of the study was to replace the enzyme in the CNS with cerliponase alfa, a recombinant form of TPP1. Twenty-four children aged 3-16 years received 30 mg, 100 mg, or 300 mg intraventricular infusions every 2 weeks during the dose-finding phase of the open-label trial; they were then switched to 300 mg infused over 4 hours every 14 days for at least 96 weeks. One child dropped out after the first dose in the study, but the others continued.
The investigators used Ommaya or Rickham ventricular reservoirs to deliver the enzyme, which were more convenient than intrathecal administration, said investigator Emily de Los Reyes, MD, a pediatric neurologist at Nationwide Children’s Hospital, Columbus, Ohio.
The primary outcome was the time until a 2-point decline on the motor and language scores of the CLN2 Clinical Rating Scale, with 0 representing no function and 6 representing normal function in both domains. The mean unadjusted rate of decline in the motor-language score per 48-week period was 0.27 points in treated patients, versus 2.12 points in 42 historical controls (P less than .001). The treatment difference at 96 weeks was about 3.3 points. There was also a decrease in seizure severity and frequency.
All but one child experienced convulsions, over two-thirds pyrexia, and almost two-thirds vomiting and hypersensitivity. About half developed upper respiratory tract infections, and about half had increased CSF white-cell counts. There were also cases of device leakage, and two children developed infections detected by CSF monitoring, without symptoms of meningitis. Both continued treatment after removal of the intraventricular device, followed by antibiotics, and device replacement.
Fourteen patients (58%) had at least one grade 3 adverse event, and there was one grade 4 event: status epilepticus deemed unrelated to the study. Side effects resolved on their own or responded to medical management. There were no deaths, study discontinuations, or dose reductions.
The mean age in the study was 60 months, about two-thirds of the patients were girls, and CLN2 diagnosis was confirmed by genotyping. Almost all the children had seizure histories. The majority were moderately advanced at baseline, with motor-language scores of 3 out of 6 in 11 patients.
An audience member asked Dr. de Los Reyes if there would be even more benefit by starting treatment before children became symptomatic. “I think all the neurologists in this group, we know that the earlier the treatment for rare diseases, the better the response,” she said.
The results were published simultaneously in the New England Journal of Medicine.
BioMarin Pharmaceutical funded the work, along with grants from the German Federal Ministry of Education and Research, the European Union’s Horizon 2020 Research and Innovation Program, and the National Institute for Health Research. Several authors were BioMarin employees. Dr. de Los Reyes is a consultant and reported a grant from the company.
SOURCE: Schulz A et al. N Engl J Med. 2018 Apr 24. doi: 10.1056/NEJMoa1712649.
LOS ANGELES – Intraventricular administration of cerliponase alfa seemed to slow the rate of motor and language decline in an open-label trial of 23 children with neuronal ceroid lipofuscinosis type 2 disease.
Neuronal ceroid lipofuscinosis type 2 disease (CLN2), a form of Batten’s disease, is a rare lysosomal storage disorder that causes progressive dementia in children. Patients have pathogenic variants in the gene encoding lysosomal enzyme tripeptidyl peptidase 1 (TPP1). Without functioning enzyme, lysosomal storage material accumulates in neurons throughout the CNS and retina.
Symptoms start at 2-4 years with seizures and language delays, followed by rapid motor, language, and cognitive declines, and blindness. Children die in early adolescence. Treatment is symptomatic; there are no approved therapies.
The idea of the study was to replace the enzyme in the CNS with cerliponase alfa, a recombinant form of TPP1. Twenty-four children aged 3-16 years received 30 mg, 100 mg, or 300 mg intraventricular infusions every 2 weeks during the dose-finding phase of the open-label trial; they were then switched to 300 mg infused over 4 hours every 14 days for at least 96 weeks. One child dropped out after the first dose in the study, but the others continued.
The investigators used Ommaya or Rickham ventricular reservoirs to deliver the enzyme, which were more convenient than intrathecal administration, said investigator Emily de Los Reyes, MD, a pediatric neurologist at Nationwide Children’s Hospital, Columbus, Ohio.
