User login
Hormone therapy raises diabetes risk in breast cancer survivors
Hormone therapy for breast cancer more than doubles a woman’s risk for developing type 2 diabetes, results of a case-cohort study suggest.
Hormone therapy with tamoxifen was associated with a more than twofold increase in risk of diabetes, and aromatase inhibitors were associated with a more than fourfold increase, reported Hatem Hamood, MD, of Leumit Health Services in Karmiel, Israel, and colleagues.
Among 2,246 women with breast cancer and no diabetes at baseline, followed for a mean of 5.9 years (longest follow-up 13 years), the crude cumulative lifetime incidence rate of diabetes was 20.9%, the investigators wrote. The report was published in the Journal of Clinical Oncology.
“[Hormone therapy] is a significant risk factor of diabetes among breast cancer survivors. The underlying mechanism is unclear, and additional research is warranted. Although cessation of treatment is not recommended and progression of breast cancer often is inevitable, devised strategies aimed at lifestyle modifications in patients at high risk of diabetes could at least preserve the natural history of breast cancer,” they wrote.
Diabetes has previously been identified as a possible risk factor for breast cancer, but the potential for breast cancer therapy as a precipitating factor for diabetes is uncertain, the authors said.
“Given the detrimental impact of diabetes on breast cancer survival, additional exploration of the role of breast cancer treatment in the development of diabetes is important not only because it would add valuable information on the etiology of diabetes but also because it would help to identify high-risk patients in need of accentuated clinical care,” they wrote.
To explore the possible association between hormone therapy and diabetes risk, the investigators performed a retrospective case-cohort study of 2,246 women who had been diagnosed with primary nonmetastatic breast cancer treated with hormone therapy from 2002 through 2012.
They examined data on a randomly selected cohort of 448 breast cancer survivors and all patients in the parent (no diabetes at baseline) cohort who developed diabetes during the study period (324 patients).
They found that the prevalence of diabetes among their source population of 2,644 breast cancer survivors (including those with baseline diabetes) increased “drastically” from 6% in 2002 to 28% in 2015. The prevalence exceeded Israeli national norms from 2010 through 2013, with standardized prevalence ratios of 1.61 to 1.81 (P less than .001).
As noted, in the population without baseline diabetes, the crude cumulative incidence rate of diabetes in the presence of death as a competing risk factor was 20.9%.
In multivariate analyses controlling for demographic and socioeconomic factors, and for chemotherapy type, hypertension, outpatient visits, use of corticosteroids, thiazide diuretics, beta-blockers, statins, and year of breast cancer diagnosis, factors significantly associated with diabetes risk were use of hormone therapy (adjusted hazard ratio [HR] 2.40, P = .008), tamoxifen (aHR 2.25, P = .013), aromatase inhibitors (aHR 4.27, P = .013), therapy duration more than 1 year (aHR 2.36, P = .009), and 1 year or less (aHR 6.48, P = .004).
The investigators noted that although other reports have found no association between aromatase inhibitors and diabetes risk, those studies had small samples or offered no explanation of the lack of association.
In contrast, a 2016 joint ACS/ASCO breast cancer survivorship-care guideline notes that aromatase inhibitors may raise the risk of diabetes, the investigators noted.
The study was supported by grants from the Israeli Council for Higher Education. The investigators reported no conflicts of interest.
SOURCE: Hamood H et al. J Clin Oncol. 2018 Apr 24. doi: 10.1200/JCO.2017.76.3524.
Hormone therapy for breast cancer more than doubles a woman’s risk for developing type 2 diabetes, results of a case-cohort study suggest.
Hormone therapy with tamoxifen was associated with a more than twofold increase in risk of diabetes, and aromatase inhibitors were associated with a more than fourfold increase, reported Hatem Hamood, MD, of Leumit Health Services in Karmiel, Israel, and colleagues.
Among 2,246 women with breast cancer and no diabetes at baseline, followed for a mean of 5.9 years (longest follow-up 13 years), the crude cumulative lifetime incidence rate of diabetes was 20.9%, the investigators wrote. The report was published in the Journal of Clinical Oncology.
“[Hormone therapy] is a significant risk factor of diabetes among breast cancer survivors. The underlying mechanism is unclear, and additional research is warranted. Although cessation of treatment is not recommended and progression of breast cancer often is inevitable, devised strategies aimed at lifestyle modifications in patients at high risk of diabetes could at least preserve the natural history of breast cancer,” they wrote.
Diabetes has previously been identified as a possible risk factor for breast cancer, but the potential for breast cancer therapy as a precipitating factor for diabetes is uncertain, the authors said.
“Given the detrimental impact of diabetes on breast cancer survival, additional exploration of the role of breast cancer treatment in the development of diabetes is important not only because it would add valuable information on the etiology of diabetes but also because it would help to identify high-risk patients in need of accentuated clinical care,” they wrote.
To explore the possible association between hormone therapy and diabetes risk, the investigators performed a retrospective case-cohort study of 2,246 women who had been diagnosed with primary nonmetastatic breast cancer treated with hormone therapy from 2002 through 2012.
They examined data on a randomly selected cohort of 448 breast cancer survivors and all patients in the parent (no diabetes at baseline) cohort who developed diabetes during the study period (324 patients).
They found that the prevalence of diabetes among their source population of 2,644 breast cancer survivors (including those with baseline diabetes) increased “drastically” from 6% in 2002 to 28% in 2015. The prevalence exceeded Israeli national norms from 2010 through 2013, with standardized prevalence ratios of 1.61 to 1.81 (P less than .001).
As noted, in the population without baseline diabetes, the crude cumulative incidence rate of diabetes in the presence of death as a competing risk factor was 20.9%.
In multivariate analyses controlling for demographic and socioeconomic factors, and for chemotherapy type, hypertension, outpatient visits, use of corticosteroids, thiazide diuretics, beta-blockers, statins, and year of breast cancer diagnosis, factors significantly associated with diabetes risk were use of hormone therapy (adjusted hazard ratio [HR] 2.40, P = .008), tamoxifen (aHR 2.25, P = .013), aromatase inhibitors (aHR 4.27, P = .013), therapy duration more than 1 year (aHR 2.36, P = .009), and 1 year or less (aHR 6.48, P = .004).
The investigators noted that although other reports have found no association between aromatase inhibitors and diabetes risk, those studies had small samples or offered no explanation of the lack of association.
In contrast, a 2016 joint ACS/ASCO breast cancer survivorship-care guideline notes that aromatase inhibitors may raise the risk of diabetes, the investigators noted.
The study was supported by grants from the Israeli Council for Higher Education. The investigators reported no conflicts of interest.
SOURCE: Hamood H et al. J Clin Oncol. 2018 Apr 24. doi: 10.1200/JCO.2017.76.3524.
Hormone therapy for breast cancer more than doubles a woman’s risk for developing type 2 diabetes, results of a case-cohort study suggest.
Hormone therapy with tamoxifen was associated with a more than twofold increase in risk of diabetes, and aromatase inhibitors were associated with a more than fourfold increase, reported Hatem Hamood, MD, of Leumit Health Services in Karmiel, Israel, and colleagues.
Among 2,246 women with breast cancer and no diabetes at baseline, followed for a mean of 5.9 years (longest follow-up 13 years), the crude cumulative lifetime incidence rate of diabetes was 20.9%, the investigators wrote. The report was published in the Journal of Clinical Oncology.
“[Hormone therapy] is a significant risk factor of diabetes among breast cancer survivors. The underlying mechanism is unclear, and additional research is warranted. Although cessation of treatment is not recommended and progression of breast cancer often is inevitable, devised strategies aimed at lifestyle modifications in patients at high risk of diabetes could at least preserve the natural history of breast cancer,” they wrote.
Diabetes has previously been identified as a possible risk factor for breast cancer, but the potential for breast cancer therapy as a precipitating factor for diabetes is uncertain, the authors said.
“Given the detrimental impact of diabetes on breast cancer survival, additional exploration of the role of breast cancer treatment in the development of diabetes is important not only because it would add valuable information on the etiology of diabetes but also because it would help to identify high-risk patients in need of accentuated clinical care,” they wrote.
To explore the possible association between hormone therapy and diabetes risk, the investigators performed a retrospective case-cohort study of 2,246 women who had been diagnosed with primary nonmetastatic breast cancer treated with hormone therapy from 2002 through 2012.
They examined data on a randomly selected cohort of 448 breast cancer survivors and all patients in the parent (no diabetes at baseline) cohort who developed diabetes during the study period (324 patients).
They found that the prevalence of diabetes among their source population of 2,644 breast cancer survivors (including those with baseline diabetes) increased “drastically” from 6% in 2002 to 28% in 2015. The prevalence exceeded Israeli national norms from 2010 through 2013, with standardized prevalence ratios of 1.61 to 1.81 (P less than .001).
As noted, in the population without baseline diabetes, the crude cumulative incidence rate of diabetes in the presence of death as a competing risk factor was 20.9%.
In multivariate analyses controlling for demographic and socioeconomic factors, and for chemotherapy type, hypertension, outpatient visits, use of corticosteroids, thiazide diuretics, beta-blockers, statins, and year of breast cancer diagnosis, factors significantly associated with diabetes risk were use of hormone therapy (adjusted hazard ratio [HR] 2.40, P = .008), tamoxifen (aHR 2.25, P = .013), aromatase inhibitors (aHR 4.27, P = .013), therapy duration more than 1 year (aHR 2.36, P = .009), and 1 year or less (aHR 6.48, P = .004).
The investigators noted that although other reports have found no association between aromatase inhibitors and diabetes risk, those studies had small samples or offered no explanation of the lack of association.
In contrast, a 2016 joint ACS/ASCO breast cancer survivorship-care guideline notes that aromatase inhibitors may raise the risk of diabetes, the investigators noted.
The study was supported by grants from the Israeli Council for Higher Education. The investigators reported no conflicts of interest.
SOURCE: Hamood H et al. J Clin Oncol. 2018 Apr 24. doi: 10.1200/JCO.2017.76.3524.
