User login
Bringing you the latest news, research and reviews, exclusive interviews, podcasts, quizzes, and more.
div[contains(@class, 'header__large-screen')]
div[contains(@class, 'read-next-article')]
div[contains(@class, 'main-prefix')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
footer[@id='footer']
section[contains(@class, 'nav-hidden')]
div[contains(@class, 'ce-card-content')]
nav[contains(@class, 'nav-ce-stack')]
div[contains(@class, 'view-medstat-quiz-listing-panes')]
div[contains(@class, 'pane-article-sidebar-latest-news')]
div[contains(@class, 'medstat-accordion-set article-series')]
Why Do Investigational OA Drugs Need Better Trial Endpoints? Lorecivivint Serves as an Example
VIENNA — The hypothesis that pivotal clinical trials for osteoarthritis (OA)-modifying therapies are not using appropriate designs or endpoints appears to be consistent with the recent failure of the phase 3 trial of the investigational agent lorecivivint, according to experts tackling this issue.
For the elusive target of disease-modifying OA drugs (DMOADs), “there have been a lot of developments in the last few years but so far a lot of disappointments,” said Francis Berenbaum, MD, PhD, head of the department of rheumatology, Saint-Antoine Hospital, Paris, France.
Disagreement on the target most likely to favorably alter the natural history of disease might be the key issue. Dr. Berenbaum considers it essential to determine which changes in the joint signify a favorable drug effect and will lead to what regulatory agencies consider a clinically meaningful benefit. These include improved function and long-term preservation of the joint, as well as symptom control.
Of primary targets to modify the course of OA, cartilage is not one of them, according to Dr. Berenbaum, who spoke in a session on DMOADs and regenerative OA therapies at the annual European Congress of Rheumatology.
OA Is Not a Cartilage-Only Disease
“There is now a big consensus that osteoarthritis is not a cartilage-only disease,” he said. Rather, he addressed the inadequate appreciation of the “whole joint” pathology that underlies OA. He called for a fundamental “paradigm change” to work toward a disease-modifying effect that produces benefit on a hard endpoint.
There are multiple steps needed to work toward this goal after a consensus is reached on a meaningful surrogate endpoint, Dr. Berenbaum said. While symptom reduction is a good start, he called for evidence of disease attenuation or a regenerative effect on an important surrogate such as improved integrity of synovial tissue and improved bone health. Such surrogates are necessary to guide DMOAD development but not sufficient. The proof that a therapy is a DMOAD depends on a favorable effect on a hard endpoint. In the case of the knee, freedom from joint replacement is an example, Dr. Berenbaum said.
Philip G. Conaghan, MBBS, PhD, director of rheumatic and musculoskeletal medicine, University of Leeds, England, agreed with this general premise. Speaking just before Dr. Berenbaum in the same session, Dr. Conaghan traced this history of the effort to create DMOADs and updated those in clinical trials.

In his talk, he listed some of the many disappointments, including those which have targeted cartilage thickness, before updating the numerous ongoing development programs. There are many targets that appear viable, but none are in final stages of testing.
In remarks to this news organization, he said he generally agreed with Dr. Berenbaum about the need for greater rigor for developing drugs to meet regulatory criteria for disease-modifying effects.
Of the drugs he reviewed, Dr. Conaghan identified lorecivivint, an intra-articular CLK/DYRK inhibitor that’s thought to modulate Wnt and inflammatory pathways, as the only drug with DMOAD potential to go to a multicenter phase 3 trial so far. The drug’s negative outcome in phase 3 was particularly disappointing after the substantial promise shown in a phase 2b study published in 2021.
In the phase 3 study, lorecivivint, relative to placebo, did not achieve a significant improvement in the primary endpoint of improved medial joint space width (JSW) in the target knee as assessed at the end of a 48-week, double-blind trial.
New Follow-Up Data Support DMOAD Activity
Yet, additional extension data from the phase 3 lorecivivint trial presented in the EULAR DMOAD session challenge the conclusion even if they do not change the results.
The new data presented at EULAR is the second of two sets of extension data. The first, reported earlier, involved an analysis at 96 weeks or 48 weeks after the double-blind trial. At the beginning of this extension, lorecivivint-start patients had received a second intraarticular injection of 0.07 mg, while placebo patients were crossed over to receive their first injection.
Over the course of this first extension, the gradual loss in medial JSW observed from baseline to the end of the initial 48 weeks had plateaued in those treated with lorecivivint, but the decline continued in the placebo group. As a result, the lorecivivint-start patients had a numerical but not a statistically significant advantage for medial JSW over the placebo-switch group, according to Yusuf Yazici, MD, chief medical officer of Biosplice Therapeutics, San Diego, which developed lorecivivint.
In a second open-label extension described by Dr. Yazici at EULAR 2024, a third injection was administered to the lorecivivint-start patients and a second injection to the placebo-start patients. After 52 more weeks of follow-up, there were now 3 years of follow-up in the lorecivivint-start group and 2 years of follow-up in the placebo-start group.
At the end of this second extension, lorecivivint-start patients had a median increase in JSW that was approaching the baseline level at study entry. Although the placebo-start group had experienced a decline in the medial JSW at the end of the first extension when they had received one injection, JSW had also improved in the direction of baseline after a second injection with 2 years of follow-up. The advantage of three injections of lorecivivint over 3 years had now reached statistical significance (P = .031) despite the improvement seen in the placebo-start group following two injections over 2 years.
At 3 Years, Benefit Is Finally Potentially Significant
If placebo-treated patients had not received a second shot of lorecivivint and progressed at the rate seen before their second shot, the hypothetical trajectory would have provided lorecivivint with a highly statistically significant advantage (P < .001), said Dr. Yazici, displaying a hypothetical graph.
Along with improvements in pain and function associated with lorecivivint relative to placebo at 6 months, 12 months, and 24 months, the structural improvements in 3 years now suggest that “long-term treatment with lorecivivint has the potential to be a DMOAD for knee OA,” Dr. Yazici said.
While Dr. Berenbaum did not comment on this speculation, he did note the potential need for long-term studies to prove a disease-modifying effect in OA. This is the rationale for identifying surrogates.
To illustrate this point, Dr. Berenbaum made an analogy between OA and cardiovascular disease. In cardiovascular disease, surrogates of disease-modifying therapies, such as control of hypertension or hyperlipidemia, are accepted by regulatory agencies on the basis of their proven association with hard endpoints, such as myocardial infarction, stroke, or cardiovascular death. Like joint failure, these events can take years or decades to arise.
“For trials in OA, we need to agree on these surrogates,” Dr. Berenbaum said, although he acknowledged that they would then have to be validated. Noting that the US Food and Drug Administration has now identified OA as a serious disease for which accelerated drug approvals will be considered to address an unmet need, Dr. Berenbaum suggested there is an even greater impetus for improving strategies for DMOAD development.
Dr. Berenbaum reported financial relationships with Grünenthal, GlaxoSmithKline, Eli Lilly, Novartis, Pfizer, and Servier. Dr. Conaghan reported financial relationships with AbbVie, AstraZeneca, Eli Lilly, Galapagos, GlaxoSmithKline, Grünenthal, Janssen, Levicept, Merck, Novartis, Pfizer, Regeneron, Stryker, and UCB. Dr. Yazici is an employee of Biosplice Therapeutics, which provided funding for the OAS-07 trial.
A version of this article first appeared on Medscape.com.
VIENNA — The hypothesis that pivotal clinical trials for osteoarthritis (OA)-modifying therapies are not using appropriate designs or endpoints appears to be consistent with the recent failure of the phase 3 trial of the investigational agent lorecivivint, according to experts tackling this issue.
For the elusive target of disease-modifying OA drugs (DMOADs), “there have been a lot of developments in the last few years but so far a lot of disappointments,” said Francis Berenbaum, MD, PhD, head of the department of rheumatology, Saint-Antoine Hospital, Paris, France.
Disagreement on the target most likely to favorably alter the natural history of disease might be the key issue. Dr. Berenbaum considers it essential to determine which changes in the joint signify a favorable drug effect and will lead to what regulatory agencies consider a clinically meaningful benefit. These include improved function and long-term preservation of the joint, as well as symptom control.
Of primary targets to modify the course of OA, cartilage is not one of them, according to Dr. Berenbaum, who spoke in a session on DMOADs and regenerative OA therapies at the annual European Congress of Rheumatology.
OA Is Not a Cartilage-Only Disease
“There is now a big consensus that osteoarthritis is not a cartilage-only disease,” he said. Rather, he addressed the inadequate appreciation of the “whole joint” pathology that underlies OA. He called for a fundamental “paradigm change” to work toward a disease-modifying effect that produces benefit on a hard endpoint.
There are multiple steps needed to work toward this goal after a consensus is reached on a meaningful surrogate endpoint, Dr. Berenbaum said. While symptom reduction is a good start, he called for evidence of disease attenuation or a regenerative effect on an important surrogate such as improved integrity of synovial tissue and improved bone health. Such surrogates are necessary to guide DMOAD development but not sufficient. The proof that a therapy is a DMOAD depends on a favorable effect on a hard endpoint. In the case of the knee, freedom from joint replacement is an example, Dr. Berenbaum said.
Philip G. Conaghan, MBBS, PhD, director of rheumatic and musculoskeletal medicine, University of Leeds, England, agreed with this general premise. Speaking just before Dr. Berenbaum in the same session, Dr. Conaghan traced this history of the effort to create DMOADs and updated those in clinical trials.
In his talk, he listed some of the many disappointments, including those which have targeted cartilage thickness, before updating the numerous ongoing development programs. There are many targets that appear viable, but none are in final stages of testing.
In remarks to this news organization, he said he generally agreed with Dr. Berenbaum about the need for greater rigor for developing drugs to meet regulatory criteria for disease-modifying effects.
Of the drugs he reviewed, Dr. Conaghan identified lorecivivint, an intra-articular CLK/DYRK inhibitor that’s thought to modulate Wnt and inflammatory pathways, as the only drug with DMOAD potential to go to a multicenter phase 3 trial so far. The drug’s negative outcome in phase 3 was particularly disappointing after the substantial promise shown in a phase 2b study published in 2021.
In the phase 3 study, lorecivivint, relative to placebo, did not achieve a significant improvement in the primary endpoint of improved medial joint space width (JSW) in the target knee as assessed at the end of a 48-week, double-blind trial.
New Follow-Up Data Support DMOAD Activity
Yet, additional extension data from the phase 3 lorecivivint trial presented in the EULAR DMOAD session challenge the conclusion even if they do not change the results.
The new data presented at EULAR is the second of two sets of extension data. The first, reported earlier, involved an analysis at 96 weeks or 48 weeks after the double-blind trial. At the beginning of this extension, lorecivivint-start patients had received a second intraarticular injection of 0.07 mg, while placebo patients were crossed over to receive their first injection.
Over the course of this first extension, the gradual loss in medial JSW observed from baseline to the end of the initial 48 weeks had plateaued in those treated with lorecivivint, but the decline continued in the placebo group. As a result, the lorecivivint-start patients had a numerical but not a statistically significant advantage for medial JSW over the placebo-switch group, according to Yusuf Yazici, MD, chief medical officer of Biosplice Therapeutics, San Diego, which developed lorecivivint.
In a second open-label extension described by Dr. Yazici at EULAR 2024, a third injection was administered to the lorecivivint-start patients and a second injection to the placebo-start patients. After 52 more weeks of follow-up, there were now 3 years of follow-up in the lorecivivint-start group and 2 years of follow-up in the placebo-start group.
At the end of this second extension, lorecivivint-start patients had a median increase in JSW that was approaching the baseline level at study entry. Although the placebo-start group had experienced a decline in the medial JSW at the end of the first extension when they had received one injection, JSW had also improved in the direction of baseline after a second injection with 2 years of follow-up. The advantage of three injections of lorecivivint over 3 years had now reached statistical significance (P = .031) despite the improvement seen in the placebo-start group following two injections over 2 years.
At 3 Years, Benefit Is Finally Potentially Significant
If placebo-treated patients had not received a second shot of lorecivivint and progressed at the rate seen before their second shot, the hypothetical trajectory would have provided lorecivivint with a highly statistically significant advantage (P < .001), said Dr. Yazici, displaying a hypothetical graph.
Along with improvements in pain and function associated with lorecivivint relative to placebo at 6 months, 12 months, and 24 months, the structural improvements in 3 years now suggest that “long-term treatment with lorecivivint has the potential to be a DMOAD for knee OA,” Dr. Yazici said.
While Dr. Berenbaum did not comment on this speculation, he did note the potential need for long-term studies to prove a disease-modifying effect in OA. This is the rationale for identifying surrogates.
To illustrate this point, Dr. Berenbaum made an analogy between OA and cardiovascular disease. In cardiovascular disease, surrogates of disease-modifying therapies, such as control of hypertension or hyperlipidemia, are accepted by regulatory agencies on the basis of their proven association with hard endpoints, such as myocardial infarction, stroke, or cardiovascular death. Like joint failure, these events can take years or decades to arise.
“For trials in OA, we need to agree on these surrogates,” Dr. Berenbaum said, although he acknowledged that they would then have to be validated. Noting that the US Food and Drug Administration has now identified OA as a serious disease for which accelerated drug approvals will be considered to address an unmet need, Dr. Berenbaum suggested there is an even greater impetus for improving strategies for DMOAD development.
Dr. Berenbaum reported financial relationships with Grünenthal, GlaxoSmithKline, Eli Lilly, Novartis, Pfizer, and Servier. Dr. Conaghan reported financial relationships with AbbVie, AstraZeneca, Eli Lilly, Galapagos, GlaxoSmithKline, Grünenthal, Janssen, Levicept, Merck, Novartis, Pfizer, Regeneron, Stryker, and UCB. Dr. Yazici is an employee of Biosplice Therapeutics, which provided funding for the OAS-07 trial.
A version of this article first appeared on Medscape.com.
VIENNA — The hypothesis that pivotal clinical trials for osteoarthritis (OA)-modifying therapies are not using appropriate designs or endpoints appears to be consistent with the recent failure of the phase 3 trial of the investigational agent lorecivivint, according to experts tackling this issue.
For the elusive target of disease-modifying OA drugs (DMOADs), “there have been a lot of developments in the last few years but so far a lot of disappointments,” said Francis Berenbaum, MD, PhD, head of the department of rheumatology, Saint-Antoine Hospital, Paris, France.
Disagreement on the target most likely to favorably alter the natural history of disease might be the key issue. Dr. Berenbaum considers it essential to determine which changes in the joint signify a favorable drug effect and will lead to what regulatory agencies consider a clinically meaningful benefit. These include improved function and long-term preservation of the joint, as well as symptom control.
Of primary targets to modify the course of OA, cartilage is not one of them, according to Dr. Berenbaum, who spoke in a session on DMOADs and regenerative OA therapies at the annual European Congress of Rheumatology.
OA Is Not a Cartilage-Only Disease
“There is now a big consensus that osteoarthritis is not a cartilage-only disease,” he said. Rather, he addressed the inadequate appreciation of the “whole joint” pathology that underlies OA. He called for a fundamental “paradigm change” to work toward a disease-modifying effect that produces benefit on a hard endpoint.
There are multiple steps needed to work toward this goal after a consensus is reached on a meaningful surrogate endpoint, Dr. Berenbaum said. While symptom reduction is a good start, he called for evidence of disease attenuation or a regenerative effect on an important surrogate such as improved integrity of synovial tissue and improved bone health. Such surrogates are necessary to guide DMOAD development but not sufficient. The proof that a therapy is a DMOAD depends on a favorable effect on a hard endpoint. In the case of the knee, freedom from joint replacement is an example, Dr. Berenbaum said.
Philip G. Conaghan, MBBS, PhD, director of rheumatic and musculoskeletal medicine, University of Leeds, England, agreed with this general premise. Speaking just before Dr. Berenbaum in the same session, Dr. Conaghan traced this history of the effort to create DMOADs and updated those in clinical trials.
In his talk, he listed some of the many disappointments, including those which have targeted cartilage thickness, before updating the numerous ongoing development programs. There are many targets that appear viable, but none are in final stages of testing.
In remarks to this news organization, he said he generally agreed with Dr. Berenbaum about the need for greater rigor for developing drugs to meet regulatory criteria for disease-modifying effects.
Of the drugs he reviewed, Dr. Conaghan identified lorecivivint, an intra-articular CLK/DYRK inhibitor that’s thought to modulate Wnt and inflammatory pathways, as the only drug with DMOAD potential to go to a multicenter phase 3 trial so far. The drug’s negative outcome in phase 3 was particularly disappointing after the substantial promise shown in a phase 2b study published in 2021.
In the phase 3 study, lorecivivint, relative to placebo, did not achieve a significant improvement in the primary endpoint of improved medial joint space width (JSW) in the target knee as assessed at the end of a 48-week, double-blind trial.
New Follow-Up Data Support DMOAD Activity
Yet, additional extension data from the phase 3 lorecivivint trial presented in the EULAR DMOAD session challenge the conclusion even if they do not change the results.
The new data presented at EULAR is the second of two sets of extension data. The first, reported earlier, involved an analysis at 96 weeks or 48 weeks after the double-blind trial. At the beginning of this extension, lorecivivint-start patients had received a second intraarticular injection of 0.07 mg, while placebo patients were crossed over to receive their first injection.
Over the course of this first extension, the gradual loss in medial JSW observed from baseline to the end of the initial 48 weeks had plateaued in those treated with lorecivivint, but the decline continued in the placebo group. As a result, the lorecivivint-start patients had a numerical but not a statistically significant advantage for medial JSW over the placebo-switch group, according to Yusuf Yazici, MD, chief medical officer of Biosplice Therapeutics, San Diego, which developed lorecivivint.
In a second open-label extension described by Dr. Yazici at EULAR 2024, a third injection was administered to the lorecivivint-start patients and a second injection to the placebo-start patients. After 52 more weeks of follow-up, there were now 3 years of follow-up in the lorecivivint-start group and 2 years of follow-up in the placebo-start group.
At the end of this second extension, lorecivivint-start patients had a median increase in JSW that was approaching the baseline level at study entry. Although the placebo-start group had experienced a decline in the medial JSW at the end of the first extension when they had received one injection, JSW had also improved in the direction of baseline after a second injection with 2 years of follow-up. The advantage of three injections of lorecivivint over 3 years had now reached statistical significance (P = .031) despite the improvement seen in the placebo-start group following two injections over 2 years.
At 3 Years, Benefit Is Finally Potentially Significant
If placebo-treated patients had not received a second shot of lorecivivint and progressed at the rate seen before their second shot, the hypothetical trajectory would have provided lorecivivint with a highly statistically significant advantage (P < .001), said Dr. Yazici, displaying a hypothetical graph.
Along with improvements in pain and function associated with lorecivivint relative to placebo at 6 months, 12 months, and 24 months, the structural improvements in 3 years now suggest that “long-term treatment with lorecivivint has the potential to be a DMOAD for knee OA,” Dr. Yazici said.
While Dr. Berenbaum did not comment on this speculation, he did note the potential need for long-term studies to prove a disease-modifying effect in OA. This is the rationale for identifying surrogates.
To illustrate this point, Dr. Berenbaum made an analogy between OA and cardiovascular disease. In cardiovascular disease, surrogates of disease-modifying therapies, such as control of hypertension or hyperlipidemia, are accepted by regulatory agencies on the basis of their proven association with hard endpoints, such as myocardial infarction, stroke, or cardiovascular death. Like joint failure, these events can take years or decades to arise.
“For trials in OA, we need to agree on these surrogates,” Dr. Berenbaum said, although he acknowledged that they would then have to be validated. Noting that the US Food and Drug Administration has now identified OA as a serious disease for which accelerated drug approvals will be considered to address an unmet need, Dr. Berenbaum suggested there is an even greater impetus for improving strategies for DMOAD development.
Dr. Berenbaum reported financial relationships with Grünenthal, GlaxoSmithKline, Eli Lilly, Novartis, Pfizer, and Servier. Dr. Conaghan reported financial relationships with AbbVie, AstraZeneca, Eli Lilly, Galapagos, GlaxoSmithKline, Grünenthal, Janssen, Levicept, Merck, Novartis, Pfizer, Regeneron, Stryker, and UCB. Dr. Yazici is an employee of Biosplice Therapeutics, which provided funding for the OAS-07 trial.
A version of this article first appeared on Medscape.com.
FROM EULAR 2024
Ixekizumab Met Phase 3 Trial Endpoint in Juvenile PsA, Enthesitis-Related Arthritis
VIENNA — Ixekizumab (Taltz), an interleukin-17A inhibitor that’s already approved for the treatment of psoriatic arthritis and axial spondyloarthritis in adults appears likely to be granted the same corresponding indications for children, based on initial results from an open-label, phase 3 trial that employed adalimumab as a reference.
With a safety profile comparable with that seen in adult patients, ixekizumab “met the prespecified criterion for success at 16 weeks,” reported Athimalaipet V. Ramanan, MD, PhD, of Bristol Royal Hospital for Children and Translational Health Sciences, Bristol, England.
In this multicenter, randomized, open-label trial called COSPIRIT-JIA, which is still ongoing, investigators enrolled 101 children with active juvenile PsA (JPsA) or enthesitis-related arthritis (ERA), which is akin to spondyloarthritis in adults.
The efficacy and safety data at 16 weeks were presented as a late-breaking abstract at the annual European Congress of Rheumatology. Dr. Ramanan said that the open-label extension to 104 weeks is underway and further follow-up out to 264 weeks is planned.
Nearly 90% Achieve ACR30
The trial had an adaptive design in which the first 40 patients without biologics experience were randomized to ixekizumab or adalimumab, stratified by JPsA or ERA diagnosis, and the following 61 patients with either no biologic experience or an inadequate response or intolerance to biologics all received ixekizumab. The drugs were dosed according to weight. Dr. Ramanan explained that a placebo-controlled trial was considered unethical because of the strong evidence of benefit from biologics for JPsA and ERA.
The trial easily met its predefined threshold for success, which required ≥ 80% probability, based on Bayesian analysis, that ≥ 50% of patients would have 30% improvement in American College of Rheumatology response criteria (ACR30) at week 16. ACR30 was achieved in 88.9% of those treated with ixekizumab overall vs 95.0% of those treated with adalimumab, but the trial was not designed as a head-to-head comparison. Rather, adalimumab served as a reference.
