User login
How effective is desmopressin for primary nocturnal enuresis?
Desmopressin reduces the number of nights of primary noctural enuresis by at least 1 per week, and increases the likelihood of “cure” (defined as 14 consecutive dry nights) while treatment is continued (number needed to treat [NNT]=5–6) (strength of recommendation [SOR]: A, based on meta-analysis). Evidence suggests that the benefits of desmopressin are temporary, with a high relapse rate once treatment is discontinued (SOR: B). However, long-term therapy with occasional weaning attempts is a safe option (SOR: B). Evidence is inadequate to judge the relative efficacy of the nasal vs oral forms of desmopressin (SOR: C).
Evidence summary
Desmopressin is an analogue of the natural pituitary hormone vasopressin acetate. It produces an antidiuretic effect, resulting in increased reabsorption of water from the kidney, a reduced volume of more concentrated urine entering the bladder, and a reduced 24-hour urine production.1,2 Desmopressin is available in a nasal spray (10 μg/spray) and an oral tablet (0.2 mg), and is most often prescribed as 1 to 2 sprays per nostril or 1 to 3 tablets at bedtime, regardless of age or weight.1
A Cochrane review1 of 16 randomized controlled trials found nasal desmopressin to be better than placebo in reducing the number of wet nights per week (mean 1.34 fewer wet nights/week; 95% confidence interval, 1.11–1.57). Desmopressin at doses of 20 μg, 40 μg, and 60 μg similarly increased the likelihood of a cure (14 consecutive dry nights during treatment) in 3 trials reporting this outcome (relative risk for failure to achieve 14 dry nights with 20 μg=0.84; NNT for cure=5.6).3 No difference was found in cure rates after treatment was stopped. Data were insufficient to judge the effectiveness of the oral versus nasal route of desmopressin.1
One randomized controlled trial found a linear dose response for oral desmopressin in reducing wet nights. After 2 weeks of treatment, the number of wet nights was decreased by 27%, 30%, and 40% at doses of 0.2 mg, 0.4 mg, and 0.6 mg, respectively, compared with 10% with placebo.1
Snajderova and colleagues studied desmopressin as a long-term treatment for 55 children with primary nocturnal enuresis. Intranasal desmopressin was titrated upward until bedwetting stopped (7–21 μg; 89.1% responders); children in whom no response occurred to a maximum of 28 μg were excluded. Every 3 months, a weaning attempt was made; if relapse occurred, the previous successful dose was reinstated. At the end of each of the 3 years, the number of responders remained higher (72.7%, 70.9%, 61.6%) than the spontaneous cure rate of 15%.4
The Swedish Enuresis Trial (SWEET) demonstrated a similar outcome in an open-label study of 399 children.5
The main side effects of desmopressin are nasal discomfort, nose bleeds, headache, abdominal pain, rash, and (rare but serious) water intoxication. Restrict fluid to 240 mL (8 oz) on nights desmopressin is given.1
Recommendations from others
A University of California at San Diego Medical Group Guideline recommends using desmopressin for primary nocturnal enuresis in children aged >5 years when it occurs frequently and causes distress, as well as under specific circumstances, such as when a child shares a room or goes to camp, or a sleepover.
Therapy begins at 10 μg (1 nasal puff) each night, increasing weekly to a maximum of 40 μg. Younger children should be reassured, encouraged to limit fluids and void before bedtime, partake in the responsibility to change bedding, and be praised for dry nights.6
The American Academy of Pediatrics also emphasizes support and encouragement of the child, and reassurance that the problem will get better in time. For children aged 7 years, alarm systems or bladder-stretching exercises might help.7
David M. Bercaw, MD
Christiana Care Health System, Wilmington, Del
Primary nocturnal enuresis can be challenging for the primary care physician, frustrating for the patient’s parents, and embarrassing for the child. The physician’s role is to help the child and parents realize that almost all children eventually maintain nocturnal continence whether or not pharmacotherapy is used.
Nonpharmacologic interventions, such as behavioral modification (eg, use of a nocturnal conditioning alarm with a moisture sensor) may be more acceptable to families, at least as a first attempt at therapy. In my experience, however, many children sleep through these alarms.
The decision to use medication should be made by a well-informed and motivated child and their parents. They should understand the limitations and expectations of pharmacotherapy. The authors of this clinical inquiry have provided the physician with an excellent summary of the evidence for the efficacy of desmopressin.
Children with enuresis associated with sleep arousal disorder should theoretically respond to older forms of pharmacotherapy, such as imipramine. However, due to potential toxicity, many clinicians are reluctant to use tricyclic antidepressants in their patients. The efficacy and low toxicity of desmopressin makes it an attractive choice for pharmacotherapy in enuretic children.
1. Glazener CM, Evans JH. Desmopressin for nocturnal enuresis in children. Cochrane Database Syst Rev 2002;(3):CD002112.-
2. Hvistendahl GM, Rawashdeh YF, Kamperis K, Hansen MN, Rittig S, Djurhuus JC. The relationship between desmopressin treatment and voiding pattern in children. BJU Int 2002;89:917-922.
3. Schulman SL, Stokes A, Salzman PM. The efficacy and safety of oral desmopressin in children with primary nocturnal enuresis. J Urol 2001;166:2427-2431.
4. Snajderova M, Lehotska V, Kernova T, Kocnarova N, Archmanova E, Janda P, Lanska V. Desmopressin in a long-term treatment of children with primary nocturnal enuresis—a symptomatic therapy? Eur J Pediatr 2001;160:197-198.
5. Tullus K, Bergstrom R, Fosdal I, Winnergard I, Hjälmås K. Efficacy and safety during long-term treatment of primary monosyptomatic nocturnal enuresis with desmopressin. Swedish Enuresis Trial Group. Acta Paediatr 1999;88:1274-1278.
6. University of California at San Diego Medical Group. UCSD Outpatient Clinical Practice Guidelines. Enuresis (pediatric). San Diego, Calif: UCSD Healthcare; 1998. Available at: http://health.ucsd.edu/clinicalresources/clinres1.html. Accessed on June 12, 2003.
7. Medem Medical Library. Bed-wetting. Chicago, Ill: American Academy of Pediatrics, 2002. Available at: www.medem.com. Accessed on June 12, 2003.
Desmopressin reduces the number of nights of primary noctural enuresis by at least 1 per week, and increases the likelihood of “cure” (defined as 14 consecutive dry nights) while treatment is continued (number needed to treat [NNT]=5–6) (strength of recommendation [SOR]: A, based on meta-analysis). Evidence suggests that the benefits of desmopressin are temporary, with a high relapse rate once treatment is discontinued (SOR: B). However, long-term therapy with occasional weaning attempts is a safe option (SOR: B). Evidence is inadequate to judge the relative efficacy of the nasal vs oral forms of desmopressin (SOR: C).
Evidence summary
Desmopressin is an analogue of the natural pituitary hormone vasopressin acetate. It produces an antidiuretic effect, resulting in increased reabsorption of water from the kidney, a reduced volume of more concentrated urine entering the bladder, and a reduced 24-hour urine production.1,2 Desmopressin is available in a nasal spray (10 μg/spray) and an oral tablet (0.2 mg), and is most often prescribed as 1 to 2 sprays per nostril or 1 to 3 tablets at bedtime, regardless of age or weight.1
A Cochrane review1 of 16 randomized controlled trials found nasal desmopressin to be better than placebo in reducing the number of wet nights per week (mean 1.34 fewer wet nights/week; 95% confidence interval, 1.11–1.57). Desmopressin at doses of 20 μg, 40 μg, and 60 μg similarly increased the likelihood of a cure (14 consecutive dry nights during treatment) in 3 trials reporting this outcome (relative risk for failure to achieve 14 dry nights with 20 μg=0.84; NNT for cure=5.6).3 No difference was found in cure rates after treatment was stopped. Data were insufficient to judge the effectiveness of the oral versus nasal route of desmopressin.1
One randomized controlled trial found a linear dose response for oral desmopressin in reducing wet nights. After 2 weeks of treatment, the number of wet nights was decreased by 27%, 30%, and 40% at doses of 0.2 mg, 0.4 mg, and 0.6 mg, respectively, compared with 10% with placebo.1
Snajderova and colleagues studied desmopressin as a long-term treatment for 55 children with primary nocturnal enuresis. Intranasal desmopressin was titrated upward until bedwetting stopped (7–21 μg; 89.1% responders); children in whom no response occurred to a maximum of 28 μg were excluded. Every 3 months, a weaning attempt was made; if relapse occurred, the previous successful dose was reinstated. At the end of each of the 3 years, the number of responders remained higher (72.7%, 70.9%, 61.6%) than the spontaneous cure rate of 15%.4
The Swedish Enuresis Trial (SWEET) demonstrated a similar outcome in an open-label study of 399 children.5
The main side effects of desmopressin are nasal discomfort, nose bleeds, headache, abdominal pain, rash, and (rare but serious) water intoxication. Restrict fluid to 240 mL (8 oz) on nights desmopressin is given.1
Recommendations from others
A University of California at San Diego Medical Group Guideline recommends using desmopressin for primary nocturnal enuresis in children aged >5 years when it occurs frequently and causes distress, as well as under specific circumstances, such as when a child shares a room or goes to camp, or a sleepover.
Therapy begins at 10 μg (1 nasal puff) each night, increasing weekly to a maximum of 40 μg. Younger children should be reassured, encouraged to limit fluids and void before bedtime, partake in the responsibility to change bedding, and be praised for dry nights.6
The American Academy of Pediatrics also emphasizes support and encouragement of the child, and reassurance that the problem will get better in time. For children aged 7 years, alarm systems or bladder-stretching exercises might help.7
David M. Bercaw, MD
Christiana Care Health System, Wilmington, Del
Primary nocturnal enuresis can be challenging for the primary care physician, frustrating for the patient’s parents, and embarrassing for the child. The physician’s role is to help the child and parents realize that almost all children eventually maintain nocturnal continence whether or not pharmacotherapy is used.
Nonpharmacologic interventions, such as behavioral modification (eg, use of a nocturnal conditioning alarm with a moisture sensor) may be more acceptable to families, at least as a first attempt at therapy. In my experience, however, many children sleep through these alarms.
The decision to use medication should be made by a well-informed and motivated child and their parents. They should understand the limitations and expectations of pharmacotherapy. The authors of this clinical inquiry have provided the physician with an excellent summary of the evidence for the efficacy of desmopressin.
Children with enuresis associated with sleep arousal disorder should theoretically respond to older forms of pharmacotherapy, such as imipramine. However, due to potential toxicity, many clinicians are reluctant to use tricyclic antidepressants in their patients. The efficacy and low toxicity of desmopressin makes it an attractive choice for pharmacotherapy in enuretic children.
Desmopressin reduces the number of nights of primary noctural enuresis by at least 1 per week, and increases the likelihood of “cure” (defined as 14 consecutive dry nights) while treatment is continued (number needed to treat [NNT]=5–6) (strength of recommendation [SOR]: A, based on meta-analysis). Evidence suggests that the benefits of desmopressin are temporary, with a high relapse rate once treatment is discontinued (SOR: B). However, long-term therapy with occasional weaning attempts is a safe option (SOR: B). Evidence is inadequate to judge the relative efficacy of the nasal vs oral forms of desmopressin (SOR: C).
Evidence summary
Desmopressin is an analogue of the natural pituitary hormone vasopressin acetate. It produces an antidiuretic effect, resulting in increased reabsorption of water from the kidney, a reduced volume of more concentrated urine entering the bladder, and a reduced 24-hour urine production.1,2 Desmopressin is available in a nasal spray (10 μg/spray) and an oral tablet (0.2 mg), and is most often prescribed as 1 to 2 sprays per nostril or 1 to 3 tablets at bedtime, regardless of age or weight.1
A Cochrane review1 of 16 randomized controlled trials found nasal desmopressin to be better than placebo in reducing the number of wet nights per week (mean 1.34 fewer wet nights/week; 95% confidence interval, 1.11–1.57). Desmopressin at doses of 20 μg, 40 μg, and 60 μg similarly increased the likelihood of a cure (14 consecutive dry nights during treatment) in 3 trials reporting this outcome (relative risk for failure to achieve 14 dry nights with 20 μg=0.84; NNT for cure=5.6).3 No difference was found in cure rates after treatment was stopped. Data were insufficient to judge the effectiveness of the oral versus nasal route of desmopressin.1
One randomized controlled trial found a linear dose response for oral desmopressin in reducing wet nights. After 2 weeks of treatment, the number of wet nights was decreased by 27%, 30%, and 40% at doses of 0.2 mg, 0.4 mg, and 0.6 mg, respectively, compared with 10% with placebo.1
Snajderova and colleagues studied desmopressin as a long-term treatment for 55 children with primary nocturnal enuresis. Intranasal desmopressin was titrated upward until bedwetting stopped (7–21 μg; 89.1% responders); children in whom no response occurred to a maximum of 28 μg were excluded. Every 3 months, a weaning attempt was made; if relapse occurred, the previous successful dose was reinstated. At the end of each of the 3 years, the number of responders remained higher (72.7%, 70.9%, 61.6%) than the spontaneous cure rate of 15%.4
The Swedish Enuresis Trial (SWEET) demonstrated a similar outcome in an open-label study of 399 children.5
The main side effects of desmopressin are nasal discomfort, nose bleeds, headache, abdominal pain, rash, and (rare but serious) water intoxication. Restrict fluid to 240 mL (8 oz) on nights desmopressin is given.1
Recommendations from others
A University of California at San Diego Medical Group Guideline recommends using desmopressin for primary nocturnal enuresis in children aged >5 years when it occurs frequently and causes distress, as well as under specific circumstances, such as when a child shares a room or goes to camp, or a sleepover.
Therapy begins at 10 μg (1 nasal puff) each night, increasing weekly to a maximum of 40 μg. Younger children should be reassured, encouraged to limit fluids and void before bedtime, partake in the responsibility to change bedding, and be praised for dry nights.6
The American Academy of Pediatrics also emphasizes support and encouragement of the child, and reassurance that the problem will get better in time. For children aged 7 years, alarm systems or bladder-stretching exercises might help.7
David M. Bercaw, MD
Christiana Care Health System, Wilmington, Del
Primary nocturnal enuresis can be challenging for the primary care physician, frustrating for the patient’s parents, and embarrassing for the child. The physician’s role is to help the child and parents realize that almost all children eventually maintain nocturnal continence whether or not pharmacotherapy is used.
Nonpharmacologic interventions, such as behavioral modification (eg, use of a nocturnal conditioning alarm with a moisture sensor) may be more acceptable to families, at least as a first attempt at therapy. In my experience, however, many children sleep through these alarms.
The decision to use medication should be made by a well-informed and motivated child and their parents. They should understand the limitations and expectations of pharmacotherapy. The authors of this clinical inquiry have provided the physician with an excellent summary of the evidence for the efficacy of desmopressin.
Children with enuresis associated with sleep arousal disorder should theoretically respond to older forms of pharmacotherapy, such as imipramine. However, due to potential toxicity, many clinicians are reluctant to use tricyclic antidepressants in their patients. The efficacy and low toxicity of desmopressin makes it an attractive choice for pharmacotherapy in enuretic children.
1. Glazener CM, Evans JH. Desmopressin for nocturnal enuresis in children. Cochrane Database Syst Rev 2002;(3):CD002112.-
2. Hvistendahl GM, Rawashdeh YF, Kamperis K, Hansen MN, Rittig S, Djurhuus JC. The relationship between desmopressin treatment and voiding pattern in children. BJU Int 2002;89:917-922.
3. Schulman SL, Stokes A, Salzman PM. The efficacy and safety of oral desmopressin in children with primary nocturnal enuresis. J Urol 2001;166:2427-2431.
4. Snajderova M, Lehotska V, Kernova T, Kocnarova N, Archmanova E, Janda P, Lanska V. Desmopressin in a long-term treatment of children with primary nocturnal enuresis—a symptomatic therapy? Eur J Pediatr 2001;160:197-198.
5. Tullus K, Bergstrom R, Fosdal I, Winnergard I, Hjälmås K. Efficacy and safety during long-term treatment of primary monosyptomatic nocturnal enuresis with desmopressin. Swedish Enuresis Trial Group. Acta Paediatr 1999;88:1274-1278.
6. University of California at San Diego Medical Group. UCSD Outpatient Clinical Practice Guidelines. Enuresis (pediatric). San Diego, Calif: UCSD Healthcare; 1998. Available at: http://health.ucsd.edu/clinicalresources/clinres1.html. Accessed on June 12, 2003.
7. Medem Medical Library. Bed-wetting. Chicago, Ill: American Academy of Pediatrics, 2002. Available at: www.medem.com. Accessed on June 12, 2003.
1. Glazener CM, Evans JH. Desmopressin for nocturnal enuresis in children. Cochrane Database Syst Rev 2002;(3):CD002112.-
2. Hvistendahl GM, Rawashdeh YF, Kamperis K, Hansen MN, Rittig S, Djurhuus JC. The relationship between desmopressin treatment and voiding pattern in children. BJU Int 2002;89:917-922.
3. Schulman SL, Stokes A, Salzman PM. The efficacy and safety of oral desmopressin in children with primary nocturnal enuresis. J Urol 2001;166:2427-2431.
4. Snajderova M, Lehotska V, Kernova T, Kocnarova N, Archmanova E, Janda P, Lanska V. Desmopressin in a long-term treatment of children with primary nocturnal enuresis—a symptomatic therapy? Eur J Pediatr 2001;160:197-198.
5. Tullus K, Bergstrom R, Fosdal I, Winnergard I, Hjälmås K. Efficacy and safety during long-term treatment of primary monosyptomatic nocturnal enuresis with desmopressin. Swedish Enuresis Trial Group. Acta Paediatr 1999;88:1274-1278.
6. University of California at San Diego Medical Group. UCSD Outpatient Clinical Practice Guidelines. Enuresis (pediatric). San Diego, Calif: UCSD Healthcare; 1998. Available at: http://health.ucsd.edu/clinicalresources/clinres1.html. Accessed on June 12, 2003.
7. Medem Medical Library. Bed-wetting. Chicago, Ill: American Academy of Pediatrics, 2002. Available at: www.medem.com. Accessed on June 12, 2003.
Evidence-based answers from the Family Physicians Inquiries Network
Do imaging studies aid diagnosis of acute sinusitis?
Accurate diagnosis of acute sinusitis in both children and adults depends on the history and clinical examination of the patient. While the clinical signs and symptoms of acute sinusitis are often difficult to distinguish from viral upper respiratory infection,1,2 such an assessment remains the best approach to diagnosing acute sinusitis (strength of recommendation [SOR]: A). There is no role for imaging in the diagnosis of acute sinusitis. For patients who have persistent symptoms, or those for whom surgery is being considered, some guidelines suggest that coronal computed tomography (CT) scan of the paranasal sinuses be considered (SOR: C, expert opinion).
Evidence summary
Three recent evidence-based guidelines3,4,5 suggest that children and adults with acute sinusitis may benefit from treatment with antibiotics more than those with rhinitis. Clinicians must develop a strategy for accurately diagnosing sinusitis to make sound treatment decisions. In the absence of a clear diagnosis of acute sinusitis, antibiotics are very unlikely to improve symptoms and are, therefore, not indicated.
Clinical evaluation. Berg1 studied 150 patients with clinical diagnoses of sinusitis and found that 85% of them had positive sinus puncture. In a review of the 11 studies that met evidence-based inclusion criteria, Varonen6 concluded that clinical evaluation has a sensitivity of roughly 0.75, whereas radiographic methodologies have sensitivities >0.80. In a prospective trial and subsequent review of the literature, Lindbaek7,8,9 suggests that several key clinical signs and symptoms can provide a level of sensitivity that approaches that of CT or magnetic resonance imaging (MRI), while enhancing specificity:
- Purulent secretion reported as a symptom or found in the nasal cavity by the doctor
- Pain in the teeth
- Pain on bending forward (inconsistent findings between studies)
- Two phases in the illness history
- Elevated erythrocyte sedimentation rate or increased C-reactive protein
- Symptoms for at least 7 days
Lau and colleagues5,10 reviewed 14 studies that compared various imaging studies with clinical evaluation or sinus puncture and aspiration with culture or both. A positive aspirate for bacterial pathogens was defined as the gold standard for diagnosis of sinusitis (Table).
X-ray vs sinus puncture. Depending on the criteria used to define a diagnosis of sinusitis on plain radiograph, estimates of sensitivity in these studies ranged from 0.41 to 0.90, and specificity estimates ranged from 0.61 to 0.85. Imaging studies that included “mucous membrane thickening” as a criterion for sinusitis were more sensitive but less specific than studies defining positive radiographs as “opacification of sinus.”
CT scan, MRI, ultrasound. While a CT scan is more sensitive than plain x-ray film,11 and MRI is more sensitive than a CT scan,12,13 the specificity of these studies is unclear. For example, in children and adults without symptoms of sinusitis, the prevalence of sinusitis signs on CT and MRI is 45% and 42%, respectively.6,7,14 In light of such findings, these imaging methodologies are better reserved for patients in whom surgery is being contemplated, or for whom chronic sinusitis is a concern. In the 1980s and 1990s, ultrasound was studied enthusiastically. Variability in test performance is great.6 Since the cost of this procedure is similar to that of a sinus CT, ultrasound is not indicated in the diagnostic evaluation of the sinuses.
Though the sensitivity and specificity of a clinical evaluation possibly could be enhanced with the use of imaging studies, diagnostic accuracy of acute disease is not sufficiently improved to justify the cost or inconvenience of such interventions.
TABLE
Sensitivity and specificity of imaging modalities in sinusitis
| Diagnostic technique | Sensitivity | Specificity |
|---|---|---|
| X-ray | Variable | Variable |
| CT scan | High | Poor |
| MRI | High | Poor |
| Sinus puncture | High | High |
| Clinical evaluation | High | Moderate |
Recommendations from others
In a guideline on appropriate antibiotic use in sinusitis,4 endorsed by the Centers for Disease Control and Prevention, American Academy of Family Physicians, the American College of Physicians–American Society of Internal Medicine, and the Infectious Diseases Society of America, radiography is not recommended for the diagnosis of acute sinusitis. The guideline recommends that clinicians rely on duration of illness (at least 7 days) and severity of symptoms to make an accurate diagnosis of sinusitis.
The American Academy of Allergy, Asthma and Immunology15 guideline makes the following recommendations regarding imaging:
- The use of imaging may be appropriate when there are vague symptoms, or poor response to initial management
- Standard radiographs are insensitive, but may be used for diagnosis of acute sinus disease
- CT is preferred for preoperative evaluation of the nose and paranasal sinuses
- MRI is very sensitive for diagnosis of soft tissue disease in the frontal, maxillary, and sphenoid sinuses
- Ultrasonography has limited utility but may be applicable in pregnant women and for determining the amount of retained secretions.
The Institute for Clinical Systems Improvement recommends that radiology be used only if initial treatment has failed, and notes that a primary goal of its guideline was to reduce the number of x-rays that physicians order for this diagnosis.16
The American College of Radiology’s criteria for sinusitis in the pediatric population ranked several radiographic studies based on their appropriateness for given clinical conditions. This review17 suggests that no imaging is appropriate if symptoms have persisted <10 days. For patients with symptoms lasting >10 days and with persistent fever, CT scan is recommended.
Jon Neher, MD
Valley Medical Center Family Practice Residency, Renton, Wash
In acute bacterial sinusitis, the history and physical have somewhat limited sensitivity and specificity. Unfortunately, imaging studies add little valuable information. Primary care physicians must therefore be reconciled to some degree of diagnostic error.
The risks associated with under-diagnosis are small, since most cases of mild sinusitis will resolve spontaneously without treatment. The risks of over-diagnosis include increased antibiotic costs, side effects, allergic reactions, and the development of resistant organisms. It is prudent, therefore, to make the diagnosis only when multiple suggestive historical and exam elements are present and to avoid giving antibiotics to patients with mild, nonspecific illnesses.
1. Berg O, Carenfelt C. Analysis of symptoms and clinical signs in the maxillary sinus empyema. Acta Otolaryngol 1988;105:343-349.
2. Williams JW, Jr, Simel DL, Roberts L, Samsa GP. Clinical evaluation for sinusitis. Making the diagnosis by history and physical examination. Ann Intern Med 1992;117:705-710.
3. Clinical practice guideline: management of sinusitis. Pediatrics 2001;108:798-808.
4. Snow V, Mottur-Pilson C, Hickner JM. Principles of appropriate antibiotic use for acute sinusitis in adults. Ann Intern Med 2001;134:495-497.
5. Lau J. Diagnosis and treatment of acute bacterial rhinosinusitis. Evidence Report/Technology Assessment No. 9. Rockville, MD: Agency for Health Care Policy and Research; 1999.
6. Varonen H, Makela M, Savolainen S, Laara E, Hilden J. Comparison of ultrasound, radiography, and clinical examination in the diagnosis of acute maxillary sinusitis: a systematic review. J Clin Epidemiol 2000;53:940-948.
7. Lindbaek M, Hjortdahl P. The clinical diagnosis of acute purulent sinusitis in general practice: a review. Br J Gen Pract 2002;52:491-495.
