User login
Smoking cessation: Tactics that make a difference
- Recommend that your patients take advantage of telephone counseling—it improves both the quit rate and the long-term abstinence rate. Web-based cessation programs also support smokers in all stages of quitting.
- Encourage patients to use both pharmacotherapy and counseling to improve abstinence. Several medications—including bupropion and varenicline—achieve comparable rates of quitting and long-term abstinence.
- Train your office staff to help identify and counsel smokers.
CASE Smoker who uses OCs
Ann G. is a 34-year-old mother of two who has been coming to the office for her annual Pap smear for several years. Her medical history is significant only for her vaginal deliveries and mild gastroesophageal reflux. She takes oral contraceptives (OCs) and uses over-the-counter ranitidine hydrochloride (Zantac) as needed. On Ann’s most recent annual visit, the medical assistant, Tammy, takes her vital signs. The chart has a section about smoking status, and Tammy notes that Ann is a smoker.
During the office visit, the ObGyn explains to Ann that her smoking is a serious health risk and advises her to quit. She also informs Ann that she needs to find a new form of birth control next year, as smoking increases the risks of using OCs, especially after age 35. Ann nervously laughs off the warning.
When she returns the following year, Ann confesses to Tammy that she is still a smoker. When Tammy asks about quitting, Ann remains adamant: “No way—I can’t do it.” Nonetheless, during the office visit, the ObGyn raises the subject again, and Ann admits that she is afraid that quitting smoking will cause her to gain weight. The physician attempts to address Ann’s fears, talks about other birth control options, and gives her a 3-month prescription for OCs. Before ending the visit, the ObGyn tells Ann that they will discuss what to do about birth control when she returns in 3 months.
Ann faces an uphill battle. The amount of nicotine in cigarettes is increasing,1 making it harder to quit. The good news is that the treatment of tobacco addiction is constantly improving, and the number of tools in our arsenal is growing. In fact, there are many resources that we can try before turning to the prescription pad. However, when needed, pharmacotherapy is an important adjunct in a patient’s struggle to achieve abstinence.
“5-A” strategy sets stage for success
Treating Tobacco Use and Dependence, a useful publication from the Agency for Healthcare Research and Quality (AHRQ), offers guidelines on many aspects of tobacco cessation, from counseling to pharmacotherapy to reimbursement.2,3 The guidelines break the smoking cessation process into five A’s:
- Ask each patient about her smoking status.
- Advise each patient who smokes that she needs to stop smoking.
- Assess your patient’s willingness to make a quit attempt in the next 30 days.
- Assist your patient in making this quit attempt or encourage her to consider a quit attempt later.
- Arrange close follow-up of any quit attempts to help prevent relapse.
Take advantage of every opportunity you have to discuss the issue with patients; short conversations can make a difference. A Cochrane review of 39 trials including 31,000 smokers revealed that even brief advice—simply encouraging patients to quit—was statistically significant in helping the smoker quit (odds ratio [OR]=1.74; 95% confidence interval [CI], 1.48–2.05).5 The pooled data generated a quit rate difference of 2.5%: for every 40 people who were told to quit, one more smoker would.
Empower the office staff
Enlisting the help of the office staff can have a significant impact on the health of patients. Fiore and colleagues evaluated a proactive approach in which medical assistants, while assessing smoking status, invited all smokers to participate in a cessation study.6 (The assistants received periodic thank-you gifts for their efforts.)
Participants were randomized to self-selected treatment or nicotine replacement therapy (NRT) patches, with or without a support program. Some who received the patches and support program also received individual counseling. The result: Most smokers were open to encouragement to quit smoking. The 13% point-prevalence abstinence rate 1 year out was comparable to the rate observed (14%) in smokers volunteering for NRT studies in the Cochrane review of 39 trials noted earlier.5
Likewise, in a randomized controlled trial (RCT) involving community-based primary care clinics, Katz and associates demonstrated that intake clinicians can also play an important role in smoking cessation.7 In the study, researchers trained intake clinicians (including registered nurses, licensed practical nurses, and medical assistants) to identify smokers, provide brief counseling, and assist in their preparation to quit. Patients were offered vouchers for patches and a counselor’s business card. Intake clinicians received periodic feedback on their performance based on exit interviews of the patients. These interventions had a statistically significant effect in moderate-to-heavy smokers in quit attempts, quit rates, and continuous abstinence.
CASE…continued A change of heart
At the 3-month follow-up, Tammy learns that Ann is still smoking—but she now wants to quit. Ann says that she found a pack of cigarettes in her 14-year-old daughter’s backpack, and feels that the only way to prevent her from getting hooked is to set a good example.
Tammy gives her the state’s quitline number, suggests some online quitting programs, and works with Ann to choose her target quit date and to pick the Web-based program she is going to use. Ann likes the fact that she can go online whenever she needs support. She also likes being able to put her quit date into the system so that the program will give her timely reminders of all her reasons to quit when she logs on.
The ObGyn writes prescriptions for varenicline (Chantix) and OCs and tells Ann to come back in 4 weeks. For her part, Tammy adds Ann to the list of patients she calls and will get in touch the day after Ann’s quit date. Tammy makes this her practice with patients because she knows that one well-timed phone call can be the key to a successful quit attempt.
Outside support improves abstinence rates
Improving your patients’ chances of long-term abstinence hinges, in part, on making the most of outside support. In many cases, your patients can take advantage of it without leaving their homes.
Quitlines increase quit rates, reduce relapse
Telephone counseling is an effective support system.8 Smokers who call to a single number (800-QUITNOW)—a service provided by the National Cancer Institute (NCI)—are directed to the quitline for their state. Smokers can also call the NCI directly at its quitline (877-44U-QUIT). Calling a quitline provides smokers with real-time counseling and information about how to quit smoking. Quitlines can be appealing to patients who are uncomfortable discussing their smoking in a group—and they are free to the patient.
Evidence supports the use of such help lines. In their study of the California Smokers’ Helpline, Zhu and colleagues tested a proactive protocol where smokers were funneled into a research trial when the help line was overwhelmed.9
The smokers in the treatment arm of this RCT were assigned a counselor who called the smokers as many as six times, following a relapse-sensitive schedule. The 12-month abstinence rate increased from 4.1% to 7.5% (P.001 in the group that had close telephone contact. this improved quit rate reflects both an increase percentage of smokers who and more importantly a decrease quitters relapsed.>
Another prospective RCT enrolled patients from Veterans Affairs (VA) medical centers and involved the same proactive telephone protocol that Zhu and associates used.10 The treatment group was offered telephone counseling as well as pharmacotherapy; the control group had access to the regular smoking-cessation program of the VA system. Quit rates were similar in both groups if the participant utilized both counseling and pharmacotherapy: 12.7% in the control group and 11.9% in the treatment group. However, only 18% of patients in the control group used both services. Among patients in the treatment group, 88% utilized both counseling and medication. This led to 6-month abstinence rates of 13% in the treatment group versus 4.1% in the control group (OR=3.5; 95% CI, 1.99–6.15). Patients who were directed to and enrolled in treatment programs were therefore more likely to attempt to quit and remain abstinent for up to 6 months.
Web-based programs offer reminders
Like quitlines, Web-based programs offer smokers immediate feedback to help them quit. Many of the programs include links to quitting resources, stories from former smokers and cancer patients, live advice from counselors, and message boards (TABLE 1). Web-based programs have been shown to help improve quit rates.
One study compared two Web programs involving 11,969 smokers.11 This RCT looked at an interactive program based, in part, on the AHRQ treatment guidelines. This program generates personalized letters for the participants along with monthly e-mail reminders. A modified program, developed by a maker of NRT products, served as the control; it contained more information about nicotine than about tobacco dependence and cessation. This program was also shorter than the interactive program, which was designed to assist smoking cessation.
Both programs improved quit rates: 10.9% for the interactive program and 8% for the modified/control program, compared with 3.3% for no treatment at all. Although this study was based on participant reports of abstinence over the previous 7 days, and had low followup rates (which Internet studies tend to have), the interactive program produced one more quitter for every 26 participants than the modified (control) program did, according to an intent-to-treat analysis (14.6% vs 10.7%, P.001 or="1.43;" ci>
Another RCT looked at the use of a more extensive Web site, combining video, audio, and text.12 This program was fully automated and delivered entirely by computer. Again, using the AHRQ guidelines and other sources, researchers designed a series of five modules to simulate work with a live counselor. There were 13 different versions to match the demographics of the participant. The modules ended with a “quit calendar” for use by the participant to pick a date within the next 30 days. The program included 20 hours of video, although no participant saw every section. The intent-to-treat analysis showed a significant difference between groups: 12.3% in the treatment group versus 5% in the control group (OR=2.66; 95% CI, 1.18–5.99).
TABLE 1
Web-based support helps smokers quit
| www.quitnet.com Boston University School of Public Health | Personalized quit plans |
| www.ffsonline.org American Lung Association | “Freedom from smoking” modules to guide smokers through quit process |
| www.whyquit.com Privately supported | Support for “cold turkey” quitting |
| www.trytostop.org Massachusetts Department of Public Health | Personalized “Quit Wizard” program |
Text messages work
A short but interesting study used text messaging to target younger smokers in New Zealand.13 This RCT involved 1,705 smokers who had cell phones with text messaging. Researchers sent participants up to five messages daily around their quit date, drawing from over 100 messages that could be personalized with individual names/nicknames. The quit rate doubled 6 weeks out (28% vs 13%; relative risk=2.2; 95% CI, 1.79–2.70).
CASE…continued Support in place
Ann leaves the office with her prescription for varenicline and OCs, the state’s quitline number, and the URL for an online support program. She is eager to try varenicline: A coworker of hers is using it and doing well. Ann has tried the nicotine patch in the past, but says that it gave her nightmares. (She kept smoking while wearing it.) This time, she hopes she’ll finally be able to quit for good.
Weighing the drug treatment options
The AHRQ guidelines recommend several types of pharmacotherapy. First-line therapies include different forms of NRT and sustained-release bupropion (Zyban).2,3
Nicotine replacement therapy doubles the chance of quitting
With NRT, the nicotine in cigarettes is replaced with nicotine from another source to reduce withdrawal symptoms so that the patient is less likely to relapse. Nicotine replacement is available in several forms: gum, transdermal patches, intra-nasal spray, inhaler, and lozenges.
A Cochrane meta-analysis of NRT analyzed 123 studies that followed patients for at least 6 months after their quit date.14 The authors concluded that NRT could almost double a patient’s chance of quitting smoking. The data from various types of NRT revealed the types to be similarly effective (TABLE 2). In the treated groups, 17% were abstinent, compared with only 10% in the control groups at the various endpoints of the trials. Smokers who had higher levels of nicotine dependence, as indicated by smoking 10 or more cigarettes daily, had higher quit rates using replacement nicotine. Generally, treatment for 8 weeks was as effective as a longer course.
The Cochrane meta-analysis also revealed that:
- Duration of therapy ranges from 3 weeks to 12 months with the various forms of NRT.
- There was no benefit to tapering off the NRT, compared with abrupt withdrawal.
- Patients are much more likely to relapse after NRT in the first 3 months.
- Combining several forms of NRT may aid a relapsed smoker in another quit attempt. However, the reattempt should be delayed by a few months, as back-to-back courses are unlikely to improve quit rates.
TABLE 2
Nicotine replacement therapy: Methods are similarly effective11
| THERAPY | ODDS RATIO (95% CI) | NO. OF PARTICIPANTS/TRIALS | NNT | DURATION OF THERAPY | COST OF 4 WEEKS (BRAND/GENERIC) † |
|---|---|---|---|---|---|
| Nasal spray | 2.35 (1.63–3.38) | 887/4 | 8.3 | 3–6 months | $560/NA |
| Inhaler | 2.14 (1.44–3.18) | 976/4 | 12.5 | 3 months, then 3-month taper | $504/NA |
| Lozenges | 2.05 (1.62–2.59) | 2,739/5 | 14.3 | Up to 12 weeks | $300/$240 |
| Patch | 1.84 (1.65–2.06) | 16,228/37 | 16.7 | 8–12 weeks | $110/$92 |
| NRT (all) | 1.77 (1.66–1.88) | 39,503/105 | * | ||
| Gum | 1.66 (1.51–1.81) | 17,819/52 | 12.5 | Up to 12 weeks | 4 mg: $234/$180 2 mg: $204/$150 |
| * Numbers not available. | |||||
| † Cost based on prices from Walgreen’s and Target Pharmacies, May and September 2007. | |||||
| NNT, number needed to treat; NA, product not available. | |||||
Sustained-release bupropion: Similar results to NRT
The other first-line therapy suggested by the AHRQ guidelines is sustained-release bupropion (Wellbutrin).2,3 A separate Cochrane Review analyzed the data from 36 studies using antidepressants and revealed that two thirds of the studies used bupropion.15 The odds of quitting smoking essentially doubled in the placebo-controlled studies when the patient used bupropion. This effect is similar to that of NRT. Neither the AHRQ guidelines nor the Cochrane Review recommend bupropion over NRT, or vice versa.
According to the Cochrane Review, there was no benefit to increasing the dosage of bupropion from 150 mg to 300 mg daily.15 Although the initial multidose study of bupropion showed a difference between dosages, it was not clinically significant by the end of the study.16 A larger, open-label randomized trial of 1,524 smokers followed for 1 year had similar results.17 At the 3-month evaluation, the higher dosage had superior efficacy, but that effect was not statistically significant by the end of the study.
Lastly, there is no benefit to continuing the bupropion beyond 7 weeks after the target quit date.
With other antidepressants, results vary
The Cochrane Review also looked at other antidepressants. There were four RCTs of nortriptyline (Aventyl/Pamelor) without NRT, totaling 777 smokers followed for at least 6 months.18-21 The pooled data essentially showed a doubling of the odds of quitting from 7% among controls to 17.2% in the treated groups (OR=2.79; 95% CI, 1.70–4.59). Adding nortriptyline to NRT did increase the quit rate, but not significantly. The dosage used in these studies (75–150 mg) is much lower than that used for depression, where significant side effects often interfere with treatment. Generally, the starting dosage for smoking cessation is 25 mg at bedtime. After 1 week, the dosage is increased to 50 mg, and the following week it is increased again to 75 mg. After a week at 75 mg, the dose is titrated upward only if necessary. The titration continues at an additional 25 mg weekly.
One of the four placebo-controlled studies included both nortriptyline and bupropion arms.20 The abstinence rates, as indicated by no smoking during the final week of treatment, were comparable for the two groups that received active medication. Treatment with bupropion or nortriptyline was significantly more effective than placebo. However, the effect was lost at the 1-year continuous-abstinence mark; the two drugs did not differ from each other or placebo (TABLE 3).
Other antidepressants were evaluated in the Cochrane study.15 Long-term studies of the tricyclic antidepressants doxepin and imipramine (Tofranil) were lacking. Nor were there statistically significant differences in smaller trials. Of the selective serotonin reuptake inhibitors, only fluoxetine (Prozac) had been studied in long-term trials, and none noted statistically significant differences. Likewise, venlafaxine (Effexor) was studied in only one trial in which the confidence interval allowed for a potentially useful clinical effect, but there was no statistically significant increase in 12-month quit rates.
TABLE 3
Varenicline, nortriptyline, bupropion—strong allies in patients’ efforts to quit
| THERAPY | ODDS RATIO (95% CI) | NO. OF PARTICIPANTS/TRIALS | NNT | DURATION OF THERAPY | COST OF 4 WEEKS (BRAND/GENERIC) † |
|---|---|---|---|---|---|
| Varenicline24,25 | 2.80 (2.03–3.88) | 1,161/2 | 7.6 | 12 weeks | $120/NA |
| Nortriptyline15 | 2.79 (1.70–4.59) | 703/4 | 9.8 | 12 weeks | $814/$8 |
| Sustained-release bupropion15 | 2.06 (1.77–2.40) | 6,443/19 | 10.2 | 7–12 weeks | $210/$100 |
| Clonidine23 | 1.89 (1.30–2.74) | 776/6 | 9.4 | 3–4 weeks | $74/$4 |
| Venlafaxine15 | 1.33 (0.59–3.00) | 136/1 | 20.4 | $145/NA | |
| Diazepam23 | 1.00 (0.39–2.54) | 76/1 | No difference | $209/$27 | |
| SSRI15 | 0.90 (0.68–1.18) | 1,768/6 | 20.7 | $170/$4 | |
| Buspirone23 | 0.71 (0.34–1.48) | 201/3 | 22.1 | $280/$84 | |
| * Cost based on prices from Walgreen’s and Target Pharmacies, May and September 2007. | |||||
| NNT, number needed to treat; SSRI, selective serotonin reuptake inhibitors; NA, not available. | |||||
Clonidine is an option, but side effects are an issue
Another Cochrane Review looked at the effectiveness of clonidine (Catapres) on smoking cessation.22 Most of the studies assessed withdrawal symptoms rather than abstinence. Of those that did assess quit rates, the pooled OR for clonidine compares favorably at 1.89 (95% CI, 1.30–2.74). Unfortunately, clonidine has significant side effects: sedation and postural hypotension. The starting dosage is 0.1 mg twice daily, and it may be titrated to a maximum dose of 0.4 mg daily. It should be used for 3 to 4 weeks only to decrease withdrawal symptoms. The smoker is then weaned off the drug.
The anxiolytics were the subject of another Cochrane Review.23 This review, however, did not recommend any anxiolytics, including diazepam and buspirone, for smoking cessation.
A new category of therapy: Nicotinic receptor agonists
With US Food and Drug Administration (FDA) approval of varenicline in May 2006, a new class of drugs became available for tobacco dependence. This α4β2 nicotinic acetylcholine receptor partial agonist was designed as a smoking cessation drug. By releasing dopamine in the brain like nicotine, it prevents craving. However, it also blocks nicotine from binding, thereby preventing the reinforcing effect of continued smoking.
Two RCTs have assessed varenicline against both bupropion and placebo (TABLE 3). Jorenby and colleagues showed that varenicline-treated participants were significantly more likely to be continuously abstinent at 52 weeks than the placebo- or bupropion-treated groups (23% vs 10.3% placebo [OR= 2.66; 95% CI, 1.72–4.11; P.001 and bupropion ci>P=.004]).24 Gonzales and associates also showed that varenicline-treated smokers were more likely to be continuously abstinent at 52 weeks than the placebo group (21.9% vs 8.4% [OR=3.09; 95% CI, 1.95–4.91; P.001>25
However, when compared with varenicline, bupropion’s effects were no longer statically significant at 52 weeks (21.9% vs 16.1% [OR=1.46; 95% CI, 0.99– 2.17; P=.057]).
The patient initiating varenicline begins by taking 0.5 mg nightly for 3 nights, then increases to 0.5 mg twice a day for 4 days. The second week, the patient begins the 1-mg twice-daily dosage that is continued through treatment.
Vaccines hold promise
Several promising ideas for the treatment of tobacco dependence are in development, including several vaccines.26 When the immune system produces antibodies to nicotine in response to the vaccine, and when these antibodies bind to the nicotine, the resultant compound is too large to cross the blood–brain barrier. This prevents the reinforcing effect of nicotine. Initial studies of vaccines show that smokers decrease the amount they smoke and find abstinence easier to maintain. However, the vaccine requires frequent boosters to maintain effective antibody titers.
NicVAX from Nabi Biopharmaceuticals was placed on a fast track for approval by the FDA, which is still at least 1 year away. The other two nicotine vaccines are unlikely to be approved for several years.27
Researchers are also studying other compounds that block the euphoria associated with smoking.28 The initial studies of rimonabant (Acomplia), a cannabinoid blocker, have shown that it is no better than other treatments already available. With its indication in some European countries for weight loss, it offered promise as an important option for patients who are concerned about the weight gain associated with smoking cessation. However, the FDA did not approve rimonabant for tobacco cessation when it issued its initial approval letter for weight loss in 2006. Because of safety concerns, the manufacturer subsequently withdrew the new drug application for rimonabant in 2007.
CASE…resolved She kicks the habit
Ann begins taking varenicline the day she leaves the office, and reaches her quit date a week later.
At her 1-month follow-up, she reports that it was easy for her to stay off the cigarettes. With the varenicline, she lost the desire to smoke. The ObGyn reminds her to work on the triggers for her smoking, urging her not to light up when she makes her morning coffee or gets in the car. The physician also suggests that Ann put $4 each morning into a jar on her dresser, so she can see how much she saves now that she isn’t buying cigarettes.
At Ann’s next annual exam, she is marked in the computer as a reformed smoker. She is very proud of that label. When she is asked what she is doing with all that extra cash, she laughs: “My daughter spends it all! But not on cigarettes!”
1. Brown D. Nicotine up sharply in many cigarettes. Washington Post, August 31, 2006. Available at: www.washingtonpost.com/wp-dyn/content/article/2006/08/30/AR2006083001418.html. Accessed on September 4, 2007.
2. Agency for Healthcare Research and Quality. Clinical Practice Guideline. Treating Tobacco Use and Dependence. Rockville, Md: US Department of Health and Human Services Public Health Service; 2000. Available at: www.ncbi.nlm.nih.gov/books/bv.fcgi?rid=hstat2. chapter.7644. Accessed on September 4, 2007.
3. Tobacco Use and Dependence Clinical Practice Guideline Panel, Staff, and Consortium Representatives. A clinical practice guideline for treating tobacco use and dependence: A US Public Health Service report. JAMA. 2000;283:3244-3254.
4. Ask and Act: A Tobacco Cessation Program. Available at: www.aafp.org/online/en/home/clinical/publichealth/tobacco/askandact.html. Accessed on September 4, 2007.
5. Lancaster T, Stead LF. Physician advice for smoking cessation. Cochrane Database Syst Rev. 2004;(4):CD000165.
6. Fiore MC, McCarthy DE, Jackson TC, et al. Integrating smoking cessation treatment into primary care: an effectiveness study. Prev Med. 2004;38:412-420.
7. Katz DA, Muehlenbruch DR, Brown RL. Effectiveness of implementing the Agency for Healthcare Research and Quality Smoking Cessation Clinical Practice Guidelines: a randomized, control trial. J Natl Cancer Inst. 2004;96:594-603.
8. Stead LF, Lancaster T, Perera R. Telephone counseling for smoking cessation. Cochrane Database Syst Rev. 2003;(1):CD002850.
9. Zhu SH, Anderson CM, Tedeschi GJ, et al. Evidence of real-world effectiveness of a telephone quitline for smokers. N Engl J Med. 2002;347:1087-1093.
10. An LC, Zhu SH, Nelson DB, et al. Benefits of telephone care over primary care for smoking cessation. Arch Intern Med. 2006;166:536-542.
11. Etter JF. Comparing the efficacy of two Internet-based, computer-tailored smoking cessation programs: a randomized trial. J Med Internet Res. 2005;7(1):e2.
12. Swartz LH, Noell JW, Schroeder SW, Ary DV. A randomised control study of a fully automated internet based smoking cessation programme. Tob Control. 2006;15:7-12.
13. Rodgers A, Corbett T, Bramley D, et al. Do u smoke after txt? Results of a randomised trial of smoking cessation using mobile phone text messaging. Tob Control. 2005;14:255-261.
14. Silagy C, Lancaster T, Stead L, Mant D, Fowler G. Nicotine replacement therapy for smoking cessation. Cochrane Database Syst Rev. 2004;(4):CD000146.
15. Hughes JR, Stead LF, Lancaster T. Antidepressants for smoking cessation. Cochrane Database Syst Rev. 2004;(2):CD000031.
16. Hurt RD, Sachs DP, Glover ED, et al. A comparison of sustained-release bupropion and placebo for smoking cessation. N Engl J Med. 1997;337:1195-1202.
17. Swan GE, McAfee T, Curry SJ, et al. Effectiveness of bupropion sustained release for smoking cessation in a health care setting. Arch Intern Med. 2003;163:2337-2344.
18. da Costa CL, Younes RN, Lourenco MT. A prospective, randomized, double-blind study comparing nortriptyline to placebo. Chest. 2002;122:403-408.
19. Hall SM, Reus VI, Munoz RF, et al. Nortriptyline and cognitive-behavioral therapy in the treatment of cigarette smoking. Arch Gen Psychiatry. 1998;55:683-690.
20. Hall SM, Humfleet GL, Reus VI, et al. Psychological intervention and antidepressant treatment in smoking cessation. Arch Gen Psychiatry. 2002;59:930-936.
21. Prochazka AV, Weaver MJ, Keller RT, et al. A randomized trial of nortriptyline for smoking cessation. Arch Intern Med. 1998;158:2035-2039.
22. Gourlay SG, Stead LF, Benowitz NL. Clonidine for smoking cessation. Cochrane Database Syst Rev. 2004;(3):CD000058.
23. Hughes JR, Stead LF, Lancaster T. Anxiolytics for smoking cessation. Cochrane Database Syst Rev. 2000;(4):CD002849.
24. Jorenby DE, Hays JT, Rigotti NA. efficacy of varenicline, an α4β2 nicotinic acetylcholine receptor partial agonist, vs placebo or sustained-release bupropion for smoking cessation. JAMA. 2006;296:56-63.
25. Gonzales D, Rennard SI, Nides M. Varenicline, an α4β2 nicotinic acetylcholine receptor partial agonist, vs sustained-release bupropion and placebo for smoking cessation. JAMA. 2006;296:47-55.
26. LeHouezec J. Why a nicotine vaccine? Clin Pharmacol Ther. 2005;78:453-455.
27. Tuller D. Scientists testing vaccines to help smokers quit. New York Times, July 4, 2006.
28. Fagerström K, Balfour DJ. Neuropharmacology and potential efficacy of new treatments for tobacco dependence. Expert Opin Investig Drugs. 2005;15:107-116.
- Recommend that your patients take advantage of telephone counseling—it improves both the quit rate and the long-term abstinence rate. Web-based cessation programs also support smokers in all stages of quitting.
- Encourage patients to use both pharmacotherapy and counseling to improve abstinence. Several medications—including bupropion and varenicline—achieve comparable rates of quitting and long-term abstinence.
- Train your office staff to help identify and counsel smokers.
CASE Smoker who uses OCs
Ann G. is a 34-year-old mother of two who has been coming to the office for her annual Pap smear for several years. Her medical history is significant only for her vaginal deliveries and mild gastroesophageal reflux. She takes oral contraceptives (OCs) and uses over-the-counter ranitidine hydrochloride (Zantac) as needed. On Ann’s most recent annual visit, the medical assistant, Tammy, takes her vital signs. The chart has a section about smoking status, and Tammy notes that Ann is a smoker.
During the office visit, the ObGyn explains to Ann that her smoking is a serious health risk and advises her to quit. She also informs Ann that she needs to find a new form of birth control next year, as smoking increases the risks of using OCs, especially after age 35. Ann nervously laughs off the warning.
When she returns the following year, Ann confesses to Tammy that she is still a smoker. When Tammy asks about quitting, Ann remains adamant: “No way—I can’t do it.” Nonetheless, during the office visit, the ObGyn raises the subject again, and Ann admits that she is afraid that quitting smoking will cause her to gain weight. The physician attempts to address Ann’s fears, talks about other birth control options, and gives her a 3-month prescription for OCs. Before ending the visit, the ObGyn tells Ann that they will discuss what to do about birth control when she returns in 3 months.
Ann faces an uphill battle. The amount of nicotine in cigarettes is increasing,1 making it harder to quit. The good news is that the treatment of tobacco addiction is constantly improving, and the number of tools in our arsenal is growing. In fact, there are many resources that we can try before turning to the prescription pad. However, when needed, pharmacotherapy is an important adjunct in a patient’s struggle to achieve abstinence.
“5-A” strategy sets stage for success
Treating Tobacco Use and Dependence, a useful publication from the Agency for Healthcare Research and Quality (AHRQ), offers guidelines on many aspects of tobacco cessation, from counseling to pharmacotherapy to reimbursement.2,3 The guidelines break the smoking cessation process into five A’s:
- Ask each patient about her smoking status.
- Advise each patient who smokes that she needs to stop smoking.
- Assess your patient’s willingness to make a quit attempt in the next 30 days.
- Assist your patient in making this quit attempt or encourage her to consider a quit attempt later.
- Arrange close follow-up of any quit attempts to help prevent relapse.
Take advantage of every opportunity you have to discuss the issue with patients; short conversations can make a difference. A Cochrane review of 39 trials including 31,000 smokers revealed that even brief advice—simply encouraging patients to quit—was statistically significant in helping the smoker quit (odds ratio [OR]=1.74; 95% confidence interval [CI], 1.48–2.05).5 The pooled data generated a quit rate difference of 2.5%: for every 40 people who were told to quit, one more smoker would.
Empower the office staff
Enlisting the help of the office staff can have a significant impact on the health of patients. Fiore and colleagues evaluated a proactive approach in which medical assistants, while assessing smoking status, invited all smokers to participate in a cessation study.6 (The assistants received periodic thank-you gifts for their efforts.)
Participants were randomized to self-selected treatment or nicotine replacement therapy (NRT) patches, with or without a support program. Some who received the patches and support program also received individual counseling. The result: Most smokers were open to encouragement to quit smoking. The 13% point-prevalence abstinence rate 1 year out was comparable to the rate observed (14%) in smokers volunteering for NRT studies in the Cochrane review of 39 trials noted earlier.5
Likewise, in a randomized controlled trial (RCT) involving community-based primary care clinics, Katz and associates demonstrated that intake clinicians can also play an important role in smoking cessation.7 In the study, researchers trained intake clinicians (including registered nurses, licensed practical nurses, and medical assistants) to identify smokers, provide brief counseling, and assist in their preparation to quit. Patients were offered vouchers for patches and a counselor’s business card. Intake clinicians received periodic feedback on their performance based on exit interviews of the patients. These interventions had a statistically significant effect in moderate-to-heavy smokers in quit attempts, quit rates, and continuous abstinence.
CASE…continued A change of heart
At the 3-month follow-up, Tammy learns that Ann is still smoking—but she now wants to quit. Ann says that she found a pack of cigarettes in her 14-year-old daughter’s backpack, and feels that the only way to prevent her from getting hooked is to set a good example.
Tammy gives her the state’s quitline number, suggests some online quitting programs, and works with Ann to choose her target quit date and to pick the Web-based program she is going to use. Ann likes the fact that she can go online whenever she needs support. She also likes being able to put her quit date into the system so that the program will give her timely reminders of all her reasons to quit when she logs on.
The ObGyn writes prescriptions for varenicline (Chantix) and OCs and tells Ann to come back in 4 weeks. For her part, Tammy adds Ann to the list of patients she calls and will get in touch the day after Ann’s quit date. Tammy makes this her practice with patients because she knows that one well-timed phone call can be the key to a successful quit attempt.
Outside support improves abstinence rates
Improving your patients’ chances of long-term abstinence hinges, in part, on making the most of outside support. In many cases, your patients can take advantage of it without leaving their homes.
Quitlines increase quit rates, reduce relapse
Telephone counseling is an effective support system.8 Smokers who call to a single number (800-QUITNOW)—a service provided by the National Cancer Institute (NCI)—are directed to the quitline for their state. Smokers can also call the NCI directly at its quitline (877-44U-QUIT). Calling a quitline provides smokers with real-time counseling and information about how to quit smoking. Quitlines can be appealing to patients who are uncomfortable discussing their smoking in a group—and they are free to the patient.
Evidence supports the use of such help lines. In their study of the California Smokers’ Helpline, Zhu and colleagues tested a proactive protocol where smokers were funneled into a research trial when the help line was overwhelmed.9
The smokers in the treatment arm of this RCT were assigned a counselor who called the smokers as many as six times, following a relapse-sensitive schedule. The 12-month abstinence rate increased from 4.1% to 7.5% (P.001 in the group that had close telephone contact. this improved quit rate reflects both an increase percentage of smokers who and more importantly a decrease quitters relapsed.>
Another prospective RCT enrolled patients from Veterans Affairs (VA) medical centers and involved the same proactive telephone protocol that Zhu and associates used.10 The treatment group was offered telephone counseling as well as pharmacotherapy; the control group had access to the regular smoking-cessation program of the VA system. Quit rates were similar in both groups if the participant utilized both counseling and pharmacotherapy: 12.7% in the control group and 11.9% in the treatment group. However, only 18% of patients in the control group used both services. Among patients in the treatment group, 88% utilized both counseling and medication. This led to 6-month abstinence rates of 13% in the treatment group versus 4.1% in the control group (OR=3.5; 95% CI, 1.99–6.15). Patients who were directed to and enrolled in treatment programs were therefore more likely to attempt to quit and remain abstinent for up to 6 months.
Web-based programs offer reminders
Like quitlines, Web-based programs offer smokers immediate feedback to help them quit. Many of the programs include links to quitting resources, stories from former smokers and cancer patients, live advice from counselors, and message boards (TABLE 1). Web-based programs have been shown to help improve quit rates.
One study compared two Web programs involving 11,969 smokers.11 This RCT looked at an interactive program based, in part, on the AHRQ treatment guidelines. This program generates personalized letters for the participants along with monthly e-mail reminders. A modified program, developed by a maker of NRT products, served as the control; it contained more information about nicotine than about tobacco dependence and cessation. This program was also shorter than the interactive program, which was designed to assist smoking cessation.
Both programs improved quit rates: 10.9% for the interactive program and 8% for the modified/control program, compared with 3.3% for no treatment at all. Although this study was based on participant reports of abstinence over the previous 7 days, and had low followup rates (which Internet studies tend to have), the interactive program produced one more quitter for every 26 participants than the modified (control) program did, according to an intent-to-treat analysis (14.6% vs 10.7%, P.001 or="1.43;" ci>
Another RCT looked at the use of a more extensive Web site, combining video, audio, and text.12 This program was fully automated and delivered entirely by computer. Again, using the AHRQ guidelines and other sources, researchers designed a series of five modules to simulate work with a live counselor. There were 13 different versions to match the demographics of the participant. The modules ended with a “quit calendar” for use by the participant to pick a date within the next 30 days. The program included 20 hours of video, although no participant saw every section. The intent-to-treat analysis showed a significant difference between groups: 12.3% in the treatment group versus 5% in the control group (OR=2.66; 95% CI, 1.18–5.99).
TABLE 1
Web-based support helps smokers quit
| www.quitnet.com Boston University School of Public Health | Personalized quit plans |
| www.ffsonline.org American Lung Association | “Freedom from smoking” modules to guide smokers through quit process |
| www.whyquit.com Privately supported | Support for “cold turkey” quitting |
| www.trytostop.org Massachusetts Department of Public Health | Personalized “Quit Wizard” program |
Text messages work
A short but interesting study used text messaging to target younger smokers in New Zealand.13 This RCT involved 1,705 smokers who had cell phones with text messaging. Researchers sent participants up to five messages daily around their quit date, drawing from over 100 messages that could be personalized with individual names/nicknames. The quit rate doubled 6 weeks out (28% vs 13%; relative risk=2.2; 95% CI, 1.79–2.70).
CASE…continued Support in place
Ann leaves the office with her prescription for varenicline and OCs, the state’s quitline number, and the URL for an online support program. She is eager to try varenicline: A coworker of hers is using it and doing well. Ann has tried the nicotine patch in the past, but says that it gave her nightmares. (She kept smoking while wearing it.) This time, she hopes she’ll finally be able to quit for good.
Weighing the drug treatment options
The AHRQ guidelines recommend several types of pharmacotherapy. First-line therapies include different forms of NRT and sustained-release bupropion (Zyban).2,3
Nicotine replacement therapy doubles the chance of quitting
With NRT, the nicotine in cigarettes is replaced with nicotine from another source to reduce withdrawal symptoms so that the patient is less likely to relapse. Nicotine replacement is available in several forms: gum, transdermal patches, intra-nasal spray, inhaler, and lozenges.
A Cochrane meta-analysis of NRT analyzed 123 studies that followed patients for at least 6 months after their quit date.14 The authors concluded that NRT could almost double a patient’s chance of quitting smoking. The data from various types of NRT revealed the types to be similarly effective (TABLE 2). In the treated groups, 17% were abstinent, compared with only 10% in the control groups at the various endpoints of the trials. Smokers who had higher levels of nicotine dependence, as indicated by smoking 10 or more cigarettes daily, had higher quit rates using replacement nicotine. Generally, treatment for 8 weeks was as effective as a longer course.
The Cochrane meta-analysis also revealed that:
- Duration of therapy ranges from 3 weeks to 12 months with the various forms of NRT.
- There was no benefit to tapering off the NRT, compared with abrupt withdrawal.
- Patients are much more likely to relapse after NRT in the first 3 months.
- Combining several forms of NRT may aid a relapsed smoker in another quit attempt. However, the reattempt should be delayed by a few months, as back-to-back courses are unlikely to improve quit rates.
TABLE 2
Nicotine replacement therapy: Methods are similarly effective11
| THERAPY | ODDS RATIO (95% CI) | NO. OF PARTICIPANTS/TRIALS | NNT | DURATION OF THERAPY | COST OF 4 WEEKS (BRAND/GENERIC) † |
|---|---|---|---|---|---|
| Nasal spray | 2.35 (1.63–3.38) | 887/4 | 8.3 | 3–6 months | $560/NA |
| Inhaler | 2.14 (1.44–3.18) | 976/4 | 12.5 | 3 months, then 3-month taper | $504/NA |
| Lozenges | 2.05 (1.62–2.59) | 2,739/5 | 14.3 | Up to 12 weeks | $300/$240 |
| Patch | 1.84 (1.65–2.06) | 16,228/37 | 16.7 | 8–12 weeks | $110/$92 |
| NRT (all) | 1.77 (1.66–1.88) | 39,503/105 | * | ||
| Gum | 1.66 (1.51–1.81) | 17,819/52 | 12.5 | Up to 12 weeks | 4 mg: $234/$180 2 mg: $204/$150 |
| * Numbers not available. | |||||
| † Cost based on prices from Walgreen’s and Target Pharmacies, May and September 2007. | |||||
| NNT, number needed to treat; NA, product not available. | |||||
Sustained-release bupropion: Similar results to NRT
The other first-line therapy suggested by the AHRQ guidelines is sustained-release bupropion (Wellbutrin).2,3 A separate Cochrane Review analyzed the data from 36 studies using antidepressants and revealed that two thirds of the studies used bupropion.15 The odds of quitting smoking essentially doubled in the placebo-controlled studies when the patient used bupropion. This effect is similar to that of NRT. Neither the AHRQ guidelines nor the Cochrane Review recommend bupropion over NRT, or vice versa.
According to the Cochrane Review, there was no benefit to increasing the dosage of bupropion from 150 mg to 300 mg daily.15 Although the initial multidose study of bupropion showed a difference between dosages, it was not clinically significant by the end of the study.16 A larger, open-label randomized trial of 1,524 smokers followed for 1 year had similar results.17 At the 3-month evaluation, the higher dosage had superior efficacy, but that effect was not statistically significant by the end of the study.
Lastly, there is no benefit to continuing the bupropion beyond 7 weeks after the target quit date.
With other antidepressants, results vary
The Cochrane Review also looked at other antidepressants. There were four RCTs of nortriptyline (Aventyl/Pamelor) without NRT, totaling 777 smokers followed for at least 6 months.18-21 The pooled data essentially showed a doubling of the odds of quitting from 7% among controls to 17.2% in the treated groups (OR=2.79; 95% CI, 1.70–4.59). Adding nortriptyline to NRT did increase the quit rate, but not significantly. The dosage used in these studies (75–150 mg) is much lower than that used for depression, where significant side effects often interfere with treatment. Generally, the starting dosage for smoking cessation is 25 mg at bedtime. After 1 week, the dosage is increased to 50 mg, and the following week it is increased again to 75 mg. After a week at 75 mg, the dose is titrated upward only if necessary. The titration continues at an additional 25 mg weekly.