When compared for the distinct diseases, the ACR30 rates were also numerically lower for ixekizumab relative to adalimumab for both ERA (88.9% vs 93.8%) and JPsA (88.9% vs 100%), but all of the adalimumab patients were naive to biologics. In comparison, about 75% of patients receiving ixekizumab were biologic-therapy naive.
Response rates to ixekizumab overall were numerically higher for patients without previous biologic experience than for those with experience (90.0% vs 85.7%), and this was also the case for patients with ERA (92.5% vs 78.6%). However, in the JPsA group, biologic-experienced patients had higher numerical response rates to ixekizumab (100% vs 85.0%).
An ACR30 is not a clinical goal that satisfies most patients and clinicians, Dr. Ramanan conceded, but he noted that ACR50 was reached with ixekizumab by 81.5% with ERA and 74.1% with JPsA, and ACR70 was reached by 68.5% and 55.6%, respectively. The highest responses of ACR90 (27.8% and 33.3%) and ACR100 (14.8% and 25.9%) were lower but still substantial in the ERA and JPsA groups, respectively.
Through week 16, 58.0% of those treated with ixekizumab had an adverse event considered treatment-related. Nearly half were of mild severity, and the remainder were moderate. Only 3.7% were considered serious. No patient discontinued study treatment because of an adverse event.
In this study, the presence of at least three active peripheral joints was an inclusion criterion. The median age was about 13 years in the biologic-naive adalimumab and ixekizumab groups and 14 years in the ixekizumab biologic-experienced group. The youngest patient in the study was aged 5 years, and the oldest was aged 18 years. Although about 40% of patients were women in the two biologic-naive subgroups, it was 60% in the biologic-experienced group.
On average, patients in the biologic-naive group were entered about 1 year after diagnosis. In the experienced patients, the average duration of disease at entry was nearly 4 years. About 45% of patients remained on conventional synthetic disease-modifying antirheumatic drugs while receiving ixekizumab. The proportion was 35% in the adalimumab reference arm.
Ixekizumab Might Fulfill Need for More Options
There are several biologics that have received regulatory approval or are already widely used for the treatment of JPsA or ERA, but more options are needed, according to Dr. Ramanan and the chair of the abstract session in which these data were reported. According to Caroline Ospelt, MD, PhD, a researcher at the Center for Experimental Rheumatology, University Hospital Zurich, Switzerland, regulatory approval of ixekizumab will depend on sustained efficacy and safety in longer follow-up from the COSPIRIT-JIA trial, but this trial supports continued development.
Despite a novel mechanism of action, “the data so far suggest a level of efficacy similar to that of anti-TNF [anti-tumor necrosis factor] biologics,” said Dr. Ospelt, who, in addition to moderating the late-breaking session, served as Scientific Program Chair of EULAR 2024.
While Dr. Ospelt emphasized that she is a researcher involved in translational rheumatology studies and not a clinician, she said there was consensus within the program committee to select this abstract from other high-quality latebreaker submissions on the basis of its potential clinical significance.
Dr. Ramanan reported financial relationships with AbbVie, AstraZeneca, Novartis, Pfizer, Roche, SOBI, UCB, and Eli Lilly, which provided funding for this study. Dr. Ospelt reported no potential conflicts of interest.
A version of this article first appeared on Medscape.com.
VIENNA — Ixekizumab (Taltz), an interleukin-17A inhibitor that’s already approved for the treatment of psoriatic arthritis and axial spondyloarthritis in adults appears likely to be granted the same corresponding indications for children, based on initial results from an open-label, phase 3 trial that employed adalimumab as a reference.
With a safety profile comparable with that seen in adult patients, ixekizumab “met the prespecified criterion for success at 16 weeks,” reported Athimalaipet V. Ramanan, MD, PhD, of Bristol Royal Hospital for Children and Translational Health Sciences, Bristol, England.
In this multicenter, randomized, open-label trial called COSPIRIT-JIA, which is still ongoing, investigators enrolled 101 children with active juvenile PsA (JPsA) or enthesitis-related arthritis (ERA), which is akin to spondyloarthritis in adults.
The efficacy and safety data at 16 weeks were presented as a late-breaking abstract at the annual European Congress of Rheumatology. Dr. Ramanan said that the open-label extension to 104 weeks is underway and further follow-up out to 264 weeks is planned.
Nearly 90% Achieve ACR30
The trial had an adaptive design in which the first 40 patients without biologics experience were randomized to ixekizumab or adalimumab, stratified by JPsA or ERA diagnosis, and the following 61 patients with either no biologic experience or an inadequate response or intolerance to biologics all received ixekizumab. The drugs were dosed according to weight. Dr. Ramanan explained that a placebo-controlled trial was considered unethical because of the strong evidence of benefit from biologics for JPsA and ERA.
The trial easily met its predefined threshold for success, which required ≥ 80% probability, based on Bayesian analysis, that ≥ 50% of patients would have 30% improvement in American College of Rheumatology response criteria (ACR30) at week 16. ACR30 was achieved in 88.9% of those treated with ixekizumab overall vs 95.0% of those treated with adalimumab, but the trial was not designed as a head-to-head comparison. Rather, adalimumab served as a reference.
When compared for the distinct diseases, the ACR30 rates were also numerically lower for ixekizumab relative to adalimumab for both ERA (88.9% vs 93.8%) and JPsA (88.9% vs 100%), but all of the adalimumab patients were naive to biologics. In comparison, about 75% of patients receiving ixekizumab were biologic-therapy naive.
Response rates to ixekizumab overall were numerically higher for patients without previous biologic experience than for those with experience (90.0% vs 85.7%), and this was also the case for patients with ERA (92.5% vs 78.6%). However, in the JPsA group, biologic-experienced patients had higher numerical response rates to ixekizumab (100% vs 85.0%).
An ACR30 is not a clinical goal that satisfies most patients and clinicians, Dr. Ramanan conceded, but he noted that ACR50 was reached with ixekizumab by 81.5% with ERA and 74.1% with JPsA, and ACR70 was reached by 68.5% and 55.6%, respectively. The highest responses of ACR90 (27.8% and 33.3%) and ACR100 (14.8% and 25.9%) were lower but still substantial in the ERA and JPsA groups, respectively.
Through week 16, 58.0% of those treated with ixekizumab had an adverse event considered treatment-related. Nearly half were of mild severity, and the remainder were moderate. Only 3.7% were considered serious. No patient discontinued study treatment because of an adverse event.
In this study, the presence of at least three active peripheral joints was an inclusion criterion. The median age was about 13 years in the biologic-naive adalimumab and ixekizumab groups and 14 years in the ixekizumab biologic-experienced group. The youngest patient in the study was aged 5 years, and the oldest was aged 18 years. Although about 40% of patients were women in the two biologic-naive subgroups, it was 60% in the biologic-experienced group.
On average, patients in the biologic-naive group were entered about 1 year after diagnosis. In the experienced patients, the average duration of disease at entry was nearly 4 years. About 45% of patients remained on conventional synthetic disease-modifying antirheumatic drugs while receiving ixekizumab. The proportion was 35% in the adalimumab reference arm.
Ixekizumab Might Fulfill Need for More Options
There are several biologics that have received regulatory approval or are already widely used for the treatment of JPsA or ERA, but more options are needed, according to Dr. Ramanan and the chair of the abstract session in which these data were reported. According to Caroline Ospelt, MD, PhD, a researcher at the Center for Experimental Rheumatology, University Hospital Zurich, Switzerland, regulatory approval of ixekizumab will depend on sustained efficacy and safety in longer follow-up from the COSPIRIT-JIA trial, but this trial supports continued development.
Despite a novel mechanism of action, “the data so far suggest a level of efficacy similar to that of anti-TNF [anti-tumor necrosis factor] biologics,” said Dr. Ospelt, who, in addition to moderating the late-breaking session, served as Scientific Program Chair of EULAR 2024.
While Dr. Ospelt emphasized that she is a researcher involved in translational rheumatology studies and not a clinician, she said there was consensus within the program committee to select this abstract from other high-quality latebreaker submissions on the basis of its potential clinical significance.
Dr. Ramanan reported financial relationships with AbbVie, AstraZeneca, Novartis, Pfizer, Roche, SOBI, UCB, and Eli Lilly, which provided funding for this study. Dr. Ospelt reported no potential conflicts of interest.
A version of this article first appeared on Medscape.com.
VIENNA — Ixekizumab (Taltz), an interleukin-17A inhibitor that’s already approved for the treatment of psoriatic arthritis and axial spondyloarthritis in adults appears likely to be granted the same corresponding indications for children, based on initial results from an open-label, phase 3 trial that employed adalimumab as a reference.
With a safety profile comparable with that seen in adult patients, ixekizumab “met the prespecified criterion for success at 16 weeks,” reported Athimalaipet V. Ramanan, MD, PhD, of Bristol Royal Hospital for Children and Translational Health Sciences, Bristol, England.
In this multicenter, randomized, open-label trial called COSPIRIT-JIA, which is still ongoing, investigators enrolled 101 children with active juvenile PsA (JPsA) or enthesitis-related arthritis (ERA), which is akin to spondyloarthritis in adults.
The efficacy and safety data at 16 weeks were presented as a late-breaking abstract at the annual European Congress of Rheumatology. Dr. Ramanan said that the open-label extension to 104 weeks is underway and further follow-up out to 264 weeks is planned.
Nearly 90% Achieve ACR30
The trial had an adaptive design in which the first 40 patients without biologics experience were randomized to ixekizumab or adalimumab, stratified by JPsA or ERA diagnosis, and the following 61 patients with either no biologic experience or an inadequate response or intolerance to biologics all received ixekizumab. The drugs were dosed according to weight. Dr. Ramanan explained that a placebo-controlled trial was considered unethical because of the strong evidence of benefit from biologics for JPsA and ERA.
The trial easily met its predefined threshold for success, which required ≥ 80% probability, based on Bayesian analysis, that ≥ 50% of patients would have 30% improvement in American College of Rheumatology response criteria (ACR30) at week 16. ACR30 was achieved in 88.9% of those treated with ixekizumab overall vs 95.0% of those treated with adalimumab, but the trial was not designed as a head-to-head comparison. Rather, adalimumab served as a reference.
When compared for the distinct diseases, the ACR30 rates were also numerically lower for ixekizumab relative to adalimumab for both ERA (88.9% vs 93.8%) and JPsA (88.9% vs 100%), but all of the adalimumab patients were naive to biologics. In comparison, about 75% of patients receiving ixekizumab were biologic-therapy naive.
Response rates to ixekizumab overall were numerically higher for patients without previous biologic experience than for those with experience (90.0% vs 85.7%), and this was also the case for patients with ERA (92.5% vs 78.6%). However, in the JPsA group, biologic-experienced patients had higher numerical response rates to ixekizumab (100% vs 85.0%).
An ACR30 is not a clinical goal that satisfies most patients and clinicians, Dr. Ramanan conceded, but he noted that ACR50 was reached with ixekizumab by 81.5% with ERA and 74.1% with JPsA, and ACR70 was reached by 68.5% and 55.6%, respectively. The highest responses of ACR90 (27.8% and 33.3%) and ACR100 (14.8% and 25.9%) were lower but still substantial in the ERA and JPsA groups, respectively.
Through week 16, 58.0% of those treated with ixekizumab had an adverse event considered treatment-related. Nearly half were of mild severity, and the remainder were moderate. Only 3.7% were considered serious. No patient discontinued study treatment because of an adverse event.
In this study, the presence of at least three active peripheral joints was an inclusion criterion. The median age was about 13 years in the biologic-naive adalimumab and ixekizumab groups and 14 years in the ixekizumab biologic-experienced group. The youngest patient in the study was aged 5 years, and the oldest was aged 18 years. Although about 40% of patients were women in the two biologic-naive subgroups, it was 60% in the biologic-experienced group.
On average, patients in the biologic-naive group were entered about 1 year after diagnosis. In the experienced patients, the average duration of disease at entry was nearly 4 years. About 45% of patients remained on conventional synthetic disease-modifying antirheumatic drugs while receiving ixekizumab. The proportion was 35% in the adalimumab reference arm.
Ixekizumab Might Fulfill Need for More Options
There are several biologics that have received regulatory approval or are already widely used for the treatment of JPsA or ERA, but more options are needed, according to Dr. Ramanan and the chair of the abstract session in which these data were reported. According to Caroline Ospelt, MD, PhD, a researcher at the Center for Experimental Rheumatology, University Hospital Zurich, Switzerland, regulatory approval of ixekizumab will depend on sustained efficacy and safety in longer follow-up from the COSPIRIT-JIA trial, but this trial supports continued development.
Despite a novel mechanism of action, “the data so far suggest a level of efficacy similar to that of anti-TNF [anti-tumor necrosis factor] biologics,” said Dr. Ospelt, who, in addition to moderating the late-breaking session, served as Scientific Program Chair of EULAR 2024.
While Dr. Ospelt emphasized that she is a researcher involved in translational rheumatology studies and not a clinician, she said there was consensus within the program committee to select this abstract from other high-quality latebreaker submissions on the basis of its potential clinical significance.
Dr. Ramanan reported financial relationships with AbbVie, AstraZeneca, Novartis, Pfizer, Roche, SOBI, UCB, and Eli Lilly, which provided funding for this study. Dr. Ospelt reported no potential conflicts of interest.
A version of this article first appeared on Medscape.com.
FROM EULAR 2024
See the Medical World Through Neurodivergent Doctors’ Eyes
Some 15%-20% of the world’s population are neurodivergent, with conditions such as autism, dyslexia, Tourette syndrome, attention-deficit/hyperactivity disorder (ADHD), and others. With different strengths and challenges around learning, engaging socially, or completing certain tasks, neurodivergent people can face barriers in the workforce.
Meanwhile, studies suggest that neurodivergent people may be overrepresented in STEM fields such as medicine. The medical field may self-select for traits associated with neurodivergent conditions, researchers say, including a hyperfocus on intense interests, pattern recognition, increased curiosity and empathy, and thinking quickly under pressure.
But . They struggle with stigma, a culture of nondisclosure, and lack of accommodations, which can lead to burnout and poor mental health.
“The medical system and the mental health system are some of the spaces that are holding on tightly to some of the outdated understandings of things like autism and ADHD,” says Megan Anna Neff, PsyD, a psychologist with autism and ADHD based in Portland, Oregon.
Situations can get dire: A 2023 survey of more than 200 autistic doctors from several countries found that 77% had considered suicide and 24% had attempted it.
But here’s the crux of it: Many neurodivergent doctors believe their unique ways of thinking and outside-the-box creativity are skills and strengths that can benefit the field. And they say making medicine more inclusive — and better understanding how a neurodivergent physician’s brain works — would allow them to thrive.
Blending In and Breaking Down
The exact number of neurodivergent physicians in the workforce remains unknown. Existing studies are small and focus mainly on autism. But researchers believe the percentage could be higher than we think, because neurodiversity can be underidentified.
Although autism can sometimes be diagnosed as early as 18 months, it’s not uncommon to receive a diagnosis well into adulthood. “Like many late-identified autistic adults, I got my autism diagnosis in the context of autistic burnout,” says Melissa Houser, MD, a primary care physician who received a diagnosis in 2021. Dr. Houser, who uses the pronouns she/they, explains that her experience is common, “a consequence of chronically having your life’s demands exceed your capacity.”
Dr. Houser, who also has ADHD and dyslexia, among other neurodivergent conditions, says that before her diagnosis, she worked in a traditional practice setting. Eventually, she began to notice intense dysregulation and fatigue. “I began to have a lot more difficulties with communication and my motor planning and sequencing,” Dr. Houser says. “I was sleep-deprived, and my needs were not being met. I was in a situation where I had a complete lack of autonomy over my practice.”
Deep in burnout, Dr. Houser says she lost her ability to “mask,” a term used to describe how some neurodivergent people work to “blend in” with societal expectations. This led to further communication breakdowns with her supervisor. Finally, Dr. Houser saw a psychiatrist.
Shortly after her diagnosis, Dr. Houser quit her job and founded All Brains Belong, a nonprofit that provides neurodiversity-affirming medical care, education, and advocacy. Research has found that people with autism are at increased risk for physical health conditions, including immune conditions, gastrointestinal disorders, metabolic conditions, and increased mortality in hospital settings. Understanding these connections can “mean the difference between life and death” for neurodivergent patients, Dr. Houser says.
Yet, in a 2015 study that assessed providers’ ability to recognize autism, a high proportion were not aware that they had patients with autism spectrum disorder, and most reported lacking both the skills and the tools to care for them.
Different as a Doctor and a Patient
Bernadette Grosjean, MD, a retired associate professor of psychiatry at David Geffen School of Medicine at UCLA and a distinguished Fellow of the American Psychiatric Association, also found insight into lifelong experiences as both a doctor and a patient with her autism diagnosis, which came when she was 61.
“Looking back, I was a smart kid but kind of clumsy and different in other ways,” Dr. Grosjean says. According to a 2021 survey by Cambridge University, autistic individuals are significantly more likely to identify as LGBTQ+, and Dr. Grosjean, who is gay, says that not being fully accepted by family or friends played a role in her struggles with mental health issues.
Throughout her mental health treatment, Dr. Grosjean felt as though her providers “were expecting from me things that I didn’t know how to do or fix. I didn’t know how to be a ‘good’ patient,” she recalls.
As a psychiatrist, Dr. Grosjean started to notice that many of the women she treated for borderline personality disorder, which is categorized by unstable relationships and emotions, were autistic. “I then started asking lots of questions about myself — the fact that I’ve always been very sensitive or that I’ve been accused of being both hypersensitive and not having emotions, and I understood a lot.”
When Dr. Grosjean came across Autistic Doctors International, a group of over 800 autistic doctors worldwide, she says, “I found my tribe.” She now serves as the US lead for psychiatry for the group, which is focused on support, advocacy, research, and education around neurodiversity.
Psychiatric comorbidities can accompany neurodivergent conditions. But a growing body of research, including a 2022 study published in the European Archives of Psychiatry and Clinical Neuroscience, indicates that autism and ADHD are frequently misdiagnosed as depression or anxiety.
Dr. Neff was unaware of her conditions until one of her children was diagnosed with autism in 2021. She started to research it. “As I was learning about autism and girls, I was like, ‘Oh, my gosh, this is me,’ ” Dr. Neff recalls. Within a few weeks, she had her own diagnosis.
In hindsight, Dr. Neff has more clarity regarding her struggles in the traditional medical space. She had found it difficult to fit patients into short appointment windows and keep their notes concise. Although she loved hospital work, the environment had been overwhelming and led to burnout.
‘A Deficit-Based Lens’
Dr. Houser believes that too often, autism is viewed through a “deficit-based lens.” Stressors like sensory overload, changes in routine, or unexpected events can exacerbate behavioral challenges for neurodivergent people in the workplace. The DSM-5 criteria for autism, she points out, are largely based on autistic “stress behaviors.”
The result, Dr. Houser says, is that neurodivergent doctors are judged by their response to stressors that put them at a disadvantage rather than their capabilities under more positive circumstances. “The more dysregulated someone is,” she says, “the more likely they are to manifest those observable behaviors.”
Dr. Neff notes that medicine is a very “sensory overwhelming work environment.” Working in ob.gyn. and primary care clinics, she remembers often coming home with a headache and a low-grade fever. “I had no idea why, but I now realize it’s because I was so sensory sick.”
Fearing for her job, Dr. Neff intentionally waited until she was in private practice to disclose her neurodiversity. “I don’t think it would have been received well if I was in a hospital system,” she says. “There’s a lot of invalidation that can come when someone chooses to self-disclose, and their colleagues don’t have a framework in mind to understand.” In one instance, after revealing her diagnosis, she remembers a well-known researcher telling her she wasn’t autistic.
Dr. Grosjean has also had former colleagues invalidate her diagnosis, something she says “keeps people quiet.”
Understanding the Neurodivergent Brain
The general lack of education on how neurodivergent brains work, physicians with these conditions say, means they are not often recognized for how they can function with certain accommodations and how they could contribute in unique ways if their workplace challenges were reduced.
“What we know about autistic brains is that we are systems-thinking pattern matchers,” says Dr. Houser, who formed an interdisciplinary task force to explore medical conditions that are more common in autistic people. Through that comprehensive approach, she has worked to find best practices to treat the constellation of conditions that can arise among these patients. “My autistic brain allowed me to do that,” Dr. Houser says.
Catriona McVey, a medical student in the United Kingdom and creator of the blog Attention Deficit Doctor, points out that “ADHD brains are interest-driven; they can be very focused when you’re doing something enjoyable or new due to increased dopaminergic stimulation.” Ms. McVey speaks from personal experience. “I’ve hyperfocused before on an essay that interested me for over 10 hours,” she recalls, “so I imagine if I was interested in surgery, I could easily hyperfocus on a long operation.”
Empathy is another key part of medical practice. Contrary to stereotypes of neurodivergent people lacking empathy, current research suggests this isn’t true. A concept known as the “double empathy problem,” a term coined by British researcher Damian Milton in 2012, challenges the misconception that autistic people do not have empathy, explains Dr. Grosjean.
Mr. Milton theorized that there are two types of empathy: emotional, when you feel someone else’s pain, and cognitive, which involves critical thinking to understand someone’s emotions or thoughts. “Autistic people have, in general, a lot of emotional empathy,” Dr. Grosjean says, “but the cognitive empathy they don’t have as well.”
Dr. Neff has experienced this in her practice. “I will often feel what my clients are feeling as they’re feeling it,” she says, adding that she has always had an innate ability to analyze and connect with clients. She’s good at observing the interplay of health conditions, incorporating biology, psychology, and social conceptualizations of issues, with nuance. She feels that recognizing behavioral patterns or psychological triggers in her patients helps her see them holistically and provide better care. “That was a skill even before I realized I was autistic, but I always thought it was just intuitive to everyone,” she says.
Support Can Lead to Success
The Americans with Disabilities Act requires employers to provide reasonable accommodations to neurodivergent employees. However, getting those accommodations involves disclosure, which many physicians have reasons to avoid.
