User login
Tips for assessing, managing temper tantrums
Concerns about tantrums come up a lot in pediatric care. We all know about telling parents to ignore tantrums in toddlers and not to give in. But what about when this advice does not work?
I like to think of tantrums as emotions that go beyond the child’s control. This reframing helps families consider that not all tantrums are an attempt by the child to manipulate them. That is an important first step in avoiding a solely punitive response and instead encouraging parents to look for the source of the imbalance.

Temper tantrums are most common when a child is making developmental spurts in abilities or thinking that are typically unevenly matched with self-control. There is a lot of unevenness in children’s ability to do, say, or tolerate feelings between the early tantrums of the 9-month-old until the greater coping of the 6-year-old. For example, 87% of 18- to 24-month-olds have tantrums just as they acquire autonomy and some language, yet can’t really speak their feelings, while 91% of 30- to 36-month-olds have tantrums because they can imagine big things, but are only capable of or allowed small ones. Even at 42-48 months, more than half have tantrums, which often are associated with the stress and fatigue from dropping their nap.
Life is frustrating for kids. Young children want to try to use their new skills such as climbing, opening things, or scribbling, but parents – at first delighted – suddenly want them to stop! At first, every new word is celebrated, but then toddler talk gets routine, and toddlers may be ignored or even shushed. When the child has a strong desire, the words may not be there, or emotions may make it hard to talk at all, leading to frustration.
With the development of a sense of self, the song is “I want,” “mine,” and “no!” Sharing is not in the child’s repertoire until age 3 years or older. Temperamentally more intense children give up less easily or are not readily distracted.
The threshold for frustration depends on the child’s overall state. Is the child hungry? Tired? Stressed? In pain? Here is where the differential diagnosis of excessive tantrums needs to also include pain from a medical condition such as celiac disease, arthritis, migraine, or sickle cell disease. Children under age 7 years commonly have a low tolerance for sensations as simple as loud noises and elastic waistbands, but those with sensory integration disorder are at the extreme in what sounds, feelings, or motions they cannot bear at any age and may need specific intervention by occupational or physical therapists. Mental health conditions such as attention-deficit/hyperactivity disorder, depression, anxiety, and bipolar disorder also predispose to irritable responses to even normal stresses, often in combination with lagging skills and poor sleep. Consider these when tantrums are extreme.
An age period of tantrums may be expected and accepted by parents, thus the name “terrible twos,” but if tantrums persist, they can wear out even a patient parent. Signs that a child’s tantrums are beyond the usual range include a frequency of more than once a day, a duration of more than the typical 5 minutes, or persistence after age 6 years. When you are asked if a child’s tantrums are “normal,” these are useful parameters. It also helps to explain to parents the natural course of anger arousal that starts with a trigger, peaks within 3 minutes, then subsides rapidly (usually a total of 90 seconds), and although starting with anger, ends up with sadness. Asking parents to collect this information helps them avoid interfering with or reinforcing tantrums.
Understanding the child’s temperament and needs, and avoiding triggers, can prevent many tantrums. What was she doing just before the tantrum started? What were the triggers such as fatigue, hunger, inability to express herself, or a buildup of jealousy from repeated sibling intrusions? Are there skill deficits setting him off, especially fine motor or language delays? Management then needs to focus on avoiding these triggers, if possible, and diagnosing and treating developmental delays.
Next, parents can try to distract by jollying, making a joke, or singing. These are useful moments of modeling. Some parents are worried that distracting the child with something more fun to do will interfere with his learning to cope. If distraction works, they should use it!
Often nothing works, and the child has to explode and recover on her own. Talking, cajoling, or scolding during the fit is useless – like trying to squash dynamite after the flame has hit the powder.
While standing by silently ignoring tantrums is usually the fastest way to reduce them, some children calm down faster if held. This does not reinforce the fits as long as the child’s demand is not fulfilled. Instead, it lends adult “ego support” to reassure the child that all is well and life goes on. Children quickly go from angry to sad; older children are even embarrassed by their loss of control. Comfort is appropriate and kind, as long as at least one parent can do this authentically.
Point out that frustrations in small doses are crucial for learning frustration tolerance. Parents who overprotect their child from any little stress to avoid fits is doing him a disservice. Instead, attention, praise, or marks for little bits of self-control effort or for “using your words” builds self-control over time. Times of transitions such as coming for dinner or going to brush teeth are often times of tantrums; these deserve a 2-minute warning and praise or marks for success in “moving on.”(Stopping electronics without a fit is another . Hint: If the child has a fit, he gets no electronics the next day.)
Adult management may be reinforcing tantrums. When parents give the child what she was screaming for, or remove a demand – such as to take a bath – that had sparked a fit, they can count on having an even worse reaction the next time.
I coach parents to think together about the six main things that set off their child’s tantrums and decide in advance on which ones they will hold their ground. Then, when the child just begins to beg for that snack, the parent should decide instantly if this is a “yes” or a “no” (aiming for more yeses). Parental “giving in” before a tantrum starts models positive flexibility for the child and avoids reinforcement. When an event on the “no” list comes up, both parents are then better able to have an unequivocal response and then walk away.