One of the four placebo-controlled studies included both nortriptyline and bupropion arms.20 The abstinence rates, as indicated by no smoking during the final week of treatment, were comparable for the two groups that received active medication. Treatment with bupropion or nortriptyline was significantly more effective than placebo. However, the effect was lost at the 1-year continuous-abstinence mark; the two drugs did not differ from each other or placebo (TABLE 3).
Other antidepressants were evaluated in the Cochrane study.15 Long-term studies of the tricyclic antidepressants doxepin and imipramine (Tofranil) were lacking. Nor were there statistically significant differences in smaller trials. Of the selective serotonin reuptake inhibitors, only fluoxetine (Prozac) had been studied in long-term trials, and none noted statistically significant differences. Likewise, venlafaxine (Effexor) was studied in only one trial in which the confidence interval allowed for a potentially useful clinical effect, but there was no statistically significant increase in 12-month quit rates.
TABLE 3
Varenicline, nortriptyline, bupropion—strong allies in patients’ efforts to quit
| THERAPY | ODDS RATIO (95% CI) | NO. OF PARTICIPANTS/TRIALS | NNT | DURATION OF THERAPY | COST OF 4 WEEKS (BRAND/GENERIC) † |
|---|---|---|---|---|---|
| Varenicline24,25 | 2.80 (2.03–3.88) | 1,161/2 | 7.6 | 12 weeks | $120/NA |
| Nortriptyline15 | 2.79 (1.70–4.59) | 703/4 | 9.8 | 12 weeks | $814/$8 |
| Sustained-release bupropion15 | 2.06 (1.77–2.40) | 6,443/19 | 10.2 | 7–12 weeks | $210/$100 |
| Clonidine23 | 1.89 (1.30–2.74) | 776/6 | 9.4 | 3–4 weeks | $74/$4 |
| Venlafaxine15 | 1.33 (0.59–3.00) | 136/1 | 20.4 | $145/NA | |
| Diazepam23 | 1.00 (0.39–2.54) | 76/1 | No difference | $209/$27 | |
| SSRI15 | 0.90 (0.68–1.18) | 1,768/6 | 20.7 | $170/$4 | |
| Buspirone23 | 0.71 (0.34–1.48) | 201/3 | 22.1 | $280/$84 | |
| * Cost based on prices from Walgreen’s and Target Pharmacies, May and September 2007. | |||||
| NNT, number needed to treat; SSRI, selective serotonin reuptake inhibitors; NA, not available. | |||||
Clonidine is an option, but side effects are an issue
Another Cochrane Review looked at the effectiveness of clonidine (Catapres) on smoking cessation.22 Most of the studies assessed withdrawal symptoms rather than abstinence. Of those that did assess quit rates, the pooled OR for clonidine compares favorably at 1.89 (95% CI, 1.30–2.74). Unfortunately, clonidine has significant side effects: sedation and postural hypotension. The starting dosage is 0.1 mg twice daily, and it may be titrated to a maximum dose of 0.4 mg daily. It should be used for 3 to 4 weeks only to decrease withdrawal symptoms. The smoker is then weaned off the drug.
The anxiolytics were the subject of another Cochrane Review.23 This review, however, did not recommend any anxiolytics, including diazepam and buspirone, for smoking cessation.
A new category of therapy: Nicotinic receptor agonists
With US Food and Drug Administration (FDA) approval of varenicline in May 2006, a new class of drugs became available for tobacco dependence. This α4β2 nicotinic acetylcholine receptor partial agonist was designed as a smoking cessation drug. By releasing dopamine in the brain like nicotine, it prevents craving. However, it also blocks nicotine from binding, thereby preventing the reinforcing effect of continued smoking.
Two RCTs have assessed varenicline against both bupropion and placebo (TABLE 3). Jorenby and colleagues showed that varenicline-treated participants were significantly more likely to be continuously abstinent at 52 weeks than the placebo- or bupropion-treated groups (23% vs 10.3% placebo [OR= 2.66; 95% CI, 1.72–4.11; P.001 and bupropion ci>P=.004]).24 Gonzales and associates also showed that varenicline-treated smokers were more likely to be continuously abstinent at 52 weeks than the placebo group (21.9% vs 8.4% [OR=3.09; 95% CI, 1.95–4.91; P.001>25
However, when compared with varenicline, bupropion’s effects were no longer statically significant at 52 weeks (21.9% vs 16.1% [OR=1.46; 95% CI, 0.99– 2.17; P=.057]).
The patient initiating varenicline begins by taking 0.5 mg nightly for 3 nights, then increases to 0.5 mg twice a day for 4 days. The second week, the patient begins the 1-mg twice-daily dosage that is continued through treatment.
Vaccines hold promise
Several promising ideas for the treatment of tobacco dependence are in development, including several vaccines.26 When the immune system produces antibodies to nicotine in response to the vaccine, and when these antibodies bind to the nicotine, the resultant compound is too large to cross the blood–brain barrier. This prevents the reinforcing effect of nicotine. Initial studies of vaccines show that smokers decrease the amount they smoke and find abstinence easier to maintain. However, the vaccine requires frequent boosters to maintain effective antibody titers.
NicVAX from Nabi Biopharmaceuticals was placed on a fast track for approval by the FDA, which is still at least 1 year away. The other two nicotine vaccines are unlikely to be approved for several years.27
Researchers are also studying other compounds that block the euphoria associated with smoking.28 The initial studies of rimonabant (Acomplia), a cannabinoid blocker, have shown that it is no better than other treatments already available. With its indication in some European countries for weight loss, it offered promise as an important option for patients who are concerned about the weight gain associated with smoking cessation. However, the FDA did not approve rimonabant for tobacco cessation when it issued its initial approval letter for weight loss in 2006. Because of safety concerns, the manufacturer subsequently withdrew the new drug application for rimonabant in 2007.
CASE…resolved She kicks the habit
Ann begins taking varenicline the day she leaves the office, and reaches her quit date a week later.
At her 1-month follow-up, she reports that it was easy for her to stay off the cigarettes. With the varenicline, she lost the desire to smoke. The ObGyn reminds her to work on the triggers for her smoking, urging her not to light up when she makes her morning coffee or gets in the car. The physician also suggests that Ann put $4 each morning into a jar on her dresser, so she can see how much she saves now that she isn’t buying cigarettes.
At Ann’s next annual exam, she is marked in the computer as a reformed smoker. She is very proud of that label. When she is asked what she is doing with all that extra cash, she laughs: “My daughter spends it all! But not on cigarettes!”
- Recommend that your patients take advantage of telephone counseling—it improves both the quit rate and the long-term abstinence rate. Web-based cessation programs also support smokers in all stages of quitting.
- Encourage patients to use both pharmacotherapy and counseling to improve abstinence. Several medications—including bupropion and varenicline—achieve comparable rates of quitting and long-term abstinence.
- Train your office staff to help identify and counsel smokers.
CASE Smoker who uses OCs
Ann G. is a 34-year-old mother of two who has been coming to the office for her annual Pap smear for several years. Her medical history is significant only for her vaginal deliveries and mild gastroesophageal reflux. She takes oral contraceptives (OCs) and uses over-the-counter ranitidine hydrochloride (Zantac) as needed. On Ann’s most recent annual visit, the medical assistant, Tammy, takes her vital signs. The chart has a section about smoking status, and Tammy notes that Ann is a smoker.
During the office visit, the ObGyn explains to Ann that her smoking is a serious health risk and advises her to quit. She also informs Ann that she needs to find a new form of birth control next year, as smoking increases the risks of using OCs, especially after age 35. Ann nervously laughs off the warning.
When she returns the following year, Ann confesses to Tammy that she is still a smoker. When Tammy asks about quitting, Ann remains adamant: “No way—I can’t do it.” Nonetheless, during the office visit, the ObGyn raises the subject again, and Ann admits that she is afraid that quitting smoking will cause her to gain weight. The physician attempts to address Ann’s fears, talks about other birth control options, and gives her a 3-month prescription for OCs. Before ending the visit, the ObGyn tells Ann that they will discuss what to do about birth control when she returns in 3 months.
Ann faces an uphill battle. The amount of nicotine in cigarettes is increasing,1 making it harder to quit. The good news is that the treatment of tobacco addiction is constantly improving, and the number of tools in our arsenal is growing. In fact, there are many resources that we can try before turning to the prescription pad. However, when needed, pharmacotherapy is an important adjunct in a patient’s struggle to achieve abstinence.
“5-A” strategy sets stage for success
Treating Tobacco Use and Dependence, a useful publication from the Agency for Healthcare Research and Quality (AHRQ), offers guidelines on many aspects of tobacco cessation, from counseling to pharmacotherapy to reimbursement.2,3 The guidelines break the smoking cessation process into five A’s:
- Ask each patient about her smoking status.
- Advise each patient who smokes that she needs to stop smoking.
- Assess your patient’s willingness to make a quit attempt in the next 30 days.
- Assist your patient in making this quit attempt or encourage her to consider a quit attempt later.
- Arrange close follow-up of any quit attempts to help prevent relapse.
Take advantage of every opportunity you have to discuss the issue with patients; short conversations can make a difference. A Cochrane review of 39 trials including 31,000 smokers revealed that even brief advice—simply encouraging patients to quit—was statistically significant in helping the smoker quit (odds ratio [OR]=1.74; 95% confidence interval [CI], 1.48–2.05).5 The pooled data generated a quit rate difference of 2.5%: for every 40 people who were told to quit, one more smoker would.
Empower the office staff
Enlisting the help of the office staff can have a significant impact on the health of patients. Fiore and colleagues evaluated a proactive approach in which medical assistants, while assessing smoking status, invited all smokers to participate in a cessation study.6 (The assistants received periodic thank-you gifts for their efforts.)
Participants were randomized to self-selected treatment or nicotine replacement therapy (NRT) patches, with or without a support program. Some who received the patches and support program also received individual counseling. The result: Most smokers were open to encouragement to quit smoking. The 13% point-prevalence abstinence rate 1 year out was comparable to the rate observed (14%) in smokers volunteering for NRT studies in the Cochrane review of 39 trials noted earlier.5
Likewise, in a randomized controlled trial (RCT) involving community-based primary care clinics, Katz and associates demonstrated that intake clinicians can also play an important role in smoking cessation.7 In the study, researchers trained intake clinicians (including registered nurses, licensed practical nurses, and medical assistants) to identify smokers, provide brief counseling, and assist in their preparation to quit. Patients were offered vouchers for patches and a counselor’s business card. Intake clinicians received periodic feedback on their performance based on exit interviews of the patients. These interventions had a statistically significant effect in moderate-to-heavy smokers in quit attempts, quit rates, and continuous abstinence.
CASE…continued A change of heart
At the 3-month follow-up, Tammy learns that Ann is still smoking—but she now wants to quit. Ann says that she found a pack of cigarettes in her 14-year-old daughter’s backpack, and feels that the only way to prevent her from getting hooked is to set a good example.
Tammy gives her the state’s quitline number, suggests some online quitting programs, and works with Ann to choose her target quit date and to pick the Web-based program she is going to use. Ann likes the fact that she can go online whenever she needs support. She also likes being able to put her quit date into the system so that the program will give her timely reminders of all her reasons to quit when she logs on.
The ObGyn writes prescriptions for varenicline (Chantix) and OCs and tells Ann to come back in 4 weeks. For her part, Tammy adds Ann to the list of patients she calls and will get in touch the day after Ann’s quit date. Tammy makes this her practice with patients because she knows that one well-timed phone call can be the key to a successful quit attempt.
Outside support improves abstinence rates
Improving your patients’ chances of long-term abstinence hinges, in part, on making the most of outside support. In many cases, your patients can take advantage of it without leaving their homes.
Quitlines increase quit rates, reduce relapse
Telephone counseling is an effective support system.8 Smokers who call to a single number (800-QUITNOW)—a service provided by the National Cancer Institute (NCI)—are directed to the quitline for their state. Smokers can also call the NCI directly at its quitline (877-44U-QUIT). Calling a quitline provides smokers with real-time counseling and information about how to quit smoking. Quitlines can be appealing to patients who are uncomfortable discussing their smoking in a group—and they are free to the patient.
Evidence supports the use of such help lines. In their study of the California Smokers’ Helpline, Zhu and colleagues tested a proactive protocol where smokers were funneled into a research trial when the help line was overwhelmed.9
The smokers in the treatment arm of this RCT were assigned a counselor who called the smokers as many as six times, following a relapse-sensitive schedule. The 12-month abstinence rate increased from 4.1% to 7.5% (P.001 in the group that had close telephone contact. this improved quit rate reflects both an increase percentage of smokers who and more importantly a decrease quitters relapsed.>
Another prospective RCT enrolled patients from Veterans Affairs (VA) medical centers and involved the same proactive telephone protocol that Zhu and associates used.10 The treatment group was offered telephone counseling as well as pharmacotherapy; the control group had access to the regular smoking-cessation program of the VA system. Quit rates were similar in both groups if the participant utilized both counseling and pharmacotherapy: 12.7% in the control group and 11.9% in the treatment group. However, only 18% of patients in the control group used both services. Among patients in the treatment group, 88% utilized both counseling and medication. This led to 6-month abstinence rates of 13% in the treatment group versus 4.1% in the control group (OR=3.5; 95% CI, 1.99–6.15). Patients who were directed to and enrolled in treatment programs were therefore more likely to attempt to quit and remain abstinent for up to 6 months.
Web-based programs offer reminders
Like quitlines, Web-based programs offer smokers immediate feedback to help them quit. Many of the programs include links to quitting resources, stories from former smokers and cancer patients, live advice from counselors, and message boards (TABLE 1). Web-based programs have been shown to help improve quit rates.
One study compared two Web programs involving 11,969 smokers.11 This RCT looked at an interactive program based, in part, on the AHRQ treatment guidelines. This program generates personalized letters for the participants along with monthly e-mail reminders. A modified program, developed by a maker of NRT products, served as the control; it contained more information about nicotine than about tobacco dependence and cessation. This program was also shorter than the interactive program, which was designed to assist smoking cessation.
Both programs improved quit rates: 10.9% for the interactive program and 8% for the modified/control program, compared with 3.3% for no treatment at all. Although this study was based on participant reports of abstinence over the previous 7 days, and had low followup rates (which Internet studies tend to have), the interactive program produced one more quitter for every 26 participants than the modified (control) program did, according to an intent-to-treat analysis (14.6% vs 10.7%, P.001 or="1.43;" ci>
Another RCT looked at the use of a more extensive Web site, combining video, audio, and text.12 This program was fully automated and delivered entirely by computer. Again, using the AHRQ guidelines and other sources, researchers designed a series of five modules to simulate work with a live counselor. There were 13 different versions to match the demographics of the participant. The modules ended with a “quit calendar” for use by the participant to pick a date within the next 30 days. The program included 20 hours of video, although no participant saw every section. The intent-to-treat analysis showed a significant difference between groups: 12.3% in the treatment group versus 5% in the control group (OR=2.66; 95% CI, 1.18–5.99).
TABLE 1
Web-based support helps smokers quit
| www.quitnet.com Boston University School of Public Health | Personalized quit plans |
| www.ffsonline.org American Lung Association | “Freedom from smoking” modules to guide smokers through quit process |
| www.whyquit.com Privately supported | Support for “cold turkey” quitting |
| www.trytostop.org Massachusetts Department of Public Health | Personalized “Quit Wizard” program |
Text messages work
A short but interesting study used text messaging to target younger smokers in New Zealand.13 This RCT involved 1,705 smokers who had cell phones with text messaging. Researchers sent participants up to five messages daily around their quit date, drawing from over 100 messages that could be personalized with individual names/nicknames. The quit rate doubled 6 weeks out (28% vs 13%; relative risk=2.2; 95% CI, 1.79–2.70).
CASE…continued Support in place
Ann leaves the office with her prescription for varenicline and OCs, the state’s quitline number, and the URL for an online support program. She is eager to try varenicline: A coworker of hers is using it and doing well. Ann has tried the nicotine patch in the past, but says that it gave her nightmares. (She kept smoking while wearing it.) This time, she hopes she’ll finally be able to quit for good.
Weighing the drug treatment options
The AHRQ guidelines recommend several types of pharmacotherapy. First-line therapies include different forms of NRT and sustained-release bupropion (Zyban).2,3
Nicotine replacement therapy doubles the chance of quitting
With NRT, the nicotine in cigarettes is replaced with nicotine from another source to reduce withdrawal symptoms so that the patient is less likely to relapse. Nicotine replacement is available in several forms: gum, transdermal patches, intra-nasal spray, inhaler, and lozenges.
A Cochrane meta-analysis of NRT analyzed 123 studies that followed patients for at least 6 months after their quit date.14 The authors concluded that NRT could almost double a patient’s chance of quitting smoking. The data from various types of NRT revealed the types to be similarly effective (TABLE 2). In the treated groups, 17% were abstinent, compared with only 10% in the control groups at the various endpoints of the trials. Smokers who had higher levels of nicotine dependence, as indicated by smoking 10 or more cigarettes daily, had higher quit rates using replacement nicotine. Generally, treatment for 8 weeks was as effective as a longer course.
The Cochrane meta-analysis also revealed that:
- Duration of therapy ranges from 3 weeks to 12 months with the various forms of NRT.
- There was no benefit to tapering off the NRT, compared with abrupt withdrawal.
- Patients are much more likely to relapse after NRT in the first 3 months.
- Combining several forms of NRT may aid a relapsed smoker in another quit attempt. However, the reattempt should be delayed by a few months, as back-to-back courses are unlikely to improve quit rates.
TABLE 2
Nicotine replacement therapy: Methods are similarly effective11
| THERAPY | ODDS RATIO (95% CI) | NO. OF PARTICIPANTS/TRIALS | NNT | DURATION OF THERAPY | COST OF 4 WEEKS (BRAND/GENERIC) † |
|---|---|---|---|---|---|
| Nasal spray | 2.35 (1.63–3.38) | 887/4 | 8.3 | 3–6 months | $560/NA |
| Inhaler | 2.14 (1.44–3.18) | 976/4 | 12.5 | 3 months, then 3-month taper | $504/NA |
| Lozenges | 2.05 (1.62–2.59) | 2,739/5 | 14.3 | Up to 12 weeks | $300/$240 |
| Patch | 1.84 (1.65–2.06) | 16,228/37 | 16.7 | 8–12 weeks | $110/$92 |
| NRT (all) | 1.77 (1.66–1.88) | 39,503/105 | * | ||
| Gum | 1.66 (1.51–1.81) | 17,819/52 | 12.5 | Up to 12 weeks | 4 mg: $234/$180 2 mg: $204/$150 |
| * Numbers not available. | |||||
| † Cost based on prices from Walgreen’s and Target Pharmacies, May and September 2007. | |||||
| NNT, number needed to treat; NA, product not available. | |||||
Sustained-release bupropion: Similar results to NRT
The other first-line therapy suggested by the AHRQ guidelines is sustained-release bupropion (Wellbutrin).2,3 A separate Cochrane Review analyzed the data from 36 studies using antidepressants and revealed that two thirds of the studies used bupropion.15 The odds of quitting smoking essentially doubled in the placebo-controlled studies when the patient used bupropion. This effect is similar to that of NRT. Neither the AHRQ guidelines nor the Cochrane Review recommend bupropion over NRT, or vice versa.
According to the Cochrane Review, there was no benefit to increasing the dosage of bupropion from 150 mg to 300 mg daily.15 Although the initial multidose study of bupropion showed a difference between dosages, it was not clinically significant by the end of the study.16 A larger, open-label randomized trial of 1,524 smokers followed for 1 year had similar results.17 At the 3-month evaluation, the higher dosage had superior efficacy, but that effect was not statistically significant by the end of the study.
Lastly, there is no benefit to continuing the bupropion beyond 7 weeks after the target quit date.
With other antidepressants, results vary
The Cochrane Review also looked at other antidepressants. There were four RCTs of nortriptyline (Aventyl/Pamelor) without NRT, totaling 777 smokers followed for at least 6 months.18-21 The pooled data essentially showed a doubling of the odds of quitting from 7% among controls to 17.2% in the treated groups (OR=2.79; 95% CI, 1.70–4.59). Adding nortriptyline to NRT did increase the quit rate, but not significantly. The dosage used in these studies (75–150 mg) is much lower than that used for depression, where significant side effects often interfere with treatment. Generally, the starting dosage for smoking cessation is 25 mg at bedtime. After 1 week, the dosage is increased to 50 mg, and the following week it is increased again to 75 mg. After a week at 75 mg, the dose is titrated upward only if necessary. The titration continues at an additional 25 mg weekly.
One of the four placebo-controlled studies included both nortriptyline and bupropion arms.20 The abstinence rates, as indicated by no smoking during the final week of treatment, were comparable for the two groups that received active medication. Treatment with bupropion or nortriptyline was significantly more effective than placebo. However, the effect was lost at the 1-year continuous-abstinence mark; the two drugs did not differ from each other or placebo (TABLE 3).
Other antidepressants were evaluated in the Cochrane study.15 Long-term studies of the tricyclic antidepressants doxepin and imipramine (Tofranil) were lacking. Nor were there statistically significant differences in smaller trials. Of the selective serotonin reuptake inhibitors, only fluoxetine (Prozac) had been studied in long-term trials, and none noted statistically significant differences. Likewise, venlafaxine (Effexor) was studied in only one trial in which the confidence interval allowed for a potentially useful clinical effect, but there was no statistically significant increase in 12-month quit rates.
TABLE 3
Varenicline, nortriptyline, bupropion—strong allies in patients’ efforts to quit
| THERAPY | ODDS RATIO (95% CI) | NO. OF PARTICIPANTS/TRIALS | NNT | DURATION OF THERAPY | COST OF 4 WEEKS (BRAND/GENERIC) † |
|---|---|---|---|---|---|
| Varenicline24,25 | 2.80 (2.03–3.88) | 1,161/2 | 7.6 | 12 weeks | $120/NA |
| Nortriptyline15 | 2.79 (1.70–4.59) | 703/4 | 9.8 | 12 weeks | $814/$8 |
| Sustained-release bupropion15 | 2.06 (1.77–2.40) | 6,443/19 | 10.2 | 7–12 weeks | $210/$100 |
| Clonidine23 | 1.89 (1.30–2.74) | 776/6 | 9.4 | 3–4 weeks | $74/$4 |
| Venlafaxine15 | 1.33 (0.59–3.00) | 136/1 | 20.4 | $145/NA | |
| Diazepam23 | 1.00 (0.39–2.54) | 76/1 | No difference | $209/$27 | |
| SSRI15 | 0.90 (0.68–1.18) | 1,768/6 | 20.7 | $170/$4 | |
| Buspirone23 | 0.71 (0.34–1.48) | 201/3 | 22.1 | $280/$84 | |
| * Cost based on prices from Walgreen’s and Target Pharmacies, May and September 2007. | |||||
| NNT, number needed to treat; SSRI, selective serotonin reuptake inhibitors; NA, not available. | |||||
Clonidine is an option, but side effects are an issue
Another Cochrane Review looked at the effectiveness of clonidine (Catapres) on smoking cessation.22 Most of the studies assessed withdrawal symptoms rather than abstinence. Of those that did assess quit rates, the pooled OR for clonidine compares favorably at 1.89 (95% CI, 1.30–2.74). Unfortunately, clonidine has significant side effects: sedation and postural hypotension. The starting dosage is 0.1 mg twice daily, and it may be titrated to a maximum dose of 0.4 mg daily. It should be used for 3 to 4 weeks only to decrease withdrawal symptoms. The smoker is then weaned off the drug.
The anxiolytics were the subject of another Cochrane Review.23 This review, however, did not recommend any anxiolytics, including diazepam and buspirone, for smoking cessation.
A new category of therapy: Nicotinic receptor agonists
With US Food and Drug Administration (FDA) approval of varenicline in May 2006, a new class of drugs became available for tobacco dependence. This α4β2 nicotinic acetylcholine receptor partial agonist was designed as a smoking cessation drug. By releasing dopamine in the brain like nicotine, it prevents craving. However, it also blocks nicotine from binding, thereby preventing the reinforcing effect of continued smoking.
Two RCTs have assessed varenicline against both bupropion and placebo (TABLE 3). Jorenby and colleagues showed that varenicline-treated participants were significantly more likely to be continuously abstinent at 52 weeks than the placebo- or bupropion-treated groups (23% vs 10.3% placebo [OR= 2.66; 95% CI, 1.72–4.11; P.001 and bupropion ci>P=.004]).24 Gonzales and associates also showed that varenicline-treated smokers were more likely to be continuously abstinent at 52 weeks than the placebo group (21.9% vs 8.4% [OR=3.09; 95% CI, 1.95–4.91; P.001>25
However, when compared with varenicline, bupropion’s effects were no longer statically significant at 52 weeks (21.9% vs 16.1% [OR=1.46; 95% CI, 0.99– 2.17; P=.057]).
The patient initiating varenicline begins by taking 0.5 mg nightly for 3 nights, then increases to 0.5 mg twice a day for 4 days. The second week, the patient begins the 1-mg twice-daily dosage that is continued through treatment.
Vaccines hold promise
Several promising ideas for the treatment of tobacco dependence are in development, including several vaccines.26 When the immune system produces antibodies to nicotine in response to the vaccine, and when these antibodies bind to the nicotine, the resultant compound is too large to cross the blood–brain barrier. This prevents the reinforcing effect of nicotine. Initial studies of vaccines show that smokers decrease the amount they smoke and find abstinence easier to maintain. However, the vaccine requires frequent boosters to maintain effective antibody titers.
NicVAX from Nabi Biopharmaceuticals was placed on a fast track for approval by the FDA, which is still at least 1 year away. The other two nicotine vaccines are unlikely to be approved for several years.27
Researchers are also studying other compounds that block the euphoria associated with smoking.28 The initial studies of rimonabant (Acomplia), a cannabinoid blocker, have shown that it is no better than other treatments already available. With its indication in some European countries for weight loss, it offered promise as an important option for patients who are concerned about the weight gain associated with smoking cessation. However, the FDA did not approve rimonabant for tobacco cessation when it issued its initial approval letter for weight loss in 2006. Because of safety concerns, the manufacturer subsequently withdrew the new drug application for rimonabant in 2007.
CASE…resolved She kicks the habit
Ann begins taking varenicline the day she leaves the office, and reaches her quit date a week later.
At her 1-month follow-up, she reports that it was easy for her to stay off the cigarettes. With the varenicline, she lost the desire to smoke. The ObGyn reminds her to work on the triggers for her smoking, urging her not to light up when she makes her morning coffee or gets in the car. The physician also suggests that Ann put $4 each morning into a jar on her dresser, so she can see how much she saves now that she isn’t buying cigarettes.
At Ann’s next annual exam, she is marked in the computer as a reformed smoker. She is very proud of that label. When she is asked what she is doing with all that extra cash, she laughs: “My daughter spends it all! But not on cigarettes!”
1. Brown D. Nicotine up sharply in many cigarettes. Washington Post, August 31, 2006. Available at: www.washingtonpost.com/wp-dyn/content/article/2006/08/30/AR2006083001418.html. Accessed on September 4, 2007.
2. Agency for Healthcare Research and Quality. Clinical Practice Guideline. Treating Tobacco Use and Dependence. Rockville, Md: US Department of Health and Human Services Public Health Service; 2000. Available at: www.ncbi.nlm.nih.gov/books/bv.fcgi?rid=hstat2. chapter.7644. Accessed on September 4, 2007.
3. Tobacco Use and Dependence Clinical Practice Guideline Panel, Staff, and Consortium Representatives. A clinical practice guideline for treating tobacco use and dependence: A US Public Health Service report. JAMA. 2000;283:3244-3254.
4. Ask and Act: A Tobacco Cessation Program. Available at: www.aafp.org/online/en/home/clinical/publichealth/tobacco/askandact.html. Accessed on September 4, 2007.
5. Lancaster T, Stead LF. Physician advice for smoking cessation. Cochrane Database Syst Rev. 2004;(4):CD000165.
6. Fiore MC, McCarthy DE, Jackson TC, et al. Integrating smoking cessation treatment into primary care: an effectiveness study. Prev Med. 2004;38:412-420.
7. Katz DA, Muehlenbruch DR, Brown RL. Effectiveness of implementing the Agency for Healthcare Research and Quality Smoking Cessation Clinical Practice Guidelines: a randomized, control trial. J Natl Cancer Inst. 2004;96:594-603.
8. Stead LF, Lancaster T, Perera R. Telephone counseling for smoking cessation. Cochrane Database Syst Rev. 2003;(1):CD002850.
9. Zhu SH, Anderson CM, Tedeschi GJ, et al. Evidence of real-world effectiveness of a telephone quitline for smokers. N Engl J Med. 2002;347:1087-1093.
10. An LC, Zhu SH, Nelson DB, et al. Benefits of telephone care over primary care for smoking cessation. Arch Intern Med. 2006;166:536-542.
11. Etter JF. Comparing the efficacy of two Internet-based, computer-tailored smoking cessation programs: a randomized trial. J Med Internet Res. 2005;7(1):e2.
12. Swartz LH, Noell JW, Schroeder SW, Ary DV. A randomised control study of a fully automated internet based smoking cessation programme. Tob Control. 2006;15:7-12.
13. Rodgers A, Corbett T, Bramley D, et al. Do u smoke after txt? Results of a randomised trial of smoking cessation using mobile phone text messaging. Tob Control. 2005;14:255-261.
14. Silagy C, Lancaster T, Stead L, Mant D, Fowler G. Nicotine replacement therapy for smoking cessation. Cochrane Database Syst Rev. 2004;(4):CD000146.
15. Hughes JR, Stead LF, Lancaster T. Antidepressants for smoking cessation. Cochrane Database Syst Rev. 2004;(2):CD000031.
16. Hurt RD, Sachs DP, Glover ED, et al. A comparison of sustained-release bupropion and placebo for smoking cessation. N Engl J Med. 1997;337:1195-1202.
17. Swan GE, McAfee T, Curry SJ, et al. Effectiveness of bupropion sustained release for smoking cessation in a health care setting. Arch Intern Med. 2003;163:2337-2344.
18. da Costa CL, Younes RN, Lourenco MT. A prospective, randomized, double-blind study comparing nortriptyline to placebo. Chest. 2002;122:403-408.
19. Hall SM, Reus VI, Munoz RF, et al. Nortriptyline and cognitive-behavioral therapy in the treatment of cigarette smoking. Arch Gen Psychiatry. 1998;55:683-690.
20. Hall SM, Humfleet GL, Reus VI, et al. Psychological intervention and antidepressant treatment in smoking cessation. Arch Gen Psychiatry. 2002;59:930-936.
21. Prochazka AV, Weaver MJ, Keller RT, et al. A randomized trial of nortriptyline for smoking cessation. Arch Intern Med. 1998;158:2035-2039.
22. Gourlay SG, Stead LF, Benowitz NL. Clonidine for smoking cessation. Cochrane Database Syst Rev. 2004;(3):CD000058.
23. Hughes JR, Stead LF, Lancaster T. Anxiolytics for smoking cessation. Cochrane Database Syst Rev. 2000;(4):CD002849.
24. Jorenby DE, Hays JT, Rigotti NA. efficacy of varenicline, an α4β2 nicotinic acetylcholine receptor partial agonist, vs placebo or sustained-release bupropion for smoking cessation. JAMA. 2006;296:56-63.
25. Gonzales D, Rennard SI, Nides M. Varenicline, an α4β2 nicotinic acetylcholine receptor partial agonist, vs sustained-release bupropion and placebo for smoking cessation. JAMA. 2006;296:47-55.
26. LeHouezec J. Why a nicotine vaccine? Clin Pharmacol Ther. 2005;78:453-455.
27. Tuller D. Scientists testing vaccines to help smokers quit. New York Times, July 4, 2006.
28. Fagerström K, Balfour DJ. Neuropharmacology and potential efficacy of new treatments for tobacco dependence. Expert Opin Investig Drugs. 2005;15:107-116.
1. Brown D. Nicotine up sharply in many cigarettes. Washington Post, August 31, 2006. Available at: www.washingtonpost.com/wp-dyn/content/article/2006/08/30/AR2006083001418.html. Accessed on September 4, 2007.
2. Agency for Healthcare Research and Quality. Clinical Practice Guideline. Treating Tobacco Use and Dependence. Rockville, Md: US Department of Health and Human Services Public Health Service; 2000. Available at: www.ncbi.nlm.nih.gov/books/bv.fcgi?rid=hstat2. chapter.7644. Accessed on September 4, 2007.
3. Tobacco Use and Dependence Clinical Practice Guideline Panel, Staff, and Consortium Representatives. A clinical practice guideline for treating tobacco use and dependence: A US Public Health Service report. JAMA. 2000;283:3244-3254.
4. Ask and Act: A Tobacco Cessation Program. Available at: www.aafp.org/online/en/home/clinical/publichealth/tobacco/askandact.html. Accessed on September 4, 2007.
5. Lancaster T, Stead LF. Physician advice for smoking cessation. Cochrane Database Syst Rev. 2004;(4):CD000165.
6. Fiore MC, McCarthy DE, Jackson TC, et al. Integrating smoking cessation treatment into primary care: an effectiveness study. Prev Med. 2004;38:412-420.
7. Katz DA, Muehlenbruch DR, Brown RL. Effectiveness of implementing the Agency for Healthcare Research and Quality Smoking Cessation Clinical Practice Guidelines: a randomized, control trial. J Natl Cancer Inst. 2004;96:594-603.
8. Stead LF, Lancaster T, Perera R. Telephone counseling for smoking cessation. Cochrane Database Syst Rev. 2003;(1):CD002850.
9. Zhu SH, Anderson CM, Tedeschi GJ, et al. Evidence of real-world effectiveness of a telephone quitline for smokers. N Engl J Med. 2002;347:1087-1093.
10. An LC, Zhu SH, Nelson DB, et al. Benefits of telephone care over primary care for smoking cessation. Arch Intern Med. 2006;166:536-542.
11. Etter JF. Comparing the efficacy of two Internet-based, computer-tailored smoking cessation programs: a randomized trial. J Med Internet Res. 2005;7(1):e2.
12. Swartz LH, Noell JW, Schroeder SW, Ary DV. A randomised control study of a fully automated internet based smoking cessation programme. Tob Control. 2006;15:7-12.
13. Rodgers A, Corbett T, Bramley D, et al. Do u smoke after txt? Results of a randomised trial of smoking cessation using mobile phone text messaging. Tob Control. 2005;14:255-261.
14. Silagy C, Lancaster T, Stead L, Mant D, Fowler G. Nicotine replacement therapy for smoking cessation. Cochrane Database Syst Rev. 2004;(4):CD000146.
15. Hughes JR, Stead LF, Lancaster T. Antidepressants for smoking cessation. Cochrane Database Syst Rev. 2004;(2):CD000031.
16. Hurt RD, Sachs DP, Glover ED, et al. A comparison of sustained-release bupropion and placebo for smoking cessation. N Engl J Med. 1997;337:1195-1202.
17. Swan GE, McAfee T, Curry SJ, et al. Effectiveness of bupropion sustained release for smoking cessation in a health care setting. Arch Intern Med. 2003;163:2337-2344.
18. da Costa CL, Younes RN, Lourenco MT. A prospective, randomized, double-blind study comparing nortriptyline to placebo. Chest. 2002;122:403-408.
19. Hall SM, Reus VI, Munoz RF, et al. Nortriptyline and cognitive-behavioral therapy in the treatment of cigarette smoking. Arch Gen Psychiatry. 1998;55:683-690.
20. Hall SM, Humfleet GL, Reus VI, et al. Psychological intervention and antidepressant treatment in smoking cessation. Arch Gen Psychiatry. 2002;59:930-936.
21. Prochazka AV, Weaver MJ, Keller RT, et al. A randomized trial of nortriptyline for smoking cessation. Arch Intern Med. 1998;158:2035-2039.
22. Gourlay SG, Stead LF, Benowitz NL. Clonidine for smoking cessation. Cochrane Database Syst Rev. 2004;(3):CD000058.
23. Hughes JR, Stead LF, Lancaster T. Anxiolytics for smoking cessation. Cochrane Database Syst Rev. 2000;(4):CD002849.
24. Jorenby DE, Hays JT, Rigotti NA. efficacy of varenicline, an α4β2 nicotinic acetylcholine receptor partial agonist, vs placebo or sustained-release bupropion for smoking cessation. JAMA. 2006;296:56-63.
25. Gonzales D, Rennard SI, Nides M. Varenicline, an α4β2 nicotinic acetylcholine receptor partial agonist, vs sustained-release bupropion and placebo for smoking cessation. JAMA. 2006;296:47-55.
26. LeHouezec J. Why a nicotine vaccine? Clin Pharmacol Ther. 2005;78:453-455.
27. Tuller D. Scientists testing vaccines to help smokers quit. New York Times, July 4, 2006.
28. Fagerström K, Balfour DJ. Neuropharmacology and potential efficacy of new treatments for tobacco dependence. Expert Opin Investig Drugs. 2005;15:107-116.
Splenic Rupture During Routine Colonoscopy
Developing a VA Palliative Care Program
FERTILITY
The field of reproductive endocrinology and infertility is anything but stagnant. New technologies continue to enter the market at a brisk pace, and a greater emphasis on evidence has produced better-designed randomized controlled trials, meta-analyses, and practice guidelines. This means greater availability of standardized protocols that reflect best practice and can be tailored to a patient’s condition and needs.
Highlighted here are notable studies and guidelines from the past year, including advice on:
- preventing peritoneal adhesions
- expediting in vitro fertilization (IVF) for unexplained infertility
- counseling the patient about the real limitations of preimplantation genetic screening for aneuploidy
- informing patients that oocyte cryopreservation is unlikely to lead to live birth.
Guideline urges good surgical technique in battle against adhesions
Practice Committee of the American Society for Reproductive Medicine in collaboration with the Society of Re-productive Surgeons. Pathogenesis, consequences, and control of peritoneal adhesions in gynecologic surgery. Fertil Steril. 2007;88:21–26.
This newly released practice guideline from the American Society of Reproductive Medicine (ASRM) focuses on adhesions and their impact on fertility. The guideline reiterates that peritoneal adhesions are a common and serious complication of gynecologic surgery and emphasizes key principles to reduce their likelihood and extent. These principles include the need to:
- Perform surgery only when the benefits of doing so clearly outweigh the risks
- Handle tissue gently (this is the most important preventive technique)
- Don’t assume laparoscopy is superior to laparotomy—it will be only if less tissue injury occurs
- Be especially careful when operating on or near ovaries, which form adhesions easily.
Ovarian surgery often necessitates additional operations
Studies have demonstrated that approximately 33% of patients who undergo open abdominal or pelvic surgery are readmitted, on average, two times over the subsequent 10 years for conditions directly or possibly related to adhesions or for further surgery that could be complicated by adhesions. The highest readmission rate directly related to adhesions—7.5 for every 100 initial operations—was associated with ovarian surgery performed via laparotomy.
Adhesion-related complications of gynecologic surgery include small-bowel obstruction, which occurs in approximately 1.5% of women who have undergone abdominal hysterectomy.
The relationship between adhesions and pelvic pain is unclear, although severe bowel adhesions can cause visceral pain. The ASRM guideline notes that “the impact that lysis of bowel or adnexal adhesions may have on abdominal and pelvic pain cannot be predicted confidently.” Postoperative adhesions increase subsequent operating times and risk of bowel injury.
