User login
Contracts Need to Ensure Physicians are Free Agents
Physicians often have medical interests other than clinical practice. A restrictive employment agreement could quash those endeavors. Physician employment agreements play an integral role in establishing the legal, financial, and operational structure of the relationship between employer and physician/employee.
One clause of particular interest to many physicians is the clause defining what a physician can and cannot do outside of providing medical services on behalf of their employer—meaning, can the physician engage in such outside activities as moonlighting, volunteering, or serving as an expert witness? Moreover, if income is generated from these outside activities, who does that income belong to—the physician or the employer?
These questions should be clearly answered in the employment agreement. And if the answers in the employment agreement do not mirror the physician’s wishes, then these terms should be negotiated with the employer and memorialized in the employment agreement.
Consult Your Contract
The first question is whether the physician is even permitted under their employment agreement to participate in activities or perform services outside of employment. Some employers prohibit engagement in outside activities and services altogether, while other employers permit certain activities that do not interfere with the physician’s day-to-day responsibilities. Physicians should be aware of requirements that give the employer the right to approve or reject outside activities. If the physician wants to be able to engage in moonlighting, expert witness consultations and testimony, speaking opportunities, volunteer efforts, teaching, research, or publishing, the physician’s desired activities should be specifically identified in the employment agreement as permitted activities.
For example: Dr. A was joining a medical practice and was presented with the group’s template employment agreement. The draft agreement precluded Dr. A from participating in any medically related outside activities. In the past, Dr. A had served as a volunteer doctor for the local marathon, a medical expert witness, and was a frequent paid speaker at conferences. For Dr. A, a prohibition on outside medical activities did not align with his interests. With minimal discussion, the practice permitted Dr. A to identify the outside activities that he could conduct without violating his employment agreement:
If a physician is permitted to engage in outside activities or services, the second question is whether income generated from such activities belongs to the physician or the employer. This often is a topic of negotiation. Physician and employer frequently do not see eye to eye on this issue. Physicians, on the one hand, often view the income generated from permitted outside activities to be separate and apart from his or her services on behalf of the employer, and thus are outside the reach of the practice. This position is strengthened if the activity occurs on the physician’s own time and outside of the employer’s hours of operation. Employers, on the other hand, often view income from outside activities as part of the employment relationship with the physician. Some employers are of the belief that the physician would not have had the opportunity to participate in the outside activity but for the physician’s employment with the particular employer.
Dr. A’s employer felt that it already was conceding by allowing Dr. A to engage in outside activities and insisted that any payment received by him for these services should be remitted to the practice. Dr. A agreed to this and negotiated for the outside activity monies to be included in his collection amounts, which was a factor in calculating Dr. A’s compensation:
The last question is whether outside activities are covered by the physician’s malpractice insurance policy. If the employer provides the policy for the benefit of the physician, the employer—and the malpractice insurance carrier—may exclude activities performed by the physician outside of his or her employment with that employer. This often is an issue for physicians who want to moonlight, as moonlighting for a third party frequently is excluded from coverage. It is important that the physician consult the malpractice insurance carrier to confirm whether certain activities are covered under the policy. It may be the case that a separate policy is required to insure the physician’s outside activities, even those activities that are unpaid.
Contract clauses describing what the physician can and cannot do outside of the employment relationship are of key importance. These clauses should mirror the individual physician’s medically related and extracurricular interests, and the financial benefits of these activities—if any—should be addressed in the employment agreement. Don’t forget to check with the insurance carrier to ensure that the activity is covered by the policy, as even volunteering medical services could expose a physician. It is best to address these issues at the onset of the employer-employee relationship. That way, all parties are on the same page from the beginning.
Steven Harris is a nationally recognized healthcare attorney and a member of the law firm McDonald Hopkins LLC in Chicago. Write to him at [email protected].
Physicians often have medical interests other than clinical practice. A restrictive employment agreement could quash those endeavors. Physician employment agreements play an integral role in establishing the legal, financial, and operational structure of the relationship between employer and physician/employee.
One clause of particular interest to many physicians is the clause defining what a physician can and cannot do outside of providing medical services on behalf of their employer—meaning, can the physician engage in such outside activities as moonlighting, volunteering, or serving as an expert witness? Moreover, if income is generated from these outside activities, who does that income belong to—the physician or the employer?
These questions should be clearly answered in the employment agreement. And if the answers in the employment agreement do not mirror the physician’s wishes, then these terms should be negotiated with the employer and memorialized in the employment agreement.
Consult Your Contract
The first question is whether the physician is even permitted under their employment agreement to participate in activities or perform services outside of employment. Some employers prohibit engagement in outside activities and services altogether, while other employers permit certain activities that do not interfere with the physician’s day-to-day responsibilities. Physicians should be aware of requirements that give the employer the right to approve or reject outside activities. If the physician wants to be able to engage in moonlighting, expert witness consultations and testimony, speaking opportunities, volunteer efforts, teaching, research, or publishing, the physician’s desired activities should be specifically identified in the employment agreement as permitted activities.
For example: Dr. A was joining a medical practice and was presented with the group’s template employment agreement. The draft agreement precluded Dr. A from participating in any medically related outside activities. In the past, Dr. A had served as a volunteer doctor for the local marathon, a medical expert witness, and was a frequent paid speaker at conferences. For Dr. A, a prohibition on outside medical activities did not align with his interests. With minimal discussion, the practice permitted Dr. A to identify the outside activities that he could conduct without violating his employment agreement:
If a physician is permitted to engage in outside activities or services, the second question is whether income generated from such activities belongs to the physician or the employer. This often is a topic of negotiation. Physician and employer frequently do not see eye to eye on this issue. Physicians, on the one hand, often view the income generated from permitted outside activities to be separate and apart from his or her services on behalf of the employer, and thus are outside the reach of the practice. This position is strengthened if the activity occurs on the physician’s own time and outside of the employer’s hours of operation. Employers, on the other hand, often view income from outside activities as part of the employment relationship with the physician. Some employers are of the belief that the physician would not have had the opportunity to participate in the outside activity but for the physician’s employment with the particular employer.
Dr. A’s employer felt that it already was conceding by allowing Dr. A to engage in outside activities and insisted that any payment received by him for these services should be remitted to the practice. Dr. A agreed to this and negotiated for the outside activity monies to be included in his collection amounts, which was a factor in calculating Dr. A’s compensation:
The last question is whether outside activities are covered by the physician’s malpractice insurance policy. If the employer provides the policy for the benefit of the physician, the employer—and the malpractice insurance carrier—may exclude activities performed by the physician outside of his or her employment with that employer. This often is an issue for physicians who want to moonlight, as moonlighting for a third party frequently is excluded from coverage. It is important that the physician consult the malpractice insurance carrier to confirm whether certain activities are covered under the policy. It may be the case that a separate policy is required to insure the physician’s outside activities, even those activities that are unpaid.
Contract clauses describing what the physician can and cannot do outside of the employment relationship are of key importance. These clauses should mirror the individual physician’s medically related and extracurricular interests, and the financial benefits of these activities—if any—should be addressed in the employment agreement. Don’t forget to check with the insurance carrier to ensure that the activity is covered by the policy, as even volunteering medical services could expose a physician. It is best to address these issues at the onset of the employer-employee relationship. That way, all parties are on the same page from the beginning.
Steven Harris is a nationally recognized healthcare attorney and a member of the law firm McDonald Hopkins LLC in Chicago. Write to him at [email protected].
Physicians often have medical interests other than clinical practice. A restrictive employment agreement could quash those endeavors. Physician employment agreements play an integral role in establishing the legal, financial, and operational structure of the relationship between employer and physician/employee.
One clause of particular interest to many physicians is the clause defining what a physician can and cannot do outside of providing medical services on behalf of their employer—meaning, can the physician engage in such outside activities as moonlighting, volunteering, or serving as an expert witness? Moreover, if income is generated from these outside activities, who does that income belong to—the physician or the employer?
These questions should be clearly answered in the employment agreement. And if the answers in the employment agreement do not mirror the physician’s wishes, then these terms should be negotiated with the employer and memorialized in the employment agreement.
Consult Your Contract
The first question is whether the physician is even permitted under their employment agreement to participate in activities or perform services outside of employment. Some employers prohibit engagement in outside activities and services altogether, while other employers permit certain activities that do not interfere with the physician’s day-to-day responsibilities. Physicians should be aware of requirements that give the employer the right to approve or reject outside activities. If the physician wants to be able to engage in moonlighting, expert witness consultations and testimony, speaking opportunities, volunteer efforts, teaching, research, or publishing, the physician’s desired activities should be specifically identified in the employment agreement as permitted activities.
For example: Dr. A was joining a medical practice and was presented with the group’s template employment agreement. The draft agreement precluded Dr. A from participating in any medically related outside activities. In the past, Dr. A had served as a volunteer doctor for the local marathon, a medical expert witness, and was a frequent paid speaker at conferences. For Dr. A, a prohibition on outside medical activities did not align with his interests. With minimal discussion, the practice permitted Dr. A to identify the outside activities that he could conduct without violating his employment agreement:
If a physician is permitted to engage in outside activities or services, the second question is whether income generated from such activities belongs to the physician or the employer. This often is a topic of negotiation. Physician and employer frequently do not see eye to eye on this issue. Physicians, on the one hand, often view the income generated from permitted outside activities to be separate and apart from his or her services on behalf of the employer, and thus are outside the reach of the practice. This position is strengthened if the activity occurs on the physician’s own time and outside of the employer’s hours of operation. Employers, on the other hand, often view income from outside activities as part of the employment relationship with the physician. Some employers are of the belief that the physician would not have had the opportunity to participate in the outside activity but for the physician’s employment with the particular employer.
Dr. A’s employer felt that it already was conceding by allowing Dr. A to engage in outside activities and insisted that any payment received by him for these services should be remitted to the practice. Dr. A agreed to this and negotiated for the outside activity monies to be included in his collection amounts, which was a factor in calculating Dr. A’s compensation:
The last question is whether outside activities are covered by the physician’s malpractice insurance policy. If the employer provides the policy for the benefit of the physician, the employer—and the malpractice insurance carrier—may exclude activities performed by the physician outside of his or her employment with that employer. This often is an issue for physicians who want to moonlight, as moonlighting for a third party frequently is excluded from coverage. It is important that the physician consult the malpractice insurance carrier to confirm whether certain activities are covered under the policy. It may be the case that a separate policy is required to insure the physician’s outside activities, even those activities that are unpaid.
Contract clauses describing what the physician can and cannot do outside of the employment relationship are of key importance. These clauses should mirror the individual physician’s medically related and extracurricular interests, and the financial benefits of these activities—if any—should be addressed in the employment agreement. Don’t forget to check with the insurance carrier to ensure that the activity is covered by the policy, as even volunteering medical services could expose a physician. It is best to address these issues at the onset of the employer-employee relationship. That way, all parties are on the same page from the beginning.
Steven Harris is a nationally recognized healthcare attorney and a member of the law firm McDonald Hopkins LLC in Chicago. Write to him at [email protected].
Patient Satisfaction Critical to Hospital Value-Based Purchasing Program
Should patient satisfaction factor prominently into healthcare pay-for-performance incentives? That question recently became moot as the Centers for Medicare & Medicaid Services (CMS) began withholding 1% of hospitals’ Medicare reimbursement as part of its Hospital Value-Based Purchasing Program, restoring it to institutions based upon their quality performance. Thirty percent of the program’s financial incentive is based upon how well hospitals score on patient satisfaction, as measured by the Hospital Consumer Assessment of Healthcare Providers and Systems (HCAHPS) survey.
Despite those data having been collected and reported for years, their use as a healthcare performance indicator continues to be controversial. To win back reimbursement withholds, hospitals must earn perfect scores: The only winners are the ones for whom patients respond “always satisfied” to such questions as “How often did doctors treat you with courtesy and respect?” or “How often did doctors explain things in a way you could understand?” or “How often did hospital staff tell you what the medicine was for?”
A perfectly happy patient, skeptics say, isn’t necessarily one who has received the best medical care, and several analyses suggest that HCAHPS has unintended biases, making it a flawed accountability tool. Some of the nation’s most prestigious hospitals, for example, receive bad patient reviews despite getting high scores on clinical quality metrics.1
Conversely, many hospitals that receive high patient ratings have low clinical quality marks (e.g. significantly worse mortality rates than the national average for heart attacks, heart failure, or pneumonia).2
Safety-net hospitals perform more poorly than other hospitals on nearly every HCAHPS measure of patient experience, with gaps that are sizable and persistent. These institutions have the most fragile operating margins and are the least able to absorb the additional reimbursement cuts that will result from their low scores.3
Teaching hospitals and other large hospitals also score more poorly, on average, than do small community hospitals.4
Unexplained geographic disparities persist, with hospitals in cities and certain regions, such as the Northeast and California, scoring lower than other regions.1
Quality Requires Clarity
“These are valid criticisms. Just because someone receives the best medical care doesn’t mean they are the happiest—and vice versa,” says Peter Short, MD, senior vice president of medical affairs for Northeast Hospital Corp. in Massachusetts. “Are there biases [in the way patient satisfaction is measured]?
Absolutely. But we’re all being held accountable and we can’t wait for a perfect system.
“Any definition of high-quality medical care must take into consideration how it is perceived by patients,” he adds, particularly when “value” in healthcare means delivering high-quality, patient-friendly care at the lowest cost.
James Merlino, MD, FACS, FASCRS, chief experience officer for Cleveland Clinic, says little peer-reviewed research exists to show that HCAHPS is a robust process of measuring patient satisfaction, but he says CMS is “focusing on the right areas.”
“It’s hard to say that paying attention to the patient experience is not something we should do. And yet, many physicians and hospitals have not done a good job focusing on patient satisfaction,” Dr. Merlino says. “How well we communicate with patients goes to the heart of the patient-provider interaction: It’s crucial that patients are clearly informed what to do while they are in a hospital and after they are discharged. Poor communication can drive confusion, noncompliance, and complications.”