FROM JOURNAL OF CLINICAL ONCOLOGY
Key clinical point: Consider screening survivors of nonmetastatic breast cancer for diabetes.
Major finding: The crude lifetime incidence of diabetes following hormone therapy for breast cancer was 20.9%.
Study details: Case-cohort study of 2,246 women with nonmetastatic breast cancer and no baseline diabetes treated with hormone therapy.
Disclosures: The study was supported by grants from the Israeli Council for Higher Education. The investigators reported no conflicts of interest.
Source: Hamood H et al. J Clin Oncol. 2018 Apr 24. doi: 10.1200/JCO.2017.76.3524.
Is PASI 100 the new benchmark in psoriasis?
KAUAI, HAWAII – I think we should just do away with PASI 90 [90% improvement in Psoriasis Area and Severity Index score] and look at how well our drugs do against the metric of PASI 100. The whole ball of wax. Let’s just go for complete clearance,” Craig L. Leonardi, MD, declared in a provocative presentation at the Hawaii Dermatology Seminar provided by Skin Disease Education Foundation/Global Academy for Medical Education.
He advocates using number needed to treat (NNT) as a performance yardstick. He finds it helpful in translating sometimes-arcane clinical trial results into useful information to guide everyday practice. The NNT is the average number of patients who need to be treated with a drug or procedure in order to achieve one additional good outcome, compared with a control intervention or placebo. It’s the inverse of the absolute risk reduction. The lower the NNT, the better an intervention is performing.

He presented a chart that summarized the NNTs to achieve a PASI 100 response for various systemic agents commonly used in treating moderate to severe psoriasis. He obtained the data from Food and Drug Administration–regulated product labeling and phase 3 clinical trials.
Dr. Leonardi drew attention to the worst performers on the list: methotrexate, with an NNT of 25 to achieve a PASI 100 response, and etanercept, with an NNT of 23.3.
“Methotrexate is a drug that the insurance industry says we have to flow through on our way to biologic drugs. But if complete clearance is your goal, this is an exercise in futility. These patients will never, ever get to complete clearance – or it’s at least very unlikely. We shouldn’t be asked to go through methotrexate on our way to anything. We shouldn’t be asked to use methotrexate at all. We should be bypassing it. And some of us are working on this,” he said.
Ustekinumab and adalimumab are the current market leaders in biologic therapy for psoriasis, but they don’t stack up so well when viewed through the filter of PASI 100 response, with NNTs of 9.2 and 5.3, respectively.
“These market leaders may not be the most relevant drugs in the current era,” according to the dermatologist.
In contrast, the high-performance biologics – the interleukin-17 inhibitors secukinumab, ixekizumab, and brodalumab and the interleukin-23 antagonist guselkumab – have impressively low NNTs of 2.4-3.6 in order to achieve complete clearance.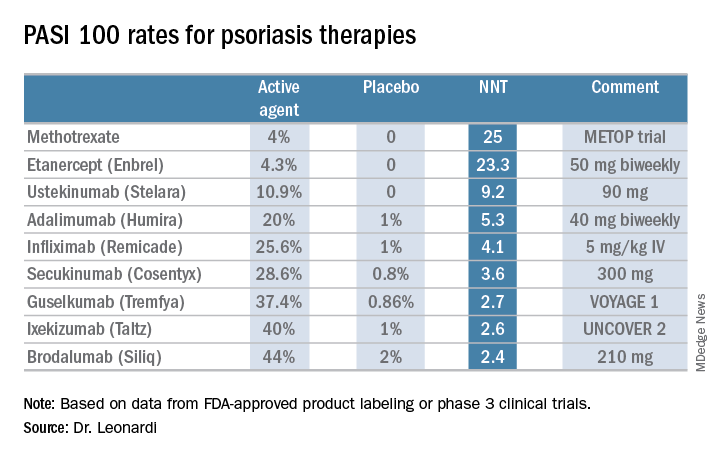
“But our IL-17 and IL-23 antagonists are markedly different from all other therapies, with NNTs of 1.3-1.1. With an NNT of 1.1, if you treated 11 patients with ixekizumab, 10 of them would achieve a PASI 75,” he explained.
“This is really quite remarkable,” Dr. Leonardi commented. “Our first drug back in 2002 was alefacept, and that drug was a ‘twenty-one percenter’: 21% of patients achieved a PASI 75. And quite frankly, we thought that was rocking voodoo science back in the day. Well, we’re really out there now. This is utterly amazing data: a PASI 75 of 81.6% for secukinumab, 86% for brodalumab, 90% for ixekizumab, and 91.2% for guselkumab. This is why we’re publishing this stuff in the best medical journals, because these results are absolutely amazing. So many different medical specialties are interested in what we’re doing with these drugs.”
He reported serving as a consultant to AbbVie, Amgen, Boehringer Ingelheim, Dermira, Eli Lilly, Janssen, Leo, Pfizer, Sandoz, and UCB and receiving research funding from 21 pharmaceutical companies.
The SDEF/Global Academy for Medical Education and this news organization are owned by the same parent company.
KAUAI, HAWAII – I think we should just do away with PASI 90 [90% improvement in Psoriasis Area and Severity Index score] and look at how well our drugs do against the metric of PASI 100. The whole ball of wax. Let’s just go for complete clearance,” Craig L. Leonardi, MD, declared in a provocative presentation at the Hawaii Dermatology Seminar provided by Skin Disease Education Foundation/Global Academy for Medical Education.
He advocates using number needed to treat (NNT) as a performance yardstick. He finds it helpful in translating sometimes-arcane clinical trial results into useful information to guide everyday practice. The NNT is the average number of patients who need to be treated with a drug or procedure in order to achieve one additional good outcome, compared with a control intervention or placebo. It’s the inverse of the absolute risk reduction. The lower the NNT, the better an intervention is performing.
He presented a chart that summarized the NNTs to achieve a PASI 100 response for various systemic agents commonly used in treating moderate to severe psoriasis. He obtained the data from Food and Drug Administration–regulated product labeling and phase 3 clinical trials.
Dr. Leonardi drew attention to the worst performers on the list: methotrexate, with an NNT of 25 to achieve a PASI 100 response, and etanercept, with an NNT of 23.3.
“Methotrexate is a drug that the insurance industry says we have to flow through on our way to biologic drugs. But if complete clearance is your goal, this is an exercise in futility. These patients will never, ever get to complete clearance – or it’s at least very unlikely. We shouldn’t be asked to go through methotrexate on our way to anything. We shouldn’t be asked to use methotrexate at all. We should be bypassing it. And some of us are working on this,” he said.
Ustekinumab and adalimumab are the current market leaders in biologic therapy for psoriasis, but they don’t stack up so well when viewed through the filter of PASI 100 response, with NNTs of 9.2 and 5.3, respectively.
“These market leaders may not be the most relevant drugs in the current era,” according to the dermatologist.
In contrast, the high-performance biologics – the interleukin-17 inhibitors secukinumab, ixekizumab, and brodalumab and the interleukin-23 antagonist guselkumab – have impressively low NNTs of 2.4-3.6 in order to achieve complete clearance.
“But our IL-17 and IL-23 antagonists are markedly different from all other therapies, with NNTs of 1.3-1.1. With an NNT of 1.1, if you treated 11 patients with ixekizumab, 10 of them would achieve a PASI 75,” he explained.
“This is really quite remarkable,” Dr. Leonardi commented. “Our first drug back in 2002 was alefacept, and that drug was a ‘twenty-one percenter’: 21% of patients achieved a PASI 75. And quite frankly, we thought that was rocking voodoo science back in the day. Well, we’re really out there now. This is utterly amazing data: a PASI 75 of 81.6% for secukinumab, 86% for brodalumab, 90% for ixekizumab, and 91.2% for guselkumab. This is why we’re publishing this stuff in the best medical journals, because these results are absolutely amazing. So many different medical specialties are interested in what we’re doing with these drugs.”
He reported serving as a consultant to AbbVie, Amgen, Boehringer Ingelheim, Dermira, Eli Lilly, Janssen, Leo, Pfizer, Sandoz, and UCB and receiving research funding from 21 pharmaceutical companies.
The SDEF/Global Academy for Medical Education and this news organization are owned by the same parent company.
KAUAI, HAWAII – I think we should just do away with PASI 90 [90% improvement in Psoriasis Area and Severity Index score] and look at how well our drugs do against the metric of PASI 100. The whole ball of wax. Let’s just go for complete clearance,” Craig L. Leonardi, MD, declared in a provocative presentation at the Hawaii Dermatology Seminar provided by Skin Disease Education Foundation/Global Academy for Medical Education.
He advocates using number needed to treat (NNT) as a performance yardstick. He finds it helpful in translating sometimes-arcane clinical trial results into useful information to guide everyday practice. The NNT is the average number of patients who need to be treated with a drug or procedure in order to achieve one additional good outcome, compared with a control intervention or placebo. It’s the inverse of the absolute risk reduction. The lower the NNT, the better an intervention is performing.
He presented a chart that summarized the NNTs to achieve a PASI 100 response for various systemic agents commonly used in treating moderate to severe psoriasis. He obtained the data from Food and Drug Administration–regulated product labeling and phase 3 clinical trials.
Dr. Leonardi drew attention to the worst performers on the list: methotrexate, with an NNT of 25 to achieve a PASI 100 response, and etanercept, with an NNT of 23.3.
“Methotrexate is a drug that the insurance industry says we have to flow through on our way to biologic drugs. But if complete clearance is your goal, this is an exercise in futility. These patients will never, ever get to complete clearance – or it’s at least very unlikely. We shouldn’t be asked to go through methotrexate on our way to anything. We shouldn’t be asked to use methotrexate at all. We should be bypassing it. And some of us are working on this,” he said.
Ustekinumab and adalimumab are the current market leaders in biologic therapy for psoriasis, but they don’t stack up so well when viewed through the filter of PASI 100 response, with NNTs of 9.2 and 5.3, respectively.
