User login
In metastatic NSCLC, better QoL outcomes tied to better outcomes
The authors, including Fabio Salomone of the University of Naples Federico II, department of clinical medicine and surgery, also observed trends toward an association between QoL improvement and PFS among patients treated with chemotherapy and immunotherapy.
The new research was presented during a poster session at European Lung Cancer Congress 2023.
“The findings of the study support the thesis that QoL and survival in patients with NSCLC are linked. Although this is documented in the literature, this study sums up the evidence of a large number of RCTs, and provides detail in the QoL/survival relationship by treatment type. The subgroup analysis by treatment type is a key strength of the study showing that the QoL/survival link is stronger and more reliable in target(ed) therapies,” George Kypriotakis, PhD, who was not involved with the study, said in an interview.
Combining efficacy and quality of life improvement is an important consideration in clinical practice. “It is important that clinicians provide therapies that are also palliative and improve QoL,” said Dr. Kypriotakis, assistant professor of behavioral sciences at University of Texas MD Anderson Cancer Center, Houston. He noted that the finding of a PFS benefit is a good indicator of overall benefit, which is important since OS outcomes require a larger number of patients and longer follow-up to determine.
“PFS can still be a valid surrogate for OS, especially when it is positively associated with QoL,” noted Dr. Kypriotakis.
The study included 81 trials. Sixteen of the studies investigated immunotherapy, 50 investigated targeted therapy, and 17 investigated chemotherapy regimens. Thirty-seven percent of the trials found an improvement in QoL in the treatment arm compared with the control arm, 59.3% found no difference between arms, and 3.7% found a worse QoL in the treatment arm. There was no statistically significant association between an improvement in OS and QoL among the trials (P = .368).
Improved QoL tied to improved PFS
The researchers found an association between improved QoL and improved PFS. Among 60 trials that showed improved PFS, 43.3% found a superior QoL in the treatment arm, 53.3% showed no difference, and 3.3% showed reduced QoL. Among 20 trials that found no improvement in PFS, 20% demonstrated an improved QoL, 75% found no change, and 5% showed worse QoL (P = .0473).
A subanalysis of 48 targeted therapy trials found a correlation between PFS and QoL improvement (P = .0196). Among 25 trials involving patients receiving epidermal growth factor receptor (EGFR) and anaplastic lymphoma kinase (ALK) inhibitors showing an improved PFS, 60% showed improved QoL, 36% showed no difference, and 4% showed worsening (P = .0077). Seven of these trials showed no PFS benefit and no change in QoL.
Industry sponsorship may affect QOL results
The researchers found potential evidence that industry sponsorship may lead to a spin on QoL outcomes. Among 51 trials that showed no QoL benefit associated with treatment, the description of the QoL outcome in 37 industry-sponsored was judged to be neutral and coherent with the study findings in 26 cases, but unjustifiably favorable in 11 cases. Among 14 with nonprofit support, descriptions of QoL results were found to be neutral in all cases (P = .0232).
“Obviously, industry may be motivated to overemphasize treatment benefits, especially in measures that also have a qualitative/subjective dimension such as QoL. Assuming that the authors used a reliable criterion to evaluate “inappropriateness,” industry may be more likely to emphasize QoL improvements as a surrogate for OS, especially when seeking drug approval,” Dr. Kypriotakis said.
The study is retrospective and cannot prove causation.
Dr. Salomone and Dr. Kypriotakis have no relevant financial disclosures.
The authors, including Fabio Salomone of the University of Naples Federico II, department of clinical medicine and surgery, also observed trends toward an association between QoL improvement and PFS among patients treated with chemotherapy and immunotherapy.
The new research was presented during a poster session at European Lung Cancer Congress 2023.
“The findings of the study support the thesis that QoL and survival in patients with NSCLC are linked. Although this is documented in the literature, this study sums up the evidence of a large number of RCTs, and provides detail in the QoL/survival relationship by treatment type. The subgroup analysis by treatment type is a key strength of the study showing that the QoL/survival link is stronger and more reliable in target(ed) therapies,” George Kypriotakis, PhD, who was not involved with the study, said in an interview.
Combining efficacy and quality of life improvement is an important consideration in clinical practice. “It is important that clinicians provide therapies that are also palliative and improve QoL,” said Dr. Kypriotakis, assistant professor of behavioral sciences at University of Texas MD Anderson Cancer Center, Houston. He noted that the finding of a PFS benefit is a good indicator of overall benefit, which is important since OS outcomes require a larger number of patients and longer follow-up to determine.
“PFS can still be a valid surrogate for OS, especially when it is positively associated with QoL,” noted Dr. Kypriotakis.
The study included 81 trials. Sixteen of the studies investigated immunotherapy, 50 investigated targeted therapy, and 17 investigated chemotherapy regimens. Thirty-seven percent of the trials found an improvement in QoL in the treatment arm compared with the control arm, 59.3% found no difference between arms, and 3.7% found a worse QoL in the treatment arm. There was no statistically significant association between an improvement in OS and QoL among the trials (P = .368).
Improved QoL tied to improved PFS
The researchers found an association between improved QoL and improved PFS. Among 60 trials that showed improved PFS, 43.3% found a superior QoL in the treatment arm, 53.3% showed no difference, and 3.3% showed reduced QoL. Among 20 trials that found no improvement in PFS, 20% demonstrated an improved QoL, 75% found no change, and 5% showed worse QoL (P = .0473).
A subanalysis of 48 targeted therapy trials found a correlation between PFS and QoL improvement (P = .0196). Among 25 trials involving patients receiving epidermal growth factor receptor (EGFR) and anaplastic lymphoma kinase (ALK) inhibitors showing an improved PFS, 60% showed improved QoL, 36% showed no difference, and 4% showed worsening (P = .0077). Seven of these trials showed no PFS benefit and no change in QoL.
Industry sponsorship may affect QOL results
The researchers found potential evidence that industry sponsorship may lead to a spin on QoL outcomes. Among 51 trials that showed no QoL benefit associated with treatment, the description of the QoL outcome in 37 industry-sponsored was judged to be neutral and coherent with the study findings in 26 cases, but unjustifiably favorable in 11 cases. Among 14 with nonprofit support, descriptions of QoL results were found to be neutral in all cases (P = .0232).
“Obviously, industry may be motivated to overemphasize treatment benefits, especially in measures that also have a qualitative/subjective dimension such as QoL. Assuming that the authors used a reliable criterion to evaluate “inappropriateness,” industry may be more likely to emphasize QoL improvements as a surrogate for OS, especially when seeking drug approval,” Dr. Kypriotakis said.
The study is retrospective and cannot prove causation.
Dr. Salomone and Dr. Kypriotakis have no relevant financial disclosures.
The authors, including Fabio Salomone of the University of Naples Federico II, department of clinical medicine and surgery, also observed trends toward an association between QoL improvement and PFS among patients treated with chemotherapy and immunotherapy.
The new research was presented during a poster session at European Lung Cancer Congress 2023.
“The findings of the study support the thesis that QoL and survival in patients with NSCLC are linked. Although this is documented in the literature, this study sums up the evidence of a large number of RCTs, and provides detail in the QoL/survival relationship by treatment type. The subgroup analysis by treatment type is a key strength of the study showing that the QoL/survival link is stronger and more reliable in target(ed) therapies,” George Kypriotakis, PhD, who was not involved with the study, said in an interview.
Combining efficacy and quality of life improvement is an important consideration in clinical practice. “It is important that clinicians provide therapies that are also palliative and improve QoL,” said Dr. Kypriotakis, assistant professor of behavioral sciences at University of Texas MD Anderson Cancer Center, Houston. He noted that the finding of a PFS benefit is a good indicator of overall benefit, which is important since OS outcomes require a larger number of patients and longer follow-up to determine.
“PFS can still be a valid surrogate for OS, especially when it is positively associated with QoL,” noted Dr. Kypriotakis.
The study included 81 trials. Sixteen of the studies investigated immunotherapy, 50 investigated targeted therapy, and 17 investigated chemotherapy regimens. Thirty-seven percent of the trials found an improvement in QoL in the treatment arm compared with the control arm, 59.3% found no difference between arms, and 3.7% found a worse QoL in the treatment arm. There was no statistically significant association between an improvement in OS and QoL among the trials (P = .368).
Improved QoL tied to improved PFS
The researchers found an association between improved QoL and improved PFS. Among 60 trials that showed improved PFS, 43.3% found a superior QoL in the treatment arm, 53.3% showed no difference, and 3.3% showed reduced QoL. Among 20 trials that found no improvement in PFS, 20% demonstrated an improved QoL, 75% found no change, and 5% showed worse QoL (P = .0473).
A subanalysis of 48 targeted therapy trials found a correlation between PFS and QoL improvement (P = .0196). Among 25 trials involving patients receiving epidermal growth factor receptor (EGFR) and anaplastic lymphoma kinase (ALK) inhibitors showing an improved PFS, 60% showed improved QoL, 36% showed no difference, and 4% showed worsening (P = .0077). Seven of these trials showed no PFS benefit and no change in QoL.
Industry sponsorship may affect QOL results
The researchers found potential evidence that industry sponsorship may lead to a spin on QoL outcomes. Among 51 trials that showed no QoL benefit associated with treatment, the description of the QoL outcome in 37 industry-sponsored was judged to be neutral and coherent with the study findings in 26 cases, but unjustifiably favorable in 11 cases. Among 14 with nonprofit support, descriptions of QoL results were found to be neutral in all cases (P = .0232).
“Obviously, industry may be motivated to overemphasize treatment benefits, especially in measures that also have a qualitative/subjective dimension such as QoL. Assuming that the authors used a reliable criterion to evaluate “inappropriateness,” industry may be more likely to emphasize QoL improvements as a surrogate for OS, especially when seeking drug approval,” Dr. Kypriotakis said.
The study is retrospective and cannot prove causation.
Dr. Salomone and Dr. Kypriotakis have no relevant financial disclosures.
FROM ELCC 2023
Refined incidence rate of HCC with alcohol-associated cirrhosis encourages surveillance
Incidence rates were higher for cohorts that underwent HCC surveillance versus those that did not undergo surveillance, suggesting that such programs offer significant benefit, lead author Daniel Q. Huang, MBBS, of the University of California, San Diego, and colleagues reported.

“A systematic review of the incidence of HCC among patients with alcohol-associated cirrhosis has not been reported,” the investigators wrote in Clinical Gastroenterology and Hepatology, prompting the present research.
Previous studies have described a broad range of annual incidence findings for HCC in this population, from 0.6% to 5.6%, suggesting that a systematic approach was needed.
To this end, Dr. Huang and colleagues analyzed data from 18 studies that involved 148,333 patients with alcohol-associated cirrhosis. The primary analysis aimed to determine cumulative incidence rates over time, while the secondary analysis characterized the impact of participation in HCC surveillance programs.
“This meta-analysis used reconstructed individual participant data, which is considered to be the gold standard for reporting survival data because it accounts for censoring of events,” the investigators noted. “The current study provides important data that are useful for clinical practice and clinical trial design.”
The cumulative incidence rates of HCC were 1%, 3%, and 9% at 1 year, 5 years, and 10 years, respectively. Among 12 of the risk factors studied, smoking, diabetes, and decompensation were all significantly associated with rate of HCC.
“Therefore, patients with alcohol-associated cirrhosis should be screened for diabetes to identify the patients at high risk for HCC development,” the investigators wrote. “In addition, patients with alcohol-associated cirrhosis should be advised to stop smoking, while patients with hepatic decompensation should be monitored carefully for the development of HCC if clinically appropriate.”
The secondary analysis showed that HCC incidence rates were higher among patients participating in HCC surveillance programs than those who did not participate (18.6 vs. 4.8 per 1,000 person-years; P = .001).
“Patients with alcohol-associated cirrhosis are known to have lower HCC surveillance rates, which may be related to poor disease awareness, clinic time constraints caused by other active medical issues, and provider beliefs regarding the likelihood of adherence,” the investigators noted.
Increased efforts are needed to promote surveillance in this population, they added, suggesting a range of communication pathways, including social media, traditional news outlets, and direct mailing.
Dr. Huang and colleagues also suggested that the findings should be validated in large prospective studies.
The study was funded by the National Institute on Alcohol Abuse and Alcoholism, the National Institute of Environmental Health Sciences, the National Center for Advancing Translational Sciences, and others. Dr. Huang disclosed funding from the Singapore Ministry of Health’s National Medical Research Council.
The association between cirrhosis and hepatocellular carcinoma (HCC) risk is well known and therefore routine surveillance is recommended by the American Association for the Study of Liver Diseases. More recent data has shown alcohol use to be an independent risk factor for HCC along with various other cancers.

Quite frequently, the focus of management in patients with alcohol-associated liver disease is alcohol cessation to prevent further decompensation, with screening often being overlooked. Previous studies have shown, however, that earlier detection is associated with improved survival. Another interesting finding of this study was that those patients who had concomitant smoking use, diabetes, and hepatic decompensation were more likely to develop HCC. When managing patients with alcohol related liver disease, confounding risk factors should be mitigated (that is, encouragement of smoking cessation, enhanced screening for diabetes, and more rigorous screening in decompensated patients).
This study brings to light the need for improved screening and concomitant risk factor mitigation for hepatocellular carcinoma given higher rates of detection in those undergoing surveillance. Larger, prospective studies are needed, however, to validate the findings in this study given the recent overall increase in rates of alcohol-associated liver disease.
Priya Maddur MD, is a visiting clinical associate professor of medicine, University of Arizona, Tucson. Dr. Maddur has no relevant disclosures.
The association between cirrhosis and hepatocellular carcinoma (HCC) risk is well known and therefore routine surveillance is recommended by the American Association for the Study of Liver Diseases. More recent data has shown alcohol use to be an independent risk factor for HCC along with various other cancers.
Quite frequently, the focus of management in patients with alcohol-associated liver disease is alcohol cessation to prevent further decompensation, with screening often being overlooked. Previous studies have shown, however, that earlier detection is associated with improved survival. Another interesting finding of this study was that those patients who had concomitant smoking use, diabetes, and hepatic decompensation were more likely to develop HCC. When managing patients with alcohol related liver disease, confounding risk factors should be mitigated (that is, encouragement of smoking cessation, enhanced screening for diabetes, and more rigorous screening in decompensated patients).
This study brings to light the need for improved screening and concomitant risk factor mitigation for hepatocellular carcinoma given higher rates of detection in those undergoing surveillance. Larger, prospective studies are needed, however, to validate the findings in this study given the recent overall increase in rates of alcohol-associated liver disease.
