Supply of the only U.S.-licensed yellow fever vaccine will be depleted by mid-2017 because of manufacturing issues, according to the Centers for Disease Control and Prevention.
Sanofi Pasteur, the manufacturer of the YF-VAX vaccine, notified the CDC and the Food and Drug Administration in 2016 there could be a shortage this year after the manufacturing complications during a factory switch over led to the loss of a large amount of vaccine supply, according to an article published online in the Morbidity and Mortality Weekly Report.
The shortage is expected to affect government workers and military personnel as well as private travelers, 8 million of whom traveled to at least one of 42 countries with endemic yellow fever virus transmission in 2015 (MMWR. 2017 Apr 28. doi: 10.15585/mmwr.mm6617e2).
The CDC, Sanofi Pasteur, and the FDA are working to supplement the shortage. The manufacturer submitted an expanded investigational new drug (eIND) application to the FDA in September 2016 for marketing permission for Stamaril, an alternative vaccine manufactured by Sanofi Pasteur France and used in around 70 countries.
The application included planning for strategic distribution sites, which the CDC is determining using a tiered system based on volume of doses ordered in 2016.
As of April 2017, 250 civilian sites have been invited to participate in the eIND program, significantly less than the 4,000 currently distributing YF-VAX.
The CDC will “monitor for critical gaps in vaccine access and collaborate to address any issues, including considering the possibility of recruiting additional clinics to participate as necessary,” according to a statement.
Supply of the only U.S.-licensed yellow fever vaccine will be depleted by mid-2017 because of manufacturing issues, according to the Centers for Disease Control and Prevention.
Sanofi Pasteur, the manufacturer of the YF-VAX vaccine, notified the CDC and the Food and Drug Administration in 2016 there could be a shortage this year after the manufacturing complications during a factory switch over led to the loss of a large amount of vaccine supply, according to an article published online in the Morbidity and Mortality Weekly Report.
The shortage is expected to affect government workers and military personnel as well as private travelers, 8 million of whom traveled to at least one of 42 countries with endemic yellow fever virus transmission in 2015 (MMWR. 2017 Apr 28. doi: 10.15585/mmwr.mm6617e2).
The CDC, Sanofi Pasteur, and the FDA are working to supplement the shortage. The manufacturer submitted an expanded investigational new drug (eIND) application to the FDA in September 2016 for marketing permission for Stamaril, an alternative vaccine manufactured by Sanofi Pasteur France and used in around 70 countries.
The application included planning for strategic distribution sites, which the CDC is determining using a tiered system based on volume of doses ordered in 2016.
As of April 2017, 250 civilian sites have been invited to participate in the eIND program, significantly less than the 4,000 currently distributing YF-VAX.
The CDC will “monitor for critical gaps in vaccine access and collaborate to address any issues, including considering the possibility of recruiting additional clinics to participate as necessary,” according to a statement.
Supply of the only U.S.-licensed yellow fever vaccine will be depleted by mid-2017 because of manufacturing issues, according to the Centers for Disease Control and Prevention.
Sanofi Pasteur, the manufacturer of the YF-VAX vaccine, notified the CDC and the Food and Drug Administration in 2016 there could be a shortage this year after the manufacturing complications during a factory switch over led to the loss of a large amount of vaccine supply, according to an article published online in the Morbidity and Mortality Weekly Report.
The shortage is expected to affect government workers and military personnel as well as private travelers, 8 million of whom traveled to at least one of 42 countries with endemic yellow fever virus transmission in 2015 (MMWR. 2017 Apr 28. doi: 10.15585/mmwr.mm6617e2).
The CDC, Sanofi Pasteur, and the FDA are working to supplement the shortage. The manufacturer submitted an expanded investigational new drug (eIND) application to the FDA in September 2016 for marketing permission for Stamaril, an alternative vaccine manufactured by Sanofi Pasteur France and used in around 70 countries.
The application included planning for strategic distribution sites, which the CDC is determining using a tiered system based on volume of doses ordered in 2016.
As of April 2017, 250 civilian sites have been invited to participate in the eIND program, significantly less than the 4,000 currently distributing YF-VAX.
The CDC will “monitor for critical gaps in vaccine access and collaborate to address any issues, including considering the possibility of recruiting additional clinics to participate as necessary,” according to a statement.
Association of inpatient antimicrobial utilization measures with antimicrobial stewardship activities and facility characteristics of Veterans Affairs medical centers
The deleterious impact of inappropriate and/or excessive antimicrobial usage is well recognized. In the United States, the Centers for Disease Control and Prevention (CDC) estimates that at least 2 million people become infected with antimicrobial-resistant bacteria with 23,000 subsequent deaths and at least $1 billion in excess medical costs per year.1
In response, many healthcare organizations have developed antimicrobial stewardship programs (ASPs). Guidelines co-sponsored by the Infectious Diseases Society of America and the Society for Healthcare Epidemiology of America, as well as recent statements from the CDC and the Transatlantic Taskforce on Antimicrobial Resistance,all recommend core ASP elements.2-5 The guidelines provide general recommendations on ASP structure, strategies, and activities. The recommended ASP structure is a team of physicians and pharmacists that collaborates with facility governing committees and other stakeholders to optimize antimicrobial use. While personnel with expertise in infectious diseases (ID) often lead ASPs, hospitalists are also recognized as key contributors, especially in quality improvement.6,7 Recommended strategies include prospective audit of antimicrobial use with intervention and feedback and formulary restriction with preauthorization. Recommended activities include education, creation of guidelines, clinical pathways, and order forms, and programs to promote de-escalation and conversion from parenteral (IV) to oral (PO) antimicrobial therapy. However, limited evidence exists regarding the effectiveness of these ASP core elements.8,9 While Cochrane reviews found clear evidence that particular stewardship strategies (eg, audit and feedback, formulary restriction, guidelines implemented with or without feedback, protocols, computerized decision support) can be effective in reducing antimicrobial usage and improving clinical outcomes over the long term, little evidence exists favoring 1 strategy over another.8 Furthermore, most individual studies of ASPs are single-center, making their conclusions less generalizable.
In 2012, the VA National Antimicrobial Stewardship Task Force (ASTF), in conjunction with the VA Healthcare Analysis and Information Group (HAIG) administered a survey on the characteristics of ASPs at all 130 acute care VA facilities (Appendix A). We used these survey results to build an implementation model and then assess associations between facility-level variables and 4 antimicrobial utilization measures.
METHODS
Survey and Data
In 2011, the ASTF was chartered to develop, deploy, and monitor a strategic plan for optimizing antimicrobial therapy management. Monthly educational webinars and sample policies were offered to all facilities, including a sample business plan for stewardship and policies to encourage de-escalation from broad-spectrum antimicrobials, promote conversion from parenteral to oral antimicrobial therapy, avoid unnecessary double anaerobic coverage, and mitigate unnecessary antimicrobial usage in the context of Clostridium difficile infection.10
At the time that ASTF was chartered, the understanding of how ASP structures across VA facilities operated was limited. Hence, to capture baseline institutional characteristics and stewardship activities, ASTF and HAIG developed an inventory assessment of ASPs that was distributed online in November 2012. All 130 VA facilities providing inpatient acute care services responded.
We derived 57 facility characteristics relevant to antimicrobial utilization and conducted a series of factor analyses to simplify the complex dataset, and identify underlying latent constructs. We categorized resulting factors into domains of evidence, context, or facilitation as guided by the Promoting Action on Research Implementation in Health Services framework.11 Briefly, the evidence domain describes how the facility uses codified and noncodified sources of knowledge (eg, research evidence, clinical experience). Organizational context comprises a facility’s characteristics that ensure a more conducive environment to put evidence into practice (eg, supportive leadership, organizational structure, evaluative systems). Facilitation emphasizes a facility personnel’s “state of preparedness” and receptivity to implementation.
Using factor analysis to identify facility factors as correlates of the outcomes, we first examined polychoric correlations among facility characteristics to assess multicollinearity. We performed independent component analysis to create latent constructs of variables that were defined by factor loadings (that indicated the proportion of variance accounted for by the construct) and uniqueness factors (that determined how well the variables were interpreted by the construct). Factors retained included variables that had uniqueness values of less than 0.7 and factor loadings greater than 0.3. Those associated with uniqueness values greater than 0.7 were left as single items, as were characteristics deemed a priori to be particularly important to antimicrobial stewardship. Factor scales that had only 2 items were converted into indices, while factor scores were generated for those factors that contained 3 or more items.12-15
Data for facility-level antimicrobial utilization measures were obtained from the VA Corporate Data Warehouse from calendar year 2012. The analysis was conducted within the VA Informatics and Computing Infrastructure. All study procedures were approved by the VA Central Institutional Review Board.
Measures
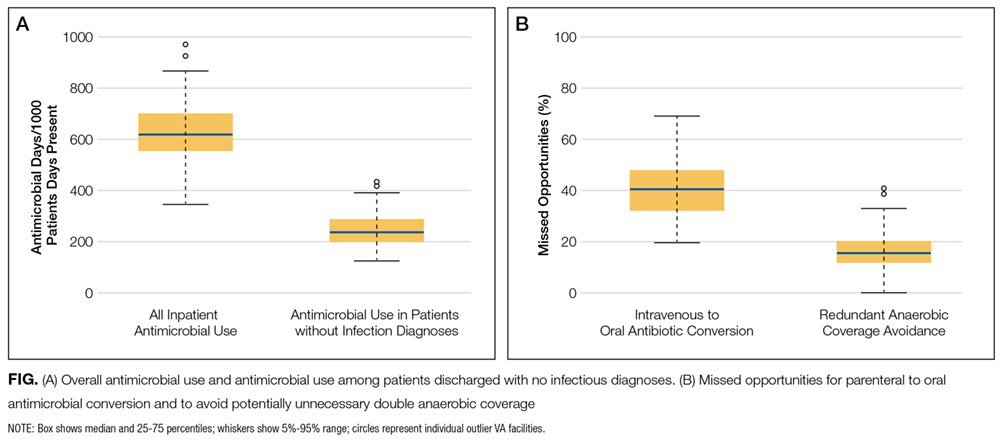
Four utilization measures were defined as dependent measures: overall antimicrobial use; antimicrobial use in patients with non-infectious discharge diagnoses; missed opportunities to convert from parenteral to oral antimicrobial therapy; and missed opportunities to avoid double anaerobic coverage with metronidazole.
Overall antimicrobial use was defined as total acute care (ie, medical/surgical/intensive care) antibacterial use for each facility aggregated as per CDC National Healthcare Safety Network Antimicrobial Use Option guidelines (antimicrobial days per 1000 patient days present). A subanalysis of overall antimicrobial use was restricted to antimicrobial use among patients without an infection-related discharge diagnosis, as we surmised that this measure may capture a greater proportion of potentially unnecessary antimicrobial use. International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM)16 codes for infectious processes were identified by a combination of those classified previously in the literature,17 and those identified by finding the descendants of all infections named in the Systematized Nomenclature of Medicine--Clinical Terms.18 Next, all remaining codes for principal discharge diagnoses for which antimicrobials were administered were reviewed for potential indications for systemic antibacterial use. Discharges were considered noninfectious if no codes were identified when systemic antimicrobials were or could be indicated. For this measure, antimicrobial days were not counted if administered on or 1 day after the calendar day of surgery warranting antimicrobial prophylaxis.
Missed opportunities for conversion from parenteral to oral (IV to PO) formulations of highly bioavailable oral antimicrobials (ciprofloxacin, levofloxacin, moxifloxacin, azithromycin, clindamycin, linezolid, metronidazole, and fluconazole) were defined as the percentage of days of unnecessary IV therapy that were given when PO therapy could have been used among patients who were not in intensive care units at the time of antimicrobial administration who were receiving other oral medications, using previously described methodology.19Missed opportunities for avoiding redundant anaerobic coverage with metronidazole were defined as the percentage of days in which patients receiving metronidazole also receivedantibiotics with activity against anaerobic bacteria, specifically beta-lactam/beta-lactamase inhibitors, carbapenems, cefotetan/cefoxitin, clindamycin, moxifloxacin, or tigecycline), using previously described methodology.20 Patients for whom C. difficile testing was either ordered or positive within the prior 28 days (indicating potential clinical concern for C. difficile infection) were excluded from this endpoint.
Analysis
The variables derived above were entered into a multivariable model for each of the 4 antimicrobial utilization measures. The least absolute shrinkage and selection operator (LASSO) regression was used to determine significant associations between variables and individual utilization measures.21 LASSO was chosen because it offers advantages over traditional subset selection approaches in large multivariable analyses by assessing covariates simultaneously rather than sequentially, supporting prediction rather than estimation of effect.22P values were not reported as they are not useful in determining statistical significance in this methodology. A tuning parameter of 0.025 was determined for the model based on a cross-validation approach. Significant variables remaining in the model were reported with the percent change in each utilization measure per unit change in the variable of interest. For binary factors, percent change was reported according to whether the variable was present or not. For ordinal variables, percent change was reported according to incremental increase in ordinal score. For continuous variables or variables represented by factor or index scores, percent change was reported per each 25% increase in the range of the score.
RESULTS
Inpatient Facility Antimicrobial Stewardship Characteristics and Antimicrobial Utilization
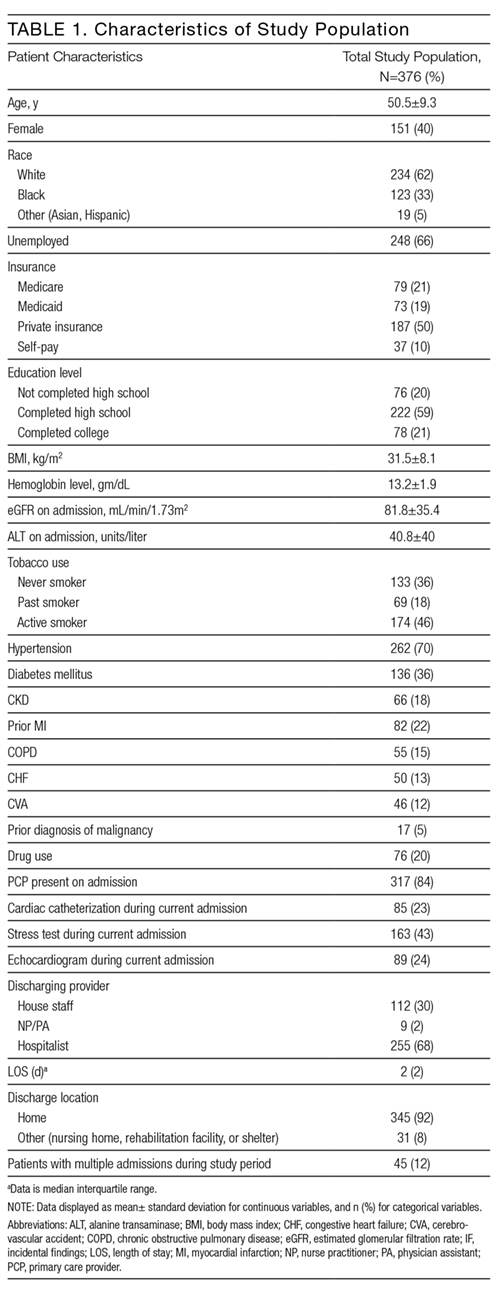
Frequencies of key facility characteristics that contributed to variable development are included in Table 1. Full survey results across all facilities are included in Appendix B. Factor analysis reduced the total number of variables to 32; however, we also included hospital size and VA complexity score. Thus, 34 variables were evaluated for association with antimicrobial utilization measures: 4 in the evidence domain, 23 in the context domain, and 7 in the facilitation domain (Table 2).
Table 1
Table 1 (continued)
Median facility antimicrobial use was 619 antimicrobial days per 1000 days present (interquartile range [IQR], 554-700; overall range, 346-974). Median facility noninfectious antimicrobial use was 236 per 1000 days present (IQR, 200-286). Missed opportunities for conversion from IV to PO antimicrobial therapy were common, with a median facility value of 40.4% (391/969) of potentially eligible days of therapy (IQR, 32.2-47.8%). Missed opportunities to avoid double anaerobic coverage were less common (median 15.3% (186/1214) of potentially eligible days of therapy (IQR, 11.8%-20.2%; Figure).
Overall Antimicrobial Use
Four variables were associated with decreased overall antimicrobial use, although with small magnitude of change: presence of postgraduate physician/pharmacy training programs (0.03% decrease per quarter increase in factor score; on the order of 0.2 antimicrobial days per 1000 patient days present), presence of pharmacists and/or ID attendings on general medicine ward teams (0.02% decrease per quarter increase in index score), frequency of systematic de-escalation review (0.01% decrease per ordinal increase in score), and degree of involvement of ID physicians and/or fellows in antimicrobial approvals (0.007% decrease per quarter increase in index score). No variables were associated with increased overall antimicrobial use.
Table 2
Table 2 (continued)
Antimicrobial Use among Discharges without Infectious Diagnoses
Six variables were associated with decreased antimicrobial use in patients without infectious discharge diagnoses, while 4 variables were associated with increased use. Variables associated with the greatest magnitude of decreased use included facility educational programs for prudent antimicrobial use (1.8% on the order of 4 antimicrobial days per 1000 patient days present), frequency of systematic de-escalation review (1.5% per incremental increase in score), and whether a facility’s lead antimicrobial stewardship pharmacist had ID training (1.3%). Also significantly associated with decreased use was a factor summarizing the presence of 4 condition-specific stewardship processes (de-escalation policies, policies for addressing antimicrobial use in the context of C. difficile infection, blood culture review, and automatic ID consults for certain conditions) (0.6% per quarter increase in factor score range), the extent to which postgraduate physician/pharmacy training programs were present (0.6% per quarter increase in factor score range), and the number of electronic antimicrobial-specific order sets present (0.4% per order set). The variables associated with increased use of antimicrobials included the presence of antimicrobial stop orders (4.6%), the degree to which non-ID physicians were involved in antimicrobial approvals (0.7% per increase in ordinal score), the level engagement with ASTF online resources (0.6% per quarter increase in factor score range), and hospital size (0.6% per 50-bed increase).
Figure
Missed Opportunities for Parenteral to Oral Antimicrobial Conversion
Missed opportunities for IV to PO antimicrobial conversion had the largest number of significant associations with organizational variables: 14 variables were associated with fewer missed opportunities, while 5 were associated with greater missed opportunities. Variables associated with the largest reductions in missed opportunities for IV to PO conversion included having guidelines for antimicrobial duration (12.8%), participating in regional stewardship collaboratives (8.1%), number of antimicrobial-specific order sets (6.0% per order set), ID training of the ASP pharmacist (4.9%), and VA facility complexity designation (4.2% per quarter increase in score indicating greater complexity).23 Variables associated with more missed opportunities included stop orders (11.7%), overall perceived receptiveness to antimicrobial stewardship among clinical services (9.4%), the degree of engagement with ASTF online resources (6.9% per quarter increase in factor score range), educational programs for prudent antimicrobial use (4.1%), and hospital size (1.0% per 50-bed increase).
Missed Opportunities for Avoidance of Double Anaerobic Coverage
Four variables were associated with more avoidance of double anaerobic coverage: ID training of the lead ASP pharmacist (8.8%), presence of pharmacists and/or ID attendings on acute care ward teams (6.2% per quarter increase in index score), degree of ID pharmacist involvement in antimicrobial approvals, ranging from not at all (score=0) to both weekdays and nights/weekends (score=2; 4.3% per ordinal increase), and the number of antimicrobial-specific order sets (1.5% per order set). No variables were associated with less avoidance of double anaerobic coverage.
Variables Associated with Multiple Favorable or Unfavorable Antimicrobial Utilization Measures
To better assess the consistency of the relationship between organizational variables and measures of antimicrobial use, we tabulated variables that were associated with at least 3 potentially favorable (ie, reduced overall or noninfectious antimicrobial use or fewer missed opportunities) measures. Altogether, 5 variables satisfied this criterion: the presence of postgraduate physician/pharmacy training programs, the number of antimicrobial-specific order sets, frequency of systematic de-escalation review, the presence of pharmacists and/or ID attendings on acute care ward teams, and formal ID training of the lead ASP pharmacist (Table 3). Three other variables were associated with at least 2 unfavorable measures: hospital size, the degree to which the facility engaged with ASTF online resources, and presence of antimicrobial stop orders.
Table 3
DISCUSSION
Variability in ASP implementation across VA allowed us to assess the relationship between ASP and facility elements and baseline patterns of antimicrobial utilization. Hospitalists and hospital policy-makers are becoming more and more engaged in inpatient antimicrobial stewardship. While our results suggest that having pharmacists and/or physicians with formal ID training participate in everyday inpatient activities can favorably improve antimicrobial utilization, considerable input into stewardship can be made by hospitalists and policy makers. In particular, based on this work, the highest yield from an organizational standpoint may be in working to develop order sets within the electronic medical record and systematic efforts to promote de-escalation of broad-spectrum therapy, as well as encouraging hospital administration to devote specific physician and pharmacy salary support to stewardship efforts.
While we noted that finding the ASTF online resources helpful was associated with potentially unfavorable antimicrobial utilization, we speculate that this may represent reverse causality due to facilities recognizing that their antimicrobial usage is suboptimal and thus seeking out sample ASTF policies to implement. The association between the presence of automatic stop orders and potentially unfavorable antimicrobial utilization is less clear since the timeframe was not specified in the survey; it may be that setting stop orders too far in advance may promote an environment in which critical thinking about antimicrobial de-escalation is not encouraged or timely. The larger magnitude of association between ASP characteristics and antimicrobial usage among patients without infectious discharge diagnoses versus overall antimicrobial usage also suggests that clinical situations where infection was of low enough suspicion to not even have the providers eventually list an infectious diagnosis on their discharge summaries may be particularly malleable to ASP interventions, though further exploration is needed in determining how useful this utilization measure may be as a marker for inappropriate antimicrobial use.
Our results complement those of Pakyz et al.24 who surveyed 44 academic medical facilities in March 2013 to develop an ASP intensity score and correlate this score and its specific components to overall and targeted antimicrobial use. This study found that the overall ASP intensity score was not significantly associated with total or targeted antimicrobial use. However, ASP strategies were more associated with decreased total and targeted antimicrobial use than were specific ASP resources. In particular, the presence of a preauthorization strategy was associated with decreased targeted antimicrobial use. Our particular findings that order set establishment and de-escalation efforts are associated with multiple antibiotic outcomes also line up with the findings of Schuts et al,who performed a meta-analysis of the effects of meeting antimicrobial stewardship objectives and found that achieving guideline concordance (such as through establishment of order sets) and successfully de-escalating antimicrobial therapy was associated with reduced mortality.25,26 This meta-analysis, however, was limited by low rigor of its studies and potential for reverse causality. While our study has the advantages of capturing an entire national network of 130 acute care facilities with a 100% response rate, it, too, is limited by a number of issues, most notably by the fact that the survey was not specifically designed for the analysis of antimicrobial utilization measures, patient-level risk stratification was not available, the VA population does not reflect the U.S. population at-large, recall bias, and that antimicrobial prescribing and stewardship practices have evolved in VA since 2012. Furthermore, all of the antimicrobial utilization measures studied are imperfect at capturing inappropriate antibiotic use; in particular, our reliance on principal ICD-9 codes for noninfectious outcomes requires prospective validation. Many survey questions were subjective and subject to misinterpretation; other unmeasured confounders may also be present. Causality cannot be inferred from association. Nevertheless, our findings support many core indicators for hospital ASP recommended by the CDC and the Transatlantic Taskforce on Antimicrobial Resistance,3,4 most notably, having personnel with ID training involved in stewardship and establishing a formal procedure for ASP review for the appropriateness of an antimicrobial at or after 48 hours from the initial order.
In summary, the VA has made efforts to advance the practice of antimicrobial stewardship system-wide, including a 2014 directive that all VA facilities have an ASP,27 since the 2012 HAIG assessment reported considerable variability in antimicrobial utilization and antimicrobial stewardship activities. Our study identifies areas of stewardship that may correlate with, positively or negatively, antimicrobial utilization measures that will require further investigation. A repeat and more detailed antimicrobial stewardship survey was recently completed and will help VA gauge ongoing effects of ASTF activities. We hope to re-evaluate our model with newer data when available.
Acknowledgments
The authors wish to thank Michael Fletcher, Jaime Lopez, and Catherine Loc-Carrillo for their administrative and organizational support of the project and Allison Kelly, MD, for her pivotal role in survey development and distribution. This work was supported by the VA Health Services Research and Development Service Collaborative Research to Enhance and Advance Transformation and Excellence (CREATE) Initiative; Cognitive Support Informatics for Antimicrobial Stewardshipproject (CRE 12-313).
Disclosure
The authors report no financial conflicts of interest.
1. Antibiotic resistance threats in the United States, 2013. Atlanta, GA: Centers for Disease Control and Prevention. http://www.cdc.gov/drugresistance/threat-report-2013/. Published 2013. Accessed January 7, 2016. 2. Dellit TH, Owens RC, McGowan JE Jr, et al. Infectious Diseases Society of America and the Society for Healthcare Epidemiology of America guidelines for developing an institutional program to enhance antimicrobial stewardship. Clin Infect Dis. 2007;44(2):159-177. PubMed 3. Centers for Disease Control and Prevention. Core elements of hospital antibiotic stewardship programs. Atlanta, GA: Centers for Disease Control and Prevention. http://www.cdc.gov/getsmart/healthcare/implementation/core-elements.html. Published 2015. Accessed January 7, 2016. 4. Pollack LA, Plachouras D, Gruhler H, Sinkowitz-Cochran R. Transatlantic taskforce on antimicrobial resistance (TATFAR) summary of the modified Delphi process for common structure and process indicators for hospital antimicrobial stewardship programs. http://www.cdc.gov/drugresistance/pdf/summary_of_tatfar_recommendation_1.pdf. Published 2015. Accessed January 7, 2016. 5. Barlam TF, Cosgrove SE, Abbo LM, MacDougal C, Schuetz AN, Septimus EJ, et al. Implementing an Antibiotic Stewardship Program: Guidelines by the Infectious Diseases Society of America and the Society for Healthcare Epidemiology of America. Clin Infect Dis. 2016;62(10):e51-e77. PubMed 6. Rohde JM, Jacobsen D, Rosenberg DJ. Role of the hospitalist in antimicrobial stewardship: a review of work completed and description of a multisite collaborative. Clin Ther. 2013;35(6):751-757. PubMed 7. Mack MR, Rohde JM, Jacobsen D, Barron JR, Ko C, Goonewardene M, et al. Engaging hospitalists in antimicrobial stewardship: lessons from a multihosopital collaborative. J Hosp Med. 2016;11(8):576-580. PubMed 8. Davey P, Brown E, Charani E, Fenelon L, Gould IM, Holmes A, et al. Interventions to improve antibiotic prescribing practices for hospital inpatients. Cochrane Database Syst Rev. 2013;4:CD003543. PubMed 9. Filice G, Drekonja D, Wilt TJ, Greer N, Butler M, Wagner B. Antimicrobial stewardship programs in inpatient settings: a systematic review. Washington, DC: Department of Veterans Affairs Health Services Research and Development. http://www.hsrd.research.va.gov/publications/esp/antimicrobial.pdf. Published 2013. Accessed January 7, 2016. 10. Graber CJ, Madaras-Kelly K, Jones MM, Neuhauser MM, Goetz MB. Unnecessary antimicrobial use in the context of Clostridium difficile infection: a call to arms for the Veterans Affairs Antimicrobial Stewardship Task Force. Infect Control Hosp Epidemiol. 2013(6);34:651-653. PubMed 11. Rycroft-Malone J. The PARIHS framework--a framework for guiding the implementation of evidence-based practice. J Nurs Care Qual. 2004;19(4):297-304. PubMed 12. Chou AF, Graber CJ, Jones MM, Zhang Y, Goetz MB, Madaras-Kelly K, et al. Specifying an implementation framework for VA antimicrobial stewardship programs. Oral presentation at the VA HSR&D/QUERI National Conference, July 8-9, 2015. Washington, DC: U.S. Department of Veterans Affairs. http://www.hsrd.research.va.gov/meetings/2015/abstract-display.cfm?RecordID=862. Accessed July 5, 2016. 13. Bartholomew DJ. Factor analysis for categorical data. J R Stat Soc. 1980;42:293-321. 14. Flanagan M, Ramanujam R, Sutherland J, Vaughn T, Diekema D, Doebbeling BN. Development and validation of measures to assess prevention and control of AMR in hospitals. Med Care. 2007;45(6): 537-544. PubMed 15. Kline P. An easy guide to factor analysis. New York: Routledge, 1994. 16. Centers for Disease Control and Prevention, National Center for Health Statistics. International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM). Atlanta GA: Centers for Disease Control and Prevention. http://www.cdc.gov/nchs/icd/icd9cm.htm. Published 2013. Accessed January 7, 2016. 17. Huttner B, Jones M, Huttner A, Rubin M, Samore MH. Antibiotic prescription practices for pneumonia, skin and soft tissue infections and urinary tract infections throughout the US Veterans Affairs system. J Antimicrob Chemother. 2013;68(10):2393-2399. PubMed 18. National Institutes of Health. SNOMED Clinical Terms (SNOMED CT). Bethesda, MD: U.S. National Library of Medicine. https://www.nlm.nih.gov/research/umls/Snomed/snomed_main.html. NIH website. Published 2009. Accessed January 7. 2016. 19. Jones M, Huttner B, Madaras-Kelly K, Nechodom K, Nielson C, Bidwell Goetz M, et al. Parenteral to oral conversion of fluoroquinolones: low-hanging fruit for antimicrobial stewardship programs? Infect Control Hosp Epidemiol 2012;33(4): 362-367. PubMed 20. Huttner B, Jones M, Rubin MA, Madaras-Kelly K, Nielson C, Goetz MB, et al. Double trouble: how big a problem is redundant anaerobic antibiotic coverage in Veterans Affairs medical centres? J Antimicrob Chemother. 2012;67(6):1537-1539. PubMed 21. Tibshirani R. Regression shrinkage and selection via the lasso. J R Stat Soc B. 1996;58:267-288. 22. Taylor J, Tibshirani RJ. Statistical learning and selective inference. Proc Natl Acad Sci U S A. 2015;112(25):7629-7634. PubMed 23. VHA Office of Productivity, Efficiency, and Staffing. Facility Complexity Levels. Department of Veterans Affairs website. http://opes.vssc.med.va.gov/FacilityComplexityLevels/Pages/default.aspx. Published 2008. Accessed January 7, 2016. 24. Pakyz AL, Moczygemba LR, Wang H, Stevens MP, Edmond MB. An evaluation of the association between an antimicrobial stewardship score and antimicrobial usage. J Antimicrob Chemother. 2015;70(5):1588-1591. PubMed 25. Schuts EC, Hulscher ME, Mouton JW, Verduin CM, Stuart JW, Overdiek HW, et al. Current evidence on hospital antimicrobial stewardship objectives: a systematic review and meta-analysis. Lancet Infect Dis. 2016;16(7):847-856. PubMed 26. Graber CJ, Goetz MB. Next steps for antimicrobial stewardship. Lancet Infect Dis. 2016;16(7):764-765. PubMed 27. Petzel RA. VHA Directive 1031: Antimicrobial stewardship programs (ASP). Washington, DC: Department of Veterans Affairs.http://www.va.gov/vhapublications/ViewPublication.asp?pub_ID=2964. Published January 22, 2014. Accessed July 5, 2016.
The deleterious impact of inappropriate and/or excessive antimicrobial usage is well recognized. In the United States, the Centers for Disease Control and Prevention (CDC) estimates that at least 2 million people become infected with antimicrobial-resistant bacteria with 23,000 subsequent deaths and at least $1 billion in excess medical costs per year.1
In response, many healthcare organizations have developed antimicrobial stewardship programs (ASPs). Guidelines co-sponsored by the Infectious Diseases Society of America and the Society for Healthcare Epidemiology of America, as well as recent statements from the CDC and the Transatlantic Taskforce on Antimicrobial Resistance,all recommend core ASP elements.2-5 The guidelines provide general recommendations on ASP structure, strategies, and activities. The recommended ASP structure is a team of physicians and pharmacists that collaborates with facility governing committees and other stakeholders to optimize antimicrobial use. While personnel with expertise in infectious diseases (ID) often lead ASPs, hospitalists are also recognized as key contributors, especially in quality improvement.6,7 Recommended strategies include prospective audit of antimicrobial use with intervention and feedback and formulary restriction with preauthorization. Recommended activities include education, creation of guidelines, clinical pathways, and order forms, and programs to promote de-escalation and conversion from parenteral (IV) to oral (PO) antimicrobial therapy. However, limited evidence exists regarding the effectiveness of these ASP core elements.8,9 While Cochrane reviews found clear evidence that particular stewardship strategies (eg, audit and feedback, formulary restriction, guidelines implemented with or without feedback, protocols, computerized decision support) can be effective in reducing antimicrobial usage and improving clinical outcomes over the long term, little evidence exists favoring 1 strategy over another.8 Furthermore, most individual studies of ASPs are single-center, making their conclusions less generalizable.
In 2012, the VA National Antimicrobial Stewardship Task Force (ASTF), in conjunction with the VA Healthcare Analysis and Information Group (HAIG) administered a survey on the characteristics of ASPs at all 130 acute care VA facilities (Appendix A). We used these survey results to build an implementation model and then assess associations between facility-level variables and 4 antimicrobial utilization measures.
METHODS
Survey and Data
In 2011, the ASTF was chartered to develop, deploy, and monitor a strategic plan for optimizing antimicrobial therapy management. Monthly educational webinars and sample policies were offered to all facilities, including a sample business plan for stewardship and policies to encourage de-escalation from broad-spectrum antimicrobials, promote conversion from parenteral to oral antimicrobial therapy, avoid unnecessary double anaerobic coverage, and mitigate unnecessary antimicrobial usage in the context of Clostridium difficile infection.10
At the time that ASTF was chartered, the understanding of how ASP structures across VA facilities operated was limited. Hence, to capture baseline institutional characteristics and stewardship activities, ASTF and HAIG developed an inventory assessment of ASPs that was distributed online in November 2012. All 130 VA facilities providing inpatient acute care services responded.
We derived 57 facility characteristics relevant to antimicrobial utilization and conducted a series of factor analyses to simplify the complex dataset, and identify underlying latent constructs. We categorized resulting factors into domains of evidence, context, or facilitation as guided by the Promoting Action on Research Implementation in Health Services framework.11 Briefly, the evidence domain describes how the facility uses codified and noncodified sources of knowledge (eg, research evidence, clinical experience). Organizational context comprises a facility’s characteristics that ensure a more conducive environment to put evidence into practice (eg, supportive leadership, organizational structure, evaluative systems). Facilitation emphasizes a facility personnel’s “state of preparedness” and receptivity to implementation.
Using factor analysis to identify facility factors as correlates of the outcomes, we first examined polychoric correlations among facility characteristics to assess multicollinearity. We performed independent component analysis to create latent constructs of variables that were defined by factor loadings (that indicated the proportion of variance accounted for by the construct) and uniqueness factors (that determined how well the variables were interpreted by the construct). Factors retained included variables that had uniqueness values of less than 0.7 and factor loadings greater than 0.3. Those associated with uniqueness values greater than 0.7 were left as single items, as were characteristics deemed a priori to be particularly important to antimicrobial stewardship. Factor scales that had only 2 items were converted into indices, while factor scores were generated for those factors that contained 3 or more items.12-15
Data for facility-level antimicrobial utilization measures were obtained from the VA Corporate Data Warehouse from calendar year 2012. The analysis was conducted within the VA Informatics and Computing Infrastructure. All study procedures were approved by the VA Central Institutional Review Board.
Measures
Four utilization measures were defined as dependent measures: overall antimicrobial use; antimicrobial use in patients with non-infectious discharge diagnoses; missed opportunities to convert from parenteral to oral antimicrobial therapy; and missed opportunities to avoid double anaerobic coverage with metronidazole.
Overall antimicrobial use was defined as total acute care (ie, medical/surgical/intensive care) antibacterial use for each facility aggregated as per CDC National Healthcare Safety Network Antimicrobial Use Option guidelines (antimicrobial days per 1000 patient days present). A subanalysis of overall antimicrobial use was restricted to antimicrobial use among patients without an infection-related discharge diagnosis, as we surmised that this measure may capture a greater proportion of potentially unnecessary antimicrobial use. International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM)16 codes for infectious processes were identified by a combination of those classified previously in the literature,17 and those identified by finding the descendants of all infections named in the Systematized Nomenclature of Medicine--Clinical Terms.18 Next, all remaining codes for principal discharge diagnoses for which antimicrobials were administered were reviewed for potential indications for systemic antibacterial use. Discharges were considered noninfectious if no codes were identified when systemic antimicrobials were or could be indicated. For this measure, antimicrobial days were not counted if administered on or 1 day after the calendar day of surgery warranting antimicrobial prophylaxis.
Missed opportunities for conversion from parenteral to oral (IV to PO) formulations of highly bioavailable oral antimicrobials (ciprofloxacin, levofloxacin, moxifloxacin, azithromycin, clindamycin, linezolid, metronidazole, and fluconazole) were defined as the percentage of days of unnecessary IV therapy that were given when PO therapy could have been used among patients who were not in intensive care units at the time of antimicrobial administration who were receiving other oral medications, using previously described methodology.19Missed opportunities for avoiding redundant anaerobic coverage with metronidazole were defined as the percentage of days in which patients receiving metronidazole also receivedantibiotics with activity against anaerobic bacteria, specifically beta-lactam/beta-lactamase inhibitors, carbapenems, cefotetan/cefoxitin, clindamycin, moxifloxacin, or tigecycline), using previously described methodology.20 Patients for whom C. difficile testing was either ordered or positive within the prior 28 days (indicating potential clinical concern for C. difficile infection) were excluded from this endpoint.
Analysis
The variables derived above were entered into a multivariable model for each of the 4 antimicrobial utilization measures. The least absolute shrinkage and selection operator (LASSO) regression was used to determine significant associations between variables and individual utilization measures.21 LASSO was chosen because it offers advantages over traditional subset selection approaches in large multivariable analyses by assessing covariates simultaneously rather than sequentially, supporting prediction rather than estimation of effect.22P values were not reported as they are not useful in determining statistical significance in this methodology. A tuning parameter of 0.025 was determined for the model based on a cross-validation approach. Significant variables remaining in the model were reported with the percent change in each utilization measure per unit change in the variable of interest. For binary factors, percent change was reported according to whether the variable was present or not. For ordinal variables, percent change was reported according to incremental increase in ordinal score. For continuous variables or variables represented by factor or index scores, percent change was reported per each 25% increase in the range of the score.
RESULTS
Inpatient Facility Antimicrobial Stewardship Characteristics and Antimicrobial Utilization
Frequencies of key facility characteristics that contributed to variable development are included in Table 1. Full survey results across all facilities are included in Appendix B. Factor analysis reduced the total number of variables to 32; however, we also included hospital size and VA complexity score. Thus, 34 variables were evaluated for association with antimicrobial utilization measures: 4 in the evidence domain, 23 in the context domain, and 7 in the facilitation domain (Table 2).
Table 1
Table 1 (continued)
Median facility antimicrobial use was 619 antimicrobial days per 1000 days present (interquartile range [IQR], 554-700; overall range, 346-974). Median facility noninfectious antimicrobial use was 236 per 1000 days present (IQR, 200-286). Missed opportunities for conversion from IV to PO antimicrobial therapy were common, with a median facility value of 40.4% (391/969) of potentially eligible days of therapy (IQR, 32.2-47.8%). Missed opportunities to avoid double anaerobic coverage were less common (median 15.3% (186/1214) of potentially eligible days of therapy (IQR, 11.8%-20.2%; Figure).
Overall Antimicrobial Use
Four variables were associated with decreased overall antimicrobial use, although with small magnitude of change: presence of postgraduate physician/pharmacy training programs (0.03% decrease per quarter increase in factor score; on the order of 0.2 antimicrobial days per 1000 patient days present), presence of pharmacists and/or ID attendings on general medicine ward teams (0.02% decrease per quarter increase in index score), frequency of systematic de-escalation review (0.01% decrease per ordinal increase in score), and degree of involvement of ID physicians and/or fellows in antimicrobial approvals (0.007% decrease per quarter increase in index score). No variables were associated with increased overall antimicrobial use.
Table 2
Table 2 (continued)
Antimicrobial Use among Discharges without Infectious Diagnoses
Six variables were associated with decreased antimicrobial use in patients without infectious discharge diagnoses, while 4 variables were associated with increased use. Variables associated with the greatest magnitude of decreased use included facility educational programs for prudent antimicrobial use (1.8% on the order of 4 antimicrobial days per 1000 patient days present), frequency of systematic de-escalation review (1.5% per incremental increase in score), and whether a facility’s lead antimicrobial stewardship pharmacist had ID training (1.3%). Also significantly associated with decreased use was a factor summarizing the presence of 4 condition-specific stewardship processes (de-escalation policies, policies for addressing antimicrobial use in the context of C. difficile infection, blood culture review, and automatic ID consults for certain conditions) (0.6% per quarter increase in factor score range), the extent to which postgraduate physician/pharmacy training programs were present (0.6% per quarter increase in factor score range), and the number of electronic antimicrobial-specific order sets present (0.4% per order set). The variables associated with increased use of antimicrobials included the presence of antimicrobial stop orders (4.6%), the degree to which non-ID physicians were involved in antimicrobial approvals (0.7% per increase in ordinal score), the level engagement with ASTF online resources (0.6% per quarter increase in factor score range), and hospital size (0.6% per 50-bed increase).
Figure
Missed Opportunities for Parenteral to Oral Antimicrobial Conversion
Missed opportunities for IV to PO antimicrobial conversion had the largest number of significant associations with organizational variables: 14 variables were associated with fewer missed opportunities, while 5 were associated with greater missed opportunities. Variables associated with the largest reductions in missed opportunities for IV to PO conversion included having guidelines for antimicrobial duration (12.8%), participating in regional stewardship collaboratives (8.1%), number of antimicrobial-specific order sets (6.0% per order set), ID training of the ASP pharmacist (4.9%), and VA facility complexity designation (4.2% per quarter increase in score indicating greater complexity).23 Variables associated with more missed opportunities included stop orders (11.7%), overall perceived receptiveness to antimicrobial stewardship among clinical services (9.4%), the degree of engagement with ASTF online resources (6.9% per quarter increase in factor score range), educational programs for prudent antimicrobial use (4.1%), and hospital size (1.0% per 50-bed increase).
Missed Opportunities for Avoidance of Double Anaerobic Coverage
Four variables were associated with more avoidance of double anaerobic coverage: ID training of the lead ASP pharmacist (8.8%), presence of pharmacists and/or ID attendings on acute care ward teams (6.2% per quarter increase in index score), degree of ID pharmacist involvement in antimicrobial approvals, ranging from not at all (score=0) to both weekdays and nights/weekends (score=2; 4.3% per ordinal increase), and the number of antimicrobial-specific order sets (1.5% per order set). No variables were associated with less avoidance of double anaerobic coverage.
Variables Associated with Multiple Favorable or Unfavorable Antimicrobial Utilization Measures
To better assess the consistency of the relationship between organizational variables and measures of antimicrobial use, we tabulated variables that were associated with at least 3 potentially favorable (ie, reduced overall or noninfectious antimicrobial use or fewer missed opportunities) measures. Altogether, 5 variables satisfied this criterion: the presence of postgraduate physician/pharmacy training programs, the number of antimicrobial-specific order sets, frequency of systematic de-escalation review, the presence of pharmacists and/or ID attendings on acute care ward teams, and formal ID training of the lead ASP pharmacist (Table 3). Three other variables were associated with at least 2 unfavorable measures: hospital size, the degree to which the facility engaged with ASTF online resources, and presence of antimicrobial stop orders.
Table 3
DISCUSSION
Variability in ASP implementation across VA allowed us to assess the relationship between ASP and facility elements and baseline patterns of antimicrobial utilization. Hospitalists and hospital policy-makers are becoming more and more engaged in inpatient antimicrobial stewardship. While our results suggest that having pharmacists and/or physicians with formal ID training participate in everyday inpatient activities can favorably improve antimicrobial utilization, considerable input into stewardship can be made by hospitalists and policy makers. In particular, based on this work, the highest yield from an organizational standpoint may be in working to develop order sets within the electronic medical record and systematic efforts to promote de-escalation of broad-spectrum therapy, as well as encouraging hospital administration to devote specific physician and pharmacy salary support to stewardship efforts.
While we noted that finding the ASTF online resources helpful was associated with potentially unfavorable antimicrobial utilization, we speculate that this may represent reverse causality due to facilities recognizing that their antimicrobial usage is suboptimal and thus seeking out sample ASTF policies to implement. The association between the presence of automatic stop orders and potentially unfavorable antimicrobial utilization is less clear since the timeframe was not specified in the survey; it may be that setting stop orders too far in advance may promote an environment in which critical thinking about antimicrobial de-escalation is not encouraged or timely. The larger magnitude of association between ASP characteristics and antimicrobial usage among patients without infectious discharge diagnoses versus overall antimicrobial usage also suggests that clinical situations where infection was of low enough suspicion to not even have the providers eventually list an infectious diagnosis on their discharge summaries may be particularly malleable to ASP interventions, though further exploration is needed in determining how useful this utilization measure may be as a marker for inappropriate antimicrobial use.
Our results complement those of Pakyz et al.24 who surveyed 44 academic medical facilities in March 2013 to develop an ASP intensity score and correlate this score and its specific components to overall and targeted antimicrobial use. This study found that the overall ASP intensity score was not significantly associated with total or targeted antimicrobial use. However, ASP strategies were more associated with decreased total and targeted antimicrobial use than were specific ASP resources. In particular, the presence of a preauthorization strategy was associated with decreased targeted antimicrobial use. Our particular findings that order set establishment and de-escalation efforts are associated with multiple antibiotic outcomes also line up with the findings of Schuts et al,who performed a meta-analysis of the effects of meeting antimicrobial stewardship objectives and found that achieving guideline concordance (such as through establishment of order sets) and successfully de-escalating antimicrobial therapy was associated with reduced mortality.25,26 This meta-analysis, however, was limited by low rigor of its studies and potential for reverse causality. While our study has the advantages of capturing an entire national network of 130 acute care facilities with a 100% response rate, it, too, is limited by a number of issues, most notably by the fact that the survey was not specifically designed for the analysis of antimicrobial utilization measures, patient-level risk stratification was not available, the VA population does not reflect the U.S. population at-large, recall bias, and that antimicrobial prescribing and stewardship practices have evolved in VA since 2012. Furthermore, all of the antimicrobial utilization measures studied are imperfect at capturing inappropriate antibiotic use; in particular, our reliance on principal ICD-9 codes for noninfectious outcomes requires prospective validation. Many survey questions were subjective and subject to misinterpretation; other unmeasured confounders may also be present. Causality cannot be inferred from association. Nevertheless, our findings support many core indicators for hospital ASP recommended by the CDC and the Transatlantic Taskforce on Antimicrobial Resistance,3,4 most notably, having personnel with ID training involved in stewardship and establishing a formal procedure for ASP review for the appropriateness of an antimicrobial at or after 48 hours from the initial order.
In summary, the VA has made efforts to advance the practice of antimicrobial stewardship system-wide, including a 2014 directive that all VA facilities have an ASP,27 since the 2012 HAIG assessment reported considerable variability in antimicrobial utilization and antimicrobial stewardship activities. Our study identifies areas of stewardship that may correlate with, positively or negatively, antimicrobial utilization measures that will require further investigation. A repeat and more detailed antimicrobial stewardship survey was recently completed and will help VA gauge ongoing effects of ASTF activities. We hope to re-evaluate our model with newer data when available.
Acknowledgments
The authors wish to thank Michael Fletcher, Jaime Lopez, and Catherine Loc-Carrillo for their administrative and organizational support of the project and Allison Kelly, MD, for her pivotal role in survey development and distribution. This work was supported by the VA Health Services Research and Development Service Collaborative Research to Enhance and Advance Transformation and Excellence (CREATE) Initiative; Cognitive Support Informatics for Antimicrobial Stewardshipproject (CRE 12-313).
Disclosure
The authors report no financial conflicts of interest.
The deleterious impact of inappropriate and/or excessive antimicrobial usage is well recognized. In the United States, the Centers for Disease Control and Prevention (CDC) estimates that at least 2 million people become infected with antimicrobial-resistant bacteria with 23,000 subsequent deaths and at least $1 billion in excess medical costs per year.1
In response, many healthcare organizations have developed antimicrobial stewardship programs (ASPs). Guidelines co-sponsored by the Infectious Diseases Society of America and the Society for Healthcare Epidemiology of America, as well as recent statements from the CDC and the Transatlantic Taskforce on Antimicrobial Resistance,all recommend core ASP elements.2-5 The guidelines provide general recommendations on ASP structure, strategies, and activities. The recommended ASP structure is a team of physicians and pharmacists that collaborates with facility governing committees and other stakeholders to optimize antimicrobial use. While personnel with expertise in infectious diseases (ID) often lead ASPs, hospitalists are also recognized as key contributors, especially in quality improvement.6,7 Recommended strategies include prospective audit of antimicrobial use with intervention and feedback and formulary restriction with preauthorization. Recommended activities include education, creation of guidelines, clinical pathways, and order forms, and programs to promote de-escalation and conversion from parenteral (IV) to oral (PO) antimicrobial therapy. However, limited evidence exists regarding the effectiveness of these ASP core elements.8,9 While Cochrane reviews found clear evidence that particular stewardship strategies (eg, audit and feedback, formulary restriction, guidelines implemented with or without feedback, protocols, computerized decision support) can be effective in reducing antimicrobial usage and improving clinical outcomes over the long term, little evidence exists favoring 1 strategy over another.8 Furthermore, most individual studies of ASPs are single-center, making their conclusions less generalizable.
In 2012, the VA National Antimicrobial Stewardship Task Force (ASTF), in conjunction with the VA Healthcare Analysis and Information Group (HAIG) administered a survey on the characteristics of ASPs at all 130 acute care VA facilities (Appendix A). We used these survey results to build an implementation model and then assess associations between facility-level variables and 4 antimicrobial utilization measures.
METHODS
Survey and Data
In 2011, the ASTF was chartered to develop, deploy, and monitor a strategic plan for optimizing antimicrobial therapy management. Monthly educational webinars and sample policies were offered to all facilities, including a sample business plan for stewardship and policies to encourage de-escalation from broad-spectrum antimicrobials, promote conversion from parenteral to oral antimicrobial therapy, avoid unnecessary double anaerobic coverage, and mitigate unnecessary antimicrobial usage in the context of Clostridium difficile infection.10
At the time that ASTF was chartered, the understanding of how ASP structures across VA facilities operated was limited. Hence, to capture baseline institutional characteristics and stewardship activities, ASTF and HAIG developed an inventory assessment of ASPs that was distributed online in November 2012. All 130 VA facilities providing inpatient acute care services responded.
We derived 57 facility characteristics relevant to antimicrobial utilization and conducted a series of factor analyses to simplify the complex dataset, and identify underlying latent constructs. We categorized resulting factors into domains of evidence, context, or facilitation as guided by the Promoting Action on Research Implementation in Health Services framework.11 Briefly, the evidence domain describes how the facility uses codified and noncodified sources of knowledge (eg, research evidence, clinical experience). Organizational context comprises a facility’s characteristics that ensure a more conducive environment to put evidence into practice (eg, supportive leadership, organizational structure, evaluative systems). Facilitation emphasizes a facility personnel’s “state of preparedness” and receptivity to implementation.
Using factor analysis to identify facility factors as correlates of the outcomes, we first examined polychoric correlations among facility characteristics to assess multicollinearity. We performed independent component analysis to create latent constructs of variables that were defined by factor loadings (that indicated the proportion of variance accounted for by the construct) and uniqueness factors (that determined how well the variables were interpreted by the construct). Factors retained included variables that had uniqueness values of less than 0.7 and factor loadings greater than 0.3. Those associated with uniqueness values greater than 0.7 were left as single items, as were characteristics deemed a priori to be particularly important to antimicrobial stewardship. Factor scales that had only 2 items were converted into indices, while factor scores were generated for those factors that contained 3 or more items.12-15
Data for facility-level antimicrobial utilization measures were obtained from the VA Corporate Data Warehouse from calendar year 2012. The analysis was conducted within the VA Informatics and Computing Infrastructure. All study procedures were approved by the VA Central Institutional Review Board.
Measures
Four utilization measures were defined as dependent measures: overall antimicrobial use; antimicrobial use in patients with non-infectious discharge diagnoses; missed opportunities to convert from parenteral to oral antimicrobial therapy; and missed opportunities to avoid double anaerobic coverage with metronidazole.
