User login
How real is resident burnout?
JACKSONVILLE, FLA. – Burnout is commonly ascribed to surgical residents, but reliable estimates of the numbers involved and a clear, comparable definition of burnout remain elusive.
A large study of general surgery residents has found that almost one in four have at least one symptom of burnout daily and more than two in five report poor psychiatric well-being, according to results of a survey reported at the Association for Academic Surgery/Society of University Surgeons Academic Surgical Congress.
“Twenty-two percent of general surgery residents report at least one symptom of burnout daily,” said Daniel “Brock” Hewitt, MD, a research fellow in the Surgical Outcomes and Quality Improvement Center in the department of surgery, Feinberg School of Medicine, Northwestern University, Chicago. “Poor resident wellness is associated with more duty-hour violations, feeling unprepared for residency, and an increase in self-reported medical errors. However, burnout is not associated with worse surgical outcomes.”
The study, undertaken with grant support from The American Board of Surgery, Accreditation of Graduate Medical Education, American College of Surgeons and Agency for Healthcare Research and Quality, provided three significant insights into resident wellness, Dr. Hewitt said. “When measuring the level of burnout, careful consideration should be given to how burnout is defined,” he said. “Secondly, wellness interventions with attention to preparedness for residency and duty-hour restrictions may help alleviate burnout. And finally, with the significant impact it does have on the individual physician, we believe that burnout needs to be addressed regardless of its impact on patient outcomes.”
The study drew on a questionnaire given to residents immediately following the 2017 American Board of Surgery In-Training Examination (ABSITE), which 3,789 general surgery residents from 115 general surgery programs completed. The survey had a 99.3% response rate. The survey evaluated two factors associated with resident wellness: burnout and poor psychiatric well-being. “Poor wellness is prevalent among physicians and trainees and is associated with depression, suicidal ideation, attrition, and absenteeism,” Dr. Hewitt said.
But to measure burnout, the researchers had to first define it. The instrument Dr. Hewitt and coauthors used is the Maslach Burnout Inventory, named for University of California at Berkley psychology professor Christina Maslach, PhD. It quantifies three different factors for burnout: emotional exhaustion; depersonalization or cynicism; and a low sense of personal accomplishment. This study defined “burnout” as having feelings of both emotional exhaustion and depersonalization, and dismissed the third measure of burnout because physicians rarely posses a low sense of personal accomplishment.
Overall, 22.3% reported one sign or symptom of burnout daily, and 56.5% did so on a weekly basis, Dr. Hewitt said.
However, Dr. Hewitt noted, burnout measurement thresholds can vary “because burnout itself is not an actual diagnosis.” Studies have calculated the burnout rate among surgeons at 28% to 69% (J Am Coll Surg. 2016:222:1230-9). A recent systematic review found up to eight different cutoffs used to define “high burnout” (Cogent Med. 2016 7 Oct; doi.org/10.1080/2331205X.2016.1237605; J Am Coll Surg, 2016:223:440-51)

How studies of physician burnout establish cutoffs and which Maslach Burnout Inventory subscales they measure has an impact on the rates of burnout they report, Dr. Hewitt said. For this study, the researchers used the Maslach scores in the top quartile in both emotional exhaustion and depersonalization to define burnout. “Burnout is probably best defined as a continuum from engagement on the one end and burnout on the other, so there’s some combination of the [Maslach] subscales that lead to burnout,” he said.
Among survey respondents, 19.5% reported high Maslach scores for emotional exhaustion and 9% of depersonalization on a daily basis (6.2% reported both)--22.3% reported at least one daily. On a weekly basis, 54.2% reported high scores for emotional exhaustion and 25.6% high scores for depersonalization, with 56.5% reporting at least one and 22.4% reporting both.
To evaluate residents’ sense of psychiatric well-being, the study used the General Health Questionnaire (Psychol Med. 1998;28:915-21). Among survey respondents, 43% met criteria for poor psychiatric well-being.
Burnout rates among men and women were identical, but a significantly higher percentage of women had poor psychiatric well-being: 48.4% to 39.7% of men.
Burnout and psychiatric well-being scores also varied depending on post-graduate year. Second- and third-year residents were significantly more likely to report burnout, compared to first-year residents, Dr. Hewitt said. Rates of poor psychiatric well-being were lowest for fourth- and fifth-year residents.
Most pronounced was the impact of 80-hour duty week violations had on residents’ sense of burnout and poor psychiatric well-being. Burnout rates were 8.4% for those who reported no monthly duty-hour violations, but doubled and quadrupled with more frequent monthly duty-hour violations: 16.1% for those who reported one to four violations a month; and 35% for those who reported five or more. Dr. Hewitt also noted wellness rates for those in the standard and flexible policy groups in Flexibility In duty hour Requirements for Surgical Trainees Trial (FIRST Trial) programs were similar.
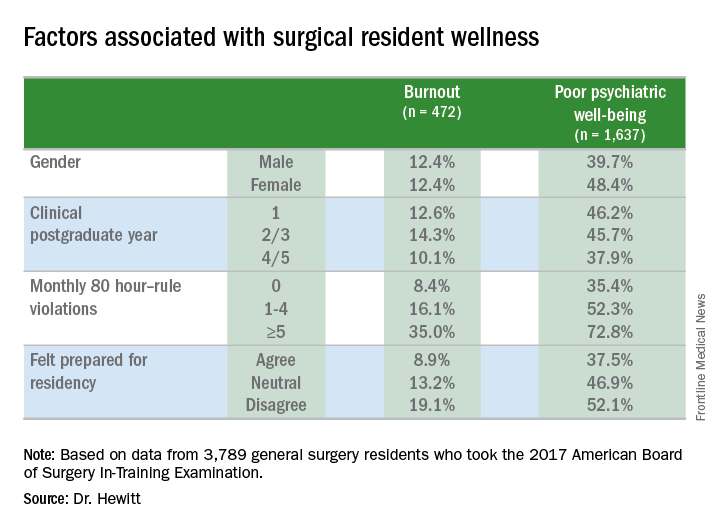
Another factor that contributed to burnout and poor psychiatric well-being was a sense of unpreparedness for residency, Dr. Hewitt said. Burnout rates for those who felt prepared were 8.9% vs. 19.1% for those who didn’t feel prepared. The disparity was less drastic, but nonetheless significant, for poor psychiatric well-being: 37.5% for those who felt prepared and 52.1% for those who didn’t.
With regard to outcomes, Dr. Hewitt said, “Residents in the highest quartile of burnout and the highest quartile of poor psychiatric well-being were significantly more likely to report a near miss or harmful medical error.” Among the burnout group, highest quartile rates were 39.3% for a near miss and 14.4% for a harmful medical error vs. 11.1% and 2.4%, respectively, for the lowest quartile. Among surgical residents who reported poor psychiatric well-being, highest quartile rates were 31.9% for a near miss and 13.2% for a harmful medical error vs. 12.5% and 2.1%, respectively, for those in the lowest quartile.
The study also analyzed outcomes for 134,877 surgical patients and found no association of overall morbidity and death or serious morbidity with resident wellness. “However,” Dr. Hewitt said, “when we look at mortality and failure to rescue, we can see an association with burnout, specifically in programs that have high levels of burnout; these patients have significantly lower odds of mortality and failure to rescue.” Each has an adjusted odds ratios of 0.81.
Among the study limitations Dr. Hewitt noted were its cross-sectional nature that led to inferences of association, not identification of causation; residents completing the survey after the ABSITE may have influenced their answers; and the fact it did not account for certain intermediate factors such as physician or nursing burnout or institutional quality measures.
The American Board of Surgery, Accreditation of Graduate Medical Education, American College of Surgeons and Agency for Healthcare Research and Quality provided grants to support the research.
SOURCE: Hewitt B et al. abstract 21.01
JACKSONVILLE, FLA. – Burnout is commonly ascribed to surgical residents, but reliable estimates of the numbers involved and a clear, comparable definition of burnout remain elusive.
A large study of general surgery residents has found that almost one in four have at least one symptom of burnout daily and more than two in five report poor psychiatric well-being, according to results of a survey reported at the Association for Academic Surgery/Society of University Surgeons Academic Surgical Congress.
“Twenty-two percent of general surgery residents report at least one symptom of burnout daily,” said Daniel “Brock” Hewitt, MD, a research fellow in the Surgical Outcomes and Quality Improvement Center in the department of surgery, Feinberg School of Medicine, Northwestern University, Chicago. “Poor resident wellness is associated with more duty-hour violations, feeling unprepared for residency, and an increase in self-reported medical errors. However, burnout is not associated with worse surgical outcomes.”
The study, undertaken with grant support from The American Board of Surgery, Accreditation of Graduate Medical Education, American College of Surgeons and Agency for Healthcare Research and Quality, provided three significant insights into resident wellness, Dr. Hewitt said. “When measuring the level of burnout, careful consideration should be given to how burnout is defined,” he said. “Secondly, wellness interventions with attention to preparedness for residency and duty-hour restrictions may help alleviate burnout. And finally, with the significant impact it does have on the individual physician, we believe that burnout needs to be addressed regardless of its impact on patient outcomes.”
The study drew on a questionnaire given to residents immediately following the 2017 American Board of Surgery In-Training Examination (ABSITE), which 3,789 general surgery residents from 115 general surgery programs completed. The survey had a 99.3% response rate. The survey evaluated two factors associated with resident wellness: burnout and poor psychiatric well-being. “Poor wellness is prevalent among physicians and trainees and is associated with depression, suicidal ideation, attrition, and absenteeism,” Dr. Hewitt said.
But to measure burnout, the researchers had to first define it. The instrument Dr. Hewitt and coauthors used is the Maslach Burnout Inventory, named for University of California at Berkley psychology professor Christina Maslach, PhD. It quantifies three different factors for burnout: emotional exhaustion; depersonalization or cynicism; and a low sense of personal accomplishment. This study defined “burnout” as having feelings of both emotional exhaustion and depersonalization, and dismissed the third measure of burnout because physicians rarely posses a low sense of personal accomplishment.
Overall, 22.3% reported one sign or symptom of burnout daily, and 56.5% did so on a weekly basis, Dr. Hewitt said.
However, Dr. Hewitt noted, burnout measurement thresholds can vary “because burnout itself is not an actual diagnosis.” Studies have calculated the burnout rate among surgeons at 28% to 69% (J Am Coll Surg. 2016:222:1230-9). A recent systematic review found up to eight different cutoffs used to define “high burnout” (Cogent Med. 2016 7 Oct; doi.org/10.1080/2331205X.2016.1237605; J Am Coll Surg, 2016:223:440-51)
How studies of physician burnout establish cutoffs and which Maslach Burnout Inventory subscales they measure has an impact on the rates of burnout they report, Dr. Hewitt said. For this study, the researchers used the Maslach scores in the top quartile in both emotional exhaustion and depersonalization to define burnout. “Burnout is probably best defined as a continuum from engagement on the one end and burnout on the other, so there’s some combination of the [Maslach] subscales that lead to burnout,” he said.
Among survey respondents, 19.5% reported high Maslach scores for emotional exhaustion and 9% of depersonalization on a daily basis (6.2% reported both)--22.3% reported at least one daily. On a weekly basis, 54.2% reported high scores for emotional exhaustion and 25.6% high scores for depersonalization, with 56.5% reporting at least one and 22.4% reporting both.
To evaluate residents’ sense of psychiatric well-being, the study used the General Health Questionnaire (Psychol Med. 1998;28:915-21). Among survey respondents, 43% met criteria for poor psychiatric well-being.
Burnout rates among men and women were identical, but a significantly higher percentage of women had poor psychiatric well-being: 48.4% to 39.7% of men.
Burnout and psychiatric well-being scores also varied depending on post-graduate year. Second- and third-year residents were significantly more likely to report burnout, compared to first-year residents, Dr. Hewitt said. Rates of poor psychiatric well-being were lowest for fourth- and fifth-year residents.
Most pronounced was the impact of 80-hour duty week violations had on residents’ sense of burnout and poor psychiatric well-being. Burnout rates were 8.4% for those who reported no monthly duty-hour violations, but doubled and quadrupled with more frequent monthly duty-hour violations: 16.1% for those who reported one to four violations a month; and 35% for those who reported five or more. Dr. Hewitt also noted wellness rates for those in the standard and flexible policy groups in Flexibility In duty hour Requirements for Surgical Trainees Trial (FIRST Trial) programs were similar.
Another factor that contributed to burnout and poor psychiatric well-being was a sense of unpreparedness for residency, Dr. Hewitt said. Burnout rates for those who felt prepared were 8.9% vs. 19.1% for those who didn’t feel prepared. The disparity was less drastic, but nonetheless significant, for poor psychiatric well-being: 37.5% for those who felt prepared and 52.1% for those who didn’t.
With regard to outcomes, Dr. Hewitt said, “Residents in the highest quartile of burnout and the highest quartile of poor psychiatric well-being were significantly more likely to report a near miss or harmful medical error.” Among the burnout group, highest quartile rates were 39.3% for a near miss and 14.4% for a harmful medical error vs. 11.1% and 2.4%, respectively, for the lowest quartile. Among surgical residents who reported poor psychiatric well-being, highest quartile rates were 31.9% for a near miss and 13.2% for a harmful medical error vs. 12.5% and 2.1%, respectively, for those in the lowest quartile.
The study also analyzed outcomes for 134,877 surgical patients and found no association of overall morbidity and death or serious morbidity with resident wellness. “However,” Dr. Hewitt said, “when we look at mortality and failure to rescue, we can see an association with burnout, specifically in programs that have high levels of burnout; these patients have significantly lower odds of mortality and failure to rescue.” Each has an adjusted odds ratios of 0.81.
Among the study limitations Dr. Hewitt noted were its cross-sectional nature that led to inferences of association, not identification of causation; residents completing the survey after the ABSITE may have influenced their answers; and the fact it did not account for certain intermediate factors such as physician or nursing burnout or institutional quality measures.
The American Board of Surgery, Accreditation of Graduate Medical Education, American College of Surgeons and Agency for Healthcare Research and Quality provided grants to support the research.
SOURCE: Hewitt B et al. abstract 21.01
JACKSONVILLE, FLA. – Burnout is commonly ascribed to surgical residents, but reliable estimates of the numbers involved and a clear, comparable definition of burnout remain elusive.
A large study of general surgery residents has found that almost one in four have at least one symptom of burnout daily and more than two in five report poor psychiatric well-being, according to results of a survey reported at the Association for Academic Surgery/Society of University Surgeons Academic Surgical Congress.
“Twenty-two percent of general surgery residents report at least one symptom of burnout daily,” said Daniel “Brock” Hewitt, MD, a research fellow in the Surgical Outcomes and Quality Improvement Center in the department of surgery, Feinberg School of Medicine, Northwestern University, Chicago. “Poor resident wellness is associated with more duty-hour violations, feeling unprepared for residency, and an increase in self-reported medical errors. However, burnout is not associated with worse surgical outcomes.”
The study, undertaken with grant support from The American Board of Surgery, Accreditation of Graduate Medical Education, American College of Surgeons and Agency for Healthcare Research and Quality, provided three significant insights into resident wellness, Dr. Hewitt said. “When measuring the level of burnout, careful consideration should be given to how burnout is defined,” he said. “Secondly, wellness interventions with attention to preparedness for residency and duty-hour restrictions may help alleviate burnout. And finally, with the significant impact it does have on the individual physician, we believe that burnout needs to be addressed regardless of its impact on patient outcomes.”
The study drew on a questionnaire given to residents immediately following the 2017 American Board of Surgery In-Training Examination (ABSITE), which 3,789 general surgery residents from 115 general surgery programs completed. The survey had a 99.3% response rate. The survey evaluated two factors associated with resident wellness: burnout and poor psychiatric well-being. “Poor wellness is prevalent among physicians and trainees and is associated with depression, suicidal ideation, attrition, and absenteeism,” Dr. Hewitt said.
But to measure burnout, the researchers had to first define it. The instrument Dr. Hewitt and coauthors used is the Maslach Burnout Inventory, named for University of California at Berkley psychology professor Christina Maslach, PhD. It quantifies three different factors for burnout: emotional exhaustion; depersonalization or cynicism; and a low sense of personal accomplishment. This study defined “burnout” as having feelings of both emotional exhaustion and depersonalization, and dismissed the third measure of burnout because physicians rarely posses a low sense of personal accomplishment.
Overall, 22.3% reported one sign or symptom of burnout daily, and 56.5% did so on a weekly basis, Dr. Hewitt said.
However, Dr. Hewitt noted, burnout measurement thresholds can vary “because burnout itself is not an actual diagnosis.” Studies have calculated the burnout rate among surgeons at 28% to 69% (J Am Coll Surg. 2016:222:1230-9). A recent systematic review found up to eight different cutoffs used to define “high burnout” (Cogent Med. 2016 7 Oct; doi.org/10.1080/2331205X.2016.1237605; J Am Coll Surg, 2016:223:440-51)
How studies of physician burnout establish cutoffs and which Maslach Burnout Inventory subscales they measure has an impact on the rates of burnout they report, Dr. Hewitt said. For this study, the researchers used the Maslach scores in the top quartile in both emotional exhaustion and depersonalization to define burnout. “Burnout is probably best defined as a continuum from engagement on the one end and burnout on the other, so there’s some combination of the [Maslach] subscales that lead to burnout,” he said.
Among survey respondents, 19.5% reported high Maslach scores for emotional exhaustion and 9% of depersonalization on a daily basis (6.2% reported both)--22.3% reported at least one daily. On a weekly basis, 54.2% reported high scores for emotional exhaustion and 25.6% high scores for depersonalization, with 56.5% reporting at least one and 22.4% reporting both.
To evaluate residents’ sense of psychiatric well-being, the study used the General Health Questionnaire (Psychol Med. 1998;28:915-21). Among survey respondents, 43% met criteria for poor psychiatric well-being.
Burnout rates among men and women were identical, but a significantly higher percentage of women had poor psychiatric well-being: 48.4% to 39.7% of men.
Burnout and psychiatric well-being scores also varied depending on post-graduate year. Second- and third-year residents were significantly more likely to report burnout, compared to first-year residents, Dr. Hewitt said. Rates of poor psychiatric well-being were lowest for fourth- and fifth-year residents.
Most pronounced was the impact of 80-hour duty week violations had on residents’ sense of burnout and poor psychiatric well-being. Burnout rates were 8.4% for those who reported no monthly duty-hour violations, but doubled and quadrupled with more frequent monthly duty-hour violations: 16.1% for those who reported one to four violations a month; and 35% for those who reported five or more. Dr. Hewitt also noted wellness rates for those in the standard and flexible policy groups in Flexibility In duty hour Requirements for Surgical Trainees Trial (FIRST Trial) programs were similar.
Another factor that contributed to burnout and poor psychiatric well-being was a sense of unpreparedness for residency, Dr. Hewitt said. Burnout rates for those who felt prepared were 8.9% vs. 19.1% for those who didn’t feel prepared. The disparity was less drastic, but nonetheless significant, for poor psychiatric well-being: 37.5% for those who felt prepared and 52.1% for those who didn’t.
