The patient's history of psoriasis, along with his current skin and scalp plaque flares, symmetrical joint symptomatology, laboratory studies, and x-rays, suggest a diagnosis of symmetrical psoriatic arthritis (PsA). The rheumatologist considers ordering additional imaging to assess for subclinical enthesitis and dactylitis, and discusses treatment next steps with the patient, given inadequate control with a TNF inhibitor.
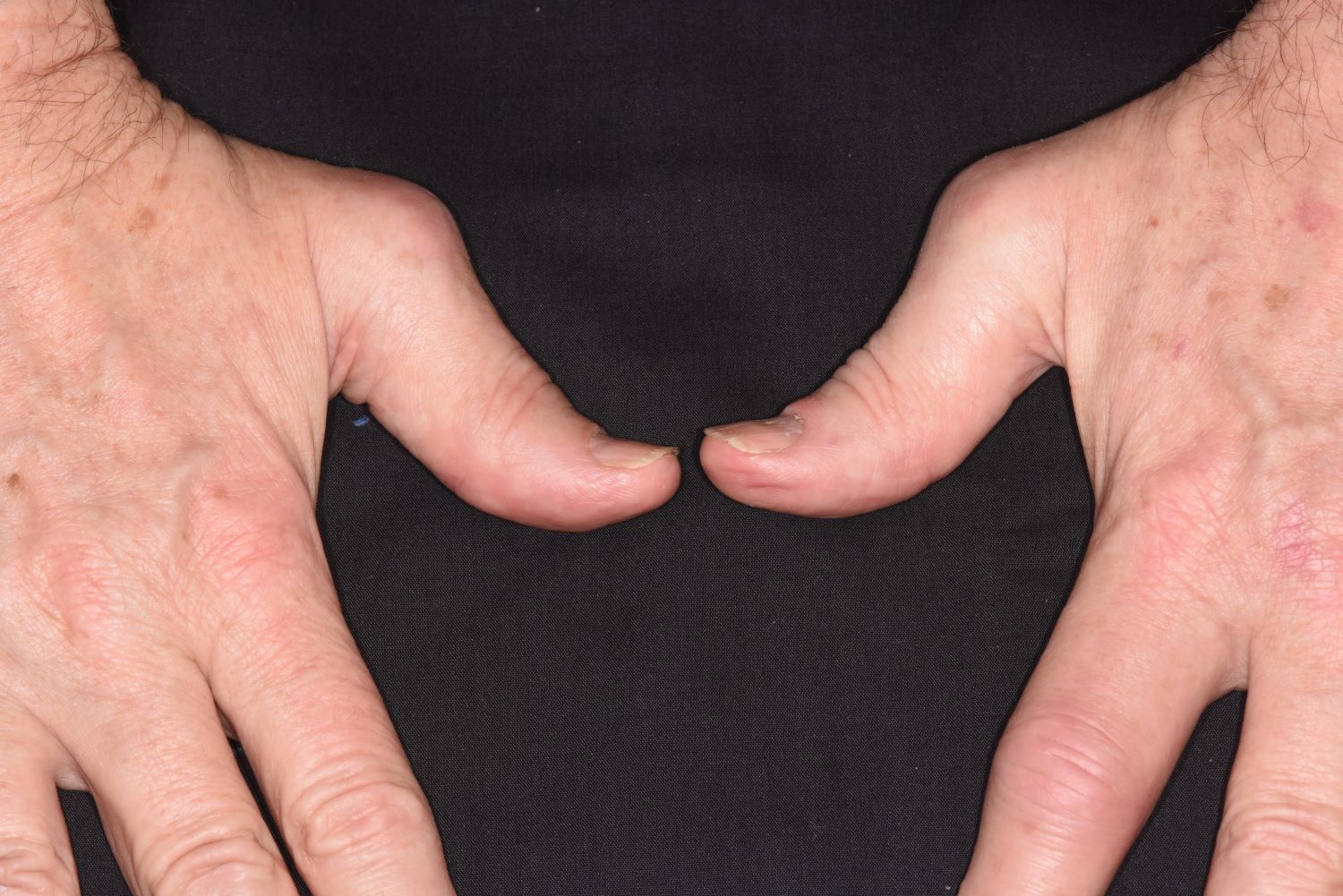
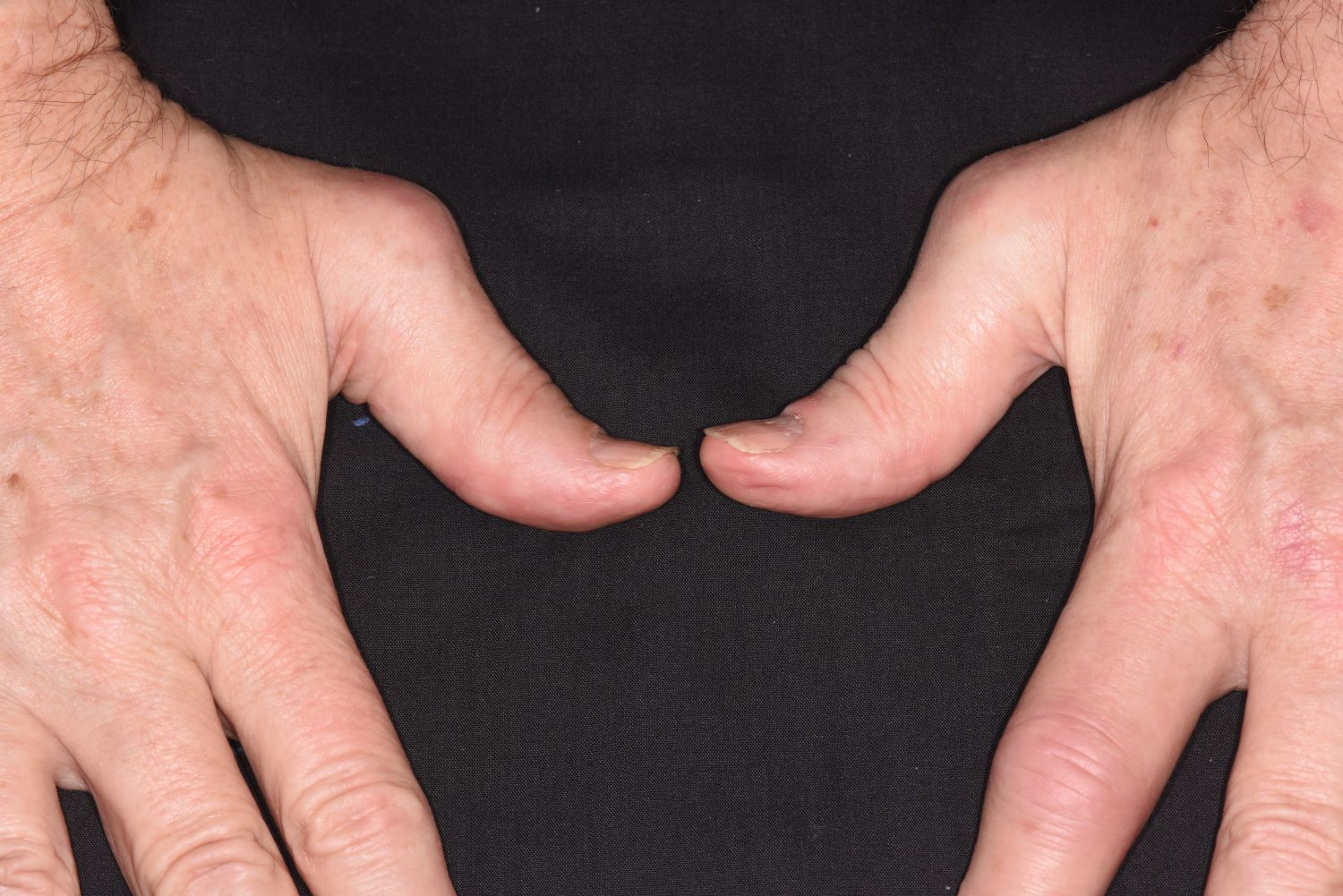
Symmetrical polyarthritis is one of the most common types of PsA and involves five or more joints in the hands, wrists, ankles, and/or feet. Among patients with PsA, 60% to 80% experience plaque psoriasis before joint-symptom onset; time to joint-symptom onset in these patients typically occurs within 10 years of a plaque psoriasis diagnosis. Involvement of DIP joints differentiates PsA from rheumatoid arthritis, as does the absence of subcutaneous nodules and a negative result for rheumatoid factor. About 30% of all people with plaque psoriasis will develop PsA, which affects an estimated 1 million people in the United States annually. Symptoms typically appear between the ages of 35 and 55 years; women are more likely than men to develop symmetrical PsA.
There are no specific diagnostic tests for PsA. Rheumatologists generally use the assessment known as the Classification Criteria for Psoriatic Arthritis, (CASPAR), which can help reveal established inflammatory articular disease through a point system based on the presence/absence of various factors. On laboratory studies, the most common characteristic abnormalities of PsA are elevated ESR and CRP levels and negative rheumatoid factor in most patients. Other abnormalities that may be present in patients with PsA include elevated serum uric acid concentration and serum immunoglobulin A, and reduced levels of circulating immune complexes. Physicians also use imaging studies, such as radiography, ultrasonography, and MRI, to help differentiate PsA from other articular diseases.
While the pathogenesis of PsA remains unclear, research has shown that disease development is associated with a complex interplay of immune-mediated inflammatory responses; genetic and environmental factors may also be involved. In addition, patients with PsA are more likely to have a high risk for comorbidities, including obesity, type 2 diabetes, hypertension, hyperlipidemia, and cardiovascular events, compared with the general population.
When patients with PsA experience both skin and joint symptoms, a multidisciplinary approach to care is advised. Multidisciplinary teams play a key role in educating patients about their treatment plans and managing their PsA symptoms. The teams also help patients determine the best approaches to exercise to help maintain current joint function, as well as helpful adjustments in daily activities that will make it easier to accommodate their disease.
Nonsteroidal anti-inflammatory drugs, whether self-prescribed or prescribed by a physician, are a common initial treatment to manage joint symptoms of PsA. Current American College of Rheumatology treatment guidelines, however, encourage early treatment with disease-modifying antirheumatic drugs (DMARDs) because approximately 40% of patients with PsA develop erosive and deforming arthritis. Several DMARDs are available, including older drugs like methotrexate, as well as newer biologic agents, such as TNF inhibitors, interleukin (IL)-17 inhibitors, IL-12/23 inhibitors, and Janus kinase inhibitors. In addition, guidelines recommend early and customized physical therapy and rehabilitation approaches for patients with PsA.
Herbert S. Diamond, MD, Professor of Medicine (retired), Temple University School of Medicine, University of Pittsburgh; Chairman, Department of Medicine Emeritus, Western Pennsylvania Hospital, Pittsburgh, PA.
Herbert S. Diamond, MD, has disclosed no relevant financial relationships.
Image Quizzes are fictional or fictionalized clinical scenarios intended to provide evidence-based educational takeaways.
The patient's history of psoriasis, along with his current skin and scalp plaque flares, symmetrical joint symptomatology, laboratory studies, and x-rays, suggest a diagnosis of symmetrical psoriatic arthritis (PsA). The rheumatologist considers ordering additional imaging to assess for subclinical enthesitis and dactylitis, and discusses treatment next steps with the patient, given inadequate control with a TNF inhibitor.
Symmetrical polyarthritis is one of the most common types of PsA and involves five or more joints in the hands, wrists, ankles, and/or feet. Among patients with PsA, 60% to 80% experience plaque psoriasis before joint-symptom onset; time to joint-symptom onset in these patients typically occurs within 10 years of a plaque psoriasis diagnosis. Involvement of DIP joints differentiates PsA from rheumatoid arthritis, as does the absence of subcutaneous nodules and a negative result for rheumatoid factor. About 30% of all people with plaque psoriasis will develop PsA, which affects an estimated 1 million people in the United States annually. Symptoms typically appear between the ages of 35 and 55 years; women are more likely than men to develop symmetrical PsA.
There are no specific diagnostic tests for PsA. Rheumatologists generally use the assessment known as the Classification Criteria for Psoriatic Arthritis, (CASPAR), which can help reveal established inflammatory articular disease through a point system based on the presence/absence of various factors. On laboratory studies, the most common characteristic abnormalities of PsA are elevated ESR and CRP levels and negative rheumatoid factor in most patients. Other abnormalities that may be present in patients with PsA include elevated serum uric acid concentration and serum immunoglobulin A, and reduced levels of circulating immune complexes. Physicians also use imaging studies, such as radiography, ultrasonography, and MRI, to help differentiate PsA from other articular diseases.
While the pathogenesis of PsA remains unclear, research has shown that disease development is associated with a complex interplay of immune-mediated inflammatory responses; genetic and environmental factors may also be involved. In addition, patients with PsA are more likely to have a high risk for comorbidities, including obesity, type 2 diabetes, hypertension, hyperlipidemia, and cardiovascular events, compared with the general population.
When patients with PsA experience both skin and joint symptoms, a multidisciplinary approach to care is advised. Multidisciplinary teams play a key role in educating patients about their treatment plans and managing their PsA symptoms. The teams also help patients determine the best approaches to exercise to help maintain current joint function, as well as helpful adjustments in daily activities that will make it easier to accommodate their disease.
Nonsteroidal anti-inflammatory drugs, whether self-prescribed or prescribed by a physician, are a common initial treatment to manage joint symptoms of PsA. Current American College of Rheumatology treatment guidelines, however, encourage early treatment with disease-modifying antirheumatic drugs (DMARDs) because approximately 40% of patients with PsA develop erosive and deforming arthritis. Several DMARDs are available, including older drugs like methotrexate, as well as newer biologic agents, such as TNF inhibitors, interleukin (IL)-17 inhibitors, IL-12/23 inhibitors, and Janus kinase inhibitors. In addition, guidelines recommend early and customized physical therapy and rehabilitation approaches for patients with PsA.
Herbert S. Diamond, MD, Professor of Medicine (retired), Temple University School of Medicine, University of Pittsburgh; Chairman, Department of Medicine Emeritus, Western Pennsylvania Hospital, Pittsburgh, PA.
Herbert S. Diamond, MD, has disclosed no relevant financial relationships.
Image Quizzes are fictional or fictionalized clinical scenarios intended to provide evidence-based educational takeaways.
The patient's history of psoriasis, along with his current skin and scalp plaque flares, symmetrical joint symptomatology, laboratory studies, and x-rays, suggest a diagnosis of symmetrical psoriatic arthritis (PsA). The rheumatologist considers ordering additional imaging to assess for subclinical enthesitis and dactylitis, and discusses treatment next steps with the patient, given inadequate control with a TNF inhibitor.
Symmetrical polyarthritis is one of the most common types of PsA and involves five or more joints in the hands, wrists, ankles, and/or feet. Among patients with PsA, 60% to 80% experience plaque psoriasis before joint-symptom onset; time to joint-symptom onset in these patients typically occurs within 10 years of a plaque psoriasis diagnosis. Involvement of DIP joints differentiates PsA from rheumatoid arthritis, as does the absence of subcutaneous nodules and a negative result for rheumatoid factor. About 30% of all people with plaque psoriasis will develop PsA, which affects an estimated 1 million people in the United States annually. Symptoms typically appear between the ages of 35 and 55 years; women are more likely than men to develop symmetrical PsA.
There are no specific diagnostic tests for PsA. Rheumatologists generally use the assessment known as the Classification Criteria for Psoriatic Arthritis, (CASPAR), which can help reveal established inflammatory articular disease through a point system based on the presence/absence of various factors. On laboratory studies, the most common characteristic abnormalities of PsA are elevated ESR and CRP levels and negative rheumatoid factor in most patients. Other abnormalities that may be present in patients with PsA include elevated serum uric acid concentration and serum immunoglobulin A, and reduced levels of circulating immune complexes. Physicians also use imaging studies, such as radiography, ultrasonography, and MRI, to help differentiate PsA from other articular diseases.
While the pathogenesis of PsA remains unclear, research has shown that disease development is associated with a complex interplay of immune-mediated inflammatory responses; genetic and environmental factors may also be involved. In addition, patients with PsA are more likely to have a high risk for comorbidities, including obesity, type 2 diabetes, hypertension, hyperlipidemia, and cardiovascular events, compared with the general population.
When patients with PsA experience both skin and joint symptoms, a multidisciplinary approach to care is advised. Multidisciplinary teams play a key role in educating patients about their treatment plans and managing their PsA symptoms. The teams also help patients determine the best approaches to exercise to help maintain current joint function, as well as helpful adjustments in daily activities that will make it easier to accommodate their disease.
Nonsteroidal anti-inflammatory drugs, whether self-prescribed or prescribed by a physician, are a common initial treatment to manage joint symptoms of PsA. Current American College of Rheumatology treatment guidelines, however, encourage early treatment with disease-modifying antirheumatic drugs (DMARDs) because approximately 40% of patients with PsA develop erosive and deforming arthritis. Several DMARDs are available, including older drugs like methotrexate, as well as newer biologic agents, such as TNF inhibitors, interleukin (IL)-17 inhibitors, IL-12/23 inhibitors, and Janus kinase inhibitors. In addition, guidelines recommend early and customized physical therapy and rehabilitation approaches for patients with PsA.
Herbert S. Diamond, MD, Professor of Medicine (retired), Temple University School of Medicine, University of Pittsburgh; Chairman, Department of Medicine Emeritus, Western Pennsylvania Hospital, Pittsburgh, PA.
Herbert S. Diamond, MD, has disclosed no relevant financial relationships.
Image Quizzes are fictional or fictionalized clinical scenarios intended to provide evidence-based educational takeaways.
A 43-year-old White man with a 5-year history of plaque psoriasis presents to a rheumatologist on referral from his dermatologist. He had been taking a tumor necrosis factor (TNF) inhibitor, which had controlled his skin and scalp plaques since diagnosis. Lately, however, some of the plaques have begun to flare up, and the patient reports new tenderness and swelling in three of the same joints on his left and right hands and extensive fatigue. Additional medical history includes type 2 diabetes, which was diagnosed 3 years ago; soon thereafter, he started taking metformin with consistent disease control. The rheumatologist conducts a physical exam and orders laboratory studies and x-rays. Results of the laboratory studies reveal elevated levels of C-reactive protein (CRP) and erythrocyte sedimentation rate (ESR). Radiographs reveal joint-space narrowing in several distal interphalangeal (DIP) joints in both hands, with mild erosive disease.
Disallow All Ads
Content Gating
No Gating (article Unlocked/Free)
Alternative CME
Disqus Comments
Default
Gate On Date
Un-Gate On Date
Consolidated Pubs: Do Not Show Source Publication Logo
Among military veterans who die by suicide, those who experience a traumatic brain injury (TBI) during service take their lives 21% sooner after deployment than those without a TBI history, a new study shows.