Overall antimicrobial use was defined as total acute care (ie, medical/surgical/intensive care) antibacterial use for each facility aggregated as per CDC National Healthcare Safety Network Antimicrobial Use Option guidelines (antimicrobial days per 1000 patient days present). A subanalysis of overall antimicrobial use was restricted to antimicrobial use among patients without an infection-related discharge diagnosis, as we surmised that this measure may capture a greater proportion of potentially unnecessary antimicrobial use. International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM)16 codes for infectious processes were identified by a combination of those classified previously in the literature,17 and those identified by finding the descendants of all infections named in the Systematized Nomenclature of Medicine--Clinical Terms.18 Next, all remaining codes for principal discharge diagnoses for which antimicrobials were administered were reviewed for potential indications for systemic antibacterial use. Discharges were considered noninfectious if no codes were identified when systemic antimicrobials were or could be indicated. For this measure, antimicrobial days were not counted if administered on or 1 day after the calendar day of surgery warranting antimicrobial prophylaxis.
Missed opportunities for conversion from parenteral to oral (IV to PO) formulations of highly bioavailable oral antimicrobials (ciprofloxacin, levofloxacin, moxifloxacin, azithromycin, clindamycin, linezolid, metronidazole, and fluconazole) were defined as the percentage of days of unnecessary IV therapy that were given when PO therapy could have been used among patients who were not in intensive care units at the time of antimicrobial administration who were receiving other oral medications, using previously described methodology.19Missed opportunities for avoiding redundant anaerobic coverage with metronidazole were defined as the percentage of days in which patients receiving metronidazole also receivedantibiotics with activity against anaerobic bacteria, specifically beta-lactam/beta-lactamase inhibitors, carbapenems, cefotetan/cefoxitin, clindamycin, moxifloxacin, or tigecycline), using previously described methodology.20 Patients for whom C. difficile testing was either ordered or positive within the prior 28 days (indicating potential clinical concern for C. difficile infection) were excluded from this endpoint.
Analysis
The variables derived above were entered into a multivariable model for each of the 4 antimicrobial utilization measures. The least absolute shrinkage and selection operator (LASSO) regression was used to determine significant associations between variables and individual utilization measures.21 LASSO was chosen because it offers advantages over traditional subset selection approaches in large multivariable analyses by assessing covariates simultaneously rather than sequentially, supporting prediction rather than estimation of effect.22P values were not reported as they are not useful in determining statistical significance in this methodology. A tuning parameter of 0.025 was determined for the model based on a cross-validation approach. Significant variables remaining in the model were reported with the percent change in each utilization measure per unit change in the variable of interest. For binary factors, percent change was reported according to whether the variable was present or not. For ordinal variables, percent change was reported according to incremental increase in ordinal score. For continuous variables or variables represented by factor or index scores, percent change was reported per each 25% increase in the range of the score.
RESULTS
Inpatient Facility Antimicrobial Stewardship Characteristics and Antimicrobial Utilization
Frequencies of key facility characteristics that contributed to variable development are included in Table 1. Full survey results across all facilities are included in Appendix B. Factor analysis reduced the total number of variables to 32; however, we also included hospital size and VA complexity score. Thus, 34 variables were evaluated for association with antimicrobial utilization measures: 4 in the evidence domain, 23 in the context domain, and 7 in the facilitation domain (Table 2).
Table 1
Table 1 (continued)
Median facility antimicrobial use was 619 antimicrobial days per 1000 days present (interquartile range [IQR], 554-700; overall range, 346-974). Median facility noninfectious antimicrobial use was 236 per 1000 days present (IQR, 200-286). Missed opportunities for conversion from IV to PO antimicrobial therapy were common, with a median facility value of 40.4% (391/969) of potentially eligible days of therapy (IQR, 32.2-47.8%). Missed opportunities to avoid double anaerobic coverage were less common (median 15.3% (186/1214) of potentially eligible days of therapy (IQR, 11.8%-20.2%; Figure).
Overall Antimicrobial Use
Four variables were associated with decreased overall antimicrobial use, although with small magnitude of change: presence of postgraduate physician/pharmacy training programs (0.03% decrease per quarter increase in factor score; on the order of 0.2 antimicrobial days per 1000 patient days present), presence of pharmacists and/or ID attendings on general medicine ward teams (0.02% decrease per quarter increase in index score), frequency of systematic de-escalation review (0.01% decrease per ordinal increase in score), and degree of involvement of ID physicians and/or fellows in antimicrobial approvals (0.007% decrease per quarter increase in index score). No variables were associated with increased overall antimicrobial use.
Table 2
Table 2 (continued)
Antimicrobial Use among Discharges without Infectious Diagnoses
Six variables were associated with decreased antimicrobial use in patients without infectious discharge diagnoses, while 4 variables were associated with increased use. Variables associated with the greatest magnitude of decreased use included facility educational programs for prudent antimicrobial use (1.8% on the order of 4 antimicrobial days per 1000 patient days present), frequency of systematic de-escalation review (1.5% per incremental increase in score), and whether a facility’s lead antimicrobial stewardship pharmacist had ID training (1.3%). Also significantly associated with decreased use was a factor summarizing the presence of 4 condition-specific stewardship processes (de-escalation policies, policies for addressing antimicrobial use in the context of C. difficile infection, blood culture review, and automatic ID consults for certain conditions) (0.6% per quarter increase in factor score range), the extent to which postgraduate physician/pharmacy training programs were present (0.6% per quarter increase in factor score range), and the number of electronic antimicrobial-specific order sets present (0.4% per order set). The variables associated with increased use of antimicrobials included the presence of antimicrobial stop orders (4.6%), the degree to which non-ID physicians were involved in antimicrobial approvals (0.7% per increase in ordinal score), the level engagement with ASTF online resources (0.6% per quarter increase in factor score range), and hospital size (0.6% per 50-bed increase).
Figure
Missed Opportunities for Parenteral to Oral Antimicrobial Conversion
Missed opportunities for IV to PO antimicrobial conversion had the largest number of significant associations with organizational variables: 14 variables were associated with fewer missed opportunities, while 5 were associated with greater missed opportunities. Variables associated with the largest reductions in missed opportunities for IV to PO conversion included having guidelines for antimicrobial duration (12.8%), participating in regional stewardship collaboratives (8.1%), number of antimicrobial-specific order sets (6.0% per order set), ID training of the ASP pharmacist (4.9%), and VA facility complexity designation (4.2% per quarter increase in score indicating greater complexity).23 Variables associated with more missed opportunities included stop orders (11.7%), overall perceived receptiveness to antimicrobial stewardship among clinical services (9.4%), the degree of engagement with ASTF online resources (6.9% per quarter increase in factor score range), educational programs for prudent antimicrobial use (4.1%), and hospital size (1.0% per 50-bed increase).
Missed Opportunities for Avoidance of Double Anaerobic Coverage
Four variables were associated with more avoidance of double anaerobic coverage: ID training of the lead ASP pharmacist (8.8%), presence of pharmacists and/or ID attendings on acute care ward teams (6.2% per quarter increase in index score), degree of ID pharmacist involvement in antimicrobial approvals, ranging from not at all (score=0) to both weekdays and nights/weekends (score=2; 4.3% per ordinal increase), and the number of antimicrobial-specific order sets (1.5% per order set). No variables were associated with less avoidance of double anaerobic coverage.
Variables Associated with Multiple Favorable or Unfavorable Antimicrobial Utilization Measures
To better assess the consistency of the relationship between organizational variables and measures of antimicrobial use, we tabulated variables that were associated with at least 3 potentially favorable (ie, reduced overall or noninfectious antimicrobial use or fewer missed opportunities) measures. Altogether, 5 variables satisfied this criterion: the presence of postgraduate physician/pharmacy training programs, the number of antimicrobial-specific order sets, frequency of systematic de-escalation review, the presence of pharmacists and/or ID attendings on acute care ward teams, and formal ID training of the lead ASP pharmacist (Table 3). Three other variables were associated with at least 2 unfavorable measures: hospital size, the degree to which the facility engaged with ASTF online resources, and presence of antimicrobial stop orders.
Table 3
DISCUSSION
Variability in ASP implementation across VA allowed us to assess the relationship between ASP and facility elements and baseline patterns of antimicrobial utilization. Hospitalists and hospital policy-makers are becoming more and more engaged in inpatient antimicrobial stewardship. While our results suggest that having pharmacists and/or physicians with formal ID training participate in everyday inpatient activities can favorably improve antimicrobial utilization, considerable input into stewardship can be made by hospitalists and policy makers. In particular, based on this work, the highest yield from an organizational standpoint may be in working to develop order sets within the electronic medical record and systematic efforts to promote de-escalation of broad-spectrum therapy, as well as encouraging hospital administration to devote specific physician and pharmacy salary support to stewardship efforts.
While we noted that finding the ASTF online resources helpful was associated with potentially unfavorable antimicrobial utilization, we speculate that this may represent reverse causality due to facilities recognizing that their antimicrobial usage is suboptimal and thus seeking out sample ASTF policies to implement. The association between the presence of automatic stop orders and potentially unfavorable antimicrobial utilization is less clear since the timeframe was not specified in the survey; it may be that setting stop orders too far in advance may promote an environment in which critical thinking about antimicrobial de-escalation is not encouraged or timely. The larger magnitude of association between ASP characteristics and antimicrobial usage among patients without infectious discharge diagnoses versus overall antimicrobial usage also suggests that clinical situations where infection was of low enough suspicion to not even have the providers eventually list an infectious diagnosis on their discharge summaries may be particularly malleable to ASP interventions, though further exploration is needed in determining how useful this utilization measure may be as a marker for inappropriate antimicrobial use.
Our results complement those of Pakyz et al.24 who surveyed 44 academic medical facilities in March 2013 to develop an ASP intensity score and correlate this score and its specific components to overall and targeted antimicrobial use. This study found that the overall ASP intensity score was not significantly associated with total or targeted antimicrobial use. However, ASP strategies were more associated with decreased total and targeted antimicrobial use than were specific ASP resources. In particular, the presence of a preauthorization strategy was associated with decreased targeted antimicrobial use. Our particular findings that order set establishment and de-escalation efforts are associated with multiple antibiotic outcomes also line up with the findings of Schuts et al,who performed a meta-analysis of the effects of meeting antimicrobial stewardship objectives and found that achieving guideline concordance (such as through establishment of order sets) and successfully de-escalating antimicrobial therapy was associated with reduced mortality.25,26 This meta-analysis, however, was limited by low rigor of its studies and potential for reverse causality. While our study has the advantages of capturing an entire national network of 130 acute care facilities with a 100% response rate, it, too, is limited by a number of issues, most notably by the fact that the survey was not specifically designed for the analysis of antimicrobial utilization measures, patient-level risk stratification was not available, the VA population does not reflect the U.S. population at-large, recall bias, and that antimicrobial prescribing and stewardship practices have evolved in VA since 2012. Furthermore, all of the antimicrobial utilization measures studied are imperfect at capturing inappropriate antibiotic use; in particular, our reliance on principal ICD-9 codes for noninfectious outcomes requires prospective validation. Many survey questions were subjective and subject to misinterpretation; other unmeasured confounders may also be present. Causality cannot be inferred from association. Nevertheless, our findings support many core indicators for hospital ASP recommended by the CDC and the Transatlantic Taskforce on Antimicrobial Resistance,3,4 most notably, having personnel with ID training involved in stewardship and establishing a formal procedure for ASP review for the appropriateness of an antimicrobial at or after 48 hours from the initial order.
In summary, the VA has made efforts to advance the practice of antimicrobial stewardship system-wide, including a 2014 directive that all VA facilities have an ASP,27 since the 2012 HAIG assessment reported considerable variability in antimicrobial utilization and antimicrobial stewardship activities. Our study identifies areas of stewardship that may correlate with, positively or negatively, antimicrobial utilization measures that will require further investigation. A repeat and more detailed antimicrobial stewardship survey was recently completed and will help VA gauge ongoing effects of ASTF activities. We hope to re-evaluate our model with newer data when available.
Acknowledgments
The authors wish to thank Michael Fletcher, Jaime Lopez, and Catherine Loc-Carrillo for their administrative and organizational support of the project and Allison Kelly, MD, for her pivotal role in survey development and distribution. This work was supported by the VA Health Services Research and Development Service Collaborative Research to Enhance and Advance Transformation and Excellence (CREATE) Initiative; Cognitive Support Informatics for Antimicrobial Stewardshipproject (CRE 12-313).
Disclosure
The authors report no financial conflicts of interest.
References
1. Antibiotic resistance threats in the United States, 2013. Atlanta, GA: Centers for Disease Control and Prevention. http://www.cdc.gov/drugresistance/threat-report-2013/. Published 2013. Accessed January 7, 2016. 2. Dellit TH, Owens RC, McGowan JE Jr, et al. Infectious Diseases Society of America and the Society for Healthcare Epidemiology of America guidelines for developing an institutional program to enhance antimicrobial stewardship. Clin Infect Dis. 2007;44(2):159-177. PubMed 3. Centers for Disease Control and Prevention. Core elements of hospital antibiotic stewardship programs. Atlanta, GA: Centers for Disease Control and Prevention. http://www.cdc.gov/getsmart/healthcare/implementation/core-elements.html. Published 2015. Accessed January 7, 2016. 4. Pollack LA, Plachouras D, Gruhler H, Sinkowitz-Cochran R. Transatlantic taskforce on antimicrobial resistance (TATFAR) summary of the modified Delphi process for common structure and process indicators for hospital antimicrobial stewardship programs. http://www.cdc.gov/drugresistance/pdf/summary_of_tatfar_recommendation_1.pdf. Published 2015. Accessed January 7, 2016. 5. Barlam TF, Cosgrove SE, Abbo LM, MacDougal C, Schuetz AN, Septimus EJ, et al. Implementing an Antibiotic Stewardship Program: Guidelines by the Infectious Diseases Society of America and the Society for Healthcare Epidemiology of America. Clin Infect Dis. 2016;62(10):e51-e77. PubMed 6. Rohde JM, Jacobsen D, Rosenberg DJ. Role of the hospitalist in antimicrobial stewardship: a review of work completed and description of a multisite collaborative. Clin Ther. 2013;35(6):751-757. PubMed 7. Mack MR, Rohde JM, Jacobsen D, Barron JR, Ko C, Goonewardene M, et al. Engaging hospitalists in antimicrobial stewardship: lessons from a multihosopital collaborative. J Hosp Med. 2016;11(8):576-580. PubMed 8. Davey P, Brown E, Charani E, Fenelon L, Gould IM, Holmes A, et al. Interventions to improve antibiotic prescribing practices for hospital inpatients. Cochrane Database Syst Rev. 2013;4:CD003543. PubMed 9. Filice G, Drekonja D, Wilt TJ, Greer N, Butler M, Wagner B. Antimicrobial stewardship programs in inpatient settings: a systematic review. Washington, DC: Department of Veterans Affairs Health Services Research and Development. http://www.hsrd.research.va.gov/publications/esp/antimicrobial.pdf. Published 2013. Accessed January 7, 2016. 10. Graber CJ, Madaras-Kelly K, Jones MM, Neuhauser MM, Goetz MB. Unnecessary antimicrobial use in the context of Clostridium difficile infection: a call to arms for the Veterans Affairs Antimicrobial Stewardship Task Force. Infect Control Hosp Epidemiol. 2013(6);34:651-653. PubMed 11. Rycroft-Malone J. The PARIHS framework--a framework for guiding the implementation of evidence-based practice. J Nurs Care Qual. 2004;19(4):297-304. PubMed 12. Chou AF, Graber CJ, Jones MM, Zhang Y, Goetz MB, Madaras-Kelly K, et al. Specifying an implementation framework for VA antimicrobial stewardship programs. Oral presentation at the VA HSR&D/QUERI National Conference, July 8-9, 2015. Washington, DC: U.S. Department of Veterans Affairs. http://www.hsrd.research.va.gov/meetings/2015/abstract-display.cfm?RecordID=862. Accessed July 5, 2016. 13. Bartholomew DJ. Factor analysis for categorical data. J R Stat Soc. 1980;42:293-321. 14. Flanagan M, Ramanujam R, Sutherland J, Vaughn T, Diekema D, Doebbeling BN. Development and validation of measures to assess prevention and control of AMR in hospitals. Med Care. 2007;45(6): 537-544. PubMed 15. Kline P. An easy guide to factor analysis. New York: Routledge, 1994. 16. Centers for Disease Control and Prevention, National Center for Health Statistics. International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM). Atlanta GA: Centers for Disease Control and Prevention. http://www.cdc.gov/nchs/icd/icd9cm.htm. Published 2013. Accessed January 7, 2016. 17. Huttner B, Jones M, Huttner A, Rubin M, Samore MH. Antibiotic prescription practices for pneumonia, skin and soft tissue infections and urinary tract infections throughout the US Veterans Affairs system. J Antimicrob Chemother. 2013;68(10):2393-2399. PubMed 18. National Institutes of Health. SNOMED Clinical Terms (SNOMED CT). Bethesda, MD: U.S. National Library of Medicine. https://www.nlm.nih.gov/research/umls/Snomed/snomed_main.html. NIH website. Published 2009. Accessed January 7. 2016. 19. Jones M, Huttner B, Madaras-Kelly K, Nechodom K, Nielson C, Bidwell Goetz M, et al. Parenteral to oral conversion of fluoroquinolones: low-hanging fruit for antimicrobial stewardship programs? Infect Control Hosp Epidemiol 2012;33(4): 362-367. PubMed 20. Huttner B, Jones M, Rubin MA, Madaras-Kelly K, Nielson C, Goetz MB, et al. Double trouble: how big a problem is redundant anaerobic antibiotic coverage in Veterans Affairs medical centres? J Antimicrob Chemother. 2012;67(6):1537-1539. PubMed 21. Tibshirani R. Regression shrinkage and selection via the lasso. J R Stat Soc B. 1996;58:267-288. 22. Taylor J, Tibshirani RJ. Statistical learning and selective inference. Proc Natl Acad Sci U S A. 2015;112(25):7629-7634. PubMed 23. VHA Office of Productivity, Efficiency, and Staffing. Facility Complexity Levels. Department of Veterans Affairs website. http://opes.vssc.med.va.gov/FacilityComplexityLevels/Pages/default.aspx. Published 2008. Accessed January 7, 2016. 24. Pakyz AL, Moczygemba LR, Wang H, Stevens MP, Edmond MB. An evaluation of the association between an antimicrobial stewardship score and antimicrobial usage. J Antimicrob Chemother. 2015;70(5):1588-1591. PubMed 25. Schuts EC, Hulscher ME, Mouton JW, Verduin CM, Stuart JW, Overdiek HW, et al. Current evidence on hospital antimicrobial stewardship objectives: a systematic review and meta-analysis. Lancet Infect Dis. 2016;16(7):847-856. PubMed 26. Graber CJ, Goetz MB. Next steps for antimicrobial stewardship. Lancet Infect Dis. 2016;16(7):764-765. PubMed 27. Petzel RA. VHA Directive 1031: Antimicrobial stewardship programs (ASP). Washington, DC: Department of Veterans Affairs.http://www.va.gov/vhapublications/ViewPublication.asp?pub_ID=2964. Published January 22, 2014. Accessed July 5, 2016.
References
1. Antibiotic resistance threats in the United States, 2013. Atlanta, GA: Centers for Disease Control and Prevention. http://www.cdc.gov/drugresistance/threat-report-2013/. Published 2013. Accessed January 7, 2016. 2. Dellit TH, Owens RC, McGowan JE Jr, et al. Infectious Diseases Society of America and the Society for Healthcare Epidemiology of America guidelines for developing an institutional program to enhance antimicrobial stewardship. Clin Infect Dis. 2007;44(2):159-177. PubMed 3. Centers for Disease Control and Prevention. Core elements of hospital antibiotic stewardship programs. Atlanta, GA: Centers for Disease Control and Prevention. http://www.cdc.gov/getsmart/healthcare/implementation/core-elements.html. Published 2015. Accessed January 7, 2016. 4. Pollack LA, Plachouras D, Gruhler H, Sinkowitz-Cochran R. Transatlantic taskforce on antimicrobial resistance (TATFAR) summary of the modified Delphi process for common structure and process indicators for hospital antimicrobial stewardship programs. http://www.cdc.gov/drugresistance/pdf/summary_of_tatfar_recommendation_1.pdf. Published 2015. Accessed January 7, 2016. 5. Barlam TF, Cosgrove SE, Abbo LM, MacDougal C, Schuetz AN, Septimus EJ, et al. Implementing an Antibiotic Stewardship Program: Guidelines by the Infectious Diseases Society of America and the Society for Healthcare Epidemiology of America. Clin Infect Dis. 2016;62(10):e51-e77. PubMed 6. Rohde JM, Jacobsen D, Rosenberg DJ. Role of the hospitalist in antimicrobial stewardship: a review of work completed and description of a multisite collaborative. Clin Ther. 2013;35(6):751-757. PubMed 7. Mack MR, Rohde JM, Jacobsen D, Barron JR, Ko C, Goonewardene M, et al. Engaging hospitalists in antimicrobial stewardship: lessons from a multihosopital collaborative. J Hosp Med. 2016;11(8):576-580. PubMed 8. Davey P, Brown E, Charani E, Fenelon L, Gould IM, Holmes A, et al. Interventions to improve antibiotic prescribing practices for hospital inpatients. Cochrane Database Syst Rev. 2013;4:CD003543. PubMed 9. Filice G, Drekonja D, Wilt TJ, Greer N, Butler M, Wagner B. Antimicrobial stewardship programs in inpatient settings: a systematic review. Washington, DC: Department of Veterans Affairs Health Services Research and Development. http://www.hsrd.research.va.gov/publications/esp/antimicrobial.pdf. Published 2013. Accessed January 7, 2016. 10. Graber CJ, Madaras-Kelly K, Jones MM, Neuhauser MM, Goetz MB. Unnecessary antimicrobial use in the context of Clostridium difficile infection: a call to arms for the Veterans Affairs Antimicrobial Stewardship Task Force. Infect Control Hosp Epidemiol. 2013(6);34:651-653. PubMed 11. Rycroft-Malone J. The PARIHS framework--a framework for guiding the implementation of evidence-based practice. J Nurs Care Qual. 2004;19(4):297-304. PubMed 12. Chou AF, Graber CJ, Jones MM, Zhang Y, Goetz MB, Madaras-Kelly K, et al. Specifying an implementation framework for VA antimicrobial stewardship programs. Oral presentation at the VA HSR&D/QUERI National Conference, July 8-9, 2015. Washington, DC: U.S. Department of Veterans Affairs. http://www.hsrd.research.va.gov/meetings/2015/abstract-display.cfm?RecordID=862. Accessed July 5, 2016. 13. Bartholomew DJ. Factor analysis for categorical data. J R Stat Soc. 1980;42:293-321. 14. Flanagan M, Ramanujam R, Sutherland J, Vaughn T, Diekema D, Doebbeling BN. Development and validation of measures to assess prevention and control of AMR in hospitals. Med Care. 2007;45(6): 537-544. PubMed 15. Kline P. An easy guide to factor analysis. New York: Routledge, 1994. 16. Centers for Disease Control and Prevention, National Center for Health Statistics. International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM). Atlanta GA: Centers for Disease Control and Prevention. http://www.cdc.gov/nchs/icd/icd9cm.htm. Published 2013. Accessed January 7, 2016. 17. Huttner B, Jones M, Huttner A, Rubin M, Samore MH. Antibiotic prescription practices for pneumonia, skin and soft tissue infections and urinary tract infections throughout the US Veterans Affairs system. J Antimicrob Chemother. 2013;68(10):2393-2399. PubMed 18. National Institutes of Health. SNOMED Clinical Terms (SNOMED CT). Bethesda, MD: U.S. National Library of Medicine. https://www.nlm.nih.gov/research/umls/Snomed/snomed_main.html. NIH website. Published 2009. Accessed January 7. 2016. 19. Jones M, Huttner B, Madaras-Kelly K, Nechodom K, Nielson C, Bidwell Goetz M, et al. Parenteral to oral conversion of fluoroquinolones: low-hanging fruit for antimicrobial stewardship programs? Infect Control Hosp Epidemiol 2012;33(4): 362-367. PubMed 20. Huttner B, Jones M, Rubin MA, Madaras-Kelly K, Nielson C, Goetz MB, et al. Double trouble: how big a problem is redundant anaerobic antibiotic coverage in Veterans Affairs medical centres? J Antimicrob Chemother. 2012;67(6):1537-1539. PubMed 21. Tibshirani R. Regression shrinkage and selection via the lasso. J R Stat Soc B. 1996;58:267-288. 22. Taylor J, Tibshirani RJ. Statistical learning and selective inference. Proc Natl Acad Sci U S A. 2015;112(25):7629-7634. PubMed 23. VHA Office of Productivity, Efficiency, and Staffing. Facility Complexity Levels. Department of Veterans Affairs website. http://opes.vssc.med.va.gov/FacilityComplexityLevels/Pages/default.aspx. Published 2008. Accessed January 7, 2016. 24. Pakyz AL, Moczygemba LR, Wang H, Stevens MP, Edmond MB. An evaluation of the association between an antimicrobial stewardship score and antimicrobial usage. J Antimicrob Chemother. 2015;70(5):1588-1591. PubMed 25. Schuts EC, Hulscher ME, Mouton JW, Verduin CM, Stuart JW, Overdiek HW, et al. Current evidence on hospital antimicrobial stewardship objectives: a systematic review and meta-analysis. Lancet Infect Dis. 2016;16(7):847-856. PubMed 26. Graber CJ, Goetz MB. Next steps for antimicrobial stewardship. Lancet Infect Dis. 2016;16(7):764-765. PubMed 27. Petzel RA. VHA Directive 1031: Antimicrobial stewardship programs (ASP). Washington, DC: Department of Veterans Affairs.http://www.va.gov/vhapublications/ViewPublication.asp?pub_ID=2964. Published January 22, 2014. Accessed July 5, 2016.
Association of inpatient antimicrobial utilization measures with antimicrobial stewardship activities and facility characteristics of Veterans Affairs medical centers
Display Headline
Association of inpatient antimicrobial utilization measures with antimicrobial stewardship activities and facility characteristics of Veterans Affairs medical centers
Address for correspondence and reprint requests: Christopher J. Graber, MD, MPH, Infectious Diseases Section, VA Greater Los Angeles Healthcare System, 11301 Wilshire Blvd, 111-F, Los Angeles, CA 90073; Telephone: 310-268-3763; Fax: 310 268-4928; E-mail: [email protected]
Content Gating
Open Access (article Unlocked/Open Access)
Alternative CME
Consolidated Pubs: Do Not Show Source Publication Logo
Older adults commonly experience insomnia and agitation during hospitalization. Unfortunately, the use of benzodiazepines and sedative hypnotics (BSH) to treat these conditions can be ineffective and expose patients to significant adverse effects.1,2 Choosing Wisely® is a campaign that promotes dialogue to reduce unnecessary medical tests, procedures, or treatments. This international campaign has highlighted BSHs as potentially harmful and has recommended against their use as first-line treatment of insomnia and agitation.3-5 Examples of harm with benzodiazepine use include cognitive impairment, impaired postural stability, and an increased incidence of falls and hip fractures in both community and acute care settings.6-8 In addition, prescriptions initiated in hospital appear to be associated with a higher risk of falls and unplanned readmission.9,10 The newer nonbenzodiazepine sedative hypnotics, commonly referred to as “z-drugs”, were initially marketed as a safer alternative in older adults due to their more favorable pharmacokinetics. Evidence has emerged that they carry similar risks.6,11,12 A study comparing benzodiazepines and zolpidem found relatively greater risk of fractures requiring hospitalization with the use of zolpidem compared to lorazepam.13
The use of benzodiazepines in the acute care setting has been evaluated in a number of studies and ranges from 20% to 45%.14-16 Few studies focus on the initiation of these medications in BSH-naïve hospitalized patients; however, reports range from 18% to 29%.17,18 Factors found to be associated with potentially inappropriate prescriptions (PIP) include Hispanic ethnicity, residing in an assisted care setting, and a greater number of BSH prescriptions prior to admission.16,19 Additionally, Cumbler et al.15 found that the presence of dementia was associated with fewer prescriptions for sleep aids in hospital. To our knowledge, there are no published studies that have investigated prescriber factors associated with the use of BSH.
The purpose of our study was to determine the frequency of PIPs of BSH in our academic hospital. Additionally, we aimed to identify patient and prescriber factors that were associated with increased likelihood of prescriptions to help guide future quality improvement initiatives.
METHODS
Study Design and Setting
This was a retrospective observational study conducted at Mount Sinai Hospital (MSH) in Toronto over a 4-month period from January 2013 to April 2013. The hospital is a 442-bed acute care academic health science center affiliated with the University of Toronto. The MSH electronic health record contains demographic data, medications and allergies, nursing documentation, and medical histories from prior encounters. It also includes computerized physician order entry (CPOE) and a detailed medication administration record. This system is integrated with an electronic pharmacy database used to monitor and dispense medications for each patient.
Patient and Medication Selection
We included inpatients over the age of 65 who were prescribed a BSH during the study period from the following services: general internal medicine, cardiology, general surgery, orthopedic surgery, and otolaryngology. To identify new exposure to BSHs, we excluded patients who were regularly prescribed a BSH prior to admission to hospital. The medications of interest included all benzodiazepines and the nonbenzodiazepine sedative hypnotic, zopiclone. Zopiclone is the most commonly used nonbenzodiazepine sedative hypnotic in Canada and the only 1 available on our hospital formulary. These were selected based on the strength of evidence to recommend against their use as first-line agents in older adults and in consultation with our geriatric medicine consultation team pharmacist.20
Data Collection
The hospital administrative database provided patient demographic information, admission service, admitting diagnosis, length of stay, and the total number of patients discharged from the study units over the study period. We then searched the pharmacy electronic database for all benzodiazepines and zopiclone prescribed during the study period for patients who met the inclusion criteria. Manual review of paper and electronic health records for this cohort of patients was conducted to extract additional variables. We used a standardized form to record data elements. Dr. Pek collected all data elements. Dr. Remfry reviewed a random sample of patient records (10%) to ensure accuracy. The agreement between reviewers was 100%.
In compliance with hospital accreditation standards, a clinical pharmacist documents a best possible medication history (BPMH) on every inpatient on admission. We used the BPMH to identify and exclude patients who were prescribed a BSH prior to hospitalization. Because all medications were ordered through the CPOE system, as-needed medication prescriptions required the selection of a specified indication. Available options included ‘agitation/anxiety’ and necessitated combining these 2 indications into 1 category. Indications were primarily extracted through electronic order entry reviews. Paper charts were reviewed when further clarification was needed.
We identified ordering physicians’ training level and familiarity with the service from administrative records obtained from medical education offices, hospital records, and relevant call schedules. Fellows were defined as trainees with a minimum of 6 years of postgraduate training.
Our primary outcome of interest was the proportion of eligible patients age 65 and older who received a PIP for a BSH. Patient variables of interest included age, sex, comorbid conditions, and a pre-admission diagnosis of dementia. Comorbid conditions and age were used to calculate the Carlson Comorbidity Index for each patient.21 Prescription variables included the medication prescribed, time of first prescription (“overnight hours” refer to prescriptions ordered after 7:00 PM and before 7:00 AM), and whether the medication was ordered as part of an admission or postoperative order set. To determine whether patients were discharged home with a prescription for a BSH, we reviewed electronic discharge prescriptions of BSH-naïve patients who received a sedative in hospital. Only medical and cardiology inpatients receive electronic discharge prescriptions, and these were available for 189 patients in our cohort. Provider variables included training level, service, and familiarity with patients. We used the provider’s training program or department of appointment to define the ‘physician on-service’ variable. As an example, a resident registered in internal medicine is defined as ‘on-service’ when prescribing sedatives for a medical inpatient. In contrast, a psychiatry resident would be considered “off-service” if he prescribed a sedative for a surgical inpatient. The familiarity of a provider was categorized as ‘regular’ if they were responsible for a patient’s care on a day-to-day basis and ‘covering’ if they were only covering on call. Other variables included admitting service and hospital length of stay.
Appropriateness Criteria
Criteria for potentially inappropriate use were modified from the American and Canadian Geriatrics Societies’ Choosing Wisely recommendations,4,5 and included insomnia and agitation. These recommendations are in line with other evidence based guidelines for safe prescribing in older adults.20 For the purposes of our study, prescriptions for “agitation/anxiety”, “agitation”, or “insomnia/sleep” were considered potentially inappropriate. Appropriate indications included alcohol withdrawal, end-of-life symptom control, preprocedural sedation, and seizure.5 Patients who were already using a BSH prior to admission for any indication, including a psychiatric diagnosis, were excluded.
Statistical Analyses
We determined the proportion of patients with at least one PIP, as well as the proportion of all prescribing events that were potentially inappropriate. We used the Chi-square statistic and 2-sample t tests to compare the unadjusted associations between patient-level characteristics and receipt of at least 1 inappropriate prescription and prescribing event-level factors with inappropriate prescriptions. Given that first-year residents are more likely to be working overnight when most PIPs are prescribed, we performed a simple logistic regression of potentially inappropriate prescribing by level of training stratified by time of prescription. A multivariable random-intercept logistic regression model was used to assess the adjusted association between patient- and prescribing event-level characteristics with inappropriate prescribing, adjusting for clustering of prescribing events within patients. Characteristics of interest were identified a priori and those with significant bivariate associations with potentially inappropriate were selected for inclusion in the model. Additionally, we included time of prescription in our model to control for potential confounding. All statistical analyses were performed using SAS 9.4 (SAS Institute Inc, Cary, North Carolina). The MSH Research Ethics Board approved the study.
RESULTS
Description of Patients Prescribed a Benzodiazepine Sedative Hypnotic
There were 1540 patients over the age of 65 discharged during the 4-month study period. We excluded the 232 patients who had been prescribed a BSH prior to admission. Of the remaining eligible 1308 BSH-naïve patients, 251 (19.2%) were prescribed a new BSH in hospital and were included in the study. Of this cohort of 251 patients, 193 (76.9%) patients were prescribed a single BSH during their admission while 58 (23.1%) received 2 or more. Of all eligible patients, 208 (15.9%) were prescribed at least 1 PIP. Approximately half of the cohort was admitted to the general internal medicine service, and the most common reason for admission was cardiovascular disease (Table 1).
Table 1
Description of Prescriptions of Benzodiazepine Sedative Hypnotic
We reviewed 328 prescriptions for BSH during the study period. The majority of these, 254 (77.4%) were potentially inappropriate (Table 2). The most common PIPs were zopiclone (167; 65.7%) and lorazepam (82; 32.3%). The PIPs were most frequently ordered on an as-needed basis (219; 86%), followed by one-time orders (30; 12%), and standing orders (5; 2%). The majority of PIPs (222; 87.4%) was prescribed for insomnia with a minority (32; 12.6%) prescribed for agitation and/or anxiety.
Table 2
Most PIP were prescribed during overnight hours (159; 62.6%) and when an in-house pharmacist was unavailable (211; 83.1%). These variables were highly correlated with prescription of sleep aid, which was defined in our criteria as potentially inappropriate. Copies of discharge prescriptions were available for 189 patients. Of these 189 patients, 19 (10.1%) were sent home with a prescription for a new sedative.
Association Between Patient/Provider Variables and Prescriptions
Patient factors associated with fewer PIPs in our bivariate analyses included older age and dementia (Table 1). A greater proportion of nighttime prescriptions were PIPs; however, this finding was not statistically significant (P = 0.067). The majority of all prescriptions was prescribed by residents in their first year of training (64.9%; Table 2), and there was a significant difference in rates of PIP across level of training (P = 0.0007). When stratified by time of prescription, there was no significant difference by level of training for nighttime prescriptions. Among daytime prescriptions, second-year residents and staff (attending physicians and fellows) were less likely to prescribe a PIP than first-year residents (odds ratio [OR], 0.24; 95% confidence interval [CI], 0.09-0.66 and OR, 0.39; 95% CI, 0.14-1.13, respectively; Table 3); however, the association between staff and first-years only approached statistical significance (P = 0.08). Interestingly, 20.4% of all PIPs were ordered routinely as part of an admission or postoperative order set.
Table 3
In our regression model, admission to a specialty or surgical service, compared to the general internal medicine service, was associated with a significantly higher likelihood of a PIP (OR, 6.61; 95% CI, 2.70-16.17; Table 4). Additionally, compared to cardiovascular admission diagnoses, neoplastic admitting diagnoses were associated with a higher likelihood of a PIP (OR, 4.43; 95% CI, 1.23-15.95). Time of prescription was a significant predictor in our multivariable regression model with nighttime prescriptions having increased odds of a PIP (OR, 4.48; 95% CI, 2.21-9.06,). When comparing prescribers at the extremes of training, attending physicians and fellows were much less likely to prescribe a PIP compared to first-year residents (OR, 0.23; 95% CI, 0.08-0.69; Table 4). However, there were no other significant differences across training levels after adjusting for patient and prescribing event characteristics.
Table 4
DISCUSSION
We found that the majority of newly prescribed BSH in hospital was for the potentially inappropriate indications of insomnia and agitation/anxiety. Medications for insomnia were primarily initiated during overnight hours. Training level of prescribers and admitting service were found to be associated with appropriateness of prescriptions.
Our study showed that 15.9% of hospitalized older adults were newly prescribed a PIP during their admission. Of all new in hospital prescriptions, 77% were deemed potentially inappropriate. These numbers are similar to those reported by other centers; however, wide ranges exist.16,19 This is likely the result of differences in appropriate use and inclusion criteria. Gillis et al.17 focused their investigation on sleep aids and showed that 26% of all admitted patients and 18% of BSH naïve patients received a prescription for insomnia. While this is similar to our findings, more than half of these patients were under the age of 65, and additional medications, such as trazodone, antihistamines, and antipsychotics were included.17 Other studies did not exclude patients who used a BSH regularly prior to admission. For example, 21% of veterans admitted to an acute care facility received a prescription for potentially inappropriate indications, but this included continuation of prior home medications.19 In contrast, we chose to focus on older adults in whom BSH pose a greater risk of harm. Exclusion of patients who regularly used a BSH prior to admission allowed us to better understand the circumstances surrounding the initiation of these medications in hospital. Furthermore, abrupt cessation of benzodiazepines can cause withdrawal and worsen confusion.22
We found that 10% of patients newly prescribed a BSH in hospital were discharged with a prescription for a BSH. The accuracy of this is limited by the lack of availability of electronic discharge prescriptions on our surgical wards; however, it is likely an underrepresentation of the true effect given the high rates of PIPs on these wards. Our study highlights the concerning practice of continuing newly prescribed BSH following discharge from hospital.
Sleep disruption and poor quality sleep in hospital is a common issue that leads to significant use of BSH.15 Nonpharmacologic interventions in older adults can be effective in improving sleep quality and reducing the need for BSH; however, they can be time-consuming to implement.23 With the exception of preventative strategies used on our Acute Care for Elders unit, formal nonpharmacologic interventions for sleep are not practiced in our hospital. We found that the majority of PIPs were prescribed as sleep aids in the overnight hours. This suggests that disruptions in sleep are leading patients and nursing staff to request pharmacologic treatments and highlights an area with significant room for improvement. Work is underway to implement and evaluate safe sleep protocols for older adults.
To our knowledge, we are the first to report an association between training level and PIP of BSH in older adults. The highest rates of PIPs were found among the first-year residents and, after controlling for patient and prescribing event characteristics, such as time of prescription, first-year residents were significantly more likely to prescribe a PIP. First-year residents are more likely to respond first to issues on the wards. There may be pressure on first-year trainees to prescribe sleep aids, as many patients and nurses may seek pharmacologic solutions for symptom management. Knowledge gaps may also be a contributing factor early in their training. A survey of physicians found that residents were more likely than attending physicians to list lack of formal education as a barrier to appropriate prescribing.24
Similarities are seen in a study of antibiotic appropriateness, where residents demonstrated gaps in knowledge of treatment of asymptomatic bacteriuria that seemed to vary by specialty.25 Interestingly, we found that patients admitted to general internal medicine were prescribed fewer PIPs. This service includes our Acute Care for Elders unit, which is staffed by trained geriatric nurses and other allied health professionals. Residents who rotated on internal medicine are also likely to have received informal teaching about medication safety in older adults. Educational interventions highlighting adverse effects of BSH and promoting nonpharmacologic solutions should be targeted at first-year residents. However, an interprofessional team approach to sleep disturbance in hospital, in combination with decision support for appropriate BSH use will achieve greater impact than education alone.
Several limitations of this study merit discussion. First, findings from a single academic center may lack generalizability. However, the demographics of our patient population and our rates of BSH use were similar to those reported in previous studies. Second, our study may be subject to observer bias, as the data collectors were not blinded. To minimize this, a strict template and clear appropriateness criteria were developed. Additionally, a second reviewer independently conducted data validation with 100% agreement among reviewers. Third, we studied prescribing patterns rather than medication administration and lacked data on filling of new BSH prescriptions in the postdischarge period. However, our primary goal is to determine risk of exposure to a BSH to minimize it. Fourth, although BSH are discouraged as “first choice for insomnia, anxiety or delirium,”4 they may be appropriate in limited situations where all nonpharmacologic strategies have failed and patient or staff safety is at risk. In our chart reviews, we were unable to determine whether all nonpharmacologic strategies were exhausted prior to prescription initiation. However, more than 20% of all PIP were routinely prescribed as part of an admission or postoperative order set, suggesting a reflexive rather than reflective approach to sedative use. Furthermore, the indications of anxiety and agitation were combined as they appear in the CPOE as a combination indication, thus leaving us unable to determine the true proportion for each indication. However, more than 87% of all PIPs were for insomnia, reflecting a clear opportunity to improve sleep management in hospital. Last, the lack of a power calculation may have resulted in the study being underpowered and thus affected the ability to detect a significant effect of covariates that have real differences on the likelihood of sedative prescriptions. For example, the low number of prescribing events by second-year residents and staff may have resulted in a type II error when comparing PIP rates with first-year residents.
We found that the majority of newly prescribed BSH among older adults in hospital were potentially inappropriate. They were most frequently prescribed by first-year residents overnight in response to insomnia. Our findings demonstrate BSH overuse remains prevalent and is associated with poor sleep in hospital. Future work will focus on implementing and evaluating safe sleep protocols and educational interventions aimed at first-year residents.
Acknowledgments
Elisabeth Pek had full access to all of the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis. Ciara Pendrith conducted and is responsible for the statistical analysis.
Disclosure
The authors report no financial conflicts of interest.
References
1. Glass J, Lanctot KL, Herrmann N, Sproule BA, Busto UE. Sedative hypnotics in older people with insomnia: meta-analysis of risks and benefits. BMJ. 2005;331(7526):1169. PubMed 2. Inouye SK. Delirium in older persons. N Engl J Med. 2006;354(11):1157-1165. PubMed 3. Morden NE, Colla CH, Sequist TD, Rosenthal MB. Choosing wisely--the politics and economics of labeling low-value services. N Engl J Med. 2014;370(7):589-592. PubMed 4. Ten Things Physicians and Patients Should Question. American Geriatrics Society 2013. Revised April 23, 2015. http://www.choosingwisely.org/societies/american-geriatrics-society/. Accessed April 30, 2016. 5. Five Things Physicians and Patients Should Question. Canadian Geriatrics Society. Released April 2, 2014. http://www.choosingwiselycanada.org/recommendations/geriatrics/. Accessed April 30, 2016. 6. de Groot MH, van Campen JP, Moek MA, Tulner LR, Beijnen JH, Lamoth CJ. The effects of fall-risk-increasing drugs on postural control: a literature review. Drugs Aging. 2013;30(11):901-920. PubMed 7. Woolcott JC, Richardson KJ, Wiens MO, et al. Meta-analysis of the impact of 9 medication classes on falls in elderly persons. Arch Intern Med. 2009;169(21):1952-1960. PubMed 8. Pariente A, Dartigues JF, Benichou J, Letenneur L, Moore N, Fourrier-Réglat A. Benzodiazepines and injurious falls in community dwelling elders. Drugs Aging. 2008;25(1):61-70. PubMed 9. Frels C, Williams P, Narayanan S, Gariballa SE. Iatrogenic causes of falls in hospitalised elderly patients: a case-control study. Postgrad Med J. 2002;78(922):487-489. PubMed 10. Pavon JM, Zhao Y, McConnell E, Hastings SN. Identifying risk of readmission in hospitalized elderly adults through inpatient medication exposure. J Am Geriatr Soc. 2014;62(6):1116-1121. PubMed 11. Kang DY, Park S, Rhee CW, et al. Zolpidem use and risk of fracture in elderly insomnia patients. J Prev Med Public Health. 2012;45(4):219-226. PubMed 12. Kolla BP, Lovely JK, Mansukhani MP, Morgenthaler TI. Zolpidem is independently associated with increased risk of inpatient falls. J Hosp Med. 2013;8(1):1-6. PubMed 13. Finkle WD, Der JS, Greenland S, et al. Risk of fractures requiring hospitalization after an initial prescription for zolpidem, alprazolam, lorazepam, or diazepam in older adults. J Am Geriatr Soc. 2011;59(10):1883-1890. PubMed 14. Elliott RA, Woodward MC, Oborne CA. Improving benzodiazepine prescribing for elderly hospital inpatients using audit and multidisciplinary feedback. Intern Med J. 2001;31(9):529-535. PubMed 15. Cumbler E, Guerrasio J, Kim J, Glasheen J. Use of medications for insomnia in the hospitalized geriatric population. J Am Geriatr Soc. 2008;56(3):579-581. PubMed 16. Somers A, Robays H, Audenaert K, Van Maele G, Bogaert M, Petrovic M. The use of hypnosedative drugs in a university hospital: has anything changed in 10 years? Eur J Clin Pharmacol. 2011;67(7):723-729. PubMed 17. Gillis CM, Poyant JO, Degrado JR, Ye L, Anger KE, Owens RL. Inpatient pharmacological sleep aid utilization is common at a tertiary medical center. J Hosp Med. 2014;9(10):652-657. PubMed 18. Frighetto L, Marra C, Bandali S, Wilbur K, Naumann T, Jewesson P. An assessment of quality of sleep and the use of drugs with sedating properties in hospitalized adult patients. Health Qual Life Outcomes. 2004;2:17. PubMed 19. Garrido MM, Prigerson HG, Penrod JD, Jones SC, Boockvar KS. Benzodiazepine and sedative-hypnotic use among older seriously Ill veterans: choosing wisely? Clin Ther. 2014;36(11):1547-1554. PubMed 20. American Geriatrics Society updated Beers Criteria for potentially inappropriate medication use in older adults: The American Geriatrics Society 2012 Beers Criteria Update Expert Panel. J Am Geriatr Soc. 2012;60(4):616-631. PubMed 21. Charlson ME, Pompei P, Ales KL, MacKenzie CR. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis. 1987;40(5):373-383. PubMed 22. Foy A, Drinkwater V, March S, Mearrick P. Confusion after admission to hospital in elderly patients using benzodiazepines. Br Med J (Clin Res Ed). 1986;293(6554):1072. PubMed 23. McDowell JA, Mion LC, Lydon TJ, Inouye SK. A nonpharmacologic sleep protocol for hospitalized older patients. J Am Geriatr Soc. 1998;46(6):700-705. PubMed 24. Ramaswamy R, Maio V, Diamond JJ, et al. Potentially inappropriate prescribing in elderly: assessing doctor knowledge, confidence and barriers. J Eval Clin Pract. 2011;17(6):1153-1159. PubMed 25. Lee MJ, Kim M, Kim NH, et al. Why is asymptomatic bacteriuria overtreated?: A tertiary care institutional survey of resident physicians. BMC Infect Dis. 2015;15:289. PubMed
Older adults commonly experience insomnia and agitation during hospitalization. Unfortunately, the use of benzodiazepines and sedative hypnotics (BSH) to treat these conditions can be ineffective and expose patients to significant adverse effects.1,2 Choosing Wisely® is a campaign that promotes dialogue to reduce unnecessary medical tests, procedures, or treatments. This international campaign has highlighted BSHs as potentially harmful and has recommended against their use as first-line treatment of insomnia and agitation.3-5 Examples of harm with benzodiazepine use include cognitive impairment, impaired postural stability, and an increased incidence of falls and hip fractures in both community and acute care settings.6-8 In addition, prescriptions initiated in hospital appear to be associated with a higher risk of falls and unplanned readmission.9,10 The newer nonbenzodiazepine sedative hypnotics, commonly referred to as “z-drugs”, were initially marketed as a safer alternative in older adults due to their more favorable pharmacokinetics. Evidence has emerged that they carry similar risks.6,11,12 A study comparing benzodiazepines and zolpidem found relatively greater risk of fractures requiring hospitalization with the use of zolpidem compared to lorazepam.13
The use of benzodiazepines in the acute care setting has been evaluated in a number of studies and ranges from 20% to 45%.14-16 Few studies focus on the initiation of these medications in BSH-naïve hospitalized patients; however, reports range from 18% to 29%.17,18 Factors found to be associated with potentially inappropriate prescriptions (PIP) include Hispanic ethnicity, residing in an assisted care setting, and a greater number of BSH prescriptions prior to admission.16,19 Additionally, Cumbler et al.15 found that the presence of dementia was associated with fewer prescriptions for sleep aids in hospital. To our knowledge, there are no published studies that have investigated prescriber factors associated with the use of BSH.
The purpose of our study was to determine the frequency of PIPs of BSH in our academic hospital. Additionally, we aimed to identify patient and prescriber factors that were associated with increased likelihood of prescriptions to help guide future quality improvement initiatives.
METHODS
Study Design and Setting
This was a retrospective observational study conducted at Mount Sinai Hospital (MSH) in Toronto over a 4-month period from January 2013 to April 2013. The hospital is a 442-bed acute care academic health science center affiliated with the University of Toronto. The MSH electronic health record contains demographic data, medications and allergies, nursing documentation, and medical histories from prior encounters. It also includes computerized physician order entry (CPOE) and a detailed medication administration record. This system is integrated with an electronic pharmacy database used to monitor and dispense medications for each patient.
Patient and Medication Selection
We included inpatients over the age of 65 who were prescribed a BSH during the study period from the following services: general internal medicine, cardiology, general surgery, orthopedic surgery, and otolaryngology. To identify new exposure to BSHs, we excluded patients who were regularly prescribed a BSH prior to admission to hospital. The medications of interest included all benzodiazepines and the nonbenzodiazepine sedative hypnotic, zopiclone. Zopiclone is the most commonly used nonbenzodiazepine sedative hypnotic in Canada and the only 1 available on our hospital formulary. These were selected based on the strength of evidence to recommend against their use as first-line agents in older adults and in consultation with our geriatric medicine consultation team pharmacist.20
Data Collection
The hospital administrative database provided patient demographic information, admission service, admitting diagnosis, length of stay, and the total number of patients discharged from the study units over the study period. We then searched the pharmacy electronic database for all benzodiazepines and zopiclone prescribed during the study period for patients who met the inclusion criteria. Manual review of paper and electronic health records for this cohort of patients was conducted to extract additional variables. We used a standardized form to record data elements. Dr. Pek collected all data elements. Dr. Remfry reviewed a random sample of patient records (10%) to ensure accuracy. The agreement between reviewers was 100%.
In compliance with hospital accreditation standards, a clinical pharmacist documents a best possible medication history (BPMH) on every inpatient on admission. We used the BPMH to identify and exclude patients who were prescribed a BSH prior to hospitalization. Because all medications were ordered through the CPOE system, as-needed medication prescriptions required the selection of a specified indication. Available options included ‘agitation/anxiety’ and necessitated combining these 2 indications into 1 category. Indications were primarily extracted through electronic order entry reviews. Paper charts were reviewed when further clarification was needed.
We identified ordering physicians’ training level and familiarity with the service from administrative records obtained from medical education offices, hospital records, and relevant call schedules. Fellows were defined as trainees with a minimum of 6 years of postgraduate training.
Our primary outcome of interest was the proportion of eligible patients age 65 and older who received a PIP for a BSH. Patient variables of interest included age, sex, comorbid conditions, and a pre-admission diagnosis of dementia. Comorbid conditions and age were used to calculate the Carlson Comorbidity Index for each patient.21 Prescription variables included the medication prescribed, time of first prescription (“overnight hours” refer to prescriptions ordered after 7:00 PM and before 7:00 AM), and whether the medication was ordered as part of an admission or postoperative order set. To determine whether patients were discharged home with a prescription for a BSH, we reviewed electronic discharge prescriptions of BSH-naïve patients who received a sedative in hospital. Only medical and cardiology inpatients receive electronic discharge prescriptions, and these were available for 189 patients in our cohort. Provider variables included training level, service, and familiarity with patients. We used the provider’s training program or department of appointment to define the ‘physician on-service’ variable. As an example, a resident registered in internal medicine is defined as ‘on-service’ when prescribing sedatives for a medical inpatient. In contrast, a psychiatry resident would be considered “off-service” if he prescribed a sedative for a surgical inpatient. The familiarity of a provider was categorized as ‘regular’ if they were responsible for a patient’s care on a day-to-day basis and ‘covering’ if they were only covering on call. Other variables included admitting service and hospital length of stay.
