User login
Making hospital medicine a lifelong, enjoyable, and engaging career
Editor’s note: Each month, the Society of Hospital Medicine puts the spotlight on some of our most active members who are making substantial contributions to hospital medicine. Visit www.hospitalmedicine.org for more information on how you can lend your expertise to help SHM improve the care of hospitalized patients.
This month, The Hospitalist spotlights Amith Skandhan, MD, FHM, a hospitalist, a director/physician liaison for clinical documentation improvement and core faculty member in the Internal Medicine Residency Program at Southeast Alabama Medical Center in Dothan, Ala., and clinical faculty member at the Alabama College of Osteopathic Medicine also in Dothan. Dr. Skandhan is the cofounder and current president of the SHM Wiregrass Chapter and is an active member of SHM’s Annual Conference and Performance Measurement Reporting committees.
When did you join SHM, and what prompted you to apply for your current committee roles?
There were many things that were not sufficiently taught during clinical training that were required in my day-to-day practice, like clinical documentation improvement, practice management, billing, coding, and so forth. I also quickly understood how vast and dynamic hospital medicine really was. While looking for an outlet to voice my questions, concerns, and curiosity, I decided to join SHM, which has helped me find and apply the techniques I’d been looking for to further my career as a hospitalist.
I’m now fortunate to be a part of SHM’s national committees, which involve hospitalists of various backgrounds and experiences, who work together to improve the overall quality of inpatient medicine. I currently serve on the Performance Reporting Measurement Committee and the Annual Conference Committee. My interests in reviewing the ever-evolving policies of health care made me apply to be a part of the Performance Reporting Measurement Committee. We work very closely with the Public Policy Committee, analyzing written policies and subsequently offering our recommendations. It’s been fulfilling to be a part of a committee that works towards developing policies that support a good quality of care on such a large scale.
My penchant for organizing events and bringing people together based on common ground led me to apply for the Annual Conference Committee. We meet every week to discuss various topics, choose and invite speakers, and help organize the entire event, which will host close to 5,000 hospitalists later this year. It has made me appreciate being a member of an organization that provides hospitalists with opportunities for education and growth. I’m hopeful that the attendees next year will find the conference to be a worthwhile experience!
As the president of SHM’s Wiregrass Chapter, how has the chapter grown since its establishment in May 2015?
Our chapter is based in Dothan, a small, rural Alabama town where Southeast Alabama Medical Center is located. The chapter covers the counties of lower Alabama and the panhandle of Florida. We named the chapter after a special species of grass that grows in this region.
When we started the chapter, our goal was to bring the best and brightest of hospital medicine to our region to give talks on hot topics in the field and also to use their expertise to guide inpatient care in our hospital system. We aggressively marketed the events to bring in large crowds of medical professionals, and we consistently average around 70-80 attendees in our meetings. Bringing in leaders from the field helped create an atmosphere of learning and inspired us to grow and develop our hospitalist program. We now closely work with hospital medicine groups in surrounding rural areas toward improving inpatient hospital care.
During these past years, we also realized that, for the further growth of our chapter, we would need to nurture an interest in hospital medicine among future generations of doctors, and this realization led to the creation of our medical student and resident wing. So far, the students have been very enthusiastic about participating in SHM-related events, and I hope that continues. We also developed a mentor-mentee program, in which we paired selected medical students with hospitalists to help guide future careers in acute care medicine. This year, we have also been helping the hospital medicine division at Southeast Alabama Medical Center create a clinical research track for medical students. To that end, we have just completed our second annual poster competition where we presented around 50 posters in the areas of clinical vignettes, quality improvement, and original research.
In addition, the chapter is very active with community activities. We took notice of the fact that many of our patients and community members were unaware of what hospitalists did because they could not understand how our work was different from that of primary care physicians. Our members have therefore participated in TV, radio, and newspaper interviews to help elucidate the role of hospitalists in patient care. We have also periodically visited primary care physician offices, nursing homes, senior citizen groups, and cancer support groups to educate these patients on various facets of health care and how hospitalists influence these areas.
In 2014, we organized a “walk with a hospitalist” event, for which we set up a half-mile “admission to discharge” scenario explaining the role of hospitalists and other departments involved in patient care. This year, in hopes of improving patient literacy in our region, we held a “shop with a doc” event, where the Southeast Alabama Medical Center hospitalists teamed up with dietitians and taught patients how food and lifestyle influenced their chronic medical illnesses. This was followed by physicians and dietitians shopping with patients in the grocery store, educating them on healthy choices and label reading.
We’re incredibly grateful for the support that we’ve received from our medical and patient communities; they’ve been critical in helping our chapter grow as much as it has, and they motivate us to work harder and do more with the chapter. We were honored to receive the SHM’s Rising Star Award at the Hospital Medicine 2017 conference in Las Vegas. We never thought that our little chapter in the American countryside would be chosen, but we’re very thankful to have our efforts recognized on the national stage!
Which SHM conferences have you attended? Tell TH about your most memorable highlights or takeaways.
When I started out as a hospitalist in 2014, I decided to attend the annual conference in Las Vegas, and I can honestly say that conference changed the course of my career. I can still remember listening to the opening speech and realizing that I was surrounded by more than 3,000 hospitalists who understood the power we had to influence inpatient care. I’ve attended all the national conferences since then and am grateful that I now get to help organize the Hospital Medicine 2018 annual conference, also known as HM18.
I had been working to find a way to improve documentation within my group, as well as change the culture and perception towards billing and coding practices, which prompted me to attend the Quality and Safety Educators Academy. During one of the problem-solving sessions, I explained the challenges that I faced to my conference group. The exercise required me to explain the problem at hand, and the players of my group then discussed their thoughts while I took notes. It was a fantastic experience, as the participants at my table offered strong solutions to my problems within a matter of minutes. Their advice led to meaningful changes in our group’s hospital documentation practices, and in turn, I’ve been promoted to physician advisor in Southeast Alabama Medical Center.
After such a great experience at Quality and Safety Educators Academy, I went on to attend SHM’s Leadership Academy, where I had the opportunity to meet some of the top leaders and pioneers in the field of hospital medicine. It’s empowering to be mentored by the very people you look up to and aspire to be like. Not only was I able to bring ideas home to my institution, but I was able to reflect and improve my own professional and personal growth. I’m happy to say that I’ve completed all three levels of Leadership Academy.
As I’ve become involved with the medical student and residency programs at my medical center, I recently attended the Academic Hospitalist Academy to help my transition into academic hospital medicine. Meeting and spending time with the faculty at Academic Hospitalist Academy made me further realize the roles that academic hospitalists play in the education of future physicians, emphasizing the idea that we can all be champions in quality and patient safety.
If you’re looking to advance your career as a hospitalist, take advantage of the conferences that SHM offers. I’ve gained so much from each experience, and I’m looking forward to returning to these conferences as a potential facilitator, in hopes of offering what I’ve learned to hospitalists looking to bring about change in their fields and careers.
What can attendees at HM18 expect to see in the area of career development, and how is this different than previous years?
Hospital medicine is only about 2 decades old, making it one of the youngest branches in medicine today. Given this fact, the Annual Conference Committee feels that it is paramount to focus on career development for both new and midcareer hospitalists alike.
One question that we wish to explore and answer this year is: “How do you make hospital medicine a life-long, enjoyable, and engaging career?” In turn, our committee has created several new additions to HM18. This includes a “Seasoning Your Career” track, which will provide ideas on how to advance in leadership, use emotional intelligence to achieve success, change your roles midcareer, and change hospitalist schedules. Another unique addition this year are career development workshops, which will aim to developing various aspects of a hospitalist’s career, such as working on leadership skills, refining presentation and communication skills, providing constructive feedback, promoting women in hospital medicine, preventing burnout, and turning ideas into clinical research. We also plan to incorporate an education track, which will focus on how hospitalists can expand their careers towards educational leadership.
Given your involvement in SHM at both the local and national levels, do you have any advice for young hospital medicine professionals looking to build their professional profiles?
I’ve frequently noticed that young hospitalists don’t realize the potential influence they hold within their own institutions or the power they have to elicit change in health care at the national level.
Though we don’t often admit it, some hospitalists feel like they are glorified residents, which definitely is not the case. As a provider on the front lines, you have the unique opportunity to implement changes pertaining to issues of cost, utilization of resources, process management, quality and patient safety, and bottlenecks in care, to name a few. These are issues that keep the administrators of your organization and leaders of hospital medicine up at night. Don’t sit around and complain about how things could be or should be; look toward creating change. Bring up possible solutions to these problems with your leaders. They will appreciate the effort, and hopefully together you can find ways to tackle these problems.
I will conclude by saying this: Hospital medicine is such a unique specialty in that it’s constantly evolving, and the pioneers of this field are still alive and practicing medicine. You can meet and interact with them during the SHM conferences and look to them as sources of inspiration or guidance. Meeting people you look up to and having them as your mentors can take you places.
Ms. Steele is the marketing communications specialist at the Society of Hospital Medicine.
Editor’s note: Each month, the Society of Hospital Medicine puts the spotlight on some of our most active members who are making substantial contributions to hospital medicine. Visit www.hospitalmedicine.org for more information on how you can lend your expertise to help SHM improve the care of hospitalized patients.
This month, The Hospitalist spotlights Amith Skandhan, MD, FHM, a hospitalist, a director/physician liaison for clinical documentation improvement and core faculty member in the Internal Medicine Residency Program at Southeast Alabama Medical Center in Dothan, Ala., and clinical faculty member at the Alabama College of Osteopathic Medicine also in Dothan. Dr. Skandhan is the cofounder and current president of the SHM Wiregrass Chapter and is an active member of SHM’s Annual Conference and Performance Measurement Reporting committees.
When did you join SHM, and what prompted you to apply for your current committee roles?
There were many things that were not sufficiently taught during clinical training that were required in my day-to-day practice, like clinical documentation improvement, practice management, billing, coding, and so forth. I also quickly understood how vast and dynamic hospital medicine really was. While looking for an outlet to voice my questions, concerns, and curiosity, I decided to join SHM, which has helped me find and apply the techniques I’d been looking for to further my career as a hospitalist.
I’m now fortunate to be a part of SHM’s national committees, which involve hospitalists of various backgrounds and experiences, who work together to improve the overall quality of inpatient medicine. I currently serve on the Performance Reporting Measurement Committee and the Annual Conference Committee. My interests in reviewing the ever-evolving policies of health care made me apply to be a part of the Performance Reporting Measurement Committee. We work very closely with the Public Policy Committee, analyzing written policies and subsequently offering our recommendations. It’s been fulfilling to be a part of a committee that works towards developing policies that support a good quality of care on such a large scale.
My penchant for organizing events and bringing people together based on common ground led me to apply for the Annual Conference Committee. We meet every week to discuss various topics, choose and invite speakers, and help organize the entire event, which will host close to 5,000 hospitalists later this year. It has made me appreciate being a member of an organization that provides hospitalists with opportunities for education and growth. I’m hopeful that the attendees next year will find the conference to be a worthwhile experience!
As the president of SHM’s Wiregrass Chapter, how has the chapter grown since its establishment in May 2015?
Our chapter is based in Dothan, a small, rural Alabama town where Southeast Alabama Medical Center is located. The chapter covers the counties of lower Alabama and the panhandle of Florida. We named the chapter after a special species of grass that grows in this region.
When we started the chapter, our goal was to bring the best and brightest of hospital medicine to our region to give talks on hot topics in the field and also to use their expertise to guide inpatient care in our hospital system. We aggressively marketed the events to bring in large crowds of medical professionals, and we consistently average around 70-80 attendees in our meetings. Bringing in leaders from the field helped create an atmosphere of learning and inspired us to grow and develop our hospitalist program. We now closely work with hospital medicine groups in surrounding rural areas toward improving inpatient hospital care.
During these past years, we also realized that, for the further growth of our chapter, we would need to nurture an interest in hospital medicine among future generations of doctors, and this realization led to the creation of our medical student and resident wing. So far, the students have been very enthusiastic about participating in SHM-related events, and I hope that continues. We also developed a mentor-mentee program, in which we paired selected medical students with hospitalists to help guide future careers in acute care medicine. This year, we have also been helping the hospital medicine division at Southeast Alabama Medical Center create a clinical research track for medical students. To that end, we have just completed our second annual poster competition where we presented around 50 posters in the areas of clinical vignettes, quality improvement, and original research.
In addition, the chapter is very active with community activities. We took notice of the fact that many of our patients and community members were unaware of what hospitalists did because they could not understand how our work was different from that of primary care physicians. Our members have therefore participated in TV, radio, and newspaper interviews to help elucidate the role of hospitalists in patient care. We have also periodically visited primary care physician offices, nursing homes, senior citizen groups, and cancer support groups to educate these patients on various facets of health care and how hospitalists influence these areas.
In 2014, we organized a “walk with a hospitalist” event, for which we set up a half-mile “admission to discharge” scenario explaining the role of hospitalists and other departments involved in patient care. This year, in hopes of improving patient literacy in our region, we held a “shop with a doc” event, where the Southeast Alabama Medical Center hospitalists teamed up with dietitians and taught patients how food and lifestyle influenced their chronic medical illnesses. This was followed by physicians and dietitians shopping with patients in the grocery store, educating them on healthy choices and label reading.
We’re incredibly grateful for the support that we’ve received from our medical and patient communities; they’ve been critical in helping our chapter grow as much as it has, and they motivate us to work harder and do more with the chapter. We were honored to receive the SHM’s Rising Star Award at the Hospital Medicine 2017 conference in Las Vegas. We never thought that our little chapter in the American countryside would be chosen, but we’re very thankful to have our efforts recognized on the national stage!
Which SHM conferences have you attended? Tell TH about your most memorable highlights or takeaways.
When I started out as a hospitalist in 2014, I decided to attend the annual conference in Las Vegas, and I can honestly say that conference changed the course of my career. I can still remember listening to the opening speech and realizing that I was surrounded by more than 3,000 hospitalists who understood the power we had to influence inpatient care. I’ve attended all the national conferences since then and am grateful that I now get to help organize the Hospital Medicine 2018 annual conference, also known as HM18.
I had been working to find a way to improve documentation within my group, as well as change the culture and perception towards billing and coding practices, which prompted me to attend the Quality and Safety Educators Academy. During one of the problem-solving sessions, I explained the challenges that I faced to my conference group. The exercise required me to explain the problem at hand, and the players of my group then discussed their thoughts while I took notes. It was a fantastic experience, as the participants at my table offered strong solutions to my problems within a matter of minutes. Their advice led to meaningful changes in our group’s hospital documentation practices, and in turn, I’ve been promoted to physician advisor in Southeast Alabama Medical Center.