How adhesions affect fertility
Adhesions may impair fertility by distorting adnexal anatomy and interfering with gamete and embryo transport. Among infertile women who have adnexal adhesions, adhesiolysis is associated with pregnancy rates of 32% at 12 months and 45% at 24 months, compared with 11% and 16%, respectively, for untreated women.1 Pregnancy rates are inversely correlated with adhesion scores on the ASRM classification system for adnexal adhesions.2
Some, but not all, adhesion-reducing measures work
According to the ASRM guideline, adhesions may be prevented, at least theoretically, by:
- minimizing peritoneal injury during surgery
- avoiding the introduction of reactive foreign bodies
- reducing the local inflammatory response
- inhibiting the coagulation cascade and promoting fibrinolysis
- placing barriers between damaged tissues.
Pharmacotherapeutic and fluid agents. ASRM found no evidence of improved pregnancy outcomes for pharmacologic and fluid agents used as an adjunct during pelvic surgery. For example, anti-inflammatory agents that have been evaluated, both locally and systemically, including dexamethasone and promethazine, have not reduced postoperative adhesions. Antibiotic solutions, 32% Dextran 70, and crystalloid solutions such as normal saline and Ringer’s lactate with or without heparin or corticosteroids have been used to separate adjacent peritoneal surfaces via “hydroflotation,” but none have reduced adhesion formation.
Surgical barriers may help decrease postoperative adhesion formation but cannot compensate for poor surgical technique. I rarely use adhesion barriers because I feel that careful tissue handling, excellent hemostasis, avoiding trauma to healthy tissue, and removal of all diseased tissue are the key ways to obtain good postsurgical results and reduce adhesions.
Hyaluronic acid agents may decrease the prevalence of adhesions and prevent the deterioration of preexisting adhesions, but because of the limited number of studies available, these data should be interpreted with caution.3 However, ASRM found no substantial evidence that they improve fertility, decrease pain, or reduce the incidence of postoperative bowel obstruction.
Averting adhesions: Surgical techniques and tools
By Togas Tulandi, MD, MHCM, and Mohammed Al-Sunaidi, MD It’s available in our archive at www.obgmanagement.com
A move from clomiphene directly to IVF may cut time to pregnancy
Reindollar RH, Regan MM, Neumann PJ, Thornton KL, Alper MM, Goldman MB. A randomized controlled trial of 503 couples assigned to conventional infertility treatment or an accelerated track to IVF: Preliminary results of the fast track and standard treatment (FASTT) trial. Fertil Steril. 2007;88(Suppl 1):S41.
This very important abstract, presented at the annual meeting of ASRM, has the potential to dramatically change fertility treatment. The multicenter randomized controlled clinical trial measured the efficacy and time to pregnancy of an accelerated treatment strategy for women 21 to 39 years old who had unexplained infertility. A similar percentage of patients—approximately 75%—became pregnant in each arm (traditional versus accelerated), with a shorter time to pregnancy in the accelerated arm.
The new paradigm for management of unexplained infertility includes:
- comprehensive fertility history and physical examination
- targeted laboratory testing and other investigation, as needed
- counseling and psychological support for the patient once the diagnosis is made
- empiric treatment with clomiphene citrate plus intrauterine insemination (IUI) for as many as three cycles
- immediate IVF for as many as six cycles.
Details of the trial
Women in the trial had attempted to conceive for 12 months and had normal ovarian reserve (and semen analysis) and no pelvic pathology. Couples already treated for infertility were excluded.
Participants were randomized to:
- a conventional treatment regimen of three cycles of clomiphene citrate with IUI, three cycles of folliclestimulating hormone (FSH) and IUI, and as many as six cycles of IVF or
- three cycles of clomiphene citrate with IUI and then as many as six cycles of IVF.
Regimen likely reduces cost, stress
Major issues affecting the eventual success rate for infertile couples are cost and psychological stress, which can cause even patients who have a good prognosis to drop out of treatment. The major complication of fertility treatment is multiple pregnancy. By avoiding the use of gonadotropins in couples with unexplained infertility and accelerating the transition to IVF, physicians can lower the cost and psychological stress of treatment. They can also reduce the likelihood of multiple pregnancy because it is easier to control the number of embryos transferred in IVF than the number of follicles that develop with gonadotropins.
In women younger than 35 years on the first IVF cycle who have a good prognosis, ASRM now recommends that only one or two day-3 embryos be transferred, and not more than one day-5 blastocyst.4 The multiple-birth rate has declined in recent years, as more and more IVF clinics place fewer embryos; the rate should continue to fall with wider application of elective single-embryo transfer.5,6
Because this accelerated protocol produces a similar number of births over a shorter period and has the potential to lower cost, psychological stress, and the multiple-birth rate, it deserves implementation for many patients and warrants further evaluation for potential benefits in other populations.
It’s no help, after all: Preimplantation genetic screening for aneuploidy
Practice Committee of the Society for Assisted Reproductive Technology and Practice Committee of the American Society for Reproductive Medicine. Preimplantation genetic testing: A Practice Committee report. Fertil Steril. 2007;88:1497–1504.
Mastenbroek S, Twisk M, van Echten-Arends J, et al. In vitro fertilization with preimplantation genetic screening. N Engl J Med. 2007;357:9–17.
Preimplantation genetic diagnosis of known single-gene defects, structural chromosomal rearrangements, X-linked disorders, and human leukocyte antigen typing is a major benefit to couples known to be at risk of passing on a heritable and debilitating genetic disease. Aneuploidy is the most common cause of early pregnancy loss, and its prevalence increases with maternal age and may increase in chromosomally normal couples who experience recurrent early pregnancy loss or repeated failure of IVF cycles. Preimplantation genetic screening (PGS) has been advocated to identify and transfer only euploid embryos and increase the chance of successful pregnancy.
New data from Mastenbroek and colleagues indicate that PGS for aneuploidy does not increase the rate of pregnancy or live birth. After several years of increasing utilization and studies suggesting that PGS has benefit, the first multicenter, randomized, doubleblind, controlled study that compared three cycles of IVF with and without PGS in women 35 to 41 years old concluded that PGS does not increase but, in fact, significantly reduces the rate of pregnancy and live birth in this group.
Findings sparked controversy
This trial generated controversy within the genetics and reproductive endocrinology specialties because it challenged the intuitive view that screening of embryos before transfer into the uterus should be beneficial—or, at least, harmless. Some now argue that the benefits of PGS, if any, cannot be intuitively assumed and assert that the burden of proof of those benefits rests with proponents of PGS.
The practice committees of the Society for Assisted Reproductive Technology (SART) and ASRM found insufficient evidence to support the use of PGS to improve the live birth rate in women of advanced age or in those who have had implantation failure or recurrent pregnancy loss (TABLE). Many physicians believe, however, that technologies under development will soon bring verifiable benefits of PGS to patients.
SART and ASRM weigh in on use of preimplantation genetic testing
| TEST | RECOMMENDATION |
|---|---|
| Pre-implantation genetic diagnosis | |
| Pre- implantation genetic screening | |
| SOURCE: Society for Assisted Reproductive Technology and American Society for Reproductive Medicine | |
Advise your patients that oocyte cryopreservation is “a long shot”
Practice Committee of the Society for Assisted Reproductive Technology and Practice Committee of the American Society for Reproductive Medicine. Essential elements of informed consent for elective oocyte cryopreservation: a practice committee opinion. Fertil Steril. 2007;88:1495–1496.
Oocyte cryopreservation is an experimental procedure that should not be offered or marketed as a means to defer reproductive aging, primarily because data on clinical outcomes are limited. That is the conclusion of this guideline from SART and ASRM. Consequently, women who may be considering the procedure should be fully informed about the process and likely outcomes and counseled by a qualified mental health professional.
Counseling is crucial
According to the SART and ASRM guideline, pretreatment counseling should include comprehensive information on a range of topics (see the box below). In addition, women considering oocyte cryopreservation should be counseled thoroughly about reproductive aging and life planning.7,8
Few alternatives for some women
Women who have cancer should receive the same counseling. Unlike healthy women, however, they may have no other options, and cryopreservation may be more appropriate for them despite experimental status.
Patients considering this procedure need comprehensive information about:
- Ovarian stimulation and oocyte retrieval
- Methods of oocyte cryopreservation
- Storage fees
- The expected thaw survival rate
- The requirement for intracytoplasmic sperm injection
- Clinic-specific data and outcomes or, in their absence, literature estimates of a 2% overall live birth rate per oocyte thawed using slow-freeze methods and 4% for vitrification, compared with age-related probabilities of success per IVF cycle using fresh nondonor oocytes
- The relatively low likelihood that a woman who cryopreserves her eggs before age 35 will ever need or use them
- State and federal screening laws for potential donation of cryopreserved oocytes
- Potential risks of basing important life decisions and expectations on a limited number of cryopreserved oocytes
- The possibility that the facility may cease operation, necessitating transfer of cryopreserved oocytes to another facility
- The possibility that cryopreserved oocytes might be lost or damaged as a result of laboratory error or other events beyond control.
1. Tulandi T, Collins JA, Burrows E, et al. Treatment-dependent and treatment-independent pregnancy among women with periadnexal adhesions. Am J Obstet Gynecol. 1990;162:354-357.
2. Marana R, Rizzi M, Muzii L, Catalano GF, Caruana P, Mancuso S. Correlation between the American Fertility Society classification of adnexal adhesions and distal tubal occlusion, salpingoscopy, and reproductive outcome in tubal surgery. Fertil Steril. 1995;64:924-929.
3. Metwally M, Gorvy D, Watson A, Li TC. Hyaluronic acid fluid agents for the prevention of adhesions after fertility-preserving gynecological surgery: a metaanalysis of randomized controlled trials. Fertil Steril. 2007;87:1139-1146.
4. Practice Committee of the Society for Assisted Reproductive Technology and the Practice Committee of the American Society for Reproductive Medicine. Guidelines on number of embryos transferred. Fertil Steril. 2006;86(Suppl 4):S51-S52.
5. Adamson GD, Baker VL. Multiple births from assisted reproductive technologies: a challenge that must be met. Fertil Steril. 2004;81:517-522.
6. Stern JE, Cedars MI, Jain T, et al. for the Society for Assisted Reproductive Technology Writing Group Assisted reproductive technology practice patterns and the impact of embryo transfer guidelines in the United States. Fertil Steril. 2007;88:275-282.
7. Menken J, Trussell J, Larsen U. Age and infertility. Science. 1986;233:1389-1394.
8. Leridon H. Can assisted reproduction technology compensate for the natural decline in fertility with age? A model assessment. Hum Reprod. 2004;19:1548-1553.
The field of reproductive endocrinology and infertility is anything but stagnant. New technologies continue to enter the market at a brisk pace, and a greater emphasis on evidence has produced better-designed randomized controlled trials, meta-analyses, and practice guidelines. This means greater availability of standardized protocols that reflect best practice and can be tailored to a patient’s condition and needs.
Highlighted here are notable studies and guidelines from the past year, including advice on:
- preventing peritoneal adhesions
- expediting in vitro fertilization (IVF) for unexplained infertility
- counseling the patient about the real limitations of preimplantation genetic screening for aneuploidy
- informing patients that oocyte cryopreservation is unlikely to lead to live birth.
Guideline urges good surgical technique in battle against adhesions
Practice Committee of the American Society for Reproductive Medicine in collaboration with the Society of Re-productive Surgeons. Pathogenesis, consequences, and control of peritoneal adhesions in gynecologic surgery. Fertil Steril. 2007;88:21–26.
This newly released practice guideline from the American Society of Reproductive Medicine (ASRM) focuses on adhesions and their impact on fertility. The guideline reiterates that peritoneal adhesions are a common and serious complication of gynecologic surgery and emphasizes key principles to reduce their likelihood and extent. These principles include the need to:
- Perform surgery only when the benefits of doing so clearly outweigh the risks
- Handle tissue gently (this is the most important preventive technique)
- Don’t assume laparoscopy is superior to laparotomy—it will be only if less tissue injury occurs
- Be especially careful when operating on or near ovaries, which form adhesions easily.
Ovarian surgery often necessitates additional operations
Studies have demonstrated that approximately 33% of patients who undergo open abdominal or pelvic surgery are readmitted, on average, two times over the subsequent 10 years for conditions directly or possibly related to adhesions or for further surgery that could be complicated by adhesions. The highest readmission rate directly related to adhesions—7.5 for every 100 initial operations—was associated with ovarian surgery performed via laparotomy.
Adhesion-related complications of gynecologic surgery include small-bowel obstruction, which occurs in approximately 1.5% of women who have undergone abdominal hysterectomy.
The relationship between adhesions and pelvic pain is unclear, although severe bowel adhesions can cause visceral pain. The ASRM guideline notes that “the impact that lysis of bowel or adnexal adhesions may have on abdominal and pelvic pain cannot be predicted confidently.” Postoperative adhesions increase subsequent operating times and risk of bowel injury.
How adhesions affect fertility
Adhesions may impair fertility by distorting adnexal anatomy and interfering with gamete and embryo transport. Among infertile women who have adnexal adhesions, adhesiolysis is associated with pregnancy rates of 32% at 12 months and 45% at 24 months, compared with 11% and 16%, respectively, for untreated women.1 Pregnancy rates are inversely correlated with adhesion scores on the ASRM classification system for adnexal adhesions.2
Some, but not all, adhesion-reducing measures work
According to the ASRM guideline, adhesions may be prevented, at least theoretically, by:
- minimizing peritoneal injury during surgery
- avoiding the introduction of reactive foreign bodies
- reducing the local inflammatory response
- inhibiting the coagulation cascade and promoting fibrinolysis
- placing barriers between damaged tissues.
Pharmacotherapeutic and fluid agents. ASRM found no evidence of improved pregnancy outcomes for pharmacologic and fluid agents used as an adjunct during pelvic surgery. For example, anti-inflammatory agents that have been evaluated, both locally and systemically, including dexamethasone and promethazine, have not reduced postoperative adhesions. Antibiotic solutions, 32% Dextran 70, and crystalloid solutions such as normal saline and Ringer’s lactate with or without heparin or corticosteroids have been used to separate adjacent peritoneal surfaces via “hydroflotation,” but none have reduced adhesion formation.
Surgical barriers may help decrease postoperative adhesion formation but cannot compensate for poor surgical technique. I rarely use adhesion barriers because I feel that careful tissue handling, excellent hemostasis, avoiding trauma to healthy tissue, and removal of all diseased tissue are the key ways to obtain good postsurgical results and reduce adhesions.
Hyaluronic acid agents may decrease the prevalence of adhesions and prevent the deterioration of preexisting adhesions, but because of the limited number of studies available, these data should be interpreted with caution.3 However, ASRM found no substantial evidence that they improve fertility, decrease pain, or reduce the incidence of postoperative bowel obstruction.
Averting adhesions: Surgical techniques and tools
By Togas Tulandi, MD, MHCM, and Mohammed Al-Sunaidi, MD It’s available in our archive at www.obgmanagement.com
A move from clomiphene directly to IVF may cut time to pregnancy
Reindollar RH, Regan MM, Neumann PJ, Thornton KL, Alper MM, Goldman MB. A randomized controlled trial of 503 couples assigned to conventional infertility treatment or an accelerated track to IVF: Preliminary results of the fast track and standard treatment (FASTT) trial. Fertil Steril. 2007;88(Suppl 1):S41.
This very important abstract, presented at the annual meeting of ASRM, has the potential to dramatically change fertility treatment. The multicenter randomized controlled clinical trial measured the efficacy and time to pregnancy of an accelerated treatment strategy for women 21 to 39 years old who had unexplained infertility. A similar percentage of patients—approximately 75%—became pregnant in each arm (traditional versus accelerated), with a shorter time to pregnancy in the accelerated arm.
The new paradigm for management of unexplained infertility includes:
- comprehensive fertility history and physical examination
- targeted laboratory testing and other investigation, as needed
- counseling and psychological support for the patient once the diagnosis is made
- empiric treatment with clomiphene citrate plus intrauterine insemination (IUI) for as many as three cycles
- immediate IVF for as many as six cycles.
Details of the trial
Women in the trial had attempted to conceive for 12 months and had normal ovarian reserve (and semen analysis) and no pelvic pathology. Couples already treated for infertility were excluded.
Participants were randomized to:
- a conventional treatment regimen of three cycles of clomiphene citrate with IUI, three cycles of folliclestimulating hormone (FSH) and IUI, and as many as six cycles of IVF or
- three cycles of clomiphene citrate with IUI and then as many as six cycles of IVF.
Regimen likely reduces cost, stress
Major issues affecting the eventual success rate for infertile couples are cost and psychological stress, which can cause even patients who have a good prognosis to drop out of treatment. The major complication of fertility treatment is multiple pregnancy. By avoiding the use of gonadotropins in couples with unexplained infertility and accelerating the transition to IVF, physicians can lower the cost and psychological stress of treatment. They can also reduce the likelihood of multiple pregnancy because it is easier to control the number of embryos transferred in IVF than the number of follicles that develop with gonadotropins.
In women younger than 35 years on the first IVF cycle who have a good prognosis, ASRM now recommends that only one or two day-3 embryos be transferred, and not more than one day-5 blastocyst.4 The multiple-birth rate has declined in recent years, as more and more IVF clinics place fewer embryos; the rate should continue to fall with wider application of elective single-embryo transfer.5,6
Because this accelerated protocol produces a similar number of births over a shorter period and has the potential to lower cost, psychological stress, and the multiple-birth rate, it deserves implementation for many patients and warrants further evaluation for potential benefits in other populations.
It’s no help, after all: Preimplantation genetic screening for aneuploidy
Practice Committee of the Society for Assisted Reproductive Technology and Practice Committee of the American Society for Reproductive Medicine. Preimplantation genetic testing: A Practice Committee report. Fertil Steril. 2007;88:1497–1504.
Mastenbroek S, Twisk M, van Echten-Arends J, et al. In vitro fertilization with preimplantation genetic screening. N Engl J Med. 2007;357:9–17.
Preimplantation genetic diagnosis of known single-gene defects, structural chromosomal rearrangements, X-linked disorders, and human leukocyte antigen typing is a major benefit to couples known to be at risk of passing on a heritable and debilitating genetic disease. Aneuploidy is the most common cause of early pregnancy loss, and its prevalence increases with maternal age and may increase in chromosomally normal couples who experience recurrent early pregnancy loss or repeated failure of IVF cycles. Preimplantation genetic screening (PGS) has been advocated to identify and transfer only euploid embryos and increase the chance of successful pregnancy.
New data from Mastenbroek and colleagues indicate that PGS for aneuploidy does not increase the rate of pregnancy or live birth. After several years of increasing utilization and studies suggesting that PGS has benefit, the first multicenter, randomized, doubleblind, controlled study that compared three cycles of IVF with and without PGS in women 35 to 41 years old concluded that PGS does not increase but, in fact, significantly reduces the rate of pregnancy and live birth in this group.
Findings sparked controversy
This trial generated controversy within the genetics and reproductive endocrinology specialties because it challenged the intuitive view that screening of embryos before transfer into the uterus should be beneficial—or, at least, harmless. Some now argue that the benefits of PGS, if any, cannot be intuitively assumed and assert that the burden of proof of those benefits rests with proponents of PGS.
The practice committees of the Society for Assisted Reproductive Technology (SART) and ASRM found insufficient evidence to support the use of PGS to improve the live birth rate in women of advanced age or in those who have had implantation failure or recurrent pregnancy loss (TABLE). Many physicians believe, however, that technologies under development will soon bring verifiable benefits of PGS to patients.
SART and ASRM weigh in on use of preimplantation genetic testing
| TEST | RECOMMENDATION |
|---|---|
| Pre-implantation genetic diagnosis | |
| Pre- implantation genetic screening | |
| SOURCE: Society for Assisted Reproductive Technology and American Society for Reproductive Medicine | |
Advise your patients that oocyte cryopreservation is “a long shot”
Practice Committee of the Society for Assisted Reproductive Technology and Practice Committee of the American Society for Reproductive Medicine. Essential elements of informed consent for elective oocyte cryopreservation: a practice committee opinion. Fertil Steril. 2007;88:1495–1496.
Oocyte cryopreservation is an experimental procedure that should not be offered or marketed as a means to defer reproductive aging, primarily because data on clinical outcomes are limited. That is the conclusion of this guideline from SART and ASRM. Consequently, women who may be considering the procedure should be fully informed about the process and likely outcomes and counseled by a qualified mental health professional.
Counseling is crucial
According to the SART and ASRM guideline, pretreatment counseling should include comprehensive information on a range of topics (see the box below). In addition, women considering oocyte cryopreservation should be counseled thoroughly about reproductive aging and life planning.7,8
Few alternatives for some women
Women who have cancer should receive the same counseling. Unlike healthy women, however, they may have no other options, and cryopreservation may be more appropriate for them despite experimental status.
Patients considering this procedure need comprehensive information about:
- Ovarian stimulation and oocyte retrieval
- Methods of oocyte cryopreservation
- Storage fees
- The expected thaw survival rate
- The requirement for intracytoplasmic sperm injection
- Clinic-specific data and outcomes or, in their absence, literature estimates of a 2% overall live birth rate per oocyte thawed using slow-freeze methods and 4% for vitrification, compared with age-related probabilities of success per IVF cycle using fresh nondonor oocytes
- The relatively low likelihood that a woman who cryopreserves her eggs before age 35 will ever need or use them
- State and federal screening laws for potential donation of cryopreserved oocytes
- Potential risks of basing important life decisions and expectations on a limited number of cryopreserved oocytes
- The possibility that the facility may cease operation, necessitating transfer of cryopreserved oocytes to another facility
- The possibility that cryopreserved oocytes might be lost or damaged as a result of laboratory error or other events beyond control.
The field of reproductive endocrinology and infertility is anything but stagnant. New technologies continue to enter the market at a brisk pace, and a greater emphasis on evidence has produced better-designed randomized controlled trials, meta-analyses, and practice guidelines. This means greater availability of standardized protocols that reflect best practice and can be tailored to a patient’s condition and needs.
Highlighted here are notable studies and guidelines from the past year, including advice on:
- preventing peritoneal adhesions
- expediting in vitro fertilization (IVF) for unexplained infertility
- counseling the patient about the real limitations of preimplantation genetic screening for aneuploidy
- informing patients that oocyte cryopreservation is unlikely to lead to live birth.
Guideline urges good surgical technique in battle against adhesions
Practice Committee of the American Society for Reproductive Medicine in collaboration with the Society of Re-productive Surgeons. Pathogenesis, consequences, and control of peritoneal adhesions in gynecologic surgery. Fertil Steril. 2007;88:21–26.
This newly released practice guideline from the American Society of Reproductive Medicine (ASRM) focuses on adhesions and their impact on fertility. The guideline reiterates that peritoneal adhesions are a common and serious complication of gynecologic surgery and emphasizes key principles to reduce their likelihood and extent. These principles include the need to:
- Perform surgery only when the benefits of doing so clearly outweigh the risks
- Handle tissue gently (this is the most important preventive technique)
- Don’t assume laparoscopy is superior to laparotomy—it will be only if less tissue injury occurs
- Be especially careful when operating on or near ovaries, which form adhesions easily.
Ovarian surgery often necessitates additional operations
Studies have demonstrated that approximately 33% of patients who undergo open abdominal or pelvic surgery are readmitted, on average, two times over the subsequent 10 years for conditions directly or possibly related to adhesions or for further surgery that could be complicated by adhesions. The highest readmission rate directly related to adhesions—7.5 for every 100 initial operations—was associated with ovarian surgery performed via laparotomy.
Adhesion-related complications of gynecologic surgery include small-bowel obstruction, which occurs in approximately 1.5% of women who have undergone abdominal hysterectomy.
The relationship between adhesions and pelvic pain is unclear, although severe bowel adhesions can cause visceral pain. The ASRM guideline notes that “the impact that lysis of bowel or adnexal adhesions may have on abdominal and pelvic pain cannot be predicted confidently.” Postoperative adhesions increase subsequent operating times and risk of bowel injury.
How adhesions affect fertility
Adhesions may impair fertility by distorting adnexal anatomy and interfering with gamete and embryo transport. Among infertile women who have adnexal adhesions, adhesiolysis is associated with pregnancy rates of 32% at 12 months and 45% at 24 months, compared with 11% and 16%, respectively, for untreated women.1 Pregnancy rates are inversely correlated with adhesion scores on the ASRM classification system for adnexal adhesions.2
Some, but not all, adhesion-reducing measures work
According to the ASRM guideline, adhesions may be prevented, at least theoretically, by:
- minimizing peritoneal injury during surgery
- avoiding the introduction of reactive foreign bodies
- reducing the local inflammatory response
- inhibiting the coagulation cascade and promoting fibrinolysis
- placing barriers between damaged tissues.
Pharmacotherapeutic and fluid agents. ASRM found no evidence of improved pregnancy outcomes for pharmacologic and fluid agents used as an adjunct during pelvic surgery. For example, anti-inflammatory agents that have been evaluated, both locally and systemically, including dexamethasone and promethazine, have not reduced postoperative adhesions. Antibiotic solutions, 32% Dextran 70, and crystalloid solutions such as normal saline and Ringer’s lactate with or without heparin or corticosteroids have been used to separate adjacent peritoneal surfaces via “hydroflotation,” but none have reduced adhesion formation.
Surgical barriers may help decrease postoperative adhesion formation but cannot compensate for poor surgical technique. I rarely use adhesion barriers because I feel that careful tissue handling, excellent hemostasis, avoiding trauma to healthy tissue, and removal of all diseased tissue are the key ways to obtain good postsurgical results and reduce adhesions.
Hyaluronic acid agents may decrease the prevalence of adhesions and prevent the deterioration of preexisting adhesions, but because of the limited number of studies available, these data should be interpreted with caution.3 However, ASRM found no substantial evidence that they improve fertility, decrease pain, or reduce the incidence of postoperative bowel obstruction.
Averting adhesions: Surgical techniques and tools
By Togas Tulandi, MD, MHCM, and Mohammed Al-Sunaidi, MD It’s available in our archive at www.obgmanagement.com
A move from clomiphene directly to IVF may cut time to pregnancy
Reindollar RH, Regan MM, Neumann PJ, Thornton KL, Alper MM, Goldman MB. A randomized controlled trial of 503 couples assigned to conventional infertility treatment or an accelerated track to IVF: Preliminary results of the fast track and standard treatment (FASTT) trial. Fertil Steril. 2007;88(Suppl 1):S41.
This very important abstract, presented at the annual meeting of ASRM, has the potential to dramatically change fertility treatment. The multicenter randomized controlled clinical trial measured the efficacy and time to pregnancy of an accelerated treatment strategy for women 21 to 39 years old who had unexplained infertility. A similar percentage of patients—approximately 75%—became pregnant in each arm (traditional versus accelerated), with a shorter time to pregnancy in the accelerated arm.
The new paradigm for management of unexplained infertility includes:
- comprehensive fertility history and physical examination
- targeted laboratory testing and other investigation, as needed
- counseling and psychological support for the patient once the diagnosis is made
- empiric treatment with clomiphene citrate plus intrauterine insemination (IUI) for as many as three cycles
- immediate IVF for as many as six cycles.
Details of the trial
Women in the trial had attempted to conceive for 12 months and had normal ovarian reserve (and semen analysis) and no pelvic pathology. Couples already treated for infertility were excluded.
Participants were randomized to:
- a conventional treatment regimen of three cycles of clomiphene citrate with IUI, three cycles of folliclestimulating hormone (FSH) and IUI, and as many as six cycles of IVF or
- three cycles of clomiphene citrate with IUI and then as many as six cycles of IVF.
Regimen likely reduces cost, stress
Major issues affecting the eventual success rate for infertile couples are cost and psychological stress, which can cause even patients who have a good prognosis to drop out of treatment. The major complication of fertility treatment is multiple pregnancy. By avoiding the use of gonadotropins in couples with unexplained infertility and accelerating the transition to IVF, physicians can lower the cost and psychological stress of treatment. They can also reduce the likelihood of multiple pregnancy because it is easier to control the number of embryos transferred in IVF than the number of follicles that develop with gonadotropins.
In women younger than 35 years on the first IVF cycle who have a good prognosis, ASRM now recommends that only one or two day-3 embryos be transferred, and not more than one day-5 blastocyst.4 The multiple-birth rate has declined in recent years, as more and more IVF clinics place fewer embryos; the rate should continue to fall with wider application of elective single-embryo transfer.5,6
Because this accelerated protocol produces a similar number of births over a shorter period and has the potential to lower cost, psychological stress, and the multiple-birth rate, it deserves implementation for many patients and warrants further evaluation for potential benefits in other populations.
It’s no help, after all: Preimplantation genetic screening for aneuploidy
Practice Committee of the Society for Assisted Reproductive Technology and Practice Committee of the American Society for Reproductive Medicine. Preimplantation genetic testing: A Practice Committee report. Fertil Steril. 2007;88:1497–1504.
Mastenbroek S, Twisk M, van Echten-Arends J, et al. In vitro fertilization with preimplantation genetic screening. N Engl J Med. 2007;357:9–17.
Preimplantation genetic diagnosis of known single-gene defects, structural chromosomal rearrangements, X-linked disorders, and human leukocyte antigen typing is a major benefit to couples known to be at risk of passing on a heritable and debilitating genetic disease. Aneuploidy is the most common cause of early pregnancy loss, and its prevalence increases with maternal age and may increase in chromosomally normal couples who experience recurrent early pregnancy loss or repeated failure of IVF cycles. Preimplantation genetic screening (PGS) has been advocated to identify and transfer only euploid embryos and increase the chance of successful pregnancy.
New data from Mastenbroek and colleagues indicate that PGS for aneuploidy does not increase the rate of pregnancy or live birth. After several years of increasing utilization and studies suggesting that PGS has benefit, the first multicenter, randomized, doubleblind, controlled study that compared three cycles of IVF with and without PGS in women 35 to 41 years old concluded that PGS does not increase but, in fact, significantly reduces the rate of pregnancy and live birth in this group.
Findings sparked controversy
This trial generated controversy within the genetics and reproductive endocrinology specialties because it challenged the intuitive view that screening of embryos before transfer into the uterus should be beneficial—or, at least, harmless. Some now argue that the benefits of PGS, if any, cannot be intuitively assumed and assert that the burden of proof of those benefits rests with proponents of PGS.
The practice committees of the Society for Assisted Reproductive Technology (SART) and ASRM found insufficient evidence to support the use of PGS to improve the live birth rate in women of advanced age or in those who have had implantation failure or recurrent pregnancy loss (TABLE). Many physicians believe, however, that technologies under development will soon bring verifiable benefits of PGS to patients.
SART and ASRM weigh in on use of preimplantation genetic testing
| TEST | RECOMMENDATION |
|---|---|
| Pre-implantation genetic diagnosis | |
| Pre- implantation genetic screening | |
| SOURCE: Society for Assisted Reproductive Technology and American Society for Reproductive Medicine | |
Advise your patients that oocyte cryopreservation is “a long shot”
Practice Committee of the Society for Assisted Reproductive Technology and Practice Committee of the American Society for Reproductive Medicine. Essential elements of informed consent for elective oocyte cryopreservation: a practice committee opinion. Fertil Steril. 2007;88:1495–1496.
Oocyte cryopreservation is an experimental procedure that should not be offered or marketed as a means to defer reproductive aging, primarily because data on clinical outcomes are limited. That is the conclusion of this guideline from SART and ASRM. Consequently, women who may be considering the procedure should be fully informed about the process and likely outcomes and counseled by a qualified mental health professional.
Counseling is crucial
According to the SART and ASRM guideline, pretreatment counseling should include comprehensive information on a range of topics (see the box below). In addition, women considering oocyte cryopreservation should be counseled thoroughly about reproductive aging and life planning.7,8
Few alternatives for some women
Women who have cancer should receive the same counseling. Unlike healthy women, however, they may have no other options, and cryopreservation may be more appropriate for them despite experimental status.
Patients considering this procedure need comprehensive information about:
- Ovarian stimulation and oocyte retrieval
- Methods of oocyte cryopreservation
- Storage fees
- The expected thaw survival rate
- The requirement for intracytoplasmic sperm injection
- Clinic-specific data and outcomes or, in their absence, literature estimates of a 2% overall live birth rate per oocyte thawed using slow-freeze methods and 4% for vitrification, compared with age-related probabilities of success per IVF cycle using fresh nondonor oocytes
- The relatively low likelihood that a woman who cryopreserves her eggs before age 35 will ever need or use them
- State and federal screening laws for potential donation of cryopreserved oocytes
- Potential risks of basing important life decisions and expectations on a limited number of cryopreserved oocytes
- The possibility that the facility may cease operation, necessitating transfer of cryopreserved oocytes to another facility
- The possibility that cryopreserved oocytes might be lost or damaged as a result of laboratory error or other events beyond control.
1. Tulandi T, Collins JA, Burrows E, et al. Treatment-dependent and treatment-independent pregnancy among women with periadnexal adhesions. Am J Obstet Gynecol. 1990;162:354-357.
2. Marana R, Rizzi M, Muzii L, Catalano GF, Caruana P, Mancuso S. Correlation between the American Fertility Society classification of adnexal adhesions and distal tubal occlusion, salpingoscopy, and reproductive outcome in tubal surgery. Fertil Steril. 1995;64:924-929.
3. Metwally M, Gorvy D, Watson A, Li TC. Hyaluronic acid fluid agents for the prevention of adhesions after fertility-preserving gynecological surgery: a metaanalysis of randomized controlled trials. Fertil Steril. 2007;87:1139-1146.
4. Practice Committee of the Society for Assisted Reproductive Technology and the Practice Committee of the American Society for Reproductive Medicine. Guidelines on number of embryos transferred. Fertil Steril. 2006;86(Suppl 4):S51-S52.
5. Adamson GD, Baker VL. Multiple births from assisted reproductive technologies: a challenge that must be met. Fertil Steril. 2004;81:517-522.
6. Stern JE, Cedars MI, Jain T, et al. for the Society for Assisted Reproductive Technology Writing Group Assisted reproductive technology practice patterns and the impact of embryo transfer guidelines in the United States. Fertil Steril. 2007;88:275-282.
7. Menken J, Trussell J, Larsen U. Age and infertility. Science. 1986;233:1389-1394.
8. Leridon H. Can assisted reproduction technology compensate for the natural decline in fertility with age? A model assessment. Hum Reprod. 2004;19:1548-1553.
1. Tulandi T, Collins JA, Burrows E, et al. Treatment-dependent and treatment-independent pregnancy among women with periadnexal adhesions. Am J Obstet Gynecol. 1990;162:354-357.
2. Marana R, Rizzi M, Muzii L, Catalano GF, Caruana P, Mancuso S. Correlation between the American Fertility Society classification of adnexal adhesions and distal tubal occlusion, salpingoscopy, and reproductive outcome in tubal surgery. Fertil Steril. 1995;64:924-929.
3. Metwally M, Gorvy D, Watson A, Li TC. Hyaluronic acid fluid agents for the prevention of adhesions after fertility-preserving gynecological surgery: a metaanalysis of randomized controlled trials. Fertil Steril. 2007;87:1139-1146.
4. Practice Committee of the Society for Assisted Reproductive Technology and the Practice Committee of the American Society for Reproductive Medicine. Guidelines on number of embryos transferred. Fertil Steril. 2006;86(Suppl 4):S51-S52.
5. Adamson GD, Baker VL. Multiple births from assisted reproductive technologies: a challenge that must be met. Fertil Steril. 2004;81:517-522.
6. Stern JE, Cedars MI, Jain T, et al. for the Society for Assisted Reproductive Technology Writing Group Assisted reproductive technology practice patterns and the impact of embryo transfer guidelines in the United States. Fertil Steril. 2007;88:275-282.
7. Menken J, Trussell J, Larsen U. Age and infertility. Science. 1986;233:1389-1394.
8. Leridon H. Can assisted reproduction technology compensate for the natural decline in fertility with age? A model assessment. Hum Reprod. 2004;19:1548-1553.
How to manage hyperthyroid disease in pregnancy
The authors report no financial relationships relevant to this article.
CASE Life on the line
A 32-year-old woman in the 24th week of her fourth pregnancy arrives at the emergency department complaining of cough and congestion, shortness of breath, and swelling in her face, hands, and feet. The swelling has become worse over the past 2 weeks, and she had several episodes of bloody vomiting the day before her visit. The patient says she has not experienced any leakage of fluid, vaginal bleeding, or contractions. She reports good fetal movement.
The patient’s medical history is unremarkable, but a review of systems reveals a 15-lb weight loss over the past 2 weeks, racing heart, worsening edema and shortness of breath, and diarrhea.
Physical findings include exophthalmia and an enlarged thyroid with a nodule on the right side, as well as bilateral rales, tachycardia, tremor, and increased deep tendon reflexes. There is no evidence of fetal cardiac failure or goiter.
A computed tomography (CT) scan of the mother shows bilateral pleural effusions indicative of high-output cardiac failure. Thyroid ultrasonography (US) reveals a diffusely enlarged thyroid gland with a right-sided mass.
The thyroid-stimulating hormone (TSH) level is undetectable. Fetal heart rate is in the 160s, with normal variability and occasional variable deceleration. Fetal US is consistent with the estimated gestational age and shows adequate amniotic fluid and no gross fetal anomalies.
What is the likely diagnosis?
This is a classic example of undiagnosed hyperthyroidism in pregnancy manifesting as thyroid storm.
As the case illustrates, uncontrolled hyperthyroidism in pregnancy poses a significant challenge for the obstetrician. The condition can cause miscarriage, preterm delivery, intrauterine growth restriction, preeclampsia, and—at its most dangerous—thyroid storm.1 Thyroid storm is a life-threatening emergency, and treatment must be initiated even before hyperthyroidism is confirmed by thyroid function testing.2 The good news is that these complications can be successfully avoided with adequate control of thyroid function.
Overt hyperthyroidism, seen in 0.2% of pregnancies, requires active intervention to avert adverse pregnancy outcome and neurologic damage to the fetus. Subclinical disease, seen in 1.7% of pregnancies, can also create serious obstetrical problems.1
The effects of hyperthyroidism in pregnancy vary in severity, ranging from the fairly innocuous, transient, and self-limited state called gestational transient thyrotoxicosis to the life-threatening emergency of thyroid storm. This review will update you on how to manage this disorder for optimal pregnancy outcome.
To screen or not to screen
Routine screening for thyroid dysfunction has been recommended for women who have infertility, menstrual disorders, or type 1 diabetes mellitus, and for pregnant women who have signs and symptoms of the disorder. Some authors recommend screening all pregnant women, but routine screening is not endorsed by the American College of Obstetricians and Gynecologists.2,3
Thyroid testing in pregnancy is recommended in women who:
- have a family history of autoimmune thyroid disease
- are on thyroid therapy
- have a goiter or
- have insulin-dependent diabetes mellitus.
Pregnant women who have a history of high-dose neck radiation, thyroid therapy, postpartum thyroiditis, or an infant born with thyroid disease should also be tested at the first prenatal visit.4
Telltale signs and laboratory tests
The signs and symptoms of hyperthyroidism can include nervousness, heat intolerance, tachycardia, palpitations, goiter, weight loss, thyromegaly, exophthalmia, increased appetite, nausea and vomiting, sweating, and tremor.1 The difficulty here? Many of these symptoms are also seen in pregnant women who have normal thyroid function, so that symptoms alone are not a reliable guide.
