User login
Open vs. endovascular for chronic mesenteric ischemia
Chronic mesenteric ischemia is best treated in an open operation.
Chronic mesenteric ischemia is a rare disorder accounting for about 1 out of 100,000 admissions.1 Because of the rarity of this disease, diagnosis is often delayed. Patients are often evaluated for other gastrointestinal diseases and/or malignancies, which in turn contributes to significant delays in diagnosis. Additionally, there are no prospective, randomized trials on which to base decisions regarding treatment; and it is unlikely that such studies will ever be undertaken.
Chronic mesenteric ischemia develops when two or more of the mesenteric vessels (celiac, superior mesenteric [SMA], or inferior mesenteric [IMA]) become occluded or develop severe stenosis. In my experience, patients most often develop occlusion (as opposed to stenosis) of their mesenteric vessels. The atherosclerotic plaque responsible for the disease originates within the aorta and the stenosis/occlusion develops at the vessel origin.

As a whole, these comorbidities would suggest that a more minimally invasive approach would be preferred. Yet, an open operation for chronic mesenteric ischemia should not be discarded as an initial operation.
Endovascular treatment of mesenteric ischemia is not without risk. As in all endovascular procedures there are complications associated with the access vessels. The orientation of the mesenteric vessels as they arise from the aorta often favors an approach from the left arm. The brachial artery is smaller than the femoral artery, and it is more difficult to apply pressure to the brachial artery to control the puncture site. This leads to a higher rate of access site complications including hemorrhage, pseudoaneurysm and thrombosis of the vessel. Bleeding or hematoma formation within the brachial neurovascular sheath can result in significant neurologic dysfunction of the arm and hand. There is risk of stroke, especially when the access vessel is the brachial artery. There are also complications directly related to the endovascular procedure.
Atheroembolism of plaque can result in occlusion of small mesenteric vessels and focal areas of bowel necrosis. Dissection of the mesenteric vessel can occur. Oderich has advocated for the use of a covered stent.2 A covered stent could cover proximal branches, and thus, in theory, the treatment itself could cause bowel ischemia or infarction. Many series that have compared open and endovascular surgery show no difference in early outcomes, but demonstrate early restenosis, decreased primary patency, and decreased assisted primary patency with endovascular treatment as compared with open operations.3-5
Another concern regarding the treatment of mesenteric ischemia is the status of the end organ, the bowel. Successful treatment of mesenteric ischemia cannot only assess the atherosclerotic lesion, but requires the surgeon to be cognizant of the condition of the bowel.
This concern is especially true for acute mesenteric ischemia,6 but the status of the bowel must also be kept in mind for chronic mesenteric ischemia. Unlike the lower extremity where the results of treatment are easily observed by inspection (color, evidence of atheroembolization), palpation (temperature, pulse), and physiologic testing (ABI), the bowel is not accessible. There are no highly accurate tests to determine if the patient has on-going bowel ischemia or has developed infarction. Should a complication occur, physical examination findings and laboratory changes often become apparent late in the course of the disease. As previously noted, these patients are often physiologically compromised and have little reserve and may not survive such complications. An open operation allows visualization of the bowel, before and after revascularization.
Traditional teaching for the surgical treatment of chronic mesenteric ischemia has emphasized that two mesenteric vessels, usually the celiac and SMA, should be revascularized.7,8 Various approaches to revascularization have been suggested including transaortic endarterectomy and an antegrade bifurcated bypass originating from the supraceliac aorta. These operations are effective in restoring flow to the mesenteric circulation, but both of these approaches involve aortic cross-clamping and are physiologically challenging for patients.
There are alternatives for open revascularization of the mesenteric vessels. The infrarenal aorta, iliac vessels, and even renal arteries can be, and have been used as the inflow source. It has been my experience that a bypass graft using an iliac artery (common or external) as the inflow source is well tolerated by patients. I have preferentially used either great saphenous vein or femoral-popliteal vein as the conduit. In many cases, the distal anastomosis is simply the SMA. However, both the celiac and SMA can be revascularized by creating a side-side anastomosis to the SMA and an end-side anastomosis to the common or proper hepatic artery. Such procedures have been durable, providing relief of symptoms and allowing patients to regain weight.9
In reality, I believe that an endovascular approach for the treatment of chronic mesenteric ischemia has a role. Vascular surgeons are uniquely positioned to carefully evaluate each patient and recommend what they feel is most appropriate. I tend to feel that an endovascular approach is less likely to be successful for patients with occluded vessels, especially those with a flush occlusion, and so will preferentially recommend an open operation for these patients. On the other hand, in my practice, I have used an endovascular approach for patients with severe stenosis, and as Dr. Harris states, know that a bypass is always an option should this be unsuccessful or ultimately fail.
References
1. Ann Vasc Surg. 1991;5:403-6
2. J Vasc Surg. 2013;58:1316-23
3. Ann Vasc Surg. 2015:29;934-40
4. World J Gastroenerol. 2013;19:1333-7
5. J Vasc Surg. 2007;45:1162-71
6. J Vasc Surg. 2015;62:767-72
7. J Vasc Surg. 2002:35:853-9
8. Surgery. 1981;90:940-6
9. J Vasc Surg. 2000;32:37-47
Eric Endean, MD, is the director of the aortic center, Gordon L. Hyde Endowed Professor and Chair, and vascular surgery section head, vascular and endovascular surgery at UK HealthCare, University of Kentucky, Lexington. He had no relevant disclosures.
Presenting the case for endovascular intervention
Chronic mesenteric ischemia (CMI) is an uncommon, but lethal, problem when left untreated. Before the endovascular era, the only option was open revascularization, which is challenging in this chronically ill, malnourished population with diffuse, systemic, atherosclerotic disease. Morbidity and mortality was relatively high because of the comorbid conditions and chronically ill status of the patients. The first mesenteric bypass was performed in 1958 by Maynard and Shaw.1
Options for open repair include transaortic endarterectomy, antegrade bypass from the supraceliac aorta or distal thoracic aorta, or retrograde bypass from the iliac artery, all of which are major abdominal procedures. Endovascular interventions are now the most commonly performed procedures for CMI in the United States based on national studies.2

Technical success with endovascular interventions can be achieved in well over 90% of patients, and multiple vessels can be treated simultaneously from either a femoral or brachial approach. The primary concern with endovascular interventions has been long-term patency, with restenosis from intimal hyperplasia or thrombosis causing recurrent symptoms in up to 30%-50% at 3-5 years.5-7 However, these rates are based on use of bare metal stents, rather than covered stents. Recent studies8 suggest that stent grafts have markedly improved outcomes over bare metal stents for ostial lesions, decreasing recurrence. Oderich found that freedom from recurrence was 92% with stent grafts as compared with 53% for bare metal stents, with primary patency rates of 92%, at 3 years8, comparable to even the best open bypass results. Schoch first reported the use of covered stents in the mesenteric circulation, and found that no patients developed recurrent stenosis at 2 years.9 Other concerns with endovascular intervention include embolization and dissection, which have not been frequently reported.
Mortality from open surgery ranges from 5% to 15%, with morbidity of 30%-40%.4 Mortality from endovascular intervention is markedly lower, in the range of 3.56% vs. 7.23%.5 Long-term survival is not different between endovascular vs. open repair (69% vs. 65%),4 with the majority of deaths related to cardiac, pulmonary, or malignancy issues. Moghadamyeghaneh, in a review of the Nationwide Inpatient Sample database, found that open surgery was one of the major predictors for higher morbidity (odds ratio, 5.07) and mortality (OR, 5.13), despite the fact that endovascular patients were older (another risk factor for adverse outcomes) and had more comorbidities in this nonrandomized, real-world study.2
Further, if one considers cost as a metric for decision making, a Markov clinical decision model by Hogendoorn et al suggests an endovascular first approach is preferred, despite the presumed higher rate of recurrence expected with use of bare metal stents, rather than covered stents, utilized for this analysis.10 Clearly, the financial advantage would be even greater for endovascular with the lower rates of recurrence with covered stents more recently reported.
If a patient develops recurrent stenosis after endovascular intervention, open bypass may be considered as an alternate to repeat endovascular intervention, dependent on the nutritional status, life expectancy, and initial intervention undertaken. Alternately, patients who undergo open repair are not immune to restenosis, with a recurrence rate of 10%-20%.11,12 Oderich found that there was a 22% mortality in those treated with repeat open interventions, with a 47% complication rate. Endovascular interventions, however, had a significantly lower rate of complications, 16%, and mortality. For patients with recurrent disease after open revascularization for CMI, the endovascular approach should also be the preferred approach.
Any lesion which is anatomically suitable for endovascular repair should first have an attempt made via this approach, utilizing covered stents. While there is a role for open revascularization, endovascular interventions can be safely performed, with minimal morbidity and mortality, and good long-term patency, even in the sickest patients. Endovascular intervention should be the procedure of choice for chronic mesenteric ischemia and recurrent chronic mesenteric ischemia.
References
1. NEJM. 1958;258:874-8
2. Am Surg. 2015;81:1149-56
3. Cardiovasc Intervent Radiol. 1980;3:43-4
4. Ann Vasc Surg. 2009;23:700-12
5. Ann Vasc Surg. 2013;27:113-22
6. J Vasc Surg. 2011;54:1422-29
7. J Vasc Surg. 2010;51:140-7
8. J Vasc Surg. 2013;58:1316-24
9. JACS. 2001;212:668-75
10. J Vasc Surg. 2014;60;715-25
11. J Vasc Surg. 200;49:1472-9
12. J Vasc Surg. 2007;45:1162-71
Linda Harris, MD, is professor of surgery; chief, division of vascular surgery; program director, vascular surgery residency & fellowship at the State University of New York at Buffalo; and an associate medical editor for Vascular Specialist. She had no relevant disclosures.
Chronic mesenteric ischemia is best treated in an open operation.
Chronic mesenteric ischemia is a rare disorder accounting for about 1 out of 100,000 admissions.1 Because of the rarity of this disease, diagnosis is often delayed. Patients are often evaluated for other gastrointestinal diseases and/or malignancies, which in turn contributes to significant delays in diagnosis. Additionally, there are no prospective, randomized trials on which to base decisions regarding treatment; and it is unlikely that such studies will ever be undertaken.
Chronic mesenteric ischemia develops when two or more of the mesenteric vessels (celiac, superior mesenteric [SMA], or inferior mesenteric [IMA]) become occluded or develop severe stenosis. In my experience, patients most often develop occlusion (as opposed to stenosis) of their mesenteric vessels. The atherosclerotic plaque responsible for the disease originates within the aorta and the stenosis/occlusion develops at the vessel origin.
As a whole, these comorbidities would suggest that a more minimally invasive approach would be preferred. Yet, an open operation for chronic mesenteric ischemia should not be discarded as an initial operation.
Endovascular treatment of mesenteric ischemia is not without risk. As in all endovascular procedures there are complications associated with the access vessels. The orientation of the mesenteric vessels as they arise from the aorta often favors an approach from the left arm. The brachial artery is smaller than the femoral artery, and it is more difficult to apply pressure to the brachial artery to control the puncture site. This leads to a higher rate of access site complications including hemorrhage, pseudoaneurysm and thrombosis of the vessel. Bleeding or hematoma formation within the brachial neurovascular sheath can result in significant neurologic dysfunction of the arm and hand. There is risk of stroke, especially when the access vessel is the brachial artery. There are also complications directly related to the endovascular procedure.
Atheroembolism of plaque can result in occlusion of small mesenteric vessels and focal areas of bowel necrosis. Dissection of the mesenteric vessel can occur. Oderich has advocated for the use of a covered stent.2 A covered stent could cover proximal branches, and thus, in theory, the treatment itself could cause bowel ischemia or infarction. Many series that have compared open and endovascular surgery show no difference in early outcomes, but demonstrate early restenosis, decreased primary patency, and decreased assisted primary patency with endovascular treatment as compared with open operations.3-5
Another concern regarding the treatment of mesenteric ischemia is the status of the end organ, the bowel. Successful treatment of mesenteric ischemia cannot only assess the atherosclerotic lesion, but requires the surgeon to be cognizant of the condition of the bowel.
This concern is especially true for acute mesenteric ischemia,6 but the status of the bowel must also be kept in mind for chronic mesenteric ischemia. Unlike the lower extremity where the results of treatment are easily observed by inspection (color, evidence of atheroembolization), palpation (temperature, pulse), and physiologic testing (ABI), the bowel is not accessible. There are no highly accurate tests to determine if the patient has on-going bowel ischemia or has developed infarction. Should a complication occur, physical examination findings and laboratory changes often become apparent late in the course of the disease. As previously noted, these patients are often physiologically compromised and have little reserve and may not survive such complications. An open operation allows visualization of the bowel, before and after revascularization.
Traditional teaching for the surgical treatment of chronic mesenteric ischemia has emphasized that two mesenteric vessels, usually the celiac and SMA, should be revascularized.7,8 Various approaches to revascularization have been suggested including transaortic endarterectomy and an antegrade bifurcated bypass originating from the supraceliac aorta. These operations are effective in restoring flow to the mesenteric circulation, but both of these approaches involve aortic cross-clamping and are physiologically challenging for patients.
There are alternatives for open revascularization of the mesenteric vessels. The infrarenal aorta, iliac vessels, and even renal arteries can be, and have been used as the inflow source. It has been my experience that a bypass graft using an iliac artery (common or external) as the inflow source is well tolerated by patients. I have preferentially used either great saphenous vein or femoral-popliteal vein as the conduit. In many cases, the distal anastomosis is simply the SMA. However, both the celiac and SMA can be revascularized by creating a side-side anastomosis to the SMA and an end-side anastomosis to the common or proper hepatic artery. Such procedures have been durable, providing relief of symptoms and allowing patients to regain weight.9
In reality, I believe that an endovascular approach for the treatment of chronic mesenteric ischemia has a role. Vascular surgeons are uniquely positioned to carefully evaluate each patient and recommend what they feel is most appropriate. I tend to feel that an endovascular approach is less likely to be successful for patients with occluded vessels, especially those with a flush occlusion, and so will preferentially recommend an open operation for these patients. On the other hand, in my practice, I have used an endovascular approach for patients with severe stenosis, and as Dr. Harris states, know that a bypass is always an option should this be unsuccessful or ultimately fail.
References
1. Ann Vasc Surg. 1991;5:403-6
2. J Vasc Surg. 2013;58:1316-23
3. Ann Vasc Surg. 2015:29;934-40
4. World J Gastroenerol. 2013;19:1333-7
5. J Vasc Surg. 2007;45:1162-71
6. J Vasc Surg. 2015;62:767-72
7. J Vasc Surg. 2002:35:853-9
8. Surgery. 1981;90:940-6
9. J Vasc Surg. 2000;32:37-47
Eric Endean, MD, is the director of the aortic center, Gordon L. Hyde Endowed Professor and Chair, and vascular surgery section head, vascular and endovascular surgery at UK HealthCare, University of Kentucky, Lexington. He had no relevant disclosures.
