User login
Bringing you the latest news, research and reviews, exclusive interviews, podcasts, quizzes, and more.
div[contains(@class, 'header__large-screen')]
div[contains(@class, 'read-next-article')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
footer[@id='footer']
div[contains(@class, 'main-prefix')]
section[contains(@class, 'nav-hidden')]
div[contains(@class, 'ce-card-content')]
nav[contains(@class, 'nav-ce-stack')]
Just gas? New study on colic suggests some longer-term implications
Pediatricians commonly are asked to see infants presenting with symptoms of colic. The frequent and intense crying associated with colic is understandably quite distressing to parents, who often worry about a serious underlying medical cause. There also is the stress of trying to soothe an irritable infant who often does not seem to respond to the typical interventions.
Conventional wisdom about colic has been that the behaviors are the result of some gastrointestinal problem that, while not perfectly understood, tends to be mercifully self-limited and not predictive of future medical or mental health problems. This perspective then leads to pediatricians typically offering mainly sympathy and reassurance at these visits.
A new study,1 however, challenges some of this traditional thinking. The data come from a remarkable longitudinal study called the Generation R Study (R being Rotterdam in the Netherlands) that has prospectively studied a group of nearly 5,000 children from before birth into adolescence. Colic symptoms were briefly assessed when infants were about 3 months old and emotional-behavioral problems have been prospectively measured at multiple time points subsequently using well-validated rating scales.

The main finding of the study was and, to a lesser extent, in adolescence. This held for both internalizing problems (like anxiety and depressive symptoms) and externalizing problems (like defiance and aggressive behavior). At age 10, participants also underwent an MRI scan and those who were excessive criers as infants were found to have a smaller amygdala, a region known for being important in regulating emotions.
The authors concluded that colicky behavior in infancy may reflect some underlying temperamental vulnerabilities and may have more predictive value than previously thought. The connection between excessive crying and a measurable brain region difference later in life is also interesting, although these kinds of brain imaging findings have been notoriously difficult to interpret clinically.
Overall, this is a solid study that deserves to be considered. Colic may reflect a bit more than most of us have been taught and shouldn’t necessarily be “shrugged off,” as the authors state in their discussion.
At the same time, however, it is important not to overinterpret the findings. The magnitude of the effects were on the small side (about 0.2 of a standard deviation) and most children with excessive crying in early infancy did not manifest high levels of mental health problems later in life. The mothers of high crying infants also had slightly higher levels of mental health problems themselves so there could be other mechanisms at work here, such as genetic differences between the two groups.
So how could a pediatrician best use this new information without taking things too far? Regardless of the question of whether the excessive crying infancy is a true risk factor for later behavior problems (in the causal sense) or whether it represents more of a marker for something else, its presence so early in life offers an opportunity. Primary care clinicians would still likely want to provide the reassurance that has typically been given in these visits but perhaps with the caveat that some of these kids go on to struggle a bit more with mental health and that they might benefit from some additional support. We are not talking about prophylactic medications here, but something like additional parenting skills. Especially if you, as the pediatrician, suspect that the parents might benefit from expanding their parenting toolkit already, here is a nice opportunity to invite them to learn some new approaches and skills — framed in a way that focuses on the temperament of the child rather than any “deficits” you perceive in the parents. Some parents may be more receptive and less defensive to the idea of participating in parent training under the framework that they are doing this because they have a temperamentally more challenging child (rather than feeling that they are deficient in basic parenting skills).
It’s always a good idea to know about what resources are available in the community when it comes to teaching parenting skills. In addition to scientifically supported books and podcasts, there has been a steady increase in reliable websites, apps, and other digital platforms related to parenting, as well as standard in-person groups and classes. This could also be a great use of an integrated behavioral health professional for practices fortunate enough to have one.
In summary, there is some new evidence that colic can represent a little more than “just gas,” and while we shouldn’t take this one study to the extreme, there may be some good opportunities here to discuss and support good parenting practices in general.
Dr. Rettew is a child and adolescent psychiatrist with Lane County Behavioral Health in Eugene, Ore., and Oregon Health & Science University, Portland. His latest book is “Parenting Made Complicated: What Science Really Knows about the Greatest Debates of Early Childhood.” You can follow him on Twitter and Facebook @PediPsych.
Reference
1. Sammallahti S et al. Excessive crying, behavior problems, and amygdala volume: A study from infancy to adolescence. J Am Acad Child Adolesc Psychiatry. 2023 Jun;62(6):675-83. doi: 10.1016/j.jaac.2023.01.014.
Pediatricians commonly are asked to see infants presenting with symptoms of colic. The frequent and intense crying associated with colic is understandably quite distressing to parents, who often worry about a serious underlying medical cause. There also is the stress of trying to soothe an irritable infant who often does not seem to respond to the typical interventions.
Conventional wisdom about colic has been that the behaviors are the result of some gastrointestinal problem that, while not perfectly understood, tends to be mercifully self-limited and not predictive of future medical or mental health problems. This perspective then leads to pediatricians typically offering mainly sympathy and reassurance at these visits.
A new study,1 however, challenges some of this traditional thinking. The data come from a remarkable longitudinal study called the Generation R Study (R being Rotterdam in the Netherlands) that has prospectively studied a group of nearly 5,000 children from before birth into adolescence. Colic symptoms were briefly assessed when infants were about 3 months old and emotional-behavioral problems have been prospectively measured at multiple time points subsequently using well-validated rating scales.
The main finding of the study was and, to a lesser extent, in adolescence. This held for both internalizing problems (like anxiety and depressive symptoms) and externalizing problems (like defiance and aggressive behavior). At age 10, participants also underwent an MRI scan and those who were excessive criers as infants were found to have a smaller amygdala, a region known for being important in regulating emotions.
The authors concluded that colicky behavior in infancy may reflect some underlying temperamental vulnerabilities and may have more predictive value than previously thought. The connection between excessive crying and a measurable brain region difference later in life is also interesting, although these kinds of brain imaging findings have been notoriously difficult to interpret clinically.
Overall, this is a solid study that deserves to be considered. Colic may reflect a bit more than most of us have been taught and shouldn’t necessarily be “shrugged off,” as the authors state in their discussion.
At the same time, however, it is important not to overinterpret the findings. The magnitude of the effects were on the small side (about 0.2 of a standard deviation) and most children with excessive crying in early infancy did not manifest high levels of mental health problems later in life. The mothers of high crying infants also had slightly higher levels of mental health problems themselves so there could be other mechanisms at work here, such as genetic differences between the two groups.
So how could a pediatrician best use this new information without taking things too far? Regardless of the question of whether the excessive crying infancy is a true risk factor for later behavior problems (in the causal sense) or whether it represents more of a marker for something else, its presence so early in life offers an opportunity. Primary care clinicians would still likely want to provide the reassurance that has typically been given in these visits but perhaps with the caveat that some of these kids go on to struggle a bit more with mental health and that they might benefit from some additional support. We are not talking about prophylactic medications here, but something like additional parenting skills. Especially if you, as the pediatrician, suspect that the parents might benefit from expanding their parenting toolkit already, here is a nice opportunity to invite them to learn some new approaches and skills — framed in a way that focuses on the temperament of the child rather than any “deficits” you perceive in the parents. Some parents may be more receptive and less defensive to the idea of participating in parent training under the framework that they are doing this because they have a temperamentally more challenging child (rather than feeling that they are deficient in basic parenting skills).
It’s always a good idea to know about what resources are available in the community when it comes to teaching parenting skills. In addition to scientifically supported books and podcasts, there has been a steady increase in reliable websites, apps, and other digital platforms related to parenting, as well as standard in-person groups and classes. This could also be a great use of an integrated behavioral health professional for practices fortunate enough to have one.
In summary, there is some new evidence that colic can represent a little more than “just gas,” and while we shouldn’t take this one study to the extreme, there may be some good opportunities here to discuss and support good parenting practices in general.
Dr. Rettew is a child and adolescent psychiatrist with Lane County Behavioral Health in Eugene, Ore., and Oregon Health & Science University, Portland. His latest book is “Parenting Made Complicated: What Science Really Knows about the Greatest Debates of Early Childhood.” You can follow him on Twitter and Facebook @PediPsych.
Reference
1. Sammallahti S et al. Excessive crying, behavior problems, and amygdala volume: A study from infancy to adolescence. J Am Acad Child Adolesc Psychiatry. 2023 Jun;62(6):675-83. doi: 10.1016/j.jaac.2023.01.014.
Pediatricians commonly are asked to see infants presenting with symptoms of colic. The frequent and intense crying associated with colic is understandably quite distressing to parents, who often worry about a serious underlying medical cause. There also is the stress of trying to soothe an irritable infant who often does not seem to respond to the typical interventions.
Conventional wisdom about colic has been that the behaviors are the result of some gastrointestinal problem that, while not perfectly understood, tends to be mercifully self-limited and not predictive of future medical or mental health problems. This perspective then leads to pediatricians typically offering mainly sympathy and reassurance at these visits.
A new study,1 however, challenges some of this traditional thinking. The data come from a remarkable longitudinal study called the Generation R Study (R being Rotterdam in the Netherlands) that has prospectively studied a group of nearly 5,000 children from before birth into adolescence. Colic symptoms were briefly assessed when infants were about 3 months old and emotional-behavioral problems have been prospectively measured at multiple time points subsequently using well-validated rating scales.
The main finding of the study was and, to a lesser extent, in adolescence. This held for both internalizing problems (like anxiety and depressive symptoms) and externalizing problems (like defiance and aggressive behavior). At age 10, participants also underwent an MRI scan and those who were excessive criers as infants were found to have a smaller amygdala, a region known for being important in regulating emotions.
The authors concluded that colicky behavior in infancy may reflect some underlying temperamental vulnerabilities and may have more predictive value than previously thought. The connection between excessive crying and a measurable brain region difference later in life is also interesting, although these kinds of brain imaging findings have been notoriously difficult to interpret clinically.
Overall, this is a solid study that deserves to be considered. Colic may reflect a bit more than most of us have been taught and shouldn’t necessarily be “shrugged off,” as the authors state in their discussion.
At the same time, however, it is important not to overinterpret the findings. The magnitude of the effects were on the small side (about 0.2 of a standard deviation) and most children with excessive crying in early infancy did not manifest high levels of mental health problems later in life. The mothers of high crying infants also had slightly higher levels of mental health problems themselves so there could be other mechanisms at work here, such as genetic differences between the two groups.
So how could a pediatrician best use this new information without taking things too far? Regardless of the question of whether the excessive crying infancy is a true risk factor for later behavior problems (in the causal sense) or whether it represents more of a marker for something else, its presence so early in life offers an opportunity. Primary care clinicians would still likely want to provide the reassurance that has typically been given in these visits but perhaps with the caveat that some of these kids go on to struggle a bit more with mental health and that they might benefit from some additional support. We are not talking about prophylactic medications here, but something like additional parenting skills. Especially if you, as the pediatrician, suspect that the parents might benefit from expanding their parenting toolkit already, here is a nice opportunity to invite them to learn some new approaches and skills — framed in a way that focuses on the temperament of the child rather than any “deficits” you perceive in the parents. Some parents may be more receptive and less defensive to the idea of participating in parent training under the framework that they are doing this because they have a temperamentally more challenging child (rather than feeling that they are deficient in basic parenting skills).
It’s always a good idea to know about what resources are available in the community when it comes to teaching parenting skills. In addition to scientifically supported books and podcasts, there has been a steady increase in reliable websites, apps, and other digital platforms related to parenting, as well as standard in-person groups and classes. This could also be a great use of an integrated behavioral health professional for practices fortunate enough to have one.
In summary, there is some new evidence that colic can represent a little more than “just gas,” and while we shouldn’t take this one study to the extreme, there may be some good opportunities here to discuss and support good parenting practices in general.
Dr. Rettew is a child and adolescent psychiatrist with Lane County Behavioral Health in Eugene, Ore., and Oregon Health & Science University, Portland. His latest book is “Parenting Made Complicated: What Science Really Knows about the Greatest Debates of Early Childhood.” You can follow him on Twitter and Facebook @PediPsych.
Reference
1. Sammallahti S et al. Excessive crying, behavior problems, and amygdala volume: A study from infancy to adolescence. J Am Acad Child Adolesc Psychiatry. 2023 Jun;62(6):675-83. doi: 10.1016/j.jaac.2023.01.014.
Adverse events in childhood alter brain function
In a meta-analysis of 83 functional magnetic resonance imaging (fMRI) studies that included more than 5000 patients, exposure to adversity was associated with higher amygdala reactivity and lower prefrontal cortical reactivity across a range of task domains.
The altered responses were only observed in studies including adult participants and were clearest in participants who had been exposed to severe threat and trauma. Children and adolescents did not show significant adversity-related differences in brain function.
“By integrating the results from 83 previous brain imaging studies, we were able to provide what is arguably the clearest evidence to date that adults who have been exposed to early life trauma have different brain responses to psychological challenges,” senior author Marco Leyton, PhD, professor of psychiatry and director of the Temperament Adversity Biology Lab at McGill University in Montreal, Quebec, Canada, said in a press release. “This includes exaggerated responses in a region that processes emotionally intense information (the amygdala) and reduced responses in a region that helps people regulate emotions and associated behaviors (the frontal cortex).”
The findings were published in JAMA Network Open.
Changes in Reactivity
“One big issue we have in psychology, and especially in neuroscience, is that single-study results are often not reproducible,” lead author Niki Hosseini-Kamkar, PhD, neuroimaging research associate at Atlas Institute for Veterans and Families at Royal Ottawa Hospital, said in an interview.
“It was very important to me to use a meta-analysis to get an overall picture of what brain regions are consistently reported across all these different studies. That is what we did here,” she added. Dr. Hosseini-Kamkar conducted this analysis while she was a postdoctoral research fellow at McGill University in Montreal.
She and her group examined adversity exposure and brain function in the following four domains of task-based fMRI: emotion processing, memory processing, inhibitory control, and reward processing. Their study included 5242 participants. The researchers used multilevel kernel density analyses (MKDA) to analyze the data more accurately.
Adversity exposure was associated with higher amygdala reactivity (P < .001) and lower prefrontal cortical reactivity (P < .001), compared with controls with no adversity exposure.
Threat types of adversity were associated with greater blood-oxygen-level-dependent (BOLD) responses in the superior temporal gyrus and lower prefrontal cortex activity in participants exposed to threat, compared with controls.
Analysis of studies of inhibitory control tasks found greater activity in the claustrum, anterior cingulate cortex, and insula in the adversity-exposed participants, compared with controls.
In addition, studies that administered emotion processing tasks showed greater amygdala reactivity and lower prefrontal cortex (superior frontal gyrus) reactivity in the adversity exposure group, compared with controls.
“The main takeaway is that there’s an exaggerated activity in the amygdala, and diminished prefrontal cortex activity, and together, this might point to a mechanism for how a history of adversity diminishes the ability to cope with later stressors and can therefore heighten susceptibility to mental illness,” said Dr. Hosseini-Kamkar.
‘Important Next Step’
“Overall, the meta-analysis by Dr. Hosseini-Kamkar and colleagues represents an important next step in understanding associations of adversity exposure with brain function while highlighting the importance of considering the role of development,” wrote Dylan G. Gee, PhD, associate professor of psychology at Yale University in New Haven, Connecticut, and Alexis Brieant, PhD, assistant professor of research or creative works at the University of Vermont in Burlington, in an accompanying commentary.
They also applauded the authors for their use of MKDA. They noted that the technique “allows inferences about the consistency and specificity of brain activation across studies and is thought to be more robust to small sample sizes than activation likelihood estimation (ALE) meta-analysis.”
Dr. Gee and Dr. Brieant also observed that a recent ALE meta-analysis failed to find a link between adversity and brain function. “Although it is important to note that the file drawer problem — by which researchers are less likely to publish null results — presents challenges to the inferences that can be drawn in the current work, the current study may provide complementary information to prior ALE meta-analyses.”
Epigenetic Changes?
Commenting on the findings for this article, Victor Fornari, MD, director of child and adolescent psychiatry at Northwell Health in Glen Oaks, New York, said, “Historically, when someone went through a traumatic event, they were told to just get over it, because somehow trauma doesn’t have a lasting impact on the brain.” Dr. Fornari was not involved in the research.
