User login
Bringing you the latest news, research and reviews, exclusive interviews, podcasts, quizzes, and more.
div[contains(@class, 'header__large-screen')]
div[contains(@class, 'read-next-article')]
div[contains(@class, 'main-prefix')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
footer[@id='footer']
section[contains(@class, 'nav-hidden')]
div[contains(@class, 'ce-card-content')]
nav[contains(@class, 'nav-ce-stack')]
div[contains(@class, 'view-medstat-quiz-listing-panes')]
div[contains(@class, 'pane-article-sidebar-latest-news')]
div[contains(@class, 'medstat-accordion-set article-series')]
Commentary: PsA in Women, February 2024

Another study investigated the persistence of targeted therapies for PsA in women compared with men. In a nationwide cohort study using administrative information from French health insurance, the study looked at 14,778 patients (57% women) with PsA who were new users of targeted therapies. The study showed that women had 20%-40% lower treatment persistence rates than men for tumour necrosis factor (TNF) inhibitors (adjusted hazard ratio [aHR] 1.4; 99% CI 1.3-1.5) and interleukin (IL)-17 inhibitors (aHR 1.2; 99% CI 1.1-1.3). However, the treatment persistence between both sexes was comparable for IL-12/23 inhibitor (aHR 1.1; 99% CI 0.9-1.3), IL-23 inhibitor (aHR 1.1; 99% CI 0.7-1.5), and Janus kinase (JAK) inhibitor (aHR 1.2; 99% CI 0.9-1.6) therapies. The paradigm that women have lower treatment persistence is based on studies done primarily in patients treated with TNF inhibitors. This study and a few other recent studies challenge this paradigm by indicating that other targeted therapies, especially JAK inhibitors, may not have lower persistence in women. Sex should be taken into consideration while choosing and counseling women about PsA therapies.
There are few studies on exercise and its impact on PsA. Functional training (FT) and resistance training (RT) may improve functional capacity and quality of life of patients with PsA. The safety of exercise is also not known, given that (micro)trauma is a risk factor for PsA. To evaluate this, Silva and colleagues conducted a 12-week, single-blind trial including 41 patients with PsA who were randomly assigned to undergo FT with elastic bands or RT with weight machines. They demonstrated that FT and RT led to similar improvements in functional capacity measured by the Bath Ankylosing Spondylitis Functional Index (P = .919), functional status measured by the Health Assessment Questionnaire for Spondyloarthritis (P = .932), disease activity measured by the Bath Ankylosing Spondylitis Disease Activity Index (P = .700), and muscle strength. No adverse events occurred in either group. Thus, FT and RT improved functional capacity, functional status, disease activity, and muscle strength to a comparable extent in patients with PsA, with no adverse events. Both modalities may be recommended for PsA patients.
Finally, a cross-sectional study that included 503 patients with PsA, of whom 160 patients underwent treatment escalation, evaluated whether the patient-reported outcome (PsA Impact of Disease questionnaire [PsAID-12]) affected treatment decisions by the treating rheumatologist. Coyle and colleagues demonstrated that although PsAID-12 scores were higher in patients who did vs did not have a treatment escalation, physicians relied more on their assessment of disease activity rather than the PsAID-12 scores when making treatment-related decisions. Of note, physicians also reported that PsAID-12 scores influenced treatment reduction decisions.
Another study investigated the persistence of targeted therapies for PsA in women compared with men. In a nationwide cohort study using administrative information from French health insurance, the study looked at 14,778 patients (57% women) with PsA who were new users of targeted therapies. The study showed that women had 20%-40% lower treatment persistence rates than men for tumour necrosis factor (TNF) inhibitors (adjusted hazard ratio [aHR] 1.4; 99% CI 1.3-1.5) and interleukin (IL)-17 inhibitors (aHR 1.2; 99% CI 1.1-1.3). However, the treatment persistence between both sexes was comparable for IL-12/23 inhibitor (aHR 1.1; 99% CI 0.9-1.3), IL-23 inhibitor (aHR 1.1; 99% CI 0.7-1.5), and Janus kinase (JAK) inhibitor (aHR 1.2; 99% CI 0.9-1.6) therapies. The paradigm that women have lower treatment persistence is based on studies done primarily in patients treated with TNF inhibitors. This study and a few other recent studies challenge this paradigm by indicating that other targeted therapies, especially JAK inhibitors, may not have lower persistence in women. Sex should be taken into consideration while choosing and counseling women about PsA therapies.
There are few studies on exercise and its impact on PsA. Functional training (FT) and resistance training (RT) may improve functional capacity and quality of life of patients with PsA. The safety of exercise is also not known, given that (micro)trauma is a risk factor for PsA. To evaluate this, Silva and colleagues conducted a 12-week, single-blind trial including 41 patients with PsA who were randomly assigned to undergo FT with elastic bands or RT with weight machines. They demonstrated that FT and RT led to similar improvements in functional capacity measured by the Bath Ankylosing Spondylitis Functional Index (P = .919), functional status measured by the Health Assessment Questionnaire for Spondyloarthritis (P = .932), disease activity measured by the Bath Ankylosing Spondylitis Disease Activity Index (P = .700), and muscle strength. No adverse events occurred in either group. Thus, FT and RT improved functional capacity, functional status, disease activity, and muscle strength to a comparable extent in patients with PsA, with no adverse events. Both modalities may be recommended for PsA patients.
Finally, a cross-sectional study that included 503 patients with PsA, of whom 160 patients underwent treatment escalation, evaluated whether the patient-reported outcome (PsA Impact of Disease questionnaire [PsAID-12]) affected treatment decisions by the treating rheumatologist. Coyle and colleagues demonstrated that although PsAID-12 scores were higher in patients who did vs did not have a treatment escalation, physicians relied more on their assessment of disease activity rather than the PsAID-12 scores when making treatment-related decisions. Of note, physicians also reported that PsAID-12 scores influenced treatment reduction decisions.
Another study investigated the persistence of targeted therapies for PsA in women compared with men. In a nationwide cohort study using administrative information from French health insurance, the study looked at 14,778 patients (57% women) with PsA who were new users of targeted therapies. The study showed that women had 20%-40% lower treatment persistence rates than men for tumour necrosis factor (TNF) inhibitors (adjusted hazard ratio [aHR] 1.4; 99% CI 1.3-1.5) and interleukin (IL)-17 inhibitors (aHR 1.2; 99% CI 1.1-1.3). However, the treatment persistence between both sexes was comparable for IL-12/23 inhibitor (aHR 1.1; 99% CI 0.9-1.3), IL-23 inhibitor (aHR 1.1; 99% CI 0.7-1.5), and Janus kinase (JAK) inhibitor (aHR 1.2; 99% CI 0.9-1.6) therapies. The paradigm that women have lower treatment persistence is based on studies done primarily in patients treated with TNF inhibitors. This study and a few other recent studies challenge this paradigm by indicating that other targeted therapies, especially JAK inhibitors, may not have lower persistence in women. Sex should be taken into consideration while choosing and counseling women about PsA therapies.
There are few studies on exercise and its impact on PsA. Functional training (FT) and resistance training (RT) may improve functional capacity and quality of life of patients with PsA. The safety of exercise is also not known, given that (micro)trauma is a risk factor for PsA. To evaluate this, Silva and colleagues conducted a 12-week, single-blind trial including 41 patients with PsA who were randomly assigned to undergo FT with elastic bands or RT with weight machines. They demonstrated that FT and RT led to similar improvements in functional capacity measured by the Bath Ankylosing Spondylitis Functional Index (P = .919), functional status measured by the Health Assessment Questionnaire for Spondyloarthritis (P = .932), disease activity measured by the Bath Ankylosing Spondylitis Disease Activity Index (P = .700), and muscle strength. No adverse events occurred in either group. Thus, FT and RT improved functional capacity, functional status, disease activity, and muscle strength to a comparable extent in patients with PsA, with no adverse events. Both modalities may be recommended for PsA patients.
Finally, a cross-sectional study that included 503 patients with PsA, of whom 160 patients underwent treatment escalation, evaluated whether the patient-reported outcome (PsA Impact of Disease questionnaire [PsAID-12]) affected treatment decisions by the treating rheumatologist. Coyle and colleagues demonstrated that although PsAID-12 scores were higher in patients who did vs did not have a treatment escalation, physicians relied more on their assessment of disease activity rather than the PsAID-12 scores when making treatment-related decisions. Of note, physicians also reported that PsAID-12 scores influenced treatment reduction decisions.
Breaking the Diagnostic Bottleneck in RA
As head of the clinical laboratory at the San Juan University Hospital in Alicante, Spain, Maria Salinas, PhD, is passionate about the role she and her colleagues can play in clinical decision-making.
Her mission is the identification of “hidden diseases,” as she calls them, chronic conditions for which early identification and intervention can change the course of the illness. Her lab has been a leader over the past decade in using technology to partner with clinicians to promote the appropriate use of testing and clinical decision-making.
An example of a disease ripe for this type of intervention is rheumatoid arthritis (RA), the most common form of autoimmune arthritis, affecting around 1.3 million people in the United States. The prognosis for patients is better the earlier treatment begins.
But the
Amy S. Kehl, MD, an attending rheumatologist at Cedars-Sinai Medical Center in Los Angeles, who also sees patients at Saint John’s Physician Partners in Santa Monica, California, recommends a workup for inflammatory arthritis for patients presenting with the new onset of joint pain and swelling, primarily of small joints, although larger joints can be involved. The workup includes markers of inflammation such as an erythrocyte sedimentation rate and C-reactive protein, which are typically elevated and can be used to monitor the progression of the disease. Similarly, the presence of anemia is consistent with RA and helpful in tracking response to treatment.
But pinning down the diagnosis requires the presence of autoimmune antibodies. Guidelines from the American College of Rheumatology require a positive result for either rheumatoid factor (RF) or anti-cyclic citrullinated peptide (anti-CCP) antibody to definitively determine whether a patient has RA (Table).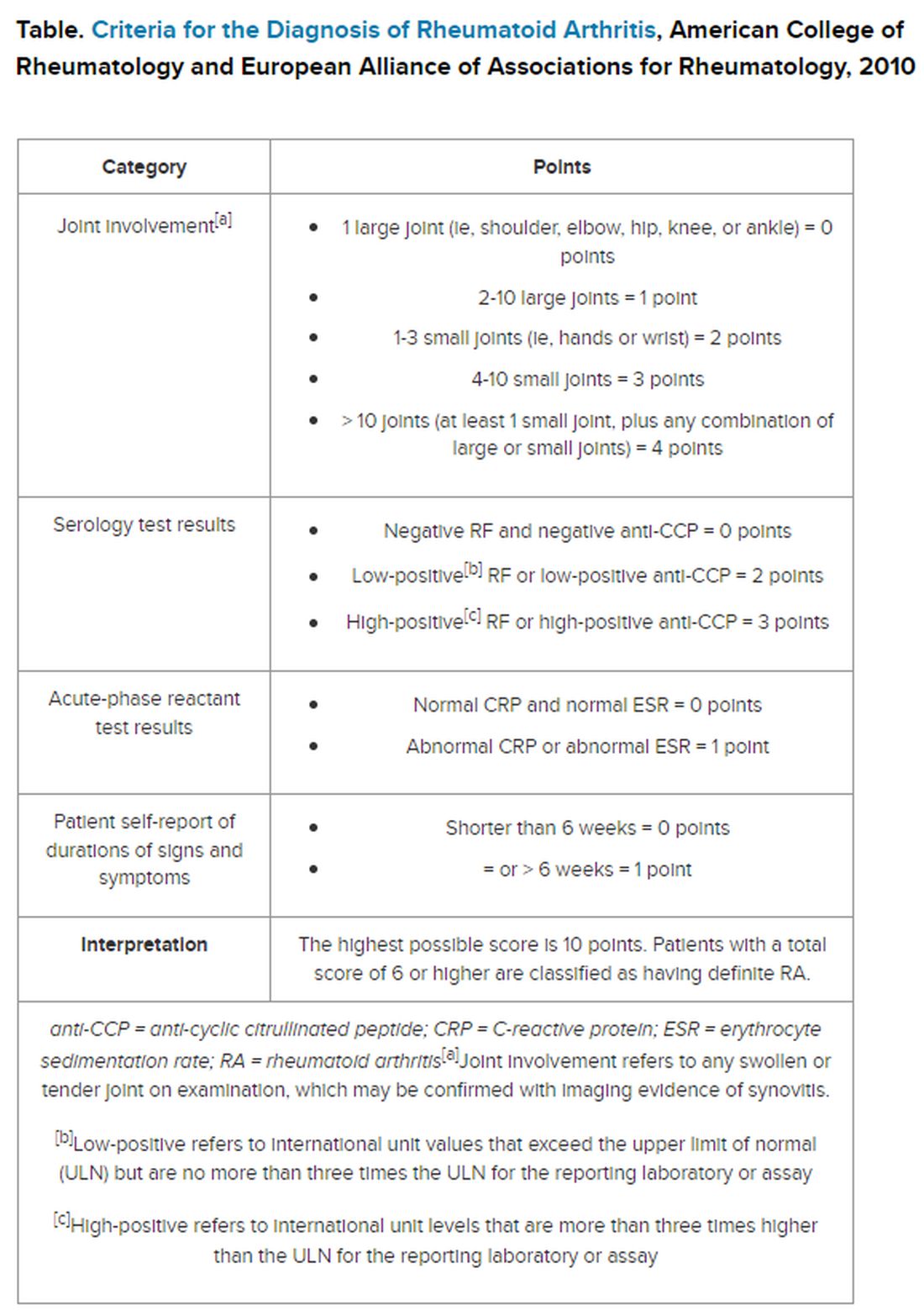
“Classically, I find that the primary care physicians include a rheumatoid factor, not always a CCP, and may include other antibodies, including an ANA [antinuclear antibody] test, as part of that workup,” Dr. Kehl said. The problem with that strategy is that although the RF test does detect 60%-80% of patients with RA, it is positive in many other autoimmune conditions. Although the ANA might be positive in patients with RA, it is nonspecific and does not confirm the diagnosis of RA.
Up to 50% of autoimmune antibody tests are inappropriately ordered. And for rheumatologists, that leads to unnecessary referrals of patients with musculoskeletal complaints who do not meet objective clinical criteria for joint disease.
“These tests get ordered almost reflexively, and sometimes they’re ordered as part of a panel that includes a rheumatoid factor and an ANA, and it’s not necessarily going to be a high-yield test,” Dr. Kehl said. Superfluous tests and referrals often cause unnecessary anxiety in patients, as well as drive up costs, she added.
Dr. Salinas made the same observation in her hospital lab, which also serves nine primary care centers. She documented an upward trend in orders for RF testing in her hospital lab between 2011 and 2019. Dr. Salinas also noted that the anti-CCP antibody test was not commonly requested, although it has more utility in the diagnosis. Like the RF, it detects 50%-70% of patients with RA but has 95% specificity, resulting in far fewer false-positive results.