After such a great experience at Quality and Safety Educators Academy, I went on to attend SHM’s Leadership Academy, where I had the opportunity to meet some of the top leaders and pioneers in the field of hospital medicine. It’s empowering to be mentored by the very people you look up to and aspire to be like. Not only was I able to bring ideas home to my institution, but I was able to reflect and improve my own professional and personal growth. I’m happy to say that I’ve completed all three levels of Leadership Academy.
As I’ve become involved with the medical student and residency programs at my medical center, I recently attended the Academic Hospitalist Academy to help my transition into academic hospital medicine. Meeting and spending time with the faculty at Academic Hospitalist Academy made me further realize the roles that academic hospitalists play in the education of future physicians, emphasizing the idea that we can all be champions in quality and patient safety.
If you’re looking to advance your career as a hospitalist, take advantage of the conferences that SHM offers. I’ve gained so much from each experience, and I’m looking forward to returning to these conferences as a potential facilitator, in hopes of offering what I’ve learned to hospitalists looking to bring about change in their fields and careers.
What can attendees at HM18 expect to see in the area of career development, and how is this different than previous years?
Hospital medicine is only about 2 decades old, making it one of the youngest branches in medicine today. Given this fact, the Annual Conference Committee feels that it is paramount to focus on career development for both new and midcareer hospitalists alike.
One question that we wish to explore and answer this year is: “How do you make hospital medicine a life-long, enjoyable, and engaging career?” In turn, our committee has created several new additions to HM18. This includes a “Seasoning Your Career” track, which will provide ideas on how to advance in leadership, use emotional intelligence to achieve success, change your roles midcareer, and change hospitalist schedules. Another unique addition this year are career development workshops, which will aim to developing various aspects of a hospitalist’s career, such as working on leadership skills, refining presentation and communication skills, providing constructive feedback, promoting women in hospital medicine, preventing burnout, and turning ideas into clinical research. We also plan to incorporate an education track, which will focus on how hospitalists can expand their careers towards educational leadership.
Given your involvement in SHM at both the local and national levels, do you have any advice for young hospital medicine professionals looking to build their professional profiles?
I’ve frequently noticed that young hospitalists don’t realize the potential influence they hold within their own institutions or the power they have to elicit change in health care at the national level.
Though we don’t often admit it, some hospitalists feel like they are glorified residents, which definitely is not the case. As a provider on the front lines, you have the unique opportunity to implement changes pertaining to issues of cost, utilization of resources, process management, quality and patient safety, and bottlenecks in care, to name a few. These are issues that keep the administrators of your organization and leaders of hospital medicine up at night. Don’t sit around and complain about how things could be or should be; look toward creating change. Bring up possible solutions to these problems with your leaders. They will appreciate the effort, and hopefully together you can find ways to tackle these problems.
I will conclude by saying this: Hospital medicine is such a unique specialty in that it’s constantly evolving, and the pioneers of this field are still alive and practicing medicine. You can meet and interact with them during the SHM conferences and look to them as sources of inspiration or guidance. Meeting people you look up to and having them as your mentors can take you places.
Ms. Steele is the marketing communications specialist at the Society of Hospital Medicine.
Editor’s note: Each month, the Society of Hospital Medicine puts the spotlight on some of our most active members who are making substantial contributions to hospital medicine. Visit www.hospitalmedicine.org for more information on how you can lend your expertise to help SHM improve the care of hospitalized patients.
This month, The Hospitalist spotlights Amith Skandhan, MD, FHM, a hospitalist, a director/physician liaison for clinical documentation improvement and core faculty member in the Internal Medicine Residency Program at Southeast Alabama Medical Center in Dothan, Ala., and clinical faculty member at the Alabama College of Osteopathic Medicine also in Dothan. Dr. Skandhan is the cofounder and current president of the SHM Wiregrass Chapter and is an active member of SHM’s Annual Conference and Performance Measurement Reporting committees.
When did you join SHM, and what prompted you to apply for your current committee roles?
There were many things that were not sufficiently taught during clinical training that were required in my day-to-day practice, like clinical documentation improvement, practice management, billing, coding, and so forth. I also quickly understood how vast and dynamic hospital medicine really was. While looking for an outlet to voice my questions, concerns, and curiosity, I decided to join SHM, which has helped me find and apply the techniques I’d been looking for to further my career as a hospitalist.
I’m now fortunate to be a part of SHM’s national committees, which involve hospitalists of various backgrounds and experiences, who work together to improve the overall quality of inpatient medicine. I currently serve on the Performance Reporting Measurement Committee and the Annual Conference Committee. My interests in reviewing the ever-evolving policies of health care made me apply to be a part of the Performance Reporting Measurement Committee. We work very closely with the Public Policy Committee, analyzing written policies and subsequently offering our recommendations. It’s been fulfilling to be a part of a committee that works towards developing policies that support a good quality of care on such a large scale.
My penchant for organizing events and bringing people together based on common ground led me to apply for the Annual Conference Committee. We meet every week to discuss various topics, choose and invite speakers, and help organize the entire event, which will host close to 5,000 hospitalists later this year. It has made me appreciate being a member of an organization that provides hospitalists with opportunities for education and growth. I’m hopeful that the attendees next year will find the conference to be a worthwhile experience!
As the president of SHM’s Wiregrass Chapter, how has the chapter grown since its establishment in May 2015?
Our chapter is based in Dothan, a small, rural Alabama town where Southeast Alabama Medical Center is located. The chapter covers the counties of lower Alabama and the panhandle of Florida. We named the chapter after a special species of grass that grows in this region.
When we started the chapter, our goal was to bring the best and brightest of hospital medicine to our region to give talks on hot topics in the field and also to use their expertise to guide inpatient care in our hospital system. We aggressively marketed the events to bring in large crowds of medical professionals, and we consistently average around 70-80 attendees in our meetings. Bringing in leaders from the field helped create an atmosphere of learning and inspired us to grow and develop our hospitalist program. We now closely work with hospital medicine groups in surrounding rural areas toward improving inpatient hospital care.
During these past years, we also realized that, for the further growth of our chapter, we would need to nurture an interest in hospital medicine among future generations of doctors, and this realization led to the creation of our medical student and resident wing. So far, the students have been very enthusiastic about participating in SHM-related events, and I hope that continues. We also developed a mentor-mentee program, in which we paired selected medical students with hospitalists to help guide future careers in acute care medicine. This year, we have also been helping the hospital medicine division at Southeast Alabama Medical Center create a clinical research track for medical students. To that end, we have just completed our second annual poster competition where we presented around 50 posters in the areas of clinical vignettes, quality improvement, and original research.
In addition, the chapter is very active with community activities. We took notice of the fact that many of our patients and community members were unaware of what hospitalists did because they could not understand how our work was different from that of primary care physicians. Our members have therefore participated in TV, radio, and newspaper interviews to help elucidate the role of hospitalists in patient care. We have also periodically visited primary care physician offices, nursing homes, senior citizen groups, and cancer support groups to educate these patients on various facets of health care and how hospitalists influence these areas.
In 2014, we organized a “walk with a hospitalist” event, for which we set up a half-mile “admission to discharge” scenario explaining the role of hospitalists and other departments involved in patient care. This year, in hopes of improving patient literacy in our region, we held a “shop with a doc” event, where the Southeast Alabama Medical Center hospitalists teamed up with dietitians and taught patients how food and lifestyle influenced their chronic medical illnesses. This was followed by physicians and dietitians shopping with patients in the grocery store, educating them on healthy choices and label reading.
We’re incredibly grateful for the support that we’ve received from our medical and patient communities; they’ve been critical in helping our chapter grow as much as it has, and they motivate us to work harder and do more with the chapter. We were honored to receive the SHM’s Rising Star Award at the Hospital Medicine 2017 conference in Las Vegas. We never thought that our little chapter in the American countryside would be chosen, but we’re very thankful to have our efforts recognized on the national stage!
Which SHM conferences have you attended? Tell TH about your most memorable highlights or takeaways.
When I started out as a hospitalist in 2014, I decided to attend the annual conference in Las Vegas, and I can honestly say that conference changed the course of my career. I can still remember listening to the opening speech and realizing that I was surrounded by more than 3,000 hospitalists who understood the power we had to influence inpatient care. I’ve attended all the national conferences since then and am grateful that I now get to help organize the Hospital Medicine 2018 annual conference, also known as HM18.
I had been working to find a way to improve documentation within my group, as well as change the culture and perception towards billing and coding practices, which prompted me to attend the Quality and Safety Educators Academy. During one of the problem-solving sessions, I explained the challenges that I faced to my conference group. The exercise required me to explain the problem at hand, and the players of my group then discussed their thoughts while I took notes. It was a fantastic experience, as the participants at my table offered strong solutions to my problems within a matter of minutes. Their advice led to meaningful changes in our group’s hospital documentation practices, and in turn, I’ve been promoted to physician advisor in Southeast Alabama Medical Center.
After such a great experience at Quality and Safety Educators Academy, I went on to attend SHM’s Leadership Academy, where I had the opportunity to meet some of the top leaders and pioneers in the field of hospital medicine. It’s empowering to be mentored by the very people you look up to and aspire to be like. Not only was I able to bring ideas home to my institution, but I was able to reflect and improve my own professional and personal growth. I’m happy to say that I’ve completed all three levels of Leadership Academy.
As I’ve become involved with the medical student and residency programs at my medical center, I recently attended the Academic Hospitalist Academy to help my transition into academic hospital medicine. Meeting and spending time with the faculty at Academic Hospitalist Academy made me further realize the roles that academic hospitalists play in the education of future physicians, emphasizing the idea that we can all be champions in quality and patient safety.
If you’re looking to advance your career as a hospitalist, take advantage of the conferences that SHM offers. I’ve gained so much from each experience, and I’m looking forward to returning to these conferences as a potential facilitator, in hopes of offering what I’ve learned to hospitalists looking to bring about change in their fields and careers.
What can attendees at HM18 expect to see in the area of career development, and how is this different than previous years?
Hospital medicine is only about 2 decades old, making it one of the youngest branches in medicine today. Given this fact, the Annual Conference Committee feels that it is paramount to focus on career development for both new and midcareer hospitalists alike.
One question that we wish to explore and answer this year is: “How do you make hospital medicine a life-long, enjoyable, and engaging career?” In turn, our committee has created several new additions to HM18. This includes a “Seasoning Your Career” track, which will provide ideas on how to advance in leadership, use emotional intelligence to achieve success, change your roles midcareer, and change hospitalist schedules. Another unique addition this year are career development workshops, which will aim to developing various aspects of a hospitalist’s career, such as working on leadership skills, refining presentation and communication skills, providing constructive feedback, promoting women in hospital medicine, preventing burnout, and turning ideas into clinical research. We also plan to incorporate an education track, which will focus on how hospitalists can expand their careers towards educational leadership.
Given your involvement in SHM at both the local and national levels, do you have any advice for young hospital medicine professionals looking to build their professional profiles?
I’ve frequently noticed that young hospitalists don’t realize the potential influence they hold within their own institutions or the power they have to elicit change in health care at the national level.
Though we don’t often admit it, some hospitalists feel like they are glorified residents, which definitely is not the case. As a provider on the front lines, you have the unique opportunity to implement changes pertaining to issues of cost, utilization of resources, process management, quality and patient safety, and bottlenecks in care, to name a few. These are issues that keep the administrators of your organization and leaders of hospital medicine up at night. Don’t sit around and complain about how things could be or should be; look toward creating change. Bring up possible solutions to these problems with your leaders. They will appreciate the effort, and hopefully together you can find ways to tackle these problems.
I will conclude by saying this: Hospital medicine is such a unique specialty in that it’s constantly evolving, and the pioneers of this field are still alive and practicing medicine. You can meet and interact with them during the SHM conferences and look to them as sources of inspiration or guidance. Meeting people you look up to and having them as your mentors can take you places.
Ms. Steele is the marketing communications specialist at the Society of Hospital Medicine.

Spray-dried plasma inches toward clinical trials
SAN DIEGO – Spray-dried plasma compared well with fresh frozen plasma in two in vitro studies, but clinical studies are needed to confirm the findings, researchers reported at the annual meeting of the American Association of Blood Banks.
The product’s logistical benefits include ease of transport, stability at room temperature, and the ability to be rapidly reconstituted – attributes that make it particularly useful in combat situations and prehospital settings where it is impractical to administer fresh frozen plasma (FFP).
The advantages of reconstituted blood products in combat settings have prompted recent efforts to speed their availability. The Food and Drug Administration and the Department of Defense recently announced a joint program to expedite the FDA’s review of products that could diagnose, treat, or prevent life-threatening conditions facing U.S. military personnel. It would be a fast-track process similar to how the FDA handles the breakthrough designation program.
In the first study, the investigators compared spray-dried plasma (SpDP) and FFP in reconstituted whole blood to test their hypothesis that SpDP is not inferior to FFP in facilitating platelet adhesion and thrombus formation, as evaluated by using a microfusion assay.
“Trauma is frequently associated with the use of plasma,” said Rachel S. Bercovitz, MD, MS, of the BloodCenter of Wisconsin and associate professor of pediatrics (hematology, oncology, and stem cell transplantation) at Northwestern University, Chicago.
Compared with FFP, SpDP can be reconstituted in 5 minutes and has more than 80% of the procoagulation and anticoagulation proteins, she explained. “Factor 8 levels were lower in the spray-dried plasma and were about at the 70% level of FFP. The other factor that was reduced, as compared to the FFP, was the von Willebrand factor (vWF), which was about 60% in SpDP compared to FFP.”
Whole blood was obtained from healthy volunteers and red blood cells (RBCs) were separated from platelet-rich plasma, and following standard procedures, resuspended in either SpDP or FFP and recombined with the packed red blood cells to create reconstituted whole blood with hematocrit of 34%-40% and 150,000-250,000 platelets per mcL.
After fluorescent labeling, the samples were flowed through a type I collagen-coated microchannel and still images of adherent platelets and thrombi were captured in order to calculate surface area coverage along the length of the channel. Next, the investigators used a ratio paired t-test to compare surface area coverage in SpDP versus FFP. The margin of noninferiority was 20% (SpDP/FFP greater than 0.8).
A total of six batches of SpDP and FFP were evaluated with 17 donors, and there was no statistical difference between the SpDP versus FFP pairs (P = .7558).
The mean ratio of SpDP versus FFP was 1.21 with a 95% confidence interval of 0.84-1.57. The surface area coverage in samples that were reconstituted with SpDP were, on average, 20% greater than in samples reconstituted with FFP. The lower limit of the 95% confidence interval was a difference of 16%, and therefore lower than the a priori determined margin of noninferiority of 20%.
“We found that SpDP is not inferior to FFP in supporting platelet adhesion and thrombus formation in our in vitro model,” Dr. Bercovitz said. “We feel that these in vitro assays support further in vivo studies of safety and efficacy of spray dried plasma.”