It also means more work. Requesting and putting adjustments in place can take a lot of time and energy to organize. Ms. McVey says they can be “long-winded, multistep tasks” that are not very compatible with ADHD. “Some doctors report that service pressures and funding are used as excuses to refuse adjustments,” she adds.
Ms. McVey lists several workplace accommodations that could be helpful, including flexible working hours, a quiet space to complete paperwork, dictation software, and extra time for medical students to complete written exams.
Neurodivergent physicians have also called for increased diversity of senior leadership and utilizing “cognitive apprenticeship models,” where employees explain their thought processes and receive timely feedback.
But far too often, there is little intervention until a doctor reaches a crisis point. “I look forward to the day when we don’t have to wait until people are profoundly depleted to discover how their brains work,” says Dr. Houser.
Beyond logistical and structural changes in the medical field, Dr. Grosjean speaks of the simple need to listen to colleagues with an open mind and believe them when they express their feelings and experiences. “Everyone has a role to play in challenging stigma, misconceptions, and stereotypes,” Ms. McVey agrees. Ask yourself the old question, she suggests: “If not me, then who? If not now, then when?”
A version of this article first appeared on Medscape.com.
Some 15%-20% of the world’s population are neurodivergent, with conditions such as autism, dyslexia, Tourette syndrome, attention-deficit/hyperactivity disorder (ADHD), and others. With different strengths and challenges around learning, engaging socially, or completing certain tasks, neurodivergent people can face barriers in the workforce.
Meanwhile, studies suggest that neurodivergent people may be overrepresented in STEM fields such as medicine. The medical field may self-select for traits associated with neurodivergent conditions, researchers say, including a hyperfocus on intense interests, pattern recognition, increased curiosity and empathy, and thinking quickly under pressure.
But . They struggle with stigma, a culture of nondisclosure, and lack of accommodations, which can lead to burnout and poor mental health.
“The medical system and the mental health system are some of the spaces that are holding on tightly to some of the outdated understandings of things like autism and ADHD,” says Megan Anna Neff, PsyD, a psychologist with autism and ADHD based in Portland, Oregon.
Situations can get dire: A 2023 survey of more than 200 autistic doctors from several countries found that 77% had considered suicide and 24% had attempted it.
But here’s the crux of it: Many neurodivergent doctors believe their unique ways of thinking and outside-the-box creativity are skills and strengths that can benefit the field. And they say making medicine more inclusive — and better understanding how a neurodivergent physician’s brain works — would allow them to thrive.
Blending In and Breaking Down
The exact number of neurodivergent physicians in the workforce remains unknown. Existing studies are small and focus mainly on autism. But researchers believe the percentage could be higher than we think, because neurodiversity can be underidentified.
Although autism can sometimes be diagnosed as early as 18 months, it’s not uncommon to receive a diagnosis well into adulthood. “Like many late-identified autistic adults, I got my autism diagnosis in the context of autistic burnout,” says Melissa Houser, MD, a primary care physician who received a diagnosis in 2021. Dr. Houser, who uses the pronouns she/they, explains that her experience is common, “a consequence of chronically having your life’s demands exceed your capacity.”
Dr. Houser, who also has ADHD and dyslexia, among other neurodivergent conditions, says that before her diagnosis, she worked in a traditional practice setting. Eventually, she began to notice intense dysregulation and fatigue. “I began to have a lot more difficulties with communication and my motor planning and sequencing,” Dr. Houser says. “I was sleep-deprived, and my needs were not being met. I was in a situation where I had a complete lack of autonomy over my practice.”
Deep in burnout, Dr. Houser says she lost her ability to “mask,” a term used to describe how some neurodivergent people work to “blend in” with societal expectations. This led to further communication breakdowns with her supervisor. Finally, Dr. Houser saw a psychiatrist.
Shortly after her diagnosis, Dr. Houser quit her job and founded All Brains Belong, a nonprofit that provides neurodiversity-affirming medical care, education, and advocacy. Research has found that people with autism are at increased risk for physical health conditions, including immune conditions, gastrointestinal disorders, metabolic conditions, and increased mortality in hospital settings. Understanding these connections can “mean the difference between life and death” for neurodivergent patients, Dr. Houser says.
Yet, in a 2015 study that assessed providers’ ability to recognize autism, a high proportion were not aware that they had patients with autism spectrum disorder, and most reported lacking both the skills and the tools to care for them.
Different as a Doctor and a Patient
Bernadette Grosjean, MD, a retired associate professor of psychiatry at David Geffen School of Medicine at UCLA and a distinguished Fellow of the American Psychiatric Association, also found insight into lifelong experiences as both a doctor and a patient with her autism diagnosis, which came when she was 61.
“Looking back, I was a smart kid but kind of clumsy and different in other ways,” Dr. Grosjean says. According to a 2021 survey by Cambridge University, autistic individuals are significantly more likely to identify as LGBTQ+, and Dr. Grosjean, who is gay, says that not being fully accepted by family or friends played a role in her struggles with mental health issues.
Throughout her mental health treatment, Dr. Grosjean felt as though her providers “were expecting from me things that I didn’t know how to do or fix. I didn’t know how to be a ‘good’ patient,” she recalls.
As a psychiatrist, Dr. Grosjean started to notice that many of the women she treated for borderline personality disorder, which is categorized by unstable relationships and emotions, were autistic. “I then started asking lots of questions about myself — the fact that I’ve always been very sensitive or that I’ve been accused of being both hypersensitive and not having emotions, and I understood a lot.”
When Dr. Grosjean came across Autistic Doctors International, a group of over 800 autistic doctors worldwide, she says, “I found my tribe.” She now serves as the US lead for psychiatry for the group, which is focused on support, advocacy, research, and education around neurodiversity.
Psychiatric comorbidities can accompany neurodivergent conditions. But a growing body of research, including a 2022 study published in the European Archives of Psychiatry and Clinical Neuroscience, indicates that autism and ADHD are frequently misdiagnosed as depression or anxiety.
Dr. Neff was unaware of her conditions until one of her children was diagnosed with autism in 2021. She started to research it. “As I was learning about autism and girls, I was like, ‘Oh, my gosh, this is me,’ ” Dr. Neff recalls. Within a few weeks, she had her own diagnosis.
In hindsight, Dr. Neff has more clarity regarding her struggles in the traditional medical space. She had found it difficult to fit patients into short appointment windows and keep their notes concise. Although she loved hospital work, the environment had been overwhelming and led to burnout.
‘A Deficit-Based Lens’
Dr. Houser believes that too often, autism is viewed through a “deficit-based lens.” Stressors like sensory overload, changes in routine, or unexpected events can exacerbate behavioral challenges for neurodivergent people in the workplace. The DSM-5 criteria for autism, she points out, are largely based on autistic “stress behaviors.”
The result, Dr. Houser says, is that neurodivergent doctors are judged by their response to stressors that put them at a disadvantage rather than their capabilities under more positive circumstances. “The more dysregulated someone is,” she says, “the more likely they are to manifest those observable behaviors.”
Dr. Neff notes that medicine is a very “sensory overwhelming work environment.” Working in ob.gyn. and primary care clinics, she remembers often coming home with a headache and a low-grade fever. “I had no idea why, but I now realize it’s because I was so sensory sick.”
Fearing for her job, Dr. Neff intentionally waited until she was in private practice to disclose her neurodiversity. “I don’t think it would have been received well if I was in a hospital system,” she says. “There’s a lot of invalidation that can come when someone chooses to self-disclose, and their colleagues don’t have a framework in mind to understand.” In one instance, after revealing her diagnosis, she remembers a well-known researcher telling her she wasn’t autistic.
Dr. Grosjean has also had former colleagues invalidate her diagnosis, something she says “keeps people quiet.”
Understanding the Neurodivergent Brain
The general lack of education on how neurodivergent brains work, physicians with these conditions say, means they are not often recognized for how they can function with certain accommodations and how they could contribute in unique ways if their workplace challenges were reduced.
“What we know about autistic brains is that we are systems-thinking pattern matchers,” says Dr. Houser, who formed an interdisciplinary task force to explore medical conditions that are more common in autistic people. Through that comprehensive approach, she has worked to find best practices to treat the constellation of conditions that can arise among these patients. “My autistic brain allowed me to do that,” Dr. Houser says.
Catriona McVey, a medical student in the United Kingdom and creator of the blog Attention Deficit Doctor, points out that “ADHD brains are interest-driven; they can be very focused when you’re doing something enjoyable or new due to increased dopaminergic stimulation.” Ms. McVey speaks from personal experience. “I’ve hyperfocused before on an essay that interested me for over 10 hours,” she recalls, “so I imagine if I was interested in surgery, I could easily hyperfocus on a long operation.”
Empathy is another key part of medical practice. Contrary to stereotypes of neurodivergent people lacking empathy, current research suggests this isn’t true. A concept known as the “double empathy problem,” a term coined by British researcher Damian Milton in 2012, challenges the misconception that autistic people do not have empathy, explains Dr. Grosjean.
Mr. Milton theorized that there are two types of empathy: emotional, when you feel someone else’s pain, and cognitive, which involves critical thinking to understand someone’s emotions or thoughts. “Autistic people have, in general, a lot of emotional empathy,” Dr. Grosjean says, “but the cognitive empathy they don’t have as well.”
Dr. Neff has experienced this in her practice. “I will often feel what my clients are feeling as they’re feeling it,” she says, adding that she has always had an innate ability to analyze and connect with clients. She’s good at observing the interplay of health conditions, incorporating biology, psychology, and social conceptualizations of issues, with nuance. She feels that recognizing behavioral patterns or psychological triggers in her patients helps her see them holistically and provide better care. “That was a skill even before I realized I was autistic, but I always thought it was just intuitive to everyone,” she says.
Support Can Lead to Success
The Americans with Disabilities Act requires employers to provide reasonable accommodations to neurodivergent employees. However, getting those accommodations involves disclosure, which many physicians have reasons to avoid.
It also means more work. Requesting and putting adjustments in place can take a lot of time and energy to organize. Ms. McVey says they can be “long-winded, multistep tasks” that are not very compatible with ADHD. “Some doctors report that service pressures and funding are used as excuses to refuse adjustments,” she adds.
Ms. McVey lists several workplace accommodations that could be helpful, including flexible working hours, a quiet space to complete paperwork, dictation software, and extra time for medical students to complete written exams.
Neurodivergent physicians have also called for increased diversity of senior leadership and utilizing “cognitive apprenticeship models,” where employees explain their thought processes and receive timely feedback.
But far too often, there is little intervention until a doctor reaches a crisis point. “I look forward to the day when we don’t have to wait until people are profoundly depleted to discover how their brains work,” says Dr. Houser.
Beyond logistical and structural changes in the medical field, Dr. Grosjean speaks of the simple need to listen to colleagues with an open mind and believe them when they express their feelings and experiences. “Everyone has a role to play in challenging stigma, misconceptions, and stereotypes,” Ms. McVey agrees. Ask yourself the old question, she suggests: “If not me, then who? If not now, then when?”
A version of this article first appeared on Medscape.com.
Some 15%-20% of the world’s population are neurodivergent, with conditions such as autism, dyslexia, Tourette syndrome, attention-deficit/hyperactivity disorder (ADHD), and others. With different strengths and challenges around learning, engaging socially, or completing certain tasks, neurodivergent people can face barriers in the workforce.
Meanwhile, studies suggest that neurodivergent people may be overrepresented in STEM fields such as medicine. The medical field may self-select for traits associated with neurodivergent conditions, researchers say, including a hyperfocus on intense interests, pattern recognition, increased curiosity and empathy, and thinking quickly under pressure.
But . They struggle with stigma, a culture of nondisclosure, and lack of accommodations, which can lead to burnout and poor mental health.
“The medical system and the mental health system are some of the spaces that are holding on tightly to some of the outdated understandings of things like autism and ADHD,” says Megan Anna Neff, PsyD, a psychologist with autism and ADHD based in Portland, Oregon.
Situations can get dire: A 2023 survey of more than 200 autistic doctors from several countries found that 77% had considered suicide and 24% had attempted it.
But here’s the crux of it: Many neurodivergent doctors believe their unique ways of thinking and outside-the-box creativity are skills and strengths that can benefit the field. And they say making medicine more inclusive — and better understanding how a neurodivergent physician’s brain works — would allow them to thrive.
Blending In and Breaking Down
The exact number of neurodivergent physicians in the workforce remains unknown. Existing studies are small and focus mainly on autism. But researchers believe the percentage could be higher than we think, because neurodiversity can be underidentified.
Although autism can sometimes be diagnosed as early as 18 months, it’s not uncommon to receive a diagnosis well into adulthood. “Like many late-identified autistic adults, I got my autism diagnosis in the context of autistic burnout,” says Melissa Houser, MD, a primary care physician who received a diagnosis in 2021. Dr. Houser, who uses the pronouns she/they, explains that her experience is common, “a consequence of chronically having your life’s demands exceed your capacity.”
Dr. Houser, who also has ADHD and dyslexia, among other neurodivergent conditions, says that before her diagnosis, she worked in a traditional practice setting. Eventually, she began to notice intense dysregulation and fatigue. “I began to have a lot more difficulties with communication and my motor planning and sequencing,” Dr. Houser says. “I was sleep-deprived, and my needs were not being met. I was in a situation where I had a complete lack of autonomy over my practice.”
Deep in burnout, Dr. Houser says she lost her ability to “mask,” a term used to describe how some neurodivergent people work to “blend in” with societal expectations. This led to further communication breakdowns with her supervisor. Finally, Dr. Houser saw a psychiatrist.
Shortly after her diagnosis, Dr. Houser quit her job and founded All Brains Belong, a nonprofit that provides neurodiversity-affirming medical care, education, and advocacy. Research has found that people with autism are at increased risk for physical health conditions, including immune conditions, gastrointestinal disorders, metabolic conditions, and increased mortality in hospital settings. Understanding these connections can “mean the difference between life and death” for neurodivergent patients, Dr. Houser says.
Yet, in a 2015 study that assessed providers’ ability to recognize autism, a high proportion were not aware that they had patients with autism spectrum disorder, and most reported lacking both the skills and the tools to care for them.
Different as a Doctor and a Patient
Bernadette Grosjean, MD, a retired associate professor of psychiatry at David Geffen School of Medicine at UCLA and a distinguished Fellow of the American Psychiatric Association, also found insight into lifelong experiences as both a doctor and a patient with her autism diagnosis, which came when she was 61.
“Looking back, I was a smart kid but kind of clumsy and different in other ways,” Dr. Grosjean says. According to a 2021 survey by Cambridge University, autistic individuals are significantly more likely to identify as LGBTQ+, and Dr. Grosjean, who is gay, says that not being fully accepted by family or friends played a role in her struggles with mental health issues.
Throughout her mental health treatment, Dr. Grosjean felt as though her providers “were expecting from me things that I didn’t know how to do or fix. I didn’t know how to be a ‘good’ patient,” she recalls.
As a psychiatrist, Dr. Grosjean started to notice that many of the women she treated for borderline personality disorder, which is categorized by unstable relationships and emotions, were autistic. “I then started asking lots of questions about myself — the fact that I’ve always been very sensitive or that I’ve been accused of being both hypersensitive and not having emotions, and I understood a lot.”
When Dr. Grosjean came across Autistic Doctors International, a group of over 800 autistic doctors worldwide, she says, “I found my tribe.” She now serves as the US lead for psychiatry for the group, which is focused on support, advocacy, research, and education around neurodiversity.
Psychiatric comorbidities can accompany neurodivergent conditions. But a growing body of research, including a 2022 study published in the European Archives of Psychiatry and Clinical Neuroscience, indicates that autism and ADHD are frequently misdiagnosed as depression or anxiety.
Dr. Neff was unaware of her conditions until one of her children was diagnosed with autism in 2021. She started to research it. “As I was learning about autism and girls, I was like, ‘Oh, my gosh, this is me,’ ” Dr. Neff recalls. Within a few weeks, she had her own diagnosis.
In hindsight, Dr. Neff has more clarity regarding her struggles in the traditional medical space. She had found it difficult to fit patients into short appointment windows and keep their notes concise. Although she loved hospital work, the environment had been overwhelming and led to burnout.
‘A Deficit-Based Lens’
Dr. Houser believes that too often, autism is viewed through a “deficit-based lens.” Stressors like sensory overload, changes in routine, or unexpected events can exacerbate behavioral challenges for neurodivergent people in the workplace. The DSM-5 criteria for autism, she points out, are largely based on autistic “stress behaviors.”
The result, Dr. Houser says, is that neurodivergent doctors are judged by their response to stressors that put them at a disadvantage rather than their capabilities under more positive circumstances. “The more dysregulated someone is,” she says, “the more likely they are to manifest those observable behaviors.”
Dr. Neff notes that medicine is a very “sensory overwhelming work environment.” Working in ob.gyn. and primary care clinics, she remembers often coming home with a headache and a low-grade fever. “I had no idea why, but I now realize it’s because I was so sensory sick.”
Fearing for her job, Dr. Neff intentionally waited until she was in private practice to disclose her neurodiversity. “I don’t think it would have been received well if I was in a hospital system,” she says. “There’s a lot of invalidation that can come when someone chooses to self-disclose, and their colleagues don’t have a framework in mind to understand.” In one instance, after revealing her diagnosis, she remembers a well-known researcher telling her she wasn’t autistic.
Dr. Grosjean has also had former colleagues invalidate her diagnosis, something she says “keeps people quiet.”
Understanding the Neurodivergent Brain
The general lack of education on how neurodivergent brains work, physicians with these conditions say, means they are not often recognized for how they can function with certain accommodations and how they could contribute in unique ways if their workplace challenges were reduced.
“What we know about autistic brains is that we are systems-thinking pattern matchers,” says Dr. Houser, who formed an interdisciplinary task force to explore medical conditions that are more common in autistic people. Through that comprehensive approach, she has worked to find best practices to treat the constellation of conditions that can arise among these patients. “My autistic brain allowed me to do that,” Dr. Houser says.
Catriona McVey, a medical student in the United Kingdom and creator of the blog Attention Deficit Doctor, points out that “ADHD brains are interest-driven; they can be very focused when you’re doing something enjoyable or new due to increased dopaminergic stimulation.” Ms. McVey speaks from personal experience. “I’ve hyperfocused before on an essay that interested me for over 10 hours,” she recalls, “so I imagine if I was interested in surgery, I could easily hyperfocus on a long operation.”
Empathy is another key part of medical practice. Contrary to stereotypes of neurodivergent people lacking empathy, current research suggests this isn’t true. A concept known as the “double empathy problem,” a term coined by British researcher Damian Milton in 2012, challenges the misconception that autistic people do not have empathy, explains Dr. Grosjean.
Mr. Milton theorized that there are two types of empathy: emotional, when you feel someone else’s pain, and cognitive, which involves critical thinking to understand someone’s emotions or thoughts. “Autistic people have, in general, a lot of emotional empathy,” Dr. Grosjean says, “but the cognitive empathy they don’t have as well.”
Dr. Neff has experienced this in her practice. “I will often feel what my clients are feeling as they’re feeling it,” she says, adding that she has always had an innate ability to analyze and connect with clients. She’s good at observing the interplay of health conditions, incorporating biology, psychology, and social conceptualizations of issues, with nuance. She feels that recognizing behavioral patterns or psychological triggers in her patients helps her see them holistically and provide better care. “That was a skill even before I realized I was autistic, but I always thought it was just intuitive to everyone,” she says.
Support Can Lead to Success
The Americans with Disabilities Act requires employers to provide reasonable accommodations to neurodivergent employees. However, getting those accommodations involves disclosure, which many physicians have reasons to avoid.
It also means more work. Requesting and putting adjustments in place can take a lot of time and energy to organize. Ms. McVey says they can be “long-winded, multistep tasks” that are not very compatible with ADHD. “Some doctors report that service pressures and funding are used as excuses to refuse adjustments,” she adds.
Ms. McVey lists several workplace accommodations that could be helpful, including flexible working hours, a quiet space to complete paperwork, dictation software, and extra time for medical students to complete written exams.
Neurodivergent physicians have also called for increased diversity of senior leadership and utilizing “cognitive apprenticeship models,” where employees explain their thought processes and receive timely feedback.
But far too often, there is little intervention until a doctor reaches a crisis point. “I look forward to the day when we don’t have to wait until people are profoundly depleted to discover how their brains work,” says Dr. Houser.
Beyond logistical and structural changes in the medical field, Dr. Grosjean speaks of the simple need to listen to colleagues with an open mind and believe them when they express their feelings and experiences. “Everyone has a role to play in challenging stigma, misconceptions, and stereotypes,” Ms. McVey agrees. Ask yourself the old question, she suggests: “If not me, then who? If not now, then when?”
A version of this article first appeared on Medscape.com.
Evolving Treatment of Nonradiographic Axial Spondyloarthritis
Nonradiographic axial spondyloarthritis (nr-axSpA) shares many characteristics with radiographic disease and responds to the same treatments, yet it has fewer FDA-approved options.
As Dr Marina Magrey, from Case Western Reserve University School of Medicine, in Cleveland, Ohio, explains, the TNF inhibitor certolizumab has been approved on the basis of results from the C-axSpAnd study.
Similarly, the IL-17 inhibitors secukinumab and ixekizumab are also options, and the results of the COAST-X and PREVENT studies show them to be safe and efficacious.
In closing, Dr Magrey outlines the SELECT-AXIS 2 study showing benefit from the JAK inhibitor upadacitinib for nr-axSpA, with no additional safety signals.
--
Professor of Rheumatology, Case Western Reserve University School of Medicine; Chief, Division of Rheumatology, University Hospitals, Cleveland, Ohio
Marina N. Magrey, MD, has disclosed the following relevant financial relationships:
Serve(d) as a director, officer, partner, employee, advisor, consultant, or trustee for: Novartis; AbbVie; UCB Pharma; Pfizer; Eli Lilly; Janssen; Bristol Myers Squibb
Received research grant from: AbbVie; Bristol Myers Squibb; Amgen
Nonradiographic axial spondyloarthritis (nr-axSpA) shares many characteristics with radiographic disease and responds to the same treatments, yet it has fewer FDA-approved options.