“We have certainly learned so much more over the past decade about early adversity and that it does have a profound impact on the brain and probably even epigenetic changes in our genes,” Dr. Fornari said.
“This is a very important avenue of investigation. People are really trying to understand if there are biological markers that we can actually measure in the brain that will offer us a window to better understand the consequence of adversity, as well as possible avenues of treatment.”
No funding source for this study was reported. Dr. Leyton, Dr. Hosseini-Kamkar, and Dr. Fornari report no relevant financial relationships. Gee reports receiving grants from the National Science Foundation and National Institutes of Health outside the submitted work. Dr. Brieant reports receiving grants from the National Institute of Mental Health outside the submitted work.
A version of this article appeared on Medscape.com.
In a meta-analysis of 83 functional magnetic resonance imaging (fMRI) studies that included more than 5000 patients, exposure to adversity was associated with higher amygdala reactivity and lower prefrontal cortical reactivity across a range of task domains.
The altered responses were only observed in studies including adult participants and were clearest in participants who had been exposed to severe threat and trauma. Children and adolescents did not show significant adversity-related differences in brain function.
“By integrating the results from 83 previous brain imaging studies, we were able to provide what is arguably the clearest evidence to date that adults who have been exposed to early life trauma have different brain responses to psychological challenges,” senior author Marco Leyton, PhD, professor of psychiatry and director of the Temperament Adversity Biology Lab at McGill University in Montreal, Quebec, Canada, said in a press release. “This includes exaggerated responses in a region that processes emotionally intense information (the amygdala) and reduced responses in a region that helps people regulate emotions and associated behaviors (the frontal cortex).”
The findings were published in JAMA Network Open.
Changes in Reactivity
“One big issue we have in psychology, and especially in neuroscience, is that single-study results are often not reproducible,” lead author Niki Hosseini-Kamkar, PhD, neuroimaging research associate at Atlas Institute for Veterans and Families at Royal Ottawa Hospital, said in an interview.
“It was very important to me to use a meta-analysis to get an overall picture of what brain regions are consistently reported across all these different studies. That is what we did here,” she added. Dr. Hosseini-Kamkar conducted this analysis while she was a postdoctoral research fellow at McGill University in Montreal.
She and her group examined adversity exposure and brain function in the following four domains of task-based fMRI: emotion processing, memory processing, inhibitory control, and reward processing. Their study included 5242 participants. The researchers used multilevel kernel density analyses (MKDA) to analyze the data more accurately.
Adversity exposure was associated with higher amygdala reactivity (P < .001) and lower prefrontal cortical reactivity (P < .001), compared with controls with no adversity exposure.
Threat types of adversity were associated with greater blood-oxygen-level-dependent (BOLD) responses in the superior temporal gyrus and lower prefrontal cortex activity in participants exposed to threat, compared with controls.
Analysis of studies of inhibitory control tasks found greater activity in the claustrum, anterior cingulate cortex, and insula in the adversity-exposed participants, compared with controls.
In addition, studies that administered emotion processing tasks showed greater amygdala reactivity and lower prefrontal cortex (superior frontal gyrus) reactivity in the adversity exposure group, compared with controls.
“The main takeaway is that there’s an exaggerated activity in the amygdala, and diminished prefrontal cortex activity, and together, this might point to a mechanism for how a history of adversity diminishes the ability to cope with later stressors and can therefore heighten susceptibility to mental illness,” said Dr. Hosseini-Kamkar.
‘Important Next Step’
“Overall, the meta-analysis by Dr. Hosseini-Kamkar and colleagues represents an important next step in understanding associations of adversity exposure with brain function while highlighting the importance of considering the role of development,” wrote Dylan G. Gee, PhD, associate professor of psychology at Yale University in New Haven, Connecticut, and Alexis Brieant, PhD, assistant professor of research or creative works at the University of Vermont in Burlington, in an accompanying commentary.
They also applauded the authors for their use of MKDA. They noted that the technique “allows inferences about the consistency and specificity of brain activation across studies and is thought to be more robust to small sample sizes than activation likelihood estimation (ALE) meta-analysis.”
Dr. Gee and Dr. Brieant also observed that a recent ALE meta-analysis failed to find a link between adversity and brain function. “Although it is important to note that the file drawer problem — by which researchers are less likely to publish null results — presents challenges to the inferences that can be drawn in the current work, the current study may provide complementary information to prior ALE meta-analyses.”
Epigenetic Changes?
Commenting on the findings for this article, Victor Fornari, MD, director of child and adolescent psychiatry at Northwell Health in Glen Oaks, New York, said, “Historically, when someone went through a traumatic event, they were told to just get over it, because somehow trauma doesn’t have a lasting impact on the brain.” Dr. Fornari was not involved in the research.
“We have certainly learned so much more over the past decade about early adversity and that it does have a profound impact on the brain and probably even epigenetic changes in our genes,” Dr. Fornari said.
“This is a very important avenue of investigation. People are really trying to understand if there are biological markers that we can actually measure in the brain that will offer us a window to better understand the consequence of adversity, as well as possible avenues of treatment.”
No funding source for this study was reported. Dr. Leyton, Dr. Hosseini-Kamkar, and Dr. Fornari report no relevant financial relationships. Gee reports receiving grants from the National Science Foundation and National Institutes of Health outside the submitted work. Dr. Brieant reports receiving grants from the National Institute of Mental Health outside the submitted work.
A version of this article appeared on Medscape.com.
In a meta-analysis of 83 functional magnetic resonance imaging (fMRI) studies that included more than 5000 patients, exposure to adversity was associated with higher amygdala reactivity and lower prefrontal cortical reactivity across a range of task domains.
The altered responses were only observed in studies including adult participants and were clearest in participants who had been exposed to severe threat and trauma. Children and adolescents did not show significant adversity-related differences in brain function.
“By integrating the results from 83 previous brain imaging studies, we were able to provide what is arguably the clearest evidence to date that adults who have been exposed to early life trauma have different brain responses to psychological challenges,” senior author Marco Leyton, PhD, professor of psychiatry and director of the Temperament Adversity Biology Lab at McGill University in Montreal, Quebec, Canada, said in a press release. “This includes exaggerated responses in a region that processes emotionally intense information (the amygdala) and reduced responses in a region that helps people regulate emotions and associated behaviors (the frontal cortex).”
The findings were published in JAMA Network Open.
Changes in Reactivity
“One big issue we have in psychology, and especially in neuroscience, is that single-study results are often not reproducible,” lead author Niki Hosseini-Kamkar, PhD, neuroimaging research associate at Atlas Institute for Veterans and Families at Royal Ottawa Hospital, said in an interview.
“It was very important to me to use a meta-analysis to get an overall picture of what brain regions are consistently reported across all these different studies. That is what we did here,” she added. Dr. Hosseini-Kamkar conducted this analysis while she was a postdoctoral research fellow at McGill University in Montreal.
She and her group examined adversity exposure and brain function in the following four domains of task-based fMRI: emotion processing, memory processing, inhibitory control, and reward processing. Their study included 5242 participants. The researchers used multilevel kernel density analyses (MKDA) to analyze the data more accurately.
Adversity exposure was associated with higher amygdala reactivity (P < .001) and lower prefrontal cortical reactivity (P < .001), compared with controls with no adversity exposure.
Threat types of adversity were associated with greater blood-oxygen-level-dependent (BOLD) responses in the superior temporal gyrus and lower prefrontal cortex activity in participants exposed to threat, compared with controls.
Analysis of studies of inhibitory control tasks found greater activity in the claustrum, anterior cingulate cortex, and insula in the adversity-exposed participants, compared with controls.
In addition, studies that administered emotion processing tasks showed greater amygdala reactivity and lower prefrontal cortex (superior frontal gyrus) reactivity in the adversity exposure group, compared with controls.
“The main takeaway is that there’s an exaggerated activity in the amygdala, and diminished prefrontal cortex activity, and together, this might point to a mechanism for how a history of adversity diminishes the ability to cope with later stressors and can therefore heighten susceptibility to mental illness,” said Dr. Hosseini-Kamkar.
‘Important Next Step’
“Overall, the meta-analysis by Dr. Hosseini-Kamkar and colleagues represents an important next step in understanding associations of adversity exposure with brain function while highlighting the importance of considering the role of development,” wrote Dylan G. Gee, PhD, associate professor of psychology at Yale University in New Haven, Connecticut, and Alexis Brieant, PhD, assistant professor of research or creative works at the University of Vermont in Burlington, in an accompanying commentary.
They also applauded the authors for their use of MKDA. They noted that the technique “allows inferences about the consistency and specificity of brain activation across studies and is thought to be more robust to small sample sizes than activation likelihood estimation (ALE) meta-analysis.”
Dr. Gee and Dr. Brieant also observed that a recent ALE meta-analysis failed to find a link between adversity and brain function. “Although it is important to note that the file drawer problem — by which researchers are less likely to publish null results — presents challenges to the inferences that can be drawn in the current work, the current study may provide complementary information to prior ALE meta-analyses.”
Epigenetic Changes?
Commenting on the findings for this article, Victor Fornari, MD, director of child and adolescent psychiatry at Northwell Health in Glen Oaks, New York, said, “Historically, when someone went through a traumatic event, they were told to just get over it, because somehow trauma doesn’t have a lasting impact on the brain.” Dr. Fornari was not involved in the research.
“We have certainly learned so much more over the past decade about early adversity and that it does have a profound impact on the brain and probably even epigenetic changes in our genes,” Dr. Fornari said.
“This is a very important avenue of investigation. People are really trying to understand if there are biological markers that we can actually measure in the brain that will offer us a window to better understand the consequence of adversity, as well as possible avenues of treatment.”
No funding source for this study was reported. Dr. Leyton, Dr. Hosseini-Kamkar, and Dr. Fornari report no relevant financial relationships. Gee reports receiving grants from the National Science Foundation and National Institutes of Health outside the submitted work. Dr. Brieant reports receiving grants from the National Institute of Mental Health outside the submitted work.
A version of this article appeared on Medscape.com.
FROM JAMA NETWORK OPEN
New cardiology certification board: What’s the plan?
The proposal by the major cardiovascular societies in the US to form a new board of cardiovascular medicine to manage initial and ongoing certification of cardiologists represents something of a revolution in the field of continuing medical education and assessment of competency.
Five US cardiovascular societies — the American College of Cardiology (ACC), the American Heart Association (AHA), the Heart Failure Society of America (HFSA), the Heart Rhythm Society (HRS), and the Society for Cardiovascular Angiography & Interventions (SCAI) — have now joined forces to propose a new professional certification board for cardiovascular medicine, to be known as the American Board of Cardiovascular Medicine (ABCVM).
The ABCVM would be independent of the American Board of Internal Medicine (ABIM), the current organization providing maintenance of certification for cardiologists as well as many other internal medicine subspecialties. The ABIM’s maintenance of certification process has been widely criticized for many years and has been described as “needlessly burdensome and expensive.”
, according to Jeffrey Kuvin, MD, a trustee of the ACC, who has been heading up the working group to develop this plan.
Dr. Kuvin, who is chair of the cardiology at Northwell Health, Manhasset, New York, a large academic healthcare system, explained that maintenance of certification has been a topic of discussion across the cardiovascular community for many years, and the ACC has a working group focused on the next steps for evaluation of competency, which he chairs.
“The topic of evaluation of competence has been on the mind of the ACC for many years and hence a work group was developed to focus on this,” Dr. Kuvin noted. “A lot of evolution of the concepts and next steps have been drawn out of this working group. And now other cardiovascular societies have joined to show unification across the house of cardiology and that this is indeed the way that the cardiovascular profession should move.”
“Time to Separate from Internal Medicine”
The general concept behind the new cardiology board is to separate cardiology from the ABIM.
“This is rooted from the concept that cardiology has evolved so much over the last few decades into such a large multidimensional specialty that it really does demarcate itself from internal medicine, and as such, it deserves a separate board governed by cardiologists with collaboration across the entirely of cardiology,” Dr. Kuvin said.
Cardiology has had significant growth and expansion of technology, tools, medications, and the approach to patients in many specialities and subspecialties, he added. “We have defined training programs in many different areas within cardiology; we have our own guidelines, our own competency statements, and in many cases, cardiology exists as its own department outside of medicine in many institutions. It’s just time to separate cardiology from the umbrella of internal medicine.”
The new cardiology board would be separate from, and not report to, the ABIM; rather, it would report directly to the American Board of Medical Specialties (ABMS), the only recognized medical certification body in the US.
What Are the Proposed Changes
Under the present system, managed by the ABIM, clinicians must undergo two stages of certification to be a cardiologist. First, they have to pass the initial certification exam in general cardiology, and then exams in one of four subspecialties if they plan to enter one of these, including interventional cardiology, electrophysiology, advanced heart failure or adult congenital heart disease.
Next, clinicians enter the maintenance of certification phase, which can take three different forms: 1) taking another recertification exam every 10 years; 2) the collaborative maintenance pathway — a collaboration between ACC and ABIM, which includes evaluation, learning and a certified exam each year; or 3) longitudinal knowledge and assessment — in which the program interacts with the clinician on an ongoing basis, sending secured questions regularly.
All three of these pathways for maintenance of certification involve high stakes questions and a set bar for passing or failing.
Under the proposed new cardiology board, an initial certification exam would still be required after fellowship training, but the maintenance of certification process would be completely restructured, with the new approach taking the form of continuous learning and assessment of competency.
“This is an iterative process, but we envision with a new American Board of Cardiovascular Medicine, we will pick up where the ABIM left off,” Dr. Kuvin notes. “That includes an initial certifying examination for the five areas that already exist under the ABIM system but with the opportunities to expand that to further specialties as well.”
He points out that there are several areas in cardiology that are currently not represented by these five areas that warrant some discussion, including multimodality imaging, vascular heart disease, and cardio-oncology.
“At present, everybody has to pass the general cardiology exam and then some may wish to further train and get certified in one of the other four other specific areas. But one topic that has been discussed over many years is how do we maintain competency in the areas in which clinicians practice over their lifetime as a cardiologist,” Dr. Kuvin commented.
He said the proposed cardiology board would like to adhere to some basic principles that are fundamental to the practice of medicine.
“We want to make sure that we are practicing medicine so that our patients derive the most benefit from seeing a cardiologist,” he said. “We also want to make sure, however, that this is a supportive process, supporting cardiologists to learn what they know and more importantly what they don’t know; to identify knowledge gaps in specific area; to help the cardiologist fill those knowledge gaps; to acknowledge those gaps have been filled; and then move on to another area of interest. This will be the focus of this new and improved model of continuous competency.”
The proposed new board also says it wants to make sure this is appropriate to the area in which the clinician is practicing.
“To take a closed book certified exam every 10 years on the world of cardiology as happens at the current time – or the assessments conducted in the other two pathways – is often meaningless to the cardiologist,” Dr. Kuvin says. “All three current pathways involve high stakes questions that are often irrelevant to one’s clinical practice.”
Lifelong Learning
“The crux of the changes we are proposing will be away from the focus of passing a test towards a model of helping the individual with their competency, with continuous learning and evaluation of competency to help the clinician fill in their knowledge gaps,” he explains.
He described the new approach as “lifelong learning,” adding that, instead of it being “a punitive pass/fail environment with no feedback, which causes a lot of discontent among clinicians,” it will be a supportive process, where a clinician will be helped in filling their knowledge gaps.
“I think this would be a welcome change not just for cardiology but across medical specialties,” Dr. Kuvin said.
He also pointed out the ABMS itself is considering a continuous competency approach, and the proposed new cardiology board aims to work with the ABMS to make sure that their goals of continuous competency assessment are matched.
“The world has changed. The ability to access information has changed. It is no longer imperative for a clinician to have every piece of knowledge in their brain, but rather to know how to get knowledge and to incorporate that knowledge into clinical practice,” Dr. Kuvin noted. “Competency should not involve knowledge alone as in a closed book exam. It is more about understanding the world that we live in, how to synthesize information, where we need to improve knowledge and how to do that.”
Dr. Kuvin acknowledged that asking clinicians questions is a very helpful tool to identify their knowledge base and their knowledge gaps. “But we believe the clinician needs to be given resources — that could be a conference, an article, a simulation — to fill that knowledge gap. Then we could ask clinicians some different questions and if they get those right then we have provided a service.”