—John Wasson, MD, emeritus professor of community and family medicine at Dartmouth Medical School
Proven Improvements
Hospitalists will be leaders in driving patient satisfaction, Dr. Merlino says, given their central role in managing patients across the continuum of care. That role gives them great responsibility—and opportunity—to champion practices at their institutions that improve the hospital experience of their patients, many of whom have complicated illnesses requiring a potentially bewildering array of tests and procedures.

Several “best practices” have proven successful in boosting patient-satisfaction scores and can be readily adapted to a variety of local hospital settings, says Dr. Short, who is a speaker in SHM’s Hospital Value-Based Program Toolkit webinar series (see “Best Practices,”).
Cleveland Clinic has greatly boosted its physician communication scores by sharing HCAHPS performance data with physicians and by gleaning best practices from its high-scoring physicians, which include, for example, ensuring that residents and fellows speak with attendings before rounding with patients to ensure staff alignment and care coordination, Dr. Merlino explains.
Cleveland Clinic also is rolling out to its entire medical staff a communication training program taught by a carefully selected team of peer physicians, which Dr. Merlino says is proving to be very effective in boosting patient satisfaction and improving care by enhancing patient-physician conversations. The program features Kaiser Permanente’s “Four Habits” model to help organize medical interviews with patients:
- Invest in the beginning by creating rapport quickly, and let the patient know what to expect.
- Get the patient’s perspective by asking for their ideas concerning the meaning of symptoms and the request for care.
- Demonstrate empathy by being open to the patient’s emotions and conveying empathy verbally and nonverbally.
- Invest in the end by delivering diagnostic information, explaining the rationale for tests and treatments, involving the patient in decision-making, and reviewing the next steps.5
“Organizations have to evolve in an increasingly value-based healthcare environment by developing a culture that can adapt to any set of questions or regulations that CMS mandates,” Dr. Merlino adds.
Next-Generation Patient Satisfaction Measures
Tools to guide patients and healthcare/hospitalist teams toward more satisfying dialogues with patients—as well as tools to improve their outcomes—are becoming increasingly available, says John Wasson, MD, emeritus professor of community and family medicine at Dartmouth Medical School and a member of The Dartmouth Institute Patient-Reported Measure Trust, which is developing and testing next-generation, patient-reported healthcare measures.
One example is Howsyourhealth.org, a family of communication-enhancement tools designed to build patient confidence in managing and controlling their health problems by helping them “get what they want and need exactly when and how they want and need it,” Dr. Wasson says.
“Hospitalists and their teams might begin to think about processes that enhance a patient’s health confidence, which is very strongly associated with many outcomes,” he notes. The hospital version of the tool—at Howsyourcare.org—immediately provides information tailored to patients’ needs, as well as a summary hospitalists can review with their teams in order to improve patient/caregiver confidence for successful management of conditions when discharged, Dr. Wasson says.
“Overall patient satisfaction is not particularly useful for predicting health confidence,” he says. “Information quality tailored to patient need is what boosts patients’ health confidence—and has real power to improve patients’ clinical outcomes.”
Christopher Guadagnino is a freelance medical journalist in Philadelphia.
References
- Rau J. When TLC doesn't satisfy patients, elite hospitals may pay a price. Kaiser Health News website. Available at: http://www.kaiserhealthnews.org/stories/2011/november/08/patient-ratings-hospital-medicare-reimbursements.aspx. Accessed Aug. 15, 2012.
- Sternberg S, Schnaars C. Medicare data can help patients fill perception gap. USA Today website. Available at: http://www.usatoday.com/yourlife/health/healthcare/hospitals/2011-08-04-hospitals-patients-death-rates-Medicare_n.htm. Accessed Aug. 15, 2012.
- Chatterjee P, Joynt KE, Orav EJ, Jha AK. Patient experience in safety-net hospitals: implications for improving care and value-based purchasing. Arch Intern Med. 2012 Jul 16:1-7. doi: 10.1001/archinternmed.2012.3158 [Epub ahead of print].
- Rau J, Medicare to begin basing hospital payments on patient-satisfaction scores. Kaiser Health News website.. Available at: http://www.kaiserhealthnews.org/stories/2011/april/28/medicare-hospital-patient-satisfaction.aspx. Accessed Aug. 15, 2011.
- Frankel RM, Stein T. Getting the most out of the clinical encounter: the four habits model. The Permanente Journal website. Available at: http://xnet.kp.org/permanentejournal/fall99pj/habits.html. Accessed Aug. 15, 2012.
Should patient satisfaction factor prominently into healthcare pay-for-performance incentives? That question recently became moot as the Centers for Medicare & Medicaid Services (CMS) began withholding 1% of hospitals’ Medicare reimbursement as part of its Hospital Value-Based Purchasing Program, restoring it to institutions based upon their quality performance. Thirty percent of the program’s financial incentive is based upon how well hospitals score on patient satisfaction, as measured by the Hospital Consumer Assessment of Healthcare Providers and Systems (HCAHPS) survey.
Despite those data having been collected and reported for years, their use as a healthcare performance indicator continues to be controversial. To win back reimbursement withholds, hospitals must earn perfect scores: The only winners are the ones for whom patients respond “always satisfied” to such questions as “How often did doctors treat you with courtesy and respect?” or “How often did doctors explain things in a way you could understand?” or “How often did hospital staff tell you what the medicine was for?”
A perfectly happy patient, skeptics say, isn’t necessarily one who has received the best medical care, and several analyses suggest that HCAHPS has unintended biases, making it a flawed accountability tool. Some of the nation’s most prestigious hospitals, for example, receive bad patient reviews despite getting high scores on clinical quality metrics.1
Conversely, many hospitals that receive high patient ratings have low clinical quality marks (e.g. significantly worse mortality rates than the national average for heart attacks, heart failure, or pneumonia).2
Safety-net hospitals perform more poorly than other hospitals on nearly every HCAHPS measure of patient experience, with gaps that are sizable and persistent. These institutions have the most fragile operating margins and are the least able to absorb the additional reimbursement cuts that will result from their low scores.3
Teaching hospitals and other large hospitals also score more poorly, on average, than do small community hospitals.4
Unexplained geographic disparities persist, with hospitals in cities and certain regions, such as the Northeast and California, scoring lower than other regions.1
Quality Requires Clarity
“These are valid criticisms. Just because someone receives the best medical care doesn’t mean they are the happiest—and vice versa,” says Peter Short, MD, senior vice president of medical affairs for Northeast Hospital Corp. in Massachusetts. “Are there biases [in the way patient satisfaction is measured]?
Absolutely. But we’re all being held accountable and we can’t wait for a perfect system.
“Any definition of high-quality medical care must take into consideration how it is perceived by patients,” he adds, particularly when “value” in healthcare means delivering high-quality, patient-friendly care at the lowest cost.
James Merlino, MD, FACS, FASCRS, chief experience officer for Cleveland Clinic, says little peer-reviewed research exists to show that HCAHPS is a robust process of measuring patient satisfaction, but he says CMS is “focusing on the right areas.”
“It’s hard to say that paying attention to the patient experience is not something we should do. And yet, many physicians and hospitals have not done a good job focusing on patient satisfaction,” Dr. Merlino says. “How well we communicate with patients goes to the heart of the patient-provider interaction: It’s crucial that patients are clearly informed what to do while they are in a hospital and after they are discharged. Poor communication can drive confusion, noncompliance, and complications.”
—John Wasson, MD, emeritus professor of community and family medicine at Dartmouth Medical School
Proven Improvements
Hospitalists will be leaders in driving patient satisfaction, Dr. Merlino says, given their central role in managing patients across the continuum of care. That role gives them great responsibility—and opportunity—to champion practices at their institutions that improve the hospital experience of their patients, many of whom have complicated illnesses requiring a potentially bewildering array of tests and procedures.
Several “best practices” have proven successful in boosting patient-satisfaction scores and can be readily adapted to a variety of local hospital settings, says Dr. Short, who is a speaker in SHM’s Hospital Value-Based Program Toolkit webinar series (see “Best Practices,”).
Cleveland Clinic has greatly boosted its physician communication scores by sharing HCAHPS performance data with physicians and by gleaning best practices from its high-scoring physicians, which include, for example, ensuring that residents and fellows speak with attendings before rounding with patients to ensure staff alignment and care coordination, Dr. Merlino explains.
Cleveland Clinic also is rolling out to its entire medical staff a communication training program taught by a carefully selected team of peer physicians, which Dr. Merlino says is proving to be very effective in boosting patient satisfaction and improving care by enhancing patient-physician conversations. The program features Kaiser Permanente’s “Four Habits” model to help organize medical interviews with patients:
- Invest in the beginning by creating rapport quickly, and let the patient know what to expect.
- Get the patient’s perspective by asking for their ideas concerning the meaning of symptoms and the request for care.
- Demonstrate empathy by being open to the patient’s emotions and conveying empathy verbally and nonverbally.
- Invest in the end by delivering diagnostic information, explaining the rationale for tests and treatments, involving the patient in decision-making, and reviewing the next steps.5
“Organizations have to evolve in an increasingly value-based healthcare environment by developing a culture that can adapt to any set of questions or regulations that CMS mandates,” Dr. Merlino adds.
Next-Generation Patient Satisfaction Measures
Tools to guide patients and healthcare/hospitalist teams toward more satisfying dialogues with patients—as well as tools to improve their outcomes—are becoming increasingly available, says John Wasson, MD, emeritus professor of community and family medicine at Dartmouth Medical School and a member of The Dartmouth Institute Patient-Reported Measure Trust, which is developing and testing next-generation, patient-reported healthcare measures.
One example is Howsyourhealth.org, a family of communication-enhancement tools designed to build patient confidence in managing and controlling their health problems by helping them “get what they want and need exactly when and how they want and need it,” Dr. Wasson says.
“Hospitalists and their teams might begin to think about processes that enhance a patient’s health confidence, which is very strongly associated with many outcomes,” he notes. The hospital version of the tool—at Howsyourcare.org—immediately provides information tailored to patients’ needs, as well as a summary hospitalists can review with their teams in order to improve patient/caregiver confidence for successful management of conditions when discharged, Dr. Wasson says.
“Overall patient satisfaction is not particularly useful for predicting health confidence,” he says. “Information quality tailored to patient need is what boosts patients’ health confidence—and has real power to improve patients’ clinical outcomes.”
Christopher Guadagnino is a freelance medical journalist in Philadelphia.
References
- Rau J. When TLC doesn't satisfy patients, elite hospitals may pay a price. Kaiser Health News website. Available at: http://www.kaiserhealthnews.org/stories/2011/november/08/patient-ratings-hospital-medicare-reimbursements.aspx. Accessed Aug. 15, 2012.
- Sternberg S, Schnaars C. Medicare data can help patients fill perception gap. USA Today website. Available at: http://www.usatoday.com/yourlife/health/healthcare/hospitals/2011-08-04-hospitals-patients-death-rates-Medicare_n.htm. Accessed Aug. 15, 2012.
- Chatterjee P, Joynt KE, Orav EJ, Jha AK. Patient experience in safety-net hospitals: implications for improving care and value-based purchasing. Arch Intern Med. 2012 Jul 16:1-7. doi: 10.1001/archinternmed.2012.3158 [Epub ahead of print].
- Rau J, Medicare to begin basing hospital payments on patient-satisfaction scores. Kaiser Health News website.. Available at: http://www.kaiserhealthnews.org/stories/2011/april/28/medicare-hospital-patient-satisfaction.aspx. Accessed Aug. 15, 2011.
- Frankel RM, Stein T. Getting the most out of the clinical encounter: the four habits model. The Permanente Journal website. Available at: http://xnet.kp.org/permanentejournal/fall99pj/habits.html. Accessed Aug. 15, 2012.
Should patient satisfaction factor prominently into healthcare pay-for-performance incentives? That question recently became moot as the Centers for Medicare & Medicaid Services (CMS) began withholding 1% of hospitals’ Medicare reimbursement as part of its Hospital Value-Based Purchasing Program, restoring it to institutions based upon their quality performance. Thirty percent of the program’s financial incentive is based upon how well hospitals score on patient satisfaction, as measured by the Hospital Consumer Assessment of Healthcare Providers and Systems (HCAHPS) survey.
Despite those data having been collected and reported for years, their use as a healthcare performance indicator continues to be controversial. To win back reimbursement withholds, hospitals must earn perfect scores: The only winners are the ones for whom patients respond “always satisfied” to such questions as “How often did doctors treat you with courtesy and respect?” or “How often did doctors explain things in a way you could understand?” or “How often did hospital staff tell you what the medicine was for?”
A perfectly happy patient, skeptics say, isn’t necessarily one who has received the best medical care, and several analyses suggest that HCAHPS has unintended biases, making it a flawed accountability tool. Some of the nation’s most prestigious hospitals, for example, receive bad patient reviews despite getting high scores on clinical quality metrics.1
Conversely, many hospitals that receive high patient ratings have low clinical quality marks (e.g. significantly worse mortality rates than the national average for heart attacks, heart failure, or pneumonia).2
Safety-net hospitals perform more poorly than other hospitals on nearly every HCAHPS measure of patient experience, with gaps that are sizable and persistent. These institutions have the most fragile operating margins and are the least able to absorb the additional reimbursement cuts that will result from their low scores.3
Teaching hospitals and other large hospitals also score more poorly, on average, than do small community hospitals.4
Unexplained geographic disparities persist, with hospitals in cities and certain regions, such as the Northeast and California, scoring lower than other regions.1
Quality Requires Clarity
“These are valid criticisms. Just because someone receives the best medical care doesn’t mean they are the happiest—and vice versa,” says Peter Short, MD, senior vice president of medical affairs for Northeast Hospital Corp. in Massachusetts. “Are there biases [in the way patient satisfaction is measured]?
Absolutely. But we’re all being held accountable and we can’t wait for a perfect system.
“Any definition of high-quality medical care must take into consideration how it is perceived by patients,” he adds, particularly when “value” in healthcare means delivering high-quality, patient-friendly care at the lowest cost.
James Merlino, MD, FACS, FASCRS, chief experience officer for Cleveland Clinic, says little peer-reviewed research exists to show that HCAHPS is a robust process of measuring patient satisfaction, but he says CMS is “focusing on the right areas.”