As Dr Marina Magrey, from Case Western Reserve University School of Medicine, in Cleveland, Ohio, explains, the TNF inhibitor certolizumab has been approved on the basis of results from the C-axSpAnd study.
Similarly, the IL-17 inhibitors secukinumab and ixekizumab are also options, and the results of the COAST-X and PREVENT studies show them to be safe and efficacious.
In closing, Dr Magrey outlines the SELECT-AXIS 2 study showing benefit from the JAK inhibitor upadacitinib for nr-axSpA, with no additional safety signals.
--
Professor of Rheumatology, Case Western Reserve University School of Medicine; Chief, Division of Rheumatology, University Hospitals, Cleveland, Ohio
Marina N. Magrey, MD, has disclosed the following relevant financial relationships:
Serve(d) as a director, officer, partner, employee, advisor, consultant, or trustee for: Novartis; AbbVie; UCB Pharma; Pfizer; Eli Lilly; Janssen; Bristol Myers Squibb
Received research grant from: AbbVie; Bristol Myers Squibb; Amgen
Nonradiographic axial spondyloarthritis (nr-axSpA) shares many characteristics with radiographic disease and responds to the same treatments, yet it has fewer FDA-approved options.
As Dr Marina Magrey, from Case Western Reserve University School of Medicine, in Cleveland, Ohio, explains, the TNF inhibitor certolizumab has been approved on the basis of results from the C-axSpAnd study.
Similarly, the IL-17 inhibitors secukinumab and ixekizumab are also options, and the results of the COAST-X and PREVENT studies show them to be safe and efficacious.
In closing, Dr Magrey outlines the SELECT-AXIS 2 study showing benefit from the JAK inhibitor upadacitinib for nr-axSpA, with no additional safety signals.
--
Professor of Rheumatology, Case Western Reserve University School of Medicine; Chief, Division of Rheumatology, University Hospitals, Cleveland, Ohio
Marina N. Magrey, MD, has disclosed the following relevant financial relationships:
Serve(d) as a director, officer, partner, employee, advisor, consultant, or trustee for: Novartis; AbbVie; UCB Pharma; Pfizer; Eli Lilly; Janssen; Bristol Myers Squibb
Received research grant from: AbbVie; Bristol Myers Squibb; Amgen

US Hospitals Prone to Cyberattacks Like One That Impacted Patient Care at Ascension, Experts Say
In the wake of a debilitating cyberattack against one of the nation’s largest health care systems, Marvin Ruckle, a nurse at an Ascension hospital in Wichita, Kansas, said he had a frightening experience: He nearly gave a baby “the wrong dose of narcotic” because of confusing paperwork.
A May 8 ransomware attack against Ascension, a Catholic health system with 140 hospitals in at least 10 states, locked providers out of systems that track and coordinate nearly every aspect of patient care. They include its systems for electronic health records, some phones, and ones “utilized to order certain tests, procedures and medications,” the company said in a May 9 statement.
More than a dozen doctors and nurses who work for the sprawling health system told Michigan Public and KFF Health News that patient care at its hospitals across the nation was compromised in the fallout of the cyberattack over the past several weeks. Clinicians working for hospitals in three states described harrowing lapses, including delayed or lost lab results, medication errors, and an absence of routine safety checks via technology to prevent potentially fatal mistakes.
Despite a precipitous rise in cyberattacks against the health sector in recent years, a weeks-long disruption of this magnitude is beyond what most health systems are prepared for, said John S. Clark, an associate chief pharmacy officer at the University of Michigan health system.
“I don’t believe that anyone is fully prepared,” he said. Most emergency management plans “are designed around long-term downtimes that are into one, two, or three days.”
Ascension in a public statement May 9 said its care teams were “trained for these kinds of disruptions,” but did not respond to questions in early June about whether it had prepared for longer periods of downtime. Ascension said June 14 it had restored access to electronic health records across its network, but that patient “medical records and other information collected between May 8” and when the service was restored “may be temporarily inaccessible as we work to update the portal with information collected during the system downtime.”
Ruckle said he “had no training” for the cyberattack.
Back to Paper
Lisa Watson, an intensive care unit nurse at Ascension Via Christi St. Francis hospital in Wichita, described her own close call. She said she nearly administered the wrong medication to a critically ill patient because she couldn’t scan it as she normally would. “My patient probably would have passed away had I not caught it,” she said.
Watson is no stranger to using paper for patients’ medical charts, saying she did so “for probably half of my career,” before electronic health records became ubiquitous in hospitals. What happened after the cyberattack was “by no means the same.”
“When we paper-charted, we had systems in place to get those orders to other departments in a timely manner,” she said, “and those have all gone away.”
Melissa LaRue, an ICU nurse at Ascension Saint Agnes Hospital in Baltimore, described a close call with “administering the wrong dosage” of a patient’s blood pressure medication. “Luckily,” she said, it was “triple-checked and remedied before that could happen. But I think the potential for harm is there when you have so much information and paperwork that you have to go through.”
Clinicians say their hospitals have relied on slapdash workarounds, using handwritten notes, faxes, sticky notes, and basic computer spreadsheets — many devised on the fly by doctors and nurses — to care for patients.
More than a dozen other nurses and doctors, some of them without union protections, at Ascension hospitals in Michigan recounted situations in which they say patient care was compromised. Those clinicians spoke on the condition that they not be named for fear of retaliation by their employer.
An Ascension hospital emergency room doctor in Detroit said a man on the city’s east side was given a dangerous narcotic intended for another patient because of a paperwork mix-up. As a result, the patient’s breathing slowed to the point that he had to be put on a ventilator. “We intubated him and we sent him to the ICU because he got the wrong medication.”
A nurse in a Michigan Ascension hospital ER said a woman with low blood sugar and “altered mental status” went into cardiac arrest and died after staff said they waited four hours for lab results they needed to determine how to treat her, but never received. “If I started having crushing chest pain in the middle of work and thought I was having a big one, I would grab someone to drive me down the street to another hospital,” the same ER nurse said.
Similar concerns reportedly led a travel nurse at an Ascension hospital in Indiana to quit. “I just want to warn those patients that are coming to any of the Ascension facilities that there will be delays in care. There is potential for error and for harm,” Justin Neisser told CBS4 in Indianapolis in May.
Several nurses and doctors at Ascension hospitals said they feared the errors they’ve witnessed since the cyberattack began could threaten their professional licenses. “This is how a RaDonda Vaught happens,” one nurse said, referring to the Tennessee nurse who was convicted of criminally negligent homicide in 2022 for a fatal drug error.
Reporters were not able to review records to verify clinicians’ claims because of privacy laws surrounding patients’ medical information that apply to health care professionals.
Ascension declined to answer questions about claims that care has been affected by the ransomware attack. “As we have made clear throughout this cyber attack which has impacted our system and our dedicated clinical providers, caring for our patients is our highest priority,” Sean Fitzpatrick, Ascension’s vice president of external communications, said via email on June 3. “We are confident that our care providers in our hospitals and facilities continue to provide quality medical care.”
The federal government requires hospitals to protect patients’ sensitive health data, according to cybersecurity experts. However, there are no federal requirements for hospitals to prevent or prepare for cyberattacks that could compromise their electronic systems.
Hospitals: ‘The No.1 Target of Ransomware’
“We’ve started to think about these as public health issues and disasters on the scale of earthquakes or hurricanes,” said Jeff Tully, a co-director of the Center for Healthcare Cybersecurity at the University of California-San Diego. “These types of cybersecurity incidents should be thought of as a matter of when, and not if.”
Josh Corman, a cybersecurity expert and advocate, said ransom crews regard hospitals as the perfect prey: “They have terrible security and they’ll pay. So almost immediately, hospitals went to the No. 1 target of ransomware.”
In 2023, the health sector experienced the largest share of ransomware attacks of 16 infrastructure sectors considered vital to national security or safety, according to an FBI report on internet crimes. In March, the federal Department of Health and Human Services said reported large breaches involving ransomware had jumped by 264% over the past five years.
A cyberattack this year on Change Healthcare, a unit of UnitedHealth Group’s Optum division that processes billions of health care transactions every year, crippled the business of providers, pharmacies, and hospitals.
In May, UnitedHealth Group CEO Andrew Witty told lawmakers the company paid a $22 million ransom as a result of the Change Healthcare attack — which occurred after hackers accessed a company portal that didn’t have multifactor authentication, a basic cybersecurity tool.
The Biden administration in recent months has pushed to bolster health care cybersecurity standards, but it’s not clear which new measures will be required.
In January, HHS nudged companies to improve email security, add multifactor authentication, and institute cybersecurity training and testing, among other voluntary measures. The Centers for Medicare & Medicaid Services is expected to release new requirements for hospitals, but the scope and timing are unclear. The same is true of an update HHS is expected to make to patient privacy regulations.
HHS said the voluntary measures “will inform the creation of new enforceable cybersecurity standards,” department spokesperson Jeff Nesbit said in a statement.
“The recent cyberattack at Ascension only underscores the need for everyone in the health care ecosystem to do their part to secure their systems and protect patients,” Nesbit said.
Meanwhile, lobbyists for the hospital industry contend cybersecurity mandates or penalties are misplaced and would curtail hospitals’ resources to fend off attacks.
“Hospitals and health systems are not the primary source of cyber risk exposure facing the health care sector,” the American Hospital Association, the largest lobbying group for U.S. hospitals, said in an April statement prepared for U.S. House lawmakers. Most large data breaches that hit hospitals in 2023 originated with third-party “business associates” or other health entities, including CMS itself, the AHA statement said.
Hospitals consolidating into large multistate health systems face increased risk of data breaches and ransomware attacks, according to one study. Ascension in 2022 was the third-largest hospital chain in the U.S. by number of beds, according to the most recent data from the federal Agency for Healthcare Research and Quality.
And while cybersecurity regulations can quickly become outdated, they can at least make it clear that if health systems fail to implement basic protections there “should be consequences for that,” Jim Bagian, a former director of the National Center for Patient Safety at the Veterans Health Administration, told Michigan Public’s Stateside.
Patients can pay the price when lapses occur. Those in hospital care face a greater likelihood of death during a cyberattack, according to researchers at the University of Minnesota School of Public Health.
Workers concerned about patient safety at Ascension hospitals in Michigan have called for the company to make changes.
“We implore Ascension to recognize the internal problems that continue to plague its hospitals, both publicly and transparently,” said Dina Carlisle, a nurse and the president of the OPEIU Local 40 union, which represents nurses at Ascension Providence Rochester. At least 125 staff members at that Ascension hospital have signed a petition asking administrators to temporarily reduce elective surgeries and nonemergency patient admissions, like under the protocols many hospitals adopted early in the covid-19 pandemic.
Watson, the Kansas ICU nurse, said in late May that nurses had urged management to bring in more nurses to help manage the workflow. “Everything that we say has fallen on deaf ears,” she said.
“It is very hard to be a nurse at Ascension right now,” Watson said in late May. “It is very hard to be a patient at Ascension right now.”
If you’re a patient or worker at an Ascension hospital and would like to tell KFF Health News about your experiences, click here to share your story with us.
KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF—an independent source of health policy research, polling, and journalism. Learn more about KFF.
In the wake of a debilitating cyberattack against one of the nation’s largest health care systems, Marvin Ruckle, a nurse at an Ascension hospital in Wichita, Kansas, said he had a frightening experience: He nearly gave a baby “the wrong dose of narcotic” because of confusing paperwork.
A May 8 ransomware attack against Ascension, a Catholic health system with 140 hospitals in at least 10 states, locked providers out of systems that track and coordinate nearly every aspect of patient care. They include its systems for electronic health records, some phones, and ones “utilized to order certain tests, procedures and medications,” the company said in a May 9 statement.
More than a dozen doctors and nurses who work for the sprawling health system told Michigan Public and KFF Health News that patient care at its hospitals across the nation was compromised in the fallout of the cyberattack over the past several weeks. Clinicians working for hospitals in three states described harrowing lapses, including delayed or lost lab results, medication errors, and an absence of routine safety checks via technology to prevent potentially fatal mistakes.
Despite a precipitous rise in cyberattacks against the health sector in recent years, a weeks-long disruption of this magnitude is beyond what most health systems are prepared for, said John S. Clark, an associate chief pharmacy officer at the University of Michigan health system.
“I don’t believe that anyone is fully prepared,” he said. Most emergency management plans “are designed around long-term downtimes that are into one, two, or three days.”
Ascension in a public statement May 9 said its care teams were “trained for these kinds of disruptions,” but did not respond to questions in early June about whether it had prepared for longer periods of downtime. Ascension said June 14 it had restored access to electronic health records across its network, but that patient “medical records and other information collected between May 8” and when the service was restored “may be temporarily inaccessible as we work to update the portal with information collected during the system downtime.”
Ruckle said he “had no training” for the cyberattack.
Back to Paper
Lisa Watson, an intensive care unit nurse at Ascension Via Christi St. Francis hospital in Wichita, described her own close call. She said she nearly administered the wrong medication to a critically ill patient because she couldn’t scan it as she normally would. “My patient probably would have passed away had I not caught it,” she said.
Watson is no stranger to using paper for patients’ medical charts, saying she did so “for probably half of my career,” before electronic health records became ubiquitous in hospitals. What happened after the cyberattack was “by no means the same.”
“When we paper-charted, we had systems in place to get those orders to other departments in a timely manner,” she said, “and those have all gone away.”
Melissa LaRue, an ICU nurse at Ascension Saint Agnes Hospital in Baltimore, described a close call with “administering the wrong dosage” of a patient’s blood pressure medication. “Luckily,” she said, it was “triple-checked and remedied before that could happen. But I think the potential for harm is there when you have so much information and paperwork that you have to go through.”
Clinicians say their hospitals have relied on slapdash workarounds, using handwritten notes, faxes, sticky notes, and basic computer spreadsheets — many devised on the fly by doctors and nurses — to care for patients.
More than a dozen other nurses and doctors, some of them without union protections, at Ascension hospitals in Michigan recounted situations in which they say patient care was compromised. Those clinicians spoke on the condition that they not be named for fear of retaliation by their employer.
An Ascension hospital emergency room doctor in Detroit said a man on the city’s east side was given a dangerous narcotic intended for another patient because of a paperwork mix-up. As a result, the patient’s breathing slowed to the point that he had to be put on a ventilator. “We intubated him and we sent him to the ICU because he got the wrong medication.”
A nurse in a Michigan Ascension hospital ER said a woman with low blood sugar and “altered mental status” went into cardiac arrest and died after staff said they waited four hours for lab results they needed to determine how to treat her, but never received. “If I started having crushing chest pain in the middle of work and thought I was having a big one, I would grab someone to drive me down the street to another hospital,” the same ER nurse said.
Similar concerns reportedly led a travel nurse at an Ascension hospital in Indiana to quit. “I just want to warn those patients that are coming to any of the Ascension facilities that there will be delays in care. There is potential for error and for harm,” Justin Neisser told CBS4 in Indianapolis in May.
Several nurses and doctors at Ascension hospitals said they feared the errors they’ve witnessed since the cyberattack began could threaten their professional licenses. “This is how a RaDonda Vaught happens,” one nurse said, referring to the Tennessee nurse who was convicted of criminally negligent homicide in 2022 for a fatal drug error.
Reporters were not able to review records to verify clinicians’ claims because of privacy laws surrounding patients’ medical information that apply to health care professionals.
Ascension declined to answer questions about claims that care has been affected by the ransomware attack. “As we have made clear throughout this cyber attack which has impacted our system and our dedicated clinical providers, caring for our patients is our highest priority,” Sean Fitzpatrick, Ascension’s vice president of external communications, said via email on June 3. “We are confident that our care providers in our hospitals and facilities continue to provide quality medical care.”
The federal government requires hospitals to protect patients’ sensitive health data, according to cybersecurity experts. However, there are no federal requirements for hospitals to prevent or prepare for cyberattacks that could compromise their electronic systems.
Hospitals: ‘The No.1 Target of Ransomware’
“We’ve started to think about these as public health issues and disasters on the scale of earthquakes or hurricanes,” said Jeff Tully, a co-director of the Center for Healthcare Cybersecurity at the University of California-San Diego. “These types of cybersecurity incidents should be thought of as a matter of when, and not if.”
Josh Corman, a cybersecurity expert and advocate, said ransom crews regard hospitals as the perfect prey: “They have terrible security and they’ll pay. So almost immediately, hospitals went to the No. 1 target of ransomware.”
In 2023, the health sector experienced the largest share of ransomware attacks of 16 infrastructure sectors considered vital to national security or safety, according to an FBI report on internet crimes. In March, the federal Department of Health and Human Services said reported large breaches involving ransomware had jumped by 264% over the past five years.
A cyberattack this year on Change Healthcare, a unit of UnitedHealth Group’s Optum division that processes billions of health care transactions every year, crippled the business of providers, pharmacies, and hospitals.
In May, UnitedHealth Group CEO Andrew Witty told lawmakers the company paid a $22 million ransom as a result of the Change Healthcare attack — which occurred after hackers accessed a company portal that didn’t have multifactor authentication, a basic cybersecurity tool.
The Biden administration in recent months has pushed to bolster health care cybersecurity standards, but it’s not clear which new measures will be required.
In January, HHS nudged companies to improve email security, add multifactor authentication, and institute cybersecurity training and testing, among other voluntary measures. The Centers for Medicare & Medicaid Services is expected to release new requirements for hospitals, but the scope and timing are unclear. The same is true of an update HHS is expected to make to patient privacy regulations.
HHS said the voluntary measures “will inform the creation of new enforceable cybersecurity standards,” department spokesperson Jeff Nesbit said in a statement.
“The recent cyberattack at Ascension only underscores the need for everyone in the health care ecosystem to do their part to secure their systems and protect patients,” Nesbit said.
Meanwhile, lobbyists for the hospital industry contend cybersecurity mandates or penalties are misplaced and would curtail hospitals’ resources to fend off attacks.
“Hospitals and health systems are not the primary source of cyber risk exposure facing the health care sector,” the American Hospital Association, the largest lobbying group for U.S. hospitals, said in an April statement prepared for U.S. House lawmakers. Most large data breaches that hit hospitals in 2023 originated with third-party “business associates” or other health entities, including CMS itself, the AHA statement said.
Hospitals consolidating into large multistate health systems face increased risk of data breaches and ransomware attacks, according to one study. Ascension in 2022 was the third-largest hospital chain in the U.S. by number of beds, according to the most recent data from the federal Agency for Healthcare Research and Quality.
And while cybersecurity regulations can quickly become outdated, they can at least make it clear that if health systems fail to implement basic protections there “should be consequences for that,” Jim Bagian, a former director of the National Center for Patient Safety at the Veterans Health Administration, told Michigan Public’s Stateside.
Patients can pay the price when lapses occur. Those in hospital care face a greater likelihood of death during a cyberattack, according to researchers at the University of Minnesota School of Public Health.
Workers concerned about patient safety at Ascension hospitals in Michigan have called for the company to make changes.
“We implore Ascension to recognize the internal problems that continue to plague its hospitals, both publicly and transparently,” said Dina Carlisle, a nurse and the president of the OPEIU Local 40 union, which represents nurses at Ascension Providence Rochester. At least 125 staff members at that Ascension hospital have signed a petition asking administrators to temporarily reduce elective surgeries and nonemergency patient admissions, like under the protocols many hospitals adopted early in the covid-19 pandemic.
Watson, the Kansas ICU nurse, said in late May that nurses had urged management to bring in more nurses to help manage the workflow. “Everything that we say has fallen on deaf ears,” she said.
“It is very hard to be a nurse at Ascension right now,” Watson said in late May. “It is very hard to be a patient at Ascension right now.”
If you’re a patient or worker at an Ascension hospital and would like to tell KFF Health News about your experiences, click here to share your story with us.
KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF—an independent source of health policy research, polling, and journalism. Learn more about KFF.
In the wake of a debilitating cyberattack against one of the nation’s largest health care systems, Marvin Ruckle, a nurse at an Ascension hospital in Wichita, Kansas, said he had a frightening experience: He nearly gave a baby “the wrong dose of narcotic” because of confusing paperwork.
A May 8 ransomware attack against Ascension, a Catholic health system with 140 hospitals in at least 10 states, locked providers out of systems that track and coordinate nearly every aspect of patient care. They include its systems for electronic health records, some phones, and ones “utilized to order certain tests, procedures and medications,” the company said in a May 9 statement.
More than a dozen doctors and nurses who work for the sprawling health system told Michigan Public and KFF Health News that patient care at its hospitals across the nation was compromised in the fallout of the cyberattack over the past several weeks. Clinicians working for hospitals in three states described harrowing lapses, including delayed or lost lab results, medication errors, and an absence of routine safety checks via technology to prevent potentially fatal mistakes.
Despite a precipitous rise in cyberattacks against the health sector in recent years, a weeks-long disruption of this magnitude is beyond what most health systems are prepared for, said John S. Clark, an associate chief pharmacy officer at the University of Michigan health system.
“I don’t believe that anyone is fully prepared,” he said. Most emergency management plans “are designed around long-term downtimes that are into one, two, or three days.”
Ascension in a public statement May 9 said its care teams were “trained for these kinds of disruptions,” but did not respond to questions in early June about whether it had prepared for longer periods of downtime. Ascension said June 14 it had restored access to electronic health records across its network, but that patient “medical records and other information collected between May 8” and when the service was restored “may be temporarily inaccessible as we work to update the portal with information collected during the system downtime.”
Ruckle said he “had no training” for the cyberattack.
Back to Paper
Lisa Watson, an intensive care unit nurse at Ascension Via Christi St. Francis hospital in Wichita, described her own close call. She said she nearly administered the wrong medication to a critically ill patient because she couldn’t scan it as she normally would. “My patient probably would have passed away had I not caught it,” she said.
Watson is no stranger to using paper for patients’ medical charts, saying she did so “for probably half of my career,” before electronic health records became ubiquitous in hospitals. What happened after the cyberattack was “by no means the same.”
“When we paper-charted, we had systems in place to get those orders to other departments in a timely manner,” she said, “and those have all gone away.”
