User login
Bringing you the latest news, research and reviews, exclusive interviews, podcasts, quizzes, and more.
div[contains(@class, 'header__large-screen')]
div[contains(@class, 'read-next-article')]
div[contains(@class, 'main-prefix')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
footer[@id='footer']
section[contains(@class, 'nav-hidden')]
div[contains(@class, 'ce-card-content')]
nav[contains(@class, 'nav-ce-stack')]
div[contains(@class, 'view-medstat-quiz-listing-panes')]
div[contains(@class, 'pane-article-sidebar-latest-news')]
div[contains(@class, 'medstat-accordion-set article-series')]
Cutaneous lupus, dermatomyositis: Excitement growing around emerging therapies
ORLANDO, FLORIDA — Advances in treating medical conditions rarely emerge in a straight line. Oftentimes, progress comes in fits and starts, and therapies to treat cutaneous lupus erythematosus (CLE) and dermatomyositis are no exception.
Beyond approved treatments that deserve more attention, like belimumab, approved by the Food and Drug Administration (FDA) for systemic lupus erythematosus (SLE) in 2011, and Octagam 10%, an intravenous immune globulin (IVIG) preparation approved for dermatomyositis in 2021, anticipation is growing for emerging therapies and their potential to provide relief to patients, Anthony Fernandez, MD, PhD, said at the ODAC Dermatology, Aesthetic & Surgical Conference. The tyrosine kinase 2 (TYK2) inhibitor deucravacitinib, Janus kinase (JAK) inhibitors brepocitinib and baricitinib, and the monoclonal antibody anifrolumab, he noted, are prime examples.
“. In my opinion, this is the start of what will be the most exciting decade in the history of these two diseases,” said Dr. Fernandez, director of medical dermatology at the Cleveland Clinic.
Emerging Treatments for Cutaneous Lupus
Although SLE can involve many organ systems, the skin is one of the most affected. There are specific cutaneous lesions categorized as either acute cutaneous lupus, subacute cutaneous lupus, or chronic cutaneous lupus.
The oral TYK2 inhibitor deucravacitinib, for example, should be able to dampen interleukin responses in people with CLE, Dr. Fernandez said. Deucravacitinib was approved by the FDA to treat psoriasis in September 2022.

A phase 2 study published in 2023 focused on this agent for relief of systemic lupus. Improvements in cutaneous disease were a secondary endpoint. The trial demonstrated that the patients treated with deucravacitinib achieved a 56%-70% CLASI-50 response, depending on dosing, compared with a 17% response among those on placebo at week 48.
Based on the trial results, recruitment has begun for a phase 2 trial to evaluate deucravacitinib, compared with placebo, in patients with discoid and/or subacute cutaneous lupus. “This may be another medicine we have available to give to any of our patients with cutaneous lupus,” Dr. Fernandez said.
Anifrolumab Appears Promising
The FDA approval of anifrolumab, a type I interferon (IFN) receptor antagonist, for treating moderate to severe SLE in July 2021, for example, is good news for dermatologists and their patients, added Dr. Fernandez. “Almost immediately after approval, case studies showed marked improvement in patients with refractory cutaneous lupus.” While the therapy was approved for treating systemic lupus, it allows for off-label treatment of the cutaneous predominant form of the disease, he said.
Furthermore, the manufacturer of anifrolumab, AstraZeneca, is launching the LAVENDER clinical trial to assess the monoclonal antibody specifically for treating CLE. “This is a big deal because we may be able to prescribe anifrolumab for our cutaneous lupus patients who don’t have systemic lupus,” Dr. Fernandez said.
Phase 3 data supported use the of anifrolumab in systemic lupus, including the TULIP-2 trial, which demonstrated its superiority to placebo for reducing severity of systemic disease and lowering corticosteroid use. A study published in March 2023 of 11 patients showed that they had a “very fast response” to the agent, Dr. Fernandez said, with a 50% or greater improvement in the Cutaneous Lupus Erythematosus Disease Area and Severity Index activity score reached by all participants at week 16. Improvements of 50% or more in this scoring system are considered clinically meaningful, he added.
Upcoming Dermatomyositis Treatments
Why highlight emerging therapies for CLE and dermatomyositis in the same ODAC presentation? Although distinct conditions, these autoimmune conditions are both mediated by type 1 IFN inflammation.
Dermatomyositis is a relatively rare immune-mediated disease that most commonly affects the skin and muscle. Doctors score disease presentation, activity, and clinical improvements on a scale similar to CLASI for cutaneous lupus, the CDASI or Cutaneous Dermatomyositis Disease Area and Severity Index. Among people with CDASI activity scores of at least 14, which is the threshold for moderate to severe disease, a 20% improvement is clinically meaningful, Dr. Fernandez said. In addition, a 40% or greater improvement correlates with significant improvements in quality of life.
There is now more evidence for the use of IVIG to treat dermatomyositis. “Among those of us who treat dermatomyositis on a regular basis, we believe IVIG is the most potent treatment. We’ve known that for a long time,” Dr. Fernandez said.
Despite this tenet, for years, there was only one placebo-controlled trial, published in 1993, that evaluated IVIG treatment for dermatomyositis, and it included only 15 participants. That was until October 2022, he said, when the New England Journal of Medicine published a study comparing a specific brand of IVIG (Octagam) with placebo in 95 people with dermatomyositis.
In the study, 79% of participants treated with IVIG had a total improvement score of at least 20 (minimal improvement), the primary endpoint, at 16 weeks, compared with 44% of those receiving a placebo. Those treated with IVIG also had significant improvements in the CDASI score, a secondary endpoint, compared with those on placebo, he said.
Based on results of this trial, the FDA approved Octagam 10% for dermatomyositis in adults. Dr. Fernandez noted the approval is restricted to the brand of IVIG in the trial, not all IVIG products. However, “the FDA approval is most important to us because it gives us ammunition to fight for insurers to approve IVIG when we feel our patients with dermatomyositis need it,” regardless of the brand.
The Potential of JAK1 Inhibitors
An open-label study of the JAK inhibitor tofacitinib, published in December 2020, showed that mean changes in CDASI activity scores at 12 weeks were statistically significant compared with baseline in 10 people with dermatomyositis. “The importance of this study is that it is proof of concept that JAK inhibition can be effective for treating dermatomyositis, especially with active skin disease,” Dr. Fernandez said.
In addition, two large phase 3 trials are evaluating JAK inhibitor safety and efficacy for treating dermatomyositis. One is the VALOR trial, currently recruiting people with recalcitrant dermatomyositis to evaluate treatment with brepocitinib. Researchers in France are looking at another JAK inhibitor, baricitinib, for treating relapsing or treatment-naive dermatomyositis. Recruitment for the BIRD clinical trial is ongoing.
Monoclonal Antibody Showing Promise
“When it comes to looking specifically at dermatomyositis cutaneous disease, it’s been found that the levels of IFN beta correlate best with not only lesional skin type 1 IFN inflammatory signatures but also overall clinical disease activity,” Dr. Fernandez said. This correlation is stronger than for any other IFN-1-type cytokine active in the disorder.
“Perhaps blocking IFN beta might be best way to get control of dermatomyositis activity,” he added.
With that in mind, a phase 2 trial of dazukibart presented at the American Academy of Dermatology 2023 annual meeting highlighted the promise of this agent that targets type 1 IFN beta.
The primary endpoint was improvement in CDASI at 12 weeks. “This medication has remarkable efficacy,” Dr. Fernandez said. “We were one of the sites for this trial. Despite being blinded, there was no question about who was receiving drug and who was receiving placebo.”
“A minimal clinical improvement in disease activity was seen in more than 90%, so almost every patient who received this medication had meaningful improvement,” he added.
Based on the results, the manufacturer, Pfizer, is recruiting participants for a phase 3 trial to further assess dazukibart in dermatomyositis and polymyositis. Dr. Fernandez said, “This is a story you should pay attention to if you treat any dermatomyositis patients at all.”
Regarding these emerging therapies for CLE and dermatomyositis, “This looks very much like the early days of psoriasis, in the early 2000s, when there was a lot of activity developing treatments,” Dr. Fernandez said. “I will predict that within 10 years, we will have multiple novel agents available that will probably work better than anything we have today.”
Dr. Fernandez reported receiving grant and/or research support from Alexion, Incyte, Mallinckrodt Pharmaceuticals, Novartis, Pfizer, and Priovant Therapeutics; acting as a consultant or advisory board member for AbbVie, Biogen, Mallinckrodt Pharmaceuticals; and being a member of the speaker bureau or receiving honoraria for non-CME from AbbVie, Kyowa Kirin, and Mallinckrodt Pharmaceuticals.
A version of this article appeared on Medscape.com.
ORLANDO, FLORIDA — Advances in treating medical conditions rarely emerge in a straight line. Oftentimes, progress comes in fits and starts, and therapies to treat cutaneous lupus erythematosus (CLE) and dermatomyositis are no exception.
Beyond approved treatments that deserve more attention, like belimumab, approved by the Food and Drug Administration (FDA) for systemic lupus erythematosus (SLE) in 2011, and Octagam 10%, an intravenous immune globulin (IVIG) preparation approved for dermatomyositis in 2021, anticipation is growing for emerging therapies and their potential to provide relief to patients, Anthony Fernandez, MD, PhD, said at the ODAC Dermatology, Aesthetic & Surgical Conference. The tyrosine kinase 2 (TYK2) inhibitor deucravacitinib, Janus kinase (JAK) inhibitors brepocitinib and baricitinib, and the monoclonal antibody anifrolumab, he noted, are prime examples.
“. In my opinion, this is the start of what will be the most exciting decade in the history of these two diseases,” said Dr. Fernandez, director of medical dermatology at the Cleveland Clinic.
Emerging Treatments for Cutaneous Lupus
Although SLE can involve many organ systems, the skin is one of the most affected. There are specific cutaneous lesions categorized as either acute cutaneous lupus, subacute cutaneous lupus, or chronic cutaneous lupus.
The oral TYK2 inhibitor deucravacitinib, for example, should be able to dampen interleukin responses in people with CLE, Dr. Fernandez said. Deucravacitinib was approved by the FDA to treat psoriasis in September 2022.
A phase 2 study published in 2023 focused on this agent for relief of systemic lupus. Improvements in cutaneous disease were a secondary endpoint. The trial demonstrated that the patients treated with deucravacitinib achieved a 56%-70% CLASI-50 response, depending on dosing, compared with a 17% response among those on placebo at week 48.
Based on the trial results, recruitment has begun for a phase 2 trial to evaluate deucravacitinib, compared with placebo, in patients with discoid and/or subacute cutaneous lupus. “This may be another medicine we have available to give to any of our patients with cutaneous lupus,” Dr. Fernandez said.
Anifrolumab Appears Promising
The FDA approval of anifrolumab, a type I interferon (IFN) receptor antagonist, for treating moderate to severe SLE in July 2021, for example, is good news for dermatologists and their patients, added Dr. Fernandez. “Almost immediately after approval, case studies showed marked improvement in patients with refractory cutaneous lupus.” While the therapy was approved for treating systemic lupus, it allows for off-label treatment of the cutaneous predominant form of the disease, he said.
Furthermore, the manufacturer of anifrolumab, AstraZeneca, is launching the LAVENDER clinical trial to assess the monoclonal antibody specifically for treating CLE. “This is a big deal because we may be able to prescribe anifrolumab for our cutaneous lupus patients who don’t have systemic lupus,” Dr. Fernandez said.
Phase 3 data supported use the of anifrolumab in systemic lupus, including the TULIP-2 trial, which demonstrated its superiority to placebo for reducing severity of systemic disease and lowering corticosteroid use. A study published in March 2023 of 11 patients showed that they had a “very fast response” to the agent, Dr. Fernandez said, with a 50% or greater improvement in the Cutaneous Lupus Erythematosus Disease Area and Severity Index activity score reached by all participants at week 16. Improvements of 50% or more in this scoring system are considered clinically meaningful, he added.
Upcoming Dermatomyositis Treatments
Why highlight emerging therapies for CLE and dermatomyositis in the same ODAC presentation? Although distinct conditions, these autoimmune conditions are both mediated by type 1 IFN inflammation.
Dermatomyositis is a relatively rare immune-mediated disease that most commonly affects the skin and muscle. Doctors score disease presentation, activity, and clinical improvements on a scale similar to CLASI for cutaneous lupus, the CDASI or Cutaneous Dermatomyositis Disease Area and Severity Index. Among people with CDASI activity scores of at least 14, which is the threshold for moderate to severe disease, a 20% improvement is clinically meaningful, Dr. Fernandez said. In addition, a 40% or greater improvement correlates with significant improvements in quality of life.
There is now more evidence for the use of IVIG to treat dermatomyositis. “Among those of us who treat dermatomyositis on a regular basis, we believe IVIG is the most potent treatment. We’ve known that for a long time,” Dr. Fernandez said.
Despite this tenet, for years, there was only one placebo-controlled trial, published in 1993, that evaluated IVIG treatment for dermatomyositis, and it included only 15 participants. That was until October 2022, he said, when the New England Journal of Medicine published a study comparing a specific brand of IVIG (Octagam) with placebo in 95 people with dermatomyositis.
In the study, 79% of participants treated with IVIG had a total improvement score of at least 20 (minimal improvement), the primary endpoint, at 16 weeks, compared with 44% of those receiving a placebo. Those treated with IVIG also had significant improvements in the CDASI score, a secondary endpoint, compared with those on placebo, he said.
Based on results of this trial, the FDA approved Octagam 10% for dermatomyositis in adults. Dr. Fernandez noted the approval is restricted to the brand of IVIG in the trial, not all IVIG products. However, “the FDA approval is most important to us because it gives us ammunition to fight for insurers to approve IVIG when we feel our patients with dermatomyositis need it,” regardless of the brand.
The Potential of JAK1 Inhibitors
An open-label study of the JAK inhibitor tofacitinib, published in December 2020, showed that mean changes in CDASI activity scores at 12 weeks were statistically significant compared with baseline in 10 people with dermatomyositis. “The importance of this study is that it is proof of concept that JAK inhibition can be effective for treating dermatomyositis, especially with active skin disease,” Dr. Fernandez said.
In addition, two large phase 3 trials are evaluating JAK inhibitor safety and efficacy for treating dermatomyositis. One is the VALOR trial, currently recruiting people with recalcitrant dermatomyositis to evaluate treatment with brepocitinib. Researchers in France are looking at another JAK inhibitor, baricitinib, for treating relapsing or treatment-naive dermatomyositis. Recruitment for the BIRD clinical trial is ongoing.
Monoclonal Antibody Showing Promise
“When it comes to looking specifically at dermatomyositis cutaneous disease, it’s been found that the levels of IFN beta correlate best with not only lesional skin type 1 IFN inflammatory signatures but also overall clinical disease activity,” Dr. Fernandez said. This correlation is stronger than for any other IFN-1-type cytokine active in the disorder.
“Perhaps blocking IFN beta might be best way to get control of dermatomyositis activity,” he added.
With that in mind, a phase 2 trial of dazukibart presented at the American Academy of Dermatology 2023 annual meeting highlighted the promise of this agent that targets type 1 IFN beta.
The primary endpoint was improvement in CDASI at 12 weeks. “This medication has remarkable efficacy,” Dr. Fernandez said. “We were one of the sites for this trial. Despite being blinded, there was no question about who was receiving drug and who was receiving placebo.”
“A minimal clinical improvement in disease activity was seen in more than 90%, so almost every patient who received this medication had meaningful improvement,” he added.
Based on the results, the manufacturer, Pfizer, is recruiting participants for a phase 3 trial to further assess dazukibart in dermatomyositis and polymyositis. Dr. Fernandez said, “This is a story you should pay attention to if you treat any dermatomyositis patients at all.”
Regarding these emerging therapies for CLE and dermatomyositis, “This looks very much like the early days of psoriasis, in the early 2000s, when there was a lot of activity developing treatments,” Dr. Fernandez said. “I will predict that within 10 years, we will have multiple novel agents available that will probably work better than anything we have today.”
Dr. Fernandez reported receiving grant and/or research support from Alexion, Incyte, Mallinckrodt Pharmaceuticals, Novartis, Pfizer, and Priovant Therapeutics; acting as a consultant or advisory board member for AbbVie, Biogen, Mallinckrodt Pharmaceuticals; and being a member of the speaker bureau or receiving honoraria for non-CME from AbbVie, Kyowa Kirin, and Mallinckrodt Pharmaceuticals.
A version of this article appeared on Medscape.com.
ORLANDO, FLORIDA — Advances in treating medical conditions rarely emerge in a straight line. Oftentimes, progress comes in fits and starts, and therapies to treat cutaneous lupus erythematosus (CLE) and dermatomyositis are no exception.
Beyond approved treatments that deserve more attention, like belimumab, approved by the Food and Drug Administration (FDA) for systemic lupus erythematosus (SLE) in 2011, and Octagam 10%, an intravenous immune globulin (IVIG) preparation approved for dermatomyositis in 2021, anticipation is growing for emerging therapies and their potential to provide relief to patients, Anthony Fernandez, MD, PhD, said at the ODAC Dermatology, Aesthetic & Surgical Conference. The tyrosine kinase 2 (TYK2) inhibitor deucravacitinib, Janus kinase (JAK) inhibitors brepocitinib and baricitinib, and the monoclonal antibody anifrolumab, he noted, are prime examples.
“. In my opinion, this is the start of what will be the most exciting decade in the history of these two diseases,” said Dr. Fernandez, director of medical dermatology at the Cleveland Clinic.
Emerging Treatments for Cutaneous Lupus
Although SLE can involve many organ systems, the skin is one of the most affected. There are specific cutaneous lesions categorized as either acute cutaneous lupus, subacute cutaneous lupus, or chronic cutaneous lupus.
The oral TYK2 inhibitor deucravacitinib, for example, should be able to dampen interleukin responses in people with CLE, Dr. Fernandez said. Deucravacitinib was approved by the FDA to treat psoriasis in September 2022.
A phase 2 study published in 2023 focused on this agent for relief of systemic lupus. Improvements in cutaneous disease were a secondary endpoint. The trial demonstrated that the patients treated with deucravacitinib achieved a 56%-70% CLASI-50 response, depending on dosing, compared with a 17% response among those on placebo at week 48.
Based on the trial results, recruitment has begun for a phase 2 trial to evaluate deucravacitinib, compared with placebo, in patients with discoid and/or subacute cutaneous lupus. “This may be another medicine we have available to give to any of our patients with cutaneous lupus,” Dr. Fernandez said.