Tactile skills for cardiologists needing to perform procedures – such as interventionalists or electrophysiologists may be incorporated by simulation in a technology-based scenario.
On how often these assessments would take place, Dr. Kuvin said that hadn’t been decided for sure.
“We certainly do not think an assessment every 10 years is appropriate. We envision, instead of an episodic model, it will be rather a lifelong journey of education and competency. This will involve frequent contact and making sure knowledge gaps are being filled. There are criteria being set out by the ABMS that there should be a certain number of touch points with individuals on an annual as well as a 5-year basis to make sure cardiologists are staying within specific guardrails. The exact nature of these is yet to be determined,” he said.
Dr. Kuvin added that it was not known yet what sort of hours would be required but added that “this will not be a significant time burden.”
What is the Timeframe?
The application to the ABMS for a separate cardiology board is still ongoing and has not yet received formal acceptance. Representatives from the five US cardiovascular societies are in the initial stages of formulating a transition board.
“The submission to the ABMS will take time for them to review. This could take up to a year or so,” Dr. Kuvin estimates.
This is the first time the ABMS has entertained the concept of a new board in many years, he noted. “It will be a paradigm shift for the whole country. I think that cardiology is really at the forefront and in a position where we can actually do this. If cardiovascular medicine is granted a new board, I think this will help change the approach of how physicians are assessed in terms of continuous competency not just in cardiology but across all specialties of medicine.”
He added: “We are confident that we can work within the construct of the ABMS guidelines that have been revised to be much more holistic in the approach of continuous competence across the board. This includes thinking beyond rote medical knowledge and thinking about the clinician as a whole and their abilities to communicate, act professionally, work within a complex medical system, utilize medical resources effectively. These all have to be part of continuous competence.”
How Much Will This Cost?
Noting that the ABIM has received criticism over the costs of the certification process, Dr. Kuvin said they intend to make this “as lean a machine as possible with the focus on reducing the financial [burden] as well as the time burden for cardiologists. It is very important that this is not cumbersome, that it is woven into clinical practice, and that it is not costly.”
But he pointed out that building a new board will have significant costs.
“We have to think about developing initial board certification examinations as well as changing the paradigm on continuous certification,” he said. “This will take some up-front costs, and our society partners have decided that they are willing to provide some start-up funds for this. We anticipate the initial certification will remain somewhat similar in price, but the cost of ongoing continuous competency assessment will be significantly reduced compared to today’s models.”
Dr. Kuvin said the collaboration of the five participating US cardiovascular societies was unprecedented. But he noted that while the transition board is beginning with representatives of these individual societies, it will ultimately be independent from these societies and have its own board of directors.
He suggested that other societies representing other parts of cardiology are also interested. “Cardiology has recognized how important this is,” he said. “Everybody is excited about this.”
A version of this article appeared on Medscape.com.
The proposal by the major cardiovascular societies in the US to form a new board of cardiovascular medicine to manage initial and ongoing certification of cardiologists represents something of a revolution in the field of continuing medical education and assessment of competency.
Five US cardiovascular societies — the American College of Cardiology (ACC), the American Heart Association (AHA), the Heart Failure Society of America (HFSA), the Heart Rhythm Society (HRS), and the Society for Cardiovascular Angiography & Interventions (SCAI) — have now joined forces to propose a new professional certification board for cardiovascular medicine, to be known as the American Board of Cardiovascular Medicine (ABCVM).
The ABCVM would be independent of the American Board of Internal Medicine (ABIM), the current organization providing maintenance of certification for cardiologists as well as many other internal medicine subspecialties. The ABIM’s maintenance of certification process has been widely criticized for many years and has been described as “needlessly burdensome and expensive.”
, according to Jeffrey Kuvin, MD, a trustee of the ACC, who has been heading up the working group to develop this plan.
Dr. Kuvin, who is chair of the cardiology at Northwell Health, Manhasset, New York, a large academic healthcare system, explained that maintenance of certification has been a topic of discussion across the cardiovascular community for many years, and the ACC has a working group focused on the next steps for evaluation of competency, which he chairs.
“The topic of evaluation of competence has been on the mind of the ACC for many years and hence a work group was developed to focus on this,” Dr. Kuvin noted. “A lot of evolution of the concepts and next steps have been drawn out of this working group. And now other cardiovascular societies have joined to show unification across the house of cardiology and that this is indeed the way that the cardiovascular profession should move.”
“Time to Separate from Internal Medicine”
The general concept behind the new cardiology board is to separate cardiology from the ABIM.
“This is rooted from the concept that cardiology has evolved so much over the last few decades into such a large multidimensional specialty that it really does demarcate itself from internal medicine, and as such, it deserves a separate board governed by cardiologists with collaboration across the entirely of cardiology,” Dr. Kuvin said.
Cardiology has had significant growth and expansion of technology, tools, medications, and the approach to patients in many specialities and subspecialties, he added. “We have defined training programs in many different areas within cardiology; we have our own guidelines, our own competency statements, and in many cases, cardiology exists as its own department outside of medicine in many institutions. It’s just time to separate cardiology from the umbrella of internal medicine.”
The new cardiology board would be separate from, and not report to, the ABIM; rather, it would report directly to the American Board of Medical Specialties (ABMS), the only recognized medical certification body in the US.
What Are the Proposed Changes
Under the present system, managed by the ABIM, clinicians must undergo two stages of certification to be a cardiologist. First, they have to pass the initial certification exam in general cardiology, and then exams in one of four subspecialties if they plan to enter one of these, including interventional cardiology, electrophysiology, advanced heart failure or adult congenital heart disease.
Next, clinicians enter the maintenance of certification phase, which can take three different forms: 1) taking another recertification exam every 10 years; 2) the collaborative maintenance pathway — a collaboration between ACC and ABIM, which includes evaluation, learning and a certified exam each year; or 3) longitudinal knowledge and assessment — in which the program interacts with the clinician on an ongoing basis, sending secured questions regularly.
All three of these pathways for maintenance of certification involve high stakes questions and a set bar for passing or failing.
Under the proposed new cardiology board, an initial certification exam would still be required after fellowship training, but the maintenance of certification process would be completely restructured, with the new approach taking the form of continuous learning and assessment of competency.
“This is an iterative process, but we envision with a new American Board of Cardiovascular Medicine, we will pick up where the ABIM left off,” Dr. Kuvin notes. “That includes an initial certifying examination for the five areas that already exist under the ABIM system but with the opportunities to expand that to further specialties as well.”
He points out that there are several areas in cardiology that are currently not represented by these five areas that warrant some discussion, including multimodality imaging, vascular heart disease, and cardio-oncology.
“At present, everybody has to pass the general cardiology exam and then some may wish to further train and get certified in one of the other four other specific areas. But one topic that has been discussed over many years is how do we maintain competency in the areas in which clinicians practice over their lifetime as a cardiologist,” Dr. Kuvin commented.
He said the proposed cardiology board would like to adhere to some basic principles that are fundamental to the practice of medicine.
“We want to make sure that we are practicing medicine so that our patients derive the most benefit from seeing a cardiologist,” he said. “We also want to make sure, however, that this is a supportive process, supporting cardiologists to learn what they know and more importantly what they don’t know; to identify knowledge gaps in specific area; to help the cardiologist fill those knowledge gaps; to acknowledge those gaps have been filled; and then move on to another area of interest. This will be the focus of this new and improved model of continuous competency.”
The proposed new board also says it wants to make sure this is appropriate to the area in which the clinician is practicing.
“To take a closed book certified exam every 10 years on the world of cardiology as happens at the current time – or the assessments conducted in the other two pathways – is often meaningless to the cardiologist,” Dr. Kuvin says. “All three current pathways involve high stakes questions that are often irrelevant to one’s clinical practice.”
Lifelong Learning
“The crux of the changes we are proposing will be away from the focus of passing a test towards a model of helping the individual with their competency, with continuous learning and evaluation of competency to help the clinician fill in their knowledge gaps,” he explains.
He described the new approach as “lifelong learning,” adding that, instead of it being “a punitive pass/fail environment with no feedback, which causes a lot of discontent among clinicians,” it will be a supportive process, where a clinician will be helped in filling their knowledge gaps.
“I think this would be a welcome change not just for cardiology but across medical specialties,” Dr. Kuvin said.
He also pointed out the ABMS itself is considering a continuous competency approach, and the proposed new cardiology board aims to work with the ABMS to make sure that their goals of continuous competency assessment are matched.
“The world has changed. The ability to access information has changed. It is no longer imperative for a clinician to have every piece of knowledge in their brain, but rather to know how to get knowledge and to incorporate that knowledge into clinical practice,” Dr. Kuvin noted. “Competency should not involve knowledge alone as in a closed book exam. It is more about understanding the world that we live in, how to synthesize information, where we need to improve knowledge and how to do that.”
Dr. Kuvin acknowledged that asking clinicians questions is a very helpful tool to identify their knowledge base and their knowledge gaps. “But we believe the clinician needs to be given resources — that could be a conference, an article, a simulation — to fill that knowledge gap. Then we could ask clinicians some different questions and if they get those right then we have provided a service.”
Tactile skills for cardiologists needing to perform procedures – such as interventionalists or electrophysiologists may be incorporated by simulation in a technology-based scenario.
On how often these assessments would take place, Dr. Kuvin said that hadn’t been decided for sure.
“We certainly do not think an assessment every 10 years is appropriate. We envision, instead of an episodic model, it will be rather a lifelong journey of education and competency. This will involve frequent contact and making sure knowledge gaps are being filled. There are criteria being set out by the ABMS that there should be a certain number of touch points with individuals on an annual as well as a 5-year basis to make sure cardiologists are staying within specific guardrails. The exact nature of these is yet to be determined,” he said.
Dr. Kuvin added that it was not known yet what sort of hours would be required but added that “this will not be a significant time burden.”
What is the Timeframe?
The application to the ABMS for a separate cardiology board is still ongoing and has not yet received formal acceptance. Representatives from the five US cardiovascular societies are in the initial stages of formulating a transition board.
“The submission to the ABMS will take time for them to review. This could take up to a year or so,” Dr. Kuvin estimates.
This is the first time the ABMS has entertained the concept of a new board in many years, he noted. “It will be a paradigm shift for the whole country. I think that cardiology is really at the forefront and in a position where we can actually do this. If cardiovascular medicine is granted a new board, I think this will help change the approach of how physicians are assessed in terms of continuous competency not just in cardiology but across all specialties of medicine.”
He added: “We are confident that we can work within the construct of the ABMS guidelines that have been revised to be much more holistic in the approach of continuous competence across the board. This includes thinking beyond rote medical knowledge and thinking about the clinician as a whole and their abilities to communicate, act professionally, work within a complex medical system, utilize medical resources effectively. These all have to be part of continuous competence.”
How Much Will This Cost?
Noting that the ABIM has received criticism over the costs of the certification process, Dr. Kuvin said they intend to make this “as lean a machine as possible with the focus on reducing the financial [burden] as well as the time burden for cardiologists. It is very important that this is not cumbersome, that it is woven into clinical practice, and that it is not costly.”
But he pointed out that building a new board will have significant costs.
“We have to think about developing initial board certification examinations as well as changing the paradigm on continuous certification,” he said. “This will take some up-front costs, and our society partners have decided that they are willing to provide some start-up funds for this. We anticipate the initial certification will remain somewhat similar in price, but the cost of ongoing continuous competency assessment will be significantly reduced compared to today’s models.”
Dr. Kuvin said the collaboration of the five participating US cardiovascular societies was unprecedented. But he noted that while the transition board is beginning with representatives of these individual societies, it will ultimately be independent from these societies and have its own board of directors.
He suggested that other societies representing other parts of cardiology are also interested. “Cardiology has recognized how important this is,” he said. “Everybody is excited about this.”
A version of this article appeared on Medscape.com.
The proposal by the major cardiovascular societies in the US to form a new board of cardiovascular medicine to manage initial and ongoing certification of cardiologists represents something of a revolution in the field of continuing medical education and assessment of competency.
Five US cardiovascular societies — the American College of Cardiology (ACC), the American Heart Association (AHA), the Heart Failure Society of America (HFSA), the Heart Rhythm Society (HRS), and the Society for Cardiovascular Angiography & Interventions (SCAI) — have now joined forces to propose a new professional certification board for cardiovascular medicine, to be known as the American Board of Cardiovascular Medicine (ABCVM).
The ABCVM would be independent of the American Board of Internal Medicine (ABIM), the current organization providing maintenance of certification for cardiologists as well as many other internal medicine subspecialties. The ABIM’s maintenance of certification process has been widely criticized for many years and has been described as “needlessly burdensome and expensive.”
, according to Jeffrey Kuvin, MD, a trustee of the ACC, who has been heading up the working group to develop this plan.
Dr. Kuvin, who is chair of the cardiology at Northwell Health, Manhasset, New York, a large academic healthcare system, explained that maintenance of certification has been a topic of discussion across the cardiovascular community for many years, and the ACC has a working group focused on the next steps for evaluation of competency, which he chairs.
“The topic of evaluation of competence has been on the mind of the ACC for many years and hence a work group was developed to focus on this,” Dr. Kuvin noted. “A lot of evolution of the concepts and next steps have been drawn out of this working group. And now other cardiovascular societies have joined to show unification across the house of cardiology and that this is indeed the way that the cardiovascular profession should move.”
“Time to Separate from Internal Medicine”
The general concept behind the new cardiology board is to separate cardiology from the ABIM.
“This is rooted from the concept that cardiology has evolved so much over the last few decades into such a large multidimensional specialty that it really does demarcate itself from internal medicine, and as such, it deserves a separate board governed by cardiologists with collaboration across the entirely of cardiology,” Dr. Kuvin said.
Cardiology has had significant growth and expansion of technology, tools, medications, and the approach to patients in many specialities and subspecialties, he added. “We have defined training programs in many different areas within cardiology; we have our own guidelines, our own competency statements, and in many cases, cardiology exists as its own department outside of medicine in many institutions. It’s just time to separate cardiology from the umbrella of internal medicine.”
The new cardiology board would be separate from, and not report to, the ABIM; rather, it would report directly to the American Board of Medical Specialties (ABMS), the only recognized medical certification body in the US.
What Are the Proposed Changes
Under the present system, managed by the ABIM, clinicians must undergo two stages of certification to be a cardiologist. First, they have to pass the initial certification exam in general cardiology, and then exams in one of four subspecialties if they plan to enter one of these, including interventional cardiology, electrophysiology, advanced heart failure or adult congenital heart disease.
Next, clinicians enter the maintenance of certification phase, which can take three different forms: 1) taking another recertification exam every 10 years; 2) the collaborative maintenance pathway — a collaboration between ACC and ABIM, which includes evaluation, learning and a certified exam each year; or 3) longitudinal knowledge and assessment — in which the program interacts with the clinician on an ongoing basis, sending secured questions regularly.
All three of these pathways for maintenance of certification involve high stakes questions and a set bar for passing or failing.
Under the proposed new cardiology board, an initial certification exam would still be required after fellowship training, but the maintenance of certification process would be completely restructured, with the new approach taking the form of continuous learning and assessment of competency.
“This is an iterative process, but we envision with a new American Board of Cardiovascular Medicine, we will pick up where the ABIM left off,” Dr. Kuvin notes. “That includes an initial certifying examination for the five areas that already exist under the ABIM system but with the opportunities to expand that to further specialties as well.”
He points out that there are several areas in cardiology that are currently not represented by these five areas that warrant some discussion, including multimodality imaging, vascular heart disease, and cardio-oncology.
“At present, everybody has to pass the general cardiology exam and then some may wish to further train and get certified in one of the other four other specific areas. But one topic that has been discussed over many years is how do we maintain competency in the areas in which clinicians practice over their lifetime as a cardiologist,” Dr. Kuvin commented.
He said the proposed cardiology board would like to adhere to some basic principles that are fundamental to the practice of medicine.
“We want to make sure that we are practicing medicine so that our patients derive the most benefit from seeing a cardiologist,” he said. “We also want to make sure, however, that this is a supportive process, supporting cardiologists to learn what they know and more importantly what they don’t know; to identify knowledge gaps in specific area; to help the cardiologist fill those knowledge gaps; to acknowledge those gaps have been filled; and then move on to another area of interest. This will be the focus of this new and improved model of continuous competency.”
