User login
Study finds etanercept biosimilar safe and effective in patients with severe plaque psoriasis
An experimental biological agent, GP2015, demonstrated equivalent efficacy and comparable safety to etanercept for moderate to severe plaque psoriasis in a manufacturer-sponsored study, according to a report published online in the British Journal of Dermatology.
These findings should contribute to the confirmation of GP2015 as an etanercept (Enbrel) biosimilar for this patient population. Proposed biosimilars such as GP2015 are follow-on versions of authorized biological products, and regulatory authorities require that they demonstrate similarity with a large body of physiochemical and clinical data before they can be confirmed as biosimilars, said Christopher Griffiths, MD, of the Dermatology Centre, Salford Royal Hospital, University of Manchester (England), and his associates.
To contribute such data, Dr. Griffiths and his associates studied the efficacy and safety of GP2015 compared with etanercept, a tumor necrosis factor blocker, in the 2-year EGALITY trial. They assessed 531 adults at 74 medical centers in 11 European countries and South Africa, all of whom had active but stable chronic plaque psoriasis affecting 10% or more of their body surface area and Psoriasis Area and Severity Index (PASI) scores of 10 or more.
The study participants were randomly assigned in approximately equal numbers in a double-blind fashion to self administer GP2015 or etanercept subcutaneously, twice weekly for 12 weeks. Those who achieved at least a 50% improvement in PASI score were then randomized to continue the same treatment once weekly or to undergo a series of three treatment “switches” between GP2015 and etanercept at 6-week intervals until week 30. During an extension phase of the study, participants could then continue to receive the same treatment they had ended on, until week 52.
The primary efficacy endpoint – the percentage of patients who showed at least a 75% improvement from baseline in PASI score (PASI 75) at 12 weeks – was 73.4% with GP2015 and 75.7% with etanercept, which demonstrated therapeutic equivalence. A secondary efficacy end point – mean change in PASI score from baseline to week 12 – also was similar between the two study drugs. In all treatment groups, both PASI mean scores and change in PASI scores over time were comparable between the two study groups, regardless of switching between the two agents. In addition, in all groups, PASI 75 and PASI 90 scores increased gradually over time until week 30, and then remained stable through week 52, the investigators said (Br J Dermatol. 2016. doi: 10.1111/bjd.15152).
The proportion of patients with at least one treatment-emergent adverse event was similar in the GP2015 and etanercept groups who did not switch agents (59.8% and 57.3%, respectively), and was also similar among those who did switch agents between GP2015 (61%) and etanercept (59.4%).
The rates of serious adverse events and of adverse events that led to withdrawal from the study were similar across all treatment groups. Immunogenicity of GP2015 was similar to etanercept.
However, the rate of “adverse events of special interest” – those referred to in special warnings and precautions on the etanercept label – was markedly higher for continued GP2015 than for continued etanercept (11.0% vs. 4.7%) and for switched GP2015 than for switched etanercept (11.0% vs. 5.2%). One patient who took etanercept throughout the trial developed malignant melanoma.
The results of the study “confirm biosimilarity that was established with all previous analytical comparisons to the reference product in that equivalent efficacy was demonstrated as well as similar safety and immunogenicity of GP2015” with etanercept, “in a highly sensitive, generally immune-competent population,” the authors concluded.
The study was funded by Hexal AG, a Sandoz company, which was involved in the study design, data collection and analysis, and manuscript preparation. Dr. Griffiths reported ties to AbbVie, BMS. Galderma, Janssen, Leo-Pharma, Lilly, MSD, Novartis, Pfizer, Regeneron, Roche, Sandoz, and UCB Pharma, and his associates reported ties to numerous industry sources.
An experimental biological agent, GP2015, demonstrated equivalent efficacy and comparable safety to etanercept for moderate to severe plaque psoriasis in a manufacturer-sponsored study, according to a report published online in the British Journal of Dermatology.
These findings should contribute to the confirmation of GP2015 as an etanercept (Enbrel) biosimilar for this patient population. Proposed biosimilars such as GP2015 are follow-on versions of authorized biological products, and regulatory authorities require that they demonstrate similarity with a large body of physiochemical and clinical data before they can be confirmed as biosimilars, said Christopher Griffiths, MD, of the Dermatology Centre, Salford Royal Hospital, University of Manchester (England), and his associates.
To contribute such data, Dr. Griffiths and his associates studied the efficacy and safety of GP2015 compared with etanercept, a tumor necrosis factor blocker, in the 2-year EGALITY trial. They assessed 531 adults at 74 medical centers in 11 European countries and South Africa, all of whom had active but stable chronic plaque psoriasis affecting 10% or more of their body surface area and Psoriasis Area and Severity Index (PASI) scores of 10 or more.
The study participants were randomly assigned in approximately equal numbers in a double-blind fashion to self administer GP2015 or etanercept subcutaneously, twice weekly for 12 weeks. Those who achieved at least a 50% improvement in PASI score were then randomized to continue the same treatment once weekly or to undergo a series of three treatment “switches” between GP2015 and etanercept at 6-week intervals until week 30. During an extension phase of the study, participants could then continue to receive the same treatment they had ended on, until week 52.
The primary efficacy endpoint – the percentage of patients who showed at least a 75% improvement from baseline in PASI score (PASI 75) at 12 weeks – was 73.4% with GP2015 and 75.7% with etanercept, which demonstrated therapeutic equivalence. A secondary efficacy end point – mean change in PASI score from baseline to week 12 – also was similar between the two study drugs. In all treatment groups, both PASI mean scores and change in PASI scores over time were comparable between the two study groups, regardless of switching between the two agents. In addition, in all groups, PASI 75 and PASI 90 scores increased gradually over time until week 30, and then remained stable through week 52, the investigators said (Br J Dermatol. 2016. doi: 10.1111/bjd.15152).
The proportion of patients with at least one treatment-emergent adverse event was similar in the GP2015 and etanercept groups who did not switch agents (59.8% and 57.3%, respectively), and was also similar among those who did switch agents between GP2015 (61%) and etanercept (59.4%).
The rates of serious adverse events and of adverse events that led to withdrawal from the study were similar across all treatment groups. Immunogenicity of GP2015 was similar to etanercept.
However, the rate of “adverse events of special interest” – those referred to in special warnings and precautions on the etanercept label – was markedly higher for continued GP2015 than for continued etanercept (11.0% vs. 4.7%) and for switched GP2015 than for switched etanercept (11.0% vs. 5.2%). One patient who took etanercept throughout the trial developed malignant melanoma.
The results of the study “confirm biosimilarity that was established with all previous analytical comparisons to the reference product in that equivalent efficacy was demonstrated as well as similar safety and immunogenicity of GP2015” with etanercept, “in a highly sensitive, generally immune-competent population,” the authors concluded.
The study was funded by Hexal AG, a Sandoz company, which was involved in the study design, data collection and analysis, and manuscript preparation. Dr. Griffiths reported ties to AbbVie, BMS. Galderma, Janssen, Leo-Pharma, Lilly, MSD, Novartis, Pfizer, Regeneron, Roche, Sandoz, and UCB Pharma, and his associates reported ties to numerous industry sources.
An experimental biological agent, GP2015, demonstrated equivalent efficacy and comparable safety to etanercept for moderate to severe plaque psoriasis in a manufacturer-sponsored study, according to a report published online in the British Journal of Dermatology.
These findings should contribute to the confirmation of GP2015 as an etanercept (Enbrel) biosimilar for this patient population. Proposed biosimilars such as GP2015 are follow-on versions of authorized biological products, and regulatory authorities require that they demonstrate similarity with a large body of physiochemical and clinical data before they can be confirmed as biosimilars, said Christopher Griffiths, MD, of the Dermatology Centre, Salford Royal Hospital, University of Manchester (England), and his associates.
To contribute such data, Dr. Griffiths and his associates studied the efficacy and safety of GP2015 compared with etanercept, a tumor necrosis factor blocker, in the 2-year EGALITY trial. They assessed 531 adults at 74 medical centers in 11 European countries and South Africa, all of whom had active but stable chronic plaque psoriasis affecting 10% or more of their body surface area and Psoriasis Area and Severity Index (PASI) scores of 10 or more.
The study participants were randomly assigned in approximately equal numbers in a double-blind fashion to self administer GP2015 or etanercept subcutaneously, twice weekly for 12 weeks. Those who achieved at least a 50% improvement in PASI score were then randomized to continue the same treatment once weekly or to undergo a series of three treatment “switches” between GP2015 and etanercept at 6-week intervals until week 30. During an extension phase of the study, participants could then continue to receive the same treatment they had ended on, until week 52.
The primary efficacy endpoint – the percentage of patients who showed at least a 75% improvement from baseline in PASI score (PASI 75) at 12 weeks – was 73.4% with GP2015 and 75.7% with etanercept, which demonstrated therapeutic equivalence. A secondary efficacy end point – mean change in PASI score from baseline to week 12 – also was similar between the two study drugs. In all treatment groups, both PASI mean scores and change in PASI scores over time were comparable between the two study groups, regardless of switching between the two agents. In addition, in all groups, PASI 75 and PASI 90 scores increased gradually over time until week 30, and then remained stable through week 52, the investigators said (Br J Dermatol. 2016. doi: 10.1111/bjd.15152).
The proportion of patients with at least one treatment-emergent adverse event was similar in the GP2015 and etanercept groups who did not switch agents (59.8% and 57.3%, respectively), and was also similar among those who did switch agents between GP2015 (61%) and etanercept (59.4%).
The rates of serious adverse events and of adverse events that led to withdrawal from the study were similar across all treatment groups. Immunogenicity of GP2015 was similar to etanercept.
However, the rate of “adverse events of special interest” – those referred to in special warnings and precautions on the etanercept label – was markedly higher for continued GP2015 than for continued etanercept (11.0% vs. 4.7%) and for switched GP2015 than for switched etanercept (11.0% vs. 5.2%). One patient who took etanercept throughout the trial developed malignant melanoma.
The results of the study “confirm biosimilarity that was established with all previous analytical comparisons to the reference product in that equivalent efficacy was demonstrated as well as similar safety and immunogenicity of GP2015” with etanercept, “in a highly sensitive, generally immune-competent population,” the authors concluded.
