User login
Losing a feisty – but grateful – patient
I’d known Jerry for over a year. When I first met him it was because he had gotten admitted with fevers and an elevation in his erythrocyte sedimentation rate. In the absence of an obvious infectious cause, I was called to see him.
He was such a character. His intelligence was evident. The day that I met him he told me that he was a retired journalist, and that he planned to write a book. His subject was to be one of the presidents, as he had a real interest in history. I particularly enjoyed hearing his "This I Believe" essay on Rhode Island’s National Public Radio about how people these days get so attached to material things, and how far removed this reality is from how he grew up.
He was feisty and opinionated. He, like many other elderly men, thought he knew best, and told everyone – doctors, nurses, his wife – how to do their jobs. He fired his primary care doctor because the doctor told him he couldn’t drive anymore. He stopped his Coumadin because he established, "after applying the scientific method" (i.e., having rechallenged himself with it), that it caused severe pruritis that he just was not willing to put up with.
In the winter of 2012, he developed what seemed to be new-onset Raynaud’s, coincident with a worsening of his thrombocytopenia and anemia. His blood pressure was too low for him to tolerate a calcium channel blocker. I suggested sildenafil, but it was not until mid-June that he came to me asking to be put on it because the condition had progressed quite rapidly, he had developed ulcerations, and he was in a lot of pain. By then we knew about the non-Hodgkin’s lymphoma on top of his preexisting myelodysplastic syndrome, and he was about to get a second opinion about getting a second bone-marrow biopsy at Dana-Farber Cancer Institute.
After the inevitable battle for insurance coverage, we managed to get the sildenafil approved for him, and it made such a huge difference that on July 26, he wrote me, by snail mail, a letter of gratitude: "The lesions are slowly vanishing, the ailing fingernails are taking deeper breaths and thickening, the fingertips are getting firmer. Your compassion, skill, and determination to aid your patients have defeated dis-ease." No doubt he really meant dis-ease, as he repeated the unusual formulation later on. He had such a way with words.
"I looked forward to another winter here with horror. But, thanks to your determination to help ... I am canceling my plans to escape to Florida."
He ended the letter with an invitation to take me to my favorite dim sum restaurant in Providence that I had recommended to him and that he liked as much as I did. He planned on taking me there in mid-August. "I don’t believe that Hippocrates would scorn such an invitation. Let me show off my fingers!"
This was not the first time that he’d invited me to dim sum, but it was the first time that I actually considered accepting the offer, having been granted imaginary permission by Hippocrates.
Jerry passed away on Aug. 1. I was too late for dim sum.
"My soul is from elsewhere, I am sure of that. And I intend to end up there." –Rumi
Dr. Chan practices rheumatology in Pawtucket, R.I.
I’d known Jerry for over a year. When I first met him it was because he had gotten admitted with fevers and an elevation in his erythrocyte sedimentation rate. In the absence of an obvious infectious cause, I was called to see him.
He was such a character. His intelligence was evident. The day that I met him he told me that he was a retired journalist, and that he planned to write a book. His subject was to be one of the presidents, as he had a real interest in history. I particularly enjoyed hearing his "This I Believe" essay on Rhode Island’s National Public Radio about how people these days get so attached to material things, and how far removed this reality is from how he grew up.
He was feisty and opinionated. He, like many other elderly men, thought he knew best, and told everyone – doctors, nurses, his wife – how to do their jobs. He fired his primary care doctor because the doctor told him he couldn’t drive anymore. He stopped his Coumadin because he established, "after applying the scientific method" (i.e., having rechallenged himself with it), that it caused severe pruritis that he just was not willing to put up with.
In the winter of 2012, he developed what seemed to be new-onset Raynaud’s, coincident with a worsening of his thrombocytopenia and anemia. His blood pressure was too low for him to tolerate a calcium channel blocker. I suggested sildenafil, but it was not until mid-June that he came to me asking to be put on it because the condition had progressed quite rapidly, he had developed ulcerations, and he was in a lot of pain. By then we knew about the non-Hodgkin’s lymphoma on top of his preexisting myelodysplastic syndrome, and he was about to get a second opinion about getting a second bone-marrow biopsy at Dana-Farber Cancer Institute.
After the inevitable battle for insurance coverage, we managed to get the sildenafil approved for him, and it made such a huge difference that on July 26, he wrote me, by snail mail, a letter of gratitude: "The lesions are slowly vanishing, the ailing fingernails are taking deeper breaths and thickening, the fingertips are getting firmer. Your compassion, skill, and determination to aid your patients have defeated dis-ease." No doubt he really meant dis-ease, as he repeated the unusual formulation later on. He had such a way with words.
"I looked forward to another winter here with horror. But, thanks to your determination to help ... I am canceling my plans to escape to Florida."
He ended the letter with an invitation to take me to my favorite dim sum restaurant in Providence that I had recommended to him and that he liked as much as I did. He planned on taking me there in mid-August. "I don’t believe that Hippocrates would scorn such an invitation. Let me show off my fingers!"
This was not the first time that he’d invited me to dim sum, but it was the first time that I actually considered accepting the offer, having been granted imaginary permission by Hippocrates.
Jerry passed away on Aug. 1. I was too late for dim sum.
"My soul is from elsewhere, I am sure of that. And I intend to end up there." –Rumi
Dr. Chan practices rheumatology in Pawtucket, R.I.
I’d known Jerry for over a year. When I first met him it was because he had gotten admitted with fevers and an elevation in his erythrocyte sedimentation rate. In the absence of an obvious infectious cause, I was called to see him.
He was such a character. His intelligence was evident. The day that I met him he told me that he was a retired journalist, and that he planned to write a book. His subject was to be one of the presidents, as he had a real interest in history. I particularly enjoyed hearing his "This I Believe" essay on Rhode Island’s National Public Radio about how people these days get so attached to material things, and how far removed this reality is from how he grew up.
He was feisty and opinionated. He, like many other elderly men, thought he knew best, and told everyone – doctors, nurses, his wife – how to do their jobs. He fired his primary care doctor because the doctor told him he couldn’t drive anymore. He stopped his Coumadin because he established, "after applying the scientific method" (i.e., having rechallenged himself with it), that it caused severe pruritis that he just was not willing to put up with.
In the winter of 2012, he developed what seemed to be new-onset Raynaud’s, coincident with a worsening of his thrombocytopenia and anemia. His blood pressure was too low for him to tolerate a calcium channel blocker. I suggested sildenafil, but it was not until mid-June that he came to me asking to be put on it because the condition had progressed quite rapidly, he had developed ulcerations, and he was in a lot of pain. By then we knew about the non-Hodgkin’s lymphoma on top of his preexisting myelodysplastic syndrome, and he was about to get a second opinion about getting a second bone-marrow biopsy at Dana-Farber Cancer Institute.
After the inevitable battle for insurance coverage, we managed to get the sildenafil approved for him, and it made such a huge difference that on July 26, he wrote me, by snail mail, a letter of gratitude: "The lesions are slowly vanishing, the ailing fingernails are taking deeper breaths and thickening, the fingertips are getting firmer. Your compassion, skill, and determination to aid your patients have defeated dis-ease." No doubt he really meant dis-ease, as he repeated the unusual formulation later on. He had such a way with words.
"I looked forward to another winter here with horror. But, thanks to your determination to help ... I am canceling my plans to escape to Florida."
He ended the letter with an invitation to take me to my favorite dim sum restaurant in Providence that I had recommended to him and that he liked as much as I did. He planned on taking me there in mid-August. "I don’t believe that Hippocrates would scorn such an invitation. Let me show off my fingers!"
This was not the first time that he’d invited me to dim sum, but it was the first time that I actually considered accepting the offer, having been granted imaginary permission by Hippocrates.
Jerry passed away on Aug. 1. I was too late for dim sum.
"My soul is from elsewhere, I am sure of that. And I intend to end up there." –Rumi
Dr. Chan practices rheumatology in Pawtucket, R.I.

The new trainee curriculum arrives
Much anticipated by many, exciting to the tech-savvy among us, and unbeknownst to others, yet equally relevant to all: The new curriculum is here. Whether you are a trainee, an educator, or a thoracic surgeon interested in the future of our specialty, the unveiling of the new curriculum is of key significance.
In 1992, at the Joint Conference on Graduate Education in Thoracic Surgery, significant emphasis was placed upon curricular change for thoracic surgical education. In response, the Thoracic Surgery Directors Association (TSDA) initiated the comprehensive thoracic surgery curriculum project in order to develop a consensus as to the content that ought to be learned during thoracic surgical training. Published in 1994, and available online, the TSDA Curriculum was intended to serve as a study guide to individual trainees and a useful resource for Program Directors. While of enormous utility over the last 2 decades, the curriculum is getting a makeover.

Being released this July is a brand-new curriculum, with updated topics and an excitingly novel platform, as a collaborative project from several organizations committed to thoracic surgical education. The Joint Council on Thoracic Surgery Education (JCTSE) has been working closely with the TSDA, with significant input from the American Board of Thoracic Surgery (ABTS), the Society of Thoracic Surgeons (STS), and the Residency Review Committee (RRC) for Thoracic Surgery. Dr. Ara Vaporciyan, Program Director at the University of Texas MD Anderson Cancer Center and 2013 Secretary/Treasurer of the TSDA, has been a key player in the development of the new curriculum.
When asked about the impetus for developing a new curriculum, Dr. Vaporciyan acknowledges that the old curriculum was an enormous advantage when first introduced, but that, now, it is somewhat outdated, and, further, new technology allows us to deliver the content better and more efficiently. Further, Dr. Vaporciyan highlights the valuable aspect of the new curriculum that links its content to expectations of the ABTS for board certification and the requirements of the Accreditation Council for Graduate Medical Education (ACGME) Milestones project.
Similar to the old curriculum, the basic architecture of the new curriculum contains 88-90 separate topics. However, within the new curriculum, the topics have been selected to cover each element of the published learning objectives provided by the ABTS.
Specific topics were identified by appointed section editors (Cardiac: Drs. James Fann and Craig Baker, Thoracic: DRs. Stephen Yang and Ara Vaporciyan, Congenital: Drs. Ram Subramanyan and Winfield Wells). Approximately 20 topic editors from all over the country have helped populate the new curriculum with content, and have additionally provided some input toward the division of topics.
For many, the most exciting feature of the new curriculum relates to the way that the educational materials will be delivered. Using WebBrain software (TheBrain, Los Angeles) for content management, all topics are organized like a mind map. For example, on the main tree, one can click on Thoracic Surgery, then neoplasm of the lung, which then explodes into three related topics: medical knowledge, patient care, and technical skills, which each branch out further. As explained by Dr. Vaporciyan, "the learning objectives of the ABTS provide the structure of the tree – its trunk and main branches – while the content components, provided by the topic editors, serve as the leaves on the ends of the branches."
So what exactly makes up those leaves at the end of the branches? The multi-media material is 100% pre-existing, coming from six different textbooks, up-to-date literature, online presentations created by the TSDA, and societal guidelines. In addition to the WebBrain content management system, the new curriculum utilizes a Moodle-based (Moodle Pty. Ltd., Perth, Australia) platform for organizing specific lessons plans and weekly curricular goals. Moodle (modular object-oriented dynamic learning environment) is an e-learning software platform, also known as a virtual learning environment.
With features such as assignment submission, quiz completion, discussion forums, file download capabilities, and opportunities for instructors to track individual trainee use, the potential opportunities for future growth are enormous. Within the new TSDA curriculum, trainees will receive a weekly email (as they have with the previous version of the curriculum). This email will direct them to a Moodle course for that week, such as "cardiac disease 1," which will provide to direct links within the WebBrain to all of the topics expected to be covered that week, ultimately providing access to the relevant multi-media materials. Once one has accessed the WebBrain, he or she can surf anywhere within the content tree.
The curriculum will be released in two phases. Phase I entails releasing the content which has been populated onto the WebBrain, utilizing Moodle as the access point. Phase II, which is expected to occur over the coming year, will include a more robust Moodle site. These courses will be fleshed out to each include a multiple-choice quiz with feedback, a wiki page, opportunities for commentary, and a means of gathering feedback from end-users regarding the curriculum. Access to these courses will be free of charge to thoracic surgical residents in the United States and Canada, as well as to program coordinators and faculty. Graduating residents will have access for 1 additional year in order to use the curriculum as a tool to prepare for Boards.
Dr. Edward Verrier, JCTSE Surgical Director of Education, explains that "the curriculum revision is a number of years in conception, preparation, organization, and now implementation. It is the combined effort of a number of dedicated educators and societies with some financial support from industry."