The proposed new board also says it wants to make sure this is appropriate to the area in which the clinician is practicing.
“To take a closed book certified exam every 10 years on the world of cardiology as happens at the current time – or the assessments conducted in the other two pathways – is often meaningless to the cardiologist,” Dr. Kuvin says. “All three current pathways involve high stakes questions that are often irrelevant to one’s clinical practice.”
Lifelong Learning
“The crux of the changes we are proposing will be away from the focus of passing a test towards a model of helping the individual with their competency, with continuous learning and evaluation of competency to help the clinician fill in their knowledge gaps,” he explains.
He described the new approach as “lifelong learning,” adding that, instead of it being “a punitive pass/fail environment with no feedback, which causes a lot of discontent among clinicians,” it will be a supportive process, where a clinician will be helped in filling their knowledge gaps.
“I think this would be a welcome change not just for cardiology but across medical specialties,” Dr. Kuvin said.
He also pointed out the ABMS itself is considering a continuous competency approach, and the proposed new cardiology board aims to work with the ABMS to make sure that their goals of continuous competency assessment are matched.
“The world has changed. The ability to access information has changed. It is no longer imperative for a clinician to have every piece of knowledge in their brain, but rather to know how to get knowledge and to incorporate that knowledge into clinical practice,” Dr. Kuvin noted. “Competency should not involve knowledge alone as in a closed book exam. It is more about understanding the world that we live in, how to synthesize information, where we need to improve knowledge and how to do that.”
Dr. Kuvin acknowledged that asking clinicians questions is a very helpful tool to identify their knowledge base and their knowledge gaps. “But we believe the clinician needs to be given resources — that could be a conference, an article, a simulation — to fill that knowledge gap. Then we could ask clinicians some different questions and if they get those right then we have provided a service.”
Tactile skills for cardiologists needing to perform procedures – such as interventionalists or electrophysiologists may be incorporated by simulation in a technology-based scenario.
On how often these assessments would take place, Dr. Kuvin said that hadn’t been decided for sure.
“We certainly do not think an assessment every 10 years is appropriate. We envision, instead of an episodic model, it will be rather a lifelong journey of education and competency. This will involve frequent contact and making sure knowledge gaps are being filled. There are criteria being set out by the ABMS that there should be a certain number of touch points with individuals on an annual as well as a 5-year basis to make sure cardiologists are staying within specific guardrails. The exact nature of these is yet to be determined,” he said.
Dr. Kuvin added that it was not known yet what sort of hours would be required but added that “this will not be a significant time burden.”
What is the Timeframe?
The application to the ABMS for a separate cardiology board is still ongoing and has not yet received formal acceptance. Representatives from the five US cardiovascular societies are in the initial stages of formulating a transition board.
“The submission to the ABMS will take time for them to review. This could take up to a year or so,” Dr. Kuvin estimates.
This is the first time the ABMS has entertained the concept of a new board in many years, he noted. “It will be a paradigm shift for the whole country. I think that cardiology is really at the forefront and in a position where we can actually do this. If cardiovascular medicine is granted a new board, I think this will help change the approach of how physicians are assessed in terms of continuous competency not just in cardiology but across all specialties of medicine.”
He added: “We are confident that we can work within the construct of the ABMS guidelines that have been revised to be much more holistic in the approach of continuous competence across the board. This includes thinking beyond rote medical knowledge and thinking about the clinician as a whole and their abilities to communicate, act professionally, work within a complex medical system, utilize medical resources effectively. These all have to be part of continuous competence.”
How Much Will This Cost?
Noting that the ABIM has received criticism over the costs of the certification process, Dr. Kuvin said they intend to make this “as lean a machine as possible with the focus on reducing the financial [burden] as well as the time burden for cardiologists. It is very important that this is not cumbersome, that it is woven into clinical practice, and that it is not costly.”
But he pointed out that building a new board will have significant costs.
“We have to think about developing initial board certification examinations as well as changing the paradigm on continuous certification,” he said. “This will take some up-front costs, and our society partners have decided that they are willing to provide some start-up funds for this. We anticipate the initial certification will remain somewhat similar in price, but the cost of ongoing continuous competency assessment will be significantly reduced compared to today’s models.”
Dr. Kuvin said the collaboration of the five participating US cardiovascular societies was unprecedented. But he noted that while the transition board is beginning with representatives of these individual societies, it will ultimately be independent from these societies and have its own board of directors.
He suggested that other societies representing other parts of cardiology are also interested. “Cardiology has recognized how important this is,” he said. “Everybody is excited about this.”
A version of this article appeared on Medscape.com.
Some reasons to get off the fence about COVID booster
Though many people remain on the fence about getting the latest COVID vaccine booster, new research suggests a strong argument for getting the shot this winter: It sharply reduces the risk for COVID.
The risk reduction was 37% for those who received two doses. Experts say the research provides a strong argument for getting the vaccine, noting that about 10% of people infected with COVID go on to have long COVID, which can be debilitating for one quarter of those with long-lasting symptoms.
The data come from a systematic literature review and meta-analysis published in October in Antimicrobial Stewardship & Epidemiology. Researchers examined 32 studies published between December 2019 and June 2023, involving 775,931 adults. Twenty-four studies, encompassing 620,221 individuals, were included in the meta-analysis.
“The body of evidence from all these different studies converge on one single reality — that vaccines reduce the risk of long COVID, and people who keep up to date on their vaccinations also fared better than people who got it once or twice and didn’t follow up,” said Ziyad Al-Aly, MD, a clinical epidemiologist at Washington University in St Louis.
Researchers have reported similar results for children. The National Institutes of Health RECOVER Initiative team found that vaccines are up to 42% effective in preventing long COVID in children, said Dr. Carlos Oliveira, MD, a pediatric infectious diseases specialist and Yale researcher who contributed to the study, which is in preprint.
Vaccines also protect children from multisystem inflammatory syndrome, a condition that can happen after COVID, as well as protect against other COVID-related problems, such as missed school days, Oliveira said. “Even if the vaccine doesn’t completely stop long COVID, it’s still good for kids to get vaccinated for all these other reasons.”
However, uptake for the latest boosters has been slow: the Centers for Disease Control and Prevention reported that by mid-November, less than 16% of people aged 18 years or older had received a shot. For children, the number was closer to 6%. A recent Kaiser Family Foundation survey found that booster rates for adults are similar to what it was 1 year ago.
The survey results suggest that people are no longer as worried about COVID, which is why there is less concerned about keeping up with boosters. Though the current mutation of the virus is not as debilitating as its predecessors, long COVID continues to be a problem: as of January 2023, 28% of people who had contracted the virus had experienced long-COVID symptoms. And though the mechanisms are still not fully understood, and researchers have yet to agree on a definition of long COVID, they are certain about this much: The best way to avoid it is to avoid getting infected to begin with.
The lack of a diagnostic test for long COVID and the fact that the symptoms mimic those of other diseases lead to inconsistency that can make studies hard to replicate. In the papers reviewed for the Antimicrobial Stewardship & Epidemiology study, long COVID was defined as having symptoms lasting from more than 4 weeks to more than 6 months. Alexandre Marra, MD, the lead author and a researcher at the Hospital Israelita Albert Einstein, in São Paulo, Brazil, and at the University of Iowa, said that a clear standard definition is needed to better understand the actual prevalence and evaluate vaccine effectiveness.
Al-Aly noted that there is a logical explanation for one finding in the paper: The percentage of individuals who had COVID and reported that long-COVID symptoms declined from 19% in June 2022 to 11% in January 2023.
Because a pandemic is a dynamic event, constantly producing different variants with different phenotypes, the prevalence of disease is naturally going to be affected. “People who got infected early in the pandemic may have a different long COVID profile and long COVID risk than people who got infected in the second or third year of the pandemic,” Al-Aly said.
Most of the studies reported data from before the Omicron-variant era. Only eight reported data during that era. Omicron was not as lethal as previous variants, and consequently, fewer patients developed long COVID during that time.
One of those who did is Yeng Chang, age 40 years, a family doctor who lives in Sherwood Park, Alberta, Canada. Chang developed long COVID during fall 2022 after getting the virus in June. By then, she’d been vaccinated three times, but she isn’t surprised that she got sick because each vaccine she had was developed before Omicron.
“When I had COVID I was really sick, but I was well enough to stay home,” she said. “I think if I didn’t have my immunizations, I might have been hospitalized, and I don’t know what would have happened.”
Long COVID has left Chang with brain fog, fatigue, and a lack of physical stamina that forced her to pause her medical practice. For the past year and a half, she’s spent more time as a patient than a physician.
Chang had her fifth COVID vaccination in the fall and recommends that others do the same. “The booster you got however many years ago was effective for the COVID of that time but there is a new COVID now. You can’t just say, ‘I had one and I’m fine forever.’”
A version of this article appeared on Medscape.com.
Though many people remain on the fence about getting the latest COVID vaccine booster, new research suggests a strong argument for getting the shot this winter: It sharply reduces the risk for COVID.
The risk reduction was 37% for those who received two doses. Experts say the research provides a strong argument for getting the vaccine, noting that about 10% of people infected with COVID go on to have long COVID, which can be debilitating for one quarter of those with long-lasting symptoms.
The data come from a systematic literature review and meta-analysis published in October in Antimicrobial Stewardship & Epidemiology. Researchers examined 32 studies published between December 2019 and June 2023, involving 775,931 adults. Twenty-four studies, encompassing 620,221 individuals, were included in the meta-analysis.
“The body of evidence from all these different studies converge on one single reality — that vaccines reduce the risk of long COVID, and people who keep up to date on their vaccinations also fared better than people who got it once or twice and didn’t follow up,” said Ziyad Al-Aly, MD, a clinical epidemiologist at Washington University in St Louis.
Researchers have reported similar results for children. The National Institutes of Health RECOVER Initiative team found that vaccines are up to 42% effective in preventing long COVID in children, said Dr. Carlos Oliveira, MD, a pediatric infectious diseases specialist and Yale researcher who contributed to the study, which is in preprint.
Vaccines also protect children from multisystem inflammatory syndrome, a condition that can happen after COVID, as well as protect against other COVID-related problems, such as missed school days, Oliveira said. “Even if the vaccine doesn’t completely stop long COVID, it’s still good for kids to get vaccinated for all these other reasons.”
However, uptake for the latest boosters has been slow: the Centers for Disease Control and Prevention reported that by mid-November, less than 16% of people aged 18 years or older had received a shot. For children, the number was closer to 6%. A recent Kaiser Family Foundation survey found that booster rates for adults are similar to what it was 1 year ago.
The survey results suggest that people are no longer as worried about COVID, which is why there is less concerned about keeping up with boosters. Though the current mutation of the virus is not as debilitating as its predecessors, long COVID continues to be a problem: as of January 2023, 28% of people who had contracted the virus had experienced long-COVID symptoms. And though the mechanisms are still not fully understood, and researchers have yet to agree on a definition of long COVID, they are certain about this much: The best way to avoid it is to avoid getting infected to begin with.
The lack of a diagnostic test for long COVID and the fact that the symptoms mimic those of other diseases lead to inconsistency that can make studies hard to replicate. In the papers reviewed for the Antimicrobial Stewardship & Epidemiology study, long COVID was defined as having symptoms lasting from more than 4 weeks to more than 6 months. Alexandre Marra, MD, the lead author and a researcher at the Hospital Israelita Albert Einstein, in São Paulo, Brazil, and at the University of Iowa, said that a clear standard definition is needed to better understand the actual prevalence and evaluate vaccine effectiveness.
Al-Aly noted that there is a logical explanation for one finding in the paper: The percentage of individuals who had COVID and reported that long-COVID symptoms declined from 19% in June 2022 to 11% in January 2023.
Because a pandemic is a dynamic event, constantly producing different variants with different phenotypes, the prevalence of disease is naturally going to be affected. “People who got infected early in the pandemic may have a different long COVID profile and long COVID risk than people who got infected in the second or third year of the pandemic,” Al-Aly said.
Most of the studies reported data from before the Omicron-variant era. Only eight reported data during that era. Omicron was not as lethal as previous variants, and consequently, fewer patients developed long COVID during that time.
One of those who did is Yeng Chang, age 40 years, a family doctor who lives in Sherwood Park, Alberta, Canada. Chang developed long COVID during fall 2022 after getting the virus in June. By then, she’d been vaccinated three times, but she isn’t surprised that she got sick because each vaccine she had was developed before Omicron.
“When I had COVID I was really sick, but I was well enough to stay home,” she said. “I think if I didn’t have my immunizations, I might have been hospitalized, and I don’t know what would have happened.”
Long COVID has left Chang with brain fog, fatigue, and a lack of physical stamina that forced her to pause her medical practice. For the past year and a half, she’s spent more time as a patient than a physician.
Chang had her fifth COVID vaccination in the fall and recommends that others do the same. “The booster you got however many years ago was effective for the COVID of that time but there is a new COVID now. You can’t just say, ‘I had one and I’m fine forever.’”
A version of this article appeared on Medscape.com.
Though many people remain on the fence about getting the latest COVID vaccine booster, new research suggests a strong argument for getting the shot this winter: It sharply reduces the risk for COVID.
The risk reduction was 37% for those who received two doses. Experts say the research provides a strong argument for getting the vaccine, noting that about 10% of people infected with COVID go on to have long COVID, which can be debilitating for one quarter of those with long-lasting symptoms.
The data come from a systematic literature review and meta-analysis published in October in Antimicrobial Stewardship & Epidemiology. Researchers examined 32 studies published between December 2019 and June 2023, involving 775,931 adults. Twenty-four studies, encompassing 620,221 individuals, were included in the meta-analysis.
“The body of evidence from all these different studies converge on one single reality — that vaccines reduce the risk of long COVID, and people who keep up to date on their vaccinations also fared better than people who got it once or twice and didn’t follow up,” said Ziyad Al-Aly, MD, a clinical epidemiologist at Washington University in St Louis.
Researchers have reported similar results for children. The National Institutes of Health RECOVER Initiative team found that vaccines are up to 42% effective in preventing long COVID in children, said Dr. Carlos Oliveira, MD, a pediatric infectious diseases specialist and Yale researcher who contributed to the study, which is in preprint.
Vaccines also protect children from multisystem inflammatory syndrome, a condition that can happen after COVID, as well as protect against other COVID-related problems, such as missed school days, Oliveira said. “Even if the vaccine doesn’t completely stop long COVID, it’s still good for kids to get vaccinated for all these other reasons.”
However, uptake for the latest boosters has been slow: the Centers for Disease Control and Prevention reported that by mid-November, less than 16% of people aged 18 years or older had received a shot. For children, the number was closer to 6%. A recent Kaiser Family Foundation survey found that booster rates for adults are similar to what it was 1 year ago.
The survey results suggest that people are no longer as worried about COVID, which is why there is less concerned about keeping up with boosters. Though the current mutation of the virus is not as debilitating as its predecessors, long COVID continues to be a problem: as of January 2023, 28% of people who had contracted the virus had experienced long-COVID symptoms. And though the mechanisms are still not fully understood, and researchers have yet to agree on a definition of long COVID, they are certain about this much: The best way to avoid it is to avoid getting infected to begin with.
The lack of a diagnostic test for long COVID and the fact that the symptoms mimic those of other diseases lead to inconsistency that can make studies hard to replicate. In the papers reviewed for the Antimicrobial Stewardship & Epidemiology study, long COVID was defined as having symptoms lasting from more than 4 weeks to more than 6 months. Alexandre Marra, MD, the lead author and a researcher at the Hospital Israelita Albert Einstein, in São Paulo, Brazil, and at the University of Iowa, said that a clear standard definition is needed to better understand the actual prevalence and evaluate vaccine effectiveness.
Al-Aly noted that there is a logical explanation for one finding in the paper: The percentage of individuals who had COVID and reported that long-COVID symptoms declined from 19% in June 2022 to 11% in January 2023.
Because a pandemic is a dynamic event, constantly producing different variants with different phenotypes, the prevalence of disease is naturally going to be affected. “People who got infected early in the pandemic may have a different long COVID profile and long COVID risk than people who got infected in the second or third year of the pandemic,” Al-Aly said.
Most of the studies reported data from before the Omicron-variant era. Only eight reported data during that era. Omicron was not as lethal as previous variants, and consequently, fewer patients developed long COVID during that time.