Anifrolumab Appears Promising
The FDA approval of anifrolumab, a type I interferon (IFN) receptor antagonist, for treating moderate to severe SLE in July 2021, for example, is good news for dermatologists and their patients, added Dr. Fernandez. “Almost immediately after approval, case studies showed marked improvement in patients with refractory cutaneous lupus.” While the therapy was approved for treating systemic lupus, it allows for off-label treatment of the cutaneous predominant form of the disease, he said.
Furthermore, the manufacturer of anifrolumab, AstraZeneca, is launching the LAVENDER clinical trial to assess the monoclonal antibody specifically for treating CLE. “This is a big deal because we may be able to prescribe anifrolumab for our cutaneous lupus patients who don’t have systemic lupus,” Dr. Fernandez said.
Phase 3 data supported use the of anifrolumab in systemic lupus, including the TULIP-2 trial, which demonstrated its superiority to placebo for reducing severity of systemic disease and lowering corticosteroid use. A study published in March 2023 of 11 patients showed that they had a “very fast response” to the agent, Dr. Fernandez said, with a 50% or greater improvement in the Cutaneous Lupus Erythematosus Disease Area and Severity Index activity score reached by all participants at week 16. Improvements of 50% or more in this scoring system are considered clinically meaningful, he added.
Upcoming Dermatomyositis Treatments
Why highlight emerging therapies for CLE and dermatomyositis in the same ODAC presentation? Although distinct conditions, these autoimmune conditions are both mediated by type 1 IFN inflammation.
Dermatomyositis is a relatively rare immune-mediated disease that most commonly affects the skin and muscle. Doctors score disease presentation, activity, and clinical improvements on a scale similar to CLASI for cutaneous lupus, the CDASI or Cutaneous Dermatomyositis Disease Area and Severity Index. Among people with CDASI activity scores of at least 14, which is the threshold for moderate to severe disease, a 20% improvement is clinically meaningful, Dr. Fernandez said. In addition, a 40% or greater improvement correlates with significant improvements in quality of life.
There is now more evidence for the use of IVIG to treat dermatomyositis. “Among those of us who treat dermatomyositis on a regular basis, we believe IVIG is the most potent treatment. We’ve known that for a long time,” Dr. Fernandez said.
Despite this tenet, for years, there was only one placebo-controlled trial, published in 1993, that evaluated IVIG treatment for dermatomyositis, and it included only 15 participants. That was until October 2022, he said, when the New England Journal of Medicine published a study comparing a specific brand of IVIG (Octagam) with placebo in 95 people with dermatomyositis.
In the study, 79% of participants treated with IVIG had a total improvement score of at least 20 (minimal improvement), the primary endpoint, at 16 weeks, compared with 44% of those receiving a placebo. Those treated with IVIG also had significant improvements in the CDASI score, a secondary endpoint, compared with those on placebo, he said.
Based on results of this trial, the FDA approved Octagam 10% for dermatomyositis in adults. Dr. Fernandez noted the approval is restricted to the brand of IVIG in the trial, not all IVIG products. However, “the FDA approval is most important to us because it gives us ammunition to fight for insurers to approve IVIG when we feel our patients with dermatomyositis need it,” regardless of the brand.
The Potential of JAK1 Inhibitors
An open-label study of the JAK inhibitor tofacitinib, published in December 2020, showed that mean changes in CDASI activity scores at 12 weeks were statistically significant compared with baseline in 10 people with dermatomyositis. “The importance of this study is that it is proof of concept that JAK inhibition can be effective for treating dermatomyositis, especially with active skin disease,” Dr. Fernandez said.
In addition, two large phase 3 trials are evaluating JAK inhibitor safety and efficacy for treating dermatomyositis. One is the VALOR trial, currently recruiting people with recalcitrant dermatomyositis to evaluate treatment with brepocitinib. Researchers in France are looking at another JAK inhibitor, baricitinib, for treating relapsing or treatment-naive dermatomyositis. Recruitment for the BIRD clinical trial is ongoing.
Monoclonal Antibody Showing Promise
“When it comes to looking specifically at dermatomyositis cutaneous disease, it’s been found that the levels of IFN beta correlate best with not only lesional skin type 1 IFN inflammatory signatures but also overall clinical disease activity,” Dr. Fernandez said. This correlation is stronger than for any other IFN-1-type cytokine active in the disorder.
“Perhaps blocking IFN beta might be best way to get control of dermatomyositis activity,” he added.
With that in mind, a phase 2 trial of dazukibart presented at the American Academy of Dermatology 2023 annual meeting highlighted the promise of this agent that targets type 1 IFN beta.
The primary endpoint was improvement in CDASI at 12 weeks. “This medication has remarkable efficacy,” Dr. Fernandez said. “We were one of the sites for this trial. Despite being blinded, there was no question about who was receiving drug and who was receiving placebo.”
“A minimal clinical improvement in disease activity was seen in more than 90%, so almost every patient who received this medication had meaningful improvement,” he added.
Based on the results, the manufacturer, Pfizer, is recruiting participants for a phase 3 trial to further assess dazukibart in dermatomyositis and polymyositis. Dr. Fernandez said, “This is a story you should pay attention to if you treat any dermatomyositis patients at all.”
Regarding these emerging therapies for CLE and dermatomyositis, “This looks very much like the early days of psoriasis, in the early 2000s, when there was a lot of activity developing treatments,” Dr. Fernandez said. “I will predict that within 10 years, we will have multiple novel agents available that will probably work better than anything we have today.”
Dr. Fernandez reported receiving grant and/or research support from Alexion, Incyte, Mallinckrodt Pharmaceuticals, Novartis, Pfizer, and Priovant Therapeutics; acting as a consultant or advisory board member for AbbVie, Biogen, Mallinckrodt Pharmaceuticals; and being a member of the speaker bureau or receiving honoraria for non-CME from AbbVie, Kyowa Kirin, and Mallinckrodt Pharmaceuticals.
A version of this article appeared on Medscape.com.
FROM ODAC 2024
Dana-Farber Moves to Retract, Correct Dozens of Cancer Papers Amid Allegations
News of the investigation follows a blog post by British molecular biologist Sholto David, MD, who flagged almost 60 papers published between 1997 and 2017 that contained image manipulation and other errors. Some of the papers were published by Dana-Farber’s chief executive officer, Laurie Glimcher, MD, and chief operating officer, William Hahn, MD, on topics including multiple myeloma and immune cells.
Mr. David, who blogs about research integrity, highlighted numerous errors and irregularities, including copying and pasting images across multiple experiments to represent different days within the same experiment, sometimes rotating or stretching images.
In one case, Mr. David equated the manipulation with tactics used by “hapless Chinese papermills” and concluded that “a swathe of research coming out of [Dana-Farber] authored by the most senior researchers and managers appears to be hopelessly corrupt with errors that are obvious from just a cursory reading the papers.”
“Imagine what mistakes might be found in the raw data if anyone was allowed to look!” he wrote.
Barrett Rollins, MD, PhD, Dana-Farber Cancer Institute’s research integrity officer, declined to comment on whether the errors represent scientific misconduct, according to STAT. Rollins told ScienceInsider that the “presence of image discrepancies in a paper is not evidence of an author’s intent to deceive.”
Access to new artificial intelligence tools is making it easier for data sleuths, like Mr. David, to unearth data manipulation and errors.
The current investigation closely follows two other investigations into the published work of Harvard University’s former president, Claudine Gay, and Stanford University’s former president, Marc Tessier-Lavigne, which led both to resign their posts.
A version of this article appeared on Medscape.com.
News of the investigation follows a blog post by British molecular biologist Sholto David, MD, who flagged almost 60 papers published between 1997 and 2017 that contained image manipulation and other errors. Some of the papers were published by Dana-Farber’s chief executive officer, Laurie Glimcher, MD, and chief operating officer, William Hahn, MD, on topics including multiple myeloma and immune cells.
Mr. David, who blogs about research integrity, highlighted numerous errors and irregularities, including copying and pasting images across multiple experiments to represent different days within the same experiment, sometimes rotating or stretching images.
In one case, Mr. David equated the manipulation with tactics used by “hapless Chinese papermills” and concluded that “a swathe of research coming out of [Dana-Farber] authored by the most senior researchers and managers appears to be hopelessly corrupt with errors that are obvious from just a cursory reading the papers.”
“Imagine what mistakes might be found in the raw data if anyone was allowed to look!” he wrote.
Barrett Rollins, MD, PhD, Dana-Farber Cancer Institute’s research integrity officer, declined to comment on whether the errors represent scientific misconduct, according to STAT. Rollins told ScienceInsider that the “presence of image discrepancies in a paper is not evidence of an author’s intent to deceive.”
Access to new artificial intelligence tools is making it easier for data sleuths, like Mr. David, to unearth data manipulation and errors.
The current investigation closely follows two other investigations into the published work of Harvard University’s former president, Claudine Gay, and Stanford University’s former president, Marc Tessier-Lavigne, which led both to resign their posts.
A version of this article appeared on Medscape.com.
News of the investigation follows a blog post by British molecular biologist Sholto David, MD, who flagged almost 60 papers published between 1997 and 2017 that contained image manipulation and other errors. Some of the papers were published by Dana-Farber’s chief executive officer, Laurie Glimcher, MD, and chief operating officer, William Hahn, MD, on topics including multiple myeloma and immune cells.
Mr. David, who blogs about research integrity, highlighted numerous errors and irregularities, including copying and pasting images across multiple experiments to represent different days within the same experiment, sometimes rotating or stretching images.
In one case, Mr. David equated the manipulation with tactics used by “hapless Chinese papermills” and concluded that “a swathe of research coming out of [Dana-Farber] authored by the most senior researchers and managers appears to be hopelessly corrupt with errors that are obvious from just a cursory reading the papers.”
“Imagine what mistakes might be found in the raw data if anyone was allowed to look!” he wrote.
Barrett Rollins, MD, PhD, Dana-Farber Cancer Institute’s research integrity officer, declined to comment on whether the errors represent scientific misconduct, according to STAT. Rollins told ScienceInsider that the “presence of image discrepancies in a paper is not evidence of an author’s intent to deceive.”
Access to new artificial intelligence tools is making it easier for data sleuths, like Mr. David, to unearth data manipulation and errors.
The current investigation closely follows two other investigations into the published work of Harvard University’s former president, Claudine Gay, and Stanford University’s former president, Marc Tessier-Lavigne, which led both to resign their posts.
A version of this article appeared on Medscape.com.
Even Intentional Weight Loss Linked With Cancer
This transcript has been edited for clarity.
As anyone who has been through medical training will tell you, some little scenes just stick with you. I had been seeing a patient in our resident clinic in West Philly for a couple of years. She was in her mid-60s with diabetes and hypertension and a distant smoking history. She was overweight and had been trying to improve her diet and lose weight since I started seeing her. One day she came in and was delighted to report that she had finally started shedding some pounds — about 15 in the past 2 months.
I enthusiastically told my preceptor that my careful dietary counseling had finally done the job. She looked through the chart for a moment and asked, “Is she up to date on her cancer screening?” A workup revealed adenocarcinoma of the lung. The patient did well, actually, but the story stuck with me.
The textbooks call it “unintentional weight loss,” often in big, scary letters, and every doctor will go just a bit pale if a patient tells them that, despite efforts not to, they are losing weight. But true unintentional weight loss is not that common. After all, most of us are at least half-heartedly trying to lose weight all the time. Should doctors be worried when we are successful?
A new study suggests that perhaps they should. We’re talking about this study, appearing in JAMA, which combined participants from two long-running observational cohorts: 120,000 women from the Nurses’ Health Study, and 50,000 men from the Health Professionals Follow-Up Study. (These cohorts started in the 1970s and 1980s, so we’ll give them a pass on the gender-specific study designs.)
The rationale of enrolling healthcare providers in these cohort studies is that they would be reliable witnesses of their own health status. If a nurse or doctor says they have pancreatic cancer, it’s likely that they truly have pancreatic cancer. Detailed health surveys were distributed to the participants every other year, and the average follow-up was more than a decade.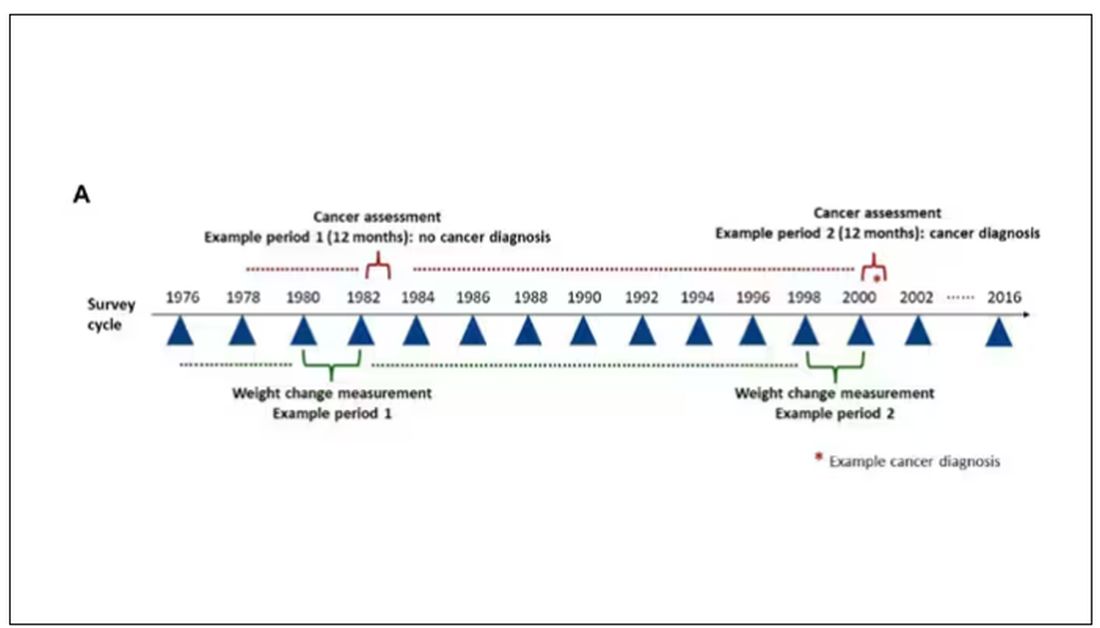
Participants recorded their weight — as an aside, a nested study found that self-reported rate was extremely well correlated with professionally measured weight — and whether they had received a cancer diagnosis since the last survey.
This allowed researchers to look at the phenomenon described above. Would weight loss precede a new diagnosis of cancer? And, more interestingly, would intentional weight loss precede a new diagnosis of cancer.
I don’t think it will surprise you to hear that individuals in the highest category of weight loss, those who lost more than 10% of their body weight over a 2-year period, had a larger risk of being diagnosed with cancer in the next year. That’s the yellow line in this graph. In fact, they had about a 40% higher risk than those who did not lose weight.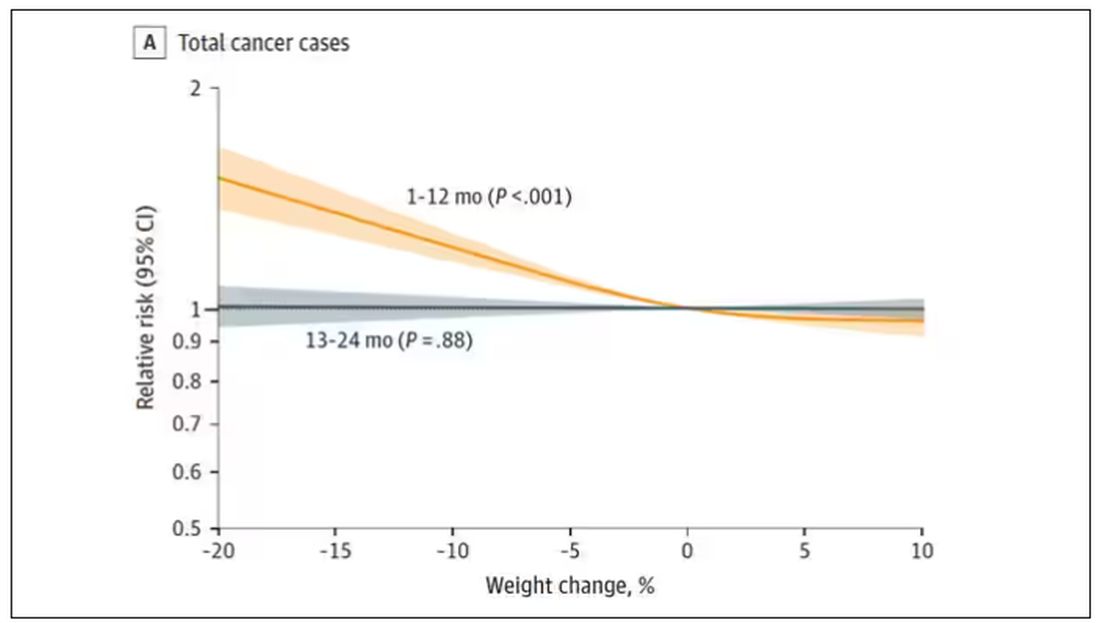
Increased risk was found across multiple cancer types, though cancers of the gastrointestinal tract, not surprisingly, were most strongly associated with antecedent weight loss.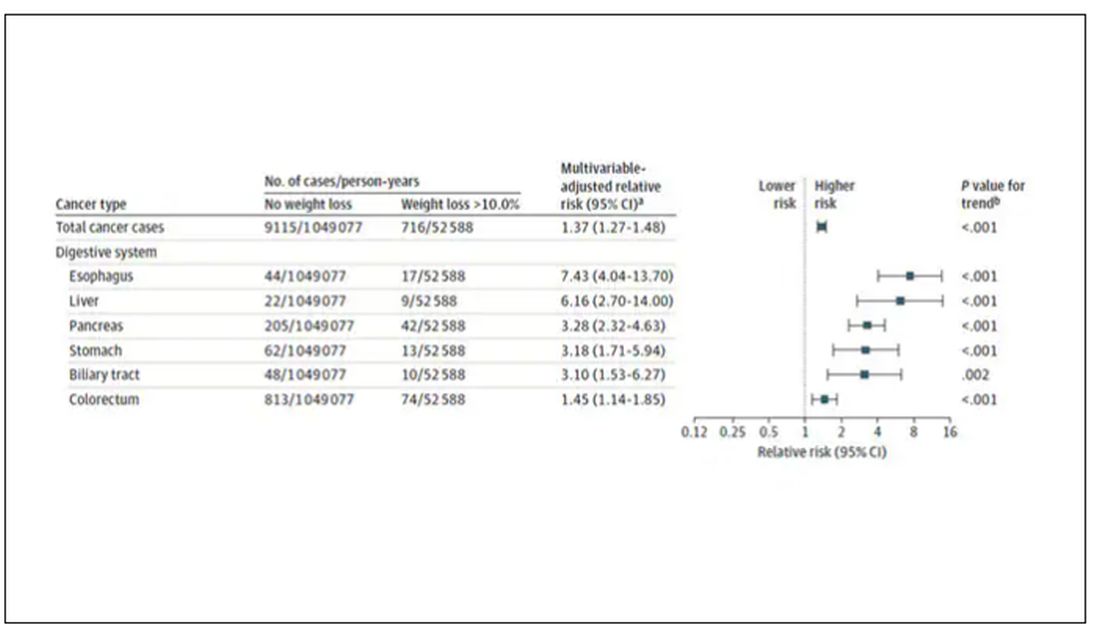
What about intentionality of weight loss? Unfortunately, the surveys did not ask participants whether they were trying to lose weight. Rather, the surveys asked about exercise and dietary habits. The researchers leveraged these responses to create three categories of participants: those who seemed to be trying to lose weight (defined as people who had increased their exercise and dietary quality); those who didn’t seem to be trying to lose weight (they changed neither exercise nor dietary behaviors); and a middle group, which changed one or the other of these behaviors but not both.