Melissa LaRue, an ICU nurse at Ascension Saint Agnes Hospital in Baltimore, described a close call with “administering the wrong dosage” of a patient’s blood pressure medication. “Luckily,” she said, it was “triple-checked and remedied before that could happen. But I think the potential for harm is there when you have so much information and paperwork that you have to go through.”
Clinicians say their hospitals have relied on slapdash workarounds, using handwritten notes, faxes, sticky notes, and basic computer spreadsheets — many devised on the fly by doctors and nurses — to care for patients.
More than a dozen other nurses and doctors, some of them without union protections, at Ascension hospitals in Michigan recounted situations in which they say patient care was compromised. Those clinicians spoke on the condition that they not be named for fear of retaliation by their employer.
An Ascension hospital emergency room doctor in Detroit said a man on the city’s east side was given a dangerous narcotic intended for another patient because of a paperwork mix-up. As a result, the patient’s breathing slowed to the point that he had to be put on a ventilator. “We intubated him and we sent him to the ICU because he got the wrong medication.”
A nurse in a Michigan Ascension hospital ER said a woman with low blood sugar and “altered mental status” went into cardiac arrest and died after staff said they waited four hours for lab results they needed to determine how to treat her, but never received. “If I started having crushing chest pain in the middle of work and thought I was having a big one, I would grab someone to drive me down the street to another hospital,” the same ER nurse said.
Similar concerns reportedly led a travel nurse at an Ascension hospital in Indiana to quit. “I just want to warn those patients that are coming to any of the Ascension facilities that there will be delays in care. There is potential for error and for harm,” Justin Neisser told CBS4 in Indianapolis in May.
Several nurses and doctors at Ascension hospitals said they feared the errors they’ve witnessed since the cyberattack began could threaten their professional licenses. “This is how a RaDonda Vaught happens,” one nurse said, referring to the Tennessee nurse who was convicted of criminally negligent homicide in 2022 for a fatal drug error.
Reporters were not able to review records to verify clinicians’ claims because of privacy laws surrounding patients’ medical information that apply to health care professionals.
Ascension declined to answer questions about claims that care has been affected by the ransomware attack. “As we have made clear throughout this cyber attack which has impacted our system and our dedicated clinical providers, caring for our patients is our highest priority,” Sean Fitzpatrick, Ascension’s vice president of external communications, said via email on June 3. “We are confident that our care providers in our hospitals and facilities continue to provide quality medical care.”
The federal government requires hospitals to protect patients’ sensitive health data, according to cybersecurity experts. However, there are no federal requirements for hospitals to prevent or prepare for cyberattacks that could compromise their electronic systems.
Hospitals: ‘The No.1 Target of Ransomware’
“We’ve started to think about these as public health issues and disasters on the scale of earthquakes or hurricanes,” said Jeff Tully, a co-director of the Center for Healthcare Cybersecurity at the University of California-San Diego. “These types of cybersecurity incidents should be thought of as a matter of when, and not if.”
Josh Corman, a cybersecurity expert and advocate, said ransom crews regard hospitals as the perfect prey: “They have terrible security and they’ll pay. So almost immediately, hospitals went to the No. 1 target of ransomware.”
In 2023, the health sector experienced the largest share of ransomware attacks of 16 infrastructure sectors considered vital to national security or safety, according to an FBI report on internet crimes. In March, the federal Department of Health and Human Services said reported large breaches involving ransomware had jumped by 264% over the past five years.
A cyberattack this year on Change Healthcare, a unit of UnitedHealth Group’s Optum division that processes billions of health care transactions every year, crippled the business of providers, pharmacies, and hospitals.
In May, UnitedHealth Group CEO Andrew Witty told lawmakers the company paid a $22 million ransom as a result of the Change Healthcare attack — which occurred after hackers accessed a company portal that didn’t have multifactor authentication, a basic cybersecurity tool.
The Biden administration in recent months has pushed to bolster health care cybersecurity standards, but it’s not clear which new measures will be required.
In January, HHS nudged companies to improve email security, add multifactor authentication, and institute cybersecurity training and testing, among other voluntary measures. The Centers for Medicare & Medicaid Services is expected to release new requirements for hospitals, but the scope and timing are unclear. The same is true of an update HHS is expected to make to patient privacy regulations.
HHS said the voluntary measures “will inform the creation of new enforceable cybersecurity standards,” department spokesperson Jeff Nesbit said in a statement.
“The recent cyberattack at Ascension only underscores the need for everyone in the health care ecosystem to do their part to secure their systems and protect patients,” Nesbit said.
Meanwhile, lobbyists for the hospital industry contend cybersecurity mandates or penalties are misplaced and would curtail hospitals’ resources to fend off attacks.
“Hospitals and health systems are not the primary source of cyber risk exposure facing the health care sector,” the American Hospital Association, the largest lobbying group for U.S. hospitals, said in an April statement prepared for U.S. House lawmakers. Most large data breaches that hit hospitals in 2023 originated with third-party “business associates” or other health entities, including CMS itself, the AHA statement said.
Hospitals consolidating into large multistate health systems face increased risk of data breaches and ransomware attacks, according to one study. Ascension in 2022 was the third-largest hospital chain in the U.S. by number of beds, according to the most recent data from the federal Agency for Healthcare Research and Quality.
And while cybersecurity regulations can quickly become outdated, they can at least make it clear that if health systems fail to implement basic protections there “should be consequences for that,” Jim Bagian, a former director of the National Center for Patient Safety at the Veterans Health Administration, told Michigan Public’s Stateside.
Patients can pay the price when lapses occur. Those in hospital care face a greater likelihood of death during a cyberattack, according to researchers at the University of Minnesota School of Public Health.
Workers concerned about patient safety at Ascension hospitals in Michigan have called for the company to make changes.
“We implore Ascension to recognize the internal problems that continue to plague its hospitals, both publicly and transparently,” said Dina Carlisle, a nurse and the president of the OPEIU Local 40 union, which represents nurses at Ascension Providence Rochester. At least 125 staff members at that Ascension hospital have signed a petition asking administrators to temporarily reduce elective surgeries and nonemergency patient admissions, like under the protocols many hospitals adopted early in the covid-19 pandemic.
Watson, the Kansas ICU nurse, said in late May that nurses had urged management to bring in more nurses to help manage the workflow. “Everything that we say has fallen on deaf ears,” she said.
“It is very hard to be a nurse at Ascension right now,” Watson said in late May. “It is very hard to be a patient at Ascension right now.”
If you’re a patient or worker at an Ascension hospital and would like to tell KFF Health News about your experiences, click here to share your story with us.
KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF—an independent source of health policy research, polling, and journalism. Learn more about KFF.
Should You Offer Medical Credit Cards?
Editor’s note: This is Dr. Eastern’s last “Managing Your Practice” column for Dermatology News. After his first column was published in 1986, Dr. Eastern continued writing his column monthly until the mid-1990s, resuming in 2005. In total, he has written over 300 columns on topics relevant to medical practice, ranging from hiring employees, selling and merging practices, complying with OSHA, and avoiding embezzlement, to electronic health records, burnout, medical assistants, negative online reviews, artificial intelligence in the office, and more. In the future, he will continue to provide commentary on practice issues with an occasional guest editorial.
Medicare reimbursement cuts, increasing overhead and staff salaries, and inflation have made running a profitable private practice increasingly challenging, particularly for rural and smaller offices. Medical credit cards are an increasingly popular choice to fill this gap.

Traditionally, these cards were used to help cover procedures insurance didn’t cover — such as cosmetic procedures — but over the years, they have been expanded to cover other healthcare charges, mostly for patients who are paying out of pocket due to inadequate insurance or other reasons.
Advantages for physicians include immediate payment from the credit card company and reduced billing and collection costs. Patients are also less likely to delay or defer treatment if they can charge the payment and pay it back in installments.
The first step in offering medical credit cards is signing up with one or more third-party card companies. CareCredit is the most common provider in the medical credit card market. Other vendors include Wells Fargo, AccessOne, Alphaeon Credit, and iCare Financial. (As always, I have no financial interest in any product or service mentioned in this column.) A member of your staff signs patients up, and the credit card company checks their credit. If approved, the card company pays you your fee and assumes responsibility for collecting from the patient.
The interest charge on medical credit cards is often deferred for a period of time, typically between 6 and 24 months. If patients pay off the debt within this time, they can avoid paying interest. But, like other credit cards, if they make late payments or have an unpaid balance once the promotional period ends, they may end up with interest and fees totaling 25%-30% or more. It is important to make it very clear to your patients that payments are interest-free only if they are all made on time and within the promotional period.

According to a Consumer Financial Protection Bureau report released earlier this year, deferred interest medical credit cards or loans were used to pay nearly $23 billion in healthcare expenses from 2018 to 2020. Individuals unable to complete payment during the promotional period paid $1 billion in deferred interest payments during that period.
Despite the growing popularity of medical credit cards among physicians, it is worth noting that some consumer groups view them as predatory financial products, marketed toward people in tough financial situations. A coalition of 60 health advocacy groups has urged the Biden Administration to ban deferred interest medical credit cards. So there is that much more reason to choose candidates for medical credit cards carefully, and to make them fully aware of what obligations they are assuming.
Patients who do not think they can pay off the balance within the interest-free time frame should probably be advised to pursue an alternative payment method, such as using a conventional credit card, taking out a personal or home-equity loan, or borrowing from a retirement savings account. Some physicians are willing to negotiate a reduced fee for patients who agree to pay cash at the time of service.
Those who do choose to apply for a medical credit card should be informed of their options, which can vary considerably depending on the product and the third-party vendor. Some medical credit products can be used only for elective procedures, but some can be used more broadly for various medical expenses. Check to make sure that each patient’s financing option can be used for his or her desired medical service.
Some payment products can only be used at specific practices or groups, while others can be used at a variety of medical offices and hospitals. If a patient arrives with a medical credit card already in hand, confirm that it is one that your office accepts.
Interest rates generally vary with each card and vendor. Make patients aware of when interest rates start accruing and if the plan offers a fixed or variable APR, or if it charges compounding interest. Confirm if there is a deferred interest option, and if so, for how long.
Different medical credit products also have varying fees and payment schedules. See that each patient reads the terms of the agreement to understand when interest may start to accrue or change, as well as when certain fees may apply. Understanding when the payments are due will help them avoid additional fees, including late fees. Some medical payment plans may also have administrative or processing fees. If so, patients should be made aware of them.
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, New Jersey. He is the author of numerous articles and textbook chapters, and is a longtime monthly columnist for Dermatology News. Write to him at [email protected].
Editor’s note: This is Dr. Eastern’s last “Managing Your Practice” column for Dermatology News. After his first column was published in 1986, Dr. Eastern continued writing his column monthly until the mid-1990s, resuming in 2005. In total, he has written over 300 columns on topics relevant to medical practice, ranging from hiring employees, selling and merging practices, complying with OSHA, and avoiding embezzlement, to electronic health records, burnout, medical assistants, negative online reviews, artificial intelligence in the office, and more. In the future, he will continue to provide commentary on practice issues with an occasional guest editorial.
Medicare reimbursement cuts, increasing overhead and staff salaries, and inflation have made running a profitable private practice increasingly challenging, particularly for rural and smaller offices. Medical credit cards are an increasingly popular choice to fill this gap.
Traditionally, these cards were used to help cover procedures insurance didn’t cover — such as cosmetic procedures — but over the years, they have been expanded to cover other healthcare charges, mostly for patients who are paying out of pocket due to inadequate insurance or other reasons.
Advantages for physicians include immediate payment from the credit card company and reduced billing and collection costs. Patients are also less likely to delay or defer treatment if they can charge the payment and pay it back in installments.
The first step in offering medical credit cards is signing up with one or more third-party card companies. CareCredit is the most common provider in the medical credit card market. Other vendors include Wells Fargo, AccessOne, Alphaeon Credit, and iCare Financial. (As always, I have no financial interest in any product or service mentioned in this column.) A member of your staff signs patients up, and the credit card company checks their credit. If approved, the card company pays you your fee and assumes responsibility for collecting from the patient.
The interest charge on medical credit cards is often deferred for a period of time, typically between 6 and 24 months. If patients pay off the debt within this time, they can avoid paying interest. But, like other credit cards, if they make late payments or have an unpaid balance once the promotional period ends, they may end up with interest and fees totaling 25%-30% or more. It is important to make it very clear to your patients that payments are interest-free only if they are all made on time and within the promotional period.
According to a Consumer Financial Protection Bureau report released earlier this year, deferred interest medical credit cards or loans were used to pay nearly $23 billion in healthcare expenses from 2018 to 2020. Individuals unable to complete payment during the promotional period paid $1 billion in deferred interest payments during that period.
Despite the growing popularity of medical credit cards among physicians, it is worth noting that some consumer groups view them as predatory financial products, marketed toward people in tough financial situations. A coalition of 60 health advocacy groups has urged the Biden Administration to ban deferred interest medical credit cards. So there is that much more reason to choose candidates for medical credit cards carefully, and to make them fully aware of what obligations they are assuming.
Patients who do not think they can pay off the balance within the interest-free time frame should probably be advised to pursue an alternative payment method, such as using a conventional credit card, taking out a personal or home-equity loan, or borrowing from a retirement savings account. Some physicians are willing to negotiate a reduced fee for patients who agree to pay cash at the time of service.
Those who do choose to apply for a medical credit card should be informed of their options, which can vary considerably depending on the product and the third-party vendor. Some medical credit products can be used only for elective procedures, but some can be used more broadly for various medical expenses. Check to make sure that each patient’s financing option can be used for his or her desired medical service.
Some payment products can only be used at specific practices or groups, while others can be used at a variety of medical offices and hospitals. If a patient arrives with a medical credit card already in hand, confirm that it is one that your office accepts.
Interest rates generally vary with each card and vendor. Make patients aware of when interest rates start accruing and if the plan offers a fixed or variable APR, or if it charges compounding interest. Confirm if there is a deferred interest option, and if so, for how long.
Different medical credit products also have varying fees and payment schedules. See that each patient reads the terms of the agreement to understand when interest may start to accrue or change, as well as when certain fees may apply. Understanding when the payments are due will help them avoid additional fees, including late fees. Some medical payment plans may also have administrative or processing fees. If so, patients should be made aware of them.
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, New Jersey. He is the author of numerous articles and textbook chapters, and is a longtime monthly columnist for Dermatology News. Write to him at [email protected].
Editor’s note: This is Dr. Eastern’s last “Managing Your Practice” column for Dermatology News. After his first column was published in 1986, Dr. Eastern continued writing his column monthly until the mid-1990s, resuming in 2005. In total, he has written over 300 columns on topics relevant to medical practice, ranging from hiring employees, selling and merging practices, complying with OSHA, and avoiding embezzlement, to electronic health records, burnout, medical assistants, negative online reviews, artificial intelligence in the office, and more. In the future, he will continue to provide commentary on practice issues with an occasional guest editorial.
Medicare reimbursement cuts, increasing overhead and staff salaries, and inflation have made running a profitable private practice increasingly challenging, particularly for rural and smaller offices. Medical credit cards are an increasingly popular choice to fill this gap.
Traditionally, these cards were used to help cover procedures insurance didn’t cover — such as cosmetic procedures — but over the years, they have been expanded to cover other healthcare charges, mostly for patients who are paying out of pocket due to inadequate insurance or other reasons.
Advantages for physicians include immediate payment from the credit card company and reduced billing and collection costs. Patients are also less likely to delay or defer treatment if they can charge the payment and pay it back in installments.
The first step in offering medical credit cards is signing up with one or more third-party card companies. CareCredit is the most common provider in the medical credit card market. Other vendors include Wells Fargo, AccessOne, Alphaeon Credit, and iCare Financial. (As always, I have no financial interest in any product or service mentioned in this column.) A member of your staff signs patients up, and the credit card company checks their credit. If approved, the card company pays you your fee and assumes responsibility for collecting from the patient.
The interest charge on medical credit cards is often deferred for a period of time, typically between 6 and 24 months. If patients pay off the debt within this time, they can avoid paying interest. But, like other credit cards, if they make late payments or have an unpaid balance once the promotional period ends, they may end up with interest and fees totaling 25%-30% or more. It is important to make it very clear to your patients that payments are interest-free only if they are all made on time and within the promotional period.
According to a Consumer Financial Protection Bureau report released earlier this year, deferred interest medical credit cards or loans were used to pay nearly $23 billion in healthcare expenses from 2018 to 2020. Individuals unable to complete payment during the promotional period paid $1 billion in deferred interest payments during that period.
Despite the growing popularity of medical credit cards among physicians, it is worth noting that some consumer groups view them as predatory financial products, marketed toward people in tough financial situations. A coalition of 60 health advocacy groups has urged the Biden Administration to ban deferred interest medical credit cards. So there is that much more reason to choose candidates for medical credit cards carefully, and to make them fully aware of what obligations they are assuming.
Patients who do not think they can pay off the balance within the interest-free time frame should probably be advised to pursue an alternative payment method, such as using a conventional credit card, taking out a personal or home-equity loan, or borrowing from a retirement savings account. Some physicians are willing to negotiate a reduced fee for patients who agree to pay cash at the time of service.
Those who do choose to apply for a medical credit card should be informed of their options, which can vary considerably depending on the product and the third-party vendor. Some medical credit products can be used only for elective procedures, but some can be used more broadly for various medical expenses. Check to make sure that each patient’s financing option can be used for his or her desired medical service.
Some payment products can only be used at specific practices or groups, while others can be used at a variety of medical offices and hospitals. If a patient arrives with a medical credit card already in hand, confirm that it is one that your office accepts.
Interest rates generally vary with each card and vendor. Make patients aware of when interest rates start accruing and if the plan offers a fixed or variable APR, or if it charges compounding interest. Confirm if there is a deferred interest option, and if so, for how long.
Different medical credit products also have varying fees and payment schedules. See that each patient reads the terms of the agreement to understand when interest may start to accrue or change, as well as when certain fees may apply. Understanding when the payments are due will help them avoid additional fees, including late fees. Some medical payment plans may also have administrative or processing fees. If so, patients should be made aware of them.
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, New Jersey. He is the author of numerous articles and textbook chapters, and is a longtime monthly columnist for Dermatology News. Write to him at [email protected].
Latest Izokibep Trial for PsA Shows Promise But Misses on Enthesitis
VIENNA — The investigational interleukin (IL)-17 inhibitor izokibep hit its mark when it came to improving overall disease activity in people with active psoriatic arthritis (PsA) in a phase 2b/3 trial, but it was no better than placebo at reducing inflammation of the entheses.
This apparent and unexpected lack of effect in the entheses was a key talking point after Philip J. Mease, MD, presented the late-breaking trial findings at the annual European Congress of Rheumatology.

At just 18.6 kilodaltons in size, izokibep is just “one tenth the size of a standard monoclonal antibody” and is classed as a small protein therapeutic, Dr. Mease said. It has a “very tight” binding affinity for IL-17A, and because it also binds to albumin, it has a prolonged half-life compared with other IL-17 inhibitors. Potentially, it should be able to “penetrate into difficult areas,” such as the entheses, he said.
Prespecified Enthesitis Analysis
However, results of a prespecified secondary analysis conducted in 209 of the 343 trial participants who had received treatment showed no significant difference in the proportions with enthesis resolution at 16 weeks, defined as a Leeds Enthesitis Index (LEI) of 0.
Comparing two dosing regimens of izokibep 160 mg once weekly (QW) vs every other week (Q2W) with placebo, enthesitis resolution was seen in 45%, 56%, and 47%, respectively, of patients.
The LEI is “sometimes subject to problems with evaluation because of placebo response, which is what we see here,” noted Dr. Mease, director of rheumatology research at the Providence Swedish Medical Center and a rheumatology professor at the University of Washington School of Medicine in Seattle.
An exploratory analysis showed that there was a better response for izokibep vs placebo if the analysis included only patients with higher LEI scores at baseline, at 8.0% (n = 12) for placebo, 22.0% (n = 9) for izokibep 160 mg QW, and 50.0% (n = 12) for izokibep 160 mg Q2W.
Main Efficacy Data
The primary endpoint for the trial was the proportion of patients who had 50% improvement in American College of Rheumatology response criteria (ACR50) at 16 weeks. This showed a clear advantage for treatment with izokibep 160 QW and Q2W compared with placebo, with a respective 40%, 43%, and 15% of patients meeting this endpoint.
Corresponding ACR20 response rates were 59%, 64%, and 35%, respectively; ACR70 response rates were a respective 25%, 23%, and 5%.
In addition to ACR70, izokibep 160 QW and Q2W met a number of other “high hurdle” efficacy endpoints better than did placebo, Dr. Mease reported. A 90% reduction from baseline in the Psoriasis Area and Severity Index (PASI90) was achieved by a respective 64%, 58%, and 12% of patients, and a 100% reduction in this index (PASI100) was achieved by a respective 51%, 47%, and 12%. And 41%, 42%, and 14% of patients, respectively, met the criteria for minimal disease activity.
Patient Population
Mease pointed out during his presentation that the trial included patients with adult-onset PsA that had been ongoing for ≥ 6 months. Patients had to have at least three tender or swollen joints and an inadequate response, intolerance, or contraindication to commonly used front-line therapies such as nonsteroidal anti-inflammatory drugs, conventional synthetic disease-modifying antirheumatic drugs (csDMARDs), and tumor necrosis factor inhibitors (TNFi).
In fact, around half of the participants across the three treatment arms had received prior csDMARDs, and almost a quarter had received a TNFi.
The mean duration of disease was around 7 years, the average age was about 50 years, and the majority of the participants were White individuals. There were more women than men in the placebo vs the izokibep arms (43.4% vs about 60.0%).
Adverse Events
Injection site reactions were the most common adverse events, most of which were mild to moderate. Very few (< 1% to 4%) led to any need to discontinue the drug.
Serious adverse events occurred at low rates in all study arms: 0.8% for placebo, 2.7% for izokibep QW, and 1.8% for izokibep Q2W.
One patient each (0.9%) in the izokibep arms developed ulcerative colitis, whereas none in the placebo group did. Only two patients developed candidiasis. One was in the placebo group and had a skin infection, and the other was an oral infection in the QW izokibep arm.
