User login
Bringing you the latest news, research and reviews, exclusive interviews, podcasts, quizzes, and more.
div[contains(@class, 'read-next-article')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
nav[contains(@class, 'nav-ce-stack nav-ce-stack__large-screen')]
header[@id='header']
div[contains(@class, 'header__large-screen')]
div[contains(@class, 'main-prefix')]
footer[@id='footer']
section[contains(@class, 'nav-hidden')]
div[contains(@class, 'ce-card-content')]
nav[contains(@class, 'nav-ce-stack')]
div[contains(@class, 'view-medstat-quiz-listing-panes')]
Diary of a rheumatologist who briefly became a COVID hospitalist
When the coronavirus pandemic hit New York City in early March, the Hospital for Special Surgery leadership decided that the best way to serve the city was to stop elective orthopedic procedures temporarily and use the facility to take on patients from its sister institution, NewYork–Presbyterian Hospital.
As in other institutions, it was all hands on deck. , other internal medicine subspecialists were asked to volunteer, including rheumatologists and primary care sports medicine doctors.
As a rheumatologist, it had been well over 10 years since I had last done any inpatient work. I was filled with trepidation, but I was also excited to dive in.
April 4:
Feeling very unmoored. I am in unfamiliar territory, and it’s terrifying. There are so many things that I no longer know how to do. Thankfully, the hospitalists are gracious, extremely supportive, and helpful.
My N95 doesn’t fit well. It’s never fit — not during residency or fellowship, not in any job I’ve had, and not today. The lady fit-testing me said she was sorry, but the look on her face said, “I’m sorry, but you’re going to die.”
April 7:
We don’t know how to treat coronavirus. I’ve sent some patients home, others I’ve sent to the ICU. Thank goodness for treatment algorithms from leadership, but we are sorely lacking good-quality data.
Our infectious disease doctor doesn’t think hydroxychloroquine works at all; I suspect he is right. The guidance right now is to give hydroxychloroquine and azithromycin to everyone who is sick enough to be admitted, but there are methodologic flaws in the early enthusiastic preprints, and so far, I’ve not noticed any demonstrable benefit.
The only thing that seems to be happening is that I am seeing more QT prolongation — not something I previously counseled my rheumatology patients on.
April 9:
The patients have been, with a few exceptions, alone in the room. They’re not allowed to have visitors and are required to wear masks all the time. Anyone who enters their rooms is fully covered up so you can barely see them. It’s anonymous and dehumanizing.
We’re instructed to take histories by phone in order to limit the time spent in each room. I buck this instruction; I still take histories in person because human contact seems more important now than ever.
Except maybe I should be smarter about this. One of my patients refuses any treatment, including oxygen support. She firmly believes this is a result of 5G networks — something I later discovered was a common conspiracy theory. She refused to wear a mask despite having a very bad cough. She coughed in my face a lot when we were chatting. My face with my ill-fitting N95 mask. Maybe the fit-testing lady’s eyes weren’t lying and I will die after all.
April 15:
On the days when I’m not working as a hospitalist, I am still doing remote visits with my rheumatology patients. It feels good to be doing something familiar and something I’m actually good at. But it is surreal to be faced with the quotidian on one hand and life and death on the other.
I recently saw a fairly new patient, and I still haven’t figured out if she has a rheumatic condition or if her symptoms all stem from an alcohol use disorder. In our previous visits, she could barely acknowledge that her drinking was an issue. On today’s visit, she told me she was 1½ months sober.
I don’t know her very well, but it was the happiest news I’d heard in a long time. I was so beside myself with joy that I cried, which says more about my current emotional state than anything else, really.
April 21:
On my panel of patients, I have three women with COVID-19 — all of whom lost their husbands to COVID-19, and none of whom were able to say their goodbyes. I cannot even begin to imagine what it must be like to survive this period of illness, isolation, and fear, only to be met on the other side by grief.
Rheumatology doesn’t lend itself too well to such existential concerns; I am not equipped for this. Perhaps my only advantage as a rheumatologist is that I know how to use IVIG, anakinra, and tocilizumab.
Someone on my panel was started on anakinra, and it turned his case around. Would he have gotten better without it anyway? We’ll never know for sure.
April 28:
Patients seem to be requiring prolonged intubation. We have now reached the stage where patients are alive but trached and PEGed. One of my patients had been intubated for close to 3 weeks. She was one of four people in her family who contracted the illness (they had had a dinner party before New York’s state of emergency was declared). We thought she might die once she was extubated, but she is still fighting. Unconscious, unarousable, but breathing on her own.
Will she ever wake up? We don’t know. We put the onus on her family to make decisions about placing a PEG tube in. They can only do so from a distance with imperfect information gleaned from periodic, brief FaceTime interactions — where no interaction happens at all.
May 4:
It’s my last day as a “COVID hospitalist.” When I first started, I felt like I was being helpful. Walking home in the middle of the 7 PM cheers for healthcare workers frequently left me teary eyed. As horrible as the situation was, I was proud of myself for volunteering to help and appreciative of a broken city’s gratitude toward all healthcare workers in general. Maybe I bought into the idea that, like many others around me, I am a hero.
I don’t feel like a hero, though. The stuff I saw was easy compared with the stuff that my colleagues in critical care saw. Our hospital accepted the more stable patient transfers from our sister hospitals. Patients who remained in the NewYork–Presbyterian system were sicker, with encephalitis, thrombotic complications, multiorgan failure, and cytokine release syndrome. It’s the doctors who took care of those patients who deserve to be called heroes.
No, I am no hero. But did my volunteering make a difference? It made a difference to me. The overwhelming feeling I am left with isn’t pride; it’s humility. I feel humbled that I could feel so unexpectedly touched by the lives of people that I had no idea I could feel touched by.
Postscript:
My patient Esther [name changed to hide her identity] died from COVID-19. She was MY patient — not a patient I met as a COVID hospitalist, but a patient with rheumatoid arthritis whom I cared for for years.
She had scleromalacia and multiple failed scleral grafts, which made her profoundly sad. She fought her anxiety fiercely and always with poise and panache. One way she dealt with her anxiety was that she constantly messaged me via our EHR portal. She ran everything by me and trusted me to be her rock.
The past month has been so busy that I just now noticed it had been a month since I last heard from her. I tried to call her but got her voicemail. It wasn’t until I exchanged messages with her ophthalmologist that I found out she had passed away from complications of COVID-19.
She was taking rituximab and mycophenolate. I wonder if these drugs made her sicker than she would have been otherwise; it fills me with sadness. I wonder if she was alone like my other COVID-19 patients. I wonder if she was afraid. I am sorry that I wasn’t able to say goodbye.
Karmela Kim Chan, MD, is an assistant professor at Weill Cornell Medical College and an attending physician at Hospital for Special Surgery and Memorial Sloan Kettering Cancer Center in New York City. Before moving to New York City, she spent 7 years in private practice in Rhode Island and was a columnist for this rheumatology publication, writing about the challenges of starting life as a full-fledged rheumatologist in a private practice.
A version of this article originally appeared on Medscape.com. This article is part of a partnership between Medscape and Hospital for Special Surgery.
When the coronavirus pandemic hit New York City in early March, the Hospital for Special Surgery leadership decided that the best way to serve the city was to stop elective orthopedic procedures temporarily and use the facility to take on patients from its sister institution, NewYork–Presbyterian Hospital.
As in other institutions, it was all hands on deck. , other internal medicine subspecialists were asked to volunteer, including rheumatologists and primary care sports medicine doctors.
As a rheumatologist, it had been well over 10 years since I had last done any inpatient work. I was filled with trepidation, but I was also excited to dive in.
April 4:
Feeling very unmoored. I am in unfamiliar territory, and it’s terrifying. There are so many things that I no longer know how to do. Thankfully, the hospitalists are gracious, extremely supportive, and helpful.
My N95 doesn’t fit well. It’s never fit — not during residency or fellowship, not in any job I’ve had, and not today. The lady fit-testing me said she was sorry, but the look on her face said, “I’m sorry, but you’re going to die.”
April 7:
We don’t know how to treat coronavirus. I’ve sent some patients home, others I’ve sent to the ICU. Thank goodness for treatment algorithms from leadership, but we are sorely lacking good-quality data.
Our infectious disease doctor doesn’t think hydroxychloroquine works at all; I suspect he is right. The guidance right now is to give hydroxychloroquine and azithromycin to everyone who is sick enough to be admitted, but there are methodologic flaws in the early enthusiastic preprints, and so far, I’ve not noticed any demonstrable benefit.
The only thing that seems to be happening is that I am seeing more QT prolongation — not something I previously counseled my rheumatology patients on.
April 9:
The patients have been, with a few exceptions, alone in the room. They’re not allowed to have visitors and are required to wear masks all the time. Anyone who enters their rooms is fully covered up so you can barely see them. It’s anonymous and dehumanizing.
We’re instructed to take histories by phone in order to limit the time spent in each room. I buck this instruction; I still take histories in person because human contact seems more important now than ever.
Except maybe I should be smarter about this. One of my patients refuses any treatment, including oxygen support. She firmly believes this is a result of 5G networks — something I later discovered was a common conspiracy theory. She refused to wear a mask despite having a very bad cough. She coughed in my face a lot when we were chatting. My face with my ill-fitting N95 mask. Maybe the fit-testing lady’s eyes weren’t lying and I will die after all.
April 15:
On the days when I’m not working as a hospitalist, I am still doing remote visits with my rheumatology patients. It feels good to be doing something familiar and something I’m actually good at. But it is surreal to be faced with the quotidian on one hand and life and death on the other.
I recently saw a fairly new patient, and I still haven’t figured out if she has a rheumatic condition or if her symptoms all stem from an alcohol use disorder. In our previous visits, she could barely acknowledge that her drinking was an issue. On today’s visit, she told me she was 1½ months sober.
I don’t know her very well, but it was the happiest news I’d heard in a long time. I was so beside myself with joy that I cried, which says more about my current emotional state than anything else, really.
April 21:
On my panel of patients, I have three women with COVID-19 — all of whom lost their husbands to COVID-19, and none of whom were able to say their goodbyes. I cannot even begin to imagine what it must be like to survive this period of illness, isolation, and fear, only to be met on the other side by grief.
Rheumatology doesn’t lend itself too well to such existential concerns; I am not equipped for this. Perhaps my only advantage as a rheumatologist is that I know how to use IVIG, anakinra, and tocilizumab.
Someone on my panel was started on anakinra, and it turned his case around. Would he have gotten better without it anyway? We’ll never know for sure.
April 28:
Patients seem to be requiring prolonged intubation. We have now reached the stage where patients are alive but trached and PEGed. One of my patients had been intubated for close to 3 weeks. She was one of four people in her family who contracted the illness (they had had a dinner party before New York’s state of emergency was declared). We thought she might die once she was extubated, but she is still fighting. Unconscious, unarousable, but breathing on her own.
Will she ever wake up? We don’t know. We put the onus on her family to make decisions about placing a PEG tube in. They can only do so from a distance with imperfect information gleaned from periodic, brief FaceTime interactions — where no interaction happens at all.
May 4:
It’s my last day as a “COVID hospitalist.” When I first started, I felt like I was being helpful. Walking home in the middle of the 7 PM cheers for healthcare workers frequently left me teary eyed. As horrible as the situation was, I was proud of myself for volunteering to help and appreciative of a broken city’s gratitude toward all healthcare workers in general. Maybe I bought into the idea that, like many others around me, I am a hero.
I don’t feel like a hero, though. The stuff I saw was easy compared with the stuff that my colleagues in critical care saw. Our hospital accepted the more stable patient transfers from our sister hospitals. Patients who remained in the NewYork–Presbyterian system were sicker, with encephalitis, thrombotic complications, multiorgan failure, and cytokine release syndrome. It’s the doctors who took care of those patients who deserve to be called heroes.
No, I am no hero. But did my volunteering make a difference? It made a difference to me. The overwhelming feeling I am left with isn’t pride; it’s humility. I feel humbled that I could feel so unexpectedly touched by the lives of people that I had no idea I could feel touched by.
Postscript:
My patient Esther [name changed to hide her identity] died from COVID-19. She was MY patient — not a patient I met as a COVID hospitalist, but a patient with rheumatoid arthritis whom I cared for for years.
She had scleromalacia and multiple failed scleral grafts, which made her profoundly sad. She fought her anxiety fiercely and always with poise and panache. One way she dealt with her anxiety was that she constantly messaged me via our EHR portal. She ran everything by me and trusted me to be her rock.
The past month has been so busy that I just now noticed it had been a month since I last heard from her. I tried to call her but got her voicemail. It wasn’t until I exchanged messages with her ophthalmologist that I found out she had passed away from complications of COVID-19.
She was taking rituximab and mycophenolate. I wonder if these drugs made her sicker than she would have been otherwise; it fills me with sadness. I wonder if she was alone like my other COVID-19 patients. I wonder if she was afraid. I am sorry that I wasn’t able to say goodbye.
Karmela Kim Chan, MD, is an assistant professor at Weill Cornell Medical College and an attending physician at Hospital for Special Surgery and Memorial Sloan Kettering Cancer Center in New York City. Before moving to New York City, she spent 7 years in private practice in Rhode Island and was a columnist for this rheumatology publication, writing about the challenges of starting life as a full-fledged rheumatologist in a private practice.
A version of this article originally appeared on Medscape.com. This article is part of a partnership between Medscape and Hospital for Special Surgery.
When the coronavirus pandemic hit New York City in early March, the Hospital for Special Surgery leadership decided that the best way to serve the city was to stop elective orthopedic procedures temporarily and use the facility to take on patients from its sister institution, NewYork–Presbyterian Hospital.
As in other institutions, it was all hands on deck. , other internal medicine subspecialists were asked to volunteer, including rheumatologists and primary care sports medicine doctors.
As a rheumatologist, it had been well over 10 years since I had last done any inpatient work. I was filled with trepidation, but I was also excited to dive in.
April 4:
Feeling very unmoored. I am in unfamiliar territory, and it’s terrifying. There are so many things that I no longer know how to do. Thankfully, the hospitalists are gracious, extremely supportive, and helpful.
My N95 doesn’t fit well. It’s never fit — not during residency or fellowship, not in any job I’ve had, and not today. The lady fit-testing me said she was sorry, but the look on her face said, “I’m sorry, but you’re going to die.”
April 7:
We don’t know how to treat coronavirus. I’ve sent some patients home, others I’ve sent to the ICU. Thank goodness for treatment algorithms from leadership, but we are sorely lacking good-quality data.
Our infectious disease doctor doesn’t think hydroxychloroquine works at all; I suspect he is right. The guidance right now is to give hydroxychloroquine and azithromycin to everyone who is sick enough to be admitted, but there are methodologic flaws in the early enthusiastic preprints, and so far, I’ve not noticed any demonstrable benefit.
The only thing that seems to be happening is that I am seeing more QT prolongation — not something I previously counseled my rheumatology patients on.
April 9:
The patients have been, with a few exceptions, alone in the room. They’re not allowed to have visitors and are required to wear masks all the time. Anyone who enters their rooms is fully covered up so you can barely see them. It’s anonymous and dehumanizing.
We’re instructed to take histories by phone in order to limit the time spent in each room. I buck this instruction; I still take histories in person because human contact seems more important now than ever.
Except maybe I should be smarter about this. One of my patients refuses any treatment, including oxygen support. She firmly believes this is a result of 5G networks — something I later discovered was a common conspiracy theory. She refused to wear a mask despite having a very bad cough. She coughed in my face a lot when we were chatting. My face with my ill-fitting N95 mask. Maybe the fit-testing lady’s eyes weren’t lying and I will die after all.
April 15:
On the days when I’m not working as a hospitalist, I am still doing remote visits with my rheumatology patients. It feels good to be doing something familiar and something I’m actually good at. But it is surreal to be faced with the quotidian on one hand and life and death on the other.
I recently saw a fairly new patient, and I still haven’t figured out if she has a rheumatic condition or if her symptoms all stem from an alcohol use disorder. In our previous visits, she could barely acknowledge that her drinking was an issue. On today’s visit, she told me she was 1½ months sober.
I don’t know her very well, but it was the happiest news I’d heard in a long time. I was so beside myself with joy that I cried, which says more about my current emotional state than anything else, really.
April 21:
On my panel of patients, I have three women with COVID-19 — all of whom lost their husbands to COVID-19, and none of whom were able to say their goodbyes. I cannot even begin to imagine what it must be like to survive this period of illness, isolation, and fear, only to be met on the other side by grief.
Rheumatology doesn’t lend itself too well to such existential concerns; I am not equipped for this. Perhaps my only advantage as a rheumatologist is that I know how to use IVIG, anakinra, and tocilizumab.
Someone on my panel was started on anakinra, and it turned his case around. Would he have gotten better without it anyway? We’ll never know for sure.
April 28:
Patients seem to be requiring prolonged intubation. We have now reached the stage where patients are alive but trached and PEGed. One of my patients had been intubated for close to 3 weeks. She was one of four people in her family who contracted the illness (they had had a dinner party before New York’s state of emergency was declared). We thought she might die once she was extubated, but she is still fighting. Unconscious, unarousable, but breathing on her own.
Will she ever wake up? We don’t know. We put the onus on her family to make decisions about placing a PEG tube in. They can only do so from a distance with imperfect information gleaned from periodic, brief FaceTime interactions — where no interaction happens at all.
May 4:
It’s my last day as a “COVID hospitalist.” When I first started, I felt like I was being helpful. Walking home in the middle of the 7 PM cheers for healthcare workers frequently left me teary eyed. As horrible as the situation was, I was proud of myself for volunteering to help and appreciative of a broken city’s gratitude toward all healthcare workers in general. Maybe I bought into the idea that, like many others around me, I am a hero.
I don’t feel like a hero, though. The stuff I saw was easy compared with the stuff that my colleagues in critical care saw. Our hospital accepted the more stable patient transfers from our sister hospitals. Patients who remained in the NewYork–Presbyterian system were sicker, with encephalitis, thrombotic complications, multiorgan failure, and cytokine release syndrome. It’s the doctors who took care of those patients who deserve to be called heroes.
No, I am no hero. But did my volunteering make a difference? It made a difference to me. The overwhelming feeling I am left with isn’t pride; it’s humility. I feel humbled that I could feel so unexpectedly touched by the lives of people that I had no idea I could feel touched by.
Postscript:
My patient Esther [name changed to hide her identity] died from COVID-19. She was MY patient — not a patient I met as a COVID hospitalist, but a patient with rheumatoid arthritis whom I cared for for years.
She had scleromalacia and multiple failed scleral grafts, which made her profoundly sad. She fought her anxiety fiercely and always with poise and panache. One way she dealt with her anxiety was that she constantly messaged me via our EHR portal. She ran everything by me and trusted me to be her rock.
The past month has been so busy that I just now noticed it had been a month since I last heard from her. I tried to call her but got her voicemail. It wasn’t until I exchanged messages with her ophthalmologist that I found out she had passed away from complications of COVID-19.
She was taking rituximab and mycophenolate. I wonder if these drugs made her sicker than she would have been otherwise; it fills me with sadness. I wonder if she was alone like my other COVID-19 patients. I wonder if she was afraid. I am sorry that I wasn’t able to say goodbye.
Karmela Kim Chan, MD, is an assistant professor at Weill Cornell Medical College and an attending physician at Hospital for Special Surgery and Memorial Sloan Kettering Cancer Center in New York City. Before moving to New York City, she spent 7 years in private practice in Rhode Island and was a columnist for this rheumatology publication, writing about the challenges of starting life as a full-fledged rheumatologist in a private practice.
A version of this article originally appeared on Medscape.com. This article is part of a partnership between Medscape and Hospital for Special Surgery.
COVID-19 fears would keep most Hispanics with stroke, MI symptoms home
More than half of Hispanic adults would be afraid to go to a hospital for a possible heart attack or stroke because they might get infected with SARS-CoV-2, according to a new survey from the American Heart Association.
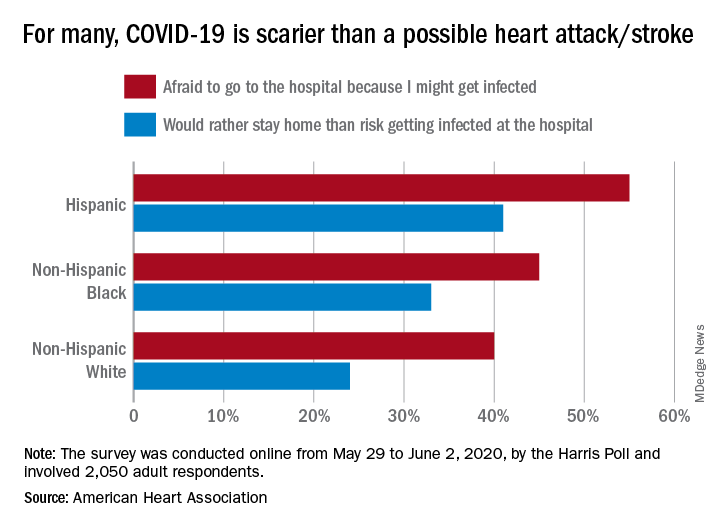
Compared with Hispanic respondents, 55% of whom said they feared COVID-19, significantly fewer Blacks (45%) and Whites (40%) would be scared to go to the hospital if they thought they were having a heart attack or stroke, the AHA said based on the survey of 2,050 adults, which was conducted May 29 to June 2, 2020, by the Harris Poll.
