User login
ONLINE EXCLUSIVE: HM pioneer Bob Wachter, MD, MHM, discusses the growing trend of specialist-hospitalists
Bob Wachter, MD, MHM, has watched the hospitalist movement grow from its infancy in the mid-1990s to more than 30,000 hospitalists practicing nationwide today. As professor and chief of the Division of Hospital Medicine and associate chairman of the Department of Medicine at the University of California at San Francisco, and chief of the medical service at UCSF Medical Center, Dr. Wachter also has watched the HM model spread to other medical specialties, including a handful of departments in his own hospital. The Hospitalist caught up with Dr. Wachter and found out what he thinks about the spread of the HM model.
Question: Do specialist-hospitalist programs threaten to siphon off your medical hospitalist workforce, or are they a boon?
Answer: Having specialized physicians focus on hospital care is a powerful model. Not only are they available all the time, but they are keeping up with innovations in their field. More importantly, they get involved in system improvement in a way that the part-time hospital person will not.

—Bob Wachter, MD, MHM
Q: Are there direct benefits to the hospitalist on the floor?
A: I think it creates a vehicle for collegiality, interchange, and learning across the specialties, which is harder to come by when we’re in the hospital all the time, but the consults we’re interacting with may not be.
Q: Aren’t hospitalists already comanaging patients with neurosurgery, hematology/oncology, and orthopedics at your institution? How are specialist hospitalists different?
A: Neurohospitalists focus their professional practice on the hospitalized care of patients with neurological diseases—they perform the same function for those patients as we do for medical patients. That is, they admit patients, supervise their overall care, and discharge them. On our neurosurgery service, which has a census of 50 patients, the surgeons are in the operating room much of the day. Their post-surgical patients often have multiple medical comorbidities (heart failure, high blood pressures, diabetes, etc.), which is where the medical hospitalist comes in to comanage and coordinate their medical care.
We probably need new lingo to distinguish between medical hospitalists comanaging specialty patients and specialty hospitalists, because it can be confusing to people.
Q: Is this model sustainable in the community and rural settings, where specialists are in short supply?
A: There is a size below which you probably cannot support a specialty hospitalist. But larger places can, and their value is not only what they do at that individual hospital, but the fact that they can teach and do research and (quality improvement) that may help influence care beyond their organization’s walls.
—GH
Bob Wachter, MD, MHM, has watched the hospitalist movement grow from its infancy in the mid-1990s to more than 30,000 hospitalists practicing nationwide today. As professor and chief of the Division of Hospital Medicine and associate chairman of the Department of Medicine at the University of California at San Francisco, and chief of the medical service at UCSF Medical Center, Dr. Wachter also has watched the HM model spread to other medical specialties, including a handful of departments in his own hospital. The Hospitalist caught up with Dr. Wachter and found out what he thinks about the spread of the HM model.
Question: Do specialist-hospitalist programs threaten to siphon off your medical hospitalist workforce, or are they a boon?
Answer: Having specialized physicians focus on hospital care is a powerful model. Not only are they available all the time, but they are keeping up with innovations in their field. More importantly, they get involved in system improvement in a way that the part-time hospital person will not.
—Bob Wachter, MD, MHM
Q: Are there direct benefits to the hospitalist on the floor?
A: I think it creates a vehicle for collegiality, interchange, and learning across the specialties, which is harder to come by when we’re in the hospital all the time, but the consults we’re interacting with may not be.
Q: Aren’t hospitalists already comanaging patients with neurosurgery, hematology/oncology, and orthopedics at your institution? How are specialist hospitalists different?
A: Neurohospitalists focus their professional practice on the hospitalized care of patients with neurological diseases—they perform the same function for those patients as we do for medical patients. That is, they admit patients, supervise their overall care, and discharge them. On our neurosurgery service, which has a census of 50 patients, the surgeons are in the operating room much of the day. Their post-surgical patients often have multiple medical comorbidities (heart failure, high blood pressures, diabetes, etc.), which is where the medical hospitalist comes in to comanage and coordinate their medical care.
We probably need new lingo to distinguish between medical hospitalists comanaging specialty patients and specialty hospitalists, because it can be confusing to people.
Q: Is this model sustainable in the community and rural settings, where specialists are in short supply?
A: There is a size below which you probably cannot support a specialty hospitalist. But larger places can, and their value is not only what they do at that individual hospital, but the fact that they can teach and do research and (quality improvement) that may help influence care beyond their organization’s walls.
—GH
Bob Wachter, MD, MHM, has watched the hospitalist movement grow from its infancy in the mid-1990s to more than 30,000 hospitalists practicing nationwide today. As professor and chief of the Division of Hospital Medicine and associate chairman of the Department of Medicine at the University of California at San Francisco, and chief of the medical service at UCSF Medical Center, Dr. Wachter also has watched the HM model spread to other medical specialties, including a handful of departments in his own hospital. The Hospitalist caught up with Dr. Wachter and found out what he thinks about the spread of the HM model.
Question: Do specialist-hospitalist programs threaten to siphon off your medical hospitalist workforce, or are they a boon?
Answer: Having specialized physicians focus on hospital care is a powerful model. Not only are they available all the time, but they are keeping up with innovations in their field. More importantly, they get involved in system improvement in a way that the part-time hospital person will not.
—Bob Wachter, MD, MHM
Q: Are there direct benefits to the hospitalist on the floor?
A: I think it creates a vehicle for collegiality, interchange, and learning across the specialties, which is harder to come by when we’re in the hospital all the time, but the consults we’re interacting with may not be.
Q: Aren’t hospitalists already comanaging patients with neurosurgery, hematology/oncology, and orthopedics at your institution? How are specialist hospitalists different?
A: Neurohospitalists focus their professional practice on the hospitalized care of patients with neurological diseases—they perform the same function for those patients as we do for medical patients. That is, they admit patients, supervise their overall care, and discharge them. On our neurosurgery service, which has a census of 50 patients, the surgeons are in the operating room much of the day. Their post-surgical patients often have multiple medical comorbidities (heart failure, high blood pressures, diabetes, etc.), which is where the medical hospitalist comes in to comanage and coordinate their medical care.
We probably need new lingo to distinguish between medical hospitalists comanaging specialty patients and specialty hospitalists, because it can be confusing to people.
Q: Is this model sustainable in the community and rural settings, where specialists are in short supply?
A: There is a size below which you probably cannot support a specialty hospitalist. But larger places can, and their value is not only what they do at that individual hospital, but the fact that they can teach and do research and (quality improvement) that may help influence care beyond their organization’s walls.
—GH
Innovative Use of Scribes in the Inpatient Setting
Over the past couple of decades, the ever-increasing medical-legal, financial, and patient-safety demands have led to a mushrooming of the amount of documentation needed during patient care, especially in the inpatient setting. With the advent of HM, that burden simply shifted to hospitalists, along with rapidly expanding patient loads as PCPs started delegating inpatient care. The problem was further compounded in teaching hospitals by a gradual decline in resident support as patient caps and work-hour limits were instituted.
Not surprisingly, the quality and accuracy of physicians’ progress notes started to suffer. It became frequently difficult to remember the details of encounters from earlier in the day, and fatigue sometimes led to details essential to continuity of care being left out completely.
A potential—and very intriguing—solution presented itself, however, as we were designing family-centered team rounds. Apparently, the ED group at the adjacent Abbott-Northwestern Hospital in Minneapolis had been using scribes for several years. The scribes captured the providers’ notes during each encounter, and the group had developed a polished system of scribe recruitment and training (mostly pre-med students awaiting acceptance to medical schools).
But would this model work in the inpatient setting where workflow was completely different? This was a total unknown, given that there has been no precedent in the literature about inpatient scribe utilization. Although relatively meager in number, the published articles about outpatient use of scribes were generally favorable, with the authors noting improved productivity and increased patient and staff satisfaction.1,2,3,4
Operationally, the main difference between inpatient and outpatient scribe use lied in the rounding mechanism itself; it was not just a provider-patient interaction, as in the ED, but rather a sometimes cacophonous collection of multiple inputs from families, providers, students, residents, nurses, and ancillary staff. The challenge here was to train the scribes (natural ability played a significant role) to produce a coherent document out of this interaction; the document had to accurately reflect current status and plans of care. The first step was to create a template for the daily progress notes with all the necessary headings, as well as age-appropriate normal exams, with the ability to directly import from the EMR such dynamic data as vital signs, medication lists, and lab results.
Each morning prior to rounds, the scribe was provided a list of patients to be rounded on, and the scribe spent about 30 minutes creating partial notes on each patient, as well as a brief patient identification statement. This proved to be a significant time-saver during rounds and allowed the scribes to keep up with the care team. Each note was pre-pended with the following statements, as recommended by the hospital’s risk-management team:
- I, (scribe name), am serving as a scribe to document services personally performed by (hospitalist name), MD, based on my observation and the provider’s statements to me.
- I, (hospitalist name), MD, attest that (scribe name) is acting in a scribe capacity, has observed my performance of the services, and has documented them in accordance with my direction.
A computer-on-wheels (COW) station was assigned to the scribes and accompanied the rounding team into the patient rooms, making it possible for them to follow the interactions in real time. The scribes were encouraged to hold their hands up and interrupt the conversation at any time if they needed clarification, something that happened rather infrequently. On the other hand, the care team was directed to speak clearly and the residents were instructed to present their cases using the same format as the progress-note template, thus minimizing guesswork on the part of the scribes. The only part of the interaction the scribes could not transcribe directly was the physical examination, and typically the attending physician dictated abnormal findings as well as systems not assessed, if any, at the end. All the scribe-generated notes were forwarded to the rounding provider’s EMR inbox and reviewed by the latter, amended when necessary, and signed electronically. The review of the scribe-generated notes proved to be initially a time-consuming process, typically two hours. However, as the scribes gained experience, the time commitment on the part of the providers decreased rapidly; after about three months, the time spent was about 30 minutes on busy days, even less otherwise, with a concomitant increase in satisfaction with the scribing process.
Not too unexpectedly, our transcription service initially pushed back on this idea because of their fear of job loss. However, this issue was resolved by eliminating the need for outsourcing overflow dictations. In addition, the relative terseness of the scribed notes did not sit well initially with some of our colleagues used to excessive verbosity, and this issue again gradually faded away as physicians realized that all the necessary information for care was preserved.
Does a scribe program make sense in all situations? Not likely. This kind of setup will work best in busy tertiary-care centers with residency programs and family-centered team rounds. Furthermore, a nearby college or university is a must if cost-efficient hiring of pre-med students is to be possible.
Walid Maalouli, MD, FAAP,
medical director, hospitalist department,
Children’s Hospitals & Clinics of Minnesota, Minneapolis
References
- Arya R, Salovich DM, Ohman-Strickland P, Merlin MA. Impact of scribes on performance indicators in the emergency department. Acad Emerg Med. 2010;17(5):490- 494.
- Koshy S, Feustel PJ, Hong M, Kogan BA. Scribes in an ambulatory urology practice: patient and physician satisfaction. J Urol. 2010;184(1):258-262.
- Conn J. Getting it in writing. Docs using scribes to ease the transition to EHRs. Mod Healthc. 2010;40(6):30,32.
- Expanded scribe role boosts staff morale. ED Manag. 2009;21(7):75-77.
Over the past couple of decades, the ever-increasing medical-legal, financial, and patient-safety demands have led to a mushrooming of the amount of documentation needed during patient care, especially in the inpatient setting. With the advent of HM, that burden simply shifted to hospitalists, along with rapidly expanding patient loads as PCPs started delegating inpatient care. The problem was further compounded in teaching hospitals by a gradual decline in resident support as patient caps and work-hour limits were instituted.
Not surprisingly, the quality and accuracy of physicians’ progress notes started to suffer. It became frequently difficult to remember the details of encounters from earlier in the day, and fatigue sometimes led to details essential to continuity of care being left out completely.
A potential—and very intriguing—solution presented itself, however, as we were designing family-centered team rounds. Apparently, the ED group at the adjacent Abbott-Northwestern Hospital in Minneapolis had been using scribes for several years. The scribes captured the providers’ notes during each encounter, and the group had developed a polished system of scribe recruitment and training (mostly pre-med students awaiting acceptance to medical schools).
But would this model work in the inpatient setting where workflow was completely different? This was a total unknown, given that there has been no precedent in the literature about inpatient scribe utilization. Although relatively meager in number, the published articles about outpatient use of scribes were generally favorable, with the authors noting improved productivity and increased patient and staff satisfaction.1,2,3,4
Operationally, the main difference between inpatient and outpatient scribe use lied in the rounding mechanism itself; it was not just a provider-patient interaction, as in the ED, but rather a sometimes cacophonous collection of multiple inputs from families, providers, students, residents, nurses, and ancillary staff. The challenge here was to train the scribes (natural ability played a significant role) to produce a coherent document out of this interaction; the document had to accurately reflect current status and plans of care. The first step was to create a template for the daily progress notes with all the necessary headings, as well as age-appropriate normal exams, with the ability to directly import from the EMR such dynamic data as vital signs, medication lists, and lab results.
Each morning prior to rounds, the scribe was provided a list of patients to be rounded on, and the scribe spent about 30 minutes creating partial notes on each patient, as well as a brief patient identification statement. This proved to be a significant time-saver during rounds and allowed the scribes to keep up with the care team. Each note was pre-pended with the following statements, as recommended by the hospital’s risk-management team:
- I, (scribe name), am serving as a scribe to document services personally performed by (hospitalist name), MD, based on my observation and the provider’s statements to me.
- I, (hospitalist name), MD, attest that (scribe name) is acting in a scribe capacity, has observed my performance of the services, and has documented them in accordance with my direction.
A computer-on-wheels (COW) station was assigned to the scribes and accompanied the rounding team into the patient rooms, making it possible for them to follow the interactions in real time. The scribes were encouraged to hold their hands up and interrupt the conversation at any time if they needed clarification, something that happened rather infrequently. On the other hand, the care team was directed to speak clearly and the residents were instructed to present their cases using the same format as the progress-note template, thus minimizing guesswork on the part of the scribes. The only part of the interaction the scribes could not transcribe directly was the physical examination, and typically the attending physician dictated abnormal findings as well as systems not assessed, if any, at the end. All the scribe-generated notes were forwarded to the rounding provider’s EMR inbox and reviewed by the latter, amended when necessary, and signed electronically. The review of the scribe-generated notes proved to be initially a time-consuming process, typically two hours. However, as the scribes gained experience, the time commitment on the part of the providers decreased rapidly; after about three months, the time spent was about 30 minutes on busy days, even less otherwise, with a concomitant increase in satisfaction with the scribing process.
Not too unexpectedly, our transcription service initially pushed back on this idea because of their fear of job loss. However, this issue was resolved by eliminating the need for outsourcing overflow dictations. In addition, the relative terseness of the scribed notes did not sit well initially with some of our colleagues used to excessive verbosity, and this issue again gradually faded away as physicians realized that all the necessary information for care was preserved.
Does a scribe program make sense in all situations? Not likely. This kind of setup will work best in busy tertiary-care centers with residency programs and family-centered team rounds. Furthermore, a nearby college or university is a must if cost-efficient hiring of pre-med students is to be possible.
Walid Maalouli, MD, FAAP,
medical director, hospitalist department,
Children’s Hospitals & Clinics of Minnesota, Minneapolis
References
- Arya R, Salovich DM, Ohman-Strickland P, Merlin MA. Impact of scribes on performance indicators in the emergency department. Acad Emerg Med. 2010;17(5):490- 494.
- Koshy S, Feustel PJ, Hong M, Kogan BA. Scribes in an ambulatory urology practice: patient and physician satisfaction. J Urol. 2010;184(1):258-262.
- Conn J. Getting it in writing. Docs using scribes to ease the transition to EHRs. Mod Healthc. 2010;40(6):30,32.
- Expanded scribe role boosts staff morale. ED Manag. 2009;21(7):75-77.
Over the past couple of decades, the ever-increasing medical-legal, financial, and patient-safety demands have led to a mushrooming of the amount of documentation needed during patient care, especially in the inpatient setting. With the advent of HM, that burden simply shifted to hospitalists, along with rapidly expanding patient loads as PCPs started delegating inpatient care. The problem was further compounded in teaching hospitals by a gradual decline in resident support as patient caps and work-hour limits were instituted.
Not surprisingly, the quality and accuracy of physicians’ progress notes started to suffer. It became frequently difficult to remember the details of encounters from earlier in the day, and fatigue sometimes led to details essential to continuity of care being left out completely.
A potential—and very intriguing—solution presented itself, however, as we were designing family-centered team rounds. Apparently, the ED group at the adjacent Abbott-Northwestern Hospital in Minneapolis had been using scribes for several years. The scribes captured the providers’ notes during each encounter, and the group had developed a polished system of scribe recruitment and training (mostly pre-med students awaiting acceptance to medical schools).
But would this model work in the inpatient setting where workflow was completely different? This was a total unknown, given that there has been no precedent in the literature about inpatient scribe utilization. Although relatively meager in number, the published articles about outpatient use of scribes were generally favorable, with the authors noting improved productivity and increased patient and staff satisfaction.1,2,3,4
Operationally, the main difference between inpatient and outpatient scribe use lied in the rounding mechanism itself; it was not just a provider-patient interaction, as in the ED, but rather a sometimes cacophonous collection of multiple inputs from families, providers, students, residents, nurses, and ancillary staff. The challenge here was to train the scribes (natural ability played a significant role) to produce a coherent document out of this interaction; the document had to accurately reflect current status and plans of care. The first step was to create a template for the daily progress notes with all the necessary headings, as well as age-appropriate normal exams, with the ability to directly import from the EMR such dynamic data as vital signs, medication lists, and lab results.
Each morning prior to rounds, the scribe was provided a list of patients to be rounded on, and the scribe spent about 30 minutes creating partial notes on each patient, as well as a brief patient identification statement. This proved to be a significant time-saver during rounds and allowed the scribes to keep up with the care team. Each note was pre-pended with the following statements, as recommended by the hospital’s risk-management team:
- I, (scribe name), am serving as a scribe to document services personally performed by (hospitalist name), MD, based on my observation and the provider’s statements to me.
- I, (hospitalist name), MD, attest that (scribe name) is acting in a scribe capacity, has observed my performance of the services, and has documented them in accordance with my direction.
A computer-on-wheels (COW) station was assigned to the scribes and accompanied the rounding team into the patient rooms, making it possible for them to follow the interactions in real time. The scribes were encouraged to hold their hands up and interrupt the conversation at any time if they needed clarification, something that happened rather infrequently. On the other hand, the care team was directed to speak clearly and the residents were instructed to present their cases using the same format as the progress-note template, thus minimizing guesswork on the part of the scribes. The only part of the interaction the scribes could not transcribe directly was the physical examination, and typically the attending physician dictated abnormal findings as well as systems not assessed, if any, at the end. All the scribe-generated notes were forwarded to the rounding provider’s EMR inbox and reviewed by the latter, amended when necessary, and signed electronically. The review of the scribe-generated notes proved to be initially a time-consuming process, typically two hours. However, as the scribes gained experience, the time commitment on the part of the providers decreased rapidly; after about three months, the time spent was about 30 minutes on busy days, even less otherwise, with a concomitant increase in satisfaction with the scribing process.
Not too unexpectedly, our transcription service initially pushed back on this idea because of their fear of job loss. However, this issue was resolved by eliminating the need for outsourcing overflow dictations. In addition, the relative terseness of the scribed notes did not sit well initially with some of our colleagues used to excessive verbosity, and this issue again gradually faded away as physicians realized that all the necessary information for care was preserved.
Does a scribe program make sense in all situations? Not likely. This kind of setup will work best in busy tertiary-care centers with residency programs and family-centered team rounds. Furthermore, a nearby college or university is a must if cost-efficient hiring of pre-med students is to be possible.
Walid Maalouli, MD, FAAP,
medical director, hospitalist department,
Children’s Hospitals & Clinics of Minnesota, Minneapolis
References
- Arya R, Salovich DM, Ohman-Strickland P, Merlin MA. Impact of scribes on performance indicators in the emergency department. Acad Emerg Med. 2010;17(5):490- 494.
- Koshy S, Feustel PJ, Hong M, Kogan BA. Scribes in an ambulatory urology practice: patient and physician satisfaction. J Urol. 2010;184(1):258-262.
- Conn J. Getting it in writing. Docs using scribes to ease the transition to EHRs. Mod Healthc. 2010;40(6):30,32.
- Expanded scribe role boosts staff morale. ED Manag. 2009;21(7):75-77.
Can You Hear Me Now?
In the past three years, SHM has brought in-depth quality-improvement (QI) programs to nearly every state in the country.
Between its three major mentored implementation projects—Project BOOST (Better Outcomes for Older Adults through Safe Transitions), Glycemic Control Mentored Implemen-tation, and the Venous Thromboembolism (VTE) Collaborative—SHM has worked with more than 100 hospitals across the country and in Canada. SHM is expanding these three programs to additional hospitals and actively developing other QI initiatives.
“SHM’s quality-improvement programs focus on real change, and they have made a substantial impact,” says Joe Miller, SHM’s senior vice president and chief solutions officer. “Hospitalists using SHM’s quality-improvement methods have impacted the care of tens of thousands of hospitalized patients.”
SHM’s programs all use a mix of in-depth mentoring led by national experts and specially designed resource toolkits that enable hospitalists to lead major initiatives within their hospitals. The programs also facilitate “peer learning,” allowing hospitalists to learn from one another.
Project BOOST, which is designed to reduce unplanned readmissions to the hospital, has received national attention. In early 2010, SHM teamed with Blue Cross/Blue Shield of Michigan and the University of Michigan to bring the program to more than a dozen hospitals in that state. SHM also announced a new collaboration with the California HealthCare Foundation to implement Project BOOST in more than 20 hospitals in California.
“Healthcare reform is creating a new focus on quality improvement,” Miller says. “SHM is bringing a multidisciplinary approach to transforming inpatient care to hospitals across the country.” TH
Chapter Updates
Milwaukee/SE Wisconsin
The Milwaukee/SE Wisconsin chapter held a meeting June 10 at Bacchus Restaurant in Milwaukee, at which congratulations were doled out to chapter member Eric Siegal, MD, SFHM, on his election to SHM’s board of directors. As chair of SHM’s Public Policy Committee, Dr. Siegal advocates for such issues as the Physician Quality Reporting Initiative (PQRI).
The chapter also acknowledged Dr. Len Scarpinato of St. Luke’s Hospital, who achieved Senior Fellow in Hospital Medicine (SFHM) designation and was honored at HM10 in April in Washington, D.C. As the regional director of Cogent Healthcare in southeast Wisconsin, Dr. Scarpinato has been instrumental in bringing hospitalists together to network and exchange innovative ideas.
Chapter member Jeanette Kalupa, DNP, ACNP-BC, APNP, of St. Luke’s was mentioned in the opening presentation at HM10 for her work as co-chair of the Nonphysician Providers Committee. Despite a busy HM10 schedule, Drs. Don Lee, Wes Lafferty, Scarpinato, Betty Tucker, and Peter Quandt took time out for a White House tour.
Greater Baltimore Area
The Greater Baltimore Area chapter of SHM met June 16 at Linwood’s Restaurant in Owings Mills, Md. Dr. Suzanne Mitchell spoke on “Relating to the Patient.” The meeting, sponsored by Merck, attracted 50 hospitalists and guests from 10 HM groups.
Los Angeles
The latest Los Angeles chapter meeting was held July 29. The featured speaker was Darrell Harrington, MD, associate medical director for Graduate Medical Education and chief of the division of general internal medicine at Harbor-UCLA Medical Center. Dr. Harrington delivered a presentation about maximizing DVT and PE quality measures. The chapter’s next meeting will be held in the fall.
Fellow in Hospital Medicine Spotlight
James C. Pile, MD, FACP, SFHM

Dr. Pile is an associate professor of medicine, interim director of hospital medicine, and associate program director of the internal residency program at the MetroHealth Campus of Case Western Reserve University in Cleveland. As a 10-year SHM member, he has been heavily involved in the growth of the Journal of Hospital Medicine, for which he is now deputy editor. He is an active member of the Annual Meeting and Education committees, and is former physician editor of The Hospitalist.
Undergraduate: Kings College in Briarcliff Manor, N.Y.
Medical school: Ohio State University College of Medicine, Columbus.
Internship and residency: University Hospitals of Cleveland.
Fellowship: Infectious Disease, National Naval Medicine Center, Bethesda, Md.
Notable: Prior to working as a hospitalist, Dr. Pile served as a battalion surgeon with Marine infantry on the front lines of the first Gulf War. He also worked as a general practitioner and infectious-disease specialist. His current interests lie in medical education, anti-microbial stewardship, and perioperative medicine.
Quotable: “I continue to see hospital medicine being front and center in patient safety in this country. … That is our whole reason for being, essentially. I anticipate us continuing to grow and develop into the real national leaders in quality improvement in the inpatient setting.”
FYI: Dr. Pile is an avid cyclist. He recently completed a one-day, 200-mile ride, and during his time in medical school, he biked from Seattle to New York City. He loves traveling and spending time with his wife and two daughters.
— Sarah Gelotte
SHAPE the Landscape of Academic Hospital Medicine: Participate in the Academic Hospitalist Survey
The recently released State of Hospital Medicine: 2010 Report Based on 2009 Data provides an unprecedented look at the factors shaping the specialty. However, for academic hospitalists, the picture can be very different. That is why SHM and the Medical Group Management Association (MGMA) are embarking on their first joint survey of academic hospitalists.

Academic HM groups—including groups at community-based teaching hospitals—can participate in the survey now through Nov. 5 by logging on to www6.mgma.com, or by contacting MGMA’s Survey Operations Department at 877-275-6462, Ext. 1895.
“Academic hospitalists and executive leaders at academic institutions need to know how they stack up against their peers in the field,” says Leslie Flores, SHM’s senior advisor for practice management. “Participating in this survey is the first step in providing an in-depth resource that identifies the major trends in academic hospital medicine.”
