User login
2018 Resident Writer’s Award Information
The 2018 Resident Writer’s Award competition is sponsored by Johnson & Johnson. Orthopedic residents are invited to submit original studies, review papers, or case reports for publication. Papers published in 2018 will be judged by The American Journal of Orthopedics Editorial Board. Honoraria will be presented to the winners at the 2019 AAOS annual meeting.
- $1,500 for the First-Place Award
- $1,000 for the Second-Place Award
- $500 for the Third-Place Award
To quality for consideration, papers must have the resident as the first-listed author and must be accepted through the journal’s standard blinded-review process. Papers submitted in 2018 but not published until 2019 will automatically qualify for the 2019 competition. Manuscripts should be prepared according to our Information for the Authors and submitted via our online submission system, Editorial Manager®, at www.editorialmanager.com/AmJOrthop.
Read more about this year's RWA winners.
Supported by Johnson & Johnson
The 2018 Resident Writer’s Award competition is sponsored by Johnson & Johnson. Orthopedic residents are invited to submit original studies, review papers, or case reports for publication. Papers published in 2018 will be judged by The American Journal of Orthopedics Editorial Board. Honoraria will be presented to the winners at the 2019 AAOS annual meeting.
- $1,500 for the First-Place Award
- $1,000 for the Second-Place Award
- $500 for the Third-Place Award
To quality for consideration, papers must have the resident as the first-listed author and must be accepted through the journal’s standard blinded-review process. Papers submitted in 2018 but not published until 2019 will automatically qualify for the 2019 competition. Manuscripts should be prepared according to our Information for the Authors and submitted via our online submission system, Editorial Manager®, at www.editorialmanager.com/AmJOrthop.
Read more about this year's RWA winners.
Supported by Johnson & Johnson
The 2018 Resident Writer’s Award competition is sponsored by Johnson & Johnson. Orthopedic residents are invited to submit original studies, review papers, or case reports for publication. Papers published in 2018 will be judged by The American Journal of Orthopedics Editorial Board. Honoraria will be presented to the winners at the 2019 AAOS annual meeting.
- $1,500 for the First-Place Award
- $1,000 for the Second-Place Award
- $500 for the Third-Place Award
To quality for consideration, papers must have the resident as the first-listed author and must be accepted through the journal’s standard blinded-review process. Papers submitted in 2018 but not published until 2019 will automatically qualify for the 2019 competition. Manuscripts should be prepared according to our Information for the Authors and submitted via our online submission system, Editorial Manager®, at www.editorialmanager.com/AmJOrthop.
Read more about this year's RWA winners.
Supported by Johnson & Johnson
VIDEOS: High-priced drugs, out-of-pocket costs raise challenges for neurologists
LOS ANGELES – Neurologists can play an important role in helping patients gain access to high-cost, breakthrough drugs, while at the same time guiding patients to lower-cost options whenever possible, speakers said at the annual meeting of the American Academy of Neurology.
The use of the Orphan Drug approval pathway established in 1983 has gained a great deal of steam for rare neurologic diseases in recent years with the approval of a number of drugs, such as nusinersen (Spinraza) for spinal muscular atrophy, eteplirsen (Exondys 51) for Duchenne muscular dystrophy, and edaravone (Radicava) for amyotrophic lateral sclerosis, said Nicholas Johnson, MD, a pediatric neuromuscular disease specialist at the University of Utah, Salt Lake City.
But given that only 2% of U.S. physicians are neurologists, yet 18% of rare diseases are neurologic and 11% of drugs in development overall are for neurologic diseases, there are a great deal of challenges arising for neurologists in getting access to these new high-priced drugs for their patients, said Dr. Johnson, who leads the AAN’s Neurology Drug Pricing Task Force and is also chair of the AAN Government Relations Committee.
These challenges range from increased administrative burden on staff, getting insurance approval, finding administration sites, and the ability to perform special patient assessments, he said in an interview.
Dr. Nicholas Johnson’s interview:
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
Dr. Brian Callaghan’s interview:
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
Many high-priced drugs commonly prescribed for chronic neurologic conditions and diagnostic tests also have high out-of-pocket costs for patients, but it is remarkably hard even for well-informed experts to find the actual costs that patients will pay out of pocket for such drugs and tests, according to Brian Callaghan, MD, a neuromuscular disease specialist at the University of Michigan, Ann Arbor.
Neurologist can seek to find more affordable alternatives to drugs when the out-of-pocket expenses are too great, said Dr. Callaghan, who also serves on the Neurology Drug Pricing Task Force. It may be advisable to put certain drugs lower on a list of potential treatment options than others for a chronic condition such as epilepsy because of their out-of-pocket costs, but it can be frustratingly hard to determine these costs in advance.
The University of Michigan Health System is unique in having drug cost data provided as part of information presented to physicians in electronic health records, but this is not the case in most other clinics. Until doctors can regularly access patient-specific drug and diagnostic testing out-of-pocket costs through EHRs, finding the best affordable medications for patients will remain a costly and time-consuming process, he said in an interview.
LOS ANGELES – Neurologists can play an important role in helping patients gain access to high-cost, breakthrough drugs, while at the same time guiding patients to lower-cost options whenever possible, speakers said at the annual meeting of the American Academy of Neurology.
The use of the Orphan Drug approval pathway established in 1983 has gained a great deal of steam for rare neurologic diseases in recent years with the approval of a number of drugs, such as nusinersen (Spinraza) for spinal muscular atrophy, eteplirsen (Exondys 51) for Duchenne muscular dystrophy, and edaravone (Radicava) for amyotrophic lateral sclerosis, said Nicholas Johnson, MD, a pediatric neuromuscular disease specialist at the University of Utah, Salt Lake City.
But given that only 2% of U.S. physicians are neurologists, yet 18% of rare diseases are neurologic and 11% of drugs in development overall are for neurologic diseases, there are a great deal of challenges arising for neurologists in getting access to these new high-priced drugs for their patients, said Dr. Johnson, who leads the AAN’s Neurology Drug Pricing Task Force and is also chair of the AAN Government Relations Committee.
These challenges range from increased administrative burden on staff, getting insurance approval, finding administration sites, and the ability to perform special patient assessments, he said in an interview.
Dr. Nicholas Johnson’s interview:
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
Dr. Brian Callaghan’s interview:
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
Many high-priced drugs commonly prescribed for chronic neurologic conditions and diagnostic tests also have high out-of-pocket costs for patients, but it is remarkably hard even for well-informed experts to find the actual costs that patients will pay out of pocket for such drugs and tests, according to Brian Callaghan, MD, a neuromuscular disease specialist at the University of Michigan, Ann Arbor.
Neurologist can seek to find more affordable alternatives to drugs when the out-of-pocket expenses are too great, said Dr. Callaghan, who also serves on the Neurology Drug Pricing Task Force. It may be advisable to put certain drugs lower on a list of potential treatment options than others for a chronic condition such as epilepsy because of their out-of-pocket costs, but it can be frustratingly hard to determine these costs in advance.
The University of Michigan Health System is unique in having drug cost data provided as part of information presented to physicians in electronic health records, but this is not the case in most other clinics. Until doctors can regularly access patient-specific drug and diagnostic testing out-of-pocket costs through EHRs, finding the best affordable medications for patients will remain a costly and time-consuming process, he said in an interview.
LOS ANGELES – Neurologists can play an important role in helping patients gain access to high-cost, breakthrough drugs, while at the same time guiding patients to lower-cost options whenever possible, speakers said at the annual meeting of the American Academy of Neurology.
The use of the Orphan Drug approval pathway established in 1983 has gained a great deal of steam for rare neurologic diseases in recent years with the approval of a number of drugs, such as nusinersen (Spinraza) for spinal muscular atrophy, eteplirsen (Exondys 51) for Duchenne muscular dystrophy, and edaravone (Radicava) for amyotrophic lateral sclerosis, said Nicholas Johnson, MD, a pediatric neuromuscular disease specialist at the University of Utah, Salt Lake City.
But given that only 2% of U.S. physicians are neurologists, yet 18% of rare diseases are neurologic and 11% of drugs in development overall are for neurologic diseases, there are a great deal of challenges arising for neurologists in getting access to these new high-priced drugs for their patients, said Dr. Johnson, who leads the AAN’s Neurology Drug Pricing Task Force and is also chair of the AAN Government Relations Committee.
These challenges range from increased administrative burden on staff, getting insurance approval, finding administration sites, and the ability to perform special patient assessments, he said in an interview.
Dr. Nicholas Johnson’s interview:
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
Dr. Brian Callaghan’s interview:
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
Many high-priced drugs commonly prescribed for chronic neurologic conditions and diagnostic tests also have high out-of-pocket costs for patients, but it is remarkably hard even for well-informed experts to find the actual costs that patients will pay out of pocket for such drugs and tests, according to Brian Callaghan, MD, a neuromuscular disease specialist at the University of Michigan, Ann Arbor.
Neurologist can seek to find more affordable alternatives to drugs when the out-of-pocket expenses are too great, said Dr. Callaghan, who also serves on the Neurology Drug Pricing Task Force. It may be advisable to put certain drugs lower on a list of potential treatment options than others for a chronic condition such as epilepsy because of their out-of-pocket costs, but it can be frustratingly hard to determine these costs in advance.
The University of Michigan Health System is unique in having drug cost data provided as part of information presented to physicians in electronic health records, but this is not the case in most other clinics. Until doctors can regularly access patient-specific drug and diagnostic testing out-of-pocket costs through EHRs, finding the best affordable medications for patients will remain a costly and time-consuming process, he said in an interview.
REPORTING FROM AAN 2018

Speakers at FDA advisory meetings have hidden conflicts
Nearly a quarter of public speakers at meetings of a Food and Drug Administration advisory committee had conflicts of interest, about 20% of which are undisclosed, a study finds.
Matthew S. McCoy, PhD., of the University of Pennsylvania, Philadelphia, and his colleagues analyzed the public speakers at 15 meetings of the FDA Anesthetic and Analgesic Drug Products Advisory Committee from September 2009 to April 2017 related to the approval of drug products. (The committee advises the FDA on anesthesiology and pain management drug products.)
Investigators evaluated meeting transcripts to learn whether speakers reported chronic pain; had received the drug under review; reported an organization affiliation; reported a conflict of interest; and expressed support, opposition or were neutral with respect to drug approval. Of the 112 speakers studied, about 20% disclosed a conflict of interest, 5% had an undisclosed financial association with the sponsor that existed prior to the meeting and 13% had an undisclosed financial association of indeterminate date,the researchers reported in JAMA Internal Medicine on April 23.
Of those 112 speakers, 20 reported having experienced chronic pain and 11 reported receiving the drug under review. Overall, about 70% of speakers (76 out of 112) supported drug approval, the study found. Speakers who disclosed a conflict of interest were significantly more likely to support drug approval. When financial associations of indeterminate date were classified as conflicts of interest, speakers with a conflict were more than eight times as likely to support drug approval.
Dr. McCoy and his colleagues noted that the findings raise concerns about pro–sponsor bias among speakers at advisory committee meetings. They propose that the FDA should require – rather than only encourage – speakers to disclose conflicts of interest at all of the agency’s advisory committee meetings.
SOURCE: McCoy MS et al. JAMA Intern Med. 2018 Apr 23. doi:10.1001/jamainternmed.2018.1324
The influence of pharmaceutical companies permeates the open public hearing, even though these firms already have highlighted their products during the sponsor presentation.
Currently, pharmaceutical and medical device companies publicly report specified types of payments to physicians through the federal Open Payments program. In my view, these companies also should be required to publicly report payments to professional associations, patient groups, and other nongovernmental organizations.
Dr. McCoy and his colleagues recommend that the Food and Drug Administration require – not merely encourage – public speakers to disclose their conflicts of interest. This is a recommendation with which I disagree. Advisory committee members fill out forms related to conflicts of interest under penalty of perjury. In contrast, speakers at the open public hearing often sign up to speak on the day of the advisory committee meeting, and no documentation is provided, giving FDA staff no opportunity to corroborate any disclosures (or lack thereof). The chair of the FDA advisory committee simply encourages public speakers to disclose any conflicts. It does not seem consistent with the spirit of inclusiveness that should characterize the open public hearing to exclude a speaker who does not disclose whether he or she has conflicts. Nonetheless, the chair should directly query any speaker who fails to disclose whether he or she has conflicts and the subsequent testimony be should be considered in the light of any refusal to disclose.
Peter Lurie, MD, is president of the Center for Science in the Public Interest, Washington. Dr Lurie reports that he worked at the FDA during 2009-2017, including as associate commissioner for public health strategy and analysis from 2014 to 2017. His comments were made in an editorial accompanying Dr. McCoy’s study (JAMA Intern Med. doi:10.1001/jamainternmed.2018.1324).
The influence of pharmaceutical companies permeates the open public hearing, even though these firms already have highlighted their products during the sponsor presentation.
Currently, pharmaceutical and medical device companies publicly report specified types of payments to physicians through the federal Open Payments program. In my view, these companies also should be required to publicly report payments to professional associations, patient groups, and other nongovernmental organizations.
Dr. McCoy and his colleagues recommend that the Food and Drug Administration require – not merely encourage – public speakers to disclose their conflicts of interest. This is a recommendation with which I disagree. Advisory committee members fill out forms related to conflicts of interest under penalty of perjury. In contrast, speakers at the open public hearing often sign up to speak on the day of the advisory committee meeting, and no documentation is provided, giving FDA staff no opportunity to corroborate any disclosures (or lack thereof). The chair of the FDA advisory committee simply encourages public speakers to disclose any conflicts. It does not seem consistent with the spirit of inclusiveness that should characterize the open public hearing to exclude a speaker who does not disclose whether he or she has conflicts. Nonetheless, the chair should directly query any speaker who fails to disclose whether he or she has conflicts and the subsequent testimony be should be considered in the light of any refusal to disclose.
Peter Lurie, MD, is president of the Center for Science in the Public Interest, Washington. Dr Lurie reports that he worked at the FDA during 2009-2017, including as associate commissioner for public health strategy and analysis from 2014 to 2017. His comments were made in an editorial accompanying Dr. McCoy’s study (JAMA Intern Med. doi:10.1001/jamainternmed.2018.1324).
The influence of pharmaceutical companies permeates the open public hearing, even though these firms already have highlighted their products during the sponsor presentation.
Currently, pharmaceutical and medical device companies publicly report specified types of payments to physicians through the federal Open Payments program. In my view, these companies also should be required to publicly report payments to professional associations, patient groups, and other nongovernmental organizations.