The study was funded by Hexal AG, a Sandoz company, which was involved in the study design, data collection and analysis, and manuscript preparation. Dr. Griffiths reported ties to AbbVie, BMS. Galderma, Janssen, Leo-Pharma, Lilly, MSD, Novartis, Pfizer, Regeneron, Roche, Sandoz, and UCB Pharma, and his associates reported ties to numerous industry sources.
FROM THE BRITISH JOURNAL OF DERMATOLOGY
Key clinical point: GP2015, a proposed etanercept biosimilar, demonstrated equivalent efficacy and comparable safety to etanercept for severe plaque psoriasis.
Major finding: The primary efficacy end point – the percentage of patients who showed at least a 75% improvement from baseline in PASI score at 12 weeks – was 73.4% with GP2015 and 75.7% with etanercept.
Data source: An international randomized double-blind study of 531 patients with moderate to severe chronic plaque psoriasis.
Disclosures: Hexal AG, a Sandoz company, funded the study. Hexal AG was involved in the study design, data collection and analysis, and manuscript preparation. Dr. Griffiths reported ties to AbbVie, BMS, Galderma, Janssen, Leo Pharma, Lilly, MSD, Novartis, Pfizer, Regeneron, Roche, Sandoz, and UCB Pharma, and his associates reported ties to numerous industry sources.
Benefit of self-administered vaginal lidocaine gel in IUD placement
Fear of potential pain caused by insertion of an intrauterine device (IUD) prevents some women from using this highly effective and safe contraceptive method. Recently, investigators conducted a randomized, placebo-controlled trial to assess whether vaginal lidocaine gel administered shortly before IUD placement was associated with a decrease from baseline in patient-reported pain scores.1
In this blinded trial, Rapkinand colleagues randomly assigned nulliparous women presenting for IUD placement (either the copper T380A IUD or the 52-mg levonorgestrel-releasing IUD) at faculty and resident clinics at a US urban academic center to place 4 mL of 2% lidocaine gel or placebo gel vaginally (using an applicator) 5 to 15 minutes prior to IUD placement.1 A 100-mm visual analog scale (VAS) was used to assess pain at each step of the procedure, including at baseline (before speculum insertion), after speculum placement, tenaculum placement, uterine sound, IUD insertion, and 5 minutes after speculum removal.
Among the 58 evaluable participants, the mean age was 23 years in the lidocaine group and 24 years in the placebo group; more than 80% of the women were white.
The study’s primary outcome was change in pain experience from baseline to IUD insertion. Pain was measured on a VAS from 0 mm (no pain) to 100 mm (worst pain in my life). Secondary outcomes included patient acceptability of gel self-insertion, physician-reported ease of IUD insertion, and need for pain medication for up to 7 days after IUD insertion.
Related article:
Liletta gets a new inserter: Steps for successful placement
What the investigators found
The mean change in pain scores with IUD placement was 61 mm for the lidocaine group and 69 mm for the placebo group (P = .06). Thus, no difference in the primary outcome was found between the 2 groups. However, women who received the lidocaine gel treatment experiencedsignificantly less pain with tenaculum placement than those who received placebo gel (32 mm vs 56 mm; P = .02), and they were substantially less likely to require cervical dilation (3.3% vs 34.5%; P = .002), an often painful procedure.
Related article:
Does the injection of ketorolac prior to IUD placement reduce pain?
Patient acceptability and satisfaction. Five minutes after the IUD placement procedure, approximately two-thirds of women in both groups indicated that they experienced an acceptable level of discomfort, and more than three-quarters indicated that they were satisfied with the placement procedure. Fully 67% of the lidocaine group and 68% of the placebo group indicated definitely or probably yes when asked if the level of discomfort they experienced was acceptable, with 27% and 21%, respectively, responding as neutral. When asked if getting the IUD was worth the level of discomfort experienced, 73% of the lidocaine group and 82% of the placebo group responded “yes,” while 23% and 18%, respectively, were unsure.
Pearls for practice
As this study showed, self-administered lidocaine vaginal gel did not alter the primary outcome (pain with IUD placement), but the reduced need for cervical dilation is a promising finding and warrants additional study.
Tip. Interestingly, the placebo-treated women experienced pain intensity with cervical tenaculum placement similar to that associated with IUD placement. This finding illuminates the fact that IUD placement is not the only action that can produce pain. For this reason, I use a finer, single-tooth tenaculum designed for use with sonohysterograms (Goldstein Grasp Cervical Stabilizer).2 This instrument appears to cause less pain and bleeding than conventional tenacula.
Related article:
How to identify and localize IUDs on ultrasound
Share your thoughts! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
- Rapkin RB, Achilles SL, Schwarz B, et al. Self-administered lidocaine gel for intrauterine device insertion in nulliparous women: a randomized controlled trial. Obstet Gynecol. 2016;128(3):621–628.
- Goldstein Grasp Cervical Stabilzer. CooperSurgical, Inc. website. http://www.coopersurgical.com/Products/Detail/Goldstein-Grasp-Cervical-Stabilizer. Accessed November 16, 2016.

The author reports that he serves on advisory boards for Bayer and Medicines360 and consults for Allergan.
The author reports that he serves on advisory boards for Bayer and Medicines360 and consults for Allergan.
The author reports that he serves on advisory boards for Bayer and Medicines360 and consults for Allergan.
Fear of potential pain caused by insertion of an intrauterine device (IUD) prevents some women from using this highly effective and safe contraceptive method. Recently, investigators conducted a randomized, placebo-controlled trial to assess whether vaginal lidocaine gel administered shortly before IUD placement was associated with a decrease from baseline in patient-reported pain scores.1
In this blinded trial, Rapkinand colleagues randomly assigned nulliparous women presenting for IUD placement (either the copper T380A IUD or the 52-mg levonorgestrel-releasing IUD) at faculty and resident clinics at a US urban academic center to place 4 mL of 2% lidocaine gel or placebo gel vaginally (using an applicator) 5 to 15 minutes prior to IUD placement.1 A 100-mm visual analog scale (VAS) was used to assess pain at each step of the procedure, including at baseline (before speculum insertion), after speculum placement, tenaculum placement, uterine sound, IUD insertion, and 5 minutes after speculum removal.
Among the 58 evaluable participants, the mean age was 23 years in the lidocaine group and 24 years in the placebo group; more than 80% of the women were white.
The study’s primary outcome was change in pain experience from baseline to IUD insertion. Pain was measured on a VAS from 0 mm (no pain) to 100 mm (worst pain in my life). Secondary outcomes included patient acceptability of gel self-insertion, physician-reported ease of IUD insertion, and need for pain medication for up to 7 days after IUD insertion.
Related article:
Liletta gets a new inserter: Steps for successful placement
What the investigators found
The mean change in pain scores with IUD placement was 61 mm for the lidocaine group and 69 mm for the placebo group (P = .06). Thus, no difference in the primary outcome was found between the 2 groups. However, women who received the lidocaine gel treatment experiencedsignificantly less pain with tenaculum placement than those who received placebo gel (32 mm vs 56 mm; P = .02), and they were substantially less likely to require cervical dilation (3.3% vs 34.5%; P = .002), an often painful procedure.
Related article:
Does the injection of ketorolac prior to IUD placement reduce pain?
Patient acceptability and satisfaction. Five minutes after the IUD placement procedure, approximately two-thirds of women in both groups indicated that they experienced an acceptable level of discomfort, and more than three-quarters indicated that they were satisfied with the placement procedure. Fully 67% of the lidocaine group and 68% of the placebo group indicated definitely or probably yes when asked if the level of discomfort they experienced was acceptable, with 27% and 21%, respectively, responding as neutral. When asked if getting the IUD was worth the level of discomfort experienced, 73% of the lidocaine group and 82% of the placebo group responded “yes,” while 23% and 18%, respectively, were unsure.
Pearls for practice
As this study showed, self-administered lidocaine vaginal gel did not alter the primary outcome (pain with IUD placement), but the reduced need for cervical dilation is a promising finding and warrants additional study.
Tip. Interestingly, the placebo-treated women experienced pain intensity with cervical tenaculum placement similar to that associated with IUD placement. This finding illuminates the fact that IUD placement is not the only action that can produce pain. For this reason, I use a finer, single-tooth tenaculum designed for use with sonohysterograms (Goldstein Grasp Cervical Stabilizer).2 This instrument appears to cause less pain and bleeding than conventional tenacula.
Related article:
How to identify and localize IUDs on ultrasound
Share your thoughts! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
Fear of potential pain caused by insertion of an intrauterine device (IUD) prevents some women from using this highly effective and safe contraceptive method. Recently, investigators conducted a randomized, placebo-controlled trial to assess whether vaginal lidocaine gel administered shortly before IUD placement was associated with a decrease from baseline in patient-reported pain scores.1
In this blinded trial, Rapkinand colleagues randomly assigned nulliparous women presenting for IUD placement (either the copper T380A IUD or the 52-mg levonorgestrel-releasing IUD) at faculty and resident clinics at a US urban academic center to place 4 mL of 2% lidocaine gel or placebo gel vaginally (using an applicator) 5 to 15 minutes prior to IUD placement.1 A 100-mm visual analog scale (VAS) was used to assess pain at each step of the procedure, including at baseline (before speculum insertion), after speculum placement, tenaculum placement, uterine sound, IUD insertion, and 5 minutes after speculum removal.
Among the 58 evaluable participants, the mean age was 23 years in the lidocaine group and 24 years in the placebo group; more than 80% of the women were white.
The study’s primary outcome was change in pain experience from baseline to IUD insertion. Pain was measured on a VAS from 0 mm (no pain) to 100 mm (worst pain in my life). Secondary outcomes included patient acceptability of gel self-insertion, physician-reported ease of IUD insertion, and need for pain medication for up to 7 days after IUD insertion.
Related article:
Liletta gets a new inserter: Steps for successful placement
What the investigators found
The mean change in pain scores with IUD placement was 61 mm for the lidocaine group and 69 mm for the placebo group (P = .06). Thus, no difference in the primary outcome was found between the 2 groups. However, women who received the lidocaine gel treatment experiencedsignificantly less pain with tenaculum placement than those who received placebo gel (32 mm vs 56 mm; P = .02), and they were substantially less likely to require cervical dilation (3.3% vs 34.5%; P = .002), an often painful procedure.