Appropriateness Criteria
Criteria for potentially inappropriate use were modified from the American and Canadian Geriatrics Societies’ Choosing Wisely recommendations,4,5 and included insomnia and agitation. These recommendations are in line with other evidence based guidelines for safe prescribing in older adults.20 For the purposes of our study, prescriptions for “agitation/anxiety”, “agitation”, or “insomnia/sleep” were considered potentially inappropriate. Appropriate indications included alcohol withdrawal, end-of-life symptom control, preprocedural sedation, and seizure.5 Patients who were already using a BSH prior to admission for any indication, including a psychiatric diagnosis, were excluded.
Statistical Analyses
We determined the proportion of patients with at least one PIP, as well as the proportion of all prescribing events that were potentially inappropriate. We used the Chi-square statistic and 2-sample t tests to compare the unadjusted associations between patient-level characteristics and receipt of at least 1 inappropriate prescription and prescribing event-level factors with inappropriate prescriptions. Given that first-year residents are more likely to be working overnight when most PIPs are prescribed, we performed a simple logistic regression of potentially inappropriate prescribing by level of training stratified by time of prescription. A multivariable random-intercept logistic regression model was used to assess the adjusted association between patient- and prescribing event-level characteristics with inappropriate prescribing, adjusting for clustering of prescribing events within patients. Characteristics of interest were identified a priori and those with significant bivariate associations with potentially inappropriate were selected for inclusion in the model. Additionally, we included time of prescription in our model to control for potential confounding. All statistical analyses were performed using SAS 9.4 (SAS Institute Inc, Cary, North Carolina). The MSH Research Ethics Board approved the study.
RESULTS
Description of Patients Prescribed a Benzodiazepine Sedative Hypnotic
There were 1540 patients over the age of 65 discharged during the 4-month study period. We excluded the 232 patients who had been prescribed a BSH prior to admission. Of the remaining eligible 1308 BSH-naïve patients, 251 (19.2%) were prescribed a new BSH in hospital and were included in the study. Of this cohort of 251 patients, 193 (76.9%) patients were prescribed a single BSH during their admission while 58 (23.1%) received 2 or more. Of all eligible patients, 208 (15.9%) were prescribed at least 1 PIP. Approximately half of the cohort was admitted to the general internal medicine service, and the most common reason for admission was cardiovascular disease (Table 1).
Table 1
Description of Prescriptions of Benzodiazepine Sedative Hypnotic
We reviewed 328 prescriptions for BSH during the study period. The majority of these, 254 (77.4%) were potentially inappropriate (Table 2). The most common PIPs were zopiclone (167; 65.7%) and lorazepam (82; 32.3%). The PIPs were most frequently ordered on an as-needed basis (219; 86%), followed by one-time orders (30; 12%), and standing orders (5; 2%). The majority of PIPs (222; 87.4%) was prescribed for insomnia with a minority (32; 12.6%) prescribed for agitation and/or anxiety.
Table 2
Most PIP were prescribed during overnight hours (159; 62.6%) and when an in-house pharmacist was unavailable (211; 83.1%). These variables were highly correlated with prescription of sleep aid, which was defined in our criteria as potentially inappropriate. Copies of discharge prescriptions were available for 189 patients. Of these 189 patients, 19 (10.1%) were sent home with a prescription for a new sedative.
Association Between Patient/Provider Variables and Prescriptions
Patient factors associated with fewer PIPs in our bivariate analyses included older age and dementia (Table 1). A greater proportion of nighttime prescriptions were PIPs; however, this finding was not statistically significant (P = 0.067). The majority of all prescriptions was prescribed by residents in their first year of training (64.9%; Table 2), and there was a significant difference in rates of PIP across level of training (P = 0.0007). When stratified by time of prescription, there was no significant difference by level of training for nighttime prescriptions. Among daytime prescriptions, second-year residents and staff (attending physicians and fellows) were less likely to prescribe a PIP than first-year residents (odds ratio [OR], 0.24; 95% confidence interval [CI], 0.09-0.66 and OR, 0.39; 95% CI, 0.14-1.13, respectively; Table 3); however, the association between staff and first-years only approached statistical significance (P = 0.08). Interestingly, 20.4% of all PIPs were ordered routinely as part of an admission or postoperative order set.
Table 3
In our regression model, admission to a specialty or surgical service, compared to the general internal medicine service, was associated with a significantly higher likelihood of a PIP (OR, 6.61; 95% CI, 2.70-16.17; Table 4). Additionally, compared to cardiovascular admission diagnoses, neoplastic admitting diagnoses were associated with a higher likelihood of a PIP (OR, 4.43; 95% CI, 1.23-15.95). Time of prescription was a significant predictor in our multivariable regression model with nighttime prescriptions having increased odds of a PIP (OR, 4.48; 95% CI, 2.21-9.06,). When comparing prescribers at the extremes of training, attending physicians and fellows were much less likely to prescribe a PIP compared to first-year residents (OR, 0.23; 95% CI, 0.08-0.69; Table 4). However, there were no other significant differences across training levels after adjusting for patient and prescribing event characteristics.
Table 4
DISCUSSION
We found that the majority of newly prescribed BSH in hospital was for the potentially inappropriate indications of insomnia and agitation/anxiety. Medications for insomnia were primarily initiated during overnight hours. Training level of prescribers and admitting service were found to be associated with appropriateness of prescriptions.
Our study showed that 15.9% of hospitalized older adults were newly prescribed a PIP during their admission. Of all new in hospital prescriptions, 77% were deemed potentially inappropriate. These numbers are similar to those reported by other centers; however, wide ranges exist.16,19 This is likely the result of differences in appropriate use and inclusion criteria. Gillis et al.17 focused their investigation on sleep aids and showed that 26% of all admitted patients and 18% of BSH naïve patients received a prescription for insomnia. While this is similar to our findings, more than half of these patients were under the age of 65, and additional medications, such as trazodone, antihistamines, and antipsychotics were included.17 Other studies did not exclude patients who used a BSH regularly prior to admission. For example, 21% of veterans admitted to an acute care facility received a prescription for potentially inappropriate indications, but this included continuation of prior home medications.19 In contrast, we chose to focus on older adults in whom BSH pose a greater risk of harm. Exclusion of patients who regularly used a BSH prior to admission allowed us to better understand the circumstances surrounding the initiation of these medications in hospital. Furthermore, abrupt cessation of benzodiazepines can cause withdrawal and worsen confusion.22
We found that 10% of patients newly prescribed a BSH in hospital were discharged with a prescription for a BSH. The accuracy of this is limited by the lack of availability of electronic discharge prescriptions on our surgical wards; however, it is likely an underrepresentation of the true effect given the high rates of PIPs on these wards. Our study highlights the concerning practice of continuing newly prescribed BSH following discharge from hospital.
Sleep disruption and poor quality sleep in hospital is a common issue that leads to significant use of BSH.15 Nonpharmacologic interventions in older adults can be effective in improving sleep quality and reducing the need for BSH; however, they can be time-consuming to implement.23 With the exception of preventative strategies used on our Acute Care for Elders unit, formal nonpharmacologic interventions for sleep are not practiced in our hospital. We found that the majority of PIPs were prescribed as sleep aids in the overnight hours. This suggests that disruptions in sleep are leading patients and nursing staff to request pharmacologic treatments and highlights an area with significant room for improvement. Work is underway to implement and evaluate safe sleep protocols for older adults.
To our knowledge, we are the first to report an association between training level and PIP of BSH in older adults. The highest rates of PIPs were found among the first-year residents and, after controlling for patient and prescribing event characteristics, such as time of prescription, first-year residents were significantly more likely to prescribe a PIP. First-year residents are more likely to respond first to issues on the wards. There may be pressure on first-year trainees to prescribe sleep aids, as many patients and nurses may seek pharmacologic solutions for symptom management. Knowledge gaps may also be a contributing factor early in their training. A survey of physicians found that residents were more likely than attending physicians to list lack of formal education as a barrier to appropriate prescribing.24
Similarities are seen in a study of antibiotic appropriateness, where residents demonstrated gaps in knowledge of treatment of asymptomatic bacteriuria that seemed to vary by specialty.25 Interestingly, we found that patients admitted to general internal medicine were prescribed fewer PIPs. This service includes our Acute Care for Elders unit, which is staffed by trained geriatric nurses and other allied health professionals. Residents who rotated on internal medicine are also likely to have received informal teaching about medication safety in older adults. Educational interventions highlighting adverse effects of BSH and promoting nonpharmacologic solutions should be targeted at first-year residents. However, an interprofessional team approach to sleep disturbance in hospital, in combination with decision support for appropriate BSH use will achieve greater impact than education alone.
Several limitations of this study merit discussion. First, findings from a single academic center may lack generalizability. However, the demographics of our patient population and our rates of BSH use were similar to those reported in previous studies. Second, our study may be subject to observer bias, as the data collectors were not blinded. To minimize this, a strict template and clear appropriateness criteria were developed. Additionally, a second reviewer independently conducted data validation with 100% agreement among reviewers. Third, we studied prescribing patterns rather than medication administration and lacked data on filling of new BSH prescriptions in the postdischarge period. However, our primary goal is to determine risk of exposure to a BSH to minimize it. Fourth, although BSH are discouraged as “first choice for insomnia, anxiety or delirium,”4 they may be appropriate in limited situations where all nonpharmacologic strategies have failed and patient or staff safety is at risk. In our chart reviews, we were unable to determine whether all nonpharmacologic strategies were exhausted prior to prescription initiation. However, more than 20% of all PIP were routinely prescribed as part of an admission or postoperative order set, suggesting a reflexive rather than reflective approach to sedative use. Furthermore, the indications of anxiety and agitation were combined as they appear in the CPOE as a combination indication, thus leaving us unable to determine the true proportion for each indication. However, more than 87% of all PIPs were for insomnia, reflecting a clear opportunity to improve sleep management in hospital. Last, the lack of a power calculation may have resulted in the study being underpowered and thus affected the ability to detect a significant effect of covariates that have real differences on the likelihood of sedative prescriptions. For example, the low number of prescribing events by second-year residents and staff may have resulted in a type II error when comparing PIP rates with first-year residents.
We found that the majority of newly prescribed BSH among older adults in hospital were potentially inappropriate. They were most frequently prescribed by first-year residents overnight in response to insomnia. Our findings demonstrate BSH overuse remains prevalent and is associated with poor sleep in hospital. Future work will focus on implementing and evaluating safe sleep protocols and educational interventions aimed at first-year residents.
Acknowledgments
Elisabeth Pek had full access to all of the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis. Ciara Pendrith conducted and is responsible for the statistical analysis.
Disclosure
The authors report no financial conflicts of interest.
Older adults commonly experience insomnia and agitation during hospitalization. Unfortunately, the use of benzodiazepines and sedative hypnotics (BSH) to treat these conditions can be ineffective and expose patients to significant adverse effects.1,2 Choosing Wisely® is a campaign that promotes dialogue to reduce unnecessary medical tests, procedures, or treatments. This international campaign has highlighted BSHs as potentially harmful and has recommended against their use as first-line treatment of insomnia and agitation.3-5 Examples of harm with benzodiazepine use include cognitive impairment, impaired postural stability, and an increased incidence of falls and hip fractures in both community and acute care settings.6-8 In addition, prescriptions initiated in hospital appear to be associated with a higher risk of falls and unplanned readmission.9,10 The newer nonbenzodiazepine sedative hypnotics, commonly referred to as “z-drugs”, were initially marketed as a safer alternative in older adults due to their more favorable pharmacokinetics. Evidence has emerged that they carry similar risks.6,11,12 A study comparing benzodiazepines and zolpidem found relatively greater risk of fractures requiring hospitalization with the use of zolpidem compared to lorazepam.13
The use of benzodiazepines in the acute care setting has been evaluated in a number of studies and ranges from 20% to 45%.14-16 Few studies focus on the initiation of these medications in BSH-naïve hospitalized patients; however, reports range from 18% to 29%.17,18 Factors found to be associated with potentially inappropriate prescriptions (PIP) include Hispanic ethnicity, residing in an assisted care setting, and a greater number of BSH prescriptions prior to admission.16,19 Additionally, Cumbler et al.15 found that the presence of dementia was associated with fewer prescriptions for sleep aids in hospital. To our knowledge, there are no published studies that have investigated prescriber factors associated with the use of BSH.
The purpose of our study was to determine the frequency of PIPs of BSH in our academic hospital. Additionally, we aimed to identify patient and prescriber factors that were associated with increased likelihood of prescriptions to help guide future quality improvement initiatives.
METHODS
Study Design and Setting
This was a retrospective observational study conducted at Mount Sinai Hospital (MSH) in Toronto over a 4-month period from January 2013 to April 2013. The hospital is a 442-bed acute care academic health science center affiliated with the University of Toronto. The MSH electronic health record contains demographic data, medications and allergies, nursing documentation, and medical histories from prior encounters. It also includes computerized physician order entry (CPOE) and a detailed medication administration record. This system is integrated with an electronic pharmacy database used to monitor and dispense medications for each patient.
Patient and Medication Selection
We included inpatients over the age of 65 who were prescribed a BSH during the study period from the following services: general internal medicine, cardiology, general surgery, orthopedic surgery, and otolaryngology. To identify new exposure to BSHs, we excluded patients who were regularly prescribed a BSH prior to admission to hospital. The medications of interest included all benzodiazepines and the nonbenzodiazepine sedative hypnotic, zopiclone. Zopiclone is the most commonly used nonbenzodiazepine sedative hypnotic in Canada and the only 1 available on our hospital formulary. These were selected based on the strength of evidence to recommend against their use as first-line agents in older adults and in consultation with our geriatric medicine consultation team pharmacist.20
Data Collection
The hospital administrative database provided patient demographic information, admission service, admitting diagnosis, length of stay, and the total number of patients discharged from the study units over the study period. We then searched the pharmacy electronic database for all benzodiazepines and zopiclone prescribed during the study period for patients who met the inclusion criteria. Manual review of paper and electronic health records for this cohort of patients was conducted to extract additional variables. We used a standardized form to record data elements. Dr. Pek collected all data elements. Dr. Remfry reviewed a random sample of patient records (10%) to ensure accuracy. The agreement between reviewers was 100%.
In compliance with hospital accreditation standards, a clinical pharmacist documents a best possible medication history (BPMH) on every inpatient on admission. We used the BPMH to identify and exclude patients who were prescribed a BSH prior to hospitalization. Because all medications were ordered through the CPOE system, as-needed medication prescriptions required the selection of a specified indication. Available options included ‘agitation/anxiety’ and necessitated combining these 2 indications into 1 category. Indications were primarily extracted through electronic order entry reviews. Paper charts were reviewed when further clarification was needed.
We identified ordering physicians’ training level and familiarity with the service from administrative records obtained from medical education offices, hospital records, and relevant call schedules. Fellows were defined as trainees with a minimum of 6 years of postgraduate training.
Our primary outcome of interest was the proportion of eligible patients age 65 and older who received a PIP for a BSH. Patient variables of interest included age, sex, comorbid conditions, and a pre-admission diagnosis of dementia. Comorbid conditions and age were used to calculate the Carlson Comorbidity Index for each patient.21 Prescription variables included the medication prescribed, time of first prescription (“overnight hours” refer to prescriptions ordered after 7:00 PM and before 7:00 AM), and whether the medication was ordered as part of an admission or postoperative order set. To determine whether patients were discharged home with a prescription for a BSH, we reviewed electronic discharge prescriptions of BSH-naïve patients who received a sedative in hospital. Only medical and cardiology inpatients receive electronic discharge prescriptions, and these were available for 189 patients in our cohort. Provider variables included training level, service, and familiarity with patients. We used the provider’s training program or department of appointment to define the ‘physician on-service’ variable. As an example, a resident registered in internal medicine is defined as ‘on-service’ when prescribing sedatives for a medical inpatient. In contrast, a psychiatry resident would be considered “off-service” if he prescribed a sedative for a surgical inpatient. The familiarity of a provider was categorized as ‘regular’ if they were responsible for a patient’s care on a day-to-day basis and ‘covering’ if they were only covering on call. Other variables included admitting service and hospital length of stay.
Appropriateness Criteria
Criteria for potentially inappropriate use were modified from the American and Canadian Geriatrics Societies’ Choosing Wisely recommendations,4,5 and included insomnia and agitation. These recommendations are in line with other evidence based guidelines for safe prescribing in older adults.20 For the purposes of our study, prescriptions for “agitation/anxiety”, “agitation”, or “insomnia/sleep” were considered potentially inappropriate. Appropriate indications included alcohol withdrawal, end-of-life symptom control, preprocedural sedation, and seizure.5 Patients who were already using a BSH prior to admission for any indication, including a psychiatric diagnosis, were excluded.
Statistical Analyses
We determined the proportion of patients with at least one PIP, as well as the proportion of all prescribing events that were potentially inappropriate. We used the Chi-square statistic and 2-sample t tests to compare the unadjusted associations between patient-level characteristics and receipt of at least 1 inappropriate prescription and prescribing event-level factors with inappropriate prescriptions. Given that first-year residents are more likely to be working overnight when most PIPs are prescribed, we performed a simple logistic regression of potentially inappropriate prescribing by level of training stratified by time of prescription. A multivariable random-intercept logistic regression model was used to assess the adjusted association between patient- and prescribing event-level characteristics with inappropriate prescribing, adjusting for clustering of prescribing events within patients. Characteristics of interest were identified a priori and those with significant bivariate associations with potentially inappropriate were selected for inclusion in the model. Additionally, we included time of prescription in our model to control for potential confounding. All statistical analyses were performed using SAS 9.4 (SAS Institute Inc, Cary, North Carolina). The MSH Research Ethics Board approved the study.
RESULTS
Description of Patients Prescribed a Benzodiazepine Sedative Hypnotic
There were 1540 patients over the age of 65 discharged during the 4-month study period. We excluded the 232 patients who had been prescribed a BSH prior to admission. Of the remaining eligible 1308 BSH-naïve patients, 251 (19.2%) were prescribed a new BSH in hospital and were included in the study. Of this cohort of 251 patients, 193 (76.9%) patients were prescribed a single BSH during their admission while 58 (23.1%) received 2 or more. Of all eligible patients, 208 (15.9%) were prescribed at least 1 PIP. Approximately half of the cohort was admitted to the general internal medicine service, and the most common reason for admission was cardiovascular disease (Table 1).
Table 1
Description of Prescriptions of Benzodiazepine Sedative Hypnotic
We reviewed 328 prescriptions for BSH during the study period. The majority of these, 254 (77.4%) were potentially inappropriate (Table 2). The most common PIPs were zopiclone (167; 65.7%) and lorazepam (82; 32.3%). The PIPs were most frequently ordered on an as-needed basis (219; 86%), followed by one-time orders (30; 12%), and standing orders (5; 2%). The majority of PIPs (222; 87.4%) was prescribed for insomnia with a minority (32; 12.6%) prescribed for agitation and/or anxiety.
Table 2
Most PIP were prescribed during overnight hours (159; 62.6%) and when an in-house pharmacist was unavailable (211; 83.1%). These variables were highly correlated with prescription of sleep aid, which was defined in our criteria as potentially inappropriate. Copies of discharge prescriptions were available for 189 patients. Of these 189 patients, 19 (10.1%) were sent home with a prescription for a new sedative.
Association Between Patient/Provider Variables and Prescriptions
Patient factors associated with fewer PIPs in our bivariate analyses included older age and dementia (Table 1). A greater proportion of nighttime prescriptions were PIPs; however, this finding was not statistically significant (P = 0.067). The majority of all prescriptions was prescribed by residents in their first year of training (64.9%; Table 2), and there was a significant difference in rates of PIP across level of training (P = 0.0007). When stratified by time of prescription, there was no significant difference by level of training for nighttime prescriptions. Among daytime prescriptions, second-year residents and staff (attending physicians and fellows) were less likely to prescribe a PIP than first-year residents (odds ratio [OR], 0.24; 95% confidence interval [CI], 0.09-0.66 and OR, 0.39; 95% CI, 0.14-1.13, respectively; Table 3); however, the association between staff and first-years only approached statistical significance (P = 0.08). Interestingly, 20.4% of all PIPs were ordered routinely as part of an admission or postoperative order set.
Table 3
In our regression model, admission to a specialty or surgical service, compared to the general internal medicine service, was associated with a significantly higher likelihood of a PIP (OR, 6.61; 95% CI, 2.70-16.17; Table 4). Additionally, compared to cardiovascular admission diagnoses, neoplastic admitting diagnoses were associated with a higher likelihood of a PIP (OR, 4.43; 95% CI, 1.23-15.95). Time of prescription was a significant predictor in our multivariable regression model with nighttime prescriptions having increased odds of a PIP (OR, 4.48; 95% CI, 2.21-9.06,). When comparing prescribers at the extremes of training, attending physicians and fellows were much less likely to prescribe a PIP compared to first-year residents (OR, 0.23; 95% CI, 0.08-0.69; Table 4). However, there were no other significant differences across training levels after adjusting for patient and prescribing event characteristics.
Table 4
DISCUSSION
We found that the majority of newly prescribed BSH in hospital was for the potentially inappropriate indications of insomnia and agitation/anxiety. Medications for insomnia were primarily initiated during overnight hours. Training level of prescribers and admitting service were found to be associated with appropriateness of prescriptions.
Our study showed that 15.9% of hospitalized older adults were newly prescribed a PIP during their admission. Of all new in hospital prescriptions, 77% were deemed potentially inappropriate. These numbers are similar to those reported by other centers; however, wide ranges exist.16,19 This is likely the result of differences in appropriate use and inclusion criteria. Gillis et al.17 focused their investigation on sleep aids and showed that 26% of all admitted patients and 18% of BSH naïve patients received a prescription for insomnia. While this is similar to our findings, more than half of these patients were under the age of 65, and additional medications, such as trazodone, antihistamines, and antipsychotics were included.17 Other studies did not exclude patients who used a BSH regularly prior to admission. For example, 21% of veterans admitted to an acute care facility received a prescription for potentially inappropriate indications, but this included continuation of prior home medications.19 In contrast, we chose to focus on older adults in whom BSH pose a greater risk of harm. Exclusion of patients who regularly used a BSH prior to admission allowed us to better understand the circumstances surrounding the initiation of these medications in hospital. Furthermore, abrupt cessation of benzodiazepines can cause withdrawal and worsen confusion.22
We found that 10% of patients newly prescribed a BSH in hospital were discharged with a prescription for a BSH. The accuracy of this is limited by the lack of availability of electronic discharge prescriptions on our surgical wards; however, it is likely an underrepresentation of the true effect given the high rates of PIPs on these wards. Our study highlights the concerning practice of continuing newly prescribed BSH following discharge from hospital.
Sleep disruption and poor quality sleep in hospital is a common issue that leads to significant use of BSH.15 Nonpharmacologic interventions in older adults can be effective in improving sleep quality and reducing the need for BSH; however, they can be time-consuming to implement.23 With the exception of preventative strategies used on our Acute Care for Elders unit, formal nonpharmacologic interventions for sleep are not practiced in our hospital. We found that the majority of PIPs were prescribed as sleep aids in the overnight hours. This suggests that disruptions in sleep are leading patients and nursing staff to request pharmacologic treatments and highlights an area with significant room for improvement. Work is underway to implement and evaluate safe sleep protocols for older adults.
To our knowledge, we are the first to report an association between training level and PIP of BSH in older adults. The highest rates of PIPs were found among the first-year residents and, after controlling for patient and prescribing event characteristics, such as time of prescription, first-year residents were significantly more likely to prescribe a PIP. First-year residents are more likely to respond first to issues on the wards. There may be pressure on first-year trainees to prescribe sleep aids, as many patients and nurses may seek pharmacologic solutions for symptom management. Knowledge gaps may also be a contributing factor early in their training. A survey of physicians found that residents were more likely than attending physicians to list lack of formal education as a barrier to appropriate prescribing.24
Similarities are seen in a study of antibiotic appropriateness, where residents demonstrated gaps in knowledge of treatment of asymptomatic bacteriuria that seemed to vary by specialty.25 Interestingly, we found that patients admitted to general internal medicine were prescribed fewer PIPs. This service includes our Acute Care for Elders unit, which is staffed by trained geriatric nurses and other allied health professionals. Residents who rotated on internal medicine are also likely to have received informal teaching about medication safety in older adults. Educational interventions highlighting adverse effects of BSH and promoting nonpharmacologic solutions should be targeted at first-year residents. However, an interprofessional team approach to sleep disturbance in hospital, in combination with decision support for appropriate BSH use will achieve greater impact than education alone.
Several limitations of this study merit discussion. First, findings from a single academic center may lack generalizability. However, the demographics of our patient population and our rates of BSH use were similar to those reported in previous studies. Second, our study may be subject to observer bias, as the data collectors were not blinded. To minimize this, a strict template and clear appropriateness criteria were developed. Additionally, a second reviewer independently conducted data validation with 100% agreement among reviewers. Third, we studied prescribing patterns rather than medication administration and lacked data on filling of new BSH prescriptions in the postdischarge period. However, our primary goal is to determine risk of exposure to a BSH to minimize it. Fourth, although BSH are discouraged as “first choice for insomnia, anxiety or delirium,”4 they may be appropriate in limited situations where all nonpharmacologic strategies have failed and patient or staff safety is at risk. In our chart reviews, we were unable to determine whether all nonpharmacologic strategies were exhausted prior to prescription initiation. However, more than 20% of all PIP were routinely prescribed as part of an admission or postoperative order set, suggesting a reflexive rather than reflective approach to sedative use. Furthermore, the indications of anxiety and agitation were combined as they appear in the CPOE as a combination indication, thus leaving us unable to determine the true proportion for each indication. However, more than 87% of all PIPs were for insomnia, reflecting a clear opportunity to improve sleep management in hospital. Last, the lack of a power calculation may have resulted in the study being underpowered and thus affected the ability to detect a significant effect of covariates that have real differences on the likelihood of sedative prescriptions. For example, the low number of prescribing events by second-year residents and staff may have resulted in a type II error when comparing PIP rates with first-year residents.
We found that the majority of newly prescribed BSH among older adults in hospital were potentially inappropriate. They were most frequently prescribed by first-year residents overnight in response to insomnia. Our findings demonstrate BSH overuse remains prevalent and is associated with poor sleep in hospital. Future work will focus on implementing and evaluating safe sleep protocols and educational interventions aimed at first-year residents.
Acknowledgments
Elisabeth Pek had full access to all of the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis. Ciara Pendrith conducted and is responsible for the statistical analysis.
Disclosure
The authors report no financial conflicts of interest.
References
1. Glass J, Lanctot KL, Herrmann N, Sproule BA, Busto UE. Sedative hypnotics in older people with insomnia: meta-analysis of risks and benefits. BMJ. 2005;331(7526):1169. PubMed 2. Inouye SK. Delirium in older persons. N Engl J Med. 2006;354(11):1157-1165. PubMed 3. Morden NE, Colla CH, Sequist TD, Rosenthal MB. Choosing wisely--the politics and economics of labeling low-value services. N Engl J Med. 2014;370(7):589-592. PubMed 4. Ten Things Physicians and Patients Should Question. American Geriatrics Society 2013. Revised April 23, 2015. http://www.choosingwisely.org/societies/american-geriatrics-society/. Accessed April 30, 2016. 5. Five Things Physicians and Patients Should Question. Canadian Geriatrics Society. Released April 2, 2014. http://www.choosingwiselycanada.org/recommendations/geriatrics/. Accessed April 30, 2016. 6. de Groot MH, van Campen JP, Moek MA, Tulner LR, Beijnen JH, Lamoth CJ. The effects of fall-risk-increasing drugs on postural control: a literature review. Drugs Aging. 2013;30(11):901-920. PubMed 7. Woolcott JC, Richardson KJ, Wiens MO, et al. Meta-analysis of the impact of 9 medication classes on falls in elderly persons. Arch Intern Med. 2009;169(21):1952-1960. PubMed 8. Pariente A, Dartigues JF, Benichou J, Letenneur L, Moore N, Fourrier-Réglat A. Benzodiazepines and injurious falls in community dwelling elders. Drugs Aging. 2008;25(1):61-70. PubMed 9. Frels C, Williams P, Narayanan S, Gariballa SE. Iatrogenic causes of falls in hospitalised elderly patients: a case-control study. Postgrad Med J. 2002;78(922):487-489. PubMed 10. Pavon JM, Zhao Y, McConnell E, Hastings SN. Identifying risk of readmission in hospitalized elderly adults through inpatient medication exposure. J Am Geriatr Soc. 2014;62(6):1116-1121. PubMed 11. Kang DY, Park S, Rhee CW, et al. Zolpidem use and risk of fracture in elderly insomnia patients. J Prev Med Public Health. 2012;45(4):219-226. PubMed 12. Kolla BP, Lovely JK, Mansukhani MP, Morgenthaler TI. Zolpidem is independently associated with increased risk of inpatient falls. J Hosp Med. 2013;8(1):1-6. PubMed 13. Finkle WD, Der JS, Greenland S, et al. Risk of fractures requiring hospitalization after an initial prescription for zolpidem, alprazolam, lorazepam, or diazepam in older adults. J Am Geriatr Soc. 2011;59(10):1883-1890. PubMed 14. Elliott RA, Woodward MC, Oborne CA. Improving benzodiazepine prescribing for elderly hospital inpatients using audit and multidisciplinary feedback. Intern Med J. 2001;31(9):529-535. PubMed 15. Cumbler E, Guerrasio J, Kim J, Glasheen J. Use of medications for insomnia in the hospitalized geriatric population. J Am Geriatr Soc. 2008;56(3):579-581. PubMed 16. Somers A, Robays H, Audenaert K, Van Maele G, Bogaert M, Petrovic M. The use of hypnosedative drugs in a university hospital: has anything changed in 10 years? Eur J Clin Pharmacol. 2011;67(7):723-729. PubMed 17. Gillis CM, Poyant JO, Degrado JR, Ye L, Anger KE, Owens RL. Inpatient pharmacological sleep aid utilization is common at a tertiary medical center. J Hosp Med. 2014;9(10):652-657. PubMed 18. Frighetto L, Marra C, Bandali S, Wilbur K, Naumann T, Jewesson P. An assessment of quality of sleep and the use of drugs with sedating properties in hospitalized adult patients. Health Qual Life Outcomes. 2004;2:17. PubMed 19. Garrido MM, Prigerson HG, Penrod JD, Jones SC, Boockvar KS. Benzodiazepine and sedative-hypnotic use among older seriously Ill veterans: choosing wisely? Clin Ther. 2014;36(11):1547-1554. PubMed 20. American Geriatrics Society updated Beers Criteria for potentially inappropriate medication use in older adults: The American Geriatrics Society 2012 Beers Criteria Update Expert Panel. J Am Geriatr Soc. 2012;60(4):616-631. PubMed 21. Charlson ME, Pompei P, Ales KL, MacKenzie CR. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis. 1987;40(5):373-383. PubMed 22. Foy A, Drinkwater V, March S, Mearrick P. Confusion after admission to hospital in elderly patients using benzodiazepines. Br Med J (Clin Res Ed). 1986;293(6554):1072. PubMed 23. McDowell JA, Mion LC, Lydon TJ, Inouye SK. A nonpharmacologic sleep protocol for hospitalized older patients. J Am Geriatr Soc. 1998;46(6):700-705. PubMed 24. Ramaswamy R, Maio V, Diamond JJ, et al. Potentially inappropriate prescribing in elderly: assessing doctor knowledge, confidence and barriers. J Eval Clin Pract. 2011;17(6):1153-1159. PubMed 25. Lee MJ, Kim M, Kim NH, et al. Why is asymptomatic bacteriuria overtreated?: A tertiary care institutional survey of resident physicians. BMC Infect Dis. 2015;15:289. PubMed
References
1. Glass J, Lanctot KL, Herrmann N, Sproule BA, Busto UE. Sedative hypnotics in older people with insomnia: meta-analysis of risks and benefits. BMJ. 2005;331(7526):1169. PubMed 2. Inouye SK. Delirium in older persons. N Engl J Med. 2006;354(11):1157-1165. PubMed 3. Morden NE, Colla CH, Sequist TD, Rosenthal MB. Choosing wisely--the politics and economics of labeling low-value services. N Engl J Med. 2014;370(7):589-592. PubMed 4. Ten Things Physicians and Patients Should Question. American Geriatrics Society 2013. Revised April 23, 2015. http://www.choosingwisely.org/societies/american-geriatrics-society/. Accessed April 30, 2016. 5. Five Things Physicians and Patients Should Question. Canadian Geriatrics Society. Released April 2, 2014. http://www.choosingwiselycanada.org/recommendations/geriatrics/. Accessed April 30, 2016. 6. de Groot MH, van Campen JP, Moek MA, Tulner LR, Beijnen JH, Lamoth CJ. The effects of fall-risk-increasing drugs on postural control: a literature review. Drugs Aging. 2013;30(11):901-920. PubMed 7. Woolcott JC, Richardson KJ, Wiens MO, et al. Meta-analysis of the impact of 9 medication classes on falls in elderly persons. Arch Intern Med. 2009;169(21):1952-1960. PubMed 8. Pariente A, Dartigues JF, Benichou J, Letenneur L, Moore N, Fourrier-Réglat A. Benzodiazepines and injurious falls in community dwelling elders. Drugs Aging. 2008;25(1):61-70. PubMed 9. Frels C, Williams P, Narayanan S, Gariballa SE. Iatrogenic causes of falls in hospitalised elderly patients: a case-control study. Postgrad Med J. 2002;78(922):487-489. PubMed 10. Pavon JM, Zhao Y, McConnell E, Hastings SN. Identifying risk of readmission in hospitalized elderly adults through inpatient medication exposure. J Am Geriatr Soc. 2014;62(6):1116-1121. PubMed 11. Kang DY, Park S, Rhee CW, et al. Zolpidem use and risk of fracture in elderly insomnia patients. J Prev Med Public Health. 2012;45(4):219-226. PubMed 12. Kolla BP, Lovely JK, Mansukhani MP, Morgenthaler TI. Zolpidem is independently associated with increased risk of inpatient falls. J Hosp Med. 2013;8(1):1-6. PubMed 13. Finkle WD, Der JS, Greenland S, et al. Risk of fractures requiring hospitalization after an initial prescription for zolpidem, alprazolam, lorazepam, or diazepam in older adults. J Am Geriatr Soc. 2011;59(10):1883-1890. PubMed 14. Elliott RA, Woodward MC, Oborne CA. Improving benzodiazepine prescribing for elderly hospital inpatients using audit and multidisciplinary feedback. Intern Med J. 2001;31(9):529-535. PubMed 15. Cumbler E, Guerrasio J, Kim J, Glasheen J. Use of medications for insomnia in the hospitalized geriatric population. J Am Geriatr Soc. 2008;56(3):579-581. PubMed 16. Somers A, Robays H, Audenaert K, Van Maele G, Bogaert M, Petrovic M. The use of hypnosedative drugs in a university hospital: has anything changed in 10 years? Eur J Clin Pharmacol. 2011;67(7):723-729. PubMed 17. Gillis CM, Poyant JO, Degrado JR, Ye L, Anger KE, Owens RL. Inpatient pharmacological sleep aid utilization is common at a tertiary medical center. J Hosp Med. 2014;9(10):652-657. PubMed 18. Frighetto L, Marra C, Bandali S, Wilbur K, Naumann T, Jewesson P. An assessment of quality of sleep and the use of drugs with sedating properties in hospitalized adult patients. Health Qual Life Outcomes. 2004;2:17. PubMed 19. Garrido MM, Prigerson HG, Penrod JD, Jones SC, Boockvar KS. Benzodiazepine and sedative-hypnotic use among older seriously Ill veterans: choosing wisely? Clin Ther. 2014;36(11):1547-1554. PubMed 20. American Geriatrics Society updated Beers Criteria for potentially inappropriate medication use in older adults: The American Geriatrics Society 2012 Beers Criteria Update Expert Panel. J Am Geriatr Soc. 2012;60(4):616-631. PubMed 21. Charlson ME, Pompei P, Ales KL, MacKenzie CR. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis. 1987;40(5):373-383. PubMed 22. Foy A, Drinkwater V, March S, Mearrick P. Confusion after admission to hospital in elderly patients using benzodiazepines. Br Med J (Clin Res Ed). 1986;293(6554):1072. PubMed 23. McDowell JA, Mion LC, Lydon TJ, Inouye SK. A nonpharmacologic sleep protocol for hospitalized older patients. J Am Geriatr Soc. 1998;46(6):700-705. PubMed 24. Ramaswamy R, Maio V, Diamond JJ, et al. Potentially inappropriate prescribing in elderly: assessing doctor knowledge, confidence and barriers. J Eval Clin Pract. 2011;17(6):1153-1159. PubMed 25. Lee MJ, Kim M, Kim NH, et al. Why is asymptomatic bacteriuria overtreated?: A tertiary care institutional survey of resident physicians. BMC Infect Dis. 2015;15:289. PubMed
Hospital-acquired anemia (HAA) is defined as having a normal hemoglobin value upon admission but developing anemia during the course of hospitalization. The condition is common, with an incidence ranging from approximately 25% when defined by using the hemoglobin value prior to discharge to 74% when using the nadir hemoglobin value during hospitalization.1-5 While there are many potential etiologies for HAA, given that iatrogenic blood loss from phlebotomy may lead to its development,6,7 HAA has been postulated to be a hazard of hospitalization that is potentially preventable.8 However, it is unclear whether the development of HAA portends worse outcomes after hospital discharge.
The limited number of studies on the association between HAA and postdischarge outcomes has been restricted to patients hospitalized for acute myocardial infarction (AMI).3,9,10 Among this subpopulation, HAA is independently associated with greater morbidity and mortality following hospital discharge.3,9,10 In a more broadly representative population of hospitalized adults, Koch et al.2 found that the development of HAA is associated with greater length of stay (LOS), hospital charges, and inpatient mortality. However, given that HAA was defined by the lowest hemoglobin level during hospitalization (and not necessarily the last value prior to discharge), it is unclear if the worse outcomes observed were the cause of the HAA, rather than its effect, since hospital LOS is a robust predictor for the development of HAA, as well as a major driver of hospital costs and a prognostic marker for inpatient mortality.3,9 Furthermore, this study evaluated outcomes only during the index hospitalization, so it is unclear if patients who develop HAA have worse clinical outcomes after discharge.
Therefore, in this study, we used clinically granular electronic health record (EHR) data from a diverse cohort of consecutive medicine inpatients hospitalized for any reason at 1 of 6 hospitals to: 1) describe the epidemiology of HAA; 2) identify predictors of its development; and 3) examine its association with 30-day postdischarge adverse outcomes. We hypothesized that the development of HAA would be independently associated with 30-day readmission and mortality in a dose-dependent fashion, with increasing severity of HAA associated with worse outcomes.
METHODS
Study Design, Population, and Data Sources
We conducted a retrospective observational cohort study using EHR data collected from November 1, 2009 to October 30, 2010 from 6 hospitals in the north Texas region. One site was a university-affiliated safety-net hospital; the remaining 5 community hospitals were a mix of teaching and nonteaching sites. All hospitals used the Epic EHR system (Epic Systems Corporation, Verona, Wisconsin). Details of this cohort have been published.11,12This study included consecutive hospitalizations among adults age 18 years or older who were discharged from a medicine inpatient service with any diagnosis. We excluded hospitalizations by individuals who were anemic within the first 24 hours of admission (hematocrit less than 36% for women and less than 40% for men), were missing a hematocrit value within the first 24 hours of hospitalization or a repeat hematocrit value prior to discharge, had a hospitalization in the preceding 30 days (ie, index hospitalization was considered a readmission), died in the hospital, were transferred to another hospital, or left against medical advice. For individuals with multiple eligible hospitalizations during the study period, we included only the first hospitalization. We also excluded those discharged to hospice, given that this population of individuals may have intentionally desired less aggressive care.
Definition of Hospital-Acquired Anemia
HAA was defined as having a normal hematocrit value (36% or greater for women and 40% or greater for men) within the first 24 hours of admission and a hematocrit value at the time of hospital discharge lower than the World Health Organization’s sex-specific cut points.13 If there was more than 1 hematocrit value on the same day, we chose the lowest value. Based on prior studies, HAA was further categorized by severity as mild (hematocrit greater than 33% and less than 36% in women; and greater than 33% and less than 40% in men), moderate (hematocrit greater than 27% and 33% or less for all), or severe (hematocrit 27% or less for all).2,14
Characteristics
We extracted information on sociodemographic characteristics, comorbidities, LOS, procedures, blood transfusions, and laboratory values from the EHR. Hospitalizations in the 12 months preceding the index hospitalization were ascertained from the EHR and from an all-payer regional hospitalization database that captures hospitalizations from 75 acute care hospitals within a 100-mile radius of Dallas-Fort Worth. International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) discharge diagnosis codes were categorized according to the Agency for Healthcare Research and Quality (AHRQ) Clinical Classifications Software (CCS).15 We defined a diagnosis for hemorrhage and coagulation, and hemorrhagic disorder as the presence of any ICD-9-CM code (primary or secondary) that mapped to the AHRQ CCS diagnoses 60 and 153, and 62, respectively. Procedures were categorized as minor diagnostic, minor therapeutic, major diagnostic, and major therapeutic using the AHRQ Healthcare Cost and Utilization Procedure Classes tool.16
Outcomes
The primary outcome was a composite of death or readmission within 30 days of hospital discharge. Hospital readmissions were ascertained at the index hospital and at any of 75 acute care hospitals in the region as described earlier. Death was ascertained from each of the hospitals’ EHR and administrative data and the Social Security Death Index. Individuals who had both outcomes (eg, a 30-day readmission and death) were considered to have only 1 occurrence of the composite primary outcome measure. Our secondary outcomes were death and readmission within 30 days of discharge, considered as separate outcomes.
Statistical Analysis
We used logistic regression models to evaluate predictors of HAA and to estimate the association of HAA on subsequent 30-day adverse outcomes after hospital discharge. All models accounted for clustering of patients by hospital. For the outcomes analyses, models were adjusted for potential confounders based on prior literature and our group’s expertise, which included age, sex, race/ethnicity, Charlson comorbidity index, prior hospitalizations, nonelective admission status, creatinine level on admission, blood urea nitrogen (BUN) to creatinine ratio of more than 20:1 on admission, LOS, receipt of a major diagnostic or therapeutic procedure during the index hospitalization, a discharge diagnosis for hemorrhage, and a discharge diagnosis for a coagulation or hemorrhagic disorder. For the mortality analyses, given the limited number of 30-day deaths after hospital discharge in our cohort, we collapsed moderate and severe HAA into a single category. In sensitivity analyses, we repeated the adjusted model, but excluded patients in our cohort who had received at least 1 blood transfusion during the index hospitalization (2.6%) given its potential for harm, and patients with a primary discharge diagnosis for AMI (3.1%).17
The functional forms of continuous variables were assessed using restricted cubic splines and locally weighted scatterplot smoothing techniques. All analyses were performed using STATA statistical software version 12.0 (StataCorp, College Station, Texas). The University of Texas Southwestern Medical Center institutional review board approved this study.
Figure
RESULTS
Of 53,995 consecutive medicine hospitalizations among adults age 18 years or older during our study period, 11,309 index hospitalizations were included in our study cohort (Supplemental Figure 1). The majority of patients excluded were because of having documented anemia within the first 24 hours of admission (n=24,950). With increasing severity of HAA, patients were older, more likely to be female, non-Hispanic white, electively admitted, have fewer comorbidities, less likely to be hospitalized in the past year, more likely to have had a major procedure, receive a blood transfusion, have a longer LOS, and have a primary or secondary discharge diagnosis for a hemorrhage or a coagulation or hemorrhagic disorder (Table 1).
Table 1
Epidemiology of HAA
Among this cohort of patients without anemia on admission, the median hematocrit value on admission was 40.6 g/dL and on discharge was 38.9 g/dL. One-third of patients with normal hematocrit value at admission developed HAA, with 21.6% developing mild HAA, 10.1% developing moderate HAA, and 1.4% developing severe HAA. The median discharge hematocrit value was 36 g/dL (interquartile range [IQR]), 35-38 g/dL) for the group of patients who developed mild HAA, 31 g/dL (IQR, 30-32 g/dL) for moderate HAA, and 26 g/dL (IQR, 25-27 g/dL) for severe HAA (Supplemental Figure 2). Among the severe HAA group, 135 of the 159 patients (85%) had a major procedure (n=123, accounting for 219 unique major procedures), a diagnosis for hemorrhage (n=30), and/or a diagnosis for a coagulation or hemorrhagic disorder (n=23) during the index hospitalization. Of the 219 major procedures among patients with severe HAA, most were musculoskeletal (92 procedures), cardiovascular (61 procedures), or digestive system-related (41 procedures). The most common types of procedures were coronary artery bypass graft (36 procedures), hip replacement (25 procedures), knee replacement (17 procedures), and femur fracture reduction (15 procedures). The 10 most common principal discharge diagnoses of the index hospitalization by HAA group are shown in Supplemental Table 1. For the severe HAA group, the most common diagnosis was hip fracture (20.8%).
Predictors of HAA
Compared to no or mild HAA, female sex, elective admission status, serum creatinine on admission, BUN to creatinine ratio greater than 20 to 1, hospital LOS, and undergoing a major diagnostic or therapeutic procedure were predictors for the development of moderate or severe HAA (Table 2). The model explained 23% of the variance (McFadden’s pseudo R2).
Table 2
Incidence of Postdischarge Outcomes by Severity of HAA
The severity of HAA was associated with a dose-dependent increase in the incidence of 30-day adverse outcomes, such that patients with increasing severity of HAA had greater 30-day composite, mortality, and readmission outcomes (P < 0.001; Figure). The 30-day postdischarge composite outcome was primarily driven by hospital readmissions given the low mortality rate in our cohort. Patients who did not develop HAA had an incidence of 9.7% for the composite outcome, whereas patients with severe HAA had an incidence of 16.4%. Among the 24 patients with severe HAA but who had not undergone a major procedure or had a discharge diagnosis for hemorrhage or for a coagulation or hemorrhagic disorder, only 3 (12.5%) had a composite postdischarge adverse outcome (2 readmissions and 1 death). The median time to readmission was similar between groups, but more patients with severe HAA had an early readmission within 7 days of hospital discharge than patients who did not develop HAA (6.9% vs. 2.9%, P = 0.001; Supplemental Table 2).
Association of HAA and Postdischarge Outcomes
In unadjusted analyses, compared to not developing HAA, mild, moderate, and severe HAA were associated with a 29%, 61%, and 81% increase in the odds for a composite outcome, respectively (Table 3). After adjustment for confounders, the effect size for HAA attenuated and was no longer statistically significant for mild and moderate HAA. However, severe HAA was significantly associated with a 39% increase in the odds for the composite outcome and a 41% increase in the odds for 30-day readmission (P = 0.008 and P = 0.02, respectively).
Table 3
In sensitivity analyses, the exclusion of individuals who received at least 1 blood transfusion during the index hospitalization (n=298) and individuals who had a primary discharge diagnosis for AMI (n=353) did not substantively change the estimates of the association between severe HAA and postdischarge outcomes (Supplemental Tables 3 and 4). However, because of the fewer number of adverse events for each analysis, the confidence intervals were wider and the association of severe HAA and the composite outcome and readmission were no longer statistically significant in these subcohorts.
DISCUSSION
In this large and diverse sample of medical inpatients, we found that HAA occurs in one-third of adults with normal hematocrit value at admission, where 10.1% of the cohort developed moderately severe HAA and 1.4% developed severe HAA by the time of discharge. Length of stay and undergoing a major diagnostic or therapeutic procedure were the 2 strongest potentially modifiable predictors of developing moderate or severe HAA. Severe HAA was independently associated with a 39% increase in the odds of being readmitted or dying within 30 days after hospital discharge compared to not developing HAA. However, the associations between mild or moderate HAA with adverse outcomes were attenuated after adjusting for confounders and were no longer statistically significant.
To our knowledge, this is the first study on the postdischarge adverse outcomes of HAA among a diverse cohort of medical inpatients hospitalized for any reason. In a more restricted population, Salisbury et al.3 found that patients hospitalized for AMI who developed moderate to severe HAA (hemoglobin value at discharge of 11 g/dL or less) had greater 1-year mortality than those without HAA (8.4% vs. 2.6%, P < 0.001), and had an 82% increase in the hazard for mortality (95% confidence interval, hazard ratio 1.11-2.98). Others have similarly shown that HAA is common among patients hospitalized with AMI and is associated with greater mortality.5,9,18 Our study extends upon this prior research by showing that severe HAA increases the risk for adverse outcomes for all adult inpatients, not only those hospitalized for AMI or among those receiving blood transfusions.
Despite the increased harm associated with severe HAA, it is unclear whether HAA is a preventable hazard of hospitalization, as suggested by others.6,8 Most patients in our cohort who developed severe HAA underwent a major procedure, had a discharge diagnosis for hemorrhage, and/or had a discharge diagnosis for a coagulation or hemorrhagic disorder. Thus, blood loss due to phlebotomy, 1 of the more modifiable etiologies of HAA, was unlikely to have been the primary driver for most patients who developed severe HAA. Since it has been estimated to take 15 days of daily phlebotomy of 53 mL of whole blood in females of average body weight (and 20 days for average weight males) with no bone marrow synthesis for severe anemia to develop, it is even less likely that phlebotomy was the principal etiology given an 8-day median LOS among patients with severe HAA.19,20 However, since the etiology of HAA can be multifactorial, limiting blood loss due to phlebotomy by using smaller volume tubes, blood conservation devices, or reducing unnecessary testing may mitigate the development of severe HAA.21,22 Additionally, since more than three-quarters of patients who developed severe HAA underwent a major procedure, more care and attention to minimizing operative blood loss could lessen the severity of HAA and facilitate better recovery. If minimizing blood loss is not feasible, in the absence of symptoms related to anemia or ongoing blood loss, randomized controlled trials overwhelmingly support a restrictive transfusion strategy using a hemoglobin value threshold of 7 mg/dL, even in the postoperative setting.23-25
The implications of mild to moderate HAA are less clear. The odds ratios for mild and moderate HAA, while not statistically significant, suggest a small increase in harm compared to not developing HAA. Furthermore, the upper boundary of the confidence intervals for mild and moderate HAA cannot exclude a possible 30% and 56% increase in the odds for the 30-day composite outcome, respectively. Thus, a better powered study, including more patients and extending the time interval for ascertaining postdischarge adverse events beyond 30 days, may reveal a harmful association. Lastly, our study assessed only the association of HAA with 30-day readmission and mortality. Examining the association between HAA and other patient-centered outcomes such as fatigue, functional impairment, and prolonged posthospitalization recovery time may uncover other important adverse effects of mild and moderate HAA, both of which occur far more frequently than severe HAA.
Our findings should be interpreted in the context of several limitations. First, although we included a diverse group of patients from a multihospital cohort, generalizability to other settings is uncertain. Second, as this was a retrospective study using EHR data, we had limited information to infer the precise mechanism of HAA for each patient. However, procedure codes and discharge diagnoses enabled us to assess which patients underwent a major procedure or had a hemorrhage or hemorrhagic disorder during the hospitalization. Third, given the relatively few number of patients with severe HAA in our cohort, we were unable to assess if the association of severe HAA differed by suspected etiology. Lastly, because we were unable to ascertain the timing of the hematocrit values within the first 24 hours of admission, we excluded both patients with preexisting anemia on admission and those who developed HAA within the first 24 hours of admission, which is not uncommon.26 Thus, we were unable to assess the effect of acute on chronic anemia arising during hospitalization and HAA that develops within the first 24 hours, both of which may also be harmful.18,27,28
In conclusion, severe HAA occurs in 1.4% of all medical hospitalizations and is associated with increased odds of death or readmission within 30 days. Since most patients with severe HAA had undergone a major procedure or had a discharge diagnosis of hemorrhage or a coagulation or hemorrhagic disorder, it is unclear if severe HAA is potentially preventable through preventing blood loss from phlebotomy or by reducing iatrogenic injury during procedures. Future research should assess the potential preventability of severe HAA, and examine other patient-centered outcomes potentially related to anemia, including fatigue, functional impairment, and trajectory of posthospital recovery.