8. Lindbaek M, Hjortdahl P, Johnsen UL. Use of symptoms, signs, and blood tests to diagnose acute sinus infections in primary care: comparison with computed tomography. Fam Med 1996;28:183-188.
9. Lindbaek M, Johnsen UL, Kaastad E, et al. CT findings in general practice patients with suspected acute sinusitis. Acta Radiol 1996;37:708-713.
10. Benninger MS, Sedory Holzer SE, Lau J. Diagnosis and treatment of uncomplicated acute bacterial rhinosinusitis: summary of the Agency for Health Care Policy and Research evidence-based report. Otolaryngol Head Neck Surg 2000;122:1-7.
11. Cotter CS, Stringer S, Rust KR, Mancuso A. The role of computed tomography scans in evaluating sinus disease in pediatric patients. Int J Pediatr Otorhinolaryngol 1999;50:63-68.
12. Gordts F, Clement PA, Destryker A, Desprechins B, Kaufman L. Prevalence of sinusitis signs on MRI in a non-ENT paediatric population. Rhinology 1997;35:154-157.
13. Chong VF, Fan YF. Comparison of CT and MRI features in sinusitis. Eur J Radiol 1998;29:47-54.
14. Patel K, Chavda SV, Violaris N, Pahor AL. Incidental paranasal sinus inflammatory changes in a British population. J Laryngol Otol 1996;110:649-651.
15. Joint Task Force on Practice Parameters in Allergy, Asthma and Immunology : Joint Task Force summary statements on diagnosis and management of sinusitis.
16. Acute Sinusitis in Adults. Bloomington, Minn: Institute for Clinical Systems Improvement (ICSI), 2002. Available at: www.icsi.org. Accessed on June 17, 2003.
17. McAlister WH, Parker BR, Kushner DC, et al. Sinusitis in the pediatric population. American College of Radiology. ACR Appropriateness Criteria. Radiology 2000;215(Suppl):811-818.
Accurate diagnosis of acute sinusitis in both children and adults depends on the history and clinical examination of the patient. While the clinical signs and symptoms of acute sinusitis are often difficult to distinguish from viral upper respiratory infection,1,2 such an assessment remains the best approach to diagnosing acute sinusitis (strength of recommendation [SOR]: A). There is no role for imaging in the diagnosis of acute sinusitis. For patients who have persistent symptoms, or those for whom surgery is being considered, some guidelines suggest that coronal computed tomography (CT) scan of the paranasal sinuses be considered (SOR: C, expert opinion).
Evidence summary
Three recent evidence-based guidelines3,4,5 suggest that children and adults with acute sinusitis may benefit from treatment with antibiotics more than those with rhinitis. Clinicians must develop a strategy for accurately diagnosing sinusitis to make sound treatment decisions. In the absence of a clear diagnosis of acute sinusitis, antibiotics are very unlikely to improve symptoms and are, therefore, not indicated.
Clinical evaluation. Berg1 studied 150 patients with clinical diagnoses of sinusitis and found that 85% of them had positive sinus puncture. In a review of the 11 studies that met evidence-based inclusion criteria, Varonen6 concluded that clinical evaluation has a sensitivity of roughly 0.75, whereas radiographic methodologies have sensitivities >0.80. In a prospective trial and subsequent review of the literature, Lindbaek7,8,9 suggests that several key clinical signs and symptoms can provide a level of sensitivity that approaches that of CT or magnetic resonance imaging (MRI), while enhancing specificity:
- Purulent secretion reported as a symptom or found in the nasal cavity by the doctor
- Pain in the teeth
- Pain on bending forward (inconsistent findings between studies)
- Two phases in the illness history
- Elevated erythrocyte sedimentation rate or increased C-reactive protein
- Symptoms for at least 7 days
Lau and colleagues5,10 reviewed 14 studies that compared various imaging studies with clinical evaluation or sinus puncture and aspiration with culture or both. A positive aspirate for bacterial pathogens was defined as the gold standard for diagnosis of sinusitis (Table).
X-ray vs sinus puncture. Depending on the criteria used to define a diagnosis of sinusitis on plain radiograph, estimates of sensitivity in these studies ranged from 0.41 to 0.90, and specificity estimates ranged from 0.61 to 0.85. Imaging studies that included “mucous membrane thickening” as a criterion for sinusitis were more sensitive but less specific than studies defining positive radiographs as “opacification of sinus.”
CT scan, MRI, ultrasound. While a CT scan is more sensitive than plain x-ray film,11 and MRI is more sensitive than a CT scan,12,13 the specificity of these studies is unclear. For example, in children and adults without symptoms of sinusitis, the prevalence of sinusitis signs on CT and MRI is 45% and 42%, respectively.6,7,14 In light of such findings, these imaging methodologies are better reserved for patients in whom surgery is being contemplated, or for whom chronic sinusitis is a concern. In the 1980s and 1990s, ultrasound was studied enthusiastically. Variability in test performance is great.6 Since the cost of this procedure is similar to that of a sinus CT, ultrasound is not indicated in the diagnostic evaluation of the sinuses.
Though the sensitivity and specificity of a clinical evaluation possibly could be enhanced with the use of imaging studies, diagnostic accuracy of acute disease is not sufficiently improved to justify the cost or inconvenience of such interventions.
TABLE
Sensitivity and specificity of imaging modalities in sinusitis
| Diagnostic technique | Sensitivity | Specificity |
|---|---|---|
| X-ray | Variable | Variable |
| CT scan | High | Poor |
| MRI | High | Poor |
| Sinus puncture | High | High |
| Clinical evaluation | High | Moderate |
Recommendations from others
In a guideline on appropriate antibiotic use in sinusitis,4 endorsed by the Centers for Disease Control and Prevention, American Academy of Family Physicians, the American College of Physicians–American Society of Internal Medicine, and the Infectious Diseases Society of America, radiography is not recommended for the diagnosis of acute sinusitis. The guideline recommends that clinicians rely on duration of illness (at least 7 days) and severity of symptoms to make an accurate diagnosis of sinusitis.
The American Academy of Allergy, Asthma and Immunology15 guideline makes the following recommendations regarding imaging:
- The use of imaging may be appropriate when there are vague symptoms, or poor response to initial management
- Standard radiographs are insensitive, but may be used for diagnosis of acute sinus disease
- CT is preferred for preoperative evaluation of the nose and paranasal sinuses
- MRI is very sensitive for diagnosis of soft tissue disease in the frontal, maxillary, and sphenoid sinuses
- Ultrasonography has limited utility but may be applicable in pregnant women and for determining the amount of retained secretions.
The Institute for Clinical Systems Improvement recommends that radiology be used only if initial treatment has failed, and notes that a primary goal of its guideline was to reduce the number of x-rays that physicians order for this diagnosis.16
The American College of Radiology’s criteria for sinusitis in the pediatric population ranked several radiographic studies based on their appropriateness for given clinical conditions. This review17 suggests that no imaging is appropriate if symptoms have persisted <10 days. For patients with symptoms lasting >10 days and with persistent fever, CT scan is recommended.
Jon Neher, MD
Valley Medical Center Family Practice Residency, Renton, Wash
In acute bacterial sinusitis, the history and physical have somewhat limited sensitivity and specificity. Unfortunately, imaging studies add little valuable information. Primary care physicians must therefore be reconciled to some degree of diagnostic error.
The risks associated with under-diagnosis are small, since most cases of mild sinusitis will resolve spontaneously without treatment. The risks of over-diagnosis include increased antibiotic costs, side effects, allergic reactions, and the development of resistant organisms. It is prudent, therefore, to make the diagnosis only when multiple suggestive historical and exam elements are present and to avoid giving antibiotics to patients with mild, nonspecific illnesses.
Accurate diagnosis of acute sinusitis in both children and adults depends on the history and clinical examination of the patient. While the clinical signs and symptoms of acute sinusitis are often difficult to distinguish from viral upper respiratory infection,1,2 such an assessment remains the best approach to diagnosing acute sinusitis (strength of recommendation [SOR]: A). There is no role for imaging in the diagnosis of acute sinusitis. For patients who have persistent symptoms, or those for whom surgery is being considered, some guidelines suggest that coronal computed tomography (CT) scan of the paranasal sinuses be considered (SOR: C, expert opinion).
Evidence summary
Three recent evidence-based guidelines3,4,5 suggest that children and adults with acute sinusitis may benefit from treatment with antibiotics more than those with rhinitis. Clinicians must develop a strategy for accurately diagnosing sinusitis to make sound treatment decisions. In the absence of a clear diagnosis of acute sinusitis, antibiotics are very unlikely to improve symptoms and are, therefore, not indicated.
Clinical evaluation. Berg1 studied 150 patients with clinical diagnoses of sinusitis and found that 85% of them had positive sinus puncture. In a review of the 11 studies that met evidence-based inclusion criteria, Varonen6 concluded that clinical evaluation has a sensitivity of roughly 0.75, whereas radiographic methodologies have sensitivities >0.80. In a prospective trial and subsequent review of the literature, Lindbaek7,8,9 suggests that several key clinical signs and symptoms can provide a level of sensitivity that approaches that of CT or magnetic resonance imaging (MRI), while enhancing specificity:
- Purulent secretion reported as a symptom or found in the nasal cavity by the doctor
- Pain in the teeth
- Pain on bending forward (inconsistent findings between studies)
- Two phases in the illness history
- Elevated erythrocyte sedimentation rate or increased C-reactive protein
- Symptoms for at least 7 days
Lau and colleagues5,10 reviewed 14 studies that compared various imaging studies with clinical evaluation or sinus puncture and aspiration with culture or both. A positive aspirate for bacterial pathogens was defined as the gold standard for diagnosis of sinusitis (Table).
X-ray vs sinus puncture. Depending on the criteria used to define a diagnosis of sinusitis on plain radiograph, estimates of sensitivity in these studies ranged from 0.41 to 0.90, and specificity estimates ranged from 0.61 to 0.85. Imaging studies that included “mucous membrane thickening” as a criterion for sinusitis were more sensitive but less specific than studies defining positive radiographs as “opacification of sinus.”
CT scan, MRI, ultrasound. While a CT scan is more sensitive than plain x-ray film,11 and MRI is more sensitive than a CT scan,12,13 the specificity of these studies is unclear. For example, in children and adults without symptoms of sinusitis, the prevalence of sinusitis signs on CT and MRI is 45% and 42%, respectively.6,7,14 In light of such findings, these imaging methodologies are better reserved for patients in whom surgery is being contemplated, or for whom chronic sinusitis is a concern. In the 1980s and 1990s, ultrasound was studied enthusiastically. Variability in test performance is great.6 Since the cost of this procedure is similar to that of a sinus CT, ultrasound is not indicated in the diagnostic evaluation of the sinuses.
Though the sensitivity and specificity of a clinical evaluation possibly could be enhanced with the use of imaging studies, diagnostic accuracy of acute disease is not sufficiently improved to justify the cost or inconvenience of such interventions.
TABLE
Sensitivity and specificity of imaging modalities in sinusitis
| Diagnostic technique | Sensitivity | Specificity |
|---|---|---|
| X-ray | Variable | Variable |
| CT scan | High | Poor |
| MRI | High | Poor |
| Sinus puncture | High | High |
| Clinical evaluation | High | Moderate |
Recommendations from others
In a guideline on appropriate antibiotic use in sinusitis,4 endorsed by the Centers for Disease Control and Prevention, American Academy of Family Physicians, the American College of Physicians–American Society of Internal Medicine, and the Infectious Diseases Society of America, radiography is not recommended for the diagnosis of acute sinusitis. The guideline recommends that clinicians rely on duration of illness (at least 7 days) and severity of symptoms to make an accurate diagnosis of sinusitis.
The American Academy of Allergy, Asthma and Immunology15 guideline makes the following recommendations regarding imaging:
- The use of imaging may be appropriate when there are vague symptoms, or poor response to initial management
- Standard radiographs are insensitive, but may be used for diagnosis of acute sinus disease
- CT is preferred for preoperative evaluation of the nose and paranasal sinuses
- MRI is very sensitive for diagnosis of soft tissue disease in the frontal, maxillary, and sphenoid sinuses
- Ultrasonography has limited utility but may be applicable in pregnant women and for determining the amount of retained secretions.
The Institute for Clinical Systems Improvement recommends that radiology be used only if initial treatment has failed, and notes that a primary goal of its guideline was to reduce the number of x-rays that physicians order for this diagnosis.16
The American College of Radiology’s criteria for sinusitis in the pediatric population ranked several radiographic studies based on their appropriateness for given clinical conditions. This review17 suggests that no imaging is appropriate if symptoms have persisted <10 days. For patients with symptoms lasting >10 days and with persistent fever, CT scan is recommended.
Jon Neher, MD
Valley Medical Center Family Practice Residency, Renton, Wash
In acute bacterial sinusitis, the history and physical have somewhat limited sensitivity and specificity. Unfortunately, imaging studies add little valuable information. Primary care physicians must therefore be reconciled to some degree of diagnostic error.
The risks associated with under-diagnosis are small, since most cases of mild sinusitis will resolve spontaneously without treatment. The risks of over-diagnosis include increased antibiotic costs, side effects, allergic reactions, and the development of resistant organisms. It is prudent, therefore, to make the diagnosis only when multiple suggestive historical and exam elements are present and to avoid giving antibiotics to patients with mild, nonspecific illnesses.
1. Berg O, Carenfelt C. Analysis of symptoms and clinical signs in the maxillary sinus empyema. Acta Otolaryngol 1988;105:343-349.
2. Williams JW, Jr, Simel DL, Roberts L, Samsa GP. Clinical evaluation for sinusitis. Making the diagnosis by history and physical examination. Ann Intern Med 1992;117:705-710.
3. Clinical practice guideline: management of sinusitis. Pediatrics 2001;108:798-808.
4. Snow V, Mottur-Pilson C, Hickner JM. Principles of appropriate antibiotic use for acute sinusitis in adults. Ann Intern Med 2001;134:495-497.
5. Lau J. Diagnosis and treatment of acute bacterial rhinosinusitis. Evidence Report/Technology Assessment No. 9. Rockville, MD: Agency for Health Care Policy and Research; 1999.
6. Varonen H, Makela M, Savolainen S, Laara E, Hilden J. Comparison of ultrasound, radiography, and clinical examination in the diagnosis of acute maxillary sinusitis: a systematic review. J Clin Epidemiol 2000;53:940-948.
7. Lindbaek M, Hjortdahl P. The clinical diagnosis of acute purulent sinusitis in general practice: a review. Br J Gen Pract 2002;52:491-495.
8. Lindbaek M, Hjortdahl P, Johnsen UL. Use of symptoms, signs, and blood tests to diagnose acute sinus infections in primary care: comparison with computed tomography. Fam Med 1996;28:183-188.
9. Lindbaek M, Johnsen UL, Kaastad E, et al. CT findings in general practice patients with suspected acute sinusitis. Acta Radiol 1996;37:708-713.
10. Benninger MS, Sedory Holzer SE, Lau J. Diagnosis and treatment of uncomplicated acute bacterial rhinosinusitis: summary of the Agency for Health Care Policy and Research evidence-based report. Otolaryngol Head Neck Surg 2000;122:1-7.
11. Cotter CS, Stringer S, Rust KR, Mancuso A. The role of computed tomography scans in evaluating sinus disease in pediatric patients. Int J Pediatr Otorhinolaryngol 1999;50:63-68.
12. Gordts F, Clement PA, Destryker A, Desprechins B, Kaufman L. Prevalence of sinusitis signs on MRI in a non-ENT paediatric population. Rhinology 1997;35:154-157.
13. Chong VF, Fan YF. Comparison of CT and MRI features in sinusitis. Eur J Radiol 1998;29:47-54.
14. Patel K, Chavda SV, Violaris N, Pahor AL. Incidental paranasal sinus inflammatory changes in a British population. J Laryngol Otol 1996;110:649-651.
15. Joint Task Force on Practice Parameters in Allergy, Asthma and Immunology : Joint Task Force summary statements on diagnosis and management of sinusitis.
16. Acute Sinusitis in Adults. Bloomington, Minn: Institute for Clinical Systems Improvement (ICSI), 2002. Available at: www.icsi.org. Accessed on June 17, 2003.
17. McAlister WH, Parker BR, Kushner DC, et al. Sinusitis in the pediatric population. American College of Radiology. ACR Appropriateness Criteria. Radiology 2000;215(Suppl):811-818.
1. Berg O, Carenfelt C. Analysis of symptoms and clinical signs in the maxillary sinus empyema. Acta Otolaryngol 1988;105:343-349.
2. Williams JW, Jr, Simel DL, Roberts L, Samsa GP. Clinical evaluation for sinusitis. Making the diagnosis by history and physical examination. Ann Intern Med 1992;117:705-710.
3. Clinical practice guideline: management of sinusitis. Pediatrics 2001;108:798-808.
4. Snow V, Mottur-Pilson C, Hickner JM. Principles of appropriate antibiotic use for acute sinusitis in adults. Ann Intern Med 2001;134:495-497.
5. Lau J. Diagnosis and treatment of acute bacterial rhinosinusitis. Evidence Report/Technology Assessment No. 9. Rockville, MD: Agency for Health Care Policy and Research; 1999.
6. Varonen H, Makela M, Savolainen S, Laara E, Hilden J. Comparison of ultrasound, radiography, and clinical examination in the diagnosis of acute maxillary sinusitis: a systematic review. J Clin Epidemiol 2000;53:940-948.
7. Lindbaek M, Hjortdahl P. The clinical diagnosis of acute purulent sinusitis in general practice: a review. Br J Gen Pract 2002;52:491-495.
8. Lindbaek M, Hjortdahl P, Johnsen UL. Use of symptoms, signs, and blood tests to diagnose acute sinus infections in primary care: comparison with computed tomography. Fam Med 1996;28:183-188.
9. Lindbaek M, Johnsen UL, Kaastad E, et al. CT findings in general practice patients with suspected acute sinusitis. Acta Radiol 1996;37:708-713.
10. Benninger MS, Sedory Holzer SE, Lau J. Diagnosis and treatment of uncomplicated acute bacterial rhinosinusitis: summary of the Agency for Health Care Policy and Research evidence-based report. Otolaryngol Head Neck Surg 2000;122:1-7.
11. Cotter CS, Stringer S, Rust KR, Mancuso A. The role of computed tomography scans in evaluating sinus disease in pediatric patients. Int J Pediatr Otorhinolaryngol 1999;50:63-68.
12. Gordts F, Clement PA, Destryker A, Desprechins B, Kaufman L. Prevalence of sinusitis signs on MRI in a non-ENT paediatric population. Rhinology 1997;35:154-157.
13. Chong VF, Fan YF. Comparison of CT and MRI features in sinusitis. Eur J Radiol 1998;29:47-54.
14. Patel K, Chavda SV, Violaris N, Pahor AL. Incidental paranasal sinus inflammatory changes in a British population. J Laryngol Otol 1996;110:649-651.
15. Joint Task Force on Practice Parameters in Allergy, Asthma and Immunology : Joint Task Force summary statements on diagnosis and management of sinusitis.
16. Acute Sinusitis in Adults. Bloomington, Minn: Institute for Clinical Systems Improvement (ICSI), 2002. Available at: www.icsi.org. Accessed on June 17, 2003.
17. McAlister WH, Parker BR, Kushner DC, et al. Sinusitis in the pediatric population. American College of Radiology. ACR Appropriateness Criteria. Radiology 2000;215(Suppl):811-818.
Evidence-based answers from the Family Physicians Inquiries Network
What findings distinguish acute bacterial sinusitis?
No combination of clinical findings can reliably distinguish acute viral rhinosinusitis from acute bacterial rhinosinusitis in primary care. Although unreliable, the best clinical predictor of acute bacterial sinusitis is the combination of unilateral nasal discharge and unilateral pain (positive likelihood ratio [LR+], 4.5; negative likelihood ratio [LR–], 0.25) (strength of recommendation [SOR]: B).1 History of purulent rhinorrhea (LR+, 1.5–1.9), maxillary tooth pain (LR+, 2.1–2.5), and purulent secretions in the nasal cavity (LR+, 2.1–5.5) may increase the likelihood of acute bacterial rhinosinusitis. Illness that starts as the common cold and pain on bending forward were not predictors of acute bacterial rhinosinusitis (SOR: B).2,3,4
Evidence summary
In one series, 87% of patients with the common cold had an abnormal computed tomography (CT) scan of the sinuses 48 to 96 hours after onset. Abnormalities visible on the CT scan persisted in 20% of patients at 2 weeks, yet epidemiological studies have shown that acute bacterial rhinosinusitis develops in only 0.5% to 2% of upper respiratory infections in adults. In primary care, only half of patients with a clinical diagnosis of acute bacterial rhinosinusitis have it proven upon aspiration.5
Two studies compared clinical findings with sinus puncture, the reference standard for acute bacterial rhinosinusitis. Berg found 4 independent predictors of aspirate purulence in Swedish emergency room patients with “paranasal” symptoms lasting <3 months (Table).1 Together, unilateral purulent nasal discharge and predominantly unilateral pain predicated purulence on aspiration (sensitivity 79%, specificity 83%, positive predictive value [PPV], 80%). Clinical exam by an otolaryngologist had a PPV of 72%.
While emergency and primary care patients may differ, this study’s rate of aspiration-proven sinusitis (43%) is closer to that seen in primary care (50%) than in referral practices (70%–80%). This study’s limitations included unclear referral criteria, overlapping clinical predictors, and lack of culture data.
In a study of general practice patients in the United Kingdom with clinically diagnosed acute maxillary sinusitis, no signs or symptoms were independently associated with their illness.6 The authors concluded that the clinical examination was more or less worthless. Only patients with positive findings on CT scan underwent aspiration in this study. Less differentiated, less severe symptoms and a less stringent definition of positive aspiration in this study may account for the different results. Additionally, one third of patients eligible for this study refused participation or withdrew prior to sinus puncture.6
Other primary care studies used less accurate reference tests such as CT2 (sensitivity and specificity unknown),5 x-ray3 (sensitivity 41%–90%, specificity 61%–85%),5 and ultrasound4 (sensitivity 76%, specificity 76%).7
Williams found 5 independent predictors of x-ray findings consistent with sinusitis in 247 male veterans:
- maxillary toothache (LR+, 2.5)
- no improvement with decongestants (LR+, 2.1)
- purulent secretions on exam (LR+, 2.1)
- abnormal transillumination (LR+, 1.6)
- colored nasal discharge (LR+, 1.5).3
In at least 2 of these 4 studies, purulent secretions in the nasal cavity (LR+, 2.1–5.5),2,3 maxillary tooth pain (LR+, 2.1–2.5)3,4 and purulent rhinorrhea (LR+, 1.5–1.9)2,3,4 increased the likelihood of acute bacterial rhinosinusitis.
Finding purulent secretions in the nasal cavity is highly specific for acute bacterial rhinosinusitis (specificity 79%–100%)1,2,3 but is uncommon and difficult to assess, requiring the use of a nasal speculum and possibly topical decongestants. The primary care physician’s overall clinical impression was accurate in Williams’ study but not in others.2,4,6 Illness starting as the common cold and pain on bending forward were not predictors of acute bacterial rhinosinusitis.2,3,4 Headache, bilateral maxillary pain, frontal sinus pain, fever, sinus tenderness on exam, and purulent pharyngeal discharge have not been shown to be useful in acute bacterial rhinosinusitis diagnosis.7
TABLE
Clinical prediction rule for acute bacterial rhinosinusitis
| Symptoms | PPV |
|---|---|
| Local pain, unilateral predominance | 41% |
| Purulent rhinorrhea, unilateral predominance | 48% |
| Purulent rhinorrhea, bilateral | 15% |
| Presence of pus in the nasal cavity | 17% |
| Clinical prediction rule: 3/4 positive: positive likelihood ratio = 6.75, negative likelihood ratio = 0.21 | |
| PPV, positive predictive value | |
Recommendations from others
A recommendation from the Agency for Health Care Policy and Research suggests using symptomatic treatment initially when the prevalence of acute bacterial rhinosinusitis in patients with upper respiratory infection is <25%, and using clinical criteria (see Table) for acute bacterial rhinosinusitis diagnosis when prevalence is higher.5
The Centers for Disease Control and Prevention recommends reserving the diagnosis of acute bacterial rhinosinusitis for patients with symptoms lasting ≥7 days with maxillary pain or tenderness in the face or teeth (especially unilateral) and purulent nasal secretions.8
An otolaryngology guideline recommends considering acute bacterial rhinosinusitis when viral upper respiratory infection persists beyond 10 days or worsens after 5 to 7 days with similar symptoms.9 The 7-to-10-day specification is based on the natural history of rhinovirus infections (SOR: C).
A Canadian Medical Association evidence-based review recommended a score based on Williams’ 5 independent predictor symptoms:
- fewer than 2 symptoms rule out acute bacterial rhinosinusitis (PPV, <40%)
- 4 or more symptoms rule in acute bacterial rhinosinusitis (PPV, 81%) (level of evidence [LOE]: 4)
- 2 or 3 symptoms (PPV, 40%–63%) may benefit from radiography (SOR: C).10
Jacob M. Reider, MD
Department of Family and Community Medicine, Albany Medical College, Albany, NY
This summary emphasizes inconsistencies in the literature and the limited predictive value of clinical findings when diagnosing sinusitis. But there is a way to sidestep this problem. When a patient presents complaining of “sinusitis,” I ask about their expectations for the visit and their understanding of their symptoms’ possible causes, and then I often show the patient a picture of sinus anatomy. By demonstrating that the osteomeatal complex is small, and focusing on obstruction rather than infection, I am able to avoid any confrontation about antibiotics entirely. Then I can recommend irrigation, hydration, and analgesia. For patients whose symptoms persist beyond 10 to 14 days, and for whom these initial interventions have failed, a trial of antibiotics may be indicated.