The primary outcome was the time until a 2-point decline on the motor and language scores of the CLN2 Clinical Rating Scale, with 0 representing no function and 6 representing normal function in both domains. The mean unadjusted rate of decline in the motor-language score per 48-week period was 0.27 points in treated patients, versus 2.12 points in 42 historical controls (P less than .001). The treatment difference at 96 weeks was about 3.3 points. There was also a decrease in seizure severity and frequency.
All but one child experienced convulsions, over two-thirds pyrexia, and almost two-thirds vomiting and hypersensitivity. About half developed upper respiratory tract infections, and about half had increased CSF white-cell counts. There were also cases of device leakage, and two children developed infections detected by CSF monitoring, without symptoms of meningitis. Both continued treatment after removal of the intraventricular device, followed by antibiotics, and device replacement.
Fourteen patients (58%) had at least one grade 3 adverse event, and there was one grade 4 event: status epilepticus deemed unrelated to the study. Side effects resolved on their own or responded to medical management. There were no deaths, study discontinuations, or dose reductions.
The mean age in the study was 60 months, about two-thirds of the patients were girls, and CLN2 diagnosis was confirmed by genotyping. Almost all the children had seizure histories. The majority were moderately advanced at baseline, with motor-language scores of 3 out of 6 in 11 patients.
An audience member asked Dr. de Los Reyes if there would be even more benefit by starting treatment before children became symptomatic. “I think all the neurologists in this group, we know that the earlier the treatment for rare diseases, the better the response,” she said.
The results were published simultaneously in the New England Journal of Medicine.
BioMarin Pharmaceutical funded the work, along with grants from the German Federal Ministry of Education and Research, the European Union’s Horizon 2020 Research and Innovation Program, and the National Institute for Health Research. Several authors were BioMarin employees. Dr. de Los Reyes is a consultant and reported a grant from the company.
SOURCE: Schulz A et al. N Engl J Med. 2018 Apr 24. doi: 10.1056/NEJMoa1712649.
REPORTING FROM AAN 2018
Key clinical point: Intraventricular administration of cerliponase alfa seemed to slow the rate of motor and language decline in 23 children with neuronal ceroid lipofuscinosis type 2 disease.
Major finding: The mean unadjusted rate of decline in the motor-language score per 48-week period was 0.27 points in treated patients, versus 2.12 points in 42 historical controls (P less than .001).
Study details: Open-label trial of 23 children.
Disclosures: BioMarin Pharmaceutical funded the work, along with grants from the German Federal Ministry of Education and Research, the European Union’s Horizon 2020 Research and Innovation Program, and the National Institute for Health Research. Several authors were BioMarin employees. The presenter is a consultant to BioMarin and reported a grant from the company.
Source: Schulz A et al. N Engl J Med. 2018 Apr 24. doi: 10.1056/NEJMoa1712649.
Fecal microbiota transplantation by capsule effective in preventing recurrent C. difficile
Clinical question: Is fecal microbiota transplantation (FMT) by oral capsule noninferior to administration via colonoscopy in preventing recurrent Clostridium difficile infection (RCDI)?
Background: Approximately 20% of patients with an initial episode of C. difficile develop recurrent disease. FMT is the most effective treatment for RCDI. Currently, it is believed that there is a higher rate of success with FMT by colonoscopy, but this is based on studies lacking a control group. The cost of administering FMT by colonoscopy is more than double the cost via oral capsule, and efficacy between the two routes has not been studied in a randomized fashion. If oral capsule delivery is noninferior, then wait times, cost, and procedure risk would be reduced.
Study design: Randomized, unblinded, noninferiority trial.
Setting: Three academic medical centers in Alberta, Ca.

Synopsis: Patients with at least three documented episodes of C. difficile infection were randomized to receive FMT by either oral capsule or colonoscopy. Exclusion criteria included complicated C. difficile infections, cancer undergoing therapy, and conditions requiring antibiotics. The primary outcome was RCDI within 12 weeks after FMT. A total of 105 patients completed the trial, with 96.2% (51/53) of patients in the capsule group and 96.2% (50/52) of patients in the colonoscopy group remaining free of RCDI at the 12-week follow-up. This met the –15% noninferiority margin and suggests that oral capsule may be an effective route of delivery for FMT. Limitations of the study are exclusion of complicated RCDI patients, lack of blinding, and no placebo control (which would have been helpful since the prevention rates were so high and recurrent diarrhea was self-reported among participants, leading to a subjective outcome).