There were no cases of uveitis, suicidal ideation, or deaths reported.
Comments on the Study
During the discussion that followed the presentation, Walter P. Maksymowych, MBChB, of the University of Alberta in Edmonton, Alberta, Canada, addressed the dosing regimens used.

“Looking at the side effect profile and then looking at the response rate, comparing the weekly dosing and every 2 weeks, do you think, in hindsight, you might be remiss that there wasn’t an additional dosing on a monthly basis, especially since this is a construct that is meant to prolong the half-life of the molecule?” he asked, adding that perhaps this should be something to consider in future studies.
Mease responded that there had been a fourth dosing arm in the trial — izokibep 80 mg once a month — but because there were only eight patients, the data were not sufficiently robust to analyze.
Commenting on the study, Laura C. Coates, MBChB, PhD, said: “It’s a pretty standard phase 2b/3 study,” and the outcomes were not wildly different from what has been seen with other IL-17A inhibitors.
“In phase 2, the enthesitis data looked really good; in phase 3, the enthesitis data looks the same as for any other IL-17 inhibitor,” Dr. Coates said.

More and longer-term data are needed to see if “the theoretical biological difference in the drug design translates to a different clinical outcome or whether it’s another IL-17,” added Dr. Coates, a clinician scientist and senior clinical research fellow at the University of Oxford in England.
Dennis McGonagle, MB MCH BAO, PhD, of the University of Leeds, England, also picked up on the enthesitis data, echoing the conclusion that the phase 2 enthesitis data were “spectacular” and noting that “it’s a real inversion of what was expected, given the small molecule.”
The study was funded by Acelyrin. Dr. Mease disclosed ties with Acelyrin and other pharmaceutical companies. Dr. Maksymowych, Dr. Coates, and Dr. McGonagle reported having a variety of financial relationships with pharmaceutical companies outside of this study.
A version of this article appeared on Medscape.com.
VIENNA — The investigational interleukin (IL)-17 inhibitor izokibep hit its mark when it came to improving overall disease activity in people with active psoriatic arthritis (PsA) in a phase 2b/3 trial, but it was no better than placebo at reducing inflammation of the entheses.
This apparent and unexpected lack of effect in the entheses was a key talking point after Philip J. Mease, MD, presented the late-breaking trial findings at the annual European Congress of Rheumatology.
At just 18.6 kilodaltons in size, izokibep is just “one tenth the size of a standard monoclonal antibody” and is classed as a small protein therapeutic, Dr. Mease said. It has a “very tight” binding affinity for IL-17A, and because it also binds to albumin, it has a prolonged half-life compared with other IL-17 inhibitors. Potentially, it should be able to “penetrate into difficult areas,” such as the entheses, he said.
Prespecified Enthesitis Analysis
However, results of a prespecified secondary analysis conducted in 209 of the 343 trial participants who had received treatment showed no significant difference in the proportions with enthesis resolution at 16 weeks, defined as a Leeds Enthesitis Index (LEI) of 0.
Comparing two dosing regimens of izokibep 160 mg once weekly (QW) vs every other week (Q2W) with placebo, enthesitis resolution was seen in 45%, 56%, and 47%, respectively, of patients.
The LEI is “sometimes subject to problems with evaluation because of placebo response, which is what we see here,” noted Dr. Mease, director of rheumatology research at the Providence Swedish Medical Center and a rheumatology professor at the University of Washington School of Medicine in Seattle.
An exploratory analysis showed that there was a better response for izokibep vs placebo if the analysis included only patients with higher LEI scores at baseline, at 8.0% (n = 12) for placebo, 22.0% (n = 9) for izokibep 160 mg QW, and 50.0% (n = 12) for izokibep 160 mg Q2W.
Main Efficacy Data
The primary endpoint for the trial was the proportion of patients who had 50% improvement in American College of Rheumatology response criteria (ACR50) at 16 weeks. This showed a clear advantage for treatment with izokibep 160 QW and Q2W compared with placebo, with a respective 40%, 43%, and 15% of patients meeting this endpoint.
Corresponding ACR20 response rates were 59%, 64%, and 35%, respectively; ACR70 response rates were a respective 25%, 23%, and 5%.
In addition to ACR70, izokibep 160 QW and Q2W met a number of other “high hurdle” efficacy endpoints better than did placebo, Dr. Mease reported. A 90% reduction from baseline in the Psoriasis Area and Severity Index (PASI90) was achieved by a respective 64%, 58%, and 12% of patients, and a 100% reduction in this index (PASI100) was achieved by a respective 51%, 47%, and 12%. And 41%, 42%, and 14% of patients, respectively, met the criteria for minimal disease activity.
Patient Population
Mease pointed out during his presentation that the trial included patients with adult-onset PsA that had been ongoing for ≥ 6 months. Patients had to have at least three tender or swollen joints and an inadequate response, intolerance, or contraindication to commonly used front-line therapies such as nonsteroidal anti-inflammatory drugs, conventional synthetic disease-modifying antirheumatic drugs (csDMARDs), and tumor necrosis factor inhibitors (TNFi).
In fact, around half of the participants across the three treatment arms had received prior csDMARDs, and almost a quarter had received a TNFi.
The mean duration of disease was around 7 years, the average age was about 50 years, and the majority of the participants were White individuals. There were more women than men in the placebo vs the izokibep arms (43.4% vs about 60.0%).
Adverse Events
Injection site reactions were the most common adverse events, most of which were mild to moderate. Very few (< 1% to 4%) led to any need to discontinue the drug.
Serious adverse events occurred at low rates in all study arms: 0.8% for placebo, 2.7% for izokibep QW, and 1.8% for izokibep Q2W.
One patient each (0.9%) in the izokibep arms developed ulcerative colitis, whereas none in the placebo group did. Only two patients developed candidiasis. One was in the placebo group and had a skin infection, and the other was an oral infection in the QW izokibep arm.
There were no cases of uveitis, suicidal ideation, or deaths reported.
Comments on the Study
During the discussion that followed the presentation, Walter P. Maksymowych, MBChB, of the University of Alberta in Edmonton, Alberta, Canada, addressed the dosing regimens used.
“Looking at the side effect profile and then looking at the response rate, comparing the weekly dosing and every 2 weeks, do you think, in hindsight, you might be remiss that there wasn’t an additional dosing on a monthly basis, especially since this is a construct that is meant to prolong the half-life of the molecule?” he asked, adding that perhaps this should be something to consider in future studies.
Mease responded that there had been a fourth dosing arm in the trial — izokibep 80 mg once a month — but because there were only eight patients, the data were not sufficiently robust to analyze.
Commenting on the study, Laura C. Coates, MBChB, PhD, said: “It’s a pretty standard phase 2b/3 study,” and the outcomes were not wildly different from what has been seen with other IL-17A inhibitors.
“In phase 2, the enthesitis data looked really good; in phase 3, the enthesitis data looks the same as for any other IL-17 inhibitor,” Dr. Coates said.
More and longer-term data are needed to see if “the theoretical biological difference in the drug design translates to a different clinical outcome or whether it’s another IL-17,” added Dr. Coates, a clinician scientist and senior clinical research fellow at the University of Oxford in England.
Dennis McGonagle, MB MCH BAO, PhD, of the University of Leeds, England, also picked up on the enthesitis data, echoing the conclusion that the phase 2 enthesitis data were “spectacular” and noting that “it’s a real inversion of what was expected, given the small molecule.”
The study was funded by Acelyrin. Dr. Mease disclosed ties with Acelyrin and other pharmaceutical companies. Dr. Maksymowych, Dr. Coates, and Dr. McGonagle reported having a variety of financial relationships with pharmaceutical companies outside of this study.
A version of this article appeared on Medscape.com.
VIENNA — The investigational interleukin (IL)-17 inhibitor izokibep hit its mark when it came to improving overall disease activity in people with active psoriatic arthritis (PsA) in a phase 2b/3 trial, but it was no better than placebo at reducing inflammation of the entheses.
This apparent and unexpected lack of effect in the entheses was a key talking point after Philip J. Mease, MD, presented the late-breaking trial findings at the annual European Congress of Rheumatology.
At just 18.6 kilodaltons in size, izokibep is just “one tenth the size of a standard monoclonal antibody” and is classed as a small protein therapeutic, Dr. Mease said. It has a “very tight” binding affinity for IL-17A, and because it also binds to albumin, it has a prolonged half-life compared with other IL-17 inhibitors. Potentially, it should be able to “penetrate into difficult areas,” such as the entheses, he said.
Prespecified Enthesitis Analysis
However, results of a prespecified secondary analysis conducted in 209 of the 343 trial participants who had received treatment showed no significant difference in the proportions with enthesis resolution at 16 weeks, defined as a Leeds Enthesitis Index (LEI) of 0.
Comparing two dosing regimens of izokibep 160 mg once weekly (QW) vs every other week (Q2W) with placebo, enthesitis resolution was seen in 45%, 56%, and 47%, respectively, of patients.
The LEI is “sometimes subject to problems with evaluation because of placebo response, which is what we see here,” noted Dr. Mease, director of rheumatology research at the Providence Swedish Medical Center and a rheumatology professor at the University of Washington School of Medicine in Seattle.
An exploratory analysis showed that there was a better response for izokibep vs placebo if the analysis included only patients with higher LEI scores at baseline, at 8.0% (n = 12) for placebo, 22.0% (n = 9) for izokibep 160 mg QW, and 50.0% (n = 12) for izokibep 160 mg Q2W.
Main Efficacy Data
The primary endpoint for the trial was the proportion of patients who had 50% improvement in American College of Rheumatology response criteria (ACR50) at 16 weeks. This showed a clear advantage for treatment with izokibep 160 QW and Q2W compared with placebo, with a respective 40%, 43%, and 15% of patients meeting this endpoint.
Corresponding ACR20 response rates were 59%, 64%, and 35%, respectively; ACR70 response rates were a respective 25%, 23%, and 5%.
In addition to ACR70, izokibep 160 QW and Q2W met a number of other “high hurdle” efficacy endpoints better than did placebo, Dr. Mease reported. A 90% reduction from baseline in the Psoriasis Area and Severity Index (PASI90) was achieved by a respective 64%, 58%, and 12% of patients, and a 100% reduction in this index (PASI100) was achieved by a respective 51%, 47%, and 12%. And 41%, 42%, and 14% of patients, respectively, met the criteria for minimal disease activity.
Patient Population
Mease pointed out during his presentation that the trial included patients with adult-onset PsA that had been ongoing for ≥ 6 months. Patients had to have at least three tender or swollen joints and an inadequate response, intolerance, or contraindication to commonly used front-line therapies such as nonsteroidal anti-inflammatory drugs, conventional synthetic disease-modifying antirheumatic drugs (csDMARDs), and tumor necrosis factor inhibitors (TNFi).
In fact, around half of the participants across the three treatment arms had received prior csDMARDs, and almost a quarter had received a TNFi.
The mean duration of disease was around 7 years, the average age was about 50 years, and the majority of the participants were White individuals. There were more women than men in the placebo vs the izokibep arms (43.4% vs about 60.0%).
Adverse Events
Injection site reactions were the most common adverse events, most of which were mild to moderate. Very few (< 1% to 4%) led to any need to discontinue the drug.
Serious adverse events occurred at low rates in all study arms: 0.8% for placebo, 2.7% for izokibep QW, and 1.8% for izokibep Q2W.
One patient each (0.9%) in the izokibep arms developed ulcerative colitis, whereas none in the placebo group did. Only two patients developed candidiasis. One was in the placebo group and had a skin infection, and the other was an oral infection in the QW izokibep arm.
There were no cases of uveitis, suicidal ideation, or deaths reported.
Comments on the Study
During the discussion that followed the presentation, Walter P. Maksymowych, MBChB, of the University of Alberta in Edmonton, Alberta, Canada, addressed the dosing regimens used.
“Looking at the side effect profile and then looking at the response rate, comparing the weekly dosing and every 2 weeks, do you think, in hindsight, you might be remiss that there wasn’t an additional dosing on a monthly basis, especially since this is a construct that is meant to prolong the half-life of the molecule?” he asked, adding that perhaps this should be something to consider in future studies.
Mease responded that there had been a fourth dosing arm in the trial — izokibep 80 mg once a month — but because there were only eight patients, the data were not sufficiently robust to analyze.
Commenting on the study, Laura C. Coates, MBChB, PhD, said: “It’s a pretty standard phase 2b/3 study,” and the outcomes were not wildly different from what has been seen with other IL-17A inhibitors.
“In phase 2, the enthesitis data looked really good; in phase 3, the enthesitis data looks the same as for any other IL-17 inhibitor,” Dr. Coates said.
More and longer-term data are needed to see if “the theoretical biological difference in the drug design translates to a different clinical outcome or whether it’s another IL-17,” added Dr. Coates, a clinician scientist and senior clinical research fellow at the University of Oxford in England.
Dennis McGonagle, MB MCH BAO, PhD, of the University of Leeds, England, also picked up on the enthesitis data, echoing the conclusion that the phase 2 enthesitis data were “spectacular” and noting that “it’s a real inversion of what was expected, given the small molecule.”
The study was funded by Acelyrin. Dr. Mease disclosed ties with Acelyrin and other pharmaceutical companies. Dr. Maksymowych, Dr. Coates, and Dr. McGonagle reported having a variety of financial relationships with pharmaceutical companies outside of this study.
A version of this article appeared on Medscape.com.
FROM EULAR 2024
Selective JAK 1 Inhibitor for RA Proves Promising in Phase 3 Trial
VIENNA — The highly selective oral Janus kinase (JAK) inhibitor SHR0302 (ivarmacitinib) enables more patients with active rheumatoid arthritis to meet American College of Rheumatology (ACR) response criteria than placebo, the results of a phase 3 trial showed.
After 24 weeks of daily treatment, the primary endpoint of an ACR20 response was met by 40.4% of those who had been given placebo, 70.4% who had received a 4-mg dose, and 75.1% given an 8-mg dose. At the same time point, ACR50 responses were a respective 15.4%, 46.0%, and 57.1%, and ACR70 responses were 6.9%, 22.2%, and 31.7%. All analyses comparing SHR0302 vs placebo were highly significant (P < .0001).
First Phase 3 Trial in China
“This is the first highly selective JAK inhibitor originally developed, and a phase 3 clinical trial conducted, [exclusively] in China,” Jinjing Liu, from the department of rheumatology at Peking Union Medical College Hospital in Beijing, China, said in an interview.

Ms. Liu presented the results at the European Alliance of Associations for Rheumatology (EULAR) 2024 Annual Meeting, during the Abstract Plenary, which highlights the best-scored abstracts of the meeting.
“We are working our best to provide more choices for Chinese patients,” Ms. Liu said, which includes lowering the financial cost of treatments. A locally developed JAK inhibitor could potentially be a much cheaper option than other alternatives that are currently available, she said.
But it is more than that, Ms. Liu said. “The selectivity of SHR0302 for JAK 1 is nine times greater than for JAK 2, so it surpasses either tofacitinib or baricitinib.” The theory is that this higher selectivity for JAK 1 over JAK 2 could lead to fewer adverse events (AEs).
“Maybe it will result in lower JAK 2–associated hematologic side effects,” Ms. Liu said.
“We have noticed that, throughout the clinical trial, the most commonly reported AEs in the drug groups were upper extremity infection [21.7%-22.8% vs 13.8% for placebo] and hyperlipidemia [12.2%-15.3% vs 5.3%].” And for the control group, she said that anemia was the second highest reported AE, at 11.7% vs 6.3% and 7.4% for SHR0302 4 and 8 mg, respectively.
Standard Design
The trial design was typical for a phase 3 study: Multicenter, randomized, placebo controlled, and double blind for the first 24 weeks, followed by an extension period out to 52 weeks. For inclusion in the study, patients had to be aged 18-75 years and have active rheumatoid arthritis and an inadequate response to previous treatment with conventional synthetic disease-modifying antirheumatic drugs.
Of 1085 patients who were initially screened, 566 were randomly allocated to receive placebo (n = 188), SHR0302 4 mg (n = 189), or SHR0302 8 mg (n = 189). The average age of patients was 51 years, and 13.3% of patients were older than 65 years.
Additional Results
Alongside improvements in ACR responses, Ms Liu reported that a significantly higher proportion of patients treated with SHR0302 vs placebo achieved a Disease Activity Score in 28 joints based on C-reactive protein less than 2.6 (29.6% with 4 mg and 39.2% with 8 mg vs 4.2% with placebo; both P < .0001) and at least 3.2 (57.1% and 46.0% vs 15.4%; both P < .0001) at 24 weeks.
There were also greater improvements seen in Health Assessment Questionnaire-Disability Index, 36-item Short-Form (SF36) physical component summary, and SF36 mental component summary scores for active vs placebo treatment.
As for AEs, there were no surprises. During the main 24-week trial period, 81.5%, 90.5%, and 79.3% of patients treated with SHR0302 4 and 8 mg and placebo, respectively, experienced any AE.
Infection-related treatment-emergent adverse effects occurred slightly more often in the SHR0302-treated groups (40.2% for 4 mg and 40.7% for 8 mg) than in the placebo group (34.0%). There was a single case of serious infection that required treatment in the SHR0302 8 mg–treated group but no cases of systemic opportunistic infection.
There was one thromboembolic event and one major cardiovascular event in the 24-week period, both occurring in patients treated with SHR0302 8 mg. There were also single cases of each reported during the extension phase of the trial, but both were in the placebo arm.
Two cases of liver function abnormality — one each in the SHR0302 4- and 8-mg groups — were recorded during the main part of the trial and two cases — both in the SHR0302 4-mg group — during the extension phase.
As for malignancy, there was a single, newly diagnosed case in the SHR0302 4 mg group in the first part of the trial and two cases, both in the SHR0302 4-mg group, during the extension phase.
“We hope this [JAK inhibitor] will be for everybody. But, you know, if it’s for patients, globally, more clinical trials would be required,” Ms. Liu said in an interview. The future, she added, was to start accumulating some real-world data and perhaps do a trial comparing SHR0302 with another JAK inhibitor or a tumor necrosis factor inhibitor.
Another JAK in the Box?
Following her presentation, Ms. Liu at EULAR 2024 was quizzed as to why there were so many screening failures. She responded that she did not have the full data to answer the question but noted that some patients in her center had been worried about being randomized to a placebo. This trial has also been conducted during the COVID-19 pandemic, so that may have been a contributing factor with patients unable to get to their follow-up appointments.

Iain B. McInnes, MD, PhD, vice principal, professor of rheumatology, and head of the College of Medical, Veterinary & Life Sciences at the University of Glasgow, Glasgow, Scotland, commented on the study, saying: “The JAK field is in evolution. We need to understand the broader toxicities. There is an unexplained mechanism driving potential cardiovascular and malignant risk in a small proportion of patients receiving the drugs.”
Dr. McInnes added, “It’s really unclear whether the solution is going to be greater selectivity and potency, or whether we need to think really about selecting the right patients for a JAK inhibitor.”
The study was funded by Jiangsu Hengrui Pharmaceuticals. Two of the 18 authors of the abstract were employees of the sponsoring company, but Ms. Liu reported having no conflicts of interest. Dr. McInnes reported serving on speaker’s bureaus for AbbVie and UCB; receiving consulting fees received from AbbVie, Amgen, AstraZeneca, Bristol-Myers Squibb, Causeway Therapeutics, Cabaletta Bio, Compugen, Eli Lilly, Evelo, Gilead, Janssen, Novartis, MoonLake Immunotherapeutics, Pfizer, Sanofi Regeneron, and UCB; and receiving grant/research support from GlaxoSmithKline, AstraZeneca, Bristol-Myers Squibb, Eli Lilly, Janssen, Novartis, and UCB.
A version of this article appeared on Medscape.com.
VIENNA — The highly selective oral Janus kinase (JAK) inhibitor SHR0302 (ivarmacitinib) enables more patients with active rheumatoid arthritis to meet American College of Rheumatology (ACR) response criteria than placebo, the results of a phase 3 trial showed.
After 24 weeks of daily treatment, the primary endpoint of an ACR20 response was met by 40.4% of those who had been given placebo, 70.4% who had received a 4-mg dose, and 75.1% given an 8-mg dose. At the same time point, ACR50 responses were a respective 15.4%, 46.0%, and 57.1%, and ACR70 responses were 6.9%, 22.2%, and 31.7%. All analyses comparing SHR0302 vs placebo were highly significant (P < .0001).
First Phase 3 Trial in China
“This is the first highly selective JAK inhibitor originally developed, and a phase 3 clinical trial conducted, [exclusively] in China,” Jinjing Liu, from the department of rheumatology at Peking Union Medical College Hospital in Beijing, China, said in an interview.
Ms. Liu presented the results at the European Alliance of Associations for Rheumatology (EULAR) 2024 Annual Meeting, during the Abstract Plenary, which highlights the best-scored abstracts of the meeting.
“We are working our best to provide more choices for Chinese patients,” Ms. Liu said, which includes lowering the financial cost of treatments. A locally developed JAK inhibitor could potentially be a much cheaper option than other alternatives that are currently available, she said.
But it is more than that, Ms. Liu said. “The selectivity of SHR0302 for JAK 1 is nine times greater than for JAK 2, so it surpasses either tofacitinib or baricitinib.” The theory is that this higher selectivity for JAK 1 over JAK 2 could lead to fewer adverse events (AEs).
“Maybe it will result in lower JAK 2–associated hematologic side effects,” Ms. Liu said.
“We have noticed that, throughout the clinical trial, the most commonly reported AEs in the drug groups were upper extremity infection [21.7%-22.8% vs 13.8% for placebo] and hyperlipidemia [12.2%-15.3% vs 5.3%].” And for the control group, she said that anemia was the second highest reported AE, at 11.7% vs 6.3% and 7.4% for SHR0302 4 and 8 mg, respectively.
Standard Design
The trial design was typical for a phase 3 study: Multicenter, randomized, placebo controlled, and double blind for the first 24 weeks, followed by an extension period out to 52 weeks. For inclusion in the study, patients had to be aged 18-75 years and have active rheumatoid arthritis and an inadequate response to previous treatment with conventional synthetic disease-modifying antirheumatic drugs.