With regard to outcomes, Dr. Hewitt said, “Residents in the highest quartile of burnout and the highest quartile of poor psychiatric well-being were significantly more likely to report a near miss or harmful medical error.” Among the burnout group, highest quartile rates were 39.3% for a near miss and 14.4% for a harmful medical error vs. 11.1% and 2.4%, respectively, for the lowest quartile. Among surgical residents who reported poor psychiatric well-being, highest quartile rates were 31.9% for a near miss and 13.2% for a harmful medical error vs. 12.5% and 2.1%, respectively, for those in the lowest quartile.
The study also analyzed outcomes for 134,877 surgical patients and found no association of overall morbidity and death or serious morbidity with resident wellness. “However,” Dr. Hewitt said, “when we look at mortality and failure to rescue, we can see an association with burnout, specifically in programs that have high levels of burnout; these patients have significantly lower odds of mortality and failure to rescue.” Each has an adjusted odds ratios of 0.81.
Among the study limitations Dr. Hewitt noted were its cross-sectional nature that led to inferences of association, not identification of causation; residents completing the survey after the ABSITE may have influenced their answers; and the fact it did not account for certain intermediate factors such as physician or nursing burnout or institutional quality measures.
The American Board of Surgery, Accreditation of Graduate Medical Education, American College of Surgeons and Agency for Healthcare Research and Quality provided grants to support the research.
SOURCE: Hewitt B et al. abstract 21.01
AT THE ANNUAL ACADEMIC SURGICAL CONGRESS
Key clinical point: Almost one in four surgical residents manifest a daily symptom of burnout.
Major finding: Overall 22.8% of daily and 44.3% had poor psychiatric well-being scores.
Study details: Surveys completed by 3,789 general surgery residents during the American Board of Surgery In-Training Examination in January 2017.
Disclosures: The American Board of Surgery, Accreditation of Graduate Medical Education, American College of Surgeons and Agency for Healthcare Research and Quality provided grants to support the research.
Source: Hewitt B et al. abstract 21.01
Experts review the year in rheumatology ... and what lies ahead
MAUI, HAWAII – Arthur Kavanaugh, MD, program director for the Rheumatology Winter Clinical Symposium, likes to close out the meeting each year in high style by assembling selected conference faculty to offer their personal picks for the top developments in the field during the past year and make predictions about the year to come.
Here’s how they called it:
The top events in rheumatology during the last year
The rise of oral small molecules: The Janus kinase (JAK) inhibitors and other oral small molecules that have begun reaching the marketplace, with many more in development, will bring a paradigm shift in the treatment not only of rheumatic diseases, but in inflammatory bowel disease and skin diseases as well, predicted Alvin F. Wells, MD, PhD, a rheumatologist at Duke University in Durham, N.C., who is also director of the Rheumatology and Immunotherapy Center in Franklin, Wisc.
“The challenge is whether Medicare will cover the pills the way they cover the infusions and the other things we do,” according to Dr. Wells.

A bevy of new drugs for psoriatic arthritis and psoriasis: “I think the most important advance in the past year was the approval of a profusion of drugs for psoriatic arthritis and psoriasis. It’s really opened up the landscape for us in terms of treatment options. The downside is it’s going to take us a while to sort through which drugs fit where,” noted Eric J. Ruderman, MD, professor of medicine and associate chief of clinical affairs in the division of rheumatology at Northwestern University in Chicago.
“The drug I was most impressed with was tofacitinib [Xeljanz, an oral JAK inhibitor], not just by its effectiveness but by its potential to change the game, and particularly the data in tumor necrosis factor inhibitor inadequate responders. That was pretty solid data. It really opens the way to oral small molecules for joint diseases,” he added.
Interleukin-18 binding protein for monogenic inflammasome diseases: The biggest recent breakthrough in pediatric rheumatology was the Food and Drug Administration’s April 2017 designation of Breakthrough Therapy status for the recombinant human IL-18 binding protein known as tadekinig alfa for monogenic IL-18-associated autoinflammatory conditions, as well as the biologic’s Orphan Drug Designation for treatment of hemophagocytic lymphohistiocytosis, according to Anne M. Stevens, MD, PhD, professor of pediatrics at the University of Washington, Seattle, and chief of pediatric rheumatology at Seattle Children’s Hospital.

Novel treatment concept emerges in severe SLE: The study that knocked the socks off of Martin J. Bergman, MD, in 2017 was the Dutch SymBiose study, presented at both the European League Against Rheumatism and American College of Rheumatology annual meetings. It included just 14 patients with severe refractory SLE – including 10 with lupus nephritis – and tested a treatment strategy of rituximab (Rituxan) followed a few weeks later by a course of belimumab (Benlysta).
“The results were very dramatic, to say the least,” said Dr. Bergman of Drexel University in Philadelphia. Indeed, this one-two therapeutic punch resulted in sharply reduced levels of pathogenic autoantibodies and immune complex-mediated neutrophil extracellular traps while also knocking down very high baseline Systemic Lupus Erythematosus Disease Activity Index (SLEDAI) scores to near zero, even while enabling patients to discontinue systemic corticosteroids and mycophenolate mofetil (CellCept). Several much larger clinical trials of this regimen and other similar ones are ongoing in an effort to duplicate the results.
Dr. Kavanaugh said the SymBiose study was one of his own top picks for study of the year as well.

Mainstream use of dupilumab (Dupixent) for moderate to severe atopic dermatitis: “This is a total game changer. It’s really changed a lot of people’s lives,” commented George M. Martin, MD, a dermatologist in private practice on Maui.
“Interestingly, historically drugs that started out in your realm later made their way to dermatology, but now we’re seeing the IL-23 inhibitors starting with us and then making their way into rheumatology and gastroenterology. The IL-23 inhibitors are very powerful drugs; when we’re seeing half of our psoriasis patients achieve PASI 100 responses, it’s very exciting. And these are durable responses,” he noted.
The opioid crisis: What’s the most important recent event in rheumatology?
“That’s easy: The biggest thing in all of medicine is the opioid crisis. Whether you recognize it or not, it’s gigantic. It’s $500 billion of the U.S. economy, every year. Forty percent of rheumatoid arthritis patients and 30% with ankylosing spondylitis are on opioids, and what goes along with that is a lot of ugly stuff,” said John J. Cush, MD, professor of medicine and rheumatology at Baylor University in Dallas.
Moreover, the FDA is now so leery of opioids that the agency has set the bar unrealistically high for approval of newer agents offering reduced abuse potential.
“I’ve been involved with or watched at least six FDA advisory panels looking at new, lower abuse-potential opioids in the last couple years. Only one agent got through,” according to Dr. Cush.
Dr. Troum commented, “I really think this whole opioid epidemic started with the campaign to make pain the fifth vital sign back in the 1990s. Some of the pharmaceutical companies took that concept and really ran with it.”
Rapamycin for inclusion body myositis: Dr. Kavanaugh’s pick for study of the year was what he described as “a brilliant presentation” of a French multicenter, placebo-controlled clinical trial of rapamycin for patients with inclusion body myositis at the 2017 ACR annual meeting.
“The French group considers IBM [inclusion body myositis] to be essentially Alzheimer’s disease of the muscle, marked by amyloid deposition. They chose to study rapamycin, which not only has immunosuppressive properties because it binds to mTOR [the mammalian target of rapamycin], but it also has the ability to inhibit amyloid protein deposition,” he explained.
The investigators reported improved 6-minute-walk distance and pulmonary function in the rapamycin group, whereas placebo-treated controls rapidly deteriorated.
“This is an approved drug for other indications, and we scratch our heads with IBM. It’s super nice to have something like that,” Dr. Kavanaugh observed.
A look at what’s in store
More tele-rheumatology: “I think the biggest thing is going to be more tele-rheumatology, more tele-ultrasound. Kaiser Permanente said 49% of their visits last year were virtual visits; that number is just going to grow,” predicted Dr. Wells.
Especially in medically underserved areas of the country, including large rural expanses, demand for remote tele-rheumatologic consults with high-quality imaging is going to increase, he added.
Here come cannabinoids for pain control: Dr. Troum predicted that in the depths of the national opioid epidemic, in a climate that discourages legitimate prescribing of traditional pain medications, rheumatologists can anticipate growing patient demand for cannabidiol and other cannabinoids for pain relief.
“I have patients coming in their 60s, 70s, and 80s – these are not young people – who are whispering to me, ‘Can I use this for my chronic pain?’ I think there’s going to be a big push for ways other than opioids to treat our patients’ pain,” according to Dr. Troum.
Tipping point nears for JAK inhibitors: In 2018, it will become clear just how seriously the Food and Drug Administration views the signal of possible increased venous thromboembolic risk associated with the oral JAK inhibitors for rheumatoid arthritis. The agency is expected to rule on Eli Lilly and Incyte’s resubmitted application for marketing approval for the JAK inhibitor baricitinib, which was tripped up earlier based in part upon VTE concerns.
“I think the big story in 2018 will be how the JAK story shakes out – whether this VTE thing has legs,” Dr. Ruderman predicted. “A sea change could be coming in our field, and it’s not coming next year or the year after, but 10 years from now: Are we going to move past the era of methotrexate and use generic small molecules instead? We’re going to find out within the next year whether that’s going to happen.”
Phase 3 results coming on tocilizumab for systemic sclerosis: “I think we’re going to see some really exciting systemic sclerosis data coming out this year,” Dr. Stevens said. Based upon the positive phase 2 results presented for tocilizumab (Actemra) last year, she’s optimistic that the ongoing phase 3 randomized trial will demonstrate a significant advantage over placebo in lung function. Also, ongoing separate clinical trials are evaluating an antifibrotic drug and rapamycin for systemic sclerosis.
Dr. Bergman, too, has high hopes for these studies: “I think we may finally be getting to a place where we can see effective drugs in systemic sclerosis.”
Amazon, Berkshire Hathaway, and JPMorgan Chase form a nonprofit to improve employee health care: In a recent press conference, the three CEOs weren’t specific about their plans, but Dr. Martin predicted the companies are likely to self-insure, bypassing Cigna and the other major health insurance companies and then contracting with physicians. He forecast that “probably within the next 5 years, what they do is going to affect everybody in this room.”
Rheumatologists will need to master a new mindset: Many rheumatologists have gotten comfortable with an all-tumor necrosis factor inhibitor treatment menu for their patients with moderate or severe rheumatoid arthritis. That’s got to change, according to Dr. Cush.
“We now have two IL-6 inhibitors, two IL-17 inhibitors, and we’ll soon have two JAK inhibitors. That’s going to be a direct threat to the not right- or left-brain, but the TNF-brain rheumatologist who now writes prescriptions for three TNF inhibitors in a row before questioning the efficacy. The idea is you will now be using drugs with other mechanisms of action first-line, or at the very least, second-line, and that’s going to be a paradigm shift for a lot of people,” he explained.
None of the speakers reported having financial conflicts regarding their comments.
MAUI, HAWAII – Arthur Kavanaugh, MD, program director for the Rheumatology Winter Clinical Symposium, likes to close out the meeting each year in high style by assembling selected conference faculty to offer their personal picks for the top developments in the field during the past year and make predictions about the year to come.
Here’s how they called it:
The top events in rheumatology during the last year
The rise of oral small molecules: The Janus kinase (JAK) inhibitors and other oral small molecules that have begun reaching the marketplace, with many more in development, will bring a paradigm shift in the treatment not only of rheumatic diseases, but in inflammatory bowel disease and skin diseases as well, predicted Alvin F. Wells, MD, PhD, a rheumatologist at Duke University in Durham, N.C., who is also director of the Rheumatology and Immunotherapy Center in Franklin, Wisc.
“The challenge is whether Medicare will cover the pills the way they cover the infusions and the other things we do,” according to Dr. Wells.
A bevy of new drugs for psoriatic arthritis and psoriasis: “I think the most important advance in the past year was the approval of a profusion of drugs for psoriatic arthritis and psoriasis. It’s really opened up the landscape for us in terms of treatment options. The downside is it’s going to take us a while to sort through which drugs fit where,” noted Eric J. Ruderman, MD, professor of medicine and associate chief of clinical affairs in the division of rheumatology at Northwestern University in Chicago.
“The drug I was most impressed with was tofacitinib [Xeljanz, an oral JAK inhibitor], not just by its effectiveness but by its potential to change the game, and particularly the data in tumor necrosis factor inhibitor inadequate responders. That was pretty solid data. It really opens the way to oral small molecules for joint diseases,” he added.
Interleukin-18 binding protein for monogenic inflammasome diseases: The biggest recent breakthrough in pediatric rheumatology was the Food and Drug Administration’s April 2017 designation of Breakthrough Therapy status for the recombinant human IL-18 binding protein known as tadekinig alfa for monogenic IL-18-associated autoinflammatory conditions, as well as the biologic’s Orphan Drug Designation for treatment of hemophagocytic lymphohistiocytosis, according to Anne M. Stevens, MD, PhD, professor of pediatrics at the University of Washington, Seattle, and chief of pediatric rheumatology at Seattle Children’s Hospital.
Novel treatment concept emerges in severe SLE: The study that knocked the socks off of Martin J. Bergman, MD, in 2017 was the Dutch SymBiose study, presented at both the European League Against Rheumatism and American College of Rheumatology annual meetings. It included just 14 patients with severe refractory SLE – including 10 with lupus nephritis – and tested a treatment strategy of rituximab (Rituxan) followed a few weeks later by a course of belimumab (Benlysta).
“The results were very dramatic, to say the least,” said Dr. Bergman of Drexel University in Philadelphia. Indeed, this one-two therapeutic punch resulted in sharply reduced levels of pathogenic autoantibodies and immune complex-mediated neutrophil extracellular traps while also knocking down very high baseline Systemic Lupus Erythematosus Disease Activity Index (SLEDAI) scores to near zero, even while enabling patients to discontinue systemic corticosteroids and mycophenolate mofetil (CellCept). Several much larger clinical trials of this regimen and other similar ones are ongoing in an effort to duplicate the results.
Dr. Kavanaugh said the SymBiose study was one of his own top picks for study of the year as well.
Mainstream use of dupilumab (Dupixent) for moderate to severe atopic dermatitis: “This is a total game changer. It’s really changed a lot of people’s lives,” commented George M. Martin, MD, a dermatologist in private practice on Maui.
“Interestingly, historically drugs that started out in your realm later made their way to dermatology, but now we’re seeing the IL-23 inhibitors starting with us and then making their way into rheumatology and gastroenterology. The IL-23 inhibitors are very powerful drugs; when we’re seeing half of our psoriasis patients achieve PASI 100 responses, it’s very exciting. And these are durable responses,” he noted.
The opioid crisis: What’s the most important recent event in rheumatology?
“That’s easy: The biggest thing in all of medicine is the opioid crisis. Whether you recognize it or not, it’s gigantic. It’s $500 billion of the U.S. economy, every year. Forty percent of rheumatoid arthritis patients and 30% with ankylosing spondylitis are on opioids, and what goes along with that is a lot of ugly stuff,” said John J. Cush, MD, professor of medicine and rheumatology at Baylor University in Dallas.
Moreover, the FDA is now so leery of opioids that the agency has set the bar unrealistically high for approval of newer agents offering reduced abuse potential.
“I’ve been involved with or watched at least six FDA advisory panels looking at new, lower abuse-potential opioids in the last couple years. Only one agent got through,” according to Dr. Cush.
Dr. Troum commented, “I really think this whole opioid epidemic started with the campaign to make pain the fifth vital sign back in the 1990s. Some of the pharmaceutical companies took that concept and really ran with it.”
Rapamycin for inclusion body myositis: Dr. Kavanaugh’s pick for study of the year was what he described as “a brilliant presentation” of a French multicenter, placebo-controlled clinical trial of rapamycin for patients with inclusion body myositis at the 2017 ACR annual meeting.
“The French group considers IBM [inclusion body myositis] to be essentially Alzheimer’s disease of the muscle, marked by amyloid deposition. They chose to study rapamycin, which not only has immunosuppressive properties because it binds to mTOR [the mammalian target of rapamycin], but it also has the ability to inhibit amyloid protein deposition,” he explained.
The investigators reported improved 6-minute-walk distance and pulmonary function in the rapamycin group, whereas placebo-treated controls rapidly deteriorated.
“This is an approved drug for other indications, and we scratch our heads with IBM. It’s super nice to have something like that,” Dr. Kavanaugh observed.
A look at what’s in store
More tele-rheumatology: “I think the biggest thing is going to be more tele-rheumatology, more tele-ultrasound. Kaiser Permanente said 49% of their visits last year were virtual visits; that number is just going to grow,” predicted Dr. Wells.
Especially in medically underserved areas of the country, including large rural expanses, demand for remote tele-rheumatologic consults with high-quality imaging is going to increase, he added.
Here come cannabinoids for pain control: Dr. Troum predicted that in the depths of the national opioid epidemic, in a climate that discourages legitimate prescribing of traditional pain medications, rheumatologists can anticipate growing patient demand for cannabidiol and other cannabinoids for pain relief.
“I have patients coming in their 60s, 70s, and 80s – these are not young people – who are whispering to me, ‘Can I use this for my chronic pain?’ I think there’s going to be a big push for ways other than opioids to treat our patients’ pain,” according to Dr. Troum.
Tipping point nears for JAK inhibitors: In 2018, it will become clear just how seriously the Food and Drug Administration views the signal of possible increased venous thromboembolic risk associated with the oral JAK inhibitors for rheumatoid arthritis. The agency is expected to rule on Eli Lilly and Incyte’s resubmitted application for marketing approval for the JAK inhibitor baricitinib, which was tripped up earlier based in part upon VTE concerns.
“I think the big story in 2018 will be how the JAK story shakes out – whether this VTE thing has legs,” Dr. Ruderman predicted. “A sea change could be coming in our field, and it’s not coming next year or the year after, but 10 years from now: Are we going to move past the era of methotrexate and use generic small molecules instead? We’re going to find out within the next year whether that’s going to happen.”
Phase 3 results coming on tocilizumab for systemic sclerosis: “I think we’re going to see some really exciting systemic sclerosis data coming out this year,” Dr. Stevens said. Based upon the positive phase 2 results presented for tocilizumab (Actemra) last year, she’s optimistic that the ongoing phase 3 randomized trial will demonstrate a significant advantage over placebo in lung function. Also, ongoing separate clinical trials are evaluating an antifibrotic drug and rapamycin for systemic sclerosis.
Dr. Bergman, too, has high hopes for these studies: “I think we may finally be getting to a place where we can see effective drugs in systemic sclerosis.”
Amazon, Berkshire Hathaway, and JPMorgan Chase form a nonprofit to improve employee health care: In a recent press conference, the three CEOs weren’t specific about their plans, but Dr. Martin predicted the companies are likely to self-insure, bypassing Cigna and the other major health insurance companies and then contracting with physicians. He forecast that “probably within the next 5 years, what they do is going to affect everybody in this room.”