“It’s hard to say that paying attention to the patient experience is not something we should do. And yet, many physicians and hospitals have not done a good job focusing on patient satisfaction,” Dr. Merlino says. “How well we communicate with patients goes to the heart of the patient-provider interaction: It’s crucial that patients are clearly informed what to do while they are in a hospital and after they are discharged. Poor communication can drive confusion, noncompliance, and complications.”
—John Wasson, MD, emeritus professor of community and family medicine at Dartmouth Medical School
Proven Improvements
Hospitalists will be leaders in driving patient satisfaction, Dr. Merlino says, given their central role in managing patients across the continuum of care. That role gives them great responsibility—and opportunity—to champion practices at their institutions that improve the hospital experience of their patients, many of whom have complicated illnesses requiring a potentially bewildering array of tests and procedures.
Several “best practices” have proven successful in boosting patient-satisfaction scores and can be readily adapted to a variety of local hospital settings, says Dr. Short, who is a speaker in SHM’s Hospital Value-Based Program Toolkit webinar series (see “Best Practices,”).
Cleveland Clinic has greatly boosted its physician communication scores by sharing HCAHPS performance data with physicians and by gleaning best practices from its high-scoring physicians, which include, for example, ensuring that residents and fellows speak with attendings before rounding with patients to ensure staff alignment and care coordination, Dr. Merlino explains.
Cleveland Clinic also is rolling out to its entire medical staff a communication training program taught by a carefully selected team of peer physicians, which Dr. Merlino says is proving to be very effective in boosting patient satisfaction and improving care by enhancing patient-physician conversations. The program features Kaiser Permanente’s “Four Habits” model to help organize medical interviews with patients:
- Invest in the beginning by creating rapport quickly, and let the patient know what to expect.
- Get the patient’s perspective by asking for their ideas concerning the meaning of symptoms and the request for care.
- Demonstrate empathy by being open to the patient’s emotions and conveying empathy verbally and nonverbally.
- Invest in the end by delivering diagnostic information, explaining the rationale for tests and treatments, involving the patient in decision-making, and reviewing the next steps.5
“Organizations have to evolve in an increasingly value-based healthcare environment by developing a culture that can adapt to any set of questions or regulations that CMS mandates,” Dr. Merlino adds.
Next-Generation Patient Satisfaction Measures
Tools to guide patients and healthcare/hospitalist teams toward more satisfying dialogues with patients—as well as tools to improve their outcomes—are becoming increasingly available, says John Wasson, MD, emeritus professor of community and family medicine at Dartmouth Medical School and a member of The Dartmouth Institute Patient-Reported Measure Trust, which is developing and testing next-generation, patient-reported healthcare measures.
One example is Howsyourhealth.org, a family of communication-enhancement tools designed to build patient confidence in managing and controlling their health problems by helping them “get what they want and need exactly when and how they want and need it,” Dr. Wasson says.
“Hospitalists and their teams might begin to think about processes that enhance a patient’s health confidence, which is very strongly associated with many outcomes,” he notes. The hospital version of the tool—at Howsyourcare.org—immediately provides information tailored to patients’ needs, as well as a summary hospitalists can review with their teams in order to improve patient/caregiver confidence for successful management of conditions when discharged, Dr. Wasson says.
“Overall patient satisfaction is not particularly useful for predicting health confidence,” he says. “Information quality tailored to patient need is what boosts patients’ health confidence—and has real power to improve patients’ clinical outcomes.”
Christopher Guadagnino is a freelance medical journalist in Philadelphia.
References
- Rau J. When TLC doesn't satisfy patients, elite hospitals may pay a price. Kaiser Health News website. Available at: http://www.kaiserhealthnews.org/stories/2011/november/08/patient-ratings-hospital-medicare-reimbursements.aspx. Accessed Aug. 15, 2012.
- Sternberg S, Schnaars C. Medicare data can help patients fill perception gap. USA Today website. Available at: http://www.usatoday.com/yourlife/health/healthcare/hospitals/2011-08-04-hospitals-patients-death-rates-Medicare_n.htm. Accessed Aug. 15, 2012.
- Chatterjee P, Joynt KE, Orav EJ, Jha AK. Patient experience in safety-net hospitals: implications for improving care and value-based purchasing. Arch Intern Med. 2012 Jul 16:1-7. doi: 10.1001/archinternmed.2012.3158 [Epub ahead of print].
- Rau J, Medicare to begin basing hospital payments on patient-satisfaction scores. Kaiser Health News website.. Available at: http://www.kaiserhealthnews.org/stories/2011/april/28/medicare-hospital-patient-satisfaction.aspx. Accessed Aug. 15, 2011.
- Frankel RM, Stein T. Getting the most out of the clinical encounter: the four habits model. The Permanente Journal website. Available at: http://xnet.kp.org/permanentejournal/fall99pj/habits.html. Accessed Aug. 15, 2012.
ICU Hospitalist Model Improves Quality of Care for Critically Ill Patients
Despite calls for board-certified intensivists to manage all critically ill patients, only a third of hospitalized ICU patients currently are seen by such a specialist—mostly because there are not enough of them to go around.1,2 More and more hospitalists, especially those in community hospitals, are working in ICUs (see “The Critical-Care Debate,”). With the proper training, that can be a good thing for patients and hospitalists, according to a Research, Innovations, and Clinical Vignettes (RIV) abstract presented at HM12 in San Diego.3
Lead author and hospitalist Mark Krivopal, MD, SFHM, formerly with TeamHealth in California and now vice president and medical director of clinical integration and hospital medicine at Steward Health Care in Boston, outlined a program at California’s Lodi Memorial Hospital that identified a group of hospitalists who had experience in caring for critically ill patients and credentials to perform such procedures as central-line placements, intubations, and ventilator management. The select group of TeamHealth hospitalists completed a two-day “Fundamentals of Critical Care Support” course offered by the Society of Critical Care Medicine (www.sccm.org), then began covering the ICU in shifts from 7 a.m. to 7 p.m. The program was so successful early on that hospital administration requested that it expand to a 24-hour service.
An ICU hospitalist program needs to be a partnership, Dr. Krivopal says. Essential oversight at Lodi Memorial is provided by the hospital’s sole pulmonologist.
Preliminary data showed a 35% reduction in ventilator days and 22% reduction in ICU stays, Dr. Krivopal says. The hospital also reports high satisfaction from nurses and other staff. Additional metrics, such as cost savings and patient satisfaction, are under review.
“So long as the level of training is sufficient, this is an approach that definitely should be explored,” he says, adding that young internists have many of the skills needed for ICU work. “But if you don’t keep those skills up [with practice] after residency, you lose them.”
References
- The Leapfrog Group. ICU physician staffing fact sheet. The Leapfrog Group website. Available at: http://www.leapfroggroup.org/media/file/Leapfrog-ICU_Physician_Staffing_Fact_Sheet.pdf. Accessed Aug. 29, 2012.
- Health Resources & Services Administration. Report to Congress: The critical care workforce: a study of the supply and demand for critical care physicians. U.S. Department of Health & Human Services website. Available at: http://bhpr.hrsa.gov/healthworkforce/reports/studycriticalcarephys.pdf. Accessed Aug. 29, 2012.
- Krivopal M, Hlaing M, Felber R, Himebaugh R. ICU hospitalist: a novel method of care for the critically ill patients in economically lean times. J Hosp Med. 2012;7(Suppl 2):192.
Despite calls for board-certified intensivists to manage all critically ill patients, only a third of hospitalized ICU patients currently are seen by such a specialist—mostly because there are not enough of them to go around.1,2 More and more hospitalists, especially those in community hospitals, are working in ICUs (see “The Critical-Care Debate,”). With the proper training, that can be a good thing for patients and hospitalists, according to a Research, Innovations, and Clinical Vignettes (RIV) abstract presented at HM12 in San Diego.3
Lead author and hospitalist Mark Krivopal, MD, SFHM, formerly with TeamHealth in California and now vice president and medical director of clinical integration and hospital medicine at Steward Health Care in Boston, outlined a program at California’s Lodi Memorial Hospital that identified a group of hospitalists who had experience in caring for critically ill patients and credentials to perform such procedures as central-line placements, intubations, and ventilator management. The select group of TeamHealth hospitalists completed a two-day “Fundamentals of Critical Care Support” course offered by the Society of Critical Care Medicine (www.sccm.org), then began covering the ICU in shifts from 7 a.m. to 7 p.m. The program was so successful early on that hospital administration requested that it expand to a 24-hour service.
An ICU hospitalist program needs to be a partnership, Dr. Krivopal says. Essential oversight at Lodi Memorial is provided by the hospital’s sole pulmonologist.
Preliminary data showed a 35% reduction in ventilator days and 22% reduction in ICU stays, Dr. Krivopal says. The hospital also reports high satisfaction from nurses and other staff. Additional metrics, such as cost savings and patient satisfaction, are under review.
“So long as the level of training is sufficient, this is an approach that definitely should be explored,” he says, adding that young internists have many of the skills needed for ICU work. “But if you don’t keep those skills up [with practice] after residency, you lose them.”
References
- The Leapfrog Group. ICU physician staffing fact sheet. The Leapfrog Group website. Available at: http://www.leapfroggroup.org/media/file/Leapfrog-ICU_Physician_Staffing_Fact_Sheet.pdf. Accessed Aug. 29, 2012.
- Health Resources & Services Administration. Report to Congress: The critical care workforce: a study of the supply and demand for critical care physicians. U.S. Department of Health & Human Services website. Available at: http://bhpr.hrsa.gov/healthworkforce/reports/studycriticalcarephys.pdf. Accessed Aug. 29, 2012.
- Krivopal M, Hlaing M, Felber R, Himebaugh R. ICU hospitalist: a novel method of care for the critically ill patients in economically lean times. J Hosp Med. 2012;7(Suppl 2):192.
Despite calls for board-certified intensivists to manage all critically ill patients, only a third of hospitalized ICU patients currently are seen by such a specialist—mostly because there are not enough of them to go around.1,2 More and more hospitalists, especially those in community hospitals, are working in ICUs (see “The Critical-Care Debate,”). With the proper training, that can be a good thing for patients and hospitalists, according to a Research, Innovations, and Clinical Vignettes (RIV) abstract presented at HM12 in San Diego.3
Lead author and hospitalist Mark Krivopal, MD, SFHM, formerly with TeamHealth in California and now vice president and medical director of clinical integration and hospital medicine at Steward Health Care in Boston, outlined a program at California’s Lodi Memorial Hospital that identified a group of hospitalists who had experience in caring for critically ill patients and credentials to perform such procedures as central-line placements, intubations, and ventilator management. The select group of TeamHealth hospitalists completed a two-day “Fundamentals of Critical Care Support” course offered by the Society of Critical Care Medicine (www.sccm.org), then began covering the ICU in shifts from 7 a.m. to 7 p.m. The program was so successful early on that hospital administration requested that it expand to a 24-hour service.
An ICU hospitalist program needs to be a partnership, Dr. Krivopal says. Essential oversight at Lodi Memorial is provided by the hospital’s sole pulmonologist.
Preliminary data showed a 35% reduction in ventilator days and 22% reduction in ICU stays, Dr. Krivopal says. The hospital also reports high satisfaction from nurses and other staff. Additional metrics, such as cost savings and patient satisfaction, are under review.
“So long as the level of training is sufficient, this is an approach that definitely should be explored,” he says, adding that young internists have many of the skills needed for ICU work. “But if you don’t keep those skills up [with practice] after residency, you lose them.”
References
- The Leapfrog Group. ICU physician staffing fact sheet. The Leapfrog Group website. Available at: http://www.leapfroggroup.org/media/file/Leapfrog-ICU_Physician_Staffing_Fact_Sheet.pdf. Accessed Aug. 29, 2012.
- Health Resources & Services Administration. Report to Congress: The critical care workforce: a study of the supply and demand for critical care physicians. U.S. Department of Health & Human Services website. Available at: http://bhpr.hrsa.gov/healthworkforce/reports/studycriticalcarephys.pdf. Accessed Aug. 29, 2012.
- Krivopal M, Hlaing M, Felber R, Himebaugh R. ICU hospitalist: a novel method of care for the critically ill patients in economically lean times. J Hosp Med. 2012;7(Suppl 2):192.
Sharp Rise in Imaging Test Rates has Slowed
A new study tracking the growth of advanced diagnostic imaging techniques found that the rate of growth for such tests is slowing dramatically, even as the total number of tests performed continues to grow.1 Starting in 2007, the rate of growth dropped sharply to about 1% to 3% from more than 6% per year during the previous decade.
Frank Levy, PhD, professor of urban economics at Massachusetts Institute of Technology in Cambridge, Mass., and one of the study’s authors, suggests that the previous growth of the technology could have been partly attributable to such nonmedical factors as profitability for hospitals and fear of malpractice by physicians. The slowdown, Dr. Levy says, also might reflect increased pushback from insurers, recognition of the cost and waste issues, and growing concerns about radiation exposure.
“There are many medical reasons for using these procedures—and many nonmedical reasons,” Dr. Levy says. “To use healthcare resources more efficiently, you should make sure your reason for ordering these tests is medical.”
SHM is working on a short list of sometimes unnecessary but commonly performed medical procedures, which it plans to submit to the American Board of Internal Medicine’s Choosing Wisely campaign this fall. One of the tests being considered for this list is serial chest X-rays for hospitalized patients outside of the ICU who are clinically stable, says Wendy Nickel, associate vice president of SHM’s Center for Hospital Innovation and Improvement. Unnecessary imaging tests are both a safety and a waste issue, she adds.
In related news, a study in the Journal of the National Cancer Institute found that 95.9% of patients 65 and older who have Stage IV cancer received at least one high-cost advanced imaging procedure (e.g. PET or nuclear medicine), with their utilization rates rising more rapidly than for earlier stages of disease.2 Such tests can lead to appropriate palliative measures but also can “distract patients from focusing on achievable end-of-life goals,” explain researchers from the Dana-Farber Cancer Institute in Boston.
References
- Lee D, Levy F. The sharp slowdown in growth of medical imaging: an early analysis suggests combination of policies was the cause. Health Affairs website. Available at: http://www.healthaffairs.org/alert_link.php?url=http://content.healthaffairs.org/content/early/2012/07/24/hlthaff.2011.1034&t=h&id=1590. Accessed Aug. 29, 2012.