Dr. McCoy and his colleagues recommend that the Food and Drug Administration require – not merely encourage – public speakers to disclose their conflicts of interest. This is a recommendation with which I disagree. Advisory committee members fill out forms related to conflicts of interest under penalty of perjury. In contrast, speakers at the open public hearing often sign up to speak on the day of the advisory committee meeting, and no documentation is provided, giving FDA staff no opportunity to corroborate any disclosures (or lack thereof). The chair of the FDA advisory committee simply encourages public speakers to disclose any conflicts. It does not seem consistent with the spirit of inclusiveness that should characterize the open public hearing to exclude a speaker who does not disclose whether he or she has conflicts. Nonetheless, the chair should directly query any speaker who fails to disclose whether he or she has conflicts and the subsequent testimony be should be considered in the light of any refusal to disclose.
Peter Lurie, MD, is president of the Center for Science in the Public Interest, Washington. Dr Lurie reports that he worked at the FDA during 2009-2017, including as associate commissioner for public health strategy and analysis from 2014 to 2017. His comments were made in an editorial accompanying Dr. McCoy’s study (JAMA Intern Med. doi:10.1001/jamainternmed.2018.1324).
Nearly a quarter of public speakers at meetings of a Food and Drug Administration advisory committee had conflicts of interest, about 20% of which are undisclosed, a study finds.
Matthew S. McCoy, PhD., of the University of Pennsylvania, Philadelphia, and his colleagues analyzed the public speakers at 15 meetings of the FDA Anesthetic and Analgesic Drug Products Advisory Committee from September 2009 to April 2017 related to the approval of drug products. (The committee advises the FDA on anesthesiology and pain management drug products.)
Investigators evaluated meeting transcripts to learn whether speakers reported chronic pain; had received the drug under review; reported an organization affiliation; reported a conflict of interest; and expressed support, opposition or were neutral with respect to drug approval. Of the 112 speakers studied, about 20% disclosed a conflict of interest, 5% had an undisclosed financial association with the sponsor that existed prior to the meeting and 13% had an undisclosed financial association of indeterminate date,the researchers reported in JAMA Internal Medicine on April 23.
Of those 112 speakers, 20 reported having experienced chronic pain and 11 reported receiving the drug under review. Overall, about 70% of speakers (76 out of 112) supported drug approval, the study found. Speakers who disclosed a conflict of interest were significantly more likely to support drug approval. When financial associations of indeterminate date were classified as conflicts of interest, speakers with a conflict were more than eight times as likely to support drug approval.
Dr. McCoy and his colleagues noted that the findings raise concerns about pro–sponsor bias among speakers at advisory committee meetings. They propose that the FDA should require – rather than only encourage – speakers to disclose conflicts of interest at all of the agency’s advisory committee meetings.
SOURCE: McCoy MS et al. JAMA Intern Med. 2018 Apr 23. doi:10.1001/jamainternmed.2018.1324
Nearly a quarter of public speakers at meetings of a Food and Drug Administration advisory committee had conflicts of interest, about 20% of which are undisclosed, a study finds.
Matthew S. McCoy, PhD., of the University of Pennsylvania, Philadelphia, and his colleagues analyzed the public speakers at 15 meetings of the FDA Anesthetic and Analgesic Drug Products Advisory Committee from September 2009 to April 2017 related to the approval of drug products. (The committee advises the FDA on anesthesiology and pain management drug products.)
Investigators evaluated meeting transcripts to learn whether speakers reported chronic pain; had received the drug under review; reported an organization affiliation; reported a conflict of interest; and expressed support, opposition or were neutral with respect to drug approval. Of the 112 speakers studied, about 20% disclosed a conflict of interest, 5% had an undisclosed financial association with the sponsor that existed prior to the meeting and 13% had an undisclosed financial association of indeterminate date,the researchers reported in JAMA Internal Medicine on April 23.
Of those 112 speakers, 20 reported having experienced chronic pain and 11 reported receiving the drug under review. Overall, about 70% of speakers (76 out of 112) supported drug approval, the study found. Speakers who disclosed a conflict of interest were significantly more likely to support drug approval. When financial associations of indeterminate date were classified as conflicts of interest, speakers with a conflict were more than eight times as likely to support drug approval.
Dr. McCoy and his colleagues noted that the findings raise concerns about pro–sponsor bias among speakers at advisory committee meetings. They propose that the FDA should require – rather than only encourage – speakers to disclose conflicts of interest at all of the agency’s advisory committee meetings.
SOURCE: McCoy MS et al. JAMA Intern Med. 2018 Apr 23. doi:10.1001/jamainternmed.2018.1324
Key clinical point: A significant portion of public speakers at certain FDA advisory committee meetings have conflicts of interest.
Major finding: Of 112 speakers, about 25% had a conflict of interest, of which about 20% were undisclosed.
Study details: A study of public speakers at 15 Anesthetic and Analgesic Drug Products Advisory Committee (AADPAC) meetings from September 2009 through April 2017 related to the approval of drug products.
Disclosures: Dr. McCoy reports that his spouse is employed by a cancer patient advocacy organization. Dr Litman reports that he is a member of AADPAC. No other disclosures were reported.
Source: McCoy et al. JAMA Intern Med. 2018 Apr 23. doi:10.1001/jamainternmed.2018.1324.
Self-harm
Nonsuicidal self-injury (NSSI) has become more prevalent in youth over recent years and has many inherent risks. In the Diagnostic and Statistical Manual, Fifth Edition (DSM-5), NSSI is a diagnosis suggested for further study, and criteria include engaging in self-injury for 5 or more days without suicidal intent as well as self-injury associated with at least 1 of the following: obtaining relief from negative thoughts or feelings, resolving interpersonal challenges, inducing positive feelings. It is associated with interpersonal difficulties or negative thoughts/feelings. The behavior causes significant impairment in functioning and is not better explained by another condition.1
Estimates of lifetime prevalence in community-based samples of youth range from 15% to 20%. Individuals often start during early adolescence. It can pose many risks including infection, permanent scarring or disfigurement, decreased self-esteem, interpersonal conflict, severe injury, or death. Reasons for engaging in self-harm can vary and include attempts to regulate negative affect, to manage feelings of emptiness/numbness, regain a sense of control over body, feelings, etc., or to provide a consequence for perceived faults. Youth often may start to engage in self-harm covertly, and it may first become apparent in emergency or primary care settings. However, upon discovery, the response given also may affect future behavior.
Efforts also have been underway to distinguish between youth who engage in self-harm with and without suicidal ideation. Girls are more likely than are boys to report NSSI, although male NSSI may present differently. In addition to cutting or more stereotypical self-injury, they may punch walls or engage in fights or other risky behaviors as a proxy for self-harm. Risk factors for boys with regard to suicide attempts include hopelessness and history of sexual abuse. Maladaptive eating patterns and hopelessness were the two most significant factors for girls.4
With regard to issues of confidentiality, it will be important to carefully gauge level of safety and to clearly communicate with the patient (and family) limits of confidentiality. This may result in working within shades of gray to help maintain the therapeutic relationship and the patient’s comfort in being able to disclose potentially sensitive information.

Families can struggle with how to manage this, and it can generate fear as well as other strong emotions.
Tips for parents and guardians
- Validate the underlying emotions while not validating the behavior. Self-injury is a coping strategy. Focus on the driving forces for the actions rather than the actions themselves.
- Approach your child from a nonjudgmental stance.
- Recognize that change may not happen overnight, and that there may be periods of regression.
- Acknowledge successes when they occur.
- Make yourself available for open communication. Open-ended questions may facilitate more dialogue.
- Take care of yourself as well. Ensure you use your supports and are engaging in healthy self-care.
- Take the behavior seriously. While this behavior is relatively common, do not assume it is “just a phase.”
- While remaining supportive, it is important to maintain a parental role and to keep expectations rather than “walking on eggshells.”
- Involve the child in identifying what can be of support.
- Become aware of local crisis resources in your community. National resources include Call 1-800-273-TALK for the national suicide hotline or Text 741741 to connect with a crisis counselor.
Things to avoid
- Avoid taking a punitive stance. While the behavior can be provocative, most likely the primary purpose is not for attention.
- Avoid engaging in power struggles.
- Avoid creating increased isolation for the child. This can be a delicate balance with regard to peer groups, but encouraging healthy social interactions and activities is a way to help build resilience.
- Avoid taking the behavior personally.5
In working with youth who engage in self-harm, it is important to work within a team, which may include family, primary care, mental health support, school, and potentially other community supports. Treatment evidence is relatively limited, but there is some evidence to support use of cognitive behavioral therapy, dialectical behavior therapy, and mentalization-based therapy. Regardless, work will likely be long term and at times intensive in addressing the problems leading to self-harm behavior.6
Dr. Strange is an assistant professor in the department of psychiatry at the University of Vermont Medical Center and University of Vermont Robert Larner College of Medicine, both in Burlington. She works with children and adolescents. She has no relevant financial disclosures.
References
1. Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (Arlington, Va.: American Psychiatric Association Publishing, 2013)
2. J Adolesc. 2014 Dec;37(8):1335-44.
3. Behav Ther. 2017 May; 48(3):366-79.
4. Acad Pediatr. 2012 May-Jun;12(3):205-13.
5. “Information for parents: What you need to know about self-injury.” The Fact Sheet Series, Cornell Research Program on Self-Injury and Recovery. 2009.
6. Clin Pediatr. 2016 Sep 13;55(11):1012-9.
Nonsuicidal self-injury (NSSI) has become more prevalent in youth over recent years and has many inherent risks. In the Diagnostic and Statistical Manual, Fifth Edition (DSM-5), NSSI is a diagnosis suggested for further study, and criteria include engaging in self-injury for 5 or more days without suicidal intent as well as self-injury associated with at least 1 of the following: obtaining relief from negative thoughts or feelings, resolving interpersonal challenges, inducing positive feelings. It is associated with interpersonal difficulties or negative thoughts/feelings. The behavior causes significant impairment in functioning and is not better explained by another condition.1
Estimates of lifetime prevalence in community-based samples of youth range from 15% to 20%. Individuals often start during early adolescence. It can pose many risks including infection, permanent scarring or disfigurement, decreased self-esteem, interpersonal conflict, severe injury, or death. Reasons for engaging in self-harm can vary and include attempts to regulate negative affect, to manage feelings of emptiness/numbness, regain a sense of control over body, feelings, etc., or to provide a consequence for perceived faults. Youth often may start to engage in self-harm covertly, and it may first become apparent in emergency or primary care settings. However, upon discovery, the response given also may affect future behavior.
Efforts also have been underway to distinguish between youth who engage in self-harm with and without suicidal ideation. Girls are more likely than are boys to report NSSI, although male NSSI may present differently. In addition to cutting or more stereotypical self-injury, they may punch walls or engage in fights or other risky behaviors as a proxy for self-harm. Risk factors for boys with regard to suicide attempts include hopelessness and history of sexual abuse. Maladaptive eating patterns and hopelessness were the two most significant factors for girls.4
With regard to issues of confidentiality, it will be important to carefully gauge level of safety and to clearly communicate with the patient (and family) limits of confidentiality. This may result in working within shades of gray to help maintain the therapeutic relationship and the patient’s comfort in being able to disclose potentially sensitive information.
Families can struggle with how to manage this, and it can generate fear as well as other strong emotions.
Tips for parents and guardians
- Validate the underlying emotions while not validating the behavior. Self-injury is a coping strategy. Focus on the driving forces for the actions rather than the actions themselves.
- Approach your child from a nonjudgmental stance.
- Recognize that change may not happen overnight, and that there may be periods of regression.
- Acknowledge successes when they occur.
- Make yourself available for open communication. Open-ended questions may facilitate more dialogue.
- Take care of yourself as well. Ensure you use your supports and are engaging in healthy self-care.
- Take the behavior seriously. While this behavior is relatively common, do not assume it is “just a phase.”
- While remaining supportive, it is important to maintain a parental role and to keep expectations rather than “walking on eggshells.”
- Involve the child in identifying what can be of support.
- Become aware of local crisis resources in your community. National resources include Call 1-800-273-TALK for the national suicide hotline or Text 741741 to connect with a crisis counselor.
Things to avoid
- Avoid taking a punitive stance. While the behavior can be provocative, most likely the primary purpose is not for attention.
- Avoid engaging in power struggles.
- Avoid creating increased isolation for the child. This can be a delicate balance with regard to peer groups, but encouraging healthy social interactions and activities is a way to help build resilience.
- Avoid taking the behavior personally.5
In working with youth who engage in self-harm, it is important to work within a team, which may include family, primary care, mental health support, school, and potentially other community supports. Treatment evidence is relatively limited, but there is some evidence to support use of cognitive behavioral therapy, dialectical behavior therapy, and mentalization-based therapy. Regardless, work will likely be long term and at times intensive in addressing the problems leading to self-harm behavior.6
Dr. Strange is an assistant professor in the department of psychiatry at the University of Vermont Medical Center and University of Vermont Robert Larner College of Medicine, both in Burlington. She works with children and adolescents. She has no relevant financial disclosures.
References
1. Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (Arlington, Va.: American Psychiatric Association Publishing, 2013)
2. J Adolesc. 2014 Dec;37(8):1335-44.
3. Behav Ther. 2017 May; 48(3):366-79.
4. Acad Pediatr. 2012 May-Jun;12(3):205-13.
5. “Information for parents: What you need to know about self-injury.” The Fact Sheet Series, Cornell Research Program on Self-Injury and Recovery. 2009.
6. Clin Pediatr. 2016 Sep 13;55(11):1012-9.
Nonsuicidal self-injury (NSSI) has become more prevalent in youth over recent years and has many inherent risks. In the Diagnostic and Statistical Manual, Fifth Edition (DSM-5), NSSI is a diagnosis suggested for further study, and criteria include engaging in self-injury for 5 or more days without suicidal intent as well as self-injury associated with at least 1 of the following: obtaining relief from negative thoughts or feelings, resolving interpersonal challenges, inducing positive feelings. It is associated with interpersonal difficulties or negative thoughts/feelings. The behavior causes significant impairment in functioning and is not better explained by another condition.1
Estimates of lifetime prevalence in community-based samples of youth range from 15% to 20%. Individuals often start during early adolescence. It can pose many risks including infection, permanent scarring or disfigurement, decreased self-esteem, interpersonal conflict, severe injury, or death. Reasons for engaging in self-harm can vary and include attempts to regulate negative affect, to manage feelings of emptiness/numbness, regain a sense of control over body, feelings, etc., or to provide a consequence for perceived faults. Youth often may start to engage in self-harm covertly, and it may first become apparent in emergency or primary care settings. However, upon discovery, the response given also may affect future behavior.
