User login
Common infections are potent risk factor for MI, stroke
ORLANDO – , according to a “big data” registry study from the United Kingdom.
“Our data show infection was just as much a risk factor or more compared with the traditional atherosclerotic cardiovascular disease risk factors,” Paul Carter, MD, said at the annual meeting of the American College of Cardiology.

Dr. Carter of Aston Medical School in Birmingham, England, presented a retrospective analysis from the ACALM (Algorithm for Comorbidities Associated with Length of stay and Mortality) study of administrative data on all of the more than 1.22 million patients admitted to seven U.K. hospitals in 2000-2013. His analysis included all 34,027 adults aged 40 years or older admitted with a urinary tract or respiratory infection on their index hospitalization who had no history of ischemic heart disease or ischemic stroke.
These patients, with a mean age of 73 years, 59% of whom were women, were compared with an equal number of age- and gender-matched adults whose index hospitalization was for reasons other than ischemic heart disease, stroke, urinary tract infection (UTI), or respiratory infection – the two most common infections resulting in hospitalization in the United Kingdom.
Patients with a respiratory infection or UTI had a 9.9% incidence of new-onset ischemic heart disease and a 4.1% rate of ischemic stroke during follow-up starting upon discharge from their index hospitalization, significantly higher than the 5.9% and 1.5% rates in controls. In a multivariate logistic regression analysis adjusted for demographics, standard cardiovascular risk factors, and the top 10 causes of mortality in the United Kingdom, patients with respiratory infection or UTI as their admitting diagnosis had a 1.36-fold increased likelihood of developing ischemic heart disease post discharge and a 2.5-fold greater risk of ischemic stroke than matched controls.
Moreover, mortality following diagnosis of ischemic heart disease was 75.2% in patients whose index hospitalization was for infection, compared with 51.1% in controls who developed ischemic heart disease without a history of hospitalization for infection, for an adjusted 2.98-fold increased likelihood of death. Similarly, mortality after an ischemic stroke was 59.8% in patients with a prior severe infection, compared with 30.8% in controls, which translated to an adjusted 3.1-fold increased risk of death post stroke in patients with a prior hospitalization for infection.
In the multivariate analysis, hospitalization for infection was a stronger risk factor for subsequent ischemic stroke than was atrial fibrillation, heart failure, type 1 or type 2 diabetes, hypertension, or hyperlipidemia. The risk of ischemic heart disease in patients with an infectious disease hospitalization was similar to the risks associated with most of those recognized risk factors.
Two possible mechanisms by which infection might predispose to subsequent ischemic heart disease and stroke are via a direct effect whereby pathogens such as Chlamydia pneumoniae are taken up into arterial plaques, where they cause a local inflammatory response, or an indirect effect in which systemic inflammation primes the atherosclerotic plaque through distribution of inflammatory cytokines, according to Dr. Carter.
He said the ACALM findings are particularly intriguing when considered in the context of the 2017 results of the landmark CANTOS trial, in which canakinumab (Ilaris), a targeted anti-inflammatory agent that inhibits the interleukin-1 beta innate immunity pathway, reduced recurrent ischemic events in post-MI patients who had high systemic inflammation as evidenced by their elevated C-reactive protein level but a normal-range LDL cholesterol (N Engl J Med. 2017 Aug 27. doi: 10.1056/NEJMoa1707914).
“If atherosclerosis is an inflammatory condition, this begs the question of whether other inflammatory conditions, like infection, which induces a large systemic inflammatory response, might drive atherosclerosis,” Dr. Carter commented.
“It’s now very well understood that inflammatory mediators, cells, and processes are involved in every step from the initial endothelial dysfunction that leads to uptake of LDL, inflammatory cells, and monocytes all the way through to plaque progression and rupture, where Th1 cytokines have been implicated in causing that rupture, and ultimately in patient presentation at the hospital,” he added.
He sees the ACALM findings as hypothesis generating, serving to help lay the groundwork for future clinical trials of vaccine or anti-inflammatory antibiotic therapies.
Dr. Carter reported having no financial conflicts related to his presentation.
SOURCE: Carter P. ACC 2018, Abstract 1325M-0.
ORLANDO – , according to a “big data” registry study from the United Kingdom.
“Our data show infection was just as much a risk factor or more compared with the traditional atherosclerotic cardiovascular disease risk factors,” Paul Carter, MD, said at the annual meeting of the American College of Cardiology.
Dr. Carter of Aston Medical School in Birmingham, England, presented a retrospective analysis from the ACALM (Algorithm for Comorbidities Associated with Length of stay and Mortality) study of administrative data on all of the more than 1.22 million patients admitted to seven U.K. hospitals in 2000-2013. His analysis included all 34,027 adults aged 40 years or older admitted with a urinary tract or respiratory infection on their index hospitalization who had no history of ischemic heart disease or ischemic stroke.
These patients, with a mean age of 73 years, 59% of whom were women, were compared with an equal number of age- and gender-matched adults whose index hospitalization was for reasons other than ischemic heart disease, stroke, urinary tract infection (UTI), or respiratory infection – the two most common infections resulting in hospitalization in the United Kingdom.
Patients with a respiratory infection or UTI had a 9.9% incidence of new-onset ischemic heart disease and a 4.1% rate of ischemic stroke during follow-up starting upon discharge from their index hospitalization, significantly higher than the 5.9% and 1.5% rates in controls. In a multivariate logistic regression analysis adjusted for demographics, standard cardiovascular risk factors, and the top 10 causes of mortality in the United Kingdom, patients with respiratory infection or UTI as their admitting diagnosis had a 1.36-fold increased likelihood of developing ischemic heart disease post discharge and a 2.5-fold greater risk of ischemic stroke than matched controls.
Moreover, mortality following diagnosis of ischemic heart disease was 75.2% in patients whose index hospitalization was for infection, compared with 51.1% in controls who developed ischemic heart disease without a history of hospitalization for infection, for an adjusted 2.98-fold increased likelihood of death. Similarly, mortality after an ischemic stroke was 59.8% in patients with a prior severe infection, compared with 30.8% in controls, which translated to an adjusted 3.1-fold increased risk of death post stroke in patients with a prior hospitalization for infection.
In the multivariate analysis, hospitalization for infection was a stronger risk factor for subsequent ischemic stroke than was atrial fibrillation, heart failure, type 1 or type 2 diabetes, hypertension, or hyperlipidemia. The risk of ischemic heart disease in patients with an infectious disease hospitalization was similar to the risks associated with most of those recognized risk factors.
Two possible mechanisms by which infection might predispose to subsequent ischemic heart disease and stroke are via a direct effect whereby pathogens such as Chlamydia pneumoniae are taken up into arterial plaques, where they cause a local inflammatory response, or an indirect effect in which systemic inflammation primes the atherosclerotic plaque through distribution of inflammatory cytokines, according to Dr. Carter.
He said the ACALM findings are particularly intriguing when considered in the context of the 2017 results of the landmark CANTOS trial, in which canakinumab (Ilaris), a targeted anti-inflammatory agent that inhibits the interleukin-1 beta innate immunity pathway, reduced recurrent ischemic events in post-MI patients who had high systemic inflammation as evidenced by their elevated C-reactive protein level but a normal-range LDL cholesterol (N Engl J Med. 2017 Aug 27. doi: 10.1056/NEJMoa1707914).
“If atherosclerosis is an inflammatory condition, this begs the question of whether other inflammatory conditions, like infection, which induces a large systemic inflammatory response, might drive atherosclerosis,” Dr. Carter commented.
“It’s now very well understood that inflammatory mediators, cells, and processes are involved in every step from the initial endothelial dysfunction that leads to uptake of LDL, inflammatory cells, and monocytes all the way through to plaque progression and rupture, where Th1 cytokines have been implicated in causing that rupture, and ultimately in patient presentation at the hospital,” he added.
He sees the ACALM findings as hypothesis generating, serving to help lay the groundwork for future clinical trials of vaccine or anti-inflammatory antibiotic therapies.
Dr. Carter reported having no financial conflicts related to his presentation.
SOURCE: Carter P. ACC 2018, Abstract 1325M-0.
ORLANDO – , according to a “big data” registry study from the United Kingdom.
“Our data show infection was just as much a risk factor or more compared with the traditional atherosclerotic cardiovascular disease risk factors,” Paul Carter, MD, said at the annual meeting of the American College of Cardiology.
Dr. Carter of Aston Medical School in Birmingham, England, presented a retrospective analysis from the ACALM (Algorithm for Comorbidities Associated with Length of stay and Mortality) study of administrative data on all of the more than 1.22 million patients admitted to seven U.K. hospitals in 2000-2013. His analysis included all 34,027 adults aged 40 years or older admitted with a urinary tract or respiratory infection on their index hospitalization who had no history of ischemic heart disease or ischemic stroke.
These patients, with a mean age of 73 years, 59% of whom were women, were compared with an equal number of age- and gender-matched adults whose index hospitalization was for reasons other than ischemic heart disease, stroke, urinary tract infection (UTI), or respiratory infection – the two most common infections resulting in hospitalization in the United Kingdom.
Patients with a respiratory infection or UTI had a 9.9% incidence of new-onset ischemic heart disease and a 4.1% rate of ischemic stroke during follow-up starting upon discharge from their index hospitalization, significantly higher than the 5.9% and 1.5% rates in controls. In a multivariate logistic regression analysis adjusted for demographics, standard cardiovascular risk factors, and the top 10 causes of mortality in the United Kingdom, patients with respiratory infection or UTI as their admitting diagnosis had a 1.36-fold increased likelihood of developing ischemic heart disease post discharge and a 2.5-fold greater risk of ischemic stroke than matched controls.
Moreover, mortality following diagnosis of ischemic heart disease was 75.2% in patients whose index hospitalization was for infection, compared with 51.1% in controls who developed ischemic heart disease without a history of hospitalization for infection, for an adjusted 2.98-fold increased likelihood of death. Similarly, mortality after an ischemic stroke was 59.8% in patients with a prior severe infection, compared with 30.8% in controls, which translated to an adjusted 3.1-fold increased risk of death post stroke in patients with a prior hospitalization for infection.
In the multivariate analysis, hospitalization for infection was a stronger risk factor for subsequent ischemic stroke than was atrial fibrillation, heart failure, type 1 or type 2 diabetes, hypertension, or hyperlipidemia. The risk of ischemic heart disease in patients with an infectious disease hospitalization was similar to the risks associated with most of those recognized risk factors.
Two possible mechanisms by which infection might predispose to subsequent ischemic heart disease and stroke are via a direct effect whereby pathogens such as Chlamydia pneumoniae are taken up into arterial plaques, where they cause a local inflammatory response, or an indirect effect in which systemic inflammation primes the atherosclerotic plaque through distribution of inflammatory cytokines, according to Dr. Carter.
He said the ACALM findings are particularly intriguing when considered in the context of the 2017 results of the landmark CANTOS trial, in which canakinumab (Ilaris), a targeted anti-inflammatory agent that inhibits the interleukin-1 beta innate immunity pathway, reduced recurrent ischemic events in post-MI patients who had high systemic inflammation as evidenced by their elevated C-reactive protein level but a normal-range LDL cholesterol (N Engl J Med. 2017 Aug 27. doi: 10.1056/NEJMoa1707914).
“If atherosclerosis is an inflammatory condition, this begs the question of whether other inflammatory conditions, like infection, which induces a large systemic inflammatory response, might drive atherosclerosis,” Dr. Carter commented.
“It’s now very well understood that inflammatory mediators, cells, and processes are involved in every step from the initial endothelial dysfunction that leads to uptake of LDL, inflammatory cells, and monocytes all the way through to plaque progression and rupture, where Th1 cytokines have been implicated in causing that rupture, and ultimately in patient presentation at the hospital,” he added.
He sees the ACALM findings as hypothesis generating, serving to help lay the groundwork for future clinical trials of vaccine or anti-inflammatory antibiotic therapies.
Dr. Carter reported having no financial conflicts related to his presentation.
SOURCE: Carter P. ACC 2018, Abstract 1325M-0.
REPORTING FROM ACC 2018
Key clinical point: Once patients have been hospitalized for a respiratory infection or UTI, their postdischarge risk of ischemic stroke is 2.5-fold greater than in those without such a history.
Major finding: Patients with a history of hospitalization for UTI or a respiratory infection who later develop ischemic heart disease or stroke have a threefold higher mortality risk than those without such a hospitalization.
Study details: This was a retrospective study of more than 68,000 subjects in the U.K. ACALM registry study.
Disclosures: The study presenter reported having no financial conflicts of interest.
Source: Carter P. ACC 2018, Abstract 1325M-0.
Carboxytherapy caused small yet transient subcutaneous fat reduction
DALLAS – , a small randomized, controlled trial demonstrated.
“Carboxytherapy has been previously used therapeutically to reduce fat, and studies of carboxytherapy have been done in the past as well,” the study’s senior author, Murad Alam, MD, said in an interview in advance of a poster session at the annual conference of the American Society for Laser Medicine and Surgery Inc. “However, earlier studies have not been controlled trials.”
For the split-body study, he and his associates enrolled 16 adults and randomized one side of their body to receive infusions of 1,000 cc of CO2 every week for 5 weeks in the flank region, while the contralateral side received sham treatments. Outcomes of interest included fat layer thickness using a diagnostic ultrasound, total circumference, and body weight, said Dr. Alam, vice-chair of the department of dermatology and chief of the division of cutaneous and aesthetic surgery at Northwestern University, Chicago. He reported that a significant difference in fat thickness was observed in the carboxytherapy-treated side 1 week after the last treatment (P = .011), but this difference was not maintained at 28 weeks as measured by diagnostic ultrasound. Total circumference decreased nominally but not significantly. Body weights did not significantly change throughout the study.

Dr. Alam acknowledged that the study’s small sample size is a limitation. “We do think we did enough treatments, five per side, to obtain an effect if one were to be seen,” he said. The researchers reported having no financial disclosures.
DALLAS – , a small randomized, controlled trial demonstrated.
“Carboxytherapy has been previously used therapeutically to reduce fat, and studies of carboxytherapy have been done in the past as well,” the study’s senior author, Murad Alam, MD, said in an interview in advance of a poster session at the annual conference of the American Society for Laser Medicine and Surgery Inc. “However, earlier studies have not been controlled trials.”
For the split-body study, he and his associates enrolled 16 adults and randomized one side of their body to receive infusions of 1,000 cc of CO2 every week for 5 weeks in the flank region, while the contralateral side received sham treatments. Outcomes of interest included fat layer thickness using a diagnostic ultrasound, total circumference, and body weight, said Dr. Alam, vice-chair of the department of dermatology and chief of the division of cutaneous and aesthetic surgery at Northwestern University, Chicago. He reported that a significant difference in fat thickness was observed in the carboxytherapy-treated side 1 week after the last treatment (P = .011), but this difference was not maintained at 28 weeks as measured by diagnostic ultrasound. Total circumference decreased nominally but not significantly. Body weights did not significantly change throughout the study.
Dr. Alam acknowledged that the study’s small sample size is a limitation. “We do think we did enough treatments, five per side, to obtain an effect if one were to be seen,” he said. The researchers reported having no financial disclosures.
DALLAS – , a small randomized, controlled trial demonstrated.
“Carboxytherapy has been previously used therapeutically to reduce fat, and studies of carboxytherapy have been done in the past as well,” the study’s senior author, Murad Alam, MD, said in an interview in advance of a poster session at the annual conference of the American Society for Laser Medicine and Surgery Inc. “However, earlier studies have not been controlled trials.”
For the split-body study, he and his associates enrolled 16 adults and randomized one side of their body to receive infusions of 1,000 cc of CO2 every week for 5 weeks in the flank region, while the contralateral side received sham treatments. Outcomes of interest included fat layer thickness using a diagnostic ultrasound, total circumference, and body weight, said Dr. Alam, vice-chair of the department of dermatology and chief of the division of cutaneous and aesthetic surgery at Northwestern University, Chicago. He reported that a significant difference in fat thickness was observed in the carboxytherapy-treated side 1 week after the last treatment (P = .011), but this difference was not maintained at 28 weeks as measured by diagnostic ultrasound. Total circumference decreased nominally but not significantly. Body weights did not significantly change throughout the study.
Dr. Alam acknowledged that the study’s small sample size is a limitation. “We do think we did enough treatments, five per side, to obtain an effect if one were to be seen,” he said. The researchers reported having no financial disclosures.
REPORTING FROM ASLMS 2018
Key clinical point: Carboxytherapy yielded a modest reduction in fat that went away after a few months.
Major finding: A significant difference in fat thickness was observed in the carboxytherapy-treated flank region 1 week after the last treatment (P = .011).
Study details: A randomized, split-body study of 16 adults.
Disclosures: Dr. Alam reported having no financial disclosures.
Short-Term Storage of Platelet-Rich Plasma at Room Temperature Does Not Affect Growth Factor or Catabolic Cytokine Concentration
ABSTRACT
The aim of this study was to provide clinical recommendations about the use of platelet-rich plasma (PRP) that was subjected to short-term storage at room temperature. We determined bioactive growth factor and cytokine concentrations as indicators of platelet and white blood cell degranulation in blood and PRP. Additionally, this study sought to validate the use of manual, direct smear analysis as an alternative to automated methods for platelet quantification in PRP.
Blood was used to generate low-leukocyte PRP (Llo PRP) or high-leukocyte PRP (Lhi PRP). Blood was either processed immediately or kept at room temperature for 2 or 4 hours prior to generation of PRP, which was then held at room temperature for 0, 1, 2, or 4 hours. Subsequently, bioactive transforming growth factor beta-1 and matrix metalloproteinase-9 were measured by ELISA (enzyme-linked immunosorbent assay). Manual and automated platelet counts were performed on all blood and PRP samples.
There were no differences in growth factor or cytokine concentration when blood or Llo PRP or Lhi PRP was retained at room temperature for up to 4 hours. Manual, direct smear analysis for platelet quantification was not different from the use of automated machine counting for PRP samples, but in the starting blood samples, manual platelet counts were significantly higher than those generated using automated technology.
When there is a delay of up to 4 hours in the generation of PRP from blood or in the application of PRP to the patient, bioactive growth factor and cytokine concentrations remain stable in both blood and PRP. A manual direct counting method is a simple, cost-effective, and valid method to measure the contents of the PRP product being delivered to the patient.
Platelet-rich plasma (PRP) is used to promote healing in many areas of medicine, such as dental surgery,1,2 soft-tissue injury,3,4 orthopedic surgery,5,6 wound healing,7 and veterinary medicine.8,9 Despite its extensive use, there are still questions about the clinical efficacy of PRP.10-12 Due to biological heterogeneity between patients13,14 and differences between available manufacturing kits,13,15 PRP can be highly variable between patients. There are classification schemes to categorize the various types of PRP,16-18 which can be divided broadly into low-leukocyte PRP (Llo PRP) and high-leukocyte PRP (Lhi PRP). PRP can be used as a point of care therapy, prepared and used immediately, or it can be used during a surgical procedure. In some institutions, blood is drawn by a phlebotomist, processed in the hospital laboratory, and then delivered to the operating room. In other instances, PRP is generated patient-side by the primary attending physician’s team, who draws the blood and processes it for immediate use.5,19 Delays at any step in these various scenarios could lead to the blood or the resultant PRP remaining at room temperature from minutes to several hours prior to administration to the patient. This variability in PRP protocols between clinical and surgical settings adds to concerns regarding the stability and efficacy of the biologic.
Continue to: When performing clinical or research...
When performing clinical or research studies using PRP, it is important to report the contents of the PRP delivered to the patient. By documenting the cellular content of the PRP delivered to the patient, the common questions of optimal platelet dose and the importance of leukocytes in PRP can begin to be answered. There are some known factors that contribute to PRP variability, such as patient biology and operator technique, but there are many other unknown factors. In some instances, there is a failure to generate PRP, defined as a lower platelet count in the PRP preparation than in the starting blood sample.13,14 To measure the platelet and cellular contents of the starting blood and PRP, samples can be submitted to a clinical pathology laboratory for a complete blood count, which adds cost to the patient above the typically unreimbursed cost of the PRP injection itself. An alternative method for measuring platelet concentrations is the use of direct smear analysis on glass slides. The use of direct smears to measure platelet concentration is well validated for blood,20,21 but the use of direct smears of PRP for determining platelet concentrations has not been previously validated. The use of manual platelet counts would provide an alternative to automated platelet counting for clinical and preclinical research studies to characterize the type of PRP administered to the patient.