Like the new State of Hospital Medicine report, the academic report will provide data on hospitalist compensation and productivity, staffing information, and financial support. It also will examine the organizational structure of academic hospitalist practices and how academic hospitalists allocate their time between clinical, research, and teaching responsibilities. The new report also will feature information about medical-school and research funding.
MGMA will publish its standard academic survey results early next spring. Hospitalist-specific data will also be published in the 2011 State of Hospital Medicine report, to be released next summer.
In the past three years, SHM has brought in-depth quality-improvement (QI) programs to nearly every state in the country.
Between its three major mentored implementation projects—Project BOOST (Better Outcomes for Older Adults through Safe Transitions), Glycemic Control Mentored Implemen-tation, and the Venous Thromboembolism (VTE) Collaborative—SHM has worked with more than 100 hospitals across the country and in Canada. SHM is expanding these three programs to additional hospitals and actively developing other QI initiatives.
“SHM’s quality-improvement programs focus on real change, and they have made a substantial impact,” says Joe Miller, SHM’s senior vice president and chief solutions officer. “Hospitalists using SHM’s quality-improvement methods have impacted the care of tens of thousands of hospitalized patients.”
SHM’s programs all use a mix of in-depth mentoring led by national experts and specially designed resource toolkits that enable hospitalists to lead major initiatives within their hospitals. The programs also facilitate “peer learning,” allowing hospitalists to learn from one another.
Project BOOST, which is designed to reduce unplanned readmissions to the hospital, has received national attention. In early 2010, SHM teamed with Blue Cross/Blue Shield of Michigan and the University of Michigan to bring the program to more than a dozen hospitals in that state. SHM also announced a new collaboration with the California HealthCare Foundation to implement Project BOOST in more than 20 hospitals in California.
“Healthcare reform is creating a new focus on quality improvement,” Miller says. “SHM is bringing a multidisciplinary approach to transforming inpatient care to hospitals across the country.” TH
Chapter Updates
Milwaukee/SE Wisconsin
The Milwaukee/SE Wisconsin chapter held a meeting June 10 at Bacchus Restaurant in Milwaukee, at which congratulations were doled out to chapter member Eric Siegal, MD, SFHM, on his election to SHM’s board of directors. As chair of SHM’s Public Policy Committee, Dr. Siegal advocates for such issues as the Physician Quality Reporting Initiative (PQRI).
The chapter also acknowledged Dr. Len Scarpinato of St. Luke’s Hospital, who achieved Senior Fellow in Hospital Medicine (SFHM) designation and was honored at HM10 in April in Washington, D.C. As the regional director of Cogent Healthcare in southeast Wisconsin, Dr. Scarpinato has been instrumental in bringing hospitalists together to network and exchange innovative ideas.
Chapter member Jeanette Kalupa, DNP, ACNP-BC, APNP, of St. Luke’s was mentioned in the opening presentation at HM10 for her work as co-chair of the Nonphysician Providers Committee. Despite a busy HM10 schedule, Drs. Don Lee, Wes Lafferty, Scarpinato, Betty Tucker, and Peter Quandt took time out for a White House tour.
Greater Baltimore Area
The Greater Baltimore Area chapter of SHM met June 16 at Linwood’s Restaurant in Owings Mills, Md. Dr. Suzanne Mitchell spoke on “Relating to the Patient.” The meeting, sponsored by Merck, attracted 50 hospitalists and guests from 10 HM groups.
Los Angeles
The latest Los Angeles chapter meeting was held July 29. The featured speaker was Darrell Harrington, MD, associate medical director for Graduate Medical Education and chief of the division of general internal medicine at Harbor-UCLA Medical Center. Dr. Harrington delivered a presentation about maximizing DVT and PE quality measures. The chapter’s next meeting will be held in the fall.
Fellow in Hospital Medicine Spotlight
James C. Pile, MD, FACP, SFHM
Dr. Pile is an associate professor of medicine, interim director of hospital medicine, and associate program director of the internal residency program at the MetroHealth Campus of Case Western Reserve University in Cleveland. As a 10-year SHM member, he has been heavily involved in the growth of the Journal of Hospital Medicine, for which he is now deputy editor. He is an active member of the Annual Meeting and Education committees, and is former physician editor of The Hospitalist.
Undergraduate: Kings College in Briarcliff Manor, N.Y.
Medical school: Ohio State University College of Medicine, Columbus.
Internship and residency: University Hospitals of Cleveland.
Fellowship: Infectious Disease, National Naval Medicine Center, Bethesda, Md.
Notable: Prior to working as a hospitalist, Dr. Pile served as a battalion surgeon with Marine infantry on the front lines of the first Gulf War. He also worked as a general practitioner and infectious-disease specialist. His current interests lie in medical education, anti-microbial stewardship, and perioperative medicine.
Quotable: “I continue to see hospital medicine being front and center in patient safety in this country. … That is our whole reason for being, essentially. I anticipate us continuing to grow and develop into the real national leaders in quality improvement in the inpatient setting.”
FYI: Dr. Pile is an avid cyclist. He recently completed a one-day, 200-mile ride, and during his time in medical school, he biked from Seattle to New York City. He loves traveling and spending time with his wife and two daughters.
— Sarah Gelotte
SHAPE the Landscape of Academic Hospital Medicine: Participate in the Academic Hospitalist Survey
The recently released State of Hospital Medicine: 2010 Report Based on 2009 Data provides an unprecedented look at the factors shaping the specialty. However, for academic hospitalists, the picture can be very different. That is why SHM and the Medical Group Management Association (MGMA) are embarking on their first joint survey of academic hospitalists.
Academic HM groups—including groups at community-based teaching hospitals—can participate in the survey now through Nov. 5 by logging on to www6.mgma.com, or by contacting MGMA’s Survey Operations Department at 877-275-6462, Ext. 1895.
“Academic hospitalists and executive leaders at academic institutions need to know how they stack up against their peers in the field,” says Leslie Flores, SHM’s senior advisor for practice management. “Participating in this survey is the first step in providing an in-depth resource that identifies the major trends in academic hospital medicine.”
Like the new State of Hospital Medicine report, the academic report will provide data on hospitalist compensation and productivity, staffing information, and financial support. It also will examine the organizational structure of academic hospitalist practices and how academic hospitalists allocate their time between clinical, research, and teaching responsibilities. The new report also will feature information about medical-school and research funding.
MGMA will publish its standard academic survey results early next spring. Hospitalist-specific data will also be published in the 2011 State of Hospital Medicine report, to be released next summer.
In the past three years, SHM has brought in-depth quality-improvement (QI) programs to nearly every state in the country.
Between its three major mentored implementation projects—Project BOOST (Better Outcomes for Older Adults through Safe Transitions), Glycemic Control Mentored Implemen-tation, and the Venous Thromboembolism (VTE) Collaborative—SHM has worked with more than 100 hospitals across the country and in Canada. SHM is expanding these three programs to additional hospitals and actively developing other QI initiatives.
“SHM’s quality-improvement programs focus on real change, and they have made a substantial impact,” says Joe Miller, SHM’s senior vice president and chief solutions officer. “Hospitalists using SHM’s quality-improvement methods have impacted the care of tens of thousands of hospitalized patients.”
SHM’s programs all use a mix of in-depth mentoring led by national experts and specially designed resource toolkits that enable hospitalists to lead major initiatives within their hospitals. The programs also facilitate “peer learning,” allowing hospitalists to learn from one another.
Project BOOST, which is designed to reduce unplanned readmissions to the hospital, has received national attention. In early 2010, SHM teamed with Blue Cross/Blue Shield of Michigan and the University of Michigan to bring the program to more than a dozen hospitals in that state. SHM also announced a new collaboration with the California HealthCare Foundation to implement Project BOOST in more than 20 hospitals in California.
“Healthcare reform is creating a new focus on quality improvement,” Miller says. “SHM is bringing a multidisciplinary approach to transforming inpatient care to hospitals across the country.” TH
Chapter Updates
Milwaukee/SE Wisconsin
The Milwaukee/SE Wisconsin chapter held a meeting June 10 at Bacchus Restaurant in Milwaukee, at which congratulations were doled out to chapter member Eric Siegal, MD, SFHM, on his election to SHM’s board of directors. As chair of SHM’s Public Policy Committee, Dr. Siegal advocates for such issues as the Physician Quality Reporting Initiative (PQRI).
The chapter also acknowledged Dr. Len Scarpinato of St. Luke’s Hospital, who achieved Senior Fellow in Hospital Medicine (SFHM) designation and was honored at HM10 in April in Washington, D.C. As the regional director of Cogent Healthcare in southeast Wisconsin, Dr. Scarpinato has been instrumental in bringing hospitalists together to network and exchange innovative ideas.
Chapter member Jeanette Kalupa, DNP, ACNP-BC, APNP, of St. Luke’s was mentioned in the opening presentation at HM10 for her work as co-chair of the Nonphysician Providers Committee. Despite a busy HM10 schedule, Drs. Don Lee, Wes Lafferty, Scarpinato, Betty Tucker, and Peter Quandt took time out for a White House tour.
Greater Baltimore Area
The Greater Baltimore Area chapter of SHM met June 16 at Linwood’s Restaurant in Owings Mills, Md. Dr. Suzanne Mitchell spoke on “Relating to the Patient.” The meeting, sponsored by Merck, attracted 50 hospitalists and guests from 10 HM groups.
Los Angeles
The latest Los Angeles chapter meeting was held July 29. The featured speaker was Darrell Harrington, MD, associate medical director for Graduate Medical Education and chief of the division of general internal medicine at Harbor-UCLA Medical Center. Dr. Harrington delivered a presentation about maximizing DVT and PE quality measures. The chapter’s next meeting will be held in the fall.
Fellow in Hospital Medicine Spotlight
James C. Pile, MD, FACP, SFHM
Dr. Pile is an associate professor of medicine, interim director of hospital medicine, and associate program director of the internal residency program at the MetroHealth Campus of Case Western Reserve University in Cleveland. As a 10-year SHM member, he has been heavily involved in the growth of the Journal of Hospital Medicine, for which he is now deputy editor. He is an active member of the Annual Meeting and Education committees, and is former physician editor of The Hospitalist.
Undergraduate: Kings College in Briarcliff Manor, N.Y.
Medical school: Ohio State University College of Medicine, Columbus.
Internship and residency: University Hospitals of Cleveland.
Fellowship: Infectious Disease, National Naval Medicine Center, Bethesda, Md.
Notable: Prior to working as a hospitalist, Dr. Pile served as a battalion surgeon with Marine infantry on the front lines of the first Gulf War. He also worked as a general practitioner and infectious-disease specialist. His current interests lie in medical education, anti-microbial stewardship, and perioperative medicine.
Quotable: “I continue to see hospital medicine being front and center in patient safety in this country. … That is our whole reason for being, essentially. I anticipate us continuing to grow and develop into the real national leaders in quality improvement in the inpatient setting.”
FYI: Dr. Pile is an avid cyclist. He recently completed a one-day, 200-mile ride, and during his time in medical school, he biked from Seattle to New York City. He loves traveling and spending time with his wife and two daughters.
— Sarah Gelotte
SHAPE the Landscape of Academic Hospital Medicine: Participate in the Academic Hospitalist Survey
The recently released State of Hospital Medicine: 2010 Report Based on 2009 Data provides an unprecedented look at the factors shaping the specialty. However, for academic hospitalists, the picture can be very different. That is why SHM and the Medical Group Management Association (MGMA) are embarking on their first joint survey of academic hospitalists.
Academic HM groups—including groups at community-based teaching hospitals—can participate in the survey now through Nov. 5 by logging on to www6.mgma.com, or by contacting MGMA’s Survey Operations Department at 877-275-6462, Ext. 1895.
“Academic hospitalists and executive leaders at academic institutions need to know how they stack up against their peers in the field,” says Leslie Flores, SHM’s senior advisor for practice management. “Participating in this survey is the first step in providing an in-depth resource that identifies the major trends in academic hospital medicine.”
Like the new State of Hospital Medicine report, the academic report will provide data on hospitalist compensation and productivity, staffing information, and financial support. It also will examine the organizational structure of academic hospitalist practices and how academic hospitalists allocate their time between clinical, research, and teaching responsibilities. The new report also will feature information about medical-school and research funding.
MGMA will publish its standard academic survey results early next spring. Hospitalist-specific data will also be published in the 2011 State of Hospital Medicine report, to be released next summer.
Market Watch
New Generics
- Anastrazole tablets (generic Arimidex)1
- Azelastine hydrochloride ophthalmic solution 0.05% (generic Optivar)2
- Aztreonam for injection in single-dose vials of 1 g/20 mL and 2 g/30 mL (generic Azactam)3
- Bupropion hydrochloride extended-release 150-mg tablets (generic Zyban)4
- Meropenem injection, USP, IV, 500-mg and 1-g vials (generic Merrem IV)5
- Levetiracetam injection in 100 mg/1 mL and 500 mg/5 mL single-use vials (generic Keppra injection)6
- Tacrolimus 5-mg capsules (generic Prograf)7
- Trandolapril/verapamil tablets (generic Tarka)8
- Valacyclovir hydrochloride tablets, USP (generic Valtrex)9
- Venlafaxine extended-release capsules (generic Effexor XR)10
New Drugs, Indications, Approval Recommendations
- The Alair Bronchial Thermoplasty System is the first device to be FDA-approved for treating severe and persistent asthma.11 It is to be used by adults who are still symptomatic despite treatment with high-dose inhaled corticosteroids (ICS) and long-acting beta-agonists (LABAs). Radiofrequency signals are converted into heat that warms the lining of targeted airways via bronchoscope. There are a number of contraindications and warnings for this device. Treatment is delivered using a standard bronchoscope under moderate sedation.
- Buprenorphine Transdermal System (Butrans) is FDA-approved to treat moderate to severe chronic pain in patients requiring continuous, around-the-clock opioid analgesia for an extended period of time.12 It is a Schedule III controlled substance and will be available in early 2011 in 5 mcg/hour, 10 mcg/hour, and 20 mcg/hour dosage strengths. Patches continuously release the drug over seven days.
- Denosumab injection (Prolia) has been approved by the FDA for treating postmenopausal women with osteoporosis at high risk for fractures.13
- Fingolimod (FTY720), an oral sphingosine 1-phosphate receptor (S1PR) modulator and disease-modifying treatment for relapsing-remitting multiple sclerosis (RRMS), has received a positive review by an FDA Advisory Committee.14 The committee voted 25-0, stating that in clinical trials to date that FTY720 has demonstrated substantial evidence of effectiveness in patients with RRMS, reducing the frequency of clinical exacerbations. This agent works by retaining lymphocytes in the lymph nodes, preventing them from entering the central nervous system to cause damage. This lymphocyte retention is reversible, allowing circulating lymphocytes to regain normal levels if treatment is stopped.
- Ketorolac tromethamine intranasal (Sprix) is FDA-approved for treating acute moderate to moderately severe pain requiring opioid-level analgesia for up to five days.15 Even though it is administered intranasally, gastrointestinal hemorrhage, bleeding, and cardiovascular risks are included in the labeling as adverse events.
- HCV Rapid Antibody Test (OraQuick) has been approved by the FDA for use in patients 15 and older to identify hepatitis C virus (HCV) antibodies.16 Available as a test strip, it identifies HCV antibodies within 20 minutes, which allows patients to more quickly present for evaluation and treatment.
- Lopinavir/ritonavir (Kaletra) has been approved by the FDA for once-daily dosing for treatment-experienced HIV patients.17 The agent had been approved for once-daily treatment for therapy-naive patients.
Pipeline
- HPV vaccine (Gardasil) is being evaluated by the FDA in order to potentially expand its indication to include women 27 to 45 years old.18 A decision is expected by the end of the year.
- Roflumilast is a phosphodiesterase 4 (PDE4) enzyme inhibitor that targets underlying inflammation in COPD patients.19 The FDA has issued a complete response letter for Roflumilast, which was filed as a potential treatment to reduce COPD exacerbations associated with chronic bronchitis in patients at risk for exacerbations. No new clinical trials have been requested.
Product Discontinuation
- Estradiol vaginal tablets 10 mcg (Vagifem) will replace estradiol vaginal tablets 25 mcg to treat the symptoms of atrophic vaginitis due to menopause.20 Sales of the 25-mcg formulation were discontinued July 31.
Medication Safety
GlaxoSmithKline has received reports of dispensing errors related to rosiglitazone (Avandia), glimepiride (Amaryl), rosiglitazone/metformin (Avandamet), candesartan (Atacand), and warfarin (Coumadin). In some instances, the patient received the wrong medication (one severe case led to impaired mental status). Errors likely occurred due to illegible written prescriptions and/or incorrectly interpreted, labeled, and filled prescriptions. Some of these products have similar dosage strengths and also look alike, leading to the errors.21
Michele B. Kaufman, PharmD, BSc, RPh, is a freelance medical writer based in New York City and a clinical pharmacist at New York Downtown Hospital.
References
- Teva gets FDA approval for generic cancer drug. Forbes.com website. Available at: http://www.forbes.com/feeds/ap/2010/06/28/business-health-care-us-teva-pharmaceutical-industries-fda_7726375.html. Accessed June 29, 2010.
- Sun Pharma bags FDA approval for generic Optivar. Pharmaceutical Business Review website. Available at: http://regulatoryaffairs.pharmaceutical-business-review.com/news/sun_pharma_bags_fda_approval_for_generic_optivar_100622/. Accessed June 25, 2010.
- APP Pharmaceuticals Inc receives FDA approval for generic Aztreonam for injection, USP. TradingMarkets.com website. Available at: http://www.tradingmarkets.com/news/stock-alert/appx_apcvz_app-pharmaceuticals-inc-receives-fda-approval-for-generic-aztreonam-for-injection-usp-995249.html. Accessed June 24, 2010.
- Mylan gets FDA approval for generic Zyban. Forbes.com website. Available at: http://www.forbes.com/feeds/prnewswire/2010/05/04/prnewswire201005040700PR_NEWS_USPR_____NE98210.html. Accessed June 25, 2010.
- Hospira receives FDA approval for Meropenem for injection, USP (I.V.) Medical News Today website. Available at: http://www.medicalnewstoday.com/articles/192733.php. Accessed June 24, 2010.
- Sun Pharma announces USFDA approval for generic Keppra injection. Medical News Today website. Available at: http://www.medicalnewstoday.com/articles/192275.php. Accessed June 24, 2010.
- Watson’s generic Prograf 5 mg receives FDA approval. Watson website. Available at: http://ir.watson.com/phoenix.zhtml?c=65778&p=irol-newsArticle&ID=1443895. Accessed July 7, 2010.
- Glenmark arm gets US FDA nod for Tarka generic; stk up. Money Control website. Available at: http://www.moneycontrol.com/news/buzzing-stocks/glenmark-gets-us-fda-nod-for-tarka-generic-stk-up_460856.html. Accessed June 25, 2010.
- Watson’s generic Valtrex 500 mg and 1000 mg receives FDA approval. Watson website. Available at: http://ir.watson.com/phoenix.zhtml?c=65778&p=irol-newsArticle&ID=1430538&highlight=. Accessed June 25, 2010.
- Walsh S. FDA approves first generic Effexor extended release capsules to treat major depressive disorder. U.S. Food and Drug Administration website. Available at: www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm217624.htm Accessed June 29, 2010.
- Waknine Y. FDA approves first non-drug treatment for severe, persistent asthma. Medscape website. Available at: www.medscape.com/viewarticle/720922. Accessed June 30, 2010.
- Butrans transdermal system approved for chronic pain. Monthly Prescribing Reference website. Available at: www.empr.com/butrans-transdermal-system-approved-for-chronic-pain/article/173803/. Accessed July 7, 2010.
- Amgen’s Prolia garners FDA approval. FirstWord website. Available at: www.firstwordplus.com/Fws.do?articleid=BDE45B4D9F3F4C4A9326074859FF661F&logRowId=366890. Accessed June 30, 2010.
- FDA advisory committee unanimously recommends approval of Novartis investigational treatment FTY720 to treat relapsing remitting MS. Novartis Pharmaceuticals Corporation website. Available at: www.pharma.us.novartis.com/newsroom/press-release.jsp?PRID=2284. Accessed June 29, 2010.
- Roxro announces FDA approval of Sprix. Sprix website. Available at: www.sprix.com/docs/SPRIX-approval-press-release.pdf. Accessed June 29, 2010.
- FDA approves rapid test for antibodies to hepatitis C virus. U.S. Food and Drug Administration website. Available at: www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm217318. Accessed July 7, 2010.
- Abbott receives FDA approval for once-daily dosing of Kaletra (lopinavir/ritonavir) for treatment-experienced patients. Abbott website. Available at: www.abbott.com/global/url/pressRelease/en_US/60.5:5/Press_Release_0849.htm. Accessed June 30, 2010.
- Dane L. FDA extends review of Merck & Co.’s Gardasil for use in older women. FirstWord website. Available at: www.firstwordplus.com/Fws.do?articleid=2843FE3BFE2B44C5B463DBA787F213ED&logRowId=369474. Accessed July 7, 2010.
- Forest Laboratories and Nycomed receive complete response letter for Roflumilast. Forest Laboratories website. Available at: www.frx.com/news/PressRelease.aspx?ID=1428047. Accessed July 25, 2010.
- Vagifem 10 mcg to replace Vagifem 25 mcg formulation for atrophic vaginitis due to menopause. Novo Nordisk website. Available at: http://press.novonordisk-us.com/index.php?s=43&item=252. Accessed June 29, 2010.
- Dear Pharmacist Letter, June 2010. Important Drug Warnings: Medication Dispensing Errors; GlaxoSmithKline.
- New Jersey State Board of Pharmacy News, April 2010;24:2-3.
New Generics
- Anastrazole tablets (generic Arimidex)1
- Azelastine hydrochloride ophthalmic solution 0.05% (generic Optivar)2
- Aztreonam for injection in single-dose vials of 1 g/20 mL and 2 g/30 mL (generic Azactam)3
- Bupropion hydrochloride extended-release 150-mg tablets (generic Zyban)4
- Meropenem injection, USP, IV, 500-mg and 1-g vials (generic Merrem IV)5
- Levetiracetam injection in 100 mg/1 mL and 500 mg/5 mL single-use vials (generic Keppra injection)6
- Tacrolimus 5-mg capsules (generic Prograf)7
- Trandolapril/verapamil tablets (generic Tarka)8
- Valacyclovir hydrochloride tablets, USP (generic Valtrex)9
- Venlafaxine extended-release capsules (generic Effexor XR)10
New Drugs, Indications, Approval Recommendations
- The Alair Bronchial Thermoplasty System is the first device to be FDA-approved for treating severe and persistent asthma.11 It is to be used by adults who are still symptomatic despite treatment with high-dose inhaled corticosteroids (ICS) and long-acting beta-agonists (LABAs). Radiofrequency signals are converted into heat that warms the lining of targeted airways via bronchoscope. There are a number of contraindications and warnings for this device. Treatment is delivered using a standard bronchoscope under moderate sedation.
- Buprenorphine Transdermal System (Butrans) is FDA-approved to treat moderate to severe chronic pain in patients requiring continuous, around-the-clock opioid analgesia for an extended period of time.12 It is a Schedule III controlled substance and will be available in early 2011 in 5 mcg/hour, 10 mcg/hour, and 20 mcg/hour dosage strengths. Patches continuously release the drug over seven days.
- Denosumab injection (Prolia) has been approved by the FDA for treating postmenopausal women with osteoporosis at high risk for fractures.13
- Fingolimod (FTY720), an oral sphingosine 1-phosphate receptor (S1PR) modulator and disease-modifying treatment for relapsing-remitting multiple sclerosis (RRMS), has received a positive review by an FDA Advisory Committee.14 The committee voted 25-0, stating that in clinical trials to date that FTY720 has demonstrated substantial evidence of effectiveness in patients with RRMS, reducing the frequency of clinical exacerbations. This agent works by retaining lymphocytes in the lymph nodes, preventing them from entering the central nervous system to cause damage. This lymphocyte retention is reversible, allowing circulating lymphocytes to regain normal levels if treatment is stopped.
- Ketorolac tromethamine intranasal (Sprix) is FDA-approved for treating acute moderate to moderately severe pain requiring opioid-level analgesia for up to five days.15 Even though it is administered intranasally, gastrointestinal hemorrhage, bleeding, and cardiovascular risks are included in the labeling as adverse events.
- HCV Rapid Antibody Test (OraQuick) has been approved by the FDA for use in patients 15 and older to identify hepatitis C virus (HCV) antibodies.16 Available as a test strip, it identifies HCV antibodies within 20 minutes, which allows patients to more quickly present for evaluation and treatment.
- Lopinavir/ritonavir (Kaletra) has been approved by the FDA for once-daily dosing for treatment-experienced HIV patients.17 The agent had been approved for once-daily treatment for therapy-naive patients.
Pipeline
- HPV vaccine (Gardasil) is being evaluated by the FDA in order to potentially expand its indication to include women 27 to 45 years old.18 A decision is expected by the end of the year.
- Roflumilast is a phosphodiesterase 4 (PDE4) enzyme inhibitor that targets underlying inflammation in COPD patients.19 The FDA has issued a complete response letter for Roflumilast, which was filed as a potential treatment to reduce COPD exacerbations associated with chronic bronchitis in patients at risk for exacerbations. No new clinical trials have been requested.
Product Discontinuation
- Estradiol vaginal tablets 10 mcg (Vagifem) will replace estradiol vaginal tablets 25 mcg to treat the symptoms of atrophic vaginitis due to menopause.20 Sales of the 25-mcg formulation were discontinued July 31.
Medication Safety
GlaxoSmithKline has received reports of dispensing errors related to rosiglitazone (Avandia), glimepiride (Amaryl), rosiglitazone/metformin (Avandamet), candesartan (Atacand), and warfarin (Coumadin). In some instances, the patient received the wrong medication (one severe case led to impaired mental status). Errors likely occurred due to illegible written prescriptions and/or incorrectly interpreted, labeled, and filled prescriptions. Some of these products have similar dosage strengths and also look alike, leading to the errors.21
Michele B. Kaufman, PharmD, BSc, RPh, is a freelance medical writer based in New York City and a clinical pharmacist at New York Downtown Hospital.