Bottom line: FMT by oral capsule may be noninferior to FMT by colonoscopy in preventing RCDI at 12 weeks.
Citation: Kao D et al. Effect of oral capsule- vs. colonoscopy-delivered fecal microbiota transplantation on recurrent Clostridium difficile infection: A randomized clinical trial. JAMA. 2017 Nov 28;318(20):1985-93.
Dr. Mehra is assistant professor of medicine, division of hospital medicine, University of Virginia.
Clinical question: Is fecal microbiota transplantation (FMT) by oral capsule noninferior to administration via colonoscopy in preventing recurrent Clostridium difficile infection (RCDI)?
Background: Approximately 20% of patients with an initial episode of C. difficile develop recurrent disease. FMT is the most effective treatment for RCDI. Currently, it is believed that there is a higher rate of success with FMT by colonoscopy, but this is based on studies lacking a control group. The cost of administering FMT by colonoscopy is more than double the cost via oral capsule, and efficacy between the two routes has not been studied in a randomized fashion. If oral capsule delivery is noninferior, then wait times, cost, and procedure risk would be reduced.
Study design: Randomized, unblinded, noninferiority trial.
Setting: Three academic medical centers in Alberta, Ca.
Synopsis: Patients with at least three documented episodes of C. difficile infection were randomized to receive FMT by either oral capsule or colonoscopy. Exclusion criteria included complicated C. difficile infections, cancer undergoing therapy, and conditions requiring antibiotics. The primary outcome was RCDI within 12 weeks after FMT. A total of 105 patients completed the trial, with 96.2% (51/53) of patients in the capsule group and 96.2% (50/52) of patients in the colonoscopy group remaining free of RCDI at the 12-week follow-up. This met the –15% noninferiority margin and suggests that oral capsule may be an effective route of delivery for FMT. Limitations of the study are exclusion of complicated RCDI patients, lack of blinding, and no placebo control (which would have been helpful since the prevention rates were so high and recurrent diarrhea was self-reported among participants, leading to a subjective outcome).
Bottom line: FMT by oral capsule may be noninferior to FMT by colonoscopy in preventing RCDI at 12 weeks.
Citation: Kao D et al. Effect of oral capsule- vs. colonoscopy-delivered fecal microbiota transplantation on recurrent Clostridium difficile infection: A randomized clinical trial. JAMA. 2017 Nov 28;318(20):1985-93.
Dr. Mehra is assistant professor of medicine, division of hospital medicine, University of Virginia.
Clinical question: Is fecal microbiota transplantation (FMT) by oral capsule noninferior to administration via colonoscopy in preventing recurrent Clostridium difficile infection (RCDI)?
Background: Approximately 20% of patients with an initial episode of C. difficile develop recurrent disease. FMT is the most effective treatment for RCDI. Currently, it is believed that there is a higher rate of success with FMT by colonoscopy, but this is based on studies lacking a control group. The cost of administering FMT by colonoscopy is more than double the cost via oral capsule, and efficacy between the two routes has not been studied in a randomized fashion. If oral capsule delivery is noninferior, then wait times, cost, and procedure risk would be reduced.
Study design: Randomized, unblinded, noninferiority trial.
Setting: Three academic medical centers in Alberta, Ca.
Synopsis: Patients with at least three documented episodes of C. difficile infection were randomized to receive FMT by either oral capsule or colonoscopy. Exclusion criteria included complicated C. difficile infections, cancer undergoing therapy, and conditions requiring antibiotics. The primary outcome was RCDI within 12 weeks after FMT. A total of 105 patients completed the trial, with 96.2% (51/53) of patients in the capsule group and 96.2% (50/52) of patients in the colonoscopy group remaining free of RCDI at the 12-week follow-up. This met the –15% noninferiority margin and suggests that oral capsule may be an effective route of delivery for FMT. Limitations of the study are exclusion of complicated RCDI patients, lack of blinding, and no placebo control (which would have been helpful since the prevention rates were so high and recurrent diarrhea was self-reported among participants, leading to a subjective outcome).
Bottom line: FMT by oral capsule may be noninferior to FMT by colonoscopy in preventing RCDI at 12 weeks.
Citation: Kao D et al. Effect of oral capsule- vs. colonoscopy-delivered fecal microbiota transplantation on recurrent Clostridium difficile infection: A randomized clinical trial. JAMA. 2017 Nov 28;318(20):1985-93.