The primary aim of this study was to determine if retention of blood or PRP at room temperature for various time intervals had an effect on final growth factor or catabolic cytokine concentration. Bioactive transforming growth factor-β1 (TGF-β1) and matrix metalloproteinase-9 (MMP-9) were measured as representatives of growth factors and catabolic cytokines, respectively. The secondary aim was to identify if manual platelet counts were an accurate reflection of automated counts. The outcomes of these experiments should provide immediately relevant information for the clinical application of PRP.
MATERIALS AND METHODS
Blood Collection and Generation of PRP
Under Institutional Review Board approval, blood (105 mL) was collected from healthy human volunteers (N = 5) into a syringe containing acid citrate dextrose anticoagulant to a final concentration of 10% acid citrate dextrose. Three 15-mL aliquots of blood were used to generate Llo PRP (Autologous Conditioned Plasma Double Syringe, Arthrex) and three 20-mL aliquots were used to generate Lhi PRP (SmartPReP 2, Harvest Technologies) (Figure 1). 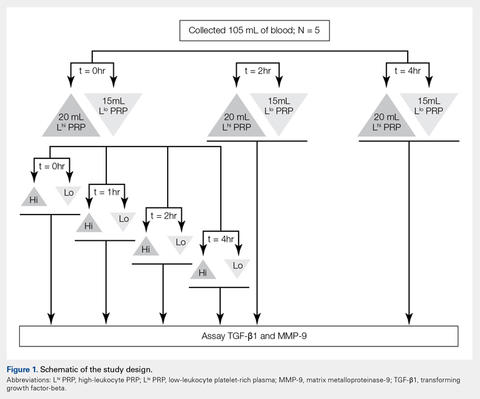
Automated and Manual Counts
Automated complete blood counts were performed by a board certified clinical pathologist in the clinical pathology department of Cornell University on all blood, Llo PRP, and Lhi PRP samples. A manual platelet count, using a modified Giemsa stain,22 was performed on smears of all blood and PRP samples (Video). Slides were scanned at 10x magnification to identify an area where many red blood cells were present while maintaining a clear field of view (Figure 2A). The magnification was then increased to 100x using oil immersion, and the total number of platelets was counted in 10 fields of view (Figure 2B). 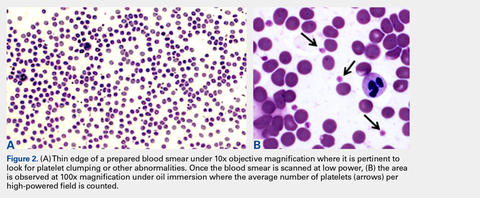
Growth Factor and Catabolic Cytokine Measurements
Blood and PRP samples were thawed for ELISA (enzyme-linked immunosorbent assay) analysis. TGF-β1 concentration was determined using the TGF-β1 Emax ImmunoAssay System (Promega Corporation), which measures biologically active TGF-β1. We chose TGF-β1 because it is commonly measured in PRP studies as an anabolic cytokine with multiple effects on tissue healing. The functions of TGF-β1 include stimulation of undifferentiated mesenchymal cell proliferation; regulation of endothelial, fibroblast, and osteoblast mitogenesis; coordination of collagen synthesis; promotion of endothelial chemotaxis and angiogenesis; activation of extracellular matrix synthesis in cartilage; and reduction of the catabolic activity of interluekin-1 and MMPs.23-25 In addition, TGF-β1 concentration strongly correlates with platelet concentration.26 MMP-9 concentration was determined using the MMP-9 Biotrak Activity Assay (GE Healthcare Biosciences) which measures both active and pro- forms of MMP-9. In PRP, MMP-9 was measured as an indicator of white blood cell (WBC) concentration.26 A catabolic cytokine capable of degrading collagen,13,27 MMP-9 has been linked to poor healing.28 For both assays, samples were measured in duplicate using a multiple detection plate reader (Tecan Safire).
Continue to: Statistical Analysis...
Statistical Analysis
Data were tested for the normal distribution to determine the appropriate statistical test. Manual and automated platelet counts were compared to each other in whole blood, Llo PRP, and Lhi PRP samples using a paired t test. Bioactive TGF-β1 concentrations in blood, Llo PRP, and Lhi PRP, were compared using a Kruskal-Wallis one-way analysis of variance (ANOVA) with Dunn’s all-pairwise comparison. Bioactive and pro-MMP-9 concentrations measured in the retained blood or PRP samples were compared using a one-way ANOVA with Tukey’s all-pairwise comparison. Statistical analyses were performed using Statistix 9 software (Analytical Software). A P value of <0.05 was considered significant.
RESULTS
Validation of PRP
PRP, as defined by an increase in platelet concentration in PRP compared with blood, was successfully generated in all samples by both systems. There was an average 1.98 ± 0.14-fold increase in platelet concentration in Llo PRP and an average 3.06 ± 0.24-fold increase in Lhi PRP. Platelet concentration was significantly higher in Lhi PRP than in Llo PRP (P = 0.001). Compared to whole blood, WBC concentration was 0.47 ± 0.07-fold lower in Llo PRP and 1.98 ± 0.14-fold greater in Lhi PRP. Similar to platelets, WBCs were significantly greater in Lhi PRP than in Llo PRP (P = 0.02).
Bioactive TGF-β1 and MMP-9 Concentration in Blood Retained at Room Temperature
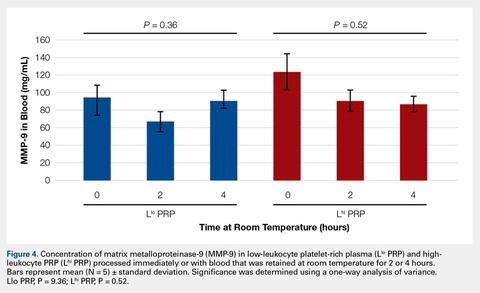
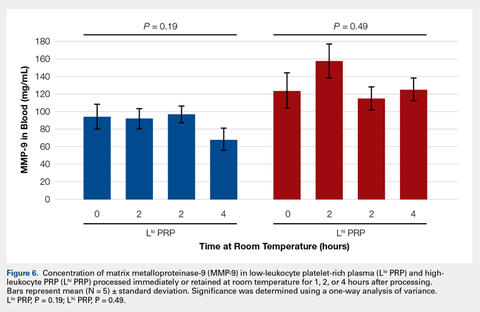
To reflect the clinical situation where blood would be drawn from a patient, but there would be a delay in processing the blood to generate PRP, blood samples were retained at room temperature for up to 4 hours prior to analysis. Neither bioactive TGF-β1 (Figure 3) nor bioactive/pro-MMP-9 concentrations (Figure 4) changed significantly over time when blood was retained at room temperature prior to centrifugation to generate PRP. 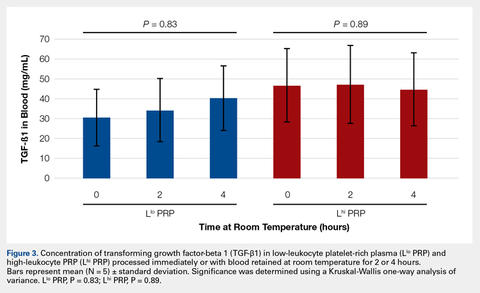
Bioactive TGF-β1 and MMP-9 Concentration in PRP Retained at Room Temperature
In order to mimic the clinical situation where PRP would be generated but might sit out prior to being administered to the patient, PRP samples were retained at room temperature for up to 4 hours prior to analysis. In these samples, bioactive TGF-β1 concentrations were not significantly different between PRP products analyzed immediately and those samples retained at room temperature for up to 4 hours (Figure 5). 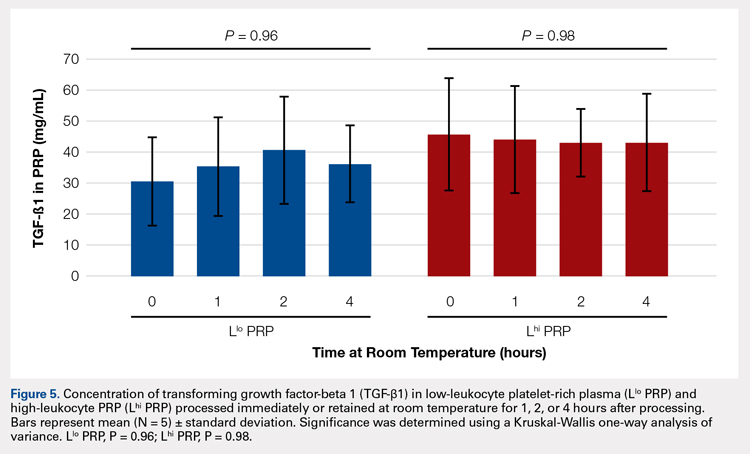
Automatic vs Manual Platelet Count
Manual platelet counts were compared to automated platelet counts to determine if a manual platelet smear analysis could be a reliable method for analyzing PRP in clinical and pre-clinical studies. There was a significant difference between the automated and manual platelet counts in blood samples (Table) (P = 0.05, N = 5) with the manual platelet count having a higher average (99.1 thou/uL) platelet concentration than automated counts. Platelet clumping was identified in 2 automated counts, which falsely decreased platelet concentration by an unknown quantity. Manual platelet counts for both Llo PRP (n = 30) and Lhi PRP (n = 30) were not different from automated platelet counts. Platelet clumping was not reported on any manual platelet counts performed on PRP samples.
Table. Platelet Concentrations of Whole Blood, Llo PRP, and Lhi PRP (N = 5)
| |||||
| Automated Count | Manual Count | P Value | ||
| Mean ± SD | Range | Mean ± SD | Range |
|
Blood | 111.8 ± 59.5 | 54-202 | 210.9 ± 59.4 | 144-297 | 0.05 |
Llo PRP | 421.4 ± 132.8 | 319-620 | 410.1 ± 94.2 | 318-543 | 0.61 |
Lhi PRP | 634.4 ± 88.8 | 517-766 | 635.4 ± 176.6 | 491-933 | 0.99 |
A paired t test was performed to compare results obtained from an automated platelet count and those obtained from a manual count.
Abbreviations: Lhi PRP, high-leukocyte platelet-rich plasma; Llo PRP, low-leukocyte platelet-rich plasma; SD, standard deviation.
Continue to:The primary aim of this study...
DISCUSSION
The primary aim of this study was to improve the clinical use of PRP by characterizing changes that might occur due to extended preparation times. Physicians commonly question the stability of blood or PRP if it is retained at room temperature prior to being administered to the patient. Clinical recommendations to optimize PRP preparation can be derived from a better understanding of the stability of platelets and WBCs, which contribute to the anabolic and catabolic cytokines in PRP.
The results of this study suggest that platelets and WBCs remain stable in blood and both Llo PRP and Lhi PRP for up to 4 hours. The use of bioactive ELISAs to measure TGF-β1 and MMP-9 allows for determination of stability of the PRP product retained at room temperature for up to 4 hours. This provides a time buffer to allow for delays from either institutional logistics or unanticipated clinical delays, without adverse effects on the generation of the final PRP product. As with all biologics, there are many factors that contribute to variability, but a relatively short delay of up to 4 hours in either generation of PRP from blood or in administration of PRP to the patient does not appear to contribute to that variability. Similar studies have been performed on equine PRP and suggest that growth factor concentrations remain stable for up to 6 hours after preparation of PRP29 and in human PRP, which implies that although samples degrade over time, platelet integrity might be acceptable for clinical use for up to 5 days after preparation, particularly if stored in oxygen.30 In contrast to this study, neither of the previously published reports used assays to measure biological activity in the stored PRP. Regardless of the variability between the studies with respect to the type of PRP evaluated and the outcome measures used, all of the studies support the concept that PRP can be stored at room temperature for at least a few hours before clinical use.
Centrifugation of blood does not guarantee the generation of PRP.13,14 In some cases, platelet counts in PRP are similar to or even less than that in the starting whole blood sample. To determine whether a clinical outcome is attributed to PRP, it is vital to know the platelet concentration and, arguably, the WBC concentration in the blood used to generate PRP and in the PRP sample administered to the patient. The platelet concentration in blood and PRP samples can be quantified using automated or manual methods. The use of automated methods can add significant cost to a study or procedure. Manually evaluating a blood smear is an accepted, though more time consuming, method of analyzing cellular components of a blood sample. Depending on the standard operating procedure of the laboratory, manual smears are often done in conjunction with an automated count. This identifies abnormalities in cellular shape or size, or platelet clumping, which are not consistently recognized by automated methods. Manually evaluating a blood smear does take some training, but the material cost is very low, which has added value for clinical or preclinical research studies. Interestingly, the results of this study indicate that manual platelet counts in blood may be more accurate than the count generated from an automated counter because the automated platelet counts were falsely low due to platelet clumping. Platelet clumping can occur as early as 1 hour after blood collection, regardless of the type of anticoagulant used.31
LIMITATIONS
The sample size of this study was small. However, variability in PRP has been well documented in multiple other studies using slightly larger sample sizes.13,14,16 Another potential limitation of this study could be that only one growth factor, TGF-β1, and one catabolic cytokine, MMP-9, were used as surrogate measures to represent platelet and WBC stability, respectively. We chose TGF-β1 because it is correlated with platelet concentrations14,15,26 and MMP-9 because it is an indicator of catabolic factors in PRP that have been correlated with WBC concentrations.26
CONCLUSION
This study illustrated that growth factor and cytokine concentrations in both Llo PRP and Lhi PRP are stable for up to 4 hours. The clinical implications of these results suggest that if the generation or administration of PRP is delayed by up to 4 hours, the resultant PRP retains its bioactivity and is acceptable for clinical application. However, given the known variability of PRP generated due to patient and manufacturer variability,13,14 it is still important to ensure that the product is indeed PRP, with an increase in platelet number over the starting sample of blood. This validation can be performed with a simple and cost-effective manual smear analysis of blood and PRP. The results of this study provide information that can be immediately translated into clinical, surgical, and research practices.
1. Nikolidakis D, Jansen JA. The biology of platelet-rich plasma and its application in oral surgery: Literature review. Tissue Eng Part B Rev. 2008;14(3):249-258. doi:10.1089/ten.teb.2008.0062.
2. Sánchez AR, Sheridan PJ, Kupp LI. Is platelet-rich plasma the perfect enhancement factor? A current review. Int J Oral Maxillofac Implants. 2003;18(1):93-103.
3. Monto RR. Platelet rich plasma treatment for chronic achilles tendinosis. Foot Ankle Int. 2012;33(5):379-385. doi:10.3113/FAI.2012.0379.
4. Owens RF, Ginnetti J, Conti SF, Latona C. Clinical and magnetic resonance imaging outcomes following platelet rich plasma injection for chronic midsubstance Achilles tendinopathy. Foot ankle Int. 2011;32(11):1032-1039. doi:10.3113/FAI.2011.1032.
5. Sánchez M, Anitua E, Azofra J, Andía I, Padilla S, Mujika I. Comparison of surgically repaired achilles tendon tears using platelet-rich fibrin matrices. Am J Sports Med. 2007;35(2):245-251. doi:10.1177/0363546506294078.
6. Silva A, Sampaio R. Anatomic ACL reconstruction: does the platelet-rich plasma accelerate tendon healing? Knee Surg Sports Traumatol Arthrosc. 2009;17(6):676-682. doi:10.1007/s00167-009-0762-8.
7. Fréchette JP, Martineau I, Gagnon G. Platelet-rich plasmas: growth factor content and roles in wound healing. J Dent Res. 2005;84(5):434-439. doi:10.1177/154405910508400507.
8. Bosch G, René van Weeren P, Barneveld A, van Schie HTM. Computerised analysis of standardised ultrasonographic images to monitor the repair of surgically created core lesions in equine superficial digital flexor tendons following treatment with intratendinous platelet rich plasma or placebo. Vet J. 2011;187(1):92-98. doi:10.1016/j.tvjl.2009.10.014.
9. Torricelli P, Fini M, Filardo G, et al. Regenerative medicine for the treatment of musculoskeletal overuse injuries in competition horses. Int Orthop. 2011;35(10):1569-1576. doi:10.1007/s00264-011-1237-3.
10. Sampson S, Gerhardt M, Mandelbaum B. Platelet rich plasma injection grafts for musculoskeletal injuries: a review. Curr Rev Musculoskelet Med. 2008;1(3-4):165-174. doi:10.1007/s12178-008-9032-5.
11. Sheth U, Simunovic N, Klein G, et al. Efficacy of autologous platelet-rich plasma use for orthopaedic indications: a meta-analysis. J Bone Joint Surg Am. 2012;94(4):298-307. doi:10.2106/JBJS.K.00154.
12. Vannini F, Di Matteo B, Filardo G, Kon E, Marcacci M, Giannini S. Platelet-rich plasma for foot and ankle pathologies: a systematic review. Foot Ankle Surg. 2014;20(1):2-9. doi:10.1016/j.fas.2013.08.001.
13. Boswell SG, Cole BJ, Sundman EA, Karas V, Fortier LA. Platelet-rich plasma: a milieu of bioactive factors. Arthroscopy. 2012;28(3):429-439. doi:10.1016/j.arthro.2011.10.018.
14. Mazzocca AD, McCarthy MBR, Chowaniec DM, et al. Platelet-rich plasma differs according to preparation method and human variability. J Bone Joint Surg Am. 2012;94(4):308-316. doi:10.2106/JBJS.K.00430.
15. Castillo TN, Pouliot MA, Kim HJ, Dragoo JL. Comparison of growth factor and platelet concentration from commercial platelet-rich plasma separation systems. Am J Sports Med. 2011;39(2):266-271. doi:10.1177/0363546510387517.
16. Arnoczky SP, Sheibani-Rad S, Shebani-Rad S. The basic science of platelet-rich plasma (PRP): what clinicians need to know. Sports Med Arthrosc. 2013;21(4):180-185. doi:10.1097/JSA.0b013e3182999712.
17. Dohan Ehrenfest DM, Bielecki T, Corso M Del, Inchingolo F, Sammartino G. Shedding light in the controversial terminology for platelet-rich products: Platelet-rich plasma (PRP), platelet-rich fibrin (PRF), platelet-leukocyte gel (PLG), preparation rich in growth factors (PRGF), classification and commercialism. J Biomed Mater Res Part A. 2010;95A(4):1280-1282. doi:10.1002/jbm.a.32894.
18. Dohan Ehrenfest DM, Rasmusson L, Albrektsson T. Classification of platelet concentrates: from pure platelet-rich plasma (P-PRP) to leucocyte- and platelet-rich fibrin (L-PRF). Trends Biotechnol. 2009;27(3):158-167. doi:10.1016/j.tibtech.2008.11.009.
19. Everts PA, Knape JT, Weibrich G, et al. Platelet-rich plasma and platelet gel: a review. J Extra Corpor Technol. 2006;38(2):174-187.
20. Malok M, Titchener EH, Bridgers C, Lee BY, Bamberg R. Comparison of two platelet count estimation methodologies for peripheral blood smears. Clin Lab Sci. 2007;20(3):154-160.
21. Gulati G, Uppal G, Florea AD, Gong J. Detection of platelet clumps on peripheral blood smears by CellaVision DM96 System and Microscopic Review. Lab Med. 2014;45(4):368-371. doi:10.1309/LM604RQVKVLRFXOR.
22. Gulati G, Song J, Florea AD, Gong J. Purpose and criteria for blood smear scan, blood smear examination, and blood smear review. Ann Lab Med. 2013;33(1):1-7. doi:10.3343/alm.2013.33.1.1.
23. Barrientos S, Stojadinovic O, Golinko MS, Brem H, Tomic-Canic M. Perspective article: Growth factors and cytokines in wound healing. Wound Repair Regen. 2008;16(5):585-601. doi:10.1111/j.1524-475X.2008.00410.x.