Rheumatologists will need to master a new mindset: Many rheumatologists have gotten comfortable with an all-tumor necrosis factor inhibitor treatment menu for their patients with moderate or severe rheumatoid arthritis. That’s got to change, according to Dr. Cush.
“We now have two IL-6 inhibitors, two IL-17 inhibitors, and we’ll soon have two JAK inhibitors. That’s going to be a direct threat to the not right- or left-brain, but the TNF-brain rheumatologist who now writes prescriptions for three TNF inhibitors in a row before questioning the efficacy. The idea is you will now be using drugs with other mechanisms of action first-line, or at the very least, second-line, and that’s going to be a paradigm shift for a lot of people,” he explained.
None of the speakers reported having financial conflicts regarding their comments.
MAUI, HAWAII – Arthur Kavanaugh, MD, program director for the Rheumatology Winter Clinical Symposium, likes to close out the meeting each year in high style by assembling selected conference faculty to offer their personal picks for the top developments in the field during the past year and make predictions about the year to come.
Here’s how they called it:
The top events in rheumatology during the last year
The rise of oral small molecules: The Janus kinase (JAK) inhibitors and other oral small molecules that have begun reaching the marketplace, with many more in development, will bring a paradigm shift in the treatment not only of rheumatic diseases, but in inflammatory bowel disease and skin diseases as well, predicted Alvin F. Wells, MD, PhD, a rheumatologist at Duke University in Durham, N.C., who is also director of the Rheumatology and Immunotherapy Center in Franklin, Wisc.
“The challenge is whether Medicare will cover the pills the way they cover the infusions and the other things we do,” according to Dr. Wells.
A bevy of new drugs for psoriatic arthritis and psoriasis: “I think the most important advance in the past year was the approval of a profusion of drugs for psoriatic arthritis and psoriasis. It’s really opened up the landscape for us in terms of treatment options. The downside is it’s going to take us a while to sort through which drugs fit where,” noted Eric J. Ruderman, MD, professor of medicine and associate chief of clinical affairs in the division of rheumatology at Northwestern University in Chicago.
“The drug I was most impressed with was tofacitinib [Xeljanz, an oral JAK inhibitor], not just by its effectiveness but by its potential to change the game, and particularly the data in tumor necrosis factor inhibitor inadequate responders. That was pretty solid data. It really opens the way to oral small molecules for joint diseases,” he added.
Interleukin-18 binding protein for monogenic inflammasome diseases: The biggest recent breakthrough in pediatric rheumatology was the Food and Drug Administration’s April 2017 designation of Breakthrough Therapy status for the recombinant human IL-18 binding protein known as tadekinig alfa for monogenic IL-18-associated autoinflammatory conditions, as well as the biologic’s Orphan Drug Designation for treatment of hemophagocytic lymphohistiocytosis, according to Anne M. Stevens, MD, PhD, professor of pediatrics at the University of Washington, Seattle, and chief of pediatric rheumatology at Seattle Children’s Hospital.
Novel treatment concept emerges in severe SLE: The study that knocked the socks off of Martin J. Bergman, MD, in 2017 was the Dutch SymBiose study, presented at both the European League Against Rheumatism and American College of Rheumatology annual meetings. It included just 14 patients with severe refractory SLE – including 10 with lupus nephritis – and tested a treatment strategy of rituximab (Rituxan) followed a few weeks later by a course of belimumab (Benlysta).
“The results were very dramatic, to say the least,” said Dr. Bergman of Drexel University in Philadelphia. Indeed, this one-two therapeutic punch resulted in sharply reduced levels of pathogenic autoantibodies and immune complex-mediated neutrophil extracellular traps while also knocking down very high baseline Systemic Lupus Erythematosus Disease Activity Index (SLEDAI) scores to near zero, even while enabling patients to discontinue systemic corticosteroids and mycophenolate mofetil (CellCept). Several much larger clinical trials of this regimen and other similar ones are ongoing in an effort to duplicate the results.
Dr. Kavanaugh said the SymBiose study was one of his own top picks for study of the year as well.
Mainstream use of dupilumab (Dupixent) for moderate to severe atopic dermatitis: “This is a total game changer. It’s really changed a lot of people’s lives,” commented George M. Martin, MD, a dermatologist in private practice on Maui.
“Interestingly, historically drugs that started out in your realm later made their way to dermatology, but now we’re seeing the IL-23 inhibitors starting with us and then making their way into rheumatology and gastroenterology. The IL-23 inhibitors are very powerful drugs; when we’re seeing half of our psoriasis patients achieve PASI 100 responses, it’s very exciting. And these are durable responses,” he noted.
The opioid crisis: What’s the most important recent event in rheumatology?
“That’s easy: The biggest thing in all of medicine is the opioid crisis. Whether you recognize it or not, it’s gigantic. It’s $500 billion of the U.S. economy, every year. Forty percent of rheumatoid arthritis patients and 30% with ankylosing spondylitis are on opioids, and what goes along with that is a lot of ugly stuff,” said John J. Cush, MD, professor of medicine and rheumatology at Baylor University in Dallas.
Moreover, the FDA is now so leery of opioids that the agency has set the bar unrealistically high for approval of newer agents offering reduced abuse potential.
“I’ve been involved with or watched at least six FDA advisory panels looking at new, lower abuse-potential opioids in the last couple years. Only one agent got through,” according to Dr. Cush.
Dr. Troum commented, “I really think this whole opioid epidemic started with the campaign to make pain the fifth vital sign back in the 1990s. Some of the pharmaceutical companies took that concept and really ran with it.”
Rapamycin for inclusion body myositis: Dr. Kavanaugh’s pick for study of the year was what he described as “a brilliant presentation” of a French multicenter, placebo-controlled clinical trial of rapamycin for patients with inclusion body myositis at the 2017 ACR annual meeting.
“The French group considers IBM [inclusion body myositis] to be essentially Alzheimer’s disease of the muscle, marked by amyloid deposition. They chose to study rapamycin, which not only has immunosuppressive properties because it binds to mTOR [the mammalian target of rapamycin], but it also has the ability to inhibit amyloid protein deposition,” he explained.
The investigators reported improved 6-minute-walk distance and pulmonary function in the rapamycin group, whereas placebo-treated controls rapidly deteriorated.
“This is an approved drug for other indications, and we scratch our heads with IBM. It’s super nice to have something like that,” Dr. Kavanaugh observed.
A look at what’s in store
More tele-rheumatology: “I think the biggest thing is going to be more tele-rheumatology, more tele-ultrasound. Kaiser Permanente said 49% of their visits last year were virtual visits; that number is just going to grow,” predicted Dr. Wells.
Especially in medically underserved areas of the country, including large rural expanses, demand for remote tele-rheumatologic consults with high-quality imaging is going to increase, he added.
Here come cannabinoids for pain control: Dr. Troum predicted that in the depths of the national opioid epidemic, in a climate that discourages legitimate prescribing of traditional pain medications, rheumatologists can anticipate growing patient demand for cannabidiol and other cannabinoids for pain relief.
“I have patients coming in their 60s, 70s, and 80s – these are not young people – who are whispering to me, ‘Can I use this for my chronic pain?’ I think there’s going to be a big push for ways other than opioids to treat our patients’ pain,” according to Dr. Troum.
Tipping point nears for JAK inhibitors: In 2018, it will become clear just how seriously the Food and Drug Administration views the signal of possible increased venous thromboembolic risk associated with the oral JAK inhibitors for rheumatoid arthritis. The agency is expected to rule on Eli Lilly and Incyte’s resubmitted application for marketing approval for the JAK inhibitor baricitinib, which was tripped up earlier based in part upon VTE concerns.
“I think the big story in 2018 will be how the JAK story shakes out – whether this VTE thing has legs,” Dr. Ruderman predicted. “A sea change could be coming in our field, and it’s not coming next year or the year after, but 10 years from now: Are we going to move past the era of methotrexate and use generic small molecules instead? We’re going to find out within the next year whether that’s going to happen.”
Phase 3 results coming on tocilizumab for systemic sclerosis: “I think we’re going to see some really exciting systemic sclerosis data coming out this year,” Dr. Stevens said. Based upon the positive phase 2 results presented for tocilizumab (Actemra) last year, she’s optimistic that the ongoing phase 3 randomized trial will demonstrate a significant advantage over placebo in lung function. Also, ongoing separate clinical trials are evaluating an antifibrotic drug and rapamycin for systemic sclerosis.
Dr. Bergman, too, has high hopes for these studies: “I think we may finally be getting to a place where we can see effective drugs in systemic sclerosis.”
Amazon, Berkshire Hathaway, and JPMorgan Chase form a nonprofit to improve employee health care: In a recent press conference, the three CEOs weren’t specific about their plans, but Dr. Martin predicted the companies are likely to self-insure, bypassing Cigna and the other major health insurance companies and then contracting with physicians. He forecast that “probably within the next 5 years, what they do is going to affect everybody in this room.”
Rheumatologists will need to master a new mindset: Many rheumatologists have gotten comfortable with an all-tumor necrosis factor inhibitor treatment menu for their patients with moderate or severe rheumatoid arthritis. That’s got to change, according to Dr. Cush.
“We now have two IL-6 inhibitors, two IL-17 inhibitors, and we’ll soon have two JAK inhibitors. That’s going to be a direct threat to the not right- or left-brain, but the TNF-brain rheumatologist who now writes prescriptions for three TNF inhibitors in a row before questioning the efficacy. The idea is you will now be using drugs with other mechanisms of action first-line, or at the very least, second-line, and that’s going to be a paradigm shift for a lot of people,” he explained.
None of the speakers reported having financial conflicts regarding their comments.
EXPERT ANALYSIS FROM RWCS 2018

Supplemental oxygen use for suspected myocardial infarction without hypoxemia
Background: Clinical guidelines recommend supplemental oxygen in patients with suspected acute myocardial infarction but data to support its use in patients without hypoxemia are limited.
Study design: Open-label, registry based randomized clinical trial.
Setting: Thirty-five hospitals in Sweden with acute cardiac care facilities.
Synopsis: Authors included 6,629 patients aged 30 and older who presented with symptoms suggestive of myocardial infarction. Patients with oxygen saturations 90% or greater were enrolled in the study and randomly assigned to either 6 liters per minute of face mask oxygen for 6-12 hours or ambient air. Median oxygen saturation was 99% in the treatment group and 97% in the ambient air group (P less than .0001). In an intention-to-treat model, 1 year after randomization there was no significant difference in all-cause mortality between the oxygen (5.0%) and ambient air (5.1%) groups (P = .80). There was no difference in the rate of rehospitalization with myocardial infarction or the composite endpoint of all-cause mortality and rehospitalizations for myocardial infarction at 30 days and 1 year. Limitations of this study include lower power than anticipated since calculations were based on a higher mortality rate than observed in this study, and the open-label protocol.
Bottom line: In patients who present with a suspected myocardial infarction without hypoxemia, oxygen therapy is not associated with improved all-cause mortality or decreased rehospitalizations for myocardial infarction.
Citation: Hofmann R, Jernberg T, Erlinge D, et al. Oxygen therapy in suspected acute myocardial infarction. N Engl J Med. 2017;377:1240-9.

Dr. Gala is a hospitalist, Beth Israel Deaconess Medical Center, and instructor in medicine, Harvard Medical School, Boston.
Background: Clinical guidelines recommend supplemental oxygen in patients with suspected acute myocardial infarction but data to support its use in patients without hypoxemia are limited.
Study design: Open-label, registry based randomized clinical trial.
Setting: Thirty-five hospitals in Sweden with acute cardiac care facilities.
Synopsis: Authors included 6,629 patients aged 30 and older who presented with symptoms suggestive of myocardial infarction. Patients with oxygen saturations 90% or greater were enrolled in the study and randomly assigned to either 6 liters per minute of face mask oxygen for 6-12 hours or ambient air. Median oxygen saturation was 99% in the treatment group and 97% in the ambient air group (P less than .0001). In an intention-to-treat model, 1 year after randomization there was no significant difference in all-cause mortality between the oxygen (5.0%) and ambient air (5.1%) groups (P = .80). There was no difference in the rate of rehospitalization with myocardial infarction or the composite endpoint of all-cause mortality and rehospitalizations for myocardial infarction at 30 days and 1 year. Limitations of this study include lower power than anticipated since calculations were based on a higher mortality rate than observed in this study, and the open-label protocol.
Bottom line: In patients who present with a suspected myocardial infarction without hypoxemia, oxygen therapy is not associated with improved all-cause mortality or decreased rehospitalizations for myocardial infarction.
Citation: Hofmann R, Jernberg T, Erlinge D, et al. Oxygen therapy in suspected acute myocardial infarction. N Engl J Med. 2017;377:1240-9.
Dr. Gala is a hospitalist, Beth Israel Deaconess Medical Center, and instructor in medicine, Harvard Medical School, Boston.
Background: Clinical guidelines recommend supplemental oxygen in patients with suspected acute myocardial infarction but data to support its use in patients without hypoxemia are limited.
Study design: Open-label, registry based randomized clinical trial.
Setting: Thirty-five hospitals in Sweden with acute cardiac care facilities.
Synopsis: Authors included 6,629 patients aged 30 and older who presented with symptoms suggestive of myocardial infarction. Patients with oxygen saturations 90% or greater were enrolled in the study and randomly assigned to either 6 liters per minute of face mask oxygen for 6-12 hours or ambient air. Median oxygen saturation was 99% in the treatment group and 97% in the ambient air group (P less than .0001). In an intention-to-treat model, 1 year after randomization there was no significant difference in all-cause mortality between the oxygen (5.0%) and ambient air (5.1%) groups (P = .80). There was no difference in the rate of rehospitalization with myocardial infarction or the composite endpoint of all-cause mortality and rehospitalizations for myocardial infarction at 30 days and 1 year. Limitations of this study include lower power than anticipated since calculations were based on a higher mortality rate than observed in this study, and the open-label protocol.
Bottom line: In patients who present with a suspected myocardial infarction without hypoxemia, oxygen therapy is not associated with improved all-cause mortality or decreased rehospitalizations for myocardial infarction.
Citation: Hofmann R, Jernberg T, Erlinge D, et al. Oxygen therapy in suspected acute myocardial infarction. N Engl J Med. 2017;377:1240-9.
Dr. Gala is a hospitalist, Beth Israel Deaconess Medical Center, and instructor in medicine, Harvard Medical School, Boston.
VIDEO: Select atopic dermatitis patients need patch testing
SAN DIEGO – Patch testing may be in order for some patients with atopic dermatitis, according to Jonathan Silverberg, MD, PhD, of the department of dermatology, Northwestern University, Chicago.
Allergic contact dermatitis is a common comorbid condition in people with AD “and sometimes, can flare up the severity of the disease,” he said in a video interview at the American Academy of Dermatology annual meeting.
Patch testing can ferret out a trigger in atopic dermatitis patients with atypical disease distribution or refractory disease, and help avoid the need for systemic therapy, Dr. Silverman pointed out.
In the interview, he discussed these and other clinical scenarios, as well as how patch testing differs in these patients and what screening series to consider using.
Dr. Silverberg had no relevant financial disclosures.
SOURCE: Silverberg, J. et al, Session 061.
SAN DIEGO – Patch testing may be in order for some patients with atopic dermatitis, according to Jonathan Silverberg, MD, PhD, of the department of dermatology, Northwestern University, Chicago.
Allergic contact dermatitis is a common comorbid condition in people with AD “and sometimes, can flare up the severity of the disease,” he said in a video interview at the American Academy of Dermatology annual meeting.
Patch testing can ferret out a trigger in atopic dermatitis patients with atypical disease distribution or refractory disease, and help avoid the need for systemic therapy, Dr. Silverman pointed out.
In the interview, he discussed these and other clinical scenarios, as well as how patch testing differs in these patients and what screening series to consider using.
Dr. Silverberg had no relevant financial disclosures.
SOURCE: Silverberg, J. et al, Session 061.
SAN DIEGO – Patch testing may be in order for some patients with atopic dermatitis, according to Jonathan Silverberg, MD, PhD, of the department of dermatology, Northwestern University, Chicago.
Allergic contact dermatitis is a common comorbid condition in people with AD “and sometimes, can flare up the severity of the disease,” he said in a video interview at the American Academy of Dermatology annual meeting.
Patch testing can ferret out a trigger in atopic dermatitis patients with atypical disease distribution or refractory disease, and help avoid the need for systemic therapy, Dr. Silverman pointed out.
In the interview, he discussed these and other clinical scenarios, as well as how patch testing differs in these patients and what screening series to consider using.
Dr. Silverberg had no relevant financial disclosures.
SOURCE: Silverberg, J. et al, Session 061.
REPORTING FROM AAD 18

VIDEO: Vulvar disorders in preadolescent patients
SAN DIEGO – Over the past few years, pediatric dermatologist Kalyani Marathe, MD, has been seeing young patients with vulvar diseases in a multidisciplinary vulvar dermatology clinic at Children’s National Health System, in Washington, DC.
When Dr. Marathe started, it was her first experience treating such patients and there still are not much data in this population. She and Veronica Gomez-Lobo, MD, a pediatric and adolescent gynecologist at Children’s, “have now been doing the clinic every month for the last three and a half years,” and counsel and treat patients together. With longitudinal follow-up, “we’re learning so much about these conditions in children,” most of whom are about ages 3-11 years.
In a video interview at the annual meeting of the American Academy of Dermatology, Dr. Marathe discussed some of what she and Dr. Gomez-Lobo have learned over the past 3 years, with algorithms for treatment for the most common conditions they encounter in the clinic: non-specific vulvovaginitis, lichen sclerosus, and vitiligo.
Dr. Marathe had no relevant disclosures. She is a Dermatology News editorial board advisor.
SOURCE: Marathe, K. et al, Session U018
SAN DIEGO – Over the past few years, pediatric dermatologist Kalyani Marathe, MD, has been seeing young patients with vulvar diseases in a multidisciplinary vulvar dermatology clinic at Children’s National Health System, in Washington, DC.
When Dr. Marathe started, it was her first experience treating such patients and there still are not much data in this population. She and Veronica Gomez-Lobo, MD, a pediatric and adolescent gynecologist at Children’s, “have now been doing the clinic every month for the last three and a half years,” and counsel and treat patients together. With longitudinal follow-up, “we’re learning so much about these conditions in children,” most of whom are about ages 3-11 years.
In a video interview at the annual meeting of the American Academy of Dermatology, Dr. Marathe discussed some of what she and Dr. Gomez-Lobo have learned over the past 3 years, with algorithms for treatment for the most common conditions they encounter in the clinic: non-specific vulvovaginitis, lichen sclerosus, and vitiligo.
Dr. Marathe had no relevant disclosures. She is a Dermatology News editorial board advisor.
SOURCE: Marathe, K. et al, Session U018
SAN DIEGO – Over the past few years, pediatric dermatologist Kalyani Marathe, MD, has been seeing young patients with vulvar diseases in a multidisciplinary vulvar dermatology clinic at Children’s National Health System, in Washington, DC.
