User login
A focus on women with diabetes and their offspring
In 2021, diabetes and related complications was the 8th leading cause of death in the United States.1 As of 2022, more than 11% of the U.S. population had diabetes and 38% of the adult U.S. population had prediabetes.2 Diabetes is the most expensive chronic condition in the United States, where $1 of every $4 in health care costs is spent on care.3
Where this is most concerning is diabetes in pregnancy. While childbirth rates in the United States have decreased since the 2007 high of 4.32 million births4 to 3.66 million in 2021,5 the incidence of diabetes in pregnancy – both pregestational and gestational – has increased. The rate of pregestational diabetes in 2021 was 10.9 per 1,000 births, a 27% increase from 2016 (8.6 per 1,000).6 The percentage of those giving birth who also were diagnosed with gestational diabetes mellitus (GDM) was 8.3% in 2021, up from 6.0% in 2016.7
Adverse outcomes for an infant born to a mother with diabetes include a higher risk of obesity and diabetes as adults, potentially leading to a forward-feeding cycle.

We and our colleagues established the Diabetes in Pregnancy Study Group of North America in 1997 because we had witnessed too frequently the devastating diabetes-induced pregnancy complications in our patients. The mission we set forth was to provide a forum for dialogue among maternal-fetal medicine subspecialists. The three main goals we set forth to support this mission were to provide a catalyst for research, contribute to the creation and refinement of medical policies, and influence professional practices in diabetes in pregnancy.8
In the last quarter century, DPSG-NA, through its annual and biennial meetings, has brought together several hundred practitioners that include physicians, nurses, statisticians, researchers, nutritionists, and allied health professionals, among others. As a group, it has improved the detection and management of diabetes in pregnant women and their offspring through knowledge sharing and influencing policies on GDM screening, diagnosis, management, and treatment. Our members have shown that preconceptional counseling for women with diabetes can significantly reduce congenital malformation and perinatal mortality compared with those women with pregestational diabetes who receive no counseling.9,10
We have addressed a wide variety of topics including the paucity of data in determining the timing of delivery for women with diabetes and the Institute of Medicine/National Academy of Medicine recommendations of gestational weight gain and risks of not adhering to them. We have learned about new scientific discoveries that reveal underlying mechanisms to diabetes-related birth defects and potential therapeutic targets; and we have discussed the health literacy requirements, ethics, and opportunities for lifestyle intervention.11-16
But we need to do more.
Two risk factors are at play: Women continue to choose to have babies at later ages and their pregnancies continue to be complicated by the rising incidence of obesity (see Figure 1 and Figure 2). 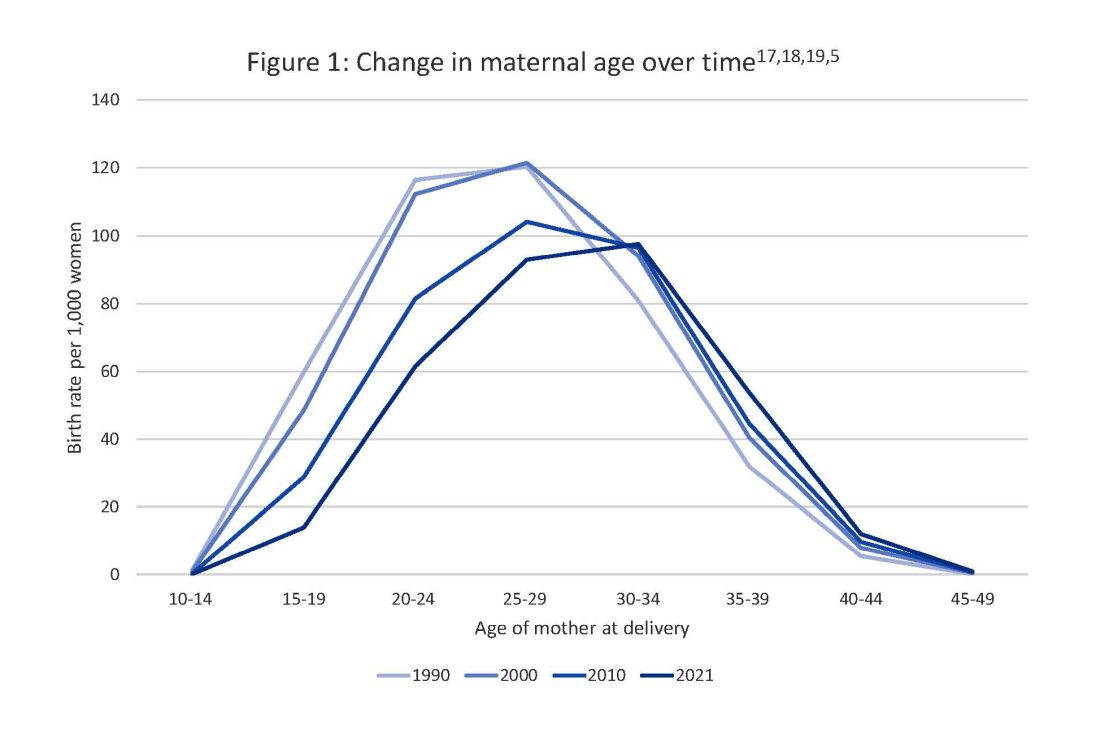
The global obesity epidemic has become a significant concern for all aspects of health and particularly for diabetes in pregnancy. 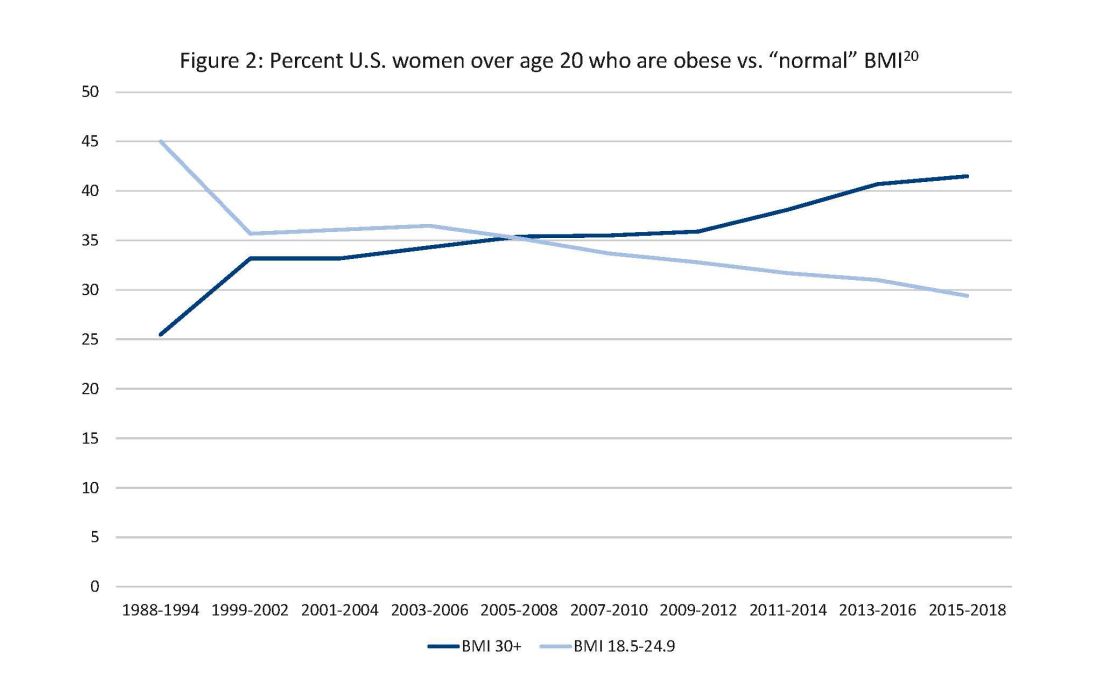
In 1990, 24.9% of women in the United States were obese; in 2010, 35.8%; and now more than 41%. Some experts project that by 2030 more than 80% of women in the United States will be overweight or obese.21
If we are to stop this cycle of diabetes begets more diabetes, now more than ever we need to come together and accelerate the research and education around the diabetes in pregnancy. Join us at this year’s DPSG-NA meeting Oct. 26-28 to take part in the knowledge sharing, discussions, and planning. More information can be found online at https://events.dpsg-na.com/home.
Dr. Miodovnik is adjunct professor of obstetrics, gynecology, and reproductive sciences at University of Maryland School of Medicine. Dr. Reece is professor of obstetrics, gynecology, and reproductive sciences and senior scientist at the Center for Birth Defects Research at University of Maryland School of Medicine.
References
1. Xu J et al. Mortality in the United States, 2021. NCHS Data Brief. 2022 Dec;(456):1-8. PMID: 36598387.
2. Centers for Disease Control and Prevention, diabetes data and statistics.
3. American Diabetes Association. The Cost of Diabetes.
4. Martin JA et al. Births: Final data for 2007. Natl Vital Stat Rep. 2010 Aug 9;58(24):1-85. PMID: 21254725.
5. Osterman MJK et al. Births: Final data for 2021. Natl Vital Stat Rep. 2023 Jan;72(1):1-53. PMID: 36723449.
6. Gregory ECW and Ely DM. Trends and characteristics in prepregnancy diabetes: United States, 2016-2021. Natl Vital Stat Rep. 2023 May;72(6):1-13. PMID: 37256333.
7. QuickStats: Percentage of mothers with gestational diabetes, by maternal age – National Vital Statistics System, United States, 2016 and 2021. MMWR Morb Mortal Wkly Rep. 2023 Jan 6;72(1):16. doi: 10.15585/mmwr.mm7201a4.
8. Langer O et al. The Diabetes in Pregnancy Study Group of North America – Introduction and summary statement. Prenat Neonat Med. 1998;3(6):514-6.
9. Willhoite MB et al. The impact of preconception counseling on pregnancy outcomes. The experience of the Maine Diabetes in Pregnancy Program. Diabetes Care. 1993 Feb;16(2):450-5. doi: 10.2337/diacare.16.2.450.
10. McElvy SS et al. A focused preconceptional and early pregnancy program in women with type 1 diabetes reduces perinatal mortality and malformation rates to general population levels. J Matern Fetal Med. 2000 Jan-Feb;9(1):14-20. doi: 10.1002/(SICI)1520-6661(200001/02)9:1<14::AID-MFM5>3.0.CO;2-K.
11. Rosen JA et al. The history and contributions of the Diabetes in Pregnancy Study Group of North America (1997-2015). Am J Perinatol. 2016 Nov;33(13):1223-6. doi: 10.1055/s-0036-1585082.
12. Driggers RW and Baschat A. The 12th meeting of the Diabetes in Pregnancy Study Group of North America (DPSG-NA): Introduction and overview. J Matern Fetal Neonatal Med. 2012 Jan;25(1):3-4. doi: 10.3109/14767058.2012.626917.
13. Langer O et al. The proceedings of the Diabetes in Pregnancy Study Group of North America 2009 conference. J Matern Fetal Neonatal Med. 2010 Mar;23(3):196-8. doi: 10.3109/14767050903550634.
14. Reece EA et al. A consensus report of the Diabetes in Pregnancy Study Group of North America Conference, Little Rock, Ark., May 2002. J Matern Fetal Neonatal Med. 2002 Dec;12(6):362-4. doi: 10.1080/jmf.12.6.362.364.
15. Reece EA and Maulik D. A consensus conference of the Diabetes in Pregnancy Study Group of North America. J Matern Fetal Neonatal Med. 2002 Dec;12(6):361. doi: 10.1080/jmf.12.6.361.361.
16. Gabbe SG. Summation of the second meeting of the Diabetes in Pregnancy Study Group of North America (DPSG-NA). J Matern Fetal Med. 2000 Jan-Feb;9(1):3-9.
17. Vital Statistics of the United States 1990: Volume I – Natality.
18. Martin JA et al. Births: final data for 2000. Natl Vital Stat Rep. 2002 Feb 12;50(5):1-101. PMID: 11876093.
19. Martin JA et al. Births: final data for 2010. Natl Vital Stat Rep. 2012 Aug 28;61(1):1-72. PMID: 24974589.
20. CDC Website. Normal weight, overweight, and obesity among adults aged 20 and over, by selected characteristics: United States.
21. Wang Y et al. Has the prevalence of overweight, obesity, and central obesity levelled off in the United States? Trends, patterns, disparities, and future projections for the obesity epidemic. Int J Epidemiol. 2020 Jun 1;49(3):810-23. doi: 10.1093/ije/dyz273.
In 2021, diabetes and related complications was the 8th leading cause of death in the United States.1 As of 2022, more than 11% of the U.S. population had diabetes and 38% of the adult U.S. population had prediabetes.2 Diabetes is the most expensive chronic condition in the United States, where $1 of every $4 in health care costs is spent on care.3
Where this is most concerning is diabetes in pregnancy. While childbirth rates in the United States have decreased since the 2007 high of 4.32 million births4 to 3.66 million in 2021,5 the incidence of diabetes in pregnancy – both pregestational and gestational – has increased. The rate of pregestational diabetes in 2021 was 10.9 per 1,000 births, a 27% increase from 2016 (8.6 per 1,000).6 The percentage of those giving birth who also were diagnosed with gestational diabetes mellitus (GDM) was 8.3% in 2021, up from 6.0% in 2016.7
Adverse outcomes for an infant born to a mother with diabetes include a higher risk of obesity and diabetes as adults, potentially leading to a forward-feeding cycle.
We and our colleagues established the Diabetes in Pregnancy Study Group of North America in 1997 because we had witnessed too frequently the devastating diabetes-induced pregnancy complications in our patients. The mission we set forth was to provide a forum for dialogue among maternal-fetal medicine subspecialists. The three main goals we set forth to support this mission were to provide a catalyst for research, contribute to the creation and refinement of medical policies, and influence professional practices in diabetes in pregnancy.8
In the last quarter century, DPSG-NA, through its annual and biennial meetings, has brought together several hundred practitioners that include physicians, nurses, statisticians, researchers, nutritionists, and allied health professionals, among others. As a group, it has improved the detection and management of diabetes in pregnant women and their offspring through knowledge sharing and influencing policies on GDM screening, diagnosis, management, and treatment. Our members have shown that preconceptional counseling for women with diabetes can significantly reduce congenital malformation and perinatal mortality compared with those women with pregestational diabetes who receive no counseling.9,10
We have addressed a wide variety of topics including the paucity of data in determining the timing of delivery for women with diabetes and the Institute of Medicine/National Academy of Medicine recommendations of gestational weight gain and risks of not adhering to them. We have learned about new scientific discoveries that reveal underlying mechanisms to diabetes-related birth defects and potential therapeutic targets; and we have discussed the health literacy requirements, ethics, and opportunities for lifestyle intervention.11-16
But we need to do more.
Two risk factors are at play: Women continue to choose to have babies at later ages and their pregnancies continue to be complicated by the rising incidence of obesity (see Figure 1 and Figure 2).
The global obesity epidemic has become a significant concern for all aspects of health and particularly for diabetes in pregnancy.
In 1990, 24.9% of women in the United States were obese; in 2010, 35.8%; and now more than 41%. Some experts project that by 2030 more than 80% of women in the United States will be overweight or obese.21
If we are to stop this cycle of diabetes begets more diabetes, now more than ever we need to come together and accelerate the research and education around the diabetes in pregnancy. Join us at this year’s DPSG-NA meeting Oct. 26-28 to take part in the knowledge sharing, discussions, and planning. More information can be found online at https://events.dpsg-na.com/home.
Dr. Miodovnik is adjunct professor of obstetrics, gynecology, and reproductive sciences at University of Maryland School of Medicine. Dr. Reece is professor of obstetrics, gynecology, and reproductive sciences and senior scientist at the Center for Birth Defects Research at University of Maryland School of Medicine.
References
1. Xu J et al. Mortality in the United States, 2021. NCHS Data Brief. 2022 Dec;(456):1-8. PMID: 36598387.
2. Centers for Disease Control and Prevention, diabetes data and statistics.
3. American Diabetes Association. The Cost of Diabetes.
4. Martin JA et al. Births: Final data for 2007. Natl Vital Stat Rep. 2010 Aug 9;58(24):1-85. PMID: 21254725.
5. Osterman MJK et al. Births: Final data for 2021. Natl Vital Stat Rep. 2023 Jan;72(1):1-53. PMID: 36723449.
6. Gregory ECW and Ely DM. Trends and characteristics in prepregnancy diabetes: United States, 2016-2021. Natl Vital Stat Rep. 2023 May;72(6):1-13. PMID: 37256333.
7. QuickStats: Percentage of mothers with gestational diabetes, by maternal age – National Vital Statistics System, United States, 2016 and 2021. MMWR Morb Mortal Wkly Rep. 2023 Jan 6;72(1):16. doi: 10.15585/mmwr.mm7201a4.
8. Langer O et al. The Diabetes in Pregnancy Study Group of North America – Introduction and summary statement. Prenat Neonat Med. 1998;3(6):514-6.
9. Willhoite MB et al. The impact of preconception counseling on pregnancy outcomes. The experience of the Maine Diabetes in Pregnancy Program. Diabetes Care. 1993 Feb;16(2):450-5. doi: 10.2337/diacare.16.2.450.
10. McElvy SS et al. A focused preconceptional and early pregnancy program in women with type 1 diabetes reduces perinatal mortality and malformation rates to general population levels. J Matern Fetal Med. 2000 Jan-Feb;9(1):14-20. doi: 10.1002/(SICI)1520-6661(200001/02)9:1<14::AID-MFM5>3.0.CO;2-K.
11. Rosen JA et al. The history and contributions of the Diabetes in Pregnancy Study Group of North America (1997-2015). Am J Perinatol. 2016 Nov;33(13):1223-6. doi: 10.1055/s-0036-1585082.
12. Driggers RW and Baschat A. The 12th meeting of the Diabetes in Pregnancy Study Group of North America (DPSG-NA): Introduction and overview. J Matern Fetal Neonatal Med. 2012 Jan;25(1):3-4. doi: 10.3109/14767058.2012.626917.
13. Langer O et al. The proceedings of the Diabetes in Pregnancy Study Group of North America 2009 conference. J Matern Fetal Neonatal Med. 2010 Mar;23(3):196-8. doi: 10.3109/14767050903550634.
14. Reece EA et al. A consensus report of the Diabetes in Pregnancy Study Group of North America Conference, Little Rock, Ark., May 2002. J Matern Fetal Neonatal Med. 2002 Dec;12(6):362-4. doi: 10.1080/jmf.12.6.362.364.
15. Reece EA and Maulik D. A consensus conference of the Diabetes in Pregnancy Study Group of North America. J Matern Fetal Neonatal Med. 2002 Dec;12(6):361. doi: 10.1080/jmf.12.6.361.361.
16. Gabbe SG. Summation of the second meeting of the Diabetes in Pregnancy Study Group of North America (DPSG-NA). J Matern Fetal Med. 2000 Jan-Feb;9(1):3-9.