“But when should we teach him a lesson?” parents often ask. If parents interpret a tantrum as manipulative, a moral failing, or an evil tendency, they tend to react with anger and even loss of control themselves. Be alert for risks of excessive punishment in these cases. Not only is their response a poor model and scary for the child, it can even become an exciting, reinforcing display. If parents are depressed or tend to ignore the child as a norm, it may be worth it to the child to throw a fit to bring them to life. You can emphasize that positive attention to good behavior and silent ignoring of fits is more effective and avoids these side effects.
Parents may experience tantrums as a battle of wills that they are not willing to lose, imagining a future rebellious teen. They need education on the normal imbalances of childhood and on both prevention and intervention strategies. What they can lose in the present is their child’s confidence in adult kindness, the opportunity to model flexibility and self-control, and a relationship with their child that conveys acceptance.
Dr. Howard is assistant professor of pediatrics at the Johns Hopkins University School of Medicine, Baltimore, and creator of CHADIS (www.CHADIS.com). She has no other relevant disclosures. Dr. Howard’s contribution to this publication was as a paid expert to Frontline Medical Communications.
Concerns about tantrums come up a lot in pediatric care. We all know about telling parents to ignore tantrums in toddlers and not to give in. But what about when this advice does not work?
I like to think of tantrums as emotions that go beyond the child’s control. This reframing helps families consider that not all tantrums are an attempt by the child to manipulate them. That is an important first step in avoiding a solely punitive response and instead encouraging parents to look for the source of the imbalance.
Temper tantrums are most common when a child is making developmental spurts in abilities or thinking that are typically unevenly matched with self-control. There is a lot of unevenness in children’s ability to do, say, or tolerate feelings between the early tantrums of the 9-month-old until the greater coping of the 6-year-old. For example, 87% of 18- to 24-month-olds have tantrums just as they acquire autonomy and some language, yet can’t really speak their feelings, while 91% of 30- to 36-month-olds have tantrums because they can imagine big things, but are only capable of or allowed small ones. Even at 42-48 months, more than half have tantrums, which often are associated with the stress and fatigue from dropping their nap.
Life is frustrating for kids. Young children want to try to use their new skills such as climbing, opening things, or scribbling, but parents – at first delighted – suddenly want them to stop! At first, every new word is celebrated, but then toddler talk gets routine, and toddlers may be ignored or even shushed. When the child has a strong desire, the words may not be there, or emotions may make it hard to talk at all, leading to frustration.
With the development of a sense of self, the song is “I want,” “mine,” and “no!” Sharing is not in the child’s repertoire until age 3 years or older. Temperamentally more intense children give up less easily or are not readily distracted.
The threshold for frustration depends on the child’s overall state. Is the child hungry? Tired? Stressed? In pain? Here is where the differential diagnosis of excessive tantrums needs to also include pain from a medical condition such as celiac disease, arthritis, migraine, or sickle cell disease. Children under age 7 years commonly have a low tolerance for sensations as simple as loud noises and elastic waistbands, but those with sensory integration disorder are at the extreme in what sounds, feelings, or motions they cannot bear at any age and may need specific intervention by occupational or physical therapists. Mental health conditions such as attention-deficit/hyperactivity disorder, depression, anxiety, and bipolar disorder also predispose to irritable responses to even normal stresses, often in combination with lagging skills and poor sleep. Consider these when tantrums are extreme.
An age period of tantrums may be expected and accepted by parents, thus the name “terrible twos,” but if tantrums persist, they can wear out even a patient parent. Signs that a child’s tantrums are beyond the usual range include a frequency of more than once a day, a duration of more than the typical 5 minutes, or persistence after age 6 years. When you are asked if a child’s tantrums are “normal,” these are useful parameters. It also helps to explain to parents the natural course of anger arousal that starts with a trigger, peaks within 3 minutes, then subsides rapidly (usually a total of 90 seconds), and although starting with anger, ends up with sadness. Asking parents to collect this information helps them avoid interfering with or reinforcing tantrums.
Understanding the child’s temperament and needs, and avoiding triggers, can prevent many tantrums. What was she doing just before the tantrum started? What were the triggers such as fatigue, hunger, inability to express herself, or a buildup of jealousy from repeated sibling intrusions? Are there skill deficits setting him off, especially fine motor or language delays? Management then needs to focus on avoiding these triggers, if possible, and diagnosing and treating developmental delays.
Next, parents can try to distract by jollying, making a joke, or singing. These are useful moments of modeling. Some parents are worried that distracting the child with something more fun to do will interfere with his learning to cope. If distraction works, they should use it!
Often nothing works, and the child has to explode and recover on her own. Talking, cajoling, or scolding during the fit is useless – like trying to squash dynamite after the flame has hit the powder.