Hispanics also were significantly more likely to stay home if they thought they were experiencing a heart attack or stroke (41%), rather than risk getting infected at the hospital, than were Blacks (33%), who were significantly more likely than Whites (24%) to stay home, the AHA reported.
White respondents, on the other hand, were the most likely to believe (89%) that a hospital would give them the same quality of care provided to everyone else. Hispanics and Blacks had significantly lower rates, at 78% and 74%, respectively, the AHA noted.
These findings are “yet another challenge for Black and Hispanic communities, who are more likely to have underlying health conditions such as cardiovascular disease and diabetes and dying of COVID-19 at disproportionately high rates,” Rafael Ortiz, MD, American Heart Association volunteer medical expert and chief of neuro-endovascular surgery at Lenox Hill Hospital, New York, said in the AHA statement.
The survey was performed in conjunction with the AHA’s “Don’t Die of Doubt” campaign, which “reminds Americans, especially in Hispanic and Black communities, that the hospital remains the safest place to be if experiencing symptoms of a heart attack or a stroke.”
Among all the survey respondents, 57% said they would feel better if hospitals treated COVID-19 patients in a separate area. A number of other possible precautions ranked lower in helping them feel better:
- Screen all visitors, patients, and staff for COVID-19 symptoms when they enter the hospital: 39%.
- Require all patients, visitors, and staff to wear masks: 30%.
- Put increased cleaning protocols in place to disinfect multiple times per day: 23%.
- “Nothing would make me feel comfortable”: 6%.
Despite all the concerns about the risk of coronavirus infection, however, most Americans (77%) still believe that hospitals are the safest place to be in the event of a medical emergency, and 84% said that hospitals are prepared to safely treat emergencies that are not related to the pandemic, the AHA reported.
“Health care professionals know what to do even when things seem chaotic, and emergency departments have made plans behind the scenes to keep patients and healthcare workers safe even during a pandemic,” Dr. Ortiz pointed out.
More than half of Hispanic adults would be afraid to go to a hospital for a possible heart attack or stroke because they might get infected with SARS-CoV-2, according to a new survey from the American Heart Association.
Compared with Hispanic respondents, 55% of whom said they feared COVID-19, significantly fewer Blacks (45%) and Whites (40%) would be scared to go to the hospital if they thought they were having a heart attack or stroke, the AHA said based on the survey of 2,050 adults, which was conducted May 29 to June 2, 2020, by the Harris Poll.
Hispanics also were significantly more likely to stay home if they thought they were experiencing a heart attack or stroke (41%), rather than risk getting infected at the hospital, than were Blacks (33%), who were significantly more likely than Whites (24%) to stay home, the AHA reported.
White respondents, on the other hand, were the most likely to believe (89%) that a hospital would give them the same quality of care provided to everyone else. Hispanics and Blacks had significantly lower rates, at 78% and 74%, respectively, the AHA noted.
These findings are “yet another challenge for Black and Hispanic communities, who are more likely to have underlying health conditions such as cardiovascular disease and diabetes and dying of COVID-19 at disproportionately high rates,” Rafael Ortiz, MD, American Heart Association volunteer medical expert and chief of neuro-endovascular surgery at Lenox Hill Hospital, New York, said in the AHA statement.
The survey was performed in conjunction with the AHA’s “Don’t Die of Doubt” campaign, which “reminds Americans, especially in Hispanic and Black communities, that the hospital remains the safest place to be if experiencing symptoms of a heart attack or a stroke.”
Among all the survey respondents, 57% said they would feel better if hospitals treated COVID-19 patients in a separate area. A number of other possible precautions ranked lower in helping them feel better:
- Screen all visitors, patients, and staff for COVID-19 symptoms when they enter the hospital: 39%.
- Require all patients, visitors, and staff to wear masks: 30%.
- Put increased cleaning protocols in place to disinfect multiple times per day: 23%.
- “Nothing would make me feel comfortable”: 6%.
Despite all the concerns about the risk of coronavirus infection, however, most Americans (77%) still believe that hospitals are the safest place to be in the event of a medical emergency, and 84% said that hospitals are prepared to safely treat emergencies that are not related to the pandemic, the AHA reported.
“Health care professionals know what to do even when things seem chaotic, and emergency departments have made plans behind the scenes to keep patients and healthcare workers safe even during a pandemic,” Dr. Ortiz pointed out.
More than half of Hispanic adults would be afraid to go to a hospital for a possible heart attack or stroke because they might get infected with SARS-CoV-2, according to a new survey from the American Heart Association.
Compared with Hispanic respondents, 55% of whom said they feared COVID-19, significantly fewer Blacks (45%) and Whites (40%) would be scared to go to the hospital if they thought they were having a heart attack or stroke, the AHA said based on the survey of 2,050 adults, which was conducted May 29 to June 2, 2020, by the Harris Poll.
Hispanics also were significantly more likely to stay home if they thought they were experiencing a heart attack or stroke (41%), rather than risk getting infected at the hospital, than were Blacks (33%), who were significantly more likely than Whites (24%) to stay home, the AHA reported.
White respondents, on the other hand, were the most likely to believe (89%) that a hospital would give them the same quality of care provided to everyone else. Hispanics and Blacks had significantly lower rates, at 78% and 74%, respectively, the AHA noted.
These findings are “yet another challenge for Black and Hispanic communities, who are more likely to have underlying health conditions such as cardiovascular disease and diabetes and dying of COVID-19 at disproportionately high rates,” Rafael Ortiz, MD, American Heart Association volunteer medical expert and chief of neuro-endovascular surgery at Lenox Hill Hospital, New York, said in the AHA statement.
The survey was performed in conjunction with the AHA’s “Don’t Die of Doubt” campaign, which “reminds Americans, especially in Hispanic and Black communities, that the hospital remains the safest place to be if experiencing symptoms of a heart attack or a stroke.”
Among all the survey respondents, 57% said they would feel better if hospitals treated COVID-19 patients in a separate area. A number of other possible precautions ranked lower in helping them feel better:
- Screen all visitors, patients, and staff for COVID-19 symptoms when they enter the hospital: 39%.
- Require all patients, visitors, and staff to wear masks: 30%.
- Put increased cleaning protocols in place to disinfect multiple times per day: 23%.
- “Nothing would make me feel comfortable”: 6%.
Despite all the concerns about the risk of coronavirus infection, however, most Americans (77%) still believe that hospitals are the safest place to be in the event of a medical emergency, and 84% said that hospitals are prepared to safely treat emergencies that are not related to the pandemic, the AHA reported.
“Health care professionals know what to do even when things seem chaotic, and emergency departments have made plans behind the scenes to keep patients and healthcare workers safe even during a pandemic,” Dr. Ortiz pointed out.
AMA urges change after dramatic increase in illicit opioid fatalities
In the past 5 years, there has been a significant drop in the use of prescription opioids and in deaths associated with such use; but at the same time there’s been a dramatic increase in fatalities involving illicit opioids and stimulants, a new report from the American Medical Association (AMA) Opioid Task Force shows.

Although the medical community has made some important progress against the opioid epidemic, with a 37% reduction in opioid prescribing since 2013, illicit drugs are now the dominant reason why drug overdoses kill more than 70,000 people each year, the report says.
In an effort to improve the situation, the AMA Opioid Task Force is urging the removal of barriers to evidence-based care for patients who have pain and for those who have substance use disorders (SUDs). The report notes that “red tape and misguided policies are grave dangers” to these patients.
“It is critically important as we see drug overdoses increasing that we work towards reducing barriers of care for substance use abusers,” Task Force Chair Patrice A. Harris, MD, said in an interview.
“At present, the status quo is killing far too many of our loved ones and wreaking havoc in our communities,” she said.
Dr. Harris noted that “a more coordinated/integrated approach” is needed to help individuals with SUDs.
“It is vitally important that these individuals can get access to treatment. Everyone deserves the opportunity for care,” she added.
Dramatic increases
The report cites figures from the Centers for Disease Control and Prevention that indicate the following regarding the period from the beginning of 2015 to the end of 2019:
- Deaths involving illicitly manufactured and fentanyl analogues increased from 5,766 to 36,509.
- Deaths involving stimulants such as increased from 4,402 to 16,279.
- Deaths involving cocaine increased from 5,496 to 15,974.
- Deaths involving heroin increased from 10,788 to 14,079.
- Deaths involving prescription opioids decreased from 12,269 to 11,904.
The report notes that deaths involving prescription opioids peaked in July 2017 at 15,003.
Some good news
In addition to the 37% reduction in opioid prescribing in recent years, the AMA lists other points of progress, such as a large increase in prescription drug monitoring program registrations. More than 1.8 million physicians and other healthcare professionals now participate in these programs.
Also, more physicians are now certified to treat opioid use disorder. More than 85,000 physicians, as well as a growing number of nurse practitioners and physician assistants, are now certified to treat patients in the office with buprenorphine. This represents an increase of more than 50,000 from 2017.
Access to naloxone is also increasing. More than 1 million naloxone prescriptions were dispensed in 2019 – nearly double the amount in 2018. This represents a 649% increase from 2017.
“We have made some good progress, but we can’t declare victory, and there are far too many barriers to getting treatment for substance use disorder,” Dr. Harris said.
“Policymakers, public health officials, and insurance companies need to come together to create a system where there are no barriers to care for people with substance use disorder and for those needing pain medications,” she added.
At present, prior authorization is often needed before these patients can receive medication. “This involves quite a bit of administration, filling in forms, making phone calls, and this is stopping people getting the care they need,” said Dr. Harris.
“This is a highly regulated environment. There are also regulations on the amount of methadone that can be prescribed and for the prescription of buprenorphine, which has to be initiated in person,” she said.
Will COVID-19 bring change?
Dr. Harris noted that some of these regulations have been relaxed during the COVID-19 crisis so that physicians could ensure that patients have continued access to medication, and she suggested that this may pave the way for the future.
“We need now to look at this carefully and have a conversation about whether these relaxations can be continued. But this would have to be evidence based. Perhaps we can use experience from the COVID-19 period to guide future policy on this,” she said.
The report highlights that despite medical society and patient advocacy, only 21 states and the District of Columbia have enacted laws that limit public and private insurers from imposing prior authorization requirements on SUD services or medications.
The Task Force urges removal of remaining prior authorizations, step therapy, and other inappropriate administrative burdens that delay or deny care for Food and Drug Administration–approved medications used as part of medication-assisted treatment for opioid use disorder.
The organization is also calling for better implementation of mental health and substance use disorder parity laws that require health insurers to provide the same level of benefits for mental health and SUD treatment and services that they do for medical/surgical care.
At present, only a few states have taken meaningful action to enact or enforce those laws, the report notes.
The Task Force also recommends the implementation of systems to track overdose and mortality trends to provide equitable public health interventions. These measures would include comprehensive, disaggregated racial and ethnic data collection related to testing, hospitalization, and mortality associated with opioids and other substances.
“We know that ending the drug overdose epidemic will not be easy, but if policymakers allow the status quo to continue, it will be impossible,” Dr. Harris said.
“ Physicians will continue to do our part. We urge policymakers to do theirs,” she added.
A version of this article originally appeared on Medscape.com.
In the past 5 years, there has been a significant drop in the use of prescription opioids and in deaths associated with such use; but at the same time there’s been a dramatic increase in fatalities involving illicit opioids and stimulants, a new report from the American Medical Association (AMA) Opioid Task Force shows.
Although the medical community has made some important progress against the opioid epidemic, with a 37% reduction in opioid prescribing since 2013, illicit drugs are now the dominant reason why drug overdoses kill more than 70,000 people each year, the report says.
In an effort to improve the situation, the AMA Opioid Task Force is urging the removal of barriers to evidence-based care for patients who have pain and for those who have substance use disorders (SUDs). The report notes that “red tape and misguided policies are grave dangers” to these patients.
“It is critically important as we see drug overdoses increasing that we work towards reducing barriers of care for substance use abusers,” Task Force Chair Patrice A. Harris, MD, said in an interview.
“At present, the status quo is killing far too many of our loved ones and wreaking havoc in our communities,” she said.
Dr. Harris noted that “a more coordinated/integrated approach” is needed to help individuals with SUDs.
“It is vitally important that these individuals can get access to treatment. Everyone deserves the opportunity for care,” she added.
Dramatic increases
The report cites figures from the Centers for Disease Control and Prevention that indicate the following regarding the period from the beginning of 2015 to the end of 2019:
- Deaths involving illicitly manufactured and fentanyl analogues increased from 5,766 to 36,509.
- Deaths involving stimulants such as increased from 4,402 to 16,279.
- Deaths involving cocaine increased from 5,496 to 15,974.
- Deaths involving heroin increased from 10,788 to 14,079.
- Deaths involving prescription opioids decreased from 12,269 to 11,904.
The report notes that deaths involving prescription opioids peaked in July 2017 at 15,003.
Some good news
In addition to the 37% reduction in opioid prescribing in recent years, the AMA lists other points of progress, such as a large increase in prescription drug monitoring program registrations. More than 1.8 million physicians and other healthcare professionals now participate in these programs.
Also, more physicians are now certified to treat opioid use disorder. More than 85,000 physicians, as well as a growing number of nurse practitioners and physician assistants, are now certified to treat patients in the office with buprenorphine. This represents an increase of more than 50,000 from 2017.
Access to naloxone is also increasing. More than 1 million naloxone prescriptions were dispensed in 2019 – nearly double the amount in 2018. This represents a 649% increase from 2017.
“We have made some good progress, but we can’t declare victory, and there are far too many barriers to getting treatment for substance use disorder,” Dr. Harris said.
“Policymakers, public health officials, and insurance companies need to come together to create a system where there are no barriers to care for people with substance use disorder and for those needing pain medications,” she added.
At present, prior authorization is often needed before these patients can receive medication. “This involves quite a bit of administration, filling in forms, making phone calls, and this is stopping people getting the care they need,” said Dr. Harris.
“This is a highly regulated environment. There are also regulations on the amount of methadone that can be prescribed and for the prescription of buprenorphine, which has to be initiated in person,” she said.
Will COVID-19 bring change?
Dr. Harris noted that some of these regulations have been relaxed during the COVID-19 crisis so that physicians could ensure that patients have continued access to medication, and she suggested that this may pave the way for the future.
“We need now to look at this carefully and have a conversation about whether these relaxations can be continued. But this would have to be evidence based. Perhaps we can use experience from the COVID-19 period to guide future policy on this,” she said.
The report highlights that despite medical society and patient advocacy, only 21 states and the District of Columbia have enacted laws that limit public and private insurers from imposing prior authorization requirements on SUD services or medications.
The Task Force urges removal of remaining prior authorizations, step therapy, and other inappropriate administrative burdens that delay or deny care for Food and Drug Administration–approved medications used as part of medication-assisted treatment for opioid use disorder.
The organization is also calling for better implementation of mental health and substance use disorder parity laws that require health insurers to provide the same level of benefits for mental health and SUD treatment and services that they do for medical/surgical care.
At present, only a few states have taken meaningful action to enact or enforce those laws, the report notes.
The Task Force also recommends the implementation of systems to track overdose and mortality trends to provide equitable public health interventions. These measures would include comprehensive, disaggregated racial and ethnic data collection related to testing, hospitalization, and mortality associated with opioids and other substances.
“We know that ending the drug overdose epidemic will not be easy, but if policymakers allow the status quo to continue, it will be impossible,” Dr. Harris said.
“ Physicians will continue to do our part. We urge policymakers to do theirs,” she added.
A version of this article originally appeared on Medscape.com.
In the past 5 years, there has been a significant drop in the use of prescription opioids and in deaths associated with such use; but at the same time there’s been a dramatic increase in fatalities involving illicit opioids and stimulants, a new report from the American Medical Association (AMA) Opioid Task Force shows.
Although the medical community has made some important progress against the opioid epidemic, with a 37% reduction in opioid prescribing since 2013, illicit drugs are now the dominant reason why drug overdoses kill more than 70,000 people each year, the report says.
In an effort to improve the situation, the AMA Opioid Task Force is urging the removal of barriers to evidence-based care for patients who have pain and for those who have substance use disorders (SUDs). The report notes that “red tape and misguided policies are grave dangers” to these patients.
“It is critically important as we see drug overdoses increasing that we work towards reducing barriers of care for substance use abusers,” Task Force Chair Patrice A. Harris, MD, said in an interview.
“At present, the status quo is killing far too many of our loved ones and wreaking havoc in our communities,” she said.
Dr. Harris noted that “a more coordinated/integrated approach” is needed to help individuals with SUDs.
“It is vitally important that these individuals can get access to treatment. Everyone deserves the opportunity for care,” she added.
Dramatic increases
The report cites figures from the Centers for Disease Control and Prevention that indicate the following regarding the period from the beginning of 2015 to the end of 2019:
- Deaths involving illicitly manufactured and fentanyl analogues increased from 5,766 to 36,509.
- Deaths involving stimulants such as increased from 4,402 to 16,279.
- Deaths involving cocaine increased from 5,496 to 15,974.
- Deaths involving heroin increased from 10,788 to 14,079.
- Deaths involving prescription opioids decreased from 12,269 to 11,904.
The report notes that deaths involving prescription opioids peaked in July 2017 at 15,003.
Some good news
In addition to the 37% reduction in opioid prescribing in recent years, the AMA lists other points of progress, such as a large increase in prescription drug monitoring program registrations. More than 1.8 million physicians and other healthcare professionals now participate in these programs.
Also, more physicians are now certified to treat opioid use disorder. More than 85,000 physicians, as well as a growing number of nurse practitioners and physician assistants, are now certified to treat patients in the office with buprenorphine. This represents an increase of more than 50,000 from 2017.
Access to naloxone is also increasing. More than 1 million naloxone prescriptions were dispensed in 2019 – nearly double the amount in 2018. This represents a 649% increase from 2017.
“We have made some good progress, but we can’t declare victory, and there are far too many barriers to getting treatment for substance use disorder,” Dr. Harris said.
“Policymakers, public health officials, and insurance companies need to come together to create a system where there are no barriers to care for people with substance use disorder and for those needing pain medications,” she added.
At present, prior authorization is often needed before these patients can receive medication. “This involves quite a bit of administration, filling in forms, making phone calls, and this is stopping people getting the care they need,” said Dr. Harris.
“This is a highly regulated environment. There are also regulations on the amount of methadone that can be prescribed and for the prescription of buprenorphine, which has to be initiated in person,” she said.
Will COVID-19 bring change?
Dr. Harris noted that some of these regulations have been relaxed during the COVID-19 crisis so that physicians could ensure that patients have continued access to medication, and she suggested that this may pave the way for the future.
“We need now to look at this carefully and have a conversation about whether these relaxations can be continued. But this would have to be evidence based. Perhaps we can use experience from the COVID-19 period to guide future policy on this,” she said.
The report highlights that despite medical society and patient advocacy, only 21 states and the District of Columbia have enacted laws that limit public and private insurers from imposing prior authorization requirements on SUD services or medications.
The Task Force urges removal of remaining prior authorizations, step therapy, and other inappropriate administrative burdens that delay or deny care for Food and Drug Administration–approved medications used as part of medication-assisted treatment for opioid use disorder.
The organization is also calling for better implementation of mental health and substance use disorder parity laws that require health insurers to provide the same level of benefits for mental health and SUD treatment and services that they do for medical/surgical care.
At present, only a few states have taken meaningful action to enact or enforce those laws, the report notes.
The Task Force also recommends the implementation of systems to track overdose and mortality trends to provide equitable public health interventions. These measures would include comprehensive, disaggregated racial and ethnic data collection related to testing, hospitalization, and mortality associated with opioids and other substances.
“We know that ending the drug overdose epidemic will not be easy, but if policymakers allow the status quo to continue, it will be impossible,” Dr. Harris said.
“ Physicians will continue to do our part. We urge policymakers to do theirs,” she added.
A version of this article originally appeared on Medscape.com.
Combination therapy quells COVID-19 cytokine storm
Treatment with high-dose methylprednisolone plus tocilizumab (Actemra, Genentech) as needed was associated with faster respiratory recovery, a lower likelihood of mechanical ventilation, and fewer in-hospital deaths compared with supportive care alone among people with COVID-19 experiencing a hyperinflammatory state known as a cytokine storm.

Compared with historic controls, participants in the treatment group were 79% more likely to achieve at least a two-stage improvement in respiratory status, for example.
“COVID-19-associated cytokine storm syndrome [CSS] is an important complication of severe acute respiratory syndrome coronavirus-2 infection in up to 25% of the patients,” lead author Sofia Ramiro, MD, PhD, said in an interview.
Furthermore, CSS often leads to death in this population, said Dr. Ramiro, a consultant rheumatologist and senior researcher at Leiden University Medical Center and Zuyderland Medical Center in Heerlen, the Netherlands.
Results of the COVID High-Intensity Immunosuppression in Cytokine Storm Syndrome (CHIC) study were published online July 20 in Annals of the Rheumatic Diseases.
Contrary to guidance?