Referencing Salman Kahn in The One World Schoolhouse: Education Reimagined, Dr. Verrier continues: "We believe that this educational tool, using both a learning management and content management electronic based platform, has the potential to ‘flip the classroom.’ With work hour restrictions for residents, a constantly increasing body of knowledge, and the challenges of teaching in the operating room, we believe the new Thoracic Surgery Curriculum has the potential to transform our current approach to surgical education."
So what does this mean for trainees? As stated by Dr. Vaporciyan, "the biggest benefit to the trainees is that, with this content and related quizzes, individuals will have the ability to assess their own needs, have immediate access to relevant content that is free of charge, and, importantly, it is the ABTS intent to ultimately derive the examination material from this new electronic curriculum." Yes, it’s true. The board has agreed that the new curriculum will serve as a template of the content for both the written and oral examinations, making this curriculum the ideal study source for trainees. Dr. John Calhoon, chair of the ABTS, reports that "it is our goal to make sure that we draw questions in the future from the content that is called for in our outline and encompassed by the efforts of this new curriculum’s editors." (And did I mention that it’s free and immediately accessible on the Internet?)
And what about for the educators out there – what does this mean for you? Vaporciyan highlights three key advantages for the teachers: 1) the curriculum is completely malleable, so you can take whatever topic you want your learners to focus upon, and you can add to it or separate topics in any way, such as rotation preparation or linear knowledge acquisition; 2) through learner management aspects of Moodle, you can track all of your learners’ progress; 3) the curriculum is linked to Milestones, which should dramatically assist with meeting this requirement of the ACGME.
As mentioned by Dr. Vaporciyan, the Milestones Project is an important recent endeavor of the ACGME, mandating that all specialty groups develop outcome-based goals for resident performance within the six domains of clinical competence. The milestones will be used by the ACGME to demonstrate accountability of effectiveness of education within ACGME-accredited programs, and, looking ahead, resident performance on milestones will become a source of normative data for the RRC to use in assessing residency programs and facilitating improvements. Linking the new curriculum to milestones will render it a great tool to program directors in ACGME-accredited programs. As explained by Dr. Calhoon, "the RRC is working with the Milestones effort to align the individual curricular modules so that residency training programs will find further synergy and utility in adapting or frankly using the curriculum ‘right off the shelf.’"
When asked about the new curriculum, President of the TSDA Dr. David Fullerton shares with us that "along with the other organizations within our specialty, the TSDA is committed to the education of our residents. The TSDA feels that the consolidation of our specialty’s curricular efforts in this way is a significant advance in thoracic surgical education." Further, Dr. Fullerton acknowledges that the new curriculum "will afford our residents immediate electronic access to important educational materials and will be flexible enough for adaption in individual programs." With gratitude on behalf of the TSDA, Dr. Fullerton congratulates all of the individuals who have contributed to making the Thoracic Surgery Curriculum a reality.
Clearly, this new curriculum has much to offer, for both the teacher and the student. It will be of significant interest to track use and observe associated relationships with subsequent board examination success.
In anticipation of an Aug. 1 launch, notifications regarding accessing the site were provided to residents and program directors via email throughout the month of July. More information on the new curriculum, as well as an introductory video, is found at www.tsda.org/education/thoracic-surgery-curricula.
And we will continue to follow and discuss the new curriculum in these pages of the Residents’ Corner.
Much anticipated by many, exciting to the tech-savvy among us, and unbeknownst to others, yet equally relevant to all: The new curriculum is here. Whether you are a trainee, an educator, or a thoracic surgeon interested in the future of our specialty, the unveiling of the new curriculum is of key significance.
In 1992, at the Joint Conference on Graduate Education in Thoracic Surgery, significant emphasis was placed upon curricular change for thoracic surgical education. In response, the Thoracic Surgery Directors Association (TSDA) initiated the comprehensive thoracic surgery curriculum project in order to develop a consensus as to the content that ought to be learned during thoracic surgical training. Published in 1994, and available online, the TSDA Curriculum was intended to serve as a study guide to individual trainees and a useful resource for Program Directors. While of enormous utility over the last 2 decades, the curriculum is getting a makeover.
Being released this July is a brand-new curriculum, with updated topics and an excitingly novel platform, as a collaborative project from several organizations committed to thoracic surgical education. The Joint Council on Thoracic Surgery Education (JCTSE) has been working closely with the TSDA, with significant input from the American Board of Thoracic Surgery (ABTS), the Society of Thoracic Surgeons (STS), and the Residency Review Committee (RRC) for Thoracic Surgery. Dr. Ara Vaporciyan, Program Director at the University of Texas MD Anderson Cancer Center and 2013 Secretary/Treasurer of the TSDA, has been a key player in the development of the new curriculum.
When asked about the impetus for developing a new curriculum, Dr. Vaporciyan acknowledges that the old curriculum was an enormous advantage when first introduced, but that, now, it is somewhat outdated, and, further, new technology allows us to deliver the content better and more efficiently. Further, Dr. Vaporciyan highlights the valuable aspect of the new curriculum that links its content to expectations of the ABTS for board certification and the requirements of the Accreditation Council for Graduate Medical Education (ACGME) Milestones project.
Similar to the old curriculum, the basic architecture of the new curriculum contains 88-90 separate topics. However, within the new curriculum, the topics have been selected to cover each element of the published learning objectives provided by the ABTS.
Specific topics were identified by appointed section editors (Cardiac: Drs. James Fann and Craig Baker, Thoracic: DRs. Stephen Yang and Ara Vaporciyan, Congenital: Drs. Ram Subramanyan and Winfield Wells). Approximately 20 topic editors from all over the country have helped populate the new curriculum with content, and have additionally provided some input toward the division of topics.
For many, the most exciting feature of the new curriculum relates to the way that the educational materials will be delivered. Using WebBrain software (TheBrain, Los Angeles) for content management, all topics are organized like a mind map. For example, on the main tree, one can click on Thoracic Surgery, then neoplasm of the lung, which then explodes into three related topics: medical knowledge, patient care, and technical skills, which each branch out further. As explained by Dr. Vaporciyan, "the learning objectives of the ABTS provide the structure of the tree – its trunk and main branches – while the content components, provided by the topic editors, serve as the leaves on the ends of the branches."
So what exactly makes up those leaves at the end of the branches? The multi-media material is 100% pre-existing, coming from six different textbooks, up-to-date literature, online presentations created by the TSDA, and societal guidelines. In addition to the WebBrain content management system, the new curriculum utilizes a Moodle-based (Moodle Pty. Ltd., Perth, Australia) platform for organizing specific lessons plans and weekly curricular goals. Moodle (modular object-oriented dynamic learning environment) is an e-learning software platform, also known as a virtual learning environment.
With features such as assignment submission, quiz completion, discussion forums, file download capabilities, and opportunities for instructors to track individual trainee use, the potential opportunities for future growth are enormous. Within the new TSDA curriculum, trainees will receive a weekly email (as they have with the previous version of the curriculum). This email will direct them to a Moodle course for that week, such as "cardiac disease 1," which will provide to direct links within the WebBrain to all of the topics expected to be covered that week, ultimately providing access to the relevant multi-media materials. Once one has accessed the WebBrain, he or she can surf anywhere within the content tree.
The curriculum will be released in two phases. Phase I entails releasing the content which has been populated onto the WebBrain, utilizing Moodle as the access point. Phase II, which is expected to occur over the coming year, will include a more robust Moodle site. These courses will be fleshed out to each include a multiple-choice quiz with feedback, a wiki page, opportunities for commentary, and a means of gathering feedback from end-users regarding the curriculum. Access to these courses will be free of charge to thoracic surgical residents in the United States and Canada, as well as to program coordinators and faculty. Graduating residents will have access for 1 additional year in order to use the curriculum as a tool to prepare for Boards.
Dr. Edward Verrier, JCTSE Surgical Director of Education, explains that "the curriculum revision is a number of years in conception, preparation, organization, and now implementation. It is the combined effort of a number of dedicated educators and societies with some financial support from industry."
Referencing Salman Kahn in The One World Schoolhouse: Education Reimagined, Dr. Verrier continues: "We believe that this educational tool, using both a learning management and content management electronic based platform, has the potential to ‘flip the classroom.’ With work hour restrictions for residents, a constantly increasing body of knowledge, and the challenges of teaching in the operating room, we believe the new Thoracic Surgery Curriculum has the potential to transform our current approach to surgical education."
So what does this mean for trainees? As stated by Dr. Vaporciyan, "the biggest benefit to the trainees is that, with this content and related quizzes, individuals will have the ability to assess their own needs, have immediate access to relevant content that is free of charge, and, importantly, it is the ABTS intent to ultimately derive the examination material from this new electronic curriculum." Yes, it’s true. The board has agreed that the new curriculum will serve as a template of the content for both the written and oral examinations, making this curriculum the ideal study source for trainees. Dr. John Calhoon, chair of the ABTS, reports that "it is our goal to make sure that we draw questions in the future from the content that is called for in our outline and encompassed by the efforts of this new curriculum’s editors." (And did I mention that it’s free and immediately accessible on the Internet?)
And what about for the educators out there – what does this mean for you? Vaporciyan highlights three key advantages for the teachers: 1) the curriculum is completely malleable, so you can take whatever topic you want your learners to focus upon, and you can add to it or separate topics in any way, such as rotation preparation or linear knowledge acquisition; 2) through learner management aspects of Moodle, you can track all of your learners’ progress; 3) the curriculum is linked to Milestones, which should dramatically assist with meeting this requirement of the ACGME.
As mentioned by Dr. Vaporciyan, the Milestones Project is an important recent endeavor of the ACGME, mandating that all specialty groups develop outcome-based goals for resident performance within the six domains of clinical competence. The milestones will be used by the ACGME to demonstrate accountability of effectiveness of education within ACGME-accredited programs, and, looking ahead, resident performance on milestones will become a source of normative data for the RRC to use in assessing residency programs and facilitating improvements. Linking the new curriculum to milestones will render it a great tool to program directors in ACGME-accredited programs. As explained by Dr. Calhoon, "the RRC is working with the Milestones effort to align the individual curricular modules so that residency training programs will find further synergy and utility in adapting or frankly using the curriculum ‘right off the shelf.’"
When asked about the new curriculum, President of the TSDA Dr. David Fullerton shares with us that "along with the other organizations within our specialty, the TSDA is committed to the education of our residents. The TSDA feels that the consolidation of our specialty’s curricular efforts in this way is a significant advance in thoracic surgical education." Further, Dr. Fullerton acknowledges that the new curriculum "will afford our residents immediate electronic access to important educational materials and will be flexible enough for adaption in individual programs." With gratitude on behalf of the TSDA, Dr. Fullerton congratulates all of the individuals who have contributed to making the Thoracic Surgery Curriculum a reality.
Clearly, this new curriculum has much to offer, for both the teacher and the student. It will be of significant interest to track use and observe associated relationships with subsequent board examination success.
In anticipation of an Aug. 1 launch, notifications regarding accessing the site were provided to residents and program directors via email throughout the month of July. More information on the new curriculum, as well as an introductory video, is found at www.tsda.org/education/thoracic-surgery-curricula.
And we will continue to follow and discuss the new curriculum in these pages of the Residents’ Corner.
Much anticipated by many, exciting to the tech-savvy among us, and unbeknownst to others, yet equally relevant to all: The new curriculum is here. Whether you are a trainee, an educator, or a thoracic surgeon interested in the future of our specialty, the unveiling of the new curriculum is of key significance.
In 1992, at the Joint Conference on Graduate Education in Thoracic Surgery, significant emphasis was placed upon curricular change for thoracic surgical education. In response, the Thoracic Surgery Directors Association (TSDA) initiated the comprehensive thoracic surgery curriculum project in order to develop a consensus as to the content that ought to be learned during thoracic surgical training. Published in 1994, and available online, the TSDA Curriculum was intended to serve as a study guide to individual trainees and a useful resource for Program Directors. While of enormous utility over the last 2 decades, the curriculum is getting a makeover.
Being released this July is a brand-new curriculum, with updated topics and an excitingly novel platform, as a collaborative project from several organizations committed to thoracic surgical education. The Joint Council on Thoracic Surgery Education (JCTSE) has been working closely with the TSDA, with significant input from the American Board of Thoracic Surgery (ABTS), the Society of Thoracic Surgeons (STS), and the Residency Review Committee (RRC) for Thoracic Surgery. Dr. Ara Vaporciyan, Program Director at the University of Texas MD Anderson Cancer Center and 2013 Secretary/Treasurer of the TSDA, has been a key player in the development of the new curriculum.