24. Crane D, Everts P. Platelet rich plasma (PRP) matrix grafts. Pract Pain Manag. 2008;8(1):12-26.
25. Fortier LA, Barker JU, Strauss EJ, McCarrel TM, Cole BJ. The role of growth factors in cartilage repair. Clin Orthop Relat Res. 2011;469(10):2706-2715. doi:10.1007/s11999-011-1857-3.
26. Sundman EA, Cole BJ, Fortier LA. Growth factor and catabolic cytokine concentrations are influenced by the cellular composition of platelet-rich plasma. Am J Sports Med. 2011;39(10):2135-2140. doi:10.1177/0363546511417792.
27. Vu TH, Shipley JM, Bergers G, et al. MMP-9/gelatinase B is a key regulator of growth plate angiogenesis and apoptosis of hypertrophic chondrocytes. Cell. 1998;93(3):411-422.
28. Watelet JB, Demetter P, Claeys C, Van Cauwenberge P, Cuvelier C, Bachert C. Neutrophil-derived metalloproteinase-9 predicts healing quality after sinus surgery. Laryngoscope. 2005;115(1):56-61. doi:10.1097/01.mlg.0000150674.30237.3f.
29. Hauschild G, Geburek F, Gosheger G, et al. Short term storage stability at room temperature of two different platelet-rich plasma preparations from equine donors and potential impact on growth factor concentrations. BMC Vet Res. 2017;13(1):7. doi:10.1186/s12917-016-0920-4.
30. Moore GW, Maloney JC, Archer RA, et al. Platelet-rich plasma for tissue regeneration can be stored at room temperature for at least five days. Br J Biomed Sci. 2017;74(2):71-77. doi:10.1080/09674845.2016.1233792.
31. McShine RL, Sibinga S, Brozovic B. Differences between the effects of EDTA and citrate anticoagulants on platelet count and mean platelet volume. Clin Lab Haematol. 1990;12(3):277-285.
ABSTRACT
The aim of this study was to provide clinical recommendations about the use of platelet-rich plasma (PRP) that was subjected to short-term storage at room temperature. We determined bioactive growth factor and cytokine concentrations as indicators of platelet and white blood cell degranulation in blood and PRP. Additionally, this study sought to validate the use of manual, direct smear analysis as an alternative to automated methods for platelet quantification in PRP.
Blood was used to generate low-leukocyte PRP (Llo PRP) or high-leukocyte PRP (Lhi PRP). Blood was either processed immediately or kept at room temperature for 2 or 4 hours prior to generation of PRP, which was then held at room temperature for 0, 1, 2, or 4 hours. Subsequently, bioactive transforming growth factor beta-1 and matrix metalloproteinase-9 were measured by ELISA (enzyme-linked immunosorbent assay). Manual and automated platelet counts were performed on all blood and PRP samples.
There were no differences in growth factor or cytokine concentration when blood or Llo PRP or Lhi PRP was retained at room temperature for up to 4 hours. Manual, direct smear analysis for platelet quantification was not different from the use of automated machine counting for PRP samples, but in the starting blood samples, manual platelet counts were significantly higher than those generated using automated technology.
When there is a delay of up to 4 hours in the generation of PRP from blood or in the application of PRP to the patient, bioactive growth factor and cytokine concentrations remain stable in both blood and PRP. A manual direct counting method is a simple, cost-effective, and valid method to measure the contents of the PRP product being delivered to the patient.
Platelet-rich plasma (PRP) is used to promote healing in many areas of medicine, such as dental surgery,1,2 soft-tissue injury,3,4 orthopedic surgery,5,6 wound healing,7 and veterinary medicine.8,9 Despite its extensive use, there are still questions about the clinical efficacy of PRP.10-12 Due to biological heterogeneity between patients13,14 and differences between available manufacturing kits,13,15 PRP can be highly variable between patients. There are classification schemes to categorize the various types of PRP,16-18 which can be divided broadly into low-leukocyte PRP (Llo PRP) and high-leukocyte PRP (Lhi PRP). PRP can be used as a point of care therapy, prepared and used immediately, or it can be used during a surgical procedure. In some institutions, blood is drawn by a phlebotomist, processed in the hospital laboratory, and then delivered to the operating room. In other instances, PRP is generated patient-side by the primary attending physician’s team, who draws the blood and processes it for immediate use.5,19 Delays at any step in these various scenarios could lead to the blood or the resultant PRP remaining at room temperature from minutes to several hours prior to administration to the patient. This variability in PRP protocols between clinical and surgical settings adds to concerns regarding the stability and efficacy of the biologic.
Continue to: When performing clinical or research...
When performing clinical or research studies using PRP, it is important to report the contents of the PRP delivered to the patient. By documenting the cellular content of the PRP delivered to the patient, the common questions of optimal platelet dose and the importance of leukocytes in PRP can begin to be answered. There are some known factors that contribute to PRP variability, such as patient biology and operator technique, but there are many other unknown factors. In some instances, there is a failure to generate PRP, defined as a lower platelet count in the PRP preparation than in the starting blood sample.13,14 To measure the platelet and cellular contents of the starting blood and PRP, samples can be submitted to a clinical pathology laboratory for a complete blood count, which adds cost to the patient above the typically unreimbursed cost of the PRP injection itself. An alternative method for measuring platelet concentrations is the use of direct smear analysis on glass slides. The use of direct smears to measure platelet concentration is well validated for blood,20,21 but the use of direct smears of PRP for determining platelet concentrations has not been previously validated. The use of manual platelet counts would provide an alternative to automated platelet counting for clinical and preclinical research studies to characterize the type of PRP administered to the patient.
The primary aim of this study was to determine if retention of blood or PRP at room temperature for various time intervals had an effect on final growth factor or catabolic cytokine concentration. Bioactive transforming growth factor-β1 (TGF-β1) and matrix metalloproteinase-9 (MMP-9) were measured as representatives of growth factors and catabolic cytokines, respectively. The secondary aim was to identify if manual platelet counts were an accurate reflection of automated counts. The outcomes of these experiments should provide immediately relevant information for the clinical application of PRP.
MATERIALS AND METHODS
Blood Collection and Generation of PRP
Under Institutional Review Board approval, blood (105 mL) was collected from healthy human volunteers (N = 5) into a syringe containing acid citrate dextrose anticoagulant to a final concentration of 10% acid citrate dextrose. Three 15-mL aliquots of blood were used to generate Llo PRP (Autologous Conditioned Plasma Double Syringe, Arthrex) and three 20-mL aliquots were used to generate Lhi PRP (SmartPReP 2, Harvest Technologies) (Figure 1).
Automated and Manual Counts
Automated complete blood counts were performed by a board certified clinical pathologist in the clinical pathology department of Cornell University on all blood, Llo PRP, and Lhi PRP samples. A manual platelet count, using a modified Giemsa stain,22 was performed on smears of all blood and PRP samples (Video). Slides were scanned at 10x magnification to identify an area where many red blood cells were present while maintaining a clear field of view (Figure 2A). The magnification was then increased to 100x using oil immersion, and the total number of platelets was counted in 10 fields of view (Figure 2B).
Growth Factor and Catabolic Cytokine Measurements
Blood and PRP samples were thawed for ELISA (enzyme-linked immunosorbent assay) analysis. TGF-β1 concentration was determined using the TGF-β1 Emax ImmunoAssay System (Promega Corporation), which measures biologically active TGF-β1. We chose TGF-β1 because it is commonly measured in PRP studies as an anabolic cytokine with multiple effects on tissue healing. The functions of TGF-β1 include stimulation of undifferentiated mesenchymal cell proliferation; regulation of endothelial, fibroblast, and osteoblast mitogenesis; coordination of collagen synthesis; promotion of endothelial chemotaxis and angiogenesis; activation of extracellular matrix synthesis in cartilage; and reduction of the catabolic activity of interluekin-1 and MMPs.23-25 In addition, TGF-β1 concentration strongly correlates with platelet concentration.26 MMP-9 concentration was determined using the MMP-9 Biotrak Activity Assay (GE Healthcare Biosciences) which measures both active and pro- forms of MMP-9. In PRP, MMP-9 was measured as an indicator of white blood cell (WBC) concentration.26 A catabolic cytokine capable of degrading collagen,13,27 MMP-9 has been linked to poor healing.28 For both assays, samples were measured in duplicate using a multiple detection plate reader (Tecan Safire).
Continue to: Statistical Analysis...
Statistical Analysis
Data were tested for the normal distribution to determine the appropriate statistical test. Manual and automated platelet counts were compared to each other in whole blood, Llo PRP, and Lhi PRP samples using a paired t test. Bioactive TGF-β1 concentrations in blood, Llo PRP, and Lhi PRP, were compared using a Kruskal-Wallis one-way analysis of variance (ANOVA) with Dunn’s all-pairwise comparison. Bioactive and pro-MMP-9 concentrations measured in the retained blood or PRP samples were compared using a one-way ANOVA with Tukey’s all-pairwise comparison. Statistical analyses were performed using Statistix 9 software (Analytical Software). A P value of <0.05 was considered significant.
RESULTS
Validation of PRP
PRP, as defined by an increase in platelet concentration in PRP compared with blood, was successfully generated in all samples by both systems. There was an average 1.98 ± 0.14-fold increase in platelet concentration in Llo PRP and an average 3.06 ± 0.24-fold increase in Lhi PRP. Platelet concentration was significantly higher in Lhi PRP than in Llo PRP (P = 0.001). Compared to whole blood, WBC concentration was 0.47 ± 0.07-fold lower in Llo PRP and 1.98 ± 0.14-fold greater in Lhi PRP. Similar to platelets, WBCs were significantly greater in Lhi PRP than in Llo PRP (P = 0.02).
Bioactive TGF-β1 and MMP-9 Concentration in Blood Retained at Room Temperature
To reflect the clinical situation where blood would be drawn from a patient, but there would be a delay in processing the blood to generate PRP, blood samples were retained at room temperature for up to 4 hours prior to analysis. Neither bioactive TGF-β1 (Figure 3) nor bioactive/pro-MMP-9 concentrations (Figure 4) changed significantly over time when blood was retained at room temperature prior to centrifugation to generate PRP.
Bioactive TGF-β1 and MMP-9 Concentration in PRP Retained at Room Temperature
In order to mimic the clinical situation where PRP would be generated but might sit out prior to being administered to the patient, PRP samples were retained at room temperature for up to 4 hours prior to analysis. In these samples, bioactive TGF-β1 concentrations were not significantly different between PRP products analyzed immediately and those samples retained at room temperature for up to 4 hours (Figure 5).
Automatic vs Manual Platelet Count
Manual platelet counts were compared to automated platelet counts to determine if a manual platelet smear analysis could be a reliable method for analyzing PRP in clinical and pre-clinical studies. There was a significant difference between the automated and manual platelet counts in blood samples (Table) (P = 0.05, N = 5) with the manual platelet count having a higher average (99.1 thou/uL) platelet concentration than automated counts. Platelet clumping was identified in 2 automated counts, which falsely decreased platelet concentration by an unknown quantity. Manual platelet counts for both Llo PRP (n = 30) and Lhi PRP (n = 30) were not different from automated platelet counts. Platelet clumping was not reported on any manual platelet counts performed on PRP samples.
Table. Platelet Concentrations of Whole Blood, Llo PRP, and Lhi PRP (N = 5)
| |||||
| Automated Count | Manual Count | P Value | ||
| Mean ± SD | Range | Mean ± SD | Range |
|
Blood | 111.8 ± 59.5 | 54-202 | 210.9 ± 59.4 | 144-297 | 0.05 |
Llo PRP | 421.4 ± 132.8 | 319-620 | 410.1 ± 94.2 | 318-543 | 0.61 |
Lhi PRP | 634.4 ± 88.8 | 517-766 | 635.4 ± 176.6 | 491-933 | 0.99 |
A paired t test was performed to compare results obtained from an automated platelet count and those obtained from a manual count.
Abbreviations: Lhi PRP, high-leukocyte platelet-rich plasma; Llo PRP, low-leukocyte platelet-rich plasma; SD, standard deviation.
Continue to:The primary aim of this study...
DISCUSSION
The primary aim of this study was to improve the clinical use of PRP by characterizing changes that might occur due to extended preparation times. Physicians commonly question the stability of blood or PRP if it is retained at room temperature prior to being administered to the patient. Clinical recommendations to optimize PRP preparation can be derived from a better understanding of the stability of platelets and WBCs, which contribute to the anabolic and catabolic cytokines in PRP.
The results of this study suggest that platelets and WBCs remain stable in blood and both Llo PRP and Lhi PRP for up to 4 hours. The use of bioactive ELISAs to measure TGF-β1 and MMP-9 allows for determination of stability of the PRP product retained at room temperature for up to 4 hours. This provides a time buffer to allow for delays from either institutional logistics or unanticipated clinical delays, without adverse effects on the generation of the final PRP product. As with all biologics, there are many factors that contribute to variability, but a relatively short delay of up to 4 hours in either generation of PRP from blood or in administration of PRP to the patient does not appear to contribute to that variability. Similar studies have been performed on equine PRP and suggest that growth factor concentrations remain stable for up to 6 hours after preparation of PRP29 and in human PRP, which implies that although samples degrade over time, platelet integrity might be acceptable for clinical use for up to 5 days after preparation, particularly if stored in oxygen.30 In contrast to this study, neither of the previously published reports used assays to measure biological activity in the stored PRP. Regardless of the variability between the studies with respect to the type of PRP evaluated and the outcome measures used, all of the studies support the concept that PRP can be stored at room temperature for at least a few hours before clinical use.
Centrifugation of blood does not guarantee the generation of PRP.13,14 In some cases, platelet counts in PRP are similar to or even less than that in the starting whole blood sample. To determine whether a clinical outcome is attributed to PRP, it is vital to know the platelet concentration and, arguably, the WBC concentration in the blood used to generate PRP and in the PRP sample administered to the patient. The platelet concentration in blood and PRP samples can be quantified using automated or manual methods. The use of automated methods can add significant cost to a study or procedure. Manually evaluating a blood smear is an accepted, though more time consuming, method of analyzing cellular components of a blood sample. Depending on the standard operating procedure of the laboratory, manual smears are often done in conjunction with an automated count. This identifies abnormalities in cellular shape or size, or platelet clumping, which are not consistently recognized by automated methods. Manually evaluating a blood smear does take some training, but the material cost is very low, which has added value for clinical or preclinical research studies. Interestingly, the results of this study indicate that manual platelet counts in blood may be more accurate than the count generated from an automated counter because the automated platelet counts were falsely low due to platelet clumping. Platelet clumping can occur as early as 1 hour after blood collection, regardless of the type of anticoagulant used.31
LIMITATIONS
The sample size of this study was small. However, variability in PRP has been well documented in multiple other studies using slightly larger sample sizes.13,14,16 Another potential limitation of this study could be that only one growth factor, TGF-β1, and one catabolic cytokine, MMP-9, were used as surrogate measures to represent platelet and WBC stability, respectively. We chose TGF-β1 because it is correlated with platelet concentrations14,15,26 and MMP-9 because it is an indicator of catabolic factors in PRP that have been correlated with WBC concentrations.26
CONCLUSION
This study illustrated that growth factor and cytokine concentrations in both Llo PRP and Lhi PRP are stable for up to 4 hours. The clinical implications of these results suggest that if the generation or administration of PRP is delayed by up to 4 hours, the resultant PRP retains its bioactivity and is acceptable for clinical application. However, given the known variability of PRP generated due to patient and manufacturer variability,13,14 it is still important to ensure that the product is indeed PRP, with an increase in platelet number over the starting sample of blood. This validation can be performed with a simple and cost-effective manual smear analysis of blood and PRP. The results of this study provide information that can be immediately translated into clinical, surgical, and research practices.
ABSTRACT
The aim of this study was to provide clinical recommendations about the use of platelet-rich plasma (PRP) that was subjected to short-term storage at room temperature. We determined bioactive growth factor and cytokine concentrations as indicators of platelet and white blood cell degranulation in blood and PRP. Additionally, this study sought to validate the use of manual, direct smear analysis as an alternative to automated methods for platelet quantification in PRP.
Blood was used to generate low-leukocyte PRP (Llo PRP) or high-leukocyte PRP (Lhi PRP). Blood was either processed immediately or kept at room temperature for 2 or 4 hours prior to generation of PRP, which was then held at room temperature for 0, 1, 2, or 4 hours. Subsequently, bioactive transforming growth factor beta-1 and matrix metalloproteinase-9 were measured by ELISA (enzyme-linked immunosorbent assay). Manual and automated platelet counts were performed on all blood and PRP samples.
There were no differences in growth factor or cytokine concentration when blood or Llo PRP or Lhi PRP was retained at room temperature for up to 4 hours. Manual, direct smear analysis for platelet quantification was not different from the use of automated machine counting for PRP samples, but in the starting blood samples, manual platelet counts were significantly higher than those generated using automated technology.
When there is a delay of up to 4 hours in the generation of PRP from blood or in the application of PRP to the patient, bioactive growth factor and cytokine concentrations remain stable in both blood and PRP. A manual direct counting method is a simple, cost-effective, and valid method to measure the contents of the PRP product being delivered to the patient.
Platelet-rich plasma (PRP) is used to promote healing in many areas of medicine, such as dental surgery,1,2 soft-tissue injury,3,4 orthopedic surgery,5,6 wound healing,7 and veterinary medicine.8,9 Despite its extensive use, there are still questions about the clinical efficacy of PRP.10-12 Due to biological heterogeneity between patients13,14 and differences between available manufacturing kits,13,15 PRP can be highly variable between patients. There are classification schemes to categorize the various types of PRP,16-18 which can be divided broadly into low-leukocyte PRP (Llo PRP) and high-leukocyte PRP (Lhi PRP). PRP can be used as a point of care therapy, prepared and used immediately, or it can be used during a surgical procedure. In some institutions, blood is drawn by a phlebotomist, processed in the hospital laboratory, and then delivered to the operating room. In other instances, PRP is generated patient-side by the primary attending physician’s team, who draws the blood and processes it for immediate use.5,19 Delays at any step in these various scenarios could lead to the blood or the resultant PRP remaining at room temperature from minutes to several hours prior to administration to the patient. This variability in PRP protocols between clinical and surgical settings adds to concerns regarding the stability and efficacy of the biologic.
Continue to: When performing clinical or research...
When performing clinical or research studies using PRP, it is important to report the contents of the PRP delivered to the patient. By documenting the cellular content of the PRP delivered to the patient, the common questions of optimal platelet dose and the importance of leukocytes in PRP can begin to be answered. There are some known factors that contribute to PRP variability, such as patient biology and operator technique, but there are many other unknown factors. In some instances, there is a failure to generate PRP, defined as a lower platelet count in the PRP preparation than in the starting blood sample.13,14 To measure the platelet and cellular contents of the starting blood and PRP, samples can be submitted to a clinical pathology laboratory for a complete blood count, which adds cost to the patient above the typically unreimbursed cost of the PRP injection itself. An alternative method for measuring platelet concentrations is the use of direct smear analysis on glass slides. The use of direct smears to measure platelet concentration is well validated for blood,20,21 but the use of direct smears of PRP for determining platelet concentrations has not been previously validated. The use of manual platelet counts would provide an alternative to automated platelet counting for clinical and preclinical research studies to characterize the type of PRP administered to the patient.
The primary aim of this study was to determine if retention of blood or PRP at room temperature for various time intervals had an effect on final growth factor or catabolic cytokine concentration. Bioactive transforming growth factor-β1 (TGF-β1) and matrix metalloproteinase-9 (MMP-9) were measured as representatives of growth factors and catabolic cytokines, respectively. The secondary aim was to identify if manual platelet counts were an accurate reflection of automated counts. The outcomes of these experiments should provide immediately relevant information for the clinical application of PRP.
MATERIALS AND METHODS
Blood Collection and Generation of PRP
Under Institutional Review Board approval, blood (105 mL) was collected from healthy human volunteers (N = 5) into a syringe containing acid citrate dextrose anticoagulant to a final concentration of 10% acid citrate dextrose. Three 15-mL aliquots of blood were used to generate Llo PRP (Autologous Conditioned Plasma Double Syringe, Arthrex) and three 20-mL aliquots were used to generate Lhi PRP (SmartPReP 2, Harvest Technologies) (Figure 1).