Let’s look at those who really seemed to be trying to lose weight. Over 2 years, they got more exercise and improved their diet.
If they succeeded in losing 10% or more of their body weight, they still had a higher risk for cancer than those who had not lost weight — about 30% higher, which is not that different from the 40% increased risk when you include those folks who weren’t changing their lifestyle.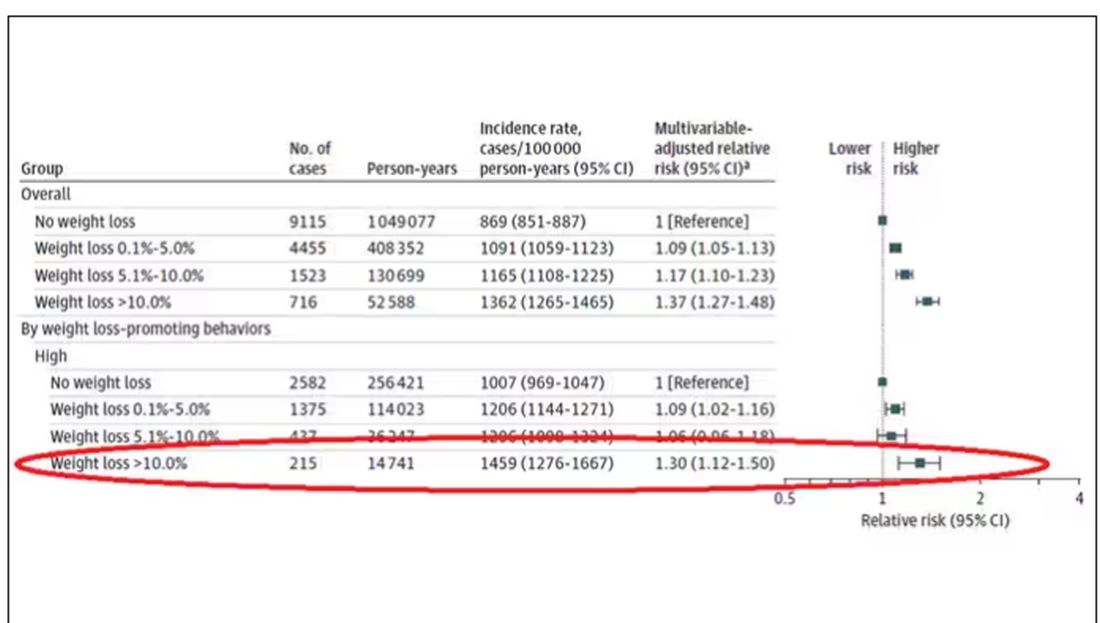
This is why this study is important. The classic teaching is that unintentional weight loss is a bad thing and needs a workup. That’s fine. But we live in a world where perhaps the majority of people are, at any given time, trying to lose weight.
We need to be careful here. I am not by any means trying to say that people who have successfully lost weight have cancer. Both of the following statements can be true:
Significant weight loss, whether intentional or not, is associated with a higher risk for cancer.
Most people with significant weight loss will not have cancer.
Both of these can be true because cancer is, fortunately, rare. Of people who lose weight, the vast majority will lose weight because they are engaging in healthier behaviors. A small number may lose weight because something else is wrong. It’s just hard to tell the two apart.
Out of the nearly 200,000 people in this study, only around 16,000 developed cancer during follow-up. Again, although the chance of having cancer is slightly higher if someone has experienced weight loss, the chance is still very low.
We also need to avoid suggesting that weight loss causes cancer. Some people lose weight because of an existing, as of yet undiagnosed cancer and its metabolic effects. This is borne out if you look at the risk of being diagnosed with cancer as you move further away from the interval of weight loss.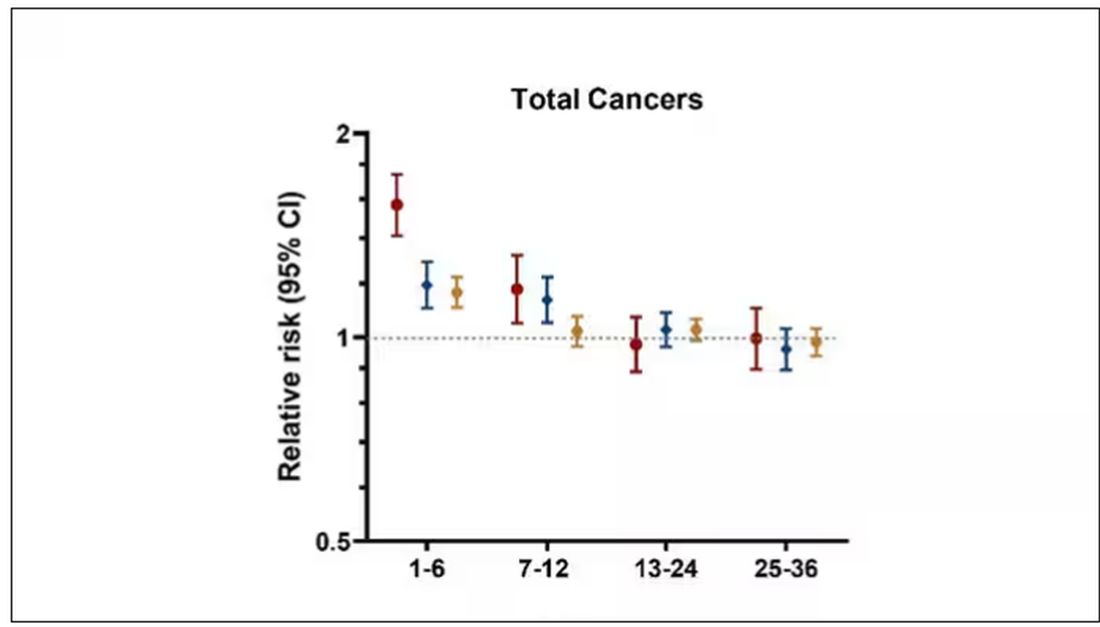
The further you get from the year of that 10% weight loss, the less likely you are to be diagnosed with cancer. Most of these cancers are diagnosed within a year of losing weight. In other words, if you’re reading this and getting worried that you lost weight 10 years ago, you’re probably out of the woods. That was, most likely, just you getting healthier.
Last thing: We have methods for weight loss now that are way more effective than diet or exercise. I’m looking at you, Ozempic. But aside from the weight loss wonder drugs, we have surgery and other interventions. This study did not capture any of that data. Ozempic wasn’t even on the market during this study, so we can’t say anything about the relationship between weight loss and cancer among people using nonlifestyle mechanisms to lose weight.
It’s a complicated system. But the clinically actionable point here is to notice if patients have lost weight. If they’ve lost it without trying, further workup is reasonable. If they’ve lost it but were trying to lose it, tell them “good job.” And consider a workup anyway.
Dr. Wilson is associate professor of medicine and public health and director of the Clinical and Translational Research Accelerator at Yale University, New Haven, Conn. He has disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
This transcript has been edited for clarity.
As anyone who has been through medical training will tell you, some little scenes just stick with you. I had been seeing a patient in our resident clinic in West Philly for a couple of years. She was in her mid-60s with diabetes and hypertension and a distant smoking history. She was overweight and had been trying to improve her diet and lose weight since I started seeing her. One day she came in and was delighted to report that she had finally started shedding some pounds — about 15 in the past 2 months.
I enthusiastically told my preceptor that my careful dietary counseling had finally done the job. She looked through the chart for a moment and asked, “Is she up to date on her cancer screening?” A workup revealed adenocarcinoma of the lung. The patient did well, actually, but the story stuck with me.
The textbooks call it “unintentional weight loss,” often in big, scary letters, and every doctor will go just a bit pale if a patient tells them that, despite efforts not to, they are losing weight. But true unintentional weight loss is not that common. After all, most of us are at least half-heartedly trying to lose weight all the time. Should doctors be worried when we are successful?
A new study suggests that perhaps they should. We’re talking about this study, appearing in JAMA, which combined participants from two long-running observational cohorts: 120,000 women from the Nurses’ Health Study, and 50,000 men from the Health Professionals Follow-Up Study. (These cohorts started in the 1970s and 1980s, so we’ll give them a pass on the gender-specific study designs.)
The rationale of enrolling healthcare providers in these cohort studies is that they would be reliable witnesses of their own health status. If a nurse or doctor says they have pancreatic cancer, it’s likely that they truly have pancreatic cancer. Detailed health surveys were distributed to the participants every other year, and the average follow-up was more than a decade.
Participants recorded their weight — as an aside, a nested study found that self-reported rate was extremely well correlated with professionally measured weight — and whether they had received a cancer diagnosis since the last survey.
This allowed researchers to look at the phenomenon described above. Would weight loss precede a new diagnosis of cancer? And, more interestingly, would intentional weight loss precede a new diagnosis of cancer.
I don’t think it will surprise you to hear that individuals in the highest category of weight loss, those who lost more than 10% of their body weight over a 2-year period, had a larger risk of being diagnosed with cancer in the next year. That’s the yellow line in this graph. In fact, they had about a 40% higher risk than those who did not lose weight.
Increased risk was found across multiple cancer types, though cancers of the gastrointestinal tract, not surprisingly, were most strongly associated with antecedent weight loss.
What about intentionality of weight loss? Unfortunately, the surveys did not ask participants whether they were trying to lose weight. Rather, the surveys asked about exercise and dietary habits. The researchers leveraged these responses to create three categories of participants: those who seemed to be trying to lose weight (defined as people who had increased their exercise and dietary quality); those who didn’t seem to be trying to lose weight (they changed neither exercise nor dietary behaviors); and a middle group, which changed one or the other of these behaviors but not both.
Let’s look at those who really seemed to be trying to lose weight. Over 2 years, they got more exercise and improved their diet.
If they succeeded in losing 10% or more of their body weight, they still had a higher risk for cancer than those who had not lost weight — about 30% higher, which is not that different from the 40% increased risk when you include those folks who weren’t changing their lifestyle.
This is why this study is important. The classic teaching is that unintentional weight loss is a bad thing and needs a workup. That’s fine. But we live in a world where perhaps the majority of people are, at any given time, trying to lose weight.
We need to be careful here. I am not by any means trying to say that people who have successfully lost weight have cancer. Both of the following statements can be true:
Significant weight loss, whether intentional or not, is associated with a higher risk for cancer.
Most people with significant weight loss will not have cancer.
Both of these can be true because cancer is, fortunately, rare. Of people who lose weight, the vast majority will lose weight because they are engaging in healthier behaviors. A small number may lose weight because something else is wrong. It’s just hard to tell the two apart.
Out of the nearly 200,000 people in this study, only around 16,000 developed cancer during follow-up. Again, although the chance of having cancer is slightly higher if someone has experienced weight loss, the chance is still very low.
We also need to avoid suggesting that weight loss causes cancer. Some people lose weight because of an existing, as of yet undiagnosed cancer and its metabolic effects. This is borne out if you look at the risk of being diagnosed with cancer as you move further away from the interval of weight loss.
The further you get from the year of that 10% weight loss, the less likely you are to be diagnosed with cancer. Most of these cancers are diagnosed within a year of losing weight. In other words, if you’re reading this and getting worried that you lost weight 10 years ago, you’re probably out of the woods. That was, most likely, just you getting healthier.
Last thing: We have methods for weight loss now that are way more effective than diet or exercise. I’m looking at you, Ozempic. But aside from the weight loss wonder drugs, we have surgery and other interventions. This study did not capture any of that data. Ozempic wasn’t even on the market during this study, so we can’t say anything about the relationship between weight loss and cancer among people using nonlifestyle mechanisms to lose weight.
It’s a complicated system. But the clinically actionable point here is to notice if patients have lost weight. If they’ve lost it without trying, further workup is reasonable. If they’ve lost it but were trying to lose it, tell them “good job.” And consider a workup anyway.
Dr. Wilson is associate professor of medicine and public health and director of the Clinical and Translational Research Accelerator at Yale University, New Haven, Conn. He has disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
This transcript has been edited for clarity.
As anyone who has been through medical training will tell you, some little scenes just stick with you. I had been seeing a patient in our resident clinic in West Philly for a couple of years. She was in her mid-60s with diabetes and hypertension and a distant smoking history. She was overweight and had been trying to improve her diet and lose weight since I started seeing her. One day she came in and was delighted to report that she had finally started shedding some pounds — about 15 in the past 2 months.
I enthusiastically told my preceptor that my careful dietary counseling had finally done the job. She looked through the chart for a moment and asked, “Is she up to date on her cancer screening?” A workup revealed adenocarcinoma of the lung. The patient did well, actually, but the story stuck with me.
The textbooks call it “unintentional weight loss,” often in big, scary letters, and every doctor will go just a bit pale if a patient tells them that, despite efforts not to, they are losing weight. But true unintentional weight loss is not that common. After all, most of us are at least half-heartedly trying to lose weight all the time. Should doctors be worried when we are successful?
A new study suggests that perhaps they should. We’re talking about this study, appearing in JAMA, which combined participants from two long-running observational cohorts: 120,000 women from the Nurses’ Health Study, and 50,000 men from the Health Professionals Follow-Up Study. (These cohorts started in the 1970s and 1980s, so we’ll give them a pass on the gender-specific study designs.)
The rationale of enrolling healthcare providers in these cohort studies is that they would be reliable witnesses of their own health status. If a nurse or doctor says they have pancreatic cancer, it’s likely that they truly have pancreatic cancer. Detailed health surveys were distributed to the participants every other year, and the average follow-up was more than a decade.
Participants recorded their weight — as an aside, a nested study found that self-reported rate was extremely well correlated with professionally measured weight — and whether they had received a cancer diagnosis since the last survey.
This allowed researchers to look at the phenomenon described above. Would weight loss precede a new diagnosis of cancer? And, more interestingly, would intentional weight loss precede a new diagnosis of cancer.
I don’t think it will surprise you to hear that individuals in the highest category of weight loss, those who lost more than 10% of their body weight over a 2-year period, had a larger risk of being diagnosed with cancer in the next year. That’s the yellow line in this graph. In fact, they had about a 40% higher risk than those who did not lose weight.
Increased risk was found across multiple cancer types, though cancers of the gastrointestinal tract, not surprisingly, were most strongly associated with antecedent weight loss.
What about intentionality of weight loss? Unfortunately, the surveys did not ask participants whether they were trying to lose weight. Rather, the surveys asked about exercise and dietary habits. The researchers leveraged these responses to create three categories of participants: those who seemed to be trying to lose weight (defined as people who had increased their exercise and dietary quality); those who didn’t seem to be trying to lose weight (they changed neither exercise nor dietary behaviors); and a middle group, which changed one or the other of these behaviors but not both.
Let’s look at those who really seemed to be trying to lose weight. Over 2 years, they got more exercise and improved their diet.
If they succeeded in losing 10% or more of their body weight, they still had a higher risk for cancer than those who had not lost weight — about 30% higher, which is not that different from the 40% increased risk when you include those folks who weren’t changing their lifestyle.
This is why this study is important. The classic teaching is that unintentional weight loss is a bad thing and needs a workup. That’s fine. But we live in a world where perhaps the majority of people are, at any given time, trying to lose weight.
We need to be careful here. I am not by any means trying to say that people who have successfully lost weight have cancer. Both of the following statements can be true:
Significant weight loss, whether intentional or not, is associated with a higher risk for cancer.
Most people with significant weight loss will not have cancer.
Both of these can be true because cancer is, fortunately, rare. Of people who lose weight, the vast majority will lose weight because they are engaging in healthier behaviors. A small number may lose weight because something else is wrong. It’s just hard to tell the two apart.
Out of the nearly 200,000 people in this study, only around 16,000 developed cancer during follow-up. Again, although the chance of having cancer is slightly higher if someone has experienced weight loss, the chance is still very low.
We also need to avoid suggesting that weight loss causes cancer. Some people lose weight because of an existing, as of yet undiagnosed cancer and its metabolic effects. This is borne out if you look at the risk of being diagnosed with cancer as you move further away from the interval of weight loss.
The further you get from the year of that 10% weight loss, the less likely you are to be diagnosed with cancer. Most of these cancers are diagnosed within a year of losing weight. In other words, if you’re reading this and getting worried that you lost weight 10 years ago, you’re probably out of the woods. That was, most likely, just you getting healthier.
Last thing: We have methods for weight loss now that are way more effective than diet or exercise. I’m looking at you, Ozempic. But aside from the weight loss wonder drugs, we have surgery and other interventions. This study did not capture any of that data. Ozempic wasn’t even on the market during this study, so we can’t say anything about the relationship between weight loss and cancer among people using nonlifestyle mechanisms to lose weight.
It’s a complicated system. But the clinically actionable point here is to notice if patients have lost weight. If they’ve lost it without trying, further workup is reasonable. If they’ve lost it but were trying to lose it, tell them “good job.” And consider a workup anyway.
Dr. Wilson is associate professor of medicine and public health and director of the Clinical and Translational Research Accelerator at Yale University, New Haven, Conn. He has disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
Corticosteroid Injections Don’t Move Blood Sugar for Most
TOPLINE:
Intra-articular corticosteroid (IACS) injections pose a minimal risk of accelerating diabetes for most people, despite temporarily elevating blood glucose levels, according to a study published in Clinical Diabetes.
METHODOLOGY:
- Almost half of Americans with diabetes have arthritis, so glycemic control is a concern for many receiving IACS injections.
- IACS injections are known to cause short-term hyperglycemia, but their long-term effects on glycemic control are not well studied.
- For the retrospective cohort study, researchers at Mayo Clinic in Rochester, Minnesota, used electronic health records from 1169 adults who had received an IACS injection in one large joint between 2012 and 2018.