While standing by silently ignoring tantrums is usually the fastest way to reduce them, some children calm down faster if held. This does not reinforce the fits as long as the child’s demand is not fulfilled. Instead, it lends adult “ego support” to reassure the child that all is well and life goes on. Children quickly go from angry to sad; older children are even embarrassed by their loss of control. Comfort is appropriate and kind, as long as at least one parent can do this authentically.
Point out that frustrations in small doses are crucial for learning frustration tolerance. Parents who overprotect their child from any little stress to avoid fits is doing him a disservice. Instead, attention, praise, or marks for little bits of self-control effort or for “using your words” builds self-control over time. Times of transitions such as coming for dinner or going to brush teeth are often times of tantrums; these deserve a 2-minute warning and praise or marks for success in “moving on.”(Stopping electronics without a fit is another . Hint: If the child has a fit, he gets no electronics the next day.)
Adult management may be reinforcing tantrums. When parents give the child what she was screaming for, or remove a demand – such as to take a bath – that had sparked a fit, they can count on having an even worse reaction the next time.
I coach parents to think together about the six main things that set off their child’s tantrums and decide in advance on which ones they will hold their ground. Then, when the child just begins to beg for that snack, the parent should decide instantly if this is a “yes” or a “no” (aiming for more yeses). Parental “giving in” before a tantrum starts models positive flexibility for the child and avoids reinforcement. When an event on the “no” list comes up, both parents are then better able to have an unequivocal response and then walk away.
“But when should we teach him a lesson?” parents often ask. If parents interpret a tantrum as manipulative, a moral failing, or an evil tendency, they tend to react with anger and even loss of control themselves. Be alert for risks of excessive punishment in these cases. Not only is their response a poor model and scary for the child, it can even become an exciting, reinforcing display. If parents are depressed or tend to ignore the child as a norm, it may be worth it to the child to throw a fit to bring them to life. You can emphasize that positive attention to good behavior and silent ignoring of fits is more effective and avoids these side effects.
Parents may experience tantrums as a battle of wills that they are not willing to lose, imagining a future rebellious teen. They need education on the normal imbalances of childhood and on both prevention and intervention strategies. What they can lose in the present is their child’s confidence in adult kindness, the opportunity to model flexibility and self-control, and a relationship with their child that conveys acceptance.
Dr. Howard is assistant professor of pediatrics at the Johns Hopkins University School of Medicine, Baltimore, and creator of CHADIS (www.CHADIS.com). She has no other relevant disclosures. Dr. Howard’s contribution to this publication was as a paid expert to Frontline Medical Communications.
Concerns about tantrums come up a lot in pediatric care. We all know about telling parents to ignore tantrums in toddlers and not to give in. But what about when this advice does not work?
I like to think of tantrums as emotions that go beyond the child’s control. This reframing helps families consider that not all tantrums are an attempt by the child to manipulate them. That is an important first step in avoiding a solely punitive response and instead encouraging parents to look for the source of the imbalance.
Temper tantrums are most common when a child is making developmental spurts in abilities or thinking that are typically unevenly matched with self-control. There is a lot of unevenness in children’s ability to do, say, or tolerate feelings between the early tantrums of the 9-month-old until the greater coping of the 6-year-old. For example, 87% of 18- to 24-month-olds have tantrums just as they acquire autonomy and some language, yet can’t really speak their feelings, while 91% of 30- to 36-month-olds have tantrums because they can imagine big things, but are only capable of or allowed small ones. Even at 42-48 months, more than half have tantrums, which often are associated with the stress and fatigue from dropping their nap.
Life is frustrating for kids. Young children want to try to use their new skills such as climbing, opening things, or scribbling, but parents – at first delighted – suddenly want them to stop! At first, every new word is celebrated, but then toddler talk gets routine, and toddlers may be ignored or even shushed. When the child has a strong desire, the words may not be there, or emotions may make it hard to talk at all, leading to frustration.
With the development of a sense of self, the song is “I want,” “mine,” and “no!” Sharing is not in the child’s repertoire until age 3 years or older. Temperamentally more intense children give up less easily or are not readily distracted.
The threshold for frustration depends on the child’s overall state. Is the child hungry? Tired? Stressed? In pain? Here is where the differential diagnosis of excessive tantrums needs to also include pain from a medical condition such as celiac disease, arthritis, migraine, or sickle cell disease. Children under age 7 years commonly have a low tolerance for sensations as simple as loud noises and elastic waistbands, but those with sensory integration disorder are at the extreme in what sounds, feelings, or motions they cannot bear at any age and may need specific intervention by occupational or physical therapists. Mental health conditions such as attention-deficit/hyperactivity disorder, depression, anxiety, and bipolar disorder also predispose to irritable responses to even normal stresses, often in combination with lagging skills and poor sleep. Consider these when tantrums are extreme.