Automated and Manual Counts
Automated complete blood counts were performed by a board certified clinical pathologist in the clinical pathology department of Cornell University on all blood, Llo PRP, and Lhi PRP samples. A manual platelet count, using a modified Giemsa stain,22 was performed on smears of all blood and PRP samples (Video). Slides were scanned at 10x magnification to identify an area where many red blood cells were present while maintaining a clear field of view (Figure 2A). The magnification was then increased to 100x using oil immersion, and the total number of platelets was counted in 10 fields of view (Figure 2B).
Growth Factor and Catabolic Cytokine Measurements
Blood and PRP samples were thawed for ELISA (enzyme-linked immunosorbent assay) analysis. TGF-β1 concentration was determined using the TGF-β1 Emax ImmunoAssay System (Promega Corporation), which measures biologically active TGF-β1. We chose TGF-β1 because it is commonly measured in PRP studies as an anabolic cytokine with multiple effects on tissue healing. The functions of TGF-β1 include stimulation of undifferentiated mesenchymal cell proliferation; regulation of endothelial, fibroblast, and osteoblast mitogenesis; coordination of collagen synthesis; promotion of endothelial chemotaxis and angiogenesis; activation of extracellular matrix synthesis in cartilage; and reduction of the catabolic activity of interluekin-1 and MMPs.23-25 In addition, TGF-β1 concentration strongly correlates with platelet concentration.26 MMP-9 concentration was determined using the MMP-9 Biotrak Activity Assay (GE Healthcare Biosciences) which measures both active and pro- forms of MMP-9. In PRP, MMP-9 was measured as an indicator of white blood cell (WBC) concentration.26 A catabolic cytokine capable of degrading collagen,13,27 MMP-9 has been linked to poor healing.28 For both assays, samples were measured in duplicate using a multiple detection plate reader (Tecan Safire).
Continue to: Statistical Analysis...
Statistical Analysis
Data were tested for the normal distribution to determine the appropriate statistical test. Manual and automated platelet counts were compared to each other in whole blood, Llo PRP, and Lhi PRP samples using a paired t test. Bioactive TGF-β1 concentrations in blood, Llo PRP, and Lhi PRP, were compared using a Kruskal-Wallis one-way analysis of variance (ANOVA) with Dunn’s all-pairwise comparison. Bioactive and pro-MMP-9 concentrations measured in the retained blood or PRP samples were compared using a one-way ANOVA with Tukey’s all-pairwise comparison. Statistical analyses were performed using Statistix 9 software (Analytical Software). A P value of <0.05 was considered significant.
RESULTS
Validation of PRP
PRP, as defined by an increase in platelet concentration in PRP compared with blood, was successfully generated in all samples by both systems. There was an average 1.98 ± 0.14-fold increase in platelet concentration in Llo PRP and an average 3.06 ± 0.24-fold increase in Lhi PRP. Platelet concentration was significantly higher in Lhi PRP than in Llo PRP (P = 0.001). Compared to whole blood, WBC concentration was 0.47 ± 0.07-fold lower in Llo PRP and 1.98 ± 0.14-fold greater in Lhi PRP. Similar to platelets, WBCs were significantly greater in Lhi PRP than in Llo PRP (P = 0.02).
Bioactive TGF-β1 and MMP-9 Concentration in Blood Retained at Room Temperature
To reflect the clinical situation where blood would be drawn from a patient, but there would be a delay in processing the blood to generate PRP, blood samples were retained at room temperature for up to 4 hours prior to analysis. Neither bioactive TGF-β1 (Figure 3) nor bioactive/pro-MMP-9 concentrations (Figure 4) changed significantly over time when blood was retained at room temperature prior to centrifugation to generate PRP.
Bioactive TGF-β1 and MMP-9 Concentration in PRP Retained at Room Temperature
In order to mimic the clinical situation where PRP would be generated but might sit out prior to being administered to the patient, PRP samples were retained at room temperature for up to 4 hours prior to analysis. In these samples, bioactive TGF-β1 concentrations were not significantly different between PRP products analyzed immediately and those samples retained at room temperature for up to 4 hours (Figure 5).
Automatic vs Manual Platelet Count
Manual platelet counts were compared to automated platelet counts to determine if a manual platelet smear analysis could be a reliable method for analyzing PRP in clinical and pre-clinical studies. There was a significant difference between the automated and manual platelet counts in blood samples (Table) (P = 0.05, N = 5) with the manual platelet count having a higher average (99.1 thou/uL) platelet concentration than automated counts. Platelet clumping was identified in 2 automated counts, which falsely decreased platelet concentration by an unknown quantity. Manual platelet counts for both Llo PRP (n = 30) and Lhi PRP (n = 30) were not different from automated platelet counts. Platelet clumping was not reported on any manual platelet counts performed on PRP samples.
Table. Platelet Concentrations of Whole Blood, Llo PRP, and Lhi PRP (N = 5)
| |||||
| Automated Count | Manual Count | P Value | ||
| Mean ± SD | Range | Mean ± SD | Range |
|
Blood | 111.8 ± 59.5 | 54-202 | 210.9 ± 59.4 | 144-297 | 0.05 |
Llo PRP | 421.4 ± 132.8 | 319-620 | 410.1 ± 94.2 | 318-543 | 0.61 |
Lhi PRP | 634.4 ± 88.8 | 517-766 | 635.4 ± 176.6 | 491-933 | 0.99 |
A paired t test was performed to compare results obtained from an automated platelet count and those obtained from a manual count.
Abbreviations: Lhi PRP, high-leukocyte platelet-rich plasma; Llo PRP, low-leukocyte platelet-rich plasma; SD, standard deviation.
Continue to:The primary aim of this study...
DISCUSSION
The primary aim of this study was to improve the clinical use of PRP by characterizing changes that might occur due to extended preparation times. Physicians commonly question the stability of blood or PRP if it is retained at room temperature prior to being administered to the patient. Clinical recommendations to optimize PRP preparation can be derived from a better understanding of the stability of platelets and WBCs, which contribute to the anabolic and catabolic cytokines in PRP.
The results of this study suggest that platelets and WBCs remain stable in blood and both Llo PRP and Lhi PRP for up to 4 hours. The use of bioactive ELISAs to measure TGF-β1 and MMP-9 allows for determination of stability of the PRP product retained at room temperature for up to 4 hours. This provides a time buffer to allow for delays from either institutional logistics or unanticipated clinical delays, without adverse effects on the generation of the final PRP product. As with all biologics, there are many factors that contribute to variability, but a relatively short delay of up to 4 hours in either generation of PRP from blood or in administration of PRP to the patient does not appear to contribute to that variability. Similar studies have been performed on equine PRP and suggest that growth factor concentrations remain stable for up to 6 hours after preparation of PRP29 and in human PRP, which implies that although samples degrade over time, platelet integrity might be acceptable for clinical use for up to 5 days after preparation, particularly if stored in oxygen.30 In contrast to this study, neither of the previously published reports used assays to measure biological activity in the stored PRP. Regardless of the variability between the studies with respect to the type of PRP evaluated and the outcome measures used, all of the studies support the concept that PRP can be stored at room temperature for at least a few hours before clinical use.
Centrifugation of blood does not guarantee the generation of PRP.13,14 In some cases, platelet counts in PRP are similar to or even less than that in the starting whole blood sample. To determine whether a clinical outcome is attributed to PRP, it is vital to know the platelet concentration and, arguably, the WBC concentration in the blood used to generate PRP and in the PRP sample administered to the patient. The platelet concentration in blood and PRP samples can be quantified using automated or manual methods. The use of automated methods can add significant cost to a study or procedure. Manually evaluating a blood smear is an accepted, though more time consuming, method of analyzing cellular components of a blood sample. Depending on the standard operating procedure of the laboratory, manual smears are often done in conjunction with an automated count. This identifies abnormalities in cellular shape or size, or platelet clumping, which are not consistently recognized by automated methods. Manually evaluating a blood smear does take some training, but the material cost is very low, which has added value for clinical or preclinical research studies. Interestingly, the results of this study indicate that manual platelet counts in blood may be more accurate than the count generated from an automated counter because the automated platelet counts were falsely low due to platelet clumping. Platelet clumping can occur as early as 1 hour after blood collection, regardless of the type of anticoagulant used.31
LIMITATIONS
The sample size of this study was small. However, variability in PRP has been well documented in multiple other studies using slightly larger sample sizes.13,14,16 Another potential limitation of this study could be that only one growth factor, TGF-β1, and one catabolic cytokine, MMP-9, were used as surrogate measures to represent platelet and WBC stability, respectively. We chose TGF-β1 because it is correlated with platelet concentrations14,15,26 and MMP-9 because it is an indicator of catabolic factors in PRP that have been correlated with WBC concentrations.26
CONCLUSION
This study illustrated that growth factor and cytokine concentrations in both Llo PRP and Lhi PRP are stable for up to 4 hours. The clinical implications of these results suggest that if the generation or administration of PRP is delayed by up to 4 hours, the resultant PRP retains its bioactivity and is acceptable for clinical application. However, given the known variability of PRP generated due to patient and manufacturer variability,13,14 it is still important to ensure that the product is indeed PRP, with an increase in platelet number over the starting sample of blood. This validation can be performed with a simple and cost-effective manual smear analysis of blood and PRP. The results of this study provide information that can be immediately translated into clinical, surgical, and research practices.
1. Nikolidakis D, Jansen JA. The biology of platelet-rich plasma and its application in oral surgery: Literature review. Tissue Eng Part B Rev. 2008;14(3):249-258. doi:10.1089/ten.teb.2008.0062.
2. Sánchez AR, Sheridan PJ, Kupp LI. Is platelet-rich plasma the perfect enhancement factor? A current review. Int J Oral Maxillofac Implants. 2003;18(1):93-103.
3. Monto RR. Platelet rich plasma treatment for chronic achilles tendinosis. Foot Ankle Int. 2012;33(5):379-385. doi:10.3113/FAI.2012.0379.
4. Owens RF, Ginnetti J, Conti SF, Latona C. Clinical and magnetic resonance imaging outcomes following platelet rich plasma injection for chronic midsubstance Achilles tendinopathy. Foot ankle Int. 2011;32(11):1032-1039. doi:10.3113/FAI.2011.1032.
5. Sánchez M, Anitua E, Azofra J, Andía I, Padilla S, Mujika I. Comparison of surgically repaired achilles tendon tears using platelet-rich fibrin matrices. Am J Sports Med. 2007;35(2):245-251. doi:10.1177/0363546506294078.
6. Silva A, Sampaio R. Anatomic ACL reconstruction: does the platelet-rich plasma accelerate tendon healing? Knee Surg Sports Traumatol Arthrosc. 2009;17(6):676-682. doi:10.1007/s00167-009-0762-8.
7. Fréchette JP, Martineau I, Gagnon G. Platelet-rich plasmas: growth factor content and roles in wound healing. J Dent Res. 2005;84(5):434-439. doi:10.1177/154405910508400507.
8. Bosch G, René van Weeren P, Barneveld A, van Schie HTM. Computerised analysis of standardised ultrasonographic images to monitor the repair of surgically created core lesions in equine superficial digital flexor tendons following treatment with intratendinous platelet rich plasma or placebo. Vet J. 2011;187(1):92-98. doi:10.1016/j.tvjl.2009.10.014.
9. Torricelli P, Fini M, Filardo G, et al. Regenerative medicine for the treatment of musculoskeletal overuse injuries in competition horses. Int Orthop. 2011;35(10):1569-1576. doi:10.1007/s00264-011-1237-3.
10. Sampson S, Gerhardt M, Mandelbaum B. Platelet rich plasma injection grafts for musculoskeletal injuries: a review. Curr Rev Musculoskelet Med. 2008;1(3-4):165-174. doi:10.1007/s12178-008-9032-5.
11. Sheth U, Simunovic N, Klein G, et al. Efficacy of autologous platelet-rich plasma use for orthopaedic indications: a meta-analysis. J Bone Joint Surg Am. 2012;94(4):298-307. doi:10.2106/JBJS.K.00154.
12. Vannini F, Di Matteo B, Filardo G, Kon E, Marcacci M, Giannini S. Platelet-rich plasma for foot and ankle pathologies: a systematic review. Foot Ankle Surg. 2014;20(1):2-9. doi:10.1016/j.fas.2013.08.001.
13. Boswell SG, Cole BJ, Sundman EA, Karas V, Fortier LA. Platelet-rich plasma: a milieu of bioactive factors. Arthroscopy. 2012;28(3):429-439. doi:10.1016/j.arthro.2011.10.018.
14. Mazzocca AD, McCarthy MBR, Chowaniec DM, et al. Platelet-rich plasma differs according to preparation method and human variability. J Bone Joint Surg Am. 2012;94(4):308-316. doi:10.2106/JBJS.K.00430.
15. Castillo TN, Pouliot MA, Kim HJ, Dragoo JL. Comparison of growth factor and platelet concentration from commercial platelet-rich plasma separation systems. Am J Sports Med. 2011;39(2):266-271. doi:10.1177/0363546510387517.
16. Arnoczky SP, Sheibani-Rad S, Shebani-Rad S. The basic science of platelet-rich plasma (PRP): what clinicians need to know. Sports Med Arthrosc. 2013;21(4):180-185. doi:10.1097/JSA.0b013e3182999712.
17. Dohan Ehrenfest DM, Bielecki T, Corso M Del, Inchingolo F, Sammartino G. Shedding light in the controversial terminology for platelet-rich products: Platelet-rich plasma (PRP), platelet-rich fibrin (PRF), platelet-leukocyte gel (PLG), preparation rich in growth factors (PRGF), classification and commercialism. J Biomed Mater Res Part A. 2010;95A(4):1280-1282. doi:10.1002/jbm.a.32894.
18. Dohan Ehrenfest DM, Rasmusson L, Albrektsson T. Classification of platelet concentrates: from pure platelet-rich plasma (P-PRP) to leucocyte- and platelet-rich fibrin (L-PRF). Trends Biotechnol. 2009;27(3):158-167. doi:10.1016/j.tibtech.2008.11.009.
19. Everts PA, Knape JT, Weibrich G, et al. Platelet-rich plasma and platelet gel: a review. J Extra Corpor Technol. 2006;38(2):174-187.
20. Malok M, Titchener EH, Bridgers C, Lee BY, Bamberg R. Comparison of two platelet count estimation methodologies for peripheral blood smears. Clin Lab Sci. 2007;20(3):154-160.
21. Gulati G, Uppal G, Florea AD, Gong J. Detection of platelet clumps on peripheral blood smears by CellaVision DM96 System and Microscopic Review. Lab Med. 2014;45(4):368-371. doi:10.1309/LM604RQVKVLRFXOR.
22. Gulati G, Song J, Florea AD, Gong J. Purpose and criteria for blood smear scan, blood smear examination, and blood smear review. Ann Lab Med. 2013;33(1):1-7. doi:10.3343/alm.2013.33.1.1.
23. Barrientos S, Stojadinovic O, Golinko MS, Brem H, Tomic-Canic M. Perspective article: Growth factors and cytokines in wound healing. Wound Repair Regen. 2008;16(5):585-601. doi:10.1111/j.1524-475X.2008.00410.x.
24. Crane D, Everts P. Platelet rich plasma (PRP) matrix grafts. Pract Pain Manag. 2008;8(1):12-26.
25. Fortier LA, Barker JU, Strauss EJ, McCarrel TM, Cole BJ. The role of growth factors in cartilage repair. Clin Orthop Relat Res. 2011;469(10):2706-2715. doi:10.1007/s11999-011-1857-3.
26. Sundman EA, Cole BJ, Fortier LA. Growth factor and catabolic cytokine concentrations are influenced by the cellular composition of platelet-rich plasma. Am J Sports Med. 2011;39(10):2135-2140. doi:10.1177/0363546511417792.
27. Vu TH, Shipley JM, Bergers G, et al. MMP-9/gelatinase B is a key regulator of growth plate angiogenesis and apoptosis of hypertrophic chondrocytes. Cell. 1998;93(3):411-422.
28. Watelet JB, Demetter P, Claeys C, Van Cauwenberge P, Cuvelier C, Bachert C. Neutrophil-derived metalloproteinase-9 predicts healing quality after sinus surgery. Laryngoscope. 2005;115(1):56-61. doi:10.1097/01.mlg.0000150674.30237.3f.
29. Hauschild G, Geburek F, Gosheger G, et al. Short term storage stability at room temperature of two different platelet-rich plasma preparations from equine donors and potential impact on growth factor concentrations. BMC Vet Res. 2017;13(1):7. doi:10.1186/s12917-016-0920-4.
30. Moore GW, Maloney JC, Archer RA, et al. Platelet-rich plasma for tissue regeneration can be stored at room temperature for at least five days. Br J Biomed Sci. 2017;74(2):71-77. doi:10.1080/09674845.2016.1233792.
31. McShine RL, Sibinga S, Brozovic B. Differences between the effects of EDTA and citrate anticoagulants on platelet count and mean platelet volume. Clin Lab Haematol. 1990;12(3):277-285.
1. Nikolidakis D, Jansen JA. The biology of platelet-rich plasma and its application in oral surgery: Literature review. Tissue Eng Part B Rev. 2008;14(3):249-258. doi:10.1089/ten.teb.2008.0062.
2. Sánchez AR, Sheridan PJ, Kupp LI. Is platelet-rich plasma the perfect enhancement factor? A current review. Int J Oral Maxillofac Implants. 2003;18(1):93-103.
3. Monto RR. Platelet rich plasma treatment for chronic achilles tendinosis. Foot Ankle Int. 2012;33(5):379-385. doi:10.3113/FAI.2012.0379.
4. Owens RF, Ginnetti J, Conti SF, Latona C. Clinical and magnetic resonance imaging outcomes following platelet rich plasma injection for chronic midsubstance Achilles tendinopathy. Foot ankle Int. 2011;32(11):1032-1039. doi:10.3113/FAI.2011.1032.
5. Sánchez M, Anitua E, Azofra J, Andía I, Padilla S, Mujika I. Comparison of surgically repaired achilles tendon tears using platelet-rich fibrin matrices. Am J Sports Med. 2007;35(2):245-251. doi:10.1177/0363546506294078.
6. Silva A, Sampaio R. Anatomic ACL reconstruction: does the platelet-rich plasma accelerate tendon healing? Knee Surg Sports Traumatol Arthrosc. 2009;17(6):676-682. doi:10.1007/s00167-009-0762-8.
7. Fréchette JP, Martineau I, Gagnon G. Platelet-rich plasmas: growth factor content and roles in wound healing. J Dent Res. 2005;84(5):434-439. doi:10.1177/154405910508400507.
8. Bosch G, René van Weeren P, Barneveld A, van Schie HTM. Computerised analysis of standardised ultrasonographic images to monitor the repair of surgically created core lesions in equine superficial digital flexor tendons following treatment with intratendinous platelet rich plasma or placebo. Vet J. 2011;187(1):92-98. doi:10.1016/j.tvjl.2009.10.014.
9. Torricelli P, Fini M, Filardo G, et al. Regenerative medicine for the treatment of musculoskeletal overuse injuries in competition horses. Int Orthop. 2011;35(10):1569-1576. doi:10.1007/s00264-011-1237-3.
10. Sampson S, Gerhardt M, Mandelbaum B. Platelet rich plasma injection grafts for musculoskeletal injuries: a review. Curr Rev Musculoskelet Med. 2008;1(3-4):165-174. doi:10.1007/s12178-008-9032-5.
11. Sheth U, Simunovic N, Klein G, et al. Efficacy of autologous platelet-rich plasma use for orthopaedic indications: a meta-analysis. J Bone Joint Surg Am. 2012;94(4):298-307. doi:10.2106/JBJS.K.00154.
12. Vannini F, Di Matteo B, Filardo G, Kon E, Marcacci M, Giannini S. Platelet-rich plasma for foot and ankle pathologies: a systematic review. Foot Ankle Surg. 2014;20(1):2-9. doi:10.1016/j.fas.2013.08.001.
13. Boswell SG, Cole BJ, Sundman EA, Karas V, Fortier LA. Platelet-rich plasma: a milieu of bioactive factors. Arthroscopy. 2012;28(3):429-439. doi:10.1016/j.arthro.2011.10.018.