References
- Teva gets FDA approval for generic cancer drug. Forbes.com website. Available at: http://www.forbes.com/feeds/ap/2010/06/28/business-health-care-us-teva-pharmaceutical-industries-fda_7726375.html. Accessed June 29, 2010.
- Sun Pharma bags FDA approval for generic Optivar. Pharmaceutical Business Review website. Available at: http://regulatoryaffairs.pharmaceutical-business-review.com/news/sun_pharma_bags_fda_approval_for_generic_optivar_100622/. Accessed June 25, 2010.
- APP Pharmaceuticals Inc receives FDA approval for generic Aztreonam for injection, USP. TradingMarkets.com website. Available at: http://www.tradingmarkets.com/news/stock-alert/appx_apcvz_app-pharmaceuticals-inc-receives-fda-approval-for-generic-aztreonam-for-injection-usp-995249.html. Accessed June 24, 2010.
- Mylan gets FDA approval for generic Zyban. Forbes.com website. Available at: http://www.forbes.com/feeds/prnewswire/2010/05/04/prnewswire201005040700PR_NEWS_USPR_____NE98210.html. Accessed June 25, 2010.
- Hospira receives FDA approval for Meropenem for injection, USP (I.V.) Medical News Today website. Available at: http://www.medicalnewstoday.com/articles/192733.php. Accessed June 24, 2010.
- Sun Pharma announces USFDA approval for generic Keppra injection. Medical News Today website. Available at: http://www.medicalnewstoday.com/articles/192275.php. Accessed June 24, 2010.
- Watson’s generic Prograf 5 mg receives FDA approval. Watson website. Available at: http://ir.watson.com/phoenix.zhtml?c=65778&p=irol-newsArticle&ID=1443895. Accessed July 7, 2010.
- Glenmark arm gets US FDA nod for Tarka generic; stk up. Money Control website. Available at: http://www.moneycontrol.com/news/buzzing-stocks/glenmark-gets-us-fda-nod-for-tarka-generic-stk-up_460856.html. Accessed June 25, 2010.
- Watson’s generic Valtrex 500 mg and 1000 mg receives FDA approval. Watson website. Available at: http://ir.watson.com/phoenix.zhtml?c=65778&p=irol-newsArticle&ID=1430538&highlight=. Accessed June 25, 2010.
- Walsh S. FDA approves first generic Effexor extended release capsules to treat major depressive disorder. U.S. Food and Drug Administration website. Available at: www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm217624.htm Accessed June 29, 2010.
- Waknine Y. FDA approves first non-drug treatment for severe, persistent asthma. Medscape website. Available at: www.medscape.com/viewarticle/720922. Accessed June 30, 2010.
- Butrans transdermal system approved for chronic pain. Monthly Prescribing Reference website. Available at: www.empr.com/butrans-transdermal-system-approved-for-chronic-pain/article/173803/. Accessed July 7, 2010.
- Amgen’s Prolia garners FDA approval. FirstWord website. Available at: www.firstwordplus.com/Fws.do?articleid=BDE45B4D9F3F4C4A9326074859FF661F&logRowId=366890. Accessed June 30, 2010.
- FDA advisory committee unanimously recommends approval of Novartis investigational treatment FTY720 to treat relapsing remitting MS. Novartis Pharmaceuticals Corporation website. Available at: www.pharma.us.novartis.com/newsroom/press-release.jsp?PRID=2284. Accessed June 29, 2010.
- Roxro announces FDA approval of Sprix. Sprix website. Available at: www.sprix.com/docs/SPRIX-approval-press-release.pdf. Accessed June 29, 2010.
- FDA approves rapid test for antibodies to hepatitis C virus. U.S. Food and Drug Administration website. Available at: www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm217318. Accessed July 7, 2010.
- Abbott receives FDA approval for once-daily dosing of Kaletra (lopinavir/ritonavir) for treatment-experienced patients. Abbott website. Available at: www.abbott.com/global/url/pressRelease/en_US/60.5:5/Press_Release_0849.htm. Accessed June 30, 2010.
- Dane L. FDA extends review of Merck & Co.’s Gardasil for use in older women. FirstWord website. Available at: www.firstwordplus.com/Fws.do?articleid=2843FE3BFE2B44C5B463DBA787F213ED&logRowId=369474. Accessed July 7, 2010.
- Forest Laboratories and Nycomed receive complete response letter for Roflumilast. Forest Laboratories website. Available at: www.frx.com/news/PressRelease.aspx?ID=1428047. Accessed July 25, 2010.
- Vagifem 10 mcg to replace Vagifem 25 mcg formulation for atrophic vaginitis due to menopause. Novo Nordisk website. Available at: http://press.novonordisk-us.com/index.php?s=43&item=252. Accessed June 29, 2010.
- Dear Pharmacist Letter, June 2010. Important Drug Warnings: Medication Dispensing Errors; GlaxoSmithKline.
- New Jersey State Board of Pharmacy News, April 2010;24:2-3.
New Generics
- Anastrazole tablets (generic Arimidex)1
- Azelastine hydrochloride ophthalmic solution 0.05% (generic Optivar)2
- Aztreonam for injection in single-dose vials of 1 g/20 mL and 2 g/30 mL (generic Azactam)3
- Bupropion hydrochloride extended-release 150-mg tablets (generic Zyban)4
- Meropenem injection, USP, IV, 500-mg and 1-g vials (generic Merrem IV)5
- Levetiracetam injection in 100 mg/1 mL and 500 mg/5 mL single-use vials (generic Keppra injection)6
- Tacrolimus 5-mg capsules (generic Prograf)7
- Trandolapril/verapamil tablets (generic Tarka)8
- Valacyclovir hydrochloride tablets, USP (generic Valtrex)9
- Venlafaxine extended-release capsules (generic Effexor XR)10
New Drugs, Indications, Approval Recommendations
- The Alair Bronchial Thermoplasty System is the first device to be FDA-approved for treating severe and persistent asthma.11 It is to be used by adults who are still symptomatic despite treatment with high-dose inhaled corticosteroids (ICS) and long-acting beta-agonists (LABAs). Radiofrequency signals are converted into heat that warms the lining of targeted airways via bronchoscope. There are a number of contraindications and warnings for this device. Treatment is delivered using a standard bronchoscope under moderate sedation.
- Buprenorphine Transdermal System (Butrans) is FDA-approved to treat moderate to severe chronic pain in patients requiring continuous, around-the-clock opioid analgesia for an extended period of time.12 It is a Schedule III controlled substance and will be available in early 2011 in 5 mcg/hour, 10 mcg/hour, and 20 mcg/hour dosage strengths. Patches continuously release the drug over seven days.
- Denosumab injection (Prolia) has been approved by the FDA for treating postmenopausal women with osteoporosis at high risk for fractures.13
- Fingolimod (FTY720), an oral sphingosine 1-phosphate receptor (S1PR) modulator and disease-modifying treatment for relapsing-remitting multiple sclerosis (RRMS), has received a positive review by an FDA Advisory Committee.14 The committee voted 25-0, stating that in clinical trials to date that FTY720 has demonstrated substantial evidence of effectiveness in patients with RRMS, reducing the frequency of clinical exacerbations. This agent works by retaining lymphocytes in the lymph nodes, preventing them from entering the central nervous system to cause damage. This lymphocyte retention is reversible, allowing circulating lymphocytes to regain normal levels if treatment is stopped.
- Ketorolac tromethamine intranasal (Sprix) is FDA-approved for treating acute moderate to moderately severe pain requiring opioid-level analgesia for up to five days.15 Even though it is administered intranasally, gastrointestinal hemorrhage, bleeding, and cardiovascular risks are included in the labeling as adverse events.
- HCV Rapid Antibody Test (OraQuick) has been approved by the FDA for use in patients 15 and older to identify hepatitis C virus (HCV) antibodies.16 Available as a test strip, it identifies HCV antibodies within 20 minutes, which allows patients to more quickly present for evaluation and treatment.
- Lopinavir/ritonavir (Kaletra) has been approved by the FDA for once-daily dosing for treatment-experienced HIV patients.17 The agent had been approved for once-daily treatment for therapy-naive patients.
Pipeline
- HPV vaccine (Gardasil) is being evaluated by the FDA in order to potentially expand its indication to include women 27 to 45 years old.18 A decision is expected by the end of the year.
- Roflumilast is a phosphodiesterase 4 (PDE4) enzyme inhibitor that targets underlying inflammation in COPD patients.19 The FDA has issued a complete response letter for Roflumilast, which was filed as a potential treatment to reduce COPD exacerbations associated with chronic bronchitis in patients at risk for exacerbations. No new clinical trials have been requested.
Product Discontinuation
- Estradiol vaginal tablets 10 mcg (Vagifem) will replace estradiol vaginal tablets 25 mcg to treat the symptoms of atrophic vaginitis due to menopause.20 Sales of the 25-mcg formulation were discontinued July 31.
Medication Safety
GlaxoSmithKline has received reports of dispensing errors related to rosiglitazone (Avandia), glimepiride (Amaryl), rosiglitazone/metformin (Avandamet), candesartan (Atacand), and warfarin (Coumadin). In some instances, the patient received the wrong medication (one severe case led to impaired mental status). Errors likely occurred due to illegible written prescriptions and/or incorrectly interpreted, labeled, and filled prescriptions. Some of these products have similar dosage strengths and also look alike, leading to the errors.21
Michele B. Kaufman, PharmD, BSc, RPh, is a freelance medical writer based in New York City and a clinical pharmacist at New York Downtown Hospital.
References
- Teva gets FDA approval for generic cancer drug. Forbes.com website. Available at: http://www.forbes.com/feeds/ap/2010/06/28/business-health-care-us-teva-pharmaceutical-industries-fda_7726375.html. Accessed June 29, 2010.
- Sun Pharma bags FDA approval for generic Optivar. Pharmaceutical Business Review website. Available at: http://regulatoryaffairs.pharmaceutical-business-review.com/news/sun_pharma_bags_fda_approval_for_generic_optivar_100622/. Accessed June 25, 2010.
- APP Pharmaceuticals Inc receives FDA approval for generic Aztreonam for injection, USP. TradingMarkets.com website. Available at: http://www.tradingmarkets.com/news/stock-alert/appx_apcvz_app-pharmaceuticals-inc-receives-fda-approval-for-generic-aztreonam-for-injection-usp-995249.html. Accessed June 24, 2010.
- Mylan gets FDA approval for generic Zyban. Forbes.com website. Available at: http://www.forbes.com/feeds/prnewswire/2010/05/04/prnewswire201005040700PR_NEWS_USPR_____NE98210.html. Accessed June 25, 2010.
- Hospira receives FDA approval for Meropenem for injection, USP (I.V.) Medical News Today website. Available at: http://www.medicalnewstoday.com/articles/192733.php. Accessed June 24, 2010.
- Sun Pharma announces USFDA approval for generic Keppra injection. Medical News Today website. Available at: http://www.medicalnewstoday.com/articles/192275.php. Accessed June 24, 2010.
- Watson’s generic Prograf 5 mg receives FDA approval. Watson website. Available at: http://ir.watson.com/phoenix.zhtml?c=65778&p=irol-newsArticle&ID=1443895. Accessed July 7, 2010.
- Glenmark arm gets US FDA nod for Tarka generic; stk up. Money Control website. Available at: http://www.moneycontrol.com/news/buzzing-stocks/glenmark-gets-us-fda-nod-for-tarka-generic-stk-up_460856.html. Accessed June 25, 2010.
- Watson’s generic Valtrex 500 mg and 1000 mg receives FDA approval. Watson website. Available at: http://ir.watson.com/phoenix.zhtml?c=65778&p=irol-newsArticle&ID=1430538&highlight=. Accessed June 25, 2010.
- Walsh S. FDA approves first generic Effexor extended release capsules to treat major depressive disorder. U.S. Food and Drug Administration website. Available at: www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm217624.htm Accessed June 29, 2010.
- Waknine Y. FDA approves first non-drug treatment for severe, persistent asthma. Medscape website. Available at: www.medscape.com/viewarticle/720922. Accessed June 30, 2010.
- Butrans transdermal system approved for chronic pain. Monthly Prescribing Reference website. Available at: www.empr.com/butrans-transdermal-system-approved-for-chronic-pain/article/173803/. Accessed July 7, 2010.
- Amgen’s Prolia garners FDA approval. FirstWord website. Available at: www.firstwordplus.com/Fws.do?articleid=BDE45B4D9F3F4C4A9326074859FF661F&logRowId=366890. Accessed June 30, 2010.
- FDA advisory committee unanimously recommends approval of Novartis investigational treatment FTY720 to treat relapsing remitting MS. Novartis Pharmaceuticals Corporation website. Available at: www.pharma.us.novartis.com/newsroom/press-release.jsp?PRID=2284. Accessed June 29, 2010.
- Roxro announces FDA approval of Sprix. Sprix website. Available at: www.sprix.com/docs/SPRIX-approval-press-release.pdf. Accessed June 29, 2010.
- FDA approves rapid test for antibodies to hepatitis C virus. U.S. Food and Drug Administration website. Available at: www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm217318. Accessed July 7, 2010.
- Abbott receives FDA approval for once-daily dosing of Kaletra (lopinavir/ritonavir) for treatment-experienced patients. Abbott website. Available at: www.abbott.com/global/url/pressRelease/en_US/60.5:5/Press_Release_0849.htm. Accessed June 30, 2010.
- Dane L. FDA extends review of Merck & Co.’s Gardasil for use in older women. FirstWord website. Available at: www.firstwordplus.com/Fws.do?articleid=2843FE3BFE2B44C5B463DBA787F213ED&logRowId=369474. Accessed July 7, 2010.
- Forest Laboratories and Nycomed receive complete response letter for Roflumilast. Forest Laboratories website. Available at: www.frx.com/news/PressRelease.aspx?ID=1428047. Accessed July 25, 2010.
- Vagifem 10 mcg to replace Vagifem 25 mcg formulation for atrophic vaginitis due to menopause. Novo Nordisk website. Available at: http://press.novonordisk-us.com/index.php?s=43&item=252. Accessed June 29, 2010.
- Dear Pharmacist Letter, June 2010. Important Drug Warnings: Medication Dispensing Errors; GlaxoSmithKline.
- New Jersey State Board of Pharmacy News, April 2010;24:2-3.
In the Literature: HM-Related Research You Need to Know
In This Edition
Literature at a Glance
A guide to this month’s studies
- Effect of early follow-up on readmission rates
- Heart rate control and outcomes in atrial fibrillation
- Pneumococcal vaccine to prevent stroke and MI
- Long-term outcomes of endovascular repair of AAA
- Insurance and outcomes in myocardial infarction
- Risk of gastrointestinal bleeding and cardiovascular outcomes with concurrent PPI and clopidogrel use
- CT in patients with suspected coronary artery disease
Reduced 30-Day Readmission Rate for Patients Discharged from Hospitals with Higher Rates of Early Follow-Up
Clinical question: Is early follow-up after discharge for heart failure associated with a reduction in readmission rates?
Background: Readmission for heart failure is very frequent and often unplanned. Early follow-up visits after discharge have been hypothesized to reduce readmissions but have been undefined.
Study design: Retrospective cohort study.
Setting: Patients with Medicare inpatient claims data linked to the OPTIMIZE-HF and GWTG-HF registries.
Synopsis: The study included 30,136 patients >65 years old with the principal discharge diagnosis of heart failure from 2003 to 2006. Hospitals were stratified into quartiles based upon the median arrival rate to “early” (within one week after discharge) follow-up appointments. Ranges of arrival rates to these appointments ranged from Quartile 1 (Q1) (<32.4% of patients) to Q4 (>44.5%). Readmission rates were highest in the lowest quartile of “early” follow-up (Q1: 23.3%; Q2: 20.5%; Q3: 20.5%; Q4: 20.5%, P<0.001). No mortality difference was seen.
The study also examined whether the physician following the patient after discharge impacted the readmission rate for these same quartiles, comparing cardiologists to generalists and comparing the same physician at discharge and follow-up (defined as “continuity”) versus different physicians. Follow-up with continuity or a cardiologist did not reduce readmissions.
Interestingly, nearly all markers of quality were best in Q1 and Q2 hospitals, which had the lowest arrival rates to appointments, which might reflect patient-centered rather than hospital-centered issues.
Bottom line: Hospitals with low “early” follow-up appointment rates after discharge have a higher readmission rate, although causality is not established.
Citation: Hernandez AF, Greiner MA, Fonarow GC, et al. Relationship between early physician follow-up and 30-day readmission among Medicare beneficiaries hospitalized for heart failure. JAMA. 2010;303 (17):1716-1722.
Strict Heart Rate Control Is Not Necessary in Management of Chronic Atrial Fibrillation
Clinical question: Is lenient heart rate control inferior to strict heart rate control in preventing cardiovascular events in patients with chronic atrial fibrillation?
Background: Guidelines generally call for the use of medications to achieve strict heart rate control in the management of chronic atrial fibrillation, but the optimal level of heart rate control necessary to avoid cardiovascular events remains uncertain.
Study design: Prospectively randomized, noninferiority trial.
Setting: Thirty-three medical centers in the Netherlands.
Synopsis: The study looked at 614 patients with permanent atrial fibrillation; 311 patients were randomized to lenient control and 303 to strict control. Calcium channel blockers, beta-blockers, or digoxin were dose-adjusted to control heart rate below 110 beats per minute (bpm) in the lenient control group versus 80 bpm in the strict control group.
Thirty-eight patients (12.9%) in the lenient control group and 43 (14.9%) in the strict control group reached the primary composite outcome of significant cardiovascular events (death, heart failure, stroke, embolism, major bleeding, major arrhythmia, need for pacemaker, or severe drug adverse event). Although no statistical difference in the frequency of these events between groups was detected, the study was dramatically underpowered due to unanticipated low event rates.
Bottom line: Although the lenient control group had far fewer outpatient visits and a trend toward improved outcomes, no definite conclusion regarding the management of permanent atrial fibrillation can be drawn from this underpowered noninferiority trial.
Citation: Van Gelder IC, Groenveld HF, Crijns HJ, et al. Lenient versus strict rate control in patients with atrial fibrillation. N Engl J Med. 2010;362(15):1363-1373.
Pneumococcal Vaccine Does Not Reduce the Risk of Stroke or Myocardial Infarction
Clinical question: Does pneumococcal vaccination reduce the risk of acute myocardial infarction (MI) and stroke?
Background: Studies have demonstrated that influenza vaccination reduces the risk of cardiac and cerebrovascular events. A single study has shown similar outcomes for the pneumococcal vaccination, although the study was limited by confounders and selection bias.
Study design: Retrospective cohort.
Setting: Large HMO in California.
Synopsis: More than 84,000 men participating in the California Men’s Health Study (CMHS) and enrolled in the Kaiser Permanente health plan were categorized as unvaccinated or vaccinated with the pneumococcal vaccine. Vaccinated patients had 10.73 first MIs and 5.30 strokes per 1,000 person-years, compared with unvaccinated patients who incurred 6.07 MIs and 1.90 strokes per 1,000 unvaccinated person-years based on ICD-9 codes.
Even with propensity scoring to minimize selection bias, no clear evidence of benefit was observed. One significant limitation is that 80% of the unvaccinated patients were younger than 60 years old, whereas 74% of the vaccinated patients were 60 or older; this might represent selection bias that cannot be overcome with propensity scoring.
Bottom line: In a population of men older than age 45, pneumococcal vaccination does not appear to reduce the risk of acute MI or stroke.
Citation: Tseng HF, Slezak JM, Quinn VP, et al. Pneumococcal vaccination and risk of acute myocardial infarction and stroke in men. JAMA. 2010;303(17):1699-1706.
No Durable Mortality Benefit from Endovascular Repair of Enlarged Abdominal Aortic Aneurysm
Clinical question: What is the cost and mortality benefit of endovascular versus open repair of abdominal aneurysms?
Background: Previous studies demonstrated a 30-day mortality benefit using endovascular repair over open surgical repair of large abdominal aortic aneurysms. Limited longer-term data are available assessing the durability of these findings.
Study design: Randomized controlled trial.
Setting: Thirty-seven hospitals in the United Kingdom.
Synopsis: Researchers looked at 1,252 patients who were at least 60 years old with a large abdominal aortic aneurysm (>5.5 cm) on CT scan. The patients were randomized to open versus endovascular repair and followed for a median of six years postoperatively. An early, postoperative, all-cause mortality benefit was observed for endovascular repair (1.8%) compared with open repair (4.3%), but no benefit was seen after six months of follow-up, driven by secondary aneurysm ruptures with endovascular grafts. Graft-related complications in all time periods were higher in the endovascular repair group, highest from 0 to 6 months (nearly 50% of patients), and were associated with an increased cost.
Bottom line: Immediate postoperative mortality benefit of endovascular repair is not sustained for abdominal aortic aneurysm beyond six months postoperatively.
Citation: The United Kingdom EVAR trial investigators. Endovascular versus open repair of abdominal aortic aneurysm. N Engl J Med. 2010:362(20):1863-1870.
Financial Constraints Delay Presentation in Patients Suffering from Acute Myocardial Infarction
Clinical question: Does being underinsured or uninsured delay individuals from seeking treatment for emergency medical care?
Background: The number of underinsured or uninsured Americans is growing. Studies have shown that patients with financial concerns avoid routine preventive and chronic medical care; however, similar avoidance has not been defined clearly for patients seeking emergent care.
Study design: Prospective cohort study.
Setting: Twenty-four urban hospitals in the U.S. included in a multisite, acute myocardial infarction (AMI) registry.
Synopsis: Of the 3,721 patients enrolled in the AMI registry, 61.7% of the cohort was insured and without financial concerns that prevented them from seeking care. These patients were less likely to have delays in care related to AMI compared with patients who were insured with financial concerns (18.5% of the cohort; OR 1.22; 95% confidence interval [CI], 1.06-1.40) or uninsured (19.8%; OR 1.30; 95% CI, 1.12-1.51) in all time frames after symptom onset. Patients were less likely to undergo PCI or thrombolysis if the delay to presentation was more than six hours.
After adjustment for confounding factors, the authors concluded that uninsured and underinsured patients were likely to delay presentation to the hospital. Despite these findings, alternative etiologies for delays in care are likely to be more significant, as insurance considerations only account for an 8% difference between the well-insured group (39.3% delayed seeking care >6 hours) and the uninsured group (48.6%). These etiologies are ill-defined.
Bottom line: Underinsured or uninsured patients have a small but significant delay in seeking treatment for AMI due to financial concerns.
Citation: Smolderen KG, Spertus JA, Nallamothu BK, et al. Health care insurance, financial concerns in accessing care, and delays to hospital presentation in acute myocardial infarction. JAMA. 2010;303 (14):1392-1400.
Concurrent Use of PPIs and Clopidogrel Decrease Hospitalizations for Gastroduodenal Bleeding without Significant Increase in Adverse Cardiovascular Events
Clinical question: Does concomitant use of proton-pump inhibitors (PPIs) and clopidogrel affect the risks of hospitalizations for gastroduodenal bleeding and serious cardiovascular events?
Background: PPIs commonly are prescribed with clopidogrel to reduce the risk of serious gastroduodenal bleeding. Recent observational studies suggest that concurrent PPI and clopidogrel administration might increase the risk of cardiovascular events compared with clopidogrel alone.
Study design: Retrospective cohort.
Setting: Tennessee Medicaid program.
Synopsis: Researchers identified 20,596 patients hospitalized for acute MI, revascularization, or unstable angina, and prescribed clopidogrel. Of this cohort, 7,593 were initial concurrent PPI users—62% used pantoprazole and 9% used omeprazole. Hospitalizations for gastroduodenal bleeding were reduced by 50% (HR 0.50 [95% CI, 0.39-0.65]) in concurrent users of PPIs and clopidogrel, compared with nonusers of PPIs.
Concurrent use was not associated with a statistically significant increase in serious cardiovascular diseases (HR, 0.99 [95% CI, 0.82-1.19]), defined as acute MI, sudden cardiac death, nonfatal or fatal stroke, or other cardiovascular deaths.
Subgroup analyses of individual PPIs and patients undergoing percutaneous coronary interventions also showed no increased risk of serious cardiovascular events. This study could differ from previous observational studies because far fewer patients were on omeprazole, the most potent inhibitor of clopidogrel.
Bottom line: In patients treated with clopidogrel, PPI users had 50% fewer hospitalizations for gastroduodenal bleeding compared with nonusers. Concurrent use of clopidogrel and PPIs, most of which was pantoprazole, was not associated with a significant increase in serious cardiovascular events.
Citation: Ray WA, Murray KT, Griffin MR, et al. Outcomes with concurrent use of clopidogrel and proton-pump inhibitors. Ann Intern Med. 2010;152(6):337-345.
CTCA a Promising, Noninvasive Option in Evaluating Patients with Suspected Coronary Artery Disease
Clinical question: How does computed tomography coronary angiography (CTCA) compare to noninvasive stress testing for diagnosing coronary artery disease (CAD)?
Background: CTCA is a newer, noninvasive test that has a high diagnostic accuracy for CAD, but its clinical role in the evaluation of patients with chest symptoms is unclear.
Study design: Observational study.
Setting: Single academic center in the Netherlands.
Synopsis: Five hundred seventeen eligible patients were evaluated with stress testing and CTCA. The patients were classified as having a low (<20%), intermediate (20%-80%), or high (>80%) pretest probability of CAD based on the Duke clinical score. Using coronary angiography as the gold standard, stress-testing was found to be less accurate than CTCA in all of the patient groups. In patients with low and intermediate pretest probabilities, a negative CTCA had a post-test probability of 0% and 1%, respectively. On the other hand, patients with an intermediate pretest probability and a positive CTCA had a post-test probability of 94% (CI, 89%-97%). In patients with an initial high pretest probability, stress-testing and CTCA confirmed disease in most cases.