One of those who did is Yeng Chang, age 40 years, a family doctor who lives in Sherwood Park, Alberta, Canada. Chang developed long COVID during fall 2022 after getting the virus in June. By then, she’d been vaccinated three times, but she isn’t surprised that she got sick because each vaccine she had was developed before Omicron.
“When I had COVID I was really sick, but I was well enough to stay home,” she said. “I think if I didn’t have my immunizations, I might have been hospitalized, and I don’t know what would have happened.”
Long COVID has left Chang with brain fog, fatigue, and a lack of physical stamina that forced her to pause her medical practice. For the past year and a half, she’s spent more time as a patient than a physician.
Chang had her fifth COVID vaccination in the fall and recommends that others do the same. “The booster you got however many years ago was effective for the COVID of that time but there is a new COVID now. You can’t just say, ‘I had one and I’m fine forever.’”
A version of this article appeared on Medscape.com.
Global measles deaths increased by 43% in 2022
The number of total reported cases rose by 18% over the same period, accounting for approximately 9 million cases and 136,000 deaths globally, mostly among children. This information comes from a new report by the World Health Organization (WHO), published in partnership with the US Centers for Disease Control and Prevention (CDC).
More Measles Outbreaks
The report also notes an increase in the number of countries experiencing significant measles outbreaks. There were 37 such countries in 2022, compared with 22 the previous year. The most affected continents were Africa and Asia.
“The rise in measles outbreaks and deaths is impressive but, unfortunately, not surprising, given the decline in vaccination rates in recent years,” said John Vertefeuille, PhD, director of the CDC’s Global Immunization Division.
Vertefeuille emphasized that measles cases anywhere in the world pose a risk to “countries and communities where people are undervaccinated.” In recent years, several regions have fallen short of their immunization targets.
Vaccination Trends
In 2022, there was a slight increase in measles vaccination after a decline exacerbated by the COVID-19 pandemic and its impact on global healthcare systems. However, 33 million children did not receive at least one dose of the vaccine last year: 22 million missed the first dose, and 11 million missed the second.
For communities to be considered protected against outbreaks, immunization coverage with the full vaccine cycle should be at least 95%. The global coverage rate for the first dose was 83%, and for the second, it was 74%.
Nevertheless, immunization recovery has not reached the poorest countries, where the immunization rate stands at 66%. Brazil is among the top 10 countries where more children missed the first dose in 2022. These nations account for over half of the 22 million unadministered vaccines. According to the report, half a million children did not receive the vaccine in Brazil.
Measles in Brazil
Brazil’s results highlight setbacks in vaccination efforts. In 2016, the country was certified to have eliminated measles, but after experiencing outbreaks in 2018, the certification was lost in 2019. In 2018, Brazil confirmed 9325 cases. The situation worsened in 2019 with 20,901 diagnoses. Since then, numbers have been decreasing: 8100 in 2020, 676 in 2021, and 44 in 2022.
Last year, four Brazilian states reported confirmed virus cases: Rio de Janeiro, Pará, São Paulo, and Amapá. Ministry of Health data indicated no confirmed measles cases in Brazil as of June 15, 2023.
Vaccination in Brazil
Vaccination coverage in Brazil, which once reached 95%, has sharply declined in recent years. The rate of patients receiving the full immunization scheme was 59% in 2021.
Globally, although the COVID-19 pandemic affected measles vaccination, measures like social isolation and mask use potentially contributed to reducing measles cases. The incidence of the disease decreased in 2020 and 2021 but is now rising again.
“From 2021 to 2022, reported measles cases increased by 67% worldwide, and the number of countries experiencing large or disruptive outbreaks increased by 68%,” the report stated.
Because of these data, the WHO and the CDC urge increased efforts for vaccination, along with improvements in epidemiological surveillance systems, especially in developing nations. “Children everywhere have the right to be protected by the lifesaving measles vaccine, no matter where they live,” said Kate O’Brien, MD, director of immunization, vaccines, and biologicals at the WHO.
“Measles is called the virus of inequality for a good reason. It is the disease that will find and attack those who are not protected.”
This article was translated from the Medscape Portuguese edition.
The number of total reported cases rose by 18% over the same period, accounting for approximately 9 million cases and 136,000 deaths globally, mostly among children. This information comes from a new report by the World Health Organization (WHO), published in partnership with the US Centers for Disease Control and Prevention (CDC).
More Measles Outbreaks
The report also notes an increase in the number of countries experiencing significant measles outbreaks. There were 37 such countries in 2022, compared with 22 the previous year. The most affected continents were Africa and Asia.
“The rise in measles outbreaks and deaths is impressive but, unfortunately, not surprising, given the decline in vaccination rates in recent years,” said John Vertefeuille, PhD, director of the CDC’s Global Immunization Division.
Vertefeuille emphasized that measles cases anywhere in the world pose a risk to “countries and communities where people are undervaccinated.” In recent years, several regions have fallen short of their immunization targets.
Vaccination Trends
In 2022, there was a slight increase in measles vaccination after a decline exacerbated by the COVID-19 pandemic and its impact on global healthcare systems. However, 33 million children did not receive at least one dose of the vaccine last year: 22 million missed the first dose, and 11 million missed the second.
For communities to be considered protected against outbreaks, immunization coverage with the full vaccine cycle should be at least 95%. The global coverage rate for the first dose was 83%, and for the second, it was 74%.
Nevertheless, immunization recovery has not reached the poorest countries, where the immunization rate stands at 66%. Brazil is among the top 10 countries where more children missed the first dose in 2022. These nations account for over half of the 22 million unadministered vaccines. According to the report, half a million children did not receive the vaccine in Brazil.
Measles in Brazil
Brazil’s results highlight setbacks in vaccination efforts. In 2016, the country was certified to have eliminated measles, but after experiencing outbreaks in 2018, the certification was lost in 2019. In 2018, Brazil confirmed 9325 cases. The situation worsened in 2019 with 20,901 diagnoses. Since then, numbers have been decreasing: 8100 in 2020, 676 in 2021, and 44 in 2022.
Last year, four Brazilian states reported confirmed virus cases: Rio de Janeiro, Pará, São Paulo, and Amapá. Ministry of Health data indicated no confirmed measles cases in Brazil as of June 15, 2023.
Vaccination in Brazil
Vaccination coverage in Brazil, which once reached 95%, has sharply declined in recent years. The rate of patients receiving the full immunization scheme was 59% in 2021.
Globally, although the COVID-19 pandemic affected measles vaccination, measures like social isolation and mask use potentially contributed to reducing measles cases. The incidence of the disease decreased in 2020 and 2021 but is now rising again.
“From 2021 to 2022, reported measles cases increased by 67% worldwide, and the number of countries experiencing large or disruptive outbreaks increased by 68%,” the report stated.
Because of these data, the WHO and the CDC urge increased efforts for vaccination, along with improvements in epidemiological surveillance systems, especially in developing nations. “Children everywhere have the right to be protected by the lifesaving measles vaccine, no matter where they live,” said Kate O’Brien, MD, director of immunization, vaccines, and biologicals at the WHO.
“Measles is called the virus of inequality for a good reason. It is the disease that will find and attack those who are not protected.”
This article was translated from the Medscape Portuguese edition.
The number of total reported cases rose by 18% over the same period, accounting for approximately 9 million cases and 136,000 deaths globally, mostly among children. This information comes from a new report by the World Health Organization (WHO), published in partnership with the US Centers for Disease Control and Prevention (CDC).
More Measles Outbreaks
The report also notes an increase in the number of countries experiencing significant measles outbreaks. There were 37 such countries in 2022, compared with 22 the previous year. The most affected continents were Africa and Asia.
“The rise in measles outbreaks and deaths is impressive but, unfortunately, not surprising, given the decline in vaccination rates in recent years,” said John Vertefeuille, PhD, director of the CDC’s Global Immunization Division.
Vertefeuille emphasized that measles cases anywhere in the world pose a risk to “countries and communities where people are undervaccinated.” In recent years, several regions have fallen short of their immunization targets.
Vaccination Trends
In 2022, there was a slight increase in measles vaccination after a decline exacerbated by the COVID-19 pandemic and its impact on global healthcare systems. However, 33 million children did not receive at least one dose of the vaccine last year: 22 million missed the first dose, and 11 million missed the second.
For communities to be considered protected against outbreaks, immunization coverage with the full vaccine cycle should be at least 95%. The global coverage rate for the first dose was 83%, and for the second, it was 74%.
Nevertheless, immunization recovery has not reached the poorest countries, where the immunization rate stands at 66%. Brazil is among the top 10 countries where more children missed the first dose in 2022. These nations account for over half of the 22 million unadministered vaccines. According to the report, half a million children did not receive the vaccine in Brazil.
Measles in Brazil
Brazil’s results highlight setbacks in vaccination efforts. In 2016, the country was certified to have eliminated measles, but after experiencing outbreaks in 2018, the certification was lost in 2019. In 2018, Brazil confirmed 9325 cases. The situation worsened in 2019 with 20,901 diagnoses. Since then, numbers have been decreasing: 8100 in 2020, 676 in 2021, and 44 in 2022.
Last year, four Brazilian states reported confirmed virus cases: Rio de Janeiro, Pará, São Paulo, and Amapá. Ministry of Health data indicated no confirmed measles cases in Brazil as of June 15, 2023.
Vaccination in Brazil
Vaccination coverage in Brazil, which once reached 95%, has sharply declined in recent years. The rate of patients receiving the full immunization scheme was 59% in 2021.
Globally, although the COVID-19 pandemic affected measles vaccination, measures like social isolation and mask use potentially contributed to reducing measles cases. The incidence of the disease decreased in 2020 and 2021 but is now rising again.
“From 2021 to 2022, reported measles cases increased by 67% worldwide, and the number of countries experiencing large or disruptive outbreaks increased by 68%,” the report stated.
Because of these data, the WHO and the CDC urge increased efforts for vaccination, along with improvements in epidemiological surveillance systems, especially in developing nations. “Children everywhere have the right to be protected by the lifesaving measles vaccine, no matter where they live,” said Kate O’Brien, MD, director of immunization, vaccines, and biologicals at the WHO.
“Measles is called the virus of inequality for a good reason. It is the disease that will find and attack those who are not protected.”
This article was translated from the Medscape Portuguese edition.
Patients with hypermobile Ehlers-Danlos syndrome report skin laxity, scarring
.
The genetic cause of hEDS, a common inherited connective tissue disorder, remains unknown, wrote Alan Snyder, MD, of the department of dermatology and dermatologic surgery at Medical University of South Carolina, Charleston, and colleagues.
Previous research suggests that changes in dermal mechanics predispose these patients to a range of skin conditions including mast cell activation disorder (MCAD) spectrum and chronic spontaneous urticaria, abnormal scars or wound healing, piezogenic papules, dyshidrosis, skin laxity or softness, easy bruising, local anesthesia resistance, keratosis pilaris, striae, and hidradenitis suppurativa, the researchers wrote.
However, data on these and other dermatologic manifestations of hEDS are limited, they said.
The diagnosis of hEDS will continue to be made more frequently and carefully, as the condition becomes more recognized and understood in the medical community, especially with anticipated capabilities of genetic testing, Dr. Snyder said in an interview.
“Being able to be aware of disease-specific comorbidities, such as those discovered in this study, allows providers to better stratify phenotypes and improve patient disease co-management,” he said.
In the study, published in the Journal of the American Academy of Dermatology, the researchers reviewed data on 1,364 patients with ICD-10 or ICD-9 codes for hEDS or EDS unspecified who were seen at a single institution between June 2005 and May 2022. Most of the patients were White (95.4%) and female (86.7%); the average age was 29.2 years.
Of the 1,364 patients included in the chart review, 497 (36.4%) had documented skin manifestations. Of these, 118 (24.2%) had disorders of follicular occlusion (12 had hidradenitis suppurativa, 32 had folliculitis, and 74 had acne); 112 (23%) had eczema or atopic dermatitis, 98 (19.7%) had mast cell disorder, 32 (6.4%) had psoriasis, and 32 (6.4%) had wound healing issues (16 had hypertrophic keloids/scarring, 5 had abscesses, 3 had abnormal bruising, and 8 had other would healing issues).
The study also included results of a multiple-choice patient survey from 1,354 individuals. In the survey, approximately two-thirds of patients reported abnormal scarring, abnormal wound healing, and cutaneous laxity (61.7%, 69.0%, and 71.0%, respectively).
The findings were limited by several factors including the retrospective study design, lack of testing to confirm hEDS diagnosis, and the potential interdisciplinary selection bias for diagnoses, the authors noted.
However, the results support previous studies showing increased rates of occlusive conditions in hEDS and higher rates of acne, folliculitis, and psoriasis, and highlight the need for clinician education to manage patients and promote better outcomes, the researchers concluded.
Data Enhance Clinical Awareness
“Given the increasingly understood relation between TH2-directed and mast-cell mediated diseases and hEDS, it was not necessarily a surprise to find the increased prevalence of atopy and mast cell disease, but rather an interesting confirmation, within the limitations that exist with retrospective chart review,” Dr. Snyder told this news organization. “While it may make some intuitive sense that certain cohorts with higher risk of HS may have a higher risk of acne, this had not been reported in the literature to date,” he noted. “Given the high levels of patient reported issues with scarring and wound healing, I was surprised that so few analogous diagnoses were physician-reported in the medical records.”
In clinical practice, “health care professionals and patients need to be aware hEDS is associated with high rates of eczematous, mast-cell mediated and follicular occlusive cutaneous disorders,” Dr. Snyder said in an interview. “There seems to be a discrepancy between patients and physician awareness of scarring or wound healing issues in this patient population,” he added.
Looking ahead, “we need to better research and characterize the various hEDS phenotypes to understand who is at highest risk for various TH2-mediated or follicular occlusive disorders,” said Dr. Snyder. “Moreover, a greater understanding is needed of the wound healing inadequacies that predispose these patients to poor outcomes during dermatologic surgery,” he said.
The study was supported by the Ehlers-Danlos Society and the Milton and Tamar Maltz Family Foundation. The researchers had no financial conflicts to disclose.
.
The genetic cause of hEDS, a common inherited connective tissue disorder, remains unknown, wrote Alan Snyder, MD, of the department of dermatology and dermatologic surgery at Medical University of South Carolina, Charleston, and colleagues.
Previous research suggests that changes in dermal mechanics predispose these patients to a range of skin conditions including mast cell activation disorder (MCAD) spectrum and chronic spontaneous urticaria, abnormal scars or wound healing, piezogenic papules, dyshidrosis, skin laxity or softness, easy bruising, local anesthesia resistance, keratosis pilaris, striae, and hidradenitis suppurativa, the researchers wrote.
However, data on these and other dermatologic manifestations of hEDS are limited, they said.
The diagnosis of hEDS will continue to be made more frequently and carefully, as the condition becomes more recognized and understood in the medical community, especially with anticipated capabilities of genetic testing, Dr. Snyder said in an interview.
“Being able to be aware of disease-specific comorbidities, such as those discovered in this study, allows providers to better stratify phenotypes and improve patient disease co-management,” he said.
In the study, published in the Journal of the American Academy of Dermatology, the researchers reviewed data on 1,364 patients with ICD-10 or ICD-9 codes for hEDS or EDS unspecified who were seen at a single institution between June 2005 and May 2022. Most of the patients were White (95.4%) and female (86.7%); the average age was 29.2 years.
Of the 1,364 patients included in the chart review, 497 (36.4%) had documented skin manifestations. Of these, 118 (24.2%) had disorders of follicular occlusion (12 had hidradenitis suppurativa, 32 had folliculitis, and 74 had acne); 112 (23%) had eczema or atopic dermatitis, 98 (19.7%) had mast cell disorder, 32 (6.4%) had psoriasis, and 32 (6.4%) had wound healing issues (16 had hypertrophic keloids/scarring, 5 had abscesses, 3 had abnormal bruising, and 8 had other would healing issues).
The study also included results of a multiple-choice patient survey from 1,354 individuals. In the survey, approximately two-thirds of patients reported abnormal scarring, abnormal wound healing, and cutaneous laxity (61.7%, 69.0%, and 71.0%, respectively).
The findings were limited by several factors including the retrospective study design, lack of testing to confirm hEDS diagnosis, and the potential interdisciplinary selection bias for diagnoses, the authors noted.