17. Vital Statistics of the United States 1990: Volume I – Natality.
18. Martin JA et al. Births: final data for 2000. Natl Vital Stat Rep. 2002 Feb 12;50(5):1-101. PMID: 11876093.
19. Martin JA et al. Births: final data for 2010. Natl Vital Stat Rep. 2012 Aug 28;61(1):1-72. PMID: 24974589.
20. CDC Website. Normal weight, overweight, and obesity among adults aged 20 and over, by selected characteristics: United States.
21. Wang Y et al. Has the prevalence of overweight, obesity, and central obesity levelled off in the United States? Trends, patterns, disparities, and future projections for the obesity epidemic. Int J Epidemiol. 2020 Jun 1;49(3):810-23. doi: 10.1093/ije/dyz273.
In 2021, diabetes and related complications was the 8th leading cause of death in the United States.1 As of 2022, more than 11% of the U.S. population had diabetes and 38% of the adult U.S. population had prediabetes.2 Diabetes is the most expensive chronic condition in the United States, where $1 of every $4 in health care costs is spent on care.3
Where this is most concerning is diabetes in pregnancy. While childbirth rates in the United States have decreased since the 2007 high of 4.32 million births4 to 3.66 million in 2021,5 the incidence of diabetes in pregnancy – both pregestational and gestational – has increased. The rate of pregestational diabetes in 2021 was 10.9 per 1,000 births, a 27% increase from 2016 (8.6 per 1,000).6 The percentage of those giving birth who also were diagnosed with gestational diabetes mellitus (GDM) was 8.3% in 2021, up from 6.0% in 2016.7
Adverse outcomes for an infant born to a mother with diabetes include a higher risk of obesity and diabetes as adults, potentially leading to a forward-feeding cycle.
We and our colleagues established the Diabetes in Pregnancy Study Group of North America in 1997 because we had witnessed too frequently the devastating diabetes-induced pregnancy complications in our patients. The mission we set forth was to provide a forum for dialogue among maternal-fetal medicine subspecialists. The three main goals we set forth to support this mission were to provide a catalyst for research, contribute to the creation and refinement of medical policies, and influence professional practices in diabetes in pregnancy.8
In the last quarter century, DPSG-NA, through its annual and biennial meetings, has brought together several hundred practitioners that include physicians, nurses, statisticians, researchers, nutritionists, and allied health professionals, among others. As a group, it has improved the detection and management of diabetes in pregnant women and their offspring through knowledge sharing and influencing policies on GDM screening, diagnosis, management, and treatment. Our members have shown that preconceptional counseling for women with diabetes can significantly reduce congenital malformation and perinatal mortality compared with those women with pregestational diabetes who receive no counseling.9,10
We have addressed a wide variety of topics including the paucity of data in determining the timing of delivery for women with diabetes and the Institute of Medicine/National Academy of Medicine recommendations of gestational weight gain and risks of not adhering to them. We have learned about new scientific discoveries that reveal underlying mechanisms to diabetes-related birth defects and potential therapeutic targets; and we have discussed the health literacy requirements, ethics, and opportunities for lifestyle intervention.11-16
But we need to do more.
Two risk factors are at play: Women continue to choose to have babies at later ages and their pregnancies continue to be complicated by the rising incidence of obesity (see Figure 1 and Figure 2).
The global obesity epidemic has become a significant concern for all aspects of health and particularly for diabetes in pregnancy.
In 1990, 24.9% of women in the United States were obese; in 2010, 35.8%; and now more than 41%. Some experts project that by 2030 more than 80% of women in the United States will be overweight or obese.21
If we are to stop this cycle of diabetes begets more diabetes, now more than ever we need to come together and accelerate the research and education around the diabetes in pregnancy. Join us at this year’s DPSG-NA meeting Oct. 26-28 to take part in the knowledge sharing, discussions, and planning. More information can be found online at https://events.dpsg-na.com/home.
Dr. Miodovnik is adjunct professor of obstetrics, gynecology, and reproductive sciences at University of Maryland School of Medicine. Dr. Reece is professor of obstetrics, gynecology, and reproductive sciences and senior scientist at the Center for Birth Defects Research at University of Maryland School of Medicine.
References
1. Xu J et al. Mortality in the United States, 2021. NCHS Data Brief. 2022 Dec;(456):1-8. PMID: 36598387.
2. Centers for Disease Control and Prevention, diabetes data and statistics.
3. American Diabetes Association. The Cost of Diabetes.
4. Martin JA et al. Births: Final data for 2007. Natl Vital Stat Rep. 2010 Aug 9;58(24):1-85. PMID: 21254725.
5. Osterman MJK et al. Births: Final data for 2021. Natl Vital Stat Rep. 2023 Jan;72(1):1-53. PMID: 36723449.
6. Gregory ECW and Ely DM. Trends and characteristics in prepregnancy diabetes: United States, 2016-2021. Natl Vital Stat Rep. 2023 May;72(6):1-13. PMID: 37256333.
7. QuickStats: Percentage of mothers with gestational diabetes, by maternal age – National Vital Statistics System, United States, 2016 and 2021. MMWR Morb Mortal Wkly Rep. 2023 Jan 6;72(1):16. doi: 10.15585/mmwr.mm7201a4.
8. Langer O et al. The Diabetes in Pregnancy Study Group of North America – Introduction and summary statement. Prenat Neonat Med. 1998;3(6):514-6.
9. Willhoite MB et al. The impact of preconception counseling on pregnancy outcomes. The experience of the Maine Diabetes in Pregnancy Program. Diabetes Care. 1993 Feb;16(2):450-5. doi: 10.2337/diacare.16.2.450.
10. McElvy SS et al. A focused preconceptional and early pregnancy program in women with type 1 diabetes reduces perinatal mortality and malformation rates to general population levels. J Matern Fetal Med. 2000 Jan-Feb;9(1):14-20. doi: 10.1002/(SICI)1520-6661(200001/02)9:1<14::AID-MFM5>3.0.CO;2-K.
11. Rosen JA et al. The history and contributions of the Diabetes in Pregnancy Study Group of North America (1997-2015). Am J Perinatol. 2016 Nov;33(13):1223-6. doi: 10.1055/s-0036-1585082.
12. Driggers RW and Baschat A. The 12th meeting of the Diabetes in Pregnancy Study Group of North America (DPSG-NA): Introduction and overview. J Matern Fetal Neonatal Med. 2012 Jan;25(1):3-4. doi: 10.3109/14767058.2012.626917.
13. Langer O et al. The proceedings of the Diabetes in Pregnancy Study Group of North America 2009 conference. J Matern Fetal Neonatal Med. 2010 Mar;23(3):196-8. doi: 10.3109/14767050903550634.
14. Reece EA et al. A consensus report of the Diabetes in Pregnancy Study Group of North America Conference, Little Rock, Ark., May 2002. J Matern Fetal Neonatal Med. 2002 Dec;12(6):362-4. doi: 10.1080/jmf.12.6.362.364.
15. Reece EA and Maulik D. A consensus conference of the Diabetes in Pregnancy Study Group of North America. J Matern Fetal Neonatal Med. 2002 Dec;12(6):361. doi: 10.1080/jmf.12.6.361.361.
16. Gabbe SG. Summation of the second meeting of the Diabetes in Pregnancy Study Group of North America (DPSG-NA). J Matern Fetal Med. 2000 Jan-Feb;9(1):3-9.
17. Vital Statistics of the United States 1990: Volume I – Natality.
18. Martin JA et al. Births: final data for 2000. Natl Vital Stat Rep. 2002 Feb 12;50(5):1-101. PMID: 11876093.
19. Martin JA et al. Births: final data for 2010. Natl Vital Stat Rep. 2012 Aug 28;61(1):1-72. PMID: 24974589.
20. CDC Website. Normal weight, overweight, and obesity among adults aged 20 and over, by selected characteristics: United States.
21. Wang Y et al. Has the prevalence of overweight, obesity, and central obesity levelled off in the United States? Trends, patterns, disparities, and future projections for the obesity epidemic. Int J Epidemiol. 2020 Jun 1;49(3):810-23. doi: 10.1093/ije/dyz273.
Antidepressants ‘don’t blunt’ semaglutide and weight loss
in a post hoc analysis of the Semaglutide Treatment Effect in People with Obesity (STEP) program.
Adverse events, including psychiatric events, were slightly more usual in the patients on antidepressants, Robert Kushner, MD, noted, in an oral session at the annual meeting of the Obesity Society.
“It is very common that patients who present for weight management are taking antidepressants for various reasons, including depression, anxiety, insomnia, or chronic pain,”Dr. Kushner, from Northwestern University in Chicago, said in an email. “We wanted to see if these participants responded differently to semaglutide, compared to those not on antidepressants.”
“We found that antidepressants do not blunt the effect of semaglutide for weight loss,” he said. “However, there is a slight increase in reported adverse effects.”
“Semaglutide 2.4 mg provides an effective treatment option for weight management, regardless of antidepressant use at baseline,” Dr. Kushner summarized. “Clinicians should be assured that we can use semaglutide in this population of patients.”
Jack Yanovski, MD, PhD, said this was a “great presentation,” noting that “it’s really important that we understand what goes on in patients with depression.”
“Of course, all these trials still had rules that prevent the folks with the most severe depressive symptoms or past suicidality to participate,” added Dr. Yanovski, chief of the Growth and Obesity Section, Eunice Kennedy Shriver National Institute of Child Health and Human Development, Rockville, Md. “We need specific trials to know exactly how well we do.”
Dr. Kushner agreed, but also noted that, ever since some earlier antidepressants were associated with risk for suicidal ideation and death, strict guidelines were put in place that exclude certain patients from participating in clinical trials.
Dr. Yanovski suggested that now that the drugs are approved, it would be possible to study this, and the information would be important for clinicians.
Dr. Kushner said he hopes that such studies are forthcoming. In the meantime, “data like this will add some support and understanding,” he suggested.
36,000 Patients with obesity, 500 on antidepressants
Many people living with obesity report taking antidepressants for depression, anxiety, chronic pain, obsessive-compulsive disorder, sleep disturbance, neuropathy, panic disorder, or posttraumatic stress disorder, Dr. Kushner noted.
However, some of these medications can cause weight gain, and little is known about treatment outcomes for people with obesity who are on antidepressants, since most weight-loss studies exclude people with active major depressive disorder.
The researchers analyzed data from 1,961 patients in STEP 1 and 807 patients in STEP 2 as well as 611 patients in STEP 3 and 304 patients in STEP 5 – 3,683 participants in total, of which 539 were on antidepressants at baseline.
The patients were randomly assigned to 2.4 mg semaglutide vs. placebo plus a lifestyle intervention (STEP 1, 2, and 5) or intensive behavioral therapy (STEP 3 only), for 68 weeks, except STEP 5, which was 104 weeks.
Patients were included if they were aged 18 or older with a body mass index ≥30 kg/m2, or ≥27 kg/m2 with more than one weight-related complication (STEP 1, 3, and 5) or BMI ≥27 kg/m2 with type 2 diabetes (STEP 2 only), and at least one self-reported unsuccessful effort to lose weight by diet.
They were excluded if they had active major depressive disorder within 2 years prior to screening (or other severe psychiatric disorders such as schizophrenia or bipolar disorder) or a Patient Health Questionnaire-9 score of 15 or higher (indicating moderately severe or severe depression), or suicide ideation (type 4 or 5 on the Columbia Suicide Severity Rating Scale) or suicide behavior, within 30 days of screening.
From baseline to week 68, patients on semaglutide (with/without baseline antidepressant use) had a significantly greater change in weight vs. patients on placebo (with/without baseline antidepressant use), respectively:
- STEP 1: –15.7% / –14.7% vs. –0.2% / –2.8%
- STEP 2: –10.7% / –9.5% vs. –3.3% / –3.4%
- STEP 3: –16.2% / –15.9% vs. –5.0% / –5.9%
- STEP 5: –19.0% / –14.1% vs. +1.6% / – 4.0%.
The proportion of reported adverse events was generally slightly greater in patients receiving semaglutide (with/without baseline antidepressant use) than those on placebo (with/without baseline antidepressant use), respectively:
- STEP 1: 97.7% vs 88.6% and 92.9% vs. 86%
- STEP 2: 97.6% vs 86.5% and 88.6% vs. 77.2%
- STEP 3: 97.6% vs 95.3% and 100% vs. 95.8%
- STEP 5: 100% vs 94.8% and 95.5% vs. 89.2%.
Gastrointestinal adverse events were more frequently reported in the semaglutide group and in patients on antidepressants at baseline. The proportion of patients with psychiatric adverse events was greater in participants on antidepressants at baseline. There were no differences in suicidal ideation/behavior in patients with/without antidepressant use at baseline.
The STEP trials were funded by Novo Nordisk. Dr. Kushner discloses that he served as a consultant for Novo Nordisk, WeightWatchers, Eli Lilly, and Pfizer, and received a research grant from Epitomee.
A version of this article appeared on Medscape.com.
in a post hoc analysis of the Semaglutide Treatment Effect in People with Obesity (STEP) program.
Adverse events, including psychiatric events, were slightly more usual in the patients on antidepressants, Robert Kushner, MD, noted, in an oral session at the annual meeting of the Obesity Society.
“It is very common that patients who present for weight management are taking antidepressants for various reasons, including depression, anxiety, insomnia, or chronic pain,”Dr. Kushner, from Northwestern University in Chicago, said in an email. “We wanted to see if these participants responded differently to semaglutide, compared to those not on antidepressants.”
“We found that antidepressants do not blunt the effect of semaglutide for weight loss,” he said. “However, there is a slight increase in reported adverse effects.”
“Semaglutide 2.4 mg provides an effective treatment option for weight management, regardless of antidepressant use at baseline,” Dr. Kushner summarized. “Clinicians should be assured that we can use semaglutide in this population of patients.”
Jack Yanovski, MD, PhD, said this was a “great presentation,” noting that “it’s really important that we understand what goes on in patients with depression.”
“Of course, all these trials still had rules that prevent the folks with the most severe depressive symptoms or past suicidality to participate,” added Dr. Yanovski, chief of the Growth and Obesity Section, Eunice Kennedy Shriver National Institute of Child Health and Human Development, Rockville, Md. “We need specific trials to know exactly how well we do.”
Dr. Kushner agreed, but also noted that, ever since some earlier antidepressants were associated with risk for suicidal ideation and death, strict guidelines were put in place that exclude certain patients from participating in clinical trials.
Dr. Yanovski suggested that now that the drugs are approved, it would be possible to study this, and the information would be important for clinicians.
Dr. Kushner said he hopes that such studies are forthcoming. In the meantime, “data like this will add some support and understanding,” he suggested.
36,000 Patients with obesity, 500 on antidepressants
Many people living with obesity report taking antidepressants for depression, anxiety, chronic pain, obsessive-compulsive disorder, sleep disturbance, neuropathy, panic disorder, or posttraumatic stress disorder, Dr. Kushner noted.
However, some of these medications can cause weight gain, and little is known about treatment outcomes for people with obesity who are on antidepressants, since most weight-loss studies exclude people with active major depressive disorder.
The researchers analyzed data from 1,961 patients in STEP 1 and 807 patients in STEP 2 as well as 611 patients in STEP 3 and 304 patients in STEP 5 – 3,683 participants in total, of which 539 were on antidepressants at baseline.
The patients were randomly assigned to 2.4 mg semaglutide vs. placebo plus a lifestyle intervention (STEP 1, 2, and 5) or intensive behavioral therapy (STEP 3 only), for 68 weeks, except STEP 5, which was 104 weeks.
Patients were included if they were aged 18 or older with a body mass index ≥30 kg/m2, or ≥27 kg/m2 with more than one weight-related complication (STEP 1, 3, and 5) or BMI ≥27 kg/m2 with type 2 diabetes (STEP 2 only), and at least one self-reported unsuccessful effort to lose weight by diet.
They were excluded if they had active major depressive disorder within 2 years prior to screening (or other severe psychiatric disorders such as schizophrenia or bipolar disorder) or a Patient Health Questionnaire-9 score of 15 or higher (indicating moderately severe or severe depression), or suicide ideation (type 4 or 5 on the Columbia Suicide Severity Rating Scale) or suicide behavior, within 30 days of screening.
From baseline to week 68, patients on semaglutide (with/without baseline antidepressant use) had a significantly greater change in weight vs. patients on placebo (with/without baseline antidepressant use), respectively:
- STEP 1: –15.7% / –14.7% vs. –0.2% / –2.8%
- STEP 2: –10.7% / –9.5% vs. –3.3% / –3.4%
- STEP 3: –16.2% / –15.9% vs. –5.0% / –5.9%
- STEP 5: –19.0% / –14.1% vs. +1.6% / – 4.0%.
The proportion of reported adverse events was generally slightly greater in patients receiving semaglutide (with/without baseline antidepressant use) than those on placebo (with/without baseline antidepressant use), respectively:
- STEP 1: 97.7% vs 88.6% and 92.9% vs. 86%
- STEP 2: 97.6% vs 86.5% and 88.6% vs. 77.2%
- STEP 3: 97.6% vs 95.3% and 100% vs. 95.8%
- STEP 5: 100% vs 94.8% and 95.5% vs. 89.2%.
Gastrointestinal adverse events were more frequently reported in the semaglutide group and in patients on antidepressants at baseline. The proportion of patients with psychiatric adverse events was greater in participants on antidepressants at baseline. There were no differences in suicidal ideation/behavior in patients with/without antidepressant use at baseline.
The STEP trials were funded by Novo Nordisk. Dr. Kushner discloses that he served as a consultant for Novo Nordisk, WeightWatchers, Eli Lilly, and Pfizer, and received a research grant from Epitomee.
A version of this article appeared on Medscape.com.
in a post hoc analysis of the Semaglutide Treatment Effect in People with Obesity (STEP) program.
Adverse events, including psychiatric events, were slightly more usual in the patients on antidepressants, Robert Kushner, MD, noted, in an oral session at the annual meeting of the Obesity Society.
“It is very common that patients who present for weight management are taking antidepressants for various reasons, including depression, anxiety, insomnia, or chronic pain,”Dr. Kushner, from Northwestern University in Chicago, said in an email. “We wanted to see if these participants responded differently to semaglutide, compared to those not on antidepressants.”
“We found that antidepressants do not blunt the effect of semaglutide for weight loss,” he said. “However, there is a slight increase in reported adverse effects.”
“Semaglutide 2.4 mg provides an effective treatment option for weight management, regardless of antidepressant use at baseline,” Dr. Kushner summarized. “Clinicians should be assured that we can use semaglutide in this population of patients.”
Jack Yanovski, MD, PhD, said this was a “great presentation,” noting that “it’s really important that we understand what goes on in patients with depression.”
“Of course, all these trials still had rules that prevent the folks with the most severe depressive symptoms or past suicidality to participate,” added Dr. Yanovski, chief of the Growth and Obesity Section, Eunice Kennedy Shriver National Institute of Child Health and Human Development, Rockville, Md. “We need specific trials to know exactly how well we do.”
Dr. Kushner agreed, but also noted that, ever since some earlier antidepressants were associated with risk for suicidal ideation and death, strict guidelines were put in place that exclude certain patients from participating in clinical trials.
