User login
Obituary: Laura Mirkinson, MD, MSc, FAAP
Laura Mirkinson, MD, MSc, FAAP, pediatric hospitalist and a founder of the American Academy of Pediatrics’ (AAP) Section on Hospital Medicine Executive Committee, died April 29 of ovarian cancer. She was 60.
Dr. Mirkinson received her medical degree from Uniformed Services University of the Health Sciences (USUHS) in Bethesda, Md., before serving her pediatrics residency at Bethesda Naval Hospital and Walter Reed Army Medical Center. She served as an active-duty medical officer in the U.S. Naval Medical Corps Reserves before retiring as a captain in 2000. She then worked at Children’s Hospital of Washington and the pediatric hospitalist group at Holy Cross Hospital in Silver Spring, Md.
Dr. Mirkinson played a role in the development of pediatric hospital medicine during and after her military service. In 2007, she was elected chief of pediatrics at Blythedale Children’s Hospital in Valhalla, N.Y. She also served as director of education for the AAP’s Section on Hospital Medicine and was its second chairperson, following the section’s co-founder Jack Percelay, MD, FAAP. Through this work, she helped promote the AAP Section on Hospital Medicine newsletter, as well as the Hospital Pediatrics journal.
Dr. Mirkinson’s colleagues and students remember her as a caring, insightful teacher and mentor who offered wise advice on all matters professional and personal. Her devotion to patient care was evident throughout her career. Even in her administrative roles, she would often practice clinical medicine to help fill scheduling gaps or cover other physicians’ vacations.
Laura Mirkinson, MD, MSc, FAAP, pediatric hospitalist and a founder of the American Academy of Pediatrics’ (AAP) Section on Hospital Medicine Executive Committee, died April 29 of ovarian cancer. She was 60.
Dr. Mirkinson received her medical degree from Uniformed Services University of the Health Sciences (USUHS) in Bethesda, Md., before serving her pediatrics residency at Bethesda Naval Hospital and Walter Reed Army Medical Center. She served as an active-duty medical officer in the U.S. Naval Medical Corps Reserves before retiring as a captain in 2000. She then worked at Children’s Hospital of Washington and the pediatric hospitalist group at Holy Cross Hospital in Silver Spring, Md.
Dr. Mirkinson played a role in the development of pediatric hospital medicine during and after her military service. In 2007, she was elected chief of pediatrics at Blythedale Children’s Hospital in Valhalla, N.Y. She also served as director of education for the AAP’s Section on Hospital Medicine and was its second chairperson, following the section’s co-founder Jack Percelay, MD, FAAP. Through this work, she helped promote the AAP Section on Hospital Medicine newsletter, as well as the Hospital Pediatrics journal.
Dr. Mirkinson’s colleagues and students remember her as a caring, insightful teacher and mentor who offered wise advice on all matters professional and personal. Her devotion to patient care was evident throughout her career. Even in her administrative roles, she would often practice clinical medicine to help fill scheduling gaps or cover other physicians’ vacations.
Laura Mirkinson, MD, MSc, FAAP, pediatric hospitalist and a founder of the American Academy of Pediatrics’ (AAP) Section on Hospital Medicine Executive Committee, died April 29 of ovarian cancer. She was 60.
Dr. Mirkinson received her medical degree from Uniformed Services University of the Health Sciences (USUHS) in Bethesda, Md., before serving her pediatrics residency at Bethesda Naval Hospital and Walter Reed Army Medical Center. She served as an active-duty medical officer in the U.S. Naval Medical Corps Reserves before retiring as a captain in 2000. She then worked at Children’s Hospital of Washington and the pediatric hospitalist group at Holy Cross Hospital in Silver Spring, Md.
Dr. Mirkinson played a role in the development of pediatric hospital medicine during and after her military service. In 2007, she was elected chief of pediatrics at Blythedale Children’s Hospital in Valhalla, N.Y. She also served as director of education for the AAP’s Section on Hospital Medicine and was its second chairperson, following the section’s co-founder Jack Percelay, MD, FAAP. Through this work, she helped promote the AAP Section on Hospital Medicine newsletter, as well as the Hospital Pediatrics journal.
Dr. Mirkinson’s colleagues and students remember her as a caring, insightful teacher and mentor who offered wise advice on all matters professional and personal. Her devotion to patient care was evident throughout her career. Even in her administrative roles, she would often practice clinical medicine to help fill scheduling gaps or cover other physicians’ vacations.
Movers and Shakers in Hospital Medicine

Chris Brown, MD, MPH, was elected one of Columbus Business First’s members of the Forty Under 40 class of 2013. Dr. Brown is the medical director of hospital medicine at Memorial Hospital of Union County in Marysville, Ohio. The designation recognizes members of the Columbus, Ohio, community who demonstrate superior professional development, community involvement, and other awards and recognitions. Dr. Brown’s colleagues describe him as “a collaborative, attentive, and detailed physician as well as a capable leader.”
Thomas Gallagher, MD, is the University of Washington’s (UW) new director of the program in hospital medicine. This new position in UW’s division of general internal medicine will oversee all of the hospitalist programs at UW Medicine and Harborview Medical Center in Seattle. Dr. Gallagher also is a UW professor of medicine and bioethics and humanities.
Pawan Dhawan, MD, has been appointed medical director of the hospitalist programs at Trident Medical Center in Charleston, S.C., and Summerville Medical Center in Summerville, S.C. Dr. Dhawan comes to Trident Health System from Bay Hospitalists in Newark, Del. Dr. Dhawan served on SHM’s Leadership Committee in 2011.
OB Hospitalist Group (OBHG) in Mauldin, S.C., has announced new medical directors of operations (MDOs) for five of its regions. Nicholas Kulbida, MD, MDO for OBHG’s northeast region, works at Bellevue Women’s Center in Niskayuna, N.Y. Susie Wilson, MD, one of two MDOs for the southeast region, is team leader at Summerville Medical Center in Summerville, S.C. Sue Smith, MD, the other MDO for OBHG’s southeast region, works for Winter Haven Hospital-Regency Medical Center in Winter Haven, Fla. Matthew Conrad, MD, MDO for the Great Lakes region, serves as an OB hospitalist at both Holmes Regional Medical Center in Melbourne, Fla., and Osceola Regional Medical Center in Kissimmee, Fla. Charlie Jaynes, MD, OBHG’s MDO for the south-central region, is an OB hospitalist at North Austin Medical Center in Austin, Texas, and Baylor All Saints Andrews Women’s Hospital in Fort Worth, Texas. Michael White, MD, the West Coast MDO, works as a hospitalist at Hoag Memorial Hospital in Newport Beach, Calif.
Jetinder Singh-Marjara, MD, is the new hospital medicine program director at Golden Valley Memorial Hospital in Clinton, Mo. Dr. Singh-Marjara has worked in Kansas City, Mo., and throughout the Midwest as a hospitalist for more than 10 years since completing his residency in internal medicine at the University of Illinois in Chicago.

Boghara, MD Tien Vo, MD
Fred Guyer, MD, recently was awarded the Northeast Florida Pediatric Society’s Pediatric Hospitalist of the Year award. Dr. Guyer is a hospitalist at Nemours Children’s Clinic in Jacksonville. Dr. Guyer is faculty at the University of Florida College of Medicine.
TeamHealth of Knoxville, Tenn., has announced three new medical directors.
Shelley Lenamond, DO, FHM, is the new facility medical director for TeamHealth’s hospitalist program at Methodist Mansfield Medical Center in Mansfield, Texas.
Haresh Boghara, MD, is the new facility medical director of hospitalist services at Methodist Charlton Medical Center in Dallas.
Tien Vo, MD, is TeamHealth’s new facility medical director of its hospitalist program at El Centro Regional Medical Center in El Centro, Calif.
Michael O'Neal is a freelance writer in New York.
Chris Brown, MD, MPH, was elected one of Columbus Business First’s members of the Forty Under 40 class of 2013. Dr. Brown is the medical director of hospital medicine at Memorial Hospital of Union County in Marysville, Ohio. The designation recognizes members of the Columbus, Ohio, community who demonstrate superior professional development, community involvement, and other awards and recognitions. Dr. Brown’s colleagues describe him as “a collaborative, attentive, and detailed physician as well as a capable leader.”
Thomas Gallagher, MD, is the University of Washington’s (UW) new director of the program in hospital medicine. This new position in UW’s division of general internal medicine will oversee all of the hospitalist programs at UW Medicine and Harborview Medical Center in Seattle. Dr. Gallagher also is a UW professor of medicine and bioethics and humanities.
Pawan Dhawan, MD, has been appointed medical director of the hospitalist programs at Trident Medical Center in Charleston, S.C., and Summerville Medical Center in Summerville, S.C. Dr. Dhawan comes to Trident Health System from Bay Hospitalists in Newark, Del. Dr. Dhawan served on SHM’s Leadership Committee in 2011.
OB Hospitalist Group (OBHG) in Mauldin, S.C., has announced new medical directors of operations (MDOs) for five of its regions. Nicholas Kulbida, MD, MDO for OBHG’s northeast region, works at Bellevue Women’s Center in Niskayuna, N.Y. Susie Wilson, MD, one of two MDOs for the southeast region, is team leader at Summerville Medical Center in Summerville, S.C. Sue Smith, MD, the other MDO for OBHG’s southeast region, works for Winter Haven Hospital-Regency Medical Center in Winter Haven, Fla. Matthew Conrad, MD, MDO for the Great Lakes region, serves as an OB hospitalist at both Holmes Regional Medical Center in Melbourne, Fla., and Osceola Regional Medical Center in Kissimmee, Fla. Charlie Jaynes, MD, OBHG’s MDO for the south-central region, is an OB hospitalist at North Austin Medical Center in Austin, Texas, and Baylor All Saints Andrews Women’s Hospital in Fort Worth, Texas. Michael White, MD, the West Coast MDO, works as a hospitalist at Hoag Memorial Hospital in Newport Beach, Calif.
Jetinder Singh-Marjara, MD, is the new hospital medicine program director at Golden Valley Memorial Hospital in Clinton, Mo. Dr. Singh-Marjara has worked in Kansas City, Mo., and throughout the Midwest as a hospitalist for more than 10 years since completing his residency in internal medicine at the University of Illinois in Chicago.
Boghara, MD Tien Vo, MD
Fred Guyer, MD, recently was awarded the Northeast Florida Pediatric Society’s Pediatric Hospitalist of the Year award. Dr. Guyer is a hospitalist at Nemours Children’s Clinic in Jacksonville. Dr. Guyer is faculty at the University of Florida College of Medicine.
TeamHealth of Knoxville, Tenn., has announced three new medical directors.
Shelley Lenamond, DO, FHM, is the new facility medical director for TeamHealth’s hospitalist program at Methodist Mansfield Medical Center in Mansfield, Texas.
Haresh Boghara, MD, is the new facility medical director of hospitalist services at Methodist Charlton Medical Center in Dallas.
Tien Vo, MD, is TeamHealth’s new facility medical director of its hospitalist program at El Centro Regional Medical Center in El Centro, Calif.
Michael O'Neal is a freelance writer in New York.
Chris Brown, MD, MPH, was elected one of Columbus Business First’s members of the Forty Under 40 class of 2013. Dr. Brown is the medical director of hospital medicine at Memorial Hospital of Union County in Marysville, Ohio. The designation recognizes members of the Columbus, Ohio, community who demonstrate superior professional development, community involvement, and other awards and recognitions. Dr. Brown’s colleagues describe him as “a collaborative, attentive, and detailed physician as well as a capable leader.”
Thomas Gallagher, MD, is the University of Washington’s (UW) new director of the program in hospital medicine. This new position in UW’s division of general internal medicine will oversee all of the hospitalist programs at UW Medicine and Harborview Medical Center in Seattle. Dr. Gallagher also is a UW professor of medicine and bioethics and humanities.
Pawan Dhawan, MD, has been appointed medical director of the hospitalist programs at Trident Medical Center in Charleston, S.C., and Summerville Medical Center in Summerville, S.C. Dr. Dhawan comes to Trident Health System from Bay Hospitalists in Newark, Del. Dr. Dhawan served on SHM’s Leadership Committee in 2011.
OB Hospitalist Group (OBHG) in Mauldin, S.C., has announced new medical directors of operations (MDOs) for five of its regions. Nicholas Kulbida, MD, MDO for OBHG’s northeast region, works at Bellevue Women’s Center in Niskayuna, N.Y. Susie Wilson, MD, one of two MDOs for the southeast region, is team leader at Summerville Medical Center in Summerville, S.C. Sue Smith, MD, the other MDO for OBHG’s southeast region, works for Winter Haven Hospital-Regency Medical Center in Winter Haven, Fla. Matthew Conrad, MD, MDO for the Great Lakes region, serves as an OB hospitalist at both Holmes Regional Medical Center in Melbourne, Fla., and Osceola Regional Medical Center in Kissimmee, Fla. Charlie Jaynes, MD, OBHG’s MDO for the south-central region, is an OB hospitalist at North Austin Medical Center in Austin, Texas, and Baylor All Saints Andrews Women’s Hospital in Fort Worth, Texas. Michael White, MD, the West Coast MDO, works as a hospitalist at Hoag Memorial Hospital in Newport Beach, Calif.
Jetinder Singh-Marjara, MD, is the new hospital medicine program director at Golden Valley Memorial Hospital in Clinton, Mo. Dr. Singh-Marjara has worked in Kansas City, Mo., and throughout the Midwest as a hospitalist for more than 10 years since completing his residency in internal medicine at the University of Illinois in Chicago.
Boghara, MD Tien Vo, MD
Fred Guyer, MD, recently was awarded the Northeast Florida Pediatric Society’s Pediatric Hospitalist of the Year award. Dr. Guyer is a hospitalist at Nemours Children’s Clinic in Jacksonville. Dr. Guyer is faculty at the University of Florida College of Medicine.
TeamHealth of Knoxville, Tenn., has announced three new medical directors.
Shelley Lenamond, DO, FHM, is the new facility medical director for TeamHealth’s hospitalist program at Methodist Mansfield Medical Center in Mansfield, Texas.
Haresh Boghara, MD, is the new facility medical director of hospitalist services at Methodist Charlton Medical Center in Dallas.