When asked about the impetus for developing a new curriculum, Dr. Vaporciyan acknowledges that the old curriculum was an enormous advantage when first introduced, but that, now, it is somewhat outdated, and, further, new technology allows us to deliver the content better and more efficiently. Further, Dr. Vaporciyan highlights the valuable aspect of the new curriculum that links its content to expectations of the ABTS for board certification and the requirements of the Accreditation Council for Graduate Medical Education (ACGME) Milestones project.
Similar to the old curriculum, the basic architecture of the new curriculum contains 88-90 separate topics. However, within the new curriculum, the topics have been selected to cover each element of the published learning objectives provided by the ABTS.
Specific topics were identified by appointed section editors (Cardiac: Drs. James Fann and Craig Baker, Thoracic: DRs. Stephen Yang and Ara Vaporciyan, Congenital: Drs. Ram Subramanyan and Winfield Wells). Approximately 20 topic editors from all over the country have helped populate the new curriculum with content, and have additionally provided some input toward the division of topics.
For many, the most exciting feature of the new curriculum relates to the way that the educational materials will be delivered. Using WebBrain software (TheBrain, Los Angeles) for content management, all topics are organized like a mind map. For example, on the main tree, one can click on Thoracic Surgery, then neoplasm of the lung, which then explodes into three related topics: medical knowledge, patient care, and technical skills, which each branch out further. As explained by Dr. Vaporciyan, "the learning objectives of the ABTS provide the structure of the tree – its trunk and main branches – while the content components, provided by the topic editors, serve as the leaves on the ends of the branches."
So what exactly makes up those leaves at the end of the branches? The multi-media material is 100% pre-existing, coming from six different textbooks, up-to-date literature, online presentations created by the TSDA, and societal guidelines. In addition to the WebBrain content management system, the new curriculum utilizes a Moodle-based (Moodle Pty. Ltd., Perth, Australia) platform for organizing specific lessons plans and weekly curricular goals. Moodle (modular object-oriented dynamic learning environment) is an e-learning software platform, also known as a virtual learning environment.
With features such as assignment submission, quiz completion, discussion forums, file download capabilities, and opportunities for instructors to track individual trainee use, the potential opportunities for future growth are enormous. Within the new TSDA curriculum, trainees will receive a weekly email (as they have with the previous version of the curriculum). This email will direct them to a Moodle course for that week, such as "cardiac disease 1," which will provide to direct links within the WebBrain to all of the topics expected to be covered that week, ultimately providing access to the relevant multi-media materials. Once one has accessed the WebBrain, he or she can surf anywhere within the content tree.
The curriculum will be released in two phases. Phase I entails releasing the content which has been populated onto the WebBrain, utilizing Moodle as the access point. Phase II, which is expected to occur over the coming year, will include a more robust Moodle site. These courses will be fleshed out to each include a multiple-choice quiz with feedback, a wiki page, opportunities for commentary, and a means of gathering feedback from end-users regarding the curriculum. Access to these courses will be free of charge to thoracic surgical residents in the United States and Canada, as well as to program coordinators and faculty. Graduating residents will have access for 1 additional year in order to use the curriculum as a tool to prepare for Boards.
Dr. Edward Verrier, JCTSE Surgical Director of Education, explains that "the curriculum revision is a number of years in conception, preparation, organization, and now implementation. It is the combined effort of a number of dedicated educators and societies with some financial support from industry."
Referencing Salman Kahn in The One World Schoolhouse: Education Reimagined, Dr. Verrier continues: "We believe that this educational tool, using both a learning management and content management electronic based platform, has the potential to ‘flip the classroom.’ With work hour restrictions for residents, a constantly increasing body of knowledge, and the challenges of teaching in the operating room, we believe the new Thoracic Surgery Curriculum has the potential to transform our current approach to surgical education."
So what does this mean for trainees? As stated by Dr. Vaporciyan, "the biggest benefit to the trainees is that, with this content and related quizzes, individuals will have the ability to assess their own needs, have immediate access to relevant content that is free of charge, and, importantly, it is the ABTS intent to ultimately derive the examination material from this new electronic curriculum." Yes, it’s true. The board has agreed that the new curriculum will serve as a template of the content for both the written and oral examinations, making this curriculum the ideal study source for trainees. Dr. John Calhoon, chair of the ABTS, reports that "it is our goal to make sure that we draw questions in the future from the content that is called for in our outline and encompassed by the efforts of this new curriculum’s editors." (And did I mention that it’s free and immediately accessible on the Internet?)
And what about for the educators out there – what does this mean for you? Vaporciyan highlights three key advantages for the teachers: 1) the curriculum is completely malleable, so you can take whatever topic you want your learners to focus upon, and you can add to it or separate topics in any way, such as rotation preparation or linear knowledge acquisition; 2) through learner management aspects of Moodle, you can track all of your learners’ progress; 3) the curriculum is linked to Milestones, which should dramatically assist with meeting this requirement of the ACGME.
As mentioned by Dr. Vaporciyan, the Milestones Project is an important recent endeavor of the ACGME, mandating that all specialty groups develop outcome-based goals for resident performance within the six domains of clinical competence. The milestones will be used by the ACGME to demonstrate accountability of effectiveness of education within ACGME-accredited programs, and, looking ahead, resident performance on milestones will become a source of normative data for the RRC to use in assessing residency programs and facilitating improvements. Linking the new curriculum to milestones will render it a great tool to program directors in ACGME-accredited programs. As explained by Dr. Calhoon, "the RRC is working with the Milestones effort to align the individual curricular modules so that residency training programs will find further synergy and utility in adapting or frankly using the curriculum ‘right off the shelf.’"
When asked about the new curriculum, President of the TSDA Dr. David Fullerton shares with us that "along with the other organizations within our specialty, the TSDA is committed to the education of our residents. The TSDA feels that the consolidation of our specialty’s curricular efforts in this way is a significant advance in thoracic surgical education." Further, Dr. Fullerton acknowledges that the new curriculum "will afford our residents immediate electronic access to important educational materials and will be flexible enough for adaption in individual programs." With gratitude on behalf of the TSDA, Dr. Fullerton congratulates all of the individuals who have contributed to making the Thoracic Surgery Curriculum a reality.
Clearly, this new curriculum has much to offer, for both the teacher and the student. It will be of significant interest to track use and observe associated relationships with subsequent board examination success.
In anticipation of an Aug. 1 launch, notifications regarding accessing the site were provided to residents and program directors via email throughout the month of July. More information on the new curriculum, as well as an introductory video, is found at www.tsda.org/education/thoracic-surgery-curricula.
And we will continue to follow and discuss the new curriculum in these pages of the Residents’ Corner.

Current recs for JE-VC extended
Japanese encephalitis virus is a leading cause of encephalitis in Asia. The disease is mosquito borne where humans are incidental hosts who do not develop high-enough bloodstream concentrations to infect feeding mosquitoes. Culex tritaeniorhynchus mosquitos, an evening- and nighttime-biting mosquito, is the most important vector for transmission to humans.
Japanese encephalitis (JE) occurs primarily in rural agricultural areas, specifically in areas of rice production using flood irrigation. Although primarily rural, these ecologic conditions can be found near urban areas. Virus transmission is seasonal, with peak incidence in summer and fall. JE occurs throughout most of Asia and parts of the Western Pacific. The largest numbers of cases have been among people traveling to Thailand, followed by China, Indonesia, and the Philippines.
JE is primarily a disease of children in endemic countries, with annual incidences of 5-50 cases per 100,000 children. However, as adult travelers are both greater in number and lack protective antibody, they represent the majority of travel-acquired cases. Between 1973 and 2012, 65 cases of travel-associated JE among persons from nonendemic areas were reported in the literature. There was a median of 1 case per year, with 6 (9%) in children under 17 years of age. Among the six pediatric cases, the median age was 9 years, with a range of 1-11 years. Cases occurred most commonly between June and August, although they were reported year-round.

Symptomatic disease is often severe; however, the majority of cases are asymptomatic. Current estimates are 68,000 cases annually, with case fatality rates of 20%-30%. Thirty percent to 50% of survivors have significant neurologic, cognitive, or behavioral sequelae.
JE-VC, a formalin-inactivated vaccine derived from an attenuated virus strain and propagated in Vero cells, was licensed for use in children beginning at 2 months of age in May 2013. This is the only JE vaccine currently licensed and available in the United States. The JE-VC vaccine, manufactured as IXIARO, was licensed for use in adults in the United States, Europe, and Australia in 2009. The primary immunization series is two doses administered intramuscularly at 0 and 28 days.
The Centers for Disease Control and Prevention Advisory Committee on Immunization Practices (ACIP) reviewed the relevant data for a June 2013 meeting. The working group concluded that the overall risk of JE for most travelers to Asia is very low, but that the risk varies based on destination, duration, season, and activities. Prolonged travel in rural areas with active JE virus transmission may confer risks to travelers that are similar to risks in susceptible resident populations. Shorter-term travelers may still be at risk if their itinerary includes outdoor or nighttime exposure in rural areas during periods of active transmission. Short-term travel restricted to major urban areas confers minimal risk of JE.
ACIP recommendations for adults 17 years of age and older were approved in June 2009, and a booster dose recommendation was approved in February 2011. Recommendations state that health providers who are considering the use of JE vaccines for travelers must weigh the risk of travel-associated JE with the benefits and potential risks of the JE vaccine.
JE is a severe disease with substantial morbidity and mortality, and there is no specific treatment. A safe and effective vaccine is available; however, the vaccine is relatively expensive and the possibility of rare, serious adverse events cannot be excluded. The 2009 and 2011 recommendations for adults included the following:
• Travelers to JE-endemic countries should be advised of the risks of JE disease and the importance of measures to reduce mosquito bites.
• JE vaccine is recommended for travelers who plan to spend a month or longer in endemic areas during the JE virus transmission season.
• JE vaccine should be considered for short-term travelers to endemic areas if they will travel outside of an urban area, and if their activities will increase the risk of JE virus exposure.
• JE vaccine is not recommended for short-term travelers whose visit will be restricted to urban areas or times outside of a well-defined JE virus transmission season.
• If it has been 1 year since the primary series, a booster dose may be given prior to potential JE virus exposure.
• Data on the need for and timing of additional booster doses are not available.
A recommendation to expand the recommended use of JE-VC to children aged 2 months was approved by ACIP in June 2013. Their recommendation was based on the data demonstrating a high rate of seroconversion in children following the two-dose primary series, low rates of serious or systemic adverse events, and the lack of therapy for a serious disease.
In summary, JE-VC is recommended for travelers who plan to spend a month or longer in endemic areas during the JE virus transmission season. This includes long-term travelers, recurrent travelers, or expatriates who will be based in urban areas but are likely to visit endemic rural or agricultural areas during a high-risk season; the vaccine also should be considered for short-term travelers to rural endemic areas during virus transmission season, as well when there are outbreaks.
Dr. Pelton is chief of pediatric infectious disease and also is the coordinator of the maternal-child HIV program at Boston Medical Center. Dr. Pelton said he has attended and received honoraria for Novartis advisory board meetings on vaccines, although JE-VC has not been discussed. E-mail him at [email protected].
Japanese encephalitis (JE) occurs primarily in rural agricultural areas, specifically in areas of rice production using flood irrigation. Although primarily rural, these ecologic conditions can be found near urban areas. Virus transmission is seasonal, with peak incidence in summer and fall. JE occurs throughout most of Asia and parts of the Western Pacific. The largest numbers of cases have been among people traveling to Thailand, followed by China, Indonesia, and the Philippines.
Japanese encephalitis virus is a leading cause of encephalitis in Asia. The disease is mosquito borne where humans are incidental hosts who do not develop high-enough bloodstream concentrations to infect feeding mosquitoes. Culex tritaeniorhynchus mosquitos, an evening- and nighttime-biting mosquito, is the most important vector for transmission to humans.
Japanese encephalitis (JE) occurs primarily in rural agricultural areas, specifically in areas of rice production using flood irrigation. Although primarily rural, these ecologic conditions can be found near urban areas. Virus transmission is seasonal, with peak incidence in summer and fall. JE occurs throughout most of Asia and parts of the Western Pacific. The largest numbers of cases have been among people traveling to Thailand, followed by China, Indonesia, and the Philippines.
JE is primarily a disease of children in endemic countries, with annual incidences of 5-50 cases per 100,000 children. However, as adult travelers are both greater in number and lack protective antibody, they represent the majority of travel-acquired cases. Between 1973 and 2012, 65 cases of travel-associated JE among persons from nonendemic areas were reported in the literature. There was a median of 1 case per year, with 6 (9%) in children under 17 years of age. Among the six pediatric cases, the median age was 9 years, with a range of 1-11 years. Cases occurred most commonly between June and August, although they were reported year-round.