Efforts also have been underway to distinguish between youth who engage in self-harm with and without suicidal ideation. Girls are more likely than are boys to report NSSI, although male NSSI may present differently. In addition to cutting or more stereotypical self-injury, they may punch walls or engage in fights or other risky behaviors as a proxy for self-harm. Risk factors for boys with regard to suicide attempts include hopelessness and history of sexual abuse. Maladaptive eating patterns and hopelessness were the two most significant factors for girls.4
With regard to issues of confidentiality, it will be important to carefully gauge level of safety and to clearly communicate with the patient (and family) limits of confidentiality. This may result in working within shades of gray to help maintain the therapeutic relationship and the patient’s comfort in being able to disclose potentially sensitive information.
Families can struggle with how to manage this, and it can generate fear as well as other strong emotions.
Tips for parents and guardians
- Validate the underlying emotions while not validating the behavior. Self-injury is a coping strategy. Focus on the driving forces for the actions rather than the actions themselves.
- Approach your child from a nonjudgmental stance.
- Recognize that change may not happen overnight, and that there may be periods of regression.
- Acknowledge successes when they occur.
- Make yourself available for open communication. Open-ended questions may facilitate more dialogue.
- Take care of yourself as well. Ensure you use your supports and are engaging in healthy self-care.
- Take the behavior seriously. While this behavior is relatively common, do not assume it is “just a phase.”
- While remaining supportive, it is important to maintain a parental role and to keep expectations rather than “walking on eggshells.”
- Involve the child in identifying what can be of support.
- Become aware of local crisis resources in your community. National resources include Call 1-800-273-TALK for the national suicide hotline or Text 741741 to connect with a crisis counselor.
Things to avoid
- Avoid taking a punitive stance. While the behavior can be provocative, most likely the primary purpose is not for attention.
- Avoid engaging in power struggles.
- Avoid creating increased isolation for the child. This can be a delicate balance with regard to peer groups, but encouraging healthy social interactions and activities is a way to help build resilience.
- Avoid taking the behavior personally.5
In working with youth who engage in self-harm, it is important to work within a team, which may include family, primary care, mental health support, school, and potentially other community supports. Treatment evidence is relatively limited, but there is some evidence to support use of cognitive behavioral therapy, dialectical behavior therapy, and mentalization-based therapy. Regardless, work will likely be long term and at times intensive in addressing the problems leading to self-harm behavior.6
Dr. Strange is an assistant professor in the department of psychiatry at the University of Vermont Medical Center and University of Vermont Robert Larner College of Medicine, both in Burlington. She works with children and adolescents. She has no relevant financial disclosures.
References
1. Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (Arlington, Va.: American Psychiatric Association Publishing, 2013)
2. J Adolesc. 2014 Dec;37(8):1335-44.
3. Behav Ther. 2017 May; 48(3):366-79.
4. Acad Pediatr. 2012 May-Jun;12(3):205-13.
5. “Information for parents: What you need to know about self-injury.” The Fact Sheet Series, Cornell Research Program on Self-Injury and Recovery. 2009.
6. Clin Pediatr. 2016 Sep 13;55(11):1012-9.
Suicide on the minds of many Utah teens
according to the Centers for Disease Control and Prevention.
Prevalence of suicidal ideation in 2015 was significantly higher among female students (25.5% vs. 13.7% for males), nonwhite students (23.4% vs. 18.7% for whites), those who were less religious (27.4% vs. 16.1% for religious students), and nonmembers of the Church of Latter Day Saints (27.1% vs. 15.3% for Mormons), Marissa L. Zwald, PhD, of the CDC’s Epidemic Intelligence Service and her associates reported in the Morbidity and Mortality Weekly Report.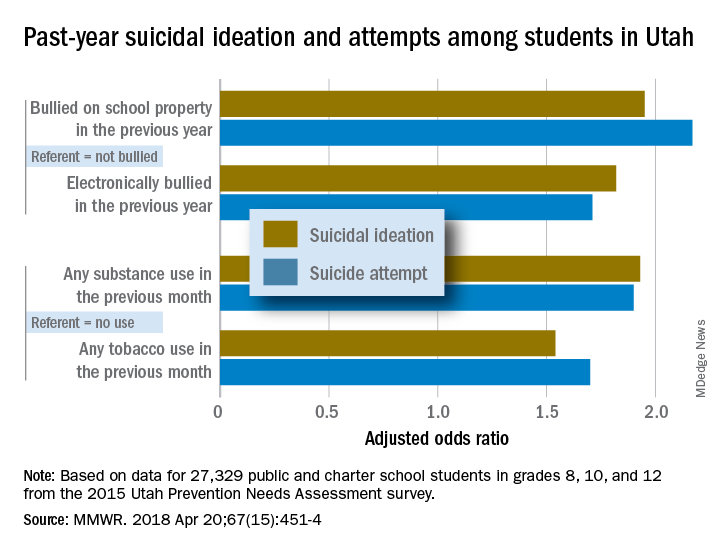
Risk factors included being bullied on school property in the previous year (adjusted odds ratios 1.95 for suicidal ideation and 2.17 for a suicide attempt, compared with those who were not bullied) and being electronically bullied (AOR of 1.82 for suicidal ideation and 1.71 for suicide attempt). Students who reported illicit substance use in the past month were more likely than nonusers to have suicidal ideation (AOR, 1.93) and to make a suicide attempt (AOR, 1.9); past-month use of tobacco, including e-cigarettes, increased risk, compared with no use, with an adjusted odds ratios of 1.54 for suicidal ideation and 1.7 for an attempt, the investigators reported.
They also looked at a number of possible protective factors, with a supportive family environment showing significance for both suicidal ideation and suicide attempts; the same was not true for prosocial behaviors or supportive community, school, or peer environments. “Possible prevention strategies to consider could include integrating family members and the home setting into existing or new interventions and identifying and addressing the needs of youths exhibiting risk factors identified in this investigation,” Dr. Zwald and her associates wrote.
SOURCE: Zwald ML et al. MMWR. 2018 Apr 20;67(15):451-4.
according to the Centers for Disease Control and Prevention.
Prevalence of suicidal ideation in 2015 was significantly higher among female students (25.5% vs. 13.7% for males), nonwhite students (23.4% vs. 18.7% for whites), those who were less religious (27.4% vs. 16.1% for religious students), and nonmembers of the Church of Latter Day Saints (27.1% vs. 15.3% for Mormons), Marissa L. Zwald, PhD, of the CDC’s Epidemic Intelligence Service and her associates reported in the Morbidity and Mortality Weekly Report.
Risk factors included being bullied on school property in the previous year (adjusted odds ratios 1.95 for suicidal ideation and 2.17 for a suicide attempt, compared with those who were not bullied) and being electronically bullied (AOR of 1.82 for suicidal ideation and 1.71 for suicide attempt). Students who reported illicit substance use in the past month were more likely than nonusers to have suicidal ideation (AOR, 1.93) and to make a suicide attempt (AOR, 1.9); past-month use of tobacco, including e-cigarettes, increased risk, compared with no use, with an adjusted odds ratios of 1.54 for suicidal ideation and 1.7 for an attempt, the investigators reported.
They also looked at a number of possible protective factors, with a supportive family environment showing significance for both suicidal ideation and suicide attempts; the same was not true for prosocial behaviors or supportive community, school, or peer environments. “Possible prevention strategies to consider could include integrating family members and the home setting into existing or new interventions and identifying and addressing the needs of youths exhibiting risk factors identified in this investigation,” Dr. Zwald and her associates wrote.
SOURCE: Zwald ML et al. MMWR. 2018 Apr 20;67(15):451-4.
according to the Centers for Disease Control and Prevention.
Prevalence of suicidal ideation in 2015 was significantly higher among female students (25.5% vs. 13.7% for males), nonwhite students (23.4% vs. 18.7% for whites), those who were less religious (27.4% vs. 16.1% for religious students), and nonmembers of the Church of Latter Day Saints (27.1% vs. 15.3% for Mormons), Marissa L. Zwald, PhD, of the CDC’s Epidemic Intelligence Service and her associates reported in the Morbidity and Mortality Weekly Report.
Risk factors included being bullied on school property in the previous year (adjusted odds ratios 1.95 for suicidal ideation and 2.17 for a suicide attempt, compared with those who were not bullied) and being electronically bullied (AOR of 1.82 for suicidal ideation and 1.71 for suicide attempt). Students who reported illicit substance use in the past month were more likely than nonusers to have suicidal ideation (AOR, 1.93) and to make a suicide attempt (AOR, 1.9); past-month use of tobacco, including e-cigarettes, increased risk, compared with no use, with an adjusted odds ratios of 1.54 for suicidal ideation and 1.7 for an attempt, the investigators reported.
They also looked at a number of possible protective factors, with a supportive family environment showing significance for both suicidal ideation and suicide attempts; the same was not true for prosocial behaviors or supportive community, school, or peer environments. “Possible prevention strategies to consider could include integrating family members and the home setting into existing or new interventions and identifying and addressing the needs of youths exhibiting risk factors identified in this investigation,” Dr. Zwald and her associates wrote.
SOURCE: Zwald ML et al. MMWR. 2018 Apr 20;67(15):451-4.
FROM MMWR
Proximal Humerus Fracture 3-D Modeling
ABSTRACT
The objective of this study is to determine the reproducibility and feasibility of using 3-dimensional (3-D) computer simulation of proximal humerus fracture computed tomography (CT) scans for fracture reduction. We hypothesized that anatomic reconstruction with 3-D models would be anatomically accurate and reproducible.
Preoperative CT scans of 28 patients with 3- and 4-part (AO classification 11-B1, 11-B2, 11-C1, 11-C2) proximal humerus fractures who were treated by hemiarthroplasty were converted into 3-D computer models. The displaced fractured fragments were anatomically reduced with computer simulation by 2 fellowship-trained shoulder surgeons, and measurements were made of the reconstructed proximal humerus.
The measurements of the reconstructed models had very good to excellent interobserver and intraobserver reliability. The reconstructions of these humerus fractures showed interclass correlation coefficients ranging from 0.71 to 0.93 between 1 observer and from 0.82 to 0.98 between 2 different observers. The fracture reduction was judged against normal proximal humerus geometry to determine reduction accuracy.
The 3-D modeling techniques used to reconstruct 3- and 4-part proximal humerus fractures were reliable and accurate. This technique of modeling and reconstructing proximal humerus fractures could be used to enhance the preoperative planning of open reduction and internal fixation or hemiarthroplasty for 3- and 4-part proximal humerus fractures.
The treatment of proximal humerus fractures is influenced by multiple factors, including patient age, associated injuries, bone quality, and fracture pattern. Three- and 4-part fractures are among the more severe of these fractures, which may result in vascular compromise to the humeral head, leading to avascular necrosis. Surgical goals for the management of these fractures are to optimize functional outcomes by re-creating a stable construct with a functional rotator cuff by open reduction and internal fixation (ORIF), hemiarthroplasty with tuberosity ORIF, or reverse shoulder replacement. Achieving a good outcome following hemiarthroplasty is dependent on many factors, including anatomic tuberosity healing and component positioning.1,2,3 Repairing the greater tuberosity in a near-anatomic position has been shown to greatly affect the results of hemiarthroplasty for fracture.3,4
Continue to: Three-dimensional (3-D) modeling...
Three-dimensional (3-D) modeling is increasingly being used in preoperative planning of shoulder arthroplasty and determining proper proximal humeral fracture treatment. 5 However, no studies have examined the reconstruction of a fractured proximal humerus into native anatomy using computer simulation. The purpose of this study is to determine the accuracy and reliability of anatomically reconstructing the preinjury proximal humerus using 3-D computer models created from postinjury computed tomography (CT) scans. The results of this study could lead to useful techniques employing CT–based models for patient-specific preoperative planning of proximal humeral fracture ORIF and during tuberosity reduction and fixation during hemiarthroplasty for fracture. We hypothesize that it is feasible to reconstruct the original anatomy of the proximal humerus by using 3-D computer modeling of proximal humerus fractures with high reliability based on interobserver and intraobserver review.
METHODS
After Institutional Review Board approval was obtained, we reviewed the medical records of consecutive patients with a diagnosis of proximal humeral fracture and the treatment codes for hemiarthroplasty from 2000 to 2013. Inclusion criteria included 3- and 4-part fractures (AO classifications 11-B1, 11-B2, 11-C1, 11-C2). CT scans with insufficient quality to differentiate bone from soft tissue (inadequate signal-to-noise ratio) were excluded from the study. A total of 28 patients with adequate CT scans met the criteria for inclusion in this study.