The World Health Organization (WHO) cautions against administering corticosteroids to some critically ill patients with COVID-19. “WHO recommends against the routine use of systemic corticosteroids for treatment of viral pneumonia,” according to an interim guidance document on the clinical management of COVID-19 published May 27.
Dr. Ramiro and colleagues make a distinction, however, noting “the risk profile of such a short course of glucocorticoid for treatment of CSS needs to be separated from preexisting chronic use of glucocorticoid for conditions like rheumatic and musculoskeletal diseases.”
Participants in the current study tolerated immunosuppressive therapy well without evidence of impaired viral clearance or bacterial superinfection, they added.
Other experts disagree with recent recommendations to use corticosteroids to treat a hyperimmune response or suspected adrenal insufficiency in the setting of refractory shock in patients with COVID-19.
Information about immunosuppressive therapy and CSS linked to COVID-19 remains anecdotal, however, Dr. Ramiro and colleagues noted.
The researchers assessed outcomes of 86 individuals with COVID-19-associated CSS treated with high-dose methylprednisolone plus/minus tocilizumab, an anti-interleukin-6 receptor monoclonal antibody. They compared them with another 86 patients with COVID-19 treated with supportive care before initiation of the combination therapy protocol.
Participants with CSS had an oxygen saturation of 94% or lower at rest or tachypnea exceeding 30 breaths per minute.
They also had at least two of the following: C-reactive protein > 100 mg/L; serum ferritin > 900 mcg/L at one occasion or a twofold increase at admission within 48 hours; or D-dimer levels > 1,500 mcg/L.
The treatment group received methylprednisolone 250 mg intravenously on day 1, followed by 80 mg intravenously on days 2-5. Investigators permitted a 2-day extension if indicated.
Those who failed to clinically improve or experienced respiratory decline could also receive intravenous tocilizumab on day 2 or after. The agent was dosed at 8 mg/kg body weight during a single infusion from day 2-5 up to a maximum of 800 mg.
In all, 37 participants received tocilizumab, including two participants who received a second dose 5 days after initial treatment.
Except for one patient in the treatment group, all participants also received antibiotic treatment and nearly 80% received chloroquine.
Mechanical ventilation and mortality
The primary outcome of at least a two-stage improvement in respiratory status on a WHO scale associated with treatment yielded a hazard ratio (HR) of 1.79. The treatment group achieved this improvement a median 7 days earlier than controls.
Mechanical ventilation to treat respiratory deterioration was 71% less likely for the treatment group versus controls (HR, 0.29).
The treatment group were also 65% less likely to die in hospital (HR, 0.35) than were controls.
The researchers also reported a significant difference in the number of deaths at day 14 in the treatment vs. control group, at 10 vs. 33 patients (P < .0001).
Glucocorticoid sufficient for many
In a sensitivity analysis excluding patients who received tocilizumab, the benefits of treatment remained statistically significant, “suggesting that a clinically relevant treatment effect can be reached by high-dose glucocorticoids alone,” the researchers noted.
This finding suggests “that the timely administration of high-dose glucocorticoids alone may provide significant benefit in more than half of the patients, and that tocilizumab is only needed in those cases that had insufficient clinical improvement on methylprednisolone alone,” they added.
“This is an important finding given the limited availability of tocilizumab in many countries and tocilizumab’s high costs.”
Complications were fairly balanced between groups. For example, bacterial infections during hospitalization were diagnosed in eight patients in the treatment group versus seven in the control group.
In addition, cardiac arrhythmias occurred in both groups, but slightly less frequently in the treatment group (P = .265), and there was a trend towards more pulmonary embolisms in the treatment group (P = .059).
Strengths and limitations
“A treatment with high-dose glucocorticoids is a convenient choice since glucocorticoids are safe, widely available, and inexpensive,” the researchers noted. “Longer follow-up, however, is needed to give final resolution about the safety and efficacy of the strategy.”
A strength of the study was “meticulous selection of those patients more likely to benefit from immunosuppressive treatment, namely patients with a CSS,” she added.
The study featured a prospective, observational design for the treatment group and retrospective analysis of the historic controls. “Methodologically, the main limitation of the study is not being a randomized controlled trial,” she noted.
“Ethically it has shown to be very rewarding to consciously decide against a randomized control trial, as we are talking about a disease that if only treated with supportive care can lead to mortality up to almost 50% from COVID-19-associated CSS,” Dr. Ramiro said.
Going forward, Dr. Ramiro plans to continue monitoring patients who experienced CSS to assess their outcome post-COVID-19 infection. “We want to focus on cardiorespiratory, functional, and quality of life outcomes,” she said. “We will also compare the outcomes between patients that have received immunosuppression with those that haven’t.”
‘Quite interesting’ results
“We desperately need better evidence to guide the management of patients hospitalized with COVID-19,” Nihar R. Desai, MD, MPH, who was not affiliated with the study, said in an interview.
“These data from the Netherlands are quite interesting and provide another signal to support the use of corticosteroids, with tocilizumab if needed, among hospitalized patients with COVID-19 to improve outcomes,” added Dr. Desai, associate professor of medicine and investigator at the Center for Outcomes Research and Evaluation, Yale University, New Haven, Conn.
“While these data are not randomized and have a relatively small sample size, we had recently seen the results of the RECOVERY trial, a UK-based randomized trial demonstrating the benefit of steroids in COVID-19,” he said.
“Taken together, these studies seem to suggest that there is a benefit with steroid therapy.” Further validation of these results is warranted, he added.
“While not a randomized clinical trial, and thus susceptible to unmeasured bias, the study adds to mounting evidence that supports targeting the excessive inflammation found in some patients with COVID-19,” Jared Radbel, MD, a pulmonologist, critical care specialist, and assistant professor of medicine at Rutgers Robert Wood Johnson Medical School, New Brunswick, N.J., said in an interview.
Dr. Radbel added that he is part of a multicenter group that has submitted a manuscript examining outcomes of critically ill patients with COVID-19 treated with tocilizumab.
Dr. Ramiro, Dr. Desai, and Dr. Radbel have disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
Treatment with high-dose methylprednisolone plus tocilizumab (Actemra, Genentech) as needed was associated with faster respiratory recovery, a lower likelihood of mechanical ventilation, and fewer in-hospital deaths compared with supportive care alone among people with COVID-19 experiencing a hyperinflammatory state known as a cytokine storm.
Compared with historic controls, participants in the treatment group were 79% more likely to achieve at least a two-stage improvement in respiratory status, for example.
“COVID-19-associated cytokine storm syndrome [CSS] is an important complication of severe acute respiratory syndrome coronavirus-2 infection in up to 25% of the patients,” lead author Sofia Ramiro, MD, PhD, said in an interview.
Furthermore, CSS often leads to death in this population, said Dr. Ramiro, a consultant rheumatologist and senior researcher at Leiden University Medical Center and Zuyderland Medical Center in Heerlen, the Netherlands.
Results of the COVID High-Intensity Immunosuppression in Cytokine Storm Syndrome (CHIC) study were published online July 20 in Annals of the Rheumatic Diseases.
Contrary to guidance?
The World Health Organization (WHO) cautions against administering corticosteroids to some critically ill patients with COVID-19. “WHO recommends against the routine use of systemic corticosteroids for treatment of viral pneumonia,” according to an interim guidance document on the clinical management of COVID-19 published May 27.
Dr. Ramiro and colleagues make a distinction, however, noting “the risk profile of such a short course of glucocorticoid for treatment of CSS needs to be separated from preexisting chronic use of glucocorticoid for conditions like rheumatic and musculoskeletal diseases.”
Participants in the current study tolerated immunosuppressive therapy well without evidence of impaired viral clearance or bacterial superinfection, they added.
Other experts disagree with recent recommendations to use corticosteroids to treat a hyperimmune response or suspected adrenal insufficiency in the setting of refractory shock in patients with COVID-19.
Information about immunosuppressive therapy and CSS linked to COVID-19 remains anecdotal, however, Dr. Ramiro and colleagues noted.
The researchers assessed outcomes of 86 individuals with COVID-19-associated CSS treated with high-dose methylprednisolone plus/minus tocilizumab, an anti-interleukin-6 receptor monoclonal antibody. They compared them with another 86 patients with COVID-19 treated with supportive care before initiation of the combination therapy protocol.
Participants with CSS had an oxygen saturation of 94% or lower at rest or tachypnea exceeding 30 breaths per minute.
They also had at least two of the following: C-reactive protein > 100 mg/L; serum ferritin > 900 mcg/L at one occasion or a twofold increase at admission within 48 hours; or D-dimer levels > 1,500 mcg/L.
The treatment group received methylprednisolone 250 mg intravenously on day 1, followed by 80 mg intravenously on days 2-5. Investigators permitted a 2-day extension if indicated.
Those who failed to clinically improve or experienced respiratory decline could also receive intravenous tocilizumab on day 2 or after. The agent was dosed at 8 mg/kg body weight during a single infusion from day 2-5 up to a maximum of 800 mg.
In all, 37 participants received tocilizumab, including two participants who received a second dose 5 days after initial treatment.
Except for one patient in the treatment group, all participants also received antibiotic treatment and nearly 80% received chloroquine.
Mechanical ventilation and mortality
The primary outcome of at least a two-stage improvement in respiratory status on a WHO scale associated with treatment yielded a hazard ratio (HR) of 1.79. The treatment group achieved this improvement a median 7 days earlier than controls.
Mechanical ventilation to treat respiratory deterioration was 71% less likely for the treatment group versus controls (HR, 0.29).
The treatment group were also 65% less likely to die in hospital (HR, 0.35) than were controls.
The researchers also reported a significant difference in the number of deaths at day 14 in the treatment vs. control group, at 10 vs. 33 patients (P < .0001).
Glucocorticoid sufficient for many
In a sensitivity analysis excluding patients who received tocilizumab, the benefits of treatment remained statistically significant, “suggesting that a clinically relevant treatment effect can be reached by high-dose glucocorticoids alone,” the researchers noted.
This finding suggests “that the timely administration of high-dose glucocorticoids alone may provide significant benefit in more than half of the patients, and that tocilizumab is only needed in those cases that had insufficient clinical improvement on methylprednisolone alone,” they added.
“This is an important finding given the limited availability of tocilizumab in many countries and tocilizumab’s high costs.”
Complications were fairly balanced between groups. For example, bacterial infections during hospitalization were diagnosed in eight patients in the treatment group versus seven in the control group.
In addition, cardiac arrhythmias occurred in both groups, but slightly less frequently in the treatment group (P = .265), and there was a trend towards more pulmonary embolisms in the treatment group (P = .059).
Strengths and limitations
“A treatment with high-dose glucocorticoids is a convenient choice since glucocorticoids are safe, widely available, and inexpensive,” the researchers noted. “Longer follow-up, however, is needed to give final resolution about the safety and efficacy of the strategy.”
A strength of the study was “meticulous selection of those patients more likely to benefit from immunosuppressive treatment, namely patients with a CSS,” she added.
The study featured a prospective, observational design for the treatment group and retrospective analysis of the historic controls. “Methodologically, the main limitation of the study is not being a randomized controlled trial,” she noted.
“Ethically it has shown to be very rewarding to consciously decide against a randomized control trial, as we are talking about a disease that if only treated with supportive care can lead to mortality up to almost 50% from COVID-19-associated CSS,” Dr. Ramiro said.
Going forward, Dr. Ramiro plans to continue monitoring patients who experienced CSS to assess their outcome post-COVID-19 infection. “We want to focus on cardiorespiratory, functional, and quality of life outcomes,” she said. “We will also compare the outcomes between patients that have received immunosuppression with those that haven’t.”
‘Quite interesting’ results
“We desperately need better evidence to guide the management of patients hospitalized with COVID-19,” Nihar R. Desai, MD, MPH, who was not affiliated with the study, said in an interview.
“These data from the Netherlands are quite interesting and provide another signal to support the use of corticosteroids, with tocilizumab if needed, among hospitalized patients with COVID-19 to improve outcomes,” added Dr. Desai, associate professor of medicine and investigator at the Center for Outcomes Research and Evaluation, Yale University, New Haven, Conn.
“While these data are not randomized and have a relatively small sample size, we had recently seen the results of the RECOVERY trial, a UK-based randomized trial demonstrating the benefit of steroids in COVID-19,” he said.
“Taken together, these studies seem to suggest that there is a benefit with steroid therapy.” Further validation of these results is warranted, he added.
“While not a randomized clinical trial, and thus susceptible to unmeasured bias, the study adds to mounting evidence that supports targeting the excessive inflammation found in some patients with COVID-19,” Jared Radbel, MD, a pulmonologist, critical care specialist, and assistant professor of medicine at Rutgers Robert Wood Johnson Medical School, New Brunswick, N.J., said in an interview.
Dr. Radbel added that he is part of a multicenter group that has submitted a manuscript examining outcomes of critically ill patients with COVID-19 treated with tocilizumab.
Dr. Ramiro, Dr. Desai, and Dr. Radbel have disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
Treatment with high-dose methylprednisolone plus tocilizumab (Actemra, Genentech) as needed was associated with faster respiratory recovery, a lower likelihood of mechanical ventilation, and fewer in-hospital deaths compared with supportive care alone among people with COVID-19 experiencing a hyperinflammatory state known as a cytokine storm.
Compared with historic controls, participants in the treatment group were 79% more likely to achieve at least a two-stage improvement in respiratory status, for example.
“COVID-19-associated cytokine storm syndrome [CSS] is an important complication of severe acute respiratory syndrome coronavirus-2 infection in up to 25% of the patients,” lead author Sofia Ramiro, MD, PhD, said in an interview.
Furthermore, CSS often leads to death in this population, said Dr. Ramiro, a consultant rheumatologist and senior researcher at Leiden University Medical Center and Zuyderland Medical Center in Heerlen, the Netherlands.
Results of the COVID High-Intensity Immunosuppression in Cytokine Storm Syndrome (CHIC) study were published online July 20 in Annals of the Rheumatic Diseases.
Contrary to guidance?
The World Health Organization (WHO) cautions against administering corticosteroids to some critically ill patients with COVID-19. “WHO recommends against the routine use of systemic corticosteroids for treatment of viral pneumonia,” according to an interim guidance document on the clinical management of COVID-19 published May 27.
Dr. Ramiro and colleagues make a distinction, however, noting “the risk profile of such a short course of glucocorticoid for treatment of CSS needs to be separated from preexisting chronic use of glucocorticoid for conditions like rheumatic and musculoskeletal diseases.”
Participants in the current study tolerated immunosuppressive therapy well without evidence of impaired viral clearance or bacterial superinfection, they added.
Other experts disagree with recent recommendations to use corticosteroids to treat a hyperimmune response or suspected adrenal insufficiency in the setting of refractory shock in patients with COVID-19.
Information about immunosuppressive therapy and CSS linked to COVID-19 remains anecdotal, however, Dr. Ramiro and colleagues noted.
The researchers assessed outcomes of 86 individuals with COVID-19-associated CSS treated with high-dose methylprednisolone plus/minus tocilizumab, an anti-interleukin-6 receptor monoclonal antibody. They compared them with another 86 patients with COVID-19 treated with supportive care before initiation of the combination therapy protocol.
Participants with CSS had an oxygen saturation of 94% or lower at rest or tachypnea exceeding 30 breaths per minute.
They also had at least two of the following: C-reactive protein > 100 mg/L; serum ferritin > 900 mcg/L at one occasion or a twofold increase at admission within 48 hours; or D-dimer levels > 1,500 mcg/L.
The treatment group received methylprednisolone 250 mg intravenously on day 1, followed by 80 mg intravenously on days 2-5. Investigators permitted a 2-day extension if indicated.
Those who failed to clinically improve or experienced respiratory decline could also receive intravenous tocilizumab on day 2 or after. The agent was dosed at 8 mg/kg body weight during a single infusion from day 2-5 up to a maximum of 800 mg.
In all, 37 participants received tocilizumab, including two participants who received a second dose 5 days after initial treatment.
Except for one patient in the treatment group, all participants also received antibiotic treatment and nearly 80% received chloroquine.
Mechanical ventilation and mortality
The primary outcome of at least a two-stage improvement in respiratory status on a WHO scale associated with treatment yielded a hazard ratio (HR) of 1.79. The treatment group achieved this improvement a median 7 days earlier than controls.
Mechanical ventilation to treat respiratory deterioration was 71% less likely for the treatment group versus controls (HR, 0.29).
The treatment group were also 65% less likely to die in hospital (HR, 0.35) than were controls.
The researchers also reported a significant difference in the number of deaths at day 14 in the treatment vs. control group, at 10 vs. 33 patients (P < .0001).
Glucocorticoid sufficient for many
In a sensitivity analysis excluding patients who received tocilizumab, the benefits of treatment remained statistically significant, “suggesting that a clinically relevant treatment effect can be reached by high-dose glucocorticoids alone,” the researchers noted.
This finding suggests “that the timely administration of high-dose glucocorticoids alone may provide significant benefit in more than half of the patients, and that tocilizumab is only needed in those cases that had insufficient clinical improvement on methylprednisolone alone,” they added.
“This is an important finding given the limited availability of tocilizumab in many countries and tocilizumab’s high costs.”
Complications were fairly balanced between groups. For example, bacterial infections during hospitalization were diagnosed in eight patients in the treatment group versus seven in the control group.
In addition, cardiac arrhythmias occurred in both groups, but slightly less frequently in the treatment group (P = .265), and there was a trend towards more pulmonary embolisms in the treatment group (P = .059).
Strengths and limitations
“A treatment with high-dose glucocorticoids is a convenient choice since glucocorticoids are safe, widely available, and inexpensive,” the researchers noted. “Longer follow-up, however, is needed to give final resolution about the safety and efficacy of the strategy.”
A strength of the study was “meticulous selection of those patients more likely to benefit from immunosuppressive treatment, namely patients with a CSS,” she added.
The study featured a prospective, observational design for the treatment group and retrospective analysis of the historic controls. “Methodologically, the main limitation of the study is not being a randomized controlled trial,” she noted.
“Ethically it has shown to be very rewarding to consciously decide against a randomized control trial, as we are talking about a disease that if only treated with supportive care can lead to mortality up to almost 50% from COVID-19-associated CSS,” Dr. Ramiro said.
Going forward, Dr. Ramiro plans to continue monitoring patients who experienced CSS to assess their outcome post-COVID-19 infection. “We want to focus on cardiorespiratory, functional, and quality of life outcomes,” she said. “We will also compare the outcomes between patients that have received immunosuppression with those that haven’t.”
‘Quite interesting’ results
“We desperately need better evidence to guide the management of patients hospitalized with COVID-19,” Nihar R. Desai, MD, MPH, who was not affiliated with the study, said in an interview.
“These data from the Netherlands are quite interesting and provide another signal to support the use of corticosteroids, with tocilizumab if needed, among hospitalized patients with COVID-19 to improve outcomes,” added Dr. Desai, associate professor of medicine and investigator at the Center for Outcomes Research and Evaluation, Yale University, New Haven, Conn.
“While these data are not randomized and have a relatively small sample size, we had recently seen the results of the RECOVERY trial, a UK-based randomized trial demonstrating the benefit of steroids in COVID-19,” he said.
“Taken together, these studies seem to suggest that there is a benefit with steroid therapy.” Further validation of these results is warranted, he added.
“While not a randomized clinical trial, and thus susceptible to unmeasured bias, the study adds to mounting evidence that supports targeting the excessive inflammation found in some patients with COVID-19,” Jared Radbel, MD, a pulmonologist, critical care specialist, and assistant professor of medicine at Rutgers Robert Wood Johnson Medical School, New Brunswick, N.J., said in an interview.
Dr. Radbel added that he is part of a multicenter group that has submitted a manuscript examining outcomes of critically ill patients with COVID-19 treated with tocilizumab.
Dr. Ramiro, Dr. Desai, and Dr. Radbel have disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
One-third of outpatients with COVID-19 are unwell weeks later
, according to survey results in Morbidity and Mortality Weekly Report from the Centers for Disease Control and Prevention.
Mark W. Tenforde, MD, PhD, for the CDC-COVID-19 Response Team, and colleagues conducted a multistate telephone survey of symptomatic adults who tested positive for SARS-CoV-2. The researchers found that 35% had not returned to their usual state of wellness when they were interviewed 2-3 weeks after testing.
Among the 270 of 274 people interviewed for whom there were data on return to health, 175 (65%) reported that they had returned to baseline health an average of 7 days from the date of testing.
Among the 274 symptomatic outpatients, the median number of symptoms was seven. Fatigue (71%), cough (61%), and headache (61%) were the most commonly reported symptoms.
Prolonged illness is well described in adults hospitalized with severe COVID-19, especially among the older adult population, but little is known about other groups.
The proportion who had not returned to health differed by age: 26% of interviewees aged 18-34 years, 32% of those aged 35-49 years, and 47% of those at least 50 years old reported not having returned to their usual health (P = .010) within 14-21 days after receiving positive test results.
Among respondents aged 18-34 years who had no chronic medical condition, 19% (9 of 48) reported not having returned to their usual state of health during that time.
Public health messaging targeting younger adults, a group who might not be expected to be sick for weeks with mild disease, is particularly important, the authors wrote.