An age period of tantrums may be expected and accepted by parents, thus the name “terrible twos,” but if tantrums persist, they can wear out even a patient parent. Signs that a child’s tantrums are beyond the usual range include a frequency of more than once a day, a duration of more than the typical 5 minutes, or persistence after age 6 years. When you are asked if a child’s tantrums are “normal,” these are useful parameters. It also helps to explain to parents the natural course of anger arousal that starts with a trigger, peaks within 3 minutes, then subsides rapidly (usually a total of 90 seconds), and although starting with anger, ends up with sadness. Asking parents to collect this information helps them avoid interfering with or reinforcing tantrums.
Understanding the child’s temperament and needs, and avoiding triggers, can prevent many tantrums. What was she doing just before the tantrum started? What were the triggers such as fatigue, hunger, inability to express herself, or a buildup of jealousy from repeated sibling intrusions? Are there skill deficits setting him off, especially fine motor or language delays? Management then needs to focus on avoiding these triggers, if possible, and diagnosing and treating developmental delays.
Next, parents can try to distract by jollying, making a joke, or singing. These are useful moments of modeling. Some parents are worried that distracting the child with something more fun to do will interfere with his learning to cope. If distraction works, they should use it!
Often nothing works, and the child has to explode and recover on her own. Talking, cajoling, or scolding during the fit is useless – like trying to squash dynamite after the flame has hit the powder.
While standing by silently ignoring tantrums is usually the fastest way to reduce them, some children calm down faster if held. This does not reinforce the fits as long as the child’s demand is not fulfilled. Instead, it lends adult “ego support” to reassure the child that all is well and life goes on. Children quickly go from angry to sad; older children are even embarrassed by their loss of control. Comfort is appropriate and kind, as long as at least one parent can do this authentically.
Point out that frustrations in small doses are crucial for learning frustration tolerance. Parents who overprotect their child from any little stress to avoid fits is doing him a disservice. Instead, attention, praise, or marks for little bits of self-control effort or for “using your words” builds self-control over time. Times of transitions such as coming for dinner or going to brush teeth are often times of tantrums; these deserve a 2-minute warning and praise or marks for success in “moving on.”(Stopping electronics without a fit is another . Hint: If the child has a fit, he gets no electronics the next day.)
Adult management may be reinforcing tantrums. When parents give the child what she was screaming for, or remove a demand – such as to take a bath – that had sparked a fit, they can count on having an even worse reaction the next time.
I coach parents to think together about the six main things that set off their child’s tantrums and decide in advance on which ones they will hold their ground. Then, when the child just begins to beg for that snack, the parent should decide instantly if this is a “yes” or a “no” (aiming for more yeses). Parental “giving in” before a tantrum starts models positive flexibility for the child and avoids reinforcement. When an event on the “no” list comes up, both parents are then better able to have an unequivocal response and then walk away.
“But when should we teach him a lesson?” parents often ask. If parents interpret a tantrum as manipulative, a moral failing, or an evil tendency, they tend to react with anger and even loss of control themselves. Be alert for risks of excessive punishment in these cases. Not only is their response a poor model and scary for the child, it can even become an exciting, reinforcing display. If parents are depressed or tend to ignore the child as a norm, it may be worth it to the child to throw a fit to bring them to life. You can emphasize that positive attention to good behavior and silent ignoring of fits is more effective and avoids these side effects.
Parents may experience tantrums as a battle of wills that they are not willing to lose, imagining a future rebellious teen. They need education on the normal imbalances of childhood and on both prevention and intervention strategies. What they can lose in the present is their child’s confidence in adult kindness, the opportunity to model flexibility and self-control, and a relationship with their child that conveys acceptance.
Dr. Howard is assistant professor of pediatrics at the Johns Hopkins University School of Medicine, Baltimore, and creator of CHADIS (www.CHADIS.com). She has no other relevant disclosures. Dr. Howard’s contribution to this publication was as a paid expert to Frontline Medical Communications.

Electronic communications and liability exposure
On a recent rerun of the 1960s TV series, “The Addams Family,” Thing, the disembodied hand that lived without a body, came down with a cold. So Morticia Addams contacted a doctor who agreed to see Thing during a house call. While the need for convenient access to a physician has not changed in 50 years, technology is offering new solutions to fill the need for patient/physician interaction that range from e-mail to text messaging to video chat, offering both promises and pitfalls. In this article we will explore some of the emerging liability issues that these new forms of patient evaluation present.
Today, there are essentially three types of interactions between patients and physicians: in office/hospital visits, telephone conferences, and electronic communications. The first two interactions have been long practiced and physicians have a good sense of the parameters of their use. Electronic communication is new and has become popular within the past few years. Clinicians often do not have a well-honed sense of the boundaries of interaction with these new mediums and, unfortunately, electronic communications have created another avenue for physician liability.

