User login
Pending Tests at Discharge
The period following discharge is a vulnerable time for patientsthe prevalence of medical errors related to this transition is high and has important patient safety and medico‐legal ramifications.13 Factors contributing to this vulnerability include complexity of hospitalized patients, shorter lengths of stay, and increased discontinuity of care. Hospitalists have recognized this threat to patient safety and have worked toward improving information exchange between inpatient and outpatient providers at hospital discharge.46 Nonetheless, the evidence suggests that more work is necessary. A recent study found that discharge summaries are often incomplete, and do not contain important information requiring follow‐up, such as pending tests.7 Additionally, a review by Kripalani et al. characterizing information deficits at hospital discharge found few interventions which specifically improve communication of pending tests at hospital discharge.8
In a prior study we determined that 41% of patients left the hospital before all laboratory and radiology test results were finalized. Of these results, 9.4% were potentially actionable and could have altered management. Physicians were aware of only 38% of post‐discharge test results.9 This awareness gap is a consequence of several factors including the lack of systems to track and alert providers of test results finalized post discharge. Also, it is unclear who is responsible for pending tests at discharge, since these tests are ordered by the inpatient physicians but often reported in the time period between hospital discharge and the patient's first follow‐up appointment with the primary care physician (PCP). Because responsibility is not explicitly made in the final communication between physicians at discharge, such test results may not be reviewed in a timely manner, potentially resulting in delays in treatment, a need for readmission, or other unfavorable outcomes.
Even in integrated health systems with advanced electronic health records, missed test results which result in treatment delays remain prevalent.10, 11 Test result management applications aid clinicians in reviewing and acting upon results as they become available and such systems may provide solutions to this problem. At Partners Healthcare in Boston, the Results Manager (RM) application was developed to help clinicians in the ambulatory setting safely, reliably, and efficiently review and act upon test results. The application enables clinicians to prioritize test results, utilize guidelines, and generate letters to patients. This system also prompts physicians to set reminders for future testing.12 In a 2.5‐year study evaluating the impact of this intervention, PCPs at 26 adult primary care practices were able to expedite communication of outpatient laboratory and imaging test results to patients with the help of RM. Patients of physicians who participated in the project reported greater satisfaction with test result communication and with information provided about their condition than did a control group of similar patients.13 RM has not yet been studied in the inpatient setting or at care transitions. We describe an attempt at modifying the Partners RM application to help inpatient physicians manage pending tests at hospital discharge.
Methods
Study Setting and Participants
We piloted our application at 2 major academic medical centers (hospitals A and B) associated with Partners Healthcare, an integrated regional health delivery network in eastern Massachusetts, from October 2004 to March 2005. Both centers use the longitudinal medical record (LMR), the electronic medical record (EMR), for nearly all ambulatory practices. The LMR is an internally developed full‐featured EMR, including a repository of laboratory and radiology reports, discharge summaries, ambulatory care notes, medication lists, problem lists, coded allergies, and other patient data. Both centers also have their own inpatient results viewing and order entry systems which provide clinicians caring for patients in the hospital the ability to review results and write orders. Although possible, clinicians caring for patients in the inpatient setting do not routinely access LMR to view test results. Inpatient physician use of the LMR is generally limited to review of the outpatient record, medication lists, and ambulatory notes at admission.
At hospital A, the hospitalist attending physician is typically responsible for all communication to outpatient physicians at discharge, as well as for follow‐up on all test results that return after discharge. Hospital B has 2 types of hospitalist services. One is staffed only by hospitalist and nonhospitalist attending physicians. Nonhospitalist attending physicians were excluded because they care for their own patients in the inpatient and ambulatory setting and typically use RM to manage test results. The other hospitalist service at hospital B is a teaching service consisting of an attending physician, resident, and interns. For this service, the resident is responsible for communication at discharge and follow‐up on all pending tests. For purposes of this study inpatient physicians refers to those physicians responsible for communication with PCPs and follow‐up on pending tests. All inpatient physicians were eligible to participate during the study period.
Test Result Management Application
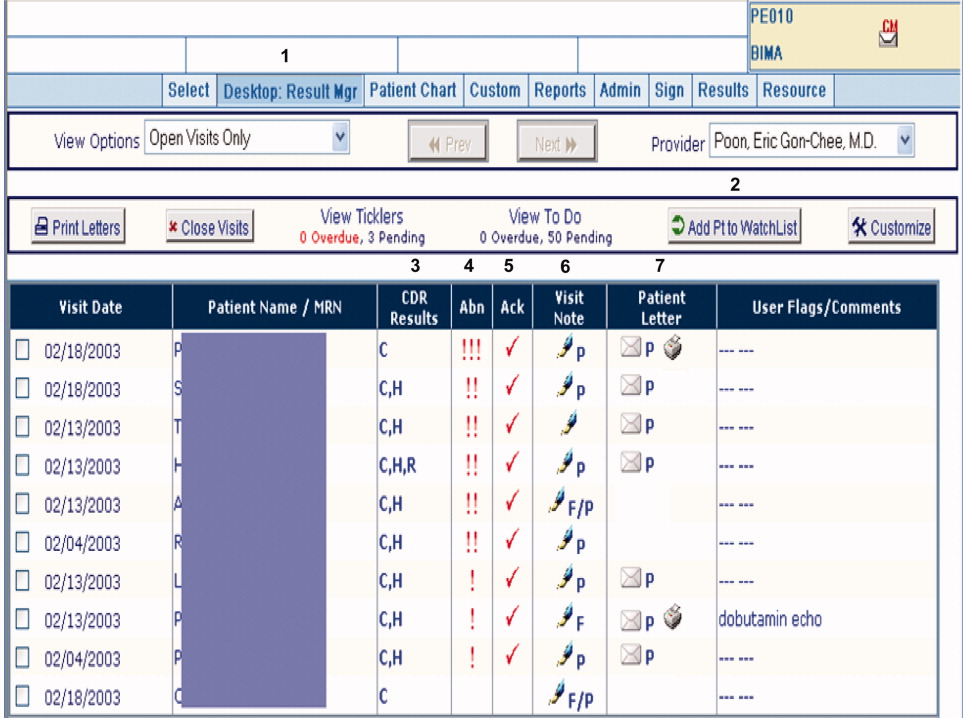
RM was originally developed by Partners Healthcare to improve timely review and appropriate management of test results in the ambulatory setting. RM was developed for and vetted by primarily ambulatory physicians. The application is browser‐based, provider‐centric, and embedded in the LMR to help ambulatory clinicians review and act upon test results in a safe, reliable, and efficient manner. Although RM has access to all inpatient and outpatient data in the Partners Clinical Data Repository (CDR), given the volume of inpatient tests ordered, hospital‐based results are suppressed by default to limit inundating ambulatory clinicians' queues. Therefore, users of RM only receive results of laboratory and radiology tests ordered in the ambulatory setting. They can track these tests for specific patients for a designated period of time by placing the patient on a watch list. Finally, RM incorporates extensive decision support features to classify the degree of abnormality for each result, presents guidelines to help clinicians manage abnormal results, allows clinicians to generate result letters to patients using predefined, context‐sensitive templates, and prompts physicians to set reminders for future testing. Because RM was developed from the ambulatory perspective, there was limited input from hospitalist physicians with regard to inpatient workflow in the original design of the module.12 See Figure 1 for a screen shot of RM and a description of its features.
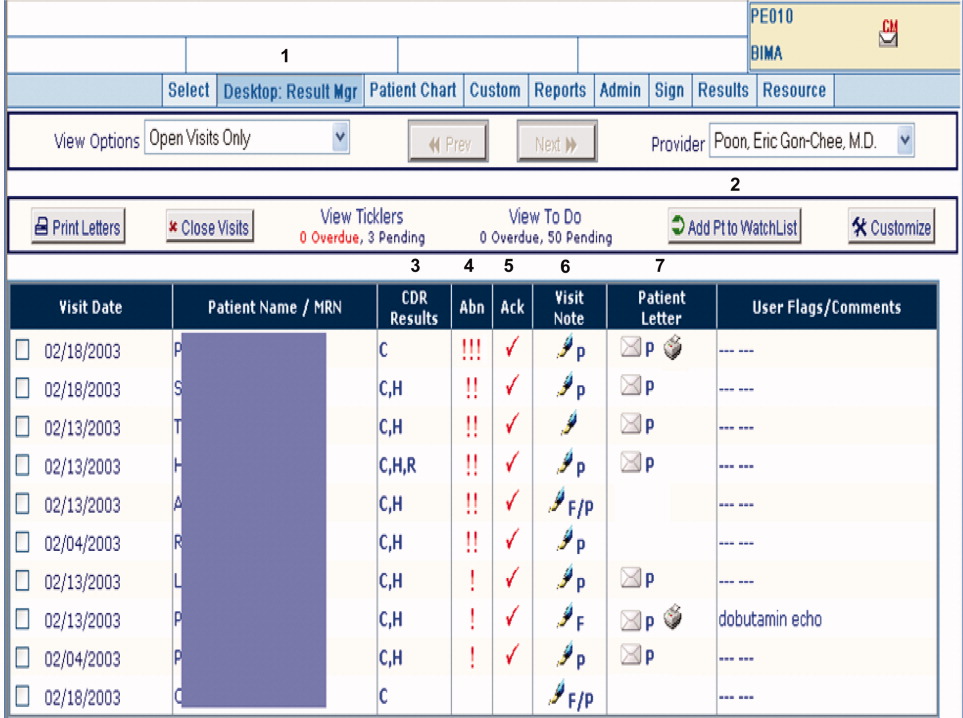
figure can be viewed in the online issue, which is available at wileyonlinelibrary.com.]
For purposes of this pilot, we modified RM to allow results of tests ordered in the inpatient setting to be available for viewing (Hospitalist Results Manager, HRM). This feature was turned on only for inpatient physicians as previously defined. Inpatient tests, including pending tests at discharge, continued to be suppressed from PCP's RM queue (however, any physician could access a patient's test result(s) directly from the Partners CDR). Inpatient physicians could track laboratory and radiology results finalized after discharge by keeping discharged patients on their HRM watch list for a designated period of time. The finalized results would become available for review in their HRM queue and abnormal results were displayed prominently at the top of this queue. Inpatient physicians were trained to use HRM in a series of meetings and demonstrations. Although HRM could be accessed from inpatient clinical workstations, it was not part of the inpatient clinical information system.
Surveys
Study surveys were developed and refined through an iterative process and pilot tested among inpatient physicians at both centers for clarity. We surveyed inpatient physicians five months after HRM implementation. Inpatient physicians were asked how often they used HRM, what barriers they faced (respondents asked to quantify agreement to statements on a 5‐point Likert scale), and which elements of an ideal system they would prefer. Finally, we solicited comments regarding perceived obstacles and suggestions for improvement. Because HRM was targeted to inpatient physicians, and because RM has been evaluated from the ambulatory perspective in a prior study,13 PCPs were not surveyed. See Supporting Information Appendix for the survey instrument used in the study.
Results
A total of 35 inpatient physicians participated in the pilot. Among 649 patients discharged during the study period, there were 1075 tests pending of which 555 were subsequently flagged as abnormal in HRM. Study surveys were sent to the 35 inpatient physician participants and 29 were completed, including partial responses (83% survey response rate). The 35 inpatient physician participants had the following characteristics: 22 were male, 13 were female; 21 were trainees and 14 were nontrainees/faculty. All 21 trainees were PGY2s. Nontrainees and faculty varied in experience level (PGY 15: 5, PGY 610: 7, PGY 1120: 1, PGY 21+: 1). Of 29 survey respondents, 7 were from hospital A and 22 were from hospital B; 19 were trainees and 10 were nontrainees/faculty. Of the 6 nonrespondents, 2 were from hospital A and 4 were from hospital B; 2 were trainees and 4 were nontrainees/faculty.
Table 1 shows the results of our survey of inpatient physicians regarding usage of HRM. Of 29 survey respondents, 14 (48%) reported never using HRM. Thirteen (45%) reported using HRM 1 to 2 times per week. None of the respondents used it more than 4 times per week. The frequency of usage was similar for hospitals A and B. Table 2 details barriers to using HRM. Twenty‐three inpatient physicians (79%) reported barriers. Seventeen (59%) thought that results in their HRM queue were not clinically relevant, 16 (55%) felt that HRM did not fit into their daily workflow, 14 (48%) had limited time to use HRM, and 12 (41%) noted that too many results in their HRM queue were on other physician's patients. Seven (24%) reported operational issues and 3 (10%) reported technical issues prohibiting use of HRM. With regard to preferred elements of an ideal results manager system, 21 (72%) inpatient physician respondents wanted to receive notification of abnormal and clinician‐designated pending test results. Four (14%) wanted to receive only abnormal results and 1 (3%) wanted to receive all results. Twenty‐seven (93%) physicians agreed that an ideally designed computerized test result management application would be valuable for managing pending tests at discharge.
| Frequency | Number of Inpatient Physicians Using HRM, n (%) | ||
|---|---|---|---|
| Overall | Hospital A | Hospital B | |
| |||
| Never | 14 (48) | 3 (43) | 11 (50) |
| 12 times per week | 13 (45) | 3 (43) | 10 (45.5) |
| 34 times per week | 2 (7) | 1 (14) | 1 (4.5) |
| 57 times per week | 0 | 0 | 0 |
| >7 times per week | 0 | 0 | 0 |
| Barrier | Overall, n (%) | Hospital A, n (%) | Hospital B, n (%) |
|---|---|---|---|
| |||
| Forgot to use HRM | 23 (79) | 7 (100) | 16 (73) |
| Results not clinically relevant | 17 (59) | 7 (100) | 10 (45) |
| Did not fit daily workflow | 16 (55) | 7 (100) | 9 (41) |
| Too little time to use HRM | 14 (48) | 6 (86) | 8 (46) |
| Results on others' patients | 12 (41) | 6 (86) | 6 (27) |
| HRM was difficult to use | 7 (24) | 2 (29) | 5 (23) |
| Had technical difficulties | 3 (10) | 0 (0) | 3 (14) |
Table 3 provides comments from inpatient physician respondents regarding obstacles prohibiting use of HRM and suggestions for future systems.
|
| Suggestions |
| Would be more useful if accessible from (the inpatient clinical information system). |
| Email notification (would have been useful). |
| At time of discharge, if there is a way to find pending labs at discharge, this would be of great utility. |
| Linking responsibility for follow‐up to test ordering (would have been useful). |
| Smarter system for filtering results so less important results are filtered out (is desirable). |
| Can the system be tied into PCP's email somehow? |
| Obstacles |
| Blood cultures, abnormal films can be difficult and time‐consuming to look up. |
| A big problem is results that automatically trigger even though they're not clinically relevant. |
| Keeping a record of patients that left with tests pending (is often difficult to do). |
| Addressing pending results is very time consuming. |
Discussion
We describe a pilot implementation of a computerized application for the management of pending tests at hospital discharge. From responses to post‐implementation surveys, we were able to identify multiple factors prohibiting successful implementation of the application. These observations may help inform future interventions and evaluations.
Almost half of inpatient physicians reported never using HRM despite training and reminders. The feedback provided by physicians in our study suggested that HRM was not ideally designed from an inpatient physician perspective. We discovered several barriers to its use: (1) HRM overburdened physicians with clinically irrelevant test results, suggesting that more robust filtering of abnormal but low importance test results may be required (eg, a borderline electrolyte abnormality or low but stable hematocrit); (2) HRM did not integrate well into inpatient workflowthe system was not integrated into the inpatient results viewing and computerized physician order entry (CPOE) applications, and therefore required an extra step to access; (3) there was no mechanism of alerting inpatient physicians that finalized test results were available for viewing in their HRM queues (eg, by email or by an alert in the inpatient computer system); (4) because responsibility for these results was unclear, most inpatient physicians had no formal method of managing them, and for many, using HRM represented an additional task; and finally (5) several physicians commented on finding results in their HRM queue that belonged to other physician's patients, implying that the hospital databases were inaccurate in identifying the discharging physician or that rotation schedules, and therefore patient responsibility, had changed in the intervening period. Table 4 summarizes the advantages and respective limitations of features of HRM available to inpatient physicians.
| Advantages | Limitations |
|---|---|
| |
| Creates a physician‐managed queue of pending test results by patient | Does not provide alert or push notification when new results available for patients |
| Filters test results by severity with most critical results appearing at the top of the queue | Severity filter set for outpatients; not restrictive enough for post‐discharge period, resulting in excessive alerting |
| Independent, voluntary acknowledgement of results by user | Active acknowledgment not required; no audit trail, feedback, or escalation if result not acknowledged |
| Embedded within LMR (the ambulatory EMR) | LMR not routinely used by many inpatient physicians |
| Offers patient communication tools (eg, pre‐populated patient results letter) | Tools not optimized for post‐discharge test result communication by inpatient physicians (eg, a tool for PCP result notification and acknowledgment) |
In the literature, there is little information regarding optimal features of a test result management system for transitions from the inpatient to ambulatory care setting. Prior studies outline important functions for results management systems developed for noninpatient sites of care, including the ambulatory and emergency room setting.12, 14, 15 These include a method of prioritizing by degree of abnormality, the ability to reliably and efficiently act upon results, and an automated alerting system for abnormal results. Findings from our study provide insight in defining core functions for result management systems which focus on transitions from the inpatient to ambulatory care setting. These functions include tight integration with applications used by inpatient physicians, clear assignment of responsibility for test results finalized after hospital discharge (as well as a mechanism to reassign responsibility), automated alerts to responsible providers of test results finalized post‐discharge, and ways to automatically filter test results to avoid over‐burdening physicians with clinically irrelevant results.
Almost all surveyed inpatient physicians agreed that an ideally designed electronic post‐discharge results management system would be valuable. For such systems to be successfully adopted, we offer several principles to help guide future work. These include: (1) clarifying responsibility at the time a test is ordered and again at discharge, (2) understanding workflow and communication patterns among inpatient and outpatient clinicians, and (3) integrating technological solutions into existing systems to minimize workflow disruptions. For example, if the primary responsibility for post‐discharge result follow‐up lies with the ordering physician, the system should be integrated within the EMR most often used by inpatient physicians and become part of inpatient physician workflow. If the system depends on administrative databases to identify the responsible providers, these must be accurate. Alternatively, in organizations with computerized provider order entry, responsibility for the result could be assigned when the test is ordered and confirmed at discharge (ie, the results management system would be integrated into the discharge order such that pending tests are reviewed at the time of discharge). The discharging physician should have the ability to assign responsibility for each pending test and select preferred mode(s) of notification once its result is finalized (eg, e‐mail, alphanumeric page, etc.). The system should have the ability to generate an automatic notification to the inpatient and PCP (and perhaps other designated providers involved in the patient's inpatient care), but it should not burden busy clinicians with unnecessary alerts and warnings. Finally, the rules by which results are prioritized must be robust enough to filter out less urgent results, and should be modified to reflect the severity of illness of recently discharged patients. In essence, in consideration of the time constraints of busy clinicians, an ideal results management system should achieve automated notification of test results while minimizing the risk of alert fatigue from the potentially large volume of alerts generated.
Our study has several important limitations. First, although our survey response rate was high, the sample size of actual participants was small. Second, because the study was conducted in 2 similar, tertiary care academic centers, it may not generalize to other settings (we note that hospital B included a nonteaching service similar to those in nonacademic medical centers). This may be particularly true in assessing the importance of specific barriers to use of results management systems, which may vary at different institutions. Third, the representation of survey respondents were skeweda majority of the responses were from trainees (all post‐graduate level [PGY] level 2) and from hospital B. Fourth, we did not actively monitor physician interaction with the test result management application, and therefore, we depended heavily on physician recollection of use of the system when responding to surveys. Finally, we did not convene focus groups of key individuals with regard to the factors facilitating or prohibiting adoption of the system. Use of semi‐structured, key informant interviews (ie, focus groups) before and after implementation of an electronic results management application, have been shown to be effective in evaluating potential barriers and facilitators of adoption.16 Focus groups of and/or interviews with inpatient and PCPs, physician extenders, and housestaff could have been useful to better characterize the potential barriers and facilitators of adoption noted by survey respondents in our study.
In summary, we offer several lessons from our attempt to implement a system to manage pending tests at hospital discharge. The success of implementing future systems to address this patient safety concern will rely on accurately assigning responsibility for these test results, integrating the system within clinical information systems commonly used by the inpatient physician, addressing workflow issues and time constraints, maximizing appropriateness of alerting, and minimizing alert fatigue.
- ,,,,.The incidence and severity of adverse events affecting patients after discharge from the hospital.Ann Intern Med.2003;138(3):161–167.
- ,,,.Medical errors related to discontinuity of care from an inpatient to an outpatient setting.J Gen Intern Med.2003;18(8):646–651.
- .Key legal principles for hospitalists.Am J Med.2001;111(9B):5S–9S.
- ,,.Passing the clinical baton: 6 principles to guide the hospitalist.Am J Med.2001;111(9B):36S–39S.
- ,.Lost in transition: challenges and opportunities for improving the quality of transitional care.Ann Intern Med.2004;141(7):533–536.
- ,,,.Promoting effective transitions of care at hospital discharge: a review of key issues for hospitalists.J Hosp Med.2007;2(5):314–323.
- ,,, et al.Adequacy of hospital discharge summaries in documenting tests with pending results and outpatient follow‐up providers.J Gen Intern Med.2009;24(9):1002–1006.
- ,,,,,.Deficits in communication and information transfer between hospital‐based and primary care physicians: Implications for patient safety and continuity of care.JAMA.2007;297(8):831–841.
- ,,, et al.Patient safety concerns arising from test results that return after hospital discharge.Ann Intern Med.2005;143(2):121–128.
- ,,.The continuing problem of missed test results in an integrated health system with an advanced electronic medical record.Jt Comm J Qual Patient Saf.2007;33(8):485–492.
- ,.The frequency of missed test results and associated treatment delays in a highly computerized health system.BMC Fam Pract.2007;8:32.
- ,,,,.Design and implementation of a comprehensive outpatient results manager.J Biomed Inform.2003;36(1–2):80–91.
- ,,, et al.Impact of an automated test results management system on patients' satisfaction about test result communication.Arch Intern Med.2007;167(20):2233–2239.
- ,,,,,.“I wish I had seen this test result earlier!”: dissatisfaction with test result management systems in primary care.Arch Intern Med.2004;164(20):2223–2228.
- ,,.Potential impact of a computerized system to report late‐arriving laboratory results in the emergency department.Pediatr Emerg Care.2000;16(5):313–315.
- ,,, et al.Electronic results management in pediatric ambulatory care: Qualitative assessment.Pediatrics.2009;123Suppl 2:S85–S91.
The period following discharge is a vulnerable time for patientsthe prevalence of medical errors related to this transition is high and has important patient safety and medico‐legal ramifications.13 Factors contributing to this vulnerability include complexity of hospitalized patients, shorter lengths of stay, and increased discontinuity of care. Hospitalists have recognized this threat to patient safety and have worked toward improving information exchange between inpatient and outpatient providers at hospital discharge.46 Nonetheless, the evidence suggests that more work is necessary. A recent study found that discharge summaries are often incomplete, and do not contain important information requiring follow‐up, such as pending tests.7 Additionally, a review by Kripalani et al. characterizing information deficits at hospital discharge found few interventions which specifically improve communication of pending tests at hospital discharge.8
In a prior study we determined that 41% of patients left the hospital before all laboratory and radiology test results were finalized. Of these results, 9.4% were potentially actionable and could have altered management. Physicians were aware of only 38% of post‐discharge test results.9 This awareness gap is a consequence of several factors including the lack of systems to track and alert providers of test results finalized post discharge. Also, it is unclear who is responsible for pending tests at discharge, since these tests are ordered by the inpatient physicians but often reported in the time period between hospital discharge and the patient's first follow‐up appointment with the primary care physician (PCP). Because responsibility is not explicitly made in the final communication between physicians at discharge, such test results may not be reviewed in a timely manner, potentially resulting in delays in treatment, a need for readmission, or other unfavorable outcomes.
Even in integrated health systems with advanced electronic health records, missed test results which result in treatment delays remain prevalent.10, 11 Test result management applications aid clinicians in reviewing and acting upon results as they become available and such systems may provide solutions to this problem. At Partners Healthcare in Boston, the Results Manager (RM) application was developed to help clinicians in the ambulatory setting safely, reliably, and efficiently review and act upon test results. The application enables clinicians to prioritize test results, utilize guidelines, and generate letters to patients. This system also prompts physicians to set reminders for future testing.12 In a 2.5‐year study evaluating the impact of this intervention, PCPs at 26 adult primary care practices were able to expedite communication of outpatient laboratory and imaging test results to patients with the help of RM. Patients of physicians who participated in the project reported greater satisfaction with test result communication and with information provided about their condition than did a control group of similar patients.13 RM has not yet been studied in the inpatient setting or at care transitions. We describe an attempt at modifying the Partners RM application to help inpatient physicians manage pending tests at hospital discharge.
Methods
Study Setting and Participants
We piloted our application at 2 major academic medical centers (hospitals A and B) associated with Partners Healthcare, an integrated regional health delivery network in eastern Massachusetts, from October 2004 to March 2005. Both centers use the longitudinal medical record (LMR), the electronic medical record (EMR), for nearly all ambulatory practices. The LMR is an internally developed full‐featured EMR, including a repository of laboratory and radiology reports, discharge summaries, ambulatory care notes, medication lists, problem lists, coded allergies, and other patient data. Both centers also have their own inpatient results viewing and order entry systems which provide clinicians caring for patients in the hospital the ability to review results and write orders. Although possible, clinicians caring for patients in the inpatient setting do not routinely access LMR to view test results. Inpatient physician use of the LMR is generally limited to review of the outpatient record, medication lists, and ambulatory notes at admission.
At hospital A, the hospitalist attending physician is typically responsible for all communication to outpatient physicians at discharge, as well as for follow‐up on all test results that return after discharge. Hospital B has 2 types of hospitalist services. One is staffed only by hospitalist and nonhospitalist attending physicians. Nonhospitalist attending physicians were excluded because they care for their own patients in the inpatient and ambulatory setting and typically use RM to manage test results. The other hospitalist service at hospital B is a teaching service consisting of an attending physician, resident, and interns. For this service, the resident is responsible for communication at discharge and follow‐up on all pending tests. For purposes of this study inpatient physicians refers to those physicians responsible for communication with PCPs and follow‐up on pending tests. All inpatient physicians were eligible to participate during the study period.
Test Result Management Application
RM was originally developed by Partners Healthcare to improve timely review and appropriate management of test results in the ambulatory setting. RM was developed for and vetted by primarily ambulatory physicians. The application is browser‐based, provider‐centric, and embedded in the LMR to help ambulatory clinicians review and act upon test results in a safe, reliable, and efficient manner. Although RM has access to all inpatient and outpatient data in the Partners Clinical Data Repository (CDR), given the volume of inpatient tests ordered, hospital‐based results are suppressed by default to limit inundating ambulatory clinicians' queues. Therefore, users of RM only receive results of laboratory and radiology tests ordered in the ambulatory setting. They can track these tests for specific patients for a designated period of time by placing the patient on a watch list. Finally, RM incorporates extensive decision support features to classify the degree of abnormality for each result, presents guidelines to help clinicians manage abnormal results, allows clinicians to generate result letters to patients using predefined, context‐sensitive templates, and prompts physicians to set reminders for future testing. Because RM was developed from the ambulatory perspective, there was limited input from hospitalist physicians with regard to inpatient workflow in the original design of the module.12 See Figure 1 for a screen shot of RM and a description of its features.
figure can be viewed in the online issue, which is available at wileyonlinelibrary.com.]
For purposes of this pilot, we modified RM to allow results of tests ordered in the inpatient setting to be available for viewing (Hospitalist Results Manager, HRM). This feature was turned on only for inpatient physicians as previously defined. Inpatient tests, including pending tests at discharge, continued to be suppressed from PCP's RM queue (however, any physician could access a patient's test result(s) directly from the Partners CDR). Inpatient physicians could track laboratory and radiology results finalized after discharge by keeping discharged patients on their HRM watch list for a designated period of time. The finalized results would become available for review in their HRM queue and abnormal results were displayed prominently at the top of this queue. Inpatient physicians were trained to use HRM in a series of meetings and demonstrations. Although HRM could be accessed from inpatient clinical workstations, it was not part of the inpatient clinical information system.