Presenting the case for endovascular intervention
Chronic mesenteric ischemia (CMI) is an uncommon, but lethal, problem when left untreated. Before the endovascular era, the only option was open revascularization, which is challenging in this chronically ill, malnourished population with diffuse, systemic, atherosclerotic disease. Morbidity and mortality was relatively high because of the comorbid conditions and chronically ill status of the patients. The first mesenteric bypass was performed in 1958 by Maynard and Shaw.1
Options for open repair include transaortic endarterectomy, antegrade bypass from the supraceliac aorta or distal thoracic aorta, or retrograde bypass from the iliac artery, all of which are major abdominal procedures. Endovascular interventions are now the most commonly performed procedures for CMI in the United States based on national studies.2
Technical success with endovascular interventions can be achieved in well over 90% of patients, and multiple vessels can be treated simultaneously from either a femoral or brachial approach. The primary concern with endovascular interventions has been long-term patency, with restenosis from intimal hyperplasia or thrombosis causing recurrent symptoms in up to 30%-50% at 3-5 years.5-7 However, these rates are based on use of bare metal stents, rather than covered stents. Recent studies8 suggest that stent grafts have markedly improved outcomes over bare metal stents for ostial lesions, decreasing recurrence. Oderich found that freedom from recurrence was 92% with stent grafts as compared with 53% for bare metal stents, with primary patency rates of 92%, at 3 years8, comparable to even the best open bypass results. Schoch first reported the use of covered stents in the mesenteric circulation, and found that no patients developed recurrent stenosis at 2 years.9 Other concerns with endovascular intervention include embolization and dissection, which have not been frequently reported.
Mortality from open surgery ranges from 5% to 15%, with morbidity of 30%-40%.4 Mortality from endovascular intervention is markedly lower, in the range of 3.56% vs. 7.23%.5 Long-term survival is not different between endovascular vs. open repair (69% vs. 65%),4 with the majority of deaths related to cardiac, pulmonary, or malignancy issues. Moghadamyeghaneh, in a review of the Nationwide Inpatient Sample database, found that open surgery was one of the major predictors for higher morbidity (odds ratio, 5.07) and mortality (OR, 5.13), despite the fact that endovascular patients were older (another risk factor for adverse outcomes) and had more comorbidities in this nonrandomized, real-world study.2
Further, if one considers cost as a metric for decision making, a Markov clinical decision model by Hogendoorn et al suggests an endovascular first approach is preferred, despite the presumed higher rate of recurrence expected with use of bare metal stents, rather than covered stents, utilized for this analysis.10 Clearly, the financial advantage would be even greater for endovascular with the lower rates of recurrence with covered stents more recently reported.
If a patient develops recurrent stenosis after endovascular intervention, open bypass may be considered as an alternate to repeat endovascular intervention, dependent on the nutritional status, life expectancy, and initial intervention undertaken. Alternately, patients who undergo open repair are not immune to restenosis, with a recurrence rate of 10%-20%.11,12 Oderich found that there was a 22% mortality in those treated with repeat open interventions, with a 47% complication rate. Endovascular interventions, however, had a significantly lower rate of complications, 16%, and mortality. For patients with recurrent disease after open revascularization for CMI, the endovascular approach should also be the preferred approach.
Any lesion which is anatomically suitable for endovascular repair should first have an attempt made via this approach, utilizing covered stents. While there is a role for open revascularization, endovascular interventions can be safely performed, with minimal morbidity and mortality, and good long-term patency, even in the sickest patients. Endovascular intervention should be the procedure of choice for chronic mesenteric ischemia and recurrent chronic mesenteric ischemia.
References
1. NEJM. 1958;258:874-8
2. Am Surg. 2015;81:1149-56
3. Cardiovasc Intervent Radiol. 1980;3:43-4
4. Ann Vasc Surg. 2009;23:700-12
5. Ann Vasc Surg. 2013;27:113-22
6. J Vasc Surg. 2011;54:1422-29
7. J Vasc Surg. 2010;51:140-7
8. J Vasc Surg. 2013;58:1316-24
9. JACS. 2001;212:668-75
10. J Vasc Surg. 2014;60;715-25
11. J Vasc Surg. 200;49:1472-9
12. J Vasc Surg. 2007;45:1162-71
Linda Harris, MD, is professor of surgery; chief, division of vascular surgery; program director, vascular surgery residency & fellowship at the State University of New York at Buffalo; and an associate medical editor for Vascular Specialist. She had no relevant disclosures.
Chronic mesenteric ischemia is best treated in an open operation.
Chronic mesenteric ischemia is a rare disorder accounting for about 1 out of 100,000 admissions.1 Because of the rarity of this disease, diagnosis is often delayed. Patients are often evaluated for other gastrointestinal diseases and/or malignancies, which in turn contributes to significant delays in diagnosis. Additionally, there are no prospective, randomized trials on which to base decisions regarding treatment; and it is unlikely that such studies will ever be undertaken.
Chronic mesenteric ischemia develops when two or more of the mesenteric vessels (celiac, superior mesenteric [SMA], or inferior mesenteric [IMA]) become occluded or develop severe stenosis. In my experience, patients most often develop occlusion (as opposed to stenosis) of their mesenteric vessels. The atherosclerotic plaque responsible for the disease originates within the aorta and the stenosis/occlusion develops at the vessel origin.
As a whole, these comorbidities would suggest that a more minimally invasive approach would be preferred. Yet, an open operation for chronic mesenteric ischemia should not be discarded as an initial operation.
Endovascular treatment of mesenteric ischemia is not without risk. As in all endovascular procedures there are complications associated with the access vessels. The orientation of the mesenteric vessels as they arise from the aorta often favors an approach from the left arm. The brachial artery is smaller than the femoral artery, and it is more difficult to apply pressure to the brachial artery to control the puncture site. This leads to a higher rate of access site complications including hemorrhage, pseudoaneurysm and thrombosis of the vessel. Bleeding or hematoma formation within the brachial neurovascular sheath can result in significant neurologic dysfunction of the arm and hand. There is risk of stroke, especially when the access vessel is the brachial artery. There are also complications directly related to the endovascular procedure.
Atheroembolism of plaque can result in occlusion of small mesenteric vessels and focal areas of bowel necrosis. Dissection of the mesenteric vessel can occur. Oderich has advocated for the use of a covered stent.2 A covered stent could cover proximal branches, and thus, in theory, the treatment itself could cause bowel ischemia or infarction. Many series that have compared open and endovascular surgery show no difference in early outcomes, but demonstrate early restenosis, decreased primary patency, and decreased assisted primary patency with endovascular treatment as compared with open operations.3-5
Another concern regarding the treatment of mesenteric ischemia is the status of the end organ, the bowel. Successful treatment of mesenteric ischemia cannot only assess the atherosclerotic lesion, but requires the surgeon to be cognizant of the condition of the bowel.
This concern is especially true for acute mesenteric ischemia,6 but the status of the bowel must also be kept in mind for chronic mesenteric ischemia. Unlike the lower extremity where the results of treatment are easily observed by inspection (color, evidence of atheroembolization), palpation (temperature, pulse), and physiologic testing (ABI), the bowel is not accessible. There are no highly accurate tests to determine if the patient has on-going bowel ischemia or has developed infarction. Should a complication occur, physical examination findings and laboratory changes often become apparent late in the course of the disease. As previously noted, these patients are often physiologically compromised and have little reserve and may not survive such complications. An open operation allows visualization of the bowel, before and after revascularization.
Traditional teaching for the surgical treatment of chronic mesenteric ischemia has emphasized that two mesenteric vessels, usually the celiac and SMA, should be revascularized.7,8 Various approaches to revascularization have been suggested including transaortic endarterectomy and an antegrade bifurcated bypass originating from the supraceliac aorta. These operations are effective in restoring flow to the mesenteric circulation, but both of these approaches involve aortic cross-clamping and are physiologically challenging for patients.
There are alternatives for open revascularization of the mesenteric vessels. The infrarenal aorta, iliac vessels, and even renal arteries can be, and have been used as the inflow source. It has been my experience that a bypass graft using an iliac artery (common or external) as the inflow source is well tolerated by patients. I have preferentially used either great saphenous vein or femoral-popliteal vein as the conduit. In many cases, the distal anastomosis is simply the SMA. However, both the celiac and SMA can be revascularized by creating a side-side anastomosis to the SMA and an end-side anastomosis to the common or proper hepatic artery. Such procedures have been durable, providing relief of symptoms and allowing patients to regain weight.9
In reality, I believe that an endovascular approach for the treatment of chronic mesenteric ischemia has a role. Vascular surgeons are uniquely positioned to carefully evaluate each patient and recommend what they feel is most appropriate. I tend to feel that an endovascular approach is less likely to be successful for patients with occluded vessels, especially those with a flush occlusion, and so will preferentially recommend an open operation for these patients. On the other hand, in my practice, I have used an endovascular approach for patients with severe stenosis, and as Dr. Harris states, know that a bypass is always an option should this be unsuccessful or ultimately fail.
References
1. Ann Vasc Surg. 1991;5:403-6
2. J Vasc Surg. 2013;58:1316-23
3. Ann Vasc Surg. 2015:29;934-40
4. World J Gastroenerol. 2013;19:1333-7
5. J Vasc Surg. 2007;45:1162-71
6. J Vasc Surg. 2015;62:767-72
7. J Vasc Surg. 2002:35:853-9
8. Surgery. 1981;90:940-6
9. J Vasc Surg. 2000;32:37-47
Eric Endean, MD, is the director of the aortic center, Gordon L. Hyde Endowed Professor and Chair, and vascular surgery section head, vascular and endovascular surgery at UK HealthCare, University of Kentucky, Lexington. He had no relevant disclosures.
Presenting the case for endovascular intervention
Chronic mesenteric ischemia (CMI) is an uncommon, but lethal, problem when left untreated. Before the endovascular era, the only option was open revascularization, which is challenging in this chronically ill, malnourished population with diffuse, systemic, atherosclerotic disease. Morbidity and mortality was relatively high because of the comorbid conditions and chronically ill status of the patients. The first mesenteric bypass was performed in 1958 by Maynard and Shaw.1
Options for open repair include transaortic endarterectomy, antegrade bypass from the supraceliac aorta or distal thoracic aorta, or retrograde bypass from the iliac artery, all of which are major abdominal procedures. Endovascular interventions are now the most commonly performed procedures for CMI in the United States based on national studies.2
Technical success with endovascular interventions can be achieved in well over 90% of patients, and multiple vessels can be treated simultaneously from either a femoral or brachial approach. The primary concern with endovascular interventions has been long-term patency, with restenosis from intimal hyperplasia or thrombosis causing recurrent symptoms in up to 30%-50% at 3-5 years.5-7 However, these rates are based on use of bare metal stents, rather than covered stents. Recent studies8 suggest that stent grafts have markedly improved outcomes over bare metal stents for ostial lesions, decreasing recurrence. Oderich found that freedom from recurrence was 92% with stent grafts as compared with 53% for bare metal stents, with primary patency rates of 92%, at 3 years8, comparable to even the best open bypass results. Schoch first reported the use of covered stents in the mesenteric circulation, and found that no patients developed recurrent stenosis at 2 years.9 Other concerns with endovascular intervention include embolization and dissection, which have not been frequently reported.
Mortality from open surgery ranges from 5% to 15%, with morbidity of 30%-40%.4 Mortality from endovascular intervention is markedly lower, in the range of 3.56% vs. 7.23%.5 Long-term survival is not different between endovascular vs. open repair (69% vs. 65%),4 with the majority of deaths related to cardiac, pulmonary, or malignancy issues. Moghadamyeghaneh, in a review of the Nationwide Inpatient Sample database, found that open surgery was one of the major predictors for higher morbidity (odds ratio, 5.07) and mortality (OR, 5.13), despite the fact that endovascular patients were older (another risk factor for adverse outcomes) and had more comorbidities in this nonrandomized, real-world study.2
Further, if one considers cost as a metric for decision making, a Markov clinical decision model by Hogendoorn et al suggests an endovascular first approach is preferred, despite the presumed higher rate of recurrence expected with use of bare metal stents, rather than covered stents, utilized for this analysis.10 Clearly, the financial advantage would be even greater for endovascular with the lower rates of recurrence with covered stents more recently reported.
If a patient develops recurrent stenosis after endovascular intervention, open bypass may be considered as an alternate to repeat endovascular intervention, dependent on the nutritional status, life expectancy, and initial intervention undertaken. Alternately, patients who undergo open repair are not immune to restenosis, with a recurrence rate of 10%-20%.11,12 Oderich found that there was a 22% mortality in those treated with repeat open interventions, with a 47% complication rate. Endovascular interventions, however, had a significantly lower rate of complications, 16%, and mortality. For patients with recurrent disease after open revascularization for CMI, the endovascular approach should also be the preferred approach.
Any lesion which is anatomically suitable for endovascular repair should first have an attempt made via this approach, utilizing covered stents. While there is a role for open revascularization, endovascular interventions can be safely performed, with minimal morbidity and mortality, and good long-term patency, even in the sickest patients. Endovascular intervention should be the procedure of choice for chronic mesenteric ischemia and recurrent chronic mesenteric ischemia.
References
1. NEJM. 1958;258:874-8
2. Am Surg. 2015;81:1149-56
3. Cardiovasc Intervent Radiol. 1980;3:43-4
4. Ann Vasc Surg. 2009;23:700-12
5. Ann Vasc Surg. 2013;27:113-22
6. J Vasc Surg. 2011;54:1422-29
7. J Vasc Surg. 2010;51:140-7
8. J Vasc Surg. 2013;58:1316-24
9. JACS. 2001;212:668-75
10. J Vasc Surg. 2014;60;715-25
11. J Vasc Surg. 200;49:1472-9
12. J Vasc Surg. 2007;45:1162-71
Linda Harris, MD, is professor of surgery; chief, division of vascular surgery; program director, vascular surgery residency & fellowship at the State University of New York at Buffalo; and an associate medical editor for Vascular Specialist. She had no relevant disclosures.
Perioperative infliximab does not increase serious infection risk
Administration of infliximab within 4 weeks of elective knee or hip arthroplasty did not have any significant effect on patients’ risk of serious infection after surgery, whereas the use of glucocorticoids increased that risk, in an analysis of a Medicare claims database.
“This increased risk with glucocorticoids has been suggested by previous studies [and] although this risk may be related in part to increased disease severity among glucocorticoid treated patients, a direct medication effect is likely. [These data suggest] that prolonged interruptions in infliximab therapy prior to surgery may be counterproductive if higher dose glucocorticoid therapy is used in substitution,” wrote the authors of the new study, led by Michael D. George, MD, of the University of Pennsylvania in Philadelphia.
Dr. George and his colleagues examined data from the U.S. Medicare claims system on 4,288 elective knee or hip arthroplasties in individuals with rheumatoid arthritis, inflammatory bowel disease, psoriasis, psoriatic arthritis, or ankylosing spondylitis who received infliximab within 6 months prior to the operation during 2007-2013 (Arthritis Care Res. 2017 Jan 27. doi: 10.1002/acr.23209).
The patients had to have received infliximab at least three times within a year of their procedure to establish that they were receiving stable therapy over a long-term period. The investigators also looked at oral prednisone, prednisolone, and methylprednisolone prescriptions and used data on average dosing to determine how much was administered to each subject.