Kyle Annen, DO, medical director of transfusion services and patient blood management at Children’s Hospital Colorado and assistant professor of pathology at the University of Colorado, Denver, said in an interview that an important message is that delayed recovery (symptoms of fatigue, cough, and shortness of breath) was evident in nearly a quarter of 18- to 34-year-olds and in a third of 35- to 49-year-olds who were not sick enough to require hospitalization.
“This should impact the perception of this being a mild illness in the young adult population and encourage them to comply with recommendations of social distancing, masking, and hand washing,” she said.
Recovery time of more than 2 weeks will affect work and school performance, especially prolonged fatigue, she noted. This was one of the prominent symptoms that were reported to be slow to dissipate.
“I think the most interesting point in this study is that of underlying conditions; psychiatric conditions were significantly correlated with prolonged recovery. I don’t think that many people think of depression and anxiety as an underlying medical condition in regards to COVID-19 risk. This could potentially have an impact, as depression and anxiety rates will likely increase as COVID-19 continues,” she said.
Buddy Creech, MD, MPH, said in an interview that it is “important to realize that the spectrum of disease with COVID is wide, including mild disease, severe disease, and prolonged disease. This report helps us understand some of the risk factors for those with prolonged symptoms and may allow us to refine even more clearly how we prioritize treatment and vaccine administration, once available.
“It also highlights the challenge of dealing with this virus. Not only do the symptoms vary widely, but so do the incubation period, the duration of symptoms, and the residual symptoms that sometimes occur. Clearly, there is much we still need to understand about this virus,” he said.
The interviews were conducted from April 15 to June 25 with a random sample of adults at least 18 years old who had received a first positive test result for SARS-CoV-2 at an outpatient visit at one of 14 US academic healthcare systems in 13 states.
A version of this article originally appeared on Medscape.com.
, according to survey results in Morbidity and Mortality Weekly Report from the Centers for Disease Control and Prevention.
Mark W. Tenforde, MD, PhD, for the CDC-COVID-19 Response Team, and colleagues conducted a multistate telephone survey of symptomatic adults who tested positive for SARS-CoV-2. The researchers found that 35% had not returned to their usual state of wellness when they were interviewed 2-3 weeks after testing.
Among the 270 of 274 people interviewed for whom there were data on return to health, 175 (65%) reported that they had returned to baseline health an average of 7 days from the date of testing.
Among the 274 symptomatic outpatients, the median number of symptoms was seven. Fatigue (71%), cough (61%), and headache (61%) were the most commonly reported symptoms.
Prolonged illness is well described in adults hospitalized with severe COVID-19, especially among the older adult population, but little is known about other groups.
The proportion who had not returned to health differed by age: 26% of interviewees aged 18-34 years, 32% of those aged 35-49 years, and 47% of those at least 50 years old reported not having returned to their usual health (P = .010) within 14-21 days after receiving positive test results.
Among respondents aged 18-34 years who had no chronic medical condition, 19% (9 of 48) reported not having returned to their usual state of health during that time.
Public health messaging targeting younger adults, a group who might not be expected to be sick for weeks with mild disease, is particularly important, the authors wrote.
Kyle Annen, DO, medical director of transfusion services and patient blood management at Children’s Hospital Colorado and assistant professor of pathology at the University of Colorado, Denver, said in an interview that an important message is that delayed recovery (symptoms of fatigue, cough, and shortness of breath) was evident in nearly a quarter of 18- to 34-year-olds and in a third of 35- to 49-year-olds who were not sick enough to require hospitalization.
“This should impact the perception of this being a mild illness in the young adult population and encourage them to comply with recommendations of social distancing, masking, and hand washing,” she said.
Recovery time of more than 2 weeks will affect work and school performance, especially prolonged fatigue, she noted. This was one of the prominent symptoms that were reported to be slow to dissipate.
“I think the most interesting point in this study is that of underlying conditions; psychiatric conditions were significantly correlated with prolonged recovery. I don’t think that many people think of depression and anxiety as an underlying medical condition in regards to COVID-19 risk. This could potentially have an impact, as depression and anxiety rates will likely increase as COVID-19 continues,” she said.
Buddy Creech, MD, MPH, said in an interview that it is “important to realize that the spectrum of disease with COVID is wide, including mild disease, severe disease, and prolonged disease. This report helps us understand some of the risk factors for those with prolonged symptoms and may allow us to refine even more clearly how we prioritize treatment and vaccine administration, once available.
“It also highlights the challenge of dealing with this virus. Not only do the symptoms vary widely, but so do the incubation period, the duration of symptoms, and the residual symptoms that sometimes occur. Clearly, there is much we still need to understand about this virus,” he said.
The interviews were conducted from April 15 to June 25 with a random sample of adults at least 18 years old who had received a first positive test result for SARS-CoV-2 at an outpatient visit at one of 14 US academic healthcare systems in 13 states.
A version of this article originally appeared on Medscape.com.
, according to survey results in Morbidity and Mortality Weekly Report from the Centers for Disease Control and Prevention.
Mark W. Tenforde, MD, PhD, for the CDC-COVID-19 Response Team, and colleagues conducted a multistate telephone survey of symptomatic adults who tested positive for SARS-CoV-2. The researchers found that 35% had not returned to their usual state of wellness when they were interviewed 2-3 weeks after testing.
Among the 270 of 274 people interviewed for whom there were data on return to health, 175 (65%) reported that they had returned to baseline health an average of 7 days from the date of testing.
Among the 274 symptomatic outpatients, the median number of symptoms was seven. Fatigue (71%), cough (61%), and headache (61%) were the most commonly reported symptoms.
Prolonged illness is well described in adults hospitalized with severe COVID-19, especially among the older adult population, but little is known about other groups.
The proportion who had not returned to health differed by age: 26% of interviewees aged 18-34 years, 32% of those aged 35-49 years, and 47% of those at least 50 years old reported not having returned to their usual health (P = .010) within 14-21 days after receiving positive test results.
Among respondents aged 18-34 years who had no chronic medical condition, 19% (9 of 48) reported not having returned to their usual state of health during that time.
Public health messaging targeting younger adults, a group who might not be expected to be sick for weeks with mild disease, is particularly important, the authors wrote.
Kyle Annen, DO, medical director of transfusion services and patient blood management at Children’s Hospital Colorado and assistant professor of pathology at the University of Colorado, Denver, said in an interview that an important message is that delayed recovery (symptoms of fatigue, cough, and shortness of breath) was evident in nearly a quarter of 18- to 34-year-olds and in a third of 35- to 49-year-olds who were not sick enough to require hospitalization.
“This should impact the perception of this being a mild illness in the young adult population and encourage them to comply with recommendations of social distancing, masking, and hand washing,” she said.
Recovery time of more than 2 weeks will affect work and school performance, especially prolonged fatigue, she noted. This was one of the prominent symptoms that were reported to be slow to dissipate.
“I think the most interesting point in this study is that of underlying conditions; psychiatric conditions were significantly correlated with prolonged recovery. I don’t think that many people think of depression and anxiety as an underlying medical condition in regards to COVID-19 risk. This could potentially have an impact, as depression and anxiety rates will likely increase as COVID-19 continues,” she said.
Buddy Creech, MD, MPH, said in an interview that it is “important to realize that the spectrum of disease with COVID is wide, including mild disease, severe disease, and prolonged disease. This report helps us understand some of the risk factors for those with prolonged symptoms and may allow us to refine even more clearly how we prioritize treatment and vaccine administration, once available.
“It also highlights the challenge of dealing with this virus. Not only do the symptoms vary widely, but so do the incubation period, the duration of symptoms, and the residual symptoms that sometimes occur. Clearly, there is much we still need to understand about this virus,” he said.
The interviews were conducted from April 15 to June 25 with a random sample of adults at least 18 years old who had received a first positive test result for SARS-CoV-2 at an outpatient visit at one of 14 US academic healthcare systems in 13 states.
A version of this article originally appeared on Medscape.com.
Small NY study: Mother-baby transmission of COVID-19 not seen
according to a study out of New York-Presbyterian Hospital.

“It is suggested in the cumulative data that the virus does not confer additional risk to the fetus during labor or during the early postnatal period in both preterm and term infants,” concluded Jeffrey Perlman, MB ChB, and colleagues in Pediatrics.
But other experts suggest substantial gaps remain in our understanding of maternal transmission of SARS-CoV-2.
“Much more needs to be known,” Munish Gupta, MD, and colleagues from Beth Israel Deaconess Medical Center and Harvard Medical School, Boston, said in an accompanying editorial.
The prospective study is the first to describe a cohort of U.S. COVID-19–related deliveries, with the prior neonatal impact of COVID-19 “almost exclusively” reported from China, noted the authors. They included a cohort of 326 women who were tested for SARS-CoV-2 on admission to labor and delivery at New York-Presbyterian Hospital between March 22 and April 15th, 2020. Of the 31 (10%) mothers who tested positive, 15 (48%) were asymptomatic and 16 (52%) were symptomatic.
Two babies were born prematurely (one by Cesarean) and were isolated in negative pressure rooms with continuous positive airway pressure. Both were moved out of isolation after two negative test results and “have exhibited an unremarkable clinical course,” the authors reported.
The other 29 term babies were cared for in their mothers’ rooms, with breastfeeding allowed, if desired. These babies and their mothers were discharged from the hospital between 24 and 48 hours after delivery.
“Visitor restriction for mothers who were positive for COVID-19 included 14 days of no visitation from the start of symptoms,” noted the team.
They added “since the prepublication release there have been a total of 47 mothers positive for COVID-19, resulting in 47 infants; 4 have been admitted to neonatal intensive care. In addition, 32 other infants have been tested for a variety of indications within the unit. All infants test results have been negative.”
The brief report outlined the institution’s checklist for delivery preparedness in either the operating room or labor delivery room, including personal protective equipment, resuscitation, transportation to the neonatal intensive care unit, and early postresuscitation care. “Suspected or confirmed COVID-19 alone in an otherwise uncomplicated pregnancy is not an indication for the resuscitation team or the neonatal fellow,” they noted, adding delivery room preparation and management should include contact precautions. “With scrupulous attention to infectious precautions, horizontal viral transmission should be minimized,” they advised.
Dr. Perlman and associates emphasized that rapid turnaround SARSCoV-2 testing is “crucial to minimize the likelihood of a provider becoming infected and/or infecting the infant.”
Although the findings are “clearly reassuring,” Dr. Gupta and colleagues have reservations. “To what extent does this report address concerns for infection risk with a rooming-in approach to care?” they asked in their accompanying editorial. “The answer is likely some, but not much.”
Many questions remain, they said, including: “What precautions were used to minimize infection risk during the postbirth hospital course? What was the approach to skin-to-skin care and direct mother-newborn contact? Were restrictions placed on family members? Were changes made to routine interventions such as hearing screens or circumcisions? What practices were in place around environmental cleaning? Most important, how did the newborns do after discharge?”
The current uncertainty around neonatal COVID-19 infection risk has led to “disparate” variations in care recommendations, they pointed out. Whereas China’s consensus guidelines recommend a 14-day separation of COVID-19–positive mothers from their healthy infants, a practice supported by the American Academy of Pediatrics “when possible,” the Italian Society of Neonatology, the Royal College of Paediatrics and Child Health, and the Canadian Paediatric Society advise “rooming-in and breastfeeding with appropriate infection prevention measures.”
Dr. Gupta and colleagues pointed to the following as at least three “critical and time-sensitive needs for research around neonatal care and outcomes related to COVID-19”:
- Studies need to have much larger sample sizes and include diverse populations. This will allow for reliable measurement of outcomes.
- Descriptions of care practices must be in detail, especially about infection prevention; these should be presented in a way to compare the efficacy of different approaches.
- There needs to be follow-up information on outcomes of both the mother and the neonate after the birth hospitalization.
Asked to comment, Lillian Beard, MD, of George Washington University in Washington welcomed the data as “good news.”

“Although small, the study was done during a 3-week peak period at the hottest spot of the pandemic in the United States during that period. It illustrates how delivery room preparedness, adequate personal protective equipment, and carefully planned infection control precautions can positively impact outcomes even during a seemingly impossible period,” she said.
“Although there are many uncertainties about maternal COVID-19 transmission and neonatal infection risks ... in my opinion, during the after birth hospitalization, the inherent benefits of rooming in for breast feeding and the opportunities for the demonstration and teaching of infection prevention practices for the family home, far outweigh the risks of disease transmission,” said Dr. Beard, who was not involved with the study.
The study and the commentary emphasize the likely low risk of vertical transmission of the virus, with horizontal transmission being the greater risk. However, cases of transplacental transmission have been reported, and the lead investigator of one recent placental study cautions against complacency.
“Neonates can get infected in both ways. The majority of cases seem to be horizontal, but those who have been infected or highly suspected to be vertically infected are not a small percentage either,” said Daniele de Luca, MD, PhD, president-elect of the European Society for Pediatric and Neonatal Intensive Care (ESPNIC) and a neonatologist at Antoine Béclère Hospital in Clamart, France.
“Perlman’s data are interesting and consistent with other reports around the world. However, two things must be remembered,” he said in an interview. “First, newborn infants are at relatively low risk from SARS-CoV-2 infections, but this is very far from zero risk. Neonatal SARS-CoV-2 infections do exist and have been described around the world. While they have a mild course in the majority of cases, neonatologists should not forget them and should be prepared to offer the best care to these babies.”
“Second, how this can be balanced with the need to promote breastfeeding and avoid overtreatment or separation from the mother is a question far from being answered. Gupta et al. in their commentary are right in saying that we have more questions than answers. While waiting for the results of large initiatives (such as the ESPNIC EPICENTRE Registry that they cite) to answer these open points, the best we can do is to provide a personalised case by case approach, transparent information to parents, and an open counselling informing clinical decisions.”
The study received no external funding. Dr. Perlman and associates had no financial disclosures. Dr. Gupta and colleagues had no relevant financial disclosures. Neither Dr. Beard nor Dr. de Luca had any relevant financial disclosures.
SOURCE: Perlman J et al. Pediatrics. 2020;146(2):e20201567.
according to a study out of New York-Presbyterian Hospital.
“It is suggested in the cumulative data that the virus does not confer additional risk to the fetus during labor or during the early postnatal period in both preterm and term infants,” concluded Jeffrey Perlman, MB ChB, and colleagues in Pediatrics.
But other experts suggest substantial gaps remain in our understanding of maternal transmission of SARS-CoV-2.
“Much more needs to be known,” Munish Gupta, MD, and colleagues from Beth Israel Deaconess Medical Center and Harvard Medical School, Boston, said in an accompanying editorial.
The prospective study is the first to describe a cohort of U.S. COVID-19–related deliveries, with the prior neonatal impact of COVID-19 “almost exclusively” reported from China, noted the authors. They included a cohort of 326 women who were tested for SARS-CoV-2 on admission to labor and delivery at New York-Presbyterian Hospital between March 22 and April 15th, 2020. Of the 31 (10%) mothers who tested positive, 15 (48%) were asymptomatic and 16 (52%) were symptomatic.
Two babies were born prematurely (one by Cesarean) and were isolated in negative pressure rooms with continuous positive airway pressure. Both were moved out of isolation after two negative test results and “have exhibited an unremarkable clinical course,” the authors reported.
The other 29 term babies were cared for in their mothers’ rooms, with breastfeeding allowed, if desired. These babies and their mothers were discharged from the hospital between 24 and 48 hours after delivery.
“Visitor restriction for mothers who were positive for COVID-19 included 14 days of no visitation from the start of symptoms,” noted the team.
They added “since the prepublication release there have been a total of 47 mothers positive for COVID-19, resulting in 47 infants; 4 have been admitted to neonatal intensive care. In addition, 32 other infants have been tested for a variety of indications within the unit. All infants test results have been negative.”
The brief report outlined the institution’s checklist for delivery preparedness in either the operating room or labor delivery room, including personal protective equipment, resuscitation, transportation to the neonatal intensive care unit, and early postresuscitation care. “Suspected or confirmed COVID-19 alone in an otherwise uncomplicated pregnancy is not an indication for the resuscitation team or the neonatal fellow,” they noted, adding delivery room preparation and management should include contact precautions. “With scrupulous attention to infectious precautions, horizontal viral transmission should be minimized,” they advised.
Dr. Perlman and associates emphasized that rapid turnaround SARSCoV-2 testing is “crucial to minimize the likelihood of a provider becoming infected and/or infecting the infant.”
Although the findings are “clearly reassuring,” Dr. Gupta and colleagues have reservations. “To what extent does this report address concerns for infection risk with a rooming-in approach to care?” they asked in their accompanying editorial. “The answer is likely some, but not much.”
Many questions remain, they said, including: “What precautions were used to minimize infection risk during the postbirth hospital course? What was the approach to skin-to-skin care and direct mother-newborn contact? Were restrictions placed on family members? Were changes made to routine interventions such as hearing screens or circumcisions? What practices were in place around environmental cleaning? Most important, how did the newborns do after discharge?”
The current uncertainty around neonatal COVID-19 infection risk has led to “disparate” variations in care recommendations, they pointed out. Whereas China’s consensus guidelines recommend a 14-day separation of COVID-19–positive mothers from their healthy infants, a practice supported by the American Academy of Pediatrics “when possible,” the Italian Society of Neonatology, the Royal College of Paediatrics and Child Health, and the Canadian Paediatric Society advise “rooming-in and breastfeeding with appropriate infection prevention measures.”
Dr. Gupta and colleagues pointed to the following as at least three “critical and time-sensitive needs for research around neonatal care and outcomes related to COVID-19”:
- Studies need to have much larger sample sizes and include diverse populations. This will allow for reliable measurement of outcomes.
- Descriptions of care practices must be in detail, especially about infection prevention; these should be presented in a way to compare the efficacy of different approaches.
- There needs to be follow-up information on outcomes of both the mother and the neonate after the birth hospitalization.
Asked to comment, Lillian Beard, MD, of George Washington University in Washington welcomed the data as “good news.”
“Although small, the study was done during a 3-week peak period at the hottest spot of the pandemic in the United States during that period. It illustrates how delivery room preparedness, adequate personal protective equipment, and carefully planned infection control precautions can positively impact outcomes even during a seemingly impossible period,” she said.
“Although there are many uncertainties about maternal COVID-19 transmission and neonatal infection risks ... in my opinion, during the after birth hospitalization, the inherent benefits of rooming in for breast feeding and the opportunities for the demonstration and teaching of infection prevention practices for the family home, far outweigh the risks of disease transmission,” said Dr. Beard, who was not involved with the study.
The study and the commentary emphasize the likely low risk of vertical transmission of the virus, with horizontal transmission being the greater risk. However, cases of transplacental transmission have been reported, and the lead investigator of one recent placental study cautions against complacency.
“Neonates can get infected in both ways. The majority of cases seem to be horizontal, but those who have been infected or highly suspected to be vertically infected are not a small percentage either,” said Daniele de Luca, MD, PhD, president-elect of the European Society for Pediatric and Neonatal Intensive Care (ESPNIC) and a neonatologist at Antoine Béclère Hospital in Clamart, France.
“Perlman’s data are interesting and consistent with other reports around the world. However, two things must be remembered,” he said in an interview. “First, newborn infants are at relatively low risk from SARS-CoV-2 infections, but this is very far from zero risk. Neonatal SARS-CoV-2 infections do exist and have been described around the world. While they have a mild course in the majority of cases, neonatologists should not forget them and should be prepared to offer the best care to these babies.”
“Second, how this can be balanced with the need to promote breastfeeding and avoid overtreatment or separation from the mother is a question far from being answered. Gupta et al. in their commentary are right in saying that we have more questions than answers. While waiting for the results of large initiatives (such as the ESPNIC EPICENTRE Registry that they cite) to answer these open points, the best we can do is to provide a personalised case by case approach, transparent information to parents, and an open counselling informing clinical decisions.”
The study received no external funding. Dr. Perlman and associates had no financial disclosures. Dr. Gupta and colleagues had no relevant financial disclosures. Neither Dr. Beard nor Dr. de Luca had any relevant financial disclosures.
SOURCE: Perlman J et al. Pediatrics. 2020;146(2):e20201567.
according to a study out of New York-Presbyterian Hospital.
“It is suggested in the cumulative data that the virus does not confer additional risk to the fetus during labor or during the early postnatal period in both preterm and term infants,” concluded Jeffrey Perlman, MB ChB, and colleagues in Pediatrics.
But other experts suggest substantial gaps remain in our understanding of maternal transmission of SARS-CoV-2.
“Much more needs to be known,” Munish Gupta, MD, and colleagues from Beth Israel Deaconess Medical Center and Harvard Medical School, Boston, said in an accompanying editorial.
The prospective study is the first to describe a cohort of U.S. COVID-19–related deliveries, with the prior neonatal impact of COVID-19 “almost exclusively” reported from China, noted the authors. They included a cohort of 326 women who were tested for SARS-CoV-2 on admission to labor and delivery at New York-Presbyterian Hospital between March 22 and April 15th, 2020. Of the 31 (10%) mothers who tested positive, 15 (48%) were asymptomatic and 16 (52%) were symptomatic.
Two babies were born prematurely (one by Cesarean) and were isolated in negative pressure rooms with continuous positive airway pressure. Both were moved out of isolation after two negative test results and “have exhibited an unremarkable clinical course,” the authors reported.