Investigators also found that increases in new mental health diagnoses are significantly higher in soldiers with a history of TBI – in some cases, strikingly higher. For example, cases of substance use disorder rose by 100% among veterans with TBI compared to just 14.5% in those with no brain injury.
Veterans Health Administration
Dr. Lisa Brenner
“We had had pieces of these findings for a long time but to be able to lay out this longitudinal story over time is the part that’s new and important to really switch the focus to people’s whole lives and things that happen over time, both psychological and physical,” lead author Lisa Brenner, PhD, director of the Veterans Health Administration (VHA) Rocky Mountain Mental Illness Research Education and Clinical Center, Aurora, Colo., said in an interview.
“If we take that life-course view, it’s a very different way about thinking about conceptualizing exposures and conceptualizing risk and it’s a different way of thinking about treatment and prevention,” added Dr. Brenner, professor of physical medicine and rehabilitation, psychiatry, and neurology at the University of Colorado, Aurora. “I think that definitely applies to civilian populations.”
Researchers have long suspected that TBI and a higher rate of new mental illness and a shorter time to suicide are all somehow linked. But this study examined all three components longitudinally, in what is thought to be the largest and longest study on the topic to date, including more than 860,000 people who were followed for up to a decade.
Investigators studied health data from the Substance Use and Psychological Injury Combat Study database on 860,892 U.S. Army soldiers who returned from deployment in Iraq or Afghanistan between 2008 and 2014 and were 18-24 years old at the end of that deployment. They then examined new mental health diagnoses and suicide trends over time.
Nearly 109,000 (12.6%) experienced a TBI during deployment, and 2,695 had died by suicide through the end of 2018.
New-onset diagnoses of anxiety, mood disorders, posttraumatic stress disorder, alcohol use, and substance use disorder (SUD) after deployment were all more common in soldiers who experienced PTSD while serving compared with those with no history of TBI.
There was a 67.7% increase in mood disorders in participants with TBI compared with a 37.5% increase in those without TBI. The increase in new cases of alcohol use disorder was also greater in the TBI group (a 31.9% increase vs. a 10.3% increase).
But the sharpest difference was the increase in substance use disorder among those with TBI, which rose 100% compared with a 14.5% increase in solders with no history of TBI.
Sharp differences in time to suicide
Death by suicide was only slightly more common in those with TBI compared with those without (0.4% vs. 0.3%, respectively). But those with a brain injury committed suicide 21.3% sooner than did those without a head injury, after the researchers controlled for sex, age, race, ethnicity, and fiscal year of return from deployment.
Time to suicide was faster in those with a TBI and two or more new mental health diagnoses and fastest among those with TBI and a new SUD diagnosis, who took their own lives 62.8% faster than did those without a TBI.
The findings offer an important message to medical professionals in many different specialties, Dr. Brenner said.
“Folks in mental health probably have a lot of patients who have brain injury in their practice, and they don’t know it and that’s an important thing to know,” she said, adding that “neurologists should screen for depression and other mental health conditions and make sure those people have evidence-based treatments for those mental health conditions while they’re addressing the TBI-related symptoms.”
Applicable to civilians?
“The complex interplay between TBI, its potential effects on mental health, and risk of suicide remains a vexing focus of ongoing investigations and academic inquiry,” Ross Zafonte, DO, president of Spaulding Rehabilitation Hospital Network and professor and chair of physical medicine and rehabilitation at Harvard Medical School, Boston, and colleagues, wrote in an accompanying editorial.
The study builds on earlier work, they added, and praised the study’s longitudinal design and large cohort as key to the findings. The data on increased rates of new-onset substance use disorder, which was also associated with a faster time to suicide in the TBI group, were of particular interest.
“In this work, Brenner and colleagues identified substance use disorder as a key factor in faster time to suicide for active-duty service members with a history of TBI compared with those without TBI and theorized that a multiple stress or exposure burden may enhance risk,” they wrote. “This theory is reasonable and has been postulated among individuals with medical sequelae linked to TBI.”
However, the authors caution against applying these findings in military veterans to civilians.
“While this work is critical in the military population, caution should be given to avoid direct generalization to other populations, such as athletes, for whom the linkage to suicidal ideation is less understood,” they wrote.
The study was funded by National Institute of Mental Health and Office of the Director at National Institutes of Health. Dr. Brenner has received personal fees from Wolters Kluwer, Rand, American Psychological Association, and Oxford University Press and serves as a consultant to sports leagues via her university affiliation. Dr. Zafonte reported receiving royalties from Springer/Demos; serving as a member of the editorial boards of Journal of Neurotrauma and Frontiers in Neurology and scientific advisory boards of Myomo, Nanodiagnostics, Onecare.ai, and Kisbee; and evaluating patients in the MGH Brain and Body-TRUST Program, which is funded by the National Football League Players Association.
A version of this article first appeared on Medscape.com.
Among military veterans who die by suicide, those who experience a traumatic brain injury (TBI) during service take their lives 21% sooner after deployment than those without a TBI history, a new study shows.
Investigators also found that increases in new mental health diagnoses are significantly higher in soldiers with a history of TBI – in some cases, strikingly higher. For example, cases of substance use disorder rose by 100% among veterans with TBI compared to just 14.5% in those with no brain injury.
Veterans Health Administration
Dr. Lisa Brenner
“We had had pieces of these findings for a long time but to be able to lay out this longitudinal story over time is the part that’s new and important to really switch the focus to people’s whole lives and things that happen over time, both psychological and physical,” lead author Lisa Brenner, PhD, director of the Veterans Health Administration (VHA) Rocky Mountain Mental Illness Research Education and Clinical Center, Aurora, Colo., said in an interview.
“If we take that life-course view, it’s a very different way about thinking about conceptualizing exposures and conceptualizing risk and it’s a different way of thinking about treatment and prevention,” added Dr. Brenner, professor of physical medicine and rehabilitation, psychiatry, and neurology at the University of Colorado, Aurora. “I think that definitely applies to civilian populations.”
Researchers have long suspected that TBI and a higher rate of new mental illness and a shorter time to suicide are all somehow linked. But this study examined all three components longitudinally, in what is thought to be the largest and longest study on the topic to date, including more than 860,000 people who were followed for up to a decade.
Investigators studied health data from the Substance Use and Psychological Injury Combat Study database on 860,892 U.S. Army soldiers who returned from deployment in Iraq or Afghanistan between 2008 and 2014 and were 18-24 years old at the end of that deployment. They then examined new mental health diagnoses and suicide trends over time.
Nearly 109,000 (12.6%) experienced a TBI during deployment, and 2,695 had died by suicide through the end of 2018.
New-onset diagnoses of anxiety, mood disorders, posttraumatic stress disorder, alcohol use, and substance use disorder (SUD) after deployment were all more common in soldiers who experienced PTSD while serving compared with those with no history of TBI.
There was a 67.7% increase in mood disorders in participants with TBI compared with a 37.5% increase in those without TBI. The increase in new cases of alcohol use disorder was also greater in the TBI group (a 31.9% increase vs. a 10.3% increase).
But the sharpest difference was the increase in substance use disorder among those with TBI, which rose 100% compared with a 14.5% increase in solders with no history of TBI.
Sharp differences in time to suicide
Death by suicide was only slightly more common in those with TBI compared with those without (0.4% vs. 0.3%, respectively). But those with a brain injury committed suicide 21.3% sooner than did those without a head injury, after the researchers controlled for sex, age, race, ethnicity, and fiscal year of return from deployment.
Time to suicide was faster in those with a TBI and two or more new mental health diagnoses and fastest among those with TBI and a new SUD diagnosis, who took their own lives 62.8% faster than did those without a TBI.
The findings offer an important message to medical professionals in many different specialties, Dr. Brenner said.
“Folks in mental health probably have a lot of patients who have brain injury in their practice, and they don’t know it and that’s an important thing to know,” she said, adding that “neurologists should screen for depression and other mental health conditions and make sure those people have evidence-based treatments for those mental health conditions while they’re addressing the TBI-related symptoms.”
Applicable to civilians?
“The complex interplay between TBI, its potential effects on mental health, and risk of suicide remains a vexing focus of ongoing investigations and academic inquiry,” Ross Zafonte, DO, president of Spaulding Rehabilitation Hospital Network and professor and chair of physical medicine and rehabilitation at Harvard Medical School, Boston, and colleagues, wrote in an accompanying editorial.
The study builds on earlier work, they added, and praised the study’s longitudinal design and large cohort as key to the findings. The data on increased rates of new-onset substance use disorder, which was also associated with a faster time to suicide in the TBI group, were of particular interest.
“In this work, Brenner and colleagues identified substance use disorder as a key factor in faster time to suicide for active-duty service members with a history of TBI compared with those without TBI and theorized that a multiple stress or exposure burden may enhance risk,” they wrote. “This theory is reasonable and has been postulated among individuals with medical sequelae linked to TBI.”
However, the authors caution against applying these findings in military veterans to civilians.
“While this work is critical in the military population, caution should be given to avoid direct generalization to other populations, such as athletes, for whom the linkage to suicidal ideation is less understood,” they wrote.
The study was funded by National Institute of Mental Health and Office of the Director at National Institutes of Health. Dr. Brenner has received personal fees from Wolters Kluwer, Rand, American Psychological Association, and Oxford University Press and serves as a consultant to sports leagues via her university affiliation. Dr. Zafonte reported receiving royalties from Springer/Demos; serving as a member of the editorial boards of Journal of Neurotrauma and Frontiers in Neurology and scientific advisory boards of Myomo, Nanodiagnostics, Onecare.ai, and Kisbee; and evaluating patients in the MGH Brain and Body-TRUST Program, which is funded by the National Football League Players Association.
A version of this article first appeared on Medscape.com.
Among military veterans who die by suicide, those who experience a traumatic brain injury (TBI) during service take their lives 21% sooner after deployment than those without a TBI history, a new study shows.
Investigators also found that increases in new mental health diagnoses are significantly higher in soldiers with a history of TBI – in some cases, strikingly higher. For example, cases of substance use disorder rose by 100% among veterans with TBI compared to just 14.5% in those with no brain injury.
Veterans Health Administration
Dr. Lisa Brenner
“We had had pieces of these findings for a long time but to be able to lay out this longitudinal story over time is the part that’s new and important to really switch the focus to people’s whole lives and things that happen over time, both psychological and physical,” lead author Lisa Brenner, PhD, director of the Veterans Health Administration (VHA) Rocky Mountain Mental Illness Research Education and Clinical Center, Aurora, Colo., said in an interview.
“If we take that life-course view, it’s a very different way about thinking about conceptualizing exposures and conceptualizing risk and it’s a different way of thinking about treatment and prevention,” added Dr. Brenner, professor of physical medicine and rehabilitation, psychiatry, and neurology at the University of Colorado, Aurora. “I think that definitely applies to civilian populations.”
Researchers have long suspected that TBI and a higher rate of new mental illness and a shorter time to suicide are all somehow linked. But this study examined all three components longitudinally, in what is thought to be the largest and longest study on the topic to date, including more than 860,000 people who were followed for up to a decade.
Investigators studied health data from the Substance Use and Psychological Injury Combat Study database on 860,892 U.S. Army soldiers who returned from deployment in Iraq or Afghanistan between 2008 and 2014 and were 18-24 years old at the end of that deployment. They then examined new mental health diagnoses and suicide trends over time.
Nearly 109,000 (12.6%) experienced a TBI during deployment, and 2,695 had died by suicide through the end of 2018.
New-onset diagnoses of anxiety, mood disorders, posttraumatic stress disorder, alcohol use, and substance use disorder (SUD) after deployment were all more common in soldiers who experienced PTSD while serving compared with those with no history of TBI.
There was a 67.7% increase in mood disorders in participants with TBI compared with a 37.5% increase in those without TBI. The increase in new cases of alcohol use disorder was also greater in the TBI group (a 31.9% increase vs. a 10.3% increase).
But the sharpest difference was the increase in substance use disorder among those with TBI, which rose 100% compared with a 14.5% increase in solders with no history of TBI.
Sharp differences in time to suicide
Death by suicide was only slightly more common in those with TBI compared with those without (0.4% vs. 0.3%, respectively). But those with a brain injury committed suicide 21.3% sooner than did those without a head injury, after the researchers controlled for sex, age, race, ethnicity, and fiscal year of return from deployment.
Time to suicide was faster in those with a TBI and two or more new mental health diagnoses and fastest among those with TBI and a new SUD diagnosis, who took their own lives 62.8% faster than did those without a TBI.
The findings offer an important message to medical professionals in many different specialties, Dr. Brenner said.
“Folks in mental health probably have a lot of patients who have brain injury in their practice, and they don’t know it and that’s an important thing to know,” she said, adding that “neurologists should screen for depression and other mental health conditions and make sure those people have evidence-based treatments for those mental health conditions while they’re addressing the TBI-related symptoms.”
Applicable to civilians?
“The complex interplay between TBI, its potential effects on mental health, and risk of suicide remains a vexing focus of ongoing investigations and academic inquiry,” Ross Zafonte, DO, president of Spaulding Rehabilitation Hospital Network and professor and chair of physical medicine and rehabilitation at Harvard Medical School, Boston, and colleagues, wrote in an accompanying editorial.
The study builds on earlier work, they added, and praised the study’s longitudinal design and large cohort as key to the findings. The data on increased rates of new-onset substance use disorder, which was also associated with a faster time to suicide in the TBI group, were of particular interest.
“In this work, Brenner and colleagues identified substance use disorder as a key factor in faster time to suicide for active-duty service members with a history of TBI compared with those without TBI and theorized that a multiple stress or exposure burden may enhance risk,” they wrote. “This theory is reasonable and has been postulated among individuals with medical sequelae linked to TBI.”
However, the authors caution against applying these findings in military veterans to civilians.
“While this work is critical in the military population, caution should be given to avoid direct generalization to other populations, such as athletes, for whom the linkage to suicidal ideation is less understood,” they wrote.
The study was funded by National Institute of Mental Health and Office of the Director at National Institutes of Health. Dr. Brenner has received personal fees from Wolters Kluwer, Rand, American Psychological Association, and Oxford University Press and serves as a consultant to sports leagues via her university affiliation. Dr. Zafonte reported receiving royalties from Springer/Demos; serving as a member of the editorial boards of Journal of Neurotrauma and Frontiers in Neurology and scientific advisory boards of Myomo, Nanodiagnostics, Onecare.ai, and Kisbee; and evaluating patients in the MGH Brain and Body-TRUST Program, which is funded by the National Football League Players Association.
A version of this article first appeared on Medscape.com.
Presenting obesity as a chronic medical condition, rather than as a failure to eat less and move more, may improve self-esteem among patients with obesity and enhance their relationships with their doctors, a new study suggests.
In an online study, patients with obesity reported significantly less internalized weight bias and significantly enhanced perceptions of positive communication with their medical providers after watching a video of a doctor who framed obesity as a treatable medical condition, compared with a video of a doctor who emphasized willpower.
“Recent research has identified the dominant role that biology (both genetics as well as homeostatic, hedonic, and executive brain systems) and environment, rather than willpower, play in the development of obesity and the resistance to weight loss,” wrote study authors Sara English, a medical student, and Michael Vallis, MD, associate professor of family medicine, both at Dalhousie University, Halifax, N.S. “Yet the false narrative that ideal or goal weight can be achieved by eating less and moving more using willpower continues to dominate the public narrative.”
The public discussion generally places all responsibility for the health outcomes of obesity on the patient. As a result, patients with obesity face bias and stigma from the public and the health care system, wrote the authors.
This stigmatization contributes to increased mortality and morbidity by promoting maladaptive eating behaviors and stress. It also causes mistrust of health care professionals, which, in turn, leads to worse health outcomes and increased health care costs.
The 2020 Canadian clinical practice guidelines for obesity management in adults emphasize that obesity is complex and that nonbehavioral factors strongly influence it. They recommend that treatment focus on improving patient-centered health outcomes and address the root causes of obesity, instead of focusing on weight loss alone.
In the present study, Ms. English and Dr. Vallis evaluated how presenting obesity as a treatable medical condition affected participants’ internalized weight bias and their perceived relationship with their health care provider. They asked 61 patients with obesity (average age, 49 years; average body mass index, 41 kg/m2) to watch two videos, the first showing a doctor endorsing the traditional “eat less, move more approach,” and the second showing a doctor describing obesity as a chronic, treatable medical condition.
Nearly half (49.5%) of participants reported that their health care provider rarely or never discusses weight loss, and almost two-thirds of participants (64%) reported feeling stigmatized by their health care provider because of their weight at least some of the time.
After having watched each video, participants were asked to imagine that they were being treated by the corresponding doctor and to complete two measures: the Weight Bias Internalization Scale (WBIS), which measures the degree to which a respondent believes the negative stereotypes about obese people, and the Patient-Health Care Provider Communication Scale (PHCPCS), which assesses the quality of patient–health care provider communication.
Virtually all participants preferred the care provider in the video with the revised presentation of obesity. Only one preferred the traditional video. The video with the revised presentation was associated with significant reductions in internalized weight bias. Participants’ WBIS total score decreased from 4.49 to 3.36 (P < .001). The revised narrative video also had a positive effect on patients’ perception of their health care providers. The PHCPCS total score increased from 2.65 to 4.20 (P < .001).
A chronic disease
In a comment, Yoni Freedhoff, MD, associate professor of family medicine at the University of Ottawa, said: “If you’re asking me if it is a good idea to treat obesity like a chronic disease, the answer would be yes, we absolutely should. It is a chronic disease, and it shouldn’t have a treatment paradigm different from the other chronic diseases.” Dr. Freedhoff did not participate in the study.
“We certainly don’t blame patients for having other chronic conditions,” Dr. Freedhoff added. “We don’t have a narrative that, in order for them to qualify for medication or other treatment options, they have to audition for them by failing lifestyle approaches first. And yet, I’d say at least 85% of chronic noncommunicable diseases have lifestyle factors, but obesity is the only one where we consider that there is a necessity for these lifestyle changes, as if there have been studies demonstrating durable and reproducible outcomes for lifestyle in obesity. There have not.”
Telling patients and doctors that obesity is a chronic disease driven by biology, not a failure of willpower, is going to reduce stigma, “which is what this study was able to demonstrate to some degree,” Dr. Freedhoff said.
“What is more stigmatizing? Being told that if you just try hard enough, you’ll succeed, and if you don’t succeed, the corollary, of course, is that you did not try hard enough? Versus, you’ve got a medical condition where you’ve got biological drivers beyond your locus of control, affecting behaviors that, in turn, contribute to your adiposity? I’m pretty sure the second statement will have far less impact on a person’s internalized weight bias than what we’ve unfortunately been doing up until now with the focus on willpower,” Dr. Freedhoff said.
No funding for the study was reported. Ms. English and Dr. Vallis reported no relevant financial relationships. Dr. Freedhoff reported receiving clinical grants from Novo Nordisk.
A version of this article first appeared on Medscape.com.
Presenting obesity as a chronic medical condition, rather than as a failure to eat less and move more, may improve self-esteem among patients with obesity and enhance their relationships with their doctors, a new study suggests.