“Although previous studies have treated TNF stopping vs. not stopping as a dichotomous exposure based on an arbitrary (and variable) stopping definition, in this study the primary analysis evaluated stop timing as a more general categorical exposure using 4-week intervals (half the standard rheumatoid arthritis dosing interval) to allow better assessment of the optimal stop timing,” the authors explained.
Stopping infliximab within 4 weeks of the operation did not significantly influence the rate of serious infection within 30 days (adjusted odds ratio, 0.90; 95% CI, 0.60-1.34) and neither did stopping within 4-8 weeks (OR, 0.95; 95% CI, 0.62-1.36) when compared against stopping 8-12 weeks before surgery. Of the 4,288 arthroplasties, 270 serious infections (6.3%) occurred within 30 days of the operation.
There also was no significant difference between stopping within 4 weeks and 8-12 weeks in the rate of prosthetic joint infection within 1 year of the operation (hazard ratio, 0.98; 95% CI, 0.52-1.87). Overall, prosthetic joint infection occurred 2.9 times per 100 person-years.
However, glucocorticoid doses of more than 10 mg per day were risky. The odds for a serious infection within 30 days after surgery more than doubled with that level of use (OR, 2.11; 95% CI, 1.30-3.40), while the risk for a prosthetic joint infection within 1 year of the surgery also rose significantly (HR, 2.70; 95% CI, 1.30-5.60).

“This is a very well done paper that adds important observational data to our understanding of perioperative medication risk,” Dr. Goodman said.
But the study results will not, at least initially, bring about any changes to the proposed guidelines for perioperative management of patients taking antirheumatic drugs that were described at the 2016 annual meeting of the American College of Rheumatology, she said.
“We were aware of the abstract, which was also presented at the ACR last fall at the time the current perioperative medication management guidelines were presented, and it won’t change guidelines at this point,” said Dr. Goodman, who is one of the lead authors of the proposed guidelines. “[But] I think [the study] could provide important background information to use in a randomized clinical trial to compare infection on [and] not on TNF inhibitors.”
The proposed guidelines conditionally recommend that all biologics should be withheld prior to surgery in patients with inflammatory arthritis, that surgery should be planned for the end of the dosing cycle, and that current daily doses of glucocorticoids, rather than supraphysiologic doses, should be continued in adults with rheumatoid arthritis, lupus, or inflammatory arthritis.
The National Institutes of Health, the Rheumatology Research Foundation, and the Department of Veterans Affairs funded the study. Dr. George did not report any relevant financial disclosures. Two coauthors disclosed receiving research grants or consulting fees from pharmaceutical companies for unrelated work.
Administration of infliximab within 4 weeks of elective knee or hip arthroplasty did not have any significant effect on patients’ risk of serious infection after surgery, whereas the use of glucocorticoids increased that risk, in an analysis of a Medicare claims database.
“This increased risk with glucocorticoids has been suggested by previous studies [and] although this risk may be related in part to increased disease severity among glucocorticoid treated patients, a direct medication effect is likely. [These data suggest] that prolonged interruptions in infliximab therapy prior to surgery may be counterproductive if higher dose glucocorticoid therapy is used in substitution,” wrote the authors of the new study, led by Michael D. George, MD, of the University of Pennsylvania in Philadelphia.
Dr. George and his colleagues examined data from the U.S. Medicare claims system on 4,288 elective knee or hip arthroplasties in individuals with rheumatoid arthritis, inflammatory bowel disease, psoriasis, psoriatic arthritis, or ankylosing spondylitis who received infliximab within 6 months prior to the operation during 2007-2013 (Arthritis Care Res. 2017 Jan 27. doi: 10.1002/acr.23209).
The patients had to have received infliximab at least three times within a year of their procedure to establish that they were receiving stable therapy over a long-term period. The investigators also looked at oral prednisone, prednisolone, and methylprednisolone prescriptions and used data on average dosing to determine how much was administered to each subject.
“Although previous studies have treated TNF stopping vs. not stopping as a dichotomous exposure based on an arbitrary (and variable) stopping definition, in this study the primary analysis evaluated stop timing as a more general categorical exposure using 4-week intervals (half the standard rheumatoid arthritis dosing interval) to allow better assessment of the optimal stop timing,” the authors explained.
Stopping infliximab within 4 weeks of the operation did not significantly influence the rate of serious infection within 30 days (adjusted odds ratio, 0.90; 95% CI, 0.60-1.34) and neither did stopping within 4-8 weeks (OR, 0.95; 95% CI, 0.62-1.36) when compared against stopping 8-12 weeks before surgery. Of the 4,288 arthroplasties, 270 serious infections (6.3%) occurred within 30 days of the operation.
There also was no significant difference between stopping within 4 weeks and 8-12 weeks in the rate of prosthetic joint infection within 1 year of the operation (hazard ratio, 0.98; 95% CI, 0.52-1.87). Overall, prosthetic joint infection occurred 2.9 times per 100 person-years.
However, glucocorticoid doses of more than 10 mg per day were risky. The odds for a serious infection within 30 days after surgery more than doubled with that level of use (OR, 2.11; 95% CI, 1.30-3.40), while the risk for a prosthetic joint infection within 1 year of the surgery also rose significantly (HR, 2.70; 95% CI, 1.30-5.60).
“This is a very well done paper that adds important observational data to our understanding of perioperative medication risk,” Dr. Goodman said.
But the study results will not, at least initially, bring about any changes to the proposed guidelines for perioperative management of patients taking antirheumatic drugs that were described at the 2016 annual meeting of the American College of Rheumatology, she said.
“We were aware of the abstract, which was also presented at the ACR last fall at the time the current perioperative medication management guidelines were presented, and it won’t change guidelines at this point,” said Dr. Goodman, who is one of the lead authors of the proposed guidelines. “[But] I think [the study] could provide important background information to use in a randomized clinical trial to compare infection on [and] not on TNF inhibitors.”
The proposed guidelines conditionally recommend that all biologics should be withheld prior to surgery in patients with inflammatory arthritis, that surgery should be planned for the end of the dosing cycle, and that current daily doses of glucocorticoids, rather than supraphysiologic doses, should be continued in adults with rheumatoid arthritis, lupus, or inflammatory arthritis.
The National Institutes of Health, the Rheumatology Research Foundation, and the Department of Veterans Affairs funded the study. Dr. George did not report any relevant financial disclosures. Two coauthors disclosed receiving research grants or consulting fees from pharmaceutical companies for unrelated work.
Administration of infliximab within 4 weeks of elective knee or hip arthroplasty did not have any significant effect on patients’ risk of serious infection after surgery, whereas the use of glucocorticoids increased that risk, in an analysis of a Medicare claims database.
“This increased risk with glucocorticoids has been suggested by previous studies [and] although this risk may be related in part to increased disease severity among glucocorticoid treated patients, a direct medication effect is likely. [These data suggest] that prolonged interruptions in infliximab therapy prior to surgery may be counterproductive if higher dose glucocorticoid therapy is used in substitution,” wrote the authors of the new study, led by Michael D. George, MD, of the University of Pennsylvania in Philadelphia.
Dr. George and his colleagues examined data from the U.S. Medicare claims system on 4,288 elective knee or hip arthroplasties in individuals with rheumatoid arthritis, inflammatory bowel disease, psoriasis, psoriatic arthritis, or ankylosing spondylitis who received infliximab within 6 months prior to the operation during 2007-2013 (Arthritis Care Res. 2017 Jan 27. doi: 10.1002/acr.23209).
The patients had to have received infliximab at least three times within a year of their procedure to establish that they were receiving stable therapy over a long-term period. The investigators also looked at oral prednisone, prednisolone, and methylprednisolone prescriptions and used data on average dosing to determine how much was administered to each subject.
“Although previous studies have treated TNF stopping vs. not stopping as a dichotomous exposure based on an arbitrary (and variable) stopping definition, in this study the primary analysis evaluated stop timing as a more general categorical exposure using 4-week intervals (half the standard rheumatoid arthritis dosing interval) to allow better assessment of the optimal stop timing,” the authors explained.
Stopping infliximab within 4 weeks of the operation did not significantly influence the rate of serious infection within 30 days (adjusted odds ratio, 0.90; 95% CI, 0.60-1.34) and neither did stopping within 4-8 weeks (OR, 0.95; 95% CI, 0.62-1.36) when compared against stopping 8-12 weeks before surgery. Of the 4,288 arthroplasties, 270 serious infections (6.3%) occurred within 30 days of the operation.
There also was no significant difference between stopping within 4 weeks and 8-12 weeks in the rate of prosthetic joint infection within 1 year of the operation (hazard ratio, 0.98; 95% CI, 0.52-1.87). Overall, prosthetic joint infection occurred 2.9 times per 100 person-years.
However, glucocorticoid doses of more than 10 mg per day were risky. The odds for a serious infection within 30 days after surgery more than doubled with that level of use (OR, 2.11; 95% CI, 1.30-3.40), while the risk for a prosthetic joint infection within 1 year of the surgery also rose significantly (HR, 2.70; 95% CI, 1.30-5.60).
“This is a very well done paper that adds important observational data to our understanding of perioperative medication risk,” Dr. Goodman said.
But the study results will not, at least initially, bring about any changes to the proposed guidelines for perioperative management of patients taking antirheumatic drugs that were described at the 2016 annual meeting of the American College of Rheumatology, she said.
“We were aware of the abstract, which was also presented at the ACR last fall at the time the current perioperative medication management guidelines were presented, and it won’t change guidelines at this point,” said Dr. Goodman, who is one of the lead authors of the proposed guidelines. “[But] I think [the study] could provide important background information to use in a randomized clinical trial to compare infection on [and] not on TNF inhibitors.”
The proposed guidelines conditionally recommend that all biologics should be withheld prior to surgery in patients with inflammatory arthritis, that surgery should be planned for the end of the dosing cycle, and that current daily doses of glucocorticoids, rather than supraphysiologic doses, should be continued in adults with rheumatoid arthritis, lupus, or inflammatory arthritis.
The National Institutes of Health, the Rheumatology Research Foundation, and the Department of Veterans Affairs funded the study. Dr. George did not report any relevant financial disclosures. Two coauthors disclosed receiving research grants or consulting fees from pharmaceutical companies for unrelated work.
FROM ARTHRITIS CARE & RESEARCH
Key clinical point:
Major finding: Subjects on glucocorticoids had an OR of 2.11 (95% CI 1.30-3.40) for serious infection within 30 days and an HR of 2.70 (95% CI 1.30-5.60) for prosthetic joint infection within 1 year.
Data source: Retrospective cohort study of 4,288 elective knee and hip arthroplasties in Medicare patients with rheumatoid arthritis, inflammatory bowel disease, psoriasis, psoriatic arthritis, or ankylosing spondylitis during 2007-2013.
Disclosures: The National Institutes of Health, the Rheumatology Research Foundation, and the Department of Veterans Affairs funded the study. Dr. George did not report any relevant financial disclosures. Two coauthors disclosed receiving research grants or consulting fees from pharmaceutical companies for unrelated work.
Novel Treatment Shows Promise for Acute Lymphoblastic Leukemia
Thanks to gene-editing treatment, 2 babies who had leukemia have a longer lease on life. Researchers from University College London, Great Ormond Street Hospital National Health Service Trust, King’s College, and Sheffield Children’s Hospital, in the United Kingdom used genetically engineered white blood cells from healthy individuals to target the cancer cells.
Related: New Treatments for Chronic Lymphocytic Leukemia
One infant was 11 months old, and the second was 16 months old. Both had refractory relapsed B-cell acute lymphoblastic leukemia and had undergone multidrug treatments. Although the potential of the method has been demonstrated in autologous and human-leukocyte-antigen–matched allogeneic settings, the researchers say, “the infrastructure and expertise required to produce personalized cell products present challenges, and low T cell counts in heavily treated individuals may preclude autologous approaches.”
The treatment involves lymphodepleting chemotherapy and anti-CD52 serotherapy, followed by a single-dose infusion of universal CAR19 cells (autologous T cells engineered to express chimeric antigen receptor against the B-cell antigen CD19). This “bridge-to-transplantation strategy” demonstrates the therapeutic potential of gene-editing technology, the researchers say.
Related: Six Open Clinical Trials That Are Expanding Our Understanding of Immunotherapies
Just 28 days after the treatment, molecular markers showed remission in both infants. The treatments were well tolerated. The first infant had an immune reaction (cytopenia and graft-vs-host disease [GVHD] in skin and marrow) in the 2 months after the infusion and was treated with steroids and bone marrow transplantation. The other baby had no adverse reactions apart from mild skin GVHD that reversed “promptly” with topical steroids and an episode of “unexplained irritability” in the 3 weeks after infusion.
The first and second infant remained cancer free 18 and 12 months later.
Source:
Qasim W, Zhan H, Samarasinghe S, et al. Sci Transl Med. 2017;9(374):pii: eaaj2013.
doi: 10.1126/scitranslmed.aaj2013.
Thanks to gene-editing treatment, 2 babies who had leukemia have a longer lease on life. Researchers from University College London, Great Ormond Street Hospital National Health Service Trust, King’s College, and Sheffield Children’s Hospital, in the United Kingdom used genetically engineered white blood cells from healthy individuals to target the cancer cells.
Related: New Treatments for Chronic Lymphocytic Leukemia
One infant was 11 months old, and the second was 16 months old. Both had refractory relapsed B-cell acute lymphoblastic leukemia and had undergone multidrug treatments. Although the potential of the method has been demonstrated in autologous and human-leukocyte-antigen–matched allogeneic settings, the researchers say, “the infrastructure and expertise required to produce personalized cell products present challenges, and low T cell counts in heavily treated individuals may preclude autologous approaches.”
The treatment involves lymphodepleting chemotherapy and anti-CD52 serotherapy, followed by a single-dose infusion of universal CAR19 cells (autologous T cells engineered to express chimeric antigen receptor against the B-cell antigen CD19). This “bridge-to-transplantation strategy” demonstrates the therapeutic potential of gene-editing technology, the researchers say.
Related: Six Open Clinical Trials That Are Expanding Our Understanding of Immunotherapies
Just 28 days after the treatment, molecular markers showed remission in both infants. The treatments were well tolerated. The first infant had an immune reaction (cytopenia and graft-vs-host disease [GVHD] in skin and marrow) in the 2 months after the infusion and was treated with steroids and bone marrow transplantation. The other baby had no adverse reactions apart from mild skin GVHD that reversed “promptly” with topical steroids and an episode of “unexplained irritability” in the 3 weeks after infusion.
The first and second infant remained cancer free 18 and 12 months later.
Source:
Qasim W, Zhan H, Samarasinghe S, et al. Sci Transl Med. 2017;9(374):pii: eaaj2013.
doi: 10.1126/scitranslmed.aaj2013.
Thanks to gene-editing treatment, 2 babies who had leukemia have a longer lease on life. Researchers from University College London, Great Ormond Street Hospital National Health Service Trust, King’s College, and Sheffield Children’s Hospital, in the United Kingdom used genetically engineered white blood cells from healthy individuals to target the cancer cells.
Related: New Treatments for Chronic Lymphocytic Leukemia
One infant was 11 months old, and the second was 16 months old. Both had refractory relapsed B-cell acute lymphoblastic leukemia and had undergone multidrug treatments. Although the potential of the method has been demonstrated in autologous and human-leukocyte-antigen–matched allogeneic settings, the researchers say, “the infrastructure and expertise required to produce personalized cell products present challenges, and low T cell counts in heavily treated individuals may preclude autologous approaches.”