Related article:
Does the injection of ketorolac prior to IUD placement reduce pain?
Patient acceptability and satisfaction. Five minutes after the IUD placement procedure, approximately two-thirds of women in both groups indicated that they experienced an acceptable level of discomfort, and more than three-quarters indicated that they were satisfied with the placement procedure. Fully 67% of the lidocaine group and 68% of the placebo group indicated definitely or probably yes when asked if the level of discomfort they experienced was acceptable, with 27% and 21%, respectively, responding as neutral. When asked if getting the IUD was worth the level of discomfort experienced, 73% of the lidocaine group and 82% of the placebo group responded “yes,” while 23% and 18%, respectively, were unsure.
Pearls for practice
As this study showed, self-administered lidocaine vaginal gel did not alter the primary outcome (pain with IUD placement), but the reduced need for cervical dilation is a promising finding and warrants additional study.
Tip. Interestingly, the placebo-treated women experienced pain intensity with cervical tenaculum placement similar to that associated with IUD placement. This finding illuminates the fact that IUD placement is not the only action that can produce pain. For this reason, I use a finer, single-tooth tenaculum designed for use with sonohysterograms (Goldstein Grasp Cervical Stabilizer).2 This instrument appears to cause less pain and bleeding than conventional tenacula.
Related article:
How to identify and localize IUDs on ultrasound
Share your thoughts! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
- Rapkin RB, Achilles SL, Schwarz B, et al. Self-administered lidocaine gel for intrauterine device insertion in nulliparous women: a randomized controlled trial. Obstet Gynecol. 2016;128(3):621–628.
- Goldstein Grasp Cervical Stabilzer. CooperSurgical, Inc. website. http://www.coopersurgical.com/Products/Detail/Goldstein-Grasp-Cervical-Stabilizer. Accessed November 16, 2016.
- Rapkin RB, Achilles SL, Schwarz B, et al. Self-administered lidocaine gel for intrauterine device insertion in nulliparous women: a randomized controlled trial. Obstet Gynecol. 2016;128(3):621–628.
- Goldstein Grasp Cervical Stabilzer. CooperSurgical, Inc. website. http://www.coopersurgical.com/Products/Detail/Goldstein-Grasp-Cervical-Stabilizer. Accessed November 16, 2016.
In this article

Early-onset preeclampsia more likely to occur in women with lupus
WASHINGTON – Women with systemic lupus erythematosus are nine times more likely to develop early-onset preeclampsia during a first pregnancy than are women without the disease, according a study of two Swedish national population-based registries.
The risk of preeclampsia occurring before 34 weeks’ gestation declined with subsequent pregnancies, but it remained significantly elevated above the background risk, Julia F. Simard, ScD, said at the annual meeting of the American College of Rheumatology.
During the study period, 742 births to women with SLE were matched with 10,484 births to women without the disease. The mean age of the patients was 31 years.
Of the women with SLE, 5% had pregestational hypertension and 3% had pregestational diabetes. Antiphospholipid antibodies were present in 2%. Among the controls, less than 1% had pregestational hypertension, and 1.3% had pregestational diabetes. There were no healthy controls with antiphospholipid antibodies.
In the entire cohort, there were 438 cases of preeclampsia: 82 in the SLE group and 356 in the control group. In the fully adjusted model, this translated to nearly a tripling of relative risk (RR, 2.7).
Preeclampsia more commonly occurred in first births, based on 56 cases in the SLE group and 225 in the control group. SLE patients in their first pregnancy also had a tripling of risk (RR, 3.2). Among subsequent births, there were 157 cases: 26 in the SLE group and 131 in the control group. The relative risk for preeclampsia was lower, but still significantly elevated (RR, 2).
There were 87 cases of early-onset preeclampsia: 32 in the SLE group and 55 in the control group. Women with SLE were more than six times more likely to develop the disorder (RR, 6.3). Early-onset preeclampsia was more common in first births for both groups: 24 in the SLE group and 34 in the control group, for a ninefold increased risk (RR, 9.3).
Again, the incidence decreased with subsequent births in both groups: 8 cases in the SLE group and 21 in the control group. But SLE patients still faced a significant threefold increase in risk (RR, 2.8).
“Antiphospholipid antibodies appear to be an important risk factor that needs to more fully understood,” Dr. Simard said. “But the risk seems to be independent of other traditional risk factors, like pregestational hypertension, body mass index, and smoking.”
She and her associates had no financial disclosures.
[email protected]
On Twitter @alz_gal
WASHINGTON – Women with systemic lupus erythematosus are nine times more likely to develop early-onset preeclampsia during a first pregnancy than are women without the disease, according a study of two Swedish national population-based registries.
The risk of preeclampsia occurring before 34 weeks’ gestation declined with subsequent pregnancies, but it remained significantly elevated above the background risk, Julia F. Simard, ScD, said at the annual meeting of the American College of Rheumatology.
During the study period, 742 births to women with SLE were matched with 10,484 births to women without the disease. The mean age of the patients was 31 years.
Of the women with SLE, 5% had pregestational hypertension and 3% had pregestational diabetes. Antiphospholipid antibodies were present in 2%. Among the controls, less than 1% had pregestational hypertension, and 1.3% had pregestational diabetes. There were no healthy controls with antiphospholipid antibodies.
In the entire cohort, there were 438 cases of preeclampsia: 82 in the SLE group and 356 in the control group. In the fully adjusted model, this translated to nearly a tripling of relative risk (RR, 2.7).
Preeclampsia more commonly occurred in first births, based on 56 cases in the SLE group and 225 in the control group. SLE patients in their first pregnancy also had a tripling of risk (RR, 3.2). Among subsequent births, there were 157 cases: 26 in the SLE group and 131 in the control group. The relative risk for preeclampsia was lower, but still significantly elevated (RR, 2).
There were 87 cases of early-onset preeclampsia: 32 in the SLE group and 55 in the control group. Women with SLE were more than six times more likely to develop the disorder (RR, 6.3). Early-onset preeclampsia was more common in first births for both groups: 24 in the SLE group and 34 in the control group, for a ninefold increased risk (RR, 9.3).
Again, the incidence decreased with subsequent births in both groups: 8 cases in the SLE group and 21 in the control group. But SLE patients still faced a significant threefold increase in risk (RR, 2.8).
“Antiphospholipid antibodies appear to be an important risk factor that needs to more fully understood,” Dr. Simard said. “But the risk seems to be independent of other traditional risk factors, like pregestational hypertension, body mass index, and smoking.”
She and her associates had no financial disclosures.
[email protected]
On Twitter @alz_gal
WASHINGTON – Women with systemic lupus erythematosus are nine times more likely to develop early-onset preeclampsia during a first pregnancy than are women without the disease, according a study of two Swedish national population-based registries.
The risk of preeclampsia occurring before 34 weeks’ gestation declined with subsequent pregnancies, but it remained significantly elevated above the background risk, Julia F. Simard, ScD, said at the annual meeting of the American College of Rheumatology.
During the study period, 742 births to women with SLE were matched with 10,484 births to women without the disease. The mean age of the patients was 31 years.
Of the women with SLE, 5% had pregestational hypertension and 3% had pregestational diabetes. Antiphospholipid antibodies were present in 2%. Among the controls, less than 1% had pregestational hypertension, and 1.3% had pregestational diabetes. There were no healthy controls with antiphospholipid antibodies.
In the entire cohort, there were 438 cases of preeclampsia: 82 in the SLE group and 356 in the control group. In the fully adjusted model, this translated to nearly a tripling of relative risk (RR, 2.7).
Preeclampsia more commonly occurred in first births, based on 56 cases in the SLE group and 225 in the control group. SLE patients in their first pregnancy also had a tripling of risk (RR, 3.2). Among subsequent births, there were 157 cases: 26 in the SLE group and 131 in the control group. The relative risk for preeclampsia was lower, but still significantly elevated (RR, 2).
There were 87 cases of early-onset preeclampsia: 32 in the SLE group and 55 in the control group. Women with SLE were more than six times more likely to develop the disorder (RR, 6.3). Early-onset preeclampsia was more common in first births for both groups: 24 in the SLE group and 34 in the control group, for a ninefold increased risk (RR, 9.3).
Again, the incidence decreased with subsequent births in both groups: 8 cases in the SLE group and 21 in the control group. But SLE patients still faced a significant threefold increase in risk (RR, 2.8).
“Antiphospholipid antibodies appear to be an important risk factor that needs to more fully understood,” Dr. Simard said. “But the risk seems to be independent of other traditional risk factors, like pregestational hypertension, body mass index, and smoking.”
She and her associates had no financial disclosures.
[email protected]
On Twitter @alz_gal
ACR ANNUAL MEETING
Key clinical point:
Major finding: Women with SLE in a first pregnancy had a ninefold greater risk of early-onset preeclampsia than did healthy control patients in their first pregnancy.
Data source: The data were extracted from two Swedish national population-based registries.
Disclosures: Dr, Simard and her associates had no financial disclosures.
Early paternal emotional involvement tied to children’s preadolescent behavior
Children whose fathers have a positive emotional response to parenting and provide a sense of security early on are less likely to exhibit behavioral problems at age 9, a cohort study of more than 13,000 children shows. However, the researchers found no association between behavioral problems and paternal involvement with child care and household tasks.
The researchers used data from the Avon Longitudinal Study of Parents and Children, a birth cohort study of children in southwest England that is also known as Children of the 90s. In this study, the children’s fathers completed questionnaires at 8 weeks (37 questions) and 8 months (21 questions) after the birth. They were asked to rate their level of agreement with 58 statements related to several issues, including direct care, household tasks, attitudes about parenting, and relationships with the child. The mothers were interviewed at child age 9 (N = 6,898) and 11 (N = 6,328) to determine the presence or absence of behavioral problems, which were measured via the total difficulties score of the Strengths and Difficulties Questionnaire.
Previous studies have tended toward the assumption that paternal involvement with the child is unidimensional, which might explain why other studies have not found a clear association with behavioral problems. This study is the first to look at paternal involvement as multidimensional, reported Charles Opondo, PhD, of the University of Oxford (England), and his colleagues (BMJ Open. 2016;6:e012034. doi: 10.1136/bmjopen-2016-012034).