The appearance of both RF and anti-CCP antibodies often predicts a rapid progression to clinical disease. Dr. Kehl wants symptomatic patients with positive results for both markers to be seen right away by a rheumatologist. “We do know from studies that bony erosions can develop as early as a month or months after the onset of an inflammatory arthritis,” she said.
To address this need, Dr. Salinas worked with rheumatologists and primary care clinicians to develop an algorithm that called for reflex testing of samples from patients with positive RF results (> 30 IU/mL) for anti-CCP antibodies. If the anti-CCP antibody result was > 40 IU/mL, a comment in the lab report suggested rheumatology referral. The lab turned down requests to test sample for RF if the patient had a negative result in the previous 12 months — but it would perform the test if the clinician repeated the request.
The results were encouraging, Dr. Salinas said. “The main result in this study was that we really identified more hidden cases of patients with rheumatoid arthritis,” she told this news organization.
Compared with baseline trends, during the study period from April 2019 to January 2021 her lab demonstrated:
- Reduced RF tests conducted by canceling 16% of tests ordered for patients with negative RF result in the previous 12 months
- Fewer unnecessary referrals, from 22% in the baseline period to 8% during the intervention period
- A smaller percentage of missed patients, from 21% to 16%
To be sure, pre- and post-implementation comparisons are difficult when the implementation period happens to coincide with the emergence of SARS-CoV-2.
Although fewer patients were seen and fewer lab tests were ordered overall in Alicante during the COVID-19 pandemic, the proportion of tests ordered for RF testing dropped, and all the patients identified with double positives for RF and anti-CCP antibodies were referred to rheumatology, suggesting evidence of benefit.
Dr. Kehl said the practice of using clinical decision support systems could be used in the United States. “I thought this was an important study,” she said. Electronic health records systems “have all these capabilities where we can include best practice alerts when you order a test to make sure that it’s clinically warranted and cost-effective.”
Dr. Salinas and Dr. Kehl reported no relevant financial relationships.
A version of this article appeared on Medscape.com.
As head of the clinical laboratory at the San Juan University Hospital in Alicante, Spain, Maria Salinas, PhD, is passionate about the role she and her colleagues can play in clinical decision-making.
Her mission is the identification of “hidden diseases,” as she calls them, chronic conditions for which early identification and intervention can change the course of the illness. Her lab has been a leader over the past decade in using technology to partner with clinicians to promote the appropriate use of testing and clinical decision-making.
An example of a disease ripe for this type of intervention is rheumatoid arthritis (RA), the most common form of autoimmune arthritis, affecting around 1.3 million people in the United States. The prognosis for patients is better the earlier treatment begins.
But the
Amy S. Kehl, MD, an attending rheumatologist at Cedars-Sinai Medical Center in Los Angeles, who also sees patients at Saint John’s Physician Partners in Santa Monica, California, recommends a workup for inflammatory arthritis for patients presenting with the new onset of joint pain and swelling, primarily of small joints, although larger joints can be involved. The workup includes markers of inflammation such as an erythrocyte sedimentation rate and C-reactive protein, which are typically elevated and can be used to monitor the progression of the disease. Similarly, the presence of anemia is consistent with RA and helpful in tracking response to treatment.
But pinning down the diagnosis requires the presence of autoimmune antibodies. Guidelines from the American College of Rheumatology require a positive result for either rheumatoid factor (RF) or anti-cyclic citrullinated peptide (anti-CCP) antibody to definitively determine whether a patient has RA (Table).
“Classically, I find that the primary care physicians include a rheumatoid factor, not always a CCP, and may include other antibodies, including an ANA [antinuclear antibody] test, as part of that workup,” Dr. Kehl said. The problem with that strategy is that although the RF test does detect 60%-80% of patients with RA, it is positive in many other autoimmune conditions. Although the ANA might be positive in patients with RA, it is nonspecific and does not confirm the diagnosis of RA.
Up to 50% of autoimmune antibody tests are inappropriately ordered. And for rheumatologists, that leads to unnecessary referrals of patients with musculoskeletal complaints who do not meet objective clinical criteria for joint disease.
“These tests get ordered almost reflexively, and sometimes they’re ordered as part of a panel that includes a rheumatoid factor and an ANA, and it’s not necessarily going to be a high-yield test,” Dr. Kehl said. Superfluous tests and referrals often cause unnecessary anxiety in patients, as well as drive up costs, she added.
Dr. Salinas made the same observation in her hospital lab, which also serves nine primary care centers. She documented an upward trend in orders for RF testing in her hospital lab between 2011 and 2019. Dr. Salinas also noted that the anti-CCP antibody test was not commonly requested, although it has more utility in the diagnosis. Like the RF, it detects 50%-70% of patients with RA but has 95% specificity, resulting in far fewer false-positive results.
The appearance of both RF and anti-CCP antibodies often predicts a rapid progression to clinical disease. Dr. Kehl wants symptomatic patients with positive results for both markers to be seen right away by a rheumatologist. “We do know from studies that bony erosions can develop as early as a month or months after the onset of an inflammatory arthritis,” she said.
To address this need, Dr. Salinas worked with rheumatologists and primary care clinicians to develop an algorithm that called for reflex testing of samples from patients with positive RF results (> 30 IU/mL) for anti-CCP antibodies. If the anti-CCP antibody result was > 40 IU/mL, a comment in the lab report suggested rheumatology referral. The lab turned down requests to test sample for RF if the patient had a negative result in the previous 12 months — but it would perform the test if the clinician repeated the request.
The results were encouraging, Dr. Salinas said. “The main result in this study was that we really identified more hidden cases of patients with rheumatoid arthritis,” she told this news organization.
Compared with baseline trends, during the study period from April 2019 to January 2021 her lab demonstrated:
- Reduced RF tests conducted by canceling 16% of tests ordered for patients with negative RF result in the previous 12 months
- Fewer unnecessary referrals, from 22% in the baseline period to 8% during the intervention period
- A smaller percentage of missed patients, from 21% to 16%
To be sure, pre- and post-implementation comparisons are difficult when the implementation period happens to coincide with the emergence of SARS-CoV-2.
Although fewer patients were seen and fewer lab tests were ordered overall in Alicante during the COVID-19 pandemic, the proportion of tests ordered for RF testing dropped, and all the patients identified with double positives for RF and anti-CCP antibodies were referred to rheumatology, suggesting evidence of benefit.
Dr. Kehl said the practice of using clinical decision support systems could be used in the United States. “I thought this was an important study,” she said. Electronic health records systems “have all these capabilities where we can include best practice alerts when you order a test to make sure that it’s clinically warranted and cost-effective.”
Dr. Salinas and Dr. Kehl reported no relevant financial relationships.
A version of this article appeared on Medscape.com.
As head of the clinical laboratory at the San Juan University Hospital in Alicante, Spain, Maria Salinas, PhD, is passionate about the role she and her colleagues can play in clinical decision-making.
Her mission is the identification of “hidden diseases,” as she calls them, chronic conditions for which early identification and intervention can change the course of the illness. Her lab has been a leader over the past decade in using technology to partner with clinicians to promote the appropriate use of testing and clinical decision-making.
An example of a disease ripe for this type of intervention is rheumatoid arthritis (RA), the most common form of autoimmune arthritis, affecting around 1.3 million people in the United States. The prognosis for patients is better the earlier treatment begins.
But the
Amy S. Kehl, MD, an attending rheumatologist at Cedars-Sinai Medical Center in Los Angeles, who also sees patients at Saint John’s Physician Partners in Santa Monica, California, recommends a workup for inflammatory arthritis for patients presenting with the new onset of joint pain and swelling, primarily of small joints, although larger joints can be involved. The workup includes markers of inflammation such as an erythrocyte sedimentation rate and C-reactive protein, which are typically elevated and can be used to monitor the progression of the disease. Similarly, the presence of anemia is consistent with RA and helpful in tracking response to treatment.
But pinning down the diagnosis requires the presence of autoimmune antibodies. Guidelines from the American College of Rheumatology require a positive result for either rheumatoid factor (RF) or anti-cyclic citrullinated peptide (anti-CCP) antibody to definitively determine whether a patient has RA (Table).
“Classically, I find that the primary care physicians include a rheumatoid factor, not always a CCP, and may include other antibodies, including an ANA [antinuclear antibody] test, as part of that workup,” Dr. Kehl said. The problem with that strategy is that although the RF test does detect 60%-80% of patients with RA, it is positive in many other autoimmune conditions. Although the ANA might be positive in patients with RA, it is nonspecific and does not confirm the diagnosis of RA.
Up to 50% of autoimmune antibody tests are inappropriately ordered. And for rheumatologists, that leads to unnecessary referrals of patients with musculoskeletal complaints who do not meet objective clinical criteria for joint disease.
“These tests get ordered almost reflexively, and sometimes they’re ordered as part of a panel that includes a rheumatoid factor and an ANA, and it’s not necessarily going to be a high-yield test,” Dr. Kehl said. Superfluous tests and referrals often cause unnecessary anxiety in patients, as well as drive up costs, she added.
Dr. Salinas made the same observation in her hospital lab, which also serves nine primary care centers. She documented an upward trend in orders for RF testing in her hospital lab between 2011 and 2019. Dr. Salinas also noted that the anti-CCP antibody test was not commonly requested, although it has more utility in the diagnosis. Like the RF, it detects 50%-70% of patients with RA but has 95% specificity, resulting in far fewer false-positive results.
The appearance of both RF and anti-CCP antibodies often predicts a rapid progression to clinical disease. Dr. Kehl wants symptomatic patients with positive results for both markers to be seen right away by a rheumatologist. “We do know from studies that bony erosions can develop as early as a month or months after the onset of an inflammatory arthritis,” she said.
To address this need, Dr. Salinas worked with rheumatologists and primary care clinicians to develop an algorithm that called for reflex testing of samples from patients with positive RF results (> 30 IU/mL) for anti-CCP antibodies. If the anti-CCP antibody result was > 40 IU/mL, a comment in the lab report suggested rheumatology referral. The lab turned down requests to test sample for RF if the patient had a negative result in the previous 12 months — but it would perform the test if the clinician repeated the request.
The results were encouraging, Dr. Salinas said. “The main result in this study was that we really identified more hidden cases of patients with rheumatoid arthritis,” she told this news organization.
Compared with baseline trends, during the study period from April 2019 to January 2021 her lab demonstrated:
- Reduced RF tests conducted by canceling 16% of tests ordered for patients with negative RF result in the previous 12 months
- Fewer unnecessary referrals, from 22% in the baseline period to 8% during the intervention period
- A smaller percentage of missed patients, from 21% to 16%
To be sure, pre- and post-implementation comparisons are difficult when the implementation period happens to coincide with the emergence of SARS-CoV-2.
Although fewer patients were seen and fewer lab tests were ordered overall in Alicante during the COVID-19 pandemic, the proportion of tests ordered for RF testing dropped, and all the patients identified with double positives for RF and anti-CCP antibodies were referred to rheumatology, suggesting evidence of benefit.
Dr. Kehl said the practice of using clinical decision support systems could be used in the United States. “I thought this was an important study,” she said. Electronic health records systems “have all these capabilities where we can include best practice alerts when you order a test to make sure that it’s clinically warranted and cost-effective.”
Dr. Salinas and Dr. Kehl reported no relevant financial relationships.
A version of this article appeared on Medscape.com.
Doctors With Limited Vacation Have Increased Burnout Risk
A recent study sheds light on the heightened risk for burnout among physicians who take infrequent vacations and engage in patient-related work during their time off.
Conducted by the American Medical Association (AMA), the study focuses on the United States, where labor regulations regarding vacation days and compensation differ from German norms. Despite this distinction, it provides valuable insights into the vacation behavior of doctors and its potential impact on burnout risk.
Christine A. Sinsky, MD, study author and senior physician advisor for physician satisfaction at the AMA, and her colleagues invited more than 90,000 physicians to participate in a survey that used postal and computer-based methods. In all, 3024 physicians, mainly those contacted by mail, filled out the questionnaire.
Limited Vacation Days
A significant proportion (59.6%) of respondents reported having taken fewer than 15 vacation days in the previous year, with nearly 20% taking fewer than 5 days off. Even when officially on vacation, most (70.4%) found themselves dealing with patient-related tasks. For one-third, these tasks consumed at least 30 minutes on a typical vacation day, often longer. This phenomenon was noted especially among female physicians.
Doctors who took less vacation and worked during their time off displayed higher emotional exhaustion and reported feeling less fulfilled in their profession.
Administrative Tasks
Administrative tasks, though no longer confined to paper, significantly influenced physicians’ vacation behavior. In the United States, handling messages from patients through the electronic health records (EHR) inbox demands a considerable amount of time.
Courses and tutorials on EHR inbox management are on the rise. A 2023 review linked electronic health records management to an increased burnout risk in the US medical community.
Lack of Coverage
Many physicians lack coverage for their EHR inbox during their absence. Less than half (49.1%) stated that someone else manages their inbox while they are on vacation.
Difficulty in finding coverage, whether for the EHR inbox or patient care, is a leading reason why many physicians seldom take more than 3 weeks of vacation per year. Financial considerations also contribute to this decision, as revealed in the survey.
Vacation Lowers Risk
Further analysis showed that doctors who took more than 3 weeks of vacation per year, which is not common, had a lower risk of developing burnout. Having coverage for vacation was also associated with reduced burnout risk and increased professional fulfillment.
However, these benefits applied only when physicians truly took a break during their vacation. Respondents who spent 30 minutes or more per day on patient-related work had a higher burnout risk. The risk was 1.58 times greater for 30-60 minutes, 1.97 times greater for 60-90 minutes, and 1.92 times greater for more than 90 minutes.
System-Level Interventions
The vacation behavior observed in this study likely exacerbates the effects of chronic workplace overload that are associated with long working hours, thus increasing the risk for burnout, according to the researchers.
“System-level measures must be implemented to ensure physicians take an appropriate number of vacation days,” wrote the researchers. “This includes having coverage available to handle clinical activities and administrative tasks, such as managing the EHR inbox. This could potentially reduce the burnout rate among physicians.”
This article was translated from the Medscape German edition. A version of this article appeared on Medscape.com.
A recent study sheds light on the heightened risk for burnout among physicians who take infrequent vacations and engage in patient-related work during their time off.
Conducted by the American Medical Association (AMA), the study focuses on the United States, where labor regulations regarding vacation days and compensation differ from German norms. Despite this distinction, it provides valuable insights into the vacation behavior of doctors and its potential impact on burnout risk.
Christine A. Sinsky, MD, study author and senior physician advisor for physician satisfaction at the AMA, and her colleagues invited more than 90,000 physicians to participate in a survey that used postal and computer-based methods. In all, 3024 physicians, mainly those contacted by mail, filled out the questionnaire.