The other 29 term babies were cared for in their mothers’ rooms, with breastfeeding allowed, if desired. These babies and their mothers were discharged from the hospital between 24 and 48 hours after delivery.
“Visitor restriction for mothers who were positive for COVID-19 included 14 days of no visitation from the start of symptoms,” noted the team.
They added “since the prepublication release there have been a total of 47 mothers positive for COVID-19, resulting in 47 infants; 4 have been admitted to neonatal intensive care. In addition, 32 other infants have been tested for a variety of indications within the unit. All infants test results have been negative.”
The brief report outlined the institution’s checklist for delivery preparedness in either the operating room or labor delivery room, including personal protective equipment, resuscitation, transportation to the neonatal intensive care unit, and early postresuscitation care. “Suspected or confirmed COVID-19 alone in an otherwise uncomplicated pregnancy is not an indication for the resuscitation team or the neonatal fellow,” they noted, adding delivery room preparation and management should include contact precautions. “With scrupulous attention to infectious precautions, horizontal viral transmission should be minimized,” they advised.
Dr. Perlman and associates emphasized that rapid turnaround SARSCoV-2 testing is “crucial to minimize the likelihood of a provider becoming infected and/or infecting the infant.”
Although the findings are “clearly reassuring,” Dr. Gupta and colleagues have reservations. “To what extent does this report address concerns for infection risk with a rooming-in approach to care?” they asked in their accompanying editorial. “The answer is likely some, but not much.”
Many questions remain, they said, including: “What precautions were used to minimize infection risk during the postbirth hospital course? What was the approach to skin-to-skin care and direct mother-newborn contact? Were restrictions placed on family members? Were changes made to routine interventions such as hearing screens or circumcisions? What practices were in place around environmental cleaning? Most important, how did the newborns do after discharge?”
The current uncertainty around neonatal COVID-19 infection risk has led to “disparate” variations in care recommendations, they pointed out. Whereas China’s consensus guidelines recommend a 14-day separation of COVID-19–positive mothers from their healthy infants, a practice supported by the American Academy of Pediatrics “when possible,” the Italian Society of Neonatology, the Royal College of Paediatrics and Child Health, and the Canadian Paediatric Society advise “rooming-in and breastfeeding with appropriate infection prevention measures.”
Dr. Gupta and colleagues pointed to the following as at least three “critical and time-sensitive needs for research around neonatal care and outcomes related to COVID-19”:
- Studies need to have much larger sample sizes and include diverse populations. This will allow for reliable measurement of outcomes.
- Descriptions of care practices must be in detail, especially about infection prevention; these should be presented in a way to compare the efficacy of different approaches.
- There needs to be follow-up information on outcomes of both the mother and the neonate after the birth hospitalization.
Asked to comment, Lillian Beard, MD, of George Washington University in Washington welcomed the data as “good news.”
“Although small, the study was done during a 3-week peak period at the hottest spot of the pandemic in the United States during that period. It illustrates how delivery room preparedness, adequate personal protective equipment, and carefully planned infection control precautions can positively impact outcomes even during a seemingly impossible period,” she said.
“Although there are many uncertainties about maternal COVID-19 transmission and neonatal infection risks ... in my opinion, during the after birth hospitalization, the inherent benefits of rooming in for breast feeding and the opportunities for the demonstration and teaching of infection prevention practices for the family home, far outweigh the risks of disease transmission,” said Dr. Beard, who was not involved with the study.
The study and the commentary emphasize the likely low risk of vertical transmission of the virus, with horizontal transmission being the greater risk. However, cases of transplacental transmission have been reported, and the lead investigator of one recent placental study cautions against complacency.
“Neonates can get infected in both ways. The majority of cases seem to be horizontal, but those who have been infected or highly suspected to be vertically infected are not a small percentage either,” said Daniele de Luca, MD, PhD, president-elect of the European Society for Pediatric and Neonatal Intensive Care (ESPNIC) and a neonatologist at Antoine Béclère Hospital in Clamart, France.
“Perlman’s data are interesting and consistent with other reports around the world. However, two things must be remembered,” he said in an interview. “First, newborn infants are at relatively low risk from SARS-CoV-2 infections, but this is very far from zero risk. Neonatal SARS-CoV-2 infections do exist and have been described around the world. While they have a mild course in the majority of cases, neonatologists should not forget them and should be prepared to offer the best care to these babies.”
“Second, how this can be balanced with the need to promote breastfeeding and avoid overtreatment or separation from the mother is a question far from being answered. Gupta et al. in their commentary are right in saying that we have more questions than answers. While waiting for the results of large initiatives (such as the ESPNIC EPICENTRE Registry that they cite) to answer these open points, the best we can do is to provide a personalised case by case approach, transparent information to parents, and an open counselling informing clinical decisions.”
The study received no external funding. Dr. Perlman and associates had no financial disclosures. Dr. Gupta and colleagues had no relevant financial disclosures. Neither Dr. Beard nor Dr. de Luca had any relevant financial disclosures.
SOURCE: Perlman J et al. Pediatrics. 2020;146(2):e20201567.
FROM PEDIATRICS

Men occupy most leadership roles in medicine
Since the early 2000s, approximately half of medical students in the United States – and in many years, more than half – have been women, but according to an update provided at the virtual Pediatric Hospital Medicine.
In pediatrics, a specialty in which approximately 70% of physicians are now women, there has been progress, but still less than 30% of pediatric department chairs are female, said Vincent Chiang, MD, chief medical officer of Boston Children’s Hospital, during a presentation at the virtual meeting sponsored by the Society of Hospital Medicine, the American Academy of Pediatrics, and the Academic Pediatric Association.
Citing published data and a survey he personally conducted of the top children’s hospitals identified by the U.S. News and World Report, Dr. Chiang said a minority of division chiefs, chief medical officers, chief financial officers, and other leaders are female. At his institution, only 2 of 16 division chiefs are female.
“No matter how you slice it, women are underrepresented in leadership positions,” he noted.
The problem is certainly not confined to medicine. Dr. Chiang cited data showing that women and men have reached “near parity” in workforce participation in the United States even though the 20% earnings gap has changed little over time.
According to 2020 data from the World Economic Forum, the United States ranked 51 for the gender gap calculated on the basis of economic, political, educational, and health attainment. Even if this places the United States in the top third of the rankings, it is far behind Iceland and the Scandinavian countries that lead the list.
Efforts to reduce structural biases are part of the fix, but Dr. Chiang cautioned that fundamental changes might never occur if the plan is to wait for an approach based on meritocracy. He said that existing structural biases are “slanted away from women,” who are not necessarily granted the opportunities that are readily available to men.
“A meritocracy only works if the initial playing field was level. Otherwise, it just perpetuates the inequalities,” he said.
The problem is not a shortage of women with the skills to lead. In a study by Zenger/Folkman, a consulting company that works on leadership skill development, women performed better than men in 16 of 18 leadership categories, according to Dr. Chiang.
“There is certainly no shortage of capable women,” he noted.
Of the many issues, Dr. Chiang highlighted two. The first is the challenge of placing women on leadership pathways. This is likely to require proactive strategies, such as fast-track advancement programs that guide female candidates toward leadership roles.
The second is more nuanced. According to Dr. Chiang, women who want to assume a leadership role should think more actively about how and who is making decisions at their institution so they can position themselves appropriately. This is nuanced because “there is a certain amount of gamesmanship,” he said. The rise to leadership “has never been a pure meritocracy.”
Importantly, many of the key decisions in any institution involve money, according to Dr. Chiang. As a result, he advised those seeking leadership roles to join audit committees or otherwise take on responsibility for profit-and-loss management. Even in a nonprofit institution, “you need to make the numbers work,” he said, citing the common catchphrase: “No margin, no mission.”
However, Dr. Chiang acknowledged the many obstacles that prevent women from working their way into positions of leadership. For example, networking is important, but women are not necessarily attracted or invited to some of the social engagements, such as golf outings, where strong relationships are created.
In a survey of 100,000 people working at Fortune 500 companies, “82% of women say they feel excluded at work and much of that comes from that informal networking,” Dr. Chiang said. “Whereas 92% of men think they are not excluding women in their daily work.”
There is no single solution, but Dr. Chiang believes that concrete structural changes are needed. Female doctors remain grossly underrepresented in leadership roles even as they now represent more than half of the workforce for many specialties. Based on the need for proactive approaches outlined by Dr. Chiang, it appears unlikely that gender inequality will ever resolve itself.
Lisa S. Rotenstein, MD, who has written on fixing the gender imbalance in health care, including for the Harvard Business Review, said she agreed during an interview that structural changes are critical.
“In order to address current disparities, leaders should be thinking about how to remove both the formal and informal obstacles that prevent women and minorities from getting into the rooms where these decisions are being made,” said Dr. Rotenstein, who is an instructor in medicine at Brigham and Women’s Hospital, Harvard Medical School in Boston.
“This will need to involve sponsorship that gets women invited to the right committees or in positions with responsibility for profit-and-loss management,” she added.
Dr. Rotenstein spoke about improving “access to the pipeline” that leads to leadership roles. The ways in which women are excluded from opportunities is often subtle and difficult to penetrate without fundamental changes, she explained.
“Institutions need to understand the processes that lead to leadership roles and make the changes that allow women and minorities to participate,” she said. It is not enough to recognize the problem, according to Dr. Rotenstein.
Like Dr. Chiang, she noted that changes are needed in the methods that move underrepresented groups into leadership roles.
Dr. Chiang reported no potential conflicts of interest relevant to this study.
Since the early 2000s, approximately half of medical students in the United States – and in many years, more than half – have been women, but according to an update provided at the virtual Pediatric Hospital Medicine.
In pediatrics, a specialty in which approximately 70% of physicians are now women, there has been progress, but still less than 30% of pediatric department chairs are female, said Vincent Chiang, MD, chief medical officer of Boston Children’s Hospital, during a presentation at the virtual meeting sponsored by the Society of Hospital Medicine, the American Academy of Pediatrics, and the Academic Pediatric Association.
Citing published data and a survey he personally conducted of the top children’s hospitals identified by the U.S. News and World Report, Dr. Chiang said a minority of division chiefs, chief medical officers, chief financial officers, and other leaders are female. At his institution, only 2 of 16 division chiefs are female.
“No matter how you slice it, women are underrepresented in leadership positions,” he noted.
The problem is certainly not confined to medicine. Dr. Chiang cited data showing that women and men have reached “near parity” in workforce participation in the United States even though the 20% earnings gap has changed little over time.
According to 2020 data from the World Economic Forum, the United States ranked 51 for the gender gap calculated on the basis of economic, political, educational, and health attainment. Even if this places the United States in the top third of the rankings, it is far behind Iceland and the Scandinavian countries that lead the list.
Efforts to reduce structural biases are part of the fix, but Dr. Chiang cautioned that fundamental changes might never occur if the plan is to wait for an approach based on meritocracy. He said that existing structural biases are “slanted away from women,” who are not necessarily granted the opportunities that are readily available to men.
“A meritocracy only works if the initial playing field was level. Otherwise, it just perpetuates the inequalities,” he said.
The problem is not a shortage of women with the skills to lead. In a study by Zenger/Folkman, a consulting company that works on leadership skill development, women performed better than men in 16 of 18 leadership categories, according to Dr. Chiang.
“There is certainly no shortage of capable women,” he noted.
Of the many issues, Dr. Chiang highlighted two. The first is the challenge of placing women on leadership pathways. This is likely to require proactive strategies, such as fast-track advancement programs that guide female candidates toward leadership roles.
The second is more nuanced. According to Dr. Chiang, women who want to assume a leadership role should think more actively about how and who is making decisions at their institution so they can position themselves appropriately. This is nuanced because “there is a certain amount of gamesmanship,” he said. The rise to leadership “has never been a pure meritocracy.”
Importantly, many of the key decisions in any institution involve money, according to Dr. Chiang. As a result, he advised those seeking leadership roles to join audit committees or otherwise take on responsibility for profit-and-loss management. Even in a nonprofit institution, “you need to make the numbers work,” he said, citing the common catchphrase: “No margin, no mission.”
However, Dr. Chiang acknowledged the many obstacles that prevent women from working their way into positions of leadership. For example, networking is important, but women are not necessarily attracted or invited to some of the social engagements, such as golf outings, where strong relationships are created.
In a survey of 100,000 people working at Fortune 500 companies, “82% of women say they feel excluded at work and much of that comes from that informal networking,” Dr. Chiang said. “Whereas 92% of men think they are not excluding women in their daily work.”
There is no single solution, but Dr. Chiang believes that concrete structural changes are needed. Female doctors remain grossly underrepresented in leadership roles even as they now represent more than half of the workforce for many specialties. Based on the need for proactive approaches outlined by Dr. Chiang, it appears unlikely that gender inequality will ever resolve itself.
Lisa S. Rotenstein, MD, who has written on fixing the gender imbalance in health care, including for the Harvard Business Review, said she agreed during an interview that structural changes are critical.
“In order to address current disparities, leaders should be thinking about how to remove both the formal and informal obstacles that prevent women and minorities from getting into the rooms where these decisions are being made,” said Dr. Rotenstein, who is an instructor in medicine at Brigham and Women’s Hospital, Harvard Medical School in Boston.
“This will need to involve sponsorship that gets women invited to the right committees or in positions with responsibility for profit-and-loss management,” she added.
Dr. Rotenstein spoke about improving “access to the pipeline” that leads to leadership roles. The ways in which women are excluded from opportunities is often subtle and difficult to penetrate without fundamental changes, she explained.
“Institutions need to understand the processes that lead to leadership roles and make the changes that allow women and minorities to participate,” she said. It is not enough to recognize the problem, according to Dr. Rotenstein.
Like Dr. Chiang, she noted that changes are needed in the methods that move underrepresented groups into leadership roles.
Dr. Chiang reported no potential conflicts of interest relevant to this study.
Since the early 2000s, approximately half of medical students in the United States – and in many years, more than half – have been women, but according to an update provided at the virtual Pediatric Hospital Medicine.
In pediatrics, a specialty in which approximately 70% of physicians are now women, there has been progress, but still less than 30% of pediatric department chairs are female, said Vincent Chiang, MD, chief medical officer of Boston Children’s Hospital, during a presentation at the virtual meeting sponsored by the Society of Hospital Medicine, the American Academy of Pediatrics, and the Academic Pediatric Association.
Citing published data and a survey he personally conducted of the top children’s hospitals identified by the U.S. News and World Report, Dr. Chiang said a minority of division chiefs, chief medical officers, chief financial officers, and other leaders are female. At his institution, only 2 of 16 division chiefs are female.
“No matter how you slice it, women are underrepresented in leadership positions,” he noted.
The problem is certainly not confined to medicine. Dr. Chiang cited data showing that women and men have reached “near parity” in workforce participation in the United States even though the 20% earnings gap has changed little over time.
According to 2020 data from the World Economic Forum, the United States ranked 51 for the gender gap calculated on the basis of economic, political, educational, and health attainment. Even if this places the United States in the top third of the rankings, it is far behind Iceland and the Scandinavian countries that lead the list.
Efforts to reduce structural biases are part of the fix, but Dr. Chiang cautioned that fundamental changes might never occur if the plan is to wait for an approach based on meritocracy. He said that existing structural biases are “slanted away from women,” who are not necessarily granted the opportunities that are readily available to men.
“A meritocracy only works if the initial playing field was level. Otherwise, it just perpetuates the inequalities,” he said.
The problem is not a shortage of women with the skills to lead. In a study by Zenger/Folkman, a consulting company that works on leadership skill development, women performed better than men in 16 of 18 leadership categories, according to Dr. Chiang.
“There is certainly no shortage of capable women,” he noted.
Of the many issues, Dr. Chiang highlighted two. The first is the challenge of placing women on leadership pathways. This is likely to require proactive strategies, such as fast-track advancement programs that guide female candidates toward leadership roles.
The second is more nuanced. According to Dr. Chiang, women who want to assume a leadership role should think more actively about how and who is making decisions at their institution so they can position themselves appropriately. This is nuanced because “there is a certain amount of gamesmanship,” he said. The rise to leadership “has never been a pure meritocracy.”
Importantly, many of the key decisions in any institution involve money, according to Dr. Chiang. As a result, he advised those seeking leadership roles to join audit committees or otherwise take on responsibility for profit-and-loss management. Even in a nonprofit institution, “you need to make the numbers work,” he said, citing the common catchphrase: “No margin, no mission.”
However, Dr. Chiang acknowledged the many obstacles that prevent women from working their way into positions of leadership. For example, networking is important, but women are not necessarily attracted or invited to some of the social engagements, such as golf outings, where strong relationships are created.
In a survey of 100,000 people working at Fortune 500 companies, “82% of women say they feel excluded at work and much of that comes from that informal networking,” Dr. Chiang said. “Whereas 92% of men think they are not excluding women in their daily work.”
There is no single solution, but Dr. Chiang believes that concrete structural changes are needed. Female doctors remain grossly underrepresented in leadership roles even as they now represent more than half of the workforce for many specialties. Based on the need for proactive approaches outlined by Dr. Chiang, it appears unlikely that gender inequality will ever resolve itself.
Lisa S. Rotenstein, MD, who has written on fixing the gender imbalance in health care, including for the Harvard Business Review, said she agreed during an interview that structural changes are critical.
“In order to address current disparities, leaders should be thinking about how to remove both the formal and informal obstacles that prevent women and minorities from getting into the rooms where these decisions are being made,” said Dr. Rotenstein, who is an instructor in medicine at Brigham and Women’s Hospital, Harvard Medical School in Boston.
“This will need to involve sponsorship that gets women invited to the right committees or in positions with responsibility for profit-and-loss management,” she added.
Dr. Rotenstein spoke about improving “access to the pipeline” that leads to leadership roles. The ways in which women are excluded from opportunities is often subtle and difficult to penetrate without fundamental changes, she explained.
“Institutions need to understand the processes that lead to leadership roles and make the changes that allow women and minorities to participate,” she said. It is not enough to recognize the problem, according to Dr. Rotenstein.
Like Dr. Chiang, she noted that changes are needed in the methods that move underrepresented groups into leadership roles.
Dr. Chiang reported no potential conflicts of interest relevant to this study.
FROM PHM20
Learn to anticipate, resolve difficult interactions with patients
Every physician encounters difficult or challenging patients during their career, but learning how to anticipate and handle these interactions is not something taught in medical school or residency, according to Donald W. Black, MD, MS.

Difficult or challenging encounters with patients are not only unavoidable, they should be expected, Dr. Black said in a virtual meeting presented by Current Psychiatry and the American Academy of Clinical Psychiatrists.
“Every doctor I know has had challenging interactions,” he said. About 15% of encounters were deemed “difficult” in a prospective study of patients by Jeffrey L. Jackson, MD, MPH, and Kurt Kroenke, MD. A depressive or anxiety disorder was present in 29% of patients, with 11% experiencing two or more disorders. Major depression was present in 8.4%, other depressive disorders in 17.4%, panic disorder in 1.4%, and other anxiety disorders in 14.2% of patients. Dr. Jackson and Dr. Kroenke found that difficult patients demonstrated disrespect and anger, made threats, and locked themselves in rooms (Arch Intern Med. 1999 May 24;159[10]:1069-75). “Rest assured, you are not the only psychiatrist to face this type of issue,” Dr. Black said at the meeting, presented by Global Academy for Medical Education.
Common scenarios can include patients who want certain tests performed after researching symptoms online, threats of legal or social media action after feeling like they are not being listened to, a demand for a second opinion after not agreeing with a physician’s diagnosis, mistrust of doctors after presenting with symptoms and not being diagnosed, patients who focus on negative outcomes, and those who do not comply with treatment. These patients can often appear angry, defensive, frightened or resistant, or manipulative; may provide vague or exaggerated symptoms; or may inappropriately rely on hospital or clinic staff for emotional and physical support.
To complicate matters, the patients’ condition also might contribute to difficult interactions, such as in patients who have conditions like chronic pain or fibromyalgia.
“These often contribute because patients never feel that their problems are being appropriately addressed,” said Dr. Black, professor of psychiatry at the University of Iowa in Iowa City. Patients with psychiatric disorders can also present unique challenges that may result in difficult encounters. Patients with anxiety might not be able to be reassured by their doctor, for example, or patients with eating disorders might refuse treatment recommendations, he said.
Difficult encounters can lead to physicians feeling angry, upset, stressed, disrespected, abused, or fearful. But “it’s not just about the patient,” Dr. Black said. Physicians can become angry or defensive because of burnout, stress, or frustration, which can lead to them snapping at patients. Physicians are also overworked, sleep-deprived, and busier than they’d like to be, he added. Personal problems can contribute, and a physician’s belief system can cause a bad interaction with a patient. If physicians “label” one of their patients, that might end up becoming a “self-fulfilling prophecy” for that patient, Dr. Black said. Poor communication, such as not conveying bad news appropriately or with empathy, seeing a patient but never making eye contact, and using medical jargon that could be confusing to the patient, also can contribute to a challenging encounter, he added.
Situational issues also might create a bad experience for the patient. For example, a patient might find it hard to make an appointment, or the clinic might be busy or have a lack of privacy or encounter administrative issues. For patients who do not speak English as their native language, not having access to an interpreter can lead to frustration on the part of both the physician and the patient. “Bad interactions are not good for patient care,” Dr. Black said.