Instead, the diagnosis of overt hyperthyroidism is made on the basis of laboratory tests indicating suppressed TSH and elevated levels of free thyroxine (FT4) and free triiodothyronine (FT3). Subclinical hyperthyroidism is defined as a suppressed TSH level with normal FT4 and FT3 levels.2
The effects of hyperthyroidism on laboratory values are shown in TABLE 1. A form of hyperthyroidism called the T3– toxicosis syndrome is diagnosed by suppressed TSH, normal FT4, and elevated FT3 levels.4
TABLE 1
Is your pregnant patient hyperthyroid? Five-test lab panel offers a guide
| TEST AND RESULT | |||||
|---|---|---|---|---|---|
| THYROID-STIMULATING HORMONE | FREE TRI-IODOTHYRONINE | FREE THYROXINE | TOTAL TRI-IODOTHYRONINE | TOTAL THYROXINE | THEN THE MOTHER’S CONDITION IS … |
| No change | No change | ↑ | ↑ | ↑ | Pregnancy |
| ↓ | ↑ | ↑ | ↑ | ↑ | Hyperthyroidism |
| ↓ | No change | No change | No change | No change | Subclinical hyperthyroidism |
What are the causes?
The most common cause of hyperthyroidism in pregnancy—accounting for some 95% of cases—is Graves’ disease.2 This autoimmune disorder is characterized by autoantibodies that activate the TSH receptor. These autoantibodies cross the placenta and can cause fetal and neonatal thyroid dysfunction even when the mother herself is in a euthyroid condition.4
Far less often, hyperthyroidism in pregnancy has a cause other than Graves’ disease; TABLE 2 summarizes the possibilities.1 Other causes of hyperthyroidism in early pregnancy include choriocarcinoma and gestational trophoblastic disease (partial and complete moles) (TABLE 3).
TABLE 2
Causes of hyperthyroidism in pregnancy
| Graves’ disease |
| Adenoma |
| Toxic nodular goiter |
| Thyroiditis |
| Excessive thyroid hormone intake |
| Choriocarcinoma |
| Molar pregnancy |
TABLE 3
What causes severe hyperthyroidism before 20 weeks’ gestation?
| Gestational transient thyrotoxicosis |
| Choriocarcinoma |
Gestational trophoblastic disease
|
Signs and symptoms of Graves’ disease
Women who have Graves’ disease usually have thyroid nodules and may have exophthalmia, pretibial myxedema, and tachycardia. They also display other classic signs and symptoms of hyperthyroidism, such as muscle weakness, tremor, and warm and moist skin.
During pregnancy, Graves’ disease usually becomes worse during the first trimester and postpartum period; symptoms resolve during the second and third trimesters.1
Thyrotoxin receptor and antithyroid antibodies
Antithyroid antibodies are common in patients with autoimmune thyroid disease, as a response to thyroid antigens. The two most common antithyroid antibodies are thyroglobulin and thyroid peroxidase (anti-TPO). Anti-TPO antibodies are associated with postpartum thyroiditis and fetal and neonatal hyperthyroidism. TSH-receptor antibodies include thyroid-stimulating immunoglobulin (TSI) and TSH-receptor antibody. TSI is associated with Graves’ disease. TSH-receptor antibody is associated with fetal goiter, congenital hypothyroidism, and chronic thyroiditis without goiter.4
Who do you test for antibodies? Test for maternal thyroid antibodies in patients who:
- had Graves’ disease with fetal or neonatal hyperthyroidism in a previous pregnancy
- have active Graves’ disease being treated with antithyroid drugs
- are euthyroid or have undergone ablative therapy and have fetal tachycardia or intrauterine growth restriction
- have chronic thyroiditis without goiter
- have fetal goiter on ultrasound.
Newborns who have congenital hypothyroidism should also be screened for thyroid antibodies.4
What are the consequences?
Hyperthyroidism can have multiple effects on the pregnant patient and her fetus, ranging in severity from the minimal to the catastrophic.
Gestational transient thyrotoxicosis
This condition is presumably related to high levels of human chorionic gonadotropin, a substance known to stimulate TSH receptors. Unhappily for your patient, the condition is usually heralded by severe bouts of nausea and vomiting starting at 4 to 8 weeks’ gestation. Laboratory tests show significantly elevated levels of FT4 and FT3 and suppressed TSH. Despite this significant derangement, patients generally have no evidence of a hypermetabolic state.
This condition resolves by 14 to 20 weeks of gestation, is not associated with poor pregnancy outcomes, and does not require treatment with antithyroid medication.1
Adverse pregnancy outcomes
Pregnant women who have uncontrolled hyperthyroidism are at increased risk of spontaneous miscarriage, congestive heart failure, preterm delivery, intrauterine growth restriction, and preeclampsia.1 Studies that evaluated pregnancy outcomes in 239 women with overt hyperthyroidism showed increased risk of adverse pregnancy outcomes, compared with treated, euthyroid women (FIGURE 1).5-7
FIGURE 1 Consequences of uncontrolled hyperthyroidism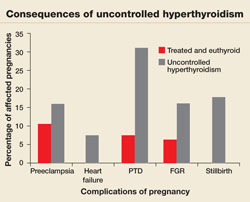
Several studies have found a much higher risk of pregnancy complications in women who have uncontrolled hyperthyroidism, compared with their treated and euthyroid peers.5-7
PTD=preterm delivery; FGR=fetal growth restrictions.
Fetal and neonatal hyperthyroidism
Hyperthyroidism in the fetus or newborn is caused by placental transfer of maternal immunoglobulin antibodies (TSI) to the fetus and is associated with maternal Graves’ disease. The incidence of neonatal hyperthyroidism is less than 1%. It can be predicted by rising levels of maternal TSI antibodies, to the point where levels in the third trimester are three to five times higher than they were at the beginning of pregnancy.4
Fetal hyperthyroidism develops at about 22 to 24 weeks’ gestation in mothers with a history of Graves’ disease who have been treated surgically or with ablative therapy prior to pregnancy. Even when these therapies achieve a euthyroid state in the mother, TSI levels may remain elevated and lead to fetal hyperthyroidism.
Characteristics of hyperthyroidism in the fetus include tachycardia, intrauterine growth restriction, congestive heart failure, oligohydramnios, and goiter. Treating the mother with antithyroid medications will ameliorate symptoms in the fetus.4
Thyroid storm
This is the worst-case scenario—a rare but potentially lethal complication of uncontrolled hyperthyroidism. Thyroid storm is a hypermetabolic state characterized by fever, nausea, vomiting, diarrhea, tachycardia, altered mental status, restlessness, nervousness, seizures, coma, and cardiac arrhythmias. It occurs in 1% to 2% of patients receiving thioamide therapy.8
In most instances, thyroid storm is a complication of uncontrolled hyperthyroidism, but it can also be precipitated by infection, surgery, thromboembolism, preeclampsia, labor, and delivery.
Thyroid storm is a medical emergency
This manifestation of uncontrolled hyperthyroidism is so urgent that treatment should be initiated before the results of TSH, FT4, and FT3 tests are available.2,8 Delivery should be avoided, if possible, until the mother’s condition can be stabilized but, if the status of the fetus is compromised, delivery is indicated.
Treatment of thyroid storm begins with stabilization of the patient, followed by initiation of a stepwise management approach (FIGURE 2).
FIGURE 2 Management of thyroid storm
Aggressive management of thyroid storm is indicated, following a stepwise approach. Each medication used to treat thyroid storm plays a specific role in suppressing thyroid function. Propylthiouracil (PTU) blocks additional synthesis of thyroid hormone and inhibits the conversion of thyroxine (T4) to triiodothyronine (T3). Methimazole blocks additional synthesis of thyroid hormones. Saturated solution of potassium iodide (SSKI), Lugol’s solution, and sodium iodide block the release of thyroid hormone from the gland. Dexamethasone is used to decrease thyroid hormone release and peripheral conversion of T4 to T3. Propranolol is used to treat maternal tachycardia by inhibiting the adrenergic effects of excessive thyroid hormones. Finally, phenobarbital is used to treat maternal agitation and restlessness caused by the increased catabolism of thyroid hormones.
SOURCE: Adapted from ACOG.2
Treatment of hyperthyroidism in pregnancy
Two medications are available to treat hyperthyroidism in pregnancy: propylthiouracil (PTU) and methimazole. These medications are known as thioamides.1,2
PTU blocks the oxidation of iodine in the thyroid gland, thereby preventing the synthesis of T4 and T3. The initial dosage for hyperthyroid women who are not pregnant is usually 300 to 450 mg/day in three divided doses every 8 hours, and this dosing strategy can also be applied to the pregnant patient. Maintenance therapy is usually achieved with 100 to 150 mg/day in divided doses every 8 to 12 hours.9
Methimazole works by blocking the organification of iodide, which decreases thyroid hormone production. The usual dosing, given in three divided doses every 8 hours, is 15 mg/day for mild hyperthyroidism, 30 to 40 mg/day for moderately severe hyperthyroidism, and 60 mg/day for severe hyperthyroidism. Maintenance therapy with methimazole is usually given at a dosage of 5 to 15 mg/day.9
In the past, PTU was considered the drug of choice for treatment of hyperthyroidism in pregnancy because clinicians believed it crossed the placenta to a lesser degree than did methimazole, and because methimazole was associated with fetal esophageal and choanal atresia and fetal cutis aplasia (congenital skin defect of the scalp).1,2 Available evidence does not, however, support these conclusions.8,10 Whatever medication regimen you choose, thyroid function should be monitored 1) every 4 weeks until TSH and FT4 levels are within normal limits and 2) every trimester thereafter. FIGURE 3 presents an algorithm for managing hyperthyroidism in pregnancy.
FIGURE 3 Management of hyperthyroidism in pregnancy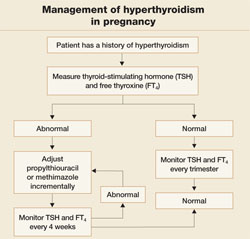
CASE Resolved
The patient in thyroid storm described at the beginning of this article requires aggressive management, as outlined in the algorithm in FIGURE 2. As her symptoms diminish, fetal tachycardia resolves. The patient’s FT4 level begins to decline, consistent with appropriate treatment, and she is discharged home and instructed to continue PTU and labetalol and to follow up at the endocrinology and high-risk obstetrics clinics as soon as possible.
The patient does not follow this advice. Consequently, she presents at 33 5/7 weeks in a hypertensive crisis, with symptoms similar to those she first exhibited plus acute pulmonary edema. Fetal heart rate is initially in the 130s, with good variability and occasional decelerations (FIGURE 4A), but decelerations then become worse (FIGURE 4B) and emergency cesarean section is performed.
A male infant is delivered, weighing 2,390 g. Apgar scores are 0 at 1 minute and 9 at 5 minutes. A 25% placental abruption is noted at the time of delivery.
Mother and fetus are stabilized and discharged.
FIGURE 4 Weakening fetal status in a mother who is in thyroid storm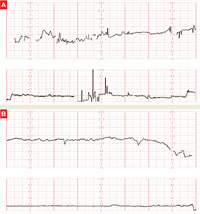
Fetal heart rate is initially in the 130s with good variability and occasional decelerations (A), but then deteriorates, with increasing decelerations (B), an indication for immediate delivery.
1. Casey BM, Leveno KJ. Thyroid disease in pregnancy. Obstet Gynecol. 2006;108:1283-1292.
2. American College of Obstetrics and Gynecology. ACOG Practice Bulletin. Clinical management guidelines for obstetrician-gynecologists. Number 37, August 2002. (Replaces Practice Bulletin Number 32, November 2001). Thyroid disease in pregnancy. Obstet Gynecol. 2002;100:387-396.
3. Mitchell ML, Klein RZ. The sequelae of untreated maternal hypothyroidism. Eur J Endocrinol. 2004;151 Suppl 3:U45-48.
4. Mestman JH. Endocrine diseases in pregnancy. In: Gabbe S, Niebyl JR, eds. Obstetrics: Normal and Problem Pregnancies. 4th ed. Philadelphia: Churchill Livingstone; 2002:1117-1168.
5. Davis LE, Leveno KJ, Cunningham FG. Hypothyroidism complicating pregnancy. Obstet Gynecol. 1988;72:108-112.
6. Davis LE, Lucas MJ, Hankins GD, Roark ML, Cunningham FG. Thyrotoxicosis complicating pregnancy. Am J Obstet Gynecol. 1989;160:63-70.
7. Kriplani A, Buckshee K, Bhargava VL, Takkar D, Ammini AC. Maternal and perinatal outcome in thyrotoxicosis complicating pregnancy. Eur J Obstet Gynecol Reprod Biol. 1994;54:159-163.
8. Belford MA. Navigating a thyroid storm. Contemporary OB/GYN. 2006; October:38–46.
9. Lazarus JH, Othman S. Thyroid disease in relation to pregnancy. Clin Endocrinol (Oxf). 1991;34:91-98.
10. Kent GN, Stuckey BG, Allen JR, Lambert T, Gee V. Postpartum thyroid dysfunction: clinical assessment and relationship to psychiatric affective morbidity. Clin Endocrinol (Oxf). 1999;51:429-438.
The authors report no financial relationships relevant to this article.
CASE Life on the line
A 32-year-old woman in the 24th week of her fourth pregnancy arrives at the emergency department complaining of cough and congestion, shortness of breath, and swelling in her face, hands, and feet. The swelling has become worse over the past 2 weeks, and she had several episodes of bloody vomiting the day before her visit. The patient says she has not experienced any leakage of fluid, vaginal bleeding, or contractions. She reports good fetal movement.
The patient’s medical history is unremarkable, but a review of systems reveals a 15-lb weight loss over the past 2 weeks, racing heart, worsening edema and shortness of breath, and diarrhea.
Physical findings include exophthalmia and an enlarged thyroid with a nodule on the right side, as well as bilateral rales, tachycardia, tremor, and increased deep tendon reflexes. There is no evidence of fetal cardiac failure or goiter.
A computed tomography (CT) scan of the mother shows bilateral pleural effusions indicative of high-output cardiac failure. Thyroid ultrasonography (US) reveals a diffusely enlarged thyroid gland with a right-sided mass.
The thyroid-stimulating hormone (TSH) level is undetectable. Fetal heart rate is in the 160s, with normal variability and occasional variable deceleration. Fetal US is consistent with the estimated gestational age and shows adequate amniotic fluid and no gross fetal anomalies.
What is the likely diagnosis?
This is a classic example of undiagnosed hyperthyroidism in pregnancy manifesting as thyroid storm.
As the case illustrates, uncontrolled hyperthyroidism in pregnancy poses a significant challenge for the obstetrician. The condition can cause miscarriage, preterm delivery, intrauterine growth restriction, preeclampsia, and—at its most dangerous—thyroid storm.1 Thyroid storm is a life-threatening emergency, and treatment must be initiated even before hyperthyroidism is confirmed by thyroid function testing.2 The good news is that these complications can be successfully avoided with adequate control of thyroid function.
Overt hyperthyroidism, seen in 0.2% of pregnancies, requires active intervention to avert adverse pregnancy outcome and neurologic damage to the fetus. Subclinical disease, seen in 1.7% of pregnancies, can also create serious obstetrical problems.1
The effects of hyperthyroidism in pregnancy vary in severity, ranging from the fairly innocuous, transient, and self-limited state called gestational transient thyrotoxicosis to the life-threatening emergency of thyroid storm. This review will update you on how to manage this disorder for optimal pregnancy outcome.
To screen or not to screen
Routine screening for thyroid dysfunction has been recommended for women who have infertility, menstrual disorders, or type 1 diabetes mellitus, and for pregnant women who have signs and symptoms of the disorder. Some authors recommend screening all pregnant women, but routine screening is not endorsed by the American College of Obstetricians and Gynecologists.2,3
Thyroid testing in pregnancy is recommended in women who:
- have a family history of autoimmune thyroid disease
- are on thyroid therapy
- have a goiter or
- have insulin-dependent diabetes mellitus.
Pregnant women who have a history of high-dose neck radiation, thyroid therapy, postpartum thyroiditis, or an infant born with thyroid disease should also be tested at the first prenatal visit.4
Telltale signs and laboratory tests
The signs and symptoms of hyperthyroidism can include nervousness, heat intolerance, tachycardia, palpitations, goiter, weight loss, thyromegaly, exophthalmia, increased appetite, nausea and vomiting, sweating, and tremor.1 The difficulty here? Many of these symptoms are also seen in pregnant women who have normal thyroid function, so that symptoms alone are not a reliable guide.
Instead, the diagnosis of overt hyperthyroidism is made on the basis of laboratory tests indicating suppressed TSH and elevated levels of free thyroxine (FT4) and free triiodothyronine (FT3). Subclinical hyperthyroidism is defined as a suppressed TSH level with normal FT4 and FT3 levels.2
The effects of hyperthyroidism on laboratory values are shown in TABLE 1. A form of hyperthyroidism called the T3– toxicosis syndrome is diagnosed by suppressed TSH, normal FT4, and elevated FT3 levels.4
TABLE 1
Is your pregnant patient hyperthyroid? Five-test lab panel offers a guide
| TEST AND RESULT | |||||
|---|---|---|---|---|---|
| THYROID-STIMULATING HORMONE | FREE TRI-IODOTHYRONINE | FREE THYROXINE | TOTAL TRI-IODOTHYRONINE | TOTAL THYROXINE | THEN THE MOTHER’S CONDITION IS … |
| No change | No change | ↑ | ↑ | ↑ | Pregnancy |
| ↓ | ↑ | ↑ | ↑ | ↑ | Hyperthyroidism |
| ↓ | No change | No change | No change | No change | Subclinical hyperthyroidism |
What are the causes?
The most common cause of hyperthyroidism in pregnancy—accounting for some 95% of cases—is Graves’ disease.2 This autoimmune disorder is characterized by autoantibodies that activate the TSH receptor. These autoantibodies cross the placenta and can cause fetal and neonatal thyroid dysfunction even when the mother herself is in a euthyroid condition.4
Far less often, hyperthyroidism in pregnancy has a cause other than Graves’ disease; TABLE 2 summarizes the possibilities.1 Other causes of hyperthyroidism in early pregnancy include choriocarcinoma and gestational trophoblastic disease (partial and complete moles) (TABLE 3).
TABLE 2
Causes of hyperthyroidism in pregnancy
| Graves’ disease |
| Adenoma |
| Toxic nodular goiter |
| Thyroiditis |
| Excessive thyroid hormone intake |
| Choriocarcinoma |
| Molar pregnancy |
TABLE 3
What causes severe hyperthyroidism before 20 weeks’ gestation?
| Gestational transient thyrotoxicosis |
| Choriocarcinoma |
Gestational trophoblastic disease
|
Signs and symptoms of Graves’ disease
Women who have Graves’ disease usually have thyroid nodules and may have exophthalmia, pretibial myxedema, and tachycardia. They also display other classic signs and symptoms of hyperthyroidism, such as muscle weakness, tremor, and warm and moist skin.
During pregnancy, Graves’ disease usually becomes worse during the first trimester and postpartum period; symptoms resolve during the second and third trimesters.1
Thyrotoxin receptor and antithyroid antibodies
Antithyroid antibodies are common in patients with autoimmune thyroid disease, as a response to thyroid antigens. The two most common antithyroid antibodies are thyroglobulin and thyroid peroxidase (anti-TPO). Anti-TPO antibodies are associated with postpartum thyroiditis and fetal and neonatal hyperthyroidism. TSH-receptor antibodies include thyroid-stimulating immunoglobulin (TSI) and TSH-receptor antibody. TSI is associated with Graves’ disease. TSH-receptor antibody is associated with fetal goiter, congenital hypothyroidism, and chronic thyroiditis without goiter.4
Who do you test for antibodies? Test for maternal thyroid antibodies in patients who:
- had Graves’ disease with fetal or neonatal hyperthyroidism in a previous pregnancy
- have active Graves’ disease being treated with antithyroid drugs
- are euthyroid or have undergone ablative therapy and have fetal tachycardia or intrauterine growth restriction
- have chronic thyroiditis without goiter
- have fetal goiter on ultrasound.
Newborns who have congenital hypothyroidism should also be screened for thyroid antibodies.4
What are the consequences?
Hyperthyroidism can have multiple effects on the pregnant patient and her fetus, ranging in severity from the minimal to the catastrophic.
Gestational transient thyrotoxicosis
This condition is presumably related to high levels of human chorionic gonadotropin, a substance known to stimulate TSH receptors. Unhappily for your patient, the condition is usually heralded by severe bouts of nausea and vomiting starting at 4 to 8 weeks’ gestation. Laboratory tests show significantly elevated levels of FT4 and FT3 and suppressed TSH. Despite this significant derangement, patients generally have no evidence of a hypermetabolic state.
This condition resolves by 14 to 20 weeks of gestation, is not associated with poor pregnancy outcomes, and does not require treatment with antithyroid medication.1
Adverse pregnancy outcomes
Pregnant women who have uncontrolled hyperthyroidism are at increased risk of spontaneous miscarriage, congestive heart failure, preterm delivery, intrauterine growth restriction, and preeclampsia.1 Studies that evaluated pregnancy outcomes in 239 women with overt hyperthyroidism showed increased risk of adverse pregnancy outcomes, compared with treated, euthyroid women (FIGURE 1).5-7
FIGURE 1 Consequences of uncontrolled hyperthyroidism
Several studies have found a much higher risk of pregnancy complications in women who have uncontrolled hyperthyroidism, compared with their treated and euthyroid peers.5-7
PTD=preterm delivery; FGR=fetal growth restrictions.
Fetal and neonatal hyperthyroidism
Hyperthyroidism in the fetus or newborn is caused by placental transfer of maternal immunoglobulin antibodies (TSI) to the fetus and is associated with maternal Graves’ disease. The incidence of neonatal hyperthyroidism is less than 1%. It can be predicted by rising levels of maternal TSI antibodies, to the point where levels in the third trimester are three to five times higher than they were at the beginning of pregnancy.4
Fetal hyperthyroidism develops at about 22 to 24 weeks’ gestation in mothers with a history of Graves’ disease who have been treated surgically or with ablative therapy prior to pregnancy. Even when these therapies achieve a euthyroid state in the mother, TSI levels may remain elevated and lead to fetal hyperthyroidism.
Characteristics of hyperthyroidism in the fetus include tachycardia, intrauterine growth restriction, congestive heart failure, oligohydramnios, and goiter. Treating the mother with antithyroid medications will ameliorate symptoms in the fetus.4
Thyroid storm
This is the worst-case scenario—a rare but potentially lethal complication of uncontrolled hyperthyroidism. Thyroid storm is a hypermetabolic state characterized by fever, nausea, vomiting, diarrhea, tachycardia, altered mental status, restlessness, nervousness, seizures, coma, and cardiac arrhythmias. It occurs in 1% to 2% of patients receiving thioamide therapy.8
In most instances, thyroid storm is a complication of uncontrolled hyperthyroidism, but it can also be precipitated by infection, surgery, thromboembolism, preeclampsia, labor, and delivery.
Thyroid storm is a medical emergency
This manifestation of uncontrolled hyperthyroidism is so urgent that treatment should be initiated before the results of TSH, FT4, and FT3 tests are available.2,8 Delivery should be avoided, if possible, until the mother’s condition can be stabilized but, if the status of the fetus is compromised, delivery is indicated.
Treatment of thyroid storm begins with stabilization of the patient, followed by initiation of a stepwise management approach (FIGURE 2).
FIGURE 2 Management of thyroid storm
Aggressive management of thyroid storm is indicated, following a stepwise approach. Each medication used to treat thyroid storm plays a specific role in suppressing thyroid function. Propylthiouracil (PTU) blocks additional synthesis of thyroid hormone and inhibits the conversion of thyroxine (T4) to triiodothyronine (T3). Methimazole blocks additional synthesis of thyroid hormones. Saturated solution of potassium iodide (SSKI), Lugol’s solution, and sodium iodide block the release of thyroid hormone from the gland. Dexamethasone is used to decrease thyroid hormone release and peripheral conversion of T4 to T3. Propranolol is used to treat maternal tachycardia by inhibiting the adrenergic effects of excessive thyroid hormones. Finally, phenobarbital is used to treat maternal agitation and restlessness caused by the increased catabolism of thyroid hormones.
SOURCE: Adapted from ACOG.2
Treatment of hyperthyroidism in pregnancy
Two medications are available to treat hyperthyroidism in pregnancy: propylthiouracil (PTU) and methimazole. These medications are known as thioamides.1,2
PTU blocks the oxidation of iodine in the thyroid gland, thereby preventing the synthesis of T4 and T3. The initial dosage for hyperthyroid women who are not pregnant is usually 300 to 450 mg/day in three divided doses every 8 hours, and this dosing strategy can also be applied to the pregnant patient. Maintenance therapy is usually achieved with 100 to 150 mg/day in divided doses every 8 to 12 hours.9
Methimazole works by blocking the organification of iodide, which decreases thyroid hormone production. The usual dosing, given in three divided doses every 8 hours, is 15 mg/day for mild hyperthyroidism, 30 to 40 mg/day for moderately severe hyperthyroidism, and 60 mg/day for severe hyperthyroidism. Maintenance therapy with methimazole is usually given at a dosage of 5 to 15 mg/day.9
In the past, PTU was considered the drug of choice for treatment of hyperthyroidism in pregnancy because clinicians believed it crossed the placenta to a lesser degree than did methimazole, and because methimazole was associated with fetal esophageal and choanal atresia and fetal cutis aplasia (congenital skin defect of the scalp).1,2 Available evidence does not, however, support these conclusions.8,10 Whatever medication regimen you choose, thyroid function should be monitored 1) every 4 weeks until TSH and FT4 levels are within normal limits and 2) every trimester thereafter. FIGURE 3 presents an algorithm for managing hyperthyroidism in pregnancy.
FIGURE 3 Management of hyperthyroidism in pregnancy
CASE Resolved
The patient in thyroid storm described at the beginning of this article requires aggressive management, as outlined in the algorithm in FIGURE 2. As her symptoms diminish, fetal tachycardia resolves. The patient’s FT4 level begins to decline, consistent with appropriate treatment, and she is discharged home and instructed to continue PTU and labetalol and to follow up at the endocrinology and high-risk obstetrics clinics as soon as possible.
The patient does not follow this advice. Consequently, she presents at 33 5/7 weeks in a hypertensive crisis, with symptoms similar to those she first exhibited plus acute pulmonary edema. Fetal heart rate is initially in the 130s, with good variability and occasional decelerations (FIGURE 4A), but decelerations then become worse (FIGURE 4B) and emergency cesarean section is performed.
A male infant is delivered, weighing 2,390 g. Apgar scores are 0 at 1 minute and 9 at 5 minutes. A 25% placental abruption is noted at the time of delivery.
Mother and fetus are stabilized and discharged.
FIGURE 4 Weakening fetal status in a mother who is in thyroid storm
Fetal heart rate is initially in the 130s with good variability and occasional decelerations (A), but then deteriorates, with increasing decelerations (B), an indication for immediate delivery.
The authors report no financial relationships relevant to this article.
CASE Life on the line
A 32-year-old woman in the 24th week of her fourth pregnancy arrives at the emergency department complaining of cough and congestion, shortness of breath, and swelling in her face, hands, and feet. The swelling has become worse over the past 2 weeks, and she had several episodes of bloody vomiting the day before her visit. The patient says she has not experienced any leakage of fluid, vaginal bleeding, or contractions. She reports good fetal movement.
The patient’s medical history is unremarkable, but a review of systems reveals a 15-lb weight loss over the past 2 weeks, racing heart, worsening edema and shortness of breath, and diarrhea.
Physical findings include exophthalmia and an enlarged thyroid with a nodule on the right side, as well as bilateral rales, tachycardia, tremor, and increased deep tendon reflexes. There is no evidence of fetal cardiac failure or goiter.
A computed tomography (CT) scan of the mother shows bilateral pleural effusions indicative of high-output cardiac failure. Thyroid ultrasonography (US) reveals a diffusely enlarged thyroid gland with a right-sided mass.
The thyroid-stimulating hormone (TSH) level is undetectable. Fetal heart rate is in the 160s, with normal variability and occasional variable deceleration. Fetal US is consistent with the estimated gestational age and shows adequate amniotic fluid and no gross fetal anomalies.
What is the likely diagnosis?
This is a classic example of undiagnosed hyperthyroidism in pregnancy manifesting as thyroid storm.
As the case illustrates, uncontrolled hyperthyroidism in pregnancy poses a significant challenge for the obstetrician. The condition can cause miscarriage, preterm delivery, intrauterine growth restriction, preeclampsia, and—at its most dangerous—thyroid storm.1 Thyroid storm is a life-threatening emergency, and treatment must be initiated even before hyperthyroidism is confirmed by thyroid function testing.2 The good news is that these complications can be successfully avoided with adequate control of thyroid function.
Overt hyperthyroidism, seen in 0.2% of pregnancies, requires active intervention to avert adverse pregnancy outcome and neurologic damage to the fetus. Subclinical disease, seen in 1.7% of pregnancies, can also create serious obstetrical problems.1
The effects of hyperthyroidism in pregnancy vary in severity, ranging from the fairly innocuous, transient, and self-limited state called gestational transient thyrotoxicosis to the life-threatening emergency of thyroid storm. This review will update you on how to manage this disorder for optimal pregnancy outcome.
To screen or not to screen
Routine screening for thyroid dysfunction has been recommended for women who have infertility, menstrual disorders, or type 1 diabetes mellitus, and for pregnant women who have signs and symptoms of the disorder. Some authors recommend screening all pregnant women, but routine screening is not endorsed by the American College of Obstetricians and Gynecologists.2,3
Thyroid testing in pregnancy is recommended in women who:
- have a family history of autoimmune thyroid disease
- are on thyroid therapy
- have a goiter or
- have insulin-dependent diabetes mellitus.
Pregnant women who have a history of high-dose neck radiation, thyroid therapy, postpartum thyroiditis, or an infant born with thyroid disease should also be tested at the first prenatal visit.4
Telltale signs and laboratory tests
The signs and symptoms of hyperthyroidism can include nervousness, heat intolerance, tachycardia, palpitations, goiter, weight loss, thyromegaly, exophthalmia, increased appetite, nausea and vomiting, sweating, and tremor.1 The difficulty here? Many of these symptoms are also seen in pregnant women who have normal thyroid function, so that symptoms alone are not a reliable guide.
Instead, the diagnosis of overt hyperthyroidism is made on the basis of laboratory tests indicating suppressed TSH and elevated levels of free thyroxine (FT4) and free triiodothyronine (FT3). Subclinical hyperthyroidism is defined as a suppressed TSH level with normal FT4 and FT3 levels.2
The effects of hyperthyroidism on laboratory values are shown in TABLE 1. A form of hyperthyroidism called the T3– toxicosis syndrome is diagnosed by suppressed TSH, normal FT4, and elevated FT3 levels.4
TABLE 1
Is your pregnant patient hyperthyroid? Five-test lab panel offers a guide
| TEST AND RESULT | |||||
|---|---|---|---|---|---|
| THYROID-STIMULATING HORMONE | FREE TRI-IODOTHYRONINE | FREE THYROXINE | TOTAL TRI-IODOTHYRONINE | TOTAL THYROXINE | THEN THE MOTHER’S CONDITION IS … |
| No change | No change | ↑ | ↑ | ↑ | Pregnancy |
| ↓ | ↑ | ↑ | ↑ | ↑ | Hyperthyroidism |
| ↓ | No change | No change | No change | No change | Subclinical hyperthyroidism |
What are the causes?
The most common cause of hyperthyroidism in pregnancy—accounting for some 95% of cases—is Graves’ disease.2 This autoimmune disorder is characterized by autoantibodies that activate the TSH receptor. These autoantibodies cross the placenta and can cause fetal and neonatal thyroid dysfunction even when the mother herself is in a euthyroid condition.4
Far less often, hyperthyroidism in pregnancy has a cause other than Graves’ disease; TABLE 2 summarizes the possibilities.1 Other causes of hyperthyroidism in early pregnancy include choriocarcinoma and gestational trophoblastic disease (partial and complete moles) (TABLE 3).
TABLE 2
Causes of hyperthyroidism in pregnancy
| Graves’ disease |
| Adenoma |
| Toxic nodular goiter |
| Thyroiditis |
| Excessive thyroid hormone intake |
| Choriocarcinoma |
| Molar pregnancy |
TABLE 3
What causes severe hyperthyroidism before 20 weeks’ gestation?
| Gestational transient thyrotoxicosis |
| Choriocarcinoma |
Gestational trophoblastic disease
|
Signs and symptoms of Graves’ disease
Women who have Graves’ disease usually have thyroid nodules and may have exophthalmia, pretibial myxedema, and tachycardia. They also display other classic signs and symptoms of hyperthyroidism, such as muscle weakness, tremor, and warm and moist skin.
During pregnancy, Graves’ disease usually becomes worse during the first trimester and postpartum period; symptoms resolve during the second and third trimesters.1
Thyrotoxin receptor and antithyroid antibodies
Antithyroid antibodies are common in patients with autoimmune thyroid disease, as a response to thyroid antigens. The two most common antithyroid antibodies are thyroglobulin and thyroid peroxidase (anti-TPO). Anti-TPO antibodies are associated with postpartum thyroiditis and fetal and neonatal hyperthyroidism. TSH-receptor antibodies include thyroid-stimulating immunoglobulin (TSI) and TSH-receptor antibody. TSI is associated with Graves’ disease. TSH-receptor antibody is associated with fetal goiter, congenital hypothyroidism, and chronic thyroiditis without goiter.4
Who do you test for antibodies? Test for maternal thyroid antibodies in patients who:
- had Graves’ disease with fetal or neonatal hyperthyroidism in a previous pregnancy
- have active Graves’ disease being treated with antithyroid drugs
- are euthyroid or have undergone ablative therapy and have fetal tachycardia or intrauterine growth restriction
- have chronic thyroiditis without goiter
- have fetal goiter on ultrasound.
Newborns who have congenital hypothyroidism should also be screened for thyroid antibodies.4
What are the consequences?
Hyperthyroidism can have multiple effects on the pregnant patient and her fetus, ranging in severity from the minimal to the catastrophic.
Gestational transient thyrotoxicosis
This condition is presumably related to high levels of human chorionic gonadotropin, a substance known to stimulate TSH receptors. Unhappily for your patient, the condition is usually heralded by severe bouts of nausea and vomiting starting at 4 to 8 weeks’ gestation. Laboratory tests show significantly elevated levels of FT4 and FT3 and suppressed TSH. Despite this significant derangement, patients generally have no evidence of a hypermetabolic state.
This condition resolves by 14 to 20 weeks of gestation, is not associated with poor pregnancy outcomes, and does not require treatment with antithyroid medication.1
Adverse pregnancy outcomes
Pregnant women who have uncontrolled hyperthyroidism are at increased risk of spontaneous miscarriage, congestive heart failure, preterm delivery, intrauterine growth restriction, and preeclampsia.1 Studies that evaluated pregnancy outcomes in 239 women with overt hyperthyroidism showed increased risk of adverse pregnancy outcomes, compared with treated, euthyroid women (FIGURE 1).5-7
FIGURE 1 Consequences of uncontrolled hyperthyroidism
Several studies have found a much higher risk of pregnancy complications in women who have uncontrolled hyperthyroidism, compared with their treated and euthyroid peers.5-7
PTD=preterm delivery; FGR=fetal growth restrictions.
Fetal and neonatal hyperthyroidism
Hyperthyroidism in the fetus or newborn is caused by placental transfer of maternal immunoglobulin antibodies (TSI) to the fetus and is associated with maternal Graves’ disease. The incidence of neonatal hyperthyroidism is less than 1%. It can be predicted by rising levels of maternal TSI antibodies, to the point where levels in the third trimester are three to five times higher than they were at the beginning of pregnancy.4
Fetal hyperthyroidism develops at about 22 to 24 weeks’ gestation in mothers with a history of Graves’ disease who have been treated surgically or with ablative therapy prior to pregnancy. Even when these therapies achieve a euthyroid state in the mother, TSI levels may remain elevated and lead to fetal hyperthyroidism.
Characteristics of hyperthyroidism in the fetus include tachycardia, intrauterine growth restriction, congestive heart failure, oligohydramnios, and goiter. Treating the mother with antithyroid medications will ameliorate symptoms in the fetus.4
Thyroid storm
This is the worst-case scenario—a rare but potentially lethal complication of uncontrolled hyperthyroidism. Thyroid storm is a hypermetabolic state characterized by fever, nausea, vomiting, diarrhea, tachycardia, altered mental status, restlessness, nervousness, seizures, coma, and cardiac arrhythmias. It occurs in 1% to 2% of patients receiving thioamide therapy.8
In most instances, thyroid storm is a complication of uncontrolled hyperthyroidism, but it can also be precipitated by infection, surgery, thromboembolism, preeclampsia, labor, and delivery.
Thyroid storm is a medical emergency
This manifestation of uncontrolled hyperthyroidism is so urgent that treatment should be initiated before the results of TSH, FT4, and FT3 tests are available.2,8 Delivery should be avoided, if possible, until the mother’s condition can be stabilized but, if the status of the fetus is compromised, delivery is indicated.
Treatment of thyroid storm begins with stabilization of the patient, followed by initiation of a stepwise management approach (FIGURE 2).
FIGURE 2 Management of thyroid storm
Aggressive management of thyroid storm is indicated, following a stepwise approach. Each medication used to treat thyroid storm plays a specific role in suppressing thyroid function. Propylthiouracil (PTU) blocks additional synthesis of thyroid hormone and inhibits the conversion of thyroxine (T4) to triiodothyronine (T3). Methimazole blocks additional synthesis of thyroid hormones. Saturated solution of potassium iodide (SSKI), Lugol’s solution, and sodium iodide block the release of thyroid hormone from the gland. Dexamethasone is used to decrease thyroid hormone release and peripheral conversion of T4 to T3. Propranolol is used to treat maternal tachycardia by inhibiting the adrenergic effects of excessive thyroid hormones. Finally, phenobarbital is used to treat maternal agitation and restlessness caused by the increased catabolism of thyroid hormones.
SOURCE: Adapted from ACOG.2
Treatment of hyperthyroidism in pregnancy
Two medications are available to treat hyperthyroidism in pregnancy: propylthiouracil (PTU) and methimazole. These medications are known as thioamides.1,2
PTU blocks the oxidation of iodine in the thyroid gland, thereby preventing the synthesis of T4 and T3. The initial dosage for hyperthyroid women who are not pregnant is usually 300 to 450 mg/day in three divided doses every 8 hours, and this dosing strategy can also be applied to the pregnant patient. Maintenance therapy is usually achieved with 100 to 150 mg/day in divided doses every 8 to 12 hours.9
Methimazole works by blocking the organification of iodide, which decreases thyroid hormone production. The usual dosing, given in three divided doses every 8 hours, is 15 mg/day for mild hyperthyroidism, 30 to 40 mg/day for moderately severe hyperthyroidism, and 60 mg/day for severe hyperthyroidism. Maintenance therapy with methimazole is usually given at a dosage of 5 to 15 mg/day.9
In the past, PTU was considered the drug of choice for treatment of hyperthyroidism in pregnancy because clinicians believed it crossed the placenta to a lesser degree than did methimazole, and because methimazole was associated with fetal esophageal and choanal atresia and fetal cutis aplasia (congenital skin defect of the scalp).1,2 Available evidence does not, however, support these conclusions.8,10 Whatever medication regimen you choose, thyroid function should be monitored 1) every 4 weeks until TSH and FT4 levels are within normal limits and 2) every trimester thereafter. FIGURE 3 presents an algorithm for managing hyperthyroidism in pregnancy.