When a physician sees a patient in person, the physician assesses the patient’s subjective complaints and objectively evaluates the patient. While it has been said that 90% of the diagnosis is arrived at through the taking of a careful history, I think we would all agree that a physical exam is an important part of a complete evaluation, and, depending upon the presenting problem and the differential diagnosis, it may be an essential part of the evaluation. When a physician interacts with a patient over the phone, that physician’s ability to evaluate the patient’s complaints through physical contact is removed, but the physician still has the ability to hear the patient’s voice and engage the patient. Voice inflections – a slight tremor in the voice of a tearful patient, the sense of heightened concern from the mother of a sick 5-year-old – can give insight into the severity of illness beyond what was conveyed by the words themselves. The conversation, in person or on the phone, allows for an iterative exchange of information, with one piece of information allowing the physician to ask the next important question, and so on. When a physician interacts with a patient through electronic communication via e-mail or text message, the tools that the physician uses to evaluate the patient objectively are removed.
Though patients are pushing for fewer in-person interactions with health care providers and have become used to electronic communications, clinicians need to be careful not to relinquish the opportunity for robust two-way conversations that allow them to obtain the information necessary to formulate a thoughtful diagnosis and plan. Recently, we have seen an important increase in lawsuits stemming from electronic interactions. In most cases, liability stems from the lack of an objective evaluation of the patient or perception of a lack of caring by the health care provider.
In a lawsuit we (G.C.) recently defended, a husband and wife had been seeing their primary care physician for 15 years. During one of the husband’s visits with the physician, the husband complained of weight loss and fatigue. The husband’s initial complaints were not concerning. However, at the next visit, the husband complained of new symptoms including chills, cramping, fatigue, and a poor appetite. A urinalysis did not point to a clear diagnosis. Thereafter, all communications between the husband and physician were conducted solely through e-mail. In those correspondences, the husband continued to make ambiguous complaints of the same symptoms. Without asking the patient to come into the office, the physician diagnosed the husband with a viral infection. Multiple e-mail exchanges ensued thereafter and, without ever setting eyes on the patient, the physician continued to assure the couple that the husband would get better over time. Meanwhile, the husband was developing endocarditis during the course of these e-mail exchanges that eventually led to his death.
What happened in this case was an unfortunate misinterpretation of the e-mails, which led to confusion, misdiagnosis, harm to the patient, and, ultimately, a lawsuit against the physician. While endocarditis is rare and difficult to diagnose under any circumstances, that physician did not ensure that he had the opportunity to evaluate the patient fully, to see with his own eyes how sick the patient might have looked, or to listen for a new murmur, or spot a Janeway lesion, all signs of more serious disease that may or may not have been apparent during a full evaluation. The uncritical use of e-mail made it easy to assume that the original diagnosis of a viral syndrome was correct, without providing the opportunity to critically reassess the patient’s concerns.
In this case, in addition to the missed diagnosis, there was an apparent violation of HIPAA. The e-mail address used by the physician was a personal e-mail account. HIPAA precludes physicians from discussing medical information through a means of communication that a non–health care provider might have access to. In an electronic age with multiple modes of communication, we have to be ever more careful to have a well thought out approach to the protection of patient privacy. It is easy to send a quick text message or e-mail to a patient, but it is important to understand that HIPAA applies even when a communication seems trivial or benign in nature.
In summary, society realizes that primary care physicians need to communicate at times other than at scheduled visits, and there is no longer an expectation that the physician will make house calls like the doctor in “The Addam’s Family” episode did 50 years ago. Society, and the courts, recognize that e-mail and text messaging are potentially useful forms of quick, convenient communication. We want to conclude with two important points. First, when using e-mails and texts to communicate with patients, use a secure HIPAA-compliant technology. Second, we need to be cautious that these convenient technologies do not creep into areas where they don’t belong, such as in making a diagnosis when doing so requires more interactive discussion and a physical exam. E-mail and text messaging are emerging as useful mediums for communication with patients, but as with any new technology, we need to be careful and thoughtful in their use.
Dr. Skolnik is associate director of the family medicine residency program at Abington (Pa.) Memorial Hospital and professor of family and community medicine at Temple University in Philadelphia. Mr. Cannon is an attorney at Marshall Dennehey Warner Coleman & Goggin in Pittsburgh.
On a recent rerun of the 1960s TV series, “The Addams Family,” Thing, the disembodied hand that lived without a body, came down with a cold. So Morticia Addams contacted a doctor who agreed to see Thing during a house call. While the need for convenient access to a physician has not changed in 50 years, technology is offering new solutions to fill the need for patient/physician interaction that range from e-mail to text messaging to video chat, offering both promises and pitfalls. In this article we will explore some of the emerging liability issues that these new forms of patient evaluation present.
Today, there are essentially three types of interactions between patients and physicians: in office/hospital visits, telephone conferences, and electronic communications. The first two interactions have been long practiced and physicians have a good sense of the parameters of their use. Electronic communication is new and has become popular within the past few years. Clinicians often do not have a well-honed sense of the boundaries of interaction with these new mediums and, unfortunately, electronic communications have created another avenue for physician liability.