Acknowledgments
The authors would like to acknowledge Ruben Amarasingham, MD, MBA, President and Chief Executive Officer of the Parkland Center for Clinical Innovation, and Ferdinand Velasco, MD, Chief Health Information Officer at Texas Health Resources, for their assistance in assembling the 6 hospital cohort used in this study. The authors would also like to thank Valy Fontil, MD, MAS, Assistant Professor of Medicine at the University of California San Francisco School of Medicine, and Elizabeth Rogers, MD, MAS, Assistant Professor of Internal Medicine and Pediatrics at the University of Minnesota Medical School, for their constructive feedback on an earlier version of this manuscript.
Disclosures
This work was supported by the Agency for Healthcare Research and Quality-funded UT Southwestern Center for Patient-Centered Outcomes Research (R24 HS022418-01); the Commonwealth Foundation (#20100323); the UT Southwestern KL2 Scholars Program supported by the National Institutes of Health (KL2 TR001103); the National Center for Advancing Translational Sciences at the National Institute of Health (U54 RFA-TR-12-006); and the National Institute on Aging (K23AG052603). The study sponsors had no role in design and conduct of the study; collection, management, analysis, and interpretation of the data; and preparation, review, or approval of the manuscript. The authors have no financial conflicts of interest to disclose.
1. Kurniali PC, Curry S, Brennan KW, et al. A retrospective study investigating the incidence and predisposing factors of hospital-acquired anemia. Anemia. 2014;2014:634582. PubMed 2. Koch CG, Li L, Sun Z, et al. Hospital-acquired anemia: prevalence, outcomes, and healthcare implications. J Hosp Med. 2013;8(9):506-512. PubMed 3. Salisbury AC, Alexander KP, Reid KJ, et al. Incidence, correlates, and outcomes of acute, hospital-acquired anemia in patients with acute myocardial infarction. Circ Cardiovasc Qual Outcomes. 2010;3(4):337-346. PubMed 4. Salisbury AC, Amin AP, Reid KJ, et al. Hospital-acquired anemia and in-hospital mortality in patients with acute myocardial infarction. Am Heart J. 2011;162(2):300-309 e303. PubMed 5. Meroño O, Cladellas M, Recasens L, et al. In-hospital acquired anemia in acute coronary syndrome. Predictors, in-hospital prognosis and one-year mortality. Rev Esp Cardiol (Engl Ed). 2012;65(8):742-748. PubMed 6. Salisbury AC, Reid KJ, Alexander KP, et al. Diagnostic blood loss from phlebotomy and hospital-acquired anemia during acute myocardial infarction. Arch Intern Med. 2011;171(18):1646-1653. PubMed 7. Thavendiranathan P, Bagai A, Ebidia A, Detsky AS, Choudhry NK. Do blood tests cause anemia in hospitalized patients? The effect of diagnostic phlebotomy on hemoglobin and hematocrit levels. J Gen Intern Med. 2005;20(6):520-524. PubMed 8. Rennke S, Fang MC. Hazards of hospitalization: more than just “never events”. Arch Intern Med. 2011;171(18):1653-1654. PubMed 9. Choi JS, Kim YA, Kang YU, et al. Clinical impact of hospital-acquired anemia in association with acute kidney injury and chronic kidney disease in patients with acute myocardial infarction. PLoS One. 2013;8(9):e75583. PubMed 10. Salisbury AC, Kosiborod M, Amin AP, et al. Recovery from hospital-acquired anemia after acute myocardial infarction and effect on outcomes. Am J Cardiol. 2011;108(7):949-954. PubMed 11. Nguyen OK, Makam AN, Clark C, et al. Predicting all-cause readmissions using electronic health record data from the entire hospitalization: Model development and comparison. J Hosp Med. 2016;11(7):473-480. PubMed 12. Amarasingham R, Velasco F, Xie B, et al. Electronic medical record-based multicondition models to predict the risk of 30 day readmission or death among adult medicine patients: validation and comparison to existing models. BMC Med Inform Decis Mak. 2015;15:39. PubMed 13. World Health Organization. Hemoglobin concentrations for the diagnosis of anaemia and assessment of severity. http://www.who.int/vmnis/indicators/haemoglobin.pdf. Accessed March 15, 2016. 14. Martin ND, Scantling D. Hospital-acquired anemia: a contemporary review of etiologies and prevention strategies. J Infus Nurs. 2015;38(5):330-338. PubMed 15. Agency for Healthcare Research and Quality, Rockville, MD. Clinical classification software (CCS) for ICD-9-CM. Healthcare Cost and Utilization Project. 2015 http://www.hcup-us.ahrq.gov/toolssoftware/ccs/ccs.jsp. Accessed November 18, 2015. 16. Agency for Healthcare Research and Quality, Rockville, MD. Procedure classes2015. Healthcare Cost and Utilization Project. 2015. https://www.hcup-us.ahrq.gov/toolssoftware/procedure/procedure.jsp. Accessed November 18, 2015. 17. Corwin HL, Gettinger A, Pearl RG, et al. The CRIT Study: Anemia and blood transfusion in the critically ill--current clinical practice in the United States. Crit Care Med. 2004;32(1):39-52. PubMed 18. Aronson D, Suleiman M, Agmon Y, et al. Changes in haemoglobin levels during hospital course and long-term outcome after acute myocardial infarction. Eur Heart J. 2007;28(11):1289-1296. PubMed 19. Lyon AW, Chin AC, Slotsve GA, Lyon ME. Simulation of repetitive diagnostic blood loss and onset of iatrogenic anemia in critical care patients with a mathematical model. Comput Biol Med. 2013;43(2):84-90. PubMed 20. van der Bom JG, Cannegieter SC. Hospital-acquired anemia: the contribution of diagnostic blood loss. J Thromb Haemost. 2015;13(6):1157-1159. PubMed 21. Sanchez-Giron F, Alvarez-Mora F. Reduction of blood loss from laboratory testing in hospitalized adult patients using small-volume (pediatric) tubes. Arch Pathol Lab Med. 2008;132(12):1916-1919. PubMed 22. Smoller BR, Kruskall MS. Phlebotomy for diagnostic laboratory tests in adults. Pattern of use and effect on transfusion requirements. N Engl J Med. 1986;314(19):1233-1235. PubMed 23. Carson JL, Carless PA, Hebert PC. Transfusion thresholds and other strategies for guiding allogeneic red blood cell transfusion. Cochrane Database Syst Rev. 2012(4):CD002042. PubMed 24. Carson JL, Carless PA, Hébert PC. Outcomes using lower vs higher hemoglobin thresholds for red blood cell transfusion. JAMA. 2013;309(1):83-84. PubMed 25. Carson JL, Sieber F, Cook DR, et al. Liberal versus restrictive blood transfusion strategy: 3-year survival and cause of death results from the FOCUS randomised controlled trial. Lancet. 2015;385(9974):1183-1189. PubMed 26. Rajkomar A, McCulloch CE, Fang MC. Low diagnostic utility of rechecking hemoglobins within 24 hours in hospitalized patients. Am J Med. 2016;129(11):1194-1197. PubMed 27. Reade MC, Weissfeld L, Angus DC, Kellum JA, Milbrandt EB. The prevalence of anemia and its association with 90-day mortality in hospitalized community-acquired pneumonia. BMC Pulm Med. 2010;10:15. PubMed 28. Halm EA, Wang JJ, Boockvar K, et al. The effect of perioperative anemia on clinical and functional outcomes in patients with hip fracture. J Orthop Trauma. 2004;18(6):369-374. PubMed
Hospital-acquired anemia (HAA) is defined as having a normal hemoglobin value upon admission but developing anemia during the course of hospitalization. The condition is common, with an incidence ranging from approximately 25% when defined by using the hemoglobin value prior to discharge to 74% when using the nadir hemoglobin value during hospitalization.1-5 While there are many potential etiologies for HAA, given that iatrogenic blood loss from phlebotomy may lead to its development,6,7 HAA has been postulated to be a hazard of hospitalization that is potentially preventable.8 However, it is unclear whether the development of HAA portends worse outcomes after hospital discharge.
The limited number of studies on the association between HAA and postdischarge outcomes has been restricted to patients hospitalized for acute myocardial infarction (AMI).3,9,10 Among this subpopulation, HAA is independently associated with greater morbidity and mortality following hospital discharge.3,9,10 In a more broadly representative population of hospitalized adults, Koch et al.2 found that the development of HAA is associated with greater length of stay (LOS), hospital charges, and inpatient mortality. However, given that HAA was defined by the lowest hemoglobin level during hospitalization (and not necessarily the last value prior to discharge), it is unclear if the worse outcomes observed were the cause of the HAA, rather than its effect, since hospital LOS is a robust predictor for the development of HAA, as well as a major driver of hospital costs and a prognostic marker for inpatient mortality.3,9 Furthermore, this study evaluated outcomes only during the index hospitalization, so it is unclear if patients who develop HAA have worse clinical outcomes after discharge.
Therefore, in this study, we used clinically granular electronic health record (EHR) data from a diverse cohort of consecutive medicine inpatients hospitalized for any reason at 1 of 6 hospitals to: 1) describe the epidemiology of HAA; 2) identify predictors of its development; and 3) examine its association with 30-day postdischarge adverse outcomes. We hypothesized that the development of HAA would be independently associated with 30-day readmission and mortality in a dose-dependent fashion, with increasing severity of HAA associated with worse outcomes.
METHODS
Study Design, Population, and Data Sources
We conducted a retrospective observational cohort study using EHR data collected from November 1, 2009 to October 30, 2010 from 6 hospitals in the north Texas region. One site was a university-affiliated safety-net hospital; the remaining 5 community hospitals were a mix of teaching and nonteaching sites. All hospitals used the Epic EHR system (Epic Systems Corporation, Verona, Wisconsin). Details of this cohort have been published.11,12This study included consecutive hospitalizations among adults age 18 years or older who were discharged from a medicine inpatient service with any diagnosis. We excluded hospitalizations by individuals who were anemic within the first 24 hours of admission (hematocrit less than 36% for women and less than 40% for men), were missing a hematocrit value within the first 24 hours of hospitalization or a repeat hematocrit value prior to discharge, had a hospitalization in the preceding 30 days (ie, index hospitalization was considered a readmission), died in the hospital, were transferred to another hospital, or left against medical advice. For individuals with multiple eligible hospitalizations during the study period, we included only the first hospitalization. We also excluded those discharged to hospice, given that this population of individuals may have intentionally desired less aggressive care.
Definition of Hospital-Acquired Anemia
HAA was defined as having a normal hematocrit value (36% or greater for women and 40% or greater for men) within the first 24 hours of admission and a hematocrit value at the time of hospital discharge lower than the World Health Organization’s sex-specific cut points.13 If there was more than 1 hematocrit value on the same day, we chose the lowest value. Based on prior studies, HAA was further categorized by severity as mild (hematocrit greater than 33% and less than 36% in women; and greater than 33% and less than 40% in men), moderate (hematocrit greater than 27% and 33% or less for all), or severe (hematocrit 27% or less for all).2,14
Characteristics
We extracted information on sociodemographic characteristics, comorbidities, LOS, procedures, blood transfusions, and laboratory values from the EHR. Hospitalizations in the 12 months preceding the index hospitalization were ascertained from the EHR and from an all-payer regional hospitalization database that captures hospitalizations from 75 acute care hospitals within a 100-mile radius of Dallas-Fort Worth. International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) discharge diagnosis codes were categorized according to the Agency for Healthcare Research and Quality (AHRQ) Clinical Classifications Software (CCS).15 We defined a diagnosis for hemorrhage and coagulation, and hemorrhagic disorder as the presence of any ICD-9-CM code (primary or secondary) that mapped to the AHRQ CCS diagnoses 60 and 153, and 62, respectively. Procedures were categorized as minor diagnostic, minor therapeutic, major diagnostic, and major therapeutic using the AHRQ Healthcare Cost and Utilization Procedure Classes tool.16
Outcomes
The primary outcome was a composite of death or readmission within 30 days of hospital discharge. Hospital readmissions were ascertained at the index hospital and at any of 75 acute care hospitals in the region as described earlier. Death was ascertained from each of the hospitals’ EHR and administrative data and the Social Security Death Index. Individuals who had both outcomes (eg, a 30-day readmission and death) were considered to have only 1 occurrence of the composite primary outcome measure. Our secondary outcomes were death and readmission within 30 days of discharge, considered as separate outcomes.
Statistical Analysis
We used logistic regression models to evaluate predictors of HAA and to estimate the association of HAA on subsequent 30-day adverse outcomes after hospital discharge. All models accounted for clustering of patients by hospital. For the outcomes analyses, models were adjusted for potential confounders based on prior literature and our group’s expertise, which included age, sex, race/ethnicity, Charlson comorbidity index, prior hospitalizations, nonelective admission status, creatinine level on admission, blood urea nitrogen (BUN) to creatinine ratio of more than 20:1 on admission, LOS, receipt of a major diagnostic or therapeutic procedure during the index hospitalization, a discharge diagnosis for hemorrhage, and a discharge diagnosis for a coagulation or hemorrhagic disorder. For the mortality analyses, given the limited number of 30-day deaths after hospital discharge in our cohort, we collapsed moderate and severe HAA into a single category. In sensitivity analyses, we repeated the adjusted model, but excluded patients in our cohort who had received at least 1 blood transfusion during the index hospitalization (2.6%) given its potential for harm, and patients with a primary discharge diagnosis for AMI (3.1%).17
The functional forms of continuous variables were assessed using restricted cubic splines and locally weighted scatterplot smoothing techniques. All analyses were performed using STATA statistical software version 12.0 (StataCorp, College Station, Texas). The University of Texas Southwestern Medical Center institutional review board approved this study.
Figure
RESULTS
Of 53,995 consecutive medicine hospitalizations among adults age 18 years or older during our study period, 11,309 index hospitalizations were included in our study cohort (Supplemental Figure 1). The majority of patients excluded were because of having documented anemia within the first 24 hours of admission (n=24,950). With increasing severity of HAA, patients were older, more likely to be female, non-Hispanic white, electively admitted, have fewer comorbidities, less likely to be hospitalized in the past year, more likely to have had a major procedure, receive a blood transfusion, have a longer LOS, and have a primary or secondary discharge diagnosis for a hemorrhage or a coagulation or hemorrhagic disorder (Table 1).
Table 1
Epidemiology of HAA
Among this cohort of patients without anemia on admission, the median hematocrit value on admission was 40.6 g/dL and on discharge was 38.9 g/dL. One-third of patients with normal hematocrit value at admission developed HAA, with 21.6% developing mild HAA, 10.1% developing moderate HAA, and 1.4% developing severe HAA. The median discharge hematocrit value was 36 g/dL (interquartile range [IQR]), 35-38 g/dL) for the group of patients who developed mild HAA, 31 g/dL (IQR, 30-32 g/dL) for moderate HAA, and 26 g/dL (IQR, 25-27 g/dL) for severe HAA (Supplemental Figure 2). Among the severe HAA group, 135 of the 159 patients (85%) had a major procedure (n=123, accounting for 219 unique major procedures), a diagnosis for hemorrhage (n=30), and/or a diagnosis for a coagulation or hemorrhagic disorder (n=23) during the index hospitalization. Of the 219 major procedures among patients with severe HAA, most were musculoskeletal (92 procedures), cardiovascular (61 procedures), or digestive system-related (41 procedures). The most common types of procedures were coronary artery bypass graft (36 procedures), hip replacement (25 procedures), knee replacement (17 procedures), and femur fracture reduction (15 procedures). The 10 most common principal discharge diagnoses of the index hospitalization by HAA group are shown in Supplemental Table 1. For the severe HAA group, the most common diagnosis was hip fracture (20.8%).
Predictors of HAA
Compared to no or mild HAA, female sex, elective admission status, serum creatinine on admission, BUN to creatinine ratio greater than 20 to 1, hospital LOS, and undergoing a major diagnostic or therapeutic procedure were predictors for the development of moderate or severe HAA (Table 2). The model explained 23% of the variance (McFadden’s pseudo R2).
Table 2
Incidence of Postdischarge Outcomes by Severity of HAA
The severity of HAA was associated with a dose-dependent increase in the incidence of 30-day adverse outcomes, such that patients with increasing severity of HAA had greater 30-day composite, mortality, and readmission outcomes (P < 0.001; Figure). The 30-day postdischarge composite outcome was primarily driven by hospital readmissions given the low mortality rate in our cohort. Patients who did not develop HAA had an incidence of 9.7% for the composite outcome, whereas patients with severe HAA had an incidence of 16.4%. Among the 24 patients with severe HAA but who had not undergone a major procedure or had a discharge diagnosis for hemorrhage or for a coagulation or hemorrhagic disorder, only 3 (12.5%) had a composite postdischarge adverse outcome (2 readmissions and 1 death). The median time to readmission was similar between groups, but more patients with severe HAA had an early readmission within 7 days of hospital discharge than patients who did not develop HAA (6.9% vs. 2.9%, P = 0.001; Supplemental Table 2).
Association of HAA and Postdischarge Outcomes
In unadjusted analyses, compared to not developing HAA, mild, moderate, and severe HAA were associated with a 29%, 61%, and 81% increase in the odds for a composite outcome, respectively (Table 3). After adjustment for confounders, the effect size for HAA attenuated and was no longer statistically significant for mild and moderate HAA. However, severe HAA was significantly associated with a 39% increase in the odds for the composite outcome and a 41% increase in the odds for 30-day readmission (P = 0.008 and P = 0.02, respectively).
Table 3
In sensitivity analyses, the exclusion of individuals who received at least 1 blood transfusion during the index hospitalization (n=298) and individuals who had a primary discharge diagnosis for AMI (n=353) did not substantively change the estimates of the association between severe HAA and postdischarge outcomes (Supplemental Tables 3 and 4). However, because of the fewer number of adverse events for each analysis, the confidence intervals were wider and the association of severe HAA and the composite outcome and readmission were no longer statistically significant in these subcohorts.
DISCUSSION
In this large and diverse sample of medical inpatients, we found that HAA occurs in one-third of adults with normal hematocrit value at admission, where 10.1% of the cohort developed moderately severe HAA and 1.4% developed severe HAA by the time of discharge. Length of stay and undergoing a major diagnostic or therapeutic procedure were the 2 strongest potentially modifiable predictors of developing moderate or severe HAA. Severe HAA was independently associated with a 39% increase in the odds of being readmitted or dying within 30 days after hospital discharge compared to not developing HAA. However, the associations between mild or moderate HAA with adverse outcomes were attenuated after adjusting for confounders and were no longer statistically significant.
To our knowledge, this is the first study on the postdischarge adverse outcomes of HAA among a diverse cohort of medical inpatients hospitalized for any reason. In a more restricted population, Salisbury et al.3 found that patients hospitalized for AMI who developed moderate to severe HAA (hemoglobin value at discharge of 11 g/dL or less) had greater 1-year mortality than those without HAA (8.4% vs. 2.6%, P < 0.001), and had an 82% increase in the hazard for mortality (95% confidence interval, hazard ratio 1.11-2.98). Others have similarly shown that HAA is common among patients hospitalized with AMI and is associated with greater mortality.5,9,18 Our study extends upon this prior research by showing that severe HAA increases the risk for adverse outcomes for all adult inpatients, not only those hospitalized for AMI or among those receiving blood transfusions.
Despite the increased harm associated with severe HAA, it is unclear whether HAA is a preventable hazard of hospitalization, as suggested by others.6,8 Most patients in our cohort who developed severe HAA underwent a major procedure, had a discharge diagnosis for hemorrhage, and/or had a discharge diagnosis for a coagulation or hemorrhagic disorder. Thus, blood loss due to phlebotomy, 1 of the more modifiable etiologies of HAA, was unlikely to have been the primary driver for most patients who developed severe HAA. Since it has been estimated to take 15 days of daily phlebotomy of 53 mL of whole blood in females of average body weight (and 20 days for average weight males) with no bone marrow synthesis for severe anemia to develop, it is even less likely that phlebotomy was the principal etiology given an 8-day median LOS among patients with severe HAA.19,20 However, since the etiology of HAA can be multifactorial, limiting blood loss due to phlebotomy by using smaller volume tubes, blood conservation devices, or reducing unnecessary testing may mitigate the development of severe HAA.21,22 Additionally, since more than three-quarters of patients who developed severe HAA underwent a major procedure, more care and attention to minimizing operative blood loss could lessen the severity of HAA and facilitate better recovery. If minimizing blood loss is not feasible, in the absence of symptoms related to anemia or ongoing blood loss, randomized controlled trials overwhelmingly support a restrictive transfusion strategy using a hemoglobin value threshold of 7 mg/dL, even in the postoperative setting.23-25
The implications of mild to moderate HAA are less clear. The odds ratios for mild and moderate HAA, while not statistically significant, suggest a small increase in harm compared to not developing HAA. Furthermore, the upper boundary of the confidence intervals for mild and moderate HAA cannot exclude a possible 30% and 56% increase in the odds for the 30-day composite outcome, respectively. Thus, a better powered study, including more patients and extending the time interval for ascertaining postdischarge adverse events beyond 30 days, may reveal a harmful association. Lastly, our study assessed only the association of HAA with 30-day readmission and mortality. Examining the association between HAA and other patient-centered outcomes such as fatigue, functional impairment, and prolonged posthospitalization recovery time may uncover other important adverse effects of mild and moderate HAA, both of which occur far more frequently than severe HAA.
Our findings should be interpreted in the context of several limitations. First, although we included a diverse group of patients from a multihospital cohort, generalizability to other settings is uncertain. Second, as this was a retrospective study using EHR data, we had limited information to infer the precise mechanism of HAA for each patient. However, procedure codes and discharge diagnoses enabled us to assess which patients underwent a major procedure or had a hemorrhage or hemorrhagic disorder during the hospitalization. Third, given the relatively few number of patients with severe HAA in our cohort, we were unable to assess if the association of severe HAA differed by suspected etiology. Lastly, because we were unable to ascertain the timing of the hematocrit values within the first 24 hours of admission, we excluded both patients with preexisting anemia on admission and those who developed HAA within the first 24 hours of admission, which is not uncommon.26 Thus, we were unable to assess the effect of acute on chronic anemia arising during hospitalization and HAA that develops within the first 24 hours, both of which may also be harmful.18,27,28
In conclusion, severe HAA occurs in 1.4% of all medical hospitalizations and is associated with increased odds of death or readmission within 30 days. Since most patients with severe HAA had undergone a major procedure or had a discharge diagnosis of hemorrhage or a coagulation or hemorrhagic disorder, it is unclear if severe HAA is potentially preventable through preventing blood loss from phlebotomy or by reducing iatrogenic injury during procedures. Future research should assess the potential preventability of severe HAA, and examine other patient-centered outcomes potentially related to anemia, including fatigue, functional impairment, and trajectory of posthospital recovery.
Acknowledgments
The authors would like to acknowledge Ruben Amarasingham, MD, MBA, President and Chief Executive Officer of the Parkland Center for Clinical Innovation, and Ferdinand Velasco, MD, Chief Health Information Officer at Texas Health Resources, for their assistance in assembling the 6 hospital cohort used in this study. The authors would also like to thank Valy Fontil, MD, MAS, Assistant Professor of Medicine at the University of California San Francisco School of Medicine, and Elizabeth Rogers, MD, MAS, Assistant Professor of Internal Medicine and Pediatrics at the University of Minnesota Medical School, for their constructive feedback on an earlier version of this manuscript.
Disclosures
This work was supported by the Agency for Healthcare Research and Quality-funded UT Southwestern Center for Patient-Centered Outcomes Research (R24 HS022418-01); the Commonwealth Foundation (#20100323); the UT Southwestern KL2 Scholars Program supported by the National Institutes of Health (KL2 TR001103); the National Center for Advancing Translational Sciences at the National Institute of Health (U54 RFA-TR-12-006); and the National Institute on Aging (K23AG052603). The study sponsors had no role in design and conduct of the study; collection, management, analysis, and interpretation of the data; and preparation, review, or approval of the manuscript. The authors have no financial conflicts of interest to disclose.
Hospital-acquired anemia (HAA) is defined as having a normal hemoglobin value upon admission but developing anemia during the course of hospitalization. The condition is common, with an incidence ranging from approximately 25% when defined by using the hemoglobin value prior to discharge to 74% when using the nadir hemoglobin value during hospitalization.1-5 While there are many potential etiologies for HAA, given that iatrogenic blood loss from phlebotomy may lead to its development,6,7 HAA has been postulated to be a hazard of hospitalization that is potentially preventable.8 However, it is unclear whether the development of HAA portends worse outcomes after hospital discharge.
The limited number of studies on the association between HAA and postdischarge outcomes has been restricted to patients hospitalized for acute myocardial infarction (AMI).3,9,10 Among this subpopulation, HAA is independently associated with greater morbidity and mortality following hospital discharge.3,9,10 In a more broadly representative population of hospitalized adults, Koch et al.2 found that the development of HAA is associated with greater length of stay (LOS), hospital charges, and inpatient mortality. However, given that HAA was defined by the lowest hemoglobin level during hospitalization (and not necessarily the last value prior to discharge), it is unclear if the worse outcomes observed were the cause of the HAA, rather than its effect, since hospital LOS is a robust predictor for the development of HAA, as well as a major driver of hospital costs and a prognostic marker for inpatient mortality.3,9 Furthermore, this study evaluated outcomes only during the index hospitalization, so it is unclear if patients who develop HAA have worse clinical outcomes after discharge.
Therefore, in this study, we used clinically granular electronic health record (EHR) data from a diverse cohort of consecutive medicine inpatients hospitalized for any reason at 1 of 6 hospitals to: 1) describe the epidemiology of HAA; 2) identify predictors of its development; and 3) examine its association with 30-day postdischarge adverse outcomes. We hypothesized that the development of HAA would be independently associated with 30-day readmission and mortality in a dose-dependent fashion, with increasing severity of HAA associated with worse outcomes.
METHODS
Study Design, Population, and Data Sources
We conducted a retrospective observational cohort study using EHR data collected from November 1, 2009 to October 30, 2010 from 6 hospitals in the north Texas region. One site was a university-affiliated safety-net hospital; the remaining 5 community hospitals were a mix of teaching and nonteaching sites. All hospitals used the Epic EHR system (Epic Systems Corporation, Verona, Wisconsin). Details of this cohort have been published.11,12This study included consecutive hospitalizations among adults age 18 years or older who were discharged from a medicine inpatient service with any diagnosis. We excluded hospitalizations by individuals who were anemic within the first 24 hours of admission (hematocrit less than 36% for women and less than 40% for men), were missing a hematocrit value within the first 24 hours of hospitalization or a repeat hematocrit value prior to discharge, had a hospitalization in the preceding 30 days (ie, index hospitalization was considered a readmission), died in the hospital, were transferred to another hospital, or left against medical advice. For individuals with multiple eligible hospitalizations during the study period, we included only the first hospitalization. We also excluded those discharged to hospice, given that this population of individuals may have intentionally desired less aggressive care.
Definition of Hospital-Acquired Anemia
HAA was defined as having a normal hematocrit value (36% or greater for women and 40% or greater for men) within the first 24 hours of admission and a hematocrit value at the time of hospital discharge lower than the World Health Organization’s sex-specific cut points.13 If there was more than 1 hematocrit value on the same day, we chose the lowest value. Based on prior studies, HAA was further categorized by severity as mild (hematocrit greater than 33% and less than 36% in women; and greater than 33% and less than 40% in men), moderate (hematocrit greater than 27% and 33% or less for all), or severe (hematocrit 27% or less for all).2,14
Characteristics
We extracted information on sociodemographic characteristics, comorbidities, LOS, procedures, blood transfusions, and laboratory values from the EHR. Hospitalizations in the 12 months preceding the index hospitalization were ascertained from the EHR and from an all-payer regional hospitalization database that captures hospitalizations from 75 acute care hospitals within a 100-mile radius of Dallas-Fort Worth. International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) discharge diagnosis codes were categorized according to the Agency for Healthcare Research and Quality (AHRQ) Clinical Classifications Software (CCS).15 We defined a diagnosis for hemorrhage and coagulation, and hemorrhagic disorder as the presence of any ICD-9-CM code (primary or secondary) that mapped to the AHRQ CCS diagnoses 60 and 153, and 62, respectively. Procedures were categorized as minor diagnostic, minor therapeutic, major diagnostic, and major therapeutic using the AHRQ Healthcare Cost and Utilization Procedure Classes tool.16
Outcomes
The primary outcome was a composite of death or readmission within 30 days of hospital discharge. Hospital readmissions were ascertained at the index hospital and at any of 75 acute care hospitals in the region as described earlier. Death was ascertained from each of the hospitals’ EHR and administrative data and the Social Security Death Index. Individuals who had both outcomes (eg, a 30-day readmission and death) were considered to have only 1 occurrence of the composite primary outcome measure. Our secondary outcomes were death and readmission within 30 days of discharge, considered as separate outcomes.
Statistical Analysis
We used logistic regression models to evaluate predictors of HAA and to estimate the association of HAA on subsequent 30-day adverse outcomes after hospital discharge. All models accounted for clustering of patients by hospital. For the outcomes analyses, models were adjusted for potential confounders based on prior literature and our group’s expertise, which included age, sex, race/ethnicity, Charlson comorbidity index, prior hospitalizations, nonelective admission status, creatinine level on admission, blood urea nitrogen (BUN) to creatinine ratio of more than 20:1 on admission, LOS, receipt of a major diagnostic or therapeutic procedure during the index hospitalization, a discharge diagnosis for hemorrhage, and a discharge diagnosis for a coagulation or hemorrhagic disorder. For the mortality analyses, given the limited number of 30-day deaths after hospital discharge in our cohort, we collapsed moderate and severe HAA into a single category. In sensitivity analyses, we repeated the adjusted model, but excluded patients in our cohort who had received at least 1 blood transfusion during the index hospitalization (2.6%) given its potential for harm, and patients with a primary discharge diagnosis for AMI (3.1%).17
The functional forms of continuous variables were assessed using restricted cubic splines and locally weighted scatterplot smoothing techniques. All analyses were performed using STATA statistical software version 12.0 (StataCorp, College Station, Texas). The University of Texas Southwestern Medical Center institutional review board approved this study.
Figure
RESULTS
Of 53,995 consecutive medicine hospitalizations among adults age 18 years or older during our study period, 11,309 index hospitalizations were included in our study cohort (Supplemental Figure 1). The majority of patients excluded were because of having documented anemia within the first 24 hours of admission (n=24,950). With increasing severity of HAA, patients were older, more likely to be female, non-Hispanic white, electively admitted, have fewer comorbidities, less likely to be hospitalized in the past year, more likely to have had a major procedure, receive a blood transfusion, have a longer LOS, and have a primary or secondary discharge diagnosis for a hemorrhage or a coagulation or hemorrhagic disorder (Table 1).
Table 1
Epidemiology of HAA
Among this cohort of patients without anemia on admission, the median hematocrit value on admission was 40.6 g/dL and on discharge was 38.9 g/dL. One-third of patients with normal hematocrit value at admission developed HAA, with 21.6% developing mild HAA, 10.1% developing moderate HAA, and 1.4% developing severe HAA. The median discharge hematocrit value was 36 g/dL (interquartile range [IQR]), 35-38 g/dL) for the group of patients who developed mild HAA, 31 g/dL (IQR, 30-32 g/dL) for moderate HAA, and 26 g/dL (IQR, 25-27 g/dL) for severe HAA (Supplemental Figure 2). Among the severe HAA group, 135 of the 159 patients (85%) had a major procedure (n=123, accounting for 219 unique major procedures), a diagnosis for hemorrhage (n=30), and/or a diagnosis for a coagulation or hemorrhagic disorder (n=23) during the index hospitalization. Of the 219 major procedures among patients with severe HAA, most were musculoskeletal (92 procedures), cardiovascular (61 procedures), or digestive system-related (41 procedures). The most common types of procedures were coronary artery bypass graft (36 procedures), hip replacement (25 procedures), knee replacement (17 procedures), and femur fracture reduction (15 procedures). The 10 most common principal discharge diagnoses of the index hospitalization by HAA group are shown in Supplemental Table 1. For the severe HAA group, the most common diagnosis was hip fracture (20.8%).
Predictors of HAA
Compared to no or mild HAA, female sex, elective admission status, serum creatinine on admission, BUN to creatinine ratio greater than 20 to 1, hospital LOS, and undergoing a major diagnostic or therapeutic procedure were predictors for the development of moderate or severe HAA (Table 2). The model explained 23% of the variance (McFadden’s pseudo R2).
Table 2
Incidence of Postdischarge Outcomes by Severity of HAA
The severity of HAA was associated with a dose-dependent increase in the incidence of 30-day adverse outcomes, such that patients with increasing severity of HAA had greater 30-day composite, mortality, and readmission outcomes (P < 0.001; Figure). The 30-day postdischarge composite outcome was primarily driven by hospital readmissions given the low mortality rate in our cohort. Patients who did not develop HAA had an incidence of 9.7% for the composite outcome, whereas patients with severe HAA had an incidence of 16.4%. Among the 24 patients with severe HAA but who had not undergone a major procedure or had a discharge diagnosis for hemorrhage or for a coagulation or hemorrhagic disorder, only 3 (12.5%) had a composite postdischarge adverse outcome (2 readmissions and 1 death). The median time to readmission was similar between groups, but more patients with severe HAA had an early readmission within 7 days of hospital discharge than patients who did not develop HAA (6.9% vs. 2.9%, P = 0.001; Supplemental Table 2).
Association of HAA and Postdischarge Outcomes
In unadjusted analyses, compared to not developing HAA, mild, moderate, and severe HAA were associated with a 29%, 61%, and 81% increase in the odds for a composite outcome, respectively (Table 3). After adjustment for confounders, the effect size for HAA attenuated and was no longer statistically significant for mild and moderate HAA. However, severe HAA was significantly associated with a 39% increase in the odds for the composite outcome and a 41% increase in the odds for 30-day readmission (P = 0.008 and P = 0.02, respectively).
Table 3
In sensitivity analyses, the exclusion of individuals who received at least 1 blood transfusion during the index hospitalization (n=298) and individuals who had a primary discharge diagnosis for AMI (n=353) did not substantively change the estimates of the association between severe HAA and postdischarge outcomes (Supplemental Tables 3 and 4). However, because of the fewer number of adverse events for each analysis, the confidence intervals were wider and the association of severe HAA and the composite outcome and readmission were no longer statistically significant in these subcohorts.
DISCUSSION
In this large and diverse sample of medical inpatients, we found that HAA occurs in one-third of adults with normal hematocrit value at admission, where 10.1% of the cohort developed moderately severe HAA and 1.4% developed severe HAA by the time of discharge. Length of stay and undergoing a major diagnostic or therapeutic procedure were the 2 strongest potentially modifiable predictors of developing moderate or severe HAA. Severe HAA was independently associated with a 39% increase in the odds of being readmitted or dying within 30 days after hospital discharge compared to not developing HAA. However, the associations between mild or moderate HAA with adverse outcomes were attenuated after adjusting for confounders and were no longer statistically significant.
To our knowledge, this is the first study on the postdischarge adverse outcomes of HAA among a diverse cohort of medical inpatients hospitalized for any reason. In a more restricted population, Salisbury et al.3 found that patients hospitalized for AMI who developed moderate to severe HAA (hemoglobin value at discharge of 11 g/dL or less) had greater 1-year mortality than those without HAA (8.4% vs. 2.6%, P < 0.001), and had an 82% increase in the hazard for mortality (95% confidence interval, hazard ratio 1.11-2.98). Others have similarly shown that HAA is common among patients hospitalized with AMI and is associated with greater mortality.5,9,18 Our study extends upon this prior research by showing that severe HAA increases the risk for adverse outcomes for all adult inpatients, not only those hospitalized for AMI or among those receiving blood transfusions.
Despite the increased harm associated with severe HAA, it is unclear whether HAA is a preventable hazard of hospitalization, as suggested by others.6,8 Most patients in our cohort who developed severe HAA underwent a major procedure, had a discharge diagnosis for hemorrhage, and/or had a discharge diagnosis for a coagulation or hemorrhagic disorder. Thus, blood loss due to phlebotomy, 1 of the more modifiable etiologies of HAA, was unlikely to have been the primary driver for most patients who developed severe HAA. Since it has been estimated to take 15 days of daily phlebotomy of 53 mL of whole blood in females of average body weight (and 20 days for average weight males) with no bone marrow synthesis for severe anemia to develop, it is even less likely that phlebotomy was the principal etiology given an 8-day median LOS among patients with severe HAA.19,20 However, since the etiology of HAA can be multifactorial, limiting blood loss due to phlebotomy by using smaller volume tubes, blood conservation devices, or reducing unnecessary testing may mitigate the development of severe HAA.21,22 Additionally, since more than three-quarters of patients who developed severe HAA underwent a major procedure, more care and attention to minimizing operative blood loss could lessen the severity of HAA and facilitate better recovery. If minimizing blood loss is not feasible, in the absence of symptoms related to anemia or ongoing blood loss, randomized controlled trials overwhelmingly support a restrictive transfusion strategy using a hemoglobin value threshold of 7 mg/dL, even in the postoperative setting.23-25
The implications of mild to moderate HAA are less clear. The odds ratios for mild and moderate HAA, while not statistically significant, suggest a small increase in harm compared to not developing HAA. Furthermore, the upper boundary of the confidence intervals for mild and moderate HAA cannot exclude a possible 30% and 56% increase in the odds for the 30-day composite outcome, respectively. Thus, a better powered study, including more patients and extending the time interval for ascertaining postdischarge adverse events beyond 30 days, may reveal a harmful association. Lastly, our study assessed only the association of HAA with 30-day readmission and mortality. Examining the association between HAA and other patient-centered outcomes such as fatigue, functional impairment, and prolonged posthospitalization recovery time may uncover other important adverse effects of mild and moderate HAA, both of which occur far more frequently than severe HAA.
Our findings should be interpreted in the context of several limitations. First, although we included a diverse group of patients from a multihospital cohort, generalizability to other settings is uncertain. Second, as this was a retrospective study using EHR data, we had limited information to infer the precise mechanism of HAA for each patient. However, procedure codes and discharge diagnoses enabled us to assess which patients underwent a major procedure or had a hemorrhage or hemorrhagic disorder during the hospitalization. Third, given the relatively few number of patients with severe HAA in our cohort, we were unable to assess if the association of severe HAA differed by suspected etiology. Lastly, because we were unable to ascertain the timing of the hematocrit values within the first 24 hours of admission, we excluded both patients with preexisting anemia on admission and those who developed HAA within the first 24 hours of admission, which is not uncommon.26 Thus, we were unable to assess the effect of acute on chronic anemia arising during hospitalization and HAA that develops within the first 24 hours, both of which may also be harmful.18,27,28
In conclusion, severe HAA occurs in 1.4% of all medical hospitalizations and is associated with increased odds of death or readmission within 30 days. Since most patients with severe HAA had undergone a major procedure or had a discharge diagnosis of hemorrhage or a coagulation or hemorrhagic disorder, it is unclear if severe HAA is potentially preventable through preventing blood loss from phlebotomy or by reducing iatrogenic injury during procedures. Future research should assess the potential preventability of severe HAA, and examine other patient-centered outcomes potentially related to anemia, including fatigue, functional impairment, and trajectory of posthospital recovery.
Acknowledgments
The authors would like to acknowledge Ruben Amarasingham, MD, MBA, President and Chief Executive Officer of the Parkland Center for Clinical Innovation, and Ferdinand Velasco, MD, Chief Health Information Officer at Texas Health Resources, for their assistance in assembling the 6 hospital cohort used in this study. The authors would also like to thank Valy Fontil, MD, MAS, Assistant Professor of Medicine at the University of California San Francisco School of Medicine, and Elizabeth Rogers, MD, MAS, Assistant Professor of Internal Medicine and Pediatrics at the University of Minnesota Medical School, for their constructive feedback on an earlier version of this manuscript.
Disclosures
This work was supported by the Agency for Healthcare Research and Quality-funded UT Southwestern Center for Patient-Centered Outcomes Research (R24 HS022418-01); the Commonwealth Foundation (#20100323); the UT Southwestern KL2 Scholars Program supported by the National Institutes of Health (KL2 TR001103); the National Center for Advancing Translational Sciences at the National Institute of Health (U54 RFA-TR-12-006); and the National Institute on Aging (K23AG052603). The study sponsors had no role in design and conduct of the study; collection, management, analysis, and interpretation of the data; and preparation, review, or approval of the manuscript. The authors have no financial conflicts of interest to disclose.
References
1. Kurniali PC, Curry S, Brennan KW, et al. A retrospective study investigating the incidence and predisposing factors of hospital-acquired anemia. Anemia. 2014;2014:634582. PubMed 2. Koch CG, Li L, Sun Z, et al. Hospital-acquired anemia: prevalence, outcomes, and healthcare implications. J Hosp Med. 2013;8(9):506-512. PubMed 3. Salisbury AC, Alexander KP, Reid KJ, et al. Incidence, correlates, and outcomes of acute, hospital-acquired anemia in patients with acute myocardial infarction. Circ Cardiovasc Qual Outcomes. 2010;3(4):337-346. PubMed 4. Salisbury AC, Amin AP, Reid KJ, et al. Hospital-acquired anemia and in-hospital mortality in patients with acute myocardial infarction. Am Heart J. 2011;162(2):300-309 e303. PubMed 5. Meroño O, Cladellas M, Recasens L, et al. In-hospital acquired anemia in acute coronary syndrome. Predictors, in-hospital prognosis and one-year mortality. Rev Esp Cardiol (Engl Ed). 2012;65(8):742-748. PubMed 6. Salisbury AC, Reid KJ, Alexander KP, et al. Diagnostic blood loss from phlebotomy and hospital-acquired anemia during acute myocardial infarction. Arch Intern Med. 2011;171(18):1646-1653. PubMed 7. Thavendiranathan P, Bagai A, Ebidia A, Detsky AS, Choudhry NK. Do blood tests cause anemia in hospitalized patients? The effect of diagnostic phlebotomy on hemoglobin and hematocrit levels. J Gen Intern Med. 2005;20(6):520-524. PubMed 8. Rennke S, Fang MC. Hazards of hospitalization: more than just “never events”. Arch Intern Med. 2011;171(18):1653-1654. PubMed 9. Choi JS, Kim YA, Kang YU, et al. Clinical impact of hospital-acquired anemia in association with acute kidney injury and chronic kidney disease in patients with acute myocardial infarction. PLoS One. 2013;8(9):e75583. PubMed 10. Salisbury AC, Kosiborod M, Amin AP, et al. Recovery from hospital-acquired anemia after acute myocardial infarction and effect on outcomes. Am J Cardiol. 2011;108(7):949-954. PubMed 11. Nguyen OK, Makam AN, Clark C, et al. Predicting all-cause readmissions using electronic health record data from the entire hospitalization: Model development and comparison. J Hosp Med. 2016;11(7):473-480. PubMed 12. Amarasingham R, Velasco F, Xie B, et al. Electronic medical record-based multicondition models to predict the risk of 30 day readmission or death among adult medicine patients: validation and comparison to existing models. BMC Med Inform Decis Mak. 2015;15:39. PubMed 13. World Health Organization. Hemoglobin concentrations for the diagnosis of anaemia and assessment of severity. http://www.who.int/vmnis/indicators/haemoglobin.pdf. Accessed March 15, 2016. 14. Martin ND, Scantling D. Hospital-acquired anemia: a contemporary review of etiologies and prevention strategies. J Infus Nurs. 2015;38(5):330-338. PubMed 15. Agency for Healthcare Research and Quality, Rockville, MD. Clinical classification software (CCS) for ICD-9-CM. Healthcare Cost and Utilization Project. 2015 http://www.hcup-us.ahrq.gov/toolssoftware/ccs/ccs.jsp. Accessed November 18, 2015. 16. Agency for Healthcare Research and Quality, Rockville, MD. Procedure classes2015. Healthcare Cost and Utilization Project. 2015. https://www.hcup-us.ahrq.gov/toolssoftware/procedure/procedure.jsp. Accessed November 18, 2015. 17. Corwin HL, Gettinger A, Pearl RG, et al. The CRIT Study: Anemia and blood transfusion in the critically ill--current clinical practice in the United States. Crit Care Med. 2004;32(1):39-52. PubMed 18. Aronson D, Suleiman M, Agmon Y, et al. Changes in haemoglobin levels during hospital course and long-term outcome after acute myocardial infarction. Eur Heart J. 2007;28(11):1289-1296. PubMed 19. Lyon AW, Chin AC, Slotsve GA, Lyon ME. Simulation of repetitive diagnostic blood loss and onset of iatrogenic anemia in critical care patients with a mathematical model. Comput Biol Med. 2013;43(2):84-90. PubMed 20. van der Bom JG, Cannegieter SC. Hospital-acquired anemia: the contribution of diagnostic blood loss. J Thromb Haemost. 2015;13(6):1157-1159. PubMed 21. Sanchez-Giron F, Alvarez-Mora F. Reduction of blood loss from laboratory testing in hospitalized adult patients using small-volume (pediatric) tubes. Arch Pathol Lab Med. 2008;132(12):1916-1919. PubMed 22. Smoller BR, Kruskall MS. Phlebotomy for diagnostic laboratory tests in adults. Pattern of use and effect on transfusion requirements. N Engl J Med. 1986;314(19):1233-1235. PubMed 23. Carson JL, Carless PA, Hebert PC. Transfusion thresholds and other strategies for guiding allogeneic red blood cell transfusion. Cochrane Database Syst Rev. 2012(4):CD002042. PubMed 24. Carson JL, Carless PA, Hébert PC. Outcomes using lower vs higher hemoglobin thresholds for red blood cell transfusion. JAMA. 2013;309(1):83-84. PubMed 25. Carson JL, Sieber F, Cook DR, et al. Liberal versus restrictive blood transfusion strategy: 3-year survival and cause of death results from the FOCUS randomised controlled trial. Lancet. 2015;385(9974):1183-1189. PubMed 26. Rajkomar A, McCulloch CE, Fang MC. Low diagnostic utility of rechecking hemoglobins within 24 hours in hospitalized patients. Am J Med. 2016;129(11):1194-1197. PubMed 27. Reade MC, Weissfeld L, Angus DC, Kellum JA, Milbrandt EB. The prevalence of anemia and its association with 90-day mortality in hospitalized community-acquired pneumonia. BMC Pulm Med. 2010;10:15. PubMed 28. Halm EA, Wang JJ, Boockvar K, et al. The effect of perioperative anemia on clinical and functional outcomes in patients with hip fracture. J Orthop Trauma. 2004;18(6):369-374. PubMed
References
1. Kurniali PC, Curry S, Brennan KW, et al. A retrospective study investigating the incidence and predisposing factors of hospital-acquired anemia. Anemia. 2014;2014:634582. PubMed 2. Koch CG, Li L, Sun Z, et al. Hospital-acquired anemia: prevalence, outcomes, and healthcare implications. J Hosp Med. 2013;8(9):506-512. PubMed 3. Salisbury AC, Alexander KP, Reid KJ, et al. Incidence, correlates, and outcomes of acute, hospital-acquired anemia in patients with acute myocardial infarction. Circ Cardiovasc Qual Outcomes. 2010;3(4):337-346. PubMed 4. Salisbury AC, Amin AP, Reid KJ, et al. Hospital-acquired anemia and in-hospital mortality in patients with acute myocardial infarction. Am Heart J. 2011;162(2):300-309 e303. PubMed 5. Meroño O, Cladellas M, Recasens L, et al. In-hospital acquired anemia in acute coronary syndrome. Predictors, in-hospital prognosis and one-year mortality. Rev Esp Cardiol (Engl Ed). 2012;65(8):742-748. PubMed 6. Salisbury AC, Reid KJ, Alexander KP, et al. Diagnostic blood loss from phlebotomy and hospital-acquired anemia during acute myocardial infarction. Arch Intern Med. 2011;171(18):1646-1653. PubMed 7. Thavendiranathan P, Bagai A, Ebidia A, Detsky AS, Choudhry NK. Do blood tests cause anemia in hospitalized patients? The effect of diagnostic phlebotomy on hemoglobin and hematocrit levels. J Gen Intern Med. 2005;20(6):520-524. PubMed 8. Rennke S, Fang MC. Hazards of hospitalization: more than just “never events”. Arch Intern Med. 2011;171(18):1653-1654. PubMed 9. Choi JS, Kim YA, Kang YU, et al. Clinical impact of hospital-acquired anemia in association with acute kidney injury and chronic kidney disease in patients with acute myocardial infarction. PLoS One. 2013;8(9):e75583. PubMed 10. Salisbury AC, Kosiborod M, Amin AP, et al. Recovery from hospital-acquired anemia after acute myocardial infarction and effect on outcomes. Am J Cardiol. 2011;108(7):949-954. PubMed 11. Nguyen OK, Makam AN, Clark C, et al. Predicting all-cause readmissions using electronic health record data from the entire hospitalization: Model development and comparison. J Hosp Med. 2016;11(7):473-480. PubMed 12. Amarasingham R, Velasco F, Xie B, et al. Electronic medical record-based multicondition models to predict the risk of 30 day readmission or death among adult medicine patients: validation and comparison to existing models. BMC Med Inform Decis Mak. 2015;15:39. PubMed 13. World Health Organization. Hemoglobin concentrations for the diagnosis of anaemia and assessment of severity. http://www.who.int/vmnis/indicators/haemoglobin.pdf. Accessed March 15, 2016. 14. Martin ND, Scantling D. Hospital-acquired anemia: a contemporary review of etiologies and prevention strategies. J Infus Nurs. 2015;38(5):330-338. PubMed 15. Agency for Healthcare Research and Quality, Rockville, MD. Clinical classification software (CCS) for ICD-9-CM. Healthcare Cost and Utilization Project. 2015 http://www.hcup-us.ahrq.gov/toolssoftware/ccs/ccs.jsp. Accessed November 18, 2015. 16. Agency for Healthcare Research and Quality, Rockville, MD. Procedure classes2015. Healthcare Cost and Utilization Project. 2015. https://www.hcup-us.ahrq.gov/toolssoftware/procedure/procedure.jsp. Accessed November 18, 2015. 17. Corwin HL, Gettinger A, Pearl RG, et al. The CRIT Study: Anemia and blood transfusion in the critically ill--current clinical practice in the United States. Crit Care Med. 2004;32(1):39-52. PubMed 18. Aronson D, Suleiman M, Agmon Y, et al. Changes in haemoglobin levels during hospital course and long-term outcome after acute myocardial infarction. Eur Heart J. 2007;28(11):1289-1296. PubMed 19. Lyon AW, Chin AC, Slotsve GA, Lyon ME. Simulation of repetitive diagnostic blood loss and onset of iatrogenic anemia in critical care patients with a mathematical model. Comput Biol Med. 2013;43(2):84-90. PubMed 20. van der Bom JG, Cannegieter SC. Hospital-acquired anemia: the contribution of diagnostic blood loss. J Thromb Haemost. 2015;13(6):1157-1159. PubMed 21. Sanchez-Giron F, Alvarez-Mora F. Reduction of blood loss from laboratory testing in hospitalized adult patients using small-volume (pediatric) tubes. Arch Pathol Lab Med. 2008;132(12):1916-1919. PubMed 22. Smoller BR, Kruskall MS. Phlebotomy for diagnostic laboratory tests in adults. Pattern of use and effect on transfusion requirements. N Engl J Med. 1986;314(19):1233-1235. PubMed 23. Carson JL, Carless PA, Hebert PC. Transfusion thresholds and other strategies for guiding allogeneic red blood cell transfusion. Cochrane Database Syst Rev. 2012(4):CD002042. PubMed 24. Carson JL, Carless PA, Hébert PC. Outcomes using lower vs higher hemoglobin thresholds for red blood cell transfusion. JAMA. 2013;309(1):83-84. PubMed 25. Carson JL, Sieber F, Cook DR, et al. Liberal versus restrictive blood transfusion strategy: 3-year survival and cause of death results from the FOCUS randomised controlled trial. Lancet. 2015;385(9974):1183-1189. PubMed 26. Rajkomar A, McCulloch CE, Fang MC. Low diagnostic utility of rechecking hemoglobins within 24 hours in hospitalized patients. Am J Med. 2016;129(11):1194-1197. PubMed 27. Reade MC, Weissfeld L, Angus DC, Kellum JA, Milbrandt EB. The prevalence of anemia and its association with 90-day mortality in hospitalized community-acquired pneumonia. BMC Pulm Med. 2010;10:15. PubMed 28. Halm EA, Wang JJ, Boockvar K, et al. The effect of perioperative anemia on clinical and functional outcomes in patients with hip fracture. J Orthop Trauma. 2004;18(6):369-374. PubMed
Diagnostic imaging is an integral part of patient evaluation in acute care settings. The use of imaging for presenting complaints of chest pain, abdominal pain, and injuries has increased in emergency departments across the United States without an increase in detection of acute pathologic conditions.1,2 An unintended consequence of this increase in diagnostic imaging is the discovery of incidental findings (IFs).