- Hu YY, Kwok AC, Jiang W, et al. High-cost imaging in elderly patients with Stage IV cancer. J Natl Cancer Inst. 2012;104(15):1165-1173.
A new study tracking the growth of advanced diagnostic imaging techniques found that the rate of growth for such tests is slowing dramatically, even as the total number of tests performed continues to grow.1 Starting in 2007, the rate of growth dropped sharply to about 1% to 3% from more than 6% per year during the previous decade.
Frank Levy, PhD, professor of urban economics at Massachusetts Institute of Technology in Cambridge, Mass., and one of the study’s authors, suggests that the previous growth of the technology could have been partly attributable to such nonmedical factors as profitability for hospitals and fear of malpractice by physicians. The slowdown, Dr. Levy says, also might reflect increased pushback from insurers, recognition of the cost and waste issues, and growing concerns about radiation exposure.
“There are many medical reasons for using these procedures—and many nonmedical reasons,” Dr. Levy says. “To use healthcare resources more efficiently, you should make sure your reason for ordering these tests is medical.”
SHM is working on a short list of sometimes unnecessary but commonly performed medical procedures, which it plans to submit to the American Board of Internal Medicine’s Choosing Wisely campaign this fall. One of the tests being considered for this list is serial chest X-rays for hospitalized patients outside of the ICU who are clinically stable, says Wendy Nickel, associate vice president of SHM’s Center for Hospital Innovation and Improvement. Unnecessary imaging tests are both a safety and a waste issue, she adds.
In related news, a study in the Journal of the National Cancer Institute found that 95.9% of patients 65 and older who have Stage IV cancer received at least one high-cost advanced imaging procedure (e.g. PET or nuclear medicine), with their utilization rates rising more rapidly than for earlier stages of disease.2 Such tests can lead to appropriate palliative measures but also can “distract patients from focusing on achievable end-of-life goals,” explain researchers from the Dana-Farber Cancer Institute in Boston.
References
- Lee D, Levy F. The sharp slowdown in growth of medical imaging: an early analysis suggests combination of policies was the cause. Health Affairs website. Available at: http://www.healthaffairs.org/alert_link.php?url=http://content.healthaffairs.org/content/early/2012/07/24/hlthaff.2011.1034&t=h&id=1590. Accessed Aug. 29, 2012.
- Hu YY, Kwok AC, Jiang W, et al. High-cost imaging in elderly patients with Stage IV cancer. J Natl Cancer Inst. 2012;104(15):1165-1173.
A new study tracking the growth of advanced diagnostic imaging techniques found that the rate of growth for such tests is slowing dramatically, even as the total number of tests performed continues to grow.1 Starting in 2007, the rate of growth dropped sharply to about 1% to 3% from more than 6% per year during the previous decade.
Frank Levy, PhD, professor of urban economics at Massachusetts Institute of Technology in Cambridge, Mass., and one of the study’s authors, suggests that the previous growth of the technology could have been partly attributable to such nonmedical factors as profitability for hospitals and fear of malpractice by physicians. The slowdown, Dr. Levy says, also might reflect increased pushback from insurers, recognition of the cost and waste issues, and growing concerns about radiation exposure.
“There are many medical reasons for using these procedures—and many nonmedical reasons,” Dr. Levy says. “To use healthcare resources more efficiently, you should make sure your reason for ordering these tests is medical.”
SHM is working on a short list of sometimes unnecessary but commonly performed medical procedures, which it plans to submit to the American Board of Internal Medicine’s Choosing Wisely campaign this fall. One of the tests being considered for this list is serial chest X-rays for hospitalized patients outside of the ICU who are clinically stable, says Wendy Nickel, associate vice president of SHM’s Center for Hospital Innovation and Improvement. Unnecessary imaging tests are both a safety and a waste issue, she adds.
In related news, a study in the Journal of the National Cancer Institute found that 95.9% of patients 65 and older who have Stage IV cancer received at least one high-cost advanced imaging procedure (e.g. PET or nuclear medicine), with their utilization rates rising more rapidly than for earlier stages of disease.2 Such tests can lead to appropriate palliative measures but also can “distract patients from focusing on achievable end-of-life goals,” explain researchers from the Dana-Farber Cancer Institute in Boston.
References
- Lee D, Levy F. The sharp slowdown in growth of medical imaging: an early analysis suggests combination of policies was the cause. Health Affairs website. Available at: http://www.healthaffairs.org/alert_link.php?url=http://content.healthaffairs.org/content/early/2012/07/24/hlthaff.2011.1034&t=h&id=1590. Accessed Aug. 29, 2012.
- Hu YY, Kwok AC, Jiang W, et al. High-cost imaging in elderly patients with Stage IV cancer. J Natl Cancer Inst. 2012;104(15):1165-1173.
Noisy Hospitals Impede Sleep
Sleep-disturbing noise in the hospital is a big problem “that can really compromise a patient’s recovery process,” according to Orfeu Buxton, PhD, associate neuroscientist in the Division of Sleep Medicine at Brigham & Women’s Hospital in Boston.1
Researchers exposed a dozen healthy volunteers to typical nocturnal hospital noise while monitoring their sleep patterns and heart rates, systematically quantifying the disruptive capacity of a range of hospital sounds on sleep. Hospitalized patients routinely cite noise as a major factor that negatively affects quality of care, the researchers note. An Aug. 2 New York Times blog post by Pauline Chen, MD, suggests that government policies linking hospital reimbursement to patient satisfaction might finally turn hospital administrators’ focus on the need to bring this noise under better control.2
References
- Buxton OM, Ellenbogen JM, Wang W, et al. Sleep disruption due to hospital noises: a prospective evaluation. Ann Intern Med. 2012;157(3):170-179.
- Chen P. The clatter of the hospital room. New York Times website. Available at: http://well.blogs.nytimes.com/2012/08/02/the-clatter-of-the-hospital-room/. Accessed Aug. 29, 2012.
Sleep-disturbing noise in the hospital is a big problem “that can really compromise a patient’s recovery process,” according to Orfeu Buxton, PhD, associate neuroscientist in the Division of Sleep Medicine at Brigham & Women’s Hospital in Boston.1
Researchers exposed a dozen healthy volunteers to typical nocturnal hospital noise while monitoring their sleep patterns and heart rates, systematically quantifying the disruptive capacity of a range of hospital sounds on sleep. Hospitalized patients routinely cite noise as a major factor that negatively affects quality of care, the researchers note. An Aug. 2 New York Times blog post by Pauline Chen, MD, suggests that government policies linking hospital reimbursement to patient satisfaction might finally turn hospital administrators’ focus on the need to bring this noise under better control.2
References
- Buxton OM, Ellenbogen JM, Wang W, et al. Sleep disruption due to hospital noises: a prospective evaluation. Ann Intern Med. 2012;157(3):170-179.
- Chen P. The clatter of the hospital room. New York Times website. Available at: http://well.blogs.nytimes.com/2012/08/02/the-clatter-of-the-hospital-room/. Accessed Aug. 29, 2012.
Sleep-disturbing noise in the hospital is a big problem “that can really compromise a patient’s recovery process,” according to Orfeu Buxton, PhD, associate neuroscientist in the Division of Sleep Medicine at Brigham & Women’s Hospital in Boston.1
Researchers exposed a dozen healthy volunteers to typical nocturnal hospital noise while monitoring their sleep patterns and heart rates, systematically quantifying the disruptive capacity of a range of hospital sounds on sleep. Hospitalized patients routinely cite noise as a major factor that negatively affects quality of care, the researchers note. An Aug. 2 New York Times blog post by Pauline Chen, MD, suggests that government policies linking hospital reimbursement to patient satisfaction might finally turn hospital administrators’ focus on the need to bring this noise under better control.2
References
- Buxton OM, Ellenbogen JM, Wang W, et al. Sleep disruption due to hospital noises: a prospective evaluation. Ann Intern Med. 2012;157(3):170-179.
- Chen P. The clatter of the hospital room. New York Times website. Available at: http://well.blogs.nytimes.com/2012/08/02/the-clatter-of-the-hospital-room/. Accessed Aug. 29, 2012.
77 Million U.S. Residents Have Difficulty Understanding Basic Health Information
The number of U.S. residents who have difficulty understanding basic health information, according to a report developed by the University of California at San Francisco and San Francisco General Hospital and published by the Institute of Medicine.1 The report also suggests ways to bridge the gaps to understanding, such as how to make this a priority at every level of the health organization, avoid stigmatizing patients over literacy issues, and adopt proven educational techniques such as teach-back (see “Teach-Back,” September 2012).
Reference
The number of U.S. residents who have difficulty understanding basic health information, according to a report developed by the University of California at San Francisco and San Francisco General Hospital and published by the Institute of Medicine.1 The report also suggests ways to bridge the gaps to understanding, such as how to make this a priority at every level of the health organization, avoid stigmatizing patients over literacy issues, and adopt proven educational techniques such as teach-back (see “Teach-Back,” September 2012).
Reference
The number of U.S. residents who have difficulty understanding basic health information, according to a report developed by the University of California at San Francisco and San Francisco General Hospital and published by the Institute of Medicine.1 The report also suggests ways to bridge the gaps to understanding, such as how to make this a priority at every level of the health organization, avoid stigmatizing patients over literacy issues, and adopt proven educational techniques such as teach-back (see “Teach-Back,” September 2012).
Reference
Win Whitcomb: Hospital Readmissions Penalties Start Now

The uproar and confusion over readmissions penalties has consumed umpteen hours of senior leaders’ time (especially that of CFOs), not to mention that of front-line nurses, case managers, quality-improvement (QI) coordinators, hospitalists, and others involved in discharge planning and ensuring a safe transition for patients out of the hospital. For many, the math is fuzzy, and for most, the return on investment is even fuzzier. After all, avoided readmissions are lost revenue to those who are running a business known as an acute-care hospital.
Let me start with the conclusion: Eliminating avoidable readmissions is the right thing to do, period. But the financial downside to doing so is probably greater than any upside realized through avoidance of the penalties that began affecting hospital payments on Oct. 1—at least in the fee-for-service world we live in. At some point in the future, when most patients are under a global payment, the math might be clearer, but today, penalties probably won’t offset lost revenue from reduced readmissions added to the cost of paying lots of people to work in meetings (and at the bedside) to devise better care transitions. (Caveat: If your hospital is bursting at the seams with full occupancy, reducing readmissions and replacing them with higher-reimbursing patients, such as those undergoing elective major surgery, likely will be a net financial gain for your hospital.)
Part of the Affordable Care Act (ACA), the Hospital Readmissions Reduction Program (HRRP) will reduce total Medicare DRG reimbursement for hospitals beginning in fiscal-year 2013 based on actual 30-day readmission rates for myocardial infarction (MI), heart failure (HF), and pneumonia that are in excess of risk-adjusted expected rates. The reduction is capped at 1% in 2013, 2% in 2014, and 3% in 2015 and beyond. Hospital readmission rates are based on calculated baseline rates using Medicare data from July 1, 2008, to June 30, 2011.
Cost of a Readmissions-Reduction Program
How much does it cost for a hospital to implement a care-transitions program—such as SHM’s Project BOOST—to reduce readmissions? Last year, I interviewed a dozen hospitals that successfully implemented SHM’s formal mentored implementation program. The result? In the first year of the program, hospitals spent about $170,000 on training and staff time devoted to the project.
Lost Revenue
Let’s look at a sample penalty calculation, then examine a scenario sizing up how revenue is lost when a hospital is successful in reducing readmissions. The ACA defines the payments for excess readmissions as:
The number of patients with the applicable condition (HF, MI, or pneumonia) multiplied by the base DRG payment made for those patients multiplied by the percentage of readmissions beyond the expected.
As an example, let’s take a hospital that treats 500 pneumonia patients (# with the applicable condition), has a base DRG payment for pneumonia of $5,000, and a readmission rate that is 4% higher than expected (in this example, the actual rate is 25% and the expected rate is 24%; 1/25=4%). The penalty is 500 X $5,000 X .04, or $100,000. We’ll assume that the readmission rate for myocardial infarction and heart failure are less than expected, so the total penalty is $100,000.
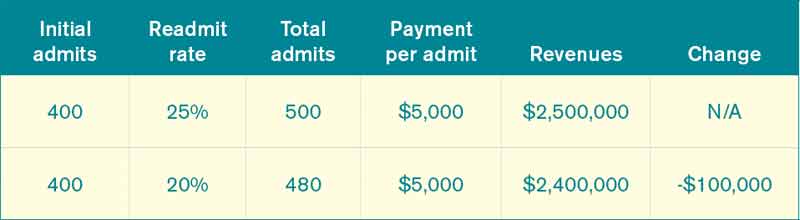
Let’s say the hospital works hard to decrease pneumonia readmissions from 25% to 20% and avoids the penalty. As outlined in Table 1, the hospital will lose $100,000 in revenue (admittedly, reducing readmissions to 20% from 25% represents a big jump, but this is for illustration purposes—we haven’t added in lost revenue from reduced readmissions for other conditions). What’s the final cost of avoiding the $100,000 readmission penalty? Lost revenue of $100,000 plus the cost of implementing the readmission reduction program of $170,000=$270,000.
Why Are We Doing This?
I see the value in care transitions and readmissions-reduction programs, such as Project BOOST, first and foremost as a way to improve patient safety; as such, if implemented effectively, they are likely worth the investment. Second, their value lies in the preparation all hospitals and health systems should be undergoing to remain market-competitive and solvent under global payment systems. Because the penalties in the HRRP might come with lost revenues and the costs of program implementation, be clear about your team’s motivation for reducing readmissions. Your CFO will see to it if I don’t.
Dr. Whitcomb is medical director of healthcare quality at Baystate Medical Center in Springfield, Mass. He is a co-founder and past president of SHM. Email him at [email protected].
The View From

SHM is an advocate for the move toward more global payment systems, as well as payment methodologies that reward good outcomes and processes over volume. System improvements require leadership and front-line physicians who are able to implement and evaluate new care-delivery models. SHM offers resources and tools to support the HM community in this era of change through leadership training (www.hospitalmedicine.com/leadership), professional development and mentoring in QI programs (www.hospitalmedicine.org/QI), and other practical tools, such as the value-based purchasing toolkit (www.hospitalmedicine.org/HVBP).