Limited Vacation Days
A significant proportion (59.6%) of respondents reported having taken fewer than 15 vacation days in the previous year, with nearly 20% taking fewer than 5 days off. Even when officially on vacation, most (70.4%) found themselves dealing with patient-related tasks. For one-third, these tasks consumed at least 30 minutes on a typical vacation day, often longer. This phenomenon was noted especially among female physicians.
Doctors who took less vacation and worked during their time off displayed higher emotional exhaustion and reported feeling less fulfilled in their profession.
Administrative Tasks
Administrative tasks, though no longer confined to paper, significantly influenced physicians’ vacation behavior. In the United States, handling messages from patients through the electronic health records (EHR) inbox demands a considerable amount of time.
Courses and tutorials on EHR inbox management are on the rise. A 2023 review linked electronic health records management to an increased burnout risk in the US medical community.
Lack of Coverage
Many physicians lack coverage for their EHR inbox during their absence. Less than half (49.1%) stated that someone else manages their inbox while they are on vacation.
Difficulty in finding coverage, whether for the EHR inbox or patient care, is a leading reason why many physicians seldom take more than 3 weeks of vacation per year. Financial considerations also contribute to this decision, as revealed in the survey.
Vacation Lowers Risk
Further analysis showed that doctors who took more than 3 weeks of vacation per year, which is not common, had a lower risk of developing burnout. Having coverage for vacation was also associated with reduced burnout risk and increased professional fulfillment.
However, these benefits applied only when physicians truly took a break during their vacation. Respondents who spent 30 minutes or more per day on patient-related work had a higher burnout risk. The risk was 1.58 times greater for 30-60 minutes, 1.97 times greater for 60-90 minutes, and 1.92 times greater for more than 90 minutes.
System-Level Interventions
The vacation behavior observed in this study likely exacerbates the effects of chronic workplace overload that are associated with long working hours, thus increasing the risk for burnout, according to the researchers.
“System-level measures must be implemented to ensure physicians take an appropriate number of vacation days,” wrote the researchers. “This includes having coverage available to handle clinical activities and administrative tasks, such as managing the EHR inbox. This could potentially reduce the burnout rate among physicians.”
This article was translated from the Medscape German edition. A version of this article appeared on Medscape.com.
A recent study sheds light on the heightened risk for burnout among physicians who take infrequent vacations and engage in patient-related work during their time off.
Conducted by the American Medical Association (AMA), the study focuses on the United States, where labor regulations regarding vacation days and compensation differ from German norms. Despite this distinction, it provides valuable insights into the vacation behavior of doctors and its potential impact on burnout risk.
Christine A. Sinsky, MD, study author and senior physician advisor for physician satisfaction at the AMA, and her colleagues invited more than 90,000 physicians to participate in a survey that used postal and computer-based methods. In all, 3024 physicians, mainly those contacted by mail, filled out the questionnaire.
Limited Vacation Days
A significant proportion (59.6%) of respondents reported having taken fewer than 15 vacation days in the previous year, with nearly 20% taking fewer than 5 days off. Even when officially on vacation, most (70.4%) found themselves dealing with patient-related tasks. For one-third, these tasks consumed at least 30 minutes on a typical vacation day, often longer. This phenomenon was noted especially among female physicians.
Doctors who took less vacation and worked during their time off displayed higher emotional exhaustion and reported feeling less fulfilled in their profession.
Administrative Tasks
Administrative tasks, though no longer confined to paper, significantly influenced physicians’ vacation behavior. In the United States, handling messages from patients through the electronic health records (EHR) inbox demands a considerable amount of time.
Courses and tutorials on EHR inbox management are on the rise. A 2023 review linked electronic health records management to an increased burnout risk in the US medical community.
Lack of Coverage
Many physicians lack coverage for their EHR inbox during their absence. Less than half (49.1%) stated that someone else manages their inbox while they are on vacation.
Difficulty in finding coverage, whether for the EHR inbox or patient care, is a leading reason why many physicians seldom take more than 3 weeks of vacation per year. Financial considerations also contribute to this decision, as revealed in the survey.
Vacation Lowers Risk
Further analysis showed that doctors who took more than 3 weeks of vacation per year, which is not common, had a lower risk of developing burnout. Having coverage for vacation was also associated with reduced burnout risk and increased professional fulfillment.
However, these benefits applied only when physicians truly took a break during their vacation. Respondents who spent 30 minutes or more per day on patient-related work had a higher burnout risk. The risk was 1.58 times greater for 30-60 minutes, 1.97 times greater for 60-90 minutes, and 1.92 times greater for more than 90 minutes.
System-Level Interventions
The vacation behavior observed in this study likely exacerbates the effects of chronic workplace overload that are associated with long working hours, thus increasing the risk for burnout, according to the researchers.
“System-level measures must be implemented to ensure physicians take an appropriate number of vacation days,” wrote the researchers. “This includes having coverage available to handle clinical activities and administrative tasks, such as managing the EHR inbox. This could potentially reduce the burnout rate among physicians.”
This article was translated from the Medscape German edition. A version of this article appeared on Medscape.com.
How to Motivate Pain Patients to Try Nondrug Options
This transcript has been edited for clarity.
Neha Pathak, MD: Hello. Today, we’re talking to Dr. Daniel Clauw, a professor at the University of Michigan in Ann Arbor, who is running a major trial on treatments for chronic back pain. We’re talking today about managing back pain in the post-opioid world. Thank you so much, Dr. Clauw, for taking the time to be our resident pain consultant today. Managing chronic pain can lead to a large amount of burnout and helplessness in the clinic setting. That’s the reality with some of the modalities that patients are requesting; there is still confusion about what is optimal for a particular type of patient, this feeling that we’re not really helping people get better, and whenever patients come in, that’s always still their chief complaint.
How would you advise providers to think about that and to settle into their role as communicators about better strategies without the burnout?
Daniel Clauw, MD: The first thing is to broaden the number of other providers that you get involved in these individuals’ care as the evidence base for all of these nonpharmacologic therapies being effective in chronic pain increases and increases. As third-party payers begin to reimburse for more and more of these therapies, it’s really difficult to manage chronic pain patients if you’re trying to do it alone on an island.
If you can, identify the good physical therapists in your community that are going to really work with people to give them an exercise program that they can use at home; find a pain psychologist that can offer some cognitive-behavioral therapy (CBT) for insomnia and some CBT for pain; and in the subset of patients with trauma, give them the emotional awareness of the neural reprocessing therapy for that specific subset.
As you start to identify more and more of these nonpharmacologic therapies that you want your patients to try, each of those has a set of providers and they can be incredibly helpful so that you, as the primary care provider (PCP), don’t really feel overwhelmed that you’re it, that you’re the only one.
Many of these individuals have more time to spend, and they have more one-on-one in-person time than you do as a primary care physician in the current healthcare system. Many of those providers have become really good at doing amateur CBT, goal-setting, and some of the other things that you need to do when you manage chronic pain patients. Try to find that other group of people that you can send your patients to that are going to be offering some of these nonpharmacologic therapies, and they’ll really help you manage these individuals.
Dr. Pathak: I think a couple of things come up for me. One is that we have to maybe broaden thinking about pain management, not only as multimodal strategies but also as multidisciplinary strategies. To your point, I think that’s really important. I also worry and wonder about health equity concerns, because just as overburdened as many PCPs are, we’re seeing it’s very difficult to get into physical therapy or to get into a setting where you’d be able to receive CBT for your pain. Any thoughts on those types of considerations?
Dr. Clauw: That’s a huge problem. Our group and many other groups in the pain space are developing websites, smartphone apps, and things like that to try to get some of these things directly to individuals with pain, not only for the reasons that you stated but also so that persons with pain don’t have to become patients. Our healthcare systems often make pain worse rather than better.
There were some great articles in The Lancet about 5 years ago talking about low back pain and that in different countries, the healthcare systems, for different reasons, have a tendency to actually make low back pain worse because they do too much surgery, immobilize people, or things like that rather than just not make them better. I think we’ve overmedicalized chronic pain in some settings, and much of what we’re trying to lead people to are things that are parts of wellness programs. The NIH National Center for Complementary and Integrative Health director talks about whole person health often.
I think that these interdisciplinary, integrative approaches are what we have to be using for chronic pain patients. I tell pain patients that, among acupuncture, acupressure, mindfulness, five different forms of CBT, yoga, and tai chi, I don’t know which of those is going to work, but I know that about 1 in 3 individuals that tries each of those therapies gets a benefit. What I really should be doing most is incentivizing people and motivating people to keep trying some of those nonpharmacologic approaches that they haven’t yet tried, because when they find one that works for them, then they will integrate it into their day-to-day life.
The other trick I would use for primary care physicians or anyone managing chronic pain patients is, don’t try to incentivize a pain patient to go try a new nonpharmacologic therapy or start an exercise program because you want their pain score to go from a 6 to a 3. Incentivize them by asking them, what are two or three things that you’re not able to do now because you have chronic pain that you’d really like to be able to do?
You’d like to play nine holes of golf; you’d like to be able to hug your grandchild; or you’d like to be able to do something else. Use those functional goals that are patient0driven to motivate your patients to do these things, because that will work much better. Again, any of us are inherently more likely to take the time and the effort to do some of these nonpharmacologic therapies if it’s for a reason that internally motivates us.
Dr. Pathak: I think that’s great. I’m very privileged to work within the Veterans Affairs (VA) healthcare system. I think that there’s been a huge shift within VA healthcare to provide these ancillary services, whether it’s yoga, tai chi, or acupuncture, as an adjunct to the pain management strategy.
Also, what comes up for me, as you’re saying, is grounding the point that instead of relying on a pain score — which can be objective and different from patient to patient and even within a patient — we should choose a smart goal that is almost more objective when it’s functional. Your goal is to walk two blocks to the mailbox. Can we achieve that as part of your pain control strategy?
I so appreciate your taking the time to be our pain consultant today. I really appreciate our discussion, and I’d like to hand it over to you for any final thoughts.
Dr. Clauw: I’d add that when you’re seeing chronic pain patients, many of them are going to have comorbid sleep problems. They’re going to have comorbid problems with fatigue and memory problems, especially the central nervous system–driven forms of pain that we now call nociplastic pain. Look at those as therapeutic targets.
If you’re befuddled because you’ve tried many different things for pain in this individual you’ve been seeing for a while, focus on their sleep and focus on getting them more active. Don’t use the word exercise — because that scares chronic pain patients — but focus on getting them more active.
There are many different tactics and strategies that you can use to motivate the patients to try some of these new nonpharmacologic approaches as the evidence base continues to increase.
Dr. Pathak: Thank you so much, again, to Dr. Clauw for joining us and being our pain consultant, really helping us to think about managing back pain in the postopioid world.
Dr. Pathak is Chief Physician Editor, Health and Lifestyle Medicine, WebMD. She has disclosed no relevant financial relationships. Dr. Clauw is Director, Chronic Pain and Fatigue Research Center, Department of Anesthesia, University of Michigan, Ann Arbor. He disclosed ties with Tonix and Viatris.
A version of this article appeared on Medscape.com.
This transcript has been edited for clarity.
Neha Pathak, MD: Hello. Today, we’re talking to Dr. Daniel Clauw, a professor at the University of Michigan in Ann Arbor, who is running a major trial on treatments for chronic back pain. We’re talking today about managing back pain in the post-opioid world. Thank you so much, Dr. Clauw, for taking the time to be our resident pain consultant today. Managing chronic pain can lead to a large amount of burnout and helplessness in the clinic setting. That’s the reality with some of the modalities that patients are requesting; there is still confusion about what is optimal for a particular type of patient, this feeling that we’re not really helping people get better, and whenever patients come in, that’s always still their chief complaint.
How would you advise providers to think about that and to settle into their role as communicators about better strategies without the burnout?
Daniel Clauw, MD: The first thing is to broaden the number of other providers that you get involved in these individuals’ care as the evidence base for all of these nonpharmacologic therapies being effective in chronic pain increases and increases. As third-party payers begin to reimburse for more and more of these therapies, it’s really difficult to manage chronic pain patients if you’re trying to do it alone on an island.
If you can, identify the good physical therapists in your community that are going to really work with people to give them an exercise program that they can use at home; find a pain psychologist that can offer some cognitive-behavioral therapy (CBT) for insomnia and some CBT for pain; and in the subset of patients with trauma, give them the emotional awareness of the neural reprocessing therapy for that specific subset.
As you start to identify more and more of these nonpharmacologic therapies that you want your patients to try, each of those has a set of providers and they can be incredibly helpful so that you, as the primary care provider (PCP), don’t really feel overwhelmed that you’re it, that you’re the only one.
Many of these individuals have more time to spend, and they have more one-on-one in-person time than you do as a primary care physician in the current healthcare system. Many of those providers have become really good at doing amateur CBT, goal-setting, and some of the other things that you need to do when you manage chronic pain patients. Try to find that other group of people that you can send your patients to that are going to be offering some of these nonpharmacologic therapies, and they’ll really help you manage these individuals.
Dr. Pathak: I think a couple of things come up for me. One is that we have to maybe broaden thinking about pain management, not only as multimodal strategies but also as multidisciplinary strategies. To your point, I think that’s really important. I also worry and wonder about health equity concerns, because just as overburdened as many PCPs are, we’re seeing it’s very difficult to get into physical therapy or to get into a setting where you’d be able to receive CBT for your pain. Any thoughts on those types of considerations?
Dr. Clauw: That’s a huge problem. Our group and many other groups in the pain space are developing websites, smartphone apps, and things like that to try to get some of these things directly to individuals with pain, not only for the reasons that you stated but also so that persons with pain don’t have to become patients. Our healthcare systems often make pain worse rather than better.
There were some great articles in The Lancet about 5 years ago talking about low back pain and that in different countries, the healthcare systems, for different reasons, have a tendency to actually make low back pain worse because they do too much surgery, immobilize people, or things like that rather than just not make them better. I think we’ve overmedicalized chronic pain in some settings, and much of what we’re trying to lead people to are things that are parts of wellness programs. The NIH National Center for Complementary and Integrative Health director talks about whole person health often.
I think that these interdisciplinary, integrative approaches are what we have to be using for chronic pain patients. I tell pain patients that, among acupuncture, acupressure, mindfulness, five different forms of CBT, yoga, and tai chi, I don’t know which of those is going to work, but I know that about 1 in 3 individuals that tries each of those therapies gets a benefit. What I really should be doing most is incentivizing people and motivating people to keep trying some of those nonpharmacologic approaches that they haven’t yet tried, because when they find one that works for them, then they will integrate it into their day-to-day life.
The other trick I would use for primary care physicians or anyone managing chronic pain patients is, don’t try to incentivize a pain patient to go try a new nonpharmacologic therapy or start an exercise program because you want their pain score to go from a 6 to a 3. Incentivize them by asking them, what are two or three things that you’re not able to do now because you have chronic pain that you’d really like to be able to do?