Dr. Yanovski suggested that now that the drugs are approved, it would be possible to study this, and the information would be important for clinicians.
Dr. Kushner said he hopes that such studies are forthcoming. In the meantime, “data like this will add some support and understanding,” he suggested.
36,000 Patients with obesity, 500 on antidepressants
Many people living with obesity report taking antidepressants for depression, anxiety, chronic pain, obsessive-compulsive disorder, sleep disturbance, neuropathy, panic disorder, or posttraumatic stress disorder, Dr. Kushner noted.
However, some of these medications can cause weight gain, and little is known about treatment outcomes for people with obesity who are on antidepressants, since most weight-loss studies exclude people with active major depressive disorder.
The researchers analyzed data from 1,961 patients in STEP 1 and 807 patients in STEP 2 as well as 611 patients in STEP 3 and 304 patients in STEP 5 – 3,683 participants in total, of which 539 were on antidepressants at baseline.
The patients were randomly assigned to 2.4 mg semaglutide vs. placebo plus a lifestyle intervention (STEP 1, 2, and 5) or intensive behavioral therapy (STEP 3 only), for 68 weeks, except STEP 5, which was 104 weeks.
Patients were included if they were aged 18 or older with a body mass index ≥30 kg/m2, or ≥27 kg/m2 with more than one weight-related complication (STEP 1, 3, and 5) or BMI ≥27 kg/m2 with type 2 diabetes (STEP 2 only), and at least one self-reported unsuccessful effort to lose weight by diet.
They were excluded if they had active major depressive disorder within 2 years prior to screening (or other severe psychiatric disorders such as schizophrenia or bipolar disorder) or a Patient Health Questionnaire-9 score of 15 or higher (indicating moderately severe or severe depression), or suicide ideation (type 4 or 5 on the Columbia Suicide Severity Rating Scale) or suicide behavior, within 30 days of screening.
From baseline to week 68, patients on semaglutide (with/without baseline antidepressant use) had a significantly greater change in weight vs. patients on placebo (with/without baseline antidepressant use), respectively:
- STEP 1: –15.7% / –14.7% vs. –0.2% / –2.8%
- STEP 2: –10.7% / –9.5% vs. –3.3% / –3.4%
- STEP 3: –16.2% / –15.9% vs. –5.0% / –5.9%
- STEP 5: –19.0% / –14.1% vs. +1.6% / – 4.0%.
The proportion of reported adverse events was generally slightly greater in patients receiving semaglutide (with/without baseline antidepressant use) than those on placebo (with/without baseline antidepressant use), respectively:
- STEP 1: 97.7% vs 88.6% and 92.9% vs. 86%
- STEP 2: 97.6% vs 86.5% and 88.6% vs. 77.2%
- STEP 3: 97.6% vs 95.3% and 100% vs. 95.8%
- STEP 5: 100% vs 94.8% and 95.5% vs. 89.2%.
Gastrointestinal adverse events were more frequently reported in the semaglutide group and in patients on antidepressants at baseline. The proportion of patients with psychiatric adverse events was greater in participants on antidepressants at baseline. There were no differences in suicidal ideation/behavior in patients with/without antidepressant use at baseline.
The STEP trials were funded by Novo Nordisk. Dr. Kushner discloses that he served as a consultant for Novo Nordisk, WeightWatchers, Eli Lilly, and Pfizer, and received a research grant from Epitomee.
A version of this article appeared on Medscape.com.
FROM OBESITYWEEK® 2023
Real-time, blood-sensing capsule accurately diagnoses UGIB in 7 minutes and may help patient triage
COPENHAGEN – , according to results from the first U.S.-based open-label, single-arm comparative clinical trial of a novel bleeding sensor for patients with suspected UGIB. It is also the largest such trial.
The capsule (PillSense, EnteraSense) is rapidly deployed, safe to use, and easy to interpret, study researchers say. In under 7 minutes, it correctly detected the presence of blood in 26 of 28 patients and its absence in 87 of 96 patients, as confirmed afterward by esophagogastroduodenoscopy (EGD).
“The use of the PillSense system will positively impact patient outcomes by providing early diagnosis, triaging, and directing care for UGIB,” said Karl Akiki, MD, study lead, who is in the division of gastroenterology and hepatology at the Mayo Clinic, Rochester, Minn. He presented the results at the annual United European Gastroenterology Week.
“Due to its ability to rapidly diagnose UGIB, it helps us, as doctors, expedite accurate clinical decision-making while also optimizing services to ensure the maximum number of patients obtain the best outcome,” he told this news organization.
“There are some pre-endoscopic assessment scores, like the Rockell or the Glasgow-Blatchford score, but they have limited clinical utility in predicting and confirming bleeding in suspected patients,” explained Dr. Akiki. He highlighted the need for a novel device that is rapid, accurate, and safe to use. He also pointed out that despite being the gold standard for diagnosis, EGD remains challenging in terms of time, personnel, and resources.
“The results of our study show the PillSense is a good diagnostic tool that will aid triage,” he said. He noted that PillSense and EGD supplement each other in patient care.
It’s not a device to replace the EGD itself,” he explained, but given the results from the capsule, it will act “as a kind of a bridge that helps us to determine which patients should undergo EGD.”
Optical sensing technology
The researchers aimed to assess the safety and efficacy of the PillSense system for patients with suspected UGIB. They enrolled 131 patients (mean age, 62 years), 60% of whom were men. The most common presenting symptoms for UGIB were melena (52%), anemia (41%), and hematemesis (15%). Five participants withdrew consent before capsule ingestion, and for two patients, primary endpoint data were missing. This left an intent-to-treat population of 124 patients; 110 completed the study.
Patients were asked to swallow the capsule and to lay on their left side. The PillSense is based on optical sensing technology that uses an optical signature of blood in the gut. The device differentiates blood from any other liquids that may be present. After 5-7 minutes, the device gathers and transmits data wirelessly to an external, handheld receiver that processes binary data and indicates either “blood detected” or “no blood detected” in the upper GI tract, explained Dr. Akiki.
Following the capsule reading, patients underwent EGD within 4 hours. This enabled the researchers to compare data between the two modalities. Follow-up visits were conducted on days 7, 14, and 21 to ensure the capsule had passed from the body. Endoscopists were blinded to the capsule result when reading the EGD.
Primary endpoints were the sensitivity and specificity of the device; secondary endpoints were positive predictive value, negative predictive value, successful passage of the capsule, and safety.
Rapid and accurate
The researchers determined the efficiency of the capsule in correctly detecting a UGIB. The capsule’s positive and negative predictive values were 74.3% and 97.8%, respectively.
“We achieved a sensitivity of around 93% (92.9%; P = 0.024) with the PillSense capsule and a specificity of 91% (90.6%; P < .001]), which were pretty good. We also detected a range from minimal bleeding – so, speckles of blood to large amounts of active bleeding covering the entire stomach,” reported Dr. Akiki.
There were no differences in terms of patient demographics, laboratory results, or concomitant use of medications. PillSense recording time was a mean of 6.71 minutes, the time from capsule ingestion to EGD was a mean of 55 minutes, and the time to capsule passage through the GI tract was 3.6 days. Most bleeds were found to be in the stomach (18/30; 60%), followed by the duodenum (5/30; 16.6%).
Various capsules for detecting UGIB are under development or are already available, but unlike some of the others, “[the PillSense] is not a video capsule,” said Dr. Akiki. “It does not take pictures at all but is more of a photo sensor capsule that measures the absorption of wavelengths.”
This explains why the PillSense was so rapid – results were available in around 7 minutes and did not require an interpretation by a physician, he explained. “Trained non-physician personnel can use it, and this is where it differs from other devices, such as video capsules that require someone highly trained to interpret the output. It’s an easy procedure and process to follow.”
The PillSense has value in improving workflow, Dr. Akiki said. “If we had someone come in during the night with a suspected upper GI bleed, we could give them the capsule, determine if they need an EGD or not, and potentially postpone it to a time – say, the morning, when more resources are available – freeing up the night for emergency cases. It helps me, as a physician, to determine which patients to send to EGD immediately or which to wait.”
He added that more studies are needed in the postmarketing phase to understand optimal use of the device and to define the exact clinical pathway for optimal implementation.
The device was approved by the U.S. Food and Drug Administration in February. Dr. Akiki noted that there were no adverse events or deaths related to the capsule.
Co-moderator, Philip Chiu, MD, a gastroenterologist from the Chinese University of Hong Kong, said, “It’s an interesting study, because sometimes we can’t differentiate by clinical symptoms as to whether this is a problem of continuous bleeding or something else. The capsule might help us in our decision-making in this respect and help determine whether we should scope the patients or just manage conservatively.”
Dr. Akiki and Dr. Chiu have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
COPENHAGEN – , according to results from the first U.S.-based open-label, single-arm comparative clinical trial of a novel bleeding sensor for patients with suspected UGIB. It is also the largest such trial.
The capsule (PillSense, EnteraSense) is rapidly deployed, safe to use, and easy to interpret, study researchers say. In under 7 minutes, it correctly detected the presence of blood in 26 of 28 patients and its absence in 87 of 96 patients, as confirmed afterward by esophagogastroduodenoscopy (EGD).
“The use of the PillSense system will positively impact patient outcomes by providing early diagnosis, triaging, and directing care for UGIB,” said Karl Akiki, MD, study lead, who is in the division of gastroenterology and hepatology at the Mayo Clinic, Rochester, Minn. He presented the results at the annual United European Gastroenterology Week.
“Due to its ability to rapidly diagnose UGIB, it helps us, as doctors, expedite accurate clinical decision-making while also optimizing services to ensure the maximum number of patients obtain the best outcome,” he told this news organization.
“There are some pre-endoscopic assessment scores, like the Rockell or the Glasgow-Blatchford score, but they have limited clinical utility in predicting and confirming bleeding in suspected patients,” explained Dr. Akiki. He highlighted the need for a novel device that is rapid, accurate, and safe to use. He also pointed out that despite being the gold standard for diagnosis, EGD remains challenging in terms of time, personnel, and resources.
“The results of our study show the PillSense is a good diagnostic tool that will aid triage,” he said. He noted that PillSense and EGD supplement each other in patient care.
It’s not a device to replace the EGD itself,” he explained, but given the results from the capsule, it will act “as a kind of a bridge that helps us to determine which patients should undergo EGD.”
Optical sensing technology
The researchers aimed to assess the safety and efficacy of the PillSense system for patients with suspected UGIB. They enrolled 131 patients (mean age, 62 years), 60% of whom were men. The most common presenting symptoms for UGIB were melena (52%), anemia (41%), and hematemesis (15%). Five participants withdrew consent before capsule ingestion, and for two patients, primary endpoint data were missing. This left an intent-to-treat population of 124 patients; 110 completed the study.
Patients were asked to swallow the capsule and to lay on their left side. The PillSense is based on optical sensing technology that uses an optical signature of blood in the gut. The device differentiates blood from any other liquids that may be present. After 5-7 minutes, the device gathers and transmits data wirelessly to an external, handheld receiver that processes binary data and indicates either “blood detected” or “no blood detected” in the upper GI tract, explained Dr. Akiki.
Following the capsule reading, patients underwent EGD within 4 hours. This enabled the researchers to compare data between the two modalities. Follow-up visits were conducted on days 7, 14, and 21 to ensure the capsule had passed from the body. Endoscopists were blinded to the capsule result when reading the EGD.
Primary endpoints were the sensitivity and specificity of the device; secondary endpoints were positive predictive value, negative predictive value, successful passage of the capsule, and safety.
Rapid and accurate
The researchers determined the efficiency of the capsule in correctly detecting a UGIB. The capsule’s positive and negative predictive values were 74.3% and 97.8%, respectively.
“We achieved a sensitivity of around 93% (92.9%; P = 0.024) with the PillSense capsule and a specificity of 91% (90.6%; P < .001]), which were pretty good. We also detected a range from minimal bleeding – so, speckles of blood to large amounts of active bleeding covering the entire stomach,” reported Dr. Akiki.
There were no differences in terms of patient demographics, laboratory results, or concomitant use of medications. PillSense recording time was a mean of 6.71 minutes, the time from capsule ingestion to EGD was a mean of 55 minutes, and the time to capsule passage through the GI tract was 3.6 days. Most bleeds were found to be in the stomach (18/30; 60%), followed by the duodenum (5/30; 16.6%).
Various capsules for detecting UGIB are under development or are already available, but unlike some of the others, “[the PillSense] is not a video capsule,” said Dr. Akiki. “It does not take pictures at all but is more of a photo sensor capsule that measures the absorption of wavelengths.”
This explains why the PillSense was so rapid – results were available in around 7 minutes and did not require an interpretation by a physician, he explained. “Trained non-physician personnel can use it, and this is where it differs from other devices, such as video capsules that require someone highly trained to interpret the output. It’s an easy procedure and process to follow.”
The PillSense has value in improving workflow, Dr. Akiki said. “If we had someone come in during the night with a suspected upper GI bleed, we could give them the capsule, determine if they need an EGD or not, and potentially postpone it to a time – say, the morning, when more resources are available – freeing up the night for emergency cases. It helps me, as a physician, to determine which patients to send to EGD immediately or which to wait.”
He added that more studies are needed in the postmarketing phase to understand optimal use of the device and to define the exact clinical pathway for optimal implementation.
The device was approved by the U.S. Food and Drug Administration in February. Dr. Akiki noted that there were no adverse events or deaths related to the capsule.
Co-moderator, Philip Chiu, MD, a gastroenterologist from the Chinese University of Hong Kong, said, “It’s an interesting study, because sometimes we can’t differentiate by clinical symptoms as to whether this is a problem of continuous bleeding or something else. The capsule might help us in our decision-making in this respect and help determine whether we should scope the patients or just manage conservatively.”
Dr. Akiki and Dr. Chiu have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
COPENHAGEN – , according to results from the first U.S.-based open-label, single-arm comparative clinical trial of a novel bleeding sensor for patients with suspected UGIB. It is also the largest such trial.
The capsule (PillSense, EnteraSense) is rapidly deployed, safe to use, and easy to interpret, study researchers say. In under 7 minutes, it correctly detected the presence of blood in 26 of 28 patients and its absence in 87 of 96 patients, as confirmed afterward by esophagogastroduodenoscopy (EGD).
“The use of the PillSense system will positively impact patient outcomes by providing early diagnosis, triaging, and directing care for UGIB,” said Karl Akiki, MD, study lead, who is in the division of gastroenterology and hepatology at the Mayo Clinic, Rochester, Minn. He presented the results at the annual United European Gastroenterology Week.
“Due to its ability to rapidly diagnose UGIB, it helps us, as doctors, expedite accurate clinical decision-making while also optimizing services to ensure the maximum number of patients obtain the best outcome,” he told this news organization.
“There are some pre-endoscopic assessment scores, like the Rockell or the Glasgow-Blatchford score, but they have limited clinical utility in predicting and confirming bleeding in suspected patients,” explained Dr. Akiki. He highlighted the need for a novel device that is rapid, accurate, and safe to use. He also pointed out that despite being the gold standard for diagnosis, EGD remains challenging in terms of time, personnel, and resources.
“The results of our study show the PillSense is a good diagnostic tool that will aid triage,” he said. He noted that PillSense and EGD supplement each other in patient care.
It’s not a device to replace the EGD itself,” he explained, but given the results from the capsule, it will act “as a kind of a bridge that helps us to determine which patients should undergo EGD.”
Optical sensing technology
The researchers aimed to assess the safety and efficacy of the PillSense system for patients with suspected UGIB. They enrolled 131 patients (mean age, 62 years), 60% of whom were men. The most common presenting symptoms for UGIB were melena (52%), anemia (41%), and hematemesis (15%). Five participants withdrew consent before capsule ingestion, and for two patients, primary endpoint data were missing. This left an intent-to-treat population of 124 patients; 110 completed the study.
Patients were asked to swallow the capsule and to lay on their left side. The PillSense is based on optical sensing technology that uses an optical signature of blood in the gut. The device differentiates blood from any other liquids that may be present. After 5-7 minutes, the device gathers and transmits data wirelessly to an external, handheld receiver that processes binary data and indicates either “blood detected” or “no blood detected” in the upper GI tract, explained Dr. Akiki.
Following the capsule reading, patients underwent EGD within 4 hours. This enabled the researchers to compare data between the two modalities. Follow-up visits were conducted on days 7, 14, and 21 to ensure the capsule had passed from the body. Endoscopists were blinded to the capsule result when reading the EGD.
Primary endpoints were the sensitivity and specificity of the device; secondary endpoints were positive predictive value, negative predictive value, successful passage of the capsule, and safety.
Rapid and accurate
The researchers determined the efficiency of the capsule in correctly detecting a UGIB. The capsule’s positive and negative predictive values were 74.3% and 97.8%, respectively.
“We achieved a sensitivity of around 93% (92.9%; P = 0.024) with the PillSense capsule and a specificity of 91% (90.6%; P < .001]), which were pretty good. We also detected a range from minimal bleeding – so, speckles of blood to large amounts of active bleeding covering the entire stomach,” reported Dr. Akiki.
There were no differences in terms of patient demographics, laboratory results, or concomitant use of medications. PillSense recording time was a mean of 6.71 minutes, the time from capsule ingestion to EGD was a mean of 55 minutes, and the time to capsule passage through the GI tract was 3.6 days. Most bleeds were found to be in the stomach (18/30; 60%), followed by the duodenum (5/30; 16.6%).
Various capsules for detecting UGIB are under development or are already available, but unlike some of the others, “[the PillSense] is not a video capsule,” said Dr. Akiki. “It does not take pictures at all but is more of a photo sensor capsule that measures the absorption of wavelengths.”
This explains why the PillSense was so rapid – results were available in around 7 minutes and did not require an interpretation by a physician, he explained. “Trained non-physician personnel can use it, and this is where it differs from other devices, such as video capsules that require someone highly trained to interpret the output. It’s an easy procedure and process to follow.”
The PillSense has value in improving workflow, Dr. Akiki said. “If we had someone come in during the night with a suspected upper GI bleed, we could give them the capsule, determine if they need an EGD or not, and potentially postpone it to a time – say, the morning, when more resources are available – freeing up the night for emergency cases. It helps me, as a physician, to determine which patients to send to EGD immediately or which to wait.”
He added that more studies are needed in the postmarketing phase to understand optimal use of the device and to define the exact clinical pathway for optimal implementation.
The device was approved by the U.S. Food and Drug Administration in February. Dr. Akiki noted that there were no adverse events or deaths related to the capsule.
Co-moderator, Philip Chiu, MD, a gastroenterologist from the Chinese University of Hong Kong, said, “It’s an interesting study, because sometimes we can’t differentiate by clinical symptoms as to whether this is a problem of continuous bleeding or something else. The capsule might help us in our decision-making in this respect and help determine whether we should scope the patients or just manage conservatively.”