1. Berg O, Carenfelt C. Analysis of symptoms and clinical signs in the maxillary sinus empyema. Acta Otolaryngol 1988;105:343-349.
2. Lindbaek M, Hjortdahl P, Johnsen UL. Use of symptoms, signs, and blood tests to diagnose acute sinus infections in primary care: comparison with computed tomography. Fam Med 1996;28:183-188.
3. Williams JW, Jr, Simel DL, Roberts L, Samsa GP. Clinical evaluation for sinusitis. Making the diagnosis by history and physical examination. Ann Intern Med 1992;117:705-710.
4. van Duijn NP, Brouwer HJ, Lamberts H. Use of symptoms and signs to diagnose maxillary sinusitis in general practice: comparison with ultrasonography. BMJ 1992;305:684-687.
5. Lau J, Zucker D, Engels EA, et al. Diagnosis and treatment of acute bacterial rhinosinusitis. Evidence Report/Technology Assessment No. 9. Rockville, Md: Agency for Health Care Policy and Research; 1999.
6. Hansen JG, Schmidt H, Rosborg J, Lund E. Predicting acute maxillary sinusitis in a general practice population. BMJ 1995;311:233-236.
7. Lindbaek M, Hjortdahl P. The clinical diagnosis of acute purulent sinusitis in general practice—a review. Br J Gen Pract 2002;52:491-495.
8. Hickner JM, Bartlett JG, Besser RE, Gonzales R, Hoffman JR, Sande MA. Principles of appropriate antibiotic use for acute rhinosinusitis in adults: background. Ann Emerg Med 2001;37:703-710.
9. Antimicrobial treatment guidelines for acute bacterial rhinosinusitis. Sinus and Allergy Health Partnership. Otolaryngol Head Neck Surg 2000;123(1 Pt 2):5-31.
10. Low DE, Desrosiers M, McSherry J, et al. A practical guide for the diagnosis and treatment of acute sinusitis. CMAJ 1997;156 (Suppl 6):S1-S14.
No combination of clinical findings can reliably distinguish acute viral rhinosinusitis from acute bacterial rhinosinusitis in primary care. Although unreliable, the best clinical predictor of acute bacterial sinusitis is the combination of unilateral nasal discharge and unilateral pain (positive likelihood ratio [LR+], 4.5; negative likelihood ratio [LR–], 0.25) (strength of recommendation [SOR]: B).1 History of purulent rhinorrhea (LR+, 1.5–1.9), maxillary tooth pain (LR+, 2.1–2.5), and purulent secretions in the nasal cavity (LR+, 2.1–5.5) may increase the likelihood of acute bacterial rhinosinusitis. Illness that starts as the common cold and pain on bending forward were not predictors of acute bacterial rhinosinusitis (SOR: B).2,3,4
Evidence summary
In one series, 87% of patients with the common cold had an abnormal computed tomography (CT) scan of the sinuses 48 to 96 hours after onset. Abnormalities visible on the CT scan persisted in 20% of patients at 2 weeks, yet epidemiological studies have shown that acute bacterial rhinosinusitis develops in only 0.5% to 2% of upper respiratory infections in adults. In primary care, only half of patients with a clinical diagnosis of acute bacterial rhinosinusitis have it proven upon aspiration.5
Two studies compared clinical findings with sinus puncture, the reference standard for acute bacterial rhinosinusitis. Berg found 4 independent predictors of aspirate purulence in Swedish emergency room patients with “paranasal” symptoms lasting <3 months (Table).1 Together, unilateral purulent nasal discharge and predominantly unilateral pain predicated purulence on aspiration (sensitivity 79%, specificity 83%, positive predictive value [PPV], 80%). Clinical exam by an otolaryngologist had a PPV of 72%.
While emergency and primary care patients may differ, this study’s rate of aspiration-proven sinusitis (43%) is closer to that seen in primary care (50%) than in referral practices (70%–80%). This study’s limitations included unclear referral criteria, overlapping clinical predictors, and lack of culture data.
In a study of general practice patients in the United Kingdom with clinically diagnosed acute maxillary sinusitis, no signs or symptoms were independently associated with their illness.6 The authors concluded that the clinical examination was more or less worthless. Only patients with positive findings on CT scan underwent aspiration in this study. Less differentiated, less severe symptoms and a less stringent definition of positive aspiration in this study may account for the different results. Additionally, one third of patients eligible for this study refused participation or withdrew prior to sinus puncture.6
Other primary care studies used less accurate reference tests such as CT2 (sensitivity and specificity unknown),5 x-ray3 (sensitivity 41%–90%, specificity 61%–85%),5 and ultrasound4 (sensitivity 76%, specificity 76%).7
Williams found 5 independent predictors of x-ray findings consistent with sinusitis in 247 male veterans:
- maxillary toothache (LR+, 2.5)
- no improvement with decongestants (LR+, 2.1)
- purulent secretions on exam (LR+, 2.1)
- abnormal transillumination (LR+, 1.6)
- colored nasal discharge (LR+, 1.5).3
In at least 2 of these 4 studies, purulent secretions in the nasal cavity (LR+, 2.1–5.5),2,3 maxillary tooth pain (LR+, 2.1–2.5)3,4 and purulent rhinorrhea (LR+, 1.5–1.9)2,3,4 increased the likelihood of acute bacterial rhinosinusitis.
Finding purulent secretions in the nasal cavity is highly specific for acute bacterial rhinosinusitis (specificity 79%–100%)1,2,3 but is uncommon and difficult to assess, requiring the use of a nasal speculum and possibly topical decongestants. The primary care physician’s overall clinical impression was accurate in Williams’ study but not in others.2,4,6 Illness starting as the common cold and pain on bending forward were not predictors of acute bacterial rhinosinusitis.2,3,4 Headache, bilateral maxillary pain, frontal sinus pain, fever, sinus tenderness on exam, and purulent pharyngeal discharge have not been shown to be useful in acute bacterial rhinosinusitis diagnosis.7
TABLE
Clinical prediction rule for acute bacterial rhinosinusitis
| Symptoms | PPV |
|---|---|
| Local pain, unilateral predominance | 41% |
| Purulent rhinorrhea, unilateral predominance | 48% |
| Purulent rhinorrhea, bilateral | 15% |
| Presence of pus in the nasal cavity | 17% |
| Clinical prediction rule: 3/4 positive: positive likelihood ratio = 6.75, negative likelihood ratio = 0.21 | |
| PPV, positive predictive value | |
Recommendations from others
A recommendation from the Agency for Health Care Policy and Research suggests using symptomatic treatment initially when the prevalence of acute bacterial rhinosinusitis in patients with upper respiratory infection is <25%, and using clinical criteria (see Table) for acute bacterial rhinosinusitis diagnosis when prevalence is higher.5
The Centers for Disease Control and Prevention recommends reserving the diagnosis of acute bacterial rhinosinusitis for patients with symptoms lasting ≥7 days with maxillary pain or tenderness in the face or teeth (especially unilateral) and purulent nasal secretions.8
An otolaryngology guideline recommends considering acute bacterial rhinosinusitis when viral upper respiratory infection persists beyond 10 days or worsens after 5 to 7 days with similar symptoms.9 The 7-to-10-day specification is based on the natural history of rhinovirus infections (SOR: C).
A Canadian Medical Association evidence-based review recommended a score based on Williams’ 5 independent predictor symptoms:
- fewer than 2 symptoms rule out acute bacterial rhinosinusitis (PPV, <40%)
- 4 or more symptoms rule in acute bacterial rhinosinusitis (PPV, 81%) (level of evidence [LOE]: 4)
- 2 or 3 symptoms (PPV, 40%–63%) may benefit from radiography (SOR: C).10
Jacob M. Reider, MD
Department of Family and Community Medicine, Albany Medical College, Albany, NY
This summary emphasizes inconsistencies in the literature and the limited predictive value of clinical findings when diagnosing sinusitis. But there is a way to sidestep this problem. When a patient presents complaining of “sinusitis,” I ask about their expectations for the visit and their understanding of their symptoms’ possible causes, and then I often show the patient a picture of sinus anatomy. By demonstrating that the osteomeatal complex is small, and focusing on obstruction rather than infection, I am able to avoid any confrontation about antibiotics entirely. Then I can recommend irrigation, hydration, and analgesia. For patients whose symptoms persist beyond 10 to 14 days, and for whom these initial interventions have failed, a trial of antibiotics may be indicated.
No combination of clinical findings can reliably distinguish acute viral rhinosinusitis from acute bacterial rhinosinusitis in primary care. Although unreliable, the best clinical predictor of acute bacterial sinusitis is the combination of unilateral nasal discharge and unilateral pain (positive likelihood ratio [LR+], 4.5; negative likelihood ratio [LR–], 0.25) (strength of recommendation [SOR]: B).1 History of purulent rhinorrhea (LR+, 1.5–1.9), maxillary tooth pain (LR+, 2.1–2.5), and purulent secretions in the nasal cavity (LR+, 2.1–5.5) may increase the likelihood of acute bacterial rhinosinusitis. Illness that starts as the common cold and pain on bending forward were not predictors of acute bacterial rhinosinusitis (SOR: B).2,3,4
Evidence summary
In one series, 87% of patients with the common cold had an abnormal computed tomography (CT) scan of the sinuses 48 to 96 hours after onset. Abnormalities visible on the CT scan persisted in 20% of patients at 2 weeks, yet epidemiological studies have shown that acute bacterial rhinosinusitis develops in only 0.5% to 2% of upper respiratory infections in adults. In primary care, only half of patients with a clinical diagnosis of acute bacterial rhinosinusitis have it proven upon aspiration.5
Two studies compared clinical findings with sinus puncture, the reference standard for acute bacterial rhinosinusitis. Berg found 4 independent predictors of aspirate purulence in Swedish emergency room patients with “paranasal” symptoms lasting <3 months (Table).1 Together, unilateral purulent nasal discharge and predominantly unilateral pain predicated purulence on aspiration (sensitivity 79%, specificity 83%, positive predictive value [PPV], 80%). Clinical exam by an otolaryngologist had a PPV of 72%.
While emergency and primary care patients may differ, this study’s rate of aspiration-proven sinusitis (43%) is closer to that seen in primary care (50%) than in referral practices (70%–80%). This study’s limitations included unclear referral criteria, overlapping clinical predictors, and lack of culture data.
In a study of general practice patients in the United Kingdom with clinically diagnosed acute maxillary sinusitis, no signs or symptoms were independently associated with their illness.6 The authors concluded that the clinical examination was more or less worthless. Only patients with positive findings on CT scan underwent aspiration in this study. Less differentiated, less severe symptoms and a less stringent definition of positive aspiration in this study may account for the different results. Additionally, one third of patients eligible for this study refused participation or withdrew prior to sinus puncture.6
Other primary care studies used less accurate reference tests such as CT2 (sensitivity and specificity unknown),5 x-ray3 (sensitivity 41%–90%, specificity 61%–85%),5 and ultrasound4 (sensitivity 76%, specificity 76%).7
Williams found 5 independent predictors of x-ray findings consistent with sinusitis in 247 male veterans:
- maxillary toothache (LR+, 2.5)
- no improvement with decongestants (LR+, 2.1)
- purulent secretions on exam (LR+, 2.1)
- abnormal transillumination (LR+, 1.6)
- colored nasal discharge (LR+, 1.5).3
In at least 2 of these 4 studies, purulent secretions in the nasal cavity (LR+, 2.1–5.5),2,3 maxillary tooth pain (LR+, 2.1–2.5)3,4 and purulent rhinorrhea (LR+, 1.5–1.9)2,3,4 increased the likelihood of acute bacterial rhinosinusitis.
Finding purulent secretions in the nasal cavity is highly specific for acute bacterial rhinosinusitis (specificity 79%–100%)1,2,3 but is uncommon and difficult to assess, requiring the use of a nasal speculum and possibly topical decongestants. The primary care physician’s overall clinical impression was accurate in Williams’ study but not in others.2,4,6 Illness starting as the common cold and pain on bending forward were not predictors of acute bacterial rhinosinusitis.2,3,4 Headache, bilateral maxillary pain, frontal sinus pain, fever, sinus tenderness on exam, and purulent pharyngeal discharge have not been shown to be useful in acute bacterial rhinosinusitis diagnosis.7
TABLE
Clinical prediction rule for acute bacterial rhinosinusitis
| Symptoms | PPV |
|---|---|
| Local pain, unilateral predominance | 41% |
| Purulent rhinorrhea, unilateral predominance | 48% |
| Purulent rhinorrhea, bilateral | 15% |
| Presence of pus in the nasal cavity | 17% |
| Clinical prediction rule: 3/4 positive: positive likelihood ratio = 6.75, negative likelihood ratio = 0.21 | |
| PPV, positive predictive value | |
Recommendations from others
A recommendation from the Agency for Health Care Policy and Research suggests using symptomatic treatment initially when the prevalence of acute bacterial rhinosinusitis in patients with upper respiratory infection is <25%, and using clinical criteria (see Table) for acute bacterial rhinosinusitis diagnosis when prevalence is higher.5
The Centers for Disease Control and Prevention recommends reserving the diagnosis of acute bacterial rhinosinusitis for patients with symptoms lasting ≥7 days with maxillary pain or tenderness in the face or teeth (especially unilateral) and purulent nasal secretions.8
An otolaryngology guideline recommends considering acute bacterial rhinosinusitis when viral upper respiratory infection persists beyond 10 days or worsens after 5 to 7 days with similar symptoms.9 The 7-to-10-day specification is based on the natural history of rhinovirus infections (SOR: C).
A Canadian Medical Association evidence-based review recommended a score based on Williams’ 5 independent predictor symptoms:
- fewer than 2 symptoms rule out acute bacterial rhinosinusitis (PPV, <40%)
- 4 or more symptoms rule in acute bacterial rhinosinusitis (PPV, 81%) (level of evidence [LOE]: 4)
- 2 or 3 symptoms (PPV, 40%–63%) may benefit from radiography (SOR: C).10
Jacob M. Reider, MD
Department of Family and Community Medicine, Albany Medical College, Albany, NY
This summary emphasizes inconsistencies in the literature and the limited predictive value of clinical findings when diagnosing sinusitis. But there is a way to sidestep this problem. When a patient presents complaining of “sinusitis,” I ask about their expectations for the visit and their understanding of their symptoms’ possible causes, and then I often show the patient a picture of sinus anatomy. By demonstrating that the osteomeatal complex is small, and focusing on obstruction rather than infection, I am able to avoid any confrontation about antibiotics entirely. Then I can recommend irrigation, hydration, and analgesia. For patients whose symptoms persist beyond 10 to 14 days, and for whom these initial interventions have failed, a trial of antibiotics may be indicated.
1. Berg O, Carenfelt C. Analysis of symptoms and clinical signs in the maxillary sinus empyema. Acta Otolaryngol 1988;105:343-349.
2. Lindbaek M, Hjortdahl P, Johnsen UL. Use of symptoms, signs, and blood tests to diagnose acute sinus infections in primary care: comparison with computed tomography. Fam Med 1996;28:183-188.
3. Williams JW, Jr, Simel DL, Roberts L, Samsa GP. Clinical evaluation for sinusitis. Making the diagnosis by history and physical examination. Ann Intern Med 1992;117:705-710.
4. van Duijn NP, Brouwer HJ, Lamberts H. Use of symptoms and signs to diagnose maxillary sinusitis in general practice: comparison with ultrasonography. BMJ 1992;305:684-687.
5. Lau J, Zucker D, Engels EA, et al. Diagnosis and treatment of acute bacterial rhinosinusitis. Evidence Report/Technology Assessment No. 9. Rockville, Md: Agency for Health Care Policy and Research; 1999.
6. Hansen JG, Schmidt H, Rosborg J, Lund E. Predicting acute maxillary sinusitis in a general practice population. BMJ 1995;311:233-236.
7. Lindbaek M, Hjortdahl P. The clinical diagnosis of acute purulent sinusitis in general practice—a review. Br J Gen Pract 2002;52:491-495.
8. Hickner JM, Bartlett JG, Besser RE, Gonzales R, Hoffman JR, Sande MA. Principles of appropriate antibiotic use for acute rhinosinusitis in adults: background. Ann Emerg Med 2001;37:703-710.
9. Antimicrobial treatment guidelines for acute bacterial rhinosinusitis. Sinus and Allergy Health Partnership. Otolaryngol Head Neck Surg 2000;123(1 Pt 2):5-31.
10. Low DE, Desrosiers M, McSherry J, et al. A practical guide for the diagnosis and treatment of acute sinusitis. CMAJ 1997;156 (Suppl 6):S1-S14.
1. Berg O, Carenfelt C. Analysis of symptoms and clinical signs in the maxillary sinus empyema. Acta Otolaryngol 1988;105:343-349.
2. Lindbaek M, Hjortdahl P, Johnsen UL. Use of symptoms, signs, and blood tests to diagnose acute sinus infections in primary care: comparison with computed tomography. Fam Med 1996;28:183-188.
3. Williams JW, Jr, Simel DL, Roberts L, Samsa GP. Clinical evaluation for sinusitis. Making the diagnosis by history and physical examination. Ann Intern Med 1992;117:705-710.
4. van Duijn NP, Brouwer HJ, Lamberts H. Use of symptoms and signs to diagnose maxillary sinusitis in general practice: comparison with ultrasonography. BMJ 1992;305:684-687.
5. Lau J, Zucker D, Engels EA, et al. Diagnosis and treatment of acute bacterial rhinosinusitis. Evidence Report/Technology Assessment No. 9. Rockville, Md: Agency for Health Care Policy and Research; 1999.
6. Hansen JG, Schmidt H, Rosborg J, Lund E. Predicting acute maxillary sinusitis in a general practice population. BMJ 1995;311:233-236.
7. Lindbaek M, Hjortdahl P. The clinical diagnosis of acute purulent sinusitis in general practice—a review. Br J Gen Pract 2002;52:491-495.
8. Hickner JM, Bartlett JG, Besser RE, Gonzales R, Hoffman JR, Sande MA. Principles of appropriate antibiotic use for acute rhinosinusitis in adults: background. Ann Emerg Med 2001;37:703-710.
9. Antimicrobial treatment guidelines for acute bacterial rhinosinusitis. Sinus and Allergy Health Partnership. Otolaryngol Head Neck Surg 2000;123(1 Pt 2):5-31.
10. Low DE, Desrosiers M, McSherry J, et al. A practical guide for the diagnosis and treatment of acute sinusitis. CMAJ 1997;156 (Suppl 6):S1-S14.
Evidence-based answers from the Family Physicians Inquiries Network
Is neurosurgery referral warranted for small brain aneurysms?
The risk of rupture of a small cerebral aneurysm (<10 mm) is very low in asymptomatic patients who have never had a subarachnoid hemorrhage. Because the risk of morbidity and mortality from surgical intervention significantly exceeds that of nonsurgical monitoring for this group, primary care physicians do not need to refer patients with this condition to a neurosurgeon for clipping (strength of recommendation [SOR]: B, based on cohort and case-control studies). For patients managed conservatively, annual office follow-up and imaging evaluation should be considered, and is necessary if a specific symptom should arise (SOR: C, based on expert opinion).
Evidence summary
Intracranial aneurysms are not rare. Based on autopsy data, prevalence has been estimated to be 0.2% to 9.9% of the population.1 Ten to 15 million Americans may have unruptured intracranial aneurysms, most of which remain undiagnosed.2
Conditions leading to the diagnosis of unruptured intracranial aneurysms include:
- headache (in 36% of patients)
- ischemic cerebrovascular disease (17.6%)
- cranial nerve deficits (15.4 %)
- aneurysmal mass effect (5.7%)
- ill-defined “spells” (4.8%)
- convulsive disorder (4.2%)
- subdural or intracerebral hemorrhage (2.7%)
- brain tumor (1.7%)
- nervous system degenerative disease (0.5%).2
No randomized controlled trials have examined whether unruptured intracranial aneurysms should be treated surgically. In the absence of a clinical trial, the evidence to answer this question is based on observational, cohort, and case-control studies, where the risks of the natural history of the condition are weighed against the risks of surgical intervention.3
One study of the natural history of unruptured cerebral aneurysm included 130 patients with 161 unruptured intracranial aneurysms who were followed for a mean of 8.3 years.4,5 This prospective investigation found that 15 patients suffered an intracranial hemorrhage. There were no ruptures of the 102 aneurysms that were ≤10 mm in diameter at the time of discovery.4,5
In the largest cohort study to date, patients without a history of subarachnoid hemorrhage had an overall risk of rupture of 0.05% per year over 7.5 years. This study also found that surgery-related morbidity and mortality at 1 year among patients aged <45 years was 6.5%, compared with 14.4% for those aged 45 to 64 years, and 32% for those aged >64 years.2
Recommendations from others
The Stroke Council of the American Heart Association recommends that observation is generally appropriate for incidental, small (<10-mm) aneurysms in patients without previous subarachnoid hemorrhage. However, special consideration for treatment should be given to young patients in this group, small aneurysms approaching the 10-mm size, and aneurysms with daughter sac formation ( Figure). In addition, patients with a family history of aneurysm or aneurysmal subarachnoid hemorrhage deserve special consideration for treatment.
For patients managed conservatively, periodic follow-up imaging should be considered; imaging is necessary if a specific symptom should arise. If changes in aneurysmal size or configuration are observed, special consideration for treatment should be made.6
Aneurysm with daughter sac
Wail Malaty, MD
Mountain Area Health Education Center Hendersonville, NC
Department of Family Medicine, University of North Carolina Chapel Hill
Asymptomatic cerebral aneurysms are potentially disastrous, since rupture can result in permanent neurologic disability or death. The diagnosis causes anxiety and fear in many patients. I try to explain to them, in clear and simple language, the minimal risk of rupture if the aneurysm is observed vs the higher risk of surgical intervention. I allow patients to express their fear and anxiety. I also elicit their input into the decision to refer. If their fear and anxiety cannot be allayed, I will refer them to a neurosurgeon. I invite them to return after the referral to discuss any further course of action.
1. Raaymakers TW, Rinkel GJ, Limburg M, Algra A. Mortality and morbidity of surgery for unruptured intracranial aneurysms: a meta-analysis. Stroke 1998;29:1531-1538.
2. International Study of Unruptured Intracranial Aneurysms Investigators. Unruptured intracranial aneurysms—risk of rupture and risks of surgical intervention. N Engl J Med 1998;339:1725-1733.
3. Brennan JW, Schwartz ML. Unruptured intracranial aneurysms: appraisal of the literature and suggested recommendations for surgery, using evidence-based medicine criteria. Neurosurgery 2000;47:1359-1372.
4. Wiebers DO, Whisnant JP, O’Fallon WM. The natural history of unruptured intracranial aneurysms. N Engl J Med 1981;304:696-698.
5. Wiebers DO, Whisnant JP, Sundt TM, Jr, O’Fallon WM. The significance of unruptured intracranial saccular aneurysms. J Neurosurg 1987;66:23-29.
6. Bederson JB, Awad IA, Wiebers DO, et al. Recommendations for the management of patients with unruptured intracranial aneurysms: A statement for healthcare professionals from the Stroke Council of the American Heart Association. Circulation 2000;102:2300-2308.
The risk of rupture of a small cerebral aneurysm (<10 mm) is very low in asymptomatic patients who have never had a subarachnoid hemorrhage. Because the risk of morbidity and mortality from surgical intervention significantly exceeds that of nonsurgical monitoring for this group, primary care physicians do not need to refer patients with this condition to a neurosurgeon for clipping (strength of recommendation [SOR]: B, based on cohort and case-control studies). For patients managed conservatively, annual office follow-up and imaging evaluation should be considered, and is necessary if a specific symptom should arise (SOR: C, based on expert opinion).
Evidence summary
Intracranial aneurysms are not rare. Based on autopsy data, prevalence has been estimated to be 0.2% to 9.9% of the population.1 Ten to 15 million Americans may have unruptured intracranial aneurysms, most of which remain undiagnosed.2
Conditions leading to the diagnosis of unruptured intracranial aneurysms include:
- headache (in 36% of patients)
- ischemic cerebrovascular disease (17.6%)
- cranial nerve deficits (15.4 %)
- aneurysmal mass effect (5.7%)
- ill-defined “spells” (4.8%)
- convulsive disorder (4.2%)
- subdural or intracerebral hemorrhage (2.7%)
- brain tumor (1.7%)
- nervous system degenerative disease (0.5%).2
No randomized controlled trials have examined whether unruptured intracranial aneurysms should be treated surgically. In the absence of a clinical trial, the evidence to answer this question is based on observational, cohort, and case-control studies, where the risks of the natural history of the condition are weighed against the risks of surgical intervention.3
One study of the natural history of unruptured cerebral aneurysm included 130 patients with 161 unruptured intracranial aneurysms who were followed for a mean of 8.3 years.4,5 This prospective investigation found that 15 patients suffered an intracranial hemorrhage. There were no ruptures of the 102 aneurysms that were ≤10 mm in diameter at the time of discovery.4,5
In the largest cohort study to date, patients without a history of subarachnoid hemorrhage had an overall risk of rupture of 0.05% per year over 7.5 years. This study also found that surgery-related morbidity and mortality at 1 year among patients aged <45 years was 6.5%, compared with 14.4% for those aged 45 to 64 years, and 32% for those aged >64 years.2
Recommendations from others
The Stroke Council of the American Heart Association recommends that observation is generally appropriate for incidental, small (<10-mm) aneurysms in patients without previous subarachnoid hemorrhage. However, special consideration for treatment should be given to young patients in this group, small aneurysms approaching the 10-mm size, and aneurysms with daughter sac formation ( Figure). In addition, patients with a family history of aneurysm or aneurysmal subarachnoid hemorrhage deserve special consideration for treatment.