You’d like to play nine holes of golf; you’d like to be able to hug your grandchild; or you’d like to be able to do something else. Use those functional goals that are patient0driven to motivate your patients to do these things, because that will work much better. Again, any of us are inherently more likely to take the time and the effort to do some of these nonpharmacologic therapies if it’s for a reason that internally motivates us.
Dr. Pathak: I think that’s great. I’m very privileged to work within the Veterans Affairs (VA) healthcare system. I think that there’s been a huge shift within VA healthcare to provide these ancillary services, whether it’s yoga, tai chi, or acupuncture, as an adjunct to the pain management strategy.
Also, what comes up for me, as you’re saying, is grounding the point that instead of relying on a pain score — which can be objective and different from patient to patient and even within a patient — we should choose a smart goal that is almost more objective when it’s functional. Your goal is to walk two blocks to the mailbox. Can we achieve that as part of your pain control strategy?
I so appreciate your taking the time to be our pain consultant today. I really appreciate our discussion, and I’d like to hand it over to you for any final thoughts.
Dr. Clauw: I’d add that when you’re seeing chronic pain patients, many of them are going to have comorbid sleep problems. They’re going to have comorbid problems with fatigue and memory problems, especially the central nervous system–driven forms of pain that we now call nociplastic pain. Look at those as therapeutic targets.
If you’re befuddled because you’ve tried many different things for pain in this individual you’ve been seeing for a while, focus on their sleep and focus on getting them more active. Don’t use the word exercise — because that scares chronic pain patients — but focus on getting them more active.
There are many different tactics and strategies that you can use to motivate the patients to try some of these new nonpharmacologic approaches as the evidence base continues to increase.
Dr. Pathak: Thank you so much, again, to Dr. Clauw for joining us and being our pain consultant, really helping us to think about managing back pain in the postopioid world.
Dr. Pathak is Chief Physician Editor, Health and Lifestyle Medicine, WebMD. She has disclosed no relevant financial relationships. Dr. Clauw is Director, Chronic Pain and Fatigue Research Center, Department of Anesthesia, University of Michigan, Ann Arbor. He disclosed ties with Tonix and Viatris.
A version of this article appeared on Medscape.com.
This transcript has been edited for clarity.
Neha Pathak, MD: Hello. Today, we’re talking to Dr. Daniel Clauw, a professor at the University of Michigan in Ann Arbor, who is running a major trial on treatments for chronic back pain. We’re talking today about managing back pain in the post-opioid world. Thank you so much, Dr. Clauw, for taking the time to be our resident pain consultant today. Managing chronic pain can lead to a large amount of burnout and helplessness in the clinic setting. That’s the reality with some of the modalities that patients are requesting; there is still confusion about what is optimal for a particular type of patient, this feeling that we’re not really helping people get better, and whenever patients come in, that’s always still their chief complaint.
How would you advise providers to think about that and to settle into their role as communicators about better strategies without the burnout?
Daniel Clauw, MD: The first thing is to broaden the number of other providers that you get involved in these individuals’ care as the evidence base for all of these nonpharmacologic therapies being effective in chronic pain increases and increases. As third-party payers begin to reimburse for more and more of these therapies, it’s really difficult to manage chronic pain patients if you’re trying to do it alone on an island.
If you can, identify the good physical therapists in your community that are going to really work with people to give them an exercise program that they can use at home; find a pain psychologist that can offer some cognitive-behavioral therapy (CBT) for insomnia and some CBT for pain; and in the subset of patients with trauma, give them the emotional awareness of the neural reprocessing therapy for that specific subset.
As you start to identify more and more of these nonpharmacologic therapies that you want your patients to try, each of those has a set of providers and they can be incredibly helpful so that you, as the primary care provider (PCP), don’t really feel overwhelmed that you’re it, that you’re the only one.
Many of these individuals have more time to spend, and they have more one-on-one in-person time than you do as a primary care physician in the current healthcare system. Many of those providers have become really good at doing amateur CBT, goal-setting, and some of the other things that you need to do when you manage chronic pain patients. Try to find that other group of people that you can send your patients to that are going to be offering some of these nonpharmacologic therapies, and they’ll really help you manage these individuals.
Dr. Pathak: I think a couple of things come up for me. One is that we have to maybe broaden thinking about pain management, not only as multimodal strategies but also as multidisciplinary strategies. To your point, I think that’s really important. I also worry and wonder about health equity concerns, because just as overburdened as many PCPs are, we’re seeing it’s very difficult to get into physical therapy or to get into a setting where you’d be able to receive CBT for your pain. Any thoughts on those types of considerations?
Dr. Clauw: That’s a huge problem. Our group and many other groups in the pain space are developing websites, smartphone apps, and things like that to try to get some of these things directly to individuals with pain, not only for the reasons that you stated but also so that persons with pain don’t have to become patients. Our healthcare systems often make pain worse rather than better.
There were some great articles in The Lancet about 5 years ago talking about low back pain and that in different countries, the healthcare systems, for different reasons, have a tendency to actually make low back pain worse because they do too much surgery, immobilize people, or things like that rather than just not make them better. I think we’ve overmedicalized chronic pain in some settings, and much of what we’re trying to lead people to are things that are parts of wellness programs. The NIH National Center for Complementary and Integrative Health director talks about whole person health often.
I think that these interdisciplinary, integrative approaches are what we have to be using for chronic pain patients. I tell pain patients that, among acupuncture, acupressure, mindfulness, five different forms of CBT, yoga, and tai chi, I don’t know which of those is going to work, but I know that about 1 in 3 individuals that tries each of those therapies gets a benefit. What I really should be doing most is incentivizing people and motivating people to keep trying some of those nonpharmacologic approaches that they haven’t yet tried, because when they find one that works for them, then they will integrate it into their day-to-day life.
The other trick I would use for primary care physicians or anyone managing chronic pain patients is, don’t try to incentivize a pain patient to go try a new nonpharmacologic therapy or start an exercise program because you want their pain score to go from a 6 to a 3. Incentivize them by asking them, what are two or three things that you’re not able to do now because you have chronic pain that you’d really like to be able to do?
You’d like to play nine holes of golf; you’d like to be able to hug your grandchild; or you’d like to be able to do something else. Use those functional goals that are patient0driven to motivate your patients to do these things, because that will work much better. Again, any of us are inherently more likely to take the time and the effort to do some of these nonpharmacologic therapies if it’s for a reason that internally motivates us.
Dr. Pathak: I think that’s great. I’m very privileged to work within the Veterans Affairs (VA) healthcare system. I think that there’s been a huge shift within VA healthcare to provide these ancillary services, whether it’s yoga, tai chi, or acupuncture, as an adjunct to the pain management strategy.
Also, what comes up for me, as you’re saying, is grounding the point that instead of relying on a pain score — which can be objective and different from patient to patient and even within a patient — we should choose a smart goal that is almost more objective when it’s functional. Your goal is to walk two blocks to the mailbox. Can we achieve that as part of your pain control strategy?
I so appreciate your taking the time to be our pain consultant today. I really appreciate our discussion, and I’d like to hand it over to you for any final thoughts.
Dr. Clauw: I’d add that when you’re seeing chronic pain patients, many of them are going to have comorbid sleep problems. They’re going to have comorbid problems with fatigue and memory problems, especially the central nervous system–driven forms of pain that we now call nociplastic pain. Look at those as therapeutic targets.
If you’re befuddled because you’ve tried many different things for pain in this individual you’ve been seeing for a while, focus on their sleep and focus on getting them more active. Don’t use the word exercise — because that scares chronic pain patients — but focus on getting them more active.
There are many different tactics and strategies that you can use to motivate the patients to try some of these new nonpharmacologic approaches as the evidence base continues to increase.
Dr. Pathak: Thank you so much, again, to Dr. Clauw for joining us and being our pain consultant, really helping us to think about managing back pain in the postopioid world.
Dr. Pathak is Chief Physician Editor, Health and Lifestyle Medicine, WebMD. She has disclosed no relevant financial relationships. Dr. Clauw is Director, Chronic Pain and Fatigue Research Center, Department of Anesthesia, University of Michigan, Ann Arbor. He disclosed ties with Tonix and Viatris.
A version of this article appeared on Medscape.com.
Medical Aid in Dying Should Be Legal, Says Ethicist
This transcript has been edited for clarity.
Hi. I’m Art Caplan. I’m at the Division of Medical Ethics at the NYU Grossman School of Medicine.
Right now, there are 10 states and the District of Columbia that have had some version of medical assistance in dying approved and on the books. That basically means that about 20% of Americans have access where they live to a physician who can prescribe a lethal dose of medication to them if they’re terminally ill and can ingest the medication themselves. That leaves many Americans not covered by this kind of access to this kind of service.
Many of you watching this may live in states where it is legal, like Oregon, Washington, New Jersey, Colorado, and Hawaii. I know many doctors say, “I’m not going to do that.” It’s not something that anyone is compelling a doctor to do. For some Americans, access is not just about where they live but whether there is a doctor willing to participate with them in bringing about their accelerated death, knowing that they’re inevitably going to die.
There’s not much we can do about that. It’s up to the conscience of each physician as to what they’re comfortable with. Certainly, there are other things that can be done to extend the possibility of having this available.
One thing that’s taking place is that, after lawsuits were filed, Vermont and Oregon have given up on their residency requirement, so you don’t have to be there 6 months or a year in order to use this opportunity. It’s legal now to move to the state or visit the state, and as soon as you get there, sign up for this kind of end-of-life intervention.
New Jersey is also being sued. I’ll predict that every state that has a residency requirement, when sued in court, is going to lose because we’ve long recognized the right of Americans to seek out healthcare in the United States, wherever they want to go.
If some states have made this a legitimate medical procedure, courts are going to say you can’t restrict it only to state residents. If someone wants to use a service, they’re entitled to show up from another state or another place and use it. I’m not sure about foreign nationals, but I’m very sure that Americans can go state to state in search of legitimate medical procedures.
The other bills that are out there, however, are basically saying they want to emulate Oregon, Washington, and the other states and say that the terminally ill, with severe restrictions, are going to be able to get this service without going anywhere.
The restrictions include a diagnosis of terminal illness and that you have to be deemed mentally competent. You can’t use this if you have Alzheimer’s or severe depression. You have to make a request twice with a week or two in between to make sure that your request is authentic. And obviously, everyone is on board to make sure that you’re not being coerced or pushed somehow into requesting a somewhat earlier death than you would have experienced without having the availability of the pills.
You also have to take the pills yourself or be able to pull a switch so that you could use a feeding tube–type administration. If you can’t do that, say due to ALS, you’re not eligible to use medical aid in dying. It’s a pretty restricted intervention.
Many people who get pills after going through these restrictions in the states that permit it don’t use it. As many as one third say they like having it there as a safety valve or a parachute, but once they know they could end their life sooner, then they’re going to stick it out.
Should states make this legal? New York, Massachusetts, Florida, and many other states have bills that are moving through. I’m going to say yes. We’ve had Oregon and Washington since the late 1990s with medical aid in dying on the books. There doesn’t seem to be any evidence of pushing people to use this, of bias against the disabled, or bigotry against particular ethnic or racial groups being used to encourage people to end their life sooner.
I think it is an option that Americans want. I think it’s an option that makes some sense. I’m well aware that we also have to make sure that people know about hospice. In some of these states, medical aid in dying is offered as a part of hospice — not all, but a few. Not everybody wants hospice once they realize that they’re dying and that it is coming relatively soon. They may want to leave with family present, with a ceremony, or with a quality of life that they desire.
Past experience says let’s continue to expand availability in each state. Let’s also realize that we have to keep the restrictions in place on how it’s used because they have protected us against abuse. Let’s understand that every doctor has an option to do this or not do this. It’s a matter of conscience and a matter of comfort.
I think legalization is the direction we’re going to be going in. Getting rid of the residency requirements that have been around, as I think courts are going to overturn them, also gives a push to the idea that once the service is in this many states, it’s something that should be available if there are doctors willing to do it.
I’m Art Caplan at the Division of Medical Ethics at NYU Grossman School of Medicine. New York, NY. Thank you for watching.
Arthur L. Caplan, PhD, has disclosed the following relevant financial relationships:
- Served as a director, officer, partner, employee, advisor, consultant, or trustee for: Johnson & Johnson’s Panel for Compassionate Drug Use (unpaid position)
- Serves as a contributing author and adviser for: Medscape
A version of this article appeared on Medscape.com.
This transcript has been edited for clarity.
Hi. I’m Art Caplan. I’m at the Division of Medical Ethics at the NYU Grossman School of Medicine.
Right now, there are 10 states and the District of Columbia that have had some version of medical assistance in dying approved and on the books. That basically means that about 20% of Americans have access where they live to a physician who can prescribe a lethal dose of medication to them if they’re terminally ill and can ingest the medication themselves. That leaves many Americans not covered by this kind of access to this kind of service.
Many of you watching this may live in states where it is legal, like Oregon, Washington, New Jersey, Colorado, and Hawaii. I know many doctors say, “I’m not going to do that.” It’s not something that anyone is compelling a doctor to do. For some Americans, access is not just about where they live but whether there is a doctor willing to participate with them in bringing about their accelerated death, knowing that they’re inevitably going to die.
There’s not much we can do about that. It’s up to the conscience of each physician as to what they’re comfortable with. Certainly, there are other things that can be done to extend the possibility of having this available.
One thing that’s taking place is that, after lawsuits were filed, Vermont and Oregon have given up on their residency requirement, so you don’t have to be there 6 months or a year in order to use this opportunity. It’s legal now to move to the state or visit the state, and as soon as you get there, sign up for this kind of end-of-life intervention.
New Jersey is also being sued. I’ll predict that every state that has a residency requirement, when sued in court, is going to lose because we’ve long recognized the right of Americans to seek out healthcare in the United States, wherever they want to go.
If some states have made this a legitimate medical procedure, courts are going to say you can’t restrict it only to state residents. If someone wants to use a service, they’re entitled to show up from another state or another place and use it. I’m not sure about foreign nationals, but I’m very sure that Americans can go state to state in search of legitimate medical procedures.
The other bills that are out there, however, are basically saying they want to emulate Oregon, Washington, and the other states and say that the terminally ill, with severe restrictions, are going to be able to get this service without going anywhere.
The restrictions include a diagnosis of terminal illness and that you have to be deemed mentally competent. You can’t use this if you have Alzheimer’s or severe depression. You have to make a request twice with a week or two in between to make sure that your request is authentic. And obviously, everyone is on board to make sure that you’re not being coerced or pushed somehow into requesting a somewhat earlier death than you would have experienced without having the availability of the pills.
You also have to take the pills yourself or be able to pull a switch so that you could use a feeding tube–type administration. If you can’t do that, say due to ALS, you’re not eligible to use medical aid in dying. It’s a pretty restricted intervention.