The results of this study suggest that CTCA is particularly useful in evaluating patients with an intermediate pretest probability.
Patients were ineligible in this study if they had acute coronary syndromes, previous coronary stent placement, coronary artery bypass surgery, or myocardial infarction. It is important to note that because anatomic lesions seen on imaging (CTCA and coronary angiography) are not always functionally significant, CTCA might have seemed more accurate and clinically useful than it actually is. The investigators also acknowledge that further studies are necessary before CTCA can be accepted as a first-line diagnostic test.
Bottom line: In patients with an intermediate pretest probability of CAD, a negative CTCA is valuable in excluding coronary artery disease, thereby reducing the need for invasive coronary angiography in this group.
Citation: Weustink AC, Mollet NR, Neefjes LA, et al. Diagnostic accuracy and clinical utility of noninvasive testing for coronary artery disease. Ann Intern Med. 2010;152(10):630-639. TH
PEDIATRIC HM LITerature
Neonatal Nonhemolytic Hyperbilirubinemia Not Associated with Long-Term Cognitive or Neuropsychiatric Disability

Clinical question: Is exposure to neonatal nonhemolytic hyperbilirubinemia associated with negative long-term cognitive effects?
Background: Guidelines for the treatment of neonatal hyperbilirubinemia focus on the prevention of rare but potentially devastating consequences: bilirubin encephalopathy and subsequent kernicterus. Small studies have raised concerns regarding the potential for long-term cognitive disability in infants exposed to severe hyperbilirubinemia without kernicterus. This association primarily has been noted in patients with severe hemolytic hyperbilirubinemia; the relationship in nonhemolytic cases is less clear.
Study design: Retrospective, population-based cohort study.
Setting: Fifth Military Conscription District of Denmark.
Synopsis: All 18-year-old male conscripts born from 1977 to 1983 had data extracted from a national discharge registry with respect to maximum total serum bilirubin (TSB-max) and other clinical details. Infants born <35 weeks or of multiple gestation, age >14 days at TSB-max, or with hemolytic disease were excluded. TSB-max was analyzed as a categorical and dichotomous variable. Data were then compared to a validated Danish intelligence test administered at military draft conscription and the presence of neuropsychiatric diagnoses.
Of those examined, 463 men exceeded the cutoff for TSB-max, compared with 12,718 controls. There were no significant differences between groups with respect to the presence of neuropsychiatric diagnoses or cognitive performance.
This study benefits from its population-based design and use of an inclusive national database. However, cognitive performance is notoriously difficult to study, owing to the numerous potential confounders, many of which could not be ascertained retrospectively from the registry. Additional limitations were that the Danish thresholds for phototherapy and exchange transfusion were 240 μmol/L and 340 μmol/L (or approximately 14 mg/dL and 20 mg/dL), respectively, and only 25 newborns were exposed to levels greater than 340 μmol/L.
Although no dose response association was noted between 240 μmol/L and 340 μmol/L, no conclusions may be drawn regarding significantly higher levels.
Bottom line: Neonatal nonhemolytic hyperbilirubinemia requiring phototherapy is unlikely to be associated with long-term cognitive or neuropsychiatric disability.
Citation: Ebbesen F, Ehrenstein V, Traeger M, Nielsen GL. Neonatal non-hemolytic hyperbilirubinemia: a prevalence study of adult neuropsychiatric disability and cognitive function in 463 male Danish conscripts. Arch Dis Child. 2010;95(8):583-587.
In This Edition
Literature at a Glance
A guide to this month’s studies
- Effect of early follow-up on readmission rates
- Heart rate control and outcomes in atrial fibrillation
- Pneumococcal vaccine to prevent stroke and MI
- Long-term outcomes of endovascular repair of AAA
- Insurance and outcomes in myocardial infarction
- Risk of gastrointestinal bleeding and cardiovascular outcomes with concurrent PPI and clopidogrel use
- CT in patients with suspected coronary artery disease
Reduced 30-Day Readmission Rate for Patients Discharged from Hospitals with Higher Rates of Early Follow-Up
Clinical question: Is early follow-up after discharge for heart failure associated with a reduction in readmission rates?
Background: Readmission for heart failure is very frequent and often unplanned. Early follow-up visits after discharge have been hypothesized to reduce readmissions but have been undefined.
Study design: Retrospective cohort study.
Setting: Patients with Medicare inpatient claims data linked to the OPTIMIZE-HF and GWTG-HF registries.
Synopsis: The study included 30,136 patients >65 years old with the principal discharge diagnosis of heart failure from 2003 to 2006. Hospitals were stratified into quartiles based upon the median arrival rate to “early” (within one week after discharge) follow-up appointments. Ranges of arrival rates to these appointments ranged from Quartile 1 (Q1) (<32.4% of patients) to Q4 (>44.5%). Readmission rates were highest in the lowest quartile of “early” follow-up (Q1: 23.3%; Q2: 20.5%; Q3: 20.5%; Q4: 20.5%, P<0.001). No mortality difference was seen.
The study also examined whether the physician following the patient after discharge impacted the readmission rate for these same quartiles, comparing cardiologists to generalists and comparing the same physician at discharge and follow-up (defined as “continuity”) versus different physicians. Follow-up with continuity or a cardiologist did not reduce readmissions.
Interestingly, nearly all markers of quality were best in Q1 and Q2 hospitals, which had the lowest arrival rates to appointments, which might reflect patient-centered rather than hospital-centered issues.
Bottom line: Hospitals with low “early” follow-up appointment rates after discharge have a higher readmission rate, although causality is not established.
Citation: Hernandez AF, Greiner MA, Fonarow GC, et al. Relationship between early physician follow-up and 30-day readmission among Medicare beneficiaries hospitalized for heart failure. JAMA. 2010;303 (17):1716-1722.
Strict Heart Rate Control Is Not Necessary in Management of Chronic Atrial Fibrillation
Clinical question: Is lenient heart rate control inferior to strict heart rate control in preventing cardiovascular events in patients with chronic atrial fibrillation?
Background: Guidelines generally call for the use of medications to achieve strict heart rate control in the management of chronic atrial fibrillation, but the optimal level of heart rate control necessary to avoid cardiovascular events remains uncertain.
Study design: Prospectively randomized, noninferiority trial.
Setting: Thirty-three medical centers in the Netherlands.
Synopsis: The study looked at 614 patients with permanent atrial fibrillation; 311 patients were randomized to lenient control and 303 to strict control. Calcium channel blockers, beta-blockers, or digoxin were dose-adjusted to control heart rate below 110 beats per minute (bpm) in the lenient control group versus 80 bpm in the strict control group.
Thirty-eight patients (12.9%) in the lenient control group and 43 (14.9%) in the strict control group reached the primary composite outcome of significant cardiovascular events (death, heart failure, stroke, embolism, major bleeding, major arrhythmia, need for pacemaker, or severe drug adverse event). Although no statistical difference in the frequency of these events between groups was detected, the study was dramatically underpowered due to unanticipated low event rates.
Bottom line: Although the lenient control group had far fewer outpatient visits and a trend toward improved outcomes, no definite conclusion regarding the management of permanent atrial fibrillation can be drawn from this underpowered noninferiority trial.
Citation: Van Gelder IC, Groenveld HF, Crijns HJ, et al. Lenient versus strict rate control in patients with atrial fibrillation. N Engl J Med. 2010;362(15):1363-1373.
Pneumococcal Vaccine Does Not Reduce the Risk of Stroke or Myocardial Infarction
Clinical question: Does pneumococcal vaccination reduce the risk of acute myocardial infarction (MI) and stroke?
Background: Studies have demonstrated that influenza vaccination reduces the risk of cardiac and cerebrovascular events. A single study has shown similar outcomes for the pneumococcal vaccination, although the study was limited by confounders and selection bias.
Study design: Retrospective cohort.
Setting: Large HMO in California.
Synopsis: More than 84,000 men participating in the California Men’s Health Study (CMHS) and enrolled in the Kaiser Permanente health plan were categorized as unvaccinated or vaccinated with the pneumococcal vaccine. Vaccinated patients had 10.73 first MIs and 5.30 strokes per 1,000 person-years, compared with unvaccinated patients who incurred 6.07 MIs and 1.90 strokes per 1,000 unvaccinated person-years based on ICD-9 codes.
Even with propensity scoring to minimize selection bias, no clear evidence of benefit was observed. One significant limitation is that 80% of the unvaccinated patients were younger than 60 years old, whereas 74% of the vaccinated patients were 60 or older; this might represent selection bias that cannot be overcome with propensity scoring.
Bottom line: In a population of men older than age 45, pneumococcal vaccination does not appear to reduce the risk of acute MI or stroke.
Citation: Tseng HF, Slezak JM, Quinn VP, et al. Pneumococcal vaccination and risk of acute myocardial infarction and stroke in men. JAMA. 2010;303(17):1699-1706.
No Durable Mortality Benefit from Endovascular Repair of Enlarged Abdominal Aortic Aneurysm
Clinical question: What is the cost and mortality benefit of endovascular versus open repair of abdominal aneurysms?
Background: Previous studies demonstrated a 30-day mortality benefit using endovascular repair over open surgical repair of large abdominal aortic aneurysms. Limited longer-term data are available assessing the durability of these findings.
Study design: Randomized controlled trial.
Setting: Thirty-seven hospitals in the United Kingdom.
Synopsis: Researchers looked at 1,252 patients who were at least 60 years old with a large abdominal aortic aneurysm (>5.5 cm) on CT scan. The patients were randomized to open versus endovascular repair and followed for a median of six years postoperatively. An early, postoperative, all-cause mortality benefit was observed for endovascular repair (1.8%) compared with open repair (4.3%), but no benefit was seen after six months of follow-up, driven by secondary aneurysm ruptures with endovascular grafts. Graft-related complications in all time periods were higher in the endovascular repair group, highest from 0 to 6 months (nearly 50% of patients), and were associated with an increased cost.
Bottom line: Immediate postoperative mortality benefit of endovascular repair is not sustained for abdominal aortic aneurysm beyond six months postoperatively.
Citation: The United Kingdom EVAR trial investigators. Endovascular versus open repair of abdominal aortic aneurysm. N Engl J Med. 2010:362(20):1863-1870.
Financial Constraints Delay Presentation in Patients Suffering from Acute Myocardial Infarction
Clinical question: Does being underinsured or uninsured delay individuals from seeking treatment for emergency medical care?
Background: The number of underinsured or uninsured Americans is growing. Studies have shown that patients with financial concerns avoid routine preventive and chronic medical care; however, similar avoidance has not been defined clearly for patients seeking emergent care.
Study design: Prospective cohort study.
Setting: Twenty-four urban hospitals in the U.S. included in a multisite, acute myocardial infarction (AMI) registry.
Synopsis: Of the 3,721 patients enrolled in the AMI registry, 61.7% of the cohort was insured and without financial concerns that prevented them from seeking care. These patients were less likely to have delays in care related to AMI compared with patients who were insured with financial concerns (18.5% of the cohort; OR 1.22; 95% confidence interval [CI], 1.06-1.40) or uninsured (19.8%; OR 1.30; 95% CI, 1.12-1.51) in all time frames after symptom onset. Patients were less likely to undergo PCI or thrombolysis if the delay to presentation was more than six hours.
After adjustment for confounding factors, the authors concluded that uninsured and underinsured patients were likely to delay presentation to the hospital. Despite these findings, alternative etiologies for delays in care are likely to be more significant, as insurance considerations only account for an 8% difference between the well-insured group (39.3% delayed seeking care >6 hours) and the uninsured group (48.6%). These etiologies are ill-defined.
Bottom line: Underinsured or uninsured patients have a small but significant delay in seeking treatment for AMI due to financial concerns.
Citation: Smolderen KG, Spertus JA, Nallamothu BK, et al. Health care insurance, financial concerns in accessing care, and delays to hospital presentation in acute myocardial infarction. JAMA. 2010;303 (14):1392-1400.
Concurrent Use of PPIs and Clopidogrel Decrease Hospitalizations for Gastroduodenal Bleeding without Significant Increase in Adverse Cardiovascular Events
Clinical question: Does concomitant use of proton-pump inhibitors (PPIs) and clopidogrel affect the risks of hospitalizations for gastroduodenal bleeding and serious cardiovascular events?
Background: PPIs commonly are prescribed with clopidogrel to reduce the risk of serious gastroduodenal bleeding. Recent observational studies suggest that concurrent PPI and clopidogrel administration might increase the risk of cardiovascular events compared with clopidogrel alone.
Study design: Retrospective cohort.
Setting: Tennessee Medicaid program.
Synopsis: Researchers identified 20,596 patients hospitalized for acute MI, revascularization, or unstable angina, and prescribed clopidogrel. Of this cohort, 7,593 were initial concurrent PPI users—62% used pantoprazole and 9% used omeprazole. Hospitalizations for gastroduodenal bleeding were reduced by 50% (HR 0.50 [95% CI, 0.39-0.65]) in concurrent users of PPIs and clopidogrel, compared with nonusers of PPIs.
Concurrent use was not associated with a statistically significant increase in serious cardiovascular diseases (HR, 0.99 [95% CI, 0.82-1.19]), defined as acute MI, sudden cardiac death, nonfatal or fatal stroke, or other cardiovascular deaths.
Subgroup analyses of individual PPIs and patients undergoing percutaneous coronary interventions also showed no increased risk of serious cardiovascular events. This study could differ from previous observational studies because far fewer patients were on omeprazole, the most potent inhibitor of clopidogrel.
Bottom line: In patients treated with clopidogrel, PPI users had 50% fewer hospitalizations for gastroduodenal bleeding compared with nonusers. Concurrent use of clopidogrel and PPIs, most of which was pantoprazole, was not associated with a significant increase in serious cardiovascular events.
Citation: Ray WA, Murray KT, Griffin MR, et al. Outcomes with concurrent use of clopidogrel and proton-pump inhibitors. Ann Intern Med. 2010;152(6):337-345.
CTCA a Promising, Noninvasive Option in Evaluating Patients with Suspected Coronary Artery Disease
Clinical question: How does computed tomography coronary angiography (CTCA) compare to noninvasive stress testing for diagnosing coronary artery disease (CAD)?
Background: CTCA is a newer, noninvasive test that has a high diagnostic accuracy for CAD, but its clinical role in the evaluation of patients with chest symptoms is unclear.
Study design: Observational study.
Setting: Single academic center in the Netherlands.
Synopsis: Five hundred seventeen eligible patients were evaluated with stress testing and CTCA. The patients were classified as having a low (<20%), intermediate (20%-80%), or high (>80%) pretest probability of CAD based on the Duke clinical score. Using coronary angiography as the gold standard, stress-testing was found to be less accurate than CTCA in all of the patient groups. In patients with low and intermediate pretest probabilities, a negative CTCA had a post-test probability of 0% and 1%, respectively. On the other hand, patients with an intermediate pretest probability and a positive CTCA had a post-test probability of 94% (CI, 89%-97%). In patients with an initial high pretest probability, stress-testing and CTCA confirmed disease in most cases.
The results of this study suggest that CTCA is particularly useful in evaluating patients with an intermediate pretest probability.
Patients were ineligible in this study if they had acute coronary syndromes, previous coronary stent placement, coronary artery bypass surgery, or myocardial infarction. It is important to note that because anatomic lesions seen on imaging (CTCA and coronary angiography) are not always functionally significant, CTCA might have seemed more accurate and clinically useful than it actually is. The investigators also acknowledge that further studies are necessary before CTCA can be accepted as a first-line diagnostic test.
Bottom line: In patients with an intermediate pretest probability of CAD, a negative CTCA is valuable in excluding coronary artery disease, thereby reducing the need for invasive coronary angiography in this group.
Citation: Weustink AC, Mollet NR, Neefjes LA, et al. Diagnostic accuracy and clinical utility of noninvasive testing for coronary artery disease. Ann Intern Med. 2010;152(10):630-639. TH
PEDIATRIC HM LITerature
Neonatal Nonhemolytic Hyperbilirubinemia Not Associated with Long-Term Cognitive or Neuropsychiatric Disability
Clinical question: Is exposure to neonatal nonhemolytic hyperbilirubinemia associated with negative long-term cognitive effects?
Background: Guidelines for the treatment of neonatal hyperbilirubinemia focus on the prevention of rare but potentially devastating consequences: bilirubin encephalopathy and subsequent kernicterus. Small studies have raised concerns regarding the potential for long-term cognitive disability in infants exposed to severe hyperbilirubinemia without kernicterus. This association primarily has been noted in patients with severe hemolytic hyperbilirubinemia; the relationship in nonhemolytic cases is less clear.
Study design: Retrospective, population-based cohort study.
Setting: Fifth Military Conscription District of Denmark.
Synopsis: All 18-year-old male conscripts born from 1977 to 1983 had data extracted from a national discharge registry with respect to maximum total serum bilirubin (TSB-max) and other clinical details. Infants born <35 weeks or of multiple gestation, age >14 days at TSB-max, or with hemolytic disease were excluded. TSB-max was analyzed as a categorical and dichotomous variable. Data were then compared to a validated Danish intelligence test administered at military draft conscription and the presence of neuropsychiatric diagnoses.
Of those examined, 463 men exceeded the cutoff for TSB-max, compared with 12,718 controls. There were no significant differences between groups with respect to the presence of neuropsychiatric diagnoses or cognitive performance.
This study benefits from its population-based design and use of an inclusive national database. However, cognitive performance is notoriously difficult to study, owing to the numerous potential confounders, many of which could not be ascertained retrospectively from the registry. Additional limitations were that the Danish thresholds for phototherapy and exchange transfusion were 240 μmol/L and 340 μmol/L (or approximately 14 mg/dL and 20 mg/dL), respectively, and only 25 newborns were exposed to levels greater than 340 μmol/L.
Although no dose response association was noted between 240 μmol/L and 340 μmol/L, no conclusions may be drawn regarding significantly higher levels.
Bottom line: Neonatal nonhemolytic hyperbilirubinemia requiring phototherapy is unlikely to be associated with long-term cognitive or neuropsychiatric disability.
Citation: Ebbesen F, Ehrenstein V, Traeger M, Nielsen GL. Neonatal non-hemolytic hyperbilirubinemia: a prevalence study of adult neuropsychiatric disability and cognitive function in 463 male Danish conscripts. Arch Dis Child. 2010;95(8):583-587.
In This Edition
Literature at a Glance
A guide to this month’s studies
- Effect of early follow-up on readmission rates
- Heart rate control and outcomes in atrial fibrillation
- Pneumococcal vaccine to prevent stroke and MI
- Long-term outcomes of endovascular repair of AAA
- Insurance and outcomes in myocardial infarction
- Risk of gastrointestinal bleeding and cardiovascular outcomes with concurrent PPI and clopidogrel use
- CT in patients with suspected coronary artery disease
Reduced 30-Day Readmission Rate for Patients Discharged from Hospitals with Higher Rates of Early Follow-Up
Clinical question: Is early follow-up after discharge for heart failure associated with a reduction in readmission rates?
Background: Readmission for heart failure is very frequent and often unplanned. Early follow-up visits after discharge have been hypothesized to reduce readmissions but have been undefined.
Study design: Retrospective cohort study.
Setting: Patients with Medicare inpatient claims data linked to the OPTIMIZE-HF and GWTG-HF registries.
Synopsis: The study included 30,136 patients >65 years old with the principal discharge diagnosis of heart failure from 2003 to 2006. Hospitals were stratified into quartiles based upon the median arrival rate to “early” (within one week after discharge) follow-up appointments. Ranges of arrival rates to these appointments ranged from Quartile 1 (Q1) (<32.4% of patients) to Q4 (>44.5%). Readmission rates were highest in the lowest quartile of “early” follow-up (Q1: 23.3%; Q2: 20.5%; Q3: 20.5%; Q4: 20.5%, P<0.001). No mortality difference was seen.
The study also examined whether the physician following the patient after discharge impacted the readmission rate for these same quartiles, comparing cardiologists to generalists and comparing the same physician at discharge and follow-up (defined as “continuity”) versus different physicians. Follow-up with continuity or a cardiologist did not reduce readmissions.
Interestingly, nearly all markers of quality were best in Q1 and Q2 hospitals, which had the lowest arrival rates to appointments, which might reflect patient-centered rather than hospital-centered issues.
Bottom line: Hospitals with low “early” follow-up appointment rates after discharge have a higher readmission rate, although causality is not established.
Citation: Hernandez AF, Greiner MA, Fonarow GC, et al. Relationship between early physician follow-up and 30-day readmission among Medicare beneficiaries hospitalized for heart failure. JAMA. 2010;303 (17):1716-1722.
Strict Heart Rate Control Is Not Necessary in Management of Chronic Atrial Fibrillation
Clinical question: Is lenient heart rate control inferior to strict heart rate control in preventing cardiovascular events in patients with chronic atrial fibrillation?
Background: Guidelines generally call for the use of medications to achieve strict heart rate control in the management of chronic atrial fibrillation, but the optimal level of heart rate control necessary to avoid cardiovascular events remains uncertain.
Study design: Prospectively randomized, noninferiority trial.
Setting: Thirty-three medical centers in the Netherlands.
Synopsis: The study looked at 614 patients with permanent atrial fibrillation; 311 patients were randomized to lenient control and 303 to strict control. Calcium channel blockers, beta-blockers, or digoxin were dose-adjusted to control heart rate below 110 beats per minute (bpm) in the lenient control group versus 80 bpm in the strict control group.
Thirty-eight patients (12.9%) in the lenient control group and 43 (14.9%) in the strict control group reached the primary composite outcome of significant cardiovascular events (death, heart failure, stroke, embolism, major bleeding, major arrhythmia, need for pacemaker, or severe drug adverse event). Although no statistical difference in the frequency of these events between groups was detected, the study was dramatically underpowered due to unanticipated low event rates.
Bottom line: Although the lenient control group had far fewer outpatient visits and a trend toward improved outcomes, no definite conclusion regarding the management of permanent atrial fibrillation can be drawn from this underpowered noninferiority trial.
Citation: Van Gelder IC, Groenveld HF, Crijns HJ, et al. Lenient versus strict rate control in patients with atrial fibrillation. N Engl J Med. 2010;362(15):1363-1373.
Pneumococcal Vaccine Does Not Reduce the Risk of Stroke or Myocardial Infarction
Clinical question: Does pneumococcal vaccination reduce the risk of acute myocardial infarction (MI) and stroke?
Background: Studies have demonstrated that influenza vaccination reduces the risk of cardiac and cerebrovascular events. A single study has shown similar outcomes for the pneumococcal vaccination, although the study was limited by confounders and selection bias.
Study design: Retrospective cohort.
Setting: Large HMO in California.
Synopsis: More than 84,000 men participating in the California Men’s Health Study (CMHS) and enrolled in the Kaiser Permanente health plan were categorized as unvaccinated or vaccinated with the pneumococcal vaccine. Vaccinated patients had 10.73 first MIs and 5.30 strokes per 1,000 person-years, compared with unvaccinated patients who incurred 6.07 MIs and 1.90 strokes per 1,000 unvaccinated person-years based on ICD-9 codes.
Even with propensity scoring to minimize selection bias, no clear evidence of benefit was observed. One significant limitation is that 80% of the unvaccinated patients were younger than 60 years old, whereas 74% of the vaccinated patients were 60 or older; this might represent selection bias that cannot be overcome with propensity scoring.
Bottom line: In a population of men older than age 45, pneumococcal vaccination does not appear to reduce the risk of acute MI or stroke.
Citation: Tseng HF, Slezak JM, Quinn VP, et al. Pneumococcal vaccination and risk of acute myocardial infarction and stroke in men. JAMA. 2010;303(17):1699-1706.
No Durable Mortality Benefit from Endovascular Repair of Enlarged Abdominal Aortic Aneurysm
Clinical question: What is the cost and mortality benefit of endovascular versus open repair of abdominal aneurysms?
Background: Previous studies demonstrated a 30-day mortality benefit using endovascular repair over open surgical repair of large abdominal aortic aneurysms. Limited longer-term data are available assessing the durability of these findings.
Study design: Randomized controlled trial.
Setting: Thirty-seven hospitals in the United Kingdom.
Synopsis: Researchers looked at 1,252 patients who were at least 60 years old with a large abdominal aortic aneurysm (>5.5 cm) on CT scan. The patients were randomized to open versus endovascular repair and followed for a median of six years postoperatively. An early, postoperative, all-cause mortality benefit was observed for endovascular repair (1.8%) compared with open repair (4.3%), but no benefit was seen after six months of follow-up, driven by secondary aneurysm ruptures with endovascular grafts. Graft-related complications in all time periods were higher in the endovascular repair group, highest from 0 to 6 months (nearly 50% of patients), and were associated with an increased cost.
Bottom line: Immediate postoperative mortality benefit of endovascular repair is not sustained for abdominal aortic aneurysm beyond six months postoperatively.
Citation: The United Kingdom EVAR trial investigators. Endovascular versus open repair of abdominal aortic aneurysm. N Engl J Med. 2010:362(20):1863-1870.
Financial Constraints Delay Presentation in Patients Suffering from Acute Myocardial Infarction
Clinical question: Does being underinsured or uninsured delay individuals from seeking treatment for emergency medical care?
Background: The number of underinsured or uninsured Americans is growing. Studies have shown that patients with financial concerns avoid routine preventive and chronic medical care; however, similar avoidance has not been defined clearly for patients seeking emergent care.
Study design: Prospective cohort study.
Setting: Twenty-four urban hospitals in the U.S. included in a multisite, acute myocardial infarction (AMI) registry.
Synopsis: Of the 3,721 patients enrolled in the AMI registry, 61.7% of the cohort was insured and without financial concerns that prevented them from seeking care. These patients were less likely to have delays in care related to AMI compared with patients who were insured with financial concerns (18.5% of the cohort; OR 1.22; 95% confidence interval [CI], 1.06-1.40) or uninsured (19.8%; OR 1.30; 95% CI, 1.12-1.51) in all time frames after symptom onset. Patients were less likely to undergo PCI or thrombolysis if the delay to presentation was more than six hours.