Of 1085 patients who were initially screened, 566 were randomly allocated to receive placebo (n = 188), SHR0302 4 mg (n = 189), or SHR0302 8 mg (n = 189). The average age of patients was 51 years, and 13.3% of patients were older than 65 years.
Additional Results
Alongside improvements in ACR responses, Ms Liu reported that a significantly higher proportion of patients treated with SHR0302 vs placebo achieved a Disease Activity Score in 28 joints based on C-reactive protein less than 2.6 (29.6% with 4 mg and 39.2% with 8 mg vs 4.2% with placebo; both P < .0001) and at least 3.2 (57.1% and 46.0% vs 15.4%; both P < .0001) at 24 weeks.
There were also greater improvements seen in Health Assessment Questionnaire-Disability Index, 36-item Short-Form (SF36) physical component summary, and SF36 mental component summary scores for active vs placebo treatment.
As for AEs, there were no surprises. During the main 24-week trial period, 81.5%, 90.5%, and 79.3% of patients treated with SHR0302 4 and 8 mg and placebo, respectively, experienced any AE.
Infection-related treatment-emergent adverse effects occurred slightly more often in the SHR0302-treated groups (40.2% for 4 mg and 40.7% for 8 mg) than in the placebo group (34.0%). There was a single case of serious infection that required treatment in the SHR0302 8 mg–treated group but no cases of systemic opportunistic infection.
There was one thromboembolic event and one major cardiovascular event in the 24-week period, both occurring in patients treated with SHR0302 8 mg. There were also single cases of each reported during the extension phase of the trial, but both were in the placebo arm.
Two cases of liver function abnormality — one each in the SHR0302 4- and 8-mg groups — were recorded during the main part of the trial and two cases — both in the SHR0302 4-mg group — during the extension phase.
As for malignancy, there was a single, newly diagnosed case in the SHR0302 4 mg group in the first part of the trial and two cases, both in the SHR0302 4-mg group, during the extension phase.
“We hope this [JAK inhibitor] will be for everybody. But, you know, if it’s for patients, globally, more clinical trials would be required,” Ms. Liu said in an interview. The future, she added, was to start accumulating some real-world data and perhaps do a trial comparing SHR0302 with another JAK inhibitor or a tumor necrosis factor inhibitor.
Another JAK in the Box?
Following her presentation, Ms. Liu at EULAR 2024 was quizzed as to why there were so many screening failures. She responded that she did not have the full data to answer the question but noted that some patients in her center had been worried about being randomized to a placebo. This trial has also been conducted during the COVID-19 pandemic, so that may have been a contributing factor with patients unable to get to their follow-up appointments.
Iain B. McInnes, MD, PhD, vice principal, professor of rheumatology, and head of the College of Medical, Veterinary & Life Sciences at the University of Glasgow, Glasgow, Scotland, commented on the study, saying: “The JAK field is in evolution. We need to understand the broader toxicities. There is an unexplained mechanism driving potential cardiovascular and malignant risk in a small proportion of patients receiving the drugs.”
Dr. McInnes added, “It’s really unclear whether the solution is going to be greater selectivity and potency, or whether we need to think really about selecting the right patients for a JAK inhibitor.”
The study was funded by Jiangsu Hengrui Pharmaceuticals. Two of the 18 authors of the abstract were employees of the sponsoring company, but Ms. Liu reported having no conflicts of interest. Dr. McInnes reported serving on speaker’s bureaus for AbbVie and UCB; receiving consulting fees received from AbbVie, Amgen, AstraZeneca, Bristol-Myers Squibb, Causeway Therapeutics, Cabaletta Bio, Compugen, Eli Lilly, Evelo, Gilead, Janssen, Novartis, MoonLake Immunotherapeutics, Pfizer, Sanofi Regeneron, and UCB; and receiving grant/research support from GlaxoSmithKline, AstraZeneca, Bristol-Myers Squibb, Eli Lilly, Janssen, Novartis, and UCB.
A version of this article appeared on Medscape.com.
VIENNA — The highly selective oral Janus kinase (JAK) inhibitor SHR0302 (ivarmacitinib) enables more patients with active rheumatoid arthritis to meet American College of Rheumatology (ACR) response criteria than placebo, the results of a phase 3 trial showed.
After 24 weeks of daily treatment, the primary endpoint of an ACR20 response was met by 40.4% of those who had been given placebo, 70.4% who had received a 4-mg dose, and 75.1% given an 8-mg dose. At the same time point, ACR50 responses were a respective 15.4%, 46.0%, and 57.1%, and ACR70 responses were 6.9%, 22.2%, and 31.7%. All analyses comparing SHR0302 vs placebo were highly significant (P < .0001).
First Phase 3 Trial in China
“This is the first highly selective JAK inhibitor originally developed, and a phase 3 clinical trial conducted, [exclusively] in China,” Jinjing Liu, from the department of rheumatology at Peking Union Medical College Hospital in Beijing, China, said in an interview.
Ms. Liu presented the results at the European Alliance of Associations for Rheumatology (EULAR) 2024 Annual Meeting, during the Abstract Plenary, which highlights the best-scored abstracts of the meeting.
“We are working our best to provide more choices for Chinese patients,” Ms. Liu said, which includes lowering the financial cost of treatments. A locally developed JAK inhibitor could potentially be a much cheaper option than other alternatives that are currently available, she said.
But it is more than that, Ms. Liu said. “The selectivity of SHR0302 for JAK 1 is nine times greater than for JAK 2, so it surpasses either tofacitinib or baricitinib.” The theory is that this higher selectivity for JAK 1 over JAK 2 could lead to fewer adverse events (AEs).
“Maybe it will result in lower JAK 2–associated hematologic side effects,” Ms. Liu said.
“We have noticed that, throughout the clinical trial, the most commonly reported AEs in the drug groups were upper extremity infection [21.7%-22.8% vs 13.8% for placebo] and hyperlipidemia [12.2%-15.3% vs 5.3%].” And for the control group, she said that anemia was the second highest reported AE, at 11.7% vs 6.3% and 7.4% for SHR0302 4 and 8 mg, respectively.
Standard Design
The trial design was typical for a phase 3 study: Multicenter, randomized, placebo controlled, and double blind for the first 24 weeks, followed by an extension period out to 52 weeks. For inclusion in the study, patients had to be aged 18-75 years and have active rheumatoid arthritis and an inadequate response to previous treatment with conventional synthetic disease-modifying antirheumatic drugs.
Of 1085 patients who were initially screened, 566 were randomly allocated to receive placebo (n = 188), SHR0302 4 mg (n = 189), or SHR0302 8 mg (n = 189). The average age of patients was 51 years, and 13.3% of patients were older than 65 years.
Additional Results
Alongside improvements in ACR responses, Ms Liu reported that a significantly higher proportion of patients treated with SHR0302 vs placebo achieved a Disease Activity Score in 28 joints based on C-reactive protein less than 2.6 (29.6% with 4 mg and 39.2% with 8 mg vs 4.2% with placebo; both P < .0001) and at least 3.2 (57.1% and 46.0% vs 15.4%; both P < .0001) at 24 weeks.
There were also greater improvements seen in Health Assessment Questionnaire-Disability Index, 36-item Short-Form (SF36) physical component summary, and SF36 mental component summary scores for active vs placebo treatment.
As for AEs, there were no surprises. During the main 24-week trial period, 81.5%, 90.5%, and 79.3% of patients treated with SHR0302 4 and 8 mg and placebo, respectively, experienced any AE.
Infection-related treatment-emergent adverse effects occurred slightly more often in the SHR0302-treated groups (40.2% for 4 mg and 40.7% for 8 mg) than in the placebo group (34.0%). There was a single case of serious infection that required treatment in the SHR0302 8 mg–treated group but no cases of systemic opportunistic infection.
There was one thromboembolic event and one major cardiovascular event in the 24-week period, both occurring in patients treated with SHR0302 8 mg. There were also single cases of each reported during the extension phase of the trial, but both were in the placebo arm.
Two cases of liver function abnormality — one each in the SHR0302 4- and 8-mg groups — were recorded during the main part of the trial and two cases — both in the SHR0302 4-mg group — during the extension phase.
As for malignancy, there was a single, newly diagnosed case in the SHR0302 4 mg group in the first part of the trial and two cases, both in the SHR0302 4-mg group, during the extension phase.
“We hope this [JAK inhibitor] will be for everybody. But, you know, if it’s for patients, globally, more clinical trials would be required,” Ms. Liu said in an interview. The future, she added, was to start accumulating some real-world data and perhaps do a trial comparing SHR0302 with another JAK inhibitor or a tumor necrosis factor inhibitor.
Another JAK in the Box?
Following her presentation, Ms. Liu at EULAR 2024 was quizzed as to why there were so many screening failures. She responded that she did not have the full data to answer the question but noted that some patients in her center had been worried about being randomized to a placebo. This trial has also been conducted during the COVID-19 pandemic, so that may have been a contributing factor with patients unable to get to their follow-up appointments.
Iain B. McInnes, MD, PhD, vice principal, professor of rheumatology, and head of the College of Medical, Veterinary & Life Sciences at the University of Glasgow, Glasgow, Scotland, commented on the study, saying: “The JAK field is in evolution. We need to understand the broader toxicities. There is an unexplained mechanism driving potential cardiovascular and malignant risk in a small proportion of patients receiving the drugs.”
Dr. McInnes added, “It’s really unclear whether the solution is going to be greater selectivity and potency, or whether we need to think really about selecting the right patients for a JAK inhibitor.”
The study was funded by Jiangsu Hengrui Pharmaceuticals. Two of the 18 authors of the abstract were employees of the sponsoring company, but Ms. Liu reported having no conflicts of interest. Dr. McInnes reported serving on speaker’s bureaus for AbbVie and UCB; receiving consulting fees received from AbbVie, Amgen, AstraZeneca, Bristol-Myers Squibb, Causeway Therapeutics, Cabaletta Bio, Compugen, Eli Lilly, Evelo, Gilead, Janssen, Novartis, MoonLake Immunotherapeutics, Pfizer, Sanofi Regeneron, and UCB; and receiving grant/research support from GlaxoSmithKline, AstraZeneca, Bristol-Myers Squibb, Eli Lilly, Janssen, Novartis, and UCB.
A version of this article appeared on Medscape.com.
FROM EULAR 2024
VEXAS Syndrome: Study Highlights Cutaneous Symptoms
Additionally, the most common histologic findings include leukocytoclastic vasculitis, neutrophilic dermatosis, and perivascular dermatitis; different variants in the UBA1 gene are associated with specific skin manifestations.
Those are key findings from a cohort study of 112 patients with VEXAS published online in JAMA Dermatology. The study, conducted by researchers at the National Institutes of Health (NIH) and several other institutions, aimed to define the spectrum of cutaneous manifestations in VEXAS in association with genetic, histologic, and other clinical findings.
First described in 2020, VEXAS syndrome is an adult-onset multisystem disease that can pose a diagnostic challenge to clinicians, the study’s corresponding author, Edward W. Cowen, MD, MHSc, of the dermatology branch at the National Institute of Arthritis and Musculoskeletal and Skin Diseases (NIAMS), said in an interview. The disease is caused by pathogenic variants in the UBA1 gene, located on the X chromosome. Affected individuals exhibit a wide range of manifestations, including cytopenia/myelodysplasia, multiorgan systemic inflammation, and cutaneous involvement.
“Patients may present to a variety of disease specialists depending on their symptoms and providers may not immediately consider a genetic etiology in an older individual,” Dr. Cowen said in an interview. “Although skin involvement occurs in more than 80% of patients, it is pleomorphic and may resemble a variety of other conditions such as vasculitis and Sweet syndrome.”
To better understand the cutaneous manifestations of VEXAS syndrome, the researchers evaluated data from 112 patients with VEXAS-defining genetic variants in the UBA1 gene between 2019 and 2023. Of the 112 patients, 73 underwent medical record review only, and 39 were prospectively evaluated at NIH. All but one of the patients were men, 94% were White individuals, and their mean age was 64 years. Skin involvement occurred in 83% of cases and was the most common presenting feature of VEXAS in 61% of cases.
Of the 64 histopathologic reports available from 60 patients, the main skin histopathologic findings were leukocytoclastic vasculitis in 23 patients (36%), neutrophilic dermatosis in 22 patients (34%), and perivascular dermatitis in 19 patients (30%). According to Dr. Cowen, one key histologic finding was a distinct pattern of “histiocytoid” dermal neutrophilic inflammation, which was present in 13 of 15 specimens (86%) that underwent central re-review. “This pattern can occasionally also be seen in patients with Sweet syndrome, unrelated to VEXAS, but was a hallmark feature found in the majority of skin biopsies of patients with VEXAS,” he said.
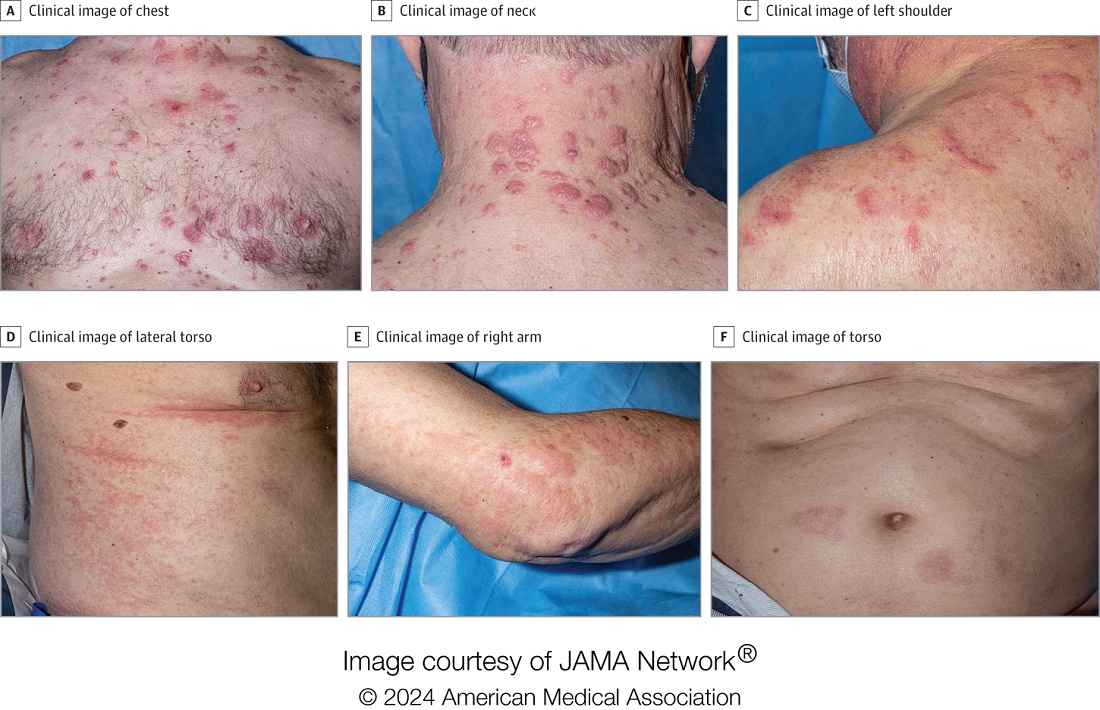
“Together with another pathologic finding, leukocytoclasia, these features can be useful clues to alert the pathologist to a potential diagnosis of VEXAS. This myeloid predominant pattern of skin inflammation was also most strongly associated with the leucine pathogenic variant of the UBA1 gene.” In contrast, cutaneous vasculitis was most strongly associated with the valine pathogenic variant of UBA1. “This is important because the valine variant has been previously independently linked to decreased survival,” he said.
In findings related to pathogenic genetic variants, the researchers observed that the p.Met41Leu variant was most frequently associated with neutrophilic dermal infiltrates in 14 of 17 patients (82%) with this variant and often resembled histiocytoid Sweet syndrome. In addition, the p.Met41Val variant was associated with vasculitic lesions in 11 of 20 patients (55%) with this variant and with a mixed leukocytic infiltrate in 17 of these 20 patients (85%).
Treatment Outcomes
In the realm of therapies, skin manifestations improved in 67 of 73 patients (92%) treated with oral prednisone, while treatment with the interleukin-1 receptor antagonist anakinra improved cutaneous disease in 9 of the 16 (56%) who received it. However, 12 (75%) of those who received anakinra developed severe injection-site reactions, including ulceration in two patients and abscess formation in one patient.
Dr. Cowen noted that VEXAS is associated with high mortality (22% in this cohort), and a high degree of suspicion is required to diagnose patients with VEXAS before significant end organ damage has occurred. “This diagnosis should be considered in all older male patients who present with neutrophilic dermatosis — particularly histiocytoid Sweet syndrome, vasculitis, or leukocytoclasia without vasculitis. Patients who appear to have isolated skin involvement may have cytopenias and acute phase reactants. Therefore, complete blood count with differential and ESR and CRP should be considered to investigate for macrocytosis, cytopenias, and systemic inflammation.”
He acknowledged certain limitations of the study, including the fact that many patients were first evaluated at the NIH after having disease symptoms for many months or years. “It is possible that patients with VEXAS referred to the NIH, either for genetic testing or in person evaluation, represent a population with more aggressive disease.”
Christine Ko, MD, professor of dermatology and pathology at Yale University, New Haven, Connecticut, who was asked to comment on the study, emphasized the importance of the UBA1 mutation in the diagnosis of this complex syndrome. “Dermatologists should be aware of VEXAS syndrome as the majority of patients present with skin lesions, which can range from urticarial to Sweet syndrome–like to palpable purpura,” Dr. Ko said.
“Chondritis and periorbital edema, sometimes unilateral, are also associated. Histopathologic clues include a predominantly histiocytoid infiltrate,” she noted. In addition, “the prominent myxoid stroma around blood vessels and adnexal structures as a clue to VEXAS syndrome surprised me; I had not read that before.”
The study was supported by the Intramural Research Program of NIAMS. One of the study authors reported personal fees from Alexion, Novartis, and Sobi outside of the submitted work. No other disclosures were reported. Dr. Ko reported having no disclosures.
A version of this article appeared on Medscape.com .
Additionally, the most common histologic findings include leukocytoclastic vasculitis, neutrophilic dermatosis, and perivascular dermatitis; different variants in the UBA1 gene are associated with specific skin manifestations.
Those are key findings from a cohort study of 112 patients with VEXAS published online in JAMA Dermatology. The study, conducted by researchers at the National Institutes of Health (NIH) and several other institutions, aimed to define the spectrum of cutaneous manifestations in VEXAS in association with genetic, histologic, and other clinical findings.
First described in 2020, VEXAS syndrome is an adult-onset multisystem disease that can pose a diagnostic challenge to clinicians, the study’s corresponding author, Edward W. Cowen, MD, MHSc, of the dermatology branch at the National Institute of Arthritis and Musculoskeletal and Skin Diseases (NIAMS), said in an interview. The disease is caused by pathogenic variants in the UBA1 gene, located on the X chromosome. Affected individuals exhibit a wide range of manifestations, including cytopenia/myelodysplasia, multiorgan systemic inflammation, and cutaneous involvement.
“Patients may present to a variety of disease specialists depending on their symptoms and providers may not immediately consider a genetic etiology in an older individual,” Dr. Cowen said in an interview. “Although skin involvement occurs in more than 80% of patients, it is pleomorphic and may resemble a variety of other conditions such as vasculitis and Sweet syndrome.”
To better understand the cutaneous manifestations of VEXAS syndrome, the researchers evaluated data from 112 patients with VEXAS-defining genetic variants in the UBA1 gene between 2019 and 2023. Of the 112 patients, 73 underwent medical record review only, and 39 were prospectively evaluated at NIH. All but one of the patients were men, 94% were White individuals, and their mean age was 64 years. Skin involvement occurred in 83% of cases and was the most common presenting feature of VEXAS in 61% of cases.
Of the 64 histopathologic reports available from 60 patients, the main skin histopathologic findings were leukocytoclastic vasculitis in 23 patients (36%), neutrophilic dermatosis in 22 patients (34%), and perivascular dermatitis in 19 patients (30%). According to Dr. Cowen, one key histologic finding was a distinct pattern of “histiocytoid” dermal neutrophilic inflammation, which was present in 13 of 15 specimens (86%) that underwent central re-review. “This pattern can occasionally also be seen in patients with Sweet syndrome, unrelated to VEXAS, but was a hallmark feature found in the majority of skin biopsies of patients with VEXAS,” he said.
“Together with another pathologic finding, leukocytoclasia, these features can be useful clues to alert the pathologist to a potential diagnosis of VEXAS. This myeloid predominant pattern of skin inflammation was also most strongly associated with the leucine pathogenic variant of the UBA1 gene.” In contrast, cutaneous vasculitis was most strongly associated with the valine pathogenic variant of UBA1. “This is important because the valine variant has been previously independently linked to decreased survival,” he said.
In findings related to pathogenic genetic variants, the researchers observed that the p.Met41Leu variant was most frequently associated with neutrophilic dermal infiltrates in 14 of 17 patients (82%) with this variant and often resembled histiocytoid Sweet syndrome. In addition, the p.Met41Val variant was associated with vasculitic lesions in 11 of 20 patients (55%) with this variant and with a mixed leukocytic infiltrate in 17 of these 20 patients (85%).
Treatment Outcomes
In the realm of therapies, skin manifestations improved in 67 of 73 patients (92%) treated with oral prednisone, while treatment with the interleukin-1 receptor antagonist anakinra improved cutaneous disease in 9 of the 16 (56%) who received it. However, 12 (75%) of those who received anakinra developed severe injection-site reactions, including ulceration in two patients and abscess formation in one patient.
Dr. Cowen noted that VEXAS is associated with high mortality (22% in this cohort), and a high degree of suspicion is required to diagnose patients with VEXAS before significant end organ damage has occurred. “This diagnosis should be considered in all older male patients who present with neutrophilic dermatosis — particularly histiocytoid Sweet syndrome, vasculitis, or leukocytoclasia without vasculitis. Patients who appear to have isolated skin involvement may have cytopenias and acute phase reactants. Therefore, complete blood count with differential and ESR and CRP should be considered to investigate for macrocytosis, cytopenias, and systemic inflammation.”