Tien Vo, MD, is TeamHealth’s new facility medical director of its hospitalist program at El Centro Regional Medical Center in El Centro, Calif.
Michael O'Neal is a freelance writer in New York.
SHM Fellow in Hospital Medicine Spotlight: Tosha Wetterneck, MD, MS, FACP, SFHM

Dr. Wetterneck is an associate professor of medicine at the University of Wisconsin School of Medicine and Public Health in Madison. She is an affiliate faculty member in the university’s department of industrial and systems engineering and a faculty researcher at the Center for Quality and Productivity Improvement. Named a senior fellow by SHM in 2012, she is a member of the society’s career satisfaction and work-life survey team and a quality-improvement (QI) mentor for the SHM-sponsored medication reconciliation QI study (MARQUIS), which is funded by the Agency for Healthcare Research and Quality (AHRQ).
Undergraduate education: University of Wisconsin at Milwaukee.
Medical school: Medical College of Wisconsin, Milwaukee.
Notable: In 2012, Dr. Wetterneck won the AMA’s Women Physicians Congress Physician Mentor Recognition Program Award. As president of the Wisconsin Medical Society, she advocates for hospitalists in AMA meetings; her current goal is to pass a resolution that focuses on care reimbursements for hospitalists. Because of her quality and safety expertise and focus on human specialized engineering, she has created a quality and safety curriculum for third- and fourth-year medical students and developed methods to proactively design hospitalist programs that prevent burnout.
FYI: Her love of dolls while growing up has inspired Dr. Wetterneck to collect all types of Raggedy Ann and Andy memorabilia.
Quotable: “The fact that SHM recognizes hospitalists is important because it recognizes those who want to stay in hospital medicine and give back to their profession.” TH
Dr. Wetterneck is an associate professor of medicine at the University of Wisconsin School of Medicine and Public Health in Madison. She is an affiliate faculty member in the university’s department of industrial and systems engineering and a faculty researcher at the Center for Quality and Productivity Improvement. Named a senior fellow by SHM in 2012, she is a member of the society’s career satisfaction and work-life survey team and a quality-improvement (QI) mentor for the SHM-sponsored medication reconciliation QI study (MARQUIS), which is funded by the Agency for Healthcare Research and Quality (AHRQ).
Undergraduate education: University of Wisconsin at Milwaukee.
Medical school: Medical College of Wisconsin, Milwaukee.
Notable: In 2012, Dr. Wetterneck won the AMA’s Women Physicians Congress Physician Mentor Recognition Program Award. As president of the Wisconsin Medical Society, she advocates for hospitalists in AMA meetings; her current goal is to pass a resolution that focuses on care reimbursements for hospitalists. Because of her quality and safety expertise and focus on human specialized engineering, she has created a quality and safety curriculum for third- and fourth-year medical students and developed methods to proactively design hospitalist programs that prevent burnout.
FYI: Her love of dolls while growing up has inspired Dr. Wetterneck to collect all types of Raggedy Ann and Andy memorabilia.
Quotable: “The fact that SHM recognizes hospitalists is important because it recognizes those who want to stay in hospital medicine and give back to their profession.” TH
Dr. Wetterneck is an associate professor of medicine at the University of Wisconsin School of Medicine and Public Health in Madison. She is an affiliate faculty member in the university’s department of industrial and systems engineering and a faculty researcher at the Center for Quality and Productivity Improvement. Named a senior fellow by SHM in 2012, she is a member of the society’s career satisfaction and work-life survey team and a quality-improvement (QI) mentor for the SHM-sponsored medication reconciliation QI study (MARQUIS), which is funded by the Agency for Healthcare Research and Quality (AHRQ).
Undergraduate education: University of Wisconsin at Milwaukee.
Medical school: Medical College of Wisconsin, Milwaukee.
Notable: In 2012, Dr. Wetterneck won the AMA’s Women Physicians Congress Physician Mentor Recognition Program Award. As president of the Wisconsin Medical Society, she advocates for hospitalists in AMA meetings; her current goal is to pass a resolution that focuses on care reimbursements for hospitalists. Because of her quality and safety expertise and focus on human specialized engineering, she has created a quality and safety curriculum for third- and fourth-year medical students and developed methods to proactively design hospitalist programs that prevent burnout.
FYI: Her love of dolls while growing up has inspired Dr. Wetterneck to collect all types of Raggedy Ann and Andy memorabilia.
Quotable: “The fact that SHM recognizes hospitalists is important because it recognizes those who want to stay in hospital medicine and give back to their profession.” TH
Nonphysician Practice Administrators More Common as Hospital Medicine Groups Expand

I can remember a time not so long ago when it was rare for me to encounter a dedicated nonphysician practice manager when visiting a hospital medicine group (HMG). Most groups had no nonphysician management support at all, or maybe just a part-time clerical person to help sort mail and post charges. In some cases, a single person supported the hospitalists and also worked with several other physician groups; this person spent only a small portion of their time with the hospitalist practice.
We all can acknowledge that most HMGs have grown much larger and more complex in recent years. SHM’s 2012 State of Hospital Medicine report suggests that one outcome of this growth is the increasing presence of nonphysician practice administrators: Fully 75% of all respondent HMGs serving adults only reported having a nonphysician administrator.
Interestingly, group size appears to have little impact on HMG administration. HMGs with four or fewer FTEs were just as likely to have an administrator as groups with 30 or more FTEs. The prevalence of administrators was highest in the South region (87%) and lowest in the West (48%). And it was highest among multistate hospitalist companies (84%) and lowest among private multispecialty or primary-care medical groups (45%).
The median time allocation for practice administrators was 1.0 FTE (the mean was 0.79 FTE). Again, very small groups are just as likely to have a full-time administrator as very large groups.
In my experience, extremely wide variation exists in nonphysician practice administrators’ roles, backgrounds, and qualifications. The survey attempted to categorize administrator roles in a meaningful way that might correlate with level of responsibility and compensation by asking about the incumbent’s management level:
- Senior management (e.g. CEO, president, executive director);
- Middle management (e.g. director, administrator, manager); or
- First-line management (e.g. supervisor or coordinator).
The majority of practice administrators were classified as middle management, as shown in Figure 1.
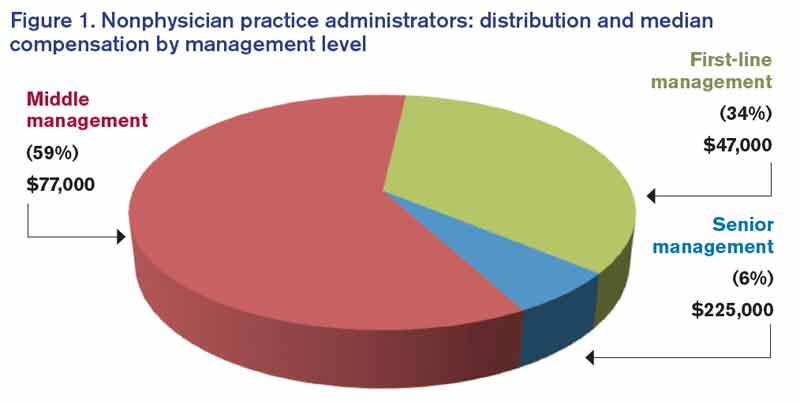
The survey collected information about compensation for practice administrators by management level. Senior management positions earned a median of $225,000 annually per FTE (though the sample size, n=10, was very small). Middle managers earned a median of $77,000, and first-line managers earned a median of $47,000.
SHM has worked diligently to reach out to nonphysician practice administrators and support them with a wide variety of tools and resources. SHM currently counts about 450 administrators as members and offers membership discounts for nonphysicians.
SHM’s Administrators’ Committee offers a series of quarterly roundtables via webinar; last year, it developed the white paper Core Competencies for a Hospitalist Practice Administrator, which can be downloaded at www.hospitalmedicine.org/Graphics/Administrators_White_Paper.pdf. And this year, for the first time, administrators became eligible for induction as Fellows in Hospital Medicine.
If you are a nonphysician practice administrator working for an HMG, or if you have one in your practice, I encourage you to get involved. Take advantage of the resources available to administrators through SHM. And please be sure that information about your administrator job gets included in the next State of Hospital Medicine survey, which will be conducted in early 2014.
Leslie Flores is a partner in Nelson Flores Hospital Medicine Consultants and a member of SHM's Practice Analysis Committee.
I can remember a time not so long ago when it was rare for me to encounter a dedicated nonphysician practice manager when visiting a hospital medicine group (HMG). Most groups had no nonphysician management support at all, or maybe just a part-time clerical person to help sort mail and post charges. In some cases, a single person supported the hospitalists and also worked with several other physician groups; this person spent only a small portion of their time with the hospitalist practice.
We all can acknowledge that most HMGs have grown much larger and more complex in recent years. SHM’s 2012 State of Hospital Medicine report suggests that one outcome of this growth is the increasing presence of nonphysician practice administrators: Fully 75% of all respondent HMGs serving adults only reported having a nonphysician administrator.
Interestingly, group size appears to have little impact on HMG administration. HMGs with four or fewer FTEs were just as likely to have an administrator as groups with 30 or more FTEs. The prevalence of administrators was highest in the South region (87%) and lowest in the West (48%). And it was highest among multistate hospitalist companies (84%) and lowest among private multispecialty or primary-care medical groups (45%).
The median time allocation for practice administrators was 1.0 FTE (the mean was 0.79 FTE). Again, very small groups are just as likely to have a full-time administrator as very large groups.
In my experience, extremely wide variation exists in nonphysician practice administrators’ roles, backgrounds, and qualifications. The survey attempted to categorize administrator roles in a meaningful way that might correlate with level of responsibility and compensation by asking about the incumbent’s management level:
- Senior management (e.g. CEO, president, executive director);
- Middle management (e.g. director, administrator, manager); or
- First-line management (e.g. supervisor or coordinator).
The majority of practice administrators were classified as middle management, as shown in Figure 1.
The survey collected information about compensation for practice administrators by management level. Senior management positions earned a median of $225,000 annually per FTE (though the sample size, n=10, was very small). Middle managers earned a median of $77,000, and first-line managers earned a median of $47,000.
SHM has worked diligently to reach out to nonphysician practice administrators and support them with a wide variety of tools and resources. SHM currently counts about 450 administrators as members and offers membership discounts for nonphysicians.
SHM’s Administrators’ Committee offers a series of quarterly roundtables via webinar; last year, it developed the white paper Core Competencies for a Hospitalist Practice Administrator, which can be downloaded at www.hospitalmedicine.org/Graphics/Administrators_White_Paper.pdf. And this year, for the first time, administrators became eligible for induction as Fellows in Hospital Medicine.
If you are a nonphysician practice administrator working for an HMG, or if you have one in your practice, I encourage you to get involved. Take advantage of the resources available to administrators through SHM. And please be sure that information about your administrator job gets included in the next State of Hospital Medicine survey, which will be conducted in early 2014.
Leslie Flores is a partner in Nelson Flores Hospital Medicine Consultants and a member of SHM's Practice Analysis Committee.
I can remember a time not so long ago when it was rare for me to encounter a dedicated nonphysician practice manager when visiting a hospital medicine group (HMG). Most groups had no nonphysician management support at all, or maybe just a part-time clerical person to help sort mail and post charges. In some cases, a single person supported the hospitalists and also worked with several other physician groups; this person spent only a small portion of their time with the hospitalist practice.
We all can acknowledge that most HMGs have grown much larger and more complex in recent years. SHM’s 2012 State of Hospital Medicine report suggests that one outcome of this growth is the increasing presence of nonphysician practice administrators: Fully 75% of all respondent HMGs serving adults only reported having a nonphysician administrator.
Interestingly, group size appears to have little impact on HMG administration. HMGs with four or fewer FTEs were just as likely to have an administrator as groups with 30 or more FTEs. The prevalence of administrators was highest in the South region (87%) and lowest in the West (48%). And it was highest among multistate hospitalist companies (84%) and lowest among private multispecialty or primary-care medical groups (45%).
The median time allocation for practice administrators was 1.0 FTE (the mean was 0.79 FTE). Again, very small groups are just as likely to have a full-time administrator as very large groups.
In my experience, extremely wide variation exists in nonphysician practice administrators’ roles, backgrounds, and qualifications. The survey attempted to categorize administrator roles in a meaningful way that might correlate with level of responsibility and compensation by asking about the incumbent’s management level:
- Senior management (e.g. CEO, president, executive director);
- Middle management (e.g. director, administrator, manager); or
- First-line management (e.g. supervisor or coordinator).
The majority of practice administrators were classified as middle management, as shown in Figure 1.
The survey collected information about compensation for practice administrators by management level. Senior management positions earned a median of $225,000 annually per FTE (though the sample size, n=10, was very small). Middle managers earned a median of $77,000, and first-line managers earned a median of $47,000.
SHM has worked diligently to reach out to nonphysician practice administrators and support them with a wide variety of tools and resources. SHM currently counts about 450 administrators as members and offers membership discounts for nonphysicians.
SHM’s Administrators’ Committee offers a series of quarterly roundtables via webinar; last year, it developed the white paper Core Competencies for a Hospitalist Practice Administrator, which can be downloaded at www.hospitalmedicine.org/Graphics/Administrators_White_Paper.pdf. And this year, for the first time, administrators became eligible for induction as Fellows in Hospital Medicine.
If you are a nonphysician practice administrator working for an HMG, or if you have one in your practice, I encourage you to get involved. Take advantage of the resources available to administrators through SHM. And please be sure that information about your administrator job gets included in the next State of Hospital Medicine survey, which will be conducted in early 2014.
Leslie Flores is a partner in Nelson Flores Hospital Medicine Consultants and a member of SHM's Practice Analysis Committee.
Can Medicare Pay for Value?
Can quality measurement and comparisons serve as the backbone for a major shift in the Medicare payment system to reward value instead of volume? That is the question being explored over the next few years as the Physician Quality Reporting System (PQRS) and, by extension, the physician value-based payment modifier (VBPM) come fully into effect for all physicians.
There seems to be a consensus in the policy community that the fee-for-service model of payment is past its prime and needs to be replaced with a more dynamic and responsive payment system. Medicare hopes that PQRS and the VBPM will enable adjustments to physician payments to reward high-quality and low-cost care. Although these programs currently are add-ons to the fee-for-service system, they likely will serve as stepping stones to more radical departures from the existing payment system.