However, the results support previous studies showing increased rates of occlusive conditions in hEDS and higher rates of acne, folliculitis, and psoriasis, and highlight the need for clinician education to manage patients and promote better outcomes, the researchers concluded.
Data Enhance Clinical Awareness
“Given the increasingly understood relation between TH2-directed and mast-cell mediated diseases and hEDS, it was not necessarily a surprise to find the increased prevalence of atopy and mast cell disease, but rather an interesting confirmation, within the limitations that exist with retrospective chart review,” Dr. Snyder told this news organization. “While it may make some intuitive sense that certain cohorts with higher risk of HS may have a higher risk of acne, this had not been reported in the literature to date,” he noted. “Given the high levels of patient reported issues with scarring and wound healing, I was surprised that so few analogous diagnoses were physician-reported in the medical records.”
In clinical practice, “health care professionals and patients need to be aware hEDS is associated with high rates of eczematous, mast-cell mediated and follicular occlusive cutaneous disorders,” Dr. Snyder said in an interview. “There seems to be a discrepancy between patients and physician awareness of scarring or wound healing issues in this patient population,” he added.
Looking ahead, “we need to better research and characterize the various hEDS phenotypes to understand who is at highest risk for various TH2-mediated or follicular occlusive disorders,” said Dr. Snyder. “Moreover, a greater understanding is needed of the wound healing inadequacies that predispose these patients to poor outcomes during dermatologic surgery,” he said.
The study was supported by the Ehlers-Danlos Society and the Milton and Tamar Maltz Family Foundation. The researchers had no financial conflicts to disclose.
.
The genetic cause of hEDS, a common inherited connective tissue disorder, remains unknown, wrote Alan Snyder, MD, of the department of dermatology and dermatologic surgery at Medical University of South Carolina, Charleston, and colleagues.
Previous research suggests that changes in dermal mechanics predispose these patients to a range of skin conditions including mast cell activation disorder (MCAD) spectrum and chronic spontaneous urticaria, abnormal scars or wound healing, piezogenic papules, dyshidrosis, skin laxity or softness, easy bruising, local anesthesia resistance, keratosis pilaris, striae, and hidradenitis suppurativa, the researchers wrote.
However, data on these and other dermatologic manifestations of hEDS are limited, they said.
The diagnosis of hEDS will continue to be made more frequently and carefully, as the condition becomes more recognized and understood in the medical community, especially with anticipated capabilities of genetic testing, Dr. Snyder said in an interview.
“Being able to be aware of disease-specific comorbidities, such as those discovered in this study, allows providers to better stratify phenotypes and improve patient disease co-management,” he said.
In the study, published in the Journal of the American Academy of Dermatology, the researchers reviewed data on 1,364 patients with ICD-10 or ICD-9 codes for hEDS or EDS unspecified who were seen at a single institution between June 2005 and May 2022. Most of the patients were White (95.4%) and female (86.7%); the average age was 29.2 years.
Of the 1,364 patients included in the chart review, 497 (36.4%) had documented skin manifestations. Of these, 118 (24.2%) had disorders of follicular occlusion (12 had hidradenitis suppurativa, 32 had folliculitis, and 74 had acne); 112 (23%) had eczema or atopic dermatitis, 98 (19.7%) had mast cell disorder, 32 (6.4%) had psoriasis, and 32 (6.4%) had wound healing issues (16 had hypertrophic keloids/scarring, 5 had abscesses, 3 had abnormal bruising, and 8 had other would healing issues).
The study also included results of a multiple-choice patient survey from 1,354 individuals. In the survey, approximately two-thirds of patients reported abnormal scarring, abnormal wound healing, and cutaneous laxity (61.7%, 69.0%, and 71.0%, respectively).
The findings were limited by several factors including the retrospective study design, lack of testing to confirm hEDS diagnosis, and the potential interdisciplinary selection bias for diagnoses, the authors noted.
However, the results support previous studies showing increased rates of occlusive conditions in hEDS and higher rates of acne, folliculitis, and psoriasis, and highlight the need for clinician education to manage patients and promote better outcomes, the researchers concluded.
Data Enhance Clinical Awareness
“Given the increasingly understood relation between TH2-directed and mast-cell mediated diseases and hEDS, it was not necessarily a surprise to find the increased prevalence of atopy and mast cell disease, but rather an interesting confirmation, within the limitations that exist with retrospective chart review,” Dr. Snyder told this news organization. “While it may make some intuitive sense that certain cohorts with higher risk of HS may have a higher risk of acne, this had not been reported in the literature to date,” he noted. “Given the high levels of patient reported issues with scarring and wound healing, I was surprised that so few analogous diagnoses were physician-reported in the medical records.”
In clinical practice, “health care professionals and patients need to be aware hEDS is associated with high rates of eczematous, mast-cell mediated and follicular occlusive cutaneous disorders,” Dr. Snyder said in an interview. “There seems to be a discrepancy between patients and physician awareness of scarring or wound healing issues in this patient population,” he added.
Looking ahead, “we need to better research and characterize the various hEDS phenotypes to understand who is at highest risk for various TH2-mediated or follicular occlusive disorders,” said Dr. Snyder. “Moreover, a greater understanding is needed of the wound healing inadequacies that predispose these patients to poor outcomes during dermatologic surgery,” he said.
The study was supported by the Ehlers-Danlos Society and the Milton and Tamar Maltz Family Foundation. The researchers had no financial conflicts to disclose.
FROM THE JOURNAL OF THE AMERICAN ACADEMY OF DERMATOLOGY
An alternative to walking out
Organized labor seems to be experiencing a rebirth of sorts. In October 2022 a strike by railroad workers was averted when a tentative agreement about wages, working conditions, health insurance, and medical leave was hammered out. This past fall, strikes by auto workers that threatened to paralyze the big three manufacturers have now been resolved with agreements that meet many of the workers’ demands. The President even made an appearance on a picket line. Baristas at coffee shops, screenwriters, and actors have all been involved in work actions around the country.
While the health care industry has been relatively immune to threatened work stoppages, there are a growing number of hospitals and clinics where nurses and physicians are exploring the possibility of organizing to give themselves a stronger voice in how health care is being delivered. The realities that come when you transition from owner to employee are finally beginning to sink in for physicians, whether they are specialists or primary care providers.

One of the most significant efforts toward unionization recently occurred in Minnesota and Wisconsin. About 400 physicians and 150 physician’s assistants and nurse practitioners employed at Allina Health System voted to unionize and join the Doctors Council.
In an interview with Jacobin, a publication that offers a socialist perspective, three of the providers involved in the process that led to the vote shared their observations. The physicians claim that the first steps toward unionization came after multiple efforts to work with the Allina’s administration were rebuffed. As primary care physicians, their initial demands focused on getting help with hiring staffing and getting support with paperwork and administrative obligations.
The organizers complained that while Medicare hoped to bolster primary care by paying the providers more, the funds went to the companies, who then distributed them in a way that often did little to help the overworked providers. In addition to achieving a more equitable distribution of the monies, one of the organizers sees unionization as a way to provide a layer of protection when providers feel they must speak out about situations which clearly put quality of care at risk.
The organizers say the idea of unionization has been particularly appealing to the younger providers who are feeling threatened by burnout. When these new physicians look to their older coworkers for advice, they often find that the seasoned employees are as stressed as they are. Realizing that things aren’t going to improve with time, acting now to strengthen their voices sounds appealing.
With the vote for unionization behind them, the organizers are now ready to formulate a prioritized list of demands. Those of you who are regular readers of Letters from Maine know that I have been urging primary care physicians to find their voices. Unfortunately, unionization seems to be becoming a more common fall-back strategy when other avenues have failed to reach a sympathetic ear in the corporate boardrooms.
As more unions form, it will be interesting to see how the organizers structure their demands and job actions. While walkouts and strikes can certainly be effective in gaining attention, that attention can carry a risk of counter productivity sometimes by alienating patients, who should become allies.
Since an unsustainable burden of paperwork and administrative demands seems to be at the top of everyone’s priority list, it might make sense to adopt this message as a scaffolding on which to built a work action. Instead of walking off the job or marching on a picket line, why not stay in the hospital and continue to see patients but only for part of the work day. The remainder of the day would be spent doing all the clerical work that has become so onerous.
Providers would agree to see patients in the mornings, saving up the clerical work and administrative obligations for the afternoon. The definition of “morning” could vary depending on local conditions.
The important message to the public and the patients would be that the providers were not abandoning them by walking out. The patients’ access to face-to-face care was being limited not because the doctors didn’t want to see them but because the providers were being forced to accept other responsibilities by the administration. The physicians would always be on site in case of a crisis, but until reasonable demands for support from the company were met, a certain portion of the providers’ day would be spent doing things not directly related to face-to-face patient care. This burden of meaningless work is the reality as it stands already. Why not organize it in a way that makes it startlingly visible to the patients and the public.
There would be no video clips of physicians walking the picket lines carrying signs. Any images released to the media would be of empty waiting rooms while providers sat hunched over their computers or talking on the phone to insurance companies.
The strategy needs a catchy phrase like “a paperwork-in” but I’m still struggling with a name. Let me know if you have a better one or even a better strategy.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Other than a Littman stethoscope he accepted as a first-year medical student in 1966, Dr. Wilkoff reports having nothing to disclose. Email him at [email protected].
Organized labor seems to be experiencing a rebirth of sorts. In October 2022 a strike by railroad workers was averted when a tentative agreement about wages, working conditions, health insurance, and medical leave was hammered out. This past fall, strikes by auto workers that threatened to paralyze the big three manufacturers have now been resolved with agreements that meet many of the workers’ demands. The President even made an appearance on a picket line. Baristas at coffee shops, screenwriters, and actors have all been involved in work actions around the country.
While the health care industry has been relatively immune to threatened work stoppages, there are a growing number of hospitals and clinics where nurses and physicians are exploring the possibility of organizing to give themselves a stronger voice in how health care is being delivered. The realities that come when you transition from owner to employee are finally beginning to sink in for physicians, whether they are specialists or primary care providers.
One of the most significant efforts toward unionization recently occurred in Minnesota and Wisconsin. About 400 physicians and 150 physician’s assistants and nurse practitioners employed at Allina Health System voted to unionize and join the Doctors Council.
In an interview with Jacobin, a publication that offers a socialist perspective, three of the providers involved in the process that led to the vote shared their observations. The physicians claim that the first steps toward unionization came after multiple efforts to work with the Allina’s administration were rebuffed. As primary care physicians, their initial demands focused on getting help with hiring staffing and getting support with paperwork and administrative obligations.
The organizers complained that while Medicare hoped to bolster primary care by paying the providers more, the funds went to the companies, who then distributed them in a way that often did little to help the overworked providers. In addition to achieving a more equitable distribution of the monies, one of the organizers sees unionization as a way to provide a layer of protection when providers feel they must speak out about situations which clearly put quality of care at risk.
The organizers say the idea of unionization has been particularly appealing to the younger providers who are feeling threatened by burnout. When these new physicians look to their older coworkers for advice, they often find that the seasoned employees are as stressed as they are. Realizing that things aren’t going to improve with time, acting now to strengthen their voices sounds appealing.
With the vote for unionization behind them, the organizers are now ready to formulate a prioritized list of demands. Those of you who are regular readers of Letters from Maine know that I have been urging primary care physicians to find their voices. Unfortunately, unionization seems to be becoming a more common fall-back strategy when other avenues have failed to reach a sympathetic ear in the corporate boardrooms.
As more unions form, it will be interesting to see how the organizers structure their demands and job actions. While walkouts and strikes can certainly be effective in gaining attention, that attention can carry a risk of counter productivity sometimes by alienating patients, who should become allies.
Since an unsustainable burden of paperwork and administrative demands seems to be at the top of everyone’s priority list, it might make sense to adopt this message as a scaffolding on which to built a work action. Instead of walking off the job or marching on a picket line, why not stay in the hospital and continue to see patients but only for part of the work day. The remainder of the day would be spent doing all the clerical work that has become so onerous.
Providers would agree to see patients in the mornings, saving up the clerical work and administrative obligations for the afternoon. The definition of “morning” could vary depending on local conditions.
The important message to the public and the patients would be that the providers were not abandoning them by walking out. The patients’ access to face-to-face care was being limited not because the doctors didn’t want to see them but because the providers were being forced to accept other responsibilities by the administration. The physicians would always be on site in case of a crisis, but until reasonable demands for support from the company were met, a certain portion of the providers’ day would be spent doing things not directly related to face-to-face patient care. This burden of meaningless work is the reality as it stands already. Why not organize it in a way that makes it startlingly visible to the patients and the public.
There would be no video clips of physicians walking the picket lines carrying signs. Any images released to the media would be of empty waiting rooms while providers sat hunched over their computers or talking on the phone to insurance companies.
The strategy needs a catchy phrase like “a paperwork-in” but I’m still struggling with a name. Let me know if you have a better one or even a better strategy.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Other than a Littman stethoscope he accepted as a first-year medical student in 1966, Dr. Wilkoff reports having nothing to disclose. Email him at [email protected].
Organized labor seems to be experiencing a rebirth of sorts. In October 2022 a strike by railroad workers was averted when a tentative agreement about wages, working conditions, health insurance, and medical leave was hammered out. This past fall, strikes by auto workers that threatened to paralyze the big three manufacturers have now been resolved with agreements that meet many of the workers’ demands. The President even made an appearance on a picket line. Baristas at coffee shops, screenwriters, and actors have all been involved in work actions around the country.
While the health care industry has been relatively immune to threatened work stoppages, there are a growing number of hospitals and clinics where nurses and physicians are exploring the possibility of organizing to give themselves a stronger voice in how health care is being delivered. The realities that come when you transition from owner to employee are finally beginning to sink in for physicians, whether they are specialists or primary care providers.
One of the most significant efforts toward unionization recently occurred in Minnesota and Wisconsin. About 400 physicians and 150 physician’s assistants and nurse practitioners employed at Allina Health System voted to unionize and join the Doctors Council.
In an interview with Jacobin, a publication that offers a socialist perspective, three of the providers involved in the process that led to the vote shared their observations. The physicians claim that the first steps toward unionization came after multiple efforts to work with the Allina’s administration were rebuffed. As primary care physicians, their initial demands focused on getting help with hiring staffing and getting support with paperwork and administrative obligations.
The organizers complained that while Medicare hoped to bolster primary care by paying the providers more, the funds went to the companies, who then distributed them in a way that often did little to help the overworked providers. In addition to achieving a more equitable distribution of the monies, one of the organizers sees unionization as a way to provide a layer of protection when providers feel they must speak out about situations which clearly put quality of care at risk.
The organizers say the idea of unionization has been particularly appealing to the younger providers who are feeling threatened by burnout. When these new physicians look to their older coworkers for advice, they often find that the seasoned employees are as stressed as they are. Realizing that things aren’t going to improve with time, acting now to strengthen their voices sounds appealing.
With the vote for unionization behind them, the organizers are now ready to formulate a prioritized list of demands. Those of you who are regular readers of Letters from Maine know that I have been urging primary care physicians to find their voices. Unfortunately, unionization seems to be becoming a more common fall-back strategy when other avenues have failed to reach a sympathetic ear in the corporate boardrooms.
As more unions form, it will be interesting to see how the organizers structure their demands and job actions. While walkouts and strikes can certainly be effective in gaining attention, that attention can carry a risk of counter productivity sometimes by alienating patients, who should become allies.
Since an unsustainable burden of paperwork and administrative demands seems to be at the top of everyone’s priority list, it might make sense to adopt this message as a scaffolding on which to built a work action. Instead of walking off the job or marching on a picket line, why not stay in the hospital and continue to see patients but only for part of the work day. The remainder of the day would be spent doing all the clerical work that has become so onerous.
Providers would agree to see patients in the mornings, saving up the clerical work and administrative obligations for the afternoon. The definition of “morning” could vary depending on local conditions.
The important message to the public and the patients would be that the providers were not abandoning them by walking out. The patients’ access to face-to-face care was being limited not because the doctors didn’t want to see them but because the providers were being forced to accept other responsibilities by the administration. The physicians would always be on site in case of a crisis, but until reasonable demands for support from the company were met, a certain portion of the providers’ day would be spent doing things not directly related to face-to-face patient care. This burden of meaningless work is the reality as it stands already. Why not organize it in a way that makes it startlingly visible to the patients and the public.