Symptomatic disease is often severe; however, the majority of cases are asymptomatic. Current estimates are 68,000 cases annually, with case fatality rates of 20%-30%. Thirty percent to 50% of survivors have significant neurologic, cognitive, or behavioral sequelae.
JE-VC, a formalin-inactivated vaccine derived from an attenuated virus strain and propagated in Vero cells, was licensed for use in children beginning at 2 months of age in May 2013. This is the only JE vaccine currently licensed and available in the United States. The JE-VC vaccine, manufactured as IXIARO, was licensed for use in adults in the United States, Europe, and Australia in 2009. The primary immunization series is two doses administered intramuscularly at 0 and 28 days.
The Centers for Disease Control and Prevention Advisory Committee on Immunization Practices (ACIP) reviewed the relevant data for a June 2013 meeting. The working group concluded that the overall risk of JE for most travelers to Asia is very low, but that the risk varies based on destination, duration, season, and activities. Prolonged travel in rural areas with active JE virus transmission may confer risks to travelers that are similar to risks in susceptible resident populations. Shorter-term travelers may still be at risk if their itinerary includes outdoor or nighttime exposure in rural areas during periods of active transmission. Short-term travel restricted to major urban areas confers minimal risk of JE.
ACIP recommendations for adults 17 years of age and older were approved in June 2009, and a booster dose recommendation was approved in February 2011. Recommendations state that health providers who are considering the use of JE vaccines for travelers must weigh the risk of travel-associated JE with the benefits and potential risks of the JE vaccine.
JE is a severe disease with substantial morbidity and mortality, and there is no specific treatment. A safe and effective vaccine is available; however, the vaccine is relatively expensive and the possibility of rare, serious adverse events cannot be excluded. The 2009 and 2011 recommendations for adults included the following:
• Travelers to JE-endemic countries should be advised of the risks of JE disease and the importance of measures to reduce mosquito bites.
• JE vaccine is recommended for travelers who plan to spend a month or longer in endemic areas during the JE virus transmission season.
• JE vaccine should be considered for short-term travelers to endemic areas if they will travel outside of an urban area, and if their activities will increase the risk of JE virus exposure.
• JE vaccine is not recommended for short-term travelers whose visit will be restricted to urban areas or times outside of a well-defined JE virus transmission season.
• If it has been 1 year since the primary series, a booster dose may be given prior to potential JE virus exposure.
• Data on the need for and timing of additional booster doses are not available.
A recommendation to expand the recommended use of JE-VC to children aged 2 months was approved by ACIP in June 2013. Their recommendation was based on the data demonstrating a high rate of seroconversion in children following the two-dose primary series, low rates of serious or systemic adverse events, and the lack of therapy for a serious disease.
In summary, JE-VC is recommended for travelers who plan to spend a month or longer in endemic areas during the JE virus transmission season. This includes long-term travelers, recurrent travelers, or expatriates who will be based in urban areas but are likely to visit endemic rural or agricultural areas during a high-risk season; the vaccine also should be considered for short-term travelers to rural endemic areas during virus transmission season, as well when there are outbreaks.
Dr. Pelton is chief of pediatric infectious disease and also is the coordinator of the maternal-child HIV program at Boston Medical Center. Dr. Pelton said he has attended and received honoraria for Novartis advisory board meetings on vaccines, although JE-VC has not been discussed. E-mail him at [email protected].
Japanese encephalitis virus is a leading cause of encephalitis in Asia. The disease is mosquito borne where humans are incidental hosts who do not develop high-enough bloodstream concentrations to infect feeding mosquitoes. Culex tritaeniorhynchus mosquitos, an evening- and nighttime-biting mosquito, is the most important vector for transmission to humans.
Japanese encephalitis (JE) occurs primarily in rural agricultural areas, specifically in areas of rice production using flood irrigation. Although primarily rural, these ecologic conditions can be found near urban areas. Virus transmission is seasonal, with peak incidence in summer and fall. JE occurs throughout most of Asia and parts of the Western Pacific. The largest numbers of cases have been among people traveling to Thailand, followed by China, Indonesia, and the Philippines.
JE is primarily a disease of children in endemic countries, with annual incidences of 5-50 cases per 100,000 children. However, as adult travelers are both greater in number and lack protective antibody, they represent the majority of travel-acquired cases. Between 1973 and 2012, 65 cases of travel-associated JE among persons from nonendemic areas were reported in the literature. There was a median of 1 case per year, with 6 (9%) in children under 17 years of age. Among the six pediatric cases, the median age was 9 years, with a range of 1-11 years. Cases occurred most commonly between June and August, although they were reported year-round.
Symptomatic disease is often severe; however, the majority of cases are asymptomatic. Current estimates are 68,000 cases annually, with case fatality rates of 20%-30%. Thirty percent to 50% of survivors have significant neurologic, cognitive, or behavioral sequelae.
JE-VC, a formalin-inactivated vaccine derived from an attenuated virus strain and propagated in Vero cells, was licensed for use in children beginning at 2 months of age in May 2013. This is the only JE vaccine currently licensed and available in the United States. The JE-VC vaccine, manufactured as IXIARO, was licensed for use in adults in the United States, Europe, and Australia in 2009. The primary immunization series is two doses administered intramuscularly at 0 and 28 days.
The Centers for Disease Control and Prevention Advisory Committee on Immunization Practices (ACIP) reviewed the relevant data for a June 2013 meeting. The working group concluded that the overall risk of JE for most travelers to Asia is very low, but that the risk varies based on destination, duration, season, and activities. Prolonged travel in rural areas with active JE virus transmission may confer risks to travelers that are similar to risks in susceptible resident populations. Shorter-term travelers may still be at risk if their itinerary includes outdoor or nighttime exposure in rural areas during periods of active transmission. Short-term travel restricted to major urban areas confers minimal risk of JE.
ACIP recommendations for adults 17 years of age and older were approved in June 2009, and a booster dose recommendation was approved in February 2011. Recommendations state that health providers who are considering the use of JE vaccines for travelers must weigh the risk of travel-associated JE with the benefits and potential risks of the JE vaccine.
JE is a severe disease with substantial morbidity and mortality, and there is no specific treatment. A safe and effective vaccine is available; however, the vaccine is relatively expensive and the possibility of rare, serious adverse events cannot be excluded. The 2009 and 2011 recommendations for adults included the following:
• Travelers to JE-endemic countries should be advised of the risks of JE disease and the importance of measures to reduce mosquito bites.
• JE vaccine is recommended for travelers who plan to spend a month or longer in endemic areas during the JE virus transmission season.
• JE vaccine should be considered for short-term travelers to endemic areas if they will travel outside of an urban area, and if their activities will increase the risk of JE virus exposure.
• JE vaccine is not recommended for short-term travelers whose visit will be restricted to urban areas or times outside of a well-defined JE virus transmission season.
• If it has been 1 year since the primary series, a booster dose may be given prior to potential JE virus exposure.
• Data on the need for and timing of additional booster doses are not available.
A recommendation to expand the recommended use of JE-VC to children aged 2 months was approved by ACIP in June 2013. Their recommendation was based on the data demonstrating a high rate of seroconversion in children following the two-dose primary series, low rates of serious or systemic adverse events, and the lack of therapy for a serious disease.
In summary, JE-VC is recommended for travelers who plan to spend a month or longer in endemic areas during the JE virus transmission season. This includes long-term travelers, recurrent travelers, or expatriates who will be based in urban areas but are likely to visit endemic rural or agricultural areas during a high-risk season; the vaccine also should be considered for short-term travelers to rural endemic areas during virus transmission season, as well when there are outbreaks.
Dr. Pelton is chief of pediatric infectious disease and also is the coordinator of the maternal-child HIV program at Boston Medical Center. Dr. Pelton said he has attended and received honoraria for Novartis advisory board meetings on vaccines, although JE-VC has not been discussed. E-mail him at [email protected].
Japanese encephalitis (JE) occurs primarily in rural agricultural areas, specifically in areas of rice production using flood irrigation. Although primarily rural, these ecologic conditions can be found near urban areas. Virus transmission is seasonal, with peak incidence in summer and fall. JE occurs throughout most of Asia and parts of the Western Pacific. The largest numbers of cases have been among people traveling to Thailand, followed by China, Indonesia, and the Philippines.
Japanese encephalitis (JE) occurs primarily in rural agricultural areas, specifically in areas of rice production using flood irrigation. Although primarily rural, these ecologic conditions can be found near urban areas. Virus transmission is seasonal, with peak incidence in summer and fall. JE occurs throughout most of Asia and parts of the Western Pacific. The largest numbers of cases have been among people traveling to Thailand, followed by China, Indonesia, and the Philippines.
Health IT coordinator moving on
Upset about the federal government’s meaningful use standards? Don’t take your complaints to Dr. Farzad Mostashari. He’s stepping down from his post as national coordinator for health information technology sometime this fall.
His departure comes as physicians and hospitals are moving toward adoption of Stage 2 of meaningful use, part of the Medicare Electronic Health Record (EHR) incentive program. Dr. Mostashari also has been called to Capitol Hill in recent weeks to field questions from lawmakers on why it is taking so long to make EHR systems talk to one another.

In an e-mail to agency staff on Aug. 6, Health and Human Services Secretary Kathleen Sebelius praised Dr. Mostashari for his work in linking the meaningful use of EHRs to population health goals and laying a "strong foundation" for increasing the interoperability of health records.
Dr. Mostashari, who became national coordinator in 2011, will stay on in his current post for a little while as HHS officials search for a replacement. As for his plans after leaving HHS, Dr. Mostashari said that he’s not sure.
"It is difficult for me to announce that I am leaving," he wrote in an e-mail to staff at the Office of the National Coordinator of Health Information Technology. "I don’t know what I will be doing after I leave public service, but be assured that I will be by your side as we continue to battle for healthcare transformation, cheering you on."
–By Mary Ellen Schneider
On Twitter @MaryEllenNY
Upset about the federal government’s meaningful use standards? Don’t take your complaints to Dr. Farzad Mostashari. He’s stepping down from his post as national coordinator for health information technology sometime this fall.
His departure comes as physicians and hospitals are moving toward adoption of Stage 2 of meaningful use, part of the Medicare Electronic Health Record (EHR) incentive program. Dr. Mostashari also has been called to Capitol Hill in recent weeks to field questions from lawmakers on why it is taking so long to make EHR systems talk to one another.
In an e-mail to agency staff on Aug. 6, Health and Human Services Secretary Kathleen Sebelius praised Dr. Mostashari for his work in linking the meaningful use of EHRs to population health goals and laying a "strong foundation" for increasing the interoperability of health records.
Dr. Mostashari, who became national coordinator in 2011, will stay on in his current post for a little while as HHS officials search for a replacement. As for his plans after leaving HHS, Dr. Mostashari said that he’s not sure.
"It is difficult for me to announce that I am leaving," he wrote in an e-mail to staff at the Office of the National Coordinator of Health Information Technology. "I don’t know what I will be doing after I leave public service, but be assured that I will be by your side as we continue to battle for healthcare transformation, cheering you on."
–By Mary Ellen Schneider
On Twitter @MaryEllenNY
Upset about the federal government’s meaningful use standards? Don’t take your complaints to Dr. Farzad Mostashari. He’s stepping down from his post as national coordinator for health information technology sometime this fall.
His departure comes as physicians and hospitals are moving toward adoption of Stage 2 of meaningful use, part of the Medicare Electronic Health Record (EHR) incentive program. Dr. Mostashari also has been called to Capitol Hill in recent weeks to field questions from lawmakers on why it is taking so long to make EHR systems talk to one another.
In an e-mail to agency staff on Aug. 6, Health and Human Services Secretary Kathleen Sebelius praised Dr. Mostashari for his work in linking the meaningful use of EHRs to population health goals and laying a "strong foundation" for increasing the interoperability of health records.
Dr. Mostashari, who became national coordinator in 2011, will stay on in his current post for a little while as HHS officials search for a replacement. As for his plans after leaving HHS, Dr. Mostashari said that he’s not sure.
"It is difficult for me to announce that I am leaving," he wrote in an e-mail to staff at the Office of the National Coordinator of Health Information Technology. "I don’t know what I will be doing after I leave public service, but be assured that I will be by your side as we continue to battle for healthcare transformation, cheering you on."
–By Mary Ellen Schneider
On Twitter @MaryEllenNY

EHR Report: Reflections from our readers
In response to our request for comments, readers have graciously flooded our inbox with a variety of e-mails full of opinions on electronic health records.