After adjustment for confounding factors, the authors concluded that uninsured and underinsured patients were likely to delay presentation to the hospital. Despite these findings, alternative etiologies for delays in care are likely to be more significant, as insurance considerations only account for an 8% difference between the well-insured group (39.3% delayed seeking care >6 hours) and the uninsured group (48.6%). These etiologies are ill-defined.
Bottom line: Underinsured or uninsured patients have a small but significant delay in seeking treatment for AMI due to financial concerns.
Citation: Smolderen KG, Spertus JA, Nallamothu BK, et al. Health care insurance, financial concerns in accessing care, and delays to hospital presentation in acute myocardial infarction. JAMA. 2010;303 (14):1392-1400.
Concurrent Use of PPIs and Clopidogrel Decrease Hospitalizations for Gastroduodenal Bleeding without Significant Increase in Adverse Cardiovascular Events
Clinical question: Does concomitant use of proton-pump inhibitors (PPIs) and clopidogrel affect the risks of hospitalizations for gastroduodenal bleeding and serious cardiovascular events?
Background: PPIs commonly are prescribed with clopidogrel to reduce the risk of serious gastroduodenal bleeding. Recent observational studies suggest that concurrent PPI and clopidogrel administration might increase the risk of cardiovascular events compared with clopidogrel alone.
Study design: Retrospective cohort.
Setting: Tennessee Medicaid program.
Synopsis: Researchers identified 20,596 patients hospitalized for acute MI, revascularization, or unstable angina, and prescribed clopidogrel. Of this cohort, 7,593 were initial concurrent PPI users—62% used pantoprazole and 9% used omeprazole. Hospitalizations for gastroduodenal bleeding were reduced by 50% (HR 0.50 [95% CI, 0.39-0.65]) in concurrent users of PPIs and clopidogrel, compared with nonusers of PPIs.
Concurrent use was not associated with a statistically significant increase in serious cardiovascular diseases (HR, 0.99 [95% CI, 0.82-1.19]), defined as acute MI, sudden cardiac death, nonfatal or fatal stroke, or other cardiovascular deaths.
Subgroup analyses of individual PPIs and patients undergoing percutaneous coronary interventions also showed no increased risk of serious cardiovascular events. This study could differ from previous observational studies because far fewer patients were on omeprazole, the most potent inhibitor of clopidogrel.
Bottom line: In patients treated with clopidogrel, PPI users had 50% fewer hospitalizations for gastroduodenal bleeding compared with nonusers. Concurrent use of clopidogrel and PPIs, most of which was pantoprazole, was not associated with a significant increase in serious cardiovascular events.
Citation: Ray WA, Murray KT, Griffin MR, et al. Outcomes with concurrent use of clopidogrel and proton-pump inhibitors. Ann Intern Med. 2010;152(6):337-345.
CTCA a Promising, Noninvasive Option in Evaluating Patients with Suspected Coronary Artery Disease
Clinical question: How does computed tomography coronary angiography (CTCA) compare to noninvasive stress testing for diagnosing coronary artery disease (CAD)?
Background: CTCA is a newer, noninvasive test that has a high diagnostic accuracy for CAD, but its clinical role in the evaluation of patients with chest symptoms is unclear.
Study design: Observational study.
Setting: Single academic center in the Netherlands.
Synopsis: Five hundred seventeen eligible patients were evaluated with stress testing and CTCA. The patients were classified as having a low (<20%), intermediate (20%-80%), or high (>80%) pretest probability of CAD based on the Duke clinical score. Using coronary angiography as the gold standard, stress-testing was found to be less accurate than CTCA in all of the patient groups. In patients with low and intermediate pretest probabilities, a negative CTCA had a post-test probability of 0% and 1%, respectively. On the other hand, patients with an intermediate pretest probability and a positive CTCA had a post-test probability of 94% (CI, 89%-97%). In patients with an initial high pretest probability, stress-testing and CTCA confirmed disease in most cases.
The results of this study suggest that CTCA is particularly useful in evaluating patients with an intermediate pretest probability.
Patients were ineligible in this study if they had acute coronary syndromes, previous coronary stent placement, coronary artery bypass surgery, or myocardial infarction. It is important to note that because anatomic lesions seen on imaging (CTCA and coronary angiography) are not always functionally significant, CTCA might have seemed more accurate and clinically useful than it actually is. The investigators also acknowledge that further studies are necessary before CTCA can be accepted as a first-line diagnostic test.
Bottom line: In patients with an intermediate pretest probability of CAD, a negative CTCA is valuable in excluding coronary artery disease, thereby reducing the need for invasive coronary angiography in this group.
Citation: Weustink AC, Mollet NR, Neefjes LA, et al. Diagnostic accuracy and clinical utility of noninvasive testing for coronary artery disease. Ann Intern Med. 2010;152(10):630-639. TH
PEDIATRIC HM LITerature
Neonatal Nonhemolytic Hyperbilirubinemia Not Associated with Long-Term Cognitive or Neuropsychiatric Disability
Clinical question: Is exposure to neonatal nonhemolytic hyperbilirubinemia associated with negative long-term cognitive effects?
Background: Guidelines for the treatment of neonatal hyperbilirubinemia focus on the prevention of rare but potentially devastating consequences: bilirubin encephalopathy and subsequent kernicterus. Small studies have raised concerns regarding the potential for long-term cognitive disability in infants exposed to severe hyperbilirubinemia without kernicterus. This association primarily has been noted in patients with severe hemolytic hyperbilirubinemia; the relationship in nonhemolytic cases is less clear.
Study design: Retrospective, population-based cohort study.
Setting: Fifth Military Conscription District of Denmark.
Synopsis: All 18-year-old male conscripts born from 1977 to 1983 had data extracted from a national discharge registry with respect to maximum total serum bilirubin (TSB-max) and other clinical details. Infants born <35 weeks or of multiple gestation, age >14 days at TSB-max, or with hemolytic disease were excluded. TSB-max was analyzed as a categorical and dichotomous variable. Data were then compared to a validated Danish intelligence test administered at military draft conscription and the presence of neuropsychiatric diagnoses.
Of those examined, 463 men exceeded the cutoff for TSB-max, compared with 12,718 controls. There were no significant differences between groups with respect to the presence of neuropsychiatric diagnoses or cognitive performance.
This study benefits from its population-based design and use of an inclusive national database. However, cognitive performance is notoriously difficult to study, owing to the numerous potential confounders, many of which could not be ascertained retrospectively from the registry. Additional limitations were that the Danish thresholds for phototherapy and exchange transfusion were 240 μmol/L and 340 μmol/L (or approximately 14 mg/dL and 20 mg/dL), respectively, and only 25 newborns were exposed to levels greater than 340 μmol/L.
Although no dose response association was noted between 240 μmol/L and 340 μmol/L, no conclusions may be drawn regarding significantly higher levels.
Bottom line: Neonatal nonhemolytic hyperbilirubinemia requiring phototherapy is unlikely to be associated with long-term cognitive or neuropsychiatric disability.
Citation: Ebbesen F, Ehrenstein V, Traeger M, Nielsen GL. Neonatal non-hemolytic hyperbilirubinemia: a prevalence study of adult neuropsychiatric disability and cognitive function in 463 male Danish conscripts. Arch Dis Child. 2010;95(8):583-587.
What Should I Do If I Get a Needlestick?
Case
While placing a central line, you sustain a needlestick. You’ve washed the area thoroughly with soap and water, but you are concerned about contracting a bloodborne pathogen. What is the risk of contracting such a pathogen, and what can be done to reduce this risk?
Overview
Needlestick injuries are a common occupational hazard in the hospital setting. According to the International Health Care Worker Safety Center (IHCWSC), approximately 295,000 hospital-based healthcare workers experience occupational percutaneous injuries annually. In 1991, Mangione et al surveyed internal-medicine house staff and found an annual incidence of 674 needlestick injuries per 1,000 participants.1 Other retrospective data estimate this risk to be as high as 839 per 1,000 healthcare workers annually.2 Evidence from the Centers for Disease Control and Prevention (CDC) in 2004 suggests that because these are only self-reported injuries, the annual incidence of such injuries is in fact much higher than the current estimates suggest.2,3,4

More than 20 bloodborne pathogens (see Table 1, right) might be transmitted from contaminated needles or sharps, including human immunodeficiency virus (HIV), hepatitis B virus (HBV), and hepatitis C virus (HCV). A quick and appropriate response to a needlestick injury can greatly decrease the risk of disease transmission following an occupational exposure to potentially infectious materials.
Review of the Data
After any needlestick injury, an affected healthcare worker should wash the area with soap and water immediately. There is no contraindication to using antiseptic solutions, but there is also no evidence to suggest that this reduces the rates of disease transmission.
As decisions for post-exposure prophylaxis often need to be made within hours, a healthcare worker should seek care in the facility areas responsible for managing occupational exposures. Healthcare providers should always be encouraged and supported to report all sharps-related injuries to such departments.
The source patient should be identified and evaluated for potentially transmissible diseases, including HIV, HBV, and HCV. If indicated, the source patient should then undergo appropriate serological testing, and any indicated antiviral prophylaxis should be initiated (see Table 2, p. 19).
Risk of Seroconversion
For all bloodborne pathogens, a needlestick injury carries a greater risk for transmission than other occupational exposures (e.g. mucous membrane exposure). If a needlestick injury occurs in the setting of an infected patient source, the risk of disease transmission varies for HIV, HBV, and HCV (see Table 3, p. 19). In general, risk for seroconversion is increased with a deep injury, an injury with a device visibly contaminated with the source patient’s blood, or an injury involving a needle placed in the source patient’s artery or vein.3,5,6
Human immunodeficiency virus. Contracting HIV after needlestick injury is rare. From 1981 to 2006, the CDC documented only 57 cases of HIV/AIDS in healthcare workers following occupational exposure and identified an additional “possible” 140 cases post-exposure.5,6 Of the 57 documented cases, 48 sustained a percutaneous injury.
Following needlestick injury involving a known HIV-positive source, the one-year risk of seroconversion has been estimated to be 0.3%.5,6 In 1997, Cardo and colleagues identified four factors associated with increased risk for seroconversion after a needlestick/sharps injury from a known positive-HIV source:
- Deep injury;
- Injury with a device visibly contaminated with the source patient’s blood;
- A procedure involving a needle placed in the source patient’s artery or vein; and
- Exposure to a source patient who died of AIDS in the two months following the occupational exposure.5
Hepatitis B virus. Wides-pread immunization of healthcare workers has led to a dramatic decline in occupationally acquired HBV. The CDC estimated that in 1985, approximately 12,500 new HBV infections occurred in healthcare workers.3 This estimate plummeted to approximately 500 new occupationally acquired HBV infections in 1997.3
Despite this, hospital-based healthcare personnel remain at risk for HBV transmission after a needlestick injury from a known positive patient source. Few studies have evaluated the occupational risk of HBV transmission after a needlestick injury. Buergler et al reported that following a needlestick injury involving a known HBV-positive source, the one-year risk of seroconversion was 0.76% to 7.35% for nonimmunized surgeons, and 0.23% to 2.28% for nonimmunized anesthesiologists.7
In the absence of post-exposure prophylaxis, an exposed healthcare worker has a 6% to 30% risk of becoming infected with HBV.3,8 The risk is greatest if the patient source is known to be hepatitis B e antigen-positive, a marker for greater disease infectivity. When given within one week of injury, post-exposure prophylaxis (PEP) with multiple doses of hepatitis B immune globulin (HBIG) provides an estimated 75% protection from transmission.
Healthcare workers who have received the hepatitis B vaccine and developed immunity have virtually no risk for infection.6,7
Hepatitis C virus. Prospective evaluation has demonstrated that the average risk of HCV transmission after percutaneous exposure to a known HCV-positive source is from 0% to 7%.3 The Italian Study Group on Occupational Risk of HIV and Other Bloodborne Infections evaluated HCV seroconversion within six months of a reported exposure with enzyme immunoassay and immunoblot assay. In this study, the authors found a seroconversion rate of 1.2%.9
Further, they suggested that HCV seroconversion only occurred from hollow-bore needles, as no seroconversions were noted in healthcare workers who sustained injuries with solid sharp objects.
Post-Exposure Management
The CDC does not recommend prophylaxis when source fluids make contact with intact skin. However, if a percutaneous occupational exposure has occurred, PEPs exist for HIV and HBV but not for HCV.3,6 If a source patient’s HIV, HBV, and HCV statuses are unknown, occupational-health personnel can interview the patient to evaluate his or her risks and initiate testing. Specific information about the time and nature of exposure should be documented.
When testing is indicated, it should be done following institutional and state-specific exposure-control policies and informed consent guidelines. In all situations, the decision to begin antiviral PEP should be carefully considered, weighing benefits of PEP versus the risks and toxicity of treatment.
Human immunodeficiency virus. If a source patient is known to be HIV-positive, has a positive rapid HIV test, or if HIV status cannot be quickly determined, PEP is indicated. Healthcare providers should be aware of rare cases in which the source patient initially tested HIV-seronegative but was subsequently found to have primary HIV infection.
Per 2004 CDC recommendations, PEP is indicated for all healthcare workers who sustain a percuanteous injury from a known HIV-positive source.3,8 For a less severe injury (e.g. solid needle or superficial injury), PEP with either a basic two-drug or three-drug regimen is indicated, depending on the source patient’s viral load.3,5,6,8
If the source patient has unknown HIV status, two-drug PEP is indicated based on the source patient’s HIV risk factors. In such patients, rapid HIV testing also is indicated to aid in determining the need for PEP. When the source HIV status is unknown, PEP is indicated in settings where exposure to HIV-infected persons is likely.
If PEP is indicated, it should be started as quickly as possible. The 2005 U.S. Public Health Service Recommendations for PEP recommend initiating two nucleosides for low-risk exposures and two nucleosides plus a boosted protease inhibitor for high-risk exposures.
Examples of commonly used dual nucleoside regimens are Zidovudine plus Lamivudine (coformulated as Combivir) or Tenofovir plus Emtricitabine (coformulated as Truvada). Current recommendations indicate that PEP should be continued for four weeks, with concurrent clinical and laboratory evaluation for drug toxicity.
Hepatitis B virus. Numerous prospective studies have evaluated the post-exposure effectiveness of HBIG. When administered within 24 hours of exposure, HBIG might offer immediate passive protection against HBV infection. Additionally, if initiated within one week of percutaneous injury with a known HBV-positive source, multiple doses of HGIB provide an estimated 75% protection from transmission.
Although the combination of HBIG and the hepatitis vaccine B series has not been evaluated as PEP in the occupational setting, evidence in the perinatal setting suggests this regimen is more effective than HBIG alone.3,6,8
Hepatitis C virus. No PEP exists for HCV, and current recommendations for post-exposure management focus on early identification and treatment of chronic disease. There are insufficient data for a treatment recommendation for patients with acute HCV infection with no evidence of disease; the appropriate dosing of such a regimen is unknown. Further, evidence suggests that treatment started early in the course of chronic infection could be just as effective and might eliminate the need to treat persons whose infection will spontaneously resolve.7
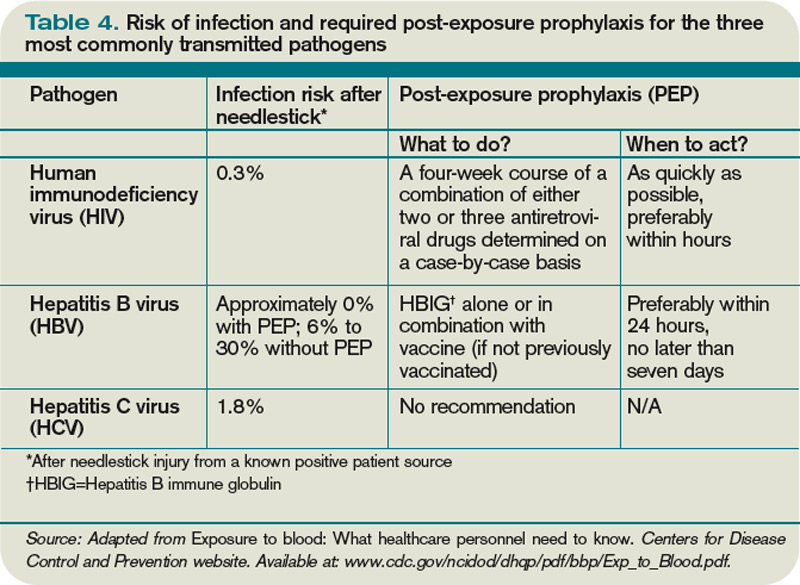
Back to the Case
Your needlestick occurred while using a hollow-bore needle to cannulate a source patient’s vein, placing you at higher risk for seroconversion. You immediately reported the exposure to the department of occupational health at your hospital. The source patient’s HIV, HBV, and HCV serological statuses were tested, and the patient was found to be HBV-positive. After appropriate counseling, you decide to receive HGIB prophylaxis to reduce your chances of becoming infected with HBV infection.
Bottom Line
Healthcare workers who suffer occupational needlestick injuries require immediate identification and attention to avoid transmission of such infectious diseases as HIV, HBV, and HCV. Source patients should undergo rapid serological testing to determine appropriate PEP. TH
Dr. Zehnder is a hospitalist in the Section of Hospital Medicine at the University of Colorado Denver.
References
- Mangione CM, Gerberding JL, Cummings, SR. Occupational exposure to HIV: Frequency and rates of underreporting of percutaneous and mucocutaneous exposures by medical housestaff. Am J Med. 1991;90(1):85-90.
- Lee JM, Botteman MF, Nicklasson L, et al. Needlestick injury in acute care nurses caring for patients with diabetes mellitus: a retrospective study. Curr Med Res Opinion. 2005;21(5):741-747.
- Workbook for designing, implementing, and evaluating a sharps injury prevention program. Centers for Disease Control and Prevention website. Available at: www.cdc.gov/sharpssafety/pdf/WorkbookComplete.pdf. Accessed Sept. 13, 2010.
- Lee JM, Botteman MF, Xanthakos N, Nicklasson L. Needlestick injuries in the United States. Epidemiologic, economic, and quality of life issues. AAOHN J. 2005;53(3):117-133.
- Cardo DM, Culver DH, Ciesielski CA, et al. A case-control study of HIV seroconversion in health care workers after percutaneous exposure. Centers for Disease Control and Prevention Needlestick Surveillance Group. N Engl J Med. 1997;337(21):1485-1490.
- Exposure to blood: What healthcare personnel need to know. CDC website. Available at: www.cdc.gov/ncidod /dhqp/pdf/bbp/Exp_to_Blood.pdf. Accessed Aug. 31, 2010.
- Buergler JM, Kim R, Thisted RA, Cohn SJ, Lichtor JL, Roizen MF. Risk of human immunodeficiency virus in surgeons, anesthesiologists, and medical students. Anesth Analg. 1992;75(1):118-124.
- Updated U.S. Public Health Service guidelines for the management of occupational exposures to HBV, HCV, and HIV and recommendations for postexposure prophylaxis. CDC website. Available at: www.cdc.gov/mmwr/preview/mmwrhtml/rr5011a1.htm. Accessed Aug. 31, 2010.
- Puro V, Petrosillo N, Ippolito G. Risk of hepatitis C seroconversion after occupational exposure in health care workers. Italian Study Group on Occupational Risk of HIV and Other Bloodborne Infections. Am J Infect Control. 1995;23(5):273-277.
Case
While placing a central line, you sustain a needlestick. You’ve washed the area thoroughly with soap and water, but you are concerned about contracting a bloodborne pathogen. What is the risk of contracting such a pathogen, and what can be done to reduce this risk?
Overview
Needlestick injuries are a common occupational hazard in the hospital setting. According to the International Health Care Worker Safety Center (IHCWSC), approximately 295,000 hospital-based healthcare workers experience occupational percutaneous injuries annually. In 1991, Mangione et al surveyed internal-medicine house staff and found an annual incidence of 674 needlestick injuries per 1,000 participants.1 Other retrospective data estimate this risk to be as high as 839 per 1,000 healthcare workers annually.2 Evidence from the Centers for Disease Control and Prevention (CDC) in 2004 suggests that because these are only self-reported injuries, the annual incidence of such injuries is in fact much higher than the current estimates suggest.2,3,4
More than 20 bloodborne pathogens (see Table 1, right) might be transmitted from contaminated needles or sharps, including human immunodeficiency virus (HIV), hepatitis B virus (HBV), and hepatitis C virus (HCV). A quick and appropriate response to a needlestick injury can greatly decrease the risk of disease transmission following an occupational exposure to potentially infectious materials.
Review of the Data
After any needlestick injury, an affected healthcare worker should wash the area with soap and water immediately. There is no contraindication to using antiseptic solutions, but there is also no evidence to suggest that this reduces the rates of disease transmission.
As decisions for post-exposure prophylaxis often need to be made within hours, a healthcare worker should seek care in the facility areas responsible for managing occupational exposures. Healthcare providers should always be encouraged and supported to report all sharps-related injuries to such departments.
The source patient should be identified and evaluated for potentially transmissible diseases, including HIV, HBV, and HCV. If indicated, the source patient should then undergo appropriate serological testing, and any indicated antiviral prophylaxis should be initiated (see Table 2, p. 19).
Risk of Seroconversion
For all bloodborne pathogens, a needlestick injury carries a greater risk for transmission than other occupational exposures (e.g. mucous membrane exposure). If a needlestick injury occurs in the setting of an infected patient source, the risk of disease transmission varies for HIV, HBV, and HCV (see Table 3, p. 19). In general, risk for seroconversion is increased with a deep injury, an injury with a device visibly contaminated with the source patient’s blood, or an injury involving a needle placed in the source patient’s artery or vein.3,5,6
Human immunodeficiency virus. Contracting HIV after needlestick injury is rare. From 1981 to 2006, the CDC documented only 57 cases of HIV/AIDS in healthcare workers following occupational exposure and identified an additional “possible” 140 cases post-exposure.5,6 Of the 57 documented cases, 48 sustained a percutaneous injury.
Following needlestick injury involving a known HIV-positive source, the one-year risk of seroconversion has been estimated to be 0.3%.5,6 In 1997, Cardo and colleagues identified four factors associated with increased risk for seroconversion after a needlestick/sharps injury from a known positive-HIV source:
- Deep injury;
- Injury with a device visibly contaminated with the source patient’s blood;
- A procedure involving a needle placed in the source patient’s artery or vein; and
- Exposure to a source patient who died of AIDS in the two months following the occupational exposure.5
Hepatitis B virus. Wides-pread immunization of healthcare workers has led to a dramatic decline in occupationally acquired HBV. The CDC estimated that in 1985, approximately 12,500 new HBV infections occurred in healthcare workers.3 This estimate plummeted to approximately 500 new occupationally acquired HBV infections in 1997.3
Despite this, hospital-based healthcare personnel remain at risk for HBV transmission after a needlestick injury from a known positive patient source. Few studies have evaluated the occupational risk of HBV transmission after a needlestick injury. Buergler et al reported that following a needlestick injury involving a known HBV-positive source, the one-year risk of seroconversion was 0.76% to 7.35% for nonimmunized surgeons, and 0.23% to 2.28% for nonimmunized anesthesiologists.7
In the absence of post-exposure prophylaxis, an exposed healthcare worker has a 6% to 30% risk of becoming infected with HBV.3,8 The risk is greatest if the patient source is known to be hepatitis B e antigen-positive, a marker for greater disease infectivity. When given within one week of injury, post-exposure prophylaxis (PEP) with multiple doses of hepatitis B immune globulin (HBIG) provides an estimated 75% protection from transmission.
Healthcare workers who have received the hepatitis B vaccine and developed immunity have virtually no risk for infection.6,7
Hepatitis C virus. Prospective evaluation has demonstrated that the average risk of HCV transmission after percutaneous exposure to a known HCV-positive source is from 0% to 7%.3 The Italian Study Group on Occupational Risk of HIV and Other Bloodborne Infections evaluated HCV seroconversion within six months of a reported exposure with enzyme immunoassay and immunoblot assay. In this study, the authors found a seroconversion rate of 1.2%.9
Further, they suggested that HCV seroconversion only occurred from hollow-bore needles, as no seroconversions were noted in healthcare workers who sustained injuries with solid sharp objects.
Post-Exposure Management
The CDC does not recommend prophylaxis when source fluids make contact with intact skin. However, if a percutaneous occupational exposure has occurred, PEPs exist for HIV and HBV but not for HCV.3,6 If a source patient’s HIV, HBV, and HCV statuses are unknown, occupational-health personnel can interview the patient to evaluate his or her risks and initiate testing. Specific information about the time and nature of exposure should be documented.
When testing is indicated, it should be done following institutional and state-specific exposure-control policies and informed consent guidelines. In all situations, the decision to begin antiviral PEP should be carefully considered, weighing benefits of PEP versus the risks and toxicity of treatment.
Human immunodeficiency virus. If a source patient is known to be HIV-positive, has a positive rapid HIV test, or if HIV status cannot be quickly determined, PEP is indicated. Healthcare providers should be aware of rare cases in which the source patient initially tested HIV-seronegative but was subsequently found to have primary HIV infection.
Per 2004 CDC recommendations, PEP is indicated for all healthcare workers who sustain a percuanteous injury from a known HIV-positive source.3,8 For a less severe injury (e.g. solid needle or superficial injury), PEP with either a basic two-drug or three-drug regimen is indicated, depending on the source patient’s viral load.3,5,6,8
If the source patient has unknown HIV status, two-drug PEP is indicated based on the source patient’s HIV risk factors. In such patients, rapid HIV testing also is indicated to aid in determining the need for PEP. When the source HIV status is unknown, PEP is indicated in settings where exposure to HIV-infected persons is likely.
If PEP is indicated, it should be started as quickly as possible. The 2005 U.S. Public Health Service Recommendations for PEP recommend initiating two nucleosides for low-risk exposures and two nucleosides plus a boosted protease inhibitor for high-risk exposures.
