User login
It takes work-arounds to make EHRs “work”
Dr. Hickner’s editorial “EHRs: Something’s gotta give” (J Fam Pract. 2014;63:558) prompted me to reflect on the elements of electronic health records (EHRs) that cannot change and the ones that can.
The EHR system I use allows the EHR to serve as a quality recorder, and it appears this is the most important part, because the reminders of what needs to be documented come first and are color-coded. From a reimbursement point of view, what is important is not the narrative, but the expanded “elements” that make it a billing document. I believe this will not change.
What can change is how the note information is organized, and I think the organization should be different for specific roles. At intake, a medical assistant can review allergies, medication lists, and preventive services; update family history; and take vital signs and history of present illness (HPI). As the physician, I want the note to show the information in the order that I process it during the visit: 1) allergies/medication list, 2) concerns/complaints with brief documentation, 3) vitals, 4) physical, 5) assessment, and 6) plan.
After the note is signed off on, I want a different format for review purposes: 1) assessment/plan (because this is what I look at first for follow-up), 2) HPI/review of systems, 3) physical, 4) allergies, 5) medication list, 6) past medical history, and 7) quality reminders (if they show up at all after the visit is complete).
Is it asking too much for a programmer to make the EHR organize information in this manner?
Edward Friedler, MD
Annandale, Va
I still dictate my notes and they very much tell a story that an EHR cannot. I have been audited repeatedly and I always have all the bullet points and essentials that the insurance company wants, but this information is in a format that everyone—including patients—can read and appreciate.
The move to APSO (assessment, plan, subjective, objective) from SOAP (subjective, objective, assessment, plan) is an example of the tail wagging the dog. Rather than fix the note so the time-honored SOAP format works, we acknowledge that no one actually reads the long template notes and they want to get to the bottom line (ie, the assessment and plan).
My dream is to return to the days when we only listed the positive findings, the assumption being that a competent physician did the exam that was required and it’s unnecessary to state that the examined anatomy was normal. Unfortunately, so much of what we must do is driven by lawyers and insurance companies—not by doctors.
David M. Brill, DO
Rocky River, Ohio
I now take photos of all of the ludicrous choices our EHR tosses at me, such as “laceration of third eyelid” or “injury, crushed by falling aircraft due to terrorist.” Most of my EHR entries now say, “See scanned handwritten note for accuracy.”
The issue of EHRs needs to be kept on the front burner. It is destroying doctor/patient relationships and quality diagnostic care while hiding the important findings in the garbage.
Jay Hammett, MD
Knoxville, Tenn
I’m in a group practice of 10 family physicians and in a typical workday, each of us sees 23 to 25 patients, answers e-mails/phone calls, and reviews labs/studies, which leaves no time for anything else. There’s a constant struggle to stay on top of the quality of the notes. I have preserved the quality of my own notes by free typing. I free type a differential next to my assessment or on the first line of the plan. I don’t use templates; they slow me down too much.
Kelly Luba, DO
Phoenix, Ariz
I was a civil service physician working for the Department of the Navy in 2005 when EHRs were thrust upon me. The system was not particularly user-friendly. Free texting was highly discouraged and it was strongly preferred that we used structured text embedded in the program.
I couldn’t use the program as envisioned, so I found a work-around. I would paste the 4 sections of the SOAP note directly into the appropriate free text sections of the electronic record. My assessment included the correct diagnosis, and I would pick a general EHR diagnosis from the dropdown list. Visually, my records did not look any different from those of other health care providers who used structured text.
I used this method until my civil service retirement in 2014. All of my record peer reviews were outstanding, and I was told that my records were easy to understand. I finally let on to all that I never used structured text and that all of my records were really written the old-fashioned way. I still used a clipboard during the patient visit, and completed all records after the patient left.
David F. Scaccia, DO, MPH
Kittery, Maine
Dr. Hickner’s editorial “EHRs: Something’s gotta give” (J Fam Pract. 2014;63:558) prompted me to reflect on the elements of electronic health records (EHRs) that cannot change and the ones that can.
The EHR system I use allows the EHR to serve as a quality recorder, and it appears this is the most important part, because the reminders of what needs to be documented come first and are color-coded. From a reimbursement point of view, what is important is not the narrative, but the expanded “elements” that make it a billing document. I believe this will not change.
What can change is how the note information is organized, and I think the organization should be different for specific roles. At intake, a medical assistant can review allergies, medication lists, and preventive services; update family history; and take vital signs and history of present illness (HPI). As the physician, I want the note to show the information in the order that I process it during the visit: 1) allergies/medication list, 2) concerns/complaints with brief documentation, 3) vitals, 4) physical, 5) assessment, and 6) plan.
After the note is signed off on, I want a different format for review purposes: 1) assessment/plan (because this is what I look at first for follow-up), 2) HPI/review of systems, 3) physical, 4) allergies, 5) medication list, 6) past medical history, and 7) quality reminders (if they show up at all after the visit is complete).
Is it asking too much for a programmer to make the EHR organize information in this manner?
Edward Friedler, MD
Annandale, Va
I still dictate my notes and they very much tell a story that an EHR cannot. I have been audited repeatedly and I always have all the bullet points and essentials that the insurance company wants, but this information is in a format that everyone—including patients—can read and appreciate.
The move to APSO (assessment, plan, subjective, objective) from SOAP (subjective, objective, assessment, plan) is an example of the tail wagging the dog. Rather than fix the note so the time-honored SOAP format works, we acknowledge that no one actually reads the long template notes and they want to get to the bottom line (ie, the assessment and plan).
My dream is to return to the days when we only listed the positive findings, the assumption being that a competent physician did the exam that was required and it’s unnecessary to state that the examined anatomy was normal. Unfortunately, so much of what we must do is driven by lawyers and insurance companies—not by doctors.
David M. Brill, DO
Rocky River, Ohio
I now take photos of all of the ludicrous choices our EHR tosses at me, such as “laceration of third eyelid” or “injury, crushed by falling aircraft due to terrorist.” Most of my EHR entries now say, “See scanned handwritten note for accuracy.”
The issue of EHRs needs to be kept on the front burner. It is destroying doctor/patient relationships and quality diagnostic care while hiding the important findings in the garbage.
Jay Hammett, MD
Knoxville, Tenn
I’m in a group practice of 10 family physicians and in a typical workday, each of us sees 23 to 25 patients, answers e-mails/phone calls, and reviews labs/studies, which leaves no time for anything else. There’s a constant struggle to stay on top of the quality of the notes. I have preserved the quality of my own notes by free typing. I free type a differential next to my assessment or on the first line of the plan. I don’t use templates; they slow me down too much.
Kelly Luba, DO
Phoenix, Ariz
I was a civil service physician working for the Department of the Navy in 2005 when EHRs were thrust upon me. The system was not particularly user-friendly. Free texting was highly discouraged and it was strongly preferred that we used structured text embedded in the program.
I couldn’t use the program as envisioned, so I found a work-around. I would paste the 4 sections of the SOAP note directly into the appropriate free text sections of the electronic record. My assessment included the correct diagnosis, and I would pick a general EHR diagnosis from the dropdown list. Visually, my records did not look any different from those of other health care providers who used structured text.
I used this method until my civil service retirement in 2014. All of my record peer reviews were outstanding, and I was told that my records were easy to understand. I finally let on to all that I never used structured text and that all of my records were really written the old-fashioned way. I still used a clipboard during the patient visit, and completed all records after the patient left.
David F. Scaccia, DO, MPH
Kittery, Maine
Dr. Hickner’s editorial “EHRs: Something’s gotta give” (J Fam Pract. 2014;63:558) prompted me to reflect on the elements of electronic health records (EHRs) that cannot change and the ones that can.
The EHR system I use allows the EHR to serve as a quality recorder, and it appears this is the most important part, because the reminders of what needs to be documented come first and are color-coded. From a reimbursement point of view, what is important is not the narrative, but the expanded “elements” that make it a billing document. I believe this will not change.
What can change is how the note information is organized, and I think the organization should be different for specific roles. At intake, a medical assistant can review allergies, medication lists, and preventive services; update family history; and take vital signs and history of present illness (HPI). As the physician, I want the note to show the information in the order that I process it during the visit: 1) allergies/medication list, 2) concerns/complaints with brief documentation, 3) vitals, 4) physical, 5) assessment, and 6) plan.
After the note is signed off on, I want a different format for review purposes: 1) assessment/plan (because this is what I look at first for follow-up), 2) HPI/review of systems, 3) physical, 4) allergies, 5) medication list, 6) past medical history, and 7) quality reminders (if they show up at all after the visit is complete).
Is it asking too much for a programmer to make the EHR organize information in this manner?
Edward Friedler, MD
Annandale, Va
I still dictate my notes and they very much tell a story that an EHR cannot. I have been audited repeatedly and I always have all the bullet points and essentials that the insurance company wants, but this information is in a format that everyone—including patients—can read and appreciate.
The move to APSO (assessment, plan, subjective, objective) from SOAP (subjective, objective, assessment, plan) is an example of the tail wagging the dog. Rather than fix the note so the time-honored SOAP format works, we acknowledge that no one actually reads the long template notes and they want to get to the bottom line (ie, the assessment and plan).
My dream is to return to the days when we only listed the positive findings, the assumption being that a competent physician did the exam that was required and it’s unnecessary to state that the examined anatomy was normal. Unfortunately, so much of what we must do is driven by lawyers and insurance companies—not by doctors.
David M. Brill, DO
Rocky River, Ohio
I now take photos of all of the ludicrous choices our EHR tosses at me, such as “laceration of third eyelid” or “injury, crushed by falling aircraft due to terrorist.” Most of my EHR entries now say, “See scanned handwritten note for accuracy.”
The issue of EHRs needs to be kept on the front burner. It is destroying doctor/patient relationships and quality diagnostic care while hiding the important findings in the garbage.
Jay Hammett, MD
Knoxville, Tenn
I’m in a group practice of 10 family physicians and in a typical workday, each of us sees 23 to 25 patients, answers e-mails/phone calls, and reviews labs/studies, which leaves no time for anything else. There’s a constant struggle to stay on top of the quality of the notes. I have preserved the quality of my own notes by free typing. I free type a differential next to my assessment or on the first line of the plan. I don’t use templates; they slow me down too much.
Kelly Luba, DO
Phoenix, Ariz
I was a civil service physician working for the Department of the Navy in 2005 when EHRs were thrust upon me. The system was not particularly user-friendly. Free texting was highly discouraged and it was strongly preferred that we used structured text embedded in the program.
I couldn’t use the program as envisioned, so I found a work-around. I would paste the 4 sections of the SOAP note directly into the appropriate free text sections of the electronic record. My assessment included the correct diagnosis, and I would pick a general EHR diagnosis from the dropdown list. Visually, my records did not look any different from those of other health care providers who used structured text.
I used this method until my civil service retirement in 2014. All of my record peer reviews were outstanding, and I was told that my records were easy to understand. I finally let on to all that I never used structured text and that all of my records were really written the old-fashioned way. I still used a clipboard during the patient visit, and completed all records after the patient left.
David F. Scaccia, DO, MPH
Kittery, Maine
Bilateral hand cramping and weakness • broad fingers • coarse facial features • Dx?
THE CASE
A 37-year-old right-hand dominant woman came to our clinic seeking treatment for bilateral generalized hand cramping and weakness that she had been experiencing for approximately 2 to 3 years. She was dropping objects and had finger locking, yet had no numbness, tingling, or morning stiffness.
Ten months earlier, she had given birth to a healthy 3715 g girl. Our patient’s prenatal glucose tolerance test had been normal. Her pregnancy and delivery had been significant for oligohydramnios, failed post-term (41 weeks 4 days) induction, and emergent low transverse cesarean section due to fetal bradycardia. Since giving birth, our patient had 3 menstrual periods while breastfeeding. She had a copper intrauterine device inserted at her 6-week postpartum visit. She also had 2 truncal acrochordons removed 3 months postpartum. She had no history of neck trauma, overuse injury, or occupational exposures.
Her blood pressure and vital signs were within normal limits. Physical exam was notable for subtly coarse facial features and broad fingers (FIGURE 1).

She had normal wrist and hand joint range of motion; her wrist and hand strengths, including grip strength, were 5 out of 5. Tinel’s sign, Phalen’s maneuver, and Finkelstein’s test were negative.
Her upper extremity neurovascular exams were completely normal. Initial laboratory studies—including a comprehensive metabolic panel—were normal. The only exception was her creatine kinase, which was 265 U/L (normal, 24-195 U/L).
At a follow-up appointment 7 weeks later, we gathered a more detailed history and learned that over the past 2 to 3 years, the patient had noticed that her shoe and ring sizes had been increasing. She also mentioned some mild weight gain following her pregnancy.
Occasionally, she had generalized hand swelling, headaches, and saw floaters, but she denied losing peripheral vision. Additional lab work at this time revealed a fasting growth hormone (GH) level of 27.3 ng/mL (normal, 0.05-8 ng/mL) and an insulin-like growth factor 1 (IGF-1) level of 848 ng/mL (normal, 106-368 ng/mL). An anterior pituitary hormone panel and cortisol level were normal. A urine pregnancy test was negative.
THE DIAGNOSIS
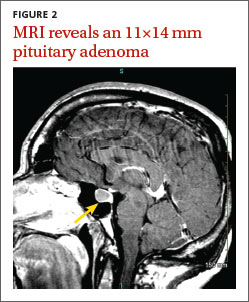
Magnetic resonance imaging (MRI) of our patient’s brain revealed a pituitary adenoma (FIGURE 2). Based on that and the patient’s elevated GH and IGF-1 levels, we diagnosed acromegaly due to a pituitary adenoma.
DISCUSSION
Acromegaly is a rare, progressively disfiguring disease with a prevalence of 40 cases per million people.1 It affects middle-aged adults, with no gender difference.2 In most cases, the cause is a benign pituitary adenoma.1-4
Physical changes include coarse facial features, generalized expansion of the skull, brow protrusion, ocular distension, prognathism, macroglossia, acral overgrowth, and dental malocclusion; these changes typically occur slowly over a long time period.1-5 For example, when we looked at the 3-year-old photo on our patient’s driver’s license, we noticed only subtle changes from her current appearance. Common clinical manifestations include headache, hyperpigmentation, hypertrichosis, hyperhidrosis, goiter, arthropathy, carpal tunnel syndrome, visual disturbances, and acrochordons.1,5
Acromegaly is associated with an increased risk of cardiovascular disease, metabolic disorders, infertility, sleep apnea, arthritis, thyroid tumors, colon adenomas, and carcinoma.1,2,4,5 Due to the insidious progression of acromegaly’s clinical manifestations, diagnosis is delayed for 4 to 10 years, on average.1 The diagnosis of acromegaly is typically based on an elevation of GH and IGF-1 levels.1,5 A brain MRI is essential in the diagnosis of a pituitary adenoma.1
Pregnancy among patients with acromegaly is uncommon. In fact, fewer than 150 cases have been reported in the literature.2,6 In most cases, it appears that pregnancy among patients with acromegaly is safe for mothers and newborns.6,7
The goals of treatment for acromegaly caused by a pituitary adenoma are to remove/ reduce the tumor and its mechanical effects, relieve symptoms, reduce serum GH and IGF-1, and restore pituitary function. Transsphenoidal surgical resection is the preferred treatment for pituitary adenomas.1,2,4 Radiation therapy and pharmacologic treatment may be necessary as adjuncts to surgery or for patients for whom surgery is contraindicated.1,4,5
Pharmacologic management of acromegaly includes dopamine agonists (cabergoline), somatostatin analogues (octreotide, lanreotide), and GH receptor antagonists (pegvisomant).1,3 Patients who receive effective early treatment of acromegaly have a life expectancy similar to that of the general population.1,5
Our patient
Our patient was referred to Neurosurgery and underwent transnasal transsphenoidal resection of the pituitary adenoma. Two weeks postop, her GH level had decreased to 0.66 ng/mL and her IGF-1 level was down to 386 ng/mL. Four months later, her GH (2.32 ng/mL) and IGF-1 levels (277 ng/mL) were within normal range and our patient reported improvement in all of her symptoms.
THE TAKEAWAY
Because it may take years for the classical clinical features of acromegaly such as coarse facial features, protruding jaw, and broad fingers to become apparent, diligent history taking is essential to diagnose the condition early. Patients may present with nonspecific and confusing symptoms such as muscle weakness.8 Early nonspecific symptoms and signs in the presence of normal basic laboratory tests should warrant an evaluation of fasting GH and IGF-1. Early treatment with surgery, radiation therapy, or pharmacotherapy may prevent or decrease the intensity of rheumatologic, cardiovascular, respiratory, and metabolic complications of acromegaly.1
1. Scacchi M, Cavagnini F. Acromegaly. Pituitary. 2006;9: 297-303.
2. Hossain B, Drake WM. Acromegaly. Medicine. 2009;37: 407-410.
3. Chan MR, Ziebert M, Maas DL, et al. “My rings won’t fit anymore”. Ectopic growth hormone-secreting tumor. Am Fam Physician. 2005;71:1766-1767.
4. Lake MG, Krook LS, Cruz SV. Pituitary adenomas: an overview. Am Fam Physician. 2013;88:319-327.
5. Vilar L, Valenzuela A, Ribeiro-Oliveira A Jr, et al. Multiple facets in the control of acromegaly. Pituitary. 2014;17 suppl 1:S11-S17.
6. Cheng V, Faiman C, Kennedy L, et al. Pregnancy and acromegaly: a review. Pituitary. 2012;15:59-63.
7. Caron P, Broussaud S, Bertherat J, et al. Acromegaly and pregnancy: a retrospective multicenter study of 59 pregnancies in 46 women. J Clin Endocrinol Metab. 2010;95:4680-4687.
8. Saguil A. Evaluation of the patient with muscle weakness. Am Fam Physician. 2005;71:1327-1336.
THE CASE
A 37-year-old right-hand dominant woman came to our clinic seeking treatment for bilateral generalized hand cramping and weakness that she had been experiencing for approximately 2 to 3 years. She was dropping objects and had finger locking, yet had no numbness, tingling, or morning stiffness.