This has been an overwhelmingly positive and educational experience. Through your comments, we have been reminded that health information technology is a field rife with debate. Here, unlike most other areas of medicine, it is still impossible to define a single best practice that can reliably be employed in every EHR implementation.
Although we are convinced that it is the timeliness of the subject matter that actually drives readership, we truly appreciate the personal words of affirmation we receive every month. And though we do try to respond to feedback individually whenever possible, we think it is important to again say thank you to everyone who has cared enough to read and respond. You help us to better navigate the murky waters of electronic health records and help make sure that our comments are grounded in the day-to-day experiences of a wide range of users.

Over thenext few columns (with the permission of the authors), we will be publishing many of the comments we have received. Not surprisingly, the majority of messages discuss negative experiences, with an occasional e-mail that speaks to the benefits of the EHR. The focus has really been on how the transition to electronic health records has changed the physician/patient experience and the efficiencies – or inefficiencies – introduced by the use of EHRs. Many respondents expressed appreciation for the opportunity to vent their frustrations, and this further underscores the need for better, more open discussion on the topic.
One letter that reflects a balanced sentiment, yet captures the overall flavor of the thoughts expressed by our fellow physicians, came from Dr. Marc D. Grobman, a solo family physician in Wilmington, Del. Dr. Grobman adopted Practice Fusion, a free ad-supported EHR that we mentioned in a previous column. He relates his experience before and after the EHR, and how it has affected his practice:
"So let’s start with my routine before EMR [electronic medical records]. I would arrive at the office at 8:30 a.m. after seeing my kids off at the school bus. I would greet my staff and start seeing patients at 9:00 a.m. During the day, messages would pile up in the little basket for me, and I would quickly jot answers to questions or requests and hand them back to my staff between patients. During lunch, I would quickly eat ... and then jump to the mail, sign everything then enter into a Word file for the patient (the poor-man’s EMR) and then bring it to the staff for filing. The filing would often take days to accomplish because, being solo, I have only two other staff members.
"Now my days at the office begin at 7:45 a.m. (after rising at 5:30 a.m. to shower, eat, and check the EMR for prescription renewals, use the Delaware Health Information Network [DHIN] to look for admissions to the local hospitals and download the lab results, H&Ps, consults, radiology reports, and so on) with a grab of incoming faxes off the fax machine. I then race to my desk and turn on the computer and scanner to scan everything. Then I race to upload the material before the patients start at 9:00 a.m. Between patients, or most often at lunch, I answer "Messages" on the EMR, write Rx’s and handle any other things that come up. During lunch I also take time to scan and upload as quickly as possible. Same routine after lunch. Before I go home @ 6 or 7 p.m., I make sure everything is scanned so I can upload after dinner at home. No filing any more for the staff, since I scan and upload everything."
On first glance, Dr. Grobman’s experience seems quite discouraging, as he has seemingly transitioned his job description from physician to staff. He even goes on to admit being "baffled" by trying to find any meaning in meaningful use. But his closing thoughts do not express regret. Instead, he shares this:
"I do like using the EMR. I like being green and not needing paper, files, folders, stickers. ... I do find it worthwhile to have [an electronic] copy of the paper forms I do fill out for prior authorizations or pre-exclusion questions or legal request-just in case, you know, someone on the other end loses it. Is the trade-off worth it? In the end I am just more than slightly positive about this whole process."
This letter does a wonderful job of articulating some of the advantages and irritations of a successful EHR implementation. Dr. Grobman also alludes to another interesting theme: frustration with the meaningful use incentive program. Again, he is not alone here. Some readers, like Dr. Michael Laidlaw of Rocklin, Calif., admit to rejecting the government incentive program altogether. Dr. Laidlaw writes:
"What made me abandon the incentive this year (I qualified for and was reimbursed for stage 1) is when I realized that I spent the first 2-5 minutes of each visit endlessly clicking a bunch of garbage to make all the green lights show up on the [meaningful use] meter. I said to myself: ‘I’m not wasting precious seconds of my life and my patients’ time to ensure some database gets filled with data. I didn’t go into medicine for this. It is not benefiting my patients or me. I hate it.’ I actually refused to take the $10K+ this year. I have even accepted that I would rather be penalized in the future. What is worth the most to me is AUTONOMY."
In reviewing all of the feedback we’ve received, this idea seems to come up again and again. Physicians are willing to accept the time-consuming idiosyncrasies of electronic health records but are offended by the idea of technologic or governmental intrusion into the physician-patient relationship. We will continue to explore this idea in the coming months as we share more reader comments and response to the column.
Dr. Skolnik is associate director of the family medicine residency program at Abington (Pa.) Memorial Hospital and professor of family and community medicine at Temple University, Philadelphia. He is editor in chief of Redi-Reference, a company that creates mobile apps. Dr. Notte practices family medicine and health care informatics at Abington Memorial. They are partners in EHR Practice Consultants. Contact them at [email protected].
In response to our request for comments, readers have graciously flooded our inbox with a variety of e-mails full of opinions on electronic health records.
This has been an overwhelmingly positive and educational experience. Through your comments, we have been reminded that health information technology is a field rife with debate. Here, unlike most other areas of medicine, it is still impossible to define a single best practice that can reliably be employed in every EHR implementation.
Although we are convinced that it is the timeliness of the subject matter that actually drives readership, we truly appreciate the personal words of affirmation we receive every month. And though we do try to respond to feedback individually whenever possible, we think it is important to again say thank you to everyone who has cared enough to read and respond. You help us to better navigate the murky waters of electronic health records and help make sure that our comments are grounded in the day-to-day experiences of a wide range of users.
Over thenext few columns (with the permission of the authors), we will be publishing many of the comments we have received. Not surprisingly, the majority of messages discuss negative experiences, with an occasional e-mail that speaks to the benefits of the EHR. The focus has really been on how the transition to electronic health records has changed the physician/patient experience and the efficiencies – or inefficiencies – introduced by the use of EHRs. Many respondents expressed appreciation for the opportunity to vent their frustrations, and this further underscores the need for better, more open discussion on the topic.
One letter that reflects a balanced sentiment, yet captures the overall flavor of the thoughts expressed by our fellow physicians, came from Dr. Marc D. Grobman, a solo family physician in Wilmington, Del. Dr. Grobman adopted Practice Fusion, a free ad-supported EHR that we mentioned in a previous column. He relates his experience before and after the EHR, and how it has affected his practice:
"So let’s start with my routine before EMR [electronic medical records]. I would arrive at the office at 8:30 a.m. after seeing my kids off at the school bus. I would greet my staff and start seeing patients at 9:00 a.m. During the day, messages would pile up in the little basket for me, and I would quickly jot answers to questions or requests and hand them back to my staff between patients. During lunch, I would quickly eat ... and then jump to the mail, sign everything then enter into a Word file for the patient (the poor-man’s EMR) and then bring it to the staff for filing. The filing would often take days to accomplish because, being solo, I have only two other staff members.
"Now my days at the office begin at 7:45 a.m. (after rising at 5:30 a.m. to shower, eat, and check the EMR for prescription renewals, use the Delaware Health Information Network [DHIN] to look for admissions to the local hospitals and download the lab results, H&Ps, consults, radiology reports, and so on) with a grab of incoming faxes off the fax machine. I then race to my desk and turn on the computer and scanner to scan everything. Then I race to upload the material before the patients start at 9:00 a.m. Between patients, or most often at lunch, I answer "Messages" on the EMR, write Rx’s and handle any other things that come up. During lunch I also take time to scan and upload as quickly as possible. Same routine after lunch. Before I go home @ 6 or 7 p.m., I make sure everything is scanned so I can upload after dinner at home. No filing any more for the staff, since I scan and upload everything."
On first glance, Dr. Grobman’s experience seems quite discouraging, as he has seemingly transitioned his job description from physician to staff. He even goes on to admit being "baffled" by trying to find any meaning in meaningful use. But his closing thoughts do not express regret. Instead, he shares this:
"I do like using the EMR. I like being green and not needing paper, files, folders, stickers. ... I do find it worthwhile to have [an electronic] copy of the paper forms I do fill out for prior authorizations or pre-exclusion questions or legal request-just in case, you know, someone on the other end loses it. Is the trade-off worth it? In the end I am just more than slightly positive about this whole process."
This letter does a wonderful job of articulating some of the advantages and irritations of a successful EHR implementation. Dr. Grobman also alludes to another interesting theme: frustration with the meaningful use incentive program. Again, he is not alone here. Some readers, like Dr. Michael Laidlaw of Rocklin, Calif., admit to rejecting the government incentive program altogether. Dr. Laidlaw writes:
"What made me abandon the incentive this year (I qualified for and was reimbursed for stage 1) is when I realized that I spent the first 2-5 minutes of each visit endlessly clicking a bunch of garbage to make all the green lights show up on the [meaningful use] meter. I said to myself: ‘I’m not wasting precious seconds of my life and my patients’ time to ensure some database gets filled with data. I didn’t go into medicine for this. It is not benefiting my patients or me. I hate it.’ I actually refused to take the $10K+ this year. I have even accepted that I would rather be penalized in the future. What is worth the most to me is AUTONOMY."
In reviewing all of the feedback we’ve received, this idea seems to come up again and again. Physicians are willing to accept the time-consuming idiosyncrasies of electronic health records but are offended by the idea of technologic or governmental intrusion into the physician-patient relationship. We will continue to explore this idea in the coming months as we share more reader comments and response to the column.
Dr. Skolnik is associate director of the family medicine residency program at Abington (Pa.) Memorial Hospital and professor of family and community medicine at Temple University, Philadelphia. He is editor in chief of Redi-Reference, a company that creates mobile apps. Dr. Notte practices family medicine and health care informatics at Abington Memorial. They are partners in EHR Practice Consultants. Contact them at [email protected].
In response to our request for comments, readers have graciously flooded our inbox with a variety of e-mails full of opinions on electronic health records.
This has been an overwhelmingly positive and educational experience. Through your comments, we have been reminded that health information technology is a field rife with debate. Here, unlike most other areas of medicine, it is still impossible to define a single best practice that can reliably be employed in every EHR implementation.
Although we are convinced that it is the timeliness of the subject matter that actually drives readership, we truly appreciate the personal words of affirmation we receive every month. And though we do try to respond to feedback individually whenever possible, we think it is important to again say thank you to everyone who has cared enough to read and respond. You help us to better navigate the murky waters of electronic health records and help make sure that our comments are grounded in the day-to-day experiences of a wide range of users.
Over thenext few columns (with the permission of the authors), we will be publishing many of the comments we have received. Not surprisingly, the majority of messages discuss negative experiences, with an occasional e-mail that speaks to the benefits of the EHR. The focus has really been on how the transition to electronic health records has changed the physician/patient experience and the efficiencies – or inefficiencies – introduced by the use of EHRs. Many respondents expressed appreciation for the opportunity to vent their frustrations, and this further underscores the need for better, more open discussion on the topic.
One letter that reflects a balanced sentiment, yet captures the overall flavor of the thoughts expressed by our fellow physicians, came from Dr. Marc D. Grobman, a solo family physician in Wilmington, Del. Dr. Grobman adopted Practice Fusion, a free ad-supported EHR that we mentioned in a previous column. He relates his experience before and after the EHR, and how it has affected his practice:
"So let’s start with my routine before EMR [electronic medical records]. I would arrive at the office at 8:30 a.m. after seeing my kids off at the school bus. I would greet my staff and start seeing patients at 9:00 a.m. During the day, messages would pile up in the little basket for me, and I would quickly jot answers to questions or requests and hand them back to my staff between patients. During lunch, I would quickly eat ... and then jump to the mail, sign everything then enter into a Word file for the patient (the poor-man’s EMR) and then bring it to the staff for filing. The filing would often take days to accomplish because, being solo, I have only two other staff members.
"Now my days at the office begin at 7:45 a.m. (after rising at 5:30 a.m. to shower, eat, and check the EMR for prescription renewals, use the Delaware Health Information Network [DHIN] to look for admissions to the local hospitals and download the lab results, H&Ps, consults, radiology reports, and so on) with a grab of incoming faxes off the fax machine. I then race to my desk and turn on the computer and scanner to scan everything. Then I race to upload the material before the patients start at 9:00 a.m. Between patients, or most often at lunch, I answer "Messages" on the EMR, write Rx’s and handle any other things that come up. During lunch I also take time to scan and upload as quickly as possible. Same routine after lunch. Before I go home @ 6 or 7 p.m., I make sure everything is scanned so I can upload after dinner at home. No filing any more for the staff, since I scan and upload everything."