In an online study, patients with obesity reported significantly less internalized weight bias and significantly enhanced perceptions of positive communication with their medical providers after watching a video of a doctor who framed obesity as a treatable medical condition, compared with a video of a doctor who emphasized willpower.
“Recent research has identified the dominant role that biology (both genetics as well as homeostatic, hedonic, and executive brain systems) and environment, rather than willpower, play in the development of obesity and the resistance to weight loss,” wrote study authors Sara English, a medical student, and Michael Vallis, MD, associate professor of family medicine, both at Dalhousie University, Halifax, N.S. “Yet the false narrative that ideal or goal weight can be achieved by eating less and moving more using willpower continues to dominate the public narrative.”
The public discussion generally places all responsibility for the health outcomes of obesity on the patient. As a result, patients with obesity face bias and stigma from the public and the health care system, wrote the authors.
This stigmatization contributes to increased mortality and morbidity by promoting maladaptive eating behaviors and stress. It also causes mistrust of health care professionals, which, in turn, leads to worse health outcomes and increased health care costs.
The 2020 Canadian clinical practice guidelines for obesity management in adults emphasize that obesity is complex and that nonbehavioral factors strongly influence it. They recommend that treatment focus on improving patient-centered health outcomes and address the root causes of obesity, instead of focusing on weight loss alone.
In the present study, Ms. English and Dr. Vallis evaluated how presenting obesity as a treatable medical condition affected participants’ internalized weight bias and their perceived relationship with their health care provider. They asked 61 patients with obesity (average age, 49 years; average body mass index, 41 kg/m2) to watch two videos, the first showing a doctor endorsing the traditional “eat less, move more approach,” and the second showing a doctor describing obesity as a chronic, treatable medical condition.
Nearly half (49.5%) of participants reported that their health care provider rarely or never discusses weight loss, and almost two-thirds of participants (64%) reported feeling stigmatized by their health care provider because of their weight at least some of the time.
After having watched each video, participants were asked to imagine that they were being treated by the corresponding doctor and to complete two measures: the Weight Bias Internalization Scale (WBIS), which measures the degree to which a respondent believes the negative stereotypes about obese people, and the Patient-Health Care Provider Communication Scale (PHCPCS), which assesses the quality of patient–health care provider communication.
Virtually all participants preferred the care provider in the video with the revised presentation of obesity. Only one preferred the traditional video. The video with the revised presentation was associated with significant reductions in internalized weight bias. Participants’ WBIS total score decreased from 4.49 to 3.36 (P < .001). The revised narrative video also had a positive effect on patients’ perception of their health care providers. The PHCPCS total score increased from 2.65 to 4.20 (P < .001).
A chronic disease
In a comment, Yoni Freedhoff, MD, associate professor of family medicine at the University of Ottawa, said: “If you’re asking me if it is a good idea to treat obesity like a chronic disease, the answer would be yes, we absolutely should. It is a chronic disease, and it shouldn’t have a treatment paradigm different from the other chronic diseases.” Dr. Freedhoff did not participate in the study.
“We certainly don’t blame patients for having other chronic conditions,” Dr. Freedhoff added. “We don’t have a narrative that, in order for them to qualify for medication or other treatment options, they have to audition for them by failing lifestyle approaches first. And yet, I’d say at least 85% of chronic noncommunicable diseases have lifestyle factors, but obesity is the only one where we consider that there is a necessity for these lifestyle changes, as if there have been studies demonstrating durable and reproducible outcomes for lifestyle in obesity. There have not.”
Telling patients and doctors that obesity is a chronic disease driven by biology, not a failure of willpower, is going to reduce stigma, “which is what this study was able to demonstrate to some degree,” Dr. Freedhoff said.
“What is more stigmatizing? Being told that if you just try hard enough, you’ll succeed, and if you don’t succeed, the corollary, of course, is that you did not try hard enough? Versus, you’ve got a medical condition where you’ve got biological drivers beyond your locus of control, affecting behaviors that, in turn, contribute to your adiposity? I’m pretty sure the second statement will have far less impact on a person’s internalized weight bias than what we’ve unfortunately been doing up until now with the focus on willpower,” Dr. Freedhoff said.
No funding for the study was reported. Ms. English and Dr. Vallis reported no relevant financial relationships. Dr. Freedhoff reported receiving clinical grants from Novo Nordisk.
A version of this article first appeared on Medscape.com.
Presenting obesity as a chronic medical condition, rather than as a failure to eat less and move more, may improve self-esteem among patients with obesity and enhance their relationships with their doctors, a new study suggests.
In an online study, patients with obesity reported significantly less internalized weight bias and significantly enhanced perceptions of positive communication with their medical providers after watching a video of a doctor who framed obesity as a treatable medical condition, compared with a video of a doctor who emphasized willpower.
“Recent research has identified the dominant role that biology (both genetics as well as homeostatic, hedonic, and executive brain systems) and environment, rather than willpower, play in the development of obesity and the resistance to weight loss,” wrote study authors Sara English, a medical student, and Michael Vallis, MD, associate professor of family medicine, both at Dalhousie University, Halifax, N.S. “Yet the false narrative that ideal or goal weight can be achieved by eating less and moving more using willpower continues to dominate the public narrative.”
The public discussion generally places all responsibility for the health outcomes of obesity on the patient. As a result, patients with obesity face bias and stigma from the public and the health care system, wrote the authors.
This stigmatization contributes to increased mortality and morbidity by promoting maladaptive eating behaviors and stress. It also causes mistrust of health care professionals, which, in turn, leads to worse health outcomes and increased health care costs.
The 2020 Canadian clinical practice guidelines for obesity management in adults emphasize that obesity is complex and that nonbehavioral factors strongly influence it. They recommend that treatment focus on improving patient-centered health outcomes and address the root causes of obesity, instead of focusing on weight loss alone.
In the present study, Ms. English and Dr. Vallis evaluated how presenting obesity as a treatable medical condition affected participants’ internalized weight bias and their perceived relationship with their health care provider. They asked 61 patients with obesity (average age, 49 years; average body mass index, 41 kg/m2) to watch two videos, the first showing a doctor endorsing the traditional “eat less, move more approach,” and the second showing a doctor describing obesity as a chronic, treatable medical condition.
Nearly half (49.5%) of participants reported that their health care provider rarely or never discusses weight loss, and almost two-thirds of participants (64%) reported feeling stigmatized by their health care provider because of their weight at least some of the time.
After having watched each video, participants were asked to imagine that they were being treated by the corresponding doctor and to complete two measures: the Weight Bias Internalization Scale (WBIS), which measures the degree to which a respondent believes the negative stereotypes about obese people, and the Patient-Health Care Provider Communication Scale (PHCPCS), which assesses the quality of patient–health care provider communication.
Virtually all participants preferred the care provider in the video with the revised presentation of obesity. Only one preferred the traditional video. The video with the revised presentation was associated with significant reductions in internalized weight bias. Participants’ WBIS total score decreased from 4.49 to 3.36 (P < .001). The revised narrative video also had a positive effect on patients’ perception of their health care providers. The PHCPCS total score increased from 2.65 to 4.20 (P < .001).
A chronic disease
In a comment, Yoni Freedhoff, MD, associate professor of family medicine at the University of Ottawa, said: “If you’re asking me if it is a good idea to treat obesity like a chronic disease, the answer would be yes, we absolutely should. It is a chronic disease, and it shouldn’t have a treatment paradigm different from the other chronic diseases.” Dr. Freedhoff did not participate in the study.
“We certainly don’t blame patients for having other chronic conditions,” Dr. Freedhoff added. “We don’t have a narrative that, in order for them to qualify for medication or other treatment options, they have to audition for them by failing lifestyle approaches first. And yet, I’d say at least 85% of chronic noncommunicable diseases have lifestyle factors, but obesity is the only one where we consider that there is a necessity for these lifestyle changes, as if there have been studies demonstrating durable and reproducible outcomes for lifestyle in obesity. There have not.”
Telling patients and doctors that obesity is a chronic disease driven by biology, not a failure of willpower, is going to reduce stigma, “which is what this study was able to demonstrate to some degree,” Dr. Freedhoff said.
“What is more stigmatizing? Being told that if you just try hard enough, you’ll succeed, and if you don’t succeed, the corollary, of course, is that you did not try hard enough? Versus, you’ve got a medical condition where you’ve got biological drivers beyond your locus of control, affecting behaviors that, in turn, contribute to your adiposity? I’m pretty sure the second statement will have far less impact on a person’s internalized weight bias than what we’ve unfortunately been doing up until now with the focus on willpower,” Dr. Freedhoff said.
No funding for the study was reported. Ms. English and Dr. Vallis reported no relevant financial relationships. Dr. Freedhoff reported receiving clinical grants from Novo Nordisk.
A version of this article first appeared on Medscape.com.
Yeung LK, Alschuler DM, Wall M, et al. Multivitamin supplementation improves memory in older adults: a randomized clinical trial. Am J Clin Nutrition. 2023;118:273-282. doi:10.1016/j.ajcnut.2023.05.011.
EXPERT COMMENTARY
Preservation of function, both physical and cognitive, is key to long-term health and well-being. Age-related loss of function drives millions of people to spend an enormous amount of money each year on unregulated therapies—vitamins, supplements, infusions, hormones, and “natural” products—all toward the promise of improvement or preservation of physical strength, sexual function, and maintenance of lean body mass and cognitive abilities. Yeung and colleagues set out to determine whether the daily use of a multivitamin/mineral supplement (Centrum Silver) would impact memory in older adults.1
PHOTO: KLAVDIYAV/SHUTTERSTOCK
Details of the study
The COSMOS-Web study was designed to test the authors’ primary hypothesis that daily dietary flavanols would improve memory over 1 year.1 This study was embedded within the larger COSMOS (COcoa Supplement and Multivitamin Outcomes Study) trial, in which 21,442 people were recruited to assess the impact of flavanols and multivitamin supplements on cardiovascular and cancer outcomes.
Results of another ancillary study, the COSMOS-Mind trial (n = 2,262, average age 73, 60% female), reported no improvement with flavanols compared with placebo on a battery of tests of cognitive function administered by phone. In COSMOS-Mind, however, it was concluded that a daily multivitamin/mineral supplement improved the composite score of cognitive tests compared with placebo, particularly in participants with a history of cardiovascular disease.2
The COSMOS-Web trial recruited an additional cohort within the larger COSMOS trial from 2016–2017 (n = 3,562, average age 71, 67% female) to participate in this study specifically geared to assess memory, using the web-based ModRey test (a test of memory validated for use in a nonimpaired population). To qualify for enrollment, participants had to have access to an internet-connected computer. They were randomly assigned in a 2 x 2 study design to receive a daily multivitamin supplement or placebo; each of these cohorts was further divided into a flavanol supplementation or a placebo group. Analysis of the data showed no association between flavanol use and performance on any of the measures of memory or cognitive function.3
The COSMOS-Web trial assessed episodic recall, a function of hippocampus-mediated cognition that is particularly vulnerable to the effects of aging as demonstrated previously by neuroimaging and neuropsychological studies. The authors deployed a battery of 3 tests via a web platform for patients to complete online and independently.
The prespecified primary outcome was performance on episodic recall as measured by the ModRey test after 1 year of supplementation with multivitamins versus placebo. The ModRey test presents a series of 20 words at 3-second intervals to participants. At the conclusion of the last word, participants were asked to recall as many words as they could; after completing the 2 additional tasks, participants were asked again to recall the words. A secondary outcome of this test is the ratio of delayed to immediate recall.
Two additional tests were administered to assess cognitive performance related to different brain regions, the ModBent test (assessing novel object recognition) and the Flanker task (a measure of executive function). There was a placebo run-in phase during which participants’ adherence to daily supplement intake was ascertained. Participants were excluded if they demonstrated less than 75% adherence to study pills during the run-in placebo phase. The cognitive tasks were presented at study initiation and at yearly intervals for 3 years. The authors chose to use the results at 1 year as their primary outcome to assess the impact of supplementation during the period when adherence would be highest.
Results.At baseline, the placebo cohort recalled 7.2 words of 20 compared with 7.1 in the supplement group. In both groups there was a practice effect, with improvement in scores in the placebo group to 7.65 words and in the multivitamin group to 7.81 words. The improvement from baseline was statistically significantly better (0.71 words) in the multivitamin cohort than in the placebo group (0.45 words). There was no improvement in either group in the ModRey memory retention test (ability to recall the words after 15 minutes) or in the ModBent or Flanker tests. At 3 years of treatment, the placebo group improved by 0.92 words (SD, 3.22) whereas the multivitamin group improved by 1.13 words (SD, 3.39). These changes remained statistically significant.
The group with cardiovascular disease had lower baseline performance on the ModRey test. With supplementation, however, the improvement in this cohort was significantly greater than in those without cardiovascular disease at 1 year. The authors acknowledged that the changes were small and may not have been noticeable to the individuals, but they argued that even small changes as demonstrated in this study can have large health benefits at a population level.
The results of the COSMOS-Web trial corroborate the findings of the COSMOS-Mind study with respect to the benefits of multivitamin/mineral supplementation on cognitive test performance, particularly in a population with preexisting cardiovascular disease. The tests used across the 2 studies were different, which lends greater reliability to the findings.
Study strengths and limitations
A major strength of this study is its careful, rigorous design as a double-blind, placebo-controlled trial in a large patient population. Great care was devoted to ensuring study medication adherence. Another strength is that the cognitive tests chosen for the COSMOS-Web trial have been validated in cognitively normal populations, not those already impaired.
A limitation, however, is in the demographics of the study. The patient population was overwhelmingly White (93%), 67% were female, and they were well educated (94.8% having completed some college or beyond). Their baseline health was good; only 4.7% had a history of cardiovascular disease. Although generalizability of the study results from this population may be concerning,relative benefits of supplementation in this healthy, generally well-nourished and educated group may be lower than might be expected in a more nutritionally and educationally challenged population.
Finally, the difference between the placebo and active supplementation groups was small. Whether this less-than-1-word difference in immediate memory recall is noticeable by a patient is questionable. Both groups improved in their test performance over time—a consequence of serial cognitive tests of any kind. Although the authors calculated that the difference in recall translates to a 3-year reduction in age-related memory decline, it is hard to reconcile that with the fact that both groups actually improved over the 3 years of the study. ●
Acknowledgement
The author would like to thank JoAnn Manson, MD, DrPH, NCMP, for her assistance in evaluating the study.
WHAT THIS EVIDENCE MEANS FOR PRACTICE
In this well-designed, randomized controlled trial by Yeung and colleagues, multivitamin/mineral supplementation improved performance on a test of immediate episodic memory at 1, 2, and 3 years compared with placebo. Given the simplicity and safety of this intervention, even with a small effect size, it makes sense to advise older patients that daily multivitamin use provides micronutrients and vitamins that may be absent in the diet or poorly absorbed by older adults. Whether this highly specific improvement in a test of hippocampal function translates into overall cognitive performance with aging remains a question.
BARBARA LEVY, MD
References
Yeung LK, Alschuler DM, Wall M, et al. Multivitamin supplementation improves memory in older adults: a randomized clinical trial. Am J Clin Nutrition. 2023;118:273282. doi:10.1016/j.ajcnut.2023.05.011.
Baker LD, Manson JE, Rapp SR, et al. Effects of cocoa extract and a multivitamin on cognitive function: a randomized clinical trial. Alzheimers Dement. 2023;19:1308-1319. doi:10.1002/alz.12767.
Brickman AM, Yeung LK, Alshuler DM, et al. Dietary flavanols restore hippocampal-dependent memory in older adults with lower diet quality and lower habitual flavanol consumption. Proc Natl Acad Sci USA. 2023:120:e2216932120. doi:10.1073/ pnas.2216932120.
Barbara Levy, MD, is Clinical Professor of Obstetrics and Gynecology, George Washington University School of Medicine and Health Sciences, Washington, DC, and Voluntary Clinical Professor of Obstetrics, Gynecology and Reproductive Sciences, UC San Diego School of Medicine. She serves on the OBG Management Board of Editors.
The author reports no financial relationships relevant to this article.
Barbara Levy, MD, is Clinical Professor of Obstetrics and Gynecology, George Washington University School of Medicine and Health Sciences, Washington, DC, and Voluntary Clinical Professor of Obstetrics, Gynecology and Reproductive Sciences, UC San Diego School of Medicine. She serves on the OBG Management Board of Editors.
The author reports no financial relationships relevant to this article.
Author and Disclosure Information
Barbara Levy, MD, is Clinical Professor of Obstetrics and Gynecology, George Washington University School of Medicine and Health Sciences, Washington, DC, and Voluntary Clinical Professor of Obstetrics, Gynecology and Reproductive Sciences, UC San Diego School of Medicine. She serves on the OBG Management Board of Editors.
The author reports no financial relationships relevant to this article.
Yeung LK, Alschuler DM, Wall M, et al. Multivitamin supplementation improves memory in older adults: a randomized clinical trial. Am J Clin Nutrition. 2023;118:273-282. doi:10.1016/j.ajcnut.2023.05.011.
EXPERT COMMENTARY
Preservation of function, both physical and cognitive, is key to long-term health and well-being. Age-related loss of function drives millions of people to spend an enormous amount of money each year on unregulated therapies—vitamins, supplements, infusions, hormones, and “natural” products—all toward the promise of improvement or preservation of physical strength, sexual function, and maintenance of lean body mass and cognitive abilities. Yeung and colleagues set out to determine whether the daily use of a multivitamin/mineral supplement (Centrum Silver) would impact memory in older adults.1
PHOTO: KLAVDIYAV/SHUTTERSTOCK
Details of the study
The COSMOS-Web study was designed to test the authors’ primary hypothesis that daily dietary flavanols would improve memory over 1 year.1 This study was embedded within the larger COSMOS (COcoa Supplement and Multivitamin Outcomes Study) trial, in which 21,442 people were recruited to assess the impact of flavanols and multivitamin supplements on cardiovascular and cancer outcomes.
Results of another ancillary study, the COSMOS-Mind trial (n = 2,262, average age 73, 60% female), reported no improvement with flavanols compared with placebo on a battery of tests of cognitive function administered by phone. In COSMOS-Mind, however, it was concluded that a daily multivitamin/mineral supplement improved the composite score of cognitive tests compared with placebo, particularly in participants with a history of cardiovascular disease.2
The COSMOS-Web trial recruited an additional cohort within the larger COSMOS trial from 2016–2017 (n = 3,562, average age 71, 67% female) to participate in this study specifically geared to assess memory, using the web-based ModRey test (a test of memory validated for use in a nonimpaired population). To qualify for enrollment, participants had to have access to an internet-connected computer. They were randomly assigned in a 2 x 2 study design to receive a daily multivitamin supplement or placebo; each of these cohorts was further divided into a flavanol supplementation or a placebo group. Analysis of the data showed no association between flavanol use and performance on any of the measures of memory or cognitive function.3
The COSMOS-Web trial assessed episodic recall, a function of hippocampus-mediated cognition that is particularly vulnerable to the effects of aging as demonstrated previously by neuroimaging and neuropsychological studies. The authors deployed a battery of 3 tests via a web platform for patients to complete online and independently.