- They analyzed data on A1C levels for study participants from 18 months before and after the injections.
- Researchers assessed if participants had a greater-than-expected (defined as an increase of more than 0.5% above expected) concentration of A1C after the injection, and examined rates of diabetic ketoacidosis and hyperosmolar hyperglycemic syndrome in the 30 days following an injection.
TAKEAWAY:
- Nearly 16% of people experienced a greater-than-expected A1C level after receiving an injection.
- A1C levels rose by an average of 1.2% in the greater-than-expected group, but decreased by an average of 0.2% in the average group.
- One patient had an episode of severe hyperglycemia that was linked to the injection.
- A baseline level of A1C above 8% was the only factor associated with a greater-than-expected increase in the marker after an IACS injection.
IN PRACTICE:
“Although most patients do not experience an increase in A1C after IACS, clinicians should counsel patients with suboptimally controlled diabetes about risks of further hyperglycemia after IACS administration,” the researchers wrote.
SOURCE:
The study was led by Terin T. Sytsma, MD, of Mayo Clinic in Rochester, Minnesota.
LIMITATIONS:
The study was retrospective and could not establish causation. In addition, the population was of residents from one county in Minnesota, and was not racially or ethnically diverse. Details about the injection, such as location and total dose, were not available. The study also did not include a control group.
DISCLOSURES:
The study was funded by Mayo Clinic and the National Center for Advancing Translational Sciences. The authors reported no relevant disclosures.
A version of this article first appeared on Medscape.com.
TOPLINE:
Intra-articular corticosteroid (IACS) injections pose a minimal risk of accelerating diabetes for most people, despite temporarily elevating blood glucose levels, according to a study published in Clinical Diabetes.
METHODOLOGY:
- Almost half of Americans with diabetes have arthritis, so glycemic control is a concern for many receiving IACS injections.
- IACS injections are known to cause short-term hyperglycemia, but their long-term effects on glycemic control are not well studied.
- For the retrospective cohort study, researchers at Mayo Clinic in Rochester, Minnesota, used electronic health records from 1169 adults who had received an IACS injection in one large joint between 2012 and 2018.
- They analyzed data on A1C levels for study participants from 18 months before and after the injections.
- Researchers assessed if participants had a greater-than-expected (defined as an increase of more than 0.5% above expected) concentration of A1C after the injection, and examined rates of diabetic ketoacidosis and hyperosmolar hyperglycemic syndrome in the 30 days following an injection.
TAKEAWAY:
- Nearly 16% of people experienced a greater-than-expected A1C level after receiving an injection.
- A1C levels rose by an average of 1.2% in the greater-than-expected group, but decreased by an average of 0.2% in the average group.
- One patient had an episode of severe hyperglycemia that was linked to the injection.
- A baseline level of A1C above 8% was the only factor associated with a greater-than-expected increase in the marker after an IACS injection.
IN PRACTICE:
“Although most patients do not experience an increase in A1C after IACS, clinicians should counsel patients with suboptimally controlled diabetes about risks of further hyperglycemia after IACS administration,” the researchers wrote.
SOURCE:
The study was led by Terin T. Sytsma, MD, of Mayo Clinic in Rochester, Minnesota.
LIMITATIONS:
The study was retrospective and could not establish causation. In addition, the population was of residents from one county in Minnesota, and was not racially or ethnically diverse. Details about the injection, such as location and total dose, were not available. The study also did not include a control group.
DISCLOSURES:
The study was funded by Mayo Clinic and the National Center for Advancing Translational Sciences. The authors reported no relevant disclosures.
A version of this article first appeared on Medscape.com.
TOPLINE:
Intra-articular corticosteroid (IACS) injections pose a minimal risk of accelerating diabetes for most people, despite temporarily elevating blood glucose levels, according to a study published in Clinical Diabetes.
METHODOLOGY:
- Almost half of Americans with diabetes have arthritis, so glycemic control is a concern for many receiving IACS injections.
- IACS injections are known to cause short-term hyperglycemia, but their long-term effects on glycemic control are not well studied.
- For the retrospective cohort study, researchers at Mayo Clinic in Rochester, Minnesota, used electronic health records from 1169 adults who had received an IACS injection in one large joint between 2012 and 2018.
- They analyzed data on A1C levels for study participants from 18 months before and after the injections.
- Researchers assessed if participants had a greater-than-expected (defined as an increase of more than 0.5% above expected) concentration of A1C after the injection, and examined rates of diabetic ketoacidosis and hyperosmolar hyperglycemic syndrome in the 30 days following an injection.
TAKEAWAY:
- Nearly 16% of people experienced a greater-than-expected A1C level after receiving an injection.
- A1C levels rose by an average of 1.2% in the greater-than-expected group, but decreased by an average of 0.2% in the average group.
- One patient had an episode of severe hyperglycemia that was linked to the injection.
- A baseline level of A1C above 8% was the only factor associated with a greater-than-expected increase in the marker after an IACS injection.
IN PRACTICE:
“Although most patients do not experience an increase in A1C after IACS, clinicians should counsel patients with suboptimally controlled diabetes about risks of further hyperglycemia after IACS administration,” the researchers wrote.
SOURCE:
The study was led by Terin T. Sytsma, MD, of Mayo Clinic in Rochester, Minnesota.
LIMITATIONS:
The study was retrospective and could not establish causation. In addition, the population was of residents from one county in Minnesota, and was not racially or ethnically diverse. Details about the injection, such as location and total dose, were not available. The study also did not include a control group.
DISCLOSURES:
The study was funded by Mayo Clinic and the National Center for Advancing Translational Sciences. The authors reported no relevant disclosures.
A version of this article first appeared on Medscape.com.
Hypocalcemia Risk Warning Added to Osteoporosis Drug
The US Food and Drug Administration (FDA) has added a boxed warning to the label of the osteoporosis drug denosumab (Prolia) about increased risk for severe hypocalcemia in patients with advanced chronic kidney disease (CKD).
Denosumab is a monoclonal antibody, indicated for the treatment of postmenopausal women with osteoporosis who are at increased risk for fracture for whom other treatments aren’t effective or can’t be tolerated. It’s also indicated to increase bone mass in men with osteoporosis at high risk for fracture, treat glucocorticoid-induced osteoporosis in men and women at high risk for fracture, increase bone mass in men at high risk for fracture receiving androgen-deprivation therapy for nonmetastatic prostate cancer, and increase bone mass in women at high risk for fracture receiving adjuvant aromatase inhibitor therapy for breast cancer.
This new warning updates a November 2022 alert based on preliminary evidence for a “substantial risk” for hypocalcemia in patients with CKD on dialysis.
Upon further examination of the data from two trials including more than 500,000 denosumab-treated women with CKD, the FDA concluded that severe hypocalcemia appears to be more common in those with CKD who also have mineral and bone disorder (CKD-MBD). And, for patients with advanced CKD taking denosumab, “severe hypocalcemia resulted in serious harm, including hospitalization, life-threatening events, and death.”
Most of the severe hypocalcemia events occurred 2-10 weeks after denosumab injection, with the greatest risk during weeks 2-5.
The new warning advises healthcare professionals to assess patients’ kidney function before prescribing denosumab, and for those with advanced CKD, “consider the risk of severe hypocalcemia with Prolia in the context of other available treatments for osteoporosis.”
If the drug is still being considered for those patients for initial or continued use, calcium blood levels should be checked, and patients should be evaluated for CKD-MBD. Prior to prescribing denosumab in these patients, CKD-MBD should be properly managed, hypocalcemia corrected, and patients supplemented with calcium and activated vitamin D to decrease the risk for severe hypocalcemia and associated complications.
“Treatment with denosumab in patients with advanced CKD, including those on dialysis, and particularly patients with diagnosed CKD-MBD should involve a health care provider with expertise in the diagnosis and management of CKD-MBD,” the FDA advises.
Once denosumab is administered, close monitoring of blood calcium levels and prompt hypocalcemia management is essential to prevent complications including seizures or arrythmias. Patients should be advised to promptly report symptoms that could be consistent with hypocalcemia, including confusion, seizures, irregular heartbeat, fainting, muscle spasms or weakness, face twitching, tingling, or numbness anywhere in the body.
In 2022, an estimated 2.2 million Prolia prefilled syringes were sold by the manufacturer to US healthcare settings.
A version of this article appeared on Medscape.com.
The US Food and Drug Administration (FDA) has added a boxed warning to the label of the osteoporosis drug denosumab (Prolia) about increased risk for severe hypocalcemia in patients with advanced chronic kidney disease (CKD).
Denosumab is a monoclonal antibody, indicated for the treatment of postmenopausal women with osteoporosis who are at increased risk for fracture for whom other treatments aren’t effective or can’t be tolerated. It’s also indicated to increase bone mass in men with osteoporosis at high risk for fracture, treat glucocorticoid-induced osteoporosis in men and women at high risk for fracture, increase bone mass in men at high risk for fracture receiving androgen-deprivation therapy for nonmetastatic prostate cancer, and increase bone mass in women at high risk for fracture receiving adjuvant aromatase inhibitor therapy for breast cancer.
This new warning updates a November 2022 alert based on preliminary evidence for a “substantial risk” for hypocalcemia in patients with CKD on dialysis.
Upon further examination of the data from two trials including more than 500,000 denosumab-treated women with CKD, the FDA concluded that severe hypocalcemia appears to be more common in those with CKD who also have mineral and bone disorder (CKD-MBD). And, for patients with advanced CKD taking denosumab, “severe hypocalcemia resulted in serious harm, including hospitalization, life-threatening events, and death.”
Most of the severe hypocalcemia events occurred 2-10 weeks after denosumab injection, with the greatest risk during weeks 2-5.
The new warning advises healthcare professionals to assess patients’ kidney function before prescribing denosumab, and for those with advanced CKD, “consider the risk of severe hypocalcemia with Prolia in the context of other available treatments for osteoporosis.”
If the drug is still being considered for those patients for initial or continued use, calcium blood levels should be checked, and patients should be evaluated for CKD-MBD. Prior to prescribing denosumab in these patients, CKD-MBD should be properly managed, hypocalcemia corrected, and patients supplemented with calcium and activated vitamin D to decrease the risk for severe hypocalcemia and associated complications.
“Treatment with denosumab in patients with advanced CKD, including those on dialysis, and particularly patients with diagnosed CKD-MBD should involve a health care provider with expertise in the diagnosis and management of CKD-MBD,” the FDA advises.
Once denosumab is administered, close monitoring of blood calcium levels and prompt hypocalcemia management is essential to prevent complications including seizures or arrythmias. Patients should be advised to promptly report symptoms that could be consistent with hypocalcemia, including confusion, seizures, irregular heartbeat, fainting, muscle spasms or weakness, face twitching, tingling, or numbness anywhere in the body.
In 2022, an estimated 2.2 million Prolia prefilled syringes were sold by the manufacturer to US healthcare settings.
A version of this article appeared on Medscape.com.
The US Food and Drug Administration (FDA) has added a boxed warning to the label of the osteoporosis drug denosumab (Prolia) about increased risk for severe hypocalcemia in patients with advanced chronic kidney disease (CKD).
Denosumab is a monoclonal antibody, indicated for the treatment of postmenopausal women with osteoporosis who are at increased risk for fracture for whom other treatments aren’t effective or can’t be tolerated. It’s also indicated to increase bone mass in men with osteoporosis at high risk for fracture, treat glucocorticoid-induced osteoporosis in men and women at high risk for fracture, increase bone mass in men at high risk for fracture receiving androgen-deprivation therapy for nonmetastatic prostate cancer, and increase bone mass in women at high risk for fracture receiving adjuvant aromatase inhibitor therapy for breast cancer.
This new warning updates a November 2022 alert based on preliminary evidence for a “substantial risk” for hypocalcemia in patients with CKD on dialysis.
Upon further examination of the data from two trials including more than 500,000 denosumab-treated women with CKD, the FDA concluded that severe hypocalcemia appears to be more common in those with CKD who also have mineral and bone disorder (CKD-MBD). And, for patients with advanced CKD taking denosumab, “severe hypocalcemia resulted in serious harm, including hospitalization, life-threatening events, and death.”
Most of the severe hypocalcemia events occurred 2-10 weeks after denosumab injection, with the greatest risk during weeks 2-5.
The new warning advises healthcare professionals to assess patients’ kidney function before prescribing denosumab, and for those with advanced CKD, “consider the risk of severe hypocalcemia with Prolia in the context of other available treatments for osteoporosis.”
If the drug is still being considered for those patients for initial or continued use, calcium blood levels should be checked, and patients should be evaluated for CKD-MBD. Prior to prescribing denosumab in these patients, CKD-MBD should be properly managed, hypocalcemia corrected, and patients supplemented with calcium and activated vitamin D to decrease the risk for severe hypocalcemia and associated complications.
“Treatment with denosumab in patients with advanced CKD, including those on dialysis, and particularly patients with diagnosed CKD-MBD should involve a health care provider with expertise in the diagnosis and management of CKD-MBD,” the FDA advises.
Once denosumab is administered, close monitoring of blood calcium levels and prompt hypocalcemia management is essential to prevent complications including seizures or arrythmias. Patients should be advised to promptly report symptoms that could be consistent with hypocalcemia, including confusion, seizures, irregular heartbeat, fainting, muscle spasms or weakness, face twitching, tingling, or numbness anywhere in the body.
In 2022, an estimated 2.2 million Prolia prefilled syringes were sold by the manufacturer to US healthcare settings.
A version of this article appeared on Medscape.com.
A Look at the Evidence Linking Diet to Skin Conditions
ORLANDO, FLORIDA — Amid all the hype, claims, and confusion, there is evidence linking some foods and drinks to an increased risk for acne, psoriasis, atopic dermatitis, rosacea, and other common skin conditions. So, what is the connection in each case? And how can people with any of these skin conditions potentially improve their health and quality of life with dietary changes?

What is clear is that there has been an explosion of interest in learning which foods can improve or worsen skin issues in recent years. It’s a good idea to familiarize yourself with the research and also to Google ‘diet’ and ‘skin’, said Vivian Shi, MD, associate professor of dermatology at the University of Arkansas for Medical Sciences, Little Rock. “As practitioners, we should be well prepared to talk about what patients want to talk about.”
Acne
One of the major areas of interest is diet and acne. “We’ve all heard sugar and dairy are bad, and the Western diet is high in sugar and dairy,” Dr. Shi said at the ODAC Dermatology, Aesthetic & Surgical Conference.
Dairy, red meat, and carbohydrates can break down into leucine, an essential amino acid found in protein. Leucine and sugar together, in turn, can produce insulin and insulin-like growth factor 1 (IGF-1), which, through different pathways, can reach the androgen receptors throughout the body, including the skin. This results in sebogenesis, lipogenesis, and keratinization, which triggers follicular inflammation and results in more of the acne-causing bacteria Cutibacterium acnes.
Milk and other dairy products also can increase IGF-1 levels, which can alter hormonal mediators and increase acne.
Not all types of dairy milk are created equal, however, when it comes to acne. Dr. Shi wondered why 2% milk has overall color and nutritional content very similar to that of whole milk. “I looked into this.” She discovered that when milk manufacturers remove the fat, they often add whey proteins to restore some nutrients. Whey protein can increase acne, Dr. Shi added.
“So, if you’re going to choose any milk to drink, I think from an acne perspective, it’s better to use whole milk. If you can get it organic, even better.” Skim milk is the most acnegenic, she said.
Psoriasis
A systematic review of 55 studies evaluating diet and psoriasis found obesity can be an exacerbating factor. The strongest evidence for dietary weight reduction points to a hypocaloric diet in people with overweight or obesity, according to the review. Other evidence suggests alcohol can lower response to treatment and is linked with more severe psoriasis. Furthermore, a gluten-free diet or vitamin D supplements can help some subpopulations of people with psoriasis.
“An overwhelming majority of our psoriasis patients are vitamin D deficient,” Dr. Shi said.
The National Psoriasis Foundation (NPF) publishes dietary modification guidelines, updated as recently as November 2023. The NPF states that “there is no diet that will cure psoriatic disease, but there are many ways in which eating healthful food may lessen the severity of symptoms and play a role in lowering the likelihood of developing comorbidities.”
Healthier choices include fruits, vegetables, whole grains, and fat-free or low-fat dairy products. Include lean meats, poultry, fish, beans, eggs, and nuts. Adherence to a Mediterranean diet has been linked to a lower severity of psoriasis.
Atopic Dermatitis
Atopic dermatitis (AD) is “one of the prototypical diseases related to diet,” Dr. Shi said. A different meta-analysis looked at randomized controlled trials of synbiotics (a combination of prebiotics and probiotics) for treatment of AD.
These researchers found that synbiotics do not prevent AD, but they can help treat it in adults and children older than 1 year. In addition, synbiotics are more beneficial than probiotics in treating the condition, although there are no head-to-head comparison studies. In addition, the meta-analysis found that prebiotics alone can lower AD severity.
However, Dr. Shi said, there are no recommendations from the American Academy of Dermatology (AAD) on prebiotics or probiotics for AD, and the AAD does not recommend any supplement or essential oil for AD.
In a 2022 review, investigators ranked the efficacy of different supplements for AD based on available evidence. They found the greatest benefit associated with vitamin D supplementation, followed by vitamin E, probiotics, hemp seed oil, histidine, and oolong tea. They also noted the ‘Six Food Elimination Diet and Autoimmune Protocol’ featured the least amount of evidence to back it up.
Rosacea
Rosacea appears to be caused by “all the fun things in life” like sunlight, alcohol, chocolate, spicy foods, and caffeine, Dr. Shi said. In people with rosacea, they can cause facial flushing, edema, burning, and an inflammatory response.
Certain foods can activate skin receptors and sensory neurons, which can release neuropeptides that act on mast cells in blood that lead to flushing. The skin-gut axis may also be involved, evidence suggests. “And that is why food has a pretty profound impact on rosacea,” Dr. Shi said.
Dr. Shi reported no relevant financial relationships.
A version of this article appeared on Medscape.com.
ORLANDO, FLORIDA — Amid all the hype, claims, and confusion, there is evidence linking some foods and drinks to an increased risk for acne, psoriasis, atopic dermatitis, rosacea, and other common skin conditions. So, what is the connection in each case? And how can people with any of these skin conditions potentially improve their health and quality of life with dietary changes?
What is clear is that there has been an explosion of interest in learning which foods can improve or worsen skin issues in recent years. It’s a good idea to familiarize yourself with the research and also to Google ‘diet’ and ‘skin’, said Vivian Shi, MD, associate professor of dermatology at the University of Arkansas for Medical Sciences, Little Rock. “As practitioners, we should be well prepared to talk about what patients want to talk about.”