Dr. Mehra is assistant professor of medicine, division of hospital medicine, University of Virginia.
DAAs open up organ donation from HCV patients
BOSTON – There was no sign of HCV infection more than a year after 10 patients at Johns Hopkins University, Baltimore, received kidneys from HCV-infected donors.
The patients were treated with prophylactic direct-acting antivirals (DAAs) before and after the procedure. Low levels of hepatitis C RNA were detected shortly after transplant in five patients, but it became undetectable within a week. None of the patients developed any clinical signs of chronic hepatitis C infection, and the transplanted kidneys functioned well.

The number of organs from HCV–infected people is on the rise because of the opioid epidemic. Organ donations from drug overdoses used to be rare, but about 10% of transplanted organs are now from an overdose death, and about 30% of people who overdose have HCV. “These are young people who could donate hearts, lungs, and kidneys, and their parents and families want them to be able to make that gift of life,” said lead investigator Christine Durand, MD, of Johns Hopkins University, Baltimore.
DAAs make that possible because they cure HCV. “If the success of these transplants continues, it could pave the way for other hepatitis C–positive organs, including hearts and livers, to be transplanted as well,” Dr. Durand and her colleagues said in a press release from Johns Hopkins.
The 10 patients were over age 50 years, with a mean age of 71 years, and had been on the kidney transplant list for an average of 4 months. The HCV-positive donors were 13-50 years old with no evidence of kidney disease (Ann Intern Med. 2018 Mar 6. doi: 10.7326/M17-2871)..
Each recipient received a dose of grazoprevir/elbasvir (Zepatier) before transplant and stayed on the medication daily for 12 weeks postop. Three patients also took a daily dose of sofosbuvir (Sovaldi) because of the strain of HCV in the donor kidney. Maybe 8 weeks of treatment, or even 4, is enough, Dr. Durand said at the Conference on Retroviruses and Opportunistic Infections.
“I am thrilled to report that at 1 year post transplant 10 out of 10 of these recipients are HCV free, and they are doing very well. Prophylactic treatment may mean that more individuals can receive transplants from hepatitis C–infected donors without transmission of infection. The use of organs from infected donors can help everyone on the transplant list by shortening wait times and shortening the wait list,” she said.
“I’m not surprised by the results of the study because these DAAs are highly effective, but I was surprised by how willing patients were to sign up for the study. They said it was a no-brainer. In our region, if you need a kidney, you are going to wait for up to 5 years, and you may die while you are waiting. If you can accept a hepatitis C–positive donor organ, you will get transplanted in a matter of weeks,” she said.
“I hope providers tell their patients with HCV that they can register as organ donors,” she said.
The work is being supported primarily by Merck Sharp & Dohme. Dr. Durand is an advisor to Bristol-Meyers Squibb, Gilead Sciences, and Merck Pharmaceuticals and has research funding from the companies.
SOURCE: Durand CM et al. Ann Intern Med. 2018 Mar 6. doi: 10.7326/M17-2871.
BOSTON – There was no sign of HCV infection more than a year after 10 patients at Johns Hopkins University, Baltimore, received kidneys from HCV-infected donors.
The patients were treated with prophylactic direct-acting antivirals (DAAs) before and after the procedure. Low levels of hepatitis C RNA were detected shortly after transplant in five patients, but it became undetectable within a week. None of the patients developed any clinical signs of chronic hepatitis C infection, and the transplanted kidneys functioned well.
The number of organs from HCV–infected people is on the rise because of the opioid epidemic. Organ donations from drug overdoses used to be rare, but about 10% of transplanted organs are now from an overdose death, and about 30% of people who overdose have HCV. “These are young people who could donate hearts, lungs, and kidneys, and their parents and families want them to be able to make that gift of life,” said lead investigator Christine Durand, MD, of Johns Hopkins University, Baltimore.
DAAs make that possible because they cure HCV. “If the success of these transplants continues, it could pave the way for other hepatitis C–positive organs, including hearts and livers, to be transplanted as well,” Dr. Durand and her colleagues said in a press release from Johns Hopkins.