Surveys
Study surveys were developed and refined through an iterative process and pilot tested among inpatient physicians at both centers for clarity. We surveyed inpatient physicians five months after HRM implementation. Inpatient physicians were asked how often they used HRM, what barriers they faced (respondents asked to quantify agreement to statements on a 5‐point Likert scale), and which elements of an ideal system they would prefer. Finally, we solicited comments regarding perceived obstacles and suggestions for improvement. Because HRM was targeted to inpatient physicians, and because RM has been evaluated from the ambulatory perspective in a prior study,13 PCPs were not surveyed. See Supporting Information Appendix for the survey instrument used in the study.
Results
A total of 35 inpatient physicians participated in the pilot. Among 649 patients discharged during the study period, there were 1075 tests pending of which 555 were subsequently flagged as abnormal in HRM. Study surveys were sent to the 35 inpatient physician participants and 29 were completed, including partial responses (83% survey response rate). The 35 inpatient physician participants had the following characteristics: 22 were male, 13 were female; 21 were trainees and 14 were nontrainees/faculty. All 21 trainees were PGY2s. Nontrainees and faculty varied in experience level (PGY 15: 5, PGY 610: 7, PGY 1120: 1, PGY 21+: 1). Of 29 survey respondents, 7 were from hospital A and 22 were from hospital B; 19 were trainees and 10 were nontrainees/faculty. Of the 6 nonrespondents, 2 were from hospital A and 4 were from hospital B; 2 were trainees and 4 were nontrainees/faculty.
Table 1 shows the results of our survey of inpatient physicians regarding usage of HRM. Of 29 survey respondents, 14 (48%) reported never using HRM. Thirteen (45%) reported using HRM 1 to 2 times per week. None of the respondents used it more than 4 times per week. The frequency of usage was similar for hospitals A and B. Table 2 details barriers to using HRM. Twenty‐three inpatient physicians (79%) reported barriers. Seventeen (59%) thought that results in their HRM queue were not clinically relevant, 16 (55%) felt that HRM did not fit into their daily workflow, 14 (48%) had limited time to use HRM, and 12 (41%) noted that too many results in their HRM queue were on other physician's patients. Seven (24%) reported operational issues and 3 (10%) reported technical issues prohibiting use of HRM. With regard to preferred elements of an ideal results manager system, 21 (72%) inpatient physician respondents wanted to receive notification of abnormal and clinician‐designated pending test results. Four (14%) wanted to receive only abnormal results and 1 (3%) wanted to receive all results. Twenty‐seven (93%) physicians agreed that an ideally designed computerized test result management application would be valuable for managing pending tests at discharge.
| Frequency | Number of Inpatient Physicians Using HRM, n (%) | ||
|---|---|---|---|
| Overall | Hospital A | Hospital B | |
| |||
| Never | 14 (48) | 3 (43) | 11 (50) |
| 12 times per week | 13 (45) | 3 (43) | 10 (45.5) |
| 34 times per week | 2 (7) | 1 (14) | 1 (4.5) |
| 57 times per week | 0 | 0 | 0 |
| >7 times per week | 0 | 0 | 0 |
| Barrier | Overall, n (%) | Hospital A, n (%) | Hospital B, n (%) |
|---|---|---|---|
| |||
| Forgot to use HRM | 23 (79) | 7 (100) | 16 (73) |
| Results not clinically relevant | 17 (59) | 7 (100) | 10 (45) |
| Did not fit daily workflow | 16 (55) | 7 (100) | 9 (41) |
| Too little time to use HRM | 14 (48) | 6 (86) | 8 (46) |
| Results on others' patients | 12 (41) | 6 (86) | 6 (27) |
| HRM was difficult to use | 7 (24) | 2 (29) | 5 (23) |
| Had technical difficulties | 3 (10) | 0 (0) | 3 (14) |
Table 3 provides comments from inpatient physician respondents regarding obstacles prohibiting use of HRM and suggestions for future systems.
|
| Suggestions |
| Would be more useful if accessible from (the inpatient clinical information system). |
| Email notification (would have been useful). |
| At time of discharge, if there is a way to find pending labs at discharge, this would be of great utility. |
| Linking responsibility for follow‐up to test ordering (would have been useful). |
| Smarter system for filtering results so less important results are filtered out (is desirable). |
| Can the system be tied into PCP's email somehow? |
| Obstacles |
| Blood cultures, abnormal films can be difficult and time‐consuming to look up. |
| A big problem is results that automatically trigger even though they're not clinically relevant. |
| Keeping a record of patients that left with tests pending (is often difficult to do). |
| Addressing pending results is very time consuming. |
Discussion
We describe a pilot implementation of a computerized application for the management of pending tests at hospital discharge. From responses to post‐implementation surveys, we were able to identify multiple factors prohibiting successful implementation of the application. These observations may help inform future interventions and evaluations.
Almost half of inpatient physicians reported never using HRM despite training and reminders. The feedback provided by physicians in our study suggested that HRM was not ideally designed from an inpatient physician perspective. We discovered several barriers to its use: (1) HRM overburdened physicians with clinically irrelevant test results, suggesting that more robust filtering of abnormal but low importance test results may be required (eg, a borderline electrolyte abnormality or low but stable hematocrit); (2) HRM did not integrate well into inpatient workflowthe system was not integrated into the inpatient results viewing and computerized physician order entry (CPOE) applications, and therefore required an extra step to access; (3) there was no mechanism of alerting inpatient physicians that finalized test results were available for viewing in their HRM queues (eg, by email or by an alert in the inpatient computer system); (4) because responsibility for these results was unclear, most inpatient physicians had no formal method of managing them, and for many, using HRM represented an additional task; and finally (5) several physicians commented on finding results in their HRM queue that belonged to other physician's patients, implying that the hospital databases were inaccurate in identifying the discharging physician or that rotation schedules, and therefore patient responsibility, had changed in the intervening period. Table 4 summarizes the advantages and respective limitations of features of HRM available to inpatient physicians.
| Advantages | Limitations |
|---|---|
| |
| Creates a physician‐managed queue of pending test results by patient | Does not provide alert or push notification when new results available for patients |
| Filters test results by severity with most critical results appearing at the top of the queue | Severity filter set for outpatients; not restrictive enough for post‐discharge period, resulting in excessive alerting |
| Independent, voluntary acknowledgement of results by user | Active acknowledgment not required; no audit trail, feedback, or escalation if result not acknowledged |
| Embedded within LMR (the ambulatory EMR) | LMR not routinely used by many inpatient physicians |
| Offers patient communication tools (eg, pre‐populated patient results letter) | Tools not optimized for post‐discharge test result communication by inpatient physicians (eg, a tool for PCP result notification and acknowledgment) |
In the literature, there is little information regarding optimal features of a test result management system for transitions from the inpatient to ambulatory care setting. Prior studies outline important functions for results management systems developed for noninpatient sites of care, including the ambulatory and emergency room setting.12, 14, 15 These include a method of prioritizing by degree of abnormality, the ability to reliably and efficiently act upon results, and an automated alerting system for abnormal results. Findings from our study provide insight in defining core functions for result management systems which focus on transitions from the inpatient to ambulatory care setting. These functions include tight integration with applications used by inpatient physicians, clear assignment of responsibility for test results finalized after hospital discharge (as well as a mechanism to reassign responsibility), automated alerts to responsible providers of test results finalized post‐discharge, and ways to automatically filter test results to avoid over‐burdening physicians with clinically irrelevant results.
Almost all surveyed inpatient physicians agreed that an ideally designed electronic post‐discharge results management system would be valuable. For such systems to be successfully adopted, we offer several principles to help guide future work. These include: (1) clarifying responsibility at the time a test is ordered and again at discharge, (2) understanding workflow and communication patterns among inpatient and outpatient clinicians, and (3) integrating technological solutions into existing systems to minimize workflow disruptions. For example, if the primary responsibility for post‐discharge result follow‐up lies with the ordering physician, the system should be integrated within the EMR most often used by inpatient physicians and become part of inpatient physician workflow. If the system depends on administrative databases to identify the responsible providers, these must be accurate. Alternatively, in organizations with computerized provider order entry, responsibility for the result could be assigned when the test is ordered and confirmed at discharge (ie, the results management system would be integrated into the discharge order such that pending tests are reviewed at the time of discharge). The discharging physician should have the ability to assign responsibility for each pending test and select preferred mode(s) of notification once its result is finalized (eg, e‐mail, alphanumeric page, etc.). The system should have the ability to generate an automatic notification to the inpatient and PCP (and perhaps other designated providers involved in the patient's inpatient care), but it should not burden busy clinicians with unnecessary alerts and warnings. Finally, the rules by which results are prioritized must be robust enough to filter out less urgent results, and should be modified to reflect the severity of illness of recently discharged patients. In essence, in consideration of the time constraints of busy clinicians, an ideal results management system should achieve automated notification of test results while minimizing the risk of alert fatigue from the potentially large volume of alerts generated.
Our study has several important limitations. First, although our survey response rate was high, the sample size of actual participants was small. Second, because the study was conducted in 2 similar, tertiary care academic centers, it may not generalize to other settings (we note that hospital B included a nonteaching service similar to those in nonacademic medical centers). This may be particularly true in assessing the importance of specific barriers to use of results management systems, which may vary at different institutions. Third, the representation of survey respondents were skeweda majority of the responses were from trainees (all post‐graduate level [PGY] level 2) and from hospital B. Fourth, we did not actively monitor physician interaction with the test result management application, and therefore, we depended heavily on physician recollection of use of the system when responding to surveys. Finally, we did not convene focus groups of key individuals with regard to the factors facilitating or prohibiting adoption of the system. Use of semi‐structured, key informant interviews (ie, focus groups) before and after implementation of an electronic results management application, have been shown to be effective in evaluating potential barriers and facilitators of adoption.16 Focus groups of and/or interviews with inpatient and PCPs, physician extenders, and housestaff could have been useful to better characterize the potential barriers and facilitators of adoption noted by survey respondents in our study.
In summary, we offer several lessons from our attempt to implement a system to manage pending tests at hospital discharge. The success of implementing future systems to address this patient safety concern will rely on accurately assigning responsibility for these test results, integrating the system within clinical information systems commonly used by the inpatient physician, addressing workflow issues and time constraints, maximizing appropriateness of alerting, and minimizing alert fatigue.
The period following discharge is a vulnerable time for patientsthe prevalence of medical errors related to this transition is high and has important patient safety and medico‐legal ramifications.13 Factors contributing to this vulnerability include complexity of hospitalized patients, shorter lengths of stay, and increased discontinuity of care. Hospitalists have recognized this threat to patient safety and have worked toward improving information exchange between inpatient and outpatient providers at hospital discharge.46 Nonetheless, the evidence suggests that more work is necessary. A recent study found that discharge summaries are often incomplete, and do not contain important information requiring follow‐up, such as pending tests.7 Additionally, a review by Kripalani et al. characterizing information deficits at hospital discharge found few interventions which specifically improve communication of pending tests at hospital discharge.8
In a prior study we determined that 41% of patients left the hospital before all laboratory and radiology test results were finalized. Of these results, 9.4% were potentially actionable and could have altered management. Physicians were aware of only 38% of post‐discharge test results.9 This awareness gap is a consequence of several factors including the lack of systems to track and alert providers of test results finalized post discharge. Also, it is unclear who is responsible for pending tests at discharge, since these tests are ordered by the inpatient physicians but often reported in the time period between hospital discharge and the patient's first follow‐up appointment with the primary care physician (PCP). Because responsibility is not explicitly made in the final communication between physicians at discharge, such test results may not be reviewed in a timely manner, potentially resulting in delays in treatment, a need for readmission, or other unfavorable outcomes.
Even in integrated health systems with advanced electronic health records, missed test results which result in treatment delays remain prevalent.10, 11 Test result management applications aid clinicians in reviewing and acting upon results as they become available and such systems may provide solutions to this problem. At Partners Healthcare in Boston, the Results Manager (RM) application was developed to help clinicians in the ambulatory setting safely, reliably, and efficiently review and act upon test results. The application enables clinicians to prioritize test results, utilize guidelines, and generate letters to patients. This system also prompts physicians to set reminders for future testing.12 In a 2.5‐year study evaluating the impact of this intervention, PCPs at 26 adult primary care practices were able to expedite communication of outpatient laboratory and imaging test results to patients with the help of RM. Patients of physicians who participated in the project reported greater satisfaction with test result communication and with information provided about their condition than did a control group of similar patients.13 RM has not yet been studied in the inpatient setting or at care transitions. We describe an attempt at modifying the Partners RM application to help inpatient physicians manage pending tests at hospital discharge.
Methods
Study Setting and Participants
We piloted our application at 2 major academic medical centers (hospitals A and B) associated with Partners Healthcare, an integrated regional health delivery network in eastern Massachusetts, from October 2004 to March 2005. Both centers use the longitudinal medical record (LMR), the electronic medical record (EMR), for nearly all ambulatory practices. The LMR is an internally developed full‐featured EMR, including a repository of laboratory and radiology reports, discharge summaries, ambulatory care notes, medication lists, problem lists, coded allergies, and other patient data. Both centers also have their own inpatient results viewing and order entry systems which provide clinicians caring for patients in the hospital the ability to review results and write orders. Although possible, clinicians caring for patients in the inpatient setting do not routinely access LMR to view test results. Inpatient physician use of the LMR is generally limited to review of the outpatient record, medication lists, and ambulatory notes at admission.
At hospital A, the hospitalist attending physician is typically responsible for all communication to outpatient physicians at discharge, as well as for follow‐up on all test results that return after discharge. Hospital B has 2 types of hospitalist services. One is staffed only by hospitalist and nonhospitalist attending physicians. Nonhospitalist attending physicians were excluded because they care for their own patients in the inpatient and ambulatory setting and typically use RM to manage test results. The other hospitalist service at hospital B is a teaching service consisting of an attending physician, resident, and interns. For this service, the resident is responsible for communication at discharge and follow‐up on all pending tests. For purposes of this study inpatient physicians refers to those physicians responsible for communication with PCPs and follow‐up on pending tests. All inpatient physicians were eligible to participate during the study period.
Test Result Management Application
RM was originally developed by Partners Healthcare to improve timely review and appropriate management of test results in the ambulatory setting. RM was developed for and vetted by primarily ambulatory physicians. The application is browser‐based, provider‐centric, and embedded in the LMR to help ambulatory clinicians review and act upon test results in a safe, reliable, and efficient manner. Although RM has access to all inpatient and outpatient data in the Partners Clinical Data Repository (CDR), given the volume of inpatient tests ordered, hospital‐based results are suppressed by default to limit inundating ambulatory clinicians' queues. Therefore, users of RM only receive results of laboratory and radiology tests ordered in the ambulatory setting. They can track these tests for specific patients for a designated period of time by placing the patient on a watch list. Finally, RM incorporates extensive decision support features to classify the degree of abnormality for each result, presents guidelines to help clinicians manage abnormal results, allows clinicians to generate result letters to patients using predefined, context‐sensitive templates, and prompts physicians to set reminders for future testing. Because RM was developed from the ambulatory perspective, there was limited input from hospitalist physicians with regard to inpatient workflow in the original design of the module.12 See Figure 1 for a screen shot of RM and a description of its features.
figure can be viewed in the online issue, which is available at wileyonlinelibrary.com.]
For purposes of this pilot, we modified RM to allow results of tests ordered in the inpatient setting to be available for viewing (Hospitalist Results Manager, HRM). This feature was turned on only for inpatient physicians as previously defined. Inpatient tests, including pending tests at discharge, continued to be suppressed from PCP's RM queue (however, any physician could access a patient's test result(s) directly from the Partners CDR). Inpatient physicians could track laboratory and radiology results finalized after discharge by keeping discharged patients on their HRM watch list for a designated period of time. The finalized results would become available for review in their HRM queue and abnormal results were displayed prominently at the top of this queue. Inpatient physicians were trained to use HRM in a series of meetings and demonstrations. Although HRM could be accessed from inpatient clinical workstations, it was not part of the inpatient clinical information system.
Surveys
Study surveys were developed and refined through an iterative process and pilot tested among inpatient physicians at both centers for clarity. We surveyed inpatient physicians five months after HRM implementation. Inpatient physicians were asked how often they used HRM, what barriers they faced (respondents asked to quantify agreement to statements on a 5‐point Likert scale), and which elements of an ideal system they would prefer. Finally, we solicited comments regarding perceived obstacles and suggestions for improvement. Because HRM was targeted to inpatient physicians, and because RM has been evaluated from the ambulatory perspective in a prior study,13 PCPs were not surveyed. See Supporting Information Appendix for the survey instrument used in the study.
Results
A total of 35 inpatient physicians participated in the pilot. Among 649 patients discharged during the study period, there were 1075 tests pending of which 555 were subsequently flagged as abnormal in HRM. Study surveys were sent to the 35 inpatient physician participants and 29 were completed, including partial responses (83% survey response rate). The 35 inpatient physician participants had the following characteristics: 22 were male, 13 were female; 21 were trainees and 14 were nontrainees/faculty. All 21 trainees were PGY2s. Nontrainees and faculty varied in experience level (PGY 15: 5, PGY 610: 7, PGY 1120: 1, PGY 21+: 1). Of 29 survey respondents, 7 were from hospital A and 22 were from hospital B; 19 were trainees and 10 were nontrainees/faculty. Of the 6 nonrespondents, 2 were from hospital A and 4 were from hospital B; 2 were trainees and 4 were nontrainees/faculty.
Table 1 shows the results of our survey of inpatient physicians regarding usage of HRM. Of 29 survey respondents, 14 (48%) reported never using HRM. Thirteen (45%) reported using HRM 1 to 2 times per week. None of the respondents used it more than 4 times per week. The frequency of usage was similar for hospitals A and B. Table 2 details barriers to using HRM. Twenty‐three inpatient physicians (79%) reported barriers. Seventeen (59%) thought that results in their HRM queue were not clinically relevant, 16 (55%) felt that HRM did not fit into their daily workflow, 14 (48%) had limited time to use HRM, and 12 (41%) noted that too many results in their HRM queue were on other physician's patients. Seven (24%) reported operational issues and 3 (10%) reported technical issues prohibiting use of HRM. With regard to preferred elements of an ideal results manager system, 21 (72%) inpatient physician respondents wanted to receive notification of abnormal and clinician‐designated pending test results. Four (14%) wanted to receive only abnormal results and 1 (3%) wanted to receive all results. Twenty‐seven (93%) physicians agreed that an ideally designed computerized test result management application would be valuable for managing pending tests at discharge.
| Frequency | Number of Inpatient Physicians Using HRM, n (%) | ||
|---|---|---|---|
| Overall | Hospital A | Hospital B | |
| |||
| Never | 14 (48) | 3 (43) | 11 (50) |
| 12 times per week | 13 (45) | 3 (43) | 10 (45.5) |
| 34 times per week | 2 (7) | 1 (14) | 1 (4.5) |
| 57 times per week | 0 | 0 | 0 |
| >7 times per week | 0 | 0 | 0 |
| Barrier | Overall, n (%) | Hospital A, n (%) | Hospital B, n (%) |
|---|---|---|---|
| |||
| Forgot to use HRM | 23 (79) | 7 (100) | 16 (73) |
| Results not clinically relevant | 17 (59) | 7 (100) | 10 (45) |
| Did not fit daily workflow | 16 (55) | 7 (100) | 9 (41) |
| Too little time to use HRM | 14 (48) | 6 (86) | 8 (46) |
| Results on others' patients | 12 (41) | 6 (86) | 6 (27) |
| HRM was difficult to use | 7 (24) | 2 (29) | 5 (23) |
| Had technical difficulties | 3 (10) | 0 (0) | 3 (14) |
Table 3 provides comments from inpatient physician respondents regarding obstacles prohibiting use of HRM and suggestions for future systems.
|
| Suggestions |
| Would be more useful if accessible from (the inpatient clinical information system). |
| Email notification (would have been useful). |
| At time of discharge, if there is a way to find pending labs at discharge, this would be of great utility. |
| Linking responsibility for follow‐up to test ordering (would have been useful). |
| Smarter system for filtering results so less important results are filtered out (is desirable). |
| Can the system be tied into PCP's email somehow? |
| Obstacles |
| Blood cultures, abnormal films can be difficult and time‐consuming to look up. |
| A big problem is results that automatically trigger even though they're not clinically relevant. |
| Keeping a record of patients that left with tests pending (is often difficult to do). |
| Addressing pending results is very time consuming. |
Discussion
We describe a pilot implementation of a computerized application for the management of pending tests at hospital discharge. From responses to post‐implementation surveys, we were able to identify multiple factors prohibiting successful implementation of the application. These observations may help inform future interventions and evaluations.
Almost half of inpatient physicians reported never using HRM despite training and reminders. The feedback provided by physicians in our study suggested that HRM was not ideally designed from an inpatient physician perspective. We discovered several barriers to its use: (1) HRM overburdened physicians with clinically irrelevant test results, suggesting that more robust filtering of abnormal but low importance test results may be required (eg, a borderline electrolyte abnormality or low but stable hematocrit); (2) HRM did not integrate well into inpatient workflowthe system was not integrated into the inpatient results viewing and computerized physician order entry (CPOE) applications, and therefore required an extra step to access; (3) there was no mechanism of alerting inpatient physicians that finalized test results were available for viewing in their HRM queues (eg, by email or by an alert in the inpatient computer system); (4) because responsibility for these results was unclear, most inpatient physicians had no formal method of managing them, and for many, using HRM represented an additional task; and finally (5) several physicians commented on finding results in their HRM queue that belonged to other physician's patients, implying that the hospital databases were inaccurate in identifying the discharging physician or that rotation schedules, and therefore patient responsibility, had changed in the intervening period. Table 4 summarizes the advantages and respective limitations of features of HRM available to inpatient physicians.
| Advantages | Limitations |
|---|---|
| |
| Creates a physician‐managed queue of pending test results by patient | Does not provide alert or push notification when new results available for patients |
| Filters test results by severity with most critical results appearing at the top of the queue | Severity filter set for outpatients; not restrictive enough for post‐discharge period, resulting in excessive alerting |
| Independent, voluntary acknowledgement of results by user | Active acknowledgment not required; no audit trail, feedback, or escalation if result not acknowledged |
| Embedded within LMR (the ambulatory EMR) | LMR not routinely used by many inpatient physicians |
| Offers patient communication tools (eg, pre‐populated patient results letter) | Tools not optimized for post‐discharge test result communication by inpatient physicians (eg, a tool for PCP result notification and acknowledgment) |
In the literature, there is little information regarding optimal features of a test result management system for transitions from the inpatient to ambulatory care setting. Prior studies outline important functions for results management systems developed for noninpatient sites of care, including the ambulatory and emergency room setting.12, 14, 15 These include a method of prioritizing by degree of abnormality, the ability to reliably and efficiently act upon results, and an automated alerting system for abnormal results. Findings from our study provide insight in defining core functions for result management systems which focus on transitions from the inpatient to ambulatory care setting. These functions include tight integration with applications used by inpatient physicians, clear assignment of responsibility for test results finalized after hospital discharge (as well as a mechanism to reassign responsibility), automated alerts to responsible providers of test results finalized post‐discharge, and ways to automatically filter test results to avoid over‐burdening physicians with clinically irrelevant results.
Almost all surveyed inpatient physicians agreed that an ideally designed electronic post‐discharge results management system would be valuable. For such systems to be successfully adopted, we offer several principles to help guide future work. These include: (1) clarifying responsibility at the time a test is ordered and again at discharge, (2) understanding workflow and communication patterns among inpatient and outpatient clinicians, and (3) integrating technological solutions into existing systems to minimize workflow disruptions. For example, if the primary responsibility for post‐discharge result follow‐up lies with the ordering physician, the system should be integrated within the EMR most often used by inpatient physicians and become part of inpatient physician workflow. If the system depends on administrative databases to identify the responsible providers, these must be accurate. Alternatively, in organizations with computerized provider order entry, responsibility for the result could be assigned when the test is ordered and confirmed at discharge (ie, the results management system would be integrated into the discharge order such that pending tests are reviewed at the time of discharge). The discharging physician should have the ability to assign responsibility for each pending test and select preferred mode(s) of notification once its result is finalized (eg, e‐mail, alphanumeric page, etc.). The system should have the ability to generate an automatic notification to the inpatient and PCP (and perhaps other designated providers involved in the patient's inpatient care), but it should not burden busy clinicians with unnecessary alerts and warnings. Finally, the rules by which results are prioritized must be robust enough to filter out less urgent results, and should be modified to reflect the severity of illness of recently discharged patients. In essence, in consideration of the time constraints of busy clinicians, an ideal results management system should achieve automated notification of test results while minimizing the risk of alert fatigue from the potentially large volume of alerts generated.
Our study has several important limitations. First, although our survey response rate was high, the sample size of actual participants was small. Second, because the study was conducted in 2 similar, tertiary care academic centers, it may not generalize to other settings (we note that hospital B included a nonteaching service similar to those in nonacademic medical centers). This may be particularly true in assessing the importance of specific barriers to use of results management systems, which may vary at different institutions. Third, the representation of survey respondents were skeweda majority of the responses were from trainees (all post‐graduate level [PGY] level 2) and from hospital B. Fourth, we did not actively monitor physician interaction with the test result management application, and therefore, we depended heavily on physician recollection of use of the system when responding to surveys. Finally, we did not convene focus groups of key individuals with regard to the factors facilitating or prohibiting adoption of the system. Use of semi‐structured, key informant interviews (ie, focus groups) before and after implementation of an electronic results management application, have been shown to be effective in evaluating potential barriers and facilitators of adoption.16 Focus groups of and/or interviews with inpatient and PCPs, physician extenders, and housestaff could have been useful to better characterize the potential barriers and facilitators of adoption noted by survey respondents in our study.
In summary, we offer several lessons from our attempt to implement a system to manage pending tests at hospital discharge. The success of implementing future systems to address this patient safety concern will rely on accurately assigning responsibility for these test results, integrating the system within clinical information systems commonly used by the inpatient physician, addressing workflow issues and time constraints, maximizing appropriateness of alerting, and minimizing alert fatigue.
- ,,,,.The incidence and severity of adverse events affecting patients after discharge from the hospital.Ann Intern Med.2003;138(3):161–167.
- ,,,.Medical errors related to discontinuity of care from an inpatient to an outpatient setting.J Gen Intern Med.2003;18(8):646–651.
- .Key legal principles for hospitalists.Am J Med.2001;111(9B):5S–9S.
- ,,.Passing the clinical baton: 6 principles to guide the hospitalist.Am J Med.2001;111(9B):36S–39S.
- ,.Lost in transition: challenges and opportunities for improving the quality of transitional care.Ann Intern Med.2004;141(7):533–536.
- ,,,.Promoting effective transitions of care at hospital discharge: a review of key issues for hospitalists.J Hosp Med.2007;2(5):314–323.
- ,,, et al.Adequacy of hospital discharge summaries in documenting tests with pending results and outpatient follow‐up providers.J Gen Intern Med.2009;24(9):1002–1006.
- ,,,,,.Deficits in communication and information transfer between hospital‐based and primary care physicians: Implications for patient safety and continuity of care.JAMA.2007;297(8):831–841.
- ,,, et al.Patient safety concerns arising from test results that return after hospital discharge.Ann Intern Med.2005;143(2):121–128.
- ,,.The continuing problem of missed test results in an integrated health system with an advanced electronic medical record.Jt Comm J Qual Patient Saf.2007;33(8):485–492.
- ,.The frequency of missed test results and associated treatment delays in a highly computerized health system.BMC Fam Pract.2007;8:32.
- ,,,,.Design and implementation of a comprehensive outpatient results manager.J Biomed Inform.2003;36(1–2):80–91.
- ,,, et al.Impact of an automated test results management system on patients' satisfaction about test result communication.Arch Intern Med.2007;167(20):2233–2239.
- ,,,,,.“I wish I had seen this test result earlier!”: dissatisfaction with test result management systems in primary care.Arch Intern Med.2004;164(20):2223–2228.
- ,,.Potential impact of a computerized system to report late‐arriving laboratory results in the emergency department.Pediatr Emerg Care.2000;16(5):313–315.
- ,,, et al.Electronic results management in pediatric ambulatory care: Qualitative assessment.Pediatrics.2009;123Suppl 2:S85–S91.
- ,,,,.The incidence and severity of adverse events affecting patients after discharge from the hospital.Ann Intern Med.2003;138(3):161–167.
- ,,,.Medical errors related to discontinuity of care from an inpatient to an outpatient setting.J Gen Intern Med.2003;18(8):646–651.
- .Key legal principles for hospitalists.Am J Med.2001;111(9B):5S–9S.