On first glance, Dr. Grobman’s experience seems quite discouraging, as he has seemingly transitioned his job description from physician to staff. He even goes on to admit being "baffled" by trying to find any meaning in meaningful use. But his closing thoughts do not express regret. Instead, he shares this:
"I do like using the EMR. I like being green and not needing paper, files, folders, stickers. ... I do find it worthwhile to have [an electronic] copy of the paper forms I do fill out for prior authorizations or pre-exclusion questions or legal request-just in case, you know, someone on the other end loses it. Is the trade-off worth it? In the end I am just more than slightly positive about this whole process."
This letter does a wonderful job of articulating some of the advantages and irritations of a successful EHR implementation. Dr. Grobman also alludes to another interesting theme: frustration with the meaningful use incentive program. Again, he is not alone here. Some readers, like Dr. Michael Laidlaw of Rocklin, Calif., admit to rejecting the government incentive program altogether. Dr. Laidlaw writes:
"What made me abandon the incentive this year (I qualified for and was reimbursed for stage 1) is when I realized that I spent the first 2-5 minutes of each visit endlessly clicking a bunch of garbage to make all the green lights show up on the [meaningful use] meter. I said to myself: ‘I’m not wasting precious seconds of my life and my patients’ time to ensure some database gets filled with data. I didn’t go into medicine for this. It is not benefiting my patients or me. I hate it.’ I actually refused to take the $10K+ this year. I have even accepted that I would rather be penalized in the future. What is worth the most to me is AUTONOMY."
In reviewing all of the feedback we’ve received, this idea seems to come up again and again. Physicians are willing to accept the time-consuming idiosyncrasies of electronic health records but are offended by the idea of technologic or governmental intrusion into the physician-patient relationship. We will continue to explore this idea in the coming months as we share more reader comments and response to the column.
Dr. Skolnik is associate director of the family medicine residency program at Abington (Pa.) Memorial Hospital and professor of family and community medicine at Temple University, Philadelphia. He is editor in chief of Redi-Reference, a company that creates mobile apps. Dr. Notte practices family medicine and health care informatics at Abington Memorial. They are partners in EHR Practice Consultants. Contact them at [email protected].

JOURNAL SCANSummary of Key ArticlesExploring the Role of Metanx® in Diabetic Neuropathy
Summary of Key Articles
Exploring the Role of Metanx® in Diabetic Neuropathy
A supplement to Internal Medicine News. This supplement was sponsored by Nestlé Health Science-Pamlab, Inc.

- Introduction
- Prevalence and Etiology
- Signs and Symptoms
- Disease Progression
- Shortcomings of Available Palliative Prescription Therapies
- Role of Metanx® in Diabetic Neuropathy
- A Randomized Trial of Metanx® in Patients with Type 2 Diabetes and Peripheral Neuropathy
- Efficacy of Metanx® in Treating Peripheral Neuropathy and Increasing Nerve Fiber Density in Zucker Diabetic Fatty Rats
Faculty/Faculty Disclosures
Aaron I. Vinik, MD, PhD
Professor of Medicine/Pathology/Neurobiology
Director of Research and Neuroendocrine Unit
Murray Waitzer Endowed Chair of Diabetes Research
Strelitz Diabetes Center for Endocrine and Metabolic Disorders
Eastern Virginia Medical School
Norfolk, Virginia
Dr Vinik has received compensation from Nestlé Health Science-Pamlab, Inc., for his participation in preparing this supplement.
Vivian Fonseca, MD
Tullis–Tulane Alumni Chair in Diabetes
Professor of Medicine
Chief, Section of Endocrinology
Tulane University School of Medicine
New Orleans, Louisiana
Dr Fonseca reports that he has served as a consultant for Nestlé Health Science-Pamlab, Inc., and has received compensation from Nestlé Health Science-Pamlab, Inc., for his participation in preparing this supplement.
A supplement to Internal Medicine News. This supplement was sponsored by Nestlé Health Science-Pamlab, Inc.
- Introduction
- Prevalence and Etiology
- Signs and Symptoms
- Disease Progression
- Shortcomings of Available Palliative Prescription Therapies
- Role of Metanx® in Diabetic Neuropathy
- A Randomized Trial of Metanx® in Patients with Type 2 Diabetes and Peripheral Neuropathy
- Efficacy of Metanx® in Treating Peripheral Neuropathy and Increasing Nerve Fiber Density in Zucker Diabetic Fatty Rats
Faculty/Faculty Disclosures
Aaron I. Vinik, MD, PhD
Professor of Medicine/Pathology/Neurobiology
Director of Research and Neuroendocrine Unit
Murray Waitzer Endowed Chair of Diabetes Research
Strelitz Diabetes Center for Endocrine and Metabolic Disorders
Eastern Virginia Medical School
Norfolk, Virginia
Dr Vinik has received compensation from Nestlé Health Science-Pamlab, Inc., for his participation in preparing this supplement.
Vivian Fonseca, MD
Tullis–Tulane Alumni Chair in Diabetes
Professor of Medicine
Chief, Section of Endocrinology
Tulane University School of Medicine
New Orleans, Louisiana
Dr Fonseca reports that he has served as a consultant for Nestlé Health Science-Pamlab, Inc., and has received compensation from Nestlé Health Science-Pamlab, Inc., for his participation in preparing this supplement.
A supplement to Internal Medicine News. This supplement was sponsored by Nestlé Health Science-Pamlab, Inc.
- Introduction
- Prevalence and Etiology
- Signs and Symptoms
- Disease Progression
- Shortcomings of Available Palliative Prescription Therapies
- Role of Metanx® in Diabetic Neuropathy
- A Randomized Trial of Metanx® in Patients with Type 2 Diabetes and Peripheral Neuropathy
- Efficacy of Metanx® in Treating Peripheral Neuropathy and Increasing Nerve Fiber Density in Zucker Diabetic Fatty Rats
Faculty/Faculty Disclosures
Aaron I. Vinik, MD, PhD
Professor of Medicine/Pathology/Neurobiology
Director of Research and Neuroendocrine Unit
Murray Waitzer Endowed Chair of Diabetes Research
Strelitz Diabetes Center for Endocrine and Metabolic Disorders
Eastern Virginia Medical School
Norfolk, Virginia
Dr Vinik has received compensation from Nestlé Health Science-Pamlab, Inc., for his participation in preparing this supplement.
Vivian Fonseca, MD
Tullis–Tulane Alumni Chair in Diabetes
Professor of Medicine
Chief, Section of Endocrinology
Tulane University School of Medicine
New Orleans, Louisiana
Dr Fonseca reports that he has served as a consultant for Nestlé Health Science-Pamlab, Inc., and has received compensation from Nestlé Health Science-Pamlab, Inc., for his participation in preparing this supplement.
Summary of Key Articles
Exploring the Role of Metanx® in Diabetic Neuropathy
Summary of Key Articles
Exploring the Role of Metanx® in Diabetic Neuropathy
JOURNAL SCAN Summary of Key ArticlesExploring the Role of Metanx® in Diabetic Neuropathy
Summary of Key Articles
Exploring the Role of Metanx® in Diabetic Neuropathy
A supplement to Family Practice News. This supplement was sponsored by Nestlé Health Science-Pamlab, Inc.

Topics
- Introduction
- Prevalence and Etiology
- Signs and Symptoms
- Disease Progression
- Shortcomings of Available Palliative Prescription Therapies
- Role of Metanx® in Diabetic Neuropathy
- A Randomized Trial of Metanx® in Patients with Type 2 Diabetes and Peripheral Neuropathy
- Efficacy of Metanx® in Treating Peripheral Neuropathy and Increasing Nerve Fiber Density in Zucker Diabetic Fatty Rats
Faculty/Faculty Disclosures
Aaron I. Vinik, MD, PhD
Professor of Medicine/Pathology/Neurobiology
Director of Research and Neuroendocrine Unit
Murray Waitzer Endowed Chair of Diabetes Research
Strelitz Diabetes Center for Endocrine and Metabolic Disorders
Eastern Virginia Medical School
Norfolk, Virginia
Dr Vinik has received compensation from Nestlé Health Science-Pamlab, Inc., for his participation in preparing this supplement.
Vivian Fonseca, MD
Tullis–Tulane Alumni Chair in Diabetes
Professor of Medicine
Chief, Section of Endocrinology
Tulane University School of Medicine
New Orleans, Louisiana
Dr Fonseca reports that he has served as a consultant for Nestlé Health Science-Pamlab, Inc., and has received compensation from Nestlé Health Science-Pamlab, Inc., for his participation in preparing this supplement.
A supplement to Family Practice News. This supplement was sponsored by Nestlé Health Science-Pamlab, Inc.
Topics
- Introduction
- Prevalence and Etiology
- Signs and Symptoms
- Disease Progression
- Shortcomings of Available Palliative Prescription Therapies
- Role of Metanx® in Diabetic Neuropathy
- A Randomized Trial of Metanx® in Patients with Type 2 Diabetes and Peripheral Neuropathy
- Efficacy of Metanx® in Treating Peripheral Neuropathy and Increasing Nerve Fiber Density in Zucker Diabetic Fatty Rats
Faculty/Faculty Disclosures
Aaron I. Vinik, MD, PhD
Professor of Medicine/Pathology/Neurobiology
Director of Research and Neuroendocrine Unit
Murray Waitzer Endowed Chair of Diabetes Research
Strelitz Diabetes Center for Endocrine and Metabolic Disorders
Eastern Virginia Medical School
Norfolk, Virginia
Dr Vinik has received compensation from Nestlé Health Science-Pamlab, Inc., for his participation in preparing this supplement.
Vivian Fonseca, MD
Tullis–Tulane Alumni Chair in Diabetes
Professor of Medicine
Chief, Section of Endocrinology
Tulane University School of Medicine
New Orleans, Louisiana
Dr Fonseca reports that he has served as a consultant for Nestlé Health Science-Pamlab, Inc., and has received compensation from Nestlé Health Science-Pamlab, Inc., for his participation in preparing this supplement.
A supplement to Family Practice News. This supplement was sponsored by Nestlé Health Science-Pamlab, Inc.
Topics
- Introduction
- Prevalence and Etiology
- Signs and Symptoms
- Disease Progression
- Shortcomings of Available Palliative Prescription Therapies
- Role of Metanx® in Diabetic Neuropathy
- A Randomized Trial of Metanx® in Patients with Type 2 Diabetes and Peripheral Neuropathy
- Efficacy of Metanx® in Treating Peripheral Neuropathy and Increasing Nerve Fiber Density in Zucker Diabetic Fatty Rats
Faculty/Faculty Disclosures
Aaron I. Vinik, MD, PhD
Professor of Medicine/Pathology/Neurobiology
Director of Research and Neuroendocrine Unit
Murray Waitzer Endowed Chair of Diabetes Research
Strelitz Diabetes Center for Endocrine and Metabolic Disorders
Eastern Virginia Medical School
Norfolk, Virginia
Dr Vinik has received compensation from Nestlé Health Science-Pamlab, Inc., for his participation in preparing this supplement.
Vivian Fonseca, MD
Tullis–Tulane Alumni Chair in Diabetes
Professor of Medicine
Chief, Section of Endocrinology
Tulane University School of Medicine
New Orleans, Louisiana
Dr Fonseca reports that he has served as a consultant for Nestlé Health Science-Pamlab, Inc., and has received compensation from Nestlé Health Science-Pamlab, Inc., for his participation in preparing this supplement.
Summary of Key Articles
Exploring the Role of Metanx® in Diabetic Neuropathy
Summary of Key Articles
Exploring the Role of Metanx® in Diabetic Neuropathy

JOURNAL SCANSummary of Key ArticlesExploring the Role of Metanx® in Diabetic Neuropathy
Summary of Key Articles
Exploring the Role of Metanx® in Diabetic Neuropathy
A supplement to Clinical Endocrinology News. This supplement was sponsored by Nestlé Health Science-Pamlab, Inc.

Topics
- Introduction
- Prevalence and Etiology
- Signs and Symptoms
- Disease Progression
- Shortcomings of Available Palliative Prescription Therapies
- Role of Metanx® in Diabetic Neuropathy
- A Randomized Trial of Metanx® in Patients with Type 2 Diabetes and Peripheral Neuropathy
- Efficacy of Metanx® in Treating Peripheral Neuropathy and Increasing Nerve Fiber Density in Zucker Diabetic Fatty Rats
Faculty/Faculty Disclosures
Aaron I. Vinik, MD, PhD
Professor of Medicine/Pathology/Neurobiology
Director of Research and Neuroendocrine Unit
Murray Waitzer Endowed Chair of Diabetes Research
Strelitz Diabetes Center for Endocrine and Metabolic Disorders
Eastern Virginia Medical School
Norfolk, Virginia
Dr Vinik has received compensation from Nestlé Health Science-Pamlab, Inc., for his participation in preparing this supplement.