SHM advocates refinements to policies for PQRS and similar programs to make them more meaningful and productive for both hospitalists and the broader health-care system. Each year, SHM submits comments on the Physician Fee Schedule Rule, which creates and updates the regulatory framework for PQRS and the VBPM. SHM also provided feedback on Quality and Resource Use Reports (QRURs), the report cards for the modifier that were being tested over the past year.
From a practical standpoint, SHM engages with measure development and endorsement processes to ensure there are reportable quality measures in PQRS that fit hospitalist practice. In addition, SHM is helping to increase accessibility to PQRS reporting by offering members reduced fare access to registry reporting through the PQRI Wizard.
The comments range from the technical aspects of individual quality measures in PQRS to how hospitalists appear to be performing in these programs. SHM firmly believes that the unique positioning of hospitalists within the health-care system presents challenges for their identification and evaluation in Medicare programs. In some sense, hospitalists exist on the line between the inpatient and outpatient worlds, a location not adequately captured in pay-for-performance programs.
It’s imperative that pay-for-performance programs have reasonable and actionable outcomes for providers. If quality measures are not clinically meaningful and do not capture a plurality of the care provided by an individual hospitalist, it is difficult for the program to meet its stated aims. If payment is to be influenced by performance on quality measures, it follows that those measures should be relevant to the care provided.
There is a long way to go toward creating quality measurement and evaluation programs that are relevant and actionable for clinical quality improvement (QI). By becoming involved in SHM’s policy efforts, members are able to share their experiences and impressions of programs with SHM and lawmakers. This partnership helps create more responsive and intuitive programs, which in turn leads to greater participation and, hopefully, improved patient outcomes. As these programs continue to evolve and more health professionals are required to participate, SHM will be looking to its membership for their perspectives.
Join the grassroots network to stay involved and up to date by registering at www.hospitalmedicine.org/grassroots.
Joshua Lapps is SHM’s government relations specialist.
Can quality measurement and comparisons serve as the backbone for a major shift in the Medicare payment system to reward value instead of volume? That is the question being explored over the next few years as the Physician Quality Reporting System (PQRS) and, by extension, the physician value-based payment modifier (VBPM) come fully into effect for all physicians.
There seems to be a consensus in the policy community that the fee-for-service model of payment is past its prime and needs to be replaced with a more dynamic and responsive payment system. Medicare hopes that PQRS and the VBPM will enable adjustments to physician payments to reward high-quality and low-cost care. Although these programs currently are add-ons to the fee-for-service system, they likely will serve as stepping stones to more radical departures from the existing payment system.
SHM advocates refinements to policies for PQRS and similar programs to make them more meaningful and productive for both hospitalists and the broader health-care system. Each year, SHM submits comments on the Physician Fee Schedule Rule, which creates and updates the regulatory framework for PQRS and the VBPM. SHM also provided feedback on Quality and Resource Use Reports (QRURs), the report cards for the modifier that were being tested over the past year.
From a practical standpoint, SHM engages with measure development and endorsement processes to ensure there are reportable quality measures in PQRS that fit hospitalist practice. In addition, SHM is helping to increase accessibility to PQRS reporting by offering members reduced fare access to registry reporting through the PQRI Wizard.
The comments range from the technical aspects of individual quality measures in PQRS to how hospitalists appear to be performing in these programs. SHM firmly believes that the unique positioning of hospitalists within the health-care system presents challenges for their identification and evaluation in Medicare programs. In some sense, hospitalists exist on the line between the inpatient and outpatient worlds, a location not adequately captured in pay-for-performance programs.
It’s imperative that pay-for-performance programs have reasonable and actionable outcomes for providers. If quality measures are not clinically meaningful and do not capture a plurality of the care provided by an individual hospitalist, it is difficult for the program to meet its stated aims. If payment is to be influenced by performance on quality measures, it follows that those measures should be relevant to the care provided.
There is a long way to go toward creating quality measurement and evaluation programs that are relevant and actionable for clinical quality improvement (QI). By becoming involved in SHM’s policy efforts, members are able to share their experiences and impressions of programs with SHM and lawmakers. This partnership helps create more responsive and intuitive programs, which in turn leads to greater participation and, hopefully, improved patient outcomes. As these programs continue to evolve and more health professionals are required to participate, SHM will be looking to its membership for their perspectives.
Join the grassroots network to stay involved and up to date by registering at www.hospitalmedicine.org/grassroots.
Joshua Lapps is SHM’s government relations specialist.
Can quality measurement and comparisons serve as the backbone for a major shift in the Medicare payment system to reward value instead of volume? That is the question being explored over the next few years as the Physician Quality Reporting System (PQRS) and, by extension, the physician value-based payment modifier (VBPM) come fully into effect for all physicians.
There seems to be a consensus in the policy community that the fee-for-service model of payment is past its prime and needs to be replaced with a more dynamic and responsive payment system. Medicare hopes that PQRS and the VBPM will enable adjustments to physician payments to reward high-quality and low-cost care. Although these programs currently are add-ons to the fee-for-service system, they likely will serve as stepping stones to more radical departures from the existing payment system.
SHM advocates refinements to policies for PQRS and similar programs to make them more meaningful and productive for both hospitalists and the broader health-care system. Each year, SHM submits comments on the Physician Fee Schedule Rule, which creates and updates the regulatory framework for PQRS and the VBPM. SHM also provided feedback on Quality and Resource Use Reports (QRURs), the report cards for the modifier that were being tested over the past year.
From a practical standpoint, SHM engages with measure development and endorsement processes to ensure there are reportable quality measures in PQRS that fit hospitalist practice. In addition, SHM is helping to increase accessibility to PQRS reporting by offering members reduced fare access to registry reporting through the PQRI Wizard.
The comments range from the technical aspects of individual quality measures in PQRS to how hospitalists appear to be performing in these programs. SHM firmly believes that the unique positioning of hospitalists within the health-care system presents challenges for their identification and evaluation in Medicare programs. In some sense, hospitalists exist on the line between the inpatient and outpatient worlds, a location not adequately captured in pay-for-performance programs.
It’s imperative that pay-for-performance programs have reasonable and actionable outcomes for providers. If quality measures are not clinically meaningful and do not capture a plurality of the care provided by an individual hospitalist, it is difficult for the program to meet its stated aims. If payment is to be influenced by performance on quality measures, it follows that those measures should be relevant to the care provided.
There is a long way to go toward creating quality measurement and evaluation programs that are relevant and actionable for clinical quality improvement (QI). By becoming involved in SHM’s policy efforts, members are able to share their experiences and impressions of programs with SHM and lawmakers. This partnership helps create more responsive and intuitive programs, which in turn leads to greater participation and, hopefully, improved patient outcomes. As these programs continue to evolve and more health professionals are required to participate, SHM will be looking to its membership for their perspectives.
Join the grassroots network to stay involved and up to date by registering at www.hospitalmedicine.org/grassroots.
Joshua Lapps is SHM’s government relations specialist.
SHM Leadership Academy Prepares Hospitalists for the Business of Medicine
Tiered training prepares hospitalists for the business of medicine
Hospitalists often leave residency feeling prepared for clinical work, but they quickly realize that the clinical side of hospitalist work is only one part of a larger spectrum of skill sets needed to succeed. Leading teams, addressing conflict, and understanding the financial implications of hospital care are important parts of life in hospital medicine, but rarely are they taught in academic life.
The demand for these skills help explain the popularity of SHM’s Leadership Academy, which has trained more than 1,000 hospitalists in financial storytelling, meta-leadership, and the mindset of a hospital CEO.
For the first time, in October, SHM will present all three levels of its leadership courses concurrently:
Foundations for Effective Leadership.
This four-day course serves as a prerequisite to all other academy courses. Attendees learn how to evaluate personal leadership strengths and weaknesses, create and execute a communication strategy for key team members, understand key hospital drivers, examine how hospital metrics are derived, and more.
Advanced Leadership: Strategies and Tools for Personal Leadership Excellence.
Through world-renowned faculty and applied exercises, this course builds skills around driving culture change through specific leadership behaviors and actions, financial storytelling, engaging in effective professional negotiation activities with proven techniques, and more.
Advanced Leadership: Developing a Winning Team and Strengthening Your Organization.
Developed in response to high demand from academy attendees, this course focuses on strengthening teams and institutions. Participants learn how to critically assess program growth opportunities and develop operational plans; lead, manage, and motivate teams in complex hospital environments; and effective communication strategies.
In addition to career-building skills, participants in each course will learn about SHM’s Certificate of Leadership in Hospital Medicine. Drs. Thomas McIlraith and Sameh Naseib received SHM’s inaugural Certificates of Leadership in Hospital Medicine on stage during the plenary session at HM13.
For academy courses, faculty, and registration information, visit www.hospitalmedicine.org/leadership.
Tiered training prepares hospitalists for the business of medicine
Hospitalists often leave residency feeling prepared for clinical work, but they quickly realize that the clinical side of hospitalist work is only one part of a larger spectrum of skill sets needed to succeed. Leading teams, addressing conflict, and understanding the financial implications of hospital care are important parts of life in hospital medicine, but rarely are they taught in academic life.
The demand for these skills help explain the popularity of SHM’s Leadership Academy, which has trained more than 1,000 hospitalists in financial storytelling, meta-leadership, and the mindset of a hospital CEO.
For the first time, in October, SHM will present all three levels of its leadership courses concurrently:
Foundations for Effective Leadership.
This four-day course serves as a prerequisite to all other academy courses. Attendees learn how to evaluate personal leadership strengths and weaknesses, create and execute a communication strategy for key team members, understand key hospital drivers, examine how hospital metrics are derived, and more.
Advanced Leadership: Strategies and Tools for Personal Leadership Excellence.
Through world-renowned faculty and applied exercises, this course builds skills around driving culture change through specific leadership behaviors and actions, financial storytelling, engaging in effective professional negotiation activities with proven techniques, and more.
Advanced Leadership: Developing a Winning Team and Strengthening Your Organization.
Developed in response to high demand from academy attendees, this course focuses on strengthening teams and institutions. Participants learn how to critically assess program growth opportunities and develop operational plans; lead, manage, and motivate teams in complex hospital environments; and effective communication strategies.
In addition to career-building skills, participants in each course will learn about SHM’s Certificate of Leadership in Hospital Medicine. Drs. Thomas McIlraith and Sameh Naseib received SHM’s inaugural Certificates of Leadership in Hospital Medicine on stage during the plenary session at HM13.
For academy courses, faculty, and registration information, visit www.hospitalmedicine.org/leadership.
Tiered training prepares hospitalists for the business of medicine
Hospitalists often leave residency feeling prepared for clinical work, but they quickly realize that the clinical side of hospitalist work is only one part of a larger spectrum of skill sets needed to succeed. Leading teams, addressing conflict, and understanding the financial implications of hospital care are important parts of life in hospital medicine, but rarely are they taught in academic life.
The demand for these skills help explain the popularity of SHM’s Leadership Academy, which has trained more than 1,000 hospitalists in financial storytelling, meta-leadership, and the mindset of a hospital CEO.
For the first time, in October, SHM will present all three levels of its leadership courses concurrently:
Foundations for Effective Leadership.
This four-day course serves as a prerequisite to all other academy courses. Attendees learn how to evaluate personal leadership strengths and weaknesses, create and execute a communication strategy for key team members, understand key hospital drivers, examine how hospital metrics are derived, and more.
Advanced Leadership: Strategies and Tools for Personal Leadership Excellence.
Through world-renowned faculty and applied exercises, this course builds skills around driving culture change through specific leadership behaviors and actions, financial storytelling, engaging in effective professional negotiation activities with proven techniques, and more.
Advanced Leadership: Developing a Winning Team and Strengthening Your Organization.
Developed in response to high demand from academy attendees, this course focuses on strengthening teams and institutions. Participants learn how to critically assess program growth opportunities and develop operational plans; lead, manage, and motivate teams in complex hospital environments; and effective communication strategies.
In addition to career-building skills, participants in each course will learn about SHM’s Certificate of Leadership in Hospital Medicine. Drs. Thomas McIlraith and Sameh Naseib received SHM’s inaugural Certificates of Leadership in Hospital Medicine on stage during the plenary session at HM13.
For academy courses, faculty, and registration information, visit www.hospitalmedicine.org/leadership.
Three Easy Ways to Get Ahead in Hospital Medicine
Getting involved—and getting ahead—in hospital medicine has never been easier, with just some planning and preparation. Here are three ways to move your hospital—and your career—forward this month.
1. Add “award-winning” to your CV: SHM’s Awards of Excellence deadline is Sept. 16.
Although 2013’s award-winners are still fresh in hospitalists’ minds, now is the time to put together award applications for the 2014 Awards of Excellence.
Each year, SHM presents six different awards that recognize individuals and one award to a team that is transforming health care and revolutionizing patient care for hospitalized patients:
- Excellence in Research Award;
- Excellence in Hospital Medicine for Non-Physicians;
- Award for Excellence in Teaching;
- Award for Outstanding Service in Hospital Medicine;
- Award for Clinical Excellence; and
- Excellence in Teamwork in Quality Improvement.
Last year, SHM received award nominations from a diverse group of hospitalists and looks forward to receiving even more this year. Each winner receives an all-expenses-paid trip to HM14 in Las Vegas, including complimentary meeting registration.
The deadline for applications for SHM’s five individual awards is Sept. 16. The deadline for the Excellence in Teamwork in Quality Improvement is Oct. 15. All SHM members are eligible, and nominees can be self-nominated.
For more information, visit www.hospital medicine.org/awards.
2. Bring the experts in reducing readmissions to your hospital: Apply now for Project BOOST.
There is still time to apply for SHM’s Project BOOST, which helps hospitals design discharge programs to reduce readmissions. SHM will accept applications for Project BOOST until the end of August.
Project BOOST is based on SHM’s award-winning mentored implementation model that brings individualized attention from national experts in reducing readmissions to hospitals across the country. Each Project BOOST site receives:
- A comprehensive intervention developed by a panel of nationally recognized experts based on the best available evidence.
- A comprehensive implementation guide that provides step-by-step instructions and project-management tools, such as the teachback training curriculum, to help interdisciplinary teams redesign workflow and plan, implement, and evaluate the intervention.