The prespecified primary outcome was performance on episodic recall as measured by the ModRey test after 1 year of supplementation with multivitamins versus placebo. The ModRey test presents a series of 20 words at 3-second intervals to participants. At the conclusion of the last word, participants were asked to recall as many words as they could; after completing the 2 additional tasks, participants were asked again to recall the words. A secondary outcome of this test is the ratio of delayed to immediate recall.
Two additional tests were administered to assess cognitive performance related to different brain regions, the ModBent test (assessing novel object recognition) and the Flanker task (a measure of executive function). There was a placebo run-in phase during which participants’ adherence to daily supplement intake was ascertained. Participants were excluded if they demonstrated less than 75% adherence to study pills during the run-in placebo phase. The cognitive tasks were presented at study initiation and at yearly intervals for 3 years. The authors chose to use the results at 1 year as their primary outcome to assess the impact of supplementation during the period when adherence would be highest.
Results.At baseline, the placebo cohort recalled 7.2 words of 20 compared with 7.1 in the supplement group. In both groups there was a practice effect, with improvement in scores in the placebo group to 7.65 words and in the multivitamin group to 7.81 words. The improvement from baseline was statistically significantly better (0.71 words) in the multivitamin cohort than in the placebo group (0.45 words). There was no improvement in either group in the ModRey memory retention test (ability to recall the words after 15 minutes) or in the ModBent or Flanker tests. At 3 years of treatment, the placebo group improved by 0.92 words (SD, 3.22) whereas the multivitamin group improved by 1.13 words (SD, 3.39). These changes remained statistically significant.
The group with cardiovascular disease had lower baseline performance on the ModRey test. With supplementation, however, the improvement in this cohort was significantly greater than in those without cardiovascular disease at 1 year. The authors acknowledged that the changes were small and may not have been noticeable to the individuals, but they argued that even small changes as demonstrated in this study can have large health benefits at a population level.
The results of the COSMOS-Web trial corroborate the findings of the COSMOS-Mind study with respect to the benefits of multivitamin/mineral supplementation on cognitive test performance, particularly in a population with preexisting cardiovascular disease. The tests used across the 2 studies were different, which lends greater reliability to the findings.
Study strengths and limitations
A major strength of this study is its careful, rigorous design as a double-blind, placebo-controlled trial in a large patient population. Great care was devoted to ensuring study medication adherence. Another strength is that the cognitive tests chosen for the COSMOS-Web trial have been validated in cognitively normal populations, not those already impaired.
A limitation, however, is in the demographics of the study. The patient population was overwhelmingly White (93%), 67% were female, and they were well educated (94.8% having completed some college or beyond). Their baseline health was good; only 4.7% had a history of cardiovascular disease. Although generalizability of the study results from this population may be concerning,relative benefits of supplementation in this healthy, generally well-nourished and educated group may be lower than might be expected in a more nutritionally and educationally challenged population.
Finally, the difference between the placebo and active supplementation groups was small. Whether this less-than-1-word difference in immediate memory recall is noticeable by a patient is questionable. Both groups improved in their test performance over time—a consequence of serial cognitive tests of any kind. Although the authors calculated that the difference in recall translates to a 3-year reduction in age-related memory decline, it is hard to reconcile that with the fact that both groups actually improved over the 3 years of the study. ●
Acknowledgement
The author would like to thank JoAnn Manson, MD, DrPH, NCMP, for her assistance in evaluating the study.
WHAT THIS EVIDENCE MEANS FOR PRACTICE
In this well-designed, randomized controlled trial by Yeung and colleagues, multivitamin/mineral supplementation improved performance on a test of immediate episodic memory at 1, 2, and 3 years compared with placebo. Given the simplicity and safety of this intervention, even with a small effect size, it makes sense to advise older patients that daily multivitamin use provides micronutrients and vitamins that may be absent in the diet or poorly absorbed by older adults. Whether this highly specific improvement in a test of hippocampal function translates into overall cognitive performance with aging remains a question.
BARBARA LEVY, MD
Yeung LK, Alschuler DM, Wall M, et al. Multivitamin supplementation improves memory in older adults: a randomized clinical trial. Am J Clin Nutrition. 2023;118:273-282. doi:10.1016/j.ajcnut.2023.05.011.
EXPERT COMMENTARY
Preservation of function, both physical and cognitive, is key to long-term health and well-being. Age-related loss of function drives millions of people to spend an enormous amount of money each year on unregulated therapies—vitamins, supplements, infusions, hormones, and “natural” products—all toward the promise of improvement or preservation of physical strength, sexual function, and maintenance of lean body mass and cognitive abilities. Yeung and colleagues set out to determine whether the daily use of a multivitamin/mineral supplement (Centrum Silver) would impact memory in older adults.1
PHOTO: KLAVDIYAV/SHUTTERSTOCK
Details of the study
The COSMOS-Web study was designed to test the authors’ primary hypothesis that daily dietary flavanols would improve memory over 1 year.1 This study was embedded within the larger COSMOS (COcoa Supplement and Multivitamin Outcomes Study) trial, in which 21,442 people were recruited to assess the impact of flavanols and multivitamin supplements on cardiovascular and cancer outcomes.
Results of another ancillary study, the COSMOS-Mind trial (n = 2,262, average age 73, 60% female), reported no improvement with flavanols compared with placebo on a battery of tests of cognitive function administered by phone. In COSMOS-Mind, however, it was concluded that a daily multivitamin/mineral supplement improved the composite score of cognitive tests compared with placebo, particularly in participants with a history of cardiovascular disease.2
The COSMOS-Web trial recruited an additional cohort within the larger COSMOS trial from 2016–2017 (n = 3,562, average age 71, 67% female) to participate in this study specifically geared to assess memory, using the web-based ModRey test (a test of memory validated for use in a nonimpaired population). To qualify for enrollment, participants had to have access to an internet-connected computer. They were randomly assigned in a 2 x 2 study design to receive a daily multivitamin supplement or placebo; each of these cohorts was further divided into a flavanol supplementation or a placebo group. Analysis of the data showed no association between flavanol use and performance on any of the measures of memory or cognitive function.3
The COSMOS-Web trial assessed episodic recall, a function of hippocampus-mediated cognition that is particularly vulnerable to the effects of aging as demonstrated previously by neuroimaging and neuropsychological studies. The authors deployed a battery of 3 tests via a web platform for patients to complete online and independently.
The prespecified primary outcome was performance on episodic recall as measured by the ModRey test after 1 year of supplementation with multivitamins versus placebo. The ModRey test presents a series of 20 words at 3-second intervals to participants. At the conclusion of the last word, participants were asked to recall as many words as they could; after completing the 2 additional tasks, participants were asked again to recall the words. A secondary outcome of this test is the ratio of delayed to immediate recall.
Two additional tests were administered to assess cognitive performance related to different brain regions, the ModBent test (assessing novel object recognition) and the Flanker task (a measure of executive function). There was a placebo run-in phase during which participants’ adherence to daily supplement intake was ascertained. Participants were excluded if they demonstrated less than 75% adherence to study pills during the run-in placebo phase. The cognitive tasks were presented at study initiation and at yearly intervals for 3 years. The authors chose to use the results at 1 year as their primary outcome to assess the impact of supplementation during the period when adherence would be highest.
Results.At baseline, the placebo cohort recalled 7.2 words of 20 compared with 7.1 in the supplement group. In both groups there was a practice effect, with improvement in scores in the placebo group to 7.65 words and in the multivitamin group to 7.81 words. The improvement from baseline was statistically significantly better (0.71 words) in the multivitamin cohort than in the placebo group (0.45 words). There was no improvement in either group in the ModRey memory retention test (ability to recall the words after 15 minutes) or in the ModBent or Flanker tests. At 3 years of treatment, the placebo group improved by 0.92 words (SD, 3.22) whereas the multivitamin group improved by 1.13 words (SD, 3.39). These changes remained statistically significant.
The group with cardiovascular disease had lower baseline performance on the ModRey test. With supplementation, however, the improvement in this cohort was significantly greater than in those without cardiovascular disease at 1 year. The authors acknowledged that the changes were small and may not have been noticeable to the individuals, but they argued that even small changes as demonstrated in this study can have large health benefits at a population level.
The results of the COSMOS-Web trial corroborate the findings of the COSMOS-Mind study with respect to the benefits of multivitamin/mineral supplementation on cognitive test performance, particularly in a population with preexisting cardiovascular disease. The tests used across the 2 studies were different, which lends greater reliability to the findings.
Study strengths and limitations
A major strength of this study is its careful, rigorous design as a double-blind, placebo-controlled trial in a large patient population. Great care was devoted to ensuring study medication adherence. Another strength is that the cognitive tests chosen for the COSMOS-Web trial have been validated in cognitively normal populations, not those already impaired.
A limitation, however, is in the demographics of the study. The patient population was overwhelmingly White (93%), 67% were female, and they were well educated (94.8% having completed some college or beyond). Their baseline health was good; only 4.7% had a history of cardiovascular disease. Although generalizability of the study results from this population may be concerning,relative benefits of supplementation in this healthy, generally well-nourished and educated group may be lower than might be expected in a more nutritionally and educationally challenged population.
Finally, the difference between the placebo and active supplementation groups was small. Whether this less-than-1-word difference in immediate memory recall is noticeable by a patient is questionable. Both groups improved in their test performance over time—a consequence of serial cognitive tests of any kind. Although the authors calculated that the difference in recall translates to a 3-year reduction in age-related memory decline, it is hard to reconcile that with the fact that both groups actually improved over the 3 years of the study. ●
Acknowledgement
The author would like to thank JoAnn Manson, MD, DrPH, NCMP, for her assistance in evaluating the study.
WHAT THIS EVIDENCE MEANS FOR PRACTICE
In this well-designed, randomized controlled trial by Yeung and colleagues, multivitamin/mineral supplementation improved performance on a test of immediate episodic memory at 1, 2, and 3 years compared with placebo. Given the simplicity and safety of this intervention, even with a small effect size, it makes sense to advise older patients that daily multivitamin use provides micronutrients and vitamins that may be absent in the diet or poorly absorbed by older adults. Whether this highly specific improvement in a test of hippocampal function translates into overall cognitive performance with aging remains a question.
BARBARA LEVY, MD
References
Yeung LK, Alschuler DM, Wall M, et al. Multivitamin supplementation improves memory in older adults: a randomized clinical trial. Am J Clin Nutrition. 2023;118:273282. doi:10.1016/j.ajcnut.2023.05.011.
Baker LD, Manson JE, Rapp SR, et al. Effects of cocoa extract and a multivitamin on cognitive function: a randomized clinical trial. Alzheimers Dement. 2023;19:1308-1319. doi:10.1002/alz.12767.
Brickman AM, Yeung LK, Alshuler DM, et al. Dietary flavanols restore hippocampal-dependent memory in older adults with lower diet quality and lower habitual flavanol consumption. Proc Natl Acad Sci USA. 2023:120:e2216932120. doi:10.1073/ pnas.2216932120.
References
Yeung LK, Alschuler DM, Wall M, et al. Multivitamin supplementation improves memory in older adults: a randomized clinical trial. Am J Clin Nutrition. 2023;118:273282. doi:10.1016/j.ajcnut.2023.05.011.
Baker LD, Manson JE, Rapp SR, et al. Effects of cocoa extract and a multivitamin on cognitive function: a randomized clinical trial. Alzheimers Dement. 2023;19:1308-1319. doi:10.1002/alz.12767.
Brickman AM, Yeung LK, Alshuler DM, et al. Dietary flavanols restore hippocampal-dependent memory in older adults with lower diet quality and lower habitual flavanol consumption. Proc Natl Acad Sci USA. 2023:120:e2216932120. doi:10.1073/ pnas.2216932120.
Given the patient's diagnosis of stage IV MCL, the presentation of diffuse skin lesions, and the histopathologic and immunophenotyping results of those lesions, this patient is diagnosed with secondary cutaneous MCL. The hematologist-oncologist discusses the findings with the patient and presents potential next steps and treatment options.
MCL is a type of B-cell neoplasm that, with advancements in the understanding of non-Hodgkin lymphoma (NHL) in the past 30 years, has been defined as its own clinicopathologic entity by the Revised European-American Lymphoma and World Health Organization classifications. Up to 10% of all NHLs are MCL. Clinical presentation includes advanced disease with B symptoms (eg, night sweats, fever, weight loss), generalized lymphadenopathy, abdominal distention associated with hepatosplenomegaly, and fatigue. Skin manifestations are not as common as other extranodal manifestations. Primary cutaneous MCL occurs in up to 6% of patients with MCL; secondary cutaneous involvement is slightly more common, occurring in 17% of patients with MCL. Secondary cutaneous MCL usually presents in late-stage disease. Men are more likely to present with MCL than are women by a ratio of 3:1. Median age at presentation is 67 years.
Diagnosing MCL is a multipronged approach. Physical examination may reveal lymphadenopathy and hepatosplenomegaly. Lymph node biopsy and aspiration with immunophenotyping in MCL reveals monoclonal B cells expressing surface immunoglobulin (Ig), IgM, or IgD, that are characteristically CD5+ and pan B-cell antigen–positive (eg, CD19, CD20, CD22) but lack expression of CD10 and CD23 and overexpress cyclin D1. Bone marrow aspirate/biopsy are used more for staging than for diagnosis. Blood studies, including anemia and cytopenias secondary to bone marrow infiltration (with up to 40% of cases showing lymphocytosis > 4000/μL), abnormal liver function tests, and a negative Coombs test also help diagnose MCL. Secondary cutaneous MCL is diagnosed on the basis of an MCL diagnosis along with diffuse infiltration of the skin, with multiple erythematous papules and nodules coalescing to form plaques; skin biopsy and immunohistopathology showing monotonous proliferation of small- to medium-sized lymphoid cells with scant cytoplasm; irregular cleaved nuclei with coarse chromatin; and inconspicuous nucleoli as well as a spared papillary dermis.
Pathogenesis of MCL involves disordered lymphoproliferation in a subset of naive pregerminal center cells in primary follicles or in the mantle region of secondary follicles. Most cases are linked with translocation of chromosome 14 and 11, which induces overexpression of protein cyclin D1. Viral infection (Epstein-Barr virus, HIV, human T-lymphotropic virus type 1, human herpes virus 6), environmental factors, and primary and secondary immunodeficiency are also associated with the development of NHL.
Patient education should include detailed information about clinical trials, available treatment options, and associated adverse events as well as psychosocial and nutrition counseling.
Chemoimmunotherapy is standard initial treatment for MCL, but relapse is expected. Chemotherapy-free regimens with biologic targets, which were once used in second-line treatment, have increasingly become an important first-line treatment given their efficacy in the relapsed/refractory setting. Chimeric antigen receptor T-cell therapy is also a second-line treatment option. In patients with MCL and a TP53 mutation, clinical trial participation is encouraged because of poor prognosis.
Timothy J. Voorhees, MD, MSCR, Assistant Professor of Internal Medicine - Clinical, Division of Hematology, The Ohio State University James Comprehensive Cancer Center, Columbus, OH.
Timothy J. Voorhees, MD, MSCR, has disclosed the following relevant financial relationships: Received research grants from: AstraZeneca; Morphosys; Incyte; Recordati.
Image Quizzes are fictional or fictionalized clinical scenarios intended to provide evidence-based educational takeaways.
Given the patient's diagnosis of stage IV MCL, the presentation of diffuse skin lesions, and the histopathologic and immunophenotyping results of those lesions, this patient is diagnosed with secondary cutaneous MCL. The hematologist-oncologist discusses the findings with the patient and presents potential next steps and treatment options.
MCL is a type of B-cell neoplasm that, with advancements in the understanding of non-Hodgkin lymphoma (NHL) in the past 30 years, has been defined as its own clinicopathologic entity by the Revised European-American Lymphoma and World Health Organization classifications. Up to 10% of all NHLs are MCL. Clinical presentation includes advanced disease with B symptoms (eg, night sweats, fever, weight loss), generalized lymphadenopathy, abdominal distention associated with hepatosplenomegaly, and fatigue. Skin manifestations are not as common as other extranodal manifestations. Primary cutaneous MCL occurs in up to 6% of patients with MCL; secondary cutaneous involvement is slightly more common, occurring in 17% of patients with MCL. Secondary cutaneous MCL usually presents in late-stage disease. Men are more likely to present with MCL than are women by a ratio of 3:1. Median age at presentation is 67 years.
Diagnosing MCL is a multipronged approach. Physical examination may reveal lymphadenopathy and hepatosplenomegaly. Lymph node biopsy and aspiration with immunophenotyping in MCL reveals monoclonal B cells expressing surface immunoglobulin (Ig), IgM, or IgD, that are characteristically CD5+ and pan B-cell antigen–positive (eg, CD19, CD20, CD22) but lack expression of CD10 and CD23 and overexpress cyclin D1. Bone marrow aspirate/biopsy are used more for staging than for diagnosis. Blood studies, including anemia and cytopenias secondary to bone marrow infiltration (with up to 40% of cases showing lymphocytosis > 4000/μL), abnormal liver function tests, and a negative Coombs test also help diagnose MCL. Secondary cutaneous MCL is diagnosed on the basis of an MCL diagnosis along with diffuse infiltration of the skin, with multiple erythematous papules and nodules coalescing to form plaques; skin biopsy and immunohistopathology showing monotonous proliferation of small- to medium-sized lymphoid cells with scant cytoplasm; irregular cleaved nuclei with coarse chromatin; and inconspicuous nucleoli as well as a spared papillary dermis.
Pathogenesis of MCL involves disordered lymphoproliferation in a subset of naive pregerminal center cells in primary follicles or in the mantle region of secondary follicles. Most cases are linked with translocation of chromosome 14 and 11, which induces overexpression of protein cyclin D1. Viral infection (Epstein-Barr virus, HIV, human T-lymphotropic virus type 1, human herpes virus 6), environmental factors, and primary and secondary immunodeficiency are also associated with the development of NHL.
Patient education should include detailed information about clinical trials, available treatment options, and associated adverse events as well as psychosocial and nutrition counseling.
Chemoimmunotherapy is standard initial treatment for MCL, but relapse is expected. Chemotherapy-free regimens with biologic targets, which were once used in second-line treatment, have increasingly become an important first-line treatment given their efficacy in the relapsed/refractory setting. Chimeric antigen receptor T-cell therapy is also a second-line treatment option. In patients with MCL and a TP53 mutation, clinical trial participation is encouraged because of poor prognosis.
Timothy J. Voorhees, MD, MSCR, Assistant Professor of Internal Medicine - Clinical, Division of Hematology, The Ohio State University James Comprehensive Cancer Center, Columbus, OH.