Priya Maddur MD, is a visiting clinical associate professor of medicine, University of Arizona, Tucson. Dr. Maddur has no relevant disclosures.
The association between cirrhosis and hepatocellular carcinoma (HCC) risk is well known and therefore routine surveillance is recommended by the American Association for the Study of Liver Diseases. More recent data has shown alcohol use to be an independent risk factor for HCC along with various other cancers.
Quite frequently, the focus of management in patients with alcohol-associated liver disease is alcohol cessation to prevent further decompensation, with screening often being overlooked. Previous studies have shown, however, that earlier detection is associated with improved survival. Another interesting finding of this study was that those patients who had concomitant smoking use, diabetes, and hepatic decompensation were more likely to develop HCC. When managing patients with alcohol related liver disease, confounding risk factors should be mitigated (that is, encouragement of smoking cessation, enhanced screening for diabetes, and more rigorous screening in decompensated patients).
This study brings to light the need for improved screening and concomitant risk factor mitigation for hepatocellular carcinoma given higher rates of detection in those undergoing surveillance. Larger, prospective studies are needed, however, to validate the findings in this study given the recent overall increase in rates of alcohol-associated liver disease.
Priya Maddur MD, is a visiting clinical associate professor of medicine, University of Arizona, Tucson. Dr. Maddur has no relevant disclosures.
Incidence rates were higher for cohorts that underwent HCC surveillance versus those that did not undergo surveillance, suggesting that such programs offer significant benefit, lead author Daniel Q. Huang, MBBS, of the University of California, San Diego, and colleagues reported.
“A systematic review of the incidence of HCC among patients with alcohol-associated cirrhosis has not been reported,” the investigators wrote in Clinical Gastroenterology and Hepatology, prompting the present research.
Previous studies have described a broad range of annual incidence findings for HCC in this population, from 0.6% to 5.6%, suggesting that a systematic approach was needed.
To this end, Dr. Huang and colleagues analyzed data from 18 studies that involved 148,333 patients with alcohol-associated cirrhosis. The primary analysis aimed to determine cumulative incidence rates over time, while the secondary analysis characterized the impact of participation in HCC surveillance programs.
“This meta-analysis used reconstructed individual participant data, which is considered to be the gold standard for reporting survival data because it accounts for censoring of events,” the investigators noted. “The current study provides important data that are useful for clinical practice and clinical trial design.”
The cumulative incidence rates of HCC were 1%, 3%, and 9% at 1 year, 5 years, and 10 years, respectively. Among 12 of the risk factors studied, smoking, diabetes, and decompensation were all significantly associated with rate of HCC.
“Therefore, patients with alcohol-associated cirrhosis should be screened for diabetes to identify the patients at high risk for HCC development,” the investigators wrote. “In addition, patients with alcohol-associated cirrhosis should be advised to stop smoking, while patients with hepatic decompensation should be monitored carefully for the development of HCC if clinically appropriate.”
The secondary analysis showed that HCC incidence rates were higher among patients participating in HCC surveillance programs than those who did not participate (18.6 vs. 4.8 per 1,000 person-years; P = .001).
“Patients with alcohol-associated cirrhosis are known to have lower HCC surveillance rates, which may be related to poor disease awareness, clinic time constraints caused by other active medical issues, and provider beliefs regarding the likelihood of adherence,” the investigators noted.
Increased efforts are needed to promote surveillance in this population, they added, suggesting a range of communication pathways, including social media, traditional news outlets, and direct mailing.
Dr. Huang and colleagues also suggested that the findings should be validated in large prospective studies.
The study was funded by the National Institute on Alcohol Abuse and Alcoholism, the National Institute of Environmental Health Sciences, the National Center for Advancing Translational Sciences, and others. Dr. Huang disclosed funding from the Singapore Ministry of Health’s National Medical Research Council.
Incidence rates were higher for cohorts that underwent HCC surveillance versus those that did not undergo surveillance, suggesting that such programs offer significant benefit, lead author Daniel Q. Huang, MBBS, of the University of California, San Diego, and colleagues reported.
“A systematic review of the incidence of HCC among patients with alcohol-associated cirrhosis has not been reported,” the investigators wrote in Clinical Gastroenterology and Hepatology, prompting the present research.
Previous studies have described a broad range of annual incidence findings for HCC in this population, from 0.6% to 5.6%, suggesting that a systematic approach was needed.
To this end, Dr. Huang and colleagues analyzed data from 18 studies that involved 148,333 patients with alcohol-associated cirrhosis. The primary analysis aimed to determine cumulative incidence rates over time, while the secondary analysis characterized the impact of participation in HCC surveillance programs.
“This meta-analysis used reconstructed individual participant data, which is considered to be the gold standard for reporting survival data because it accounts for censoring of events,” the investigators noted. “The current study provides important data that are useful for clinical practice and clinical trial design.”
The cumulative incidence rates of HCC were 1%, 3%, and 9% at 1 year, 5 years, and 10 years, respectively. Among 12 of the risk factors studied, smoking, diabetes, and decompensation were all significantly associated with rate of HCC.
“Therefore, patients with alcohol-associated cirrhosis should be screened for diabetes to identify the patients at high risk for HCC development,” the investigators wrote. “In addition, patients with alcohol-associated cirrhosis should be advised to stop smoking, while patients with hepatic decompensation should be monitored carefully for the development of HCC if clinically appropriate.”
The secondary analysis showed that HCC incidence rates were higher among patients participating in HCC surveillance programs than those who did not participate (18.6 vs. 4.8 per 1,000 person-years; P = .001).
“Patients with alcohol-associated cirrhosis are known to have lower HCC surveillance rates, which may be related to poor disease awareness, clinic time constraints caused by other active medical issues, and provider beliefs regarding the likelihood of adherence,” the investigators noted.
Increased efforts are needed to promote surveillance in this population, they added, suggesting a range of communication pathways, including social media, traditional news outlets, and direct mailing.
Dr. Huang and colleagues also suggested that the findings should be validated in large prospective studies.
The study was funded by the National Institute on Alcohol Abuse and Alcoholism, the National Institute of Environmental Health Sciences, the National Center for Advancing Translational Sciences, and others. Dr. Huang disclosed funding from the Singapore Ministry of Health’s National Medical Research Council.
FROM CLINICAL GASTROENTEROLOGY AND HEPATOLOGY
Antibiotic pretreatment reduces liver ischemia/reperfusion injury
Antibiotic pretreatment may protect against liver ischemia/reperfusion (I/R) injury through altered gut microbiota, glutamine levels, and glutamine downstream products in circulation, according to a recent study in Cellular and Molecular Gastroenterology and Hepatology.
The findings show that , wrote Tianfei Lu, with the Abdominal Transplant Surgery Center at Ruijin Hospital and Shanghai Jiao Tong University, China, and colleagues.
“Potential therapies that target macrophage metabolism, including antibiotic therapies and novel immunometabolism modulators, can be exploited for the treatment of liver I/R injury,” the authors wrote.
Liver I/R injury is a common complication of liver resection, transplantation, trauma, and hemorrhagic shock. Previous studies have noted the important role of gut microbiota in liver disease progression, yet the mechanisms in liver I/R injury remain unknown.
The researchers pretreated mice with an antibiotic cocktail to modify the gut microbiome. They found that the pretreatment showed protective effects against hepatic I/R injury, with reductions in serum alanine aminotransferase (ALT), interleukin-1 beta, tumor necrosis factor–alpha, IL-6, IL-12b, and CXCL10.
Through histologic analysis of liver tissues, they also found that the area of necrosis, the degree of congestion and edema, and the presence of vacuole-like lesions were alleviated in the preconditioned mice. Inflammation and necrosis of the liver were also lower, according to both qualitative and quantitative data.
Then, through fecal microbiota transplantation into germ-free mice, they found that the protection from I/R injury was transferable. This finding indicated that the altered gut microbiome, rather than the antibiotic treatment itself, exerted the protective effect.
Because altered gut microbiota can cause changes in metabolites, the researchers used ultra-performance liquid chromatography coupled to tandem mass spectrometry to explore the changes of gut microbiota and metabolites in both feces and portal blood, as well as analyze the mechanisms underlying their protective effects in liver I/R injury.
The researchers found that glutamine and its downstream product called alpha-ketoglutarate (AKG) were present in higher concentrations in feces and blood in the mice with antibiotic pretreatment. Glutamate levels were significantly lower, indicating that glutamine is converted into AKG through glutamate after entering the blood.
In addition, there were increased levels of intermediate products of the tricarboxylic acid (TCA) cycle, as well as pyruvate produced by glycolysis. That led to an increase in M2 macrophages, which are responsible for anti-inflammatory processes and tissue repair.
The authors concluded that elevated glutamine levels in the intestine cause an increase in AKG levels in the blood, and AKG can promote M2 macrophage polarization by fueling the TCA cycle. In turn, the increased number of M2 macrophages can repair hepatic I/R injury.
Finally, the researchers tested oligomycin A, which can block the OXPHOS metabolic pathway and inhibit the mitochondrial ATP synthase. As expected, they wrote, the protective effect of antibiotic pretreatment reversed, M2 macrophages decreased, and serum ALT levels increased.
“The immunometabolism and polarization of macrophages play an important role in host homeostasis and the development of various diseases,” the authors wrote. “The relationship between antibiotics treatment, altered gut microbiota, and liver I/R injury are complex and worthy of further study.”
The study was supported by the China National Science and Technology Major Project, National Natural Science Foundation of China, and Natural Science Foundation exploration project of Zhejiang Province. The authors disclosed no conflicts.
In modern clinical practice, multiple conditions can cause ischemia and reperfusion injury to the liver, including surgical liver resection, liver transplantation, and physical trauma to the organ. Liver damage due to hypoxia is followed by reperfusion injury, resulting in a pre-proinflammatory environment. Liver resident macrophages called Kupffer cells are major mediators of this response, initiating a signaling cascade that leads to recruitment of neutrophils, natural killer cells, and circulating macrophages, which attack sinusoidal endothelial cells and hepatocytes.

In the current issue of CMGH, Lu and colleagues address the question of to what extent do the gut microbiome and its metabolite products, which reach the liver via the portal circulation, play a role in the severity of ischemia and reperfusion injury (Cell Mol Gastroenterol Hepatol. 2023 Jan 24. doi: 10.1016/j.jcmgh.2023.01.004). This topic is of clinical relevance, as the microbial load of the gut lumen can be easily reduced by several orders of magnitude using non-absorbed antibiotics. Thus, it is important to establish if pretreatment of patients scheduled for liver resection or transplantation might benefit from preprocedure antibiotic treatment.
Remarkably, Lu and colleagues find that antibiotic preconditioning significantly reduces ischemia and reperfusion injury in an animal model. Mechanistically, they linked the protective effects to a shift of macrophage polarization to the protective M phenotype, which is known to promote tissue repair. These findings suggest that the antibiotic preconditioning of patients who are undergoing procedures with significant ischemia and reperfusion injury should be evaluated in future clinical trials.
Klaus H. Kaestner, PhD, MS, is the Thomas and Evelyn Suor Butterworth Professor in Genetics and associate director of the Penn Diabetes Research Center at the University of Pennsylvania, Philadelphia. He has no relevant financial relationships.
In modern clinical practice, multiple conditions can cause ischemia and reperfusion injury to the liver, including surgical liver resection, liver transplantation, and physical trauma to the organ. Liver damage due to hypoxia is followed by reperfusion injury, resulting in a pre-proinflammatory environment. Liver resident macrophages called Kupffer cells are major mediators of this response, initiating a signaling cascade that leads to recruitment of neutrophils, natural killer cells, and circulating macrophages, which attack sinusoidal endothelial cells and hepatocytes.
In the current issue of CMGH, Lu and colleagues address the question of to what extent do the gut microbiome and its metabolite products, which reach the liver via the portal circulation, play a role in the severity of ischemia and reperfusion injury (Cell Mol Gastroenterol Hepatol. 2023 Jan 24. doi: 10.1016/j.jcmgh.2023.01.004). This topic is of clinical relevance, as the microbial load of the gut lumen can be easily reduced by several orders of magnitude using non-absorbed antibiotics. Thus, it is important to establish if pretreatment of patients scheduled for liver resection or transplantation might benefit from preprocedure antibiotic treatment.
Remarkably, Lu and colleagues find that antibiotic preconditioning significantly reduces ischemia and reperfusion injury in an animal model. Mechanistically, they linked the protective effects to a shift of macrophage polarization to the protective M phenotype, which is known to promote tissue repair. These findings suggest that the antibiotic preconditioning of patients who are undergoing procedures with significant ischemia and reperfusion injury should be evaluated in future clinical trials.
Klaus H. Kaestner, PhD, MS, is the Thomas and Evelyn Suor Butterworth Professor in Genetics and associate director of the Penn Diabetes Research Center at the University of Pennsylvania, Philadelphia. He has no relevant financial relationships.
In modern clinical practice, multiple conditions can cause ischemia and reperfusion injury to the liver, including surgical liver resection, liver transplantation, and physical trauma to the organ. Liver damage due to hypoxia is followed by reperfusion injury, resulting in a pre-proinflammatory environment. Liver resident macrophages called Kupffer cells are major mediators of this response, initiating a signaling cascade that leads to recruitment of neutrophils, natural killer cells, and circulating macrophages, which attack sinusoidal endothelial cells and hepatocytes.
In the current issue of CMGH, Lu and colleagues address the question of to what extent do the gut microbiome and its metabolite products, which reach the liver via the portal circulation, play a role in the severity of ischemia and reperfusion injury (Cell Mol Gastroenterol Hepatol. 2023 Jan 24. doi: 10.1016/j.jcmgh.2023.01.004). This topic is of clinical relevance, as the microbial load of the gut lumen can be easily reduced by several orders of magnitude using non-absorbed antibiotics. Thus, it is important to establish if pretreatment of patients scheduled for liver resection or transplantation might benefit from preprocedure antibiotic treatment.
Remarkably, Lu and colleagues find that antibiotic preconditioning significantly reduces ischemia and reperfusion injury in an animal model. Mechanistically, they linked the protective effects to a shift of macrophage polarization to the protective M phenotype, which is known to promote tissue repair. These findings suggest that the antibiotic preconditioning of patients who are undergoing procedures with significant ischemia and reperfusion injury should be evaluated in future clinical trials.
Klaus H. Kaestner, PhD, MS, is the Thomas and Evelyn Suor Butterworth Professor in Genetics and associate director of the Penn Diabetes Research Center at the University of Pennsylvania, Philadelphia. He has no relevant financial relationships.