The CT scan protocol included 0.5-mm axial cuts with inclusion of the proximal humerus in the Digital Imaging and Communications in Medicine format. These CT scans were converted into patient-specific 3-D computer models of the shoulder using Mimics software (Materialise Inc.). The use of this software to produce anatomically accurate models has previously been verified in a shoulder model.6,7 The tuberosity fragments were then individually separated from each other using the voxel-selecting capabilities of 3-D software and manipulated with translation and rotation for anatomic reduction (Figures 1A-1D, Figure 2). 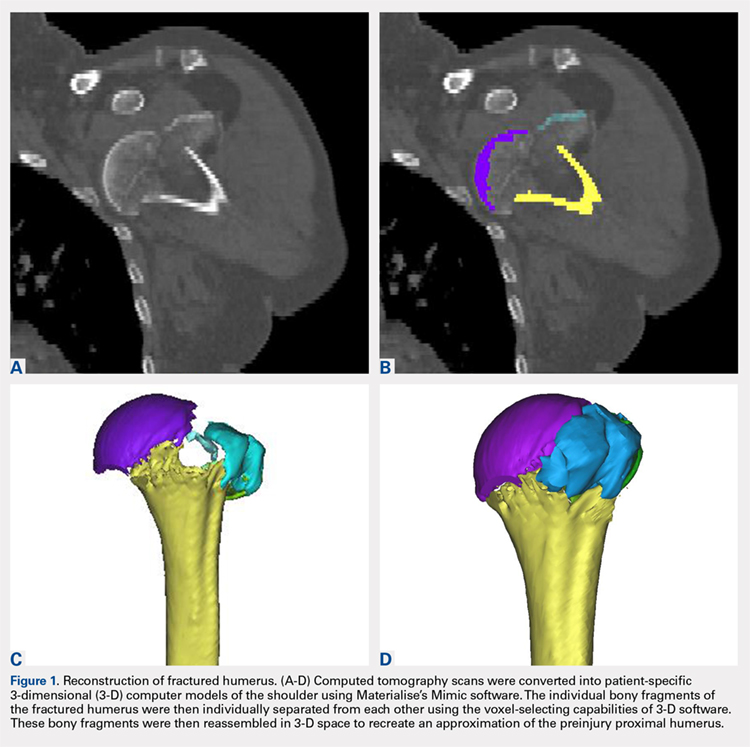
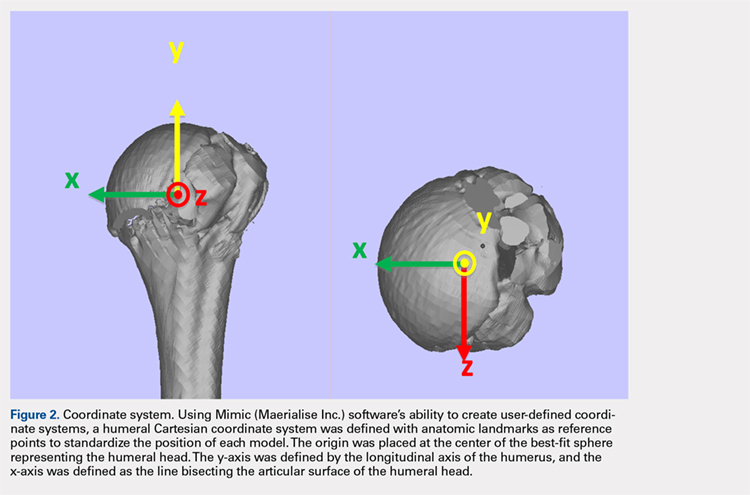
The de-identified anatomically reconstructed shoulder models were then uploaded into Materialise’s Magics rapid prototyping software, and a user-defined humeral Cartesian coordinate system was defined with anatomic landmarks as reference points to standardize the position of each model (Figure 3).8,9 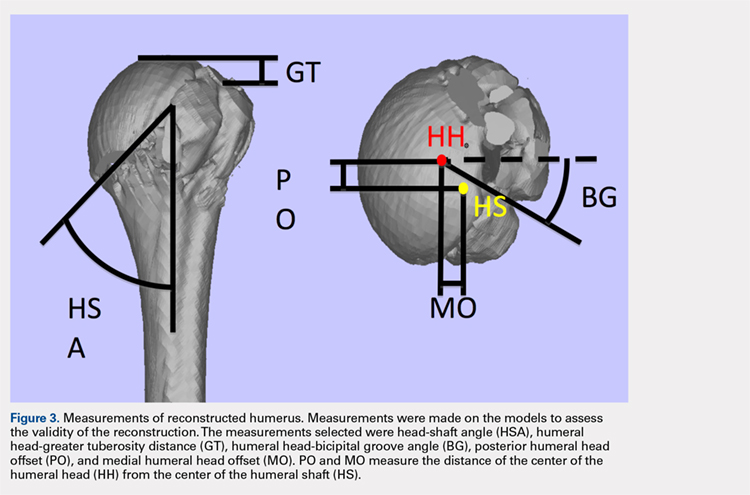
A series of measurements were made on these models to assess the validity and reliability of the reassembly. The bicipital groove at the anatomic neck was used to measure humeral head version as described by Kummer and colleagues.10 The head-shaft angle, humeral head-greater tuberosity distance, humeral head-bicipital groove angle, and posterior and medial humeral head offset were measured directly on the reconstructed humerus.
Continue to: Two fellowship-trained shoulder...
Two fellowship-trained shoulder surgeons independently reassembled these fracture fragments via computer simulation. Interobserver reliability testing was conducted on these reconstructions by measuring the geometry between the 2 different surgeons’ reconstructions. Intraobserver reliability testing was conducted by 1 surgeon repeating the reconstructions with 4-week intervals between trials and measuring the geometry between the 2 different trials. The average dimensions of the reconstructed proximal humerus fractures were compared with the geometry of normal humeri reported in previously conducted anatomic studies.11,12,13
STATISTICS
The measured dimensions of the 28 reassembled proximal humeri models were averaged across all trials between the 2 fellowship-trained surgeons and compared with the range of normal dimensions of a healthy proximal humerus using the 2 one-sided tests (TOST) method for equivalence between 2 means given a range. The interobserver and intraobserver reliabilities were quantified using the interclass correlation coefficient. An excellent correlation was defined as a correlation coefficient >0.81; very good was defined as 0.61 to 0.80; and good was defined as 0.41 to 0.60.
RESULTS
Of the patients studied, 9 (32.1%) were male, and the average age at the time of CT scanning was 72 years. Of the 28 patients with fracture, 18 (64.2%) had 3-part fractures (AO classifications 11-B1, 11-B2), and 10 (35.8%) had 4-part fractures (AO classifications 11-C1, 11-C2). When examining the location of the intertubercular fracture line, we found that 13 (46.4%) fractures went through the bicipital groove. Of the remaining fracture lines, 9 (32.1%) extended into the greater tuberosity and 6 (21.4%) extended into the lesser tuberosity.
All users were able to reconstruct all 28 fractures using this technique. The average measured dimensions fell within the range of dimensions of a normal healthy proximal humerus specified in the literature to within a 95% confidence interval using the TOST for equivalence, in which we compared measured values with ranges reported in the literature (Table).11,12,13
Table. Dimensions of Proximal Humerus Geometry
| Normal Parameters | Average Dimensions From Trials | Dimensions From Literature |
| Head shaft angle | 43.5° ± 1° | 42.5° ± 12.5° |
| Head to greater tuberosity distance | 4.9 mm ± 0.4 mm | 8 mm ± 3.2 mm |
Head to bicipital groove angle (anatomic neck) | 26.4° ± 2° | 27.3° ± 14° |
| Posterior humeral head offset | 1.6 mm ± 0.3 mm | 4 mm ± 6 mm |
| Medial humeral head offset | 4.5 mm ± 0.3 mm | 9 mm ± 5 mm |
The reconstructions of these humerus fractures showed intraclass correlation coefficients ranging from 0.71 to 0.93 in 1 observer and interclass correlation coefficients from 0.82 to 0.98 between 2 different observers (Table).
DISCUSSION
This study demonstrates that it is feasible to reliably and accurately reconstruct the original anatomy of the proximal humerus by using 3-D computer modeling of proximal humerus fractures. Poor outcomes after hemiarthroplasty for proximal humerus fractures are mostly related to tuberosity malpositioning, resorption, or failure of fixation and resultant dysfunction of the rotator cuff.14,15,16 These studies highlight the importance of accurate tuberosity reduction during surgical care of these fractures.
Continue to: The 3-D computer model...
The 3-D computer model reconstruction of 3- and 4-part proximal humerus fractures were reliable and valid. The interclass correlation coefficients showed very good to excellent interobserver and intraobserver reliability for all measurements conducted. The averaged dimensions from all trials fell within the appropriate range of dimensions for a normal healthy humerus reported in the literature, as verified by the TOST method.11,12,13 The 3-D modeling capabilities demonstrated in this study allowed a greater understanding of the fracture patterns present in 3- and 4-part (AO classifications 11-B1, 11-B2, 11-C1, 11-C2) humerus fractures.
Overreduction of greater tuberosity to create cortical overlap with the lateral shaft may be used to promote bony union. As a result of this distalization, there may be extra strains placed on the rotator cuff, making the patient more prone to rotator cuff tear, as well as improperly balancing the dynamic stabilizers of the shoulder. Poor clinical outcomes in hemiarthroplasty for proximal humerus fractures have been correlated with a greater tuberosity placed distal relative to the humeral head by 1 cm in a study2 and by 2 cm in another.3
This study has several limitations. The first is the assumption that our injured patients had preinjury proximal humerus geometry within the range of normal dimensions of a healthy humerus. Unfortunately, because we were unable to obtain CT scans of the contralateral shoulder, we had to use standard proximal humerus geometry as the control. Another limitation, inherent in the technique, is that only cortical and dense trabecular bone was modeled, so that comminuted or osteoporotic bone was not well modeled. This study did not correlate the findings from these models with clinical outcomes. A prospective study is needed to evaluate the impact of this 3-D modeling on fracture reductions and clinical outcomes.
This study demonstrates that patient-specific modeling of proximal humerus fracture 3-D CT scans may help surgeons reliably and accurately reconstruct fractures. This technique may have utility in the preoperative planning of tuberosity fracture reduction and hemiarthroplasty. It gives surgeons the ability to visualize fracture fragments, and the process of reconstructing the fragments may help surgeons understand the required maneuvers for reduction at the time of surgery. This technique also provides dimensions of the patient’s native humerus, thus potentially improving the anatomic accuracy of the reduction or hemiarthroplasty reconstruction. With the new trend toward patient-specific instrumentation, this study also provides a means of planning the size of the humeral prostheses as well as the version relative to the biceps groove and intertubercular fracture line.
CONCLUSION
This study demonstrates the feasibility of using 3-D computer modeling of complex proximal humerus fractures in anatomic reconstruction. These techniques of computer-simulated 3-D models are valid and reliable. We believe that this technique of modeling and reconstructing proximal humerus fractures could be used to enhance the preoperative planning of hemiarthroplasty for 3- and 4-part proximal humerus fractures by providing improved understanding of the patient’s native humeral geometry and tuberosity reduction.
1. Boileau P, Krishnan SG, Tinsi L, Walch G, Coste JS, Mole D. Tuberosity malposition and migration: reasons for poor outcomes after hemiarthroplasty for displaced fractures of the proximal humerus. J Shoulder Elbow Surg. 2002;11(5):401-412. doi:10.1067/mse.2002.124527.
2. Mighell MA, Kolm GP, Collinge CA, Frankle MA. Outcomes of hemiarthroplasty for fractures of the proximal humerus. J Shoulder Elbow Surg. 2003;12(6):569-577. doi:10.1016/S1058274603002131.
3. Greiner SH, Kaab MJ, Kroning I, Scheibel M, Perka C. Reconstruction of humeral length and centering of the prosthetic head in hemiarthroplasty for proximal humeral fractures. J Shoulder Elbow Surg. 2008;17(5):709-714. doi:10.1016/j.jse.2008.03.004.
4. Smith AM, Mardones RM, Sperling JW, Cofield RH. Early complications of operatively treated proximal humeral fractures. J Shoulder Elbow Surg. 2007;16(1):14-24. doi:10.1016/j.jse.2006.05.008.
5. Scalise JJ, Codsi MJ, Bryan J, Iannotti JP. The three-dimensional glenoid vault model can estimate normal glenoid version in osteoarthritis. J Shoulder Elbow Surg. 2008;17(3):487-491. doi:10.1016/j.jse.2007.09.006.
6. Bryce CD, Pennypacker JL, Kulkarni N, et al. Validation of three-dimensional models of in situ scapulae. J Shoulder Elbow Surg. 2008;17(5):825-832. doi:10.1016/j.jse.2008.01.141.
7. Yongpravat C, Kim HM, Gardner TR, Bigliani LU, Levine WN, Ahmad CS. Glenoid implant orientation and cement failure in total shoulder arthroplasty: a finite element analysis. J Shoulder Elbow Surg. 2013;22(7):940-947. doi:10.1016/j.jse.2012.09.007.
8. Boileau P, Walch G. The three-dimensional geometry of the proximal humerus. Implications for surgical technique and prosthetic design. J Bone Joint Surg Br. 1997;79(5):857-865. doi:10.1302/0301-620X.79B5.0790857.
9. Wu G, van der Helm FC, Veeger HE, et al. ISB recommendation on definitions of joint coordinate systems of various joints for the reporting of human joint motion--Part II: shoulder, elbow, wrist and hand. J Biomech. 2005;38(5):981-992.
10. Kummer FJ, Perkins R, Zuckerman JD. The use of the bicipital groove for alignment of the humeral stem in shoulder arthroplasty. J Shoulder Elbow Surg. 1998;7(2):144-146. doi:10.1016/S1058-2746(98)90225-7.
11. Iannotti JP, Gabriel JP, Schneck SL, Evans BG, Misra S. The normal glenohumeral relationships. An anatomical study of one hundred and forty shoulders. J Bone Joint Surg Am. 1992;74(4):491-500.
12. Pearl ML, Volk AG. Coronal plane geometry of the proximal humerus relevant to prosthetic arthroplasty. J Shoulder Elbow Surg. 1996;5(4):320-326. doi:10.1016/S1058-2746(96)80060-7.
13. Pearl ML. Proximal humeral anatomy in shoulder arthroplasty: Implications for prosthetic design and surgical technique. J Shoulder Elbow Surg. 2005;14(1 Suppl S):99S-104S. doi:10.1016/j.jse.2004.09.025.
14. Prakash U, McGurty DW, Dent JA. Hemiarthroplasty for severe fractures of the proximal humerus. J Shoulder Elbow Surg. 2002;11(5):428-430. doi:10.1067/mse.2002.126615.
15. Robinson CM, Page RS, Hill RM, Sanders DL, Court-Brown CM, Wakefield AE. Primary hemiarthroplasty for treatment of proximal humeral fractures. J Bone Joint Surg Am. 2003;85-A(7):1215-1223.
16. Zyto K, Wallace WA, Frostick SP, Preston BJ. Outcome after hemiarthroplasty for three- and four-part fractures of the proximal humerus. J Shoulder Elbow Surg. 1998;7(2):85-89. doi:10.1016/S1058-2746(98)90215-4.
ABSTRACT
The objective of this study is to determine the reproducibility and feasibility of using 3-dimensional (3-D) computer simulation of proximal humerus fracture computed tomography (CT) scans for fracture reduction. We hypothesized that anatomic reconstruction with 3-D models would be anatomically accurate and reproducible.
Preoperative CT scans of 28 patients with 3- and 4-part (AO classification 11-B1, 11-B2, 11-C1, 11-C2) proximal humerus fractures who were treated by hemiarthroplasty were converted into 3-D computer models. The displaced fractured fragments were anatomically reduced with computer simulation by 2 fellowship-trained shoulder surgeons, and measurements were made of the reconstructed proximal humerus.
The measurements of the reconstructed models had very good to excellent interobserver and intraobserver reliability. The reconstructions of these humerus fractures showed interclass correlation coefficients ranging from 0.71 to 0.93 between 1 observer and from 0.82 to 0.98 between 2 different observers. The fracture reduction was judged against normal proximal humerus geometry to determine reduction accuracy.
The 3-D modeling techniques used to reconstruct 3- and 4-part proximal humerus fractures were reliable and accurate. This technique of modeling and reconstructing proximal humerus fractures could be used to enhance the preoperative planning of open reduction and internal fixation or hemiarthroplasty for 3- and 4-part proximal humerus fractures.