The questions for fathers related to emotional response to the childhood, how often fathers participated in domestic and child care activity, and feelings of security about their paternal role.
Children of fathers who scored high on questions about emotional response were less likely to have behavioral problems at age 9 (odds ratio, 0.86; 95% confidence interval, 0.79-0.94; P = .001), as were children of fathers who scored high on their sense of security (OR, 0.87; 95% CI, 0.79-0.96; P = .006). The same patterns were true at age 11.
The impact of paternal involvement on mothers could be an important factor. “There is evidence that fathers’ involvement can also alleviate the impact of factors such as maternal depression, which are known to increase children’s risk of behavioral problems,” the researchers wrote.
Meanwhile, Dr. Opondo and his colleagues found no significant relationship between behavioral problems, and time spent in domestic and child care activity at either age.
“The findings of this research study suggest that it is psychological and emotional aspects of paternal involvement in a child’s infancy that are most powerful in influencing later child behavior and not the amount of time that fathers are engaged in child care or domestic tasks in the household,” Dr. Opondo and his colleagues said.
The researchers cited several limitations. The study was observational, for example, and could be subject to unobserved confounders. In addition, the study relied on self-reporting, which can produce bias.
The Policy Research Program in the Department of Health, England, funded the study. The authors reported having no financial disclosures.
Children whose fathers have a positive emotional response to parenting and provide a sense of security early on are less likely to exhibit behavioral problems at age 9, a cohort study of more than 13,000 children shows. However, the researchers found no association between behavioral problems and paternal involvement with child care and household tasks.
The researchers used data from the Avon Longitudinal Study of Parents and Children, a birth cohort study of children in southwest England that is also known as Children of the 90s. In this study, the children’s fathers completed questionnaires at 8 weeks (37 questions) and 8 months (21 questions) after the birth. They were asked to rate their level of agreement with 58 statements related to several issues, including direct care, household tasks, attitudes about parenting, and relationships with the child. The mothers were interviewed at child age 9 (N = 6,898) and 11 (N = 6,328) to determine the presence or absence of behavioral problems, which were measured via the total difficulties score of the Strengths and Difficulties Questionnaire.
Previous studies have tended toward the assumption that paternal involvement with the child is unidimensional, which might explain why other studies have not found a clear association with behavioral problems. This study is the first to look at paternal involvement as multidimensional, reported Charles Opondo, PhD, of the University of Oxford (England), and his colleagues (BMJ Open. 2016;6:e012034. doi: 10.1136/bmjopen-2016-012034).
The questions for fathers related to emotional response to the childhood, how often fathers participated in domestic and child care activity, and feelings of security about their paternal role.
Children of fathers who scored high on questions about emotional response were less likely to have behavioral problems at age 9 (odds ratio, 0.86; 95% confidence interval, 0.79-0.94; P = .001), as were children of fathers who scored high on their sense of security (OR, 0.87; 95% CI, 0.79-0.96; P = .006). The same patterns were true at age 11.
The impact of paternal involvement on mothers could be an important factor. “There is evidence that fathers’ involvement can also alleviate the impact of factors such as maternal depression, which are known to increase children’s risk of behavioral problems,” the researchers wrote.
Meanwhile, Dr. Opondo and his colleagues found no significant relationship between behavioral problems, and time spent in domestic and child care activity at either age.
“The findings of this research study suggest that it is psychological and emotional aspects of paternal involvement in a child’s infancy that are most powerful in influencing later child behavior and not the amount of time that fathers are engaged in child care or domestic tasks in the household,” Dr. Opondo and his colleagues said.
The researchers cited several limitations. The study was observational, for example, and could be subject to unobserved confounders. In addition, the study relied on self-reporting, which can produce bias.
The Policy Research Program in the Department of Health, England, funded the study. The authors reported having no financial disclosures.
Children whose fathers have a positive emotional response to parenting and provide a sense of security early on are less likely to exhibit behavioral problems at age 9, a cohort study of more than 13,000 children shows. However, the researchers found no association between behavioral problems and paternal involvement with child care and household tasks.
The researchers used data from the Avon Longitudinal Study of Parents and Children, a birth cohort study of children in southwest England that is also known as Children of the 90s. In this study, the children’s fathers completed questionnaires at 8 weeks (37 questions) and 8 months (21 questions) after the birth. They were asked to rate their level of agreement with 58 statements related to several issues, including direct care, household tasks, attitudes about parenting, and relationships with the child. The mothers were interviewed at child age 9 (N = 6,898) and 11 (N = 6,328) to determine the presence or absence of behavioral problems, which were measured via the total difficulties score of the Strengths and Difficulties Questionnaire.
Previous studies have tended toward the assumption that paternal involvement with the child is unidimensional, which might explain why other studies have not found a clear association with behavioral problems. This study is the first to look at paternal involvement as multidimensional, reported Charles Opondo, PhD, of the University of Oxford (England), and his colleagues (BMJ Open. 2016;6:e012034. doi: 10.1136/bmjopen-2016-012034).
The questions for fathers related to emotional response to the childhood, how often fathers participated in domestic and child care activity, and feelings of security about their paternal role.
Children of fathers who scored high on questions about emotional response were less likely to have behavioral problems at age 9 (odds ratio, 0.86; 95% confidence interval, 0.79-0.94; P = .001), as were children of fathers who scored high on their sense of security (OR, 0.87; 95% CI, 0.79-0.96; P = .006). The same patterns were true at age 11.
The impact of paternal involvement on mothers could be an important factor. “There is evidence that fathers’ involvement can also alleviate the impact of factors such as maternal depression, which are known to increase children’s risk of behavioral problems,” the researchers wrote.
Meanwhile, Dr. Opondo and his colleagues found no significant relationship between behavioral problems, and time spent in domestic and child care activity at either age.
“The findings of this research study suggest that it is psychological and emotional aspects of paternal involvement in a child’s infancy that are most powerful in influencing later child behavior and not the amount of time that fathers are engaged in child care or domestic tasks in the household,” Dr. Opondo and his colleagues said.
The researchers cited several limitations. The study was observational, for example, and could be subject to unobserved confounders. In addition, the study relied on self-reporting, which can produce bias.
The Policy Research Program in the Department of Health, England, funded the study. The authors reported having no financial disclosures.
Key clinical point:
Major finding: The children of fathers who reported strong emotional attachment and security as a parent had a lower risk of behavioral problems.
Data source: Cohort study of 14,440 children in southwest England.
Disclosures: The Policy Research Program in the Department of Health, England, funded the study. The authors reported having no financial disclosures.
Abuse-Deterrent Opioids: What Practitioners Need to Know
Opioid Abuse-Deterrent Formulations
The meaning of the term abuse-deterrent is often misunderstood to mean abuse-proof. The FDA defines abuse-deterrent properties as those properties expected to meaningfully deter abuse even if they do not fully prevent abuse. Abuse-deterrent properties make certain types of abuse, such as crushing in order to snort or dissolving in order to inject, more difficult or less rewarding. However, this does not mean that the product is impossible to abuse or that these properties will necessarily prevent addiction, overdose, or death.
Of note, currently marketed abuse-deterrent formulation technologies do not effectively deter one of the most common forms of opioid abuse—simply swallowing a number of intact tablets or capsules. Abuse-deterrent opioids do not reduce the risk for opioid addiction, and they carry the same warnings about the risk for addiction as do conventional opioids.
Abuse and Misuse Data
The FDA is encouraging pharmaceutical industry efforts to develop pain medicines that are more difficult to abuse and to prioritize the need for data and study methods that will help evaluate the impact of abuse-deterrent opioids on misuse and abuse in the community. To collect this important information, the FDA requires that all companies that have brand-name opioids with labeling describing abuse-deterrent properties conduct postmarketing studies to determine the impact of abuse-deterrent formulation technologies in the real world. Each company is given a time line to which they must adhere. These types of studies take several years to conduct and analyze. Data collected will include the amount prescribed for each product; adverse events related to the use, abuse, and misuse of the products; and epidemiologic data on the rates of abuse and misuse and their consequences (addiction, overdose, and death). These studies should allow the FDA to assess the impact in the community, if any, attributable to the abuse-deterrent properties.
The science of abuse deterrence is relatively new, and both the formulation technologies and the analytical, clinical, and statistical methods for evaluating those technologies ar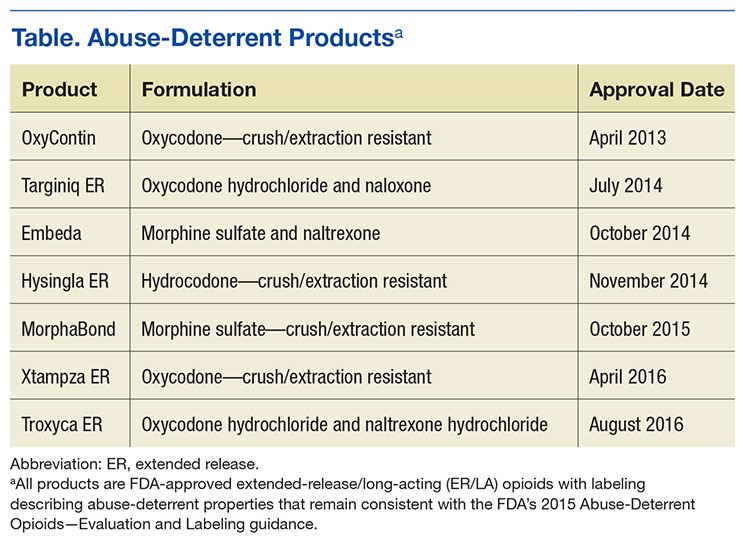
Key Points for Practitioners
The FDA’s work to facilitate the safe use of opioids is taking place within a larger policy framework aimed at addressing opioid abuse while ensuring appropriate access to pain treatment. The FDA has undertaken several efforts helpful to clinicians. The FDA’s Extended-Release and Long-Acting Opioid Analgesics Risk Evaluation and Mitigation Strategy (ER/LA REMS) Program is required for all companies who make these products. The program’s goal is to reduce serious adverse outcomes of inappropriate prescribing, misuse, and abuse of ER/LA opioid analgesics while maintaining patient access to pain medications. Adverse outcomes of concern include addiction, unintentional overdose, and death.