Antibiotic pretreatment may protect against liver ischemia/reperfusion (I/R) injury through altered gut microbiota, glutamine levels, and glutamine downstream products in circulation, according to a recent study in Cellular and Molecular Gastroenterology and Hepatology.
The findings show that , wrote Tianfei Lu, with the Abdominal Transplant Surgery Center at Ruijin Hospital and Shanghai Jiao Tong University, China, and colleagues.
“Potential therapies that target macrophage metabolism, including antibiotic therapies and novel immunometabolism modulators, can be exploited for the treatment of liver I/R injury,” the authors wrote.
Liver I/R injury is a common complication of liver resection, transplantation, trauma, and hemorrhagic shock. Previous studies have noted the important role of gut microbiota in liver disease progression, yet the mechanisms in liver I/R injury remain unknown.
The researchers pretreated mice with an antibiotic cocktail to modify the gut microbiome. They found that the pretreatment showed protective effects against hepatic I/R injury, with reductions in serum alanine aminotransferase (ALT), interleukin-1 beta, tumor necrosis factor–alpha, IL-6, IL-12b, and CXCL10.
Through histologic analysis of liver tissues, they also found that the area of necrosis, the degree of congestion and edema, and the presence of vacuole-like lesions were alleviated in the preconditioned mice. Inflammation and necrosis of the liver were also lower, according to both qualitative and quantitative data.
Then, through fecal microbiota transplantation into germ-free mice, they found that the protection from I/R injury was transferable. This finding indicated that the altered gut microbiome, rather than the antibiotic treatment itself, exerted the protective effect.
Because altered gut microbiota can cause changes in metabolites, the researchers used ultra-performance liquid chromatography coupled to tandem mass spectrometry to explore the changes of gut microbiota and metabolites in both feces and portal blood, as well as analyze the mechanisms underlying their protective effects in liver I/R injury.
The researchers found that glutamine and its downstream product called alpha-ketoglutarate (AKG) were present in higher concentrations in feces and blood in the mice with antibiotic pretreatment. Glutamate levels were significantly lower, indicating that glutamine is converted into AKG through glutamate after entering the blood.
In addition, there were increased levels of intermediate products of the tricarboxylic acid (TCA) cycle, as well as pyruvate produced by glycolysis. That led to an increase in M2 macrophages, which are responsible for anti-inflammatory processes and tissue repair.
The authors concluded that elevated glutamine levels in the intestine cause an increase in AKG levels in the blood, and AKG can promote M2 macrophage polarization by fueling the TCA cycle. In turn, the increased number of M2 macrophages can repair hepatic I/R injury.
Finally, the researchers tested oligomycin A, which can block the OXPHOS metabolic pathway and inhibit the mitochondrial ATP synthase. As expected, they wrote, the protective effect of antibiotic pretreatment reversed, M2 macrophages decreased, and serum ALT levels increased.
“The immunometabolism and polarization of macrophages play an important role in host homeostasis and the development of various diseases,” the authors wrote. “The relationship between antibiotics treatment, altered gut microbiota, and liver I/R injury are complex and worthy of further study.”
The study was supported by the China National Science and Technology Major Project, National Natural Science Foundation of China, and Natural Science Foundation exploration project of Zhejiang Province. The authors disclosed no conflicts.
Antibiotic pretreatment may protect against liver ischemia/reperfusion (I/R) injury through altered gut microbiota, glutamine levels, and glutamine downstream products in circulation, according to a recent study in Cellular and Molecular Gastroenterology and Hepatology.
The findings show that , wrote Tianfei Lu, with the Abdominal Transplant Surgery Center at Ruijin Hospital and Shanghai Jiao Tong University, China, and colleagues.
“Potential therapies that target macrophage metabolism, including antibiotic therapies and novel immunometabolism modulators, can be exploited for the treatment of liver I/R injury,” the authors wrote.
Liver I/R injury is a common complication of liver resection, transplantation, trauma, and hemorrhagic shock. Previous studies have noted the important role of gut microbiota in liver disease progression, yet the mechanisms in liver I/R injury remain unknown.
The researchers pretreated mice with an antibiotic cocktail to modify the gut microbiome. They found that the pretreatment showed protective effects against hepatic I/R injury, with reductions in serum alanine aminotransferase (ALT), interleukin-1 beta, tumor necrosis factor–alpha, IL-6, IL-12b, and CXCL10.
Through histologic analysis of liver tissues, they also found that the area of necrosis, the degree of congestion and edema, and the presence of vacuole-like lesions were alleviated in the preconditioned mice. Inflammation and necrosis of the liver were also lower, according to both qualitative and quantitative data.
Then, through fecal microbiota transplantation into germ-free mice, they found that the protection from I/R injury was transferable. This finding indicated that the altered gut microbiome, rather than the antibiotic treatment itself, exerted the protective effect.
Because altered gut microbiota can cause changes in metabolites, the researchers used ultra-performance liquid chromatography coupled to tandem mass spectrometry to explore the changes of gut microbiota and metabolites in both feces and portal blood, as well as analyze the mechanisms underlying their protective effects in liver I/R injury.
The researchers found that glutamine and its downstream product called alpha-ketoglutarate (AKG) were present in higher concentrations in feces and blood in the mice with antibiotic pretreatment. Glutamate levels were significantly lower, indicating that glutamine is converted into AKG through glutamate after entering the blood.
In addition, there were increased levels of intermediate products of the tricarboxylic acid (TCA) cycle, as well as pyruvate produced by glycolysis. That led to an increase in M2 macrophages, which are responsible for anti-inflammatory processes and tissue repair.
The authors concluded that elevated glutamine levels in the intestine cause an increase in AKG levels in the blood, and AKG can promote M2 macrophage polarization by fueling the TCA cycle. In turn, the increased number of M2 macrophages can repair hepatic I/R injury.
Finally, the researchers tested oligomycin A, which can block the OXPHOS metabolic pathway and inhibit the mitochondrial ATP synthase. As expected, they wrote, the protective effect of antibiotic pretreatment reversed, M2 macrophages decreased, and serum ALT levels increased.
“The immunometabolism and polarization of macrophages play an important role in host homeostasis and the development of various diseases,” the authors wrote. “The relationship between antibiotics treatment, altered gut microbiota, and liver I/R injury are complex and worthy of further study.”
The study was supported by the China National Science and Technology Major Project, National Natural Science Foundation of China, and Natural Science Foundation exploration project of Zhejiang Province. The authors disclosed no conflicts.
FROM CELLULAR AND MOLECULAR GASTROENTEROLOGY AND HEPATOLOGY
New guidelines for cannabis in chronic pain management released
New clinical practice guidelines for cannabis in chronic pain management have been released.
Developed by a group of Canadian researchers, clinicians, and patients, the guidelines note that cannabinoid-based medicines (CBM) may help clinicians offer an effective, less addictive, alternative to opioids in patients with chronic noncancer pain and comorbid conditions.
“We don’t recommend using CBM first line for anything pretty much because there are other alternatives that may be more effective and also offer fewer side effects,” lead guideline author Alan Bell, MD, assistant professor of family and community medicine at the University of Toronto, told this news organization.

“But I would strongly argue that I would use cannabis-based medicine over opioids every time. Why would you use a high potency-high toxicity agent when there’s a low potency-low toxicity alternative?” he said.
The guidelines were published online in the journal Cannabis and Cannabinoid Research.
Examining the evidence
A consistent criticism of CBM has been the lack of quality research supporting its therapeutic utility. To develop the current recommendations, the task force reviewed 47 pain management studies enrolling more than 11,000 patients. Almost half of the studies (n = 22) were randomized controlled trials (RCTs) and 12 of the 19 included systematic reviews focused solely on RCTs.
Overall, 38 of the 47 included studies demonstrated that CBM provided at least moderate benefits for chronic pain, resulting in a “strong” recommendation – mostly as an adjunct or replacement treatment in individuals living with chronic pain.
Overall, the guidelines place a high value on improving chronic pain and functionality, and addressing co-occurring conditions such as insomnia, anxiety and depression, mobility, and inflammation. They also provide practical dosing and formulation tips to support the use of CBM in the clinical setting.
When it comes to chronic pain, CBM is not a panacea. However, prior research suggests cannabinoids and opioids share several pharmacologic properties, including independent but possibly related mechanisms for antinociception, making them an intriguing combination.
In the current guidelines, all of the four studies specifically addressing combined opioids and vaporized cannabis flower demonstrated further pain reduction, reinforcing the conclusion that the benefits of CBM for improving pain control in patients taking opioids outweigh the risk of nonserious adverse events (AEs), such as dry mouth, dizziness, increased appetite, sedation, and concentration difficulties.
The recommendations also highlighted evidence demonstrating that a majority of participants were able to reduce use of routine pain medications with concomitant CBM/opioid administration, while simultaneously offering secondary benefits such as improved sleep, anxiety, and mood, as well as prevention of opioid tolerance and dose escalation.
Importantly, the guidelines offer an evidence-based algorithm with a clear framework for tapering patients off opioids, especially those who are on > 50 mg MED, which places them with a twofold greater risk for fatal overdose.
An effective alternative
Commenting on the new guidelines, Mark Wallace, MD, who has extensive experience researching and treating pain patients with medical cannabis, said the genesis of his interest in medical cannabis mirrors the guidelines’ focus.
“What got me interested in medical cannabis was trying to get patients off of opioids,” said Dr. Wallace, professor of anesthesiology and chief of the division of pain medicine in the department of anesthesiology at the University of California, San Diego. Dr. Wallace, who was not involved in the guidelines’ development study, said that he’s “titrated hundreds of patients off of opioids using cannabis.”
Dr. Wallace said he found the guidelines’ dosing recommendations helpful.
“If you stay within the 1- to 5-mg dosing range, the risks are so incredibly low, you’re not going to harm the patient.”
While there are patients who abuse cannabis and CBMs, Dr. Wallace noted that he has seen only one patient in the past 20 years who was overusing the medical cannabis. He added that his patient population does not use medical cannabis to get high and, in fact, wants to avoid doses that produce that effect at all costs.
Also commenting on the guidelines, Christopher Gilligan, MD, MBA, associate chief medical officer and a pain medicine physician at Brigham and Women’s Hospital in Boston, who was not involved in the guidelines’ development, points to the risks.

“When we have an opportunity to use cannabinoids in place of opioids for our patients, I think that that’s a positive thing ... and a wise choice in terms of risk benefit,” Dr. Gilligan said.
On the other hand, he cautioned that “freely prescribing” cannabinoids for chronic pain in patients who aren’t on opioids is not good practice.
“We have to take seriously the potential adverse effects of [cannabis], including marijuana use disorder, interference with learning, memory impairment, and psychotic breakthroughs,” said Dr. Gilligan.
Given the current climate, it would appear that CBM is a long way from being endorsed by the Food and Drug Administration, but for clinicians interested in trying CBM for chronic pain patients, the guidelines may offer a roadmap for initiation and an alternative to prescribing opioids.
Dr. Bell, Dr. Gilligan, and Dr. Wallace report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
New clinical practice guidelines for cannabis in chronic pain management have been released.
Developed by a group of Canadian researchers, clinicians, and patients, the guidelines note that cannabinoid-based medicines (CBM) may help clinicians offer an effective, less addictive, alternative to opioids in patients with chronic noncancer pain and comorbid conditions.
“We don’t recommend using CBM first line for anything pretty much because there are other alternatives that may be more effective and also offer fewer side effects,” lead guideline author Alan Bell, MD, assistant professor of family and community medicine at the University of Toronto, told this news organization.
“But I would strongly argue that I would use cannabis-based medicine over opioids every time. Why would you use a high potency-high toxicity agent when there’s a low potency-low toxicity alternative?” he said.
The guidelines were published online in the journal Cannabis and Cannabinoid Research.
Examining the evidence
A consistent criticism of CBM has been the lack of quality research supporting its therapeutic utility. To develop the current recommendations, the task force reviewed 47 pain management studies enrolling more than 11,000 patients. Almost half of the studies (n = 22) were randomized controlled trials (RCTs) and 12 of the 19 included systematic reviews focused solely on RCTs.
Overall, 38 of the 47 included studies demonstrated that CBM provided at least moderate benefits for chronic pain, resulting in a “strong” recommendation – mostly as an adjunct or replacement treatment in individuals living with chronic pain.
Overall, the guidelines place a high value on improving chronic pain and functionality, and addressing co-occurring conditions such as insomnia, anxiety and depression, mobility, and inflammation. They also provide practical dosing and formulation tips to support the use of CBM in the clinical setting.
When it comes to chronic pain, CBM is not a panacea. However, prior research suggests cannabinoids and opioids share several pharmacologic properties, including independent but possibly related mechanisms for antinociception, making them an intriguing combination.
In the current guidelines, all of the four studies specifically addressing combined opioids and vaporized cannabis flower demonstrated further pain reduction, reinforcing the conclusion that the benefits of CBM for improving pain control in patients taking opioids outweigh the risk of nonserious adverse events (AEs), such as dry mouth, dizziness, increased appetite, sedation, and concentration difficulties.
The recommendations also highlighted evidence demonstrating that a majority of participants were able to reduce use of routine pain medications with concomitant CBM/opioid administration, while simultaneously offering secondary benefits such as improved sleep, anxiety, and mood, as well as prevention of opioid tolerance and dose escalation.
Importantly, the guidelines offer an evidence-based algorithm with a clear framework for tapering patients off opioids, especially those who are on > 50 mg MED, which places them with a twofold greater risk for fatal overdose.
An effective alternative
Commenting on the new guidelines, Mark Wallace, MD, who has extensive experience researching and treating pain patients with medical cannabis, said the genesis of his interest in medical cannabis mirrors the guidelines’ focus.
“What got me interested in medical cannabis was trying to get patients off of opioids,” said Dr. Wallace, professor of anesthesiology and chief of the division of pain medicine in the department of anesthesiology at the University of California, San Diego. Dr. Wallace, who was not involved in the guidelines’ development study, said that he’s “titrated hundreds of patients off of opioids using cannabis.”
Dr. Wallace said he found the guidelines’ dosing recommendations helpful.
“If you stay within the 1- to 5-mg dosing range, the risks are so incredibly low, you’re not going to harm the patient.”
While there are patients who abuse cannabis and CBMs, Dr. Wallace noted that he has seen only one patient in the past 20 years who was overusing the medical cannabis. He added that his patient population does not use medical cannabis to get high and, in fact, wants to avoid doses that produce that effect at all costs.
Also commenting on the guidelines, Christopher Gilligan, MD, MBA, associate chief medical officer and a pain medicine physician at Brigham and Women’s Hospital in Boston, who was not involved in the guidelines’ development, points to the risks.