Examples of commonly used dual nucleoside regimens are Zidovudine plus Lamivudine (coformulated as Combivir) or Tenofovir plus Emtricitabine (coformulated as Truvada). Current recommendations indicate that PEP should be continued for four weeks, with concurrent clinical and laboratory evaluation for drug toxicity.
Hepatitis B virus. Numerous prospective studies have evaluated the post-exposure effectiveness of HBIG. When administered within 24 hours of exposure, HBIG might offer immediate passive protection against HBV infection. Additionally, if initiated within one week of percutaneous injury with a known HBV-positive source, multiple doses of HGIB provide an estimated 75% protection from transmission.
Although the combination of HBIG and the hepatitis vaccine B series has not been evaluated as PEP in the occupational setting, evidence in the perinatal setting suggests this regimen is more effective than HBIG alone.3,6,8
Hepatitis C virus. No PEP exists for HCV, and current recommendations for post-exposure management focus on early identification and treatment of chronic disease. There are insufficient data for a treatment recommendation for patients with acute HCV infection with no evidence of disease; the appropriate dosing of such a regimen is unknown. Further, evidence suggests that treatment started early in the course of chronic infection could be just as effective and might eliminate the need to treat persons whose infection will spontaneously resolve.7
Back to the Case
Your needlestick occurred while using a hollow-bore needle to cannulate a source patient’s vein, placing you at higher risk for seroconversion. You immediately reported the exposure to the department of occupational health at your hospital. The source patient’s HIV, HBV, and HCV serological statuses were tested, and the patient was found to be HBV-positive. After appropriate counseling, you decide to receive HGIB prophylaxis to reduce your chances of becoming infected with HBV infection.
Bottom Line
Healthcare workers who suffer occupational needlestick injuries require immediate identification and attention to avoid transmission of such infectious diseases as HIV, HBV, and HCV. Source patients should undergo rapid serological testing to determine appropriate PEP. TH
Dr. Zehnder is a hospitalist in the Section of Hospital Medicine at the University of Colorado Denver.
References
- Mangione CM, Gerberding JL, Cummings, SR. Occupational exposure to HIV: Frequency and rates of underreporting of percutaneous and mucocutaneous exposures by medical housestaff. Am J Med. 1991;90(1):85-90.
- Lee JM, Botteman MF, Nicklasson L, et al. Needlestick injury in acute care nurses caring for patients with diabetes mellitus: a retrospective study. Curr Med Res Opinion. 2005;21(5):741-747.
- Workbook for designing, implementing, and evaluating a sharps injury prevention program. Centers for Disease Control and Prevention website. Available at: www.cdc.gov/sharpssafety/pdf/WorkbookComplete.pdf. Accessed Sept. 13, 2010.
- Lee JM, Botteman MF, Xanthakos N, Nicklasson L. Needlestick injuries in the United States. Epidemiologic, economic, and quality of life issues. AAOHN J. 2005;53(3):117-133.
- Cardo DM, Culver DH, Ciesielski CA, et al. A case-control study of HIV seroconversion in health care workers after percutaneous exposure. Centers for Disease Control and Prevention Needlestick Surveillance Group. N Engl J Med. 1997;337(21):1485-1490.
- Exposure to blood: What healthcare personnel need to know. CDC website. Available at: www.cdc.gov/ncidod /dhqp/pdf/bbp/Exp_to_Blood.pdf. Accessed Aug. 31, 2010.
- Buergler JM, Kim R, Thisted RA, Cohn SJ, Lichtor JL, Roizen MF. Risk of human immunodeficiency virus in surgeons, anesthesiologists, and medical students. Anesth Analg. 1992;75(1):118-124.
- Updated U.S. Public Health Service guidelines for the management of occupational exposures to HBV, HCV, and HIV and recommendations for postexposure prophylaxis. CDC website. Available at: www.cdc.gov/mmwr/preview/mmwrhtml/rr5011a1.htm. Accessed Aug. 31, 2010.
- Puro V, Petrosillo N, Ippolito G. Risk of hepatitis C seroconversion after occupational exposure in health care workers. Italian Study Group on Occupational Risk of HIV and Other Bloodborne Infections. Am J Infect Control. 1995;23(5):273-277.
Case
While placing a central line, you sustain a needlestick. You’ve washed the area thoroughly with soap and water, but you are concerned about contracting a bloodborne pathogen. What is the risk of contracting such a pathogen, and what can be done to reduce this risk?
Overview
Needlestick injuries are a common occupational hazard in the hospital setting. According to the International Health Care Worker Safety Center (IHCWSC), approximately 295,000 hospital-based healthcare workers experience occupational percutaneous injuries annually. In 1991, Mangione et al surveyed internal-medicine house staff and found an annual incidence of 674 needlestick injuries per 1,000 participants.1 Other retrospective data estimate this risk to be as high as 839 per 1,000 healthcare workers annually.2 Evidence from the Centers for Disease Control and Prevention (CDC) in 2004 suggests that because these are only self-reported injuries, the annual incidence of such injuries is in fact much higher than the current estimates suggest.2,3,4
More than 20 bloodborne pathogens (see Table 1, right) might be transmitted from contaminated needles or sharps, including human immunodeficiency virus (HIV), hepatitis B virus (HBV), and hepatitis C virus (HCV). A quick and appropriate response to a needlestick injury can greatly decrease the risk of disease transmission following an occupational exposure to potentially infectious materials.
Review of the Data
After any needlestick injury, an affected healthcare worker should wash the area with soap and water immediately. There is no contraindication to using antiseptic solutions, but there is also no evidence to suggest that this reduces the rates of disease transmission.
As decisions for post-exposure prophylaxis often need to be made within hours, a healthcare worker should seek care in the facility areas responsible for managing occupational exposures. Healthcare providers should always be encouraged and supported to report all sharps-related injuries to such departments.
The source patient should be identified and evaluated for potentially transmissible diseases, including HIV, HBV, and HCV. If indicated, the source patient should then undergo appropriate serological testing, and any indicated antiviral prophylaxis should be initiated (see Table 2, p. 19).
Risk of Seroconversion
For all bloodborne pathogens, a needlestick injury carries a greater risk for transmission than other occupational exposures (e.g. mucous membrane exposure). If a needlestick injury occurs in the setting of an infected patient source, the risk of disease transmission varies for HIV, HBV, and HCV (see Table 3, p. 19). In general, risk for seroconversion is increased with a deep injury, an injury with a device visibly contaminated with the source patient’s blood, or an injury involving a needle placed in the source patient’s artery or vein.3,5,6
Human immunodeficiency virus. Contracting HIV after needlestick injury is rare. From 1981 to 2006, the CDC documented only 57 cases of HIV/AIDS in healthcare workers following occupational exposure and identified an additional “possible” 140 cases post-exposure.5,6 Of the 57 documented cases, 48 sustained a percutaneous injury.
Following needlestick injury involving a known HIV-positive source, the one-year risk of seroconversion has been estimated to be 0.3%.5,6 In 1997, Cardo and colleagues identified four factors associated with increased risk for seroconversion after a needlestick/sharps injury from a known positive-HIV source:
- Deep injury;
- Injury with a device visibly contaminated with the source patient’s blood;
- A procedure involving a needle placed in the source patient’s artery or vein; and
- Exposure to a source patient who died of AIDS in the two months following the occupational exposure.5
Hepatitis B virus. Wides-pread immunization of healthcare workers has led to a dramatic decline in occupationally acquired HBV. The CDC estimated that in 1985, approximately 12,500 new HBV infections occurred in healthcare workers.3 This estimate plummeted to approximately 500 new occupationally acquired HBV infections in 1997.3
Despite this, hospital-based healthcare personnel remain at risk for HBV transmission after a needlestick injury from a known positive patient source. Few studies have evaluated the occupational risk of HBV transmission after a needlestick injury. Buergler et al reported that following a needlestick injury involving a known HBV-positive source, the one-year risk of seroconversion was 0.76% to 7.35% for nonimmunized surgeons, and 0.23% to 2.28% for nonimmunized anesthesiologists.7
In the absence of post-exposure prophylaxis, an exposed healthcare worker has a 6% to 30% risk of becoming infected with HBV.3,8 The risk is greatest if the patient source is known to be hepatitis B e antigen-positive, a marker for greater disease infectivity. When given within one week of injury, post-exposure prophylaxis (PEP) with multiple doses of hepatitis B immune globulin (HBIG) provides an estimated 75% protection from transmission.
Healthcare workers who have received the hepatitis B vaccine and developed immunity have virtually no risk for infection.6,7
Hepatitis C virus. Prospective evaluation has demonstrated that the average risk of HCV transmission after percutaneous exposure to a known HCV-positive source is from 0% to 7%.3 The Italian Study Group on Occupational Risk of HIV and Other Bloodborne Infections evaluated HCV seroconversion within six months of a reported exposure with enzyme immunoassay and immunoblot assay. In this study, the authors found a seroconversion rate of 1.2%.9
Further, they suggested that HCV seroconversion only occurred from hollow-bore needles, as no seroconversions were noted in healthcare workers who sustained injuries with solid sharp objects.
Post-Exposure Management
The CDC does not recommend prophylaxis when source fluids make contact with intact skin. However, if a percutaneous occupational exposure has occurred, PEPs exist for HIV and HBV but not for HCV.3,6 If a source patient’s HIV, HBV, and HCV statuses are unknown, occupational-health personnel can interview the patient to evaluate his or her risks and initiate testing. Specific information about the time and nature of exposure should be documented.
When testing is indicated, it should be done following institutional and state-specific exposure-control policies and informed consent guidelines. In all situations, the decision to begin antiviral PEP should be carefully considered, weighing benefits of PEP versus the risks and toxicity of treatment.
Human immunodeficiency virus. If a source patient is known to be HIV-positive, has a positive rapid HIV test, or if HIV status cannot be quickly determined, PEP is indicated. Healthcare providers should be aware of rare cases in which the source patient initially tested HIV-seronegative but was subsequently found to have primary HIV infection.
Per 2004 CDC recommendations, PEP is indicated for all healthcare workers who sustain a percuanteous injury from a known HIV-positive source.3,8 For a less severe injury (e.g. solid needle or superficial injury), PEP with either a basic two-drug or three-drug regimen is indicated, depending on the source patient’s viral load.3,5,6,8
If the source patient has unknown HIV status, two-drug PEP is indicated based on the source patient’s HIV risk factors. In such patients, rapid HIV testing also is indicated to aid in determining the need for PEP. When the source HIV status is unknown, PEP is indicated in settings where exposure to HIV-infected persons is likely.
If PEP is indicated, it should be started as quickly as possible. The 2005 U.S. Public Health Service Recommendations for PEP recommend initiating two nucleosides for low-risk exposures and two nucleosides plus a boosted protease inhibitor for high-risk exposures.
Examples of commonly used dual nucleoside regimens are Zidovudine plus Lamivudine (coformulated as Combivir) or Tenofovir plus Emtricitabine (coformulated as Truvada). Current recommendations indicate that PEP should be continued for four weeks, with concurrent clinical and laboratory evaluation for drug toxicity.
Hepatitis B virus. Numerous prospective studies have evaluated the post-exposure effectiveness of HBIG. When administered within 24 hours of exposure, HBIG might offer immediate passive protection against HBV infection. Additionally, if initiated within one week of percutaneous injury with a known HBV-positive source, multiple doses of HGIB provide an estimated 75% protection from transmission.
Although the combination of HBIG and the hepatitis vaccine B series has not been evaluated as PEP in the occupational setting, evidence in the perinatal setting suggests this regimen is more effective than HBIG alone.3,6,8
Hepatitis C virus. No PEP exists for HCV, and current recommendations for post-exposure management focus on early identification and treatment of chronic disease. There are insufficient data for a treatment recommendation for patients with acute HCV infection with no evidence of disease; the appropriate dosing of such a regimen is unknown. Further, evidence suggests that treatment started early in the course of chronic infection could be just as effective and might eliminate the need to treat persons whose infection will spontaneously resolve.7
Back to the Case
Your needlestick occurred while using a hollow-bore needle to cannulate a source patient’s vein, placing you at higher risk for seroconversion. You immediately reported the exposure to the department of occupational health at your hospital. The source patient’s HIV, HBV, and HCV serological statuses were tested, and the patient was found to be HBV-positive. After appropriate counseling, you decide to receive HGIB prophylaxis to reduce your chances of becoming infected with HBV infection.
Bottom Line
Healthcare workers who suffer occupational needlestick injuries require immediate identification and attention to avoid transmission of such infectious diseases as HIV, HBV, and HCV. Source patients should undergo rapid serological testing to determine appropriate PEP. TH
Dr. Zehnder is a hospitalist in the Section of Hospital Medicine at the University of Colorado Denver.
References
- Mangione CM, Gerberding JL, Cummings, SR. Occupational exposure to HIV: Frequency and rates of underreporting of percutaneous and mucocutaneous exposures by medical housestaff. Am J Med. 1991;90(1):85-90.
- Lee JM, Botteman MF, Nicklasson L, et al. Needlestick injury in acute care nurses caring for patients with diabetes mellitus: a retrospective study. Curr Med Res Opinion. 2005;21(5):741-747.
- Workbook for designing, implementing, and evaluating a sharps injury prevention program. Centers for Disease Control and Prevention website. Available at: www.cdc.gov/sharpssafety/pdf/WorkbookComplete.pdf. Accessed Sept. 13, 2010.
- Lee JM, Botteman MF, Xanthakos N, Nicklasson L. Needlestick injuries in the United States. Epidemiologic, economic, and quality of life issues. AAOHN J. 2005;53(3):117-133.
- Cardo DM, Culver DH, Ciesielski CA, et al. A case-control study of HIV seroconversion in health care workers after percutaneous exposure. Centers for Disease Control and Prevention Needlestick Surveillance Group. N Engl J Med. 1997;337(21):1485-1490.
- Exposure to blood: What healthcare personnel need to know. CDC website. Available at: www.cdc.gov/ncidod /dhqp/pdf/bbp/Exp_to_Blood.pdf. Accessed Aug. 31, 2010.
- Buergler JM, Kim R, Thisted RA, Cohn SJ, Lichtor JL, Roizen MF. Risk of human immunodeficiency virus in surgeons, anesthesiologists, and medical students. Anesth Analg. 1992;75(1):118-124.
- Updated U.S. Public Health Service guidelines for the management of occupational exposures to HBV, HCV, and HIV and recommendations for postexposure prophylaxis. CDC website. Available at: www.cdc.gov/mmwr/preview/mmwrhtml/rr5011a1.htm. Accessed Aug. 31, 2010.
- Puro V, Petrosillo N, Ippolito G. Risk of hepatitis C seroconversion after occupational exposure in health care workers. Italian Study Group on Occupational Risk of HIV and Other Bloodborne Infections. Am J Infect Control. 1995;23(5):273-277.
Back to Basics
Let’s examine a documentation case for hospitalists providing daily care: A 65-year-old male patient is admitted with a left hip fracture. The patient also has hypertension and Type 2 diabetes, which might complicate his care. The orthopedic surgeon manages the patient’s perioperative course for the fracture while the hospitalist provides daily post-op care for hypertension and diabetes.
A common scenario is the hospitalist will provide concurrent care, along with a varying number of specialists, depending on the complexity of the patient’s presenting problems and existing comorbidities. Payors define concurrent care as more than one physician providing care to the same patient on the same date, or during the same hospitalization. Payors often consider two key principles before reimbursing concurrent care:
- Does the patient’s condition warrant more than one physician? and
- Are the services provided by each physician reasonable and necessary?1
When more than one medical condition exists and each physician actively treats the condition related to their expertise, each physician can demonstrate medical necessity. As in the above example, the orthopedic surgeon cares for the patient’s fracture while the hospitalist oversees diabetes and hypertension management. Claim submission follows the same logic. Report each subsequent hospital care code (99231-99233) with the corresponding diagnosis each physician primarily manages (i.e., orthopedic surgeon: 9923x with 820.8; hospitalist: 9923x with 250.00, 401.1).
When each physician assigns a different primary diagnosis code to the visit code, each is more likely to receive payment. Because each of these physicians are in different specialties and different provider groups, most payors do not require modifier 25 (separately identifiable E/M service on the same day as a procedure or other service) appended to the visit code. However, some managed-care payors require each physician to append modifier 25 to the concurrent E/M visit code (i.e., 99232-25) despite claim submission under different tax identification numbers.
Unfortunately, the physicians might not realize this until a claim rejection has been issued. Furthermore, payors might want to see the proof before rendering payment. In other words, they pay the first claim received and deny any subsequent claim in order to confirm medical necessity of the concurrent visit. Appeal denied such claims rejections with supporting documentation that distinguishes each physician visit, if possible. This assists the payors in understanding each physician’s contribution to care.
Reasons for Denial
Concurrent care services are more easily distinguished when separate diagnoses are reported with each service. Conversely, payors are likely to deny services that are hard to differentiate. Furthermore, payors frequently deny concurrent care services for the following reasons:
- Services exceed normal frequency or duration for a given condition without documented circumstances requiring additional care; or
- Services by one physician duplicate or overlap those of another provider without recognizable distinction.2
For example, a hospitalist might be involved in the post-op care of patients with fractures and no other identifiable chronic or acute conditions or complications. In these cases, the hospitalist’s continued involvement might constitute a facility policy (e.g., quality of care, risk reduction, etc.) rather than active clinical management. Claim submission could erroneously occur with each physician reporting 9923x for 820.8. Payors deny medically unnecessary services, or request refunds for inappropriate payments.
Hospitalists might attempt to negotiate other terms with the facility to account for the unpaid time and effort directed toward these types of cases.
Group Practice
Physicians in the same group practice with the same specialty designation must report, and are paid, as a single physician. Multiple visits to the same patient can occur on the same day by members of the same group (e.g., hospitalist A evaluates the patient in the morning, and hospitalist B reviews test results and the resulting course of treatment in the afternoon). However, only one subsequent hospital care service can be reported for the day.
The hospitalists should select the visit level representative of the combined services and submit one appropriately determined code (e.g., 99233), thereby capturing the medically necessary efforts of each physician. To complicate matters, the hospitalists must determine which name to report on the claim: the physician who provided the first encounter, or the physician who provided the most extensive or best-documented encounter.
Tracking productivity for these cases proves challenging. Some practices develop an internal accounting system and credit each physician for their medically necessary efforts (a labor-intensive task for administrators and physicians). TH
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center in Philadelphia. She is faculty for SHM’s inpatient coding course.
References
- Medicare Benefit Policy Manual: Concurrent Care. Chapter 15, Section 30.E. CMS website. Available at: www.cms.gov/manuals/Downloads/bp102c15.pdf. Accessed July 9, 2010.
- Medicare Claims Processing Manual: Physicians in Group Practice. Chapter 12, Section 30.6.5. CMS website. Available at: www.cms.gov/manuals/downloads/clm104c12.pdf. Accessed July 9, 2010.
- Pohlig, C. Daily care conundrums. The Hospitalist website. Available at: www.the-hospitalist.org/details/article/188735/Daily_Care_Conundrums_.html. Accessed July 9, 2010.
- Medicare Claims Processing Manual: Hospital Visits Same Day But by Different Physicians. Chapter 12, Section 30.6.9.C. CMS website. Available at: www.cms.gov/manuals/downloads/clm104c12.pdf. Accessed July 9, 2010.
- Abraham M, Beebe M, Dalton J, Evans D, Glenn R. Current Procedural Terminology Professional Edition. Chicago: American Medical Association Press; 2010:15.
Let’s examine a documentation case for hospitalists providing daily care: A 65-year-old male patient is admitted with a left hip fracture. The patient also has hypertension and Type 2 diabetes, which might complicate his care. The orthopedic surgeon manages the patient’s perioperative course for the fracture while the hospitalist provides daily post-op care for hypertension and diabetes.
A common scenario is the hospitalist will provide concurrent care, along with a varying number of specialists, depending on the complexity of the patient’s presenting problems and existing comorbidities. Payors define concurrent care as more than one physician providing care to the same patient on the same date, or during the same hospitalization. Payors often consider two key principles before reimbursing concurrent care:
- Does the patient’s condition warrant more than one physician? and
- Are the services provided by each physician reasonable and necessary?1
When more than one medical condition exists and each physician actively treats the condition related to their expertise, each physician can demonstrate medical necessity. As in the above example, the orthopedic surgeon cares for the patient’s fracture while the hospitalist oversees diabetes and hypertension management. Claim submission follows the same logic. Report each subsequent hospital care code (99231-99233) with the corresponding diagnosis each physician primarily manages (i.e., orthopedic surgeon: 9923x with 820.8; hospitalist: 9923x with 250.00, 401.1).
When each physician assigns a different primary diagnosis code to the visit code, each is more likely to receive payment. Because each of these physicians are in different specialties and different provider groups, most payors do not require modifier 25 (separately identifiable E/M service on the same day as a procedure or other service) appended to the visit code. However, some managed-care payors require each physician to append modifier 25 to the concurrent E/M visit code (i.e., 99232-25) despite claim submission under different tax identification numbers.
Unfortunately, the physicians might not realize this until a claim rejection has been issued. Furthermore, payors might want to see the proof before rendering payment. In other words, they pay the first claim received and deny any subsequent claim in order to confirm medical necessity of the concurrent visit. Appeal denied such claims rejections with supporting documentation that distinguishes each physician visit, if possible. This assists the payors in understanding each physician’s contribution to care.
Reasons for Denial
Concurrent care services are more easily distinguished when separate diagnoses are reported with each service. Conversely, payors are likely to deny services that are hard to differentiate. Furthermore, payors frequently deny concurrent care services for the following reasons:
- Services exceed normal frequency or duration for a given condition without documented circumstances requiring additional care; or
- Services by one physician duplicate or overlap those of another provider without recognizable distinction.2
For example, a hospitalist might be involved in the post-op care of patients with fractures and no other identifiable chronic or acute conditions or complications. In these cases, the hospitalist’s continued involvement might constitute a facility policy (e.g., quality of care, risk reduction, etc.) rather than active clinical management. Claim submission could erroneously occur with each physician reporting 9923x for 820.8. Payors deny medically unnecessary services, or request refunds for inappropriate payments.
Hospitalists might attempt to negotiate other terms with the facility to account for the unpaid time and effort directed toward these types of cases.
Group Practice
Physicians in the same group practice with the same specialty designation must report, and are paid, as a single physician. Multiple visits to the same patient can occur on the same day by members of the same group (e.g., hospitalist A evaluates the patient in the morning, and hospitalist B reviews test results and the resulting course of treatment in the afternoon). However, only one subsequent hospital care service can be reported for the day.
The hospitalists should select the visit level representative of the combined services and submit one appropriately determined code (e.g., 99233), thereby capturing the medically necessary efforts of each physician. To complicate matters, the hospitalists must determine which name to report on the claim: the physician who provided the first encounter, or the physician who provided the most extensive or best-documented encounter.
Tracking productivity for these cases proves challenging. Some practices develop an internal accounting system and credit each physician for their medically necessary efforts (a labor-intensive task for administrators and physicians). TH
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center in Philadelphia. She is faculty for SHM’s inpatient coding course.
References
- Medicare Benefit Policy Manual: Concurrent Care. Chapter 15, Section 30.E. CMS website. Available at: www.cms.gov/manuals/Downloads/bp102c15.pdf. Accessed July 9, 2010.
- Medicare Claims Processing Manual: Physicians in Group Practice. Chapter 12, Section 30.6.5. CMS website. Available at: www.cms.gov/manuals/downloads/clm104c12.pdf. Accessed July 9, 2010.
- Pohlig, C. Daily care conundrums. The Hospitalist website. Available at: www.the-hospitalist.org/details/article/188735/Daily_Care_Conundrums_.html. Accessed July 9, 2010.
- Medicare Claims Processing Manual: Hospital Visits Same Day But by Different Physicians. Chapter 12, Section 30.6.9.C. CMS website. Available at: www.cms.gov/manuals/downloads/clm104c12.pdf. Accessed July 9, 2010.
- Abraham M, Beebe M, Dalton J, Evans D, Glenn R. Current Procedural Terminology Professional Edition. Chicago: American Medical Association Press; 2010:15.
Let’s examine a documentation case for hospitalists providing daily care: A 65-year-old male patient is admitted with a left hip fracture. The patient also has hypertension and Type 2 diabetes, which might complicate his care. The orthopedic surgeon manages the patient’s perioperative course for the fracture while the hospitalist provides daily post-op care for hypertension and diabetes.
A common scenario is the hospitalist will provide concurrent care, along with a varying number of specialists, depending on the complexity of the patient’s presenting problems and existing comorbidities. Payors define concurrent care as more than one physician providing care to the same patient on the same date, or during the same hospitalization. Payors often consider two key principles before reimbursing concurrent care:
- Does the patient’s condition warrant more than one physician? and
- Are the services provided by each physician reasonable and necessary?1
When more than one medical condition exists and each physician actively treats the condition related to their expertise, each physician can demonstrate medical necessity. As in the above example, the orthopedic surgeon cares for the patient’s fracture while the hospitalist oversees diabetes and hypertension management. Claim submission follows the same logic. Report each subsequent hospital care code (99231-99233) with the corresponding diagnosis each physician primarily manages (i.e., orthopedic surgeon: 9923x with 820.8; hospitalist: 9923x with 250.00, 401.1).
When each physician assigns a different primary diagnosis code to the visit code, each is more likely to receive payment. Because each of these physicians are in different specialties and different provider groups, most payors do not require modifier 25 (separately identifiable E/M service on the same day as a procedure or other service) appended to the visit code. However, some managed-care payors require each physician to append modifier 25 to the concurrent E/M visit code (i.e., 99232-25) despite claim submission under different tax identification numbers.
Unfortunately, the physicians might not realize this until a claim rejection has been issued. Furthermore, payors might want to see the proof before rendering payment. In other words, they pay the first claim received and deny any subsequent claim in order to confirm medical necessity of the concurrent visit. Appeal denied such claims rejections with supporting documentation that distinguishes each physician visit, if possible. This assists the payors in understanding each physician’s contribution to care.