Incidental findings are unexpected findings (eg, nodules) noted on diagnostic imaging that are not related to the presenting complaint.3 The increasing use of diagnostic imaging and increased sensitivity of these tests have led to a higher burden of radiologic IFs.4 In a tertiary level hospital, Lumbreras et al.5 found that the overall incidence of IFs for all radiologic imaging for inpatients and outpatients was 15%, while Orme et al.6 found that the incidence in imaging research was 39.8%. The existing evidence base suggests that the identification of radiologic IFs has financial,5,7 clinical,6 ethical, and legal implications.8 Also, IFs increase workload for healthcare professionals, including that related to follow-up and surveillance.9
In the field of radiology, the burden of radiologic IFs is a well-accepted fact and various white papers have been published by the American College of Radiology on how to address them.4,7 Hospitalized patients are a population that undergoes a substantial number of diagnostic tests. In the era of accountable care organizations10 with an emphasis on population health and high-value care, radiologic IFs pose a particular challenge to healthcare providers.
Chest pain is one of the most common reasons for emergency department visits in the United States.11 In this study, we report on radiologic IFs and factors associated with these among patients hospitalized for chest pain of suspected cardiac origin, and we evaluate the hypothesis that radiologic IFs are associated with an increase in LOS in this population.
METHODS
We conducted a secondary analysis of data from the Chest Pain and Cocaine Study (CPAC). The CPAC study is a cross sectional study of all patients hospitalized with chest pain to our urban academic medical center. Medical records were reviewed to generate a database of all such patients during the study period. The main focus of CPAC was to look at healthcare disparities and resource utilization in patients with or without a concomitant diagnosis of cocaine use.12
Figure
Study Population
The Figure shows the selection of the study sample for this analysis. The CPaC Study identified 1811 consecutive admissions for chest pain/angina pectoris (based on admitting diagnosis ICD-9-CM codes: 411.x; 413.x, 414.x; and 786.5x) over 24 months. Per the CPaC Study protocol, patients older than 65 years were excluded (n=567 admissions). After chart review, all admissions diagnosed with acute myocardial infarction (n=97) or noncardiac chest pain (n=655) were excluded. For this analysis, we excluded 39 additional admissions of patients who had known prior radiologic IFs, leading to a sample size of 453 admissions. Three hundred and seventy six patients had accounted for 453 admissions during the study period, and we included1 of these admissions in the analysis using the following process: If a patient had a radiologic IF on any admission during the study period, that patient was included in the “IF” group for the analysis, and data from the first admission with an IF were used for the analysis. If a patient had no radiologic IFs on any admission during the study period, that patient was included in the “no IF” group, and the data from the first admission in the database were used for analysis.
Measurements
Data collection was completed retrospectively by medical record review using a standardized CPaC Study protocol. The database was created and maintained using REDCap (Research Electronic Data Capture; Vanderbilt University, Knoxville, Tennessee) electronic data capture tool hosted at Johns Hopkins University.13 All data were manually abstracted into REDCap from electronic medical records. All missing values and inconsistent data were reviewed by multiple physicians to ensure data integrity.
We defined all diagnostic (noninterventional; nonlaboratory) testing done during a patient’s hospitalization as “diagnostic” tests, except cardiac stress testing and echocardiogram. We defined diagnostic tests as “primary” tests if they were done in response to patients’ presenting complaint. We defined diagnostic tests as “secondary” tests if they were done by providers due to IFs. Cardiac computed tomography was included in diagnostic tests. Cardiac testing (echocardiogram, cardiac stress testing, cardiac catheterization and pacemaker placement) was considered separate from the “diagnostic tests” since these were focused cardiac imaging that are interventional in nature with low yield on extra-cardiac radiologic IFs.
Incidental findings were defined as any unexpected findings on diagnostic imaging unrelated to the reason for admission, and were classified based on organ systems and their clinical significance as major, moderate, or minor using a classification previously published by Lumbreras et al.14 All radiologic IFs data underwent sequential dual review by investigators for accuracy of documentation. Individuals with multiple radiologic IFs belonging to more than one category of clinical significance were categorized with the IFs group of highest clinical significance. Ten percent of the patients with no IFs were reviewed again, and no errors found.
Demographic variables at the time of admission included age, sex, race, level of education, employment status, insurance status, body mass index (BMI), and smoking status. Comorbid conditions at the time of admission consisted of the following: hypertension, diabetes mellitus, chronic kidney disease (CKD), chronic obstructive pulmonary disease (COPD), history of myocardial infarction, cerebrovascular accident (CVA), congestive heart failure (CHF), drug use and malignancy or history of it. Initial laboratory values were extracted from electronic medical records and included hemoglobin, creatinine, blood urea nitrogen (BUN), aspartate transaminase, alanine transaminase, and alkaline phosphatase. We calculated the estimated glomerular filtration rate (eGFR) using the MDRD (Modification of Diet in Renal Disease) equation.15 Admission and discharge information as well as whether the patient had a primary care provider, were obtained from medical records. The length of hospital stay was calculated by subtracting date of admission from date of discharge.
Statistical Analysis
We conducted 2 main analyses: 1) a descriptive analysis of the association between patient characteristics (independent variables) and identification of IFs during admission (primary outcome) and 2) an analysis of the association between identification of incidental findings during admission (independent variable) and LOS (primary outcome).
For the descriptive analysis of radiologic IFs, we compared the characteristics of patients with and without radiologic IFs during admission using a t-test (for normally distributed continuous variables) or Mann-Whitney test (for nonnormally distributed continuous variables) and a chi-square or Fisher exact test for categorical variables based on the number of observations. We included variables significantly associated with the occurrence of radiologic IFs (P < 0.05) in a multiple logistic regression model to identify characteristics independently associated with presence of radiologic IFs.
Length of stay was right-skewed even after natural logarithm transformation and, therefore, we used negative binomial regression for the analysis of the association between the identification of radiologic IFs during admission and LOS. We included potential confounding variables in the multiple negative binomial regression model based on plausibility of confounding and association with both the exposure (identification of radiologic IFs during admission) and outcome (LOS) at a level of P < 0.3. Age, education level, history of drug use, history of CHF, history of CKD, lower eGFR, higher serum creatinine/BUN, hemoglobin, occurrence of cardiac catheterization, stress testing, and multiple admissions during the study period were identified as confounders. For correlated variables (eg, hemoglobin and hematocrit), the variable with the strongest statistical association (lowest P value) was included in the model.In sensitivity analysis, we dropped patients with extreme LOS (longer than 10 days). All analyses were performed using STATA 13 (Stata Statistical Software: Release 13; StataCorp., College Station, Texas).
Table 1
RESULTS
Table 1 shows the characteristics of the 376 patients included in this study. Overall mean age was 50.5 years, 40% were females, 62% were Caucasian, 66% were unemployed, 84% identified a primary care provider upon admission, and 68% were cared for by a hospitalist. Overall median LOS was 2 days (interquartile range [IQR] = 2). Of the 376 patients in the study, 197 (52%) had new radiologic IFs. Comparing the patients with radiologic IFs and no IFs, it was evident that more radiological tests were performed in the IF group (2.2 tests per patient) in comparison with the no IF group (1.26 tests per patient). Looking at patient characteristics, patients with radiologic IFs were older (52 years vs. 48.8 years; P < 0.001), reported a lower education level and lower hemoglobin levels on admission (12.0 gm/dL vs. 13.4 gm/dL; P = 0.029), but were more likely to be unemployed (72% vs. 59%; P = 0.009), have COPD (19% vs. 10%; P = 0.007), and a history of malignancy (7% vs. 2%, P = 0.04). In addition, patients in the radiologic IF group had lower rates of cardiac catheterization (18% vs. 28%; P = 0.02), were more likely to be readmitted more than once during the study period (17% vs. 7%; P = 0.02) and be discharged by hospitalists (75% vs. 60%; P = 0.003; Supplemental Table 1).
Overall, 658 diagnostic tests were performed in the study population; of these, 268 (40.7%) tests revealed 364 new radiologic IFs (Supplement Table 2). Of these radiologic IFs, 27 (7.4%) were of major clinical significance, 154 (42%) were of moderate clinical significance, and 183 (50%) were of minor clinical significance (Supplement Table 3). Computed tomography (CT) scans yielded more IFs compared to any other imaging modalities. Of the radiologic IFs of major clinical significance, 3 malignant/premalignant lesions were found. While pulmonary nodules were the most common moderate clinically significant findings, atelectasis and spinal degenerative changes were the most common radiologic IFs of minor clinical significance (Supplement Table 4).
Table 2 Results of the logistic regression models testing the association between patient characteristics and radiologic IFs are displayed in Table 2. Only age and repeat admissions remained significantly associated with radiologic IFs in the fully adjusted model (adjusted odds ratio [OR], 1.04; 95% confidence interval [CI], 1.01-1.06 and 2.68; 95% CI, 1.60-4.44, respectively).
Median LOS was 2 days (IQR=1) for patients with no IFs and 2 days (IQR=2) for patient with radiologic IFs (P = 0.08). Unadjusted negative binomial regression analysis revealed that identification of any radiologic IFs during admission (vs. none) was associated with an increased LOS by 24% (unadjusted IRR, 1.24; 95% CI, 1.06-1.45). After adjustment for confounders, identification of any radiologic IFs during admission remained significantly associated with a longer LOS (adjusted IRR, 1.26; 95% CI, 1.07-1.49). Results remained significant on a sensitivity analysis excluding admissions lasting longer than 10 days (adjusted IRR, 1.21; 95% CI, 1.03-1.42; Supplement Table 5).
Table 3
Incidental findings of minor and moderate clinical significance were associated with increase in LOS on multiple negative binomial regression (adjusted IRR, 1.27; 95% CI, 1.03-1.57 and 1.24; 95% CI, 1.02-1.52, respectively; Table 3); however, upon dropping length of hospitalization outliers, only radiologic IFs with major clinical significance were associated with increase in length of hospitalization (adjusted IRR, 1.39; 95% CI, 1.04-1.87; Table 3).
Supplemental chart review revealed that 26 patients accounted for the 27 radiologic IFs of major clinical significance. This group had 54% women, median LOS remained 2 days (IQR 2) and, on average, had about 3 diagnostic tests performed per patient. Cardiac testing was performed less on these patients compared to others (Supplement Table S6). Review also revealed that, of the 26 patients, 2 had abnormal labs, 2 had drug abuse/psychiatric issues, and another 2 had radiologic IFs that warranted further consultations, imaging, and longer LOS.
DISCUSSION
Radiologic IFs in patients admitted with chest pain of suspected cardiac origin are a common occurrence as shown in our study. Similar to prior studies, 41% of all radiologic tests done in our study population revealed IFs.6 The majority of the IFs were of minor to moderate clinical significance and, as reported in the literature, were more common with older age and CT imaging.14,16 In addition, an IF diagnosed during admission for chest pain was associated with a 26% increase in length of hospital stay.
To our knowledge, we present the first study on the impact of identification of radiologic IFs in hospitalized patients on length of hospital stay and specifically in patients hospitalized with chest pain of suspected cardiac origin. Trends over the past decade have shown a decrease in LOS and hospitalizations but with an increase in health resource utilization.17,18 Association of radiologic IFs with increase in LOS is significant as this potentially increases hospital-acquired conditions such as infections and resource utilization leading to increase in costs of hospitalizations.19 This in return is a concern for patient safety.
The positive association between LOS and radiologic IFs, interestingly, continued to exist despite sensitivity analysis. Incidental findings of major clinical significance were associated with longer LOS in the sensitivity analysis. Supplemental chart review of patients with major clinical findings suggested more extra-cardiac workup compared to patients with minor/moderate radiologic IFs. This could indicate that the presence of clinically significant radiologic IFs could have led to further inpatient work-up and consultations. The downstream healthcare expenditure associated with workup of IFs in individual radiologic tests is well established.20 In case of cardiac CT, Goehler et al.21 found that the healthcare expenditure was high following incidentally detected pulmonary nodules with an overall small reduction in lung cancer mortality. Incidental findings also increase the burden of reporting and concern for medico-legal issues for providers.4 These concerns are likely valid for hospitalized patients as well.
The socioeconomic trends in the study population were consistent with data from the Bureau of Labor Statistics in that low education is associated with higher unemployment.22 Although, overall, gender, race and insurance mix were similar in both groups, we did see trends of socioeconomic differences in the patients with radiologic IFs of major clinical significance that might not have been statistically significant owing to the small sample size. Despite the population being relatively of younger age (given our cut off age was 65 years) there was still a positive association with age and presence of radiologic IFs. The higher number of patients with COPD or history of malignancy in the radiologic IF group suggests that an association with IFs could exist for these disease cohorts; however, after adjustment for multiple covariates, such an association did not transpire. Interestingly, patients with no radiologic IFs underwent cardiac catheterization or stress testing more often than patients with discovered IFs. This speaks of 2 possibilities; first, that both tests probably do not yield many extra-cardiac IFs, or, secondly, that these patients did not require further workup. More patients in the IF group had more than 1 admission during the study period, and this was associated with increased odds of detecting radiologic IFs. We hypothesize that this might have occurred because of the diagnostic dilemma in these patients who have multiple admissions for the same reason leading to wider array of diagnostic workup. Indeed, we did not note upon chart review alternative diagnoses in these patients but only more IFs. There are several study limitations to consider. First, the fact that this is a single center study sets limitations to interpretation and generalizability of the data. Second, we cannot exclude the possibility of residual confounding. Third, the small number of patients included in this study precludes definitive identification of more factors potentially associated with IFs. However, this study sheds light on a yet unidentified problem within the realm of inpatient management especially for the internists and hospitalists. We tried to limit bias to the extent possible by including only 1 presenting complaint and age-restricting the population.
CONCLUSION
Incidental findings are both clinical and financial challenges to the medical field. This study attempted to shed light on impact of radiologic IFs on care and resource utilization in patients admitted with chest pain of suspected cardiac origin. The positive association between radiologic IFs and length of hospital stay implies that the presence of IFs is associated with increase in LOS and indirectly a likely increase in overall healthcare expenditure. Given the high incidence of radiologic IFs, assuming that these will be present on radiologic tests, should be more a norm than an exception. Providers should know that radiologic testing, especially CT, is associated with detection of IFs.16 By avoiding inappropriate ordering of imaging, the issue of IFs could be mitigated.
While radiologists have recommendations about necessary follow-up for some IFs,7 no clear follow-up guidelines exist for most IFs arising in hospitalized patients. Further prospective and cost analysis studies are needed to assess the overall impact of IFs on other hospitalized patient populations and on the healthcare system in general.
1. Korley FK, Pham JC, Kirsch TD. Use of advanced radiology during visits to US emergency departments for injury-related conditions, 1998-2007. JAMA. 2010;304(13):1465-1471. PubMed 2. Pines JM. Trends in the rates of radiography use and important diagnoses in emergency department patients with abdominal pain. Med Care. 2009;47(7):782-786. PubMed 3. McGraw-Hill Concise Dictionary of Modern Medicine. Incidentalomas. http://medical-dictionary.thefreedictionary.com/Incidental+findings. Updated 2002. Accessed April 13, 2017. 4. Berland LL, Silverman SG, Gore RM, et al. Managing incidental findings on abdominal CT: White paper of the ACR incidental findings committee. J Am Coll Radiol. 2010;7(10):754-773. PubMed 5. Lumbreras B, González-Alvárez I, Lorente MF, Calbo J, Aranaz J, Hernández-Aguado I. Unexpected findings at imaging: Predicting frequency in various types of studies. Eur J Radiol. 2010;74(1):269-274. PubMed 6. Orme NM, Fletcher JG, Siddiki HA, et al. Incidental findings in imaging research: Evaluating incidence, benefit, and burden. Arch Intern Med. 2010;170(17):1525-1532. PubMed 7. Berland LL. Overview of white papers of the ACR incidental findings committee II on adnexal, vascular, splenic, nodal, gallbladder, and biliary findings. J Am Coll Radiol. 2013;10(9):672-674. PubMed 8. Booth TC, Jackson A, Wardlaw JM, Taylor SA, Waldman AD. Incidental findings found in “healthy” volunteers during imaging performed for research: Current legal and ethical implications. Br J Radiol. 2010;83(990):456-465. PubMed 9. Kelly ME, Heeney A, Redmond CE, et al. Incidental findings detected on emergency abdominal CT scans: A 1-year review. Abdom Imaging. 2015;40(6):1853-1857. PubMed 10. Centers for Medicare and Medicaid Services. Accountable care organizations (ACO). https://www.cms.gov/Medicare/Medicare-Fee-for-Service-Payment/ACO/index.html?redirect=/aco. Baltimore, Maryland. Updated 01/06/2015. 11. Weiss AJ (Truven Health Analytics), Wier LM (Truven Health Analytics), Stocks C (AHRQ), Blanchard J (RAND). Overview of Emergency Department Visits in the United States, 2011. HCUP Statistical Brief #174. June 2014. Agency for Healthcare Research and Quality, Rockville, MD. http://www.hcup-us.ahrq.gov/reports/statbriefs/sb174-Emergency-Department-Visits-Overview.pdf. 12. Chibungu A, Gundareddy V, Wright SM, Nwabuo C, Bollampally P, Landis R, Eid SM. Management of cocaine-induced myocardial infarction: 4-year experience at an urban medical center. South Med J. 2016;109(3):185-190. PubMed 13. Harris PA, Taylor R, Thielke R, Payne J, Gonzalez N, Conde JG. Research electronic data capture (REDCap)--a metadata-driven methodology and workflow process for providing translational research informatics support. J Biomed Inform. 2009;42(2):377-381. PubMed 14. Lumbreras B, Donat L, Hernández-Aguado I. Incidental findings in imaging diagnostic tests: a systematic review. Br J Radiol. 2010;83(988):276-289. PubMed 15. Fontela PC, Winkelmann ER, Ott JN, Uggeri DP. Estimated glomerular filtration rate in patients with type 2 diabetes mellitus. Rev Assoc Méd Bras (1992). 2014;60(6):531-537. PubMed 16. Samim M, Goss S, Luty S, Weinreb J, Moore C. Incidental findings on CT for suspected renal colic in emergency department patients: prevalence and types in 5,383 consecutive examinations. J Am Coll Radiol. 2015;12(1):63-69. PubMed 17. Avalere Health for the American Health Association. TrendWatch ChartBook 2014; trends affecting hospitals and health systems. 2014. http://www.aha.org/research/reports/tw/chartbook/2014/14chartbook.pdf. 18. Weiss AJ, Elixhauser A. Overview of hospital stays in the United States, 2012. HCUP statistical brief #180. https://www.hcup-us.ahrq.gov/reports/statbriefs/sb180-Hospitalizations-United-States-2012.jsp. Accessed April 13, 2017. 19. Hauck K, Zhao X. How dangerous is a day in hospital?: A model of adverse events and length of stay for medical inpatients. Med Care. 2011;49(12):1068-1075. PubMed 20. Ding A, Eisenberg JD, Pandharipande PV. The economic burden of incidentally detected findings. Radiol Clin North Am. 2011;49(2):257-265. PubMed 21. Goehler A, McMahon PM, Lumish HS, et al. Cost-effectiveness of follow-up of pulmonary nodules incidentally detected on cardiac computed tomographic angiography in patients with suspected coronary artery disease. Circulation. 2014;130(8):668-675. PubMed 22. U.S. Department of Labor. Bureau of Labor Statistics. Employment projections. Earning and unemployment rates by educational attainment, 2015. http://www.bls.gov/emp/ep_chart_001.htm. Updated March 15, 2016. Accessed April 13, 2017
Diagnostic imaging is an integral part of patient evaluation in acute care settings. The use of imaging for presenting complaints of chest pain, abdominal pain, and injuries has increased in emergency departments across the United States without an increase in detection of acute pathologic conditions.1,2 An unintended consequence of this increase in diagnostic imaging is the discovery of incidental findings (IFs).
Incidental findings are unexpected findings (eg, nodules) noted on diagnostic imaging that are not related to the presenting complaint.3 The increasing use of diagnostic imaging and increased sensitivity of these tests have led to a higher burden of radiologic IFs.4 In a tertiary level hospital, Lumbreras et al.5 found that the overall incidence of IFs for all radiologic imaging for inpatients and outpatients was 15%, while Orme et al.6 found that the incidence in imaging research was 39.8%. The existing evidence base suggests that the identification of radiologic IFs has financial,5,7 clinical,6 ethical, and legal implications.8 Also, IFs increase workload for healthcare professionals, including that related to follow-up and surveillance.9
In the field of radiology, the burden of radiologic IFs is a well-accepted fact and various white papers have been published by the American College of Radiology on how to address them.4,7 Hospitalized patients are a population that undergoes a substantial number of diagnostic tests. In the era of accountable care organizations10 with an emphasis on population health and high-value care, radiologic IFs pose a particular challenge to healthcare providers.
Chest pain is one of the most common reasons for emergency department visits in the United States.11 In this study, we report on radiologic IFs and factors associated with these among patients hospitalized for chest pain of suspected cardiac origin, and we evaluate the hypothesis that radiologic IFs are associated with an increase in LOS in this population.
METHODS
We conducted a secondary analysis of data from the Chest Pain and Cocaine Study (CPAC). The CPAC study is a cross sectional study of all patients hospitalized with chest pain to our urban academic medical center. Medical records were reviewed to generate a database of all such patients during the study period. The main focus of CPAC was to look at healthcare disparities and resource utilization in patients with or without a concomitant diagnosis of cocaine use.12
Figure
Study Population
The Figure shows the selection of the study sample for this analysis. The CPaC Study identified 1811 consecutive admissions for chest pain/angina pectoris (based on admitting diagnosis ICD-9-CM codes: 411.x; 413.x, 414.x; and 786.5x) over 24 months. Per the CPaC Study protocol, patients older than 65 years were excluded (n=567 admissions). After chart review, all admissions diagnosed with acute myocardial infarction (n=97) or noncardiac chest pain (n=655) were excluded. For this analysis, we excluded 39 additional admissions of patients who had known prior radiologic IFs, leading to a sample size of 453 admissions. Three hundred and seventy six patients had accounted for 453 admissions during the study period, and we included1 of these admissions in the analysis using the following process: If a patient had a radiologic IF on any admission during the study period, that patient was included in the “IF” group for the analysis, and data from the first admission with an IF were used for the analysis. If a patient had no radiologic IFs on any admission during the study period, that patient was included in the “no IF” group, and the data from the first admission in the database were used for analysis.
Measurements
Data collection was completed retrospectively by medical record review using a standardized CPaC Study protocol. The database was created and maintained using REDCap (Research Electronic Data Capture; Vanderbilt University, Knoxville, Tennessee) electronic data capture tool hosted at Johns Hopkins University.13 All data were manually abstracted into REDCap from electronic medical records. All missing values and inconsistent data were reviewed by multiple physicians to ensure data integrity.
We defined all diagnostic (noninterventional; nonlaboratory) testing done during a patient’s hospitalization as “diagnostic” tests, except cardiac stress testing and echocardiogram. We defined diagnostic tests as “primary” tests if they were done in response to patients’ presenting complaint. We defined diagnostic tests as “secondary” tests if they were done by providers due to IFs. Cardiac computed tomography was included in diagnostic tests. Cardiac testing (echocardiogram, cardiac stress testing, cardiac catheterization and pacemaker placement) was considered separate from the “diagnostic tests” since these were focused cardiac imaging that are interventional in nature with low yield on extra-cardiac radiologic IFs.
Incidental findings were defined as any unexpected findings on diagnostic imaging unrelated to the reason for admission, and were classified based on organ systems and their clinical significance as major, moderate, or minor using a classification previously published by Lumbreras et al.14 All radiologic IFs data underwent sequential dual review by investigators for accuracy of documentation. Individuals with multiple radiologic IFs belonging to more than one category of clinical significance were categorized with the IFs group of highest clinical significance. Ten percent of the patients with no IFs were reviewed again, and no errors found.
Demographic variables at the time of admission included age, sex, race, level of education, employment status, insurance status, body mass index (BMI), and smoking status. Comorbid conditions at the time of admission consisted of the following: hypertension, diabetes mellitus, chronic kidney disease (CKD), chronic obstructive pulmonary disease (COPD), history of myocardial infarction, cerebrovascular accident (CVA), congestive heart failure (CHF), drug use and malignancy or history of it. Initial laboratory values were extracted from electronic medical records and included hemoglobin, creatinine, blood urea nitrogen (BUN), aspartate transaminase, alanine transaminase, and alkaline phosphatase. We calculated the estimated glomerular filtration rate (eGFR) using the MDRD (Modification of Diet in Renal Disease) equation.15 Admission and discharge information as well as whether the patient had a primary care provider, were obtained from medical records. The length of hospital stay was calculated by subtracting date of admission from date of discharge.
Statistical Analysis
We conducted 2 main analyses: 1) a descriptive analysis of the association between patient characteristics (independent variables) and identification of IFs during admission (primary outcome) and 2) an analysis of the association between identification of incidental findings during admission (independent variable) and LOS (primary outcome).
For the descriptive analysis of radiologic IFs, we compared the characteristics of patients with and without radiologic IFs during admission using a t-test (for normally distributed continuous variables) or Mann-Whitney test (for nonnormally distributed continuous variables) and a chi-square or Fisher exact test for categorical variables based on the number of observations. We included variables significantly associated with the occurrence of radiologic IFs (P < 0.05) in a multiple logistic regression model to identify characteristics independently associated with presence of radiologic IFs.
Length of stay was right-skewed even after natural logarithm transformation and, therefore, we used negative binomial regression for the analysis of the association between the identification of radiologic IFs during admission and LOS. We included potential confounding variables in the multiple negative binomial regression model based on plausibility of confounding and association with both the exposure (identification of radiologic IFs during admission) and outcome (LOS) at a level of P < 0.3. Age, education level, history of drug use, history of CHF, history of CKD, lower eGFR, higher serum creatinine/BUN, hemoglobin, occurrence of cardiac catheterization, stress testing, and multiple admissions during the study period were identified as confounders. For correlated variables (eg, hemoglobin and hematocrit), the variable with the strongest statistical association (lowest P value) was included in the model.In sensitivity analysis, we dropped patients with extreme LOS (longer than 10 days). All analyses were performed using STATA 13 (Stata Statistical Software: Release 13; StataCorp., College Station, Texas).
Table 1
RESULTS
Table 1 shows the characteristics of the 376 patients included in this study. Overall mean age was 50.5 years, 40% were females, 62% were Caucasian, 66% were unemployed, 84% identified a primary care provider upon admission, and 68% were cared for by a hospitalist. Overall median LOS was 2 days (interquartile range [IQR] = 2). Of the 376 patients in the study, 197 (52%) had new radiologic IFs. Comparing the patients with radiologic IFs and no IFs, it was evident that more radiological tests were performed in the IF group (2.2 tests per patient) in comparison with the no IF group (1.26 tests per patient). Looking at patient characteristics, patients with radiologic IFs were older (52 years vs. 48.8 years; P < 0.001), reported a lower education level and lower hemoglobin levels on admission (12.0 gm/dL vs. 13.4 gm/dL; P = 0.029), but were more likely to be unemployed (72% vs. 59%; P = 0.009), have COPD (19% vs. 10%; P = 0.007), and a history of malignancy (7% vs. 2%, P = 0.04). In addition, patients in the radiologic IF group had lower rates of cardiac catheterization (18% vs. 28%; P = 0.02), were more likely to be readmitted more than once during the study period (17% vs. 7%; P = 0.02) and be discharged by hospitalists (75% vs. 60%; P = 0.003; Supplemental Table 1).
Overall, 658 diagnostic tests were performed in the study population; of these, 268 (40.7%) tests revealed 364 new radiologic IFs (Supplement Table 2). Of these radiologic IFs, 27 (7.4%) were of major clinical significance, 154 (42%) were of moderate clinical significance, and 183 (50%) were of minor clinical significance (Supplement Table 3). Computed tomography (CT) scans yielded more IFs compared to any other imaging modalities. Of the radiologic IFs of major clinical significance, 3 malignant/premalignant lesions were found. While pulmonary nodules were the most common moderate clinically significant findings, atelectasis and spinal degenerative changes were the most common radiologic IFs of minor clinical significance (Supplement Table 4).
Table 2 Results of the logistic regression models testing the association between patient characteristics and radiologic IFs are displayed in Table 2. Only age and repeat admissions remained significantly associated with radiologic IFs in the fully adjusted model (adjusted odds ratio [OR], 1.04; 95% confidence interval [CI], 1.01-1.06 and 2.68; 95% CI, 1.60-4.44, respectively).
Median LOS was 2 days (IQR=1) for patients with no IFs and 2 days (IQR=2) for patient with radiologic IFs (P = 0.08). Unadjusted negative binomial regression analysis revealed that identification of any radiologic IFs during admission (vs. none) was associated with an increased LOS by 24% (unadjusted IRR, 1.24; 95% CI, 1.06-1.45). After adjustment for confounders, identification of any radiologic IFs during admission remained significantly associated with a longer LOS (adjusted IRR, 1.26; 95% CI, 1.07-1.49). Results remained significant on a sensitivity analysis excluding admissions lasting longer than 10 days (adjusted IRR, 1.21; 95% CI, 1.03-1.42; Supplement Table 5).
Table 3
Incidental findings of minor and moderate clinical significance were associated with increase in LOS on multiple negative binomial regression (adjusted IRR, 1.27; 95% CI, 1.03-1.57 and 1.24; 95% CI, 1.02-1.52, respectively; Table 3); however, upon dropping length of hospitalization outliers, only radiologic IFs with major clinical significance were associated with increase in length of hospitalization (adjusted IRR, 1.39; 95% CI, 1.04-1.87; Table 3).
Supplemental chart review revealed that 26 patients accounted for the 27 radiologic IFs of major clinical significance. This group had 54% women, median LOS remained 2 days (IQR 2) and, on average, had about 3 diagnostic tests performed per patient. Cardiac testing was performed less on these patients compared to others (Supplement Table S6). Review also revealed that, of the 26 patients, 2 had abnormal labs, 2 had drug abuse/psychiatric issues, and another 2 had radiologic IFs that warranted further consultations, imaging, and longer LOS.
DISCUSSION
Radiologic IFs in patients admitted with chest pain of suspected cardiac origin are a common occurrence as shown in our study. Similar to prior studies, 41% of all radiologic tests done in our study population revealed IFs.6 The majority of the IFs were of minor to moderate clinical significance and, as reported in the literature, were more common with older age and CT imaging.14,16 In addition, an IF diagnosed during admission for chest pain was associated with a 26% increase in length of hospital stay.
To our knowledge, we present the first study on the impact of identification of radiologic IFs in hospitalized patients on length of hospital stay and specifically in patients hospitalized with chest pain of suspected cardiac origin. Trends over the past decade have shown a decrease in LOS and hospitalizations but with an increase in health resource utilization.17,18 Association of radiologic IFs with increase in LOS is significant as this potentially increases hospital-acquired conditions such as infections and resource utilization leading to increase in costs of hospitalizations.19 This in return is a concern for patient safety.
The positive association between LOS and radiologic IFs, interestingly, continued to exist despite sensitivity analysis. Incidental findings of major clinical significance were associated with longer LOS in the sensitivity analysis. Supplemental chart review of patients with major clinical findings suggested more extra-cardiac workup compared to patients with minor/moderate radiologic IFs. This could indicate that the presence of clinically significant radiologic IFs could have led to further inpatient work-up and consultations. The downstream healthcare expenditure associated with workup of IFs in individual radiologic tests is well established.20 In case of cardiac CT, Goehler et al.21 found that the healthcare expenditure was high following incidentally detected pulmonary nodules with an overall small reduction in lung cancer mortality. Incidental findings also increase the burden of reporting and concern for medico-legal issues for providers.4 These concerns are likely valid for hospitalized patients as well.
The socioeconomic trends in the study population were consistent with data from the Bureau of Labor Statistics in that low education is associated with higher unemployment.22 Although, overall, gender, race and insurance mix were similar in both groups, we did see trends of socioeconomic differences in the patients with radiologic IFs of major clinical significance that might not have been statistically significant owing to the small sample size. Despite the population being relatively of younger age (given our cut off age was 65 years) there was still a positive association with age and presence of radiologic IFs. The higher number of patients with COPD or history of malignancy in the radiologic IF group suggests that an association with IFs could exist for these disease cohorts; however, after adjustment for multiple covariates, such an association did not transpire. Interestingly, patients with no radiologic IFs underwent cardiac catheterization or stress testing more often than patients with discovered IFs. This speaks of 2 possibilities; first, that both tests probably do not yield many extra-cardiac IFs, or, secondly, that these patients did not require further workup. More patients in the IF group had more than 1 admission during the study period, and this was associated with increased odds of detecting radiologic IFs. We hypothesize that this might have occurred because of the diagnostic dilemma in these patients who have multiple admissions for the same reason leading to wider array of diagnostic workup. Indeed, we did not note upon chart review alternative diagnoses in these patients but only more IFs. There are several study limitations to consider. First, the fact that this is a single center study sets limitations to interpretation and generalizability of the data. Second, we cannot exclude the possibility of residual confounding. Third, the small number of patients included in this study precludes definitive identification of more factors potentially associated with IFs. However, this study sheds light on a yet unidentified problem within the realm of inpatient management especially for the internists and hospitalists. We tried to limit bias to the extent possible by including only 1 presenting complaint and age-restricting the population.
CONCLUSION
Incidental findings are both clinical and financial challenges to the medical field. This study attempted to shed light on impact of radiologic IFs on care and resource utilization in patients admitted with chest pain of suspected cardiac origin. The positive association between radiologic IFs and length of hospital stay implies that the presence of IFs is associated with increase in LOS and indirectly a likely increase in overall healthcare expenditure. Given the high incidence of radiologic IFs, assuming that these will be present on radiologic tests, should be more a norm than an exception. Providers should know that radiologic testing, especially CT, is associated with detection of IFs.16 By avoiding inappropriate ordering of imaging, the issue of IFs could be mitigated.
While radiologists have recommendations about necessary follow-up for some IFs,7 no clear follow-up guidelines exist for most IFs arising in hospitalized patients. Further prospective and cost analysis studies are needed to assess the overall impact of IFs on other hospitalized patient populations and on the healthcare system in general.
Disclosure
The authors report no conflicts of interest.
Diagnostic imaging is an integral part of patient evaluation in acute care settings. The use of imaging for presenting complaints of chest pain, abdominal pain, and injuries has increased in emergency departments across the United States without an increase in detection of acute pathologic conditions.1,2 An unintended consequence of this increase in diagnostic imaging is the discovery of incidental findings (IFs).
Incidental findings are unexpected findings (eg, nodules) noted on diagnostic imaging that are not related to the presenting complaint.3 The increasing use of diagnostic imaging and increased sensitivity of these tests have led to a higher burden of radiologic IFs.4 In a tertiary level hospital, Lumbreras et al.5 found that the overall incidence of IFs for all radiologic imaging for inpatients and outpatients was 15%, while Orme et al.6 found that the incidence in imaging research was 39.8%. The existing evidence base suggests that the identification of radiologic IFs has financial,5,7 clinical,6 ethical, and legal implications.8 Also, IFs increase workload for healthcare professionals, including that related to follow-up and surveillance.9
In the field of radiology, the burden of radiologic IFs is a well-accepted fact and various white papers have been published by the American College of Radiology on how to address them.4,7 Hospitalized patients are a population that undergoes a substantial number of diagnostic tests. In the era of accountable care organizations10 with an emphasis on population health and high-value care, radiologic IFs pose a particular challenge to healthcare providers.
Chest pain is one of the most common reasons for emergency department visits in the United States.11 In this study, we report on radiologic IFs and factors associated with these among patients hospitalized for chest pain of suspected cardiac origin, and we evaluate the hypothesis that radiologic IFs are associated with an increase in LOS in this population.
METHODS
We conducted a secondary analysis of data from the Chest Pain and Cocaine Study (CPAC). The CPAC study is a cross sectional study of all patients hospitalized with chest pain to our urban academic medical center. Medical records were reviewed to generate a database of all such patients during the study period. The main focus of CPAC was to look at healthcare disparities and resource utilization in patients with or without a concomitant diagnosis of cocaine use.12
Figure
Study Population
The Figure shows the selection of the study sample for this analysis. The CPaC Study identified 1811 consecutive admissions for chest pain/angina pectoris (based on admitting diagnosis ICD-9-CM codes: 411.x; 413.x, 414.x; and 786.5x) over 24 months. Per the CPaC Study protocol, patients older than 65 years were excluded (n=567 admissions). After chart review, all admissions diagnosed with acute myocardial infarction (n=97) or noncardiac chest pain (n=655) were excluded. For this analysis, we excluded 39 additional admissions of patients who had known prior radiologic IFs, leading to a sample size of 453 admissions. Three hundred and seventy six patients had accounted for 453 admissions during the study period, and we included1 of these admissions in the analysis using the following process: If a patient had a radiologic IF on any admission during the study period, that patient was included in the “IF” group for the analysis, and data from the first admission with an IF were used for the analysis. If a patient had no radiologic IFs on any admission during the study period, that patient was included in the “no IF” group, and the data from the first admission in the database were used for analysis.
Measurements
Data collection was completed retrospectively by medical record review using a standardized CPaC Study protocol. The database was created and maintained using REDCap (Research Electronic Data Capture; Vanderbilt University, Knoxville, Tennessee) electronic data capture tool hosted at Johns Hopkins University.13 All data were manually abstracted into REDCap from electronic medical records. All missing values and inconsistent data were reviewed by multiple physicians to ensure data integrity.
We defined all diagnostic (noninterventional; nonlaboratory) testing done during a patient’s hospitalization as “diagnostic” tests, except cardiac stress testing and echocardiogram. We defined diagnostic tests as “primary” tests if they were done in response to patients’ presenting complaint. We defined diagnostic tests as “secondary” tests if they were done by providers due to IFs. Cardiac computed tomography was included in diagnostic tests. Cardiac testing (echocardiogram, cardiac stress testing, cardiac catheterization and pacemaker placement) was considered separate from the “diagnostic tests” since these were focused cardiac imaging that are interventional in nature with low yield on extra-cardiac radiologic IFs.
Incidental findings were defined as any unexpected findings on diagnostic imaging unrelated to the reason for admission, and were classified based on organ systems and their clinical significance as major, moderate, or minor using a classification previously published by Lumbreras et al.14 All radiologic IFs data underwent sequential dual review by investigators for accuracy of documentation. Individuals with multiple radiologic IFs belonging to more than one category of clinical significance were categorized with the IFs group of highest clinical significance. Ten percent of the patients with no IFs were reviewed again, and no errors found.
Demographic variables at the time of admission included age, sex, race, level of education, employment status, insurance status, body mass index (BMI), and smoking status. Comorbid conditions at the time of admission consisted of the following: hypertension, diabetes mellitus, chronic kidney disease (CKD), chronic obstructive pulmonary disease (COPD), history of myocardial infarction, cerebrovascular accident (CVA), congestive heart failure (CHF), drug use and malignancy or history of it. Initial laboratory values were extracted from electronic medical records and included hemoglobin, creatinine, blood urea nitrogen (BUN), aspartate transaminase, alanine transaminase, and alkaline phosphatase. We calculated the estimated glomerular filtration rate (eGFR) using the MDRD (Modification of Diet in Renal Disease) equation.15 Admission and discharge information as well as whether the patient had a primary care provider, were obtained from medical records. The length of hospital stay was calculated by subtracting date of admission from date of discharge.
Statistical Analysis
We conducted 2 main analyses: 1) a descriptive analysis of the association between patient characteristics (independent variables) and identification of IFs during admission (primary outcome) and 2) an analysis of the association between identification of incidental findings during admission (independent variable) and LOS (primary outcome).
For the descriptive analysis of radiologic IFs, we compared the characteristics of patients with and without radiologic IFs during admission using a t-test (for normally distributed continuous variables) or Mann-Whitney test (for nonnormally distributed continuous variables) and a chi-square or Fisher exact test for categorical variables based on the number of observations. We included variables significantly associated with the occurrence of radiologic IFs (P < 0.05) in a multiple logistic regression model to identify characteristics independently associated with presence of radiologic IFs.
Length of stay was right-skewed even after natural logarithm transformation and, therefore, we used negative binomial regression for the analysis of the association between the identification of radiologic IFs during admission and LOS. We included potential confounding variables in the multiple negative binomial regression model based on plausibility of confounding and association with both the exposure (identification of radiologic IFs during admission) and outcome (LOS) at a level of P < 0.3. Age, education level, history of drug use, history of CHF, history of CKD, lower eGFR, higher serum creatinine/BUN, hemoglobin, occurrence of cardiac catheterization, stress testing, and multiple admissions during the study period were identified as confounders. For correlated variables (eg, hemoglobin and hematocrit), the variable with the strongest statistical association (lowest P value) was included in the model.In sensitivity analysis, we dropped patients with extreme LOS (longer than 10 days). All analyses were performed using STATA 13 (Stata Statistical Software: Release 13; StataCorp., College Station, Texas).
Table 1
RESULTS
Table 1 shows the characteristics of the 376 patients included in this study. Overall mean age was 50.5 years, 40% were females, 62% were Caucasian, 66% were unemployed, 84% identified a primary care provider upon admission, and 68% were cared for by a hospitalist. Overall median LOS was 2 days (interquartile range [IQR] = 2). Of the 376 patients in the study, 197 (52%) had new radiologic IFs. Comparing the patients with radiologic IFs and no IFs, it was evident that more radiological tests were performed in the IF group (2.2 tests per patient) in comparison with the no IF group (1.26 tests per patient). Looking at patient characteristics, patients with radiologic IFs were older (52 years vs. 48.8 years; P < 0.001), reported a lower education level and lower hemoglobin levels on admission (12.0 gm/dL vs. 13.4 gm/dL; P = 0.029), but were more likely to be unemployed (72% vs. 59%; P = 0.009), have COPD (19% vs. 10%; P = 0.007), and a history of malignancy (7% vs. 2%, P = 0.04). In addition, patients in the radiologic IF group had lower rates of cardiac catheterization (18% vs. 28%; P = 0.02), were more likely to be readmitted more than once during the study period (17% vs. 7%; P = 0.02) and be discharged by hospitalists (75% vs. 60%; P = 0.003; Supplemental Table 1).
Overall, 658 diagnostic tests were performed in the study population; of these, 268 (40.7%) tests revealed 364 new radiologic IFs (Supplement Table 2). Of these radiologic IFs, 27 (7.4%) were of major clinical significance, 154 (42%) were of moderate clinical significance, and 183 (50%) were of minor clinical significance (Supplement Table 3). Computed tomography (CT) scans yielded more IFs compared to any other imaging modalities. Of the radiologic IFs of major clinical significance, 3 malignant/premalignant lesions were found. While pulmonary nodules were the most common moderate clinically significant findings, atelectasis and spinal degenerative changes were the most common radiologic IFs of minor clinical significance (Supplement Table 4).
Table 2 Results of the logistic regression models testing the association between patient characteristics and radiologic IFs are displayed in Table 2. Only age and repeat admissions remained significantly associated with radiologic IFs in the fully adjusted model (adjusted odds ratio [OR], 1.04; 95% confidence interval [CI], 1.01-1.06 and 2.68; 95% CI, 1.60-4.44, respectively).
Median LOS was 2 days (IQR=1) for patients with no IFs and 2 days (IQR=2) for patient with radiologic IFs (P = 0.08). Unadjusted negative binomial regression analysis revealed that identification of any radiologic IFs during admission (vs. none) was associated with an increased LOS by 24% (unadjusted IRR, 1.24; 95% CI, 1.06-1.45). After adjustment for confounders, identification of any radiologic IFs during admission remained significantly associated with a longer LOS (adjusted IRR, 1.26; 95% CI, 1.07-1.49). Results remained significant on a sensitivity analysis excluding admissions lasting longer than 10 days (adjusted IRR, 1.21; 95% CI, 1.03-1.42; Supplement Table 5).
Table 3
Incidental findings of minor and moderate clinical significance were associated with increase in LOS on multiple negative binomial regression (adjusted IRR, 1.27; 95% CI, 1.03-1.57 and 1.24; 95% CI, 1.02-1.52, respectively; Table 3); however, upon dropping length of hospitalization outliers, only radiologic IFs with major clinical significance were associated with increase in length of hospitalization (adjusted IRR, 1.39; 95% CI, 1.04-1.87; Table 3).
Supplemental chart review revealed that 26 patients accounted for the 27 radiologic IFs of major clinical significance. This group had 54% women, median LOS remained 2 days (IQR 2) and, on average, had about 3 diagnostic tests performed per patient. Cardiac testing was performed less on these patients compared to others (Supplement Table S6). Review also revealed that, of the 26 patients, 2 had abnormal labs, 2 had drug abuse/psychiatric issues, and another 2 had radiologic IFs that warranted further consultations, imaging, and longer LOS.
DISCUSSION
Radiologic IFs in patients admitted with chest pain of suspected cardiac origin are a common occurrence as shown in our study. Similar to prior studies, 41% of all radiologic tests done in our study population revealed IFs.6 The majority of the IFs were of minor to moderate clinical significance and, as reported in the literature, were more common with older age and CT imaging.14,16 In addition, an IF diagnosed during admission for chest pain was associated with a 26% increase in length of hospital stay.
To our knowledge, we present the first study on the impact of identification of radiologic IFs in hospitalized patients on length of hospital stay and specifically in patients hospitalized with chest pain of suspected cardiac origin. Trends over the past decade have shown a decrease in LOS and hospitalizations but with an increase in health resource utilization.17,18 Association of radiologic IFs with increase in LOS is significant as this potentially increases hospital-acquired conditions such as infections and resource utilization leading to increase in costs of hospitalizations.19 This in return is a concern for patient safety.
The positive association between LOS and radiologic IFs, interestingly, continued to exist despite sensitivity analysis. Incidental findings of major clinical significance were associated with longer LOS in the sensitivity analysis. Supplemental chart review of patients with major clinical findings suggested more extra-cardiac workup compared to patients with minor/moderate radiologic IFs. This could indicate that the presence of clinically significant radiologic IFs could have led to further inpatient work-up and consultations. The downstream healthcare expenditure associated with workup of IFs in individual radiologic tests is well established.20 In case of cardiac CT, Goehler et al.21 found that the healthcare expenditure was high following incidentally detected pulmonary nodules with an overall small reduction in lung cancer mortality. Incidental findings also increase the burden of reporting and concern for medico-legal issues for providers.4 These concerns are likely valid for hospitalized patients as well.
The socioeconomic trends in the study population were consistent with data from the Bureau of Labor Statistics in that low education is associated with higher unemployment.22 Although, overall, gender, race and insurance mix were similar in both groups, we did see trends of socioeconomic differences in the patients with radiologic IFs of major clinical significance that might not have been statistically significant owing to the small sample size. Despite the population being relatively of younger age (given our cut off age was 65 years) there was still a positive association with age and presence of radiologic IFs. The higher number of patients with COPD or history of malignancy in the radiologic IF group suggests that an association with IFs could exist for these disease cohorts; however, after adjustment for multiple covariates, such an association did not transpire. Interestingly, patients with no radiologic IFs underwent cardiac catheterization or stress testing more often than patients with discovered IFs. This speaks of 2 possibilities; first, that both tests probably do not yield many extra-cardiac IFs, or, secondly, that these patients did not require further workup. More patients in the IF group had more than 1 admission during the study period, and this was associated with increased odds of detecting radiologic IFs. We hypothesize that this might have occurred because of the diagnostic dilemma in these patients who have multiple admissions for the same reason leading to wider array of diagnostic workup. Indeed, we did not note upon chart review alternative diagnoses in these patients but only more IFs. There are several study limitations to consider. First, the fact that this is a single center study sets limitations to interpretation and generalizability of the data. Second, we cannot exclude the possibility of residual confounding. Third, the small number of patients included in this study precludes definitive identification of more factors potentially associated with IFs. However, this study sheds light on a yet unidentified problem within the realm of inpatient management especially for the internists and hospitalists. We tried to limit bias to the extent possible by including only 1 presenting complaint and age-restricting the population.
CONCLUSION
Incidental findings are both clinical and financial challenges to the medical field. This study attempted to shed light on impact of radiologic IFs on care and resource utilization in patients admitted with chest pain of suspected cardiac origin. The positive association between radiologic IFs and length of hospital stay implies that the presence of IFs is associated with increase in LOS and indirectly a likely increase in overall healthcare expenditure. Given the high incidence of radiologic IFs, assuming that these will be present on radiologic tests, should be more a norm than an exception. Providers should know that radiologic testing, especially CT, is associated with detection of IFs.16 By avoiding inappropriate ordering of imaging, the issue of IFs could be mitigated.
While radiologists have recommendations about necessary follow-up for some IFs,7 no clear follow-up guidelines exist for most IFs arising in hospitalized patients. Further prospective and cost analysis studies are needed to assess the overall impact of IFs on other hospitalized patient populations and on the healthcare system in general.
Disclosure
The authors report no conflicts of interest.