Dr. Akiki and Dr. Chiu have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
AT UEG WEEK 2023
Endoscopic remission doubled with risankizumab vs. ustekinumab in Crohn’s disease
AT UEG WEEK 2023
COPENHAGEN – (CD) who have failed one or more anti–tumor necrosis factor (anti-TNF) therapies, according to the results of the phase 3 SEQUENCE trial.
Secondary endpoints – presented for the first time at the United European Gastroenterology Week 2023 – also showed superiority of risankizumab (Skyrizi, AbbVie), an interleulin-23 inhibitor, over ustekinumab (Stelara), an IL-12 and IL-23 inhibitor, for clinical remission at week 48 (60.8% vs. 40.8%) and a statistically significant endoscopic response also favoring risankizumab at weeks 24 and 48.
“With endoscopic remission we see that with a single agent we have doubled the endoscopic remission rate by moving from 16% to 31% with risankizumab [at week 48],” said Laurent Peyrin-Biroulet, MD, PhD, a gastroenterologist specializing in inflammatory bowel disease at Nancy University Hospital, France. “Superiority for sure was met.”
“This sort of thing happens once in your career,” noted Dr. Peyrin-Biroulet, who presented the results of the study at the meeting. “It’s totally amazing that everything you see here was in favor of risankizumab.
“Already we see the efficacy signal in the proportion of premature discontinuations at 2% vs. 13% due to lack of efficacy [in risankizumab and ustekinumab, respectively],” he said. “This is due to drug failure.”
Risankizumab is an IL-23 inhibitor that selectively blocks the cytokine IL-23, thought to be linked to a number of chronic immune-mediated diseases, by binding to its p19 subunit. It is the first IL-23 inhibitor to receive approval from the U.S. Food and Drug Administration in June 2022 for moderately to severely active CD based on data from the ADVANCE, MOTIVATE, and FORTIFY trials.
Risankizumab and ustekinumab head-to-head
The phase 3, open-label, multicenter, randomized, clinical trial evaluated risankizumab vs. ustekinumab through week 48 in patients with moderately to severely active CD.
Participants were required to have a CD Activity Index (CDAI) score of 220 to 450 at baseline, a Simple Endoscopic Score for Crohn’s Disease (SES-CD) of 6 or more for ileocolonic or colonic disease (and of 4 or more for isolated ileal disease), excluding the presence of a narrowing component, plus an average daily stool frequency of four or more and/or average daily abdominal pain score of 2 or more. They were also required to have previously failed one or more anti-TNF therapies.
Randomization was stratified by the number of anti-TNF therapies failed (one or more than one), and steroid use at baseline; steroids were then tapered from week 2. Two primary endpoints comprised clinical remission at week 24 (defined as CDAI < 150, noninferiority margin within 10% of risankizumab vs ustekinumab in 50% of participants), and also endoscopic remission (SES-CD of 4 or less, and at least a 2-point reduction vs. baseline and no subscore greater than 1 in any individual component) at week 48 demonstrating superiority of risankizumab vs ustekinumab.
Secondary endpoints included clinical remission at week 48, endoscopic response at weeks 48 and 24, steroid-free endoscopic remission at week 48, and steroid-free clinical remission at week 48 (all tested for superiority of risankizumab vs ustekinumab).
Intravenous risankizumab at 600 mg was given at weeks 0, 4 , and 8 followed by subcutaneous risankizumab at a 360-mg maintenance dose every 8 weeks through week 48 (n = 255). Participants who completed the week-48 visit continued on subcutaneous risankizumab for up to an additional 220 weeks. Ustekinumab was given as a weight-based, intravenous induction dose at week 0 followed by a 90-mg subcutaneous dose every 8 weeks, starting at week 8 through week 48 (n = 265). Participants received open-label drug administration but efficacy assessment was blinded.
Superiority of risankizumab
Both primary endpoints were met. For clinical remission at week 24, in half of the patients enrolled, rates were 58.6% (75/128) for risankizumab and 39.5% (54/137) for ustekinumab, for a difference of 18.4% [95% confidence interval, 6.6-30.3], meaning that noninferiority was met within the predefined margin of 10%. The second primary endpoint of endoscopic remission at week 48 showed rates of 31.8% (81/255) for risankizumab and 16.2% (43/265) for ustekinumab (P < .0001 for superiority).
Risankizumab was found to be superior to ustekinumab for all secondary endpoints (all with P < .0001). Steroid-free endoscopic remission at week 48 showed a 16% difference, and steroid-free clinical remission at week 48 showed a 20% difference – both in favor of risankizumab.
In addition, more participants on risankizumab completed the study (89.4%) than those on ustekinumab (74.0%), Dr. Peyrin-Biroulet reported.
Adverse event rates (events per 100 person-years) were comparable between the two drugs at 341.2 for risankizumab and 282.7 for ustekinumab. For risankizumab, no new safety risks were observed, and those recorded were consistent with the known safety profile. Serious adverse events occurred in 10% of risankizumab-treated patients, and 17% of ustekinumab-treated patients.
“We know the safety of IL-23 inhibitors is good,” said Dr. Peyrin-Biroulet. “If we look at all adverse events there was no difference across arms, and in terms of serious adverse events, it was in favor of risankizumab because a CD flare is considered a serious adverse event.”
Session comoderator, Alessandro Armuzzi, MD, head of the Inflammatory Bowel Disease Center at the IRCCS Humanitas Research Hospital in Milan, commented on the findings. “The results look in favor of risankizumab – all the endpoints were met, not only the co-endpoints but also the secondary endpoints too,” he said.
These results, showing a preference for risankizumab, have value in helping clinicians with the sequence of therapies when patients with Crohn’s disease have failed one or more TNF inhibitor, said Dr. Armuzzi.
No funding for this study was disclosed. Dr. Peyrin-Biroulet has disclosed receiving fees from Galapagos, AbbVie, Janssen, Genentech, Alimentiv, Ferring, Tillots, Celltrion, Takeda, Pfizer, Index, Sandoz, Celgene, Biogen, SamsungBioepis, Inotrem, Allergan, MSD, Roche, Arena, Gilead, Amgen, BMS, Vifor, Norgine, Mylan, Lilly, Fresenius Kabi, OSEImmunotherapeutics, Enthera, Theravance, Pandion, Gossamer, Viatris, ThermoFisher, ONOPharma, Mopac, Cytoki, Morphic, Prometheus, and Applied MolecularTransport. Dr. Armuzzi disclosed consulting/advisory board fees from AbbVie, Amgen, Arena, Biogen, Boehringer Ingelheim, Bristol-Myers Squibb, Celgene, Celltrion, Eli-Lilly, Ferring, Galapagos, Gilead, Janssen, Lionhealth, MSD, Nestlé, Pfizer, Protagonist Therapeutics, Roche, Samsung Bioepis, Sandoz, Takeda, and Tillots Pharma; speaker’s fees from AbbVie, Amgen, Arena, Biogen, Bristol-Myers Squibb, Eli-Lilly, Ferring, Galapagos, Gilead, Janssen, Lionhealth, MSD, Novartis, Pfizer, Roche, Samsung Bioepis, Sandoz, and Takeda; and research grants from MSD, Takeda, Pfizer, and Biogen.
A version of this article first appeared on Medscape.com.
AT UEG WEEK 2023
COPENHAGEN – (CD) who have failed one or more anti–tumor necrosis factor (anti-TNF) therapies, according to the results of the phase 3 SEQUENCE trial.
Secondary endpoints – presented for the first time at the United European Gastroenterology Week 2023 – also showed superiority of risankizumab (Skyrizi, AbbVie), an interleulin-23 inhibitor, over ustekinumab (Stelara), an IL-12 and IL-23 inhibitor, for clinical remission at week 48 (60.8% vs. 40.8%) and a statistically significant endoscopic response also favoring risankizumab at weeks 24 and 48.
“With endoscopic remission we see that with a single agent we have doubled the endoscopic remission rate by moving from 16% to 31% with risankizumab [at week 48],” said Laurent Peyrin-Biroulet, MD, PhD, a gastroenterologist specializing in inflammatory bowel disease at Nancy University Hospital, France. “Superiority for sure was met.”
“This sort of thing happens once in your career,” noted Dr. Peyrin-Biroulet, who presented the results of the study at the meeting. “It’s totally amazing that everything you see here was in favor of risankizumab.
“Already we see the efficacy signal in the proportion of premature discontinuations at 2% vs. 13% due to lack of efficacy [in risankizumab and ustekinumab, respectively],” he said. “This is due to drug failure.”
Risankizumab is an IL-23 inhibitor that selectively blocks the cytokine IL-23, thought to be linked to a number of chronic immune-mediated diseases, by binding to its p19 subunit. It is the first IL-23 inhibitor to receive approval from the U.S. Food and Drug Administration in June 2022 for moderately to severely active CD based on data from the ADVANCE, MOTIVATE, and FORTIFY trials.
Risankizumab and ustekinumab head-to-head
The phase 3, open-label, multicenter, randomized, clinical trial evaluated risankizumab vs. ustekinumab through week 48 in patients with moderately to severely active CD.
Participants were required to have a CD Activity Index (CDAI) score of 220 to 450 at baseline, a Simple Endoscopic Score for Crohn’s Disease (SES-CD) of 6 or more for ileocolonic or colonic disease (and of 4 or more for isolated ileal disease), excluding the presence of a narrowing component, plus an average daily stool frequency of four or more and/or average daily abdominal pain score of 2 or more. They were also required to have previously failed one or more anti-TNF therapies.
Randomization was stratified by the number of anti-TNF therapies failed (one or more than one), and steroid use at baseline; steroids were then tapered from week 2. Two primary endpoints comprised clinical remission at week 24 (defined as CDAI < 150, noninferiority margin within 10% of risankizumab vs ustekinumab in 50% of participants), and also endoscopic remission (SES-CD of 4 or less, and at least a 2-point reduction vs. baseline and no subscore greater than 1 in any individual component) at week 48 demonstrating superiority of risankizumab vs ustekinumab.
Secondary endpoints included clinical remission at week 48, endoscopic response at weeks 48 and 24, steroid-free endoscopic remission at week 48, and steroid-free clinical remission at week 48 (all tested for superiority of risankizumab vs ustekinumab).
Intravenous risankizumab at 600 mg was given at weeks 0, 4 , and 8 followed by subcutaneous risankizumab at a 360-mg maintenance dose every 8 weeks through week 48 (n = 255). Participants who completed the week-48 visit continued on subcutaneous risankizumab for up to an additional 220 weeks. Ustekinumab was given as a weight-based, intravenous induction dose at week 0 followed by a 90-mg subcutaneous dose every 8 weeks, starting at week 8 through week 48 (n = 265). Participants received open-label drug administration but efficacy assessment was blinded.
Superiority of risankizumab
Both primary endpoints were met. For clinical remission at week 24, in half of the patients enrolled, rates were 58.6% (75/128) for risankizumab and 39.5% (54/137) for ustekinumab, for a difference of 18.4% [95% confidence interval, 6.6-30.3], meaning that noninferiority was met within the predefined margin of 10%. The second primary endpoint of endoscopic remission at week 48 showed rates of 31.8% (81/255) for risankizumab and 16.2% (43/265) for ustekinumab (P < .0001 for superiority).
Risankizumab was found to be superior to ustekinumab for all secondary endpoints (all with P < .0001). Steroid-free endoscopic remission at week 48 showed a 16% difference, and steroid-free clinical remission at week 48 showed a 20% difference – both in favor of risankizumab.
In addition, more participants on risankizumab completed the study (89.4%) than those on ustekinumab (74.0%), Dr. Peyrin-Biroulet reported.
Adverse event rates (events per 100 person-years) were comparable between the two drugs at 341.2 for risankizumab and 282.7 for ustekinumab. For risankizumab, no new safety risks were observed, and those recorded were consistent with the known safety profile. Serious adverse events occurred in 10% of risankizumab-treated patients, and 17% of ustekinumab-treated patients.
“We know the safety of IL-23 inhibitors is good,” said Dr. Peyrin-Biroulet. “If we look at all adverse events there was no difference across arms, and in terms of serious adverse events, it was in favor of risankizumab because a CD flare is considered a serious adverse event.”
Session comoderator, Alessandro Armuzzi, MD, head of the Inflammatory Bowel Disease Center at the IRCCS Humanitas Research Hospital in Milan, commented on the findings. “The results look in favor of risankizumab – all the endpoints were met, not only the co-endpoints but also the secondary endpoints too,” he said.
These results, showing a preference for risankizumab, have value in helping clinicians with the sequence of therapies when patients with Crohn’s disease have failed one or more TNF inhibitor, said Dr. Armuzzi.
No funding for this study was disclosed. Dr. Peyrin-Biroulet has disclosed receiving fees from Galapagos, AbbVie, Janssen, Genentech, Alimentiv, Ferring, Tillots, Celltrion, Takeda, Pfizer, Index, Sandoz, Celgene, Biogen, SamsungBioepis, Inotrem, Allergan, MSD, Roche, Arena, Gilead, Amgen, BMS, Vifor, Norgine, Mylan, Lilly, Fresenius Kabi, OSEImmunotherapeutics, Enthera, Theravance, Pandion, Gossamer, Viatris, ThermoFisher, ONOPharma, Mopac, Cytoki, Morphic, Prometheus, and Applied MolecularTransport. Dr. Armuzzi disclosed consulting/advisory board fees from AbbVie, Amgen, Arena, Biogen, Boehringer Ingelheim, Bristol-Myers Squibb, Celgene, Celltrion, Eli-Lilly, Ferring, Galapagos, Gilead, Janssen, Lionhealth, MSD, Nestlé, Pfizer, Protagonist Therapeutics, Roche, Samsung Bioepis, Sandoz, Takeda, and Tillots Pharma; speaker’s fees from AbbVie, Amgen, Arena, Biogen, Bristol-Myers Squibb, Eli-Lilly, Ferring, Galapagos, Gilead, Janssen, Lionhealth, MSD, Novartis, Pfizer, Roche, Samsung Bioepis, Sandoz, and Takeda; and research grants from MSD, Takeda, Pfizer, and Biogen.
A version of this article first appeared on Medscape.com.
AT UEG WEEK 2023
COPENHAGEN – (CD) who have failed one or more anti–tumor necrosis factor (anti-TNF) therapies, according to the results of the phase 3 SEQUENCE trial.
Secondary endpoints – presented for the first time at the United European Gastroenterology Week 2023 – also showed superiority of risankizumab (Skyrizi, AbbVie), an interleulin-23 inhibitor, over ustekinumab (Stelara), an IL-12 and IL-23 inhibitor, for clinical remission at week 48 (60.8% vs. 40.8%) and a statistically significant endoscopic response also favoring risankizumab at weeks 24 and 48.
“With endoscopic remission we see that with a single agent we have doubled the endoscopic remission rate by moving from 16% to 31% with risankizumab [at week 48],” said Laurent Peyrin-Biroulet, MD, PhD, a gastroenterologist specializing in inflammatory bowel disease at Nancy University Hospital, France. “Superiority for sure was met.”
“This sort of thing happens once in your career,” noted Dr. Peyrin-Biroulet, who presented the results of the study at the meeting. “It’s totally amazing that everything you see here was in favor of risankizumab.
“Already we see the efficacy signal in the proportion of premature discontinuations at 2% vs. 13% due to lack of efficacy [in risankizumab and ustekinumab, respectively],” he said. “This is due to drug failure.”
Risankizumab is an IL-23 inhibitor that selectively blocks the cytokine IL-23, thought to be linked to a number of chronic immune-mediated diseases, by binding to its p19 subunit. It is the first IL-23 inhibitor to receive approval from the U.S. Food and Drug Administration in June 2022 for moderately to severely active CD based on data from the ADVANCE, MOTIVATE, and FORTIFY trials.
Risankizumab and ustekinumab head-to-head
The phase 3, open-label, multicenter, randomized, clinical trial evaluated risankizumab vs. ustekinumab through week 48 in patients with moderately to severely active CD.
Participants were required to have a CD Activity Index (CDAI) score of 220 to 450 at baseline, a Simple Endoscopic Score for Crohn’s Disease (SES-CD) of 6 or more for ileocolonic or colonic disease (and of 4 or more for isolated ileal disease), excluding the presence of a narrowing component, plus an average daily stool frequency of four or more and/or average daily abdominal pain score of 2 or more. They were also required to have previously failed one or more anti-TNF therapies.
Randomization was stratified by the number of anti-TNF therapies failed (one or more than one), and steroid use at baseline; steroids were then tapered from week 2. Two primary endpoints comprised clinical remission at week 24 (defined as CDAI < 150, noninferiority margin within 10% of risankizumab vs ustekinumab in 50% of participants), and also endoscopic remission (SES-CD of 4 or less, and at least a 2-point reduction vs. baseline and no subscore greater than 1 in any individual component) at week 48 demonstrating superiority of risankizumab vs ustekinumab.
Secondary endpoints included clinical remission at week 48, endoscopic response at weeks 48 and 24, steroid-free endoscopic remission at week 48, and steroid-free clinical remission at week 48 (all tested for superiority of risankizumab vs ustekinumab).
Intravenous risankizumab at 600 mg was given at weeks 0, 4 , and 8 followed by subcutaneous risankizumab at a 360-mg maintenance dose every 8 weeks through week 48 (n = 255). Participants who completed the week-48 visit continued on subcutaneous risankizumab for up to an additional 220 weeks. Ustekinumab was given as a weight-based, intravenous induction dose at week 0 followed by a 90-mg subcutaneous dose every 8 weeks, starting at week 8 through week 48 (n = 265). Participants received open-label drug administration but efficacy assessment was blinded.
Superiority of risankizumab
Both primary endpoints were met. For clinical remission at week 24, in half of the patients enrolled, rates were 58.6% (75/128) for risankizumab and 39.5% (54/137) for ustekinumab, for a difference of 18.4% [95% confidence interval, 6.6-30.3], meaning that noninferiority was met within the predefined margin of 10%. The second primary endpoint of endoscopic remission at week 48 showed rates of 31.8% (81/255) for risankizumab and 16.2% (43/265) for ustekinumab (P < .0001 for superiority).
Risankizumab was found to be superior to ustekinumab for all secondary endpoints (all with P < .0001). Steroid-free endoscopic remission at week 48 showed a 16% difference, and steroid-free clinical remission at week 48 showed a 20% difference – both in favor of risankizumab.
In addition, more participants on risankizumab completed the study (89.4%) than those on ustekinumab (74.0%), Dr. Peyrin-Biroulet reported.
Adverse event rates (events per 100 person-years) were comparable between the two drugs at 341.2 for risankizumab and 282.7 for ustekinumab. For risankizumab, no new safety risks were observed, and those recorded were consistent with the known safety profile. Serious adverse events occurred in 10% of risankizumab-treated patients, and 17% of ustekinumab-treated patients.
“We know the safety of IL-23 inhibitors is good,” said Dr. Peyrin-Biroulet. “If we look at all adverse events there was no difference across arms, and in terms of serious adverse events, it was in favor of risankizumab because a CD flare is considered a serious adverse event.”