“When we have an opportunity to use cannabinoids in place of opioids for our patients, I think that that’s a positive thing ... and a wise choice in terms of risk benefit,” Dr. Gilligan said.
On the other hand, he cautioned that “freely prescribing” cannabinoids for chronic pain in patients who aren’t on opioids is not good practice.
“We have to take seriously the potential adverse effects of [cannabis], including marijuana use disorder, interference with learning, memory impairment, and psychotic breakthroughs,” said Dr. Gilligan.
Given the current climate, it would appear that CBM is a long way from being endorsed by the Food and Drug Administration, but for clinicians interested in trying CBM for chronic pain patients, the guidelines may offer a roadmap for initiation and an alternative to prescribing opioids.
Dr. Bell, Dr. Gilligan, and Dr. Wallace report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
New clinical practice guidelines for cannabis in chronic pain management have been released.
Developed by a group of Canadian researchers, clinicians, and patients, the guidelines note that cannabinoid-based medicines (CBM) may help clinicians offer an effective, less addictive, alternative to opioids in patients with chronic noncancer pain and comorbid conditions.
“We don’t recommend using CBM first line for anything pretty much because there are other alternatives that may be more effective and also offer fewer side effects,” lead guideline author Alan Bell, MD, assistant professor of family and community medicine at the University of Toronto, told this news organization.
“But I would strongly argue that I would use cannabis-based medicine over opioids every time. Why would you use a high potency-high toxicity agent when there’s a low potency-low toxicity alternative?” he said.
The guidelines were published online in the journal Cannabis and Cannabinoid Research.
Examining the evidence
A consistent criticism of CBM has been the lack of quality research supporting its therapeutic utility. To develop the current recommendations, the task force reviewed 47 pain management studies enrolling more than 11,000 patients. Almost half of the studies (n = 22) were randomized controlled trials (RCTs) and 12 of the 19 included systematic reviews focused solely on RCTs.
Overall, 38 of the 47 included studies demonstrated that CBM provided at least moderate benefits for chronic pain, resulting in a “strong” recommendation – mostly as an adjunct or replacement treatment in individuals living with chronic pain.
Overall, the guidelines place a high value on improving chronic pain and functionality, and addressing co-occurring conditions such as insomnia, anxiety and depression, mobility, and inflammation. They also provide practical dosing and formulation tips to support the use of CBM in the clinical setting.
When it comes to chronic pain, CBM is not a panacea. However, prior research suggests cannabinoids and opioids share several pharmacologic properties, including independent but possibly related mechanisms for antinociception, making them an intriguing combination.
In the current guidelines, all of the four studies specifically addressing combined opioids and vaporized cannabis flower demonstrated further pain reduction, reinforcing the conclusion that the benefits of CBM for improving pain control in patients taking opioids outweigh the risk of nonserious adverse events (AEs), such as dry mouth, dizziness, increased appetite, sedation, and concentration difficulties.
The recommendations also highlighted evidence demonstrating that a majority of participants were able to reduce use of routine pain medications with concomitant CBM/opioid administration, while simultaneously offering secondary benefits such as improved sleep, anxiety, and mood, as well as prevention of opioid tolerance and dose escalation.
Importantly, the guidelines offer an evidence-based algorithm with a clear framework for tapering patients off opioids, especially those who are on > 50 mg MED, which places them with a twofold greater risk for fatal overdose.
An effective alternative
Commenting on the new guidelines, Mark Wallace, MD, who has extensive experience researching and treating pain patients with medical cannabis, said the genesis of his interest in medical cannabis mirrors the guidelines’ focus.
“What got me interested in medical cannabis was trying to get patients off of opioids,” said Dr. Wallace, professor of anesthesiology and chief of the division of pain medicine in the department of anesthesiology at the University of California, San Diego. Dr. Wallace, who was not involved in the guidelines’ development study, said that he’s “titrated hundreds of patients off of opioids using cannabis.”
Dr. Wallace said he found the guidelines’ dosing recommendations helpful.
“If you stay within the 1- to 5-mg dosing range, the risks are so incredibly low, you’re not going to harm the patient.”
While there are patients who abuse cannabis and CBMs, Dr. Wallace noted that he has seen only one patient in the past 20 years who was overusing the medical cannabis. He added that his patient population does not use medical cannabis to get high and, in fact, wants to avoid doses that produce that effect at all costs.
Also commenting on the guidelines, Christopher Gilligan, MD, MBA, associate chief medical officer and a pain medicine physician at Brigham and Women’s Hospital in Boston, who was not involved in the guidelines’ development, points to the risks.
“When we have an opportunity to use cannabinoids in place of opioids for our patients, I think that that’s a positive thing ... and a wise choice in terms of risk benefit,” Dr. Gilligan said.
On the other hand, he cautioned that “freely prescribing” cannabinoids for chronic pain in patients who aren’t on opioids is not good practice.
“We have to take seriously the potential adverse effects of [cannabis], including marijuana use disorder, interference with learning, memory impairment, and psychotic breakthroughs,” said Dr. Gilligan.
Given the current climate, it would appear that CBM is a long way from being endorsed by the Food and Drug Administration, but for clinicians interested in trying CBM for chronic pain patients, the guidelines may offer a roadmap for initiation and an alternative to prescribing opioids.
Dr. Bell, Dr. Gilligan, and Dr. Wallace report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM CANNABIS AND CANNABINOID RESEARCH
Study highlights potential skin cancer risk of UV nail polish dryers
Results of a study recently published in Nature Communications suggests that According to two experts, these findings raise concerns regarding the safety of frequent use of these nail dryers.
In the study, human and mouse cells were exposed to radiation from UV nail dryers. Exposing human and mice skin cells to UVA light for 20 minutes resulted in the death of 20%-30% of cells; three consecutive 20-minute sessions resulted in the death of 65%-70% of cells. Additionally, surviving cells suffered oxidative damage to their DNA and mitochondria, with mutational patterns similar to those seen in skin cancer, study investigator Maria Zhivagui, PhD, of the University of California, San Diego, and associates reported.

“This study showed that irradiation of human and mouse cell lines using UV nail polish dryers resulted in DNA damage and genome mutations,” Shari Lipner, MD, PhD, director of the nail division at New York–Presbyterian Hospital/Weill Cornell Medicine, New York, said in an interview. The study “ties together exposure to UV light from nail polish dryers and genetic mutations that are associated with skin cancers,” added Dr. Lipner, who was not involved with the study.
UV nail lamps are commonly used to dry and harden gel nail polish formulas. Often referred to as “mini tanning beds,” these devices emit UVA radiation, classified as a Group 1 Carcinogen by the International Agency for Research on Cancer.
“Both UVA and UVB are main drivers of both melanoma and keratinocyte carcinomas (basal cell carcinoma and squamous cell carcinoma),” said Anthony Rossi, MD, a dermatologic surgeon at Memorial Sloan Kettering Cancer Center, New York, who was also not a study investigator. UV irradiance “produces DNA mutations that are specific to forming types of skin cancer,” he said in an interview.
UVA wavelengths commonly used in nail dryers can penetrate all layers of the epidermis, the top layer of the skin, potentially affecting stem cells in the skin, according to the study.
Dr. Lipner noted that “there have been several case reports of patients with histories of gel manicures using UV nail polish dryers who later developed squamous cell carcinomas on the dorsal hands, fingers, and nails, and articles describing high UV emissions from nail polish dryers, but the direct connection between UV dryers and skin cancer development was tenuous.” The first of its kind, the new study investigated the impact of UV nail drying devices at a cellular level.
The results of this study, in combination with previous case reports suggesting the development of skin cancers following UVA dryer use, raise concern regarding the safety of these commonly used devices. The study, the authors wrote, “does not provide direct evidence for an increased cancer risk in human beings,” but their findings and “prior evidence strongly suggest that radiation emitted by UV nail polish dryers may cause cancers of the hand and that UV nail polish dryers, similar to tanning beds, may increase the risk of early onset skin cancer.”

Dr. Rossi said that, “while this study shows that the UV exposure does affect human cells and causes mutations, the study was not done in vivo in human beings, so further studies are needed to know at what dose and frequency gel manicures would be needed to cause detrimental effects.” However, for people who regularly receive gel manicures involving UV nail dryers, both Dr. Lipner and Dr. Rossi recommend applying a broad-spectrum sunscreen to protect the dorsal hands, fingertips, and skin surrounding the nails, or wearing UV-protective gloves.
The study was supported by an Alfred B. Sloan Research Fellowship to one of the authors and grants from the National Institutes of Health to two authors. One author reported being a compensated consultant and having an equity interest in io9. Dr. Lipner and Dr. Rossi reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Results of a study recently published in Nature Communications suggests that According to two experts, these findings raise concerns regarding the safety of frequent use of these nail dryers.
In the study, human and mouse cells were exposed to radiation from UV nail dryers. Exposing human and mice skin cells to UVA light for 20 minutes resulted in the death of 20%-30% of cells; three consecutive 20-minute sessions resulted in the death of 65%-70% of cells. Additionally, surviving cells suffered oxidative damage to their DNA and mitochondria, with mutational patterns similar to those seen in skin cancer, study investigator Maria Zhivagui, PhD, of the University of California, San Diego, and associates reported.
“This study showed that irradiation of human and mouse cell lines using UV nail polish dryers resulted in DNA damage and genome mutations,” Shari Lipner, MD, PhD, director of the nail division at New York–Presbyterian Hospital/Weill Cornell Medicine, New York, said in an interview. The study “ties together exposure to UV light from nail polish dryers and genetic mutations that are associated with skin cancers,” added Dr. Lipner, who was not involved with the study.
UV nail lamps are commonly used to dry and harden gel nail polish formulas. Often referred to as “mini tanning beds,” these devices emit UVA radiation, classified as a Group 1 Carcinogen by the International Agency for Research on Cancer.
“Both UVA and UVB are main drivers of both melanoma and keratinocyte carcinomas (basal cell carcinoma and squamous cell carcinoma),” said Anthony Rossi, MD, a dermatologic surgeon at Memorial Sloan Kettering Cancer Center, New York, who was also not a study investigator. UV irradiance “produces DNA mutations that are specific to forming types of skin cancer,” he said in an interview.
UVA wavelengths commonly used in nail dryers can penetrate all layers of the epidermis, the top layer of the skin, potentially affecting stem cells in the skin, according to the study.
Dr. Lipner noted that “there have been several case reports of patients with histories of gel manicures using UV nail polish dryers who later developed squamous cell carcinomas on the dorsal hands, fingers, and nails, and articles describing high UV emissions from nail polish dryers, but the direct connection between UV dryers and skin cancer development was tenuous.” The first of its kind, the new study investigated the impact of UV nail drying devices at a cellular level.
The results of this study, in combination with previous case reports suggesting the development of skin cancers following UVA dryer use, raise concern regarding the safety of these commonly used devices. The study, the authors wrote, “does not provide direct evidence for an increased cancer risk in human beings,” but their findings and “prior evidence strongly suggest that radiation emitted by UV nail polish dryers may cause cancers of the hand and that UV nail polish dryers, similar to tanning beds, may increase the risk of early onset skin cancer.”
Dr. Rossi said that, “while this study shows that the UV exposure does affect human cells and causes mutations, the study was not done in vivo in human beings, so further studies are needed to know at what dose and frequency gel manicures would be needed to cause detrimental effects.” However, for people who regularly receive gel manicures involving UV nail dryers, both Dr. Lipner and Dr. Rossi recommend applying a broad-spectrum sunscreen to protect the dorsal hands, fingertips, and skin surrounding the nails, or wearing UV-protective gloves.
The study was supported by an Alfred B. Sloan Research Fellowship to one of the authors and grants from the National Institutes of Health to two authors. One author reported being a compensated consultant and having an equity interest in io9. Dr. Lipner and Dr. Rossi reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Results of a study recently published in Nature Communications suggests that According to two experts, these findings raise concerns regarding the safety of frequent use of these nail dryers.
In the study, human and mouse cells were exposed to radiation from UV nail dryers. Exposing human and mice skin cells to UVA light for 20 minutes resulted in the death of 20%-30% of cells; three consecutive 20-minute sessions resulted in the death of 65%-70% of cells. Additionally, surviving cells suffered oxidative damage to their DNA and mitochondria, with mutational patterns similar to those seen in skin cancer, study investigator Maria Zhivagui, PhD, of the University of California, San Diego, and associates reported.
“This study showed that irradiation of human and mouse cell lines using UV nail polish dryers resulted in DNA damage and genome mutations,” Shari Lipner, MD, PhD, director of the nail division at New York–Presbyterian Hospital/Weill Cornell Medicine, New York, said in an interview. The study “ties together exposure to UV light from nail polish dryers and genetic mutations that are associated with skin cancers,” added Dr. Lipner, who was not involved with the study.
UV nail lamps are commonly used to dry and harden gel nail polish formulas. Often referred to as “mini tanning beds,” these devices emit UVA radiation, classified as a Group 1 Carcinogen by the International Agency for Research on Cancer.
“Both UVA and UVB are main drivers of both melanoma and keratinocyte carcinomas (basal cell carcinoma and squamous cell carcinoma),” said Anthony Rossi, MD, a dermatologic surgeon at Memorial Sloan Kettering Cancer Center, New York, who was also not a study investigator. UV irradiance “produces DNA mutations that are specific to forming types of skin cancer,” he said in an interview.
UVA wavelengths commonly used in nail dryers can penetrate all layers of the epidermis, the top layer of the skin, potentially affecting stem cells in the skin, according to the study.
Dr. Lipner noted that “there have been several case reports of patients with histories of gel manicures using UV nail polish dryers who later developed squamous cell carcinomas on the dorsal hands, fingers, and nails, and articles describing high UV emissions from nail polish dryers, but the direct connection between UV dryers and skin cancer development was tenuous.” The first of its kind, the new study investigated the impact of UV nail drying devices at a cellular level.
The results of this study, in combination with previous case reports suggesting the development of skin cancers following UVA dryer use, raise concern regarding the safety of these commonly used devices. The study, the authors wrote, “does not provide direct evidence for an increased cancer risk in human beings,” but their findings and “prior evidence strongly suggest that radiation emitted by UV nail polish dryers may cause cancers of the hand and that UV nail polish dryers, similar to tanning beds, may increase the risk of early onset skin cancer.”