References
1. Korley FK, Pham JC, Kirsch TD. Use of advanced radiology during visits to US emergency departments for injury-related conditions, 1998-2007. JAMA. 2010;304(13):1465-1471. PubMed 2. Pines JM. Trends in the rates of radiography use and important diagnoses in emergency department patients with abdominal pain. Med Care. 2009;47(7):782-786. PubMed 3. McGraw-Hill Concise Dictionary of Modern Medicine. Incidentalomas. http://medical-dictionary.thefreedictionary.com/Incidental+findings. Updated 2002. Accessed April 13, 2017. 4. Berland LL, Silverman SG, Gore RM, et al. Managing incidental findings on abdominal CT: White paper of the ACR incidental findings committee. J Am Coll Radiol. 2010;7(10):754-773. PubMed 5. Lumbreras B, González-Alvárez I, Lorente MF, Calbo J, Aranaz J, Hernández-Aguado I. Unexpected findings at imaging: Predicting frequency in various types of studies. Eur J Radiol. 2010;74(1):269-274. PubMed 6. Orme NM, Fletcher JG, Siddiki HA, et al. Incidental findings in imaging research: Evaluating incidence, benefit, and burden. Arch Intern Med. 2010;170(17):1525-1532. PubMed 7. Berland LL. Overview of white papers of the ACR incidental findings committee II on adnexal, vascular, splenic, nodal, gallbladder, and biliary findings. J Am Coll Radiol. 2013;10(9):672-674. PubMed 8. Booth TC, Jackson A, Wardlaw JM, Taylor SA, Waldman AD. Incidental findings found in “healthy” volunteers during imaging performed for research: Current legal and ethical implications. Br J Radiol. 2010;83(990):456-465. PubMed 9. Kelly ME, Heeney A, Redmond CE, et al. Incidental findings detected on emergency abdominal CT scans: A 1-year review. Abdom Imaging. 2015;40(6):1853-1857. PubMed 10. Centers for Medicare and Medicaid Services. Accountable care organizations (ACO). https://www.cms.gov/Medicare/Medicare-Fee-for-Service-Payment/ACO/index.html?redirect=/aco. Baltimore, Maryland. Updated 01/06/2015. 11. Weiss AJ (Truven Health Analytics), Wier LM (Truven Health Analytics), Stocks C (AHRQ), Blanchard J (RAND). Overview of Emergency Department Visits in the United States, 2011. HCUP Statistical Brief #174. June 2014. Agency for Healthcare Research and Quality, Rockville, MD. http://www.hcup-us.ahrq.gov/reports/statbriefs/sb174-Emergency-Department-Visits-Overview.pdf. 12. Chibungu A, Gundareddy V, Wright SM, Nwabuo C, Bollampally P, Landis R, Eid SM. Management of cocaine-induced myocardial infarction: 4-year experience at an urban medical center. South Med J. 2016;109(3):185-190. PubMed 13. Harris PA, Taylor R, Thielke R, Payne J, Gonzalez N, Conde JG. Research electronic data capture (REDCap)--a metadata-driven methodology and workflow process for providing translational research informatics support. J Biomed Inform. 2009;42(2):377-381. PubMed 14. Lumbreras B, Donat L, Hernández-Aguado I. Incidental findings in imaging diagnostic tests: a systematic review. Br J Radiol. 2010;83(988):276-289. PubMed 15. Fontela PC, Winkelmann ER, Ott JN, Uggeri DP. Estimated glomerular filtration rate in patients with type 2 diabetes mellitus. Rev Assoc Méd Bras (1992). 2014;60(6):531-537. PubMed 16. Samim M, Goss S, Luty S, Weinreb J, Moore C. Incidental findings on CT for suspected renal colic in emergency department patients: prevalence and types in 5,383 consecutive examinations. J Am Coll Radiol. 2015;12(1):63-69. PubMed 17. Avalere Health for the American Health Association. TrendWatch ChartBook 2014; trends affecting hospitals and health systems. 2014. http://www.aha.org/research/reports/tw/chartbook/2014/14chartbook.pdf. 18. Weiss AJ, Elixhauser A. Overview of hospital stays in the United States, 2012. HCUP statistical brief #180. https://www.hcup-us.ahrq.gov/reports/statbriefs/sb180-Hospitalizations-United-States-2012.jsp. Accessed April 13, 2017. 19. Hauck K, Zhao X. How dangerous is a day in hospital?: A model of adverse events and length of stay for medical inpatients. Med Care. 2011;49(12):1068-1075. PubMed 20. Ding A, Eisenberg JD, Pandharipande PV. The economic burden of incidentally detected findings. Radiol Clin North Am. 2011;49(2):257-265. PubMed 21. Goehler A, McMahon PM, Lumish HS, et al. Cost-effectiveness of follow-up of pulmonary nodules incidentally detected on cardiac computed tomographic angiography in patients with suspected coronary artery disease. Circulation. 2014;130(8):668-675. PubMed 22. U.S. Department of Labor. Bureau of Labor Statistics. Employment projections. Earning and unemployment rates by educational attainment, 2015. http://www.bls.gov/emp/ep_chart_001.htm. Updated March 15, 2016. Accessed April 13, 2017
References
1. Korley FK, Pham JC, Kirsch TD. Use of advanced radiology during visits to US emergency departments for injury-related conditions, 1998-2007. JAMA. 2010;304(13):1465-1471. PubMed 2. Pines JM. Trends in the rates of radiography use and important diagnoses in emergency department patients with abdominal pain. Med Care. 2009;47(7):782-786. PubMed 3. McGraw-Hill Concise Dictionary of Modern Medicine. Incidentalomas. http://medical-dictionary.thefreedictionary.com/Incidental+findings. Updated 2002. Accessed April 13, 2017. 4. Berland LL, Silverman SG, Gore RM, et al. Managing incidental findings on abdominal CT: White paper of the ACR incidental findings committee. J Am Coll Radiol. 2010;7(10):754-773. PubMed 5. Lumbreras B, González-Alvárez I, Lorente MF, Calbo J, Aranaz J, Hernández-Aguado I. Unexpected findings at imaging: Predicting frequency in various types of studies. Eur J Radiol. 2010;74(1):269-274. PubMed 6. Orme NM, Fletcher JG, Siddiki HA, et al. Incidental findings in imaging research: Evaluating incidence, benefit, and burden. Arch Intern Med. 2010;170(17):1525-1532. PubMed 7. Berland LL. Overview of white papers of the ACR incidental findings committee II on adnexal, vascular, splenic, nodal, gallbladder, and biliary findings. J Am Coll Radiol. 2013;10(9):672-674. PubMed 8. Booth TC, Jackson A, Wardlaw JM, Taylor SA, Waldman AD. Incidental findings found in “healthy” volunteers during imaging performed for research: Current legal and ethical implications. Br J Radiol. 2010;83(990):456-465. PubMed 9. Kelly ME, Heeney A, Redmond CE, et al. Incidental findings detected on emergency abdominal CT scans: A 1-year review. Abdom Imaging. 2015;40(6):1853-1857. PubMed 10. Centers for Medicare and Medicaid Services. Accountable care organizations (ACO). https://www.cms.gov/Medicare/Medicare-Fee-for-Service-Payment/ACO/index.html?redirect=/aco. Baltimore, Maryland. Updated 01/06/2015. 11. Weiss AJ (Truven Health Analytics), Wier LM (Truven Health Analytics), Stocks C (AHRQ), Blanchard J (RAND). Overview of Emergency Department Visits in the United States, 2011. HCUP Statistical Brief #174. June 2014. Agency for Healthcare Research and Quality, Rockville, MD. http://www.hcup-us.ahrq.gov/reports/statbriefs/sb174-Emergency-Department-Visits-Overview.pdf. 12. Chibungu A, Gundareddy V, Wright SM, Nwabuo C, Bollampally P, Landis R, Eid SM. Management of cocaine-induced myocardial infarction: 4-year experience at an urban medical center. South Med J. 2016;109(3):185-190. PubMed 13. Harris PA, Taylor R, Thielke R, Payne J, Gonzalez N, Conde JG. Research electronic data capture (REDCap)--a metadata-driven methodology and workflow process for providing translational research informatics support. J Biomed Inform. 2009;42(2):377-381. PubMed 14. Lumbreras B, Donat L, Hernández-Aguado I. Incidental findings in imaging diagnostic tests: a systematic review. Br J Radiol. 2010;83(988):276-289. PubMed 15. Fontela PC, Winkelmann ER, Ott JN, Uggeri DP. Estimated glomerular filtration rate in patients with type 2 diabetes mellitus. Rev Assoc Méd Bras (1992). 2014;60(6):531-537. PubMed 16. Samim M, Goss S, Luty S, Weinreb J, Moore C. Incidental findings on CT for suspected renal colic in emergency department patients: prevalence and types in 5,383 consecutive examinations. J Am Coll Radiol. 2015;12(1):63-69. PubMed 17. Avalere Health for the American Health Association. TrendWatch ChartBook 2014; trends affecting hospitals and health systems. 2014. http://www.aha.org/research/reports/tw/chartbook/2014/14chartbook.pdf. 18. Weiss AJ, Elixhauser A. Overview of hospital stays in the United States, 2012. HCUP statistical brief #180. https://www.hcup-us.ahrq.gov/reports/statbriefs/sb180-Hospitalizations-United-States-2012.jsp. Accessed April 13, 2017. 19. Hauck K, Zhao X. How dangerous is a day in hospital?: A model of adverse events and length of stay for medical inpatients. Med Care. 2011;49(12):1068-1075. PubMed 20. Ding A, Eisenberg JD, Pandharipande PV. The economic burden of incidentally detected findings. Radiol Clin North Am. 2011;49(2):257-265. PubMed 21. Goehler A, McMahon PM, Lumish HS, et al. Cost-effectiveness of follow-up of pulmonary nodules incidentally detected on cardiac computed tomographic angiography in patients with suspected coronary artery disease. Circulation. 2014;130(8):668-675. PubMed 22. U.S. Department of Labor. Bureau of Labor Statistics. Employment projections. Earning and unemployment rates by educational attainment, 2015. http://www.bls.gov/emp/ep_chart_001.htm. Updated March 15, 2016. Accessed April 13, 2017
Address for correspondence and reprint requests: Venkat Pradeep Gundareddy, MD, MPH; Johns Hopkins University School of Medicine; Division of Hospital Medicine, Johns Hopkins Bayview Medical Center, 5200 Eastern Ave, MFL West 6th Floor, Baltimore, MD 21224; Telephone: 410-550-5018; Fax: 410-550-2972; E-mail: [email protected]
2017 Society of Hospital Medicine DOI
Content Gating
Gated (full article locked unless allowed per User)
The ability of serum troponin measurement in the diagnosis of acute myocardial infarction (AMI) was validated in patients with at least a moderate pretest probability for the disease.1 The diagnostic yield of troponin testing in clinical trials has been between 20% and 50%, excluded patients thought unlikely to have AMI. In practice, physicians often encounter low-risk patients and patients in whom the diagnosis on initial presentation is unclear. Several noncardiac diagnoses, such as pneumonia and respiratory failure, are associated with an elevated troponin level in the absence of AMI, but patients can present with symptoms similar or identical to those of patients who present with AMI.2-4 Elevated troponin level in sepsis has been associated with worsened prognosis, though there is no evidence that this finding alters management. An American College of Cardiology Foundation opinion published in 2012 expressly recommends against troponin testing in patients with sepsis.4
The only guideline-based indication for troponin testing is the diagnosis or exclusion of AMI.5 We conducted a comprehensive review of troponin testing in our healthcare system to see whether testing might be used in clinical settings in which AMI was unlikely.
METHODS
We retrospectively obtained data on all visits to 14 hospitals in an integrated healthcare system in Texas between June 2013 and June 2014. We analyzed data for all hospital encounters during which a troponin assay was ordered and a troponin level reported—including qualitative point-of-care assays and quantitative laboratory troponin I measurements. We identified 93,436 visits. Quantitative measurements were divided into negative (<0.05 ng/mL), indeterminate (0.05-0.09 ng/mL), and elevated (>0.09 ng/mL), based on the reference ranges reported to physicians. We associated troponin levels with ICD-9 (International Classification of Diseases, Ninth Revision) primary and secondary diagnoses, grouping ICD-9 codes 410 (AMI), 411 (other acute or subacute forms of ischemic heart disease [IHD]), 412 (old myocardial infarction), 413 (angina pectoris), and 414 (other forms of chronic IHD) as representing IHD diagnoses.
To further evaluate troponin testing, we constructed 2 contingency matrices (Table).6 We included visits for which both primary and secondary diagnoses were available for review and for which quantitative troponin I measurements were available; 92,445 encounters met criteria for inclusion in matrix calculations. In the first matrix (part A of Table), a primary diagnosis of any AMI (ICD-9 code 410) was used as “positive” and all others “negative.” In the second matrix (part B of Table), “positive” includes any primary or secondary diagnosis of AMI.
Table
RESULTS
We identified a total of 93,436 hospital visits associated with troponin testing; 179,239 troponin measurements were associated with these visits (an average of 1.81 per encounter). Of these visits, 59,897 (64.1%) were associated with a single measurement. Of the 179,239 measurements, 147,051 (82.1%) were negative, 21,881 (12.1%) indeterminate, and 10,307 (5.8%) positive. Primary diagnoses of hypertension, dizziness, abdominal pain, anxiety, dehydration, and headache associated with troponin testing comprised 6127 encounters and had no associated elevated troponin levels. Several non-cardiac primary diagnoses were associated with significant numbers of elevated troponin values including septicemia (27%), acute respiratory failure (28%), and cerebrovascular accident (10%). Seventy-six percent of encounters associated with troponin testing had no primary or secondary IHD diagnosis. Only 2% of 16,941 visits with a primary diagnosis of chest pain were associated with abnormal troponin levels (Figure).
Figure
Analysis of contingency matrices revealed AMI prevalence of 2.6% when primary AMI diagnoses were considered and 3.5% when any AMI diagnoses were considered. Sensitivity and specificity were high (>90%), and negative predictive value extremely high (>99%) in each circumstance. However, positive predictive values were low (21.7% and 28.8%, respectively), indicating the majority of patients with elevated troponin levels were not reported to have AMI by attending physicians.
DISCUSSION
We were surprised to find that troponin level was measured only once during 64% of the hospital encounters. Although there are clinical scenarios in which a single measurement might be indicated, detecting a rise or fall in troponin level is integral to the diagnosis of AMI, which is why guidelines recommend serial measurement.4 We were also surprised to find a low rate of either primary or secondary AMI in patients tested. As others have found,2,3 elevated troponin levels were associated with noncardiac primary diagnoses, such as sepsis, respiratory failure, and stroke. Of interest, the majority (72%) of patients with elevated troponin levels did not receive a primary or secondary diagnosis of AMI.
Determining the appropriate level of use for a diagnostic laboratory test can be difficult. Primary diagnostic codes, including codes for headache and dizziness, accounted for thousands of tested patients but were associated with no elevated troponin levels. On the other hand, sepsis, pneumonia, and stroke were associated with high rates of elevated troponin levels. Elevated troponin levels likely precipitate cardiology consultation and testing, which increase cost of care perhaps without improving either quality or value of care. However, evidence for the potential prognostic value of testing has led to ongoing research at our institution to evaluate whether troponin measurement might guide better management of such patients.
Appropriate use criteria have been developed for many diagnostic studies, including echocardiography, stress testing, and cardiac catheterization, but not for laboratory testing. Our data suggest possible overuse of troponin testing in our healthcare system. The low AMI incidence we found (2.6%-3.5%) indicates that many patients without AMI are being tested.
Although it is impossible to accurately estimate sensitivity and specificity of testing post hoc, it is reassuring to see that measured sensitivity, specificity, and negative predictive values were all high and consistent with published values from prospective clinical trials.7,8
As potential roles for troponin testing develop for patients without primary cardiac disease, it becomes even more important to develop guidelines for testing and to avoid universal testing of all hospitalized patients. The high negative predictive value of troponin testing (99%) is attractive to physicians who want to avoid missing AMI. Electronic order sets allow troponin testing to be included alongside “standard” testing, such as complete blood cell counts and comprehensive metabolic panels, and may contribute to overuse.
The troponin assays used in our healthcare system in 2014 likely will be replaced with high-sensitivity assays currently being used in Europe.9,10 These high-sensitivity assays can improve sensitivity but cannot be expected to increase positive predictive value or reduce false detection rates. When performed as single measurements, hs troponin has the potential to increase the number of elevated troponins detected that are not associated with AMI.
On the basis of our data, we have initiated a system-wide program to improve performance of troponin testing in our healthcare system. We are working with hospitalists and critical care and emergency department physicians to ensure that serial measurements are being performed and that the correct patients are being tested. Future data collection will help determine the success or failure of these efforts.
Disclosure
Nothing to report.
References
1. Thygesen K, Alpert JS, Jaffe AS, et al. Third universal definition of myocardial infarction. Circulation. 2012;126(16):2020-2035. PubMed 2. Hamm CW, Giannitsis E, Katus HA. Cardiac troponin elevations in patients without acute coronary syndrome. Circulation. 2002;106(23):2871-2872. PubMed 3. Roongsritong C, Warraich I, Bradley C. Common causes of troponin elevations in the absence of acute myocardial infarction: incidence and clinical significance. Chest. 2004;125(5):1877-1884. PubMed 4. Newby LK, Jesse RL, Babb JD, et al. ACCF 2012 expert consensus document on practical clinical considerations in the interpretation of troponin elevations: a report of the American College of Cardiology Foundation Task Force on Clinical Consensus Documents. J Am Coll Cardiol. 2012;60(23):2427-2463. PubMed 5. Amsterdam EA, Wenger NK, Brindis RG, et al; American College of Cardiology; American Heart Association Task Force on Practice Guidelines; Society for Cardiovascular Angiography and Interventions; Society of Thoracic Surgeons; American Association for Clinical Chemistry. 2014 AHA/ACC Guideline for the Management of Patients With Non-ST-Elevation Acute Coronary Syndromes: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. 2014;64(24):e139-e228. 6. Pearson K. On the Theory of Contingency and Its Relationship to Association and Normal Correlation. Mathematical Contributions to the Theory of Evolution. London, England: Dulau & Co; 1904. 7. Katus HA, Remppis A, Neumann FJ, et al. Diagnostic efficiency of troponin T measurements in acute myocardial infarction. Circulation. 1991;83(3):902-912. PubMed 8. Olatidoye AG, Wu AH, Feng YJ, Waters D. Prognostic role of troponin T versus troponin I in unstable angina pectoris for cardiac events with meta-analysis comparing published studies. Am J Cardiol. 1998;81(12):1405-1410. PubMed 9. Reichlin T, Hochholzer W, Bassetti S, et al. Early diagnosis of myocardial infarction with sensitive cardiac troponin assays. N Engl J Med. 2009;361(9):858-867. PubMed 10. Keller T, Zeller T, Peetz D, et al. Sensitive troponin I assay in early diagnosis of acute myocardial infarction. N Engl J Med. 2009;361(9):868-877. PubMed
The ability of serum troponin measurement in the diagnosis of acute myocardial infarction (AMI) was validated in patients with at least a moderate pretest probability for the disease.1 The diagnostic yield of troponin testing in clinical trials has been between 20% and 50%, excluded patients thought unlikely to have AMI. In practice, physicians often encounter low-risk patients and patients in whom the diagnosis on initial presentation is unclear. Several noncardiac diagnoses, such as pneumonia and respiratory failure, are associated with an elevated troponin level in the absence of AMI, but patients can present with symptoms similar or identical to those of patients who present with AMI.2-4 Elevated troponin level in sepsis has been associated with worsened prognosis, though there is no evidence that this finding alters management. An American College of Cardiology Foundation opinion published in 2012 expressly recommends against troponin testing in patients with sepsis.4
The only guideline-based indication for troponin testing is the diagnosis or exclusion of AMI.5 We conducted a comprehensive review of troponin testing in our healthcare system to see whether testing might be used in clinical settings in which AMI was unlikely.
METHODS
We retrospectively obtained data on all visits to 14 hospitals in an integrated healthcare system in Texas between June 2013 and June 2014. We analyzed data for all hospital encounters during which a troponin assay was ordered and a troponin level reported—including qualitative point-of-care assays and quantitative laboratory troponin I measurements. We identified 93,436 visits. Quantitative measurements were divided into negative (<0.05 ng/mL), indeterminate (0.05-0.09 ng/mL), and elevated (>0.09 ng/mL), based on the reference ranges reported to physicians. We associated troponin levels with ICD-9 (International Classification of Diseases, Ninth Revision) primary and secondary diagnoses, grouping ICD-9 codes 410 (AMI), 411 (other acute or subacute forms of ischemic heart disease [IHD]), 412 (old myocardial infarction), 413 (angina pectoris), and 414 (other forms of chronic IHD) as representing IHD diagnoses.
To further evaluate troponin testing, we constructed 2 contingency matrices (Table).6 We included visits for which both primary and secondary diagnoses were available for review and for which quantitative troponin I measurements were available; 92,445 encounters met criteria for inclusion in matrix calculations. In the first matrix (part A of Table), a primary diagnosis of any AMI (ICD-9 code 410) was used as “positive” and all others “negative.” In the second matrix (part B of Table), “positive” includes any primary or secondary diagnosis of AMI.
Table
RESULTS
We identified a total of 93,436 hospital visits associated with troponin testing; 179,239 troponin measurements were associated with these visits (an average of 1.81 per encounter). Of these visits, 59,897 (64.1%) were associated with a single measurement. Of the 179,239 measurements, 147,051 (82.1%) were negative, 21,881 (12.1%) indeterminate, and 10,307 (5.8%) positive. Primary diagnoses of hypertension, dizziness, abdominal pain, anxiety, dehydration, and headache associated with troponin testing comprised 6127 encounters and had no associated elevated troponin levels. Several non-cardiac primary diagnoses were associated with significant numbers of elevated troponin values including septicemia (27%), acute respiratory failure (28%), and cerebrovascular accident (10%). Seventy-six percent of encounters associated with troponin testing had no primary or secondary IHD diagnosis. Only 2% of 16,941 visits with a primary diagnosis of chest pain were associated with abnormal troponin levels (Figure).
Figure
Analysis of contingency matrices revealed AMI prevalence of 2.6% when primary AMI diagnoses were considered and 3.5% when any AMI diagnoses were considered. Sensitivity and specificity were high (>90%), and negative predictive value extremely high (>99%) in each circumstance. However, positive predictive values were low (21.7% and 28.8%, respectively), indicating the majority of patients with elevated troponin levels were not reported to have AMI by attending physicians.
DISCUSSION
We were surprised to find that troponin level was measured only once during 64% of the hospital encounters. Although there are clinical scenarios in which a single measurement might be indicated, detecting a rise or fall in troponin level is integral to the diagnosis of AMI, which is why guidelines recommend serial measurement.4 We were also surprised to find a low rate of either primary or secondary AMI in patients tested. As others have found,2,3 elevated troponin levels were associated with noncardiac primary diagnoses, such as sepsis, respiratory failure, and stroke. Of interest, the majority (72%) of patients with elevated troponin levels did not receive a primary or secondary diagnosis of AMI.
Determining the appropriate level of use for a diagnostic laboratory test can be difficult. Primary diagnostic codes, including codes for headache and dizziness, accounted for thousands of tested patients but were associated with no elevated troponin levels. On the other hand, sepsis, pneumonia, and stroke were associated with high rates of elevated troponin levels. Elevated troponin levels likely precipitate cardiology consultation and testing, which increase cost of care perhaps without improving either quality or value of care. However, evidence for the potential prognostic value of testing has led to ongoing research at our institution to evaluate whether troponin measurement might guide better management of such patients.
Appropriate use criteria have been developed for many diagnostic studies, including echocardiography, stress testing, and cardiac catheterization, but not for laboratory testing. Our data suggest possible overuse of troponin testing in our healthcare system. The low AMI incidence we found (2.6%-3.5%) indicates that many patients without AMI are being tested.
Although it is impossible to accurately estimate sensitivity and specificity of testing post hoc, it is reassuring to see that measured sensitivity, specificity, and negative predictive values were all high and consistent with published values from prospective clinical trials.7,8
As potential roles for troponin testing develop for patients without primary cardiac disease, it becomes even more important to develop guidelines for testing and to avoid universal testing of all hospitalized patients. The high negative predictive value of troponin testing (99%) is attractive to physicians who want to avoid missing AMI. Electronic order sets allow troponin testing to be included alongside “standard” testing, such as complete blood cell counts and comprehensive metabolic panels, and may contribute to overuse.
The troponin assays used in our healthcare system in 2014 likely will be replaced with high-sensitivity assays currently being used in Europe.9,10 These high-sensitivity assays can improve sensitivity but cannot be expected to increase positive predictive value or reduce false detection rates. When performed as single measurements, hs troponin has the potential to increase the number of elevated troponins detected that are not associated with AMI.
On the basis of our data, we have initiated a system-wide program to improve performance of troponin testing in our healthcare system. We are working with hospitalists and critical care and emergency department physicians to ensure that serial measurements are being performed and that the correct patients are being tested. Future data collection will help determine the success or failure of these efforts.
Disclosure
Nothing to report.
The ability of serum troponin measurement in the diagnosis of acute myocardial infarction (AMI) was validated in patients with at least a moderate pretest probability for the disease.1 The diagnostic yield of troponin testing in clinical trials has been between 20% and 50%, excluded patients thought unlikely to have AMI. In practice, physicians often encounter low-risk patients and patients in whom the diagnosis on initial presentation is unclear. Several noncardiac diagnoses, such as pneumonia and respiratory failure, are associated with an elevated troponin level in the absence of AMI, but patients can present with symptoms similar or identical to those of patients who present with AMI.2-4 Elevated troponin level in sepsis has been associated with worsened prognosis, though there is no evidence that this finding alters management. An American College of Cardiology Foundation opinion published in 2012 expressly recommends against troponin testing in patients with sepsis.4
The only guideline-based indication for troponin testing is the diagnosis or exclusion of AMI.5 We conducted a comprehensive review of troponin testing in our healthcare system to see whether testing might be used in clinical settings in which AMI was unlikely.
METHODS
We retrospectively obtained data on all visits to 14 hospitals in an integrated healthcare system in Texas between June 2013 and June 2014. We analyzed data for all hospital encounters during which a troponin assay was ordered and a troponin level reported—including qualitative point-of-care assays and quantitative laboratory troponin I measurements. We identified 93,436 visits. Quantitative measurements were divided into negative (<0.05 ng/mL), indeterminate (0.05-0.09 ng/mL), and elevated (>0.09 ng/mL), based on the reference ranges reported to physicians. We associated troponin levels with ICD-9 (International Classification of Diseases, Ninth Revision) primary and secondary diagnoses, grouping ICD-9 codes 410 (AMI), 411 (other acute or subacute forms of ischemic heart disease [IHD]), 412 (old myocardial infarction), 413 (angina pectoris), and 414 (other forms of chronic IHD) as representing IHD diagnoses.
To further evaluate troponin testing, we constructed 2 contingency matrices (Table).6 We included visits for which both primary and secondary diagnoses were available for review and for which quantitative troponin I measurements were available; 92,445 encounters met criteria for inclusion in matrix calculations. In the first matrix (part A of Table), a primary diagnosis of any AMI (ICD-9 code 410) was used as “positive” and all others “negative.” In the second matrix (part B of Table), “positive” includes any primary or secondary diagnosis of AMI.
Table
RESULTS
We identified a total of 93,436 hospital visits associated with troponin testing; 179,239 troponin measurements were associated with these visits (an average of 1.81 per encounter). Of these visits, 59,897 (64.1%) were associated with a single measurement. Of the 179,239 measurements, 147,051 (82.1%) were negative, 21,881 (12.1%) indeterminate, and 10,307 (5.8%) positive. Primary diagnoses of hypertension, dizziness, abdominal pain, anxiety, dehydration, and headache associated with troponin testing comprised 6127 encounters and had no associated elevated troponin levels. Several non-cardiac primary diagnoses were associated with significant numbers of elevated troponin values including septicemia (27%), acute respiratory failure (28%), and cerebrovascular accident (10%). Seventy-six percent of encounters associated with troponin testing had no primary or secondary IHD diagnosis. Only 2% of 16,941 visits with a primary diagnosis of chest pain were associated with abnormal troponin levels (Figure).
Figure
Analysis of contingency matrices revealed AMI prevalence of 2.6% when primary AMI diagnoses were considered and 3.5% when any AMI diagnoses were considered. Sensitivity and specificity were high (>90%), and negative predictive value extremely high (>99%) in each circumstance. However, positive predictive values were low (21.7% and 28.8%, respectively), indicating the majority of patients with elevated troponin levels were not reported to have AMI by attending physicians.
DISCUSSION
We were surprised to find that troponin level was measured only once during 64% of the hospital encounters. Although there are clinical scenarios in which a single measurement might be indicated, detecting a rise or fall in troponin level is integral to the diagnosis of AMI, which is why guidelines recommend serial measurement.4 We were also surprised to find a low rate of either primary or secondary AMI in patients tested. As others have found,2,3 elevated troponin levels were associated with noncardiac primary diagnoses, such as sepsis, respiratory failure, and stroke. Of interest, the majority (72%) of patients with elevated troponin levels did not receive a primary or secondary diagnosis of AMI.
Determining the appropriate level of use for a diagnostic laboratory test can be difficult. Primary diagnostic codes, including codes for headache and dizziness, accounted for thousands of tested patients but were associated with no elevated troponin levels. On the other hand, sepsis, pneumonia, and stroke were associated with high rates of elevated troponin levels. Elevated troponin levels likely precipitate cardiology consultation and testing, which increase cost of care perhaps without improving either quality or value of care. However, evidence for the potential prognostic value of testing has led to ongoing research at our institution to evaluate whether troponin measurement might guide better management of such patients.
Appropriate use criteria have been developed for many diagnostic studies, including echocardiography, stress testing, and cardiac catheterization, but not for laboratory testing. Our data suggest possible overuse of troponin testing in our healthcare system. The low AMI incidence we found (2.6%-3.5%) indicates that many patients without AMI are being tested.
Although it is impossible to accurately estimate sensitivity and specificity of testing post hoc, it is reassuring to see that measured sensitivity, specificity, and negative predictive values were all high and consistent with published values from prospective clinical trials.7,8
As potential roles for troponin testing develop for patients without primary cardiac disease, it becomes even more important to develop guidelines for testing and to avoid universal testing of all hospitalized patients. The high negative predictive value of troponin testing (99%) is attractive to physicians who want to avoid missing AMI. Electronic order sets allow troponin testing to be included alongside “standard” testing, such as complete blood cell counts and comprehensive metabolic panels, and may contribute to overuse.
The troponin assays used in our healthcare system in 2014 likely will be replaced with high-sensitivity assays currently being used in Europe.9,10 These high-sensitivity assays can improve sensitivity but cannot be expected to increase positive predictive value or reduce false detection rates. When performed as single measurements, hs troponin has the potential to increase the number of elevated troponins detected that are not associated with AMI.
On the basis of our data, we have initiated a system-wide program to improve performance of troponin testing in our healthcare system. We are working with hospitalists and critical care and emergency department physicians to ensure that serial measurements are being performed and that the correct patients are being tested. Future data collection will help determine the success or failure of these efforts.
Disclosure
Nothing to report.
References
1. Thygesen K, Alpert JS, Jaffe AS, et al. Third universal definition of myocardial infarction. Circulation. 2012;126(16):2020-2035. PubMed 2. Hamm CW, Giannitsis E, Katus HA. Cardiac troponin elevations in patients without acute coronary syndrome. Circulation. 2002;106(23):2871-2872. PubMed 3. Roongsritong C, Warraich I, Bradley C. Common causes of troponin elevations in the absence of acute myocardial infarction: incidence and clinical significance. Chest. 2004;125(5):1877-1884. PubMed 4. Newby LK, Jesse RL, Babb JD, et al. ACCF 2012 expert consensus document on practical clinical considerations in the interpretation of troponin elevations: a report of the American College of Cardiology Foundation Task Force on Clinical Consensus Documents. J Am Coll Cardiol. 2012;60(23):2427-2463. PubMed 5. Amsterdam EA, Wenger NK, Brindis RG, et al; American College of Cardiology; American Heart Association Task Force on Practice Guidelines; Society for Cardiovascular Angiography and Interventions; Society of Thoracic Surgeons; American Association for Clinical Chemistry. 2014 AHA/ACC Guideline for the Management of Patients With Non-ST-Elevation Acute Coronary Syndromes: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. 2014;64(24):e139-e228. 6. Pearson K. On the Theory of Contingency and Its Relationship to Association and Normal Correlation. Mathematical Contributions to the Theory of Evolution. London, England: Dulau & Co; 1904. 7. Katus HA, Remppis A, Neumann FJ, et al. Diagnostic efficiency of troponin T measurements in acute myocardial infarction. Circulation. 1991;83(3):902-912. PubMed 8. Olatidoye AG, Wu AH, Feng YJ, Waters D. Prognostic role of troponin T versus troponin I in unstable angina pectoris for cardiac events with meta-analysis comparing published studies. Am J Cardiol. 1998;81(12):1405-1410. PubMed 9. Reichlin T, Hochholzer W, Bassetti S, et al. Early diagnosis of myocardial infarction with sensitive cardiac troponin assays. N Engl J Med. 2009;361(9):858-867. PubMed 10. Keller T, Zeller T, Peetz D, et al. Sensitive troponin I assay in early diagnosis of acute myocardial infarction. N Engl J Med. 2009;361(9):868-877. PubMed
References
1. Thygesen K, Alpert JS, Jaffe AS, et al. Third universal definition of myocardial infarction. Circulation. 2012;126(16):2020-2035. PubMed 2. Hamm CW, Giannitsis E, Katus HA. Cardiac troponin elevations in patients without acute coronary syndrome. Circulation. 2002;106(23):2871-2872. PubMed 3. Roongsritong C, Warraich I, Bradley C. Common causes of troponin elevations in the absence of acute myocardial infarction: incidence and clinical significance. Chest. 2004;125(5):1877-1884. PubMed 4. Newby LK, Jesse RL, Babb JD, et al. ACCF 2012 expert consensus document on practical clinical considerations in the interpretation of troponin elevations: a report of the American College of Cardiology Foundation Task Force on Clinical Consensus Documents. J Am Coll Cardiol. 2012;60(23):2427-2463. PubMed 5. Amsterdam EA, Wenger NK, Brindis RG, et al; American College of Cardiology; American Heart Association Task Force on Practice Guidelines; Society for Cardiovascular Angiography and Interventions; Society of Thoracic Surgeons; American Association for Clinical Chemistry. 2014 AHA/ACC Guideline for the Management of Patients With Non-ST-Elevation Acute Coronary Syndromes: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. 2014;64(24):e139-e228. 6. Pearson K. On the Theory of Contingency and Its Relationship to Association and Normal Correlation. Mathematical Contributions to the Theory of Evolution. London, England: Dulau & Co; 1904. 7. Katus HA, Remppis A, Neumann FJ, et al. Diagnostic efficiency of troponin T measurements in acute myocardial infarction. Circulation. 1991;83(3):902-912. PubMed 8. Olatidoye AG, Wu AH, Feng YJ, Waters D. Prognostic role of troponin T versus troponin I in unstable angina pectoris for cardiac events with meta-analysis comparing published studies. Am J Cardiol. 1998;81(12):1405-1410. PubMed 9. Reichlin T, Hochholzer W, Bassetti S, et al. Early diagnosis of myocardial infarction with sensitive cardiac troponin assays. N Engl J Med. 2009;361(9):858-867. PubMed 10. Keller T, Zeller T, Peetz D, et al. Sensitive troponin I assay in early diagnosis of acute myocardial infarction. N Engl J Med. 2009;361(9):868-877. PubMed
Address for correspondence and reprint requests: Jeffrey Michel, MD, FACC, Department of Cardiology, Scott and White Memorial Hospital, 2410 S 31st St, MS-33-ST156, Temple, TX 76508; Telephone: 512-568-2494; Fax: 254-724-9854; E-mail: [email protected]
Content Gating
Gated (full article locked unless allowed per User)
Electronic consultation (e-consult) in the outpatient setting allows subspecialists to provide assessment and recommendations for patients without in-person visits.1 An e-consult is an asynchronous communication that uses the electronic medical record (EMR) and typically involves an electronic order from a requesting provider and an electronic note from a consulting provider. The initial motivation for developing this consultation modality was to improve access to subspecialty care for patients in the primary care setting, and findings of studies at several sites support this claim.1-4 In addition, e-consult may also reduce cost because converting unnecessary face-to-face encounters into e-consults reduces patients’ travel costs and healthcare organizations’ expensive subspecialty clinic time.3,5 Moreover, instead of addressing less complex clinical questions in informal, undocumented face-to-face or telephone “curbside” consultations with specialists, providers can instead ask for e-consults and thereby ensure thorough chart review and proper documentation.6
Use of e-consults in the inpatient setting is relatively novel.7 In addition to having the advantages already mentioned, e-consults are faster than in-person bedside consultations and may be beneficial in the fast-moving inpatient care setting. Finally, healthcare systems with multiple hospital sites may not have the capacity to physically locate subspecialists at each site, which makes e-consults attractive for avoiding unnecessary travel time.
In this article, we describe how we developed an inpatient e-consult protocol for a new, remote hospital within our healthcare system and explore data on safety and physician attitudes after e-consult implementation.
METHODS
The Institutional Review Board of the University of California San Francisco (UCSF) approved this study.
Setting
In February 2015, UCSF opened a new hospital in the Mission Bay neighborhood of San Francisco, 4 miles from the existing hospital. The new hospital is home to several adult inpatient services: urology, otolaryngology, colorectal surgery, obstetrics, and gynecologic surgery. A hospitalist is on-site 24 hours a day to provide consultation for these services around issues that relate to internal medicine. A hospitalist who requires subspecialty expertise to answer a clinical question can request a consultation by in-person visit, video telemedicine, or e-consult, each of which is available 24/7. Almost all of the medicine subspecialists work on the existing campus, not in Mission Bay.
Protocol Development and Implementation
The protocol for the e-consult program was developed over several months by an interdisciplinary group that included 3 hospitalists, 1 obstetrician, 1 project manager, and 1 informaticist. The group outlined the process for requesting and completing an e-consult (Figure), designed a note template for consultants to use for EMR documentation, conducted outreach with subspecialty groups to discuss the protocol, and developed an EMR report to track e-consult use and content over time. As our medical center does not bill payers for inpatient e-consults, e-consult note tracking is used to provide reimbursement internally, from the medical center to the respective departments of the consultants. Reimbursement is made at a set rate per e-consult note, with the rate set to approximate the reimbursement of a low-acuity in-person consult on the main campus.
Figure
The workflow of an e-consult is as follows: (1) When a primary team requires a consultation on an issue that falls within the purview of internal medicine, it pages the on-site hospitalist. (2) The hospitalist accepts the consultation by phone, reviews the chart, and examines the patient. (3) If the hospitalist requires subspecialty assistance to answer a clinical question, he or she contacts the appropriate subspecialty service by pager. (4) The subspecialist speaks with the hospitalist about the consultation question, and together they decide if an e-consult is appropriate, based on the complexity of the clinical scenario. (5) The subspecialist reviews the patient’s chart and documents their care plan recommendations in an e-consult note. Consultants can use e-consult for both initial and follow-up assessment, and there is no strict requirement that they also contact the hospitalist or the primary team by phone in addition to consultation note. Given their novelty, almost all e-consults are performed by subspecialist attendings, not residents or fellows.
Evaluation
Each month, we tracked e-consult use using an EMR report built as part of the implementation of the program. For the first four months of implementation, every patient who received an e-consult also had a manual chart review of the period around the e-consult, performed by a hospitalist, in order to audit for any potential safety issues. These issues included, for example, an e-consult performed for a patient whose complexity or severity of illness was felt to be too great to defer an in-person visit, or a patient who received e-consult recommendations that were significantly retracted in a follow-up in-person note.
Eight months after the program started, we assessed experience by electronically surveying the 9 hospitalists and 11 consultants who had requested or performed at least 2 e-consults.8 Survey items were measured on a 5-point Likert scale: strongly disagree to strongly agree. The items, which related to ease of calling for a consultation, quality of e-consults, impact on clinical care, safety concerns, and satisfaction, were inspired by themes identified in a systematic review of the literature on e-consults in the outpatient setting.2 We sent 2 reminders to responders. Data were summarized using descriptive statistics. Analysis was performed in SPSS version 22.0 (IBM).
RESULTS
There were 143 initial subspecialty consultations by e-consult between program launch in February 2015 and manuscript preparation in February 2016, an average of 11 e-consults per month. There were 313 total e-consult notes (these included both initial and follow-up e-consult notes). By comparison, 240 initial in-person consultations occurred during the same period, and there were 435 total in-person consultation notes (46% new or initial notes, 54% follow-up notes). The top 5 subspecialties by volume of e-consults were infectious disease (35%), hematology (20%), endocrinology (14%), nephrology (13%), and cardiology (8%). For reference, e-consults are also available from psychiatry, neurology, oncology, gastroenterology, pulmonology, and rheumatology. Percentage of consultations performed during daytime hours (defined as 8 a.m. to 5 p.m.) was 92% for e-consults and 96% for in-person consultations.
There were no e-consult–related patient safety issues reported through the medical center’s incident reporting system during the study period. There were also no patient safety issues identified in the manual audits of 80 charts during the first 4 months of the program.
Seven (78%) of 9 hospitalists and 7 (64%) of 11 consultants completed the survey. Both groups agreed that e-consults were easy to use and efficient (Table). All hospitalists were satisfied with the quality of e-consult recommendations, but only 3 (43%) of the 7 consultants agreed they could provide high-quality consultation by e-consult. In their comments, 2 consultants expressed concerns. One concern was about missing crucial information by performing only a chart review, and the other was about being tempted to perform an e-consult simply because it is expedient.
Table
DISCUSSION
Although use of e-consults in the outpatient setting is relatively commonplace, our program represents a novel use of e-consults in safely and efficiently providing subspecialty consultation to inpatients at a remote hospital.
For hospitalists, an e-consult system offers numerous benefits. Clinical questions beyond an internists’ scope of practice come up often, and simple questions might traditionally result in an informal curbside consult. While a curbside consult provides answers faster than an in-person visit, it creates risks for the requesting hospitalists: the consultants only know what they are told, whether the information is incomplete or erroneous; their opinions are given without documentation or compensation, which reduces a sense of accountability; and the lack of documentation does not allow their advice to persist in the chart as a reference for future providers.9 Our e-consult program solves these problems by requiring that consultants perform chart review and provide documentation as well as obligating the medical center to pay a small compensation to consultants for their time. We hope this lowers the bar to requesting consultation for remote sites, where the alternative would be burdensome travel time to do an in-person visit.
In our study, hospitalists were universally pleased with the quality of e-consult recommendations, but only 43% of consultants agreed. These findings correlate with the literature on e-consults in the outpatient setting.2 Unfortunately, our survey comments did not shed further light on this sentiment. In the outpatient literature, consultants were most concerned with having a clear clinical question, facing the liability of providing recommendations without performing an examination, and receiving appropriate compensation for answering e-consults.
The generalizability of our program findings is limited most significantly by the particular arrangement of our clinical services: Our remote site is home to a select group of adult inpatient services, a hospitalist is available on-site for these services 24 hours a day, and the distance to the remote site can be overcome with modest effort should a patient require an in-person visit in the initial or follow-up period. The generalizability of our safety findings is limited by the use of a single reviewer for chart auditing.
Given the rise of accountable care organizations and the prevalence of hospital mergers in the healthcare landscape, we believe that healthcare systems that operate remote sites under constrained budgets could look to e-consults to more cost-effectively extend subspecialty expertise across the inpatient enterprise. With improvements in health information exchange, it may also become feasible for consultants to offer e-consults to hospitals outside a medical center’s network. Our study showed that inpatient e-consult programs can be developed and implemented, that they appear not to pose any significant safety issues, and that they can facilitate delivery of timely clinical care.
Acknowledgment
The authors thank Raphaela Levy-Moore for creating and implementing the e-consult note template for our electronic medical record.
Disclosure
Nothing to report.
References
1. Chen AH, Murphy EJ, Yee HF Jr. eReferral—a new model for integrated care. N Engl J Med. 2013;368(26):2450-2453. PubMed 2. Vimalananda VG, Gupte G, Seraj SM, et al. Electronic consultations (e-consults) to improve access to specialty care: a systematic review and narrative synthesis. J Telemed Telecare. 2015;21(6):323-330. PubMed 3. Kirsh S, Carey E, Aron DC, et al. Impact of a national specialty e-consultation implementation project on access. Am J Manag Care. 2015;21(12):e648-e654. PubMed 4. Bergman J, Neuhausen K, Chamie K, et al. Building a medical neighborhood in the safety net: an innovative technology improves hematuria workups. Urology. 2013;82(6):1277-1282. PubMed 5. Wasfy JH, Rao SK, Chittle MD, Gallen KM, Isselbacher EM, Ferris TG. Initial results of a cardiac e-consult pilot program. J Am Coll Cardiol. 2014;64(24):2706-2707. PubMed 6. Perley CM. Physician use of the curbside consultation to address information needs: report on a collective case study. J Med Libr Assoc. 2006;94(2):137-144. PubMed 7. Gupte G, Vimalananda V, Simon SR, DeVito K, Clark J, Orlander JD. Disruptive innovation: implementation of electronic consultations in a Veterans Affairs health care system. JMIR Med Inform. 2016;4(1):e6. PubMed 8. REDCap. Vanderbilt University website. http://www.project-redcap.org. 2015. Accessed March 3, 2016. 9. Burden M, Sarcone E, Keniston A, et al. Prospective comparison of curbside versus formal consultations. J Hosp Med. 2013;8(1):31-35. PubMed
Electronic consultation (e-consult) in the outpatient setting allows subspecialists to provide assessment and recommendations for patients without in-person visits.1 An e-consult is an asynchronous communication that uses the electronic medical record (EMR) and typically involves an electronic order from a requesting provider and an electronic note from a consulting provider. The initial motivation for developing this consultation modality was to improve access to subspecialty care for patients in the primary care setting, and findings of studies at several sites support this claim.1-4 In addition, e-consult may also reduce cost because converting unnecessary face-to-face encounters into e-consults reduces patients’ travel costs and healthcare organizations’ expensive subspecialty clinic time.3,5 Moreover, instead of addressing less complex clinical questions in informal, undocumented face-to-face or telephone “curbside” consultations with specialists, providers can instead ask for e-consults and thereby ensure thorough chart review and proper documentation.6
Use of e-consults in the inpatient setting is relatively novel.7 In addition to having the advantages already mentioned, e-consults are faster than in-person bedside consultations and may be beneficial in the fast-moving inpatient care setting. Finally, healthcare systems with multiple hospital sites may not have the capacity to physically locate subspecialists at each site, which makes e-consults attractive for avoiding unnecessary travel time.
In this article, we describe how we developed an inpatient e-consult protocol for a new, remote hospital within our healthcare system and explore data on safety and physician attitudes after e-consult implementation.
METHODS
The Institutional Review Board of the University of California San Francisco (UCSF) approved this study.
Setting
In February 2015, UCSF opened a new hospital in the Mission Bay neighborhood of San Francisco, 4 miles from the existing hospital. The new hospital is home to several adult inpatient services: urology, otolaryngology, colorectal surgery, obstetrics, and gynecologic surgery. A hospitalist is on-site 24 hours a day to provide consultation for these services around issues that relate to internal medicine. A hospitalist who requires subspecialty expertise to answer a clinical question can request a consultation by in-person visit, video telemedicine, or e-consult, each of which is available 24/7. Almost all of the medicine subspecialists work on the existing campus, not in Mission Bay.
Protocol Development and Implementation
The protocol for the e-consult program was developed over several months by an interdisciplinary group that included 3 hospitalists, 1 obstetrician, 1 project manager, and 1 informaticist. The group outlined the process for requesting and completing an e-consult (Figure), designed a note template for consultants to use for EMR documentation, conducted outreach with subspecialty groups to discuss the protocol, and developed an EMR report to track e-consult use and content over time. As our medical center does not bill payers for inpatient e-consults, e-consult note tracking is used to provide reimbursement internally, from the medical center to the respective departments of the consultants. Reimbursement is made at a set rate per e-consult note, with the rate set to approximate the reimbursement of a low-acuity in-person consult on the main campus.
Figure
The workflow of an e-consult is as follows: (1) When a primary team requires a consultation on an issue that falls within the purview of internal medicine, it pages the on-site hospitalist. (2) The hospitalist accepts the consultation by phone, reviews the chart, and examines the patient. (3) If the hospitalist requires subspecialty assistance to answer a clinical question, he or she contacts the appropriate subspecialty service by pager. (4) The subspecialist speaks with the hospitalist about the consultation question, and together they decide if an e-consult is appropriate, based on the complexity of the clinical scenario. (5) The subspecialist reviews the patient’s chart and documents their care plan recommendations in an e-consult note. Consultants can use e-consult for both initial and follow-up assessment, and there is no strict requirement that they also contact the hospitalist or the primary team by phone in addition to consultation note. Given their novelty, almost all e-consults are performed by subspecialist attendings, not residents or fellows.
Evaluation
Each month, we tracked e-consult use using an EMR report built as part of the implementation of the program. For the first four months of implementation, every patient who received an e-consult also had a manual chart review of the period around the e-consult, performed by a hospitalist, in order to audit for any potential safety issues. These issues included, for example, an e-consult performed for a patient whose complexity or severity of illness was felt to be too great to defer an in-person visit, or a patient who received e-consult recommendations that were significantly retracted in a follow-up in-person note.
Eight months after the program started, we assessed experience by electronically surveying the 9 hospitalists and 11 consultants who had requested or performed at least 2 e-consults.8 Survey items were measured on a 5-point Likert scale: strongly disagree to strongly agree. The items, which related to ease of calling for a consultation, quality of e-consults, impact on clinical care, safety concerns, and satisfaction, were inspired by themes identified in a systematic review of the literature on e-consults in the outpatient setting.2 We sent 2 reminders to responders. Data were summarized using descriptive statistics. Analysis was performed in SPSS version 22.0 (IBM).
RESULTS
There were 143 initial subspecialty consultations by e-consult between program launch in February 2015 and manuscript preparation in February 2016, an average of 11 e-consults per month. There were 313 total e-consult notes (these included both initial and follow-up e-consult notes). By comparison, 240 initial in-person consultations occurred during the same period, and there were 435 total in-person consultation notes (46% new or initial notes, 54% follow-up notes). The top 5 subspecialties by volume of e-consults were infectious disease (35%), hematology (20%), endocrinology (14%), nephrology (13%), and cardiology (8%). For reference, e-consults are also available from psychiatry, neurology, oncology, gastroenterology, pulmonology, and rheumatology. Percentage of consultations performed during daytime hours (defined as 8 a.m. to 5 p.m.) was 92% for e-consults and 96% for in-person consultations.
There were no e-consult–related patient safety issues reported through the medical center’s incident reporting system during the study period. There were also no patient safety issues identified in the manual audits of 80 charts during the first 4 months of the program.
Seven (78%) of 9 hospitalists and 7 (64%) of 11 consultants completed the survey. Both groups agreed that e-consults were easy to use and efficient (Table). All hospitalists were satisfied with the quality of e-consult recommendations, but only 3 (43%) of the 7 consultants agreed they could provide high-quality consultation by e-consult. In their comments, 2 consultants expressed concerns. One concern was about missing crucial information by performing only a chart review, and the other was about being tempted to perform an e-consult simply because it is expedient.
Table
DISCUSSION
Although use of e-consults in the outpatient setting is relatively commonplace, our program represents a novel use of e-consults in safely and efficiently providing subspecialty consultation to inpatients at a remote hospital.
For hospitalists, an e-consult system offers numerous benefits. Clinical questions beyond an internists’ scope of practice come up often, and simple questions might traditionally result in an informal curbside consult. While a curbside consult provides answers faster than an in-person visit, it creates risks for the requesting hospitalists: the consultants only know what they are told, whether the information is incomplete or erroneous; their opinions are given without documentation or compensation, which reduces a sense of accountability; and the lack of documentation does not allow their advice to persist in the chart as a reference for future providers.9 Our e-consult program solves these problems by requiring that consultants perform chart review and provide documentation as well as obligating the medical center to pay a small compensation to consultants for their time. We hope this lowers the bar to requesting consultation for remote sites, where the alternative would be burdensome travel time to do an in-person visit.
In our study, hospitalists were universally pleased with the quality of e-consult recommendations, but only 43% of consultants agreed. These findings correlate with the literature on e-consults in the outpatient setting.2 Unfortunately, our survey comments did not shed further light on this sentiment. In the outpatient literature, consultants were most concerned with having a clear clinical question, facing the liability of providing recommendations without performing an examination, and receiving appropriate compensation for answering e-consults.
The generalizability of our program findings is limited most significantly by the particular arrangement of our clinical services: Our remote site is home to a select group of adult inpatient services, a hospitalist is available on-site for these services 24 hours a day, and the distance to the remote site can be overcome with modest effort should a patient require an in-person visit in the initial or follow-up period. The generalizability of our safety findings is limited by the use of a single reviewer for chart auditing.
Given the rise of accountable care organizations and the prevalence of hospital mergers in the healthcare landscape, we believe that healthcare systems that operate remote sites under constrained budgets could look to e-consults to more cost-effectively extend subspecialty expertise across the inpatient enterprise. With improvements in health information exchange, it may also become feasible for consultants to offer e-consults to hospitals outside a medical center’s network. Our study showed that inpatient e-consult programs can be developed and implemented, that they appear not to pose any significant safety issues, and that they can facilitate delivery of timely clinical care.
Acknowledgment
The authors thank Raphaela Levy-Moore for creating and implementing the e-consult note template for our electronic medical record.
Disclosure
Nothing to report.
Electronic consultation (e-consult) in the outpatient setting allows subspecialists to provide assessment and recommendations for patients without in-person visits.1 An e-consult is an asynchronous communication that uses the electronic medical record (EMR) and typically involves an electronic order from a requesting provider and an electronic note from a consulting provider. The initial motivation for developing this consultation modality was to improve access to subspecialty care for patients in the primary care setting, and findings of studies at several sites support this claim.1-4 In addition, e-consult may also reduce cost because converting unnecessary face-to-face encounters into e-consults reduces patients’ travel costs and healthcare organizations’ expensive subspecialty clinic time.3,5 Moreover, instead of addressing less complex clinical questions in informal, undocumented face-to-face or telephone “curbside” consultations with specialists, providers can instead ask for e-consults and thereby ensure thorough chart review and proper documentation.6
Use of e-consults in the inpatient setting is relatively novel.7 In addition to having the advantages already mentioned, e-consults are faster than in-person bedside consultations and may be beneficial in the fast-moving inpatient care setting. Finally, healthcare systems with multiple hospital sites may not have the capacity to physically locate subspecialists at each site, which makes e-consults attractive for avoiding unnecessary travel time.
In this article, we describe how we developed an inpatient e-consult protocol for a new, remote hospital within our healthcare system and explore data on safety and physician attitudes after e-consult implementation.
METHODS
The Institutional Review Board of the University of California San Francisco (UCSF) approved this study.
Setting
In February 2015, UCSF opened a new hospital in the Mission Bay neighborhood of San Francisco, 4 miles from the existing hospital. The new hospital is home to several adult inpatient services: urology, otolaryngology, colorectal surgery, obstetrics, and gynecologic surgery. A hospitalist is on-site 24 hours a day to provide consultation for these services around issues that relate to internal medicine. A hospitalist who requires subspecialty expertise to answer a clinical question can request a consultation by in-person visit, video telemedicine, or e-consult, each of which is available 24/7. Almost all of the medicine subspecialists work on the existing campus, not in Mission Bay.
Protocol Development and Implementation
The protocol for the e-consult program was developed over several months by an interdisciplinary group that included 3 hospitalists, 1 obstetrician, 1 project manager, and 1 informaticist. The group outlined the process for requesting and completing an e-consult (Figure), designed a note template for consultants to use for EMR documentation, conducted outreach with subspecialty groups to discuss the protocol, and developed an EMR report to track e-consult use and content over time. As our medical center does not bill payers for inpatient e-consults, e-consult note tracking is used to provide reimbursement internally, from the medical center to the respective departments of the consultants. Reimbursement is made at a set rate per e-consult note, with the rate set to approximate the reimbursement of a low-acuity in-person consult on the main campus.