When Dr. Marathe started, it was her first experience treating such patients and there still are not much data in this population. She and Veronica Gomez-Lobo, MD, a pediatric and adolescent gynecologist at Children’s, “have now been doing the clinic every month for the last three and a half years,” and counsel and treat patients together. With longitudinal follow-up, “we’re learning so much about these conditions in children,” most of whom are about ages 3-11 years.
In a video interview at the annual meeting of the American Academy of Dermatology, Dr. Marathe discussed some of what she and Dr. Gomez-Lobo have learned over the past 3 years, with algorithms for treatment for the most common conditions they encounter in the clinic: non-specific vulvovaginitis, lichen sclerosus, and vitiligo.
Dr. Marathe had no relevant disclosures. She is a Dermatology News editorial board advisor.
SOURCE: Marathe, K. et al, Session U018
REPORTING FROM AAD 18

Risankizumab outpaced ustekinumab for complete clearance of plaque psoriasis
SAN DIEGO – Risankizumab outperformed ustekinumab in two phase 3 trials investigating the IL-23 blocker for moderate to severe plaque psoriasis.
In two year-long studies, 56% and 59% of those taking risankizumab and 21% and 30% of those taking ustekinumab achieved completely clear skin, Kenneth B. Gordon, MD, said at the annual meeting of the American Academy of Dermatology.

“One of the things we are striving for now is complete skin clearance,” said Dr. Gordon, chair of the dermatology department the Medical College of Wisconsin, Milwaukee. “In the past, people have said that it wasn’t important to reach that, yet here we are, getting more than 50% of patients to that point.”
Risankizumab is an investigational monoclonal antibody that selectively blocks IL-23, a key inflammatory protein. The drug is also in phase 3 trials for Crohn's disease, and being investigated for psoriatic arthritis. AbbVie, which is developing risankizumab, plans future trials for treating ulcerative colitis.
Dr. Gordon reported the results of UltIMMa-1 and UltIMMa-2, identical three-armed studies that randomized a total of 797 patients with moderate to severe plaque psoriasis to risankizumab 150 mg, ustekinumab 45 mg or 90 mg (based on weight), or to a crossover group that took placebo for the first 16 weeks of the study and then were switched to risankizumab 150 mg for the remainder of the study. Study drugs were delivered at weeks 0, 4, 16, 28, and 40.
The coprimary endpoints were at least a 90% improvement in the Psoriasis Area Severity Index score (PASI 90) at week 16 and a score of 0 or 1 on the Static Physicians’ Assessment scale (sPGA 0/1) at week 16, compared with placebo. Key secondary endpoints compared risankizumab with ustekinumab: PASI 90, sPGA score of clear (sPGA 0), sPGA 0/1, and Dermatology Quality of Life (DLQI) score of 0/1 at week 16, and PASI 90, PASI 100 and sPGA 0 at week 52.
In both trials, patients were 48 years old on average; about 20% had severe plaque psoriasis. The mean PASI score was about 20 at trial entry. Prior therapy included biologics in 30%-43%, depending on the trial, and TNF-alpha inhibitors in about 25%.
Patient retention in the study was good, Dr. Gordon noted, with 95% of risankizumab patients still taking the drug at 52 weeks. Patients also stayed on ustekinumab, with 94% of UltIMMa-1 patients and 91% of UltIMMa-2 patients still taking the drug at 52 weeks.
At week 16, risankizumab was clearly superior to placebo in both endpoints. In both studies, 75% of actively treated patients achieved PASI 90, compared to 5% of those taking placebo. In UltIMMa-1, a clear or almost clear sPGA was seen in 88% of risankizumab patients as compared to 8% of those taking placebo. In UltIMMa-2, these numbers were 84% and 5%, respectively.
In the secondary comparison of the two active drugs, risankizumab significantly outperformed ustekinumab on PASI90 at 16 weeks in UltIMMa-1 (75% vs. 42%) and in UltIMMa-2 (75% vs. 47%). The PASI90 outcomes similarly favored risankizumab at 52 weeks in UltIMMa-1 (82% vs. 44%) and in UltIMMa-2 (81% vs. 50%).
As compared with ustekinumab, risankizumab aced the secondary endpoint of complete skin clearance in UltIMMa-1 and (36% vs. 12%) and UltIMMa-2 (51% vs. 24%). The results similarly favored risankizumab at 52 weeks in both trials (56% vs. 21% and 59% vs. 30%).
Another secondary endpoint looked at how the crossover group fared. At week 51, the PASI90 for this group was 78% in UltIMMa-1 and 85% in UltIMMa-2; the PASI100 at 52 weeks for these patients was 55% and 67%.
A responder time curve demonstrated just how quickly the crossover patients made up for lost time after switching to risankizumab. Although these patients made no progress toward disease clearance during their placebo period, they quickly caught up with the primary risankizumab group. At 16 weeks, 5% in this group had a PASI 90; by week 28, 51% did; and by week 52, PASI 90 topped out at 78%.
“The time course seen in this trial is very important,” Dr. Gordon said. “By 8 weeks, almost 44% [of the primary risankizumab group] was already at PASI90. They reached an extremely high level of response that was very consistent over 1 year. In the ustekinumab group, we saw some saw-toothing of response, indicating that people were losing effectiveness at the end of the dosing period. With risankizumab, we did not see that, indicating that the once every 12 weeks dosing period is effective.”
The DLQI 0/1 outcome occurred at 16 and 52 weeks in significantly more patients taking risankizumab in both studies. By week 52 in UltIMMa-1, 75% of patients on risankizumab had achieved a DLQ1 0/1, compared with 47% of the ustekinumab group. In UltIMMa-2, these numbers were 71% and 44%, with the crossover group posting scores similar to the primary risankizumab group in both studies (62% and 68%).
Risankizumab proved safe and well tolerated, Dr. Gordon said. Less than 1% of patients discontinued the medication due to an adverse event. In both the UltIMMa-1 and UltIMMa-2 trials, the most frequently reported treatment-emergent adverse event in the risankizumab groups was upper respiratory tract infection. In UltIMMa-1, one patient receiving risankizumab presented with latent tuberculosis and was treated with rifampicin. There were no new cases of tuberculosis.
The serious adverse event rate hovered between 2%-3% in both trials. The rate of serious infection was 1%. The rate of malignancy was 0.3%, but fell to 0 when nonmelanoma skin cancer was excluded. There were no major cardiovascular events.
"Not only do these data show significant rates of clear skin, but because we know the burden of psoriasis extends beyond the skin, we are encouraged by the patient-reported improvement in quality of life after one year of treatment," he said. "Given the significant impact of psoriasis, it is important to continue to investigate additional treatment options."
AbbVie sponsored the trials. Dr. Gordon is a consultant for the company.
SOURCE: Gordon et al. AAD, Abstract 6495
SAN DIEGO – Risankizumab outperformed ustekinumab in two phase 3 trials investigating the IL-23 blocker for moderate to severe plaque psoriasis.
In two year-long studies, 56% and 59% of those taking risankizumab and 21% and 30% of those taking ustekinumab achieved completely clear skin, Kenneth B. Gordon, MD, said at the annual meeting of the American Academy of Dermatology.
“One of the things we are striving for now is complete skin clearance,” said Dr. Gordon, chair of the dermatology department the Medical College of Wisconsin, Milwaukee. “In the past, people have said that it wasn’t important to reach that, yet here we are, getting more than 50% of patients to that point.”
Risankizumab is an investigational monoclonal antibody that selectively blocks IL-23, a key inflammatory protein. The drug is also in phase 3 trials for Crohn's disease, and being investigated for psoriatic arthritis. AbbVie, which is developing risankizumab, plans future trials for treating ulcerative colitis.
Dr. Gordon reported the results of UltIMMa-1 and UltIMMa-2, identical three-armed studies that randomized a total of 797 patients with moderate to severe plaque psoriasis to risankizumab 150 mg, ustekinumab 45 mg or 90 mg (based on weight), or to a crossover group that took placebo for the first 16 weeks of the study and then were switched to risankizumab 150 mg for the remainder of the study. Study drugs were delivered at weeks 0, 4, 16, 28, and 40.
The coprimary endpoints were at least a 90% improvement in the Psoriasis Area Severity Index score (PASI 90) at week 16 and a score of 0 or 1 on the Static Physicians’ Assessment scale (sPGA 0/1) at week 16, compared with placebo. Key secondary endpoints compared risankizumab with ustekinumab: PASI 90, sPGA score of clear (sPGA 0), sPGA 0/1, and Dermatology Quality of Life (DLQI) score of 0/1 at week 16, and PASI 90, PASI 100 and sPGA 0 at week 52.
In both trials, patients were 48 years old on average; about 20% had severe plaque psoriasis. The mean PASI score was about 20 at trial entry. Prior therapy included biologics in 30%-43%, depending on the trial, and TNF-alpha inhibitors in about 25%.
Patient retention in the study was good, Dr. Gordon noted, with 95% of risankizumab patients still taking the drug at 52 weeks. Patients also stayed on ustekinumab, with 94% of UltIMMa-1 patients and 91% of UltIMMa-2 patients still taking the drug at 52 weeks.
At week 16, risankizumab was clearly superior to placebo in both endpoints. In both studies, 75% of actively treated patients achieved PASI 90, compared to 5% of those taking placebo. In UltIMMa-1, a clear or almost clear sPGA was seen in 88% of risankizumab patients as compared to 8% of those taking placebo. In UltIMMa-2, these numbers were 84% and 5%, respectively.
In the secondary comparison of the two active drugs, risankizumab significantly outperformed ustekinumab on PASI90 at 16 weeks in UltIMMa-1 (75% vs. 42%) and in UltIMMa-2 (75% vs. 47%). The PASI90 outcomes similarly favored risankizumab at 52 weeks in UltIMMa-1 (82% vs. 44%) and in UltIMMa-2 (81% vs. 50%).
As compared with ustekinumab, risankizumab aced the secondary endpoint of complete skin clearance in UltIMMa-1 and (36% vs. 12%) and UltIMMa-2 (51% vs. 24%). The results similarly favored risankizumab at 52 weeks in both trials (56% vs. 21% and 59% vs. 30%).
Another secondary endpoint looked at how the crossover group fared. At week 51, the PASI90 for this group was 78% in UltIMMa-1 and 85% in UltIMMa-2; the PASI100 at 52 weeks for these patients was 55% and 67%.
A responder time curve demonstrated just how quickly the crossover patients made up for lost time after switching to risankizumab. Although these patients made no progress toward disease clearance during their placebo period, they quickly caught up with the primary risankizumab group. At 16 weeks, 5% in this group had a PASI 90; by week 28, 51% did; and by week 52, PASI 90 topped out at 78%.
“The time course seen in this trial is very important,” Dr. Gordon said. “By 8 weeks, almost 44% [of the primary risankizumab group] was already at PASI90. They reached an extremely high level of response that was very consistent over 1 year. In the ustekinumab group, we saw some saw-toothing of response, indicating that people were losing effectiveness at the end of the dosing period. With risankizumab, we did not see that, indicating that the once every 12 weeks dosing period is effective.”
The DLQI 0/1 outcome occurred at 16 and 52 weeks in significantly more patients taking risankizumab in both studies. By week 52 in UltIMMa-1, 75% of patients on risankizumab had achieved a DLQ1 0/1, compared with 47% of the ustekinumab group. In UltIMMa-2, these numbers were 71% and 44%, with the crossover group posting scores similar to the primary risankizumab group in both studies (62% and 68%).
Risankizumab proved safe and well tolerated, Dr. Gordon said. Less than 1% of patients discontinued the medication due to an adverse event. In both the UltIMMa-1 and UltIMMa-2 trials, the most frequently reported treatment-emergent adverse event in the risankizumab groups was upper respiratory tract infection. In UltIMMa-1, one patient receiving risankizumab presented with latent tuberculosis and was treated with rifampicin. There were no new cases of tuberculosis.
The serious adverse event rate hovered between 2%-3% in both trials. The rate of serious infection was 1%. The rate of malignancy was 0.3%, but fell to 0 when nonmelanoma skin cancer was excluded. There were no major cardiovascular events.
"Not only do these data show significant rates of clear skin, but because we know the burden of psoriasis extends beyond the skin, we are encouraged by the patient-reported improvement in quality of life after one year of treatment," he said. "Given the significant impact of psoriasis, it is important to continue to investigate additional treatment options."
AbbVie sponsored the trials. Dr. Gordon is a consultant for the company.
SOURCE: Gordon et al. AAD, Abstract 6495
SAN DIEGO – Risankizumab outperformed ustekinumab in two phase 3 trials investigating the IL-23 blocker for moderate to severe plaque psoriasis.
In two year-long studies, 56% and 59% of those taking risankizumab and 21% and 30% of those taking ustekinumab achieved completely clear skin, Kenneth B. Gordon, MD, said at the annual meeting of the American Academy of Dermatology.
“One of the things we are striving for now is complete skin clearance,” said Dr. Gordon, chair of the dermatology department the Medical College of Wisconsin, Milwaukee. “In the past, people have said that it wasn’t important to reach that, yet here we are, getting more than 50% of patients to that point.”
Risankizumab is an investigational monoclonal antibody that selectively blocks IL-23, a key inflammatory protein. The drug is also in phase 3 trials for Crohn's disease, and being investigated for psoriatic arthritis. AbbVie, which is developing risankizumab, plans future trials for treating ulcerative colitis.
Dr. Gordon reported the results of UltIMMa-1 and UltIMMa-2, identical three-armed studies that randomized a total of 797 patients with moderate to severe plaque psoriasis to risankizumab 150 mg, ustekinumab 45 mg or 90 mg (based on weight), or to a crossover group that took placebo for the first 16 weeks of the study and then were switched to risankizumab 150 mg for the remainder of the study. Study drugs were delivered at weeks 0, 4, 16, 28, and 40.
The coprimary endpoints were at least a 90% improvement in the Psoriasis Area Severity Index score (PASI 90) at week 16 and a score of 0 or 1 on the Static Physicians’ Assessment scale (sPGA 0/1) at week 16, compared with placebo. Key secondary endpoints compared risankizumab with ustekinumab: PASI 90, sPGA score of clear (sPGA 0), sPGA 0/1, and Dermatology Quality of Life (DLQI) score of 0/1 at week 16, and PASI 90, PASI 100 and sPGA 0 at week 52.
In both trials, patients were 48 years old on average; about 20% had severe plaque psoriasis. The mean PASI score was about 20 at trial entry. Prior therapy included biologics in 30%-43%, depending on the trial, and TNF-alpha inhibitors in about 25%.
Patient retention in the study was good, Dr. Gordon noted, with 95% of risankizumab patients still taking the drug at 52 weeks. Patients also stayed on ustekinumab, with 94% of UltIMMa-1 patients and 91% of UltIMMa-2 patients still taking the drug at 52 weeks.
At week 16, risankizumab was clearly superior to placebo in both endpoints. In both studies, 75% of actively treated patients achieved PASI 90, compared to 5% of those taking placebo. In UltIMMa-1, a clear or almost clear sPGA was seen in 88% of risankizumab patients as compared to 8% of those taking placebo. In UltIMMa-2, these numbers were 84% and 5%, respectively.
In the secondary comparison of the two active drugs, risankizumab significantly outperformed ustekinumab on PASI90 at 16 weeks in UltIMMa-1 (75% vs. 42%) and in UltIMMa-2 (75% vs. 47%). The PASI90 outcomes similarly favored risankizumab at 52 weeks in UltIMMa-1 (82% vs. 44%) and in UltIMMa-2 (81% vs. 50%).
As compared with ustekinumab, risankizumab aced the secondary endpoint of complete skin clearance in UltIMMa-1 and (36% vs. 12%) and UltIMMa-2 (51% vs. 24%). The results similarly favored risankizumab at 52 weeks in both trials (56% vs. 21% and 59% vs. 30%).
Another secondary endpoint looked at how the crossover group fared. At week 51, the PASI90 for this group was 78% in UltIMMa-1 and 85% in UltIMMa-2; the PASI100 at 52 weeks for these patients was 55% and 67%.
A responder time curve demonstrated just how quickly the crossover patients made up for lost time after switching to risankizumab. Although these patients made no progress toward disease clearance during their placebo period, they quickly caught up with the primary risankizumab group. At 16 weeks, 5% in this group had a PASI 90; by week 28, 51% did; and by week 52, PASI 90 topped out at 78%.
“The time course seen in this trial is very important,” Dr. Gordon said. “By 8 weeks, almost 44% [of the primary risankizumab group] was already at PASI90. They reached an extremely high level of response that was very consistent over 1 year. In the ustekinumab group, we saw some saw-toothing of response, indicating that people were losing effectiveness at the end of the dosing period. With risankizumab, we did not see that, indicating that the once every 12 weeks dosing period is effective.”
The DLQI 0/1 outcome occurred at 16 and 52 weeks in significantly more patients taking risankizumab in both studies. By week 52 in UltIMMa-1, 75% of patients on risankizumab had achieved a DLQ1 0/1, compared with 47% of the ustekinumab group. In UltIMMa-2, these numbers were 71% and 44%, with the crossover group posting scores similar to the primary risankizumab group in both studies (62% and 68%).
Risankizumab proved safe and well tolerated, Dr. Gordon said. Less than 1% of patients discontinued the medication due to an adverse event. In both the UltIMMa-1 and UltIMMa-2 trials, the most frequently reported treatment-emergent adverse event in the risankizumab groups was upper respiratory tract infection. In UltIMMa-1, one patient receiving risankizumab presented with latent tuberculosis and was treated with rifampicin. There were no new cases of tuberculosis.
The serious adverse event rate hovered between 2%-3% in both trials. The rate of serious infection was 1%. The rate of malignancy was 0.3%, but fell to 0 when nonmelanoma skin cancer was excluded. There were no major cardiovascular events.
"Not only do these data show significant rates of clear skin, but because we know the burden of psoriasis extends beyond the skin, we are encouraged by the patient-reported improvement in quality of life after one year of treatment," he said. "Given the significant impact of psoriasis, it is important to continue to investigate additional treatment options."
AbbVie sponsored the trials. Dr. Gordon is a consultant for the company.
SOURCE: Gordon et al. AAD, Abstract 6495
REPORTING FROM AAD 18
Key clinical point: Risankizumab outperformed placebo and the active comparator ustekinumab.
Major finding: In the two studies, 56% and 59% of those taking risankizumab had clear skin as compared to 21% and 30% of those taking ustekinumab.
Study details: The twin placebo-crossover active comparator trials randomized 797 patients.
Disclosures: AbbVie sponsored the studies. Dr. Gordon is a consultant for the company.
Source: Gordon et al. AAD abstract 6495
Thank you to our top Community contributors
2017 was a busy year in the AGA Community, our member-only discussion forum. Some of our favorite discussions included challenging clinical cases you shared, remembering your colleague Dr. Marv Sleisenger and first-hand recaps of AGA’s Advocacy Day experiences.
Thank you to everyone who contributed to the conversations in 2017, making the AGA Community a hub for collaboration to ever-expand the field of GI.