The treatment of proximal humerus fractures is influenced by multiple factors, including patient age, associated injuries, bone quality, and fracture pattern. Three- and 4-part fractures are among the more severe of these fractures, which may result in vascular compromise to the humeral head, leading to avascular necrosis. Surgical goals for the management of these fractures are to optimize functional outcomes by re-creating a stable construct with a functional rotator cuff by open reduction and internal fixation (ORIF), hemiarthroplasty with tuberosity ORIF, or reverse shoulder replacement. Achieving a good outcome following hemiarthroplasty is dependent on many factors, including anatomic tuberosity healing and component positioning.1,2,3 Repairing the greater tuberosity in a near-anatomic position has been shown to greatly affect the results of hemiarthroplasty for fracture.3,4
Continue to: Three-dimensional (3-D) modeling...
Three-dimensional (3-D) modeling is increasingly being used in preoperative planning of shoulder arthroplasty and determining proper proximal humeral fracture treatment. 5 However, no studies have examined the reconstruction of a fractured proximal humerus into native anatomy using computer simulation. The purpose of this study is to determine the accuracy and reliability of anatomically reconstructing the preinjury proximal humerus using 3-D computer models created from postinjury computed tomography (CT) scans. The results of this study could lead to useful techniques employing CT–based models for patient-specific preoperative planning of proximal humeral fracture ORIF and during tuberosity reduction and fixation during hemiarthroplasty for fracture. We hypothesize that it is feasible to reconstruct the original anatomy of the proximal humerus by using 3-D computer modeling of proximal humerus fractures with high reliability based on interobserver and intraobserver review.
METHODS
After Institutional Review Board approval was obtained, we reviewed the medical records of consecutive patients with a diagnosis of proximal humeral fracture and the treatment codes for hemiarthroplasty from 2000 to 2013. Inclusion criteria included 3- and 4-part fractures (AO classifications 11-B1, 11-B2, 11-C1, 11-C2). CT scans with insufficient quality to differentiate bone from soft tissue (inadequate signal-to-noise ratio) were excluded from the study. A total of 28 patients with adequate CT scans met the criteria for inclusion in this study.
The CT scan protocol included 0.5-mm axial cuts with inclusion of the proximal humerus in the Digital Imaging and Communications in Medicine format. These CT scans were converted into patient-specific 3-D computer models of the shoulder using Mimics software (Materialise Inc.). The use of this software to produce anatomically accurate models has previously been verified in a shoulder model.6,7 The tuberosity fragments were then individually separated from each other using the voxel-selecting capabilities of 3-D software and manipulated with translation and rotation for anatomic reduction (Figures 1A-1D, Figure 2).
The de-identified anatomically reconstructed shoulder models were then uploaded into Materialise’s Magics rapid prototyping software, and a user-defined humeral Cartesian coordinate system was defined with anatomic landmarks as reference points to standardize the position of each model (Figure 3).8,9
A series of measurements were made on these models to assess the validity and reliability of the reassembly. The bicipital groove at the anatomic neck was used to measure humeral head version as described by Kummer and colleagues.10 The head-shaft angle, humeral head-greater tuberosity distance, humeral head-bicipital groove angle, and posterior and medial humeral head offset were measured directly on the reconstructed humerus.
Continue to: Two fellowship-trained shoulder...
Two fellowship-trained shoulder surgeons independently reassembled these fracture fragments via computer simulation. Interobserver reliability testing was conducted on these reconstructions by measuring the geometry between the 2 different surgeons’ reconstructions. Intraobserver reliability testing was conducted by 1 surgeon repeating the reconstructions with 4-week intervals between trials and measuring the geometry between the 2 different trials. The average dimensions of the reconstructed proximal humerus fractures were compared with the geometry of normal humeri reported in previously conducted anatomic studies.11,12,13
STATISTICS
The measured dimensions of the 28 reassembled proximal humeri models were averaged across all trials between the 2 fellowship-trained surgeons and compared with the range of normal dimensions of a healthy proximal humerus using the 2 one-sided tests (TOST) method for equivalence between 2 means given a range. The interobserver and intraobserver reliabilities were quantified using the interclass correlation coefficient. An excellent correlation was defined as a correlation coefficient >0.81; very good was defined as 0.61 to 0.80; and good was defined as 0.41 to 0.60.
RESULTS
Of the patients studied, 9 (32.1%) were male, and the average age at the time of CT scanning was 72 years. Of the 28 patients with fracture, 18 (64.2%) had 3-part fractures (AO classifications 11-B1, 11-B2), and 10 (35.8%) had 4-part fractures (AO classifications 11-C1, 11-C2). When examining the location of the intertubercular fracture line, we found that 13 (46.4%) fractures went through the bicipital groove. Of the remaining fracture lines, 9 (32.1%) extended into the greater tuberosity and 6 (21.4%) extended into the lesser tuberosity.
All users were able to reconstruct all 28 fractures using this technique. The average measured dimensions fell within the range of dimensions of a normal healthy proximal humerus specified in the literature to within a 95% confidence interval using the TOST for equivalence, in which we compared measured values with ranges reported in the literature (Table).11,12,13
Table. Dimensions of Proximal Humerus Geometry
| Normal Parameters | Average Dimensions From Trials | Dimensions From Literature |
| Head shaft angle | 43.5° ± 1° | 42.5° ± 12.5° |
| Head to greater tuberosity distance | 4.9 mm ± 0.4 mm | 8 mm ± 3.2 mm |
Head to bicipital groove angle (anatomic neck) | 26.4° ± 2° | 27.3° ± 14° |
| Posterior humeral head offset | 1.6 mm ± 0.3 mm | 4 mm ± 6 mm |
| Medial humeral head offset | 4.5 mm ± 0.3 mm | 9 mm ± 5 mm |
The reconstructions of these humerus fractures showed intraclass correlation coefficients ranging from 0.71 to 0.93 in 1 observer and interclass correlation coefficients from 0.82 to 0.98 between 2 different observers (Table).
DISCUSSION
This study demonstrates that it is feasible to reliably and accurately reconstruct the original anatomy of the proximal humerus by using 3-D computer modeling of proximal humerus fractures. Poor outcomes after hemiarthroplasty for proximal humerus fractures are mostly related to tuberosity malpositioning, resorption, or failure of fixation and resultant dysfunction of the rotator cuff.14,15,16 These studies highlight the importance of accurate tuberosity reduction during surgical care of these fractures.
Continue to: The 3-D computer model...
The 3-D computer model reconstruction of 3- and 4-part proximal humerus fractures were reliable and valid. The interclass correlation coefficients showed very good to excellent interobserver and intraobserver reliability for all measurements conducted. The averaged dimensions from all trials fell within the appropriate range of dimensions for a normal healthy humerus reported in the literature, as verified by the TOST method.11,12,13 The 3-D modeling capabilities demonstrated in this study allowed a greater understanding of the fracture patterns present in 3- and 4-part (AO classifications 11-B1, 11-B2, 11-C1, 11-C2) humerus fractures.
Overreduction of greater tuberosity to create cortical overlap with the lateral shaft may be used to promote bony union. As a result of this distalization, there may be extra strains placed on the rotator cuff, making the patient more prone to rotator cuff tear, as well as improperly balancing the dynamic stabilizers of the shoulder. Poor clinical outcomes in hemiarthroplasty for proximal humerus fractures have been correlated with a greater tuberosity placed distal relative to the humeral head by 1 cm in a study2 and by 2 cm in another.3
This study has several limitations. The first is the assumption that our injured patients had preinjury proximal humerus geometry within the range of normal dimensions of a healthy humerus. Unfortunately, because we were unable to obtain CT scans of the contralateral shoulder, we had to use standard proximal humerus geometry as the control. Another limitation, inherent in the technique, is that only cortical and dense trabecular bone was modeled, so that comminuted or osteoporotic bone was not well modeled. This study did not correlate the findings from these models with clinical outcomes. A prospective study is needed to evaluate the impact of this 3-D modeling on fracture reductions and clinical outcomes.
This study demonstrates that patient-specific modeling of proximal humerus fracture 3-D CT scans may help surgeons reliably and accurately reconstruct fractures. This technique may have utility in the preoperative planning of tuberosity fracture reduction and hemiarthroplasty. It gives surgeons the ability to visualize fracture fragments, and the process of reconstructing the fragments may help surgeons understand the required maneuvers for reduction at the time of surgery. This technique also provides dimensions of the patient’s native humerus, thus potentially improving the anatomic accuracy of the reduction or hemiarthroplasty reconstruction. With the new trend toward patient-specific instrumentation, this study also provides a means of planning the size of the humeral prostheses as well as the version relative to the biceps groove and intertubercular fracture line.
CONCLUSION
This study demonstrates the feasibility of using 3-D computer modeling of complex proximal humerus fractures in anatomic reconstruction. These techniques of computer-simulated 3-D models are valid and reliable. We believe that this technique of modeling and reconstructing proximal humerus fractures could be used to enhance the preoperative planning of hemiarthroplasty for 3- and 4-part proximal humerus fractures by providing improved understanding of the patient’s native humeral geometry and tuberosity reduction.
ABSTRACT
The objective of this study is to determine the reproducibility and feasibility of using 3-dimensional (3-D) computer simulation of proximal humerus fracture computed tomography (CT) scans for fracture reduction. We hypothesized that anatomic reconstruction with 3-D models would be anatomically accurate and reproducible.
Preoperative CT scans of 28 patients with 3- and 4-part (AO classification 11-B1, 11-B2, 11-C1, 11-C2) proximal humerus fractures who were treated by hemiarthroplasty were converted into 3-D computer models. The displaced fractured fragments were anatomically reduced with computer simulation by 2 fellowship-trained shoulder surgeons, and measurements were made of the reconstructed proximal humerus.
The measurements of the reconstructed models had very good to excellent interobserver and intraobserver reliability. The reconstructions of these humerus fractures showed interclass correlation coefficients ranging from 0.71 to 0.93 between 1 observer and from 0.82 to 0.98 between 2 different observers. The fracture reduction was judged against normal proximal humerus geometry to determine reduction accuracy.
The 3-D modeling techniques used to reconstruct 3- and 4-part proximal humerus fractures were reliable and accurate. This technique of modeling and reconstructing proximal humerus fractures could be used to enhance the preoperative planning of open reduction and internal fixation or hemiarthroplasty for 3- and 4-part proximal humerus fractures.
The treatment of proximal humerus fractures is influenced by multiple factors, including patient age, associated injuries, bone quality, and fracture pattern. Three- and 4-part fractures are among the more severe of these fractures, which may result in vascular compromise to the humeral head, leading to avascular necrosis. Surgical goals for the management of these fractures are to optimize functional outcomes by re-creating a stable construct with a functional rotator cuff by open reduction and internal fixation (ORIF), hemiarthroplasty with tuberosity ORIF, or reverse shoulder replacement. Achieving a good outcome following hemiarthroplasty is dependent on many factors, including anatomic tuberosity healing and component positioning.1,2,3 Repairing the greater tuberosity in a near-anatomic position has been shown to greatly affect the results of hemiarthroplasty for fracture.3,4
Continue to: Three-dimensional (3-D) modeling...
Three-dimensional (3-D) modeling is increasingly being used in preoperative planning of shoulder arthroplasty and determining proper proximal humeral fracture treatment. 5 However, no studies have examined the reconstruction of a fractured proximal humerus into native anatomy using computer simulation. The purpose of this study is to determine the accuracy and reliability of anatomically reconstructing the preinjury proximal humerus using 3-D computer models created from postinjury computed tomography (CT) scans. The results of this study could lead to useful techniques employing CT–based models for patient-specific preoperative planning of proximal humeral fracture ORIF and during tuberosity reduction and fixation during hemiarthroplasty for fracture. We hypothesize that it is feasible to reconstruct the original anatomy of the proximal humerus by using 3-D computer modeling of proximal humerus fractures with high reliability based on interobserver and intraobserver review.
METHODS
After Institutional Review Board approval was obtained, we reviewed the medical records of consecutive patients with a diagnosis of proximal humeral fracture and the treatment codes for hemiarthroplasty from 2000 to 2013. Inclusion criteria included 3- and 4-part fractures (AO classifications 11-B1, 11-B2, 11-C1, 11-C2). CT scans with insufficient quality to differentiate bone from soft tissue (inadequate signal-to-noise ratio) were excluded from the study. A total of 28 patients with adequate CT scans met the criteria for inclusion in this study.
The CT scan protocol included 0.5-mm axial cuts with inclusion of the proximal humerus in the Digital Imaging and Communications in Medicine format. These CT scans were converted into patient-specific 3-D computer models of the shoulder using Mimics software (Materialise Inc.). The use of this software to produce anatomically accurate models has previously been verified in a shoulder model.6,7 The tuberosity fragments were then individually separated from each other using the voxel-selecting capabilities of 3-D software and manipulated with translation and rotation for anatomic reduction (Figures 1A-1D, Figure 2).
The de-identified anatomically reconstructed shoulder models were then uploaded into Materialise’s Magics rapid prototyping software, and a user-defined humeral Cartesian coordinate system was defined with anatomic landmarks as reference points to standardize the position of each model (Figure 3).8,9
A series of measurements were made on these models to assess the validity and reliability of the reassembly. The bicipital groove at the anatomic neck was used to measure humeral head version as described by Kummer and colleagues.10 The head-shaft angle, humeral head-greater tuberosity distance, humeral head-bicipital groove angle, and posterior and medial humeral head offset were measured directly on the reconstructed humerus.
Continue to: Two fellowship-trained shoulder...
Two fellowship-trained shoulder surgeons independently reassembled these fracture fragments via computer simulation. Interobserver reliability testing was conducted on these reconstructions by measuring the geometry between the 2 different surgeons’ reconstructions. Intraobserver reliability testing was conducted by 1 surgeon repeating the reconstructions with 4-week intervals between trials and measuring the geometry between the 2 different trials. The average dimensions of the reconstructed proximal humerus fractures were compared with the geometry of normal humeri reported in previously conducted anatomic studies.11,12,13
STATISTICS
The measured dimensions of the 28 reassembled proximal humeri models were averaged across all trials between the 2 fellowship-trained surgeons and compared with the range of normal dimensions of a healthy proximal humerus using the 2 one-sided tests (TOST) method for equivalence between 2 means given a range. The interobserver and intraobserver reliabilities were quantified using the interclass correlation coefficient. An excellent correlation was defined as a correlation coefficient >0.81; very good was defined as 0.61 to 0.80; and good was defined as 0.41 to 0.60.
RESULTS
Of the patients studied, 9 (32.1%) were male, and the average age at the time of CT scanning was 72 years. Of the 28 patients with fracture, 18 (64.2%) had 3-part fractures (AO classifications 11-B1, 11-B2), and 10 (35.8%) had 4-part fractures (AO classifications 11-C1, 11-C2). When examining the location of the intertubercular fracture line, we found that 13 (46.4%) fractures went through the bicipital groove. Of the remaining fracture lines, 9 (32.1%) extended into the greater tuberosity and 6 (21.4%) extended into the lesser tuberosity.