There would be no video clips of physicians walking the picket lines carrying signs. Any images released to the media would be of empty waiting rooms while providers sat hunched over their computers or talking on the phone to insurance companies.
The strategy needs a catchy phrase like “a paperwork-in” but I’m still struggling with a name. Let me know if you have a better one or even a better strategy.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Other than a Littman stethoscope he accepted as a first-year medical student in 1966, Dr. Wilkoff reports having nothing to disclose. Email him at [email protected].
FDA mandates five changes to iPLEDGE program for isotretinoin
In a letter dated Nov. 30, 2023, the .
The development follows a March 2023 joint meeting of the FDA’s Drug Safety and Risk Management Advisory Committee and the Dermatologic and Ophthalmic Drugs Advisory Committee about iPLEDGE REMS requirements, which included feedback from patients and dermatologists and recommendations for changes to the REMS program, aimed at minimizing the burden of the program on patients, pharmacies, and prescribers while continuing to maintain safe use of the highly teratogenic drug for patients.
The five changes include the following:
- Remove the requirement that pregnancy tests must be performed in a specially certified (i.e., Clinical Laboratory Improvement Amendments [CLIA]) laboratory. In the opinion of John S. Barbieri, MD, MBA, director of the Advanced Acne Therapeutics Clinic at Brigham and Women’s Hospital, Boston, this change “may make it easier to perform pregnancy tests in a clinic setting without needing to send the patient to a separate lab,” he said in an interview.
- Allow prescribers the option of using home pregnancy testing for their patients during and after isotretinoin treatment. Prescribers who rely on the patient to perform a home pregnancy test need to take steps to minimize patients falsifying the results of these tests. According to Dr. Barbieri, this means that two pregnancy tests prior to starting isotretinoin must be done in a lab or office setting. “However, all the pregnancy tests on therapy can be either in a medical setting or using a home pregnancy test,” he told this news organization. “This option facilitates the use of telemedicine so that patients would not need to come in; they can just share a pregnancy test with their name and date with their dermatologist.”
- Remove the waiting period requirement — also known as the “19-day lockout” — for patients if they do not obtain isotretinoin within the first 7-day prescription window. According to Dr. Barbieri, this change helps to ensure that patients can begin isotretinoin in a timely manner. “Insurance and pharmacy delays that are no fault of the patient can commonly cause missed initial window periods,” he said. “Allowing for immediate repeat of a pregnancy test to start a new window period, rather than requiring the patient to wait 19 more days, can ensure patient safety and pregnancy prevention without negatively impacting access.”
- Revise the pregnancy registry requirement to remove the objective to document the pregnancy and fetal outcomes for each pregnancy.
- Revise the requirement for prescribers to document patient counseling in patients who cannot become pregnant from monthly to only at enrollment. Dr. Barbieri characterized this change as “major” and said that it could eliminate the need for monthly visits for persons of non–childbearing potential. “This could substantially reduce logistical burdens for patients and reduce wait times to see a dermatologist,” he said.
Future changes to iPLEDGE that Dr. Barbieri would like to see include allowing for home pregnancy tests prior to starting therapy — particularly the test after the 30-day window period. “In addition, it would be good to be able to reduce the 30-day waiting period prior to therapy to something shorter,” such as 14 days, which would still “reliably exclude pregnancy, particularly for those on stable long-acting reversible contraception,” he said. There are also opportunities to improve the iPLEDGE website functionality and to ensure that the website is accessible to patients with limited English proficiency, he added.
He also recommended greater transparency by the Isotretinoin Products Manufacturers Group and inclusion of input from diverse stakeholders such as dermatologists, patients, and pharmacists.
Dr. Barbieri reported personal fees from Dexcel Pharma.
In a letter dated Nov. 30, 2023, the .
The development follows a March 2023 joint meeting of the FDA’s Drug Safety and Risk Management Advisory Committee and the Dermatologic and Ophthalmic Drugs Advisory Committee about iPLEDGE REMS requirements, which included feedback from patients and dermatologists and recommendations for changes to the REMS program, aimed at minimizing the burden of the program on patients, pharmacies, and prescribers while continuing to maintain safe use of the highly teratogenic drug for patients.
The five changes include the following:
- Remove the requirement that pregnancy tests must be performed in a specially certified (i.e., Clinical Laboratory Improvement Amendments [CLIA]) laboratory. In the opinion of John S. Barbieri, MD, MBA, director of the Advanced Acne Therapeutics Clinic at Brigham and Women’s Hospital, Boston, this change “may make it easier to perform pregnancy tests in a clinic setting without needing to send the patient to a separate lab,” he said in an interview.
- Allow prescribers the option of using home pregnancy testing for their patients during and after isotretinoin treatment. Prescribers who rely on the patient to perform a home pregnancy test need to take steps to minimize patients falsifying the results of these tests. According to Dr. Barbieri, this means that two pregnancy tests prior to starting isotretinoin must be done in a lab or office setting. “However, all the pregnancy tests on therapy can be either in a medical setting or using a home pregnancy test,” he told this news organization. “This option facilitates the use of telemedicine so that patients would not need to come in; they can just share a pregnancy test with their name and date with their dermatologist.”
- Remove the waiting period requirement — also known as the “19-day lockout” — for patients if they do not obtain isotretinoin within the first 7-day prescription window. According to Dr. Barbieri, this change helps to ensure that patients can begin isotretinoin in a timely manner. “Insurance and pharmacy delays that are no fault of the patient can commonly cause missed initial window periods,” he said. “Allowing for immediate repeat of a pregnancy test to start a new window period, rather than requiring the patient to wait 19 more days, can ensure patient safety and pregnancy prevention without negatively impacting access.”
- Revise the pregnancy registry requirement to remove the objective to document the pregnancy and fetal outcomes for each pregnancy.
- Revise the requirement for prescribers to document patient counseling in patients who cannot become pregnant from monthly to only at enrollment. Dr. Barbieri characterized this change as “major” and said that it could eliminate the need for monthly visits for persons of non–childbearing potential. “This could substantially reduce logistical burdens for patients and reduce wait times to see a dermatologist,” he said.
Future changes to iPLEDGE that Dr. Barbieri would like to see include allowing for home pregnancy tests prior to starting therapy — particularly the test after the 30-day window period. “In addition, it would be good to be able to reduce the 30-day waiting period prior to therapy to something shorter,” such as 14 days, which would still “reliably exclude pregnancy, particularly for those on stable long-acting reversible contraception,” he said. There are also opportunities to improve the iPLEDGE website functionality and to ensure that the website is accessible to patients with limited English proficiency, he added.
He also recommended greater transparency by the Isotretinoin Products Manufacturers Group and inclusion of input from diverse stakeholders such as dermatologists, patients, and pharmacists.
Dr. Barbieri reported personal fees from Dexcel Pharma.
In a letter dated Nov. 30, 2023, the .
The development follows a March 2023 joint meeting of the FDA’s Drug Safety and Risk Management Advisory Committee and the Dermatologic and Ophthalmic Drugs Advisory Committee about iPLEDGE REMS requirements, which included feedback from patients and dermatologists and recommendations for changes to the REMS program, aimed at minimizing the burden of the program on patients, pharmacies, and prescribers while continuing to maintain safe use of the highly teratogenic drug for patients.
The five changes include the following:
- Remove the requirement that pregnancy tests must be performed in a specially certified (i.e., Clinical Laboratory Improvement Amendments [CLIA]) laboratory. In the opinion of John S. Barbieri, MD, MBA, director of the Advanced Acne Therapeutics Clinic at Brigham and Women’s Hospital, Boston, this change “may make it easier to perform pregnancy tests in a clinic setting without needing to send the patient to a separate lab,” he said in an interview.
- Allow prescribers the option of using home pregnancy testing for their patients during and after isotretinoin treatment. Prescribers who rely on the patient to perform a home pregnancy test need to take steps to minimize patients falsifying the results of these tests. According to Dr. Barbieri, this means that two pregnancy tests prior to starting isotretinoin must be done in a lab or office setting. “However, all the pregnancy tests on therapy can be either in a medical setting or using a home pregnancy test,” he told this news organization. “This option facilitates the use of telemedicine so that patients would not need to come in; they can just share a pregnancy test with their name and date with their dermatologist.”
- Remove the waiting period requirement — also known as the “19-day lockout” — for patients if they do not obtain isotretinoin within the first 7-day prescription window. According to Dr. Barbieri, this change helps to ensure that patients can begin isotretinoin in a timely manner. “Insurance and pharmacy delays that are no fault of the patient can commonly cause missed initial window periods,” he said. “Allowing for immediate repeat of a pregnancy test to start a new window period, rather than requiring the patient to wait 19 more days, can ensure patient safety and pregnancy prevention without negatively impacting access.”
- Revise the pregnancy registry requirement to remove the objective to document the pregnancy and fetal outcomes for each pregnancy.
- Revise the requirement for prescribers to document patient counseling in patients who cannot become pregnant from monthly to only at enrollment. Dr. Barbieri characterized this change as “major” and said that it could eliminate the need for monthly visits for persons of non–childbearing potential. “This could substantially reduce logistical burdens for patients and reduce wait times to see a dermatologist,” he said.
Future changes to iPLEDGE that Dr. Barbieri would like to see include allowing for home pregnancy tests prior to starting therapy — particularly the test after the 30-day window period. “In addition, it would be good to be able to reduce the 30-day waiting period prior to therapy to something shorter,” such as 14 days, which would still “reliably exclude pregnancy, particularly for those on stable long-acting reversible contraception,” he said. There are also opportunities to improve the iPLEDGE website functionality and to ensure that the website is accessible to patients with limited English proficiency, he added.
He also recommended greater transparency by the Isotretinoin Products Manufacturers Group and inclusion of input from diverse stakeholders such as dermatologists, patients, and pharmacists.
Dr. Barbieri reported personal fees from Dexcel Pharma.
Are you sure your patient is alive?
This transcript has been edited for clarity.
Much of my research focuses on what is known as clinical decision support — prompts and messages to providers to help them make good decisions for their patients. I know that these things can be annoying, which is exactly why I study them — to figure out which ones actually help.
When I got started on this about 10 years ago, we were learning a lot about how best to message providers about their patients. My team had developed a simple alert for acute kidney injury (AKI). We knew that providers often missed the diagnosis, so maybe letting them know would improve patient outcomes.
As we tested the alert, we got feedback, and I have kept an email from an ICU doctor from those early days. It read:
Dear Dr. Wilson: Thank you for the automated alert informing me that my patient had AKI. Regrettably, the alert fired about an hour after the patient had died. I feel that the information is less than actionable at this time.
Our early system had neglected to add a conditional flag ensuring that the patient was still alive at the time it sent the alert message. A small oversight, but one that had very large implications. Future studies would show that “false positive” alerts like this seriously degrade physician confidence in the system. And why wouldn’t they?
Not knowing the vital status of a patient can have major consequences.
Health systems send messages to their patients all the time: reminders of appointments, reminders for preventive care, reminders for vaccinations, and so on.
But what if the patient being reminded has died? It’s a waste of resources, of course, but more than that, it can be painful for their families and reflects poorly on the health care system. Of all the people who should know whether someone is alive or dead, shouldn’t their doctor be at the top of the list?
A new study in JAMA Internal Medicine quantifies this very phenomenon.
Researchers examined 11,658 primary care patients in their health system who met the criteria of being “seriously ill” and followed them for 2 years. During that period of time, 25% were recorded as deceased in the electronic health record. But 30.8% had died. That left 676 patients who had died, but were not known to have died, left in the system.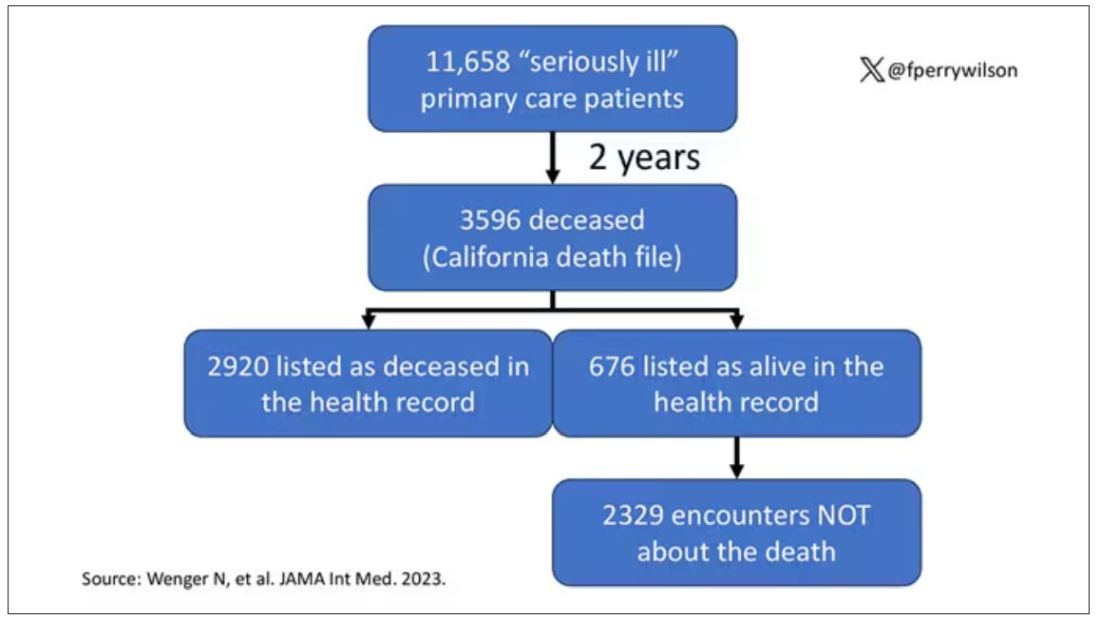
And those 676 were not left to rest in peace. They received 221 telephone and 338 health portal messages not related to death, and 920 letters reminding them about unmet primary care metrics like flu shots and cancer screening. Orders were entered into the health record for things like vaccines and routine screenings for 158 patients, and 310 future appointments — destined to be no-shows — were still on the books. One can only imagine the frustration of families checking their mail and finding yet another letter reminding their deceased loved one to get a mammogram.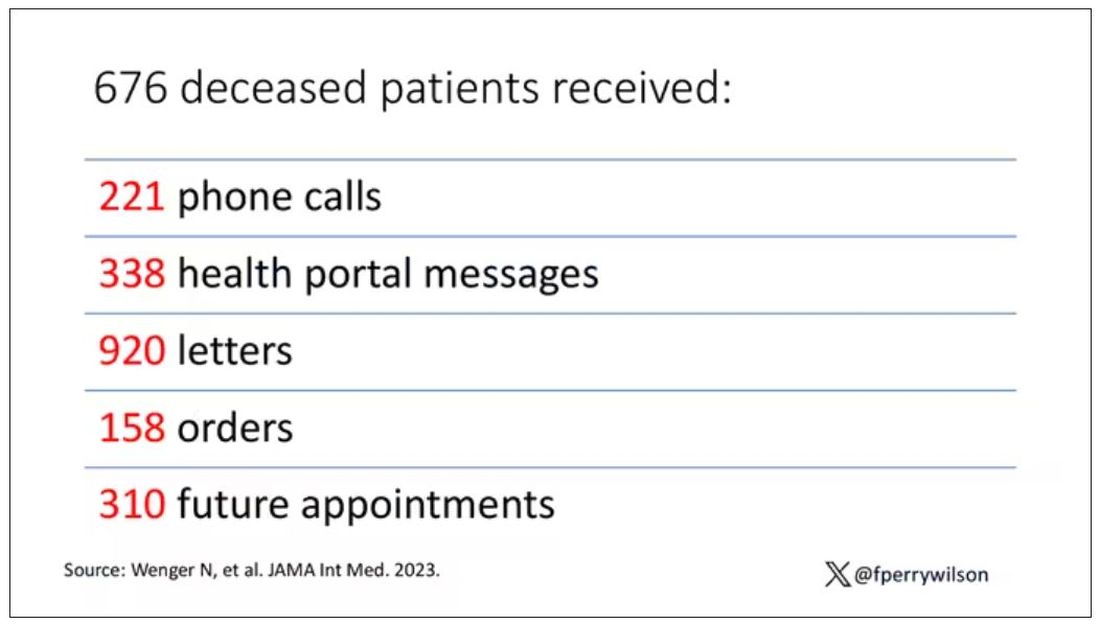
How did the researchers figure out who had died? It turns out it’s not that hard. California keeps a record of all deaths in the state; they simply had to search it. Like all state death records, they tend to lag a bit so it’s not clinically terribly useful, but it works. California and most other states also have a very accurate and up-to-date death file which can only be used by law enforcement to investigate criminal activity and fraud; health care is left in the lurch.