Ten months earlier, she had given birth to a healthy 3715 g girl. Our patient’s prenatal glucose tolerance test had been normal. Her pregnancy and delivery had been significant for oligohydramnios, failed post-term (41 weeks 4 days) induction, and emergent low transverse cesarean section due to fetal bradycardia. Since giving birth, our patient had 3 menstrual periods while breastfeeding. She had a copper intrauterine device inserted at her 6-week postpartum visit. She also had 2 truncal acrochordons removed 3 months postpartum. She had no history of neck trauma, overuse injury, or occupational exposures.
Her blood pressure and vital signs were within normal limits. Physical exam was notable for subtly coarse facial features and broad fingers (FIGURE 1).
She had normal wrist and hand joint range of motion; her wrist and hand strengths, including grip strength, were 5 out of 5. Tinel’s sign, Phalen’s maneuver, and Finkelstein’s test were negative.
Her upper extremity neurovascular exams were completely normal. Initial laboratory studies—including a comprehensive metabolic panel—were normal. The only exception was her creatine kinase, which was 265 U/L (normal, 24-195 U/L).
At a follow-up appointment 7 weeks later, we gathered a more detailed history and learned that over the past 2 to 3 years, the patient had noticed that her shoe and ring sizes had been increasing. She also mentioned some mild weight gain following her pregnancy.
Occasionally, she had generalized hand swelling, headaches, and saw floaters, but she denied losing peripheral vision. Additional lab work at this time revealed a fasting growth hormone (GH) level of 27.3 ng/mL (normal, 0.05-8 ng/mL) and an insulin-like growth factor 1 (IGF-1) level of 848 ng/mL (normal, 106-368 ng/mL). An anterior pituitary hormone panel and cortisol level were normal. A urine pregnancy test was negative.
THE DIAGNOSIS
Magnetic resonance imaging (MRI) of our patient’s brain revealed a pituitary adenoma (FIGURE 2). Based on that and the patient’s elevated GH and IGF-1 levels, we diagnosed acromegaly due to a pituitary adenoma.
DISCUSSION
Acromegaly is a rare, progressively disfiguring disease with a prevalence of 40 cases per million people.1 It affects middle-aged adults, with no gender difference.2 In most cases, the cause is a benign pituitary adenoma.1-4
Physical changes include coarse facial features, generalized expansion of the skull, brow protrusion, ocular distension, prognathism, macroglossia, acral overgrowth, and dental malocclusion; these changes typically occur slowly over a long time period.1-5 For example, when we looked at the 3-year-old photo on our patient’s driver’s license, we noticed only subtle changes from her current appearance. Common clinical manifestations include headache, hyperpigmentation, hypertrichosis, hyperhidrosis, goiter, arthropathy, carpal tunnel syndrome, visual disturbances, and acrochordons.1,5
Acromegaly is associated with an increased risk of cardiovascular disease, metabolic disorders, infertility, sleep apnea, arthritis, thyroid tumors, colon adenomas, and carcinoma.1,2,4,5 Due to the insidious progression of acromegaly’s clinical manifestations, diagnosis is delayed for 4 to 10 years, on average.1 The diagnosis of acromegaly is typically based on an elevation of GH and IGF-1 levels.1,5 A brain MRI is essential in the diagnosis of a pituitary adenoma.1
Pregnancy among patients with acromegaly is uncommon. In fact, fewer than 150 cases have been reported in the literature.2,6 In most cases, it appears that pregnancy among patients with acromegaly is safe for mothers and newborns.6,7
The goals of treatment for acromegaly caused by a pituitary adenoma are to remove/ reduce the tumor and its mechanical effects, relieve symptoms, reduce serum GH and IGF-1, and restore pituitary function. Transsphenoidal surgical resection is the preferred treatment for pituitary adenomas.1,2,4 Radiation therapy and pharmacologic treatment may be necessary as adjuncts to surgery or for patients for whom surgery is contraindicated.1,4,5
Pharmacologic management of acromegaly includes dopamine agonists (cabergoline), somatostatin analogues (octreotide, lanreotide), and GH receptor antagonists (pegvisomant).1,3 Patients who receive effective early treatment of acromegaly have a life expectancy similar to that of the general population.1,5
Our patient
Our patient was referred to Neurosurgery and underwent transnasal transsphenoidal resection of the pituitary adenoma. Two weeks postop, her GH level had decreased to 0.66 ng/mL and her IGF-1 level was down to 386 ng/mL. Four months later, her GH (2.32 ng/mL) and IGF-1 levels (277 ng/mL) were within normal range and our patient reported improvement in all of her symptoms.
THE TAKEAWAY
Because it may take years for the classical clinical features of acromegaly such as coarse facial features, protruding jaw, and broad fingers to become apparent, diligent history taking is essential to diagnose the condition early. Patients may present with nonspecific and confusing symptoms such as muscle weakness.8 Early nonspecific symptoms and signs in the presence of normal basic laboratory tests should warrant an evaluation of fasting GH and IGF-1. Early treatment with surgery, radiation therapy, or pharmacotherapy may prevent or decrease the intensity of rheumatologic, cardiovascular, respiratory, and metabolic complications of acromegaly.1
THE CASE
A 37-year-old right-hand dominant woman came to our clinic seeking treatment for bilateral generalized hand cramping and weakness that she had been experiencing for approximately 2 to 3 years. She was dropping objects and had finger locking, yet had no numbness, tingling, or morning stiffness.
Ten months earlier, she had given birth to a healthy 3715 g girl. Our patient’s prenatal glucose tolerance test had been normal. Her pregnancy and delivery had been significant for oligohydramnios, failed post-term (41 weeks 4 days) induction, and emergent low transverse cesarean section due to fetal bradycardia. Since giving birth, our patient had 3 menstrual periods while breastfeeding. She had a copper intrauterine device inserted at her 6-week postpartum visit. She also had 2 truncal acrochordons removed 3 months postpartum. She had no history of neck trauma, overuse injury, or occupational exposures.
Her blood pressure and vital signs were within normal limits. Physical exam was notable for subtly coarse facial features and broad fingers (FIGURE 1).
She had normal wrist and hand joint range of motion; her wrist and hand strengths, including grip strength, were 5 out of 5. Tinel’s sign, Phalen’s maneuver, and Finkelstein’s test were negative.
Her upper extremity neurovascular exams were completely normal. Initial laboratory studies—including a comprehensive metabolic panel—were normal. The only exception was her creatine kinase, which was 265 U/L (normal, 24-195 U/L).
At a follow-up appointment 7 weeks later, we gathered a more detailed history and learned that over the past 2 to 3 years, the patient had noticed that her shoe and ring sizes had been increasing. She also mentioned some mild weight gain following her pregnancy.
Occasionally, she had generalized hand swelling, headaches, and saw floaters, but she denied losing peripheral vision. Additional lab work at this time revealed a fasting growth hormone (GH) level of 27.3 ng/mL (normal, 0.05-8 ng/mL) and an insulin-like growth factor 1 (IGF-1) level of 848 ng/mL (normal, 106-368 ng/mL). An anterior pituitary hormone panel and cortisol level were normal. A urine pregnancy test was negative.
THE DIAGNOSIS
Magnetic resonance imaging (MRI) of our patient’s brain revealed a pituitary adenoma (FIGURE 2). Based on that and the patient’s elevated GH and IGF-1 levels, we diagnosed acromegaly due to a pituitary adenoma.
DISCUSSION
Acromegaly is a rare, progressively disfiguring disease with a prevalence of 40 cases per million people.1 It affects middle-aged adults, with no gender difference.2 In most cases, the cause is a benign pituitary adenoma.1-4
Physical changes include coarse facial features, generalized expansion of the skull, brow protrusion, ocular distension, prognathism, macroglossia, acral overgrowth, and dental malocclusion; these changes typically occur slowly over a long time period.1-5 For example, when we looked at the 3-year-old photo on our patient’s driver’s license, we noticed only subtle changes from her current appearance. Common clinical manifestations include headache, hyperpigmentation, hypertrichosis, hyperhidrosis, goiter, arthropathy, carpal tunnel syndrome, visual disturbances, and acrochordons.1,5
Acromegaly is associated with an increased risk of cardiovascular disease, metabolic disorders, infertility, sleep apnea, arthritis, thyroid tumors, colon adenomas, and carcinoma.1,2,4,5 Due to the insidious progression of acromegaly’s clinical manifestations, diagnosis is delayed for 4 to 10 years, on average.1 The diagnosis of acromegaly is typically based on an elevation of GH and IGF-1 levels.1,5 A brain MRI is essential in the diagnosis of a pituitary adenoma.1
Pregnancy among patients with acromegaly is uncommon. In fact, fewer than 150 cases have been reported in the literature.2,6 In most cases, it appears that pregnancy among patients with acromegaly is safe for mothers and newborns.6,7
The goals of treatment for acromegaly caused by a pituitary adenoma are to remove/ reduce the tumor and its mechanical effects, relieve symptoms, reduce serum GH and IGF-1, and restore pituitary function. Transsphenoidal surgical resection is the preferred treatment for pituitary adenomas.1,2,4 Radiation therapy and pharmacologic treatment may be necessary as adjuncts to surgery or for patients for whom surgery is contraindicated.1,4,5
Pharmacologic management of acromegaly includes dopamine agonists (cabergoline), somatostatin analogues (octreotide, lanreotide), and GH receptor antagonists (pegvisomant).1,3 Patients who receive effective early treatment of acromegaly have a life expectancy similar to that of the general population.1,5
Our patient
Our patient was referred to Neurosurgery and underwent transnasal transsphenoidal resection of the pituitary adenoma. Two weeks postop, her GH level had decreased to 0.66 ng/mL and her IGF-1 level was down to 386 ng/mL. Four months later, her GH (2.32 ng/mL) and IGF-1 levels (277 ng/mL) were within normal range and our patient reported improvement in all of her symptoms.
THE TAKEAWAY
Because it may take years for the classical clinical features of acromegaly such as coarse facial features, protruding jaw, and broad fingers to become apparent, diligent history taking is essential to diagnose the condition early. Patients may present with nonspecific and confusing symptoms such as muscle weakness.8 Early nonspecific symptoms and signs in the presence of normal basic laboratory tests should warrant an evaluation of fasting GH and IGF-1. Early treatment with surgery, radiation therapy, or pharmacotherapy may prevent or decrease the intensity of rheumatologic, cardiovascular, respiratory, and metabolic complications of acromegaly.1
1. Scacchi M, Cavagnini F. Acromegaly. Pituitary. 2006;9: 297-303.
2. Hossain B, Drake WM. Acromegaly. Medicine. 2009;37: 407-410.
3. Chan MR, Ziebert M, Maas DL, et al. “My rings won’t fit anymore”. Ectopic growth hormone-secreting tumor. Am Fam Physician. 2005;71:1766-1767.
4. Lake MG, Krook LS, Cruz SV. Pituitary adenomas: an overview. Am Fam Physician. 2013;88:319-327.
5. Vilar L, Valenzuela A, Ribeiro-Oliveira A Jr, et al. Multiple facets in the control of acromegaly. Pituitary. 2014;17 suppl 1:S11-S17.
6. Cheng V, Faiman C, Kennedy L, et al. Pregnancy and acromegaly: a review. Pituitary. 2012;15:59-63.
7. Caron P, Broussaud S, Bertherat J, et al. Acromegaly and pregnancy: a retrospective multicenter study of 59 pregnancies in 46 women. J Clin Endocrinol Metab. 2010;95:4680-4687.
8. Saguil A. Evaluation of the patient with muscle weakness. Am Fam Physician. 2005;71:1327-1336.
1. Scacchi M, Cavagnini F. Acromegaly. Pituitary. 2006;9: 297-303.
2. Hossain B, Drake WM. Acromegaly. Medicine. 2009;37: 407-410.
3. Chan MR, Ziebert M, Maas DL, et al. “My rings won’t fit anymore”. Ectopic growth hormone-secreting tumor. Am Fam Physician. 2005;71:1766-1767.
4. Lake MG, Krook LS, Cruz SV. Pituitary adenomas: an overview. Am Fam Physician. 2013;88:319-327.
5. Vilar L, Valenzuela A, Ribeiro-Oliveira A Jr, et al. Multiple facets in the control of acromegaly. Pituitary. 2014;17 suppl 1:S11-S17.
6. Cheng V, Faiman C, Kennedy L, et al. Pregnancy and acromegaly: a review. Pituitary. 2012;15:59-63.
7. Caron P, Broussaud S, Bertherat J, et al. Acromegaly and pregnancy: a retrospective multicenter study of 59 pregnancies in 46 women. J Clin Endocrinol Metab. 2010;95:4680-4687.
8. Saguil A. Evaluation of the patient with muscle weakness. Am Fam Physician. 2005;71:1327-1336.

Prescribing statins for patients with ACS? No need to wait
Prescribe a high-dose statin before any patient with acute coronary syndrome (ACS) undergoes percutaneous coronary intervention (PCI); it may be reasonable to extend this to patients being evaluated for ACS.1
Strength of recommendation
A: Based on a meta-analysis
Navarese EP, Kowalewski M, Andreotti F, et al. Meta-analysis of time-related benefits of statin therapy in patients with acute coronary syndrome undergoing percutaneous coronary intervention. Am J Cardiol. 2014;113:1753-1764.
Illustrative case
A 48-year-old man comes to the emergency department with chest pain and is diagnosed with ACS. He is scheduled to have PCI within the next 24 hours. When should you start him on a statin?
Statins are the mainstay pharmaceutical treatment for hyperlipidemia, and are used for primary and secondary prevention of coronary artery disease and stroke.2,3 Well-known for their cholesterol-lowering effect, they also have benefits that are independent of their effects on lipids, including improving endothelial function, decreasing oxidative stress, and decreasing vascular inflammation.4-6
Compared to patients with stable angina, patients with ACS experience markedly higher rates of coronary events, especially immediately before and after PCI and during the subsequent 30 days.1 American College of Cardiology/American Heart Association (ACC/AHA) guidelines for the management of non-ST elevation myocardial infarction (NSTEMI) advocate starting statins before patients are discharged from the hospital, but they don’t specify precisely when.7
Considering the higher risk of coronary events before and after PCI and statins’ pleiotropic effects, it is reasonable to investigate the optimal time for starting statins in patients with ACS.
STUDY SUMMARY: Meta-analysis of 20 RCTs shows statins before PCI cuts risk of MI
Navarese et al1 performed a systematic review and meta-analysis of studies comparing the clinical outcomes of patients with ACS who received statins before or after PCI (statins group) vs those who received low-dose statins or no statins (control group). The authors searched PubMed, Cochrane, Google Scholar, and CINAHL databases as well as key conference proceedings for studies published before November 2013. Using reasonable inclusion and exclusion criteria and appropriate statistical methods, they analyzed the results of 20 randomized controlled trials that included 8750 patients. Four studies enrolled only patients with ST elevation MI, 8 were restricted to NSTEMI, and the remaining 8 studies enrolled patients with any type of MI or unstable angina.
For patients who were started on a statin before PCI, the mean timing of administration was 0.53 ± 0.42 days before. For those started after PCI, the average time to administration was 3.18 ± 3.56 days after.
Whether administered before or after PCI, statins reduced the incidence of MIs. The overall 30-day incidence of MIs was 3.4% (123 of 3621) in the statins group and 5% (179 of 3577) in the control group. This resulted in an absolute risk reduction of 1.6% (number needed to treat=62.5), and a reduction of the odds of MI by 33% (odds ratio [OR]=0.67; 95% confidence interval [CI], 0.53-0.84; P=.0007). There was also a trend toward reduced mortality in the statin group (OR=0.66; 95% CI, 0.43-1.02; P=.06).
In addition, administering statins before PCI resulted in a greater reduction in the odds of MI at 30 days (OR=0.38; 95% CI, 0.24-0.59; P<.0001) than starting them post-PCI (OR=0.85; 95% CI, 0.64-1.13; P=.28) when compared to the controls. The difference between the pre-PCI OR and the post-PCI OR was statistically significant (P=.002). These findings persisted past 30 days (P=.06).
WHAT'S NEW: Early statin administration is most effective
According to ACC/AHA guidelines, all patients with ACS should be receiving a statin by the time they are discharged. However, when to start the statin is not specified. This meta-analysis is the first report to show that administering a statin before PCI can significantly reduce the risk of subsequent MI.
CAVEATS: Benefits might vary with different statins
The studies evaluated in this meta-analysis used various statins and dosing regimens, which could have affected the results. However, sensitivity analyses found similar benefits across different types of statins. In addition, most of the included trials used high doses of statins, which minimized the potential discrepancy in outcomes from various dosing regimens. And while the included studies were not perfect, Navarese et al1 used reasonable methods to identify potential biases.
CHALLENGES TO IMPLEMENTATION: No barriers to starting statins earlier
Implementing this intervention may be as simple as editing a standard order. This meta-analysis also suggests that the earlier the intervention, the greater the benefit, which may be an argument for starting a statin when a patient first presents for evaluation for ACS, since the risks of taking a statin are quite low. We believe it would be beneficial if the next update of the ACC/AHA guidelines7 included this recommendation.
ACKNOWLEDGEMENT
The PURLs Surveillance System was supported in part by Grant Number UL1RR024999 from the National Center For Research Resources, a Clinical Translational Science Award to the University of Chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center For Research Resources or the National Institutes of Health.
1. Navarese EP, Kowalewski M, Andreotti F, et al. Meta-analysis of time-related benefits of statin therapy in patients with acute coronary syndrome undergoing percutaneous coronary intervention. Am J Cardiol. 2014;113:1753-1764.
2. Pignone M, Phillips C, Mulrow C. Use of lipid lowering drugs for primary prevention of coronary heart disease: meta-analysis of randomised trials. BMJ. 2000;321:983-986.
3. Prevention of cardiovascular events and death with pravastatin in patients with coronary heart disease and a broad range of initial cholesterol levels. The Long-Term Intervention with Pravastatin in Ischaemic Disease (LIPID) Study Group. N Engl J Med. 1998;339:1349-1357.