Figure
The workflow of an e-consult is as follows: (1) When a primary team requires a consultation on an issue that falls within the purview of internal medicine, it pages the on-site hospitalist. (2) The hospitalist accepts the consultation by phone, reviews the chart, and examines the patient. (3) If the hospitalist requires subspecialty assistance to answer a clinical question, he or she contacts the appropriate subspecialty service by pager. (4) The subspecialist speaks with the hospitalist about the consultation question, and together they decide if an e-consult is appropriate, based on the complexity of the clinical scenario. (5) The subspecialist reviews the patient’s chart and documents their care plan recommendations in an e-consult note. Consultants can use e-consult for both initial and follow-up assessment, and there is no strict requirement that they also contact the hospitalist or the primary team by phone in addition to consultation note. Given their novelty, almost all e-consults are performed by subspecialist attendings, not residents or fellows.
Evaluation
Each month, we tracked e-consult use using an EMR report built as part of the implementation of the program. For the first four months of implementation, every patient who received an e-consult also had a manual chart review of the period around the e-consult, performed by a hospitalist, in order to audit for any potential safety issues. These issues included, for example, an e-consult performed for a patient whose complexity or severity of illness was felt to be too great to defer an in-person visit, or a patient who received e-consult recommendations that were significantly retracted in a follow-up in-person note.
Eight months after the program started, we assessed experience by electronically surveying the 9 hospitalists and 11 consultants who had requested or performed at least 2 e-consults.8 Survey items were measured on a 5-point Likert scale: strongly disagree to strongly agree. The items, which related to ease of calling for a consultation, quality of e-consults, impact on clinical care, safety concerns, and satisfaction, were inspired by themes identified in a systematic review of the literature on e-consults in the outpatient setting.2 We sent 2 reminders to responders. Data were summarized using descriptive statistics. Analysis was performed in SPSS version 22.0 (IBM).
RESULTS
There were 143 initial subspecialty consultations by e-consult between program launch in February 2015 and manuscript preparation in February 2016, an average of 11 e-consults per month. There were 313 total e-consult notes (these included both initial and follow-up e-consult notes). By comparison, 240 initial in-person consultations occurred during the same period, and there were 435 total in-person consultation notes (46% new or initial notes, 54% follow-up notes). The top 5 subspecialties by volume of e-consults were infectious disease (35%), hematology (20%), endocrinology (14%), nephrology (13%), and cardiology (8%). For reference, e-consults are also available from psychiatry, neurology, oncology, gastroenterology, pulmonology, and rheumatology. Percentage of consultations performed during daytime hours (defined as 8 a.m. to 5 p.m.) was 92% for e-consults and 96% for in-person consultations.
There were no e-consult–related patient safety issues reported through the medical center’s incident reporting system during the study period. There were also no patient safety issues identified in the manual audits of 80 charts during the first 4 months of the program.
Seven (78%) of 9 hospitalists and 7 (64%) of 11 consultants completed the survey. Both groups agreed that e-consults were easy to use and efficient (Table). All hospitalists were satisfied with the quality of e-consult recommendations, but only 3 (43%) of the 7 consultants agreed they could provide high-quality consultation by e-consult. In their comments, 2 consultants expressed concerns. One concern was about missing crucial information by performing only a chart review, and the other was about being tempted to perform an e-consult simply because it is expedient.
Table
DISCUSSION
Although use of e-consults in the outpatient setting is relatively commonplace, our program represents a novel use of e-consults in safely and efficiently providing subspecialty consultation to inpatients at a remote hospital.
For hospitalists, an e-consult system offers numerous benefits. Clinical questions beyond an internists’ scope of practice come up often, and simple questions might traditionally result in an informal curbside consult. While a curbside consult provides answers faster than an in-person visit, it creates risks for the requesting hospitalists: the consultants only know what they are told, whether the information is incomplete or erroneous; their opinions are given without documentation or compensation, which reduces a sense of accountability; and the lack of documentation does not allow their advice to persist in the chart as a reference for future providers.9 Our e-consult program solves these problems by requiring that consultants perform chart review and provide documentation as well as obligating the medical center to pay a small compensation to consultants for their time. We hope this lowers the bar to requesting consultation for remote sites, where the alternative would be burdensome travel time to do an in-person visit.
In our study, hospitalists were universally pleased with the quality of e-consult recommendations, but only 43% of consultants agreed. These findings correlate with the literature on e-consults in the outpatient setting.2 Unfortunately, our survey comments did not shed further light on this sentiment. In the outpatient literature, consultants were most concerned with having a clear clinical question, facing the liability of providing recommendations without performing an examination, and receiving appropriate compensation for answering e-consults.
The generalizability of our program findings is limited most significantly by the particular arrangement of our clinical services: Our remote site is home to a select group of adult inpatient services, a hospitalist is available on-site for these services 24 hours a day, and the distance to the remote site can be overcome with modest effort should a patient require an in-person visit in the initial or follow-up period. The generalizability of our safety findings is limited by the use of a single reviewer for chart auditing.
Given the rise of accountable care organizations and the prevalence of hospital mergers in the healthcare landscape, we believe that healthcare systems that operate remote sites under constrained budgets could look to e-consults to more cost-effectively extend subspecialty expertise across the inpatient enterprise. With improvements in health information exchange, it may also become feasible for consultants to offer e-consults to hospitals outside a medical center’s network. Our study showed that inpatient e-consult programs can be developed and implemented, that they appear not to pose any significant safety issues, and that they can facilitate delivery of timely clinical care.
Acknowledgment
The authors thank Raphaela Levy-Moore for creating and implementing the e-consult note template for our electronic medical record.
Disclosure
Nothing to report.
References
1. Chen AH, Murphy EJ, Yee HF Jr. eReferral—a new model for integrated care. N Engl J Med. 2013;368(26):2450-2453. PubMed 2. Vimalananda VG, Gupte G, Seraj SM, et al. Electronic consultations (e-consults) to improve access to specialty care: a systematic review and narrative synthesis. J Telemed Telecare. 2015;21(6):323-330. PubMed 3. Kirsh S, Carey E, Aron DC, et al. Impact of a national specialty e-consultation implementation project on access. Am J Manag Care. 2015;21(12):e648-e654. PubMed 4. Bergman J, Neuhausen K, Chamie K, et al. Building a medical neighborhood in the safety net: an innovative technology improves hematuria workups. Urology. 2013;82(6):1277-1282. PubMed 5. Wasfy JH, Rao SK, Chittle MD, Gallen KM, Isselbacher EM, Ferris TG. Initial results of a cardiac e-consult pilot program. J Am Coll Cardiol. 2014;64(24):2706-2707. PubMed 6. Perley CM. Physician use of the curbside consultation to address information needs: report on a collective case study. J Med Libr Assoc. 2006;94(2):137-144. PubMed 7. Gupte G, Vimalananda V, Simon SR, DeVito K, Clark J, Orlander JD. Disruptive innovation: implementation of electronic consultations in a Veterans Affairs health care system. JMIR Med Inform. 2016;4(1):e6. PubMed 8. REDCap. Vanderbilt University website. http://www.project-redcap.org. 2015. Accessed March 3, 2016. 9. Burden M, Sarcone E, Keniston A, et al. Prospective comparison of curbside versus formal consultations. J Hosp Med. 2013;8(1):31-35. PubMed
References
1. Chen AH, Murphy EJ, Yee HF Jr. eReferral—a new model for integrated care. N Engl J Med. 2013;368(26):2450-2453. PubMed 2. Vimalananda VG, Gupte G, Seraj SM, et al. Electronic consultations (e-consults) to improve access to specialty care: a systematic review and narrative synthesis. J Telemed Telecare. 2015;21(6):323-330. PubMed 3. Kirsh S, Carey E, Aron DC, et al. Impact of a national specialty e-consultation implementation project on access. Am J Manag Care. 2015;21(12):e648-e654. PubMed 4. Bergman J, Neuhausen K, Chamie K, et al. Building a medical neighborhood in the safety net: an innovative technology improves hematuria workups. Urology. 2013;82(6):1277-1282. PubMed 5. Wasfy JH, Rao SK, Chittle MD, Gallen KM, Isselbacher EM, Ferris TG. Initial results of a cardiac e-consult pilot program. J Am Coll Cardiol. 2014;64(24):2706-2707. PubMed 6. Perley CM. Physician use of the curbside consultation to address information needs: report on a collective case study. J Med Libr Assoc. 2006;94(2):137-144. PubMed 7. Gupte G, Vimalananda V, Simon SR, DeVito K, Clark J, Orlander JD. Disruptive innovation: implementation of electronic consultations in a Veterans Affairs health care system. JMIR Med Inform. 2016;4(1):e6. PubMed 8. REDCap. Vanderbilt University website. http://www.project-redcap.org. 2015. Accessed March 3, 2016. 9. Burden M, Sarcone E, Keniston A, et al. Prospective comparison of curbside versus formal consultations. J Hosp Med. 2013;8(1):31-35. PubMed
Address for correspondence and reprint requests: Nader Najafi, MD, Division of Hospital Medicine, University of California San Francisco, 505 Parnassus Ave, M1283, San Francisco, CA 94143-0131; Telephone: 415-476-2223; Fax: 415-502-1963; E-mail: [email protected]
Content Gating
Gated (full article locked unless allowed per User)
Avoiding repeated complete blood count (CBC) tests in the face of clinical and lab stability is a focus of the Choosing Wisely® initiatives launched by the American Board of Internal Medicine Foundation1 and endorsed by the Society of Hospital Medicine.2 However, specific scenarios in which daily morning labs can be safely avoided have not been identified. The goal of this study was to identify situations in which routine CBC testing can be avoided in patients with community-acquired pneumonia (CAP), one of the most common reasons for hospital admission.3
METHODS
This was a retrospective study of 50 patients with CAP discharged from our hospital between February 1, 2015 and May 1, 2015. We performed chart abstractions collecting daily vital signs, lab results, provider notes including assessments and plans (A&Ps), and order entry logs, as well as documentation indicating whether a lab result or clinical finding appeared to affect clinical management (eg, a new order or documentation of changing plans). Both escalations and de-escalations were included as management changes. For example, if the note stated “Persistent leukocytosis, add vancomycin,” then the clinical action of expanded antibiotic coverage would be attributed to the CBC.
We defined clinical stability based on Definition B of the Pneumonia Patient Outcomes Research Team (PORT) study criteria.4 We used descriptive statistics and likelihood ratios to characterize the utility of CBC testing in terms of producing clinical management changes. Likelihood ratios were calculated with the “test” representing a CBC being ordered or not ordered and the outcome being any change in management independent of whether it was due to the CBC.
RESULTS
Of 50 patients, 33 (66%) were female, the mean age was 75 years, the mean length of stay was 2.8 days, and the median CURB-65 score,5 an estimate of mortality in CAP used for decision-making about inpatient versus outpatient treatment, was 1 (25th to 75th interquartile range: 1, 2); no patients had a CURB score greater than 3 (Table 1). Forty-one (82%) patients met PORT clinical stability criteria prior to discharge, and 30 (75% of stable patients) had CBCs obtained.
Table 1
On days after admission, 94 subsequent CBCs were obtained. Of these CBCs, 6 (6.4%) were associated with management changes indicated in documentation or orders (Table 2). In 2 of the 6 patients, management changes were likely relevant to pneumonia. In the first case, the patient had a white blood cell count (WBC) of 15.4 on the planned day of discharge but no accompanying clinical changes. Her discharge was potentially delayed pending a repeat CBC which again showed a WBC 14.7; the patient was then discharged without any additional changes in plan. In the second case, the patient experienced new-onset altered mental status on hospital day 3 and increasing O2 requirement with a rising WBC noted on hospital day 4. Repeat chest x-ray, repeat blood cultures, and an ultrasound for parapneumonic effusion were obtained, and the patient’s symptoms and signs resolved over a period of days without changes in treatment. In the 4 other cases, available documentation suggested the hemoglobin abnormalities found represented chronic or incidental illnesses, specifically iron deficiency anemia, iatrogenic anemia due to fluid resuscitation and hemodilution, previously known chronic lymphocytic leukemia, and thrombocytopenia due to acute infection. In all 6 instances, CBC values improved without treatment intervention.
Table 2 Among all patients, the positive likelihood ratio of CBCs obtained after admission in terms of being followed by a change in clinical management was very poor (1.12, 95% confidence interval [CI], 0.86-1.44). For clinically unstable patients, there were 64 CBCs ordered, and the likelihood ratio was similar at 0.98 (95% CI, 0.75-1.29). The positive likelihood ratio among clinically stable patients, who had 30 CBCs ordered, was still quite weak, though confidence intervals were wider (1.23, 95% CI, 0.66-2.29).
DISCUSSION
Though small, our initial study suggests the potential opportunity for savings if Choosing Wisely® recommendations for CBC testing were implemented in patients with community-acquired pneumonia.
Our study has several limitations. Note-writing practices and ordering patterns likely varied between providers, and documentation bias may play a role in our results. However, we defined whether a CBC was associated with changes in clinical decision-making or management by incorporating a number of mutually reinforcing elements of the medical record. We recognize, however, that our approach may not capture undocumented clinical issues or other cognitive (eg, reassurance of clinical resolution) reasons why CBCs were obtained.
Even with these limitations, the likelihood of a CBC value meaningfully changing clinical management among patients with CAP appears to be quite low as evidenced by the case descriptions, particularly when obtained in stable patients by PORT criteria and on the day of discharge. Whether clinical stability as measured by PORT score can be used to target patients in whom CBC testing is unnecessary is difficult to discern from our data, as the overall utility of CBCs obtained after admission was quite low and the rate of changes in management was also low. However, even if CBCs are not particularly costly, unnecessary testing may produce harm in the form of prolonged length of stay, making even one unnecessary CBC potentially extremely expensive. More research involving larger-scale studies are needed to determine the “number needed to screen” for the daily CBC in CAP to determine if the cost savings from overtesting and treatment outweigh the potential benefit of a single CBC that changes management.
Disclosure
Nothing to report.
References
1. Choosing Wisely. Promoting conversations between providers and patients. Choosing Wisely. http://www.choosingwisely.org/. Accessed March 28, 2016. 2. Beresford L. The Society of Hospital Medicine’s “Choosing Wisely” Recommendations for Hospitalists. 2013. http://www.the-hospitalist.org/article/the-society-of-hospital-medicines-choosing-wisely-recommendations-for-hospitalists/. Accessed March 28, 2016. 3. File TM Jr, Marrie TJ. Burden of community-acquired pneumonia in North American adults. Postgrad Med. 2010;122(2):130-141. PubMed 4. Halm EA, Fine MJ, Marrie TJ, et al. Time to clinical stability in patients hospitalized with community-acquired pneumonia: Implications for practice guidelines. JAMA. 1998;279(18):1452-1457. PubMed 5. Lim W, van der Eerden MM, Laing R, et al. Defining community acquired pneumonia severity on presentation to hospital: an international derivation and validation study. Thorax. 2003;58(5):377-382. PubMed
Avoiding repeated complete blood count (CBC) tests in the face of clinical and lab stability is a focus of the Choosing Wisely® initiatives launched by the American Board of Internal Medicine Foundation1 and endorsed by the Society of Hospital Medicine.2 However, specific scenarios in which daily morning labs can be safely avoided have not been identified. The goal of this study was to identify situations in which routine CBC testing can be avoided in patients with community-acquired pneumonia (CAP), one of the most common reasons for hospital admission.3
METHODS
This was a retrospective study of 50 patients with CAP discharged from our hospital between February 1, 2015 and May 1, 2015. We performed chart abstractions collecting daily vital signs, lab results, provider notes including assessments and plans (A&Ps), and order entry logs, as well as documentation indicating whether a lab result or clinical finding appeared to affect clinical management (eg, a new order or documentation of changing plans). Both escalations and de-escalations were included as management changes. For example, if the note stated “Persistent leukocytosis, add vancomycin,” then the clinical action of expanded antibiotic coverage would be attributed to the CBC.
We defined clinical stability based on Definition B of the Pneumonia Patient Outcomes Research Team (PORT) study criteria.4 We used descriptive statistics and likelihood ratios to characterize the utility of CBC testing in terms of producing clinical management changes. Likelihood ratios were calculated with the “test” representing a CBC being ordered or not ordered and the outcome being any change in management independent of whether it was due to the CBC.
RESULTS
Of 50 patients, 33 (66%) were female, the mean age was 75 years, the mean length of stay was 2.8 days, and the median CURB-65 score,5 an estimate of mortality in CAP used for decision-making about inpatient versus outpatient treatment, was 1 (25th to 75th interquartile range: 1, 2); no patients had a CURB score greater than 3 (Table 1). Forty-one (82%) patients met PORT clinical stability criteria prior to discharge, and 30 (75% of stable patients) had CBCs obtained.
Table 1
On days after admission, 94 subsequent CBCs were obtained. Of these CBCs, 6 (6.4%) were associated with management changes indicated in documentation or orders (Table 2). In 2 of the 6 patients, management changes were likely relevant to pneumonia. In the first case, the patient had a white blood cell count (WBC) of 15.4 on the planned day of discharge but no accompanying clinical changes. Her discharge was potentially delayed pending a repeat CBC which again showed a WBC 14.7; the patient was then discharged without any additional changes in plan. In the second case, the patient experienced new-onset altered mental status on hospital day 3 and increasing O2 requirement with a rising WBC noted on hospital day 4. Repeat chest x-ray, repeat blood cultures, and an ultrasound for parapneumonic effusion were obtained, and the patient’s symptoms and signs resolved over a period of days without changes in treatment. In the 4 other cases, available documentation suggested the hemoglobin abnormalities found represented chronic or incidental illnesses, specifically iron deficiency anemia, iatrogenic anemia due to fluid resuscitation and hemodilution, previously known chronic lymphocytic leukemia, and thrombocytopenia due to acute infection. In all 6 instances, CBC values improved without treatment intervention.
Table 2 Among all patients, the positive likelihood ratio of CBCs obtained after admission in terms of being followed by a change in clinical management was very poor (1.12, 95% confidence interval [CI], 0.86-1.44). For clinically unstable patients, there were 64 CBCs ordered, and the likelihood ratio was similar at 0.98 (95% CI, 0.75-1.29). The positive likelihood ratio among clinically stable patients, who had 30 CBCs ordered, was still quite weak, though confidence intervals were wider (1.23, 95% CI, 0.66-2.29).
DISCUSSION
Though small, our initial study suggests the potential opportunity for savings if Choosing Wisely® recommendations for CBC testing were implemented in patients with community-acquired pneumonia.
Our study has several limitations. Note-writing practices and ordering patterns likely varied between providers, and documentation bias may play a role in our results. However, we defined whether a CBC was associated with changes in clinical decision-making or management by incorporating a number of mutually reinforcing elements of the medical record. We recognize, however, that our approach may not capture undocumented clinical issues or other cognitive (eg, reassurance of clinical resolution) reasons why CBCs were obtained.
Even with these limitations, the likelihood of a CBC value meaningfully changing clinical management among patients with CAP appears to be quite low as evidenced by the case descriptions, particularly when obtained in stable patients by PORT criteria and on the day of discharge. Whether clinical stability as measured by PORT score can be used to target patients in whom CBC testing is unnecessary is difficult to discern from our data, as the overall utility of CBCs obtained after admission was quite low and the rate of changes in management was also low. However, even if CBCs are not particularly costly, unnecessary testing may produce harm in the form of prolonged length of stay, making even one unnecessary CBC potentially extremely expensive. More research involving larger-scale studies are needed to determine the “number needed to screen” for the daily CBC in CAP to determine if the cost savings from overtesting and treatment outweigh the potential benefit of a single CBC that changes management.
Disclosure
Nothing to report.
Avoiding repeated complete blood count (CBC) tests in the face of clinical and lab stability is a focus of the Choosing Wisely® initiatives launched by the American Board of Internal Medicine Foundation1 and endorsed by the Society of Hospital Medicine.2 However, specific scenarios in which daily morning labs can be safely avoided have not been identified. The goal of this study was to identify situations in which routine CBC testing can be avoided in patients with community-acquired pneumonia (CAP), one of the most common reasons for hospital admission.3
METHODS
This was a retrospective study of 50 patients with CAP discharged from our hospital between February 1, 2015 and May 1, 2015. We performed chart abstractions collecting daily vital signs, lab results, provider notes including assessments and plans (A&Ps), and order entry logs, as well as documentation indicating whether a lab result or clinical finding appeared to affect clinical management (eg, a new order or documentation of changing plans). Both escalations and de-escalations were included as management changes. For example, if the note stated “Persistent leukocytosis, add vancomycin,” then the clinical action of expanded antibiotic coverage would be attributed to the CBC.
We defined clinical stability based on Definition B of the Pneumonia Patient Outcomes Research Team (PORT) study criteria.4 We used descriptive statistics and likelihood ratios to characterize the utility of CBC testing in terms of producing clinical management changes. Likelihood ratios were calculated with the “test” representing a CBC being ordered or not ordered and the outcome being any change in management independent of whether it was due to the CBC.
RESULTS
Of 50 patients, 33 (66%) were female, the mean age was 75 years, the mean length of stay was 2.8 days, and the median CURB-65 score,5 an estimate of mortality in CAP used for decision-making about inpatient versus outpatient treatment, was 1 (25th to 75th interquartile range: 1, 2); no patients had a CURB score greater than 3 (Table 1). Forty-one (82%) patients met PORT clinical stability criteria prior to discharge, and 30 (75% of stable patients) had CBCs obtained.
Table 1
On days after admission, 94 subsequent CBCs were obtained. Of these CBCs, 6 (6.4%) were associated with management changes indicated in documentation or orders (Table 2). In 2 of the 6 patients, management changes were likely relevant to pneumonia. In the first case, the patient had a white blood cell count (WBC) of 15.4 on the planned day of discharge but no accompanying clinical changes. Her discharge was potentially delayed pending a repeat CBC which again showed a WBC 14.7; the patient was then discharged without any additional changes in plan. In the second case, the patient experienced new-onset altered mental status on hospital day 3 and increasing O2 requirement with a rising WBC noted on hospital day 4. Repeat chest x-ray, repeat blood cultures, and an ultrasound for parapneumonic effusion were obtained, and the patient’s symptoms and signs resolved over a period of days without changes in treatment. In the 4 other cases, available documentation suggested the hemoglobin abnormalities found represented chronic or incidental illnesses, specifically iron deficiency anemia, iatrogenic anemia due to fluid resuscitation and hemodilution, previously known chronic lymphocytic leukemia, and thrombocytopenia due to acute infection. In all 6 instances, CBC values improved without treatment intervention.
Table 2 Among all patients, the positive likelihood ratio of CBCs obtained after admission in terms of being followed by a change in clinical management was very poor (1.12, 95% confidence interval [CI], 0.86-1.44). For clinically unstable patients, there were 64 CBCs ordered, and the likelihood ratio was similar at 0.98 (95% CI, 0.75-1.29). The positive likelihood ratio among clinically stable patients, who had 30 CBCs ordered, was still quite weak, though confidence intervals were wider (1.23, 95% CI, 0.66-2.29).
DISCUSSION
Though small, our initial study suggests the potential opportunity for savings if Choosing Wisely® recommendations for CBC testing were implemented in patients with community-acquired pneumonia.
Our study has several limitations. Note-writing practices and ordering patterns likely varied between providers, and documentation bias may play a role in our results. However, we defined whether a CBC was associated with changes in clinical decision-making or management by incorporating a number of mutually reinforcing elements of the medical record. We recognize, however, that our approach may not capture undocumented clinical issues or other cognitive (eg, reassurance of clinical resolution) reasons why CBCs were obtained.
Even with these limitations, the likelihood of a CBC value meaningfully changing clinical management among patients with CAP appears to be quite low as evidenced by the case descriptions, particularly when obtained in stable patients by PORT criteria and on the day of discharge. Whether clinical stability as measured by PORT score can be used to target patients in whom CBC testing is unnecessary is difficult to discern from our data, as the overall utility of CBCs obtained after admission was quite low and the rate of changes in management was also low. However, even if CBCs are not particularly costly, unnecessary testing may produce harm in the form of prolonged length of stay, making even one unnecessary CBC potentially extremely expensive. More research involving larger-scale studies are needed to determine the “number needed to screen” for the daily CBC in CAP to determine if the cost savings from overtesting and treatment outweigh the potential benefit of a single CBC that changes management.
Disclosure
Nothing to report.
References
1. Choosing Wisely. Promoting conversations between providers and patients. Choosing Wisely. http://www.choosingwisely.org/. Accessed March 28, 2016. 2. Beresford L. The Society of Hospital Medicine’s “Choosing Wisely” Recommendations for Hospitalists. 2013. http://www.the-hospitalist.org/article/the-society-of-hospital-medicines-choosing-wisely-recommendations-for-hospitalists/. Accessed March 28, 2016. 3. File TM Jr, Marrie TJ. Burden of community-acquired pneumonia in North American adults. Postgrad Med. 2010;122(2):130-141. PubMed 4. Halm EA, Fine MJ, Marrie TJ, et al. Time to clinical stability in patients hospitalized with community-acquired pneumonia: Implications for practice guidelines. JAMA. 1998;279(18):1452-1457. PubMed 5. Lim W, van der Eerden MM, Laing R, et al. Defining community acquired pneumonia severity on presentation to hospital: an international derivation and validation study. Thorax. 2003;58(5):377-382. PubMed
References
1. Choosing Wisely. Promoting conversations between providers and patients. Choosing Wisely. http://www.choosingwisely.org/. Accessed March 28, 2016. 2. Beresford L. The Society of Hospital Medicine’s “Choosing Wisely” Recommendations for Hospitalists. 2013. http://www.the-hospitalist.org/article/the-society-of-hospital-medicines-choosing-wisely-recommendations-for-hospitalists/. Accessed March 28, 2016. 3. File TM Jr, Marrie TJ. Burden of community-acquired pneumonia in North American adults. Postgrad Med. 2010;122(2):130-141. PubMed 4. Halm EA, Fine MJ, Marrie TJ, et al. Time to clinical stability in patients hospitalized with community-acquired pneumonia: Implications for practice guidelines. JAMA. 1998;279(18):1452-1457. PubMed 5. Lim W, van der Eerden MM, Laing R, et al. Defining community acquired pneumonia severity on presentation to hospital: an international derivation and validation study. Thorax. 2003;58(5):377-382. PubMed
Addiction is a national epidemic that represents both a pressing need and a significant burden to the healthcare system.1 Hospitals are increasingly filled with people admitted for medical complications of substance use disorders (SUD).2People with SUD have longer lengths of stay (LOS) and high readmission rates.3 Hospitalization often does not address the root cause—the SUD. For example, many hospitals replace heart valves and deliver prolonged courses of intravenous (IV) antibiotics for endocarditis from injection drug use but do not offer addiction medicine consultation, medication for addiction treatment (MAT), or linkage to posthospital SUD treatment.4,5
Hospitalization can provide reachable moments for initiating addiction care.6 Medications for opioid7 and alcohol use disorders8 can be started during hospitalization, promoting engagement in outpatient SUD care7 and increased uptake of MAT,7-9 and reducing readmissions.8,10 Yet, medications for SUD are underprescribed,11,12 and most hospitals lack inpatient addiction medicine services and pathways to timely SUD care after discharge. Furthermore, traditional SUD treatment programs are often not equipped to manage medically complex patients or they have long waitlists.13 Most behavioral-physical health integration occurs in ambulatory settings. This fails to engage patients who do not access primary care. There is an urgent need for models that can improve care for hospitalized patients with SUD.
Here, we describe our experience using patient needs assessment to engage stakeholders and drive local systems change. We also describe the resulting care model, the Improving Addiction Care Team (IMPACT). Our experience provides a potentially useful example to other hospitals and communities seeking to address the national SUD epidemic.
METHODS
Setting
In 2012, Oregon transformed its Medicaid system by establishing 16 regional “coordinated care organizations” (CCOs) to improve outcomes and slow healthcare spending.14 In a CCO environment, hospitals assume increased financial risk, yet reforms have focused on the outpatient setting. Therefore, executive leadership at Oregon Health & Science University (OHSU), an urban academic medical center, asked clinician-leaders to design point-of-care improvements for Medicaid-funded adults and build on existing models to improve care for socioeconomically vulnerable adults.15,16 One priority that emerged was to make improvements for hospitalized adults with SUD. Of the adult inpatients at OHSU, 30% have Medicaid and 15% have SUD by administrative data alone. Before we started our work, OHSU lacked inpatient addiction medicine services.
Local Needs Assessment
To understand local needs and opportunities, we surveyed hospitalized adults with SUD. We used the electronic health record to generate a list of inpatients flagged by nurses for risky alcohol or drug use. A research assistant screened consecutive adults (≥18 years old) and invited those who screened positive for alcohol use (Alcohol Use Disorders Identification Test–Consumption [AUDIT-C])17 or drug use (single-item screener)18 to participate. We excluded non-English speakers, incarcerated adults, people using only marijuana or tobacco, psychiatry inpatients, and people unable to consent. Surveys assessed social and demographic factors, healthcare utilization, substance use severity, and treatment experience. Participants who reported high-risk illicit drug or alcohol use19 were asked to indicate their readiness to change on a 3-point scale developed for this study. Response range included: no interest, interest in cutting back, or interest in quitting. A subset of participants completed in-depth qualitative interviews exploring patient perceptions of substance use treatment needs.20 We obtained hospital administrative data from hospital financial services.
Partner Engagement
We identified community partners with which we had an individual or organizational relationship and a common interest and potential for collaboration. All invited partners agreed to attend initial meetings. We convened leadership and frontline staff across partners. OHSU staff included hospital nursing and social work leaders; infectious disease, hospitalist, and addiction physicians; and health services researchers. Community organizations included Central City Concern (CCC), a community organization serving people facing homelessness and addiction; CODA, Inc., a nonprofit SUD treatment agency; and Coram/CVS infusion pharmacy.
Collectively, we reviewed needs assessment findings and examples from the literature7-9 to develop strategies to address patient and system needs. We used patient narratives to foster alignment and prioritized areas in which integration could improve quality and costs. We assumed we would petition OHSU and/or Medicaid CCOs to finance efforts and saved potentially challenging budget discussions for later, when partnerships would be more developed. Our task force attended more than 3 large-group meetings and numerous small-group meetings to develop IMPACT.
RESULTS
Needs Assessment
Between September 2014 and April 2015, a research assistant approached 326 patients. Of these, 235 (72%) met study inclusion criteria, and 185 (78%) agreed to participate (Table 1). Of people who reported any substance use within the preceding 3 months, 58% of alcohol users and 67% of drug users said they were interested in cutting back or quitting. Fifty-four percent of participants with moderate- to high-risk opioid use and 16% with moderate- to high-risk alcohol use reported strong interest in MAT. In qualitative interviews, participants described inadequately treated withdrawal, the importance of trust and choice, and long wait times as a barriers to entering treatment after hospital discharge.20
Table 1
Administrative data revealed high rates of hospital readmissions and longer than expected LOS (Figure). Mean LOS was 10.26 days—4 days more than medicine patients’. Mean LOS was high among participants who required long-term IV antibiotics, particularly those with endocarditis or osteomyelitis (21.75 days; range, 1.00-51.00 days). We excluded one outlier with a 116-day hospitalization.
Intervention Design
Mapping needs to intervention components. We mapped needs assessment findings to 3 main IMPACT components: inpatient addiction medicine consultation service, pathways to posthospital SUD treatment, and medically enhanced residential treatment (MERT) (Table 2).
Figure
Inpatient addiction medicine consultation service. We developed this service to address patients’ report of high readiness to change and interest in starting MAT in the hospital. Community partners highlighted the need for peers to increase engagement and trust. Therefore, we included a physician, a social worker, and two peers on our team. The inpatient service engages patients, advises on withdrawal and pain, performs SUD assessments, initiates MAT, and provides counseling and treatment.
Table 2 Pathways to posthospital SUD treatment. As pathways from hospital to community SUD treatment were lacking, and long administrative wait times limited access to community treatment, we employed “in-reach” liaisons—community SUD treatment staff who perform in-hospital assessments to triage and coordinate care across systems. Given that patients value having treatment choices, we linked pathways to an array of MAT and abstinence-based treatments, including office-based, intensive outpatient and residential levels of care. For patients who live outside the Portland area, we developed relationships with rural stakeholders and engaged the help of the Oregon State Opioid Authority in introducing our program to SUD treatment providers around the state.
Medically Enhanced Residential Treatment (MERT). In many cases where patients required prolonged courses of IV antibiotics, hospital stays were longer for two reasons: At-home central-line self-administration of antibiotics was deemed unsafe, and patients were denied admission to a skilled nursing facility due to history of substance use. These long LOS create an opportunity to initiate and engage patients in treatment, and to render savings by shifting care to a residential addiction treatment setting that can accommodate IV antibiotic administration and MAT. We increased residential staffing and collaborated with a home infusion pharmacy to administer daily infusions on site.
Funding the Intervention
We used administrative data to estimate potential savings and tailored a business case to CCO and hospital payers. The CCO business case centered on hospitalization as an opportunity to engage out-of-treatment adults and potentially reduce high-cost readmissions by managing physical and behavioral health needs. Working within budgeting time lines, we used data from the first 165 participants. These participants had 137 readmissions over a mean observation period of 4.5 months. Mean charge per readmission was $31,157 (range, $699-$206,596) and was highest for people with endocarditis (mean, $55,493; range, $23,204-$145,066) and osteomyelitis (mean, $68,774; range, $29,359-$124,481). We estimated that a 10% reduction in 6-month readmissions could avoid $674,863 in charges.
For the hospital, the primary financial incentive was reduced LOS. Given the possibility of shortening hospitalization through MERT, we estimated a 20% mean LOS reduction; for budgeting, we estimated a conservative 10% reduction. A 10% mean LOS reduction would free 205 bed-days (10% × 10.26 days mean LOS × 200 patients) and create space for another 32 inpatient admissions in year 1, assuming no change from medical patients’ 6.26 days mean LOS. The future of bundled payments further bolstered our business case, as did the potential to improve care quality, reduce nonproductive staff time, and increase institutional learning about SUD. Overall program costs approximated projected savings, and the hospital and a local CCO agreed to equally share the costs of the intervention (Table 2).
DISCUSSION
We have described an innovative approach to developing an SUD intervention for hospitalized adults. Using a process of broad stakeholder engagement, data-driven understanding of population needs, and analysis of financial incentives, we built consensus and secured funding for a multicomponent intervention across hospital and post–acute care settings. Other studies have demonstrated the feasibility and efficacy of starting a single medication for a specific indication7-9 (eg, methadone for opioid use disorder), yet strategies for expanding SUD services in hospitals and facilitating posthospital treatment linkages remain scarce.21 Our model addresses a widespread need and could be adapted to other hospitals, SUD treatment organizations, and Medicaid payers.
Our experience has several limitations. First, it took place at a single academic medical center in Oregon, a Medicaid expansion state. Second, our needs assessment involved a convenience sample of limited racial/ethnic diversity. Third, almost all patients had insurance, which could limit generalizability. Fourth, to secure funding, it was essential we had a clinical champion who was persuasive with hospital and CCO leadership; though increasing disease burden and skyrocketing costs2 may drive administrators’ increased demand for ways to address SUD in hospitalized adults.
Our experience has several key implications. First, diverse partners were vital at all stages of program design, suggesting hospitals should look beyond traditional healthcare partners to address the SUD epidemic. Second, an interprofessional team that includes physicians, social workers, and peers may better engage patients and address complex system needs. Finally, a planned IMPACT evaluation will assess effects on substance use, healthcare use, and costs.
The United States faces a burgeoning SUD epidemic. Our experience describes an innovative care model and supports the idea that hospitals may play a leading role in convening partners, providing treatment, and driving population health improvements for adults with SUD.
Acknowledgment
The authors would like to acknowledge Peter Rapp and Thomas Yackel for leadership support; Tara Williams for administrative data support; Sarann Bielavitz and Naomi Wright for project management support, and Lynn Smith-Stott and Maria Michalczyk for help with model design. This work was presented at the American Society of Addiction Medicine national conference in Baltimore, MD in April 2016.
Disclosure
This work was funded by Oregon Health & Science University and CareOregon. The authors have no conflicts of interest to disclose.
References
1. Volkow N, Frieden TR, Hyde PS, Cha SS. Medication-assisted therapies—Tackling the opioid-overdose epidemic. N Engl J Med. 2014; 370:2063-2066.PubMed 2. Ronan MV, Herzig SJ. Hospitalizations related to opioid abuse/dependence and associated serious infections increased sharply, 2002-12. Health Aff (Millwood). 2016;35(5):832-837. PubMed 3. Walley AY, Paasche-Orlow M, Lee EC, et al. Acute care hospital utilization among medical inpatients discharged with a substance use disorder diagnosis. J Addict Med. 2012;6(1):50-56. PubMed 4. Rosenthal ES, Karchmer AW, Thiesen-Toupal J, Castillo RA, Rowley CF. Suboptimal addiction interventions for patients hospitalized with injection drug use-associated infective endocarditis. Am J Med. 2016;129(5):481-485. PubMed 5. Fanucchi L, Lofwall MR. Putting parity into practice—integrating opioid-use disorder treatment into the hospital setting. N Engl J Med. 2016;379(9):811-813. PubMed 6. Pollini RA, O’Toole TP, Ford D, Bigelow G. Does this patient really want treatment? Factors associated with baseline and evolving readiness for change among hospitalized substance using adults interested in treatment. Addict Behav. 2006;31(10):1904-1918. PubMed 7. Liebschutz JM, Crooks D, Herman D, et al. Buprenorphine treatment for hospitalized, opioid-dependent patients: a randomized clinical trial. JAMA Intern Med. 2014;174(8):1369-1376. PubMed 8. Wei J, Defries T, Lozada M, Young N, Huen W, Tulsky J. An inpatient treatment and discharge planning protocol for alcohol and dependence: efficacy in reducing 30-day readmissions and emergency department visits. J Gen Intern Med. 2015;30(3):365-370. PubMed 9. Shanahan CW, Beers D, Alford DP, Brigandi E, Samet JH. A transitional opioid program to engage hospitalized drug users. J Gen Intern Med. 2010;25(8):803-808. PubMed 10. Pecoraro A, Horton T, Ewen E, et al. Early data from Project Engage: a program to identify and transition medically hospitalized patients into addictions treatment. Addict Sci Clin Pract. 2012;7:20. PubMed 11. National Center on Addiction and Substance Abuse; Addiction Medicine: Closing the Gap between Science and Practice. June 2012. http://www.centeronaddiction.org/addiction-research/reports/addiction-medicine-closing-gap-between-science-and-practice. Accessed May 2, 2016. 12. Center for Behavioral Health Statistics and Quality, Substance Abuse and Mental Health Services Administration, US Department of Health and Human Services. Results From the 2010 National Survey on Drug Use and Health: Summary of National Findings. Rockville, MD: Center for Behavioral Health Statistics and Quality, Substance Abuse and Mental Health Services Administration, US Dept of Health and Human Services; 2011. NSDUH series H-41, HHS publication SMA 11-4658. https://www.samhsa.gov/data/sites/default/files/NSDUHNationalFindingsResults2010-web/2k10ResultsRev/NSDUHresultsRev2010.pdf. Published September 2011. Accessed March 31, 2017. 13. Vestal C. Few doctors are willing, able to prescribe powerful anti-addiction drugs. http://www.pewtrusts.org/en/research-and-analysis/blogs/stateline/2016/01/15/few-doctors-are-willing-able-to-prescribe-powerful-anti-addiction-drugs. Published January 15, 2016. Accessed May 2, 2016. 14. McConnell KJ. Oregon’s Medicaid coordinated care organizations. JAMA. 2016;315(9):869-870. PubMed 15. Englander H, Kansagara D. Planning and designing the Care Transitions Innovation (C-TraIn) for uninsured and Medicaid patients. J Hosp Med. 2012;7(7):524-529. PubMed 16. Englander H, Michaels L, Chan B, Kansagara D. The Care Transitions Innovation (C-TraIn) for socioeconomically disadvantaged adults: results of a cluster randomized controlled trial. J Gen Intern Med. 2014;29(11):1460-1467. PubMed 17. Bush K, Kivlahan DR, McDonell MB, Fihn SD, Bradley KA. The AUDIT alcohol consumption questions (AUDIT-C): an effective brief screening test for problem drinking. Ambulatory Care Quality Improvement Project (ACQUIP). Alcohol Use Disorders Identification Test. Arch Intern Med. 1998;158(16):1789-1795. PubMed 18. Smith PC, Schmidt SM, Allensworth-Davies D, Saitz R. A single-question screening test for drug use in primary care. Arch Intern Med. 2010;170(13):1155-1160. PubMed 19. Humeniuk R, Ali R, Babor TF, et al. Validation of the Alcohol, Smoking and Substance Involvement Screening Test (ASSIST). Addiction. 2008;103(6):1039-1047. PubMed 20. Velez CM, Nicolaidis C, Korthuis PT, Englander H. “It’s been an experience, a life learning experience”: a qualitative study of hospitalized patients with substance use disorders. J Gen Intern Med. 2017;32(3):296-303. PubMed 21. Gryczynski J, Schwartz RP, O’Grady KE, Restivo L, Mitchell SG, Jaffe JH. Understanding patterns of high-cost health care use across different substance user groups. Health Aff (Millwood). 2016.;35(1):12-19. PubMed
Addiction is a national epidemic that represents both a pressing need and a significant burden to the healthcare system.1 Hospitals are increasingly filled with people admitted for medical complications of substance use disorders (SUD).2People with SUD have longer lengths of stay (LOS) and high readmission rates.3 Hospitalization often does not address the root cause—the SUD. For example, many hospitals replace heart valves and deliver prolonged courses of intravenous (IV) antibiotics for endocarditis from injection drug use but do not offer addiction medicine consultation, medication for addiction treatment (MAT), or linkage to posthospital SUD treatment.4,5
Hospitalization can provide reachable moments for initiating addiction care.6 Medications for opioid7 and alcohol use disorders8 can be started during hospitalization, promoting engagement in outpatient SUD care7 and increased uptake of MAT,7-9 and reducing readmissions.8,10 Yet, medications for SUD are underprescribed,11,12 and most hospitals lack inpatient addiction medicine services and pathways to timely SUD care after discharge. Furthermore, traditional SUD treatment programs are often not equipped to manage medically complex patients or they have long waitlists.13 Most behavioral-physical health integration occurs in ambulatory settings. This fails to engage patients who do not access primary care. There is an urgent need for models that can improve care for hospitalized patients with SUD.
Here, we describe our experience using patient needs assessment to engage stakeholders and drive local systems change. We also describe the resulting care model, the Improving Addiction Care Team (IMPACT). Our experience provides a potentially useful example to other hospitals and communities seeking to address the national SUD epidemic.
METHODS
Setting
In 2012, Oregon transformed its Medicaid system by establishing 16 regional “coordinated care organizations” (CCOs) to improve outcomes and slow healthcare spending.14 In a CCO environment, hospitals assume increased financial risk, yet reforms have focused on the outpatient setting. Therefore, executive leadership at Oregon Health & Science University (OHSU), an urban academic medical center, asked clinician-leaders to design point-of-care improvements for Medicaid-funded adults and build on existing models to improve care for socioeconomically vulnerable adults.15,16 One priority that emerged was to make improvements for hospitalized adults with SUD. Of the adult inpatients at OHSU, 30% have Medicaid and 15% have SUD by administrative data alone. Before we started our work, OHSU lacked inpatient addiction medicine services.
Local Needs Assessment
To understand local needs and opportunities, we surveyed hospitalized adults with SUD. We used the electronic health record to generate a list of inpatients flagged by nurses for risky alcohol or drug use. A research assistant screened consecutive adults (≥18 years old) and invited those who screened positive for alcohol use (Alcohol Use Disorders Identification Test–Consumption [AUDIT-C])17 or drug use (single-item screener)18 to participate. We excluded non-English speakers, incarcerated adults, people using only marijuana or tobacco, psychiatry inpatients, and people unable to consent. Surveys assessed social and demographic factors, healthcare utilization, substance use severity, and treatment experience. Participants who reported high-risk illicit drug or alcohol use19 were asked to indicate their readiness to change on a 3-point scale developed for this study. Response range included: no interest, interest in cutting back, or interest in quitting. A subset of participants completed in-depth qualitative interviews exploring patient perceptions of substance use treatment needs.20 We obtained hospital administrative data from hospital financial services.
Partner Engagement
We identified community partners with which we had an individual or organizational relationship and a common interest and potential for collaboration. All invited partners agreed to attend initial meetings. We convened leadership and frontline staff across partners. OHSU staff included hospital nursing and social work leaders; infectious disease, hospitalist, and addiction physicians; and health services researchers. Community organizations included Central City Concern (CCC), a community organization serving people facing homelessness and addiction; CODA, Inc., a nonprofit SUD treatment agency; and Coram/CVS infusion pharmacy.
Collectively, we reviewed needs assessment findings and examples from the literature7-9 to develop strategies to address patient and system needs. We used patient narratives to foster alignment and prioritized areas in which integration could improve quality and costs. We assumed we would petition OHSU and/or Medicaid CCOs to finance efforts and saved potentially challenging budget discussions for later, when partnerships would be more developed. Our task force attended more than 3 large-group meetings and numerous small-group meetings to develop IMPACT.
RESULTS
Needs Assessment
Between September 2014 and April 2015, a research assistant approached 326 patients. Of these, 235 (72%) met study inclusion criteria, and 185 (78%) agreed to participate (Table 1). Of people who reported any substance use within the preceding 3 months, 58% of alcohol users and 67% of drug users said they were interested in cutting back or quitting. Fifty-four percent of participants with moderate- to high-risk opioid use and 16% with moderate- to high-risk alcohol use reported strong interest in MAT. In qualitative interviews, participants described inadequately treated withdrawal, the importance of trust and choice, and long wait times as a barriers to entering treatment after hospital discharge.20
Table 1
Administrative data revealed high rates of hospital readmissions and longer than expected LOS (Figure). Mean LOS was 10.26 days—4 days more than medicine patients’. Mean LOS was high among participants who required long-term IV antibiotics, particularly those with endocarditis or osteomyelitis (21.75 days; range, 1.00-51.00 days). We excluded one outlier with a 116-day hospitalization.
Intervention Design
Mapping needs to intervention components. We mapped needs assessment findings to 3 main IMPACT components: inpatient addiction medicine consultation service, pathways to posthospital SUD treatment, and medically enhanced residential treatment (MERT) (Table 2).
Figure
Inpatient addiction medicine consultation service. We developed this service to address patients’ report of high readiness to change and interest in starting MAT in the hospital. Community partners highlighted the need for peers to increase engagement and trust. Therefore, we included a physician, a social worker, and two peers on our team. The inpatient service engages patients, advises on withdrawal and pain, performs SUD assessments, initiates MAT, and provides counseling and treatment.
Table 2 Pathways to posthospital SUD treatment. As pathways from hospital to community SUD treatment were lacking, and long administrative wait times limited access to community treatment, we employed “in-reach” liaisons—community SUD treatment staff who perform in-hospital assessments to triage and coordinate care across systems. Given that patients value having treatment choices, we linked pathways to an array of MAT and abstinence-based treatments, including office-based, intensive outpatient and residential levels of care. For patients who live outside the Portland area, we developed relationships with rural stakeholders and engaged the help of the Oregon State Opioid Authority in introducing our program to SUD treatment providers around the state.
Medically Enhanced Residential Treatment (MERT). In many cases where patients required prolonged courses of IV antibiotics, hospital stays were longer for two reasons: At-home central-line self-administration of antibiotics was deemed unsafe, and patients were denied admission to a skilled nursing facility due to history of substance use. These long LOS create an opportunity to initiate and engage patients in treatment, and to render savings by shifting care to a residential addiction treatment setting that can accommodate IV antibiotic administration and MAT. We increased residential staffing and collaborated with a home infusion pharmacy to administer daily infusions on site.
Funding the Intervention
We used administrative data to estimate potential savings and tailored a business case to CCO and hospital payers. The CCO business case centered on hospitalization as an opportunity to engage out-of-treatment adults and potentially reduce high-cost readmissions by managing physical and behavioral health needs. Working within budgeting time lines, we used data from the first 165 participants. These participants had 137 readmissions over a mean observation period of 4.5 months. Mean charge per readmission was $31,157 (range, $699-$206,596) and was highest for people with endocarditis (mean, $55,493; range, $23,204-$145,066) and osteomyelitis (mean, $68,774; range, $29,359-$124,481). We estimated that a 10% reduction in 6-month readmissions could avoid $674,863 in charges.
For the hospital, the primary financial incentive was reduced LOS. Given the possibility of shortening hospitalization through MERT, we estimated a 20% mean LOS reduction; for budgeting, we estimated a conservative 10% reduction. A 10% mean LOS reduction would free 205 bed-days (10% × 10.26 days mean LOS × 200 patients) and create space for another 32 inpatient admissions in year 1, assuming no change from medical patients’ 6.26 days mean LOS. The future of bundled payments further bolstered our business case, as did the potential to improve care quality, reduce nonproductive staff time, and increase institutional learning about SUD. Overall program costs approximated projected savings, and the hospital and a local CCO agreed to equally share the costs of the intervention (Table 2).
DISCUSSION
We have described an innovative approach to developing an SUD intervention for hospitalized adults. Using a process of broad stakeholder engagement, data-driven understanding of population needs, and analysis of financial incentives, we built consensus and secured funding for a multicomponent intervention across hospital and post–acute care settings. Other studies have demonstrated the feasibility and efficacy of starting a single medication for a specific indication7-9 (eg, methadone for opioid use disorder), yet strategies for expanding SUD services in hospitals and facilitating posthospital treatment linkages remain scarce.21 Our model addresses a widespread need and could be adapted to other hospitals, SUD treatment organizations, and Medicaid payers.
Our experience has several limitations. First, it took place at a single academic medical center in Oregon, a Medicaid expansion state. Second, our needs assessment involved a convenience sample of limited racial/ethnic diversity. Third, almost all patients had insurance, which could limit generalizability. Fourth, to secure funding, it was essential we had a clinical champion who was persuasive with hospital and CCO leadership; though increasing disease burden and skyrocketing costs2 may drive administrators’ increased demand for ways to address SUD in hospitalized adults.
Our experience has several key implications. First, diverse partners were vital at all stages of program design, suggesting hospitals should look beyond traditional healthcare partners to address the SUD epidemic. Second, an interprofessional team that includes physicians, social workers, and peers may better engage patients and address complex system needs. Finally, a planned IMPACT evaluation will assess effects on substance use, healthcare use, and costs.
The United States faces a burgeoning SUD epidemic. Our experience describes an innovative care model and supports the idea that hospitals may play a leading role in convening partners, providing treatment, and driving population health improvements for adults with SUD.
Acknowledgment
The authors would like to acknowledge Peter Rapp and Thomas Yackel for leadership support; Tara Williams for administrative data support; Sarann Bielavitz and Naomi Wright for project management support, and Lynn Smith-Stott and Maria Michalczyk for help with model design. This work was presented at the American Society of Addiction Medicine national conference in Baltimore, MD in April 2016.
Disclosure
This work was funded by Oregon Health & Science University and CareOregon. The authors have no conflicts of interest to disclose.
Addiction is a national epidemic that represents both a pressing need and a significant burden to the healthcare system.1 Hospitals are increasingly filled with people admitted for medical complications of substance use disorders (SUD).2People with SUD have longer lengths of stay (LOS) and high readmission rates.3 Hospitalization often does not address the root cause—the SUD. For example, many hospitals replace heart valves and deliver prolonged courses of intravenous (IV) antibiotics for endocarditis from injection drug use but do not offer addiction medicine consultation, medication for addiction treatment (MAT), or linkage to posthospital SUD treatment.4,5
Hospitalization can provide reachable moments for initiating addiction care.6 Medications for opioid7 and alcohol use disorders8 can be started during hospitalization, promoting engagement in outpatient SUD care7 and increased uptake of MAT,7-9 and reducing readmissions.8,10 Yet, medications for SUD are underprescribed,11,12 and most hospitals lack inpatient addiction medicine services and pathways to timely SUD care after discharge. Furthermore, traditional SUD treatment programs are often not equipped to manage medically complex patients or they have long waitlists.13 Most behavioral-physical health integration occurs in ambulatory settings. This fails to engage patients who do not access primary care. There is an urgent need for models that can improve care for hospitalized patients with SUD.