Reasons for Denial
Concurrent care services are more easily distinguished when separate diagnoses are reported with each service. Conversely, payors are likely to deny services that are hard to differentiate. Furthermore, payors frequently deny concurrent care services for the following reasons:
- Services exceed normal frequency or duration for a given condition without documented circumstances requiring additional care; or
- Services by one physician duplicate or overlap those of another provider without recognizable distinction.2
For example, a hospitalist might be involved in the post-op care of patients with fractures and no other identifiable chronic or acute conditions or complications. In these cases, the hospitalist’s continued involvement might constitute a facility policy (e.g., quality of care, risk reduction, etc.) rather than active clinical management. Claim submission could erroneously occur with each physician reporting 9923x for 820.8. Payors deny medically unnecessary services, or request refunds for inappropriate payments.
Hospitalists might attempt to negotiate other terms with the facility to account for the unpaid time and effort directed toward these types of cases.
Group Practice
Physicians in the same group practice with the same specialty designation must report, and are paid, as a single physician. Multiple visits to the same patient can occur on the same day by members of the same group (e.g., hospitalist A evaluates the patient in the morning, and hospitalist B reviews test results and the resulting course of treatment in the afternoon). However, only one subsequent hospital care service can be reported for the day.
The hospitalists should select the visit level representative of the combined services and submit one appropriately determined code (e.g., 99233), thereby capturing the medically necessary efforts of each physician. To complicate matters, the hospitalists must determine which name to report on the claim: the physician who provided the first encounter, or the physician who provided the most extensive or best-documented encounter.
Tracking productivity for these cases proves challenging. Some practices develop an internal accounting system and credit each physician for their medically necessary efforts (a labor-intensive task for administrators and physicians). TH
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center in Philadelphia. She is faculty for SHM’s inpatient coding course.
References
- Medicare Benefit Policy Manual: Concurrent Care. Chapter 15, Section 30.E. CMS website. Available at: www.cms.gov/manuals/Downloads/bp102c15.pdf. Accessed July 9, 2010.
- Medicare Claims Processing Manual: Physicians in Group Practice. Chapter 12, Section 30.6.5. CMS website. Available at: www.cms.gov/manuals/downloads/clm104c12.pdf. Accessed July 9, 2010.
- Pohlig, C. Daily care conundrums. The Hospitalist website. Available at: www.the-hospitalist.org/details/article/188735/Daily_Care_Conundrums_.html. Accessed July 9, 2010.
- Medicare Claims Processing Manual: Hospital Visits Same Day But by Different Physicians. Chapter 12, Section 30.6.9.C. CMS website. Available at: www.cms.gov/manuals/downloads/clm104c12.pdf. Accessed July 9, 2010.
- Abraham M, Beebe M, Dalton J, Evans D, Glenn R. Current Procedural Terminology Professional Edition. Chicago: American Medical Association Press; 2010:15.
Endangered Species?
The 1961 classic “The Ecology of Medical Care,” published in the New England Journal of Medicine, mapped out the broad features of the American healthcare landscape.1 For every 1,000 adult, the study suggested, 750 reported an illness, 250 consulted a doctor, and nine were admitted to a hospital in any given month. The subsequent arrival of Medicare and Medicaid fundamentally changed the U.S. healthcare system. And yet an updated version of the study, released in 2001, yielded surprisingly similar numbers, with 800 residents experiencing symptoms, 217 visiting a physician’s office, and eight being hospitalized in an average month.2
“It helps kind of put in perspective where the bulk of care really occurs,” says Ann O’Malley, MD, a senior researcher at the Washington, D.C.-based Center for Studying Health System Change. “It’s in outpatient provider offices, mostly primary-care provider offices.”
Dr. O’Malley and a host of other observers, however, are warning that the keystone members of this healthcare ecosystem are in serious trouble. As organizations such as SHM have likewise made clear, the accelerating shortage of general internists, family practitioners, and other PCPs has created sizable cracks in the supports of the entire healthcare infrastructure.
How big are the cracks? The number of medical school students pursuing a primary-care career has dropped by more than half since 1997, according to the American Academy of Family Physicians. And with the number of medical students entering the field unable to keep up with attrition, the remaining doctors are facing increasingly difficult working conditions. “Overloaded primary-care practices, whose doctors are aptly compared to hamsters on a treadmill, struggle to provide prompt access and high-quality care,” asserted a 2009 op-ed in the New England Journal of Medicine.3 The result: a vicious circle of decline leading to an anticipated shortfall of roughly 21,000 PCPs by 2015, according to the Association of American Medical Colleges.
Many primary-care providers had already stopped taking new patients when June’s Medicare reimbursement rate fiasco allowed the sustainable growth rate (SGR) formula’s mandated 21.2 percent rate cut to temporarily go into effect. Legislators eventually plugged the hole, but not before a new round of jitters seized the nation’s physicians, and reports proliferated throughout the summer about Medicare beneficiaries being unable to find a doctor willing to see them. The recession hasn’t helped, with more privately insured patients waiting longer to see their doctors to avoid copays, and with hospital emergency departments becoming de facto primary-care centers for those patients who have waited too long or have no other alternatives.
Uneven Challenges
Not only is there an acute shortage of primary-care physicians, Dr. O’Malley says, but there is also a distinctly uneven distribution throughout the country. For hospitalists, she says, the implications could be profound. “Hospitalists are increasingly going to be evaluated around issues such as avoiding hospital readmissions and [reducing] length of stay,” she says, “and if they want to improve both of those things, one of the keys is improving chronic care management in the outpatient setting, and improving follow-up post discharge.”
Both metrics will require the involvement of outpatient care providers, underscoring the importance of good communication and mutual respect. Despite the longstanding support of hospitalists for their primary-care counterparts, however, leaders are still being forced to address the perception that HM is somehow bad for what ails PCPs.
In a recent online article posted on the Becker’s Hospital Review website, SHM President Jeff Wiese, MD, SFHM, responded to one such criticism: that hospitalists make primary care less attractive for physicians. Hospitalists are not to blame for the decrease in interest, he asserted, but are actually complementary to the PCP role. And with millions more Americans about to be newly insured, that complementary relationship will be even more important. “It’s a tremendous waste of resources to use a primary-care provider for [a hospital visit]. We need to move into proactive mode, not reactive mode,” Dr. Wiese said. “More PCPs are going to need even more time in the clinic to handle the increased number of patients, and you lose the luxury to run back and forth between the clinic and the hospital. For those that can develop a trusting relationship with a hospitalist, you can work together to see more patients and provide more care.”
So what’s the real root of the problem? Money. According to recent surveys, PCPs earn about half the salary of dermatologists and an even smaller fraction of an average cardiologist’s pay. With medical school debt routinely reaching $200,000, Dr. O’Malley and other analysts say, many doctors simply can’t afford to go into primary care.
“It all comes down to payment, basically,” she says. “At present, our payment system for physician services and for medical procedures is quite skewed. It overcompensates for certain types of diagnostics and procedures, and it undercompensates for the more cognitive type of care that primary-care providers provide.”
The Road Ahead
Fortunately, some relief is trickling in. One measure strongly supported by SHM and included in the Affordable Care Act is a 10% Medicare reimbursement bonus for primary care delivered by qualified doctors, slated to begin next year. In June, U.S. Department of Health and Human Services Secretary Kathleen Sebelius announced a separate, $250 million initiative to boost the primary-care workforce. The money would help train PCPs by creating more residency slots, and offer new support for physician assistants, nurses, and nurse practitioners. Among the measures included in last year’s stimulus package, an expansion of the National Health Service Corps will provide more debt-relief opportunities for PCPs. And in mid-September, HHS tapped stimulus funds to award another $50.3 million for primary care training programs and loan repayment.
The Obama administration has claimed its combined actions “will support the training and development of more than 16,000 new primary-care providers over the next five years,” according to a June 16 HHS press release.
Observers say those measures alone are unlikely to be enough to stem the tide, however. “It’s definitely a step in the right direction,” Dr. O’Malley says of the Medicare bonus. “I don’t think it’s going to solve the primary-care workforce issue, because a 10% bonus, given how low primary-care physician salaries are compared to their specialist counterparts, is not going to be that much of an increase. Among the physicians that I’ve talked to and other healthcare providers, few feel that that’s sufficient enough to really encourage a lot of people to pursue primary care.”
Several other efforts now underway might help:
- Texas Tech University Health Sciences Center unveiled a new Family Medicine Accelerated Track program, which will allow primary-care medical students to complete a degree in three years. Certain students will receive a one-year scholarship, meaning that overall debt for some could be half that of the standard four-year program.
- Reid Hospital and Health Care Services in Richmond, Ind., successfully reversed a downward trend in primary-care referrals by forming its own nonprofit subsidiary corporation, Reid Physician Associates. The nonprofit will include about 50 employed outpatient providers by year’s end to complement the 233-bed hospital’s inpatient staff.
- Danville, Pa.-based Geisinger Health System has begun paying the salaries of extra nurses for both in-network and independent primary-care practices. The nurses manage patients’ chronic conditions, ensure that they are following prescribed treatments, and communicate with hospitalists and other providers about transitions of care. Although still in its early stages, the experiment suggests the nurses are helping to spot problems, prevent unnecessary hospitalizations, and save money.
The Geisinger experiment is among the first steps toward a patient-centered medical home model of care. An eventual Medicare-led expansion of such medical homes and accountable-care organizations, now in the early experimental stages, could provide even more direct support to PCPs. To be successful, though, Dr. O’Malley says the models will need to focus on paying providers fairly for the value they bring to the system. “Obviously, payment reform is what we need if we’re ever going to develop a sustainable primary-care workforce in this country,” she says. TH
Bryn Nelson is a freelance medical writer based in Seattle.
References
- White KL, Williams TF, Greenberg BG. The ecology of medical care. N Engl J Med. 1961;265:885-992.
- Green LA, Fryer GE Jr., Yawn BP, Lanier D, Dovey SM. The ecology of medical care revisited. N Engl J Med. 2001;344(26):2021-2025.
- Bodenheimer T, Grumbach K, Berenson RA. A lifeline for primary care. N Engl J Med. 2009;360(26):2693-2696.
The 1961 classic “The Ecology of Medical Care,” published in the New England Journal of Medicine, mapped out the broad features of the American healthcare landscape.1 For every 1,000 adult, the study suggested, 750 reported an illness, 250 consulted a doctor, and nine were admitted to a hospital in any given month. The subsequent arrival of Medicare and Medicaid fundamentally changed the U.S. healthcare system. And yet an updated version of the study, released in 2001, yielded surprisingly similar numbers, with 800 residents experiencing symptoms, 217 visiting a physician’s office, and eight being hospitalized in an average month.2
“It helps kind of put in perspective where the bulk of care really occurs,” says Ann O’Malley, MD, a senior researcher at the Washington, D.C.-based Center for Studying Health System Change. “It’s in outpatient provider offices, mostly primary-care provider offices.”
Dr. O’Malley and a host of other observers, however, are warning that the keystone members of this healthcare ecosystem are in serious trouble. As organizations such as SHM have likewise made clear, the accelerating shortage of general internists, family practitioners, and other PCPs has created sizable cracks in the supports of the entire healthcare infrastructure.
How big are the cracks? The number of medical school students pursuing a primary-care career has dropped by more than half since 1997, according to the American Academy of Family Physicians. And with the number of medical students entering the field unable to keep up with attrition, the remaining doctors are facing increasingly difficult working conditions. “Overloaded primary-care practices, whose doctors are aptly compared to hamsters on a treadmill, struggle to provide prompt access and high-quality care,” asserted a 2009 op-ed in the New England Journal of Medicine.3 The result: a vicious circle of decline leading to an anticipated shortfall of roughly 21,000 PCPs by 2015, according to the Association of American Medical Colleges.
Many primary-care providers had already stopped taking new patients when June’s Medicare reimbursement rate fiasco allowed the sustainable growth rate (SGR) formula’s mandated 21.2 percent rate cut to temporarily go into effect. Legislators eventually plugged the hole, but not before a new round of jitters seized the nation’s physicians, and reports proliferated throughout the summer about Medicare beneficiaries being unable to find a doctor willing to see them. The recession hasn’t helped, with more privately insured patients waiting longer to see their doctors to avoid copays, and with hospital emergency departments becoming de facto primary-care centers for those patients who have waited too long or have no other alternatives.
Uneven Challenges
Not only is there an acute shortage of primary-care physicians, Dr. O’Malley says, but there is also a distinctly uneven distribution throughout the country. For hospitalists, she says, the implications could be profound. “Hospitalists are increasingly going to be evaluated around issues such as avoiding hospital readmissions and [reducing] length of stay,” she says, “and if they want to improve both of those things, one of the keys is improving chronic care management in the outpatient setting, and improving follow-up post discharge.”
Both metrics will require the involvement of outpatient care providers, underscoring the importance of good communication and mutual respect. Despite the longstanding support of hospitalists for their primary-care counterparts, however, leaders are still being forced to address the perception that HM is somehow bad for what ails PCPs.
In a recent online article posted on the Becker’s Hospital Review website, SHM President Jeff Wiese, MD, SFHM, responded to one such criticism: that hospitalists make primary care less attractive for physicians. Hospitalists are not to blame for the decrease in interest, he asserted, but are actually complementary to the PCP role. And with millions more Americans about to be newly insured, that complementary relationship will be even more important. “It’s a tremendous waste of resources to use a primary-care provider for [a hospital visit]. We need to move into proactive mode, not reactive mode,” Dr. Wiese said. “More PCPs are going to need even more time in the clinic to handle the increased number of patients, and you lose the luxury to run back and forth between the clinic and the hospital. For those that can develop a trusting relationship with a hospitalist, you can work together to see more patients and provide more care.”
So what’s the real root of the problem? Money. According to recent surveys, PCPs earn about half the salary of dermatologists and an even smaller fraction of an average cardiologist’s pay. With medical school debt routinely reaching $200,000, Dr. O’Malley and other analysts say, many doctors simply can’t afford to go into primary care.
“It all comes down to payment, basically,” she says. “At present, our payment system for physician services and for medical procedures is quite skewed. It overcompensates for certain types of diagnostics and procedures, and it undercompensates for the more cognitive type of care that primary-care providers provide.”
The Road Ahead
Fortunately, some relief is trickling in. One measure strongly supported by SHM and included in the Affordable Care Act is a 10% Medicare reimbursement bonus for primary care delivered by qualified doctors, slated to begin next year. In June, U.S. Department of Health and Human Services Secretary Kathleen Sebelius announced a separate, $250 million initiative to boost the primary-care workforce. The money would help train PCPs by creating more residency slots, and offer new support for physician assistants, nurses, and nurse practitioners. Among the measures included in last year’s stimulus package, an expansion of the National Health Service Corps will provide more debt-relief opportunities for PCPs. And in mid-September, HHS tapped stimulus funds to award another $50.3 million for primary care training programs and loan repayment.
The Obama administration has claimed its combined actions “will support the training and development of more than 16,000 new primary-care providers over the next five years,” according to a June 16 HHS press release.
Observers say those measures alone are unlikely to be enough to stem the tide, however. “It’s definitely a step in the right direction,” Dr. O’Malley says of the Medicare bonus. “I don’t think it’s going to solve the primary-care workforce issue, because a 10% bonus, given how low primary-care physician salaries are compared to their specialist counterparts, is not going to be that much of an increase. Among the physicians that I’ve talked to and other healthcare providers, few feel that that’s sufficient enough to really encourage a lot of people to pursue primary care.”
Several other efforts now underway might help:
- Texas Tech University Health Sciences Center unveiled a new Family Medicine Accelerated Track program, which will allow primary-care medical students to complete a degree in three years. Certain students will receive a one-year scholarship, meaning that overall debt for some could be half that of the standard four-year program.
- Reid Hospital and Health Care Services in Richmond, Ind., successfully reversed a downward trend in primary-care referrals by forming its own nonprofit subsidiary corporation, Reid Physician Associates. The nonprofit will include about 50 employed outpatient providers by year’s end to complement the 233-bed hospital’s inpatient staff.
- Danville, Pa.-based Geisinger Health System has begun paying the salaries of extra nurses for both in-network and independent primary-care practices. The nurses manage patients’ chronic conditions, ensure that they are following prescribed treatments, and communicate with hospitalists and other providers about transitions of care. Although still in its early stages, the experiment suggests the nurses are helping to spot problems, prevent unnecessary hospitalizations, and save money.
The Geisinger experiment is among the first steps toward a patient-centered medical home model of care. An eventual Medicare-led expansion of such medical homes and accountable-care organizations, now in the early experimental stages, could provide even more direct support to PCPs. To be successful, though, Dr. O’Malley says the models will need to focus on paying providers fairly for the value they bring to the system. “Obviously, payment reform is what we need if we’re ever going to develop a sustainable primary-care workforce in this country,” she says. TH
Bryn Nelson is a freelance medical writer based in Seattle.
References
- White KL, Williams TF, Greenberg BG. The ecology of medical care. N Engl J Med. 1961;265:885-992.
- Green LA, Fryer GE Jr., Yawn BP, Lanier D, Dovey SM. The ecology of medical care revisited. N Engl J Med. 2001;344(26):2021-2025.
- Bodenheimer T, Grumbach K, Berenson RA. A lifeline for primary care. N Engl J Med. 2009;360(26):2693-2696.
The 1961 classic “The Ecology of Medical Care,” published in the New England Journal of Medicine, mapped out the broad features of the American healthcare landscape.1 For every 1,000 adult, the study suggested, 750 reported an illness, 250 consulted a doctor, and nine were admitted to a hospital in any given month. The subsequent arrival of Medicare and Medicaid fundamentally changed the U.S. healthcare system. And yet an updated version of the study, released in 2001, yielded surprisingly similar numbers, with 800 residents experiencing symptoms, 217 visiting a physician’s office, and eight being hospitalized in an average month.2
“It helps kind of put in perspective where the bulk of care really occurs,” says Ann O’Malley, MD, a senior researcher at the Washington, D.C.-based Center for Studying Health System Change. “It’s in outpatient provider offices, mostly primary-care provider offices.”
Dr. O’Malley and a host of other observers, however, are warning that the keystone members of this healthcare ecosystem are in serious trouble. As organizations such as SHM have likewise made clear, the accelerating shortage of general internists, family practitioners, and other PCPs has created sizable cracks in the supports of the entire healthcare infrastructure.
How big are the cracks? The number of medical school students pursuing a primary-care career has dropped by more than half since 1997, according to the American Academy of Family Physicians. And with the number of medical students entering the field unable to keep up with attrition, the remaining doctors are facing increasingly difficult working conditions. “Overloaded primary-care practices, whose doctors are aptly compared to hamsters on a treadmill, struggle to provide prompt access and high-quality care,” asserted a 2009 op-ed in the New England Journal of Medicine.3 The result: a vicious circle of decline leading to an anticipated shortfall of roughly 21,000 PCPs by 2015, according to the Association of American Medical Colleges.
Many primary-care providers had already stopped taking new patients when June’s Medicare reimbursement rate fiasco allowed the sustainable growth rate (SGR) formula’s mandated 21.2 percent rate cut to temporarily go into effect. Legislators eventually plugged the hole, but not before a new round of jitters seized the nation’s physicians, and reports proliferated throughout the summer about Medicare beneficiaries being unable to find a doctor willing to see them. The recession hasn’t helped, with more privately insured patients waiting longer to see their doctors to avoid copays, and with hospital emergency departments becoming de facto primary-care centers for those patients who have waited too long or have no other alternatives.
Uneven Challenges
Not only is there an acute shortage of primary-care physicians, Dr. O’Malley says, but there is also a distinctly uneven distribution throughout the country. For hospitalists, she says, the implications could be profound. “Hospitalists are increasingly going to be evaluated around issues such as avoiding hospital readmissions and [reducing] length of stay,” she says, “and if they want to improve both of those things, one of the keys is improving chronic care management in the outpatient setting, and improving follow-up post discharge.”
Both metrics will require the involvement of outpatient care providers, underscoring the importance of good communication and mutual respect. Despite the longstanding support of hospitalists for their primary-care counterparts, however, leaders are still being forced to address the perception that HM is somehow bad for what ails PCPs.
In a recent online article posted on the Becker’s Hospital Review website, SHM President Jeff Wiese, MD, SFHM, responded to one such criticism: that hospitalists make primary care less attractive for physicians. Hospitalists are not to blame for the decrease in interest, he asserted, but are actually complementary to the PCP role. And with millions more Americans about to be newly insured, that complementary relationship will be even more important. “It’s a tremendous waste of resources to use a primary-care provider for [a hospital visit]. We need to move into proactive mode, not reactive mode,” Dr. Wiese said. “More PCPs are going to need even more time in the clinic to handle the increased number of patients, and you lose the luxury to run back and forth between the clinic and the hospital. For those that can develop a trusting relationship with a hospitalist, you can work together to see more patients and provide more care.”
So what’s the real root of the problem? Money. According to recent surveys, PCPs earn about half the salary of dermatologists and an even smaller fraction of an average cardiologist’s pay. With medical school debt routinely reaching $200,000, Dr. O’Malley and other analysts say, many doctors simply can’t afford to go into primary care.
“It all comes down to payment, basically,” she says. “At present, our payment system for physician services and for medical procedures is quite skewed. It overcompensates for certain types of diagnostics and procedures, and it undercompensates for the more cognitive type of care that primary-care providers provide.”
The Road Ahead
Fortunately, some relief is trickling in. One measure strongly supported by SHM and included in the Affordable Care Act is a 10% Medicare reimbursement bonus for primary care delivered by qualified doctors, slated to begin next year. In June, U.S. Department of Health and Human Services Secretary Kathleen Sebelius announced a separate, $250 million initiative to boost the primary-care workforce. The money would help train PCPs by creating more residency slots, and offer new support for physician assistants, nurses, and nurse practitioners. Among the measures included in last year’s stimulus package, an expansion of the National Health Service Corps will provide more debt-relief opportunities for PCPs. And in mid-September, HHS tapped stimulus funds to award another $50.3 million for primary care training programs and loan repayment.
The Obama administration has claimed its combined actions “will support the training and development of more than 16,000 new primary-care providers over the next five years,” according to a June 16 HHS press release.
Observers say those measures alone are unlikely to be enough to stem the tide, however. “It’s definitely a step in the right direction,” Dr. O’Malley says of the Medicare bonus. “I don’t think it’s going to solve the primary-care workforce issue, because a 10% bonus, given how low primary-care physician salaries are compared to their specialist counterparts, is not going to be that much of an increase. Among the physicians that I’ve talked to and other healthcare providers, few feel that that’s sufficient enough to really encourage a lot of people to pursue primary care.”
Several other efforts now underway might help:
- Texas Tech University Health Sciences Center unveiled a new Family Medicine Accelerated Track program, which will allow primary-care medical students to complete a degree in three years. Certain students will receive a one-year scholarship, meaning that overall debt for some could be half that of the standard four-year program.
- Reid Hospital and Health Care Services in Richmond, Ind., successfully reversed a downward trend in primary-care referrals by forming its own nonprofit subsidiary corporation, Reid Physician Associates. The nonprofit will include about 50 employed outpatient providers by year’s end to complement the 233-bed hospital’s inpatient staff.
- Danville, Pa.-based Geisinger Health System has begun paying the salaries of extra nurses for both in-network and independent primary-care practices. The nurses manage patients’ chronic conditions, ensure that they are following prescribed treatments, and communicate with hospitalists and other providers about transitions of care. Although still in its early stages, the experiment suggests the nurses are helping to spot problems, prevent unnecessary hospitalizations, and save money.
The Geisinger experiment is among the first steps toward a patient-centered medical home model of care. An eventual Medicare-led expansion of such medical homes and accountable-care organizations, now in the early experimental stages, could provide even more direct support to PCPs. To be successful, though, Dr. O’Malley says the models will need to focus on paying providers fairly for the value they bring to the system. “Obviously, payment reform is what we need if we’re ever going to develop a sustainable primary-care workforce in this country,” she says. TH
Bryn Nelson is a freelance medical writer based in Seattle.
References
- White KL, Williams TF, Greenberg BG. The ecology of medical care. N Engl J Med. 1961;265:885-992.
- Green LA, Fryer GE Jr., Yawn BP, Lanier D, Dovey SM. The ecology of medical care revisited. N Engl J Med. 2001;344(26):2021-2025.
- Bodenheimer T, Grumbach K, Berenson RA. A lifeline for primary care. N Engl J Med. 2009;360(26):2693-2696.
Management Material
Eric Howell, MD, SFHM, is the first to admit how quickly it happened. Shortly after he became a hospitalist in 2000 at Johns Hopkins Bayview Medical Center in Baltimore, lower- and midlevel managers began to notice the quality of his daily clinical work. They reported their observations up the line, and soon Dr. Howell was rewarded with a small leadership role. He succeeded in that role, was given more responsibility, and in six short years he had worked his way up the management chain, becoming director of the medical center’s HM division.
“In hospital medicine, it’s fairly common to see young physicians stepping up into management,” says Patrick Cawley, MD, SFHM, a former SHM president who now directs the hospitalist program at the Medical University of South Carolina in Charleston and serves as medical director of the Medical University Hospital Authority. “The bottom line is they are there and they are getting noticed.”
On average, it takes about five years for a hospitalist to move into management; the average time for physicians in more established medical fields is 15 years or more, Dr. Cawley says. Part of the reason for the quick management rise in HM has to do with demographics. Because most hospitalists are younger, there is greater occasion for younger physicians who want to be in management to advance, says Timothy Keogh, PhD, an adjunct associate professor in the Department of Health Systems Management at Tulane University’s School of Public Health and Tropical Medicine in New Orleans, where he also directs the Master of Health Administration Program.
Another reason is that because hospitalists work in the hospital every day, they have innumerable opportunities to make an impression, Dr. Cawley says. They also know hospital culture, which gives them an advantage. “This is why hospitalists often get leadership positions,” he says. “Only by knowing the culture can you change the culture.”