The key to resolving these issues is to focus on the goal, Dr. Black said. “We all want the same thing. We want to help the patient get better; we want to keep patients healthy; we want to keep them happy; we want to be fulfilled; [and] we want to manage our time and make a living – and meet our professional expectations.”
Begin by recognizing the difficult situation and assessing how the patient, the environment, or you might be contributing to the problem. “You have to step back and say what’s going on with this, and what are the factors that are combining to create this situation,” Dr. Black said. It is important to be calm and professional and not argue or talk over the patient. The goal is to work with the patient to find a solution.
One technique is to verbalize the problem without blaming the patient, the physician, or the environment (“We both have very different views about how your symptoms should be investigated, and that’s causing some difficulty between us. Do you agree?”).
There also might be alternative explanations for a patient’s behavior. For example, anger could be misdirected at a physician because of anxiety surrounding an unrelated event. In this case, it is important to listen to the patient and empathize, which will help the patient feel supported and build a rapport that can aid in resolving the problem encounter, Dr. Black said. Finding common ground when patients and physicians have different ideas on treatment or diagnosis is another way to help resolve a difficult encounter.
However, setting boundaries also is important, he noted. If, after remediation or if patients demonstrate signs of threatening or abusive behavior, initiate sexual advances, refuse to follow a treatment plan, fail to pay their bills, or are potentially putting themselves in harm’s way through noncompliance, a physician might consider terminating the relationship. Terminating the patient relationship should be done after attempting to work with the patient through a case manager and team members, and clearly advising a patient about behavior that could lead to termination of the patient-provider relationship.
Global Academy and this news organization are owned by the same parent company. Dr. Black reported that he is a consultant for Otsuka and receives royalties from American Psychiatric Publishing, Oxford University Press, and UpToDate. In addition, he receives funding from Nellie Ball Trust, the National Institute on Drug Abuse, the National Institute on Aging, and the National Center for Responsible Gaming.
Every physician encounters difficult or challenging patients during their career, but learning how to anticipate and handle these interactions is not something taught in medical school or residency, according to Donald W. Black, MD, MS.
Difficult or challenging encounters with patients are not only unavoidable, they should be expected, Dr. Black said in a virtual meeting presented by Current Psychiatry and the American Academy of Clinical Psychiatrists.
“Every doctor I know has had challenging interactions,” he said. About 15% of encounters were deemed “difficult” in a prospective study of patients by Jeffrey L. Jackson, MD, MPH, and Kurt Kroenke, MD. A depressive or anxiety disorder was present in 29% of patients, with 11% experiencing two or more disorders. Major depression was present in 8.4%, other depressive disorders in 17.4%, panic disorder in 1.4%, and other anxiety disorders in 14.2% of patients. Dr. Jackson and Dr. Kroenke found that difficult patients demonstrated disrespect and anger, made threats, and locked themselves in rooms (Arch Intern Med. 1999 May 24;159[10]:1069-75). “Rest assured, you are not the only psychiatrist to face this type of issue,” Dr. Black said at the meeting, presented by Global Academy for Medical Education.
Common scenarios can include patients who want certain tests performed after researching symptoms online, threats of legal or social media action after feeling like they are not being listened to, a demand for a second opinion after not agreeing with a physician’s diagnosis, mistrust of doctors after presenting with symptoms and not being diagnosed, patients who focus on negative outcomes, and those who do not comply with treatment. These patients can often appear angry, defensive, frightened or resistant, or manipulative; may provide vague or exaggerated symptoms; or may inappropriately rely on hospital or clinic staff for emotional and physical support.
To complicate matters, the patients’ condition also might contribute to difficult interactions, such as in patients who have conditions like chronic pain or fibromyalgia.
“These often contribute because patients never feel that their problems are being appropriately addressed,” said Dr. Black, professor of psychiatry at the University of Iowa in Iowa City. Patients with psychiatric disorders can also present unique challenges that may result in difficult encounters. Patients with anxiety might not be able to be reassured by their doctor, for example, or patients with eating disorders might refuse treatment recommendations, he said.
Difficult encounters can lead to physicians feeling angry, upset, stressed, disrespected, abused, or fearful. But “it’s not just about the patient,” Dr. Black said. Physicians can become angry or defensive because of burnout, stress, or frustration, which can lead to them snapping at patients. Physicians are also overworked, sleep-deprived, and busier than they’d like to be, he added. Personal problems can contribute, and a physician’s belief system can cause a bad interaction with a patient. If physicians “label” one of their patients, that might end up becoming a “self-fulfilling prophecy” for that patient, Dr. Black said. Poor communication, such as not conveying bad news appropriately or with empathy, seeing a patient but never making eye contact, and using medical jargon that could be confusing to the patient, also can contribute to a challenging encounter, he added.
Situational issues also might create a bad experience for the patient. For example, a patient might find it hard to make an appointment, or the clinic might be busy or have a lack of privacy or encounter administrative issues. For patients who do not speak English as their native language, not having access to an interpreter can lead to frustration on the part of both the physician and the patient. “Bad interactions are not good for patient care,” Dr. Black said.
The key to resolving these issues is to focus on the goal, Dr. Black said. “We all want the same thing. We want to help the patient get better; we want to keep patients healthy; we want to keep them happy; we want to be fulfilled; [and] we want to manage our time and make a living – and meet our professional expectations.”
Begin by recognizing the difficult situation and assessing how the patient, the environment, or you might be contributing to the problem. “You have to step back and say what’s going on with this, and what are the factors that are combining to create this situation,” Dr. Black said. It is important to be calm and professional and not argue or talk over the patient. The goal is to work with the patient to find a solution.
One technique is to verbalize the problem without blaming the patient, the physician, or the environment (“We both have very different views about how your symptoms should be investigated, and that’s causing some difficulty between us. Do you agree?”).
There also might be alternative explanations for a patient’s behavior. For example, anger could be misdirected at a physician because of anxiety surrounding an unrelated event. In this case, it is important to listen to the patient and empathize, which will help the patient feel supported and build a rapport that can aid in resolving the problem encounter, Dr. Black said. Finding common ground when patients and physicians have different ideas on treatment or diagnosis is another way to help resolve a difficult encounter.
However, setting boundaries also is important, he noted. If, after remediation or if patients demonstrate signs of threatening or abusive behavior, initiate sexual advances, refuse to follow a treatment plan, fail to pay their bills, or are potentially putting themselves in harm’s way through noncompliance, a physician might consider terminating the relationship. Terminating the patient relationship should be done after attempting to work with the patient through a case manager and team members, and clearly advising a patient about behavior that could lead to termination of the patient-provider relationship.
Global Academy and this news organization are owned by the same parent company. Dr. Black reported that he is a consultant for Otsuka and receives royalties from American Psychiatric Publishing, Oxford University Press, and UpToDate. In addition, he receives funding from Nellie Ball Trust, the National Institute on Drug Abuse, the National Institute on Aging, and the National Center for Responsible Gaming.
Every physician encounters difficult or challenging patients during their career, but learning how to anticipate and handle these interactions is not something taught in medical school or residency, according to Donald W. Black, MD, MS.
Difficult or challenging encounters with patients are not only unavoidable, they should be expected, Dr. Black said in a virtual meeting presented by Current Psychiatry and the American Academy of Clinical Psychiatrists.
“Every doctor I know has had challenging interactions,” he said. About 15% of encounters were deemed “difficult” in a prospective study of patients by Jeffrey L. Jackson, MD, MPH, and Kurt Kroenke, MD. A depressive or anxiety disorder was present in 29% of patients, with 11% experiencing two or more disorders. Major depression was present in 8.4%, other depressive disorders in 17.4%, panic disorder in 1.4%, and other anxiety disorders in 14.2% of patients. Dr. Jackson and Dr. Kroenke found that difficult patients demonstrated disrespect and anger, made threats, and locked themselves in rooms (Arch Intern Med. 1999 May 24;159[10]:1069-75). “Rest assured, you are not the only psychiatrist to face this type of issue,” Dr. Black said at the meeting, presented by Global Academy for Medical Education.
Common scenarios can include patients who want certain tests performed after researching symptoms online, threats of legal or social media action after feeling like they are not being listened to, a demand for a second opinion after not agreeing with a physician’s diagnosis, mistrust of doctors after presenting with symptoms and not being diagnosed, patients who focus on negative outcomes, and those who do not comply with treatment. These patients can often appear angry, defensive, frightened or resistant, or manipulative; may provide vague or exaggerated symptoms; or may inappropriately rely on hospital or clinic staff for emotional and physical support.
To complicate matters, the patients’ condition also might contribute to difficult interactions, such as in patients who have conditions like chronic pain or fibromyalgia.
“These often contribute because patients never feel that their problems are being appropriately addressed,” said Dr. Black, professor of psychiatry at the University of Iowa in Iowa City. Patients with psychiatric disorders can also present unique challenges that may result in difficult encounters. Patients with anxiety might not be able to be reassured by their doctor, for example, or patients with eating disorders might refuse treatment recommendations, he said.
Difficult encounters can lead to physicians feeling angry, upset, stressed, disrespected, abused, or fearful. But “it’s not just about the patient,” Dr. Black said. Physicians can become angry or defensive because of burnout, stress, or frustration, which can lead to them snapping at patients. Physicians are also overworked, sleep-deprived, and busier than they’d like to be, he added. Personal problems can contribute, and a physician’s belief system can cause a bad interaction with a patient. If physicians “label” one of their patients, that might end up becoming a “self-fulfilling prophecy” for that patient, Dr. Black said. Poor communication, such as not conveying bad news appropriately or with empathy, seeing a patient but never making eye contact, and using medical jargon that could be confusing to the patient, also can contribute to a challenging encounter, he added.
Situational issues also might create a bad experience for the patient. For example, a patient might find it hard to make an appointment, or the clinic might be busy or have a lack of privacy or encounter administrative issues. For patients who do not speak English as their native language, not having access to an interpreter can lead to frustration on the part of both the physician and the patient. “Bad interactions are not good for patient care,” Dr. Black said.
The key to resolving these issues is to focus on the goal, Dr. Black said. “We all want the same thing. We want to help the patient get better; we want to keep patients healthy; we want to keep them happy; we want to be fulfilled; [and] we want to manage our time and make a living – and meet our professional expectations.”
Begin by recognizing the difficult situation and assessing how the patient, the environment, or you might be contributing to the problem. “You have to step back and say what’s going on with this, and what are the factors that are combining to create this situation,” Dr. Black said. It is important to be calm and professional and not argue or talk over the patient. The goal is to work with the patient to find a solution.
One technique is to verbalize the problem without blaming the patient, the physician, or the environment (“We both have very different views about how your symptoms should be investigated, and that’s causing some difficulty between us. Do you agree?”).
There also might be alternative explanations for a patient’s behavior. For example, anger could be misdirected at a physician because of anxiety surrounding an unrelated event. In this case, it is important to listen to the patient and empathize, which will help the patient feel supported and build a rapport that can aid in resolving the problem encounter, Dr. Black said. Finding common ground when patients and physicians have different ideas on treatment or diagnosis is another way to help resolve a difficult encounter.
However, setting boundaries also is important, he noted. If, after remediation or if patients demonstrate signs of threatening or abusive behavior, initiate sexual advances, refuse to follow a treatment plan, fail to pay their bills, or are potentially putting themselves in harm’s way through noncompliance, a physician might consider terminating the relationship. Terminating the patient relationship should be done after attempting to work with the patient through a case manager and team members, and clearly advising a patient about behavior that could lead to termination of the patient-provider relationship.
Global Academy and this news organization are owned by the same parent company. Dr. Black reported that he is a consultant for Otsuka and receives royalties from American Psychiatric Publishing, Oxford University Press, and UpToDate. In addition, he receives funding from Nellie Ball Trust, the National Institute on Drug Abuse, the National Institute on Aging, and the National Center for Responsible Gaming.
FROM CP/AACP PSYCHIATRY UPDATE
Experts call for immediate suspension of ECT, others push back
Experts are calling for the immediate suspension of electroconvulsive therapy (ECT) for major depression.
A new review by investigators led by John Read, PhD, University of East London, conclude there is no evidence to show that ECT is effective in either its target demographic or its target diagnostic group. They say its use should be suspended until more robust research proves it is safe and effective.
However, the review’s conclusions have been met with passionate opposition from expert psychiatrists who say ECT can be a lifesaving treatment for patients, many of whom have exhausted all other treatment options. Other clinicians maintain that the review itself is fraught with methodologic shortcomings that invalidate its conclusions.
“We’ve concluded there is no adequate research on which to base an answer to the question, ‘Does ECT work?,’ ” Read told Medscape Medical News. “We’re not actually saying ECT doesn’t work. We’re saying there’s no way to know whether it works or not on the basis of the current research, which, after 80 years of the treatment being used, is pretty amazing.”
On the other hand, Read said there is substantial evidence to suggest ECT causes significant adverse events. “Depending who you ask, the psychiatrists or the patients, somewhere between 12% and 55% of patients get permanent or persistent memory loss,” he said.
“So there is a very serious cost to its use, and if there’s a serious cost, you ... have to know that there’s a very strong efficacy benefit, and we just don’t know that. That’s why we’re calling for suspension until there is adequate research,” Read added.
The study was published in a recent issue of Ethical Human Psychology and Psychiatry.
Widespread use
ECT remains a popular treatment modality for resistant depression. Global data show that it is used to treat almost a million patients every year. Although ECT continues to be the subject of comparative research, the investigators say that most of these studies do not adhere to the same standards that govern clinical trials of other psychiatric medications and medical interventions.
The investigators also note that to date, only 11 placebo-controlled studies of the efficacy of ECT have been conducted. They write that the last study to compare ECT with sham or simulated ECT (SECT) – in which a general anesthetic was administered but the electricity was not – was performed in 1985. Nevertheless, this relatively small body of evidence has been the basis of many meta-analyses.
In the current review, the authors evaluated the impartiality and robustness of these previous meta-analyses and the quality of the studies that were included.
“The primary goal is not to assess whether or not ECT is effective,” they write. “The intent, instead, is to determine whether the available evidence is robust enough to answer that question.”
For Read, the decision to analyze the current state of ECT research was both personal and professional.
“As a young nursing attendant in a Bronx hospital, I had the job of sitting with people as they came around from ECT. It was my job to try to explain why they didn’t know who they were, where they were, why their head was throbbing, and why people would do something like that to them,” he said.
“On the research side, this is my sixth review, and in each one we’ve reached the same conclusion,” Read added.
Other research stands in direct opposition to the current review’s findings. Many studies have concluded that ECT is safe and effective for patients with depression.
Ongoing debate
A 2018 registry analysis showed no additional risk for cognitive impairment in patients who underwent ECT up to 40 years after therapy. A 2018 study also showed that ECT was efficacious and cost-effective for patients with treatment-resistant depression.
However, the ECT debate continues. As reported early last year, there seems to be little common ground between clinicians who believe in the utility of ECT for depression and those who vehemently do not.
For the current review, Read and colleagues performed a Medline search for meta-analyses of the efficacy of ECT for depression. Meta-analyses were only included if they comprised placebo-controlled trials that compared ECT with SECT.
Once the meta-analyses were identified, investigators assessed their component studies. This assessment was conducted by two independent reviewers who used a 24-point quality scale developed by the authors. This scale, the authors note, combines the “risk of bias” domains of the Cochrane Handbook Risk of Bias Tool with criteria related to quality of study design and reporting, as well as several criteria specific to ECT research.
The two reviewers were blinded to each other’s ratings. Interrater differences were resolved collectively.
The literature search yielded 83 potential articles; after exclusion criteria were applied, 14 remained. Three of these articles were literature reviews, one discussed different types of statistical analyses used in ECT research, one was a meta-analysis in Hungarian, one was a meta-analysis that compared ECT with SECT in a selected population of elderly people, and three focused on transcranial magnetic stimulation.
This left five meta-analyses for the review. These included from 1 to 7 of the 11 studies in question:
- Janicak et al, 1985
- Kho, van Vreewijk, Simpson, & Zwinderman, 2003
- Mutz et al, 2019
- Pagnin, de Queiroz, Pini, & Cassano, 2004
- UK ECT Review Group, 2003
The review revealed shortcomings with both the meta-analyses and the studies they included. The investigators found that the mean quality scores of the 11 studies (10.27 ± 2.45 and 11.91 ± 2.91) were not statistically different between the two raters (P = .17), whose scores were significantly correlated (P = .001).
Among the 264 total ratings, the investigators found 55 inconsistencies, which were all resolved by discussion. The mean final quality score for the 11 studies included in the review was 12.27 ± 3.20/24; eight scored 13 or less.
The results of these studies do little to support the benefits of ECT relative to SECT, the reviewers note. Indeed, only four concluded that ECT is significantly superior to SECT. Five found no significant difference, and the remaining two had mixed results.
What’s more, only two of what the investigators describe as “higher quality” studies reported follow-up data. Of these, one produced an effect size of 0.065 favoring ECT, the other showed a small benefit in favor of SECT (effect size, 0.299).
The investigators describe the five meta-analyses included in the review as “flawed,” stating that the meta-analyses “pay little or no attention to the multiple limitations of the studies they include.”
These limitations include the number of patients included in the studies (which average 37 patients); lack of a description of randomization and blinding processes; lack of patient ratings; selective reporting of findings; and the absence of assessment of patient quality of life. Furthermore, the authors note that none of the 11 studies “convincingly” demonstrate double-blinding.
Given these shortcomings, the investigators say the meta-analyses of ECT fail to prove the following:
- The short- and long-term efficacy benefits of ECT over SECT;
- Whether ECT is effective among patients who have failed other treatments for depression;
- Whether ECT prevents ;
- Whether ECT improves patients’ quality of life;
- Whether ECT is more effective in women than men;
- Whether ECT is effective in children or adolescents.
“Shoddy” research
The authors conclude that the review’s findings demonstrate the weakness of evidence that currently supports the use of ECT for depression.
“I would never have guessed how shoddy some of this research was,” said review coauthor Irving Kirsch, PhD, a lecturer on medicine at Beth Israel Deaconess Medical Center, Boston. Many of these shortcomings, Kirsch said, involve blinding and placebo effects.
“It’s not clear how you could ever run a truly blinded trial of ECT, given how pronounced the immediate side effects are,” he told Medscape Medical News. “And one of the things that’s underappreciated is the pronounced responses to placebo treatment with depression and severe depression. These can last for a very long time.”
Kirsch noted that more invasive placebo treatments, such as SECT, tend to have more pronounced effects.
“Not all placebos are created equal. We know, for example, that placebo injections are more effective than placebo pills and that placebo surgery can be extremely powerful,” he said.
The authors call for an immediate suspension of ECT until new studies address these research shortcomings.
“The doctors who perform ECT aren’t evil or stupid, they’re just ignorant of the research. What they see is very temporary benefit in some of the patients. The research suggests that about a third – half at most – get a very temporary lift in mood, which seems to be the sort of euphoria you get from mild brain injury,” Read explained.
“I have seen people who haven’t spoken or eaten for several weeks start speaking and eating, but we know that 4 weeks later, they’re going to be just as depressed as they were, or worse. And now they’re going to have brain damage as well,” said Read.
He added that physicians often don’t see long-term patient outcomes, just the immediate effect of ECT.
A “lifesaver”
No recent randomized controlled trials regarding ECT have been conducted because “no IRB [institutional review board] on planet earth will allow such a trial because of the overwhelming evidence of efficacy and the risk of anesthesia with no ECT,” noted Mark S. George, MD, the Layton McCurdy Endowed Chair in Psychiatry at the Medical University of South Carolina, Charleston.
It is a “logical fallacy” to conclude that ECT does not work because the trials were flawed, said George, who was not involved with the current review
“This is not supported by anything they have looked at,” he told Medscape Medical News. “It’s not really a scientific study when you make conclusions that aren’t based on your data, or not what you set out to do. That’s what I find egregious here.”
The way he sees it, the utility of ECT is unquestionable. “It is our most effective acute treatment for depression, and it’s our most effective treatment for suicide,” he said.
“The authors of this review don’t see the patients that I see every day, who are catatonic, who can’t eat, who are suicidal. For those people, ECT is a lifesaver,” George added.
FDA’s position
Sameer Jauhar, MBChB, PhD, a consultant psychiatrist at the South London and Maudsley NHS Foundation Trust, London, was equally unimpressed with the quality of the review.
“I try to approach everything with an open mind,” he said. “But as a doctor, if I’m reading about evidence, I expect a well-conducted meta-analysis and/or very clear systematic review with an adequate level of peer review.”
The current review, said Jauhar, doesn’t meet these criteria. He said the article reads more like a narrative review, one in which the authors dictated their own arbitrary criteria of study quality.
Most important, he said, is the fact that ECT has been the focus of a great deal of research. “The best quality synthesis of the evidence I’ve come across is the UK ECT Review Group’s 2003 meta-analysis, published in The Lancet, which asked this very question. None of the studies has changed since then.”
Jauhar also noted that in 2018, the Food and Drug Administration reclassified ECT from class III (higher risk) to class II (moderate risk). Use of ECT was also limited to treatment of “catatonia or a severe major depressive episode associated with major depressive disorder or bipolar disorder in patients age 13 years and older who are treatment-resistant or who require a rapid response treatment due to the severity of their psychiatric or medical condition.”