4. Liao JK. Beyond lipid lowering: the role of statins in vascular protection. Int J Cardiol. 2002;86:5-18.
5. Li J, Li JJ, He JG, et al. Atorvastatin decreases C-reactive protein-induced inflammatory response in pulmonary artery smooth muscle cells by inhibiting nuclear factor-kappaB pathway. Cardiovasc Ther. 2010;28:8-14.
6. Tandon V, Bano G, Khajuria V, et al. Pleiotropic effects of statins. Indian J Pharmacol. 2005;37:77-85.
7. Wright RS, Anderson JL, Adams CD, et al; American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. 2011 ACCF/AHA focused update incorporated into the ACC/AHA 2007 Guidelines for the Management of Patients with Unstable Angina/Non-ST-Elevation Myocardial Infarction: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines developed in collaboration with the American Academy of Family Physicians, Society for Cardiovascular Angiography and Interventions, and the Society of Thoracic Surgeons. J Am Coll Cardiol. 2011;57:e215-e367.
Prescribe a high-dose statin before any patient with acute coronary syndrome (ACS) undergoes percutaneous coronary intervention (PCI); it may be reasonable to extend this to patients being evaluated for ACS.1
Strength of recommendation
A: Based on a meta-analysis
Navarese EP, Kowalewski M, Andreotti F, et al. Meta-analysis of time-related benefits of statin therapy in patients with acute coronary syndrome undergoing percutaneous coronary intervention. Am J Cardiol. 2014;113:1753-1764.
Illustrative case
A 48-year-old man comes to the emergency department with chest pain and is diagnosed with ACS. He is scheduled to have PCI within the next 24 hours. When should you start him on a statin?
Statins are the mainstay pharmaceutical treatment for hyperlipidemia, and are used for primary and secondary prevention of coronary artery disease and stroke.2,3 Well-known for their cholesterol-lowering effect, they also have benefits that are independent of their effects on lipids, including improving endothelial function, decreasing oxidative stress, and decreasing vascular inflammation.4-6
Compared to patients with stable angina, patients with ACS experience markedly higher rates of coronary events, especially immediately before and after PCI and during the subsequent 30 days.1 American College of Cardiology/American Heart Association (ACC/AHA) guidelines for the management of non-ST elevation myocardial infarction (NSTEMI) advocate starting statins before patients are discharged from the hospital, but they don’t specify precisely when.7
Considering the higher risk of coronary events before and after PCI and statins’ pleiotropic effects, it is reasonable to investigate the optimal time for starting statins in patients with ACS.
STUDY SUMMARY: Meta-analysis of 20 RCTs shows statins before PCI cuts risk of MI
Navarese et al1 performed a systematic review and meta-analysis of studies comparing the clinical outcomes of patients with ACS who received statins before or after PCI (statins group) vs those who received low-dose statins or no statins (control group). The authors searched PubMed, Cochrane, Google Scholar, and CINAHL databases as well as key conference proceedings for studies published before November 2013. Using reasonable inclusion and exclusion criteria and appropriate statistical methods, they analyzed the results of 20 randomized controlled trials that included 8750 patients. Four studies enrolled only patients with ST elevation MI, 8 were restricted to NSTEMI, and the remaining 8 studies enrolled patients with any type of MI or unstable angina.
For patients who were started on a statin before PCI, the mean timing of administration was 0.53 ± 0.42 days before. For those started after PCI, the average time to administration was 3.18 ± 3.56 days after.
Whether administered before or after PCI, statins reduced the incidence of MIs. The overall 30-day incidence of MIs was 3.4% (123 of 3621) in the statins group and 5% (179 of 3577) in the control group. This resulted in an absolute risk reduction of 1.6% (number needed to treat=62.5), and a reduction of the odds of MI by 33% (odds ratio [OR]=0.67; 95% confidence interval [CI], 0.53-0.84; P=.0007). There was also a trend toward reduced mortality in the statin group (OR=0.66; 95% CI, 0.43-1.02; P=.06).
In addition, administering statins before PCI resulted in a greater reduction in the odds of MI at 30 days (OR=0.38; 95% CI, 0.24-0.59; P<.0001) than starting them post-PCI (OR=0.85; 95% CI, 0.64-1.13; P=.28) when compared to the controls. The difference between the pre-PCI OR and the post-PCI OR was statistically significant (P=.002). These findings persisted past 30 days (P=.06).
WHAT'S NEW: Early statin administration is most effective
According to ACC/AHA guidelines, all patients with ACS should be receiving a statin by the time they are discharged. However, when to start the statin is not specified. This meta-analysis is the first report to show that administering a statin before PCI can significantly reduce the risk of subsequent MI.
CAVEATS: Benefits might vary with different statins
The studies evaluated in this meta-analysis used various statins and dosing regimens, which could have affected the results. However, sensitivity analyses found similar benefits across different types of statins. In addition, most of the included trials used high doses of statins, which minimized the potential discrepancy in outcomes from various dosing regimens. And while the included studies were not perfect, Navarese et al1 used reasonable methods to identify potential biases.
CHALLENGES TO IMPLEMENTATION: No barriers to starting statins earlier
Implementing this intervention may be as simple as editing a standard order. This meta-analysis also suggests that the earlier the intervention, the greater the benefit, which may be an argument for starting a statin when a patient first presents for evaluation for ACS, since the risks of taking a statin are quite low. We believe it would be beneficial if the next update of the ACC/AHA guidelines7 included this recommendation.
ACKNOWLEDGEMENT
The PURLs Surveillance System was supported in part by Grant Number UL1RR024999 from the National Center For Research Resources, a Clinical Translational Science Award to the University of Chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center For Research Resources or the National Institutes of Health.
Prescribe a high-dose statin before any patient with acute coronary syndrome (ACS) undergoes percutaneous coronary intervention (PCI); it may be reasonable to extend this to patients being evaluated for ACS.1
Strength of recommendation
A: Based on a meta-analysis
Navarese EP, Kowalewski M, Andreotti F, et al. Meta-analysis of time-related benefits of statin therapy in patients with acute coronary syndrome undergoing percutaneous coronary intervention. Am J Cardiol. 2014;113:1753-1764.
Illustrative case
A 48-year-old man comes to the emergency department with chest pain and is diagnosed with ACS. He is scheduled to have PCI within the next 24 hours. When should you start him on a statin?
Statins are the mainstay pharmaceutical treatment for hyperlipidemia, and are used for primary and secondary prevention of coronary artery disease and stroke.2,3 Well-known for their cholesterol-lowering effect, they also have benefits that are independent of their effects on lipids, including improving endothelial function, decreasing oxidative stress, and decreasing vascular inflammation.4-6
Compared to patients with stable angina, patients with ACS experience markedly higher rates of coronary events, especially immediately before and after PCI and during the subsequent 30 days.1 American College of Cardiology/American Heart Association (ACC/AHA) guidelines for the management of non-ST elevation myocardial infarction (NSTEMI) advocate starting statins before patients are discharged from the hospital, but they don’t specify precisely when.7
Considering the higher risk of coronary events before and after PCI and statins’ pleiotropic effects, it is reasonable to investigate the optimal time for starting statins in patients with ACS.
STUDY SUMMARY: Meta-analysis of 20 RCTs shows statins before PCI cuts risk of MI
Navarese et al1 performed a systematic review and meta-analysis of studies comparing the clinical outcomes of patients with ACS who received statins before or after PCI (statins group) vs those who received low-dose statins or no statins (control group). The authors searched PubMed, Cochrane, Google Scholar, and CINAHL databases as well as key conference proceedings for studies published before November 2013. Using reasonable inclusion and exclusion criteria and appropriate statistical methods, they analyzed the results of 20 randomized controlled trials that included 8750 patients. Four studies enrolled only patients with ST elevation MI, 8 were restricted to NSTEMI, and the remaining 8 studies enrolled patients with any type of MI or unstable angina.
For patients who were started on a statin before PCI, the mean timing of administration was 0.53 ± 0.42 days before. For those started after PCI, the average time to administration was 3.18 ± 3.56 days after.
Whether administered before or after PCI, statins reduced the incidence of MIs. The overall 30-day incidence of MIs was 3.4% (123 of 3621) in the statins group and 5% (179 of 3577) in the control group. This resulted in an absolute risk reduction of 1.6% (number needed to treat=62.5), and a reduction of the odds of MI by 33% (odds ratio [OR]=0.67; 95% confidence interval [CI], 0.53-0.84; P=.0007). There was also a trend toward reduced mortality in the statin group (OR=0.66; 95% CI, 0.43-1.02; P=.06).
In addition, administering statins before PCI resulted in a greater reduction in the odds of MI at 30 days (OR=0.38; 95% CI, 0.24-0.59; P<.0001) than starting them post-PCI (OR=0.85; 95% CI, 0.64-1.13; P=.28) when compared to the controls. The difference between the pre-PCI OR and the post-PCI OR was statistically significant (P=.002). These findings persisted past 30 days (P=.06).
WHAT'S NEW: Early statin administration is most effective
According to ACC/AHA guidelines, all patients with ACS should be receiving a statin by the time they are discharged. However, when to start the statin is not specified. This meta-analysis is the first report to show that administering a statin before PCI can significantly reduce the risk of subsequent MI.
CAVEATS: Benefits might vary with different statins
The studies evaluated in this meta-analysis used various statins and dosing regimens, which could have affected the results. However, sensitivity analyses found similar benefits across different types of statins. In addition, most of the included trials used high doses of statins, which minimized the potential discrepancy in outcomes from various dosing regimens. And while the included studies were not perfect, Navarese et al1 used reasonable methods to identify potential biases.
CHALLENGES TO IMPLEMENTATION: No barriers to starting statins earlier
Implementing this intervention may be as simple as editing a standard order. This meta-analysis also suggests that the earlier the intervention, the greater the benefit, which may be an argument for starting a statin when a patient first presents for evaluation for ACS, since the risks of taking a statin are quite low. We believe it would be beneficial if the next update of the ACC/AHA guidelines7 included this recommendation.
ACKNOWLEDGEMENT
The PURLs Surveillance System was supported in part by Grant Number UL1RR024999 from the National Center For Research Resources, a Clinical Translational Science Award to the University of Chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center For Research Resources or the National Institutes of Health.
1. Navarese EP, Kowalewski M, Andreotti F, et al. Meta-analysis of time-related benefits of statin therapy in patients with acute coronary syndrome undergoing percutaneous coronary intervention. Am J Cardiol. 2014;113:1753-1764.
2. Pignone M, Phillips C, Mulrow C. Use of lipid lowering drugs for primary prevention of coronary heart disease: meta-analysis of randomised trials. BMJ. 2000;321:983-986.
3. Prevention of cardiovascular events and death with pravastatin in patients with coronary heart disease and a broad range of initial cholesterol levels. The Long-Term Intervention with Pravastatin in Ischaemic Disease (LIPID) Study Group. N Engl J Med. 1998;339:1349-1357.
4. Liao JK. Beyond lipid lowering: the role of statins in vascular protection. Int J Cardiol. 2002;86:5-18.
5. Li J, Li JJ, He JG, et al. Atorvastatin decreases C-reactive protein-induced inflammatory response in pulmonary artery smooth muscle cells by inhibiting nuclear factor-kappaB pathway. Cardiovasc Ther. 2010;28:8-14.
6. Tandon V, Bano G, Khajuria V, et al. Pleiotropic effects of statins. Indian J Pharmacol. 2005;37:77-85.
7. Wright RS, Anderson JL, Adams CD, et al; American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. 2011 ACCF/AHA focused update incorporated into the ACC/AHA 2007 Guidelines for the Management of Patients with Unstable Angina/Non-ST-Elevation Myocardial Infarction: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines developed in collaboration with the American Academy of Family Physicians, Society for Cardiovascular Angiography and Interventions, and the Society of Thoracic Surgeons. J Am Coll Cardiol. 2011;57:e215-e367.
1. Navarese EP, Kowalewski M, Andreotti F, et al. Meta-analysis of time-related benefits of statin therapy in patients with acute coronary syndrome undergoing percutaneous coronary intervention. Am J Cardiol. 2014;113:1753-1764.
2. Pignone M, Phillips C, Mulrow C. Use of lipid lowering drugs for primary prevention of coronary heart disease: meta-analysis of randomised trials. BMJ. 2000;321:983-986.
3. Prevention of cardiovascular events and death with pravastatin in patients with coronary heart disease and a broad range of initial cholesterol levels. The Long-Term Intervention with Pravastatin in Ischaemic Disease (LIPID) Study Group. N Engl J Med. 1998;339:1349-1357.
4. Liao JK. Beyond lipid lowering: the role of statins in vascular protection. Int J Cardiol. 2002;86:5-18.
5. Li J, Li JJ, He JG, et al. Atorvastatin decreases C-reactive protein-induced inflammatory response in pulmonary artery smooth muscle cells by inhibiting nuclear factor-kappaB pathway. Cardiovasc Ther. 2010;28:8-14.
6. Tandon V, Bano G, Khajuria V, et al. Pleiotropic effects of statins. Indian J Pharmacol. 2005;37:77-85.
7. Wright RS, Anderson JL, Adams CD, et al; American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. 2011 ACCF/AHA focused update incorporated into the ACC/AHA 2007 Guidelines for the Management of Patients with Unstable Angina/Non-ST-Elevation Myocardial Infarction: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines developed in collaboration with the American Academy of Family Physicians, Society for Cardiovascular Angiography and Interventions, and the Society of Thoracic Surgeons. J Am Coll Cardiol. 2011;57:e215-e367.
Copyright © 2014 Family Physicians Inquiries Network. All rights reserved.
Pneumococcal vaccines for older adults: Getting the timing right
In August 2014, the Advisory Committee on Immunization Practices (ACIP) decided to add the 13-valent pneumococcal conjugate vaccine (PCV13) to the routine immunization schedule for adults ages 65 years and older; previously, it had recommended that these patients receive only the 23-valent pneumococcal polysaccharide vaccine (PPSV23).1 The US Food and Drug Administration (FDA) had approved PCV13 for use in adults ages 50 years and older in late 2011. The delay between FDA approval and this new ACIP recommendation occurred for 2 reasons: The epidemiology of pneumococcal disease (pneumonia, meningitis, and bacteremia) in older adults is evolving due to the widespread use of PCV13 in children, and a large clinical trial looking at the efficacy of this vaccine in individuals 65 and older was still underway.
Pneumococcal disease in older adults remains a problem
Routine use of the 7-valent pneumococcal conjugate vaccine (PCV7) in children began in 2000. In 2010, the vaccine was expanded to include 6 more antigens (PCV13). The routine use of this vaccine has markedly reduced pneumococcal disease in children and, by way of indirect protection, in adults. Between 2010 and 2013, the incidence of invasive pneumococcal disease (eg, meningitis and bacteremia) caused by the 13 serotypes in the vaccine had decreased by 50% in adults ages 65 years and older.1 However, in this age group, there are still more than 13,000 cases of invasive pneumococcal disease each year.1 Approximately 20% of these cases—and 10% of cases community-acquired pneumonia (CAP) in this age group—are still caused by one of the PCV13 serotypes. This epidemiology left ACIP to consider whether to recommend PCV13 for older adults even though the incidence of pneumococcal disease was declining without the use of the vaccine. ACIP took a middle-of-the-road position on August 13, 2014 by recommending the vaccine now but agreeing to reexamine the issue again in 2018.1
PCV13 substantially cuts the rate of pneumococcal disease
In June 2014, ACIP reviewed the results of a large randomized, placebo-controlled clinical trial of PCV13 in 85,000 adults ages 65 years and older that was conducted in the Netherlands from 2008 to 2013.1 PCV13 reduced the rate of disease caused by the vaccine serotypes by 45.6% for pneumonia and 75% for invasive pneumococcal disease.
Because the population in this study was PPSV23-naïve, the added advantage of PCV13 in patients who have been vaccinated with PPSV23 has not been determined. Twelve of the 13 serotypes in PCV13 are in PPSV23. And while PPSV23 can protect against invasive pneumococcal disease, its effectiveness against CAP is less well proven.
Using modeling that took into consideration anticipated rates of vaccination with both PCV13 and PPSV23 in adults and children, the Centers for Disease Control and Prevention estimated that adding PCV13 to the adult immunization schedule would prevent 230 cases of invasive pneumococcal disease and 12,000 cases of CAP over the lifetime of a cohort of 65 year olds.1 With time, however, and the increasing indirect protection from routine use of PCV13 in children, these numbers would decline.
Timing of administration depends on patients’ vaccine history
Adults 65 years of age and older should receive both PCV13 and PPSV23, but not at the same time. In those who have not received any pneumococcal vaccine, the preferred sequence is to first administer PCV13 and then PPSV23 6 to 12 months later (FIGURE); the minimum acceptable interval between PCV13 and PPSV23 is 8 weeks.1 If PPSV23 is administered first, PCV13 should not be given until at least 12 months after the PPSV23 dose. This is because the immune response to PCV13 is not as robust when PCV13 follows PPSV23.
For patients who have been vaccinated with PPSV23 before age 65, PCV13 should be administered at least 12 months after PPSV23, followed by another dose of PPSV23 that should be administered 6 to 12 months after PCV13, but no sooner than 5 years since the previous PPSV23 (FIGURE).
Coadministration of PCV13 with trivalent influenza vaccine results in a slight decrease in the immune response to each vaccine;1 this is unlikely to be clinically important. Coadministration with other vaccines has not been studied.

Who’ll reimburse for the PCV13 vaccine? One issue that could delay the use of both vaccines in older adults is that currently, Medicare pays for only one pneumococcal vaccine in patients who are 65 and older. The Centers for Medicare and Medicaid Services will attempt to amend this policy, but how quickly this will occur is unknown.
Different recommendations for patients at higher risk
There are 2 sets of recommendations for use of pneumococcal vaccines: one for routine use for most patients, and a separate set of recommendations for those with conditions that put them at higher risk of infections and/or complications from pneumococcal disease.1-4 PPSV23 is recommended for children (starting at age 2 years) and adults with certain high-risk medical conditions, such as chronic heart, lung, or liver disease, and diabetes; functional or anatomical asplenia; or immunocompromising conditions such as human immunodeficiency virus infection, chronic renal failure, leukemia, or lymphoma.3 PPSV23 should be repeated 5 years after the first dose in patients with asplenia, those who are immunocompromised, and for everyone age 65 and older who received it before age 65. No more than 3 doses of PPSV23 should be given to anyone.