All users were able to reconstruct all 28 fractures using this technique. The average measured dimensions fell within the range of dimensions of a normal healthy proximal humerus specified in the literature to within a 95% confidence interval using the TOST for equivalence, in which we compared measured values with ranges reported in the literature (Table).11,12,13
Table. Dimensions of Proximal Humerus Geometry
| Normal Parameters | Average Dimensions From Trials | Dimensions From Literature |
| Head shaft angle | 43.5° ± 1° | 42.5° ± 12.5° |
| Head to greater tuberosity distance | 4.9 mm ± 0.4 mm | 8 mm ± 3.2 mm |
Head to bicipital groove angle (anatomic neck) | 26.4° ± 2° | 27.3° ± 14° |
| Posterior humeral head offset | 1.6 mm ± 0.3 mm | 4 mm ± 6 mm |
| Medial humeral head offset | 4.5 mm ± 0.3 mm | 9 mm ± 5 mm |
The reconstructions of these humerus fractures showed intraclass correlation coefficients ranging from 0.71 to 0.93 in 1 observer and interclass correlation coefficients from 0.82 to 0.98 between 2 different observers (Table).
DISCUSSION
This study demonstrates that it is feasible to reliably and accurately reconstruct the original anatomy of the proximal humerus by using 3-D computer modeling of proximal humerus fractures. Poor outcomes after hemiarthroplasty for proximal humerus fractures are mostly related to tuberosity malpositioning, resorption, or failure of fixation and resultant dysfunction of the rotator cuff.14,15,16 These studies highlight the importance of accurate tuberosity reduction during surgical care of these fractures.
Continue to: The 3-D computer model...
The 3-D computer model reconstruction of 3- and 4-part proximal humerus fractures were reliable and valid. The interclass correlation coefficients showed very good to excellent interobserver and intraobserver reliability for all measurements conducted. The averaged dimensions from all trials fell within the appropriate range of dimensions for a normal healthy humerus reported in the literature, as verified by the TOST method.11,12,13 The 3-D modeling capabilities demonstrated in this study allowed a greater understanding of the fracture patterns present in 3- and 4-part (AO classifications 11-B1, 11-B2, 11-C1, 11-C2) humerus fractures.
Overreduction of greater tuberosity to create cortical overlap with the lateral shaft may be used to promote bony union. As a result of this distalization, there may be extra strains placed on the rotator cuff, making the patient more prone to rotator cuff tear, as well as improperly balancing the dynamic stabilizers of the shoulder. Poor clinical outcomes in hemiarthroplasty for proximal humerus fractures have been correlated with a greater tuberosity placed distal relative to the humeral head by 1 cm in a study2 and by 2 cm in another.3
This study has several limitations. The first is the assumption that our injured patients had preinjury proximal humerus geometry within the range of normal dimensions of a healthy humerus. Unfortunately, because we were unable to obtain CT scans of the contralateral shoulder, we had to use standard proximal humerus geometry as the control. Another limitation, inherent in the technique, is that only cortical and dense trabecular bone was modeled, so that comminuted or osteoporotic bone was not well modeled. This study did not correlate the findings from these models with clinical outcomes. A prospective study is needed to evaluate the impact of this 3-D modeling on fracture reductions and clinical outcomes.
This study demonstrates that patient-specific modeling of proximal humerus fracture 3-D CT scans may help surgeons reliably and accurately reconstruct fractures. This technique may have utility in the preoperative planning of tuberosity fracture reduction and hemiarthroplasty. It gives surgeons the ability to visualize fracture fragments, and the process of reconstructing the fragments may help surgeons understand the required maneuvers for reduction at the time of surgery. This technique also provides dimensions of the patient’s native humerus, thus potentially improving the anatomic accuracy of the reduction or hemiarthroplasty reconstruction. With the new trend toward patient-specific instrumentation, this study also provides a means of planning the size of the humeral prostheses as well as the version relative to the biceps groove and intertubercular fracture line.
CONCLUSION
This study demonstrates the feasibility of using 3-D computer modeling of complex proximal humerus fractures in anatomic reconstruction. These techniques of computer-simulated 3-D models are valid and reliable. We believe that this technique of modeling and reconstructing proximal humerus fractures could be used to enhance the preoperative planning of hemiarthroplasty for 3- and 4-part proximal humerus fractures by providing improved understanding of the patient’s native humeral geometry and tuberosity reduction.
1. Boileau P, Krishnan SG, Tinsi L, Walch G, Coste JS, Mole D. Tuberosity malposition and migration: reasons for poor outcomes after hemiarthroplasty for displaced fractures of the proximal humerus. J Shoulder Elbow Surg. 2002;11(5):401-412. doi:10.1067/mse.2002.124527.
2. Mighell MA, Kolm GP, Collinge CA, Frankle MA. Outcomes of hemiarthroplasty for fractures of the proximal humerus. J Shoulder Elbow Surg. 2003;12(6):569-577. doi:10.1016/S1058274603002131.
3. Greiner SH, Kaab MJ, Kroning I, Scheibel M, Perka C. Reconstruction of humeral length and centering of the prosthetic head in hemiarthroplasty for proximal humeral fractures. J Shoulder Elbow Surg. 2008;17(5):709-714. doi:10.1016/j.jse.2008.03.004.
4. Smith AM, Mardones RM, Sperling JW, Cofield RH. Early complications of operatively treated proximal humeral fractures. J Shoulder Elbow Surg. 2007;16(1):14-24. doi:10.1016/j.jse.2006.05.008.
5. Scalise JJ, Codsi MJ, Bryan J, Iannotti JP. The three-dimensional glenoid vault model can estimate normal glenoid version in osteoarthritis. J Shoulder Elbow Surg. 2008;17(3):487-491. doi:10.1016/j.jse.2007.09.006.
6. Bryce CD, Pennypacker JL, Kulkarni N, et al. Validation of three-dimensional models of in situ scapulae. J Shoulder Elbow Surg. 2008;17(5):825-832. doi:10.1016/j.jse.2008.01.141.
7. Yongpravat C, Kim HM, Gardner TR, Bigliani LU, Levine WN, Ahmad CS. Glenoid implant orientation and cement failure in total shoulder arthroplasty: a finite element analysis. J Shoulder Elbow Surg. 2013;22(7):940-947. doi:10.1016/j.jse.2012.09.007.
8. Boileau P, Walch G. The three-dimensional geometry of the proximal humerus. Implications for surgical technique and prosthetic design. J Bone Joint Surg Br. 1997;79(5):857-865. doi:10.1302/0301-620X.79B5.0790857.
9. Wu G, van der Helm FC, Veeger HE, et al. ISB recommendation on definitions of joint coordinate systems of various joints for the reporting of human joint motion--Part II: shoulder, elbow, wrist and hand. J Biomech. 2005;38(5):981-992.
10. Kummer FJ, Perkins R, Zuckerman JD. The use of the bicipital groove for alignment of the humeral stem in shoulder arthroplasty. J Shoulder Elbow Surg. 1998;7(2):144-146. doi:10.1016/S1058-2746(98)90225-7.
11. Iannotti JP, Gabriel JP, Schneck SL, Evans BG, Misra S. The normal glenohumeral relationships. An anatomical study of one hundred and forty shoulders. J Bone Joint Surg Am. 1992;74(4):491-500.
12. Pearl ML, Volk AG. Coronal plane geometry of the proximal humerus relevant to prosthetic arthroplasty. J Shoulder Elbow Surg. 1996;5(4):320-326. doi:10.1016/S1058-2746(96)80060-7.
13. Pearl ML. Proximal humeral anatomy in shoulder arthroplasty: Implications for prosthetic design and surgical technique. J Shoulder Elbow Surg. 2005;14(1 Suppl S):99S-104S. doi:10.1016/j.jse.2004.09.025.
14. Prakash U, McGurty DW, Dent JA. Hemiarthroplasty for severe fractures of the proximal humerus. J Shoulder Elbow Surg. 2002;11(5):428-430. doi:10.1067/mse.2002.126615.
15. Robinson CM, Page RS, Hill RM, Sanders DL, Court-Brown CM, Wakefield AE. Primary hemiarthroplasty for treatment of proximal humeral fractures. J Bone Joint Surg Am. 2003;85-A(7):1215-1223.
16. Zyto K, Wallace WA, Frostick SP, Preston BJ. Outcome after hemiarthroplasty for three- and four-part fractures of the proximal humerus. J Shoulder Elbow Surg. 1998;7(2):85-89. doi:10.1016/S1058-2746(98)90215-4.
1. Boileau P, Krishnan SG, Tinsi L, Walch G, Coste JS, Mole D. Tuberosity malposition and migration: reasons for poor outcomes after hemiarthroplasty for displaced fractures of the proximal humerus. J Shoulder Elbow Surg. 2002;11(5):401-412. doi:10.1067/mse.2002.124527.
2. Mighell MA, Kolm GP, Collinge CA, Frankle MA. Outcomes of hemiarthroplasty for fractures of the proximal humerus. J Shoulder Elbow Surg. 2003;12(6):569-577. doi:10.1016/S1058274603002131.
3. Greiner SH, Kaab MJ, Kroning I, Scheibel M, Perka C. Reconstruction of humeral length and centering of the prosthetic head in hemiarthroplasty for proximal humeral fractures. J Shoulder Elbow Surg. 2008;17(5):709-714. doi:10.1016/j.jse.2008.03.004.
4. Smith AM, Mardones RM, Sperling JW, Cofield RH. Early complications of operatively treated proximal humeral fractures. J Shoulder Elbow Surg. 2007;16(1):14-24. doi:10.1016/j.jse.2006.05.008.
5. Scalise JJ, Codsi MJ, Bryan J, Iannotti JP. The three-dimensional glenoid vault model can estimate normal glenoid version in osteoarthritis. J Shoulder Elbow Surg. 2008;17(3):487-491. doi:10.1016/j.jse.2007.09.006.
6. Bryce CD, Pennypacker JL, Kulkarni N, et al. Validation of three-dimensional models of in situ scapulae. J Shoulder Elbow Surg. 2008;17(5):825-832. doi:10.1016/j.jse.2008.01.141.
7. Yongpravat C, Kim HM, Gardner TR, Bigliani LU, Levine WN, Ahmad CS. Glenoid implant orientation and cement failure in total shoulder arthroplasty: a finite element analysis. J Shoulder Elbow Surg. 2013;22(7):940-947. doi:10.1016/j.jse.2012.09.007.
8. Boileau P, Walch G. The three-dimensional geometry of the proximal humerus. Implications for surgical technique and prosthetic design. J Bone Joint Surg Br. 1997;79(5):857-865. doi:10.1302/0301-620X.79B5.0790857.
9. Wu G, van der Helm FC, Veeger HE, et al. ISB recommendation on definitions of joint coordinate systems of various joints for the reporting of human joint motion--Part II: shoulder, elbow, wrist and hand. J Biomech. 2005;38(5):981-992.
10. Kummer FJ, Perkins R, Zuckerman JD. The use of the bicipital groove for alignment of the humeral stem in shoulder arthroplasty. J Shoulder Elbow Surg. 1998;7(2):144-146. doi:10.1016/S1058-2746(98)90225-7.
11. Iannotti JP, Gabriel JP, Schneck SL, Evans BG, Misra S. The normal glenohumeral relationships. An anatomical study of one hundred and forty shoulders. J Bone Joint Surg Am. 1992;74(4):491-500.
12. Pearl ML, Volk AG. Coronal plane geometry of the proximal humerus relevant to prosthetic arthroplasty. J Shoulder Elbow Surg. 1996;5(4):320-326. doi:10.1016/S1058-2746(96)80060-7.
13. Pearl ML. Proximal humeral anatomy in shoulder arthroplasty: Implications for prosthetic design and surgical technique. J Shoulder Elbow Surg. 2005;14(1 Suppl S):99S-104S. doi:10.1016/j.jse.2004.09.025.
14. Prakash U, McGurty DW, Dent JA. Hemiarthroplasty for severe fractures of the proximal humerus. J Shoulder Elbow Surg. 2002;11(5):428-430. doi:10.1067/mse.2002.126615.
15. Robinson CM, Page RS, Hill RM, Sanders DL, Court-Brown CM, Wakefield AE. Primary hemiarthroplasty for treatment of proximal humeral fractures. J Bone Joint Surg Am. 2003;85-A(7):1215-1223.
16. Zyto K, Wallace WA, Frostick SP, Preston BJ. Outcome after hemiarthroplasty for three- and four-part fractures of the proximal humerus. J Shoulder Elbow Surg. 1998;7(2):85-89. doi:10.1016/S1058-2746(98)90215-4.
TAKE-HOME POINTS
- Proximal humerus fractures may be better understood with 3-D CT imaging.
- 3-D computer modeling of complex proximal humerus fractures allows an understanding of tuebroisty reduction durring ORIF or hemiarthroplasty.
- 3-D modeling enhances preoperative planning for hemiarthroplasty implant size and position relative to the repaired tuberosity fragments.
- 3-D modeling of fracture reduction can help surgeons understand the patient’s native humeral geometry and anatomy.
- Preoperative evaluation of fracture characteristics and fragment reduction help surgeons better understand surgical solutions.
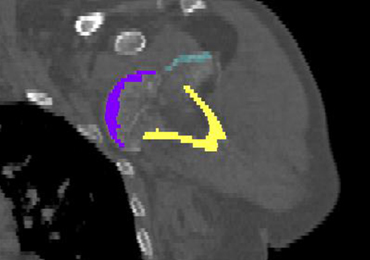
Real-world data so far support pimavanserin trial results
LOS ANGELES – Two studies of real-world use of pimavanserin after its approval in March 2016 for the treatment of Parkinson’s disease–associated psychosis indicate its effectiveness, tolerability, and safety in line with clinical trial results, according to reports presented at the annual meeting of the American Academy of Neurology.
In the first study, 102 patients were prescribed pimavanserin (Nuplazid) during May 2016-March 2018. Of the 88 patients who actually took the drug, 83% had Parkinson’s, and 78% were men. Participants’ mean age was 79 years. Nearly a third had deep brain stimulation.
About two-thirds of the patients started taking pimavanserin after failing prior antipsychotic therapy, whereas the other third had not previously taken an antipsychotic. Quetiapine had been used by 91% of previous antipsychotic users, and another 20% had taken clozapine. Other antipsychotics were less commonly used.