Timothy J. Voorhees, MD, MSCR, has disclosed the following relevant financial relationships: Received research grants from: AstraZeneca; Morphosys; Incyte; Recordati.
Image Quizzes are fictional or fictionalized clinical scenarios intended to provide evidence-based educational takeaways.
Given the patient's diagnosis of stage IV MCL, the presentation of diffuse skin lesions, and the histopathologic and immunophenotyping results of those lesions, this patient is diagnosed with secondary cutaneous MCL. The hematologist-oncologist discusses the findings with the patient and presents potential next steps and treatment options.
MCL is a type of B-cell neoplasm that, with advancements in the understanding of non-Hodgkin lymphoma (NHL) in the past 30 years, has been defined as its own clinicopathologic entity by the Revised European-American Lymphoma and World Health Organization classifications. Up to 10% of all NHLs are MCL. Clinical presentation includes advanced disease with B symptoms (eg, night sweats, fever, weight loss), generalized lymphadenopathy, abdominal distention associated with hepatosplenomegaly, and fatigue. Skin manifestations are not as common as other extranodal manifestations. Primary cutaneous MCL occurs in up to 6% of patients with MCL; secondary cutaneous involvement is slightly more common, occurring in 17% of patients with MCL. Secondary cutaneous MCL usually presents in late-stage disease. Men are more likely to present with MCL than are women by a ratio of 3:1. Median age at presentation is 67 years.
Diagnosing MCL is a multipronged approach. Physical examination may reveal lymphadenopathy and hepatosplenomegaly. Lymph node biopsy and aspiration with immunophenotyping in MCL reveals monoclonal B cells expressing surface immunoglobulin (Ig), IgM, or IgD, that are characteristically CD5+ and pan B-cell antigen–positive (eg, CD19, CD20, CD22) but lack expression of CD10 and CD23 and overexpress cyclin D1. Bone marrow aspirate/biopsy are used more for staging than for diagnosis. Blood studies, including anemia and cytopenias secondary to bone marrow infiltration (with up to 40% of cases showing lymphocytosis > 4000/μL), abnormal liver function tests, and a negative Coombs test also help diagnose MCL. Secondary cutaneous MCL is diagnosed on the basis of an MCL diagnosis along with diffuse infiltration of the skin, with multiple erythematous papules and nodules coalescing to form plaques; skin biopsy and immunohistopathology showing monotonous proliferation of small- to medium-sized lymphoid cells with scant cytoplasm; irregular cleaved nuclei with coarse chromatin; and inconspicuous nucleoli as well as a spared papillary dermis.
Pathogenesis of MCL involves disordered lymphoproliferation in a subset of naive pregerminal center cells in primary follicles or in the mantle region of secondary follicles. Most cases are linked with translocation of chromosome 14 and 11, which induces overexpression of protein cyclin D1. Viral infection (Epstein-Barr virus, HIV, human T-lymphotropic virus type 1, human herpes virus 6), environmental factors, and primary and secondary immunodeficiency are also associated with the development of NHL.
Patient education should include detailed information about clinical trials, available treatment options, and associated adverse events as well as psychosocial and nutrition counseling.
Chemoimmunotherapy is standard initial treatment for MCL, but relapse is expected. Chemotherapy-free regimens with biologic targets, which were once used in second-line treatment, have increasingly become an important first-line treatment given their efficacy in the relapsed/refractory setting. Chimeric antigen receptor T-cell therapy is also a second-line treatment option. In patients with MCL and a TP53 mutation, clinical trial participation is encouraged because of poor prognosis.
Timothy J. Voorhees, MD, MSCR, Assistant Professor of Internal Medicine - Clinical, Division of Hematology, The Ohio State University James Comprehensive Cancer Center, Columbus, OH.
Timothy J. Voorhees, MD, MSCR, has disclosed the following relevant financial relationships: Received research grants from: AstraZeneca; Morphosys; Incyte; Recordati.
Image Quizzes are fictional or fictionalized clinical scenarios intended to provide evidence-based educational takeaways.
A 72-year-old man presents to his hematologist-oncologist with red ulcerative nodules on both legs. Six months before, the patient was diagnosed with stage IV mantle cell lymphoma (MCL) and began chemotherapy with rituximab, cyclophosphamide, doxorubicin, vincristine, and prednisone (R-CHOP). Initial patient reports at diagnosis were abdominal distention, generalized lymphadenopathy, night sweats, and fatigue; he received a referral to hematology-oncology after his complete blood count with differential revealed anemia and cytopenias. Additional blood studies showed lymphocytosis > 4000/μL, elevated lactate dehydrogenase levels, abnormal liver function tests, and a negative result on the Coombs test. Ultrasound of the abdomen revealed hepatosplenomegaly and abdominal lymphadenopathy. The hematologist-oncologist ordered a lymph node biopsy and aspiration. Immunophenotyping showed CD5 and CD20 expression but a lack of CD23 and CD10 expression; cyclin D1 was overexpressed. Bone marrow biopsy revealed hypercellular marrow spaces showing infiltration by sheets of atypical lymphoid cells.
Because the patient presents with red ulcerative nodules on both legs, the hematologist-oncologist orders a skin biopsy of the lesions. Histopathologic evaluation shows monotonous proliferation of small- to medium-sized lymphoid cells with scant cytoplasm, irregular cleaved nuclei with coarse chromatin, and inconspicuous nucleoli as well as a spared papillary dermis. Immunophenotyping shows CD5 and CD20 expression but a lack of CD23 and CD10 expression; cyclin D1 is overexpressed.
Disallow All Ads
Content Gating
No Gating (article Unlocked/Free)
Alternative CME
Disqus Comments
Default
Gate On Date
Un-Gate On Date
Consolidated Pubs: Do Not Show Source Publication Logo
Just one in five American adults with opioid use disorder (OUD) in 2021 received medication for the condition, a new study shows.
Using data from the 2021 National Survey on Drug Use and Health (NSDUH), investigators found that of the 2.5 million adults with OUD in that year, 35.6% received some kind of substance abuse treatment, but only 22.3% received recommended medications for the condition, such as methadone, buprenorphine, or extended-release naltrexone.
“More than 80,000 people are dying of a drug overdose involving an opioid every year, while safe and effective medicines to treat opioid use disorder are sitting on the shelf unused,” senior author Wilson Compton, MD, MPE, deputy director of the National Institute on Drug Abuse (NIDA), said in a statement. “This study adds to the growing evidence that telehealth services are an important strategy that could help us bridge this gap, supporting the delivery of safe, effective, and lifesaving care for people with opioid use disorder.”
The findings were published online as a research letter in JAMA Network Open.
The study included 47,291 adults aged 18 years or older in the 2021 NSDUH, which provides nationally representative data of the U.S. civilian, noninstitutionalized population based on past-year OUD.
Men, people aged 35 years or older, urban residents, and non-Hispanic Whites were the most likely to receive medication for opioid use disorder (MOUD). MOUD use was more common among those who received substance use treatment via telehealth, those with severe OUD, and people with annual incomes below $50,000.
Black people, women, unemployed individuals, those living in rural areas, and people with past-year cannabis use disorder were less likely to receive MOUD.
“It is not a matter of whether we should address health disparities and inequities that many racial/ethnic minority groups face when trying to access substance use treatment,” lead author Christopher M. Jones, PharmD, MPH, DrPH, director of the National Center for Injury Prevention and Control in the Centers for Disease Control and Prevention, said in a statement. “We must address these issues if we hope to reverse the trend of increasing drug overdose deaths.”
The study was funded by the Centers for Disease Control and Prevention and the National Institutes of Health. Dr. Compton reported long-term stock holdings in General Electric, 3M Companies, and Pfizer outside the submitted work.
A version of this article first appeared on Medscape.com.
Just one in five American adults with opioid use disorder (OUD) in 2021 received medication for the condition, a new study shows.
Using data from the 2021 National Survey on Drug Use and Health (NSDUH), investigators found that of the 2.5 million adults with OUD in that year, 35.6% received some kind of substance abuse treatment, but only 22.3% received recommended medications for the condition, such as methadone, buprenorphine, or extended-release naltrexone.
“More than 80,000 people are dying of a drug overdose involving an opioid every year, while safe and effective medicines to treat opioid use disorder are sitting on the shelf unused,” senior author Wilson Compton, MD, MPE, deputy director of the National Institute on Drug Abuse (NIDA), said in a statement. “This study adds to the growing evidence that telehealth services are an important strategy that could help us bridge this gap, supporting the delivery of safe, effective, and lifesaving care for people with opioid use disorder.”
The findings were published online as a research letter in JAMA Network Open.
The study included 47,291 adults aged 18 years or older in the 2021 NSDUH, which provides nationally representative data of the U.S. civilian, noninstitutionalized population based on past-year OUD.
Men, people aged 35 years or older, urban residents, and non-Hispanic Whites were the most likely to receive medication for opioid use disorder (MOUD). MOUD use was more common among those who received substance use treatment via telehealth, those with severe OUD, and people with annual incomes below $50,000.
Black people, women, unemployed individuals, those living in rural areas, and people with past-year cannabis use disorder were less likely to receive MOUD.
“It is not a matter of whether we should address health disparities and inequities that many racial/ethnic minority groups face when trying to access substance use treatment,” lead author Christopher M. Jones, PharmD, MPH, DrPH, director of the National Center for Injury Prevention and Control in the Centers for Disease Control and Prevention, said in a statement. “We must address these issues if we hope to reverse the trend of increasing drug overdose deaths.”
The study was funded by the Centers for Disease Control and Prevention and the National Institutes of Health. Dr. Compton reported long-term stock holdings in General Electric, 3M Companies, and Pfizer outside the submitted work.
A version of this article first appeared on Medscape.com.
Just one in five American adults with opioid use disorder (OUD) in 2021 received medication for the condition, a new study shows.
Using data from the 2021 National Survey on Drug Use and Health (NSDUH), investigators found that of the 2.5 million adults with OUD in that year, 35.6% received some kind of substance abuse treatment, but only 22.3% received recommended medications for the condition, such as methadone, buprenorphine, or extended-release naltrexone.
“More than 80,000 people are dying of a drug overdose involving an opioid every year, while safe and effective medicines to treat opioid use disorder are sitting on the shelf unused,” senior author Wilson Compton, MD, MPE, deputy director of the National Institute on Drug Abuse (NIDA), said in a statement. “This study adds to the growing evidence that telehealth services are an important strategy that could help us bridge this gap, supporting the delivery of safe, effective, and lifesaving care for people with opioid use disorder.”
The findings were published online as a research letter in JAMA Network Open.
The study included 47,291 adults aged 18 years or older in the 2021 NSDUH, which provides nationally representative data of the U.S. civilian, noninstitutionalized population based on past-year OUD.
Men, people aged 35 years or older, urban residents, and non-Hispanic Whites were the most likely to receive medication for opioid use disorder (MOUD). MOUD use was more common among those who received substance use treatment via telehealth, those with severe OUD, and people with annual incomes below $50,000.
Black people, women, unemployed individuals, those living in rural areas, and people with past-year cannabis use disorder were less likely to receive MOUD.
“It is not a matter of whether we should address health disparities and inequities that many racial/ethnic minority groups face when trying to access substance use treatment,” lead author Christopher M. Jones, PharmD, MPH, DrPH, director of the National Center for Injury Prevention and Control in the Centers for Disease Control and Prevention, said in a statement. “We must address these issues if we hope to reverse the trend of increasing drug overdose deaths.”
The study was funded by the Centers for Disease Control and Prevention and the National Institutes of Health. Dr. Compton reported long-term stock holdings in General Electric, 3M Companies, and Pfizer outside the submitted work.
A version of this article first appeared on Medscape.com.
The patient's history, symptomatology, and assessments suggest a diagnosis of nonalcoholic fatty liver disease (NAFLD). The primary care physician recommends referral to a hepatologist for evaluation and possible liver biopsy.
NAFLD involves an accumulation of triglycerides and other fats in the liver (unrelated to alcohol consumption and other liver disease), with the presence of hepatic steatosis in more than 5% of hepatocytes. NAFLD affects 25% to 35% of the general population, making it the most common cause of chronic liver disease. The rate increases among patients with obesity, 80% of whom are affected by NAFLD.
NAFLD should be considered in patients with unexplained elevations in serum aminotransferases (without positive viral markers or autoantibodies and no history of alcohol use) and a high risk for steatohepatitis, including obesity. The standard NAFLD assessment for biopsy specimens is the Brunt system, and disease stage is determined using the NAFLD activity score and the amount of fibrosis present.
A study of the natural history of NAFLD in patients who were followed for 3 years showed that without pharmacologic intervention, one third experienced disease progression, one third remained stable, and one third improved. An independent risk factor for progression of nonalcoholic steatohepatitis was abnormal glucose tolerance testing. In another natural history study, a 10% higher rate of mortality over 10 years was demonstrated among those with NAFLD vs controls, with the top three causes of death being cancer, heart disease, and liver-related disease. Prevalence of chronic liver disease and cirrhosis has been shown to be elevated in Latino and Japanese American populations.
Patients with NAFLD should be seen regularly to assess for disease progression and receive guidance on weight management interventions and exercise. A weight loss of more than 5% has been shown to reduce liver fat and provide cardiometabolic benefits; a weight reduction of more than 10% can help reverse steatohepatitis or liver fibrosis. In addition to weight loss management strategies, physicians should discuss the importance of controlling hyperlipidemia, insulin resistance, and T2D with their patients and share the importance of avoiding alcohol and other hepatotoxic substances.
According to the American Association of Clinical Endocrinology Clinical Practice Guideline: "There are no U.S. Food and Drug Administration-approved medications for the treatment of NAFLD; however, some diabetes and anti-obesity medications can be beneficial. Bariatric surgery is also effective for weight loss and reducing liver fat in persons with severe obesity."
Courtney Whittle, MD, MSW, Diplomate of ABOM, Pediatric Lead, Obesity Champion, TSPMG, Weight A Minute Clinic, Atlanta, Georgia.
Courtney Whittle, MD, MSW, Diplomate of ABOM, has disclosed no relevant financial relationships.
Image Quizzes are fictional or fictionalized clinical scenarios intended to provide evidence-based educational takeaways.
Author and Disclosure Information
Reviewed by Courtney Whittle, MD, MSW, Diplomate of ABOM
Reviewed by Courtney Whittle, MD, MSW, Diplomate of ABOM
Author and Disclosure Information
Reviewed by Courtney Whittle, MD, MSW, Diplomate of ABOM
The patient's history, symptomatology, and assessments suggest a diagnosis of nonalcoholic fatty liver disease (NAFLD). The primary care physician recommends referral to a hepatologist for evaluation and possible liver biopsy.
NAFLD involves an accumulation of triglycerides and other fats in the liver (unrelated to alcohol consumption and other liver disease), with the presence of hepatic steatosis in more than 5% of hepatocytes. NAFLD affects 25% to 35% of the general population, making it the most common cause of chronic liver disease. The rate increases among patients with obesity, 80% of whom are affected by NAFLD.
NAFLD should be considered in patients with unexplained elevations in serum aminotransferases (without positive viral markers or autoantibodies and no history of alcohol use) and a high risk for steatohepatitis, including obesity. The standard NAFLD assessment for biopsy specimens is the Brunt system, and disease stage is determined using the NAFLD activity score and the amount of fibrosis present.
A study of the natural history of NAFLD in patients who were followed for 3 years showed that without pharmacologic intervention, one third experienced disease progression, one third remained stable, and one third improved. An independent risk factor for progression of nonalcoholic steatohepatitis was abnormal glucose tolerance testing. In another natural history study, a 10% higher rate of mortality over 10 years was demonstrated among those with NAFLD vs controls, with the top three causes of death being cancer, heart disease, and liver-related disease. Prevalence of chronic liver disease and cirrhosis has been shown to be elevated in Latino and Japanese American populations.
Patients with NAFLD should be seen regularly to assess for disease progression and receive guidance on weight management interventions and exercise. A weight loss of more than 5% has been shown to reduce liver fat and provide cardiometabolic benefits; a weight reduction of more than 10% can help reverse steatohepatitis or liver fibrosis. In addition to weight loss management strategies, physicians should discuss the importance of controlling hyperlipidemia, insulin resistance, and T2D with their patients and share the importance of avoiding alcohol and other hepatotoxic substances.
According to the American Association of Clinical Endocrinology Clinical Practice Guideline: "There are no U.S. Food and Drug Administration-approved medications for the treatment of NAFLD; however, some diabetes and anti-obesity medications can be beneficial. Bariatric surgery is also effective for weight loss and reducing liver fat in persons with severe obesity."
Courtney Whittle, MD, MSW, Diplomate of ABOM, Pediatric Lead, Obesity Champion, TSPMG, Weight A Minute Clinic, Atlanta, Georgia.
Courtney Whittle, MD, MSW, Diplomate of ABOM, has disclosed no relevant financial relationships.
Image Quizzes are fictional or fictionalized clinical scenarios intended to provide evidence-based educational takeaways.
The patient's history, symptomatology, and assessments suggest a diagnosis of nonalcoholic fatty liver disease (NAFLD). The primary care physician recommends referral to a hepatologist for evaluation and possible liver biopsy.
NAFLD involves an accumulation of triglycerides and other fats in the liver (unrelated to alcohol consumption and other liver disease), with the presence of hepatic steatosis in more than 5% of hepatocytes. NAFLD affects 25% to 35% of the general population, making it the most common cause of chronic liver disease. The rate increases among patients with obesity, 80% of whom are affected by NAFLD.
NAFLD should be considered in patients with unexplained elevations in serum aminotransferases (without positive viral markers or autoantibodies and no history of alcohol use) and a high risk for steatohepatitis, including obesity. The standard NAFLD assessment for biopsy specimens is the Brunt system, and disease stage is determined using the NAFLD activity score and the amount of fibrosis present.
A study of the natural history of NAFLD in patients who were followed for 3 years showed that without pharmacologic intervention, one third experienced disease progression, one third remained stable, and one third improved. An independent risk factor for progression of nonalcoholic steatohepatitis was abnormal glucose tolerance testing. In another natural history study, a 10% higher rate of mortality over 10 years was demonstrated among those with NAFLD vs controls, with the top three causes of death being cancer, heart disease, and liver-related disease. Prevalence of chronic liver disease and cirrhosis has been shown to be elevated in Latino and Japanese American populations.
Patients with NAFLD should be seen regularly to assess for disease progression and receive guidance on weight management interventions and exercise. A weight loss of more than 5% has been shown to reduce liver fat and provide cardiometabolic benefits; a weight reduction of more than 10% can help reverse steatohepatitis or liver fibrosis. In addition to weight loss management strategies, physicians should discuss the importance of controlling hyperlipidemia, insulin resistance, and T2D with their patients and share the importance of avoiding alcohol and other hepatotoxic substances.