Acne
One of the major areas of interest is diet and acne. “We’ve all heard sugar and dairy are bad, and the Western diet is high in sugar and dairy,” Dr. Shi said at the ODAC Dermatology, Aesthetic & Surgical Conference.
Dairy, red meat, and carbohydrates can break down into leucine, an essential amino acid found in protein. Leucine and sugar together, in turn, can produce insulin and insulin-like growth factor 1 (IGF-1), which, through different pathways, can reach the androgen receptors throughout the body, including the skin. This results in sebogenesis, lipogenesis, and keratinization, which triggers follicular inflammation and results in more of the acne-causing bacteria Cutibacterium acnes.
Milk and other dairy products also can increase IGF-1 levels, which can alter hormonal mediators and increase acne.
Not all types of dairy milk are created equal, however, when it comes to acne. Dr. Shi wondered why 2% milk has overall color and nutritional content very similar to that of whole milk. “I looked into this.” She discovered that when milk manufacturers remove the fat, they often add whey proteins to restore some nutrients. Whey protein can increase acne, Dr. Shi added.
“So, if you’re going to choose any milk to drink, I think from an acne perspective, it’s better to use whole milk. If you can get it organic, even better.” Skim milk is the most acnegenic, she said.
Psoriasis
A systematic review of 55 studies evaluating diet and psoriasis found obesity can be an exacerbating factor. The strongest evidence for dietary weight reduction points to a hypocaloric diet in people with overweight or obesity, according to the review. Other evidence suggests alcohol can lower response to treatment and is linked with more severe psoriasis. Furthermore, a gluten-free diet or vitamin D supplements can help some subpopulations of people with psoriasis.
“An overwhelming majority of our psoriasis patients are vitamin D deficient,” Dr. Shi said.
The National Psoriasis Foundation (NPF) publishes dietary modification guidelines, updated as recently as November 2023. The NPF states that “there is no diet that will cure psoriatic disease, but there are many ways in which eating healthful food may lessen the severity of symptoms and play a role in lowering the likelihood of developing comorbidities.”
Healthier choices include fruits, vegetables, whole grains, and fat-free or low-fat dairy products. Include lean meats, poultry, fish, beans, eggs, and nuts. Adherence to a Mediterranean diet has been linked to a lower severity of psoriasis.
Atopic Dermatitis
Atopic dermatitis (AD) is “one of the prototypical diseases related to diet,” Dr. Shi said. A different meta-analysis looked at randomized controlled trials of synbiotics (a combination of prebiotics and probiotics) for treatment of AD.
These researchers found that synbiotics do not prevent AD, but they can help treat it in adults and children older than 1 year. In addition, synbiotics are more beneficial than probiotics in treating the condition, although there are no head-to-head comparison studies. In addition, the meta-analysis found that prebiotics alone can lower AD severity.
However, Dr. Shi said, there are no recommendations from the American Academy of Dermatology (AAD) on prebiotics or probiotics for AD, and the AAD does not recommend any supplement or essential oil for AD.
In a 2022 review, investigators ranked the efficacy of different supplements for AD based on available evidence. They found the greatest benefit associated with vitamin D supplementation, followed by vitamin E, probiotics, hemp seed oil, histidine, and oolong tea. They also noted the ‘Six Food Elimination Diet and Autoimmune Protocol’ featured the least amount of evidence to back it up.
Rosacea
Rosacea appears to be caused by “all the fun things in life” like sunlight, alcohol, chocolate, spicy foods, and caffeine, Dr. Shi said. In people with rosacea, they can cause facial flushing, edema, burning, and an inflammatory response.
Certain foods can activate skin receptors and sensory neurons, which can release neuropeptides that act on mast cells in blood that lead to flushing. The skin-gut axis may also be involved, evidence suggests. “And that is why food has a pretty profound impact on rosacea,” Dr. Shi said.
Dr. Shi reported no relevant financial relationships.
A version of this article appeared on Medscape.com.
ORLANDO, FLORIDA — Amid all the hype, claims, and confusion, there is evidence linking some foods and drinks to an increased risk for acne, psoriasis, atopic dermatitis, rosacea, and other common skin conditions. So, what is the connection in each case? And how can people with any of these skin conditions potentially improve their health and quality of life with dietary changes?
What is clear is that there has been an explosion of interest in learning which foods can improve or worsen skin issues in recent years. It’s a good idea to familiarize yourself with the research and also to Google ‘diet’ and ‘skin’, said Vivian Shi, MD, associate professor of dermatology at the University of Arkansas for Medical Sciences, Little Rock. “As practitioners, we should be well prepared to talk about what patients want to talk about.”
Acne
One of the major areas of interest is diet and acne. “We’ve all heard sugar and dairy are bad, and the Western diet is high in sugar and dairy,” Dr. Shi said at the ODAC Dermatology, Aesthetic & Surgical Conference.
Dairy, red meat, and carbohydrates can break down into leucine, an essential amino acid found in protein. Leucine and sugar together, in turn, can produce insulin and insulin-like growth factor 1 (IGF-1), which, through different pathways, can reach the androgen receptors throughout the body, including the skin. This results in sebogenesis, lipogenesis, and keratinization, which triggers follicular inflammation and results in more of the acne-causing bacteria Cutibacterium acnes.
Milk and other dairy products also can increase IGF-1 levels, which can alter hormonal mediators and increase acne.
Not all types of dairy milk are created equal, however, when it comes to acne. Dr. Shi wondered why 2% milk has overall color and nutritional content very similar to that of whole milk. “I looked into this.” She discovered that when milk manufacturers remove the fat, they often add whey proteins to restore some nutrients. Whey protein can increase acne, Dr. Shi added.
“So, if you’re going to choose any milk to drink, I think from an acne perspective, it’s better to use whole milk. If you can get it organic, even better.” Skim milk is the most acnegenic, she said.
Psoriasis
A systematic review of 55 studies evaluating diet and psoriasis found obesity can be an exacerbating factor. The strongest evidence for dietary weight reduction points to a hypocaloric diet in people with overweight or obesity, according to the review. Other evidence suggests alcohol can lower response to treatment and is linked with more severe psoriasis. Furthermore, a gluten-free diet or vitamin D supplements can help some subpopulations of people with psoriasis.
“An overwhelming majority of our psoriasis patients are vitamin D deficient,” Dr. Shi said.
The National Psoriasis Foundation (NPF) publishes dietary modification guidelines, updated as recently as November 2023. The NPF states that “there is no diet that will cure psoriatic disease, but there are many ways in which eating healthful food may lessen the severity of symptoms and play a role in lowering the likelihood of developing comorbidities.”
Healthier choices include fruits, vegetables, whole grains, and fat-free or low-fat dairy products. Include lean meats, poultry, fish, beans, eggs, and nuts. Adherence to a Mediterranean diet has been linked to a lower severity of psoriasis.
Atopic Dermatitis
Atopic dermatitis (AD) is “one of the prototypical diseases related to diet,” Dr. Shi said. A different meta-analysis looked at randomized controlled trials of synbiotics (a combination of prebiotics and probiotics) for treatment of AD.
These researchers found that synbiotics do not prevent AD, but they can help treat it in adults and children older than 1 year. In addition, synbiotics are more beneficial than probiotics in treating the condition, although there are no head-to-head comparison studies. In addition, the meta-analysis found that prebiotics alone can lower AD severity.
However, Dr. Shi said, there are no recommendations from the American Academy of Dermatology (AAD) on prebiotics or probiotics for AD, and the AAD does not recommend any supplement or essential oil for AD.
In a 2022 review, investigators ranked the efficacy of different supplements for AD based on available evidence. They found the greatest benefit associated with vitamin D supplementation, followed by vitamin E, probiotics, hemp seed oil, histidine, and oolong tea. They also noted the ‘Six Food Elimination Diet and Autoimmune Protocol’ featured the least amount of evidence to back it up.
Rosacea
Rosacea appears to be caused by “all the fun things in life” like sunlight, alcohol, chocolate, spicy foods, and caffeine, Dr. Shi said. In people with rosacea, they can cause facial flushing, edema, burning, and an inflammatory response.
Certain foods can activate skin receptors and sensory neurons, which can release neuropeptides that act on mast cells in blood that lead to flushing. The skin-gut axis may also be involved, evidence suggests. “And that is why food has a pretty profound impact on rosacea,” Dr. Shi said.
Dr. Shi reported no relevant financial relationships.
A version of this article appeared on Medscape.com.
Why Don’t Physicians Call In Sick?
I began practicing medicine on July 1, 1981. In the 43-plus years since then,
There are several reasons, both good and bad, why this is so: (1) like most physicians, I am a terrible patient; (2) as a solo practitioner, there was (until recently — I’ll get to that in a minute) no one else to see an office full of patients who had waited significant amounts of time for their appointments and in many cases had taken off work themselves to keep them; and (3) there is an unspoken rule against it. Taking sick days is highly frowned upon in the medical world. As a medical student, intern, and resident I was told in so many words not to call in sick, no matter how serious the illness might be.

Apparently, I was not the only doctor-in-training to receive that message. In a survey reported in JAMA Pediatrics several years ago, 95% of the physicians and advanced practice clinicians (APCs) surveyed believed that working while sick put patients at risk — yet 83% reported working sick at least one time over the prior year. They understood the risks, but did it anyway.
There is no question that this practice does put patients’ health at risk. The JAMA study linked numerous reports of outbreaks traceable to symptomatic healthcare workers. Some outbreaks of flu, staph infections, norovirus, and pertussis were shown to originate from a sick physician or supporting staff member. These associations have led to increased morbidity and mortality, as well as excess costs. Those of us who treat immunocompromised patients on a regular basis risk inducing a life-threatening illness by unnecessarily exposing them to pathogens.
The JAMA survey results also confirmed my own observation that many physicians feel boxed in by their institutions or practice situations. “The study illustrates the complex social and logistic factors that cause this behavior,” the authors wrote. “These results may inform efforts to design systems at our hospital to provide support for attending physicians and APCs and help them make the right choice to keep their patients and colleagues safe while caring for themselves.”
What might those efforts look like? For one thing, we can take the obvious and necessary steps to avoid getting sick in the first place, such as staying fit and hydrated, and eating well. We can keep up with routine health visits and measures such as colorectal screening, pap smears, and mammograms, and stay up to date with flu shots and all other essential immunizations.
Next, we can minimize the risk of spreading any illnesses we encounter in the course of our work by practicing the basic infectious disease prevention measures driven home so forcefully by the recent COVID-19 pandemic — washing our hands, using hand sanitizers, and, when appropriate, wearing gloves and masks.
Finally, we can work to overcome this institutional taboo against staying home when we do get sick. Work out a system of mutual coverage for such situations. Two years ago, I merged my solo practice with a local, larger group. I did it for a variety of reasons, but a principal one was to assure that a partner could cover for me if I became ill. Practitioners who choose to remain solo or in small groups should contact colleagues and work out a coverage agreement.
Now, during flu season, it is especially important to resist the temptation to work while sick. The CDC has guidelines for employees specific for the flu, which notes that “persons with the flu are most contagious during the first 3 days of their illness,” and should remain at home until at least 24 hours after their fever subsides (without the use of fever-reducing medications) or after symptoms have improved (at least 4-5 days after they started) — or, if they do not have a fever, after symptoms improve “for at least 4-5 days after the onset of symptoms.”
Of course, we need to remember that COVID-19 is still with us. With the constant evolution of new strains, it is especially important to avoid exposing patients and colleagues to the disease should you become infected. The most recent advice from the CDC includes the recommendation that those who are mildly ill and not moderately or severely immunocompromised should isolate after SARS-CoV-2 infection for at least 5 days after symptom onset (day 0 is the day symptoms appeared, and day 1 is the next full day thereafter) if fever has resolved for at least 24 hours (without taking fever-reducing medications) and other symptoms are improving. In addition, “a high-quality mask should be worn around others at home and in public through day 10.”
We should also extend these rules to our support staff, starting with providing them with adequate sick leave and encouraging them to use it when necessary. Research has found a direct correlation between preventative health care and the number of paid sick leave days a worker gets. In a study of over 3000 US workers, those with 10 paid sick days or more annually accessed preventative care more frequently than those without paid sick days.
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, N.J. He is the author of numerous articles and textbook chapters, and is a longtime monthly columnist for Dermatology News. Write to him at [email protected].
I began practicing medicine on July 1, 1981. In the 43-plus years since then,
There are several reasons, both good and bad, why this is so: (1) like most physicians, I am a terrible patient; (2) as a solo practitioner, there was (until recently — I’ll get to that in a minute) no one else to see an office full of patients who had waited significant amounts of time for their appointments and in many cases had taken off work themselves to keep them; and (3) there is an unspoken rule against it. Taking sick days is highly frowned upon in the medical world. As a medical student, intern, and resident I was told in so many words not to call in sick, no matter how serious the illness might be.
Apparently, I was not the only doctor-in-training to receive that message. In a survey reported in JAMA Pediatrics several years ago, 95% of the physicians and advanced practice clinicians (APCs) surveyed believed that working while sick put patients at risk — yet 83% reported working sick at least one time over the prior year. They understood the risks, but did it anyway.
There is no question that this practice does put patients’ health at risk. The JAMA study linked numerous reports of outbreaks traceable to symptomatic healthcare workers. Some outbreaks of flu, staph infections, norovirus, and pertussis were shown to originate from a sick physician or supporting staff member. These associations have led to increased morbidity and mortality, as well as excess costs. Those of us who treat immunocompromised patients on a regular basis risk inducing a life-threatening illness by unnecessarily exposing them to pathogens.
The JAMA survey results also confirmed my own observation that many physicians feel boxed in by their institutions or practice situations. “The study illustrates the complex social and logistic factors that cause this behavior,” the authors wrote. “These results may inform efforts to design systems at our hospital to provide support for attending physicians and APCs and help them make the right choice to keep their patients and colleagues safe while caring for themselves.”
What might those efforts look like? For one thing, we can take the obvious and necessary steps to avoid getting sick in the first place, such as staying fit and hydrated, and eating well. We can keep up with routine health visits and measures such as colorectal screening, pap smears, and mammograms, and stay up to date with flu shots and all other essential immunizations.
Next, we can minimize the risk of spreading any illnesses we encounter in the course of our work by practicing the basic infectious disease prevention measures driven home so forcefully by the recent COVID-19 pandemic — washing our hands, using hand sanitizers, and, when appropriate, wearing gloves and masks.
Finally, we can work to overcome this institutional taboo against staying home when we do get sick. Work out a system of mutual coverage for such situations. Two years ago, I merged my solo practice with a local, larger group. I did it for a variety of reasons, but a principal one was to assure that a partner could cover for me if I became ill. Practitioners who choose to remain solo or in small groups should contact colleagues and work out a coverage agreement.
Now, during flu season, it is especially important to resist the temptation to work while sick. The CDC has guidelines for employees specific for the flu, which notes that “persons with the flu are most contagious during the first 3 days of their illness,” and should remain at home until at least 24 hours after their fever subsides (without the use of fever-reducing medications) or after symptoms have improved (at least 4-5 days after they started) — or, if they do not have a fever, after symptoms improve “for at least 4-5 days after the onset of symptoms.”
Of course, we need to remember that COVID-19 is still with us. With the constant evolution of new strains, it is especially important to avoid exposing patients and colleagues to the disease should you become infected. The most recent advice from the CDC includes the recommendation that those who are mildly ill and not moderately or severely immunocompromised should isolate after SARS-CoV-2 infection for at least 5 days after symptom onset (day 0 is the day symptoms appeared, and day 1 is the next full day thereafter) if fever has resolved for at least 24 hours (without taking fever-reducing medications) and other symptoms are improving. In addition, “a high-quality mask should be worn around others at home and in public through day 10.”
We should also extend these rules to our support staff, starting with providing them with adequate sick leave and encouraging them to use it when necessary. Research has found a direct correlation between preventative health care and the number of paid sick leave days a worker gets. In a study of over 3000 US workers, those with 10 paid sick days or more annually accessed preventative care more frequently than those without paid sick days.
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, N.J. He is the author of numerous articles and textbook chapters, and is a longtime monthly columnist for Dermatology News. Write to him at [email protected].
I began practicing medicine on July 1, 1981. In the 43-plus years since then,
There are several reasons, both good and bad, why this is so: (1) like most physicians, I am a terrible patient; (2) as a solo practitioner, there was (until recently — I’ll get to that in a minute) no one else to see an office full of patients who had waited significant amounts of time for their appointments and in many cases had taken off work themselves to keep them; and (3) there is an unspoken rule against it. Taking sick days is highly frowned upon in the medical world. As a medical student, intern, and resident I was told in so many words not to call in sick, no matter how serious the illness might be.
Apparently, I was not the only doctor-in-training to receive that message. In a survey reported in JAMA Pediatrics several years ago, 95% of the physicians and advanced practice clinicians (APCs) surveyed believed that working while sick put patients at risk — yet 83% reported working sick at least one time over the prior year. They understood the risks, but did it anyway.
There is no question that this practice does put patients’ health at risk. The JAMA study linked numerous reports of outbreaks traceable to symptomatic healthcare workers. Some outbreaks of flu, staph infections, norovirus, and pertussis were shown to originate from a sick physician or supporting staff member. These associations have led to increased morbidity and mortality, as well as excess costs. Those of us who treat immunocompromised patients on a regular basis risk inducing a life-threatening illness by unnecessarily exposing them to pathogens.
The JAMA survey results also confirmed my own observation that many physicians feel boxed in by their institutions or practice situations. “The study illustrates the complex social and logistic factors that cause this behavior,” the authors wrote. “These results may inform efforts to design systems at our hospital to provide support for attending physicians and APCs and help them make the right choice to keep their patients and colleagues safe while caring for themselves.”
What might those efforts look like? For one thing, we can take the obvious and necessary steps to avoid getting sick in the first place, such as staying fit and hydrated, and eating well. We can keep up with routine health visits and measures such as colorectal screening, pap smears, and mammograms, and stay up to date with flu shots and all other essential immunizations.
Next, we can minimize the risk of spreading any illnesses we encounter in the course of our work by practicing the basic infectious disease prevention measures driven home so forcefully by the recent COVID-19 pandemic — washing our hands, using hand sanitizers, and, when appropriate, wearing gloves and masks.
Finally, we can work to overcome this institutional taboo against staying home when we do get sick. Work out a system of mutual coverage for such situations. Two years ago, I merged my solo practice with a local, larger group. I did it for a variety of reasons, but a principal one was to assure that a partner could cover for me if I became ill. Practitioners who choose to remain solo or in small groups should contact colleagues and work out a coverage agreement.