There was no consistent strategy implemented for starting pimavanserin: 17 stopped or were advised to stop their other antipsychotic before starting pimavanserin, 15 were told to taper off their other antipsychotic for 1 week or for up to 3 months, and 22 were told to keep taking their other antipsychotic after starting pimavanserin.
The mean treatment duration has been nearly 11 months for the two-thirds of patients who remain on pimavanserin, including 38 who take it alone and another 20 who take it with another antipsychotic.
A total of 10 patients were unable to tolerate pimavanserin because of adverse events, 5 of whom had generalized weakness/gait instability. This adverse event was the only difference in adverse events that was seen from the clinical trials, said lead author Jessie Sellers, a nurse practitioner at Vanderbilt University Medical Center in Nashville, Tenn.
“But overall the drug was really well tolerated and was effective,” she said.
There also was no increase in mortality detected in users, providing evidence against an association with mortality in older people with dementia-related psychosis that previously led to a boxed warning for atypical antipsychotics, noted senior author Daniel O. Claassen, MD. A total of 6 of the 88 patients died, compared with 5 of the 14 patients who never started the drug.
Patients who stopped pimavanserin and started another antipsychotic had only limited success. Of 11 patients who stopped pimavanserin and started another antipsychotic, only 5 were successful. Another six who stopped pimavanserin did not take another antipsychotic drug, primarily because of the resolution of their symptoms.
The pimavanserin status was unknown for four patients, and another three patients who stopped the drug had not returned for follow-up.
Abhimanyu Mahajan, MD, and other researchers from Henry Ford Hospital in Detroit reported similar results with pimavanserin at the AAN annual meeting in a separate, smaller, retrospective chart review of 16 patients with Parkinson’s disease–associated psychosis and 1 with Lewy body dementia.
These patients had a mean duration of parkinsonism of nearly 12 years and more than 2 years of psychotic symptoms, which consisted of daily or continuous hallucinations in all but one patient.
Telephone interviews with patients and caregivers revealed that 10 of 14 had improvement in hallucinations, and 3 had stopped taking it because of either no benefit or remission. Of six patients who took pimavanserin monotherapy, half improved from severe to mild hallucination severity (less than one episode per week), two had no change, and one improved from severe to moderate. For the other eight patients who took pimavanserin with another antipsychotic, two had no change in hallucination severity, two went from severe to mild, three improved from severe to moderate, and one went from moderate to mild. The patients reported no major adverse events.
Ms. Sellers and another author had no disclosures. Dr. Claassen disclosed personal compensation for consulting, serving on a scientific advisory board, speaking, or other activities with several companies, including Acadia, which markets pimavanserin.
Two of the authors of Dr. Mahajan’s study reported financial ties to Acadia and other companies.
SOURCE: Sellers J et al. AAN 2018, abstract P1.040 and Mahajan A et al. AAN 2018, abstract P5.065
LOS ANGELES – Two studies of real-world use of pimavanserin after its approval in March 2016 for the treatment of Parkinson’s disease–associated psychosis indicate its effectiveness, tolerability, and safety in line with clinical trial results, according to reports presented at the annual meeting of the American Academy of Neurology.
In the first study, 102 patients were prescribed pimavanserin (Nuplazid) during May 2016-March 2018. Of the 88 patients who actually took the drug, 83% had Parkinson’s, and 78% were men. Participants’ mean age was 79 years. Nearly a third had deep brain stimulation.
About two-thirds of the patients started taking pimavanserin after failing prior antipsychotic therapy, whereas the other third had not previously taken an antipsychotic. Quetiapine had been used by 91% of previous antipsychotic users, and another 20% had taken clozapine. Other antipsychotics were less commonly used.
There was no consistent strategy implemented for starting pimavanserin: 17 stopped or were advised to stop their other antipsychotic before starting pimavanserin, 15 were told to taper off their other antipsychotic for 1 week or for up to 3 months, and 22 were told to keep taking their other antipsychotic after starting pimavanserin.
The mean treatment duration has been nearly 11 months for the two-thirds of patients who remain on pimavanserin, including 38 who take it alone and another 20 who take it with another antipsychotic.
A total of 10 patients were unable to tolerate pimavanserin because of adverse events, 5 of whom had generalized weakness/gait instability. This adverse event was the only difference in adverse events that was seen from the clinical trials, said lead author Jessie Sellers, a nurse practitioner at Vanderbilt University Medical Center in Nashville, Tenn.
“But overall the drug was really well tolerated and was effective,” she said.
There also was no increase in mortality detected in users, providing evidence against an association with mortality in older people with dementia-related psychosis that previously led to a boxed warning for atypical antipsychotics, noted senior author Daniel O. Claassen, MD. A total of 6 of the 88 patients died, compared with 5 of the 14 patients who never started the drug.
Patients who stopped pimavanserin and started another antipsychotic had only limited success. Of 11 patients who stopped pimavanserin and started another antipsychotic, only 5 were successful. Another six who stopped pimavanserin did not take another antipsychotic drug, primarily because of the resolution of their symptoms.
The pimavanserin status was unknown for four patients, and another three patients who stopped the drug had not returned for follow-up.
Abhimanyu Mahajan, MD, and other researchers from Henry Ford Hospital in Detroit reported similar results with pimavanserin at the AAN annual meeting in a separate, smaller, retrospective chart review of 16 patients with Parkinson’s disease–associated psychosis and 1 with Lewy body dementia.
These patients had a mean duration of parkinsonism of nearly 12 years and more than 2 years of psychotic symptoms, which consisted of daily or continuous hallucinations in all but one patient.
Telephone interviews with patients and caregivers revealed that 10 of 14 had improvement in hallucinations, and 3 had stopped taking it because of either no benefit or remission. Of six patients who took pimavanserin monotherapy, half improved from severe to mild hallucination severity (less than one episode per week), two had no change, and one improved from severe to moderate. For the other eight patients who took pimavanserin with another antipsychotic, two had no change in hallucination severity, two went from severe to mild, three improved from severe to moderate, and one went from moderate to mild. The patients reported no major adverse events.
Ms. Sellers and another author had no disclosures. Dr. Claassen disclosed personal compensation for consulting, serving on a scientific advisory board, speaking, or other activities with several companies, including Acadia, which markets pimavanserin.
Two of the authors of Dr. Mahajan’s study reported financial ties to Acadia and other companies.
SOURCE: Sellers J et al. AAN 2018, abstract P1.040 and Mahajan A et al. AAN 2018, abstract P5.065
LOS ANGELES – Two studies of real-world use of pimavanserin after its approval in March 2016 for the treatment of Parkinson’s disease–associated psychosis indicate its effectiveness, tolerability, and safety in line with clinical trial results, according to reports presented at the annual meeting of the American Academy of Neurology.
In the first study, 102 patients were prescribed pimavanserin (Nuplazid) during May 2016-March 2018. Of the 88 patients who actually took the drug, 83% had Parkinson’s, and 78% were men. Participants’ mean age was 79 years. Nearly a third had deep brain stimulation.
About two-thirds of the patients started taking pimavanserin after failing prior antipsychotic therapy, whereas the other third had not previously taken an antipsychotic. Quetiapine had been used by 91% of previous antipsychotic users, and another 20% had taken clozapine. Other antipsychotics were less commonly used.
There was no consistent strategy implemented for starting pimavanserin: 17 stopped or were advised to stop their other antipsychotic before starting pimavanserin, 15 were told to taper off their other antipsychotic for 1 week or for up to 3 months, and 22 were told to keep taking their other antipsychotic after starting pimavanserin.
The mean treatment duration has been nearly 11 months for the two-thirds of patients who remain on pimavanserin, including 38 who take it alone and another 20 who take it with another antipsychotic.
A total of 10 patients were unable to tolerate pimavanserin because of adverse events, 5 of whom had generalized weakness/gait instability. This adverse event was the only difference in adverse events that was seen from the clinical trials, said lead author Jessie Sellers, a nurse practitioner at Vanderbilt University Medical Center in Nashville, Tenn.
“But overall the drug was really well tolerated and was effective,” she said.
There also was no increase in mortality detected in users, providing evidence against an association with mortality in older people with dementia-related psychosis that previously led to a boxed warning for atypical antipsychotics, noted senior author Daniel O. Claassen, MD. A total of 6 of the 88 patients died, compared with 5 of the 14 patients who never started the drug.
Patients who stopped pimavanserin and started another antipsychotic had only limited success. Of 11 patients who stopped pimavanserin and started another antipsychotic, only 5 were successful. Another six who stopped pimavanserin did not take another antipsychotic drug, primarily because of the resolution of their symptoms.
The pimavanserin status was unknown for four patients, and another three patients who stopped the drug had not returned for follow-up.
Abhimanyu Mahajan, MD, and other researchers from Henry Ford Hospital in Detroit reported similar results with pimavanserin at the AAN annual meeting in a separate, smaller, retrospective chart review of 16 patients with Parkinson’s disease–associated psychosis and 1 with Lewy body dementia.
These patients had a mean duration of parkinsonism of nearly 12 years and more than 2 years of psychotic symptoms, which consisted of daily or continuous hallucinations in all but one patient.
Telephone interviews with patients and caregivers revealed that 10 of 14 had improvement in hallucinations, and 3 had stopped taking it because of either no benefit or remission. Of six patients who took pimavanserin monotherapy, half improved from severe to mild hallucination severity (less than one episode per week), two had no change, and one improved from severe to moderate. For the other eight patients who took pimavanserin with another antipsychotic, two had no change in hallucination severity, two went from severe to mild, three improved from severe to moderate, and one went from moderate to mild. The patients reported no major adverse events.
Ms. Sellers and another author had no disclosures. Dr. Claassen disclosed personal compensation for consulting, serving on a scientific advisory board, speaking, or other activities with several companies, including Acadia, which markets pimavanserin.
Two of the authors of Dr. Mahajan’s study reported financial ties to Acadia and other companies.
SOURCE: Sellers J et al. AAN 2018, abstract P1.040 and Mahajan A et al. AAN 2018, abstract P5.065
REPORTING FROM AAN 2018
Key clinical point:
Major finding: Psychotic symptoms improved in 71%-88% of patients taking pimavanserin.
Study details: Two retrospective chart reviews totaling 105 patients who took pimavanserin.
Disclosures: One or more authors in each study reported financial ties to Acadia, which markets pimavanserin.
Source: Sellers J et al. AAN 2018, abstract P1.040, and Mahajan A et al. AAN 2018, abstract P5.065.
MenB vaccine receives breakthrough therapy designation for children aged 1-9 years
according to an April 23, 2018, press statement from the vaccine’s manufacturer.
Trumenba is the first Neisseria meningitidis group B (MenB) vaccine to receive this designation for children as young as 1 year in the United States. In 2014, it became the first MenB vaccine to receive approval in the United States for older patients – aged 10-25 years. “As of 2016, the burden of MenB is highest in adolescents/young adults (32%) and infants (20%), followed by children ages 1 to 4 years (12%) and children ages 5 to 10 years (4%),” according to the statement.
The 2014 approval letter required the vaccine’s manufacturer, Pfizer, to assess the efficacy and safety of Trumenba among children aged 1-9 years. Data from the resulting phase 2 studies supported Pfizer’s request for a breakthrough therapy designation for use of the MenB vaccine in that age group.
For more information, read Pfizer’s full press statement.
according to an April 23, 2018, press statement from the vaccine’s manufacturer.
Trumenba is the first Neisseria meningitidis group B (MenB) vaccine to receive this designation for children as young as 1 year in the United States. In 2014, it became the first MenB vaccine to receive approval in the United States for older patients – aged 10-25 years. “As of 2016, the burden of MenB is highest in adolescents/young adults (32%) and infants (20%), followed by children ages 1 to 4 years (12%) and children ages 5 to 10 years (4%),” according to the statement.
The 2014 approval letter required the vaccine’s manufacturer, Pfizer, to assess the efficacy and safety of Trumenba among children aged 1-9 years. Data from the resulting phase 2 studies supported Pfizer’s request for a breakthrough therapy designation for use of the MenB vaccine in that age group.
For more information, read Pfizer’s full press statement.
according to an April 23, 2018, press statement from the vaccine’s manufacturer.
Trumenba is the first Neisseria meningitidis group B (MenB) vaccine to receive this designation for children as young as 1 year in the United States. In 2014, it became the first MenB vaccine to receive approval in the United States for older patients – aged 10-25 years. “As of 2016, the burden of MenB is highest in adolescents/young adults (32%) and infants (20%), followed by children ages 1 to 4 years (12%) and children ages 5 to 10 years (4%),” according to the statement.
The 2014 approval letter required the vaccine’s manufacturer, Pfizer, to assess the efficacy and safety of Trumenba among children aged 1-9 years. Data from the resulting phase 2 studies supported Pfizer’s request for a breakthrough therapy designation for use of the MenB vaccine in that age group.
For more information, read Pfizer’s full press statement.
VIDEO: AAN MS guidelines aim to help clinicians weigh expanding drug choices
LOS ANGELES – A new clinical guideline for adults with multiple sclerosis is designed to help clinicians navigate an increasingly complex landscape of treatment options, its authors say.
The new American Academy of Neurology (AAN) guideline includes some 30 recommendations related to starting a disease-modifying therapy (DMT), switching therapies, or stopping treatment. The guideline, presented April 23 at the AAN annual meeting and published online simultaneously in Neurology, is the first full MS practice guideline issued by AAN since 2002, when only a handful of medications were licensed for use in MS.
The new guideline does not present a hierarchy of DMTs to start but instead weighs evidence for 21 medications or formulations, including 8 used off label, with the idea that clinicians will tailor their choices by considering patient needs, preferences, potential adverse affects, cost of medicines, comorbidities (including depression), and likelihood of adherence, among other factors addressed.
“It’s a dramatically different landscape of the choices clinicians have,” guideline lead author Alexander Rae-Grant, MD, of the Cleveland Clinic, said at a press conference announcing the guideline.
The guideline encourages clinicians and patients “to have a detailed discussion of the risks and benefits of different therapies,” guideline coauthor Ruth Ann Marrie, MD, PhD, of the University of Manitoba, Winnipeg, said at the press conference. “You need to have that informed ... discussion to share decision making – the guideline provides information for each provider-patient dyad to make decisions specific to that patient.”
The guideline incorporates findings from nearly 50 randomized trials, although few of these were head-to-head comparisons of therapies. The authors graded evidence for each DMT as compared with placebo or other DMTs in lowering relapse rate, taking into consideration study design and size. The guideline reflects changes to diagnostic criteria made in 2010, and a classification scheme issued in 2014 for MS subtypes, both of which have complicated the extension of clinical trial findings to some patient groups. It stresses early treatment, recommending that clinicians start DMTs in people with a single clinical demyelinating event and two or more brain lesions characteristic of MS.