Dr. Rossi said that, “while this study shows that the UV exposure does affect human cells and causes mutations, the study was not done in vivo in human beings, so further studies are needed to know at what dose and frequency gel manicures would be needed to cause detrimental effects.” However, for people who regularly receive gel manicures involving UV nail dryers, both Dr. Lipner and Dr. Rossi recommend applying a broad-spectrum sunscreen to protect the dorsal hands, fingertips, and skin surrounding the nails, or wearing UV-protective gloves.
The study was supported by an Alfred B. Sloan Research Fellowship to one of the authors and grants from the National Institutes of Health to two authors. One author reported being a compensated consultant and having an equity interest in io9. Dr. Lipner and Dr. Rossi reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM NATURE COMMUNICATIONS
What are the clinical implications of recent skin dysbiosis discoveries?
NEW ORLEANS – .
“There’s still a lot for us to learn,” Adam Friedman, MD, professor and chair of dermatology at George Washington University, Washington, said at the annual meeting of the American Academy of Dermatology. “Multiple factors contribute to the variability in the skin microbiota, including age, sex, environment, immune system, host genotype, lifestyle, and pathobiology. The question becomes, when do these factors or impacts on the microbiota become clinically significant?”
According to Dr. Friedman, there are 10 times more bacteria cells than human cells in the human body, “but it’s not a fight to the finish; it’s not us versus them,” he said. “Together, we are a super organism.” There are also more than 500 species of bacteria on human skin excluding viruses and fungi, and each person carries up to 5 pounds of bacteria, which is akin to finding a new organ in the body.
“What’s so unique is that we each have our own bacterial fingerprint,” he said. “Whoever is sitting next to you? Their microbiota makeup is different than yours.”
Beyond genetics and environment, activities that can contribute to alterations in skin flora or skin dysbiosis include topical application of steroids, antibiotics, retinoids, harsh soaps, chemical and physical exfoliants, and resurfacing techniques. “With anything we apply or do to the skin, we are literally changing the home of many microorganisms, for good or bad,” he said.
In the realm of atopic dermatitis (AD), Staphylococcus aureus has been implicated as an offender in the pathophysiology of the disease. “It’s not about one single species of Staphylococcus, though,” said Dr. Friedman, who also is director of translational research at George Washington University. “We’re finding out that, depending on the severity of disease, Staph. epidermis may be part of the problem as opposed to it just being about Staph. aureus. Furthermore, and more importantly, these changes in the microbiota, specifically a decrease in microbial diversity, has been shown to precede a disease flare, highlighting the central role of maintaining microbial diversity and by definition, supporting the living barrier in our management of AD.”
With this in mind, researchers in one study used high-throughput sequencing to evaluate the microbial communities associated with affected and unaffected skin of 49 patients with AD before and after emollient treatment. Following 84 days of emollient application, clinical symptoms of AD improved in 72% of the study population and Stenotrophomonas species were significantly more abundant among responders.
Prebiotics, probiotics
“Our treatments certainly can positively impact the microbiota, as we have seen even recently with some of our new targeted therapies, but we can also directly provide support,” he continued. Prebiotics, which he defined as supplements or foods that contain a nondigestible ingredient that selectively stimulates the growth and/or activity of indigenous bacteria, can be found in many over-the-counter moisturizers.

For example, colloidal oatmeal has been found to support the growth of S. epidermidis and enhance the production of lactic acid. “We really don’t know much about what these induced changes mean from a clinical perspective; that has yet to be elucidated,” Dr. Friedman said.
In light of the recent attention to the early application of moisturizers in infants at high risk of developing AD in an effort to prevent or limit AD, “maybe part of this has to do with applying something that’s nurturing an evolving microbiota,” Dr. Friedman noted. “It’s something to think about.”
Yet another area of study involves the use of probiotics, which Dr. Friedman defined as supplements or foods that contain viable microorganisms that alter the microflora of the host. In a first-of-its-kind trial, researchers evaluated the safety and efficacy of self-administered topical Roseomonas mucosa in 10 adults and 5 children with AD. No adverse events or treatment complications were observed, and the topical R. mucosa was associated with significant decreases in measures of disease severity, topical steroid requirement, and S. aureus burden
In a more recent randomized trial of 11 patients with AD, Richard L. Gallo, MD, PhD, chair of dermatology, University of California, San Diego, and colleagues found that application of a personalized topical cream formulated from coagulase-negative Staphylococcus with antimicrobial activity against S. aureus reduced colonization of S. aureus and improved disease severity.
And in another randomized, controlled trial, Italian researchers enrolled 80 adults with mild to severe AD to receive a placebo or a supplement that was a mixture of lactobacilli for 56 days. They found that adults in the treatment arm showed an improvement in skin smoothness, skin moisturization, self-perception, and a decrease in the SCORing Atopic Dermatitis (SCORAD) index as well as in levels of inflammatory markers associated with AD.
Dr. Friedman also discussed postbiotics, nonviable bacterial products or metabolic byproducts from probiotic microorganisms that have biologic activity in the host. In one trial, French researchers enrolled 75 people with AD who ranged in age from 6 to 70 years to receive a cream containing a 5% lysate of the nonpathogenic bacteria Vitreoscilla filiformis, or a vehicle cream for 30 days. They found that compared with the vehicle, V. filiformis lysate significantly decreased SCORAD levels and pruritus; active cream was shown to significantly decrease loss of sleep from day 0 to day 29.
Dr. Friedman characterized these novel approaches to AD as “an exciting area, one we need to pay attention to. But what I really want to know is, aside from these purposefully made and marketed products that have pre- and postprobiotics, is there a difference with some of the products we use already? My assumption is that there is, but we need to see that data.”
Dr. Friedman disclosed that he is a consultant and/or advisory board member for Medscape/SanovaWorks, Oakstone Institute, L’Oréal, La Roche Posay, Galderma, Aveeno, Ortho Dermatologic, Microcures, Pfizer, Novartis, Lilly, Hoth Therapeutics, Zylo Therapeutics, BMS, Vial, Janssen, Novocure, Dermavant, Regeneron/Sanofi, and Incyte. He has also received grants from Pfizer, the Dermatology Foundation, Lilly, Janssen, Incyte, and Galderma.
NEW ORLEANS – .
“There’s still a lot for us to learn,” Adam Friedman, MD, professor and chair of dermatology at George Washington University, Washington, said at the annual meeting of the American Academy of Dermatology. “Multiple factors contribute to the variability in the skin microbiota, including age, sex, environment, immune system, host genotype, lifestyle, and pathobiology. The question becomes, when do these factors or impacts on the microbiota become clinically significant?”
According to Dr. Friedman, there are 10 times more bacteria cells than human cells in the human body, “but it’s not a fight to the finish; it’s not us versus them,” he said. “Together, we are a super organism.” There are also more than 500 species of bacteria on human skin excluding viruses and fungi, and each person carries up to 5 pounds of bacteria, which is akin to finding a new organ in the body.
“What’s so unique is that we each have our own bacterial fingerprint,” he said. “Whoever is sitting next to you? Their microbiota makeup is different than yours.”
Beyond genetics and environment, activities that can contribute to alterations in skin flora or skin dysbiosis include topical application of steroids, antibiotics, retinoids, harsh soaps, chemical and physical exfoliants, and resurfacing techniques. “With anything we apply or do to the skin, we are literally changing the home of many microorganisms, for good or bad,” he said.
In the realm of atopic dermatitis (AD), Staphylococcus aureus has been implicated as an offender in the pathophysiology of the disease. “It’s not about one single species of Staphylococcus, though,” said Dr. Friedman, who also is director of translational research at George Washington University. “We’re finding out that, depending on the severity of disease, Staph. epidermis may be part of the problem as opposed to it just being about Staph. aureus. Furthermore, and more importantly, these changes in the microbiota, specifically a decrease in microbial diversity, has been shown to precede a disease flare, highlighting the central role of maintaining microbial diversity and by definition, supporting the living barrier in our management of AD.”
With this in mind, researchers in one study used high-throughput sequencing to evaluate the microbial communities associated with affected and unaffected skin of 49 patients with AD before and after emollient treatment. Following 84 days of emollient application, clinical symptoms of AD improved in 72% of the study population and Stenotrophomonas species were significantly more abundant among responders.
Prebiotics, probiotics
“Our treatments certainly can positively impact the microbiota, as we have seen even recently with some of our new targeted therapies, but we can also directly provide support,” he continued. Prebiotics, which he defined as supplements or foods that contain a nondigestible ingredient that selectively stimulates the growth and/or activity of indigenous bacteria, can be found in many over-the-counter moisturizers.
For example, colloidal oatmeal has been found to support the growth of S. epidermidis and enhance the production of lactic acid. “We really don’t know much about what these induced changes mean from a clinical perspective; that has yet to be elucidated,” Dr. Friedman said.
In light of the recent attention to the early application of moisturizers in infants at high risk of developing AD in an effort to prevent or limit AD, “maybe part of this has to do with applying something that’s nurturing an evolving microbiota,” Dr. Friedman noted. “It’s something to think about.”
Yet another area of study involves the use of probiotics, which Dr. Friedman defined as supplements or foods that contain viable microorganisms that alter the microflora of the host. In a first-of-its-kind trial, researchers evaluated the safety and efficacy of self-administered topical Roseomonas mucosa in 10 adults and 5 children with AD. No adverse events or treatment complications were observed, and the topical R. mucosa was associated with significant decreases in measures of disease severity, topical steroid requirement, and S. aureus burden
In a more recent randomized trial of 11 patients with AD, Richard L. Gallo, MD, PhD, chair of dermatology, University of California, San Diego, and colleagues found that application of a personalized topical cream formulated from coagulase-negative Staphylococcus with antimicrobial activity against S. aureus reduced colonization of S. aureus and improved disease severity.
And in another randomized, controlled trial, Italian researchers enrolled 80 adults with mild to severe AD to receive a placebo or a supplement that was a mixture of lactobacilli for 56 days. They found that adults in the treatment arm showed an improvement in skin smoothness, skin moisturization, self-perception, and a decrease in the SCORing Atopic Dermatitis (SCORAD) index as well as in levels of inflammatory markers associated with AD.
Dr. Friedman also discussed postbiotics, nonviable bacterial products or metabolic byproducts from probiotic microorganisms that have biologic activity in the host. In one trial, French researchers enrolled 75 people with AD who ranged in age from 6 to 70 years to receive a cream containing a 5% lysate of the nonpathogenic bacteria Vitreoscilla filiformis, or a vehicle cream for 30 days. They found that compared with the vehicle, V. filiformis lysate significantly decreased SCORAD levels and pruritus; active cream was shown to significantly decrease loss of sleep from day 0 to day 29.
Dr. Friedman characterized these novel approaches to AD as “an exciting area, one we need to pay attention to. But what I really want to know is, aside from these purposefully made and marketed products that have pre- and postprobiotics, is there a difference with some of the products we use already? My assumption is that there is, but we need to see that data.”
Dr. Friedman disclosed that he is a consultant and/or advisory board member for Medscape/SanovaWorks, Oakstone Institute, L’Oréal, La Roche Posay, Galderma, Aveeno, Ortho Dermatologic, Microcures, Pfizer, Novartis, Lilly, Hoth Therapeutics, Zylo Therapeutics, BMS, Vial, Janssen, Novocure, Dermavant, Regeneron/Sanofi, and Incyte. He has also received grants from Pfizer, the Dermatology Foundation, Lilly, Janssen, Incyte, and Galderma.
NEW ORLEANS – .
“There’s still a lot for us to learn,” Adam Friedman, MD, professor and chair of dermatology at George Washington University, Washington, said at the annual meeting of the American Academy of Dermatology. “Multiple factors contribute to the variability in the skin microbiota, including age, sex, environment, immune system, host genotype, lifestyle, and pathobiology. The question becomes, when do these factors or impacts on the microbiota become clinically significant?”
According to Dr. Friedman, there are 10 times more bacteria cells than human cells in the human body, “but it’s not a fight to the finish; it’s not us versus them,” he said. “Together, we are a super organism.” There are also more than 500 species of bacteria on human skin excluding viruses and fungi, and each person carries up to 5 pounds of bacteria, which is akin to finding a new organ in the body.
“What’s so unique is that we each have our own bacterial fingerprint,” he said. “Whoever is sitting next to you? Their microbiota makeup is different than yours.”
Beyond genetics and environment, activities that can contribute to alterations in skin flora or skin dysbiosis include topical application of steroids, antibiotics, retinoids, harsh soaps, chemical and physical exfoliants, and resurfacing techniques. “With anything we apply or do to the skin, we are literally changing the home of many microorganisms, for good or bad,” he said.
In the realm of atopic dermatitis (AD), Staphylococcus aureus has been implicated as an offender in the pathophysiology of the disease. “It’s not about one single species of Staphylococcus, though,” said Dr. Friedman, who also is director of translational research at George Washington University. “We’re finding out that, depending on the severity of disease, Staph. epidermis may be part of the problem as opposed to it just being about Staph. aureus. Furthermore, and more importantly, these changes in the microbiota, specifically a decrease in microbial diversity, has been shown to precede a disease flare, highlighting the central role of maintaining microbial diversity and by definition, supporting the living barrier in our management of AD.”
With this in mind, researchers in one study used high-throughput sequencing to evaluate the microbial communities associated with affected and unaffected skin of 49 patients with AD before and after emollient treatment. Following 84 days of emollient application, clinical symptoms of AD improved in 72% of the study population and Stenotrophomonas species were significantly more abundant among responders.
Prebiotics, probiotics
“Our treatments certainly can positively impact the microbiota, as we have seen even recently with some of our new targeted therapies, but we can also directly provide support,” he continued. Prebiotics, which he defined as supplements or foods that contain a nondigestible ingredient that selectively stimulates the growth and/or activity of indigenous bacteria, can be found in many over-the-counter moisturizers.
For example, colloidal oatmeal has been found to support the growth of S. epidermidis and enhance the production of lactic acid. “We really don’t know much about what these induced changes mean from a clinical perspective; that has yet to be elucidated,” Dr. Friedman said.
In light of the recent attention to the early application of moisturizers in infants at high risk of developing AD in an effort to prevent or limit AD, “maybe part of this has to do with applying something that’s nurturing an evolving microbiota,” Dr. Friedman noted. “It’s something to think about.”
Yet another area of study involves the use of probiotics, which Dr. Friedman defined as supplements or foods that contain viable microorganisms that alter the microflora of the host. In a first-of-its-kind trial, researchers evaluated the safety and efficacy of self-administered topical Roseomonas mucosa in 10 adults and 5 children with AD. No adverse events or treatment complications were observed, and the topical R. mucosa was associated with significant decreases in measures of disease severity, topical steroid requirement, and S. aureus burden
In a more recent randomized trial of 11 patients with AD, Richard L. Gallo, MD, PhD, chair of dermatology, University of California, San Diego, and colleagues found that application of a personalized topical cream formulated from coagulase-negative Staphylococcus with antimicrobial activity against S. aureus reduced colonization of S. aureus and improved disease severity.