The 10 patients were over age 50 years, with a mean age of 71 years, and had been on the kidney transplant list for an average of 4 months. The HCV-positive donors were 13-50 years old with no evidence of kidney disease (Ann Intern Med. 2018 Mar 6. doi: 10.7326/M17-2871)..
Each recipient received a dose of grazoprevir/elbasvir (Zepatier) before transplant and stayed on the medication daily for 12 weeks postop. Three patients also took a daily dose of sofosbuvir (Sovaldi) because of the strain of HCV in the donor kidney. Maybe 8 weeks of treatment, or even 4, is enough, Dr. Durand said at the Conference on Retroviruses and Opportunistic Infections.
“I am thrilled to report that at 1 year post transplant 10 out of 10 of these recipients are HCV free, and they are doing very well. Prophylactic treatment may mean that more individuals can receive transplants from hepatitis C–infected donors without transmission of infection. The use of organs from infected donors can help everyone on the transplant list by shortening wait times and shortening the wait list,” she said.
“I’m not surprised by the results of the study because these DAAs are highly effective, but I was surprised by how willing patients were to sign up for the study. They said it was a no-brainer. In our region, if you need a kidney, you are going to wait for up to 5 years, and you may die while you are waiting. If you can accept a hepatitis C–positive donor organ, you will get transplanted in a matter of weeks,” she said.
“I hope providers tell their patients with HCV that they can register as organ donors,” she said.
The work is being supported primarily by Merck Sharp & Dohme. Dr. Durand is an advisor to Bristol-Meyers Squibb, Gilead Sciences, and Merck Pharmaceuticals and has research funding from the companies.
SOURCE: Durand CM et al. Ann Intern Med. 2018 Mar 6. doi: 10.7326/M17-2871.
BOSTON – There was no sign of HCV infection more than a year after 10 patients at Johns Hopkins University, Baltimore, received kidneys from HCV-infected donors.
The patients were treated with prophylactic direct-acting antivirals (DAAs) before and after the procedure. Low levels of hepatitis C RNA were detected shortly after transplant in five patients, but it became undetectable within a week. None of the patients developed any clinical signs of chronic hepatitis C infection, and the transplanted kidneys functioned well.
The number of organs from HCV–infected people is on the rise because of the opioid epidemic. Organ donations from drug overdoses used to be rare, but about 10% of transplanted organs are now from an overdose death, and about 30% of people who overdose have HCV. “These are young people who could donate hearts, lungs, and kidneys, and their parents and families want them to be able to make that gift of life,” said lead investigator Christine Durand, MD, of Johns Hopkins University, Baltimore.
DAAs make that possible because they cure HCV. “If the success of these transplants continues, it could pave the way for other hepatitis C–positive organs, including hearts and livers, to be transplanted as well,” Dr. Durand and her colleagues said in a press release from Johns Hopkins.
The 10 patients were over age 50 years, with a mean age of 71 years, and had been on the kidney transplant list for an average of 4 months. The HCV-positive donors were 13-50 years old with no evidence of kidney disease (Ann Intern Med. 2018 Mar 6. doi: 10.7326/M17-2871)..
Each recipient received a dose of grazoprevir/elbasvir (Zepatier) before transplant and stayed on the medication daily for 12 weeks postop. Three patients also took a daily dose of sofosbuvir (Sovaldi) because of the strain of HCV in the donor kidney. Maybe 8 weeks of treatment, or even 4, is enough, Dr. Durand said at the Conference on Retroviruses and Opportunistic Infections.
“I am thrilled to report that at 1 year post transplant 10 out of 10 of these recipients are HCV free, and they are doing very well. Prophylactic treatment may mean that more individuals can receive transplants from hepatitis C–infected donors without transmission of infection. The use of organs from infected donors can help everyone on the transplant list by shortening wait times and shortening the wait list,” she said.
“I’m not surprised by the results of the study because these DAAs are highly effective, but I was surprised by how willing patients were to sign up for the study. They said it was a no-brainer. In our region, if you need a kidney, you are going to wait for up to 5 years, and you may die while you are waiting. If you can accept a hepatitis C–positive donor organ, you will get transplanted in a matter of weeks,” she said.
“I hope providers tell their patients with HCV that they can register as organ donors,” she said.
The work is being supported primarily by Merck Sharp & Dohme. Dr. Durand is an advisor to Bristol-Meyers Squibb, Gilead Sciences, and Merck Pharmaceuticals and has research funding from the companies.