Tied for the title of top contributor in 2017 were Dmitriy Kedrin, MD, PhD, of Elliot Hospital in Manchester, N.H., and Sunanda Kane, MD, MSPH, AGAF, of Mayo Clinic in Rochester, MN.
Both are key influencers in the forum, especially with helping colleagues manage challenging patient cases. Learn more about each contributor and why keeping up with the Community is an important part of their regular routines in this brief Q&A.
Thanks for being such an active member of the AGA Community! Why do you contribute?
Dr. Kane: “You are welcome! I contribute because I feel I have helpful suggestions and recommendations for managing difficult patient scenarios as well as for professional issues.”
Dr. Kedrin: “I think it is important for GI docs to be a part of a larger community, stay informed on latest guidelines, research publications and approaches to difficult cases, where more than one road can be taken. I feel that it is a great forum for someone like me, relatively junior gastroenterologist.”
Why do you enjoy being part of the AGA Community?
Kane: “I feel engaged with my colleagues who I otherwise do not see on a regular basis, and get to ‘meet’ new ones.”
Kedrin: “I find the case discussions informative. I learn a great deal about current trends and opinions on important topics in the GI world.”
What do you like to do in your free time?
Kane: “I enjoy cooking and binge-watching Netflix.”
Kedrin: “I bake bread and run a gastroenterology literature review podcast called ‘GI Pearls.’”
What’s your approach to handling a difficult patient case you come across in your practice?
Kane: “I reach out to as many of my colleagues as I think appropriate who may have some experience or thoughts about how to help a difficult patient.”
Kedrin: “I often seek advice of other clinicians, some with more expertise in a particular area. I also go to the literature and try to learn more that way, help expand my differential as well as figure out the best therapeutic approach.”
Was there a conversation in the AGA Community in 2017 that was your favorite?
Kane: “All conversations have merit, none stick out as a favorite.”
Kedrin: “Oh, there are several. I recall a patient case where there were several thought leaders in the field who had a disagreement about the best approach to treatment. The work-life balance conversation [Early Career Group members only] was also very good. I also enjoyed reading about different opinions regarding the values of randomized versus observational trials that happened a while back.”
View the top discussions and contributors from 2017 on the AGA Community homepage, for a limited time.
2017 was a busy year in the AGA Community, our member-only discussion forum. Some of our favorite discussions included challenging clinical cases you shared, remembering your colleague Dr. Marv Sleisenger and first-hand recaps of AGA’s Advocacy Day experiences.
Thank you to everyone who contributed to the conversations in 2017, making the AGA Community a hub for collaboration to ever-expand the field of GI.
Tied for the title of top contributor in 2017 were Dmitriy Kedrin, MD, PhD, of Elliot Hospital in Manchester, N.H., and Sunanda Kane, MD, MSPH, AGAF, of Mayo Clinic in Rochester, MN.
Both are key influencers in the forum, especially with helping colleagues manage challenging patient cases. Learn more about each contributor and why keeping up with the Community is an important part of their regular routines in this brief Q&A.
Thanks for being such an active member of the AGA Community! Why do you contribute?
Dr. Kane: “You are welcome! I contribute because I feel I have helpful suggestions and recommendations for managing difficult patient scenarios as well as for professional issues.”
Dr. Kedrin: “I think it is important for GI docs to be a part of a larger community, stay informed on latest guidelines, research publications and approaches to difficult cases, where more than one road can be taken. I feel that it is a great forum for someone like me, relatively junior gastroenterologist.”
Why do you enjoy being part of the AGA Community?
Kane: “I feel engaged with my colleagues who I otherwise do not see on a regular basis, and get to ‘meet’ new ones.”
Kedrin: “I find the case discussions informative. I learn a great deal about current trends and opinions on important topics in the GI world.”
What do you like to do in your free time?
Kane: “I enjoy cooking and binge-watching Netflix.”
Kedrin: “I bake bread and run a gastroenterology literature review podcast called ‘GI Pearls.’”
What’s your approach to handling a difficult patient case you come across in your practice?
Kane: “I reach out to as many of my colleagues as I think appropriate who may have some experience or thoughts about how to help a difficult patient.”
Kedrin: “I often seek advice of other clinicians, some with more expertise in a particular area. I also go to the literature and try to learn more that way, help expand my differential as well as figure out the best therapeutic approach.”
Was there a conversation in the AGA Community in 2017 that was your favorite?
Kane: “All conversations have merit, none stick out as a favorite.”
Kedrin: “Oh, there are several. I recall a patient case where there were several thought leaders in the field who had a disagreement about the best approach to treatment. The work-life balance conversation [Early Career Group members only] was also very good. I also enjoyed reading about different opinions regarding the values of randomized versus observational trials that happened a while back.”
View the top discussions and contributors from 2017 on the AGA Community homepage, for a limited time.
2017 was a busy year in the AGA Community, our member-only discussion forum. Some of our favorite discussions included challenging clinical cases you shared, remembering your colleague Dr. Marv Sleisenger and first-hand recaps of AGA’s Advocacy Day experiences.
Thank you to everyone who contributed to the conversations in 2017, making the AGA Community a hub for collaboration to ever-expand the field of GI.
Tied for the title of top contributor in 2017 were Dmitriy Kedrin, MD, PhD, of Elliot Hospital in Manchester, N.H., and Sunanda Kane, MD, MSPH, AGAF, of Mayo Clinic in Rochester, MN.
Both are key influencers in the forum, especially with helping colleagues manage challenging patient cases. Learn more about each contributor and why keeping up with the Community is an important part of their regular routines in this brief Q&A.
Thanks for being such an active member of the AGA Community! Why do you contribute?
Dr. Kane: “You are welcome! I contribute because I feel I have helpful suggestions and recommendations for managing difficult patient scenarios as well as for professional issues.”
Dr. Kedrin: “I think it is important for GI docs to be a part of a larger community, stay informed on latest guidelines, research publications and approaches to difficult cases, where more than one road can be taken. I feel that it is a great forum for someone like me, relatively junior gastroenterologist.”
Why do you enjoy being part of the AGA Community?
Kane: “I feel engaged with my colleagues who I otherwise do not see on a regular basis, and get to ‘meet’ new ones.”
Kedrin: “I find the case discussions informative. I learn a great deal about current trends and opinions on important topics in the GI world.”
What do you like to do in your free time?
Kane: “I enjoy cooking and binge-watching Netflix.”
Kedrin: “I bake bread and run a gastroenterology literature review podcast called ‘GI Pearls.’”
What’s your approach to handling a difficult patient case you come across in your practice?
Kane: “I reach out to as many of my colleagues as I think appropriate who may have some experience or thoughts about how to help a difficult patient.”
Kedrin: “I often seek advice of other clinicians, some with more expertise in a particular area. I also go to the literature and try to learn more that way, help expand my differential as well as figure out the best therapeutic approach.”
Was there a conversation in the AGA Community in 2017 that was your favorite?
Kane: “All conversations have merit, none stick out as a favorite.”
Kedrin: “Oh, there are several. I recall a patient case where there were several thought leaders in the field who had a disagreement about the best approach to treatment. The work-life balance conversation [Early Career Group members only] was also very good. I also enjoyed reading about different opinions regarding the values of randomized versus observational trials that happened a while back.”
View the top discussions and contributors from 2017 on the AGA Community homepage, for a limited time.
Nd:YAG laser treatment improves the appearance of facial wrinkles
wrote Eric F. Bernstein, MD, a laser surgeon in private practice in Ardmore, Pa., and his associates.
In the study, two fractionated lasers were each combined with a specially designed “holographic beam-splitting optic” to treat mild to moderate facial wrinkles in 24 patients aged 18-75 years with Fitzpatrick skin types I-VI; 14 patients received five monthly treatments with the 1,064 nm laser, while the other 10 patients received four monthly treatments with the 532 nm laser.
Blinded evaluators assessed images taken at baseline and at 12 weeks after treatment. The evaluators found improvements of greater than 20% in 56.9% of the evaluated images, with no statistically significant difference between the two wavelengths. Of those treated with the 1,064 nm laser, 12 of 14 patients were “satisfied” or “very satisfied”; of those treated with the 532 nm laser, 8 of the 10 were “satisfied” or “very satisfied,” Dr. Bernstein and his colleagues wrote in the Journal of Drugs in Dermatology.
Patients experienced only mild to moderate discomfort during the laser treatment. Side effects were mild and were limited to erythema and edema in almost all patients; fewer than half the patients developed petechiae. Side effects generally resolved within a few days of treatment.
Dr. Bernstein and some of the other authors reported relationships with Syneron Candela, which provided funding for and loaned equipment used in the study.
Source: Bernstein EF et al. J Drugs Dermatol. 2017 Nov 1;16(11):1077-82.
wrote Eric F. Bernstein, MD, a laser surgeon in private practice in Ardmore, Pa., and his associates.
In the study, two fractionated lasers were each combined with a specially designed “holographic beam-splitting optic” to treat mild to moderate facial wrinkles in 24 patients aged 18-75 years with Fitzpatrick skin types I-VI; 14 patients received five monthly treatments with the 1,064 nm laser, while the other 10 patients received four monthly treatments with the 532 nm laser.
Blinded evaluators assessed images taken at baseline and at 12 weeks after treatment. The evaluators found improvements of greater than 20% in 56.9% of the evaluated images, with no statistically significant difference between the two wavelengths. Of those treated with the 1,064 nm laser, 12 of 14 patients were “satisfied” or “very satisfied”; of those treated with the 532 nm laser, 8 of the 10 were “satisfied” or “very satisfied,” Dr. Bernstein and his colleagues wrote in the Journal of Drugs in Dermatology.
Patients experienced only mild to moderate discomfort during the laser treatment. Side effects were mild and were limited to erythema and edema in almost all patients; fewer than half the patients developed petechiae. Side effects generally resolved within a few days of treatment.
Dr. Bernstein and some of the other authors reported relationships with Syneron Candela, which provided funding for and loaned equipment used in the study.
Source: Bernstein EF et al. J Drugs Dermatol. 2017 Nov 1;16(11):1077-82.
wrote Eric F. Bernstein, MD, a laser surgeon in private practice in Ardmore, Pa., and his associates.
In the study, two fractionated lasers were each combined with a specially designed “holographic beam-splitting optic” to treat mild to moderate facial wrinkles in 24 patients aged 18-75 years with Fitzpatrick skin types I-VI; 14 patients received five monthly treatments with the 1,064 nm laser, while the other 10 patients received four monthly treatments with the 532 nm laser.
Blinded evaluators assessed images taken at baseline and at 12 weeks after treatment. The evaluators found improvements of greater than 20% in 56.9% of the evaluated images, with no statistically significant difference between the two wavelengths. Of those treated with the 1,064 nm laser, 12 of 14 patients were “satisfied” or “very satisfied”; of those treated with the 532 nm laser, 8 of the 10 were “satisfied” or “very satisfied,” Dr. Bernstein and his colleagues wrote in the Journal of Drugs in Dermatology.
Patients experienced only mild to moderate discomfort during the laser treatment. Side effects were mild and were limited to erythema and edema in almost all patients; fewer than half the patients developed petechiae. Side effects generally resolved within a few days of treatment.
Dr. Bernstein and some of the other authors reported relationships with Syneron Candela, which provided funding for and loaned equipment used in the study.
Source: Bernstein EF et al. J Drugs Dermatol. 2017 Nov 1;16(11):1077-82.
FROM THE JOURNAL OF DRUGS IN DERMATOLOGY
Addressing the Needs of Patients With Chronic Pain
Chronic pain is a common health care problem that remains a significant burden for the VHA.1,2 Some reports indicate that nearly 50% of VA patients report chronic pain.3,4 Both within and outside the VHA, primary care providers (PCPs) generally manage patients with chronic pain.5,6 Historically, a biomedical approach to chronic pain also included the use of opioid medications, which may have contributed to increased opioid-related morbidity and mortality especially among the veteran patient population.7-9 The use of opioids also is controversial due to concerns about adverse effects (AEs), long-term efficacy, functional outcomes, and the potential for drug abuse and addiction.10 Consequently, alternative treatment options that incorporate an interdisciplinary approach have gained significant interest among pain care providers.11 Interdisciplinary programs have been shown to improve functional status and psychological well-being and to reduce pain severity and opioid use.12-14 These benefits may persist for a decade or longer.15
Background
The Stepped Care Model for Pain Management (SCM-PM) is a specific pain treatment approach promoted by the VA National Pain Management Directive.16 This systematically adjusted approach is associated with improved patient satisfaction and health outcomes for pain and depression.17,18 At its core, the model promotes engaging patients as active participants in their care along with a team of doctors who can offer an integrated, evidence-based, multimodal, interdisciplinary treatment plan.
To successfully implement this strategy at the VA, patient aligned care teams (PACT) assess and manage patients with common pain conditions through collaboration with mental health, complementary and integrative health services, physical therapy, and other programs, such as opioid renewal clinics and pain schools.19 This collaborative care approach, which the PCP initiates, is step 1 of the SCM-PM. If initial treatment is not successful and patients are not improving as expected, specialty care consultation and collaborative comanagement through interdisciplinary pain specialty teams are sought (step 2). Finally, step 3 involves tertiary, interdisciplinary care, including access to advanced diagnostic and pain rehabilitation programs accredited by the Commission for Accreditation of Rehabilitation Facilities (CARF).
Although the advantages of interdisciplinary pain programs are clear, resource limitations as well as challenges related to competencies of the PCPs, nurses, and associated health care professionals in pain assessment and management can make implementation of these programs, including the SCM-PM, difficult for many clinics and facilities. Thus, identifying effective chronic pain models and strategies, incorporating the philosophy and key elements of interdisciplinary programs, and accounting for facility resources and capacity are all important.
At the Ann Arbor VAMC, development of a comprehensive interdisciplinary team started with the implementation of joint sessions with a clinical pharmacist and health psychologist embedded in primary care to enhance access to behavioral pain management interventions.20 This program was subsequently expanded to include a pain physician, 2 pain-focused physical therapists (PTs) and a pain nurse.
This article describes a novel team approach for providing more comprehensive, interdisciplinary care for patients with chronic pain along with the initial results for the patients who were part of an outpatient pain group program (OPGP).
Methods
Developing a more interdisciplinary pain management program included integrating different services and creating a strategy for comprehensive evaluation and management of patients with chronic pain. After patients were referred to the interdisciplinary pain clinic by their PCP, they received a systematically structured multidimensional assessment. The primary focus of this assessment was to create an individually directed treatment approach based on the patient’s responses to previous treatments and information collected from several questionnaires administered prior to evaluation. This information helped guide individual patient decision making and actively engaged patients in their care, thus following one of the central tenants of the SCM-PM model. Moreover, functional restoration was at the core of each patient’s evaluation and management. The primary focus was on nonpharmacologic treatment options that included psychological, physical, and occupational therapy; self-management; education; and complementary and alternative therapies. These modalities were offered either individually or in a group setting.
The first step after referral was an evaluation that followed the main core principles for complex disease management described by Tauben and Theodore.21 All new patients were asked to complete a 2-question pain intensity and pain interference measure, the 4-question Patient Health Questionnaire (PHQ-4), 4-question Primary Care-PTSD screening tool (PC-PTSD), and the STOP-BANG questionnaire to assess the risk for obstructive sleep apnea.22-24 Each measure allowed the physician to identify specific problem areas and formulate a treatment plan that would incorporate PTs or occupational therapists, psychologists and/or clinical specialists, and pharmacists if needed.
Patients who were found to have or expressed significant disability because of pain and who wished to learn pain self-management strategies could participate in an 8-week OPGP. This program included the use of cognitive behavioral therapy (CBT) strategies along with group physical therapy classes. Some patients also received individual therapies concurrently with the 8-week OPGP. Patients were excluded from participating in the OPGP only if their current medical or psychiatric status precluded them from full engagement and maximum benefit as determined by the pain physician and psychologist.
Participants and Intervention
Program participants were patients with a chronic pain diagnosis who enrolled in the interdisciplinary pain team OPGP between April 2016 and April 2017. Most patients were referred by their PCPs due to chronic low back, neck, joint or neuropathic pain, although many presented with multiple pain areas. The onset of pain often was a result of a service-related injury or overuse, or the etiology was unknown.
A board-certified pain physician, licensed clinical psychologist, 2 licensed PTs, and a clinical pharmacist led the OPGP sessions. The program was composed of 3-hour-long sessions held weekly for 8 consecutive weeks. Each week, a member of the team covered a specific topic (Table 1). 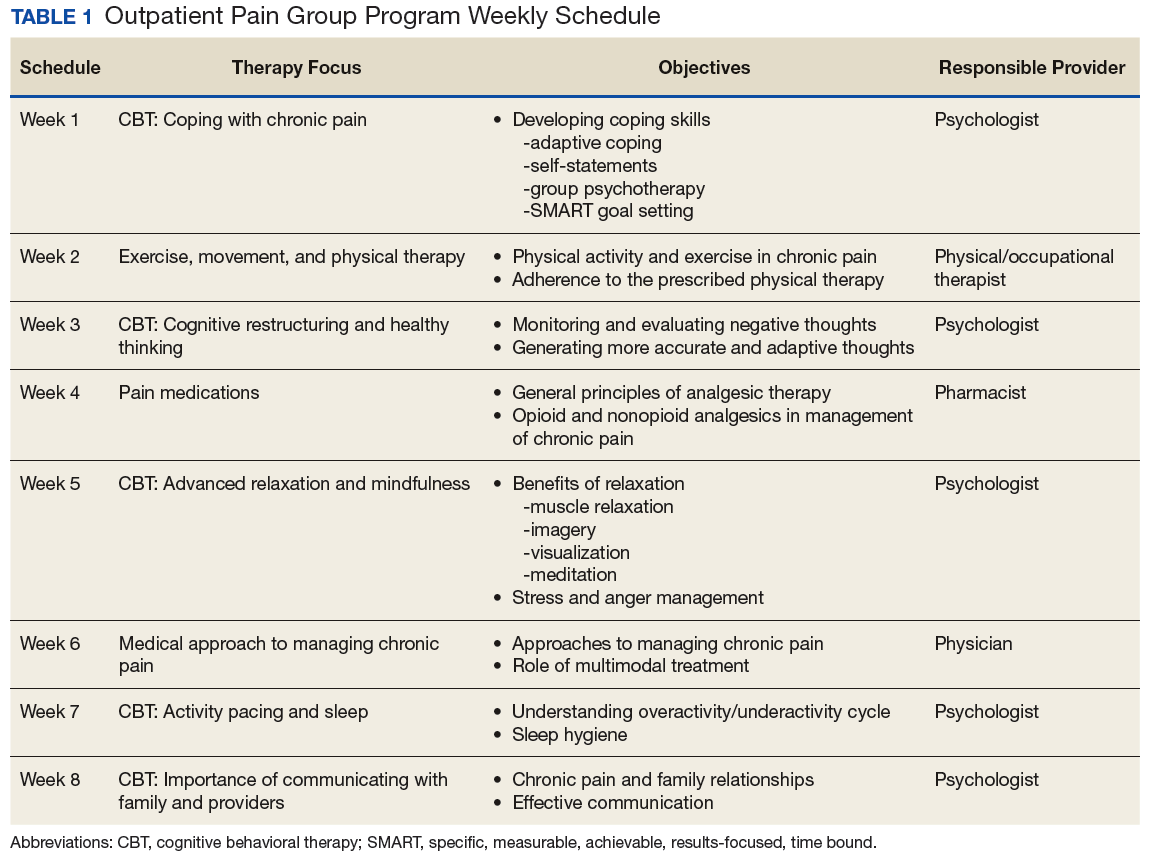
These sessions focused on the importance of exercise, movement, and physical therapy; appropriate use of medications for managing chronic pain; pacing activities and body mechanics; and the medical approach to managing chronic pain. In addition to didactic presentations, interaction and therapeutic dialogue was encouraged among patients. The education portion of each weekly session lasted about 90 minutes, including a short break. Then, following another short break, patients proceeded to the physical therapy area and engaged in an individualized, monitored exercise program, conducted by the team PTs. Patients also were issued pedometers and encouraged to track their steps each day. Education in improving posture and body mechanics was a key component of the exercise portion of the program so patients could resume their normal daily activities and regain enjoyment in their life. Pain outcomemeasures were collected at admission and immediately before discharge.