- Longitudinal technical assistance providing face-to-face training and a year of expert mentoring and coaching to implement BOOST interventions that build a culture that supports safe and complete transitions. The mentoring program provides a training DVD and curriculum for nurses and case managers on using the teachback process, as well as webinars that target the educational needs of other team members, including administrators, data analysts, physicians, nurses, and others.
- Collaboration that allows sites to communicate with and learn from each other via the BOOST community site and quarterly all-site teleconferences and webinars.
- The BOOST data center, an online resource that allows sites to store and benchmark data against control units and other sites and generates reports.
For more information, visit www.hospital medicine.org/boost.
3. Start Choosing Wisely today.
In 2014, as part of a grant from the ABIM Foundation, SHM will begin its first Choosing Wisely case-study competition to highlight hospitalists’ best practices within the popular campaign.
But in order to have a successful case study next year, some preparation is in order now. Developing goals, gathering a team, and, perhaps most important, developing benchmarking data on a project motivated by Choosing Wisely will all be important parts of a compelling case study.
To start brainstorming your project to implement Choosing Wisely recommendations at your hospital, visit www.hospitalmedicine.org/choosingwisely.
Brendon Shank is SHM’s associate vice president of communications.
Getting involved—and getting ahead—in hospital medicine has never been easier, with just some planning and preparation. Here are three ways to move your hospital—and your career—forward this month.
1. Add “award-winning” to your CV: SHM’s Awards of Excellence deadline is Sept. 16.
Although 2013’s award-winners are still fresh in hospitalists’ minds, now is the time to put together award applications for the 2014 Awards of Excellence.
Each year, SHM presents six different awards that recognize individuals and one award to a team that is transforming health care and revolutionizing patient care for hospitalized patients:
- Excellence in Research Award;
- Excellence in Hospital Medicine for Non-Physicians;
- Award for Excellence in Teaching;
- Award for Outstanding Service in Hospital Medicine;
- Award for Clinical Excellence; and
- Excellence in Teamwork in Quality Improvement.
Last year, SHM received award nominations from a diverse group of hospitalists and looks forward to receiving even more this year. Each winner receives an all-expenses-paid trip to HM14 in Las Vegas, including complimentary meeting registration.
The deadline for applications for SHM’s five individual awards is Sept. 16. The deadline for the Excellence in Teamwork in Quality Improvement is Oct. 15. All SHM members are eligible, and nominees can be self-nominated.
For more information, visit www.hospital medicine.org/awards.
2. Bring the experts in reducing readmissions to your hospital: Apply now for Project BOOST.
There is still time to apply for SHM’s Project BOOST, which helps hospitals design discharge programs to reduce readmissions. SHM will accept applications for Project BOOST until the end of August.
Project BOOST is based on SHM’s award-winning mentored implementation model that brings individualized attention from national experts in reducing readmissions to hospitals across the country. Each Project BOOST site receives:
- A comprehensive intervention developed by a panel of nationally recognized experts based on the best available evidence.
- A comprehensive implementation guide that provides step-by-step instructions and project-management tools, such as the teachback training curriculum, to help interdisciplinary teams redesign workflow and plan, implement, and evaluate the intervention.
- Longitudinal technical assistance providing face-to-face training and a year of expert mentoring and coaching to implement BOOST interventions that build a culture that supports safe and complete transitions. The mentoring program provides a training DVD and curriculum for nurses and case managers on using the teachback process, as well as webinars that target the educational needs of other team members, including administrators, data analysts, physicians, nurses, and others.
- Collaboration that allows sites to communicate with and learn from each other via the BOOST community site and quarterly all-site teleconferences and webinars.
- The BOOST data center, an online resource that allows sites to store and benchmark data against control units and other sites and generates reports.
For more information, visit www.hospital medicine.org/boost.
3. Start Choosing Wisely today.
In 2014, as part of a grant from the ABIM Foundation, SHM will begin its first Choosing Wisely case-study competition to highlight hospitalists’ best practices within the popular campaign.
But in order to have a successful case study next year, some preparation is in order now. Developing goals, gathering a team, and, perhaps most important, developing benchmarking data on a project motivated by Choosing Wisely will all be important parts of a compelling case study.
To start brainstorming your project to implement Choosing Wisely recommendations at your hospital, visit www.hospitalmedicine.org/choosingwisely.
Brendon Shank is SHM’s associate vice president of communications.
Getting involved—and getting ahead—in hospital medicine has never been easier, with just some planning and preparation. Here are three ways to move your hospital—and your career—forward this month.
1. Add “award-winning” to your CV: SHM’s Awards of Excellence deadline is Sept. 16.
Although 2013’s award-winners are still fresh in hospitalists’ minds, now is the time to put together award applications for the 2014 Awards of Excellence.
Each year, SHM presents six different awards that recognize individuals and one award to a team that is transforming health care and revolutionizing patient care for hospitalized patients:
- Excellence in Research Award;
- Excellence in Hospital Medicine for Non-Physicians;
- Award for Excellence in Teaching;
- Award for Outstanding Service in Hospital Medicine;
- Award for Clinical Excellence; and
- Excellence in Teamwork in Quality Improvement.
Last year, SHM received award nominations from a diverse group of hospitalists and looks forward to receiving even more this year. Each winner receives an all-expenses-paid trip to HM14 in Las Vegas, including complimentary meeting registration.
The deadline for applications for SHM’s five individual awards is Sept. 16. The deadline for the Excellence in Teamwork in Quality Improvement is Oct. 15. All SHM members are eligible, and nominees can be self-nominated.
For more information, visit www.hospital medicine.org/awards.
2. Bring the experts in reducing readmissions to your hospital: Apply now for Project BOOST.
There is still time to apply for SHM’s Project BOOST, which helps hospitals design discharge programs to reduce readmissions. SHM will accept applications for Project BOOST until the end of August.
Project BOOST is based on SHM’s award-winning mentored implementation model that brings individualized attention from national experts in reducing readmissions to hospitals across the country. Each Project BOOST site receives:
- A comprehensive intervention developed by a panel of nationally recognized experts based on the best available evidence.
- A comprehensive implementation guide that provides step-by-step instructions and project-management tools, such as the teachback training curriculum, to help interdisciplinary teams redesign workflow and plan, implement, and evaluate the intervention.
- Longitudinal technical assistance providing face-to-face training and a year of expert mentoring and coaching to implement BOOST interventions that build a culture that supports safe and complete transitions. The mentoring program provides a training DVD and curriculum for nurses and case managers on using the teachback process, as well as webinars that target the educational needs of other team members, including administrators, data analysts, physicians, nurses, and others.
- Collaboration that allows sites to communicate with and learn from each other via the BOOST community site and quarterly all-site teleconferences and webinars.
- The BOOST data center, an online resource that allows sites to store and benchmark data against control units and other sites and generates reports.
For more information, visit www.hospital medicine.org/boost.
3. Start Choosing Wisely today.
In 2014, as part of a grant from the ABIM Foundation, SHM will begin its first Choosing Wisely case-study competition to highlight hospitalists’ best practices within the popular campaign.
But in order to have a successful case study next year, some preparation is in order now. Developing goals, gathering a team, and, perhaps most important, developing benchmarking data on a project motivated by Choosing Wisely will all be important parts of a compelling case study.
To start brainstorming your project to implement Choosing Wisely recommendations at your hospital, visit www.hospitalmedicine.org/choosingwisely.
Brendon Shank is SHM’s associate vice president of communications.
SHM Microsites Help Focused-Practice Specialists Work Together

The hospitalist model of providing care in the hospital has spread beyond internal medicine, pediatrics, and family medicine. Specialists in a number of other fields have adopted HM principles and adapted them to such medical specialties as orthopedics, surgery, psychiatry, OBGYN, and neurology.
Leaders in those hospital-focused-practice specialties now can work together to share best practices and identify opportunities to improve hospital-based care delivery through SHM, which has dedicated a section of its website (www.hospitalmedicine.org/hfp) to providing hospital-focused-practice caregivers some of the first resources in the specialty.
“SHM has created these Web areas as a place to convene and develop these emerging specialties in hospital medicine,” SHM CEO Larry Wellikson, MD, SFHM, says in a video on the website. He says that the new Web areas give specialty hospitalists the chance to “put their practice on the map, begin to share data, post relevant articles, and use social networks to share ideas.”
The site highlights five emerging specialties:
- Orthopedic HM;
- Surgical/acute-care surgery;
- Psychiatric HM;
- OBGYN HM; and
- Neurohospitalists.
Each of the listed specialties has its own section of the website that describes the practice, provides relevant articles, and lists events specific to the practice. Later, SHM expects to include access to a hospital-focused-practice community on its popular Hospital Medicine Exchange (HMX) online collaboration site.
Specialty hospitalists can literally put their practice on the map by filling out a practice profile form, which then enters the practice information on a map for other specialty hospitalists to see.
High-level conversations among hospitalists and hospital executives about hospital-focused practice began to take shape at a 2011 conference hosted by SHM. In 2012, the American Hospital Association’s Physician Leadership Forum and SHM published the first report on the subject, “Creating the Hospital of the Future: The Implications for Hospital-Focused Physician Practice,” which was sponsored by Apogee Physicians, Delphi Healthcare Partners Inc., and Eagle Hospital Physicians.
Dr. Wellikson says now is the time for these pioneer hospitalists to come together.
“This is your opportunity to create your new specialty,” he says, “and SHM is happy to be a part of this.”
Brendon Shank is SHM’s associate vice president of communications.
The hospitalist model of providing care in the hospital has spread beyond internal medicine, pediatrics, and family medicine. Specialists in a number of other fields have adopted HM principles and adapted them to such medical specialties as orthopedics, surgery, psychiatry, OBGYN, and neurology.
Leaders in those hospital-focused-practice specialties now can work together to share best practices and identify opportunities to improve hospital-based care delivery through SHM, which has dedicated a section of its website (www.hospitalmedicine.org/hfp) to providing hospital-focused-practice caregivers some of the first resources in the specialty.
“SHM has created these Web areas as a place to convene and develop these emerging specialties in hospital medicine,” SHM CEO Larry Wellikson, MD, SFHM, says in a video on the website. He says that the new Web areas give specialty hospitalists the chance to “put their practice on the map, begin to share data, post relevant articles, and use social networks to share ideas.”
The site highlights five emerging specialties:
- Orthopedic HM;
- Surgical/acute-care surgery;
- Psychiatric HM;
- OBGYN HM; and
- Neurohospitalists.
Each of the listed specialties has its own section of the website that describes the practice, provides relevant articles, and lists events specific to the practice. Later, SHM expects to include access to a hospital-focused-practice community on its popular Hospital Medicine Exchange (HMX) online collaboration site.
Specialty hospitalists can literally put their practice on the map by filling out a practice profile form, which then enters the practice information on a map for other specialty hospitalists to see.
High-level conversations among hospitalists and hospital executives about hospital-focused practice began to take shape at a 2011 conference hosted by SHM. In 2012, the American Hospital Association’s Physician Leadership Forum and SHM published the first report on the subject, “Creating the Hospital of the Future: The Implications for Hospital-Focused Physician Practice,” which was sponsored by Apogee Physicians, Delphi Healthcare Partners Inc., and Eagle Hospital Physicians.
Dr. Wellikson says now is the time for these pioneer hospitalists to come together.
“This is your opportunity to create your new specialty,” he says, “and SHM is happy to be a part of this.”
Brendon Shank is SHM’s associate vice president of communications.
The hospitalist model of providing care in the hospital has spread beyond internal medicine, pediatrics, and family medicine. Specialists in a number of other fields have adopted HM principles and adapted them to such medical specialties as orthopedics, surgery, psychiatry, OBGYN, and neurology.
Leaders in those hospital-focused-practice specialties now can work together to share best practices and identify opportunities to improve hospital-based care delivery through SHM, which has dedicated a section of its website (www.hospitalmedicine.org/hfp) to providing hospital-focused-practice caregivers some of the first resources in the specialty.
“SHM has created these Web areas as a place to convene and develop these emerging specialties in hospital medicine,” SHM CEO Larry Wellikson, MD, SFHM, says in a video on the website. He says that the new Web areas give specialty hospitalists the chance to “put their practice on the map, begin to share data, post relevant articles, and use social networks to share ideas.”
The site highlights five emerging specialties:
- Orthopedic HM;
- Surgical/acute-care surgery;
- Psychiatric HM;
- OBGYN HM; and
- Neurohospitalists.
Each of the listed specialties has its own section of the website that describes the practice, provides relevant articles, and lists events specific to the practice. Later, SHM expects to include access to a hospital-focused-practice community on its popular Hospital Medicine Exchange (HMX) online collaboration site.
Specialty hospitalists can literally put their practice on the map by filling out a practice profile form, which then enters the practice information on a map for other specialty hospitalists to see.
High-level conversations among hospitalists and hospital executives about hospital-focused practice began to take shape at a 2011 conference hosted by SHM. In 2012, the American Hospital Association’s Physician Leadership Forum and SHM published the first report on the subject, “Creating the Hospital of the Future: The Implications for Hospital-Focused Physician Practice,” which was sponsored by Apogee Physicians, Delphi Healthcare Partners Inc., and Eagle Hospital Physicians.
Dr. Wellikson says now is the time for these pioneer hospitalists to come together.
“This is your opportunity to create your new specialty,” he says, “and SHM is happy to be a part of this.”
Brendon Shank is SHM’s associate vice president of communications.
Reviews of Research on Steroids and VTE Risk, Epidural Catheterization, and Beta-Blockers During Noncardiac Surgery
In This Edition
Literature At A Glance
A guide to this month’s studies
- Steroids may increase VTE risk
- Mortality rates rise at critical-care hospitals
- Physicians don’t discuss advance-care planning with elderly, families
- Ultrasound imaging for lumbar puncture, epidural catheterization
- Financial impact of surgical complications on hospitals
- Lab test fees and frequency of test ordering
- Inpatient elderly multidisciplinary teams reduce readmissions
- Use of beta-blockers in high-risk patients during noncardiac surgery
- Patient-centered decision-making and health-care outcomes
- Adverse surgical outcomes in patients with schizophrenia
Steroids May Increase VTE Risk
Clinical question: Is exogenous glucocorticoid administration associated with an increased risk of VTE?