Session comoderator, Alessandro Armuzzi, MD, head of the Inflammatory Bowel Disease Center at the IRCCS Humanitas Research Hospital in Milan, commented on the findings. “The results look in favor of risankizumab – all the endpoints were met, not only the co-endpoints but also the secondary endpoints too,” he said.
These results, showing a preference for risankizumab, have value in helping clinicians with the sequence of therapies when patients with Crohn’s disease have failed one or more TNF inhibitor, said Dr. Armuzzi.
No funding for this study was disclosed. Dr. Peyrin-Biroulet has disclosed receiving fees from Galapagos, AbbVie, Janssen, Genentech, Alimentiv, Ferring, Tillots, Celltrion, Takeda, Pfizer, Index, Sandoz, Celgene, Biogen, SamsungBioepis, Inotrem, Allergan, MSD, Roche, Arena, Gilead, Amgen, BMS, Vifor, Norgine, Mylan, Lilly, Fresenius Kabi, OSEImmunotherapeutics, Enthera, Theravance, Pandion, Gossamer, Viatris, ThermoFisher, ONOPharma, Mopac, Cytoki, Morphic, Prometheus, and Applied MolecularTransport. Dr. Armuzzi disclosed consulting/advisory board fees from AbbVie, Amgen, Arena, Biogen, Boehringer Ingelheim, Bristol-Myers Squibb, Celgene, Celltrion, Eli-Lilly, Ferring, Galapagos, Gilead, Janssen, Lionhealth, MSD, Nestlé, Pfizer, Protagonist Therapeutics, Roche, Samsung Bioepis, Sandoz, Takeda, and Tillots Pharma; speaker’s fees from AbbVie, Amgen, Arena, Biogen, Bristol-Myers Squibb, Eli-Lilly, Ferring, Galapagos, Gilead, Janssen, Lionhealth, MSD, Novartis, Pfizer, Roche, Samsung Bioepis, Sandoz, and Takeda; and research grants from MSD, Takeda, Pfizer, and Biogen.
A version of this article first appeared on Medscape.com.
Taking a new obesity drug and birth control pills? Be careful
For women who are obese, daily life is wrought with landmines. Whether it’s the challenges of air travel because plane seats are too small, the need to shield themselves from the world’s discriminating eyes, or the great lengths many will go to achieve better health and the promise of longevity, navigating life as an obese person requires a thick skin.
So, it’s no wonder so many are willing to pay more than $1,000 a month out of pocket to get their hands on drugs like semaglutide (Ozempic and Wegovy) or tirzepatide (Mounjaro). The benefits of these drugs, which are part of a new class called glucagonlike peptide–1 (GLP-1) receptor agonists, include significant and rapid weight loss, blood sugar control, and improved life quality; they are unprecedented in a setting where surgery has long been considered the most effective long-term option.
On the flip side, the desire for rapid weight loss and better blood sugar control also comes with an unexpected cost. , making an unintended pregnancy more likely.
Neel Shah, MD, an endocrinologist and associate professor at the University of Texas Health Science Center at Houston, said he has had several patients become pregnant without intending to.
“It was when Mounjaro came out on the market when we started using it,” he said of the drug the Food and Drug Administration approved for type 2 diabetes in 2022. “It [the warning] was in the product insert, but clinically speaking, I don’t know if it was at the top of providers’ minds when they were prescribing Mounjaro.”
When asked if he believed that we were going to be seeing a significant increase in so-called Mounjaro babies, Dr. Shah was sure in his response.
“Absolutely. We will because the sheer volume [of patients] will increase,” he said.
It’s all in the gut
One of the ways that drugs like Mounjaro work is by delaying the time that it takes for food to move from the stomach to the small intestine. Although data are still evolving, it is believed that this process – delayed gastric emptying – may affect the absorption of birth control pills.
Dr. Shah said another theory is that vomiting, which is a common side effect of these types of drugs, also affects the pills’ ability to prevent pregnancy.
And “there’s a prolonged period of ramping up the dose because of the GI side effects,” said Pinar Kodaman, MD, PhD, a reproductive endocrinologist and assistant professor of gynecology at Yale University in New Haven, Conn.
“Initially, at the lowest dose, there may not be a lot of potential effect on absorption and gastric emptying. But as the dose goes up, it becomes more common, and it can cause diarrhea, which is another condition that can affect the absorption of any medication,” she said.
Unanticipated outcomes, extra prevention
Roughly 42% of women in the United States are obese, 40% of whom are between the ages of 20 and 39. Although these new drugs can improve fertility outcomes for women who are obese (especially those with polycystic ovary syndrome, or PCOS), only one – Mounjaro – currently carries a warning about birth control pill effectiveness on its label. Unfortunately, it appears that some doctors are unaware or not counseling patients about this risk, and the data are unclear about whether other drugs in this class, like Ozempic and Wegovy, have the same risks.
“To date, it hasn’t been a typical thing that we counsel about,” said Dr. Kodaman. “It’s all fairly new, but when we have patients on birth control pills, we do review other medications that they are on because some can affect efficacy, and it’s something to keep in mind.”
It’s also unclear if other forms of birth control – for example, birth control patches that deliver through the skin – might carry similar pregnancy risks. Dr. Shah said some of his patients who became pregnant without intending to were using these patches. This raises even more questions, since they deliver drugs through the skin directly into the bloodstream and not through the GI system.
What can women do to help ensure that they don’t become pregnant while using these drugs?
“I really think that if patients want to protect themselves from an unplanned pregnancy, that as soon as they start the GLP receptor agonists, it wouldn’t be a bad idea to use condoms, because the onset of action is pretty quick,” said Dr. Kodaman, noting also that “at the lowest dose there may not be a lot of potential effect on gastric emptying. But as the dose goes up, it becomes much more common or can cause diarrhea.”
Dr. Shah said that in his practice he’s “been telling patients to add barrier contraception” 4 weeks before they start their first dose “and at any dose adjustment.”
Zoobia Chaudhry, an obesity medicine doctor and assistant professor of medicine at Johns Hopkins University in Baltimore, recommends that “patients just make sure that the injection and medication that they take are at least 1 hour apart.”
“Most of the time, patients do take birth control before bedtime, so if the two are spaced, it should be OK,” she said.
Another option is for women to speak to their doctors about other contraceptive options like IUDs or implantable rods, where gastric absorption is not going to be an issue.
“There’s very little research on this class of drugs,” said Emily Goodstein, a 40-year-old small-business owner in Washington, who recently switched from Ozempic to Mounjaro. “Being a person who lives in a larger body is such a horrifying experience because of the way that the world discriminates against you.”
She appreciates the feeling of being proactive that these new drugs grant. It has “opened up a bunch of opportunities for me to be seen as a full individual by the medical establishment,” she said. “I was willing to take the risk, knowing that I would be on these drugs for the rest of my life.”
In addition to being what Dr. Goodstein refers to as a guinea pig, she said she made sure that her primary care doctor was aware that she was not trying or planning to become pregnant again. (She has a 3-year-old child.) Still, her doctor mentioned only the most common side effects linked to these drugs, like nausea, vomiting, and diarrhea, and did not mention the risk of pregnancy.
“Folks are really not talking about the reproductive implications,” she said, referring to members of a Facebook group on these drugs that she belongs to.
Like patients themselves, many doctors are just beginning to get their arms around these agents. “Awareness, education, provider involvement, and having a multidisciplinary team could help patients achieve the goals that they set out for themselves,” said Dr. Shah.
Clear conversations are key.
A version of this article first appeared on WebMD.com.
For women who are obese, daily life is wrought with landmines. Whether it’s the challenges of air travel because plane seats are too small, the need to shield themselves from the world’s discriminating eyes, or the great lengths many will go to achieve better health and the promise of longevity, navigating life as an obese person requires a thick skin.
So, it’s no wonder so many are willing to pay more than $1,000 a month out of pocket to get their hands on drugs like semaglutide (Ozempic and Wegovy) or tirzepatide (Mounjaro). The benefits of these drugs, which are part of a new class called glucagonlike peptide–1 (GLP-1) receptor agonists, include significant and rapid weight loss, blood sugar control, and improved life quality; they are unprecedented in a setting where surgery has long been considered the most effective long-term option.
On the flip side, the desire for rapid weight loss and better blood sugar control also comes with an unexpected cost. , making an unintended pregnancy more likely.
Neel Shah, MD, an endocrinologist and associate professor at the University of Texas Health Science Center at Houston, said he has had several patients become pregnant without intending to.
“It was when Mounjaro came out on the market when we started using it,” he said of the drug the Food and Drug Administration approved for type 2 diabetes in 2022. “It [the warning] was in the product insert, but clinically speaking, I don’t know if it was at the top of providers’ minds when they were prescribing Mounjaro.”
When asked if he believed that we were going to be seeing a significant increase in so-called Mounjaro babies, Dr. Shah was sure in his response.
“Absolutely. We will because the sheer volume [of patients] will increase,” he said.
It’s all in the gut
One of the ways that drugs like Mounjaro work is by delaying the time that it takes for food to move from the stomach to the small intestine. Although data are still evolving, it is believed that this process – delayed gastric emptying – may affect the absorption of birth control pills.
Dr. Shah said another theory is that vomiting, which is a common side effect of these types of drugs, also affects the pills’ ability to prevent pregnancy.
And “there’s a prolonged period of ramping up the dose because of the GI side effects,” said Pinar Kodaman, MD, PhD, a reproductive endocrinologist and assistant professor of gynecology at Yale University in New Haven, Conn.
“Initially, at the lowest dose, there may not be a lot of potential effect on absorption and gastric emptying. But as the dose goes up, it becomes more common, and it can cause diarrhea, which is another condition that can affect the absorption of any medication,” she said.
Unanticipated outcomes, extra prevention
Roughly 42% of women in the United States are obese, 40% of whom are between the ages of 20 and 39. Although these new drugs can improve fertility outcomes for women who are obese (especially those with polycystic ovary syndrome, or PCOS), only one – Mounjaro – currently carries a warning about birth control pill effectiveness on its label. Unfortunately, it appears that some doctors are unaware or not counseling patients about this risk, and the data are unclear about whether other drugs in this class, like Ozempic and Wegovy, have the same risks.
“To date, it hasn’t been a typical thing that we counsel about,” said Dr. Kodaman. “It’s all fairly new, but when we have patients on birth control pills, we do review other medications that they are on because some can affect efficacy, and it’s something to keep in mind.”
It’s also unclear if other forms of birth control – for example, birth control patches that deliver through the skin – might carry similar pregnancy risks. Dr. Shah said some of his patients who became pregnant without intending to were using these patches. This raises even more questions, since they deliver drugs through the skin directly into the bloodstream and not through the GI system.
What can women do to help ensure that they don’t become pregnant while using these drugs?
“I really think that if patients want to protect themselves from an unplanned pregnancy, that as soon as they start the GLP receptor agonists, it wouldn’t be a bad idea to use condoms, because the onset of action is pretty quick,” said Dr. Kodaman, noting also that “at the lowest dose there may not be a lot of potential effect on gastric emptying. But as the dose goes up, it becomes much more common or can cause diarrhea.”
Dr. Shah said that in his practice he’s “been telling patients to add barrier contraception” 4 weeks before they start their first dose “and at any dose adjustment.”
Zoobia Chaudhry, an obesity medicine doctor and assistant professor of medicine at Johns Hopkins University in Baltimore, recommends that “patients just make sure that the injection and medication that they take are at least 1 hour apart.”
“Most of the time, patients do take birth control before bedtime, so if the two are spaced, it should be OK,” she said.
Another option is for women to speak to their doctors about other contraceptive options like IUDs or implantable rods, where gastric absorption is not going to be an issue.
“There’s very little research on this class of drugs,” said Emily Goodstein, a 40-year-old small-business owner in Washington, who recently switched from Ozempic to Mounjaro. “Being a person who lives in a larger body is such a horrifying experience because of the way that the world discriminates against you.”
She appreciates the feeling of being proactive that these new drugs grant. It has “opened up a bunch of opportunities for me to be seen as a full individual by the medical establishment,” she said. “I was willing to take the risk, knowing that I would be on these drugs for the rest of my life.”
In addition to being what Dr. Goodstein refers to as a guinea pig, she said she made sure that her primary care doctor was aware that she was not trying or planning to become pregnant again. (She has a 3-year-old child.) Still, her doctor mentioned only the most common side effects linked to these drugs, like nausea, vomiting, and diarrhea, and did not mention the risk of pregnancy.
“Folks are really not talking about the reproductive implications,” she said, referring to members of a Facebook group on these drugs that she belongs to.
Like patients themselves, many doctors are just beginning to get their arms around these agents. “Awareness, education, provider involvement, and having a multidisciplinary team could help patients achieve the goals that they set out for themselves,” said Dr. Shah.
Clear conversations are key.
A version of this article first appeared on WebMD.com.
For women who are obese, daily life is wrought with landmines. Whether it’s the challenges of air travel because plane seats are too small, the need to shield themselves from the world’s discriminating eyes, or the great lengths many will go to achieve better health and the promise of longevity, navigating life as an obese person requires a thick skin.
So, it’s no wonder so many are willing to pay more than $1,000 a month out of pocket to get their hands on drugs like semaglutide (Ozempic and Wegovy) or tirzepatide (Mounjaro). The benefits of these drugs, which are part of a new class called glucagonlike peptide–1 (GLP-1) receptor agonists, include significant and rapid weight loss, blood sugar control, and improved life quality; they are unprecedented in a setting where surgery has long been considered the most effective long-term option.
On the flip side, the desire for rapid weight loss and better blood sugar control also comes with an unexpected cost. , making an unintended pregnancy more likely.
Neel Shah, MD, an endocrinologist and associate professor at the University of Texas Health Science Center at Houston, said he has had several patients become pregnant without intending to.
“It was when Mounjaro came out on the market when we started using it,” he said of the drug the Food and Drug Administration approved for type 2 diabetes in 2022. “It [the warning] was in the product insert, but clinically speaking, I don’t know if it was at the top of providers’ minds when they were prescribing Mounjaro.”
When asked if he believed that we were going to be seeing a significant increase in so-called Mounjaro babies, Dr. Shah was sure in his response.
“Absolutely. We will because the sheer volume [of patients] will increase,” he said.
It’s all in the gut
One of the ways that drugs like Mounjaro work is by delaying the time that it takes for food to move from the stomach to the small intestine. Although data are still evolving, it is believed that this process – delayed gastric emptying – may affect the absorption of birth control pills.
Dr. Shah said another theory is that vomiting, which is a common side effect of these types of drugs, also affects the pills’ ability to prevent pregnancy.
And “there’s a prolonged period of ramping up the dose because of the GI side effects,” said Pinar Kodaman, MD, PhD, a reproductive endocrinologist and assistant professor of gynecology at Yale University in New Haven, Conn.
“Initially, at the lowest dose, there may not be a lot of potential effect on absorption and gastric emptying. But as the dose goes up, it becomes more common, and it can cause diarrhea, which is another condition that can affect the absorption of any medication,” she said.
Unanticipated outcomes, extra prevention
Roughly 42% of women in the United States are obese, 40% of whom are between the ages of 20 and 39. Although these new drugs can improve fertility outcomes for women who are obese (especially those with polycystic ovary syndrome, or PCOS), only one – Mounjaro – currently carries a warning about birth control pill effectiveness on its label. Unfortunately, it appears that some doctors are unaware or not counseling patients about this risk, and the data are unclear about whether other drugs in this class, like Ozempic and Wegovy, have the same risks.
“To date, it hasn’t been a typical thing that we counsel about,” said Dr. Kodaman. “It’s all fairly new, but when we have patients on birth control pills, we do review other medications that they are on because some can affect efficacy, and it’s something to keep in mind.”
It’s also unclear if other forms of birth control – for example, birth control patches that deliver through the skin – might carry similar pregnancy risks. Dr. Shah said some of his patients who became pregnant without intending to were using these patches. This raises even more questions, since they deliver drugs through the skin directly into the bloodstream and not through the GI system.
What can women do to help ensure that they don’t become pregnant while using these drugs?
“I really think that if patients want to protect themselves from an unplanned pregnancy, that as soon as they start the GLP receptor agonists, it wouldn’t be a bad idea to use condoms, because the onset of action is pretty quick,” said Dr. Kodaman, noting also that “at the lowest dose there may not be a lot of potential effect on gastric emptying. But as the dose goes up, it becomes much more common or can cause diarrhea.”
Dr. Shah said that in his practice he’s “been telling patients to add barrier contraception” 4 weeks before they start their first dose “and at any dose adjustment.”
Zoobia Chaudhry, an obesity medicine doctor and assistant professor of medicine at Johns Hopkins University in Baltimore, recommends that “patients just make sure that the injection and medication that they take are at least 1 hour apart.”
“Most of the time, patients do take birth control before bedtime, so if the two are spaced, it should be OK,” she said.
Another option is for women to speak to their doctors about other contraceptive options like IUDs or implantable rods, where gastric absorption is not going to be an issue.
“There’s very little research on this class of drugs,” said Emily Goodstein, a 40-year-old small-business owner in Washington, who recently switched from Ozempic to Mounjaro. “Being a person who lives in a larger body is such a horrifying experience because of the way that the world discriminates against you.”
She appreciates the feeling of being proactive that these new drugs grant. It has “opened up a bunch of opportunities for me to be seen as a full individual by the medical establishment,” she said. “I was willing to take the risk, knowing that I would be on these drugs for the rest of my life.”
In addition to being what Dr. Goodstein refers to as a guinea pig, she said she made sure that her primary care doctor was aware that she was not trying or planning to become pregnant again. (She has a 3-year-old child.) Still, her doctor mentioned only the most common side effects linked to these drugs, like nausea, vomiting, and diarrhea, and did not mention the risk of pregnancy.
“Folks are really not talking about the reproductive implications,” she said, referring to members of a Facebook group on these drugs that she belongs to.
Like patients themselves, many doctors are just beginning to get their arms around these agents. “Awareness, education, provider involvement, and having a multidisciplinary team could help patients achieve the goals that they set out for themselves,” said Dr. Shah.
Clear conversations are key.
A version of this article first appeared on WebMD.com.
Employed physicians: A survival guide
The strike by health care workers at Kaiser Permanente may not involve physicians (yet). But as more doctors in the United States are finding themselves working as salaried employees, physicians can – and probably will – become a powerful force for change in a health care system that has shown itself to be increasingly hostile to employee concerns over issues involving patient care, wages and benefits, safety, and well-being.
Salaried employment has its challenges. Physician-employees may have less autonomy and voice in decision-making that affects patients. They may splinter into fragmented work groups; feel isolated; and have different imperatives based on who they are, what they want, and where they work. They may feel more removed from their patients and struggle to build strong relationships, with their employers in the way.
Yet important opportunities exist for doctors when embracing their employee side. Examples of these interests include adequate compensation, wellness, job security, patient and worker safety, health care quality, reasonable workloads and schedules, and fair treatment by employers, including the need to exhibit a strong collective voice in organizational decision-making.