Medication management also was an important part of the program for some patients and included tapering off opioids and other drugs and implementing trials of adjuvant pain medications shown to help chronic pain. For some patients, this medication management continued after the patient completed the program.
Measures
The Pain Outcome Questionnaire (POQ) is a 19-item, self-report measure of pain treatment outcomes. Pain rating, mobility, activities of daily living, vitality, negative effect, and fear are the functioning domains evaluated, and the subscale scores are added to produce a total score. The POQ was developed from samples of veterans undergoing inpatient or outpatient pain treatment at VA facilities. For each of the subscales and the total score, higher values indicate poorer outcomes. In normative outpatient VA samples, a total score of 71 is at the 25th percentile, and 120 is at the 75th percentile. The POQ has been shown to have good reliability and validity among veterans in an outpatient setting.25
The Pain Catastrophizing Scale (PCS) is a 13-item scale designed to measure various levels of pain catastrophizing.26 Each item is rated on a 5-point Likert-type scale, from 0 (not at all) to 4 (all the time). The PCS consists of 3 subscale domains: rumination, 4 items; magnification, 3 items; and helplessness, 6 items. Responses to all items also can be added to produce a total score from 0 to 52, with higher scores indicating a higher level of catastrophic thinking related to pain. This project evaluated both the total score and the 3 subscale scores.
The Pain Self-Efficacy Questionnaire (PSEQ) is a 10-item questionnaire that assesses confidence in an individual’s ability to cope or to perform activities despite the pain.27 The PSEQ covers a range of functions, including household chores, socializing, work, as well as coping with pain without medications. Each question has a 7-point Likert scale response: 0 = not at all confident, and 7 = completely confident, to produce a total score from 0 to 60. Higher scores indicate stronger pain self-efficacy, which has been shown to be associated with return to work and maintenance of functional gains.
The Patient Health Questionnaire-4 (PHQ-4) is a 4-item instrument used to screen for depression and anxiety in outpatient medical settings.22 Patients indicate how often they have been bothered by certain problems on a 4-point Likert scale, from 0 (not at all) to 3 (nearly every day). The PHQ-4 provides a total score (0-12) with scores of 6 to 8 indicating moderate and 9 to 12 indicating severe psychological distress; 2 subscale scores, 1 for anxiety (2 questions) and 1 for depression (2 questions). For this analysis, the total PHQ-4 score has been dichotomized with 1 indicating a score in the moderate or severe range vs 0 for a score of mild or no psychological distress. Likewise, each of the subscale scores have been dichotomized with 1 indicating a score of 3 or greater, which is considered a positive screen.
The 6-minute walk test (6MWT) measures the distance (in feet) an individual can walk over a total of 6 minutes on a hard, flat surface.28 Even though the individual can walk at a self-selected pace and rest if needed during the test, the goal is for the patient to walk as far as possible over the course of 6 minutes. The 6MWT provides information regarding functional capacity, response to therapy, and prognosis across a range of chronic conditions, including pain.
Data Analysis
Data analysis included the use of both descriptive and comparative statistics. A descriptive analysis was conducted to examine the characteristics of patients who did and did not complete the OPGP. Specific outcomes for those individuals who completed the program, and thus had complete pre- and post-OPGP information, then were compared. Paired t tests were used to compare differences in continuous measures between baseline (pre-OPGP) and the 8-week follow-up (post-OPGP). Comparisons involving dichotomous measures were made using the Fisher exact test. A 2-sided α with a P value .05 was considered statistically significant. All statistical analyses were conducted using STATA version 14.1 (StataCorp, College Station, TX).
Results
A total of 36 patients enrolled, and 28 (77%) completed the OPGP. Patients who did not complete the program (n = 8) either self-discharged due to lack of interest or had difficulty in consistently making their appointments and decided not to continue (Table 2). 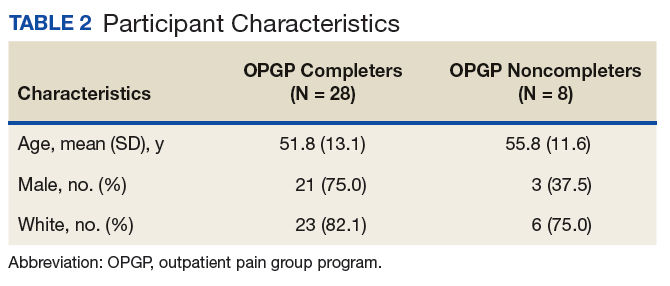
Outcomes for OPGP Completers
Improvements were observed for all outcome domains among patients who completed the program (eTable). 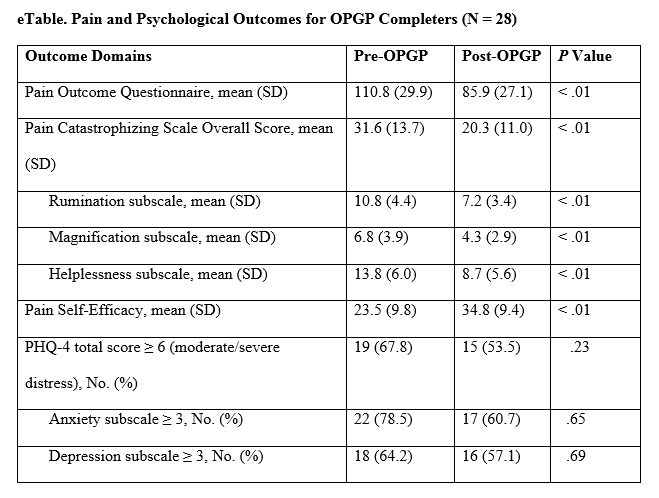
Discussion
This report describes the novel model for improving delivery of chronic pain management services implemented at the Ann Arbor VAMC through the development of a multidisciplinary pain PACT. The program included using a systematically structured multidimensional approach to identify appropriate treatments and delivery of interdisciplinary care for patients with chronic pain through an OPGP. The authors’ findings establish the feasibility and acceptability of the OPGP. More than 75% of those enrolled completed the program, indicating the promising potential of this approach with significant improvements observed for several pain-related outcomes among those who completed the 8-week program.
Stepped care is a well-established approach to managing complex chronic pain conditions. The approach adds increased levels of treatment intensity when there is no improvement after initial, simple measures are instituted (eg, over-the-counter pain medications, physical therapy, life style changes). Understanding the complexity of the pain experience while treating the patient and not simply the pain has the highest likelihood of helping patients with chronic pain. Given the prevalence of chronic pain among patients in primary care nationally, measurement-based pain care potentially could result in an earlier referral to appropriate care well before pain becomes intractable and chronic.
Growing evidence shows that multidisciplinary treatments reduce pain symptoms and intensity, medication, health care provider use, and improve quality of life.11-15,29,30 A systematic review by van Tulder and colleagues, for example, noted improvements in physical parameters, such as range of motion and flexibility and behavioral health parameters, including anxiety, depression, and cognition.29 Similarly, the cohort of patients who participated in the OPGP showed statistically significant improvements in several domains of pain-related distress and functioning following treatment, including pain catastrophizing, pain self-efficacy, and the multicomponent pain outcomes questionnaires. Functional improvement also was observed by comparing the distance walked in 6 minutes before and after program completion.
There is significant variation in duration of rehabilitation programs lasting from 2 weeks to 12 weeks or longer. These sessions consist of half days, daily sessions, weekly sessions, and monthly sessions. Inconsistencies also exist among programs that use 3 to 280 professional contact hours. Although it has been shown that programs with more than 100 hours of professional contact tended to have better outcomes than did those with less than 30 hours of contact, Stratton and colleagues reported that a 6-week group program was equivalent or better than a 12- and 10-week group program among veterans.11,31 These findings along with staffing and resource constraints led to the implementation of the 8-week OPGP with fewer than 30 hours of contact time per group. These results have important practical implications, as shorter treatments may offer comparable therapeutic impact than do longer, more time-intensive protocols.
Limitations
These findings were derived from a quality improvement project within one institution, and several limitations exist. Although the broader purpose of the article was to show how the fundamentals of creating a cohesive multidisciplinary chronic pain team can be implemented within the VA setting, the highlighted outcomes were primarily from participants in the OPGP Since this was not a controlled or experimental study and given potential sample size and selections issues as well as the lack of longer-term follow-up information, further study is needed to draw definitive conclusions about program effectiveness, despite promising preliminary results. In addition, medication use, such as opioids either before or after completion of the program, was not included as part of this evaluation. As previously discussed, medication management for some patients continued beyond the 8-week time frame of the OPGP. Nonetheless, understanding the impact of this team approach on opioid use also is an important topic for future research.
Despite these limitations, the described model could be a feasible option for improving pain management in outpatient practices not only within the VA but in community settings.
Conclusion
These results suggest that the use of short-term, structured therapeutic protocols could be a potentially effective strategy for the behavioral treatment of chronic pain conditions among veterans. The development and implementation of effective, innovative, evidence-based practice to address the needs of patients with chronic pain is an important priority for maximizing clinical service delivery and meeting the needs of the nation’s veterans.
Acknowledgments
The authors thank the previous Associate Chief of Staff, Ambulatory Care, Clinton Greenstone, MD, and Director of Primary Care Adam Tremblay, MD, for their vision, leadership, and support of the team and its efforts.
This work was supported in part through a Department of Veterans Affairs Health Services Research and Development Service Research Career Scientist Award (RCS 11-222) awarded to Sarah Krein, PhD.
1. Kerns RD, Otis J, Rosenberg R, Reid MC. Veterans’ reports of pain and associations with ratings of health, health-risk behaviors, affective distress, and use of the healthcare system. J Rehabil Res Dev. 2003;40(5):371-379.
2. Yu W, Ravelo A, Wagner TH, et al. Prevalence and cost of chronic conditions in the VA health care system. Med Care Res Rev. 2003;60(suppl 3):146S-167S.
3. Gironda RJ, Clark ME, Massengale JP, Walker RL. Pain among veterans of operations Enduring Freedom and Iraqi Freedom. Pain Med. 2006;7(4):339-343.
4. Cifu DX, Taylor BC, Carne WF, et al. Traumatic brain injury, posttraumatic stress disorder, and pain diagnoses in OIF/OEF/OND veterans. J Rehabil Res Dev. 2013;50(9):1169-1176.
5. Breuer B, Cruciani R, Portenoy RK. Pain management by primary care physicians, pain physicians, chiropractors, and acupuncturists: a national survey. South Med J. 2010;103(8):738-747.
6. Bergman AA, Matthias MS, Coffing JM, Krebs EE. Contrasting tensions between patients and PCPs in chronic pain management: a qualitative study. Pain Med. 2013;14(11):1689-1697.
7. Caudill-Slosberg MA, Schwartz LM, Woloshin S. Office visits and analgesic prescriptions for musculoskeletal pain in US: 1980 vs. 2000. Pain. 2004;109(3):514-519.
8. Zedler B, Xie L, Wang L, et al. Risk factors for serious prescription opioid-related toxicity or overdose among Veterans Health Administration patients. Pain Med. 2014;15(11):1911-1929.
9. Bohnert AS, Valenstein M, Bair MJ, et al. Association between opioid prescribing patterns and opioid overdose-related deaths. JAMA. 2011;305(13):1315-1321.
10. Chou R, Clark E, Helfand M. Comparative efficacy and safety of long-acting oral opioids for chronic non-cancer pain: a systematic review. J Pain Symptom Manage. 2003;26(5):1026-1048.
11. Guzmán J, Esmail R, Karjalainen K, Malmivaara A, Irvin E, Bombardier C. Multidisciplinary rehabilitation for chronic low back pain: systematic review. BMJ. 2001;322(7301):1511-1516.
12. Gatchel RJ, Okifuji A. Evidence-based scientific data documenting the treatment and cost-effectiveness of comprehensive pain programs for chronic nonmalignant pain. J Pain. 2006;7(11):779-793.
13. Flor H, Fydrich T, Turk DC. Efficacy of multidisciplinary pain treatment centers: a meta-analytic review. Pain. 1992;49(2):221-230.
14. Scascighini L, Toma V, Dober-Spielmann S, Sprott H. Multidisciplinary treatment for chronic pain: a systematic review of interventions and outcomes. Rheumatology (Oxford). 2008;47(5):670-678.
15. Patrick LE, Altmaier EM, Found EM. Long-term outcomes in multidisciplinary treatment of chronic low back pain: results of a 13-year follow-up. Spine (Phila Pa 1976). 2004;29(8):850-855.
16. Moore BA, Anderson D, Dorflinger L, et al. Stepped care model for pain management and quality of pain care in long-term opioid therapy. J Rehabil Res Dev. 2016;53(1):137-146.
17. Anderson DR, Zlateva I, Coman EN, Khatri K, Tian T, Kerns RD. Improving pain care through implementation of the stepped care model at a multisite community health center. J Pain Res. 2016;9:1021-1029.
18. Scott EL, Kroenke K, Wu J, Yu Z. Beneficial effects of improvement in depression, pain catastrophizing, and anxiety on pain outcomes: a 12-month longitudinal analysis. J Pain. 2016;17(2):215-222.
19. Kerns RD, Philip EJ, Lee AW, Rosenberger PH. Implementation of the Veterans Health Administration national pain management strategy. Transl Behav Med. 2011;1(4):635-643.
20. Bloor LE, Fisher C, Grix B, Zaleon CR, Wice S. Conjoint sessions with clinical pharmacy and health psychology for chronic pain. Fed Pract. 2017;34(4):35-41.
21. Tauben D, Theodore BR. Measurement-based stepped care approach to interdisciplinary chronic pain management. In: Benzon HT, Rathmell JP, Wu CL, et al, eds. Practical Management of Pain. 5th ed. Philadelphia, PA: Elsevier Mosby; 2013:37-46.
22. Kroenke K, Spitzer RL, Williams JB, Löwe B. An ultra-brief screening scale for anxiety and depression: the PHQ-4. Psychosomatics. 2009;50(6):613-621.
23. Ouimette P, Wade M, Prins A, Schohn M. Identifying PTSD in primary care: comparison of the primary care-PTSD screen (PC-PTSD) and the general health questionnaire-12 (GHQ). J Anxiety Disord. 2008;22(2):337-343.
24. Chung F, Yegneswaran B, Liao P, et al. STOP questionnaire: a tool to screen patients for obstructive sleep apnea. Anesthesiology. 2008;108(5):812-821.
25. Clark ME, Gironda RJ, Young RW. Development and validation of the pain outcomes questionnaire-VA. J Rehabil Res Dev. 2003;40(5):381-395.
26. Sullivan MJL, Bishop SR, Pivik J. The pain catastrophizing scale: development and validation. Psychol Assess. 1995;7(4):524-532.
27. Nicholas MK. The pain self-efficacy questionnaire: taking pain into account. Eur J Pain. 2007;11(2):153-163.
28. Peppin JF, Marcum S, Kirsh KL. The chronic pain patient and functional assessment: use of the 6-minute walk test in a multidisciplinary pain clinic. Curr Med Res Opin. 2014;30(3):361-365.
29. van Tulder MW, Ostelo R, Vlaeyen JW, Linton SJ, Morley SJ, Assendelft WJ. Behavioral treatment for chronic low back pain: a systematic review within the framework of the Cochrane back review group. Spine (Phila Pa 1976). 2000;25(20):2688-2699.
30. Sanders SH, Harden RN, Vicente PJ. Evidence-based clinical practice guidelines for interdisciplinary rehabilitation of chronic nonmalignant pain syndrome patients. Pain Pract. 2005;5(4):303-315.
31. Stratton KJ, Bender MC, Cameron JJ, Pickett TC. Development and evaluation of a behavioral pain management treatment program in a veterans affairs medical center. Mil Med. 2015;180(3):263-268.
Chronic pain is a common health care problem that remains a significant burden for the VHA.1,2 Some reports indicate that nearly 50% of VA patients report chronic pain.3,4 Both within and outside the VHA, primary care providers (PCPs) generally manage patients with chronic pain.5,6 Historically, a biomedical approach to chronic pain also included the use of opioid medications, which may have contributed to increased opioid-related morbidity and mortality especially among the veteran patient population.7-9 The use of opioids also is controversial due to concerns about adverse effects (AEs), long-term efficacy, functional outcomes, and the potential for drug abuse and addiction.10 Consequently, alternative treatment options that incorporate an interdisciplinary approach have gained significant interest among pain care providers.11 Interdisciplinary programs have been shown to improve functional status and psychological well-being and to reduce pain severity and opioid use.12-14 These benefits may persist for a decade or longer.15
Background
The Stepped Care Model for Pain Management (SCM-PM) is a specific pain treatment approach promoted by the VA National Pain Management Directive.16 This systematically adjusted approach is associated with improved patient satisfaction and health outcomes for pain and depression.17,18 At its core, the model promotes engaging patients as active participants in their care along with a team of doctors who can offer an integrated, evidence-based, multimodal, interdisciplinary treatment plan.
To successfully implement this strategy at the VA, patient aligned care teams (PACT) assess and manage patients with common pain conditions through collaboration with mental health, complementary and integrative health services, physical therapy, and other programs, such as opioid renewal clinics and pain schools.19 This collaborative care approach, which the PCP initiates, is step 1 of the SCM-PM. If initial treatment is not successful and patients are not improving as expected, specialty care consultation and collaborative comanagement through interdisciplinary pain specialty teams are sought (step 2). Finally, step 3 involves tertiary, interdisciplinary care, including access to advanced diagnostic and pain rehabilitation programs accredited by the Commission for Accreditation of Rehabilitation Facilities (CARF).
Although the advantages of interdisciplinary pain programs are clear, resource limitations as well as challenges related to competencies of the PCPs, nurses, and associated health care professionals in pain assessment and management can make implementation of these programs, including the SCM-PM, difficult for many clinics and facilities. Thus, identifying effective chronic pain models and strategies, incorporating the philosophy and key elements of interdisciplinary programs, and accounting for facility resources and capacity are all important.