Many people who get pills after going through these restrictions in the states that permit it don’t use it. As many as one third say they like having it there as a safety valve or a parachute, but once they know they could end their life sooner, then they’re going to stick it out.
Should states make this legal? New York, Massachusetts, Florida, and many other states have bills that are moving through. I’m going to say yes. We’ve had Oregon and Washington since the late 1990s with medical aid in dying on the books. There doesn’t seem to be any evidence of pushing people to use this, of bias against the disabled, or bigotry against particular ethnic or racial groups being used to encourage people to end their life sooner.
I think it is an option that Americans want. I think it’s an option that makes some sense. I’m well aware that we also have to make sure that people know about hospice. In some of these states, medical aid in dying is offered as a part of hospice — not all, but a few. Not everybody wants hospice once they realize that they’re dying and that it is coming relatively soon. They may want to leave with family present, with a ceremony, or with a quality of life that they desire.
Past experience says let’s continue to expand availability in each state. Let’s also realize that we have to keep the restrictions in place on how it’s used because they have protected us against abuse. Let’s understand that every doctor has an option to do this or not do this. It’s a matter of conscience and a matter of comfort.
I think legalization is the direction we’re going to be going in. Getting rid of the residency requirements that have been around, as I think courts are going to overturn them, also gives a push to the idea that once the service is in this many states, it’s something that should be available if there are doctors willing to do it.
I’m Art Caplan at the Division of Medical Ethics at NYU Grossman School of Medicine. New York, NY. Thank you for watching.
Arthur L. Caplan, PhD, has disclosed the following relevant financial relationships:
- Served as a director, officer, partner, employee, advisor, consultant, or trustee for: Johnson & Johnson’s Panel for Compassionate Drug Use (unpaid position)
- Serves as a contributing author and adviser for: Medscape
A version of this article appeared on Medscape.com.
This transcript has been edited for clarity.
Hi. I’m Art Caplan. I’m at the Division of Medical Ethics at the NYU Grossman School of Medicine.
Right now, there are 10 states and the District of Columbia that have had some version of medical assistance in dying approved and on the books. That basically means that about 20% of Americans have access where they live to a physician who can prescribe a lethal dose of medication to them if they’re terminally ill and can ingest the medication themselves. That leaves many Americans not covered by this kind of access to this kind of service.
Many of you watching this may live in states where it is legal, like Oregon, Washington, New Jersey, Colorado, and Hawaii. I know many doctors say, “I’m not going to do that.” It’s not something that anyone is compelling a doctor to do. For some Americans, access is not just about where they live but whether there is a doctor willing to participate with them in bringing about their accelerated death, knowing that they’re inevitably going to die.
There’s not much we can do about that. It’s up to the conscience of each physician as to what they’re comfortable with. Certainly, there are other things that can be done to extend the possibility of having this available.
One thing that’s taking place is that, after lawsuits were filed, Vermont and Oregon have given up on their residency requirement, so you don’t have to be there 6 months or a year in order to use this opportunity. It’s legal now to move to the state or visit the state, and as soon as you get there, sign up for this kind of end-of-life intervention.
New Jersey is also being sued. I’ll predict that every state that has a residency requirement, when sued in court, is going to lose because we’ve long recognized the right of Americans to seek out healthcare in the United States, wherever they want to go.
If some states have made this a legitimate medical procedure, courts are going to say you can’t restrict it only to state residents. If someone wants to use a service, they’re entitled to show up from another state or another place and use it. I’m not sure about foreign nationals, but I’m very sure that Americans can go state to state in search of legitimate medical procedures.
The other bills that are out there, however, are basically saying they want to emulate Oregon, Washington, and the other states and say that the terminally ill, with severe restrictions, are going to be able to get this service without going anywhere.
The restrictions include a diagnosis of terminal illness and that you have to be deemed mentally competent. You can’t use this if you have Alzheimer’s or severe depression. You have to make a request twice with a week or two in between to make sure that your request is authentic. And obviously, everyone is on board to make sure that you’re not being coerced or pushed somehow into requesting a somewhat earlier death than you would have experienced without having the availability of the pills.
You also have to take the pills yourself or be able to pull a switch so that you could use a feeding tube–type administration. If you can’t do that, say due to ALS, you’re not eligible to use medical aid in dying. It’s a pretty restricted intervention.
Many people who get pills after going through these restrictions in the states that permit it don’t use it. As many as one third say they like having it there as a safety valve or a parachute, but once they know they could end their life sooner, then they’re going to stick it out.
Should states make this legal? New York, Massachusetts, Florida, and many other states have bills that are moving through. I’m going to say yes. We’ve had Oregon and Washington since the late 1990s with medical aid in dying on the books. There doesn’t seem to be any evidence of pushing people to use this, of bias against the disabled, or bigotry against particular ethnic or racial groups being used to encourage people to end their life sooner.
I think it is an option that Americans want. I think it’s an option that makes some sense. I’m well aware that we also have to make sure that people know about hospice. In some of these states, medical aid in dying is offered as a part of hospice — not all, but a few. Not everybody wants hospice once they realize that they’re dying and that it is coming relatively soon. They may want to leave with family present, with a ceremony, or with a quality of life that they desire.
Past experience says let’s continue to expand availability in each state. Let’s also realize that we have to keep the restrictions in place on how it’s used because they have protected us against abuse. Let’s understand that every doctor has an option to do this or not do this. It’s a matter of conscience and a matter of comfort.
I think legalization is the direction we’re going to be going in. Getting rid of the residency requirements that have been around, as I think courts are going to overturn them, also gives a push to the idea that once the service is in this many states, it’s something that should be available if there are doctors willing to do it.
I’m Art Caplan at the Division of Medical Ethics at NYU Grossman School of Medicine. New York, NY. Thank you for watching.
Arthur L. Caplan, PhD, has disclosed the following relevant financial relationships:
- Served as a director, officer, partner, employee, advisor, consultant, or trustee for: Johnson & Johnson’s Panel for Compassionate Drug Use (unpaid position)
- Serves as a contributing author and adviser for: Medscape
A version of this article appeared on Medscape.com.
The Emerging Physician-Scientist Crisis in America
Recent reporting has shown that That’s a problem, because physician-scientists are uniquely equipped to make scientific discoveries in the laboratory and translate them to the clinic. Indeed, many of the discoveries that have transformed medicine for the better were made by physician-scientists. For example, Jonas Salk developed the polio vaccine, Timothy Ley sequenced the first cancer genome, and Anthony Fauci coordinated public health responses to both the HIV/AIDS and COVID-19 pandemics. Indicative of their sheer impact, at least a third and as many as half of all Nobel Prizes and Lasker Awards in physiology/medicine have gone to physician-scientists.
So why is the supply of physician-scientists shrinking so precipitously at a time when medical discoveries are being made at a record-high rate? Immunotherapy and proton therapy are transforming cancer care; RNA technology led to COVID vaccines; CRISPR is facilitating gene editing and treatment of diseases like sickle cell anemia. Yet, as exciting as medical science has become, only 1.5% of American doctors work as physician-scientists, more than a threefold drop compared with 30 years ago when the figure was a more robust 4.7%. What’s going on?
Residency training programs at prestigious academic medical centers have standard infolded research years; for example, neurosurgery residents at academic medical centers will often get 2 years of protected research time. And the National Institutes of Health has training grants dedicated to physician-scientists, such as the K08 award program. Several foundations are also dedicated to supporting early-career physician-scientists. Yet, the number of physicians deciding to become physician-scientists remains low, and, more troubling, the attrition rate of those who do decide to go this route is quite high.
The underlying issue is multifold. First, funding rates from the federal government for grants have become competitive to the point of being unrealistic. For example, the current funding rate for the flagship R01 program from the National Cancer Institute is only 12%. Promotions are typically tied to these grant awards, which means physician-scientists who are unable to acquire substantial grant funding are unable to pay for their research or win promotion — and often exit the physician-scientist track altogether.
Compounding this issue is a lack of mentorship for early-career physician-scientists. With the rise of “careerism” in medicine, senior-level physician-scientists may have less incentive to mentor those who are earlier in their careers. Rather, there seems to be greater reward to “managing up” — that is, spending time to please hospital administrators and departmental leadership. Being involved in countless committees appears to carry more value in advancing an established investigator’s career than does mentorship.
Finally, physician-scientists typically earn less than their clinician colleagues, despite juggling both scientific and clinical responsibilities. While many are comfortable with this arrangement when embarking on this track, the disparity may become untenable after a while, especially as departmental leadership will often turn to physician-scientists to fill clinical coverage gaps when faculty leave the department, or as the medical center expands to satellite centers outside the primary hospital. Indeed, physician-scientists get pulled in several directions, which can lead to burnout and attrition, with many who are highly equipped for this track ultimately hanging up their cleats and seeking more clinical or private industry–oriented opportunities.
Every academic medical center operates differently. Some clearly have done a better job than others promoting and fostering physician-scientists. What we find in the centers that manage to retain physician-scientists is leadership plays a major role: If a medical center values the importance of physician-scientists, they will do things to foster the success of those people, such as assembling mentorship committees, establishing clear criteria for promotion and career advancement, protecting research time while maintaining some level of pay equity, advocating for team science approaches, and supporting investigators in cases of gaps in federal funding. Different countries also have different models for physician-scientist training, with Germany, for example, allowing medical residents to have 3 years of protected time to engage in research after their second year of residency.
The stakes here are high. If we can’t address the physician-scientist recruitment and retention crisis in America now, we risk falling behind other countries in our ability to innovate and deliver world-class care.
Dr Chaudhuri is a tenure-track physician-scientist at Washington University in St. Louis, a Paul and Daisy Soros Fellow, and a Public Voices Fellow of The OpEd Project.
Aadel Chaudhuri, MD, PhD, has disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
Recent reporting has shown that That’s a problem, because physician-scientists are uniquely equipped to make scientific discoveries in the laboratory and translate them to the clinic. Indeed, many of the discoveries that have transformed medicine for the better were made by physician-scientists. For example, Jonas Salk developed the polio vaccine, Timothy Ley sequenced the first cancer genome, and Anthony Fauci coordinated public health responses to both the HIV/AIDS and COVID-19 pandemics. Indicative of their sheer impact, at least a third and as many as half of all Nobel Prizes and Lasker Awards in physiology/medicine have gone to physician-scientists.
So why is the supply of physician-scientists shrinking so precipitously at a time when medical discoveries are being made at a record-high rate? Immunotherapy and proton therapy are transforming cancer care; RNA technology led to COVID vaccines; CRISPR is facilitating gene editing and treatment of diseases like sickle cell anemia. Yet, as exciting as medical science has become, only 1.5% of American doctors work as physician-scientists, more than a threefold drop compared with 30 years ago when the figure was a more robust 4.7%. What’s going on?
Residency training programs at prestigious academic medical centers have standard infolded research years; for example, neurosurgery residents at academic medical centers will often get 2 years of protected research time. And the National Institutes of Health has training grants dedicated to physician-scientists, such as the K08 award program. Several foundations are also dedicated to supporting early-career physician-scientists. Yet, the number of physicians deciding to become physician-scientists remains low, and, more troubling, the attrition rate of those who do decide to go this route is quite high.
The underlying issue is multifold. First, funding rates from the federal government for grants have become competitive to the point of being unrealistic. For example, the current funding rate for the flagship R01 program from the National Cancer Institute is only 12%. Promotions are typically tied to these grant awards, which means physician-scientists who are unable to acquire substantial grant funding are unable to pay for their research or win promotion — and often exit the physician-scientist track altogether.
Compounding this issue is a lack of mentorship for early-career physician-scientists. With the rise of “careerism” in medicine, senior-level physician-scientists may have less incentive to mentor those who are earlier in their careers. Rather, there seems to be greater reward to “managing up” — that is, spending time to please hospital administrators and departmental leadership. Being involved in countless committees appears to carry more value in advancing an established investigator’s career than does mentorship.
Finally, physician-scientists typically earn less than their clinician colleagues, despite juggling both scientific and clinical responsibilities. While many are comfortable with this arrangement when embarking on this track, the disparity may become untenable after a while, especially as departmental leadership will often turn to physician-scientists to fill clinical coverage gaps when faculty leave the department, or as the medical center expands to satellite centers outside the primary hospital. Indeed, physician-scientists get pulled in several directions, which can lead to burnout and attrition, with many who are highly equipped for this track ultimately hanging up their cleats and seeking more clinical or private industry–oriented opportunities.
Every academic medical center operates differently. Some clearly have done a better job than others promoting and fostering physician-scientists. What we find in the centers that manage to retain physician-scientists is leadership plays a major role: If a medical center values the importance of physician-scientists, they will do things to foster the success of those people, such as assembling mentorship committees, establishing clear criteria for promotion and career advancement, protecting research time while maintaining some level of pay equity, advocating for team science approaches, and supporting investigators in cases of gaps in federal funding. Different countries also have different models for physician-scientist training, with Germany, for example, allowing medical residents to have 3 years of protected time to engage in research after their second year of residency.
The stakes here are high. If we can’t address the physician-scientist recruitment and retention crisis in America now, we risk falling behind other countries in our ability to innovate and deliver world-class care.
Dr Chaudhuri is a tenure-track physician-scientist at Washington University in St. Louis, a Paul and Daisy Soros Fellow, and a Public Voices Fellow of The OpEd Project.
Aadel Chaudhuri, MD, PhD, has disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
Recent reporting has shown that That’s a problem, because physician-scientists are uniquely equipped to make scientific discoveries in the laboratory and translate them to the clinic. Indeed, many of the discoveries that have transformed medicine for the better were made by physician-scientists. For example, Jonas Salk developed the polio vaccine, Timothy Ley sequenced the first cancer genome, and Anthony Fauci coordinated public health responses to both the HIV/AIDS and COVID-19 pandemics. Indicative of their sheer impact, at least a third and as many as half of all Nobel Prizes and Lasker Awards in physiology/medicine have gone to physician-scientists.
So why is the supply of physician-scientists shrinking so precipitously at a time when medical discoveries are being made at a record-high rate? Immunotherapy and proton therapy are transforming cancer care; RNA technology led to COVID vaccines; CRISPR is facilitating gene editing and treatment of diseases like sickle cell anemia. Yet, as exciting as medical science has become, only 1.5% of American doctors work as physician-scientists, more than a threefold drop compared with 30 years ago when the figure was a more robust 4.7%. What’s going on?
Residency training programs at prestigious academic medical centers have standard infolded research years; for example, neurosurgery residents at academic medical centers will often get 2 years of protected research time. And the National Institutes of Health has training grants dedicated to physician-scientists, such as the K08 award program. Several foundations are also dedicated to supporting early-career physician-scientists. Yet, the number of physicians deciding to become physician-scientists remains low, and, more troubling, the attrition rate of those who do decide to go this route is quite high.