For patients managed conservatively, periodic follow-up imaging should be considered; imaging is necessary if a specific symptom should arise. If changes in aneurysmal size or configuration are observed, special consideration for treatment should be made.6
Aneurysm with daughter sac
Wail Malaty, MD
Mountain Area Health Education Center Hendersonville, NC
Department of Family Medicine, University of North Carolina Chapel Hill
Asymptomatic cerebral aneurysms are potentially disastrous, since rupture can result in permanent neurologic disability or death. The diagnosis causes anxiety and fear in many patients. I try to explain to them, in clear and simple language, the minimal risk of rupture if the aneurysm is observed vs the higher risk of surgical intervention. I allow patients to express their fear and anxiety. I also elicit their input into the decision to refer. If their fear and anxiety cannot be allayed, I will refer them to a neurosurgeon. I invite them to return after the referral to discuss any further course of action.
The risk of rupture of a small cerebral aneurysm (<10 mm) is very low in asymptomatic patients who have never had a subarachnoid hemorrhage. Because the risk of morbidity and mortality from surgical intervention significantly exceeds that of nonsurgical monitoring for this group, primary care physicians do not need to refer patients with this condition to a neurosurgeon for clipping (strength of recommendation [SOR]: B, based on cohort and case-control studies). For patients managed conservatively, annual office follow-up and imaging evaluation should be considered, and is necessary if a specific symptom should arise (SOR: C, based on expert opinion).
Evidence summary
Intracranial aneurysms are not rare. Based on autopsy data, prevalence has been estimated to be 0.2% to 9.9% of the population.1 Ten to 15 million Americans may have unruptured intracranial aneurysms, most of which remain undiagnosed.2
Conditions leading to the diagnosis of unruptured intracranial aneurysms include:
- headache (in 36% of patients)
- ischemic cerebrovascular disease (17.6%)
- cranial nerve deficits (15.4 %)
- aneurysmal mass effect (5.7%)
- ill-defined “spells” (4.8%)
- convulsive disorder (4.2%)
- subdural or intracerebral hemorrhage (2.7%)
- brain tumor (1.7%)
- nervous system degenerative disease (0.5%).2
No randomized controlled trials have examined whether unruptured intracranial aneurysms should be treated surgically. In the absence of a clinical trial, the evidence to answer this question is based on observational, cohort, and case-control studies, where the risks of the natural history of the condition are weighed against the risks of surgical intervention.3
One study of the natural history of unruptured cerebral aneurysm included 130 patients with 161 unruptured intracranial aneurysms who were followed for a mean of 8.3 years.4,5 This prospective investigation found that 15 patients suffered an intracranial hemorrhage. There were no ruptures of the 102 aneurysms that were ≤10 mm in diameter at the time of discovery.4,5
In the largest cohort study to date, patients without a history of subarachnoid hemorrhage had an overall risk of rupture of 0.05% per year over 7.5 years. This study also found that surgery-related morbidity and mortality at 1 year among patients aged <45 years was 6.5%, compared with 14.4% for those aged 45 to 64 years, and 32% for those aged >64 years.2
Recommendations from others
The Stroke Council of the American Heart Association recommends that observation is generally appropriate for incidental, small (<10-mm) aneurysms in patients without previous subarachnoid hemorrhage. However, special consideration for treatment should be given to young patients in this group, small aneurysms approaching the 10-mm size, and aneurysms with daughter sac formation ( Figure). In addition, patients with a family history of aneurysm or aneurysmal subarachnoid hemorrhage deserve special consideration for treatment.
For patients managed conservatively, periodic follow-up imaging should be considered; imaging is necessary if a specific symptom should arise. If changes in aneurysmal size or configuration are observed, special consideration for treatment should be made.6
Aneurysm with daughter sac
Wail Malaty, MD
Mountain Area Health Education Center Hendersonville, NC
Department of Family Medicine, University of North Carolina Chapel Hill
Asymptomatic cerebral aneurysms are potentially disastrous, since rupture can result in permanent neurologic disability or death. The diagnosis causes anxiety and fear in many patients. I try to explain to them, in clear and simple language, the minimal risk of rupture if the aneurysm is observed vs the higher risk of surgical intervention. I allow patients to express their fear and anxiety. I also elicit their input into the decision to refer. If their fear and anxiety cannot be allayed, I will refer them to a neurosurgeon. I invite them to return after the referral to discuss any further course of action.
1. Raaymakers TW, Rinkel GJ, Limburg M, Algra A. Mortality and morbidity of surgery for unruptured intracranial aneurysms: a meta-analysis. Stroke 1998;29:1531-1538.
2. International Study of Unruptured Intracranial Aneurysms Investigators. Unruptured intracranial aneurysms—risk of rupture and risks of surgical intervention. N Engl J Med 1998;339:1725-1733.
3. Brennan JW, Schwartz ML. Unruptured intracranial aneurysms: appraisal of the literature and suggested recommendations for surgery, using evidence-based medicine criteria. Neurosurgery 2000;47:1359-1372.
4. Wiebers DO, Whisnant JP, O’Fallon WM. The natural history of unruptured intracranial aneurysms. N Engl J Med 1981;304:696-698.
5. Wiebers DO, Whisnant JP, Sundt TM, Jr, O’Fallon WM. The significance of unruptured intracranial saccular aneurysms. J Neurosurg 1987;66:23-29.
6. Bederson JB, Awad IA, Wiebers DO, et al. Recommendations for the management of patients with unruptured intracranial aneurysms: A statement for healthcare professionals from the Stroke Council of the American Heart Association. Circulation 2000;102:2300-2308.
1. Raaymakers TW, Rinkel GJ, Limburg M, Algra A. Mortality and morbidity of surgery for unruptured intracranial aneurysms: a meta-analysis. Stroke 1998;29:1531-1538.
2. International Study of Unruptured Intracranial Aneurysms Investigators. Unruptured intracranial aneurysms—risk of rupture and risks of surgical intervention. N Engl J Med 1998;339:1725-1733.
3. Brennan JW, Schwartz ML. Unruptured intracranial aneurysms: appraisal of the literature and suggested recommendations for surgery, using evidence-based medicine criteria. Neurosurgery 2000;47:1359-1372.
4. Wiebers DO, Whisnant JP, O’Fallon WM. The natural history of unruptured intracranial aneurysms. N Engl J Med 1981;304:696-698.
5. Wiebers DO, Whisnant JP, Sundt TM, Jr, O’Fallon WM. The significance of unruptured intracranial saccular aneurysms. J Neurosurg 1987;66:23-29.
6. Bederson JB, Awad IA, Wiebers DO, et al. Recommendations for the management of patients with unruptured intracranial aneurysms: A statement for healthcare professionals from the Stroke Council of the American Heart Association. Circulation 2000;102:2300-2308.
Evidence-based answers from the Family Physicians Inquiries Network
What is the prognosis of postherpetic neuralgia?
Postherpetic neuralgia occurs rarely among patients aged <50 years with herpes zoster. The incidence, duration, and severity of post-herpetic neuralgia increases with age, but older patients usually have only mild pain. Most cases resolve spontaneously within 3 months.1,2
Even in the highest-risk group, people aged >70 years, 25% had some pain at 3 months, but only 10% had pain at 1 year, and none had severe pain. Only a few patients have pain that persists for years (strength of recommendation: A, based on a well-done prospective cohort study).
Evidence summary
Postherpetic neuralgia is defined as pain that persists more than 1 month following onset of herpes zoster. The annual incidence of herpes zoster in population-based studies ranges from 1/1000 to 2/1000.1,3 Among adults aged >60 years, the annual incidence increases to 3.6/1000 for men and 5.6/1000 for women.1
In a prospective study performed in a primary care setting in Iceland, all cases of herpes zoster and postherpetic neuralgia occurring over 4.5 years in a population of 100,000 were identified, and all cases of postherpetic neuralgia were followed for up to 7.6 years. Few patients (4%) received antiviral medication.
In this study, postherpetic neuralgia followed herpes zoster in 2% of patients under age 40, 21% between the ages of 40 and 60, and in 40% of those over age 60.1,2 Subjects self-described pain as none, mild, moderate, or severe. Patients aged >60 years had the worst prognosis: 18% still had mild pain at 3 months and 6% had moderate or severe pain. At 1 year, 8% had mild pain and 2% had moderate pain. No patients had severe pain after 12 months.1,2
Among the 14 patients with pain persisting >12 months, 7 had complete resolution of pain, 5 had persisting pain that either improved or remained mild, 1 had ongoing moderate pain at 7 years, and 1 was lost to follow-up.2 (See Table.) Although postherpetic neuralgia can recur after resolution,4 no recurrence of pain was found among 183 randomly selected patients who had had resolution by 1 year.2
These results are similar to those found in an analysis of a retrospective cohort drawn from a large general practice network database,5 as well as other population-based studies.6,7 The prognosis is better than that reported in the placebo arms of trials of acute herpes zoster treatment.4 Patients in such trials are more likely to have severe disease than those seen in primary care settings.
TABLE
Risk of postherpetic neuralgia by age
| Age (y) | Pain at 3 mo | Pain at 1 y |
|---|---|---|
| >50 | 3% mild | 0% |
| 50–59 | 4% mild | 4% mild |
| 60–69 | 9% mild | 3% mild |
| 4% moderate to severe | 1% moderate | |
| ≥70 | 18% mild | 8% mild |
| 6% moderate to severe | 2% moderate |
Recommendations from others
A British guideline states that 5% of herpes zoster patients have postherpetic neuralgia 1 year after shingles.8 A review in the New England Journal of Medicine states that 48% of herpes zoster patients aged >70 years have postherpetic neuralgia at 1 year.9 This prevalence comes from a retrospective cohort study that combined patients presenting to a referral center with herpes zoster or postherpetic neuralgia into a single cohort, thus overestimating the prevalence of postherpetic neuralgia and providing a less reliable prognosis.10
Larry Halverson, MD
Cox Health Systems Family Practice Residency Program, Springfield, Missouri
Knowing the overall good prognosis for postherpetic neuralgia is helpful as I encounter patients with shingles. This answer is consistent with my experience. Fear of potential interminable pain and anecdotal experience with prolonged patient suffering has seduced me to start medications to “prevent” this problem. In some cases, my unnecessary (and unproven) “preventive” medications have produced new problems. Future research should focus on effective pain treatment options instead of prevention of a condition that usually resolves with time.
1. Helgason S, Sigurdsson JA, Gudmundsson S. The clinical course of herpes zoster: a prospective study in primary care. Eur J Gen Pract 1996;2:12-16.
2. Helgason S, Peturrson G, Gudmundsson S, Sigurdsson JA. Prevalence of postherpetic neuralgia after a single episode of herpes zoster: prospective study with long term follow up. BMJ 2000;321:1-4.
3. MacDonald BK, Cockerell OC, Sander JW, Shorvon SD. The incidence and lifetime prevalence of neurological disorders in a prospective community-based study in the UK. Brain 2000;123:665-676.
4. Alper BS, Lewis PR. Does treatment of acute herpes zoster prevent or shorten postherpetic neuralgia? J Fam Pract 2000;49:255-264.
5. Opstelten W, Mauritz J, de Wit N, van Wijck A, Stalman W. Herpes zoster and postherpetic neuralgia: incidence and risk indicators using a general practice research database. Fam Pract 2002;19:471-475.
6. Ragozzino MW, Melton LJ, Kurland LT, Chu CP, Perry HO. Population-based study of herpes zoster and its sequelae. Medicine (Baltimore) 1982;61:310-316.
7. Choo PW, Galil K, Donahue JG, Walker AM, Spiegelman D, Platt R. Risk factors for postherpetic neuralgia. Arch Intern Med 1997;157:1217-1224.
8. Guidelines for the management of shingles. Report of a working group of the British Society for the Study of Infection (BSSI). J Infect 1995;30:193-200.
9. Wood AJJ. Postherpetic neuralgia—pathogenesis, treatment and prevention. N Engl J Med 1996;335:32-41.
10. Morgas JM, Kierland RR. The outcome of patients with herpes zoster. Arch Dermatol 1957;75:193-196.
Postherpetic neuralgia occurs rarely among patients aged <50 years with herpes zoster. The incidence, duration, and severity of post-herpetic neuralgia increases with age, but older patients usually have only mild pain. Most cases resolve spontaneously within 3 months.1,2
Even in the highest-risk group, people aged >70 years, 25% had some pain at 3 months, but only 10% had pain at 1 year, and none had severe pain. Only a few patients have pain that persists for years (strength of recommendation: A, based on a well-done prospective cohort study).
Evidence summary
Postherpetic neuralgia is defined as pain that persists more than 1 month following onset of herpes zoster. The annual incidence of herpes zoster in population-based studies ranges from 1/1000 to 2/1000.1,3 Among adults aged >60 years, the annual incidence increases to 3.6/1000 for men and 5.6/1000 for women.1
In a prospective study performed in a primary care setting in Iceland, all cases of herpes zoster and postherpetic neuralgia occurring over 4.5 years in a population of 100,000 were identified, and all cases of postherpetic neuralgia were followed for up to 7.6 years. Few patients (4%) received antiviral medication.
In this study, postherpetic neuralgia followed herpes zoster in 2% of patients under age 40, 21% between the ages of 40 and 60, and in 40% of those over age 60.1,2 Subjects self-described pain as none, mild, moderate, or severe. Patients aged >60 years had the worst prognosis: 18% still had mild pain at 3 months and 6% had moderate or severe pain. At 1 year, 8% had mild pain and 2% had moderate pain. No patients had severe pain after 12 months.1,2
Among the 14 patients with pain persisting >12 months, 7 had complete resolution of pain, 5 had persisting pain that either improved or remained mild, 1 had ongoing moderate pain at 7 years, and 1 was lost to follow-up.2 (See Table.) Although postherpetic neuralgia can recur after resolution,4 no recurrence of pain was found among 183 randomly selected patients who had had resolution by 1 year.2
These results are similar to those found in an analysis of a retrospective cohort drawn from a large general practice network database,5 as well as other population-based studies.6,7 The prognosis is better than that reported in the placebo arms of trials of acute herpes zoster treatment.4 Patients in such trials are more likely to have severe disease than those seen in primary care settings.
TABLE
Risk of postherpetic neuralgia by age
| Age (y) | Pain at 3 mo | Pain at 1 y |
|---|---|---|
| >50 | 3% mild | 0% |
| 50–59 | 4% mild | 4% mild |
| 60–69 | 9% mild | 3% mild |
| 4% moderate to severe | 1% moderate | |
| ≥70 | 18% mild | 8% mild |
| 6% moderate to severe | 2% moderate |
Recommendations from others
A British guideline states that 5% of herpes zoster patients have postherpetic neuralgia 1 year after shingles.8 A review in the New England Journal of Medicine states that 48% of herpes zoster patients aged >70 years have postherpetic neuralgia at 1 year.9 This prevalence comes from a retrospective cohort study that combined patients presenting to a referral center with herpes zoster or postherpetic neuralgia into a single cohort, thus overestimating the prevalence of postherpetic neuralgia and providing a less reliable prognosis.10
Larry Halverson, MD
Cox Health Systems Family Practice Residency Program, Springfield, Missouri
Knowing the overall good prognosis for postherpetic neuralgia is helpful as I encounter patients with shingles. This answer is consistent with my experience. Fear of potential interminable pain and anecdotal experience with prolonged patient suffering has seduced me to start medications to “prevent” this problem. In some cases, my unnecessary (and unproven) “preventive” medications have produced new problems. Future research should focus on effective pain treatment options instead of prevention of a condition that usually resolves with time.
Postherpetic neuralgia occurs rarely among patients aged <50 years with herpes zoster. The incidence, duration, and severity of post-herpetic neuralgia increases with age, but older patients usually have only mild pain. Most cases resolve spontaneously within 3 months.1,2
Even in the highest-risk group, people aged >70 years, 25% had some pain at 3 months, but only 10% had pain at 1 year, and none had severe pain. Only a few patients have pain that persists for years (strength of recommendation: A, based on a well-done prospective cohort study).
Evidence summary
Postherpetic neuralgia is defined as pain that persists more than 1 month following onset of herpes zoster. The annual incidence of herpes zoster in population-based studies ranges from 1/1000 to 2/1000.1,3 Among adults aged >60 years, the annual incidence increases to 3.6/1000 for men and 5.6/1000 for women.1
In a prospective study performed in a primary care setting in Iceland, all cases of herpes zoster and postherpetic neuralgia occurring over 4.5 years in a population of 100,000 were identified, and all cases of postherpetic neuralgia were followed for up to 7.6 years. Few patients (4%) received antiviral medication.
In this study, postherpetic neuralgia followed herpes zoster in 2% of patients under age 40, 21% between the ages of 40 and 60, and in 40% of those over age 60.1,2 Subjects self-described pain as none, mild, moderate, or severe. Patients aged >60 years had the worst prognosis: 18% still had mild pain at 3 months and 6% had moderate or severe pain. At 1 year, 8% had mild pain and 2% had moderate pain. No patients had severe pain after 12 months.1,2
Among the 14 patients with pain persisting >12 months, 7 had complete resolution of pain, 5 had persisting pain that either improved or remained mild, 1 had ongoing moderate pain at 7 years, and 1 was lost to follow-up.2 (See Table.) Although postherpetic neuralgia can recur after resolution,4 no recurrence of pain was found among 183 randomly selected patients who had had resolution by 1 year.2
These results are similar to those found in an analysis of a retrospective cohort drawn from a large general practice network database,5 as well as other population-based studies.6,7 The prognosis is better than that reported in the placebo arms of trials of acute herpes zoster treatment.4 Patients in such trials are more likely to have severe disease than those seen in primary care settings.
TABLE
Risk of postherpetic neuralgia by age
| Age (y) | Pain at 3 mo | Pain at 1 y |
|---|---|---|
| >50 | 3% mild | 0% |
| 50–59 | 4% mild | 4% mild |
| 60–69 | 9% mild | 3% mild |
| 4% moderate to severe | 1% moderate | |
| ≥70 | 18% mild | 8% mild |
| 6% moderate to severe | 2% moderate |
Recommendations from others
A British guideline states that 5% of herpes zoster patients have postherpetic neuralgia 1 year after shingles.8 A review in the New England Journal of Medicine states that 48% of herpes zoster patients aged >70 years have postherpetic neuralgia at 1 year.9 This prevalence comes from a retrospective cohort study that combined patients presenting to a referral center with herpes zoster or postherpetic neuralgia into a single cohort, thus overestimating the prevalence of postherpetic neuralgia and providing a less reliable prognosis.10
Larry Halverson, MD
Cox Health Systems Family Practice Residency Program, Springfield, Missouri
Knowing the overall good prognosis for postherpetic neuralgia is helpful as I encounter patients with shingles. This answer is consistent with my experience. Fear of potential interminable pain and anecdotal experience with prolonged patient suffering has seduced me to start medications to “prevent” this problem. In some cases, my unnecessary (and unproven) “preventive” medications have produced new problems. Future research should focus on effective pain treatment options instead of prevention of a condition that usually resolves with time.
1. Helgason S, Sigurdsson JA, Gudmundsson S. The clinical course of herpes zoster: a prospective study in primary care. Eur J Gen Pract 1996;2:12-16.
2. Helgason S, Peturrson G, Gudmundsson S, Sigurdsson JA. Prevalence of postherpetic neuralgia after a single episode of herpes zoster: prospective study with long term follow up. BMJ 2000;321:1-4.
3. MacDonald BK, Cockerell OC, Sander JW, Shorvon SD. The incidence and lifetime prevalence of neurological disorders in a prospective community-based study in the UK. Brain 2000;123:665-676.
4. Alper BS, Lewis PR. Does treatment of acute herpes zoster prevent or shorten postherpetic neuralgia? J Fam Pract 2000;49:255-264.
5. Opstelten W, Mauritz J, de Wit N, van Wijck A, Stalman W. Herpes zoster and postherpetic neuralgia: incidence and risk indicators using a general practice research database. Fam Pract 2002;19:471-475.
6. Ragozzino MW, Melton LJ, Kurland LT, Chu CP, Perry HO. Population-based study of herpes zoster and its sequelae. Medicine (Baltimore) 1982;61:310-316.
7. Choo PW, Galil K, Donahue JG, Walker AM, Spiegelman D, Platt R. Risk factors for postherpetic neuralgia. Arch Intern Med 1997;157:1217-1224.
8. Guidelines for the management of shingles. Report of a working group of the British Society for the Study of Infection (BSSI). J Infect 1995;30:193-200.
9. Wood AJJ. Postherpetic neuralgia—pathogenesis, treatment and prevention. N Engl J Med 1996;335:32-41.
10. Morgas JM, Kierland RR. The outcome of patients with herpes zoster. Arch Dermatol 1957;75:193-196.
1. Helgason S, Sigurdsson JA, Gudmundsson S. The clinical course of herpes zoster: a prospective study in primary care. Eur J Gen Pract 1996;2:12-16.
2. Helgason S, Peturrson G, Gudmundsson S, Sigurdsson JA. Prevalence of postherpetic neuralgia after a single episode of herpes zoster: prospective study with long term follow up. BMJ 2000;321:1-4.
3. MacDonald BK, Cockerell OC, Sander JW, Shorvon SD. The incidence and lifetime prevalence of neurological disorders in a prospective community-based study in the UK. Brain 2000;123:665-676.
4. Alper BS, Lewis PR. Does treatment of acute herpes zoster prevent or shorten postherpetic neuralgia? J Fam Pract 2000;49:255-264.
5. Opstelten W, Mauritz J, de Wit N, van Wijck A, Stalman W. Herpes zoster and postherpetic neuralgia: incidence and risk indicators using a general practice research database. Fam Pract 2002;19:471-475.
6. Ragozzino MW, Melton LJ, Kurland LT, Chu CP, Perry HO. Population-based study of herpes zoster and its sequelae. Medicine (Baltimore) 1982;61:310-316.
7. Choo PW, Galil K, Donahue JG, Walker AM, Spiegelman D, Platt R. Risk factors for postherpetic neuralgia. Arch Intern Med 1997;157:1217-1224.
8. Guidelines for the management of shingles. Report of a working group of the British Society for the Study of Infection (BSSI). J Infect 1995;30:193-200.
9. Wood AJJ. Postherpetic neuralgia—pathogenesis, treatment and prevention. N Engl J Med 1996;335:32-41.
10. Morgas JM, Kierland RR. The outcome of patients with herpes zoster. Arch Dermatol 1957;75:193-196.
Evidence-based answers from the Family Physicians Inquiries Network
What is the most effective nicotine replacement therapy?
No single nicotine replacement therapy is most effective for all smokers. All forms of nicotine replacement therapy (gum, transdermal patch, spray, inhaler, and lozenge) are equally effective, increasing smoking cessation rates by about 150% to 200%.1,2
A Cochrane Review found that 17% of smokers who had used nicotine replacement therapy successfully quit at follow-up vs 10% of smokers in the control group.1 Except in special circumstances (medical contraindications, smoking <10 cigarettes daily, pregnancy, or breastfeeding), all smokers attempting to quit should be offered nicotine replacement therapy (strength of recommendation [SOR]: A).3
Higher doses of nicotine gum or lozenge (4 mg vs 2 mg) increase quit rates in heavy smokers.1,2 Use of high-dose patches (>21 mg) may benefit heavy smokers or those relapsing due to nicotine withdrawal (SOR: B).3 For relapsed smokers, combination therapy improves long-term abstinence rates (estimated abstinence 28.6% vs 17.4% for monotherapy) (SOR: B).3
Evidence summary
A Cochrane Review of 110 trials evaluating the efficacy of nicotine replacement therapy in 35,600 smokers found higher quit rates among heavy smokers using 4-mg compared with 2-mg nicotine gum (odds ratio [OR], 2.67; 95% confidence interval [CI], 1.69–4.22).1 However, patients often chew too few pieces of nicotine gum daily, resulting in underdosing.3 Smokers should use the gum on a fixed schedule (at least 1 piece every 1 to 2 hours).3
The Cochrane Review finds borderline evidence of a small benefit in abstinence rates (OR, 1.21; 95% CI, 1.03–1.42) with higher-dose nicotine patches (>21 mg/24 hr or 15 mg/16 hr) for heavy or relapsed smokers.1 Combining methods that maintain constant drug levels (transdermal patch) with those having more rapid effects (gum, spray, inhaler, lozenge) is more effective than monotherapy (OR, 1.9; 95% CI, 1.3–2.6).3 Reserve combination therapy for smokers who relapse following monotherapy.