PCV13 is recommended for previously unvaccinated children and adults who have cochlear implants, cerebrospinal fluid leaks, functional or anatomical asplenia, or are immunocompromised.
1. Tomczyk S, Bennett NM, Stoecker C, et al; Centers for Disease Control and Prevention (CDC). Use of 13-valent pneumococcal conjugate vaccine and 23-valent pneumococcal polysaccharide vaccine among adults aged ≥65 years: recommendations of the Advisory Committee on Immunization Practices (ACIP). MMWR Morb Mortal Wkly Rep. 2014;63:822-825.
2. Centers for Disease Control and Prevention (CDC). Use of 13-valent pneumococcal conjugate vaccine and 23-valent pneumococcal polysaccharide vaccine for adults with immunocompromising conditions: recommendations of the Advisory Committee on Immunization Practices (ACIP). MMWR Morb Mortal Wkly Rep. 2012;61:816-819.
3. Centers for Disease Control and Prevention (CDC). Use of 13-valent pneumococcal conjugate vaccine and 23-valent pneumococcal polysaccharide vaccine among children aged 6-18 years with immunocompromising conditions: recommendations of the Advisory Committee on Immunization Practices (ACIP). MMWR Morb Mortal Wkly Rep. 2013;62:521-524.
4. Nuorti JP, Whitney CG; Centers for Disease Control and Prevention (CDC). Prevention of pneumococcal disease among infants and children - Use of 13-valent pneumococcal conjugate vaccine and 23-valent pneumococcal polysaccharide vaccine - Recommendations of the Advisory Committee on Immunization Practices (ACIP). MMWR Recomm Rep. 2010;59:1-18.
In August 2014, the Advisory Committee on Immunization Practices (ACIP) decided to add the 13-valent pneumococcal conjugate vaccine (PCV13) to the routine immunization schedule for adults ages 65 years and older; previously, it had recommended that these patients receive only the 23-valent pneumococcal polysaccharide vaccine (PPSV23).1 The US Food and Drug Administration (FDA) had approved PCV13 for use in adults ages 50 years and older in late 2011. The delay between FDA approval and this new ACIP recommendation occurred for 2 reasons: The epidemiology of pneumococcal disease (pneumonia, meningitis, and bacteremia) in older adults is evolving due to the widespread use of PCV13 in children, and a large clinical trial looking at the efficacy of this vaccine in individuals 65 and older was still underway.
Pneumococcal disease in older adults remains a problem
Routine use of the 7-valent pneumococcal conjugate vaccine (PCV7) in children began in 2000. In 2010, the vaccine was expanded to include 6 more antigens (PCV13). The routine use of this vaccine has markedly reduced pneumococcal disease in children and, by way of indirect protection, in adults. Between 2010 and 2013, the incidence of invasive pneumococcal disease (eg, meningitis and bacteremia) caused by the 13 serotypes in the vaccine had decreased by 50% in adults ages 65 years and older.1 However, in this age group, there are still more than 13,000 cases of invasive pneumococcal disease each year.1 Approximately 20% of these cases—and 10% of cases community-acquired pneumonia (CAP) in this age group—are still caused by one of the PCV13 serotypes. This epidemiology left ACIP to consider whether to recommend PCV13 for older adults even though the incidence of pneumococcal disease was declining without the use of the vaccine. ACIP took a middle-of-the-road position on August 13, 2014 by recommending the vaccine now but agreeing to reexamine the issue again in 2018.1
PCV13 substantially cuts the rate of pneumococcal disease
In June 2014, ACIP reviewed the results of a large randomized, placebo-controlled clinical trial of PCV13 in 85,000 adults ages 65 years and older that was conducted in the Netherlands from 2008 to 2013.1 PCV13 reduced the rate of disease caused by the vaccine serotypes by 45.6% for pneumonia and 75% for invasive pneumococcal disease.
Because the population in this study was PPSV23-naïve, the added advantage of PCV13 in patients who have been vaccinated with PPSV23 has not been determined. Twelve of the 13 serotypes in PCV13 are in PPSV23. And while PPSV23 can protect against invasive pneumococcal disease, its effectiveness against CAP is less well proven.
Using modeling that took into consideration anticipated rates of vaccination with both PCV13 and PPSV23 in adults and children, the Centers for Disease Control and Prevention estimated that adding PCV13 to the adult immunization schedule would prevent 230 cases of invasive pneumococcal disease and 12,000 cases of CAP over the lifetime of a cohort of 65 year olds.1 With time, however, and the increasing indirect protection from routine use of PCV13 in children, these numbers would decline.
Timing of administration depends on patients’ vaccine history
Adults 65 years of age and older should receive both PCV13 and PPSV23, but not at the same time. In those who have not received any pneumococcal vaccine, the preferred sequence is to first administer PCV13 and then PPSV23 6 to 12 months later (FIGURE); the minimum acceptable interval between PCV13 and PPSV23 is 8 weeks.1 If PPSV23 is administered first, PCV13 should not be given until at least 12 months after the PPSV23 dose. This is because the immune response to PCV13 is not as robust when PCV13 follows PPSV23.
For patients who have been vaccinated with PPSV23 before age 65, PCV13 should be administered at least 12 months after PPSV23, followed by another dose of PPSV23 that should be administered 6 to 12 months after PCV13, but no sooner than 5 years since the previous PPSV23 (FIGURE).
Coadministration of PCV13 with trivalent influenza vaccine results in a slight decrease in the immune response to each vaccine;1 this is unlikely to be clinically important. Coadministration with other vaccines has not been studied.
Who’ll reimburse for the PCV13 vaccine? One issue that could delay the use of both vaccines in older adults is that currently, Medicare pays for only one pneumococcal vaccine in patients who are 65 and older. The Centers for Medicare and Medicaid Services will attempt to amend this policy, but how quickly this will occur is unknown.
Different recommendations for patients at higher risk
There are 2 sets of recommendations for use of pneumococcal vaccines: one for routine use for most patients, and a separate set of recommendations for those with conditions that put them at higher risk of infections and/or complications from pneumococcal disease.1-4 PPSV23 is recommended for children (starting at age 2 years) and adults with certain high-risk medical conditions, such as chronic heart, lung, or liver disease, and diabetes; functional or anatomical asplenia; or immunocompromising conditions such as human immunodeficiency virus infection, chronic renal failure, leukemia, or lymphoma.3 PPSV23 should be repeated 5 years after the first dose in patients with asplenia, those who are immunocompromised, and for everyone age 65 and older who received it before age 65. No more than 3 doses of PPSV23 should be given to anyone.
PCV13 is recommended for previously unvaccinated children and adults who have cochlear implants, cerebrospinal fluid leaks, functional or anatomical asplenia, or are immunocompromised.
In August 2014, the Advisory Committee on Immunization Practices (ACIP) decided to add the 13-valent pneumococcal conjugate vaccine (PCV13) to the routine immunization schedule for adults ages 65 years and older; previously, it had recommended that these patients receive only the 23-valent pneumococcal polysaccharide vaccine (PPSV23).1 The US Food and Drug Administration (FDA) had approved PCV13 for use in adults ages 50 years and older in late 2011. The delay between FDA approval and this new ACIP recommendation occurred for 2 reasons: The epidemiology of pneumococcal disease (pneumonia, meningitis, and bacteremia) in older adults is evolving due to the widespread use of PCV13 in children, and a large clinical trial looking at the efficacy of this vaccine in individuals 65 and older was still underway.
Pneumococcal disease in older adults remains a problem
Routine use of the 7-valent pneumococcal conjugate vaccine (PCV7) in children began in 2000. In 2010, the vaccine was expanded to include 6 more antigens (PCV13). The routine use of this vaccine has markedly reduced pneumococcal disease in children and, by way of indirect protection, in adults. Between 2010 and 2013, the incidence of invasive pneumococcal disease (eg, meningitis and bacteremia) caused by the 13 serotypes in the vaccine had decreased by 50% in adults ages 65 years and older.1 However, in this age group, there are still more than 13,000 cases of invasive pneumococcal disease each year.1 Approximately 20% of these cases—and 10% of cases community-acquired pneumonia (CAP) in this age group—are still caused by one of the PCV13 serotypes. This epidemiology left ACIP to consider whether to recommend PCV13 for older adults even though the incidence of pneumococcal disease was declining without the use of the vaccine. ACIP took a middle-of-the-road position on August 13, 2014 by recommending the vaccine now but agreeing to reexamine the issue again in 2018.1
PCV13 substantially cuts the rate of pneumococcal disease
In June 2014, ACIP reviewed the results of a large randomized, placebo-controlled clinical trial of PCV13 in 85,000 adults ages 65 years and older that was conducted in the Netherlands from 2008 to 2013.1 PCV13 reduced the rate of disease caused by the vaccine serotypes by 45.6% for pneumonia and 75% for invasive pneumococcal disease.
Because the population in this study was PPSV23-naïve, the added advantage of PCV13 in patients who have been vaccinated with PPSV23 has not been determined. Twelve of the 13 serotypes in PCV13 are in PPSV23. And while PPSV23 can protect against invasive pneumococcal disease, its effectiveness against CAP is less well proven.
Using modeling that took into consideration anticipated rates of vaccination with both PCV13 and PPSV23 in adults and children, the Centers for Disease Control and Prevention estimated that adding PCV13 to the adult immunization schedule would prevent 230 cases of invasive pneumococcal disease and 12,000 cases of CAP over the lifetime of a cohort of 65 year olds.1 With time, however, and the increasing indirect protection from routine use of PCV13 in children, these numbers would decline.
Timing of administration depends on patients’ vaccine history
Adults 65 years of age and older should receive both PCV13 and PPSV23, but not at the same time. In those who have not received any pneumococcal vaccine, the preferred sequence is to first administer PCV13 and then PPSV23 6 to 12 months later (FIGURE); the minimum acceptable interval between PCV13 and PPSV23 is 8 weeks.1 If PPSV23 is administered first, PCV13 should not be given until at least 12 months after the PPSV23 dose. This is because the immune response to PCV13 is not as robust when PCV13 follows PPSV23.
For patients who have been vaccinated with PPSV23 before age 65, PCV13 should be administered at least 12 months after PPSV23, followed by another dose of PPSV23 that should be administered 6 to 12 months after PCV13, but no sooner than 5 years since the previous PPSV23 (FIGURE).
Coadministration of PCV13 with trivalent influenza vaccine results in a slight decrease in the immune response to each vaccine;1 this is unlikely to be clinically important. Coadministration with other vaccines has not been studied.
Who’ll reimburse for the PCV13 vaccine? One issue that could delay the use of both vaccines in older adults is that currently, Medicare pays for only one pneumococcal vaccine in patients who are 65 and older. The Centers for Medicare and Medicaid Services will attempt to amend this policy, but how quickly this will occur is unknown.
Different recommendations for patients at higher risk
There are 2 sets of recommendations for use of pneumococcal vaccines: one for routine use for most patients, and a separate set of recommendations for those with conditions that put them at higher risk of infections and/or complications from pneumococcal disease.1-4 PPSV23 is recommended for children (starting at age 2 years) and adults with certain high-risk medical conditions, such as chronic heart, lung, or liver disease, and diabetes; functional or anatomical asplenia; or immunocompromising conditions such as human immunodeficiency virus infection, chronic renal failure, leukemia, or lymphoma.3 PPSV23 should be repeated 5 years after the first dose in patients with asplenia, those who are immunocompromised, and for everyone age 65 and older who received it before age 65. No more than 3 doses of PPSV23 should be given to anyone.
PCV13 is recommended for previously unvaccinated children and adults who have cochlear implants, cerebrospinal fluid leaks, functional or anatomical asplenia, or are immunocompromised.
1. Tomczyk S, Bennett NM, Stoecker C, et al; Centers for Disease Control and Prevention (CDC). Use of 13-valent pneumococcal conjugate vaccine and 23-valent pneumococcal polysaccharide vaccine among adults aged ≥65 years: recommendations of the Advisory Committee on Immunization Practices (ACIP). MMWR Morb Mortal Wkly Rep. 2014;63:822-825.
2. Centers for Disease Control and Prevention (CDC). Use of 13-valent pneumococcal conjugate vaccine and 23-valent pneumococcal polysaccharide vaccine for adults with immunocompromising conditions: recommendations of the Advisory Committee on Immunization Practices (ACIP). MMWR Morb Mortal Wkly Rep. 2012;61:816-819.
3. Centers for Disease Control and Prevention (CDC). Use of 13-valent pneumococcal conjugate vaccine and 23-valent pneumococcal polysaccharide vaccine among children aged 6-18 years with immunocompromising conditions: recommendations of the Advisory Committee on Immunization Practices (ACIP). MMWR Morb Mortal Wkly Rep. 2013;62:521-524.
4. Nuorti JP, Whitney CG; Centers for Disease Control and Prevention (CDC). Prevention of pneumococcal disease among infants and children - Use of 13-valent pneumococcal conjugate vaccine and 23-valent pneumococcal polysaccharide vaccine - Recommendations of the Advisory Committee on Immunization Practices (ACIP). MMWR Recomm Rep. 2010;59:1-18.
1. Tomczyk S, Bennett NM, Stoecker C, et al; Centers for Disease Control and Prevention (CDC). Use of 13-valent pneumococcal conjugate vaccine and 23-valent pneumococcal polysaccharide vaccine among adults aged ≥65 years: recommendations of the Advisory Committee on Immunization Practices (ACIP). MMWR Morb Mortal Wkly Rep. 2014;63:822-825.
2. Centers for Disease Control and Prevention (CDC). Use of 13-valent pneumococcal conjugate vaccine and 23-valent pneumococcal polysaccharide vaccine for adults with immunocompromising conditions: recommendations of the Advisory Committee on Immunization Practices (ACIP). MMWR Morb Mortal Wkly Rep. 2012;61:816-819.
3. Centers for Disease Control and Prevention (CDC). Use of 13-valent pneumococcal conjugate vaccine and 23-valent pneumococcal polysaccharide vaccine among children aged 6-18 years with immunocompromising conditions: recommendations of the Advisory Committee on Immunization Practices (ACIP). MMWR Morb Mortal Wkly Rep. 2013;62:521-524.
4. Nuorti JP, Whitney CG; Centers for Disease Control and Prevention (CDC). Prevention of pneumococcal disease among infants and children - Use of 13-valent pneumococcal conjugate vaccine and 23-valent pneumococcal polysaccharide vaccine - Recommendations of the Advisory Committee on Immunization Practices (ACIP). MMWR Recomm Rep. 2010;59:1-18.
Which risk factors and signs and symptoms are associated with coccidioidomycosis?
EVIDENCE-BASED ANSWER:
Risk factors for coccidioidomycosis, or valley fever, include lower respiratory tract symptoms lasting longer than 14 days, chest pain, rash, having lived in endemic areas fewer than 10 years, and diabetes mellitus or immunosuppressive conditions (strength of recommendation [SOR]: B, several prospective cohort and case-control studies).
The most common signs and symptoms include cough (74%), fever (56%), night sweats (35%), pleuritic chest pain (33%), chills (28%), dyspnea (27%), weight loss (21%), and rash (14%) (SOR: B, retrospective cohort study).
EVIDENCE SUMMARY
A 2013 surveillance report by the Centers for Disease Control and Prevention that included 111,717 patients in 28 states and the District of Columbia found an 8-fold increase in reported coccidioidomycosis in endemic areas from 1998 to 2011 (age-adjusted incidence rates: 5.3 per 100,000 in 1998 and 42.6 per 100,000 in 2011). Cases in nonendemic states increased 40-fold in the same time period, from 6 cases to 240.1 The disease is endemic in the southwest United States and northwest Mexico.
Risk factors include persistent symptoms, chest pain, diabetes, immunosuppression
A 2008 case-control study of 136 patients in Phoenix, Arizona (an endemic area) found that 15% of the patients diagnosed with community-acquired pneumonia (CAP) had coccidioidomycosis on serologic testing. Risk factors for CAP caused by coccidioidomycosis in this population were symptom duration longer than 14 days (odds ratio [OR]=5.0; 95% confidence interval [CI], 2.1-15.7), age younger than 18 years (OR=5.5; 95% CI, 2.1-15.3), chest pain (OR=4.6; 95% CI, 1.8-11.8), and diabetes mellitus or an immunosuppressive condition (OR=3.8; 95% CI, 1.0-16.5).2
Abnormal chest X-rays, myalgia— and a rash
A 2006 prospective cohort study of 55 patients in Tucson, Arizona, which is part of the endemic area, found that 29% of patients diagnosed with CAP tested serologically positive for coccidioidomycosis. Risk factors included fewer than 10 years of exposure to an endemic area (OR=4.11; 95% CI, 1.01-16.8). Chest radiograph abnormalities were more common in patients with CAP caused by coccidioidomycosis than patients without coccidioidomycosis (75% vs 25%, P=.005). Myalgia is more common when coccidioidal pneumonia is present (69% vs 23%, P=.0022).3
A 2009 prospective cohort study of 35 patients with CAP in Phoenix, Arizona found that 6 patients (17%) tested positive for coccidioidomycosis. Only 1 statistically significant risk factor was identified—half of patients with coccidioidomycosis exhibited a rash, while there were no rashes in the group without the disease (P=.002).4
Other common signs and symptoms
A retrospective cohort study in San Diego, California in 2004 evaluated and stratified 223 patients with known coccidioidomycosis for presenting symptoms, exam findings, and radiographic findings. The most common signs and symptoms at time of seropositive testing were cough (74%), fever (56%), night sweats (35%), pleuritic chest pain (33%), chills (28%), weight loss (21%), rash (14%), and arthralgia or myalgia (13% and 12%, respectively).5
Airspace opacity was the most common radiographic abnormality (58.8%); the second most common was pulmonary nodules (22.8%).5 The study didn’t compare the frequency of these findings with noncoccidioidal pneumonia.