When a physician sees a patient in person, the physician assesses the patient’s subjective complaints and objectively evaluates the patient. While it has been said that 90% of the diagnosis is arrived at through the taking of a careful history, I think we would all agree that a physical exam is an important part of a complete evaluation, and, depending upon the presenting problem and the differential diagnosis, it may be an essential part of the evaluation. When a physician interacts with a patient over the phone, that physician’s ability to evaluate the patient’s complaints through physical contact is removed, but the physician still has the ability to hear the patient’s voice and engage the patient. Voice inflections – a slight tremor in the voice of a tearful patient, the sense of heightened concern from the mother of a sick 5-year-old – can give insight into the severity of illness beyond what was conveyed by the words themselves. The conversation, in person or on the phone, allows for an iterative exchange of information, with one piece of information allowing the physician to ask the next important question, and so on. When a physician interacts with a patient through electronic communication via e-mail or text message, the tools that the physician uses to evaluate the patient objectively are removed.
Though patients are pushing for fewer in-person interactions with health care providers and have become used to electronic communications, clinicians need to be careful not to relinquish the opportunity for robust two-way conversations that allow them to obtain the information necessary to formulate a thoughtful diagnosis and plan. Recently, we have seen an important increase in lawsuits stemming from electronic interactions. In most cases, liability stems from the lack of an objective evaluation of the patient or perception of a lack of caring by the health care provider.
In a lawsuit we (G.C.) recently defended, a husband and wife had been seeing their primary care physician for 15 years. During one of the husband’s visits with the physician, the husband complained of weight loss and fatigue. The husband’s initial complaints were not concerning. However, at the next visit, the husband complained of new symptoms including chills, cramping, fatigue, and a poor appetite. A urinalysis did not point to a clear diagnosis. Thereafter, all communications between the husband and physician were conducted solely through e-mail. In those correspondences, the husband continued to make ambiguous complaints of the same symptoms. Without asking the patient to come into the office, the physician diagnosed the husband with a viral infection. Multiple e-mail exchanges ensued thereafter and, without ever setting eyes on the patient, the physician continued to assure the couple that the husband would get better over time. Meanwhile, the husband was developing endocarditis during the course of these e-mail exchanges that eventually led to his death.
What happened in this case was an unfortunate misinterpretation of the e-mails, which led to confusion, misdiagnosis, harm to the patient, and, ultimately, a lawsuit against the physician. While endocarditis is rare and difficult to diagnose under any circumstances, that physician did not ensure that he had the opportunity to evaluate the patient fully, to see with his own eyes how sick the patient might have looked, or to listen for a new murmur, or spot a Janeway lesion, all signs of more serious disease that may or may not have been apparent during a full evaluation. The uncritical use of e-mail made it easy to assume that the original diagnosis of a viral syndrome was correct, without providing the opportunity to critically reassess the patient’s concerns.
In this case, in addition to the missed diagnosis, there was an apparent violation of HIPAA. The e-mail address used by the physician was a personal e-mail account. HIPAA precludes physicians from discussing medical information through a means of communication that a non–health care provider might have access to. In an electronic age with multiple modes of communication, we have to be ever more careful to have a well thought out approach to the protection of patient privacy. It is easy to send a quick text message or e-mail to a patient, but it is important to understand that HIPAA applies even when a communication seems trivial or benign in nature.
In summary, society realizes that primary care physicians need to communicate at times other than at scheduled visits, and there is no longer an expectation that the physician will make house calls like the doctor in “The Addam’s Family” episode did 50 years ago. Society, and the courts, recognize that e-mail and text messaging are potentially useful forms of quick, convenient communication. We want to conclude with two important points. First, when using e-mails and texts to communicate with patients, use a secure HIPAA-compliant technology. Second, we need to be cautious that these convenient technologies do not creep into areas where they don’t belong, such as in making a diagnosis when doing so requires more interactive discussion and a physical exam. E-mail and text messaging are emerging as useful mediums for communication with patients, but as with any new technology, we need to be careful and thoughtful in their use.
Dr. Skolnik is associate director of the family medicine residency program at Abington (Pa.) Memorial Hospital and professor of family and community medicine at Temple University in Philadelphia. Mr. Cannon is an attorney at Marshall Dennehey Warner Coleman & Goggin in Pittsburgh.
On a recent rerun of the 1960s TV series, “The Addams Family,” Thing, the disembodied hand that lived without a body, came down with a cold. So Morticia Addams contacted a doctor who agreed to see Thing during a house call. While the need for convenient access to a physician has not changed in 50 years, technology is offering new solutions to fill the need for patient/physician interaction that range from e-mail to text messaging to video chat, offering both promises and pitfalls. In this article we will explore some of the emerging liability issues that these new forms of patient evaluation present.
Today, there are essentially three types of interactions between patients and physicians: in office/hospital visits, telephone conferences, and electronic communications. The first two interactions have been long practiced and physicians have a good sense of the parameters of their use. Electronic communication is new and has become popular within the past few years. Clinicians often do not have a well-honed sense of the boundaries of interaction with these new mediums and, unfortunately, electronic communications have created another avenue for physician liability.