FIGURE 3 Management of hyperthyroidism in pregnancy
CASE Resolved
The patient in thyroid storm described at the beginning of this article requires aggressive management, as outlined in the algorithm in FIGURE 2. As her symptoms diminish, fetal tachycardia resolves. The patient’s FT4 level begins to decline, consistent with appropriate treatment, and she is discharged home and instructed to continue PTU and labetalol and to follow up at the endocrinology and high-risk obstetrics clinics as soon as possible.
The patient does not follow this advice. Consequently, she presents at 33 5/7 weeks in a hypertensive crisis, with symptoms similar to those she first exhibited plus acute pulmonary edema. Fetal heart rate is initially in the 130s, with good variability and occasional decelerations (FIGURE 4A), but decelerations then become worse (FIGURE 4B) and emergency cesarean section is performed.
A male infant is delivered, weighing 2,390 g. Apgar scores are 0 at 1 minute and 9 at 5 minutes. A 25% placental abruption is noted at the time of delivery.
Mother and fetus are stabilized and discharged.
FIGURE 4 Weakening fetal status in a mother who is in thyroid storm
Fetal heart rate is initially in the 130s with good variability and occasional decelerations (A), but then deteriorates, with increasing decelerations (B), an indication for immediate delivery.
1. Casey BM, Leveno KJ. Thyroid disease in pregnancy. Obstet Gynecol. 2006;108:1283-1292.
2. American College of Obstetrics and Gynecology. ACOG Practice Bulletin. Clinical management guidelines for obstetrician-gynecologists. Number 37, August 2002. (Replaces Practice Bulletin Number 32, November 2001). Thyroid disease in pregnancy. Obstet Gynecol. 2002;100:387-396.
3. Mitchell ML, Klein RZ. The sequelae of untreated maternal hypothyroidism. Eur J Endocrinol. 2004;151 Suppl 3:U45-48.
4. Mestman JH. Endocrine diseases in pregnancy. In: Gabbe S, Niebyl JR, eds. Obstetrics: Normal and Problem Pregnancies. 4th ed. Philadelphia: Churchill Livingstone; 2002:1117-1168.
5. Davis LE, Leveno KJ, Cunningham FG. Hypothyroidism complicating pregnancy. Obstet Gynecol. 1988;72:108-112.
6. Davis LE, Lucas MJ, Hankins GD, Roark ML, Cunningham FG. Thyrotoxicosis complicating pregnancy. Am J Obstet Gynecol. 1989;160:63-70.
7. Kriplani A, Buckshee K, Bhargava VL, Takkar D, Ammini AC. Maternal and perinatal outcome in thyrotoxicosis complicating pregnancy. Eur J Obstet Gynecol Reprod Biol. 1994;54:159-163.
8. Belford MA. Navigating a thyroid storm. Contemporary OB/GYN. 2006; October:38–46.
9. Lazarus JH, Othman S. Thyroid disease in relation to pregnancy. Clin Endocrinol (Oxf). 1991;34:91-98.
10. Kent GN, Stuckey BG, Allen JR, Lambert T, Gee V. Postpartum thyroid dysfunction: clinical assessment and relationship to psychiatric affective morbidity. Clin Endocrinol (Oxf). 1999;51:429-438.
1. Casey BM, Leveno KJ. Thyroid disease in pregnancy. Obstet Gynecol. 2006;108:1283-1292.
2. American College of Obstetrics and Gynecology. ACOG Practice Bulletin. Clinical management guidelines for obstetrician-gynecologists. Number 37, August 2002. (Replaces Practice Bulletin Number 32, November 2001). Thyroid disease in pregnancy. Obstet Gynecol. 2002;100:387-396.
3. Mitchell ML, Klein RZ. The sequelae of untreated maternal hypothyroidism. Eur J Endocrinol. 2004;151 Suppl 3:U45-48.
4. Mestman JH. Endocrine diseases in pregnancy. In: Gabbe S, Niebyl JR, eds. Obstetrics: Normal and Problem Pregnancies. 4th ed. Philadelphia: Churchill Livingstone; 2002:1117-1168.
5. Davis LE, Leveno KJ, Cunningham FG. Hypothyroidism complicating pregnancy. Obstet Gynecol. 1988;72:108-112.
6. Davis LE, Lucas MJ, Hankins GD, Roark ML, Cunningham FG. Thyrotoxicosis complicating pregnancy. Am J Obstet Gynecol. 1989;160:63-70.
7. Kriplani A, Buckshee K, Bhargava VL, Takkar D, Ammini AC. Maternal and perinatal outcome in thyrotoxicosis complicating pregnancy. Eur J Obstet Gynecol Reprod Biol. 1994;54:159-163.
8. Belford MA. Navigating a thyroid storm. Contemporary OB/GYN. 2006; October:38–46.
9. Lazarus JH, Othman S. Thyroid disease in relation to pregnancy. Clin Endocrinol (Oxf). 1991;34:91-98.
10. Kent GN, Stuckey BG, Allen JR, Lambert T, Gee V. Postpartum thyroid dysfunction: clinical assessment and relationship to psychiatric affective morbidity. Clin Endocrinol (Oxf). 1999;51:429-438.
Posttraumatic Stress Disorder in Veterans: Inpatient Assessment and Management
Recurrent Otic Barotrauma in a Student Naval Aviator
Morton Neuroma
Aromatase inhibitors, a new option for inducing ovulation
Dr. Mitwally holds patents licensed to Serono for use of aromatase inhibitors for infertility treatment.
Dr. Casper has a licensing agreement with Ares-Serono for use of aromatase inhibitors in assisted reproduction.
CASE 1 Ovulation begins, but pregnancy does not follow
U.Y. is a 32-year-old woman who has been trying to conceive for 3 years. Her infertility is caused by anovulation associated with polycystic ovary syndrome (PCOS). All other variables are within physiologic limits—she has patent tubes and an unremarkable uterus, and her partner has a normal semen analysis.
She has undergone six cycles of treatment with clomiphene citrate, with ovulation documented each time by ultrasonography (US) and measurement of luteal-phase progesterone levels. Her endometrial thickness is 4 to 6 mm around the day of ovulation.
Would an aromatase inhibitor increase her chances of conceiving?
This patient is an excellent candidate for ovulation induction using an aromatase inhibitor (AI).
The primary reason? She is unlikely to benefit from an increased dosage of clomiphene citrate because the dosage that triggers ovulation is believed to be most appropriate—an increase above that level is not expected to improve the chance of pregnancy. Moreover, conception is less likely after more than six cycles of clomiphene citrate.1,2
In this article, we describe the induction of ovulation using AIs—a relatively new, and off-label, application (TABLES 1 and 2). The strategies presented here are suitable for general ObGyns and do not require sophisticated technology such as rapid hormonal assays or transvaginal US.
Because this application is so new, with limited data published so far, much of the information presented here is based on our personal experience rather than level-1 evidence, which is sorely needed.
Of course, induction of ovulation is appropriate only after other specific causes of anovulation or ovulatory dysfunction are excluded, such as thyroid disorders, hyperprolactinemia, severe insulin resistance, and ovarian failure.
Concerns about teratogenicity of AIs appear to be largely unfounded (see below).
TABLE 1
Aromatase inhibitors work best in these applications
| APPLICATION | EVIDENCE |
|---|---|
Induction of ovulation, particularly in women with polycystic ovary syndrome:
See case 1 and case 2 |
|
| Ovarian stimulation (superovulation) in ovulatory women with unexplained or endometriosis-related infertility See case 3 | Strong evidence from several clinical trials |
| Use in conjunction with controlled ovarian hyperstimulation by gonadotropins with intrauterine insemination and assisted reproduction | Accumulating evidence of several advantages when used with gonadotropins:
|
TABLE 2
Avoid AIs in these situations
| SITUATION | JUSTIFICATION |
|---|---|
| When clomiphene citrate fails to induce ovulation in a woman with insulin resistance See case 2 | First try insulin sensitizers and other measures to improve insulin action (weight loss, exercise, and dietary modifications) |
| When other causes of infertility (besides ovulatory dysfunction) are likely | Pregnancy is unlikely |
| When the patient has hypothalamic/hypopituitary anovulation or ovarian failure | Ovarian stimulation is dependent on capacity to produce endogenous gonadotropins and presence of responding ovarian follicles |
Ovulation is good, but pregnancy is better
In women undergoing induction of ovulation, there are two levels of success: ovulation and pregnancy.
Clearly, the presence of other, nonovulatory infertility factors—e.g., male infertility and tubal-uterine problems—can prevent successful ovulation induction from translating into pregnancy.
We have reported3-9 on the successful use of AIs to stimulate the ovary and achieve pregnancy—even in women who fail to conceive after several treatment trials with clomiphene citrate.4
Other authors have conducted further investigations that have confirmed our findings and have recommended use of these agents for other aspects of infertility treatment, such as assisted reproduction.10-19
Latest generation of AIs is more benign
Many AIs have been developed over the past 30 years. The most recent are third-generation agents that were approved mainly to suppress estrogen production in postmenopausal women with breast cancer. Clinical failure of earlier generations of AIs for their approved indication was mainly due to significant adverse effects, lack of satisfactory potency, or lack of specificity in inhibiting the aromatase enzyme without inhibiting other enzymes of steroidogenesis.20
Third-generation AIs that are commercially available in North America, Europe, and other parts of the world include:
- two nonsteroidal preparations: anastrozole (Arimidex) and letrozole (Femara)
- one steroidal agent: exemestane (Aromasin).
Letrozole and anastrozole are reversible, competitive agents with considerably greater potency (more than 1,000 times greater) than the first-generation AI aminoglutethimide. At a dosage of 1 to 5 mg/day, they reduce estrogen levels by 97% to more than 99%.
AIs are completely absorbed after oral administration, with a mean terminal half-life of approximately 45 hours (range: 30–60 hours). Exemestane has a shorter circulating half-life of approximately 9 hours, but may have a longer effect because it is irreversible.21
Mild gastrointestinal (GI) disturbances account for most of the adverse events, and rarely limit therapy.
How AIs work
Although we continue to accrue data on the use of AIs to induce ovulation, the underlying mechanism of action has not been studied. However, we believe that AIs work both centrally (at the level of the hypothalamus and pituitary) and peripherally (at the level of the ovaries).22-28
At the central level, AIs suppress estrogen production by directly, specifically, and potently inhibiting the aromatase enzyme (i.e., estrogen synthase, the enzyme responsible for the synthesis of estrogen). Because the aromatase enzyme is expressed in various tissues and organs—most notably, the ovaries, brain, and fat29—AIs suppress estrogen production in all of those tissues, leading to a low serum estrogen level and low local estrogen level. Low estrogen levels are thought to release the hypothalamus and pituitary gland from their negative-feedback mechanism, thereby increasing production of endogenous gonadotropins from the pituitary gland and stimulating ovarian follicular development and ovulation (FIGURE).
At the peripheral level, the aromatase enzyme catalyzes the terminal step in the steroidogenesis cascade that converts androgens into estrogen. When that enzyme is inhibited, enzyme substrate (androgens) is thought to accumulate. Contrary to the general belief that androgens are deleterious to ovarian follicles, studies in primates have demonstrated that androgens actually up-regulate the expression of gonadotropin receptors, particularly follicle-stimulating hormone (FSH) receptors.30 This renders the ovaries more sensitive to gonadotropin stimulation—whether the gonadotropins are endogenous or exogenous.22-28
FIGURE Aromatase inhibitors promote follicle development, then fade from the scene in time to prevent hyperovulation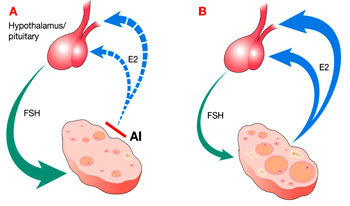
Administration of an aromatase inhibitor (AI) on cycle days 3 to 7 suppresses ovarian estradiol (E2) secretion, as shown in A, which reduces estrogen-negative feedback at the hypothalamus and pituitary. As a result, follicle-stimulating hormone (FSH) secretion increases, fostering growth of multiple ovarian follicles. The growing follicles, shown in B, cause estrogen levels to rise again, depressing FSH, and leading to monofollicular ovulation in most cases.
Why AIs are superior to clomiphene
Clomiphene citrate is a selective estrogen receptor modulator (SERM) that is believed to induce ovulation through its antiestrogenic properties at the level of the hypothalamus or pituitary gland, or both. Clomiphene down-regulates estrogen receptors at this level, and the hypothalamus and pituitary gland react as though the estrogen level is very low. This reverses the suppression of endogenous gonadotropins by estrogen, and gonadotropin levels rise, stimulating ovarian follicular development.
The down-regulation of estrogen receptors with clomiphene administration is not limited to the hypothalamus and pituitary gland, but also occurs peripherally at the endometrium and cervix, where it is not so desirable. When the cervix is affected, it becomes an unfavorable environment for sperm to penetrate, and when the endometrium is affected, its hypoestrogenic status may reduce the likelihood of embryo implantation—or may increase the risk of pregnancy loss if implantation occurs.
These peripheral antiestrogenic prop erties of clomiphene citrate may account for the discrepancy between high ovulation and low pregnancy rates.22-28 Several strategies to overcome this problem—e.g., adding estrogen, starting clomiphene citrate earlier in the menstrual period, or using another SERM, such as tamoxifen—have been largely unsuccessful. With clomiphene citrate, depletion of estrogen receptors has long-term effects because of the drug’s relatively long half-life (several days).31
In contrast, AIs do not appear to affect the expression of estrogen receptors in different body tissues, such as the endometrium and cervix. AIs have a shorter half-life (8 hours to 2 days), and nonsteroidal third-generation agents have a reversible inhibitory effect on the aromatase enzyme. Moreover, the rise in endogenous gonadotropins stimulates the production of more aromatase enzyme. This newly formed aromatase enzyme, and the return of a normal aromatase level after a short half-life of AI, leads the maturing ovarian follicles to secrete estrogen, which reaches a physiologic level soon after the last administration of AI. The rising estrogen level allows development of a more hospitable uterine environment (endometrium and cervical mucus).22-28
Early evidence confirms efficacy of AIs
After our pioneering reports of successful ovulation induction3-9 and improved ovarian response to stimulation by gonadotropins5-7 using AIs in small, nonrandomized, controlled trials, several larger and better designed clinical trials followed and supported our findings.10-19
Clinical trials comparing AIs with clomiphene citrate have consistently reported a universal “trend” toward superiority of AIs in achieving pregnancy despite comparable levels of success in achieving ovulation.10,11,14,16-19 However, these published clinical trials lacked adequate sample size to definitively confirm the superiority of AIs in achieving clinical pregnancy. We believe AIs are superior because, in our experience, they have helped women achieve pregnancy even after failure of several cycles of clomiphene treatment.4,15
Should an AI follow a trial of clomiphene?
U.Y., the patient described at the opening of this article, has two main options now that she has completed six cycles of clomiphene citrate without conceiving. The usual strategy would be a shift to more sophisticated treatment using gonadotropin injection. However, exogenous gonadotropins have several disadvantages:
- the drugs must be injected (orally inactive)
- they are more expensive than clomiphene citrate and AIs
- they require close monitoring by an infertility specialist with expensive and sophisticated technology
- they carry a risk of severe ovarian hyperstimulation, which is unlikely with clomiphene citrate and unreported with AIs
- multiple pregnancy is likely, particularly in conjunction with intrauterine insemination
- the risk of ovarian hyperstimulation with gonadotropin injection is much higher in women with PCOS, such as U.Y., as is the likelihood of multiple pregnancy.
The reason U.Y. has not conceived after six cycles of clomiphene citrate is likely related to the drug’s antiestrogenic effects on the endometrium, which appeared to be very thin (4–6 mm) on US imaging around the day of ovulation. If she fails to conceive with AIs, she will probably not become pregnant after a switch to gonadotropin injection unless more advanced treatment is included, such as in vitro fertilization (IVF) and embryo transfer. Other causes of her infertility—besides ovulatory dysfunction—may explain the failure to conceive.
Comparable pregnancy rates have been observed for AIs and gonadotropin injection, although further study is needed—specifically, clinical trials comparing gonadotropin and AIs in conjunction with timed intercourse or intrauterine insemination, or both.
CASE 2 No response to clomiphene citrate
G.A., 28 years old, has been trying to conceive for 3 years. She reports having irregular menstrual periods indicative of anovulation, and body temperature charts and progesterone levels support that diagnosis. She undergoes three cycles of clomiphene citrate at dosages ranging from 50 to 150 mg/day for 5 days starting on day 3 of the menstrual cycle. Despite treatment, she fails to ovulate.
Would an AI increase her chance of ovulating and conceiving?
Failure to ovulate after treatment with clomiphene citrate may have any of several causes, including inappropriate patient selection and resistance to the drug.
An example of inappropriate patient selection would be a woman with hypothalamic/hypopituitary anovulation; this type of patient often has insufficient levels of endogenous gonadotropins (luteinizing hormone and FSH). Another example would be a woman with reduced ovarian reserve; this type of patient is often unresponsive to clomiphene citrate and may have substantially elevated gonadotropin levels, most notably high FSH on day 3 of the menstrual cycle.
AIs are unlikely to induce ovulation in either of these patients. For the first type of patient, exogenous gonadotropin injection would be appropriate, as would be a gonadotropin-releasing hormone (GnRH) pump. For a woman with reduced ovarian reserve, an oocyte donor and IVF are the best treatment option.
Success with an AI is unlikely when there is no appropriate indication for clomiphene citrate. For example, a woman with severe insulin resistance who fails to ovulate in response to clomiphene citrate is unlikely to ovulate in response to an AI. In that case, an insulin sensitizer—alone or in combination with clomiphene citrate or an AI—would be the appropriate option. Other measures to reduce insulin resistance, such as weight loss, exercise, and dietary modification, may also be helpful.
CASE 3 Ovulatory patient with endometriosis fails to conceive on clomiphene
R.C., 34 years old, has been trying to conceive for 2 years. Her basic infertility workup, which included a hysterosalpingogram and semen analysis, did not reveal any abnormalities. She has regular menstrual cycles suggestive of ovulation. In addition, luteal-phase progesterone levels and biphasic body temperature charts both indicate regular ovulation.
After six cycles of clomiphene citrate, her gynecologist performs diagnostic laparoscopy. Other than minimal, stage 1 endometriosis, confirmed by pathologic examination of peritoneal biopsies, there are no remarkable findings. Methylene blue tubal perfusion confirms patent fallopian tubes during the operation. The gynecologist fulgurates the minimal endometriotic implants using carbon dioxide laser. Two months after the procedure, the patient undergoes three more cycles of clomiphene citrate, without success.
Would an AI help her conceive?
Most of the data on successful treatment with clomiphene citrate come from anovulatory women with PCOS in whom anovulation is the main cause of infertility. Evidence is weaker when the patient is ovulatory and has unexplained or endometriosis-associated infertility.32
A recent nonrandomized, controlled study that included women with a medical history comparable to R.C.’s found treatment with clomiphene citrate to significantly reduce the chance of pregnancy, compared with timed intercourse without clomiphene or other forms of ovarian stimulation, following conservative laparoscopic surgery for their endometriosis.33 We believe that clomiphene citrate is in-appropriate in women with endometriosis-related infertility—and may activate underlying endometriotic lesions.
For R.C., treatment with an AI is a viable option, particularly in light of recent data showing that the aromatase enzyme is expressed in endometriotic lesions.34 An AI could also enhance conception by further suppressing endometriosis through its effects on circulating estrogen levels and local estrogen production. This is an unproven extrapolation that seems scientifically appropriate to us, but needs confirmation by randomized clinical trials.
CASE 4 Woman with unexplained—and uninvestigated—infertility
E.D., 31 years old, has been trying to conceive for 1 year. Neither she nor her husband has undergone any study of their infertility problem.
Would empiric treatment with an AI be appropriate?
No treatment should begin until the patient and her partner have undergone the basic workup (TABLE 3). If a specific cause of infertility is determined, the patient should be treated accordingly. If no explanation for the infertility can be found, or anovulation is the likely cause, empirical ovarian stimulation with timed intercourse or intrauterine insemination is reasonable, provided:
- semen analysis is within normal limits
- ovarian function is present—i.e., the patient is expected to ovulate in response to ovarian stimulation
- at least one tube is patent and functional
- uterus has no serious abnormalities.
If ovarian stimulation fails to trigger ovulation or pregnancy, consider the options listed in TABLE 4
TABLE 3
Basic infertility workup
|
|
|
|
|
TABLE 4
When ovarian stimulation fails, next step depends on several variables
| LEVEL OF FAILURE | CLOMIPHENE CITRATE | AROMATASE INHIBITORS |
|---|---|---|
| 1–No ovulation | Is indication appropriate? Neither clomiphene citrate nor AIs are appropriate for hypothalamic/hypopituitary anovulation or ovarian failure Is severe insulin resistance present? If so, consider insulin sensitizers and encourage exercise, dietary changes, and weight loss | |
| Other options: Change to AI or retry clomiphene citrate in conjunction with an insulin sensitizer. If treatment fails after 3 to 6 additional cycles, consider an injectable gonadotropin | Other options: Try adding an insulin sensitizer. If treatment fails after 3 to 6 additional cycles, consider an injectable gonadotropin | |
| 2–Ovulation but no pregnancy | Was another cause of infertility (besides ovulatory dysfunction) overlooked? Investigate further, if necessary Options: Consider AIs before injectable gonadotropins, especially when there is evidence, with clomiphene citrate, of a persistent antiestrogenic effect, such as thin endometrium around the time of ovulation; endometriosis; or unexplained infertility. Move to gonadotropins if AIs fail | |
Minimal adverse effects
AIs are generally well tolerated. The most common adverse effects are hot flushes, GI disturbances (nausea and vomiting), and leg cramps. In clinical trials involving postmenopausal women with breast cancer who were taking an AI, very few withdrew because of drug-related adverse effects.35 Those women took an AI on a daily basis over several months. Fewer adverse effects would be expected among usually healthy younger women administered a short course (a few days) for ovarian stimulation. In addition, our clinical experience has been that fewer women experience side effects such as mild hot flushes and symptoms similar to premenstrual syndrome when taking an AI, compared with clomiphene citrate.3-9
When any medication is given during pregnancy, there are concerns about its effects. Drugs used to induce ovulation are no exception. In fact, clomiphene citrate is classified as pregnancy category X—a fact frequently overlooked by treating physicians. As for AIs, recent studies found no evidence of teratogenicity or clastogenicity in animal embryos when anastrozole was given. The picture is murkier for letrozole.
When used for ovarian stimulation, the short half-life of AIs and administration in the early follicular phase (several days before ovulation and fertilization occur) should ensure clearance of the drugs before implantation. Nevertheless, it is important to confirm that the patient is not pregnant before an AI is given. We recommend a pregnancy test before administering an AI for ovulation induction.
Mixed bag of data on pregnancy outcomes
Three large studies recently reported on pregnancy outcomes after infertility treatment with AIs.9,36,37 The first was a cohort study comparing outcomes of 394 pregnancies achieved after treatment with letrozole (133 pregnancies) and other ovarian-stimulation agents, including clomiphene citrate (113 pregnancies) and gonadotropins (110 pregnancies), with a control group of 38 pregnancies achieved without ovarian stimulation.9 The study encompassed three tertiary referral centers over 2 years. Pregnancies conceived after treatment with an AI had rates of miscarriage and ectopic pregnancy comparable to all other groups. In addition, letrozole was associated with a significantly lower rate of multiple gestation than was clomiphene citrate.9
The second study, presented in abstract form, compared the outcome of 150 births after treatment with letrozole to a database of 36,050 normal deliveries.36 Although the authors themselves stated that there was no statistically significant difference in the overall incidence of congenital malformation, they reported a higher incidence of locomotor malformation and cardiac anomaly in the infants conceived after treatment with letrozole.36 They did not address this discrepancy or explain how locomotor malformation was assessed.
A closer look at the abstract reveals major methodological flaws that weaken the data and conclusions presented:
- The study was not well controlled. The treated patients (n=130) were infertile women, mainly suffering from PCOS and unexplained infertility, who had a mean age of 35.2 years. The control group included a database of spontaneously conceiving women who were significantly younger (mean age: 30.5 years). The control group also included deliveries in a low-risk hospital that refers out high-risk pregnancies to secondary and tertiary hospitals. These are important distinctions because women of advanced maternal age have an increased incidence of medical illnesses, making their pregnancies higher in risk.
- The incidence of multiple gestation was significantly higher among women treated for infertility than among women in the control group. It is well known that multiple gestations are at increased risk of fetal malformation compared with singleton pregnancies.
- The incidence of cardiac anomaly among women treated with letrozole did not differ significantly from the known incidence of cardiac malformation in the general population, but the authors concluded that the rate of cardiac malformation was significantly higher in the letrozole group than among controls. This is misleading because it was the control group that developed cardiac malformation at a significantly lower rate than in the general population. Such a low incidence of cardiac anomaly in a low-risk hospital setting is not surprising, because mothers would be transferred to a tertiary-care center once an anomaly was detected.
- Data on congenital malformation in the control group were collected from delivery records available in the maternity ward of the hospital. However, a significant percentage of congenital malformations, such as cardiac anomaly, are not detected until after the neonatal period.36
When using clomiphene citrate or an aromatase inhibitor (AI):
- avoid a dosage that exceeds 100 to 150 mg/day for clomiphene citrate or 2.5 to 5 mg/day for AIs or a treatment period longer than 5 days each cycle
- do not administer an AI beyond day 7 of the menstrual cycle
- stop after three to six cycles of treatment
- do not increase the dosage once ovulation occurs
- discontinue treatment when serious adverse effects are present, such as visual side effects.
It is also interesting that the results of this abstract have not been published in a peer-reviewed journal more than a year after its presentation.
The third study, which is more recent, compared the incidence of congenital malformation in 911 newborns conceived after treatment with letrozole (n=514) or clomiphene citrate (n=397).37 It found no statistically significant difference between the groups. Congenital malformation was diagnosed in 2.4% and 4.8% of the letrozole- and clomiphene-treated groups, respectively, and major malformation occurred in 1.2% and 3% of the letrozole- and clomiphene-treated groups, respectively. These differences were not statistically significant, but there was a sevenfold increase in overall cardiac anomalies in the clomiphene-treated group, compared with the letrozole-treated group—and this difference was statistically significant. These findings warrant further investigation into the use of clomiphene citrate for induction of ovulation.
1. Dickey RP, Taylor SN, Lu PY, Sartor BM, Rye PH, Pyrzak R. Effect of diagnosis, age, sperm quality, and number of preovulatory follicles on the outcome of multiple cycles of clomiphene citrate-intrauterine insemination. Fertil Steril. 2002;78:1088-1095.
2. Imani B, Eijkemans MJ, te Velde ER, Habbema JD, Fauser BC. Predictors of chances to conceive in ovulatory patients during clomiphene citrate induction of ovulation in normogonadotropic oligomenorrheic infertility. J Clin Endocrinol Metab. 1999;84:1617-1622.
3. Mitwally MFM, Casper RF. Aromatase inhibition: a novel method of ovulation induction in women with polycystic ovarian syndrome. Reprod Technol. 2000;10:244-247.
4. Mitwally MFM, Casper RF. Use of an AI for induction of ovulation in patients with an inadequate response to clomiphene citrate. Fertil Steril. 2001;75:305-309.
5. Mitwally MFM, Casper RF. Aromatase inhibition improves ovarian response to follicle-stimulating hormone in poor responders. Fertil Steril. 2002;77:776-780.
6. Mitwally MF, Casper RF. Aromatase inhibition reduces gonadotropin dose required for controlled ovarian stimulation in women with unexplained infertility. Hum Reprod. 2003;188:1588-1597.
7. Mitwally MF, Casper RF. Aromatase inhibition reduces the dose of gonadotropin required for controlled ovarian hyperstimulation. J Soc Gynecol Investig. 2004;11:406-415.
8. Mitwally MFM, Casper RF. Single dose administration of the aromatase inhibitor, letrozole: a simple and convenient effective method of ovulation induction. Fertil Steril. 2005;83:229-231.
9. Mitwally MFM, Casper RF. Pregnancy outcome after the use of an AI for induction of ovulation. Am J Obstet Gynecol. 2005;192:381-386.
10. Fatemi HM, Kolibianakis E, Tournaye H, et al. Clomiphene citrate versus letrozole for ovarian stimulation: a pilot study. Reprod Biomed Online. 2003;75:543-546.
11. Al-Fozan H, Al-Khadouri M, Tan SL, Tulandi T. A randomized trial of letrozole versus clomiphene citrate in women undergoing superovulation. Fertil Steril. 2004;82:1561-1563.
12. Goswami SK, Das T, Chattopadhyay R, et al. A randomized single-blind controlled trial of letrozole as a low-cost IVF protocol in women with poor ovarian response: a preliminary report. Hum Reprod. 2004;19:2031-2035.
13. Garcia-Velasco JA, Moreno L, Pacheco A, et al. The aromatase inhibitor letrozole increases the concentration of intraovarian androgens and improves in vitro fertilization outcome in low responder patients: a pilot study. Fertil Steril. 2005;84:82-87.
14. Bayar U, Tanrierdi HA, Barut A, et al. Letrozole vs. clomiphene citrate in patients with ovulatory infertility. Fertil Steril. 2006;85:1045-1048.
15. Elnashar A, Fouad H, Eldosoky M, et al. Letrozole induction of ovulation in women with clomiphene citrate-resistant polycystic ovary syndrome may not depend on the period of infertility, the body mass index, or the luteinizing hormone/follicle stimulating hormone ratio. Fertil Steril. 2006;85:161-164.
16. Atay V, Cam C, Muhcu M, et al. Comparison of letrozole and clomiphene citrate in women with polycystic ovaries undergoing ovarian stimulation. J Int Med Res. 2006;34:73-76.
17. Sohrabvand F, Ansari S, Bagheri M. Efficacy of combined metformin-letrozole in comparison with metformin-clomiphene citrate in clomiphene-resistant infertile women with polycystic ovarian disease. Hum Reprod. 2006;21:1432-1435.
18. Sipe CS, Davis WA, Maifeld M, Van Voorhis BJ. A prospective randomized trial comparing anastrozole and clomiphene citrate in an ovulation induction protocol using gonadotropins. Fertil Steril. 2006;86:1676-1681.
19. Bayar U, Basaran M, Kiran S, Coskun A, Gezer S. Use of an aromatase inhibitor in patients with polycystic ovary syndrome: a prospective randomized trial. Fertil Steril. 2006;86:1447-1451.
20. Buzdar A, Howell A. Advances in aromatase inhibition: clinical efficacy and tolerability in the treatment of breast cancer. Clin Cancer Res. 2001;7:2620-2635.
21. Winer EP, Hudis C, Burstein HJ, et al. American Society of Clinical Oncology Technology Assessment on the use of aromatase inhibitors as adjuvant therapy for women with hormone receptor-positive breast cancer: status report 2002. J Clin Oncol. 2002;2015:3317-3327.
22. Mitwally MF, Casper RF. Potential of aromatase inhibitors for ovulation and superovulation induction in infertile women. Drugs. 2006;66:2149-2160.
23. Mitwally MFM, Casper RF. Letrozole for ovulation induction. Exp Rev Obstet Gynecol. 2006;1:15-27.
24. Casper RF, Mitwally MF. Review: aromatase inhibitors for ovulation induction. J Clin Endocrinol Metab. 2006;91:760-771.
25. Mitwally MF, Casper RF, Diamond MP. The role of aromatase inhibitors in ameliorating deleterious effects of ovarian stimulation on outcome of infertility treatment. Reprod Biol Endocrinol. 2005;3:54.-
26. Mitwally MF, Casper RF. Aromatase inhibitors in ovulation induction. Semin Reprod Med. 2004;22:61-78.
27. Mitwally MF, Casper RF. Aromatase inhibitors for the treatment of infertility. Expert Opin Investig Drugs. 2003;12:353-371.
28. Mitwally MF, Casper RF. Aromatase inhibition for ovarian stimulation: future avenues for infertility management. Curr Opin Obstet Gynecol. 2002;14:255-263.
29. Cole PA, Robinson CH. Mechanism and inhibition of cytochrome P-450 aromatase. J Med Chem. 1990;33:2933-2944.
30. Weil S, Vendola K, Zhou J, Bondy CA. Androgen and follicle-stimulating hormone interactions in primate ovarian follicle development. J Clin Endocrinol Metab. 1999;848:2951-2956.
31. Mikkelson TJ, Kroboth PD, Cameron WJ. Single dose pharmacokinetics of clomiphene citrate in normal volunteers. Fertil Steril. 1986;46:392-396.
32. Hughes E, Collins J, Vandekerckhove P. Clomiphene citrate for unexplained subfertility in women. Cochrane Database Syst Rev. 2000;(2):CD000057.-
33. Mitwally MF, Albuarki H, Ashraf M, Diamond MP, Abuzeid M. Clomiphene reduces chance of pregnancy in infertile women with endometriosis following laparoscopic surgery. J Soc Gynecol Investig. 2006;13(2) (suppl):abstract 646.-
34. Attar E, Bulun SE. Aromatase and other steroidogenic genes in endometriosis: translational aspects. Hum Reprod Update. 2006;12:49-56.
35. Goss PE. Risks versus benefits in the clinical application of aromatase inhibitors. Endocr Relat Cancer. 1999;6:325-332.
36. Biljan MM, Hemmings R, Brassard N. The outcome of 150 babies following the treatment with letrozole or letrozole and gonadotropins [abstract no. 1033]. Fertil Steril. 2005;84 (suppl):abstract 1033.-
37. Tulandi T, Martin J, Al-Fadhli R, et al. Congenital malformations among 911 newborns conceived after infertility treatment with letrozole or clomiphene citrate. Fertil Steril. 2006;85:1761-1765.
Dr. Mitwally holds patents licensed to Serono for use of aromatase inhibitors for infertility treatment.
Dr. Casper has a licensing agreement with Ares-Serono for use of aromatase inhibitors in assisted reproduction.
CASE 1 Ovulation begins, but pregnancy does not follow
U.Y. is a 32-year-old woman who has been trying to conceive for 3 years. Her infertility is caused by anovulation associated with polycystic ovary syndrome (PCOS). All other variables are within physiologic limits—she has patent tubes and an unremarkable uterus, and her partner has a normal semen analysis.
She has undergone six cycles of treatment with clomiphene citrate, with ovulation documented each time by ultrasonography (US) and measurement of luteal-phase progesterone levels. Her endometrial thickness is 4 to 6 mm around the day of ovulation.
Would an aromatase inhibitor increase her chances of conceiving?
This patient is an excellent candidate for ovulation induction using an aromatase inhibitor (AI).
The primary reason? She is unlikely to benefit from an increased dosage of clomiphene citrate because the dosage that triggers ovulation is believed to be most appropriate—an increase above that level is not expected to improve the chance of pregnancy. Moreover, conception is less likely after more than six cycles of clomiphene citrate.1,2
In this article, we describe the induction of ovulation using AIs—a relatively new, and off-label, application (TABLES 1 and 2). The strategies presented here are suitable for general ObGyns and do not require sophisticated technology such as rapid hormonal assays or transvaginal US.
Because this application is so new, with limited data published so far, much of the information presented here is based on our personal experience rather than level-1 evidence, which is sorely needed.
Of course, induction of ovulation is appropriate only after other specific causes of anovulation or ovulatory dysfunction are excluded, such as thyroid disorders, hyperprolactinemia, severe insulin resistance, and ovarian failure.
Concerns about teratogenicity of AIs appear to be largely unfounded (see below).
TABLE 1
Aromatase inhibitors work best in these applications
| APPLICATION | EVIDENCE |
|---|---|
Induction of ovulation, particularly in women with polycystic ovary syndrome:
See case 1 and case 2 |
|
| Ovarian stimulation (superovulation) in ovulatory women with unexplained or endometriosis-related infertility See case 3 | Strong evidence from several clinical trials |
| Use in conjunction with controlled ovarian hyperstimulation by gonadotropins with intrauterine insemination and assisted reproduction | Accumulating evidence of several advantages when used with gonadotropins:
|
TABLE 2
Avoid AIs in these situations
| SITUATION | JUSTIFICATION |
|---|---|
| When clomiphene citrate fails to induce ovulation in a woman with insulin resistance See case 2 | First try insulin sensitizers and other measures to improve insulin action (weight loss, exercise, and dietary modifications) |
| When other causes of infertility (besides ovulatory dysfunction) are likely | Pregnancy is unlikely |
| When the patient has hypothalamic/hypopituitary anovulation or ovarian failure | Ovarian stimulation is dependent on capacity to produce endogenous gonadotropins and presence of responding ovarian follicles |
Ovulation is good, but pregnancy is better
In women undergoing induction of ovulation, there are two levels of success: ovulation and pregnancy.
Clearly, the presence of other, nonovulatory infertility factors—e.g., male infertility and tubal-uterine problems—can prevent successful ovulation induction from translating into pregnancy.
We have reported3-9 on the successful use of AIs to stimulate the ovary and achieve pregnancy—even in women who fail to conceive after several treatment trials with clomiphene citrate.4
Other authors have conducted further investigations that have confirmed our findings and have recommended use of these agents for other aspects of infertility treatment, such as assisted reproduction.10-19
Latest generation of AIs is more benign
Many AIs have been developed over the past 30 years. The most recent are third-generation agents that were approved mainly to suppress estrogen production in postmenopausal women with breast cancer. Clinical failure of earlier generations of AIs for their approved indication was mainly due to significant adverse effects, lack of satisfactory potency, or lack of specificity in inhibiting the aromatase enzyme without inhibiting other enzymes of steroidogenesis.20
Third-generation AIs that are commercially available in North America, Europe, and other parts of the world include:
- two nonsteroidal preparations: anastrozole (Arimidex) and letrozole (Femara)
- one steroidal agent: exemestane (Aromasin).
Letrozole and anastrozole are reversible, competitive agents with considerably greater potency (more than 1,000 times greater) than the first-generation AI aminoglutethimide. At a dosage of 1 to 5 mg/day, they reduce estrogen levels by 97% to more than 99%.
AIs are completely absorbed after oral administration, with a mean terminal half-life of approximately 45 hours (range: 30–60 hours). Exemestane has a shorter circulating half-life of approximately 9 hours, but may have a longer effect because it is irreversible.21
Mild gastrointestinal (GI) disturbances account for most of the adverse events, and rarely limit therapy.
How AIs work
Although we continue to accrue data on the use of AIs to induce ovulation, the underlying mechanism of action has not been studied. However, we believe that AIs work both centrally (at the level of the hypothalamus and pituitary) and peripherally (at the level of the ovaries).22-28
At the central level, AIs suppress estrogen production by directly, specifically, and potently inhibiting the aromatase enzyme (i.e., estrogen synthase, the enzyme responsible for the synthesis of estrogen). Because the aromatase enzyme is expressed in various tissues and organs—most notably, the ovaries, brain, and fat29—AIs suppress estrogen production in all of those tissues, leading to a low serum estrogen level and low local estrogen level. Low estrogen levels are thought to release the hypothalamus and pituitary gland from their negative-feedback mechanism, thereby increasing production of endogenous gonadotropins from the pituitary gland and stimulating ovarian follicular development and ovulation (FIGURE).
At the peripheral level, the aromatase enzyme catalyzes the terminal step in the steroidogenesis cascade that converts androgens into estrogen. When that enzyme is inhibited, enzyme substrate (androgens) is thought to accumulate. Contrary to the general belief that androgens are deleterious to ovarian follicles, studies in primates have demonstrated that androgens actually up-regulate the expression of gonadotropin receptors, particularly follicle-stimulating hormone (FSH) receptors.30 This renders the ovaries more sensitive to gonadotropin stimulation—whether the gonadotropins are endogenous or exogenous.22-28
FIGURE Aromatase inhibitors promote follicle development, then fade from the scene in time to prevent hyperovulation
Administration of an aromatase inhibitor (AI) on cycle days 3 to 7 suppresses ovarian estradiol (E2) secretion, as shown in A, which reduces estrogen-negative feedback at the hypothalamus and pituitary. As a result, follicle-stimulating hormone (FSH) secretion increases, fostering growth of multiple ovarian follicles. The growing follicles, shown in B, cause estrogen levels to rise again, depressing FSH, and leading to monofollicular ovulation in most cases.