The treatment involves lymphodepleting chemotherapy and anti-CD52 serotherapy, followed by a single-dose infusion of universal CAR19 cells (autologous T cells engineered to express chimeric antigen receptor against the B-cell antigen CD19). This “bridge-to-transplantation strategy” demonstrates the therapeutic potential of gene-editing technology, the researchers say.
Related: Six Open Clinical Trials That Are Expanding Our Understanding of Immunotherapies
Just 28 days after the treatment, molecular markers showed remission in both infants. The treatments were well tolerated. The first infant had an immune reaction (cytopenia and graft-vs-host disease [GVHD] in skin and marrow) in the 2 months after the infusion and was treated with steroids and bone marrow transplantation. The other baby had no adverse reactions apart from mild skin GVHD that reversed “promptly” with topical steroids and an episode of “unexplained irritability” in the 3 weeks after infusion.
The first and second infant remained cancer free 18 and 12 months later.
Source:
Qasim W, Zhan H, Samarasinghe S, et al. Sci Transl Med. 2017;9(374):pii: eaaj2013.
doi: 10.1126/scitranslmed.aaj2013.
Psoriatic Arthritis Treatment: The Dermatologist’s Role


E-cigarette ‘dripping’ is up among teens
Use of electronic cigarettes among young people is on the rise, and one in four high school students report using these devices for dripping, according to a study by Suchitra Krishnan-Sarin, PhD, of Yale University, New Haven, and associates.
In the spring of 2015, 7,045 students from eight Connecticut high schools completed anonymous surveys that examined tobacco use behaviors and perceptions. Among 1,080 ever e-cigarette users, 26% of students reported ever using e-cigarettes for dripping, which involves “vaporizing the e-liquid at high temperatures by dripping a couple of drops of e-liquid directly onto an atomizer’s coil and then immediately inhaling the vapor.”
Students use dripping because it produces thicker clouds of vapor (according to 64% of respondents); because they get a stronger throat hit (28%); and because it makes the flavors taste better (39%). Curiosity was cited by 22% of the students. 
These results suggest that youth who use dripping may be those who are more familiar with and have experience with using multiple tobacco products, including e-cigarettes Pediatrics. 2017. doi: 10.1542/peds.2016-3224).
“Importantly, risk assessment models for e-cigarettes must take into consideration the prevalence rates and toxicities of these alternative e-cigarette use behaviors, especially among vulnerable youth. There is also a critical need for regulatory efforts that consider restrictions on the e-cigarette device so it cannot be easily manipulated for behaviors such as dripping,” the researchers noted. “Finally, there is an urgent need for prevention programs that educate youth about the potential dangers and toxicity of the use of e-cigarettes for dripping.”
Use of electronic cigarettes among young people is on the rise, and one in four high school students report using these devices for dripping, according to a study by Suchitra Krishnan-Sarin, PhD, of Yale University, New Haven, and associates.
In the spring of 2015, 7,045 students from eight Connecticut high schools completed anonymous surveys that examined tobacco use behaviors and perceptions. Among 1,080 ever e-cigarette users, 26% of students reported ever using e-cigarettes for dripping, which involves “vaporizing the e-liquid at high temperatures by dripping a couple of drops of e-liquid directly onto an atomizer’s coil and then immediately inhaling the vapor.”
Students use dripping because it produces thicker clouds of vapor (according to 64% of respondents); because they get a stronger throat hit (28%); and because it makes the flavors taste better (39%). Curiosity was cited by 22% of the students.
These results suggest that youth who use dripping may be those who are more familiar with and have experience with using multiple tobacco products, including e-cigarettes Pediatrics. 2017. doi: 10.1542/peds.2016-3224).
“Importantly, risk assessment models for e-cigarettes must take into consideration the prevalence rates and toxicities of these alternative e-cigarette use behaviors, especially among vulnerable youth. There is also a critical need for regulatory efforts that consider restrictions on the e-cigarette device so it cannot be easily manipulated for behaviors such as dripping,” the researchers noted. “Finally, there is an urgent need for prevention programs that educate youth about the potential dangers and toxicity of the use of e-cigarettes for dripping.”
Use of electronic cigarettes among young people is on the rise, and one in four high school students report using these devices for dripping, according to a study by Suchitra Krishnan-Sarin, PhD, of Yale University, New Haven, and associates.
In the spring of 2015, 7,045 students from eight Connecticut high schools completed anonymous surveys that examined tobacco use behaviors and perceptions. Among 1,080 ever e-cigarette users, 26% of students reported ever using e-cigarettes for dripping, which involves “vaporizing the e-liquid at high temperatures by dripping a couple of drops of e-liquid directly onto an atomizer’s coil and then immediately inhaling the vapor.”
Students use dripping because it produces thicker clouds of vapor (according to 64% of respondents); because they get a stronger throat hit (28%); and because it makes the flavors taste better (39%). Curiosity was cited by 22% of the students.
These results suggest that youth who use dripping may be those who are more familiar with and have experience with using multiple tobacco products, including e-cigarettes Pediatrics. 2017. doi: 10.1542/peds.2016-3224).
“Importantly, risk assessment models for e-cigarettes must take into consideration the prevalence rates and toxicities of these alternative e-cigarette use behaviors, especially among vulnerable youth. There is also a critical need for regulatory efforts that consider restrictions on the e-cigarette device so it cannot be easily manipulated for behaviors such as dripping,” the researchers noted. “Finally, there is an urgent need for prevention programs that educate youth about the potential dangers and toxicity of the use of e-cigarettes for dripping.”
FROM PEDIATRICS
HFNC bests conventional O2 therapy
In patients with acute respiratory failure, high-flow nasal cannula (HFNC) is more reliable than is conventional oxygen therapy at reducing rates of endotracheal intubation, although no significant difference was found when HFNC was compared with noninvasive positive pressure ventilation, a new study found.
An increasing awareness of the high rate of adverse events and mortality rates associated with invasive mechanical ventilation in hospitals has led to a rise in the use of noninvasive positive pressure ventilation (NIPPV). While this has effectively cut the use of conventional oxygen therapy (COT), its application in clinical practice is limited by a host of complications such as interface intolerance, skin damage, and other hazards. HFNC, because of its demonstrated efficacy and relatively easier application, and better tolerance in patients, also has been gaining popularity. Despite the known benefits HFNC, this therapy is not given to all adults with acute respiratory failure (ARF). This may be due to the lack of consistency in data regarding how HFNC’s effectiveness at decreasing intubation and reintubation rates compares with COT’s and NIPPV’s.
Researchers in China conducted a meta-analysis and systematic review of all superiority and nonsuperiority data on the outcomes of using HFNC, COT, and NIPPV to treat ARF. Their examination included 18 trials comprising 3,881 patients, which compared the results of receiving HFNC with the results of receiving NIPPV or COT. The study is published in CHEST (10.1016/j.chest.2017.01.004).
The investigators concluded that HFNC was associated with significantly lower rates of the need for endotracheal intubation, compared with COT (P = .01). When HFNC was compared with NIPPV, however, the rates of patients needing intubation were not statistically different from each other (P = .16). HFNC was not associated with significant improvements in mortality rates or lengths of stay in the intensive care units, when compared with both COT and NIPPV.
According to the researchers’ subgroup analysis conducted of HFNC in 2,741 patients following extubation, those patients who received HFNC had a significantly lower reintubation rate than that of those who received COT (OR = 0.39, P = .0003). In this analysis, again, no significant differences in outcomes were seen between patients who received HFNC and NIPPV (OR = 1.07, P = .60)
Bin-Miao Liang, MD, PhD, a researcher in the department of respiratory and critical care medicine at Sichuan University in China, and coauthors noted that “concomitant complications such as acute kidney dysfunction and cardiac impairment may contribute to ICU mortality and ICU [lengths-of-stay] besides respiratory status itself.” Factors such as available beds, a patient’s insurance status, and other resources may also have impacted outcomes, they said.
The researchers wrote that they found “[significant] statistical heterogeneity” in the rates of endotracheal intubation and ICU mortality between HFNC and NIPPV. A lack of raw data, which prevented a subanalysis of individual respiratory failure from being performed, is one possible cause of the statistical heterogeneity, the authors concluded.
China-Japan Friendship Hospital is continuing the search for more data on the success rates of HFNC and NIPPV at reducing intubation and mortality rates. The hospital is sponsoring a multicenter, randomized, noninferiority trial titled, “High Flow Nasal Cannula vs. NPPV in Moderate Chronic Obstructive Pulmonary Disease Exacerbation,” according to ClinicalTrials.gov. No results were available for this trial as of Feb. 6.
None of the authors had relevant disclosures.
[email protected]
On Twitter @whitneymcknight
The introduction of high-flow nasal cannula (HFNC) fundamentally has changed how patients with acute respiratory failure are treated – both in avoidance of intubation and prevention of reintubation. Its use is supported by some very high quality studies over the last few years done in a variety of types of critically-ill patients. While its clinical superiority to noninvasive ventilation (NIV) is still open to debate, the comfort and other attributes that HFNC provides increasingly are making it the first-choice modality (e.g., the patient can continue to eat, speak, and wear for longer periods of time).

Eric J. Gartman, MD , is assistant professor of medicine at Brown University, Providence, R.I. He is an editorial board member of CHEST.
The introduction of high-flow nasal cannula (HFNC) fundamentally has changed how patients with acute respiratory failure are treated – both in avoidance of intubation and prevention of reintubation. Its use is supported by some very high quality studies over the last few years done in a variety of types of critically-ill patients. While its clinical superiority to noninvasive ventilation (NIV) is still open to debate, the comfort and other attributes that HFNC provides increasingly are making it the first-choice modality (e.g., the patient can continue to eat, speak, and wear for longer periods of time).
Eric J. Gartman, MD , is assistant professor of medicine at Brown University, Providence, R.I. He is an editorial board member of CHEST.
The introduction of high-flow nasal cannula (HFNC) fundamentally has changed how patients with acute respiratory failure are treated – both in avoidance of intubation and prevention of reintubation. Its use is supported by some very high quality studies over the last few years done in a variety of types of critically-ill patients. While its clinical superiority to noninvasive ventilation (NIV) is still open to debate, the comfort and other attributes that HFNC provides increasingly are making it the first-choice modality (e.g., the patient can continue to eat, speak, and wear for longer periods of time).
Eric J. Gartman, MD , is assistant professor of medicine at Brown University, Providence, R.I. He is an editorial board member of CHEST.
In patients with acute respiratory failure, high-flow nasal cannula (HFNC) is more reliable than is conventional oxygen therapy at reducing rates of endotracheal intubation, although no significant difference was found when HFNC was compared with noninvasive positive pressure ventilation, a new study found.
An increasing awareness of the high rate of adverse events and mortality rates associated with invasive mechanical ventilation in hospitals has led to a rise in the use of noninvasive positive pressure ventilation (NIPPV). While this has effectively cut the use of conventional oxygen therapy (COT), its application in clinical practice is limited by a host of complications such as interface intolerance, skin damage, and other hazards. HFNC, because of its demonstrated efficacy and relatively easier application, and better tolerance in patients, also has been gaining popularity. Despite the known benefits HFNC, this therapy is not given to all adults with acute respiratory failure (ARF). This may be due to the lack of consistency in data regarding how HFNC’s effectiveness at decreasing intubation and reintubation rates compares with COT’s and NIPPV’s.
Researchers in China conducted a meta-analysis and systematic review of all superiority and nonsuperiority data on the outcomes of using HFNC, COT, and NIPPV to treat ARF. Their examination included 18 trials comprising 3,881 patients, which compared the results of receiving HFNC with the results of receiving NIPPV or COT. The study is published in CHEST (10.1016/j.chest.2017.01.004).
The investigators concluded that HFNC was associated with significantly lower rates of the need for endotracheal intubation, compared with COT (P = .01). When HFNC was compared with NIPPV, however, the rates of patients needing intubation were not statistically different from each other (P = .16). HFNC was not associated with significant improvements in mortality rates or lengths of stay in the intensive care units, when compared with both COT and NIPPV.
According to the researchers’ subgroup analysis conducted of HFNC in 2,741 patients following extubation, those patients who received HFNC had a significantly lower reintubation rate than that of those who received COT (OR = 0.39, P = .0003). In this analysis, again, no significant differences in outcomes were seen between patients who received HFNC and NIPPV (OR = 1.07, P = .60)
Bin-Miao Liang, MD, PhD, a researcher in the department of respiratory and critical care medicine at Sichuan University in China, and coauthors noted that “concomitant complications such as acute kidney dysfunction and cardiac impairment may contribute to ICU mortality and ICU [lengths-of-stay] besides respiratory status itself.” Factors such as available beds, a patient’s insurance status, and other resources may also have impacted outcomes, they said.
The researchers wrote that they found “[significant] statistical heterogeneity” in the rates of endotracheal intubation and ICU mortality between HFNC and NIPPV. A lack of raw data, which prevented a subanalysis of individual respiratory failure from being performed, is one possible cause of the statistical heterogeneity, the authors concluded.
China-Japan Friendship Hospital is continuing the search for more data on the success rates of HFNC and NIPPV at reducing intubation and mortality rates. The hospital is sponsoring a multicenter, randomized, noninferiority trial titled, “High Flow Nasal Cannula vs. NPPV in Moderate Chronic Obstructive Pulmonary Disease Exacerbation,” according to ClinicalTrials.gov. No results were available for this trial as of Feb. 6.
None of the authors had relevant disclosures.
[email protected]
On Twitter @whitneymcknight
In patients with acute respiratory failure, high-flow nasal cannula (HFNC) is more reliable than is conventional oxygen therapy at reducing rates of endotracheal intubation, although no significant difference was found when HFNC was compared with noninvasive positive pressure ventilation, a new study found.
An increasing awareness of the high rate of adverse events and mortality rates associated with invasive mechanical ventilation in hospitals has led to a rise in the use of noninvasive positive pressure ventilation (NIPPV). While this has effectively cut the use of conventional oxygen therapy (COT), its application in clinical practice is limited by a host of complications such as interface intolerance, skin damage, and other hazards. HFNC, because of its demonstrated efficacy and relatively easier application, and better tolerance in patients, also has been gaining popularity. Despite the known benefits HFNC, this therapy is not given to all adults with acute respiratory failure (ARF). This may be due to the lack of consistency in data regarding how HFNC’s effectiveness at decreasing intubation and reintubation rates compares with COT’s and NIPPV’s.
Researchers in China conducted a meta-analysis and systematic review of all superiority and nonsuperiority data on the outcomes of using HFNC, COT, and NIPPV to treat ARF. Their examination included 18 trials comprising 3,881 patients, which compared the results of receiving HFNC with the results of receiving NIPPV or COT. The study is published in CHEST (10.1016/j.chest.2017.01.004).
The investigators concluded that HFNC was associated with significantly lower rates of the need for endotracheal intubation, compared with COT (P = .01). When HFNC was compared with NIPPV, however, the rates of patients needing intubation were not statistically different from each other (P = .16). HFNC was not associated with significant improvements in mortality rates or lengths of stay in the intensive care units, when compared with both COT and NIPPV.