In a second study, Michael A. Meledeo, PhD, of the U.S. Army Institute of Surgical Research (coagulation and blood research), and his colleagues examined methods of reconstituting SpDP. They noted that a single unit process has been developed that produces a long-lived and readily stored SpDP product, which decreased high-molecular-weight multimers of vWF but increased low-molecular-weight multimers. vWF is critical in the process of platelet adhesion and thrombus formation, Dr. Meledeo said.
The researchers examined different reconstitution solutions: FFP, FFP with glycine, regular SpDP without pretreatment and rehydrated with glycine-hydrochloride:glycine, SpDP pretreated with glycine-HCl, or glycine-HCl:glycine and rehydrated with water.
Several in vitro analyses were performed, including measurement of vWF activity, fibrin polymerization kinetics, thrombin generation, coagulation properties and platelet adhesion to collagen.
Pretreated SpDP had better vWF activity, compared with regular SpDP (P less than .05). As compared with FFP, fibrin polymerization density was slightly lower in regular SpDP (0.879 vs. 0.742 optical density; P less than .01), although generation of thrombin was similar.
The researchers also found that the bicarbonate/base excess were lower in SpDP samples versus FFP (P less than .001). Thromboelastography results (used to measure coagulation properties) remained unchanged in plasma-only samples, but clot strength in reconstructed whole blood was reduced in all SpDP samples, compared with FFP (63.82 vs. 55-59.38; P less than .01).
Finally, platelet adhesion was equivalent in pretreated SpDP samples and FFP, while with regular SpDP, it was improved as compared with all other samples (71.53% surface coverage vs. 30.26%-43.87%; P less than .05).
“Based on these results, spray dried plasma was equivalent or superior to FFP in most of the in vitro hemostasis assays,” Dr. Meledeo said. “Reconstitution with glycine-HCl or glycine-HCl:glycine induced a superior von Willebrand function, but it was inferior in terms of supporting a flowing platelet adhesion to collagen.”
Dr. Bercovitz and Dr. Meledeo reported having no financial disclosures.
SOURCES: Bercovitz R et al. AABB 17 Abstract C20-A02B; Meledeo M et al. AABB 17 Abstract C21-A02B.
SAN DIEGO – Spray-dried plasma compared well with fresh frozen plasma in two in vitro studies, but clinical studies are needed to confirm the findings, researchers reported at the annual meeting of the American Association of Blood Banks.
The product’s logistical benefits include ease of transport, stability at room temperature, and the ability to be rapidly reconstituted – attributes that make it particularly useful in combat situations and prehospital settings where it is impractical to administer fresh frozen plasma (FFP).
The advantages of reconstituted blood products in combat settings have prompted recent efforts to speed their availability. The Food and Drug Administration and the Department of Defense recently announced a joint program to expedite the FDA’s review of products that could diagnose, treat, or prevent life-threatening conditions facing U.S. military personnel. It would be a fast-track process similar to how the FDA handles the breakthrough designation program.
In the first study, the investigators compared spray-dried plasma (SpDP) and FFP in reconstituted whole blood to test their hypothesis that SpDP is not inferior to FFP in facilitating platelet adhesion and thrombus formation, as evaluated by using a microfusion assay.
“Trauma is frequently associated with the use of plasma,” said Rachel S. Bercovitz, MD, MS, of the BloodCenter of Wisconsin and associate professor of pediatrics (hematology, oncology, and stem cell transplantation) at Northwestern University, Chicago.
Compared with FFP, SpDP can be reconstituted in 5 minutes and has more than 80% of the procoagulation and anticoagulation proteins, she explained. “Factor 8 levels were lower in the spray-dried plasma and were about at the 70% level of FFP. The other factor that was reduced, as compared to the FFP, was the von Willebrand factor (vWF), which was about 60% in SpDP compared to FFP.”
Whole blood was obtained from healthy volunteers and red blood cells (RBCs) were separated from platelet-rich plasma, and following standard procedures, resuspended in either SpDP or FFP and recombined with the packed red blood cells to create reconstituted whole blood with hematocrit of 34%-40% and 150,000-250,000 platelets per mcL.
After fluorescent labeling, the samples were flowed through a type I collagen-coated microchannel and still images of adherent platelets and thrombi were captured in order to calculate surface area coverage along the length of the channel. Next, the investigators used a ratio paired t-test to compare surface area coverage in SpDP versus FFP. The margin of noninferiority was 20% (SpDP/FFP greater than 0.8).
A total of six batches of SpDP and FFP were evaluated with 17 donors, and there was no statistical difference between the SpDP versus FFP pairs (P = .7558).
The mean ratio of SpDP versus FFP was 1.21 with a 95% confidence interval of 0.84-1.57. The surface area coverage in samples that were reconstituted with SpDP were, on average, 20% greater than in samples reconstituted with FFP. The lower limit of the 95% confidence interval was a difference of 16%, and therefore lower than the a priori determined margin of noninferiority of 20%.
“We found that SpDP is not inferior to FFP in supporting platelet adhesion and thrombus formation in our in vitro model,” Dr. Bercovitz said. “We feel that these in vitro assays support further in vivo studies of safety and efficacy of spray dried plasma.”
In a second study, Michael A. Meledeo, PhD, of the U.S. Army Institute of Surgical Research (coagulation and blood research), and his colleagues examined methods of reconstituting SpDP. They noted that a single unit process has been developed that produces a long-lived and readily stored SpDP product, which decreased high-molecular-weight multimers of vWF but increased low-molecular-weight multimers. vWF is critical in the process of platelet adhesion and thrombus formation, Dr. Meledeo said.
The researchers examined different reconstitution solutions: FFP, FFP with glycine, regular SpDP without pretreatment and rehydrated with glycine-hydrochloride:glycine, SpDP pretreated with glycine-HCl, or glycine-HCl:glycine and rehydrated with water.
Several in vitro analyses were performed, including measurement of vWF activity, fibrin polymerization kinetics, thrombin generation, coagulation properties and platelet adhesion to collagen.
Pretreated SpDP had better vWF activity, compared with regular SpDP (P less than .05). As compared with FFP, fibrin polymerization density was slightly lower in regular SpDP (0.879 vs. 0.742 optical density; P less than .01), although generation of thrombin was similar.
The researchers also found that the bicarbonate/base excess were lower in SpDP samples versus FFP (P less than .001). Thromboelastography results (used to measure coagulation properties) remained unchanged in plasma-only samples, but clot strength in reconstructed whole blood was reduced in all SpDP samples, compared with FFP (63.82 vs. 55-59.38; P less than .01).
Finally, platelet adhesion was equivalent in pretreated SpDP samples and FFP, while with regular SpDP, it was improved as compared with all other samples (71.53% surface coverage vs. 30.26%-43.87%; P less than .05).
“Based on these results, spray dried plasma was equivalent or superior to FFP in most of the in vitro hemostasis assays,” Dr. Meledeo said. “Reconstitution with glycine-HCl or glycine-HCl:glycine induced a superior von Willebrand function, but it was inferior in terms of supporting a flowing platelet adhesion to collagen.”
Dr. Bercovitz and Dr. Meledeo reported having no financial disclosures.
SOURCES: Bercovitz R et al. AABB 17 Abstract C20-A02B; Meledeo M et al. AABB 17 Abstract C21-A02B.
SAN DIEGO – Spray-dried plasma compared well with fresh frozen plasma in two in vitro studies, but clinical studies are needed to confirm the findings, researchers reported at the annual meeting of the American Association of Blood Banks.
The product’s logistical benefits include ease of transport, stability at room temperature, and the ability to be rapidly reconstituted – attributes that make it particularly useful in combat situations and prehospital settings where it is impractical to administer fresh frozen plasma (FFP).
The advantages of reconstituted blood products in combat settings have prompted recent efforts to speed their availability. The Food and Drug Administration and the Department of Defense recently announced a joint program to expedite the FDA’s review of products that could diagnose, treat, or prevent life-threatening conditions facing U.S. military personnel. It would be a fast-track process similar to how the FDA handles the breakthrough designation program.
In the first study, the investigators compared spray-dried plasma (SpDP) and FFP in reconstituted whole blood to test their hypothesis that SpDP is not inferior to FFP in facilitating platelet adhesion and thrombus formation, as evaluated by using a microfusion assay.
“Trauma is frequently associated with the use of plasma,” said Rachel S. Bercovitz, MD, MS, of the BloodCenter of Wisconsin and associate professor of pediatrics (hematology, oncology, and stem cell transplantation) at Northwestern University, Chicago.
Compared with FFP, SpDP can be reconstituted in 5 minutes and has more than 80% of the procoagulation and anticoagulation proteins, she explained. “Factor 8 levels were lower in the spray-dried plasma and were about at the 70% level of FFP. The other factor that was reduced, as compared to the FFP, was the von Willebrand factor (vWF), which was about 60% in SpDP compared to FFP.”
Whole blood was obtained from healthy volunteers and red blood cells (RBCs) were separated from platelet-rich plasma, and following standard procedures, resuspended in either SpDP or FFP and recombined with the packed red blood cells to create reconstituted whole blood with hematocrit of 34%-40% and 150,000-250,000 platelets per mcL.
After fluorescent labeling, the samples were flowed through a type I collagen-coated microchannel and still images of adherent platelets and thrombi were captured in order to calculate surface area coverage along the length of the channel. Next, the investigators used a ratio paired t-test to compare surface area coverage in SpDP versus FFP. The margin of noninferiority was 20% (SpDP/FFP greater than 0.8).
A total of six batches of SpDP and FFP were evaluated with 17 donors, and there was no statistical difference between the SpDP versus FFP pairs (P = .7558).
The mean ratio of SpDP versus FFP was 1.21 with a 95% confidence interval of 0.84-1.57. The surface area coverage in samples that were reconstituted with SpDP were, on average, 20% greater than in samples reconstituted with FFP. The lower limit of the 95% confidence interval was a difference of 16%, and therefore lower than the a priori determined margin of noninferiority of 20%.
“We found that SpDP is not inferior to FFP in supporting platelet adhesion and thrombus formation in our in vitro model,” Dr. Bercovitz said. “We feel that these in vitro assays support further in vivo studies of safety and efficacy of spray dried plasma.”
In a second study, Michael A. Meledeo, PhD, of the U.S. Army Institute of Surgical Research (coagulation and blood research), and his colleagues examined methods of reconstituting SpDP. They noted that a single unit process has been developed that produces a long-lived and readily stored SpDP product, which decreased high-molecular-weight multimers of vWF but increased low-molecular-weight multimers. vWF is critical in the process of platelet adhesion and thrombus formation, Dr. Meledeo said.
The researchers examined different reconstitution solutions: FFP, FFP with glycine, regular SpDP without pretreatment and rehydrated with glycine-hydrochloride:glycine, SpDP pretreated with glycine-HCl, or glycine-HCl:glycine and rehydrated with water.
Several in vitro analyses were performed, including measurement of vWF activity, fibrin polymerization kinetics, thrombin generation, coagulation properties and platelet adhesion to collagen.
Pretreated SpDP had better vWF activity, compared with regular SpDP (P less than .05). As compared with FFP, fibrin polymerization density was slightly lower in regular SpDP (0.879 vs. 0.742 optical density; P less than .01), although generation of thrombin was similar.
The researchers also found that the bicarbonate/base excess were lower in SpDP samples versus FFP (P less than .001). Thromboelastography results (used to measure coagulation properties) remained unchanged in plasma-only samples, but clot strength in reconstructed whole blood was reduced in all SpDP samples, compared with FFP (63.82 vs. 55-59.38; P less than .01).
Finally, platelet adhesion was equivalent in pretreated SpDP samples and FFP, while with regular SpDP, it was improved as compared with all other samples (71.53% surface coverage vs. 30.26%-43.87%; P less than .05).
“Based on these results, spray dried plasma was equivalent or superior to FFP in most of the in vitro hemostasis assays,” Dr. Meledeo said. “Reconstitution with glycine-HCl or glycine-HCl:glycine induced a superior von Willebrand function, but it was inferior in terms of supporting a flowing platelet adhesion to collagen.”
Dr. Bercovitz and Dr. Meledeo reported having no financial disclosures.
SOURCES: Bercovitz R et al. AABB 17 Abstract C20-A02B; Meledeo M et al. AABB 17 Abstract C21-A02B.
REPORTING FROM AABB 17
Key clinical point:
Major finding: Spray-dried plasma was equal to, or superior to, fresh frozen plasma in many of the in vitro assays utilized, especially when pretreated in glycine solutions.
Study details: Two in vitro assays that compared spray-dried plasma with fresh frozen plasma.
Disclosures: Dr. Bercovitz and Dr. Meledeo reported having no financial disclosures.
Sources: Bercovitz R et al. AABB 17 Abstract C20-A02B; Meledeo M et al. AABB 17 Abstract C21-A02B.
Clinical Challenges - February 2018 What's your diagnosis?
The diagnosis: Metastatic insulinoma surrounded by steatotic hepatocytes
The loss of L-FABP expression in steatotic hepatocytes is the hallmark of HNF1alpha-inactivated liver adenoma,1 and clearly suggested this diagnosis. However, the emergence of multiple steatotic lesions over a short period of time was uncommon for liver adenomas. Despite the absence of radiologically detectable metastasis, this diagnosis could not be ruled out, and the patient underwent a surgical liver biopsy (tip of the right lobe). The specimen showed a 0.2 cm greyish nodule surrounded by a steatotic map-like area of 3.5 cm in the largest dimension (Figure E). Histopathologic examination showed neuroendocrine cells (Figures F [hematoxylin and eosin staining] and G [insulin immunostaining]), confirming the diagnosis of metastatic insulinoma surrounded by steatotic hepatocytes.