Additionally, the Project BOOST toolkit (www.hospitalmedicine.org/BOOST) includes a return-on-investment calculator to use in your institution’s efforts in reducing readmissions. The calculator is built both for fee-for-service and accountable-care-organization payment models, and it can serve as an adjunct to estimates provided to your hospital of penalties for excess readmissions under HRRP.
The uproar and confusion over readmissions penalties has consumed umpteen hours of senior leaders’ time (especially that of CFOs), not to mention that of front-line nurses, case managers, quality-improvement (QI) coordinators, hospitalists, and others involved in discharge planning and ensuring a safe transition for patients out of the hospital. For many, the math is fuzzy, and for most, the return on investment is even fuzzier. After all, avoided readmissions are lost revenue to those who are running a business known as an acute-care hospital.
Let me start with the conclusion: Eliminating avoidable readmissions is the right thing to do, period. But the financial downside to doing so is probably greater than any upside realized through avoidance of the penalties that began affecting hospital payments on Oct. 1—at least in the fee-for-service world we live in. At some point in the future, when most patients are under a global payment, the math might be clearer, but today, penalties probably won’t offset lost revenue from reduced readmissions added to the cost of paying lots of people to work in meetings (and at the bedside) to devise better care transitions. (Caveat: If your hospital is bursting at the seams with full occupancy, reducing readmissions and replacing them with higher-reimbursing patients, such as those undergoing elective major surgery, likely will be a net financial gain for your hospital.)
Part of the Affordable Care Act (ACA), the Hospital Readmissions Reduction Program (HRRP) will reduce total Medicare DRG reimbursement for hospitals beginning in fiscal-year 2013 based on actual 30-day readmission rates for myocardial infarction (MI), heart failure (HF), and pneumonia that are in excess of risk-adjusted expected rates. The reduction is capped at 1% in 2013, 2% in 2014, and 3% in 2015 and beyond. Hospital readmission rates are based on calculated baseline rates using Medicare data from July 1, 2008, to June 30, 2011.
Cost of a Readmissions-Reduction Program
How much does it cost for a hospital to implement a care-transitions program—such as SHM’s Project BOOST—to reduce readmissions? Last year, I interviewed a dozen hospitals that successfully implemented SHM’s formal mentored implementation program. The result? In the first year of the program, hospitals spent about $170,000 on training and staff time devoted to the project.
Lost Revenue
Let’s look at a sample penalty calculation, then examine a scenario sizing up how revenue is lost when a hospital is successful in reducing readmissions. The ACA defines the payments for excess readmissions as:
The number of patients with the applicable condition (HF, MI, or pneumonia) multiplied by the base DRG payment made for those patients multiplied by the percentage of readmissions beyond the expected.
As an example, let’s take a hospital that treats 500 pneumonia patients (# with the applicable condition), has a base DRG payment for pneumonia of $5,000, and a readmission rate that is 4% higher than expected (in this example, the actual rate is 25% and the expected rate is 24%; 1/25=4%). The penalty is 500 X $5,000 X .04, or $100,000. We’ll assume that the readmission rate for myocardial infarction and heart failure are less than expected, so the total penalty is $100,000.
Let’s say the hospital works hard to decrease pneumonia readmissions from 25% to 20% and avoids the penalty. As outlined in Table 1, the hospital will lose $100,000 in revenue (admittedly, reducing readmissions to 20% from 25% represents a big jump, but this is for illustration purposes—we haven’t added in lost revenue from reduced readmissions for other conditions). What’s the final cost of avoiding the $100,000 readmission penalty? Lost revenue of $100,000 plus the cost of implementing the readmission reduction program of $170,000=$270,000.
Why Are We Doing This?
I see the value in care transitions and readmissions-reduction programs, such as Project BOOST, first and foremost as a way to improve patient safety; as such, if implemented effectively, they are likely worth the investment. Second, their value lies in the preparation all hospitals and health systems should be undergoing to remain market-competitive and solvent under global payment systems. Because the penalties in the HRRP might come with lost revenues and the costs of program implementation, be clear about your team’s motivation for reducing readmissions. Your CFO will see to it if I don’t.
Dr. Whitcomb is medical director of healthcare quality at Baystate Medical Center in Springfield, Mass. He is a co-founder and past president of SHM. Email him at [email protected].
The View From
SHM is an advocate for the move toward more global payment systems, as well as payment methodologies that reward good outcomes and processes over volume. System improvements require leadership and front-line physicians who are able to implement and evaluate new care-delivery models. SHM offers resources and tools to support the HM community in this era of change through leadership training (www.hospitalmedicine.com/leadership), professional development and mentoring in QI programs (www.hospitalmedicine.org/QI), and other practical tools, such as the value-based purchasing toolkit (www.hospitalmedicine.org/HVBP).
Additionally, the Project BOOST toolkit (www.hospitalmedicine.org/BOOST) includes a return-on-investment calculator to use in your institution’s efforts in reducing readmissions. The calculator is built both for fee-for-service and accountable-care-organization payment models, and it can serve as an adjunct to estimates provided to your hospital of penalties for excess readmissions under HRRP.
The uproar and confusion over readmissions penalties has consumed umpteen hours of senior leaders’ time (especially that of CFOs), not to mention that of front-line nurses, case managers, quality-improvement (QI) coordinators, hospitalists, and others involved in discharge planning and ensuring a safe transition for patients out of the hospital. For many, the math is fuzzy, and for most, the return on investment is even fuzzier. After all, avoided readmissions are lost revenue to those who are running a business known as an acute-care hospital.
Let me start with the conclusion: Eliminating avoidable readmissions is the right thing to do, period. But the financial downside to doing so is probably greater than any upside realized through avoidance of the penalties that began affecting hospital payments on Oct. 1—at least in the fee-for-service world we live in. At some point in the future, when most patients are under a global payment, the math might be clearer, but today, penalties probably won’t offset lost revenue from reduced readmissions added to the cost of paying lots of people to work in meetings (and at the bedside) to devise better care transitions. (Caveat: If your hospital is bursting at the seams with full occupancy, reducing readmissions and replacing them with higher-reimbursing patients, such as those undergoing elective major surgery, likely will be a net financial gain for your hospital.)
Part of the Affordable Care Act (ACA), the Hospital Readmissions Reduction Program (HRRP) will reduce total Medicare DRG reimbursement for hospitals beginning in fiscal-year 2013 based on actual 30-day readmission rates for myocardial infarction (MI), heart failure (HF), and pneumonia that are in excess of risk-adjusted expected rates. The reduction is capped at 1% in 2013, 2% in 2014, and 3% in 2015 and beyond. Hospital readmission rates are based on calculated baseline rates using Medicare data from July 1, 2008, to June 30, 2011.
Cost of a Readmissions-Reduction Program
How much does it cost for a hospital to implement a care-transitions program—such as SHM’s Project BOOST—to reduce readmissions? Last year, I interviewed a dozen hospitals that successfully implemented SHM’s formal mentored implementation program. The result? In the first year of the program, hospitals spent about $170,000 on training and staff time devoted to the project.
Lost Revenue
Let’s look at a sample penalty calculation, then examine a scenario sizing up how revenue is lost when a hospital is successful in reducing readmissions. The ACA defines the payments for excess readmissions as:
The number of patients with the applicable condition (HF, MI, or pneumonia) multiplied by the base DRG payment made for those patients multiplied by the percentage of readmissions beyond the expected.
As an example, let’s take a hospital that treats 500 pneumonia patients (# with the applicable condition), has a base DRG payment for pneumonia of $5,000, and a readmission rate that is 4% higher than expected (in this example, the actual rate is 25% and the expected rate is 24%; 1/25=4%). The penalty is 500 X $5,000 X .04, or $100,000. We’ll assume that the readmission rate for myocardial infarction and heart failure are less than expected, so the total penalty is $100,000.
Let’s say the hospital works hard to decrease pneumonia readmissions from 25% to 20% and avoids the penalty. As outlined in Table 1, the hospital will lose $100,000 in revenue (admittedly, reducing readmissions to 20% from 25% represents a big jump, but this is for illustration purposes—we haven’t added in lost revenue from reduced readmissions for other conditions). What’s the final cost of avoiding the $100,000 readmission penalty? Lost revenue of $100,000 plus the cost of implementing the readmission reduction program of $170,000=$270,000.
Why Are We Doing This?
I see the value in care transitions and readmissions-reduction programs, such as Project BOOST, first and foremost as a way to improve patient safety; as such, if implemented effectively, they are likely worth the investment. Second, their value lies in the preparation all hospitals and health systems should be undergoing to remain market-competitive and solvent under global payment systems. Because the penalties in the HRRP might come with lost revenues and the costs of program implementation, be clear about your team’s motivation for reducing readmissions. Your CFO will see to it if I don’t.
Dr. Whitcomb is medical director of healthcare quality at Baystate Medical Center in Springfield, Mass. He is a co-founder and past president of SHM. Email him at [email protected].
The View From
SHM is an advocate for the move toward more global payment systems, as well as payment methodologies that reward good outcomes and processes over volume. System improvements require leadership and front-line physicians who are able to implement and evaluate new care-delivery models. SHM offers resources and tools to support the HM community in this era of change through leadership training (www.hospitalmedicine.com/leadership), professional development and mentoring in QI programs (www.hospitalmedicine.org/QI), and other practical tools, such as the value-based purchasing toolkit (www.hospitalmedicine.org/HVBP).
Additionally, the Project BOOST toolkit (www.hospitalmedicine.org/BOOST) includes a return-on-investment calculator to use in your institution’s efforts in reducing readmissions. The calculator is built both for fee-for-service and accountable-care-organization payment models, and it can serve as an adjunct to estimates provided to your hospital of penalties for excess readmissions under HRRP.
Alternative Healthcare Models Aim to Boost Sagging Critical-Care Workforce
Amid the struggle to boost the country’s sagging critical-care workforce, experts have most commonly proposed creating a tiered or regionalized model of care, investing more in tele-ICU services, and augmenting the role of midlevel providers.
The University of Pittsburgh Medical Center, with 20 hospitals and roughly 500 ICU beds throughout its network, is adopting a regionalized healthcare delivery system. Some of the center’s most high-risk services, such as its big transplant programs, are centralized within the main university campus hospitals, as are about half of the ICU beds.
“In those hospitals, we’ve decided that we need 24/7 in-house, intensive-care attendings,” says Derek Angus, MD, the center’s chair of critical-care medicine. The doctors work with fellows and a rapidly growing expansion of midlevel providers.
In some of the smaller hospitals, however, some ICU patients are seen and managed by hospitalists. The medical center’s eventual goal is to be more systematic about the kinds of patients managed by intensivists as well as those managed by hospitalists. It’s a task made easier by the specialists’ close working relationship within the same department.
Dr. Angus believes telemedicine could help by providing a sort of mission control that can help track critically ill patients and those at risk of being admitted to ICUs across all 20 hospitals. He concedes, however, that telemedicine for ICU assistance has had mixed results in the medical literature, suggesting that a major key is working out the proper roles and responsibilities of those using the technology.
To improve the consistency of its own frontline providers, the Emory University Center for Critical Care in Atlanta developed a competency-based, critical-care training program for nurse practitioners (NPs) and physician assistants (PAs).
“It’s very clear that if you have a group of NP and PA providers who can do 90 percent of what the physician does, it really begins to unload the physician to focus on what I call the big-picture pieces of critical care,” says center director Timothy Buchman, PhD, MD.
That attending physician can be trained as a care executive to ensure well-coordinated care and to focus on any process that isn’t working well. “At a big academic health sciences center, that should probably be a critical-care physician,” Dr. Buchman notes. “But for the smaller community and regional hospitals that have a relatively less sick population, the person who will be well-positioned to oversee this nonphysician provider staff could well be a hospitalist who’s received additional guidance and training in critical care.”
For mild or moderate complexity of care, he says, the added training need not necessarily include a traditional two-year fellowship. Under a value-based system, sicker patients could be rapidly transferred to a higher level of care, and telemedicine could provide a “backstop” for providers in smaller hospitals who lack the training and experience of someone with a full critical-care fellowship.
Amid the struggle to boost the country’s sagging critical-care workforce, experts have most commonly proposed creating a tiered or regionalized model of care, investing more in tele-ICU services, and augmenting the role of midlevel providers.
The University of Pittsburgh Medical Center, with 20 hospitals and roughly 500 ICU beds throughout its network, is adopting a regionalized healthcare delivery system. Some of the center’s most high-risk services, such as its big transplant programs, are centralized within the main university campus hospitals, as are about half of the ICU beds.
“In those hospitals, we’ve decided that we need 24/7 in-house, intensive-care attendings,” says Derek Angus, MD, the center’s chair of critical-care medicine. The doctors work with fellows and a rapidly growing expansion of midlevel providers.
In some of the smaller hospitals, however, some ICU patients are seen and managed by hospitalists. The medical center’s eventual goal is to be more systematic about the kinds of patients managed by intensivists as well as those managed by hospitalists. It’s a task made easier by the specialists’ close working relationship within the same department.
Dr. Angus believes telemedicine could help by providing a sort of mission control that can help track critically ill patients and those at risk of being admitted to ICUs across all 20 hospitals. He concedes, however, that telemedicine for ICU assistance has had mixed results in the medical literature, suggesting that a major key is working out the proper roles and responsibilities of those using the technology.
To improve the consistency of its own frontline providers, the Emory University Center for Critical Care in Atlanta developed a competency-based, critical-care training program for nurse practitioners (NPs) and physician assistants (PAs).
“It’s very clear that if you have a group of NP and PA providers who can do 90 percent of what the physician does, it really begins to unload the physician to focus on what I call the big-picture pieces of critical care,” says center director Timothy Buchman, PhD, MD.
That attending physician can be trained as a care executive to ensure well-coordinated care and to focus on any process that isn’t working well. “At a big academic health sciences center, that should probably be a critical-care physician,” Dr. Buchman notes. “But for the smaller community and regional hospitals that have a relatively less sick population, the person who will be well-positioned to oversee this nonphysician provider staff could well be a hospitalist who’s received additional guidance and training in critical care.”