“These market leaders may not be the most relevant drugs in the current era,” according to the dermatologist.
In contrast, the high-performance biologics – the interleukin-17 inhibitors secukinumab, ixekizumab, and brodalumab and the interleukin-23 antagonist guselkumab – have impressively low NNTs of 2.4-3.6 in order to achieve complete clearance.
“But our IL-17 and IL-23 antagonists are markedly different from all other therapies, with NNTs of 1.3-1.1. With an NNT of 1.1, if you treated 11 patients with ixekizumab, 10 of them would achieve a PASI 75,” he explained.
“This is really quite remarkable,” Dr. Leonardi commented. “Our first drug back in 2002 was alefacept, and that drug was a ‘twenty-one percenter’: 21% of patients achieved a PASI 75. And quite frankly, we thought that was rocking voodoo science back in the day. Well, we’re really out there now. This is utterly amazing data: a PASI 75 of 81.6% for secukinumab, 86% for brodalumab, 90% for ixekizumab, and 91.2% for guselkumab. This is why we’re publishing this stuff in the best medical journals, because these results are absolutely amazing. So many different medical specialties are interested in what we’re doing with these drugs.”
He reported serving as a consultant to AbbVie, Amgen, Boehringer Ingelheim, Dermira, Eli Lilly, Janssen, Leo, Pfizer, Sandoz, and UCB and receiving research funding from 21 pharmaceutical companies.
The SDEF/Global Academy for Medical Education and this news organization are owned by the same parent company.
EXPERT ANALYSIS FROM SDEF HAWAII DERMATOLOGY SEMINAR
Vehicle crash risk linked to various sleep disorders
Individuals with certain sleeping disorders may have a higher risk of crashes, near-crashes or unsafe maneuvering prior to such events, suggests a study.
“The results confirm that some sleep disorders generally increase driving risk as defined by our dependent measures,” wrote Shu-Yuan Liu, a doctoral student, and two colleagues at Virginia Tech, Blacksburg (Sleep. 2018 Apr 1. doi: 10.1093/sleep/zsy023). “Furthermore, the results also provide some insights into how risk varies across specific types of sleep disorder and some moderating factors.”
The study involved licensed drivers who drove at least 3 days a week, had an eligible vehicle in good working condition, and agreed to participate for 1 to 2 years. At the start and end of the study, participants filled out a questionnaire on any medical conditions they had or had been treated for in the past year, any medications they were taking, and any aids they were using for a medical condition.
Among the conditions they were able to select were narcolepsy, sleep apnea, insomnia, shift work sleep disorder, restless legs syndrome (RLS), periodic limb movement disorder, and migraine. All of these conditions have been linked in previous studies to a higher risk of vehicle collisions.
A total of 646 participants, 18.2% of the sample, had one of those disorders: 0.14% had narcolepsy, 7.4% had sleep apnea, 4.8% had insomnia, 3.4% had RLS, 0.37% had shift work sleep disorder, 0.23% had periodic limb movement disorder, and 8.4% had migraine.
Analysis of vehicle data found that female drivers with RLS and any drivers with insomnia had a higher risk of crashes or near-crashes (adjusted odds ratio [AOR] = 2.26 and 1.49, respectively, P less than .05 for both). Drivers with narcolepsy had 9 times greater odds of being involved in a crash or near-crash, but the finding was not statistically significant (AOR = 10.24, P less than .1).
“Drivers who reported frequency of sleepy driving as ‘never,’ ‘rarely,’ and ‘sometimes’ also had higher a risk, indicating that crash or near-crash risk is also associated with sources other than these sleeping disorders,” the authors noted. These drivers’ increased odds of getting into or nearly getting into a crash ranged from 31% to 53% greater (P less than .05).
All drivers with shift work sleep disorder, except for those aged 20-24, had a crash or near-crash rate that was 7.5 times greater than that of drivers without any sleeping disorders. The rate among drivers aged 20-24 with this disorder had a 90% lower rate (risk ratio [RR] = 0.1, P less than .05) compared with control drivers.
When the researchers analyzed the drivers’ maneuvers just before a crash or near-crash, they found females with sleep apnea had a 36% greater odds of doing an unsafe maneuver in crash/near-crash circumstances (AOR = 1.36). (AOR = 3.38 and 3.53, respectively, P less than .05).
The only drivers with a sleeping disorder who were more likely to be involved in crashes of greater severity were those with periodic limb movement disorder (AOR = 1.43, P less than .05).
However, young drivers, senior drivers, and nighttime drivers also all had higher odds of being involved in more severe crashes and in performing unsafe maneuvers prior to a crash or near-crash. Nighttime drivers seemed to be most at risk for these, and they were linked to having more than 5 times greater odds of unsafely maneuvering their vehicles prior to getting into a crash or near crash (AOR = 6.71, P less than .05).
“This is a strong piece of evidence that nighttime driving is less safe than daytime driving and limiting amount of nighttime driving could be one method to moderate road risk for some individuals,” the authors wrote.
The study’s limitations include its observational nature, low numbers of participants with several of the sleeping disorders (at levels below the disorder’s prevalence in the general population), and the complexities involved in what causes a crash or near crash.
One limitation of this study was that sleep hygiene and sleep quality were not examined, even though these might contribute significantly to roadway safety, the researchers noted. This study also did not take into account what medications or other treatment (such as continuous positive airway pressure for those with sleep apnea) the participants might be receiving for their condition.
The study’s implications include the need for physicians to advise patients with insomnia or females with sleep apnea to use caution while driving without “exaggerating risks that introduce undue fear to patients with other sleep disorders and thereby limiting mobility unnecessarily,” the authors wrote. The researchers also suggested that employers consider providing alternative transportation to shift workers and/or that insurance companies offer employers lower rates for offering such alternatives.
SOURCE: Liu Shu-Yuan et al. Sleep J. 2018 Apr 1. doi: 10.1093/sleep/zsy023.
Individuals with certain sleeping disorders may have a higher risk of crashes, near-crashes or unsafe maneuvering prior to such events, suggests a study.
“The results confirm that some sleep disorders generally increase driving risk as defined by our dependent measures,” wrote Shu-Yuan Liu, a doctoral student, and two colleagues at Virginia Tech, Blacksburg (Sleep. 2018 Apr 1. doi: 10.1093/sleep/zsy023). “Furthermore, the results also provide some insights into how risk varies across specific types of sleep disorder and some moderating factors.”
The study involved licensed drivers who drove at least 3 days a week, had an eligible vehicle in good working condition, and agreed to participate for 1 to 2 years. At the start and end of the study, participants filled out a questionnaire on any medical conditions they had or had been treated for in the past year, any medications they were taking, and any aids they were using for a medical condition.
Among the conditions they were able to select were narcolepsy, sleep apnea, insomnia, shift work sleep disorder, restless legs syndrome (RLS), periodic limb movement disorder, and migraine. All of these conditions have been linked in previous studies to a higher risk of vehicle collisions.
A total of 646 participants, 18.2% of the sample, had one of those disorders: 0.14% had narcolepsy, 7.4% had sleep apnea, 4.8% had insomnia, 3.4% had RLS, 0.37% had shift work sleep disorder, 0.23% had periodic limb movement disorder, and 8.4% had migraine.
Analysis of vehicle data found that female drivers with RLS and any drivers with insomnia had a higher risk of crashes or near-crashes (adjusted odds ratio [AOR] = 2.26 and 1.49, respectively, P less than .05 for both). Drivers with narcolepsy had 9 times greater odds of being involved in a crash or near-crash, but the finding was not statistically significant (AOR = 10.24, P less than .1).
“Drivers who reported frequency of sleepy driving as ‘never,’ ‘rarely,’ and ‘sometimes’ also had higher a risk, indicating that crash or near-crash risk is also associated with sources other than these sleeping disorders,” the authors noted. These drivers’ increased odds of getting into or nearly getting into a crash ranged from 31% to 53% greater (P less than .05).
All drivers with shift work sleep disorder, except for those aged 20-24, had a crash or near-crash rate that was 7.5 times greater than that of drivers without any sleeping disorders. The rate among drivers aged 20-24 with this disorder had a 90% lower rate (risk ratio [RR] = 0.1, P less than .05) compared with control drivers.
When the researchers analyzed the drivers’ maneuvers just before a crash or near-crash, they found females with sleep apnea had a 36% greater odds of doing an unsafe maneuver in crash/near-crash circumstances (AOR = 1.36). (AOR = 3.38 and 3.53, respectively, P less than .05).
The only drivers with a sleeping disorder who were more likely to be involved in crashes of greater severity were those with periodic limb movement disorder (AOR = 1.43, P less than .05).
However, young drivers, senior drivers, and nighttime drivers also all had higher odds of being involved in more severe crashes and in performing unsafe maneuvers prior to a crash or near-crash. Nighttime drivers seemed to be most at risk for these, and they were linked to having more than 5 times greater odds of unsafely maneuvering their vehicles prior to getting into a crash or near crash (AOR = 6.71, P less than .05).
“This is a strong piece of evidence that nighttime driving is less safe than daytime driving and limiting amount of nighttime driving could be one method to moderate road risk for some individuals,” the authors wrote.
The study’s limitations include its observational nature, low numbers of participants with several of the sleeping disorders (at levels below the disorder’s prevalence in the general population), and the complexities involved in what causes a crash or near crash.
One limitation of this study was that sleep hygiene and sleep quality were not examined, even though these might contribute significantly to roadway safety, the researchers noted. This study also did not take into account what medications or other treatment (such as continuous positive airway pressure for those with sleep apnea) the participants might be receiving for their condition.
The study’s implications include the need for physicians to advise patients with insomnia or females with sleep apnea to use caution while driving without “exaggerating risks that introduce undue fear to patients with other sleep disorders and thereby limiting mobility unnecessarily,” the authors wrote. The researchers also suggested that employers consider providing alternative transportation to shift workers and/or that insurance companies offer employers lower rates for offering such alternatives.