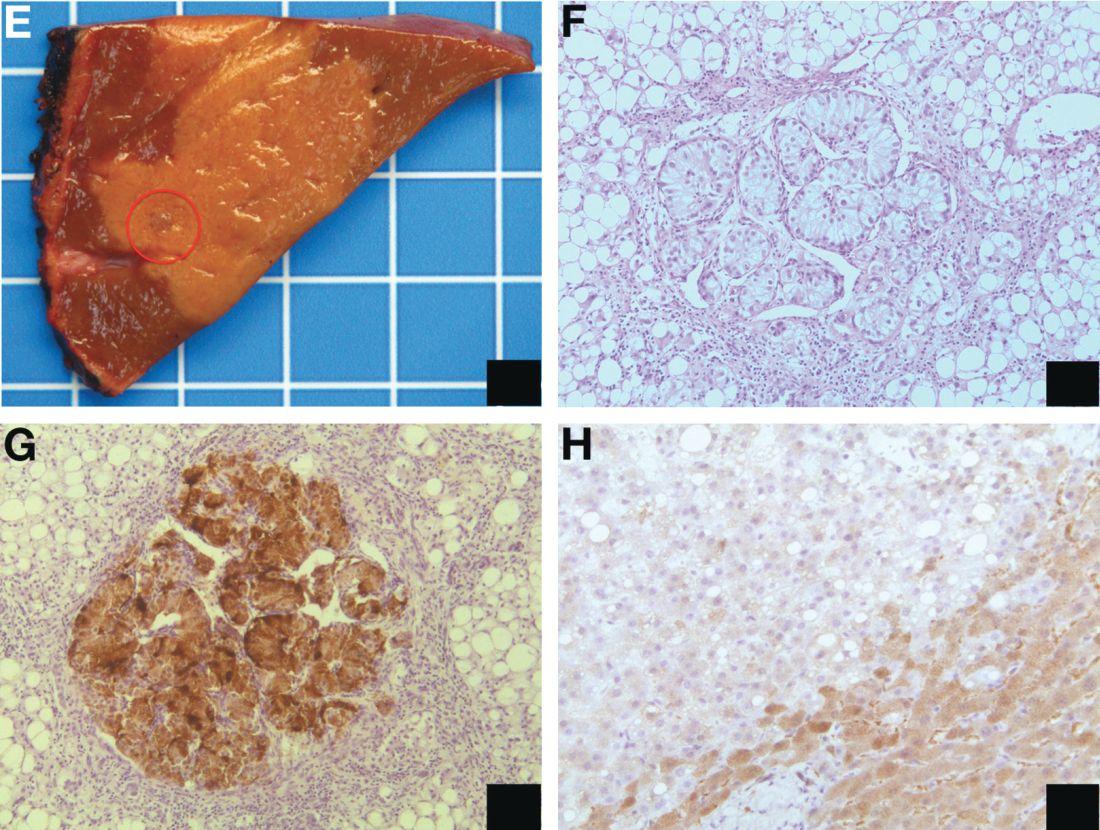
The key interest of the case is the reduction of L-FABP expression in the steatotic hepatocytes (Figure H [L-FABP immunostaining]), which was an unexpected finding and could have led to an incorrect diagnosis of HNF1α-inactivated liver adenoma.
In contrast with other functional neuroendocrine tumors, insulinomas are frequently benign tumors, and only about 10% of patients develop metastasis. In the liver, they are often surrounded by microscopic or radiologically detectable steatotic areas thanks to the paracrine effect of insulin. Such a feature has been previously described both with liver insulinoma metastases2 and after pancreatic islet transplantation.3 The reduction of L-FABP expression within the steatotic hepatocytes seems to be less frequent because it was not observed in an additional patient with G3 insulinoma (neuroendocrine carcinoma) metastases and in 3 pancreatic islet recipients (data not shown).
The present patient with multiple liver G2 insulinoma metastases illustrates 1) the potential of foci of steatosis to represent early signs of insulinoma liver metastasis, and 2) the presence of a reduction or even a loss of L-FABP expression in other liver lesions than HNF1alpha-inactivated liver adenoma.
Acknowledgment
Claudio De Vito’s current affiliation is Institute of Liver Studies, King’s College Hospital, London, UK.
The authors thank A.M.J. Shapiro from the University of Alberta, Edmonton, Canada and A. Quaglia from the King’s College Hospital, London, UK for sharing the liver samples of transplanted pancreatic islets and G3 insulinoma metastasis. They are also grateful to the members of the Geneva Hepato-Biliary and Pancreatic Center for the discussion of the case.
References
1. Bioulac-Sage P., Cubel G., Taouji S., et al. Immunohistochemical markers on needle biopsies are helpful for the diagnosis of focal nodular hyperplasia and hepatocellular adenoma subtypes. Am J Surg Pathol. 2012;36:1691-9.
2. Sohn J., Siegelman E., Osiason, A. Unusual patterns of hepatic steatosis caused by the local effect of insulin revealed on chemical shift MR imaging. AJR Am J Roentgenol. 2001;176:471-4.
3. Toso C., Isse K., Demetris A.J., et al. Histologic graft assessment after clinical islet transplantation. Transplantation. 2009;88:1286-93.
The diagnosis: Metastatic insulinoma surrounded by steatotic hepatocytes
The loss of L-FABP expression in steatotic hepatocytes is the hallmark of HNF1alpha-inactivated liver adenoma,1 and clearly suggested this diagnosis. However, the emergence of multiple steatotic lesions over a short period of time was uncommon for liver adenomas. Despite the absence of radiologically detectable metastasis, this diagnosis could not be ruled out, and the patient underwent a surgical liver biopsy (tip of the right lobe). The specimen showed a 0.2 cm greyish nodule surrounded by a steatotic map-like area of 3.5 cm in the largest dimension (Figure E). Histopathologic examination showed neuroendocrine cells (Figures F [hematoxylin and eosin staining] and G [insulin immunostaining]), confirming the diagnosis of metastatic insulinoma surrounded by steatotic hepatocytes.
The key interest of the case is the reduction of L-FABP expression in the steatotic hepatocytes (Figure H [L-FABP immunostaining]), which was an unexpected finding and could have led to an incorrect diagnosis of HNF1α-inactivated liver adenoma.
In contrast with other functional neuroendocrine tumors, insulinomas are frequently benign tumors, and only about 10% of patients develop metastasis. In the liver, they are often surrounded by microscopic or radiologically detectable steatotic areas thanks to the paracrine effect of insulin. Such a feature has been previously described both with liver insulinoma metastases2 and after pancreatic islet transplantation.3 The reduction of L-FABP expression within the steatotic hepatocytes seems to be less frequent because it was not observed in an additional patient with G3 insulinoma (neuroendocrine carcinoma) metastases and in 3 pancreatic islet recipients (data not shown).
The present patient with multiple liver G2 insulinoma metastases illustrates 1) the potential of foci of steatosis to represent early signs of insulinoma liver metastasis, and 2) the presence of a reduction or even a loss of L-FABP expression in other liver lesions than HNF1alpha-inactivated liver adenoma.
Acknowledgment
Claudio De Vito’s current affiliation is Institute of Liver Studies, King’s College Hospital, London, UK.
The authors thank A.M.J. Shapiro from the University of Alberta, Edmonton, Canada and A. Quaglia from the King’s College Hospital, London, UK for sharing the liver samples of transplanted pancreatic islets and G3 insulinoma metastasis. They are also grateful to the members of the Geneva Hepato-Biliary and Pancreatic Center for the discussion of the case.
References
1. Bioulac-Sage P., Cubel G., Taouji S., et al. Immunohistochemical markers on needle biopsies are helpful for the diagnosis of focal nodular hyperplasia and hepatocellular adenoma subtypes. Am J Surg Pathol. 2012;36:1691-9.
2. Sohn J., Siegelman E., Osiason, A. Unusual patterns of hepatic steatosis caused by the local effect of insulin revealed on chemical shift MR imaging. AJR Am J Roentgenol. 2001;176:471-4.
3. Toso C., Isse K., Demetris A.J., et al. Histologic graft assessment after clinical islet transplantation. Transplantation. 2009;88:1286-93.
The diagnosis: Metastatic insulinoma surrounded by steatotic hepatocytes
The loss of L-FABP expression in steatotic hepatocytes is the hallmark of HNF1alpha-inactivated liver adenoma,1 and clearly suggested this diagnosis. However, the emergence of multiple steatotic lesions over a short period of time was uncommon for liver adenomas. Despite the absence of radiologically detectable metastasis, this diagnosis could not be ruled out, and the patient underwent a surgical liver biopsy (tip of the right lobe). The specimen showed a 0.2 cm greyish nodule surrounded by a steatotic map-like area of 3.5 cm in the largest dimension (Figure E). Histopathologic examination showed neuroendocrine cells (Figures F [hematoxylin and eosin staining] and G [insulin immunostaining]), confirming the diagnosis of metastatic insulinoma surrounded by steatotic hepatocytes.
The key interest of the case is the reduction of L-FABP expression in the steatotic hepatocytes (Figure H [L-FABP immunostaining]), which was an unexpected finding and could have led to an incorrect diagnosis of HNF1α-inactivated liver adenoma.
In contrast with other functional neuroendocrine tumors, insulinomas are frequently benign tumors, and only about 10% of patients develop metastasis. In the liver, they are often surrounded by microscopic or radiologically detectable steatotic areas thanks to the paracrine effect of insulin. Such a feature has been previously described both with liver insulinoma metastases2 and after pancreatic islet transplantation.3 The reduction of L-FABP expression within the steatotic hepatocytes seems to be less frequent because it was not observed in an additional patient with G3 insulinoma (neuroendocrine carcinoma) metastases and in 3 pancreatic islet recipients (data not shown).
The present patient with multiple liver G2 insulinoma metastases illustrates 1) the potential of foci of steatosis to represent early signs of insulinoma liver metastasis, and 2) the presence of a reduction or even a loss of L-FABP expression in other liver lesions than HNF1alpha-inactivated liver adenoma.
Acknowledgment
Claudio De Vito’s current affiliation is Institute of Liver Studies, King’s College Hospital, London, UK.
The authors thank A.M.J. Shapiro from the University of Alberta, Edmonton, Canada and A. Quaglia from the King’s College Hospital, London, UK for sharing the liver samples of transplanted pancreatic islets and G3 insulinoma metastasis. They are also grateful to the members of the Geneva Hepato-Biliary and Pancreatic Center for the discussion of the case.
References
1. Bioulac-Sage P., Cubel G., Taouji S., et al. Immunohistochemical markers on needle biopsies are helpful for the diagnosis of focal nodular hyperplasia and hepatocellular adenoma subtypes. Am J Surg Pathol. 2012;36:1691-9.
2. Sohn J., Siegelman E., Osiason, A. Unusual patterns of hepatic steatosis caused by the local effect of insulin revealed on chemical shift MR imaging. AJR Am J Roentgenol. 2001;176:471-4.
3. Toso C., Isse K., Demetris A.J., et al. Histologic graft assessment after clinical islet transplantation. Transplantation. 2009;88:1286-93.
By Claudio De Vito, MD, PhD, Laura Rubbia-Brandt, MD, PhD, and Christian Toso, MD, PhD. Published previously in Gastroenterology (2016;151[1]32, 330).
A 22-year-old woman with no past medical history was investigated for hypoglycemia episodes. A nodule located in the head of the pancreas was identified, with radiologic features of a neuroendocrine neoplasm. The overall clinical presentation was consistent with an insulinoma. No distant lesion was detected. She underwent a Whipple procedure, and the histopathologic examination reported a 2.2-cm, well-differentiated neuroendocrine tumor (insulinoma) G2 (4% Ki-67 index), with no lymphovascular invasion or lymph node metastasis (0 of 30 lymph nodes). 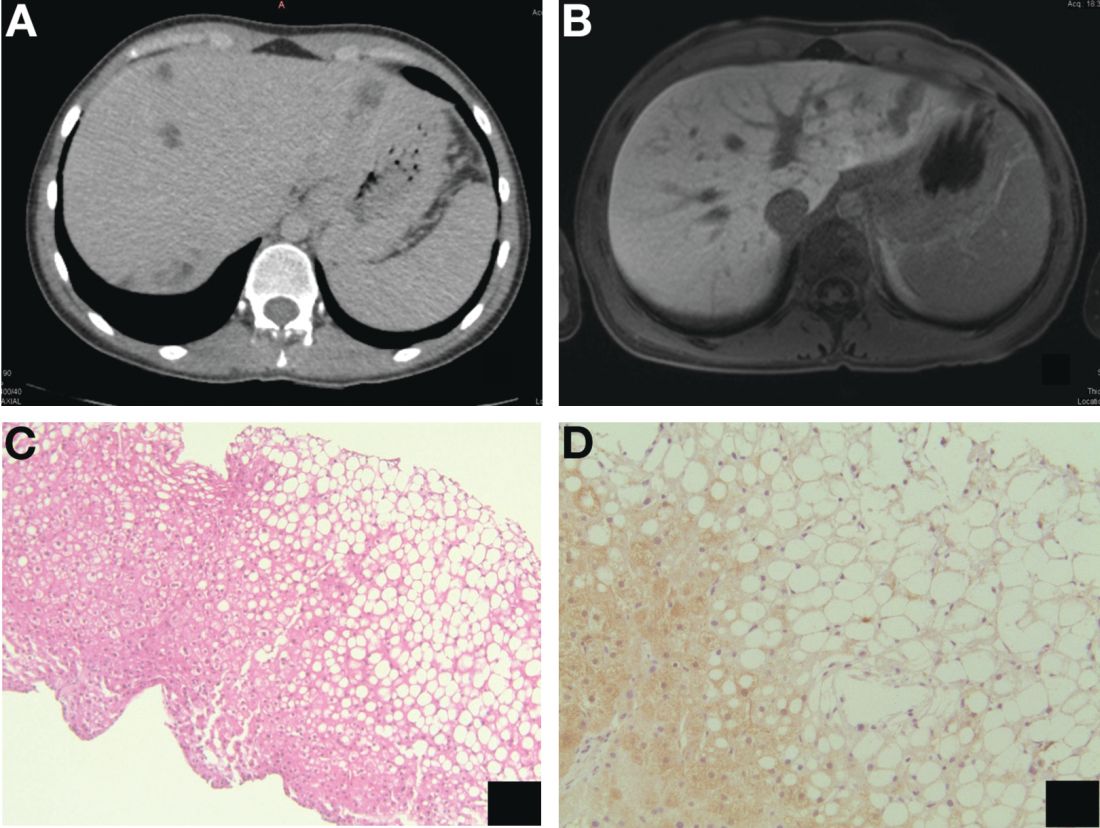
Psychiatric pharmacogenomics not ‘ready for prime time’
NEW YORK – Pharmacogenomics testing for guiding drug choices in psychiatric disease is “not completely ready for prime time,” based on a critical review of published guidelines and expert opinions on the use of those tests, according to Erika L. Nurmi, MD, PhD.
It is important to understand the limitations of such tests because many patients or family members are asking clinicians to be guided by the results of tests they have ordered on their own, said Dr. Nurmi, a researcher and clinician at the UCLA Semel Institute for Neuroscience and Human Behavior, Los Angeles.
Published guidelines and expert opinions based on objective data support these conclusions, she said. Dr. Nurmi suggested that .
“Basically, what it says is if you do not have the testing in hand, don’t order it. If you have the testing in hand when a poor metabolizer of CYP2D6 or CYP2C19 has been identified, switch to a med that is not metabolized by those enzymes. That’s it,” Dr. Nurmi reported at a pediatric psychopharmacology update held by the American Academy of Child and Adolescent Psychiatry.