Some believe that physician-employees must be unionized to maximize their rights and power as employees. Many expect physician unionization to take hold more fully over time. Medical residents, the doctors of tomorrow, are already considering unionization in greater numbers. Some are also doing it in the same employment setting alongside other health professionals, such as nurses.
Having studied doctors and their employment situations for years, I am convinced that whether through unionization or another approach, physicians must also change how they think about control; train and learn alongside other health care workers who share similar interests; and elevate at an early career stage their knowledge of the business side of health care.
Adopt a more pragmatic definition of autonomy
Doctors must embrace an updated definition of autonomy – one that matches their status as highly paid labor.
When I have spoken to physicians in my research about what autonomy means to them, many seem unable to reconceptualize it from a vague and absolute form of their profession’s strategic control over their economic fates and technical skills toward an individualized control that is situation-specific, one centered on winning the daily fights about workplace bread-and-butter issues such as those mentioned above.
But a more pragmatic definition of autonomy could get doctors focused on influencing important issues of the patient-care day and enhance their negotiating power with employers. It would allow physicians to break out of what often seems a paralysis of inaction – waiting for employers, insurers, or the government to reinstate the profession’s idealized version of control by handing it back the keys to the health care system through major regulatory, structural, and reimbursement-related changes. This fantasy is unlikely to become reality.
Physician-employees I’ve talked to over the years understand their everyday challenges. But when it comes to engaging in localized and sustained action to overcome them, they often perform less well, leading to feelings of helplessness and burnout. Valuing tactical control over their jobs and work setting will yield smaller but more impactful wins as employees intent on making their everyday work lives better.
Train alongside other health care professionals
Physicians must accept that how they are trained no longer prepares them for the employee world into which most are dropped. For instance, unless doctors are trained collaboratively alongside other health care professionals – such as nurses – they are less likely to identify closely with these colleagues once in practice. There is strength in numbers, so this mutual identification empowers both groups of employees. Yet, medical education remains largely the same: training young medical students in isolation for the first couple of years, then placing them into clerkships and residencies where true interprofessional care opportunities remain stunted and secondary to the “physician as captain of the team” mantra.
Unfortunately, the “hidden curriculum” of medicine helps convince medical students and residents early in their careers that they are the unquestioned leaders in patient care settings. This hierarchy encourages some doctors to keep their psychological distance from other members of the health care team and to resist sharing power, concerns, or insights with less skilled health care workers. This socialization harms the ability of physicians to act in a unified fashion alongside these other workers. Having physicians learn and train alongside other health professionals yields positive benefits for collective advocacy, including a shared sense of purpose, positive views on collaboration with others in the health setting, and greater development of bonds with nonphysician coworkers.
Integrate business with medical training in real time
Medical students and residents generally lack exposure to the everyday business realities of the U.S. health care system. This gap hinders their ability to understand the employee world and push for the types of changes and work conditions that benefit all health care workers. Formal business and management training should be a required part of every U.S. medical school and residency curriculum from day one. If you see it at all in medical schools now, it is mostly by accident, or given separate treatment in the form of standalone MBA or MPH degrees that rarely integrate organically and in real time with actual medical training. Not every doctor needs an MBA or MPH degree. However, all of them require a stronger contextual understanding of how the medicine they wish to practice is shaped by the economic and fiscal circumstances surrounding it – circumstances they do not control.
This is another reason why young doctors are unhappy and burned out. They cannot push for specific changes or properly critique the pros and cons of how their work is structured because they have not been made aware, in real time as they learn clinical practice, how their jobs are shaped by realities such as insurance coverage and reimbursement, the fragmentation of the care delivery system, their employer’s financial health , and the socioeconomic circumstances of their patients. They aren’t given the methods and tools related to process and quality improvement, budgeting, negotiation, risk management, leadership, and talent management that might help them navigate these undermining forces. They also get little advance exposure in their training to important workplace “soft” skills in such areas as how to work in teams, networking, communication and listening, empathy, and problem-solving – all necessary foci for bringing them closer to other health care workers and advocating alongside them effectively with health care employers.
Now is the time for physicians to embrace their identity as employees. Doing so is in their own best interest as professionals. It will help others in the health care workforce as well as patients. Moreover, it provides a needed counterbalance to the powerful corporate ethos now ascendant in U.S. health care.
Timothy Hoff, PhD, is a professor of management and healthcare systems at Northeastern University, Boston, and an associate fellow at the University of Oxford, England. He disclosed no relevant conflicts of interest.
A version of this article first appeared on Medscape.com.
The strike by health care workers at Kaiser Permanente may not involve physicians (yet). But as more doctors in the United States are finding themselves working as salaried employees, physicians can – and probably will – become a powerful force for change in a health care system that has shown itself to be increasingly hostile to employee concerns over issues involving patient care, wages and benefits, safety, and well-being.
Salaried employment has its challenges. Physician-employees may have less autonomy and voice in decision-making that affects patients. They may splinter into fragmented work groups; feel isolated; and have different imperatives based on who they are, what they want, and where they work. They may feel more removed from their patients and struggle to build strong relationships, with their employers in the way.
Yet important opportunities exist for doctors when embracing their employee side. Examples of these interests include adequate compensation, wellness, job security, patient and worker safety, health care quality, reasonable workloads and schedules, and fair treatment by employers, including the need to exhibit a strong collective voice in organizational decision-making.
Some believe that physician-employees must be unionized to maximize their rights and power as employees. Many expect physician unionization to take hold more fully over time. Medical residents, the doctors of tomorrow, are already considering unionization in greater numbers. Some are also doing it in the same employment setting alongside other health professionals, such as nurses.
Having studied doctors and their employment situations for years, I am convinced that whether through unionization or another approach, physicians must also change how they think about control; train and learn alongside other health care workers who share similar interests; and elevate at an early career stage their knowledge of the business side of health care.
Adopt a more pragmatic definition of autonomy
Doctors must embrace an updated definition of autonomy – one that matches their status as highly paid labor.
When I have spoken to physicians in my research about what autonomy means to them, many seem unable to reconceptualize it from a vague and absolute form of their profession’s strategic control over their economic fates and technical skills toward an individualized control that is situation-specific, one centered on winning the daily fights about workplace bread-and-butter issues such as those mentioned above.
But a more pragmatic definition of autonomy could get doctors focused on influencing important issues of the patient-care day and enhance their negotiating power with employers. It would allow physicians to break out of what often seems a paralysis of inaction – waiting for employers, insurers, or the government to reinstate the profession’s idealized version of control by handing it back the keys to the health care system through major regulatory, structural, and reimbursement-related changes. This fantasy is unlikely to become reality.
Physician-employees I’ve talked to over the years understand their everyday challenges. But when it comes to engaging in localized and sustained action to overcome them, they often perform less well, leading to feelings of helplessness and burnout. Valuing tactical control over their jobs and work setting will yield smaller but more impactful wins as employees intent on making their everyday work lives better.
Train alongside other health care professionals
Physicians must accept that how they are trained no longer prepares them for the employee world into which most are dropped. For instance, unless doctors are trained collaboratively alongside other health care professionals – such as nurses – they are less likely to identify closely with these colleagues once in practice. There is strength in numbers, so this mutual identification empowers both groups of employees. Yet, medical education remains largely the same: training young medical students in isolation for the first couple of years, then placing them into clerkships and residencies where true interprofessional care opportunities remain stunted and secondary to the “physician as captain of the team” mantra.
Unfortunately, the “hidden curriculum” of medicine helps convince medical students and residents early in their careers that they are the unquestioned leaders in patient care settings. This hierarchy encourages some doctors to keep their psychological distance from other members of the health care team and to resist sharing power, concerns, or insights with less skilled health care workers. This socialization harms the ability of physicians to act in a unified fashion alongside these other workers. Having physicians learn and train alongside other health professionals yields positive benefits for collective advocacy, including a shared sense of purpose, positive views on collaboration with others in the health setting, and greater development of bonds with nonphysician coworkers.
Integrate business with medical training in real time
Medical students and residents generally lack exposure to the everyday business realities of the U.S. health care system. This gap hinders their ability to understand the employee world and push for the types of changes and work conditions that benefit all health care workers. Formal business and management training should be a required part of every U.S. medical school and residency curriculum from day one. If you see it at all in medical schools now, it is mostly by accident, or given separate treatment in the form of standalone MBA or MPH degrees that rarely integrate organically and in real time with actual medical training. Not every doctor needs an MBA or MPH degree. However, all of them require a stronger contextual understanding of how the medicine they wish to practice is shaped by the economic and fiscal circumstances surrounding it – circumstances they do not control.
This is another reason why young doctors are unhappy and burned out. They cannot push for specific changes or properly critique the pros and cons of how their work is structured because they have not been made aware, in real time as they learn clinical practice, how their jobs are shaped by realities such as insurance coverage and reimbursement, the fragmentation of the care delivery system, their employer’s financial health , and the socioeconomic circumstances of their patients. They aren’t given the methods and tools related to process and quality improvement, budgeting, negotiation, risk management, leadership, and talent management that might help them navigate these undermining forces. They also get little advance exposure in their training to important workplace “soft” skills in such areas as how to work in teams, networking, communication and listening, empathy, and problem-solving – all necessary foci for bringing them closer to other health care workers and advocating alongside them effectively with health care employers.
Now is the time for physicians to embrace their identity as employees. Doing so is in their own best interest as professionals. It will help others in the health care workforce as well as patients. Moreover, it provides a needed counterbalance to the powerful corporate ethos now ascendant in U.S. health care.
Timothy Hoff, PhD, is a professor of management and healthcare systems at Northeastern University, Boston, and an associate fellow at the University of Oxford, England. He disclosed no relevant conflicts of interest.
A version of this article first appeared on Medscape.com.
The strike by health care workers at Kaiser Permanente may not involve physicians (yet). But as more doctors in the United States are finding themselves working as salaried employees, physicians can – and probably will – become a powerful force for change in a health care system that has shown itself to be increasingly hostile to employee concerns over issues involving patient care, wages and benefits, safety, and well-being.
Salaried employment has its challenges. Physician-employees may have less autonomy and voice in decision-making that affects patients. They may splinter into fragmented work groups; feel isolated; and have different imperatives based on who they are, what they want, and where they work. They may feel more removed from their patients and struggle to build strong relationships, with their employers in the way.
Yet important opportunities exist for doctors when embracing their employee side. Examples of these interests include adequate compensation, wellness, job security, patient and worker safety, health care quality, reasonable workloads and schedules, and fair treatment by employers, including the need to exhibit a strong collective voice in organizational decision-making.
Some believe that physician-employees must be unionized to maximize their rights and power as employees. Many expect physician unionization to take hold more fully over time. Medical residents, the doctors of tomorrow, are already considering unionization in greater numbers. Some are also doing it in the same employment setting alongside other health professionals, such as nurses.
Having studied doctors and their employment situations for years, I am convinced that whether through unionization or another approach, physicians must also change how they think about control; train and learn alongside other health care workers who share similar interests; and elevate at an early career stage their knowledge of the business side of health care.
Adopt a more pragmatic definition of autonomy
Doctors must embrace an updated definition of autonomy – one that matches their status as highly paid labor.
When I have spoken to physicians in my research about what autonomy means to them, many seem unable to reconceptualize it from a vague and absolute form of their profession’s strategic control over their economic fates and technical skills toward an individualized control that is situation-specific, one centered on winning the daily fights about workplace bread-and-butter issues such as those mentioned above.
But a more pragmatic definition of autonomy could get doctors focused on influencing important issues of the patient-care day and enhance their negotiating power with employers. It would allow physicians to break out of what often seems a paralysis of inaction – waiting for employers, insurers, or the government to reinstate the profession’s idealized version of control by handing it back the keys to the health care system through major regulatory, structural, and reimbursement-related changes. This fantasy is unlikely to become reality.
Physician-employees I’ve talked to over the years understand their everyday challenges. But when it comes to engaging in localized and sustained action to overcome them, they often perform less well, leading to feelings of helplessness and burnout. Valuing tactical control over their jobs and work setting will yield smaller but more impactful wins as employees intent on making their everyday work lives better.
Train alongside other health care professionals
Physicians must accept that how they are trained no longer prepares them for the employee world into which most are dropped. For instance, unless doctors are trained collaboratively alongside other health care professionals – such as nurses – they are less likely to identify closely with these colleagues once in practice. There is strength in numbers, so this mutual identification empowers both groups of employees. Yet, medical education remains largely the same: training young medical students in isolation for the first couple of years, then placing them into clerkships and residencies where true interprofessional care opportunities remain stunted and secondary to the “physician as captain of the team” mantra.
Unfortunately, the “hidden curriculum” of medicine helps convince medical students and residents early in their careers that they are the unquestioned leaders in patient care settings. This hierarchy encourages some doctors to keep their psychological distance from other members of the health care team and to resist sharing power, concerns, or insights with less skilled health care workers. This socialization harms the ability of physicians to act in a unified fashion alongside these other workers. Having physicians learn and train alongside other health professionals yields positive benefits for collective advocacy, including a shared sense of purpose, positive views on collaboration with others in the health setting, and greater development of bonds with nonphysician coworkers.
Integrate business with medical training in real time
Medical students and residents generally lack exposure to the everyday business realities of the U.S. health care system. This gap hinders their ability to understand the employee world and push for the types of changes and work conditions that benefit all health care workers. Formal business and management training should be a required part of every U.S. medical school and residency curriculum from day one. If you see it at all in medical schools now, it is mostly by accident, or given separate treatment in the form of standalone MBA or MPH degrees that rarely integrate organically and in real time with actual medical training. Not every doctor needs an MBA or MPH degree. However, all of them require a stronger contextual understanding of how the medicine they wish to practice is shaped by the economic and fiscal circumstances surrounding it – circumstances they do not control.
This is another reason why young doctors are unhappy and burned out. They cannot push for specific changes or properly critique the pros and cons of how their work is structured because they have not been made aware, in real time as they learn clinical practice, how their jobs are shaped by realities such as insurance coverage and reimbursement, the fragmentation of the care delivery system, their employer’s financial health , and the socioeconomic circumstances of their patients. They aren’t given the methods and tools related to process and quality improvement, budgeting, negotiation, risk management, leadership, and talent management that might help them navigate these undermining forces. They also get little advance exposure in their training to important workplace “soft” skills in such areas as how to work in teams, networking, communication and listening, empathy, and problem-solving – all necessary foci for bringing them closer to other health care workers and advocating alongside them effectively with health care employers.
Now is the time for physicians to embrace their identity as employees. Doing so is in their own best interest as professionals. It will help others in the health care workforce as well as patients. Moreover, it provides a needed counterbalance to the powerful corporate ethos now ascendant in U.S. health care.
Timothy Hoff, PhD, is a professor of management and healthcare systems at Northeastern University, Boston, and an associate fellow at the University of Oxford, England. He disclosed no relevant conflicts of interest.
A version of this article first appeared on Medscape.com.
Why legal pot makes this physician sick
Last year, my husband and I took a 16-day road trip from Kentucky through Massachusetts to Maine. On our first morning in Boston, we exited the Park Street Station en route to Boston Common, but instead of being greeted by the aroma of molasses, we were hit full-on with a pungent, repulsive odor. “That’s skunk weed,” my husband chuckled as we stepped right into the middle of the Boston Freedom Rally, a celebration of all things cannabis.
As we boarded a hop-on-hop-off bus, we learned that this was the one week of the year that the city skips testing tour bus drivers for tetrahydrocannabinol (THC), “because we all test positive,” the driver quipped. As our open-air bus circled the Common, a crowd of pot enthusiasts displayed signs in support of relaxed regulation for public consumption.
The 34-year-old Boston Freedom Rally is a sign that U.S. culture has transformed forever. Mary Jane is no friend of emergency physicians nor of staff on hospital wards and offices.
Toking boomers and millennials
Researchers at the University of California, San Diego, looked at cannabis-related emergency department visits from all acute-care hospitals in the state from 2005 to 2019 and found an 1,808% increase in patients aged 65 or older (that is not a typo) who were there for complications from cannabis use.
The lead author said in an interview that, “older patients taking marijuana or related products may have dizziness and falls, heart palpitations, panic attacks, confusion, anxiety or worsening of underlying lung diseases, such as asthma or [chronic obstructive pulmonary disease].”
A recent study from Canada suggests that commercialization has been associated with an increase in related hospitalizations, including cannabis-induced psychosis.
According to a National Study of Drug Use and Health, marijuana use in young adults reached an all-time high (pun intended) in 2021. Nearly 10% of eighth graders and 20% of 10th graders reported using marijuana this past year.
The full downside of any drug, legal or illegal, is largely unknown until it infiltrates the mainstream market, but these are the typical cases we see:
Let’s start with the demotivated high school honors student who dropped out of college to work at the local cinema. He stumbled and broke his clavicle outside a bar at 2 AM, but he wasn’t sure if he passed out, so a cardiology consult was requested to “rule out” arrhythmia associated with syncope. He related that his plan to become a railway conductor had been upended because he knew he would be drug tested and just couldn’t give up pot. After a normal cardiac exam, ECG, labs, a Holter, and an echocardiogram were also requested and normal at a significant cost.
Cannabinoid hyperemesis syndrome
One of my Midwest colleagues related her encounter with two middle-aged pot users with ventricular tachycardia (VT). These episodes coincided with potassium levels less than 3.0 mEq/L in the setting of repetitive vomiting. The QTc interval didn’t normalize despite a corrected potassium level in one patient. They were both informed that they should never smoke pot because vomiting would predictably drop their K+ levels again and prolong their QTc intervals. Then began “the circular argument,” as my friend described it. The patient claims, “I smoke pot to relieve my nausea,” to which she explains that “in many folks, pot use induces nausea.” Of course, the classic reply is, “Not me.” Predictably one of these stoners soon returned with more VT, more puking, and more hypokalemia. “Consider yourself ‘allergic’ to pot smoke,” my friend advised, but “was met with no meaningful hint of understanding or hope for transformative change,” she told me.
I’ve seen cannabinoid hyperemesis syndrome several times in the past few years. It occurs in daily to weekly pot users. Very rarely, it can cause cerebral edema, but it is also associated with seizures and dehydration that can lead to hypovolemic shock and kidney failure.
Heart and brain harm
Then there are the young patients who for various reasons have developed heart failure. Unfortunately, some are repetitively tox screen positive with varying trifectas of methamphetamine (meth), cocaine, and THC; opiates, meth, and THC; alcohol, meth, and THC; or heroin, meth, and THC. THC, the ever present and essential third leg of the stool of stupor. These unfortunate patients often need heart failure medications that they can’t afford or won’t take because illicit drug use is expensive and dulls their ability to prioritize their health. Some desperately need a heart transplant, but the necessary negative drug screen is a pipe dream.
And it’s not just the heart that is affected. There are data linking cannabis use to a higher risk for both ischemic and hemorrhagic stroke. A retrospective study published in Stroke, of more than 1,000 people diagnosed with an aneurysmal subarachnoid hemorrhage, found that more than half of the 46 who tested positive for THC at admission developed delayed cerebral ischemia (DCI), which increases the risk for disability or early death. This was after adjusting for several patient characteristics as well as recent exposure to other illicit substances; cocaine, meth, and tobacco use were not associated with DCI.