Regarding concerns about weight gain, all nicotine replacement therapies delay but do not prevent weight gain. There is a dose-response relationship between nicotine gum and weight gain: smokers who use more gum gain less weight.3 Although abstinence rates are comparable across the 5 available forms of nicotine replacement, smokers unwilling to give up oral and behavioral rituals of smoking may perceive the inhaler as being more helpful (Table 1).4
Decisions about the best form of therapy can be based on patient preference, on degree of nicotine dependence (a Fagerström Test of Nicotine Dependence Scale score ≥5 [Table 2], or habitually smoking the first cigarette within 30 minutes of awakening),5 or nicotine replacement therapy history, which includes number and outcome of previous quit attempts, specific method used, duration, side effects, and proper usage.
Recommendations from others
The Cochrane Review states: “All of the commercially available forms of nicotine replacement therapy are effective as part of a strategy to promote smoking cessation. They increase quit rates approximately 1.5 to 2 fold regardless of setting. Use of nicotine replacement therapy should be preferentially directed to smokers who are motivated to quit, and have high levels of nicotine dependency. Choice of which form to use should reflect patient needs, tolerability and cost considerations. Patches are likely to be easier to use than gum or nasal spray in primary care settings.”1
The US Department of Health and Human Services Clinical Practice Guideline states: “All patients attempting to quit should be encouraged to use effective pharmacotherapies for smoking cessation except in the presence of special circumstances.”3 Heavy smokers should use 4-mg nicotine gum. Combining the nicotine patch with a self-administered form of nicotine replacement therapy (gum or nicotine nasal spray) is more efficacious than a single form of therapy. Patients should be encouraged to use combined treatments if unable to quit using a single form of first-line pharmacotherapy.3
TABLE 1
Nicotine replacement therapy selection guide
| Moderate smokers (10–20 cigarettes/d) | Heavy smokers (>30 cigarettes/d) | Weight concerns | |
|---|---|---|---|
| Gum | (4 mg vs 2 mg gum enhances quit rates) | (All nicotine replacement therapies delay weight gain, specifically nicotine gum) | |
| Transdermal patch | (Small benefit of dosing >21 mg) | ||
| Inhaler | |||
| Nasal spray | |||
| Lozenge | (Reserve 4 mg for heavy smokers) | ||
| Combination |
TABLE 2
Fagerström test for level of nicotine dependence (abridged)
| How soon after waking do you smoke first cigarette? | ______ Points | |
| Less than 5 minutes: 3 points | ||
| 5 to 30 minutes: 2 points | ||
| 31 to 60 minutes: 1 point | ||
| How many cigarettes do you smoke per day? | ______ Points | |
| More than 30 per day: 3 points | ||
| 21 to 30 per day: 2 points | ||
| 11 to 20 per day: 1 point | ||
| ______ Total Points | ||
| Interpretation | ||
| Total points | Level of dependence | Nictotine replacement therapy |
| 5–6 points | heavy nicotine dependence | consider 21-mg nicotine patch |
| 3–4 points | moderate nicotine dependence | consider 14-mg nicotine patch |
| 0–2 points | light nicotine dependence | consider 7-mg nicotine patch or no patch |
Erik Lindbloom, MD, MSPH
Department of Family and Community Medicine, University of Missouri– Columbia
Now that nicotine replacement therapy is available over the counter, prescribers may not consider or discuss delivery options with patients as much as they did in the past. As this Clinical Inquiry illustrates, there are situations when one approach may be recommended over another.
For example, the relapsed smoker who has tried 1 nicotine replacement product may not even be aware that other methods, including combination therapy, are possible. Considering the enormous potential health improvement that is achieved through smoking cessation, this may be one of the most important topics to revisit regularly with patients.
1. Silagy C, Lancaster T, Stead L, Mant D, Fowler G. Nicotine replacement therapy for smoking cessation. The Cochrane Library, Volume (Issue 4), 2002.
2. Shiffman S, Dresler CM, Hajek P, Gilburt SJ, Targett DA, Strahs KR. Efficacy of a nicotine lozenge for smoking cessation. Arch Intern Med 2002;162:1267-1276.
3. Fiore MC, Bailey WC, Cohen SJ, et al. Treating Tobacco Use and Dependence. Clinical Practice Guideline. Rockville, Md: US Dept of Health and Human Services, Public Health Service, June 2000.
4. Schneider NG, Olmstead R, Nilsson F, Vaghaiwalla Mody F, Franzon M, Doan K. Efficacy of a nicotine inhaler in smoking cessation: a double-blind, placebo-controlled trial. Addiction 1996;91:1293-1306.
5. Heatherton TF, Kozlowski LT, Frecker RC, Fagerström KO. The Fagerström Test for Nicotine Dependence: a revision of the Fagerström Tolerance Questionnaire. Br J Addict 1991;86:1119-1127.
No single nicotine replacement therapy is most effective for all smokers. All forms of nicotine replacement therapy (gum, transdermal patch, spray, inhaler, and lozenge) are equally effective, increasing smoking cessation rates by about 150% to 200%.1,2
A Cochrane Review found that 17% of smokers who had used nicotine replacement therapy successfully quit at follow-up vs 10% of smokers in the control group.1 Except in special circumstances (medical contraindications, smoking <10 cigarettes daily, pregnancy, or breastfeeding), all smokers attempting to quit should be offered nicotine replacement therapy (strength of recommendation [SOR]: A).3
Higher doses of nicotine gum or lozenge (4 mg vs 2 mg) increase quit rates in heavy smokers.1,2 Use of high-dose patches (>21 mg) may benefit heavy smokers or those relapsing due to nicotine withdrawal (SOR: B).3 For relapsed smokers, combination therapy improves long-term abstinence rates (estimated abstinence 28.6% vs 17.4% for monotherapy) (SOR: B).3
Evidence summary
A Cochrane Review of 110 trials evaluating the efficacy of nicotine replacement therapy in 35,600 smokers found higher quit rates among heavy smokers using 4-mg compared with 2-mg nicotine gum (odds ratio [OR], 2.67; 95% confidence interval [CI], 1.69–4.22).1 However, patients often chew too few pieces of nicotine gum daily, resulting in underdosing.3 Smokers should use the gum on a fixed schedule (at least 1 piece every 1 to 2 hours).3
The Cochrane Review finds borderline evidence of a small benefit in abstinence rates (OR, 1.21; 95% CI, 1.03–1.42) with higher-dose nicotine patches (>21 mg/24 hr or 15 mg/16 hr) for heavy or relapsed smokers.1 Combining methods that maintain constant drug levels (transdermal patch) with those having more rapid effects (gum, spray, inhaler, lozenge) is more effective than monotherapy (OR, 1.9; 95% CI, 1.3–2.6).3 Reserve combination therapy for smokers who relapse following monotherapy.
Regarding concerns about weight gain, all nicotine replacement therapies delay but do not prevent weight gain. There is a dose-response relationship between nicotine gum and weight gain: smokers who use more gum gain less weight.3 Although abstinence rates are comparable across the 5 available forms of nicotine replacement, smokers unwilling to give up oral and behavioral rituals of smoking may perceive the inhaler as being more helpful (Table 1).4
Decisions about the best form of therapy can be based on patient preference, on degree of nicotine dependence (a Fagerström Test of Nicotine Dependence Scale score ≥5 [Table 2], or habitually smoking the first cigarette within 30 minutes of awakening),5 or nicotine replacement therapy history, which includes number and outcome of previous quit attempts, specific method used, duration, side effects, and proper usage.
Recommendations from others
The Cochrane Review states: “All of the commercially available forms of nicotine replacement therapy are effective as part of a strategy to promote smoking cessation. They increase quit rates approximately 1.5 to 2 fold regardless of setting. Use of nicotine replacement therapy should be preferentially directed to smokers who are motivated to quit, and have high levels of nicotine dependency. Choice of which form to use should reflect patient needs, tolerability and cost considerations. Patches are likely to be easier to use than gum or nasal spray in primary care settings.”1
The US Department of Health and Human Services Clinical Practice Guideline states: “All patients attempting to quit should be encouraged to use effective pharmacotherapies for smoking cessation except in the presence of special circumstances.”3 Heavy smokers should use 4-mg nicotine gum. Combining the nicotine patch with a self-administered form of nicotine replacement therapy (gum or nicotine nasal spray) is more efficacious than a single form of therapy. Patients should be encouraged to use combined treatments if unable to quit using a single form of first-line pharmacotherapy.3
TABLE 1
Nicotine replacement therapy selection guide
| Moderate smokers (10–20 cigarettes/d) | Heavy smokers (>30 cigarettes/d) | Weight concerns | |
|---|---|---|---|
| Gum | (4 mg vs 2 mg gum enhances quit rates) | (All nicotine replacement therapies delay weight gain, specifically nicotine gum) | |
| Transdermal patch | (Small benefit of dosing >21 mg) | ||
| Inhaler | |||
| Nasal spray | |||
| Lozenge | (Reserve 4 mg for heavy smokers) | ||
| Combination |
TABLE 2
Fagerström test for level of nicotine dependence (abridged)
| How soon after waking do you smoke first cigarette? | ______ Points | |
| Less than 5 minutes: 3 points | ||
| 5 to 30 minutes: 2 points | ||
| 31 to 60 minutes: 1 point | ||
| How many cigarettes do you smoke per day? | ______ Points | |
| More than 30 per day: 3 points | ||
| 21 to 30 per day: 2 points | ||
| 11 to 20 per day: 1 point | ||
| ______ Total Points | ||
| Interpretation | ||
| Total points | Level of dependence | Nictotine replacement therapy |
| 5–6 points | heavy nicotine dependence | consider 21-mg nicotine patch |
| 3–4 points | moderate nicotine dependence | consider 14-mg nicotine patch |
| 0–2 points | light nicotine dependence | consider 7-mg nicotine patch or no patch |
Erik Lindbloom, MD, MSPH
Department of Family and Community Medicine, University of Missouri– Columbia
Now that nicotine replacement therapy is available over the counter, prescribers may not consider or discuss delivery options with patients as much as they did in the past. As this Clinical Inquiry illustrates, there are situations when one approach may be recommended over another.
For example, the relapsed smoker who has tried 1 nicotine replacement product may not even be aware that other methods, including combination therapy, are possible. Considering the enormous potential health improvement that is achieved through smoking cessation, this may be one of the most important topics to revisit regularly with patients.
No single nicotine replacement therapy is most effective for all smokers. All forms of nicotine replacement therapy (gum, transdermal patch, spray, inhaler, and lozenge) are equally effective, increasing smoking cessation rates by about 150% to 200%.1,2
A Cochrane Review found that 17% of smokers who had used nicotine replacement therapy successfully quit at follow-up vs 10% of smokers in the control group.1 Except in special circumstances (medical contraindications, smoking <10 cigarettes daily, pregnancy, or breastfeeding), all smokers attempting to quit should be offered nicotine replacement therapy (strength of recommendation [SOR]: A).3
Higher doses of nicotine gum or lozenge (4 mg vs 2 mg) increase quit rates in heavy smokers.1,2 Use of high-dose patches (>21 mg) may benefit heavy smokers or those relapsing due to nicotine withdrawal (SOR: B).3 For relapsed smokers, combination therapy improves long-term abstinence rates (estimated abstinence 28.6% vs 17.4% for monotherapy) (SOR: B).3
Evidence summary
A Cochrane Review of 110 trials evaluating the efficacy of nicotine replacement therapy in 35,600 smokers found higher quit rates among heavy smokers using 4-mg compared with 2-mg nicotine gum (odds ratio [OR], 2.67; 95% confidence interval [CI], 1.69–4.22).1 However, patients often chew too few pieces of nicotine gum daily, resulting in underdosing.3 Smokers should use the gum on a fixed schedule (at least 1 piece every 1 to 2 hours).3
The Cochrane Review finds borderline evidence of a small benefit in abstinence rates (OR, 1.21; 95% CI, 1.03–1.42) with higher-dose nicotine patches (>21 mg/24 hr or 15 mg/16 hr) for heavy or relapsed smokers.1 Combining methods that maintain constant drug levels (transdermal patch) with those having more rapid effects (gum, spray, inhaler, lozenge) is more effective than monotherapy (OR, 1.9; 95% CI, 1.3–2.6).3 Reserve combination therapy for smokers who relapse following monotherapy.
Regarding concerns about weight gain, all nicotine replacement therapies delay but do not prevent weight gain. There is a dose-response relationship between nicotine gum and weight gain: smokers who use more gum gain less weight.3 Although abstinence rates are comparable across the 5 available forms of nicotine replacement, smokers unwilling to give up oral and behavioral rituals of smoking may perceive the inhaler as being more helpful (Table 1).4
Decisions about the best form of therapy can be based on patient preference, on degree of nicotine dependence (a Fagerström Test of Nicotine Dependence Scale score ≥5 [Table 2], or habitually smoking the first cigarette within 30 minutes of awakening),5 or nicotine replacement therapy history, which includes number and outcome of previous quit attempts, specific method used, duration, side effects, and proper usage.
Recommendations from others
The Cochrane Review states: “All of the commercially available forms of nicotine replacement therapy are effective as part of a strategy to promote smoking cessation. They increase quit rates approximately 1.5 to 2 fold regardless of setting. Use of nicotine replacement therapy should be preferentially directed to smokers who are motivated to quit, and have high levels of nicotine dependency. Choice of which form to use should reflect patient needs, tolerability and cost considerations. Patches are likely to be easier to use than gum or nasal spray in primary care settings.”1
The US Department of Health and Human Services Clinical Practice Guideline states: “All patients attempting to quit should be encouraged to use effective pharmacotherapies for smoking cessation except in the presence of special circumstances.”3 Heavy smokers should use 4-mg nicotine gum. Combining the nicotine patch with a self-administered form of nicotine replacement therapy (gum or nicotine nasal spray) is more efficacious than a single form of therapy. Patients should be encouraged to use combined treatments if unable to quit using a single form of first-line pharmacotherapy.3
TABLE 1
Nicotine replacement therapy selection guide
| Moderate smokers (10–20 cigarettes/d) | Heavy smokers (>30 cigarettes/d) | Weight concerns | |
|---|---|---|---|
| Gum | (4 mg vs 2 mg gum enhances quit rates) | (All nicotine replacement therapies delay weight gain, specifically nicotine gum) | |
| Transdermal patch | (Small benefit of dosing >21 mg) | ||
| Inhaler | |||
| Nasal spray | |||
| Lozenge | (Reserve 4 mg for heavy smokers) | ||
| Combination |
TABLE 2
Fagerström test for level of nicotine dependence (abridged)
| How soon after waking do you smoke first cigarette? | ______ Points | |
| Less than 5 minutes: 3 points | ||
| 5 to 30 minutes: 2 points | ||
| 31 to 60 minutes: 1 point | ||
| How many cigarettes do you smoke per day? | ______ Points | |
| More than 30 per day: 3 points | ||
| 21 to 30 per day: 2 points | ||
| 11 to 20 per day: 1 point | ||
| ______ Total Points | ||
| Interpretation | ||
| Total points | Level of dependence | Nictotine replacement therapy |
| 5–6 points | heavy nicotine dependence | consider 21-mg nicotine patch |
| 3–4 points | moderate nicotine dependence | consider 14-mg nicotine patch |
| 0–2 points | light nicotine dependence | consider 7-mg nicotine patch or no patch |
Erik Lindbloom, MD, MSPH
Department of Family and Community Medicine, University of Missouri– Columbia
Now that nicotine replacement therapy is available over the counter, prescribers may not consider or discuss delivery options with patients as much as they did in the past. As this Clinical Inquiry illustrates, there are situations when one approach may be recommended over another.
For example, the relapsed smoker who has tried 1 nicotine replacement product may not even be aware that other methods, including combination therapy, are possible. Considering the enormous potential health improvement that is achieved through smoking cessation, this may be one of the most important topics to revisit regularly with patients.
1. Silagy C, Lancaster T, Stead L, Mant D, Fowler G. Nicotine replacement therapy for smoking cessation. The Cochrane Library, Volume (Issue 4), 2002.
2. Shiffman S, Dresler CM, Hajek P, Gilburt SJ, Targett DA, Strahs KR. Efficacy of a nicotine lozenge for smoking cessation. Arch Intern Med 2002;162:1267-1276.
3. Fiore MC, Bailey WC, Cohen SJ, et al. Treating Tobacco Use and Dependence. Clinical Practice Guideline. Rockville, Md: US Dept of Health and Human Services, Public Health Service, June 2000.
4. Schneider NG, Olmstead R, Nilsson F, Vaghaiwalla Mody F, Franzon M, Doan K. Efficacy of a nicotine inhaler in smoking cessation: a double-blind, placebo-controlled trial. Addiction 1996;91:1293-1306.
5. Heatherton TF, Kozlowski LT, Frecker RC, Fagerström KO. The Fagerström Test for Nicotine Dependence: a revision of the Fagerström Tolerance Questionnaire. Br J Addict 1991;86:1119-1127.
1. Silagy C, Lancaster T, Stead L, Mant D, Fowler G. Nicotine replacement therapy for smoking cessation. The Cochrane Library, Volume (Issue 4), 2002.
2. Shiffman S, Dresler CM, Hajek P, Gilburt SJ, Targett DA, Strahs KR. Efficacy of a nicotine lozenge for smoking cessation. Arch Intern Med 2002;162:1267-1276.
3. Fiore MC, Bailey WC, Cohen SJ, et al. Treating Tobacco Use and Dependence. Clinical Practice Guideline. Rockville, Md: US Dept of Health and Human Services, Public Health Service, June 2000.
4. Schneider NG, Olmstead R, Nilsson F, Vaghaiwalla Mody F, Franzon M, Doan K. Efficacy of a nicotine inhaler in smoking cessation: a double-blind, placebo-controlled trial. Addiction 1996;91:1293-1306.
5. Heatherton TF, Kozlowski LT, Frecker RC, Fagerström KO. The Fagerström Test for Nicotine Dependence: a revision of the Fagerström Tolerance Questionnaire. Br J Addict 1991;86:1119-1127.
Evidence-based answers from the Family Physicians Inquiries Network
Are antibiotics helpful for acute maxillary sinusitis?
The inability of clinical criteria to accurately differentiate bacterial from viral disease makes routine use of antibiotics inappropriate for clinically diagnosed maxillary sinusitis (strength of recommendation [SOR]: C, based on inconsistent systematic reviews and randomized controlled trials).
Antibiotics can provide symptomatic relief, best demonstrated in patients with bacterial maxillary sinusitis confirmed by computed tomography (CT) or sinus aspiration (SOR: A, based on 1 systematic review). However, this benefit does not persist in trials that better reflect general practice by using clinical diagnostic criteria (SOR: C, inconsistent studies).
In trials showing improvement with antibiotics, symptoms decrease, at best, 2 to 3 days sooner than with placebo, and, regardless of treatment, at least two thirds of patients are improved in 14 days (SOR: A, based on multiple systematic reviews).1
No evidence suggests that antibiotics decrease complication rates. Newer broad-spectrum antibiotics are no better at relieving symptoms or improving cure rates than “firstline” agents such as amoxicillin (SOR: A, based on multiple randomized controlled trials).2,3
Evidence summary
Nearly all trials comparing placebo with antibiotics for maxillary sinusitis are confounded by the difficulty in identifying true bacterial disease. The gold standard, sinus aspiration, offers the best diagnostic accuracy. CT scanning and plain radiography lack sufficient diagnostic accuracy to be useful alone, though CT scans offer better sensitivity.
One systematic review, limited to randomized controlled trials that required either radiographic or aspiration evidence of sinusitis, found penicillin superior to placebo,4 but all patients recovered in a few weeks regardless of treatment. Given that radiographs have poor diagnostic accuracy5 and that sinus aspiration is impractical in outpatient practice, such efficacy studies are less meaningful than effectiveness studies that use clinical criteria for study entry and outcome measurement.
No accurate clinical diagnostic criteria have been established. In ear, nose, and throat practices where bacterial sinusitis prevalence is high, clinical criteria identify only 70%–80% of cases compared with the sinus aspiration.6 In general practice, where the pretest probability of bacterial disease is far lower, clinical criteria are even less reliable,1 which confounds the interpretation of most clinical trials.
Accordingly, some placebo-controlled, primary-care–based clinical trials have shown symptomatic benefit of antibiotics for maxillary sinusitis7,8,9 while others have shown no benefit whatsoever.10,11,12 In those trials that demonstrated a significant difference, antibiotics were always more likely than placebo to cause side effects, and no control group fared worse than its matched antibiotic group by the end of a follow-up period of at least 25 days.
It is likely that antibiotics would be more useful if the subgroup of patients with bacterial disease could be accurately identified in outpatient practice. For the present, given that no such reliable criteria exist, that withholding antibiotics in these patients appears to be safe, and that antibiotic overuse has clear harm to individuals and society, sinusitis symptoms should be treated without antibiotics until the clinical course strongly suggests nonviral illness.
Recommendations from others
An evidence report from the Agency for Health Care Policy and Research recommends “initial symptomatic treatment or the use of clinical criteria to guide treatment.”1 The American Academy of Family Physicians “recognizes inappropriate use of antibiotics as a risk to both personal and public health and encourages only the appropriate use of these medications,”13 but has not published sinusitis guidelines. The Centers for Disease Control and most authorities suggest that bacterial disease can be inferred in those with signs or symptoms that suggest bacterial rather than viral illness (eg, overall duration of symptoms, so-called “double-sickening,” unilateral symptoms) and justify use of antibiotics in these patients.
Debra J. Barnette, PharmD, BCPS, CDE
Coastal Area Health Education Center, Wilmington, NC
The challenge in using antibiotics appropriately for acute maxillary sinusitis is in our inability to accurately determine bacterial vs viral causes based on clinical symptoms alone. Symptoms lasting <1 week are unlikely to be bacterial in origin. Patients without persistent purulent discharge and maxillary/facial tenderness or tooth pain are unlikely to have a bacterial infection.14
The key point: most patients will improve with or without antibiotic treatment. Withholding antibiotics does not increase the risk of developing complications. Balancing this against the potential for increasing antibiotic resistance should lead to prudent use. Antibiotics should be reserved for patients with severe or prolonged symptoms. Amoxicillin, doxycycline, and trimethoprim-sulfamethoxazole are efficacious and inexpensive initial options if therapy is warranted.
1. Lau, et al. Evidence report/technology assessment: Diagnosis and treatment of acute bacterial rhinosinusitis. AHCPR Publ. No. 99-E016. Rockville, Md: Agency for Health Care Policy & Research; 1999.
2. deFerranti SD, Ioannidis JP, Lau J, Anninger WV, Barza M. Are amoxicillin and folate inhibitors as effective as other antibiotics for acute sinusitis? A meta analysis. BMJ 1998;317:632-637.
3. Piccirillo JF, Mager DE, Frisse ME, Brophy RH, Goggin A. Impact of first-line vs. second-line antibiotics for the treatment of acute uncomplicated sinusitis. JAMA 2001;286:1849-1856.
4. Williams JW, Jr, Aguilar C, Makela M, et al. Antibiotics for acute maxillary sinusitis. Cochrane Database Syst Rev 2002;CD000243-Updated quarterly.
5. Engels EA, Terrin N, Barza M, Lau J. Meta-analysis of diagnostic tests for acute sinusitis. J Clin Epidemiol 2000;53:852-862.
6. Varonen H, Makela M, Savolainen S, Laara E, Hilden J. Comparison of ultrasound, radiography, and clinical examination in the diagnosis of acute maxillary sinusitis: a systematic review. J Clin Epidemiol 2000;53:940-948.
7. De Sutter AI, DeMeyere MJ, Christiaens TC, Van Driel ML, Peersman W, De Maeseneer JM. Does amoxicillin improve outcomes in patients with purulent rhinorrhea? A pragmatic randomized double-blind controlled trial in family practice. J Fam Pract 2002;51:317-323.
8. Haye R, Lingaas E, Hoivik HO, Odegard T. Azithromycin versus placebo in acute infectious rhinitis with clinical symptoms but without radiological signs of maxillary sinusitis. Eur J Clin Microbiol Infect Dis 1998;17:309-312.
9. Lindbaek M, Hjortdahl P, Johnsen VL. Randomised, double-blind, placebo controlled trial of penicillin V and amoxycillin in treatment of acute sinus infections in adults. BMJ 1996;313:325-329.
10. Stalman W, van Essen GA, van der Graaf Y, de Melker RA. The end of antibiotic treatment in adults with acute sinusitis-like complaints in general practice? A placebo-controlled double-blind randomized doxycycline trial. Br J Gen Pract 1997;47:794-799.
11. Stalman W, van Essen GA, van der Graaf Y, de Melker RA. Maxillary sinusitis in adults: an evaluation of placebo-controlled double-blind trials. Fam Pract 1997;14:124-129.
12. Van Buchem FL, Knottnerus JA, Schrijnemaekers VJ, Peeters MF. Primary-care-based randomised placebo-controlled trial of antibiotic treatment in acute maxillary sinusitis. Lancet 1997;349:683-687.
13. American Academy of Family Physicians. Clinical recommendations. Antibiotics. Available at: http://www.aafp.org/ x2584.xml. Accessed on May 6, 2003.