The guidelines from the Clinical Pharmacogenetics Implementation Consortium (CPIC) were only modestly more detailed. Only a moderate level of evidence supported most recommendations, she said, and these were labeled optional. The exception regarded treating ultrafast metabolizers of CYP2D6 who are taking paroxetine: In these, the use of a drug metabolized by a different enzyme was strongly recommended.
Similar recommendations in the CPIC guidelines were made for fluoxetine, fluvoxamine, and sertraline. In patients on citalopram or escitalopram, ultrafast metabolizers of CYP2C19 are considered candidates for a non-CYP2C19 drug. If they are poor metabolizers, the CPIC guidelines recommended a non-CYP2C19 drug or reducing the starting dose by 50%.
However, in all of these cases, pharmacogenomics testing is best reserved for patients who have had an inadequate response to therapy or, in the case of poor metabolizers, have had unacceptable adverse events.
Of the limitations Dr. Nurmi outlined for pharmacogenomics testing, one of the most important is that these tests typically focus on a single genetic variant. According to Dr. Nurmi, the problem with a single variant is that “our bodies are more complex.” She said she believes that genetic information for drug selection will not be useful until testing is able to synthesize information from multiple genetic variants and place this in context with confounders such as age and exposure to other substances, such as hormones, caffeine, or grapefruit juice.
This complexity is likely to be mastered eventually, Dr. Nurmi said, but patients now have unrealistic expectations. For their part, clinicians need to develop an understanding of the limitations of these tests in order to provide informed counsel. As pharmacogenomics testing is being marketed directly to consumers with inflated claims about its value, clinicians often must defend their decision to use or not use this information.
“Commercially available products combine variants of widely discrepant validity using proprietary, undisclosed algorithms into sweeping treatment recommendations,” said Dr. Nurmi, who noted that she has found some of her own data misappropriated to make claims. Often, the companies that develop the tests have conducted the validation studies without any replication by independent investigators. She noted that many studies have been declared positive on the basis of secondary outcomes after the primary outcome was negative.
“There are very few positive prospective, randomized, double-blind trials,” Dr. Nurmi said. Even when such trials have been conducted, they typically are not designed to show a clinically meaningful outcome.
By attempting to look at a single or a limited number of variants in which to guide choice of medication in psychiatric disease, pharmacogenomics testing is being “vastly oversimplified,” Dr. Nurmi said. Although she said she believes this field is enormously promising and that medical records for each patient eventually will contain the genome sequence, she emphasized that, at this time, pharmacogenomics testing has a very limited role to play for the management of psychiatric diseases.
Dr. Nurmi reported she had no financial relationships relevant to this topic.
NEW YORK – Pharmacogenomics testing for guiding drug choices in psychiatric disease is “not completely ready for prime time,” based on a critical review of published guidelines and expert opinions on the use of those tests, according to Erika L. Nurmi, MD, PhD.
It is important to understand the limitations of such tests because many patients or family members are asking clinicians to be guided by the results of tests they have ordered on their own, said Dr. Nurmi, a researcher and clinician at the UCLA Semel Institute for Neuroscience and Human Behavior, Los Angeles.
Published guidelines and expert opinions based on objective data support these conclusions, she said. Dr. Nurmi suggested that .
“Basically, what it says is if you do not have the testing in hand, don’t order it. If you have the testing in hand when a poor metabolizer of CYP2D6 or CYP2C19 has been identified, switch to a med that is not metabolized by those enzymes. That’s it,” Dr. Nurmi reported at a pediatric psychopharmacology update held by the American Academy of Child and Adolescent Psychiatry.
The guidelines from the Clinical Pharmacogenetics Implementation Consortium (CPIC) were only modestly more detailed. Only a moderate level of evidence supported most recommendations, she said, and these were labeled optional. The exception regarded treating ultrafast metabolizers of CYP2D6 who are taking paroxetine: In these, the use of a drug metabolized by a different enzyme was strongly recommended.
Similar recommendations in the CPIC guidelines were made for fluoxetine, fluvoxamine, and sertraline. In patients on citalopram or escitalopram, ultrafast metabolizers of CYP2C19 are considered candidates for a non-CYP2C19 drug. If they are poor metabolizers, the CPIC guidelines recommended a non-CYP2C19 drug or reducing the starting dose by 50%.
However, in all of these cases, pharmacogenomics testing is best reserved for patients who have had an inadequate response to therapy or, in the case of poor metabolizers, have had unacceptable adverse events.
Of the limitations Dr. Nurmi outlined for pharmacogenomics testing, one of the most important is that these tests typically focus on a single genetic variant. According to Dr. Nurmi, the problem with a single variant is that “our bodies are more complex.” She said she believes that genetic information for drug selection will not be useful until testing is able to synthesize information from multiple genetic variants and place this in context with confounders such as age and exposure to other substances, such as hormones, caffeine, or grapefruit juice.
This complexity is likely to be mastered eventually, Dr. Nurmi said, but patients now have unrealistic expectations. For their part, clinicians need to develop an understanding of the limitations of these tests in order to provide informed counsel. As pharmacogenomics testing is being marketed directly to consumers with inflated claims about its value, clinicians often must defend their decision to use or not use this information.
“Commercially available products combine variants of widely discrepant validity using proprietary, undisclosed algorithms into sweeping treatment recommendations,” said Dr. Nurmi, who noted that she has found some of her own data misappropriated to make claims. Often, the companies that develop the tests have conducted the validation studies without any replication by independent investigators. She noted that many studies have been declared positive on the basis of secondary outcomes after the primary outcome was negative.
“There are very few positive prospective, randomized, double-blind trials,” Dr. Nurmi said. Even when such trials have been conducted, they typically are not designed to show a clinically meaningful outcome.
By attempting to look at a single or a limited number of variants in which to guide choice of medication in psychiatric disease, pharmacogenomics testing is being “vastly oversimplified,” Dr. Nurmi said. Although she said she believes this field is enormously promising and that medical records for each patient eventually will contain the genome sequence, she emphasized that, at this time, pharmacogenomics testing has a very limited role to play for the management of psychiatric diseases.
Dr. Nurmi reported she had no financial relationships relevant to this topic.
NEW YORK – Pharmacogenomics testing for guiding drug choices in psychiatric disease is “not completely ready for prime time,” based on a critical review of published guidelines and expert opinions on the use of those tests, according to Erika L. Nurmi, MD, PhD.
It is important to understand the limitations of such tests because many patients or family members are asking clinicians to be guided by the results of tests they have ordered on their own, said Dr. Nurmi, a researcher and clinician at the UCLA Semel Institute for Neuroscience and Human Behavior, Los Angeles.
Published guidelines and expert opinions based on objective data support these conclusions, she said. Dr. Nurmi suggested that .
“Basically, what it says is if you do not have the testing in hand, don’t order it. If you have the testing in hand when a poor metabolizer of CYP2D6 or CYP2C19 has been identified, switch to a med that is not metabolized by those enzymes. That’s it,” Dr. Nurmi reported at a pediatric psychopharmacology update held by the American Academy of Child and Adolescent Psychiatry.
The guidelines from the Clinical Pharmacogenetics Implementation Consortium (CPIC) were only modestly more detailed. Only a moderate level of evidence supported most recommendations, she said, and these were labeled optional. The exception regarded treating ultrafast metabolizers of CYP2D6 who are taking paroxetine: In these, the use of a drug metabolized by a different enzyme was strongly recommended.
Similar recommendations in the CPIC guidelines were made for fluoxetine, fluvoxamine, and sertraline. In patients on citalopram or escitalopram, ultrafast metabolizers of CYP2C19 are considered candidates for a non-CYP2C19 drug. If they are poor metabolizers, the CPIC guidelines recommended a non-CYP2C19 drug or reducing the starting dose by 50%.
However, in all of these cases, pharmacogenomics testing is best reserved for patients who have had an inadequate response to therapy or, in the case of poor metabolizers, have had unacceptable adverse events.
Of the limitations Dr. Nurmi outlined for pharmacogenomics testing, one of the most important is that these tests typically focus on a single genetic variant. According to Dr. Nurmi, the problem with a single variant is that “our bodies are more complex.” She said she believes that genetic information for drug selection will not be useful until testing is able to synthesize information from multiple genetic variants and place this in context with confounders such as age and exposure to other substances, such as hormones, caffeine, or grapefruit juice.
This complexity is likely to be mastered eventually, Dr. Nurmi said, but patients now have unrealistic expectations. For their part, clinicians need to develop an understanding of the limitations of these tests in order to provide informed counsel. As pharmacogenomics testing is being marketed directly to consumers with inflated claims about its value, clinicians often must defend their decision to use or not use this information.
“Commercially available products combine variants of widely discrepant validity using proprietary, undisclosed algorithms into sweeping treatment recommendations,” said Dr. Nurmi, who noted that she has found some of her own data misappropriated to make claims. Often, the companies that develop the tests have conducted the validation studies without any replication by independent investigators. She noted that many studies have been declared positive on the basis of secondary outcomes after the primary outcome was negative.
“There are very few positive prospective, randomized, double-blind trials,” Dr. Nurmi said. Even when such trials have been conducted, they typically are not designed to show a clinically meaningful outcome.
By attempting to look at a single or a limited number of variants in which to guide choice of medication in psychiatric disease, pharmacogenomics testing is being “vastly oversimplified,” Dr. Nurmi said. Although she said she believes this field is enormously promising and that medical records for each patient eventually will contain the genome sequence, she emphasized that, at this time, pharmacogenomics testing has a very limited role to play for the management of psychiatric diseases.
Dr. Nurmi reported she had no financial relationships relevant to this topic.
EXPERT ANALYSIS FROM THE PSYCHOPHARMACOLOGY UPDATE INSTITUTE
PCOS may influence the diversity of the gut microbiome
according to a study from the Journal of Clinical Endocrinology and Metabolism.
“This study demonstrated that Caucasian women diagnosed with PCOS using the Rotterdam criteria had a reduction in overall species richness [alpha diversity] of the gut microbiome, compared to healthy women, and changes in the composition of the microbial community [beta diversity]” wrote Pedro J. Torres and his associates. “Interestingly, our study found that the biodiversity of the microbiome strongly correlated with hyperandrogenism.”
Dr. Torres of the University of California, San Diego, and his colleagues recruited 163 women at the University of Poznan (Poland) and conducted analysis on fecal samples to determine the effects of PCOS on the gut microbiome. Each woman underwent a battery of tests to determine whether she had PCOS or polycystic ovarian morphology (PCOM). Ovarian morphology was determined from a transvaginal ultrasound evaluation. The women were assessed for body mass index and hirsutism. Blood samples were taken to test for hormonal abnormalities common with PCOS and metabolic issues, like type 2 diabetes mellitus and glucose tolerance. Fecal samples were taken to analyze the gut microbiota of each study participant; analysis of the fecal samples generated gut microbial diversity profiles for each of the 163 women. Analysis of the samples was conducted at the University of California, San Diego.
Of the subjects, 48 were healthy, 42 had PCOM, and 73 were diagnosed with PCOS. The researches noted that, compared with healthy women and those with PCOM, women with PCOS had higher levels of serum total and free testosterone, as well as higher rates of hirsutism and fewer menses per year. These women also had higher levels of serum luteinizing hormone and increased ratios of luteinizing hormone to follicle stimulating hormone.
The DNA analysis of fecal samples yielded 481 sequence variants from the fecal swabs. Women with PCOS were found to have lower alpha diversity in their gut microbiome, as evidenced by abundance (P = .04) and Faith’s phylogenetic diveristy (P = .02). The luteinizing hormone to follicle stimulating hormone ratio also appeared to affect the alpha diversity of women with PCOS, as seen in observed sequence variants and Faith’s phylogenetic diversity (P = .08).
Beta diversity analysis, or the biodiversity between samples, revealed that hyperandrogenism could be a primary driver of changes in the gut microbiome. Using permutational multivariate analysis of variance, researchers determined that hyperandrogenism significantly affected beta diversity (P = .0009).
Androgens may help affect the gut microbiome in important ways, and changes in the gut microbiome may influence how the pathology of PCOS develops, according to Mr. Torres and his colleagues; however, more studies should be conducted to determine the effects of androgens on the gut microbiome.
“If hyperandrogenism drives the microbial composition of the gut, it would be interesting to determine if treatment of PCOS with androgen antagonists or oral contraceptives results in recovery of the gut microbiome and improvement of the PCOS metabolic phenotype” wrote Mr. Torres and his colleagues. “Moreover, it would be informative to determine whether the gut microbiome of women diagnosed with PCOS using the criteria of oligomenorrhea and polycystic ovaries is distinct from that of women diagnosed with the other subtypes of PCOS that include hyperandrogenism.”
The authors had no relevant financial disclosures to report.
SOURCE: Torres PJ et al. J Clin Endocrinol Metab. 2018 Jan 23. doi: 10.1210/jc.2017-02153.
Polycystic ovarian syndrome (PCOS) can manifest itself in many ways, but this study reveals that it can directly affect the metabolism of those who have the disorder.
“We’re still early days in studying this, but this study suggests that one of the clinical characteristics of these women with this disorder – their elevated testosterone – is correlated with changes in the gut microbiome,” Varykina G. Thackray, PhD, of the department of reproductive medicine and the center for reproductive science and medicine at the University of California, San Diego, said in an interview. “That means that these women are in a different group than other people with metabolic disorders, and it potentially gives us a way to think of new therapies that might be helpful for this specific group of women.”

When asked whether fecal transplants may be a potential therapy to help treat the metabolic issues associated with PCOS, Dr. Thackray stated that she did not believe a lot of women would use that as a therapy because of the “ick” factor. She stated the goal is to identify some beneficial bacteria that could be taken as a probiotic to help restore the gut microbiome.
Unfortunately, researchers still do not understand what causes PCOS. Some studies suggest that there are environmental and genetic factors, but there is nothing definitive. Dr. Thackray stated that getting more funding and conducting more research are the best ways to understand and combat this disorder.
Dr. Thackray is an associate professor of reproductive medicine at the University of California, San Diego.
Polycystic ovarian syndrome (PCOS) can manifest itself in many ways, but this study reveals that it can directly affect the metabolism of those who have the disorder.
“We’re still early days in studying this, but this study suggests that one of the clinical characteristics of these women with this disorder – their elevated testosterone – is correlated with changes in the gut microbiome,” Varykina G. Thackray, PhD, of the department of reproductive medicine and the center for reproductive science and medicine at the University of California, San Diego, said in an interview. “That means that these women are in a different group than other people with metabolic disorders, and it potentially gives us a way to think of new therapies that might be helpful for this specific group of women.”
When asked whether fecal transplants may be a potential therapy to help treat the metabolic issues associated with PCOS, Dr. Thackray stated that she did not believe a lot of women would use that as a therapy because of the “ick” factor. She stated the goal is to identify some beneficial bacteria that could be taken as a probiotic to help restore the gut microbiome.