Natural my ...
I’m certain my anti-cannabis stance will strike a nerve with those who love their recreational THC and push for its legal sale; after all, “It’s perfectly natural.” But I counter with the fact that tornadoes, earthquakes, cyanide, and appendicitis are all natural but certainly not optimal. And what we are seeing in the vascular specialties is completely unnatural. We are treating a different mix of complications than before pot was readily accessible across several states.
Our most effective action is to educate our patients. We should encourage those who don’t currently smoke cannabis to never start and those who do to quit. People who require marijuana for improved quality of life for terminal care or true (not supposed) disorders that mainstream medicine fails should be approached with empathy and caution.
A good rule of thumb is to never breathe anything you can see. Never put anything in your body that comes off the street: Drug dealers who sell cannabis cut with fentanyl will be ecstatic to take someone’s money then merely keep scrolling when their obituary comes up.
Let’s try to reverse the rise of vascular complications, orthopedic injuries, and vomiting across America. We can start by encouraging our patients to avoid “skunk weed” and get back to the sweet smells of nature in our cities and parks.
Some details have been changed to protect the patients’ identities, but the essence of their diagnoses has been preserved.
Dr. Walton-Shirley is a retired clinical cardiologist from Nashville, Tenn. She disclosed no relevant conflicts of interest.
A version of this article first appeared on Medscape.com.
Last year, my husband and I took a 16-day road trip from Kentucky through Massachusetts to Maine. On our first morning in Boston, we exited the Park Street Station en route to Boston Common, but instead of being greeted by the aroma of molasses, we were hit full-on with a pungent, repulsive odor. “That’s skunk weed,” my husband chuckled as we stepped right into the middle of the Boston Freedom Rally, a celebration of all things cannabis.
As we boarded a hop-on-hop-off bus, we learned that this was the one week of the year that the city skips testing tour bus drivers for tetrahydrocannabinol (THC), “because we all test positive,” the driver quipped. As our open-air bus circled the Common, a crowd of pot enthusiasts displayed signs in support of relaxed regulation for public consumption.
The 34-year-old Boston Freedom Rally is a sign that U.S. culture has transformed forever. Mary Jane is no friend of emergency physicians nor of staff on hospital wards and offices.
Toking boomers and millennials
Researchers at the University of California, San Diego, looked at cannabis-related emergency department visits from all acute-care hospitals in the state from 2005 to 2019 and found an 1,808% increase in patients aged 65 or older (that is not a typo) who were there for complications from cannabis use.
The lead author said in an interview that, “older patients taking marijuana or related products may have dizziness and falls, heart palpitations, panic attacks, confusion, anxiety or worsening of underlying lung diseases, such as asthma or [chronic obstructive pulmonary disease].”
A recent study from Canada suggests that commercialization has been associated with an increase in related hospitalizations, including cannabis-induced psychosis.
According to a National Study of Drug Use and Health, marijuana use in young adults reached an all-time high (pun intended) in 2021. Nearly 10% of eighth graders and 20% of 10th graders reported using marijuana this past year.
The full downside of any drug, legal or illegal, is largely unknown until it infiltrates the mainstream market, but these are the typical cases we see:
Let’s start with the demotivated high school honors student who dropped out of college to work at the local cinema. He stumbled and broke his clavicle outside a bar at 2 AM, but he wasn’t sure if he passed out, so a cardiology consult was requested to “rule out” arrhythmia associated with syncope. He related that his plan to become a railway conductor had been upended because he knew he would be drug tested and just couldn’t give up pot. After a normal cardiac exam, ECG, labs, a Holter, and an echocardiogram were also requested and normal at a significant cost.
Cannabinoid hyperemesis syndrome
One of my Midwest colleagues related her encounter with two middle-aged pot users with ventricular tachycardia (VT). These episodes coincided with potassium levels less than 3.0 mEq/L in the setting of repetitive vomiting. The QTc interval didn’t normalize despite a corrected potassium level in one patient. They were both informed that they should never smoke pot because vomiting would predictably drop their K+ levels again and prolong their QTc intervals. Then began “the circular argument,” as my friend described it. The patient claims, “I smoke pot to relieve my nausea,” to which she explains that “in many folks, pot use induces nausea.” Of course, the classic reply is, “Not me.” Predictably one of these stoners soon returned with more VT, more puking, and more hypokalemia. “Consider yourself ‘allergic’ to pot smoke,” my friend advised, but “was met with no meaningful hint of understanding or hope for transformative change,” she told me.
I’ve seen cannabinoid hyperemesis syndrome several times in the past few years. It occurs in daily to weekly pot users. Very rarely, it can cause cerebral edema, but it is also associated with seizures and dehydration that can lead to hypovolemic shock and kidney failure.
Heart and brain harm
Then there are the young patients who for various reasons have developed heart failure. Unfortunately, some are repetitively tox screen positive with varying trifectas of methamphetamine (meth), cocaine, and THC; opiates, meth, and THC; alcohol, meth, and THC; or heroin, meth, and THC. THC, the ever present and essential third leg of the stool of stupor. These unfortunate patients often need heart failure medications that they can’t afford or won’t take because illicit drug use is expensive and dulls their ability to prioritize their health. Some desperately need a heart transplant, but the necessary negative drug screen is a pipe dream.
And it’s not just the heart that is affected. There are data linking cannabis use to a higher risk for both ischemic and hemorrhagic stroke. A retrospective study published in Stroke, of more than 1,000 people diagnosed with an aneurysmal subarachnoid hemorrhage, found that more than half of the 46 who tested positive for THC at admission developed delayed cerebral ischemia (DCI), which increases the risk for disability or early death. This was after adjusting for several patient characteristics as well as recent exposure to other illicit substances; cocaine, meth, and tobacco use were not associated with DCI.
Natural my ...
I’m certain my anti-cannabis stance will strike a nerve with those who love their recreational THC and push for its legal sale; after all, “It’s perfectly natural.” But I counter with the fact that tornadoes, earthquakes, cyanide, and appendicitis are all natural but certainly not optimal. And what we are seeing in the vascular specialties is completely unnatural. We are treating a different mix of complications than before pot was readily accessible across several states.
Our most effective action is to educate our patients. We should encourage those who don’t currently smoke cannabis to never start and those who do to quit. People who require marijuana for improved quality of life for terminal care or true (not supposed) disorders that mainstream medicine fails should be approached with empathy and caution.
A good rule of thumb is to never breathe anything you can see. Never put anything in your body that comes off the street: Drug dealers who sell cannabis cut with fentanyl will be ecstatic to take someone’s money then merely keep scrolling when their obituary comes up.
Let’s try to reverse the rise of vascular complications, orthopedic injuries, and vomiting across America. We can start by encouraging our patients to avoid “skunk weed” and get back to the sweet smells of nature in our cities and parks.
Some details have been changed to protect the patients’ identities, but the essence of their diagnoses has been preserved.
Dr. Walton-Shirley is a retired clinical cardiologist from Nashville, Tenn. She disclosed no relevant conflicts of interest.
A version of this article first appeared on Medscape.com.
Last year, my husband and I took a 16-day road trip from Kentucky through Massachusetts to Maine. On our first morning in Boston, we exited the Park Street Station en route to Boston Common, but instead of being greeted by the aroma of molasses, we were hit full-on with a pungent, repulsive odor. “That’s skunk weed,” my husband chuckled as we stepped right into the middle of the Boston Freedom Rally, a celebration of all things cannabis.
As we boarded a hop-on-hop-off bus, we learned that this was the one week of the year that the city skips testing tour bus drivers for tetrahydrocannabinol (THC), “because we all test positive,” the driver quipped. As our open-air bus circled the Common, a crowd of pot enthusiasts displayed signs in support of relaxed regulation for public consumption.
The 34-year-old Boston Freedom Rally is a sign that U.S. culture has transformed forever. Mary Jane is no friend of emergency physicians nor of staff on hospital wards and offices.
Toking boomers and millennials
Researchers at the University of California, San Diego, looked at cannabis-related emergency department visits from all acute-care hospitals in the state from 2005 to 2019 and found an 1,808% increase in patients aged 65 or older (that is not a typo) who were there for complications from cannabis use.
The lead author said in an interview that, “older patients taking marijuana or related products may have dizziness and falls, heart palpitations, panic attacks, confusion, anxiety or worsening of underlying lung diseases, such as asthma or [chronic obstructive pulmonary disease].”
A recent study from Canada suggests that commercialization has been associated with an increase in related hospitalizations, including cannabis-induced psychosis.
According to a National Study of Drug Use and Health, marijuana use in young adults reached an all-time high (pun intended) in 2021. Nearly 10% of eighth graders and 20% of 10th graders reported using marijuana this past year.
The full downside of any drug, legal or illegal, is largely unknown until it infiltrates the mainstream market, but these are the typical cases we see:
Let’s start with the demotivated high school honors student who dropped out of college to work at the local cinema. He stumbled and broke his clavicle outside a bar at 2 AM, but he wasn’t sure if he passed out, so a cardiology consult was requested to “rule out” arrhythmia associated with syncope. He related that his plan to become a railway conductor had been upended because he knew he would be drug tested and just couldn’t give up pot. After a normal cardiac exam, ECG, labs, a Holter, and an echocardiogram were also requested and normal at a significant cost.
Cannabinoid hyperemesis syndrome
One of my Midwest colleagues related her encounter with two middle-aged pot users with ventricular tachycardia (VT). These episodes coincided with potassium levels less than 3.0 mEq/L in the setting of repetitive vomiting. The QTc interval didn’t normalize despite a corrected potassium level in one patient. They were both informed that they should never smoke pot because vomiting would predictably drop their K+ levels again and prolong their QTc intervals. Then began “the circular argument,” as my friend described it. The patient claims, “I smoke pot to relieve my nausea,” to which she explains that “in many folks, pot use induces nausea.” Of course, the classic reply is, “Not me.” Predictably one of these stoners soon returned with more VT, more puking, and more hypokalemia. “Consider yourself ‘allergic’ to pot smoke,” my friend advised, but “was met with no meaningful hint of understanding or hope for transformative change,” she told me.
I’ve seen cannabinoid hyperemesis syndrome several times in the past few years. It occurs in daily to weekly pot users. Very rarely, it can cause cerebral edema, but it is also associated with seizures and dehydration that can lead to hypovolemic shock and kidney failure.
Heart and brain harm
Then there are the young patients who for various reasons have developed heart failure. Unfortunately, some are repetitively tox screen positive with varying trifectas of methamphetamine (meth), cocaine, and THC; opiates, meth, and THC; alcohol, meth, and THC; or heroin, meth, and THC. THC, the ever present and essential third leg of the stool of stupor. These unfortunate patients often need heart failure medications that they can’t afford or won’t take because illicit drug use is expensive and dulls their ability to prioritize their health. Some desperately need a heart transplant, but the necessary negative drug screen is a pipe dream.
And it’s not just the heart that is affected. There are data linking cannabis use to a higher risk for both ischemic and hemorrhagic stroke. A retrospective study published in Stroke, of more than 1,000 people diagnosed with an aneurysmal subarachnoid hemorrhage, found that more than half of the 46 who tested positive for THC at admission developed delayed cerebral ischemia (DCI), which increases the risk for disability or early death. This was after adjusting for several patient characteristics as well as recent exposure to other illicit substances; cocaine, meth, and tobacco use were not associated with DCI.
Natural my ...
I’m certain my anti-cannabis stance will strike a nerve with those who love their recreational THC and push for its legal sale; after all, “It’s perfectly natural.” But I counter with the fact that tornadoes, earthquakes, cyanide, and appendicitis are all natural but certainly not optimal. And what we are seeing in the vascular specialties is completely unnatural. We are treating a different mix of complications than before pot was readily accessible across several states.
Our most effective action is to educate our patients. We should encourage those who don’t currently smoke cannabis to never start and those who do to quit. People who require marijuana for improved quality of life for terminal care or true (not supposed) disorders that mainstream medicine fails should be approached with empathy and caution.
A good rule of thumb is to never breathe anything you can see. Never put anything in your body that comes off the street: Drug dealers who sell cannabis cut with fentanyl will be ecstatic to take someone’s money then merely keep scrolling when their obituary comes up.
Let’s try to reverse the rise of vascular complications, orthopedic injuries, and vomiting across America. We can start by encouraging our patients to avoid “skunk weed” and get back to the sweet smells of nature in our cities and parks.
Some details have been changed to protect the patients’ identities, but the essence of their diagnoses has been preserved.
Dr. Walton-Shirley is a retired clinical cardiologist from Nashville, Tenn. She disclosed no relevant conflicts of interest.
A version of this article first appeared on Medscape.com.
Addressing obesity bias in health care
Obesity is a major factor affecting the health of many Americans. It is estimated by the Centers for Disease Control and Prevention that 41% of adults and 19.7% of children in our country now meet the criteria for being obese. Obesity costs the United States approximately $147 billion annually in health care costs. While these numbers are staggering, they continue to rise.
The recent craze over medications such as Ozempic, Wegovy, and Mounjaro shows how eager people are to lose weight. Yet, many of them face bias, not just in their daily lives, but from health care professionals who should do better. No one should feel stigmatized when they come for medical help. This just drives away patients who need us and who may then suffer more severe consequences of obesity-related illnesses.
Earlier this year, the American Association of Clinical Endocrinology issued a consensus statement on the role stigma and weight bias play in the management of obesity. They proposed a staging system to address the severity of obesity and suggested stigma and bias should be assessed in all patients.
While we are good at diagnosing obesity, many of us fail at addressing it empathetically with patients. I’ve seen many patients cry about past encounters they’ve had in the health care system. We need to address the emotional effect that obesity has as well as the physical complications.
Obesity is a major contributor to many diseases such as diabetes and heart disease, but we are finding it also plays a role in other diseases such as certain cancers. Treating obesity is imperative to prevent these diseases as well as to promote better treatment outcomes. We’ve all seen the diabetic patient lose weight and have their blood glucose levels come under control.
Many patients have tried hard to lose weight yet health care providers talk to them as if they haven’t made any efforts. This is very frustrating for patients. Simply telling a patient to diet and lose weight is a setup for failure. We need to address their past efforts and see what has worked and what hasn’t. Redoing the same thing over and over again is not a recipe for success.
Additionally, the focus on “diet and exercise” fails to account for emotional factors that may be contributing to a person’s obesity. Some people eat when they are stressed or depressed. It can become a habit or even an addiction. If this contributor to obesity isn’t fixed, nothing will work.
However, no medication will work well without the basic building blocks of diet and exercise. Routinely prescribing weight-loss medications without discussing diet and exercise will not result in much weight loss. Some patients simply don’t know how to eat healthfully or what they should do for exercise. A little education can go a long way. Ancillary staff, such as nutritionists or diabetic counselors, can help and free up the doctor’s time. In small practices, we can’t afford to provide those services in house but we should learn where patients can go for these services.
The AACE guidelines do a great job staging obesity. The guidelines make it easier to measure progress and decide on treatment plans. With this system, it is no longer necessary to use terms such as “excess weight” or “morbid obesity.” Patients already know they are overweight. What they need to know are clear steps so that they can reach goals. These guidelines greatly assist with providing those steps.
Most of us can do better when treating patients with obesity, We are probably not even aware of the times we have been guilty of stigmatization or weight bias. When we start treating obesity as a serious medical problem rather than something that’s the fault of the patient, it becomes much easier. When we remind ourselves what can happen to our patients when we fail to treat their obesity, we can become more serious about trying to help them reverse this critical medical problem. Bring an end to throwing out a “lose weight” or “eat healthier” suggestion to our already stressed patients. In order to address the obesity crisis that is here, we need to look inside ourselves and ask how we are going to contribute to the solution.
Dr. Girgis practices family medicine in South River, N.J., and is a clinical assistant of medicine at Robert Wood Johnson Medical School, New Brunswick, N.J.
Obesity is a major factor affecting the health of many Americans. It is estimated by the Centers for Disease Control and Prevention that 41% of adults and 19.7% of children in our country now meet the criteria for being obese. Obesity costs the United States approximately $147 billion annually in health care costs. While these numbers are staggering, they continue to rise.
The recent craze over medications such as Ozempic, Wegovy, and Mounjaro shows how eager people are to lose weight. Yet, many of them face bias, not just in their daily lives, but from health care professionals who should do better. No one should feel stigmatized when they come for medical help. This just drives away patients who need us and who may then suffer more severe consequences of obesity-related illnesses.
Earlier this year, the American Association of Clinical Endocrinology issued a consensus statement on the role stigma and weight bias play in the management of obesity. They proposed a staging system to address the severity of obesity and suggested stigma and bias should be assessed in all patients.
While we are good at diagnosing obesity, many of us fail at addressing it empathetically with patients. I’ve seen many patients cry about past encounters they’ve had in the health care system. We need to address the emotional effect that obesity has as well as the physical complications.
Obesity is a major contributor to many diseases such as diabetes and heart disease, but we are finding it also plays a role in other diseases such as certain cancers. Treating obesity is imperative to prevent these diseases as well as to promote better treatment outcomes. We’ve all seen the diabetic patient lose weight and have their blood glucose levels come under control.
Many patients have tried hard to lose weight yet health care providers talk to them as if they haven’t made any efforts. This is very frustrating for patients. Simply telling a patient to diet and lose weight is a setup for failure. We need to address their past efforts and see what has worked and what hasn’t. Redoing the same thing over and over again is not a recipe for success.
Additionally, the focus on “diet and exercise” fails to account for emotional factors that may be contributing to a person’s obesity. Some people eat when they are stressed or depressed. It can become a habit or even an addiction. If this contributor to obesity isn’t fixed, nothing will work.
However, no medication will work well without the basic building blocks of diet and exercise. Routinely prescribing weight-loss medications without discussing diet and exercise will not result in much weight loss. Some patients simply don’t know how to eat healthfully or what they should do for exercise. A little education can go a long way. Ancillary staff, such as nutritionists or diabetic counselors, can help and free up the doctor’s time. In small practices, we can’t afford to provide those services in house but we should learn where patients can go for these services.
The AACE guidelines do a great job staging obesity. The guidelines make it easier to measure progress and decide on treatment plans. With this system, it is no longer necessary to use terms such as “excess weight” or “morbid obesity.” Patients already know they are overweight. What they need to know are clear steps so that they can reach goals. These guidelines greatly assist with providing those steps.
Most of us can do better when treating patients with obesity, We are probably not even aware of the times we have been guilty of stigmatization or weight bias. When we start treating obesity as a serious medical problem rather than something that’s the fault of the patient, it becomes much easier. When we remind ourselves what can happen to our patients when we fail to treat their obesity, we can become more serious about trying to help them reverse this critical medical problem. Bring an end to throwing out a “lose weight” or “eat healthier” suggestion to our already stressed patients. In order to address the obesity crisis that is here, we need to look inside ourselves and ask how we are going to contribute to the solution.
Dr. Girgis practices family medicine in South River, N.J., and is a clinical assistant of medicine at Robert Wood Johnson Medical School, New Brunswick, N.J.