- ,,.Passing the clinical baton: 6 principles to guide the hospitalist.Am J Med.2001;111(9B):36S–39S.
- ,.Lost in transition: challenges and opportunities for improving the quality of transitional care.Ann Intern Med.2004;141(7):533–536.
- ,,,.Promoting effective transitions of care at hospital discharge: a review of key issues for hospitalists.J Hosp Med.2007;2(5):314–323.
- ,,, et al.Adequacy of hospital discharge summaries in documenting tests with pending results and outpatient follow‐up providers.J Gen Intern Med.2009;24(9):1002–1006.
- ,,,,,.Deficits in communication and information transfer between hospital‐based and primary care physicians: Implications for patient safety and continuity of care.JAMA.2007;297(8):831–841.
- ,,, et al.Patient safety concerns arising from test results that return after hospital discharge.Ann Intern Med.2005;143(2):121–128.
- ,,.The continuing problem of missed test results in an integrated health system with an advanced electronic medical record.Jt Comm J Qual Patient Saf.2007;33(8):485–492.
- ,.The frequency of missed test results and associated treatment delays in a highly computerized health system.BMC Fam Pract.2007;8:32.
- ,,,,.Design and implementation of a comprehensive outpatient results manager.J Biomed Inform.2003;36(1–2):80–91.
- ,,, et al.Impact of an automated test results management system on patients' satisfaction about test result communication.Arch Intern Med.2007;167(20):2233–2239.
- ,,,,,.“I wish I had seen this test result earlier!”: dissatisfaction with test result management systems in primary care.Arch Intern Med.2004;164(20):2223–2228.
- ,,.Potential impact of a computerized system to report late‐arriving laboratory results in the emergency department.Pediatr Emerg Care.2000;16(5):313–315.
- ,,, et al.Electronic results management in pediatric ambulatory care: Qualitative assessment.Pediatrics.2009;123Suppl 2:S85–S91.
Copyright © 2010 Society of Hospital Medicine
BEST PRACTICES IN: Managing Eczema With Natural Ingredients
A supplement to Skin & Allergy News. This supplement was sponsored by Johnson & Johnson Consumer Products Company.

- What Role Should Colloidal Oatmeal Play?
- What Other Naturally Derived Ingredients May Benefit Patients With AD?
- The Value of 510(k) Products in Eczema
Faculty/Faculty Disclosure
Lawrence Eichenfield, MD
Chief of Pediatric and Adolescent Dermatology
Rady Children's Hospital and The University of California, San Diego School of Medicine
Professor of Clinical
Pediatrics and Medicine
(Dermatology)
The University of California
San Diego, CA
Dr. Eichenfield was a consultant to Johnson and Johnson.
Melissa Reyes Merin, MD
Clinical Fellow
Rady Children’s Hospital
San Diego, CA
Dr. Reyes Merin has nothing to disclose.
Copyright (c) 2010 Elsevier Inc.
A supplement to Skin & Allergy News. This supplement was sponsored by Johnson & Johnson Consumer Products Company.
- What Role Should Colloidal Oatmeal Play?
- What Other Naturally Derived Ingredients May Benefit Patients With AD?
- The Value of 510(k) Products in Eczema
Faculty/Faculty Disclosure
Lawrence Eichenfield, MD
Chief of Pediatric and Adolescent Dermatology
Rady Children's Hospital and The University of California, San Diego School of Medicine
Professor of Clinical
Pediatrics and Medicine
(Dermatology)
The University of California
San Diego, CA
Dr. Eichenfield was a consultant to Johnson and Johnson.
Melissa Reyes Merin, MD
Clinical Fellow
Rady Children’s Hospital
San Diego, CA
Dr. Reyes Merin has nothing to disclose.
Copyright (c) 2010 Elsevier Inc.
A supplement to Skin & Allergy News. This supplement was sponsored by Johnson & Johnson Consumer Products Company.
- What Role Should Colloidal Oatmeal Play?
- What Other Naturally Derived Ingredients May Benefit Patients With AD?
- The Value of 510(k) Products in Eczema
Faculty/Faculty Disclosure
Lawrence Eichenfield, MD
Chief of Pediatric and Adolescent Dermatology
Rady Children's Hospital and The University of California, San Diego School of Medicine
Professor of Clinical
Pediatrics and Medicine
(Dermatology)
The University of California
San Diego, CA
Dr. Eichenfield was a consultant to Johnson and Johnson.
Melissa Reyes Merin, MD
Clinical Fellow
Rady Children’s Hospital
San Diego, CA
Dr. Reyes Merin has nothing to disclose.
Copyright (c) 2010 Elsevier Inc.

New Treatment Option for AFib Patients
The FDA's approval of a new oral anticoagulant—the first in 56 years—has sparked conversation in internal-medicine circles, prompting the industry to wonder: Will the new drug unseat warfarin as the go-to therapy?
Warfarin is among the most common prescriptions written by hospitalists, but that is in part due to its status as the lone option for the prevention of strokes and embolisms in atrial fibrillation (AF) patients. But on Oct. 19, the FDA approved dabigatran etexilate (Pradaxa) for AF patients. Several other similar medications are under development.
An FDA announcement on the approval notes that in a trial of 18,000 patients, those taking dabigatran etexilate had fewer strokes than those who took warfarin. The study (N Engl J Med. 361;12:1139-1151) reported primary outcome rates were 1.69% per year in the warfarin group, compared with 1.53% per year in the group that received 110mg of dabigatran (P<0.001).
Marketers for the new drug have suggested that while physicians often are slow to accept new therapies, the elimination of blood monitoring that often increases length of stay could nudge hospitalists to adopt the treatment more quickly.
Kurt Pfeifer, MD, FACP, program director of the Internal Medicine Residency program at Medical College in Milwaukee and a bleeding-risk research follower, is not so sure. He says that until there is clinical evidence, it will be difficult to tout any potential long-term benefits of the new therapy.
"It's not time to have a funeral for warfarin," Dr. Pfeifer says.
He adds that dabigatran's initial trials have not showed him such a compelling efficacy that he would consider removing current warfarin patients from their therapy. He also says that the cost of the new medication—at least double that of warfarin, with no generics available—will be a stumbling block and could prevent it from hospital formularies.
"Even with all these alternative anticoagulants out there, there is still no doubt that warfarin will be a mainstay therapy," Dr. Pfeifer says. "There is a reason these drugs are around a long time. …They are effective and they are cheap."
The FDA's approval of a new oral anticoagulant—the first in 56 years—has sparked conversation in internal-medicine circles, prompting the industry to wonder: Will the new drug unseat warfarin as the go-to therapy?
Warfarin is among the most common prescriptions written by hospitalists, but that is in part due to its status as the lone option for the prevention of strokes and embolisms in atrial fibrillation (AF) patients. But on Oct. 19, the FDA approved dabigatran etexilate (Pradaxa) for AF patients. Several other similar medications are under development.
An FDA announcement on the approval notes that in a trial of 18,000 patients, those taking dabigatran etexilate had fewer strokes than those who took warfarin. The study (N Engl J Med. 361;12:1139-1151) reported primary outcome rates were 1.69% per year in the warfarin group, compared with 1.53% per year in the group that received 110mg of dabigatran (P<0.001).
Marketers for the new drug have suggested that while physicians often are slow to accept new therapies, the elimination of blood monitoring that often increases length of stay could nudge hospitalists to adopt the treatment more quickly.
Kurt Pfeifer, MD, FACP, program director of the Internal Medicine Residency program at Medical College in Milwaukee and a bleeding-risk research follower, is not so sure. He says that until there is clinical evidence, it will be difficult to tout any potential long-term benefits of the new therapy.
"It's not time to have a funeral for warfarin," Dr. Pfeifer says.
He adds that dabigatran's initial trials have not showed him such a compelling efficacy that he would consider removing current warfarin patients from their therapy. He also says that the cost of the new medication—at least double that of warfarin, with no generics available—will be a stumbling block and could prevent it from hospital formularies.
"Even with all these alternative anticoagulants out there, there is still no doubt that warfarin will be a mainstay therapy," Dr. Pfeifer says. "There is a reason these drugs are around a long time. …They are effective and they are cheap."
The FDA's approval of a new oral anticoagulant—the first in 56 years—has sparked conversation in internal-medicine circles, prompting the industry to wonder: Will the new drug unseat warfarin as the go-to therapy?
Warfarin is among the most common prescriptions written by hospitalists, but that is in part due to its status as the lone option for the prevention of strokes and embolisms in atrial fibrillation (AF) patients. But on Oct. 19, the FDA approved dabigatran etexilate (Pradaxa) for AF patients. Several other similar medications are under development.
An FDA announcement on the approval notes that in a trial of 18,000 patients, those taking dabigatran etexilate had fewer strokes than those who took warfarin. The study (N Engl J Med. 361;12:1139-1151) reported primary outcome rates were 1.69% per year in the warfarin group, compared with 1.53% per year in the group that received 110mg of dabigatran (P<0.001).
Marketers for the new drug have suggested that while physicians often are slow to accept new therapies, the elimination of blood monitoring that often increases length of stay could nudge hospitalists to adopt the treatment more quickly.
Kurt Pfeifer, MD, FACP, program director of the Internal Medicine Residency program at Medical College in Milwaukee and a bleeding-risk research follower, is not so sure. He says that until there is clinical evidence, it will be difficult to tout any potential long-term benefits of the new therapy.
"It's not time to have a funeral for warfarin," Dr. Pfeifer says.
He adds that dabigatran's initial trials have not showed him such a compelling efficacy that he would consider removing current warfarin patients from their therapy. He also says that the cost of the new medication—at least double that of warfarin, with no generics available—will be a stumbling block and could prevent it from hospital formularies.
"Even with all these alternative anticoagulants out there, there is still no doubt that warfarin will be a mainstay therapy," Dr. Pfeifer says. "There is a reason these drugs are around a long time. …They are effective and they are cheap."
A Boost for Pediatric Research
Pediatric Research in Inpatient Settings (PRIS), a network of pediatric hospitalists practicing at 150 academic and community hospitals, recently landed two federal stimulus grants totaling $12 million, far outstripping past support for research in the field, according to PRIS executive council chair Raj Srivastava, MD, MPH.
"Our mandate is to get federal dollars for multisite, transformative, clinical research for pediatric hospital medicine," says Dr. Srivastava, a pediatric hospitalist at Primary Children's Medical Center in Salt Lake City. "If we are going to be a real specialty, we have to conduct research to define best evidence and best practice: how to translate the evidence out into the field."
PRIS was formed in 2002 with sponsorship from SHM, the American Academy of Pediatrics, and the Academic Pediatric Association. Reorganized last year with a new executive council of active researchers, PRIS convened a strategic planning roundtable to reinvigorate the research agenda. In March, the Child Health Corporation of America, a business alliance of CEOs from 42 nonprofit children’s hospitals, awarded PRIS $1.4 million to support its infrastructure needs and a process that would prioritize research based on prevalence, cost, and variation in practice.
The federal stimulus monies, a pair of three-year grants awarded in September, will fund pediatric inpatient comparative effectiveness research. One of the grants, for $9 million, will support work to link clinical and administrative databases at six children’s hospitals. The second grant, worth $3 million, will be used to study the effectiveness of a resident handoff "bundle" of QI processes designed to enhance communication and improve signouts and transitions of care.
Dr. Srivastava says that, with the infrastructure now in place, more grant support will become possible. Adult hospitalists could use the PRIS experience as a model for building their own multisite research networks, he adds. “This kind of research matters because it is what we are all being asked to do in healthcare anyway,” he says.
Pediatric Research in Inpatient Settings (PRIS), a network of pediatric hospitalists practicing at 150 academic and community hospitals, recently landed two federal stimulus grants totaling $12 million, far outstripping past support for research in the field, according to PRIS executive council chair Raj Srivastava, MD, MPH.
"Our mandate is to get federal dollars for multisite, transformative, clinical research for pediatric hospital medicine," says Dr. Srivastava, a pediatric hospitalist at Primary Children's Medical Center in Salt Lake City. "If we are going to be a real specialty, we have to conduct research to define best evidence and best practice: how to translate the evidence out into the field."
PRIS was formed in 2002 with sponsorship from SHM, the American Academy of Pediatrics, and the Academic Pediatric Association. Reorganized last year with a new executive council of active researchers, PRIS convened a strategic planning roundtable to reinvigorate the research agenda. In March, the Child Health Corporation of America, a business alliance of CEOs from 42 nonprofit children’s hospitals, awarded PRIS $1.4 million to support its infrastructure needs and a process that would prioritize research based on prevalence, cost, and variation in practice.
The federal stimulus monies, a pair of three-year grants awarded in September, will fund pediatric inpatient comparative effectiveness research. One of the grants, for $9 million, will support work to link clinical and administrative databases at six children’s hospitals. The second grant, worth $3 million, will be used to study the effectiveness of a resident handoff "bundle" of QI processes designed to enhance communication and improve signouts and transitions of care.
Dr. Srivastava says that, with the infrastructure now in place, more grant support will become possible. Adult hospitalists could use the PRIS experience as a model for building their own multisite research networks, he adds. “This kind of research matters because it is what we are all being asked to do in healthcare anyway,” he says.
Pediatric Research in Inpatient Settings (PRIS), a network of pediatric hospitalists practicing at 150 academic and community hospitals, recently landed two federal stimulus grants totaling $12 million, far outstripping past support for research in the field, according to PRIS executive council chair Raj Srivastava, MD, MPH.
"Our mandate is to get federal dollars for multisite, transformative, clinical research for pediatric hospital medicine," says Dr. Srivastava, a pediatric hospitalist at Primary Children's Medical Center in Salt Lake City. "If we are going to be a real specialty, we have to conduct research to define best evidence and best practice: how to translate the evidence out into the field."
PRIS was formed in 2002 with sponsorship from SHM, the American Academy of Pediatrics, and the Academic Pediatric Association. Reorganized last year with a new executive council of active researchers, PRIS convened a strategic planning roundtable to reinvigorate the research agenda. In March, the Child Health Corporation of America, a business alliance of CEOs from 42 nonprofit children’s hospitals, awarded PRIS $1.4 million to support its infrastructure needs and a process that would prioritize research based on prevalence, cost, and variation in practice.
The federal stimulus monies, a pair of three-year grants awarded in September, will fund pediatric inpatient comparative effectiveness research. One of the grants, for $9 million, will support work to link clinical and administrative databases at six children’s hospitals. The second grant, worth $3 million, will be used to study the effectiveness of a resident handoff "bundle" of QI processes designed to enhance communication and improve signouts and transitions of care.
Dr. Srivastava says that, with the infrastructure now in place, more grant support will become possible. Adult hospitalists could use the PRIS experience as a model for building their own multisite research networks, he adds. “This kind of research matters because it is what we are all being asked to do in healthcare anyway,” he says.
Family CPR Training Before Discharge
Patients discharged from the hospital with coronary disease complications experience an increased risk of sudden cardiac arrest (SCA), which afflicts over 200,000 people in the United States each year with an 80% to 90% mortality rate.17 Prompt delivery of cardiopulmonary resuscitation (CPR) can triple the probability of survival from SCA, yet less than 25% of SCA victims receive bystander CPR.8 Given that 80% of SCA events occur in the home environment, hospitalization could serve as an important point of capture for family instruction in CPR. Prior investigations have suggested conducting conventional CPR training courses before discharge for family members. However, significant barriers exist to this approach, including the requirement for a certified instructor and a large time commitment for standard training.912
To address these resource and time barriers, the American Heart Association recently established a video self‐instruction (VSI) course in CPR, eliminating the need for an instructor and reducing the time requirement for training to 25 minutes. The course consists of a digital video disc (DVD) and low‐cost inflatable mannequin in a self‐contained kit.13 Several investigations have shown that CPR performance skills of students after VSI courses are similar to those of students after traditional CPR training programs.1417 This VSI program presents the unique opportunity for secondary training, given that the DVD and mannequin may be shared by primary trainees with family members or friends. This VSI approach has not been evaluated in the hospital setting or with family members of patients at risk for SCA. We sought to test the feasibility of an in‐hospital CPR training program using the VSI tool, with the hypothesis that VSI training would be well‐accepted by family members of hospitalized patients with known or suspected coronary disease. We further hypothesized that subjects would be able to perform skills adequately and would be motivated to subsequently share the VSI course with others after their family member's hospital discharge.
METHODS
This prospective, multicenter investigation was approved by the University of Pennsylvania Institutional Review Board (IRB) and represents the initial component of an ongoing longitudinal study testing different methods of CPR education in the hospital setting. Enrollment was conducted at 3 hospitals: The Hospital of the University of Pennsylvania (a 700‐bed tertiary‐care academic medical center), Penn Presbyterian Medical Center (a 300‐bed tertiary‐care and community hospital) and Pennsylvania Hospital (a 400‐bed community hospital).
Recruitment Strategy
Family members of hospitalized patients with known or suspected coronary disease were targeted in this investigation (eg, patients admitted with known myocardial infarction, or patients over 40 years old admitted with chest pain or shortness of breath who had a known history of coronary risk factors). Recruitment took place in the cardiology and telemetry wards of each hospital site by research assistants who were previously CPR trained, but not certified as CPR instructors. Subjects were considered eligible for participation if they were a family member of a current inpatient with known or suspected coronary disease and had not received CPR instruction within the past 2 years. Subjects were excluded if they were under age 18 years, felt unwell, or considered themselves physically unable to undergo CPR training. Eligible individuals were approached using an IRB‐approved recruitment script. If the family member declined participation, the research assistant collected the individual's demographic information and reason for nonparticipation.
If the targeted individual expressed willingness to undergo CPR training, the research assistant administered a pretraining questionnaire to obtain demographic information and history of prior CPR instruction. Subjects then underwent the VSI training program in a family consultation room within the hospital unit, proctored by the research assistant. The VSI program contains an instructional DVD that teaches standard CPR (30 compressions: 2 breaths), as well as the importance of recognizing a nonresponsive patient and calling 9‐1‐1. The training process, including set‐up, video review, and practice routinely took less than 45 minutes per subject. Upon completion of the VSI session, subjects were tested in their newly acquired CPR skills using a VSI or a standard CPR‐recording mannequin, with CPR data analyzed via commercial software (Skill‐Reporter ResuciAnne and Skill‐Reporter software, Laerdal Medical Corporation, Wappinger Falls, NY). Compression rate was calculated as compressions per minute, omitting pauses, with video‐recorded data abstracted and combined with objective CPR recordings. Subjects then completed a Likert scale semi‐quantitative self‐assessment to rate their perspectives on the CPR training experience. Subjects were not compensated financially, but were given the VSI kit to bring home with them at no cost, for the opportunity of performing secondary training.
Assessment of Secondary Training
In an effort to determine whether subjects shared the VSI kit with other family members, follow‐up telephone contact was made with enrollees approximately 1 month after initial CPR training. Subjects were asked to complete a brief survey that included self‐reporting of whether they shared the kit, and if so, how many individuals were trained by the subject (measurement of secondary training, defined as the mean number of people trained for each kit distributed).
Data Analysis and Statistical Calculations
All data, including compiled survey results and CPR quantitative data, were abstracted using a spreadsheet application (Excel, Microsoft Corporation, Redmond, WA). Descriptive statistics were used to compare demographics of enrolled vs. nonenrolled populations, using either student's t‐tests for continuous variables or chi square tests for categorical data. Data are presented as mean standard deviation (SD), with significance set at an alpha = 0.05.
RESULTS
Subject Characteristics and Demographics
Subjects were recruited at the 3 hospital sites between May 2009 and January 2010. A total of 756 eligible individuals were approached, and 280 accepted enrollment for CPR training, representing a 37% enrollment rate (Figure 1). Of the 280 enrolled, 136 underwent instruction using the VSI training program as described, and 144 were enrolled using an experimental method of VSI training in CPR; this second cohort will be described elsewhere. When comparing the eligible individuals who declined enrollment versus those who accepted (Table 1), no significant differences were observed with regard to age, gender or race (P = NS for each). Common reasons cited for nonparticipation included lack of interest or lack of time (data not shown).
| Enrolled (%) n = 136 | Screened/Not Enrolled (%) n = 476 | |
|---|---|---|
| ||
| Age, years | 52 15 | 46 26 |
| Female | 94 (69) | 326 (68) |
| Race | ||
| White | 101 (74) | 316 (66) |
| Black | 30 (22) | 90 (19) |
| Hispanic | 5 (4) | 8 (2) |
| Other/no response | 0 (0) | 59 (13) |
| Relationship to patient | ||
| Spouse | 49 (36) | 171 (36) |
| Immediate family* | 58 (43) | 168 (35) |
| Other | 28 (21) | 76 (16) |
| No response | 1 (1) | 61 (13) |
| Highest Education | ||
| Elementary | 1 (1) | 1 (1) |
| Middle schoo1 | 1 (1) | 7 (1) |
| High school | 46 (34) | 157 (33) |
| Some college/vocation | 36 (26) | 86 (18) |
| College | 30 (22) | 92 (19) |
| Graduate school | 22 (16) | 39 (8) |
| No response | 0 (0) | 94 (20) |
| Previous CPR training | ||
| No | 78 (57) | |
| Yes: within past 2 years | 0 (0) | |
| Yes: within past 25 years | 13 (10) | |
| Yes: within past 510 years | 5 (4) | |
| Yes: more than 10 years ago | 40 (29) | |
Demographics of the enrolled subject cohort are detailed in Table 1. The mean age of subjects was 52 15, and 94 of 136 (69%) were female. Enrolled subjects represented spouses or immediate family members of the hospitalized patient in 107 of 136 (79%) of cases, and the vast majority, 118 of 136 (87%), had either never received CPR training or had received it over 10 years prior to current enrollment.
Subject Perspectives
A posttraining survey revealed that most respondents, 101 of 136 (74%) felt comfortable or very comfortable learning CPR from the VSI kit, and 127 of 136 (93%) felt likely or very likely to share the VSI kit (Figure 2).
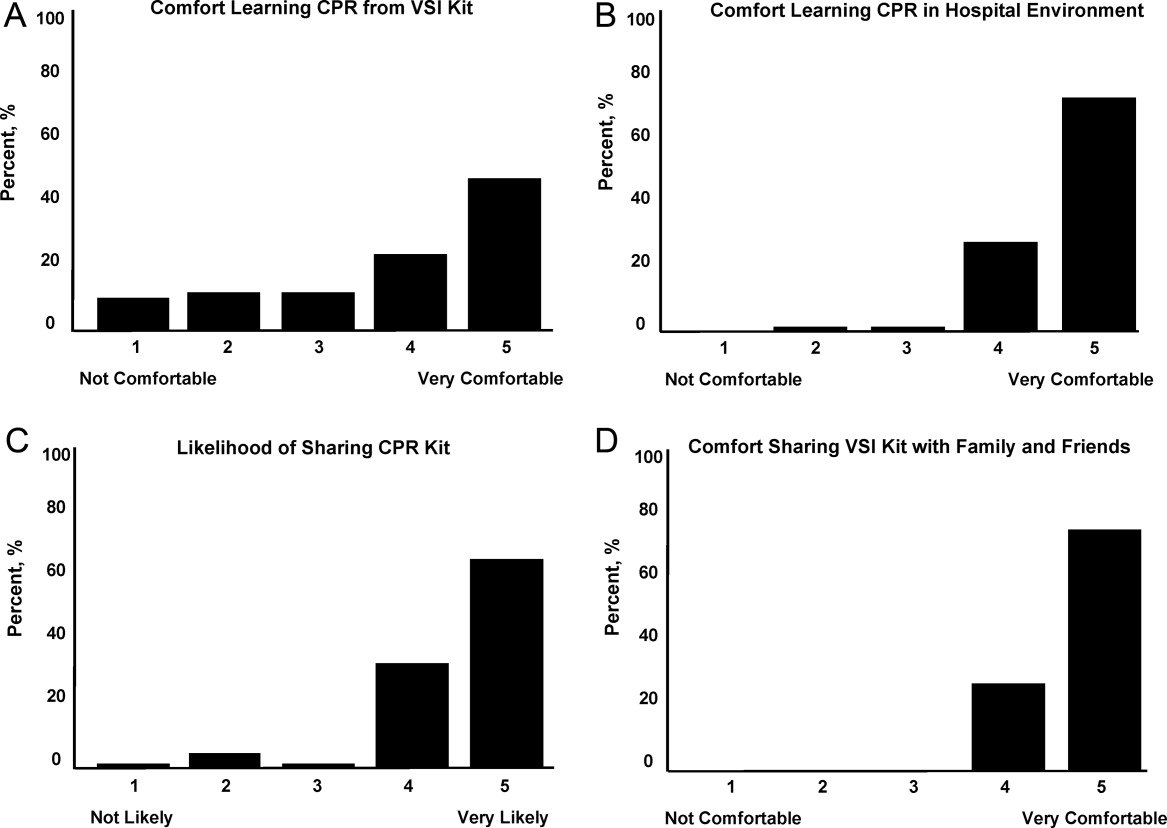
Resuscitation Skills Testing
After CPR training, subjects were asked to perform initial resuscitation actions including 2 minutes of CPR on a mannequin (Table 2). A total of 127 subjects completed these trainings, with 25 completing testing using a VSI kit and 102 using a depth‐recording mannequin; data from 9 subjects were excluded due to CPR recording technical problems. With regard to performance of initial resuscitation actions, 96 of 127 (76%) of subjects assessed responsiveness, 90 of 127 (71%) checked for breathing and 91 of 127 (72%) signaled the need to call for help. CPR was attempted by 127 of 127 (100%) subjects. The mean chest compression rate was 90 26 per minutes, and mean compression depth was 37 12 mm. The mean ventilation rate was 4 3 per minutes.
Secondary Training
Eligible subjects (n = 122) were surveyed via telephone 1 month after initial training, in which 95 individuals participated (78% response rate of those eligible for follow‐up). VSI kits were shared by 57 subjects, with a total of 132 additional individuals receiving VSI‐based CPR instruction. This represented a mean of 2.1 (median of 6) people trained per kit shared, with the actual number of people trained ranging from 1 to 15.
DISCUSSION
In the current work, we demonstrated the feasibility of using the hospital environment as a point of capture for training family members of at‐risk patients in CPR skills. Given that most SCA events occur in the home setting, family member training may hold greater potential for CPR delivery during actual events than training a similar number of younger laypersons at large. Other investigators have identified the focused identification and CPR training of populations at risk of SCA as an important and potentially efficient step to improve survival.10, 12, 18, 19 CPR education of family members before hospital discharge represents a logical extension of other cardiac risk factor‐focused health care education and services before patients are discharged home, including delivery of dietary counseling, diabetic teaching, and education regarding cardiac symptoms. To our knowledge, our work represents the first hospital‐based, adult, layperson, CPR training program using VSI as an instructional approach.
CPR training via a 25‐minute VSI program has been shown to yield CPR performance quality in trainees that is similar to that generated from formal CPR classes that require 3 hours to 4 hours.1416 While VSI training does not provide CPR certification, it is unlikely that the lack of testing and certification is a barrier to participation for the lay public. Indeed, the removal of the pressures of a formal class and testing may increase interest in CPR training through the VSI method.13, 20, 21
Several prior investigations have exploited VSI methodology as an outreach tool to teach CPR in various settings. A recent study in Norway used VSI CPR kits as refresher tools for hospital employees.22 Other work has focused on use of VSI implementation in schools.20, 21, 23 An example of this latter approach was a Danish initiative in which 35,000 VSI kits were distributed to seventh graders.20 Over 15,000 laypersons received secondary training at home by the initially trained students, highlighting a key advantage of the VSI kit approach. It has been argued that this secondary training phenomenon is among the reasons the VSI educational approach may offer a cost effective means for targeted family training.13, 20, 21
While participants in our program were able to adequately perform CPR skills and expressed self‐reported motivation and empowerment, it must be acknowledged that many trained laypersons still do not act when confronted with an actual arrest event.8 In addition, CPR quality at the time of actual performance may be variable, attenuating the survival benefit.2426 However, several population‐based observational studies have supported the notion that training more laypersons in CPR translates into improved overall survival rates from cardiac arrest.25, 27, 28 Further work will be required to follow newly trained, at‐risk family members over time to determine if SCA events occur, and if so, whether CPR was initiated.