According to the American Association of Clinical Endocrinology Clinical Practice Guideline: "There are no U.S. Food and Drug Administration-approved medications for the treatment of NAFLD; however, some diabetes and anti-obesity medications can be beneficial. Bariatric surgery is also effective for weight loss and reducing liver fat in persons with severe obesity."
Courtney Whittle, MD, MSW, Diplomate of ABOM, Pediatric Lead, Obesity Champion, TSPMG, Weight A Minute Clinic, Atlanta, Georgia.
Courtney Whittle, MD, MSW, Diplomate of ABOM, has disclosed no relevant financial relationships.
Image Quizzes are fictional or fictionalized clinical scenarios intended to provide evidence-based educational takeaways.
Simon Fraser/Freeman Hospital, Newcastle upon Tyne / Science Source
A 51-year-old Hispanic man presents to his primary care physician with fatigue and pain in the upper right abdomen. Physical exam reveals ascites and splenomegaly. His height is 5 ft 8 in and weight is 274 lb; his BMI is 41.7. For the past 5 years, the patient has seen his physician for routine annual exams, during which time he has consistently met the criteria for World Health Organization Class 3 overweight (BMI ≥ 40) and has taken metformin, with varying degrees of adherence, for type 2 diabetes (T2D). Now, given the patient's symptoms and the potential for uncontrolled diabetes, the physician orders laboratory studies and viral serologies for hepatitis. Results of these assessments exclude viral infection but demonstrate abnormal levels of fasting insulin and glucose, hypertriglyceridemia, and elevated transaminase levels that are sixfold above normal levels, with an aspartate aminotransferase-to-alanine transaminase ratio < 1:1.
Disallow All Ads
Content Gating
No Gating (article Unlocked/Free)
Alternative CME
Disqus Comments
Default
Gate On Date
Un-Gate On Date
Consolidated Pubs: Do Not Show Source Publication Logo
Higher daily step counts were associated with reduced risk of all-cause mortality and cardiovascular (CV) mortality, with benefit beginning with any amount over about 4,000 and 2,300 steps, respectively, in a new meta-analysis.
More steps were better – additional benefit was seen with increasing increments of 500 or 1,000 steps.
Leonardo Patrizi/E+/Getty Images
“One of our main aims was to overcome all the inconsistencies in previous studies, where the optimal number of daily steps for health benefits was usually between 6,000 and 10,000,” Maciej Banach, MD, PhD, of the Medical University of Lodz (Poland), said in an interview.
“As a preventive cardiologist, I saw that many of my patients were discouraged and said it’s impossible when I told them that making lifestyle changes included taking at least 7,000 daily steps,” he said.
“But our study in relatively healthy individuals, not patients, showed even a lower number – for example, around 4,000 – may be associated with a significant reduction of mortality.
“I tell people to start early, be regular, and don’t worry about the initial baseline number, because it’s important to start and it’s important to improve,” he said. “Our study showed that if we increase the number of steps per day, every 500- to 1,000-step increase might still be associated with an additional mortality reduction of 7%-15%.”
The study was published online in the European Journal of Preventive Cardiology.
Every move counts
The investigators searched the literature through June 2022 and selected 17 cohort studies with 226,889 participants and a median follow-up of 7.1 years for inclusion in the analysis: 10 studies reported all-cause mortality, 4 reported CV mortality, and 3 reported both outcomes.
The mean age of the participants was 64.4 years, and half were women. Daily step counts in the included studies were objectively measured for at least 7 consecutive days.
As noted, a 1,000-step increment was associated with a 15% decrease in risk of all-cause mortality (hazard ratio, 0.85); a 500-step increment was associated with a 7% decrease in CV mortality (HR, 0.93).
Compared with the reference quartile (median steps/day, 3,967), quartile 1 (median steps, 5,537) was associated with a 48% lower risk of all-cause mortality; quartile 2 (median steps, 7,370), with a 55% lower risk; and quartile 3 (median steps, 11,529), with a 67% risk reduction.
Similarly, compared with the lowest quartile of steps per day used as reference (median steps, 2,337), higher quartiles of steps per day (Q1, 3,982; Q2, 6,661; and Q3, 10,413) were linearly associated with a reduced risk of CV mortality (16%, 49%, and 77%, respectively).
In a restricted cubic splines model, a nonlinear dose-response association was observed between step count and all-cause and CV mortality, with a progressively lower risk of mortality with an increase in step count.
Dose-response curves were similar for men and women. However, there was a difference by age: Among people aged 60 years or older, the size of the risk reduction was smaller. Among the older adults, there was a 42% risk reduction for those who walked between 6000 and 10,000 steps daily, compared with a 49% reduction in risk among younger adults who walked between 7,000 and 13,000 steps a day.
For both groups, daily step counts higher than 5,000 resulted in a “dramatically” lower risk of all-cause mortality.
An analysis that compared the impact of climate regions on the associations showed no significant effect on all-cause mortality. People in all climate zones benefited when the daily step count exceeded approximately 5,500.
Even given the encouraging study results, “we know very well that every kind of exercise is critically important,” Dr. Banach said. It is easier to focus on step counts because the counts can be monitored and calculated with smartwatches, pedometers, and other tools. That also makes it easier to check associations and outcomes for large groups of patients.
“But in fact, we should not be focusing on one type of exercise, such as walking or running,” he said. “We can dance, ride bicycles, and do many other different exercises that mobilize our hearts.
“We also know that in all these activities, including steps, people have different capabilities – for example, some can walk more slowly, others faster and with more intensity.”
Dr. Banach recommended following the European and U.S. physical activity guidelines that advise, in addition to muscle-strengthening activities, 150 minutes of moderate-intensity aerobic training weekly, or 75 minutes of vigorous-intensity aerobic activity, or an equivalent combination of moderate- and vigorous-intensity aerobic activity.
From the results he sees in patients, he believes the combination approach is probably best for the heart.
Furthermore, it’s important to exercise regularly, something that’s easier if individuals enjoy what they’re doing. “The type of training or whether you are completely inactive or very active at the start doesn’t matter, because any improvement, any addition to the to the baseline values will have health benefits,” he concluded.
Higher goals helpful
Three experts commented on the study; all noted that the results are in line with previous studies, that the observational nature of the study is a limitation, and that additional randomized, controlled trials are needed to confirm the findings.
Evan Brittain, MD, an associate professor of medicine at Vanderbilt University Medical Center, Nashville, Tenn., expressed some additional concerns.
Dr. Brittain was principal investigator of a recent study that found that the relationship between steps per day and incident disease was inverse and linear for obesity, sleep apnea, gastroesophageal reflux disease, and major depressive disorder. Daily step counts above 8,200 were associated with protection from incident disease.
He noted that, in the current study, “the authors chose to make the least active quartile (25%) the reference group (only 3,967 steps/day for all-cause mortality and only 2,337 steps/day for CV mortality analysis), which somewhat lowers the bar for finding a significant benefit at higher step counts.
“Moreover, in the spline analyses, zero steps per day is used as the comparison, which is not a practical, real-world comparison,” he said. “As a result, those data are very hard to interpret, and I think are overstated.”
Like Dr. Banach, Dr. Brittain said he would continue to advise following guideline recommendations to get 150 minutes per week of moderate-intensity activity. However, he added that although it is reasonable to advise patients that benefits do accrue with daily step counts of less than 10,000, “I would not want patients to misconstrue from this study that getting more than only 2,330 steps per day is a beneficial goal.”
Martin Halle, MD, a professor in the department of prevention and sports medicine at the Technical University of Munich (Germany), said: “From a clinical, medical, and health perspective, the general population should aim for 5,000 steps, which is about 3-4 kilometers [about 2 miles] of walking, and intensity counts – the faster you walk, the better.
“I recommend doing 100 steps fast and 100 steps slow and then 100 steps fast and 100 steps slow,” said Dr. Halle, who is past president of the European Association of Preventive Cardiology. This approach not only motivates people, “but they improve their exercise capacity substantially and very quickly, just within weeks.”
European Society of Cardiology vice president and European Journal of Preventive Cardiology editor-in-chief Massimo Piepoli, MD, PhD, agreed that “little is better than nothing and more is even better. This applies to healthy subjects, as well as patients with chronic diseases.
“Five hundred steps is a very short distance (such as walking two blocks or walking the dog for about 10-15 minutes every day),” he said. Yet, increasing step counts in increments of 500 “is associated with a significant reduction in cardiovascular mortality both in men and women, particularly in older individuals.
“We do not need to depend on expensive gym facilities,” he added. “But at the same time, we need to live in and to promote the building of neighborhoods where it is possible to walk in a safe and healthy environment.”
The research received no external funding. Dr. Banach has reported financial relationships with Amgen, Daiichi Sankyo, Esperion, Freia Pharmaceuticals, Kogen, KRKA, Polpharma, NewAmsterdam, Novartis, Novo Nordisk, Polfarmex, Sanofi Aventis, Teva, Valeant, Viatris, and Zentiva, and is chief marketing and development officer at Longevity Group and chief marketing officer at Nomi Biotech.
A version of this article first appeared on Medscape.com.
Higher daily step counts were associated with reduced risk of all-cause mortality and cardiovascular (CV) mortality, with benefit beginning with any amount over about 4,000 and 2,300 steps, respectively, in a new meta-analysis.
More steps were better – additional benefit was seen with increasing increments of 500 or 1,000 steps.
Leonardo Patrizi/E+/Getty Images
“One of our main aims was to overcome all the inconsistencies in previous studies, where the optimal number of daily steps for health benefits was usually between 6,000 and 10,000,” Maciej Banach, MD, PhD, of the Medical University of Lodz (Poland), said in an interview.
“As a preventive cardiologist, I saw that many of my patients were discouraged and said it’s impossible when I told them that making lifestyle changes included taking at least 7,000 daily steps,” he said.
“But our study in relatively healthy individuals, not patients, showed even a lower number – for example, around 4,000 – may be associated with a significant reduction of mortality.
“I tell people to start early, be regular, and don’t worry about the initial baseline number, because it’s important to start and it’s important to improve,” he said. “Our study showed that if we increase the number of steps per day, every 500- to 1,000-step increase might still be associated with an additional mortality reduction of 7%-15%.”
The study was published online in the European Journal of Preventive Cardiology.
Every move counts
The investigators searched the literature through June 2022 and selected 17 cohort studies with 226,889 participants and a median follow-up of 7.1 years for inclusion in the analysis: 10 studies reported all-cause mortality, 4 reported CV mortality, and 3 reported both outcomes.
The mean age of the participants was 64.4 years, and half were women. Daily step counts in the included studies were objectively measured for at least 7 consecutive days.
As noted, a 1,000-step increment was associated with a 15% decrease in risk of all-cause mortality (hazard ratio, 0.85); a 500-step increment was associated with a 7% decrease in CV mortality (HR, 0.93).
Compared with the reference quartile (median steps/day, 3,967), quartile 1 (median steps, 5,537) was associated with a 48% lower risk of all-cause mortality; quartile 2 (median steps, 7,370), with a 55% lower risk; and quartile 3 (median steps, 11,529), with a 67% risk reduction.
Similarly, compared with the lowest quartile of steps per day used as reference (median steps, 2,337), higher quartiles of steps per day (Q1, 3,982; Q2, 6,661; and Q3, 10,413) were linearly associated with a reduced risk of CV mortality (16%, 49%, and 77%, respectively).
In a restricted cubic splines model, a nonlinear dose-response association was observed between step count and all-cause and CV mortality, with a progressively lower risk of mortality with an increase in step count.
Dose-response curves were similar for men and women. However, there was a difference by age: Among people aged 60 years or older, the size of the risk reduction was smaller. Among the older adults, there was a 42% risk reduction for those who walked between 6000 and 10,000 steps daily, compared with a 49% reduction in risk among younger adults who walked between 7,000 and 13,000 steps a day.
For both groups, daily step counts higher than 5,000 resulted in a “dramatically” lower risk of all-cause mortality.
An analysis that compared the impact of climate regions on the associations showed no significant effect on all-cause mortality. People in all climate zones benefited when the daily step count exceeded approximately 5,500.
Even given the encouraging study results, “we know very well that every kind of exercise is critically important,” Dr. Banach said. It is easier to focus on step counts because the counts can be monitored and calculated with smartwatches, pedometers, and other tools. That also makes it easier to check associations and outcomes for large groups of patients.
“But in fact, we should not be focusing on one type of exercise, such as walking or running,” he said. “We can dance, ride bicycles, and do many other different exercises that mobilize our hearts.
“We also know that in all these activities, including steps, people have different capabilities – for example, some can walk more slowly, others faster and with more intensity.”
Dr. Banach recommended following the European and U.S. physical activity guidelines that advise, in addition to muscle-strengthening activities, 150 minutes of moderate-intensity aerobic training weekly, or 75 minutes of vigorous-intensity aerobic activity, or an equivalent combination of moderate- and vigorous-intensity aerobic activity.
From the results he sees in patients, he believes the combination approach is probably best for the heart.
Furthermore, it’s important to exercise regularly, something that’s easier if individuals enjoy what they’re doing. “The type of training or whether you are completely inactive or very active at the start doesn’t matter, because any improvement, any addition to the to the baseline values will have health benefits,” he concluded.
Higher goals helpful
Three experts commented on the study; all noted that the results are in line with previous studies, that the observational nature of the study is a limitation, and that additional randomized, controlled trials are needed to confirm the findings.
Evan Brittain, MD, an associate professor of medicine at Vanderbilt University Medical Center, Nashville, Tenn., expressed some additional concerns.
Dr. Brittain was principal investigator of a recent study that found that the relationship between steps per day and incident disease was inverse and linear for obesity, sleep apnea, gastroesophageal reflux disease, and major depressive disorder. Daily step counts above 8,200 were associated with protection from incident disease.
He noted that, in the current study, “the authors chose to make the least active quartile (25%) the reference group (only 3,967 steps/day for all-cause mortality and only 2,337 steps/day for CV mortality analysis), which somewhat lowers the bar for finding a significant benefit at higher step counts.
“Moreover, in the spline analyses, zero steps per day is used as the comparison, which is not a practical, real-world comparison,” he said. “As a result, those data are very hard to interpret, and I think are overstated.”
Like Dr. Banach, Dr. Brittain said he would continue to advise following guideline recommendations to get 150 minutes per week of moderate-intensity activity. However, he added that although it is reasonable to advise patients that benefits do accrue with daily step counts of less than 10,000, “I would not want patients to misconstrue from this study that getting more than only 2,330 steps per day is a beneficial goal.”
Martin Halle, MD, a professor in the department of prevention and sports medicine at the Technical University of Munich (Germany), said: “From a clinical, medical, and health perspective, the general population should aim for 5,000 steps, which is about 3-4 kilometers [about 2 miles] of walking, and intensity counts – the faster you walk, the better.
“I recommend doing 100 steps fast and 100 steps slow and then 100 steps fast and 100 steps slow,” said Dr. Halle, who is past president of the European Association of Preventive Cardiology. This approach not only motivates people, “but they improve their exercise capacity substantially and very quickly, just within weeks.”
European Society of Cardiology vice president and European Journal of Preventive Cardiology editor-in-chief Massimo Piepoli, MD, PhD, agreed that “little is better than nothing and more is even better. This applies to healthy subjects, as well as patients with chronic diseases.
“Five hundred steps is a very short distance (such as walking two blocks or walking the dog for about 10-15 minutes every day),” he said. Yet, increasing step counts in increments of 500 “is associated with a significant reduction in cardiovascular mortality both in men and women, particularly in older individuals.
“We do not need to depend on expensive gym facilities,” he added. “But at the same time, we need to live in and to promote the building of neighborhoods where it is possible to walk in a safe and healthy environment.”
The research received no external funding. Dr. Banach has reported financial relationships with Amgen, Daiichi Sankyo, Esperion, Freia Pharmaceuticals, Kogen, KRKA, Polpharma, NewAmsterdam, Novartis, Novo Nordisk, Polfarmex, Sanofi Aventis, Teva, Valeant, Viatris, and Zentiva, and is chief marketing and development officer at Longevity Group and chief marketing officer at Nomi Biotech.
A version of this article first appeared on Medscape.com.
Higher daily step counts were associated with reduced risk of all-cause mortality and cardiovascular (CV) mortality, with benefit beginning with any amount over about 4,000 and 2,300 steps, respectively, in a new meta-analysis.
More steps were better – additional benefit was seen with increasing increments of 500 or 1,000 steps.
Leonardo Patrizi/E+/Getty Images
“One of our main aims was to overcome all the inconsistencies in previous studies, where the optimal number of daily steps for health benefits was usually between 6,000 and 10,000,” Maciej Banach, MD, PhD, of the Medical University of Lodz (Poland), said in an interview.
“As a preventive cardiologist, I saw that many of my patients were discouraged and said it’s impossible when I told them that making lifestyle changes included taking at least 7,000 daily steps,” he said.
“But our study in relatively healthy individuals, not patients, showed even a lower number – for example, around 4,000 – may be associated with a significant reduction of mortality.
“I tell people to start early, be regular, and don’t worry about the initial baseline number, because it’s important to start and it’s important to improve,” he said. “Our study showed that if we increase the number of steps per day, every 500- to 1,000-step increase might still be associated with an additional mortality reduction of 7%-15%.”
The study was published online in the European Journal of Preventive Cardiology.
Every move counts
The investigators searched the literature through June 2022 and selected 17 cohort studies with 226,889 participants and a median follow-up of 7.1 years for inclusion in the analysis: 10 studies reported all-cause mortality, 4 reported CV mortality, and 3 reported both outcomes.
The mean age of the participants was 64.4 years, and half were women. Daily step counts in the included studies were objectively measured for at least 7 consecutive days.
As noted, a 1,000-step increment was associated with a 15% decrease in risk of all-cause mortality (hazard ratio, 0.85); a 500-step increment was associated with a 7% decrease in CV mortality (HR, 0.93).
Compared with the reference quartile (median steps/day, 3,967), quartile 1 (median steps, 5,537) was associated with a 48% lower risk of all-cause mortality; quartile 2 (median steps, 7,370), with a 55% lower risk; and quartile 3 (median steps, 11,529), with a 67% risk reduction.
Similarly, compared with the lowest quartile of steps per day used as reference (median steps, 2,337), higher quartiles of steps per day (Q1, 3,982; Q2, 6,661; and Q3, 10,413) were linearly associated with a reduced risk of CV mortality (16%, 49%, and 77%, respectively).
In a restricted cubic splines model, a nonlinear dose-response association was observed between step count and all-cause and CV mortality, with a progressively lower risk of mortality with an increase in step count.
Dose-response curves were similar for men and women. However, there was a difference by age: Among people aged 60 years or older, the size of the risk reduction was smaller. Among the older adults, there was a 42% risk reduction for those who walked between 6000 and 10,000 steps daily, compared with a 49% reduction in risk among younger adults who walked between 7,000 and 13,000 steps a day.
For both groups, daily step counts higher than 5,000 resulted in a “dramatically” lower risk of all-cause mortality.