At the Ann Arbor VAMC, development of a comprehensive interdisciplinary team started with the implementation of joint sessions with a clinical pharmacist and health psychologist embedded in primary care to enhance access to behavioral pain management interventions.20 This program was subsequently expanded to include a pain physician, 2 pain-focused physical therapists (PTs) and a pain nurse.
This article describes a novel team approach for providing more comprehensive, interdisciplinary care for patients with chronic pain along with the initial results for the patients who were part of an outpatient pain group program (OPGP).
Methods
Developing a more interdisciplinary pain management program included integrating different services and creating a strategy for comprehensive evaluation and management of patients with chronic pain. After patients were referred to the interdisciplinary pain clinic by their PCP, they received a systematically structured multidimensional assessment. The primary focus of this assessment was to create an individually directed treatment approach based on the patient’s responses to previous treatments and information collected from several questionnaires administered prior to evaluation. This information helped guide individual patient decision making and actively engaged patients in their care, thus following one of the central tenants of the SCM-PM model. Moreover, functional restoration was at the core of each patient’s evaluation and management. The primary focus was on nonpharmacologic treatment options that included psychological, physical, and occupational therapy; self-management; education; and complementary and alternative therapies. These modalities were offered either individually or in a group setting.
The first step after referral was an evaluation that followed the main core principles for complex disease management described by Tauben and Theodore.21 All new patients were asked to complete a 2-question pain intensity and pain interference measure, the 4-question Patient Health Questionnaire (PHQ-4), 4-question Primary Care-PTSD screening tool (PC-PTSD), and the STOP-BANG questionnaire to assess the risk for obstructive sleep apnea.22-24 Each measure allowed the physician to identify specific problem areas and formulate a treatment plan that would incorporate PTs or occupational therapists, psychologists and/or clinical specialists, and pharmacists if needed.
Patients who were found to have or expressed significant disability because of pain and who wished to learn pain self-management strategies could participate in an 8-week OPGP. This program included the use of cognitive behavioral therapy (CBT) strategies along with group physical therapy classes. Some patients also received individual therapies concurrently with the 8-week OPGP. Patients were excluded from participating in the OPGP only if their current medical or psychiatric status precluded them from full engagement and maximum benefit as determined by the pain physician and psychologist.
Participants and Intervention
Program participants were patients with a chronic pain diagnosis who enrolled in the interdisciplinary pain team OPGP between April 2016 and April 2017. Most patients were referred by their PCPs due to chronic low back, neck, joint or neuropathic pain, although many presented with multiple pain areas. The onset of pain often was a result of a service-related injury or overuse, or the etiology was unknown.
A board-certified pain physician, licensed clinical psychologist, 2 licensed PTs, and a clinical pharmacist led the OPGP sessions. The program was composed of 3-hour-long sessions held weekly for 8 consecutive weeks. Each week, a member of the team covered a specific topic (Table 1).
These sessions focused on the importance of exercise, movement, and physical therapy; appropriate use of medications for managing chronic pain; pacing activities and body mechanics; and the medical approach to managing chronic pain. In addition to didactic presentations, interaction and therapeutic dialogue was encouraged among patients. The education portion of each weekly session lasted about 90 minutes, including a short break. Then, following another short break, patients proceeded to the physical therapy area and engaged in an individualized, monitored exercise program, conducted by the team PTs. Patients also were issued pedometers and encouraged to track their steps each day. Education in improving posture and body mechanics was a key component of the exercise portion of the program so patients could resume their normal daily activities and regain enjoyment in their life. Pain outcomemeasures were collected at admission and immediately before discharge.
Medication management also was an important part of the program for some patients and included tapering off opioids and other drugs and implementing trials of adjuvant pain medications shown to help chronic pain. For some patients, this medication management continued after the patient completed the program.
Measures
The Pain Outcome Questionnaire (POQ) is a 19-item, self-report measure of pain treatment outcomes. Pain rating, mobility, activities of daily living, vitality, negative effect, and fear are the functioning domains evaluated, and the subscale scores are added to produce a total score. The POQ was developed from samples of veterans undergoing inpatient or outpatient pain treatment at VA facilities. For each of the subscales and the total score, higher values indicate poorer outcomes. In normative outpatient VA samples, a total score of 71 is at the 25th percentile, and 120 is at the 75th percentile. The POQ has been shown to have good reliability and validity among veterans in an outpatient setting.25
The Pain Catastrophizing Scale (PCS) is a 13-item scale designed to measure various levels of pain catastrophizing.26 Each item is rated on a 5-point Likert-type scale, from 0 (not at all) to 4 (all the time). The PCS consists of 3 subscale domains: rumination, 4 items; magnification, 3 items; and helplessness, 6 items. Responses to all items also can be added to produce a total score from 0 to 52, with higher scores indicating a higher level of catastrophic thinking related to pain. This project evaluated both the total score and the 3 subscale scores.
The Pain Self-Efficacy Questionnaire (PSEQ) is a 10-item questionnaire that assesses confidence in an individual’s ability to cope or to perform activities despite the pain.27 The PSEQ covers a range of functions, including household chores, socializing, work, as well as coping with pain without medications. Each question has a 7-point Likert scale response: 0 = not at all confident, and 7 = completely confident, to produce a total score from 0 to 60. Higher scores indicate stronger pain self-efficacy, which has been shown to be associated with return to work and maintenance of functional gains.
The Patient Health Questionnaire-4 (PHQ-4) is a 4-item instrument used to screen for depression and anxiety in outpatient medical settings.22 Patients indicate how often they have been bothered by certain problems on a 4-point Likert scale, from 0 (not at all) to 3 (nearly every day). The PHQ-4 provides a total score (0-12) with scores of 6 to 8 indicating moderate and 9 to 12 indicating severe psychological distress; 2 subscale scores, 1 for anxiety (2 questions) and 1 for depression (2 questions). For this analysis, the total PHQ-4 score has been dichotomized with 1 indicating a score in the moderate or severe range vs 0 for a score of mild or no psychological distress. Likewise, each of the subscale scores have been dichotomized with 1 indicating a score of 3 or greater, which is considered a positive screen.
The 6-minute walk test (6MWT) measures the distance (in feet) an individual can walk over a total of 6 minutes on a hard, flat surface.28 Even though the individual can walk at a self-selected pace and rest if needed during the test, the goal is for the patient to walk as far as possible over the course of 6 minutes. The 6MWT provides information regarding functional capacity, response to therapy, and prognosis across a range of chronic conditions, including pain.
Data Analysis
Data analysis included the use of both descriptive and comparative statistics. A descriptive analysis was conducted to examine the characteristics of patients who did and did not complete the OPGP. Specific outcomes for those individuals who completed the program, and thus had complete pre- and post-OPGP information, then were compared. Paired t tests were used to compare differences in continuous measures between baseline (pre-OPGP) and the 8-week follow-up (post-OPGP). Comparisons involving dichotomous measures were made using the Fisher exact test. A 2-sided α with a P value .05 was considered statistically significant. All statistical analyses were conducted using STATA version 14.1 (StataCorp, College Station, TX).
Results
A total of 36 patients enrolled, and 28 (77%) completed the OPGP. Patients who did not complete the program (n = 8) either self-discharged due to lack of interest or had difficulty in consistently making their appointments and decided not to continue (Table 2).
Outcomes for OPGP Completers
Improvements were observed for all outcome domains among patients who completed the program (eTable).
Discussion
This report describes the novel model for improving delivery of chronic pain management services implemented at the Ann Arbor VAMC through the development of a multidisciplinary pain PACT. The program included using a systematically structured multidimensional approach to identify appropriate treatments and delivery of interdisciplinary care for patients with chronic pain through an OPGP. The authors’ findings establish the feasibility and acceptability of the OPGP. More than 75% of those enrolled completed the program, indicating the promising potential of this approach with significant improvements observed for several pain-related outcomes among those who completed the 8-week program.
Stepped care is a well-established approach to managing complex chronic pain conditions. The approach adds increased levels of treatment intensity when there is no improvement after initial, simple measures are instituted (eg, over-the-counter pain medications, physical therapy, life style changes). Understanding the complexity of the pain experience while treating the patient and not simply the pain has the highest likelihood of helping patients with chronic pain. Given the prevalence of chronic pain among patients in primary care nationally, measurement-based pain care potentially could result in an earlier referral to appropriate care well before pain becomes intractable and chronic.
Growing evidence shows that multidisciplinary treatments reduce pain symptoms and intensity, medication, health care provider use, and improve quality of life.11-15,29,30 A systematic review by van Tulder and colleagues, for example, noted improvements in physical parameters, such as range of motion and flexibility and behavioral health parameters, including anxiety, depression, and cognition.29 Similarly, the cohort of patients who participated in the OPGP showed statistically significant improvements in several domains of pain-related distress and functioning following treatment, including pain catastrophizing, pain self-efficacy, and the multicomponent pain outcomes questionnaires. Functional improvement also was observed by comparing the distance walked in 6 minutes before and after program completion.
There is significant variation in duration of rehabilitation programs lasting from 2 weeks to 12 weeks or longer. These sessions consist of half days, daily sessions, weekly sessions, and monthly sessions. Inconsistencies also exist among programs that use 3 to 280 professional contact hours. Although it has been shown that programs with more than 100 hours of professional contact tended to have better outcomes than did those with less than 30 hours of contact, Stratton and colleagues reported that a 6-week group program was equivalent or better than a 12- and 10-week group program among veterans.11,31 These findings along with staffing and resource constraints led to the implementation of the 8-week OPGP with fewer than 30 hours of contact time per group. These results have important practical implications, as shorter treatments may offer comparable therapeutic impact than do longer, more time-intensive protocols.
Limitations
These findings were derived from a quality improvement project within one institution, and several limitations exist. Although the broader purpose of the article was to show how the fundamentals of creating a cohesive multidisciplinary chronic pain team can be implemented within the VA setting, the highlighted outcomes were primarily from participants in the OPGP Since this was not a controlled or experimental study and given potential sample size and selections issues as well as the lack of longer-term follow-up information, further study is needed to draw definitive conclusions about program effectiveness, despite promising preliminary results. In addition, medication use, such as opioids either before or after completion of the program, was not included as part of this evaluation. As previously discussed, medication management for some patients continued beyond the 8-week time frame of the OPGP. Nonetheless, understanding the impact of this team approach on opioid use also is an important topic for future research.
Despite these limitations, the described model could be a feasible option for improving pain management in outpatient practices not only within the VA but in community settings.
Conclusion
These results suggest that the use of short-term, structured therapeutic protocols could be a potentially effective strategy for the behavioral treatment of chronic pain conditions among veterans. The development and implementation of effective, innovative, evidence-based practice to address the needs of patients with chronic pain is an important priority for maximizing clinical service delivery and meeting the needs of the nation’s veterans.
Acknowledgments
The authors thank the previous Associate Chief of Staff, Ambulatory Care, Clinton Greenstone, MD, and Director of Primary Care Adam Tremblay, MD, for their vision, leadership, and support of the team and its efforts.
This work was supported in part through a Department of Veterans Affairs Health Services Research and Development Service Research Career Scientist Award (RCS 11-222) awarded to Sarah Krein, PhD.
Chronic pain is a common health care problem that remains a significant burden for the VHA.1,2 Some reports indicate that nearly 50% of VA patients report chronic pain.3,4 Both within and outside the VHA, primary care providers (PCPs) generally manage patients with chronic pain.5,6 Historically, a biomedical approach to chronic pain also included the use of opioid medications, which may have contributed to increased opioid-related morbidity and mortality especially among the veteran patient population.7-9 The use of opioids also is controversial due to concerns about adverse effects (AEs), long-term efficacy, functional outcomes, and the potential for drug abuse and addiction.10 Consequently, alternative treatment options that incorporate an interdisciplinary approach have gained significant interest among pain care providers.11 Interdisciplinary programs have been shown to improve functional status and psychological well-being and to reduce pain severity and opioid use.12-14 These benefits may persist for a decade or longer.15
Background
The Stepped Care Model for Pain Management (SCM-PM) is a specific pain treatment approach promoted by the VA National Pain Management Directive.16 This systematically adjusted approach is associated with improved patient satisfaction and health outcomes for pain and depression.17,18 At its core, the model promotes engaging patients as active participants in their care along with a team of doctors who can offer an integrated, evidence-based, multimodal, interdisciplinary treatment plan.
To successfully implement this strategy at the VA, patient aligned care teams (PACT) assess and manage patients with common pain conditions through collaboration with mental health, complementary and integrative health services, physical therapy, and other programs, such as opioid renewal clinics and pain schools.19 This collaborative care approach, which the PCP initiates, is step 1 of the SCM-PM. If initial treatment is not successful and patients are not improving as expected, specialty care consultation and collaborative comanagement through interdisciplinary pain specialty teams are sought (step 2). Finally, step 3 involves tertiary, interdisciplinary care, including access to advanced diagnostic and pain rehabilitation programs accredited by the Commission for Accreditation of Rehabilitation Facilities (CARF).
Although the advantages of interdisciplinary pain programs are clear, resource limitations as well as challenges related to competencies of the PCPs, nurses, and associated health care professionals in pain assessment and management can make implementation of these programs, including the SCM-PM, difficult for many clinics and facilities. Thus, identifying effective chronic pain models and strategies, incorporating the philosophy and key elements of interdisciplinary programs, and accounting for facility resources and capacity are all important.
At the Ann Arbor VAMC, development of a comprehensive interdisciplinary team started with the implementation of joint sessions with a clinical pharmacist and health psychologist embedded in primary care to enhance access to behavioral pain management interventions.20 This program was subsequently expanded to include a pain physician, 2 pain-focused physical therapists (PTs) and a pain nurse.
This article describes a novel team approach for providing more comprehensive, interdisciplinary care for patients with chronic pain along with the initial results for the patients who were part of an outpatient pain group program (OPGP).
Methods
Developing a more interdisciplinary pain management program included integrating different services and creating a strategy for comprehensive evaluation and management of patients with chronic pain. After patients were referred to the interdisciplinary pain clinic by their PCP, they received a systematically structured multidimensional assessment. The primary focus of this assessment was to create an individually directed treatment approach based on the patient’s responses to previous treatments and information collected from several questionnaires administered prior to evaluation. This information helped guide individual patient decision making and actively engaged patients in their care, thus following one of the central tenants of the SCM-PM model. Moreover, functional restoration was at the core of each patient’s evaluation and management. The primary focus was on nonpharmacologic treatment options that included psychological, physical, and occupational therapy; self-management; education; and complementary and alternative therapies. These modalities were offered either individually or in a group setting.
The first step after referral was an evaluation that followed the main core principles for complex disease management described by Tauben and Theodore.21 All new patients were asked to complete a 2-question pain intensity and pain interference measure, the 4-question Patient Health Questionnaire (PHQ-4), 4-question Primary Care-PTSD screening tool (PC-PTSD), and the STOP-BANG questionnaire to assess the risk for obstructive sleep apnea.22-24 Each measure allowed the physician to identify specific problem areas and formulate a treatment plan that would incorporate PTs or occupational therapists, psychologists and/or clinical specialists, and pharmacists if needed.
Patients who were found to have or expressed significant disability because of pain and who wished to learn pain self-management strategies could participate in an 8-week OPGP. This program included the use of cognitive behavioral therapy (CBT) strategies along with group physical therapy classes. Some patients also received individual therapies concurrently with the 8-week OPGP. Patients were excluded from participating in the OPGP only if their current medical or psychiatric status precluded them from full engagement and maximum benefit as determined by the pain physician and psychologist.
Participants and Intervention
Program participants were patients with a chronic pain diagnosis who enrolled in the interdisciplinary pain team OPGP between April 2016 and April 2017. Most patients were referred by their PCPs due to chronic low back, neck, joint or neuropathic pain, although many presented with multiple pain areas. The onset of pain often was a result of a service-related injury or overuse, or the etiology was unknown.
A board-certified pain physician, licensed clinical psychologist, 2 licensed PTs, and a clinical pharmacist led the OPGP sessions. The program was composed of 3-hour-long sessions held weekly for 8 consecutive weeks. Each week, a member of the team covered a specific topic (Table 1).
These sessions focused on the importance of exercise, movement, and physical therapy; appropriate use of medications for managing chronic pain; pacing activities and body mechanics; and the medical approach to managing chronic pain. In addition to didactic presentations, interaction and therapeutic dialogue was encouraged among patients. The education portion of each weekly session lasted about 90 minutes, including a short break. Then, following another short break, patients proceeded to the physical therapy area and engaged in an individualized, monitored exercise program, conducted by the team PTs. Patients also were issued pedometers and encouraged to track their steps each day. Education in improving posture and body mechanics was a key component of the exercise portion of the program so patients could resume their normal daily activities and regain enjoyment in their life. Pain outcomemeasures were collected at admission and immediately before discharge.
Medication management also was an important part of the program for some patients and included tapering off opioids and other drugs and implementing trials of adjuvant pain medications shown to help chronic pain. For some patients, this medication management continued after the patient completed the program.
Measures
The Pain Outcome Questionnaire (POQ) is a 19-item, self-report measure of pain treatment outcomes. Pain rating, mobility, activities of daily living, vitality, negative effect, and fear are the functioning domains evaluated, and the subscale scores are added to produce a total score. The POQ was developed from samples of veterans undergoing inpatient or outpatient pain treatment at VA facilities. For each of the subscales and the total score, higher values indicate poorer outcomes. In normative outpatient VA samples, a total score of 71 is at the 25th percentile, and 120 is at the 75th percentile. The POQ has been shown to have good reliability and validity among veterans in an outpatient setting.25
The Pain Catastrophizing Scale (PCS) is a 13-item scale designed to measure various levels of pain catastrophizing.26 Each item is rated on a 5-point Likert-type scale, from 0 (not at all) to 4 (all the time). The PCS consists of 3 subscale domains: rumination, 4 items; magnification, 3 items; and helplessness, 6 items. Responses to all items also can be added to produce a total score from 0 to 52, with higher scores indicating a higher level of catastrophic thinking related to pain. This project evaluated both the total score and the 3 subscale scores.
The Pain Self-Efficacy Questionnaire (PSEQ) is a 10-item questionnaire that assesses confidence in an individual’s ability to cope or to perform activities despite the pain.27 The PSEQ covers a range of functions, including household chores, socializing, work, as well as coping with pain without medications. Each question has a 7-point Likert scale response: 0 = not at all confident, and 7 = completely confident, to produce a total score from 0 to 60. Higher scores indicate stronger pain self-efficacy, which has been shown to be associated with return to work and maintenance of functional gains.
The Patient Health Questionnaire-4 (PHQ-4) is a 4-item instrument used to screen for depression and anxiety in outpatient medical settings.22 Patients indicate how often they have been bothered by certain problems on a 4-point Likert scale, from 0 (not at all) to 3 (nearly every day). The PHQ-4 provides a total score (0-12) with scores of 6 to 8 indicating moderate and 9 to 12 indicating severe psychological distress; 2 subscale scores, 1 for anxiety (2 questions) and 1 for depression (2 questions). For this analysis, the total PHQ-4 score has been dichotomized with 1 indicating a score in the moderate or severe range vs 0 for a score of mild or no psychological distress. Likewise, each of the subscale scores have been dichotomized with 1 indicating a score of 3 or greater, which is considered a positive screen.