He acknowledged certain limitations of the study, including the fact that many patients were first evaluated at the NIH after having disease symptoms for many months or years. “It is possible that patients with VEXAS referred to the NIH, either for genetic testing or in person evaluation, represent a population with more aggressive disease.”
Christine Ko, MD, professor of dermatology and pathology at Yale University, New Haven, Connecticut, who was asked to comment on the study, emphasized the importance of the UBA1 mutation in the diagnosis of this complex syndrome. “Dermatologists should be aware of VEXAS syndrome as the majority of patients present with skin lesions, which can range from urticarial to Sweet syndrome–like to palpable purpura,” Dr. Ko said.
“Chondritis and periorbital edema, sometimes unilateral, are also associated. Histopathologic clues include a predominantly histiocytoid infiltrate,” she noted. In addition, “the prominent myxoid stroma around blood vessels and adnexal structures as a clue to VEXAS syndrome surprised me; I had not read that before.”
The study was supported by the Intramural Research Program of NIAMS. One of the study authors reported personal fees from Alexion, Novartis, and Sobi outside of the submitted work. No other disclosures were reported. Dr. Ko reported having no disclosures.
A version of this article appeared on Medscape.com .
Additionally, the most common histologic findings include leukocytoclastic vasculitis, neutrophilic dermatosis, and perivascular dermatitis; different variants in the UBA1 gene are associated with specific skin manifestations.
Those are key findings from a cohort study of 112 patients with VEXAS published online in JAMA Dermatology. The study, conducted by researchers at the National Institutes of Health (NIH) and several other institutions, aimed to define the spectrum of cutaneous manifestations in VEXAS in association with genetic, histologic, and other clinical findings.
First described in 2020, VEXAS syndrome is an adult-onset multisystem disease that can pose a diagnostic challenge to clinicians, the study’s corresponding author, Edward W. Cowen, MD, MHSc, of the dermatology branch at the National Institute of Arthritis and Musculoskeletal and Skin Diseases (NIAMS), said in an interview. The disease is caused by pathogenic variants in the UBA1 gene, located on the X chromosome. Affected individuals exhibit a wide range of manifestations, including cytopenia/myelodysplasia, multiorgan systemic inflammation, and cutaneous involvement.
“Patients may present to a variety of disease specialists depending on their symptoms and providers may not immediately consider a genetic etiology in an older individual,” Dr. Cowen said in an interview. “Although skin involvement occurs in more than 80% of patients, it is pleomorphic and may resemble a variety of other conditions such as vasculitis and Sweet syndrome.”
To better understand the cutaneous manifestations of VEXAS syndrome, the researchers evaluated data from 112 patients with VEXAS-defining genetic variants in the UBA1 gene between 2019 and 2023. Of the 112 patients, 73 underwent medical record review only, and 39 were prospectively evaluated at NIH. All but one of the patients were men, 94% were White individuals, and their mean age was 64 years. Skin involvement occurred in 83% of cases and was the most common presenting feature of VEXAS in 61% of cases.
Of the 64 histopathologic reports available from 60 patients, the main skin histopathologic findings were leukocytoclastic vasculitis in 23 patients (36%), neutrophilic dermatosis in 22 patients (34%), and perivascular dermatitis in 19 patients (30%). According to Dr. Cowen, one key histologic finding was a distinct pattern of “histiocytoid” dermal neutrophilic inflammation, which was present in 13 of 15 specimens (86%) that underwent central re-review. “This pattern can occasionally also be seen in patients with Sweet syndrome, unrelated to VEXAS, but was a hallmark feature found in the majority of skin biopsies of patients with VEXAS,” he said.
“Together with another pathologic finding, leukocytoclasia, these features can be useful clues to alert the pathologist to a potential diagnosis of VEXAS. This myeloid predominant pattern of skin inflammation was also most strongly associated with the leucine pathogenic variant of the UBA1 gene.” In contrast, cutaneous vasculitis was most strongly associated with the valine pathogenic variant of UBA1. “This is important because the valine variant has been previously independently linked to decreased survival,” he said.
In findings related to pathogenic genetic variants, the researchers observed that the p.Met41Leu variant was most frequently associated with neutrophilic dermal infiltrates in 14 of 17 patients (82%) with this variant and often resembled histiocytoid Sweet syndrome. In addition, the p.Met41Val variant was associated with vasculitic lesions in 11 of 20 patients (55%) with this variant and with a mixed leukocytic infiltrate in 17 of these 20 patients (85%).
Treatment Outcomes
In the realm of therapies, skin manifestations improved in 67 of 73 patients (92%) treated with oral prednisone, while treatment with the interleukin-1 receptor antagonist anakinra improved cutaneous disease in 9 of the 16 (56%) who received it. However, 12 (75%) of those who received anakinra developed severe injection-site reactions, including ulceration in two patients and abscess formation in one patient.
Dr. Cowen noted that VEXAS is associated with high mortality (22% in this cohort), and a high degree of suspicion is required to diagnose patients with VEXAS before significant end organ damage has occurred. “This diagnosis should be considered in all older male patients who present with neutrophilic dermatosis — particularly histiocytoid Sweet syndrome, vasculitis, or leukocytoclasia without vasculitis. Patients who appear to have isolated skin involvement may have cytopenias and acute phase reactants. Therefore, complete blood count with differential and ESR and CRP should be considered to investigate for macrocytosis, cytopenias, and systemic inflammation.”
He acknowledged certain limitations of the study, including the fact that many patients were first evaluated at the NIH after having disease symptoms for many months or years. “It is possible that patients with VEXAS referred to the NIH, either for genetic testing or in person evaluation, represent a population with more aggressive disease.”
Christine Ko, MD, professor of dermatology and pathology at Yale University, New Haven, Connecticut, who was asked to comment on the study, emphasized the importance of the UBA1 mutation in the diagnosis of this complex syndrome. “Dermatologists should be aware of VEXAS syndrome as the majority of patients present with skin lesions, which can range from urticarial to Sweet syndrome–like to palpable purpura,” Dr. Ko said.
“Chondritis and periorbital edema, sometimes unilateral, are also associated. Histopathologic clues include a predominantly histiocytoid infiltrate,” she noted. In addition, “the prominent myxoid stroma around blood vessels and adnexal structures as a clue to VEXAS syndrome surprised me; I had not read that before.”
The study was supported by the Intramural Research Program of NIAMS. One of the study authors reported personal fees from Alexion, Novartis, and Sobi outside of the submitted work. No other disclosures were reported. Dr. Ko reported having no disclosures.
A version of this article appeared on Medscape.com .
FROM JAMA DERMATOLOGY
A New Psychotherapeutic ‘Gold Standard’ for Chronic Pain?
, the current psychotherapeutic gold standard, a new study suggested.
Two thirds of the patients who received EAET reported at least a 30% reduction in pain compared with 17% of those who received CBT. The randomized clinical trial also showed that individuals with depression and anxiety responded more favorably to EAET, a novel finding.
The study is one of only a few to directly compare EAET with CBT.
“Most people with chronic pain don’t consider psychotherapy at all,” said study investigator Brandon C. Yarns, MD, a staff psychiatrist at the VA Greater Los Angeles Healthcare System, and clinical professor of health sciences at the Department of Psychiatry and Biobehavioral Sciences, UCLA Health.
Although patients were allowed to continue medication for pain and other comorbidities during the study, those who received EAET “had larger improvements in pain, depression, and anxiety,” Dr. Yarns said. “That suggests that the effect was due to the EAET.”
The findings were published online in JAMA Network Open.
‘Gold Standard’
EAET was first used in the early 2010s. In the therapy, patients are asked to recall a difficult or traumatic memory, engage in experiencing how the related emotions feel in the body, express those feelings in words, and release or let them go. They are taught that the brain’s perception of pain is strongly influenced by the evasion of grief, fear, rage, or guilt, Dr. Yarns said.
This contrasts with CBT — considered the current gold standard for chronic pain — which teaches patients to improve the ability to tolerate pain though guided imagery, muscle relaxation, and other exercises and to adapt their thinking to change how they think about pain.
Although prior studies suggested EAET is effective in reducing pain in fibromyalgia and chronic musculoskeletal, pelvic, and head pain, most included primarily younger, female patients.
The research is the “first full-scale evaluation of EAET, to our knowledge, in a medically or psychiatrically complex, racially and ethnically diverse, older sample comprising predominantly men,” investigators wrote.
The trial enrolled 126 veterans (92% men; 55% Black or African American) aged 60-95 years with at least 3 months of musculoskeletal pain. More than two thirds of patients had a psychiatric diagnosis, with about one third having posttraumatic stress disorder (PTSD). Almost all had back pain, and many had pain in multiple locations.
All services were delivered in-person at the US Department of Veterans Affairs Greater Los Angeles Healthcare System, Los Angeles. Half underwent CBT, while the other half received EAET.
Each patient had one 90-minute individual session and eight additional 90-minute group sessions.
Patients were asked to rate their pain using a 0-10 scale in the Brief Pain Inventory (BPI) before starting treatment, at the end of the nine sessions (at week 10), and 6 months after the sessions ended. Baseline BPI score for both groups was a mean of around 6.
Post treatment, people in the EAET versus CBT group had a mean two-point reduction versus 0.60 reduction, respectively, on the BPI scale. A clinically significant reduction in pain — defined as ≥ 30% decrease — was reported in 63% of EAET patients versus 17% of CBT patients (odds ratio [OR], 21.54; P < .001).
At 6 months, the mean reduction was 1.2 for the EAET group compared with 0.25 for the CBT group, and 40% of the EAET group reported a clinically significant reduction in pain.
A little more than a third (35%) of veterans receiving EAET reported at least a 50% reduction in pain at 10 weeks compared with 7% of those receiving CBT. At 6 months, 16% of the EAET arm reported a halving of their pain.
EAET was also superior to CBT in reducing anxiety, depression, and PTSD symptoms at the 10-week mark.
More Work Needed
In an accompanying editorial, Matthias Karst, MD, PhD, a clinician with the Pain Clinic, Hannover Medical School, in Hannover, Germany, noted that EAET’s effects “are significantly superior to those of CBT in almost all dimensions, even after 6 months.”
EAET “assigns a special place to the integration of the body into the emotional experience,” he wrote.
The study demonstrated that “the evocation and expression of emotions is superior to the mere cognitive discussion of these emotions in therapy of patients with chronic pain.”
Commenting on the findings, Traci J. Speed, MD, PhD, assistant professor of psychiatry and behavioral sciences and an attending psychiatrist of the Johns Hopkins Pain Treatment Program at Johns Hopkins University, Baltimore, called the study “ground-breaking” because it showed effectiveness in people with high rates of PTSD, anxiety, and depression.
“It is a little bit surprising how impressive the study outcomes are in terms of maintaining the effects at the end of the treatment and sustaining some of the effects on pain sensitivity even at the 6-month follow-up,” said Dr. Speed, who was not part of the study.
However, she continued, “I don’t think it changes the current standard of practice yet. CBT has decades of research and evidence that it is effective for chronic pain and that will I think continue to be the standard of care.”
Although EAET is in its infancy, chronic pain experts are interested in learning more about the therapy, Dr. Speed added.
“It blends well with the current techniques and extends the current gold standard treatment approaches,” she said. “We are starting to really appreciate the role that emotions play in pain sensitivity.”
Both Dr. Karst and Dr. Speed noted that more study is needed to determine the sustainability of treatment effects.
Dr. Yarns agreed. “We need more research on what the appropriate dose is and perhaps how one might go about personalizing that for the patient,” he said.
The study was funded by a career development award to Dr. Yarns from the VA Clinical Science Research and Development Service. Dr. Yarns reported receiving grants from the US Department of Veterans Affairs during the study. Other authors’ disclosures are in the original article. Dr. Speed reported no conflicts.
A version of this article appeared on Medscape.com.
, the current psychotherapeutic gold standard, a new study suggested.
Two thirds of the patients who received EAET reported at least a 30% reduction in pain compared with 17% of those who received CBT. The randomized clinical trial also showed that individuals with depression and anxiety responded more favorably to EAET, a novel finding.
The study is one of only a few to directly compare EAET with CBT.
“Most people with chronic pain don’t consider psychotherapy at all,” said study investigator Brandon C. Yarns, MD, a staff psychiatrist at the VA Greater Los Angeles Healthcare System, and clinical professor of health sciences at the Department of Psychiatry and Biobehavioral Sciences, UCLA Health.
Although patients were allowed to continue medication for pain and other comorbidities during the study, those who received EAET “had larger improvements in pain, depression, and anxiety,” Dr. Yarns said. “That suggests that the effect was due to the EAET.”
The findings were published online in JAMA Network Open.
‘Gold Standard’
EAET was first used in the early 2010s. In the therapy, patients are asked to recall a difficult or traumatic memory, engage in experiencing how the related emotions feel in the body, express those feelings in words, and release or let them go. They are taught that the brain’s perception of pain is strongly influenced by the evasion of grief, fear, rage, or guilt, Dr. Yarns said.
This contrasts with CBT — considered the current gold standard for chronic pain — which teaches patients to improve the ability to tolerate pain though guided imagery, muscle relaxation, and other exercises and to adapt their thinking to change how they think about pain.
Although prior studies suggested EAET is effective in reducing pain in fibromyalgia and chronic musculoskeletal, pelvic, and head pain, most included primarily younger, female patients.
The research is the “first full-scale evaluation of EAET, to our knowledge, in a medically or psychiatrically complex, racially and ethnically diverse, older sample comprising predominantly men,” investigators wrote.
The trial enrolled 126 veterans (92% men; 55% Black or African American) aged 60-95 years with at least 3 months of musculoskeletal pain. More than two thirds of patients had a psychiatric diagnosis, with about one third having posttraumatic stress disorder (PTSD). Almost all had back pain, and many had pain in multiple locations.
All services were delivered in-person at the US Department of Veterans Affairs Greater Los Angeles Healthcare System, Los Angeles. Half underwent CBT, while the other half received EAET.
Each patient had one 90-minute individual session and eight additional 90-minute group sessions.
Patients were asked to rate their pain using a 0-10 scale in the Brief Pain Inventory (BPI) before starting treatment, at the end of the nine sessions (at week 10), and 6 months after the sessions ended. Baseline BPI score for both groups was a mean of around 6.
Post treatment, people in the EAET versus CBT group had a mean two-point reduction versus 0.60 reduction, respectively, on the BPI scale. A clinically significant reduction in pain — defined as ≥ 30% decrease — was reported in 63% of EAET patients versus 17% of CBT patients (odds ratio [OR], 21.54; P < .001).
At 6 months, the mean reduction was 1.2 for the EAET group compared with 0.25 for the CBT group, and 40% of the EAET group reported a clinically significant reduction in pain.
A little more than a third (35%) of veterans receiving EAET reported at least a 50% reduction in pain at 10 weeks compared with 7% of those receiving CBT. At 6 months, 16% of the EAET arm reported a halving of their pain.
EAET was also superior to CBT in reducing anxiety, depression, and PTSD symptoms at the 10-week mark.
More Work Needed
In an accompanying editorial, Matthias Karst, MD, PhD, a clinician with the Pain Clinic, Hannover Medical School, in Hannover, Germany, noted that EAET’s effects “are significantly superior to those of CBT in almost all dimensions, even after 6 months.”
EAET “assigns a special place to the integration of the body into the emotional experience,” he wrote.
The study demonstrated that “the evocation and expression of emotions is superior to the mere cognitive discussion of these emotions in therapy of patients with chronic pain.”
Commenting on the findings, Traci J. Speed, MD, PhD, assistant professor of psychiatry and behavioral sciences and an attending psychiatrist of the Johns Hopkins Pain Treatment Program at Johns Hopkins University, Baltimore, called the study “ground-breaking” because it showed effectiveness in people with high rates of PTSD, anxiety, and depression.
“It is a little bit surprising how impressive the study outcomes are in terms of maintaining the effects at the end of the treatment and sustaining some of the effects on pain sensitivity even at the 6-month follow-up,” said Dr. Speed, who was not part of the study.
However, she continued, “I don’t think it changes the current standard of practice yet. CBT has decades of research and evidence that it is effective for chronic pain and that will I think continue to be the standard of care.”
Although EAET is in its infancy, chronic pain experts are interested in learning more about the therapy, Dr. Speed added.
“It blends well with the current techniques and extends the current gold standard treatment approaches,” she said. “We are starting to really appreciate the role that emotions play in pain sensitivity.”
Both Dr. Karst and Dr. Speed noted that more study is needed to determine the sustainability of treatment effects.
Dr. Yarns agreed. “We need more research on what the appropriate dose is and perhaps how one might go about personalizing that for the patient,” he said.
The study was funded by a career development award to Dr. Yarns from the VA Clinical Science Research and Development Service. Dr. Yarns reported receiving grants from the US Department of Veterans Affairs during the study. Other authors’ disclosures are in the original article. Dr. Speed reported no conflicts.
A version of this article appeared on Medscape.com.
, the current psychotherapeutic gold standard, a new study suggested.
Two thirds of the patients who received EAET reported at least a 30% reduction in pain compared with 17% of those who received CBT. The randomized clinical trial also showed that individuals with depression and anxiety responded more favorably to EAET, a novel finding.
The study is one of only a few to directly compare EAET with CBT.
“Most people with chronic pain don’t consider psychotherapy at all,” said study investigator Brandon C. Yarns, MD, a staff psychiatrist at the VA Greater Los Angeles Healthcare System, and clinical professor of health sciences at the Department of Psychiatry and Biobehavioral Sciences, UCLA Health.
Although patients were allowed to continue medication for pain and other comorbidities during the study, those who received EAET “had larger improvements in pain, depression, and anxiety,” Dr. Yarns said. “That suggests that the effect was due to the EAET.”
The findings were published online in JAMA Network Open.
‘Gold Standard’
EAET was first used in the early 2010s. In the therapy, patients are asked to recall a difficult or traumatic memory, engage in experiencing how the related emotions feel in the body, express those feelings in words, and release or let them go. They are taught that the brain’s perception of pain is strongly influenced by the evasion of grief, fear, rage, or guilt, Dr. Yarns said.
This contrasts with CBT — considered the current gold standard for chronic pain — which teaches patients to improve the ability to tolerate pain though guided imagery, muscle relaxation, and other exercises and to adapt their thinking to change how they think about pain.
Although prior studies suggested EAET is effective in reducing pain in fibromyalgia and chronic musculoskeletal, pelvic, and head pain, most included primarily younger, female patients.
The research is the “first full-scale evaluation of EAET, to our knowledge, in a medically or psychiatrically complex, racially and ethnically diverse, older sample comprising predominantly men,” investigators wrote.
The trial enrolled 126 veterans (92% men; 55% Black or African American) aged 60-95 years with at least 3 months of musculoskeletal pain. More than two thirds of patients had a psychiatric diagnosis, with about one third having posttraumatic stress disorder (PTSD). Almost all had back pain, and many had pain in multiple locations.
All services were delivered in-person at the US Department of Veterans Affairs Greater Los Angeles Healthcare System, Los Angeles. Half underwent CBT, while the other half received EAET.
Each patient had one 90-minute individual session and eight additional 90-minute group sessions.
Patients were asked to rate their pain using a 0-10 scale in the Brief Pain Inventory (BPI) before starting treatment, at the end of the nine sessions (at week 10), and 6 months after the sessions ended. Baseline BPI score for both groups was a mean of around 6.
Post treatment, people in the EAET versus CBT group had a mean two-point reduction versus 0.60 reduction, respectively, on the BPI scale. A clinically significant reduction in pain — defined as ≥ 30% decrease — was reported in 63% of EAET patients versus 17% of CBT patients (odds ratio [OR], 21.54; P < .001).
At 6 months, the mean reduction was 1.2 for the EAET group compared with 0.25 for the CBT group, and 40% of the EAET group reported a clinically significant reduction in pain.
A little more than a third (35%) of veterans receiving EAET reported at least a 50% reduction in pain at 10 weeks compared with 7% of those receiving CBT. At 6 months, 16% of the EAET arm reported a halving of their pain.
EAET was also superior to CBT in reducing anxiety, depression, and PTSD symptoms at the 10-week mark.
More Work Needed
In an accompanying editorial, Matthias Karst, MD, PhD, a clinician with the Pain Clinic, Hannover Medical School, in Hannover, Germany, noted that EAET’s effects “are significantly superior to those of CBT in almost all dimensions, even after 6 months.”
EAET “assigns a special place to the integration of the body into the emotional experience,” he wrote.
The study demonstrated that “the evocation and expression of emotions is superior to the mere cognitive discussion of these emotions in therapy of patients with chronic pain.”
Commenting on the findings, Traci J. Speed, MD, PhD, assistant professor of psychiatry and behavioral sciences and an attending psychiatrist of the Johns Hopkins Pain Treatment Program at Johns Hopkins University, Baltimore, called the study “ground-breaking” because it showed effectiveness in people with high rates of PTSD, anxiety, and depression.
“It is a little bit surprising how impressive the study outcomes are in terms of maintaining the effects at the end of the treatment and sustaining some of the effects on pain sensitivity even at the 6-month follow-up,” said Dr. Speed, who was not part of the study.
However, she continued, “I don’t think it changes the current standard of practice yet. CBT has decades of research and evidence that it is effective for chronic pain and that will I think continue to be the standard of care.”
Although EAET is in its infancy, chronic pain experts are interested in learning more about the therapy, Dr. Speed added.
“It blends well with the current techniques and extends the current gold standard treatment approaches,” she said. “We are starting to really appreciate the role that emotions play in pain sensitivity.”
Both Dr. Karst and Dr. Speed noted that more study is needed to determine the sustainability of treatment effects.
Dr. Yarns agreed. “We need more research on what the appropriate dose is and perhaps how one might go about personalizing that for the patient,” he said.
The study was funded by a career development award to Dr. Yarns from the VA Clinical Science Research and Development Service. Dr. Yarns reported receiving grants from the US Department of Veterans Affairs during the study. Other authors’ disclosures are in the original article. Dr. Speed reported no conflicts.
A version of this article appeared on Medscape.com.