For mild or moderate complexity of care, he says, the added training need not necessarily include a traditional two-year fellowship. Under a value-based system, sicker patients could be rapidly transferred to a higher level of care, and telemedicine could provide a “backstop” for providers in smaller hospitals who lack the training and experience of someone with a full critical-care fellowship.
Amid the struggle to boost the country’s sagging critical-care workforce, experts have most commonly proposed creating a tiered or regionalized model of care, investing more in tele-ICU services, and augmenting the role of midlevel providers.
The University of Pittsburgh Medical Center, with 20 hospitals and roughly 500 ICU beds throughout its network, is adopting a regionalized healthcare delivery system. Some of the center’s most high-risk services, such as its big transplant programs, are centralized within the main university campus hospitals, as are about half of the ICU beds.
“In those hospitals, we’ve decided that we need 24/7 in-house, intensive-care attendings,” says Derek Angus, MD, the center’s chair of critical-care medicine. The doctors work with fellows and a rapidly growing expansion of midlevel providers.
In some of the smaller hospitals, however, some ICU patients are seen and managed by hospitalists. The medical center’s eventual goal is to be more systematic about the kinds of patients managed by intensivists as well as those managed by hospitalists. It’s a task made easier by the specialists’ close working relationship within the same department.
Dr. Angus believes telemedicine could help by providing a sort of mission control that can help track critically ill patients and those at risk of being admitted to ICUs across all 20 hospitals. He concedes, however, that telemedicine for ICU assistance has had mixed results in the medical literature, suggesting that a major key is working out the proper roles and responsibilities of those using the technology.
To improve the consistency of its own frontline providers, the Emory University Center for Critical Care in Atlanta developed a competency-based, critical-care training program for nurse practitioners (NPs) and physician assistants (PAs).
“It’s very clear that if you have a group of NP and PA providers who can do 90 percent of what the physician does, it really begins to unload the physician to focus on what I call the big-picture pieces of critical care,” says center director Timothy Buchman, PhD, MD.
That attending physician can be trained as a care executive to ensure well-coordinated care and to focus on any process that isn’t working well. “At a big academic health sciences center, that should probably be a critical-care physician,” Dr. Buchman notes. “But for the smaller community and regional hospitals that have a relatively less sick population, the person who will be well-positioned to oversee this nonphysician provider staff could well be a hospitalist who’s received additional guidance and training in critical care.”
For mild or moderate complexity of care, he says, the added training need not necessarily include a traditional two-year fellowship. Under a value-based system, sicker patients could be rapidly transferred to a higher level of care, and telemedicine could provide a “backstop” for providers in smaller hospitals who lack the training and experience of someone with a full critical-care fellowship.
Guidelines Drive Optimal Care for Heart Failure Patients
Cardiologists aren’t shy about repeating it: guidelines, guidelines, guidelines. That is, follow them.
“Evidence-based, guideline-driven optimal care for heart failure truly is beneficial,” Dr. Yancy says. “Every effort should be made to strive to achieve ideal thresholds and meeting best practices.”
There is now compelling evidence that, for patients with heart failure, the higher the degree of adherence to Class I-recommended therapies, the greater the reduction in 24-month mortality risk.5
“It would seem as if practicing best quality is almost a perfunctory statement, but consistently, when we look at surveys of quality improvement and adherence to evidence-based strategies, persistent gaps remain in the broader community,” Dr. Yancy says. “We know what we need to do. We’re still striving to get closer and closer to optimal care.”
Dr. Harold says the guidelines are there to make things simpler. So take advantage of them.
“If anything, hospitalists tend to be ahead of most other groups in terms of knowing evidence-based pathways and really tracking very specific protocols,” he says. “I think one of the advantages of hospitalist care is very often, it is guideline-driven. You have less variation in terms of care and quality outcomes.”
Cardiologists aren’t shy about repeating it: guidelines, guidelines, guidelines. That is, follow them.
“Evidence-based, guideline-driven optimal care for heart failure truly is beneficial,” Dr. Yancy says. “Every effort should be made to strive to achieve ideal thresholds and meeting best practices.”
There is now compelling evidence that, for patients with heart failure, the higher the degree of adherence to Class I-recommended therapies, the greater the reduction in 24-month mortality risk.5
“It would seem as if practicing best quality is almost a perfunctory statement, but consistently, when we look at surveys of quality improvement and adherence to evidence-based strategies, persistent gaps remain in the broader community,” Dr. Yancy says. “We know what we need to do. We’re still striving to get closer and closer to optimal care.”
Dr. Harold says the guidelines are there to make things simpler. So take advantage of them.
“If anything, hospitalists tend to be ahead of most other groups in terms of knowing evidence-based pathways and really tracking very specific protocols,” he says. “I think one of the advantages of hospitalist care is very often, it is guideline-driven. You have less variation in terms of care and quality outcomes.”
Cardiologists aren’t shy about repeating it: guidelines, guidelines, guidelines. That is, follow them.
“Evidence-based, guideline-driven optimal care for heart failure truly is beneficial,” Dr. Yancy says. “Every effort should be made to strive to achieve ideal thresholds and meeting best practices.”
There is now compelling evidence that, for patients with heart failure, the higher the degree of adherence to Class I-recommended therapies, the greater the reduction in 24-month mortality risk.5
“It would seem as if practicing best quality is almost a perfunctory statement, but consistently, when we look at surveys of quality improvement and adherence to evidence-based strategies, persistent gaps remain in the broader community,” Dr. Yancy says. “We know what we need to do. We’re still striving to get closer and closer to optimal care.”
Dr. Harold says the guidelines are there to make things simpler. So take advantage of them.
“If anything, hospitalists tend to be ahead of most other groups in terms of knowing evidence-based pathways and really tracking very specific protocols,” he says. “I think one of the advantages of hospitalist care is very often, it is guideline-driven. You have less variation in terms of care and quality outcomes.”
12 Things Cardiologists Think Hospitalists Need to Know
Only about a third of ideal candidates with heart failure are currently treated with [aldosterone antagonists], even though it markedly improves outcome and is Class I-recommended in the guidelines.

—Gregg Fonarow, MD, co-chief, University of California at Los Angeles division of cardiology, chair, American Heart Association’s Get With The Guidelines program steering committee

You might not have done a fellowship in cardiology, but quite often you probably feel like a cardiologist. Hospitalists frequently attend to patients on observation for heart problems and help manage even the most complex patients.
Often, you are working alongside the cardiologist. But other times, you’re on your own. Hospitalists are expected to carry an increasingly heavy load when it comes to heart-failure patients and many other kinds of patients with specialized disorders. It can be hard to keep up with what you need to know.
Top Twelve
- Recognize the new importance of beta-blockers for heart failure, and go with the best of them.
- It’s not readmissions that are the problem—it’s avoidable readmissions.
- New interventional technologies will mean more complex patients, so be ready.
- Aldosterone antagonists, though probably underutilized, can be very effective but require caution.
- Switching from IV diuretics to an oral regimen calls for careful monitoring.
- Patients with heart failure with preserved ejection fraction have outcomes over the longer haul similar to those with heart failure with reduced ejection fraction. And in preserved ejection fraction cases, the contributing illnesses must be addressed.
- Inotropic agents can do more harm than good.
- Pay attention to the ins and outs of new antiplatelet therapies.
- Bridging anticoagulant therapy in patients going for electrophysiology procedures should be done only some, not most, of the time.
- Some non-STEMI patients might benefit from getting to the catheterization lab quickly.
- Beware the idiosyncrasies of new anticoagulants.
- Be cognizant of stent thrombosis and how to manage it.
The Hospitalist spoke to several cardiologists about the latest in treatments, technologies, and HM’s role in the system of care. The following are their suggestions for what you really need to know about treating patients with heart conditions.
1) Recognize the new importance of beta-blockers for heart failure, and go with the best of them.
Angiotensin converting enzyme inhibitors and angiotensive receptor blockers have been part of the Centers for Medicare & Medicaid Services’ (CMS) core measures for heart failure for a long time, but beta-blockers at hospital discharge only recently have been added as American College of Cardiology/American Heart Association/American Medical Association–Physician Consortium for Performance Improvement measures for heart failure.1
“For those with heart failure and reduced left ventricular ejection fraction, very old and outdated concepts would have talked about potentially holding the beta-blocker during hospitalization for heart failure—or not initiating until the patient was an outpatient,” says Gregg Fonarow, MD, co-chief of the University of California at Los Angeles’ division of cardiology and chair of the steering committee for the American Heart Association’s Get With The Guidelines program. “[But] the guidelines and evidence, and often performance measures, linked to them are now explicit about initiating or maintaining beta-blockers during the heart-failure hospitalization.”
Beta-blockers should be initiated as patients are stabilized before discharge. Dr. Fonarow suggests hospitalists use only one of the three evidence-based therapies: carvedilol, metoprolol succinate, or bisoprolol.
“Many physicians have been using metoprolol tartrate or atenolol in heart-failure patients,” Dr. Fonarow says. “These are not known to improve clinical outcomes. So here’s an example where the specific medication is absolutely, critically important.”
2) It’s not readmissions that are the problem—it’s avoidable readmissions.
“The modifier is very important,” says Clyde Yancy, MD, chief of the division of cardiology at the Northwestern University Feinberg School of Medicine in Chicago. “Heart failure continues to be a problematic disease. Many patients now do really well, but some do not. Those patients are symptomatic and may require frequent hospitalizations for stabilization. We should not disallow or misdirect those patients who need inpatient care from receiving such because of an arbitrary incentive to reduce rehospitalizations out of fear of punitive financial damages. The unforeseen risks here are real.”
Dr. Yancy says studies based on CMS data have found that institutions with higher readmission rates have lower 30-day mortality rates.2 He cautions hospitalists to be “very thoughtful about an overzealous embrace of reducing all readmissions for heart failure.” Instead, the goal should be to limit the “avoidable readmissions.”
“And for the patient that clearly has advanced disease,” he says, “rather than triaging them away from the hospital, we really should be very respectful of their disease. Keep those patients where disease-modifying interventions can be deployed, and we can work to achieve the best possible outcome for those that have the most advanced disease.”
3) New interventional technologies will mean more complex patients, so be ready.
Advances in interventional procedures, including transcatheter aortic valve replacement (TAVR) and endoscopic mitral valve repair, will translate into a new population of highly complex patients. Many of these patients will be in their 80s or 90s.
“It’s a whole new paradigm shift of technology,” says John Harold, MD, president-elect of the American College of Cardiology and past chief of staff and department of medicine clinical chief of staff at Cedars-Sinai Medical Center in Los Angeles. “Very often, the hospitalist is at the front dealing with all of these issues.”
Many of these patients have other problems, including renal insufficiency, diabetes, and the like.
“They have all sorts of other things going on simultaneously, so very often the hospitalist becomes … the point person in dealing with all of these issues,” Dr. Harold says.
4) Aldosterone antagonists, though probably underutilized, can be very effective but require caution.
Aldosterone antagonists can greatly improve outcomes and reduce hospitalization in heart-failure patients, but they have to be used with very careful dosing and patient selection, Dr. Fonarow says. And they require early follow-up once patients are discharged.
“Only about a third of ideal candidates with heart failure are currently treated with this agent, even though it markedly improves outcome and is Class I-recommended in the guidelines,” Dr. Fonarow says. “But this is one where it needs to be started at appropriate low doses, with meticulous monitoring in both the inpatient and the outpatient setting, early follow-up, and early laboratory checks.”
5) Switching from IV diuretics to an oral regimen calls for careful monitoring.
Transitioning patients from IV diuretics to oral regimens is an area rife with mistakes, Dr. Fonarow says. It requires a lot of “meticulous attention to proper potassium supplementation and monitoring of renal function and electrolyte levels,” he says.
Medication reconciliation—“med rec”—is especially important during the transition from inpatient to outpatient.
“There are common medication errors that are made during this transition,” Dr. Fonarow says. “Hospitalists, along with other [care team] members, can really play a critically important role in trying to reduce that risk.”
6) Patients with heart failure with preserved ejection
fraction have outcomes over the longer haul similar to those with heart failure with reduced ejection fraction. And in preserved ejection fraction cases, the contributing illnesses must be addressed.
“We really can’t exercise a thought economy that just says, ‘Extrapolate the evidence-based therapies for heart failure with reduced ejection fraction to heart failure with preserved ejection fraction’ and expect good outcomes,” Dr. Yancy says. “That’s not the case. We don’t have an evidence base to substantiate that.”
He says one or more common comorbidities (e.g. atrial fibrillation, hypertension, obesity, diabetes, renal insufficiency) are present in 90% of patients with preserved ejection fraction. Treatment of those comorbidities—for example, rate control in afib patients, lowering the blood pressure in hypertension patients—has to be done with care.
“We should recognize that the therapy for this condition, albeit absent any specifically indicated interventions that will change its natural history, can still be skillfully constructed,” Dr. Yancy says. “But that construct needs to reflect the recommended, guideline-driven interventions for the concomitant other comorbidities.”
7) Inotropic agents can do more harm than good.
For patients who aren’t in cardiogenic shock, using inotropic agents doesn’t help. In fact, it might actually hurt. Dr. Fonarow says studies have shown these agents can “prolong length of stay, cause complications, and increase mortality risk.”
He notes that the use of inotropes should be avoided, or if it’s being considered, a cardiologist with knowledge and experience in heart failure should be involved in the treatment and care.
Statements about avoiding inotropes in heart failure, except under very specific circumstances, have been “incredibly strengthened” recently in the American College of Cardiology and Heart Failure Society of America guidelines.3
8) Pay attention to the ins and outs of new antiplatelet therapies.

—John Harold, MD, president-elect, American College of Cardiology, former chief of staff, department of medicine, Cedars-Sinai Medical Center, Los Angeles
Hospitalists caring for acute coronary syndrome patients need to familiarize themselves with updated guidelines and additional therapies that are now available, Dr. Fonarow says. New antiplatelet therapies (e.g. prasugrel and ticagrelor) are available as part of the armamentarium, along with the mainstay clopidogrel.