The 6-minute walk test (6MWT) measures the distance (in feet) an individual can walk over a total of 6 minutes on a hard, flat surface.28 Even though the individual can walk at a self-selected pace and rest if needed during the test, the goal is for the patient to walk as far as possible over the course of 6 minutes. The 6MWT provides information regarding functional capacity, response to therapy, and prognosis across a range of chronic conditions, including pain.
Data Analysis
Data analysis included the use of both descriptive and comparative statistics. A descriptive analysis was conducted to examine the characteristics of patients who did and did not complete the OPGP. Specific outcomes for those individuals who completed the program, and thus had complete pre- and post-OPGP information, then were compared. Paired t tests were used to compare differences in continuous measures between baseline (pre-OPGP) and the 8-week follow-up (post-OPGP). Comparisons involving dichotomous measures were made using the Fisher exact test. A 2-sided α with a P value .05 was considered statistically significant. All statistical analyses were conducted using STATA version 14.1 (StataCorp, College Station, TX).
Results
A total of 36 patients enrolled, and 28 (77%) completed the OPGP. Patients who did not complete the program (n = 8) either self-discharged due to lack of interest or had difficulty in consistently making their appointments and decided not to continue (Table 2).
Outcomes for OPGP Completers
Improvements were observed for all outcome domains among patients who completed the program (eTable).
Discussion
This report describes the novel model for improving delivery of chronic pain management services implemented at the Ann Arbor VAMC through the development of a multidisciplinary pain PACT. The program included using a systematically structured multidimensional approach to identify appropriate treatments and delivery of interdisciplinary care for patients with chronic pain through an OPGP. The authors’ findings establish the feasibility and acceptability of the OPGP. More than 75% of those enrolled completed the program, indicating the promising potential of this approach with significant improvements observed for several pain-related outcomes among those who completed the 8-week program.
Stepped care is a well-established approach to managing complex chronic pain conditions. The approach adds increased levels of treatment intensity when there is no improvement after initial, simple measures are instituted (eg, over-the-counter pain medications, physical therapy, life style changes). Understanding the complexity of the pain experience while treating the patient and not simply the pain has the highest likelihood of helping patients with chronic pain. Given the prevalence of chronic pain among patients in primary care nationally, measurement-based pain care potentially could result in an earlier referral to appropriate care well before pain becomes intractable and chronic.
Growing evidence shows that multidisciplinary treatments reduce pain symptoms and intensity, medication, health care provider use, and improve quality of life.11-15,29,30 A systematic review by van Tulder and colleagues, for example, noted improvements in physical parameters, such as range of motion and flexibility and behavioral health parameters, including anxiety, depression, and cognition.29 Similarly, the cohort of patients who participated in the OPGP showed statistically significant improvements in several domains of pain-related distress and functioning following treatment, including pain catastrophizing, pain self-efficacy, and the multicomponent pain outcomes questionnaires. Functional improvement also was observed by comparing the distance walked in 6 minutes before and after program completion.
There is significant variation in duration of rehabilitation programs lasting from 2 weeks to 12 weeks or longer. These sessions consist of half days, daily sessions, weekly sessions, and monthly sessions. Inconsistencies also exist among programs that use 3 to 280 professional contact hours. Although it has been shown that programs with more than 100 hours of professional contact tended to have better outcomes than did those with less than 30 hours of contact, Stratton and colleagues reported that a 6-week group program was equivalent or better than a 12- and 10-week group program among veterans.11,31 These findings along with staffing and resource constraints led to the implementation of the 8-week OPGP with fewer than 30 hours of contact time per group. These results have important practical implications, as shorter treatments may offer comparable therapeutic impact than do longer, more time-intensive protocols.
Limitations
These findings were derived from a quality improvement project within one institution, and several limitations exist. Although the broader purpose of the article was to show how the fundamentals of creating a cohesive multidisciplinary chronic pain team can be implemented within the VA setting, the highlighted outcomes were primarily from participants in the OPGP Since this was not a controlled or experimental study and given potential sample size and selections issues as well as the lack of longer-term follow-up information, further study is needed to draw definitive conclusions about program effectiveness, despite promising preliminary results. In addition, medication use, such as opioids either before or after completion of the program, was not included as part of this evaluation. As previously discussed, medication management for some patients continued beyond the 8-week time frame of the OPGP. Nonetheless, understanding the impact of this team approach on opioid use also is an important topic for future research.
Despite these limitations, the described model could be a feasible option for improving pain management in outpatient practices not only within the VA but in community settings.
Conclusion
These results suggest that the use of short-term, structured therapeutic protocols could be a potentially effective strategy for the behavioral treatment of chronic pain conditions among veterans. The development and implementation of effective, innovative, evidence-based practice to address the needs of patients with chronic pain is an important priority for maximizing clinical service delivery and meeting the needs of the nation’s veterans.
Acknowledgments
The authors thank the previous Associate Chief of Staff, Ambulatory Care, Clinton Greenstone, MD, and Director of Primary Care Adam Tremblay, MD, for their vision, leadership, and support of the team and its efforts.
This work was supported in part through a Department of Veterans Affairs Health Services Research and Development Service Research Career Scientist Award (RCS 11-222) awarded to Sarah Krein, PhD.
1. Kerns RD, Otis J, Rosenberg R, Reid MC. Veterans’ reports of pain and associations with ratings of health, health-risk behaviors, affective distress, and use of the healthcare system. J Rehabil Res Dev. 2003;40(5):371-379.
2. Yu W, Ravelo A, Wagner TH, et al. Prevalence and cost of chronic conditions in the VA health care system. Med Care Res Rev. 2003;60(suppl 3):146S-167S.
3. Gironda RJ, Clark ME, Massengale JP, Walker RL. Pain among veterans of operations Enduring Freedom and Iraqi Freedom. Pain Med. 2006;7(4):339-343.
4. Cifu DX, Taylor BC, Carne WF, et al. Traumatic brain injury, posttraumatic stress disorder, and pain diagnoses in OIF/OEF/OND veterans. J Rehabil Res Dev. 2013;50(9):1169-1176.
5. Breuer B, Cruciani R, Portenoy RK. Pain management by primary care physicians, pain physicians, chiropractors, and acupuncturists: a national survey. South Med J. 2010;103(8):738-747.
6. Bergman AA, Matthias MS, Coffing JM, Krebs EE. Contrasting tensions between patients and PCPs in chronic pain management: a qualitative study. Pain Med. 2013;14(11):1689-1697.
7. Caudill-Slosberg MA, Schwartz LM, Woloshin S. Office visits and analgesic prescriptions for musculoskeletal pain in US: 1980 vs. 2000. Pain. 2004;109(3):514-519.
8. Zedler B, Xie L, Wang L, et al. Risk factors for serious prescription opioid-related toxicity or overdose among Veterans Health Administration patients. Pain Med. 2014;15(11):1911-1929.
9. Bohnert AS, Valenstein M, Bair MJ, et al. Association between opioid prescribing patterns and opioid overdose-related deaths. JAMA. 2011;305(13):1315-1321.
10. Chou R, Clark E, Helfand M. Comparative efficacy and safety of long-acting oral opioids for chronic non-cancer pain: a systematic review. J Pain Symptom Manage. 2003;26(5):1026-1048.
11. Guzmán J, Esmail R, Karjalainen K, Malmivaara A, Irvin E, Bombardier C. Multidisciplinary rehabilitation for chronic low back pain: systematic review. BMJ. 2001;322(7301):1511-1516.
12. Gatchel RJ, Okifuji A. Evidence-based scientific data documenting the treatment and cost-effectiveness of comprehensive pain programs for chronic nonmalignant pain. J Pain. 2006;7(11):779-793.
13. Flor H, Fydrich T, Turk DC. Efficacy of multidisciplinary pain treatment centers: a meta-analytic review. Pain. 1992;49(2):221-230.
14. Scascighini L, Toma V, Dober-Spielmann S, Sprott H. Multidisciplinary treatment for chronic pain: a systematic review of interventions and outcomes. Rheumatology (Oxford). 2008;47(5):670-678.
15. Patrick LE, Altmaier EM, Found EM. Long-term outcomes in multidisciplinary treatment of chronic low back pain: results of a 13-year follow-up. Spine (Phila Pa 1976). 2004;29(8):850-855.
16. Moore BA, Anderson D, Dorflinger L, et al. Stepped care model for pain management and quality of pain care in long-term opioid therapy. J Rehabil Res Dev. 2016;53(1):137-146.
17. Anderson DR, Zlateva I, Coman EN, Khatri K, Tian T, Kerns RD. Improving pain care through implementation of the stepped care model at a multisite community health center. J Pain Res. 2016;9:1021-1029.
18. Scott EL, Kroenke K, Wu J, Yu Z. Beneficial effects of improvement in depression, pain catastrophizing, and anxiety on pain outcomes: a 12-month longitudinal analysis. J Pain. 2016;17(2):215-222.
19. Kerns RD, Philip EJ, Lee AW, Rosenberger PH. Implementation of the Veterans Health Administration national pain management strategy. Transl Behav Med. 2011;1(4):635-643.
20. Bloor LE, Fisher C, Grix B, Zaleon CR, Wice S. Conjoint sessions with clinical pharmacy and health psychology for chronic pain. Fed Pract. 2017;34(4):35-41.
21. Tauben D, Theodore BR. Measurement-based stepped care approach to interdisciplinary chronic pain management. In: Benzon HT, Rathmell JP, Wu CL, et al, eds. Practical Management of Pain. 5th ed. Philadelphia, PA: Elsevier Mosby; 2013:37-46.
22. Kroenke K, Spitzer RL, Williams JB, Löwe B. An ultra-brief screening scale for anxiety and depression: the PHQ-4. Psychosomatics. 2009;50(6):613-621.
23. Ouimette P, Wade M, Prins A, Schohn M. Identifying PTSD in primary care: comparison of the primary care-PTSD screen (PC-PTSD) and the general health questionnaire-12 (GHQ). J Anxiety Disord. 2008;22(2):337-343.
24. Chung F, Yegneswaran B, Liao P, et al. STOP questionnaire: a tool to screen patients for obstructive sleep apnea. Anesthesiology. 2008;108(5):812-821.
25. Clark ME, Gironda RJ, Young RW. Development and validation of the pain outcomes questionnaire-VA. J Rehabil Res Dev. 2003;40(5):381-395.
26. Sullivan MJL, Bishop SR, Pivik J. The pain catastrophizing scale: development and validation. Psychol Assess. 1995;7(4):524-532.
27. Nicholas MK. The pain self-efficacy questionnaire: taking pain into account. Eur J Pain. 2007;11(2):153-163.
28. Peppin JF, Marcum S, Kirsh KL. The chronic pain patient and functional assessment: use of the 6-minute walk test in a multidisciplinary pain clinic. Curr Med Res Opin. 2014;30(3):361-365.
29. van Tulder MW, Ostelo R, Vlaeyen JW, Linton SJ, Morley SJ, Assendelft WJ. Behavioral treatment for chronic low back pain: a systematic review within the framework of the Cochrane back review group. Spine (Phila Pa 1976). 2000;25(20):2688-2699.
30. Sanders SH, Harden RN, Vicente PJ. Evidence-based clinical practice guidelines for interdisciplinary rehabilitation of chronic nonmalignant pain syndrome patients. Pain Pract. 2005;5(4):303-315.
31. Stratton KJ, Bender MC, Cameron JJ, Pickett TC. Development and evaluation of a behavioral pain management treatment program in a veterans affairs medical center. Mil Med. 2015;180(3):263-268.
1. Kerns RD, Otis J, Rosenberg R, Reid MC. Veterans’ reports of pain and associations with ratings of health, health-risk behaviors, affective distress, and use of the healthcare system. J Rehabil Res Dev. 2003;40(5):371-379.
2. Yu W, Ravelo A, Wagner TH, et al. Prevalence and cost of chronic conditions in the VA health care system. Med Care Res Rev. 2003;60(suppl 3):146S-167S.
3. Gironda RJ, Clark ME, Massengale JP, Walker RL. Pain among veterans of operations Enduring Freedom and Iraqi Freedom. Pain Med. 2006;7(4):339-343.
4. Cifu DX, Taylor BC, Carne WF, et al. Traumatic brain injury, posttraumatic stress disorder, and pain diagnoses in OIF/OEF/OND veterans. J Rehabil Res Dev. 2013;50(9):1169-1176.
5. Breuer B, Cruciani R, Portenoy RK. Pain management by primary care physicians, pain physicians, chiropractors, and acupuncturists: a national survey. South Med J. 2010;103(8):738-747.
6. Bergman AA, Matthias MS, Coffing JM, Krebs EE. Contrasting tensions between patients and PCPs in chronic pain management: a qualitative study. Pain Med. 2013;14(11):1689-1697.
7. Caudill-Slosberg MA, Schwartz LM, Woloshin S. Office visits and analgesic prescriptions for musculoskeletal pain in US: 1980 vs. 2000. Pain. 2004;109(3):514-519.
8. Zedler B, Xie L, Wang L, et al. Risk factors for serious prescription opioid-related toxicity or overdose among Veterans Health Administration patients. Pain Med. 2014;15(11):1911-1929.
9. Bohnert AS, Valenstein M, Bair MJ, et al. Association between opioid prescribing patterns and opioid overdose-related deaths. JAMA. 2011;305(13):1315-1321.
10. Chou R, Clark E, Helfand M. Comparative efficacy and safety of long-acting oral opioids for chronic non-cancer pain: a systematic review. J Pain Symptom Manage. 2003;26(5):1026-1048.
11. Guzmán J, Esmail R, Karjalainen K, Malmivaara A, Irvin E, Bombardier C. Multidisciplinary rehabilitation for chronic low back pain: systematic review. BMJ. 2001;322(7301):1511-1516.
12. Gatchel RJ, Okifuji A. Evidence-based scientific data documenting the treatment and cost-effectiveness of comprehensive pain programs for chronic nonmalignant pain. J Pain. 2006;7(11):779-793.
13. Flor H, Fydrich T, Turk DC. Efficacy of multidisciplinary pain treatment centers: a meta-analytic review. Pain. 1992;49(2):221-230.
14. Scascighini L, Toma V, Dober-Spielmann S, Sprott H. Multidisciplinary treatment for chronic pain: a systematic review of interventions and outcomes. Rheumatology (Oxford). 2008;47(5):670-678.
15. Patrick LE, Altmaier EM, Found EM. Long-term outcomes in multidisciplinary treatment of chronic low back pain: results of a 13-year follow-up. Spine (Phila Pa 1976). 2004;29(8):850-855.
16. Moore BA, Anderson D, Dorflinger L, et al. Stepped care model for pain management and quality of pain care in long-term opioid therapy. J Rehabil Res Dev. 2016;53(1):137-146.
17. Anderson DR, Zlateva I, Coman EN, Khatri K, Tian T, Kerns RD. Improving pain care through implementation of the stepped care model at a multisite community health center. J Pain Res. 2016;9:1021-1029.
18. Scott EL, Kroenke K, Wu J, Yu Z. Beneficial effects of improvement in depression, pain catastrophizing, and anxiety on pain outcomes: a 12-month longitudinal analysis. J Pain. 2016;17(2):215-222.
19. Kerns RD, Philip EJ, Lee AW, Rosenberger PH. Implementation of the Veterans Health Administration national pain management strategy. Transl Behav Med. 2011;1(4):635-643.
20. Bloor LE, Fisher C, Grix B, Zaleon CR, Wice S. Conjoint sessions with clinical pharmacy and health psychology for chronic pain. Fed Pract. 2017;34(4):35-41.
21. Tauben D, Theodore BR. Measurement-based stepped care approach to interdisciplinary chronic pain management. In: Benzon HT, Rathmell JP, Wu CL, et al, eds. Practical Management of Pain. 5th ed. Philadelphia, PA: Elsevier Mosby; 2013:37-46.
22. Kroenke K, Spitzer RL, Williams JB, Löwe B. An ultra-brief screening scale for anxiety and depression: the PHQ-4. Psychosomatics. 2009;50(6):613-621.
23. Ouimette P, Wade M, Prins A, Schohn M. Identifying PTSD in primary care: comparison of the primary care-PTSD screen (PC-PTSD) and the general health questionnaire-12 (GHQ). J Anxiety Disord. 2008;22(2):337-343.
24. Chung F, Yegneswaran B, Liao P, et al. STOP questionnaire: a tool to screen patients for obstructive sleep apnea. Anesthesiology. 2008;108(5):812-821.
25. Clark ME, Gironda RJ, Young RW. Development and validation of the pain outcomes questionnaire-VA. J Rehabil Res Dev. 2003;40(5):381-395.
26. Sullivan MJL, Bishop SR, Pivik J. The pain catastrophizing scale: development and validation. Psychol Assess. 1995;7(4):524-532.
27. Nicholas MK. The pain self-efficacy questionnaire: taking pain into account. Eur J Pain. 2007;11(2):153-163.
28. Peppin JF, Marcum S, Kirsh KL. The chronic pain patient and functional assessment: use of the 6-minute walk test in a multidisciplinary pain clinic. Curr Med Res Opin. 2014;30(3):361-365.
29. van Tulder MW, Ostelo R, Vlaeyen JW, Linton SJ, Morley SJ, Assendelft WJ. Behavioral treatment for chronic low back pain: a systematic review within the framework of the Cochrane back review group. Spine (Phila Pa 1976). 2000;25(20):2688-2699.
30. Sanders SH, Harden RN, Vicente PJ. Evidence-based clinical practice guidelines for interdisciplinary rehabilitation of chronic nonmalignant pain syndrome patients. Pain Pract. 2005;5(4):303-315.
31. Stratton KJ, Bender MC, Cameron JJ, Pickett TC. Development and evaluation of a behavioral pain management treatment program in a veterans affairs medical center. Mil Med. 2015;180(3):263-268.
MDedge Daily News: The new test for concussion
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
There’s now a blood test to diagnose concussion, elderly people are getting the least protection from the flu vaccine, concerns about VTE from JAK inhibitors may be overblown, and black women are much more likely to have a certain risk factor for preterm birth.
Listen to the MDedge Daily News podcast for all the details on today’s top news.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
There’s now a blood test to diagnose concussion, elderly people are getting the least protection from the flu vaccine, concerns about VTE from JAK inhibitors may be overblown, and black women are much more likely to have a certain risk factor for preterm birth.
Listen to the MDedge Daily News podcast for all the details on today’s top news.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
There’s now a blood test to diagnose concussion, elderly people are getting the least protection from the flu vaccine, concerns about VTE from JAK inhibitors may be overblown, and black women are much more likely to have a certain risk factor for preterm birth.
Listen to the MDedge Daily News podcast for all the details on today’s top news.