SOURCE: Liu Shu-Yuan et al. Sleep J. 2018 Apr 1. doi: 10.1093/sleep/zsy023.
Individuals with certain sleeping disorders may have a higher risk of crashes, near-crashes or unsafe maneuvering prior to such events, suggests a study.
“The results confirm that some sleep disorders generally increase driving risk as defined by our dependent measures,” wrote Shu-Yuan Liu, a doctoral student, and two colleagues at Virginia Tech, Blacksburg (Sleep. 2018 Apr 1. doi: 10.1093/sleep/zsy023). “Furthermore, the results also provide some insights into how risk varies across specific types of sleep disorder and some moderating factors.”
The study involved licensed drivers who drove at least 3 days a week, had an eligible vehicle in good working condition, and agreed to participate for 1 to 2 years. At the start and end of the study, participants filled out a questionnaire on any medical conditions they had or had been treated for in the past year, any medications they were taking, and any aids they were using for a medical condition.
Among the conditions they were able to select were narcolepsy, sleep apnea, insomnia, shift work sleep disorder, restless legs syndrome (RLS), periodic limb movement disorder, and migraine. All of these conditions have been linked in previous studies to a higher risk of vehicle collisions.
A total of 646 participants, 18.2% of the sample, had one of those disorders: 0.14% had narcolepsy, 7.4% had sleep apnea, 4.8% had insomnia, 3.4% had RLS, 0.37% had shift work sleep disorder, 0.23% had periodic limb movement disorder, and 8.4% had migraine.
Analysis of vehicle data found that female drivers with RLS and any drivers with insomnia had a higher risk of crashes or near-crashes (adjusted odds ratio [AOR] = 2.26 and 1.49, respectively, P less than .05 for both). Drivers with narcolepsy had 9 times greater odds of being involved in a crash or near-crash, but the finding was not statistically significant (AOR = 10.24, P less than .1).
“Drivers who reported frequency of sleepy driving as ‘never,’ ‘rarely,’ and ‘sometimes’ also had higher a risk, indicating that crash or near-crash risk is also associated with sources other than these sleeping disorders,” the authors noted. These drivers’ increased odds of getting into or nearly getting into a crash ranged from 31% to 53% greater (P less than .05).
All drivers with shift work sleep disorder, except for those aged 20-24, had a crash or near-crash rate that was 7.5 times greater than that of drivers without any sleeping disorders. The rate among drivers aged 20-24 with this disorder had a 90% lower rate (risk ratio [RR] = 0.1, P less than .05) compared with control drivers.
When the researchers analyzed the drivers’ maneuvers just before a crash or near-crash, they found females with sleep apnea had a 36% greater odds of doing an unsafe maneuver in crash/near-crash circumstances (AOR = 1.36). (AOR = 3.38 and 3.53, respectively, P less than .05).
The only drivers with a sleeping disorder who were more likely to be involved in crashes of greater severity were those with periodic limb movement disorder (AOR = 1.43, P less than .05).
However, young drivers, senior drivers, and nighttime drivers also all had higher odds of being involved in more severe crashes and in performing unsafe maneuvers prior to a crash or near-crash. Nighttime drivers seemed to be most at risk for these, and they were linked to having more than 5 times greater odds of unsafely maneuvering their vehicles prior to getting into a crash or near crash (AOR = 6.71, P less than .05).
“This is a strong piece of evidence that nighttime driving is less safe than daytime driving and limiting amount of nighttime driving could be one method to moderate road risk for some individuals,” the authors wrote.
The study’s limitations include its observational nature, low numbers of participants with several of the sleeping disorders (at levels below the disorder’s prevalence in the general population), and the complexities involved in what causes a crash or near crash.
One limitation of this study was that sleep hygiene and sleep quality were not examined, even though these might contribute significantly to roadway safety, the researchers noted. This study also did not take into account what medications or other treatment (such as continuous positive airway pressure for those with sleep apnea) the participants might be receiving for their condition.
The study’s implications include the need for physicians to advise patients with insomnia or females with sleep apnea to use caution while driving without “exaggerating risks that introduce undue fear to patients with other sleep disorders and thereby limiting mobility unnecessarily,” the authors wrote. The researchers also suggested that employers consider providing alternative transportation to shift workers and/or that insurance companies offer employers lower rates for offering such alternatives.
SOURCE: Liu Shu-Yuan et al. Sleep J. 2018 Apr 1. doi: 10.1093/sleep/zsy023.
FROM SLEEP
Key clinical point: Individuals with certain sleeping disorders may have a higher risk of crashes, near-crashes or unsafe maneuvering prior to such events.
Major finding: Drivers with insomnia and female drivers with sleep apnea have 49% and 126% greater odds, respectively, of a crash or near-crash.
Data source: The findings are based on an analysis of naturalistic driving data from 3,541 U.S. drivers between ages 16 and 98.
Disclosures: The data were provided by the Transportation Research Board of the National Academy of Sciences. No external funding was noted. The authors reported having no disclosures.
Source: Liu Shu-Yuan et al. Sleep J. 2018 Apr 1. doi: 10.1093/sleep/zsy023.
Drs. O'Neil, Meadows, and Patterson Earn Annual AJO Resident Writer's Awards

Bryan Hanypsiak, MD, Editor-in-Chief of The American Journal of Orthopedics, along with Darla Conrad, Senior Director, North America, and Mindy Edgar, Manager, Academic Alliances from the Johnson & Johnson Institute presented the 2017 Resident Writer’s Award to the three winners at the American Academy of Orthopaedic Surgeons (AAOS) annual meeting in New Orleans. All articles published in 2017 with a resident as the first-listed author and accepted through the journal’s standard blinded-review process were eligible for this award. The annual Resident Writer's Award is sponsored by Johnson & Johnson. Papers published in 2018 will be judged by The American Journal of Orthopedics Editorial Board, and honoraria will be presented to the winners at the 2019 AAOS annual meeting.

Joseph T. O’Neil, MD
Molly C. Meadows, MD
Joseph T. Patterson, MD
See more information about the 2018 Resident Writer's Award.
Supported by Johnson & Johnson
Bryan Hanypsiak, MD, Editor-in-Chief of The American Journal of Orthopedics, along with Darla Conrad, Senior Director, North America, and Mindy Edgar, Manager, Academic Alliances from the Johnson & Johnson Institute presented the 2017 Resident Writer’s Award to the three winners at the American Academy of Orthopaedic Surgeons (AAOS) annual meeting in New Orleans. All articles published in 2017 with a resident as the first-listed author and accepted through the journal’s standard blinded-review process were eligible for this award. The annual Resident Writer's Award is sponsored by Johnson & Johnson. Papers published in 2018 will be judged by The American Journal of Orthopedics Editorial Board, and honoraria will be presented to the winners at the 2019 AAOS annual meeting.
Joseph T. O’Neil, MD
Molly C. Meadows, MD
Joseph T. Patterson, MD
See more information about the 2018 Resident Writer's Award.
Supported by Johnson & Johnson
Bryan Hanypsiak, MD, Editor-in-Chief of The American Journal of Orthopedics, along with Darla Conrad, Senior Director, North America, and Mindy Edgar, Manager, Academic Alliances from the Johnson & Johnson Institute presented the 2017 Resident Writer’s Award to the three winners at the American Academy of Orthopaedic Surgeons (AAOS) annual meeting in New Orleans. All articles published in 2017 with a resident as the first-listed author and accepted through the journal’s standard blinded-review process were eligible for this award. The annual Resident Writer's Award is sponsored by Johnson & Johnson. Papers published in 2018 will be judged by The American Journal of Orthopedics Editorial Board, and honoraria will be presented to the winners at the 2019 AAOS annual meeting.
Joseph T. O’Neil, MD
Molly C. Meadows, MD
Joseph T. Patterson, MD
See more information about the 2018 Resident Writer's Award.
Supported by Johnson & Johnson
AJO Awards Molly C. Meadows, MD, Second-Place Resident Writer's Award
2017 AJO Resident Writer's Awards
Second-Place Award
An Original Study
Effects of Platelet-Rich Plasma and Indomethacin on Biomechanics of Rotator Cuff Repair
Molly C. Meadows, MD, David M. Levy, MD, Christopher M. Ferry, MS, Thomas R. Gardner, MCE, Takeshi Teratani, MD, and Christopher S. Ahmad, MD

Dr. Meadows is currently in her chief year of orthopedic surgery residency training at Rush University Medical Center. Prior to residency, she completed undergraduate education at Brown University and medical school at Columbia University. Dr. Meadows is beginning a sports medicine fellowship at Stanford University in August 2018, and she plans to pursue a pediatric orthopedic fellowship thereafter.
Her research interests include osteochondritis dissecans lesions, patellofemoral disorders, and other sports injuries in the skeletally immature population.
Read the full version of Dr. Meadows' original study.
2017 AJO Resident Writer's Awards
Second-Place Award
An Original Study
Effects of Platelet-Rich Plasma and Indomethacin on Biomechanics of Rotator Cuff Repair
Molly C. Meadows, MD, David M. Levy, MD, Christopher M. Ferry, MS, Thomas R. Gardner, MCE, Takeshi Teratani, MD, and Christopher S. Ahmad, MD
Dr. Meadows is currently in her chief year of orthopedic surgery residency training at Rush University Medical Center. Prior to residency, she completed undergraduate education at Brown University and medical school at Columbia University. Dr. Meadows is beginning a sports medicine fellowship at Stanford University in August 2018, and she plans to pursue a pediatric orthopedic fellowship thereafter.
Her research interests include osteochondritis dissecans lesions, patellofemoral disorders, and other sports injuries in the skeletally immature population.
Read the full version of Dr. Meadows' original study.