According to the researchers’ subgroup analysis conducted of HFNC in 2,741 patients following extubation, those patients who received HFNC had a significantly lower reintubation rate than that of those who received COT (OR = 0.39, P = .0003). In this analysis, again, no significant differences in outcomes were seen between patients who received HFNC and NIPPV (OR = 1.07, P = .60)
Bin-Miao Liang, MD, PhD, a researcher in the department of respiratory and critical care medicine at Sichuan University in China, and coauthors noted that “concomitant complications such as acute kidney dysfunction and cardiac impairment may contribute to ICU mortality and ICU [lengths-of-stay] besides respiratory status itself.” Factors such as available beds, a patient’s insurance status, and other resources may also have impacted outcomes, they said.
The researchers wrote that they found “[significant] statistical heterogeneity” in the rates of endotracheal intubation and ICU mortality between HFNC and NIPPV. A lack of raw data, which prevented a subanalysis of individual respiratory failure from being performed, is one possible cause of the statistical heterogeneity, the authors concluded.
China-Japan Friendship Hospital is continuing the search for more data on the success rates of HFNC and NIPPV at reducing intubation and mortality rates. The hospital is sponsoring a multicenter, randomized, noninferiority trial titled, “High Flow Nasal Cannula vs. NPPV in Moderate Chronic Obstructive Pulmonary Disease Exacerbation,” according to ClinicalTrials.gov. No results were available for this trial as of Feb. 6.
None of the authors had relevant disclosures.
[email protected]
On Twitter @whitneymcknight
FROM CHEST
Key clinical point:
Major finding: Endotracheal intubation rates in adults with acute respiratory failure who received HFNC and NIPPV were not significantly different from each other (P = .16).
Data source: Meta-analysis and systematic review of 18 trials with 3,881 patients.
Disclosures: None of the authors had relevant disclosures.
Early mild cognitive impairment in Parkinson’s leads to dementia in more than 40%
Developing persistent mild cognitive impairment soon after being diagnosed with Parkinson’s disease significantly increased the risk of subsequent dementia, according to a cohort study that examined the natural history of mild cognitive impairment in 178 patients over 5 years.
After the researchers controlled for age, sex, and education, patients who had persistent mild cognitive impairment (MCI) by 1 year after their Parkinson’s disease (PD) diagnosis had a 16.6-fold greater odds of subsequent dementia, compared with those who were cognitively normal (95% confidence interval, 5.1-54.7; P less than .001). Notably, early MCI significantly predicted dementia even if patients reverted to normal cognition with dopaminergic treatment, reported Kenn F. Pedersen, MD, PhD, of the Norwegian Centre for Movement Disorders at Stavanger (Norway) University Hospital, and his associates. “Early PD-MCI, regardless of persistence or reversion to normal cognition, has prognostic value for predicting dementia in patients with PD,” they concluded.
At baseline, 20% of patients had MCI. Among those who did not, cumulative incidence rates of MCI were 10% at year 1, 23% at year 3, and 29% by the end of the study after 5 years of follow-up. In all, 59% of patients with persistent MCI by year 1 developed dementia, compared with 7% of patients who retained normal cognition at 1 year. About one in four patients with MCI reverted to normal cognition by the end of the study, but they still faced a 10.7-fold greater odds of dementia at the 5-year follow-up, compared with cognitively normal patients (95% CI, 1.5-78.5; P = .02).
The Research Council of Norway, the Western Norway Regional Health Authority, and the Norwegian Parkinson’s Disease Association funded the study. Dr. Pedersen had no disclosures. One coauthor reported serving on advisory boards for Lundbeck and GlaxoSmithKline and receiving payment for lecturing from Orion Pharma and GlaxoSmithKline.
Developing persistent mild cognitive impairment soon after being diagnosed with Parkinson’s disease significantly increased the risk of subsequent dementia, according to a cohort study that examined the natural history of mild cognitive impairment in 178 patients over 5 years.
After the researchers controlled for age, sex, and education, patients who had persistent mild cognitive impairment (MCI) by 1 year after their Parkinson’s disease (PD) diagnosis had a 16.6-fold greater odds of subsequent dementia, compared with those who were cognitively normal (95% confidence interval, 5.1-54.7; P less than .001). Notably, early MCI significantly predicted dementia even if patients reverted to normal cognition with dopaminergic treatment, reported Kenn F. Pedersen, MD, PhD, of the Norwegian Centre for Movement Disorders at Stavanger (Norway) University Hospital, and his associates. “Early PD-MCI, regardless of persistence or reversion to normal cognition, has prognostic value for predicting dementia in patients with PD,” they concluded.
At baseline, 20% of patients had MCI. Among those who did not, cumulative incidence rates of MCI were 10% at year 1, 23% at year 3, and 29% by the end of the study after 5 years of follow-up. In all, 59% of patients with persistent MCI by year 1 developed dementia, compared with 7% of patients who retained normal cognition at 1 year. About one in four patients with MCI reverted to normal cognition by the end of the study, but they still faced a 10.7-fold greater odds of dementia at the 5-year follow-up, compared with cognitively normal patients (95% CI, 1.5-78.5; P = .02).
The Research Council of Norway, the Western Norway Regional Health Authority, and the Norwegian Parkinson’s Disease Association funded the study. Dr. Pedersen had no disclosures. One coauthor reported serving on advisory boards for Lundbeck and GlaxoSmithKline and receiving payment for lecturing from Orion Pharma and GlaxoSmithKline.
Developing persistent mild cognitive impairment soon after being diagnosed with Parkinson’s disease significantly increased the risk of subsequent dementia, according to a cohort study that examined the natural history of mild cognitive impairment in 178 patients over 5 years.
After the researchers controlled for age, sex, and education, patients who had persistent mild cognitive impairment (MCI) by 1 year after their Parkinson’s disease (PD) diagnosis had a 16.6-fold greater odds of subsequent dementia, compared with those who were cognitively normal (95% confidence interval, 5.1-54.7; P less than .001). Notably, early MCI significantly predicted dementia even if patients reverted to normal cognition with dopaminergic treatment, reported Kenn F. Pedersen, MD, PhD, of the Norwegian Centre for Movement Disorders at Stavanger (Norway) University Hospital, and his associates. “Early PD-MCI, regardless of persistence or reversion to normal cognition, has prognostic value for predicting dementia in patients with PD,” they concluded.
At baseline, 20% of patients had MCI. Among those who did not, cumulative incidence rates of MCI were 10% at year 1, 23% at year 3, and 29% by the end of the study after 5 years of follow-up. In all, 59% of patients with persistent MCI by year 1 developed dementia, compared with 7% of patients who retained normal cognition at 1 year. About one in four patients with MCI reverted to normal cognition by the end of the study, but they still faced a 10.7-fold greater odds of dementia at the 5-year follow-up, compared with cognitively normal patients (95% CI, 1.5-78.5; P = .02).
The Research Council of Norway, the Western Norway Regional Health Authority, and the Norwegian Parkinson’s Disease Association funded the study. Dr. Pedersen had no disclosures. One coauthor reported serving on advisory boards for Lundbeck and GlaxoSmithKline and receiving payment for lecturing from Orion Pharma and GlaxoSmithKline.
FROM NEUROLOGY
Key clinical point: Developing mild cognitive impairment early in the course of Parkinson’s disease significantly increases the risk of subsequent dementia.
Major finding: In all, 59% of patients with persistent mild cognitive impairment at 1 year and 7% of those with normal cognition later developed dementia (odds ratio, 16.6; P less than .001).
Data source: A population-based cohort study of 178 patients with newly diagnosed Parkinson’s disease.
Disclosures: The Research Council of Norway, the Western Norway Regional Health Authority, and the Norwegian Parkinson’s Disease Association funded the study. Dr. Pederson had no disclosures. One coauthor reported serving on advisory boards for Lundbeck and GlaxoSmithKline and receiving payment for lecturing from Orion Pharma and GlaxoSmithKline.
Lower C. difficile mortality with vancomycin than metronidazole
Treating Clostridium difficile infection with vancomycin achieves the same recurrence rates as does treatment with metronidazole, but with a significantly lower 30-day mortality, new research suggests.
A retrospective, propensity-matched cohort study examined U.S. Department of Veterans Affairs health care system data from 47,471 patients with C. difficile infection who were treated with either vancomycin or metronidazole, according to a report published online Feb. 6 in JAMA Internal Medicine.
“Current guidelines recommend metronidazole hydrochloride as initial therapy for most cases of mild to moderate CDI [Clostridium difficile infection],” wrote Vanessa W. Stevens, PhD, of Veterans Affairs Salt Lake City Health Care System, and her coauthors. “Although an early clinical trial found no difference in cure rates between vancomycin hydrochloride and metronidazole, subsequent observational data and clinical trials suggest that metronidazole is inferior to vancomycin for primary clinical cure, especially in severe cases.”
Their study found patients treated with vancomycin had a similar risk of recurrence compared with those treated with metronidazole (relative risk, 0.98; 95% confidence interval, 0.87 to 1.10), with an overall recurrence rate of 16%.
However, patients treated with vancomycin had a 14% reduction in 30-day mortality compared to the metronidazole-treated group. This was after adjustment for factors such as comorbidity scores, hospitalization history, receipt of chemotherapy, receipt of immunosuppressive medication or proton pump inhibitor therapy in the prior 30-days, or antibiotic use on the day of diagnosis.
The 30-day mortality was not significantly different among patients with mild to moderate CDI, but there was a significant 21% reduction among patients with severe infection. The number needed to treat to prevent one death among patients with severe infection was 25 (JAMA Intern Med. 2017 Feb 6. doi: 10.1001/jamainternmed.2016.9045).
“This is the largest study to date to compare vancomycin and metronidazole in a real-world setting and one of the few studies focused on downstream outcomes of CDI,” researchers reported.
The authors noted that despite strong evidence and guidelines supporting the use of vancomycin for severe CDI – and the fact that 42% of episodes in the study were classified as severe – only 4%-6% of patients were prescribed vancomycin.
“Although the excess treatment costs of vancomycin relative to metronidazole and the concern for vancomycin-resistant Enterococcus will likely remain barriers, improved clinical cure and mortality rates may warrant reconsideration of current prescribing practices,” they wrote. “One approach to minimizing the effects of increasing vancomycin use is to target vancomycin treatment to patients with severe disease.”
The study was supported by researcher grants from the U.S. Department of Veterans Affairs. No conflicts of interest were declared.
AGA Resource
AGA offers patient education materials to help you discuss C. diff with your patients at http://www.gastro.org/patient-care/conditions-diseases/clostridium-difficile-infection.
Treating Clostridium difficile infection with vancomycin achieves the same recurrence rates as does treatment with metronidazole, but with a significantly lower 30-day mortality, new research suggests.
A retrospective, propensity-matched cohort study examined U.S. Department of Veterans Affairs health care system data from 47,471 patients with C. difficile infection who were treated with either vancomycin or metronidazole, according to a report published online Feb. 6 in JAMA Internal Medicine.
“Current guidelines recommend metronidazole hydrochloride as initial therapy for most cases of mild to moderate CDI [Clostridium difficile infection],” wrote Vanessa W. Stevens, PhD, of Veterans Affairs Salt Lake City Health Care System, and her coauthors. “Although an early clinical trial found no difference in cure rates between vancomycin hydrochloride and metronidazole, subsequent observational data and clinical trials suggest that metronidazole is inferior to vancomycin for primary clinical cure, especially in severe cases.”
Their study found patients treated with vancomycin had a similar risk of recurrence compared with those treated with metronidazole (relative risk, 0.98; 95% confidence interval, 0.87 to 1.10), with an overall recurrence rate of 16%.
However, patients treated with vancomycin had a 14% reduction in 30-day mortality compared to the metronidazole-treated group. This was after adjustment for factors such as comorbidity scores, hospitalization history, receipt of chemotherapy, receipt of immunosuppressive medication or proton pump inhibitor therapy in the prior 30-days, or antibiotic use on the day of diagnosis.
The 30-day mortality was not significantly different among patients with mild to moderate CDI, but there was a significant 21% reduction among patients with severe infection. The number needed to treat to prevent one death among patients with severe infection was 25 (JAMA Intern Med. 2017 Feb 6. doi: 10.1001/jamainternmed.2016.9045).
“This is the largest study to date to compare vancomycin and metronidazole in a real-world setting and one of the few studies focused on downstream outcomes of CDI,” researchers reported.
The authors noted that despite strong evidence and guidelines supporting the use of vancomycin for severe CDI – and the fact that 42% of episodes in the study were classified as severe – only 4%-6% of patients were prescribed vancomycin.
“Although the excess treatment costs of vancomycin relative to metronidazole and the concern for vancomycin-resistant Enterococcus will likely remain barriers, improved clinical cure and mortality rates may warrant reconsideration of current prescribing practices,” they wrote. “One approach to minimizing the effects of increasing vancomycin use is to target vancomycin treatment to patients with severe disease.”
The study was supported by researcher grants from the U.S. Department of Veterans Affairs. No conflicts of interest were declared.
AGA Resource
AGA offers patient education materials to help you discuss C. diff with your patients at http://www.gastro.org/patient-care/conditions-diseases/clostridium-difficile-infection.
Treating Clostridium difficile infection with vancomycin achieves the same recurrence rates as does treatment with metronidazole, but with a significantly lower 30-day mortality, new research suggests.
A retrospective, propensity-matched cohort study examined U.S. Department of Veterans Affairs health care system data from 47,471 patients with C. difficile infection who were treated with either vancomycin or metronidazole, according to a report published online Feb. 6 in JAMA Internal Medicine.
“Current guidelines recommend metronidazole hydrochloride as initial therapy for most cases of mild to moderate CDI [Clostridium difficile infection],” wrote Vanessa W. Stevens, PhD, of Veterans Affairs Salt Lake City Health Care System, and her coauthors. “Although an early clinical trial found no difference in cure rates between vancomycin hydrochloride and metronidazole, subsequent observational data and clinical trials suggest that metronidazole is inferior to vancomycin for primary clinical cure, especially in severe cases.”
Their study found patients treated with vancomycin had a similar risk of recurrence compared with those treated with metronidazole (relative risk, 0.98; 95% confidence interval, 0.87 to 1.10), with an overall recurrence rate of 16%.
However, patients treated with vancomycin had a 14% reduction in 30-day mortality compared to the metronidazole-treated group. This was after adjustment for factors such as comorbidity scores, hospitalization history, receipt of chemotherapy, receipt of immunosuppressive medication or proton pump inhibitor therapy in the prior 30-days, or antibiotic use on the day of diagnosis.
The 30-day mortality was not significantly different among patients with mild to moderate CDI, but there was a significant 21% reduction among patients with severe infection. The number needed to treat to prevent one death among patients with severe infection was 25 (JAMA Intern Med. 2017 Feb 6. doi: 10.1001/jamainternmed.2016.9045).
“This is the largest study to date to compare vancomycin and metronidazole in a real-world setting and one of the few studies focused on downstream outcomes of CDI,” researchers reported.
The authors noted that despite strong evidence and guidelines supporting the use of vancomycin for severe CDI – and the fact that 42% of episodes in the study were classified as severe – only 4%-6% of patients were prescribed vancomycin.