SOURCE: Durand CM et al. Ann Intern Med. 2018 Mar 6. doi: 10.7326/M17-2871.
REPORTING FROM CROI
Key clinical point: HCV may soon no longer bar organ donation.
Major finding: There was no sign of HCV infection more than a year after 10 patients at Johns Hopkins University, Baltimore, received kidneys from HCV-infected donors.
Study details: Open-label nonrandomized trial.
Disclosures: The work is being supported primarily by Merck Sharp & Dohme. The study lead is an advisor to Bristol-Meyers Squibb, Gilead Sciences, and Merck Pharmaceuticals, and has research funding from the companies.
Source: Durand CM et al. Ann Intern Med. 2018 Mar 6. doi: 10.7326/M17-2871.
Migraine and Elevated Vascular Biomarkers Linked
Elevated vascular biomarkers were associated with migraine, a recent study found, particularly migraine with aura (MA), as well as with years of aura and number of aura attacks. Participants (300 women, 117 men) were aged 30–60 (mean 48) years, 155 MA, 128 migraine without aura (MO), and 134 were controls with no severe headaches. Plasma concentrations of fibrinogen, Factor II, D-dimer, high sensitivity C-reactive protein (hs-CRP), and von Willebrand factor antigen were compared between groups, also stratifying by sex. Researchers found:
- Fibrinogen and hs-CRP were elevated in migraineurs compared to controls.
- In logistic regression analyses, MO and MA had increased likelihood of elevated fibrinogen, and MA had increased likelihood of elevated Factor II and hs-CRP.
- Fibrinogen and Factor II were associated with MA in women but not men.
- In the migraine subgroup, the total number of years of aura, but not headache, predicted elevated hs-CRP, and the average number of aura, but not headache, attacks predicted all biomarkers but Factor II.
Migraine and vascular disease biomarkers: A population-based case-control study. Cephalalgia. 2018;38(3):511-518. doi:10.1177/0333102417698936.
Elevated vascular biomarkers were associated with migraine, a recent study found, particularly migraine with aura (MA), as well as with years of aura and number of aura attacks. Participants (300 women, 117 men) were aged 30–60 (mean 48) years, 155 MA, 128 migraine without aura (MO), and 134 were controls with no severe headaches. Plasma concentrations of fibrinogen, Factor II, D-dimer, high sensitivity C-reactive protein (hs-CRP), and von Willebrand factor antigen were compared between groups, also stratifying by sex. Researchers found:
- Fibrinogen and hs-CRP were elevated in migraineurs compared to controls.
- In logistic regression analyses, MO and MA had increased likelihood of elevated fibrinogen, and MA had increased likelihood of elevated Factor II and hs-CRP.
- Fibrinogen and Factor II were associated with MA in women but not men.
- In the migraine subgroup, the total number of years of aura, but not headache, predicted elevated hs-CRP, and the average number of aura, but not headache, attacks predicted all biomarkers but Factor II.
Migraine and vascular disease biomarkers: A population-based case-control study. Cephalalgia. 2018;38(3):511-518. doi:10.1177/0333102417698936.
Elevated vascular biomarkers were associated with migraine, a recent study found, particularly migraine with aura (MA), as well as with years of aura and number of aura attacks. Participants (300 women, 117 men) were aged 30–60 (mean 48) years, 155 MA, 128 migraine without aura (MO), and 134 were controls with no severe headaches. Plasma concentrations of fibrinogen, Factor II, D-dimer, high sensitivity C-reactive protein (hs-CRP), and von Willebrand factor antigen were compared between groups, also stratifying by sex. Researchers found:
- Fibrinogen and hs-CRP were elevated in migraineurs compared to controls.
- In logistic regression analyses, MO and MA had increased likelihood of elevated fibrinogen, and MA had increased likelihood of elevated Factor II and hs-CRP.
- Fibrinogen and Factor II were associated with MA in women but not men.
- In the migraine subgroup, the total number of years of aura, but not headache, predicted elevated hs-CRP, and the average number of aura, but not headache, attacks predicted all biomarkers but Factor II.
Migraine and vascular disease biomarkers: A population-based case-control study. Cephalalgia. 2018;38(3):511-518. doi:10.1177/0333102417698936.