The FDA also noted that “[t]he safe use of ECT for treatment of these conditions has been well studied and is better understood than other uses. Therefore, sufficient information exists to establish special controls that mitigate known risks and provide a reasonable assurance of safety and effectiveness for these two uses of ECT devices.”
As part of the FDA’s 2018 reclassification, ECT manufacturers were required to file a premarket approval application for all uses that were not reclassified. The full text of the order is available in the Federal Register.
“So the FDA has been through it, The Lancet has been through it, and the findings were clear,” said Jauhar. “It’s very easy to poke holes in studies that were conducted 30 or more years ago. But the fact is, the field has moved on.”
Jauhar acknowledged there are patients who have had bad experiences with ECT, and he accepts that such events occasionally occur. Nevertheless, he said,
Jauhar also noted that the journal in which the review was published has a 2019 CiteScore of 0.3 and ranks in the 15th percentile of the Scopus Clinical Psychology category. He further noted that Kirsch is a member of the journal’s editorial board.
“I would say that the level of peer review here was negligible at best,” Jauhar said. “In addition, the ‘findings’ are driven more by ideology than evidence.”
Asked to respond to Jauhar’s comments, Kirsch noted that although he is on the journal’s advisory board, he has not been actively involved. Kirsch added that he serves on about a dozen academic advisory boards and serves as a reviewer for many top scientific and medical journals, including The Journal of the American Medical Association and the New England Journal of Medicine.
“Our article was peer reviewed,” Kirsch said, “and we revised it following the first round of reviews.” The review process did not differ from those he has gone through with more than 250 published peer-reviewed articles on which he was an author or coauthor, he noted.
A growing movement
Despite such expert opposition, the movement to suspend ECT continues. Recently, Sarah Price Hancock, MS, CRC, CPMC, who is herself a recipient of more than 100 ECT treatments, authored an international petition to standardize, regulate, and audit the modality. Hancock hopes to present the document, which currently has more than 6600 signatures, to the American Psychiatric Association and similar international societies.
A version of the petition was presented to the UK’s National Health Service on July 2, the 59th anniversary of the death by suicide of Ernest Hemingway, who had received some 20 ECT treatments himself.
“Hopefully by his 60th anniversary, America and the world will be taking his death and the thousands living with adverse reactions more seriously by auditing, regulating, and tracking patients with a history of ECT to provide much needed comprehensive brain injury rehabilitation as necessary,” Hancock told Medscape Medical News.
Among the signatories of the petition is Sue Cunliffe, MbChB, who underwent ECT for depression in 2004, with devastating effects. “I was left really badly brain damaged, and so I’ve never been allowed to work again,” she told Medscape Medical News.
Cunliffe said the immediate effects of the treatment were profound. She said her hands shook, her balance and coordination were impaired, and her memories evaporated. However, she found a neuropsychologist who she says was able to help her recover control of her life. “Now at least I’m able to plan my life so that I can live with the brain damage.”
Kirsch acknowledged that sorting through the ECT literature can be daunting. “If you’re a physician, you try to keep up with the literature, but the problem is, the literature is so old and done in ways which would not pass muster right now. The data are really poor, and I guess it’s just that people aren’t aware of it.”
George agreed that the therapy is not without its shortcomings.
“Does ECT have cognitive side effects? Unfortunately, it does. But so do lots of lifesaving therapies in medicine, like cancer chemotherapy,” he said.
“Nobody really gets well with a single ECT session. It’s usually eight to 12 over 3 or 4 weeks. So it’s not particularly durable. That’s why we often combine ECT with other forms of brain stimulation,” George added.
He noted that the recent advent of alternative forms of ECT – including right unilateral ultrabrief pulse ECT and focal electrically administered seizure therapy – are beginning to address some of these shortcomings.
“The holy grail of brain stimulation is to be able to do things less invasively, and we’re moving slowly in that direction,” he said. “But right now, we don’t have anything that is as acutely as effective as ECT. It is our lifesaver at the moment.”
The review authors as well as George, Jauhar, Cunliffe, and Hancock report no relevant financial relationships.
This article first appeared on Medscape.com.
Experts are calling for the immediate suspension of electroconvulsive therapy (ECT) for major depression.
A new review by investigators led by John Read, PhD, University of East London, conclude there is no evidence to show that ECT is effective in either its target demographic or its target diagnostic group. They say its use should be suspended until more robust research proves it is safe and effective.
However, the review’s conclusions have been met with passionate opposition from expert psychiatrists who say ECT can be a lifesaving treatment for patients, many of whom have exhausted all other treatment options. Other clinicians maintain that the review itself is fraught with methodologic shortcomings that invalidate its conclusions.
“We’ve concluded there is no adequate research on which to base an answer to the question, ‘Does ECT work?,’ ” Read told Medscape Medical News. “We’re not actually saying ECT doesn’t work. We’re saying there’s no way to know whether it works or not on the basis of the current research, which, after 80 years of the treatment being used, is pretty amazing.”
On the other hand, Read said there is substantial evidence to suggest ECT causes significant adverse events. “Depending who you ask, the psychiatrists or the patients, somewhere between 12% and 55% of patients get permanent or persistent memory loss,” he said.
“So there is a very serious cost to its use, and if there’s a serious cost, you ... have to know that there’s a very strong efficacy benefit, and we just don’t know that. That’s why we’re calling for suspension until there is adequate research,” Read added.
The study was published in a recent issue of Ethical Human Psychology and Psychiatry.
Widespread use
ECT remains a popular treatment modality for resistant depression. Global data show that it is used to treat almost a million patients every year. Although ECT continues to be the subject of comparative research, the investigators say that most of these studies do not adhere to the same standards that govern clinical trials of other psychiatric medications and medical interventions.
The investigators also note that to date, only 11 placebo-controlled studies of the efficacy of ECT have been conducted. They write that the last study to compare ECT with sham or simulated ECT (SECT) – in which a general anesthetic was administered but the electricity was not – was performed in 1985. Nevertheless, this relatively small body of evidence has been the basis of many meta-analyses.
In the current review, the authors evaluated the impartiality and robustness of these previous meta-analyses and the quality of the studies that were included.
“The primary goal is not to assess whether or not ECT is effective,” they write. “The intent, instead, is to determine whether the available evidence is robust enough to answer that question.”
For Read, the decision to analyze the current state of ECT research was both personal and professional.
“As a young nursing attendant in a Bronx hospital, I had the job of sitting with people as they came around from ECT. It was my job to try to explain why they didn’t know who they were, where they were, why their head was throbbing, and why people would do something like that to them,” he said.
“On the research side, this is my sixth review, and in each one we’ve reached the same conclusion,” Read added.
Other research stands in direct opposition to the current review’s findings. Many studies have concluded that ECT is safe and effective for patients with depression.
Ongoing debate
A 2018 registry analysis showed no additional risk for cognitive impairment in patients who underwent ECT up to 40 years after therapy. A 2018 study also showed that ECT was efficacious and cost-effective for patients with treatment-resistant depression.
However, the ECT debate continues. As reported early last year, there seems to be little common ground between clinicians who believe in the utility of ECT for depression and those who vehemently do not.
For the current review, Read and colleagues performed a Medline search for meta-analyses of the efficacy of ECT for depression. Meta-analyses were only included if they comprised placebo-controlled trials that compared ECT with SECT.
Once the meta-analyses were identified, investigators assessed their component studies. This assessment was conducted by two independent reviewers who used a 24-point quality scale developed by the authors. This scale, the authors note, combines the “risk of bias” domains of the Cochrane Handbook Risk of Bias Tool with criteria related to quality of study design and reporting, as well as several criteria specific to ECT research.
The two reviewers were blinded to each other’s ratings. Interrater differences were resolved collectively.
The literature search yielded 83 potential articles; after exclusion criteria were applied, 14 remained. Three of these articles were literature reviews, one discussed different types of statistical analyses used in ECT research, one was a meta-analysis in Hungarian, one was a meta-analysis that compared ECT with SECT in a selected population of elderly people, and three focused on transcranial magnetic stimulation.
This left five meta-analyses for the review. These included from 1 to 7 of the 11 studies in question:
- Janicak et al, 1985
- Kho, van Vreewijk, Simpson, & Zwinderman, 2003
- Mutz et al, 2019
- Pagnin, de Queiroz, Pini, & Cassano, 2004
- UK ECT Review Group, 2003
The review revealed shortcomings with both the meta-analyses and the studies they included. The investigators found that the mean quality scores of the 11 studies (10.27 ± 2.45 and 11.91 ± 2.91) were not statistically different between the two raters (P = .17), whose scores were significantly correlated (P = .001).
Among the 264 total ratings, the investigators found 55 inconsistencies, which were all resolved by discussion. The mean final quality score for the 11 studies included in the review was 12.27 ± 3.20/24; eight scored 13 or less.
The results of these studies do little to support the benefits of ECT relative to SECT, the reviewers note. Indeed, only four concluded that ECT is significantly superior to SECT. Five found no significant difference, and the remaining two had mixed results.
What’s more, only two of what the investigators describe as “higher quality” studies reported follow-up data. Of these, one produced an effect size of 0.065 favoring ECT, the other showed a small benefit in favor of SECT (effect size, 0.299).
The investigators describe the five meta-analyses included in the review as “flawed,” stating that the meta-analyses “pay little or no attention to the multiple limitations of the studies they include.”
These limitations include the number of patients included in the studies (which average 37 patients); lack of a description of randomization and blinding processes; lack of patient ratings; selective reporting of findings; and the absence of assessment of patient quality of life. Furthermore, the authors note that none of the 11 studies “convincingly” demonstrate double-blinding.
Given these shortcomings, the investigators say the meta-analyses of ECT fail to prove the following:
- The short- and long-term efficacy benefits of ECT over SECT;
- Whether ECT is effective among patients who have failed other treatments for depression;
- Whether ECT prevents ;
- Whether ECT improves patients’ quality of life;
- Whether ECT is more effective in women than men;
- Whether ECT is effective in children or adolescents.
“Shoddy” research
The authors conclude that the review’s findings demonstrate the weakness of evidence that currently supports the use of ECT for depression.
“I would never have guessed how shoddy some of this research was,” said review coauthor Irving Kirsch, PhD, a lecturer on medicine at Beth Israel Deaconess Medical Center, Boston. Many of these shortcomings, Kirsch said, involve blinding and placebo effects.
“It’s not clear how you could ever run a truly blinded trial of ECT, given how pronounced the immediate side effects are,” he told Medscape Medical News. “And one of the things that’s underappreciated is the pronounced responses to placebo treatment with depression and severe depression. These can last for a very long time.”
Kirsch noted that more invasive placebo treatments, such as SECT, tend to have more pronounced effects.
“Not all placebos are created equal. We know, for example, that placebo injections are more effective than placebo pills and that placebo surgery can be extremely powerful,” he said.
The authors call for an immediate suspension of ECT until new studies address these research shortcomings.
“The doctors who perform ECT aren’t evil or stupid, they’re just ignorant of the research. What they see is very temporary benefit in some of the patients. The research suggests that about a third – half at most – get a very temporary lift in mood, which seems to be the sort of euphoria you get from mild brain injury,” Read explained.
“I have seen people who haven’t spoken or eaten for several weeks start speaking and eating, but we know that 4 weeks later, they’re going to be just as depressed as they were, or worse. And now they’re going to have brain damage as well,” said Read.
He added that physicians often don’t see long-term patient outcomes, just the immediate effect of ECT.
A “lifesaver”
No recent randomized controlled trials regarding ECT have been conducted because “no IRB [institutional review board] on planet earth will allow such a trial because of the overwhelming evidence of efficacy and the risk of anesthesia with no ECT,” noted Mark S. George, MD, the Layton McCurdy Endowed Chair in Psychiatry at the Medical University of South Carolina, Charleston.
It is a “logical fallacy” to conclude that ECT does not work because the trials were flawed, said George, who was not involved with the current review
“This is not supported by anything they have looked at,” he told Medscape Medical News. “It’s not really a scientific study when you make conclusions that aren’t based on your data, or not what you set out to do. That’s what I find egregious here.”
The way he sees it, the utility of ECT is unquestionable. “It is our most effective acute treatment for depression, and it’s our most effective treatment for suicide,” he said.
“The authors of this review don’t see the patients that I see every day, who are catatonic, who can’t eat, who are suicidal. For those people, ECT is a lifesaver,” George added.
FDA’s position
Sameer Jauhar, MBChB, PhD, a consultant psychiatrist at the South London and Maudsley NHS Foundation Trust, London, was equally unimpressed with the quality of the review.
“I try to approach everything with an open mind,” he said. “But as a doctor, if I’m reading about evidence, I expect a well-conducted meta-analysis and/or very clear systematic review with an adequate level of peer review.”
The current review, said Jauhar, doesn’t meet these criteria. He said the article reads more like a narrative review, one in which the authors dictated their own arbitrary criteria of study quality.
Most important, he said, is the fact that ECT has been the focus of a great deal of research. “The best quality synthesis of the evidence I’ve come across is the UK ECT Review Group’s 2003 meta-analysis, published in The Lancet, which asked this very question. None of the studies has changed since then.”
Jauhar also noted that in 2018, the Food and Drug Administration reclassified ECT from class III (higher risk) to class II (moderate risk). Use of ECT was also limited to treatment of “catatonia or a severe major depressive episode associated with major depressive disorder or bipolar disorder in patients age 13 years and older who are treatment-resistant or who require a rapid response treatment due to the severity of their psychiatric or medical condition.”
The FDA also noted that “[t]he safe use of ECT for treatment of these conditions has been well studied and is better understood than other uses. Therefore, sufficient information exists to establish special controls that mitigate known risks and provide a reasonable assurance of safety and effectiveness for these two uses of ECT devices.”
As part of the FDA’s 2018 reclassification, ECT manufacturers were required to file a premarket approval application for all uses that were not reclassified. The full text of the order is available in the Federal Register.
“So the FDA has been through it, The Lancet has been through it, and the findings were clear,” said Jauhar. “It’s very easy to poke holes in studies that were conducted 30 or more years ago. But the fact is, the field has moved on.”
Jauhar acknowledged there are patients who have had bad experiences with ECT, and he accepts that such events occasionally occur. Nevertheless, he said,
Jauhar also noted that the journal in which the review was published has a 2019 CiteScore of 0.3 and ranks in the 15th percentile of the Scopus Clinical Psychology category. He further noted that Kirsch is a member of the journal’s editorial board.
“I would say that the level of peer review here was negligible at best,” Jauhar said. “In addition, the ‘findings’ are driven more by ideology than evidence.”
Asked to respond to Jauhar’s comments, Kirsch noted that although he is on the journal’s advisory board, he has not been actively involved. Kirsch added that he serves on about a dozen academic advisory boards and serves as a reviewer for many top scientific and medical journals, including The Journal of the American Medical Association and the New England Journal of Medicine.
“Our article was peer reviewed,” Kirsch said, “and we revised it following the first round of reviews.” The review process did not differ from those he has gone through with more than 250 published peer-reviewed articles on which he was an author or coauthor, he noted.
A growing movement
Despite such expert opposition, the movement to suspend ECT continues. Recently, Sarah Price Hancock, MS, CRC, CPMC, who is herself a recipient of more than 100 ECT treatments, authored an international petition to standardize, regulate, and audit the modality. Hancock hopes to present the document, which currently has more than 6600 signatures, to the American Psychiatric Association and similar international societies.
A version of the petition was presented to the UK’s National Health Service on July 2, the 59th anniversary of the death by suicide of Ernest Hemingway, who had received some 20 ECT treatments himself.
“Hopefully by his 60th anniversary, America and the world will be taking his death and the thousands living with adverse reactions more seriously by auditing, regulating, and tracking patients with a history of ECT to provide much needed comprehensive brain injury rehabilitation as necessary,” Hancock told Medscape Medical News.
Among the signatories of the petition is Sue Cunliffe, MbChB, who underwent ECT for depression in 2004, with devastating effects. “I was left really badly brain damaged, and so I’ve never been allowed to work again,” she told Medscape Medical News.
Cunliffe said the immediate effects of the treatment were profound. She said her hands shook, her balance and coordination were impaired, and her memories evaporated. However, she found a neuropsychologist who she says was able to help her recover control of her life. “Now at least I’m able to plan my life so that I can live with the brain damage.”
Kirsch acknowledged that sorting through the ECT literature can be daunting. “If you’re a physician, you try to keep up with the literature, but the problem is, the literature is so old and done in ways which would not pass muster right now. The data are really poor, and I guess it’s just that people aren’t aware of it.”
George agreed that the therapy is not without its shortcomings.
“Does ECT have cognitive side effects? Unfortunately, it does. But so do lots of lifesaving therapies in medicine, like cancer chemotherapy,” he said.
“Nobody really gets well with a single ECT session. It’s usually eight to 12 over 3 or 4 weeks. So it’s not particularly durable. That’s why we often combine ECT with other forms of brain stimulation,” George added.
He noted that the recent advent of alternative forms of ECT – including right unilateral ultrabrief pulse ECT and focal electrically administered seizure therapy – are beginning to address some of these shortcomings.
“The holy grail of brain stimulation is to be able to do things less invasively, and we’re moving slowly in that direction,” he said. “But right now, we don’t have anything that is as acutely as effective as ECT. It is our lifesaver at the moment.”
The review authors as well as George, Jauhar, Cunliffe, and Hancock report no relevant financial relationships.
This article first appeared on Medscape.com.
Experts are calling for the immediate suspension of electroconvulsive therapy (ECT) for major depression.
A new review by investigators led by John Read, PhD, University of East London, conclude there is no evidence to show that ECT is effective in either its target demographic or its target diagnostic group. They say its use should be suspended until more robust research proves it is safe and effective.
However, the review’s conclusions have been met with passionate opposition from expert psychiatrists who say ECT can be a lifesaving treatment for patients, many of whom have exhausted all other treatment options. Other clinicians maintain that the review itself is fraught with methodologic shortcomings that invalidate its conclusions.
“We’ve concluded there is no adequate research on which to base an answer to the question, ‘Does ECT work?,’ ” Read told Medscape Medical News. “We’re not actually saying ECT doesn’t work. We’re saying there’s no way to know whether it works or not on the basis of the current research, which, after 80 years of the treatment being used, is pretty amazing.”
On the other hand, Read said there is substantial evidence to suggest ECT causes significant adverse events. “Depending who you ask, the psychiatrists or the patients, somewhere between 12% and 55% of patients get permanent or persistent memory loss,” he said.
“So there is a very serious cost to its use, and if there’s a serious cost, you ... have to know that there’s a very strong efficacy benefit, and we just don’t know that. That’s why we’re calling for suspension until there is adequate research,” Read added.
The study was published in a recent issue of Ethical Human Psychology and Psychiatry.
Widespread use
ECT remains a popular treatment modality for resistant depression. Global data show that it is used to treat almost a million patients every year. Although ECT continues to be the subject of comparative research, the investigators say that most of these studies do not adhere to the same standards that govern clinical trials of other psychiatric medications and medical interventions.
The investigators also note that to date, only 11 placebo-controlled studies of the efficacy of ECT have been conducted. They write that the last study to compare ECT with sham or simulated ECT (SECT) – in which a general anesthetic was administered but the electricity was not – was performed in 1985. Nevertheless, this relatively small body of evidence has been the basis of many meta-analyses.
In the current review, the authors evaluated the impartiality and robustness of these previous meta-analyses and the quality of the studies that were included.
“The primary goal is not to assess whether or not ECT is effective,” they write. “The intent, instead, is to determine whether the available evidence is robust enough to answer that question.”
For Read, the decision to analyze the current state of ECT research was both personal and professional.
“As a young nursing attendant in a Bronx hospital, I had the job of sitting with people as they came around from ECT. It was my job to try to explain why they didn’t know who they were, where they were, why their head was throbbing, and why people would do something like that to them,” he said.
“On the research side, this is my sixth review, and in each one we’ve reached the same conclusion,” Read added.
Other research stands in direct opposition to the current review’s findings. Many studies have concluded that ECT is safe and effective for patients with depression.
Ongoing debate
A 2018 registry analysis showed no additional risk for cognitive impairment in patients who underwent ECT up to 40 years after therapy. A 2018 study also showed that ECT was efficacious and cost-effective for patients with treatment-resistant depression.
However, the ECT debate continues. As reported early last year, there seems to be little common ground between clinicians who believe in the utility of ECT for depression and those who vehemently do not.
For the current review, Read and colleagues performed a Medline search for meta-analyses of the efficacy of ECT for depression. Meta-analyses were only included if they comprised placebo-controlled trials that compared ECT with SECT.
Once the meta-analyses were identified, investigators assessed their component studies. This assessment was conducted by two independent reviewers who used a 24-point quality scale developed by the authors. This scale, the authors note, combines the “risk of bias” domains of the Cochrane Handbook Risk of Bias Tool with criteria related to quality of study design and reporting, as well as several criteria specific to ECT research.
The two reviewers were blinded to each other’s ratings. Interrater differences were resolved collectively.