Why AIs are superior to clomiphene
Clomiphene citrate is a selective estrogen receptor modulator (SERM) that is believed to induce ovulation through its antiestrogenic properties at the level of the hypothalamus or pituitary gland, or both. Clomiphene down-regulates estrogen receptors at this level, and the hypothalamus and pituitary gland react as though the estrogen level is very low. This reverses the suppression of endogenous gonadotropins by estrogen, and gonadotropin levels rise, stimulating ovarian follicular development.
The down-regulation of estrogen receptors with clomiphene administration is not limited to the hypothalamus and pituitary gland, but also occurs peripherally at the endometrium and cervix, where it is not so desirable. When the cervix is affected, it becomes an unfavorable environment for sperm to penetrate, and when the endometrium is affected, its hypoestrogenic status may reduce the likelihood of embryo implantation—or may increase the risk of pregnancy loss if implantation occurs.
These peripheral antiestrogenic prop erties of clomiphene citrate may account for the discrepancy between high ovulation and low pregnancy rates.22-28 Several strategies to overcome this problem—e.g., adding estrogen, starting clomiphene citrate earlier in the menstrual period, or using another SERM, such as tamoxifen—have been largely unsuccessful. With clomiphene citrate, depletion of estrogen receptors has long-term effects because of the drug’s relatively long half-life (several days).31
In contrast, AIs do not appear to affect the expression of estrogen receptors in different body tissues, such as the endometrium and cervix. AIs have a shorter half-life (8 hours to 2 days), and nonsteroidal third-generation agents have a reversible inhibitory effect on the aromatase enzyme. Moreover, the rise in endogenous gonadotropins stimulates the production of more aromatase enzyme. This newly formed aromatase enzyme, and the return of a normal aromatase level after a short half-life of AI, leads the maturing ovarian follicles to secrete estrogen, which reaches a physiologic level soon after the last administration of AI. The rising estrogen level allows development of a more hospitable uterine environment (endometrium and cervical mucus).22-28
Early evidence confirms efficacy of AIs
After our pioneering reports of successful ovulation induction3-9 and improved ovarian response to stimulation by gonadotropins5-7 using AIs in small, nonrandomized, controlled trials, several larger and better designed clinical trials followed and supported our findings.10-19
Clinical trials comparing AIs with clomiphene citrate have consistently reported a universal “trend” toward superiority of AIs in achieving pregnancy despite comparable levels of success in achieving ovulation.10,11,14,16-19 However, these published clinical trials lacked adequate sample size to definitively confirm the superiority of AIs in achieving clinical pregnancy. We believe AIs are superior because, in our experience, they have helped women achieve pregnancy even after failure of several cycles of clomiphene treatment.4,15
Should an AI follow a trial of clomiphene?
U.Y., the patient described at the opening of this article, has two main options now that she has completed six cycles of clomiphene citrate without conceiving. The usual strategy would be a shift to more sophisticated treatment using gonadotropin injection. However, exogenous gonadotropins have several disadvantages:
- the drugs must be injected (orally inactive)
- they are more expensive than clomiphene citrate and AIs
- they require close monitoring by an infertility specialist with expensive and sophisticated technology
- they carry a risk of severe ovarian hyperstimulation, which is unlikely with clomiphene citrate and unreported with AIs
- multiple pregnancy is likely, particularly in conjunction with intrauterine insemination
- the risk of ovarian hyperstimulation with gonadotropin injection is much higher in women with PCOS, such as U.Y., as is the likelihood of multiple pregnancy.
The reason U.Y. has not conceived after six cycles of clomiphene citrate is likely related to the drug’s antiestrogenic effects on the endometrium, which appeared to be very thin (4–6 mm) on US imaging around the day of ovulation. If she fails to conceive with AIs, she will probably not become pregnant after a switch to gonadotropin injection unless more advanced treatment is included, such as in vitro fertilization (IVF) and embryo transfer. Other causes of her infertility—besides ovulatory dysfunction—may explain the failure to conceive.
Comparable pregnancy rates have been observed for AIs and gonadotropin injection, although further study is needed—specifically, clinical trials comparing gonadotropin and AIs in conjunction with timed intercourse or intrauterine insemination, or both.
CASE 2 No response to clomiphene citrate
G.A., 28 years old, has been trying to conceive for 3 years. She reports having irregular menstrual periods indicative of anovulation, and body temperature charts and progesterone levels support that diagnosis. She undergoes three cycles of clomiphene citrate at dosages ranging from 50 to 150 mg/day for 5 days starting on day 3 of the menstrual cycle. Despite treatment, she fails to ovulate.
Would an AI increase her chance of ovulating and conceiving?
Failure to ovulate after treatment with clomiphene citrate may have any of several causes, including inappropriate patient selection and resistance to the drug.
An example of inappropriate patient selection would be a woman with hypothalamic/hypopituitary anovulation; this type of patient often has insufficient levels of endogenous gonadotropins (luteinizing hormone and FSH). Another example would be a woman with reduced ovarian reserve; this type of patient is often unresponsive to clomiphene citrate and may have substantially elevated gonadotropin levels, most notably high FSH on day 3 of the menstrual cycle.
AIs are unlikely to induce ovulation in either of these patients. For the first type of patient, exogenous gonadotropin injection would be appropriate, as would be a gonadotropin-releasing hormone (GnRH) pump. For a woman with reduced ovarian reserve, an oocyte donor and IVF are the best treatment option.
Success with an AI is unlikely when there is no appropriate indication for clomiphene citrate. For example, a woman with severe insulin resistance who fails to ovulate in response to clomiphene citrate is unlikely to ovulate in response to an AI. In that case, an insulin sensitizer—alone or in combination with clomiphene citrate or an AI—would be the appropriate option. Other measures to reduce insulin resistance, such as weight loss, exercise, and dietary modification, may also be helpful.
CASE 3 Ovulatory patient with endometriosis fails to conceive on clomiphene
R.C., 34 years old, has been trying to conceive for 2 years. Her basic infertility workup, which included a hysterosalpingogram and semen analysis, did not reveal any abnormalities. She has regular menstrual cycles suggestive of ovulation. In addition, luteal-phase progesterone levels and biphasic body temperature charts both indicate regular ovulation.
After six cycles of clomiphene citrate, her gynecologist performs diagnostic laparoscopy. Other than minimal, stage 1 endometriosis, confirmed by pathologic examination of peritoneal biopsies, there are no remarkable findings. Methylene blue tubal perfusion confirms patent fallopian tubes during the operation. The gynecologist fulgurates the minimal endometriotic implants using carbon dioxide laser. Two months after the procedure, the patient undergoes three more cycles of clomiphene citrate, without success.
Would an AI help her conceive?
Most of the data on successful treatment with clomiphene citrate come from anovulatory women with PCOS in whom anovulation is the main cause of infertility. Evidence is weaker when the patient is ovulatory and has unexplained or endometriosis-associated infertility.32
A recent nonrandomized, controlled study that included women with a medical history comparable to R.C.’s found treatment with clomiphene citrate to significantly reduce the chance of pregnancy, compared with timed intercourse without clomiphene or other forms of ovarian stimulation, following conservative laparoscopic surgery for their endometriosis.33 We believe that clomiphene citrate is in-appropriate in women with endometriosis-related infertility—and may activate underlying endometriotic lesions.
For R.C., treatment with an AI is a viable option, particularly in light of recent data showing that the aromatase enzyme is expressed in endometriotic lesions.34 An AI could also enhance conception by further suppressing endometriosis through its effects on circulating estrogen levels and local estrogen production. This is an unproven extrapolation that seems scientifically appropriate to us, but needs confirmation by randomized clinical trials.
CASE 4 Woman with unexplained—and uninvestigated—infertility
E.D., 31 years old, has been trying to conceive for 1 year. Neither she nor her husband has undergone any study of their infertility problem.
Would empiric treatment with an AI be appropriate?
No treatment should begin until the patient and her partner have undergone the basic workup (TABLE 3). If a specific cause of infertility is determined, the patient should be treated accordingly. If no explanation for the infertility can be found, or anovulation is the likely cause, empirical ovarian stimulation with timed intercourse or intrauterine insemination is reasonable, provided:
- semen analysis is within normal limits
- ovarian function is present—i.e., the patient is expected to ovulate in response to ovarian stimulation
- at least one tube is patent and functional
- uterus has no serious abnormalities.
If ovarian stimulation fails to trigger ovulation or pregnancy, consider the options listed in TABLE 4
TABLE 3
Basic infertility workup
|
|
|
|
|
TABLE 4
When ovarian stimulation fails, next step depends on several variables
| LEVEL OF FAILURE | CLOMIPHENE CITRATE | AROMATASE INHIBITORS |
|---|---|---|
| 1–No ovulation | Is indication appropriate? Neither clomiphene citrate nor AIs are appropriate for hypothalamic/hypopituitary anovulation or ovarian failure Is severe insulin resistance present? If so, consider insulin sensitizers and encourage exercise, dietary changes, and weight loss | |
| Other options: Change to AI or retry clomiphene citrate in conjunction with an insulin sensitizer. If treatment fails after 3 to 6 additional cycles, consider an injectable gonadotropin | Other options: Try adding an insulin sensitizer. If treatment fails after 3 to 6 additional cycles, consider an injectable gonadotropin | |
| 2–Ovulation but no pregnancy | Was another cause of infertility (besides ovulatory dysfunction) overlooked? Investigate further, if necessary Options: Consider AIs before injectable gonadotropins, especially when there is evidence, with clomiphene citrate, of a persistent antiestrogenic effect, such as thin endometrium around the time of ovulation; endometriosis; or unexplained infertility. Move to gonadotropins if AIs fail | |
Minimal adverse effects
AIs are generally well tolerated. The most common adverse effects are hot flushes, GI disturbances (nausea and vomiting), and leg cramps. In clinical trials involving postmenopausal women with breast cancer who were taking an AI, very few withdrew because of drug-related adverse effects.35 Those women took an AI on a daily basis over several months. Fewer adverse effects would be expected among usually healthy younger women administered a short course (a few days) for ovarian stimulation. In addition, our clinical experience has been that fewer women experience side effects such as mild hot flushes and symptoms similar to premenstrual syndrome when taking an AI, compared with clomiphene citrate.3-9
When any medication is given during pregnancy, there are concerns about its effects. Drugs used to induce ovulation are no exception. In fact, clomiphene citrate is classified as pregnancy category X—a fact frequently overlooked by treating physicians. As for AIs, recent studies found no evidence of teratogenicity or clastogenicity in animal embryos when anastrozole was given. The picture is murkier for letrozole.
When used for ovarian stimulation, the short half-life of AIs and administration in the early follicular phase (several days before ovulation and fertilization occur) should ensure clearance of the drugs before implantation. Nevertheless, it is important to confirm that the patient is not pregnant before an AI is given. We recommend a pregnancy test before administering an AI for ovulation induction.
Mixed bag of data on pregnancy outcomes
Three large studies recently reported on pregnancy outcomes after infertility treatment with AIs.9,36,37 The first was a cohort study comparing outcomes of 394 pregnancies achieved after treatment with letrozole (133 pregnancies) and other ovarian-stimulation agents, including clomiphene citrate (113 pregnancies) and gonadotropins (110 pregnancies), with a control group of 38 pregnancies achieved without ovarian stimulation.9 The study encompassed three tertiary referral centers over 2 years. Pregnancies conceived after treatment with an AI had rates of miscarriage and ectopic pregnancy comparable to all other groups. In addition, letrozole was associated with a significantly lower rate of multiple gestation than was clomiphene citrate.9
The second study, presented in abstract form, compared the outcome of 150 births after treatment with letrozole to a database of 36,050 normal deliveries.36 Although the authors themselves stated that there was no statistically significant difference in the overall incidence of congenital malformation, they reported a higher incidence of locomotor malformation and cardiac anomaly in the infants conceived after treatment with letrozole.36 They did not address this discrepancy or explain how locomotor malformation was assessed.
A closer look at the abstract reveals major methodological flaws that weaken the data and conclusions presented:
- The study was not well controlled. The treated patients (n=130) were infertile women, mainly suffering from PCOS and unexplained infertility, who had a mean age of 35.2 years. The control group included a database of spontaneously conceiving women who were significantly younger (mean age: 30.5 years). The control group also included deliveries in a low-risk hospital that refers out high-risk pregnancies to secondary and tertiary hospitals. These are important distinctions because women of advanced maternal age have an increased incidence of medical illnesses, making their pregnancies higher in risk.
- The incidence of multiple gestation was significantly higher among women treated for infertility than among women in the control group. It is well known that multiple gestations are at increased risk of fetal malformation compared with singleton pregnancies.
- The incidence of cardiac anomaly among women treated with letrozole did not differ significantly from the known incidence of cardiac malformation in the general population, but the authors concluded that the rate of cardiac malformation was significantly higher in the letrozole group than among controls. This is misleading because it was the control group that developed cardiac malformation at a significantly lower rate than in the general population. Such a low incidence of cardiac anomaly in a low-risk hospital setting is not surprising, because mothers would be transferred to a tertiary-care center once an anomaly was detected.
- Data on congenital malformation in the control group were collected from delivery records available in the maternity ward of the hospital. However, a significant percentage of congenital malformations, such as cardiac anomaly, are not detected until after the neonatal period.36
When using clomiphene citrate or an aromatase inhibitor (AI):
- avoid a dosage that exceeds 100 to 150 mg/day for clomiphene citrate or 2.5 to 5 mg/day for AIs or a treatment period longer than 5 days each cycle
- do not administer an AI beyond day 7 of the menstrual cycle
- stop after three to six cycles of treatment
- do not increase the dosage once ovulation occurs
- discontinue treatment when serious adverse effects are present, such as visual side effects.
It is also interesting that the results of this abstract have not been published in a peer-reviewed journal more than a year after its presentation.
The third study, which is more recent, compared the incidence of congenital malformation in 911 newborns conceived after treatment with letrozole (n=514) or clomiphene citrate (n=397).37 It found no statistically significant difference between the groups. Congenital malformation was diagnosed in 2.4% and 4.8% of the letrozole- and clomiphene-treated groups, respectively, and major malformation occurred in 1.2% and 3% of the letrozole- and clomiphene-treated groups, respectively. These differences were not statistically significant, but there was a sevenfold increase in overall cardiac anomalies in the clomiphene-treated group, compared with the letrozole-treated group—and this difference was statistically significant. These findings warrant further investigation into the use of clomiphene citrate for induction of ovulation.
Dr. Mitwally holds patents licensed to Serono for use of aromatase inhibitors for infertility treatment.
Dr. Casper has a licensing agreement with Ares-Serono for use of aromatase inhibitors in assisted reproduction.
CASE 1 Ovulation begins, but pregnancy does not follow
U.Y. is a 32-year-old woman who has been trying to conceive for 3 years. Her infertility is caused by anovulation associated with polycystic ovary syndrome (PCOS). All other variables are within physiologic limits—she has patent tubes and an unremarkable uterus, and her partner has a normal semen analysis.
She has undergone six cycles of treatment with clomiphene citrate, with ovulation documented each time by ultrasonography (US) and measurement of luteal-phase progesterone levels. Her endometrial thickness is 4 to 6 mm around the day of ovulation.
Would an aromatase inhibitor increase her chances of conceiving?
This patient is an excellent candidate for ovulation induction using an aromatase inhibitor (AI).
The primary reason? She is unlikely to benefit from an increased dosage of clomiphene citrate because the dosage that triggers ovulation is believed to be most appropriate—an increase above that level is not expected to improve the chance of pregnancy. Moreover, conception is less likely after more than six cycles of clomiphene citrate.1,2
In this article, we describe the induction of ovulation using AIs—a relatively new, and off-label, application (TABLES 1 and 2). The strategies presented here are suitable for general ObGyns and do not require sophisticated technology such as rapid hormonal assays or transvaginal US.
Because this application is so new, with limited data published so far, much of the information presented here is based on our personal experience rather than level-1 evidence, which is sorely needed.
Of course, induction of ovulation is appropriate only after other specific causes of anovulation or ovulatory dysfunction are excluded, such as thyroid disorders, hyperprolactinemia, severe insulin resistance, and ovarian failure.
Concerns about teratogenicity of AIs appear to be largely unfounded (see below).
TABLE 1
Aromatase inhibitors work best in these applications
| APPLICATION | EVIDENCE |
|---|---|
Induction of ovulation, particularly in women with polycystic ovary syndrome:
See case 1 and case 2 |
|
| Ovarian stimulation (superovulation) in ovulatory women with unexplained or endometriosis-related infertility See case 3 | Strong evidence from several clinical trials |
| Use in conjunction with controlled ovarian hyperstimulation by gonadotropins with intrauterine insemination and assisted reproduction | Accumulating evidence of several advantages when used with gonadotropins:
|
TABLE 2
Avoid AIs in these situations
| SITUATION | JUSTIFICATION |
|---|---|
| When clomiphene citrate fails to induce ovulation in a woman with insulin resistance See case 2 | First try insulin sensitizers and other measures to improve insulin action (weight loss, exercise, and dietary modifications) |
| When other causes of infertility (besides ovulatory dysfunction) are likely | Pregnancy is unlikely |
| When the patient has hypothalamic/hypopituitary anovulation or ovarian failure | Ovarian stimulation is dependent on capacity to produce endogenous gonadotropins and presence of responding ovarian follicles |
Ovulation is good, but pregnancy is better
In women undergoing induction of ovulation, there are two levels of success: ovulation and pregnancy.
Clearly, the presence of other, nonovulatory infertility factors—e.g., male infertility and tubal-uterine problems—can prevent successful ovulation induction from translating into pregnancy.
We have reported3-9 on the successful use of AIs to stimulate the ovary and achieve pregnancy—even in women who fail to conceive after several treatment trials with clomiphene citrate.4
Other authors have conducted further investigations that have confirmed our findings and have recommended use of these agents for other aspects of infertility treatment, such as assisted reproduction.10-19
Latest generation of AIs is more benign
Many AIs have been developed over the past 30 years. The most recent are third-generation agents that were approved mainly to suppress estrogen production in postmenopausal women with breast cancer. Clinical failure of earlier generations of AIs for their approved indication was mainly due to significant adverse effects, lack of satisfactory potency, or lack of specificity in inhibiting the aromatase enzyme without inhibiting other enzymes of steroidogenesis.20
Third-generation AIs that are commercially available in North America, Europe, and other parts of the world include:
- two nonsteroidal preparations: anastrozole (Arimidex) and letrozole (Femara)
- one steroidal agent: exemestane (Aromasin).
Letrozole and anastrozole are reversible, competitive agents with considerably greater potency (more than 1,000 times greater) than the first-generation AI aminoglutethimide. At a dosage of 1 to 5 mg/day, they reduce estrogen levels by 97% to more than 99%.
AIs are completely absorbed after oral administration, with a mean terminal half-life of approximately 45 hours (range: 30–60 hours). Exemestane has a shorter circulating half-life of approximately 9 hours, but may have a longer effect because it is irreversible.21
Mild gastrointestinal (GI) disturbances account for most of the adverse events, and rarely limit therapy.
How AIs work
Although we continue to accrue data on the use of AIs to induce ovulation, the underlying mechanism of action has not been studied. However, we believe that AIs work both centrally (at the level of the hypothalamus and pituitary) and peripherally (at the level of the ovaries).22-28
At the central level, AIs suppress estrogen production by directly, specifically, and potently inhibiting the aromatase enzyme (i.e., estrogen synthase, the enzyme responsible for the synthesis of estrogen). Because the aromatase enzyme is expressed in various tissues and organs—most notably, the ovaries, brain, and fat29—AIs suppress estrogen production in all of those tissues, leading to a low serum estrogen level and low local estrogen level. Low estrogen levels are thought to release the hypothalamus and pituitary gland from their negative-feedback mechanism, thereby increasing production of endogenous gonadotropins from the pituitary gland and stimulating ovarian follicular development and ovulation (FIGURE).
At the peripheral level, the aromatase enzyme catalyzes the terminal step in the steroidogenesis cascade that converts androgens into estrogen. When that enzyme is inhibited, enzyme substrate (androgens) is thought to accumulate. Contrary to the general belief that androgens are deleterious to ovarian follicles, studies in primates have demonstrated that androgens actually up-regulate the expression of gonadotropin receptors, particularly follicle-stimulating hormone (FSH) receptors.30 This renders the ovaries more sensitive to gonadotropin stimulation—whether the gonadotropins are endogenous or exogenous.22-28
FIGURE Aromatase inhibitors promote follicle development, then fade from the scene in time to prevent hyperovulation
Administration of an aromatase inhibitor (AI) on cycle days 3 to 7 suppresses ovarian estradiol (E2) secretion, as shown in A, which reduces estrogen-negative feedback at the hypothalamus and pituitary. As a result, follicle-stimulating hormone (FSH) secretion increases, fostering growth of multiple ovarian follicles. The growing follicles, shown in B, cause estrogen levels to rise again, depressing FSH, and leading to monofollicular ovulation in most cases.
Why AIs are superior to clomiphene
Clomiphene citrate is a selective estrogen receptor modulator (SERM) that is believed to induce ovulation through its antiestrogenic properties at the level of the hypothalamus or pituitary gland, or both. Clomiphene down-regulates estrogen receptors at this level, and the hypothalamus and pituitary gland react as though the estrogen level is very low. This reverses the suppression of endogenous gonadotropins by estrogen, and gonadotropin levels rise, stimulating ovarian follicular development.
The down-regulation of estrogen receptors with clomiphene administration is not limited to the hypothalamus and pituitary gland, but also occurs peripherally at the endometrium and cervix, where it is not so desirable. When the cervix is affected, it becomes an unfavorable environment for sperm to penetrate, and when the endometrium is affected, its hypoestrogenic status may reduce the likelihood of embryo implantation—or may increase the risk of pregnancy loss if implantation occurs.
These peripheral antiestrogenic prop erties of clomiphene citrate may account for the discrepancy between high ovulation and low pregnancy rates.22-28 Several strategies to overcome this problem—e.g., adding estrogen, starting clomiphene citrate earlier in the menstrual period, or using another SERM, such as tamoxifen—have been largely unsuccessful. With clomiphene citrate, depletion of estrogen receptors has long-term effects because of the drug’s relatively long half-life (several days).31
In contrast, AIs do not appear to affect the expression of estrogen receptors in different body tissues, such as the endometrium and cervix. AIs have a shorter half-life (8 hours to 2 days), and nonsteroidal third-generation agents have a reversible inhibitory effect on the aromatase enzyme. Moreover, the rise in endogenous gonadotropins stimulates the production of more aromatase enzyme. This newly formed aromatase enzyme, and the return of a normal aromatase level after a short half-life of AI, leads the maturing ovarian follicles to secrete estrogen, which reaches a physiologic level soon after the last administration of AI. The rising estrogen level allows development of a more hospitable uterine environment (endometrium and cervical mucus).22-28
Early evidence confirms efficacy of AIs
After our pioneering reports of successful ovulation induction3-9 and improved ovarian response to stimulation by gonadotropins5-7 using AIs in small, nonrandomized, controlled trials, several larger and better designed clinical trials followed and supported our findings.10-19
Clinical trials comparing AIs with clomiphene citrate have consistently reported a universal “trend” toward superiority of AIs in achieving pregnancy despite comparable levels of success in achieving ovulation.10,11,14,16-19 However, these published clinical trials lacked adequate sample size to definitively confirm the superiority of AIs in achieving clinical pregnancy. We believe AIs are superior because, in our experience, they have helped women achieve pregnancy even after failure of several cycles of clomiphene treatment.4,15
Should an AI follow a trial of clomiphene?
U.Y., the patient described at the opening of this article, has two main options now that she has completed six cycles of clomiphene citrate without conceiving. The usual strategy would be a shift to more sophisticated treatment using gonadotropin injection. However, exogenous gonadotropins have several disadvantages:
- the drugs must be injected (orally inactive)
- they are more expensive than clomiphene citrate and AIs
- they require close monitoring by an infertility specialist with expensive and sophisticated technology
- they carry a risk of severe ovarian hyperstimulation, which is unlikely with clomiphene citrate and unreported with AIs
- multiple pregnancy is likely, particularly in conjunction with intrauterine insemination
- the risk of ovarian hyperstimulation with gonadotropin injection is much higher in women with PCOS, such as U.Y., as is the likelihood of multiple pregnancy.
The reason U.Y. has not conceived after six cycles of clomiphene citrate is likely related to the drug’s antiestrogenic effects on the endometrium, which appeared to be very thin (4–6 mm) on US imaging around the day of ovulation. If she fails to conceive with AIs, she will probably not become pregnant after a switch to gonadotropin injection unless more advanced treatment is included, such as in vitro fertilization (IVF) and embryo transfer. Other causes of her infertility—besides ovulatory dysfunction—may explain the failure to conceive.
Comparable pregnancy rates have been observed for AIs and gonadotropin injection, although further study is needed—specifically, clinical trials comparing gonadotropin and AIs in conjunction with timed intercourse or intrauterine insemination, or both.
CASE 2 No response to clomiphene citrate
G.A., 28 years old, has been trying to conceive for 3 years. She reports having irregular menstrual periods indicative of anovulation, and body temperature charts and progesterone levels support that diagnosis. She undergoes three cycles of clomiphene citrate at dosages ranging from 50 to 150 mg/day for 5 days starting on day 3 of the menstrual cycle. Despite treatment, she fails to ovulate.
Would an AI increase her chance of ovulating and conceiving?
Failure to ovulate after treatment with clomiphene citrate may have any of several causes, including inappropriate patient selection and resistance to the drug.
An example of inappropriate patient selection would be a woman with hypothalamic/hypopituitary anovulation; this type of patient often has insufficient levels of endogenous gonadotropins (luteinizing hormone and FSH). Another example would be a woman with reduced ovarian reserve; this type of patient is often unresponsive to clomiphene citrate and may have substantially elevated gonadotropin levels, most notably high FSH on day 3 of the menstrual cycle.
AIs are unlikely to induce ovulation in either of these patients. For the first type of patient, exogenous gonadotropin injection would be appropriate, as would be a gonadotropin-releasing hormone (GnRH) pump. For a woman with reduced ovarian reserve, an oocyte donor and IVF are the best treatment option.
Success with an AI is unlikely when there is no appropriate indication for clomiphene citrate. For example, a woman with severe insulin resistance who fails to ovulate in response to clomiphene citrate is unlikely to ovulate in response to an AI. In that case, an insulin sensitizer—alone or in combination with clomiphene citrate or an AI—would be the appropriate option. Other measures to reduce insulin resistance, such as weight loss, exercise, and dietary modification, may also be helpful.
CASE 3 Ovulatory patient with endometriosis fails to conceive on clomiphene
R.C., 34 years old, has been trying to conceive for 2 years. Her basic infertility workup, which included a hysterosalpingogram and semen analysis, did not reveal any abnormalities. She has regular menstrual cycles suggestive of ovulation. In addition, luteal-phase progesterone levels and biphasic body temperature charts both indicate regular ovulation.
After six cycles of clomiphene citrate, her gynecologist performs diagnostic laparoscopy. Other than minimal, stage 1 endometriosis, confirmed by pathologic examination of peritoneal biopsies, there are no remarkable findings. Methylene blue tubal perfusion confirms patent fallopian tubes during the operation. The gynecologist fulgurates the minimal endometriotic implants using carbon dioxide laser. Two months after the procedure, the patient undergoes three more cycles of clomiphene citrate, without success.
Would an AI help her conceive?
Most of the data on successful treatment with clomiphene citrate come from anovulatory women with PCOS in whom anovulation is the main cause of infertility. Evidence is weaker when the patient is ovulatory and has unexplained or endometriosis-associated infertility.32
A recent nonrandomized, controlled study that included women with a medical history comparable to R.C.’s found treatment with clomiphene citrate to significantly reduce the chance of pregnancy, compared with timed intercourse without clomiphene or other forms of ovarian stimulation, following conservative laparoscopic surgery for their endometriosis.33 We believe that clomiphene citrate is in-appropriate in women with endometriosis-related infertility—and may activate underlying endometriotic lesions.
For R.C., treatment with an AI is a viable option, particularly in light of recent data showing that the aromatase enzyme is expressed in endometriotic lesions.34 An AI could also enhance conception by further suppressing endometriosis through its effects on circulating estrogen levels and local estrogen production. This is an unproven extrapolation that seems scientifically appropriate to us, but needs confirmation by randomized clinical trials.
CASE 4 Woman with unexplained—and uninvestigated—infertility
E.D., 31 years old, has been trying to conceive for 1 year. Neither she nor her husband has undergone any study of their infertility problem.
Would empiric treatment with an AI be appropriate?
No treatment should begin until the patient and her partner have undergone the basic workup (TABLE 3). If a specific cause of infertility is determined, the patient should be treated accordingly. If no explanation for the infertility can be found, or anovulation is the likely cause, empirical ovarian stimulation with timed intercourse or intrauterine insemination is reasonable, provided:
- semen analysis is within normal limits
- ovarian function is present—i.e., the patient is expected to ovulate in response to ovarian stimulation
- at least one tube is patent and functional
- uterus has no serious abnormalities.
If ovarian stimulation fails to trigger ovulation or pregnancy, consider the options listed in TABLE 4
TABLE 3
Basic infertility workup
|
|
|
|
|
TABLE 4
When ovarian stimulation fails, next step depends on several variables
| LEVEL OF FAILURE | CLOMIPHENE CITRATE | AROMATASE INHIBITORS |
|---|---|---|
| 1–No ovulation | Is indication appropriate? Neither clomiphene citrate nor AIs are appropriate for hypothalamic/hypopituitary anovulation or ovarian failure Is severe insulin resistance present? If so, consider insulin sensitizers and encourage exercise, dietary changes, and weight loss | |
| Other options: Change to AI or retry clomiphene citrate in conjunction with an insulin sensitizer. If treatment fails after 3 to 6 additional cycles, consider an injectable gonadotropin | Other options: Try adding an insulin sensitizer. If treatment fails after 3 to 6 additional cycles, consider an injectable gonadotropin | |
| 2–Ovulation but no pregnancy | Was another cause of infertility (besides ovulatory dysfunction) overlooked? Investigate further, if necessary Options: Consider AIs before injectable gonadotropins, especially when there is evidence, with clomiphene citrate, of a persistent antiestrogenic effect, such as thin endometrium around the time of ovulation; endometriosis; or unexplained infertility. Move to gonadotropins if AIs fail | |
Minimal adverse effects
AIs are generally well tolerated. The most common adverse effects are hot flushes, GI disturbances (nausea and vomiting), and leg cramps. In clinical trials involving postmenopausal women with breast cancer who were taking an AI, very few withdrew because of drug-related adverse effects.35 Those women took an AI on a daily basis over several months. Fewer adverse effects would be expected among usually healthy younger women administered a short course (a few days) for ovarian stimulation. In addition, our clinical experience has been that fewer women experience side effects such as mild hot flushes and symptoms similar to premenstrual syndrome when taking an AI, compared with clomiphene citrate.3-9
When any medication is given during pregnancy, there are concerns about its effects. Drugs used to induce ovulation are no exception. In fact, clomiphene citrate is classified as pregnancy category X—a fact frequently overlooked by treating physicians. As for AIs, recent studies found no evidence of teratogenicity or clastogenicity in animal embryos when anastrozole was given. The picture is murkier for letrozole.
When used for ovarian stimulation, the short half-life of AIs and administration in the early follicular phase (several days before ovulation and fertilization occur) should ensure clearance of the drugs before implantation. Nevertheless, it is important to confirm that the patient is not pregnant before an AI is given. We recommend a pregnancy test before administering an AI for ovulation induction.
Mixed bag of data on pregnancy outcomes
Three large studies recently reported on pregnancy outcomes after infertility treatment with AIs.9,36,37 The first was a cohort study comparing outcomes of 394 pregnancies achieved after treatment with letrozole (133 pregnancies) and other ovarian-stimulation agents, including clomiphene citrate (113 pregnancies) and gonadotropins (110 pregnancies), with a control group of 38 pregnancies achieved without ovarian stimulation.9 The study encompassed three tertiary referral centers over 2 years. Pregnancies conceived after treatment with an AI had rates of miscarriage and ectopic pregnancy comparable to all other groups. In addition, letrozole was associated with a significantly lower rate of multiple gestation than was clomiphene citrate.9
The second study, presented in abstract form, compared the outcome of 150 births after treatment with letrozole to a database of 36,050 normal deliveries.36 Although the authors themselves stated that there was no statistically significant difference in the overall incidence of congenital malformation, they reported a higher incidence of locomotor malformation and cardiac anomaly in the infants conceived after treatment with letrozole.36 They did not address this discrepancy or explain how locomotor malformation was assessed.
A closer look at the abstract reveals major methodological flaws that weaken the data and conclusions presented:
- The study was not well controlled. The treated patients (n=130) were infertile women, mainly suffering from PCOS and unexplained infertility, who had a mean age of 35.2 years. The control group included a database of spontaneously conceiving women who were significantly younger (mean age: 30.5 years). The control group also included deliveries in a low-risk hospital that refers out high-risk pregnancies to secondary and tertiary hospitals. These are important distinctions because women of advanced maternal age have an increased incidence of medical illnesses, making their pregnancies higher in risk.
- The incidence of multiple gestation was significantly higher among women treated for infertility than among women in the control group. It is well known that multiple gestations are at increased risk of fetal malformation compared with singleton pregnancies.
- The incidence of cardiac anomaly among women treated with letrozole did not differ significantly from the known incidence of cardiac malformation in the general population, but the authors concluded that the rate of cardiac malformation was significantly higher in the letrozole group than among controls. This is misleading because it was the control group that developed cardiac malformation at a significantly lower rate than in the general population. Such a low incidence of cardiac anomaly in a low-risk hospital setting is not surprising, because mothers would be transferred to a tertiary-care center once an anomaly was detected.
- Data on congenital malformation in the control group were collected from delivery records available in the maternity ward of the hospital. However, a significant percentage of congenital malformations, such as cardiac anomaly, are not detected until after the neonatal period.36
When using clomiphene citrate or an aromatase inhibitor (AI):
- avoid a dosage that exceeds 100 to 150 mg/day for clomiphene citrate or 2.5 to 5 mg/day for AIs or a treatment period longer than 5 days each cycle
- do not administer an AI beyond day 7 of the menstrual cycle
- stop after three to six cycles of treatment
- do not increase the dosage once ovulation occurs
- discontinue treatment when serious adverse effects are present, such as visual side effects.
It is also interesting that the results of this abstract have not been published in a peer-reviewed journal more than a year after its presentation.
The third study, which is more recent, compared the incidence of congenital malformation in 911 newborns conceived after treatment with letrozole (n=514) or clomiphene citrate (n=397).37 It found no statistically significant difference between the groups. Congenital malformation was diagnosed in 2.4% and 4.8% of the letrozole- and clomiphene-treated groups, respectively, and major malformation occurred in 1.2% and 3% of the letrozole- and clomiphene-treated groups, respectively. These differences were not statistically significant, but there was a sevenfold increase in overall cardiac anomalies in the clomiphene-treated group, compared with the letrozole-treated group—and this difference was statistically significant. These findings warrant further investigation into the use of clomiphene citrate for induction of ovulation.
1. Dickey RP, Taylor SN, Lu PY, Sartor BM, Rye PH, Pyrzak R. Effect of diagnosis, age, sperm quality, and number of preovulatory follicles on the outcome of multiple cycles of clomiphene citrate-intrauterine insemination. Fertil Steril. 2002;78:1088-1095.
2. Imani B, Eijkemans MJ, te Velde ER, Habbema JD, Fauser BC. Predictors of chances to conceive in ovulatory patients during clomiphene citrate induction of ovulation in normogonadotropic oligomenorrheic infertility. J Clin Endocrinol Metab. 1999;84:1617-1622.
3. Mitwally MFM, Casper RF. Aromatase inhibition: a novel method of ovulation induction in women with polycystic ovarian syndrome. Reprod Technol. 2000;10:244-247.
4. Mitwally MFM, Casper RF. Use of an AI for induction of ovulation in patients with an inadequate response to clomiphene citrate. Fertil Steril. 2001;75:305-309.
5. Mitwally MFM, Casper RF. Aromatase inhibition improves ovarian response to follicle-stimulating hormone in poor responders. Fertil Steril. 2002;77:776-780.
6. Mitwally MF, Casper RF. Aromatase inhibition reduces gonadotropin dose required for controlled ovarian stimulation in women with unexplained infertility. Hum Reprod. 2003;188:1588-1597.
7. Mitwally MF, Casper RF. Aromatase inhibition reduces the dose of gonadotropin required for controlled ovarian hyperstimulation. J Soc Gynecol Investig. 2004;11:406-415.
8. Mitwally MFM, Casper RF. Single dose administration of the aromatase inhibitor, letrozole: a simple and convenient effective method of ovulation induction. Fertil Steril. 2005;83:229-231.
9. Mitwally MFM, Casper RF. Pregnancy outcome after the use of an AI for induction of ovulation. Am J Obstet Gynecol. 2005;192:381-386.
10. Fatemi HM, Kolibianakis E, Tournaye H, et al. Clomiphene citrate versus letrozole for ovarian stimulation: a pilot study. Reprod Biomed Online. 2003;75:543-546.
11. Al-Fozan H, Al-Khadouri M, Tan SL, Tulandi T. A randomized trial of letrozole versus clomiphene citrate in women undergoing superovulation. Fertil Steril. 2004;82:1561-1563.
12. Goswami SK, Das T, Chattopadhyay R, et al. A randomized single-blind controlled trial of letrozole as a low-cost IVF protocol in women with poor ovarian response: a preliminary report. Hum Reprod. 2004;19:2031-2035.
13. Garcia-Velasco JA, Moreno L, Pacheco A, et al. The aromatase inhibitor letrozole increases the concentration of intraovarian androgens and improves in vitro fertilization outcome in low responder patients: a pilot study. Fertil Steril. 2005;84:82-87.
14. Bayar U, Tanrierdi HA, Barut A, et al. Letrozole vs. clomiphene citrate in patients with ovulatory infertility. Fertil Steril. 2006;85:1045-1048.
15. Elnashar A, Fouad H, Eldosoky M, et al. Letrozole induction of ovulation in women with clomiphene citrate-resistant polycystic ovary syndrome may not depend on the period of infertility, the body mass index, or the luteinizing hormone/follicle stimulating hormone ratio. Fertil Steril. 2006;85:161-164.
16. Atay V, Cam C, Muhcu M, et al. Comparison of letrozole and clomiphene citrate in women with polycystic ovaries undergoing ovarian stimulation. J Int Med Res. 2006;34:73-76.
17. Sohrabvand F, Ansari S, Bagheri M. Efficacy of combined metformin-letrozole in comparison with metformin-clomiphene citrate in clomiphene-resistant infertile women with polycystic ovarian disease. Hum Reprod. 2006;21:1432-1435.
18. Sipe CS, Davis WA, Maifeld M, Van Voorhis BJ. A prospective randomized trial comparing anastrozole and clomiphene citrate in an ovulation induction protocol using gonadotropins. Fertil Steril. 2006;86:1676-1681.