14. Snow V, Mottur-Pilson C, Hickner JM. Principles of appropriate antibiotic use for acute sinusitis in adults. Ann Intern Med 2001;134:495-497.
The inability of clinical criteria to accurately differentiate bacterial from viral disease makes routine use of antibiotics inappropriate for clinically diagnosed maxillary sinusitis (strength of recommendation [SOR]: C, based on inconsistent systematic reviews and randomized controlled trials).
Antibiotics can provide symptomatic relief, best demonstrated in patients with bacterial maxillary sinusitis confirmed by computed tomography (CT) or sinus aspiration (SOR: A, based on 1 systematic review). However, this benefit does not persist in trials that better reflect general practice by using clinical diagnostic criteria (SOR: C, inconsistent studies).
In trials showing improvement with antibiotics, symptoms decrease, at best, 2 to 3 days sooner than with placebo, and, regardless of treatment, at least two thirds of patients are improved in 14 days (SOR: A, based on multiple systematic reviews).1
No evidence suggests that antibiotics decrease complication rates. Newer broad-spectrum antibiotics are no better at relieving symptoms or improving cure rates than “firstline” agents such as amoxicillin (SOR: A, based on multiple randomized controlled trials).2,3
Evidence summary
Nearly all trials comparing placebo with antibiotics for maxillary sinusitis are confounded by the difficulty in identifying true bacterial disease. The gold standard, sinus aspiration, offers the best diagnostic accuracy. CT scanning and plain radiography lack sufficient diagnostic accuracy to be useful alone, though CT scans offer better sensitivity.
One systematic review, limited to randomized controlled trials that required either radiographic or aspiration evidence of sinusitis, found penicillin superior to placebo,4 but all patients recovered in a few weeks regardless of treatment. Given that radiographs have poor diagnostic accuracy5 and that sinus aspiration is impractical in outpatient practice, such efficacy studies are less meaningful than effectiveness studies that use clinical criteria for study entry and outcome measurement.
No accurate clinical diagnostic criteria have been established. In ear, nose, and throat practices where bacterial sinusitis prevalence is high, clinical criteria identify only 70%–80% of cases compared with the sinus aspiration.6 In general practice, where the pretest probability of bacterial disease is far lower, clinical criteria are even less reliable,1 which confounds the interpretation of most clinical trials.
Accordingly, some placebo-controlled, primary-care–based clinical trials have shown symptomatic benefit of antibiotics for maxillary sinusitis7,8,9 while others have shown no benefit whatsoever.10,11,12 In those trials that demonstrated a significant difference, antibiotics were always more likely than placebo to cause side effects, and no control group fared worse than its matched antibiotic group by the end of a follow-up period of at least 25 days.
It is likely that antibiotics would be more useful if the subgroup of patients with bacterial disease could be accurately identified in outpatient practice. For the present, given that no such reliable criteria exist, that withholding antibiotics in these patients appears to be safe, and that antibiotic overuse has clear harm to individuals and society, sinusitis symptoms should be treated without antibiotics until the clinical course strongly suggests nonviral illness.
Recommendations from others
An evidence report from the Agency for Health Care Policy and Research recommends “initial symptomatic treatment or the use of clinical criteria to guide treatment.”1 The American Academy of Family Physicians “recognizes inappropriate use of antibiotics as a risk to both personal and public health and encourages only the appropriate use of these medications,”13 but has not published sinusitis guidelines. The Centers for Disease Control and most authorities suggest that bacterial disease can be inferred in those with signs or symptoms that suggest bacterial rather than viral illness (eg, overall duration of symptoms, so-called “double-sickening,” unilateral symptoms) and justify use of antibiotics in these patients.
Debra J. Barnette, PharmD, BCPS, CDE
Coastal Area Health Education Center, Wilmington, NC
The challenge in using antibiotics appropriately for acute maxillary sinusitis is in our inability to accurately determine bacterial vs viral causes based on clinical symptoms alone. Symptoms lasting <1 week are unlikely to be bacterial in origin. Patients without persistent purulent discharge and maxillary/facial tenderness or tooth pain are unlikely to have a bacterial infection.14
The key point: most patients will improve with or without antibiotic treatment. Withholding antibiotics does not increase the risk of developing complications. Balancing this against the potential for increasing antibiotic resistance should lead to prudent use. Antibiotics should be reserved for patients with severe or prolonged symptoms. Amoxicillin, doxycycline, and trimethoprim-sulfamethoxazole are efficacious and inexpensive initial options if therapy is warranted.
The inability of clinical criteria to accurately differentiate bacterial from viral disease makes routine use of antibiotics inappropriate for clinically diagnosed maxillary sinusitis (strength of recommendation [SOR]: C, based on inconsistent systematic reviews and randomized controlled trials).
Antibiotics can provide symptomatic relief, best demonstrated in patients with bacterial maxillary sinusitis confirmed by computed tomography (CT) or sinus aspiration (SOR: A, based on 1 systematic review). However, this benefit does not persist in trials that better reflect general practice by using clinical diagnostic criteria (SOR: C, inconsistent studies).
In trials showing improvement with antibiotics, symptoms decrease, at best, 2 to 3 days sooner than with placebo, and, regardless of treatment, at least two thirds of patients are improved in 14 days (SOR: A, based on multiple systematic reviews).1
No evidence suggests that antibiotics decrease complication rates. Newer broad-spectrum antibiotics are no better at relieving symptoms or improving cure rates than “firstline” agents such as amoxicillin (SOR: A, based on multiple randomized controlled trials).2,3
Evidence summary
Nearly all trials comparing placebo with antibiotics for maxillary sinusitis are confounded by the difficulty in identifying true bacterial disease. The gold standard, sinus aspiration, offers the best diagnostic accuracy. CT scanning and plain radiography lack sufficient diagnostic accuracy to be useful alone, though CT scans offer better sensitivity.
One systematic review, limited to randomized controlled trials that required either radiographic or aspiration evidence of sinusitis, found penicillin superior to placebo,4 but all patients recovered in a few weeks regardless of treatment. Given that radiographs have poor diagnostic accuracy5 and that sinus aspiration is impractical in outpatient practice, such efficacy studies are less meaningful than effectiveness studies that use clinical criteria for study entry and outcome measurement.
No accurate clinical diagnostic criteria have been established. In ear, nose, and throat practices where bacterial sinusitis prevalence is high, clinical criteria identify only 70%–80% of cases compared with the sinus aspiration.6 In general practice, where the pretest probability of bacterial disease is far lower, clinical criteria are even less reliable,1 which confounds the interpretation of most clinical trials.
Accordingly, some placebo-controlled, primary-care–based clinical trials have shown symptomatic benefit of antibiotics for maxillary sinusitis7,8,9 while others have shown no benefit whatsoever.10,11,12 In those trials that demonstrated a significant difference, antibiotics were always more likely than placebo to cause side effects, and no control group fared worse than its matched antibiotic group by the end of a follow-up period of at least 25 days.
It is likely that antibiotics would be more useful if the subgroup of patients with bacterial disease could be accurately identified in outpatient practice. For the present, given that no such reliable criteria exist, that withholding antibiotics in these patients appears to be safe, and that antibiotic overuse has clear harm to individuals and society, sinusitis symptoms should be treated without antibiotics until the clinical course strongly suggests nonviral illness.
Recommendations from others
An evidence report from the Agency for Health Care Policy and Research recommends “initial symptomatic treatment or the use of clinical criteria to guide treatment.”1 The American Academy of Family Physicians “recognizes inappropriate use of antibiotics as a risk to both personal and public health and encourages only the appropriate use of these medications,”13 but has not published sinusitis guidelines. The Centers for Disease Control and most authorities suggest that bacterial disease can be inferred in those with signs or symptoms that suggest bacterial rather than viral illness (eg, overall duration of symptoms, so-called “double-sickening,” unilateral symptoms) and justify use of antibiotics in these patients.
Debra J. Barnette, PharmD, BCPS, CDE
Coastal Area Health Education Center, Wilmington, NC
The challenge in using antibiotics appropriately for acute maxillary sinusitis is in our inability to accurately determine bacterial vs viral causes based on clinical symptoms alone. Symptoms lasting <1 week are unlikely to be bacterial in origin. Patients without persistent purulent discharge and maxillary/facial tenderness or tooth pain are unlikely to have a bacterial infection.14
The key point: most patients will improve with or without antibiotic treatment. Withholding antibiotics does not increase the risk of developing complications. Balancing this against the potential for increasing antibiotic resistance should lead to prudent use. Antibiotics should be reserved for patients with severe or prolonged symptoms. Amoxicillin, doxycycline, and trimethoprim-sulfamethoxazole are efficacious and inexpensive initial options if therapy is warranted.
1. Lau, et al. Evidence report/technology assessment: Diagnosis and treatment of acute bacterial rhinosinusitis. AHCPR Publ. No. 99-E016. Rockville, Md: Agency for Health Care Policy & Research; 1999.
2. deFerranti SD, Ioannidis JP, Lau J, Anninger WV, Barza M. Are amoxicillin and folate inhibitors as effective as other antibiotics for acute sinusitis? A meta analysis. BMJ 1998;317:632-637.
3. Piccirillo JF, Mager DE, Frisse ME, Brophy RH, Goggin A. Impact of first-line vs. second-line antibiotics for the treatment of acute uncomplicated sinusitis. JAMA 2001;286:1849-1856.
4. Williams JW, Jr, Aguilar C, Makela M, et al. Antibiotics for acute maxillary sinusitis. Cochrane Database Syst Rev 2002;CD000243-Updated quarterly.
5. Engels EA, Terrin N, Barza M, Lau J. Meta-analysis of diagnostic tests for acute sinusitis. J Clin Epidemiol 2000;53:852-862.
6. Varonen H, Makela M, Savolainen S, Laara E, Hilden J. Comparison of ultrasound, radiography, and clinical examination in the diagnosis of acute maxillary sinusitis: a systematic review. J Clin Epidemiol 2000;53:940-948.
7. De Sutter AI, DeMeyere MJ, Christiaens TC, Van Driel ML, Peersman W, De Maeseneer JM. Does amoxicillin improve outcomes in patients with purulent rhinorrhea? A pragmatic randomized double-blind controlled trial in family practice. J Fam Pract 2002;51:317-323.
8. Haye R, Lingaas E, Hoivik HO, Odegard T. Azithromycin versus placebo in acute infectious rhinitis with clinical symptoms but without radiological signs of maxillary sinusitis. Eur J Clin Microbiol Infect Dis 1998;17:309-312.
9. Lindbaek M, Hjortdahl P, Johnsen VL. Randomised, double-blind, placebo controlled trial of penicillin V and amoxycillin in treatment of acute sinus infections in adults. BMJ 1996;313:325-329.
10. Stalman W, van Essen GA, van der Graaf Y, de Melker RA. The end of antibiotic treatment in adults with acute sinusitis-like complaints in general practice? A placebo-controlled double-blind randomized doxycycline trial. Br J Gen Pract 1997;47:794-799.
11. Stalman W, van Essen GA, van der Graaf Y, de Melker RA. Maxillary sinusitis in adults: an evaluation of placebo-controlled double-blind trials. Fam Pract 1997;14:124-129.
12. Van Buchem FL, Knottnerus JA, Schrijnemaekers VJ, Peeters MF. Primary-care-based randomised placebo-controlled trial of antibiotic treatment in acute maxillary sinusitis. Lancet 1997;349:683-687.
13. American Academy of Family Physicians. Clinical recommendations. Antibiotics. Available at: http://www.aafp.org/ x2584.xml. Accessed on May 6, 2003.
14. Snow V, Mottur-Pilson C, Hickner JM. Principles of appropriate antibiotic use for acute sinusitis in adults. Ann Intern Med 2001;134:495-497.
1. Lau, et al. Evidence report/technology assessment: Diagnosis and treatment of acute bacterial rhinosinusitis. AHCPR Publ. No. 99-E016. Rockville, Md: Agency for Health Care Policy & Research; 1999.
2. deFerranti SD, Ioannidis JP, Lau J, Anninger WV, Barza M. Are amoxicillin and folate inhibitors as effective as other antibiotics for acute sinusitis? A meta analysis. BMJ 1998;317:632-637.
3. Piccirillo JF, Mager DE, Frisse ME, Brophy RH, Goggin A. Impact of first-line vs. second-line antibiotics for the treatment of acute uncomplicated sinusitis. JAMA 2001;286:1849-1856.
4. Williams JW, Jr, Aguilar C, Makela M, et al. Antibiotics for acute maxillary sinusitis. Cochrane Database Syst Rev 2002;CD000243-Updated quarterly.
5. Engels EA, Terrin N, Barza M, Lau J. Meta-analysis of diagnostic tests for acute sinusitis. J Clin Epidemiol 2000;53:852-862.
6. Varonen H, Makela M, Savolainen S, Laara E, Hilden J. Comparison of ultrasound, radiography, and clinical examination in the diagnosis of acute maxillary sinusitis: a systematic review. J Clin Epidemiol 2000;53:940-948.
7. De Sutter AI, DeMeyere MJ, Christiaens TC, Van Driel ML, Peersman W, De Maeseneer JM. Does amoxicillin improve outcomes in patients with purulent rhinorrhea? A pragmatic randomized double-blind controlled trial in family practice. J Fam Pract 2002;51:317-323.
8. Haye R, Lingaas E, Hoivik HO, Odegard T. Azithromycin versus placebo in acute infectious rhinitis with clinical symptoms but without radiological signs of maxillary sinusitis. Eur J Clin Microbiol Infect Dis 1998;17:309-312.
9. Lindbaek M, Hjortdahl P, Johnsen VL. Randomised, double-blind, placebo controlled trial of penicillin V and amoxycillin in treatment of acute sinus infections in adults. BMJ 1996;313:325-329.
10. Stalman W, van Essen GA, van der Graaf Y, de Melker RA. The end of antibiotic treatment in adults with acute sinusitis-like complaints in general practice? A placebo-controlled double-blind randomized doxycycline trial. Br J Gen Pract 1997;47:794-799.
11. Stalman W, van Essen GA, van der Graaf Y, de Melker RA. Maxillary sinusitis in adults: an evaluation of placebo-controlled double-blind trials. Fam Pract 1997;14:124-129.
12. Van Buchem FL, Knottnerus JA, Schrijnemaekers VJ, Peeters MF. Primary-care-based randomised placebo-controlled trial of antibiotic treatment in acute maxillary sinusitis. Lancet 1997;349:683-687.
13. American Academy of Family Physicians. Clinical recommendations. Antibiotics. Available at: http://www.aafp.org/ x2584.xml. Accessed on May 6, 2003.
14. Snow V, Mottur-Pilson C, Hickner JM. Principles of appropriate antibiotic use for acute sinusitis in adults. Ann Intern Med 2001;134:495-497.
Evidence-based answers from the Family Physicians Inquiries Network
Does daily monitoring of blood glucose predict hemoglobin A1c levels?
Hemoglobin A1c (HbA1c) levels correlate closely, though not perfectly, with blood glucose levels in patients with diabetes (strength of recommendation [SOR]: A, based on systematic reviews).
Correlation is higher for blood glucose levels later in the day than earlier in the day, higher for blood glucose levels in the most recent 30 days than from the prior 31–120 days, and higher for patients with type 2 diabetes compared with patients with type 1 diabetes (SOR: A, based on cohort studies).
Evidence summary
Four cohort studies of patients with diabetes have compared overall mean blood glucose levels with HbA1c levels.1-4 All but one4 were limited to patients with type 1 diabetes. Study periods ranged from 1 to 6 months, and frequency of blood glucose measurement ranged from 2 to 4 times per day.
Correlation coefficients between mean blood glucose levels and HbA1c levels ranged from 0.71 to 0.86, implying that 50% to 74% of the variance in HbA1c is explained by the mean blood glucose (in each study, correlation was significant [P<.02]).
We found 5 studies comparing blood glucose measurements at specific times of day with HbA1c levels see (Table). Data from 3 studies comparing blood glucose values after lunchtime with those earlier in the day suggest that the lunchtime levels are more closely associated with HbA1c levels.5,7,9 No consistent difference was shown between preprandial and postprandial blood glucose levels in their strength of association with HbA1c levels. In 1 of these studies, a blood glucose level of 150 mg/dL 2 hours after lunch predicted a HbA1c of 7% with 85% sensitivity and 85% specificity.7 One study provided only limited information on blood glucose–HbA1c correlations in relation to mealtimes but did report that the times of day at which the 2 were best correlated were in the periods from midnight to 5:00 AM and between noon and 3:00 PM.9 One study compared patients with type 1 and type 2 diabetes and found a higher correlation between blood glucose and HbA1c levels in the latter.6
The relationship between HbA1c and blood glucose levels is such that blood glucose levels from the preceding 30 days determine about 50% of the total HbA1c.10 This relationship may be altered by uremia, intake of vitamins C or E, and conditions that affect erythrocyte turnover.11
It remains unclear whether management strategies that focus on minimizing HbA1c levels are optimal for prevention of diabetic complications.
Although HbA1c levels correlate with the risk of some complications, aspects of glycemia not reflected in the HbA1c level, such as the heights of glycemic “excursions” from the mean, may independently affect the risk of complications of diabetes.12 If so, quantitative analysis of day-to-day blood glucose levels might yield a better estimation of the risk of diabetic complications than HbA1c levels.
TABLE
Correlation coefficients between blood glucose levels and hemoglobin A1c levels
| Study | Rohlfing et el, 20025 | Prendergast et al, 19946 | Prendergast et al, 19946 | Avignon et al, 19977 | Bastyr et al, 20008 | Levetan et al, 20018 |
|---|---|---|---|---|---|---|
| Diabetes type | Type 1 | Type 1 | Type 2 | Type 2 | Type 2 | Unspecified |
| N | 1439 | 104 | 234 | 66 | 135 | 44 |
| Frequency of blood glucose measurement* | Quarterly over 6.5 y | “Periodically” over 3 y† | “Periodically” over 3 y† | Once only | Twice on separate days | Continuously for 3 days |
| Correlation coefficients | ||||||
| Pre-breakfast | 0.69 | 0.38 | 0.61 | 0.62 | 0.22 | <0.30 |
| Post-breakfast | 0.67 | 0.27 | 0.51 | 0.33 | ||
| Pre-lunch | 0.72 | 0.65 | ||||
| Post-lunch | 0.77 | 0.81 | ||||
| Pre-dinner | 0.75 | 0.78 | ||||
| Post-dinner | 0.78 | 0.34 | ||||
| Bedtime | 0.76 | |||||
| *Blood glucose measurements from Avignon et al, 19977 were taken at fixed times of day; time designations are based on average mealtimes in the study population. †Frequency of blood glucose measurements not specified. | ||||||
Recommendations from others
No official statement by any organization was found relating to the quantitative relationship between blood glucose levels from daily monitoring and HbA1c levels. However, the American Diabetes Association (ADA) specifies treatment goals for both HbA1c and blood glucose levels. An ADA expert panel recently concluded, “There are insufficient data to determine accurately the relative contribution of fasting plasma glucose and postprandial plasma glucose to HbA1c.”13
Tsveti Markova, MD
Department of Family Medicine, Wayne State University, Detroit, Mich
In practice, glycemic control is fundamental in managing patients with diabetes. I believe that treatment targets need to be individualized. Patient education about the importance of both HbA1c and self blood glucose monitoring are crucial in accomplishing this goal. While HbA1c <7% is strongly associated with reduction of microvascular complications, the blood glucose results are very useful in preventing hypoglycemia, as well as adjusting medication and insulin doses, diet, and exercise. The new, minimally invasive at-home glucometers and HbA1c test kits, which were recently approved by the Food and Drug Administration, improve compliance and help patients take control of their diabetes management.
1. Hempe JM, Gomez R, McCarter RJ, Jr, Chalew SA. High and low hemoglobin glycation phenotypes in type I diabetes: a challenge for interpretation of glycemic control. J Diabetes Complications 2002;16:313-320.
2. Kovatchev BP, Cox DJ, Straume M, Farhy LS. Association of self-monitoring blood glucose profiles with glycosylated hemoglobin in patients with insulin-dependent diabetes. Methods Enzymol 2000;321:410-417.
3. Peterson CM, Jones RL, Dupuis A, Levine BS, Bernstein R, O’Shea M. Feasibility of improved blood glucose control in patients with insulin-dependent diabetes mellitus. Diabetes Care 1979;2:329-335.
4. Ditzel J, Kjaergaard JJ. Haemoglobin A1c concentrations after initial treatment for newly discovered diabetes. Br Med J 1978;1:741-742.
5. Rohlfing CL, Wiedmeyer HM, Little RR, England JD, Tennill A, Goldstein DE. Defining the relationship between plasma glucose and HbA(1c): analysis of glucose profiles and HbA(1c) in the Diabetes Control and Complications Trial. Diabetes Care 2002;25:275-278.
6. Prendergast C, Smyth O, Murray F, Cunningham SK, McKenna TJ. The relationship of blood glucose and haemoglobin A1 levels in diabetic subjects. Ir J Med Sci 1994;163:233-235.
7. Avignon A, Radauceanu A, Monnier L. Nonfasting plasma glucose is a better marker of diabetic control than fasting plasma glucose in type 2 diabetes. Diabetes Care 1997;20:1822-1826.
8. Bastyr EJ, 3rd, Stuart CA, Brodows RG, et al. Therapy focused on lowering postprandial glucose, not fasting glucose, may be superior for lowering HbA1c. Diabetes Care 2000;23:1236-1241.
9. Levetan CS, Jeng LM, Thornton KR, Want L, Ratner RE. When do glucose values best correlate with hemoglobin A1c? Diabetes 2001;50(2 suppl):A124.-
10. Tahara Y, Shima K. The response of GHb to stepwise plasma glucose change over time in diabetic patients. Diabetes Care 1993;16:1313-1314.
11. Sacks DB, Bruns DE, Goldstein DE, Maclaren NK, McDonald JM, Parrott M. Guidelines and recommendations for laboratory analysis in the diagnosis and management of diabetes mellitus. Clin Chem 2002;48:436-472.
12. Goldstein DE, Little RR, Lorenz RA, Malone JI, Nathan D, Peterson CM. Tests of glycemia in diabetes. Diabetes Care 1995;18:896-909.
13. American Diabetes Association. Postprandial blood glucose. Diabetes Care 2001;24:775-778.
Hemoglobin A1c (HbA1c) levels correlate closely, though not perfectly, with blood glucose levels in patients with diabetes (strength of recommendation [SOR]: A, based on systematic reviews).
Correlation is higher for blood glucose levels later in the day than earlier in the day, higher for blood glucose levels in the most recent 30 days than from the prior 31–120 days, and higher for patients with type 2 diabetes compared with patients with type 1 diabetes (SOR: A, based on cohort studies).
Evidence summary
Four cohort studies of patients with diabetes have compared overall mean blood glucose levels with HbA1c levels.1-4 All but one4 were limited to patients with type 1 diabetes. Study periods ranged from 1 to 6 months, and frequency of blood glucose measurement ranged from 2 to 4 times per day.
Correlation coefficients between mean blood glucose levels and HbA1c levels ranged from 0.71 to 0.86, implying that 50% to 74% of the variance in HbA1c is explained by the mean blood glucose (in each study, correlation was significant [P<.02]).
We found 5 studies comparing blood glucose measurements at specific times of day with HbA1c levels see (Table). Data from 3 studies comparing blood glucose values after lunchtime with those earlier in the day suggest that the lunchtime levels are more closely associated with HbA1c levels.5,7,9 No consistent difference was shown between preprandial and postprandial blood glucose levels in their strength of association with HbA1c levels. In 1 of these studies, a blood glucose level of 150 mg/dL 2 hours after lunch predicted a HbA1c of 7% with 85% sensitivity and 85% specificity.7 One study provided only limited information on blood glucose–HbA1c correlations in relation to mealtimes but did report that the times of day at which the 2 were best correlated were in the periods from midnight to 5:00 AM and between noon and 3:00 PM.9 One study compared patients with type 1 and type 2 diabetes and found a higher correlation between blood glucose and HbA1c levels in the latter.6
The relationship between HbA1c and blood glucose levels is such that blood glucose levels from the preceding 30 days determine about 50% of the total HbA1c.10 This relationship may be altered by uremia, intake of vitamins C or E, and conditions that affect erythrocyte turnover.11
It remains unclear whether management strategies that focus on minimizing HbA1c levels are optimal for prevention of diabetic complications.
Although HbA1c levels correlate with the risk of some complications, aspects of glycemia not reflected in the HbA1c level, such as the heights of glycemic “excursions” from the mean, may independently affect the risk of complications of diabetes.12 If so, quantitative analysis of day-to-day blood glucose levels might yield a better estimation of the risk of diabetic complications than HbA1c levels.