14. Mazzocca AD, McCarthy MBR, Chowaniec DM, et al. Platelet-rich plasma differs according to preparation method and human variability. J Bone Joint Surg Am. 2012;94(4):308-316. doi:10.2106/JBJS.K.00430.
15. Castillo TN, Pouliot MA, Kim HJ, Dragoo JL. Comparison of growth factor and platelet concentration from commercial platelet-rich plasma separation systems. Am J Sports Med. 2011;39(2):266-271. doi:10.1177/0363546510387517.
16. Arnoczky SP, Sheibani-Rad S, Shebani-Rad S. The basic science of platelet-rich plasma (PRP): what clinicians need to know. Sports Med Arthrosc. 2013;21(4):180-185. doi:10.1097/JSA.0b013e3182999712.
17. Dohan Ehrenfest DM, Bielecki T, Corso M Del, Inchingolo F, Sammartino G. Shedding light in the controversial terminology for platelet-rich products: Platelet-rich plasma (PRP), platelet-rich fibrin (PRF), platelet-leukocyte gel (PLG), preparation rich in growth factors (PRGF), classification and commercialism. J Biomed Mater Res Part A. 2010;95A(4):1280-1282. doi:10.1002/jbm.a.32894.
18. Dohan Ehrenfest DM, Rasmusson L, Albrektsson T. Classification of platelet concentrates: from pure platelet-rich plasma (P-PRP) to leucocyte- and platelet-rich fibrin (L-PRF). Trends Biotechnol. 2009;27(3):158-167. doi:10.1016/j.tibtech.2008.11.009.
19. Everts PA, Knape JT, Weibrich G, et al. Platelet-rich plasma and platelet gel: a review. J Extra Corpor Technol. 2006;38(2):174-187.
20. Malok M, Titchener EH, Bridgers C, Lee BY, Bamberg R. Comparison of two platelet count estimation methodologies for peripheral blood smears. Clin Lab Sci. 2007;20(3):154-160.
21. Gulati G, Uppal G, Florea AD, Gong J. Detection of platelet clumps on peripheral blood smears by CellaVision DM96 System and Microscopic Review. Lab Med. 2014;45(4):368-371. doi:10.1309/LM604RQVKVLRFXOR.
22. Gulati G, Song J, Florea AD, Gong J. Purpose and criteria for blood smear scan, blood smear examination, and blood smear review. Ann Lab Med. 2013;33(1):1-7. doi:10.3343/alm.2013.33.1.1.
23. Barrientos S, Stojadinovic O, Golinko MS, Brem H, Tomic-Canic M. Perspective article: Growth factors and cytokines in wound healing. Wound Repair Regen. 2008;16(5):585-601. doi:10.1111/j.1524-475X.2008.00410.x.
24. Crane D, Everts P. Platelet rich plasma (PRP) matrix grafts. Pract Pain Manag. 2008;8(1):12-26.
25. Fortier LA, Barker JU, Strauss EJ, McCarrel TM, Cole BJ. The role of growth factors in cartilage repair. Clin Orthop Relat Res. 2011;469(10):2706-2715. doi:10.1007/s11999-011-1857-3.
26. Sundman EA, Cole BJ, Fortier LA. Growth factor and catabolic cytokine concentrations are influenced by the cellular composition of platelet-rich plasma. Am J Sports Med. 2011;39(10):2135-2140. doi:10.1177/0363546511417792.
27. Vu TH, Shipley JM, Bergers G, et al. MMP-9/gelatinase B is a key regulator of growth plate angiogenesis and apoptosis of hypertrophic chondrocytes. Cell. 1998;93(3):411-422.
28. Watelet JB, Demetter P, Claeys C, Van Cauwenberge P, Cuvelier C, Bachert C. Neutrophil-derived metalloproteinase-9 predicts healing quality after sinus surgery. Laryngoscope. 2005;115(1):56-61. doi:10.1097/01.mlg.0000150674.30237.3f.
29. Hauschild G, Geburek F, Gosheger G, et al. Short term storage stability at room temperature of two different platelet-rich plasma preparations from equine donors and potential impact on growth factor concentrations. BMC Vet Res. 2017;13(1):7. doi:10.1186/s12917-016-0920-4.
30. Moore GW, Maloney JC, Archer RA, et al. Platelet-rich plasma for tissue regeneration can be stored at room temperature for at least five days. Br J Biomed Sci. 2017;74(2):71-77. doi:10.1080/09674845.2016.1233792.
31. McShine RL, Sibinga S, Brozovic B. Differences between the effects of EDTA and citrate anticoagulants on platelet count and mean platelet volume. Clin Lab Haematol. 1990;12(3):277-285.
TAKE-HOME POINTS
- Blood can be stored at room temperature for up to 4 hours before making PRP without loss in activity.
- PRP can be stored at room temperature for up to 4 hours before administration to a patient without loss in activity.
- Manual, direct smear analysis is as accurate as automated counting for measuring platelet concentration in PRP.
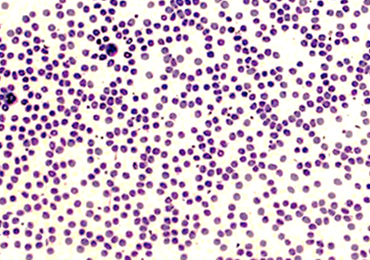
Gene strong predictor of metastasis in melanoma
CHICAGO – Investigators have identified four genes that are overexpressed in primary melanoma, including one, CXCL1, that holds promise as a strong predictor of future metastatic disease, according to study results presented at the Society of Surgical Oncology Annual Cancer Symposium.
The study implicated four genes strongly expressed in primary melanoma tumors of patients who develop distant metastases – CXCL1, CXCL2, CBL, and CD276 – said Jennifer Erdrich, MD, MPH, of Cedars Sinai Medical Center, Los Angeles. However, CXCL1 stood out. “CXCL1 overexpression is an independent predictor of developing metastatic disease. Patients with CXCL1 overexpression in the primary tumor in our study had decreased overall 5-year survival.” CXCL1 may be a useful predictive marker in primary melanoma and a potential target for immunotherapy, she said.
The rationale for analyzing the 79 genes implicated in cancer only rather than the entire array of 22,000 genes was to reduce the odds of a high false-discovery rate from 5% to 0.007%. “This is what strengthens our findings in a cohort of 37 patients,” Dr. Erdrich said.
The study analyzed pathological characteristics of the metastatic and nonmetastatic groups. Most characteristics were similar between the two groups, including location of the primary tumor in the trunk and extremities of 67% and 71%, respectively, and age of 60 years and older. The analysis noted two deviations: primary tumor size was thicker in the metastatic group (2.1 mm vs. 1.05 mm; P = .6), although Dr. Erdrich noted this was “not significantly different”; and a higher rate of ulceration in the metastatic group (50% vs. 13%; P = .05).
The genes CXCL1 and CXCL2 are both chemokines involved in growth and inflammation. “CXCL1 expression was 2.51 times greater in the metastatic group,” Dr. Erdrich said (P less than .001). Overexpression in the other three genes of interest was: CXCL2, 1.68 times greater (P less than .01); CD276, which is involved in T-cell immunity, 1.16 times greater (P = .04); and C-CBL, which is a photo-oncogene involved in the ubiquitin pathway, 1.15 times greater (P = .01). “The overexpression of all four of these was statistically significant,” she said.
Univariate analysis found ulceration of the primary along with overexpression of
the four genes to be significant predictors of metastasis. “However, in our multivariate model, three of the genes dropped out but CXCL1 remained robust,” she said.
Dr. Erdrich noted that CXCL1 is a cytokine located on chromosome 4, is secreted by macrophages, exerts its signal through CXCR2, and is one of five cytokines upregulated in lesions that respond to immunotherapy (Br J Dermatol. 2016;175:966-78).
CXCL1 compares favorably with S100, the existing blood-based biomarker for predicting recurrence in high-risk melanoma, as a predictor of metastases, Dr. Erdrich said, with an area under the curve of 0.80 versus 0.66; sensitivity of 67% versus 77%; specificity of 97% versus 61%; positive predictive value of 80% versus 40%; and negative predictive value of 94% versus 88% (Anticancer Res. 1999;19:2685-90; Cancer. 2003;97:1737-45).
The study also looked at overall survival in patients with low and high expression of CXCL1. “The patients with high expression had 5-year survival of only 50% compared to those of low expression, whose 5-year survival was 97%,” Dr. Erdrich said.
Dr. Erdrich and her coauthors reported having no financial relationships.
SOURCE: Erdrich J et al. SSO 2018, Abstract 82.
CHICAGO – Investigators have identified four genes that are overexpressed in primary melanoma, including one, CXCL1, that holds promise as a strong predictor of future metastatic disease, according to study results presented at the Society of Surgical Oncology Annual Cancer Symposium.
The study implicated four genes strongly expressed in primary melanoma tumors of patients who develop distant metastases – CXCL1, CXCL2, CBL, and CD276 – said Jennifer Erdrich, MD, MPH, of Cedars Sinai Medical Center, Los Angeles. However, CXCL1 stood out. “CXCL1 overexpression is an independent predictor of developing metastatic disease. Patients with CXCL1 overexpression in the primary tumor in our study had decreased overall 5-year survival.” CXCL1 may be a useful predictive marker in primary melanoma and a potential target for immunotherapy, she said.
The rationale for analyzing the 79 genes implicated in cancer only rather than the entire array of 22,000 genes was to reduce the odds of a high false-discovery rate from 5% to 0.007%. “This is what strengthens our findings in a cohort of 37 patients,” Dr. Erdrich said.
The study analyzed pathological characteristics of the metastatic and nonmetastatic groups. Most characteristics were similar between the two groups, including location of the primary tumor in the trunk and extremities of 67% and 71%, respectively, and age of 60 years and older. The analysis noted two deviations: primary tumor size was thicker in the metastatic group (2.1 mm vs. 1.05 mm; P = .6), although Dr. Erdrich noted this was “not significantly different”; and a higher rate of ulceration in the metastatic group (50% vs. 13%; P = .05).
The genes CXCL1 and CXCL2 are both chemokines involved in growth and inflammation. “CXCL1 expression was 2.51 times greater in the metastatic group,” Dr. Erdrich said (P less than .001). Overexpression in the other three genes of interest was: CXCL2, 1.68 times greater (P less than .01); CD276, which is involved in T-cell immunity, 1.16 times greater (P = .04); and C-CBL, which is a photo-oncogene involved in the ubiquitin pathway, 1.15 times greater (P = .01). “The overexpression of all four of these was statistically significant,” she said.
Univariate analysis found ulceration of the primary along with overexpression of
the four genes to be significant predictors of metastasis. “However, in our multivariate model, three of the genes dropped out but CXCL1 remained robust,” she said.
Dr. Erdrich noted that CXCL1 is a cytokine located on chromosome 4, is secreted by macrophages, exerts its signal through CXCR2, and is one of five cytokines upregulated in lesions that respond to immunotherapy (Br J Dermatol. 2016;175:966-78).
CXCL1 compares favorably with S100, the existing blood-based biomarker for predicting recurrence in high-risk melanoma, as a predictor of metastases, Dr. Erdrich said, with an area under the curve of 0.80 versus 0.66; sensitivity of 67% versus 77%; specificity of 97% versus 61%; positive predictive value of 80% versus 40%; and negative predictive value of 94% versus 88% (Anticancer Res. 1999;19:2685-90; Cancer. 2003;97:1737-45).
The study also looked at overall survival in patients with low and high expression of CXCL1. “The patients with high expression had 5-year survival of only 50% compared to those of low expression, whose 5-year survival was 97%,” Dr. Erdrich said.
Dr. Erdrich and her coauthors reported having no financial relationships.
SOURCE: Erdrich J et al. SSO 2018, Abstract 82.
CHICAGO – Investigators have identified four genes that are overexpressed in primary melanoma, including one, CXCL1, that holds promise as a strong predictor of future metastatic disease, according to study results presented at the Society of Surgical Oncology Annual Cancer Symposium.
The study implicated four genes strongly expressed in primary melanoma tumors of patients who develop distant metastases – CXCL1, CXCL2, CBL, and CD276 – said Jennifer Erdrich, MD, MPH, of Cedars Sinai Medical Center, Los Angeles. However, CXCL1 stood out. “CXCL1 overexpression is an independent predictor of developing metastatic disease. Patients with CXCL1 overexpression in the primary tumor in our study had decreased overall 5-year survival.” CXCL1 may be a useful predictive marker in primary melanoma and a potential target for immunotherapy, she said.
The rationale for analyzing the 79 genes implicated in cancer only rather than the entire array of 22,000 genes was to reduce the odds of a high false-discovery rate from 5% to 0.007%. “This is what strengthens our findings in a cohort of 37 patients,” Dr. Erdrich said.
The study analyzed pathological characteristics of the metastatic and nonmetastatic groups. Most characteristics were similar between the two groups, including location of the primary tumor in the trunk and extremities of 67% and 71%, respectively, and age of 60 years and older. The analysis noted two deviations: primary tumor size was thicker in the metastatic group (2.1 mm vs. 1.05 mm; P = .6), although Dr. Erdrich noted this was “not significantly different”; and a higher rate of ulceration in the metastatic group (50% vs. 13%; P = .05).
The genes CXCL1 and CXCL2 are both chemokines involved in growth and inflammation. “CXCL1 expression was 2.51 times greater in the metastatic group,” Dr. Erdrich said (P less than .001). Overexpression in the other three genes of interest was: CXCL2, 1.68 times greater (P less than .01); CD276, which is involved in T-cell immunity, 1.16 times greater (P = .04); and C-CBL, which is a photo-oncogene involved in the ubiquitin pathway, 1.15 times greater (P = .01). “The overexpression of all four of these was statistically significant,” she said.
Univariate analysis found ulceration of the primary along with overexpression of
the four genes to be significant predictors of metastasis. “However, in our multivariate model, three of the genes dropped out but CXCL1 remained robust,” she said.
Dr. Erdrich noted that CXCL1 is a cytokine located on chromosome 4, is secreted by macrophages, exerts its signal through CXCR2, and is one of five cytokines upregulated in lesions that respond to immunotherapy (Br J Dermatol. 2016;175:966-78).
CXCL1 compares favorably with S100, the existing blood-based biomarker for predicting recurrence in high-risk melanoma, as a predictor of metastases, Dr. Erdrich said, with an area under the curve of 0.80 versus 0.66; sensitivity of 67% versus 77%; specificity of 97% versus 61%; positive predictive value of 80% versus 40%; and negative predictive value of 94% versus 88% (Anticancer Res. 1999;19:2685-90; Cancer. 2003;97:1737-45).
The study also looked at overall survival in patients with low and high expression of CXCL1. “The patients with high expression had 5-year survival of only 50% compared to those of low expression, whose 5-year survival was 97%,” Dr. Erdrich said.
Dr. Erdrich and her coauthors reported having no financial relationships.
SOURCE: Erdrich J et al. SSO 2018, Abstract 82.
REPORTING FROM SSO 2018
Key clinical point: The CXCL1 gene may predict metastatic risk in primary melanoma.
Major findings: CXCL1 overexpression yielded 50% 5-year survival, almost half that of underexpression.
Study details: Gene analysis of samples from 37 patients with nonmetastatic primary melanoma who had surgical removal of primary lesion with median follow-up of 38 months.
Disclosures: Dr. Erdrich and her coauthors reported having no financial disclosures.
Source: Erdrich J et al. SSO 2018, Abstract 82.
Consider spironolactone in treatment-resistant hypertension
ORLANDO – More than one-third of patients with treatment-resistant hypertension in U.S. cardiology practices are eligible for preferential consideration of spironolactone as their fourth-line agent in accord with the practice-changing findings of the PATHWAY-2 trial, Lauren Thompson, MD, said at the annual meeting of the American College of Cardiology.
She presented a study that harnessed the ACC’s National Cardiovascular Data Registry PINNACLE Registry – the largest observational outpatient cardiovascular registry in the world – to assess the potential impact of PATHWAY-2 on the management of treatment-resistant hypertension (TRH) in U.S. cardiology practices. And as she discovered, the potential implications for daily practice are huge.

Dr. Thompson, a cardiology fellow at the University of Colorado, Denver, identified 19,044 patients in the PINNACLE registry for 2013-2014 with TRH, defined as uncontrolled blood pressure despite use of drugs from three antihypertensive classes. Of these patients, 37% met the PATHWAY-2 enrollment criteria by virtue of already being on an ACE inhibitor or angiotensin receptor blocker, a calcium channel blocker, and a thiazide diuretic, but not spironolactone. This is the large subgroup which, on the basis of PATHWAY-2, should receive serious consideration of spironolactone as the fourth drug.
The most widely prescribed antihypertensive agents in PINNACLE registry patients with TRH were beta-blockers, in 87%; ACE inhibitors, in 72%; calcium channel blockers, in 71%; and thiazide diuretics, in 69%. Of note, 27% of patients with TRH were already on spironolactone.
Audience discussion centered around the uncertainties regarding treatment adherence in patients labeled as having TRH.
“I think sometimes clinicians are afraid to prescribe spironolactone in patients that they think might be nonadherent,” one cardiologist observed.
Dr. Thompson noted that it’s not possible to look at prescription-filling rates in the PINNACLE registry.
“Unfortunately, we can’t exclude white coat hypertension or nonadherence as reasons why patients in PINNACLE end up on multiple antihypertensive medication classes. We can see that a prescription was written, but we have no way to know if it was actually filled or not,” she observed.
Also, since patients in cardiology clinics typically have multiple cardiovascular comorbidities, it’s quite possible that patients with TRH who are on a beta-blocker, for example, might not have received that drug for blood pressure control.
Dr. Thompson’s study was supported by the ACC’s National Cardiovascular Disease Registry. She reported having no financial conflicts of interest.
Source: Thompson L. ACC 18. Abstract 1324M-09.
ORLANDO – More than one-third of patients with treatment-resistant hypertension in U.S. cardiology practices are eligible for preferential consideration of spironolactone as their fourth-line agent in accord with the practice-changing findings of the PATHWAY-2 trial, Lauren Thompson, MD, said at the annual meeting of the American College of Cardiology.
She presented a study that harnessed the ACC’s National Cardiovascular Data Registry PINNACLE Registry – the largest observational outpatient cardiovascular registry in the world – to assess the potential impact of PATHWAY-2 on the management of treatment-resistant hypertension (TRH) in U.S. cardiology practices. And as she discovered, the potential implications for daily practice are huge.
Dr. Thompson, a cardiology fellow at the University of Colorado, Denver, identified 19,044 patients in the PINNACLE registry for 2013-2014 with TRH, defined as uncontrolled blood pressure despite use of drugs from three antihypertensive classes. Of these patients, 37% met the PATHWAY-2 enrollment criteria by virtue of already being on an ACE inhibitor or angiotensin receptor blocker, a calcium channel blocker, and a thiazide diuretic, but not spironolactone. This is the large subgroup which, on the basis of PATHWAY-2, should receive serious consideration of spironolactone as the fourth drug.
The most widely prescribed antihypertensive agents in PINNACLE registry patients with TRH were beta-blockers, in 87%; ACE inhibitors, in 72%; calcium channel blockers, in 71%; and thiazide diuretics, in 69%. Of note, 27% of patients with TRH were already on spironolactone.
Audience discussion centered around the uncertainties regarding treatment adherence in patients labeled as having TRH.
“I think sometimes clinicians are afraid to prescribe spironolactone in patients that they think might be nonadherent,” one cardiologist observed.
Dr. Thompson noted that it’s not possible to look at prescription-filling rates in the PINNACLE registry.
“Unfortunately, we can’t exclude white coat hypertension or nonadherence as reasons why patients in PINNACLE end up on multiple antihypertensive medication classes. We can see that a prescription was written, but we have no way to know if it was actually filled or not,” she observed.
Also, since patients in cardiology clinics typically have multiple cardiovascular comorbidities, it’s quite possible that patients with TRH who are on a beta-blocker, for example, might not have received that drug for blood pressure control.
Dr. Thompson’s study was supported by the ACC’s National Cardiovascular Disease Registry. She reported having no financial conflicts of interest.
Source: Thompson L. ACC 18. Abstract 1324M-09.