19. Bayar U, Basaran M, Kiran S, Coskun A, Gezer S. Use of an aromatase inhibitor in patients with polycystic ovary syndrome: a prospective randomized trial. Fertil Steril. 2006;86:1447-1451.
20. Buzdar A, Howell A. Advances in aromatase inhibition: clinical efficacy and tolerability in the treatment of breast cancer. Clin Cancer Res. 2001;7:2620-2635.
21. Winer EP, Hudis C, Burstein HJ, et al. American Society of Clinical Oncology Technology Assessment on the use of aromatase inhibitors as adjuvant therapy for women with hormone receptor-positive breast cancer: status report 2002. J Clin Oncol. 2002;2015:3317-3327.
22. Mitwally MF, Casper RF. Potential of aromatase inhibitors for ovulation and superovulation induction in infertile women. Drugs. 2006;66:2149-2160.
23. Mitwally MFM, Casper RF. Letrozole for ovulation induction. Exp Rev Obstet Gynecol. 2006;1:15-27.
24. Casper RF, Mitwally MF. Review: aromatase inhibitors for ovulation induction. J Clin Endocrinol Metab. 2006;91:760-771.
25. Mitwally MF, Casper RF, Diamond MP. The role of aromatase inhibitors in ameliorating deleterious effects of ovarian stimulation on outcome of infertility treatment. Reprod Biol Endocrinol. 2005;3:54.-
26. Mitwally MF, Casper RF. Aromatase inhibitors in ovulation induction. Semin Reprod Med. 2004;22:61-78.
27. Mitwally MF, Casper RF. Aromatase inhibitors for the treatment of infertility. Expert Opin Investig Drugs. 2003;12:353-371.
28. Mitwally MF, Casper RF. Aromatase inhibition for ovarian stimulation: future avenues for infertility management. Curr Opin Obstet Gynecol. 2002;14:255-263.
29. Cole PA, Robinson CH. Mechanism and inhibition of cytochrome P-450 aromatase. J Med Chem. 1990;33:2933-2944.
30. Weil S, Vendola K, Zhou J, Bondy CA. Androgen and follicle-stimulating hormone interactions in primate ovarian follicle development. J Clin Endocrinol Metab. 1999;848:2951-2956.
31. Mikkelson TJ, Kroboth PD, Cameron WJ. Single dose pharmacokinetics of clomiphene citrate in normal volunteers. Fertil Steril. 1986;46:392-396.
32. Hughes E, Collins J, Vandekerckhove P. Clomiphene citrate for unexplained subfertility in women. Cochrane Database Syst Rev. 2000;(2):CD000057.-
33. Mitwally MF, Albuarki H, Ashraf M, Diamond MP, Abuzeid M. Clomiphene reduces chance of pregnancy in infertile women with endometriosis following laparoscopic surgery. J Soc Gynecol Investig. 2006;13(2) (suppl):abstract 646.-
34. Attar E, Bulun SE. Aromatase and other steroidogenic genes in endometriosis: translational aspects. Hum Reprod Update. 2006;12:49-56.
35. Goss PE. Risks versus benefits in the clinical application of aromatase inhibitors. Endocr Relat Cancer. 1999;6:325-332.
36. Biljan MM, Hemmings R, Brassard N. The outcome of 150 babies following the treatment with letrozole or letrozole and gonadotropins [abstract no. 1033]. Fertil Steril. 2005;84 (suppl):abstract 1033.-
37. Tulandi T, Martin J, Al-Fadhli R, et al. Congenital malformations among 911 newborns conceived after infertility treatment with letrozole or clomiphene citrate. Fertil Steril. 2006;85:1761-1765.
1. Dickey RP, Taylor SN, Lu PY, Sartor BM, Rye PH, Pyrzak R. Effect of diagnosis, age, sperm quality, and number of preovulatory follicles on the outcome of multiple cycles of clomiphene citrate-intrauterine insemination. Fertil Steril. 2002;78:1088-1095.
2. Imani B, Eijkemans MJ, te Velde ER, Habbema JD, Fauser BC. Predictors of chances to conceive in ovulatory patients during clomiphene citrate induction of ovulation in normogonadotropic oligomenorrheic infertility. J Clin Endocrinol Metab. 1999;84:1617-1622.
3. Mitwally MFM, Casper RF. Aromatase inhibition: a novel method of ovulation induction in women with polycystic ovarian syndrome. Reprod Technol. 2000;10:244-247.
4. Mitwally MFM, Casper RF. Use of an AI for induction of ovulation in patients with an inadequate response to clomiphene citrate. Fertil Steril. 2001;75:305-309.
5. Mitwally MFM, Casper RF. Aromatase inhibition improves ovarian response to follicle-stimulating hormone in poor responders. Fertil Steril. 2002;77:776-780.
6. Mitwally MF, Casper RF. Aromatase inhibition reduces gonadotropin dose required for controlled ovarian stimulation in women with unexplained infertility. Hum Reprod. 2003;188:1588-1597.
7. Mitwally MF, Casper RF. Aromatase inhibition reduces the dose of gonadotropin required for controlled ovarian hyperstimulation. J Soc Gynecol Investig. 2004;11:406-415.
8. Mitwally MFM, Casper RF. Single dose administration of the aromatase inhibitor, letrozole: a simple and convenient effective method of ovulation induction. Fertil Steril. 2005;83:229-231.
9. Mitwally MFM, Casper RF. Pregnancy outcome after the use of an AI for induction of ovulation. Am J Obstet Gynecol. 2005;192:381-386.
10. Fatemi HM, Kolibianakis E, Tournaye H, et al. Clomiphene citrate versus letrozole for ovarian stimulation: a pilot study. Reprod Biomed Online. 2003;75:543-546.
11. Al-Fozan H, Al-Khadouri M, Tan SL, Tulandi T. A randomized trial of letrozole versus clomiphene citrate in women undergoing superovulation. Fertil Steril. 2004;82:1561-1563.
12. Goswami SK, Das T, Chattopadhyay R, et al. A randomized single-blind controlled trial of letrozole as a low-cost IVF protocol in women with poor ovarian response: a preliminary report. Hum Reprod. 2004;19:2031-2035.
13. Garcia-Velasco JA, Moreno L, Pacheco A, et al. The aromatase inhibitor letrozole increases the concentration of intraovarian androgens and improves in vitro fertilization outcome in low responder patients: a pilot study. Fertil Steril. 2005;84:82-87.
14. Bayar U, Tanrierdi HA, Barut A, et al. Letrozole vs. clomiphene citrate in patients with ovulatory infertility. Fertil Steril. 2006;85:1045-1048.
15. Elnashar A, Fouad H, Eldosoky M, et al. Letrozole induction of ovulation in women with clomiphene citrate-resistant polycystic ovary syndrome may not depend on the period of infertility, the body mass index, or the luteinizing hormone/follicle stimulating hormone ratio. Fertil Steril. 2006;85:161-164.
16. Atay V, Cam C, Muhcu M, et al. Comparison of letrozole and clomiphene citrate in women with polycystic ovaries undergoing ovarian stimulation. J Int Med Res. 2006;34:73-76.
17. Sohrabvand F, Ansari S, Bagheri M. Efficacy of combined metformin-letrozole in comparison with metformin-clomiphene citrate in clomiphene-resistant infertile women with polycystic ovarian disease. Hum Reprod. 2006;21:1432-1435.
18. Sipe CS, Davis WA, Maifeld M, Van Voorhis BJ. A prospective randomized trial comparing anastrozole and clomiphene citrate in an ovulation induction protocol using gonadotropins. Fertil Steril. 2006;86:1676-1681.
19. Bayar U, Basaran M, Kiran S, Coskun A, Gezer S. Use of an aromatase inhibitor in patients with polycystic ovary syndrome: a prospective randomized trial. Fertil Steril. 2006;86:1447-1451.
20. Buzdar A, Howell A. Advances in aromatase inhibition: clinical efficacy and tolerability in the treatment of breast cancer. Clin Cancer Res. 2001;7:2620-2635.
21. Winer EP, Hudis C, Burstein HJ, et al. American Society of Clinical Oncology Technology Assessment on the use of aromatase inhibitors as adjuvant therapy for women with hormone receptor-positive breast cancer: status report 2002. J Clin Oncol. 2002;2015:3317-3327.
22. Mitwally MF, Casper RF. Potential of aromatase inhibitors for ovulation and superovulation induction in infertile women. Drugs. 2006;66:2149-2160.
23. Mitwally MFM, Casper RF. Letrozole for ovulation induction. Exp Rev Obstet Gynecol. 2006;1:15-27.
24. Casper RF, Mitwally MF. Review: aromatase inhibitors for ovulation induction. J Clin Endocrinol Metab. 2006;91:760-771.
25. Mitwally MF, Casper RF, Diamond MP. The role of aromatase inhibitors in ameliorating deleterious effects of ovarian stimulation on outcome of infertility treatment. Reprod Biol Endocrinol. 2005;3:54.-
26. Mitwally MF, Casper RF. Aromatase inhibitors in ovulation induction. Semin Reprod Med. 2004;22:61-78.
27. Mitwally MF, Casper RF. Aromatase inhibitors for the treatment of infertility. Expert Opin Investig Drugs. 2003;12:353-371.
28. Mitwally MF, Casper RF. Aromatase inhibition for ovarian stimulation: future avenues for infertility management. Curr Opin Obstet Gynecol. 2002;14:255-263.
29. Cole PA, Robinson CH. Mechanism and inhibition of cytochrome P-450 aromatase. J Med Chem. 1990;33:2933-2944.
30. Weil S, Vendola K, Zhou J, Bondy CA. Androgen and follicle-stimulating hormone interactions in primate ovarian follicle development. J Clin Endocrinol Metab. 1999;848:2951-2956.
31. Mikkelson TJ, Kroboth PD, Cameron WJ. Single dose pharmacokinetics of clomiphene citrate in normal volunteers. Fertil Steril. 1986;46:392-396.
32. Hughes E, Collins J, Vandekerckhove P. Clomiphene citrate for unexplained subfertility in women. Cochrane Database Syst Rev. 2000;(2):CD000057.-
33. Mitwally MF, Albuarki H, Ashraf M, Diamond MP, Abuzeid M. Clomiphene reduces chance of pregnancy in infertile women with endometriosis following laparoscopic surgery. J Soc Gynecol Investig. 2006;13(2) (suppl):abstract 646.-
34. Attar E, Bulun SE. Aromatase and other steroidogenic genes in endometriosis: translational aspects. Hum Reprod Update. 2006;12:49-56.
35. Goss PE. Risks versus benefits in the clinical application of aromatase inhibitors. Endocr Relat Cancer. 1999;6:325-332.
36. Biljan MM, Hemmings R, Brassard N. The outcome of 150 babies following the treatment with letrozole or letrozole and gonadotropins [abstract no. 1033]. Fertil Steril. 2005;84 (suppl):abstract 1033.-
37. Tulandi T, Martin J, Al-Fadhli R, et al. Congenital malformations among 911 newborns conceived after infertility treatment with letrozole or clomiphene citrate. Fertil Steril. 2006;85:1761-1765.
Can safety and efficacy go hand in hand? Contraception for medically complex patients
The author reports no financial relationships relevant to this article.
CASE Multiple morbidities complicate choice of contraceptive
D.M. is a 27-year-old woman who has sickle cell disease, which led to a mild stroke during adolescence. She also has mild renal insufficiency and was given a diagnosis in adulthood of systemic lupus erythematosus, for which she takes prednisone on a maintenance basis.
D.M. is sexually active with her long-term boyfriend, and has undergone salpingectomy for ectopic pregnancy. Recently, she underwent exploratory laparotomy after a ruptured hemorrhagic ovarian cyst caused an intraperitoneal hemorrhage.
What method of birth control would be most appropriate for this patient?
The question is a daunting one, but it’s imperative for health-care providers to understand the nature and magnitude of contraceptive risks in medically complex women and provide the answers that these patients need.
In this article, I describe important considerations and sift the evidence regarding each of what I refer to here as highly effective contraceptive methods:
- safe hormonal contraceptives
- intrauterine contraceptives
- minimally invasive surgical sterilization.
These methods have given medically complex women greater control over their reproductive function and health, and a number of them offer benefits beyond contraception.
With some methods, such as progestin-only contraception, prospective data are lacking but retrospective studies show no elevated risk of cardiovascular events. And although combination hormonal contraceptives carry an elevated relative risk of cardiovascular events, absolute risk is very low.
First, who are these patients?
Women who have an extreme chronic medical condition, such as pulmonary hypertension, cardiomyopathy, or a dilated aortic root (>40 mm), face pregnancy-associated mortality as high as 10% to 50%—making unplanned pregnancy significantly more dangerous than any contraceptive. And even women who have a less severe medical condition stand to benefit from careful pregnancy timing: Those who have diabetes, lupus, or inflammatory bowel disease often need to optimize their medical condition before becoming pregnant. Still others may need to discontinue a teratogenic medication or treatment.
As for women who have multiple serious medical conditions, such as the patient described above, there is critical need to understand and prepare for the risks of pregnancy. These women deserve a contraceptive that has an efficacy rate approaching 100%.
All too often, however, these women settle for less effective barrier methods— or no method at all—out of concern that contraceptive and personal medical risks may interact adversely. Medical interests may drive these choices, but the unplanned pregnancies that result can pose more health risks than the rejected contraceptives.
A tool to weigh contraceptive risks
The World Health Organization (WHO) has categorized a large number of medical conditions according to their level of risk in regard to specific contraceptives.1 The four categories established by WHO range from no restrictions (category 1) to unacceptable health risks (category 4) (TABLE 1). With this system, you have a streamlined resource for weighing a contraceptive’s risks and benefits and finding an appropriate method for your patients.
TABLE 1
Four levels of risk in WHO categories
| CATEGORY | WHAT IT MEANS |
|---|---|
| 1 | A condition for which there is no restriction on the use of the contraceptive method |
| 2 | A condition in which the advantages of using the method generally outweigh the theoretical or proven risks |
| 3 | A condition in which the theoretical or proven risks usually outweigh the advantages of using the method |
| 4 | A condition that represents an unacceptable health risk if the contraceptive method is used |
Sifting risks and benefits of hormonal contraceptives
With typical use, hormonal contraceptive pills and injections prevent pregnancy in 92% to 97% of women who use one of these methods for 1 year.2 They also may decrease dysmenorrhea and menorrhagia, reduce the incidence of functional ovarian cysts, improve menstrual symptoms, and help prevent ovarian and endometrial cancers.2,3 In surveys in selected developed countries, the majority of women have used hormonal contraceptives at some time in their reproductive lives.2
Hormonal contraceptives also carry rare but potentially serious health risks that may deter their use—at times, inappropriately. Combined oral contraceptives (OCs) may double or triple the risk of myocardial infarction (MI)4 and stroke5,6 and triple or quadruple the risk of deep venous thrombosis (DVT) and venous thromboembolism (VTE).7
Recent data on the combined contraceptive patch suggest that it carries a risk of VTE twice as high as combined OCs.8 (Rates of MI and stroke were too small to compare accurately.8) We lack data on the vaginal ring contraceptive, but its medical risks are assumed to be similar to those of combined oral contraceptives.1
Putting the risks of OCs in context
It is very important to interpret these risks in light of the overall rarity of cardiovascular events and the opposing risks of pregnancy. TABLE 2 shows the low incidence of MI, stroke, and VTE among nonpregnant and pregnant women.
For every 100,000 woman-years, combined OCs are estimated to contribute three additional cases of MI, four additional cases of stroke, and 10 to 20 additional cases of VTE.3,5,9 For these severe conditions, the baseline incidence plus additional cases attributed to use of combination OCs still does not approach the risk of pregnancy itself. One study showed that women face a higher risk of cardiovascular death in pregnancy than when taking combined OCs, with the exception of smokers over the age of 35 years.9
For most women, combined OCs pose no greater cardiovascular risk than pregnancy does—but baseline cardiovascular risk factors augment that risk. Women who have hypertension, those who smoke, and those over age 35 face higher risks of MI and stroke while taking combined OCs.4,10 Diabetes and hypercholesterolemia further elevate the risk of MI,4 and migraine headache and thrombophilia raise the risk of stroke.6,11-13 Women with thrombophilia, a history of a clotting disorder, elevated body mass index (BMI), and, possibly, those who smoke face a higher risk of VTE when using a combined hormonal contraceptive.14-17
Because of these risks, the WHO classifies significant cardiovascular risk factors as category 4 (contraindicated) in regard to combined OCs (TABLE 3).
These risk factors include:
- known vascular disease
- ischemic heart disease
- history of stroke
- known thrombotic mutation
- complicated valvular disease.
When systolic blood pressure exceeds 160 mm Hg or diastolic blood pressure surpasses 100 mm Hg, combined OCs are again contraindicated. Use of combined OCs in women who have milder blood pressure elevations and adequately controlled hypertension is classified as category 3—theoretical or proven risks usually outweigh the advantages of using the method. Individual risk factors such as hyperlipidemia or uncomplicated diabetes are classified as category 3 in regard to combined OCs—unless multiple factors coexist, in which case they fall into category 4.
TABLE 2
Incidence of major cardiovascular events per 100,000 woman-years
| GROUP | MYOCARDIAL INFARCTION | STROKE | VENOUS THROMBOEMBOLISM3 |
|---|---|---|---|
| Nonpregnant | 0.2–530 | 4–1430 | 5 |
| Additional cases attributed to oral contraceptive use | 0.6–39 | 4.15 | 10–20 |
| Pregnant | 2.731 –6.232 | 2033 | 60 |
TABLE 3
Risk states in which combined hormonal contraceptives are contraindicated
| CARDIOVASCULAR RISK |
Multiple cardiovascular risk factors
|
| Systolic blood pressure >160 mm Hg |
| Diastolic blood pressure >100 mm Hg |
| Current vascular disease |
| History of ischemic heart disease |
Advanced diabetes
|
| CLOTTING RISK |
| History of deep venous thrombosis or pulmonary embolism |
| Major surgery with prolonged immobilization |
| Known thrombophilia |
| Complicated valvular heart disease |
| STROKE RISK |
| History of stroke |
| Migraine over age 35 |
| Migraine with aura |
| GASTROINTESTINAL ILLNESS |
| Active viral hepatitis |
| Decompensated cirrhosis |
| Liver tumor |
| CANCER RISK |
| Current breast cancer |
| SOURCE: World Health Organization |
Obese women may benefit from OCs—but efficacy may decline
Although obesity increases the risk of VTE17 and possibly MI4 during use of combined OCs, the WHO classifies it as category 2 in regard to this contraceptive method—advantages generally outweigh the theoretical or proven risks. This rating is based on the low number of major adverse events associated with use of low-dose combined OCs in obese women.1
However, combined OCs appear to be less effective in obese women than in their normal-weight peers. A recent case-control study showed diminished efficacy for women with a BMI over 27, and an even higher rate of contraceptive failure for those with a BMI over 32.18 Nevertheless, it is important for clinicians and patients to recognize the benefits likely to accrue from this method—probably at a higher rate than is seen with most barrier methods.
Obese women who suffer from oligoovulation may also benefit from the progestin in combined OCs, which can mitigate the effects of unopposed estrogen.
Nevertheless, it may be wise, when counseling these women, to consider a more effective method that carries less risk, such as a progestin-releasing intrauterine contraceptive.
Stroke risk in migraine sufferers may render OC option unwise
Patients who experience migraine have a higher risk of stroke than their migraine-free peers. The risk is even higher when the migraine is preceded by an aura (a 5- to 10-minute episode of moving lights in a visual field, speech disturbance, paresthesias, or weakness that precedes the headache).12,19 Risk is especially elevated when women who suffer migraines use a combined OC, with an odds ratio for stroke ranging from 6.6 to 8.7.
Because of these heightened risks, the WHO classifies migraine with aura as category 4 (contraindicated) for combined OCs. When no aura is present, the advisability of OC use depends on the woman’s age and whether her symptoms predate hormone use. Migraine without aura falls into category 4 for women over age 35 whose symptoms develop while on the contraceptive. It falls into category 2 if the woman is under age 35 and her symptoms predate contraceptive use. In other situations, migraine without aura falls into category 3.
Progestin-only options may be safer in women with cardiovascular risk
Women who face an unacceptable level of cardiovascular risk with combined OCs may still be candidates for progestin-only contraceptives. Although data are thin regarding the risks of progestins in the absence of estrogen, an international WHO study found no increased cardiovascular risk with the use of oral or injectable progestins.20
Current breast cancer is the only medical condition in which progestin-only contraception is contraindicated (category 4). Significant or multiple cardiac risk factors are classified as category 3 in regard to depot medroxyprogesterone acetate, and as category 1 or 2 for progestin-only pills.
Current DVT or VTE is classified as category 3 in regard to progestin-only contraception. A history of DVT or VTE is category 2 (TABLE 4).
TABLE 4
Risks of progestin-only contraceptives may outweigh benefits in these conditions
| CATEGORY 4 – CONTRAINDICATED |
| Current breast cancer |
| CATEGORY 3 – RISKS GENERALLY OUTWEIGH BENEFITS |
| Cardiovascular risk (for depot medroxyprogesterone acetate) |
Multiple CV risk factors
|
| Systolic BP >160 mm Hg |
| Diastolic BP >100 mm Hg |
| Current vascular disease |
Advanced diabetes
|
| Cardiovascular risk (for all progestin-only contraceptives) |
| History of ischemic heart disease while on the contraceptive |
| Clotting risk |
| Current deep venous thrombosis or pulmonary embolism |
| Stroke risk |
| History of stroke while on the contraceptive |
| Migraine with aura developing while on contraceptive |
| Gastrointestinal illness |
| Active viral hepatitis |
| Liver tumor |
| Decompensated cirrhosis |
| Cancer risk |
| History of breast cancer, remission up to 5 years |
| Unexplained vaginal bleeding |
| CV=cardiovascular |
| SOURCE: World Health Organization |
Liver disease, cancer may rule out use of hormones
Estrogens and progestins are metabolized by the liver, and women with significant liver dysfunction may accumulate medication. Hormones are also contraindicated in the setting of hormone-sensitive tumors, such as liver adenomas and breast cancer.
In addition, hormones may interact with—and should be avoided during use of—drugs that affect metabolic enzymes, such as certain anticonvulsants, rifampin, and some antiretrovirals.1
Intrauterine option is underused
Two types of intrauterine contraception (IUC) are available in the United States: the CuT-380A and the LNG-20. The former uses copper, whereas the latter delivers the progestin levonorgestrel directly to the endometrium. Both methods are extremely effective, with cumulative failure rates below 1% to 2% over 5 to 10 years.21 Unlike most hormonal contraceptives, IUCs do not require patient compliance, and the LNG-20 has the additional benefit of decreasing menstrual blood loss.21
Despite these advantages, fear of uterine infection has led to underuse of IUC in the United States.22 A worldwide review of prospective studies of IUC revealed that the risk of infection is limited to the first 20 days after insertion, when the risk of pelvic inflammatory disease (PID) is approximately 1%.23 Thereafter, the risk of infection is significantly lower and can be linked to other PID risk factors, such as young age and multiple partners.23,24 The risk may be even lower with the LNG-20 than with the copper system.25 The IUC’s safety and high level of effectiveness make it an excellent choice for many women with chronic medical conditions.
Picture is murky in immunocompromised women
Infection caused by IUC may be unlikely in a healthy woman, but use of IUC in immunocompromised patients carries uncertain risk. Data from HIV-infected women in Africa have been reassuring, demonstrating an acceptably low risk of infection.26 However, no studies have evaluated IUC among women on immunosuppressive drugs or those with otherwise impaired immune systems, and the WHO does not make formal recommendations for these patients. Two case reports of IUC failure in transplant patients led some to theorize that immune-mediated inflammation is necessary for IUC function, but this has not been proven.27
When immunocompromised women do not qualify for other highly effective contraceptives, the benefit of IUC may outweigh any theoretical risks. In this case, the LNG-20 may be preferable for its possibly lower risk of infection and decreased reliance on an inflammatory mechanism of action.
Contraindications to IUC include breast cancer, pelvic infection
Although the LNG-20 contains a hormone, the amount of levonorgestrel entering the circulation is very low, so the method is not restricted in women with cardiovascular risk factors. The only contraindications to IUC are:
- pelvic infection or sepsis
- pregnancy
- undiagnosed abnormal uterine bleeding or gynecologic cancer
- distorted uterine cavity
- breast cancer (for the LNG-20)
- Wilson’s disease (for the CuT-380A).
Sterilization is a safe option
For women ready to forego future childbearing, surgical sterilization is an excellent option. It requires no compliance or follow-up on the part of the patient, and efficacy rates approach that of IUC—at 98% to 99% or higher.
Beyond regret and sterilization failure, the risks of sterilization are limited to those of the surgical procedure itself. These may be negligible if tubal ligation is performed at the time of another indicated surgery, such as cesarean section.
Interval sterilization with laparoscopic tubal ligation is usually performed with general anesthesia. The rate of major morbidity is approximately 0.9%, including major bleeding, need for laparotomy, organ injury, and major infection. Complications may be higher in women with diabetes, a history of major surgery, and obesity.28
The WHO advises caution when using this method in the setting of severe diabetes, sickle cell disease, coagulopathy, severe renal disease, cardiovascular disease, or pulmonary disease.1
Insertion of intratubal coils is less invasive than tubal ligation
Hysteroscopic tubal sterilization with placement of titanium–Dacron intratubal coils (sold by the name Essure) is another option gaining use (FIGURE). Although large-scale studies have yet to be published, data from the largest phase III trial are consistent with smaller studies.29 In that multicenter trial, coil placement was successful in 92% of patients, and 99% of women completed the procedure without general anesthesia. Tubal perforation was identified in 1% of women, who went on to a laparoscopic procedure.
This less invasive method of permanent sterilization increases options for women who are poor laparoscopy candidates, although the 10% of women who experience technical failure will be forced to find an alternative method. Patient compliance is also an issue because the woman must use backup contraception for 3 months following the procedure, until tubal occlusion is confirmed by hysterosalpingography.
FIGURE Sterilization via insertion of intratubal coils
Delivery of the Essure device.
After 3 months, polyethylene (PET) fibers elicit ingrowth and proximal tubal occlusion.
Focusing on the patient’s partner may be the smartest approach
Male sterilization with vasectomy poses no medical risks to a woman with a complex medical history. However, long-term success requires that she keep the same sexual partner throughout her reproductive life or seek another form of contraception.
CASE RESOLVED Patient opts for progestin-only pills
Because of her sickle cell disease, D.M., the patient described at the beginning of this article, is not a good candidate for surgical sterilization, and neither is her boyfriend. According to WHO criteria, her sickle cell disease falls into category 2 in regard to combined OCs and category 1 for IUC—both effective methods. No guidance is available regarding concomitant use of steroids, which she is taking for lupus, with IUC, but her baseline risk for pelvic infection is thought to be relatively low. The noncontraceptive benefit of ovarian cyst suppression makes combined OCs even more attractive for this patient, but her history of stroke contraindicates this method (category 4). Depot medroxyprogesterone acetate may suppress ovarian function and is classified as category 3. She ultimately selects a combination of progestin-only pills and condoms and has successfully avoided pregnancy.
1. World Health Organization Medical Eligibility Criteria for Contraceptive Use. 3rd ed. Geneva: World Health Organization; 2004. Available at:www.who.int/reproductive-health/publications/mec/index.htm. Accessed Oct. 25, 2007.
2. Hatcher RA, Nelson A. Combined hormonal contraceptive methods. In: Hatcher RA et al, eds. Contraceptive Technology. 18th ed. New York: Ardent Media; 2004;391:460-
3. Faculty of Family Planning and Reproductive Health Care Clinical Effectiveness Unit First Prescription of Combined Oral Contraception. Royal College of Obstetricians and Gynaecologists: 2006.
4. Tanis BC, van den Bosch MA, Kemmeren JM, et al. Oral contraceptives and the risk of myocardial infarction. N Engl J Med. 2001;345:1787-1793.
5. Gillum LA, Mamidipudi SK, Johnston SC. Ischemic stroke risk with oral contraceptives: a meta-analysis. JAMA. 2000;284:72-78.
6. World Health Organization Collaborative Study of Cardiovascular Disease and Steroid Hormone Contraception Ischaemic stroke and combined oral contraceptives: results of an international, multicentre, case-control study. Lancet. 1996;348:498-505.
7. Vandenbroucke JP, Rosing J, Bloemenkamp KW, et al. Oral contraceptives and the risk of venous thrombosis. N Engl J Med. 2001;344:1527-1535.
8. Cole JA, Norman H, Doherty M, Walker AM. Venous thromboembolism, myocardial infarction, and stroke among transdermal contraceptive system users. Obstet Gynecol. 2007;109(2 Pt 1):339-346.
9. Schwingl PJ, Ory HW, Visness CM. Estimates of the risk of cardiovascular death attributable to low-dose oral contraceptives in the United States. Am J Obstet Gynecol. 1999;180(1 Pt 1):241-249.
10. Petitti DB, Sidney S, Quesenberry CP. Oral contraceptive use and myocardial infarction. Contraception. 1998;57:143-155.
11. Curtis KM, Mohllajee AP, Peterson HB. Use of combined oral contraceptives among women with migraine and nonmigrainous headaches: a systematic review. Contraception. 2006;73:189-194.
12. Etminan M, Takkouche B, Isorna FC, Samii A. Risk of ischaemic stroke in people with migraine: systematic review and meta-analysis of observational studies. BMJ. 2005;330:63.-
13. Slooter AJ, Rosendaal FR, Tanis BC, Kemmeren JM, van der Graaf Y, Algra A. Prothrombotic conditions, oral contraceptives, and the risk of ischemic stroke. J Thromb Haemost. 2005;3:1213-1217.
14. Mohllajee AP, Curtis KM, Martins SL, Peterson HB. Does use of hormonal contraceptives among women with thrombogenic mutations increase their risk of thromboembolism? A systematic review. Contraception. 2006;73:166-178.
15. Christiansen SC, Cannegieter SC, Koster T, Vandenbroucke JP, Rosendaal FR. Thrombophilia, clinical factors, and recurrent venous thrombotic events. JAMA. 2005;293:2352-2361.
16. World Health Organization Collaborative Study of Cardiovascular Disease and Steroid Hormone Contraception Effect of different progestagens in low oestrogen oral contraceptives on venous thromboembolic disease. Lancet. 1995;346:1582-1588.
17. Sidney S, Petitti DB, Soff GA, Cundiff DL, Tolan KK, Quesenberry CP, Jr. Venous thromboembolic disease in users of low-estrogen combined estrogen-progestin oral contraceptives. Contraception. 2004;70:3-10.
18. Holt VL, Scholes D, Wicklund KG, Cushing-Haugen KL, Daling JR. Body mass index, weight, and oral contraceptive failure risk. Obstet Gynecol. 2005;105:46-52.
19. Chang CL, Donaghy M, Poulter N. Migraine and stroke in young women: case-control study. The World Health Organisation Collaborative Study of Cardiovascular Disease and Steroid Hormone Contraception. BMJ. 1999;318:13-18.
20. World Health Organization Collaborative Study of Cardiovascular Disease and Steroid Hormone Contraception Cardiovascular disease and use of oral and injectable progestogen-only contraceptives and combined injectable contraceptives Results of an international, multicenter, case-control study. Contraception. 1998;57:315-324.
21. Grimes DA. Intrauterine devices. In: Hatcher RA et al, eds. Contraceptive Technology. 18th ed. New York: Ardent Media; 2004; 495-530.
22. Darney PD. Time to pardon the IUD? N Engl J Med. 2001;345:608-610.
23. Farley TM, Rosenberg MJ, Rowe PJ, Chen JH, Meirik O. Intrauterine devices and pelvic inflammatory disease: an international perspective. Lancet. 1992;339:785-788.
24. Lee NC, Rubin GL, Borucki R. The intrauterine device and pelvic inflammatory disease revisited: new results from the Women’s Health Study. Obstet Gynecol. 1988;72:1-6.
25. Andersson K, Odlind V, Rybo G. Levonorgestrel-releasing and copper-releasing (Nova T) IUDs during five years of use: a randomized comparative trial. Contraception. 1994;49:56-72.
26. Morrison CS, Sekadde-Kigondu C, Sinei SK, Weiner DH, Kwok C, Kokonya D. Is the intrauterine device appropriate contraception for HIV-1-infected women. BJOG. 2001;108:784-790.
27. Zerner J, Doil KL, Drewry J, Leeber DA. Intrauterine contraceptive device failures in renal transplant patients. J Reprod Med. 1981;26:99-102.
28. Jamieson DJ, Hillis SD, Duerr A, Marchbanks PA, Costello C, Peterson HB. Complications of interval laparoscopic tubal sterilization: findings from the United States Collaborative Review of Sterilization. Obstet Gynecol. 2000;96:997-1002.
29. Cooper JM, Carignan CS, Cher D, Kerin JF. Selective Tubal Occlusion Procedure Investigators Microinsert nonincisional hysteroscopic sterilization. Obstet Gynecol. 2003;102:59-67.
30. Petitti DB, Sidney S, Quesenberry CP, Jr, Bernstein A. Incidence of stroke and myocardial infarction in women of reproductive age. Stroke. 1997;28:280-283.
31. Ladner HE, Danielsen B, Gilbert WM. Acute myocardial infarction in pregnancy and the puerperium: a population-based study. Obstet Gynecol. 2005;105:480-484.
32. James AH, Jamison MG, Biswas MS, Brancazio LR, Swamy GK, Myers ER. Acute myocardial infarction in pregnancy: a United States population-based study. Circulation. 2006;113:1564-1571.
33. Kittner SJ, Stern BJ, Feeser BR, et al. Pregnancy and the risk of stroke. N Engl J Med. 1996;335:768-774.
The author reports no financial relationships relevant to this article.
CASE Multiple morbidities complicate choice of contraceptive
D.M. is a 27-year-old woman who has sickle cell disease, which led to a mild stroke during adolescence. She also has mild renal insufficiency and was given a diagnosis in adulthood of systemic lupus erythematosus, for which she takes prednisone on a maintenance basis.
D.M. is sexually active with her long-term boyfriend, and has undergone salpingectomy for ectopic pregnancy. Recently, she underwent exploratory laparotomy after a ruptured hemorrhagic ovarian cyst caused an intraperitoneal hemorrhage.
What method of birth control would be most appropriate for this patient?
The question is a daunting one, but it’s imperative for health-care providers to understand the nature and magnitude of contraceptive risks in medically complex women and provide the answers that these patients need.
In this article, I describe important considerations and sift the evidence regarding each of what I refer to here as highly effective contraceptive methods:
- safe hormonal contraceptives
- intrauterine contraceptives
- minimally invasive surgical sterilization.
These methods have given medically complex women greater control over their reproductive function and health, and a number of them offer benefits beyond contraception.
With some methods, such as progestin-only contraception, prospective data are lacking but retrospective studies show no elevated risk of cardiovascular events. And although combination hormonal contraceptives carry an elevated relative risk of cardiovascular events, absolute risk is very low.
First, who are these patients?
Women who have an extreme chronic medical condition, such as pulmonary hypertension, cardiomyopathy, or a dilated aortic root (>40 mm), face pregnancy-associated mortality as high as 10% to 50%—making unplanned pregnancy significantly more dangerous than any contraceptive. And even women who have a less severe medical condition stand to benefit from careful pregnancy timing: Those who have diabetes, lupus, or inflammatory bowel disease often need to optimize their medical condition before becoming pregnant. Still others may need to discontinue a teratogenic medication or treatment.
As for women who have multiple serious medical conditions, such as the patient described above, there is critical need to understand and prepare for the risks of pregnancy. These women deserve a contraceptive that has an efficacy rate approaching 100%.
All too often, however, these women settle for less effective barrier methods— or no method at all—out of concern that contraceptive and personal medical risks may interact adversely. Medical interests may drive these choices, but the unplanned pregnancies that result can pose more health risks than the rejected contraceptives.
A tool to weigh contraceptive risks
The World Health Organization (WHO) has categorized a large number of medical conditions according to their level of risk in regard to specific contraceptives.1 The four categories established by WHO range from no restrictions (category 1) to unacceptable health risks (category 4) (TABLE 1). With this system, you have a streamlined resource for weighing a contraceptive’s risks and benefits and finding an appropriate method for your patients.
TABLE 1
Four levels of risk in WHO categories
| CATEGORY | WHAT IT MEANS |
|---|---|
| 1 | A condition for which there is no restriction on the use of the contraceptive method |
| 2 | A condition in which the advantages of using the method generally outweigh the theoretical or proven risks |
| 3 | A condition in which the theoretical or proven risks usually outweigh the advantages of using the method |
| 4 | A condition that represents an unacceptable health risk if the contraceptive method is used |
Sifting risks and benefits of hormonal contraceptives
With typical use, hormonal contraceptive pills and injections prevent pregnancy in 92% to 97% of women who use one of these methods for 1 year.2 They also may decrease dysmenorrhea and menorrhagia, reduce the incidence of functional ovarian cysts, improve menstrual symptoms, and help prevent ovarian and endometrial cancers.2,3 In surveys in selected developed countries, the majority of women have used hormonal contraceptives at some time in their reproductive lives.2
Hormonal contraceptives also carry rare but potentially serious health risks that may deter their use—at times, inappropriately. Combined oral contraceptives (OCs) may double or triple the risk of myocardial infarction (MI)4 and stroke5,6 and triple or quadruple the risk of deep venous thrombosis (DVT) and venous thromboembolism (VTE).7
Recent data on the combined contraceptive patch suggest that it carries a risk of VTE twice as high as combined OCs.8 (Rates of MI and stroke were too small to compare accurately.8) We lack data on the vaginal ring contraceptive, but its medical risks are assumed to be similar to those of combined oral contraceptives.1
Putting the risks of OCs in context
It is very important to interpret these risks in light of the overall rarity of cardiovascular events and the opposing risks of pregnancy. TABLE 2 shows the low incidence of MI, stroke, and VTE among nonpregnant and pregnant women.
For every 100,000 woman-years, combined OCs are estimated to contribute three additional cases of MI, four additional cases of stroke, and 10 to 20 additional cases of VTE.3,5,9 For these severe conditions, the baseline incidence plus additional cases attributed to use of combination OCs still does not approach the risk of pregnancy itself. One study showed that women face a higher risk of cardiovascular death in pregnancy than when taking combined OCs, with the exception of smokers over the age of 35 years.9
For most women, combined OCs pose no greater cardiovascular risk than pregnancy does—but baseline cardiovascular risk factors augment that risk. Women who have hypertension, those who smoke, and those over age 35 face higher risks of MI and stroke while taking combined OCs.4,10 Diabetes and hypercholesterolemia further elevate the risk of MI,4 and migraine headache and thrombophilia raise the risk of stroke.6,11-13 Women with thrombophilia, a history of a clotting disorder, elevated body mass index (BMI), and, possibly, those who smoke face a higher risk of VTE when using a combined hormonal contraceptive.14-17
Because of these risks, the WHO classifies significant cardiovascular risk factors as category 4 (contraindicated) in regard to combined OCs (TABLE 3).
These risk factors include:
- known vascular disease
- ischemic heart disease
- history of stroke
- known thrombotic mutation
- complicated valvular disease.
When systolic blood pressure exceeds 160 mm Hg or diastolic blood pressure surpasses 100 mm Hg, combined OCs are again contraindicated. Use of combined OCs in women who have milder blood pressure elevations and adequately controlled hypertension is classified as category 3—theoretical or proven risks usually outweigh the advantages of using the method. Individual risk factors such as hyperlipidemia or uncomplicated diabetes are classified as category 3 in regard to combined OCs—unless multiple factors coexist, in which case they fall into category 4.