Take the First Step
Although hospitalists are well positioned to assume management positions, it doesn’t mean an opportunity is going to fall into your lap. The best recipe for getting recognized—and promoted—is “doing the job you are currently doing really well,” Dr. Howell explains. “You have to do a good job on the basics.”
Often, physicians have their eye on a long-term goal and forget to focus on succeeding at their present work, Dr. Howell adds. That includes building relationships with lower- and mid-level managers like charge nurses, unit directors, and social work managers. That said, hospitalists who want to advance have to be proactive, Dr. Keogh says.
“Leadership is not only about hard work; leadership is about seeing the big picture and going above and beyond,” says Dr. Keogh, who is a member of the SHM Leadership Academy faculty.
The best place to show initiative is on a committee, and the easiest place to start is on a quality-improvement (QI) committee, Dr. Cawley says. If hospitalists are successful in that capacity, they can move on to peer review and credentials committees. From there, the next steps could be becoming first an officer, and then president, of the hospital’s medical staff.
“If you have the leadership skills, you can move up relatively quickly,” Dr. Cawley says. “Some people don’t need a lot of leadership training because they have it innately. But this isn’t true of the vast majority of people.”
Training Opportunities
The good news for the vast majority of hospitalists seeking a managerial role is that opportunities for training abound.
Fellowships are a good idea, but it’s critical that hospitalists interested in management choose the right one, Dr. Howell says. Select a fellowship program that focuses on areas important to the hospital—say, QI projects, patient-care initiatives, and system improvement.
Hospitalist Paul Grant, MD, considers the one-year HM fellowship he completed at the Cleveland Clinic Foundation an asset because he was able to gain expertise in perioperative medicine. The fellowship has served him well at the University of Michigan Health System in Ann Arbor, where he is director of perioperative medicine and consultative medicine.
“The fellowship really gives me an advantage,” says Dr. Grant, who notes he would like to assume a larger management role in the future.
Upward-thinking hospitalists should know something about budgeting, Dr. Keogh points out. Taking a budgetary course or two at a local community or technical college will not only provide a hospitalist the basics needed to understand and prepare budgets, but it also will demonstrate their willingness to master new skills that are important at the next level, he says.
An advanced degree, such as an MBA, a master’s degree in public health (MPH), or a master’s degree in medical management (MMM), can set hospitalists apart from their colleagues, Dr. Keogh says. These courses teach hospitalists how to excel at communication, how to implement change, and how to develop effective strategies.
Hospitalists can gain management-related skills from leadership courses tailored to physicians and healthcare professionals. SHM hosts two Leadership Academies per year (www.hospitalmedicine.org/leadership), and the American College of Physician Executives (www.acpe.org) and the American College of Healthcare Executives (www.ache.org) also offer leadership training, Dr. Cawley says.
Improve Weaknesses
You might want to consider communicating with upper-level managers (e.g., CMO, chief of staff, or vice president of medical affairs), but proceed cautiously, because there are right ways and wrong ways of reaching out. If you have a suggestion, ask to meet with an upper-level manager face to face to present the idea.
“Leadership is personal,” Dr. Cawley explains. “I think e-mails aren’t as effective as coming to sit down and converse.”
E-mail, however, can be used effectively to report on your project’s success. For example, Dr. Howell says he sent an e-mail about quality indicators to the president of the Johns Hopkins health system. When things went well—as they usually did—the president saw it. When things didn’t go as well, Dr. Howell put together a corrective action plan and e-mailed it along with the indicators to show he was aware of the situation and already had a plan in place to fix it.
“A lot of times [hospitalists] won’t be able to get to the next level and they’ll wonder why,” Dr. Cawley says. “They need to ask somebody they trust to give them an honest evaluation of what they’re doing well and what they may need to improve.”
Hospitalists must be open to constructive criticism, as honest assessments of your work aren’t going to be 100% complimentary. At times, they will be critical.
“Dealing with the feedback can be difficult, but ultimately it helps the hospitalist progress,” Dr. Cawley says. TH
Lisa Ryan is a freelance writer based in New Jersey.
Eric Howell, MD, SFHM, is the first to admit how quickly it happened. Shortly after he became a hospitalist in 2000 at Johns Hopkins Bayview Medical Center in Baltimore, lower- and midlevel managers began to notice the quality of his daily clinical work. They reported their observations up the line, and soon Dr. Howell was rewarded with a small leadership role. He succeeded in that role, was given more responsibility, and in six short years he had worked his way up the management chain, becoming director of the medical center’s HM division.
“In hospital medicine, it’s fairly common to see young physicians stepping up into management,” says Patrick Cawley, MD, SFHM, a former SHM president who now directs the hospitalist program at the Medical University of South Carolina in Charleston and serves as medical director of the Medical University Hospital Authority. “The bottom line is they are there and they are getting noticed.”
On average, it takes about five years for a hospitalist to move into management; the average time for physicians in more established medical fields is 15 years or more, Dr. Cawley says. Part of the reason for the quick management rise in HM has to do with demographics. Because most hospitalists are younger, there is greater occasion for younger physicians who want to be in management to advance, says Timothy Keogh, PhD, an adjunct associate professor in the Department of Health Systems Management at Tulane University’s School of Public Health and Tropical Medicine in New Orleans, where he also directs the Master of Health Administration Program.
Another reason is that because hospitalists work in the hospital every day, they have innumerable opportunities to make an impression, Dr. Cawley says. They also know hospital culture, which gives them an advantage. “This is why hospitalists often get leadership positions,” he says. “Only by knowing the culture can you change the culture.”
Take the First Step
Although hospitalists are well positioned to assume management positions, it doesn’t mean an opportunity is going to fall into your lap. The best recipe for getting recognized—and promoted—is “doing the job you are currently doing really well,” Dr. Howell explains. “You have to do a good job on the basics.”
Often, physicians have their eye on a long-term goal and forget to focus on succeeding at their present work, Dr. Howell adds. That includes building relationships with lower- and mid-level managers like charge nurses, unit directors, and social work managers. That said, hospitalists who want to advance have to be proactive, Dr. Keogh says.
“Leadership is not only about hard work; leadership is about seeing the big picture and going above and beyond,” says Dr. Keogh, who is a member of the SHM Leadership Academy faculty.
The best place to show initiative is on a committee, and the easiest place to start is on a quality-improvement (QI) committee, Dr. Cawley says. If hospitalists are successful in that capacity, they can move on to peer review and credentials committees. From there, the next steps could be becoming first an officer, and then president, of the hospital’s medical staff.
“If you have the leadership skills, you can move up relatively quickly,” Dr. Cawley says. “Some people don’t need a lot of leadership training because they have it innately. But this isn’t true of the vast majority of people.”
Training Opportunities
The good news for the vast majority of hospitalists seeking a managerial role is that opportunities for training abound.
Fellowships are a good idea, but it’s critical that hospitalists interested in management choose the right one, Dr. Howell says. Select a fellowship program that focuses on areas important to the hospital—say, QI projects, patient-care initiatives, and system improvement.
Hospitalist Paul Grant, MD, considers the one-year HM fellowship he completed at the Cleveland Clinic Foundation an asset because he was able to gain expertise in perioperative medicine. The fellowship has served him well at the University of Michigan Health System in Ann Arbor, where he is director of perioperative medicine and consultative medicine.
“The fellowship really gives me an advantage,” says Dr. Grant, who notes he would like to assume a larger management role in the future.
Upward-thinking hospitalists should know something about budgeting, Dr. Keogh points out. Taking a budgetary course or two at a local community or technical college will not only provide a hospitalist the basics needed to understand and prepare budgets, but it also will demonstrate their willingness to master new skills that are important at the next level, he says.
An advanced degree, such as an MBA, a master’s degree in public health (MPH), or a master’s degree in medical management (MMM), can set hospitalists apart from their colleagues, Dr. Keogh says. These courses teach hospitalists how to excel at communication, how to implement change, and how to develop effective strategies.
Hospitalists can gain management-related skills from leadership courses tailored to physicians and healthcare professionals. SHM hosts two Leadership Academies per year (www.hospitalmedicine.org/leadership), and the American College of Physician Executives (www.acpe.org) and the American College of Healthcare Executives (www.ache.org) also offer leadership training, Dr. Cawley says.
Improve Weaknesses
You might want to consider communicating with upper-level managers (e.g., CMO, chief of staff, or vice president of medical affairs), but proceed cautiously, because there are right ways and wrong ways of reaching out. If you have a suggestion, ask to meet with an upper-level manager face to face to present the idea.
“Leadership is personal,” Dr. Cawley explains. “I think e-mails aren’t as effective as coming to sit down and converse.”
E-mail, however, can be used effectively to report on your project’s success. For example, Dr. Howell says he sent an e-mail about quality indicators to the president of the Johns Hopkins health system. When things went well—as they usually did—the president saw it. When things didn’t go as well, Dr. Howell put together a corrective action plan and e-mailed it along with the indicators to show he was aware of the situation and already had a plan in place to fix it.
“A lot of times [hospitalists] won’t be able to get to the next level and they’ll wonder why,” Dr. Cawley says. “They need to ask somebody they trust to give them an honest evaluation of what they’re doing well and what they may need to improve.”
Hospitalists must be open to constructive criticism, as honest assessments of your work aren’t going to be 100% complimentary. At times, they will be critical.
“Dealing with the feedback can be difficult, but ultimately it helps the hospitalist progress,” Dr. Cawley says. TH
Lisa Ryan is a freelance writer based in New Jersey.
Eric Howell, MD, SFHM, is the first to admit how quickly it happened. Shortly after he became a hospitalist in 2000 at Johns Hopkins Bayview Medical Center in Baltimore, lower- and midlevel managers began to notice the quality of his daily clinical work. They reported their observations up the line, and soon Dr. Howell was rewarded with a small leadership role. He succeeded in that role, was given more responsibility, and in six short years he had worked his way up the management chain, becoming director of the medical center’s HM division.
“In hospital medicine, it’s fairly common to see young physicians stepping up into management,” says Patrick Cawley, MD, SFHM, a former SHM president who now directs the hospitalist program at the Medical University of South Carolina in Charleston and serves as medical director of the Medical University Hospital Authority. “The bottom line is they are there and they are getting noticed.”
On average, it takes about five years for a hospitalist to move into management; the average time for physicians in more established medical fields is 15 years or more, Dr. Cawley says. Part of the reason for the quick management rise in HM has to do with demographics. Because most hospitalists are younger, there is greater occasion for younger physicians who want to be in management to advance, says Timothy Keogh, PhD, an adjunct associate professor in the Department of Health Systems Management at Tulane University’s School of Public Health and Tropical Medicine in New Orleans, where he also directs the Master of Health Administration Program.
Another reason is that because hospitalists work in the hospital every day, they have innumerable opportunities to make an impression, Dr. Cawley says. They also know hospital culture, which gives them an advantage. “This is why hospitalists often get leadership positions,” he says. “Only by knowing the culture can you change the culture.”
Take the First Step
Although hospitalists are well positioned to assume management positions, it doesn’t mean an opportunity is going to fall into your lap. The best recipe for getting recognized—and promoted—is “doing the job you are currently doing really well,” Dr. Howell explains. “You have to do a good job on the basics.”
Often, physicians have their eye on a long-term goal and forget to focus on succeeding at their present work, Dr. Howell adds. That includes building relationships with lower- and mid-level managers like charge nurses, unit directors, and social work managers. That said, hospitalists who want to advance have to be proactive, Dr. Keogh says.
“Leadership is not only about hard work; leadership is about seeing the big picture and going above and beyond,” says Dr. Keogh, who is a member of the SHM Leadership Academy faculty.
The best place to show initiative is on a committee, and the easiest place to start is on a quality-improvement (QI) committee, Dr. Cawley says. If hospitalists are successful in that capacity, they can move on to peer review and credentials committees. From there, the next steps could be becoming first an officer, and then president, of the hospital’s medical staff.
“If you have the leadership skills, you can move up relatively quickly,” Dr. Cawley says. “Some people don’t need a lot of leadership training because they have it innately. But this isn’t true of the vast majority of people.”
Training Opportunities
The good news for the vast majority of hospitalists seeking a managerial role is that opportunities for training abound.
Fellowships are a good idea, but it’s critical that hospitalists interested in management choose the right one, Dr. Howell says. Select a fellowship program that focuses on areas important to the hospital—say, QI projects, patient-care initiatives, and system improvement.
Hospitalist Paul Grant, MD, considers the one-year HM fellowship he completed at the Cleveland Clinic Foundation an asset because he was able to gain expertise in perioperative medicine. The fellowship has served him well at the University of Michigan Health System in Ann Arbor, where he is director of perioperative medicine and consultative medicine.
“The fellowship really gives me an advantage,” says Dr. Grant, who notes he would like to assume a larger management role in the future.
Upward-thinking hospitalists should know something about budgeting, Dr. Keogh points out. Taking a budgetary course or two at a local community or technical college will not only provide a hospitalist the basics needed to understand and prepare budgets, but it also will demonstrate their willingness to master new skills that are important at the next level, he says.
An advanced degree, such as an MBA, a master’s degree in public health (MPH), or a master’s degree in medical management (MMM), can set hospitalists apart from their colleagues, Dr. Keogh says. These courses teach hospitalists how to excel at communication, how to implement change, and how to develop effective strategies.
Hospitalists can gain management-related skills from leadership courses tailored to physicians and healthcare professionals. SHM hosts two Leadership Academies per year (www.hospitalmedicine.org/leadership), and the American College of Physician Executives (www.acpe.org) and the American College of Healthcare Executives (www.ache.org) also offer leadership training, Dr. Cawley says.
Improve Weaknesses
You might want to consider communicating with upper-level managers (e.g., CMO, chief of staff, or vice president of medical affairs), but proceed cautiously, because there are right ways and wrong ways of reaching out. If you have a suggestion, ask to meet with an upper-level manager face to face to present the idea.
“Leadership is personal,” Dr. Cawley explains. “I think e-mails aren’t as effective as coming to sit down and converse.”
E-mail, however, can be used effectively to report on your project’s success. For example, Dr. Howell says he sent an e-mail about quality indicators to the president of the Johns Hopkins health system. When things went well—as they usually did—the president saw it. When things didn’t go as well, Dr. Howell put together a corrective action plan and e-mailed it along with the indicators to show he was aware of the situation and already had a plan in place to fix it.
“A lot of times [hospitalists] won’t be able to get to the next level and they’ll wonder why,” Dr. Cawley says. “They need to ask somebody they trust to give them an honest evaluation of what they’re doing well and what they may need to improve.”
Hospitalists must be open to constructive criticism, as honest assessments of your work aren’t going to be 100% complimentary. At times, they will be critical.
“Dealing with the feedback can be difficult, but ultimately it helps the hospitalist progress,” Dr. Cawley says. TH
Lisa Ryan is a freelance writer based in New Jersey.
Should hospitalists accept gifts from pharmaceutical, medical device, and biotech companies?

Recent discussions on conflicts of interest in medical publications underscore the significance of the important yet fragile relationship between the pharmaceutical industry and healthcare professionals. Among these is an examination of how academic departments can maintain a relationship with the industry.1 This study suggests that if appropriate boundaries are established between industry and academia, it is possible to collaborate. However, part of the policy in this investigation included “elimination of industry-supplied meals, gifts, and favors.”2
The Institute of Medicine’s “Conflict of Interest in Medical Research, Education, and Practice” included groundbreaking recommendations.3 Among them was a call for professionals to adopt a policy that prohibits “the acceptance of items of material value from pharmaceutical, medical device, and biotechnology companies, except in specified situations.”3
Our nation has been embroiled in a healthcare debate. Questions of right versus privilege, access versus affordability, and, of course, the perpetual political overlay have monopolized most of the discourse. Some contend that healthcare reform will redefine the current relationship between pharma and physicians . . . and not a moment too soon.
Lest there be ambiguity, though, the medical profession remains a noble vocation. This notwithstanding, until 2002, physicians freely participated in golf outings, received athletic tickets, and dined at five-star restaurants. But after the pharmaceutical industry smartly adopted voluntary guidelines that restrict gifting to doctors, we are left with drug samples and, of course, the “free lunch.” Certainly, pharma can claim it has made significant contributions to furthering medical education and research. Many could argue the tangible negative effects that would follow if the funding suddenly were absent.
But let’s not kid ourselves: There is a good reason the pharmaceutical industry spends more than $12 billion per year on marketing to doctors.4 In 2006, Rep. Henry Waxman (D-Calif.) said, “It is obvious that drug companies provide these free lunches so their sales reps can get the doctor’s ear and influence the prescribing practices.”2 Most doctors would never admit any such influence. It would be, however, disingenuous for any practicing physician to say there is none.
A randomized trial conducted by Adair et al concluded the “access to drug samples in clinic influences resident prescribing decisions. This could affect resident education and increase drug costs for patients.”5 An earlier study by Chew et al concluded “the availability of drug samples led physicians to dispense and subsequently prescribe drugs that differ from their preferred drug choice. Physicians most often report using drug samples to avoid cost to the patient.”6
Sure, local culture drives some prescribing practice, but one must be mindful of the reality that the pharmaceutical industry has significant influence. Plus, free drug samples help patients in the short term. Once the samples are gone, an expensive prescription for that new drug will follow. It’s another win for the industry and another loss for the patient and the healthcare system.
Many studies have shown that gifting exerts influence, even if doctors are unwilling to admit it. But patients and doctors alike would like to state with clarity of conscience that the medication prescribed is only based on clinical evidence, not influence. TH
Dr. Pyke is a hospitalist at Geisinger Wyoming Valley Medical Systems in Mountain Top, Pa.
References
- Dubovsky SL, Kaye DL, Pristach CA, DelRegno P, Pessar L, Stiles K. Can academic departments maintain industry relationships while promoting physician professionalism? Acad Med. 2010;85(1):68-73.
- Salganik MW, Hopkins JS, Rockoff JD. Medical salesmen prescribe lunches. Catering trade feeds on rep-doctor meals. The Baltimore Sun. July 29, 2006.
- Institute of Medicine Conflict of Interest in Medical Research, Education and Practice Full Recommendations. 4-28-09.
- Wolfe SM. Why do American drug companies spend more than $12 billion a year pushing drugs? Is it education or promotion? J Gen Intern Med. 2007;11(10):637-639.
- Adair RF, Holmgren LR. Do drug samples influence resident prescribing behavior? A randomized trial. Am J Med. 2005;118(8):881-884.
- Chew LD, O’Young TS, Hazlet TK, Bradley KA, Maynard C, Lessler DS. A physician survey of the effect of drug sample availability on physicians’ behavior. J Gen Intern Med. 2000;15(7):478-483.
Recent discussions on conflicts of interest in medical publications underscore the significance of the important yet fragile relationship between the pharmaceutical industry and healthcare professionals. Among these is an examination of how academic departments can maintain a relationship with the industry.1 This study suggests that if appropriate boundaries are established between industry and academia, it is possible to collaborate. However, part of the policy in this investigation included “elimination of industry-supplied meals, gifts, and favors.”2
The Institute of Medicine’s “Conflict of Interest in Medical Research, Education, and Practice” included groundbreaking recommendations.3 Among them was a call for professionals to adopt a policy that prohibits “the acceptance of items of material value from pharmaceutical, medical device, and biotechnology companies, except in specified situations.”3
Our nation has been embroiled in a healthcare debate. Questions of right versus privilege, access versus affordability, and, of course, the perpetual political overlay have monopolized most of the discourse. Some contend that healthcare reform will redefine the current relationship between pharma and physicians . . . and not a moment too soon.
Lest there be ambiguity, though, the medical profession remains a noble vocation. This notwithstanding, until 2002, physicians freely participated in golf outings, received athletic tickets, and dined at five-star restaurants. But after the pharmaceutical industry smartly adopted voluntary guidelines that restrict gifting to doctors, we are left with drug samples and, of course, the “free lunch.” Certainly, pharma can claim it has made significant contributions to furthering medical education and research. Many could argue the tangible negative effects that would follow if the funding suddenly were absent.
But let’s not kid ourselves: There is a good reason the pharmaceutical industry spends more than $12 billion per year on marketing to doctors.4 In 2006, Rep. Henry Waxman (D-Calif.) said, “It is obvious that drug companies provide these free lunches so their sales reps can get the doctor’s ear and influence the prescribing practices.”2 Most doctors would never admit any such influence. It would be, however, disingenuous for any practicing physician to say there is none.
A randomized trial conducted by Adair et al concluded the “access to drug samples in clinic influences resident prescribing decisions. This could affect resident education and increase drug costs for patients.”5 An earlier study by Chew et al concluded “the availability of drug samples led physicians to dispense and subsequently prescribe drugs that differ from their preferred drug choice. Physicians most often report using drug samples to avoid cost to the patient.”6
Sure, local culture drives some prescribing practice, but one must be mindful of the reality that the pharmaceutical industry has significant influence. Plus, free drug samples help patients in the short term. Once the samples are gone, an expensive prescription for that new drug will follow. It’s another win for the industry and another loss for the patient and the healthcare system.
Many studies have shown that gifting exerts influence, even if doctors are unwilling to admit it. But patients and doctors alike would like to state with clarity of conscience that the medication prescribed is only based on clinical evidence, not influence. TH
Dr. Pyke is a hospitalist at Geisinger Wyoming Valley Medical Systems in Mountain Top, Pa.
References
- Dubovsky SL, Kaye DL, Pristach CA, DelRegno P, Pessar L, Stiles K. Can academic departments maintain industry relationships while promoting physician professionalism? Acad Med. 2010;85(1):68-73.
- Salganik MW, Hopkins JS, Rockoff JD. Medical salesmen prescribe lunches. Catering trade feeds on rep-doctor meals. The Baltimore Sun. July 29, 2006.
- Institute of Medicine Conflict of Interest in Medical Research, Education and Practice Full Recommendations. 4-28-09.
- Wolfe SM. Why do American drug companies spend more than $12 billion a year pushing drugs? Is it education or promotion? J Gen Intern Med. 2007;11(10):637-639.
- Adair RF, Holmgren LR. Do drug samples influence resident prescribing behavior? A randomized trial. Am J Med. 2005;118(8):881-884.
- Chew LD, O’Young TS, Hazlet TK, Bradley KA, Maynard C, Lessler DS. A physician survey of the effect of drug sample availability on physicians’ behavior. J Gen Intern Med. 2000;15(7):478-483.
Recent discussions on conflicts of interest in medical publications underscore the significance of the important yet fragile relationship between the pharmaceutical industry and healthcare professionals. Among these is an examination of how academic departments can maintain a relationship with the industry.1 This study suggests that if appropriate boundaries are established between industry and academia, it is possible to collaborate. However, part of the policy in this investigation included “elimination of industry-supplied meals, gifts, and favors.”2
The Institute of Medicine’s “Conflict of Interest in Medical Research, Education, and Practice” included groundbreaking recommendations.3 Among them was a call for professionals to adopt a policy that prohibits “the acceptance of items of material value from pharmaceutical, medical device, and biotechnology companies, except in specified situations.”3
Our nation has been embroiled in a healthcare debate. Questions of right versus privilege, access versus affordability, and, of course, the perpetual political overlay have monopolized most of the discourse. Some contend that healthcare reform will redefine the current relationship between pharma and physicians . . . and not a moment too soon.
Lest there be ambiguity, though, the medical profession remains a noble vocation. This notwithstanding, until 2002, physicians freely participated in golf outings, received athletic tickets, and dined at five-star restaurants. But after the pharmaceutical industry smartly adopted voluntary guidelines that restrict gifting to doctors, we are left with drug samples and, of course, the “free lunch.” Certainly, pharma can claim it has made significant contributions to furthering medical education and research. Many could argue the tangible negative effects that would follow if the funding suddenly were absent.
But let’s not kid ourselves: There is a good reason the pharmaceutical industry spends more than $12 billion per year on marketing to doctors.4 In 2006, Rep. Henry Waxman (D-Calif.) said, “It is obvious that drug companies provide these free lunches so their sales reps can get the doctor’s ear and influence the prescribing practices.”2 Most doctors would never admit any such influence. It would be, however, disingenuous for any practicing physician to say there is none.
A randomized trial conducted by Adair et al concluded the “access to drug samples in clinic influences resident prescribing decisions. This could affect resident education and increase drug costs for patients.”5 An earlier study by Chew et al concluded “the availability of drug samples led physicians to dispense and subsequently prescribe drugs that differ from their preferred drug choice. Physicians most often report using drug samples to avoid cost to the patient.”6
Sure, local culture drives some prescribing practice, but one must be mindful of the reality that the pharmaceutical industry has significant influence. Plus, free drug samples help patients in the short term. Once the samples are gone, an expensive prescription for that new drug will follow. It’s another win for the industry and another loss for the patient and the healthcare system.
Many studies have shown that gifting exerts influence, even if doctors are unwilling to admit it. But patients and doctors alike would like to state with clarity of conscience that the medication prescribed is only based on clinical evidence, not influence. TH
Dr. Pyke is a hospitalist at Geisinger Wyoming Valley Medical Systems in Mountain Top, Pa.
References
- Dubovsky SL, Kaye DL, Pristach CA, DelRegno P, Pessar L, Stiles K. Can academic departments maintain industry relationships while promoting physician professionalism? Acad Med. 2010;85(1):68-73.
- Salganik MW, Hopkins JS, Rockoff JD. Medical salesmen prescribe lunches. Catering trade feeds on rep-doctor meals. The Baltimore Sun. July 29, 2006.
- Institute of Medicine Conflict of Interest in Medical Research, Education and Practice Full Recommendations. 4-28-09.
- Wolfe SM. Why do American drug companies spend more than $12 billion a year pushing drugs? Is it education or promotion? J Gen Intern Med. 2007;11(10):637-639.
- Adair RF, Holmgren LR. Do drug samples influence resident prescribing behavior? A randomized trial. Am J Med. 2005;118(8):881-884.
- Chew LD, O’Young TS, Hazlet TK, Bradley KA, Maynard C, Lessler DS. A physician survey of the effect of drug sample availability on physicians’ behavior. J Gen Intern Med. 2000;15(7):478-483.