Background: Endogenous hypercortisolism is linked to increased VTE rates, and pathophysiologic data exist to suggest glucocorticoids increase clotting, but few studies have measured the clinical link between glucocorticoid administration and VTE events.
Study design: Case-control study.
Setting: Denmark.
Synopsis: The authors analyzed Danish national registries, which include information on diagnoses and prescriptions. The study selection period was Jan. 1, 2005, to Dec. 31, 2011. During this period, 38,675 cases of VTE (both DVT and pulmonary embolism) were identified in the population of Denmark. These cases were matched with 387,650 controls. Three routes of glucocorticoid use were studied: systemic (oral and intravenous), inhaled, and intestinal-acting. Cases were classified as present (within 90 days of VTE event), recent (91 to 365 days), or former (over 365 days) users of glucocorticoids. Categories were also created for new versus continuous users.
Glucocorticoid use was associated with a significant increase in VTE occurrence. The strongest link was in new and recent users, and the effect diminished over time. Key limitations of the study included its reliance on registry data, as well as the fact that cases had more comorbid conditions than controls (e.g. recent infection, chronic illnesses).
Bottom line: Recipients of glucocorticoids had an increased risk of VTE; the effect was strongest in new and recent users.
Citation: Johannesdottir SA, Horvath-Puho E, Dekkers OM, et al. Use of glucocorticoids and risk of venous thromboembolism. JAMA Intern Med. 2013;173(9):743-752.
Mortality Rates Rise at Critical-Access Hospitals
Clinical question: How have trends in mortality changed in the past decade at critical-access hospitals when compared to other hospitals?
Background: Hospitals are designated as critical-access hospitals (CAH) by meeting certain requirements—namely, rural setting, small number of beds, and minimum distance from the nearest hospital. Because of the intrinsic challenges they face, CAHs are exempt from certain quality measures. Little data exist on patient outcomes at CAHs.
Study design: Retrospective observational study.
Setting: All nonfederal hospitals in the U.S. that provide acute care to Medicare beneficiaries.
Synopsis: Using Medicare data, risk-adjusted 30-day mortality rates were calculated at critical-access hospitals and non-critical-access hospitals from 2002 to 2010 for three conditions: acute myocardial infarction, congestive heart failure, and pneumonia. Mortality trends across these conditions were compared at baseline and over time. In 2002, CAHs had mortality rates comparable with non-CAHs. From 2002 to 2010, mortality rates increased by 0.1% per year at CAHs and decreased by 0.2% per year at non-CAHs, resulting in a mortality difference between these two hospital groups at the end of the study period. The authors postulate that differences in policy initiatives, enforcement of quality measures, and access to technology may play a role.
This study is limited in its ability to explain the findings. Notably, within the CAHs, the authors found that 48% did improve from 2002 to 2010; there were no significant differences in hospital characteristics between the CAHs that did and did not improve. The reasons for the overall widening gap between CAHs and non-CAHs, therefore, merit further investigation.
Bottom line: From 2002 to 2010, mortality rates at U.S. critical-access hospitals rose while rates fell at non-critical access hospitals.
Citation: Joynt KE, Orav EJ, Jha AK. Mortality rates for Medicare beneficiaries admitted to critical access and non-critical access hospitals, 2002-2010. JAMA. 2013;309(13):1379-1387.
Physicians Fail to Discuss Advance-Care Planning with Hospitalized Elderly, Relatives
Clinical question: Do elderly patients who are at high risk for death have documented advance-care plans, and do their physicians discuss goals of care with them?
Background: While studies indicate that most sick, elderly patients prefer a better quality of life to life-sustaining treatment, many patients still die in the hospital, often in the ICU. It is unclear whether this is due to the absence of advance-care planning or the lack of communicating goals of care.
Study design: Multicenter prospective cohort study.
Setting: Canada.
Synopsis: A validated questionnaire was used to evaluate advance-care planning both before hospitalization and on admission. Patients and their families were enrolled if they were considered at high risk for dying, including patients with advanced disease, or aged >80 years. Of the 278 patients enrolled, 76.3% had thought about advance-care planning. Approximately 47.9% of patients had written an advance-care plan, and 73.3% had formally documented a surrogate health-care decision-maker. Only a quarter of patients reported that they had been asked about advance-care planning on admission to the hospital. Patients’ stated preferences for end-of-life care were notably incongruent with goals-of-care orders documented in the hospital records. While 28% of patients preferred comfort-only care, this was documented in the hospital records for only 4.5% of patients.
In this study of mostly white, English-speaking hospitalized patients, many had considered and made advance-care plans but few had discussed this with their health-care providers. Not surprisingly, the goals-of-care orders that were documented did not match patients’ previously stated end-of-life preferences.
Bottom line: Physicians routinely fail to discuss patients’ advance-care planning, which may have profound effects on their inpatient care.
Citation: Heyland DK, Barwich D, Pichora D, et al. Failure to engage hospitalized elderly patients and their families in advance care planning. JAMA Intern Med. 2013;173(9):778-787.
Ultrasound Use Reduces Lumbar Puncture and Epidural Catheterization Failure
Clinical question: Does ultrasound imaging for lumbar puncture and epidural catheterization reduce risk of procedure failures?
Background: Numerous studies have compared ultrasound-guided lumbar puncture and epidural catheterization with standard techniques, but they have been underpowered to evaluate whether ultrasound use reduces lumbar puncture and epidural catheterization failure.
Study design: Systematic review and meta-analysis of randomized controlled trials.
Setting: Hospitals in North America, Europe, and Asia.
Synopsis: Among 14 trials, a total of 1,334 patients (including one pediatric study group) were randomly assigned either to receive ultrasound imaging or to a control group (using manual palpation or loss of resistance). Ultrasound imaging comprised a preprocedure marking approach, real-time visual guidance, or both. In the 12 trials in which the primary outcome was available, ultrasound imaging significantly reduced the risk of failed procedures with a risk ratio of 0.21 (95% confidence interval 0.10 to 0.43). A total of 16 ultrasound-guided procedures were needed to avoid one procedure failure. Ultrasound guidance also reduced the number of traumatic procedures, needle reinsertions, and needle redirections. These results were consistent across multiple subgroup analyses.
Only one of the studies included in the meta-analysis was double-blind, and in all of the studies, ultrasound imaging was performed by a clinician with high-level ultrasound experience. While this study suggests that ultrasound does reduce the frequency of procedure failure, the investigators did not include cost-effectiveness analyses.
Bottom line: Ultrasound imaging likely reduces the failure of lumbar puncture and epidural catheterization, but future research will be necessary to evaluate the cost-effectiveness of ultrasound use for these procedures.
Citation: Shaikh F, Brzezinski J, Alexander S, et al. Ultrasound imaging for lumbar punctures and epidural catheterisations: systematic review and meta-analysis. BMJ. 2013;346:f1720.
Surgical Complications might Be Financially Advantageous for Hospitals
Clinical question: What is the impact of surgical complications on hospital finances?
Background: Surgical complications are common and lead to longer lengths of stay and higher costs. Strategies are available to reduce postsurgical complications but have not been universally adopted.
Study design: Observational study.
Setting: Twelve hospitals in one nonprofit Southern hospital system, which includes academic, nonacademic, and rural settings.
Synopsis: Researchers identified 34,526 patients who underwent surgery in 2010, excluding patients undergoing Caesarean section. Of those, 1,820 procedures (5.3%) were associated with at least one complication. The most frequent complications were surgical-site infection, other infections, pneumonia, and thromboembolic disease. The mortality rate for patients with complications was 12.3% compared with 0.6% for those without. Length of stay was four times longer for patients with complications.
Complications were associated with a higher total cost of hospitalization, with a differential of $37,917. This translated into a higher contribution to the margin. The cost differential varied by insurance type, with higher contributions under Medicare and private insurance but not with Medicaid.
The study had the benefit of using a large administrative database; however, this may have underestimated the actual rate of postoperative complications. The study supports the paradox in which quality-improvement (QI) programs that reduce surgical complications and improve postoperative mortality may negatively affect a hospital’s financial performance.
Bottom line: Surgical complications lead to higher mortality for patients but a financial benefit for hospitals.
Citation: Eappen S, Lane BH, Rosenberg B, et al. Relationship between occurrence of surgical complications and hospital finances. JAMA. 2013;309(5):1509-1606.
Showing Lab Test Fees May Decrease Frequency Of Test Ordering
Clinical question: Does information on the cost of a lab test lead to lowered ordering frequency among internal-medicine residents?
Background: Lab test overuse is common; some studies estimate that 70% of lab tests do not affect care. Strategies to reduce frequency of unnecessary lab tests are needed.
Study design: Randomized controlled trial.
Setting: Johns Hopkins Hospital, a 1,051-bed academic medical center in Baltimore.
Synopsis: Researchers used an administrative database to identify the 35 most frequently ordered and the 35 most expensive tests (each ordered at least 50 times). They randomized tests to an active arm, which displayed the Medicare allowable fee at the time of order entry within the computerized physician order entry, and a control arm. A total of 1,166,753 tests were ordered during the baseline and intervention period. Many more tests were ordered in the active group relative to the control group, a consequence of the randomization process. Relative to a six-month baseline period, tests in the active group were ordered 9.1% less frequently; control-group tests were ordered 5.1% more frequently. Charges decreased by $3.79 per patient-day in the active group and increased by $0.52 per patient-day in the control group.
This study reflects a low-cost strategy to reduce lab testing and associated costs. It is unknown whether only unnecessary tests were averted, or if there was any effect on the quality of care. The durability of the intervention and its applicability to other settings and with other types of providers is unclear.
Bottom line: Showing the fee associated with lab tests may decrease the frequency of ordering these tests and the resultant costs.
Citation: Feldman LS, Shihab HM, Thiemann D, et al. Impact of providing fee data on laboratory test ordering: a controlled clinical trial. JAMA Intern Med. 2013;173(10):903-908.
Inpatient Elderly Multidisciplinary-Team-Based Unit Reduces Readmissions
Clinical question: Can an inpatient unit that uses interdisciplinary rounds and a team approach reduce 30-day readmissions and lower cost compared with usual care?
Background: Elderly patients are at risk for adverse outcomes including delirium, deconditioning, and undernutrition. The Acute Care for Elders (ACE) model is designed as a team-based approach to improve communication between clinicians and to begin discharge planning soon after admission. ACE units have been shown to improve specific outcomes in older adults, but the impact on cost is less clear.
Study design: Retrospective cohort study.
Setting: University of Alabama at Birmingham Acute Care for Elders unit.
Synopsis: The analysis of cost data extrapolated from administrative sources indicated an average of $371 in variable cost savings per patient, and therefore an expected $148,400 savings for 400 patients admitted to this unit. The rate of 30-day readmissions was significantly lower in the ACE model: 7.9% versus 12.8% in patients receiving usual care.
Limitations of this study relate both to its design and single-center location. It is unclear which aspect of this ACE unit was helpful in the studied outcomes, and how this specific program would be reproduced at another institution. There were also some costs associated with the ACE-unit staffing, which may have resulted in an overestimation of the cost savings.
Bottom line: ACE units appear to improve outcomes and may lower cost, but further investigation is needed.
Citation: Flood KL, MacLennan PA, McGrew D, Green D, Dodd C, Brown CJ. Effects of an acute care for elders unit on costs and 30-day readmissions. JAMA. 2013 April 22 [Epub ahead of print].
Continue Beta-Blockers in High-Risk Patients During Noncardiac Surgery
Clinical question: Does exposure to a beta-blocker at the time of noncardiac surgery have an association with mortality, cardiac arrest, or Q-wave myocardial infarction (MI)?
Background: Exposure to beta-blockers perioperatively is controversial. The authors suggest that a randomized trial would be difficult, as one might need to withhold beta-blockers from stable patients. The American Heart Association and American College of Cardiology currently recommend continuation of pre-existing beta-blockades perioperatively.
Study design: Retrospective, propensity-matched cohort analysis.
Setting: One hundred four Veterans Affairs (VA) medical centers from January 2005 to August 2010.
Synopsis: Exposure for any reason to beta-blockers around nonvascular surgery appears to lower the risk of mortality and cardiac arrest, particularly in patients with higher revised cardiac risk index factors. Stopping beta-blockers in this same period was associated with increased mortality. The reasons for beta-blocker use in the exposed cohort were not well-established or -stratified.
Limitations include that the exposed cohort had a higher rate of cardiovascular disease and comorbidities and were generally older. Duration of exposure to beta-blockers was mixed, although more than 75% had a prescription for more than three months, with less than 2% for several days. Some of the matched cohort appears to have had beta-blocker exposure, thus diminishing the potential impact.
Bottom line: In this retrospective analysis, there is an association between beta-blocker use during noncardiac, nonvascular surgery and lower mortality, as well as lower rates of cardiac arrest and Q-wave MI, particularly among higher-risk patients.
Citation: London MJ, Hur K, Schwartz G, Henderson WG. Association of perioperative beta-blockade with mortality and cardiovascular morbidity following major noncardiac surgery. JAMA. 2013;309(16):1704-1713.
Patient-Centered Decision-Making and Health-Care Outcomes
Clinical question: Does recognition of contextual domains in the care plan lead to resolution of patients’ presenting problems?
Background: Patient-centered decision-making, or contextualization of care, adapts best evidence to the care of the individual patient. Examples of contextual domains include access to care, social support, and financial situation. Contextual errors (e.g. unrecognized domains) are, on average, more costly than errors in evidenced-based medicine.
Study design: Observational study.
Setting: VA ambulatory-care centers.
Synopsis: A total of 548 patient-derived audio recordings of physician encounters that included contextual red flags (e.g. missed appointments, HbA1c >8%) were reviewed at two VA hospital ambulatory-care centers using the content coding for contextualization of care (4C) method. Prospectively determined good and poor outcomes were derived from specific red flags (e.g. keeping next appointment, decrease in HbA1c). Of the 548 red flags, 208 were associated with contextual domains using the 4C method. Some 59% of physicians recognized contextual domains in care-plan development, leading to good outcomes in 71% of red flags. As many as 41% of physicians did not recognize contextual domains, leading to poor outcomes in 54% of red-flag instances.
Hospitalists should be aware of contextual domains and red flags (e.g. readmissions), and this study provides a method of evaluating patient-centered decision-making in the hospital setting. However, the inherently subjective 4C method may underestimate the number of contextual domains.