And in another randomized, controlled trial, Italian researchers enrolled 80 adults with mild to severe AD to receive a placebo or a supplement that was a mixture of lactobacilli for 56 days. They found that adults in the treatment arm showed an improvement in skin smoothness, skin moisturization, self-perception, and a decrease in the SCORing Atopic Dermatitis (SCORAD) index as well as in levels of inflammatory markers associated with AD.
Dr. Friedman also discussed postbiotics, nonviable bacterial products or metabolic byproducts from probiotic microorganisms that have biologic activity in the host. In one trial, French researchers enrolled 75 people with AD who ranged in age from 6 to 70 years to receive a cream containing a 5% lysate of the nonpathogenic bacteria Vitreoscilla filiformis, or a vehicle cream for 30 days. They found that compared with the vehicle, V. filiformis lysate significantly decreased SCORAD levels and pruritus; active cream was shown to significantly decrease loss of sleep from day 0 to day 29.
Dr. Friedman characterized these novel approaches to AD as “an exciting area, one we need to pay attention to. But what I really want to know is, aside from these purposefully made and marketed products that have pre- and postprobiotics, is there a difference with some of the products we use already? My assumption is that there is, but we need to see that data.”
Dr. Friedman disclosed that he is a consultant and/or advisory board member for Medscape/SanovaWorks, Oakstone Institute, L’Oréal, La Roche Posay, Galderma, Aveeno, Ortho Dermatologic, Microcures, Pfizer, Novartis, Lilly, Hoth Therapeutics, Zylo Therapeutics, BMS, Vial, Janssen, Novocure, Dermavant, Regeneron/Sanofi, and Incyte. He has also received grants from Pfizer, the Dermatology Foundation, Lilly, Janssen, Incyte, and Galderma.
AT AAD 2023

AGA guidelines, CPUs lead education at DDW® 2023
Below is a sampling of AGA’s invited-speaker sessions we’re excited about this year for clinical practitioners. To view other AGA program highlights, check out the DDW Preliminary Program.
- Guidelines Highlights 2023
- Clinical Practice Updates: Battle of the Heavyweights
- AGA Clinical Symposium
- Case Studies in Measuring Care and Improving Quality
- Optimizing Your GI Practice: Guidelines, Quality and Delivery
- AGA Postgraduate Course ($)
- Surviving the First Years in Clinical Practice: Roundtable With the Experts
Below is a sampling of AGA’s invited-speaker sessions we’re excited about this year for clinical practitioners. To view other AGA program highlights, check out the DDW Preliminary Program.
- Guidelines Highlights 2023
- Clinical Practice Updates: Battle of the Heavyweights
- AGA Clinical Symposium
- Case Studies in Measuring Care and Improving Quality
- Optimizing Your GI Practice: Guidelines, Quality and Delivery
- AGA Postgraduate Course ($)
- Surviving the First Years in Clinical Practice: Roundtable With the Experts
Below is a sampling of AGA’s invited-speaker sessions we’re excited about this year for clinical practitioners. To view other AGA program highlights, check out the DDW Preliminary Program.
- Guidelines Highlights 2023
- Clinical Practice Updates: Battle of the Heavyweights
- AGA Clinical Symposium
- Case Studies in Measuring Care and Improving Quality
- Optimizing Your GI Practice: Guidelines, Quality and Delivery
- AGA Postgraduate Course ($)
- Surviving the First Years in Clinical Practice: Roundtable With the Experts
Protect the next generation of GI investigators
Investing in research is the only way we will identify new diagnostics and treatments. However, at this time of unparalleled scientific and clinical opportunity, promising early stage investigators are leaving the field because of the instability of federal research funding.
Fortunately, the AGA Research Foundation has a proven track record of funding young investigators whose work advances the field of gastroenterology and hepatology.
Help the AGA build a community of investigators through the AGA Research Foundation.
Your donation to the AGA Research Foundation can fund future success stories by keeping young scientists working to advance our understanding of digestive diseases.
Donate today to help protect the GI research pipeline. Make a tax-deductible donation at www.foundation.gastro.org.
Investing in research is the only way we will identify new diagnostics and treatments. However, at this time of unparalleled scientific and clinical opportunity, promising early stage investigators are leaving the field because of the instability of federal research funding.
Fortunately, the AGA Research Foundation has a proven track record of funding young investigators whose work advances the field of gastroenterology and hepatology.
Help the AGA build a community of investigators through the AGA Research Foundation.
Your donation to the AGA Research Foundation can fund future success stories by keeping young scientists working to advance our understanding of digestive diseases.
Donate today to help protect the GI research pipeline. Make a tax-deductible donation at www.foundation.gastro.org.
Investing in research is the only way we will identify new diagnostics and treatments. However, at this time of unparalleled scientific and clinical opportunity, promising early stage investigators are leaving the field because of the instability of federal research funding.
Fortunately, the AGA Research Foundation has a proven track record of funding young investigators whose work advances the field of gastroenterology and hepatology.
Help the AGA build a community of investigators through the AGA Research Foundation.
Your donation to the AGA Research Foundation can fund future success stories by keeping young scientists working to advance our understanding of digestive diseases.
Donate today to help protect the GI research pipeline. Make a tax-deductible donation at www.foundation.gastro.org.
Picking up the premotor symptoms of Parkinson’s
This transcript has been edited for clarity.
Matthew F. Watto, MD: Welcome back to The Curbsiders. We had a great discussion on Parkinson’s Disease for Primary Care with Dr. Albert Hung. Paul, this was something that really made me nervous. I didn’t have a lot of comfort with it. But he taught us a lot of tips about how to recognize Parkinson’s.
I hadn’t been as aware of the premotor symptoms: constipation, hyposmia (loss of sense of smell), and rapid eye movement sleep behavior disorder. If patients have those early on and they aren’t explained by other things (especially the REM sleep behavior disorder), you should really key in because those patients are at risk of developing Parkinson’s years down the line. Those symptoms could present first, which just kind of blew my mind.
What tips do you have about how to recognize Parkinson’s? Do you want to talk about the physical exam?
Paul N. Williams, MD: You know I love the physical exam stuff, so I’m happy to talk about that.
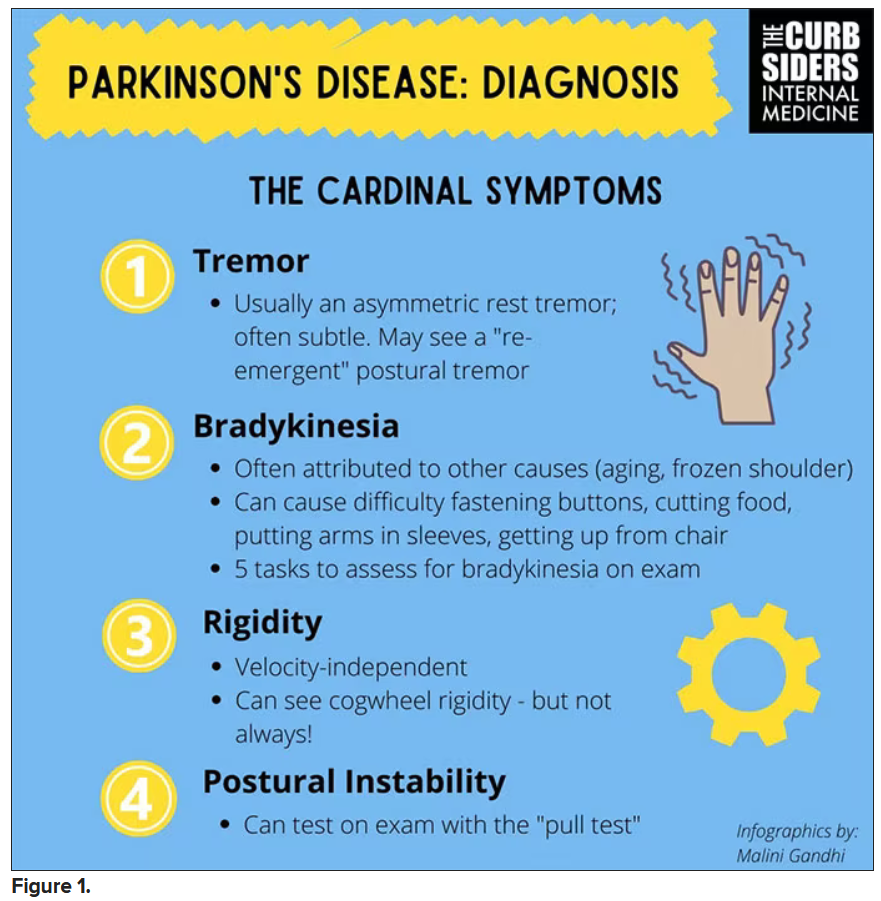
You were deeply upset that cogwheel rigidity was not pathognomonic for Parkinson’s, but you made the point – and our guest agreed – that asymmetry tends to be the key here. And I really appreciated the point about reemergent tremor. This is this idea of a resting tremor. If someone has more parkinsonian features, you might see an intention tremor with essential tremor. If they reach out, it might seem steady at first, but if they hold long enough, then the tremor may kind of reemerge. I thought that was a neat distinction.
And this idea of cogwheel rigidity is a combination of some of the cardinal features of Parkinson’s – it’s a little bit of tremor and a little bit of rigidity too. There’s a baseline increase in tone, and then the tremor is superimposed on top of that. When you’re feeling cogwheeling, that’s actually what you’re feeling on examination. Parkinson’s, with all of its physical exam findings has always fascinated me.
Dr. Watto: He also told us about some red flags.
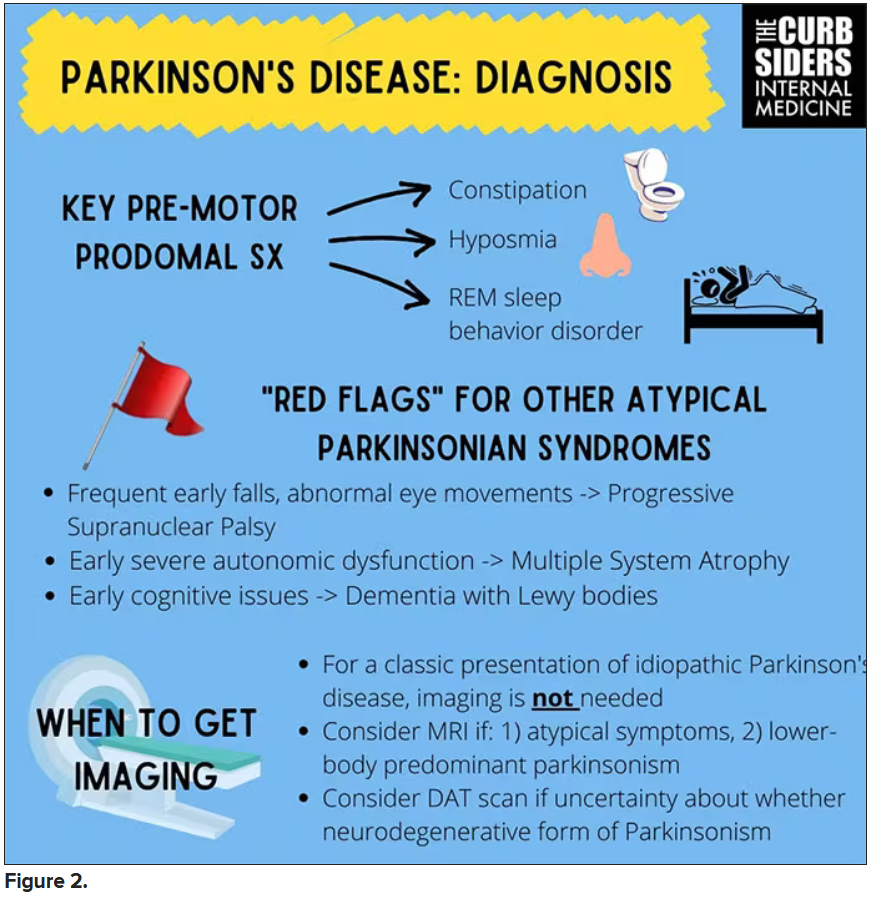
With classic idiopathic parkinsonism, there’s asymmetric involvement of the tremor. So red flags include a symmetric tremor, which might be something other than idiopathic parkinsonism. He also mentioned that one of the reasons you may want to get imaging (which is not always necessary if someone has a classic presentation), is if you see lower body–predominant symptoms of parkinsonism. These patients have rigidity or slowness of movement in their legs, but their upper bodies are not affected. They don’t have masked facies or the tremor in their hands. You might get an MRI in that case because that could be presentation of vascular dementia or vascular disease in the brain or even normal pressure hydrocephalus, which is a treatable condition. That would be one reason to get imaging.
What if the patient was exposed to a drug like a dopamine antagonist? They will get better in a couple of days, right?
Dr. Williams: This was a really fascinating point because we typically think if a patient’s symptoms are related to a drug exposure – in this case, drug-induced parkinsonism – we can just stop the medication and the symptoms will disappear in a couple of days as the drug leaves the system. But as it turns out, it might take much longer. A mistake that Dr Hung often sees is that the clinician stops the possibly offending agent, but when they don’t see an immediate relief of symptoms, they assume the drug wasn’t causing them. You really have to give the patient a fair shot off the medication to experience recovery because those symptoms can last weeks or even months after the drug is discontinued.
Dr. Watto: Dr Hung looks at the patient’s problem list and asks whether is there any reason this patient might have been exposed to one of these medications?
We’re not going to get too much into specific Parkinson’s treatment, but I was glad to hear that exercise actually improves mobility and may even have some neuroprotective effects. He mentioned ongoing trials looking at that. We always love an excuse to tell patients that they should be moving around more and being physically active.
Dr. Williams: That was one of the more shocking things I learned, that exercise might actually be good for you. That will deeply inform my practice. Many of the treatments that we use for Parkinson’s only address symptoms. They don’t address progression or fix anything, but exercise can help with that.
Dr. Watto: Paul, the last question I wanted to ask you is about our role in primary care. Patients with Parkinson’s have autonomic symptoms. They have neurocognitive symptoms. What is our role in that as primary care physicians?