RECOMMENDATIONS
In 2005 guidelines, the Infectious Diseases Society of America (IDSA) stated that the “management of coccidioidomycosis first involves recognizing that a coccidioidal infection exists, defining the extent of infection, and identifying host factors that predispose to disease severity.”6 The IDSA didn’t give specific recommendations regarding how to diagnose or differentiate coccidioidal infection from CAP.
1. Centers for Disease Control and Prevention (CDC). Increase in reported coccidioidomycosis—United States, 1998-2011. MMWR Morb Mortal Wkly Rep. 2013;62:217-221.
2. Chang DC, Anderson S, Wannemuehler K, et al. Testing for coccidioidomycosis among patients with community-acquired pneumonia. Emerg Infect Dis. 2008;14: 1053-1059.
3. Valdivia L, Nix D, Wright M, et al. Coccidioidomycosis as a common cause of community-acquired pneumonia. Emerg Infect Dis. 2006;12:958-962.
4. Kim MM, Blair JE, Carey EJ, et al. Coccidioidal pneumonia, Phoenix, Arizona, USA, 2000-2004. Emerg Infect Dis. 2009;15:397-401.
5. Crum NF, Lederman ER, Stafford CM, et al. Coccidioidomycosis: a descriptive survey of a reemerging disease. Clinical characteristics and current controversies. Medicine (Baltimore). 2004;83:149-175.
6. Galgiani JN, Ampel NM, Blair JE, et al; Infectious Disease Society of America. Coccidioidomycosis. Clin Infect Dis. 2005;41:1217-1223.
EVIDENCE-BASED ANSWER:
Risk factors for coccidioidomycosis, or valley fever, include lower respiratory tract symptoms lasting longer than 14 days, chest pain, rash, having lived in endemic areas fewer than 10 years, and diabetes mellitus or immunosuppressive conditions (strength of recommendation [SOR]: B, several prospective cohort and case-control studies).
The most common signs and symptoms include cough (74%), fever (56%), night sweats (35%), pleuritic chest pain (33%), chills (28%), dyspnea (27%), weight loss (21%), and rash (14%) (SOR: B, retrospective cohort study).
EVIDENCE SUMMARY
A 2013 surveillance report by the Centers for Disease Control and Prevention that included 111,717 patients in 28 states and the District of Columbia found an 8-fold increase in reported coccidioidomycosis in endemic areas from 1998 to 2011 (age-adjusted incidence rates: 5.3 per 100,000 in 1998 and 42.6 per 100,000 in 2011). Cases in nonendemic states increased 40-fold in the same time period, from 6 cases to 240.1 The disease is endemic in the southwest United States and northwest Mexico.
Risk factors include persistent symptoms, chest pain, diabetes, immunosuppression
A 2008 case-control study of 136 patients in Phoenix, Arizona (an endemic area) found that 15% of the patients diagnosed with community-acquired pneumonia (CAP) had coccidioidomycosis on serologic testing. Risk factors for CAP caused by coccidioidomycosis in this population were symptom duration longer than 14 days (odds ratio [OR]=5.0; 95% confidence interval [CI], 2.1-15.7), age younger than 18 years (OR=5.5; 95% CI, 2.1-15.3), chest pain (OR=4.6; 95% CI, 1.8-11.8), and diabetes mellitus or an immunosuppressive condition (OR=3.8; 95% CI, 1.0-16.5).2
Abnormal chest X-rays, myalgia— and a rash
A 2006 prospective cohort study of 55 patients in Tucson, Arizona, which is part of the endemic area, found that 29% of patients diagnosed with CAP tested serologically positive for coccidioidomycosis. Risk factors included fewer than 10 years of exposure to an endemic area (OR=4.11; 95% CI, 1.01-16.8). Chest radiograph abnormalities were more common in patients with CAP caused by coccidioidomycosis than patients without coccidioidomycosis (75% vs 25%, P=.005). Myalgia is more common when coccidioidal pneumonia is present (69% vs 23%, P=.0022).3
A 2009 prospective cohort study of 35 patients with CAP in Phoenix, Arizona found that 6 patients (17%) tested positive for coccidioidomycosis. Only 1 statistically significant risk factor was identified—half of patients with coccidioidomycosis exhibited a rash, while there were no rashes in the group without the disease (P=.002).4
Other common signs and symptoms
A retrospective cohort study in San Diego, California in 2004 evaluated and stratified 223 patients with known coccidioidomycosis for presenting symptoms, exam findings, and radiographic findings. The most common signs and symptoms at time of seropositive testing were cough (74%), fever (56%), night sweats (35%), pleuritic chest pain (33%), chills (28%), weight loss (21%), rash (14%), and arthralgia or myalgia (13% and 12%, respectively).5
Airspace opacity was the most common radiographic abnormality (58.8%); the second most common was pulmonary nodules (22.8%).5 The study didn’t compare the frequency of these findings with noncoccidioidal pneumonia.
RECOMMENDATIONS
In 2005 guidelines, the Infectious Diseases Society of America (IDSA) stated that the “management of coccidioidomycosis first involves recognizing that a coccidioidal infection exists, defining the extent of infection, and identifying host factors that predispose to disease severity.”6 The IDSA didn’t give specific recommendations regarding how to diagnose or differentiate coccidioidal infection from CAP.
EVIDENCE-BASED ANSWER:
Risk factors for coccidioidomycosis, or valley fever, include lower respiratory tract symptoms lasting longer than 14 days, chest pain, rash, having lived in endemic areas fewer than 10 years, and diabetes mellitus or immunosuppressive conditions (strength of recommendation [SOR]: B, several prospective cohort and case-control studies).
The most common signs and symptoms include cough (74%), fever (56%), night sweats (35%), pleuritic chest pain (33%), chills (28%), dyspnea (27%), weight loss (21%), and rash (14%) (SOR: B, retrospective cohort study).
EVIDENCE SUMMARY
A 2013 surveillance report by the Centers for Disease Control and Prevention that included 111,717 patients in 28 states and the District of Columbia found an 8-fold increase in reported coccidioidomycosis in endemic areas from 1998 to 2011 (age-adjusted incidence rates: 5.3 per 100,000 in 1998 and 42.6 per 100,000 in 2011). Cases in nonendemic states increased 40-fold in the same time period, from 6 cases to 240.1 The disease is endemic in the southwest United States and northwest Mexico.
Risk factors include persistent symptoms, chest pain, diabetes, immunosuppression
A 2008 case-control study of 136 patients in Phoenix, Arizona (an endemic area) found that 15% of the patients diagnosed with community-acquired pneumonia (CAP) had coccidioidomycosis on serologic testing. Risk factors for CAP caused by coccidioidomycosis in this population were symptom duration longer than 14 days (odds ratio [OR]=5.0; 95% confidence interval [CI], 2.1-15.7), age younger than 18 years (OR=5.5; 95% CI, 2.1-15.3), chest pain (OR=4.6; 95% CI, 1.8-11.8), and diabetes mellitus or an immunosuppressive condition (OR=3.8; 95% CI, 1.0-16.5).2
Abnormal chest X-rays, myalgia— and a rash
A 2006 prospective cohort study of 55 patients in Tucson, Arizona, which is part of the endemic area, found that 29% of patients diagnosed with CAP tested serologically positive for coccidioidomycosis. Risk factors included fewer than 10 years of exposure to an endemic area (OR=4.11; 95% CI, 1.01-16.8). Chest radiograph abnormalities were more common in patients with CAP caused by coccidioidomycosis than patients without coccidioidomycosis (75% vs 25%, P=.005). Myalgia is more common when coccidioidal pneumonia is present (69% vs 23%, P=.0022).3
A 2009 prospective cohort study of 35 patients with CAP in Phoenix, Arizona found that 6 patients (17%) tested positive for coccidioidomycosis. Only 1 statistically significant risk factor was identified—half of patients with coccidioidomycosis exhibited a rash, while there were no rashes in the group without the disease (P=.002).4
Other common signs and symptoms
A retrospective cohort study in San Diego, California in 2004 evaluated and stratified 223 patients with known coccidioidomycosis for presenting symptoms, exam findings, and radiographic findings. The most common signs and symptoms at time of seropositive testing were cough (74%), fever (56%), night sweats (35%), pleuritic chest pain (33%), chills (28%), weight loss (21%), rash (14%), and arthralgia or myalgia (13% and 12%, respectively).5
Airspace opacity was the most common radiographic abnormality (58.8%); the second most common was pulmonary nodules (22.8%).5 The study didn’t compare the frequency of these findings with noncoccidioidal pneumonia.
RECOMMENDATIONS
In 2005 guidelines, the Infectious Diseases Society of America (IDSA) stated that the “management of coccidioidomycosis first involves recognizing that a coccidioidal infection exists, defining the extent of infection, and identifying host factors that predispose to disease severity.”6 The IDSA didn’t give specific recommendations regarding how to diagnose or differentiate coccidioidal infection from CAP.
1. Centers for Disease Control and Prevention (CDC). Increase in reported coccidioidomycosis—United States, 1998-2011. MMWR Morb Mortal Wkly Rep. 2013;62:217-221.
2. Chang DC, Anderson S, Wannemuehler K, et al. Testing for coccidioidomycosis among patients with community-acquired pneumonia. Emerg Infect Dis. 2008;14: 1053-1059.
3. Valdivia L, Nix D, Wright M, et al. Coccidioidomycosis as a common cause of community-acquired pneumonia. Emerg Infect Dis. 2006;12:958-962.
4. Kim MM, Blair JE, Carey EJ, et al. Coccidioidal pneumonia, Phoenix, Arizona, USA, 2000-2004. Emerg Infect Dis. 2009;15:397-401.
5. Crum NF, Lederman ER, Stafford CM, et al. Coccidioidomycosis: a descriptive survey of a reemerging disease. Clinical characteristics and current controversies. Medicine (Baltimore). 2004;83:149-175.
6. Galgiani JN, Ampel NM, Blair JE, et al; Infectious Disease Society of America. Coccidioidomycosis. Clin Infect Dis. 2005;41:1217-1223.
1. Centers for Disease Control and Prevention (CDC). Increase in reported coccidioidomycosis—United States, 1998-2011. MMWR Morb Mortal Wkly Rep. 2013;62:217-221.
2. Chang DC, Anderson S, Wannemuehler K, et al. Testing for coccidioidomycosis among patients with community-acquired pneumonia. Emerg Infect Dis. 2008;14: 1053-1059.
3. Valdivia L, Nix D, Wright M, et al. Coccidioidomycosis as a common cause of community-acquired pneumonia. Emerg Infect Dis. 2006;12:958-962.
4. Kim MM, Blair JE, Carey EJ, et al. Coccidioidal pneumonia, Phoenix, Arizona, USA, 2000-2004. Emerg Infect Dis. 2009;15:397-401.
5. Crum NF, Lederman ER, Stafford CM, et al. Coccidioidomycosis: a descriptive survey of a reemerging disease. Clinical characteristics and current controversies. Medicine (Baltimore). 2004;83:149-175.
6. Galgiani JN, Ampel NM, Blair JE, et al; Infectious Disease Society of America. Coccidioidomycosis. Clin Infect Dis. 2005;41:1217-1223.
Evidence-based answers from the Family Physicians Inquiries Network
Is immediate-release topiramate an effective treatment for adult obesity?
EVIDENCE-BASED ANSWER:
Yes. Topiramate (at daily doses of 64-400 mg) produces an average 5.34 kg of additional weight loss compared with placebo (95% confidence interval [CI], -6.12 to -4.56) in overweight to obese adults for periods of 16 to 60 weeks (strength of recommendation [SOR]: A, meta-analyses of randomized controlled trials [RCTs]).
Topiramate increases the chances of losing 5% or more of baseline body weight (BBW) with a number needed to treat (NNT) of 3 (95% CI, 2-3) and 10% or more of BBW with an NNT of 4 (95% CI, 3-4). However, approximately 17% of patients discontinue the drug because of adverse effects, including paresthesia, hypoesthesia, taste perversion, and psychomotor impairment (SOR: A, meta-analyses of RCTs).
EVIDENCE SUMMARY
A meta-analysis of 10 well-done RCTs with a total of 3320 patients found that topiramate produced more weight loss than placebo.1 Studies included men and women ages 18 to 75 years, with a body mass index (BMI) of 27 to 50. Several studies included patients with hypertension, dyslipidemia, and diabetes mellitus; one study included patients with binge eating disorder. Investigators recruited subjects from sites in Europe, North America, Australia, and South Africa. The studies lasted 16 to 60 weeks and used variable doses of topiramate (64-400 mg daily). Most incorporated a structured lifestyle intervention program for both the treatment and control groups.
Patients taking topiramate lost 5.34 kg (95% CI, -6.12 to -4.56) more than subjects taking placebo. All studies showed significantly greater weight loss in the topiramate groups, regardless of dose and duration, although there was some heterogeneity among the results. The NNTs to achieve weight loss of 5% or more of BBW and 10% or more of BBW were 3 (95% CI, 2-3) and 4 (95% CI, 3-4), respectively.
No major adverse events, but some unpleasant effects
A safety analysis on 6620 subjects found no major adverse events.1 Subjects in the topiramate group were more likely to withdraw because of adverse effects (odds ratio=1.97; 95% CI, 1.64-2.29; number needed to harm=14; 95% CI, 11-18). The most common adverse effects were paresthesia, hypoesthesia, taste perversion, and psychomotor impairment, and these effects were most likely to lead to discontinuation at daily doses >96 mg.
Two formulas are effective in patients with diabetes
Investigators stopped 6 studies early because the sponsor wanted to pursue development of a controlled-release formulation of topiramate. The meta-analysis includes a single study of controlled-release topiramate, 175 mg daily in patients with diabetes, that showed equivalent efficacy and similar tolerability to immediate-release topiramate.2
Three other RCTs included in the meta-analysis specifically examined obese patients with type 2 diabetes, a population deemed more resistant to typical weight loss regimens, treated with immediate-release topiramate in dosages of 96 mg and 192 mg daily.3-5 These patients also experienced greater weight loss than patients taking placebo, comparable to what was seen in the overall meta-analysis.
FDA approval and cost of therapy
Topiramate monotherapy isn’t approved by the US Food and Drug Administration (FDA) for obesity treatment. In 2012, the FDA approved phentermine/topiramate extended-release (Qsymia) for long-term treatment of obesity; the monthly cost for a maintenance dose of 7.5 mg/46 mg daily is approximately $185.6 Topiramate immediate-release tablets cost approximately $25 per month for twice daily doses of 50 to 100 mg.7
RECOMMENDATIONS
The US Preventive Services Task Force recommends screening all adults for obesity by measuring BMI and referring patients with a BMI ≥30 for high-intensity, comprehensive behavioral interventions. It makes no recommendation for pharmacologic management.8
The Institute for Clinical Systems Improvement concludes that pharmacotherapy should be used only as part of a comprehensive obesity treatment plan. Pharmacotherapy should be considered if obese patients are unable to lose 1 pound per week with diet, physical activity, and behavior modification.9
1. Kramer CK, Leitão CB, Pinto LC, et al. Efficacy and safety of topiramate on weight loss: a meta-analysis of randomized controlled trials. Obes Rev. 2011;12:e338-e347.
2. Rosenstock J, Hollander P, Gadde KM, et al; OBD-202 Study Group. A randomized, double-blind, placebo-controlled, multicenter study to assess the efficacy and safety of topiramate controlled release in the treatment of obese type 2 diabetic patients. Diabetes Care. 2007;30:1480-1486.
3. Stenlöf K, Rössner S, Vercruysse F, et al. Topiramate in the treatment of obese subjects with drug-naive type 2 diabetes. Diabetes Obes Metab. 2007;9:360-368.
4. Toplak H, Hamann A, Moore R, et al. Efficacy and safety of topiramate in combination with metformin in the treatment of obese subjects with type 2 diabetes: a randomized, double-blind, placebo-controlled study. Int J Obes (Lond). 2007;31:138-146.
5. Eliasson B, Gudbjörnsdottir S, Cederholm J, et al. Weight loss and metabolic effects of topiramate in overweight and obese type 2 diabetic patients: randomized double-blind placebo-controlled trial. Int J Obes (Lond). 2007;31: 1140-1147.
6. Drugs.com. Qsymia. Drugs.com Web site. Available at: www.drugs.com/pro/qsymia.html. Accessed September 26, 2014.
7. Drugs.com. Topirimate prices, coupons and patient assistance programs. Drugs.com Web site. Available at: www.drugs.com/price-guide/topiramate. Accessed September 26, 2014.
8. US Preventive Services Task Force. Obesity in Adults: Screening and management. US Preventive Services Task Force Web site. Available at: www.uspreventiveservicestaskforce.org/uspstf11/obeseadult/obesers.htm. Accessed September 30, 2014.
9. Fitch A, Everling L, Fox C, et al. Prevention and management of obesity for adults. Institute for Clinical Systems Improvement Web site. Available at: www.icsi.org/_asset/s935hy/Obesity-Adults.pdf. Accessed September 30, 2014.
EVIDENCE-BASED ANSWER:
Yes. Topiramate (at daily doses of 64-400 mg) produces an average 5.34 kg of additional weight loss compared with placebo (95% confidence interval [CI], -6.12 to -4.56) in overweight to obese adults for periods of 16 to 60 weeks (strength of recommendation [SOR]: A, meta-analyses of randomized controlled trials [RCTs]).
Topiramate increases the chances of losing 5% or more of baseline body weight (BBW) with a number needed to treat (NNT) of 3 (95% CI, 2-3) and 10% or more of BBW with an NNT of 4 (95% CI, 3-4). However, approximately 17% of patients discontinue the drug because of adverse effects, including paresthesia, hypoesthesia, taste perversion, and psychomotor impairment (SOR: A, meta-analyses of RCTs).
EVIDENCE SUMMARY
A meta-analysis of 10 well-done RCTs with a total of 3320 patients found that topiramate produced more weight loss than placebo.1 Studies included men and women ages 18 to 75 years, with a body mass index (BMI) of 27 to 50. Several studies included patients with hypertension, dyslipidemia, and diabetes mellitus; one study included patients with binge eating disorder. Investigators recruited subjects from sites in Europe, North America, Australia, and South Africa. The studies lasted 16 to 60 weeks and used variable doses of topiramate (64-400 mg daily). Most incorporated a structured lifestyle intervention program for both the treatment and control groups.