2017 AJO Resident Writer's Awards
Second-Place Award
An Original Study
Effects of Platelet-Rich Plasma and Indomethacin on Biomechanics of Rotator Cuff Repair
Molly C. Meadows, MD, David M. Levy, MD, Christopher M. Ferry, MS, Thomas R. Gardner, MCE, Takeshi Teratani, MD, and Christopher S. Ahmad, MD
Dr. Meadows is currently in her chief year of orthopedic surgery residency training at Rush University Medical Center. Prior to residency, she completed undergraduate education at Brown University and medical school at Columbia University. Dr. Meadows is beginning a sports medicine fellowship at Stanford University in August 2018, and she plans to pursue a pediatric orthopedic fellowship thereafter.
Her research interests include osteochondritis dissecans lesions, patellofemoral disorders, and other sports injuries in the skeletally immature population.
Read the full version of Dr. Meadows' original study.
AJO Awards Joseph T. Patterson, MD, Third-Place Resident Writer's Award
2017 AJO Resident Writer's Awards
Third-Place Award
An Original Study
Does Preoperative Pneumonia Affect Complications of Geriatric Hip Fracture Surgery?
Joseph T. Patterson, MD, Daniel D. Bohl, MD, MPH, Bryce A. Basques, MD, Alexander H. Arzeno, MD, and Jonathan Grauer, MD

Dr. Patterson is completing his orthopedic surgery residency at the University of California San Francisco, and will continue training with a fellowship in orthopedic trauma at Harborview Medical Center. Prior to residency, he completed undergraduate education at the University of California Los Angeles and medical school at Yale University.
His research interests include geriatric hip fracture care, interdisciplinary trauma care performance improvement, and outcome assessment in orthopedic trauma.
Read the full version of Dr. Patterson's original study.
2017 AJO Resident Writer's Awards
Third-Place Award
An Original Study
Does Preoperative Pneumonia Affect Complications of Geriatric Hip Fracture Surgery?
Joseph T. Patterson, MD, Daniel D. Bohl, MD, MPH, Bryce A. Basques, MD, Alexander H. Arzeno, MD, and Jonathan Grauer, MD
Dr. Patterson is completing his orthopedic surgery residency at the University of California San Francisco, and will continue training with a fellowship in orthopedic trauma at Harborview Medical Center. Prior to residency, he completed undergraduate education at the University of California Los Angeles and medical school at Yale University.
His research interests include geriatric hip fracture care, interdisciplinary trauma care performance improvement, and outcome assessment in orthopedic trauma.
Read the full version of Dr. Patterson's original study.
2017 AJO Resident Writer's Awards
Third-Place Award
An Original Study
Does Preoperative Pneumonia Affect Complications of Geriatric Hip Fracture Surgery?
Joseph T. Patterson, MD, Daniel D. Bohl, MD, MPH, Bryce A. Basques, MD, Alexander H. Arzeno, MD, and Jonathan Grauer, MD
Dr. Patterson is completing his orthopedic surgery residency at the University of California San Francisco, and will continue training with a fellowship in orthopedic trauma at Harborview Medical Center. Prior to residency, he completed undergraduate education at the University of California Los Angeles and medical school at Yale University.
His research interests include geriatric hip fracture care, interdisciplinary trauma care performance improvement, and outcome assessment in orthopedic trauma.
Read the full version of Dr. Patterson's original study.
Ketamine formulation study is ‘groundbreaking’
It is remarkable to consider that we now have more than 30 medications approved by the Food and Drug Administration as monotherapy or augmentation for the treatment of major depressive disorder. And yet, we know very little about how these medications perform for patients at high risk for suicide.
Historically, suicidal patients have been excluded from phase 3 antidepressant trials, which provide the basis for regulatory approval. Even studies in treatment-resistant depression (TRD) have tended to exclude patients with the highest risk of suicide. Further, the FDA does not mandate that a new antidepressant medication demonstrate any benefit for suicidal ideation.

Focus on high-risk patients
The recent report by Canuso et al.3 in the American Journal of Psychiatry is a groundbreaking study: Previous placebo-controlled trials of intravenous ketamine in depressed patients with clinically significant suicidal ideation have used only one-time dose administrations4,5,6.
This phase 2, proof-of-concept trial randomized 68 adults with MDD at 11 U.S. sites, which were primarily academic medical centers. In contrast to previous ketamine studies, which recruited patients via advertisement or clinician referral, patients were identified and screened in an emergency department or an inpatient psychiatric unit. Participants had to voluntarily agree to hospitalization for 5 days following randomization, with the remainder of the study conducted on an outpatient basis. Intranasal esketamine (84 mg) or placebo was administered twice per week over 4 weeks, in addition to standard-of-care antidepressant treatment. The primary outcome was the change in the Montgomery Åsberg Depression Rating Scale (MADRS) score from baseline to 4 hours after first dose of study medication.
For the primary MADRS outcome, esketamine statistically separated from placebo at 4 hours and 24 hours, with moderate effect sizes (0.61 to 0.65). There were no significant differences at the end of the double-blind period at day 25 and at posttreatment follow-up at day 81. For the suicidal thoughts item of the MADRS, esketamine’s efficacy was greater than placebo at 4 hours, but not at 24 hours or at day 25. Clinician global judgment of suicide risk was not statistically different between groups at any time point, although the esketamine group had numerically greater improvements at 4 hours and 24 hours. There were no group differences in self-report measures (Beck Scale for Suicidal Ideation or Beck Hopelessness Scale) at any time point.
Regarding safety and tolerability, adverse events led to early termination for 5 patients in the esketamine group, compared with one in the placebo group. The most common adverse events were nausea, dizziness, dissociation, unpleasant taste, and headache, which were more frequent in the esketamine group. Transient elevations in blood pressure and dissociative symptoms generally peaked at 40 minutes after dosing and returned to baseline by 2 hours.
Putting findings in perspective
Several aspects of the trial are noteworthy. First, enrolled patients were markedly depressed, and half required additional suicide precautions in addition to hospitalization. Three patients (all in the placebo group) made suicide attempts during the follow-up period, further evidence that these patients were extremely high risk. Second, the sample was significantly more racially diverse (38% black or African American) than most previous ketamine studies. Third, psychiatric hospitalization plus the initiation of standard antidepressant medication resulted in substantial improvements for many patients randomized to intranasal placebo spray. Inflated short-term placebo responses are commonly seen even in severely depressed patients, making signal detection especially challenging for new drugs. Finally, it is difficult to compare the results of this study with the few placebo-controlled trials of intravenous ketamine for patients with MDD and significant suicidal ideation, because of differences in outcomes measures, patient populations, doses, and route of administration. This study used the Suicide Ideation and Behavior Assessment Tool, a computerized, modular instrument with patient-reported and clinician-reported assessments, which was developed specifically to measure rapid changes in suicidality and awaits further validation in ongoing studies.
Limitations of this study include the absence of reported plasma esketamine levels. Is it possible that higher doses of esketamine, or a different dosing schedule, would have had resulted in greater efficacy? The 84-mg dose used in this trial recently was found to be safe and effective in patients with TRD2, and was reported to have similar plasma levels as IV esketamine 0.2 mg/kg2. This dose, in turn, corresponds to a racemic ketamine dose of approximately 0.31 mg/kg1. Future studies will need to examine the antisuicidal and antidepressant effects of the most commonly used racemic ketamine dose (0.5 mg/kg), compared with 84 mg intranasal esketamine. The twice per week dosing schedule was supported empirically from a previous study of intravenous ketamine showing that twice weekly infusions were equally effective to thrice weekly administrations7. It is unknown, however, whether even less-frequent administrations (such as once weekly) would have been more effective than twice-weekly over the 4-week, double-blind period. Finally, the authors raise the possibility of functional unblinding, which always is a concern in ketamine studies. Although the placebo solution contained a bittering agent to simulate the taste of esketamine intranasal solution, the integrity of the blind was not reported.
Conclusion
Overall, this study is a promising start. In my view, the risk to benefit ratio for this approach is acceptable, given the morbidity and mortality associated with suicidal depression. The fact that esketamine nasal spray would be administered only under the observation of a clinician in a medical setting, and not be dispensed for at-home use, is reassuring and would mitigate the potential for abuse. In the meantime, our field awaits the results of larger phase 3 studies for patients with MDD at imminent risk for suicide.
Dr. Mathew is affiliated with the Michael E. Debakey VA Medical Center, and the Menninger Department of Psychiatry and Behavioral Sciences at the Baylor College of Medicine in Houston. Over the last 12 months, he has served as a paid consultant to Alkermes and Fortress Biotech. He also has served as an investigator on clinical trials sponsored by Janssen Research and Development, the manufacturer of intranasal esketamine, and as an investigator on a trial sponsored by NeuroRx.
References
1. Biol Psychiatry. 2016 Sep 15;80(6):424-31.
2. JAMA Psychiatry. 2018 Feb 1;75(2):139-48.
3. Am J Psychiatry. 2018 Apr 16. doi: 10.1176/appi.ajp.2018.17060720.
4. Am J Psychiatry. 2018 Apr 1;175(4]):327-35.
5. Psychol Med. 2015 Dec;45(16):3571-80.
6. Am J Psychiatry. 2018 Feb 1;175(2):150-8.
7. Am J Psychiatry. 2016 Aug 1;173(8):816-26.
It is remarkable to consider that we now have more than 30 medications approved by the Food and Drug Administration as monotherapy or augmentation for the treatment of major depressive disorder. And yet, we know very little about how these medications perform for patients at high risk for suicide.
Historically, suicidal patients have been excluded from phase 3 antidepressant trials, which provide the basis for regulatory approval. Even studies in treatment-resistant depression (TRD) have tended to exclude patients with the highest risk of suicide. Further, the FDA does not mandate that a new antidepressant medication demonstrate any benefit for suicidal ideation.
Focus on high-risk patients
The recent report by Canuso et al.3 in the American Journal of Psychiatry is a groundbreaking study: Previous placebo-controlled trials of intravenous ketamine in depressed patients with clinically significant suicidal ideation have used only one-time dose administrations4,5,6.