Bottom line: Recognition and incorporation of contextual domains in care-plan development in the ambulatory setting are associated with improved contextual red flag outcomes.
Citation: Weiner SJ, Schwartz A, Sharma G, et al. Patient-centered decision making and health care outcomes: an observational study. Ann Intern Med. 2013;158:573-579.
Adverse Surgical Outcomes in Schizophrenia Patients
Clinical question: What is the full spectrum of postoperative complications and mortality in schizophrenic patients receiving in-hospital major surgery?
Background: Schizophrenia affects an estimated 4 to 7 per 1,000 persons worldwide, and patients with schizophrenia are at increased risk of diabetes, cardiovascular disease, and stroke with subsequent increased mortality risk. The correlation between severity of mental illness and postoperative in-hospital mortality has not been validated in previous studies.
Study design: Population-based, cross-sectional study.
Setting: Taiwan hospitals.
Synopsis: Using the Taiwan National Health Insurance Research Database, researchers examined claims from 2004 to 2007 and retrospectively identified 8,967 schizophrenic patients who underwent major inpatient surgery and were hospitalized for more than one day. Primary outcomes included acute myocardial infarction, acute renal failure, stroke, and in-hospital mortality within 30 days. Postoperative complications and mortality rates were compared between schizophrenic patients and patients without mental illness.
Schizophrenic patients had higher rates of many primary outcomes, including 30-day postoperative mortality, compared with patients without mental illness, after adjusting for sex, age, surgery type, and hospital setting. The risk for 30-day mortality rose with the number of preoperative schizophrenia-related services provided. Limitations include the nature of retrospective analysis and generalizability.
Bottom line: Compared to patients without mental illness, schizophrenic patients have an increased risk of acute renal failure, pneumonia, septicemia, and 30-day mortality in the postoperative setting, with higher mortality rates in schizophrenic patients with more severe disease.
Citation: Liao CC, Shen WW, Chang CC, Chang H, Chen T. Surgical adverse outcomes in patients with schizophrenia. Ann Surg. 2013;257:433-438.
In This Edition
Literature At A Glance
A guide to this month’s studies
- Steroids may increase VTE risk
- Mortality rates rise at critical-care hospitals
- Physicians don’t discuss advance-care planning with elderly, families
- Ultrasound imaging for lumbar puncture, epidural catheterization
- Financial impact of surgical complications on hospitals
- Lab test fees and frequency of test ordering
- Inpatient elderly multidisciplinary teams reduce readmissions
- Use of beta-blockers in high-risk patients during noncardiac surgery
- Patient-centered decision-making and health-care outcomes
- Adverse surgical outcomes in patients with schizophrenia
Steroids May Increase VTE Risk
Clinical question: Is exogenous glucocorticoid administration associated with an increased risk of VTE?
Background: Endogenous hypercortisolism is linked to increased VTE rates, and pathophysiologic data exist to suggest glucocorticoids increase clotting, but few studies have measured the clinical link between glucocorticoid administration and VTE events.
Study design: Case-control study.
Setting: Denmark.
Synopsis: The authors analyzed Danish national registries, which include information on diagnoses and prescriptions. The study selection period was Jan. 1, 2005, to Dec. 31, 2011. During this period, 38,675 cases of VTE (both DVT and pulmonary embolism) were identified in the population of Denmark. These cases were matched with 387,650 controls. Three routes of glucocorticoid use were studied: systemic (oral and intravenous), inhaled, and intestinal-acting. Cases were classified as present (within 90 days of VTE event), recent (91 to 365 days), or former (over 365 days) users of glucocorticoids. Categories were also created for new versus continuous users.
Glucocorticoid use was associated with a significant increase in VTE occurrence. The strongest link was in new and recent users, and the effect diminished over time. Key limitations of the study included its reliance on registry data, as well as the fact that cases had more comorbid conditions than controls (e.g. recent infection, chronic illnesses).
Bottom line: Recipients of glucocorticoids had an increased risk of VTE; the effect was strongest in new and recent users.
Citation: Johannesdottir SA, Horvath-Puho E, Dekkers OM, et al. Use of glucocorticoids and risk of venous thromboembolism. JAMA Intern Med. 2013;173(9):743-752.
Mortality Rates Rise at Critical-Access Hospitals
Clinical question: How have trends in mortality changed in the past decade at critical-access hospitals when compared to other hospitals?
Background: Hospitals are designated as critical-access hospitals (CAH) by meeting certain requirements—namely, rural setting, small number of beds, and minimum distance from the nearest hospital. Because of the intrinsic challenges they face, CAHs are exempt from certain quality measures. Little data exist on patient outcomes at CAHs.
Study design: Retrospective observational study.
Setting: All nonfederal hospitals in the U.S. that provide acute care to Medicare beneficiaries.
Synopsis: Using Medicare data, risk-adjusted 30-day mortality rates were calculated at critical-access hospitals and non-critical-access hospitals from 2002 to 2010 for three conditions: acute myocardial infarction, congestive heart failure, and pneumonia. Mortality trends across these conditions were compared at baseline and over time. In 2002, CAHs had mortality rates comparable with non-CAHs. From 2002 to 2010, mortality rates increased by 0.1% per year at CAHs and decreased by 0.2% per year at non-CAHs, resulting in a mortality difference between these two hospital groups at the end of the study period. The authors postulate that differences in policy initiatives, enforcement of quality measures, and access to technology may play a role.
This study is limited in its ability to explain the findings. Notably, within the CAHs, the authors found that 48% did improve from 2002 to 2010; there were no significant differences in hospital characteristics between the CAHs that did and did not improve. The reasons for the overall widening gap between CAHs and non-CAHs, therefore, merit further investigation.
Bottom line: From 2002 to 2010, mortality rates at U.S. critical-access hospitals rose while rates fell at non-critical access hospitals.
Citation: Joynt KE, Orav EJ, Jha AK. Mortality rates for Medicare beneficiaries admitted to critical access and non-critical access hospitals, 2002-2010. JAMA. 2013;309(13):1379-1387.
Physicians Fail to Discuss Advance-Care Planning with Hospitalized Elderly, Relatives
Clinical question: Do elderly patients who are at high risk for death have documented advance-care plans, and do their physicians discuss goals of care with them?
Background: While studies indicate that most sick, elderly patients prefer a better quality of life to life-sustaining treatment, many patients still die in the hospital, often in the ICU. It is unclear whether this is due to the absence of advance-care planning or the lack of communicating goals of care.
Study design: Multicenter prospective cohort study.
Setting: Canada.
Synopsis: A validated questionnaire was used to evaluate advance-care planning both before hospitalization and on admission. Patients and their families were enrolled if they were considered at high risk for dying, including patients with advanced disease, or aged >80 years. Of the 278 patients enrolled, 76.3% had thought about advance-care planning. Approximately 47.9% of patients had written an advance-care plan, and 73.3% had formally documented a surrogate health-care decision-maker. Only a quarter of patients reported that they had been asked about advance-care planning on admission to the hospital. Patients’ stated preferences for end-of-life care were notably incongruent with goals-of-care orders documented in the hospital records. While 28% of patients preferred comfort-only care, this was documented in the hospital records for only 4.5% of patients.
In this study of mostly white, English-speaking hospitalized patients, many had considered and made advance-care plans but few had discussed this with their health-care providers. Not surprisingly, the goals-of-care orders that were documented did not match patients’ previously stated end-of-life preferences.
Bottom line: Physicians routinely fail to discuss patients’ advance-care planning, which may have profound effects on their inpatient care.
Citation: Heyland DK, Barwich D, Pichora D, et al. Failure to engage hospitalized elderly patients and their families in advance care planning. JAMA Intern Med. 2013;173(9):778-787.
Ultrasound Use Reduces Lumbar Puncture and Epidural Catheterization Failure
Clinical question: Does ultrasound imaging for lumbar puncture and epidural catheterization reduce risk of procedure failures?
Background: Numerous studies have compared ultrasound-guided lumbar puncture and epidural catheterization with standard techniques, but they have been underpowered to evaluate whether ultrasound use reduces lumbar puncture and epidural catheterization failure.
Study design: Systematic review and meta-analysis of randomized controlled trials.
Setting: Hospitals in North America, Europe, and Asia.
Synopsis: Among 14 trials, a total of 1,334 patients (including one pediatric study group) were randomly assigned either to receive ultrasound imaging or to a control group (using manual palpation or loss of resistance). Ultrasound imaging comprised a preprocedure marking approach, real-time visual guidance, or both. In the 12 trials in which the primary outcome was available, ultrasound imaging significantly reduced the risk of failed procedures with a risk ratio of 0.21 (95% confidence interval 0.10 to 0.43). A total of 16 ultrasound-guided procedures were needed to avoid one procedure failure. Ultrasound guidance also reduced the number of traumatic procedures, needle reinsertions, and needle redirections. These results were consistent across multiple subgroup analyses.
Only one of the studies included in the meta-analysis was double-blind, and in all of the studies, ultrasound imaging was performed by a clinician with high-level ultrasound experience. While this study suggests that ultrasound does reduce the frequency of procedure failure, the investigators did not include cost-effectiveness analyses.
Bottom line: Ultrasound imaging likely reduces the failure of lumbar puncture and epidural catheterization, but future research will be necessary to evaluate the cost-effectiveness of ultrasound use for these procedures.
Citation: Shaikh F, Brzezinski J, Alexander S, et al. Ultrasound imaging for lumbar punctures and epidural catheterisations: systematic review and meta-analysis. BMJ. 2013;346:f1720.
Surgical Complications might Be Financially Advantageous for Hospitals
Clinical question: What is the impact of surgical complications on hospital finances?
Background: Surgical complications are common and lead to longer lengths of stay and higher costs. Strategies are available to reduce postsurgical complications but have not been universally adopted.
Study design: Observational study.
Setting: Twelve hospitals in one nonprofit Southern hospital system, which includes academic, nonacademic, and rural settings.
Synopsis: Researchers identified 34,526 patients who underwent surgery in 2010, excluding patients undergoing Caesarean section. Of those, 1,820 procedures (5.3%) were associated with at least one complication. The most frequent complications were surgical-site infection, other infections, pneumonia, and thromboembolic disease. The mortality rate for patients with complications was 12.3% compared with 0.6% for those without. Length of stay was four times longer for patients with complications.
Complications were associated with a higher total cost of hospitalization, with a differential of $37,917. This translated into a higher contribution to the margin. The cost differential varied by insurance type, with higher contributions under Medicare and private insurance but not with Medicaid.
The study had the benefit of using a large administrative database; however, this may have underestimated the actual rate of postoperative complications. The study supports the paradox in which quality-improvement (QI) programs that reduce surgical complications and improve postoperative mortality may negatively affect a hospital’s financial performance.
Bottom line: Surgical complications lead to higher mortality for patients but a financial benefit for hospitals.
Citation: Eappen S, Lane BH, Rosenberg B, et al. Relationship between occurrence of surgical complications and hospital finances. JAMA. 2013;309(5):1509-1606.
Showing Lab Test Fees May Decrease Frequency Of Test Ordering
Clinical question: Does information on the cost of a lab test lead to lowered ordering frequency among internal-medicine residents?
Background: Lab test overuse is common; some studies estimate that 70% of lab tests do not affect care. Strategies to reduce frequency of unnecessary lab tests are needed.
Study design: Randomized controlled trial.
Setting: Johns Hopkins Hospital, a 1,051-bed academic medical center in Baltimore.
Synopsis: Researchers used an administrative database to identify the 35 most frequently ordered and the 35 most expensive tests (each ordered at least 50 times). They randomized tests to an active arm, which displayed the Medicare allowable fee at the time of order entry within the computerized physician order entry, and a control arm. A total of 1,166,753 tests were ordered during the baseline and intervention period. Many more tests were ordered in the active group relative to the control group, a consequence of the randomization process. Relative to a six-month baseline period, tests in the active group were ordered 9.1% less frequently; control-group tests were ordered 5.1% more frequently. Charges decreased by $3.79 per patient-day in the active group and increased by $0.52 per patient-day in the control group.
This study reflects a low-cost strategy to reduce lab testing and associated costs. It is unknown whether only unnecessary tests were averted, or if there was any effect on the quality of care. The durability of the intervention and its applicability to other settings and with other types of providers is unclear.
Bottom line: Showing the fee associated with lab tests may decrease the frequency of ordering these tests and the resultant costs.
Citation: Feldman LS, Shihab HM, Thiemann D, et al. Impact of providing fee data on laboratory test ordering: a controlled clinical trial. JAMA Intern Med. 2013;173(10):903-908.
Inpatient Elderly Multidisciplinary-Team-Based Unit Reduces Readmissions
Clinical question: Can an inpatient unit that uses interdisciplinary rounds and a team approach reduce 30-day readmissions and lower cost compared with usual care?
Background: Elderly patients are at risk for adverse outcomes including delirium, deconditioning, and undernutrition. The Acute Care for Elders (ACE) model is designed as a team-based approach to improve communication between clinicians and to begin discharge planning soon after admission. ACE units have been shown to improve specific outcomes in older adults, but the impact on cost is less clear.
Study design: Retrospective cohort study.
Setting: University of Alabama at Birmingham Acute Care for Elders unit.
Synopsis: The analysis of cost data extrapolated from administrative sources indicated an average of $371 in variable cost savings per patient, and therefore an expected $148,400 savings for 400 patients admitted to this unit. The rate of 30-day readmissions was significantly lower in the ACE model: 7.9% versus 12.8% in patients receiving usual care.
Limitations of this study relate both to its design and single-center location. It is unclear which aspect of this ACE unit was helpful in the studied outcomes, and how this specific program would be reproduced at another institution. There were also some costs associated with the ACE-unit staffing, which may have resulted in an overestimation of the cost savings.
Bottom line: ACE units appear to improve outcomes and may lower cost, but further investigation is needed.
Citation: Flood KL, MacLennan PA, McGrew D, Green D, Dodd C, Brown CJ. Effects of an acute care for elders unit on costs and 30-day readmissions. JAMA. 2013 April 22 [Epub ahead of print].
Continue Beta-Blockers in High-Risk Patients During Noncardiac Surgery
Clinical question: Does exposure to a beta-blocker at the time of noncardiac surgery have an association with mortality, cardiac arrest, or Q-wave myocardial infarction (MI)?