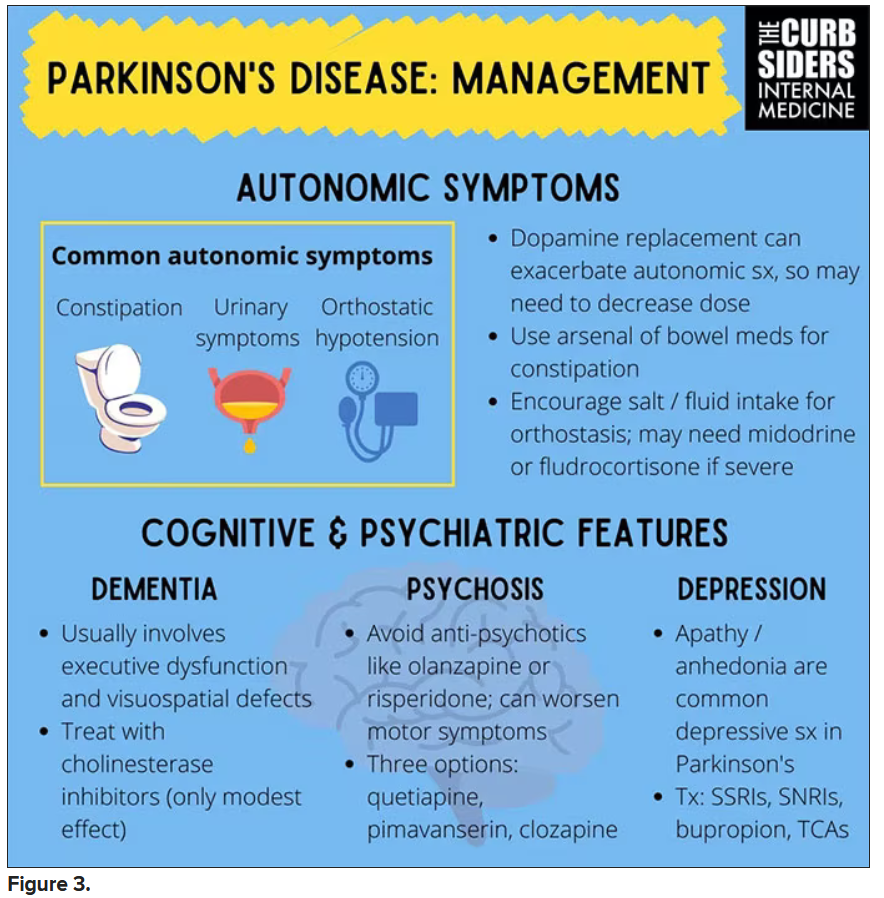
Dr. Williams: Myriad symptoms can accompany Parkinson’s, and we have experience with most of them. We should all feel fairly comfortable dealing with constipation, which can be a very bothersome symptom. And we can use our full arsenal for symptoms such as depression, anxiety, and even apathy – the anhedonia, which apparently can be the predominant feature. We do have the tools to address these problems.
This might be a situation where we might reach for bupropion or a tricyclic antidepressant, which might not be your initial choice for a patient with a possibly annoying mood disorder. But for someone with Parkinson’s disease, this actually may be very helpful. We know how to manage a lot of the symptoms that come along with Parkinson’s that are not just the motor symptoms, and we should take ownership of those things.
Dr. Watto: You can hear the rest of this podcast here. This has been another episode of The Curbsiders bringing you a little knowledge food for your brain hole. Until next time, I’ve been Dr Matthew Frank Watto.
Dr. Williams: And I’m Dr Paul Nelson Williams.
Dr. Watto is a clinical assistant professor, department of medicine, at the University of Pennsylvania, Philadelphia. Dr. Williams is Associate Professor of Clinical Medicine, Department of General Internal Medicine, at Temple University, Philadelphia. Neither Dr. Watto nor Dr. Williams reported any relevant conflicts of interest.
A version of this article first appeared on Medscape.com.
This transcript has been edited for clarity.
Matthew F. Watto, MD: Welcome back to The Curbsiders. We had a great discussion on Parkinson’s Disease for Primary Care with Dr. Albert Hung. Paul, this was something that really made me nervous. I didn’t have a lot of comfort with it. But he taught us a lot of tips about how to recognize Parkinson’s.
I hadn’t been as aware of the premotor symptoms: constipation, hyposmia (loss of sense of smell), and rapid eye movement sleep behavior disorder. If patients have those early on and they aren’t explained by other things (especially the REM sleep behavior disorder), you should really key in because those patients are at risk of developing Parkinson’s years down the line. Those symptoms could present first, which just kind of blew my mind.
What tips do you have about how to recognize Parkinson’s? Do you want to talk about the physical exam?
Paul N. Williams, MD: You know I love the physical exam stuff, so I’m happy to talk about that.
You were deeply upset that cogwheel rigidity was not pathognomonic for Parkinson’s, but you made the point – and our guest agreed – that asymmetry tends to be the key here. And I really appreciated the point about reemergent tremor. This is this idea of a resting tremor. If someone has more parkinsonian features, you might see an intention tremor with essential tremor. If they reach out, it might seem steady at first, but if they hold long enough, then the tremor may kind of reemerge. I thought that was a neat distinction.
And this idea of cogwheel rigidity is a combination of some of the cardinal features of Parkinson’s – it’s a little bit of tremor and a little bit of rigidity too. There’s a baseline increase in tone, and then the tremor is superimposed on top of that. When you’re feeling cogwheeling, that’s actually what you’re feeling on examination. Parkinson’s, with all of its physical exam findings has always fascinated me.
Dr. Watto: He also told us about some red flags.
With classic idiopathic parkinsonism, there’s asymmetric involvement of the tremor. So red flags include a symmetric tremor, which might be something other than idiopathic parkinsonism. He also mentioned that one of the reasons you may want to get imaging (which is not always necessary if someone has a classic presentation), is if you see lower body–predominant symptoms of parkinsonism. These patients have rigidity or slowness of movement in their legs, but their upper bodies are not affected. They don’t have masked facies or the tremor in their hands. You might get an MRI in that case because that could be presentation of vascular dementia or vascular disease in the brain or even normal pressure hydrocephalus, which is a treatable condition. That would be one reason to get imaging.
What if the patient was exposed to a drug like a dopamine antagonist? They will get better in a couple of days, right?
Dr. Williams: This was a really fascinating point because we typically think if a patient’s symptoms are related to a drug exposure – in this case, drug-induced parkinsonism – we can just stop the medication and the symptoms will disappear in a couple of days as the drug leaves the system. But as it turns out, it might take much longer. A mistake that Dr Hung often sees is that the clinician stops the possibly offending agent, but when they don’t see an immediate relief of symptoms, they assume the drug wasn’t causing them. You really have to give the patient a fair shot off the medication to experience recovery because those symptoms can last weeks or even months after the drug is discontinued.
Dr. Watto: Dr Hung looks at the patient’s problem list and asks whether is there any reason this patient might have been exposed to one of these medications?
We’re not going to get too much into specific Parkinson’s treatment, but I was glad to hear that exercise actually improves mobility and may even have some neuroprotective effects. He mentioned ongoing trials looking at that. We always love an excuse to tell patients that they should be moving around more and being physically active.
Dr. Williams: That was one of the more shocking things I learned, that exercise might actually be good for you. That will deeply inform my practice. Many of the treatments that we use for Parkinson’s only address symptoms. They don’t address progression or fix anything, but exercise can help with that.
Dr. Watto: Paul, the last question I wanted to ask you is about our role in primary care. Patients with Parkinson’s have autonomic symptoms. They have neurocognitive symptoms. What is our role in that as primary care physicians?
Dr. Williams: Myriad symptoms can accompany Parkinson’s, and we have experience with most of them. We should all feel fairly comfortable dealing with constipation, which can be a very bothersome symptom. And we can use our full arsenal for symptoms such as depression, anxiety, and even apathy – the anhedonia, which apparently can be the predominant feature. We do have the tools to address these problems.
This might be a situation where we might reach for bupropion or a tricyclic antidepressant, which might not be your initial choice for a patient with a possibly annoying mood disorder. But for someone with Parkinson’s disease, this actually may be very helpful. We know how to manage a lot of the symptoms that come along with Parkinson’s that are not just the motor symptoms, and we should take ownership of those things.
Dr. Watto: You can hear the rest of this podcast here. This has been another episode of The Curbsiders bringing you a little knowledge food for your brain hole. Until next time, I’ve been Dr Matthew Frank Watto.
Dr. Williams: And I’m Dr Paul Nelson Williams.
Dr. Watto is a clinical assistant professor, department of medicine, at the University of Pennsylvania, Philadelphia. Dr. Williams is Associate Professor of Clinical Medicine, Department of General Internal Medicine, at Temple University, Philadelphia. Neither Dr. Watto nor Dr. Williams reported any relevant conflicts of interest.
A version of this article first appeared on Medscape.com.
This transcript has been edited for clarity.
Matthew F. Watto, MD: Welcome back to The Curbsiders. We had a great discussion on Parkinson’s Disease for Primary Care with Dr. Albert Hung. Paul, this was something that really made me nervous. I didn’t have a lot of comfort with it. But he taught us a lot of tips about how to recognize Parkinson’s.
I hadn’t been as aware of the premotor symptoms: constipation, hyposmia (loss of sense of smell), and rapid eye movement sleep behavior disorder. If patients have those early on and they aren’t explained by other things (especially the REM sleep behavior disorder), you should really key in because those patients are at risk of developing Parkinson’s years down the line. Those symptoms could present first, which just kind of blew my mind.
What tips do you have about how to recognize Parkinson’s? Do you want to talk about the physical exam?
Paul N. Williams, MD: You know I love the physical exam stuff, so I’m happy to talk about that.
You were deeply upset that cogwheel rigidity was not pathognomonic for Parkinson’s, but you made the point – and our guest agreed – that asymmetry tends to be the key here. And I really appreciated the point about reemergent tremor. This is this idea of a resting tremor. If someone has more parkinsonian features, you might see an intention tremor with essential tremor. If they reach out, it might seem steady at first, but if they hold long enough, then the tremor may kind of reemerge. I thought that was a neat distinction.
And this idea of cogwheel rigidity is a combination of some of the cardinal features of Parkinson’s – it’s a little bit of tremor and a little bit of rigidity too. There’s a baseline increase in tone, and then the tremor is superimposed on top of that. When you’re feeling cogwheeling, that’s actually what you’re feeling on examination. Parkinson’s, with all of its physical exam findings has always fascinated me.
Dr. Watto: He also told us about some red flags.
With classic idiopathic parkinsonism, there’s asymmetric involvement of the tremor. So red flags include a symmetric tremor, which might be something other than idiopathic parkinsonism. He also mentioned that one of the reasons you may want to get imaging (which is not always necessary if someone has a classic presentation), is if you see lower body–predominant symptoms of parkinsonism. These patients have rigidity or slowness of movement in their legs, but their upper bodies are not affected. They don’t have masked facies or the tremor in their hands. You might get an MRI in that case because that could be presentation of vascular dementia or vascular disease in the brain or even normal pressure hydrocephalus, which is a treatable condition. That would be one reason to get imaging.
What if the patient was exposed to a drug like a dopamine antagonist? They will get better in a couple of days, right?
Dr. Williams: This was a really fascinating point because we typically think if a patient’s symptoms are related to a drug exposure – in this case, drug-induced parkinsonism – we can just stop the medication and the symptoms will disappear in a couple of days as the drug leaves the system. But as it turns out, it might take much longer. A mistake that Dr Hung often sees is that the clinician stops the possibly offending agent, but when they don’t see an immediate relief of symptoms, they assume the drug wasn’t causing them. You really have to give the patient a fair shot off the medication to experience recovery because those symptoms can last weeks or even months after the drug is discontinued.
Dr. Watto: Dr Hung looks at the patient’s problem list and asks whether is there any reason this patient might have been exposed to one of these medications?
We’re not going to get too much into specific Parkinson’s treatment, but I was glad to hear that exercise actually improves mobility and may even have some neuroprotective effects. He mentioned ongoing trials looking at that. We always love an excuse to tell patients that they should be moving around more and being physically active.
Dr. Williams: That was one of the more shocking things I learned, that exercise might actually be good for you. That will deeply inform my practice. Many of the treatments that we use for Parkinson’s only address symptoms. They don’t address progression or fix anything, but exercise can help with that.
Dr. Watto: Paul, the last question I wanted to ask you is about our role in primary care. Patients with Parkinson’s have autonomic symptoms. They have neurocognitive symptoms. What is our role in that as primary care physicians?
Dr. Williams: Myriad symptoms can accompany Parkinson’s, and we have experience with most of them. We should all feel fairly comfortable dealing with constipation, which can be a very bothersome symptom. And we can use our full arsenal for symptoms such as depression, anxiety, and even apathy – the anhedonia, which apparently can be the predominant feature. We do have the tools to address these problems.
This might be a situation where we might reach for bupropion or a tricyclic antidepressant, which might not be your initial choice for a patient with a possibly annoying mood disorder. But for someone with Parkinson’s disease, this actually may be very helpful. We know how to manage a lot of the symptoms that come along with Parkinson’s that are not just the motor symptoms, and we should take ownership of those things.
Dr. Watto: You can hear the rest of this podcast here. This has been another episode of The Curbsiders bringing you a little knowledge food for your brain hole. Until next time, I’ve been Dr Matthew Frank Watto.
Dr. Williams: And I’m Dr Paul Nelson Williams.
Dr. Watto is a clinical assistant professor, department of medicine, at the University of Pennsylvania, Philadelphia. Dr. Williams is Associate Professor of Clinical Medicine, Department of General Internal Medicine, at Temple University, Philadelphia. Neither Dr. Watto nor Dr. Williams reported any relevant conflicts of interest.
A version of this article first appeared on Medscape.com.
Reforming prior authorization remains AGA’s top policy priority
Reforming prior authorization polices to reduce red tape for physicians and help patients get the care they need in a timely manner is the AGA’s number one policy priority as it impacts every gastroenterologist regardless of practice setting. We have seen an increase in prior authorization policies from every major insurer. The most recent prior authorization program to impact gastroenterologists was announced by UnitedHealthcare (UHC) in March for implementation on June 1, 2023 and will require prior authorization for most colonoscopy and upper GI endoscopy procedures with the exception of screening colonoscopy.1 This policy is a step back at a time when payers should be developing innovative policies in collaboration with health care providers to improve patient care.
UHC’s GI prior authorization policy
AGA met with UHC in March to discuss their plan to require prior authorization for most GI endoscopy procedures. We stressed how this change will cause care delays for high-risk individuals, deter patients from undergoing medically recommended procedures, exacerbate existing sociodemographic disparities in care and outcomes, and add unnecessary paperwork burden to physicians who have mounting rates of burnout.