TABLE 2
Incidence of major cardiovascular events per 100,000 woman-years
| GROUP | MYOCARDIAL INFARCTION | STROKE | VENOUS THROMBOEMBOLISM3 |
|---|---|---|---|
| Nonpregnant | 0.2–530 | 4–1430 | 5 |
| Additional cases attributed to oral contraceptive use | 0.6–39 | 4.15 | 10–20 |
| Pregnant | 2.731 –6.232 | 2033 | 60 |
TABLE 3
Risk states in which combined hormonal contraceptives are contraindicated
| CARDIOVASCULAR RISK |
Multiple cardiovascular risk factors
|
| Systolic blood pressure >160 mm Hg |
| Diastolic blood pressure >100 mm Hg |
| Current vascular disease |
| History of ischemic heart disease |
Advanced diabetes
|
| CLOTTING RISK |
| History of deep venous thrombosis or pulmonary embolism |
| Major surgery with prolonged immobilization |
| Known thrombophilia |
| Complicated valvular heart disease |
| STROKE RISK |
| History of stroke |
| Migraine over age 35 |
| Migraine with aura |
| GASTROINTESTINAL ILLNESS |
| Active viral hepatitis |
| Decompensated cirrhosis |
| Liver tumor |
| CANCER RISK |
| Current breast cancer |
| SOURCE: World Health Organization |
Obese women may benefit from OCs—but efficacy may decline
Although obesity increases the risk of VTE17 and possibly MI4 during use of combined OCs, the WHO classifies it as category 2 in regard to this contraceptive method—advantages generally outweigh the theoretical or proven risks. This rating is based on the low number of major adverse events associated with use of low-dose combined OCs in obese women.1
However, combined OCs appear to be less effective in obese women than in their normal-weight peers. A recent case-control study showed diminished efficacy for women with a BMI over 27, and an even higher rate of contraceptive failure for those with a BMI over 32.18 Nevertheless, it is important for clinicians and patients to recognize the benefits likely to accrue from this method—probably at a higher rate than is seen with most barrier methods.
Obese women who suffer from oligoovulation may also benefit from the progestin in combined OCs, which can mitigate the effects of unopposed estrogen.
Nevertheless, it may be wise, when counseling these women, to consider a more effective method that carries less risk, such as a progestin-releasing intrauterine contraceptive.
Stroke risk in migraine sufferers may render OC option unwise
Patients who experience migraine have a higher risk of stroke than their migraine-free peers. The risk is even higher when the migraine is preceded by an aura (a 5- to 10-minute episode of moving lights in a visual field, speech disturbance, paresthesias, or weakness that precedes the headache).12,19 Risk is especially elevated when women who suffer migraines use a combined OC, with an odds ratio for stroke ranging from 6.6 to 8.7.
Because of these heightened risks, the WHO classifies migraine with aura as category 4 (contraindicated) for combined OCs. When no aura is present, the advisability of OC use depends on the woman’s age and whether her symptoms predate hormone use. Migraine without aura falls into category 4 for women over age 35 whose symptoms develop while on the contraceptive. It falls into category 2 if the woman is under age 35 and her symptoms predate contraceptive use. In other situations, migraine without aura falls into category 3.
Progestin-only options may be safer in women with cardiovascular risk
Women who face an unacceptable level of cardiovascular risk with combined OCs may still be candidates for progestin-only contraceptives. Although data are thin regarding the risks of progestins in the absence of estrogen, an international WHO study found no increased cardiovascular risk with the use of oral or injectable progestins.20
Current breast cancer is the only medical condition in which progestin-only contraception is contraindicated (category 4). Significant or multiple cardiac risk factors are classified as category 3 in regard to depot medroxyprogesterone acetate, and as category 1 or 2 for progestin-only pills.
Current DVT or VTE is classified as category 3 in regard to progestin-only contraception. A history of DVT or VTE is category 2 (TABLE 4).
TABLE 4
Risks of progestin-only contraceptives may outweigh benefits in these conditions
| CATEGORY 4 – CONTRAINDICATED |
| Current breast cancer |
| CATEGORY 3 – RISKS GENERALLY OUTWEIGH BENEFITS |
| Cardiovascular risk (for depot medroxyprogesterone acetate) |
Multiple CV risk factors
|
| Systolic BP >160 mm Hg |
| Diastolic BP >100 mm Hg |
| Current vascular disease |
Advanced diabetes
|
| Cardiovascular risk (for all progestin-only contraceptives) |
| History of ischemic heart disease while on the contraceptive |
| Clotting risk |
| Current deep venous thrombosis or pulmonary embolism |
| Stroke risk |
| History of stroke while on the contraceptive |
| Migraine with aura developing while on contraceptive |
| Gastrointestinal illness |
| Active viral hepatitis |
| Liver tumor |
| Decompensated cirrhosis |
| Cancer risk |
| History of breast cancer, remission up to 5 years |
| Unexplained vaginal bleeding |
| CV=cardiovascular |
| SOURCE: World Health Organization |
Liver disease, cancer may rule out use of hormones
Estrogens and progestins are metabolized by the liver, and women with significant liver dysfunction may accumulate medication. Hormones are also contraindicated in the setting of hormone-sensitive tumors, such as liver adenomas and breast cancer.
In addition, hormones may interact with—and should be avoided during use of—drugs that affect metabolic enzymes, such as certain anticonvulsants, rifampin, and some antiretrovirals.1
Intrauterine option is underused
Two types of intrauterine contraception (IUC) are available in the United States: the CuT-380A and the LNG-20. The former uses copper, whereas the latter delivers the progestin levonorgestrel directly to the endometrium. Both methods are extremely effective, with cumulative failure rates below 1% to 2% over 5 to 10 years.21 Unlike most hormonal contraceptives, IUCs do not require patient compliance, and the LNG-20 has the additional benefit of decreasing menstrual blood loss.21
Despite these advantages, fear of uterine infection has led to underuse of IUC in the United States.22 A worldwide review of prospective studies of IUC revealed that the risk of infection is limited to the first 20 days after insertion, when the risk of pelvic inflammatory disease (PID) is approximately 1%.23 Thereafter, the risk of infection is significantly lower and can be linked to other PID risk factors, such as young age and multiple partners.23,24 The risk may be even lower with the LNG-20 than with the copper system.25 The IUC’s safety and high level of effectiveness make it an excellent choice for many women with chronic medical conditions.
Picture is murky in immunocompromised women
Infection caused by IUC may be unlikely in a healthy woman, but use of IUC in immunocompromised patients carries uncertain risk. Data from HIV-infected women in Africa have been reassuring, demonstrating an acceptably low risk of infection.26 However, no studies have evaluated IUC among women on immunosuppressive drugs or those with otherwise impaired immune systems, and the WHO does not make formal recommendations for these patients. Two case reports of IUC failure in transplant patients led some to theorize that immune-mediated inflammation is necessary for IUC function, but this has not been proven.27
When immunocompromised women do not qualify for other highly effective contraceptives, the benefit of IUC may outweigh any theoretical risks. In this case, the LNG-20 may be preferable for its possibly lower risk of infection and decreased reliance on an inflammatory mechanism of action.
Contraindications to IUC include breast cancer, pelvic infection
Although the LNG-20 contains a hormone, the amount of levonorgestrel entering the circulation is very low, so the method is not restricted in women with cardiovascular risk factors. The only contraindications to IUC are:
- pelvic infection or sepsis
- pregnancy
- undiagnosed abnormal uterine bleeding or gynecologic cancer
- distorted uterine cavity
- breast cancer (for the LNG-20)
- Wilson’s disease (for the CuT-380A).
Sterilization is a safe option
For women ready to forego future childbearing, surgical sterilization is an excellent option. It requires no compliance or follow-up on the part of the patient, and efficacy rates approach that of IUC—at 98% to 99% or higher.
Beyond regret and sterilization failure, the risks of sterilization are limited to those of the surgical procedure itself. These may be negligible if tubal ligation is performed at the time of another indicated surgery, such as cesarean section.
Interval sterilization with laparoscopic tubal ligation is usually performed with general anesthesia. The rate of major morbidity is approximately 0.9%, including major bleeding, need for laparotomy, organ injury, and major infection. Complications may be higher in women with diabetes, a history of major surgery, and obesity.28
The WHO advises caution when using this method in the setting of severe diabetes, sickle cell disease, coagulopathy, severe renal disease, cardiovascular disease, or pulmonary disease.1
Insertion of intratubal coils is less invasive than tubal ligation
Hysteroscopic tubal sterilization with placement of titanium–Dacron intratubal coils (sold by the name Essure) is another option gaining use (FIGURE). Although large-scale studies have yet to be published, data from the largest phase III trial are consistent with smaller studies.29 In that multicenter trial, coil placement was successful in 92% of patients, and 99% of women completed the procedure without general anesthesia. Tubal perforation was identified in 1% of women, who went on to a laparoscopic procedure.
This less invasive method of permanent sterilization increases options for women who are poor laparoscopy candidates, although the 10% of women who experience technical failure will be forced to find an alternative method. Patient compliance is also an issue because the woman must use backup contraception for 3 months following the procedure, until tubal occlusion is confirmed by hysterosalpingography.
FIGURE Sterilization via insertion of intratubal coils
Delivery of the Essure device.
After 3 months, polyethylene (PET) fibers elicit ingrowth and proximal tubal occlusion.
Focusing on the patient’s partner may be the smartest approach
Male sterilization with vasectomy poses no medical risks to a woman with a complex medical history. However, long-term success requires that she keep the same sexual partner throughout her reproductive life or seek another form of contraception.
CASE RESOLVED Patient opts for progestin-only pills
Because of her sickle cell disease, D.M., the patient described at the beginning of this article, is not a good candidate for surgical sterilization, and neither is her boyfriend. According to WHO criteria, her sickle cell disease falls into category 2 in regard to combined OCs and category 1 for IUC—both effective methods. No guidance is available regarding concomitant use of steroids, which she is taking for lupus, with IUC, but her baseline risk for pelvic infection is thought to be relatively low. The noncontraceptive benefit of ovarian cyst suppression makes combined OCs even more attractive for this patient, but her history of stroke contraindicates this method (category 4). Depot medroxyprogesterone acetate may suppress ovarian function and is classified as category 3. She ultimately selects a combination of progestin-only pills and condoms and has successfully avoided pregnancy.
The author reports no financial relationships relevant to this article.
CASE Multiple morbidities complicate choice of contraceptive
D.M. is a 27-year-old woman who has sickle cell disease, which led to a mild stroke during adolescence. She also has mild renal insufficiency and was given a diagnosis in adulthood of systemic lupus erythematosus, for which she takes prednisone on a maintenance basis.
D.M. is sexually active with her long-term boyfriend, and has undergone salpingectomy for ectopic pregnancy. Recently, she underwent exploratory laparotomy after a ruptured hemorrhagic ovarian cyst caused an intraperitoneal hemorrhage.
What method of birth control would be most appropriate for this patient?
The question is a daunting one, but it’s imperative for health-care providers to understand the nature and magnitude of contraceptive risks in medically complex women and provide the answers that these patients need.
In this article, I describe important considerations and sift the evidence regarding each of what I refer to here as highly effective contraceptive methods:
- safe hormonal contraceptives
- intrauterine contraceptives
- minimally invasive surgical sterilization.
These methods have given medically complex women greater control over their reproductive function and health, and a number of them offer benefits beyond contraception.
With some methods, such as progestin-only contraception, prospective data are lacking but retrospective studies show no elevated risk of cardiovascular events. And although combination hormonal contraceptives carry an elevated relative risk of cardiovascular events, absolute risk is very low.
First, who are these patients?
Women who have an extreme chronic medical condition, such as pulmonary hypertension, cardiomyopathy, or a dilated aortic root (>40 mm), face pregnancy-associated mortality as high as 10% to 50%—making unplanned pregnancy significantly more dangerous than any contraceptive. And even women who have a less severe medical condition stand to benefit from careful pregnancy timing: Those who have diabetes, lupus, or inflammatory bowel disease often need to optimize their medical condition before becoming pregnant. Still others may need to discontinue a teratogenic medication or treatment.
As for women who have multiple serious medical conditions, such as the patient described above, there is critical need to understand and prepare for the risks of pregnancy. These women deserve a contraceptive that has an efficacy rate approaching 100%.
All too often, however, these women settle for less effective barrier methods— or no method at all—out of concern that contraceptive and personal medical risks may interact adversely. Medical interests may drive these choices, but the unplanned pregnancies that result can pose more health risks than the rejected contraceptives.
A tool to weigh contraceptive risks
The World Health Organization (WHO) has categorized a large number of medical conditions according to their level of risk in regard to specific contraceptives.1 The four categories established by WHO range from no restrictions (category 1) to unacceptable health risks (category 4) (TABLE 1). With this system, you have a streamlined resource for weighing a contraceptive’s risks and benefits and finding an appropriate method for your patients.
TABLE 1
Four levels of risk in WHO categories
| CATEGORY | WHAT IT MEANS |
|---|---|
| 1 | A condition for which there is no restriction on the use of the contraceptive method |
| 2 | A condition in which the advantages of using the method generally outweigh the theoretical or proven risks |
| 3 | A condition in which the theoretical or proven risks usually outweigh the advantages of using the method |
| 4 | A condition that represents an unacceptable health risk if the contraceptive method is used |
Sifting risks and benefits of hormonal contraceptives
With typical use, hormonal contraceptive pills and injections prevent pregnancy in 92% to 97% of women who use one of these methods for 1 year.2 They also may decrease dysmenorrhea and menorrhagia, reduce the incidence of functional ovarian cysts, improve menstrual symptoms, and help prevent ovarian and endometrial cancers.2,3 In surveys in selected developed countries, the majority of women have used hormonal contraceptives at some time in their reproductive lives.2
Hormonal contraceptives also carry rare but potentially serious health risks that may deter their use—at times, inappropriately. Combined oral contraceptives (OCs) may double or triple the risk of myocardial infarction (MI)4 and stroke5,6 and triple or quadruple the risk of deep venous thrombosis (DVT) and venous thromboembolism (VTE).7
Recent data on the combined contraceptive patch suggest that it carries a risk of VTE twice as high as combined OCs.8 (Rates of MI and stroke were too small to compare accurately.8) We lack data on the vaginal ring contraceptive, but its medical risks are assumed to be similar to those of combined oral contraceptives.1
Putting the risks of OCs in context
It is very important to interpret these risks in light of the overall rarity of cardiovascular events and the opposing risks of pregnancy. TABLE 2 shows the low incidence of MI, stroke, and VTE among nonpregnant and pregnant women.
For every 100,000 woman-years, combined OCs are estimated to contribute three additional cases of MI, four additional cases of stroke, and 10 to 20 additional cases of VTE.3,5,9 For these severe conditions, the baseline incidence plus additional cases attributed to use of combination OCs still does not approach the risk of pregnancy itself. One study showed that women face a higher risk of cardiovascular death in pregnancy than when taking combined OCs, with the exception of smokers over the age of 35 years.9
For most women, combined OCs pose no greater cardiovascular risk than pregnancy does—but baseline cardiovascular risk factors augment that risk. Women who have hypertension, those who smoke, and those over age 35 face higher risks of MI and stroke while taking combined OCs.4,10 Diabetes and hypercholesterolemia further elevate the risk of MI,4 and migraine headache and thrombophilia raise the risk of stroke.6,11-13 Women with thrombophilia, a history of a clotting disorder, elevated body mass index (BMI), and, possibly, those who smoke face a higher risk of VTE when using a combined hormonal contraceptive.14-17
Because of these risks, the WHO classifies significant cardiovascular risk factors as category 4 (contraindicated) in regard to combined OCs (TABLE 3).
These risk factors include:
- known vascular disease
- ischemic heart disease
- history of stroke
- known thrombotic mutation
- complicated valvular disease.
When systolic blood pressure exceeds 160 mm Hg or diastolic blood pressure surpasses 100 mm Hg, combined OCs are again contraindicated. Use of combined OCs in women who have milder blood pressure elevations and adequately controlled hypertension is classified as category 3—theoretical or proven risks usually outweigh the advantages of using the method. Individual risk factors such as hyperlipidemia or uncomplicated diabetes are classified as category 3 in regard to combined OCs—unless multiple factors coexist, in which case they fall into category 4.
TABLE 2
Incidence of major cardiovascular events per 100,000 woman-years
| GROUP | MYOCARDIAL INFARCTION | STROKE | VENOUS THROMBOEMBOLISM3 |
|---|---|---|---|
| Nonpregnant | 0.2–530 | 4–1430 | 5 |
| Additional cases attributed to oral contraceptive use | 0.6–39 | 4.15 | 10–20 |
| Pregnant | 2.731 –6.232 | 2033 | 60 |
TABLE 3
Risk states in which combined hormonal contraceptives are contraindicated
| CARDIOVASCULAR RISK |
Multiple cardiovascular risk factors
|
| Systolic blood pressure >160 mm Hg |
| Diastolic blood pressure >100 mm Hg |
| Current vascular disease |
| History of ischemic heart disease |
Advanced diabetes
|
| CLOTTING RISK |
| History of deep venous thrombosis or pulmonary embolism |
| Major surgery with prolonged immobilization |
| Known thrombophilia |
| Complicated valvular heart disease |
| STROKE RISK |
| History of stroke |
| Migraine over age 35 |
| Migraine with aura |
| GASTROINTESTINAL ILLNESS |
| Active viral hepatitis |
| Decompensated cirrhosis |
| Liver tumor |
| CANCER RISK |
| Current breast cancer |
| SOURCE: World Health Organization |
Obese women may benefit from OCs—but efficacy may decline
Although obesity increases the risk of VTE17 and possibly MI4 during use of combined OCs, the WHO classifies it as category 2 in regard to this contraceptive method—advantages generally outweigh the theoretical or proven risks. This rating is based on the low number of major adverse events associated with use of low-dose combined OCs in obese women.1
However, combined OCs appear to be less effective in obese women than in their normal-weight peers. A recent case-control study showed diminished efficacy for women with a BMI over 27, and an even higher rate of contraceptive failure for those with a BMI over 32.18 Nevertheless, it is important for clinicians and patients to recognize the benefits likely to accrue from this method—probably at a higher rate than is seen with most barrier methods.
Obese women who suffer from oligoovulation may also benefit from the progestin in combined OCs, which can mitigate the effects of unopposed estrogen.
Nevertheless, it may be wise, when counseling these women, to consider a more effective method that carries less risk, such as a progestin-releasing intrauterine contraceptive.
Stroke risk in migraine sufferers may render OC option unwise
Patients who experience migraine have a higher risk of stroke than their migraine-free peers. The risk is even higher when the migraine is preceded by an aura (a 5- to 10-minute episode of moving lights in a visual field, speech disturbance, paresthesias, or weakness that precedes the headache).12,19 Risk is especially elevated when women who suffer migraines use a combined OC, with an odds ratio for stroke ranging from 6.6 to 8.7.
Because of these heightened risks, the WHO classifies migraine with aura as category 4 (contraindicated) for combined OCs. When no aura is present, the advisability of OC use depends on the woman’s age and whether her symptoms predate hormone use. Migraine without aura falls into category 4 for women over age 35 whose symptoms develop while on the contraceptive. It falls into category 2 if the woman is under age 35 and her symptoms predate contraceptive use. In other situations, migraine without aura falls into category 3.
Progestin-only options may be safer in women with cardiovascular risk
Women who face an unacceptable level of cardiovascular risk with combined OCs may still be candidates for progestin-only contraceptives. Although data are thin regarding the risks of progestins in the absence of estrogen, an international WHO study found no increased cardiovascular risk with the use of oral or injectable progestins.20
Current breast cancer is the only medical condition in which progestin-only contraception is contraindicated (category 4). Significant or multiple cardiac risk factors are classified as category 3 in regard to depot medroxyprogesterone acetate, and as category 1 or 2 for progestin-only pills.
Current DVT or VTE is classified as category 3 in regard to progestin-only contraception. A history of DVT or VTE is category 2 (TABLE 4).
TABLE 4
Risks of progestin-only contraceptives may outweigh benefits in these conditions
| CATEGORY 4 – CONTRAINDICATED |
| Current breast cancer |
| CATEGORY 3 – RISKS GENERALLY OUTWEIGH BENEFITS |
| Cardiovascular risk (for depot medroxyprogesterone acetate) |
Multiple CV risk factors
|
| Systolic BP >160 mm Hg |
| Diastolic BP >100 mm Hg |
| Current vascular disease |
Advanced diabetes
|
| Cardiovascular risk (for all progestin-only contraceptives) |
| History of ischemic heart disease while on the contraceptive |
| Clotting risk |
| Current deep venous thrombosis or pulmonary embolism |
| Stroke risk |
| History of stroke while on the contraceptive |
| Migraine with aura developing while on contraceptive |
| Gastrointestinal illness |
| Active viral hepatitis |
| Liver tumor |
| Decompensated cirrhosis |
| Cancer risk |
| History of breast cancer, remission up to 5 years |
| Unexplained vaginal bleeding |
| CV=cardiovascular |
| SOURCE: World Health Organization |
Liver disease, cancer may rule out use of hormones
Estrogens and progestins are metabolized by the liver, and women with significant liver dysfunction may accumulate medication. Hormones are also contraindicated in the setting of hormone-sensitive tumors, such as liver adenomas and breast cancer.
In addition, hormones may interact with—and should be avoided during use of—drugs that affect metabolic enzymes, such as certain anticonvulsants, rifampin, and some antiretrovirals.1
Intrauterine option is underused
Two types of intrauterine contraception (IUC) are available in the United States: the CuT-380A and the LNG-20. The former uses copper, whereas the latter delivers the progestin levonorgestrel directly to the endometrium. Both methods are extremely effective, with cumulative failure rates below 1% to 2% over 5 to 10 years.21 Unlike most hormonal contraceptives, IUCs do not require patient compliance, and the LNG-20 has the additional benefit of decreasing menstrual blood loss.21
Despite these advantages, fear of uterine infection has led to underuse of IUC in the United States.22 A worldwide review of prospective studies of IUC revealed that the risk of infection is limited to the first 20 days after insertion, when the risk of pelvic inflammatory disease (PID) is approximately 1%.23 Thereafter, the risk of infection is significantly lower and can be linked to other PID risk factors, such as young age and multiple partners.23,24 The risk may be even lower with the LNG-20 than with the copper system.25 The IUC’s safety and high level of effectiveness make it an excellent choice for many women with chronic medical conditions.
Picture is murky in immunocompromised women
Infection caused by IUC may be unlikely in a healthy woman, but use of IUC in immunocompromised patients carries uncertain risk. Data from HIV-infected women in Africa have been reassuring, demonstrating an acceptably low risk of infection.26 However, no studies have evaluated IUC among women on immunosuppressive drugs or those with otherwise impaired immune systems, and the WHO does not make formal recommendations for these patients. Two case reports of IUC failure in transplant patients led some to theorize that immune-mediated inflammation is necessary for IUC function, but this has not been proven.27
When immunocompromised women do not qualify for other highly effective contraceptives, the benefit of IUC may outweigh any theoretical risks. In this case, the LNG-20 may be preferable for its possibly lower risk of infection and decreased reliance on an inflammatory mechanism of action.
Contraindications to IUC include breast cancer, pelvic infection
Although the LNG-20 contains a hormone, the amount of levonorgestrel entering the circulation is very low, so the method is not restricted in women with cardiovascular risk factors. The only contraindications to IUC are:
- pelvic infection or sepsis
- pregnancy
- undiagnosed abnormal uterine bleeding or gynecologic cancer
- distorted uterine cavity
- breast cancer (for the LNG-20)
- Wilson’s disease (for the CuT-380A).
Sterilization is a safe option
For women ready to forego future childbearing, surgical sterilization is an excellent option. It requires no compliance or follow-up on the part of the patient, and efficacy rates approach that of IUC—at 98% to 99% or higher.
Beyond regret and sterilization failure, the risks of sterilization are limited to those of the surgical procedure itself. These may be negligible if tubal ligation is performed at the time of another indicated surgery, such as cesarean section.
Interval sterilization with laparoscopic tubal ligation is usually performed with general anesthesia. The rate of major morbidity is approximately 0.9%, including major bleeding, need for laparotomy, organ injury, and major infection. Complications may be higher in women with diabetes, a history of major surgery, and obesity.28
The WHO advises caution when using this method in the setting of severe diabetes, sickle cell disease, coagulopathy, severe renal disease, cardiovascular disease, or pulmonary disease.1
Insertion of intratubal coils is less invasive than tubal ligation
Hysteroscopic tubal sterilization with placement of titanium–Dacron intratubal coils (sold by the name Essure) is another option gaining use (FIGURE). Although large-scale studies have yet to be published, data from the largest phase III trial are consistent with smaller studies.29 In that multicenter trial, coil placement was successful in 92% of patients, and 99% of women completed the procedure without general anesthesia. Tubal perforation was identified in 1% of women, who went on to a laparoscopic procedure.
This less invasive method of permanent sterilization increases options for women who are poor laparoscopy candidates, although the 10% of women who experience technical failure will be forced to find an alternative method. Patient compliance is also an issue because the woman must use backup contraception for 3 months following the procedure, until tubal occlusion is confirmed by hysterosalpingography.
FIGURE Sterilization via insertion of intratubal coils
Delivery of the Essure device.
After 3 months, polyethylene (PET) fibers elicit ingrowth and proximal tubal occlusion.
Focusing on the patient’s partner may be the smartest approach
Male sterilization with vasectomy poses no medical risks to a woman with a complex medical history. However, long-term success requires that she keep the same sexual partner throughout her reproductive life or seek another form of contraception.
CASE RESOLVED Patient opts for progestin-only pills
Because of her sickle cell disease, D.M., the patient described at the beginning of this article, is not a good candidate for surgical sterilization, and neither is her boyfriend. According to WHO criteria, her sickle cell disease falls into category 2 in regard to combined OCs and category 1 for IUC—both effective methods. No guidance is available regarding concomitant use of steroids, which she is taking for lupus, with IUC, but her baseline risk for pelvic infection is thought to be relatively low. The noncontraceptive benefit of ovarian cyst suppression makes combined OCs even more attractive for this patient, but her history of stroke contraindicates this method (category 4). Depot medroxyprogesterone acetate may suppress ovarian function and is classified as category 3. She ultimately selects a combination of progestin-only pills and condoms and has successfully avoided pregnancy.
1. World Health Organization Medical Eligibility Criteria for Contraceptive Use. 3rd ed. Geneva: World Health Organization; 2004. Available at:www.who.int/reproductive-health/publications/mec/index.htm. Accessed Oct. 25, 2007.
2. Hatcher RA, Nelson A. Combined hormonal contraceptive methods. In: Hatcher RA et al, eds. Contraceptive Technology. 18th ed. New York: Ardent Media; 2004;391:460-
3. Faculty of Family Planning and Reproductive Health Care Clinical Effectiveness Unit First Prescription of Combined Oral Contraception. Royal College of Obstetricians and Gynaecologists: 2006.
4. Tanis BC, van den Bosch MA, Kemmeren JM, et al. Oral contraceptives and the risk of myocardial infarction. N Engl J Med. 2001;345:1787-1793.
5. Gillum LA, Mamidipudi SK, Johnston SC. Ischemic stroke risk with oral contraceptives: a meta-analysis. JAMA. 2000;284:72-78.
6. World Health Organization Collaborative Study of Cardiovascular Disease and Steroid Hormone Contraception Ischaemic stroke and combined oral contraceptives: results of an international, multicentre, case-control study. Lancet. 1996;348:498-505.
7. Vandenbroucke JP, Rosing J, Bloemenkamp KW, et al. Oral contraceptives and the risk of venous thrombosis. N Engl J Med. 2001;344:1527-1535.
8. Cole JA, Norman H, Doherty M, Walker AM. Venous thromboembolism, myocardial infarction, and stroke among transdermal contraceptive system users. Obstet Gynecol. 2007;109(2 Pt 1):339-346.
9. Schwingl PJ, Ory HW, Visness CM. Estimates of the risk of cardiovascular death attributable to low-dose oral contraceptives in the United States. Am J Obstet Gynecol. 1999;180(1 Pt 1):241-249.
10. Petitti DB, Sidney S, Quesenberry CP. Oral contraceptive use and myocardial infarction. Contraception. 1998;57:143-155.
11. Curtis KM, Mohllajee AP, Peterson HB. Use of combined oral contraceptives among women with migraine and nonmigrainous headaches: a systematic review. Contraception. 2006;73:189-194.
12. Etminan M, Takkouche B, Isorna FC, Samii A. Risk of ischaemic stroke in people with migraine: systematic review and meta-analysis of observational studies. BMJ. 2005;330:63.-
13. Slooter AJ, Rosendaal FR, Tanis BC, Kemmeren JM, van der Graaf Y, Algra A. Prothrombotic conditions, oral contraceptives, and the risk of ischemic stroke. J Thromb Haemost. 2005;3:1213-1217.
14. Mohllajee AP, Curtis KM, Martins SL, Peterson HB. Does use of hormonal contraceptives among women with thrombogenic mutations increase their risk of thromboembolism? A systematic review. Contraception. 2006;73:166-178.
15. Christiansen SC, Cannegieter SC, Koster T, Vandenbroucke JP, Rosendaal FR. Thrombophilia, clinical factors, and recurrent venous thrombotic events. JAMA. 2005;293:2352-2361.
16. World Health Organization Collaborative Study of Cardiovascular Disease and Steroid Hormone Contraception Effect of different progestagens in low oestrogen oral contraceptives on venous thromboembolic disease. Lancet. 1995;346:1582-1588.
17. Sidney S, Petitti DB, Soff GA, Cundiff DL, Tolan KK, Quesenberry CP, Jr. Venous thromboembolic disease in users of low-estrogen combined estrogen-progestin oral contraceptives. Contraception. 2004;70:3-10.
18. Holt VL, Scholes D, Wicklund KG, Cushing-Haugen KL, Daling JR. Body mass index, weight, and oral contraceptive failure risk. Obstet Gynecol. 2005;105:46-52.
19. Chang CL, Donaghy M, Poulter N. Migraine and stroke in young women: case-control study. The World Health Organisation Collaborative Study of Cardiovascular Disease and Steroid Hormone Contraception. BMJ. 1999;318:13-18.
20. World Health Organization Collaborative Study of Cardiovascular Disease and Steroid Hormone Contraception Cardiovascular disease and use of oral and injectable progestogen-only contraceptives and combined injectable contraceptives Results of an international, multicenter, case-control study. Contraception. 1998;57:315-324.
21. Grimes DA. Intrauterine devices. In: Hatcher RA et al, eds. Contraceptive Technology. 18th ed. New York: Ardent Media; 2004; 495-530.
22. Darney PD. Time to pardon the IUD? N Engl J Med. 2001;345:608-610.
23. Farley TM, Rosenberg MJ, Rowe PJ, Chen JH, Meirik O. Intrauterine devices and pelvic inflammatory disease: an international perspective. Lancet. 1992;339:785-788.
24. Lee NC, Rubin GL, Borucki R. The intrauterine device and pelvic inflammatory disease revisited: new results from the Women’s Health Study. Obstet Gynecol. 1988;72:1-6.
25. Andersson K, Odlind V, Rybo G. Levonorgestrel-releasing and copper-releasing (Nova T) IUDs during five years of use: a randomized comparative trial. Contraception. 1994;49:56-72.
26. Morrison CS, Sekadde-Kigondu C, Sinei SK, Weiner DH, Kwok C, Kokonya D. Is the intrauterine device appropriate contraception for HIV-1-infected women. BJOG. 2001;108:784-790.
27. Zerner J, Doil KL, Drewry J, Leeber DA. Intrauterine contraceptive device failures in renal transplant patients. J Reprod Med. 1981;26:99-102.
28. Jamieson DJ, Hillis SD, Duerr A, Marchbanks PA, Costello C, Peterson HB. Complications of interval laparoscopic tubal sterilization: findings from the United States Collaborative Review of Sterilization. Obstet Gynecol. 2000;96:997-1002.
29. Cooper JM, Carignan CS, Cher D, Kerin JF. Selective Tubal Occlusion Procedure Investigators Microinsert nonincisional hysteroscopic sterilization. Obstet Gynecol. 2003;102:59-67.
30. Petitti DB, Sidney S, Quesenberry CP, Jr, Bernstein A. Incidence of stroke and myocardial infarction in women of reproductive age. Stroke. 1997;28:280-283.
31. Ladner HE, Danielsen B, Gilbert WM. Acute myocardial infarction in pregnancy and the puerperium: a population-based study. Obstet Gynecol. 2005;105:480-484.
32. James AH, Jamison MG, Biswas MS, Brancazio LR, Swamy GK, Myers ER. Acute myocardial infarction in pregnancy: a United States population-based study. Circulation. 2006;113:1564-1571.
33. Kittner SJ, Stern BJ, Feeser BR, et al. Pregnancy and the risk of stroke. N Engl J Med. 1996;335:768-774.
1. World Health Organization Medical Eligibility Criteria for Contraceptive Use. 3rd ed. Geneva: World Health Organization; 2004. Available at:www.who.int/reproductive-health/publications/mec/index.htm. Accessed Oct. 25, 2007.
2. Hatcher RA, Nelson A. Combined hormonal contraceptive methods. In: Hatcher RA et al, eds. Contraceptive Technology. 18th ed. New York: Ardent Media; 2004;391:460-
3. Faculty of Family Planning and Reproductive Health Care Clinical Effectiveness Unit First Prescription of Combined Oral Contraception. Royal College of Obstetricians and Gynaecologists: 2006.
4. Tanis BC, van den Bosch MA, Kemmeren JM, et al. Oral contraceptives and the risk of myocardial infarction. N Engl J Med. 2001;345:1787-1793.
5. Gillum LA, Mamidipudi SK, Johnston SC. Ischemic stroke risk with oral contraceptives: a meta-analysis. JAMA. 2000;284:72-78.
6. World Health Organization Collaborative Study of Cardiovascular Disease and Steroid Hormone Contraception Ischaemic stroke and combined oral contraceptives: results of an international, multicentre, case-control study. Lancet. 1996;348:498-505.
7. Vandenbroucke JP, Rosing J, Bloemenkamp KW, et al. Oral contraceptives and the risk of venous thrombosis. N Engl J Med. 2001;344:1527-1535.
8. Cole JA, Norman H, Doherty M, Walker AM. Venous thromboembolism, myocardial infarction, and stroke among transdermal contraceptive system users. Obstet Gynecol. 2007;109(2 Pt 1):339-346.
9. Schwingl PJ, Ory HW, Visness CM. Estimates of the risk of cardiovascular death attributable to low-dose oral contraceptives in the United States. Am J Obstet Gynecol. 1999;180(1 Pt 1):241-249.
10. Petitti DB, Sidney S, Quesenberry CP. Oral contraceptive use and myocardial infarction. Contraception. 1998;57:143-155.
11. Curtis KM, Mohllajee AP, Peterson HB. Use of combined oral contraceptives among women with migraine and nonmigrainous headaches: a systematic review. Contraception. 2006;73:189-194.
12. Etminan M, Takkouche B, Isorna FC, Samii A. Risk of ischaemic stroke in people with migraine: systematic review and meta-analysis of observational studies. BMJ. 2005;330:63.-
13. Slooter AJ, Rosendaal FR, Tanis BC, Kemmeren JM, van der Graaf Y, Algra A. Prothrombotic conditions, oral contraceptives, and the risk of ischemic stroke. J Thromb Haemost. 2005;3:1213-1217.
14. Mohllajee AP, Curtis KM, Martins SL, Peterson HB. Does use of hormonal contraceptives among women with thrombogenic mutations increase their risk of thromboembolism? A systematic review. Contraception. 2006;73:166-178.
15. Christiansen SC, Cannegieter SC, Koster T, Vandenbroucke JP, Rosendaal FR. Thrombophilia, clinical factors, and recurrent venous thrombotic events. JAMA. 2005;293:2352-2361.
16. World Health Organization Collaborative Study of Cardiovascular Disease and Steroid Hormone Contraception Effect of different progestagens in low oestrogen oral contraceptives on venous thromboembolic disease. Lancet. 1995;346:1582-1588.
17. Sidney S, Petitti DB, Soff GA, Cundiff DL, Tolan KK, Quesenberry CP, Jr. Venous thromboembolic disease in users of low-estrogen combined estrogen-progestin oral contraceptives. Contraception. 2004;70:3-10.
18. Holt VL, Scholes D, Wicklund KG, Cushing-Haugen KL, Daling JR. Body mass index, weight, and oral contraceptive failure risk. Obstet Gynecol. 2005;105:46-52.
19. Chang CL, Donaghy M, Poulter N. Migraine and stroke in young women: case-control study. The World Health Organisation Collaborative Study of Cardiovascular Disease and Steroid Hormone Contraception. BMJ. 1999;318:13-18.
20. World Health Organization Collaborative Study of Cardiovascular Disease and Steroid Hormone Contraception Cardiovascular disease and use of oral and injectable progestogen-only contraceptives and combined injectable contraceptives Results of an international, multicenter, case-control study. Contraception. 1998;57:315-324.
21. Grimes DA. Intrauterine devices. In: Hatcher RA et al, eds. Contraceptive Technology. 18th ed. New York: Ardent Media; 2004; 495-530.
22. Darney PD. Time to pardon the IUD? N Engl J Med. 2001;345:608-610.
23. Farley TM, Rosenberg MJ, Rowe PJ, Chen JH, Meirik O. Intrauterine devices and pelvic inflammatory disease: an international perspective. Lancet. 1992;339:785-788.
24. Lee NC, Rubin GL, Borucki R. The intrauterine device and pelvic inflammatory disease revisited: new results from the Women’s Health Study. Obstet Gynecol. 1988;72:1-6.
25. Andersson K, Odlind V, Rybo G. Levonorgestrel-releasing and copper-releasing (Nova T) IUDs during five years of use: a randomized comparative trial. Contraception. 1994;49:56-72.
26. Morrison CS, Sekadde-Kigondu C, Sinei SK, Weiner DH, Kwok C, Kokonya D. Is the intrauterine device appropriate contraception for HIV-1-infected women. BJOG. 2001;108:784-790.
27. Zerner J, Doil KL, Drewry J, Leeber DA. Intrauterine contraceptive device failures in renal transplant patients. J Reprod Med. 1981;26:99-102.
28. Jamieson DJ, Hillis SD, Duerr A, Marchbanks PA, Costello C, Peterson HB. Complications of interval laparoscopic tubal sterilization: findings from the United States Collaborative Review of Sterilization. Obstet Gynecol. 2000;96:997-1002.
29. Cooper JM, Carignan CS, Cher D, Kerin JF. Selective Tubal Occlusion Procedure Investigators Microinsert nonincisional hysteroscopic sterilization. Obstet Gynecol. 2003;102:59-67.
30. Petitti DB, Sidney S, Quesenberry CP, Jr, Bernstein A. Incidence of stroke and myocardial infarction in women of reproductive age. Stroke. 1997;28:280-283.
31. Ladner HE, Danielsen B, Gilbert WM. Acute myocardial infarction in pregnancy and the puerperium: a population-based study. Obstet Gynecol. 2005;105:480-484.
32. James AH, Jamison MG, Biswas MS, Brancazio LR, Swamy GK, Myers ER. Acute myocardial infarction in pregnancy: a United States population-based study. Circulation. 2006;113:1564-1571.
33. Kittner SJ, Stern BJ, Feeser BR, et al. Pregnancy and the risk of stroke. N Engl J Med. 1996;335:768-774.