“Although the excess treatment costs of vancomycin relative to metronidazole and the concern for vancomycin-resistant Enterococcus will likely remain barriers, improved clinical cure and mortality rates may warrant reconsideration of current prescribing practices,” they wrote. “One approach to minimizing the effects of increasing vancomycin use is to target vancomycin treatment to patients with severe disease.”
The study was supported by researcher grants from the U.S. Department of Veterans Affairs. No conflicts of interest were declared.
AGA Resource
AGA offers patient education materials to help you discuss C. diff with your patients at http://www.gastro.org/patient-care/conditions-diseases/clostridium-difficile-infection.
FROM JAMA INTERNAL MEDICINE
Key clinical point: Vancomycin therapy is associated with significantly lower 30-day mortality from severe Clostridium difficile infection compared to metronidazole.
Major finding: Treatment with vancomycin prevented one death per 25 patients with severe C. difficile infection.
Data source: A retrospective, propensity-matched cohort study of 47,471 patients with C. difficile infection.
Disclosures: The study was supported by researcher grants from the U.S. Department of Veterans Affairs. No conflicts of interest were declared.
Lower C. difficile mortality with vancomycin than metronidazole
Treating Clostridium difficile infection with vancomycin achieves the same recurrence rates as does treatment with metronidazole, but with a significantly lower 30-day mortality, new research suggests.
A retrospective, propensity-matched cohort study examined U.S. Department of Veterans Affairs health care system data from 47,471 patients with C. difficile infection who were treated with either vancomycin or metronidazole, according to a report published online Feb. 6 in JAMA Internal Medicine.
“Current guidelines recommend metronidazole hydrochloride as initial therapy for most cases of mild to moderate CDI [Clostridium difficile infection],” wrote Vanessa W. Stevens, PhD, of Veterans Affairs Salt Lake City Health Care System, and her coauthors. “Although an early clinical trial found no difference in cure rates between vancomycin hydrochloride and metronidazole, subsequent observational data and clinical trials suggest that metronidazole is inferior to vancomycin for primary clinical cure, especially in severe cases.”
Their study found patients treated with vancomycin had a similar risk of recurrence compared with those treated with metronidazole (relative risk, 0.98; 95% confidence interval, 0.87 to 1.10), with an overall recurrence rate of 16%.
However, patients treated with vancomycin had a 14% reduction in 30-day mortality compared to the metronidazole-treated group. This was after adjustment for factors such as comorbidity scores, hospitalization history, receipt of chemotherapy, receipt of immunosuppressive medication or proton pump inhibitor therapy in the prior 30-days, or antibiotic use on the day of diagnosis.
The 30-day mortality was not significantly different among patients with mild to moderate CDI, but there was a significant 21% reduction among patients with severe infection. The number needed to treat to prevent one death among patients with severe infection was 25 (JAMA Intern Med. 2017 Feb 6. doi: 10.1001/jamainternmed.2016.9045).
“This is the largest study to date to compare vancomycin and metronidazole in a real-world setting and one of the few studies focused on downstream outcomes of CDI,” researchers reported.
The authors noted that despite strong evidence and guidelines supporting the use of vancomycin for severe CDI – and the fact that 42% of episodes in the study were classified as severe – only 4%-6% of patients were prescribed vancomycin.
“Although the excess treatment costs of vancomycin relative to metronidazole and the concern for vancomycin-resistant Enterococcus will likely remain barriers, improved clinical cure and mortality rates may warrant reconsideration of current prescribing practices,” they wrote. “One approach to minimizing the effects of increasing vancomycin use is to target vancomycin treatment to patients with severe disease.”
The study was supported by researcher grants from the U.S. Department of Veterans Affairs. No conflicts of interest were declared.
Treating Clostridium difficile infection with vancomycin achieves the same recurrence rates as does treatment with metronidazole, but with a significantly lower 30-day mortality, new research suggests.
A retrospective, propensity-matched cohort study examined U.S. Department of Veterans Affairs health care system data from 47,471 patients with C. difficile infection who were treated with either vancomycin or metronidazole, according to a report published online Feb. 6 in JAMA Internal Medicine.
“Current guidelines recommend metronidazole hydrochloride as initial therapy for most cases of mild to moderate CDI [Clostridium difficile infection],” wrote Vanessa W. Stevens, PhD, of Veterans Affairs Salt Lake City Health Care System, and her coauthors. “Although an early clinical trial found no difference in cure rates between vancomycin hydrochloride and metronidazole, subsequent observational data and clinical trials suggest that metronidazole is inferior to vancomycin for primary clinical cure, especially in severe cases.”
Their study found patients treated with vancomycin had a similar risk of recurrence compared with those treated with metronidazole (relative risk, 0.98; 95% confidence interval, 0.87 to 1.10), with an overall recurrence rate of 16%.
However, patients treated with vancomycin had a 14% reduction in 30-day mortality compared to the metronidazole-treated group. This was after adjustment for factors such as comorbidity scores, hospitalization history, receipt of chemotherapy, receipt of immunosuppressive medication or proton pump inhibitor therapy in the prior 30-days, or antibiotic use on the day of diagnosis.
The 30-day mortality was not significantly different among patients with mild to moderate CDI, but there was a significant 21% reduction among patients with severe infection. The number needed to treat to prevent one death among patients with severe infection was 25 (JAMA Intern Med. 2017 Feb 6. doi: 10.1001/jamainternmed.2016.9045).
“This is the largest study to date to compare vancomycin and metronidazole in a real-world setting and one of the few studies focused on downstream outcomes of CDI,” researchers reported.
The authors noted that despite strong evidence and guidelines supporting the use of vancomycin for severe CDI – and the fact that 42% of episodes in the study were classified as severe – only 4%-6% of patients were prescribed vancomycin.
“Although the excess treatment costs of vancomycin relative to metronidazole and the concern for vancomycin-resistant Enterococcus will likely remain barriers, improved clinical cure and mortality rates may warrant reconsideration of current prescribing practices,” they wrote. “One approach to minimizing the effects of increasing vancomycin use is to target vancomycin treatment to patients with severe disease.”
The study was supported by researcher grants from the U.S. Department of Veterans Affairs. No conflicts of interest were declared.
Treating Clostridium difficile infection with vancomycin achieves the same recurrence rates as does treatment with metronidazole, but with a significantly lower 30-day mortality, new research suggests.
A retrospective, propensity-matched cohort study examined U.S. Department of Veterans Affairs health care system data from 47,471 patients with C. difficile infection who were treated with either vancomycin or metronidazole, according to a report published online Feb. 6 in JAMA Internal Medicine.
“Current guidelines recommend metronidazole hydrochloride as initial therapy for most cases of mild to moderate CDI [Clostridium difficile infection],” wrote Vanessa W. Stevens, PhD, of Veterans Affairs Salt Lake City Health Care System, and her coauthors. “Although an early clinical trial found no difference in cure rates between vancomycin hydrochloride and metronidazole, subsequent observational data and clinical trials suggest that metronidazole is inferior to vancomycin for primary clinical cure, especially in severe cases.”
Their study found patients treated with vancomycin had a similar risk of recurrence compared with those treated with metronidazole (relative risk, 0.98; 95% confidence interval, 0.87 to 1.10), with an overall recurrence rate of 16%.
However, patients treated with vancomycin had a 14% reduction in 30-day mortality compared to the metronidazole-treated group. This was after adjustment for factors such as comorbidity scores, hospitalization history, receipt of chemotherapy, receipt of immunosuppressive medication or proton pump inhibitor therapy in the prior 30-days, or antibiotic use on the day of diagnosis.
The 30-day mortality was not significantly different among patients with mild to moderate CDI, but there was a significant 21% reduction among patients with severe infection. The number needed to treat to prevent one death among patients with severe infection was 25 (JAMA Intern Med. 2017 Feb 6. doi: 10.1001/jamainternmed.2016.9045).
“This is the largest study to date to compare vancomycin and metronidazole in a real-world setting and one of the few studies focused on downstream outcomes of CDI,” researchers reported.
The authors noted that despite strong evidence and guidelines supporting the use of vancomycin for severe CDI – and the fact that 42% of episodes in the study were classified as severe – only 4%-6% of patients were prescribed vancomycin.
“Although the excess treatment costs of vancomycin relative to metronidazole and the concern for vancomycin-resistant Enterococcus will likely remain barriers, improved clinical cure and mortality rates may warrant reconsideration of current prescribing practices,” they wrote. “One approach to minimizing the effects of increasing vancomycin use is to target vancomycin treatment to patients with severe disease.”
The study was supported by researcher grants from the U.S. Department of Veterans Affairs. No conflicts of interest were declared.
FROM JAMA INTERNAL MEDICINE
Key clinical point: Vancomycin therapy is associated with significantly lower 30-day mortality from severe Clostridium difficile infection compared to metronidazole.
Major finding: Treatment with vancomycin prevented one death per 25 patients with severe C. difficile infection.
Data source: A retrospective, propensity-matched cohort study of 47,471 patients with C. difficile infection.
Disclosures: The study was supported by researcher grants from the U.S. Department of Veterans Affairs. No conflicts of interest were declared.
Resolution of Psoriatic Lesions on the Gingiva and Hard Palate Following Administration of Adalimumab for Cutaneous Psoriasis
Psoriasis is a chronic, relapsing, inflammatory systemic disorder of the skin with an incidence of 2% to 3% and is estimated to affect 125 million individuals worldwide.1 Environmental triggers of disease modulation may include cutaneous microbiota, smoking, alcohol use, drugs (ie, beta-blockers, lithium, antimalarials), stress, and trauma.2 Comorbidities associated with cutaneous lesions include psoriatic arthritis, Crohn disease, type 2 diabetes mellitus, metabolic syndrome, stroke, and cardiovascular disease.3 In some studies, patients with psoriasis also had a 24% to 27% increased propensity for periodontal bone loss versus 10% of controls.4,5
Oral psoriasis is rare and case reports have been preferentially published in dental journals, usually with regard to glossal lesions, leaving gingival and palatal psoriatic involvement infrequently reported in the dermatologic literature.6,7 In fact, oral assessments involving 535 psoriatic patients from a dermatology center only yielded cases of geographic and fissured tongue.8 Another study at a psoriasis clinic found 3.8% (21/547) of patients with geographic tongue, 3.1% (17/547) with buccal mucosal plaques, and only 0.4% (2/547) with palatal lesions.9 To extend the knowledge of oral psoriasis, we provide the clinical and histopathologic findings of a patient with synchronous oral and cutaneous psoriatic lesions that responded well to the administration of adalimumab for management of recurrent cutaneous disease.
Case Report
A 51-year-old man presented to the attending periodontist for comprehensive treatment of multiple quadrants of gingival recession. His medical history was remarkable for psoriasis; Prinzmetal angina, which led to myocardial infarction; and diverticulitis. The cutaneous psoriasis began approximately 18 years prior to the current presentation and was initially managed with various topical therapeutics. At an 11-year follow-up, the patient was experiencing poor lesional control as well as severe pruritus and was prescribed etanercept by a dermatologist. His inconsistent compliance with frequency and dosing failed to achieve satisfactory disease suppression and etanercept was discontinued after approximately 2.5 years. Two years later the patient was switched to adalimumab by a dermatologist, and around this time he had developed psoriatic arthritis of the hands and knees and pitting of the nail plates. The patient elected to discontinue adalimumab usage after 3 years due to successful management of the skin lesions, cost considerations, and his perception that the psoriasis could “remain in remission.” After a 6-month lapse, the patient resumed adalimumab due to cutaneous lesional recurrence (Figure 1A).

At the current presentation, an oral examination performed 2 days after the reinstitution of adalim-umab revealed generalized severe gingivitis with an atypical inflammatory response that extended from just beyond the mucogingival junction to the marginal gingiva. The gingiva also appeared edematous with a conspicuously granular surface (Figure 1B). The hard palate displayed multiple red macules of varying sizes (Figure 1C). A maxillary gingival biopsy demonstrated hyperkeratosis, parakeratosis, spongiosis, acanthosis, elongation of the rete ridges, numerous collections of neutrophils (Munro microabscesses), and abundant lymphocytes in the subjacent connective tissue (Figure 2). Periodic acid–Schiff staining was negative for fungal hyphae. These features were consistent with oral mucosal psoriasis.
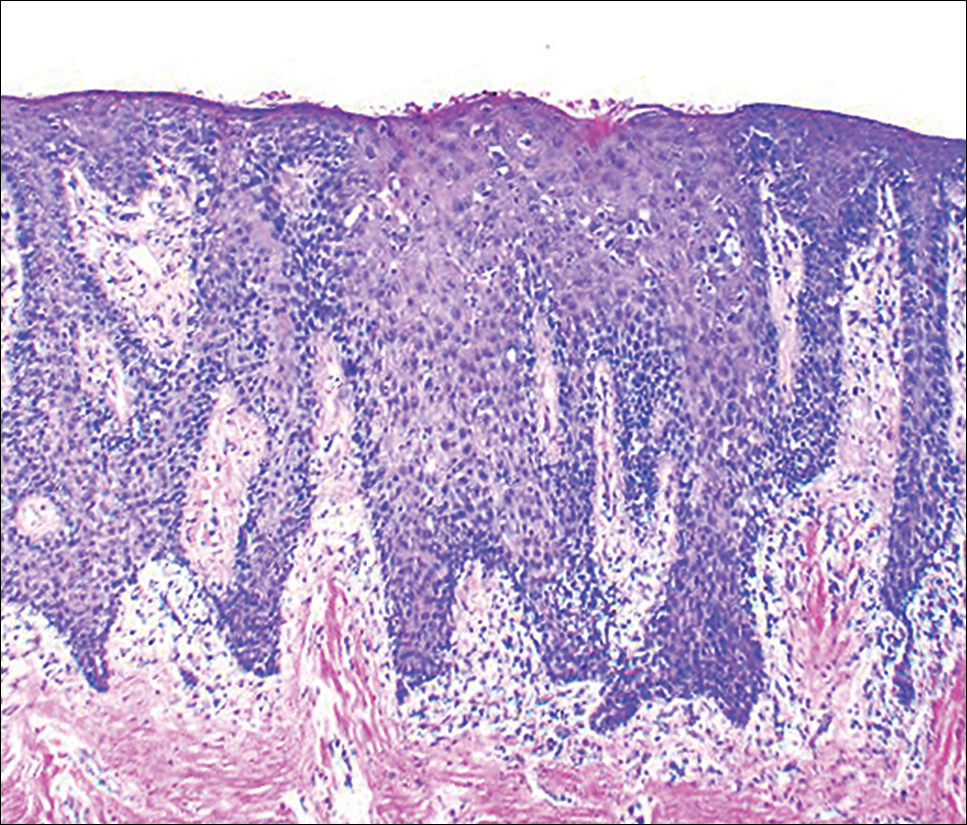
At a 2-month follow-up, the biopsy site had healed without incident and without loss of the gingival architecture. There was an almost-complete resolution of the gingival erythema (Figure 3A) and the patient has since noticed a lack of bleeding using floss. Additionally, the red macules on the palate were no longer present (Figure 3B). The cutaneous plaques were greatly reduced in size and the patient experienced a proportionate decline in pruritus. Based on the uneventful surgical biopsy procedure, the patient was advised to undergo gingival grafting and has not returned for periodontal care.