Vivian Fonseca, MD
Tullis–Tulane Alumni Chair in Diabetes
Professor of Medicine
Chief, Section of Endocrinology
Tulane University School of Medicine
New Orleans, Louisiana
Dr Fonseca reports that he has served as a consultant for Nestlé Health Science-Pamlab, Inc., and has received compensation from Nestlé Health Science-Pamlab, Inc., for his participation in preparing this supplement.
A supplement to Clinical Endocrinology News. This supplement was sponsored by Nestlé Health Science-Pamlab, Inc.
Topics
- Introduction
- Prevalence and Etiology
- Signs and Symptoms
- Disease Progression
- Shortcomings of Available Palliative Prescription Therapies
- Role of Metanx® in Diabetic Neuropathy
- A Randomized Trial of Metanx® in Patients with Type 2 Diabetes and Peripheral Neuropathy
- Efficacy of Metanx® in Treating Peripheral Neuropathy and Increasing Nerve Fiber Density in Zucker Diabetic Fatty Rats
Faculty/Faculty Disclosures
Aaron I. Vinik, MD, PhD
Professor of Medicine/Pathology/Neurobiology
Director of Research and Neuroendocrine Unit
Murray Waitzer Endowed Chair of Diabetes Research
Strelitz Diabetes Center for Endocrine and Metabolic Disorders
Eastern Virginia Medical School
Norfolk, Virginia
Dr Vinik has received compensation from Nestlé Health Science-Pamlab, Inc., for his participation in preparing this supplement.
Vivian Fonseca, MD
Tullis–Tulane Alumni Chair in Diabetes
Professor of Medicine
Chief, Section of Endocrinology
Tulane University School of Medicine
New Orleans, Louisiana
Dr Fonseca reports that he has served as a consultant for Nestlé Health Science-Pamlab, Inc., and has received compensation from Nestlé Health Science-Pamlab, Inc., for his participation in preparing this supplement.
A supplement to Clinical Endocrinology News. This supplement was sponsored by Nestlé Health Science-Pamlab, Inc.
Topics
- Introduction
- Prevalence and Etiology
- Signs and Symptoms
- Disease Progression
- Shortcomings of Available Palliative Prescription Therapies
- Role of Metanx® in Diabetic Neuropathy
- A Randomized Trial of Metanx® in Patients with Type 2 Diabetes and Peripheral Neuropathy
- Efficacy of Metanx® in Treating Peripheral Neuropathy and Increasing Nerve Fiber Density in Zucker Diabetic Fatty Rats
Faculty/Faculty Disclosures
Aaron I. Vinik, MD, PhD
Professor of Medicine/Pathology/Neurobiology
Director of Research and Neuroendocrine Unit
Murray Waitzer Endowed Chair of Diabetes Research
Strelitz Diabetes Center for Endocrine and Metabolic Disorders
Eastern Virginia Medical School
Norfolk, Virginia
Dr Vinik has received compensation from Nestlé Health Science-Pamlab, Inc., for his participation in preparing this supplement.
Vivian Fonseca, MD
Tullis–Tulane Alumni Chair in Diabetes
Professor of Medicine
Chief, Section of Endocrinology
Tulane University School of Medicine
New Orleans, Louisiana
Dr Fonseca reports that he has served as a consultant for Nestlé Health Science-Pamlab, Inc., and has received compensation from Nestlé Health Science-Pamlab, Inc., for his participation in preparing this supplement.
Summary of Key Articles
Exploring the Role of Metanx® in Diabetic Neuropathy
Summary of Key Articles
Exploring the Role of Metanx® in Diabetic Neuropathy

More than a document: The importance of the informed consent process
In a recent issue of JAMA Surgery, Dr. Jacqueline M. Garonzik-Wang and colleagues presented the results of an important study of missing surgical consent forms at Johns Hopkins Hospital. The authors tallied the absence of a surgical consent form in a patient’s medical record and the resulting delays and other impacts on the surgical services. The authors also surveyed nurses, surgical residents, and surgical faculty regarding their satisfaction with the informed consent process. The results of the study show that cases are often delayed and surgical residents are often pulled away from other activities (e.g., educational conferences) to have new consent forms signed in the preoperative area. In addition, both faculty and residents had concerns about residents obtaining informed consent for major elective procedures.
This is undoubtedly an important study in that it casts light upon an important source of delays and dissatisfaction in the preoperative setting. However, are there additional lessons about informed consent that might be gleaned from this type of analysis?
Moving beyond the study itself, other important issues arise. Consider a patient who comes to the office for evaluation of a symptomatic hernia. Once the surgeon decides that the operation is indicated, the consent process requires a description of the indications (benefits), risks, and alternatives for the patient. Even though the surgeon may be convinced that the benefits of the operation outweigh the risks, the patient still needs to be convinced. Depending on the patient and the procedure being recommended, the time necessary to explain the above to the patient so that he or she is adequately informed and willing to sign the consent form will vary greatly.
In contemporary surgical practice, the determination of when the patient has been adequately informed is made by the patient. At the point that he or she is comfortable enough with the recommendation to proceed to an operation, the informed consent process has reached its conclusion. Only at this point, is the informed consent form even relevant to the discussion. The patient’s signature on the informed consent form is designed to signify the conclusion of the informed consent process.
Although we often mix the signature on the form with the process itself, they are, in fact, markedly different. The informed consent process is an ethical requirement; whereas the signature on the form is a legal requirement. The fact that these two requirements are different can readily be seen from the Mayo Clinic experience. For years, no informed consent forms were even used at the Mayo Clinic! The discussion of the indications, risks, and alternatives was documented in the surgeon’s notes and the fact that the patient showed up for the elective operation could be taken as the evidence of the adequacy of the informed consent process. Although this practice was acceptable to both surgeons and patients for years, the Clinic ultimately changed its practice in response to federal regulations that require the patient’s signature on an informed consent form.
Certainly, there is nothing inherently wrong with the practice of obtaining a signature from a patient on a consent form at the conclusion of the informed consent process. However, the current emphasis on the form itself has had a tendency for the process to be short changed in favor of getting the signature. The fact that both practicing surgeons and surgeons in training often slip into the habit of referring to the process solely by the form can frequently be seen. How often have we or our colleagues talked about "consenting the patient" when we really mean "obtaining informed consent from a patient"?
The Hopkins study serves to remind us that if we really take the process of obtaining informed consent from surgical patients as ethically important, we must be sure to give it the attention it deserves in our practice. If obtaining informed consent is central to the ethical practice of surgery, then why do we so often depend on the least experienced member of the surgical team to carry out this task right before surgery? Perhaps this practice does not reflect our devaluation of the informed consent process as much as a realization that if a patient scheduled for elective surgery has discussed the operation with the surgeon and has chosen to come to the hospital for the procedure, we can assume that the patient has already had a satisfactory consent process. In this context, the problem of the missing consent form is less an ethical issue than a clerical one that might be solved by eliminating the paper form and depending on technology for a solution.
How might a technological fix help in this situation? Among the possibilities would be to have paper forms signed in the attending surgeon’s office at the time of the informed consent discussion. The form could then be scanned into the electronic medical record. Such an approach should significantly reduce the numbers of missing forms since the electronic version cannot be misplaced. This approach will not, however, solve the problem of the missing consent form if the patient is undecided about surgery when he or she leaves the outpatient visit. In such cases, the patient may not be back to the office or hospital until the day of surgery.
Alternatively, all of the information on the standard informed consent form could be made electronic and after the discussion with the attending surgeon, the electronic version could be signed if the patient is amenable, or printed for the patient to take home if he or she is undecided. If the patient then decides to proceed with surgery, the patient could sign in to a secure website and electronically acknowledge (that is, sign) the electronic consent form. This electronic version could then be reviewed by the preoperative nurse and the patient on the day of surgery. As long as the informed consent process that is dependent on the relationship between the surgeon and patient remains intact, there is no reason why technology might not help us eliminate the problem of the missing consent form.
Garonzik-Wang JM, Brat G, Salazar JH, et al. Missing consent forms in the preoperative area: A single-center assessment of the scope of the problem and its downstream effects. JAMA Surg. Published online July 10, 2013, E1-E4.
Dr. Angelos is an ACS Fellow; the Linda Kohler Anderson Professor of Surgery and Surgical Ethics; chief, endocrine surgery; and associate director of the MacLean Center for Clinical Medical Ethics at the University of Chicago.
In a recent issue of JAMA Surgery, Dr. Jacqueline M. Garonzik-Wang and colleagues presented the results of an important study of missing surgical consent forms at Johns Hopkins Hospital. The authors tallied the absence of a surgical consent form in a patient’s medical record and the resulting delays and other impacts on the surgical services. The authors also surveyed nurses, surgical residents, and surgical faculty regarding their satisfaction with the informed consent process. The results of the study show that cases are often delayed and surgical residents are often pulled away from other activities (e.g., educational conferences) to have new consent forms signed in the preoperative area. In addition, both faculty and residents had concerns about residents obtaining informed consent for major elective procedures.
This is undoubtedly an important study in that it casts light upon an important source of delays and dissatisfaction in the preoperative setting. However, are there additional lessons about informed consent that might be gleaned from this type of analysis?
Moving beyond the study itself, other important issues arise. Consider a patient who comes to the office for evaluation of a symptomatic hernia. Once the surgeon decides that the operation is indicated, the consent process requires a description of the indications (benefits), risks, and alternatives for the patient. Even though the surgeon may be convinced that the benefits of the operation outweigh the risks, the patient still needs to be convinced. Depending on the patient and the procedure being recommended, the time necessary to explain the above to the patient so that he or she is adequately informed and willing to sign the consent form will vary greatly.
In contemporary surgical practice, the determination of when the patient has been adequately informed is made by the patient. At the point that he or she is comfortable enough with the recommendation to proceed to an operation, the informed consent process has reached its conclusion. Only at this point, is the informed consent form even relevant to the discussion. The patient’s signature on the informed consent form is designed to signify the conclusion of the informed consent process.
Although we often mix the signature on the form with the process itself, they are, in fact, markedly different. The informed consent process is an ethical requirement; whereas the signature on the form is a legal requirement. The fact that these two requirements are different can readily be seen from the Mayo Clinic experience. For years, no informed consent forms were even used at the Mayo Clinic! The discussion of the indications, risks, and alternatives was documented in the surgeon’s notes and the fact that the patient showed up for the elective operation could be taken as the evidence of the adequacy of the informed consent process. Although this practice was acceptable to both surgeons and patients for years, the Clinic ultimately changed its practice in response to federal regulations that require the patient’s signature on an informed consent form.
Certainly, there is nothing inherently wrong with the practice of obtaining a signature from a patient on a consent form at the conclusion of the informed consent process. However, the current emphasis on the form itself has had a tendency for the process to be short changed in favor of getting the signature. The fact that both practicing surgeons and surgeons in training often slip into the habit of referring to the process solely by the form can frequently be seen. How often have we or our colleagues talked about "consenting the patient" when we really mean "obtaining informed consent from a patient"?
The Hopkins study serves to remind us that if we really take the process of obtaining informed consent from surgical patients as ethically important, we must be sure to give it the attention it deserves in our practice. If obtaining informed consent is central to the ethical practice of surgery, then why do we so often depend on the least experienced member of the surgical team to carry out this task right before surgery? Perhaps this practice does not reflect our devaluation of the informed consent process as much as a realization that if a patient scheduled for elective surgery has discussed the operation with the surgeon and has chosen to come to the hospital for the procedure, we can assume that the patient has already had a satisfactory consent process. In this context, the problem of the missing consent form is less an ethical issue than a clerical one that might be solved by eliminating the paper form and depending on technology for a solution.
How might a technological fix help in this situation? Among the possibilities would be to have paper forms signed in the attending surgeon’s office at the time of the informed consent discussion. The form could then be scanned into the electronic medical record. Such an approach should significantly reduce the numbers of missing forms since the electronic version cannot be misplaced. This approach will not, however, solve the problem of the missing consent form if the patient is undecided about surgery when he or she leaves the outpatient visit. In such cases, the patient may not be back to the office or hospital until the day of surgery.
Alternatively, all of the information on the standard informed consent form could be made electronic and after the discussion with the attending surgeon, the electronic version could be signed if the patient is amenable, or printed for the patient to take home if he or she is undecided. If the patient then decides to proceed with surgery, the patient could sign in to a secure website and electronically acknowledge (that is, sign) the electronic consent form. This electronic version could then be reviewed by the preoperative nurse and the patient on the day of surgery. As long as the informed consent process that is dependent on the relationship between the surgeon and patient remains intact, there is no reason why technology might not help us eliminate the problem of the missing consent form.