Background: Exposure to beta-blockers perioperatively is controversial. The authors suggest that a randomized trial would be difficult, as one might need to withhold beta-blockers from stable patients. The American Heart Association and American College of Cardiology currently recommend continuation of pre-existing beta-blockades perioperatively.
Study design: Retrospective, propensity-matched cohort analysis.
Setting: One hundred four Veterans Affairs (VA) medical centers from January 2005 to August 2010.
Synopsis: Exposure for any reason to beta-blockers around nonvascular surgery appears to lower the risk of mortality and cardiac arrest, particularly in patients with higher revised cardiac risk index factors. Stopping beta-blockers in this same period was associated with increased mortality. The reasons for beta-blocker use in the exposed cohort were not well-established or -stratified.
Limitations include that the exposed cohort had a higher rate of cardiovascular disease and comorbidities and were generally older. Duration of exposure to beta-blockers was mixed, although more than 75% had a prescription for more than three months, with less than 2% for several days. Some of the matched cohort appears to have had beta-blocker exposure, thus diminishing the potential impact.
Bottom line: In this retrospective analysis, there is an association between beta-blocker use during noncardiac, nonvascular surgery and lower mortality, as well as lower rates of cardiac arrest and Q-wave MI, particularly among higher-risk patients.
Citation: London MJ, Hur K, Schwartz G, Henderson WG. Association of perioperative beta-blockade with mortality and cardiovascular morbidity following major noncardiac surgery. JAMA. 2013;309(16):1704-1713.
Patient-Centered Decision-Making and Health-Care Outcomes
Clinical question: Does recognition of contextual domains in the care plan lead to resolution of patients’ presenting problems?
Background: Patient-centered decision-making, or contextualization of care, adapts best evidence to the care of the individual patient. Examples of contextual domains include access to care, social support, and financial situation. Contextual errors (e.g. unrecognized domains) are, on average, more costly than errors in evidenced-based medicine.
Study design: Observational study.
Setting: VA ambulatory-care centers.
Synopsis: A total of 548 patient-derived audio recordings of physician encounters that included contextual red flags (e.g. missed appointments, HbA1c >8%) were reviewed at two VA hospital ambulatory-care centers using the content coding for contextualization of care (4C) method. Prospectively determined good and poor outcomes were derived from specific red flags (e.g. keeping next appointment, decrease in HbA1c). Of the 548 red flags, 208 were associated with contextual domains using the 4C method. Some 59% of physicians recognized contextual domains in care-plan development, leading to good outcomes in 71% of red flags. As many as 41% of physicians did not recognize contextual domains, leading to poor outcomes in 54% of red-flag instances.
Hospitalists should be aware of contextual domains and red flags (e.g. readmissions), and this study provides a method of evaluating patient-centered decision-making in the hospital setting. However, the inherently subjective 4C method may underestimate the number of contextual domains.
Bottom line: Recognition and incorporation of contextual domains in care-plan development in the ambulatory setting are associated with improved contextual red flag outcomes.
Citation: Weiner SJ, Schwartz A, Sharma G, et al. Patient-centered decision making and health care outcomes: an observational study. Ann Intern Med. 2013;158:573-579.
Adverse Surgical Outcomes in Schizophrenia Patients
Clinical question: What is the full spectrum of postoperative complications and mortality in schizophrenic patients receiving in-hospital major surgery?
Background: Schizophrenia affects an estimated 4 to 7 per 1,000 persons worldwide, and patients with schizophrenia are at increased risk of diabetes, cardiovascular disease, and stroke with subsequent increased mortality risk. The correlation between severity of mental illness and postoperative in-hospital mortality has not been validated in previous studies.
Study design: Population-based, cross-sectional study.
Setting: Taiwan hospitals.
Synopsis: Using the Taiwan National Health Insurance Research Database, researchers examined claims from 2004 to 2007 and retrospectively identified 8,967 schizophrenic patients who underwent major inpatient surgery and were hospitalized for more than one day. Primary outcomes included acute myocardial infarction, acute renal failure, stroke, and in-hospital mortality within 30 days. Postoperative complications and mortality rates were compared between schizophrenic patients and patients without mental illness.
Schizophrenic patients had higher rates of many primary outcomes, including 30-day postoperative mortality, compared with patients without mental illness, after adjusting for sex, age, surgery type, and hospital setting. The risk for 30-day mortality rose with the number of preoperative schizophrenia-related services provided. Limitations include the nature of retrospective analysis and generalizability.
Bottom line: Compared to patients without mental illness, schizophrenic patients have an increased risk of acute renal failure, pneumonia, septicemia, and 30-day mortality in the postoperative setting, with higher mortality rates in schizophrenic patients with more severe disease.
Citation: Liao CC, Shen WW, Chang CC, Chang H, Chen T. Surgical adverse outcomes in patients with schizophrenia. Ann Surg. 2013;257:433-438.
In This Edition
Literature At A Glance
A guide to this month’s studies
- Steroids may increase VTE risk
- Mortality rates rise at critical-care hospitals
- Physicians don’t discuss advance-care planning with elderly, families
- Ultrasound imaging for lumbar puncture, epidural catheterization
- Financial impact of surgical complications on hospitals
- Lab test fees and frequency of test ordering
- Inpatient elderly multidisciplinary teams reduce readmissions
- Use of beta-blockers in high-risk patients during noncardiac surgery
- Patient-centered decision-making and health-care outcomes
- Adverse surgical outcomes in patients with schizophrenia
Steroids May Increase VTE Risk
Clinical question: Is exogenous glucocorticoid administration associated with an increased risk of VTE?
Background: Endogenous hypercortisolism is linked to increased VTE rates, and pathophysiologic data exist to suggest glucocorticoids increase clotting, but few studies have measured the clinical link between glucocorticoid administration and VTE events.
Study design: Case-control study.
Setting: Denmark.
Synopsis: The authors analyzed Danish national registries, which include information on diagnoses and prescriptions. The study selection period was Jan. 1, 2005, to Dec. 31, 2011. During this period, 38,675 cases of VTE (both DVT and pulmonary embolism) were identified in the population of Denmark. These cases were matched with 387,650 controls. Three routes of glucocorticoid use were studied: systemic (oral and intravenous), inhaled, and intestinal-acting. Cases were classified as present (within 90 days of VTE event), recent (91 to 365 days), or former (over 365 days) users of glucocorticoids. Categories were also created for new versus continuous users.
Glucocorticoid use was associated with a significant increase in VTE occurrence. The strongest link was in new and recent users, and the effect diminished over time. Key limitations of the study included its reliance on registry data, as well as the fact that cases had more comorbid conditions than controls (e.g. recent infection, chronic illnesses).
Bottom line: Recipients of glucocorticoids had an increased risk of VTE; the effect was strongest in new and recent users.
Citation: Johannesdottir SA, Horvath-Puho E, Dekkers OM, et al. Use of glucocorticoids and risk of venous thromboembolism. JAMA Intern Med. 2013;173(9):743-752.
Mortality Rates Rise at Critical-Access Hospitals
Clinical question: How have trends in mortality changed in the past decade at critical-access hospitals when compared to other hospitals?
Background: Hospitals are designated as critical-access hospitals (CAH) by meeting certain requirements—namely, rural setting, small number of beds, and minimum distance from the nearest hospital. Because of the intrinsic challenges they face, CAHs are exempt from certain quality measures. Little data exist on patient outcomes at CAHs.
Study design: Retrospective observational study.
Setting: All nonfederal hospitals in the U.S. that provide acute care to Medicare beneficiaries.
Synopsis: Using Medicare data, risk-adjusted 30-day mortality rates were calculated at critical-access hospitals and non-critical-access hospitals from 2002 to 2010 for three conditions: acute myocardial infarction, congestive heart failure, and pneumonia. Mortality trends across these conditions were compared at baseline and over time. In 2002, CAHs had mortality rates comparable with non-CAHs. From 2002 to 2010, mortality rates increased by 0.1% per year at CAHs and decreased by 0.2% per year at non-CAHs, resulting in a mortality difference between these two hospital groups at the end of the study period. The authors postulate that differences in policy initiatives, enforcement of quality measures, and access to technology may play a role.
This study is limited in its ability to explain the findings. Notably, within the CAHs, the authors found that 48% did improve from 2002 to 2010; there were no significant differences in hospital characteristics between the CAHs that did and did not improve. The reasons for the overall widening gap between CAHs and non-CAHs, therefore, merit further investigation.
Bottom line: From 2002 to 2010, mortality rates at U.S. critical-access hospitals rose while rates fell at non-critical access hospitals.
Citation: Joynt KE, Orav EJ, Jha AK. Mortality rates for Medicare beneficiaries admitted to critical access and non-critical access hospitals, 2002-2010. JAMA. 2013;309(13):1379-1387.
Physicians Fail to Discuss Advance-Care Planning with Hospitalized Elderly, Relatives
Clinical question: Do elderly patients who are at high risk for death have documented advance-care plans, and do their physicians discuss goals of care with them?
Background: While studies indicate that most sick, elderly patients prefer a better quality of life to life-sustaining treatment, many patients still die in the hospital, often in the ICU. It is unclear whether this is due to the absence of advance-care planning or the lack of communicating goals of care.
Study design: Multicenter prospective cohort study.
Setting: Canada.
Synopsis: A validated questionnaire was used to evaluate advance-care planning both before hospitalization and on admission. Patients and their families were enrolled if they were considered at high risk for dying, including patients with advanced disease, or aged >80 years. Of the 278 patients enrolled, 76.3% had thought about advance-care planning. Approximately 47.9% of patients had written an advance-care plan, and 73.3% had formally documented a surrogate health-care decision-maker. Only a quarter of patients reported that they had been asked about advance-care planning on admission to the hospital. Patients’ stated preferences for end-of-life care were notably incongruent with goals-of-care orders documented in the hospital records. While 28% of patients preferred comfort-only care, this was documented in the hospital records for only 4.5% of patients.
In this study of mostly white, English-speaking hospitalized patients, many had considered and made advance-care plans but few had discussed this with their health-care providers. Not surprisingly, the goals-of-care orders that were documented did not match patients’ previously stated end-of-life preferences.
Bottom line: Physicians routinely fail to discuss patients’ advance-care planning, which may have profound effects on their inpatient care.
Citation: Heyland DK, Barwich D, Pichora D, et al. Failure to engage hospitalized elderly patients and their families in advance care planning. JAMA Intern Med. 2013;173(9):778-787.
Ultrasound Use Reduces Lumbar Puncture and Epidural Catheterization Failure
Clinical question: Does ultrasound imaging for lumbar puncture and epidural catheterization reduce risk of procedure failures?
Background: Numerous studies have compared ultrasound-guided lumbar puncture and epidural catheterization with standard techniques, but they have been underpowered to evaluate whether ultrasound use reduces lumbar puncture and epidural catheterization failure.
Study design: Systematic review and meta-analysis of randomized controlled trials.
Setting: Hospitals in North America, Europe, and Asia.
Synopsis: Among 14 trials, a total of 1,334 patients (including one pediatric study group) were randomly assigned either to receive ultrasound imaging or to a control group (using manual palpation or loss of resistance). Ultrasound imaging comprised a preprocedure marking approach, real-time visual guidance, or both. In the 12 trials in which the primary outcome was available, ultrasound imaging significantly reduced the risk of failed procedures with a risk ratio of 0.21 (95% confidence interval 0.10 to 0.43). A total of 16 ultrasound-guided procedures were needed to avoid one procedure failure. Ultrasound guidance also reduced the number of traumatic procedures, needle reinsertions, and needle redirections. These results were consistent across multiple subgroup analyses.
Only one of the studies included in the meta-analysis was double-blind, and in all of the studies, ultrasound imaging was performed by a clinician with high-level ultrasound experience. While this study suggests that ultrasound does reduce the frequency of procedure failure, the investigators did not include cost-effectiveness analyses.
Bottom line: Ultrasound imaging likely reduces the failure of lumbar puncture and epidural catheterization, but future research will be necessary to evaluate the cost-effectiveness of ultrasound use for these procedures.
Citation: Shaikh F, Brzezinski J, Alexander S, et al. Ultrasound imaging for lumbar punctures and epidural catheterisations: systematic review and meta-analysis. BMJ. 2013;346:f1720.
Surgical Complications might Be Financially Advantageous for Hospitals
Clinical question: What is the impact of surgical complications on hospital finances?
Background: Surgical complications are common and lead to longer lengths of stay and higher costs. Strategies are available to reduce postsurgical complications but have not been universally adopted.
Study design: Observational study.
Setting: Twelve hospitals in one nonprofit Southern hospital system, which includes academic, nonacademic, and rural settings.
Synopsis: Researchers identified 34,526 patients who underwent surgery in 2010, excluding patients undergoing Caesarean section. Of those, 1,820 procedures (5.3%) were associated with at least one complication. The most frequent complications were surgical-site infection, other infections, pneumonia, and thromboembolic disease. The mortality rate for patients with complications was 12.3% compared with 0.6% for those without. Length of stay was four times longer for patients with complications.
Complications were associated with a higher total cost of hospitalization, with a differential of $37,917. This translated into a higher contribution to the margin. The cost differential varied by insurance type, with higher contributions under Medicare and private insurance but not with Medicaid.
The study had the benefit of using a large administrative database; however, this may have underestimated the actual rate of postoperative complications. The study supports the paradox in which quality-improvement (QI) programs that reduce surgical complications and improve postoperative mortality may negatively affect a hospital’s financial performance.
Bottom line: Surgical complications lead to higher mortality for patients but a financial benefit for hospitals.
Citation: Eappen S, Lane BH, Rosenberg B, et al. Relationship between occurrence of surgical complications and hospital finances. JAMA. 2013;309(5):1509-1606.
Showing Lab Test Fees May Decrease Frequency Of Test Ordering
Clinical question: Does information on the cost of a lab test lead to lowered ordering frequency among internal-medicine residents?
Background: Lab test overuse is common; some studies estimate that 70% of lab tests do not affect care. Strategies to reduce frequency of unnecessary lab tests are needed.
Study design: Randomized controlled trial.
Setting: Johns Hopkins Hospital, a 1,051-bed academic medical center in Baltimore.