ORLANDO – More than one-third of patients with treatment-resistant hypertension in U.S. cardiology practices are eligible for preferential consideration of spironolactone as their fourth-line agent in accord with the practice-changing findings of the PATHWAY-2 trial, Lauren Thompson, MD, said at the annual meeting of the American College of Cardiology.
She presented a study that harnessed the ACC’s National Cardiovascular Data Registry PINNACLE Registry – the largest observational outpatient cardiovascular registry in the world – to assess the potential impact of PATHWAY-2 on the management of treatment-resistant hypertension (TRH) in U.S. cardiology practices. And as she discovered, the potential implications for daily practice are huge.
Dr. Thompson, a cardiology fellow at the University of Colorado, Denver, identified 19,044 patients in the PINNACLE registry for 2013-2014 with TRH, defined as uncontrolled blood pressure despite use of drugs from three antihypertensive classes. Of these patients, 37% met the PATHWAY-2 enrollment criteria by virtue of already being on an ACE inhibitor or angiotensin receptor blocker, a calcium channel blocker, and a thiazide diuretic, but not spironolactone. This is the large subgroup which, on the basis of PATHWAY-2, should receive serious consideration of spironolactone as the fourth drug.
The most widely prescribed antihypertensive agents in PINNACLE registry patients with TRH were beta-blockers, in 87%; ACE inhibitors, in 72%; calcium channel blockers, in 71%; and thiazide diuretics, in 69%. Of note, 27% of patients with TRH were already on spironolactone.
Audience discussion centered around the uncertainties regarding treatment adherence in patients labeled as having TRH.
“I think sometimes clinicians are afraid to prescribe spironolactone in patients that they think might be nonadherent,” one cardiologist observed.
Dr. Thompson noted that it’s not possible to look at prescription-filling rates in the PINNACLE registry.
“Unfortunately, we can’t exclude white coat hypertension or nonadherence as reasons why patients in PINNACLE end up on multiple antihypertensive medication classes. We can see that a prescription was written, but we have no way to know if it was actually filled or not,” she observed.
Also, since patients in cardiology clinics typically have multiple cardiovascular comorbidities, it’s quite possible that patients with TRH who are on a beta-blocker, for example, might not have received that drug for blood pressure control.
Dr. Thompson’s study was supported by the ACC’s National Cardiovascular Disease Registry. She reported having no financial conflicts of interest.
Source: Thompson L. ACC 18. Abstract 1324M-09.
REPORTING FROM ACC 18
Key clinical point:
Major finding: Thirty-seven percent of patients with treatment-resistant hypertension in U.S. cardiology practices could benefit from preferential consideration of spironolactone as their fourth-line antihypertensive agent.
Study details: This retrospective study included more than 19,000 patients with treatment-resistant hypertension in U.S. cardiology practices.
Disclosures: The presenter reported having no financial conflicts regarding her study, supported by the ACC’s National Cardiovascular Data Registry.
Source: Thompson L. ACC 18. Abstract 1324M-09.
From #MeToo to troponins: Updates in hospital medicine
How do you summarize a year’s worth of hospitalist-relevant research in an hour? If you’re Cynthia Cooper, MD, and Barbara Slawski, MD, MS, SFHM, you do it with teamwork, rigor, and style.
When the two physicians signed on for the 2018 “Update in Hospital Medicine” talk, they knew the bar was high. The updates talk is a perennial crowd favorite at the Society of Hospital Medicine annual conferences, and this year’s talk, which touched on topics from #MeToo to kidney injury, didn’t disappoint.

“One of the things that made the news a lot this last year is gender bias, so we thought we’d start out with that,” said Dr. Slawski, chief of the section of perioperative medicine at the Medical College of Wisconsin in Milwaukee.
In a retrospective observational study, the investigators looked at archived grand rounds video to see how often speakers with doctoral degrees were introduced by title, rather than by first name. Mixed-gender evaluators found that females were much more likely than were males to introduce either females or males by title (P less than .001).
“Have any of you ever had this experience? Me, too,” said Dr. Slawski, to wide and prolonged applause.
Females introducing males were almost twice as likely to use the speaker’s title as when males introduced females (95% vs. 49%; P less than .001). These revelations, said Dr. Slawski, present an “opportunity for improving professional interactions in an environment of mutual respect,” a comment that the room again greeted with a round of applause.
The inpatient syncope evaluation was made a little easier with another top study presented by Dr. Slawski. Using a large multinational database, investigators looked at a subgroup of patients with syncope who were admitted to the hospital. They found that fewer than 2% of patients with syncope were diagnosed with pulmonary embolus (PE) or deep venous thrombosis within 90 days of the index admission. For Dr. Slawski, this means clinicians may be able to relax their worry about thromboembolic events just a bit: “Although this diagnosis should be considered, not all patients need evaluation,” she said.
Dr. Slawski did point out that this observational, retrospective trial differed in many ways from the earlier-published PESIT trial that found a rate of 17% for PE among patients hospitalized for syncope.
Another common clinical dilemma – how to rule out MI in low-risk patients – was addressed in a meta-analysis looking at high-sensitivity troponin T levels in patients with negative ECGs.
In patients coming to the emergency department with a suspicion of acute coronary syndrome, investigators found just a 0.49% incidence of cardiac events in patients who had no ECG evidence of new ischemia and very-low high-sensitivity troponin T. The study looked at two proposed lower limits – less than .0005 mcg/L and less than .003 mcg/L.
Between these two levels, “Sensitivity and negative predictive values were about the same; no patients had mortality within 30 days if they met the criteria,” said Dr. Slawski. However, “You have to remember that sensitivity was below the preset consensus of 99%,” she said; the pooled sensitivity was 98.7%, with fairly high heterogeneity between studies. Also, she said, “If you’re going to use this strategy as your hospital, you have to remember that these values are specific to the assay” at your particular institution.
Dr. Cooper, a nephrologist who practices hospital medicine at Massachusetts General Hospital, Boston, ran through several kidney-related studies. Among these was a retrospective study of the use of IV contrast for computerized tomography (CT), examining the risk of acute kidney injury when patients who received IV contrast were compared both with those who had a CT without contrast and with those who did not have CT. Nearly 17,000 patients were included, with propensity matching used to limit confounding.
Both in this study and in a later meta-analysis, no significant differences were seen in acute kidney injury, the need for renal replacement therapy, or mortality after CT with contrast. However, Dr. Cooper said that as a nephrologist, “This doesn’t make physiological sense to me, so I’m not convinced,” she said. “Ultimately, we need to have a randomized, controlled trial, though it’s hard to imagine” just how such a study could be structured and conducted, she said.
“Influenza H3N2 has dominated outbreaks in the United States over the last few years,” and this fact contributed significantly to the severity of the past year’s influenza season, said Dr. Cooper. Not only does this strain “seem to have greater variability in how often it mutates,” but “it’s also less likely to grow in egg media – so it’s less likely to appear in the vaccine,” she said.
Antivirals are effective only if instituted promptly, meaning that many patients who are admitted to the hospital with influenza and pulmonary infiltrates are beyond this window. Building on what was known about the theoretical efficacy of both macrolides and NSAID medications, a group of researchers in Hong Kong conducted a randomized placebo-controlled trial to compare outcomes when 500 mg of clarithromycin and 200 mg of naproxen were added on days 1 and 2 of hospitalization.
When these two interventions were added to the usual regime of amoxicillin clavulanate, oseltamivir, and esomeprazole, hospital stay was 1 day shorter. Importantly, said Dr. Cooper, 30-day and 90-day mortality rates were shorter and there was a significant reduction in viral titer. This is a strategy Dr. Cooper plans to implement. “My expectation is just like this past year, next year will likely be a bad year for influenza,” she said.
How do you summarize a year’s worth of hospitalist-relevant research in an hour? If you’re Cynthia Cooper, MD, and Barbara Slawski, MD, MS, SFHM, you do it with teamwork, rigor, and style.
When the two physicians signed on for the 2018 “Update in Hospital Medicine” talk, they knew the bar was high. The updates talk is a perennial crowd favorite at the Society of Hospital Medicine annual conferences, and this year’s talk, which touched on topics from #MeToo to kidney injury, didn’t disappoint.
“One of the things that made the news a lot this last year is gender bias, so we thought we’d start out with that,” said Dr. Slawski, chief of the section of perioperative medicine at the Medical College of Wisconsin in Milwaukee.
In a retrospective observational study, the investigators looked at archived grand rounds video to see how often speakers with doctoral degrees were introduced by title, rather than by first name. Mixed-gender evaluators found that females were much more likely than were males to introduce either females or males by title (P less than .001).
“Have any of you ever had this experience? Me, too,” said Dr. Slawski, to wide and prolonged applause.
Females introducing males were almost twice as likely to use the speaker’s title as when males introduced females (95% vs. 49%; P less than .001). These revelations, said Dr. Slawski, present an “opportunity for improving professional interactions in an environment of mutual respect,” a comment that the room again greeted with a round of applause.
The inpatient syncope evaluation was made a little easier with another top study presented by Dr. Slawski. Using a large multinational database, investigators looked at a subgroup of patients with syncope who were admitted to the hospital. They found that fewer than 2% of patients with syncope were diagnosed with pulmonary embolus (PE) or deep venous thrombosis within 90 days of the index admission. For Dr. Slawski, this means clinicians may be able to relax their worry about thromboembolic events just a bit: “Although this diagnosis should be considered, not all patients need evaluation,” she said.
Dr. Slawski did point out that this observational, retrospective trial differed in many ways from the earlier-published PESIT trial that found a rate of 17% for PE among patients hospitalized for syncope.
Another common clinical dilemma – how to rule out MI in low-risk patients – was addressed in a meta-analysis looking at high-sensitivity troponin T levels in patients with negative ECGs.
In patients coming to the emergency department with a suspicion of acute coronary syndrome, investigators found just a 0.49% incidence of cardiac events in patients who had no ECG evidence of new ischemia and very-low high-sensitivity troponin T. The study looked at two proposed lower limits – less than .0005 mcg/L and less than .003 mcg/L.
Between these two levels, “Sensitivity and negative predictive values were about the same; no patients had mortality within 30 days if they met the criteria,” said Dr. Slawski. However, “You have to remember that sensitivity was below the preset consensus of 99%,” she said; the pooled sensitivity was 98.7%, with fairly high heterogeneity between studies. Also, she said, “If you’re going to use this strategy as your hospital, you have to remember that these values are specific to the assay” at your particular institution.
Dr. Cooper, a nephrologist who practices hospital medicine at Massachusetts General Hospital, Boston, ran through several kidney-related studies. Among these was a retrospective study of the use of IV contrast for computerized tomography (CT), examining the risk of acute kidney injury when patients who received IV contrast were compared both with those who had a CT without contrast and with those who did not have CT. Nearly 17,000 patients were included, with propensity matching used to limit confounding.
Both in this study and in a later meta-analysis, no significant differences were seen in acute kidney injury, the need for renal replacement therapy, or mortality after CT with contrast. However, Dr. Cooper said that as a nephrologist, “This doesn’t make physiological sense to me, so I’m not convinced,” she said. “Ultimately, we need to have a randomized, controlled trial, though it’s hard to imagine” just how such a study could be structured and conducted, she said.
“Influenza H3N2 has dominated outbreaks in the United States over the last few years,” and this fact contributed significantly to the severity of the past year’s influenza season, said Dr. Cooper. Not only does this strain “seem to have greater variability in how often it mutates,” but “it’s also less likely to grow in egg media – so it’s less likely to appear in the vaccine,” she said.
Antivirals are effective only if instituted promptly, meaning that many patients who are admitted to the hospital with influenza and pulmonary infiltrates are beyond this window. Building on what was known about the theoretical efficacy of both macrolides and NSAID medications, a group of researchers in Hong Kong conducted a randomized placebo-controlled trial to compare outcomes when 500 mg of clarithromycin and 200 mg of naproxen were added on days 1 and 2 of hospitalization.
When these two interventions were added to the usual regime of amoxicillin clavulanate, oseltamivir, and esomeprazole, hospital stay was 1 day shorter. Importantly, said Dr. Cooper, 30-day and 90-day mortality rates were shorter and there was a significant reduction in viral titer. This is a strategy Dr. Cooper plans to implement. “My expectation is just like this past year, next year will likely be a bad year for influenza,” she said.
How do you summarize a year’s worth of hospitalist-relevant research in an hour? If you’re Cynthia Cooper, MD, and Barbara Slawski, MD, MS, SFHM, you do it with teamwork, rigor, and style.
When the two physicians signed on for the 2018 “Update in Hospital Medicine” talk, they knew the bar was high. The updates talk is a perennial crowd favorite at the Society of Hospital Medicine annual conferences, and this year’s talk, which touched on topics from #MeToo to kidney injury, didn’t disappoint.
“One of the things that made the news a lot this last year is gender bias, so we thought we’d start out with that,” said Dr. Slawski, chief of the section of perioperative medicine at the Medical College of Wisconsin in Milwaukee.
In a retrospective observational study, the investigators looked at archived grand rounds video to see how often speakers with doctoral degrees were introduced by title, rather than by first name. Mixed-gender evaluators found that females were much more likely than were males to introduce either females or males by title (P less than .001).
“Have any of you ever had this experience? Me, too,” said Dr. Slawski, to wide and prolonged applause.
Females introducing males were almost twice as likely to use the speaker’s title as when males introduced females (95% vs. 49%; P less than .001). These revelations, said Dr. Slawski, present an “opportunity for improving professional interactions in an environment of mutual respect,” a comment that the room again greeted with a round of applause.
The inpatient syncope evaluation was made a little easier with another top study presented by Dr. Slawski. Using a large multinational database, investigators looked at a subgroup of patients with syncope who were admitted to the hospital. They found that fewer than 2% of patients with syncope were diagnosed with pulmonary embolus (PE) or deep venous thrombosis within 90 days of the index admission. For Dr. Slawski, this means clinicians may be able to relax their worry about thromboembolic events just a bit: “Although this diagnosis should be considered, not all patients need evaluation,” she said.
Dr. Slawski did point out that this observational, retrospective trial differed in many ways from the earlier-published PESIT trial that found a rate of 17% for PE among patients hospitalized for syncope.
Another common clinical dilemma – how to rule out MI in low-risk patients – was addressed in a meta-analysis looking at high-sensitivity troponin T levels in patients with negative ECGs.
In patients coming to the emergency department with a suspicion of acute coronary syndrome, investigators found just a 0.49% incidence of cardiac events in patients who had no ECG evidence of new ischemia and very-low high-sensitivity troponin T. The study looked at two proposed lower limits – less than .0005 mcg/L and less than .003 mcg/L.
Between these two levels, “Sensitivity and negative predictive values were about the same; no patients had mortality within 30 days if they met the criteria,” said Dr. Slawski. However, “You have to remember that sensitivity was below the preset consensus of 99%,” she said; the pooled sensitivity was 98.7%, with fairly high heterogeneity between studies. Also, she said, “If you’re going to use this strategy as your hospital, you have to remember that these values are specific to the assay” at your particular institution.
Dr. Cooper, a nephrologist who practices hospital medicine at Massachusetts General Hospital, Boston, ran through several kidney-related studies. Among these was a retrospective study of the use of IV contrast for computerized tomography (CT), examining the risk of acute kidney injury when patients who received IV contrast were compared both with those who had a CT without contrast and with those who did not have CT. Nearly 17,000 patients were included, with propensity matching used to limit confounding.
Both in this study and in a later meta-analysis, no significant differences were seen in acute kidney injury, the need for renal replacement therapy, or mortality after CT with contrast. However, Dr. Cooper said that as a nephrologist, “This doesn’t make physiological sense to me, so I’m not convinced,” she said. “Ultimately, we need to have a randomized, controlled trial, though it’s hard to imagine” just how such a study could be structured and conducted, she said.
“Influenza H3N2 has dominated outbreaks in the United States over the last few years,” and this fact contributed significantly to the severity of the past year’s influenza season, said Dr. Cooper. Not only does this strain “seem to have greater variability in how often it mutates,” but “it’s also less likely to grow in egg media – so it’s less likely to appear in the vaccine,” she said.
Antivirals are effective only if instituted promptly, meaning that many patients who are admitted to the hospital with influenza and pulmonary infiltrates are beyond this window. Building on what was known about the theoretical efficacy of both macrolides and NSAID medications, a group of researchers in Hong Kong conducted a randomized placebo-controlled trial to compare outcomes when 500 mg of clarithromycin and 200 mg of naproxen were added on days 1 and 2 of hospitalization.
When these two interventions were added to the usual regime of amoxicillin clavulanate, oseltamivir, and esomeprazole, hospital stay was 1 day shorter. Importantly, said Dr. Cooper, 30-day and 90-day mortality rates were shorter and there was a significant reduction in viral titer. This is a strategy Dr. Cooper plans to implement. “My expectation is just like this past year, next year will likely be a bad year for influenza,” she said.

Use procalcitonin-guided algorithms to guide antibiotic therapy for acute respiratory infections to improve patient outcomes
Clinical question: How does using procalcitonin levels for adults with acute respiratory infections (ARIs) affect patient outcomes?
Background: While the ARI diagnosis encompasses bacterial, viral, and inflammatory etiologies, as many as 75% of ARIs are treated with antibiotics. Procalcitonin is a biomarker released by tissues in response to bacterial infections. Its production is also inhibited by interferon-gamma, a cytokine released in response to viral infections, therefore, making procalcitonin a biomarker of particular interest to support the use of antibiotic therapy in the treatment of ARIs.
Study design: Cochrane Review.
Setting: Medical wards, intensive care units, primary care clinics, and emergency departments across 12 countries.
Synopsis: The review included 26 randomized control trials of 6,708 immunocompetent adults with ARIs who received antibiotics either based on procalcitonin-guided antibiotic therapy or routine care. Primary endpoints evaluated included all-cause mortality and treatment failure at 30 days. Secondary endpoints were antibiotic use, antibiotic-related side effects, and length of hospital stay. There were significantly fewer deaths in the procalcitonin-guided group than in the control group (286/8.6% vs. 336/10%; adjusted odds ratio, 0.83; 95% confidence interval, 0.70-0.99; P = .037). Treatment failure was not statistically different between the procalcitonin-guided participants and the controls. Of the secondary endpoints, antibiotic use and antibiotic-related side effects were lower in the procalcitonin-guided group (5.7 days vs. 8.1 days; P less than .001; and 16.3% vs. 22.1%; P less than .001). Each of the RCTs had varying algorithms for the use of procalcitonin-guided therapy, so no specific treatment guidelines can be gleaned from this review.
Bottom line: Procalcitonin-guided algorithms are associated with lower mortality, lower antibiotic exposure, and lower antibiotic-related side effects. However, more research is needed to determine best practice algorithms for using procalcitonin levels to guide treatment decisions.
Citation: Schuetz P et al. Procalcitonin to initiate or discontinue antibiotics in acute respiratory tract infections. Cochrane Database Syst Rev. 2017 Oct 12. doi: 10.1002/14651858.cd007498.pub3.
Dr. Sundar is assistant professor of medicine in the division of hospital medicine, Emory University, Atlanta.
Clinical question: How does using procalcitonin levels for adults with acute respiratory infections (ARIs) affect patient outcomes?
Background: While the ARI diagnosis encompasses bacterial, viral, and inflammatory etiologies, as many as 75% of ARIs are treated with antibiotics. Procalcitonin is a biomarker released by tissues in response to bacterial infections. Its production is also inhibited by interferon-gamma, a cytokine released in response to viral infections, therefore, making procalcitonin a biomarker of particular interest to support the use of antibiotic therapy in the treatment of ARIs.
Study design: Cochrane Review.
Setting: Medical wards, intensive care units, primary care clinics, and emergency departments across 12 countries.
Synopsis: The review included 26 randomized control trials of 6,708 immunocompetent adults with ARIs who received antibiotics either based on procalcitonin-guided antibiotic therapy or routine care. Primary endpoints evaluated included all-cause mortality and treatment failure at 30 days. Secondary endpoints were antibiotic use, antibiotic-related side effects, and length of hospital stay. There were significantly fewer deaths in the procalcitonin-guided group than in the control group (286/8.6% vs. 336/10%; adjusted odds ratio, 0.83; 95% confidence interval, 0.70-0.99; P = .037). Treatment failure was not statistically different between the procalcitonin-guided participants and the controls. Of the secondary endpoints, antibiotic use and antibiotic-related side effects were lower in the procalcitonin-guided group (5.7 days vs. 8.1 days; P less than .001; and 16.3% vs. 22.1%; P less than .001). Each of the RCTs had varying algorithms for the use of procalcitonin-guided therapy, so no specific treatment guidelines can be gleaned from this review.