Nationwide, there is the real-time fact of death service, supported by the National Association for Public Health Statistics and Information Systems. This allows employers to verify, in real time, whether the person applying for a job is alive. Healthcare systems are not allowed to use it.
Let’s also remember that very few people die in this country without some health care agency knowing about it and recording it. But sharing of medical information is so poor in the United States that your patient could die in a hospital one city away from you and you might not find out until you’re calling them to see why they missed a scheduled follow-up appointment.
These events — the embarrassing lack of knowledge about the very vital status of our patients — highlight a huge problem with health care in our country. The fragmented health care system is terrible at data sharing, in part because of poor protocols, in part because of unfounded concerns about patient privacy, and in part because of a tendency to hoard data that might be valuable in the future. It has to stop. We need to know how our patients are doing even when they are not sitting in front of us. When it comes to life and death, the knowledge is out there; we just can’t access it. Seems like a pretty easy fix.
Dr. Wilson is associate professor of medicine and public health and director of the Clinical and Translational Research Accelerator at Yale University, New Haven, Connecticut. He has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com .
This transcript has been edited for clarity.
Much of my research focuses on what is known as clinical decision support — prompts and messages to providers to help them make good decisions for their patients. I know that these things can be annoying, which is exactly why I study them — to figure out which ones actually help.
When I got started on this about 10 years ago, we were learning a lot about how best to message providers about their patients. My team had developed a simple alert for acute kidney injury (AKI). We knew that providers often missed the diagnosis, so maybe letting them know would improve patient outcomes.
As we tested the alert, we got feedback, and I have kept an email from an ICU doctor from those early days. It read:
Dear Dr. Wilson: Thank you for the automated alert informing me that my patient had AKI. Regrettably, the alert fired about an hour after the patient had died. I feel that the information is less than actionable at this time.
Our early system had neglected to add a conditional flag ensuring that the patient was still alive at the time it sent the alert message. A small oversight, but one that had very large implications. Future studies would show that “false positive” alerts like this seriously degrade physician confidence in the system. And why wouldn’t they?
Not knowing the vital status of a patient can have major consequences.
Health systems send messages to their patients all the time: reminders of appointments, reminders for preventive care, reminders for vaccinations, and so on.
But what if the patient being reminded has died? It’s a waste of resources, of course, but more than that, it can be painful for their families and reflects poorly on the health care system. Of all the people who should know whether someone is alive or dead, shouldn’t their doctor be at the top of the list?
A new study in JAMA Internal Medicine quantifies this very phenomenon.
Researchers examined 11,658 primary care patients in their health system who met the criteria of being “seriously ill” and followed them for 2 years. During that period of time, 25% were recorded as deceased in the electronic health record. But 30.8% had died. That left 676 patients who had died, but were not known to have died, left in the system.
And those 676 were not left to rest in peace. They received 221 telephone and 338 health portal messages not related to death, and 920 letters reminding them about unmet primary care metrics like flu shots and cancer screening. Orders were entered into the health record for things like vaccines and routine screenings for 158 patients, and 310 future appointments — destined to be no-shows — were still on the books. One can only imagine the frustration of families checking their mail and finding yet another letter reminding their deceased loved one to get a mammogram.
How did the researchers figure out who had died? It turns out it’s not that hard. California keeps a record of all deaths in the state; they simply had to search it. Like all state death records, they tend to lag a bit so it’s not clinically terribly useful, but it works. California and most other states also have a very accurate and up-to-date death file which can only be used by law enforcement to investigate criminal activity and fraud; health care is left in the lurch.
Nationwide, there is the real-time fact of death service, supported by the National Association for Public Health Statistics and Information Systems. This allows employers to verify, in real time, whether the person applying for a job is alive. Healthcare systems are not allowed to use it.
Let’s also remember that very few people die in this country without some health care agency knowing about it and recording it. But sharing of medical information is so poor in the United States that your patient could die in a hospital one city away from you and you might not find out until you’re calling them to see why they missed a scheduled follow-up appointment.
These events — the embarrassing lack of knowledge about the very vital status of our patients — highlight a huge problem with health care in our country. The fragmented health care system is terrible at data sharing, in part because of poor protocols, in part because of unfounded concerns about patient privacy, and in part because of a tendency to hoard data that might be valuable in the future. It has to stop. We need to know how our patients are doing even when they are not sitting in front of us. When it comes to life and death, the knowledge is out there; we just can’t access it. Seems like a pretty easy fix.
Dr. Wilson is associate professor of medicine and public health and director of the Clinical and Translational Research Accelerator at Yale University, New Haven, Connecticut. He has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com .
This transcript has been edited for clarity.
Much of my research focuses on what is known as clinical decision support — prompts and messages to providers to help them make good decisions for their patients. I know that these things can be annoying, which is exactly why I study them — to figure out which ones actually help.
When I got started on this about 10 years ago, we were learning a lot about how best to message providers about their patients. My team had developed a simple alert for acute kidney injury (AKI). We knew that providers often missed the diagnosis, so maybe letting them know would improve patient outcomes.
As we tested the alert, we got feedback, and I have kept an email from an ICU doctor from those early days. It read:
Dear Dr. Wilson: Thank you for the automated alert informing me that my patient had AKI. Regrettably, the alert fired about an hour after the patient had died. I feel that the information is less than actionable at this time.
Our early system had neglected to add a conditional flag ensuring that the patient was still alive at the time it sent the alert message. A small oversight, but one that had very large implications. Future studies would show that “false positive” alerts like this seriously degrade physician confidence in the system. And why wouldn’t they?
Not knowing the vital status of a patient can have major consequences.
Health systems send messages to their patients all the time: reminders of appointments, reminders for preventive care, reminders for vaccinations, and so on.
But what if the patient being reminded has died? It’s a waste of resources, of course, but more than that, it can be painful for their families and reflects poorly on the health care system. Of all the people who should know whether someone is alive or dead, shouldn’t their doctor be at the top of the list?
A new study in JAMA Internal Medicine quantifies this very phenomenon.
Researchers examined 11,658 primary care patients in their health system who met the criteria of being “seriously ill” and followed them for 2 years. During that period of time, 25% were recorded as deceased in the electronic health record. But 30.8% had died. That left 676 patients who had died, but were not known to have died, left in the system.
And those 676 were not left to rest in peace. They received 221 telephone and 338 health portal messages not related to death, and 920 letters reminding them about unmet primary care metrics like flu shots and cancer screening. Orders were entered into the health record for things like vaccines and routine screenings for 158 patients, and 310 future appointments — destined to be no-shows — were still on the books. One can only imagine the frustration of families checking their mail and finding yet another letter reminding their deceased loved one to get a mammogram.
How did the researchers figure out who had died? It turns out it’s not that hard. California keeps a record of all deaths in the state; they simply had to search it. Like all state death records, they tend to lag a bit so it’s not clinically terribly useful, but it works. California and most other states also have a very accurate and up-to-date death file which can only be used by law enforcement to investigate criminal activity and fraud; health care is left in the lurch.
Nationwide, there is the real-time fact of death service, supported by the National Association for Public Health Statistics and Information Systems. This allows employers to verify, in real time, whether the person applying for a job is alive. Healthcare systems are not allowed to use it.
Let’s also remember that very few people die in this country without some health care agency knowing about it and recording it. But sharing of medical information is so poor in the United States that your patient could die in a hospital one city away from you and you might not find out until you’re calling them to see why they missed a scheduled follow-up appointment.
These events — the embarrassing lack of knowledge about the very vital status of our patients — highlight a huge problem with health care in our country. The fragmented health care system is terrible at data sharing, in part because of poor protocols, in part because of unfounded concerns about patient privacy, and in part because of a tendency to hoard data that might be valuable in the future. It has to stop. We need to know how our patients are doing even when they are not sitting in front of us. When it comes to life and death, the knowledge is out there; we just can’t access it. Seems like a pretty easy fix.
Dr. Wilson is associate professor of medicine and public health and director of the Clinical and Translational Research Accelerator at Yale University, New Haven, Connecticut. He has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com .
Early age at first period raises type 2 diabetes risk
TOPLINE:
, a retrospective study of US women under age 65 found.
METHODOLOGY:
- Researchers analyzed data from 17,377 women who were aged 20-65 years when they participated in a National Health and Nutrition Examination Survey (NHANES) from 1999 to 2018 and reported their age at first menstruation, which was classified as ≤ 10, 11, 12, 13, 14, or ≥ 15 years of age.
- In total, 0.2% of the women (1773) had type 2 diabetes; of these, 11.5% (205) had cardiovascular disease (CVD), defined as coronary heart disease (CHD), myocardial infarction, or stroke.
- Compared with women who had their first menstrual period at age 13 (the mean age in this population), those who had their period at age ≤ 10 had a significantly greater risk of having type 2 diabetes, after adjustment for age, race/ethnicity, education, parity, menopause status, family history of diabetes, smoking status, physical activity, alcohol consumption, and body mass index (odds ratio, 1.32; 95% CI, 1.03-1.69; P trend = .03).
- Among the women with diabetes, compared with those who had their first menstrual period at age 13, those who had it at age ≤ 10 had a significantly greater risk of having stroke (OR, 2.66; 95% CI, 1.07-6.64; P trend = .02), but not CVD or CHD, after adjustment for these multiple variables.
TAKEAWAY:
- In a racially and ethnically diverse national sample of US women younger than 65, “extremely early” age at first menstrual period was associated with significantly increased risk for type 2 diabetes; among the women with type 2 diabetes, it was associated with significantly increased risk for stroke but not CVD or CHD, after adjustment for multiple variables.
- Early age at menarche may be an early indicator of the cardiometabolic disease trajectory in women.
IN PRACTICE:
“Women with early-life exposures such as early age at menarche need to be further examined for diabetes and prevention research and strategies for progression of diabetes complications,” the study authors write.
SOURCE:
The authors, mainly from Tulane University School of Public Health and Tropical Medicine, New Orleans, Louisiana, and also from Harvard Medical School, Boston, Massachusetts, published their findings in BMJ Nutrition, Prevention & Health.
LIMITATIONS:
- The women who participated in NHANES may not be representative of all women in the United States (selection bias).
- The study only included women who reported the age when they had their first menstrual period (selection bias).
- This was a cross-sectional, observational study, so it cannot show causality.
- The women may have reported the wrong age at which they had their first period (recall bias and social desirability bias).
- The women may have inaccurately reported CVD and type 2 diabetes (recall bias and social desirability bias).
DISCLOSURES:
The researchers were supported by grants from the National Heart, Lung, and Blood Institute and from the National Institute of General Medical Sciences of the National Institutes of Health.
A version of this article first appeared on Medscape.com.
TOPLINE:
, a retrospective study of US women under age 65 found.
METHODOLOGY:
- Researchers analyzed data from 17,377 women who were aged 20-65 years when they participated in a National Health and Nutrition Examination Survey (NHANES) from 1999 to 2018 and reported their age at first menstruation, which was classified as ≤ 10, 11, 12, 13, 14, or ≥ 15 years of age.
- In total, 0.2% of the women (1773) had type 2 diabetes; of these, 11.5% (205) had cardiovascular disease (CVD), defined as coronary heart disease (CHD), myocardial infarction, or stroke.
- Compared with women who had their first menstrual period at age 13 (the mean age in this population), those who had their period at age ≤ 10 had a significantly greater risk of having type 2 diabetes, after adjustment for age, race/ethnicity, education, parity, menopause status, family history of diabetes, smoking status, physical activity, alcohol consumption, and body mass index (odds ratio, 1.32; 95% CI, 1.03-1.69; P trend = .03).
- Among the women with diabetes, compared with those who had their first menstrual period at age 13, those who had it at age ≤ 10 had a significantly greater risk of having stroke (OR, 2.66; 95% CI, 1.07-6.64; P trend = .02), but not CVD or CHD, after adjustment for these multiple variables.
TAKEAWAY:
- In a racially and ethnically diverse national sample of US women younger than 65, “extremely early” age at first menstrual period was associated with significantly increased risk for type 2 diabetes; among the women with type 2 diabetes, it was associated with significantly increased risk for stroke but not CVD or CHD, after adjustment for multiple variables.
- Early age at menarche may be an early indicator of the cardiometabolic disease trajectory in women.
IN PRACTICE:
“Women with early-life exposures such as early age at menarche need to be further examined for diabetes and prevention research and strategies for progression of diabetes complications,” the study authors write.
SOURCE:
The authors, mainly from Tulane University School of Public Health and Tropical Medicine, New Orleans, Louisiana, and also from Harvard Medical School, Boston, Massachusetts, published their findings in BMJ Nutrition, Prevention & Health.
LIMITATIONS:
- The women who participated in NHANES may not be representative of all women in the United States (selection bias).
- The study only included women who reported the age when they had their first menstrual period (selection bias).
- This was a cross-sectional, observational study, so it cannot show causality.
- The women may have reported the wrong age at which they had their first period (recall bias and social desirability bias).
- The women may have inaccurately reported CVD and type 2 diabetes (recall bias and social desirability bias).
DISCLOSURES:
The researchers were supported by grants from the National Heart, Lung, and Blood Institute and from the National Institute of General Medical Sciences of the National Institutes of Health.
A version of this article first appeared on Medscape.com.
TOPLINE:
, a retrospective study of US women under age 65 found.
METHODOLOGY:
- Researchers analyzed data from 17,377 women who were aged 20-65 years when they participated in a National Health and Nutrition Examination Survey (NHANES) from 1999 to 2018 and reported their age at first menstruation, which was classified as ≤ 10, 11, 12, 13, 14, or ≥ 15 years of age.
- In total, 0.2% of the women (1773) had type 2 diabetes; of these, 11.5% (205) had cardiovascular disease (CVD), defined as coronary heart disease (CHD), myocardial infarction, or stroke.
- Compared with women who had their first menstrual period at age 13 (the mean age in this population), those who had their period at age ≤ 10 had a significantly greater risk of having type 2 diabetes, after adjustment for age, race/ethnicity, education, parity, menopause status, family history of diabetes, smoking status, physical activity, alcohol consumption, and body mass index (odds ratio, 1.32; 95% CI, 1.03-1.69; P trend = .03).
- Among the women with diabetes, compared with those who had their first menstrual period at age 13, those who had it at age ≤ 10 had a significantly greater risk of having stroke (OR, 2.66; 95% CI, 1.07-6.64; P trend = .02), but not CVD or CHD, after adjustment for these multiple variables.
TAKEAWAY:
- In a racially and ethnically diverse national sample of US women younger than 65, “extremely early” age at first menstrual period was associated with significantly increased risk for type 2 diabetes; among the women with type 2 diabetes, it was associated with significantly increased risk for stroke but not CVD or CHD, after adjustment for multiple variables.
- Early age at menarche may be an early indicator of the cardiometabolic disease trajectory in women.
IN PRACTICE:
“Women with early-life exposures such as early age at menarche need to be further examined for diabetes and prevention research and strategies for progression of diabetes complications,” the study authors write.
SOURCE:
The authors, mainly from Tulane University School of Public Health and Tropical Medicine, New Orleans, Louisiana, and also from Harvard Medical School, Boston, Massachusetts, published their findings in BMJ Nutrition, Prevention & Health.
LIMITATIONS:
- The women who participated in NHANES may not be representative of all women in the United States (selection bias).
- The study only included women who reported the age when they had their first menstrual period (selection bias).
- This was a cross-sectional, observational study, so it cannot show causality.
- The women may have reported the wrong age at which they had their first period (recall bias and social desirability bias).
- The women may have inaccurately reported CVD and type 2 diabetes (recall bias and social desirability bias).
DISCLOSURES:
The researchers were supported by grants from the National Heart, Lung, and Blood Institute and from the National Institute of General Medical Sciences of the National Institutes of Health.
A version of this article first appeared on Medscape.com.