Limitations
Willingness to undergo CPR training is likely to be confounded by cultural, regional, and educational factors. Therefore, the general applicability of this 3‐hospital program to other practice environments remains an open question. In our program, the majority of screened family members still refused participation; however, we did not discern a simple relationship between willingness to participate and age, gender, or race. Furthermore, we utilized paid research assistants as subject recruiters and proctors to the VSI training; from a broader implementation perspective, it would be important to determine whether hospital volunteers or staff could perform the training. In addition, while a VSI training kit currently costs $35 and a conventional CPR course could cost from $150 to $300, a formal cost‐effectiveness analysis of VSI training has yet to be performed. Another key limitation is that the secondary training effect was measured by participant self‐report, which may be prone to recall bias; however, no specific incentives or penalties were used to encourage over‐reporting of secondary training. Finally, in this short‐term feasibility study, no direct patient outcomes nor instances of CPR performance were measured.
CONCLUSIONS
In this prospective study of hospital‐based CPR training, we have shown that targeted training of families before hospital discharge is feasible, well received by trainees, and has the benefits of secondary training in the home environment, where most SCA events take place. This program could be easily implemented in other hospital or practice settings. Through targeted CPR training programs such as the one described in this investigation, at risk populations that are underrepresented in conventional CPR training classes can be equipped with important life‐saving skills. Further work on a larger scale will be required to measure the impact of such programs on patient outcomes.
Acknowledgements
The authors wish to thank Lori Albright, Matthew Buchwald, Laura Ebbeling, Emily Esposito, Lori Ingleton, Kristy Walsh, Benjamin Weisenthal, Julie Xu and Mariana Gonzalez for subject recruitment and data collection assistance.
- ,,, et al.Heart disease and stroke statistics–2010 update: a report from the American Heart Association.Circulation.2010;121(7):e46–e215.
- ,,, et al.Regional variation in out‐of‐hospital cardiac arrest incidence and outcome.JAMA.2008;300(12):1423–1431.
- ,,, et al.Prediction of sudden cardiac death after myocardial infarction in the beta‐blocking era.J Am Coll Cardiol.2003;42(4):652–658.
- ,,, et al.Sudden death in patients with myocardial infarction and left ventricular dysfunction, heart failure, or both.N Engl J Med.2005;352(25):2581–2588.
- ,,,.One‐year health status outcomes of unstable angina versus myocardial infarction: a prospective, observational cohort study of ACS survivors.BMC Cardiovasc Disord.2007;7:28.
- ,,,,.Sudden death after myocardial infarction.JAMA.2008;300(17):2022–2029.
- ,,.Elevated admission serum creatinine predicts poor myocardial blood flow and one‐year mortality in ST‐segment elevation myocardial infarction patients undergoing primary percutaneous coronary intervention.J Invasive Cardiol.2009;21(10):493–498.
- ,,,,,.CPR training and CPR performance: do CPR‐trained bystanders perform CPR?Acad Emerg Med.2006;13(6):596–601.
- ,,, et al.Reducing barriers for implementation of bystander‐initiated cardiopulmonary resuscitation: a scientific statement from the American Heart Association for healthcare providers, policymakers, and community leaders regarding the effectiveness of cardiopulmonary resuscitation.Circulation.2008;117(5):704–709.
- ,,.Understanding and improving low bystander CPR rates: a systematic review of the literature.CJEM.2008;10(1):51–65.
- ,.Are we training the right people yet? A survey of participants in public cardiopulmonary resuscitation classes.Resuscitation.1998;37(1):21–25.
- ,,, et al.Cardiac arrest in private locations: different strategies are needed to improve outcome.Resuscitation.2003;58(2):171–176.
- ,.The American Heart Association CPR Anytime Program: the potential impact of highly accessible training in cardiopulmonary resuscitation.J Cardiopulm Rehabil.2006;26(6):346–354.
- ,,,,.Laypersons may learn basic life support in 24 min using a personal resuscitation manikin.Resuscitation.2006;69(3):435–442.
- ,,, et al.Prospective, randomized trial of the effectiveness and retention of 30‐min layperson training for cardiopulmonary resuscitation and automated external defibrillators: The American Airlines Study.Resuscitation.2007;74(2):276–285.
- ,,,,,.Effectiveness of a 30‐min CPR self‐instruction program for lay responders: a controlled randomized study.Resuscitation.2005;67(1):31–43.
- ,,, et al.Randomized, controlled trial of video self‐instruction versus traditional CPR training.Ann Emerg Med.1998;31(3):364–369.
- ,,, et al.A randomized controlled trial of chest compression only CPR for older adults‐a pilot study.Resuscitation.2003;58(2):177–185.
- ,.Estimating cost‐effectiveness of mass cardiopulmonary resuscitation training strategies to improve survival from cardiac arrest in private locations.Prehosp Emerg Care.2004;8(4):420–423.
- ,,,.Disseminating cardiopulmonary resuscitation training by distributing 35,000 personal manikins among school children.Circulation.2007;116(12):1380–1385.
- ,,.Impact of a self‐instruction CPR kit on 7th graders' and adults' skills and CPR performance.Resuscitation.2008;79(1):103–108.
- ,,,,.Hospital employees improve basic life support skills and confidence with a personal resuscitation manikin and a 24‐min video instruction.Resuscitation.2009;80(8):898–902.
- ,,.High school students as ambassadors of CPR‐‐a model for reaching the most appropriate target population?Resuscitation.2010;81(1):78–81.
- ,,,.Three‐phase model of cardiac arrest: time‐dependent benefit of bystander cardiopulmonary resuscitation.Am J Cardiol.2006;98(4):497–499.
- ,,,.Performance of chest compressions by laypersons during the Public Access Defibrillation Trial.Resuscitation.2010;81(3):293–296.
- ,,, et al.Chest compression rates during cardiopulmonary resuscitation are suboptimal: a prospective study during in‐hospital cardiac arrest.Circulation.2005;111(4):428–434.
- ,,, et al.The Save Hearts in Arizona Registry and Education (SHARE) program: who is performing CPR and where are they doing it?Resuscitation.2007;75(1):68–75.
- ,,,,.Efficacy of bystander CPR: intervention by lay people and by health care professionals.Resuscitation.2005;66(3):291–295.
Patients discharged from the hospital with coronary disease complications experience an increased risk of sudden cardiac arrest (SCA), which afflicts over 200,000 people in the United States each year with an 80% to 90% mortality rate.17 Prompt delivery of cardiopulmonary resuscitation (CPR) can triple the probability of survival from SCA, yet less than 25% of SCA victims receive bystander CPR.8 Given that 80% of SCA events occur in the home environment, hospitalization could serve as an important point of capture for family instruction in CPR. Prior investigations have suggested conducting conventional CPR training courses before discharge for family members. However, significant barriers exist to this approach, including the requirement for a certified instructor and a large time commitment for standard training.912
To address these resource and time barriers, the American Heart Association recently established a video self‐instruction (VSI) course in CPR, eliminating the need for an instructor and reducing the time requirement for training to 25 minutes. The course consists of a digital video disc (DVD) and low‐cost inflatable mannequin in a self‐contained kit.13 Several investigations have shown that CPR performance skills of students after VSI courses are similar to those of students after traditional CPR training programs.1417 This VSI program presents the unique opportunity for secondary training, given that the DVD and mannequin may be shared by primary trainees with family members or friends. This VSI approach has not been evaluated in the hospital setting or with family members of patients at risk for SCA. We sought to test the feasibility of an in‐hospital CPR training program using the VSI tool, with the hypothesis that VSI training would be well‐accepted by family members of hospitalized patients with known or suspected coronary disease. We further hypothesized that subjects would be able to perform skills adequately and would be motivated to subsequently share the VSI course with others after their family member's hospital discharge.
METHODS
This prospective, multicenter investigation was approved by the University of Pennsylvania Institutional Review Board (IRB) and represents the initial component of an ongoing longitudinal study testing different methods of CPR education in the hospital setting. Enrollment was conducted at 3 hospitals: The Hospital of the University of Pennsylvania (a 700‐bed tertiary‐care academic medical center), Penn Presbyterian Medical Center (a 300‐bed tertiary‐care and community hospital) and Pennsylvania Hospital (a 400‐bed community hospital).
Recruitment Strategy
Family members of hospitalized patients with known or suspected coronary disease were targeted in this investigation (eg, patients admitted with known myocardial infarction, or patients over 40 years old admitted with chest pain or shortness of breath who had a known history of coronary risk factors). Recruitment took place in the cardiology and telemetry wards of each hospital site by research assistants who were previously CPR trained, but not certified as CPR instructors. Subjects were considered eligible for participation if they were a family member of a current inpatient with known or suspected coronary disease and had not received CPR instruction within the past 2 years. Subjects were excluded if they were under age 18 years, felt unwell, or considered themselves physically unable to undergo CPR training. Eligible individuals were approached using an IRB‐approved recruitment script. If the family member declined participation, the research assistant collected the individual's demographic information and reason for nonparticipation.
If the targeted individual expressed willingness to undergo CPR training, the research assistant administered a pretraining questionnaire to obtain demographic information and history of prior CPR instruction. Subjects then underwent the VSI training program in a family consultation room within the hospital unit, proctored by the research assistant. The VSI program contains an instructional DVD that teaches standard CPR (30 compressions: 2 breaths), as well as the importance of recognizing a nonresponsive patient and calling 9‐1‐1. The training process, including set‐up, video review, and practice routinely took less than 45 minutes per subject. Upon completion of the VSI session, subjects were tested in their newly acquired CPR skills using a VSI or a standard CPR‐recording mannequin, with CPR data analyzed via commercial software (Skill‐Reporter ResuciAnne and Skill‐Reporter software, Laerdal Medical Corporation, Wappinger Falls, NY). Compression rate was calculated as compressions per minute, omitting pauses, with video‐recorded data abstracted and combined with objective CPR recordings. Subjects then completed a Likert scale semi‐quantitative self‐assessment to rate their perspectives on the CPR training experience. Subjects were not compensated financially, but were given the VSI kit to bring home with them at no cost, for the opportunity of performing secondary training.
Assessment of Secondary Training
In an effort to determine whether subjects shared the VSI kit with other family members, follow‐up telephone contact was made with enrollees approximately 1 month after initial CPR training. Subjects were asked to complete a brief survey that included self‐reporting of whether they shared the kit, and if so, how many individuals were trained by the subject (measurement of secondary training, defined as the mean number of people trained for each kit distributed).
Data Analysis and Statistical Calculations
All data, including compiled survey results and CPR quantitative data, were abstracted using a spreadsheet application (Excel, Microsoft Corporation, Redmond, WA). Descriptive statistics were used to compare demographics of enrolled vs. nonenrolled populations, using either student's t‐tests for continuous variables or chi square tests for categorical data. Data are presented as mean standard deviation (SD), with significance set at an alpha = 0.05.
RESULTS
Subject Characteristics and Demographics
Subjects were recruited at the 3 hospital sites between May 2009 and January 2010. A total of 756 eligible individuals were approached, and 280 accepted enrollment for CPR training, representing a 37% enrollment rate (Figure 1). Of the 280 enrolled, 136 underwent instruction using the VSI training program as described, and 144 were enrolled using an experimental method of VSI training in CPR; this second cohort will be described elsewhere. When comparing the eligible individuals who declined enrollment versus those who accepted (Table 1), no significant differences were observed with regard to age, gender or race (P = NS for each). Common reasons cited for nonparticipation included lack of interest or lack of time (data not shown).
| Enrolled (%) n = 136 | Screened/Not Enrolled (%) n = 476 | |
|---|---|---|
| ||
| Age, years | 52 15 | 46 26 |
| Female | 94 (69) | 326 (68) |
| Race | ||
| White | 101 (74) | 316 (66) |
| Black | 30 (22) | 90 (19) |
| Hispanic | 5 (4) | 8 (2) |
| Other/no response | 0 (0) | 59 (13) |
| Relationship to patient | ||
| Spouse | 49 (36) | 171 (36) |
| Immediate family* | 58 (43) | 168 (35) |
| Other | 28 (21) | 76 (16) |
| No response | 1 (1) | 61 (13) |
| Highest Education | ||
| Elementary | 1 (1) | 1 (1) |
| Middle schoo1 | 1 (1) | 7 (1) |
| High school | 46 (34) | 157 (33) |
| Some college/vocation | 36 (26) | 86 (18) |
| College | 30 (22) | 92 (19) |
| Graduate school | 22 (16) | 39 (8) |
| No response | 0 (0) | 94 (20) |
| Previous CPR training | ||
| No | 78 (57) | |
| Yes: within past 2 years | 0 (0) | |
| Yes: within past 25 years | 13 (10) | |
| Yes: within past 510 years | 5 (4) | |
| Yes: more than 10 years ago | 40 (29) | |
Demographics of the enrolled subject cohort are detailed in Table 1. The mean age of subjects was 52 15, and 94 of 136 (69%) were female. Enrolled subjects represented spouses or immediate family members of the hospitalized patient in 107 of 136 (79%) of cases, and the vast majority, 118 of 136 (87%), had either never received CPR training or had received it over 10 years prior to current enrollment.
Subject Perspectives
A posttraining survey revealed that most respondents, 101 of 136 (74%) felt comfortable or very comfortable learning CPR from the VSI kit, and 127 of 136 (93%) felt likely or very likely to share the VSI kit (Figure 2).
Resuscitation Skills Testing
After CPR training, subjects were asked to perform initial resuscitation actions including 2 minutes of CPR on a mannequin (Table 2). A total of 127 subjects completed these trainings, with 25 completing testing using a VSI kit and 102 using a depth‐recording mannequin; data from 9 subjects were excluded due to CPR recording technical problems. With regard to performance of initial resuscitation actions, 96 of 127 (76%) of subjects assessed responsiveness, 90 of 127 (71%) checked for breathing and 91 of 127 (72%) signaled the need to call for help. CPR was attempted by 127 of 127 (100%) subjects. The mean chest compression rate was 90 26 per minutes, and mean compression depth was 37 12 mm. The mean ventilation rate was 4 3 per minutes.
Secondary Training
Eligible subjects (n = 122) were surveyed via telephone 1 month after initial training, in which 95 individuals participated (78% response rate of those eligible for follow‐up). VSI kits were shared by 57 subjects, with a total of 132 additional individuals receiving VSI‐based CPR instruction. This represented a mean of 2.1 (median of 6) people trained per kit shared, with the actual number of people trained ranging from 1 to 15.
DISCUSSION
In the current work, we demonstrated the feasibility of using the hospital environment as a point of capture for training family members of at‐risk patients in CPR skills. Given that most SCA events occur in the home setting, family member training may hold greater potential for CPR delivery during actual events than training a similar number of younger laypersons at large. Other investigators have identified the focused identification and CPR training of populations at risk of SCA as an important and potentially efficient step to improve survival.10, 12, 18, 19 CPR education of family members before hospital discharge represents a logical extension of other cardiac risk factor‐focused health care education and services before patients are discharged home, including delivery of dietary counseling, diabetic teaching, and education regarding cardiac symptoms. To our knowledge, our work represents the first hospital‐based, adult, layperson, CPR training program using VSI as an instructional approach.
CPR training via a 25‐minute VSI program has been shown to yield CPR performance quality in trainees that is similar to that generated from formal CPR classes that require 3 hours to 4 hours.1416 While VSI training does not provide CPR certification, it is unlikely that the lack of testing and certification is a barrier to participation for the lay public. Indeed, the removal of the pressures of a formal class and testing may increase interest in CPR training through the VSI method.13, 20, 21
Several prior investigations have exploited VSI methodology as an outreach tool to teach CPR in various settings. A recent study in Norway used VSI CPR kits as refresher tools for hospital employees.22 Other work has focused on use of VSI implementation in schools.20, 21, 23 An example of this latter approach was a Danish initiative in which 35,000 VSI kits were distributed to seventh graders.20 Over 15,000 laypersons received secondary training at home by the initially trained students, highlighting a key advantage of the VSI kit approach. It has been argued that this secondary training phenomenon is among the reasons the VSI educational approach may offer a cost effective means for targeted family training.13, 20, 21
While participants in our program were able to adequately perform CPR skills and expressed self‐reported motivation and empowerment, it must be acknowledged that many trained laypersons still do not act when confronted with an actual arrest event.8 In addition, CPR quality at the time of actual performance may be variable, attenuating the survival benefit.2426 However, several population‐based observational studies have supported the notion that training more laypersons in CPR translates into improved overall survival rates from cardiac arrest.25, 27, 28 Further work will be required to follow newly trained, at‐risk family members over time to determine if SCA events occur, and if so, whether CPR was initiated.
Limitations
Willingness to undergo CPR training is likely to be confounded by cultural, regional, and educational factors. Therefore, the general applicability of this 3‐hospital program to other practice environments remains an open question. In our program, the majority of screened family members still refused participation; however, we did not discern a simple relationship between willingness to participate and age, gender, or race. Furthermore, we utilized paid research assistants as subject recruiters and proctors to the VSI training; from a broader implementation perspective, it would be important to determine whether hospital volunteers or staff could perform the training. In addition, while a VSI training kit currently costs $35 and a conventional CPR course could cost from $150 to $300, a formal cost‐effectiveness analysis of VSI training has yet to be performed. Another key limitation is that the secondary training effect was measured by participant self‐report, which may be prone to recall bias; however, no specific incentives or penalties were used to encourage over‐reporting of secondary training. Finally, in this short‐term feasibility study, no direct patient outcomes nor instances of CPR performance were measured.
CONCLUSIONS
In this prospective study of hospital‐based CPR training, we have shown that targeted training of families before hospital discharge is feasible, well received by trainees, and has the benefits of secondary training in the home environment, where most SCA events take place. This program could be easily implemented in other hospital or practice settings. Through targeted CPR training programs such as the one described in this investigation, at risk populations that are underrepresented in conventional CPR training classes can be equipped with important life‐saving skills. Further work on a larger scale will be required to measure the impact of such programs on patient outcomes.
Acknowledgements
The authors wish to thank Lori Albright, Matthew Buchwald, Laura Ebbeling, Emily Esposito, Lori Ingleton, Kristy Walsh, Benjamin Weisenthal, Julie Xu and Mariana Gonzalez for subject recruitment and data collection assistance.
Patients discharged from the hospital with coronary disease complications experience an increased risk of sudden cardiac arrest (SCA), which afflicts over 200,000 people in the United States each year with an 80% to 90% mortality rate.17 Prompt delivery of cardiopulmonary resuscitation (CPR) can triple the probability of survival from SCA, yet less than 25% of SCA victims receive bystander CPR.8 Given that 80% of SCA events occur in the home environment, hospitalization could serve as an important point of capture for family instruction in CPR. Prior investigations have suggested conducting conventional CPR training courses before discharge for family members. However, significant barriers exist to this approach, including the requirement for a certified instructor and a large time commitment for standard training.912
To address these resource and time barriers, the American Heart Association recently established a video self‐instruction (VSI) course in CPR, eliminating the need for an instructor and reducing the time requirement for training to 25 minutes. The course consists of a digital video disc (DVD) and low‐cost inflatable mannequin in a self‐contained kit.13 Several investigations have shown that CPR performance skills of students after VSI courses are similar to those of students after traditional CPR training programs.1417 This VSI program presents the unique opportunity for secondary training, given that the DVD and mannequin may be shared by primary trainees with family members or friends. This VSI approach has not been evaluated in the hospital setting or with family members of patients at risk for SCA. We sought to test the feasibility of an in‐hospital CPR training program using the VSI tool, with the hypothesis that VSI training would be well‐accepted by family members of hospitalized patients with known or suspected coronary disease. We further hypothesized that subjects would be able to perform skills adequately and would be motivated to subsequently share the VSI course with others after their family member's hospital discharge.
METHODS
This prospective, multicenter investigation was approved by the University of Pennsylvania Institutional Review Board (IRB) and represents the initial component of an ongoing longitudinal study testing different methods of CPR education in the hospital setting. Enrollment was conducted at 3 hospitals: The Hospital of the University of Pennsylvania (a 700‐bed tertiary‐care academic medical center), Penn Presbyterian Medical Center (a 300‐bed tertiary‐care and community hospital) and Pennsylvania Hospital (a 400‐bed community hospital).
Recruitment Strategy
Family members of hospitalized patients with known or suspected coronary disease were targeted in this investigation (eg, patients admitted with known myocardial infarction, or patients over 40 years old admitted with chest pain or shortness of breath who had a known history of coronary risk factors). Recruitment took place in the cardiology and telemetry wards of each hospital site by research assistants who were previously CPR trained, but not certified as CPR instructors. Subjects were considered eligible for participation if they were a family member of a current inpatient with known or suspected coronary disease and had not received CPR instruction within the past 2 years. Subjects were excluded if they were under age 18 years, felt unwell, or considered themselves physically unable to undergo CPR training. Eligible individuals were approached using an IRB‐approved recruitment script. If the family member declined participation, the research assistant collected the individual's demographic information and reason for nonparticipation.
If the targeted individual expressed willingness to undergo CPR training, the research assistant administered a pretraining questionnaire to obtain demographic information and history of prior CPR instruction. Subjects then underwent the VSI training program in a family consultation room within the hospital unit, proctored by the research assistant. The VSI program contains an instructional DVD that teaches standard CPR (30 compressions: 2 breaths), as well as the importance of recognizing a nonresponsive patient and calling 9‐1‐1. The training process, including set‐up, video review, and practice routinely took less than 45 minutes per subject. Upon completion of the VSI session, subjects were tested in their newly acquired CPR skills using a VSI or a standard CPR‐recording mannequin, with CPR data analyzed via commercial software (Skill‐Reporter ResuciAnne and Skill‐Reporter software, Laerdal Medical Corporation, Wappinger Falls, NY). Compression rate was calculated as compressions per minute, omitting pauses, with video‐recorded data abstracted and combined with objective CPR recordings. Subjects then completed a Likert scale semi‐quantitative self‐assessment to rate their perspectives on the CPR training experience. Subjects were not compensated financially, but were given the VSI kit to bring home with them at no cost, for the opportunity of performing secondary training.
Assessment of Secondary Training
In an effort to determine whether subjects shared the VSI kit with other family members, follow‐up telephone contact was made with enrollees approximately 1 month after initial CPR training. Subjects were asked to complete a brief survey that included self‐reporting of whether they shared the kit, and if so, how many individuals were trained by the subject (measurement of secondary training, defined as the mean number of people trained for each kit distributed).
Data Analysis and Statistical Calculations
All data, including compiled survey results and CPR quantitative data, were abstracted using a spreadsheet application (Excel, Microsoft Corporation, Redmond, WA). Descriptive statistics were used to compare demographics of enrolled vs. nonenrolled populations, using either student's t‐tests for continuous variables or chi square tests for categorical data. Data are presented as mean standard deviation (SD), with significance set at an alpha = 0.05.
RESULTS
Subject Characteristics and Demographics
Subjects were recruited at the 3 hospital sites between May 2009 and January 2010. A total of 756 eligible individuals were approached, and 280 accepted enrollment for CPR training, representing a 37% enrollment rate (Figure 1). Of the 280 enrolled, 136 underwent instruction using the VSI training program as described, and 144 were enrolled using an experimental method of VSI training in CPR; this second cohort will be described elsewhere. When comparing the eligible individuals who declined enrollment versus those who accepted (Table 1), no significant differences were observed with regard to age, gender or race (P = NS for each). Common reasons cited for nonparticipation included lack of interest or lack of time (data not shown).
| Enrolled (%) n = 136 | Screened/Not Enrolled (%) n = 476 | |
|---|---|---|
| ||
| Age, years | 52 15 | 46 26 |
| Female | 94 (69) | 326 (68) |
| Race | ||
| White | 101 (74) | 316 (66) |
| Black | 30 (22) | 90 (19) |
| Hispanic | 5 (4) | 8 (2) |
| Other/no response | 0 (0) | 59 (13) |
| Relationship to patient | ||
| Spouse | 49 (36) | 171 (36) |
| Immediate family* | 58 (43) | 168 (35) |
| Other | 28 (21) | 76 (16) |
| No response | 1 (1) | 61 (13) |
| Highest Education | ||
| Elementary | 1 (1) | 1 (1) |
| Middle schoo1 | 1 (1) | 7 (1) |
| High school | 46 (34) | 157 (33) |
| Some college/vocation | 36 (26) | 86 (18) |
| College | 30 (22) | 92 (19) |
| Graduate school | 22 (16) | 39 (8) |
| No response | 0 (0) | 94 (20) |
| Previous CPR training | ||
| No | 78 (57) | |
| Yes: within past 2 years | 0 (0) | |
| Yes: within past 25 years | 13 (10) | |
| Yes: within past 510 years | 5 (4) | |
| Yes: more than 10 years ago | 40 (29) | |
Demographics of the enrolled subject cohort are detailed in Table 1. The mean age of subjects was 52 15, and 94 of 136 (69%) were female. Enrolled subjects represented spouses or immediate family members of the hospitalized patient in 107 of 136 (79%) of cases, and the vast majority, 118 of 136 (87%), had either never received CPR training or had received it over 10 years prior to current enrollment.
Subject Perspectives
A posttraining survey revealed that most respondents, 101 of 136 (74%) felt comfortable or very comfortable learning CPR from the VSI kit, and 127 of 136 (93%) felt likely or very likely to share the VSI kit (Figure 2).
Resuscitation Skills Testing
After CPR training, subjects were asked to perform initial resuscitation actions including 2 minutes of CPR on a mannequin (Table 2). A total of 127 subjects completed these trainings, with 25 completing testing using a VSI kit and 102 using a depth‐recording mannequin; data from 9 subjects were excluded due to CPR recording technical problems. With regard to performance of initial resuscitation actions, 96 of 127 (76%) of subjects assessed responsiveness, 90 of 127 (71%) checked for breathing and 91 of 127 (72%) signaled the need to call for help. CPR was attempted by 127 of 127 (100%) subjects. The mean chest compression rate was 90 26 per minutes, and mean compression depth was 37 12 mm. The mean ventilation rate was 4 3 per minutes.
Secondary Training
Eligible subjects (n = 122) were surveyed via telephone 1 month after initial training, in which 95 individuals participated (78% response rate of those eligible for follow‐up). VSI kits were shared by 57 subjects, with a total of 132 additional individuals receiving VSI‐based CPR instruction. This represented a mean of 2.1 (median of 6) people trained per kit shared, with the actual number of people trained ranging from 1 to 15.
DISCUSSION
In the current work, we demonstrated the feasibility of using the hospital environment as a point of capture for training family members of at‐risk patients in CPR skills. Given that most SCA events occur in the home setting, family member training may hold greater potential for CPR delivery during actual events than training a similar number of younger laypersons at large. Other investigators have identified the focused identification and CPR training of populations at risk of SCA as an important and potentially efficient step to improve survival.10, 12, 18, 19 CPR education of family members before hospital discharge represents a logical extension of other cardiac risk factor‐focused health care education and services before patients are discharged home, including delivery of dietary counseling, diabetic teaching, and education regarding cardiac symptoms. To our knowledge, our work represents the first hospital‐based, adult, layperson, CPR training program using VSI as an instructional approach.
CPR training via a 25‐minute VSI program has been shown to yield CPR performance quality in trainees that is similar to that generated from formal CPR classes that require 3 hours to 4 hours.1416 While VSI training does not provide CPR certification, it is unlikely that the lack of testing and certification is a barrier to participation for the lay public. Indeed, the removal of the pressures of a formal class and testing may increase interest in CPR training through the VSI method.13, 20, 21
Several prior investigations have exploited VSI methodology as an outreach tool to teach CPR in various settings. A recent study in Norway used VSI CPR kits as refresher tools for hospital employees.22 Other work has focused on use of VSI implementation in schools.20, 21, 23 An example of this latter approach was a Danish initiative in which 35,000 VSI kits were distributed to seventh graders.20 Over 15,000 laypersons received secondary training at home by the initially trained students, highlighting a key advantage of the VSI kit approach. It has been argued that this secondary training phenomenon is among the reasons the VSI educational approach may offer a cost effective means for targeted family training.13, 20, 21
While participants in our program were able to adequately perform CPR skills and expressed self‐reported motivation and empowerment, it must be acknowledged that many trained laypersons still do not act when confronted with an actual arrest event.8 In addition, CPR quality at the time of actual performance may be variable, attenuating the survival benefit.2426 However, several population‐based observational studies have supported the notion that training more laypersons in CPR translates into improved overall survival rates from cardiac arrest.25, 27, 28 Further work will be required to follow newly trained, at‐risk family members over time to determine if SCA events occur, and if so, whether CPR was initiated.