Comment
Psoriasis of the oral cavity is rare and typically occurs on the tongue and less frequently on the hard palate, lip, buccal mucosa, and gingiva.2,7 The lesions are almost always concordant with cutaneous psoriasis, and only sporadic examples exclusive to the oral mucosa have been recognized.7,10 Gingival psoriasis usually is described as intensely erythematous and occasionally laced with white scaly streaks involving the marginal gingiva that extend toward the mucogingival junction. In general, the erythematous presentation of gingival psoriasis may not be commensurate with the degree of inflammation induced by dental plaque-based periodontal disease. Doben11 documented gingival psoriasis as appearing “deeply stippled and grainy” and commented that the tissue was “friable” and incapable of maintaining a “clean incision line” during periodontal surgery. In our patient, the gingiva also had exhibited a granular surface. Patients with oral psoriasis often report soreness or a burning sensation of the gingiva, which may easily bleed on manipulation or brushing the teeth, whereas other patients are asymptomatic,12 as in our case. Psoriasis of the hard palate usually presents as multiple painless red macules. Unlike cutaneous psoriasis, oral lesions rarely evoke pruritus.10 Histopathologically, oral psoriasis bears a striking resemblance to its cutaneous counterpart. The epithelium has a pronounced parakeratinized surface with elongated rete ridges and aggregations of Munro microabscesses. The connective tissue often is composed of dilated capillaries that closely approximate the epithelium as well as infiltrations of lymphocytes. Specimens suspected for oral psoriasis should routinely be stained with periodic acid–Schiff to rule out candidiasis coinfection. The microscopic findings of our patient were congruent with prior reports of oral psoriasis.7,10-12 Some clinicians have questioned if psoriasis can actually occur in the oral cavity, but most authorities in the field have recognized its true existence, as evidenced by various shared HLA antigens, specifically HLA-Cw.13
Another group of oral lesions collectively referred to as psoriasiform mucositis, notably geographic tongue (benign migratory glossitis, erythema migrans) and its extraglossal variant geographic stomatitis,14,15 have histopathologic features and HLAs similar to those seen in cutaneous psoriasis.13 Interestingly, geographic tongue has been found in 3.8% to 9.1% of cohorts with cutaneous psoriasis,8,9 but in the extant population, the vast majority of patients with oral psoriasiform mucositis do not have cutaneous psoriasis. Other differential diagnoses for gingival psoriasis are lichen planus, human immunodeficiency virus–associated periodontitis, desquamative gingivitis, plasma cell gingivitis, erythematous candidiasis, mucous membrane pemphigoid, pemphigus vulgaris, leukemia, systemic lupus erythematosus, granulomatosis with polyangiitis, orofacial granulomatosis, localized juvenile spongiotic gingivitis hyperplasia, and primary gingivostomatitis.
Management of gingival psoriasis focuses on strategies to reduce inflammation and discomfort and measures to achieve meticulous oral plaque control. Judicious efforts should be exercised to avoid oral soft-tissue injury when performing periodontal scaling, although it has not been established whether gingival psoriasis is associated with the Köbner phenomenon, as seen with cutaneous lesions. Adjunctive measures employed for symptomatic patients have involved the use of corticosteroids (eg, lesional injection, oral rinse, systemic) and oral rinses with retinoic acid, chlorhexidine gluconate, and warm saline.7,10,16 Prolonged utilization of corticosteroids, however, may necessitate supplemental administration of antifungal agents.
This case report represents a rare documentation of a successful outcome of gingival and palatal psoriasis subsequent to the reinstitution of adalimumab solely for treatment of recurrent cutaneous disease. There likely is a pharmacologic basis for the amelioration of oral psoriasis in our patient. Adalimumab is a bivalent IgG monoclonal antibody that binds to activated dermal dendritic cell receptors of tumor necrosis factor α, thereby attenuating a cytokine-derived inflammatory response and apoptosis.17 In fact, patients with rheumatoid arthritis showed notable reductions in both gingival inflammation and bleeding following a 3-month regimen of adalimumab.18
Conclusion
Practitioners should be aware of the phenotypic overlap of cutaneous and oral psoriasis, particularly involving the gingiva and palate. It is recommended that psoriasis patients routinely receive a dental prophylaxis and engage in oral hygiene efforts to reduce the presence of oral microbiota. Furthermore, it is emphasized that psoriatic patients who maintain an atypical erythematous presentation on the oral mucosa undergo a biopsy for identification of the lesions and correlation with disease dissemination. Prospective studies are needed to characterize the clinical courses of oral psoriasis, ascertain their correlative behavior with cutaneous flares, and determine if lesional improvement can be achieved with the use of biologic agents or other therapeutic modalities.
- Gupta R, Debbaneh MG, Liao W. Genetic epidemiology of psoriasis. Curr Dermatol Rep. 2014;3:61-78.
- Younai FS, Phelan JA. Oral mucositis with features of psoriasis: report of a case and review of the literature. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1997;84:61-67.
- Xu T, Zhang YH. Association of psoriasis with stroke and myocardial infarction: meta-analysis of cohort studies. Br J Dermatol. 2012;167:1345-1350.
- Lazaridou E, Tsikrikoni A, Fotiadou C, et al. Association of chronic plaque psoriasis and severe periodontitis: a hospital based case-control study. J Eur Acad Dermatol Venereol. 2013;27:967-972.
- Skudutyte-Rysstad R, Slevolden EM, Hansen BF, et al. Association between moderate to severe psoriasis and periodontitis in a Scandinavian population. BMC Oral Health. 2014;14:139.
- Zunt SL, Tomich CE. Erythema migrans—a psoriasiform lesion of the oral mucosa. J Dermatol Surg Oncol. 1989;15:1067-1070.
- Reis V, Artico G, Seo J, et al. Psoriasiform mucositis on the gingival and palatal mucosae treated with retinoic-acid mouthwash. Int J Dermatol. 2013;52:113-115.
- Germi L, De Giorgi V, Bergamo F, et al. Psoriasis and oral lesions: multicentric study of oral mucosa diseases Italian group (GIPMO). Dermatol Online J. 2012;18:11.
- Kaur I, Handa S, Kumar B. Oral lesions in psoriasis. Int J Dermatol. 1997;36:78-79.
- Brayshaw HA, Orban B. Psoriasis gingivae. J Periodontol. 1953;24:156-160.
- Doben DI. Psoriasis of the attached gingiva. J Periodontol. 1976;47:38-40.
- Mattsson U, Warfvinge G, Jontell M. Oral psoriasis—a diagnostic dilemma: a report of two cases and a review of the literature. Oral Surg Oral Med Oral Pathol Oral Radiol. 2015;120:e183-e189.
- Dermatologic diseases. In: Neville BW, Damm DD, Allen CM, et al, eds. Oral and Maxillofacial Pathology. 3rd ed. St. Louis, MO: Saunders/Elsevier; 2009:792-794.
- Brooks JK, Balciunas BA. Geographic stomatitis: review of the literature and report of five cases. J Am Dent Assoc. 1987;115:421-424.
- Brooks JK, Nikitakis NG. Multiple mucosal lesions. erythema migrans. Gen Dent. 2007;55:160, 163.
- Ulmansky M, Michelle R, Azaz B. Oral psoriasis: report of six new cases. J Oral Pathol Med. 1995;24:42-45.
- Lis K, Kuzawinska O, Bałkowiec-Iskra E. Tumor necrosis factor inhibitors—state of knowledge. Arch Med Sci. 2014;10:1175-1185.
- Kobayashi T, Yokoyama T, Ito S, et al. Periodontal and serum protein profiles in patients with rheumatoid arthritis treated with tumor necrosis factor inhibitor adalimumab. J Periodontol. 2014;85:1480-1488.
Psoriasis is a chronic, relapsing, inflammatory systemic disorder of the skin with an incidence of 2% to 3% and is estimated to affect 125 million individuals worldwide.1 Environmental triggers of disease modulation may include cutaneous microbiota, smoking, alcohol use, drugs (ie, beta-blockers, lithium, antimalarials), stress, and trauma.2 Comorbidities associated with cutaneous lesions include psoriatic arthritis, Crohn disease, type 2 diabetes mellitus, metabolic syndrome, stroke, and cardiovascular disease.3 In some studies, patients with psoriasis also had a 24% to 27% increased propensity for periodontal bone loss versus 10% of controls.4,5
Oral psoriasis is rare and case reports have been preferentially published in dental journals, usually with regard to glossal lesions, leaving gingival and palatal psoriatic involvement infrequently reported in the dermatologic literature.6,7 In fact, oral assessments involving 535 psoriatic patients from a dermatology center only yielded cases of geographic and fissured tongue.8 Another study at a psoriasis clinic found 3.8% (21/547) of patients with geographic tongue, 3.1% (17/547) with buccal mucosal plaques, and only 0.4% (2/547) with palatal lesions.9 To extend the knowledge of oral psoriasis, we provide the clinical and histopathologic findings of a patient with synchronous oral and cutaneous psoriatic lesions that responded well to the administration of adalimumab for management of recurrent cutaneous disease.
Case Report
A 51-year-old man presented to the attending periodontist for comprehensive treatment of multiple quadrants of gingival recession. His medical history was remarkable for psoriasis; Prinzmetal angina, which led to myocardial infarction; and diverticulitis. The cutaneous psoriasis began approximately 18 years prior to the current presentation and was initially managed with various topical therapeutics. At an 11-year follow-up, the patient was experiencing poor lesional control as well as severe pruritus and was prescribed etanercept by a dermatologist. His inconsistent compliance with frequency and dosing failed to achieve satisfactory disease suppression and etanercept was discontinued after approximately 2.5 years. Two years later the patient was switched to adalimumab by a dermatologist, and around this time he had developed psoriatic arthritis of the hands and knees and pitting of the nail plates. The patient elected to discontinue adalimumab usage after 3 years due to successful management of the skin lesions, cost considerations, and his perception that the psoriasis could “remain in remission.” After a 6-month lapse, the patient resumed adalimumab due to cutaneous lesional recurrence (Figure 1A).
At the current presentation, an oral examination performed 2 days after the reinstitution of adalim-umab revealed generalized severe gingivitis with an atypical inflammatory response that extended from just beyond the mucogingival junction to the marginal gingiva. The gingiva also appeared edematous with a conspicuously granular surface (Figure 1B). The hard palate displayed multiple red macules of varying sizes (Figure 1C). A maxillary gingival biopsy demonstrated hyperkeratosis, parakeratosis, spongiosis, acanthosis, elongation of the rete ridges, numerous collections of neutrophils (Munro microabscesses), and abundant lymphocytes in the subjacent connective tissue (Figure 2). Periodic acid–Schiff staining was negative for fungal hyphae. These features were consistent with oral mucosal psoriasis.
At a 2-month follow-up, the biopsy site had healed without incident and without loss of the gingival architecture. There was an almost-complete resolution of the gingival erythema (Figure 3A) and the patient has since noticed a lack of bleeding using floss. Additionally, the red macules on the palate were no longer present (Figure 3B). The cutaneous plaques were greatly reduced in size and the patient experienced a proportionate decline in pruritus. Based on the uneventful surgical biopsy procedure, the patient was advised to undergo gingival grafting and has not returned for periodontal care.
Comment
Psoriasis of the oral cavity is rare and typically occurs on the tongue and less frequently on the hard palate, lip, buccal mucosa, and gingiva.2,7 The lesions are almost always concordant with cutaneous psoriasis, and only sporadic examples exclusive to the oral mucosa have been recognized.7,10 Gingival psoriasis usually is described as intensely erythematous and occasionally laced with white scaly streaks involving the marginal gingiva that extend toward the mucogingival junction. In general, the erythematous presentation of gingival psoriasis may not be commensurate with the degree of inflammation induced by dental plaque-based periodontal disease. Doben11 documented gingival psoriasis as appearing “deeply stippled and grainy” and commented that the tissue was “friable” and incapable of maintaining a “clean incision line” during periodontal surgery. In our patient, the gingiva also had exhibited a granular surface. Patients with oral psoriasis often report soreness or a burning sensation of the gingiva, which may easily bleed on manipulation or brushing the teeth, whereas other patients are asymptomatic,12 as in our case. Psoriasis of the hard palate usually presents as multiple painless red macules. Unlike cutaneous psoriasis, oral lesions rarely evoke pruritus.10 Histopathologically, oral psoriasis bears a striking resemblance to its cutaneous counterpart. The epithelium has a pronounced parakeratinized surface with elongated rete ridges and aggregations of Munro microabscesses. The connective tissue often is composed of dilated capillaries that closely approximate the epithelium as well as infiltrations of lymphocytes. Specimens suspected for oral psoriasis should routinely be stained with periodic acid–Schiff to rule out candidiasis coinfection. The microscopic findings of our patient were congruent with prior reports of oral psoriasis.7,10-12 Some clinicians have questioned if psoriasis can actually occur in the oral cavity, but most authorities in the field have recognized its true existence, as evidenced by various shared HLA antigens, specifically HLA-Cw.13
Another group of oral lesions collectively referred to as psoriasiform mucositis, notably geographic tongue (benign migratory glossitis, erythema migrans) and its extraglossal variant geographic stomatitis,14,15 have histopathologic features and HLAs similar to those seen in cutaneous psoriasis.13 Interestingly, geographic tongue has been found in 3.8% to 9.1% of cohorts with cutaneous psoriasis,8,9 but in the extant population, the vast majority of patients with oral psoriasiform mucositis do not have cutaneous psoriasis. Other differential diagnoses for gingival psoriasis are lichen planus, human immunodeficiency virus–associated periodontitis, desquamative gingivitis, plasma cell gingivitis, erythematous candidiasis, mucous membrane pemphigoid, pemphigus vulgaris, leukemia, systemic lupus erythematosus, granulomatosis with polyangiitis, orofacial granulomatosis, localized juvenile spongiotic gingivitis hyperplasia, and primary gingivostomatitis.
Management of gingival psoriasis focuses on strategies to reduce inflammation and discomfort and measures to achieve meticulous oral plaque control. Judicious efforts should be exercised to avoid oral soft-tissue injury when performing periodontal scaling, although it has not been established whether gingival psoriasis is associated with the Köbner phenomenon, as seen with cutaneous lesions. Adjunctive measures employed for symptomatic patients have involved the use of corticosteroids (eg, lesional injection, oral rinse, systemic) and oral rinses with retinoic acid, chlorhexidine gluconate, and warm saline.7,10,16 Prolonged utilization of corticosteroids, however, may necessitate supplemental administration of antifungal agents.