When a physician sees a patient in person, the physician assesses the patient’s subjective complaints and objectively evaluates the patient. While it has been said that 90% of the diagnosis is arrived at through the taking of a careful history, I think we would all agree that a physical exam is an important part of a complete evaluation, and, depending upon the presenting problem and the differential diagnosis, it may be an essential part of the evaluation. When a physician interacts with a patient over the phone, that physician’s ability to evaluate the patient’s complaints through physical contact is removed, but the physician still has the ability to hear the patient’s voice and engage the patient. Voice inflections – a slight tremor in the voice of a tearful patient, the sense of heightened concern from the mother of a sick 5-year-old – can give insight into the severity of illness beyond what was conveyed by the words themselves. The conversation, in person or on the phone, allows for an iterative exchange of information, with one piece of information allowing the physician to ask the next important question, and so on. When a physician interacts with a patient through electronic communication via e-mail or text message, the tools that the physician uses to evaluate the patient objectively are removed.
Though patients are pushing for fewer in-person interactions with health care providers and have become used to electronic communications, clinicians need to be careful not to relinquish the opportunity for robust two-way conversations that allow them to obtain the information necessary to formulate a thoughtful diagnosis and plan. Recently, we have seen an important increase in lawsuits stemming from electronic interactions. In most cases, liability stems from the lack of an objective evaluation of the patient or perception of a lack of caring by the health care provider.
In a lawsuit we (G.C.) recently defended, a husband and wife had been seeing their primary care physician for 15 years. During one of the husband’s visits with the physician, the husband complained of weight loss and fatigue. The husband’s initial complaints were not concerning. However, at the next visit, the husband complained of new symptoms including chills, cramping, fatigue, and a poor appetite. A urinalysis did not point to a clear diagnosis. Thereafter, all communications between the husband and physician were conducted solely through e-mail. In those correspondences, the husband continued to make ambiguous complaints of the same symptoms. Without asking the patient to come into the office, the physician diagnosed the husband with a viral infection. Multiple e-mail exchanges ensued thereafter and, without ever setting eyes on the patient, the physician continued to assure the couple that the husband would get better over time. Meanwhile, the husband was developing endocarditis during the course of these e-mail exchanges that eventually led to his death.
What happened in this case was an unfortunate misinterpretation of the e-mails, which led to confusion, misdiagnosis, harm to the patient, and, ultimately, a lawsuit against the physician. While endocarditis is rare and difficult to diagnose under any circumstances, that physician did not ensure that he had the opportunity to evaluate the patient fully, to see with his own eyes how sick the patient might have looked, or to listen for a new murmur, or spot a Janeway lesion, all signs of more serious disease that may or may not have been apparent during a full evaluation. The uncritical use of e-mail made it easy to assume that the original diagnosis of a viral syndrome was correct, without providing the opportunity to critically reassess the patient’s concerns.
In this case, in addition to the missed diagnosis, there was an apparent violation of HIPAA. The e-mail address used by the physician was a personal e-mail account. HIPAA precludes physicians from discussing medical information through a means of communication that a non–health care provider might have access to. In an electronic age with multiple modes of communication, we have to be ever more careful to have a well thought out approach to the protection of patient privacy. It is easy to send a quick text message or e-mail to a patient, but it is important to understand that HIPAA applies even when a communication seems trivial or benign in nature.
In summary, society realizes that primary care physicians need to communicate at times other than at scheduled visits, and there is no longer an expectation that the physician will make house calls like the doctor in “The Addam’s Family” episode did 50 years ago. Society, and the courts, recognize that e-mail and text messaging are potentially useful forms of quick, convenient communication. We want to conclude with two important points. First, when using e-mails and texts to communicate with patients, use a secure HIPAA-compliant technology. Second, we need to be cautious that these convenient technologies do not creep into areas where they don’t belong, such as in making a diagnosis when doing so requires more interactive discussion and a physical exam. E-mail and text messaging are emerging as useful mediums for communication with patients, but as with any new technology, we need to be careful and thoughtful in their use.
Dr. Skolnik is associate director of the family medicine residency program at Abington (Pa.) Memorial Hospital and professor of family and community medicine at Temple University in Philadelphia. Mr. Cannon is an attorney at Marshall Dennehey Warner Coleman & Goggin in Pittsburgh.

More questions than answers?

More questions than answers?
The data presented by Wright and colleagues on the prevalence of underlying cancer in women who undergo myomectomy is disturbing and thought-provoking.
Are those in the 50-and-older age group who undergo myomectomy different from their same-aged peers with fibroids who do not undergo myomectomy? If so, why? If not, then with a 1 in 154 to 1 in 31 risk of occult malignancy, should not all women 50 years and older with fibroids undergo hysterectomy for this occult risk? This certainly has not been the standard of care for women 50 and older with asymptomatic fibroids. Thoughts?
In conclusion, it appears that power morcellation, or should I say the morcellation issue, has brought forth more questions than answers.