TABLE
Correlation coefficients between blood glucose levels and hemoglobin A1c levels
| Study | Rohlfing et el, 20025 | Prendergast et al, 19946 | Prendergast et al, 19946 | Avignon et al, 19977 | Bastyr et al, 20008 | Levetan et al, 20018 |
|---|---|---|---|---|---|---|
| Diabetes type | Type 1 | Type 1 | Type 2 | Type 2 | Type 2 | Unspecified |
| N | 1439 | 104 | 234 | 66 | 135 | 44 |
| Frequency of blood glucose measurement* | Quarterly over 6.5 y | “Periodically” over 3 y† | “Periodically” over 3 y† | Once only | Twice on separate days | Continuously for 3 days |
| Correlation coefficients | ||||||
| Pre-breakfast | 0.69 | 0.38 | 0.61 | 0.62 | 0.22 | <0.30 |
| Post-breakfast | 0.67 | 0.27 | 0.51 | 0.33 | ||
| Pre-lunch | 0.72 | 0.65 | ||||
| Post-lunch | 0.77 | 0.81 | ||||
| Pre-dinner | 0.75 | 0.78 | ||||
| Post-dinner | 0.78 | 0.34 | ||||
| Bedtime | 0.76 | |||||
| *Blood glucose measurements from Avignon et al, 19977 were taken at fixed times of day; time designations are based on average mealtimes in the study population. †Frequency of blood glucose measurements not specified. | ||||||
Recommendations from others
No official statement by any organization was found relating to the quantitative relationship between blood glucose levels from daily monitoring and HbA1c levels. However, the American Diabetes Association (ADA) specifies treatment goals for both HbA1c and blood glucose levels. An ADA expert panel recently concluded, “There are insufficient data to determine accurately the relative contribution of fasting plasma glucose and postprandial plasma glucose to HbA1c.”13
Tsveti Markova, MD
Department of Family Medicine, Wayne State University, Detroit, Mich
In practice, glycemic control is fundamental in managing patients with diabetes. I believe that treatment targets need to be individualized. Patient education about the importance of both HbA1c and self blood glucose monitoring are crucial in accomplishing this goal. While HbA1c <7% is strongly associated with reduction of microvascular complications, the blood glucose results are very useful in preventing hypoglycemia, as well as adjusting medication and insulin doses, diet, and exercise. The new, minimally invasive at-home glucometers and HbA1c test kits, which were recently approved by the Food and Drug Administration, improve compliance and help patients take control of their diabetes management.
Hemoglobin A1c (HbA1c) levels correlate closely, though not perfectly, with blood glucose levels in patients with diabetes (strength of recommendation [SOR]: A, based on systematic reviews).
Correlation is higher for blood glucose levels later in the day than earlier in the day, higher for blood glucose levels in the most recent 30 days than from the prior 31–120 days, and higher for patients with type 2 diabetes compared with patients with type 1 diabetes (SOR: A, based on cohort studies).
Evidence summary
Four cohort studies of patients with diabetes have compared overall mean blood glucose levels with HbA1c levels.1-4 All but one4 were limited to patients with type 1 diabetes. Study periods ranged from 1 to 6 months, and frequency of blood glucose measurement ranged from 2 to 4 times per day.
Correlation coefficients between mean blood glucose levels and HbA1c levels ranged from 0.71 to 0.86, implying that 50% to 74% of the variance in HbA1c is explained by the mean blood glucose (in each study, correlation was significant [P<.02]).
We found 5 studies comparing blood glucose measurements at specific times of day with HbA1c levels see (Table). Data from 3 studies comparing blood glucose values after lunchtime with those earlier in the day suggest that the lunchtime levels are more closely associated with HbA1c levels.5,7,9 No consistent difference was shown between preprandial and postprandial blood glucose levels in their strength of association with HbA1c levels. In 1 of these studies, a blood glucose level of 150 mg/dL 2 hours after lunch predicted a HbA1c of 7% with 85% sensitivity and 85% specificity.7 One study provided only limited information on blood glucose–HbA1c correlations in relation to mealtimes but did report that the times of day at which the 2 were best correlated were in the periods from midnight to 5:00 AM and between noon and 3:00 PM.9 One study compared patients with type 1 and type 2 diabetes and found a higher correlation between blood glucose and HbA1c levels in the latter.6
The relationship between HbA1c and blood glucose levels is such that blood glucose levels from the preceding 30 days determine about 50% of the total HbA1c.10 This relationship may be altered by uremia, intake of vitamins C or E, and conditions that affect erythrocyte turnover.11
It remains unclear whether management strategies that focus on minimizing HbA1c levels are optimal for prevention of diabetic complications.
Although HbA1c levels correlate with the risk of some complications, aspects of glycemia not reflected in the HbA1c level, such as the heights of glycemic “excursions” from the mean, may independently affect the risk of complications of diabetes.12 If so, quantitative analysis of day-to-day blood glucose levels might yield a better estimation of the risk of diabetic complications than HbA1c levels.
TABLE
Correlation coefficients between blood glucose levels and hemoglobin A1c levels
| Study | Rohlfing et el, 20025 | Prendergast et al, 19946 | Prendergast et al, 19946 | Avignon et al, 19977 | Bastyr et al, 20008 | Levetan et al, 20018 |
|---|---|---|---|---|---|---|
| Diabetes type | Type 1 | Type 1 | Type 2 | Type 2 | Type 2 | Unspecified |
| N | 1439 | 104 | 234 | 66 | 135 | 44 |
| Frequency of blood glucose measurement* | Quarterly over 6.5 y | “Periodically” over 3 y† | “Periodically” over 3 y† | Once only | Twice on separate days | Continuously for 3 days |
| Correlation coefficients | ||||||
| Pre-breakfast | 0.69 | 0.38 | 0.61 | 0.62 | 0.22 | <0.30 |
| Post-breakfast | 0.67 | 0.27 | 0.51 | 0.33 | ||
| Pre-lunch | 0.72 | 0.65 | ||||
| Post-lunch | 0.77 | 0.81 | ||||
| Pre-dinner | 0.75 | 0.78 | ||||
| Post-dinner | 0.78 | 0.34 | ||||
| Bedtime | 0.76 | |||||
| *Blood glucose measurements from Avignon et al, 19977 were taken at fixed times of day; time designations are based on average mealtimes in the study population. †Frequency of blood glucose measurements not specified. | ||||||
Recommendations from others
No official statement by any organization was found relating to the quantitative relationship between blood glucose levels from daily monitoring and HbA1c levels. However, the American Diabetes Association (ADA) specifies treatment goals for both HbA1c and blood glucose levels. An ADA expert panel recently concluded, “There are insufficient data to determine accurately the relative contribution of fasting plasma glucose and postprandial plasma glucose to HbA1c.”13
Tsveti Markova, MD
Department of Family Medicine, Wayne State University, Detroit, Mich
In practice, glycemic control is fundamental in managing patients with diabetes. I believe that treatment targets need to be individualized. Patient education about the importance of both HbA1c and self blood glucose monitoring are crucial in accomplishing this goal. While HbA1c <7% is strongly associated with reduction of microvascular complications, the blood glucose results are very useful in preventing hypoglycemia, as well as adjusting medication and insulin doses, diet, and exercise. The new, minimally invasive at-home glucometers and HbA1c test kits, which were recently approved by the Food and Drug Administration, improve compliance and help patients take control of their diabetes management.
1. Hempe JM, Gomez R, McCarter RJ, Jr, Chalew SA. High and low hemoglobin glycation phenotypes in type I diabetes: a challenge for interpretation of glycemic control. J Diabetes Complications 2002;16:313-320.
2. Kovatchev BP, Cox DJ, Straume M, Farhy LS. Association of self-monitoring blood glucose profiles with glycosylated hemoglobin in patients with insulin-dependent diabetes. Methods Enzymol 2000;321:410-417.
3. Peterson CM, Jones RL, Dupuis A, Levine BS, Bernstein R, O’Shea M. Feasibility of improved blood glucose control in patients with insulin-dependent diabetes mellitus. Diabetes Care 1979;2:329-335.
4. Ditzel J, Kjaergaard JJ. Haemoglobin A1c concentrations after initial treatment for newly discovered diabetes. Br Med J 1978;1:741-742.
5. Rohlfing CL, Wiedmeyer HM, Little RR, England JD, Tennill A, Goldstein DE. Defining the relationship between plasma glucose and HbA(1c): analysis of glucose profiles and HbA(1c) in the Diabetes Control and Complications Trial. Diabetes Care 2002;25:275-278.
6. Prendergast C, Smyth O, Murray F, Cunningham SK, McKenna TJ. The relationship of blood glucose and haemoglobin A1 levels in diabetic subjects. Ir J Med Sci 1994;163:233-235.
7. Avignon A, Radauceanu A, Monnier L. Nonfasting plasma glucose is a better marker of diabetic control than fasting plasma glucose in type 2 diabetes. Diabetes Care 1997;20:1822-1826.
8. Bastyr EJ, 3rd, Stuart CA, Brodows RG, et al. Therapy focused on lowering postprandial glucose, not fasting glucose, may be superior for lowering HbA1c. Diabetes Care 2000;23:1236-1241.
9. Levetan CS, Jeng LM, Thornton KR, Want L, Ratner RE. When do glucose values best correlate with hemoglobin A1c? Diabetes 2001;50(2 suppl):A124.-
10. Tahara Y, Shima K. The response of GHb to stepwise plasma glucose change over time in diabetic patients. Diabetes Care 1993;16:1313-1314.
11. Sacks DB, Bruns DE, Goldstein DE, Maclaren NK, McDonald JM, Parrott M. Guidelines and recommendations for laboratory analysis in the diagnosis and management of diabetes mellitus. Clin Chem 2002;48:436-472.
12. Goldstein DE, Little RR, Lorenz RA, Malone JI, Nathan D, Peterson CM. Tests of glycemia in diabetes. Diabetes Care 1995;18:896-909.
13. American Diabetes Association. Postprandial blood glucose. Diabetes Care 2001;24:775-778.
1. Hempe JM, Gomez R, McCarter RJ, Jr, Chalew SA. High and low hemoglobin glycation phenotypes in type I diabetes: a challenge for interpretation of glycemic control. J Diabetes Complications 2002;16:313-320.
2. Kovatchev BP, Cox DJ, Straume M, Farhy LS. Association of self-monitoring blood glucose profiles with glycosylated hemoglobin in patients with insulin-dependent diabetes. Methods Enzymol 2000;321:410-417.
3. Peterson CM, Jones RL, Dupuis A, Levine BS, Bernstein R, O’Shea M. Feasibility of improved blood glucose control in patients with insulin-dependent diabetes mellitus. Diabetes Care 1979;2:329-335.
4. Ditzel J, Kjaergaard JJ. Haemoglobin A1c concentrations after initial treatment for newly discovered diabetes. Br Med J 1978;1:741-742.
5. Rohlfing CL, Wiedmeyer HM, Little RR, England JD, Tennill A, Goldstein DE. Defining the relationship between plasma glucose and HbA(1c): analysis of glucose profiles and HbA(1c) in the Diabetes Control and Complications Trial. Diabetes Care 2002;25:275-278.
6. Prendergast C, Smyth O, Murray F, Cunningham SK, McKenna TJ. The relationship of blood glucose and haemoglobin A1 levels in diabetic subjects. Ir J Med Sci 1994;163:233-235.
7. Avignon A, Radauceanu A, Monnier L. Nonfasting plasma glucose is a better marker of diabetic control than fasting plasma glucose in type 2 diabetes. Diabetes Care 1997;20:1822-1826.
8. Bastyr EJ, 3rd, Stuart CA, Brodows RG, et al. Therapy focused on lowering postprandial glucose, not fasting glucose, may be superior for lowering HbA1c. Diabetes Care 2000;23:1236-1241.
9. Levetan CS, Jeng LM, Thornton KR, Want L, Ratner RE. When do glucose values best correlate with hemoglobin A1c? Diabetes 2001;50(2 suppl):A124.-
10. Tahara Y, Shima K. The response of GHb to stepwise plasma glucose change over time in diabetic patients. Diabetes Care 1993;16:1313-1314.
11. Sacks DB, Bruns DE, Goldstein DE, Maclaren NK, McDonald JM, Parrott M. Guidelines and recommendations for laboratory analysis in the diagnosis and management of diabetes mellitus. Clin Chem 2002;48:436-472.
12. Goldstein DE, Little RR, Lorenz RA, Malone JI, Nathan D, Peterson CM. Tests of glycemia in diabetes. Diabetes Care 1995;18:896-909.
13. American Diabetes Association. Postprandial blood glucose. Diabetes Care 2001;24:775-778.
Evidence-based answers from the Family Physicians Inquiries Network
How should we manage infants at risk for group B streptococcal disease?
Asymptomatic term infants whose mothers received adequate intrapartum antibiotic prophylaxis (defined as intravenous penicillin or ampicillin at least 4 hours before delivery) for group B streptococcal disease do not need work-up or treatment (strength of recommendation [SOR]: B, based on retrospective, population-based study). These infants should be observed for 48 hours, but may be discharged after 24 hours in circumstances where close follow-up is available (SOR: D, based on expert opinion).
Symptomatic infants, premature infants (gestational age <35 weeks) of mothers who did not receive prophylaxis, and infants whose mothers had chorioamnionitis should receive a full evaluation (complete blood count, blood culture, and chest x-ray with or without a lumbar puncture) and an initial empiric antibiotic treatment with ampicillin or penicillin and gentamycin. If a term infant is not symptomatic and maternal antibiotic prophylaxis was not adequate, opinions differ as to whether to perform limited evaluation with empiric treatment or close observation (SOR: D, based on expert opinion). See Figure.
FIGURE
Management of infants born to mothers with group B streptococcal disease–positive cultures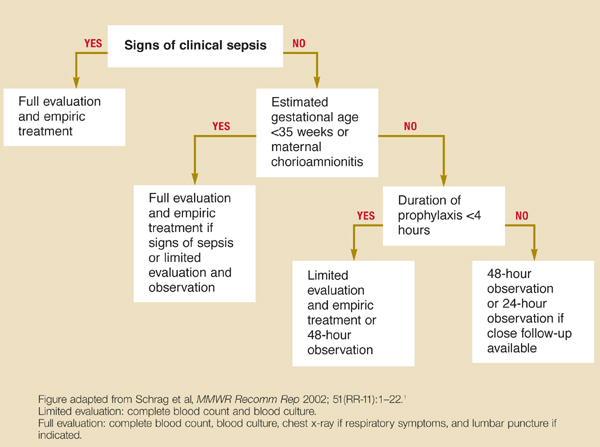
Evidence summary
Intrapartum antibiotic prophylaxis has decreased the incidence of early-onset group B streptococcal disease by 65% in the last decade.1 A multicenter population-based study demonstrated that basing prophylaxis on screening cultures is twice as effective as risk stratification, a previously recommended strategy.2
Intrapartum prophylaxis of women who had positive group B streptococcal disease screening cultures at 35 weeks will prevent 70% of earlyonset disease and 89% of fatalities.3,4 As demonstrated by multicenter retrospective studies, infants aged <35 weeks are at significantly higher risk of group B streptococcal disease than term infants (relative risk=1.5–2.07), and mortality for premature infants with early-onset disease (25%–30%) is substantially higher than for term infants with early-onset disease (2%–8%).2,5
A large retrospective study demonstrated that infants who developed early-onset disease despite intrapartum prophylaxis developed the same clinical syndrome in the same time frame (78% of early-onset disease evident in first 24 hours and 96% by 48 hours) as infants whose mothers did not receive prophylaxis.6
The duration of adequate intrapartum antibiotic prophylaxis was initially set at 4 hours, based on a study measuring antibiotic penetration into amniotic fluid.7 A recent randomized trial, enrolling more than 4500 women, has confirmed this finding. The vertical transmission rate of group B streptococcal disease, as measured by neonatal colonization (as opposed to clinical illness), is 46% when antibiotic prophylaxis is started <1 hour before delivery, 2.9% when prophylaxis is given at 2 to 4 hours, and 1.2% when given at least 4 hours before delivery.8
Implementation of these guidelines is aided by the adoption of an institution-wide policy to support point of care decision-making.9 A retrospective study after the release of the 1996 Centers for Disease Control (CDC) guidelines concluded that hospitals with established group B streptococcal disease policies had significantly fewer cases of early-onset disease (P=.038).10
Recommendations from others
The 2002 Prevention of Perinatal Group B Streptococcal Disease Revised Guidelines from the CDC states: “a healthy-appearing infant whose mother received >4 hours of [intrapartum antibiotic prophylaxis] before delivery may be discharged home as early as 24 hours after delivery, assuming other discharge criteria have been met and that a person able to comply fully with instructions for home observation will be present … if these conditions are not met, the infant should remain in the hospital for at least 48 hours of observation and until criteria for discharge are achieved.”1
These guidelines strongly support universal prenatal screening and the use of intrapartum antibiotic prophylaxis. Both the American Academy of Pediatrics and the American College Obstetrics and Gynecology have endorsed the CDC’s revised guidelines.
Richard Nicholas, MD
Rose Family Medicine Residency, Denver, Colo
The question of appropriate care of the infant exposed to group B streptococcal disease arises frequently in any practice caring for newborns. These clear, evidence-based recommendations are helpful in guiding that care. The evidence supports watchful waiting for appropriately covered newborns, providing reassurance for both parents and physicians.
Unfortunately, little evidence exists to guide care in a setting that seems to be quite common: the term, asymptomatic infant born to a mother who, in labor, received less-than-adequate intrapartum antibiotic prophylaxis. Further research for this subgroup is needed; in the meantime, physicians who provide maternity or newborn care should work together to develop protocols that ensure adequate intrapartum antibiotic coverage for mothers with group B streptococcal disease.
1. Schrag S, Gorwitz R, Fultz-Butts K, Schuchat A. Prevention of perinatal group B streptococcal disease. Revised guidelines from CDC MMWR Recomm Rep 2002;51(RR-11):1-22.
2. Schrag SJ, Zell ER, Lynfield R, et al. A population-based comparison of strategies to prevent early-onset group B streptococcal disease in neonates. N Engl J Med 2002;347:233-239.
3. Boyer KM, Gotoff SP. Prevention of early-onset neonatal group B streptococcal disease with selective intrapartum chemoprophylaxis. N Engl J Med 1986;314:1665-1669.
4. Schuchat A, Oxtoby M, Cochi S, et al. Population-based risk factors for neonatal group B streptococcal disease: results of a cohort study in metropolitan Atlanta. J Infect Dis 1990;162:672-677.
5. Cochi SL, Feldman RA. Estimating national incidence of group B streptococcal disease: the effect of adjusting for birth weight. Pediatr Infect Dis 1983;2:414-415.
6. Bromberger P, Lawrence JM, Braun D, Saunders B, Contreras R, Petitti DB. The influence of intrapartum antibiotics on the clinical spectrum of early-onset group B streptococcal infection in term infants. Pediatrics 2000;106:244-250.
7. Bray RE, Boe RW, Johnson WL. Transfer of ampicillin into fetus and amniotic fluid from maternal plasma in late pregnancy. Am J Obstet Gynecol 1966;96:938-942.
8. de Cueto M, Sanchez MJ, Sampedro A, Miranda JA, Herruzo AJ, Rosa-Fraile M. Timing of intrapartum ampicillin and prevention of vertical transmission of group B streptococcus. Obstet Gynecol 1998;91:112-114.
9. Clemens CJ, Gable EK. The development of a group B streptococcus prevention policy at a community hospital. J Perinatol 2002;22:523-525.
10. Factor SH, Whitney CG, Zywicki SS, Schuchat A. Effects of hospital policies based on 1996 group B streptococcal disease consensus guidelines. The Active Bacterial Core Surveillance Team. Obstet Gynecol 2000;95:377-382.
Asymptomatic term infants whose mothers received adequate intrapartum antibiotic prophylaxis (defined as intravenous penicillin or ampicillin at least 4 hours before delivery) for group B streptococcal disease do not need work-up or treatment (strength of recommendation [SOR]: B, based on retrospective, population-based study). These infants should be observed for 48 hours, but may be discharged after 24 hours in circumstances where close follow-up is available (SOR: D, based on expert opinion).
Symptomatic infants, premature infants (gestational age <35 weeks) of mothers who did not receive prophylaxis, and infants whose mothers had chorioamnionitis should receive a full evaluation (complete blood count, blood culture, and chest x-ray with or without a lumbar puncture) and an initial empiric antibiotic treatment with ampicillin or penicillin and gentamycin. If a term infant is not symptomatic and maternal antibiotic prophylaxis was not adequate, opinions differ as to whether to perform limited evaluation with empiric treatment or close observation (SOR: D, based on expert opinion). See Figure.
FIGURE
Management of infants born to mothers with group B streptococcal disease–positive cultures
Evidence summary
Intrapartum antibiotic prophylaxis has decreased the incidence of early-onset group B streptococcal disease by 65% in the last decade.1 A multicenter population-based study demonstrated that basing prophylaxis on screening cultures is twice as effective as risk stratification, a previously recommended strategy.2
Intrapartum prophylaxis of women who had positive group B streptococcal disease screening cultures at 35 weeks will prevent 70% of earlyonset disease and 89% of fatalities.3,4 As demonstrated by multicenter retrospective studies, infants aged <35 weeks are at significantly higher risk of group B streptococcal disease than term infants (relative risk=1.5–2.07), and mortality for premature infants with early-onset disease (25%–30%) is substantially higher than for term infants with early-onset disease (2%–8%).2,5
A large retrospective study demonstrated that infants who developed early-onset disease despite intrapartum prophylaxis developed the same clinical syndrome in the same time frame (78% of early-onset disease evident in first 24 hours and 96% by 48 hours) as infants whose mothers did not receive prophylaxis.6
The duration of adequate intrapartum antibiotic prophylaxis was initially set at 4 hours, based on a study measuring antibiotic penetration into amniotic fluid.7 A recent randomized trial, enrolling more than 4500 women, has confirmed this finding. The vertical transmission rate of group B streptococcal disease, as measured by neonatal colonization (as opposed to clinical illness), is 46% when antibiotic prophylaxis is started <1 hour before delivery, 2.9% when prophylaxis is given at 2 to 4 hours, and 1.2% when given at least 4 hours before delivery.8
Implementation of these guidelines is aided by the adoption of an institution-wide policy to support point of care decision-making.9 A retrospective study after the release of the 1996 Centers for Disease Control (CDC) guidelines concluded that hospitals with established group B streptococcal disease policies had significantly fewer cases of early-onset disease (P=.038).10
Recommendations from others
The 2002 Prevention of Perinatal Group B Streptococcal Disease Revised Guidelines from the CDC states: “a healthy-appearing infant whose mother received >4 hours of [intrapartum antibiotic prophylaxis] before delivery may be discharged home as early as 24 hours after delivery, assuming other discharge criteria have been met and that a person able to comply fully with instructions for home observation will be present … if these conditions are not met, the infant should remain in the hospital for at least 48 hours of observation and until criteria for discharge are achieved.”1
These guidelines strongly support universal prenatal screening and the use of intrapartum antibiotic prophylaxis. Both the American Academy of Pediatrics and the American College Obstetrics and Gynecology have endorsed the CDC’s revised guidelines.
Richard Nicholas, MD
Rose Family Medicine Residency, Denver, Colo
The question of appropriate care of the infant exposed to group B streptococcal disease arises frequently in any practice caring for newborns. These clear, evidence-based recommendations are helpful in guiding that care. The evidence supports watchful waiting for appropriately covered newborns, providing reassurance for both parents and physicians.
Unfortunately, little evidence exists to guide care in a setting that seems to be quite common: the term, asymptomatic infant born to a mother who, in labor, received less-than-adequate intrapartum antibiotic prophylaxis. Further research for this subgroup is needed; in the meantime, physicians who provide maternity or newborn care should work together to develop protocols that ensure adequate intrapartum antibiotic coverage for mothers with group B streptococcal disease.
Asymptomatic term infants whose mothers received adequate intrapartum antibiotic prophylaxis (defined as intravenous penicillin or ampicillin at least 4 hours before delivery) for group B streptococcal disease do not need work-up or treatment (strength of recommendation [SOR]: B, based on retrospective, population-based study). These infants should be observed for 48 hours, but may be discharged after 24 hours in circumstances where close follow-up is available (SOR: D, based on expert opinion).
Symptomatic infants, premature infants (gestational age <35 weeks) of mothers who did not receive prophylaxis, and infants whose mothers had chorioamnionitis should receive a full evaluation (complete blood count, blood culture, and chest x-ray with or without a lumbar puncture) and an initial empiric antibiotic treatment with ampicillin or penicillin and gentamycin. If a term infant is not symptomatic and maternal antibiotic prophylaxis was not adequate, opinions differ as to whether to perform limited evaluation with empiric treatment or close observation (SOR: D, based on expert opinion). See Figure.