Limitations
Willingness to undergo CPR training is likely to be confounded by cultural, regional, and educational factors. Therefore, the general applicability of this 3‐hospital program to other practice environments remains an open question. In our program, the majority of screened family members still refused participation; however, we did not discern a simple relationship between willingness to participate and age, gender, or race. Furthermore, we utilized paid research assistants as subject recruiters and proctors to the VSI training; from a broader implementation perspective, it would be important to determine whether hospital volunteers or staff could perform the training. In addition, while a VSI training kit currently costs $35 and a conventional CPR course could cost from $150 to $300, a formal cost‐effectiveness analysis of VSI training has yet to be performed. Another key limitation is that the secondary training effect was measured by participant self‐report, which may be prone to recall bias; however, no specific incentives or penalties were used to encourage over‐reporting of secondary training. Finally, in this short‐term feasibility study, no direct patient outcomes nor instances of CPR performance were measured.
CONCLUSIONS
In this prospective study of hospital‐based CPR training, we have shown that targeted training of families before hospital discharge is feasible, well received by trainees, and has the benefits of secondary training in the home environment, where most SCA events take place. This program could be easily implemented in other hospital or practice settings. Through targeted CPR training programs such as the one described in this investigation, at risk populations that are underrepresented in conventional CPR training classes can be equipped with important life‐saving skills. Further work on a larger scale will be required to measure the impact of such programs on patient outcomes.
Acknowledgements
The authors wish to thank Lori Albright, Matthew Buchwald, Laura Ebbeling, Emily Esposito, Lori Ingleton, Kristy Walsh, Benjamin Weisenthal, Julie Xu and Mariana Gonzalez for subject recruitment and data collection assistance.
- ,,, et al.Heart disease and stroke statistics–2010 update: a report from the American Heart Association.Circulation.2010;121(7):e46–e215.
- ,,, et al.Regional variation in out‐of‐hospital cardiac arrest incidence and outcome.JAMA.2008;300(12):1423–1431.
- ,,, et al.Prediction of sudden cardiac death after myocardial infarction in the beta‐blocking era.J Am Coll Cardiol.2003;42(4):652–658.
- ,,, et al.Sudden death in patients with myocardial infarction and left ventricular dysfunction, heart failure, or both.N Engl J Med.2005;352(25):2581–2588.
- ,,,.One‐year health status outcomes of unstable angina versus myocardial infarction: a prospective, observational cohort study of ACS survivors.BMC Cardiovasc Disord.2007;7:28.
- ,,,,.Sudden death after myocardial infarction.JAMA.2008;300(17):2022–2029.
- ,,.Elevated admission serum creatinine predicts poor myocardial blood flow and one‐year mortality in ST‐segment elevation myocardial infarction patients undergoing primary percutaneous coronary intervention.J Invasive Cardiol.2009;21(10):493–498.
- ,,,,,.CPR training and CPR performance: do CPR‐trained bystanders perform CPR?Acad Emerg Med.2006;13(6):596–601.
- ,,, et al.Reducing barriers for implementation of bystander‐initiated cardiopulmonary resuscitation: a scientific statement from the American Heart Association for healthcare providers, policymakers, and community leaders regarding the effectiveness of cardiopulmonary resuscitation.Circulation.2008;117(5):704–709.
- ,,.Understanding and improving low bystander CPR rates: a systematic review of the literature.CJEM.2008;10(1):51–65.
- ,.Are we training the right people yet? A survey of participants in public cardiopulmonary resuscitation classes.Resuscitation.1998;37(1):21–25.
- ,,, et al.Cardiac arrest in private locations: different strategies are needed to improve outcome.Resuscitation.2003;58(2):171–176.
- ,.The American Heart Association CPR Anytime Program: the potential impact of highly accessible training in cardiopulmonary resuscitation.J Cardiopulm Rehabil.2006;26(6):346–354.
- ,,,,.Laypersons may learn basic life support in 24 min using a personal resuscitation manikin.Resuscitation.2006;69(3):435–442.
- ,,, et al.Prospective, randomized trial of the effectiveness and retention of 30‐min layperson training for cardiopulmonary resuscitation and automated external defibrillators: The American Airlines Study.Resuscitation.2007;74(2):276–285.
- ,,,,,.Effectiveness of a 30‐min CPR self‐instruction program for lay responders: a controlled randomized study.Resuscitation.2005;67(1):31–43.
- ,,, et al.Randomized, controlled trial of video self‐instruction versus traditional CPR training.Ann Emerg Med.1998;31(3):364–369.
- ,,, et al.A randomized controlled trial of chest compression only CPR for older adults‐a pilot study.Resuscitation.2003;58(2):177–185.
- ,.Estimating cost‐effectiveness of mass cardiopulmonary resuscitation training strategies to improve survival from cardiac arrest in private locations.Prehosp Emerg Care.2004;8(4):420–423.
- ,,,.Disseminating cardiopulmonary resuscitation training by distributing 35,000 personal manikins among school children.Circulation.2007;116(12):1380–1385.
- ,,.Impact of a self‐instruction CPR kit on 7th graders' and adults' skills and CPR performance.Resuscitation.2008;79(1):103–108.
- ,,,,.Hospital employees improve basic life support skills and confidence with a personal resuscitation manikin and a 24‐min video instruction.Resuscitation.2009;80(8):898–902.
- ,,.High school students as ambassadors of CPR‐‐a model for reaching the most appropriate target population?Resuscitation.2010;81(1):78–81.
- ,,,.Three‐phase model of cardiac arrest: time‐dependent benefit of bystander cardiopulmonary resuscitation.Am J Cardiol.2006;98(4):497–499.
- ,,,.Performance of chest compressions by laypersons during the Public Access Defibrillation Trial.Resuscitation.2010;81(3):293–296.
- ,,, et al.Chest compression rates during cardiopulmonary resuscitation are suboptimal: a prospective study during in‐hospital cardiac arrest.Circulation.2005;111(4):428–434.
- ,,, et al.The Save Hearts in Arizona Registry and Education (SHARE) program: who is performing CPR and where are they doing it?Resuscitation.2007;75(1):68–75.
- ,,,,.Efficacy of bystander CPR: intervention by lay people and by health care professionals.Resuscitation.2005;66(3):291–295.
- ,,, et al.Heart disease and stroke statistics–2010 update: a report from the American Heart Association.Circulation.2010;121(7):e46–e215.
- ,,, et al.Regional variation in out‐of‐hospital cardiac arrest incidence and outcome.JAMA.2008;300(12):1423–1431.
- ,,, et al.Prediction of sudden cardiac death after myocardial infarction in the beta‐blocking era.J Am Coll Cardiol.2003;42(4):652–658.
- ,,, et al.Sudden death in patients with myocardial infarction and left ventricular dysfunction, heart failure, or both.N Engl J Med.2005;352(25):2581–2588.
- ,,,.One‐year health status outcomes of unstable angina versus myocardial infarction: a prospective, observational cohort study of ACS survivors.BMC Cardiovasc Disord.2007;7:28.
- ,,,,.Sudden death after myocardial infarction.JAMA.2008;300(17):2022–2029.
- ,,.Elevated admission serum creatinine predicts poor myocardial blood flow and one‐year mortality in ST‐segment elevation myocardial infarction patients undergoing primary percutaneous coronary intervention.J Invasive Cardiol.2009;21(10):493–498.
- ,,,,,.CPR training and CPR performance: do CPR‐trained bystanders perform CPR?Acad Emerg Med.2006;13(6):596–601.
- ,,, et al.Reducing barriers for implementation of bystander‐initiated cardiopulmonary resuscitation: a scientific statement from the American Heart Association for healthcare providers, policymakers, and community leaders regarding the effectiveness of cardiopulmonary resuscitation.Circulation.2008;117(5):704–709.
- ,,.Understanding and improving low bystander CPR rates: a systematic review of the literature.CJEM.2008;10(1):51–65.
- ,.Are we training the right people yet? A survey of participants in public cardiopulmonary resuscitation classes.Resuscitation.1998;37(1):21–25.
- ,,, et al.Cardiac arrest in private locations: different strategies are needed to improve outcome.Resuscitation.2003;58(2):171–176.
- ,.The American Heart Association CPR Anytime Program: the potential impact of highly accessible training in cardiopulmonary resuscitation.J Cardiopulm Rehabil.2006;26(6):346–354.
- ,,,,.Laypersons may learn basic life support in 24 min using a personal resuscitation manikin.Resuscitation.2006;69(3):435–442.
- ,,, et al.Prospective, randomized trial of the effectiveness and retention of 30‐min layperson training for cardiopulmonary resuscitation and automated external defibrillators: The American Airlines Study.Resuscitation.2007;74(2):276–285.
- ,,,,,.Effectiveness of a 30‐min CPR self‐instruction program for lay responders: a controlled randomized study.Resuscitation.2005;67(1):31–43.
- ,,, et al.Randomized, controlled trial of video self‐instruction versus traditional CPR training.Ann Emerg Med.1998;31(3):364–369.
- ,,, et al.A randomized controlled trial of chest compression only CPR for older adults‐a pilot study.Resuscitation.2003;58(2):177–185.
- ,.Estimating cost‐effectiveness of mass cardiopulmonary resuscitation training strategies to improve survival from cardiac arrest in private locations.Prehosp Emerg Care.2004;8(4):420–423.
- ,,,.Disseminating cardiopulmonary resuscitation training by distributing 35,000 personal manikins among school children.Circulation.2007;116(12):1380–1385.
- ,,.Impact of a self‐instruction CPR kit on 7th graders' and adults' skills and CPR performance.Resuscitation.2008;79(1):103–108.
- ,,,,.Hospital employees improve basic life support skills and confidence with a personal resuscitation manikin and a 24‐min video instruction.Resuscitation.2009;80(8):898–902.
- ,,.High school students as ambassadors of CPR‐‐a model for reaching the most appropriate target population?Resuscitation.2010;81(1):78–81.
- ,,,.Three‐phase model of cardiac arrest: time‐dependent benefit of bystander cardiopulmonary resuscitation.Am J Cardiol.2006;98(4):497–499.
- ,,,.Performance of chest compressions by laypersons during the Public Access Defibrillation Trial.Resuscitation.2010;81(3):293–296.
- ,,, et al.Chest compression rates during cardiopulmonary resuscitation are suboptimal: a prospective study during in‐hospital cardiac arrest.Circulation.2005;111(4):428–434.
- ,,, et al.The Save Hearts in Arizona Registry and Education (SHARE) program: who is performing CPR and where are they doing it?Resuscitation.2007;75(1):68–75.
- ,,,,.Efficacy of bystander CPR: intervention by lay people and by health care professionals.Resuscitation.2005;66(3):291–295.
Greater Hospitalist Role Envisioned for Cancer Patients
Hospitalists who encounter the occasional late-stage colorectal cancer patient might be perplexed as to why the patient refuses to remove food from their in-room refrigerator and often are wearing mittens. But it would be immediately clear to them once they knew that the patient was on oxaliplatin—a less-than-decade-old medication delivered via the chemotherapy regimen known as FOLFOX—and that a common side effect is neuropathy resulting in extreme sensitivity to cold.
Why wouldn’t hospitalists know this? Because, according to a medical oncologist at Memorial Sloan-Kettering Cancer Center in New York City, oncologists traditionally have tried to holistically manage the care of cancer patients. In today’s age of new treatments and increased inpatient care for patients with aggressive cancers, though, Jason Konner, MD, says it’s time for hospitalists to take a greater role in the management of cancer patients.
The upshot: Dr. Konner envisions a new breed of oncologist-hospitalists. (Check out this in-depth look at specialty physicians adopting the HM model of care.)
“Universally, the hospitalist is going to have to be part of a team with the oncologist,” says Dr. Konner, assistant professor with the Gynecological Medical Oncology Service and Developmental Therapeutic Services. “We’re going to complement each other. There are definitely things that we can do that they can’t and definitely things they can do that we can’t. Right now, it’s just being part of the team to address the diverse medical complications of cancer. But I think that increasingly, [hospitalists] are going to be the primary caregivers, sometimes solely the caregivers, of patients with cancer complications.”
The concept, which was raised during an “Oncology for the Hospitalist” presentation at the fifth annual Mid-Atlantic Hospital Medicine Symposium at Mount Sinai School of Medicine in New York City, is not new, but it is particularly relevant as cancer mortality and incidence rates continue to drop. Dr. Konner counters that while improved screening techniques—mammographies and prostate-specific antigen (PSA) tests, to note a pair—have reduced incidences, the majority of “aggressive cancers and cancers that kill people” still require intensive inpatient care.
To wit, a pilot program at Mount Sinai several years ago dedicated a hospitalist to the oncology service in the hopes of developing a staffer with a new expertise. The brief program, which yielded little data because of its small sample size, was aimed at determining the efficacy of an oncology hospitalist.
Richard Quinn is a freelance writer based in New Jersey.
Hospitalists who encounter the occasional late-stage colorectal cancer patient might be perplexed as to why the patient refuses to remove food from their in-room refrigerator and often are wearing mittens. But it would be immediately clear to them once they knew that the patient was on oxaliplatin—a less-than-decade-old medication delivered via the chemotherapy regimen known as FOLFOX—and that a common side effect is neuropathy resulting in extreme sensitivity to cold.
Why wouldn’t hospitalists know this? Because, according to a medical oncologist at Memorial Sloan-Kettering Cancer Center in New York City, oncologists traditionally have tried to holistically manage the care of cancer patients. In today’s age of new treatments and increased inpatient care for patients with aggressive cancers, though, Jason Konner, MD, says it’s time for hospitalists to take a greater role in the management of cancer patients.
The upshot: Dr. Konner envisions a new breed of oncologist-hospitalists. (Check out this in-depth look at specialty physicians adopting the HM model of care.)
“Universally, the hospitalist is going to have to be part of a team with the oncologist,” says Dr. Konner, assistant professor with the Gynecological Medical Oncology Service and Developmental Therapeutic Services. “We’re going to complement each other. There are definitely things that we can do that they can’t and definitely things they can do that we can’t. Right now, it’s just being part of the team to address the diverse medical complications of cancer. But I think that increasingly, [hospitalists] are going to be the primary caregivers, sometimes solely the caregivers, of patients with cancer complications.”
The concept, which was raised during an “Oncology for the Hospitalist” presentation at the fifth annual Mid-Atlantic Hospital Medicine Symposium at Mount Sinai School of Medicine in New York City, is not new, but it is particularly relevant as cancer mortality and incidence rates continue to drop. Dr. Konner counters that while improved screening techniques—mammographies and prostate-specific antigen (PSA) tests, to note a pair—have reduced incidences, the majority of “aggressive cancers and cancers that kill people” still require intensive inpatient care.
To wit, a pilot program at Mount Sinai several years ago dedicated a hospitalist to the oncology service in the hopes of developing a staffer with a new expertise. The brief program, which yielded little data because of its small sample size, was aimed at determining the efficacy of an oncology hospitalist.
Richard Quinn is a freelance writer based in New Jersey.
Hospitalists who encounter the occasional late-stage colorectal cancer patient might be perplexed as to why the patient refuses to remove food from their in-room refrigerator and often are wearing mittens. But it would be immediately clear to them once they knew that the patient was on oxaliplatin—a less-than-decade-old medication delivered via the chemotherapy regimen known as FOLFOX—and that a common side effect is neuropathy resulting in extreme sensitivity to cold.
Why wouldn’t hospitalists know this? Because, according to a medical oncologist at Memorial Sloan-Kettering Cancer Center in New York City, oncologists traditionally have tried to holistically manage the care of cancer patients. In today’s age of new treatments and increased inpatient care for patients with aggressive cancers, though, Jason Konner, MD, says it’s time for hospitalists to take a greater role in the management of cancer patients.
The upshot: Dr. Konner envisions a new breed of oncologist-hospitalists. (Check out this in-depth look at specialty physicians adopting the HM model of care.)
“Universally, the hospitalist is going to have to be part of a team with the oncologist,” says Dr. Konner, assistant professor with the Gynecological Medical Oncology Service and Developmental Therapeutic Services. “We’re going to complement each other. There are definitely things that we can do that they can’t and definitely things they can do that we can’t. Right now, it’s just being part of the team to address the diverse medical complications of cancer. But I think that increasingly, [hospitalists] are going to be the primary caregivers, sometimes solely the caregivers, of patients with cancer complications.”
The concept, which was raised during an “Oncology for the Hospitalist” presentation at the fifth annual Mid-Atlantic Hospital Medicine Symposium at Mount Sinai School of Medicine in New York City, is not new, but it is particularly relevant as cancer mortality and incidence rates continue to drop. Dr. Konner counters that while improved screening techniques—mammographies and prostate-specific antigen (PSA) tests, to note a pair—have reduced incidences, the majority of “aggressive cancers and cancers that kill people” still require intensive inpatient care.
To wit, a pilot program at Mount Sinai several years ago dedicated a hospitalist to the oncology service in the hopes of developing a staffer with a new expertise. The brief program, which yielded little data because of its small sample size, was aimed at determining the efficacy of an oncology hospitalist.
Richard Quinn is a freelance writer based in New Jersey.
Diabetes Rates Expected to Double
Hospitalist Jeffrey Schnipper, MD, MPH, FHM, estimated last year that a full third of his current patient census was either diabetic or hypoglycemic, a figure that might seem out of place for someone who isn’t a diabetologist.
Last week, Dr. Schnipper's estimation made perfect sense with the release of a new report from the Centers for Disease Control and Prevention (CDC) that forecasts a near-doubling of diabetic incidences in the next 40 years.
"I won't be surprised when there's a day where half of my patients have diabetes or hypoglycemia," says Dr. Schnipper, director of clinical research and associate physician in the general medicine division at Brigham and Women's Hospitalist Service in Boston. "We all have to become experts in how to comanage these patients."
The CDC data, published in Population Health Metrics on Oct. 22, state that "annual diagnosed diabetes incidence [new cases] will increase from about 8 cases per 1,000 in 2008 to about 15 in 2050" (doi: 10.1186/1478-7954-8-29). The authors note that intervention can reduce that prevalence, but won't eliminate it.
Dr. Schnipper says the exponential growth of diabetes incidence will not directly correlate to growth in patient counts, as many diabetics will be able to control their disease without admission to the hospital. However, he says, a large percentage of new cases are likely to end up as hospitalized patients heaped on HM groups' already full plates.
He suggests one response to the looming surge in diabetics might be to administer an A1c test to nearly all of your admitted patients to determine blood-glucose levels, or develop new protocols for how, who, and when to screen for diabetes.
One obvious patient group to be concerned about is the obese population, which Dr. Schnipper says is a direct cause of the diabetic incidence increase. "What we're seeing is an epidemic of obesity causing an epidemic of diabetes," he adds. "We already need to know how to manage these patients."
Hospitalist Jeffrey Schnipper, MD, MPH, FHM, estimated last year that a full third of his current patient census was either diabetic or hypoglycemic, a figure that might seem out of place for someone who isn’t a diabetologist.
Last week, Dr. Schnipper's estimation made perfect sense with the release of a new report from the Centers for Disease Control and Prevention (CDC) that forecasts a near-doubling of diabetic incidences in the next 40 years.
"I won't be surprised when there's a day where half of my patients have diabetes or hypoglycemia," says Dr. Schnipper, director of clinical research and associate physician in the general medicine division at Brigham and Women's Hospitalist Service in Boston. "We all have to become experts in how to comanage these patients."
The CDC data, published in Population Health Metrics on Oct. 22, state that "annual diagnosed diabetes incidence [new cases] will increase from about 8 cases per 1,000 in 2008 to about 15 in 2050" (doi: 10.1186/1478-7954-8-29). The authors note that intervention can reduce that prevalence, but won't eliminate it.
Dr. Schnipper says the exponential growth of diabetes incidence will not directly correlate to growth in patient counts, as many diabetics will be able to control their disease without admission to the hospital. However, he says, a large percentage of new cases are likely to end up as hospitalized patients heaped on HM groups' already full plates.
He suggests one response to the looming surge in diabetics might be to administer an A1c test to nearly all of your admitted patients to determine blood-glucose levels, or develop new protocols for how, who, and when to screen for diabetes.
One obvious patient group to be concerned about is the obese population, which Dr. Schnipper says is a direct cause of the diabetic incidence increase. "What we're seeing is an epidemic of obesity causing an epidemic of diabetes," he adds. "We already need to know how to manage these patients."
Hospitalist Jeffrey Schnipper, MD, MPH, FHM, estimated last year that a full third of his current patient census was either diabetic or hypoglycemic, a figure that might seem out of place for someone who isn’t a diabetologist.
Last week, Dr. Schnipper's estimation made perfect sense with the release of a new report from the Centers for Disease Control and Prevention (CDC) that forecasts a near-doubling of diabetic incidences in the next 40 years.
"I won't be surprised when there's a day where half of my patients have diabetes or hypoglycemia," says Dr. Schnipper, director of clinical research and associate physician in the general medicine division at Brigham and Women's Hospitalist Service in Boston. "We all have to become experts in how to comanage these patients."
The CDC data, published in Population Health Metrics on Oct. 22, state that "annual diagnosed diabetes incidence [new cases] will increase from about 8 cases per 1,000 in 2008 to about 15 in 2050" (doi: 10.1186/1478-7954-8-29). The authors note that intervention can reduce that prevalence, but won't eliminate it.
Dr. Schnipper says the exponential growth of diabetes incidence will not directly correlate to growth in patient counts, as many diabetics will be able to control their disease without admission to the hospital. However, he says, a large percentage of new cases are likely to end up as hospitalized patients heaped on HM groups' already full plates.
He suggests one response to the looming surge in diabetics might be to administer an A1c test to nearly all of your admitted patients to determine blood-glucose levels, or develop new protocols for how, who, and when to screen for diabetes.
One obvious patient group to be concerned about is the obese population, which Dr. Schnipper says is a direct cause of the diabetic incidence increase. "What we're seeing is an epidemic of obesity causing an epidemic of diabetes," he adds. "We already need to know how to manage these patients."
In the Literature: Research You Need to Know
Clinical question: Are beta-blockers safe to use in patients with chest pain and recent cocaine use?
Background: Beta-blockers are known to improve outcomes after myocardial infarction, yet are contraindicated in chest pain associated with recent cocaine use. Recommendations against beta-blocker use in the setting of cocaine-induced chest pain are based on case reports, small human experiments, and the theoretical concern that beta-blockers may potentiate cocaine toxicity by creating unopposed alpha-adrenergic stimulation. Clinical outcomes of beta-blocker use in patients with cocaine use and chest pain are unknown.
Study design: Retrospective cohort study.
Setting: San Francisco General Hospital, San Francisco.
Synopsis: Three hundred thirty-one patients with chest pain and positive urine toxicologic screening for cocaine were admitted during the study period. One hundred fifty-one (46%) received a beta-blocker in the ED, per the discretion of the treating physicians. There were no differences in ECG abnormalities, troponin levels, length of stay, intubation, ventricular arrhythmias, use of vasopressors, or death in those patients who did and who did not receive a beta-blocker. Over a median follow-up of 972 days, patients who had been discharged on a beta-blocker did have a significant reduction in cardiovascular death (hazard ratio 0.29, 95% CI, 0.09-0.98, P=0.047).
Because this was an observational study and post-discharge data were limited only to vital status, definitive conclusions regarding the safety of beta-blockers in cocaine-associated chest pain cannot be made. The authors acknowledge that more rigorous study is indicated given the potential benefit of beta-blockers in this population.
Bottom line: Use of beta-blockers in patients with chest pain and positive urine drug screen for cocaine is not associated with immediate adverse outcomes and might actually reduce cardiovascular mortality over time.
Citation: Rangel C, Shu RG, Lazar LD, Vittinghoff E, Hsue PY, Marcus GM. Beta-blockers for chest pain associated with recent cocaine use. Arch Intern Med. 2010;170(10):874-879.
Reviewed for TH eWire by Kelly Cunningham MD, Joshua LaBrin, MD, Amanda Salanitro, MD, MSPH, Kelly Sopko, MD, Shelley Ellis, MD, MPH, and Elizabeth Rice MD, Section of Hospital Medicine, Vanderbilt University.
For more physician reviews of literature, visit our website.
Clinical question: Are beta-blockers safe to use in patients with chest pain and recent cocaine use?
Background: Beta-blockers are known to improve outcomes after myocardial infarction, yet are contraindicated in chest pain associated with recent cocaine use. Recommendations against beta-blocker use in the setting of cocaine-induced chest pain are based on case reports, small human experiments, and the theoretical concern that beta-blockers may potentiate cocaine toxicity by creating unopposed alpha-adrenergic stimulation. Clinical outcomes of beta-blocker use in patients with cocaine use and chest pain are unknown.
Study design: Retrospective cohort study.
Setting: San Francisco General Hospital, San Francisco.
Synopsis: Three hundred thirty-one patients with chest pain and positive urine toxicologic screening for cocaine were admitted during the study period. One hundred fifty-one (46%) received a beta-blocker in the ED, per the discretion of the treating physicians. There were no differences in ECG abnormalities, troponin levels, length of stay, intubation, ventricular arrhythmias, use of vasopressors, or death in those patients who did and who did not receive a beta-blocker. Over a median follow-up of 972 days, patients who had been discharged on a beta-blocker did have a significant reduction in cardiovascular death (hazard ratio 0.29, 95% CI, 0.09-0.98, P=0.047).
Because this was an observational study and post-discharge data were limited only to vital status, definitive conclusions regarding the safety of beta-blockers in cocaine-associated chest pain cannot be made. The authors acknowledge that more rigorous study is indicated given the potential benefit of beta-blockers in this population.
Bottom line: Use of beta-blockers in patients with chest pain and positive urine drug screen for cocaine is not associated with immediate adverse outcomes and might actually reduce cardiovascular mortality over time.
Citation: Rangel C, Shu RG, Lazar LD, Vittinghoff E, Hsue PY, Marcus GM. Beta-blockers for chest pain associated with recent cocaine use. Arch Intern Med. 2010;170(10):874-879.
Reviewed for TH eWire by Kelly Cunningham MD, Joshua LaBrin, MD, Amanda Salanitro, MD, MSPH, Kelly Sopko, MD, Shelley Ellis, MD, MPH, and Elizabeth Rice MD, Section of Hospital Medicine, Vanderbilt University.
For more physician reviews of literature, visit our website.
Clinical question: Are beta-blockers safe to use in patients with chest pain and recent cocaine use?
Background: Beta-blockers are known to improve outcomes after myocardial infarction, yet are contraindicated in chest pain associated with recent cocaine use. Recommendations against beta-blocker use in the setting of cocaine-induced chest pain are based on case reports, small human experiments, and the theoretical concern that beta-blockers may potentiate cocaine toxicity by creating unopposed alpha-adrenergic stimulation. Clinical outcomes of beta-blocker use in patients with cocaine use and chest pain are unknown.
Study design: Retrospective cohort study.
Setting: San Francisco General Hospital, San Francisco.
Synopsis: Three hundred thirty-one patients with chest pain and positive urine toxicologic screening for cocaine were admitted during the study period. One hundred fifty-one (46%) received a beta-blocker in the ED, per the discretion of the treating physicians. There were no differences in ECG abnormalities, troponin levels, length of stay, intubation, ventricular arrhythmias, use of vasopressors, or death in those patients who did and who did not receive a beta-blocker. Over a median follow-up of 972 days, patients who had been discharged on a beta-blocker did have a significant reduction in cardiovascular death (hazard ratio 0.29, 95% CI, 0.09-0.98, P=0.047).
Because this was an observational study and post-discharge data were limited only to vital status, definitive conclusions regarding the safety of beta-blockers in cocaine-associated chest pain cannot be made. The authors acknowledge that more rigorous study is indicated given the potential benefit of beta-blockers in this population.
Bottom line: Use of beta-blockers in patients with chest pain and positive urine drug screen for cocaine is not associated with immediate adverse outcomes and might actually reduce cardiovascular mortality over time.
Citation: Rangel C, Shu RG, Lazar LD, Vittinghoff E, Hsue PY, Marcus GM. Beta-blockers for chest pain associated with recent cocaine use. Arch Intern Med. 2010;170(10):874-879.
Reviewed for TH eWire by Kelly Cunningham MD, Joshua LaBrin, MD, Amanda Salanitro, MD, MSPH, Kelly Sopko, MD, Shelley Ellis, MD, MPH, and Elizabeth Rice MD, Section of Hospital Medicine, Vanderbilt University.
For more physician reviews of literature, visit our website.