The underlying issue is multifold. First, funding rates from the federal government for grants have become competitive to the point of being unrealistic. For example, the current funding rate for the flagship R01 program from the National Cancer Institute is only 12%. Promotions are typically tied to these grant awards, which means physician-scientists who are unable to acquire substantial grant funding are unable to pay for their research or win promotion — and often exit the physician-scientist track altogether.
Compounding this issue is a lack of mentorship for early-career physician-scientists. With the rise of “careerism” in medicine, senior-level physician-scientists may have less incentive to mentor those who are earlier in their careers. Rather, there seems to be greater reward to “managing up” — that is, spending time to please hospital administrators and departmental leadership. Being involved in countless committees appears to carry more value in advancing an established investigator’s career than does mentorship.
Finally, physician-scientists typically earn less than their clinician colleagues, despite juggling both scientific and clinical responsibilities. While many are comfortable with this arrangement when embarking on this track, the disparity may become untenable after a while, especially as departmental leadership will often turn to physician-scientists to fill clinical coverage gaps when faculty leave the department, or as the medical center expands to satellite centers outside the primary hospital. Indeed, physician-scientists get pulled in several directions, which can lead to burnout and attrition, with many who are highly equipped for this track ultimately hanging up their cleats and seeking more clinical or private industry–oriented opportunities.
Every academic medical center operates differently. Some clearly have done a better job than others promoting and fostering physician-scientists. What we find in the centers that manage to retain physician-scientists is leadership plays a major role: If a medical center values the importance of physician-scientists, they will do things to foster the success of those people, such as assembling mentorship committees, establishing clear criteria for promotion and career advancement, protecting research time while maintaining some level of pay equity, advocating for team science approaches, and supporting investigators in cases of gaps in federal funding. Different countries also have different models for physician-scientist training, with Germany, for example, allowing medical residents to have 3 years of protected time to engage in research after their second year of residency.
The stakes here are high. If we can’t address the physician-scientist recruitment and retention crisis in America now, we risk falling behind other countries in our ability to innovate and deliver world-class care.
Dr Chaudhuri is a tenure-track physician-scientist at Washington University in St. Louis, a Paul and Daisy Soros Fellow, and a Public Voices Fellow of The OpEd Project.
Aadel Chaudhuri, MD, PhD, has disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
Five Bold Predictions for Long COVID in 2024
With a number of large-scale clinical trials underway and researchers on the hunt for new therapies, long COVID scientists are hopeful that this is the year patients — and doctors who care for them — will finally see improvements in treating their symptoms.
Here are five bold predictions — all based on encouraging research — that could happen in 2024. At the very least, they are promising signs of progress against a debilitating and frustrating disease.
#1: We’ll gain a better understanding of each long COVID phenotype
This past year, a wide breadth of research began showing that long COVID can be defined by a number of different disease phenotypes that present a range of symptoms.
Researchers identified four clinical phenotypes: Chronic fatigue-like syndrome, headache, and memory loss; respiratory syndrome, which includes cough and difficulty breathing; chronic pain; and neurosensorial syndrome, which causes an altered sense of taste and smell.
Identifying specific diagnostic criteria for each phenotype would lead to better health outcomes for patients instead of treating them as if it were a “one-size-fits-all disease,” said Nisha Viswanathan, MD, director of the long COVID program at UCLA Health, Los Angeles, California.
Ultimately, she hopes that this year her patients will receive treatments based on the type of long COVID they’re personally experiencing, and the symptoms they have, leading to improved health outcomes and more rapid relief.
“Many new medications are focused on different pathways of long COVID, and the challenge becomes which drug is the right drug for each treatment,” said Dr. Viswanathan.
#2: Monoclonal antibodies may change the game
We’re starting to have a better understanding that what’s been called “viral persistence” as a main cause of long COVID may potentially be treated with monoclonal antibodies. These are antibodies produced by cloning unique white blood cells to target the circulating spike proteins in the blood that hang out in viral reservoirs and cause the immune system to react as if it’s still fighting acute COVID-19.
Smaller-scale studies have already shown promising results. A January 2024 study published in The American Journal of Emergency Medicine followed three patients who completely recovered from long COVID after taking monoclonal antibodies. “Remission occurred despite dissimilar past histories, sex, age, and illness duration,” wrote the study authors.
Larger clinical trials are underway at the University of California, San Francisco, California, to test targeted monoclonal antibodies. If the results of the larger study show that monoclonal antibodies are beneficial, then it could be a game changer for a large swath of patients around the world, said David F. Putrino, PhD, who runs the long COVID clinic at Mount Sinai Health System in New York City.
“The idea is that the downstream damage caused by viral persistence will resolve itself once you wipe out the virus,” said Dr. Putrino.
#3: Paxlovid could prove effective for long COVID
The US Food and Drug Administration granted approval for Paxlovid last May for the treatment of mild to moderate COVID-19 in adults at a high risk for severe disease. The medication is made up of two drugs packaged together. The first, nirmatrelvir, works by blocking a key enzyme required for virus replication. The second, ritonavir, is an antiviral that’s been used in patients with HIV and helps boost levels of antivirals in the body.
In a large-scale trial headed up by Dr. Putrino and his team, the oral antiviral is being studied for use in the post-viral stage in patients who test negative for acute COVID-19 but have persisting symptoms of long COVID.
Similar to monoclonal antibodies, the idea is to quell viral persistence. If patients have long COVID because they can’t clear SAR-CoV-2 from their bodies, Paxlovid could help. But unlike monoclonal antibodies that quash the virus, Paxlovid stops the virus from replicating. It’s a different mechanism with the same end goal.
It’s been a controversial treatment because it’s life-changing for some patients and ineffective for others. In addition, it can cause a range of side effects such as diarrhea, nausea, vomiting, and an impaired sense of taste. The goal of the trial is to see which patients with long COVID are most likely to benefit from the treatment.
#4: Anti-inflammatories like metformin could prove useful
Many of the inflammatory markers persistent in patients with long COVID were similarly present in patients with autoimmune diseases like rheumatoid arthritis, according to a July 2023 study published in JAMA.
The hope is that anti-inflammatory medications may be used to reduce inflammation causing long COVID symptoms. But drugs used to treat rheumatoid arthritis like abatacept and infliximabcan also have serious side effects, including increased risk for infection, flu-like symptoms, and burning of the skin.
“Powerful anti-inflammatories can change a number of pathways in the immune system,” said Grace McComsey, MD, who leads the long COVID RECOVER study at University Hospitals Health System in Cleveland, Ohio. Anti-inflammatories hold promise but, Dr. McComsey said, “some are more toxic with many side effects, so even if they work, there’s still a question about who should take them.”
Still, other anti-inflammatories that could work don’t have as many side effects. For example, a study published in The Lancet Infectious Diseases found that the diabetes drug metformin reduced a patient’s risk for long COVID up to 40% when the drug was taken during the acute stage.
Metformin, compared to other anti-inflammatories (also known as immune modulators), is an inexpensive and widely available drug with relatively few side effects compared with other medications.
#5: Serotonin levels — and selective serotonin reuptake inhibitors (SSRIs) — may be keys to unlocking long COVID
One of the most groundbreaking studies of the year came last November. A study published in the journal Cell found lower circulating serotonin levels in patents with long COVID than in those who did not have the condition. The study also found that the SSRI fluoxetine improved cognitive function in rat models infected with the virus.
Researchers found that the reduction in serotonin levels was partially caused by the body’s inability to absorb tryptophan, an amino acid that’s a precursor to serotonin. Overactivated blood platelets may also have played a role.
Michael Peluso, MD, an assistant research professor of infectious medicine at the UCSF School of Medicine, San Francisco, California, hopes to take the finding a step further, investigating whether increased serotonin levels in patients with long COVID will lead to improvements in symptoms.
“What we need now is a good clinical trial to see whether altering levels of serotonin in people with long COVID will lead to symptom relief,” Dr. Peluso said last month in an interview with this news organization.
If patients show an improvement in symptoms, then the next step is looking into whether SSRIs boost serotonin levels in patients and, as a result, reduce their symptoms.
A version of this article appeared on Medscape.com.
With a number of large-scale clinical trials underway and researchers on the hunt for new therapies, long COVID scientists are hopeful that this is the year patients — and doctors who care for them — will finally see improvements in treating their symptoms.
Here are five bold predictions — all based on encouraging research — that could happen in 2024. At the very least, they are promising signs of progress against a debilitating and frustrating disease.
#1: We’ll gain a better understanding of each long COVID phenotype
This past year, a wide breadth of research began showing that long COVID can be defined by a number of different disease phenotypes that present a range of symptoms.
Researchers identified four clinical phenotypes: Chronic fatigue-like syndrome, headache, and memory loss; respiratory syndrome, which includes cough and difficulty breathing; chronic pain; and neurosensorial syndrome, which causes an altered sense of taste and smell.
Identifying specific diagnostic criteria for each phenotype would lead to better health outcomes for patients instead of treating them as if it were a “one-size-fits-all disease,” said Nisha Viswanathan, MD, director of the long COVID program at UCLA Health, Los Angeles, California.
Ultimately, she hopes that this year her patients will receive treatments based on the type of long COVID they’re personally experiencing, and the symptoms they have, leading to improved health outcomes and more rapid relief.
“Many new medications are focused on different pathways of long COVID, and the challenge becomes which drug is the right drug for each treatment,” said Dr. Viswanathan.
#2: Monoclonal antibodies may change the game
We’re starting to have a better understanding that what’s been called “viral persistence” as a main cause of long COVID may potentially be treated with monoclonal antibodies. These are antibodies produced by cloning unique white blood cells to target the circulating spike proteins in the blood that hang out in viral reservoirs and cause the immune system to react as if it’s still fighting acute COVID-19.
Smaller-scale studies have already shown promising results. A January 2024 study published in The American Journal of Emergency Medicine followed three patients who completely recovered from long COVID after taking monoclonal antibodies. “Remission occurred despite dissimilar past histories, sex, age, and illness duration,” wrote the study authors.
Larger clinical trials are underway at the University of California, San Francisco, California, to test targeted monoclonal antibodies. If the results of the larger study show that monoclonal antibodies are beneficial, then it could be a game changer for a large swath of patients around the world, said David F. Putrino, PhD, who runs the long COVID clinic at Mount Sinai Health System in New York City.
“The idea is that the downstream damage caused by viral persistence will resolve itself once you wipe out the virus,” said Dr. Putrino.
#3: Paxlovid could prove effective for long COVID
The US Food and Drug Administration granted approval for Paxlovid last May for the treatment of mild to moderate COVID-19 in adults at a high risk for severe disease. The medication is made up of two drugs packaged together. The first, nirmatrelvir, works by blocking a key enzyme required for virus replication. The second, ritonavir, is an antiviral that’s been used in patients with HIV and helps boost levels of antivirals in the body.
In a large-scale trial headed up by Dr. Putrino and his team, the oral antiviral is being studied for use in the post-viral stage in patients who test negative for acute COVID-19 but have persisting symptoms of long COVID.
Similar to monoclonal antibodies, the idea is to quell viral persistence. If patients have long COVID because they can’t clear SAR-CoV-2 from their bodies, Paxlovid could help. But unlike monoclonal antibodies that quash the virus, Paxlovid stops the virus from replicating. It’s a different mechanism with the same end goal.
It’s been a controversial treatment because it’s life-changing for some patients and ineffective for others. In addition, it can cause a range of side effects such as diarrhea, nausea, vomiting, and an impaired sense of taste. The goal of the trial is to see which patients with long COVID are most likely to benefit from the treatment.
#4: Anti-inflammatories like metformin could prove useful
Many of the inflammatory markers persistent in patients with long COVID were similarly present in patients with autoimmune diseases like rheumatoid arthritis, according to a July 2023 study published in JAMA.
The hope is that anti-inflammatory medications may be used to reduce inflammation causing long COVID symptoms. But drugs used to treat rheumatoid arthritis like abatacept and infliximabcan also have serious side effects, including increased risk for infection, flu-like symptoms, and burning of the skin.
“Powerful anti-inflammatories can change a number of pathways in the immune system,” said Grace McComsey, MD, who leads the long COVID RECOVER study at University Hospitals Health System in Cleveland, Ohio. Anti-inflammatories hold promise but, Dr. McComsey said, “some are more toxic with many side effects, so even if they work, there’s still a question about who should take them.”
Still, other anti-inflammatories that could work don’t have as many side effects. For example, a study published in The Lancet Infectious Diseases found that the diabetes drug metformin reduced a patient’s risk for long COVID up to 40% when the drug was taken during the acute stage.
Metformin, compared to other anti-inflammatories (also known as immune modulators), is an inexpensive and widely available drug with relatively few side effects compared with other medications.
#5: Serotonin levels — and selective serotonin reuptake inhibitors (SSRIs) — may be keys to unlocking long COVID
One of the most groundbreaking studies of the year came last November. A study published in the journal Cell found lower circulating serotonin levels in patents with long COVID than in those who did not have the condition. The study also found that the SSRI fluoxetine improved cognitive function in rat models infected with the virus.
Researchers found that the reduction in serotonin levels was partially caused by the body’s inability to absorb tryptophan, an amino acid that’s a precursor to serotonin. Overactivated blood platelets may also have played a role.
Michael Peluso, MD, an assistant research professor of infectious medicine at the UCSF School of Medicine, San Francisco, California, hopes to take the finding a step further, investigating whether increased serotonin levels in patients with long COVID will lead to improvements in symptoms.
“What we need now is a good clinical trial to see whether altering levels of serotonin in people with long COVID will lead to symptom relief,” Dr. Peluso said last month in an interview with this news organization.
If patients show an improvement in symptoms, then the next step is looking into whether SSRIs boost serotonin levels in patients and, as a result, reduce their symptoms.
A version of this article appeared on Medscape.com.
With a number of large-scale clinical trials underway and researchers on the hunt for new therapies, long COVID scientists are hopeful that this is the year patients — and doctors who care for them — will finally see improvements in treating their symptoms.
Here are five bold predictions — all based on encouraging research — that could happen in 2024. At the very least, they are promising signs of progress against a debilitating and frustrating disease.
#1: We’ll gain a better understanding of each long COVID phenotype
This past year, a wide breadth of research began showing that long COVID can be defined by a number of different disease phenotypes that present a range of symptoms.
Researchers identified four clinical phenotypes: Chronic fatigue-like syndrome, headache, and memory loss; respiratory syndrome, which includes cough and difficulty breathing; chronic pain; and neurosensorial syndrome, which causes an altered sense of taste and smell.
Identifying specific diagnostic criteria for each phenotype would lead to better health outcomes for patients instead of treating them as if it were a “one-size-fits-all disease,” said Nisha Viswanathan, MD, director of the long COVID program at UCLA Health, Los Angeles, California.