Bottom line: Procalcitonin-guided algorithms are associated with lower mortality, lower antibiotic exposure, and lower antibiotic-related side effects. However, more research is needed to determine best practice algorithms for using procalcitonin levels to guide treatment decisions.
Citation: Schuetz P et al. Procalcitonin to initiate or discontinue antibiotics in acute respiratory tract infections. Cochrane Database Syst Rev. 2017 Oct 12. doi: 10.1002/14651858.cd007498.pub3.
Dr. Sundar is assistant professor of medicine in the division of hospital medicine, Emory University, Atlanta.
Clinical question: How does using procalcitonin levels for adults with acute respiratory infections (ARIs) affect patient outcomes?
Background: While the ARI diagnosis encompasses bacterial, viral, and inflammatory etiologies, as many as 75% of ARIs are treated with antibiotics. Procalcitonin is a biomarker released by tissues in response to bacterial infections. Its production is also inhibited by interferon-gamma, a cytokine released in response to viral infections, therefore, making procalcitonin a biomarker of particular interest to support the use of antibiotic therapy in the treatment of ARIs.
Study design: Cochrane Review.
Setting: Medical wards, intensive care units, primary care clinics, and emergency departments across 12 countries.
Synopsis: The review included 26 randomized control trials of 6,708 immunocompetent adults with ARIs who received antibiotics either based on procalcitonin-guided antibiotic therapy or routine care. Primary endpoints evaluated included all-cause mortality and treatment failure at 30 days. Secondary endpoints were antibiotic use, antibiotic-related side effects, and length of hospital stay. There were significantly fewer deaths in the procalcitonin-guided group than in the control group (286/8.6% vs. 336/10%; adjusted odds ratio, 0.83; 95% confidence interval, 0.70-0.99; P = .037). Treatment failure was not statistically different between the procalcitonin-guided participants and the controls. Of the secondary endpoints, antibiotic use and antibiotic-related side effects were lower in the procalcitonin-guided group (5.7 days vs. 8.1 days; P less than .001; and 16.3% vs. 22.1%; P less than .001). Each of the RCTs had varying algorithms for the use of procalcitonin-guided therapy, so no specific treatment guidelines can be gleaned from this review.
Bottom line: Procalcitonin-guided algorithms are associated with lower mortality, lower antibiotic exposure, and lower antibiotic-related side effects. However, more research is needed to determine best practice algorithms for using procalcitonin levels to guide treatment decisions.
Citation: Schuetz P et al. Procalcitonin to initiate or discontinue antibiotics in acute respiratory tract infections. Cochrane Database Syst Rev. 2017 Oct 12. doi: 10.1002/14651858.cd007498.pub3.
Dr. Sundar is assistant professor of medicine in the division of hospital medicine, Emory University, Atlanta.
Mixed outcomes in analysis of NSAIDs and IBD exacerbation
The relationship between nonsteroidal anti-inflammatory drug (NSAID) use and exacerbations of inflammatory bowel disease (IBD) may not be as clear-cut as previously thought, according to the results of a systematic review and meta-analysis.
The report was published online in Alimentary Pharmacology and Therapeutics.
The researchers presented their analysis of 18 studies examining the association between acetaminophen, NSAIDs, and cyclo-oxygenase-2 (COX-2) inhibitors, and the risk of Crohn’s disease, ulcerative colitis flares, and IBD.
Five studies looked at the association between NSAIDS – such as naproxen and indomethacin – and the risk of Crohn’s disease exacerbation. While this showed a 42% increased risk of exacerbation with NSAID use, the authors noted that they saw substantial heterogeneity across the studies.
For example, two nonrandomized trials comparing NSAIDs and acetaminophen in patients with quiescent disease found NSAIDs were associated with frequent, early clinical relapse of IBD. But another study comparing patients with symptom flares and those in clinical remission found no difference between the two groups in the frequency of NSAID use.
Researchers also conducted a meta-analysis of studies involving acetaminophen, which found a statistically significant 56% increase in the risk of IBD exacerbation with acetaminophen. However, in the systematic review, there were two nonrandomized clinical trials which showed only one disease exacerbation in 46 patients with quiescent IBD, which was lower than the rate seen in the NSAID group.
Given the heterogeneity seen across the studies, the authors conducted an analysis limited to studies that scored seven or above on the Newcastle-Ottowa Scale for assessing the quality of nonrandomized studies. In this analysis, the risk of Crohn’s disease exacerbations increased significantly with NSAID use (RR = 1.53; 95% confidence interval, 1.08-2.16) but they did not see an association between NSAID use and the risk of ulcerative colitis or other IBD exacerbations.
Similarly, when they restricted their analysis to studies with a low risk of bias, the researchers found there was an increased risk of Crohn’s disease exacerbations, but not ulcerative colitis, with NSAID use.
“American College of Gastroenterology guidelines for management of IBD recognise NSAIDs as potential triggers for disease exacerbation, highlighting the ongoing concern regarding the use of these medications in patients with established disease,” wrote Dr. Oluwatoba Moninuola of Harvard University T.H. Chan School of Public Health, and coauthors.
“Although, it’s well established that NSAIDs may cause de novo damage throughout the gastrointestinal tract, the precise mechanism through which NSAIDs promote IBD exacerbation remains largely unknown.”
They said previous research suggested COX-1 and COX-2 inhibitors may be responsible for the inhibition of intestinal prostaglandin synthesis.
The authors also noted that wide variations in the definition of disease exacerbation may have contributed to the heterogeneity of the studies included, and that there may have been confounding by the indication for acetaminophen and NSAID use.
“We recognise that IBD is a heterogeneous disease and therefore, there may be subgroups of patients particularly at risk of disease exacerbations with use of NSAIDs.”
One author was supported by the American Gastroenterological Association and by the National Institute of Diabetes and Digestive and Kidney Diseases, and declared consulting and research funding from the pharmaceutical industry. No other conflicts of interest were declared.
SOURCE: Moninuola O et al. Aliment Pharmacol Ther. 2018 Apr 5. doi: 10.1111/apt.14606.
The relationship between nonsteroidal anti-inflammatory drug (NSAID) use and exacerbations of inflammatory bowel disease (IBD) may not be as clear-cut as previously thought, according to the results of a systematic review and meta-analysis.
The report was published online in Alimentary Pharmacology and Therapeutics.
The researchers presented their analysis of 18 studies examining the association between acetaminophen, NSAIDs, and cyclo-oxygenase-2 (COX-2) inhibitors, and the risk of Crohn’s disease, ulcerative colitis flares, and IBD.
Five studies looked at the association between NSAIDS – such as naproxen and indomethacin – and the risk of Crohn’s disease exacerbation. While this showed a 42% increased risk of exacerbation with NSAID use, the authors noted that they saw substantial heterogeneity across the studies.
For example, two nonrandomized trials comparing NSAIDs and acetaminophen in patients with quiescent disease found NSAIDs were associated with frequent, early clinical relapse of IBD. But another study comparing patients with symptom flares and those in clinical remission found no difference between the two groups in the frequency of NSAID use.
Researchers also conducted a meta-analysis of studies involving acetaminophen, which found a statistically significant 56% increase in the risk of IBD exacerbation with acetaminophen. However, in the systematic review, there were two nonrandomized clinical trials which showed only one disease exacerbation in 46 patients with quiescent IBD, which was lower than the rate seen in the NSAID group.
Given the heterogeneity seen across the studies, the authors conducted an analysis limited to studies that scored seven or above on the Newcastle-Ottowa Scale for assessing the quality of nonrandomized studies. In this analysis, the risk of Crohn’s disease exacerbations increased significantly with NSAID use (RR = 1.53; 95% confidence interval, 1.08-2.16) but they did not see an association between NSAID use and the risk of ulcerative colitis or other IBD exacerbations.
Similarly, when they restricted their analysis to studies with a low risk of bias, the researchers found there was an increased risk of Crohn’s disease exacerbations, but not ulcerative colitis, with NSAID use.
“American College of Gastroenterology guidelines for management of IBD recognise NSAIDs as potential triggers for disease exacerbation, highlighting the ongoing concern regarding the use of these medications in patients with established disease,” wrote Dr. Oluwatoba Moninuola of Harvard University T.H. Chan School of Public Health, and coauthors.
“Although, it’s well established that NSAIDs may cause de novo damage throughout the gastrointestinal tract, the precise mechanism through which NSAIDs promote IBD exacerbation remains largely unknown.”
They said previous research suggested COX-1 and COX-2 inhibitors may be responsible for the inhibition of intestinal prostaglandin synthesis.
The authors also noted that wide variations in the definition of disease exacerbation may have contributed to the heterogeneity of the studies included, and that there may have been confounding by the indication for acetaminophen and NSAID use.
“We recognise that IBD is a heterogeneous disease and therefore, there may be subgroups of patients particularly at risk of disease exacerbations with use of NSAIDs.”
One author was supported by the American Gastroenterological Association and by the National Institute of Diabetes and Digestive and Kidney Diseases, and declared consulting and research funding from the pharmaceutical industry. No other conflicts of interest were declared.
SOURCE: Moninuola O et al. Aliment Pharmacol Ther. 2018 Apr 5. doi: 10.1111/apt.14606.
The relationship between nonsteroidal anti-inflammatory drug (NSAID) use and exacerbations of inflammatory bowel disease (IBD) may not be as clear-cut as previously thought, according to the results of a systematic review and meta-analysis.
The report was published online in Alimentary Pharmacology and Therapeutics.
The researchers presented their analysis of 18 studies examining the association between acetaminophen, NSAIDs, and cyclo-oxygenase-2 (COX-2) inhibitors, and the risk of Crohn’s disease, ulcerative colitis flares, and IBD.
Five studies looked at the association between NSAIDS – such as naproxen and indomethacin – and the risk of Crohn’s disease exacerbation. While this showed a 42% increased risk of exacerbation with NSAID use, the authors noted that they saw substantial heterogeneity across the studies.
For example, two nonrandomized trials comparing NSAIDs and acetaminophen in patients with quiescent disease found NSAIDs were associated with frequent, early clinical relapse of IBD. But another study comparing patients with symptom flares and those in clinical remission found no difference between the two groups in the frequency of NSAID use.
Researchers also conducted a meta-analysis of studies involving acetaminophen, which found a statistically significant 56% increase in the risk of IBD exacerbation with acetaminophen. However, in the systematic review, there were two nonrandomized clinical trials which showed only one disease exacerbation in 46 patients with quiescent IBD, which was lower than the rate seen in the NSAID group.
Given the heterogeneity seen across the studies, the authors conducted an analysis limited to studies that scored seven or above on the Newcastle-Ottowa Scale for assessing the quality of nonrandomized studies. In this analysis, the risk of Crohn’s disease exacerbations increased significantly with NSAID use (RR = 1.53; 95% confidence interval, 1.08-2.16) but they did not see an association between NSAID use and the risk of ulcerative colitis or other IBD exacerbations.
Similarly, when they restricted their analysis to studies with a low risk of bias, the researchers found there was an increased risk of Crohn’s disease exacerbations, but not ulcerative colitis, with NSAID use.
“American College of Gastroenterology guidelines for management of IBD recognise NSAIDs as potential triggers for disease exacerbation, highlighting the ongoing concern regarding the use of these medications in patients with established disease,” wrote Dr. Oluwatoba Moninuola of Harvard University T.H. Chan School of Public Health, and coauthors.
“Although, it’s well established that NSAIDs may cause de novo damage throughout the gastrointestinal tract, the precise mechanism through which NSAIDs promote IBD exacerbation remains largely unknown.”
They said previous research suggested COX-1 and COX-2 inhibitors may be responsible for the inhibition of intestinal prostaglandin synthesis.
The authors also noted that wide variations in the definition of disease exacerbation may have contributed to the heterogeneity of the studies included, and that there may have been confounding by the indication for acetaminophen and NSAID use.
“We recognise that IBD is a heterogeneous disease and therefore, there may be subgroups of patients particularly at risk of disease exacerbations with use of NSAIDs.”
One author was supported by the American Gastroenterological Association and by the National Institute of Diabetes and Digestive and Kidney Diseases, and declared consulting and research funding from the pharmaceutical industry. No other conflicts of interest were declared.
SOURCE: Moninuola O et al. Aliment Pharmacol Ther. 2018 Apr 5. doi: 10.1111/apt.14606.
FROM ALIMENTARY PHARMACOLOGY AND THERAPEUTICS
Key clinical point: Nonsteroidal anti-inflammatory drugs may increase the risk of some inflammatory bowel diseases.
Major finding: NSAIDs are associated with a 42% increased risk of Crohn’s disease exacerbation.
Study details: Systematic review and meta-analysis of 18 studies.
Disclosures: One author was supported by the American Gastroenterological Association and by the National Institute of Diabetes and Digestive and Kidney Diseases, and declared consulting and research funding from the pharmaceutical industry. No other conflicts of interest were declared.
Source: Moninuola O et al. Aliment Pharmacol Ther. 2018 Apr 5. doi: 10.1111/apt.14606.
Launching into the future
Hospital Medicine: 10 years ago
My first Society of Hospital Medicine Annual Conference was HM08, and it changed the course of my professional career.
I was a first-year hospitalist from an academic program of fewer than 10 physicians. My knowledge about my field did not extend much beyond the clinical practice of hospital medicine. I remember sitting at the airport on my way to HM08 and excitedly looking over the schedule for the meeting. I diligently circled the sessions that I was looking forward to attending, the majority of which focused on the clinical tracks. But by the end of the meeting, in additional to valuable medical knowledge, I walked away with novel insights that launched me into my future.

New ideas in HM: In 2008, comanagement was still a new concept. As I attended sessions and spoke with hospitalists from across the country, it became clear that this was a collaboration that would be core to our specialty. Within a couple of months of returning home from the annual conference, I was approached by the chair of neurosurgery at my institution with a proposal to develop a quality program for his group. While at that time I was considering other competing interests, my experience at HM08 helped me recognize that this was a unique opportunity to build bridges across specialties and to collaborate. I subsequently became the executive director of quality for neurosurgery and over the years was able to create a strong relationship between our departments that led to building a nationally recognized program with exceptional performance in hospital-based quality.
Side note: If you’re interested in resources on comanagement, please check out SHM’s Resources for Effective Co-Management of Hospitalized Patients at https://www.hospitalmedicine.org/comanagement .
Emerging themes and trends in health care: While the quality movement had launched about a decade before HM08, many institutions still did not have robust programs. As I attended sessions during the annual meeting and spoke with thought leaders, one message became clear: Hospitalists would have to lead the quality movement at their institutions. When I returned home, I began learning about quality improvement and started to lead various initiatives. These efforts led to my appointment as associate chief medical officer for the health system. This position enabled me to leverage my knowledge of hospital-based care and collaborate across various specialties to reduce our mortality and readmission rates in the organization.
Side note: If you’re interested in learning more about quality improvement educational and mentorship opportunities, please visit https://www.hospitalmedicine.org/qi and look at the resources for each specific topic.
And, most importantly, friendships: By far the most important thing I took away from HM08 was the friendships that started at that meeting and have developed over the years since. A decade later, I continue to rely on, grow from, and be challenged by the same people I met at that meeting. They are the colleagues I call when I find myself in a tough spot at work and need advice, the collaborators I work with on grants and projects, and the friends I text when I travel to a new town and want to grab a bite to eat.
Side note: If you’re interested in connecting with colleagues who share similar interests, please visit https://www.hospitalmedicine.org/sigs and review SHM’s Special Interest Groups to find ones that are right for you. To connect on a more local level, find an SHM Chapter near you at https://www.hospitalmedicine.org/chapters.
I’ve shared these stories with you because for me my journey with our society has been a deeply personal one. And I feel indebted to SHM and the incredible people who drawn to it for helping me develop and enjoy a rich and rewarding career thus far. So, as I look forward to the next decade, I wanted to share my thoughts on HM and emerging themes in health care with you.
Hospital medicine: The next decade
New ideas in HM: Population health management
Building on our strong culture of collaboration as we move forward into this next decade, we have to define how we deliver value in the context of population health management. As hospitalists, we have to push the boundaries of the hospital and provide high-value care beyond our four walls.
How can we do that? I think technology will play a critical role in extending our reach beyond the hospital. As we move toward delivering greater value to our patients, lower acuity patients will receive care in their homes. Telehealth will enable us to monitor and manage these patients remotely while transferring our bedside management to patients’ bedrooms in their own homes. Virtual hospitals will further enable us to evaluate, triage, monitor, and manage patients remotely. Our active engagement in these efforts is critical to ensure the continued growth and value we bring to our patients, our organizations, and our society.
Emerging themes and trends in health care: Transitioning from quality to value
In the next decade, value will prevail. This is not a novel concept – much like how quality was not a new idea in 2008.
Value has been around for a while: There are some robust programs nationally, there is research around the topic, and there are policies with implications for reimbursements. However, the full potential of value has not yet been realized by health care – it exists in individual programs, not in everything we do. The unprecedented number of mergers and acquisitions in health care in 2018 support the fact that the future will belong to those institutions that can deliver the highest quality of care at the most appropriate cost throughout the entire continuum of care.
What are some of the tools that will help us get there? Artificial intelligence and machine learning will improve the predictive value for the care we deliver to individual patients; some preliminary work in this area has already revealed that factors that we previously associated with higher risk of readmissions are not truly predictive. Another emerging technology is blockchain: By creating a single source of truth for our patients’ medical information, it enables us to have dynamic, high-integrity records regardless of which health systems and EHRs have cared for those patients.
I wish you an energizing journey as you launch your future into the next dynamic decade of health care, and I look forward to connecting with you as we continue to build a society that prepares us for the challenges and opportunities ahead.
Dr. Afsar is the president of the Society of Hospital Medicine and the chief ambulatory officer and chief medical officer for the accountable care organizations at UC Irvine Health.
Hospital Medicine: 10 years ago
My first Society of Hospital Medicine Annual Conference was HM08, and it changed the course of my professional career.
I was a first-year hospitalist from an academic program of fewer than 10 physicians. My knowledge about my field did not extend much beyond the clinical practice of hospital medicine. I remember sitting at the airport on my way to HM08 and excitedly looking over the schedule for the meeting. I diligently circled the sessions that I was looking forward to attending, the majority of which focused on the clinical tracks. But by the end of the meeting, in additional to valuable medical knowledge, I walked away with novel insights that launched me into my future.
New ideas in HM: In 2008, comanagement was still a new concept. As I attended sessions and spoke with hospitalists from across the country, it became clear that this was a collaboration that would be core to our specialty. Within a couple of months of returning home from the annual conference, I was approached by the chair of neurosurgery at my institution with a proposal to develop a quality program for his group. While at that time I was considering other competing interests, my experience at HM08 helped me recognize that this was a unique opportunity to build bridges across specialties and to collaborate. I subsequently became the executive director of quality for neurosurgery and over the years was able to create a strong relationship between our departments that led to building a nationally recognized program with exceptional performance in hospital-based quality.
Side note: If you’re interested in resources on comanagement, please check out SHM’s Resources for Effective Co-Management of Hospitalized Patients at https://www.hospitalmedicine.org/comanagement .
Emerging themes and trends in health care: While the quality movement had launched about a decade before HM08, many institutions still did not have robust programs. As I attended sessions during the annual meeting and spoke with thought leaders, one message became clear: Hospitalists would have to lead the quality movement at their institutions. When I returned home, I began learning about quality improvement and started to lead various initiatives. These efforts led to my appointment as associate chief medical officer for the health system. This position enabled me to leverage my knowledge of hospital-based care and collaborate across various specialties to reduce our mortality and readmission rates in the organization.
Side note: If you’re interested in learning more about quality improvement educational and mentorship opportunities, please visit https://www.hospitalmedicine.org/qi and look at the resources for each specific topic.