This phase 2, proof-of-concept trial randomized 68 adults with MDD at 11 U.S. sites, which were primarily academic medical centers. In contrast to previous ketamine studies, which recruited patients via advertisement or clinician referral, patients were identified and screened in an emergency department or an inpatient psychiatric unit. Participants had to voluntarily agree to hospitalization for 5 days following randomization, with the remainder of the study conducted on an outpatient basis. Intranasal esketamine (84 mg) or placebo was administered twice per week over 4 weeks, in addition to standard-of-care antidepressant treatment. The primary outcome was the change in the Montgomery Åsberg Depression Rating Scale (MADRS) score from baseline to 4 hours after first dose of study medication.
For the primary MADRS outcome, esketamine statistically separated from placebo at 4 hours and 24 hours, with moderate effect sizes (0.61 to 0.65). There were no significant differences at the end of the double-blind period at day 25 and at posttreatment follow-up at day 81. For the suicidal thoughts item of the MADRS, esketamine’s efficacy was greater than placebo at 4 hours, but not at 24 hours or at day 25. Clinician global judgment of suicide risk was not statistically different between groups at any time point, although the esketamine group had numerically greater improvements at 4 hours and 24 hours. There were no group differences in self-report measures (Beck Scale for Suicidal Ideation or Beck Hopelessness Scale) at any time point.
Regarding safety and tolerability, adverse events led to early termination for 5 patients in the esketamine group, compared with one in the placebo group. The most common adverse events were nausea, dizziness, dissociation, unpleasant taste, and headache, which were more frequent in the esketamine group. Transient elevations in blood pressure and dissociative symptoms generally peaked at 40 minutes after dosing and returned to baseline by 2 hours.
Putting findings in perspective
Several aspects of the trial are noteworthy. First, enrolled patients were markedly depressed, and half required additional suicide precautions in addition to hospitalization. Three patients (all in the placebo group) made suicide attempts during the follow-up period, further evidence that these patients were extremely high risk. Second, the sample was significantly more racially diverse (38% black or African American) than most previous ketamine studies. Third, psychiatric hospitalization plus the initiation of standard antidepressant medication resulted in substantial improvements for many patients randomized to intranasal placebo spray. Inflated short-term placebo responses are commonly seen even in severely depressed patients, making signal detection especially challenging for new drugs. Finally, it is difficult to compare the results of this study with the few placebo-controlled trials of intravenous ketamine for patients with MDD and significant suicidal ideation, because of differences in outcomes measures, patient populations, doses, and route of administration. This study used the Suicide Ideation and Behavior Assessment Tool, a computerized, modular instrument with patient-reported and clinician-reported assessments, which was developed specifically to measure rapid changes in suicidality and awaits further validation in ongoing studies.
Limitations of this study include the absence of reported plasma esketamine levels. Is it possible that higher doses of esketamine, or a different dosing schedule, would have had resulted in greater efficacy? The 84-mg dose used in this trial recently was found to be safe and effective in patients with TRD2, and was reported to have similar plasma levels as IV esketamine 0.2 mg/kg2. This dose, in turn, corresponds to a racemic ketamine dose of approximately 0.31 mg/kg1. Future studies will need to examine the antisuicidal and antidepressant effects of the most commonly used racemic ketamine dose (0.5 mg/kg), compared with 84 mg intranasal esketamine. The twice per week dosing schedule was supported empirically from a previous study of intravenous ketamine showing that twice weekly infusions were equally effective to thrice weekly administrations7. It is unknown, however, whether even less-frequent administrations (such as once weekly) would have been more effective than twice-weekly over the 4-week, double-blind period. Finally, the authors raise the possibility of functional unblinding, which always is a concern in ketamine studies. Although the placebo solution contained a bittering agent to simulate the taste of esketamine intranasal solution, the integrity of the blind was not reported.
Conclusion
Overall, this study is a promising start. In my view, the risk to benefit ratio for this approach is acceptable, given the morbidity and mortality associated with suicidal depression. The fact that esketamine nasal spray would be administered only under the observation of a clinician in a medical setting, and not be dispensed for at-home use, is reassuring and would mitigate the potential for abuse. In the meantime, our field awaits the results of larger phase 3 studies for patients with MDD at imminent risk for suicide.
Dr. Mathew is affiliated with the Michael E. Debakey VA Medical Center, and the Menninger Department of Psychiatry and Behavioral Sciences at the Baylor College of Medicine in Houston. Over the last 12 months, he has served as a paid consultant to Alkermes and Fortress Biotech. He also has served as an investigator on clinical trials sponsored by Janssen Research and Development, the manufacturer of intranasal esketamine, and as an investigator on a trial sponsored by NeuroRx.
References
1. Biol Psychiatry. 2016 Sep 15;80(6):424-31.
2. JAMA Psychiatry. 2018 Feb 1;75(2):139-48.
3. Am J Psychiatry. 2018 Apr 16. doi: 10.1176/appi.ajp.2018.17060720.
4. Am J Psychiatry. 2018 Apr 1;175(4]):327-35.
5. Psychol Med. 2015 Dec;45(16):3571-80.
6. Am J Psychiatry. 2018 Feb 1;175(2):150-8.
7. Am J Psychiatry. 2016 Aug 1;173(8):816-26.
It is remarkable to consider that we now have more than 30 medications approved by the Food and Drug Administration as monotherapy or augmentation for the treatment of major depressive disorder. And yet, we know very little about how these medications perform for patients at high risk for suicide.
Historically, suicidal patients have been excluded from phase 3 antidepressant trials, which provide the basis for regulatory approval. Even studies in treatment-resistant depression (TRD) have tended to exclude patients with the highest risk of suicide. Further, the FDA does not mandate that a new antidepressant medication demonstrate any benefit for suicidal ideation.
Focus on high-risk patients
The recent report by Canuso et al.3 in the American Journal of Psychiatry is a groundbreaking study: Previous placebo-controlled trials of intravenous ketamine in depressed patients with clinically significant suicidal ideation have used only one-time dose administrations4,5,6.
This phase 2, proof-of-concept trial randomized 68 adults with MDD at 11 U.S. sites, which were primarily academic medical centers. In contrast to previous ketamine studies, which recruited patients via advertisement or clinician referral, patients were identified and screened in an emergency department or an inpatient psychiatric unit. Participants had to voluntarily agree to hospitalization for 5 days following randomization, with the remainder of the study conducted on an outpatient basis. Intranasal esketamine (84 mg) or placebo was administered twice per week over 4 weeks, in addition to standard-of-care antidepressant treatment. The primary outcome was the change in the Montgomery Åsberg Depression Rating Scale (MADRS) score from baseline to 4 hours after first dose of study medication.
For the primary MADRS outcome, esketamine statistically separated from placebo at 4 hours and 24 hours, with moderate effect sizes (0.61 to 0.65). There were no significant differences at the end of the double-blind period at day 25 and at posttreatment follow-up at day 81. For the suicidal thoughts item of the MADRS, esketamine’s efficacy was greater than placebo at 4 hours, but not at 24 hours or at day 25. Clinician global judgment of suicide risk was not statistically different between groups at any time point, although the esketamine group had numerically greater improvements at 4 hours and 24 hours. There were no group differences in self-report measures (Beck Scale for Suicidal Ideation or Beck Hopelessness Scale) at any time point.
Regarding safety and tolerability, adverse events led to early termination for 5 patients in the esketamine group, compared with one in the placebo group. The most common adverse events were nausea, dizziness, dissociation, unpleasant taste, and headache, which were more frequent in the esketamine group. Transient elevations in blood pressure and dissociative symptoms generally peaked at 40 minutes after dosing and returned to baseline by 2 hours.
Putting findings in perspective
Several aspects of the trial are noteworthy. First, enrolled patients were markedly depressed, and half required additional suicide precautions in addition to hospitalization. Three patients (all in the placebo group) made suicide attempts during the follow-up period, further evidence that these patients were extremely high risk. Second, the sample was significantly more racially diverse (38% black or African American) than most previous ketamine studies. Third, psychiatric hospitalization plus the initiation of standard antidepressant medication resulted in substantial improvements for many patients randomized to intranasal placebo spray. Inflated short-term placebo responses are commonly seen even in severely depressed patients, making signal detection especially challenging for new drugs. Finally, it is difficult to compare the results of this study with the few placebo-controlled trials of intravenous ketamine for patients with MDD and significant suicidal ideation, because of differences in outcomes measures, patient populations, doses, and route of administration. This study used the Suicide Ideation and Behavior Assessment Tool, a computerized, modular instrument with patient-reported and clinician-reported assessments, which was developed specifically to measure rapid changes in suicidality and awaits further validation in ongoing studies.
Limitations of this study include the absence of reported plasma esketamine levels. Is it possible that higher doses of esketamine, or a different dosing schedule, would have had resulted in greater efficacy? The 84-mg dose used in this trial recently was found to be safe and effective in patients with TRD2, and was reported to have similar plasma levels as IV esketamine 0.2 mg/kg2. This dose, in turn, corresponds to a racemic ketamine dose of approximately 0.31 mg/kg1. Future studies will need to examine the antisuicidal and antidepressant effects of the most commonly used racemic ketamine dose (0.5 mg/kg), compared with 84 mg intranasal esketamine. The twice per week dosing schedule was supported empirically from a previous study of intravenous ketamine showing that twice weekly infusions were equally effective to thrice weekly administrations7. It is unknown, however, whether even less-frequent administrations (such as once weekly) would have been more effective than twice-weekly over the 4-week, double-blind period. Finally, the authors raise the possibility of functional unblinding, which always is a concern in ketamine studies. Although the placebo solution contained a bittering agent to simulate the taste of esketamine intranasal solution, the integrity of the blind was not reported.
Conclusion
Overall, this study is a promising start. In my view, the risk to benefit ratio for this approach is acceptable, given the morbidity and mortality associated with suicidal depression. The fact that esketamine nasal spray would be administered only under the observation of a clinician in a medical setting, and not be dispensed for at-home use, is reassuring and would mitigate the potential for abuse. In the meantime, our field awaits the results of larger phase 3 studies for patients with MDD at imminent risk for suicide.