An analysis that compared the impact of climate regions on the associations showed no significant effect on all-cause mortality. People in all climate zones benefited when the daily step count exceeded approximately 5,500.
Even given the encouraging study results, “we know very well that every kind of exercise is critically important,” Dr. Banach said. It is easier to focus on step counts because the counts can be monitored and calculated with smartwatches, pedometers, and other tools. That also makes it easier to check associations and outcomes for large groups of patients.
“But in fact, we should not be focusing on one type of exercise, such as walking or running,” he said. “We can dance, ride bicycles, and do many other different exercises that mobilize our hearts.
“We also know that in all these activities, including steps, people have different capabilities – for example, some can walk more slowly, others faster and with more intensity.”
Dr. Banach recommended following the European and U.S. physical activity guidelines that advise, in addition to muscle-strengthening activities, 150 minutes of moderate-intensity aerobic training weekly, or 75 minutes of vigorous-intensity aerobic activity, or an equivalent combination of moderate- and vigorous-intensity aerobic activity.
From the results he sees in patients, he believes the combination approach is probably best for the heart.
Furthermore, it’s important to exercise regularly, something that’s easier if individuals enjoy what they’re doing. “The type of training or whether you are completely inactive or very active at the start doesn’t matter, because any improvement, any addition to the to the baseline values will have health benefits,” he concluded.
Higher goals helpful
Three experts commented on the study; all noted that the results are in line with previous studies, that the observational nature of the study is a limitation, and that additional randomized, controlled trials are needed to confirm the findings.
Evan Brittain, MD, an associate professor of medicine at Vanderbilt University Medical Center, Nashville, Tenn., expressed some additional concerns.
Dr. Brittain was principal investigator of a recent study that found that the relationship between steps per day and incident disease was inverse and linear for obesity, sleep apnea, gastroesophageal reflux disease, and major depressive disorder. Daily step counts above 8,200 were associated with protection from incident disease.
He noted that, in the current study, “the authors chose to make the least active quartile (25%) the reference group (only 3,967 steps/day for all-cause mortality and only 2,337 steps/day for CV mortality analysis), which somewhat lowers the bar for finding a significant benefit at higher step counts.
“Moreover, in the spline analyses, zero steps per day is used as the comparison, which is not a practical, real-world comparison,” he said. “As a result, those data are very hard to interpret, and I think are overstated.”
Like Dr. Banach, Dr. Brittain said he would continue to advise following guideline recommendations to get 150 minutes per week of moderate-intensity activity. However, he added that although it is reasonable to advise patients that benefits do accrue with daily step counts of less than 10,000, “I would not want patients to misconstrue from this study that getting more than only 2,330 steps per day is a beneficial goal.”
Martin Halle, MD, a professor in the department of prevention and sports medicine at the Technical University of Munich (Germany), said: “From a clinical, medical, and health perspective, the general population should aim for 5,000 steps, which is about 3-4 kilometers [about 2 miles] of walking, and intensity counts – the faster you walk, the better.
“I recommend doing 100 steps fast and 100 steps slow and then 100 steps fast and 100 steps slow,” said Dr. Halle, who is past president of the European Association of Preventive Cardiology. This approach not only motivates people, “but they improve their exercise capacity substantially and very quickly, just within weeks.”
European Society of Cardiology vice president and European Journal of Preventive Cardiology editor-in-chief Massimo Piepoli, MD, PhD, agreed that “little is better than nothing and more is even better. This applies to healthy subjects, as well as patients with chronic diseases.
“Five hundred steps is a very short distance (such as walking two blocks or walking the dog for about 10-15 minutes every day),” he said. Yet, increasing step counts in increments of 500 “is associated with a significant reduction in cardiovascular mortality both in men and women, particularly in older individuals.
“We do not need to depend on expensive gym facilities,” he added. “But at the same time, we need to live in and to promote the building of neighborhoods where it is possible to walk in a safe and healthy environment.”
The research received no external funding. Dr. Banach has reported financial relationships with Amgen, Daiichi Sankyo, Esperion, Freia Pharmaceuticals, Kogen, KRKA, Polpharma, NewAmsterdam, Novartis, Novo Nordisk, Polfarmex, Sanofi Aventis, Teva, Valeant, Viatris, and Zentiva, and is chief marketing and development officer at Longevity Group and chief marketing officer at Nomi Biotech.
A version of this article first appeared on Medscape.com.
Datascope/Maquet/Getinge has announced a recall of the Cardiosave Hybrid and Rescue Intra-Aortic Balloon Pumps (IABPs) because they may shut down unexpectedly due to electrical failures in the power management board or solenoid board (power source path).
“Using an affected pump may cause serious adverse health events, including unstable blood pressure, injury (e.g., inadequate blood supply or a vital organ injury), and death,” the Food and Drug Administration said in the recall notice.
The FDA has identified this as a class I recall, the most serious type of recall due to the risk for serious injury or death. To date, Datascope/Maquet/Getinge received 26 complaints, but no reports of injuries or death.
The devices are indicated for acute coronary syndrome, cardiac and noncardiac surgery, and complications of heart failure in adults.
The recall includes a total of 4,586 Cardiosave Hybrid or Rescue IABP units distributed from March 2, 2012, to May 19, 2023. Product model numbers for the recalled Cardiosave Hybrid and Cardiosave Rescue are available online.
On June 5, Datascope/Maquet/Getinge sent an “important medical device advisory” to all affected customers. The letter advises customers to be sure there is an alternative IABP available to continue therapy and provide alternative hemodynamic support if there is no other means to continue counterpulsation therapy.
Customers with questions about this recall should contact their company representative or call technical support at 1-888-943-8872, Monday through Friday, between 8:00 a.m. and 6:00 p.m. ET.
Last March, Datascope/Getinge recalled 2,300 Cardiosave Hybrid or Rescue IABPs because the coiled cable connecting the display and base on some units may fail, causing an unexpected shutdown without warnings or alarms to alert the user.
Any adverse events or suspected adverse events related to the recalled Cardiosave Hybrid/Rescue IABPs should be reported to the FDA through MedWatch, its adverse event reporting program.
A version of this article appeared on Medscape.com.
Datascope/Maquet/Getinge has announced a recall of the Cardiosave Hybrid and Rescue Intra-Aortic Balloon Pumps (IABPs) because they may shut down unexpectedly due to electrical failures in the power management board or solenoid board (power source path).
“Using an affected pump may cause serious adverse health events, including unstable blood pressure, injury (e.g., inadequate blood supply or a vital organ injury), and death,” the Food and Drug Administration said in the recall notice.
The FDA has identified this as a class I recall, the most serious type of recall due to the risk for serious injury or death. To date, Datascope/Maquet/Getinge received 26 complaints, but no reports of injuries or death.
The devices are indicated for acute coronary syndrome, cardiac and noncardiac surgery, and complications of heart failure in adults.
The recall includes a total of 4,586 Cardiosave Hybrid or Rescue IABP units distributed from March 2, 2012, to May 19, 2023. Product model numbers for the recalled Cardiosave Hybrid and Cardiosave Rescue are available online.
On June 5, Datascope/Maquet/Getinge sent an “important medical device advisory” to all affected customers. The letter advises customers to be sure there is an alternative IABP available to continue therapy and provide alternative hemodynamic support if there is no other means to continue counterpulsation therapy.
Customers with questions about this recall should contact their company representative or call technical support at 1-888-943-8872, Monday through Friday, between 8:00 a.m. and 6:00 p.m. ET.
Last March, Datascope/Getinge recalled 2,300 Cardiosave Hybrid or Rescue IABPs because the coiled cable connecting the display and base on some units may fail, causing an unexpected shutdown without warnings or alarms to alert the user.
Any adverse events or suspected adverse events related to the recalled Cardiosave Hybrid/Rescue IABPs should be reported to the FDA through MedWatch, its adverse event reporting program.
A version of this article appeared on Medscape.com.
Datascope/Maquet/Getinge has announced a recall of the Cardiosave Hybrid and Rescue Intra-Aortic Balloon Pumps (IABPs) because they may shut down unexpectedly due to electrical failures in the power management board or solenoid board (power source path).
“Using an affected pump may cause serious adverse health events, including unstable blood pressure, injury (e.g., inadequate blood supply or a vital organ injury), and death,” the Food and Drug Administration said in the recall notice.
The FDA has identified this as a class I recall, the most serious type of recall due to the risk for serious injury or death. To date, Datascope/Maquet/Getinge received 26 complaints, but no reports of injuries or death.
The devices are indicated for acute coronary syndrome, cardiac and noncardiac surgery, and complications of heart failure in adults.
The recall includes a total of 4,586 Cardiosave Hybrid or Rescue IABP units distributed from March 2, 2012, to May 19, 2023. Product model numbers for the recalled Cardiosave Hybrid and Cardiosave Rescue are available online.
On June 5, Datascope/Maquet/Getinge sent an “important medical device advisory” to all affected customers. The letter advises customers to be sure there is an alternative IABP available to continue therapy and provide alternative hemodynamic support if there is no other means to continue counterpulsation therapy.
Customers with questions about this recall should contact their company representative or call technical support at 1-888-943-8872, Monday through Friday, between 8:00 a.m. and 6:00 p.m. ET.
Last March, Datascope/Getinge recalled 2,300 Cardiosave Hybrid or Rescue IABPs because the coiled cable connecting the display and base on some units may fail, causing an unexpected shutdown without warnings or alarms to alert the user.
Any adverse events or suspected adverse events related to the recalled Cardiosave Hybrid/Rescue IABPs should be reported to the FDA through MedWatch, its adverse event reporting program.
A version of this article appeared on Medscape.com.
The utility of artificial intelligence in pulmonology has focused mainly on using image datasets to detect and diagnose lung malignancies, but now a growing number of AI models are emerging that apply machine learning to improve predictability for other pulmonary conditions, including pulmonary infections, pulmonary fibrosis, and chronic obstructive pulmonary disease (COPD).
These applications are moving beyond the traditional AI model of collecting data from a multitude of images to cast a wider data net that includes electronic health records.
Also on the horizon, ChatGPT technology is poised to have an impact. But pulmonologists and their practices have a number of barriers to clear before they feel a meaningful impact from AI.
The imperative, said AI researcher Ishanu Chattopadhyay, PhD, is to create transformative models that can detect lung disease early on. Dr. Chattopadhyay, an assistant professor of medicine at the University of Chicago and its Institute for Genomics and Systems Biology, and fellow researchers developed an AI algorithm that uses comorbidity signatures in electronic health records to screen for idiopathic pulmonary fibrosis (IPF) (Nature Med. 2022 Sep 29. doi: 10.1038/s41591-022-02010-y).
“If you could do this when somebody walks into a primary care setting and they are barely suspecting something is going on with them or when they don’t have the typical risk factors, there is a certain fraction of these people who do have IPF and they will almost invariably be diagnosed late and/or misdiagnosed,” Dr. Chattopadhyay said, citing a study that found 55% of patients with IPF have had at least one misdiagnosis and 38% have two or more misdiagnoses (BMC Pulm Med. 2018 Jan 17. doi: 10.1186/s12890-017-0560-x).
Harnessing massive data sets
AI models cull data sets, whether banks of radiographic images or files in an EHR, to extract telltale signatures of a disease state. Dr. Chattopadhyay and his team’s model used three databases with almost 3 million participants and 54,247 positive cases of IPF. Hospitals in Scotland have deployed what they’ve claimed are the first AI models to predict COPD built with 55,000 patient records from a regional National Health Service database. Another AI model for staging COPD, developed by researchers in the United States and Romania, used more than 18,000 medical records from 588 patients to identify physiological signals predictive of COPD (Advanced Sci. 2023 Feb 19. doi: 10.1002/advs.202203485).
Said Dr. Chattopadhyay: “If I can bring in AI which doesn’t just look at radiological images but actually gets it back where someone walks into primary care using only the information that is available at that point in the patient files and asking for nothing more, it raises a flag reliably that gets you a pulmonary referral that will hopefully reduce the misdiagnosis and late diagnosis.”
Dr. Tseng
Victor Tseng, MD, medical director for pulmonology at Ansible Health in Mountain View, Calif., who’s researching the potential of AI in pulmonology, speculated on what functions AI can perform in the clinic. “I think you will start to see much more interventional sort of clinically patient care–facing applications,” he said. That would include acting as a triage layer to direct patient queries to a nurse, physician, or another practitioner, providing patient instructions, serving as therapeutic software, coordinating care, integrating supply chain issues,” he said.
AI vs. spirometry for COPD
Researchers in the United States and Romania, led by Paul Bogdan, PhD, at the University of Southern California Viterbi School of Engineering, developed a model that predicted COPD with an accuracy of almost 99% (98.66%) and avoids many of the shortcomings of spirometry, Dr. Bogdan said.
USC Viterbi School of Engineering
Dr. Bogdan
The models developed by Dr. Bogdan and collaborators use a different principle than existing AI platforms, Dr. Bogdan said. They analyze the properties of the data. As he explained it, they exploit what he called the “geometry of these data” to make inferences and decisions on a patient’s risk for COPD.
“Deep learning is very good for images, for videos, but it doesn’t work that well for signals,” said Mihai Udrescu, PhD, one of the Romanian collaborators. “But if we process the data with the technique brought up by Paul [Bogdan] and his team at USC, deep learning also works well on physiological signals.”
Dr. Paul Bogdan
Dr. Paul Bogdan, (left) and research associate Chenzhong Yin are standing in front of a summary of their research.
Said Dr. Bogdan, “Nobody thought about using physiological signals to predict COPD before this work. They used spirometry, but spirometry is cumbersome and several steps have to be performed in order to have an accurate spirometry.” His team’s AI models extract and analyze risk data based on 10 minutes of monitoring.
Dr. Udrescu
This technology also has the potential to improve accessibility of COPD screening, Dr. Udrescu said. “It can democratize the access to the health care because you don’t need to travel for 100 or 200 miles to see a specialist,” he said. “You just send an app to the mobile phone of a patient, the person puts on a smart watch and wears it for a couple of minutes and the data is either recorded locally or is transmitted and it is analyzed.” The computations can be done locally and in a matter of minutes, he said.
In Scotland, a 12-month feasibility study is underway to evaluate an AI model to identify COPD patients at greatest risk for adverse events. A press release from Lenus, the company developing the technology, said the study will use a COPD multidisciplinary team to consider real-time AI model outputs to enable proactive patient encounters and reduce emergency care visits.
Researchers in Paris built an AI model that showed a 68% accuracy in distinguishing people with asthma from people with COPD in administrative medical databases (BMC Pulmon Med. 2022 Sep 20. doi: 10.1186/s12890-022-02144-2). They found that asthma patients were younger than those with COPD (a mean of 49.9 vs. 72.1 years) and that COPD occurred mostly in men (68% vs. 33%). And an international team of researchers reported that an AI model that used chest CT scans determined that ever-smokers with COPD who met the imaging criteria for bronchiectasis were more prone to disease exacerbations (Radiology. 2022 Dec 13. doi: 10.1148/radiol.221109).
AI in idiopathic pulmonary fibrosis
The AI model that Dr. Chattopadhyay and collaborators developed had an 88% accuracy in predicting IPF. The model, known as the zero-burden comorbidity risk score for IPF (ZCoR-IPF), identified IPF cases in adults age 45 and older 1-4 years sooner than in a variety of pulmonology practice settings.
The model accounted for about 700 different features of IPF, Dr. Chattopadhyay said, but it deviated from standard AI risk models in that it used a machine learning algorithm to extract disease features that aren’t well understood or even known. “We do not know what all the risk factors of IPF are,” he said. “People who don’t have all the risk factors still get IPF. So we have to step back from the raw EHR data from where the features are being generated automatically, and then you can apply standard ML tools.”
Researchers at Nagoya University in Japan also reported on an AI algorithm for predicting IPF that used 646,800 high-resolution CT images and medical records data from 1,068 patients. Their algorithm had an average diagnostic accuracy of 83.6% and, they reported, demonstrated good accuracy even in patients with signs of interstitial pneumonia or who had surgical lung biopsies (Respirology. 2022 Dec 13. doi: 10.1111/resp.14310).
Chat GPT: The next frontier in AI
Dr. Tseng last year led a group of researchers that fed questions from the United States Medical Licensing Exam to a ChatGPT model, which found it answered 60%-65% of questions correctly (PLOS Digit Health. 2023 Feb 9. doi: 10.1371/journal.pdig.0000198). As Dr. Tseng pointed out, that’s good enough to get a medical license.
It may be a matter of time before ChatGPT technology finds its way into the clinic, Dr. Tseng said. A quick ChatGPT query of how it could be used in medicine yielded 12 different answers, from patient triage to providing basic first aid instructions in an emergency.
Dr. Tseng, who’s pulmonology practice places an emphasis on virtual care delivery, went deeper than the ChatGPT answer. “If you’re a respiratory therapist and you’re trying to execute a complicated medical care plan written by a physician, there’s a natural disconnect between our language and their language,” he said. “What we have found is that GPT has significantly harmonized the care plan. And that’s amazing because you end up with this single-stream understanding of the care plan, where the language is halfway between a bedside clinician, like the respiratory therapist or nurse, and is also something that a physician can understand and take the bigger sort of direction of care from.”
Barriers to AI in clinic
Numerous barriers face widespread adoption of AI tools in the clinic, Dr. Tseng said, including physician and staff anxiety about learning new technology. “AI tools, for all purposes, are supposed to allay the cognitive burden and the tedium burden on clinicians, but end up actually costing more time,” he said.
Dr. Novak
Health care organizations will also need to retool for AI, a group of medical informatics and digital health experts, led by Laurie Lovett Novak, PhD, reported (JAMIA Open. 2023 May 3. doi: 10.1093/jamiaopen/ooad028). But it’s coming nonetheless, Dr. Novak, an associate professor of biomedical informatics at Vanderbilt University Medical Center in Nashville, Tenn., said in an interview.
“In the near future, managers in clinics and inpatient units will be overseeing care that involves numerous AI-based technologies, including predictive analytics, imaging tools, language models, and others,” she said. “Organizations need to support managers by implementing capabilities for algorithmo-vigilance.”
That would include dealing with what she called “algorithmic drift” – when the accuracy of an AI model wanes because of changes in the underlying data – and ensuring that models are unbiased and aren’t used in a way that contributes to inequities in health care. “These new organizational capabilities will demand new tools and new competencies,” she said. That would include policies and processes drawing guidance from medical societies for legal and regulatory direction for managers, staff training, and software documentation.
Dr. Tseng envisioned how AI would work in the clinic. “I personally think that, at some time in the near future, AI-driven care coordination, where the AI basically handles appointment scheduling, patient motivation, patient engagement and acts as their health navigator, will be superior to any human health navigator on the whole, only for the reason that AI is indefatigable,” Dr. Tseng said. “It doesn’t get tired, it doesn’t get burned out, and these health navigation care coordination roles are notoriously difficult.”