Now, during flu season, it is especially important to resist the temptation to work while sick. The CDC has guidelines for employees specific for the flu, which notes that “persons with the flu are most contagious during the first 3 days of their illness,” and should remain at home until at least 24 hours after their fever subsides (without the use of fever-reducing medications) or after symptoms have improved (at least 4-5 days after they started) — or, if they do not have a fever, after symptoms improve “for at least 4-5 days after the onset of symptoms.”
Of course, we need to remember that COVID-19 is still with us. With the constant evolution of new strains, it is especially important to avoid exposing patients and colleagues to the disease should you become infected. The most recent advice from the CDC includes the recommendation that those who are mildly ill and not moderately or severely immunocompromised should isolate after SARS-CoV-2 infection for at least 5 days after symptom onset (day 0 is the day symptoms appeared, and day 1 is the next full day thereafter) if fever has resolved for at least 24 hours (without taking fever-reducing medications) and other symptoms are improving. In addition, “a high-quality mask should be worn around others at home and in public through day 10.”
We should also extend these rules to our support staff, starting with providing them with adequate sick leave and encouraging them to use it when necessary. Research has found a direct correlation between preventative health care and the number of paid sick leave days a worker gets. In a study of over 3000 US workers, those with 10 paid sick days or more annually accessed preventative care more frequently than those without paid sick days.
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, N.J. He is the author of numerous articles and textbook chapters, and is a longtime monthly columnist for Dermatology News. Write to him at [email protected].

Best Practices for Hiring, Training, Retaining Rheumatology Advanced Practice Providers
Once considered a luxury, hiring a nurse, nurse practitioner, or physician assistant is becoming a necessity in many rheumatology practices.
Seeing the wait lists pile up in her Florida practice, Stacy Yonker, MBA, chief executive officer of Sarasota Arthritis Center, knew she had to make some changes. “Everyone’s aging in the boomer generations. Particularly in Florida, we have a lot of people who retire here. In the more southern demographics, it is a very difficult challenge for practices to get new patients in,” she said.

Ms. Yonker is in the process of hiring several nurse practitioners (NPs) to assist in the clinics and infusion suites, lightening the load for the practice’s 11 rheumatologists.
Hiring an advanced practice provider (APP) to support the practice is just a first step. Getting these additional personnel up to speed means an investment in education and fostering good working relationships with NPs, PAs, and the staff’s physicians. Even more importantly, practices need to set realistic expectations on workload for these new hires.

“I tried to hire them, but I couldn’t keep them,” is a statement Christine A. Stamatos, DNP, ANP-C, hears all the time from rheumatologists. Oftentimes it’s because the practice saddles the new hire with 20 patients a day, said Dr. Stamatos, director of the Fibromyalgia Wellness Center within the division of rheumatology at Northwell Health in Huntington, New York. She is also an assistant professor at Hofstra Northwell School of Graduate Nursing and Physician Assistant Studies in Hempstead, New York.
“Twenty patients a day is too much,” Dr. Stamatos said. Overload someone, and they won’t stay. Offer them the support, mentoring, and tools they need to practice in their setting — and they will.
Why the Profession Needs APPs
Rheumatology is a much smaller specialty than most, with only a set number of rheumatologists in the field that can provide care to patients. A growing shortage is also looming. Reports from the American College of Rheumatology have projected troubling shortfalls in rheumatologists over the next decade in all regions of the United States.
Many of them aging into retirement “poses a significant issue on being able to continue providing care for the population that experiences the rheumatic disease,” said Ms. Yonker, a director of the National Organization of Rheumatology Management (NORM), a forum that promotes education and advocacy for rheumatology practice managers. People are also living longer, which means more patients are developing arthritis and autoimmune diseases.
Julia M. Swafford, PA-C, a rheumatology physician assistant in Battle Creek, Michigan, sees many advantages of hiring NPs and PAs, and not just from a financial perspective.

Salaries for PAs and NPs aren’t as high and they’re also more accessible than a rheumatologist. “You could train an NP or PA a lot quicker during that same time frame it would take to find a new rheumatology provider,” she offered. And while they may not be as experienced as rheumatologists, “you can kind of mold me on how you like to practice, what medications you may like to use, how you like to treat your patients,” Ms. Swafford said.
Hiring Someone With Experience
Recruiting and retaining APPs is not without its challenges.
Finding individuals compatible with this specialty isn’t easy, noted Mark Box, MD, medical director of Carondelet Rheumatology in Kansas City, Missouri. Ideally, APPs should be inquisitive, compassionate, and ready to learn. “Rheumatology is a cognitive specialty where you have to fit many pieces together. You need an APP who wants to embrace that,” he said.
The profession isn’t that “sexy” either, noted Katie Taylor, Carondelet’s practice manager. Patients are often in head-to-toe pain, and miserable. Many have been to other specialists without answers to their questions. For these reasons, rheumatology can be a hard sell for some PAs and NPs.

Nurse practitioners aren’t always comfortable with administering things such as controlled medications, for example. “It’s a hard patient population, and it’s a specialty of exclusion. You’ve got to be really smart to understand our diseases and our processes and our drugs,” Ms. Taylor said. In other words, it’s a difficult environment for an NP to walk into if their previous experience has been limited to upper respiratory issues and urinary tract infections in the primary care setting.
When hiring an APP, rheumatologists should look for someone who demonstrates an interest in lifelong learning, because the field is changing every day. They should exhibit good scores in educational training and have experience working in an emergency department or another field that translates well into rheumatology such as critical care, immunology, hematology, and orthopedics, she said.
Carondelet Rheumatology was specifically looking for an NP with rheumatology experience to support Dr. Box’s solo practice.
He was facing enormous pressure to be in the office every single day of the week. The practice had to cancel patients for its infusion suite on a regular basis when he was out of the office, Ms. Taylor said. “We couldn’t see new patients, and he wasn’t able to touch as many patients as he wanted to. The doctor takes the oath of touching as many in your community as possible, and you’re limited when you’re a one-man show.”
The practice eventually found an NP who already knew how to do joint injections. “We started her with easier diagnoses for things like osteoporosis and gout. She had an orthopedic background, so she was familiar with some of those diseases,” she said.
Even so, she often leaves with questions every day. “It’s a commitment for her to understand and learn so much,” Ms. Taylor said.
New hires will need support from the practice to get comfortable with rheumatology, Dr. Stamatos said. Responsibility should come in gradual steps.
Instead of loading an NP with 20 patients a day, 2 or 3 patients in the first quarter, eventually graduating to 6-8 patients is a more realistic expectation, Dr. Stamatos advised.
Shadowing the Physician
Partnerships with physicians is a critical component to this onboarding process.
A nurse practitioner recently hired at Dr. Stamatos’ practice works alongside a physician to manage a panel of 25 patients. “We make sure she gets her training, the resources she needs. I personally meet with her to make sure her education is moving forward, connecting her with radiology, pulmonary, hematology,” and other areas of the practice relevant to her training, she added.
The NP also attends weekly grand rounds and case conferences with the fellows. This is the type of well-rounded support any APP needs, she stressed. “Without proper training, you lose people.”
At Sarasota Arthritis Center, NPs help cover the suites but also get assigned to specific physicians so that they can familiarize themselves with that physician’s panel of patients.
“When we start an APP, they shadow for about twice as long as a new physician would. Usually, they’re shadowing for about 6 weeks, just kind of learning the space. There’s a lot of nurse practitioners or PAs who may not have prior rheumatology experience, so we’re essentially training them from the ground up on rheumatology,” Ms. Yonker said.
Pairing them with one provider often directs what type of disease state they focus on, she continued. This dynamic relationship helps guide decisions on whether to include these NPs in the care of patients with more complex diseases.
At least in her practice, the NPs do not see any new patients. They are simply part of the larger care team. “That’s kind of how we present it to our patients, and it makes them feel more comfortable just because they know that they’re not necessarily being handed off to somebody — that the doctor is still overseeing their care,” Ms. Yonker said.
At the same time, the NPs know that they’re supported, that they too have access to tools and mentorship if they need it, she added.
The new NP at Carondelet Rheumatology piggybacked on the doctor’s schedule for 3 months, slowly taking on infusion patients so she could get familiar with their diseases and respective drugs. Eventually, she got her own schedule and was able to take on new patients.
It’s a team effort, Ms. Taylor noted. The NP does the preliminary workup and then the physician comes in and greets the new patient. Together, they develop a follow-up plan for the patient.
Education Resources for Practices
In the case of Dr. Box’s one-physician practice, he was looking for an NP who was willing to be independent and cover things in his absence. “The training has to be there to accomplish that,” said Dr. Box, who likened the training of APPs to a medical residency.
Encouraging them to ask questions, do continuing medical education online and outside reading, are important steps, he added.
In a recent editorial, rheumatologists Eli M. Miloslavsky, MD, and Bethany Marston, MD, offered some strategies for better prepping the APP workforce to meet the demands of rheumatology practices. “Consideration should be given to formal curricula or training programs to help APPs achieve both competence and confidence in treating rheumatologic conditions,” they offered, suggesting an online curriculum developed by the ACR for such a purpose. Fellowship training should also focus on working effectively with APPs, they added.
“Finally, incorporating APPs more effectively into rheumatology professional societies and supporting practices in hiring and training APPs will all be important steps in addressing the rheumatology workforce shortage,” Dr. Miloslavsky and Dr. Marston wrote.
Ms. Yonker said all her APPs take various courses that the ACR and other organizations provide for rheumatology-specific, midlevel positions. “We provide as much training as possible for them to feel comfortable in this space. They are set directly with a physician for a long time and then eventually go into their own space.”
In addition to ACR, the Rheumatology Nurses Society and the Association of Women in Rheumatology offer excellent online training resources for APPs, Ms. Yonker said. “Also, the Bone Health and Osteoporosis Foundation offers an osteoporosis fracture liaison certification which we put APPs through as well,” she added.
Rheumatology practices should also look into an important clinical training grant program from the Rheumatology Research Foundation, Dr. Stamatos advised.
To date, they have “funded almost everyone that applies,” she said. Each grantee receives $25,000 to support training and education involved in onboarding an APP to a rheumatology practice. The money covers attendance at a live rheumatology conference, online educational programs, textbooks, and any society memberships while defraying the cost of training this employee. To increase awareness of the program, the foundation has since expanded the number of available submission dates and the number of grant awardees per year. Currently, the application deadlines for the grants are December 1 and March 1.
For her own health system, Dr. Stamatos has been working on a rheumatology fellowship program for APPs. Through simulation labs, leadership exercises, and other activities, these APPs will learn how to transition from being a new provider to someone who can become part of a practice, she said.
APPs themselves can also get proactive in this learning cycle, Ms. Swafford said. In her view, both APPs and rheumatologists should be conducting didactic lectures and organizing elective rotations with medical students to get them excited about the field. This would establish a good education base that would encourage PAs and NPs to choose rheumatology.
“That’s a huge thing that’s probably missing,” Ms. Swafford said.
Buy-in From the Doctor
No recruitment effort is going to work if the rheumatologists in the practice aren’t committed to the model of having an APP, Ms. Yonker said. “Everybody wants to know their purpose in their company and that they’re valued and they’re needed. And so, I think a pitfall would be if your rheumatologist is not sold on the model of expanding the care team. Because this takes work on behalf of the doctor.”
Rheumatologists are very busy, so it’s a hard sell for them to take time out of their busy clinics to train somebody to do a good job taking care of their patients, Ms. Taylor agreed. “I think that we need the physicians that have had success with this and allow them to coach the physicians that are still resistant.”
In his small practice, Dr. Box has encouraged his NP to assist with practice improvements, working with the office manager. These workers are providers and need to be treated as such, he said. “They need to feel like they contribute to the practice more than just grinding through patients.”
Peer support is another successful ingredient for these workers. Ms. Taylor’s NP finds the time to commiserate with her fellow nurse practitioners — other rheumatology nurses who are also learning the ropes. Rheumatologists are smart, and they can be very intimidating, Ms. Taylor said. In their small office, the rheumatologist is her only peer.
“She likes to get out and sort of integrate with other nurse practitioners that are learning too.”
When APPs Make a Difference
Practices that take on APPs are reporting positive metrics — mainly, shorter wait times for patients. Ms. Yonker’s physicians have been able to add on one to two new patients a day. Wait times have since dwindled from a 5-month to a 3-month wait with the addition of the NPs. “Three months is still long, but we’re working on getting it to that ideal 6-week wait period, which we’re hoping we can accomplish. So we’re able to get more new patients in for sure,” she said.
Prior to hiring an NP, Ms. Taylor’s practice had to defer acceptances for new patients by at least a year. Now, they’re able to accept about half of all new patient referrals. With the NP on board, “We can get them in within 30 days,” she said.
Sometimes, an APP will go beyond their scope of work to make a difference and better support patients.
Patients with rheumatic and osteopathic conditions are often underdiagnosed in the primary care space. As a result, they are not treated as often as they should be. Seeing a need for specialty care, Ms. Swafford took action.
She currently runs the only bone health clinic in southwest Michigan, coordinating with rheumatologists, NPs, urgent care, hospitalists, and interventional radiologists to attend to these patients more quickly and reduce wait times for care. Specialists will flag things such as nontraumatic hip fractures and vertebral fractures and refer them to Ms. Swafford’s clinic, which is part of Bronson Rheumatology Specialists.
The clinic gets quite a few referrals, and the practice is growing. “Usually, they don’t take as long as a rheumatology referral for a workup, so we can see them a little bit quicker,” usually within 3 weeks, she added.
APPs have an opportunity to make their mark in rheumatology at a time when the profession is experiencing significant gaps in care, Ms. Swafford continued. “Unless we find a way to fill that niche, we’re going to be in a world of trouble in the next 10, 20 years.”
None of the sources reported any disclosures or conflicts of interest.
Once considered a luxury, hiring a nurse, nurse practitioner, or physician assistant is becoming a necessity in many rheumatology practices.
Seeing the wait lists pile up in her Florida practice, Stacy Yonker, MBA, chief executive officer of Sarasota Arthritis Center, knew she had to make some changes. “Everyone’s aging in the boomer generations. Particularly in Florida, we have a lot of people who retire here. In the more southern demographics, it is a very difficult challenge for practices to get new patients in,” she said.
Ms. Yonker is in the process of hiring several nurse practitioners (NPs) to assist in the clinics and infusion suites, lightening the load for the practice’s 11 rheumatologists.
Hiring an advanced practice provider (APP) to support the practice is just a first step. Getting these additional personnel up to speed means an investment in education and fostering good working relationships with NPs, PAs, and the staff’s physicians. Even more importantly, practices need to set realistic expectations on workload for these new hires.
“I tried to hire them, but I couldn’t keep them,” is a statement Christine A. Stamatos, DNP, ANP-C, hears all the time from rheumatologists. Oftentimes it’s because the practice saddles the new hire with 20 patients a day, said Dr. Stamatos, director of the Fibromyalgia Wellness Center within the division of rheumatology at Northwell Health in Huntington, New York. She is also an assistant professor at Hofstra Northwell School of Graduate Nursing and Physician Assistant Studies in Hempstead, New York.
“Twenty patients a day is too much,” Dr. Stamatos said. Overload someone, and they won’t stay. Offer them the support, mentoring, and tools they need to practice in their setting — and they will.
Why the Profession Needs APPs
Rheumatology is a much smaller specialty than most, with only a set number of rheumatologists in the field that can provide care to patients. A growing shortage is also looming. Reports from the American College of Rheumatology have projected troubling shortfalls in rheumatologists over the next decade in all regions of the United States.
Many of them aging into retirement “poses a significant issue on being able to continue providing care for the population that experiences the rheumatic disease,” said Ms. Yonker, a director of the National Organization of Rheumatology Management (NORM), a forum that promotes education and advocacy for rheumatology practice managers. People are also living longer, which means more patients are developing arthritis and autoimmune diseases.
Julia M. Swafford, PA-C, a rheumatology physician assistant in Battle Creek, Michigan, sees many advantages of hiring NPs and PAs, and not just from a financial perspective.
Salaries for PAs and NPs aren’t as high and they’re also more accessible than a rheumatologist. “You could train an NP or PA a lot quicker during that same time frame it would take to find a new rheumatology provider,” she offered. And while they may not be as experienced as rheumatologists, “you can kind of mold me on how you like to practice, what medications you may like to use, how you like to treat your patients,” Ms. Swafford said.
Hiring Someone With Experience
Recruiting and retaining APPs is not without its challenges.
Finding individuals compatible with this specialty isn’t easy, noted Mark Box, MD, medical director of Carondelet Rheumatology in Kansas City, Missouri. Ideally, APPs should be inquisitive, compassionate, and ready to learn. “Rheumatology is a cognitive specialty where you have to fit many pieces together. You need an APP who wants to embrace that,” he said.
The profession isn’t that “sexy” either, noted Katie Taylor, Carondelet’s practice manager. Patients are often in head-to-toe pain, and miserable. Many have been to other specialists without answers to their questions. For these reasons, rheumatology can be a hard sell for some PAs and NPs.
Nurse practitioners aren’t always comfortable with administering things such as controlled medications, for example. “It’s a hard patient population, and it’s a specialty of exclusion. You’ve got to be really smart to understand our diseases and our processes and our drugs,” Ms. Taylor said. In other words, it’s a difficult environment for an NP to walk into if their previous experience has been limited to upper respiratory issues and urinary tract infections in the primary care setting.
When hiring an APP, rheumatologists should look for someone who demonstrates an interest in lifelong learning, because the field is changing every day. They should exhibit good scores in educational training and have experience working in an emergency department or another field that translates well into rheumatology such as critical care, immunology, hematology, and orthopedics, she said.
Carondelet Rheumatology was specifically looking for an NP with rheumatology experience to support Dr. Box’s solo practice.
He was facing enormous pressure to be in the office every single day of the week. The practice had to cancel patients for its infusion suite on a regular basis when he was out of the office, Ms. Taylor said. “We couldn’t see new patients, and he wasn’t able to touch as many patients as he wanted to. The doctor takes the oath of touching as many in your community as possible, and you’re limited when you’re a one-man show.”
The practice eventually found an NP who already knew how to do joint injections. “We started her with easier diagnoses for things like osteoporosis and gout. She had an orthopedic background, so she was familiar with some of those diseases,” she said.
Even so, she often leaves with questions every day. “It’s a commitment for her to understand and learn so much,” Ms. Taylor said.
New hires will need support from the practice to get comfortable with rheumatology, Dr. Stamatos said. Responsibility should come in gradual steps.
Instead of loading an NP with 20 patients a day, 2 or 3 patients in the first quarter, eventually graduating to 6-8 patients is a more realistic expectation, Dr. Stamatos advised.
Shadowing the Physician
Partnerships with physicians is a critical component to this onboarding process.