Here, we describe our experience using patient needs assessment to engage stakeholders and drive local systems change. We also describe the resulting care model, the Improving Addiction Care Team (IMPACT). Our experience provides a potentially useful example to other hospitals and communities seeking to address the national SUD epidemic.
METHODS
Setting
In 2012, Oregon transformed its Medicaid system by establishing 16 regional “coordinated care organizations” (CCOs) to improve outcomes and slow healthcare spending.14 In a CCO environment, hospitals assume increased financial risk, yet reforms have focused on the outpatient setting. Therefore, executive leadership at Oregon Health & Science University (OHSU), an urban academic medical center, asked clinician-leaders to design point-of-care improvements for Medicaid-funded adults and build on existing models to improve care for socioeconomically vulnerable adults.15,16 One priority that emerged was to make improvements for hospitalized adults with SUD. Of the adult inpatients at OHSU, 30% have Medicaid and 15% have SUD by administrative data alone. Before we started our work, OHSU lacked inpatient addiction medicine services.
Local Needs Assessment
To understand local needs and opportunities, we surveyed hospitalized adults with SUD. We used the electronic health record to generate a list of inpatients flagged by nurses for risky alcohol or drug use. A research assistant screened consecutive adults (≥18 years old) and invited those who screened positive for alcohol use (Alcohol Use Disorders Identification Test–Consumption [AUDIT-C])17 or drug use (single-item screener)18 to participate. We excluded non-English speakers, incarcerated adults, people using only marijuana or tobacco, psychiatry inpatients, and people unable to consent. Surveys assessed social and demographic factors, healthcare utilization, substance use severity, and treatment experience. Participants who reported high-risk illicit drug or alcohol use19 were asked to indicate their readiness to change on a 3-point scale developed for this study. Response range included: no interest, interest in cutting back, or interest in quitting. A subset of participants completed in-depth qualitative interviews exploring patient perceptions of substance use treatment needs.20 We obtained hospital administrative data from hospital financial services.
Partner Engagement
We identified community partners with which we had an individual or organizational relationship and a common interest and potential for collaboration. All invited partners agreed to attend initial meetings. We convened leadership and frontline staff across partners. OHSU staff included hospital nursing and social work leaders; infectious disease, hospitalist, and addiction physicians; and health services researchers. Community organizations included Central City Concern (CCC), a community organization serving people facing homelessness and addiction; CODA, Inc., a nonprofit SUD treatment agency; and Coram/CVS infusion pharmacy.
Collectively, we reviewed needs assessment findings and examples from the literature7-9 to develop strategies to address patient and system needs. We used patient narratives to foster alignment and prioritized areas in which integration could improve quality and costs. We assumed we would petition OHSU and/or Medicaid CCOs to finance efforts and saved potentially challenging budget discussions for later, when partnerships would be more developed. Our task force attended more than 3 large-group meetings and numerous small-group meetings to develop IMPACT.
RESULTS
Needs Assessment
Between September 2014 and April 2015, a research assistant approached 326 patients. Of these, 235 (72%) met study inclusion criteria, and 185 (78%) agreed to participate (Table 1). Of people who reported any substance use within the preceding 3 months, 58% of alcohol users and 67% of drug users said they were interested in cutting back or quitting. Fifty-four percent of participants with moderate- to high-risk opioid use and 16% with moderate- to high-risk alcohol use reported strong interest in MAT. In qualitative interviews, participants described inadequately treated withdrawal, the importance of trust and choice, and long wait times as a barriers to entering treatment after hospital discharge.20
Table 1
Administrative data revealed high rates of hospital readmissions and longer than expected LOS (Figure). Mean LOS was 10.26 days—4 days more than medicine patients’. Mean LOS was high among participants who required long-term IV antibiotics, particularly those with endocarditis or osteomyelitis (21.75 days; range, 1.00-51.00 days). We excluded one outlier with a 116-day hospitalization.
Intervention Design
Mapping needs to intervention components. We mapped needs assessment findings to 3 main IMPACT components: inpatient addiction medicine consultation service, pathways to posthospital SUD treatment, and medically enhanced residential treatment (MERT) (Table 2).
Figure
Inpatient addiction medicine consultation service. We developed this service to address patients’ report of high readiness to change and interest in starting MAT in the hospital. Community partners highlighted the need for peers to increase engagement and trust. Therefore, we included a physician, a social worker, and two peers on our team. The inpatient service engages patients, advises on withdrawal and pain, performs SUD assessments, initiates MAT, and provides counseling and treatment.
Table 2 Pathways to posthospital SUD treatment. As pathways from hospital to community SUD treatment were lacking, and long administrative wait times limited access to community treatment, we employed “in-reach” liaisons—community SUD treatment staff who perform in-hospital assessments to triage and coordinate care across systems. Given that patients value having treatment choices, we linked pathways to an array of MAT and abstinence-based treatments, including office-based, intensive outpatient and residential levels of care. For patients who live outside the Portland area, we developed relationships with rural stakeholders and engaged the help of the Oregon State Opioid Authority in introducing our program to SUD treatment providers around the state.
Medically Enhanced Residential Treatment (MERT). In many cases where patients required prolonged courses of IV antibiotics, hospital stays were longer for two reasons: At-home central-line self-administration of antibiotics was deemed unsafe, and patients were denied admission to a skilled nursing facility due to history of substance use. These long LOS create an opportunity to initiate and engage patients in treatment, and to render savings by shifting care to a residential addiction treatment setting that can accommodate IV antibiotic administration and MAT. We increased residential staffing and collaborated with a home infusion pharmacy to administer daily infusions on site.
Funding the Intervention
We used administrative data to estimate potential savings and tailored a business case to CCO and hospital payers. The CCO business case centered on hospitalization as an opportunity to engage out-of-treatment adults and potentially reduce high-cost readmissions by managing physical and behavioral health needs. Working within budgeting time lines, we used data from the first 165 participants. These participants had 137 readmissions over a mean observation period of 4.5 months. Mean charge per readmission was $31,157 (range, $699-$206,596) and was highest for people with endocarditis (mean, $55,493; range, $23,204-$145,066) and osteomyelitis (mean, $68,774; range, $29,359-$124,481). We estimated that a 10% reduction in 6-month readmissions could avoid $674,863 in charges.
For the hospital, the primary financial incentive was reduced LOS. Given the possibility of shortening hospitalization through MERT, we estimated a 20% mean LOS reduction; for budgeting, we estimated a conservative 10% reduction. A 10% mean LOS reduction would free 205 bed-days (10% × 10.26 days mean LOS × 200 patients) and create space for another 32 inpatient admissions in year 1, assuming no change from medical patients’ 6.26 days mean LOS. The future of bundled payments further bolstered our business case, as did the potential to improve care quality, reduce nonproductive staff time, and increase institutional learning about SUD. Overall program costs approximated projected savings, and the hospital and a local CCO agreed to equally share the costs of the intervention (Table 2).
DISCUSSION
We have described an innovative approach to developing an SUD intervention for hospitalized adults. Using a process of broad stakeholder engagement, data-driven understanding of population needs, and analysis of financial incentives, we built consensus and secured funding for a multicomponent intervention across hospital and post–acute care settings. Other studies have demonstrated the feasibility and efficacy of starting a single medication for a specific indication7-9 (eg, methadone for opioid use disorder), yet strategies for expanding SUD services in hospitals and facilitating posthospital treatment linkages remain scarce.21 Our model addresses a widespread need and could be adapted to other hospitals, SUD treatment organizations, and Medicaid payers.
Our experience has several limitations. First, it took place at a single academic medical center in Oregon, a Medicaid expansion state. Second, our needs assessment involved a convenience sample of limited racial/ethnic diversity. Third, almost all patients had insurance, which could limit generalizability. Fourth, to secure funding, it was essential we had a clinical champion who was persuasive with hospital and CCO leadership; though increasing disease burden and skyrocketing costs2 may drive administrators’ increased demand for ways to address SUD in hospitalized adults.
Our experience has several key implications. First, diverse partners were vital at all stages of program design, suggesting hospitals should look beyond traditional healthcare partners to address the SUD epidemic. Second, an interprofessional team that includes physicians, social workers, and peers may better engage patients and address complex system needs. Finally, a planned IMPACT evaluation will assess effects on substance use, healthcare use, and costs.
The United States faces a burgeoning SUD epidemic. Our experience describes an innovative care model and supports the idea that hospitals may play a leading role in convening partners, providing treatment, and driving population health improvements for adults with SUD.
Acknowledgment
The authors would like to acknowledge Peter Rapp and Thomas Yackel for leadership support; Tara Williams for administrative data support; Sarann Bielavitz and Naomi Wright for project management support, and Lynn Smith-Stott and Maria Michalczyk for help with model design. This work was presented at the American Society of Addiction Medicine national conference in Baltimore, MD in April 2016.
Disclosure
This work was funded by Oregon Health & Science University and CareOregon. The authors have no conflicts of interest to disclose.
References
1. Volkow N, Frieden TR, Hyde PS, Cha SS. Medication-assisted therapies—Tackling the opioid-overdose epidemic. N Engl J Med. 2014; 370:2063-2066.PubMed 2. Ronan MV, Herzig SJ. Hospitalizations related to opioid abuse/dependence and associated serious infections increased sharply, 2002-12. Health Aff (Millwood). 2016;35(5):832-837. PubMed 3. Walley AY, Paasche-Orlow M, Lee EC, et al. Acute care hospital utilization among medical inpatients discharged with a substance use disorder diagnosis. J Addict Med. 2012;6(1):50-56. PubMed 4. Rosenthal ES, Karchmer AW, Thiesen-Toupal J, Castillo RA, Rowley CF. Suboptimal addiction interventions for patients hospitalized with injection drug use-associated infective endocarditis. Am J Med. 2016;129(5):481-485. PubMed 5. Fanucchi L, Lofwall MR. Putting parity into practice—integrating opioid-use disorder treatment into the hospital setting. N Engl J Med. 2016;379(9):811-813. PubMed 6. Pollini RA, O’Toole TP, Ford D, Bigelow G. Does this patient really want treatment? Factors associated with baseline and evolving readiness for change among hospitalized substance using adults interested in treatment. Addict Behav. 2006;31(10):1904-1918. PubMed 7. Liebschutz JM, Crooks D, Herman D, et al. Buprenorphine treatment for hospitalized, opioid-dependent patients: a randomized clinical trial. JAMA Intern Med. 2014;174(8):1369-1376. PubMed 8. Wei J, Defries T, Lozada M, Young N, Huen W, Tulsky J. An inpatient treatment and discharge planning protocol for alcohol and dependence: efficacy in reducing 30-day readmissions and emergency department visits. J Gen Intern Med. 2015;30(3):365-370. PubMed 9. Shanahan CW, Beers D, Alford DP, Brigandi E, Samet JH. A transitional opioid program to engage hospitalized drug users. J Gen Intern Med. 2010;25(8):803-808. PubMed 10. Pecoraro A, Horton T, Ewen E, et al. Early data from Project Engage: a program to identify and transition medically hospitalized patients into addictions treatment. Addict Sci Clin Pract. 2012;7:20. PubMed 11. National Center on Addiction and Substance Abuse; Addiction Medicine: Closing the Gap between Science and Practice. June 2012. http://www.centeronaddiction.org/addiction-research/reports/addiction-medicine-closing-gap-between-science-and-practice. Accessed May 2, 2016. 12. Center for Behavioral Health Statistics and Quality, Substance Abuse and Mental Health Services Administration, US Department of Health and Human Services. Results From the 2010 National Survey on Drug Use and Health: Summary of National Findings. Rockville, MD: Center for Behavioral Health Statistics and Quality, Substance Abuse and Mental Health Services Administration, US Dept of Health and Human Services; 2011. NSDUH series H-41, HHS publication SMA 11-4658. https://www.samhsa.gov/data/sites/default/files/NSDUHNationalFindingsResults2010-web/2k10ResultsRev/NSDUHresultsRev2010.pdf. Published September 2011. Accessed March 31, 2017. 13. Vestal C. Few doctors are willing, able to prescribe powerful anti-addiction drugs. http://www.pewtrusts.org/en/research-and-analysis/blogs/stateline/2016/01/15/few-doctors-are-willing-able-to-prescribe-powerful-anti-addiction-drugs. Published January 15, 2016. Accessed May 2, 2016. 14. McConnell KJ. Oregon’s Medicaid coordinated care organizations. JAMA. 2016;315(9):869-870. PubMed 15. Englander H, Kansagara D. Planning and designing the Care Transitions Innovation (C-TraIn) for uninsured and Medicaid patients. J Hosp Med. 2012;7(7):524-529. PubMed 16. Englander H, Michaels L, Chan B, Kansagara D. The Care Transitions Innovation (C-TraIn) for socioeconomically disadvantaged adults: results of a cluster randomized controlled trial. J Gen Intern Med. 2014;29(11):1460-1467. PubMed 17. Bush K, Kivlahan DR, McDonell MB, Fihn SD, Bradley KA. The AUDIT alcohol consumption questions (AUDIT-C): an effective brief screening test for problem drinking. Ambulatory Care Quality Improvement Project (ACQUIP). Alcohol Use Disorders Identification Test. Arch Intern Med. 1998;158(16):1789-1795. PubMed 18. Smith PC, Schmidt SM, Allensworth-Davies D, Saitz R. A single-question screening test for drug use in primary care. Arch Intern Med. 2010;170(13):1155-1160. PubMed 19. Humeniuk R, Ali R, Babor TF, et al. Validation of the Alcohol, Smoking and Substance Involvement Screening Test (ASSIST). Addiction. 2008;103(6):1039-1047. PubMed 20. Velez CM, Nicolaidis C, Korthuis PT, Englander H. “It’s been an experience, a life learning experience”: a qualitative study of hospitalized patients with substance use disorders. J Gen Intern Med. 2017;32(3):296-303. PubMed 21. Gryczynski J, Schwartz RP, O’Grady KE, Restivo L, Mitchell SG, Jaffe JH. Understanding patterns of high-cost health care use across different substance user groups. Health Aff (Millwood). 2016.;35(1):12-19. PubMed
References
1. Volkow N, Frieden TR, Hyde PS, Cha SS. Medication-assisted therapies—Tackling the opioid-overdose epidemic. N Engl J Med. 2014; 370:2063-2066.PubMed 2. Ronan MV, Herzig SJ. Hospitalizations related to opioid abuse/dependence and associated serious infections increased sharply, 2002-12. Health Aff (Millwood). 2016;35(5):832-837. PubMed 3. Walley AY, Paasche-Orlow M, Lee EC, et al. Acute care hospital utilization among medical inpatients discharged with a substance use disorder diagnosis. J Addict Med. 2012;6(1):50-56. PubMed 4. Rosenthal ES, Karchmer AW, Thiesen-Toupal J, Castillo RA, Rowley CF. Suboptimal addiction interventions for patients hospitalized with injection drug use-associated infective endocarditis. Am J Med. 2016;129(5):481-485. PubMed 5. Fanucchi L, Lofwall MR. Putting parity into practice—integrating opioid-use disorder treatment into the hospital setting. N Engl J Med. 2016;379(9):811-813. PubMed 6. Pollini RA, O’Toole TP, Ford D, Bigelow G. Does this patient really want treatment? Factors associated with baseline and evolving readiness for change among hospitalized substance using adults interested in treatment. Addict Behav. 2006;31(10):1904-1918. PubMed 7. Liebschutz JM, Crooks D, Herman D, et al. Buprenorphine treatment for hospitalized, opioid-dependent patients: a randomized clinical trial. JAMA Intern Med. 2014;174(8):1369-1376. PubMed 8. Wei J, Defries T, Lozada M, Young N, Huen W, Tulsky J. An inpatient treatment and discharge planning protocol for alcohol and dependence: efficacy in reducing 30-day readmissions and emergency department visits. J Gen Intern Med. 2015;30(3):365-370. PubMed 9. Shanahan CW, Beers D, Alford DP, Brigandi E, Samet JH. A transitional opioid program to engage hospitalized drug users. J Gen Intern Med. 2010;25(8):803-808. PubMed 10. Pecoraro A, Horton T, Ewen E, et al. Early data from Project Engage: a program to identify and transition medically hospitalized patients into addictions treatment. Addict Sci Clin Pract. 2012;7:20. PubMed 11. National Center on Addiction and Substance Abuse; Addiction Medicine: Closing the Gap between Science and Practice. June 2012. http://www.centeronaddiction.org/addiction-research/reports/addiction-medicine-closing-gap-between-science-and-practice. Accessed May 2, 2016. 12. Center for Behavioral Health Statistics and Quality, Substance Abuse and Mental Health Services Administration, US Department of Health and Human Services. Results From the 2010 National Survey on Drug Use and Health: Summary of National Findings. Rockville, MD: Center for Behavioral Health Statistics and Quality, Substance Abuse and Mental Health Services Administration, US Dept of Health and Human Services; 2011. NSDUH series H-41, HHS publication SMA 11-4658. https://www.samhsa.gov/data/sites/default/files/NSDUHNationalFindingsResults2010-web/2k10ResultsRev/NSDUHresultsRev2010.pdf. Published September 2011. Accessed March 31, 2017. 13. Vestal C. Few doctors are willing, able to prescribe powerful anti-addiction drugs. http://www.pewtrusts.org/en/research-and-analysis/blogs/stateline/2016/01/15/few-doctors-are-willing-able-to-prescribe-powerful-anti-addiction-drugs. Published January 15, 2016. Accessed May 2, 2016. 14. McConnell KJ. Oregon’s Medicaid coordinated care organizations. JAMA. 2016;315(9):869-870. PubMed 15. Englander H, Kansagara D. Planning and designing the Care Transitions Innovation (C-TraIn) for uninsured and Medicaid patients. J Hosp Med. 2012;7(7):524-529. PubMed 16. Englander H, Michaels L, Chan B, Kansagara D. The Care Transitions Innovation (C-TraIn) for socioeconomically disadvantaged adults: results of a cluster randomized controlled trial. J Gen Intern Med. 2014;29(11):1460-1467. PubMed 17. Bush K, Kivlahan DR, McDonell MB, Fihn SD, Bradley KA. The AUDIT alcohol consumption questions (AUDIT-C): an effective brief screening test for problem drinking. Ambulatory Care Quality Improvement Project (ACQUIP). Alcohol Use Disorders Identification Test. Arch Intern Med. 1998;158(16):1789-1795. PubMed 18. Smith PC, Schmidt SM, Allensworth-Davies D, Saitz R. A single-question screening test for drug use in primary care. Arch Intern Med. 2010;170(13):1155-1160. PubMed 19. Humeniuk R, Ali R, Babor TF, et al. Validation of the Alcohol, Smoking and Substance Involvement Screening Test (ASSIST). Addiction. 2008;103(6):1039-1047. PubMed 20. Velez CM, Nicolaidis C, Korthuis PT, Englander H. “It’s been an experience, a life learning experience”: a qualitative study of hospitalized patients with substance use disorders. J Gen Intern Med. 2017;32(3):296-303. PubMed 21. Gryczynski J, Schwartz RP, O’Grady KE, Restivo L, Mitchell SG, Jaffe JH. Understanding patterns of high-cost health care use across different substance user groups. Health Aff (Millwood). 2016.;35(1):12-19. PubMed
Address for correspondence and reprint requests: Honora Englander, MD, Mail Code BTE 119, Oregon Health & Science University, 3181 SW Sam Jackson Park Rd, Portland, OR 97239; Telephone: 971-404-5725; Fax: 503-494-1159
Content Gating
Gated (full article locked unless allowed per User)
The “Things We Do for No Reason” series reviews practices which have become common parts of hospital care but which may provide little value to our patients. Practices reviewed in the TWDFNR series do not represent “black and white” conclusions or clinical practice standards, but are meant as a starting place for research and active discussions among hospitalists and patients. We invite you to be part of that discussion. https://www.choosingwisely.org/
Acute interstitial nephritis (AIN) is an important cause of acute kidney injury (AKI) in the hospital setting. However, the diagnosis of AIN is challenging because of its nonspecific clinical manifestations and the invasiveness of kidney biopsy, the gold standard for diagnosis. Urine eosinophils (UEs) emerged several decades ago as a noninvasive alternative for diagnosing AIN. Initial studies found UEs had a significant diagnostic value, but these studies had small sample sizes, and the diagnosis of AIN was made on clinical grounds only, without biopsy confirmation. In this article, we review the literature on the diagnostic value of UEs in the diagnosis of AIN.
CASE REPORT
A 62-year-old woman with type 2 diabetes mellitus, systemic hypertension, coronary artery disease, and obesity is admitted for AKI found on routine laboratory testing. She has been taking amoxicillin and doxycycline for left leg cellulitis the past 5 days, but improvement has been minimal. On admission, blood pressure is 120/74 mm Hg, and heart rate is 89 beats per minute. Serum creatinine level is increased, from 0.7 mg/dL at baseline to 3.6 mg/dL on admission. Complete urinalysis reveals 1+ protein and presence of white blood cells and isormorphic red blood cells. No casts or crystals are seen. Given the possibility of AIN, UE testing is ordered. UEs are positive at 25%. Does this result significantly increase the patient’s posttest probability of having AIN?
WHY YOU MIGHT THINK ORDERING URINE EOSINOPHILS IN THE EVALUATION OF AIN IS HELPFUL
AKI occurs in more than 1 in 5 hospitalizations and is associated with a more than 4-fold increased likelihood of in-hospital mortality at 21 days.1 AIN is an important cause of AKI and has been found in 6% to 30% of AKI patients who had biopsies performed.2-4 AIN is characterized by infiltration of inflammatory cells in the kidney interstitium and is more commonly caused by drugs, especially beta-lactam antibiotics, and less commonly by autoimmune or systemic diseases and infections. As the signs and symptoms of AIN are nonspecific, and the gold-standard test is renal biopsy, diagnosticians have sought a noninvasive test, such as UEs.
In 1978, Galpin et al.5 found that UEs comprised 10% to 60% of urine white blood cells in 9 of 9 patients with methicillin-induced interstitial nephritis; 6 of the 9 had biopsy-proven AIN. In 1980, Linton et al.6 found UEs in 6 of 9 patients with drug-induced AIN; 8 of the 9 had biopsy-proven AIN. In 1986, Nolan et al.7 reported that, compared with Wright stain, Hansel stain was more sensitive in visualizing UEs; they did not use biopsy for confirmation. Wright-stain detection of UEs is limited by the variable staining characteristics of “eosinophilic” granules in body fluids other than blood. With Hansel stain, UEs are readily identified by their brilliant red-pink granules. These 3 small studies helped make UEs the go-to noninvasive test for assessing for AIN.8
WHY THERE IS LITTLE REASON TO ORDER URINE EOSINOPHILS IN PATIENTS WITH SUSPICION FOR AIN
While initial studies indicated UEs might be diagnostically helpful, subsequent studies did not. In 1985, Corwin et al.9 used Wright stain and found UEs in 65 of 470 adults with AKI. Only 9 (14%) of the 65 had a diagnosis of AIN, which was made mostly on clinical grounds. These findings showed that UEs were produced by other renal or urinary tract abnormalities, such as urinary tract infections, acute tubular necrosis, and glomerulonephritis. In a second study, Corwin et al.10 found that Hansel stain (vs Wright stain) improved the sensitivity of UEs for AIN diagnosis, from 25% to 62.5%. Sensitivity was improved at the expense of specificity, as Hansel stain was positive in other diagnoses as well. The AIN diagnosis was not confirmed by kidney biopsy in the large majority of patients in this study. Lack of confirmation by biopsy, the gold-standard diagnostic test, was a methodologic flaw of this study and others.
Sutton11 reviewed data from 10 studies and found AIN could not be reliably excluded in the absence of UEs (only 19 of 32 biopsy-confirmed AIN cases had UEs present). In addition, Ruffing et al.12 used Hansel stain and concluded that the positive predictive value of UEs was inadequate in diagnosing AIN. Only 6 of their 15 patients with AIN had positive UEs. Urine eosinophils were also present in patients with other diagnoses (glomerulonephritis, chronic kidney disease, acute pyelonephritis, prerenal azotemia). Like many other investigators, Ruffing et al. made the AIN diagnosis on clinical grounds in the large majority of cases.
Muriithi et al.13 reported similarly negative results in their retrospective AKI study involving 566 Mayo Clinic patients and spanning almost 2 decades. The study included patients who underwent both Hansel-stain UE testing and kidney biopsy within a week of each other. Only 28 (30%) of 91 biopsy-proven AIN cases were positive for UEs. Using the 1% cutoff for a positive UE test yielded only 30.8% sensitivity and 68.2% specificity. Using the 5% cutoff increased specificity to 91.2%, at the expense of sensitivity (19.2%); positive predictive value improved to only 30%, and negative predictive value remained relatively unchanged, at 85.6%. In short, Muriithi et al. found that UE testing had no utility in AIN diagnosis.
In summary, initial studies, such as those by Corwin et al,9,10 supported the conclusion that UEs are useful in AIN diagnosis but had questionable validity owing to methodologic issues, including small sample size and lack of biopsy confirmation of AIN. On the other hand, more recent studies, such as the one conducted by Muriithi et al.,13 had larger sample sizes and biopsy-proven diagnoses and confirmed the poor diagnostic value of UEs in AIN.
The poor sensitivity and specificity of UE tests can have important consequences. A false positive test may cause the clinician to incorrectly diagnose the patient with AIN and prompt the clinician to remove medications that may be vitally important. The clinician may also consider treating the patient with steroids empirically. A false negative test may inappropriately reassure the clinician that the patient does not have AIN and does not need cessation of the culprit drug. This may also lead the clinician to forego a necessary kidney biopsy.
WHAT YOU SHOULD DO INSTEAD
A history of recent exposure to a classic offending drug (eg, beta-lactam, proton pump inhibitor, nonsteroidal anti-inflammatory drug) in combination with the classic triad of fever, rash, and peripheral eosinophilia suggests an AIN diagnosis. However, less than 5% to 10% of patients present with this triad.14,15 Regardless of the triad’s presence, if other causes of AKI have been excluded, stopping a potential offending agent and monitoring for improvement are recommended. If a culprit drug cannot be safely discontinued, renal biopsy may be necessary for confirmation of the diagnosis. Moreover, if kidney function continues to deteriorate, a nephrology consultation may be warranted for guidance on the risks and benefits of performing a kidney biopsy to confirm the diagnosis and/or the use of corticosteroids.
RECOMMENDATIONS
Urine eosinophils should not be used in the diagnosis of AIN.
The clinical diagnosis of drug-associated AIN should be based on excluding other possible likely etiologies of AKI and confirming the history of drug exposure. This is reinforced when kidney function improves upon discontinuation of offending agent.
Kidney biopsy is the gold standard for AIN and should be performed if the clinical picture is unclear or the renal function is not improving upon discontinuation of offending agent.
Table
CONCLUSION
Since the mid-1980s, studies have found that UEs are too insensitive and nonspecific to confirm or exclude the diagnosis of AIN in patients with AKI (Table). UEs are seen in other AKI etiologies, such as pyelonephritis, acute tubular necrosis, atheroembolic renal disease, and glomerulonephritis. Current evidence-based medicine does not support use of UEs as a biomarker for AIN. False-positive and false-negative results confuse the overall picture and result either in discontinuation of important medications and unnecessary steroid treatment or in delayed removal of a culprit medication.16
Our case’s positive UE test does not affect the posttest probability that our patient has AIN. Presence of a culprit drug and absence of clinical data suggesting an alternative diagnosis would lead most clinicians to change antibiotic therapy and observe for improvement in renal function.
Disclosure
Nothing to report.
Do you think this is a low-value practice? Is this truly a “Thing We Do for No Reason?” Share what you do in your practice and join in the conversation online by retweeting it on Twitter (#TWDFNR) and Liking It on Facebook. We invite you to propose ideas for other “Things We Do for No Reason” topics by emailing [email protected].
References
1. Wang HE, Muntner P, Chertow GM, Warnock DG. Acute kidney injury and mortality in hospitalized patients. Am J Nephrol. 2012;35(4):349-355. 2. Farrington K, Levison DA, Greenwood RN, Cattell WR, Baker LR. Renal biopsy in patients with unexplained renal impairment and normal kidney size. Q J Med. 1989;70(263):221-233. 3. Michel DM, Kelly CJ. Acute interstitial nephritis. J Am Soc Nephrol. 1998;9(3):506-515. 4. Neilson EG. Pathogenesis and therapy of interstitial nephritis. Kidney Int. 1989;35(5):1257-1270. 5. Galpin JE, Shinaberger JH, Stanley TM, et al. Acute interstitial nephritis due to methicillin. Am J Med. 1978;65(5):756-765. 6. Linton AL, Clark WF, Driedger AA, Turnbull DI, Lindsay RM. Acute interstitial nephritis due to drugs: review of the literature with a report of nine cases. Ann Intern Med. 1980;93(5):735-741. 7. Nolan CR 3rd, Anger MS, Kelleher SP. Eosinophiluria—a new method of detection and definition of the clinical spectrum. N Engl J Med. 1986;315(24):1516-1519. 8. Perazella MA, Bomback AS. Urinary eosinophils in AIN: farewell to an old biomarker? Clin J Am Soc Nephrol. 2013;8(11):1841-1843. 9. Corwin HL, Korbet SM, Schwartz MM. Clinical correlates of eosinophiluria. Arch Intern Med. 1985;145(6):1097-1099. 10. Corwin HL, Bray RA, Haber MH. The detection and interpretation of urinary eosinophils. Arch Pathol Lab Med. 1989;113(11):1256-1258. 11. Sutton JM. Urinary eosinophils. Arch Intern Med. 1986;146(11):2243-2244. 12. Ruffing KA, Hoppes P, Blend D, Cugino A, Jarjoura D, Whittier FC. Eosinophils in urine revisited. Clin Nephrol. 1994;41(3):163-166. 13. Muriithi AK, Nasr SH, Leung N. Utility of urine eosinophils in the diagnosis of acute interstitial nephritis. Clin J Am Soc Nephrol. 2013;8(11):1857-1862. 14. Clarkson MR, Giblin L, O’Connell FP, et al. Acute interstitial nephritis: clinical features and response to corticosteroid therapy. Nephrol Dial Transplant. 2004;19(11):2778-2783. 15. Rossert J. Drug-induced acute interstitial nephritis. Kidney Int. 2001;60(2):804-817. 16. Fletcher A. Eosinophiluria and acute interstitial nephritis. N Engl J Med. 2008;358(16):1760-1761.
The “Things We Do for No Reason” series reviews practices which have become common parts of hospital care but which may provide little value to our patients. Practices reviewed in the TWDFNR series do not represent “black and white” conclusions or clinical practice standards, but are meant as a starting place for research and active discussions among hospitalists and patients. We invite you to be part of that discussion. https://www.choosingwisely.org/
Acute interstitial nephritis (AIN) is an important cause of acute kidney injury (AKI) in the hospital setting. However, the diagnosis of AIN is challenging because of its nonspecific clinical manifestations and the invasiveness of kidney biopsy, the gold standard for diagnosis. Urine eosinophils (UEs) emerged several decades ago as a noninvasive alternative for diagnosing AIN. Initial studies found UEs had a significant diagnostic value, but these studies had small sample sizes, and the diagnosis of AIN was made on clinical grounds only, without biopsy confirmation. In this article, we review the literature on the diagnostic value of UEs in the diagnosis of AIN.
CASE REPORT
A 62-year-old woman with type 2 diabetes mellitus, systemic hypertension, coronary artery disease, and obesity is admitted for AKI found on routine laboratory testing. She has been taking amoxicillin and doxycycline for left leg cellulitis the past 5 days, but improvement has been minimal. On admission, blood pressure is 120/74 mm Hg, and heart rate is 89 beats per minute. Serum creatinine level is increased, from 0.7 mg/dL at baseline to 3.6 mg/dL on admission. Complete urinalysis reveals 1+ protein and presence of white blood cells and isormorphic red blood cells. No casts or crystals are seen. Given the possibility of AIN, UE testing is ordered. UEs are positive at 25%. Does this result significantly increase the patient’s posttest probability of having AIN?
WHY YOU MIGHT THINK ORDERING URINE EOSINOPHILS IN THE EVALUATION OF AIN IS HELPFUL
AKI occurs in more than 1 in 5 hospitalizations and is associated with a more than 4-fold increased likelihood of in-hospital mortality at 21 days.1 AIN is an important cause of AKI and has been found in 6% to 30% of AKI patients who had biopsies performed.2-4 AIN is characterized by infiltration of inflammatory cells in the kidney interstitium and is more commonly caused by drugs, especially beta-lactam antibiotics, and less commonly by autoimmune or systemic diseases and infections. As the signs and symptoms of AIN are nonspecific, and the gold-standard test is renal biopsy, diagnosticians have sought a noninvasive test, such as UEs.
In 1978, Galpin et al.5 found that UEs comprised 10% to 60% of urine white blood cells in 9 of 9 patients with methicillin-induced interstitial nephritis; 6 of the 9 had biopsy-proven AIN. In 1980, Linton et al.6 found UEs in 6 of 9 patients with drug-induced AIN; 8 of the 9 had biopsy-proven AIN. In 1986, Nolan et al.7 reported that, compared with Wright stain, Hansel stain was more sensitive in visualizing UEs; they did not use biopsy for confirmation. Wright-stain detection of UEs is limited by the variable staining characteristics of “eosinophilic” granules in body fluids other than blood. With Hansel stain, UEs are readily identified by their brilliant red-pink granules. These 3 small studies helped make UEs the go-to noninvasive test for assessing for AIN.8
WHY THERE IS LITTLE REASON TO ORDER URINE EOSINOPHILS IN PATIENTS WITH SUSPICION FOR AIN
While initial studies indicated UEs might be diagnostically helpful, subsequent studies did not. In 1985, Corwin et al.9 used Wright stain and found UEs in 65 of 470 adults with AKI. Only 9 (14%) of the 65 had a diagnosis of AIN, which was made mostly on clinical grounds. These findings showed that UEs were produced by other renal or urinary tract abnormalities, such as urinary tract infections, acute tubular necrosis, and glomerulonephritis. In a second study, Corwin et al.10 found that Hansel stain (vs Wright stain) improved the sensitivity of UEs for AIN diagnosis, from 25% to 62.5%. Sensitivity was improved at the expense of specificity, as Hansel stain was positive in other diagnoses as well. The AIN diagnosis was not confirmed by kidney biopsy in the large majority of patients in this study. Lack of confirmation by biopsy, the gold-standard diagnostic test, was a methodologic flaw of this study and others.
Sutton11 reviewed data from 10 studies and found AIN could not be reliably excluded in the absence of UEs (only 19 of 32 biopsy-confirmed AIN cases had UEs present). In addition, Ruffing et al.12 used Hansel stain and concluded that the positive predictive value of UEs was inadequate in diagnosing AIN. Only 6 of their 15 patients with AIN had positive UEs. Urine eosinophils were also present in patients with other diagnoses (glomerulonephritis, chronic kidney disease, acute pyelonephritis, prerenal azotemia). Like many other investigators, Ruffing et al. made the AIN diagnosis on clinical grounds in the large majority of cases.
Muriithi et al.13 reported similarly negative results in their retrospective AKI study involving 566 Mayo Clinic patients and spanning almost 2 decades. The study included patients who underwent both Hansel-stain UE testing and kidney biopsy within a week of each other. Only 28 (30%) of 91 biopsy-proven AIN cases were positive for UEs. Using the 1% cutoff for a positive UE test yielded only 30.8% sensitivity and 68.2% specificity. Using the 5% cutoff increased specificity to 91.2%, at the expense of sensitivity (19.2%); positive predictive value improved to only 30%, and negative predictive value remained relatively unchanged, at 85.6%. In short, Muriithi et al. found that UE testing had no utility in AIN diagnosis.
In summary, initial studies, such as those by Corwin et al,9,10 supported the conclusion that UEs are useful in AIN diagnosis but had questionable validity owing to methodologic issues, including small sample size and lack of biopsy confirmation of AIN. On the other hand, more recent studies, such as the one conducted by Muriithi et al.,13 had larger sample sizes and biopsy-proven diagnoses and confirmed the poor diagnostic value of UEs in AIN.
The poor sensitivity and specificity of UE tests can have important consequences. A false positive test may cause the clinician to incorrectly diagnose the patient with AIN and prompt the clinician to remove medications that may be vitally important. The clinician may also consider treating the patient with steroids empirically. A false negative test may inappropriately reassure the clinician that the patient does not have AIN and does not need cessation of the culprit drug. This may also lead the clinician to forego a necessary kidney biopsy.
WHAT YOU SHOULD DO INSTEAD
A history of recent exposure to a classic offending drug (eg, beta-lactam, proton pump inhibitor, nonsteroidal anti-inflammatory drug) in combination with the classic triad of fever, rash, and peripheral eosinophilia suggests an AIN diagnosis. However, less than 5% to 10% of patients present with this triad.14,15 Regardless of the triad’s presence, if other causes of AKI have been excluded, stopping a potential offending agent and monitoring for improvement are recommended. If a culprit drug cannot be safely discontinued, renal biopsy may be necessary for confirmation of the diagnosis. Moreover, if kidney function continues to deteriorate, a nephrology consultation may be warranted for guidance on the risks and benefits of performing a kidney biopsy to confirm the diagnosis and/or the use of corticosteroids.
RECOMMENDATIONS
Urine eosinophils should not be used in the diagnosis of AIN.
The clinical diagnosis of drug-associated AIN should be based on excluding other possible likely etiologies of AKI and confirming the history of drug exposure. This is reinforced when kidney function improves upon discontinuation of offending agent.
Kidney biopsy is the gold standard for AIN and should be performed if the clinical picture is unclear or the renal function is not improving upon discontinuation of offending agent.
Table
CONCLUSION
Since the mid-1980s, studies have found that UEs are too insensitive and nonspecific to confirm or exclude the diagnosis of AIN in patients with AKI (Table). UEs are seen in other AKI etiologies, such as pyelonephritis, acute tubular necrosis, atheroembolic renal disease, and glomerulonephritis. Current evidence-based medicine does not support use of UEs as a biomarker for AIN. False-positive and false-negative results confuse the overall picture and result either in discontinuation of important medications and unnecessary steroid treatment or in delayed removal of a culprit medication.16
Our case’s positive UE test does not affect the posttest probability that our patient has AIN. Presence of a culprit drug and absence of clinical data suggesting an alternative diagnosis would lead most clinicians to change antibiotic therapy and observe for improvement in renal function.
Disclosure
Nothing to report.
Do you think this is a low-value practice? Is this truly a “Thing We Do for No Reason?” Share what you do in your practice and join in the conversation online by retweeting it on Twitter (#TWDFNR) and Liking It on Facebook. We invite you to propose ideas for other “Things We Do for No Reason” topics by emailing [email protected].
The “Things We Do for No Reason” series reviews practices which have become common parts of hospital care but which may provide little value to our patients. Practices reviewed in the TWDFNR series do not represent “black and white” conclusions or clinical practice standards, but are meant as a starting place for research and active discussions among hospitalists and patients. We invite you to be part of that discussion. https://www.choosingwisely.org/
Acute interstitial nephritis (AIN) is an important cause of acute kidney injury (AKI) in the hospital setting. However, the diagnosis of AIN is challenging because of its nonspecific clinical manifestations and the invasiveness of kidney biopsy, the gold standard for diagnosis. Urine eosinophils (UEs) emerged several decades ago as a noninvasive alternative for diagnosing AIN. Initial studies found UEs had a significant diagnostic value, but these studies had small sample sizes, and the diagnosis of AIN was made on clinical grounds only, without biopsy confirmation. In this article, we review the literature on the diagnostic value of UEs in the diagnosis of AIN.
CASE REPORT
A 62-year-old woman with type 2 diabetes mellitus, systemic hypertension, coronary artery disease, and obesity is admitted for AKI found on routine laboratory testing. She has been taking amoxicillin and doxycycline for left leg cellulitis the past 5 days, but improvement has been minimal. On admission, blood pressure is 120/74 mm Hg, and heart rate is 89 beats per minute. Serum creatinine level is increased, from 0.7 mg/dL at baseline to 3.6 mg/dL on admission. Complete urinalysis reveals 1+ protein and presence of white blood cells and isormorphic red blood cells. No casts or crystals are seen. Given the possibility of AIN, UE testing is ordered. UEs are positive at 25%. Does this result significantly increase the patient’s posttest probability of having AIN?
WHY YOU MIGHT THINK ORDERING URINE EOSINOPHILS IN THE EVALUATION OF AIN IS HELPFUL
AKI occurs in more than 1 in 5 hospitalizations and is associated with a more than 4-fold increased likelihood of in-hospital mortality at 21 days.1 AIN is an important cause of AKI and has been found in 6% to 30% of AKI patients who had biopsies performed.2-4 AIN is characterized by infiltration of inflammatory cells in the kidney interstitium and is more commonly caused by drugs, especially beta-lactam antibiotics, and less commonly by autoimmune or systemic diseases and infections. As the signs and symptoms of AIN are nonspecific, and the gold-standard test is renal biopsy, diagnosticians have sought a noninvasive test, such as UEs.
In 1978, Galpin et al.5 found that UEs comprised 10% to 60% of urine white blood cells in 9 of 9 patients with methicillin-induced interstitial nephritis; 6 of the 9 had biopsy-proven AIN. In 1980, Linton et al.6 found UEs in 6 of 9 patients with drug-induced AIN; 8 of the 9 had biopsy-proven AIN. In 1986, Nolan et al.7 reported that, compared with Wright stain, Hansel stain was more sensitive in visualizing UEs; they did not use biopsy for confirmation. Wright-stain detection of UEs is limited by the variable staining characteristics of “eosinophilic” granules in body fluids other than blood. With Hansel stain, UEs are readily identified by their brilliant red-pink granules. These 3 small studies helped make UEs the go-to noninvasive test for assessing for AIN.8
WHY THERE IS LITTLE REASON TO ORDER URINE EOSINOPHILS IN PATIENTS WITH SUSPICION FOR AIN
While initial studies indicated UEs might be diagnostically helpful, subsequent studies did not. In 1985, Corwin et al.9 used Wright stain and found UEs in 65 of 470 adults with AKI. Only 9 (14%) of the 65 had a diagnosis of AIN, which was made mostly on clinical grounds. These findings showed that UEs were produced by other renal or urinary tract abnormalities, such as urinary tract infections, acute tubular necrosis, and glomerulonephritis. In a second study, Corwin et al.10 found that Hansel stain (vs Wright stain) improved the sensitivity of UEs for AIN diagnosis, from 25% to 62.5%. Sensitivity was improved at the expense of specificity, as Hansel stain was positive in other diagnoses as well. The AIN diagnosis was not confirmed by kidney biopsy in the large majority of patients in this study. Lack of confirmation by biopsy, the gold-standard diagnostic test, was a methodologic flaw of this study and others.
Sutton11 reviewed data from 10 studies and found AIN could not be reliably excluded in the absence of UEs (only 19 of 32 biopsy-confirmed AIN cases had UEs present). In addition, Ruffing et al.12 used Hansel stain and concluded that the positive predictive value of UEs was inadequate in diagnosing AIN. Only 6 of their 15 patients with AIN had positive UEs. Urine eosinophils were also present in patients with other diagnoses (glomerulonephritis, chronic kidney disease, acute pyelonephritis, prerenal azotemia). Like many other investigators, Ruffing et al. made the AIN diagnosis on clinical grounds in the large majority of cases.
Muriithi et al.13 reported similarly negative results in their retrospective AKI study involving 566 Mayo Clinic patients and spanning almost 2 decades. The study included patients who underwent both Hansel-stain UE testing and kidney biopsy within a week of each other. Only 28 (30%) of 91 biopsy-proven AIN cases were positive for UEs. Using the 1% cutoff for a positive UE test yielded only 30.8% sensitivity and 68.2% specificity. Using the 5% cutoff increased specificity to 91.2%, at the expense of sensitivity (19.2%); positive predictive value improved to only 30%, and negative predictive value remained relatively unchanged, at 85.6%. In short, Muriithi et al. found that UE testing had no utility in AIN diagnosis.
In summary, initial studies, such as those by Corwin et al,9,10 supported the conclusion that UEs are useful in AIN diagnosis but had questionable validity owing to methodologic issues, including small sample size and lack of biopsy confirmation of AIN. On the other hand, more recent studies, such as the one conducted by Muriithi et al.,13 had larger sample sizes and biopsy-proven diagnoses and confirmed the poor diagnostic value of UEs in AIN.
The poor sensitivity and specificity of UE tests can have important consequences. A false positive test may cause the clinician to incorrectly diagnose the patient with AIN and prompt the clinician to remove medications that may be vitally important. The clinician may also consider treating the patient with steroids empirically. A false negative test may inappropriately reassure the clinician that the patient does not have AIN and does not need cessation of the culprit drug. This may also lead the clinician to forego a necessary kidney biopsy.
WHAT YOU SHOULD DO INSTEAD
A history of recent exposure to a classic offending drug (eg, beta-lactam, proton pump inhibitor, nonsteroidal anti-inflammatory drug) in combination with the classic triad of fever, rash, and peripheral eosinophilia suggests an AIN diagnosis. However, less than 5% to 10% of patients present with this triad.14,15 Regardless of the triad’s presence, if other causes of AKI have been excluded, stopping a potential offending agent and monitoring for improvement are recommended. If a culprit drug cannot be safely discontinued, renal biopsy may be necessary for confirmation of the diagnosis. Moreover, if kidney function continues to deteriorate, a nephrology consultation may be warranted for guidance on the risks and benefits of performing a kidney biopsy to confirm the diagnosis and/or the use of corticosteroids.
RECOMMENDATIONS
Urine eosinophils should not be used in the diagnosis of AIN.
The clinical diagnosis of drug-associated AIN should be based on excluding other possible likely etiologies of AKI and confirming the history of drug exposure. This is reinforced when kidney function improves upon discontinuation of offending agent.
Kidney biopsy is the gold standard for AIN and should be performed if the clinical picture is unclear or the renal function is not improving upon discontinuation of offending agent.
Table
CONCLUSION
Since the mid-1980s, studies have found that UEs are too insensitive and nonspecific to confirm or exclude the diagnosis of AIN in patients with AKI (Table). UEs are seen in other AKI etiologies, such as pyelonephritis, acute tubular necrosis, atheroembolic renal disease, and glomerulonephritis. Current evidence-based medicine does not support use of UEs as a biomarker for AIN. False-positive and false-negative results confuse the overall picture and result either in discontinuation of important medications and unnecessary steroid treatment or in delayed removal of a culprit medication.16
Our case’s positive UE test does not affect the posttest probability that our patient has AIN. Presence of a culprit drug and absence of clinical data suggesting an alternative diagnosis would lead most clinicians to change antibiotic therapy and observe for improvement in renal function.
Disclosure
Nothing to report.
Do you think this is a low-value practice? Is this truly a “Thing We Do for No Reason?” Share what you do in your practice and join in the conversation online by retweeting it on Twitter (#TWDFNR) and Liking It on Facebook. We invite you to propose ideas for other “Things We Do for No Reason” topics by emailing [email protected].
References
1. Wang HE, Muntner P, Chertow GM, Warnock DG. Acute kidney injury and mortality in hospitalized patients. Am J Nephrol. 2012;35(4):349-355. 2. Farrington K, Levison DA, Greenwood RN, Cattell WR, Baker LR. Renal biopsy in patients with unexplained renal impairment and normal kidney size. Q J Med. 1989;70(263):221-233. 3. Michel DM, Kelly CJ. Acute interstitial nephritis. J Am Soc Nephrol. 1998;9(3):506-515. 4. Neilson EG. Pathogenesis and therapy of interstitial nephritis. Kidney Int. 1989;35(5):1257-1270. 5. Galpin JE, Shinaberger JH, Stanley TM, et al. Acute interstitial nephritis due to methicillin. Am J Med. 1978;65(5):756-765. 6. Linton AL, Clark WF, Driedger AA, Turnbull DI, Lindsay RM. Acute interstitial nephritis due to drugs: review of the literature with a report of nine cases. Ann Intern Med. 1980;93(5):735-741. 7. Nolan CR 3rd, Anger MS, Kelleher SP. Eosinophiluria—a new method of detection and definition of the clinical spectrum. N Engl J Med. 1986;315(24):1516-1519. 8. Perazella MA, Bomback AS. Urinary eosinophils in AIN: farewell to an old biomarker? Clin J Am Soc Nephrol. 2013;8(11):1841-1843. 9. Corwin HL, Korbet SM, Schwartz MM. Clinical correlates of eosinophiluria. Arch Intern Med. 1985;145(6):1097-1099. 10. Corwin HL, Bray RA, Haber MH. The detection and interpretation of urinary eosinophils. Arch Pathol Lab Med. 1989;113(11):1256-1258. 11. Sutton JM. Urinary eosinophils. Arch Intern Med. 1986;146(11):2243-2244. 12. Ruffing KA, Hoppes P, Blend D, Cugino A, Jarjoura D, Whittier FC. Eosinophils in urine revisited. Clin Nephrol. 1994;41(3):163-166. 13. Muriithi AK, Nasr SH, Leung N. Utility of urine eosinophils in the diagnosis of acute interstitial nephritis. Clin J Am Soc Nephrol. 2013;8(11):1857-1862. 14. Clarkson MR, Giblin L, O’Connell FP, et al. Acute interstitial nephritis: clinical features and response to corticosteroid therapy. Nephrol Dial Transplant. 2004;19(11):2778-2783. 15. Rossert J. Drug-induced acute interstitial nephritis. Kidney Int. 2001;60(2):804-817. 16. Fletcher A. Eosinophiluria and acute interstitial nephritis. N Engl J Med. 2008;358(16):1760-1761.
References
1. Wang HE, Muntner P, Chertow GM, Warnock DG. Acute kidney injury and mortality in hospitalized patients. Am J Nephrol. 2012;35(4):349-355. 2. Farrington K, Levison DA, Greenwood RN, Cattell WR, Baker LR. Renal biopsy in patients with unexplained renal impairment and normal kidney size. Q J Med. 1989;70(263):221-233. 3. Michel DM, Kelly CJ. Acute interstitial nephritis. J Am Soc Nephrol. 1998;9(3):506-515. 4. Neilson EG. Pathogenesis and therapy of interstitial nephritis. Kidney Int. 1989;35(5):1257-1270. 5. Galpin JE, Shinaberger JH, Stanley TM, et al. Acute interstitial nephritis due to methicillin. Am J Med. 1978;65(5):756-765. 6. Linton AL, Clark WF, Driedger AA, Turnbull DI, Lindsay RM. Acute interstitial nephritis due to drugs: review of the literature with a report of nine cases. Ann Intern Med. 1980;93(5):735-741. 7. Nolan CR 3rd, Anger MS, Kelleher SP. Eosinophiluria—a new method of detection and definition of the clinical spectrum. N Engl J Med. 1986;315(24):1516-1519. 8. Perazella MA, Bomback AS. Urinary eosinophils in AIN: farewell to an old biomarker? Clin J Am Soc Nephrol. 2013;8(11):1841-1843. 9. Corwin HL, Korbet SM, Schwartz MM. Clinical correlates of eosinophiluria. Arch Intern Med. 1985;145(6):1097-1099. 10. Corwin HL, Bray RA, Haber MH. The detection and interpretation of urinary eosinophils. Arch Pathol Lab Med. 1989;113(11):1256-1258. 11. Sutton JM. Urinary eosinophils. Arch Intern Med. 1986;146(11):2243-2244. 12. Ruffing KA, Hoppes P, Blend D, Cugino A, Jarjoura D, Whittier FC. Eosinophils in urine revisited. Clin Nephrol. 1994;41(3):163-166. 13. Muriithi AK, Nasr SH, Leung N. Utility of urine eosinophils in the diagnosis of acute interstitial nephritis. Clin J Am Soc Nephrol. 2013;8(11):1857-1862. 14. Clarkson MR, Giblin L, O’Connell FP, et al. Acute interstitial nephritis: clinical features and response to corticosteroid therapy. Nephrol Dial Transplant. 2004;19(11):2778-2783. 15. Rossert J. Drug-induced acute interstitial nephritis. Kidney Int. 2001;60(2):804-817. 16. Fletcher A. Eosinophiluria and acute interstitial nephritis. N Engl J Med. 2008;358(16):1760-1761.
Address for correspondence and reprint requests: Helbert Rondon-Berrios, MD, Renal-Electrolyte Division, Department of Medicine, University of Pittsburgh School of Medicine, A915 Scaife Hall, 3550 Terrace St, Pittsburgh, PA 15213; Telephone: 412-647-3120; Fax: 412-647-6222; E-mail: [email protected]
Content Gating
Open Access (article Unlocked/Open Access)
Alternative CME
Consolidated Pubs: Do Not Show Source Publication Logo

")

")