As part of the REMS, all ER/LA opioid analgesic pharmaceutical companies must provide education for prescribers of their medications through accredited continuing education activities that are supported by independent educational grants. Companies must also provide information that prescribers can use when counseling patients about the risks and benefits associated with ER/LA opioid analgesic use.
The FDA has developed core messages that are communicated to prescribers in the Blueprint for Prescriber Education. The Blueprint is directed to prescribers of ER/LA opioid analgesics but also may be relevant for other health care professionals (eg, pharmacists). Companies involved in the ER/LA Opioid Analgesics REMS Program have collaborated to implement a single shared REMS. This group provides a list of REMS-compliant continuing education activities, which can be found at http://www.er-la-opioidrems.com.
It is important for practitioners to understand that all currently approved abuse-deterrent opioid products still can be abused, and as scheduled controlled substances, they are addictive. The abuse-deterrent properties are expected to deter but do not wholly prevent abuse. Because in the end opioid medications must be able to deliver the opioid to the patient, there probably always will be potential for abuse of these products. Consequently, practitioners should counsel their patients on the following:
- Keep medicines in a secure location out of the reach and out of sight of children and pets. Put away medicines after every use. Accidental exposure to medicine in the home is a major source of unintentional poisonings in the U.S.
- If medicines are no longer needed, dispose of them properly. Disposing of all unused opioid analgesics reduces access to these medications by family members and household guests seeking opioids for abuse.
- The FDA recommends returning most prescription medications through a local or U.S. Drug Enforcement Administration (DEA)-sponsored take-back program or DEA-authorized collector. For opioid analgesics, the FDA recommends immediate removal from the home by flushing them down the toilet or sink.
Opioids Action Plan
In February 2016, FDA Commissioner Robert Califf (then the deputy commissioner for medical products and tobacco) announced the FDA Opioids Action Plan. The plan focuses on policies aimed at reversing the opioid epidemic while still providing patients in pain access to effective pain relief. The FDA actions include:
- Convening an expert advisory committee before approving any new drug application for an opioid that does not have abuse-deterrent properties;
- Consulting with the Pediatric Advisory Committee about a framework for pediatric opioid labeling before any new labeling is approved;
- Updating the REMS requirements for ER/LA opioid analgesics after considering the advisory committee’s recommendations from a meeting held in May 2016 and reviewing existing requirements;
- Improving access to naloxone (by facilitating the development of an over-the-counter version of naloxone, which is currently available only by prescription, thereby making it more accessible to treat opioid overdose), and medication-assisted treatment options for patients with opioid use disorders; and
- Supporting better pain management options, including alternative, nonaddictive treatments for pain.
The FDA is conducting research on pain measurements for conditions such as chronic low back pain, osteoarthritis, diabetic neuropathy, postherpetic neuralgia, and fibromyalgia. The FDA is also working to support the development of nonopioid options for these patients.
Consistent with the plan, in March 2016, the FDA announced that it was requiring changes to the labeling on immediate-release opioids, including additional warnings and safety information that incorporate elements similar to the ER/LA opioid analgesics labeling. Furthermore, among other steps, the FDA has contracted with the National Academy of Medicine to provide advice on how to incorporate current evidence about the public health impact of opioid use (for patients who are prescribed opioids as well as for nonpatients) into regulatory activities concerning opioids.
The FDA shares the responsibility of keeping patients safe. Working with the health care community and federal and state partners to help reduce opioid misuse and abuse and improve appropriate opioid prescribing while ensuring that patients in pain continue to have appropriate access to opioid analgesics is a top priority for the FDA and part of the targeted approach of the HHS focused on prevention, treatment, and intervention.
Opioid Abuse-Deterrent Formulations
The meaning of the term abuse-deterrent is often misunderstood to mean abuse-proof. The FDA defines abuse-deterrent properties as those properties expected to meaningfully deter abuse even if they do not fully prevent abuse. Abuse-deterrent properties make certain types of abuse, such as crushing in order to snort or dissolving in order to inject, more difficult or less rewarding. However, this does not mean that the product is impossible to abuse or that these properties will necessarily prevent addiction, overdose, or death.
Of note, currently marketed abuse-deterrent formulation technologies do not effectively deter one of the most common forms of opioid abuse—simply swallowing a number of intact tablets or capsules. Abuse-deterrent opioids do not reduce the risk for opioid addiction, and they carry the same warnings about the risk for addiction as do conventional opioids.
Abuse and Misuse Data
The FDA is encouraging pharmaceutical industry efforts to develop pain medicines that are more difficult to abuse and to prioritize the need for data and study methods that will help evaluate the impact of abuse-deterrent opioids on misuse and abuse in the community. To collect this important information, the FDA requires that all companies that have brand-name opioids with labeling describing abuse-deterrent properties conduct postmarketing studies to determine the impact of abuse-deterrent formulation technologies in the real world. Each company is given a time line to which they must adhere. These types of studies take several years to conduct and analyze. Data collected will include the amount prescribed for each product; adverse events related to the use, abuse, and misuse of the products; and epidemiologic data on the rates of abuse and misuse and their consequences (addiction, overdose, and death). These studies should allow the FDA to assess the impact in the community, if any, attributable to the abuse-deterrent properties.
The science of abuse deterrence is relatively new, and both the formulation technologies and the analytical, clinical, and statistical methods for evaluating those technologies ar
Key Points for Practitioners
The FDA’s work to facilitate the safe use of opioids is taking place within a larger policy framework aimed at addressing opioid abuse while ensuring appropriate access to pain treatment. The FDA has undertaken several efforts helpful to clinicians. The FDA’s Extended-Release and Long-Acting Opioid Analgesics Risk Evaluation and Mitigation Strategy (ER/LA REMS) Program is required for all companies who make these products. The program’s goal is to reduce serious adverse outcomes of inappropriate prescribing, misuse, and abuse of ER/LA opioid analgesics while maintaining patient access to pain medications. Adverse outcomes of concern include addiction, unintentional overdose, and death.
As part of the REMS, all ER/LA opioid analgesic pharmaceutical companies must provide education for prescribers of their medications through accredited continuing education activities that are supported by independent educational grants. Companies must also provide information that prescribers can use when counseling patients about the risks and benefits associated with ER/LA opioid analgesic use.
The FDA has developed core messages that are communicated to prescribers in the Blueprint for Prescriber Education. The Blueprint is directed to prescribers of ER/LA opioid analgesics but also may be relevant for other health care professionals (eg, pharmacists). Companies involved in the ER/LA Opioid Analgesics REMS Program have collaborated to implement a single shared REMS. This group provides a list of REMS-compliant continuing education activities, which can be found at http://www.er-la-opioidrems.com.
It is important for practitioners to understand that all currently approved abuse-deterrent opioid products still can be abused, and as scheduled controlled substances, they are addictive. The abuse-deterrent properties are expected to deter but do not wholly prevent abuse. Because in the end opioid medications must be able to deliver the opioid to the patient, there probably always will be potential for abuse of these products. Consequently, practitioners should counsel their patients on the following:
- Keep medicines in a secure location out of the reach and out of sight of children and pets. Put away medicines after every use. Accidental exposure to medicine in the home is a major source of unintentional poisonings in the U.S.
- If medicines are no longer needed, dispose of them properly. Disposing of all unused opioid analgesics reduces access to these medications by family members and household guests seeking opioids for abuse.
- The FDA recommends returning most prescription medications through a local or U.S. Drug Enforcement Administration (DEA)-sponsored take-back program or DEA-authorized collector. For opioid analgesics, the FDA recommends immediate removal from the home by flushing them down the toilet or sink.
Opioids Action Plan
In February 2016, FDA Commissioner Robert Califf (then the deputy commissioner for medical products and tobacco) announced the FDA Opioids Action Plan. The plan focuses on policies aimed at reversing the opioid epidemic while still providing patients in pain access to effective pain relief. The FDA actions include:
- Convening an expert advisory committee before approving any new drug application for an opioid that does not have abuse-deterrent properties;
- Consulting with the Pediatric Advisory Committee about a framework for pediatric opioid labeling before any new labeling is approved;
- Updating the REMS requirements for ER/LA opioid analgesics after considering the advisory committee’s recommendations from a meeting held in May 2016 and reviewing existing requirements;
- Improving access to naloxone (by facilitating the development of an over-the-counter version of naloxone, which is currently available only by prescription, thereby making it more accessible to treat opioid overdose), and medication-assisted treatment options for patients with opioid use disorders; and
- Supporting better pain management options, including alternative, nonaddictive treatments for pain.
The FDA is conducting research on pain measurements for conditions such as chronic low back pain, osteoarthritis, diabetic neuropathy, postherpetic neuralgia, and fibromyalgia. The FDA is also working to support the development of nonopioid options for these patients.
Consistent with the plan, in March 2016, the FDA announced that it was requiring changes to the labeling on immediate-release opioids, including additional warnings and safety information that incorporate elements similar to the ER/LA opioid analgesics labeling. Furthermore, among other steps, the FDA has contracted with the National Academy of Medicine to provide advice on how to incorporate current evidence about the public health impact of opioid use (for patients who are prescribed opioids as well as for nonpatients) into regulatory activities concerning opioids.
The FDA shares the responsibility of keeping patients safe. Working with the health care community and federal and state partners to help reduce opioid misuse and abuse and improve appropriate opioid prescribing while ensuring that patients in pain continue to have appropriate access to opioid analgesics is a top priority for the FDA and part of the targeted approach of the HHS focused on prevention, treatment, and intervention.
Opioid Abuse-Deterrent Formulations
The meaning of the term abuse-deterrent is often misunderstood to mean abuse-proof. The FDA defines abuse-deterrent properties as those properties expected to meaningfully deter abuse even if they do not fully prevent abuse. Abuse-deterrent properties make certain types of abuse, such as crushing in order to snort or dissolving in order to inject, more difficult or less rewarding. However, this does not mean that the product is impossible to abuse or that these properties will necessarily prevent addiction, overdose, or death.