And, most importantly, friendships: By far the most important thing I took away from HM08 was the friendships that started at that meeting and have developed over the years since. A decade later, I continue to rely on, grow from, and be challenged by the same people I met at that meeting. They are the colleagues I call when I find myself in a tough spot at work and need advice, the collaborators I work with on grants and projects, and the friends I text when I travel to a new town and want to grab a bite to eat.
Side note: If you’re interested in connecting with colleagues who share similar interests, please visit https://www.hospitalmedicine.org/sigs and review SHM’s Special Interest Groups to find ones that are right for you. To connect on a more local level, find an SHM Chapter near you at https://www.hospitalmedicine.org/chapters.
I’ve shared these stories with you because for me my journey with our society has been a deeply personal one. And I feel indebted to SHM and the incredible people who drawn to it for helping me develop and enjoy a rich and rewarding career thus far. So, as I look forward to the next decade, I wanted to share my thoughts on HM and emerging themes in health care with you.
Hospital medicine: The next decade
New ideas in HM: Population health management
Building on our strong culture of collaboration as we move forward into this next decade, we have to define how we deliver value in the context of population health management. As hospitalists, we have to push the boundaries of the hospital and provide high-value care beyond our four walls.
How can we do that? I think technology will play a critical role in extending our reach beyond the hospital. As we move toward delivering greater value to our patients, lower acuity patients will receive care in their homes. Telehealth will enable us to monitor and manage these patients remotely while transferring our bedside management to patients’ bedrooms in their own homes. Virtual hospitals will further enable us to evaluate, triage, monitor, and manage patients remotely. Our active engagement in these efforts is critical to ensure the continued growth and value we bring to our patients, our organizations, and our society.
Emerging themes and trends in health care: Transitioning from quality to value
In the next decade, value will prevail. This is not a novel concept – much like how quality was not a new idea in 2008.
Value has been around for a while: There are some robust programs nationally, there is research around the topic, and there are policies with implications for reimbursements. However, the full potential of value has not yet been realized by health care – it exists in individual programs, not in everything we do. The unprecedented number of mergers and acquisitions in health care in 2018 support the fact that the future will belong to those institutions that can deliver the highest quality of care at the most appropriate cost throughout the entire continuum of care.
What are some of the tools that will help us get there? Artificial intelligence and machine learning will improve the predictive value for the care we deliver to individual patients; some preliminary work in this area has already revealed that factors that we previously associated with higher risk of readmissions are not truly predictive. Another emerging technology is blockchain: By creating a single source of truth for our patients’ medical information, it enables us to have dynamic, high-integrity records regardless of which health systems and EHRs have cared for those patients.
I wish you an energizing journey as you launch your future into the next dynamic decade of health care, and I look forward to connecting with you as we continue to build a society that prepares us for the challenges and opportunities ahead.
Dr. Afsar is the president of the Society of Hospital Medicine and the chief ambulatory officer and chief medical officer for the accountable care organizations at UC Irvine Health.
Hospital Medicine: 10 years ago
My first Society of Hospital Medicine Annual Conference was HM08, and it changed the course of my professional career.
I was a first-year hospitalist from an academic program of fewer than 10 physicians. My knowledge about my field did not extend much beyond the clinical practice of hospital medicine. I remember sitting at the airport on my way to HM08 and excitedly looking over the schedule for the meeting. I diligently circled the sessions that I was looking forward to attending, the majority of which focused on the clinical tracks. But by the end of the meeting, in additional to valuable medical knowledge, I walked away with novel insights that launched me into my future.
New ideas in HM: In 2008, comanagement was still a new concept. As I attended sessions and spoke with hospitalists from across the country, it became clear that this was a collaboration that would be core to our specialty. Within a couple of months of returning home from the annual conference, I was approached by the chair of neurosurgery at my institution with a proposal to develop a quality program for his group. While at that time I was considering other competing interests, my experience at HM08 helped me recognize that this was a unique opportunity to build bridges across specialties and to collaborate. I subsequently became the executive director of quality for neurosurgery and over the years was able to create a strong relationship between our departments that led to building a nationally recognized program with exceptional performance in hospital-based quality.
Side note: If you’re interested in resources on comanagement, please check out SHM’s Resources for Effective Co-Management of Hospitalized Patients at https://www.hospitalmedicine.org/comanagement .
Emerging themes and trends in health care: While the quality movement had launched about a decade before HM08, many institutions still did not have robust programs. As I attended sessions during the annual meeting and spoke with thought leaders, one message became clear: Hospitalists would have to lead the quality movement at their institutions. When I returned home, I began learning about quality improvement and started to lead various initiatives. These efforts led to my appointment as associate chief medical officer for the health system. This position enabled me to leverage my knowledge of hospital-based care and collaborate across various specialties to reduce our mortality and readmission rates in the organization.
Side note: If you’re interested in learning more about quality improvement educational and mentorship opportunities, please visit https://www.hospitalmedicine.org/qi and look at the resources for each specific topic.
And, most importantly, friendships: By far the most important thing I took away from HM08 was the friendships that started at that meeting and have developed over the years since. A decade later, I continue to rely on, grow from, and be challenged by the same people I met at that meeting. They are the colleagues I call when I find myself in a tough spot at work and need advice, the collaborators I work with on grants and projects, and the friends I text when I travel to a new town and want to grab a bite to eat.
Side note: If you’re interested in connecting with colleagues who share similar interests, please visit https://www.hospitalmedicine.org/sigs and review SHM’s Special Interest Groups to find ones that are right for you. To connect on a more local level, find an SHM Chapter near you at https://www.hospitalmedicine.org/chapters.
I’ve shared these stories with you because for me my journey with our society has been a deeply personal one. And I feel indebted to SHM and the incredible people who drawn to it for helping me develop and enjoy a rich and rewarding career thus far. So, as I look forward to the next decade, I wanted to share my thoughts on HM and emerging themes in health care with you.
Hospital medicine: The next decade
New ideas in HM: Population health management
Building on our strong culture of collaboration as we move forward into this next decade, we have to define how we deliver value in the context of population health management. As hospitalists, we have to push the boundaries of the hospital and provide high-value care beyond our four walls.
How can we do that? I think technology will play a critical role in extending our reach beyond the hospital. As we move toward delivering greater value to our patients, lower acuity patients will receive care in their homes. Telehealth will enable us to monitor and manage these patients remotely while transferring our bedside management to patients’ bedrooms in their own homes. Virtual hospitals will further enable us to evaluate, triage, monitor, and manage patients remotely. Our active engagement in these efforts is critical to ensure the continued growth and value we bring to our patients, our organizations, and our society.
Emerging themes and trends in health care: Transitioning from quality to value
In the next decade, value will prevail. This is not a novel concept – much like how quality was not a new idea in 2008.
Value has been around for a while: There are some robust programs nationally, there is research around the topic, and there are policies with implications for reimbursements. However, the full potential of value has not yet been realized by health care – it exists in individual programs, not in everything we do. The unprecedented number of mergers and acquisitions in health care in 2018 support the fact that the future will belong to those institutions that can deliver the highest quality of care at the most appropriate cost throughout the entire continuum of care.
What are some of the tools that will help us get there? Artificial intelligence and machine learning will improve the predictive value for the care we deliver to individual patients; some preliminary work in this area has already revealed that factors that we previously associated with higher risk of readmissions are not truly predictive. Another emerging technology is blockchain: By creating a single source of truth for our patients’ medical information, it enables us to have dynamic, high-integrity records regardless of which health systems and EHRs have cared for those patients.
I wish you an energizing journey as you launch your future into the next dynamic decade of health care, and I look forward to connecting with you as we continue to build a society that prepares us for the challenges and opportunities ahead.
Dr. Afsar is the president of the Society of Hospital Medicine and the chief ambulatory officer and chief medical officer for the accountable care organizations at UC Irvine Health.
Recently approved SK treatment spares melanocytes in preclinical study
A study using an ex vivo model to evaluate a seborrheic keratosis (SK) treatment shows that a topical application of 40% hydrogen peroxide is gentler on skin than a 5- or 10-second treatment with liquid nitrogen, particularly with respect to melanocytes, suggesting that the former may be less likely to produce disfiguring damage.
The 40% hydrogen peroxide solution (Eskata), also known as A-101, received Food and Drug Administration approval for the treatment of “seborrheic keratoses that are raised” in December, 2017. The study was published online in the Journal of the American Academy of Dermatology.
Melanocyte damage can lead to significant dyschromia, a poor cosmetic outcome that can have a tremendous impact on quality of life for dark-skinned patients, in whom it produces white spots. “A lot of these destructive approaches, especially liquid nitrogen, can leave more disfigurement upon treatment than the lesion itself,” the study’s lead author Adam Friedman, MD, said in an interview.
Melanocytes are particularly vulnerable to the effects of cold, so the destructive potential of liquid nitrogen is no surprise. But Dr. Friedman of the department of dermatology, George Washington University, Washington, wanted to get a better understanding of the impact of the new treatment on different skin cell types and the toxicity profile, so he approached the manufacturer, Aclaris Therapeutics, to do a study.
His team tested 40% hydrogen peroxide treatment and liquid nitrogen cryosurgery on a validated ex vivo human reconstituted full-thickness model derived from Fitzpatrick V skin, with 5 or 10 seconds of cryosurgery or 1 or 2 mcL of 40% hydrogen peroxide.
Using standard a hematoxylin and eosin stain as well as immunohistochemical staining to examine the architecture and cells types of the skin model following both treatments, the researchers found that 5- and 10-second cryosurgery resulted in significant thinning of the epidermis and increased cell death. There was also separation at the dermal-epidermal junction, which was more prominent in the 10-second cryosurgery group, although present even with a 5-second freeze cycle.
The hydrogen peroxide–treated groups showed acanthosis of the epidermis and mild pallor, but this was less noticeable than in the cryosurgery specimens. There was no epidermal clefting in the hydrogen peroxide–treated samples.
Tunel staining revealed 16.4 (plus or minus 0.6424) apoptotic cells per high-powered field in the 5-second cryosurgery experiment and 20.6 (plus or minus 0.6424) in the 10-second procedure. For the hydrogen peroxide treatment, those numbers were 8.65 (plus or minus 0.4122) in the 1 mcL experiment and 12.4 (plus or minus 0.3728) in the 2 mcL experiment.
As expected, melanocytes fared better with the hydrogen peroxide treatment. In the untreated samples, there were 2.5 melanocytes (plus or minus 0.1987) in the untreated sample and 2.0 (plus or minus 0.5000) melanocytes in the vehicle-treated sample. In the 5-second cryosurgery sample, there were 0.45 melanocytes (plus or minus 0.1535), and in the 10 second cryosurgery sample there were 0.2 (plus or minus 0.0918) melanocytes. In contrast, with the 1-mcL hydrogen peroxide-treated sample, there were 1.95 melanocytes in both the 1-mcL and 2-mcL samples (plus or minus 0.1535 for both groups).
“,” Dr. Friedman said. These results, he added, “offer us a lot of insight in terms of how damaging liquid nitrogen is, and it’s good to be reminded of that so that we don’t cause too much harm.”
The authors noted that a clinical trial evaluating the risk of hypopigmentation and hyperpigmentation with 40% hydrogen peroxide in people with darker skin types is underway. In the study, hydrogen peroxide is used to treat dermatosis papulosa nigra.
The study was funded by Aclaris Therapeutics. Senior author Adam Friedman, MD, is a consultant for Aclaris. Dr. Friedman is on the editorial board of Dermatology News.
SOURCE: Kao S et al. J Am Acad Dermatol. 2018 Mar 27. doi: 10.1016/j.jaad.2018.03.034.
A study using an ex vivo model to evaluate a seborrheic keratosis (SK) treatment shows that a topical application of 40% hydrogen peroxide is gentler on skin than a 5- or 10-second treatment with liquid nitrogen, particularly with respect to melanocytes, suggesting that the former may be less likely to produce disfiguring damage.
The 40% hydrogen peroxide solution (Eskata), also known as A-101, received Food and Drug Administration approval for the treatment of “seborrheic keratoses that are raised” in December, 2017. The study was published online in the Journal of the American Academy of Dermatology.
Melanocyte damage can lead to significant dyschromia, a poor cosmetic outcome that can have a tremendous impact on quality of life for dark-skinned patients, in whom it produces white spots. “A lot of these destructive approaches, especially liquid nitrogen, can leave more disfigurement upon treatment than the lesion itself,” the study’s lead author Adam Friedman, MD, said in an interview.
Melanocytes are particularly vulnerable to the effects of cold, so the destructive potential of liquid nitrogen is no surprise. But Dr. Friedman of the department of dermatology, George Washington University, Washington, wanted to get a better understanding of the impact of the new treatment on different skin cell types and the toxicity profile, so he approached the manufacturer, Aclaris Therapeutics, to do a study.
His team tested 40% hydrogen peroxide treatment and liquid nitrogen cryosurgery on a validated ex vivo human reconstituted full-thickness model derived from Fitzpatrick V skin, with 5 or 10 seconds of cryosurgery or 1 or 2 mcL of 40% hydrogen peroxide.
Using standard a hematoxylin and eosin stain as well as immunohistochemical staining to examine the architecture and cells types of the skin model following both treatments, the researchers found that 5- and 10-second cryosurgery resulted in significant thinning of the epidermis and increased cell death. There was also separation at the dermal-epidermal junction, which was more prominent in the 10-second cryosurgery group, although present even with a 5-second freeze cycle.
The hydrogen peroxide–treated groups showed acanthosis of the epidermis and mild pallor, but this was less noticeable than in the cryosurgery specimens. There was no epidermal clefting in the hydrogen peroxide–treated samples.
Tunel staining revealed 16.4 (plus or minus 0.6424) apoptotic cells per high-powered field in the 5-second cryosurgery experiment and 20.6 (plus or minus 0.6424) in the 10-second procedure. For the hydrogen peroxide treatment, those numbers were 8.65 (plus or minus 0.4122) in the 1 mcL experiment and 12.4 (plus or minus 0.3728) in the 2 mcL experiment.
As expected, melanocytes fared better with the hydrogen peroxide treatment. In the untreated samples, there were 2.5 melanocytes (plus or minus 0.1987) in the untreated sample and 2.0 (plus or minus 0.5000) melanocytes in the vehicle-treated sample. In the 5-second cryosurgery sample, there were 0.45 melanocytes (plus or minus 0.1535), and in the 10 second cryosurgery sample there were 0.2 (plus or minus 0.0918) melanocytes. In contrast, with the 1-mcL hydrogen peroxide-treated sample, there were 1.95 melanocytes in both the 1-mcL and 2-mcL samples (plus or minus 0.1535 for both groups).
“,” Dr. Friedman said. These results, he added, “offer us a lot of insight in terms of how damaging liquid nitrogen is, and it’s good to be reminded of that so that we don’t cause too much harm.”
The authors noted that a clinical trial evaluating the risk of hypopigmentation and hyperpigmentation with 40% hydrogen peroxide in people with darker skin types is underway. In the study, hydrogen peroxide is used to treat dermatosis papulosa nigra.
The study was funded by Aclaris Therapeutics. Senior author Adam Friedman, MD, is a consultant for Aclaris. Dr. Friedman is on the editorial board of Dermatology News.
SOURCE: Kao S et al. J Am Acad Dermatol. 2018 Mar 27. doi: 10.1016/j.jaad.2018.03.034.
A study using an ex vivo model to evaluate a seborrheic keratosis (SK) treatment shows that a topical application of 40% hydrogen peroxide is gentler on skin than a 5- or 10-second treatment with liquid nitrogen, particularly with respect to melanocytes, suggesting that the former may be less likely to produce disfiguring damage.
The 40% hydrogen peroxide solution (Eskata), also known as A-101, received Food and Drug Administration approval for the treatment of “seborrheic keratoses that are raised” in December, 2017. The study was published online in the Journal of the American Academy of Dermatology.
Melanocyte damage can lead to significant dyschromia, a poor cosmetic outcome that can have a tremendous impact on quality of life for dark-skinned patients, in whom it produces white spots. “A lot of these destructive approaches, especially liquid nitrogen, can leave more disfigurement upon treatment than the lesion itself,” the study’s lead author Adam Friedman, MD, said in an interview.
Melanocytes are particularly vulnerable to the effects of cold, so the destructive potential of liquid nitrogen is no surprise. But Dr. Friedman of the department of dermatology, George Washington University, Washington, wanted to get a better understanding of the impact of the new treatment on different skin cell types and the toxicity profile, so he approached the manufacturer, Aclaris Therapeutics, to do a study.
His team tested 40% hydrogen peroxide treatment and liquid nitrogen cryosurgery on a validated ex vivo human reconstituted full-thickness model derived from Fitzpatrick V skin, with 5 or 10 seconds of cryosurgery or 1 or 2 mcL of 40% hydrogen peroxide.
Using standard a hematoxylin and eosin stain as well as immunohistochemical staining to examine the architecture and cells types of the skin model following both treatments, the researchers found that 5- and 10-second cryosurgery resulted in significant thinning of the epidermis and increased cell death. There was also separation at the dermal-epidermal junction, which was more prominent in the 10-second cryosurgery group, although present even with a 5-second freeze cycle.
The hydrogen peroxide–treated groups showed acanthosis of the epidermis and mild pallor, but this was less noticeable than in the cryosurgery specimens. There was no epidermal clefting in the hydrogen peroxide–treated samples.
Tunel staining revealed 16.4 (plus or minus 0.6424) apoptotic cells per high-powered field in the 5-second cryosurgery experiment and 20.6 (plus or minus 0.6424) in the 10-second procedure. For the hydrogen peroxide treatment, those numbers were 8.65 (plus or minus 0.4122) in the 1 mcL experiment and 12.4 (plus or minus 0.3728) in the 2 mcL experiment.
As expected, melanocytes fared better with the hydrogen peroxide treatment. In the untreated samples, there were 2.5 melanocytes (plus or minus 0.1987) in the untreated sample and 2.0 (plus or minus 0.5000) melanocytes in the vehicle-treated sample. In the 5-second cryosurgery sample, there were 0.45 melanocytes (plus or minus 0.1535), and in the 10 second cryosurgery sample there were 0.2 (plus or minus 0.0918) melanocytes. In contrast, with the 1-mcL hydrogen peroxide-treated sample, there were 1.95 melanocytes in both the 1-mcL and 2-mcL samples (plus or minus 0.1535 for both groups).
“,” Dr. Friedman said. These results, he added, “offer us a lot of insight in terms of how damaging liquid nitrogen is, and it’s good to be reminded of that so that we don’t cause too much harm.”
The authors noted that a clinical trial evaluating the risk of hypopigmentation and hyperpigmentation with 40% hydrogen peroxide in people with darker skin types is underway. In the study, hydrogen peroxide is used to treat dermatosis papulosa nigra.
The study was funded by Aclaris Therapeutics. Senior author Adam Friedman, MD, is a consultant for Aclaris. Dr. Friedman is on the editorial board of Dermatology News.
SOURCE: Kao S et al. J Am Acad Dermatol. 2018 Mar 27. doi: 10.1016/j.jaad.2018.03.034.
FROM JOURNAL OF THE AMERICAN ACADEMY OF DERMATOLOGY
Key clinical point: The results of a preclinical study using an ex vivo model of darker skin found that a 40% hydrogen peroxide solution for treating SKs was less damaging to the skin.
Major finding: The topical hydrogen peroxide treatment left 1.95 melanocytes in place, compared with 0.2-0.4 in the liquid nitrogen samples. As expected, melanocytes fared better with the hydrogen peroxide treatment. In the untreated samples, there were 2.5 melanocytes (plus or minus 0.1987) in the untreated sample and 2.0 (plus or minus 0.5000) melanocytes in the vehicle-treated sample. In the 5-second cryosurgery sample, there were 0.45 melanocytes (plus or minus 0.1535), and in the 10-second cryosurgery sample there were 0.2 (plus or minus 0.0918) melanocytes.
Study details: The study compared the cytotoxic effects and impact on melanocytes of liquid nitrogen and 40% hydrogen peroxide solution using ex vivo human reconstituted full-thickness model.
Disclosures: The study was funded by Aclaris Therapeutics. Senior author Adam Friedman, MD, is a consultant for Aclaris.
Source: Kao S. et al. J Am Acad Dermatol. 2018 Mar 27. doi: 10.1016/j.jaad.2018.03.034.