A nurse practitioner recently hired at Dr. Stamatos’ practice works alongside a physician to manage a panel of 25 patients. “We make sure she gets her training, the resources she needs. I personally meet with her to make sure her education is moving forward, connecting her with radiology, pulmonary, hematology,” and other areas of the practice relevant to her training, she added.
The NP also attends weekly grand rounds and case conferences with the fellows. This is the type of well-rounded support any APP needs, she stressed. “Without proper training, you lose people.”
At Sarasota Arthritis Center, NPs help cover the suites but also get assigned to specific physicians so that they can familiarize themselves with that physician’s panel of patients.
“When we start an APP, they shadow for about twice as long as a new physician would. Usually, they’re shadowing for about 6 weeks, just kind of learning the space. There’s a lot of nurse practitioners or PAs who may not have prior rheumatology experience, so we’re essentially training them from the ground up on rheumatology,” Ms. Yonker said.
Pairing them with one provider often directs what type of disease state they focus on, she continued. This dynamic relationship helps guide decisions on whether to include these NPs in the care of patients with more complex diseases.
At least in her practice, the NPs do not see any new patients. They are simply part of the larger care team. “That’s kind of how we present it to our patients, and it makes them feel more comfortable just because they know that they’re not necessarily being handed off to somebody — that the doctor is still overseeing their care,” Ms. Yonker said.
At the same time, the NPs know that they’re supported, that they too have access to tools and mentorship if they need it, she added.
The new NP at Carondelet Rheumatology piggybacked on the doctor’s schedule for 3 months, slowly taking on infusion patients so she could get familiar with their diseases and respective drugs. Eventually, she got her own schedule and was able to take on new patients.
It’s a team effort, Ms. Taylor noted. The NP does the preliminary workup and then the physician comes in and greets the new patient. Together, they develop a follow-up plan for the patient.
Education Resources for Practices
In the case of Dr. Box’s one-physician practice, he was looking for an NP who was willing to be independent and cover things in his absence. “The training has to be there to accomplish that,” said Dr. Box, who likened the training of APPs to a medical residency.
Encouraging them to ask questions, do continuing medical education online and outside reading, are important steps, he added.
In a recent editorial, rheumatologists Eli M. Miloslavsky, MD, and Bethany Marston, MD, offered some strategies for better prepping the APP workforce to meet the demands of rheumatology practices. “Consideration should be given to formal curricula or training programs to help APPs achieve both competence and confidence in treating rheumatologic conditions,” they offered, suggesting an online curriculum developed by the ACR for such a purpose. Fellowship training should also focus on working effectively with APPs, they added.
“Finally, incorporating APPs more effectively into rheumatology professional societies and supporting practices in hiring and training APPs will all be important steps in addressing the rheumatology workforce shortage,” Dr. Miloslavsky and Dr. Marston wrote.
Ms. Yonker said all her APPs take various courses that the ACR and other organizations provide for rheumatology-specific, midlevel positions. “We provide as much training as possible for them to feel comfortable in this space. They are set directly with a physician for a long time and then eventually go into their own space.”
In addition to ACR, the Rheumatology Nurses Society and the Association of Women in Rheumatology offer excellent online training resources for APPs, Ms. Yonker said. “Also, the Bone Health and Osteoporosis Foundation offers an osteoporosis fracture liaison certification which we put APPs through as well,” she added.
Rheumatology practices should also look into an important clinical training grant program from the Rheumatology Research Foundation, Dr. Stamatos advised.
To date, they have “funded almost everyone that applies,” she said. Each grantee receives $25,000 to support training and education involved in onboarding an APP to a rheumatology practice. The money covers attendance at a live rheumatology conference, online educational programs, textbooks, and any society memberships while defraying the cost of training this employee. To increase awareness of the program, the foundation has since expanded the number of available submission dates and the number of grant awardees per year. Currently, the application deadlines for the grants are December 1 and March 1.
For her own health system, Dr. Stamatos has been working on a rheumatology fellowship program for APPs. Through simulation labs, leadership exercises, and other activities, these APPs will learn how to transition from being a new provider to someone who can become part of a practice, she said.
APPs themselves can also get proactive in this learning cycle, Ms. Swafford said. In her view, both APPs and rheumatologists should be conducting didactic lectures and organizing elective rotations with medical students to get them excited about the field. This would establish a good education base that would encourage PAs and NPs to choose rheumatology.
“That’s a huge thing that’s probably missing,” Ms. Swafford said.
Buy-in From the Doctor
No recruitment effort is going to work if the rheumatologists in the practice aren’t committed to the model of having an APP, Ms. Yonker said. “Everybody wants to know their purpose in their company and that they’re valued and they’re needed. And so, I think a pitfall would be if your rheumatologist is not sold on the model of expanding the care team. Because this takes work on behalf of the doctor.”
Rheumatologists are very busy, so it’s a hard sell for them to take time out of their busy clinics to train somebody to do a good job taking care of their patients, Ms. Taylor agreed. “I think that we need the physicians that have had success with this and allow them to coach the physicians that are still resistant.”
In his small practice, Dr. Box has encouraged his NP to assist with practice improvements, working with the office manager. These workers are providers and need to be treated as such, he said. “They need to feel like they contribute to the practice more than just grinding through patients.”
Peer support is another successful ingredient for these workers. Ms. Taylor’s NP finds the time to commiserate with her fellow nurse practitioners — other rheumatology nurses who are also learning the ropes. Rheumatologists are smart, and they can be very intimidating, Ms. Taylor said. In their small office, the rheumatologist is her only peer.
“She likes to get out and sort of integrate with other nurse practitioners that are learning too.”
When APPs Make a Difference
Practices that take on APPs are reporting positive metrics — mainly, shorter wait times for patients. Ms. Yonker’s physicians have been able to add on one to two new patients a day. Wait times have since dwindled from a 5-month to a 3-month wait with the addition of the NPs. “Three months is still long, but we’re working on getting it to that ideal 6-week wait period, which we’re hoping we can accomplish. So we’re able to get more new patients in for sure,” she said.
Prior to hiring an NP, Ms. Taylor’s practice had to defer acceptances for new patients by at least a year. Now, they’re able to accept about half of all new patient referrals. With the NP on board, “We can get them in within 30 days,” she said.
Sometimes, an APP will go beyond their scope of work to make a difference and better support patients.
Patients with rheumatic and osteopathic conditions are often underdiagnosed in the primary care space. As a result, they are not treated as often as they should be. Seeing a need for specialty care, Ms. Swafford took action.
She currently runs the only bone health clinic in southwest Michigan, coordinating with rheumatologists, NPs, urgent care, hospitalists, and interventional radiologists to attend to these patients more quickly and reduce wait times for care. Specialists will flag things such as nontraumatic hip fractures and vertebral fractures and refer them to Ms. Swafford’s clinic, which is part of Bronson Rheumatology Specialists.
The clinic gets quite a few referrals, and the practice is growing. “Usually, they don’t take as long as a rheumatology referral for a workup, so we can see them a little bit quicker,” usually within 3 weeks, she added.
APPs have an opportunity to make their mark in rheumatology at a time when the profession is experiencing significant gaps in care, Ms. Swafford continued. “Unless we find a way to fill that niche, we’re going to be in a world of trouble in the next 10, 20 years.”
None of the sources reported any disclosures or conflicts of interest.
Once considered a luxury, hiring a nurse, nurse practitioner, or physician assistant is becoming a necessity in many rheumatology practices.
Seeing the wait lists pile up in her Florida practice, Stacy Yonker, MBA, chief executive officer of Sarasota Arthritis Center, knew she had to make some changes. “Everyone’s aging in the boomer generations. Particularly in Florida, we have a lot of people who retire here. In the more southern demographics, it is a very difficult challenge for practices to get new patients in,” she said.
Ms. Yonker is in the process of hiring several nurse practitioners (NPs) to assist in the clinics and infusion suites, lightening the load for the practice’s 11 rheumatologists.
Hiring an advanced practice provider (APP) to support the practice is just a first step. Getting these additional personnel up to speed means an investment in education and fostering good working relationships with NPs, PAs, and the staff’s physicians. Even more importantly, practices need to set realistic expectations on workload for these new hires.
“I tried to hire them, but I couldn’t keep them,” is a statement Christine A. Stamatos, DNP, ANP-C, hears all the time from rheumatologists. Oftentimes it’s because the practice saddles the new hire with 20 patients a day, said Dr. Stamatos, director of the Fibromyalgia Wellness Center within the division of rheumatology at Northwell Health in Huntington, New York. She is also an assistant professor at Hofstra Northwell School of Graduate Nursing and Physician Assistant Studies in Hempstead, New York.
“Twenty patients a day is too much,” Dr. Stamatos said. Overload someone, and they won’t stay. Offer them the support, mentoring, and tools they need to practice in their setting — and they will.
Why the Profession Needs APPs
Rheumatology is a much smaller specialty than most, with only a set number of rheumatologists in the field that can provide care to patients. A growing shortage is also looming. Reports from the American College of Rheumatology have projected troubling shortfalls in rheumatologists over the next decade in all regions of the United States.
Many of them aging into retirement “poses a significant issue on being able to continue providing care for the population that experiences the rheumatic disease,” said Ms. Yonker, a director of the National Organization of Rheumatology Management (NORM), a forum that promotes education and advocacy for rheumatology practice managers. People are also living longer, which means more patients are developing arthritis and autoimmune diseases.
Julia M. Swafford, PA-C, a rheumatology physician assistant in Battle Creek, Michigan, sees many advantages of hiring NPs and PAs, and not just from a financial perspective.
Salaries for PAs and NPs aren’t as high and they’re also more accessible than a rheumatologist. “You could train an NP or PA a lot quicker during that same time frame it would take to find a new rheumatology provider,” she offered. And while they may not be as experienced as rheumatologists, “you can kind of mold me on how you like to practice, what medications you may like to use, how you like to treat your patients,” Ms. Swafford said.
Hiring Someone With Experience
Recruiting and retaining APPs is not without its challenges.
Finding individuals compatible with this specialty isn’t easy, noted Mark Box, MD, medical director of Carondelet Rheumatology in Kansas City, Missouri. Ideally, APPs should be inquisitive, compassionate, and ready to learn. “Rheumatology is a cognitive specialty where you have to fit many pieces together. You need an APP who wants to embrace that,” he said.
The profession isn’t that “sexy” either, noted Katie Taylor, Carondelet’s practice manager. Patients are often in head-to-toe pain, and miserable. Many have been to other specialists without answers to their questions. For these reasons, rheumatology can be a hard sell for some PAs and NPs.
Nurse practitioners aren’t always comfortable with administering things such as controlled medications, for example. “It’s a hard patient population, and it’s a specialty of exclusion. You’ve got to be really smart to understand our diseases and our processes and our drugs,” Ms. Taylor said. In other words, it’s a difficult environment for an NP to walk into if their previous experience has been limited to upper respiratory issues and urinary tract infections in the primary care setting.
When hiring an APP, rheumatologists should look for someone who demonstrates an interest in lifelong learning, because the field is changing every day. They should exhibit good scores in educational training and have experience working in an emergency department or another field that translates well into rheumatology such as critical care, immunology, hematology, and orthopedics, she said.
Carondelet Rheumatology was specifically looking for an NP with rheumatology experience to support Dr. Box’s solo practice.
He was facing enormous pressure to be in the office every single day of the week. The practice had to cancel patients for its infusion suite on a regular basis when he was out of the office, Ms. Taylor said. “We couldn’t see new patients, and he wasn’t able to touch as many patients as he wanted to. The doctor takes the oath of touching as many in your community as possible, and you’re limited when you’re a one-man show.”
The practice eventually found an NP who already knew how to do joint injections. “We started her with easier diagnoses for things like osteoporosis and gout. She had an orthopedic background, so she was familiar with some of those diseases,” she said.
Even so, she often leaves with questions every day. “It’s a commitment for her to understand and learn so much,” Ms. Taylor said.
New hires will need support from the practice to get comfortable with rheumatology, Dr. Stamatos said. Responsibility should come in gradual steps.
Instead of loading an NP with 20 patients a day, 2 or 3 patients in the first quarter, eventually graduating to 6-8 patients is a more realistic expectation, Dr. Stamatos advised.
Shadowing the Physician
Partnerships with physicians is a critical component to this onboarding process.
A nurse practitioner recently hired at Dr. Stamatos’ practice works alongside a physician to manage a panel of 25 patients. “We make sure she gets her training, the resources she needs. I personally meet with her to make sure her education is moving forward, connecting her with radiology, pulmonary, hematology,” and other areas of the practice relevant to her training, she added.
The NP also attends weekly grand rounds and case conferences with the fellows. This is the type of well-rounded support any APP needs, she stressed. “Without proper training, you lose people.”
At Sarasota Arthritis Center, NPs help cover the suites but also get assigned to specific physicians so that they can familiarize themselves with that physician’s panel of patients.
“When we start an APP, they shadow for about twice as long as a new physician would. Usually, they’re shadowing for about 6 weeks, just kind of learning the space. There’s a lot of nurse practitioners or PAs who may not have prior rheumatology experience, so we’re essentially training them from the ground up on rheumatology,” Ms. Yonker said.
Pairing them with one provider often directs what type of disease state they focus on, she continued. This dynamic relationship helps guide decisions on whether to include these NPs in the care of patients with more complex diseases.
At least in her practice, the NPs do not see any new patients. They are simply part of the larger care team. “That’s kind of how we present it to our patients, and it makes them feel more comfortable just because they know that they’re not necessarily being handed off to somebody — that the doctor is still overseeing their care,” Ms. Yonker said.
At the same time, the NPs know that they’re supported, that they too have access to tools and mentorship if they need it, she added.
The new NP at Carondelet Rheumatology piggybacked on the doctor’s schedule for 3 months, slowly taking on infusion patients so she could get familiar with their diseases and respective drugs. Eventually, she got her own schedule and was able to take on new patients.
It’s a team effort, Ms. Taylor noted. The NP does the preliminary workup and then the physician comes in and greets the new patient. Together, they develop a follow-up plan for the patient.
Education Resources for Practices
In the case of Dr. Box’s one-physician practice, he was looking for an NP who was willing to be independent and cover things in his absence. “The training has to be there to accomplish that,” said Dr. Box, who likened the training of APPs to a medical residency.
Encouraging them to ask questions, do continuing medical education online and outside reading, are important steps, he added.
In a recent editorial, rheumatologists Eli M. Miloslavsky, MD, and Bethany Marston, MD, offered some strategies for better prepping the APP workforce to meet the demands of rheumatology practices. “Consideration should be given to formal curricula or training programs to help APPs achieve both competence and confidence in treating rheumatologic conditions,” they offered, suggesting an online curriculum developed by the ACR for such a purpose. Fellowship training should also focus on working effectively with APPs, they added.
“Finally, incorporating APPs more effectively into rheumatology professional societies and supporting practices in hiring and training APPs will all be important steps in addressing the rheumatology workforce shortage,” Dr. Miloslavsky and Dr. Marston wrote.
Ms. Yonker said all her APPs take various courses that the ACR and other organizations provide for rheumatology-specific, midlevel positions. “We provide as much training as possible for them to feel comfortable in this space. They are set directly with a physician for a long time and then eventually go into their own space.”
In addition to ACR, the Rheumatology Nurses Society and the Association of Women in Rheumatology offer excellent online training resources for APPs, Ms. Yonker said. “Also, the Bone Health and Osteoporosis Foundation offers an osteoporosis fracture liaison certification which we put APPs through as well,” she added.
Rheumatology practices should also look into an important clinical training grant program from the Rheumatology Research Foundation, Dr. Stamatos advised.
To date, they have “funded almost everyone that applies,” she said. Each grantee receives $25,000 to support training and education involved in onboarding an APP to a rheumatology practice. The money covers attendance at a live rheumatology conference, online educational programs, textbooks, and any society memberships while defraying the cost of training this employee. To increase awareness of the program, the foundation has since expanded the number of available submission dates and the number of grant awardees per year. Currently, the application deadlines for the grants are December 1 and March 1.
For her own health system, Dr. Stamatos has been working on a rheumatology fellowship program for APPs. Through simulation labs, leadership exercises, and other activities, these APPs will learn how to transition from being a new provider to someone who can become part of a practice, she said.
APPs themselves can also get proactive in this learning cycle, Ms. Swafford said. In her view, both APPs and rheumatologists should be conducting didactic lectures and organizing elective rotations with medical students to get them excited about the field. This would establish a good education base that would encourage PAs and NPs to choose rheumatology.
“That’s a huge thing that’s probably missing,” Ms. Swafford said.
Buy-in From the Doctor
No recruitment effort is going to work if the rheumatologists in the practice aren’t committed to the model of having an APP, Ms. Yonker said. “Everybody wants to know their purpose in their company and that they’re valued and they’re needed. And so, I think a pitfall would be if your rheumatologist is not sold on the model of expanding the care team. Because this takes work on behalf of the doctor.”
Rheumatologists are very busy, so it’s a hard sell for them to take time out of their busy clinics to train somebody to do a good job taking care of their patients, Ms. Taylor agreed. “I think that we need the physicians that have had success with this and allow them to coach the physicians that are still resistant.”
In his small practice, Dr. Box has encouraged his NP to assist with practice improvements, working with the office manager. These workers are providers and need to be treated as such, he said. “They need to feel like they contribute to the practice more than just grinding through patients.”
Peer support is another successful ingredient for these workers. Ms. Taylor’s NP finds the time to commiserate with her fellow nurse practitioners — other rheumatology nurses who are also learning the ropes. Rheumatologists are smart, and they can be very intimidating, Ms. Taylor said. In their small office, the rheumatologist is her only peer.
“She likes to get out and sort of integrate with other nurse practitioners that are learning too.”
When APPs Make a Difference
Practices that take on APPs are reporting positive metrics — mainly, shorter wait times for patients. Ms. Yonker’s physicians have been able to add on one to two new patients a day. Wait times have since dwindled from a 5-month to a 3-month wait with the addition of the NPs. “Three months is still long, but we’re working on getting it to that ideal 6-week wait period, which we’re hoping we can accomplish. So we’re able to get more new patients in for sure,” she said.
Prior to hiring an NP, Ms. Taylor’s practice had to defer acceptances for new patients by at least a year. Now, they’re able to accept about half of all new patient referrals. With the NP on board, “We can get them in within 30 days,” she said.
Sometimes, an APP will go beyond their scope of work to make a difference and better support patients.
Patients with rheumatic and osteopathic conditions are often underdiagnosed in the primary care space. As a result, they are not treated as often as they should be. Seeing a need for specialty care, Ms. Swafford took action.