Split Personality
By the fourth year of residency, most in combined internal medicine/pediatrics (commonly known as “med-ped”) residencies come to realize that their training is heavily weighted toward inpatient and ICU settings. After all, med-ped residency programs require that all the inpatient and ICU requirements of both the American Board of Internal Medicine (ABIM) and the American Board of Pediatrics (ABP) be met. This allows med-ped graduates, numbering just over 300 each year, to sit for both boards, and potentially to be able to obtain admitting privileges for both adults and children. This seems to be the perfect training for a hospitalist-to-be, if one so desires.
But for hospitalists, there comes the dilemma: Should you concentrate on the adult or the pediatric population, or is it possible to be a med-ped hospitalist? By far, most HM job opportunities are for either purely adult hospitalists or purely pediatric hospitalists, although there are an increasing number of “off the shelf” med-ped hospitalist positions. Building a med-ped career as a hospitalist from shifts in adult and pediatric programs is a possibility but requires extra attention to scheduling, salary, and benefits.
Med-ped physicians are used to being creative about their work, but some might begin to ask themselves whether the additional effort is worth it. Seeking out knowledgeable administrators and department/division chiefs, following other med-ped hospitalists who have already blazed a trail, and being realistic about your “mix” of work are some solutions for the hybrid hospitalist.
Academia Fosters Cooperation—and Lack Thereof
An ever-increasing number of med-ped physicians seem to think being a med-peds hospitalist is possible, even desirable. Heather Toth, MD, program director for the med-ped residency program at Medical College of Wisconsin and a hospitalist at Children’s Hospital of Wisconsin, both in Milwaukee, doesn’t regret her decision to put in the extra work required to be a hospitalist for all age groups.
“[It is] absolutely a wonderful career and worth the effort to establish a combined position. There is much to be learned from each world [medicine and pediatrics] to enrich our patients’ care,” says Dr. Toth, who was a former chief resident for the med-ped program at the college. In her case, being close to the administrators of both departments played to her advantage and allowed her to craft her job “from the inside,” she says.

“The process was much smoother than anticipated,” Dr. Toth explains. “One concern was which department would own my time. This was overcome by splitting my time by months. For example, January is medicine wards, February is pediatric wards, etc., with corresponding overnight shifts/call.”
Others have experienced obstacles in carving out an academic med-peds hospitalist position. Susan Hunt, MD, a hospitalist at Brigham and Women’s Hospital in Boston, finished her med-ped residency at Duke University in 2008 and began her career as an adults-only hospitalist. However, the desire to work in pediatrics still burned, leading Dr. Hunt to seek pediatric hospitalist work within the Partners HealthCare system. Initially, her efforts were to no avail. More recently, she has been able to break into hospitalist work through the Children’s Hospital Boston’s outreach program at local community hospitals.
“Pediatric programs tend to be small and, in Boston, had very little turnover,” Dr. Hunt says. She also has a warning for pediatric hospitalist hopefuls. “Increasing pediatric time invariably results in decreased pay.”
For the most part, med-ped hospitalist positions in academic hospitals tend to be crafted from a combination of time from two distinct departments. But an academic setting does offer potential med-ped hospitalists a few advantages, such as:
- Typically more hospitalists in each department, leading to greater scheduling flexibility;
- Larger pediatric hospitalist programs that often encompass not only the “main” hospital, but also community hospitals; this leads to increased availability of hospitalist work; and
- The possibility of a med-ped residency program at the same site, which allows for the possibility of being a role model to med-ped residents.
Although the trends might be changing, there are multiple barriers to an academic med-ped hospitalist job. Often, the IM and pediatric departments are not used to working together. Determining who will pay the hospitalist’s salary and benefits, how the schedule will be coordinated, and to whom the hospitalist is responsible can be tricky. Moreover, it’s not always clear which department will take the lead in the promotion process. Departments expect hospitalists to act as good citizens by serving on committees, and it can be difficult to serve two masters.
As a result, many academic med-peds hospitalists have a primary appointment in one department and have their clinical salaries “bought down” by the other. A handful of hospital committees, including quality-improvement (QI) and information technology, allow med-ped hospitalists to serve on one committee and receive citizenship “credit” from both departments. Leonard Feldman, MD, FAAP, FACP, and Carrie Herzke, MD, have walked this tightrope at Johns Hopkins Hospital in Baltimore. Their successes in this arena have created more clinical and research opportunities for med-ped hospitalists, as the administrators and physicians have learned how to negotiate their relationship. One example of this success has been the Johns Hopkins Hospitalist Scholars Program, which provides up to $12,000 of annual funding to hospitalist faculty.
Although rare, the academic med-ped hospitalist program under a single administrative structure does exist. Allen Liles, MD, program director for the hospital medicine program at the University of North Carolina (UNC) Hospitals in Chapel Hill, has brought together a group of 17 hospitalists, six of whom are med-ped-trained.
“Both the pediatric portion and the medicine portion are administered within this one program,” states Dr. Liles. “I think this is a huge advantage to actually making it work. If I was not the director being med-peds-trained, I am not sure this would have happened.” According to Dr. Liles, it took six months of working closely with the CFO of UNC Hospitals to establish a program that he felt “managed to change the paradigm.”
“It is the hospital that derives the most benefit from a [combined] hospitalist program,” adds Dr. Liles. “And as such, they were easy to convince of the benefits of a med-ped model and expansion into pediatrics.”
The Community Setting: Challenges and Successes
Academic settings aren’t alone in their battles putting together med-ped hospitalist positions. Jacques-Bret Burgess, MD, MPH, FAAP, a hospitalist with Traverse City, Mich.-based Hospitalists of Northwest Michigan (HNM), began in April 2009 to establish a pediatric hospitalist program within his group of adult hospitalists. Since that time, med-ped-trained hospitalists have increased to five from just one out of the 30 hospitalists employed by HNM. But there have been growing pains.
“The majority of administrators and physicians just do not understand the potential, nor the efficiency, of a [med-ped] physician,” Dr. Burgess says. “Most frustrations come from trying to explain what an IM-ped physician is, what we are capable of, and then obtaining adequate support to practice both disciplines while at the same time maintaining some sense of self and family.”
In fact, it is not uncommon for med-ped hospitalists to work full time in one discipline—usually adult—and moonlight or work part time in pediatrics. Jeff Whittall, MD, a hospitalist for MultiCare Inpatient Services in Tacoma, Wash., works primarily as an adult hospitalist at Tacoma General Hospital but provides pediatric urgent care at Mary Bridge Children’s Hospital in Tacoma as well. “It is a fantastic mix,” Dr. Whittall says.
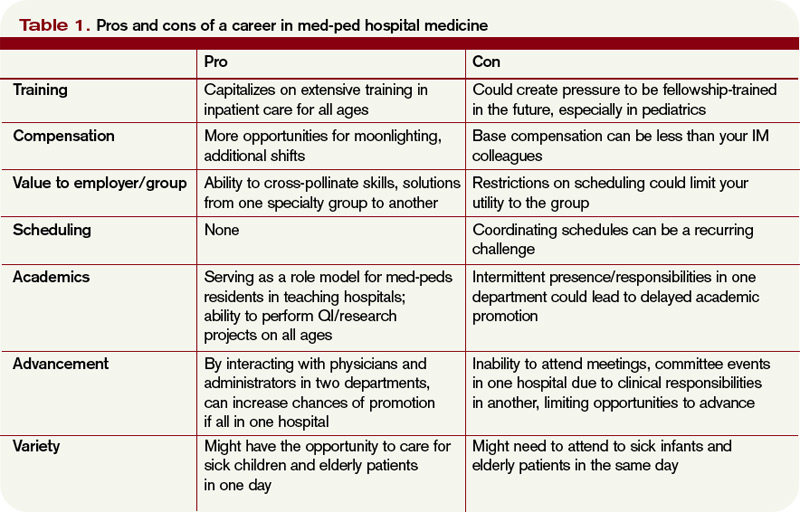
That said, other med-ped hospitalists consider such combinations to be a compromise. Many yearn for that perfect mix of adult and pediatric hospitalist work, and have even taken on additional training to do so.
Oliver Medzihradsy, MD, was a half-time adult hospitalist at Barton Memorial Hospital in South Lake Tahoe, Calif., with the other half spent in outpatient pediatrics for Tahoe Carson Valley Medical Group, until this year. In August, be became a first-year fellow at Rady Children’s Hospital in pediatric hospital medicine.
“Having been out [of] hospital-based peds for four years now, I decided that, if I wanted to get back into … [pediatrics] as a hospitalist, it would serve me well to go back for a peds hospital medicine fellowship,” said Dr. Medzihradsy. “Economically, it’s rather foolhardy to take such a salary cut, not to mention the philosophical change of becoming a trainee again, but from a clinical passion standpoint, it’s what I wish to do.”
In some cases, community hospitalist programs, many of which offer a less territorial work environment and organizational structure, have been more successful at establishing full-fledged combined med-ped hospitalist programs. Elliot Hospital in Manchester, N.H., has built from the ground up a hospitalist program utilizing both internal medicine and med-ped-trained hospitalists. Currently, Elliot Hospital employs four med-ped-trained hospitalists, who staff the pediatric inpatient unit but are available for adult inpatients when pediatric volume is low. Other community hospitalist programs utilize the pediatric skills of their med-ped hospitalists in urgent-care or ED coverage in times of low pediatric volume.
“From the perspective of our med-ped physicians, they feel that this is a unique employment opportunity that allows them to have a truly balanced 50-50 medicine/pediatrics inpatient experience,” said Anita Ritenour, MD, assistant vice president for medical affairs at Elliot Hospital. Although trained in internal medicine, her familiarity with community med-ped physicians made her an early advocate of med-ped hospitalists.
Amy Stone, MD, director of Elliot Hospital’s pediatric hospitalist program and a med-ped-trained physician, typically starts her day at 7 a.m. with sign-out from the overnight provider, then touches base with nurses about overnight events. Family-centered rounds follow, with the afternoons being occupied by ED or direct admissions and family meetings. Given their training, however, the med-ped-trained pediatric hospitalists can get called upon to help out on the internal-medicine side.
“As a med-ped hospitalist on the peds service, we get pulled occasionally to help with the internal-medicine service to admit, both during the day and at night,” adds Dr. Craig Widness, another med-peds-trained hospitalist at Elliot.
But the scope of practice and volume has ramped up for the pediatric hospitalist service at Elliot, as many community pediatric groups have opted to utilize their services. In addition, a new pediatric ICU has recently been established, managed by the pediatric hospitalist service.
As a result, the opportunities for the med-ped-trained pediatric hospitalists to help out on the adult hospitalist vortex have been increasingly rare, which seem to be a welcome development to the pediatric hospitalists.

Building the Perfect Beast
So how does a med-ped physician entering hospital medicine build a job that satisfies the need to care for both adults and children? In some cases, the perfect med-ped position is already available. More likely, however, hospitalist jobs in a specific location are limited to either one discipline or another.
In many, if not most, cases, practice in one discipline will have to be somewhat compromised to fulfill the staffing needs of the “primary” job, at least initially. In the interview and hiring process, however, hospitalists wishing to pursue med-peds must make known their desire to work in both medicine and pediatrics. The transparency will allow hospital and group administrators to build into your schedule time to work in both pursuits.
“Start trying to arrange for pediatrics early. I started before I finished residency and it took me over a year to set up,” Dr. Hunt says, noting her current position is in the academic arena. “Discuss your plans with any medicine group you intend to join. See if your FTE would be flexible or if they can help arrange things. Get in touch with local med-ped program directors, if possible, as they often know people on both sides and might be able to help get you in touch with the right people.”
When looking at community hospitalist jobs, it is critical to ensure your administrators are familiar with med-peds residency training. It helps them better understand your skills, your goals, and allows them to put you in position to care for patients in all age groups.
“When one finds administrators and leaders that understand and respect the concept [of med-peds], hold on to them,” Dr. Burgess advises. “Do not let anyone take your unique training for granted and try to categorize you as one or the other; rather, we are both. We have two sets of boards, with separate training and a unique overlap that provides synergy with our abilities. Find a group that understands the level of training you possess.”
Call Protection
As uncommon as it is to find med-ped hospitalist jobs that feature built-in coordination of work in both disciplines, one should pay attention to coordinating salary, call, vacation, and CME between the two disciplines.
“Talk with potential groups about how they cover you for call, how you will be reimbursed, and what data will they base your pay and incentives on,” Dr. Burgess says. “What will they base your CME on—two disciplines or one? What is your depth if you have a sick child and sick adult at the same time?”
Most important, med-peds must make sure administrators of both disciplines are aware of your activities on both sides. “We do not want double-call days,” Dr. Burgess adds. He also warns that overcoming the frustrations of med-pedwork “takes a great deal of patience and discussion.”
Salary might be an issue, especially as one tries to mold a position. SHM and the Medical Group Management Association (MGMA) State of Hospital Medicine: 2010 Report Based on 2009 Data lists the median national annual compensation for adult hospitalists as $215,000, and $160,038 for pediatric hospitalists. This also has implications when IM time is bought down by pediatrics in academic centers, as pediatrics might not pay as much for clinical time as medicine will.
Back Where You Belong
Either by necessity or choice, med-ped-trained hospitalists all across the country have taken jobs in one setting or another and now yearn to get back into the other discipline. It might not be as difficult as you think.
If hospitalist work in the other discipline is available in your institution, you could consider a reduction of FTE in your current job to expand into the other discipline. Keep in mind, however, the interdepartmental coordination difficulties (i.e. scheduling, benefits, maintaining privileges). Those can be even more pronounced if two or more employers are involved.
Additionally, a reduction of FTE in your current job could lead to increased clinical time on the part of your colleagues, or perhaps even hiring additional staff, so this change needs to be discussed thoroughly with administrators and colleagues well in advance of any changes.
Less dramatic changes can enable a med-ped hospitalist to get a taste of the other discipline without wholesale changes in salary and schedule. Moonlighting as an intermittent hospitalist or nocturnist, taking call in the other discipline’s call schedule, or filling in for urgent-care slots can keep skills and knowledge from getting rusty.
It also can prevent the loss of pediatric admitting and procedural privileges. A patchwork approach also could lead to a steady hospitalist job in the other discipline.
“I discussed my desire to do pediatrics with friends and acquaintances who worked as pediatricians in local community hospitals through Children’s Hospital Boston,” Dr. Hunt says. “Eventually, [it led] to the peds work.”
As is often the case in HM, med-ped programs tend to follow the tenet “if you build it, they will come.” Once a hospitalist director discovers the flexibility and skill set a med-ped hospitalist provides the group, they often look to expand—especially to staff smaller pediatric units.
Such was the case at Elliot Hospital; familiarity with med-ped moonlighters eventually led to a full-time med-ped hospitalist hire. Following the full-time hire, the HM group realized a dramatic increase in local pediatric groups referring patients to Elliot’s hospitalist group, including the largest pediatric group in Southern New Hampshire, Dartmouth-Hitchcock Clinic.
“Initial referral base from the community was sluggish as community [pediatricians] wanted to hold onto their patients,” Dr. Ritenour says. “As the acuity of what we could support as hospitalists grew, more referrals were made for kids that might have previously been transferred.”
The Future of Med-Ped Hospitalists
At the dawn of combined med-ped residencies in the early 1960s, the hospitalist movement was only a twinkle in the eye of house physicians of yore. Now that both movements have matured, will we see this hybrid of a hybrid flourish?
“I think med-peds is well suited for hospital medicine, based on solid training that includes numerous inpatient wards and critical care in both internal medicine and pediatrics,” says Dr. Toth, adding she hopes to bring additional med-ped hospitalists to her group in Milwaukee in the future.
It seems inevitable that the med-ped movement, which has grown into the largest combined residency specialty in the country, and the hospitalist movement, which has exploded as the fastest-growing medical specialty, will continue to intertwine, branch out, and evolve.
And every year, some of those med-ped residency program graduates will continue to climb those twisted trunks, as challenging as it might seem. TH
Dr. Chang is a med-peds hospitalist at the University of California at San Diego and Rady Children’s Hospital. He is a member of Team Hospitalist.
By the fourth year of residency, most in combined internal medicine/pediatrics (commonly known as “med-ped”) residencies come to realize that their training is heavily weighted toward inpatient and ICU settings. After all, med-ped residency programs require that all the inpatient and ICU requirements of both the American Board of Internal Medicine (ABIM) and the American Board of Pediatrics (ABP) be met. This allows med-ped graduates, numbering just over 300 each year, to sit for both boards, and potentially to be able to obtain admitting privileges for both adults and children. This seems to be the perfect training for a hospitalist-to-be, if one so desires.
But for hospitalists, there comes the dilemma: Should you concentrate on the adult or the pediatric population, or is it possible to be a med-ped hospitalist? By far, most HM job opportunities are for either purely adult hospitalists or purely pediatric hospitalists, although there are an increasing number of “off the shelf” med-ped hospitalist positions. Building a med-ped career as a hospitalist from shifts in adult and pediatric programs is a possibility but requires extra attention to scheduling, salary, and benefits.
Med-ped physicians are used to being creative about their work, but some might begin to ask themselves whether the additional effort is worth it. Seeking out knowledgeable administrators and department/division chiefs, following other med-ped hospitalists who have already blazed a trail, and being realistic about your “mix” of work are some solutions for the hybrid hospitalist.
Academia Fosters Cooperation—and Lack Thereof
An ever-increasing number of med-ped physicians seem to think being a med-peds hospitalist is possible, even desirable. Heather Toth, MD, program director for the med-ped residency program at Medical College of Wisconsin and a hospitalist at Children’s Hospital of Wisconsin, both in Milwaukee, doesn’t regret her decision to put in the extra work required to be a hospitalist for all age groups.
“[It is] absolutely a wonderful career and worth the effort to establish a combined position. There is much to be learned from each world [medicine and pediatrics] to enrich our patients’ care,” says Dr. Toth, who was a former chief resident for the med-ped program at the college. In her case, being close to the administrators of both departments played to her advantage and allowed her to craft her job “from the inside,” she says.
“The process was much smoother than anticipated,” Dr. Toth explains. “One concern was which department would own my time. This was overcome by splitting my time by months. For example, January is medicine wards, February is pediatric wards, etc., with corresponding overnight shifts/call.”
Others have experienced obstacles in carving out an academic med-peds hospitalist position. Susan Hunt, MD, a hospitalist at Brigham and Women’s Hospital in Boston, finished her med-ped residency at Duke University in 2008 and began her career as an adults-only hospitalist. However, the desire to work in pediatrics still burned, leading Dr. Hunt to seek pediatric hospitalist work within the Partners HealthCare system. Initially, her efforts were to no avail. More recently, she has been able to break into hospitalist work through the Children’s Hospital Boston’s outreach program at local community hospitals.
“Pediatric programs tend to be small and, in Boston, had very little turnover,” Dr. Hunt says. She also has a warning for pediatric hospitalist hopefuls. “Increasing pediatric time invariably results in decreased pay.”
For the most part, med-ped hospitalist positions in academic hospitals tend to be crafted from a combination of time from two distinct departments. But an academic setting does offer potential med-ped hospitalists a few advantages, such as:
- Typically more hospitalists in each department, leading to greater scheduling flexibility;
- Larger pediatric hospitalist programs that often encompass not only the “main” hospital, but also community hospitals; this leads to increased availability of hospitalist work; and
- The possibility of a med-ped residency program at the same site, which allows for the possibility of being a role model to med-ped residents.
Although the trends might be changing, there are multiple barriers to an academic med-ped hospitalist job. Often, the IM and pediatric departments are not used to working together. Determining who will pay the hospitalist’s salary and benefits, how the schedule will be coordinated, and to whom the hospitalist is responsible can be tricky. Moreover, it’s not always clear which department will take the lead in the promotion process. Departments expect hospitalists to act as good citizens by serving on committees, and it can be difficult to serve two masters.
As a result, many academic med-peds hospitalists have a primary appointment in one department and have their clinical salaries “bought down” by the other. A handful of hospital committees, including quality-improvement (QI) and information technology, allow med-ped hospitalists to serve on one committee and receive citizenship “credit” from both departments. Leonard Feldman, MD, FAAP, FACP, and Carrie Herzke, MD, have walked this tightrope at Johns Hopkins Hospital in Baltimore. Their successes in this arena have created more clinical and research opportunities for med-ped hospitalists, as the administrators and physicians have learned how to negotiate their relationship. One example of this success has been the Johns Hopkins Hospitalist Scholars Program, which provides up to $12,000 of annual funding to hospitalist faculty.
Although rare, the academic med-ped hospitalist program under a single administrative structure does exist. Allen Liles, MD, program director for the hospital medicine program at the University of North Carolina (UNC) Hospitals in Chapel Hill, has brought together a group of 17 hospitalists, six of whom are med-ped-trained.
“Both the pediatric portion and the medicine portion are administered within this one program,” states Dr. Liles. “I think this is a huge advantage to actually making it work. If I was not the director being med-peds-trained, I am not sure this would have happened.” According to Dr. Liles, it took six months of working closely with the CFO of UNC Hospitals to establish a program that he felt “managed to change the paradigm.”
“It is the hospital that derives the most benefit from a [combined] hospitalist program,” adds Dr. Liles. “And as such, they were easy to convince of the benefits of a med-ped model and expansion into pediatrics.”
The Community Setting: Challenges and Successes
Academic settings aren’t alone in their battles putting together med-ped hospitalist positions. Jacques-Bret Burgess, MD, MPH, FAAP, a hospitalist with Traverse City, Mich.-based Hospitalists of Northwest Michigan (HNM), began in April 2009 to establish a pediatric hospitalist program within his group of adult hospitalists. Since that time, med-ped-trained hospitalists have increased to five from just one out of the 30 hospitalists employed by HNM. But there have been growing pains.
“The majority of administrators and physicians just do not understand the potential, nor the efficiency, of a [med-ped] physician,” Dr. Burgess says. “Most frustrations come from trying to explain what an IM-ped physician is, what we are capable of, and then obtaining adequate support to practice both disciplines while at the same time maintaining some sense of self and family.”
In fact, it is not uncommon for med-ped hospitalists to work full time in one discipline—usually adult—and moonlight or work part time in pediatrics. Jeff Whittall, MD, a hospitalist for MultiCare Inpatient Services in Tacoma, Wash., works primarily as an adult hospitalist at Tacoma General Hospital but provides pediatric urgent care at Mary Bridge Children’s Hospital in Tacoma as well. “It is a fantastic mix,” Dr. Whittall says.
That said, other med-ped hospitalists consider such combinations to be a compromise. Many yearn for that perfect mix of adult and pediatric hospitalist work, and have even taken on additional training to do so.
Oliver Medzihradsy, MD, was a half-time adult hospitalist at Barton Memorial Hospital in South Lake Tahoe, Calif., with the other half spent in outpatient pediatrics for Tahoe Carson Valley Medical Group, until this year. In August, be became a first-year fellow at Rady Children’s Hospital in pediatric hospital medicine.
“Having been out [of] hospital-based peds for four years now, I decided that, if I wanted to get back into … [pediatrics] as a hospitalist, it would serve me well to go back for a peds hospital medicine fellowship,” said Dr. Medzihradsy. “Economically, it’s rather foolhardy to take such a salary cut, not to mention the philosophical change of becoming a trainee again, but from a clinical passion standpoint, it’s what I wish to do.”
In some cases, community hospitalist programs, many of which offer a less territorial work environment and organizational structure, have been more successful at establishing full-fledged combined med-ped hospitalist programs. Elliot Hospital in Manchester, N.H., has built from the ground up a hospitalist program utilizing both internal medicine and med-ped-trained hospitalists. Currently, Elliot Hospital employs four med-ped-trained hospitalists, who staff the pediatric inpatient unit but are available for adult inpatients when pediatric volume is low. Other community hospitalist programs utilize the pediatric skills of their med-ped hospitalists in urgent-care or ED coverage in times of low pediatric volume.
“From the perspective of our med-ped physicians, they feel that this is a unique employment opportunity that allows them to have a truly balanced 50-50 medicine/pediatrics inpatient experience,” said Anita Ritenour, MD, assistant vice president for medical affairs at Elliot Hospital. Although trained in internal medicine, her familiarity with community med-ped physicians made her an early advocate of med-ped hospitalists.
Amy Stone, MD, director of Elliot Hospital’s pediatric hospitalist program and a med-ped-trained physician, typically starts her day at 7 a.m. with sign-out from the overnight provider, then touches base with nurses about overnight events. Family-centered rounds follow, with the afternoons being occupied by ED or direct admissions and family meetings. Given their training, however, the med-ped-trained pediatric hospitalists can get called upon to help out on the internal-medicine side.
“As a med-ped hospitalist on the peds service, we get pulled occasionally to help with the internal-medicine service to admit, both during the day and at night,” adds Dr. Craig Widness, another med-peds-trained hospitalist at Elliot.
But the scope of practice and volume has ramped up for the pediatric hospitalist service at Elliot, as many community pediatric groups have opted to utilize their services. In addition, a new pediatric ICU has recently been established, managed by the pediatric hospitalist service.
As a result, the opportunities for the med-ped-trained pediatric hospitalists to help out on the adult hospitalist vortex have been increasingly rare, which seem to be a welcome development to the pediatric hospitalists.
Building the Perfect Beast
So how does a med-ped physician entering hospital medicine build a job that satisfies the need to care for both adults and children? In some cases, the perfect med-ped position is already available. More likely, however, hospitalist jobs in a specific location are limited to either one discipline or another.
In many, if not most, cases, practice in one discipline will have to be somewhat compromised to fulfill the staffing needs of the “primary” job, at least initially. In the interview and hiring process, however, hospitalists wishing to pursue med-peds must make known their desire to work in both medicine and pediatrics. The transparency will allow hospital and group administrators to build into your schedule time to work in both pursuits.
“Start trying to arrange for pediatrics early. I started before I finished residency and it took me over a year to set up,” Dr. Hunt says, noting her current position is in the academic arena. “Discuss your plans with any medicine group you intend to join. See if your FTE would be flexible or if they can help arrange things. Get in touch with local med-ped program directors, if possible, as they often know people on both sides and might be able to help get you in touch with the right people.”
When looking at community hospitalist jobs, it is critical to ensure your administrators are familiar with med-peds residency training. It helps them better understand your skills, your goals, and allows them to put you in position to care for patients in all age groups.
“When one finds administrators and leaders that understand and respect the concept [of med-peds], hold on to them,” Dr. Burgess advises. “Do not let anyone take your unique training for granted and try to categorize you as one or the other; rather, we are both. We have two sets of boards, with separate training and a unique overlap that provides synergy with our abilities. Find a group that understands the level of training you possess.”
Call Protection
As uncommon as it is to find med-ped hospitalist jobs that feature built-in coordination of work in both disciplines, one should pay attention to coordinating salary, call, vacation, and CME between the two disciplines.
“Talk with potential groups about how they cover you for call, how you will be reimbursed, and what data will they base your pay and incentives on,” Dr. Burgess says. “What will they base your CME on—two disciplines or one? What is your depth if you have a sick child and sick adult at the same time?”
Most important, med-peds must make sure administrators of both disciplines are aware of your activities on both sides. “We do not want double-call days,” Dr. Burgess adds. He also warns that overcoming the frustrations of med-pedwork “takes a great deal of patience and discussion.”
Salary might be an issue, especially as one tries to mold a position. SHM and the Medical Group Management Association (MGMA) State of Hospital Medicine: 2010 Report Based on 2009 Data lists the median national annual compensation for adult hospitalists as $215,000, and $160,038 for pediatric hospitalists. This also has implications when IM time is bought down by pediatrics in academic centers, as pediatrics might not pay as much for clinical time as medicine will.
Back Where You Belong
Either by necessity or choice, med-ped-trained hospitalists all across the country have taken jobs in one setting or another and now yearn to get back into the other discipline. It might not be as difficult as you think.
If hospitalist work in the other discipline is available in your institution, you could consider a reduction of FTE in your current job to expand into the other discipline. Keep in mind, however, the interdepartmental coordination difficulties (i.e. scheduling, benefits, maintaining privileges). Those can be even more pronounced if two or more employers are involved.
Additionally, a reduction of FTE in your current job could lead to increased clinical time on the part of your colleagues, or perhaps even hiring additional staff, so this change needs to be discussed thoroughly with administrators and colleagues well in advance of any changes.
Less dramatic changes can enable a med-ped hospitalist to get a taste of the other discipline without wholesale changes in salary and schedule. Moonlighting as an intermittent hospitalist or nocturnist, taking call in the other discipline’s call schedule, or filling in for urgent-care slots can keep skills and knowledge from getting rusty.
It also can prevent the loss of pediatric admitting and procedural privileges. A patchwork approach also could lead to a steady hospitalist job in the other discipline.