Synopsis: Researchers used an administrative database to identify the 35 most frequently ordered and the 35 most expensive tests (each ordered at least 50 times). They randomized tests to an active arm, which displayed the Medicare allowable fee at the time of order entry within the computerized physician order entry, and a control arm. A total of 1,166,753 tests were ordered during the baseline and intervention period. Many more tests were ordered in the active group relative to the control group, a consequence of the randomization process. Relative to a six-month baseline period, tests in the active group were ordered 9.1% less frequently; control-group tests were ordered 5.1% more frequently. Charges decreased by $3.79 per patient-day in the active group and increased by $0.52 per patient-day in the control group.
This study reflects a low-cost strategy to reduce lab testing and associated costs. It is unknown whether only unnecessary tests were averted, or if there was any effect on the quality of care. The durability of the intervention and its applicability to other settings and with other types of providers is unclear.
Bottom line: Showing the fee associated with lab tests may decrease the frequency of ordering these tests and the resultant costs.
Citation: Feldman LS, Shihab HM, Thiemann D, et al. Impact of providing fee data on laboratory test ordering: a controlled clinical trial. JAMA Intern Med. 2013;173(10):903-908.
Inpatient Elderly Multidisciplinary-Team-Based Unit Reduces Readmissions
Clinical question: Can an inpatient unit that uses interdisciplinary rounds and a team approach reduce 30-day readmissions and lower cost compared with usual care?
Background: Elderly patients are at risk for adverse outcomes including delirium, deconditioning, and undernutrition. The Acute Care for Elders (ACE) model is designed as a team-based approach to improve communication between clinicians and to begin discharge planning soon after admission. ACE units have been shown to improve specific outcomes in older adults, but the impact on cost is less clear.
Study design: Retrospective cohort study.
Setting: University of Alabama at Birmingham Acute Care for Elders unit.
Synopsis: The analysis of cost data extrapolated from administrative sources indicated an average of $371 in variable cost savings per patient, and therefore an expected $148,400 savings for 400 patients admitted to this unit. The rate of 30-day readmissions was significantly lower in the ACE model: 7.9% versus 12.8% in patients receiving usual care.
Limitations of this study relate both to its design and single-center location. It is unclear which aspect of this ACE unit was helpful in the studied outcomes, and how this specific program would be reproduced at another institution. There were also some costs associated with the ACE-unit staffing, which may have resulted in an overestimation of the cost savings.
Bottom line: ACE units appear to improve outcomes and may lower cost, but further investigation is needed.
Citation: Flood KL, MacLennan PA, McGrew D, Green D, Dodd C, Brown CJ. Effects of an acute care for elders unit on costs and 30-day readmissions. JAMA. 2013 April 22 [Epub ahead of print].
Continue Beta-Blockers in High-Risk Patients During Noncardiac Surgery
Clinical question: Does exposure to a beta-blocker at the time of noncardiac surgery have an association with mortality, cardiac arrest, or Q-wave myocardial infarction (MI)?
Background: Exposure to beta-blockers perioperatively is controversial. The authors suggest that a randomized trial would be difficult, as one might need to withhold beta-blockers from stable patients. The American Heart Association and American College of Cardiology currently recommend continuation of pre-existing beta-blockades perioperatively.
Study design: Retrospective, propensity-matched cohort analysis.
Setting: One hundred four Veterans Affairs (VA) medical centers from January 2005 to August 2010.
Synopsis: Exposure for any reason to beta-blockers around nonvascular surgery appears to lower the risk of mortality and cardiac arrest, particularly in patients with higher revised cardiac risk index factors. Stopping beta-blockers in this same period was associated with increased mortality. The reasons for beta-blocker use in the exposed cohort were not well-established or -stratified.
Limitations include that the exposed cohort had a higher rate of cardiovascular disease and comorbidities and were generally older. Duration of exposure to beta-blockers was mixed, although more than 75% had a prescription for more than three months, with less than 2% for several days. Some of the matched cohort appears to have had beta-blocker exposure, thus diminishing the potential impact.
Bottom line: In this retrospective analysis, there is an association between beta-blocker use during noncardiac, nonvascular surgery and lower mortality, as well as lower rates of cardiac arrest and Q-wave MI, particularly among higher-risk patients.
Citation: London MJ, Hur K, Schwartz G, Henderson WG. Association of perioperative beta-blockade with mortality and cardiovascular morbidity following major noncardiac surgery. JAMA. 2013;309(16):1704-1713.
Patient-Centered Decision-Making and Health-Care Outcomes
Clinical question: Does recognition of contextual domains in the care plan lead to resolution of patients’ presenting problems?
Background: Patient-centered decision-making, or contextualization of care, adapts best evidence to the care of the individual patient. Examples of contextual domains include access to care, social support, and financial situation. Contextual errors (e.g. unrecognized domains) are, on average, more costly than errors in evidenced-based medicine.
Study design: Observational study.
Setting: VA ambulatory-care centers.
Synopsis: A total of 548 patient-derived audio recordings of physician encounters that included contextual red flags (e.g. missed appointments, HbA1c >8%) were reviewed at two VA hospital ambulatory-care centers using the content coding for contextualization of care (4C) method. Prospectively determined good and poor outcomes were derived from specific red flags (e.g. keeping next appointment, decrease in HbA1c). Of the 548 red flags, 208 were associated with contextual domains using the 4C method. Some 59% of physicians recognized contextual domains in care-plan development, leading to good outcomes in 71% of red flags. As many as 41% of physicians did not recognize contextual domains, leading to poor outcomes in 54% of red-flag instances.
Hospitalists should be aware of contextual domains and red flags (e.g. readmissions), and this study provides a method of evaluating patient-centered decision-making in the hospital setting. However, the inherently subjective 4C method may underestimate the number of contextual domains.
Bottom line: Recognition and incorporation of contextual domains in care-plan development in the ambulatory setting are associated with improved contextual red flag outcomes.
Citation: Weiner SJ, Schwartz A, Sharma G, et al. Patient-centered decision making and health care outcomes: an observational study. Ann Intern Med. 2013;158:573-579.
Adverse Surgical Outcomes in Schizophrenia Patients
Clinical question: What is the full spectrum of postoperative complications and mortality in schizophrenic patients receiving in-hospital major surgery?
Background: Schizophrenia affects an estimated 4 to 7 per 1,000 persons worldwide, and patients with schizophrenia are at increased risk of diabetes, cardiovascular disease, and stroke with subsequent increased mortality risk. The correlation between severity of mental illness and postoperative in-hospital mortality has not been validated in previous studies.
Study design: Population-based, cross-sectional study.
Setting: Taiwan hospitals.
Synopsis: Using the Taiwan National Health Insurance Research Database, researchers examined claims from 2004 to 2007 and retrospectively identified 8,967 schizophrenic patients who underwent major inpatient surgery and were hospitalized for more than one day. Primary outcomes included acute myocardial infarction, acute renal failure, stroke, and in-hospital mortality within 30 days. Postoperative complications and mortality rates were compared between schizophrenic patients and patients without mental illness.
Schizophrenic patients had higher rates of many primary outcomes, including 30-day postoperative mortality, compared with patients without mental illness, after adjusting for sex, age, surgery type, and hospital setting. The risk for 30-day mortality rose with the number of preoperative schizophrenia-related services provided. Limitations include the nature of retrospective analysis and generalizability.
Bottom line: Compared to patients without mental illness, schizophrenic patients have an increased risk of acute renal failure, pneumonia, septicemia, and 30-day mortality in the postoperative setting, with higher mortality rates in schizophrenic patients with more severe disease.
Citation: Liao CC, Shen WW, Chang CC, Chang H, Chen T. Surgical adverse outcomes in patients with schizophrenia. Ann Surg. 2013;257:433-438.
Observation Status Designation in Pediatric Hospitals Is Costly

Clinical question: What are the costs associated with observation-status hospital stays compared to inpatient-status stays in pediatric hospitals?
Background: Observation status is a designation for hospitalizations that are typically shorter than 48 hours and do not meet criteria for inpatient status. It is considered to be outpatient for evaluation and management (E/M) coding. A designation of observation status for a hospital stay can have significant effects on out-of-pocket costs for patients and reimbursements to physicians and hospitals. It also can affect readmission and length-of-stay data, as observation-status hospital stays are often excluded from a hospital’s inpatient data.
Study design: Multicenter retrospective cohort study.
Setting: Thirty-three freestanding children’s hospitals.
Synopsis: Researchers reviewed data obtained from the Pediatric Health Information System (PHIS), which contains demographic and resource utilization date from 43 freestanding children’s hospitals in the U.S. Resource utilization data were reviewed from 33 of 43 hospitals in PHIS that reported data regarding observation- versus inpatient-status stays. Data were then limited to observation-status stays £2 days, which made up 97.8% of all observation-status stays. These were then compared to a corresponding cohort of inpatient-status stays of £2 days (47.5% of inpatient-status stays), excluding any patient who had spent time in an ICU.
Hospitalization costs were analyzed and separated into room and nonroom costs, as well as in aggregate. These were further subdivided into costs for four common diagnoses (asthma, gastroenteritis, bronchiolitis, and seizure) and were risk-adjusted.
Observation status was used variably between hospitals (2% to 45%) and within hospitals. There was significant overlap in costs of observation-status and inpatient-status stays, which persisted when accounting for nonroom costs and within the diagnosis subgroups. Although average severity-adjusted costs for observation-status stays were consistently less than those for inpatient-status stays, the dollar amounts were small.
Bottom line: Observation-status designation is used inconsistently in pediatric hospitals, and their costs overlap substantially with inpatient-status stays.
Citation: Fieldston ES, Shah SS, Hall M. Resource utilization for observation-status stays at children’s hospitals. Pediatrics. 2013;131;1050-1058.
Reviewed by Pediatric Editor Weijen Chang, MD, SFHM, FACP, associate clinical professor of medicine and pediatrics at the University of California at San Diego School of Medicine, and a hospitalist at both UCSD Medical Center and Rady Children’s Hospital.
Clinical question: What are the costs associated with observation-status hospital stays compared to inpatient-status stays in pediatric hospitals?
Background: Observation status is a designation for hospitalizations that are typically shorter than 48 hours and do not meet criteria for inpatient status. It is considered to be outpatient for evaluation and management (E/M) coding. A designation of observation status for a hospital stay can have significant effects on out-of-pocket costs for patients and reimbursements to physicians and hospitals. It also can affect readmission and length-of-stay data, as observation-status hospital stays are often excluded from a hospital’s inpatient data.
Study design: Multicenter retrospective cohort study.
Setting: Thirty-three freestanding children’s hospitals.
Synopsis: Researchers reviewed data obtained from the Pediatric Health Information System (PHIS), which contains demographic and resource utilization date from 43 freestanding children’s hospitals in the U.S. Resource utilization data were reviewed from 33 of 43 hospitals in PHIS that reported data regarding observation- versus inpatient-status stays. Data were then limited to observation-status stays £2 days, which made up 97.8% of all observation-status stays. These were then compared to a corresponding cohort of inpatient-status stays of £2 days (47.5% of inpatient-status stays), excluding any patient who had spent time in an ICU.
Hospitalization costs were analyzed and separated into room and nonroom costs, as well as in aggregate. These were further subdivided into costs for four common diagnoses (asthma, gastroenteritis, bronchiolitis, and seizure) and were risk-adjusted.
Observation status was used variably between hospitals (2% to 45%) and within hospitals. There was significant overlap in costs of observation-status and inpatient-status stays, which persisted when accounting for nonroom costs and within the diagnosis subgroups. Although average severity-adjusted costs for observation-status stays were consistently less than those for inpatient-status stays, the dollar amounts were small.
Bottom line: Observation-status designation is used inconsistently in pediatric hospitals, and their costs overlap substantially with inpatient-status stays.
Citation: Fieldston ES, Shah SS, Hall M. Resource utilization for observation-status stays at children’s hospitals. Pediatrics. 2013;131;1050-1058.
Reviewed by Pediatric Editor Weijen Chang, MD, SFHM, FACP, associate clinical professor of medicine and pediatrics at the University of California at San Diego School of Medicine, and a hospitalist at both UCSD Medical Center and Rady Children’s Hospital.
Clinical question: What are the costs associated with observation-status hospital stays compared to inpatient-status stays in pediatric hospitals?
Background: Observation status is a designation for hospitalizations that are typically shorter than 48 hours and do not meet criteria for inpatient status. It is considered to be outpatient for evaluation and management (E/M) coding. A designation of observation status for a hospital stay can have significant effects on out-of-pocket costs for patients and reimbursements to physicians and hospitals. It also can affect readmission and length-of-stay data, as observation-status hospital stays are often excluded from a hospital’s inpatient data.
Study design: Multicenter retrospective cohort study.
Setting: Thirty-three freestanding children’s hospitals.
Synopsis: Researchers reviewed data obtained from the Pediatric Health Information System (PHIS), which contains demographic and resource utilization date from 43 freestanding children’s hospitals in the U.S. Resource utilization data were reviewed from 33 of 43 hospitals in PHIS that reported data regarding observation- versus inpatient-status stays. Data were then limited to observation-status stays £2 days, which made up 97.8% of all observation-status stays. These were then compared to a corresponding cohort of inpatient-status stays of £2 days (47.5% of inpatient-status stays), excluding any patient who had spent time in an ICU.
Hospitalization costs were analyzed and separated into room and nonroom costs, as well as in aggregate. These were further subdivided into costs for four common diagnoses (asthma, gastroenteritis, bronchiolitis, and seizure) and were risk-adjusted.
Observation status was used variably between hospitals (2% to 45%) and within hospitals. There was significant overlap in costs of observation-status and inpatient-status stays, which persisted when accounting for nonroom costs and within the diagnosis subgroups. Although average severity-adjusted costs for observation-status stays were consistently less than those for inpatient-status stays, the dollar amounts were small.
Bottom line: Observation-status designation is used inconsistently in pediatric hospitals, and their costs overlap substantially with inpatient-status stays.
Citation: Fieldston ES, Shah SS, Hall M. Resource utilization for observation-status stays at children’s hospitals. Pediatrics. 2013;131;1050-1058.
Reviewed by Pediatric Editor Weijen Chang, MD, SFHM, FACP, associate clinical professor of medicine and pediatrics at the University of California at San Diego School of Medicine, and a hospitalist at both UCSD Medical Center and Rady Children’s Hospital.