Of note, currently marketed abuse-deterrent formulation technologies do not effectively deter one of the most common forms of opioid abuse—simply swallowing a number of intact tablets or capsules. Abuse-deterrent opioids do not reduce the risk for opioid addiction, and they carry the same warnings about the risk for addiction as do conventional opioids.
Abuse and Misuse Data
The FDA is encouraging pharmaceutical industry efforts to develop pain medicines that are more difficult to abuse and to prioritize the need for data and study methods that will help evaluate the impact of abuse-deterrent opioids on misuse and abuse in the community. To collect this important information, the FDA requires that all companies that have brand-name opioids with labeling describing abuse-deterrent properties conduct postmarketing studies to determine the impact of abuse-deterrent formulation technologies in the real world. Each company is given a time line to which they must adhere. These types of studies take several years to conduct and analyze. Data collected will include the amount prescribed for each product; adverse events related to the use, abuse, and misuse of the products; and epidemiologic data on the rates of abuse and misuse and their consequences (addiction, overdose, and death). These studies should allow the FDA to assess the impact in the community, if any, attributable to the abuse-deterrent properties.
The science of abuse deterrence is relatively new, and both the formulation technologies and the analytical, clinical, and statistical methods for evaluating those technologies ar
Key Points for Practitioners
The FDA’s work to facilitate the safe use of opioids is taking place within a larger policy framework aimed at addressing opioid abuse while ensuring appropriate access to pain treatment. The FDA has undertaken several efforts helpful to clinicians. The FDA’s Extended-Release and Long-Acting Opioid Analgesics Risk Evaluation and Mitigation Strategy (ER/LA REMS) Program is required for all companies who make these products. The program’s goal is to reduce serious adverse outcomes of inappropriate prescribing, misuse, and abuse of ER/LA opioid analgesics while maintaining patient access to pain medications. Adverse outcomes of concern include addiction, unintentional overdose, and death.
As part of the REMS, all ER/LA opioid analgesic pharmaceutical companies must provide education for prescribers of their medications through accredited continuing education activities that are supported by independent educational grants. Companies must also provide information that prescribers can use when counseling patients about the risks and benefits associated with ER/LA opioid analgesic use.
The FDA has developed core messages that are communicated to prescribers in the Blueprint for Prescriber Education. The Blueprint is directed to prescribers of ER/LA opioid analgesics but also may be relevant for other health care professionals (eg, pharmacists). Companies involved in the ER/LA Opioid Analgesics REMS Program have collaborated to implement a single shared REMS. This group provides a list of REMS-compliant continuing education activities, which can be found at http://www.er-la-opioidrems.com.
It is important for practitioners to understand that all currently approved abuse-deterrent opioid products still can be abused, and as scheduled controlled substances, they are addictive. The abuse-deterrent properties are expected to deter but do not wholly prevent abuse. Because in the end opioid medications must be able to deliver the opioid to the patient, there probably always will be potential for abuse of these products. Consequently, practitioners should counsel their patients on the following:
- Keep medicines in a secure location out of the reach and out of sight of children and pets. Put away medicines after every use. Accidental exposure to medicine in the home is a major source of unintentional poisonings in the U.S.
- If medicines are no longer needed, dispose of them properly. Disposing of all unused opioid analgesics reduces access to these medications by family members and household guests seeking opioids for abuse.
- The FDA recommends returning most prescription medications through a local or U.S. Drug Enforcement Administration (DEA)-sponsored take-back program or DEA-authorized collector. For opioid analgesics, the FDA recommends immediate removal from the home by flushing them down the toilet or sink.
Opioids Action Plan
In February 2016, FDA Commissioner Robert Califf (then the deputy commissioner for medical products and tobacco) announced the FDA Opioids Action Plan. The plan focuses on policies aimed at reversing the opioid epidemic while still providing patients in pain access to effective pain relief. The FDA actions include:
- Convening an expert advisory committee before approving any new drug application for an opioid that does not have abuse-deterrent properties;
- Consulting with the Pediatric Advisory Committee about a framework for pediatric opioid labeling before any new labeling is approved;
- Updating the REMS requirements for ER/LA opioid analgesics after considering the advisory committee’s recommendations from a meeting held in May 2016 and reviewing existing requirements;
- Improving access to naloxone (by facilitating the development of an over-the-counter version of naloxone, which is currently available only by prescription, thereby making it more accessible to treat opioid overdose), and medication-assisted treatment options for patients with opioid use disorders; and
- Supporting better pain management options, including alternative, nonaddictive treatments for pain.
The FDA is conducting research on pain measurements for conditions such as chronic low back pain, osteoarthritis, diabetic neuropathy, postherpetic neuralgia, and fibromyalgia. The FDA is also working to support the development of nonopioid options for these patients.
Consistent with the plan, in March 2016, the FDA announced that it was requiring changes to the labeling on immediate-release opioids, including additional warnings and safety information that incorporate elements similar to the ER/LA opioid analgesics labeling. Furthermore, among other steps, the FDA has contracted with the National Academy of Medicine to provide advice on how to incorporate current evidence about the public health impact of opioid use (for patients who are prescribed opioids as well as for nonpatients) into regulatory activities concerning opioids.
The FDA shares the responsibility of keeping patients safe. Working with the health care community and federal and state partners to help reduce opioid misuse and abuse and improve appropriate opioid prescribing while ensuring that patients in pain continue to have appropriate access to opioid analgesics is a top priority for the FDA and part of the targeted approach of the HHS focused on prevention, treatment, and intervention.
NICE recommends taking ibrutinib off CDF

Photo courtesy of Janssen
The National Institute for Health and Care Excellence (NICE) has issued a final appraisal determination recommending that ibrutinib come off the Cancer Drugs Fund (CDF) and be made available through the National Health Service (NHS).
Ibrutinib is a Bruton’s tyrosine kinase inhibitor approved by the European Commission treat patients with chronic lymphocytic leukemia (CLL).
NICE is recommending that ibrutinib be made available through the NHS for previously treated CLL patients and untreated CLL patients who have 17p deletion or TP53 mutation.
This means patients will no longer have to apply to the CDF to obtain ibrutinib. The CDF is money the English government sets aside to pay for cancer drugs that haven’t been approved by NICE and aren’t available within the NHS.
Though certain NICE products and services are provided to Wales, Scotland, and Northern Ireland, the governments of these countries do not have a CDF
or similar program.
Following the decision to reform the CDF earlier this year, NICE began to reappraise all drugs in the CDF in April.
New recommendation
NICE previously said it could not recommend ibrutinib for routine NHS use. However, Janssen, the company that makes ibrutinib, agreed to reduce the
price of the drug for the NHS. Because of the discount, an independent appraisal committee was able to deem ibrutinib cost-effective.
The list price for a single tablet of ibrutinib (140 mg) is £51.10 (excluding tax). The cost of a year’s course of ibrutinib treatment is £55,954.50 (excluding tax).
The discount the NHS will receive is confidential. The Department of Health said the cost of ibrutinib will not constitute an excessive administrative burden on the NHS.
NICE’s final appraisal determination on ibrutinib is now with consultees who have the opportunity to appeal against it. If there is no appeal, or an appeal is not upheld, the final appraisal determination is issued by NICE as a guidance.
Once NICE issues a final guidance on ibrutinib, the NHS must make the drug available within 3 months. ![]()
Photo courtesy of Janssen
The National Institute for Health and Care Excellence (NICE) has issued a final appraisal determination recommending that ibrutinib come off the Cancer Drugs Fund (CDF) and be made available through the National Health Service (NHS).
Ibrutinib is a Bruton’s tyrosine kinase inhibitor approved by the European Commission treat patients with chronic lymphocytic leukemia (CLL).
NICE is recommending that ibrutinib be made available through the NHS for previously treated CLL patients and untreated CLL patients who have 17p deletion or TP53 mutation.
This means patients will no longer have to apply to the CDF to obtain ibrutinib. The CDF is money the English government sets aside to pay for cancer drugs that haven’t been approved by NICE and aren’t available within the NHS.
Though certain NICE products and services are provided to Wales, Scotland, and Northern Ireland, the governments of these countries do not have a CDF
or similar program.
Following the decision to reform the CDF earlier this year, NICE began to reappraise all drugs in the CDF in April.
New recommendation
NICE previously said it could not recommend ibrutinib for routine NHS use. However, Janssen, the company that makes ibrutinib, agreed to reduce the
price of the drug for the NHS. Because of the discount, an independent appraisal committee was able to deem ibrutinib cost-effective.
The list price for a single tablet of ibrutinib (140 mg) is £51.10 (excluding tax). The cost of a year’s course of ibrutinib treatment is £55,954.50 (excluding tax).
The discount the NHS will receive is confidential. The Department of Health said the cost of ibrutinib will not constitute an excessive administrative burden on the NHS.
NICE’s final appraisal determination on ibrutinib is now with consultees who have the opportunity to appeal against it. If there is no appeal, or an appeal is not upheld, the final appraisal determination is issued by NICE as a guidance.
Once NICE issues a final guidance on ibrutinib, the NHS must make the drug available within 3 months. ![]()
Photo courtesy of Janssen
The National Institute for Health and Care Excellence (NICE) has issued a final appraisal determination recommending that ibrutinib come off the Cancer Drugs Fund (CDF) and be made available through the National Health Service (NHS).
Ibrutinib is a Bruton’s tyrosine kinase inhibitor approved by the European Commission treat patients with chronic lymphocytic leukemia (CLL).
NICE is recommending that ibrutinib be made available through the NHS for previously treated CLL patients and untreated CLL patients who have 17p deletion or TP53 mutation.
This means patients will no longer have to apply to the CDF to obtain ibrutinib. The CDF is money the English government sets aside to pay for cancer drugs that haven’t been approved by NICE and aren’t available within the NHS.
Though certain NICE products and services are provided to Wales, Scotland, and Northern Ireland, the governments of these countries do not have a CDF
or similar program.
Following the decision to reform the CDF earlier this year, NICE began to reappraise all drugs in the CDF in April.
New recommendation
NICE previously said it could not recommend ibrutinib for routine NHS use. However, Janssen, the company that makes ibrutinib, agreed to reduce the
price of the drug for the NHS. Because of the discount, an independent appraisal committee was able to deem ibrutinib cost-effective.