“I discussed my desire to do pediatrics with friends and acquaintances who worked as pediatricians in local community hospitals through Children’s Hospital Boston,” Dr. Hunt says. “Eventually, [it led] to the peds work.”
As is often the case in HM, med-ped programs tend to follow the tenet “if you build it, they will come.” Once a hospitalist director discovers the flexibility and skill set a med-ped hospitalist provides the group, they often look to expand—especially to staff smaller pediatric units.
Such was the case at Elliot Hospital; familiarity with med-ped moonlighters eventually led to a full-time med-ped hospitalist hire. Following the full-time hire, the HM group realized a dramatic increase in local pediatric groups referring patients to Elliot’s hospitalist group, including the largest pediatric group in Southern New Hampshire, Dartmouth-Hitchcock Clinic.
“Initial referral base from the community was sluggish as community [pediatricians] wanted to hold onto their patients,” Dr. Ritenour says. “As the acuity of what we could support as hospitalists grew, more referrals were made for kids that might have previously been transferred.”
The Future of Med-Ped Hospitalists
At the dawn of combined med-ped residencies in the early 1960s, the hospitalist movement was only a twinkle in the eye of house physicians of yore. Now that both movements have matured, will we see this hybrid of a hybrid flourish?
“I think med-peds is well suited for hospital medicine, based on solid training that includes numerous inpatient wards and critical care in both internal medicine and pediatrics,” says Dr. Toth, adding she hopes to bring additional med-ped hospitalists to her group in Milwaukee in the future.
It seems inevitable that the med-ped movement, which has grown into the largest combined residency specialty in the country, and the hospitalist movement, which has exploded as the fastest-growing medical specialty, will continue to intertwine, branch out, and evolve.
And every year, some of those med-ped residency program graduates will continue to climb those twisted trunks, as challenging as it might seem. TH
Dr. Chang is a med-peds hospitalist at the University of California at San Diego and Rady Children’s Hospital. He is a member of Team Hospitalist.
By the fourth year of residency, most in combined internal medicine/pediatrics (commonly known as “med-ped”) residencies come to realize that their training is heavily weighted toward inpatient and ICU settings. After all, med-ped residency programs require that all the inpatient and ICU requirements of both the American Board of Internal Medicine (ABIM) and the American Board of Pediatrics (ABP) be met. This allows med-ped graduates, numbering just over 300 each year, to sit for both boards, and potentially to be able to obtain admitting privileges for both adults and children. This seems to be the perfect training for a hospitalist-to-be, if one so desires.
But for hospitalists, there comes the dilemma: Should you concentrate on the adult or the pediatric population, or is it possible to be a med-ped hospitalist? By far, most HM job opportunities are for either purely adult hospitalists or purely pediatric hospitalists, although there are an increasing number of “off the shelf” med-ped hospitalist positions. Building a med-ped career as a hospitalist from shifts in adult and pediatric programs is a possibility but requires extra attention to scheduling, salary, and benefits.
Med-ped physicians are used to being creative about their work, but some might begin to ask themselves whether the additional effort is worth it. Seeking out knowledgeable administrators and department/division chiefs, following other med-ped hospitalists who have already blazed a trail, and being realistic about your “mix” of work are some solutions for the hybrid hospitalist.
Academia Fosters Cooperation—and Lack Thereof
An ever-increasing number of med-ped physicians seem to think being a med-peds hospitalist is possible, even desirable. Heather Toth, MD, program director for the med-ped residency program at Medical College of Wisconsin and a hospitalist at Children’s Hospital of Wisconsin, both in Milwaukee, doesn’t regret her decision to put in the extra work required to be a hospitalist for all age groups.
“[It is] absolutely a wonderful career and worth the effort to establish a combined position. There is much to be learned from each world [medicine and pediatrics] to enrich our patients’ care,” says Dr. Toth, who was a former chief resident for the med-ped program at the college. In her case, being close to the administrators of both departments played to her advantage and allowed her to craft her job “from the inside,” she says.
“The process was much smoother than anticipated,” Dr. Toth explains. “One concern was which department would own my time. This was overcome by splitting my time by months. For example, January is medicine wards, February is pediatric wards, etc., with corresponding overnight shifts/call.”
Others have experienced obstacles in carving out an academic med-peds hospitalist position. Susan Hunt, MD, a hospitalist at Brigham and Women’s Hospital in Boston, finished her med-ped residency at Duke University in 2008 and began her career as an adults-only hospitalist. However, the desire to work in pediatrics still burned, leading Dr. Hunt to seek pediatric hospitalist work within the Partners HealthCare system. Initially, her efforts were to no avail. More recently, she has been able to break into hospitalist work through the Children’s Hospital Boston’s outreach program at local community hospitals.
“Pediatric programs tend to be small and, in Boston, had very little turnover,” Dr. Hunt says. She also has a warning for pediatric hospitalist hopefuls. “Increasing pediatric time invariably results in decreased pay.”
For the most part, med-ped hospitalist positions in academic hospitals tend to be crafted from a combination of time from two distinct departments. But an academic setting does offer potential med-ped hospitalists a few advantages, such as:
- Typically more hospitalists in each department, leading to greater scheduling flexibility;
- Larger pediatric hospitalist programs that often encompass not only the “main” hospital, but also community hospitals; this leads to increased availability of hospitalist work; and
- The possibility of a med-ped residency program at the same site, which allows for the possibility of being a role model to med-ped residents.
Although the trends might be changing, there are multiple barriers to an academic med-ped hospitalist job. Often, the IM and pediatric departments are not used to working together. Determining who will pay the hospitalist’s salary and benefits, how the schedule will be coordinated, and to whom the hospitalist is responsible can be tricky. Moreover, it’s not always clear which department will take the lead in the promotion process. Departments expect hospitalists to act as good citizens by serving on committees, and it can be difficult to serve two masters.
As a result, many academic med-peds hospitalists have a primary appointment in one department and have their clinical salaries “bought down” by the other. A handful of hospital committees, including quality-improvement (QI) and information technology, allow med-ped hospitalists to serve on one committee and receive citizenship “credit” from both departments. Leonard Feldman, MD, FAAP, FACP, and Carrie Herzke, MD, have walked this tightrope at Johns Hopkins Hospital in Baltimore. Their successes in this arena have created more clinical and research opportunities for med-ped hospitalists, as the administrators and physicians have learned how to negotiate their relationship. One example of this success has been the Johns Hopkins Hospitalist Scholars Program, which provides up to $12,000 of annual funding to hospitalist faculty.
Although rare, the academic med-ped hospitalist program under a single administrative structure does exist. Allen Liles, MD, program director for the hospital medicine program at the University of North Carolina (UNC) Hospitals in Chapel Hill, has brought together a group of 17 hospitalists, six of whom are med-ped-trained.
“Both the pediatric portion and the medicine portion are administered within this one program,” states Dr. Liles. “I think this is a huge advantage to actually making it work. If I was not the director being med-peds-trained, I am not sure this would have happened.” According to Dr. Liles, it took six months of working closely with the CFO of UNC Hospitals to establish a program that he felt “managed to change the paradigm.”
“It is the hospital that derives the most benefit from a [combined] hospitalist program,” adds Dr. Liles. “And as such, they were easy to convince of the benefits of a med-ped model and expansion into pediatrics.”
The Community Setting: Challenges and Successes
Academic settings aren’t alone in their battles putting together med-ped hospitalist positions. Jacques-Bret Burgess, MD, MPH, FAAP, a hospitalist with Traverse City, Mich.-based Hospitalists of Northwest Michigan (HNM), began in April 2009 to establish a pediatric hospitalist program within his group of adult hospitalists. Since that time, med-ped-trained hospitalists have increased to five from just one out of the 30 hospitalists employed by HNM. But there have been growing pains.
“The majority of administrators and physicians just do not understand the potential, nor the efficiency, of a [med-ped] physician,” Dr. Burgess says. “Most frustrations come from trying to explain what an IM-ped physician is, what we are capable of, and then obtaining adequate support to practice both disciplines while at the same time maintaining some sense of self and family.”
In fact, it is not uncommon for med-ped hospitalists to work full time in one discipline—usually adult—and moonlight or work part time in pediatrics. Jeff Whittall, MD, a hospitalist for MultiCare Inpatient Services in Tacoma, Wash., works primarily as an adult hospitalist at Tacoma General Hospital but provides pediatric urgent care at Mary Bridge Children’s Hospital in Tacoma as well. “It is a fantastic mix,” Dr. Whittall says.
That said, other med-ped hospitalists consider such combinations to be a compromise. Many yearn for that perfect mix of adult and pediatric hospitalist work, and have even taken on additional training to do so.
Oliver Medzihradsy, MD, was a half-time adult hospitalist at Barton Memorial Hospital in South Lake Tahoe, Calif., with the other half spent in outpatient pediatrics for Tahoe Carson Valley Medical Group, until this year. In August, be became a first-year fellow at Rady Children’s Hospital in pediatric hospital medicine.
“Having been out [of] hospital-based peds for four years now, I decided that, if I wanted to get back into … [pediatrics] as a hospitalist, it would serve me well to go back for a peds hospital medicine fellowship,” said Dr. Medzihradsy. “Economically, it’s rather foolhardy to take such a salary cut, not to mention the philosophical change of becoming a trainee again, but from a clinical passion standpoint, it’s what I wish to do.”
In some cases, community hospitalist programs, many of which offer a less territorial work environment and organizational structure, have been more successful at establishing full-fledged combined med-ped hospitalist programs. Elliot Hospital in Manchester, N.H., has built from the ground up a hospitalist program utilizing both internal medicine and med-ped-trained hospitalists. Currently, Elliot Hospital employs four med-ped-trained hospitalists, who staff the pediatric inpatient unit but are available for adult inpatients when pediatric volume is low. Other community hospitalist programs utilize the pediatric skills of their med-ped hospitalists in urgent-care or ED coverage in times of low pediatric volume.
“From the perspective of our med-ped physicians, they feel that this is a unique employment opportunity that allows them to have a truly balanced 50-50 medicine/pediatrics inpatient experience,” said Anita Ritenour, MD, assistant vice president for medical affairs at Elliot Hospital. Although trained in internal medicine, her familiarity with community med-ped physicians made her an early advocate of med-ped hospitalists.
Amy Stone, MD, director of Elliot Hospital’s pediatric hospitalist program and a med-ped-trained physician, typically starts her day at 7 a.m. with sign-out from the overnight provider, then touches base with nurses about overnight events. Family-centered rounds follow, with the afternoons being occupied by ED or direct admissions and family meetings. Given their training, however, the med-ped-trained pediatric hospitalists can get called upon to help out on the internal-medicine side.
“As a med-ped hospitalist on the peds service, we get pulled occasionally to help with the internal-medicine service to admit, both during the day and at night,” adds Dr. Craig Widness, another med-peds-trained hospitalist at Elliot.
But the scope of practice and volume has ramped up for the pediatric hospitalist service at Elliot, as many community pediatric groups have opted to utilize their services. In addition, a new pediatric ICU has recently been established, managed by the pediatric hospitalist service.
As a result, the opportunities for the med-ped-trained pediatric hospitalists to help out on the adult hospitalist vortex have been increasingly rare, which seem to be a welcome development to the pediatric hospitalists.
Building the Perfect Beast
So how does a med-ped physician entering hospital medicine build a job that satisfies the need to care for both adults and children? In some cases, the perfect med-ped position is already available. More likely, however, hospitalist jobs in a specific location are limited to either one discipline or another.
In many, if not most, cases, practice in one discipline will have to be somewhat compromised to fulfill the staffing needs of the “primary” job, at least initially. In the interview and hiring process, however, hospitalists wishing to pursue med-peds must make known their desire to work in both medicine and pediatrics. The transparency will allow hospital and group administrators to build into your schedule time to work in both pursuits.
“Start trying to arrange for pediatrics early. I started before I finished residency and it took me over a year to set up,” Dr. Hunt says, noting her current position is in the academic arena. “Discuss your plans with any medicine group you intend to join. See if your FTE would be flexible or if they can help arrange things. Get in touch with local med-ped program directors, if possible, as they often know people on both sides and might be able to help get you in touch with the right people.”
When looking at community hospitalist jobs, it is critical to ensure your administrators are familiar with med-peds residency training. It helps them better understand your skills, your goals, and allows them to put you in position to care for patients in all age groups.
“When one finds administrators and leaders that understand and respect the concept [of med-peds], hold on to them,” Dr. Burgess advises. “Do not let anyone take your unique training for granted and try to categorize you as one or the other; rather, we are both. We have two sets of boards, with separate training and a unique overlap that provides synergy with our abilities. Find a group that understands the level of training you possess.”
Call Protection
As uncommon as it is to find med-ped hospitalist jobs that feature built-in coordination of work in both disciplines, one should pay attention to coordinating salary, call, vacation, and CME between the two disciplines.
“Talk with potential groups about how they cover you for call, how you will be reimbursed, and what data will they base your pay and incentives on,” Dr. Burgess says. “What will they base your CME on—two disciplines or one? What is your depth if you have a sick child and sick adult at the same time?”
Most important, med-peds must make sure administrators of both disciplines are aware of your activities on both sides. “We do not want double-call days,” Dr. Burgess adds. He also warns that overcoming the frustrations of med-pedwork “takes a great deal of patience and discussion.”
Salary might be an issue, especially as one tries to mold a position. SHM and the Medical Group Management Association (MGMA) State of Hospital Medicine: 2010 Report Based on 2009 Data lists the median national annual compensation for adult hospitalists as $215,000, and $160,038 for pediatric hospitalists. This also has implications when IM time is bought down by pediatrics in academic centers, as pediatrics might not pay as much for clinical time as medicine will.
Back Where You Belong
Either by necessity or choice, med-ped-trained hospitalists all across the country have taken jobs in one setting or another and now yearn to get back into the other discipline. It might not be as difficult as you think.
If hospitalist work in the other discipline is available in your institution, you could consider a reduction of FTE in your current job to expand into the other discipline. Keep in mind, however, the interdepartmental coordination difficulties (i.e. scheduling, benefits, maintaining privileges). Those can be even more pronounced if two or more employers are involved.
Additionally, a reduction of FTE in your current job could lead to increased clinical time on the part of your colleagues, or perhaps even hiring additional staff, so this change needs to be discussed thoroughly with administrators and colleagues well in advance of any changes.
Less dramatic changes can enable a med-ped hospitalist to get a taste of the other discipline without wholesale changes in salary and schedule. Moonlighting as an intermittent hospitalist or nocturnist, taking call in the other discipline’s call schedule, or filling in for urgent-care slots can keep skills and knowledge from getting rusty.
It also can prevent the loss of pediatric admitting and procedural privileges. A patchwork approach also could lead to a steady hospitalist job in the other discipline.
“I discussed my desire to do pediatrics with friends and acquaintances who worked as pediatricians in local community hospitals through Children’s Hospital Boston,” Dr. Hunt says. “Eventually, [it led] to the peds work.”
As is often the case in HM, med-ped programs tend to follow the tenet “if you build it, they will come.” Once a hospitalist director discovers the flexibility and skill set a med-ped hospitalist provides the group, they often look to expand—especially to staff smaller pediatric units.
Such was the case at Elliot Hospital; familiarity with med-ped moonlighters eventually led to a full-time med-ped hospitalist hire. Following the full-time hire, the HM group realized a dramatic increase in local pediatric groups referring patients to Elliot’s hospitalist group, including the largest pediatric group in Southern New Hampshire, Dartmouth-Hitchcock Clinic.
“Initial referral base from the community was sluggish as community [pediatricians] wanted to hold onto their patients,” Dr. Ritenour says. “As the acuity of what we could support as hospitalists grew, more referrals were made for kids that might have previously been transferred.”
The Future of Med-Ped Hospitalists
At the dawn of combined med-ped residencies in the early 1960s, the hospitalist movement was only a twinkle in the eye of house physicians of yore. Now that both movements have matured, will we see this hybrid of a hybrid flourish?
“I think med-peds is well suited for hospital medicine, based on solid training that includes numerous inpatient wards and critical care in both internal medicine and pediatrics,” says Dr. Toth, adding she hopes to bring additional med-ped hospitalists to her group in Milwaukee in the future.
It seems inevitable that the med-ped movement, which has grown into the largest combined residency specialty in the country, and the hospitalist movement, which has exploded as the fastest-growing medical specialty, will continue to intertwine, branch out, and evolve.
And every year, some of those med-ped residency program graduates will continue to climb those twisted trunks, as challenging as it might seem. TH
Dr. Chang is a med-peds hospitalist at the University of California at San Diego and Rady Children’s Hospital. He is a member of Team Hospitalist.
A Bundle of Nerves
In a single year, one health system saved itself more than $2 million on orthopedic, cardiology, and cardiovascular surgery procedures. Another hospital saved Medicare an estimated $750,000. Supply costs dropped, scores on quality metrics rose, and bonus payments were distributed to participating doctors.
A runaway success? Not so fast.
Encouraging, if early, results from Medicare’s Acute Care Episode (ACE) Demonstration might have strengthened the case for bundling payments around episodes of care as an effective way to rein in spiraling healthcare costs and transition from a volume-based to a value-based payment system. But broad skepticism persists over the wisdom of binding together the fates of hospitals and doctors, and critics are far from ready to drop their argument that bundling will be unworkable across wider, less-well-defined swaths of healthcare.
The current bundling and gain-sharing duo differs only superficially from the despised capitation model of the 1990s, argues Adam Singer, MD, CEO of North Hollywood, Calif.-based IPC: The Hospitalist Company. “It’s capitation in a different dress, except that instead of over a patient population, it’s done over an individual patient’s case,” he says.
Not so, says Lisa Kettering, MD, SFHM, vice president of medical affairs and CMO at Exempla St. Joseph Hospital in Denver.
“I’ve been around in medicine long enough to have been around when there was capitation,” she says. “I think the current bundling project is a vast improvement and I think it’s a very different animal from old capitation … and pivots absolutely critically on the physician involvement at the heart of quality, at the heart of decision-making. That’s never happened before.”
Amid the swirling expectations and apprehensions, what has the ACE demo taught us so far about bundling, and what does it mean for the future of hospital medicine? In essence, bundling lumps Medicare Part A and Part B reimbursements into a single payment aimed at encouraging hospitals and doctors to work together to improve efficiency, maintain high-quality care, and reduce overall expenses. Hospitals participating in the ACE Demonstration provide a roughly 5% discount to Medicare for a specific list of diagnosis-related groups (DRGs), and the Centers for Medicare & Medicaid Services (CMS) passes on half of the savings to beneficiaries who use participating hospitals for the covered procedures.
After submitting their claims, the hospitals receive a bundled Medicare payment, from which they pay doctors 100% of their Part B fees. As an incentive, some providers are eligible for bonus payments in the form of gain-sharing. CMS rules preclude any payments for referrals, cap all payments at 25% of the physician fee schedule, and mandate that any payment be based on reductions in patient care costs due to ACE activities. But participating hospitals are otherwise free to devise their own formulas and specific quality metrics that doctors must meet to gain the bonus.
SHM repeatedly has signaled its support for exploring bundling as a way to better align financial incentives among providers and reward them for quality and efficiency instead of quantity. The 10,000-member society strongly supports further testing of payment bundling methodologies prior to a national rollout, however, and has called for the integral involvement of hospitalists in developing and implementing bundling projects.
With its main focus on cardiologists, orthopedic surgeons, and cardiovascular surgeons, the ACE Demonstration has had little direct impact on hospitalists’ jobs or bank accounts—so far. That could change with an expanded pilot mandated by healthcare reform legislation. Slated to begin by Jan. 1, 2013, the project will redefine covered episodes of care to include all medical services administered three days before a hospital admission through 30 days after discharge.
CMS hasn’t yet decided which procedures will be covered, but officials say they’ve learned from past experience to begin with well-defined episodes of care. “Back in the ’90s, we did a bundled demonstration for bypass procedures and also for cataract procedures,” says Cynthia Mason, project manager with the CMS Medicare Demonstrations Group. “What we learned from that is obviously it’s easier both for Medicare, as well as for the providers, to predict utilization when you have a more standardized package of services. You also need a variety and large number of services in order to give you opportunities for looking at efficiencies and improvements in the system.”
Upfront Investment, Immediate Savings, Improved Quality
Early opinions have been mostly positive among the ACE participants. Hillcrest Medical Center in Tulsa, Okla., was first out of the gate in May 2009. Over the project’s first year, Hillcrest CEO Steve Dobbs estimates that the 490-bed hospital has saved CMS about $750,000; half of that sum has been passed along to patients. The hospital itself has spent about $550,000 in marketing, start-up costs, corporate support, and paying third-party claims. But recent investments have led to double-digit gains in patient volume (24% in cardiology and cardiovascular surgery, and a whopping 37% in orthopedics), margins in orthopedics are up, and direct negotiations between participating doctors and national vendors have netted additional savings. As a reward for help with cost-cutting, Hillcrest recently passed along two gain-sharing checks totaling $130,000 to be split among six independent orthopedists.
“What’s actually driving this program is the supply cost savings from all of our national partners,” Dobbs says. A big question is whether the negotiated savings—and hence the gain-sharing—could be maintained over a greatly expanded pilot project. “If this goes nationwide and everybody’s in it, do you get the same benefit? I don’t know the answer to that right now,” he says.
Dobbs is careful to point out that success is not measured by patient volume and supply costs alone. Hillcrest’s gain-sharing plan stipulates that physicians must reach the 90% threshold for a range of quality metrics. For one previously problematic category—stopping antibiotics 24 hours post-surgery—Dobbs says both the orthopedics and cardiovascular surgery departments have dramatically increased their compliance rates.
Baptist Health System in San Antonio, which began its own demonstration in June 2009, has reported savings of $2.2 million for its 1,275-bed, four-campus health system. So far, the roughly 20 hospitalists employed by IPC: The Hospitalist Company who work within the Baptist Health System have not directly participated in the project. But Felix Aguirre, MD, FHM, IPC’s vice president of medical affairs in San Antonio, says the demonstration has had a definite impact on efficiency.

“Since the demonstration project has come up, it seems like everybody is obeying the evidence-based guidelines now,” says Dr. Aguirre, a member of SHM’s Public Policy Committee and Team Hospitalist. “So it’s not keeping the hip replacement patient in for five days, it’s what the guidelines say: three days.”
Some kinks still need to be worked out. Baptist has had trouble with double payments and other claims-related issues, Dr. Aguirre says. Hillcrest’s Dobbs complains that he has heard virtually no feedback from CMS. Medicare’s Mason says officials have been “very pleased” with the project’s progress so far, but concedes that a delay in updating a claims processing system has pushed back the launch at two other demonstration sites until Nov. 1.
At one of those sites, 361-bed Exempla St. Joseph Hospital, the three-year demonstration will encompass only cardiology and cardiovascular surgery. Dr. Kettering, a former SHM board member who serves as executive sponsor and director of St. Joseph Hospital’s ACE demo, says the shared-savings program will be limited to cardiovascular surgery for the first year to ensure the system is running smoothly. In the second or third year, however, hospitalists who care for eligible patients could theoretically benefit from a similar gain-sharing agreement, if they meet certain agreed-upon, evidence-based metrics. In that circumstance, she says, hospitalists would begin to learn the ropes and become directly involved in quality outcomes. Extending the model beyond ACE, their primary role could expand dramatically to that of learning how to operate bundling across the continuum of care.
The eventual bundling experiences at all five demonstration sites will likely be positive, Dr. Aguirre says, given that they were carefully chosen to maximize the likelihood of success. “Where the rubber will hit the road is, how do you translate where you’re obviously going to be successful at five sites to implementing it across maybe a thousand sites and making it successful?” he asks.

All Eggs in One Basket?
One thing is certain: For bundling to expand, it will have to convince some fierce critics of its staying power. IPC’s Dr. Singer says so much emphasis has been placed on bundling that it has drowned out any discussion of other alternatives. “It seems like we as a society are hell-bent on putting this in as the method of payment, but I don’t really see all the elements that really would promote a higher-quality product that would reduce cost, which is what it should be about,” he says.
If not bundling, what? For some observers, payment-reform options follow a continuum arcing away from the fee-for-service system, though not everyone agrees on just how widely each might—or should—depart from the status quo. Some healthcare leaders, for example, contend that it would be easiest to simply devise new DRG categories for hospitalists or primary-care physicians (PCPs) to replace the existing fee-for-service CPT codes. “It’s a very simple way of aligning the doctor and the hospital without combining the doctor and the hospital into one entity, which is what bundling does,” Dr. Singer says.
Even some bundling advocates say the solution might ease some anxiety over who controls the purse strings, though such a system would need to account for critical-access hospitals, which currently don’t use the DRG system at all. Alternatively, some analysts see broadened gain-sharing rules as a good way to align incentives toward more efficient care, regardless of whether the incentive system accompanies bundling.
Although still in their formative stages, accountable-care organizations (ACOs) and patient-centered medical homes (PCMHs)—and the implicit bundling of medical services across patient populations—are being advanced as longer-term reforms. Even then, analysts argue over whether such models will be sufficiently free from a fee-for-service foundation. Despite the vigorous debate, most observers agree that Medicare officials are keen to offload more of the risk, whether onto physicians or onto hospitals. “They’re saying, ‘Here’s the dollar. You administer it. And if you end up in the negative, you do, but if it’s in the positive, you get a share of everything,’ ” Dr. Aguirre says.
HM: Front and Center
Hospitalists might be uniquely well positioned to bring more efficiency and value, as well as help hospitals manage that risk. With bundling, though, the big question is how they’ll be paid for their services amid the demands of multiple providers. “I’ve heard it described as a big potential food fight,” says Kirk Mathews, CEO of St. Louis-based Inpatient Management Inc. and a member of SHM’s Workforce Summit Committee.
In the scenario relayed to him by fearful hospitalists, a hospital administrator is seated at the table with pie in hand, with the various providers clamoring for a slice. “Everyone will be sitting there saying, ‘Here’s why we deserve this percent of the bundled payment,’” Mathews says. “Whether that’s an accurate portrayal or not, that’s the fear.”
Taken a step further, the scenario envisions hospitalists struggling to hold their own at the table against high-powered and higher-paid specialists. Some of the ACE Demonstration sites, however, have used physician-hospital organizations, or PHOs, to help decentralize the decision-making and ensure that stakeholders are represented. Similarly, if patient referrals to hospitalists from other providers drop—as they did for some of the ACE Demonstration bundles at Baptist and Hillcrest—could hospitalists lose their bargaining power through an erosion of recouped professional fees?
If bundling expands, Hillcrest’s CEO says hospitalists are instead likely to assume a more central role (see “Six Pieces of Bundling-Related Advice for Hospitalists,” right). “If we truly go to bundled payments on everything,” Dobbs says, “then I think everybody’s got to be at the table and contributing, and especially the hospitalist, because the medical DRGs, that’s going to be where the hospitalists drive the equation, and that’s going to be a huge part of this.”
As SHM’s CEO Larry Wellikson, MD, SFHM, wrote in The Hospitalist last year (see “Bundling Bedlam,” July 2009, p. 46), the bundling of Medicare Part A dollars that subsidize HM with Part B physicians’ payments might actually pave the way for a more professional discussion of the value that hospitalists deliver. With bundling, he wrote, “the need for subsidies or support could diminish or vanish.”

But that doesn’t resolve the issue of how to fairly size each bundle. Stuart Guterman, vice president of the Washington, D.C.-based Common-wealth Fund’s Program on Payment and System Reform, says one lesson from the capitation scheme of the ’90s is that an overemphasis on cost savings can lead to payments that are frequently insufficient to cover the costs of appropriate care.
“So there’s got to be more collaboration on what an appropriate amount is, and that’s a very important feature,” Guterman says. “Clearly, if you don’t pay enough, it doesn’t bode well for the success of any kind of payment approach. If you pay too much, it means you’re wasting money.”
The size and complexity of healthcare networks will influence how those bundle-related payments are negotiated. And in this case, several analysts say bigger isn’t necessarily better. “My own view is that it’s easier for a handful of hospitalists and a few community doctors in the hospital to come to an agreement on how they’re going to work within a bundle,” says Robert Berenson, MD, a senior fellow in the Urban Institute’s Health Policy Center and vice chair of the Medicare Payment Advisory Commission (MedPAC).

“My experience is that in rural communities, there’s a greater alliance of interests between the doctors and the hospitals, whereas in big urban areas they’re often competing with each other. So I don’t see that as the problem, frankly. I think this is probably better designed for smaller places where there’s already reasonably good relationships.”