Unfortunately, researchers still do not understand what causes PCOS. Some studies suggest that there are environmental and genetic factors, but there is nothing definitive. Dr. Thackray stated that getting more funding and conducting more research are the best ways to understand and combat this disorder.
Dr. Thackray is an associate professor of reproductive medicine at the University of California, San Diego.
Polycystic ovarian syndrome (PCOS) can manifest itself in many ways, but this study reveals that it can directly affect the metabolism of those who have the disorder.
“We’re still early days in studying this, but this study suggests that one of the clinical characteristics of these women with this disorder – their elevated testosterone – is correlated with changes in the gut microbiome,” Varykina G. Thackray, PhD, of the department of reproductive medicine and the center for reproductive science and medicine at the University of California, San Diego, said in an interview. “That means that these women are in a different group than other people with metabolic disorders, and it potentially gives us a way to think of new therapies that might be helpful for this specific group of women.”
When asked whether fecal transplants may be a potential therapy to help treat the metabolic issues associated with PCOS, Dr. Thackray stated that she did not believe a lot of women would use that as a therapy because of the “ick” factor. She stated the goal is to identify some beneficial bacteria that could be taken as a probiotic to help restore the gut microbiome.
Unfortunately, researchers still do not understand what causes PCOS. Some studies suggest that there are environmental and genetic factors, but there is nothing definitive. Dr. Thackray stated that getting more funding and conducting more research are the best ways to understand and combat this disorder.
Dr. Thackray is an associate professor of reproductive medicine at the University of California, San Diego.
according to a study from the Journal of Clinical Endocrinology and Metabolism.
“This study demonstrated that Caucasian women diagnosed with PCOS using the Rotterdam criteria had a reduction in overall species richness [alpha diversity] of the gut microbiome, compared to healthy women, and changes in the composition of the microbial community [beta diversity]” wrote Pedro J. Torres and his associates. “Interestingly, our study found that the biodiversity of the microbiome strongly correlated with hyperandrogenism.”
Dr. Torres of the University of California, San Diego, and his colleagues recruited 163 women at the University of Poznan (Poland) and conducted analysis on fecal samples to determine the effects of PCOS on the gut microbiome. Each woman underwent a battery of tests to determine whether she had PCOS or polycystic ovarian morphology (PCOM). Ovarian morphology was determined from a transvaginal ultrasound evaluation. The women were assessed for body mass index and hirsutism. Blood samples were taken to test for hormonal abnormalities common with PCOS and metabolic issues, like type 2 diabetes mellitus and glucose tolerance. Fecal samples were taken to analyze the gut microbiota of each study participant; analysis of the fecal samples generated gut microbial diversity profiles for each of the 163 women. Analysis of the samples was conducted at the University of California, San Diego.
Of the subjects, 48 were healthy, 42 had PCOM, and 73 were diagnosed with PCOS. The researches noted that, compared with healthy women and those with PCOM, women with PCOS had higher levels of serum total and free testosterone, as well as higher rates of hirsutism and fewer menses per year. These women also had higher levels of serum luteinizing hormone and increased ratios of luteinizing hormone to follicle stimulating hormone.
The DNA analysis of fecal samples yielded 481 sequence variants from the fecal swabs. Women with PCOS were found to have lower alpha diversity in their gut microbiome, as evidenced by abundance (P = .04) and Faith’s phylogenetic diveristy (P = .02). The luteinizing hormone to follicle stimulating hormone ratio also appeared to affect the alpha diversity of women with PCOS, as seen in observed sequence variants and Faith’s phylogenetic diversity (P = .08).
Beta diversity analysis, or the biodiversity between samples, revealed that hyperandrogenism could be a primary driver of changes in the gut microbiome. Using permutational multivariate analysis of variance, researchers determined that hyperandrogenism significantly affected beta diversity (P = .0009).
Androgens may help affect the gut microbiome in important ways, and changes in the gut microbiome may influence how the pathology of PCOS develops, according to Mr. Torres and his colleagues; however, more studies should be conducted to determine the effects of androgens on the gut microbiome.
“If hyperandrogenism drives the microbial composition of the gut, it would be interesting to determine if treatment of PCOS with androgen antagonists or oral contraceptives results in recovery of the gut microbiome and improvement of the PCOS metabolic phenotype” wrote Mr. Torres and his colleagues. “Moreover, it would be informative to determine whether the gut microbiome of women diagnosed with PCOS using the criteria of oligomenorrhea and polycystic ovaries is distinct from that of women diagnosed with the other subtypes of PCOS that include hyperandrogenism.”
The authors had no relevant financial disclosures to report.
SOURCE: Torres PJ et al. J Clin Endocrinol Metab. 2018 Jan 23. doi: 10.1210/jc.2017-02153.
according to a study from the Journal of Clinical Endocrinology and Metabolism.
“This study demonstrated that Caucasian women diagnosed with PCOS using the Rotterdam criteria had a reduction in overall species richness [alpha diversity] of the gut microbiome, compared to healthy women, and changes in the composition of the microbial community [beta diversity]” wrote Pedro J. Torres and his associates. “Interestingly, our study found that the biodiversity of the microbiome strongly correlated with hyperandrogenism.”
Dr. Torres of the University of California, San Diego, and his colleagues recruited 163 women at the University of Poznan (Poland) and conducted analysis on fecal samples to determine the effects of PCOS on the gut microbiome. Each woman underwent a battery of tests to determine whether she had PCOS or polycystic ovarian morphology (PCOM). Ovarian morphology was determined from a transvaginal ultrasound evaluation. The women were assessed for body mass index and hirsutism. Blood samples were taken to test for hormonal abnormalities common with PCOS and metabolic issues, like type 2 diabetes mellitus and glucose tolerance. Fecal samples were taken to analyze the gut microbiota of each study participant; analysis of the fecal samples generated gut microbial diversity profiles for each of the 163 women. Analysis of the samples was conducted at the University of California, San Diego.
Of the subjects, 48 were healthy, 42 had PCOM, and 73 were diagnosed with PCOS. The researches noted that, compared with healthy women and those with PCOM, women with PCOS had higher levels of serum total and free testosterone, as well as higher rates of hirsutism and fewer menses per year. These women also had higher levels of serum luteinizing hormone and increased ratios of luteinizing hormone to follicle stimulating hormone.
The DNA analysis of fecal samples yielded 481 sequence variants from the fecal swabs. Women with PCOS were found to have lower alpha diversity in their gut microbiome, as evidenced by abundance (P = .04) and Faith’s phylogenetic diveristy (P = .02). The luteinizing hormone to follicle stimulating hormone ratio also appeared to affect the alpha diversity of women with PCOS, as seen in observed sequence variants and Faith’s phylogenetic diversity (P = .08).
Beta diversity analysis, or the biodiversity between samples, revealed that hyperandrogenism could be a primary driver of changes in the gut microbiome. Using permutational multivariate analysis of variance, researchers determined that hyperandrogenism significantly affected beta diversity (P = .0009).
Androgens may help affect the gut microbiome in important ways, and changes in the gut microbiome may influence how the pathology of PCOS develops, according to Mr. Torres and his colleagues; however, more studies should be conducted to determine the effects of androgens on the gut microbiome.
“If hyperandrogenism drives the microbial composition of the gut, it would be interesting to determine if treatment of PCOS with androgen antagonists or oral contraceptives results in recovery of the gut microbiome and improvement of the PCOS metabolic phenotype” wrote Mr. Torres and his colleagues. “Moreover, it would be informative to determine whether the gut microbiome of women diagnosed with PCOS using the criteria of oligomenorrhea and polycystic ovaries is distinct from that of women diagnosed with the other subtypes of PCOS that include hyperandrogenism.”
The authors had no relevant financial disclosures to report.
SOURCE: Torres PJ et al. J Clin Endocrinol Metab. 2018 Jan 23. doi: 10.1210/jc.2017-02153.
FROM THE JOURNAL OF CLINICAL ENDOCRINOLOGY AND METABOLISM
Key clinical point: Hyperandrogenism may have an effect on the gut microbiome of women with PCOS.
Major finding: Lower bacterial diversity was observed in women with PCOS, compared with healthy women
Study details: Researchers recruited 163 women diagnosed with PCOS. Blood and fecal samples were collected, and ovaries were imaged using ultrasound.
Disclosures: The authors had no relevant financial disclosures to report.
Source: Torres PJ et al. J Clin Endocrinol Metab. 2018 Jan 23. doi: 10.1210/jc.2017-02153.
Abrupt behavior changes in autism? ID medical triggers first
NEW YORK – When treating children with autism spectrum disorder who develop an abrupt increase in symptoms, it is best to identify and treat the precipitating event or events – rather than intensify ASD drug therapy, an expert said.
“These acute behavior changes are almost always triggered by something,” Jeremy Veenstra-VanderWeele, MD, reported at a pediatric psychopharmacology update held by the American Academy of Child and Adolescent Psychiatry. Triggers are not always identifiable, but Dr. Veenstra-VanderWeele said solutions may prove simple when they are.

In ASD patients with an acute change in behavior, caregivers typically think first of environmental triggers, including adverse interactions with peers or siblings. But Dr. Veenstra-VanderWeele emphasized that medical problems should be considered first. This makes sense because of the importance of quickly resolving health problems. However, pain and discomfort, particularly in those with difficulty verbalizing these complaints, can be overlooked.
Moreover, even highly verbal ASD patients may not volunteer physical complaints without prompting, Dr. Veenstra-VanderWeele said. Among the health issues in children, constipation and other gastrointestinal issues are “incredibly common” in ASD patients. Dr. Veenstra-VanderWeele looks for clues, such as body posturing suggesting abdominal pain or flatulence, when a history is ambiguous.
“I will order an abdominal flat plate when I hear enough symptoms to make me wonder when the family is not sure,” Dr. Veenstra-VanderWeele reported. “Almost always it comes back with evidence of constipation. We treat it, and they are less irritable like all of us would be.”
All common conditions in a pediatric population, including ear infections, dental caries, and food allergies, should be considered, according to Dr. Veenstra-VanderWeele, who recommended a practice pathway for evaluating triggers in children with ASD (Pediatrics. 2016 Feb;137 Suppl 2:S136-48). A coauthor on this pathway, Dr. Veenstra-VanderWeele emphasized the importance of pursuing a systematic approach to medical issues before considering other triggers, such as psychosocial stressors.
In adolescents, headache caused by migraine and late-onset epilepsy, often in the form of complex partial seizures, should be added to the list of potential triggers for irritation or aggression, Dr. Veenstra-VanderWeele said. Epilepsy often precedes the diagnosis of ASD in young children, and Dr. Veenstra-VanderWeele noted that a second peak incidence sometimes occurs in late adolescence.
After ruling out medical problems, helping patients recognize and verbalize stressors can serve as both diagnosis and treatment. In ASD patients with limited verbal skills who are suffering from stress, “aggression is one form of communication,” Dr. Veenstra-VanderWeele said.
However, Dr. Veenstra-VanderWeele cautioned that, even if a trigger is successfully addressed, inadvertently reinforced aggression might persist.
“Aggression can be rewarded sometimes by removing the patient from the classroom, sometimes by giving in, and then that becomes a maladaptive reinforcement pattern that needs to be broken,” Dr. Veenstra-VanderWeele said. “Even if you are treating their irritability and agitation with, say, risperidone, you still need to break the maladaptive reinforcement pattern or they will keep engaging in what has become instrumental aggression.”
Dr. Veenstra-VanderWeele reported financial relationships with Hoffmann-La Roche, Novartis, Seaside Therapeutics, and SynapDx.
NEW YORK – When treating children with autism spectrum disorder who develop an abrupt increase in symptoms, it is best to identify and treat the precipitating event or events – rather than intensify ASD drug therapy, an expert said.
“These acute behavior changes are almost always triggered by something,” Jeremy Veenstra-VanderWeele, MD, reported at a pediatric psychopharmacology update held by the American Academy of Child and Adolescent Psychiatry. Triggers are not always identifiable, but Dr. Veenstra-VanderWeele said solutions may prove simple when they are.
In ASD patients with an acute change in behavior, caregivers typically think first of environmental triggers, including adverse interactions with peers or siblings. But Dr. Veenstra-VanderWeele emphasized that medical problems should be considered first. This makes sense because of the importance of quickly resolving health problems. However, pain and discomfort, particularly in those with difficulty verbalizing these complaints, can be overlooked.
Moreover, even highly verbal ASD patients may not volunteer physical complaints without prompting, Dr. Veenstra-VanderWeele said. Among the health issues in children, constipation and other gastrointestinal issues are “incredibly common” in ASD patients. Dr. Veenstra-VanderWeele looks for clues, such as body posturing suggesting abdominal pain or flatulence, when a history is ambiguous.
“I will order an abdominal flat plate when I hear enough symptoms to make me wonder when the family is not sure,” Dr. Veenstra-VanderWeele reported. “Almost always it comes back with evidence of constipation. We treat it, and they are less irritable like all of us would be.”
All common conditions in a pediatric population, including ear infections, dental caries, and food allergies, should be considered, according to Dr. Veenstra-VanderWeele, who recommended a practice pathway for evaluating triggers in children with ASD (Pediatrics. 2016 Feb;137 Suppl 2:S136-48). A coauthor on this pathway, Dr. Veenstra-VanderWeele emphasized the importance of pursuing a systematic approach to medical issues before considering other triggers, such as psychosocial stressors.
In adolescents, headache caused by migraine and late-onset epilepsy, often in the form of complex partial seizures, should be added to the list of potential triggers for irritation or aggression, Dr. Veenstra-VanderWeele said. Epilepsy often precedes the diagnosis of ASD in young children, and Dr. Veenstra-VanderWeele noted that a second peak incidence sometimes occurs in late adolescence.
After ruling out medical problems, helping patients recognize and verbalize stressors can serve as both diagnosis and treatment. In ASD patients with limited verbal skills who are suffering from stress, “aggression is one form of communication,” Dr. Veenstra-VanderWeele said.
However, Dr. Veenstra-VanderWeele cautioned that, even if a trigger is successfully addressed, inadvertently reinforced aggression might persist.
“Aggression can be rewarded sometimes by removing the patient from the classroom, sometimes by giving in, and then that becomes a maladaptive reinforcement pattern that needs to be broken,” Dr. Veenstra-VanderWeele said. “Even if you are treating their irritability and agitation with, say, risperidone, you still need to break the maladaptive reinforcement pattern or they will keep engaging in what has become instrumental aggression.”
Dr. Veenstra-VanderWeele reported financial relationships with Hoffmann-La Roche, Novartis, Seaside Therapeutics, and SynapDx.