Patients taking topiramate lost 5.34 kg (95% CI, -6.12 to -4.56) more than subjects taking placebo. All studies showed significantly greater weight loss in the topiramate groups, regardless of dose and duration, although there was some heterogeneity among the results. The NNTs to achieve weight loss of 5% or more of BBW and 10% or more of BBW were 3 (95% CI, 2-3) and 4 (95% CI, 3-4), respectively.
No major adverse events, but some unpleasant effects
A safety analysis on 6620 subjects found no major adverse events.1 Subjects in the topiramate group were more likely to withdraw because of adverse effects (odds ratio=1.97; 95% CI, 1.64-2.29; number needed to harm=14; 95% CI, 11-18). The most common adverse effects were paresthesia, hypoesthesia, taste perversion, and psychomotor impairment, and these effects were most likely to lead to discontinuation at daily doses >96 mg.
Two formulas are effective in patients with diabetes
Investigators stopped 6 studies early because the sponsor wanted to pursue development of a controlled-release formulation of topiramate. The meta-analysis includes a single study of controlled-release topiramate, 175 mg daily in patients with diabetes, that showed equivalent efficacy and similar tolerability to immediate-release topiramate.2
Three other RCTs included in the meta-analysis specifically examined obese patients with type 2 diabetes, a population deemed more resistant to typical weight loss regimens, treated with immediate-release topiramate in dosages of 96 mg and 192 mg daily.3-5 These patients also experienced greater weight loss than patients taking placebo, comparable to what was seen in the overall meta-analysis.
FDA approval and cost of therapy
Topiramate monotherapy isn’t approved by the US Food and Drug Administration (FDA) for obesity treatment. In 2012, the FDA approved phentermine/topiramate extended-release (Qsymia) for long-term treatment of obesity; the monthly cost for a maintenance dose of 7.5 mg/46 mg daily is approximately $185.6 Topiramate immediate-release tablets cost approximately $25 per month for twice daily doses of 50 to 100 mg.7
RECOMMENDATIONS
The US Preventive Services Task Force recommends screening all adults for obesity by measuring BMI and referring patients with a BMI ≥30 for high-intensity, comprehensive behavioral interventions. It makes no recommendation for pharmacologic management.8
The Institute for Clinical Systems Improvement concludes that pharmacotherapy should be used only as part of a comprehensive obesity treatment plan. Pharmacotherapy should be considered if obese patients are unable to lose 1 pound per week with diet, physical activity, and behavior modification.9
EVIDENCE-BASED ANSWER:
Yes. Topiramate (at daily doses of 64-400 mg) produces an average 5.34 kg of additional weight loss compared with placebo (95% confidence interval [CI], -6.12 to -4.56) in overweight to obese adults for periods of 16 to 60 weeks (strength of recommendation [SOR]: A, meta-analyses of randomized controlled trials [RCTs]).
Topiramate increases the chances of losing 5% or more of baseline body weight (BBW) with a number needed to treat (NNT) of 3 (95% CI, 2-3) and 10% or more of BBW with an NNT of 4 (95% CI, 3-4). However, approximately 17% of patients discontinue the drug because of adverse effects, including paresthesia, hypoesthesia, taste perversion, and psychomotor impairment (SOR: A, meta-analyses of RCTs).
EVIDENCE SUMMARY
A meta-analysis of 10 well-done RCTs with a total of 3320 patients found that topiramate produced more weight loss than placebo.1 Studies included men and women ages 18 to 75 years, with a body mass index (BMI) of 27 to 50. Several studies included patients with hypertension, dyslipidemia, and diabetes mellitus; one study included patients with binge eating disorder. Investigators recruited subjects from sites in Europe, North America, Australia, and South Africa. The studies lasted 16 to 60 weeks and used variable doses of topiramate (64-400 mg daily). Most incorporated a structured lifestyle intervention program for both the treatment and control groups.
Patients taking topiramate lost 5.34 kg (95% CI, -6.12 to -4.56) more than subjects taking placebo. All studies showed significantly greater weight loss in the topiramate groups, regardless of dose and duration, although there was some heterogeneity among the results. The NNTs to achieve weight loss of 5% or more of BBW and 10% or more of BBW were 3 (95% CI, 2-3) and 4 (95% CI, 3-4), respectively.
No major adverse events, but some unpleasant effects
A safety analysis on 6620 subjects found no major adverse events.1 Subjects in the topiramate group were more likely to withdraw because of adverse effects (odds ratio=1.97; 95% CI, 1.64-2.29; number needed to harm=14; 95% CI, 11-18). The most common adverse effects were paresthesia, hypoesthesia, taste perversion, and psychomotor impairment, and these effects were most likely to lead to discontinuation at daily doses >96 mg.
Two formulas are effective in patients with diabetes
Investigators stopped 6 studies early because the sponsor wanted to pursue development of a controlled-release formulation of topiramate. The meta-analysis includes a single study of controlled-release topiramate, 175 mg daily in patients with diabetes, that showed equivalent efficacy and similar tolerability to immediate-release topiramate.2
Three other RCTs included in the meta-analysis specifically examined obese patients with type 2 diabetes, a population deemed more resistant to typical weight loss regimens, treated with immediate-release topiramate in dosages of 96 mg and 192 mg daily.3-5 These patients also experienced greater weight loss than patients taking placebo, comparable to what was seen in the overall meta-analysis.
FDA approval and cost of therapy
Topiramate monotherapy isn’t approved by the US Food and Drug Administration (FDA) for obesity treatment. In 2012, the FDA approved phentermine/topiramate extended-release (Qsymia) for long-term treatment of obesity; the monthly cost for a maintenance dose of 7.5 mg/46 mg daily is approximately $185.6 Topiramate immediate-release tablets cost approximately $25 per month for twice daily doses of 50 to 100 mg.7
RECOMMENDATIONS
The US Preventive Services Task Force recommends screening all adults for obesity by measuring BMI and referring patients with a BMI ≥30 for high-intensity, comprehensive behavioral interventions. It makes no recommendation for pharmacologic management.8
The Institute for Clinical Systems Improvement concludes that pharmacotherapy should be used only as part of a comprehensive obesity treatment plan. Pharmacotherapy should be considered if obese patients are unable to lose 1 pound per week with diet, physical activity, and behavior modification.9
1. Kramer CK, Leitão CB, Pinto LC, et al. Efficacy and safety of topiramate on weight loss: a meta-analysis of randomized controlled trials. Obes Rev. 2011;12:e338-e347.
2. Rosenstock J, Hollander P, Gadde KM, et al; OBD-202 Study Group. A randomized, double-blind, placebo-controlled, multicenter study to assess the efficacy and safety of topiramate controlled release in the treatment of obese type 2 diabetic patients. Diabetes Care. 2007;30:1480-1486.
3. Stenlöf K, Rössner S, Vercruysse F, et al. Topiramate in the treatment of obese subjects with drug-naive type 2 diabetes. Diabetes Obes Metab. 2007;9:360-368.
4. Toplak H, Hamann A, Moore R, et al. Efficacy and safety of topiramate in combination with metformin in the treatment of obese subjects with type 2 diabetes: a randomized, double-blind, placebo-controlled study. Int J Obes (Lond). 2007;31:138-146.
5. Eliasson B, Gudbjörnsdottir S, Cederholm J, et al. Weight loss and metabolic effects of topiramate in overweight and obese type 2 diabetic patients: randomized double-blind placebo-controlled trial. Int J Obes (Lond). 2007;31: 1140-1147.
6. Drugs.com. Qsymia. Drugs.com Web site. Available at: www.drugs.com/pro/qsymia.html. Accessed September 26, 2014.
7. Drugs.com. Topirimate prices, coupons and patient assistance programs. Drugs.com Web site. Available at: www.drugs.com/price-guide/topiramate. Accessed September 26, 2014.
8. US Preventive Services Task Force. Obesity in Adults: Screening and management. US Preventive Services Task Force Web site. Available at: www.uspreventiveservicestaskforce.org/uspstf11/obeseadult/obesers.htm. Accessed September 30, 2014.
9. Fitch A, Everling L, Fox C, et al. Prevention and management of obesity for adults. Institute for Clinical Systems Improvement Web site. Available at: www.icsi.org/_asset/s935hy/Obesity-Adults.pdf. Accessed September 30, 2014.
1. Kramer CK, Leitão CB, Pinto LC, et al. Efficacy and safety of topiramate on weight loss: a meta-analysis of randomized controlled trials. Obes Rev. 2011;12:e338-e347.
2. Rosenstock J, Hollander P, Gadde KM, et al; OBD-202 Study Group. A randomized, double-blind, placebo-controlled, multicenter study to assess the efficacy and safety of topiramate controlled release in the treatment of obese type 2 diabetic patients. Diabetes Care. 2007;30:1480-1486.
3. Stenlöf K, Rössner S, Vercruysse F, et al. Topiramate in the treatment of obese subjects with drug-naive type 2 diabetes. Diabetes Obes Metab. 2007;9:360-368.
4. Toplak H, Hamann A, Moore R, et al. Efficacy and safety of topiramate in combination with metformin in the treatment of obese subjects with type 2 diabetes: a randomized, double-blind, placebo-controlled study. Int J Obes (Lond). 2007;31:138-146.
5. Eliasson B, Gudbjörnsdottir S, Cederholm J, et al. Weight loss and metabolic effects of topiramate in overweight and obese type 2 diabetic patients: randomized double-blind placebo-controlled trial. Int J Obes (Lond). 2007;31: 1140-1147.
6. Drugs.com. Qsymia. Drugs.com Web site. Available at: www.drugs.com/pro/qsymia.html. Accessed September 26, 2014.
7. Drugs.com. Topirimate prices, coupons and patient assistance programs. Drugs.com Web site. Available at: www.drugs.com/price-guide/topiramate. Accessed September 26, 2014.
8. US Preventive Services Task Force. Obesity in Adults: Screening and management. US Preventive Services Task Force Web site. Available at: www.uspreventiveservicestaskforce.org/uspstf11/obeseadult/obesers.htm. Accessed September 30, 2014.
9. Fitch A, Everling L, Fox C, et al. Prevention and management of obesity for adults. Institute for Clinical Systems Improvement Web site. Available at: www.icsi.org/_asset/s935hy/Obesity-Adults.pdf. Accessed September 30, 2014.
Evidence-based answers from the Family Physicians Inquiries Network
High failure rate seen with limited parathyroidectomy in patients with MEN-1
SAN FRANCISCO – Patients with hyperparathyroidism due to multiple endocrine neoplasia type 1 (MEN-1) have a 4 in 10 chance of persistent hyperparathyroidism if they undergo surgery that leaves at least one gland in place, according to a retrospective cohort study presented at the annual clinical congress of the American College of Surgeons.
“Limited initial parathyroidectomy in patients with MEN-1–associated primary hyperparathyroidism results in a high failure rate. Additional enlarged contralateral parathyroid glands are frequently missed by preoperative localizing studies,” commented lead investigator Dr. Naris Nilubol, a staff clinician with the endocrine oncology branch of the Center for Cancer Research, National Cancer Institute, Bethesda, Md.

“We conclude that limited parathyroidectomy in MEN-1 guided by preoperative localizing studies is associated with high failure rates and therefore should not be performed,” he maintained.
In an interview, session comoderator Dr. Marybeth S. Hughes, a staff clinician with the thoracic and gastrointestinal oncology branch, Center for Cancer Research, National Cancer Institute, commented, “In general, I would say that the data presented just reiterates the standard of care, that MEN-1 patients should have bilateral neck exploration with [removal of] three and half glands, or four glands with autotransplantation. So it just basically solidifies what is being done standardly. I don’t think there is a compelling argument to change the standard.”
Dr. Nilubol and colleagues reviewed the charts of 99 patients with MEN-1 who underwent at least one parathyroidectomy at the National Institutes of Health (NIH).
Of the 64 patients who had initial surgery at NIH and had preoperative localizing studies done, 32 had only a single enlarged gland identified by the tests, suggesting they would be good candidates for limited surgery, according to Dr. Nilubol. Bilateral neck dissection at the time of parathyroidectomy showed that in 22 (69%) of these 32 patients, the studies had correctly identified the largest gland; however, in 19 (87%) of those 22, it missed another enlarged gland on the contralateral side. Furthermore, in 5 (16%) of the 32, the largest gland was found on the contralateral side.
With a median follow-up of 23 months, the risk of persistent hyperparathyroidism was 41% for patients who had limited parathyroidectomy (three or fewer glands removed) at initial surgery, significantly and sharply higher than the 6% seen in patients who had subtotal parathyroidectomy or more extensive surgery (at least three and a half glands removed).

Looking at the cumulative number of glands removed during initial and subsequent surgeries, 57% of patients having two or fewer glands removed and 45% of those having two and a half to three glands removed had persistent hyperparathyroidism – both significantly higher than the 5% of patients having at least three and a half glands removed.
Regarding complications, 10% of the patients who had their initial surgery at NIH developed permanent hypoparathyroidism, reported Dr. Nilubol, who disclosed that he had no relevant conflicts of interest.
Session attendees asked about the use of parathyroid hormone levels intraoperatively to guide surgery and what strategy surgeons follow at his institution in this patient population.
Previous research has suggested that intraoperative parathyroid hormone levels do not add any information that would change the operative plan, Dr. Nilubol replied. “Everybody at NIH has preop localizing studies as part of the clinical investigation, but it doesn’t change the way we approach it. Everybody gets a bilateral neck exploration and three and a half–gland removal,” provided all glands can be found, he said.
Session attendee Dr. Michael J. Campbell, a surgeon at the University California, Davis, commented, “A 10% permanent hypoparathyroidism rate in these patients – and they have a tendency to be young, most of them in their late teens, early 20s – that’s a major complication. So could you take your data and make exactly the opposite argument, that maybe you should be doing less to these patients to limit that fairly life-altering complication?” Permanent hypothyroidism at that age is “a significant medical problem,” Dr. Nilubol agreed. However, “at the NIH, we don’t operate on everybody just because they have primary hyperparathyroidism. They have to fulfill metabolic complications before we choose to operate on them. We want to delay the surgeries and [time] between the surgeries because if they live long enough, it will recur, so we want to operate when we can make the most difference, meaning [addressing] kidney stone, bone loss, etc. The most common reason for young patients is they have kidney stones, which leads to surgery.”
SAN FRANCISCO – Patients with hyperparathyroidism due to multiple endocrine neoplasia type 1 (MEN-1) have a 4 in 10 chance of persistent hyperparathyroidism if they undergo surgery that leaves at least one gland in place, according to a retrospective cohort study presented at the annual clinical congress of the American College of Surgeons.
“Limited initial parathyroidectomy in patients with MEN-1–associated primary hyperparathyroidism results in a high failure rate. Additional enlarged contralateral parathyroid glands are frequently missed by preoperative localizing studies,” commented lead investigator Dr. Naris Nilubol, a staff clinician with the endocrine oncology branch of the Center for Cancer Research, National Cancer Institute, Bethesda, Md.
“We conclude that limited parathyroidectomy in MEN-1 guided by preoperative localizing studies is associated with high failure rates and therefore should not be performed,” he maintained.
In an interview, session comoderator Dr. Marybeth S. Hughes, a staff clinician with the thoracic and gastrointestinal oncology branch, Center for Cancer Research, National Cancer Institute, commented, “In general, I would say that the data presented just reiterates the standard of care, that MEN-1 patients should have bilateral neck exploration with [removal of] three and half glands, or four glands with autotransplantation. So it just basically solidifies what is being done standardly. I don’t think there is a compelling argument to change the standard.”
Dr. Nilubol and colleagues reviewed the charts of 99 patients with MEN-1 who underwent at least one parathyroidectomy at the National Institutes of Health (NIH).
Of the 64 patients who had initial surgery at NIH and had preoperative localizing studies done, 32 had only a single enlarged gland identified by the tests, suggesting they would be good candidates for limited surgery, according to Dr. Nilubol. Bilateral neck dissection at the time of parathyroidectomy showed that in 22 (69%) of these 32 patients, the studies had correctly identified the largest gland; however, in 19 (87%) of those 22, it missed another enlarged gland on the contralateral side. Furthermore, in 5 (16%) of the 32, the largest gland was found on the contralateral side.
With a median follow-up of 23 months, the risk of persistent hyperparathyroidism was 41% for patients who had limited parathyroidectomy (three or fewer glands removed) at initial surgery, significantly and sharply higher than the 6% seen in patients who had subtotal parathyroidectomy or more extensive surgery (at least three and a half glands removed).
Looking at the cumulative number of glands removed during initial and subsequent surgeries, 57% of patients having two or fewer glands removed and 45% of those having two and a half to three glands removed had persistent hyperparathyroidism – both significantly higher than the 5% of patients having at least three and a half glands removed.
Regarding complications, 10% of the patients who had their initial surgery at NIH developed permanent hypoparathyroidism, reported Dr. Nilubol, who disclosed that he had no relevant conflicts of interest.
Session attendees asked about the use of parathyroid hormone levels intraoperatively to guide surgery and what strategy surgeons follow at his institution in this patient population.
Previous research has suggested that intraoperative parathyroid hormone levels do not add any information that would change the operative plan, Dr. Nilubol replied. “Everybody at NIH has preop localizing studies as part of the clinical investigation, but it doesn’t change the way we approach it. Everybody gets a bilateral neck exploration and three and a half–gland removal,” provided all glands can be found, he said.
Session attendee Dr. Michael J. Campbell, a surgeon at the University California, Davis, commented, “A 10% permanent hypoparathyroidism rate in these patients – and they have a tendency to be young, most of them in their late teens, early 20s – that’s a major complication. So could you take your data and make exactly the opposite argument, that maybe you should be doing less to these patients to limit that fairly life-altering complication?” Permanent hypothyroidism at that age is “a significant medical problem,” Dr. Nilubol agreed. However, “at the NIH, we don’t operate on everybody just because they have primary hyperparathyroidism. They have to fulfill metabolic complications before we choose to operate on them. We want to delay the surgeries and [time] between the surgeries because if they live long enough, it will recur, so we want to operate when we can make the most difference, meaning [addressing] kidney stone, bone loss, etc. The most common reason for young patients is they have kidney stones, which leads to surgery.”