This case report represents a rare documentation of a successful outcome of gingival and palatal psoriasis subsequent to the reinstitution of adalimumab solely for treatment of recurrent cutaneous disease. There likely is a pharmacologic basis for the amelioration of oral psoriasis in our patient. Adalimumab is a bivalent IgG monoclonal antibody that binds to activated dermal dendritic cell receptors of tumor necrosis factor α, thereby attenuating a cytokine-derived inflammatory response and apoptosis.17 In fact, patients with rheumatoid arthritis showed notable reductions in both gingival inflammation and bleeding following a 3-month regimen of adalimumab.18
Conclusion
Practitioners should be aware of the phenotypic overlap of cutaneous and oral psoriasis, particularly involving the gingiva and palate. It is recommended that psoriasis patients routinely receive a dental prophylaxis and engage in oral hygiene efforts to reduce the presence of oral microbiota. Furthermore, it is emphasized that psoriatic patients who maintain an atypical erythematous presentation on the oral mucosa undergo a biopsy for identification of the lesions and correlation with disease dissemination. Prospective studies are needed to characterize the clinical courses of oral psoriasis, ascertain their correlative behavior with cutaneous flares, and determine if lesional improvement can be achieved with the use of biologic agents or other therapeutic modalities.
Psoriasis is a chronic, relapsing, inflammatory systemic disorder of the skin with an incidence of 2% to 3% and is estimated to affect 125 million individuals worldwide.1 Environmental triggers of disease modulation may include cutaneous microbiota, smoking, alcohol use, drugs (ie, beta-blockers, lithium, antimalarials), stress, and trauma.2 Comorbidities associated with cutaneous lesions include psoriatic arthritis, Crohn disease, type 2 diabetes mellitus, metabolic syndrome, stroke, and cardiovascular disease.3 In some studies, patients with psoriasis also had a 24% to 27% increased propensity for periodontal bone loss versus 10% of controls.4,5
Oral psoriasis is rare and case reports have been preferentially published in dental journals, usually with regard to glossal lesions, leaving gingival and palatal psoriatic involvement infrequently reported in the dermatologic literature.6,7 In fact, oral assessments involving 535 psoriatic patients from a dermatology center only yielded cases of geographic and fissured tongue.8 Another study at a psoriasis clinic found 3.8% (21/547) of patients with geographic tongue, 3.1% (17/547) with buccal mucosal plaques, and only 0.4% (2/547) with palatal lesions.9 To extend the knowledge of oral psoriasis, we provide the clinical and histopathologic findings of a patient with synchronous oral and cutaneous psoriatic lesions that responded well to the administration of adalimumab for management of recurrent cutaneous disease.
Case Report
A 51-year-old man presented to the attending periodontist for comprehensive treatment of multiple quadrants of gingival recession. His medical history was remarkable for psoriasis; Prinzmetal angina, which led to myocardial infarction; and diverticulitis. The cutaneous psoriasis began approximately 18 years prior to the current presentation and was initially managed with various topical therapeutics. At an 11-year follow-up, the patient was experiencing poor lesional control as well as severe pruritus and was prescribed etanercept by a dermatologist. His inconsistent compliance with frequency and dosing failed to achieve satisfactory disease suppression and etanercept was discontinued after approximately 2.5 years. Two years later the patient was switched to adalimumab by a dermatologist, and around this time he had developed psoriatic arthritis of the hands and knees and pitting of the nail plates. The patient elected to discontinue adalimumab usage after 3 years due to successful management of the skin lesions, cost considerations, and his perception that the psoriasis could “remain in remission.” After a 6-month lapse, the patient resumed adalimumab due to cutaneous lesional recurrence (Figure 1A).
At the current presentation, an oral examination performed 2 days after the reinstitution of adalim-umab revealed generalized severe gingivitis with an atypical inflammatory response that extended from just beyond the mucogingival junction to the marginal gingiva. The gingiva also appeared edematous with a conspicuously granular surface (Figure 1B). The hard palate displayed multiple red macules of varying sizes (Figure 1C). A maxillary gingival biopsy demonstrated hyperkeratosis, parakeratosis, spongiosis, acanthosis, elongation of the rete ridges, numerous collections of neutrophils (Munro microabscesses), and abundant lymphocytes in the subjacent connective tissue (Figure 2). Periodic acid–Schiff staining was negative for fungal hyphae. These features were consistent with oral mucosal psoriasis.
At a 2-month follow-up, the biopsy site had healed without incident and without loss of the gingival architecture. There was an almost-complete resolution of the gingival erythema (Figure 3A) and the patient has since noticed a lack of bleeding using floss. Additionally, the red macules on the palate were no longer present (Figure 3B). The cutaneous plaques were greatly reduced in size and the patient experienced a proportionate decline in pruritus. Based on the uneventful surgical biopsy procedure, the patient was advised to undergo gingival grafting and has not returned for periodontal care.
Comment
Psoriasis of the oral cavity is rare and typically occurs on the tongue and less frequently on the hard palate, lip, buccal mucosa, and gingiva.2,7 The lesions are almost always concordant with cutaneous psoriasis, and only sporadic examples exclusive to the oral mucosa have been recognized.7,10 Gingival psoriasis usually is described as intensely erythematous and occasionally laced with white scaly streaks involving the marginal gingiva that extend toward the mucogingival junction. In general, the erythematous presentation of gingival psoriasis may not be commensurate with the degree of inflammation induced by dental plaque-based periodontal disease. Doben11 documented gingival psoriasis as appearing “deeply stippled and grainy” and commented that the tissue was “friable” and incapable of maintaining a “clean incision line” during periodontal surgery. In our patient, the gingiva also had exhibited a granular surface. Patients with oral psoriasis often report soreness or a burning sensation of the gingiva, which may easily bleed on manipulation or brushing the teeth, whereas other patients are asymptomatic,12 as in our case. Psoriasis of the hard palate usually presents as multiple painless red macules. Unlike cutaneous psoriasis, oral lesions rarely evoke pruritus.10 Histopathologically, oral psoriasis bears a striking resemblance to its cutaneous counterpart. The epithelium has a pronounced parakeratinized surface with elongated rete ridges and aggregations of Munro microabscesses. The connective tissue often is composed of dilated capillaries that closely approximate the epithelium as well as infiltrations of lymphocytes. Specimens suspected for oral psoriasis should routinely be stained with periodic acid–Schiff to rule out candidiasis coinfection. The microscopic findings of our patient were congruent with prior reports of oral psoriasis.7,10-12 Some clinicians have questioned if psoriasis can actually occur in the oral cavity, but most authorities in the field have recognized its true existence, as evidenced by various shared HLA antigens, specifically HLA-Cw.13
Another group of oral lesions collectively referred to as psoriasiform mucositis, notably geographic tongue (benign migratory glossitis, erythema migrans) and its extraglossal variant geographic stomatitis,14,15 have histopathologic features and HLAs similar to those seen in cutaneous psoriasis.13 Interestingly, geographic tongue has been found in 3.8% to 9.1% of cohorts with cutaneous psoriasis,8,9 but in the extant population, the vast majority of patients with oral psoriasiform mucositis do not have cutaneous psoriasis. Other differential diagnoses for gingival psoriasis are lichen planus, human immunodeficiency virus–associated periodontitis, desquamative gingivitis, plasma cell gingivitis, erythematous candidiasis, mucous membrane pemphigoid, pemphigus vulgaris, leukemia, systemic lupus erythematosus, granulomatosis with polyangiitis, orofacial granulomatosis, localized juvenile spongiotic gingivitis hyperplasia, and primary gingivostomatitis.
Management of gingival psoriasis focuses on strategies to reduce inflammation and discomfort and measures to achieve meticulous oral plaque control. Judicious efforts should be exercised to avoid oral soft-tissue injury when performing periodontal scaling, although it has not been established whether gingival psoriasis is associated with the Köbner phenomenon, as seen with cutaneous lesions. Adjunctive measures employed for symptomatic patients have involved the use of corticosteroids (eg, lesional injection, oral rinse, systemic) and oral rinses with retinoic acid, chlorhexidine gluconate, and warm saline.7,10,16 Prolonged utilization of corticosteroids, however, may necessitate supplemental administration of antifungal agents.
This case report represents a rare documentation of a successful outcome of gingival and palatal psoriasis subsequent to the reinstitution of adalimumab solely for treatment of recurrent cutaneous disease. There likely is a pharmacologic basis for the amelioration of oral psoriasis in our patient. Adalimumab is a bivalent IgG monoclonal antibody that binds to activated dermal dendritic cell receptors of tumor necrosis factor α, thereby attenuating a cytokine-derived inflammatory response and apoptosis.17 In fact, patients with rheumatoid arthritis showed notable reductions in both gingival inflammation and bleeding following a 3-month regimen of adalimumab.18
Conclusion
Practitioners should be aware of the phenotypic overlap of cutaneous and oral psoriasis, particularly involving the gingiva and palate. It is recommended that psoriasis patients routinely receive a dental prophylaxis and engage in oral hygiene efforts to reduce the presence of oral microbiota. Furthermore, it is emphasized that psoriatic patients who maintain an atypical erythematous presentation on the oral mucosa undergo a biopsy for identification of the lesions and correlation with disease dissemination. Prospective studies are needed to characterize the clinical courses of oral psoriasis, ascertain their correlative behavior with cutaneous flares, and determine if lesional improvement can be achieved with the use of biologic agents or other therapeutic modalities.
- Gupta R, Debbaneh MG, Liao W. Genetic epidemiology of psoriasis. Curr Dermatol Rep. 2014;3:61-78.
- Younai FS, Phelan JA. Oral mucositis with features of psoriasis: report of a case and review of the literature. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1997;84:61-67.
- Xu T, Zhang YH. Association of psoriasis with stroke and myocardial infarction: meta-analysis of cohort studies. Br J Dermatol. 2012;167:1345-1350.
- Lazaridou E, Tsikrikoni A, Fotiadou C, et al. Association of chronic plaque psoriasis and severe periodontitis: a hospital based case-control study. J Eur Acad Dermatol Venereol. 2013;27:967-972.
- Skudutyte-Rysstad R, Slevolden EM, Hansen BF, et al. Association between moderate to severe psoriasis and periodontitis in a Scandinavian population. BMC Oral Health. 2014;14:139.
- Zunt SL, Tomich CE. Erythema migrans—a psoriasiform lesion of the oral mucosa. J Dermatol Surg Oncol. 1989;15:1067-1070.
- Reis V, Artico G, Seo J, et al. Psoriasiform mucositis on the gingival and palatal mucosae treated with retinoic-acid mouthwash. Int J Dermatol. 2013;52:113-115.
- Germi L, De Giorgi V, Bergamo F, et al. Psoriasis and oral lesions: multicentric study of oral mucosa diseases Italian group (GIPMO). Dermatol Online J. 2012;18:11.
- Kaur I, Handa S, Kumar B. Oral lesions in psoriasis. Int J Dermatol. 1997;36:78-79.
- Brayshaw HA, Orban B. Psoriasis gingivae. J Periodontol. 1953;24:156-160.
- Doben DI. Psoriasis of the attached gingiva. J Periodontol. 1976;47:38-40.
- Mattsson U, Warfvinge G, Jontell M. Oral psoriasis—a diagnostic dilemma: a report of two cases and a review of the literature. Oral Surg Oral Med Oral Pathol Oral Radiol. 2015;120:e183-e189.
- Dermatologic diseases. In: Neville BW, Damm DD, Allen CM, et al, eds. Oral and Maxillofacial Pathology. 3rd ed. St. Louis, MO: Saunders/Elsevier; 2009:792-794.
- Brooks JK, Balciunas BA. Geographic stomatitis: review of the literature and report of five cases. J Am Dent Assoc. 1987;115:421-424.
- Brooks JK, Nikitakis NG. Multiple mucosal lesions. erythema migrans. Gen Dent. 2007;55:160, 163.
- Ulmansky M, Michelle R, Azaz B. Oral psoriasis: report of six new cases. J Oral Pathol Med. 1995;24:42-45.
- Lis K, Kuzawinska O, Bałkowiec-Iskra E. Tumor necrosis factor inhibitors—state of knowledge. Arch Med Sci. 2014;10:1175-1185.
- Kobayashi T, Yokoyama T, Ito S, et al. Periodontal and serum protein profiles in patients with rheumatoid arthritis treated with tumor necrosis factor inhibitor adalimumab. J Periodontol. 2014;85:1480-1488.
- Gupta R, Debbaneh MG, Liao W. Genetic epidemiology of psoriasis. Curr Dermatol Rep. 2014;3:61-78.
- Younai FS, Phelan JA. Oral mucositis with features of psoriasis: report of a case and review of the literature. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1997;84:61-67.
- Xu T, Zhang YH. Association of psoriasis with stroke and myocardial infarction: meta-analysis of cohort studies. Br J Dermatol. 2012;167:1345-1350.
- Lazaridou E, Tsikrikoni A, Fotiadou C, et al. Association of chronic plaque psoriasis and severe periodontitis: a hospital based case-control study. J Eur Acad Dermatol Venereol. 2013;27:967-972.
- Skudutyte-Rysstad R, Slevolden EM, Hansen BF, et al. Association between moderate to severe psoriasis and periodontitis in a Scandinavian population. BMC Oral Health. 2014;14:139.
- Zunt SL, Tomich CE. Erythema migrans—a psoriasiform lesion of the oral mucosa. J Dermatol Surg Oncol. 1989;15:1067-1070.
- Reis V, Artico G, Seo J, et al. Psoriasiform mucositis on the gingival and palatal mucosae treated with retinoic-acid mouthwash. Int J Dermatol. 2013;52:113-115.
- Germi L, De Giorgi V, Bergamo F, et al. Psoriasis and oral lesions: multicentric study of oral mucosa diseases Italian group (GIPMO). Dermatol Online J. 2012;18:11.
- Kaur I, Handa S, Kumar B. Oral lesions in psoriasis. Int J Dermatol. 1997;36:78-79.
- Brayshaw HA, Orban B. Psoriasis gingivae. J Periodontol. 1953;24:156-160.
- Doben DI. Psoriasis of the attached gingiva. J Periodontol. 1976;47:38-40.
- Mattsson U, Warfvinge G, Jontell M. Oral psoriasis—a diagnostic dilemma: a report of two cases and a review of the literature. Oral Surg Oral Med Oral Pathol Oral Radiol. 2015;120:e183-e189.
- Dermatologic diseases. In: Neville BW, Damm DD, Allen CM, et al, eds. Oral and Maxillofacial Pathology. 3rd ed. St. Louis, MO: Saunders/Elsevier; 2009:792-794.
- Brooks JK, Balciunas BA. Geographic stomatitis: review of the literature and report of five cases. J Am Dent Assoc. 1987;115:421-424.
- Brooks JK, Nikitakis NG. Multiple mucosal lesions. erythema migrans. Gen Dent. 2007;55:160, 163.
- Ulmansky M, Michelle R, Azaz B. Oral psoriasis: report of six new cases. J Oral Pathol Med. 1995;24:42-45.
- Lis K, Kuzawinska O, Bałkowiec-Iskra E. Tumor necrosis factor inhibitors—state of knowledge. Arch Med Sci. 2014;10:1175-1185.
- Kobayashi T, Yokoyama T, Ito S, et al. Periodontal and serum protein profiles in patients with rheumatoid arthritis treated with tumor necrosis factor inhibitor adalimumab. J Periodontol. 2014;85:1480-1488.
Practice Points
- A subset of patients with cutaneous psoriasis may be associated with oral psoriatic outbreaks.
- Oral psoriasis presents as an atypical inflammatory response, and histopathologic assessment is recommended for lesional identity.
- Use of adalimumab for management of cutaneous psoriasis may demonstrate efficacy for oral psoriasis.