NEW YORK – When treating children with autism spectrum disorder who develop an abrupt increase in symptoms, it is best to identify and treat the precipitating event or events – rather than intensify ASD drug therapy, an expert said.
“These acute behavior changes are almost always triggered by something,” Jeremy Veenstra-VanderWeele, MD, reported at a pediatric psychopharmacology update held by the American Academy of Child and Adolescent Psychiatry. Triggers are not always identifiable, but Dr. Veenstra-VanderWeele said solutions may prove simple when they are.
In ASD patients with an acute change in behavior, caregivers typically think first of environmental triggers, including adverse interactions with peers or siblings. But Dr. Veenstra-VanderWeele emphasized that medical problems should be considered first. This makes sense because of the importance of quickly resolving health problems. However, pain and discomfort, particularly in those with difficulty verbalizing these complaints, can be overlooked.
Moreover, even highly verbal ASD patients may not volunteer physical complaints without prompting, Dr. Veenstra-VanderWeele said. Among the health issues in children, constipation and other gastrointestinal issues are “incredibly common” in ASD patients. Dr. Veenstra-VanderWeele looks for clues, such as body posturing suggesting abdominal pain or flatulence, when a history is ambiguous.
“I will order an abdominal flat plate when I hear enough symptoms to make me wonder when the family is not sure,” Dr. Veenstra-VanderWeele reported. “Almost always it comes back with evidence of constipation. We treat it, and they are less irritable like all of us would be.”
All common conditions in a pediatric population, including ear infections, dental caries, and food allergies, should be considered, according to Dr. Veenstra-VanderWeele, who recommended a practice pathway for evaluating triggers in children with ASD (Pediatrics. 2016 Feb;137 Suppl 2:S136-48). A coauthor on this pathway, Dr. Veenstra-VanderWeele emphasized the importance of pursuing a systematic approach to medical issues before considering other triggers, such as psychosocial stressors.
In adolescents, headache caused by migraine and late-onset epilepsy, often in the form of complex partial seizures, should be added to the list of potential triggers for irritation or aggression, Dr. Veenstra-VanderWeele said. Epilepsy often precedes the diagnosis of ASD in young children, and Dr. Veenstra-VanderWeele noted that a second peak incidence sometimes occurs in late adolescence.
After ruling out medical problems, helping patients recognize and verbalize stressors can serve as both diagnosis and treatment. In ASD patients with limited verbal skills who are suffering from stress, “aggression is one form of communication,” Dr. Veenstra-VanderWeele said.
However, Dr. Veenstra-VanderWeele cautioned that, even if a trigger is successfully addressed, inadvertently reinforced aggression might persist.
“Aggression can be rewarded sometimes by removing the patient from the classroom, sometimes by giving in, and then that becomes a maladaptive reinforcement pattern that needs to be broken,” Dr. Veenstra-VanderWeele said. “Even if you are treating their irritability and agitation with, say, risperidone, you still need to break the maladaptive reinforcement pattern or they will keep engaging in what has become instrumental aggression.”
Dr. Veenstra-VanderWeele reported financial relationships with Hoffmann-La Roche, Novartis, Seaside Therapeutics, and SynapDx.
EXPERT ANALYSIS FROM the PSYCHOPHARMACOLOGY UPDATE INSTITUTE
No improvement in sight for Alzheimer’s drug development
Another one bites the dust.
Yet another investigational agent joins intepirdine, verubecestat, solanezumab, bapineuzumab, latrepirdine, and many others on the scrap pile of research: The complete release of trial data on idalopirdine found the drug wasn’t of clinically significant benefit in Alzheimer’s disease (JAMA. 2018;319[2]:130-42).
The numbers are bad enough that a handful of companies, including the giant Pfizer, have decided to leave Alzheimer’s drug development entirely to focus on more promising fields. And I get that. All of us – on any exhausting, fruitless, task – will reach the point where it’s time to cut our losses and move on. I don’t blame these companies for mostly leaving the field. (Pfizer is planning to form a neuroscience venture fund to support further research.)
Optimists will argue that you still learn things from a negative trial, which is true, but nothing to date is on the immediate horizon to help. The five agents we’ve had available for the past 15-20 years are all old enough to have lost their patents, and their benefits are modest, at best.
And all this going on as the overall human population, including myself, gradually ages and dementia becomes a medical-cost time bomb on the horizon. This isn’t an American problem. Every country in the world is facing it.
Politicians love to promise hope for these things: creating fast-track programs to get drugs to market faster, finding ways to bring down costs so more people can afford them, and improving methods to treat those in need. But none of those things matter if the medications don’t work.
Many of these trials test similar molecules because the evidence to date suggests they’re targeting the cause of Alzheimer’s. But so far they aren’t working. What if, as the Firesign Theatre and others have said, everything you know is wrong?

Perhaps our greatest quality as a species is resilience. We go on because we have to. The planet keeps moving around the sun as it has for almost 5 billion years, and we face tomorrow. Caregivers wake up for another day of doing their best for a faltering parent. I wake up for another day of doing my best to help them. And the researchers go back for another day hoping to find the real answer and treatment. Without trying, no treatment for anything will ever be found. We owe our patients, and ourselves, a better future than that.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.
Another one bites the dust.
Yet another investigational agent joins intepirdine, verubecestat, solanezumab, bapineuzumab, latrepirdine, and many others on the scrap pile of research: The complete release of trial data on idalopirdine found the drug wasn’t of clinically significant benefit in Alzheimer’s disease (JAMA. 2018;319[2]:130-42).
The numbers are bad enough that a handful of companies, including the giant Pfizer, have decided to leave Alzheimer’s drug development entirely to focus on more promising fields. And I get that. All of us – on any exhausting, fruitless, task – will reach the point where it’s time to cut our losses and move on. I don’t blame these companies for mostly leaving the field. (Pfizer is planning to form a neuroscience venture fund to support further research.)
Optimists will argue that you still learn things from a negative trial, which is true, but nothing to date is on the immediate horizon to help. The five agents we’ve had available for the past 15-20 years are all old enough to have lost their patents, and their benefits are modest, at best.
And all this going on as the overall human population, including myself, gradually ages and dementia becomes a medical-cost time bomb on the horizon. This isn’t an American problem. Every country in the world is facing it.
Politicians love to promise hope for these things: creating fast-track programs to get drugs to market faster, finding ways to bring down costs so more people can afford them, and improving methods to treat those in need. But none of those things matter if the medications don’t work.
Many of these trials test similar molecules because the evidence to date suggests they’re targeting the cause of Alzheimer’s. But so far they aren’t working. What if, as the Firesign Theatre and others have said, everything you know is wrong?
Perhaps our greatest quality as a species is resilience. We go on because we have to. The planet keeps moving around the sun as it has for almost 5 billion years, and we face tomorrow. Caregivers wake up for another day of doing their best for a faltering parent. I wake up for another day of doing my best to help them. And the researchers go back for another day hoping to find the real answer and treatment. Without trying, no treatment for anything will ever be found. We owe our patients, and ourselves, a better future than that.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.
Another one bites the dust.
Yet another investigational agent joins intepirdine, verubecestat, solanezumab, bapineuzumab, latrepirdine, and many others on the scrap pile of research: The complete release of trial data on idalopirdine found the drug wasn’t of clinically significant benefit in Alzheimer’s disease (JAMA. 2018;319[2]:130-42).
The numbers are bad enough that a handful of companies, including the giant Pfizer, have decided to leave Alzheimer’s drug development entirely to focus on more promising fields. And I get that. All of us – on any exhausting, fruitless, task – will reach the point where it’s time to cut our losses and move on. I don’t blame these companies for mostly leaving the field. (Pfizer is planning to form a neuroscience venture fund to support further research.)
Optimists will argue that you still learn things from a negative trial, which is true, but nothing to date is on the immediate horizon to help. The five agents we’ve had available for the past 15-20 years are all old enough to have lost their patents, and their benefits are modest, at best.
And all this going on as the overall human population, including myself, gradually ages and dementia becomes a medical-cost time bomb on the horizon. This isn’t an American problem. Every country in the world is facing it.
Politicians love to promise hope for these things: creating fast-track programs to get drugs to market faster, finding ways to bring down costs so more people can afford them, and improving methods to treat those in need. But none of those things matter if the medications don’t work.
Many of these trials test similar molecules because the evidence to date suggests they’re targeting the cause of Alzheimer’s. But so far they aren’t working. What if, as the Firesign Theatre and others have said, everything you know is wrong?
Perhaps our greatest quality as a species is resilience. We go on because we have to. The planet keeps moving around the sun as it has for almost 5 billion years, and we face tomorrow. Caregivers wake up for another day of doing their best for a faltering parent. I wake up for another day of doing my best to help them. And the researchers go back for another day hoping to find the real answer and treatment. Without trying, no treatment for anything will ever be found. We owe our patients, and ourselves, a better future than that.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.
VIDEO: Could targeting gut dysbiosis in MS prevent disease?
SAN DIEGO – Compelling findings in a genetically engineered mouse model of multiple sclerosis identify mechanisms of how adolescence and gut dysbiosis contribute to the risk of MS. In addition, disparities in gut microbiome species could explain why some people are at higher risk for developing multiple sclerosis, while others seem to enjoy a protective effect against development of this and other autoimmune diseases.
The hope is that these findings could pave the way for clinicians to potentially prevent development of multiple sclerosis in people at higher risk, perhaps through altering the gut flora and probiotic therapy, Suhayl Dhib-Jalbut, MD, said in a video interview at ACTRIMS Forum 2018, held by the Americas Committee for Treatment and Research in Multiple Sclerosis.
Dr. Dhib-Jalbut and his team discovered these findings using humanized transgenic mice – in other words, mice containing risk genes for triggering disease transferred from a patient with multiple sclerosis. The mice were more likely to develop MS-like disease at certain ages and in the presence of an altered gut microbiome or gut dysbiosis (Proc Natl Acad Sci U S A. 2017 Oct 31;114[44]:E9318-27).
Dr. Dhib-Jalbut is past president of ACTRIMS and is professor and chairman of the departments of neurology at Rutgers–Robert Wood Johnson Medical School, New Brunswick, N.J., and New Jersey Medical School, Newark. He has received research grants from Biogen and Teva, and is a consultant for Genzyme, Teva, Celgene, and, Mallinckrodt.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
SAN DIEGO – Compelling findings in a genetically engineered mouse model of multiple sclerosis identify mechanisms of how adolescence and gut dysbiosis contribute to the risk of MS. In addition, disparities in gut microbiome species could explain why some people are at higher risk for developing multiple sclerosis, while others seem to enjoy a protective effect against development of this and other autoimmune diseases.
The hope is that these findings could pave the way for clinicians to potentially prevent development of multiple sclerosis in people at higher risk, perhaps through altering the gut flora and probiotic therapy, Suhayl Dhib-Jalbut, MD, said in a video interview at ACTRIMS Forum 2018, held by the Americas Committee for Treatment and Research in Multiple Sclerosis.
Dr. Dhib-Jalbut and his team discovered these findings using humanized transgenic mice – in other words, mice containing risk genes for triggering disease transferred from a patient with multiple sclerosis. The mice were more likely to develop MS-like disease at certain ages and in the presence of an altered gut microbiome or gut dysbiosis (Proc Natl Acad Sci U S A. 2017 Oct 31;114[44]:E9318-27).
Dr. Dhib-Jalbut is past president of ACTRIMS and is professor and chairman of the departments of neurology at Rutgers–Robert Wood Johnson Medical School, New Brunswick, N.J., and New Jersey Medical School, Newark. He has received research grants from Biogen and Teva, and is a consultant for Genzyme, Teva, Celgene, and, Mallinckrodt.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
SAN DIEGO – Compelling findings in a genetically engineered mouse model of multiple sclerosis identify mechanisms of how adolescence and gut dysbiosis contribute to the risk of MS. In addition, disparities in gut microbiome species could explain why some people are at higher risk for developing multiple sclerosis, while others seem to enjoy a protective effect against development of this and other autoimmune diseases.
The hope is that these findings could pave the way for clinicians to potentially prevent development of multiple sclerosis in people at higher risk, perhaps through altering the gut flora and probiotic therapy, Suhayl Dhib-Jalbut, MD, said in a video interview at ACTRIMS Forum 2018, held by the Americas Committee for Treatment and Research in Multiple Sclerosis.
Dr. Dhib-Jalbut and his team discovered these findings using humanized transgenic mice – in other words, mice containing risk genes for triggering disease transferred from a patient with multiple sclerosis. The mice were more likely to develop MS-like disease at certain ages and in the presence of an altered gut microbiome or gut dysbiosis (Proc Natl Acad Sci U S A. 2017 Oct 31;114[44]:E9318-27).
Dr. Dhib-Jalbut is past president of ACTRIMS and is professor and chairman of the departments of neurology at Rutgers–Robert Wood Johnson Medical School, New Brunswick, N.J., and New Jersey Medical School, Newark. He has received research grants from Biogen and Teva, and is a consultant for Genzyme, Teva, Celgene, and, Mallinckrodt.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
EXPERT ANALYSIS FROM ACTRIMS FORUM 2018

Ticagrelor may be superior to clopidogrel in poor metabolizers
LOS ANGELES – In patients who had experienced a minor stroke or a transient ischemic attack with a moderate to high risk of stroke, the combination of ticagrelor and aspirin reduced the 90-day incidence of high on-treatment platelet reactivity, according to results from the PRINCE trial.
Although the combination outperformed clopidogrel (Plavix) plus aspirin, ticagrelor (Brilinta) was associated with higher bleeding risk.
The researchers also saw a trend toward a reduction in strokes that did not reach statistical significance, but the trial was halted following an interim analysis showing that the high on-treatment platelet reactivity (HOPR) endpoint, defined as P2Y12 reaction unit (PRU) greater than 208, showed a statistically significant difference. “To prove the clinical benefit, we will need a larger sample size,” study first author and presenter Yilong Wang, MD, PhD, of Beijing Tiantan Hospital, Capital Medical University, said in an interview at the International Stroke Conference, sponsored by the American Heart Association.

Previously, the SOCRATES trial found no advantage to treatment with ticagrelor over aspirin, but a prespecified exploratory analysis focusing on Asian patients (Stroke. 2017;48:167-73) found a trend toward reducing vascular events in the ticagrelor group, compared with patients taking aspirin.
In the Platelet Reactivity in Acute Stroke or Transient Ischemic Attack (PRINCE) trial, the researchers sought to examine the safety and efficacy of ticagrelor when compared with clopidogrel in 675 Asian patients (mean age 61 years, one-quarter of whom were female) from 26 centers in China and randomized them to ticagrelor plus aspirin (Tica) or clopidogrel plus aspirin (Clop). Within 24 hours of symptom onset, patients received 180 mg ticagrelor or 300 mg clopidogrel plus 100-300 mg aspirin. During days 1-21, they received 90 mg ticagrelor twice per day or 75 mg clopidogrel once per day. Both groups received 100 mg aspirin once per day. From day 21 to day 90, they received 90 mg ticagrelor twice per day or 75 mg clopidogrel once per day, with no aspirin.