SAN FRANCISCO – Patients with hyperparathyroidism due to multiple endocrine neoplasia type 1 (MEN-1) have a 4 in 10 chance of persistent hyperparathyroidism if they undergo surgery that leaves at least one gland in place, according to a retrospective cohort study presented at the annual clinical congress of the American College of Surgeons.
“Limited initial parathyroidectomy in patients with MEN-1–associated primary hyperparathyroidism results in a high failure rate. Additional enlarged contralateral parathyroid glands are frequently missed by preoperative localizing studies,” commented lead investigator Dr. Naris Nilubol, a staff clinician with the endocrine oncology branch of the Center for Cancer Research, National Cancer Institute, Bethesda, Md.
“We conclude that limited parathyroidectomy in MEN-1 guided by preoperative localizing studies is associated with high failure rates and therefore should not be performed,” he maintained.
In an interview, session comoderator Dr. Marybeth S. Hughes, a staff clinician with the thoracic and gastrointestinal oncology branch, Center for Cancer Research, National Cancer Institute, commented, “In general, I would say that the data presented just reiterates the standard of care, that MEN-1 patients should have bilateral neck exploration with [removal of] three and half glands, or four glands with autotransplantation. So it just basically solidifies what is being done standardly. I don’t think there is a compelling argument to change the standard.”
Dr. Nilubol and colleagues reviewed the charts of 99 patients with MEN-1 who underwent at least one parathyroidectomy at the National Institutes of Health (NIH).
Of the 64 patients who had initial surgery at NIH and had preoperative localizing studies done, 32 had only a single enlarged gland identified by the tests, suggesting they would be good candidates for limited surgery, according to Dr. Nilubol. Bilateral neck dissection at the time of parathyroidectomy showed that in 22 (69%) of these 32 patients, the studies had correctly identified the largest gland; however, in 19 (87%) of those 22, it missed another enlarged gland on the contralateral side. Furthermore, in 5 (16%) of the 32, the largest gland was found on the contralateral side.
With a median follow-up of 23 months, the risk of persistent hyperparathyroidism was 41% for patients who had limited parathyroidectomy (three or fewer glands removed) at initial surgery, significantly and sharply higher than the 6% seen in patients who had subtotal parathyroidectomy or more extensive surgery (at least three and a half glands removed).
Looking at the cumulative number of glands removed during initial and subsequent surgeries, 57% of patients having two or fewer glands removed and 45% of those having two and a half to three glands removed had persistent hyperparathyroidism – both significantly higher than the 5% of patients having at least three and a half glands removed.
Regarding complications, 10% of the patients who had their initial surgery at NIH developed permanent hypoparathyroidism, reported Dr. Nilubol, who disclosed that he had no relevant conflicts of interest.
Session attendees asked about the use of parathyroid hormone levels intraoperatively to guide surgery and what strategy surgeons follow at his institution in this patient population.
Previous research has suggested that intraoperative parathyroid hormone levels do not add any information that would change the operative plan, Dr. Nilubol replied. “Everybody at NIH has preop localizing studies as part of the clinical investigation, but it doesn’t change the way we approach it. Everybody gets a bilateral neck exploration and three and a half–gland removal,” provided all glands can be found, he said.
Session attendee Dr. Michael J. Campbell, a surgeon at the University California, Davis, commented, “A 10% permanent hypoparathyroidism rate in these patients – and they have a tendency to be young, most of them in their late teens, early 20s – that’s a major complication. So could you take your data and make exactly the opposite argument, that maybe you should be doing less to these patients to limit that fairly life-altering complication?” Permanent hypothyroidism at that age is “a significant medical problem,” Dr. Nilubol agreed. However, “at the NIH, we don’t operate on everybody just because they have primary hyperparathyroidism. They have to fulfill metabolic complications before we choose to operate on them. We want to delay the surgeries and [time] between the surgeries because if they live long enough, it will recur, so we want to operate when we can make the most difference, meaning [addressing] kidney stone, bone loss, etc. The most common reason for young patients is they have kidney stones, which leads to surgery.”
AT THE ACS CLINICAL CONGRESS
Key clinical point: Patients are more likely to have persistent hyperparathyroidism if a gland is left behind.
Major finding: The failure rate after initial parathyroidectomy was 41% with limited surgery versus 6% with subtotal or more extensive surgery.
Data source: A retrospective chart review of 99 patients with MEN-1–associated hyperparathyroidism.
Disclosures: Dr. Nilubol disclosed that he had no relevant conflicts of interest.

Diabetes therapy and cancer risk
To the Editor: I would like to add three points to the excellent review of diabetes therapy and cancer risk by Drs. Sun, Kashyap, and Nasr in the October 2014 issue of Cleveland Clinic Journal of Medicine.1
First, a recent 10-year prospective observational study of more than 190,000 patients showed no increase in bladder cancer with exposure to or long-term use of pioglitazone vs comparator when smoking status was controlled. Although publicly released, these 10-year data have not yet been published.
Second, a recent paper2 from the US Food and Drug Administration and European Medicine Agency reviewed the pancreatic safety of incretin-based therapies. They concluded that there is no evidence that these agents increase the risk of pancreatitis or of pancreatic cancer. So I believe that the authors’ comment that pancreatitis is a “potential side effect” of these agents is not quite accurate.
Lastly, the authors cite no substantial evidence that would support their statement to avoid using glucagon-like protein 1 (GLP-1) receptor agonists in those with a personal history of differentiated thyroid cancer. Indeed these patients, if adequately treated, should have no remnant thyroid tissue. The rodent data indicate an effect of GLP-1 agonists on rodent C cells, not thyroid follicular cells.3 In addition, the prescribing information for these agents does not advise such a limitation on their use.
- Ching Sun GE, Kashyap SR, Nasr C. Diabetes therapy and cancer risk: where do we stand when treating patients? Cleve Clin J Med 2014; 81:620–628.
- Egan AG, Blind E, Dunder K, et al. Pancreatic safety of incretin-based drugs—FDA and EMA assessment. N Engl J Med 2014; 370:794–797.
- Knudsen L, Madsen LW, Andersen S, et al. Glucagon-like peptide-1 receptor agonists activate rodent thyroid C-cells causing calcitonin release and C-cell proliferation. Endocrinology 2010; 151:1473–1486.
To the Editor: I would like to add three points to the excellent review of diabetes therapy and cancer risk by Drs. Sun, Kashyap, and Nasr in the October 2014 issue of Cleveland Clinic Journal of Medicine.1
First, a recent 10-year prospective observational study of more than 190,000 patients showed no increase in bladder cancer with exposure to or long-term use of pioglitazone vs comparator when smoking status was controlled. Although publicly released, these 10-year data have not yet been published.
Second, a recent paper2 from the US Food and Drug Administration and European Medicine Agency reviewed the pancreatic safety of incretin-based therapies. They concluded that there is no evidence that these agents increase the risk of pancreatitis or of pancreatic cancer. So I believe that the authors’ comment that pancreatitis is a “potential side effect” of these agents is not quite accurate.
Lastly, the authors cite no substantial evidence that would support their statement to avoid using glucagon-like protein 1 (GLP-1) receptor agonists in those with a personal history of differentiated thyroid cancer. Indeed these patients, if adequately treated, should have no remnant thyroid tissue. The rodent data indicate an effect of GLP-1 agonists on rodent C cells, not thyroid follicular cells.3 In addition, the prescribing information for these agents does not advise such a limitation on their use.
To the Editor: I would like to add three points to the excellent review of diabetes therapy and cancer risk by Drs. Sun, Kashyap, and Nasr in the October 2014 issue of Cleveland Clinic Journal of Medicine.1
First, a recent 10-year prospective observational study of more than 190,000 patients showed no increase in bladder cancer with exposure to or long-term use of pioglitazone vs comparator when smoking status was controlled. Although publicly released, these 10-year data have not yet been published.
Second, a recent paper2 from the US Food and Drug Administration and European Medicine Agency reviewed the pancreatic safety of incretin-based therapies. They concluded that there is no evidence that these agents increase the risk of pancreatitis or of pancreatic cancer. So I believe that the authors’ comment that pancreatitis is a “potential side effect” of these agents is not quite accurate.
Lastly, the authors cite no substantial evidence that would support their statement to avoid using glucagon-like protein 1 (GLP-1) receptor agonists in those with a personal history of differentiated thyroid cancer. Indeed these patients, if adequately treated, should have no remnant thyroid tissue. The rodent data indicate an effect of GLP-1 agonists on rodent C cells, not thyroid follicular cells.3 In addition, the prescribing information for these agents does not advise such a limitation on their use.
- Ching Sun GE, Kashyap SR, Nasr C. Diabetes therapy and cancer risk: where do we stand when treating patients? Cleve Clin J Med 2014; 81:620–628.
- Egan AG, Blind E, Dunder K, et al. Pancreatic safety of incretin-based drugs—FDA and EMA assessment. N Engl J Med 2014; 370:794–797.
- Knudsen L, Madsen LW, Andersen S, et al. Glucagon-like peptide-1 receptor agonists activate rodent thyroid C-cells causing calcitonin release and C-cell proliferation. Endocrinology 2010; 151:1473–1486.
- Ching Sun GE, Kashyap SR, Nasr C. Diabetes therapy and cancer risk: where do we stand when treating patients? Cleve Clin J Med 2014; 81:620–628.
- Egan AG, Blind E, Dunder K, et al. Pancreatic safety of incretin-based drugs—FDA and EMA assessment. N Engl J Med 2014; 370:794–797.
- Knudsen L, Madsen LW, Andersen S, et al. Glucagon-like peptide-1 receptor agonists activate rodent thyroid C-cells causing calcitonin release and C-cell proliferation. Endocrinology 2010; 151:1473–1486.
In reply: Diabetes therapy and cancer risk
In Reply: In regard to Dr. Weiss’s first point, the Kaiser Permanente Northern California diabetes registry study aimed to assess the association between bladder cancer and pioglitazone in 193,099 patients. In their 2011 interim 5-year analysis, Lewis et al reported a modest but statistically significant increased risk of bladder cancer in patients with type 2 diabetes mellitus who used pioglitazone for 2 or more years.1
We appreciate Dr. Weiss’s comment on the 10-year study conclusion data. As Dr. Weiss has indicated, the recent Takeda news release2 showed that the primary analysis found no association between pioglitazone use and bladder cancer risk. Furthermore, no association was found between bladder cancer risk and duration of use, higher cumulative doses, or time since initiation of pioglitazone.2
Regarding Dr. Weiss’s second point, we agree that at this time the cumulative data are not supportive of pancreatitis as per Egan et al.3 Recent publication of the SAVOR-TIMI trial4 of saxagliptin documented no increased risk of pancreatitis or pancreatic cancer over 2.1 years of follow-up in more than 16,000 patients over the age of 40 with type 2 diabetes. However, since amylase and lipase levels were not routinely checked in study participants, subclinical and asymptomatic cases may not have been recognized.4 Therefore, we stand by our statement that pancreatitis is a potential side effect.
It is important to recognize that although the observational data reviewed by both agencies (the US Food and Drug Administration and European Medicine Agency) in the publication by Egan et al3 are reassuring, we cannot yet say with absolute certainty that there is no associated risk. In fact, the concluding statements of the publication are as follows: “Although the totality of the data that have been reviewed provides reassurance, pancreatitis will continue to be considered a risk associated with these drugs until more data are available; both agencies continue to investigate this safety signal.”3
On September 18, 2014, the newest approved GLP-1 receptor agonist, dulaglutide, was approved with a boxed warning that it causes thyroid C-cell tumors in rats, that whether it causes thyroid C-cell tumors including medullary thyroid carcinoma (MTC) in humans is unknown, and that since relevance to humans could not be determined from clinical or nonclinical studies, dulaglutide is contraindicated in patients with a personal or family history of MTC, as well as in patients with multiple endocrine neoplasia syndrome type 2.5
It is important to recognize that despite these controversies, which have not been well-supported to date, incretin-based therapies have numerous metabolic benefits, including favorable glycemic and weight effects.
In regard to Dr. Weiss’s last point, we would like to point out the study by Gier et al6 in which GLP-1 receptor expression was found in 3 of 17 cases of human papillary thyroid cancer. The implication is that abnormal thyroid tissue does not behave the same way as normal tissue.
Furthermore, Dr. Weiss brings up the point that patients with thyroid cancer, if it is adequately treated, should have no remnant thyroid tissue. Certainly, adequate treatment would be an easy call to make if a stimulated thyroglobulin level is below the assay’s detection limit and there is no imaging evidence of residual thyroid cancer. For example, in someone with a history of thyroid cancer diagnosed more than 10 years ago without biochemical or imaging evidence of disease, any potential concerns of GLP-1 receptor agonist use in regards to thyroid cancer would be nominal. But not everyone with thyroid cancer falls into this category.
We do not suggest that these potential risks preclude the use of these agents in all patients, but rather that a discussion should occur between physician and patient. Diabetes therapy, as in treatment of other medical conditions, should be tailored to the individual patient, and all potential risk and benefits should be disclosed and considered.
- Lewis JD, Ferrara A, Peng T, et al. Risk of bladder cancer among diabetic patients treated with pioglitazone: interim report of a longitudinal cohort study. Diabetes Care 2011; 34:916–922.
- Takeda Pharmaceuticals. 2014. Takeda announces completion of the post-marketing commitment to submit data to the FDA, the EMA and the PMDA for pioglitazone containing medicines including ACTOS. [Press release]. Accessed 19 October 2014. www.takeda.us/newsroom/press_release_detail.aspx?year=2014&id=314. Accessed November 3, 2014.
- Egan AG, Blind E, Dunder K, et al. Pancreatic safety of incretin-based drugs—FDA and EMA assessment. N Engl J Med 2014; 370:794–797.
- Raz I, Bhatt DL, Hirshberg B, et al. Incidence of pancreatitis and pancreatic cancer in a randomized controlled multicenter trial (SAVOR-TIMI 53) of the dipeptidyl peptidase-4 inhibitor saxagliptin. Diabetes Care 2014; 37:2435–2441.
- Trulicity [package insert]. Indianapolis, IN: Eli Lilly & Company; 2014.
- Gier B, Butler PC, Lai CK, Kirakossian D, DeNicola MM, Yeh MW. Glucagon like peptide-1 receptor expression in the human thyroid gland. J Clin Endocrinol Metab 2012; 97:121–131.
In Reply: In regard to Dr. Weiss’s first point, the Kaiser Permanente Northern California diabetes registry study aimed to assess the association between bladder cancer and pioglitazone in 193,099 patients. In their 2011 interim 5-year analysis, Lewis et al reported a modest but statistically significant increased risk of bladder cancer in patients with type 2 diabetes mellitus who used pioglitazone for 2 or more years.1
We appreciate Dr. Weiss’s comment on the 10-year study conclusion data. As Dr. Weiss has indicated, the recent Takeda news release2 showed that the primary analysis found no association between pioglitazone use and bladder cancer risk. Furthermore, no association was found between bladder cancer risk and duration of use, higher cumulative doses, or time since initiation of pioglitazone.2
Regarding Dr. Weiss’s second point, we agree that at this time the cumulative data are not supportive of pancreatitis as per Egan et al.3 Recent publication of the SAVOR-TIMI trial4 of saxagliptin documented no increased risk of pancreatitis or pancreatic cancer over 2.1 years of follow-up in more than 16,000 patients over the age of 40 with type 2 diabetes. However, since amylase and lipase levels were not routinely checked in study participants, subclinical and asymptomatic cases may not have been recognized.4 Therefore, we stand by our statement that pancreatitis is a potential side effect.
It is important to recognize that although the observational data reviewed by both agencies (the US Food and Drug Administration and European Medicine Agency) in the publication by Egan et al3 are reassuring, we cannot yet say with absolute certainty that there is no associated risk. In fact, the concluding statements of the publication are as follows: “Although the totality of the data that have been reviewed provides reassurance, pancreatitis will continue to be considered a risk associated with these drugs until more data are available; both agencies continue to investigate this safety signal.”3
On September 18, 2014, the newest approved GLP-1 receptor agonist, dulaglutide, was approved with a boxed warning that it causes thyroid C-cell tumors in rats, that whether it causes thyroid C-cell tumors including medullary thyroid carcinoma (MTC) in humans is unknown, and that since relevance to humans could not be determined from clinical or nonclinical studies, dulaglutide is contraindicated in patients with a personal or family history of MTC, as well as in patients with multiple endocrine neoplasia syndrome type 2.5
It is important to recognize that despite these controversies, which have not been well-supported to date, incretin-based therapies have numerous metabolic benefits, including favorable glycemic and weight effects.
In regard to Dr. Weiss’s last point, we would like to point out the study by Gier et al6 in which GLP-1 receptor expression was found in 3 of 17 cases of human papillary thyroid cancer. The implication is that abnormal thyroid tissue does not behave the same way as normal tissue.
Furthermore, Dr. Weiss brings up the point that patients with thyroid cancer, if it is adequately treated, should have no remnant thyroid tissue. Certainly, adequate treatment would be an easy call to make if a stimulated thyroglobulin level is below the assay’s detection limit and there is no imaging evidence of residual thyroid cancer. For example, in someone with a history of thyroid cancer diagnosed more than 10 years ago without biochemical or imaging evidence of disease, any potential concerns of GLP-1 receptor agonist use in regards to thyroid cancer would be nominal. But not everyone with thyroid cancer falls into this category.
We do not suggest that these potential risks preclude the use of these agents in all patients, but rather that a discussion should occur between physician and patient. Diabetes therapy, as in treatment of other medical conditions, should be tailored to the individual patient, and all potential risk and benefits should be disclosed and considered.