The literature search yielded 83 potential articles; after exclusion criteria were applied, 14 remained. Three of these articles were literature reviews, one discussed different types of statistical analyses used in ECT research, one was a meta-analysis in Hungarian, one was a meta-analysis that compared ECT with SECT in a selected population of elderly people, and three focused on transcranial magnetic stimulation.
This left five meta-analyses for the review. These included from 1 to 7 of the 11 studies in question:
- Janicak et al, 1985
- Kho, van Vreewijk, Simpson, & Zwinderman, 2003
- Mutz et al, 2019
- Pagnin, de Queiroz, Pini, & Cassano, 2004
- UK ECT Review Group, 2003
The review revealed shortcomings with both the meta-analyses and the studies they included. The investigators found that the mean quality scores of the 11 studies (10.27 ± 2.45 and 11.91 ± 2.91) were not statistically different between the two raters (P = .17), whose scores were significantly correlated (P = .001).
Among the 264 total ratings, the investigators found 55 inconsistencies, which were all resolved by discussion. The mean final quality score for the 11 studies included in the review was 12.27 ± 3.20/24; eight scored 13 or less.
The results of these studies do little to support the benefits of ECT relative to SECT, the reviewers note. Indeed, only four concluded that ECT is significantly superior to SECT. Five found no significant difference, and the remaining two had mixed results.
What’s more, only two of what the investigators describe as “higher quality” studies reported follow-up data. Of these, one produced an effect size of 0.065 favoring ECT, the other showed a small benefit in favor of SECT (effect size, 0.299).
The investigators describe the five meta-analyses included in the review as “flawed,” stating that the meta-analyses “pay little or no attention to the multiple limitations of the studies they include.”
These limitations include the number of patients included in the studies (which average 37 patients); lack of a description of randomization and blinding processes; lack of patient ratings; selective reporting of findings; and the absence of assessment of patient quality of life. Furthermore, the authors note that none of the 11 studies “convincingly” demonstrate double-blinding.
Given these shortcomings, the investigators say the meta-analyses of ECT fail to prove the following:
- The short- and long-term efficacy benefits of ECT over SECT;
- Whether ECT is effective among patients who have failed other treatments for depression;
- Whether ECT prevents ;
- Whether ECT improves patients’ quality of life;
- Whether ECT is more effective in women than men;
- Whether ECT is effective in children or adolescents.
“Shoddy” research
The authors conclude that the review’s findings demonstrate the weakness of evidence that currently supports the use of ECT for depression.
“I would never have guessed how shoddy some of this research was,” said review coauthor Irving Kirsch, PhD, a lecturer on medicine at Beth Israel Deaconess Medical Center, Boston. Many of these shortcomings, Kirsch said, involve blinding and placebo effects.
“It’s not clear how you could ever run a truly blinded trial of ECT, given how pronounced the immediate side effects are,” he told Medscape Medical News. “And one of the things that’s underappreciated is the pronounced responses to placebo treatment with depression and severe depression. These can last for a very long time.”
Kirsch noted that more invasive placebo treatments, such as SECT, tend to have more pronounced effects.
“Not all placebos are created equal. We know, for example, that placebo injections are more effective than placebo pills and that placebo surgery can be extremely powerful,” he said.
The authors call for an immediate suspension of ECT until new studies address these research shortcomings.
“The doctors who perform ECT aren’t evil or stupid, they’re just ignorant of the research. What they see is very temporary benefit in some of the patients. The research suggests that about a third – half at most – get a very temporary lift in mood, which seems to be the sort of euphoria you get from mild brain injury,” Read explained.
“I have seen people who haven’t spoken or eaten for several weeks start speaking and eating, but we know that 4 weeks later, they’re going to be just as depressed as they were, or worse. And now they’re going to have brain damage as well,” said Read.
He added that physicians often don’t see long-term patient outcomes, just the immediate effect of ECT.
A “lifesaver”
No recent randomized controlled trials regarding ECT have been conducted because “no IRB [institutional review board] on planet earth will allow such a trial because of the overwhelming evidence of efficacy and the risk of anesthesia with no ECT,” noted Mark S. George, MD, the Layton McCurdy Endowed Chair in Psychiatry at the Medical University of South Carolina, Charleston.
It is a “logical fallacy” to conclude that ECT does not work because the trials were flawed, said George, who was not involved with the current review
“This is not supported by anything they have looked at,” he told Medscape Medical News. “It’s not really a scientific study when you make conclusions that aren’t based on your data, or not what you set out to do. That’s what I find egregious here.”
The way he sees it, the utility of ECT is unquestionable. “It is our most effective acute treatment for depression, and it’s our most effective treatment for suicide,” he said.
“The authors of this review don’t see the patients that I see every day, who are catatonic, who can’t eat, who are suicidal. For those people, ECT is a lifesaver,” George added.
FDA’s position
Sameer Jauhar, MBChB, PhD, a consultant psychiatrist at the South London and Maudsley NHS Foundation Trust, London, was equally unimpressed with the quality of the review.
“I try to approach everything with an open mind,” he said. “But as a doctor, if I’m reading about evidence, I expect a well-conducted meta-analysis and/or very clear systematic review with an adequate level of peer review.”
The current review, said Jauhar, doesn’t meet these criteria. He said the article reads more like a narrative review, one in which the authors dictated their own arbitrary criteria of study quality.
Most important, he said, is the fact that ECT has been the focus of a great deal of research. “The best quality synthesis of the evidence I’ve come across is the UK ECT Review Group’s 2003 meta-analysis, published in The Lancet, which asked this very question. None of the studies has changed since then.”
Jauhar also noted that in 2018, the Food and Drug Administration reclassified ECT from class III (higher risk) to class II (moderate risk). Use of ECT was also limited to treatment of “catatonia or a severe major depressive episode associated with major depressive disorder or bipolar disorder in patients age 13 years and older who are treatment-resistant or who require a rapid response treatment due to the severity of their psychiatric or medical condition.”
The FDA also noted that “[t]he safe use of ECT for treatment of these conditions has been well studied and is better understood than other uses. Therefore, sufficient information exists to establish special controls that mitigate known risks and provide a reasonable assurance of safety and effectiveness for these two uses of ECT devices.”
As part of the FDA’s 2018 reclassification, ECT manufacturers were required to file a premarket approval application for all uses that were not reclassified. The full text of the order is available in the Federal Register.
“So the FDA has been through it, The Lancet has been through it, and the findings were clear,” said Jauhar. “It’s very easy to poke holes in studies that were conducted 30 or more years ago. But the fact is, the field has moved on.”
Jauhar acknowledged there are patients who have had bad experiences with ECT, and he accepts that such events occasionally occur. Nevertheless, he said,
Jauhar also noted that the journal in which the review was published has a 2019 CiteScore of 0.3 and ranks in the 15th percentile of the Scopus Clinical Psychology category. He further noted that Kirsch is a member of the journal’s editorial board.
“I would say that the level of peer review here was negligible at best,” Jauhar said. “In addition, the ‘findings’ are driven more by ideology than evidence.”
Asked to respond to Jauhar’s comments, Kirsch noted that although he is on the journal’s advisory board, he has not been actively involved. Kirsch added that he serves on about a dozen academic advisory boards and serves as a reviewer for many top scientific and medical journals, including The Journal of the American Medical Association and the New England Journal of Medicine.
“Our article was peer reviewed,” Kirsch said, “and we revised it following the first round of reviews.” The review process did not differ from those he has gone through with more than 250 published peer-reviewed articles on which he was an author or coauthor, he noted.
A growing movement
Despite such expert opposition, the movement to suspend ECT continues. Recently, Sarah Price Hancock, MS, CRC, CPMC, who is herself a recipient of more than 100 ECT treatments, authored an international petition to standardize, regulate, and audit the modality. Hancock hopes to present the document, which currently has more than 6600 signatures, to the American Psychiatric Association and similar international societies.
A version of the petition was presented to the UK’s National Health Service on July 2, the 59th anniversary of the death by suicide of Ernest Hemingway, who had received some 20 ECT treatments himself.
“Hopefully by his 60th anniversary, America and the world will be taking his death and the thousands living with adverse reactions more seriously by auditing, regulating, and tracking patients with a history of ECT to provide much needed comprehensive brain injury rehabilitation as necessary,” Hancock told Medscape Medical News.
Among the signatories of the petition is Sue Cunliffe, MbChB, who underwent ECT for depression in 2004, with devastating effects. “I was left really badly brain damaged, and so I’ve never been allowed to work again,” she told Medscape Medical News.
Cunliffe said the immediate effects of the treatment were profound. She said her hands shook, her balance and coordination were impaired, and her memories evaporated. However, she found a neuropsychologist who she says was able to help her recover control of her life. “Now at least I’m able to plan my life so that I can live with the brain damage.”
Kirsch acknowledged that sorting through the ECT literature can be daunting. “If you’re a physician, you try to keep up with the literature, but the problem is, the literature is so old and done in ways which would not pass muster right now. The data are really poor, and I guess it’s just that people aren’t aware of it.”
George agreed that the therapy is not without its shortcomings.
“Does ECT have cognitive side effects? Unfortunately, it does. But so do lots of lifesaving therapies in medicine, like cancer chemotherapy,” he said.
“Nobody really gets well with a single ECT session. It’s usually eight to 12 over 3 or 4 weeks. So it’s not particularly durable. That’s why we often combine ECT with other forms of brain stimulation,” George added.
He noted that the recent advent of alternative forms of ECT – including right unilateral ultrabrief pulse ECT and focal electrically administered seizure therapy – are beginning to address some of these shortcomings.
“The holy grail of brain stimulation is to be able to do things less invasively, and we’re moving slowly in that direction,” he said. “But right now, we don’t have anything that is as acutely as effective as ECT. It is our lifesaver at the moment.”
The review authors as well as George, Jauhar, Cunliffe, and Hancock report no relevant financial relationships.
This article first appeared on Medscape.com.
More than half of psychiatrists have net worth under $1 million
Most psychiatrists live at or below their means, and more than half have a net worth of less than $1 million, according to the Medscape Psychiatrist Debt and Net Worth Report 2020.
An important caveat, however, is that the data for this year’s report were collected as part of the Medscape Physician Compensation Report 2020, prior to Feb. 11, 2020 – and before COVID-19 was declared a pandemic.
Although it will be some time before medical practices become accustomed to a new version of normal,
Among the lowest earners
According to the Medscape Psychiatrist Compensation Report 2020, psychiatrists are among the lowest earners of all physicians, earning $268,000 on average this year. However, that’s up somewhat from last year’s earnings of $260,000.
Among psychiatrists, 57% report a net worth (total assets minus total liabilities) of less than $1 million; 38% have a net worth between $1 million and $5 million, and 5% top $5 million in net worth.
Among specialists, orthopedists are most likely (at 19%) to top the $5 million level, followed by plastic surgeons and gastroenterologists (both at 16%), according to the overall Medscape Physician Debt and Net Worth Report 2020. The report is based on more than 17,000 physicians and spans 30 specialties.
By gender, more female than male psychiatrists have a net worth of less than $1 million (61% vs. 53%). The percentages are closer between female and male psychiatrists who have a net worth between $1 million and $5 million, at 36% and 41%, respectively. In addition, more male than female psychiatrists have a net worth above $5 million (6% vs. 3%).
As expected, the older the physician, the more money they have as earnings increase and early-career debt decreases. This is the case for psychiatrists, whose net worth over $1 million increased with age.
However, psychiatrists are among the most likely of all physicians to have a net worth of less than $500,000 (at 37%), which is on par with public health and preventive medicine physicians (also at 37%) and just below family medicine physicians (at 46%), pediatricians (44%), neurologists (41%), and internal medicine physicians (40%).
For nearly two-thirds of psychiatrists (63%), mortgage payments on their primary residence are the major expense; 39% of psychiatrists have a mortgage of $300,000 or less, and 12% have a mortgage topping $500,000; 31% have no mortgage at all. Six in 10 psychiatrists live in a house that is 3,000 sq ft or smaller.
Mortgage aside, other top ongoing expenses for psychiatrists are car payments (38%), school loan payments (28%), credit card debt (26%), and medical expenses for self or loved one (20%). At 28%, psychiatrists are toward the top of the list of all physicians when it comes to those still paying off loans for education.
Spending vs. saving
The average American has four credit cards, according to the credit reporting agency Experian. More than half of psychiatrists said they have four or fewer credit cards (35% have three or four credit cards, 20% have one or two cards, and 1% have none). A quarter of psychiatrists (25%) have five or six credit cards, and 19% have seven or more at their disposal.
Only a small percentage of psychiatrists (7%) say they live above their means; 53% live at their means, and 39% live below their means.
Most psychiatrists (62%) contribute $1,000 or more to a tax-deferred retirement or college savings account each month; 13% do not do this on a regular basis. Nearly two-thirds (65%) of psychiatrists contribute to a taxable savings account, a tool many use when tax-deferred contributions have reached their limit.
Nearly half of psychiatrists (47%) rely on a mental budget for personal expenses; 16% rely on a written budget or use software or an app for budgeting; and 37% don’t have a budget for personal expenses.
Three-quarters of psychiatrists did not experience a financial loss in 2019. Of those who did have a loss, the main causes were bad investments (6%) and practice-related problems (6%). Other factors were job loss (self or spouse/partner), real estate loss (4%), legal fees (3%), and divorce (3%).
Among psychiatrists who have joint finances with a spouse or partner, 51% pool their income to pay household expenses. For 14%, the person who earns more pays more of the bills and/or expenses. Only a small percentage divide bills and expenses equally, regardless of how much each makes (5%).
About 43% of psychiatrists currently work with a financial planner or have done so in the past, 40% never did, and 17% met with a financial planner but did not pursue working with that person.
A version of this article originally appeared on Medscape.com.
Most psychiatrists live at or below their means, and more than half have a net worth of less than $1 million, according to the Medscape Psychiatrist Debt and Net Worth Report 2020.
An important caveat, however, is that the data for this year’s report were collected as part of the Medscape Physician Compensation Report 2020, prior to Feb. 11, 2020 – and before COVID-19 was declared a pandemic.
Although it will be some time before medical practices become accustomed to a new version of normal,
Among the lowest earners
According to the Medscape Psychiatrist Compensation Report 2020, psychiatrists are among the lowest earners of all physicians, earning $268,000 on average this year. However, that’s up somewhat from last year’s earnings of $260,000.
Among psychiatrists, 57% report a net worth (total assets minus total liabilities) of less than $1 million; 38% have a net worth between $1 million and $5 million, and 5% top $5 million in net worth.
Among specialists, orthopedists are most likely (at 19%) to top the $5 million level, followed by plastic surgeons and gastroenterologists (both at 16%), according to the overall Medscape Physician Debt and Net Worth Report 2020. The report is based on more than 17,000 physicians and spans 30 specialties.
By gender, more female than male psychiatrists have a net worth of less than $1 million (61% vs. 53%). The percentages are closer between female and male psychiatrists who have a net worth between $1 million and $5 million, at 36% and 41%, respectively. In addition, more male than female psychiatrists have a net worth above $5 million (6% vs. 3%).
As expected, the older the physician, the more money they have as earnings increase and early-career debt decreases. This is the case for psychiatrists, whose net worth over $1 million increased with age.
However, psychiatrists are among the most likely of all physicians to have a net worth of less than $500,000 (at 37%), which is on par with public health and preventive medicine physicians (also at 37%) and just below family medicine physicians (at 46%), pediatricians (44%), neurologists (41%), and internal medicine physicians (40%).
For nearly two-thirds of psychiatrists (63%), mortgage payments on their primary residence are the major expense; 39% of psychiatrists have a mortgage of $300,000 or less, and 12% have a mortgage topping $500,000; 31% have no mortgage at all. Six in 10 psychiatrists live in a house that is 3,000 sq ft or smaller.
Mortgage aside, other top ongoing expenses for psychiatrists are car payments (38%), school loan payments (28%), credit card debt (26%), and medical expenses for self or loved one (20%). At 28%, psychiatrists are toward the top of the list of all physicians when it comes to those still paying off loans for education.
Spending vs. saving
The average American has four credit cards, according to the credit reporting agency Experian. More than half of psychiatrists said they have four or fewer credit cards (35% have three or four credit cards, 20% have one or two cards, and 1% have none). A quarter of psychiatrists (25%) have five or six credit cards, and 19% have seven or more at their disposal.
Only a small percentage of psychiatrists (7%) say they live above their means; 53% live at their means, and 39% live below their means.
Most psychiatrists (62%) contribute $1,000 or more to a tax-deferred retirement or college savings account each month; 13% do not do this on a regular basis. Nearly two-thirds (65%) of psychiatrists contribute to a taxable savings account, a tool many use when tax-deferred contributions have reached their limit.
Nearly half of psychiatrists (47%) rely on a mental budget for personal expenses; 16% rely on a written budget or use software or an app for budgeting; and 37% don’t have a budget for personal expenses.
Three-quarters of psychiatrists did not experience a financial loss in 2019. Of those who did have a loss, the main causes were bad investments (6%) and practice-related problems (6%). Other factors were job loss (self or spouse/partner), real estate loss (4%), legal fees (3%), and divorce (3%).
Among psychiatrists who have joint finances with a spouse or partner, 51% pool their income to pay household expenses. For 14%, the person who earns more pays more of the bills and/or expenses. Only a small percentage divide bills and expenses equally, regardless of how much each makes (5%).
About 43% of psychiatrists currently work with a financial planner or have done so in the past, 40% never did, and 17% met with a financial planner but did not pursue working with that person.
A version of this article originally appeared on Medscape.com.
Most psychiatrists live at or below their means, and more than half have a net worth of less than $1 million, according to the Medscape Psychiatrist Debt and Net Worth Report 2020.
An important caveat, however, is that the data for this year’s report were collected as part of the Medscape Physician Compensation Report 2020, prior to Feb. 11, 2020 – and before COVID-19 was declared a pandemic.
Although it will be some time before medical practices become accustomed to a new version of normal,
Among the lowest earners
According to the Medscape Psychiatrist Compensation Report 2020, psychiatrists are among the lowest earners of all physicians, earning $268,000 on average this year. However, that’s up somewhat from last year’s earnings of $260,000.
Among psychiatrists, 57% report a net worth (total assets minus total liabilities) of less than $1 million; 38% have a net worth between $1 million and $5 million, and 5% top $5 million in net worth.
Among specialists, orthopedists are most likely (at 19%) to top the $5 million level, followed by plastic surgeons and gastroenterologists (both at 16%), according to the overall Medscape Physician Debt and Net Worth Report 2020. The report is based on more than 17,000 physicians and spans 30 specialties.
By gender, more female than male psychiatrists have a net worth of less than $1 million (61% vs. 53%). The percentages are closer between female and male psychiatrists who have a net worth between $1 million and $5 million, at 36% and 41%, respectively. In addition, more male than female psychiatrists have a net worth above $5 million (6% vs. 3%).
As expected, the older the physician, the more money they have as earnings increase and early-career debt decreases. This is the case for psychiatrists, whose net worth over $1 million increased with age.
However, psychiatrists are among the most likely of all physicians to have a net worth of less than $500,000 (at 37%), which is on par with public health and preventive medicine physicians (also at 37%) and just below family medicine physicians (at 46%), pediatricians (44%), neurologists (41%), and internal medicine physicians (40%).
For nearly two-thirds of psychiatrists (63%), mortgage payments on their primary residence are the major expense; 39% of psychiatrists have a mortgage of $300,000 or less, and 12% have a mortgage topping $500,000; 31% have no mortgage at all. Six in 10 psychiatrists live in a house that is 3,000 sq ft or smaller.
Mortgage aside, other top ongoing expenses for psychiatrists are car payments (38%), school loan payments (28%), credit card debt (26%), and medical expenses for self or loved one (20%). At 28%, psychiatrists are toward the top of the list of all physicians when it comes to those still paying off loans for education.
Spending vs. saving
The average American has four credit cards, according to the credit reporting agency Experian. More than half of psychiatrists said they have four or fewer credit cards (35% have three or four credit cards, 20% have one or two cards, and 1% have none). A quarter of psychiatrists (25%) have five or six credit cards, and 19% have seven or more at their disposal.
Only a small percentage of psychiatrists (7%) say they live above their means; 53% live at their means, and 39% live below their means.
Most psychiatrists (62%) contribute $1,000 or more to a tax-deferred retirement or college savings account each month; 13% do not do this on a regular basis. Nearly two-thirds (65%) of psychiatrists contribute to a taxable savings account, a tool many use when tax-deferred contributions have reached their limit.
Nearly half of psychiatrists (47%) rely on a mental budget for personal expenses; 16% rely on a written budget or use software or an app for budgeting; and 37% don’t have a budget for personal expenses.
Three-quarters of psychiatrists did not experience a financial loss in 2019. Of those who did have a loss, the main causes were bad investments (6%) and practice-related problems (6%). Other factors were job loss (self or spouse/partner), real estate loss (4%), legal fees (3%), and divorce (3%).
Among psychiatrists who have joint finances with a spouse or partner, 51% pool their income to pay household expenses. For 14%, the person who earns more pays more of the bills and/or expenses. Only a small percentage divide bills and expenses equally, regardless of how much each makes (5%).
About 43% of psychiatrists currently work with a financial planner or have done so in the past, 40% never did, and 17% met with a financial planner but did not pursue working with that person.
A version of this article originally appeared on Medscape.com.