FIGURE
Management of infants born to mothers with group B streptococcal disease–positive cultures
Evidence summary
Intrapartum antibiotic prophylaxis has decreased the incidence of early-onset group B streptococcal disease by 65% in the last decade.1 A multicenter population-based study demonstrated that basing prophylaxis on screening cultures is twice as effective as risk stratification, a previously recommended strategy.2
Intrapartum prophylaxis of women who had positive group B streptococcal disease screening cultures at 35 weeks will prevent 70% of earlyonset disease and 89% of fatalities.3,4 As demonstrated by multicenter retrospective studies, infants aged <35 weeks are at significantly higher risk of group B streptococcal disease than term infants (relative risk=1.5–2.07), and mortality for premature infants with early-onset disease (25%–30%) is substantially higher than for term infants with early-onset disease (2%–8%).2,5
A large retrospective study demonstrated that infants who developed early-onset disease despite intrapartum prophylaxis developed the same clinical syndrome in the same time frame (78% of early-onset disease evident in first 24 hours and 96% by 48 hours) as infants whose mothers did not receive prophylaxis.6
The duration of adequate intrapartum antibiotic prophylaxis was initially set at 4 hours, based on a study measuring antibiotic penetration into amniotic fluid.7 A recent randomized trial, enrolling more than 4500 women, has confirmed this finding. The vertical transmission rate of group B streptococcal disease, as measured by neonatal colonization (as opposed to clinical illness), is 46% when antibiotic prophylaxis is started <1 hour before delivery, 2.9% when prophylaxis is given at 2 to 4 hours, and 1.2% when given at least 4 hours before delivery.8
Implementation of these guidelines is aided by the adoption of an institution-wide policy to support point of care decision-making.9 A retrospective study after the release of the 1996 Centers for Disease Control (CDC) guidelines concluded that hospitals with established group B streptococcal disease policies had significantly fewer cases of early-onset disease (P=.038).10
Recommendations from others
The 2002 Prevention of Perinatal Group B Streptococcal Disease Revised Guidelines from the CDC states: “a healthy-appearing infant whose mother received >4 hours of [intrapartum antibiotic prophylaxis] before delivery may be discharged home as early as 24 hours after delivery, assuming other discharge criteria have been met and that a person able to comply fully with instructions for home observation will be present … if these conditions are not met, the infant should remain in the hospital for at least 48 hours of observation and until criteria for discharge are achieved.”1
These guidelines strongly support universal prenatal screening and the use of intrapartum antibiotic prophylaxis. Both the American Academy of Pediatrics and the American College Obstetrics and Gynecology have endorsed the CDC’s revised guidelines.
Richard Nicholas, MD
Rose Family Medicine Residency, Denver, Colo
The question of appropriate care of the infant exposed to group B streptococcal disease arises frequently in any practice caring for newborns. These clear, evidence-based recommendations are helpful in guiding that care. The evidence supports watchful waiting for appropriately covered newborns, providing reassurance for both parents and physicians.
Unfortunately, little evidence exists to guide care in a setting that seems to be quite common: the term, asymptomatic infant born to a mother who, in labor, received less-than-adequate intrapartum antibiotic prophylaxis. Further research for this subgroup is needed; in the meantime, physicians who provide maternity or newborn care should work together to develop protocols that ensure adequate intrapartum antibiotic coverage for mothers with group B streptococcal disease.
1. Schrag S, Gorwitz R, Fultz-Butts K, Schuchat A. Prevention of perinatal group B streptococcal disease. Revised guidelines from CDC MMWR Recomm Rep 2002;51(RR-11):1-22.
2. Schrag SJ, Zell ER, Lynfield R, et al. A population-based comparison of strategies to prevent early-onset group B streptococcal disease in neonates. N Engl J Med 2002;347:233-239.
3. Boyer KM, Gotoff SP. Prevention of early-onset neonatal group B streptococcal disease with selective intrapartum chemoprophylaxis. N Engl J Med 1986;314:1665-1669.
4. Schuchat A, Oxtoby M, Cochi S, et al. Population-based risk factors for neonatal group B streptococcal disease: results of a cohort study in metropolitan Atlanta. J Infect Dis 1990;162:672-677.
5. Cochi SL, Feldman RA. Estimating national incidence of group B streptococcal disease: the effect of adjusting for birth weight. Pediatr Infect Dis 1983;2:414-415.
6. Bromberger P, Lawrence JM, Braun D, Saunders B, Contreras R, Petitti DB. The influence of intrapartum antibiotics on the clinical spectrum of early-onset group B streptococcal infection in term infants. Pediatrics 2000;106:244-250.
7. Bray RE, Boe RW, Johnson WL. Transfer of ampicillin into fetus and amniotic fluid from maternal plasma in late pregnancy. Am J Obstet Gynecol 1966;96:938-942.
8. de Cueto M, Sanchez MJ, Sampedro A, Miranda JA, Herruzo AJ, Rosa-Fraile M. Timing of intrapartum ampicillin and prevention of vertical transmission of group B streptococcus. Obstet Gynecol 1998;91:112-114.
9. Clemens CJ, Gable EK. The development of a group B streptococcus prevention policy at a community hospital. J Perinatol 2002;22:523-525.
10. Factor SH, Whitney CG, Zywicki SS, Schuchat A. Effects of hospital policies based on 1996 group B streptococcal disease consensus guidelines. The Active Bacterial Core Surveillance Team. Obstet Gynecol 2000;95:377-382.
1. Schrag S, Gorwitz R, Fultz-Butts K, Schuchat A. Prevention of perinatal group B streptococcal disease. Revised guidelines from CDC MMWR Recomm Rep 2002;51(RR-11):1-22.
2. Schrag SJ, Zell ER, Lynfield R, et al. A population-based comparison of strategies to prevent early-onset group B streptococcal disease in neonates. N Engl J Med 2002;347:233-239.
3. Boyer KM, Gotoff SP. Prevention of early-onset neonatal group B streptococcal disease with selective intrapartum chemoprophylaxis. N Engl J Med 1986;314:1665-1669.
4. Schuchat A, Oxtoby M, Cochi S, et al. Population-based risk factors for neonatal group B streptococcal disease: results of a cohort study in metropolitan Atlanta. J Infect Dis 1990;162:672-677.
5. Cochi SL, Feldman RA. Estimating national incidence of group B streptococcal disease: the effect of adjusting for birth weight. Pediatr Infect Dis 1983;2:414-415.
6. Bromberger P, Lawrence JM, Braun D, Saunders B, Contreras R, Petitti DB. The influence of intrapartum antibiotics on the clinical spectrum of early-onset group B streptococcal infection in term infants. Pediatrics 2000;106:244-250.
7. Bray RE, Boe RW, Johnson WL. Transfer of ampicillin into fetus and amniotic fluid from maternal plasma in late pregnancy. Am J Obstet Gynecol 1966;96:938-942.
8. de Cueto M, Sanchez MJ, Sampedro A, Miranda JA, Herruzo AJ, Rosa-Fraile M. Timing of intrapartum ampicillin and prevention of vertical transmission of group B streptococcus. Obstet Gynecol 1998;91:112-114.
9. Clemens CJ, Gable EK. The development of a group B streptococcus prevention policy at a community hospital. J Perinatol 2002;22:523-525.
10. Factor SH, Whitney CG, Zywicki SS, Schuchat A. Effects of hospital policies based on 1996 group B streptococcal disease consensus guidelines. The Active Bacterial Core Surveillance Team. Obstet Gynecol 2000;95:377-382.
Evidence-based answers from the Family Physicians Inquiries Network
Are tympanostomy tubes indicated for recurrent acute otitis media?
For children with recurrent acute otitis media (here defined as 3 or more episodes in 6 months, or 4 or more in a year), tympanostomy tubes are indicated if middle-ear effusion is present. Tubes reduce the frequency of recurrent acute otitis media by 2 to 3 episodes per year in these patients (strength of recommendation [SOR]: A; based on randomized controlled trials).
Further benefits include improved quality of life for both child and caregiver and greater parental satisfaction (SOR: B; based on trials that included patients with recurrent acute otitis media or otitis media with effusion).
Tympanostomy tubes do not decrease the number of recurrent acute otitis media episodes in children without middle-ear effusion (SOR: A, based on randomized controlled trials). These children run the risk of adverse outcomes of tube placement, including transient or recurrent otorrhea, tympanosclerosis, focal atrophy, perforation, and cholesteatoma (SOR: A; based on meta-analysis).
Evidence summary
Several randomized controlled trials and a meta-analysis demonstrated that the children most likely to benefit from tympanostomy tubes are those more than 6 months old with middle-ear effusion who have had 3 or more episodes of acute otitis media in 6 months, or 4 or more episodes in 12 months.1-4 Data are inadequate to determine the lowest rate of recurrence that would suggest a benefit from tube placement.
A meta-analysis of 5 randomized trials comparing no surgery with placement of tubes for recurrent acute otitis media with or without middle-ear effusion showed that the placement of tubes resulted in a mean absolute decrease in acute otitis media incidence of 1.0 per year (95% confidence interval [CI], 0.4–1.6), and a decrease in the prevalence of middle-ear effusion by 115 days per year (95% CI, 11–220).4 The benefit of tubes for recurrent acute otitis media was demonstrated only in studies in which middle-ear effusion was present:2,3 one found 3.01 (95% CI, 2.18–3.84) fewer acute episodes per year;1,4 the other found 2.27 (95% CI, 1.03–3.51) fewer.2,4
One randomized controlled trial of 264 children, aged 7 to 35 months, with a history of recurrent acute otitis media but free of middle-ear effusion, compared tubes with medical therapy and found no difference in recurrence over 2 years.3 The medical therapy arm received prophylaxis with either amoxicillin or placebo. The amoxicillin arm had 0.6 fewer episodes of acute otitis media per year compared with the other 2, a statistically significant 40% decrease (relative risk reduction=0.4).3
The average time with otitis media of any type (acute otitis media, otitis media with effusion, or ottorhea) also decreased—15.0% in the placebo group, 10.0% in the amoxicillin group, and 6.6% in the tympanostomy tube group (amoxicillin vs. placebo, P=.03; tubes vs. placebo, P<.001).3 Higher dropout rates occurred in the amoxicillin and medical treatment groups.3
In prospective studies of patients receiving tubes for recurrent acute otitis media and otitis media with effusion, measures of quality of life—physical suffering, emotional distress, activity limitation, hearing loss, speech development, caregiver concern/worry, parental post-tube satisfaction,4,5,6 and an ear symptom score6 —improved after tube placement. Within several weeks of tube placement, 79% of children had improved quality of life, 17% had trivial change, and 4% were worse.4
A meta-analysis reporting sequelae of tympanostomy tubes found an absolute complication rate of 26% for transient otorrhea and 4% for chronic otorrhea.4
Compared with nonsurgical treatment, complication rates for tube placement were reported in 0.7% of surgically treated ears.7 Complications included:
- tympanosclerosis (relative risk [RR]=3.5 [95% CI, 2.6–4.9])
- focal atrophy (RR=1.7 [95% CI, 1.1–2.7])
- perforation (RR=3.5 [95% CI, 1.5–7.1])
- 2% with short-term tubes
- 16% with long-term tubes
- cholesteatoma (RR=2.6 [95% CI, 1.5–4.4]).
Recommendations from others
The Institute for Clinical Systems Improvement 2001 guidelines for recurrent acute otitis media treatment in children recommends initial antibiotic prophylaxis with amoxicillin (20 mg/kg/day) for 2 to 6 months (based on randomized controlled trial data). If there are 2 recurrences of acute otitis media during that time, then referral to an otorhinolaryngologist for possible tympanostomy tube placement is recommended.8
Michael Fisher, MD
University of North Carolina, Chapel Hill
Of the remaining challenges to the care of children with recurrent acute otitis media, 2 major issues are accurate diagnosis and the lack of information about long-term results. Diagnosis is difficult and requires pneumotoscopy and/or tympanometry. Without those techniques, a red drum (unless it is bulging) has a <40% positive predictive value for recurrent acute otitis media with effusion. On the other hand, with pneumotoscopy or tympanometry, the positive predictive value is 78% to 85%.
We don’t want to refer children unnecessarily for tubes. Delaying referral up to 9 months in children aged 6 to 36 months with middle-ear effusion does not seem to hurt language acquisition at 3 years of age. At this point, I know of no long-term follow-up studies of randomized controlled trials of >4 years to assess differences in language acquisition and hearing.
1. Gebhart DE. Tympanostomy tubes in the otitis media prone child. Laryngoscope 1981;91:849-866.
2. Gonzalez C, Arnold JE, Woody EA, et al. Prevention of recurrent acute otitis media: chemoprophylaxis versus tympanostomy tubes. Laryngoscope 1986;96:1330-1334.
3. Casselbrant ML, Kaleida PH, Rockette HE, et al. Efficacy of antimicrobial prophylaxis and of tympanostomy tube insertion for prevention of recurrent acute otitis media: results of a randomized clinical trial. Pediatr Infect Dis J 1992;11:278-286.
4. Rosenfeld RM. Surgical prevention of otitis media. Vaccine 2000;19:S134-S139.
5. Rosenfeld RM, Bhaya MH, Bower CM, et al. Impact of tympanostomy tubes on child quality of life. Arch Otolaryngol Head Neck Surg 2000;126:585-592.
6. Richards M, Giannoni C. Quality-of-life outcomes after surgical intervention for otitis media. Arch Otolaryngol Head Neck Surg 2002;128:776-782.
7. Kay DJ, Nelson M, Rosenfeld RM. Meta-analysis of tympanostomy tube sequelae. Otolaryngol Head Neck Surg 2001;124:374-380.
8. Diagnosis and treatment of otitis media in children. Bloomington, Minn: Institute for Clinical Systems Improvement (ICSI), 2001.
For children with recurrent acute otitis media (here defined as 3 or more episodes in 6 months, or 4 or more in a year), tympanostomy tubes are indicated if middle-ear effusion is present. Tubes reduce the frequency of recurrent acute otitis media by 2 to 3 episodes per year in these patients (strength of recommendation [SOR]: A; based on randomized controlled trials).
Further benefits include improved quality of life for both child and caregiver and greater parental satisfaction (SOR: B; based on trials that included patients with recurrent acute otitis media or otitis media with effusion).
Tympanostomy tubes do not decrease the number of recurrent acute otitis media episodes in children without middle-ear effusion (SOR: A, based on randomized controlled trials). These children run the risk of adverse outcomes of tube placement, including transient or recurrent otorrhea, tympanosclerosis, focal atrophy, perforation, and cholesteatoma (SOR: A; based on meta-analysis).
Evidence summary
Several randomized controlled trials and a meta-analysis demonstrated that the children most likely to benefit from tympanostomy tubes are those more than 6 months old with middle-ear effusion who have had 3 or more episodes of acute otitis media in 6 months, or 4 or more episodes in 12 months.1-4 Data are inadequate to determine the lowest rate of recurrence that would suggest a benefit from tube placement.
A meta-analysis of 5 randomized trials comparing no surgery with placement of tubes for recurrent acute otitis media with or without middle-ear effusion showed that the placement of tubes resulted in a mean absolute decrease in acute otitis media incidence of 1.0 per year (95% confidence interval [CI], 0.4–1.6), and a decrease in the prevalence of middle-ear effusion by 115 days per year (95% CI, 11–220).4 The benefit of tubes for recurrent acute otitis media was demonstrated only in studies in which middle-ear effusion was present:2,3 one found 3.01 (95% CI, 2.18–3.84) fewer acute episodes per year;1,4 the other found 2.27 (95% CI, 1.03–3.51) fewer.2,4
One randomized controlled trial of 264 children, aged 7 to 35 months, with a history of recurrent acute otitis media but free of middle-ear effusion, compared tubes with medical therapy and found no difference in recurrence over 2 years.3 The medical therapy arm received prophylaxis with either amoxicillin or placebo. The amoxicillin arm had 0.6 fewer episodes of acute otitis media per year compared with the other 2, a statistically significant 40% decrease (relative risk reduction=0.4).3
The average time with otitis media of any type (acute otitis media, otitis media with effusion, or ottorhea) also decreased—15.0% in the placebo group, 10.0% in the amoxicillin group, and 6.6% in the tympanostomy tube group (amoxicillin vs. placebo, P=.03; tubes vs. placebo, P<.001).3 Higher dropout rates occurred in the amoxicillin and medical treatment groups.3
In prospective studies of patients receiving tubes for recurrent acute otitis media and otitis media with effusion, measures of quality of life—physical suffering, emotional distress, activity limitation, hearing loss, speech development, caregiver concern/worry, parental post-tube satisfaction,4,5,6 and an ear symptom score6 —improved after tube placement. Within several weeks of tube placement, 79% of children had improved quality of life, 17% had trivial change, and 4% were worse.4
A meta-analysis reporting sequelae of tympanostomy tubes found an absolute complication rate of 26% for transient otorrhea and 4% for chronic otorrhea.4
Compared with nonsurgical treatment, complication rates for tube placement were reported in 0.7% of surgically treated ears.7 Complications included:
- tympanosclerosis (relative risk [RR]=3.5 [95% CI, 2.6–4.9])
- focal atrophy (RR=1.7 [95% CI, 1.1–2.7])
- perforation (RR=3.5 [95% CI, 1.5–7.1])
- 2% with short-term tubes
- 16% with long-term tubes
- cholesteatoma (RR=2.6 [95% CI, 1.5–4.4]).
Recommendations from others
The Institute for Clinical Systems Improvement 2001 guidelines for recurrent acute otitis media treatment in children recommends initial antibiotic prophylaxis with amoxicillin (20 mg/kg/day) for 2 to 6 months (based on randomized controlled trial data). If there are 2 recurrences of acute otitis media during that time, then referral to an otorhinolaryngologist for possible tympanostomy tube placement is recommended.8
Michael Fisher, MD
University of North Carolina, Chapel Hill
Of the remaining challenges to the care of children with recurrent acute otitis media, 2 major issues are accurate diagnosis and the lack of information about long-term results. Diagnosis is difficult and requires pneumotoscopy and/or tympanometry. Without those techniques, a red drum (unless it is bulging) has a <40% positive predictive value for recurrent acute otitis media with effusion. On the other hand, with pneumotoscopy or tympanometry, the positive predictive value is 78% to 85%.
We don’t want to refer children unnecessarily for tubes. Delaying referral up to 9 months in children aged 6 to 36 months with middle-ear effusion does not seem to hurt language acquisition at 3 years of age. At this point, I know of no long-term follow-up studies of randomized controlled trials of >4 years to assess differences in language acquisition and hearing.
For children with recurrent acute otitis media (here defined as 3 or more episodes in 6 months, or 4 or more in a year), tympanostomy tubes are indicated if middle-ear effusion is present. Tubes reduce the frequency of recurrent acute otitis media by 2 to 3 episodes per year in these patients (strength of recommendation [SOR]: A; based on randomized controlled trials).
Further benefits include improved quality of life for both child and caregiver and greater parental satisfaction (SOR: B; based on trials that included patients with recurrent acute otitis media or otitis media with effusion).
Tympanostomy tubes do not decrease the number of recurrent acute otitis media episodes in children without middle-ear effusion (SOR: A, based on randomized controlled trials). These children run the risk of adverse outcomes of tube placement, including transient or recurrent otorrhea, tympanosclerosis, focal atrophy, perforation, and cholesteatoma (SOR: A; based on meta-analysis).
Evidence summary
Several randomized controlled trials and a meta-analysis demonstrated that the children most likely to benefit from tympanostomy tubes are those more than 6 months old with middle-ear effusion who have had 3 or more episodes of acute otitis media in 6 months, or 4 or more episodes in 12 months.1-4 Data are inadequate to determine the lowest rate of recurrence that would suggest a benefit from tube placement.
A meta-analysis of 5 randomized trials comparing no surgery with placement of tubes for recurrent acute otitis media with or without middle-ear effusion showed that the placement of tubes resulted in a mean absolute decrease in acute otitis media incidence of 1.0 per year (95% confidence interval [CI], 0.4–1.6), and a decrease in the prevalence of middle-ear effusion by 115 days per year (95% CI, 11–220).4 The benefit of tubes for recurrent acute otitis media was demonstrated only in studies in which middle-ear effusion was present:2,3 one found 3.01 (95% CI, 2.18–3.84) fewer acute episodes per year;1,4 the other found 2.27 (95% CI, 1.03–3.51) fewer.2,4
One randomized controlled trial of 264 children, aged 7 to 35 months, with a history of recurrent acute otitis media but free of middle-ear effusion, compared tubes with medical therapy and found no difference in recurrence over 2 years.3 The medical therapy arm received prophylaxis with either amoxicillin or placebo. The amoxicillin arm had 0.6 fewer episodes of acute otitis media per year compared with the other 2, a statistically significant 40% decrease (relative risk reduction=0.4).3
The average time with otitis media of any type (acute otitis media, otitis media with effusion, or ottorhea) also decreased—15.0% in the placebo group, 10.0% in the amoxicillin group, and 6.6% in the tympanostomy tube group (amoxicillin vs. placebo, P=.03; tubes vs. placebo, P<.001).3 Higher dropout rates occurred in the amoxicillin and medical treatment groups.3
In prospective studies of patients receiving tubes for recurrent acute otitis media and otitis media with effusion, measures of quality of life—physical suffering, emotional distress, activity limitation, hearing loss, speech development, caregiver concern/worry, parental post-tube satisfaction,4,5,6 and an ear symptom score6 —improved after tube placement. Within several weeks of tube placement, 79% of children had improved quality of life, 17% had trivial change, and 4% were worse.4
A meta-analysis reporting sequelae of tympanostomy tubes found an absolute complication rate of 26% for transient otorrhea and 4% for chronic otorrhea.4
Compared with nonsurgical treatment, complication rates for tube placement were reported in 0.7% of surgically treated ears.7 Complications included:
- tympanosclerosis (relative risk [RR]=3.5 [95% CI, 2.6–4.9])
- focal atrophy (RR=1.7 [95% CI, 1.1–2.7])
- perforation (RR=3.5 [95% CI, 1.5–7.1])
- 2% with short-term tubes
- 16% with long-term tubes
- cholesteatoma (RR=2.6 [95% CI, 1.5–4.4]).
Recommendations from others
The Institute for Clinical Systems Improvement 2001 guidelines for recurrent acute otitis media treatment in children recommends initial antibiotic prophylaxis with amoxicillin (20 mg/kg/day) for 2 to 6 months (based on randomized controlled trial data). If there are 2 recurrences of acute otitis media during that time, then referral to an otorhinolaryngologist for possible tympanostomy tube placement is recommended.8
Michael Fisher, MD
University of North Carolina, Chapel Hill
Of the remaining challenges to the care of children with recurrent acute otitis media, 2 major issues are accurate diagnosis and the lack of information about long-term results. Diagnosis is difficult and requires pneumotoscopy and/or tympanometry. Without those techniques, a red drum (unless it is bulging) has a <40% positive predictive value for recurrent acute otitis media with effusion. On the other hand, with pneumotoscopy or tympanometry, the positive predictive value is 78% to 85%.
We don’t want to refer children unnecessarily for tubes. Delaying referral up to 9 months in children aged 6 to 36 months with middle-ear effusion does not seem to hurt language acquisition at 3 years of age. At this point, I know of no long-term follow-up studies of randomized controlled trials of >4 years to assess differences in language acquisition and hearing.
1. Gebhart DE. Tympanostomy tubes in the otitis media prone child. Laryngoscope 1981;91:849-866.
2. Gonzalez C, Arnold JE, Woody EA, et al. Prevention of recurrent acute otitis media: chemoprophylaxis versus tympanostomy tubes. Laryngoscope 1986;96:1330-1334.
3. Casselbrant ML, Kaleida PH, Rockette HE, et al. Efficacy of antimicrobial prophylaxis and of tympanostomy tube insertion for prevention of recurrent acute otitis media: results of a randomized clinical trial. Pediatr Infect Dis J 1992;11:278-286.
4. Rosenfeld RM. Surgical prevention of otitis media. Vaccine 2000;19:S134-S139.
5. Rosenfeld RM, Bhaya MH, Bower CM, et al. Impact of tympanostomy tubes on child quality of life. Arch Otolaryngol Head Neck Surg 2000;126:585-592.
6. Richards M, Giannoni C. Quality-of-life outcomes after surgical intervention for otitis media. Arch Otolaryngol Head Neck Surg 2002;128:776-782.
7. Kay DJ, Nelson M, Rosenfeld RM. Meta-analysis of tympanostomy tube sequelae. Otolaryngol Head Neck Surg 2001;124:374-380.
8. Diagnosis and treatment of otitis media in children. Bloomington, Minn: Institute for Clinical Systems Improvement (ICSI), 2001.
1. Gebhart DE. Tympanostomy tubes in the otitis media prone child. Laryngoscope 1981;91:849-866.
2. Gonzalez C, Arnold JE, Woody EA, et al. Prevention of recurrent acute otitis media: chemoprophylaxis versus tympanostomy tubes. Laryngoscope 1986;96:1330-1334.
3. Casselbrant ML, Kaleida PH, Rockette HE, et al. Efficacy of antimicrobial prophylaxis and of tympanostomy tube insertion for prevention of recurrent acute otitis media: results of a randomized clinical trial. Pediatr Infect Dis J 1992;11:278-286.
4. Rosenfeld RM. Surgical prevention of otitis media. Vaccine 2000;19:S134-S139.
5. Rosenfeld RM, Bhaya MH, Bower CM, et al. Impact of tympanostomy tubes on child quality of life. Arch Otolaryngol Head Neck Surg 2000;126:585-592.
6. Richards M, Giannoni C. Quality-of-life outcomes after surgical intervention for otitis media. Arch Otolaryngol Head Neck Surg 2002;128:776-782.
7. Kay DJ, Nelson M, Rosenfeld RM. Meta-analysis of tympanostomy tube sequelae. Otolaryngol Head Neck Surg 2001;124:374-380.
8. Diagnosis and treatment of otitis media in children. Bloomington, Minn: Institute for Clinical Systems Improvement (ICSI), 2001.
Evidence-based answers from the Family Physicians Inquiries Network