Several drugs used off label in MS, including azathioprine and cladribine, were included in the evidence review, with cladribine described as a cost-effective option for patients without the resources to obtain approved agents.
Patients with a new diagnosis of MS should be counseled on starting DMTs not at the time of diagnosis but in a dedicated follow-up visit, the guideline says. Dr. Rae-Grant said that there’s a reasonable amount of “literature to suggest that at the time of diagnosis, what people hear after diagnosis is zero – and that deciding what medication to use is such a weighty decision, we did feel it was important to do that at a different time.”
Dr. Marrie said the AAN guideline “shares some strong similarities” with guidelines released in 2017 by the European Academy of Neurology, including recommendations for early initiation of therapy, for maintaining therapies, and for switching DMTs in individuals not responding or who have breakthrough relapses or changes on MRI.
Dr. Marrie disclosed no conflicts of interest related to her work on the guidelines. Dr. Rae-Grant disclosed income from textbooks on neurology and MS, and no other financial conflicts of interest.
SOURCE: Rae-Grant A et al. Neurology. 2018;90:777-88.
LOS ANGELES – A new clinical guideline for adults with multiple sclerosis is designed to help clinicians navigate an increasingly complex landscape of treatment options, its authors say.
The new American Academy of Neurology (AAN) guideline includes some 30 recommendations related to starting a disease-modifying therapy (DMT), switching therapies, or stopping treatment. The guideline, presented April 23 at the AAN annual meeting and published online simultaneously in Neurology, is the first full MS practice guideline issued by AAN since 2002, when only a handful of medications were licensed for use in MS.
The new guideline does not present a hierarchy of DMTs to start but instead weighs evidence for 21 medications or formulations, including 8 used off label, with the idea that clinicians will tailor their choices by considering patient needs, preferences, potential adverse affects, cost of medicines, comorbidities (including depression), and likelihood of adherence, among other factors addressed.
“It’s a dramatically different landscape of the choices clinicians have,” guideline lead author Alexander Rae-Grant, MD, of the Cleveland Clinic, said at a press conference announcing the guideline.
The guideline encourages clinicians and patients “to have a detailed discussion of the risks and benefits of different therapies,” guideline coauthor Ruth Ann Marrie, MD, PhD, of the University of Manitoba, Winnipeg, said at the press conference. “You need to have that informed ... discussion to share decision making – the guideline provides information for each provider-patient dyad to make decisions specific to that patient.”
The guideline incorporates findings from nearly 50 randomized trials, although few of these were head-to-head comparisons of therapies. The authors graded evidence for each DMT as compared with placebo or other DMTs in lowering relapse rate, taking into consideration study design and size. The guideline reflects changes to diagnostic criteria made in 2010, and a classification scheme issued in 2014 for MS subtypes, both of which have complicated the extension of clinical trial findings to some patient groups. It stresses early treatment, recommending that clinicians start DMTs in people with a single clinical demyelinating event and two or more brain lesions characteristic of MS.
Several drugs used off label in MS, including azathioprine and cladribine, were included in the evidence review, with cladribine described as a cost-effective option for patients without the resources to obtain approved agents.
Patients with a new diagnosis of MS should be counseled on starting DMTs not at the time of diagnosis but in a dedicated follow-up visit, the guideline says. Dr. Rae-Grant said that there’s a reasonable amount of “literature to suggest that at the time of diagnosis, what people hear after diagnosis is zero – and that deciding what medication to use is such a weighty decision, we did feel it was important to do that at a different time.”
Dr. Marrie said the AAN guideline “shares some strong similarities” with guidelines released in 2017 by the European Academy of Neurology, including recommendations for early initiation of therapy, for maintaining therapies, and for switching DMTs in individuals not responding or who have breakthrough relapses or changes on MRI.
Dr. Marrie disclosed no conflicts of interest related to her work on the guidelines. Dr. Rae-Grant disclosed income from textbooks on neurology and MS, and no other financial conflicts of interest.
SOURCE: Rae-Grant A et al. Neurology. 2018;90:777-88.
LOS ANGELES – A new clinical guideline for adults with multiple sclerosis is designed to help clinicians navigate an increasingly complex landscape of treatment options, its authors say.
The new American Academy of Neurology (AAN) guideline includes some 30 recommendations related to starting a disease-modifying therapy (DMT), switching therapies, or stopping treatment. The guideline, presented April 23 at the AAN annual meeting and published online simultaneously in Neurology, is the first full MS practice guideline issued by AAN since 2002, when only a handful of medications were licensed for use in MS.
The new guideline does not present a hierarchy of DMTs to start but instead weighs evidence for 21 medications or formulations, including 8 used off label, with the idea that clinicians will tailor their choices by considering patient needs, preferences, potential adverse affects, cost of medicines, comorbidities (including depression), and likelihood of adherence, among other factors addressed.
“It’s a dramatically different landscape of the choices clinicians have,” guideline lead author Alexander Rae-Grant, MD, of the Cleveland Clinic, said at a press conference announcing the guideline.
The guideline encourages clinicians and patients “to have a detailed discussion of the risks and benefits of different therapies,” guideline coauthor Ruth Ann Marrie, MD, PhD, of the University of Manitoba, Winnipeg, said at the press conference. “You need to have that informed ... discussion to share decision making – the guideline provides information for each provider-patient dyad to make decisions specific to that patient.”
The guideline incorporates findings from nearly 50 randomized trials, although few of these were head-to-head comparisons of therapies. The authors graded evidence for each DMT as compared with placebo or other DMTs in lowering relapse rate, taking into consideration study design and size. The guideline reflects changes to diagnostic criteria made in 2010, and a classification scheme issued in 2014 for MS subtypes, both of which have complicated the extension of clinical trial findings to some patient groups. It stresses early treatment, recommending that clinicians start DMTs in people with a single clinical demyelinating event and two or more brain lesions characteristic of MS.
Several drugs used off label in MS, including azathioprine and cladribine, were included in the evidence review, with cladribine described as a cost-effective option for patients without the resources to obtain approved agents.
Patients with a new diagnosis of MS should be counseled on starting DMTs not at the time of diagnosis but in a dedicated follow-up visit, the guideline says. Dr. Rae-Grant said that there’s a reasonable amount of “literature to suggest that at the time of diagnosis, what people hear after diagnosis is zero – and that deciding what medication to use is such a weighty decision, we did feel it was important to do that at a different time.”
Dr. Marrie said the AAN guideline “shares some strong similarities” with guidelines released in 2017 by the European Academy of Neurology, including recommendations for early initiation of therapy, for maintaining therapies, and for switching DMTs in individuals not responding or who have breakthrough relapses or changes on MRI.
Dr. Marrie disclosed no conflicts of interest related to her work on the guidelines. Dr. Rae-Grant disclosed income from textbooks on neurology and MS, and no other financial conflicts of interest.
SOURCE: Rae-Grant A et al. Neurology. 2018;90:777-88.
REPORTING FROM AAN 2018
Stroke patients benefited from CPAP
the results of a randomized study suggest.
Obstructive sleep apnea is present in 50%-80% of patients with stroke, previous studies show, and its presence is associated with impaired function and cognition, delirium, and longer rehabilitation time, among other negative impacts, wrote Anupama Gupta, PhD, and her coauthors from the All India Institute of Medical Sciences, New Delhi, in the Journal of Clinical Sleep Medicine. Although multiple trials have shown a positive effect of CPAP on stroke recovery, relatively few investigations have looked specifically at whether the intervention prevents subsequent vascular events.
Patients’ clinical stroke outcomes were categorized in accordance with the Modified Rankin Scale (mRS), which is most widely used to assess disability and dependence outcomes among patients with stroke.
Significantly more patients who were treated with CPAP experienced an improvement in their mRS score by at least 1 point, when assessed at both 6 and 12 months following entrance into the study. Specifically, 53% (16) of patients in the CPAP group had an improvement of at least 1 point in their mRS score at 12 months, compared with 27% (11) of patients who did not use CPAP (P = .03).
“These differences are statistically significant, as well as clinically meaningful and relevant,” Dr. Gupta and her colleagues said in their report.
This finding was consistent with what researchers have seen in some earlier studies of stroke patients who used CPAP, the researchers wrote.
Additionally, CPAP-treated patients had fewer subsequent vascular events, compared with those who did not use CPAP, though the difference did not reach statistical significance. There was only one new vascular event (3.33%) in the CPAP group at 12-month follow-up, versus six events (15%) in the non-CPAP group (P = .23).
Nevertheless, the results provide more evidence for the potential benefit of CPAP in stroke patients with obstructive sleep apnea, the researchers noted.
“Our results indicate that new vascular events may be better prevented – and significantly more patients may make good stroke recovery – with CPAP treatment as compared to only best medical treatment,” Dr. Gupta and her colleagues wrote.
Before the study started, investigators determined that they would have needed 80 patients per arm for a power of 80%. A total of 679 patients were screened, but only 116 reported for polysomnography testing, and of those, 83 had at least moderate obstructive sleep apnea.
Due to a lack of CPAP devices, only 70 of those 83 patients made it all the way to randomization, investigators reported.
Dr. Gupta and her coauthors reported no conflicts of interest related to the study.
SOURCE: Gupta A et al. J Clin Sleep Med. 2018 Mar 30. pii:jc-17-00230.
the results of a randomized study suggest.
Obstructive sleep apnea is present in 50%-80% of patients with stroke, previous studies show, and its presence is associated with impaired function and cognition, delirium, and longer rehabilitation time, among other negative impacts, wrote Anupama Gupta, PhD, and her coauthors from the All India Institute of Medical Sciences, New Delhi, in the Journal of Clinical Sleep Medicine. Although multiple trials have shown a positive effect of CPAP on stroke recovery, relatively few investigations have looked specifically at whether the intervention prevents subsequent vascular events.
Patients’ clinical stroke outcomes were categorized in accordance with the Modified Rankin Scale (mRS), which is most widely used to assess disability and dependence outcomes among patients with stroke.
Significantly more patients who were treated with CPAP experienced an improvement in their mRS score by at least 1 point, when assessed at both 6 and 12 months following entrance into the study. Specifically, 53% (16) of patients in the CPAP group had an improvement of at least 1 point in their mRS score at 12 months, compared with 27% (11) of patients who did not use CPAP (P = .03).
“These differences are statistically significant, as well as clinically meaningful and relevant,” Dr. Gupta and her colleagues said in their report.
This finding was consistent with what researchers have seen in some earlier studies of stroke patients who used CPAP, the researchers wrote.
Additionally, CPAP-treated patients had fewer subsequent vascular events, compared with those who did not use CPAP, though the difference did not reach statistical significance. There was only one new vascular event (3.33%) in the CPAP group at 12-month follow-up, versus six events (15%) in the non-CPAP group (P = .23).
Nevertheless, the results provide more evidence for the potential benefit of CPAP in stroke patients with obstructive sleep apnea, the researchers noted.
“Our results indicate that new vascular events may be better prevented – and significantly more patients may make good stroke recovery – with CPAP treatment as compared to only best medical treatment,” Dr. Gupta and her colleagues wrote.
Before the study started, investigators determined that they would have needed 80 patients per arm for a power of 80%. A total of 679 patients were screened, but only 116 reported for polysomnography testing, and of those, 83 had at least moderate obstructive sleep apnea.
Due to a lack of CPAP devices, only 70 of those 83 patients made it all the way to randomization, investigators reported.
Dr. Gupta and her coauthors reported no conflicts of interest related to the study.
SOURCE: Gupta A et al. J Clin Sleep Med. 2018 Mar 30. pii:jc-17-00230.
the results of a randomized study suggest.
Obstructive sleep apnea is present in 50%-80% of patients with stroke, previous studies show, and its presence is associated with impaired function and cognition, delirium, and longer rehabilitation time, among other negative impacts, wrote Anupama Gupta, PhD, and her coauthors from the All India Institute of Medical Sciences, New Delhi, in the Journal of Clinical Sleep Medicine. Although multiple trials have shown a positive effect of CPAP on stroke recovery, relatively few investigations have looked specifically at whether the intervention prevents subsequent vascular events.
Patients’ clinical stroke outcomes were categorized in accordance with the Modified Rankin Scale (mRS), which is most widely used to assess disability and dependence outcomes among patients with stroke.
Significantly more patients who were treated with CPAP experienced an improvement in their mRS score by at least 1 point, when assessed at both 6 and 12 months following entrance into the study. Specifically, 53% (16) of patients in the CPAP group had an improvement of at least 1 point in their mRS score at 12 months, compared with 27% (11) of patients who did not use CPAP (P = .03).
“These differences are statistically significant, as well as clinically meaningful and relevant,” Dr. Gupta and her colleagues said in their report.
This finding was consistent with what researchers have seen in some earlier studies of stroke patients who used CPAP, the researchers wrote.
Additionally, CPAP-treated patients had fewer subsequent vascular events, compared with those who did not use CPAP, though the difference did not reach statistical significance. There was only one new vascular event (3.33%) in the CPAP group at 12-month follow-up, versus six events (15%) in the non-CPAP group (P = .23).
Nevertheless, the results provide more evidence for the potential benefit of CPAP in stroke patients with obstructive sleep apnea, the researchers noted.
“Our results indicate that new vascular events may be better prevented – and significantly more patients may make good stroke recovery – with CPAP treatment as compared to only best medical treatment,” Dr. Gupta and her colleagues wrote.
Before the study started, investigators determined that they would have needed 80 patients per arm for a power of 80%. A total of 679 patients were screened, but only 116 reported for polysomnography testing, and of those, 83 had at least moderate obstructive sleep apnea.
Due to a lack of CPAP devices, only 70 of those 83 patients made it all the way to randomization, investigators reported.
Dr. Gupta and her coauthors reported no conflicts of interest related to the study.
SOURCE: Gupta A et al. J Clin Sleep Med. 2018 Mar 30. pii:jc-17-00230.
FROM THE JOURNAL OF CLINICAL SLEEP MEDICINE
Key clinical point: Continuous positive airway pressure (CPAP) treatment may prevent vascular events in patients with stroke who have OSA.
Major finding: There was one vascular event (3.33%) at 12 months for CPAP-treated patients, versus six events (15%) in non-CPAP patients, though the difference was not significant (P = .23).
Study details: A single-blind, randomized, controlled trial including 70 patients with imaging-confirmed first arterial stroke and OSA.
Disclosures: The authors reported no conflicts of interest related to the study.
Source: Gupta A et al. J Clin Sleep Med. 2018 Mar 30. pii:jc-17-00230.