Ultimately, she hopes that this year her patients will receive treatments based on the type of long COVID they’re personally experiencing, and the symptoms they have, leading to improved health outcomes and more rapid relief.
“Many new medications are focused on different pathways of long COVID, and the challenge becomes which drug is the right drug for each treatment,” said Dr. Viswanathan.
#2: Monoclonal antibodies may change the game
We’re starting to have a better understanding that what’s been called “viral persistence” as a main cause of long COVID may potentially be treated with monoclonal antibodies. These are antibodies produced by cloning unique white blood cells to target the circulating spike proteins in the blood that hang out in viral reservoirs and cause the immune system to react as if it’s still fighting acute COVID-19.
Smaller-scale studies have already shown promising results. A January 2024 study published in The American Journal of Emergency Medicine followed three patients who completely recovered from long COVID after taking monoclonal antibodies. “Remission occurred despite dissimilar past histories, sex, age, and illness duration,” wrote the study authors.
Larger clinical trials are underway at the University of California, San Francisco, California, to test targeted monoclonal antibodies. If the results of the larger study show that monoclonal antibodies are beneficial, then it could be a game changer for a large swath of patients around the world, said David F. Putrino, PhD, who runs the long COVID clinic at Mount Sinai Health System in New York City.
“The idea is that the downstream damage caused by viral persistence will resolve itself once you wipe out the virus,” said Dr. Putrino.
#3: Paxlovid could prove effective for long COVID
The US Food and Drug Administration granted approval for Paxlovid last May for the treatment of mild to moderate COVID-19 in adults at a high risk for severe disease. The medication is made up of two drugs packaged together. The first, nirmatrelvir, works by blocking a key enzyme required for virus replication. The second, ritonavir, is an antiviral that’s been used in patients with HIV and helps boost levels of antivirals in the body.
In a large-scale trial headed up by Dr. Putrino and his team, the oral antiviral is being studied for use in the post-viral stage in patients who test negative for acute COVID-19 but have persisting symptoms of long COVID.
Similar to monoclonal antibodies, the idea is to quell viral persistence. If patients have long COVID because they can’t clear SAR-CoV-2 from their bodies, Paxlovid could help. But unlike monoclonal antibodies that quash the virus, Paxlovid stops the virus from replicating. It’s a different mechanism with the same end goal.
It’s been a controversial treatment because it’s life-changing for some patients and ineffective for others. In addition, it can cause a range of side effects such as diarrhea, nausea, vomiting, and an impaired sense of taste. The goal of the trial is to see which patients with long COVID are most likely to benefit from the treatment.
#4: Anti-inflammatories like metformin could prove useful
Many of the inflammatory markers persistent in patients with long COVID were similarly present in patients with autoimmune diseases like rheumatoid arthritis, according to a July 2023 study published in JAMA.
The hope is that anti-inflammatory medications may be used to reduce inflammation causing long COVID symptoms. But drugs used to treat rheumatoid arthritis like abatacept and infliximabcan also have serious side effects, including increased risk for infection, flu-like symptoms, and burning of the skin.
“Powerful anti-inflammatories can change a number of pathways in the immune system,” said Grace McComsey, MD, who leads the long COVID RECOVER study at University Hospitals Health System in Cleveland, Ohio. Anti-inflammatories hold promise but, Dr. McComsey said, “some are more toxic with many side effects, so even if they work, there’s still a question about who should take them.”
Still, other anti-inflammatories that could work don’t have as many side effects. For example, a study published in The Lancet Infectious Diseases found that the diabetes drug metformin reduced a patient’s risk for long COVID up to 40% when the drug was taken during the acute stage.
Metformin, compared to other anti-inflammatories (also known as immune modulators), is an inexpensive and widely available drug with relatively few side effects compared with other medications.
#5: Serotonin levels — and selective serotonin reuptake inhibitors (SSRIs) — may be keys to unlocking long COVID
One of the most groundbreaking studies of the year came last November. A study published in the journal Cell found lower circulating serotonin levels in patents with long COVID than in those who did not have the condition. The study also found that the SSRI fluoxetine improved cognitive function in rat models infected with the virus.
Researchers found that the reduction in serotonin levels was partially caused by the body’s inability to absorb tryptophan, an amino acid that’s a precursor to serotonin. Overactivated blood platelets may also have played a role.
Michael Peluso, MD, an assistant research professor of infectious medicine at the UCSF School of Medicine, San Francisco, California, hopes to take the finding a step further, investigating whether increased serotonin levels in patients with long COVID will lead to improvements in symptoms.
“What we need now is a good clinical trial to see whether altering levels of serotonin in people with long COVID will lead to symptom relief,” Dr. Peluso said last month in an interview with this news organization.
If patients show an improvement in symptoms, then the next step is looking into whether SSRIs boost serotonin levels in patients and, as a result, reduce their symptoms.
A version of this article appeared on Medscape.com.
A Paradox? Higher Male Fertility Seen With Inflammatory Arthritis
TOPLINE:
Men with an inflammatory arthritis (IA) diagnosis are less likely to be childless than healthy comparators, according to an epidemiological study.
METHODS:
- 10,865 men in the Norwegian Arthritis Registry were compared with 54,325 men without IA, matched by age and location.
- In the arthritis group, 37% had rheumatoid arthritis, 33% had psoriatic arthritis, and 30% had spondyloarthritis.
- Researchers used childlessness and number of children as proxies for male fertility.
TAKEAWAY:
- 21% of men with IA were childless compared with 27% in the healthy cohort (P < .001).
- On an average, a man with IA had 1.80 children whereas a man in the control group had 1.69 children (P < .001).
- These findings were consistent over time, but the most pronounced difference between groups was seen in men diagnosed after the year 2000.
IN PRACTICE:
The finding “is novel and generates new hypotheses regarding associations between fertility, inflammatory rheumatic diseases, and immune-modulating drugs,” the authors wrote.
SOURCE:
First author Gudrun David Sigmo, of the department of rheumatology at Stavanger (Norway) University Hospital, and colleagues had their work published online on January 23, 2024, in Annals of the Rheumatic Diseases.
LIMITATIONS:
The analysis relied on administrative data, and researchers did not have data on confounding factors.
DISCLOSURES:
The study was funded by the nonprofit organizations Aslaug Anders fond, Astri og Edvard Riisøens legat, Det alminnelige medisinske forskningsfond, Pahles legat, and Fagsenter for medisins-ke kvalitetsregistre i Helse Vest. The authors declared no relevant conflicts of interest.
A version of this article first appeared on Medscape.com.
TOPLINE:
Men with an inflammatory arthritis (IA) diagnosis are less likely to be childless than healthy comparators, according to an epidemiological study.
METHODS:
- 10,865 men in the Norwegian Arthritis Registry were compared with 54,325 men without IA, matched by age and location.
- In the arthritis group, 37% had rheumatoid arthritis, 33% had psoriatic arthritis, and 30% had spondyloarthritis.
- Researchers used childlessness and number of children as proxies for male fertility.
TAKEAWAY:
- 21% of men with IA were childless compared with 27% in the healthy cohort (P < .001).
- On an average, a man with IA had 1.80 children whereas a man in the control group had 1.69 children (P < .001).
- These findings were consistent over time, but the most pronounced difference between groups was seen in men diagnosed after the year 2000.
IN PRACTICE:
The finding “is novel and generates new hypotheses regarding associations between fertility, inflammatory rheumatic diseases, and immune-modulating drugs,” the authors wrote.
SOURCE:
First author Gudrun David Sigmo, of the department of rheumatology at Stavanger (Norway) University Hospital, and colleagues had their work published online on January 23, 2024, in Annals of the Rheumatic Diseases.
LIMITATIONS:
The analysis relied on administrative data, and researchers did not have data on confounding factors.
DISCLOSURES:
The study was funded by the nonprofit organizations Aslaug Anders fond, Astri og Edvard Riisøens legat, Det alminnelige medisinske forskningsfond, Pahles legat, and Fagsenter for medisins-ke kvalitetsregistre i Helse Vest. The authors declared no relevant conflicts of interest.
A version of this article first appeared on Medscape.com.
TOPLINE:
Men with an inflammatory arthritis (IA) diagnosis are less likely to be childless than healthy comparators, according to an epidemiological study.
METHODS:
- 10,865 men in the Norwegian Arthritis Registry were compared with 54,325 men without IA, matched by age and location.
- In the arthritis group, 37% had rheumatoid arthritis, 33% had psoriatic arthritis, and 30% had spondyloarthritis.
- Researchers used childlessness and number of children as proxies for male fertility.
TAKEAWAY:
- 21% of men with IA were childless compared with 27% in the healthy cohort (P < .001).
- On an average, a man with IA had 1.80 children whereas a man in the control group had 1.69 children (P < .001).
- These findings were consistent over time, but the most pronounced difference between groups was seen in men diagnosed after the year 2000.
IN PRACTICE:
The finding “is novel and generates new hypotheses regarding associations between fertility, inflammatory rheumatic diseases, and immune-modulating drugs,” the authors wrote.
SOURCE:
First author Gudrun David Sigmo, of the department of rheumatology at Stavanger (Norway) University Hospital, and colleagues had their work published online on January 23, 2024, in Annals of the Rheumatic Diseases.
LIMITATIONS:
The analysis relied on administrative data, and researchers did not have data on confounding factors.
DISCLOSURES:
The study was funded by the nonprofit organizations Aslaug Anders fond, Astri og Edvard Riisøens legat, Det alminnelige medisinske forskningsfond, Pahles legat, and Fagsenter for medisins-ke kvalitetsregistre i Helse Vest. The authors declared no relevant conflicts of interest.
A version of this article first appeared on Medscape.com.
Vibrating Belt Receives Approval to Help Women With Osteopenia Keep Bone Strength
The US Food and Drug Administration (FDA) has approved a wearable belt device for postmenopausal women with osteopenia, the precursor to osteoporosis, according to the company’s manufacturer, Bone Health Technologies.
According to the company, the device (Osteoboost) is the first nonpharmacologic device-based, prescription-only treatment for postmenopausal women with low bone density. It has not been tested for ability to reduce fracture risk.

The device is worn around the hips and delivers calibrated mild vibrations to the hips and lumbar spine to help preserve bone strength and density. A vibration pack is mounted to the back of the belt.
FDA approval, announced on January 18, was based on the findings of a National Institutes of Health–funded double-blinded, sham-controlled study of 126 women with low bone density conducted at the University of Nebraska Medical Center in Omaha. The data were shared at the 2023 Endocrine Society and American Society for Bone and Mineral Research annual meetings and published in the Journal of the Endocrine Society.
Lead investigator Laura D. Bilek, PT, PhD, associate dean for research and associate professor at the University of Nebraska, and colleagues wrote that the primary outcome measurement was the change in vertebral strength measured by CT scans for women who used the device a minimum of three times per week compared with a sham group who wore a belt that emitted sound but had no vibrations.
Compressive strength and volumetric density of the first lumbar vertebra were analyzed.
In the active-belt group, women lost, on average, 0.48% bone strength, while those in the sham group lost nearly 2.84% (P = .014), about five times as much. Results also showed that participants in the active treatment group who used the device three times per week lost 0.29% bone mineral density (BMD) compared with the 1.97% BMD lost in the control group. No adverse events were reported in the study.
Sonali Khandelwal, MD, a rheumatologist at Rush University in Chicago, told this news organization there’s considerable fear among some patients about long-term use of available medications for bone health, “so any modality that is nontherapeutic — not a pill — is always exciting.”
The endpoints of the study are one good measure, she said, but she emphasized that it will be important to show that the improved bone density from the belt that is described in this study “is a true marker of decreased fracture risk.”
Because there are no apparent side effects, she said it may be effective in combination with weight-bearing exercise, vitamin D and calcium, and/or medication, depending on severity of bone loss.
Current medications on the market for osteoporosis have been shown to improve bone strength and reduce fracture risk, she noted.
“It could help; I just don’t think we have enough evidence that it will completely treat the bone loss,” Dr. Khandelwal said.
She said she sees the potential population most interested in the belt as premenopausal women with a family history of bone loss who may not meet the level of bone loss for medical management but are interested in prevention.
“I also think of individuals who might already meet medication needs but are completely averse to being on medication,” she said. The bulk of her practice is treating bone loss, she said, estimating that 20% of her patients do not want to be on medication.
Bone Health Technologies CEO Laura Yecies, MBA, told this news organization the company has not yet set the price for the device and noted that because it will be available by prescription only, out-of-pocket costs and copays will differ. She said the company expects to begin shipping later this year. Requests for update notifications can be made at the company’s website.
Dr. Bilek told this news organization the device was tested for a year, so it’s unclear how long people with osteopenia would need to wear the belt for maximum benefit.
The theory behind the mechanism of action, she said, “is that the vibration actually inhibits the cells [osteoclasts] that take away bone mass.”
The researchers included only postmenopausal women with osteopenia in the study, but Dr. Bilek said she would like to test the device on other groups, such as men with prostate cancer getting testosterone-blocking therapy, which can result in loss of bone density. An estimated 34 million people in the United States have osteopenia.
Dr. Bilek said a next step for the study is to enroll a more diverse cohort at an additional center to test the device because most of the women in this one were White.
She noted that women’s bone mass peaks at age 30 and then starts to decline.
“When women hit menopause, there’s a really rapid decline [in bone strength] for the next 5-7 years and then the decline levels off. If we can slow that decline, hopefully that woman’s bone density is maintained at a higher level throughout their life,” Dr. Bilek said.
Dr. Bilek is a scientific adviser to Bone Health Technologies. She and many coauthors of the study received grants or fees from the company and own stock in or are employees of the company. Ms. Yecies is the founder and CEO of Bone Health Technologies. Dr. Khandelwal had no relevant financial relationships.
A version of this article first appeared on Medscape.com.
The US Food and Drug Administration (FDA) has approved a wearable belt device for postmenopausal women with osteopenia, the precursor to osteoporosis, according to the company’s manufacturer, Bone Health Technologies.
According to the company, the device (Osteoboost) is the first nonpharmacologic device-based, prescription-only treatment for postmenopausal women with low bone density. It has not been tested for ability to reduce fracture risk.
The device is worn around the hips and delivers calibrated mild vibrations to the hips and lumbar spine to help preserve bone strength and density. A vibration pack is mounted to the back of the belt.
FDA approval, announced on January 18, was based on the findings of a National Institutes of Health–funded double-blinded, sham-controlled study of 126 women with low bone density conducted at the University of Nebraska Medical Center in Omaha. The data were shared at the 2023 Endocrine Society and American Society for Bone and Mineral Research annual meetings and published in the Journal of the Endocrine Society.
Lead investigator Laura D. Bilek, PT, PhD, associate dean for research and associate professor at the University of Nebraska, and colleagues wrote that the primary outcome measurement was the change in vertebral strength measured by CT scans for women who used the device a minimum of three times per week compared with a sham group who wore a belt that emitted sound but had no vibrations.