The physicians and researchers interviewed for this report had no relevant relationships to disclose.
The utility of artificial intelligence in pulmonology has focused mainly on using image datasets to detect and diagnose lung malignancies, but now a growing number of AI models are emerging that apply machine learning to improve predictability for other pulmonary conditions, including pulmonary infections, pulmonary fibrosis, and chronic obstructive pulmonary disease (COPD).
These applications are moving beyond the traditional AI model of collecting data from a multitude of images to cast a wider data net that includes electronic health records.
Also on the horizon, ChatGPT technology is poised to have an impact. But pulmonologists and their practices have a number of barriers to clear before they feel a meaningful impact from AI.
The imperative, said AI researcher Ishanu Chattopadhyay, PhD, is to create transformative models that can detect lung disease early on. Dr. Chattopadhyay, an assistant professor of medicine at the University of Chicago and its Institute for Genomics and Systems Biology, and fellow researchers developed an AI algorithm that uses comorbidity signatures in electronic health records to screen for idiopathic pulmonary fibrosis (IPF) (Nature Med. 2022 Sep 29. doi: 10.1038/s41591-022-02010-y).
“If you could do this when somebody walks into a primary care setting and they are barely suspecting something is going on with them or when they don’t have the typical risk factors, there is a certain fraction of these people who do have IPF and they will almost invariably be diagnosed late and/or misdiagnosed,” Dr. Chattopadhyay said, citing a study that found 55% of patients with IPF have had at least one misdiagnosis and 38% have two or more misdiagnoses (BMC Pulm Med. 2018 Jan 17. doi: 10.1186/s12890-017-0560-x).
Harnessing massive data sets
AI models cull data sets, whether banks of radiographic images or files in an EHR, to extract telltale signatures of a disease state. Dr. Chattopadhyay and his team’s model used three databases with almost 3 million participants and 54,247 positive cases of IPF. Hospitals in Scotland have deployed what they’ve claimed are the first AI models to predict COPD built with 55,000 patient records from a regional National Health Service database. Another AI model for staging COPD, developed by researchers in the United States and Romania, used more than 18,000 medical records from 588 patients to identify physiological signals predictive of COPD (Advanced Sci. 2023 Feb 19. doi: 10.1002/advs.202203485).
Said Dr. Chattopadhyay: “If I can bring in AI which doesn’t just look at radiological images but actually gets it back where someone walks into primary care using only the information that is available at that point in the patient files and asking for nothing more, it raises a flag reliably that gets you a pulmonary referral that will hopefully reduce the misdiagnosis and late diagnosis.”
Dr. Tseng
Victor Tseng, MD, medical director for pulmonology at Ansible Health in Mountain View, Calif., who’s researching the potential of AI in pulmonology, speculated on what functions AI can perform in the clinic. “I think you will start to see much more interventional sort of clinically patient care–facing applications,” he said. That would include acting as a triage layer to direct patient queries to a nurse, physician, or another practitioner, providing patient instructions, serving as therapeutic software, coordinating care, integrating supply chain issues,” he said.
AI vs. spirometry for COPD
Researchers in the United States and Romania, led by Paul Bogdan, PhD, at the University of Southern California Viterbi School of Engineering, developed a model that predicted COPD with an accuracy of almost 99% (98.66%) and avoids many of the shortcomings of spirometry, Dr. Bogdan said.
USC Viterbi School of Engineering
Dr. Bogdan
The models developed by Dr. Bogdan and collaborators use a different principle than existing AI platforms, Dr. Bogdan said. They analyze the properties of the data. As he explained it, they exploit what he called the “geometry of these data” to make inferences and decisions on a patient’s risk for COPD.
“Deep learning is very good for images, for videos, but it doesn’t work that well for signals,” said Mihai Udrescu, PhD, one of the Romanian collaborators. “But if we process the data with the technique brought up by Paul [Bogdan] and his team at USC, deep learning also works well on physiological signals.”
Dr. Paul Bogdan
Dr. Paul Bogdan, (left) and research associate Chenzhong Yin are standing in front of a summary of their research.
Said Dr. Bogdan, “Nobody thought about using physiological signals to predict COPD before this work. They used spirometry, but spirometry is cumbersome and several steps have to be performed in order to have an accurate spirometry.” His team’s AI models extract and analyze risk data based on 10 minutes of monitoring.
Dr. Udrescu
This technology also has the potential to improve accessibility of COPD screening, Dr. Udrescu said. “It can democratize the access to the health care because you don’t need to travel for 100 or 200 miles to see a specialist,” he said. “You just send an app to the mobile phone of a patient, the person puts on a smart watch and wears it for a couple of minutes and the data is either recorded locally or is transmitted and it is analyzed.” The computations can be done locally and in a matter of minutes, he said.
In Scotland, a 12-month feasibility study is underway to evaluate an AI model to identify COPD patients at greatest risk for adverse events. A press release from Lenus, the company developing the technology, said the study will use a COPD multidisciplinary team to consider real-time AI model outputs to enable proactive patient encounters and reduce emergency care visits.
Researchers in Paris built an AI model that showed a 68% accuracy in distinguishing people with asthma from people with COPD in administrative medical databases (BMC Pulmon Med. 2022 Sep 20. doi: 10.1186/s12890-022-02144-2). They found that asthma patients were younger than those with COPD (a mean of 49.9 vs. 72.1 years) and that COPD occurred mostly in men (68% vs. 33%). And an international team of researchers reported that an AI model that used chest CT scans determined that ever-smokers with COPD who met the imaging criteria for bronchiectasis were more prone to disease exacerbations (Radiology. 2022 Dec 13. doi: 10.1148/radiol.221109).
AI in idiopathic pulmonary fibrosis
The AI model that Dr. Chattopadhyay and collaborators developed had an 88% accuracy in predicting IPF. The model, known as the zero-burden comorbidity risk score for IPF (ZCoR-IPF), identified IPF cases in adults age 45 and older 1-4 years sooner than in a variety of pulmonology practice settings.
The model accounted for about 700 different features of IPF, Dr. Chattopadhyay said, but it deviated from standard AI risk models in that it used a machine learning algorithm to extract disease features that aren’t well understood or even known. “We do not know what all the risk factors of IPF are,” he said. “People who don’t have all the risk factors still get IPF. So we have to step back from the raw EHR data from where the features are being generated automatically, and then you can apply standard ML tools.”
Researchers at Nagoya University in Japan also reported on an AI algorithm for predicting IPF that used 646,800 high-resolution CT images and medical records data from 1,068 patients. Their algorithm had an average diagnostic accuracy of 83.6% and, they reported, demonstrated good accuracy even in patients with signs of interstitial pneumonia or who had surgical lung biopsies (Respirology. 2022 Dec 13. doi: 10.1111/resp.14310).
Chat GPT: The next frontier in AI
Dr. Tseng last year led a group of researchers that fed questions from the United States Medical Licensing Exam to a ChatGPT model, which found it answered 60%-65% of questions correctly (PLOS Digit Health. 2023 Feb 9. doi: 10.1371/journal.pdig.0000198). As Dr. Tseng pointed out, that’s good enough to get a medical license.
It may be a matter of time before ChatGPT technology finds its way into the clinic, Dr. Tseng said. A quick ChatGPT query of how it could be used in medicine yielded 12 different answers, from patient triage to providing basic first aid instructions in an emergency.
Dr. Tseng, who’s pulmonology practice places an emphasis on virtual care delivery, went deeper than the ChatGPT answer. “If you’re a respiratory therapist and you’re trying to execute a complicated medical care plan written by a physician, there’s a natural disconnect between our language and their language,” he said. “What we have found is that GPT has significantly harmonized the care plan. And that’s amazing because you end up with this single-stream understanding of the care plan, where the language is halfway between a bedside clinician, like the respiratory therapist or nurse, and is also something that a physician can understand and take the bigger sort of direction of care from.”
Barriers to AI in clinic
Numerous barriers face widespread adoption of AI tools in the clinic, Dr. Tseng said, including physician and staff anxiety about learning new technology. “AI tools, for all purposes, are supposed to allay the cognitive burden and the tedium burden on clinicians, but end up actually costing more time,” he said.
Dr. Novak
Health care organizations will also need to retool for AI, a group of medical informatics and digital health experts, led by Laurie Lovett Novak, PhD, reported (JAMIA Open. 2023 May 3. doi: 10.1093/jamiaopen/ooad028). But it’s coming nonetheless, Dr. Novak, an associate professor of biomedical informatics at Vanderbilt University Medical Center in Nashville, Tenn., said in an interview.
“In the near future, managers in clinics and inpatient units will be overseeing care that involves numerous AI-based technologies, including predictive analytics, imaging tools, language models, and others,” she said. “Organizations need to support managers by implementing capabilities for algorithmo-vigilance.”
That would include dealing with what she called “algorithmic drift” – when the accuracy of an AI model wanes because of changes in the underlying data – and ensuring that models are unbiased and aren’t used in a way that contributes to inequities in health care. “These new organizational capabilities will demand new tools and new competencies,” she said. That would include policies and processes drawing guidance from medical societies for legal and regulatory direction for managers, staff training, and software documentation.
Dr. Tseng envisioned how AI would work in the clinic. “I personally think that, at some time in the near future, AI-driven care coordination, where the AI basically handles appointment scheduling, patient motivation, patient engagement and acts as their health navigator, will be superior to any human health navigator on the whole, only for the reason that AI is indefatigable,” Dr. Tseng said. “It doesn’t get tired, it doesn’t get burned out, and these health navigation care coordination roles are notoriously difficult.”
The physicians and researchers interviewed for this report had no relevant relationships to disclose.
The utility of artificial intelligence in pulmonology has focused mainly on using image datasets to detect and diagnose lung malignancies, but now a growing number of AI models are emerging that apply machine learning to improve predictability for other pulmonary conditions, including pulmonary infections, pulmonary fibrosis, and chronic obstructive pulmonary disease (COPD).
These applications are moving beyond the traditional AI model of collecting data from a multitude of images to cast a wider data net that includes electronic health records.
Also on the horizon, ChatGPT technology is poised to have an impact. But pulmonologists and their practices have a number of barriers to clear before they feel a meaningful impact from AI.
The imperative, said AI researcher Ishanu Chattopadhyay, PhD, is to create transformative models that can detect lung disease early on. Dr. Chattopadhyay, an assistant professor of medicine at the University of Chicago and its Institute for Genomics and Systems Biology, and fellow researchers developed an AI algorithm that uses comorbidity signatures in electronic health records to screen for idiopathic pulmonary fibrosis (IPF) (Nature Med. 2022 Sep 29. doi: 10.1038/s41591-022-02010-y).
“If you could do this when somebody walks into a primary care setting and they are barely suspecting something is going on with them or when they don’t have the typical risk factors, there is a certain fraction of these people who do have IPF and they will almost invariably be diagnosed late and/or misdiagnosed,” Dr. Chattopadhyay said, citing a study that found 55% of patients with IPF have had at least one misdiagnosis and 38% have two or more misdiagnoses (BMC Pulm Med. 2018 Jan 17. doi: 10.1186/s12890-017-0560-x).
Harnessing massive data sets
AI models cull data sets, whether banks of radiographic images or files in an EHR, to extract telltale signatures of a disease state. Dr. Chattopadhyay and his team’s model used three databases with almost 3 million participants and 54,247 positive cases of IPF. Hospitals in Scotland have deployed what they’ve claimed are the first AI models to predict COPD built with 55,000 patient records from a regional National Health Service database. Another AI model for staging COPD, developed by researchers in the United States and Romania, used more than 18,000 medical records from 588 patients to identify physiological signals predictive of COPD (Advanced Sci. 2023 Feb 19. doi: 10.1002/advs.202203485).
Said Dr. Chattopadhyay: “If I can bring in AI which doesn’t just look at radiological images but actually gets it back where someone walks into primary care using only the information that is available at that point in the patient files and asking for nothing more, it raises a flag reliably that gets you a pulmonary referral that will hopefully reduce the misdiagnosis and late diagnosis.”
Dr. Tseng
Victor Tseng, MD, medical director for pulmonology at Ansible Health in Mountain View, Calif., who’s researching the potential of AI in pulmonology, speculated on what functions AI can perform in the clinic. “I think you will start to see much more interventional sort of clinically patient care–facing applications,” he said. That would include acting as a triage layer to direct patient queries to a nurse, physician, or another practitioner, providing patient instructions, serving as therapeutic software, coordinating care, integrating supply chain issues,” he said.
AI vs. spirometry for COPD
Researchers in the United States and Romania, led by Paul Bogdan, PhD, at the University of Southern California Viterbi School of Engineering, developed a model that predicted COPD with an accuracy of almost 99% (98.66%) and avoids many of the shortcomings of spirometry, Dr. Bogdan said.
USC Viterbi School of Engineering
Dr. Bogdan
The models developed by Dr. Bogdan and collaborators use a different principle than existing AI platforms, Dr. Bogdan said. They analyze the properties of the data. As he explained it, they exploit what he called the “geometry of these data” to make inferences and decisions on a patient’s risk for COPD.
“Deep learning is very good for images, for videos, but it doesn’t work that well for signals,” said Mihai Udrescu, PhD, one of the Romanian collaborators. “But if we process the data with the technique brought up by Paul [Bogdan] and his team at USC, deep learning also works well on physiological signals.”
Dr. Paul Bogdan
Dr. Paul Bogdan, (left) and research associate Chenzhong Yin are standing in front of a summary of their research.
Said Dr. Bogdan, “Nobody thought about using physiological signals to predict COPD before this work. They used spirometry, but spirometry is cumbersome and several steps have to be performed in order to have an accurate spirometry.” His team’s AI models extract and analyze risk data based on 10 minutes of monitoring.
Dr. Udrescu
This technology also has the potential to improve accessibility of COPD screening, Dr. Udrescu said. “It can democratize the access to the health care because you don’t need to travel for 100 or 200 miles to see a specialist,” he said. “You just send an app to the mobile phone of a patient, the person puts on a smart watch and wears it for a couple of minutes and the data is either recorded locally or is transmitted and it is analyzed.” The computations can be done locally and in a matter of minutes, he said.
In Scotland, a 12-month feasibility study is underway to evaluate an AI model to identify COPD patients at greatest risk for adverse events. A press release from Lenus, the company developing the technology, said the study will use a COPD multidisciplinary team to consider real-time AI model outputs to enable proactive patient encounters and reduce emergency care visits.
Researchers in Paris built an AI model that showed a 68% accuracy in distinguishing people with asthma from people with COPD in administrative medical databases (BMC Pulmon Med. 2022 Sep 20. doi: 10.1186/s12890-022-02144-2). They found that asthma patients were younger than those with COPD (a mean of 49.9 vs. 72.1 years) and that COPD occurred mostly in men (68% vs. 33%). And an international team of researchers reported that an AI model that used chest CT scans determined that ever-smokers with COPD who met the imaging criteria for bronchiectasis were more prone to disease exacerbations (Radiology. 2022 Dec 13. doi: 10.1148/radiol.221109).
AI in idiopathic pulmonary fibrosis
The AI model that Dr. Chattopadhyay and collaborators developed had an 88% accuracy in predicting IPF. The model, known as the zero-burden comorbidity risk score for IPF (ZCoR-IPF), identified IPF cases in adults age 45 and older 1-4 years sooner than in a variety of pulmonology practice settings.
The model accounted for about 700 different features of IPF, Dr. Chattopadhyay said, but it deviated from standard AI risk models in that it used a machine learning algorithm to extract disease features that aren’t well understood or even known. “We do not know what all the risk factors of IPF are,” he said. “People who don’t have all the risk factors still get IPF. So we have to step back from the raw EHR data from where the features are being generated automatically, and then you can apply standard ML tools.”
Researchers at Nagoya University in Japan also reported on an AI algorithm for predicting IPF that used 646,800 high-resolution CT images and medical records data from 1,068 patients. Their algorithm had an average diagnostic accuracy of 83.6% and, they reported, demonstrated good accuracy even in patients with signs of interstitial pneumonia or who had surgical lung biopsies (Respirology. 2022 Dec 13. doi: 10.1111/resp.14310).
Chat GPT: The next frontier in AI
Dr. Tseng last year led a group of researchers that fed questions from the United States Medical Licensing Exam to a ChatGPT model, which found it answered 60%-65% of questions correctly (PLOS Digit Health. 2023 Feb 9. doi: 10.1371/journal.pdig.0000198). As Dr. Tseng pointed out, that’s good enough to get a medical license.
It may be a matter of time before ChatGPT technology finds its way into the clinic, Dr. Tseng said. A quick ChatGPT query of how it could be used in medicine yielded 12 different answers, from patient triage to providing basic first aid instructions in an emergency.
Dr. Tseng, who’s pulmonology practice places an emphasis on virtual care delivery, went deeper than the ChatGPT answer. “If you’re a respiratory therapist and you’re trying to execute a complicated medical care plan written by a physician, there’s a natural disconnect between our language and their language,” he said. “What we have found is that GPT has significantly harmonized the care plan. And that’s amazing because you end up with this single-stream understanding of the care plan, where the language is halfway between a bedside clinician, like the respiratory therapist or nurse, and is also something that a physician can understand and take the bigger sort of direction of care from.”
Barriers to AI in clinic
Numerous barriers face widespread adoption of AI tools in the clinic, Dr. Tseng said, including physician and staff anxiety about learning new technology. “AI tools, for all purposes, are supposed to allay the cognitive burden and the tedium burden on clinicians, but end up actually costing more time,” he said.
Dr. Novak
Health care organizations will also need to retool for AI, a group of medical informatics and digital health experts, led by Laurie Lovett Novak, PhD, reported (JAMIA Open. 2023 May 3. doi: 10.1093/jamiaopen/ooad028). But it’s coming nonetheless, Dr. Novak, an associate professor of biomedical informatics at Vanderbilt University Medical Center in Nashville, Tenn., said in an interview.
“In the near future, managers in clinics and inpatient units will be overseeing care that involves numerous AI-based technologies, including predictive analytics, imaging tools, language models, and others,” she said. “Organizations need to support managers by implementing capabilities for algorithmo-vigilance.”
That would include dealing with what she called “algorithmic drift” – when the accuracy of an AI model wanes because of changes in the underlying data – and ensuring that models are unbiased and aren’t used in a way that contributes to inequities in health care. “These new organizational capabilities will demand new tools and new competencies,” she said. That would include policies and processes drawing guidance from medical societies for legal and regulatory direction for managers, staff training, and software documentation.
Dr. Tseng envisioned how AI would work in the clinic. “I personally think that, at some time in the near future, AI-driven care coordination, where the AI basically handles appointment scheduling, patient motivation, patient engagement and acts as their health navigator, will be superior to any human health navigator on the whole, only for the reason that AI is indefatigable,” Dr. Tseng said. “It doesn’t get tired, it doesn’t get burned out, and these health navigation care coordination roles are notoriously difficult.”
The physicians and researchers interviewed for this report had no relevant relationships to disclose.