“These therapies lower the risk of recurrent events, lowered the risk of stent thrombosis,” he says. “In the case of ticagrelor, it actually lowered all-cause mortality. These are important new therapies, with new guideline recommendations, that all hospitalists should be aware of.”
9) Bridging anticoagulant therapy in patients going for electrophysiology procedures should be done only some, not most, of the time.
“Patients getting such devices as pacemakers or implantable cardioverter defribrillators (ICD) installed tend not to need bridging,” says Joaquin Cigarroa, MD, clinical chief of cardiology at Oregon Health & Science University in Portland.
He says it’s actually “safer” to do the procedure when patients “are on oral antithrombotics than switching them from an oral agent, and bridging with low- molecular-weight- or unfractionated heparin.”
“It’s a big deal,” Dr. Cigarroa adds, because it is risky to have elderly and frail patients on multiple antithrombotics. “Hemorrhagic complications in cardiology patients still occurs very frequently, so really be attuned to estimating bleeding risk and making sure that we’re dosing antithrombotics appropriately. Bridging should be the minority of patients, not the majority of patients.”
10) Some non-STEMI patients might benefit from getting to the catheterization lab quickly.
Door-to-balloon time is recognized as critical for ST-segment elevation myocardial infarction (STEMI) patients, but more recent work—such as in the TIMACS trial—finds benefits of early revascularization for some non-STEMI patients as well.2
“This trial showed that among higher-risk patients, using a validated risk score, that those patients did benefit from an early approach, meaning going to the cath lab in the first 12 hours of hospitalization,” Dr. Fonarow says. “We now have more information about the optimal timing of coronary angiography and potential revascularization of higher-risk patients with non-ST-segment elevation MI.”

11) Beware the idiosyncrasies of new anticoagulants.
The introduction of dabigatran and rivaroxaban (and, perhaps soon, apixaban) to the array of anticoagulant therapies brings a new slate of considerations for hospitalists, Dr. Harold says.
“For the majority of these, there’s no specific way to reverse the anticoagulant effect in the event of a major bleeding event,” he says. “There’s no simple antidote. And the effect can last up to 12 to 24 hours, depending on the renal function. This is what the hospitalist will be called to deal with: bleeding complications in patients who have these newer anticoagulants on board.”
Dr. Fonarow says that the new CHA2DS2-VASc score has been found to do a better job than the traditional CHADS2 score in assessing afib stroke risk.4
12) Be cognizant of stent thrombosis and how to manage it.
Dr. Harold says that most hospitalists probably are up to date on drug-eluting stents and the risk of stopping dual antiplatelet therapy within several months of implant, but that doesn’t mean they won’t treat patients whose primary-care physicians (PCPs) aren’t up to date. He recommends working on these cases with hematologists.
“That knowledge is not widespread in terms of the internal-medicine community,” he says. “I’ve seen situations where patients have had their Plavix stopped for colonoscopies and they’ve had stent thrombosis. It’s this knowledge of cardiac patients who come in with recent deployment of drug-eluting stents who may end up having other issues.”
Tom Collins is a freelance writer in South Florida.
References
- 2009 Focused Update: ACCF/AHA Guidelines for the Diagnosis and Management of Heart Failure in Adults. Circulation. 2009;119:1977-2016 an HFSA 2010 Comprehensive Heart Failure Practice Guideline. J Cardiac Failure. 2010;16(6):475-539.
- Gorodeski EZ, Starling RC, Blackstone EH. Are all readmissions bad readmissions? N Engl J Med. 2010;363:297-298.
- Mehta SR, Granger CB, Boden WE, et al. Early versus delayed invasive intervention in acute coronary syndromes. N Engl J Med. 2009;360(21):2165-2175.
- Olesen JB, Torp-Pedersen C, Hansen ML, Lip GY. The value of the CHA2DS2-VASc score for refining stroke risk stratification in patients with atrial fibrillation with a CHADS2 score 0-1: a nationwide cohort study. Thromb Haemost. 2012;107(6):1172-1179.
- Associations between outpatient heart failure process-of-care measures and mortality. Circulation. 2011;123(15):1601-1610.
Only about a third of ideal candidates with heart failure are currently treated with [aldosterone antagonists], even though it markedly improves outcome and is Class I-recommended in the guidelines.
—Gregg Fonarow, MD, co-chief, University of California at Los Angeles division of cardiology, chair, American Heart Association’s Get With The Guidelines program steering committee
You might not have done a fellowship in cardiology, but quite often you probably feel like a cardiologist. Hospitalists frequently attend to patients on observation for heart problems and help manage even the most complex patients.
Often, you are working alongside the cardiologist. But other times, you’re on your own. Hospitalists are expected to carry an increasingly heavy load when it comes to heart-failure patients and many other kinds of patients with specialized disorders. It can be hard to keep up with what you need to know.
Top Twelve
- Recognize the new importance of beta-blockers for heart failure, and go with the best of them.
- It’s not readmissions that are the problem—it’s avoidable readmissions.
- New interventional technologies will mean more complex patients, so be ready.
- Aldosterone antagonists, though probably underutilized, can be very effective but require caution.
- Switching from IV diuretics to an oral regimen calls for careful monitoring.
- Patients with heart failure with preserved ejection fraction have outcomes over the longer haul similar to those with heart failure with reduced ejection fraction. And in preserved ejection fraction cases, the contributing illnesses must be addressed.
- Inotropic agents can do more harm than good.
- Pay attention to the ins and outs of new antiplatelet therapies.
- Bridging anticoagulant therapy in patients going for electrophysiology procedures should be done only some, not most, of the time.
- Some non-STEMI patients might benefit from getting to the catheterization lab quickly.
- Beware the idiosyncrasies of new anticoagulants.
- Be cognizant of stent thrombosis and how to manage it.
The Hospitalist spoke to several cardiologists about the latest in treatments, technologies, and HM’s role in the system of care. The following are their suggestions for what you really need to know about treating patients with heart conditions.
1) Recognize the new importance of beta-blockers for heart failure, and go with the best of them.
Angiotensin converting enzyme inhibitors and angiotensive receptor blockers have been part of the Centers for Medicare & Medicaid Services’ (CMS) core measures for heart failure for a long time, but beta-blockers at hospital discharge only recently have been added as American College of Cardiology/American Heart Association/American Medical Association–Physician Consortium for Performance Improvement measures for heart failure.1
“For those with heart failure and reduced left ventricular ejection fraction, very old and outdated concepts would have talked about potentially holding the beta-blocker during hospitalization for heart failure—or not initiating until the patient was an outpatient,” says Gregg Fonarow, MD, co-chief of the University of California at Los Angeles’ division of cardiology and chair of the steering committee for the American Heart Association’s Get With The Guidelines program. “[But] the guidelines and evidence, and often performance measures, linked to them are now explicit about initiating or maintaining beta-blockers during the heart-failure hospitalization.”
Beta-blockers should be initiated as patients are stabilized before discharge. Dr. Fonarow suggests hospitalists use only one of the three evidence-based therapies: carvedilol, metoprolol succinate, or bisoprolol.
“Many physicians have been using metoprolol tartrate or atenolol in heart-failure patients,” Dr. Fonarow says. “These are not known to improve clinical outcomes. So here’s an example where the specific medication is absolutely, critically important.”
2) It’s not readmissions that are the problem—it’s avoidable readmissions.
“The modifier is very important,” says Clyde Yancy, MD, chief of the division of cardiology at the Northwestern University Feinberg School of Medicine in Chicago. “Heart failure continues to be a problematic disease. Many patients now do really well, but some do not. Those patients are symptomatic and may require frequent hospitalizations for stabilization. We should not disallow or misdirect those patients who need inpatient care from receiving such because of an arbitrary incentive to reduce rehospitalizations out of fear of punitive financial damages. The unforeseen risks here are real.”
Dr. Yancy says studies based on CMS data have found that institutions with higher readmission rates have lower 30-day mortality rates.2 He cautions hospitalists to be “very thoughtful about an overzealous embrace of reducing all readmissions for heart failure.” Instead, the goal should be to limit the “avoidable readmissions.”
“And for the patient that clearly has advanced disease,” he says, “rather than triaging them away from the hospital, we really should be very respectful of their disease. Keep those patients where disease-modifying interventions can be deployed, and we can work to achieve the best possible outcome for those that have the most advanced disease.”
3) New interventional technologies will mean more complex patients, so be ready.
Advances in interventional procedures, including transcatheter aortic valve replacement (TAVR) and endoscopic mitral valve repair, will translate into a new population of highly complex patients. Many of these patients will be in their 80s or 90s.
“It’s a whole new paradigm shift of technology,” says John Harold, MD, president-elect of the American College of Cardiology and past chief of staff and department of medicine clinical chief of staff at Cedars-Sinai Medical Center in Los Angeles. “Very often, the hospitalist is at the front dealing with all of these issues.”
Many of these patients have other problems, including renal insufficiency, diabetes, and the like.
“They have all sorts of other things going on simultaneously, so very often the hospitalist becomes … the point person in dealing with all of these issues,” Dr. Harold says.
4) Aldosterone antagonists, though probably underutilized, can be very effective but require caution.
Aldosterone antagonists can greatly improve outcomes and reduce hospitalization in heart-failure patients, but they have to be used with very careful dosing and patient selection, Dr. Fonarow says. And they require early follow-up once patients are discharged.
“Only about a third of ideal candidates with heart failure are currently treated with this agent, even though it markedly improves outcome and is Class I-recommended in the guidelines,” Dr. Fonarow says. “But this is one where it needs to be started at appropriate low doses, with meticulous monitoring in both the inpatient and the outpatient setting, early follow-up, and early laboratory checks.”
5) Switching from IV diuretics to an oral regimen calls for careful monitoring.
Transitioning patients from IV diuretics to oral regimens is an area rife with mistakes, Dr. Fonarow says. It requires a lot of “meticulous attention to proper potassium supplementation and monitoring of renal function and electrolyte levels,” he says.
Medication reconciliation—“med rec”—is especially important during the transition from inpatient to outpatient.
“There are common medication errors that are made during this transition,” Dr. Fonarow says. “Hospitalists, along with other [care team] members, can really play a critically important role in trying to reduce that risk.”
6) Patients with heart failure with preserved ejection
fraction have outcomes over the longer haul similar to those with heart failure with reduced ejection fraction. And in preserved ejection fraction cases, the contributing illnesses must be addressed.
“We really can’t exercise a thought economy that just says, ‘Extrapolate the evidence-based therapies for heart failure with reduced ejection fraction to heart failure with preserved ejection fraction’ and expect good outcomes,” Dr. Yancy says. “That’s not the case. We don’t have an evidence base to substantiate that.”
He says one or more common comorbidities (e.g. atrial fibrillation, hypertension, obesity, diabetes, renal insufficiency) are present in 90% of patients with preserved ejection fraction. Treatment of those comorbidities—for example, rate control in afib patients, lowering the blood pressure in hypertension patients—has to be done with care.
“We should recognize that the therapy for this condition, albeit absent any specifically indicated interventions that will change its natural history, can still be skillfully constructed,” Dr. Yancy says. “But that construct needs to reflect the recommended, guideline-driven interventions for the concomitant other comorbidities.”
7) Inotropic agents can do more harm than good.
For patients who aren’t in cardiogenic shock, using inotropic agents doesn’t help. In fact, it might actually hurt. Dr. Fonarow says studies have shown these agents can “prolong length of stay, cause complications, and increase mortality risk.”
He notes that the use of inotropes should be avoided, or if it’s being considered, a cardiologist with knowledge and experience in heart failure should be involved in the treatment and care.
Statements about avoiding inotropes in heart failure, except under very specific circumstances, have been “incredibly strengthened” recently in the American College of Cardiology and Heart Failure Society of America guidelines.3
8) Pay attention to the ins and outs of new antiplatelet therapies.
—John Harold, MD, president-elect, American College of Cardiology, former chief of staff, department of medicine, Cedars-Sinai Medical Center, Los Angeles
Hospitalists caring for acute coronary syndrome patients need to familiarize themselves with updated guidelines and additional therapies that are now available, Dr. Fonarow says. New antiplatelet therapies (e.g. prasugrel and ticagrelor) are available as part of the armamentarium, along with the mainstay clopidogrel.
“These therapies lower the risk of recurrent events, lowered the risk of stent thrombosis,” he says. “In the case of ticagrelor, it actually lowered all-cause mortality. These are important new therapies, with new guideline recommendations, that all hospitalists should be aware of.”
9) Bridging anticoagulant therapy in patients going for electrophysiology procedures should be done only some, not most, of the time.
“Patients getting such devices as pacemakers or implantable cardioverter defribrillators (ICD) installed tend not to need bridging,” says Joaquin Cigarroa, MD, clinical chief of cardiology at Oregon Health & Science University in Portland.
He says it’s actually “safer” to do the procedure when patients “are on oral antithrombotics than switching them from an oral agent, and bridging with low- molecular-weight- or unfractionated heparin.”
“It’s a big deal,” Dr. Cigarroa adds, because it is risky to have elderly and frail patients on multiple antithrombotics. “Hemorrhagic complications in cardiology patients still occurs very frequently, so really be attuned to estimating bleeding risk and making sure that we’re dosing antithrombotics appropriately. Bridging should be the minority of patients, not the majority of patients.”
10) Some non-STEMI patients might benefit from getting to the catheterization lab quickly.
Door-to-balloon time is recognized as critical for ST-segment elevation myocardial infarction (STEMI) patients, but more recent work—such as in the TIMACS trial—finds benefits of early revascularization for some non-STEMI patients as well.2
“This trial showed that among higher-risk patients, using a validated risk score, that those patients did benefit from an early approach, meaning going to the cath lab in the first 12 hours of hospitalization,” Dr. Fonarow says. “We now have more information about the optimal timing of coronary angiography and potential revascularization of higher-risk patients with non-ST-segment elevation MI.”
11) Beware the idiosyncrasies of new anticoagulants.
The introduction of dabigatran and rivaroxaban (and, perhaps soon, apixaban) to the array of anticoagulant therapies brings a new slate of considerations for hospitalists, Dr. Harold says.
“For the majority of these, there’s no specific way to reverse the anticoagulant effect in the event of a major bleeding event,” he says. “There’s no simple antidote. And the effect can last up to 12 to 24 hours, depending on the renal function. This is what the hospitalist will be called to deal with: bleeding complications in patients who have these newer anticoagulants on board.”