Linda Lee, MD, medical director of endoscopy at Brigham and Women’s Hospital, Boston, recently spoke of the impact this policy will have on gastroenterologists and their patients. “We all know that requiring prior authorizations really only leads to more bureaucracy within the insurance company, as well as within each health care provider’s practice, because we need people to fill out these prior authorization forms, waste time trying to get through to their 1-800 number to speak with someone who has no clinical knowledge, then be told we need to speak with someone else who actually does have some medical knowledge about why these procedures are necessary.”
However, Dr. Lee stressed that “most importantly, this will lead to poorer patient care with delays in care as we are struggling to wade through the morass of prior authorization while patients are bleeding, not able to swallow, vomiting, and more while waiting for their insurance company to approve their potentially life-saving procedures.”
We were particularly troubled that UHC announced this policy during Colorectal Cancer Awareness Month, given the need to screen more Americans for colorectal cancer which remains the nation’s number two cancer killer. The UHC program would require a PA on surveillance colonoscopy for those patients who have previously had polyps removed and are at a higher risk for developing colorectal cancer.
“We know that patients with high-risk adenomas or advanced sessile serrated lesions have a higher risk of developing colorectal cancer and timely access to the necessary surveillance colonoscopy is critical,” said David Lieberman, MD, past president of the AGA and chair of the AGA Executive Committee on the Screening Continuum.
AGA plans to meet with UHC again to ask them to reconsider this policy, but we need your advocacy now to tell United how this will impact you and your patients.
How you can help stop UHC’s prior authorization program
Write to UHC: Tell UHC how this policy would impact you and your patients. Contact their CEO using our customizable letter2 that outlines the impact of United’s GI endoscopy prior authorization program on gastroenterologists and their patients available on the AGA Advocacy Action Center.
Use social media: Tag United (@UHC) on Twitter and tell them how this burdensome program will cause delays for high-risk individuals, deter patients from seeking treatment, and exacerbate existing disparities in care, all while saddling physicians with even more paperwork. Once you’ve tweeted, tag your colleagues and encourage them to get involved.
AGA is working to reform prior authorization
The AGA has supported federal legislation that would streamline prior authorization processes in Medicare Advantage (MA), the private insurance plans that contract with the Medicare program, given the explosion of these policies over the past several years. The Improving Seniors Timely Access to Care Act, bipartisan, bicameral legislation, would reduce prior authorization burdens by:
- Establishing an electronic prior authorization (ePA) program and require MA plans to adopt ePA capabilities.
- Requiring the Secretary of Health and Human Services to establish a list of items and services eligible for real-time decisions under an MA ePA program.
- Standardizing and streamlining the prior authorization process for routinely approved items and services.
- Ensuring prior authorization requests are reviewed by qualified medical personnel.
- Increasing transparency around MA prior authorization requirements and their use.
- Protecting beneficiaries from any disruptions in care due to prior authorization requirements as they transition between MA plans.
The Centers for Medicare & Medicaid Services (CMS) has also recognized the impact that prior authorization is having on physician wellness and how it is contributing to physician burnout. The agency recently proposed implementing many of the provisions that are outlined in the legislation, and AGA has expressed our support for moving forward with many of their proposals.
Earlier this year, Shivan Mehta, MD, MPH, met with CMS administrator Chiquita Brooks-LaSure and Surgeon General Vivek Murthy, MD, MBA, to express AGA’s support for prior authorization reform and discussed how it impacts how patients with chronic conditions like inflammatory bowel disease maintain continuity of care. He also stressed how prior authorization further exacerbates health inequities since it creates an additional barrier to care when barriers already exist.
AGA is taking a multi-pronged approach to advocating for prior authorization reform and reducing paperwork through legislative advocacy, regulatory advocacy with the CMS, and payer advocacy. We can’t do this alone. Join our AGA Advocacy Center3 and get involved in our AGA Congressional Advocates Program.4The authors have no conflicts to declare.
References
1. UnitedHealthcare (2023 Mar 01) New requirements for gastroenterology services.
2. American Gastroenterological Association (n.d.) AGA Advocacy Action Center. Tell United to Stop New Prior Auth Requirements!
3. American Gastroenterological Association (n.d.) AGA Advocacy Action Center. Advocacy & Policy. Get Involved.
4. American Gastroenterological Association (n.d.) AGA Congressional Advocates Program.
Reforming prior authorization polices to reduce red tape for physicians and help patients get the care they need in a timely manner is the AGA’s number one policy priority as it impacts every gastroenterologist regardless of practice setting. We have seen an increase in prior authorization policies from every major insurer. The most recent prior authorization program to impact gastroenterologists was announced by UnitedHealthcare (UHC) in March for implementation on June 1, 2023 and will require prior authorization for most colonoscopy and upper GI endoscopy procedures with the exception of screening colonoscopy.1 This policy is a step back at a time when payers should be developing innovative policies in collaboration with health care providers to improve patient care.
UHC’s GI prior authorization policy
AGA met with UHC in March to discuss their plan to require prior authorization for most GI endoscopy procedures. We stressed how this change will cause care delays for high-risk individuals, deter patients from undergoing medically recommended procedures, exacerbate existing sociodemographic disparities in care and outcomes, and add unnecessary paperwork burden to physicians who have mounting rates of burnout.
Linda Lee, MD, medical director of endoscopy at Brigham and Women’s Hospital, Boston, recently spoke of the impact this policy will have on gastroenterologists and their patients. “We all know that requiring prior authorizations really only leads to more bureaucracy within the insurance company, as well as within each health care provider’s practice, because we need people to fill out these prior authorization forms, waste time trying to get through to their 1-800 number to speak with someone who has no clinical knowledge, then be told we need to speak with someone else who actually does have some medical knowledge about why these procedures are necessary.”
However, Dr. Lee stressed that “most importantly, this will lead to poorer patient care with delays in care as we are struggling to wade through the morass of prior authorization while patients are bleeding, not able to swallow, vomiting, and more while waiting for their insurance company to approve their potentially life-saving procedures.”
We were particularly troubled that UHC announced this policy during Colorectal Cancer Awareness Month, given the need to screen more Americans for colorectal cancer which remains the nation’s number two cancer killer. The UHC program would require a PA on surveillance colonoscopy for those patients who have previously had polyps removed and are at a higher risk for developing colorectal cancer.
“We know that patients with high-risk adenomas or advanced sessile serrated lesions have a higher risk of developing colorectal cancer and timely access to the necessary surveillance colonoscopy is critical,” said David Lieberman, MD, past president of the AGA and chair of the AGA Executive Committee on the Screening Continuum.
AGA plans to meet with UHC again to ask them to reconsider this policy, but we need your advocacy now to tell United how this will impact you and your patients.
How you can help stop UHC’s prior authorization program
Write to UHC: Tell UHC how this policy would impact you and your patients. Contact their CEO using our customizable letter2 that outlines the impact of United’s GI endoscopy prior authorization program on gastroenterologists and their patients available on the AGA Advocacy Action Center.
Use social media: Tag United (@UHC) on Twitter and tell them how this burdensome program will cause delays for high-risk individuals, deter patients from seeking treatment, and exacerbate existing disparities in care, all while saddling physicians with even more paperwork. Once you’ve tweeted, tag your colleagues and encourage them to get involved.
AGA is working to reform prior authorization
The AGA has supported federal legislation that would streamline prior authorization processes in Medicare Advantage (MA), the private insurance plans that contract with the Medicare program, given the explosion of these policies over the past several years. The Improving Seniors Timely Access to Care Act, bipartisan, bicameral legislation, would reduce prior authorization burdens by:
- Establishing an electronic prior authorization (ePA) program and require MA plans to adopt ePA capabilities.
- Requiring the Secretary of Health and Human Services to establish a list of items and services eligible for real-time decisions under an MA ePA program.
- Standardizing and streamlining the prior authorization process for routinely approved items and services.
- Ensuring prior authorization requests are reviewed by qualified medical personnel.
- Increasing transparency around MA prior authorization requirements and their use.
- Protecting beneficiaries from any disruptions in care due to prior authorization requirements as they transition between MA plans.
The Centers for Medicare & Medicaid Services (CMS) has also recognized the impact that prior authorization is having on physician wellness and how it is contributing to physician burnout. The agency recently proposed implementing many of the provisions that are outlined in the legislation, and AGA has expressed our support for moving forward with many of their proposals.
Earlier this year, Shivan Mehta, MD, MPH, met with CMS administrator Chiquita Brooks-LaSure and Surgeon General Vivek Murthy, MD, MBA, to express AGA’s support for prior authorization reform and discussed how it impacts how patients with chronic conditions like inflammatory bowel disease maintain continuity of care. He also stressed how prior authorization further exacerbates health inequities since it creates an additional barrier to care when barriers already exist.
AGA is taking a multi-pronged approach to advocating for prior authorization reform and reducing paperwork through legislative advocacy, regulatory advocacy with the CMS, and payer advocacy. We can’t do this alone. Join our AGA Advocacy Center3 and get involved in our AGA Congressional Advocates Program.4The authors have no conflicts to declare.
References
1. UnitedHealthcare (2023 Mar 01) New requirements for gastroenterology services.
2. American Gastroenterological Association (n.d.) AGA Advocacy Action Center. Tell United to Stop New Prior Auth Requirements!
3. American Gastroenterological Association (n.d.) AGA Advocacy Action Center. Advocacy & Policy. Get Involved.
4. American Gastroenterological Association (n.d.) AGA Congressional Advocates Program.
Reforming prior authorization polices to reduce red tape for physicians and help patients get the care they need in a timely manner is the AGA’s number one policy priority as it impacts every gastroenterologist regardless of practice setting. We have seen an increase in prior authorization policies from every major insurer. The most recent prior authorization program to impact gastroenterologists was announced by UnitedHealthcare (UHC) in March for implementation on June 1, 2023 and will require prior authorization for most colonoscopy and upper GI endoscopy procedures with the exception of screening colonoscopy.1 This policy is a step back at a time when payers should be developing innovative policies in collaboration with health care providers to improve patient care.
UHC’s GI prior authorization policy
AGA met with UHC in March to discuss their plan to require prior authorization for most GI endoscopy procedures. We stressed how this change will cause care delays for high-risk individuals, deter patients from undergoing medically recommended procedures, exacerbate existing sociodemographic disparities in care and outcomes, and add unnecessary paperwork burden to physicians who have mounting rates of burnout.
Linda Lee, MD, medical director of endoscopy at Brigham and Women’s Hospital, Boston, recently spoke of the impact this policy will have on gastroenterologists and their patients. “We all know that requiring prior authorizations really only leads to more bureaucracy within the insurance company, as well as within each health care provider’s practice, because we need people to fill out these prior authorization forms, waste time trying to get through to their 1-800 number to speak with someone who has no clinical knowledge, then be told we need to speak with someone else who actually does have some medical knowledge about why these procedures are necessary.”
However, Dr. Lee stressed that “most importantly, this will lead to poorer patient care with delays in care as we are struggling to wade through the morass of prior authorization while patients are bleeding, not able to swallow, vomiting, and more while waiting for their insurance company to approve their potentially life-saving procedures.”
We were particularly troubled that UHC announced this policy during Colorectal Cancer Awareness Month, given the need to screen more Americans for colorectal cancer which remains the nation’s number two cancer killer. The UHC program would require a PA on surveillance colonoscopy for those patients who have previously had polyps removed and are at a higher risk for developing colorectal cancer.
“We know that patients with high-risk adenomas or advanced sessile serrated lesions have a higher risk of developing colorectal cancer and timely access to the necessary surveillance colonoscopy is critical,” said David Lieberman, MD, past president of the AGA and chair of the AGA Executive Committee on the Screening Continuum.
AGA plans to meet with UHC again to ask them to reconsider this policy, but we need your advocacy now to tell United how this will impact you and your patients.
How you can help stop UHC’s prior authorization program
Write to UHC: Tell UHC how this policy would impact you and your patients. Contact their CEO using our customizable letter2 that outlines the impact of United’s GI endoscopy prior authorization program on gastroenterologists and their patients available on the AGA Advocacy Action Center.
Use social media: Tag United (@UHC) on Twitter and tell them how this burdensome program will cause delays for high-risk individuals, deter patients from seeking treatment, and exacerbate existing disparities in care, all while saddling physicians with even more paperwork. Once you’ve tweeted, tag your colleagues and encourage them to get involved.
AGA is working to reform prior authorization
The AGA has supported federal legislation that would streamline prior authorization processes in Medicare Advantage (MA), the private insurance plans that contract with the Medicare program, given the explosion of these policies over the past several years. The Improving Seniors Timely Access to Care Act, bipartisan, bicameral legislation, would reduce prior authorization burdens by:
- Establishing an electronic prior authorization (ePA) program and require MA plans to adopt ePA capabilities.
- Requiring the Secretary of Health and Human Services to establish a list of items and services eligible for real-time decisions under an MA ePA program.
- Standardizing and streamlining the prior authorization process for routinely approved items and services.
- Ensuring prior authorization requests are reviewed by qualified medical personnel.
- Increasing transparency around MA prior authorization requirements and their use.
- Protecting beneficiaries from any disruptions in care due to prior authorization requirements as they transition between MA plans.
The Centers for Medicare & Medicaid Services (CMS) has also recognized the impact that prior authorization is having on physician wellness and how it is contributing to physician burnout. The agency recently proposed implementing many of the provisions that are outlined in the legislation, and AGA has expressed our support for moving forward with many of their proposals.
Earlier this year, Shivan Mehta, MD, MPH, met with CMS administrator Chiquita Brooks-LaSure and Surgeon General Vivek Murthy, MD, MBA, to express AGA’s support for prior authorization reform and discussed how it impacts how patients with chronic conditions like inflammatory bowel disease maintain continuity of care. He also stressed how prior authorization further exacerbates health inequities since it creates an additional barrier to care when barriers already exist.
AGA is taking a multi-pronged approach to advocating for prior authorization reform and reducing paperwork through legislative advocacy, regulatory advocacy with the CMS, and payer advocacy. We can’t do this alone. Join our AGA Advocacy Center3 and get involved in our AGA Congressional Advocates Program.4The authors have no conflicts to declare.
References
1. UnitedHealthcare (2023 Mar 01) New requirements for gastroenterology services.
2. American Gastroenterological Association (n.d.) AGA Advocacy Action Center. Tell United to Stop New Prior Auth Requirements!
3. American Gastroenterological Association (n.d.) AGA Advocacy Action Center. Advocacy & Policy. Get Involved.
4. American Gastroenterological Association (n.d.) AGA Congressional Advocates Program.