The list price for a single tablet of ibrutinib (140 mg) is £51.10 (excluding tax). The cost of a year’s course of ibrutinib treatment is £55,954.50 (excluding tax).
The discount the NHS will receive is confidential. The Department of Health said the cost of ibrutinib will not constitute an excessive administrative burden on the NHS.
NICE’s final appraisal determination on ibrutinib is now with consultees who have the opportunity to appeal against it. If there is no appeal, or an appeal is not upheld, the final appraisal determination is issued by NICE as a guidance.
Once NICE issues a final guidance on ibrutinib, the NHS must make the drug available within 3 months. ![]()
System could enable oral treatment of hemophilia, team says

Photo courtesy of the CDC
Researchers say they have developed biodegradable hydrophilic carriers that could provide oral delivery of factor IX (FIX) to treat hemophilia B.
Preclinical experiments have shown these carriers can be loaded with FIX and release it in response to environmental
stimuli.
Sarena Horava, PhD, of Triton Systems, Inc. in Chelmsford, Massachusetts, and her colleagues described the carriers in the International Journal of Pharmaceutics.
The current work builds on a previous delivery system devised by Dr Horova and Nicholas A. Peppas, ScD, of The University of Texas at Austin.
Although that system was successful in transporting FIX, the researchers found that modifications were needed to improve the oral bioavailability of FIX.
The team noted that FIX is delicate and unstable in the body’s various pH environments. So the new system is designed to capitalize on the body’s pH and changes in enzymes inside the gastrointestinal tract.
Specifically, the researchers developed a biodegradable, pH-responsive hydrogel microcarrier system based on the poly(methacrylic acid)-grafted-poly(ethylene glycol) [P(MAA-g-EG)].
The team said the incorporation of an enzymatically degradable peptide crosslinking agent allows for site-specific degradation by trypsin in the small intestine.
The carrier is designed to remain intact as it moves through the body. Once it reaches the small intestine, the carrier should begin to swell with the increase in pH. The carrier should then be degraded by trypsin and slowly release FIX over time.
The researchers said their experiments confirmed that the peptide crosslinked P(MAA-g-EG) microparticles are capable of loading FIX and releasing it under intestinal conditions.
They said the biodegradable component allowed for increased levels of FIX to be released, when compared to the previous system.
Furthermore, both the microparticles and the degradation products enhanced the in vitro absorption of FIX.
“Based on the current capabilities of this system, approximately 2 capsules would be equivalent to 1 injection [of FIX],” Dr Horava said. “However, we anticipate that we will make further improvements to the delivery capacity of the oral delivery system and therefore decrease the capsule amount.”
The researchers plan to conduct additional preclinical experiments with this system before starting clinical trials. ![]()
Photo courtesy of the CDC
Researchers say they have developed biodegradable hydrophilic carriers that could provide oral delivery of factor IX (FIX) to treat hemophilia B.
Preclinical experiments have shown these carriers can be loaded with FIX and release it in response to environmental
stimuli.
Sarena Horava, PhD, of Triton Systems, Inc. in Chelmsford, Massachusetts, and her colleagues described the carriers in the International Journal of Pharmaceutics.
The current work builds on a previous delivery system devised by Dr Horova and Nicholas A. Peppas, ScD, of The University of Texas at Austin.
Although that system was successful in transporting FIX, the researchers found that modifications were needed to improve the oral bioavailability of FIX.
The team noted that FIX is delicate and unstable in the body’s various pH environments. So the new system is designed to capitalize on the body’s pH and changes in enzymes inside the gastrointestinal tract.
Specifically, the researchers developed a biodegradable, pH-responsive hydrogel microcarrier system based on the poly(methacrylic acid)-grafted-poly(ethylene glycol) [P(MAA-g-EG)].
The team said the incorporation of an enzymatically degradable peptide crosslinking agent allows for site-specific degradation by trypsin in the small intestine.
The carrier is designed to remain intact as it moves through the body. Once it reaches the small intestine, the carrier should begin to swell with the increase in pH. The carrier should then be degraded by trypsin and slowly release FIX over time.
The researchers said their experiments confirmed that the peptide crosslinked P(MAA-g-EG) microparticles are capable of loading FIX and releasing it under intestinal conditions.
They said the biodegradable component allowed for increased levels of FIX to be released, when compared to the previous system.
Furthermore, both the microparticles and the degradation products enhanced the in vitro absorption of FIX.
“Based on the current capabilities of this system, approximately 2 capsules would be equivalent to 1 injection [of FIX],” Dr Horava said. “However, we anticipate that we will make further improvements to the delivery capacity of the oral delivery system and therefore decrease the capsule amount.”
The researchers plan to conduct additional preclinical experiments with this system before starting clinical trials. ![]()
Photo courtesy of the CDC
Researchers say they have developed biodegradable hydrophilic carriers that could provide oral delivery of factor IX (FIX) to treat hemophilia B.
Preclinical experiments have shown these carriers can be loaded with FIX and release it in response to environmental
stimuli.
Sarena Horava, PhD, of Triton Systems, Inc. in Chelmsford, Massachusetts, and her colleagues described the carriers in the International Journal of Pharmaceutics.
The current work builds on a previous delivery system devised by Dr Horova and Nicholas A. Peppas, ScD, of The University of Texas at Austin.
Although that system was successful in transporting FIX, the researchers found that modifications were needed to improve the oral bioavailability of FIX.
The team noted that FIX is delicate and unstable in the body’s various pH environments. So the new system is designed to capitalize on the body’s pH and changes in enzymes inside the gastrointestinal tract.
Specifically, the researchers developed a biodegradable, pH-responsive hydrogel microcarrier system based on the poly(methacrylic acid)-grafted-poly(ethylene glycol) [P(MAA-g-EG)].
The team said the incorporation of an enzymatically degradable peptide crosslinking agent allows for site-specific degradation by trypsin in the small intestine.
The carrier is designed to remain intact as it moves through the body. Once it reaches the small intestine, the carrier should begin to swell with the increase in pH. The carrier should then be degraded by trypsin and slowly release FIX over time.
The researchers said their experiments confirmed that the peptide crosslinked P(MAA-g-EG) microparticles are capable of loading FIX and releasing it under intestinal conditions.
They said the biodegradable component allowed for increased levels of FIX to be released, when compared to the previous system.
Furthermore, both the microparticles and the degradation products enhanced the in vitro absorption of FIX.
“Based on the current capabilities of this system, approximately 2 capsules would be equivalent to 1 injection [of FIX],” Dr Horava said. “However, we anticipate that we will make further improvements to the delivery capacity of the oral delivery system and therefore decrease the capsule amount.”
The researchers plan to conduct additional preclinical experiments with this system before starting clinical trials. ![]()
FDA grants full approval for ponatinib
Photo from Business Wire
The US Food and Drug Administration (FDA) has granted full approval for the kinase inhibitor ponatinib (Iclusig®) and updated the drug’s label.
Ponatinib now has full approval as a treatment for adults with chronic myeloid leukemia (CML) or Philadelphia chromosome-positive acute lymphoblastic leukemia (Ph+ ALL) when no other tyrosine kinase inhibitor is indicated.
Ponatinib is also approved to treat adults with T315I-positive CML or T315I-positive Ph+ ALL.
Ponatinib was initially approved in December 2012 under the FDA’s accelerated approval program.
This program allows the FDA to approve a drug to treat a serious or life-threatening disease based on clinical data showing the drug has an effect on a surrogate endpoint reasonably likely to predict clinical benefit to patients.
The company developing the drug must conduct post-approval research to determine if the drug provides a clinical benefit. If so, the drug can be granted full approval.
The full approval and label update for ponatinib is based on 48-month follow-up data (as of August 2015) from the phase 2 PACE trial, which enrolled heavily pretreated patients with resistant or intolerant CML or Ph+ ALL. These data were presented at the 2016 ASCO Annual Meeting.
“The longer follow up of the PACE study confirms the clinical benefit of ponatinib in this setting,” said Jorge Cortes, MD, a professor at The University of Texas MD Anderson Cancer Center in Houston and a leading investigator in the PACE trial.
“We had learned from the initial report of the high response rate with ponatinib among CML patients with resistance or intolerance to prior therapies. The 4-year follow-up and updated safety profile demonstrate durability of responses in this heavily pretreated population. These results solidify ponatinib as an important and valuable treatment option for refractory patients with CML where no other TKI therapy is appropriate, including those who have the T315I mutation.”
Past problems with ponatinib
Previous follow-up data from the PACE trial, collected in 2013, suggested ponatinib can increase the risk of thrombotic events. When these data came to light, officials in the US and European Union, where ponatinib had already been approved, began to investigate the drug.
Ponatinib was pulled from the US market for a little over 2 months, and trials of the drug were placed on partial hold while the FDA evaluated the drug’s safety. Ponatinib went back on the market in January 2014, with new safety measures in place.
Ponatinib was not pulled from the market in the European Union, but the European Medicine’s Agency released recommendations for safer use of the drug. The Committee for Medicinal Products for Human Use reviewed data on ponatinib and decided its benefits outweigh its risks. ![]()
Photo from Business Wire
The US Food and Drug Administration (FDA) has granted full approval for the kinase inhibitor ponatinib (Iclusig®) and updated the drug’s label.
Ponatinib now has full approval as a treatment for adults with chronic myeloid leukemia (CML) or Philadelphia chromosome-positive acute lymphoblastic leukemia (Ph+ ALL) when no other tyrosine kinase inhibitor is indicated.
Ponatinib is also approved to treat adults with T315I-positive CML or T315I-positive Ph+ ALL.
Ponatinib was initially approved in December 2012 under the FDA’s accelerated approval program.
This program allows the FDA to approve a drug to treat a serious or life-threatening disease based on clinical data showing the drug has an effect on a surrogate endpoint reasonably likely to predict clinical benefit to patients.
The company developing the drug must conduct post-approval research to determine if the drug provides a clinical benefit. If so, the drug can be granted full approval.
The full approval and label update for ponatinib is based on 48-month follow-up data (as of August 2015) from the phase 2 PACE trial, which enrolled heavily pretreated patients with resistant or intolerant CML or Ph+ ALL. These data were presented at the 2016 ASCO Annual Meeting.