Compressive strength and volumetric density of the first lumbar vertebra were analyzed.
In the active-belt group, women lost, on average, 0.48% bone strength, while those in the sham group lost nearly 2.84% (P = .014), about five times as much. Results also showed that participants in the active treatment group who used the device three times per week lost 0.29% bone mineral density (BMD) compared with the 1.97% BMD lost in the control group. No adverse events were reported in the study.
Sonali Khandelwal, MD, a rheumatologist at Rush University in Chicago, told this news organization there’s considerable fear among some patients about long-term use of available medications for bone health, “so any modality that is nontherapeutic — not a pill — is always exciting.”
The endpoints of the study are one good measure, she said, but she emphasized that it will be important to show that the improved bone density from the belt that is described in this study “is a true marker of decreased fracture risk.”
Because there are no apparent side effects, she said it may be effective in combination with weight-bearing exercise, vitamin D and calcium, and/or medication, depending on severity of bone loss.
Current medications on the market for osteoporosis have been shown to improve bone strength and reduce fracture risk, she noted.
“It could help; I just don’t think we have enough evidence that it will completely treat the bone loss,” Dr. Khandelwal said.
She said she sees the potential population most interested in the belt as premenopausal women with a family history of bone loss who may not meet the level of bone loss for medical management but are interested in prevention.
“I also think of individuals who might already meet medication needs but are completely averse to being on medication,” she said. The bulk of her practice is treating bone loss, she said, estimating that 20% of her patients do not want to be on medication.
Bone Health Technologies CEO Laura Yecies, MBA, told this news organization the company has not yet set the price for the device and noted that because it will be available by prescription only, out-of-pocket costs and copays will differ. She said the company expects to begin shipping later this year. Requests for update notifications can be made at the company’s website.
Dr. Bilek told this news organization the device was tested for a year, so it’s unclear how long people with osteopenia would need to wear the belt for maximum benefit.
The theory behind the mechanism of action, she said, “is that the vibration actually inhibits the cells [osteoclasts] that take away bone mass.”
The researchers included only postmenopausal women with osteopenia in the study, but Dr. Bilek said she would like to test the device on other groups, such as men with prostate cancer getting testosterone-blocking therapy, which can result in loss of bone density. An estimated 34 million people in the United States have osteopenia.
Dr. Bilek said a next step for the study is to enroll a more diverse cohort at an additional center to test the device because most of the women in this one were White.
She noted that women’s bone mass peaks at age 30 and then starts to decline.
“When women hit menopause, there’s a really rapid decline [in bone strength] for the next 5-7 years and then the decline levels off. If we can slow that decline, hopefully that woman’s bone density is maintained at a higher level throughout their life,” Dr. Bilek said.
Dr. Bilek is a scientific adviser to Bone Health Technologies. She and many coauthors of the study received grants or fees from the company and own stock in or are employees of the company. Ms. Yecies is the founder and CEO of Bone Health Technologies. Dr. Khandelwal had no relevant financial relationships.
A version of this article first appeared on Medscape.com.
The US Food and Drug Administration (FDA) has approved a wearable belt device for postmenopausal women with osteopenia, the precursor to osteoporosis, according to the company’s manufacturer, Bone Health Technologies.
According to the company, the device (Osteoboost) is the first nonpharmacologic device-based, prescription-only treatment for postmenopausal women with low bone density. It has not been tested for ability to reduce fracture risk.
The device is worn around the hips and delivers calibrated mild vibrations to the hips and lumbar spine to help preserve bone strength and density. A vibration pack is mounted to the back of the belt.
FDA approval, announced on January 18, was based on the findings of a National Institutes of Health–funded double-blinded, sham-controlled study of 126 women with low bone density conducted at the University of Nebraska Medical Center in Omaha. The data were shared at the 2023 Endocrine Society and American Society for Bone and Mineral Research annual meetings and published in the Journal of the Endocrine Society.
Lead investigator Laura D. Bilek, PT, PhD, associate dean for research and associate professor at the University of Nebraska, and colleagues wrote that the primary outcome measurement was the change in vertebral strength measured by CT scans for women who used the device a minimum of three times per week compared with a sham group who wore a belt that emitted sound but had no vibrations.
Compressive strength and volumetric density of the first lumbar vertebra were analyzed.
In the active-belt group, women lost, on average, 0.48% bone strength, while those in the sham group lost nearly 2.84% (P = .014), about five times as much. Results also showed that participants in the active treatment group who used the device three times per week lost 0.29% bone mineral density (BMD) compared with the 1.97% BMD lost in the control group. No adverse events were reported in the study.
Sonali Khandelwal, MD, a rheumatologist at Rush University in Chicago, told this news organization there’s considerable fear among some patients about long-term use of available medications for bone health, “so any modality that is nontherapeutic — not a pill — is always exciting.”
The endpoints of the study are one good measure, she said, but she emphasized that it will be important to show that the improved bone density from the belt that is described in this study “is a true marker of decreased fracture risk.”
Because there are no apparent side effects, she said it may be effective in combination with weight-bearing exercise, vitamin D and calcium, and/or medication, depending on severity of bone loss.
Current medications on the market for osteoporosis have been shown to improve bone strength and reduce fracture risk, she noted.
“It could help; I just don’t think we have enough evidence that it will completely treat the bone loss,” Dr. Khandelwal said.
She said she sees the potential population most interested in the belt as premenopausal women with a family history of bone loss who may not meet the level of bone loss for medical management but are interested in prevention.
“I also think of individuals who might already meet medication needs but are completely averse to being on medication,” she said. The bulk of her practice is treating bone loss, she said, estimating that 20% of her patients do not want to be on medication.
Bone Health Technologies CEO Laura Yecies, MBA, told this news organization the company has not yet set the price for the device and noted that because it will be available by prescription only, out-of-pocket costs and copays will differ. She said the company expects to begin shipping later this year. Requests for update notifications can be made at the company’s website.
Dr. Bilek told this news organization the device was tested for a year, so it’s unclear how long people with osteopenia would need to wear the belt for maximum benefit.
The theory behind the mechanism of action, she said, “is that the vibration actually inhibits the cells [osteoclasts] that take away bone mass.”
The researchers included only postmenopausal women with osteopenia in the study, but Dr. Bilek said she would like to test the device on other groups, such as men with prostate cancer getting testosterone-blocking therapy, which can result in loss of bone density. An estimated 34 million people in the United States have osteopenia.
Dr. Bilek said a next step for the study is to enroll a more diverse cohort at an additional center to test the device because most of the women in this one were White.
She noted that women’s bone mass peaks at age 30 and then starts to decline.
“When women hit menopause, there’s a really rapid decline [in bone strength] for the next 5-7 years and then the decline levels off. If we can slow that decline, hopefully that woman’s bone density is maintained at a higher level throughout their life,” Dr. Bilek said.
Dr. Bilek is a scientific adviser to Bone Health Technologies. She and many coauthors of the study received grants or fees from the company and own stock in or are employees of the company. Ms. Yecies is the founder and CEO of Bone Health Technologies. Dr. Khandelwal had no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Is RA Disease Activity Assessed Too Little After Starting TNFi?
TOPLINE:
Less than half of patients with rheumatoid arthritis (RA) initiating a first-line tumor necrosis factor inhibitor (TNFi) in clinical practice had a recorded composite disease activity assessment at the start of the treatment, and many remained on that treatment for years without evidence recorded in their electronic medical record of achieving low-disease activity or remission.
METHODOLOGY:
- Researchers reviewed data from 1651 adults aged 18 years and older with moderate to severe RA at baseline or follow-up in the electronic medical record database of the American Rheumatology Network, a large community network of independent practices with > 200 rheumatologists across the United States.
- Patients received a TNFi as their first advanced therapy between January 2014 and August 2021 and were assessed for measurement of disease activity with the Clinical Disease Activity Index (CDAI) or Routine Assessment of Patient Index Data 3 (RAPID3) at baseline and follow-up visits.
TAKEAWAY:
- Among the patients with moderate to severe RA, 47.2% of patients remained on first-line TNFi therapy 1 year after initiation despite no evidence of achieving treatment targets of low disease activity or remission (defined as CDAI ≤ 10 and/or RAPID3 ≤ 2).
- Approximately one third of patients remained on TNFi therapy for 2 (38.1%) or 3 (35.4%) years after initiation despite not achieving these targets. The median times to TNFi discontinuation was 30.4 months and to subsequent therapy initiation 68.3 months.
- A total of 52% discontinued their initial TNFi during the study period; among those who started a second therapy, 15% restarted the same TNFi, 45.6% started another TNFi, 27.6% started a non-TNFi biologic, and 11.5% started a Janus kinase inhibitor.
- The most common reported reasons for discontinuation were a combination of efficacy and intolerance, efficacy only, and intolerance only (26.9%, 25.3%, and 20.3%, respectively).
- Persistent pain was the most common reason for efficacy-related discontinuation (39.0%), followed by persistent inflammation/swelling and overall general discomfort (31.8% for both).
IN PRACTICE:
“Consistent monitoring of treatment response and timely switch to effective therapy as appropriate is needed in patients with RA initiating their first advanced therapies,” the researchers wrote.
SOURCE:
First author Colin Edgerton, MD, of Articularis Healthcare Group and American Rheumatology Network, Charleston, South Carolina, reported their work on January 14, 2024, in ACR Open Rheumatology.
LIMITATIONS:
The findings were limited by several factors including the retrospective design, incomplete data from electronic medical records, and reliance on physician documentation for drivers of discontinuation.
DISCLOSURES:
The study was supported by AbbVie. Lead author Edgerton also disclosed relationships with Novartis and Boehringer Ingelheim.
A version of this article first appeared on Medscape.com.
TOPLINE:
Less than half of patients with rheumatoid arthritis (RA) initiating a first-line tumor necrosis factor inhibitor (TNFi) in clinical practice had a recorded composite disease activity assessment at the start of the treatment, and many remained on that treatment for years without evidence recorded in their electronic medical record of achieving low-disease activity or remission.
METHODOLOGY:
- Researchers reviewed data from 1651 adults aged 18 years and older with moderate to severe RA at baseline or follow-up in the electronic medical record database of the American Rheumatology Network, a large community network of independent practices with > 200 rheumatologists across the United States.
- Patients received a TNFi as their first advanced therapy between January 2014 and August 2021 and were assessed for measurement of disease activity with the Clinical Disease Activity Index (CDAI) or Routine Assessment of Patient Index Data 3 (RAPID3) at baseline and follow-up visits.
TAKEAWAY:
- Among the patients with moderate to severe RA, 47.2% of patients remained on first-line TNFi therapy 1 year after initiation despite no evidence of achieving treatment targets of low disease activity or remission (defined as CDAI ≤ 10 and/or RAPID3 ≤ 2).
- Approximately one third of patients remained on TNFi therapy for 2 (38.1%) or 3 (35.4%) years after initiation despite not achieving these targets. The median times to TNFi discontinuation was 30.4 months and to subsequent therapy initiation 68.3 months.
- A total of 52% discontinued their initial TNFi during the study period; among those who started a second therapy, 15% restarted the same TNFi, 45.6% started another TNFi, 27.6% started a non-TNFi biologic, and 11.5% started a Janus kinase inhibitor.
- The most common reported reasons for discontinuation were a combination of efficacy and intolerance, efficacy only, and intolerance only (26.9%, 25.3%, and 20.3%, respectively).
- Persistent pain was the most common reason for efficacy-related discontinuation (39.0%), followed by persistent inflammation/swelling and overall general discomfort (31.8% for both).
IN PRACTICE:
“Consistent monitoring of treatment response and timely switch to effective therapy as appropriate is needed in patients with RA initiating their first advanced therapies,” the researchers wrote.
SOURCE:
First author Colin Edgerton, MD, of Articularis Healthcare Group and American Rheumatology Network, Charleston, South Carolina, reported their work on January 14, 2024, in ACR Open Rheumatology.
LIMITATIONS:
The findings were limited by several factors including the retrospective design, incomplete data from electronic medical records, and reliance on physician documentation for drivers of discontinuation.
DISCLOSURES:
The study was supported by AbbVie. Lead author Edgerton also disclosed relationships with Novartis and Boehringer Ingelheim.
A version of this article first appeared on Medscape.com.
TOPLINE:
Less than half of patients with rheumatoid arthritis (RA) initiating a first-line tumor necrosis factor inhibitor (TNFi) in clinical practice had a recorded composite disease activity assessment at the start of the treatment, and many remained on that treatment for years without evidence recorded in their electronic medical record of achieving low-disease activity or remission.
METHODOLOGY:
- Researchers reviewed data from 1651 adults aged 18 years and older with moderate to severe RA at baseline or follow-up in the electronic medical record database of the American Rheumatology Network, a large community network of independent practices with > 200 rheumatologists across the United States.
- Patients received a TNFi as their first advanced therapy between January 2014 and August 2021 and were assessed for measurement of disease activity with the Clinical Disease Activity Index (CDAI) or Routine Assessment of Patient Index Data 3 (RAPID3) at baseline and follow-up visits.
TAKEAWAY:
- Among the patients with moderate to severe RA, 47.2% of patients remained on first-line TNFi therapy 1 year after initiation despite no evidence of achieving treatment targets of low disease activity or remission (defined as CDAI ≤ 10 and/or RAPID3 ≤ 2).
- Approximately one third of patients remained on TNFi therapy for 2 (38.1%) or 3 (35.4%) years after initiation despite not achieving these targets. The median times to TNFi discontinuation was 30.4 months and to subsequent therapy initiation 68.3 months.
- A total of 52% discontinued their initial TNFi during the study period; among those who started a second therapy, 15% restarted the same TNFi, 45.6% started another TNFi, 27.6% started a non-TNFi biologic, and 11.5% started a Janus kinase inhibitor.
- The most common reported reasons for discontinuation were a combination of efficacy and intolerance, efficacy only, and intolerance only (26.9%, 25.3%, and 20.3%, respectively).
- Persistent pain was the most common reason for efficacy-related discontinuation (39.0%), followed by persistent inflammation/swelling and overall general discomfort (31.8% for both).
IN PRACTICE:
“Consistent monitoring of treatment response and timely switch to effective therapy as appropriate is needed in patients with RA initiating their first advanced therapies,” the researchers wrote.
SOURCE:
First author Colin Edgerton, MD, of Articularis Healthcare Group and American Rheumatology Network, Charleston, South Carolina, reported their work on January 14, 2024, in ACR Open Rheumatology.
LIMITATIONS:
The findings were limited by several factors including the retrospective design, incomplete data from electronic medical records, and reliance on physician documentation for drivers of discontinuation.
DISCLOSURES:
The study was supported by AbbVie. Lead author Edgerton also disclosed relationships with Novartis and Boehringer Ingelheim.
A version of this article first appeared on Medscape.com.