Dr. Fonarow says that the new CHA2DS2-VASc score has been found to do a better job than the traditional CHADS2 score in assessing afib stroke risk.4
12) Be cognizant of stent thrombosis and how to manage it.
Dr. Harold says that most hospitalists probably are up to date on drug-eluting stents and the risk of stopping dual antiplatelet therapy within several months of implant, but that doesn’t mean they won’t treat patients whose primary-care physicians (PCPs) aren’t up to date. He recommends working on these cases with hematologists.
“That knowledge is not widespread in terms of the internal-medicine community,” he says. “I’ve seen situations where patients have had their Plavix stopped for colonoscopies and they’ve had stent thrombosis. It’s this knowledge of cardiac patients who come in with recent deployment of drug-eluting stents who may end up having other issues.”
Tom Collins is a freelance writer in South Florida.
References
- 2009 Focused Update: ACCF/AHA Guidelines for the Diagnosis and Management of Heart Failure in Adults. Circulation. 2009;119:1977-2016 an HFSA 2010 Comprehensive Heart Failure Practice Guideline. J Cardiac Failure. 2010;16(6):475-539.
- Gorodeski EZ, Starling RC, Blackstone EH. Are all readmissions bad readmissions? N Engl J Med. 2010;363:297-298.
- Mehta SR, Granger CB, Boden WE, et al. Early versus delayed invasive intervention in acute coronary syndromes. N Engl J Med. 2009;360(21):2165-2175.
- Olesen JB, Torp-Pedersen C, Hansen ML, Lip GY. The value of the CHA2DS2-VASc score for refining stroke risk stratification in patients with atrial fibrillation with a CHADS2 score 0-1: a nationwide cohort study. Thromb Haemost. 2012;107(6):1172-1179.
- Associations between outpatient heart failure process-of-care measures and mortality. Circulation. 2011;123(15):1601-1610.
Only about a third of ideal candidates with heart failure are currently treated with [aldosterone antagonists], even though it markedly improves outcome and is Class I-recommended in the guidelines.
—Gregg Fonarow, MD, co-chief, University of California at Los Angeles division of cardiology, chair, American Heart Association’s Get With The Guidelines program steering committee
You might not have done a fellowship in cardiology, but quite often you probably feel like a cardiologist. Hospitalists frequently attend to patients on observation for heart problems and help manage even the most complex patients.
Often, you are working alongside the cardiologist. But other times, you’re on your own. Hospitalists are expected to carry an increasingly heavy load when it comes to heart-failure patients and many other kinds of patients with specialized disorders. It can be hard to keep up with what you need to know.
Top Twelve
- Recognize the new importance of beta-blockers for heart failure, and go with the best of them.
- It’s not readmissions that are the problem—it’s avoidable readmissions.
- New interventional technologies will mean more complex patients, so be ready.
- Aldosterone antagonists, though probably underutilized, can be very effective but require caution.
- Switching from IV diuretics to an oral regimen calls for careful monitoring.
- Patients with heart failure with preserved ejection fraction have outcomes over the longer haul similar to those with heart failure with reduced ejection fraction. And in preserved ejection fraction cases, the contributing illnesses must be addressed.
- Inotropic agents can do more harm than good.
- Pay attention to the ins and outs of new antiplatelet therapies.
- Bridging anticoagulant therapy in patients going for electrophysiology procedures should be done only some, not most, of the time.
- Some non-STEMI patients might benefit from getting to the catheterization lab quickly.
- Beware the idiosyncrasies of new anticoagulants.
- Be cognizant of stent thrombosis and how to manage it.
The Hospitalist spoke to several cardiologists about the latest in treatments, technologies, and HM’s role in the system of care. The following are their suggestions for what you really need to know about treating patients with heart conditions.
1) Recognize the new importance of beta-blockers for heart failure, and go with the best of them.
Angiotensin converting enzyme inhibitors and angiotensive receptor blockers have been part of the Centers for Medicare & Medicaid Services’ (CMS) core measures for heart failure for a long time, but beta-blockers at hospital discharge only recently have been added as American College of Cardiology/American Heart Association/American Medical Association–Physician Consortium for Performance Improvement measures for heart failure.1
“For those with heart failure and reduced left ventricular ejection fraction, very old and outdated concepts would have talked about potentially holding the beta-blocker during hospitalization for heart failure—or not initiating until the patient was an outpatient,” says Gregg Fonarow, MD, co-chief of the University of California at Los Angeles’ division of cardiology and chair of the steering committee for the American Heart Association’s Get With The Guidelines program. “[But] the guidelines and evidence, and often performance measures, linked to them are now explicit about initiating or maintaining beta-blockers during the heart-failure hospitalization.”
Beta-blockers should be initiated as patients are stabilized before discharge. Dr. Fonarow suggests hospitalists use only one of the three evidence-based therapies: carvedilol, metoprolol succinate, or bisoprolol.
“Many physicians have been using metoprolol tartrate or atenolol in heart-failure patients,” Dr. Fonarow says. “These are not known to improve clinical outcomes. So here’s an example where the specific medication is absolutely, critically important.”
2) It’s not readmissions that are the problem—it’s avoidable readmissions.
“The modifier is very important,” says Clyde Yancy, MD, chief of the division of cardiology at the Northwestern University Feinberg School of Medicine in Chicago. “Heart failure continues to be a problematic disease. Many patients now do really well, but some do not. Those patients are symptomatic and may require frequent hospitalizations for stabilization. We should not disallow or misdirect those patients who need inpatient care from receiving such because of an arbitrary incentive to reduce rehospitalizations out of fear of punitive financial damages. The unforeseen risks here are real.”
Dr. Yancy says studies based on CMS data have found that institutions with higher readmission rates have lower 30-day mortality rates.2 He cautions hospitalists to be “very thoughtful about an overzealous embrace of reducing all readmissions for heart failure.” Instead, the goal should be to limit the “avoidable readmissions.”
“And for the patient that clearly has advanced disease,” he says, “rather than triaging them away from the hospital, we really should be very respectful of their disease. Keep those patients where disease-modifying interventions can be deployed, and we can work to achieve the best possible outcome for those that have the most advanced disease.”
3) New interventional technologies will mean more complex patients, so be ready.
Advances in interventional procedures, including transcatheter aortic valve replacement (TAVR) and endoscopic mitral valve repair, will translate into a new population of highly complex patients. Many of these patients will be in their 80s or 90s.
“It’s a whole new paradigm shift of technology,” says John Harold, MD, president-elect of the American College of Cardiology and past chief of staff and department of medicine clinical chief of staff at Cedars-Sinai Medical Center in Los Angeles. “Very often, the hospitalist is at the front dealing with all of these issues.”
Many of these patients have other problems, including renal insufficiency, diabetes, and the like.
“They have all sorts of other things going on simultaneously, so very often the hospitalist becomes … the point person in dealing with all of these issues,” Dr. Harold says.
4) Aldosterone antagonists, though probably underutilized, can be very effective but require caution.
Aldosterone antagonists can greatly improve outcomes and reduce hospitalization in heart-failure patients, but they have to be used with very careful dosing and patient selection, Dr. Fonarow says. And they require early follow-up once patients are discharged.
“Only about a third of ideal candidates with heart failure are currently treated with this agent, even though it markedly improves outcome and is Class I-recommended in the guidelines,” Dr. Fonarow says. “But this is one where it needs to be started at appropriate low doses, with meticulous monitoring in both the inpatient and the outpatient setting, early follow-up, and early laboratory checks.”
5) Switching from IV diuretics to an oral regimen calls for careful monitoring.
Transitioning patients from IV diuretics to oral regimens is an area rife with mistakes, Dr. Fonarow says. It requires a lot of “meticulous attention to proper potassium supplementation and monitoring of renal function and electrolyte levels,” he says.
Medication reconciliation—“med rec”—is especially important during the transition from inpatient to outpatient.
“There are common medication errors that are made during this transition,” Dr. Fonarow says. “Hospitalists, along with other [care team] members, can really play a critically important role in trying to reduce that risk.”
6) Patients with heart failure with preserved ejection
fraction have outcomes over the longer haul similar to those with heart failure with reduced ejection fraction. And in preserved ejection fraction cases, the contributing illnesses must be addressed.
“We really can’t exercise a thought economy that just says, ‘Extrapolate the evidence-based therapies for heart failure with reduced ejection fraction to heart failure with preserved ejection fraction’ and expect good outcomes,” Dr. Yancy says. “That’s not the case. We don’t have an evidence base to substantiate that.”
He says one or more common comorbidities (e.g. atrial fibrillation, hypertension, obesity, diabetes, renal insufficiency) are present in 90% of patients with preserved ejection fraction. Treatment of those comorbidities—for example, rate control in afib patients, lowering the blood pressure in hypertension patients—has to be done with care.
“We should recognize that the therapy for this condition, albeit absent any specifically indicated interventions that will change its natural history, can still be skillfully constructed,” Dr. Yancy says. “But that construct needs to reflect the recommended, guideline-driven interventions for the concomitant other comorbidities.”
7) Inotropic agents can do more harm than good.
For patients who aren’t in cardiogenic shock, using inotropic agents doesn’t help. In fact, it might actually hurt. Dr. Fonarow says studies have shown these agents can “prolong length of stay, cause complications, and increase mortality risk.”
He notes that the use of inotropes should be avoided, or if it’s being considered, a cardiologist with knowledge and experience in heart failure should be involved in the treatment and care.
Statements about avoiding inotropes in heart failure, except under very specific circumstances, have been “incredibly strengthened” recently in the American College of Cardiology and Heart Failure Society of America guidelines.3
8) Pay attention to the ins and outs of new antiplatelet therapies.
—John Harold, MD, president-elect, American College of Cardiology, former chief of staff, department of medicine, Cedars-Sinai Medical Center, Los Angeles
Hospitalists caring for acute coronary syndrome patients need to familiarize themselves with updated guidelines and additional therapies that are now available, Dr. Fonarow says. New antiplatelet therapies (e.g. prasugrel and ticagrelor) are available as part of the armamentarium, along with the mainstay clopidogrel.
“These therapies lower the risk of recurrent events, lowered the risk of stent thrombosis,” he says. “In the case of ticagrelor, it actually lowered all-cause mortality. These are important new therapies, with new guideline recommendations, that all hospitalists should be aware of.”
9) Bridging anticoagulant therapy in patients going for electrophysiology procedures should be done only some, not most, of the time.
“Patients getting such devices as pacemakers or implantable cardioverter defribrillators (ICD) installed tend not to need bridging,” says Joaquin Cigarroa, MD, clinical chief of cardiology at Oregon Health & Science University in Portland.
He says it’s actually “safer” to do the procedure when patients “are on oral antithrombotics than switching them from an oral agent, and bridging with low- molecular-weight- or unfractionated heparin.”
“It’s a big deal,” Dr. Cigarroa adds, because it is risky to have elderly and frail patients on multiple antithrombotics. “Hemorrhagic complications in cardiology patients still occurs very frequently, so really be attuned to estimating bleeding risk and making sure that we’re dosing antithrombotics appropriately. Bridging should be the minority of patients, not the majority of patients.”
10) Some non-STEMI patients might benefit from getting to the catheterization lab quickly.
Door-to-balloon time is recognized as critical for ST-segment elevation myocardial infarction (STEMI) patients, but more recent work—such as in the TIMACS trial—finds benefits of early revascularization for some non-STEMI patients as well.2
“This trial showed that among higher-risk patients, using a validated risk score, that those patients did benefit from an early approach, meaning going to the cath lab in the first 12 hours of hospitalization,” Dr. Fonarow says. “We now have more information about the optimal timing of coronary angiography and potential revascularization of higher-risk patients with non-ST-segment elevation MI.”
11) Beware the idiosyncrasies of new anticoagulants.
The introduction of dabigatran and rivaroxaban (and, perhaps soon, apixaban) to the array of anticoagulant therapies brings a new slate of considerations for hospitalists, Dr. Harold says.
“For the majority of these, there’s no specific way to reverse the anticoagulant effect in the event of a major bleeding event,” he says. “There’s no simple antidote. And the effect can last up to 12 to 24 hours, depending on the renal function. This is what the hospitalist will be called to deal with: bleeding complications in patients who have these newer anticoagulants on board.”
Dr. Fonarow says that the new CHA2DS2-VASc score has been found to do a better job than the traditional CHADS2 score in assessing afib stroke risk.4
12) Be cognizant of stent thrombosis and how to manage it.
Dr. Harold says that most hospitalists probably are up to date on drug-eluting stents and the risk of stopping dual antiplatelet therapy within several months of implant, but that doesn’t mean they won’t treat patients whose primary-care physicians (PCPs) aren’t up to date. He recommends working on these cases with hematologists.
“That knowledge is not widespread in terms of the internal-medicine community,” he says. “I’ve seen situations where patients have had their Plavix stopped for colonoscopies and they’ve had stent thrombosis. It’s this knowledge of cardiac patients who come in with recent deployment of drug-eluting stents who may end up having other issues.”
Tom Collins is a freelance writer in South Florida.
References
- 2009 Focused Update: ACCF/AHA Guidelines for the Diagnosis and Management of Heart Failure in Adults. Circulation. 2009;119:1977-2016 an HFSA 2010 Comprehensive Heart Failure Practice Guideline. J Cardiac Failure. 2010;16(6):475-539.
- Gorodeski EZ, Starling RC, Blackstone EH. Are all readmissions bad readmissions? N Engl J Med. 2010;363:297-298.
- Mehta SR, Granger CB, Boden WE, et al. Early versus delayed invasive intervention in acute coronary syndromes. N Engl J Med. 2009;360(21):2165-2175.
- Olesen JB, Torp-Pedersen C, Hansen ML, Lip GY. The value of the CHA2DS2-VASc score for refining stroke risk stratification in patients with atrial fibrillation with a CHADS2 score 0-1: a nationwide cohort study. Thromb Haemost. 2012;107(6):1172-1179.
- Associations between outpatient heart failure process-of-care measures and mortality. Circulation. 2011;123(15):1601-1610.