Dr. Mathew is affiliated with the Michael E. Debakey VA Medical Center, and the Menninger Department of Psychiatry and Behavioral Sciences at the Baylor College of Medicine in Houston. Over the last 12 months, he has served as a paid consultant to Alkermes and Fortress Biotech. He also has served as an investigator on clinical trials sponsored by Janssen Research and Development, the manufacturer of intranasal esketamine, and as an investigator on a trial sponsored by NeuroRx.
References
1. Biol Psychiatry. 2016 Sep 15;80(6):424-31.
2. JAMA Psychiatry. 2018 Feb 1;75(2):139-48.
3. Am J Psychiatry. 2018 Apr 16. doi: 10.1176/appi.ajp.2018.17060720.
4. Am J Psychiatry. 2018 Apr 1;175(4]):327-35.
5. Psychol Med. 2015 Dec;45(16):3571-80.
6. Am J Psychiatry. 2018 Feb 1;175(2):150-8.
7. Am J Psychiatry. 2016 Aug 1;173(8):816-26.
Therapeutic endoscopy expands reach to deep GI lesions
BOSTON –
“The main difficulty with these procedures is closure,” Mouen A. Khashab, MD, said at the AGA Tech Summit, which was sponsored by the AGA Center for GI Innovation and Technology. “Sometimes you can create a large defect that you’re not sure you can close. You must have experience with large defect closure.”
In experienced hands, the endoscopic approaches spare adjacent large organs, have a complete resection rate approaching 95%, and an acceptable rate of adverse events. They can provide excellent surgical specimens that are more than adequate for histologic studies, although some cannot provide any information on margins, said Dr. Khashab, director of therapeutic endoscopy at Johns Hopkins University, Baltimore. “When doing a full-thickness endoscopic resection, you can’t comment on the margins. You’re not getting any normal tissue around the tumor, and this can create an issue with some patients.”
Dr. Khashab briefly described three endoscopic resection techniques that are suitable for the following deep GI tumors:
- Submucosal tunneling endoscopic resection. STER is most suitable for smaller tumors (4 cm or less). Tumors of this size are easily removed en bloc via the endoscopic tunnel. Larger tumors can also be resected this way, but need to be removed piecemeal after dissection off the muscle layer. This is an acceptable alternative in leiomyomas but not in gastrointestinal stromal tumors. “For this technique, you introduce the scope into the submucosal layer and create a space with tunneling,” Dr. Khashab said. “We then expose the tumor, dissect it off the wall of the muscularis propria, and pull it out of the tunnel.” A 2017 meta-analysis examined outcomes in 28 studies with data on 1,085 lesions. The pooled complete resection and en bloc resection rates were 97.5% and 94.6%, respectively. Common complications associated with STER were air leakage symptoms (15%) and perforation (5.6%). “The perforation rate is reasonable, I think. A lot of these complications can be managed intraoperatively with clipping or suturing,” Dr. Khashab noted.
- Endoscopic submucosal dissection: ESD is now being used to resect tumors that originate from the muscularis propria. “This is something I didn’t used to think was even possible,” Dr. Khashab said. “But we are seeing some literature on this now. A lot of these tumors originate from the superficial MP [muscularis propria], so we can dissect off the muscle without needing a full-thickness resection.” He presented findings from a large study comprising 143 patients with submucosal gastric or esophageal tumors that arose from the muscularis propria at the esophagogastric junction. These were large lesions, a mean 17.6 cm, but they ranged up to 50 cm. The en bloc resection rate was 94%. There were six perforations (4%), along with four pneumoperitoneum and two pneumothorax, which resolved without further surgery. There were no local recurrences or metastases when the 2012 study appeared, with a mean follow-up of 2 years.
- Endoscopic full-thickness resection: EFTR “is a technically demanding procedure, and we frequently have to work on these tumors in retroflexion,” Dr. Khashab said. He referred to a 2011 paper, which described the EFTR technique used in 26 patients with gastric cancers. The tumors (mean size, 2.8 cm) were located in the gastric corpus and in the gastric fundus. Although the procedures were lengthy, ranging from 60 to 145 minutes, they were highly successful, with a 100% complete resection rate. Nevertheless, there was also a 100% perforation rate, although all these were closed intraoperatively. There was no postoperative gastric bleeding, peritonitis sign, or abdominal abscess. No lesion residual or recurrence was found during the 6-24 month follow-up period.
Dr. Khashab is a consultant and medical advisory board member for Boston Scientific and Olympus.
BOSTON –
“The main difficulty with these procedures is closure,” Mouen A. Khashab, MD, said at the AGA Tech Summit, which was sponsored by the AGA Center for GI Innovation and Technology. “Sometimes you can create a large defect that you’re not sure you can close. You must have experience with large defect closure.”
In experienced hands, the endoscopic approaches spare adjacent large organs, have a complete resection rate approaching 95%, and an acceptable rate of adverse events. They can provide excellent surgical specimens that are more than adequate for histologic studies, although some cannot provide any information on margins, said Dr. Khashab, director of therapeutic endoscopy at Johns Hopkins University, Baltimore. “When doing a full-thickness endoscopic resection, you can’t comment on the margins. You’re not getting any normal tissue around the tumor, and this can create an issue with some patients.”
Dr. Khashab briefly described three endoscopic resection techniques that are suitable for the following deep GI tumors:
- Submucosal tunneling endoscopic resection. STER is most suitable for smaller tumors (4 cm or less). Tumors of this size are easily removed en bloc via the endoscopic tunnel. Larger tumors can also be resected this way, but need to be removed piecemeal after dissection off the muscle layer. This is an acceptable alternative in leiomyomas but not in gastrointestinal stromal tumors. “For this technique, you introduce the scope into the submucosal layer and create a space with tunneling,” Dr. Khashab said. “We then expose the tumor, dissect it off the wall of the muscularis propria, and pull it out of the tunnel.” A 2017 meta-analysis examined outcomes in 28 studies with data on 1,085 lesions. The pooled complete resection and en bloc resection rates were 97.5% and 94.6%, respectively. Common complications associated with STER were air leakage symptoms (15%) and perforation (5.6%). “The perforation rate is reasonable, I think. A lot of these complications can be managed intraoperatively with clipping or suturing,” Dr. Khashab noted.
- Endoscopic submucosal dissection: ESD is now being used to resect tumors that originate from the muscularis propria. “This is something I didn’t used to think was even possible,” Dr. Khashab said. “But we are seeing some literature on this now. A lot of these tumors originate from the superficial MP [muscularis propria], so we can dissect off the muscle without needing a full-thickness resection.” He presented findings from a large study comprising 143 patients with submucosal gastric or esophageal tumors that arose from the muscularis propria at the esophagogastric junction. These were large lesions, a mean 17.6 cm, but they ranged up to 50 cm. The en bloc resection rate was 94%. There were six perforations (4%), along with four pneumoperitoneum and two pneumothorax, which resolved without further surgery. There were no local recurrences or metastases when the 2012 study appeared, with a mean follow-up of 2 years.
- Endoscopic full-thickness resection: EFTR “is a technically demanding procedure, and we frequently have to work on these tumors in retroflexion,” Dr. Khashab said. He referred to a 2011 paper, which described the EFTR technique used in 26 patients with gastric cancers. The tumors (mean size, 2.8 cm) were located in the gastric corpus and in the gastric fundus. Although the procedures were lengthy, ranging from 60 to 145 minutes, they were highly successful, with a 100% complete resection rate. Nevertheless, there was also a 100% perforation rate, although all these were closed intraoperatively. There was no postoperative gastric bleeding, peritonitis sign, or abdominal abscess. No lesion residual or recurrence was found during the 6-24 month follow-up period.
Dr. Khashab is a consultant and medical advisory board member for Boston Scientific and Olympus.
BOSTON –
“The main difficulty with these procedures is closure,” Mouen A. Khashab, MD, said at the AGA Tech Summit, which was sponsored by the AGA Center for GI Innovation and Technology. “Sometimes you can create a large defect that you’re not sure you can close. You must have experience with large defect closure.”
In experienced hands, the endoscopic approaches spare adjacent large organs, have a complete resection rate approaching 95%, and an acceptable rate of adverse events. They can provide excellent surgical specimens that are more than adequate for histologic studies, although some cannot provide any information on margins, said Dr. Khashab, director of therapeutic endoscopy at Johns Hopkins University, Baltimore. “When doing a full-thickness endoscopic resection, you can’t comment on the margins. You’re not getting any normal tissue around the tumor, and this can create an issue with some patients.”
Dr. Khashab briefly described three endoscopic resection techniques that are suitable for the following deep GI tumors:
- Submucosal tunneling endoscopic resection. STER is most suitable for smaller tumors (4 cm or less). Tumors of this size are easily removed en bloc via the endoscopic tunnel. Larger tumors can also be resected this way, but need to be removed piecemeal after dissection off the muscle layer. This is an acceptable alternative in leiomyomas but not in gastrointestinal stromal tumors. “For this technique, you introduce the scope into the submucosal layer and create a space with tunneling,” Dr. Khashab said. “We then expose the tumor, dissect it off the wall of the muscularis propria, and pull it out of the tunnel.” A 2017 meta-analysis examined outcomes in 28 studies with data on 1,085 lesions. The pooled complete resection and en bloc resection rates were 97.5% and 94.6%, respectively. Common complications associated with STER were air leakage symptoms (15%) and perforation (5.6%). “The perforation rate is reasonable, I think. A lot of these complications can be managed intraoperatively with clipping or suturing,” Dr. Khashab noted.
- Endoscopic submucosal dissection: ESD is now being used to resect tumors that originate from the muscularis propria. “This is something I didn’t used to think was even possible,” Dr. Khashab said. “But we are seeing some literature on this now. A lot of these tumors originate from the superficial MP [muscularis propria], so we can dissect off the muscle without needing a full-thickness resection.” He presented findings from a large study comprising 143 patients with submucosal gastric or esophageal tumors that arose from the muscularis propria at the esophagogastric junction. These were large lesions, a mean 17.6 cm, but they ranged up to 50 cm. The en bloc resection rate was 94%. There were six perforations (4%), along with four pneumoperitoneum and two pneumothorax, which resolved without further surgery. There were no local recurrences or metastases when the 2012 study appeared, with a mean follow-up of 2 years.