Obesity is a major factor affecting the health of many Americans. It is estimated by the Centers for Disease Control and Prevention that 41% of adults and 19.7% of children in our country now meet the criteria for being obese. Obesity costs the United States approximately $147 billion annually in health care costs. While these numbers are staggering, they continue to rise.
The recent craze over medications such as Ozempic, Wegovy, and Mounjaro shows how eager people are to lose weight. Yet, many of them face bias, not just in their daily lives, but from health care professionals who should do better. No one should feel stigmatized when they come for medical help. This just drives away patients who need us and who may then suffer more severe consequences of obesity-related illnesses.
Earlier this year, the American Association of Clinical Endocrinology issued a consensus statement on the role stigma and weight bias play in the management of obesity. They proposed a staging system to address the severity of obesity and suggested stigma and bias should be assessed in all patients.
While we are good at diagnosing obesity, many of us fail at addressing it empathetically with patients. I’ve seen many patients cry about past encounters they’ve had in the health care system. We need to address the emotional effect that obesity has as well as the physical complications.
Obesity is a major contributor to many diseases such as diabetes and heart disease, but we are finding it also plays a role in other diseases such as certain cancers. Treating obesity is imperative to prevent these diseases as well as to promote better treatment outcomes. We’ve all seen the diabetic patient lose weight and have their blood glucose levels come under control.
Many patients have tried hard to lose weight yet health care providers talk to them as if they haven’t made any efforts. This is very frustrating for patients. Simply telling a patient to diet and lose weight is a setup for failure. We need to address their past efforts and see what has worked and what hasn’t. Redoing the same thing over and over again is not a recipe for success.
Additionally, the focus on “diet and exercise” fails to account for emotional factors that may be contributing to a person’s obesity. Some people eat when they are stressed or depressed. It can become a habit or even an addiction. If this contributor to obesity isn’t fixed, nothing will work.
However, no medication will work well without the basic building blocks of diet and exercise. Routinely prescribing weight-loss medications without discussing diet and exercise will not result in much weight loss. Some patients simply don’t know how to eat healthfully or what they should do for exercise. A little education can go a long way. Ancillary staff, such as nutritionists or diabetic counselors, can help and free up the doctor’s time. In small practices, we can’t afford to provide those services in house but we should learn where patients can go for these services.
The AACE guidelines do a great job staging obesity. The guidelines make it easier to measure progress and decide on treatment plans. With this system, it is no longer necessary to use terms such as “excess weight” or “morbid obesity.” Patients already know they are overweight. What they need to know are clear steps so that they can reach goals. These guidelines greatly assist with providing those steps.
Most of us can do better when treating patients with obesity, We are probably not even aware of the times we have been guilty of stigmatization or weight bias. When we start treating obesity as a serious medical problem rather than something that’s the fault of the patient, it becomes much easier. When we remind ourselves what can happen to our patients when we fail to treat their obesity, we can become more serious about trying to help them reverse this critical medical problem. Bring an end to throwing out a “lose weight” or “eat healthier” suggestion to our already stressed patients. In order to address the obesity crisis that is here, we need to look inside ourselves and ask how we are going to contribute to the solution.
Dr. Girgis practices family medicine in South River, N.J., and is a clinical assistant of medicine at Robert Wood Johnson Medical School, New Brunswick, N.J.
FDA approves bimekizumab for moderate to severe plaque psoriasis in adults
, the manufacturer announced in a press release.
The indication is for adults who are candidates for systemic therapy or phototherapy.
With this approval, bimekizumab becomes the only interleukin (IL)-17A and IL-17F inhibitor approved for the treatment of these patients. Psoriasis affects more than 7.5 million U.S. adults, according to the National Psoriasis Foundation.
“We have been eagerly awaiting bimekizumab,” Mark Lebwohl, MD, bimekizumab investigator and dean for clinical therapeutics at the Icahn School of Medicine at Mount Sinai, New York City, said in the press release.
Dr. Lebwohl states that bimekizumab “achieved superior levels of skin clearance at week 16 compared to placebo and three existing biologics for psoriasis, with responses being rapid and lasting up to a year. Long-term data have also shown that the majority of patients maintained high levels of clinical response through three years.”
The most common adverse reactions (occurring in at least 1% of patients) are upper respiratory infections, oral candidiasis, headache, tinea infections, gastroenteritis, herpes simplex infections, acne, folliculitis, other Candida infections, fatigue, and injection site reactions, according to the company, UCB.
Available in about 1 month in U.S.
Bimekizumab can be administered by a health care provider or it can be self-injected by a patient after training. It is available as a single-dose prefilled autoinjector and a single-dose prefilled syringe and will be available in the United States in about 1 month.
The recommended dosage of bimekizumab for patients with psoriasis is 320 mg (two subcutaneous injections of 160 mg each) at baseline, then on weeks 4, 8, 12, and 16, then every 8 weeks thereafter. For patients weighing at least 120 kg (about 265 lb), a dosage of 320 mg every 4 weeks after week 16 may be considered, the company states.
Three phase 3 trials
Approval was based on three phase 3 multicenter, randomized, placebo and/or active comparator-controlled trials: bimekizumab versus placebo and ustekinumab (BE VIVID); versus placebo (BE READY); and versus adalimumab (BE SURE).
“All studies met their co-primary endpoints and all ranked secondary endpoints,” the company reports. Secondary endpoints included the Psoriasis Area and Severity Index (PASI) 75 at week 4 and PASI 100 (complete skin clearance) at week 16.
Highlights from the trials include the following results, according to UCB:
- Clear or almost clear skin: More than 8 out of 10 patients achieved a 90% or greater reduction from baseline in the PASI 90 and an Investigator’s Global Assessment score of 0/1 at week 16.
- Complete skin clearance: About 60% of patients achieved PASI 100 at week 16.
- Time to response: More than 70% of patients achieved PASI 75 at week 4 following one 320-mg dose.
Safety information
The safety information includes the statement that bimekizumab may increase the risk for suicidal ideation and behavior, though a causal association has not been established. Prescribers should advise patients, caregivers, and families “to monitor for emergence or worsening of depression, suicidal ideation, or other mood changes,” according to the prescribing information.
Bimekizumab is being studied for other conditions, including hidradenitis suppurativa. In the European Union, it was approved for the treatment of psoriasis in 2021 and for the treatment of psoriatic arthritis and ankylosing spondylitis in June 2023.
Dr. Lebwohl is an investigator for UCB. He has not accepted any consulting payments from UCB.
A version of this article first appeared on Medscape.com.
, the manufacturer announced in a press release.
The indication is for adults who are candidates for systemic therapy or phototherapy.
With this approval, bimekizumab becomes the only interleukin (IL)-17A and IL-17F inhibitor approved for the treatment of these patients. Psoriasis affects more than 7.5 million U.S. adults, according to the National Psoriasis Foundation.
“We have been eagerly awaiting bimekizumab,” Mark Lebwohl, MD, bimekizumab investigator and dean for clinical therapeutics at the Icahn School of Medicine at Mount Sinai, New York City, said in the press release.
Dr. Lebwohl states that bimekizumab “achieved superior levels of skin clearance at week 16 compared to placebo and three existing biologics for psoriasis, with responses being rapid and lasting up to a year. Long-term data have also shown that the majority of patients maintained high levels of clinical response through three years.”
The most common adverse reactions (occurring in at least 1% of patients) are upper respiratory infections, oral candidiasis, headache, tinea infections, gastroenteritis, herpes simplex infections, acne, folliculitis, other Candida infections, fatigue, and injection site reactions, according to the company, UCB.
Available in about 1 month in U.S.
Bimekizumab can be administered by a health care provider or it can be self-injected by a patient after training. It is available as a single-dose prefilled autoinjector and a single-dose prefilled syringe and will be available in the United States in about 1 month.
The recommended dosage of bimekizumab for patients with psoriasis is 320 mg (two subcutaneous injections of 160 mg each) at baseline, then on weeks 4, 8, 12, and 16, then every 8 weeks thereafter. For patients weighing at least 120 kg (about 265 lb), a dosage of 320 mg every 4 weeks after week 16 may be considered, the company states.
Three phase 3 trials
Approval was based on three phase 3 multicenter, randomized, placebo and/or active comparator-controlled trials: bimekizumab versus placebo and ustekinumab (BE VIVID); versus placebo (BE READY); and versus adalimumab (BE SURE).
“All studies met their co-primary endpoints and all ranked secondary endpoints,” the company reports. Secondary endpoints included the Psoriasis Area and Severity Index (PASI) 75 at week 4 and PASI 100 (complete skin clearance) at week 16.
Highlights from the trials include the following results, according to UCB:
- Clear or almost clear skin: More than 8 out of 10 patients achieved a 90% or greater reduction from baseline in the PASI 90 and an Investigator’s Global Assessment score of 0/1 at week 16.
- Complete skin clearance: About 60% of patients achieved PASI 100 at week 16.
- Time to response: More than 70% of patients achieved PASI 75 at week 4 following one 320-mg dose.
Safety information
The safety information includes the statement that bimekizumab may increase the risk for suicidal ideation and behavior, though a causal association has not been established. Prescribers should advise patients, caregivers, and families “to monitor for emergence or worsening of depression, suicidal ideation, or other mood changes,” according to the prescribing information.
Bimekizumab is being studied for other conditions, including hidradenitis suppurativa. In the European Union, it was approved for the treatment of psoriasis in 2021 and for the treatment of psoriatic arthritis and ankylosing spondylitis in June 2023.
Dr. Lebwohl is an investigator for UCB. He has not accepted any consulting payments from UCB.
A version of this article first appeared on Medscape.com.
, the manufacturer announced in a press release.
The indication is for adults who are candidates for systemic therapy or phototherapy.
With this approval, bimekizumab becomes the only interleukin (IL)-17A and IL-17F inhibitor approved for the treatment of these patients. Psoriasis affects more than 7.5 million U.S. adults, according to the National Psoriasis Foundation.
“We have been eagerly awaiting bimekizumab,” Mark Lebwohl, MD, bimekizumab investigator and dean for clinical therapeutics at the Icahn School of Medicine at Mount Sinai, New York City, said in the press release.
Dr. Lebwohl states that bimekizumab “achieved superior levels of skin clearance at week 16 compared to placebo and three existing biologics for psoriasis, with responses being rapid and lasting up to a year. Long-term data have also shown that the majority of patients maintained high levels of clinical response through three years.”
The most common adverse reactions (occurring in at least 1% of patients) are upper respiratory infections, oral candidiasis, headache, tinea infections, gastroenteritis, herpes simplex infections, acne, folliculitis, other Candida infections, fatigue, and injection site reactions, according to the company, UCB.
Available in about 1 month in U.S.
Bimekizumab can be administered by a health care provider or it can be self-injected by a patient after training. It is available as a single-dose prefilled autoinjector and a single-dose prefilled syringe and will be available in the United States in about 1 month.
The recommended dosage of bimekizumab for patients with psoriasis is 320 mg (two subcutaneous injections of 160 mg each) at baseline, then on weeks 4, 8, 12, and 16, then every 8 weeks thereafter. For patients weighing at least 120 kg (about 265 lb), a dosage of 320 mg every 4 weeks after week 16 may be considered, the company states.
Three phase 3 trials
Approval was based on three phase 3 multicenter, randomized, placebo and/or active comparator-controlled trials: bimekizumab versus placebo and ustekinumab (BE VIVID); versus placebo (BE READY); and versus adalimumab (BE SURE).
“All studies met their co-primary endpoints and all ranked secondary endpoints,” the company reports. Secondary endpoints included the Psoriasis Area and Severity Index (PASI) 75 at week 4 and PASI 100 (complete skin clearance) at week 16.
Highlights from the trials include the following results, according to UCB:
- Clear or almost clear skin: More than 8 out of 10 patients achieved a 90% or greater reduction from baseline in the PASI 90 and an Investigator’s Global Assessment score of 0/1 at week 16.
- Complete skin clearance: About 60% of patients achieved PASI 100 at week 16.
- Time to response: More than 70% of patients achieved PASI 75 at week 4 following one 320-mg dose.
Safety information
The safety information includes the statement that bimekizumab may increase the risk for suicidal ideation and behavior, though a causal association has not been established. Prescribers should advise patients, caregivers, and families “to monitor for emergence or worsening of depression, suicidal ideation, or other mood changes,” according to the prescribing information.
Bimekizumab is being studied for other conditions, including hidradenitis suppurativa. In the European Union, it was approved for the treatment of psoriasis in 2021 and for the treatment of psoriatic arthritis and ankylosing spondylitis in June 2023.
Dr. Lebwohl is an investigator for UCB. He has not accepted any consulting payments from UCB.
A version of this article first appeared on Medscape.com.
Once-weekly topical therapy shows promise for moderate to severe acne
TOPLINE:
METHODOLOGY:
- Poor patient compliance with topical acne therapies is a common clinical challenge.
- In a 12-week, randomized, controlled, phase 2b trial of 181 patients 12 years of age and older, researchers investigated the safety, tolerability, and efficacy of DMT310, a powdered mixture of Spongilla lacustris for treating moderate to severe acne. (In vitro studies have found that components of S. lacustris, a freshwater sponge, have effects that include antimicrobial activity against Cutibacterium acnes and anti-inflammatory activity in human keratinocytes).
- The study’s primary efficacy endpoint was the absolute change in inflammatory lesion count from baseline to week 12.
- Endpoint success was defined as an Investigator Global Assessment (IGA) score of 0 or 1 and at least a two-grade improvement from baseline at week 12.
TAKEAWAY:
- Of the 181 patients, 91 received DMT310 (applied once a week to the face and washed off after 10-15 minutes), and 90 received placebo.
- Patients in the DMT310 arm showed a significantly greater mean reduction in the number of inflammatory lesions at week 12, compared with those in the placebo arm (–15.64 vs. –10.84, respectively; P < .001).
- Similarly, patients in the DMT310 arm showed a significantly greater mean reduction in the number of noninflammatory lesions at week 12, compared with those in the placebo arm (–18.26 vs. –12.41, respectively; P < .001).
- At week 12, endpoint success based on IGA scores also significantly favored patients in the DMT310 arm, compared with those in the placebo arm (44.40% vs. 17.78%; P < .001).
IN PRACTICE:
This study is too preliminary to have practice application. The researchers concluded that the findings “support further study of DMT310 in larger, confirmatory phase 3 trials.”
SOURCE:
Lawrence F. Eichenfield, MD, professor of dermatology and pediatrics at the University of California, San Diego, led the research. The study was published online June 7 in the Journal of the American Academy of Dermatology.
LIMITATIONS:
The analysis did not include an active comparator group and it enrolled a limited number of Asian patients.
DISCLOSURES:
Dr. Eichenfield disclosed that he is a consultant to Dermata, which is developing DMT310, as were three other authors of the study. One author is a company employee. The remaining authors disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
TOPLINE:
METHODOLOGY:
- Poor patient compliance with topical acne therapies is a common clinical challenge.
- In a 12-week, randomized, controlled, phase 2b trial of 181 patients 12 years of age and older, researchers investigated the safety, tolerability, and efficacy of DMT310, a powdered mixture of Spongilla lacustris for treating moderate to severe acne. (In vitro studies have found that components of S. lacustris, a freshwater sponge, have effects that include antimicrobial activity against Cutibacterium acnes and anti-inflammatory activity in human keratinocytes).
- The study’s primary efficacy endpoint was the absolute change in inflammatory lesion count from baseline to week 12.
- Endpoint success was defined as an Investigator Global Assessment (IGA) score of 0 or 1 and at least a two-grade improvement from baseline at week 12.
TAKEAWAY:
- Of the 181 patients, 91 received DMT310 (applied once a week to the face and washed off after 10-15 minutes), and 90 received placebo.
- Patients in the DMT310 arm showed a significantly greater mean reduction in the number of inflammatory lesions at week 12, compared with those in the placebo arm (–15.64 vs. –10.84, respectively; P < .001).
- Similarly, patients in the DMT310 arm showed a significantly greater mean reduction in the number of noninflammatory lesions at week 12, compared with those in the placebo arm (–18.26 vs. –12.41, respectively; P < .001).
- At week 12, endpoint success based on IGA scores also significantly favored patients in the DMT310 arm, compared with those in the placebo arm (44.40% vs. 17.78%; P < .001).
IN PRACTICE:
This study is too preliminary to have practice application. The researchers concluded that the findings “support further study of DMT310 in larger, confirmatory phase 3 trials.”
SOURCE:
Lawrence F. Eichenfield, MD, professor of dermatology and pediatrics at the University of California, San Diego, led the research. The study was published online June 7 in the Journal of the American Academy of Dermatology.
LIMITATIONS:
The analysis did not include an active comparator group and it enrolled a limited number of Asian patients.
DISCLOSURES:
Dr. Eichenfield disclosed that he is a consultant to Dermata, which is developing DMT310, as were three other authors of the study. One author is a company employee. The remaining authors disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
TOPLINE:
METHODOLOGY:
- Poor patient compliance with topical acne therapies is a common clinical challenge.
- In a 12-week, randomized, controlled, phase 2b trial of 181 patients 12 years of age and older, researchers investigated the safety, tolerability, and efficacy of DMT310, a powdered mixture of Spongilla lacustris for treating moderate to severe acne. (In vitro studies have found that components of S. lacustris, a freshwater sponge, have effects that include antimicrobial activity against Cutibacterium acnes and anti-inflammatory activity in human keratinocytes).
- The study’s primary efficacy endpoint was the absolute change in inflammatory lesion count from baseline to week 12.
- Endpoint success was defined as an Investigator Global Assessment (IGA) score of 0 or 1 and at least a two-grade improvement from baseline at week 12.
TAKEAWAY:
- Of the 181 patients, 91 received DMT310 (applied once a week to the face and washed off after 10-15 minutes), and 90 received placebo.
- Patients in the DMT310 arm showed a significantly greater mean reduction in the number of inflammatory lesions at week 12, compared with those in the placebo arm (–15.64 vs. –10.84, respectively; P < .001).
- Similarly, patients in the DMT310 arm showed a significantly greater mean reduction in the number of noninflammatory lesions at week 12, compared with those in the placebo arm (–18.26 vs. –12.41, respectively; P < .001).
- At week 12, endpoint success based on IGA scores also significantly favored patients in the DMT310 arm, compared with those in the placebo arm (44.40% vs. 17.78%; P < .001).
IN PRACTICE:
This study is too preliminary to have practice application. The researchers concluded that the findings “support further study of DMT310 in larger, confirmatory phase 3 trials.”
SOURCE:
Lawrence F. Eichenfield, MD, professor of dermatology and pediatrics at the University of California, San Diego, led the research. The study was published online June 7 in the Journal of the American Academy of Dermatology.
LIMITATIONS:
The analysis did not include an active comparator group and it enrolled a limited number of Asian patients.
DISCLOSURES:
Dr. Eichenfield disclosed that he is a consultant to Dermata, which is developing DMT310, as were three other authors of the study. One author is a company employee. The remaining authors disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.