L. Scott Sussman, MD, a hospitalist at Mt. Ascutney Hospital and Health Center in Windsor, Vt., agrees that bundling likely wouldn’t negatively affect the day-to-day operations of the 25-bed critical-access hospital. Almost all admitted patients have PCPs in the affiliated Mt. Ascutney Physicians Practice, aiding communication during hospitalizations and care transitions. Dr. Sussman thinks bundling fits well with the mission of hospitalists to provide quality care and help smooth their patients’ transition back to community providers. “From the reading that I’ve done on bundling, it does seem to me that if implemented properly, it really could achieve cost savings while maintaining quality care,” he says.
Nevertheless, he has plenty of questions and concerns. Bundling would be more complicated, he concedes, if most admissions were referred from private-practice physicians in the community. And because Mt. Ascutney is a critical-access hospital, patients who develop complications or require a higher level of care are transferred to a tertiary-care facility—in this case, a 22-mile drive over the state line to Dartmouth-Hitchcock Medical Center in Lebanon, N.H. “How would the payment be divided up at that point?” he asks.
To make bundling work, healthcare leaders will clearly need to blaze a trail through uncharted territory.
But if the goal is getting more from the trillions spent annually on healthcare, advocates like Guterman say it provides an important step toward a better-functioning system.
Among hospitalists, at least some observers are betting that bundling will ultimately find its way. “I think bundled payments are here to stay,” Dr. Aguirre says. “I think our goal now is to see how we can modify it or create it so it can have the best impact for us and we can have the best impact for it.” TH
Bryn Nelson is a freelance medical writer based in Seattle.
In a single year, one health system saved itself more than $2 million on orthopedic, cardiology, and cardiovascular surgery procedures. Another hospital saved Medicare an estimated $750,000. Supply costs dropped, scores on quality metrics rose, and bonus payments were distributed to participating doctors.
A runaway success? Not so fast.
Encouraging, if early, results from Medicare’s Acute Care Episode (ACE) Demonstration might have strengthened the case for bundling payments around episodes of care as an effective way to rein in spiraling healthcare costs and transition from a volume-based to a value-based payment system. But broad skepticism persists over the wisdom of binding together the fates of hospitals and doctors, and critics are far from ready to drop their argument that bundling will be unworkable across wider, less-well-defined swaths of healthcare.
The current bundling and gain-sharing duo differs only superficially from the despised capitation model of the 1990s, argues Adam Singer, MD, CEO of North Hollywood, Calif.-based IPC: The Hospitalist Company. “It’s capitation in a different dress, except that instead of over a patient population, it’s done over an individual patient’s case,” he says.
Not so, says Lisa Kettering, MD, SFHM, vice president of medical affairs and CMO at Exempla St. Joseph Hospital in Denver.
“I’ve been around in medicine long enough to have been around when there was capitation,” she says. “I think the current bundling project is a vast improvement and I think it’s a very different animal from old capitation … and pivots absolutely critically on the physician involvement at the heart of quality, at the heart of decision-making. That’s never happened before.”
Amid the swirling expectations and apprehensions, what has the ACE demo taught us so far about bundling, and what does it mean for the future of hospital medicine? In essence, bundling lumps Medicare Part A and Part B reimbursements into a single payment aimed at encouraging hospitals and doctors to work together to improve efficiency, maintain high-quality care, and reduce overall expenses. Hospitals participating in the ACE Demonstration provide a roughly 5% discount to Medicare for a specific list of diagnosis-related groups (DRGs), and the Centers for Medicare & Medicaid Services (CMS) passes on half of the savings to beneficiaries who use participating hospitals for the covered procedures.
After submitting their claims, the hospitals receive a bundled Medicare payment, from which they pay doctors 100% of their Part B fees. As an incentive, some providers are eligible for bonus payments in the form of gain-sharing. CMS rules preclude any payments for referrals, cap all payments at 25% of the physician fee schedule, and mandate that any payment be based on reductions in patient care costs due to ACE activities. But participating hospitals are otherwise free to devise their own formulas and specific quality metrics that doctors must meet to gain the bonus.
SHM repeatedly has signaled its support for exploring bundling as a way to better align financial incentives among providers and reward them for quality and efficiency instead of quantity. The 10,000-member society strongly supports further testing of payment bundling methodologies prior to a national rollout, however, and has called for the integral involvement of hospitalists in developing and implementing bundling projects.
With its main focus on cardiologists, orthopedic surgeons, and cardiovascular surgeons, the ACE Demonstration has had little direct impact on hospitalists’ jobs or bank accounts—so far. That could change with an expanded pilot mandated by healthcare reform legislation. Slated to begin by Jan. 1, 2013, the project will redefine covered episodes of care to include all medical services administered three days before a hospital admission through 30 days after discharge.
CMS hasn’t yet decided which procedures will be covered, but officials say they’ve learned from past experience to begin with well-defined episodes of care. “Back in the ’90s, we did a bundled demonstration for bypass procedures and also for cataract procedures,” says Cynthia Mason, project manager with the CMS Medicare Demonstrations Group. “What we learned from that is obviously it’s easier both for Medicare, as well as for the providers, to predict utilization when you have a more standardized package of services. You also need a variety and large number of services in order to give you opportunities for looking at efficiencies and improvements in the system.”
Upfront Investment, Immediate Savings, Improved Quality
Early opinions have been mostly positive among the ACE participants. Hillcrest Medical Center in Tulsa, Okla., was first out of the gate in May 2009. Over the project’s first year, Hillcrest CEO Steve Dobbs estimates that the 490-bed hospital has saved CMS about $750,000; half of that sum has been passed along to patients. The hospital itself has spent about $550,000 in marketing, start-up costs, corporate support, and paying third-party claims. But recent investments have led to double-digit gains in patient volume (24% in cardiology and cardiovascular surgery, and a whopping 37% in orthopedics), margins in orthopedics are up, and direct negotiations between participating doctors and national vendors have netted additional savings. As a reward for help with cost-cutting, Hillcrest recently passed along two gain-sharing checks totaling $130,000 to be split among six independent orthopedists.
“What’s actually driving this program is the supply cost savings from all of our national partners,” Dobbs says. A big question is whether the negotiated savings—and hence the gain-sharing—could be maintained over a greatly expanded pilot project. “If this goes nationwide and everybody’s in it, do you get the same benefit? I don’t know the answer to that right now,” he says.
Dobbs is careful to point out that success is not measured by patient volume and supply costs alone. Hillcrest’s gain-sharing plan stipulates that physicians must reach the 90% threshold for a range of quality metrics. For one previously problematic category—stopping antibiotics 24 hours post-surgery—Dobbs says both the orthopedics and cardiovascular surgery departments have dramatically increased their compliance rates.
Baptist Health System in San Antonio, which began its own demonstration in June 2009, has reported savings of $2.2 million for its 1,275-bed, four-campus health system. So far, the roughly 20 hospitalists employed by IPC: The Hospitalist Company who work within the Baptist Health System have not directly participated in the project. But Felix Aguirre, MD, FHM, IPC’s vice president of medical affairs in San Antonio, says the demonstration has had a definite impact on efficiency.
“Since the demonstration project has come up, it seems like everybody is obeying the evidence-based guidelines now,” says Dr. Aguirre, a member of SHM’s Public Policy Committee and Team Hospitalist. “So it’s not keeping the hip replacement patient in for five days, it’s what the guidelines say: three days.”
Some kinks still need to be worked out. Baptist has had trouble with double payments and other claims-related issues, Dr. Aguirre says. Hillcrest’s Dobbs complains that he has heard virtually no feedback from CMS. Medicare’s Mason says officials have been “very pleased” with the project’s progress so far, but concedes that a delay in updating a claims processing system has pushed back the launch at two other demonstration sites until Nov. 1.
At one of those sites, 361-bed Exempla St. Joseph Hospital, the three-year demonstration will encompass only cardiology and cardiovascular surgery. Dr. Kettering, a former SHM board member who serves as executive sponsor and director of St. Joseph Hospital’s ACE demo, says the shared-savings program will be limited to cardiovascular surgery for the first year to ensure the system is running smoothly. In the second or third year, however, hospitalists who care for eligible patients could theoretically benefit from a similar gain-sharing agreement, if they meet certain agreed-upon, evidence-based metrics. In that circumstance, she says, hospitalists would begin to learn the ropes and become directly involved in quality outcomes. Extending the model beyond ACE, their primary role could expand dramatically to that of learning how to operate bundling across the continuum of care.
The eventual bundling experiences at all five demonstration sites will likely be positive, Dr. Aguirre says, given that they were carefully chosen to maximize the likelihood of success. “Where the rubber will hit the road is, how do you translate where you’re obviously going to be successful at five sites to implementing it across maybe a thousand sites and making it successful?” he asks.
All Eggs in One Basket?
One thing is certain: For bundling to expand, it will have to convince some fierce critics of its staying power. IPC’s Dr. Singer says so much emphasis has been placed on bundling that it has drowned out any discussion of other alternatives. “It seems like we as a society are hell-bent on putting this in as the method of payment, but I don’t really see all the elements that really would promote a higher-quality product that would reduce cost, which is what it should be about,” he says.
If not bundling, what? For some observers, payment-reform options follow a continuum arcing away from the fee-for-service system, though not everyone agrees on just how widely each might—or should—depart from the status quo. Some healthcare leaders, for example, contend that it would be easiest to simply devise new DRG categories for hospitalists or primary-care physicians (PCPs) to replace the existing fee-for-service CPT codes. “It’s a very simple way of aligning the doctor and the hospital without combining the doctor and the hospital into one entity, which is what bundling does,” Dr. Singer says.
Even some bundling advocates say the solution might ease some anxiety over who controls the purse strings, though such a system would need to account for critical-access hospitals, which currently don’t use the DRG system at all. Alternatively, some analysts see broadened gain-sharing rules as a good way to align incentives toward more efficient care, regardless of whether the incentive system accompanies bundling.
Although still in their formative stages, accountable-care organizations (ACOs) and patient-centered medical homes (PCMHs)—and the implicit bundling of medical services across patient populations—are being advanced as longer-term reforms. Even then, analysts argue over whether such models will be sufficiently free from a fee-for-service foundation. Despite the vigorous debate, most observers agree that Medicare officials are keen to offload more of the risk, whether onto physicians or onto hospitals. “They’re saying, ‘Here’s the dollar. You administer it. And if you end up in the negative, you do, but if it’s in the positive, you get a share of everything,’ ” Dr. Aguirre says.
HM: Front and Center
Hospitalists might be uniquely well positioned to bring more efficiency and value, as well as help hospitals manage that risk. With bundling, though, the big question is how they’ll be paid for their services amid the demands of multiple providers. “I’ve heard it described as a big potential food fight,” says Kirk Mathews, CEO of St. Louis-based Inpatient Management Inc. and a member of SHM’s Workforce Summit Committee.
In the scenario relayed to him by fearful hospitalists, a hospital administrator is seated at the table with pie in hand, with the various providers clamoring for a slice. “Everyone will be sitting there saying, ‘Here’s why we deserve this percent of the bundled payment,’” Mathews says. “Whether that’s an accurate portrayal or not, that’s the fear.”
Taken a step further, the scenario envisions hospitalists struggling to hold their own at the table against high-powered and higher-paid specialists. Some of the ACE Demonstration sites, however, have used physician-hospital organizations, or PHOs, to help decentralize the decision-making and ensure that stakeholders are represented. Similarly, if patient referrals to hospitalists from other providers drop—as they did for some of the ACE Demonstration bundles at Baptist and Hillcrest—could hospitalists lose their bargaining power through an erosion of recouped professional fees?
If bundling expands, Hillcrest’s CEO says hospitalists are instead likely to assume a more central role (see “Six Pieces of Bundling-Related Advice for Hospitalists,” right). “If we truly go to bundled payments on everything,” Dobbs says, “then I think everybody’s got to be at the table and contributing, and especially the hospitalist, because the medical DRGs, that’s going to be where the hospitalists drive the equation, and that’s going to be a huge part of this.”
As SHM’s CEO Larry Wellikson, MD, SFHM, wrote in The Hospitalist last year (see “Bundling Bedlam,” July 2009, p. 46), the bundling of Medicare Part A dollars that subsidize HM with Part B physicians’ payments might actually pave the way for a more professional discussion of the value that hospitalists deliver. With bundling, he wrote, “the need for subsidies or support could diminish or vanish.”
But that doesn’t resolve the issue of how to fairly size each bundle. Stuart Guterman, vice president of the Washington, D.C.-based Common-wealth Fund’s Program on Payment and System Reform, says one lesson from the capitation scheme of the ’90s is that an overemphasis on cost savings can lead to payments that are frequently insufficient to cover the costs of appropriate care.
“So there’s got to be more collaboration on what an appropriate amount is, and that’s a very important feature,” Guterman says. “Clearly, if you don’t pay enough, it doesn’t bode well for the success of any kind of payment approach. If you pay too much, it means you’re wasting money.”
The size and complexity of healthcare networks will influence how those bundle-related payments are negotiated. And in this case, several analysts say bigger isn’t necessarily better. “My own view is that it’s easier for a handful of hospitalists and a few community doctors in the hospital to come to an agreement on how they’re going to work within a bundle,” says Robert Berenson, MD, a senior fellow in the Urban Institute’s Health Policy Center and vice chair of the Medicare Payment Advisory Commission (MedPAC).
“My experience is that in rural communities, there’s a greater alliance of interests between the doctors and the hospitals, whereas in big urban areas they’re often competing with each other. So I don’t see that as the problem, frankly. I think this is probably better designed for smaller places where there’s already reasonably good relationships.”
L. Scott Sussman, MD, a hospitalist at Mt. Ascutney Hospital and Health Center in Windsor, Vt., agrees that bundling likely wouldn’t negatively affect the day-to-day operations of the 25-bed critical-access hospital. Almost all admitted patients have PCPs in the affiliated Mt. Ascutney Physicians Practice, aiding communication during hospitalizations and care transitions. Dr. Sussman thinks bundling fits well with the mission of hospitalists to provide quality care and help smooth their patients’ transition back to community providers. “From the reading that I’ve done on bundling, it does seem to me that if implemented properly, it really could achieve cost savings while maintaining quality care,” he says.
Nevertheless, he has plenty of questions and concerns. Bundling would be more complicated, he concedes, if most admissions were referred from private-practice physicians in the community. And because Mt. Ascutney is a critical-access hospital, patients who develop complications or require a higher level of care are transferred to a tertiary-care facility—in this case, a 22-mile drive over the state line to Dartmouth-Hitchcock Medical Center in Lebanon, N.H. “How would the payment be divided up at that point?” he asks.
To make bundling work, healthcare leaders will clearly need to blaze a trail through uncharted territory.
But if the goal is getting more from the trillions spent annually on healthcare, advocates like Guterman say it provides an important step toward a better-functioning system.
Among hospitalists, at least some observers are betting that bundling will ultimately find its way. “I think bundled payments are here to stay,” Dr. Aguirre says. “I think our goal now is to see how we can modify it or create it so it can have the best impact for us and we can have the best impact for it.” TH
Bryn Nelson is a freelance medical writer based in Seattle.
In a single year, one health system saved itself more than $2 million on orthopedic, cardiology, and cardiovascular surgery procedures. Another hospital saved Medicare an estimated $750,000. Supply costs dropped, scores on quality metrics rose, and bonus payments were distributed to participating doctors.
A runaway success? Not so fast.
Encouraging, if early, results from Medicare’s Acute Care Episode (ACE) Demonstration might have strengthened the case for bundling payments around episodes of care as an effective way to rein in spiraling healthcare costs and transition from a volume-based to a value-based payment system. But broad skepticism persists over the wisdom of binding together the fates of hospitals and doctors, and critics are far from ready to drop their argument that bundling will be unworkable across wider, less-well-defined swaths of healthcare.
The current bundling and gain-sharing duo differs only superficially from the despised capitation model of the 1990s, argues Adam Singer, MD, CEO of North Hollywood, Calif.-based IPC: The Hospitalist Company. “It’s capitation in a different dress, except that instead of over a patient population, it’s done over an individual patient’s case,” he says.
Not so, says Lisa Kettering, MD, SFHM, vice president of medical affairs and CMO at Exempla St. Joseph Hospital in Denver.
“I’ve been around in medicine long enough to have been around when there was capitation,” she says. “I think the current bundling project is a vast improvement and I think it’s a very different animal from old capitation … and pivots absolutely critically on the physician involvement at the heart of quality, at the heart of decision-making. That’s never happened before.”
Amid the swirling expectations and apprehensions, what has the ACE demo taught us so far about bundling, and what does it mean for the future of hospital medicine? In essence, bundling lumps Medicare Part A and Part B reimbursements into a single payment aimed at encouraging hospitals and doctors to work together to improve efficiency, maintain high-quality care, and reduce overall expenses. Hospitals participating in the ACE Demonstration provide a roughly 5% discount to Medicare for a specific list of diagnosis-related groups (DRGs), and the Centers for Medicare & Medicaid Services (CMS) passes on half of the savings to beneficiaries who use participating hospitals for the covered procedures.
After submitting their claims, the hospitals receive a bundled Medicare payment, from which they pay doctors 100% of their Part B fees. As an incentive, some providers are eligible for bonus payments in the form of gain-sharing. CMS rules preclude any payments for referrals, cap all payments at 25% of the physician fee schedule, and mandate that any payment be based on reductions in patient care costs due to ACE activities. But participating hospitals are otherwise free to devise their own formulas and specific quality metrics that doctors must meet to gain the bonus.
SHM repeatedly has signaled its support for exploring bundling as a way to better align financial incentives among providers and reward them for quality and efficiency instead of quantity. The 10,000-member society strongly supports further testing of payment bundling methodologies prior to a national rollout, however, and has called for the integral involvement of hospitalists in developing and implementing bundling projects.
With its main focus on cardiologists, orthopedic surgeons, and cardiovascular surgeons, the ACE Demonstration has had little direct impact on hospitalists’ jobs or bank accounts—so far. That could change with an expanded pilot mandated by healthcare reform legislation. Slated to begin by Jan. 1, 2013, the project will redefine covered episodes of care to include all medical services administered three days before a hospital admission through 30 days after discharge.
CMS hasn’t yet decided which procedures will be covered, but officials say they’ve learned from past experience to begin with well-defined episodes of care. “Back in the ’90s, we did a bundled demonstration for bypass procedures and also for cataract procedures,” says Cynthia Mason, project manager with the CMS Medicare Demonstrations Group. “What we learned from that is obviously it’s easier both for Medicare, as well as for the providers, to predict utilization when you have a more standardized package of services. You also need a variety and large number of services in order to give you opportunities for looking at efficiencies and improvements in the system.”
Upfront Investment, Immediate Savings, Improved Quality
Early opinions have been mostly positive among the ACE participants. Hillcrest Medical Center in Tulsa, Okla., was first out of the gate in May 2009. Over the project’s first year, Hillcrest CEO Steve Dobbs estimates that the 490-bed hospital has saved CMS about $750,000; half of that sum has been passed along to patients. The hospital itself has spent about $550,000 in marketing, start-up costs, corporate support, and paying third-party claims. But recent investments have led to double-digit gains in patient volume (24% in cardiology and cardiovascular surgery, and a whopping 37% in orthopedics), margins in orthopedics are up, and direct negotiations between participating doctors and national vendors have netted additional savings. As a reward for help with cost-cutting, Hillcrest recently passed along two gain-sharing checks totaling $130,000 to be split among six independent orthopedists.
“What’s actually driving this program is the supply cost savings from all of our national partners,” Dobbs says. A big question is whether the negotiated savings—and hence the gain-sharing—could be maintained over a greatly expanded pilot project. “If this goes nationwide and everybody’s in it, do you get the same benefit? I don’t know the answer to that right now,” he says.
Dobbs is careful to point out that success is not measured by patient volume and supply costs alone. Hillcrest’s gain-sharing plan stipulates that physicians must reach the 90% threshold for a range of quality metrics. For one previously problematic category—stopping antibiotics 24 hours post-surgery—Dobbs says both the orthopedics and cardiovascular surgery departments have dramatically increased their compliance rates.
Baptist Health System in San Antonio, which began its own demonstration in June 2009, has reported savings of $2.2 million for its 1,275-bed, four-campus health system. So far, the roughly 20 hospitalists employed by IPC: The Hospitalist Company who work within the Baptist Health System have not directly participated in the project. But Felix Aguirre, MD, FHM, IPC’s vice president of medical affairs in San Antonio, says the demonstration has had a definite impact on efficiency.
“Since the demonstration project has come up, it seems like everybody is obeying the evidence-based guidelines now,” says Dr. Aguirre, a member of SHM’s Public Policy Committee and Team Hospitalist. “So it’s not keeping the hip replacement patient in for five days, it’s what the guidelines say: three days.”
Some kinks still need to be worked out. Baptist has had trouble with double payments and other claims-related issues, Dr. Aguirre says. Hillcrest’s Dobbs complains that he has heard virtually no feedback from CMS. Medicare’s Mason says officials have been “very pleased” with the project’s progress so far, but concedes that a delay in updating a claims processing system has pushed back the launch at two other demonstration sites until Nov. 1.
At one of those sites, 361-bed Exempla St. Joseph Hospital, the three-year demonstration will encompass only cardiology and cardiovascular surgery. Dr. Kettering, a former SHM board member who serves as executive sponsor and director of St. Joseph Hospital’s ACE demo, says the shared-savings program will be limited to cardiovascular surgery for the first year to ensure the system is running smoothly. In the second or third year, however, hospitalists who care for eligible patients could theoretically benefit from a similar gain-sharing agreement, if they meet certain agreed-upon, evidence-based metrics. In that circumstance, she says, hospitalists would begin to learn the ropes and become directly involved in quality outcomes. Extending the model beyond ACE, their primary role could expand dramatically to that of learning how to operate bundling across the continuum of care.
The eventual bundling experiences at all five demonstration sites will likely be positive, Dr. Aguirre says, given that they were carefully chosen to maximize the likelihood of success. “Where the rubber will hit the road is, how do you translate where you’re obviously going to be successful at five sites to implementing it across maybe a thousand sites and making it successful?” he asks.
All Eggs in One Basket?
One thing is certain: For bundling to expand, it will have to convince some fierce critics of its staying power. IPC’s Dr. Singer says so much emphasis has been placed on bundling that it has drowned out any discussion of other alternatives. “It seems like we as a society are hell-bent on putting this in as the method of payment, but I don’t really see all the elements that really would promote a higher-quality product that would reduce cost, which is what it should be about,” he says.
If not bundling, what? For some observers, payment-reform options follow a continuum arcing away from the fee-for-service system, though not everyone agrees on just how widely each might—or should—depart from the status quo. Some healthcare leaders, for example, contend that it would be easiest to simply devise new DRG categories for hospitalists or primary-care physicians (PCPs) to replace the existing fee-for-service CPT codes. “It’s a very simple way of aligning the doctor and the hospital without combining the doctor and the hospital into one entity, which is what bundling does,” Dr. Singer says.
Even some bundling advocates say the solution might ease some anxiety over who controls the purse strings, though such a system would need to account for critical-access hospitals, which currently don’t use the DRG system at all. Alternatively, some analysts see broadened gain-sharing rules as a good way to align incentives toward more efficient care, regardless of whether the incentive system accompanies bundling.
Although still in their formative stages, accountable-care organizations (ACOs) and patient-centered medical homes (PCMHs)—and the implicit bundling of medical services across patient populations—are being advanced as longer-term reforms. Even then, analysts argue over whether such models will be sufficiently free from a fee-for-service foundation. Despite the vigorous debate, most observers agree that Medicare officials are keen to offload more of the risk, whether onto physicians or onto hospitals. “They’re saying, ‘Here’s the dollar. You administer it. And if you end up in the negative, you do, but if it’s in the positive, you get a share of everything,’ ” Dr. Aguirre says.
HM: Front and Center
Hospitalists might be uniquely well positioned to bring more efficiency and value, as well as help hospitals manage that risk. With bundling, though, the big question is how they’ll be paid for their services amid the demands of multiple providers. “I’ve heard it described as a big potential food fight,” says Kirk Mathews, CEO of St. Louis-based Inpatient Management Inc. and a member of SHM’s Workforce Summit Committee.
In the scenario relayed to him by fearful hospitalists, a hospital administrator is seated at the table with pie in hand, with the various providers clamoring for a slice. “Everyone will be sitting there saying, ‘Here’s why we deserve this percent of the bundled payment,’” Mathews says. “Whether that’s an accurate portrayal or not, that’s the fear.”
Taken a step further, the scenario envisions hospitalists struggling to hold their own at the table against high-powered and higher-paid specialists. Some of the ACE Demonstration sites, however, have used physician-hospital organizations, or PHOs, to help decentralize the decision-making and ensure that stakeholders are represented. Similarly, if patient referrals to hospitalists from other providers drop—as they did for some of the ACE Demonstration bundles at Baptist and Hillcrest—could hospitalists lose their bargaining power through an erosion of recouped professional fees?
If bundling expands, Hillcrest’s CEO says hospitalists are instead likely to assume a more central role (see “Six Pieces of Bundling-Related Advice for Hospitalists,” right). “If we truly go to bundled payments on everything,” Dobbs says, “then I think everybody’s got to be at the table and contributing, and especially the hospitalist, because the medical DRGs, that’s going to be where the hospitalists drive the equation, and that’s going to be a huge part of this.”
As SHM’s CEO Larry Wellikson, MD, SFHM, wrote in The Hospitalist last year (see “Bundling Bedlam,” July 2009, p. 46), the bundling of Medicare Part A dollars that subsidize HM with Part B physicians’ payments might actually pave the way for a more professional discussion of the value that hospitalists deliver. With bundling, he wrote, “the need for subsidies or support could diminish or vanish.”
But that doesn’t resolve the issue of how to fairly size each bundle. Stuart Guterman, vice president of the Washington, D.C.-based Common-wealth Fund’s Program on Payment and System Reform, says one lesson from the capitation scheme of the ’90s is that an overemphasis on cost savings can lead to payments that are frequently insufficient to cover the costs of appropriate care.
“So there’s got to be more collaboration on what an appropriate amount is, and that’s a very important feature,” Guterman says. “Clearly, if you don’t pay enough, it doesn’t bode well for the success of any kind of payment approach. If you pay too much, it means you’re wasting money.”
The size and complexity of healthcare networks will influence how those bundle-related payments are negotiated. And in this case, several analysts say bigger isn’t necessarily better. “My own view is that it’s easier for a handful of hospitalists and a few community doctors in the hospital to come to an agreement on how they’re going to work within a bundle,” says Robert Berenson, MD, a senior fellow in the Urban Institute’s Health Policy Center and vice chair of the Medicare Payment Advisory Commission (MedPAC).
“My experience is that in rural communities, there’s a greater alliance of interests between the doctors and the hospitals, whereas in big urban areas they’re often competing with each other. So I don’t see that as the problem, frankly. I think this is probably better designed for smaller places where there’s already reasonably good relationships.”
L. Scott Sussman, MD, a hospitalist at Mt. Ascutney Hospital and Health Center in Windsor, Vt., agrees that bundling likely wouldn’t negatively affect the day-to-day operations of the 25-bed critical-access hospital. Almost all admitted patients have PCPs in the affiliated Mt. Ascutney Physicians Practice, aiding communication during hospitalizations and care transitions. Dr. Sussman thinks bundling fits well with the mission of hospitalists to provide quality care and help smooth their patients’ transition back to community providers. “From the reading that I’ve done on bundling, it does seem to me that if implemented properly, it really could achieve cost savings while maintaining quality care,” he says.
Nevertheless, he has plenty of questions and concerns. Bundling would be more complicated, he concedes, if most admissions were referred from private-practice physicians in the community. And because Mt. Ascutney is a critical-access hospital, patients who develop complications or require a higher level of care are transferred to a tertiary-care facility—in this case, a 22-mile drive over the state line to Dartmouth-Hitchcock Medical Center in Lebanon, N.H. “How would the payment be divided up at that point?” he asks.
To make bundling work, healthcare leaders will clearly need to blaze a trail through uncharted territory.
But if the goal is getting more from the trillions spent annually on healthcare, advocates like Guterman say it provides an important step toward a better-functioning system.
Among hospitalists, at least some observers are betting that bundling will ultimately find its way. “I think bundled payments are here to stay,” Dr. Aguirre says. “I think our goal now is to see how we can modify it or create it so it can have the best impact for us and we can have the best impact for it.” TH
Bryn Nelson is a freelance medical writer based in Seattle.