She currently runs the only bone health clinic in southwest Michigan, coordinating with rheumatologists, NPs, urgent care, hospitalists, and interventional radiologists to attend to these patients more quickly and reduce wait times for care. Specialists will flag things such as nontraumatic hip fractures and vertebral fractures and refer them to Ms. Swafford’s clinic, which is part of Bronson Rheumatology Specialists.
The clinic gets quite a few referrals, and the practice is growing. “Usually, they don’t take as long as a rheumatology referral for a workup, so we can see them a little bit quicker,” usually within 3 weeks, she added.
APPs have an opportunity to make their mark in rheumatology at a time when the profession is experiencing significant gaps in care, Ms. Swafford continued. “Unless we find a way to fill that niche, we’re going to be in a world of trouble in the next 10, 20 years.”
None of the sources reported any disclosures or conflicts of interest.
Smoking Associated With Increased Risk for Hair Loss Among Men
, according to a new study.
In addition, the odds of developing AGA are higher among those who smoke at least 10 cigarettes per day than among those who smoke less, the study authors found.
“Men who smoke are more likely to develop and experience progression of male pattern hair loss,” lead author Aditya Gupta, MD, PhD, professor of medicine at the University of Toronto, Toronto, and director of clinical research at Mediprobe Research Inc., London, Ontario, Canada, told this news organization.
“Our patients with male pattern baldness need to be educated about the negative effects of smoking, given that this condition can have a profound negative psychological impact on those who suffer from it,” he said.
The study was published online in the Journal of Cosmetic Dermatology.
Analyzing Smoking’s Effects
Smoking generally has been accepted as a risk factor for the development and progression of AGA or the most common form of hair loss. The research evidence on this association has been inconsistent, however, the authors wrote.
The investigators conducted a review and meta-analysis of eight observational studies to understand the links between smoking and AGA. Ever-smokers were defined as current and former smokers.
Overall, based on six studies, men who have ever smoked are 1.8 times more likely (P < .05) to develop AGA.
Based on two studies, men who smoke 10 or more cigarettes daily are about twice as likely (P < .05) to develop AGA than those who smoke up to 10 cigarettes per day.
Based on four studies, ever smoking is associated with 1.3 times higher odds of AGA progressing from mild (ie, Norwood-Hamilton stages I-III) to more severe (stages IV-VII) than among those who have never smoked.
Based on two studies, there’s no association between AGA progression and smoking intensity (as defined as smoking up to 20 cigarettes daily vs smoking 20 or more cigarettes per day).
“Though our pooled analysis found no significant association between smoking intensity and severity of male AGA, a positive correlation may exist and be detected through an analysis that is statistically better powered,” said Dr. Gupta.
The investigators noted the limitations of their analysis, such as its reliance on observational studies and its lack of data about nicotine levels, smoking intensity, and smoking cessation among study participants.
Additional studies are needed to better understand the links between smoking and hair loss, said Dr. Gupta, as well as the effects of smoking cessation.
Improving Practice and Research
Commenting on the findings for this news organization, Arash Babadjouni, MD, a dermatologist at Midwestern University, Glendale, Arizona, said, “Smoking is not only a preventable cause of significant systemic disease but also affects the follicular growth cycle and fiber pigmentation. The prevalence of hair loss and premature hair graying is higher in smokers than nonsmokers.”
Dr. Babadjouni, who wasn’t involved with this study, has researched the associations between smoking and hair loss and premature hair graying.
“Evidence of this association can be used to clinically promote smoking cessation and emphasize the consequences of smoking on hair,” he said. “Smoking status should be assessed in patients who are presenting to their dermatologist and physicians alike for evaluation of alopecia and premature hair graying.”
The study was conducted without outside funding, and the authors declared no conflicts of interest. Dr. Babadjouni reported no relevant disclosures.
A version of this article appeared on Medscape.com.
, according to a new study.
In addition, the odds of developing AGA are higher among those who smoke at least 10 cigarettes per day than among those who smoke less, the study authors found.
“Men who smoke are more likely to develop and experience progression of male pattern hair loss,” lead author Aditya Gupta, MD, PhD, professor of medicine at the University of Toronto, Toronto, and director of clinical research at Mediprobe Research Inc., London, Ontario, Canada, told this news organization.
“Our patients with male pattern baldness need to be educated about the negative effects of smoking, given that this condition can have a profound negative psychological impact on those who suffer from it,” he said.
The study was published online in the Journal of Cosmetic Dermatology.
Analyzing Smoking’s Effects
Smoking generally has been accepted as a risk factor for the development and progression of AGA or the most common form of hair loss. The research evidence on this association has been inconsistent, however, the authors wrote.
The investigators conducted a review and meta-analysis of eight observational studies to understand the links between smoking and AGA. Ever-smokers were defined as current and former smokers.
Overall, based on six studies, men who have ever smoked are 1.8 times more likely (P < .05) to develop AGA.
Based on two studies, men who smoke 10 or more cigarettes daily are about twice as likely (P < .05) to develop AGA than those who smoke up to 10 cigarettes per day.
Based on four studies, ever smoking is associated with 1.3 times higher odds of AGA progressing from mild (ie, Norwood-Hamilton stages I-III) to more severe (stages IV-VII) than among those who have never smoked.
Based on two studies, there’s no association between AGA progression and smoking intensity (as defined as smoking up to 20 cigarettes daily vs smoking 20 or more cigarettes per day).
“Though our pooled analysis found no significant association between smoking intensity and severity of male AGA, a positive correlation may exist and be detected through an analysis that is statistically better powered,” said Dr. Gupta.
The investigators noted the limitations of their analysis, such as its reliance on observational studies and its lack of data about nicotine levels, smoking intensity, and smoking cessation among study participants.
Additional studies are needed to better understand the links between smoking and hair loss, said Dr. Gupta, as well as the effects of smoking cessation.
Improving Practice and Research
Commenting on the findings for this news organization, Arash Babadjouni, MD, a dermatologist at Midwestern University, Glendale, Arizona, said, “Smoking is not only a preventable cause of significant systemic disease but also affects the follicular growth cycle and fiber pigmentation. The prevalence of hair loss and premature hair graying is higher in smokers than nonsmokers.”
Dr. Babadjouni, who wasn’t involved with this study, has researched the associations between smoking and hair loss and premature hair graying.
“Evidence of this association can be used to clinically promote smoking cessation and emphasize the consequences of smoking on hair,” he said. “Smoking status should be assessed in patients who are presenting to their dermatologist and physicians alike for evaluation of alopecia and premature hair graying.”
The study was conducted without outside funding, and the authors declared no conflicts of interest. Dr. Babadjouni reported no relevant disclosures.
A version of this article appeared on Medscape.com.
, according to a new study.
In addition, the odds of developing AGA are higher among those who smoke at least 10 cigarettes per day than among those who smoke less, the study authors found.
“Men who smoke are more likely to develop and experience progression of male pattern hair loss,” lead author Aditya Gupta, MD, PhD, professor of medicine at the University of Toronto, Toronto, and director of clinical research at Mediprobe Research Inc., London, Ontario, Canada, told this news organization.
“Our patients with male pattern baldness need to be educated about the negative effects of smoking, given that this condition can have a profound negative psychological impact on those who suffer from it,” he said.
The study was published online in the Journal of Cosmetic Dermatology.
Analyzing Smoking’s Effects
Smoking generally has been accepted as a risk factor for the development and progression of AGA or the most common form of hair loss. The research evidence on this association has been inconsistent, however, the authors wrote.
The investigators conducted a review and meta-analysis of eight observational studies to understand the links between smoking and AGA. Ever-smokers were defined as current and former smokers.
Overall, based on six studies, men who have ever smoked are 1.8 times more likely (P < .05) to develop AGA.
Based on two studies, men who smoke 10 or more cigarettes daily are about twice as likely (P < .05) to develop AGA than those who smoke up to 10 cigarettes per day.
Based on four studies, ever smoking is associated with 1.3 times higher odds of AGA progressing from mild (ie, Norwood-Hamilton stages I-III) to more severe (stages IV-VII) than among those who have never smoked.
Based on two studies, there’s no association between AGA progression and smoking intensity (as defined as smoking up to 20 cigarettes daily vs smoking 20 or more cigarettes per day).
“Though our pooled analysis found no significant association between smoking intensity and severity of male AGA, a positive correlation may exist and be detected through an analysis that is statistically better powered,” said Dr. Gupta.
The investigators noted the limitations of their analysis, such as its reliance on observational studies and its lack of data about nicotine levels, smoking intensity, and smoking cessation among study participants.
Additional studies are needed to better understand the links between smoking and hair loss, said Dr. Gupta, as well as the effects of smoking cessation.
Improving Practice and Research
Commenting on the findings for this news organization, Arash Babadjouni, MD, a dermatologist at Midwestern University, Glendale, Arizona, said, “Smoking is not only a preventable cause of significant systemic disease but also affects the follicular growth cycle and fiber pigmentation. The prevalence of hair loss and premature hair graying is higher in smokers than nonsmokers.”
Dr. Babadjouni, who wasn’t involved with this study, has researched the associations between smoking and hair loss and premature hair graying.
“Evidence of this association can be used to clinically promote smoking cessation and emphasize the consequences of smoking on hair,” he said. “Smoking status should be assessed in patients who are presenting to their dermatologist and physicians alike for evaluation of alopecia and premature hair graying.”
The study was conducted without outside funding, and the authors declared no conflicts of interest. Dr. Babadjouni reported no relevant disclosures.
A version of this article appeared on Medscape.com.
FROM THE JOURNAL OF COSMETIC DERMATOLOGY
How much would you bet on a diagnosis?
“You have psoriasis,” I say all the time. I mean it when I say it, of course. But I don’t always to the same degree. Sometimes I’m trying to say, “You probably have psoriasis.” Other times I mean, “You most definitely have psoriasis.” I rarely use those terms though.
One 36-year-old man with a flaky scalp and scaly elbows wasn’t satisfied with my assessment. His dad has psoriasis. So does his older brother. He was in to see me to find out if he had psoriasis too. “Probably” was what I gave him. He pushed back, “What percent chance?” That’s a good question — must be an engineer. I’m unsure.

With the exception of the poker players, our species is notoriously bad at probabilities. We’re wired to notice the significance of events, but terrible at understanding their likelihood. This is salient in lottery ticket holders and some NFL offensive coordinators who persist despite very long odds of things working out. It’s also reflected in the language we use. Rarely do we say, there’s a sixty percent chance something will happen. Rather, we say, “it’s likely.” There are two problems here. One, we often misjudge the actual probability of something occurring and two, the terms we use are subjective and differences in interpretation can lead to misunderstandings.
Let’s take a look. A 55-year-old man with a chronic eczematous rash on his trunk and extremities is getting worse despite dupilumab. He recently had night sweats. Do you think he has atopic dermatitis or cutaneous T-cell lymphoma? If you had to place a $100 bet, would you change your answer? Immanuel Kant thinks you would. In his “Critique of Pure Reason,” the German philosopher proposes that betting helps clarify the mind, an antidote to brashness. The example Kant uses is of a physician who observes a patient and concludes he has phthisis (tuberculosis), but we really don’t know if the physician is confident. Kant proposes that if he had to bet on his conclusion, then we’d have insight into just how convinced he is of phthisis. So, what’s your bet?
If you’re a bad poker player, then you might bet he has cutaneous T-cell lymphoma. However, not having any additional information, the smart call is atopic dermatitis, which has a base rate 1000-fold higher than CTCL. It is therefore more probable to be eczema even in a case that worsens despite dupilumab or with recent night sweats, both of which could be a result of common variables such as weather and COVID. Failure to account for the base rate is a mistake we physicians sometimes make. Economists rarely do. Try to think like one before answering a likelihood question.
If you think about it, “probably” means something different even to me, depending on the situation. I might say I’ll probably go to Montana this summer and I’ll probably retire at 65. The actual likelihoods might be 95% and 70%. That’s a big difference. What about between probably and likely? Or possibly and maybe? Do they mean the same to you as to the person you’re speaking with? For much of the work we do, precise likelihoods aren’t critical. Yet, it can be important in decision making and in discussing probabilities, such as the risk of hepatitis on terbinafine or of melanoma recurrence after Mohs.
I told my patient “I say about a 70% chance you have psoriasis. I could do a biopsy today to confirm.” He thought for a second and asked, “What is the chance it’s psoriasis if the biopsy shows it?” “Eighty six percent,” I replied.
Seemed like a good bet to me.
Dr. Benabio is director of Healthcare Transformation and chief of dermatology at Kaiser Permanente San Diego. The opinions expressed in this column are his own and do not represent those of Kaiser Permanente. Dr. Benabio is @Dermdoc on X. Write to him at [email protected].
“You have psoriasis,” I say all the time. I mean it when I say it, of course. But I don’t always to the same degree. Sometimes I’m trying to say, “You probably have psoriasis.” Other times I mean, “You most definitely have psoriasis.” I rarely use those terms though.
One 36-year-old man with a flaky scalp and scaly elbows wasn’t satisfied with my assessment. His dad has psoriasis. So does his older brother. He was in to see me to find out if he had psoriasis too. “Probably” was what I gave him. He pushed back, “What percent chance?” That’s a good question — must be an engineer. I’m unsure.
With the exception of the poker players, our species is notoriously bad at probabilities. We’re wired to notice the significance of events, but terrible at understanding their likelihood. This is salient in lottery ticket holders and some NFL offensive coordinators who persist despite very long odds of things working out. It’s also reflected in the language we use. Rarely do we say, there’s a sixty percent chance something will happen. Rather, we say, “it’s likely.” There are two problems here. One, we often misjudge the actual probability of something occurring and two, the terms we use are subjective and differences in interpretation can lead to misunderstandings.
Let’s take a look. A 55-year-old man with a chronic eczematous rash on his trunk and extremities is getting worse despite dupilumab. He recently had night sweats. Do you think he has atopic dermatitis or cutaneous T-cell lymphoma? If you had to place a $100 bet, would you change your answer? Immanuel Kant thinks you would. In his “Critique of Pure Reason,” the German philosopher proposes that betting helps clarify the mind, an antidote to brashness. The example Kant uses is of a physician who observes a patient and concludes he has phthisis (tuberculosis), but we really don’t know if the physician is confident. Kant proposes that if he had to bet on his conclusion, then we’d have insight into just how convinced he is of phthisis. So, what’s your bet?
If you’re a bad poker player, then you might bet he has cutaneous T-cell lymphoma. However, not having any additional information, the smart call is atopic dermatitis, which has a base rate 1000-fold higher than CTCL. It is therefore more probable to be eczema even in a case that worsens despite dupilumab or with recent night sweats, both of which could be a result of common variables such as weather and COVID. Failure to account for the base rate is a mistake we physicians sometimes make. Economists rarely do. Try to think like one before answering a likelihood question.
If you think about it, “probably” means something different even to me, depending on the situation. I might say I’ll probably go to Montana this summer and I’ll probably retire at 65. The actual likelihoods might be 95% and 70%. That’s a big difference. What about between probably and likely? Or possibly and maybe? Do they mean the same to you as to the person you’re speaking with? For much of the work we do, precise likelihoods aren’t critical. Yet, it can be important in decision making and in discussing probabilities, such as the risk of hepatitis on terbinafine or of melanoma recurrence after Mohs.
I told my patient “I say about a 70% chance you have psoriasis. I could do a biopsy today to confirm.” He thought for a second and asked, “What is the chance it’s psoriasis if the biopsy shows it?” “Eighty six percent,” I replied.
Seemed like a good bet to me.
Dr. Benabio is director of Healthcare Transformation and chief of dermatology at Kaiser Permanente San Diego. The opinions expressed in this column are his own and do not represent those of Kaiser Permanente. Dr. Benabio is @Dermdoc on X. Write to him at [email protected].
“You have psoriasis,” I say all the time. I mean it when I say it, of course. But I don’t always to the same degree. Sometimes I’m trying to say, “You probably have psoriasis.” Other times I mean, “You most definitely have psoriasis.” I rarely use those terms though.
One 36-year-old man with a flaky scalp and scaly elbows wasn’t satisfied with my assessment. His dad has psoriasis. So does his older brother. He was in to see me to find out if he had psoriasis too. “Probably” was what I gave him. He pushed back, “What percent chance?” That’s a good question — must be an engineer. I’m unsure.
With the exception of the poker players, our species is notoriously bad at probabilities. We’re wired to notice the significance of events, but terrible at understanding their likelihood. This is salient in lottery ticket holders and some NFL offensive coordinators who persist despite very long odds of things working out. It’s also reflected in the language we use. Rarely do we say, there’s a sixty percent chance something will happen. Rather, we say, “it’s likely.” There are two problems here. One, we often misjudge the actual probability of something occurring and two, the terms we use are subjective and differences in interpretation can lead to misunderstandings.
Let’s take a look. A 55-year-old man with a chronic eczematous rash on his trunk and extremities is getting worse despite dupilumab. He recently had night sweats. Do you think he has atopic dermatitis or cutaneous T-cell lymphoma? If you had to place a $100 bet, would you change your answer? Immanuel Kant thinks you would. In his “Critique of Pure Reason,” the German philosopher proposes that betting helps clarify the mind, an antidote to brashness. The example Kant uses is of a physician who observes a patient and concludes he has phthisis (tuberculosis), but we really don’t know if the physician is confident. Kant proposes that if he had to bet on his conclusion, then we’d have insight into just how convinced he is of phthisis. So, what’s your bet?
If you’re a bad poker player, then you might bet he has cutaneous T-cell lymphoma. However, not having any additional information, the smart call is atopic dermatitis, which has a base rate 1000-fold higher than CTCL. It is therefore more probable to be eczema even in a case that worsens despite dupilumab or with recent night sweats, both of which could be a result of common variables such as weather and COVID. Failure to account for the base rate is a mistake we physicians sometimes make. Economists rarely do. Try to think like one before answering a likelihood question.
If you think about it, “probably” means something different even to me, depending on the situation. I might say I’ll probably go to Montana this summer and I’ll probably retire at 65. The actual likelihoods might be 95% and 70%. That’s a big difference. What about between probably and likely? Or possibly and maybe? Do they mean the same to you as to the person you’re speaking with? For much of the work we do, precise likelihoods aren’t critical. Yet, it can be important in decision making and in discussing probabilities, such as the risk of hepatitis on terbinafine or of melanoma recurrence after Mohs.
I told my patient “I say about a 70% chance you have psoriasis. I could do a biopsy today to confirm.” He thought for a second and asked, “What is the chance it’s psoriasis if the biopsy shows it?” “Eighty six percent,” I replied.
Seemed like a good bet to me.
Dr. Benabio is director of Healthcare Transformation and chief of dermatology at Kaiser Permanente San Diego. The opinions expressed in this column are his own and do not represent those of Kaiser Permanente. Dr. Benabio is @Dermdoc on X. Write to him at [email protected].