At 90 days, the mean PRU value was 175.44 in the Clop group, compared with 69.24 in the Tica group. Overall, 27.7% of the Clop group experienced HOPR in the first 7 days, compared with 3.9% of the Tica group. At 90 days, 29.7% of the Clop group had experienced HOPR, compared with 12.5% of the Tica group (odds ratio, 0.33; 95% confidence interval, 0.21-0.51; P less than .001).
Ticagrelor was associated with greater benefit among those with impaired ability to metabolize clopidogrel. Among poor metabolizers, HOPR occurred in 10.5% in the Tica group and 42.4% of the Clop group (OR, 0.16; 95% CI, 0.05-0.56; P = .004). A similar favorable effect was seen in intermediate metabolizers in the Tica group (OR, 0.24; 95% CI, 0.12-0.49; P less than .001).
The 90-day stroke rate was no different between the Tica and Clop groups (6.3% vs. 8.8%, respectively; P = .20).
Minimal bleeding was higher in the Tica group (19.0% vs. 10.6%; hazard ratio, 1.86; P = .003), as was any bleeding (22.3% vs. 14.2%; HR, 1.65; P = .007). There were three deaths in the Tica group and two in the Clop group.
Dyspnea was the most common cause of drug discontinuation, and occurred in 4.2% of patients taking ticagrelor but none of the patients taking clopidogrel (P = .0001).
The researchers hope to demonstrate the clinical benefits of the combination in the upcoming PRINCE 2 trial. The results will have an important impact because CYP2C19 loss of function alleles are more common in Asian population. “It’s a very big problem for us,” Dr. Wang said.
The study was funded by the National Natural Science Foundation of China, the Beijing Institute for Brain, and the Beijing Municipal Science & Technology Commission of Cerebral Vascular Disease. AstraZeneca provided study drugs. Dr. Wang reported having no financial disclosures.
SOURCE: Wang Y et al. ISC 2018, abstract LB8
LOS ANGELES – In patients who had experienced a minor stroke or a transient ischemic attack with a moderate to high risk of stroke, the combination of ticagrelor and aspirin reduced the 90-day incidence of high on-treatment platelet reactivity, according to results from the PRINCE trial.
Although the combination outperformed clopidogrel (Plavix) plus aspirin, ticagrelor (Brilinta) was associated with higher bleeding risk.
The researchers also saw a trend toward a reduction in strokes that did not reach statistical significance, but the trial was halted following an interim analysis showing that the high on-treatment platelet reactivity (HOPR) endpoint, defined as P2Y12 reaction unit (PRU) greater than 208, showed a statistically significant difference. “To prove the clinical benefit, we will need a larger sample size,” study first author and presenter Yilong Wang, MD, PhD, of Beijing Tiantan Hospital, Capital Medical University, said in an interview at the International Stroke Conference, sponsored by the American Heart Association.
Previously, the SOCRATES trial found no advantage to treatment with ticagrelor over aspirin, but a prespecified exploratory analysis focusing on Asian patients (Stroke. 2017;48:167-73) found a trend toward reducing vascular events in the ticagrelor group, compared with patients taking aspirin.
In the Platelet Reactivity in Acute Stroke or Transient Ischemic Attack (PRINCE) trial, the researchers sought to examine the safety and efficacy of ticagrelor when compared with clopidogrel in 675 Asian patients (mean age 61 years, one-quarter of whom were female) from 26 centers in China and randomized them to ticagrelor plus aspirin (Tica) or clopidogrel plus aspirin (Clop). Within 24 hours of symptom onset, patients received 180 mg ticagrelor or 300 mg clopidogrel plus 100-300 mg aspirin. During days 1-21, they received 90 mg ticagrelor twice per day or 75 mg clopidogrel once per day. Both groups received 100 mg aspirin once per day. From day 21 to day 90, they received 90 mg ticagrelor twice per day or 75 mg clopidogrel once per day, with no aspirin.
At 90 days, the mean PRU value was 175.44 in the Clop group, compared with 69.24 in the Tica group. Overall, 27.7% of the Clop group experienced HOPR in the first 7 days, compared with 3.9% of the Tica group. At 90 days, 29.7% of the Clop group had experienced HOPR, compared with 12.5% of the Tica group (odds ratio, 0.33; 95% confidence interval, 0.21-0.51; P less than .001).
Ticagrelor was associated with greater benefit among those with impaired ability to metabolize clopidogrel. Among poor metabolizers, HOPR occurred in 10.5% in the Tica group and 42.4% of the Clop group (OR, 0.16; 95% CI, 0.05-0.56; P = .004). A similar favorable effect was seen in intermediate metabolizers in the Tica group (OR, 0.24; 95% CI, 0.12-0.49; P less than .001).
The 90-day stroke rate was no different between the Tica and Clop groups (6.3% vs. 8.8%, respectively; P = .20).
Minimal bleeding was higher in the Tica group (19.0% vs. 10.6%; hazard ratio, 1.86; P = .003), as was any bleeding (22.3% vs. 14.2%; HR, 1.65; P = .007). There were three deaths in the Tica group and two in the Clop group.
Dyspnea was the most common cause of drug discontinuation, and occurred in 4.2% of patients taking ticagrelor but none of the patients taking clopidogrel (P = .0001).
The researchers hope to demonstrate the clinical benefits of the combination in the upcoming PRINCE 2 trial. The results will have an important impact because CYP2C19 loss of function alleles are more common in Asian population. “It’s a very big problem for us,” Dr. Wang said.
The study was funded by the National Natural Science Foundation of China, the Beijing Institute for Brain, and the Beijing Municipal Science & Technology Commission of Cerebral Vascular Disease. AstraZeneca provided study drugs. Dr. Wang reported having no financial disclosures.
SOURCE: Wang Y et al. ISC 2018, abstract LB8
LOS ANGELES – In patients who had experienced a minor stroke or a transient ischemic attack with a moderate to high risk of stroke, the combination of ticagrelor and aspirin reduced the 90-day incidence of high on-treatment platelet reactivity, according to results from the PRINCE trial.
Although the combination outperformed clopidogrel (Plavix) plus aspirin, ticagrelor (Brilinta) was associated with higher bleeding risk.
The researchers also saw a trend toward a reduction in strokes that did not reach statistical significance, but the trial was halted following an interim analysis showing that the high on-treatment platelet reactivity (HOPR) endpoint, defined as P2Y12 reaction unit (PRU) greater than 208, showed a statistically significant difference. “To prove the clinical benefit, we will need a larger sample size,” study first author and presenter Yilong Wang, MD, PhD, of Beijing Tiantan Hospital, Capital Medical University, said in an interview at the International Stroke Conference, sponsored by the American Heart Association.
Previously, the SOCRATES trial found no advantage to treatment with ticagrelor over aspirin, but a prespecified exploratory analysis focusing on Asian patients (Stroke. 2017;48:167-73) found a trend toward reducing vascular events in the ticagrelor group, compared with patients taking aspirin.
In the Platelet Reactivity in Acute Stroke or Transient Ischemic Attack (PRINCE) trial, the researchers sought to examine the safety and efficacy of ticagrelor when compared with clopidogrel in 675 Asian patients (mean age 61 years, one-quarter of whom were female) from 26 centers in China and randomized them to ticagrelor plus aspirin (Tica) or clopidogrel plus aspirin (Clop). Within 24 hours of symptom onset, patients received 180 mg ticagrelor or 300 mg clopidogrel plus 100-300 mg aspirin. During days 1-21, they received 90 mg ticagrelor twice per day or 75 mg clopidogrel once per day. Both groups received 100 mg aspirin once per day. From day 21 to day 90, they received 90 mg ticagrelor twice per day or 75 mg clopidogrel once per day, with no aspirin.
At 90 days, the mean PRU value was 175.44 in the Clop group, compared with 69.24 in the Tica group. Overall, 27.7% of the Clop group experienced HOPR in the first 7 days, compared with 3.9% of the Tica group. At 90 days, 29.7% of the Clop group had experienced HOPR, compared with 12.5% of the Tica group (odds ratio, 0.33; 95% confidence interval, 0.21-0.51; P less than .001).
Ticagrelor was associated with greater benefit among those with impaired ability to metabolize clopidogrel. Among poor metabolizers, HOPR occurred in 10.5% in the Tica group and 42.4% of the Clop group (OR, 0.16; 95% CI, 0.05-0.56; P = .004). A similar favorable effect was seen in intermediate metabolizers in the Tica group (OR, 0.24; 95% CI, 0.12-0.49; P less than .001).
The 90-day stroke rate was no different between the Tica and Clop groups (6.3% vs. 8.8%, respectively; P = .20).
Minimal bleeding was higher in the Tica group (19.0% vs. 10.6%; hazard ratio, 1.86; P = .003), as was any bleeding (22.3% vs. 14.2%; HR, 1.65; P = .007). There were three deaths in the Tica group and two in the Clop group.
Dyspnea was the most common cause of drug discontinuation, and occurred in 4.2% of patients taking ticagrelor but none of the patients taking clopidogrel (P = .0001).
The researchers hope to demonstrate the clinical benefits of the combination in the upcoming PRINCE 2 trial. The results will have an important impact because CYP2C19 loss of function alleles are more common in Asian population. “It’s a very big problem for us,” Dr. Wang said.
The study was funded by the National Natural Science Foundation of China, the Beijing Institute for Brain, and the Beijing Municipal Science & Technology Commission of Cerebral Vascular Disease. AstraZeneca provided study drugs. Dr. Wang reported having no financial disclosures.
SOURCE: Wang Y et al. ISC 2018, abstract LB8
REPORTING FROM ISC 2018
Key clinical point: Ticagrelor may be a better option than clopidogrel in patients with loss-of-function CYP2C19 alleles.
Major finding: Patients on ticagrelor had a lower 90-day risk of high on-treatment platelet reactivity (OR, 0.33).
Data source: Randomized, open-label trial with blinded assessments (n = 675).
Disclosures: The study was funded by the National Natural Science Foundation of China, the Beijing Institute for Brain, and the Beijing Municipal Science & Technology Commission of Cerebral Vascular Disease. AstraZeneca provided study drugs. Dr. Wang reported having no financial disclosures.
Source: Wang Y et al. ISC 2018, abstract LB8
Baby boomers are the hepatitis C generation
Increases in hepatitis C–related inpatient stays for baby boomers from 2005 to 2014 far outpaced those of older adults, while younger adults saw their admissions drop over that period, according to the Agency for Healthcare Research and Quality.
For the baby boomers (adults aged 52-72 years), the rate of inpatient stays involving hepatitis C with or without hepatitis B, HIV, or alcoholic liver disease rose from 300.7 per 100,000 population in 2005 to 503.1 per 100,000 in 2014 – an increase of over 67%. For patients aged 73 years and older, that rate went from 104.4 in 2005 to 117.1 in 2014, which translates to a 12% increase, and for patients aged 18-51 years, it dropped 15%, from 182.5 to 155.4, the AHRQ said in a statistical brief.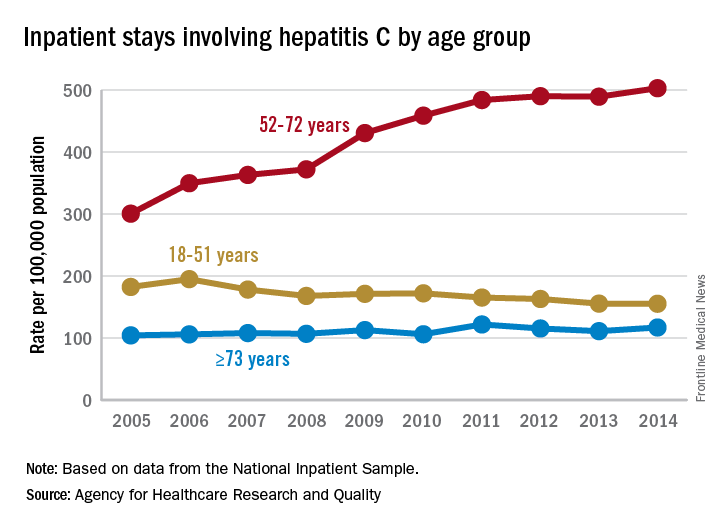
Along with the increased hospitalizations, “acute hepatitis C cases nearly tripled from 2010 through 2015,” the report noted, which was “likely the result of increasing injection drug use due to the growing opioid epidemic.”
AGA offers tools to help you become more efficient, understand quality standards, and improve the process of care for your hepatitis C patients.
Increases in hepatitis C–related inpatient stays for baby boomers from 2005 to 2014 far outpaced those of older adults, while younger adults saw their admissions drop over that period, according to the Agency for Healthcare Research and Quality.
For the baby boomers (adults aged 52-72 years), the rate of inpatient stays involving hepatitis C with or without hepatitis B, HIV, or alcoholic liver disease rose from 300.7 per 100,000 population in 2005 to 503.1 per 100,000 in 2014 – an increase of over 67%. For patients aged 73 years and older, that rate went from 104.4 in 2005 to 117.1 in 2014, which translates to a 12% increase, and for patients aged 18-51 years, it dropped 15%, from 182.5 to 155.4, the AHRQ said in a statistical brief.
Along with the increased hospitalizations, “acute hepatitis C cases nearly tripled from 2010 through 2015,” the report noted, which was “likely the result of increasing injection drug use due to the growing opioid epidemic.”
AGA offers tools to help you become more efficient, understand quality standards, and improve the process of care for your hepatitis C patients.
Increases in hepatitis C–related inpatient stays for baby boomers from 2005 to 2014 far outpaced those of older adults, while younger adults saw their admissions drop over that period, according to the Agency for Healthcare Research and Quality.
For the baby boomers (adults aged 52-72 years), the rate of inpatient stays involving hepatitis C with or without hepatitis B, HIV, or alcoholic liver disease rose from 300.7 per 100,000 population in 2005 to 503.1 per 100,000 in 2014 – an increase of over 67%. For patients aged 73 years and older, that rate went from 104.4 in 2005 to 117.1 in 2014, which translates to a 12% increase, and for patients aged 18-51 years, it dropped 15%, from 182.5 to 155.4, the AHRQ said in a statistical brief.
Along with the increased hospitalizations, “acute hepatitis C cases nearly tripled from 2010 through 2015,” the report noted, which was “likely the result of increasing injection drug use due to the growing opioid epidemic.”
AGA offers tools to help you become more efficient, understand quality standards, and improve the process of care for your hepatitis C patients.