In Reply: In regard to Dr. Weiss’s first point, the Kaiser Permanente Northern California diabetes registry study aimed to assess the association between bladder cancer and pioglitazone in 193,099 patients. In their 2011 interim 5-year analysis, Lewis et al reported a modest but statistically significant increased risk of bladder cancer in patients with type 2 diabetes mellitus who used pioglitazone for 2 or more years.1
We appreciate Dr. Weiss’s comment on the 10-year study conclusion data. As Dr. Weiss has indicated, the recent Takeda news release2 showed that the primary analysis found no association between pioglitazone use and bladder cancer risk. Furthermore, no association was found between bladder cancer risk and duration of use, higher cumulative doses, or time since initiation of pioglitazone.2
Regarding Dr. Weiss’s second point, we agree that at this time the cumulative data are not supportive of pancreatitis as per Egan et al.3 Recent publication of the SAVOR-TIMI trial4 of saxagliptin documented no increased risk of pancreatitis or pancreatic cancer over 2.1 years of follow-up in more than 16,000 patients over the age of 40 with type 2 diabetes. However, since amylase and lipase levels were not routinely checked in study participants, subclinical and asymptomatic cases may not have been recognized.4 Therefore, we stand by our statement that pancreatitis is a potential side effect.
It is important to recognize that although the observational data reviewed by both agencies (the US Food and Drug Administration and European Medicine Agency) in the publication by Egan et al3 are reassuring, we cannot yet say with absolute certainty that there is no associated risk. In fact, the concluding statements of the publication are as follows: “Although the totality of the data that have been reviewed provides reassurance, pancreatitis will continue to be considered a risk associated with these drugs until more data are available; both agencies continue to investigate this safety signal.”3
On September 18, 2014, the newest approved GLP-1 receptor agonist, dulaglutide, was approved with a boxed warning that it causes thyroid C-cell tumors in rats, that whether it causes thyroid C-cell tumors including medullary thyroid carcinoma (MTC) in humans is unknown, and that since relevance to humans could not be determined from clinical or nonclinical studies, dulaglutide is contraindicated in patients with a personal or family history of MTC, as well as in patients with multiple endocrine neoplasia syndrome type 2.5
It is important to recognize that despite these controversies, which have not been well-supported to date, incretin-based therapies have numerous metabolic benefits, including favorable glycemic and weight effects.
In regard to Dr. Weiss’s last point, we would like to point out the study by Gier et al6 in which GLP-1 receptor expression was found in 3 of 17 cases of human papillary thyroid cancer. The implication is that abnormal thyroid tissue does not behave the same way as normal tissue.
Furthermore, Dr. Weiss brings up the point that patients with thyroid cancer, if it is adequately treated, should have no remnant thyroid tissue. Certainly, adequate treatment would be an easy call to make if a stimulated thyroglobulin level is below the assay’s detection limit and there is no imaging evidence of residual thyroid cancer. For example, in someone with a history of thyroid cancer diagnosed more than 10 years ago without biochemical or imaging evidence of disease, any potential concerns of GLP-1 receptor agonist use in regards to thyroid cancer would be nominal. But not everyone with thyroid cancer falls into this category.
We do not suggest that these potential risks preclude the use of these agents in all patients, but rather that a discussion should occur between physician and patient. Diabetes therapy, as in treatment of other medical conditions, should be tailored to the individual patient, and all potential risk and benefits should be disclosed and considered.
- Lewis JD, Ferrara A, Peng T, et al. Risk of bladder cancer among diabetic patients treated with pioglitazone: interim report of a longitudinal cohort study. Diabetes Care 2011; 34:916–922.
- Takeda Pharmaceuticals. 2014. Takeda announces completion of the post-marketing commitment to submit data to the FDA, the EMA and the PMDA for pioglitazone containing medicines including ACTOS. [Press release]. Accessed 19 October 2014. www.takeda.us/newsroom/press_release_detail.aspx?year=2014&id=314. Accessed November 3, 2014.
- Egan AG, Blind E, Dunder K, et al. Pancreatic safety of incretin-based drugs—FDA and EMA assessment. N Engl J Med 2014; 370:794–797.
- Raz I, Bhatt DL, Hirshberg B, et al. Incidence of pancreatitis and pancreatic cancer in a randomized controlled multicenter trial (SAVOR-TIMI 53) of the dipeptidyl peptidase-4 inhibitor saxagliptin. Diabetes Care 2014; 37:2435–2441.
- Trulicity [package insert]. Indianapolis, IN: Eli Lilly & Company; 2014.
- Gier B, Butler PC, Lai CK, Kirakossian D, DeNicola MM, Yeh MW. Glucagon like peptide-1 receptor expression in the human thyroid gland. J Clin Endocrinol Metab 2012; 97:121–131.
- Lewis JD, Ferrara A, Peng T, et al. Risk of bladder cancer among diabetic patients treated with pioglitazone: interim report of a longitudinal cohort study. Diabetes Care 2011; 34:916–922.
- Takeda Pharmaceuticals. 2014. Takeda announces completion of the post-marketing commitment to submit data to the FDA, the EMA and the PMDA for pioglitazone containing medicines including ACTOS. [Press release]. Accessed 19 October 2014. www.takeda.us/newsroom/press_release_detail.aspx?year=2014&id=314. Accessed November 3, 2014.
- Egan AG, Blind E, Dunder K, et al. Pancreatic safety of incretin-based drugs—FDA and EMA assessment. N Engl J Med 2014; 370:794–797.
- Raz I, Bhatt DL, Hirshberg B, et al. Incidence of pancreatitis and pancreatic cancer in a randomized controlled multicenter trial (SAVOR-TIMI 53) of the dipeptidyl peptidase-4 inhibitor saxagliptin. Diabetes Care 2014; 37:2435–2441.
- Trulicity [package insert]. Indianapolis, IN: Eli Lilly & Company; 2014.
- Gier B, Butler PC, Lai CK, Kirakossian D, DeNicola MM, Yeh MW. Glucagon like peptide-1 receptor expression in the human thyroid gland. J Clin Endocrinol Metab 2012; 97:121–131.
Mutations indicate predisposition to blood cancers

Credit: Graham Colm
Two teams of researchers have identified somatic mutations that increase the likelihood a person will develop a hematologic malignancy.
This “pre-malignant” stage was detected simply by sequencing DNA from blood samples.
The researchers found that subjects carrying certain mutations had more than 10 times the risk of developing a hematologic malignancy than individuals without the mutations. And the risk increased with age.
Steven McCarroll, PhD, of Harvard Medical School in Boston, Massachusetts, and Benjamin Ebert, MD, PhD, also of Harvard Medical School, reported these findings in NEJM.
Both research teams looked at somatic mutations in DNA samples collected from the blood of subjects who had not been diagnosed with cancer or blood disorders.
Taking two very different approaches, the teams found that a surprising percentage of individuals had acquired a subset of the somatic mutations present in hematologic malignancies. And subjects with the mutations were more likely to develop these cancers.
This pre-malignant state was rare in individuals under the age of 40. But it appeared with increasing frequency with each decade of life, ultimately appearing in more than 10% of individuals over the age of 70.
The researchers believe these early mutations lie in wait for follow-on, cooperating mutations that, when they occur in the same cells as the earlier mutations, drive the cells toward cancer. The majority of mutations occurred in just 3 genes: DNMT3A, TET2, and ASXL1.
Dr Ebert’s group
Dr Ebert and his colleagues had hypothesized that, since hematologic malignancies increase with age, it might be possible to detect early somatic mutations that could be initiating the disease process, and these mutations might increase with age.
The researchers looked specifically at 160 genes known to be recurrently mutated in hematologic malignancies, using genetic data derived from approximately 17,000 blood samples originally obtained for studies on the genetics of type 2 diabetes.
The team found a roughly 11-fold increase in the risk of hematologic malignancy among subjects with the subset of somatic mutations linked to blood cancers. And there was a clear association between age and the frequency of these mutations.
Men were slightly more likely to have the mutations than women, and Hispanics were slightly less likely to have the mutations than other racial/ethnic groups.
The researchers also found an association between the presence of this pre-malignant state and the risk of overall mortality independent of malignancy. Individuals with the mutations had a higher risk of type 2 diabetes, coronary heart disease, and ischemic stroke as well.
However, additional research will be needed to determine the nature of these associations.
Dr McCarroll’s group
Dr McCarroll and his colleagues discovered the same phenomenon while trying to determine whether somatic mutations contribute to the risk of developing schizophrenia.
The team studied roughly 12,000 DNA samples from patients with schizophrenia and bipolar disorder, as well as healthy controls, searching across the whole genome at all of the protein-coding genes for patterns in somatic mutations.
The somatic mutations were concentrated in a handful of genes that turned out to be cancer genes.
So the researchers used electronic medical records to follow the patients’ medical histories, finding that subjects with these acquired mutations had a nearly 13-fold higher risk of developing a hematologic malignancy than subjects without the mutations.
The team conducted follow-up analyses on tumor samples from 2 patients who had progressed from this pre-malignant state to cancer. In both cases, the cancer developed from the same cells that had harbored the initiating mutations years earlier.
“The fact that both teams converged on strikingly similar findings, using very different approaches and looking at DNA from very different sets of patients, has given us great confidence in the results,” said study author Giulio Genovese, PhD, of the Broad Institute of MIT and Harvard in Cambridge, Massachusetts.
Next steps
The researchers emphasized that there is no clinical benefit today for testing for this pre-malignant state, as there are no treatments currently available that would address this condition in otherwise healthy people.
However, they said the results open the door to entirely new directions for research, toward early detection and even prevention of hematologic malignancies.
“The results demonstrate a way to identify high-risk cohorts—people who are at much higher than average risk of progressing to cancer—which could be a population for clinical trials of future prevention strategies,” Dr McCarroll said. “The abundance of these mutated cells could also serve as a biomarker—like LDL cholesterol is for cardiovascular disease—to test the effects of potential prevention therapies in clinical trials.”
Dr Ebert added, “A new focus of investigation will now be to develop interventions that might decrease the likelihood that individuals with these mutations will go on to develop overt malignancies, or therapeutic strategies to decrease mortality from other conditions that may be instigated by these mutations.”
This research is set to be presented on December 9 at the 56th ASH Annual Meeting in San Francisco. ![]()
Credit: Graham Colm
Two teams of researchers have identified somatic mutations that increase the likelihood a person will develop a hematologic malignancy.
This “pre-malignant” stage was detected simply by sequencing DNA from blood samples.
The researchers found that subjects carrying certain mutations had more than 10 times the risk of developing a hematologic malignancy than individuals without the mutations. And the risk increased with age.
Steven McCarroll, PhD, of Harvard Medical School in Boston, Massachusetts, and Benjamin Ebert, MD, PhD, also of Harvard Medical School, reported these findings in NEJM.
Both research teams looked at somatic mutations in DNA samples collected from the blood of subjects who had not been diagnosed with cancer or blood disorders.
Taking two very different approaches, the teams found that a surprising percentage of individuals had acquired a subset of the somatic mutations present in hematologic malignancies. And subjects with the mutations were more likely to develop these cancers.
This pre-malignant state was rare in individuals under the age of 40. But it appeared with increasing frequency with each decade of life, ultimately appearing in more than 10% of individuals over the age of 70.
The researchers believe these early mutations lie in wait for follow-on, cooperating mutations that, when they occur in the same cells as the earlier mutations, drive the cells toward cancer. The majority of mutations occurred in just 3 genes: DNMT3A, TET2, and ASXL1.
Dr Ebert’s group
Dr Ebert and his colleagues had hypothesized that, since hematologic malignancies increase with age, it might be possible to detect early somatic mutations that could be initiating the disease process, and these mutations might increase with age.
The researchers looked specifically at 160 genes known to be recurrently mutated in hematologic malignancies, using genetic data derived from approximately 17,000 blood samples originally obtained for studies on the genetics of type 2 diabetes.
The team found a roughly 11-fold increase in the risk of hematologic malignancy among subjects with the subset of somatic mutations linked to blood cancers. And there was a clear association between age and the frequency of these mutations.
Men were slightly more likely to have the mutations than women, and Hispanics were slightly less likely to have the mutations than other racial/ethnic groups.
The researchers also found an association between the presence of this pre-malignant state and the risk of overall mortality independent of malignancy. Individuals with the mutations had a higher risk of type 2 diabetes, coronary heart disease, and ischemic stroke as well.
However, additional research will be needed to determine the nature of these associations.
Dr McCarroll’s group
Dr McCarroll and his colleagues discovered the same phenomenon while trying to determine whether somatic mutations contribute to the risk of developing schizophrenia.
The team studied roughly 12,000 DNA samples from patients with schizophrenia and bipolar disorder, as well as healthy controls, searching across the whole genome at all of the protein-coding genes for patterns in somatic mutations.
The somatic mutations were concentrated in a handful of genes that turned out to be cancer genes.
So the researchers used electronic medical records to follow the patients’ medical histories, finding that subjects with these acquired mutations had a nearly 13-fold higher risk of developing a hematologic malignancy than subjects without the mutations.
The team conducted follow-up analyses on tumor samples from 2 patients who had progressed from this pre-malignant state to cancer. In both cases, the cancer developed from the same cells that had harbored the initiating mutations years earlier.
“The fact that both teams converged on strikingly similar findings, using very different approaches and looking at DNA from very different sets of patients, has given us great confidence in the results,” said study author Giulio Genovese, PhD, of the Broad Institute of MIT and Harvard in Cambridge, Massachusetts.
Next steps
The researchers emphasized that there is no clinical benefit today for testing for this pre-malignant state, as there are no treatments currently available that would address this condition in otherwise healthy people.
However, they said the results open the door to entirely new directions for research, toward early detection and even prevention of hematologic malignancies.
“The results demonstrate a way to identify high-risk cohorts—people who are at much higher than average risk of progressing to cancer—which could be a population for clinical trials of future prevention strategies,” Dr McCarroll said. “The abundance of these mutated cells could also serve as a biomarker—like LDL cholesterol is for cardiovascular disease—to test the effects of potential prevention therapies in clinical trials.”
Dr Ebert added, “A new focus of investigation will now be to develop interventions that might decrease the likelihood that individuals with these mutations will go on to develop overt malignancies, or therapeutic strategies to decrease mortality from other conditions that may be instigated by these mutations.”
This research is set to be presented on December 9 at the 56th ASH Annual Meeting in San Francisco. ![]()
Credit: Graham Colm
Two teams of researchers have identified somatic mutations that increase the likelihood a person will develop a hematologic malignancy.
This “pre-malignant” stage was detected simply by sequencing DNA from blood samples.
The researchers found that subjects carrying certain mutations had more than 10 times the risk of developing a hematologic malignancy than individuals without the mutations. And the risk increased with age.
Steven McCarroll, PhD, of Harvard Medical School in Boston, Massachusetts, and Benjamin Ebert, MD, PhD, also of Harvard Medical School, reported these findings in NEJM.
Both research teams looked at somatic mutations in DNA samples collected from the blood of subjects who had not been diagnosed with cancer or blood disorders.
Taking two very different approaches, the teams found that a surprising percentage of individuals had acquired a subset of the somatic mutations present in hematologic malignancies. And subjects with the mutations were more likely to develop these cancers.
This pre-malignant state was rare in individuals under the age of 40. But it appeared with increasing frequency with each decade of life, ultimately appearing in more than 10% of individuals over the age of 70.
The researchers believe these early mutations lie in wait for follow-on, cooperating mutations that, when they occur in the same cells as the earlier mutations, drive the cells toward cancer. The majority of mutations occurred in just 3 genes: DNMT3A, TET2, and ASXL1.
Dr Ebert’s group
Dr Ebert and his colleagues had hypothesized that, since hematologic malignancies increase with age, it might be possible to detect early somatic mutations that could be initiating the disease process, and these mutations might increase with age.
The researchers looked specifically at 160 genes known to be recurrently mutated in hematologic malignancies, using genetic data derived from approximately 17,000 blood samples originally obtained for studies on the genetics of type 2 diabetes.
The team found a roughly 11-fold increase in the risk of hematologic malignancy among subjects with the subset of somatic mutations linked to blood cancers. And there was a clear association between age and the frequency of these mutations.
Men were slightly more likely to have the mutations than women, and Hispanics were slightly less likely to have the mutations than other racial/ethnic groups.
The researchers also found an association between the presence of this pre-malignant state and the risk of overall mortality independent of malignancy. Individuals with the mutations had a higher risk of type 2 diabetes, coronary heart disease, and ischemic stroke as well.
However, additional research will be needed to determine the nature of these associations.
Dr McCarroll’s group
Dr McCarroll and his colleagues discovered the same phenomenon while trying to determine whether somatic mutations contribute to the risk of developing schizophrenia.
The team studied roughly 12,000 DNA samples from patients with schizophrenia and bipolar disorder, as well as healthy controls, searching across the whole genome at all of the protein-coding genes for patterns in somatic mutations.
The somatic mutations were concentrated in a handful of genes that turned out to be cancer genes.
So the researchers used electronic medical records to follow the patients’ medical histories, finding that subjects with these acquired mutations had a nearly 13-fold higher risk of developing a hematologic malignancy than subjects without the mutations.
The team conducted follow-up analyses on tumor samples from 2 patients who had progressed from this pre-malignant state to cancer. In both cases, the cancer developed from the same cells that had harbored the initiating mutations years earlier.
“The fact that both teams converged on strikingly similar findings, using very different approaches and looking at DNA from very different sets of patients, has given us great confidence in the results,” said study author Giulio Genovese, PhD, of the Broad Institute of MIT and Harvard in Cambridge, Massachusetts.
Next steps
The researchers emphasized that there is no clinical benefit today for testing for this pre-malignant state, as there are no treatments currently available that would address this condition in otherwise healthy people.
However, they said the results open the door to entirely new directions for research, toward early detection and even prevention of hematologic malignancies.
“The results demonstrate a way to identify high-risk cohorts—people who are at much higher than average risk of progressing to cancer—which could be a population for clinical trials of future prevention strategies,” Dr McCarroll said. “The abundance of these mutated cells could also serve as a biomarker—like LDL cholesterol is for cardiovascular disease—to test the effects of potential prevention therapies in clinical trials.”
Dr Ebert added, “A new focus of investigation will now be to develop interventions that might decrease the likelihood that individuals with these mutations will go on to develop overt malignancies, or therapeutic strategies to decrease mortality from other conditions that may be instigated by these mutations.”
This research is set to be presented on December 9 at the 56th ASH Annual Meeting in San Francisco. ![]()