- Endoscopic full-thickness resection: EFTR “is a technically demanding procedure, and we frequently have to work on these tumors in retroflexion,” Dr. Khashab said. He referred to a 2011 paper, which described the EFTR technique used in 26 patients with gastric cancers. The tumors (mean size, 2.8 cm) were located in the gastric corpus and in the gastric fundus. Although the procedures were lengthy, ranging from 60 to 145 minutes, they were highly successful, with a 100% complete resection rate. Nevertheless, there was also a 100% perforation rate, although all these were closed intraoperatively. There was no postoperative gastric bleeding, peritonitis sign, or abdominal abscess. No lesion residual or recurrence was found during the 6-24 month follow-up period.
Dr. Khashab is a consultant and medical advisory board member for Boston Scientific and Olympus.
EXPERT ANALYSIS FROM THE 2018 AGA TECH SUMMIT
AJO Awards Joseph T. O'Neil, MD, First-Place Resident Writer's Award
2017 AJO Resident Writer's Awards
First-Place Award
An Original Study
Prospective Evaluation of Opioid Consumption After Distal Radius Fracture Repair Surgery
Joseph T. O’Neil, MD, Mark L. Wang, MD, PhD, Nayoung Kim, BS, Mitchell Maltenfort, PhD, and Asif M. Ilyas, MD

Dr. O'Neil completed his orthopedic surgery residency training at Thomas Jefferson University Hospital in Philadelphia, Pennsylvania. Prior to residency, he completed undergraduate education at the University of Notre Dame and medical school at Thomas Jefferson University. He was born and raised in the Philadelphia area.
Dr. O'Neil is currently an orthopedic foot and ankle surgery fellow at Union Memorial Hospital in Baltimore, Maryland.
His research interests include total ankle arthroplasty; the diagnosis, treatment, and prevention of periprosthetic joint infection in the ankle; as well as helping to combat the opioid epidemic in the United States by better understanding patterns of prescribing and use following common orthopedic surgical procedures.
Read the full version of Dr. O'Neil's original study.
2017 AJO Resident Writer's Awards
First-Place Award
An Original Study
Prospective Evaluation of Opioid Consumption After Distal Radius Fracture Repair Surgery
Joseph T. O’Neil, MD, Mark L. Wang, MD, PhD, Nayoung Kim, BS, Mitchell Maltenfort, PhD, and Asif M. Ilyas, MD
Dr. O'Neil completed his orthopedic surgery residency training at Thomas Jefferson University Hospital in Philadelphia, Pennsylvania. Prior to residency, he completed undergraduate education at the University of Notre Dame and medical school at Thomas Jefferson University. He was born and raised in the Philadelphia area.
Dr. O'Neil is currently an orthopedic foot and ankle surgery fellow at Union Memorial Hospital in Baltimore, Maryland.
His research interests include total ankle arthroplasty; the diagnosis, treatment, and prevention of periprosthetic joint infection in the ankle; as well as helping to combat the opioid epidemic in the United States by better understanding patterns of prescribing and use following common orthopedic surgical procedures.
Read the full version of Dr. O'Neil's original study.
2017 AJO Resident Writer's Awards
First-Place Award
An Original Study
Prospective Evaluation of Opioid Consumption After Distal Radius Fracture Repair Surgery
Joseph T. O’Neil, MD, Mark L. Wang, MD, PhD, Nayoung Kim, BS, Mitchell Maltenfort, PhD, and Asif M. Ilyas, MD
Dr. O'Neil completed his orthopedic surgery residency training at Thomas Jefferson University Hospital in Philadelphia, Pennsylvania. Prior to residency, he completed undergraduate education at the University of Notre Dame and medical school at Thomas Jefferson University. He was born and raised in the Philadelphia area.
Dr. O'Neil is currently an orthopedic foot and ankle surgery fellow at Union Memorial Hospital in Baltimore, Maryland.
His research interests include total ankle arthroplasty; the diagnosis, treatment, and prevention of periprosthetic joint infection in the ankle; as well as helping to combat the opioid epidemic in the United States by better understanding patterns of prescribing and use following common orthopedic surgical procedures.
Read the full version of Dr. O'Neil's original study.
Lupus is quietly killing young women
according to researchers at the University of California, Los Angeles.
SLE was either the underlying or a contributing cause of death for 28,411 females from 2000 to 2015, when it was one of the 20 most common causes of death among females aged 5-64 years in the United States, based on an analysis of the Centers for Disease Control and Prevention’s Wide-ranging Online Data for Epidemiologic Research multiple cause-of-death database, the researchers said.
SLE was the 10th-leading cause of death in the 15- to 24-year age group (1,226 deaths), the 14th-leading cause among women aged 25-34 (2,431 deaths) and 35-44 (3,646 deaths), and the 16th-leading cause in those aged 45-54 (5,271 deaths), Eric Y. Yen, MD, and Ram R. Singh, MD, reported in Arthritis & Rheumatology.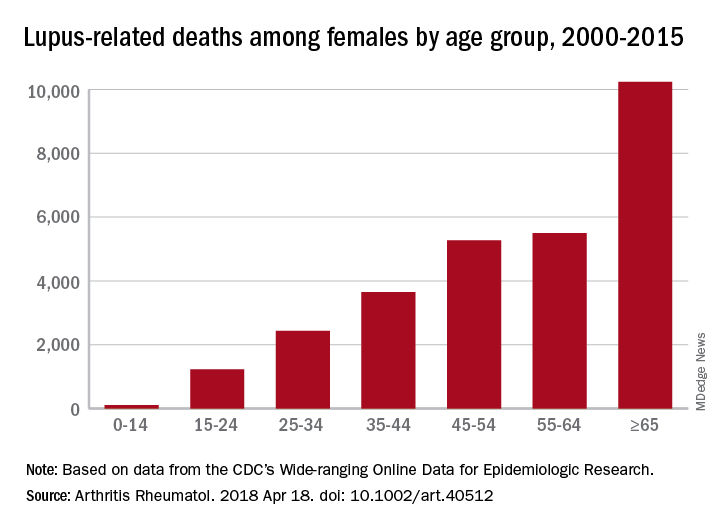
The numbers for SLE could be higher, though, since it is underreported on death certificates – by as much as 40% in one study – and other causes may be overreported. “Patients with SLE die prematurely of complications such as cardiovascular events, infections, renal failure, and respiratory diseases [and] these proximate causes of death may be perceived to be unrelated to SLE, when in fact the disease or the medications used for it predispose to them,” the investigators said.
Dr. Yen was supported by the National Institutes of Health and UCLA Children’s Discovery and Innovation Institute. Dr. Singh was supported by the NIH, the Lupus Foundation of America, and the Rheumatology Research Foundation.
SOURCE: Yen EY and Singh RR. Arthritis Rheumatol. 2018 Apr 18. doi: 10.1002/art.40512.
according to researchers at the University of California, Los Angeles.
SLE was either the underlying or a contributing cause of death for 28,411 females from 2000 to 2015, when it was one of the 20 most common causes of death among females aged 5-64 years in the United States, based on an analysis of the Centers for Disease Control and Prevention’s Wide-ranging Online Data for Epidemiologic Research multiple cause-of-death database, the researchers said.
SLE was the 10th-leading cause of death in the 15- to 24-year age group (1,226 deaths), the 14th-leading cause among women aged 25-34 (2,431 deaths) and 35-44 (3,646 deaths), and the 16th-leading cause in those aged 45-54 (5,271 deaths), Eric Y. Yen, MD, and Ram R. Singh, MD, reported in Arthritis & Rheumatology.
The numbers for SLE could be higher, though, since it is underreported on death certificates – by as much as 40% in one study – and other causes may be overreported. “Patients with SLE die prematurely of complications such as cardiovascular events, infections, renal failure, and respiratory diseases [and] these proximate causes of death may be perceived to be unrelated to SLE, when in fact the disease or the medications used for it predispose to them,” the investigators said.
Dr. Yen was supported by the National Institutes of Health and UCLA Children’s Discovery and Innovation Institute. Dr. Singh was supported by the NIH, the Lupus Foundation of America, and the Rheumatology Research Foundation.
SOURCE: Yen EY and Singh RR. Arthritis Rheumatol. 2018 Apr 18. doi: 10.1002/art.40512.
according to researchers at the University of California, Los Angeles.
SLE was either the underlying or a contributing cause of death for 28,411 females from 2000 to 2015, when it was one of the 20 most common causes of death among females aged 5-64 years in the United States, based on an analysis of the Centers for Disease Control and Prevention’s Wide-ranging Online Data for Epidemiologic Research multiple cause-of-death database, the researchers said.
SLE was the 10th-leading cause of death in the 15- to 24-year age group (1,226 deaths), the 14th-leading cause among women aged 25-34 (2,431 deaths) and 35-44 (3,646 deaths), and the 16th-leading cause in those aged 45-54 (5,271 deaths), Eric Y. Yen, MD, and Ram R. Singh, MD, reported in Arthritis & Rheumatology.
The numbers for SLE could be higher, though, since it is underreported on death certificates – by as much as 40% in one study – and other causes may be overreported. “Patients with SLE die prematurely of complications such as cardiovascular events, infections, renal failure, and respiratory diseases [and] these proximate causes of death may be perceived to be unrelated to SLE, when in fact the disease or the medications used for it predispose to them,” the investigators said.
Dr. Yen was supported by the National Institutes of Health and UCLA Children’s Discovery and Innovation Institute. Dr. Singh was supported by the NIH, the Lupus Foundation of America, and the Rheumatology Research Foundation.
SOURCE: Yen EY and Singh RR. Arthritis Rheumatol. 2018 Apr 18. doi: 10.1002/art.40512.
FROM ARTHRITIS & RHEUMATOLOGY