“The longer follow up of the PACE study confirms the clinical benefit of ponatinib in this setting,” said Jorge Cortes, MD, a professor at The University of Texas MD Anderson Cancer Center in Houston and a leading investigator in the PACE trial.
“We had learned from the initial report of the high response rate with ponatinib among CML patients with resistance or intolerance to prior therapies. The 4-year follow-up and updated safety profile demonstrate durability of responses in this heavily pretreated population. These results solidify ponatinib as an important and valuable treatment option for refractory patients with CML where no other TKI therapy is appropriate, including those who have the T315I mutation.”
Past problems with ponatinib
Previous follow-up data from the PACE trial, collected in 2013, suggested ponatinib can increase the risk of thrombotic events. When these data came to light, officials in the US and European Union, where ponatinib had already been approved, began to investigate the drug.
Ponatinib was pulled from the US market for a little over 2 months, and trials of the drug were placed on partial hold while the FDA evaluated the drug’s safety. Ponatinib went back on the market in January 2014, with new safety measures in place.
Ponatinib was not pulled from the market in the European Union, but the European Medicine’s Agency released recommendations for safer use of the drug. The Committee for Medicinal Products for Human Use reviewed data on ponatinib and decided its benefits outweigh its risks. ![]()
Photo from Business Wire
The US Food and Drug Administration (FDA) has granted full approval for the kinase inhibitor ponatinib (Iclusig®) and updated the drug’s label.
Ponatinib now has full approval as a treatment for adults with chronic myeloid leukemia (CML) or Philadelphia chromosome-positive acute lymphoblastic leukemia (Ph+ ALL) when no other tyrosine kinase inhibitor is indicated.
Ponatinib is also approved to treat adults with T315I-positive CML or T315I-positive Ph+ ALL.
Ponatinib was initially approved in December 2012 under the FDA’s accelerated approval program.
This program allows the FDA to approve a drug to treat a serious or life-threatening disease based on clinical data showing the drug has an effect on a surrogate endpoint reasonably likely to predict clinical benefit to patients.
The company developing the drug must conduct post-approval research to determine if the drug provides a clinical benefit. If so, the drug can be granted full approval.
The full approval and label update for ponatinib is based on 48-month follow-up data (as of August 2015) from the phase 2 PACE trial, which enrolled heavily pretreated patients with resistant or intolerant CML or Ph+ ALL. These data were presented at the 2016 ASCO Annual Meeting.
“The longer follow up of the PACE study confirms the clinical benefit of ponatinib in this setting,” said Jorge Cortes, MD, a professor at The University of Texas MD Anderson Cancer Center in Houston and a leading investigator in the PACE trial.
“We had learned from the initial report of the high response rate with ponatinib among CML patients with resistance or intolerance to prior therapies. The 4-year follow-up and updated safety profile demonstrate durability of responses in this heavily pretreated population. These results solidify ponatinib as an important and valuable treatment option for refractory patients with CML where no other TKI therapy is appropriate, including those who have the T315I mutation.”
Past problems with ponatinib
Previous follow-up data from the PACE trial, collected in 2013, suggested ponatinib can increase the risk of thrombotic events. When these data came to light, officials in the US and European Union, where ponatinib had already been approved, began to investigate the drug.
Ponatinib was pulled from the US market for a little over 2 months, and trials of the drug were placed on partial hold while the FDA evaluated the drug’s safety. Ponatinib went back on the market in January 2014, with new safety measures in place.
Ponatinib was not pulled from the market in the European Union, but the European Medicine’s Agency released recommendations for safer use of the drug. The Committee for Medicinal Products for Human Use reviewed data on ponatinib and decided its benefits outweigh its risks. ![]()
Resistant Hypertension
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel

Low-dose IL-2 shows promise for refractory lupus
WASHINGTON – A novel biologic treatment strategy involving subcutaneous low-dose interleukin-2 therapy for refractory systemic lupus erythematosus (SLE) showed promise in a single-center, combined phase I/IIa trial.
In 12 patients with active and refractory SLE – that is, patients with SLE disease activity index (SLEDAI) score of at least 6 who were on at least two different immunosuppressive therapies – low-dose IL-2 treatment led to an effective and cycle-dependent increase in the percentage of CD25hi cells among regulatory T cells (Treg). The increase was statistically significant (P less than .001), Jens Humrich, MD, and his colleagues reported in a late-breaking poster at the annual meeting of the American College of Rheumatology.
However, a reduction in levels of anti-dsDNA antibodies was not observed, said Dr. Humrich of University Hospital Schleswig-Holstein in Lubeck, Germany.
Treatment was safe; treatment-related adverse events were generally mild and transient, Dr. Humrich noted.
Study subjects received four treatment cycles each, with daily subcutaneous injections of recombinant human IL-2 (aldesleukin) at single doses of 0.75, 1.5, or 3.0 million IU on 5 consecutive days. Cycles were separated by a washout period of 9-16 days. Subjects were then followed for 9 weeks.
IL-2 is crucial for the growth and survival of Treg (and thus for the control of autoimmunity). Prior studies demonstrated the significance of acquired IL-2 deficiency and related Treg defects in the pathogenesis of SLE – and that compensation for IL-2 deficiency with low-dose IL-2 can correct these defects, he explained.
In the current study, the primary aim was to show at least a twofold increase in the percentage of CD25hi cells among CD3+CD4+Foxp3+CD127lo Treg cells after the fourth treatment cycle vs. baseline, and secondary aims included clinical responses assessed by SLEDAI and changes in serologic and other immunologic parameters, he said.
The findings suggest that low-dose IL-2 therapy can safely and selectively expand the Treg population and decrease disease activity in patients with active and refractory SLE.
“This study provides the basis for larger and placebo-controlled clinical studies aiming to prove the efficacy of this novel biologic treatment strategy,” the investigators concluded.
Dr. Humrich reported having no disclosures.
WASHINGTON – A novel biologic treatment strategy involving subcutaneous low-dose interleukin-2 therapy for refractory systemic lupus erythematosus (SLE) showed promise in a single-center, combined phase I/IIa trial.
In 12 patients with active and refractory SLE – that is, patients with SLE disease activity index (SLEDAI) score of at least 6 who were on at least two different immunosuppressive therapies – low-dose IL-2 treatment led to an effective and cycle-dependent increase in the percentage of CD25hi cells among regulatory T cells (Treg). The increase was statistically significant (P less than .001), Jens Humrich, MD, and his colleagues reported in a late-breaking poster at the annual meeting of the American College of Rheumatology.
However, a reduction in levels of anti-dsDNA antibodies was not observed, said Dr. Humrich of University Hospital Schleswig-Holstein in Lubeck, Germany.
Treatment was safe; treatment-related adverse events were generally mild and transient, Dr. Humrich noted.
Study subjects received four treatment cycles each, with daily subcutaneous injections of recombinant human IL-2 (aldesleukin) at single doses of 0.75, 1.5, or 3.0 million IU on 5 consecutive days. Cycles were separated by a washout period of 9-16 days. Subjects were then followed for 9 weeks.
IL-2 is crucial for the growth and survival of Treg (and thus for the control of autoimmunity). Prior studies demonstrated the significance of acquired IL-2 deficiency and related Treg defects in the pathogenesis of SLE – and that compensation for IL-2 deficiency with low-dose IL-2 can correct these defects, he explained.
In the current study, the primary aim was to show at least a twofold increase in the percentage of CD25hi cells among CD3+CD4+Foxp3+CD127lo Treg cells after the fourth treatment cycle vs. baseline, and secondary aims included clinical responses assessed by SLEDAI and changes in serologic and other immunologic parameters, he said.
The findings suggest that low-dose IL-2 therapy can safely and selectively expand the Treg population and decrease disease activity in patients with active and refractory SLE.
“This study provides the basis for larger and placebo-controlled clinical studies aiming to prove the efficacy of this novel biologic treatment strategy,” the investigators concluded.
Dr. Humrich reported having no disclosures.
WASHINGTON – A novel biologic treatment strategy involving subcutaneous low-dose interleukin-2 therapy for refractory systemic lupus erythematosus (SLE) showed promise in a single-center, combined phase I/IIa trial.
In 12 patients with active and refractory SLE – that is, patients with SLE disease activity index (SLEDAI) score of at least 6 who were on at least two different immunosuppressive therapies – low-dose IL-2 treatment led to an effective and cycle-dependent increase in the percentage of CD25hi cells among regulatory T cells (Treg). The increase was statistically significant (P less than .001), Jens Humrich, MD, and his colleagues reported in a late-breaking poster at the annual meeting of the American College of Rheumatology.
However, a reduction in levels of anti-dsDNA antibodies was not observed, said Dr. Humrich of University Hospital Schleswig-Holstein in Lubeck, Germany.
Treatment was safe; treatment-related adverse events were generally mild and transient, Dr. Humrich noted.
Study subjects received four treatment cycles each, with daily subcutaneous injections of recombinant human IL-2 (aldesleukin) at single doses of 0.75, 1.5, or 3.0 million IU on 5 consecutive days. Cycles were separated by a washout period of 9-16 days. Subjects were then followed for 9 weeks.
IL-2 is crucial for the growth and survival of Treg (and thus for the control of autoimmunity). Prior studies demonstrated the significance of acquired IL-2 deficiency and related Treg defects in the pathogenesis of SLE – and that compensation for IL-2 deficiency with low-dose IL-2 can correct these defects, he explained.
In the current study, the primary aim was to show at least a twofold increase in the percentage of CD25hi cells among CD3+CD4+Foxp3+CD127lo Treg cells after the fourth treatment cycle vs. baseline, and secondary aims included clinical responses assessed by SLEDAI and changes in serologic and other immunologic parameters, he said.
The findings suggest that low-dose IL-2 therapy can safely and selectively expand the Treg population and decrease disease activity in patients with active and refractory SLE.
“This study provides the basis for larger and placebo-controlled clinical studies aiming to prove the efficacy of this novel biologic treatment strategy,” the investigators concluded.
Dr. Humrich reported having no disclosures.
Key clinical point:
Major finding: A reduction in SLEDAI was seen in 10 patients (83.3%), and a clinical response occurred in 8 (66.7%).
Data source: A combined phase I/IIa trial involving 12 patients.
Disclosures: Dr. Humrich reported having no disclosures.