Garonzik-Wang JM, Brat G, Salazar JH, et al. Missing consent forms in the preoperative area: A single-center assessment of the scope of the problem and its downstream effects. JAMA Surg. Published online July 10, 2013, E1-E4.
Dr. Angelos is an ACS Fellow; the Linda Kohler Anderson Professor of Surgery and Surgical Ethics; chief, endocrine surgery; and associate director of the MacLean Center for Clinical Medical Ethics at the University of Chicago.
In a recent issue of JAMA Surgery, Dr. Jacqueline M. Garonzik-Wang and colleagues presented the results of an important study of missing surgical consent forms at Johns Hopkins Hospital. The authors tallied the absence of a surgical consent form in a patient’s medical record and the resulting delays and other impacts on the surgical services. The authors also surveyed nurses, surgical residents, and surgical faculty regarding their satisfaction with the informed consent process. The results of the study show that cases are often delayed and surgical residents are often pulled away from other activities (e.g., educational conferences) to have new consent forms signed in the preoperative area. In addition, both faculty and residents had concerns about residents obtaining informed consent for major elective procedures.
This is undoubtedly an important study in that it casts light upon an important source of delays and dissatisfaction in the preoperative setting. However, are there additional lessons about informed consent that might be gleaned from this type of analysis?
Moving beyond the study itself, other important issues arise. Consider a patient who comes to the office for evaluation of a symptomatic hernia. Once the surgeon decides that the operation is indicated, the consent process requires a description of the indications (benefits), risks, and alternatives for the patient. Even though the surgeon may be convinced that the benefits of the operation outweigh the risks, the patient still needs to be convinced. Depending on the patient and the procedure being recommended, the time necessary to explain the above to the patient so that he or she is adequately informed and willing to sign the consent form will vary greatly.
In contemporary surgical practice, the determination of when the patient has been adequately informed is made by the patient. At the point that he or she is comfortable enough with the recommendation to proceed to an operation, the informed consent process has reached its conclusion. Only at this point, is the informed consent form even relevant to the discussion. The patient’s signature on the informed consent form is designed to signify the conclusion of the informed consent process.
Although we often mix the signature on the form with the process itself, they are, in fact, markedly different. The informed consent process is an ethical requirement; whereas the signature on the form is a legal requirement. The fact that these two requirements are different can readily be seen from the Mayo Clinic experience. For years, no informed consent forms were even used at the Mayo Clinic! The discussion of the indications, risks, and alternatives was documented in the surgeon’s notes and the fact that the patient showed up for the elective operation could be taken as the evidence of the adequacy of the informed consent process. Although this practice was acceptable to both surgeons and patients for years, the Clinic ultimately changed its practice in response to federal regulations that require the patient’s signature on an informed consent form.
Certainly, there is nothing inherently wrong with the practice of obtaining a signature from a patient on a consent form at the conclusion of the informed consent process. However, the current emphasis on the form itself has had a tendency for the process to be short changed in favor of getting the signature. The fact that both practicing surgeons and surgeons in training often slip into the habit of referring to the process solely by the form can frequently be seen. How often have we or our colleagues talked about "consenting the patient" when we really mean "obtaining informed consent from a patient"?
The Hopkins study serves to remind us that if we really take the process of obtaining informed consent from surgical patients as ethically important, we must be sure to give it the attention it deserves in our practice. If obtaining informed consent is central to the ethical practice of surgery, then why do we so often depend on the least experienced member of the surgical team to carry out this task right before surgery? Perhaps this practice does not reflect our devaluation of the informed consent process as much as a realization that if a patient scheduled for elective surgery has discussed the operation with the surgeon and has chosen to come to the hospital for the procedure, we can assume that the patient has already had a satisfactory consent process. In this context, the problem of the missing consent form is less an ethical issue than a clerical one that might be solved by eliminating the paper form and depending on technology for a solution.
How might a technological fix help in this situation? Among the possibilities would be to have paper forms signed in the attending surgeon’s office at the time of the informed consent discussion. The form could then be scanned into the electronic medical record. Such an approach should significantly reduce the numbers of missing forms since the electronic version cannot be misplaced. This approach will not, however, solve the problem of the missing consent form if the patient is undecided about surgery when he or she leaves the outpatient visit. In such cases, the patient may not be back to the office or hospital until the day of surgery.
Alternatively, all of the information on the standard informed consent form could be made electronic and after the discussion with the attending surgeon, the electronic version could be signed if the patient is amenable, or printed for the patient to take home if he or she is undecided. If the patient then decides to proceed with surgery, the patient could sign in to a secure website and electronically acknowledge (that is, sign) the electronic consent form. This electronic version could then be reviewed by the preoperative nurse and the patient on the day of surgery. As long as the informed consent process that is dependent on the relationship between the surgeon and patient remains intact, there is no reason why technology might not help us eliminate the problem of the missing consent form.
Garonzik-Wang JM, Brat G, Salazar JH, et al. Missing consent forms in the preoperative area: A single-center assessment of the scope of the problem and its downstream effects. JAMA Surg. Published online July 10, 2013, E1-E4.
Dr. Angelos is an ACS Fellow; the Linda Kohler Anderson Professor of Surgery and Surgical Ethics; chief, endocrine surgery; and associate director of the MacLean Center for Clinical Medical Ethics at the University of Chicago.
What is causing her abdominal pain?
CASE: A healthy, nulliparous, 20-year-old woman visits her ObGyn to report a 2-day history of right lower quadrant pain. Her last menstrual period was appropriately timed and normal. She is not sexually active. Upon examination, she exhibits minimal left and right lower quadrant tenderness. Examination with the vaginal speculum reveals no vaginal or cervical abnormalities, and bimanual examination reveals a uterus of normal size, with cervical motion tenderness but no adnexal fullness or mass. For this reason, transvaginal ultrasound (TVUS) is performed. It reveals an enlarged, edematous appendix adjacent to a normal-appearing right ovary (FIGURE 1).
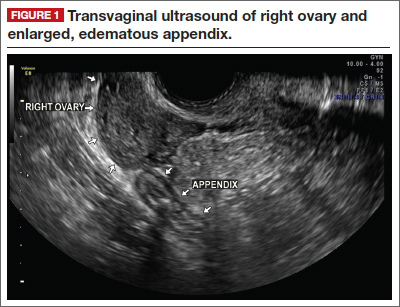
No uterine or ovarian pathology is noted. Because the appendix is enlarged on TVUS, Doppler interrogation is added, which shows abundant vascularity of the appendix (FIGURE 2).
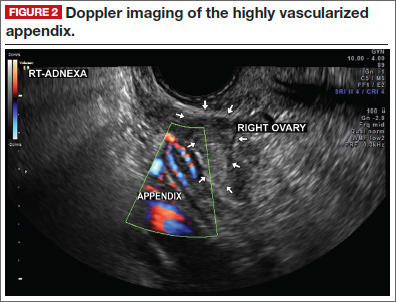
What do these findings suggest?
Acute appendicitis is the most likely diagnosis, as both the physical findings and ultrasound imaging point to it. The patient is referred to a general surgeon, who examines her, noting that she is afebrile, with tenderness in the right lower quadrant. She exhibits localized guarding at McBurneys point, with mild rebound. There is no sign of organomegaly. Bowel sounds are normal, with no distention. The patient undergoes laparoscopy, which confirms the diagnosis. The appendix is resected successfully, and rupture is averted (FIGURE 3).
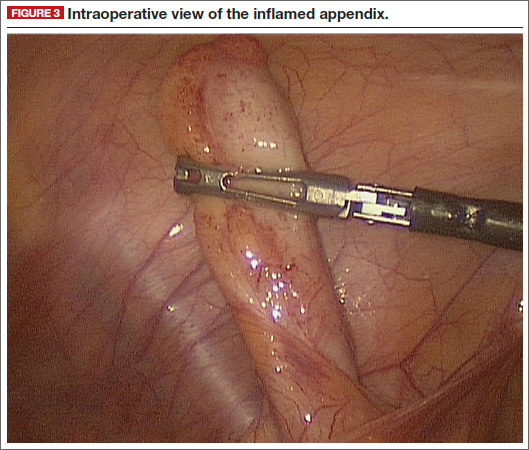
The patient is discharged home on the first postoperative day. At a follow-up visit 2 weeks later, she is fully recovered and has returned to full and normal activity.
Clinicians who are familiar with the appearance of an inflamed appendix on TVUS may be able to expedite the management of women with appendicitis, avoiding the potential delay, expense, and radiation exposure associated with computed tomography imaging of the abdomen and pelvis.
Acknowledgment
The authors are grateful to Grace J. Horton, RDMS, and Christine L. Bubier, AS, RT(R), RDMS, who generated the images in this case.
Do you have a DIAGNOSTIC IN-SIGHT?
Submit a query for your image-based case! [email protected]
CASE: A healthy, nulliparous, 20-year-old woman visits her ObGyn to report a 2-day history of right lower quadrant pain. Her last menstrual period was appropriately timed and normal. She is not sexually active. Upon examination, she exhibits minimal left and right lower quadrant tenderness. Examination with the vaginal speculum reveals no vaginal or cervical abnormalities, and bimanual examination reveals a uterus of normal size, with cervical motion tenderness but no adnexal fullness or mass. For this reason, transvaginal ultrasound (TVUS) is performed. It reveals an enlarged, edematous appendix adjacent to a normal-appearing right ovary (FIGURE 1).
No uterine or ovarian pathology is noted. Because the appendix is enlarged on TVUS, Doppler interrogation is added, which shows abundant vascularity of the appendix (FIGURE 2).
What do these findings suggest?
Acute appendicitis is the most likely diagnosis, as both the physical findings and ultrasound imaging point to it. The patient is referred to a general surgeon, who examines her, noting that she is afebrile, with tenderness in the right lower quadrant. She exhibits localized guarding at McBurneys point, with mild rebound. There is no sign of organomegaly. Bowel sounds are normal, with no distention. The patient undergoes laparoscopy, which confirms the diagnosis. The appendix is resected successfully, and rupture is averted (FIGURE 3).
The patient is discharged home on the first postoperative day. At a follow-up visit 2 weeks later, she is fully recovered and has returned to full and normal activity.
Clinicians who are familiar with the appearance of an inflamed appendix on TVUS may be able to expedite the management of women with appendicitis, avoiding the potential delay, expense, and radiation exposure associated with computed tomography imaging of the abdomen and pelvis.
Acknowledgment
The authors are grateful to Grace J. Horton, RDMS, and Christine L. Bubier, AS, RT(R), RDMS, who generated the images in this case.
Do you have a DIAGNOSTIC IN-SIGHT?
Submit a query for your image-based case! [email protected]
CASE: A healthy, nulliparous, 20-year-old woman visits her ObGyn to report a 2-day history of right lower quadrant pain. Her last menstrual period was appropriately timed and normal. She is not sexually active. Upon examination, she exhibits minimal left and right lower quadrant tenderness. Examination with the vaginal speculum reveals no vaginal or cervical abnormalities, and bimanual examination reveals a uterus of normal size, with cervical motion tenderness but no adnexal fullness or mass. For this reason, transvaginal ultrasound (TVUS) is performed. It reveals an enlarged, edematous appendix adjacent to a normal-appearing right ovary (FIGURE 1).
No uterine or ovarian pathology is noted. Because the appendix is enlarged on TVUS, Doppler interrogation is added, which shows abundant vascularity of the appendix (FIGURE 2).
What do these findings suggest?
Acute appendicitis is the most likely diagnosis, as both the physical findings and ultrasound imaging point to it. The patient is referred to a general surgeon, who examines her, noting that she is afebrile, with tenderness in the right lower quadrant. She exhibits localized guarding at McBurneys point, with mild rebound. There is no sign of organomegaly. Bowel sounds are normal, with no distention. The patient undergoes laparoscopy, which confirms the diagnosis. The appendix is resected successfully, and rupture is averted (FIGURE 3).
The patient is discharged home on the first postoperative day. At a follow-up visit 2 weeks later, she is fully recovered and has returned to full and normal activity.
Clinicians who are familiar with the appearance of an inflamed appendix on TVUS may be able to expedite the management of women with appendicitis, avoiding the potential delay, expense, and radiation exposure associated with computed tomography imaging of the abdomen and pelvis.
Acknowledgment
The authors are grateful to Grace J. Horton, RDMS, and Christine L. Bubier, AS, RT(R), RDMS, who generated the images in this case.
Do you have a DIAGNOSTIC IN-SIGHT?
Submit a query for your image-based case! [email protected]