Richard L. Myers, MD
Jacksonville, Florida
Dr. Barbieri responds
I agree with Dr. Myers: Women aged 50 and older who have fibroids and undergo myomectomy must be clinically different than women of the same age who have fibroids but do not undergo myomectomy. It is likely that the women who undergo myomectomy have larger pelvic tumors or are more symptomatic than those who do not undergo myomectomy. I think this demonstrates that gynecologists are successfully identifying those women with a pelvic mass thought to be due to fibroids with the greatest risk of occult cancer and recommending that those women undergo surgery, while simultaneously recommending expectant management for those at lowest risk of an occult cancer.
“UPDATE ON MINIMALLY INVASIVE gynecologic SURGERY”
AMY L. GARCIA, MD (APRIL 2015)
Additional tips for in-office hysteroscopy
Thank you for the excellent coverage of hysteroscopy in the April issue. For me, patient trust is extremely important. Before I begin in-office hysteroscopy, I explain how the procedure is performed and answer all questions. I reassure the patient that, if it is too painful, I will stop and we will move to the operating room. I find music to be distracting to me as I am talking and constantly reassuring her.
In addition, I don’t perform the procedure when the patient is menstruating as it decreases visibility and I don’t want the intrauterine lidocaine to enter open vessels. It is helpful to perform this procedure shortly after menses and prior to ovulation to avoid instrumenting a pregnant uterus. Even if the menses is normal in timing and flow, a pregnancy test is still performed prior to the procedure. Doing it in this time period also can offer better visibility, as the endometrium is thinner.
I prescribe oral misoprostol the night before (400 mg, or 200 mg if she has undergone a cesarean delivery). The patient also is instructed to take ibuprofen 800 mg 1 hour prior to the procedure.
I continuously tell the patient what to expect. First, I perform a bimanual exam to determine the uterine position. Then local anesthesia placed on the anterior lip of the cervix prevents pain when placing the tenaculum. A paracervical block is performed and lidocaine jelly is placed in the cervix. Using an angiocatheter, I inject 4 mL of 2% lidocaine into the uterus and then wait 3 minutes.
It is important to only use the amount of fluid necessary to avoid overdistending the uterus. I take care to avoid touching the fundus, as this increases pain. I use a 4-mm 30˚ scope. I agree that the pain is dependent on physician expertise and procedure length.
If the cavity is clean, I perform a thorough endometrial biopsy that causes minimal pain because of the intrauterine lidocaine. I recently started doing in-office diagnostic hysteroscopy again. When I did it years ago without intrauterine lidocaine, it was unacceptably painful. I have performed 25 cases, all of which were successful, including on postmenopausal patients. All of the patients reported being highly satisfied and glad to have had the procedure performed in the office.
Ray Wertheim, MD
Fairfax, Virginia
Would you approve this candidate for uterus transplantation?
Instant Poll
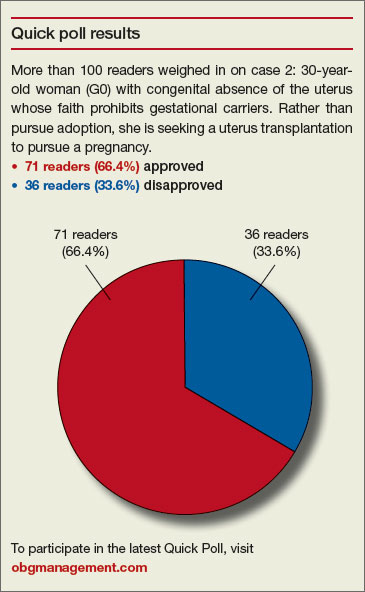
Dr. Barbieri presented 3 cases to readers in his recent editorial on uterus transplantation and asked, “Would you approve or disapprove of transplantation of the uterus in these cases?”
- 23-year-old Army sergeant (G0) injured by improvised explosive device. To save her life, military surgeons removed her uterus, which had been lacerated in the explosion. She requested uterus transplantation to pursue a pregnancy. The Department of Defense has approved her request.
- 30-year-old woman (G0) with congenital absence of the uterus who is a devout member of a religious community in which the tenets of faith prohibit gestational carriers. Rather than pursue adoption, she is seeking a uterus transplantation to pursue a pregnancy.
- 35-year-old woman (G1P1) who had her uterus removed to treat cervical cancer. She has been disease-free for 3 years. She would like a uterus transplant to pursue a pregnancy.
READERS WEIGH IN:
Concentrate on saving lives
We should be concentrating our resources on saving lives rather than on satisfying the wishes of some very genuine people.
Where will it end? Let us not compare uterine transplant with kidney, heart, and lung transplants.
Ram A. Singh, MD
Oklahoma City, Oklahoma
No to 35-year-old patient
Assuming, as stated, that the women are healthy and psychosocially approved, to which I would add, they are fully informed on the preparation, medications, procedure, postoperative recovery, and potential complications,I would approve the first 2 cases and disapprove of the last. My reasoning for denying a uterus transplant to the 35-year-old woman is that, after she goes through the process of screening and evaluation, she will be an “elderly gravida,” which in itself has risks. I would also be concerned that all the family members fully understand the potential risks of her undertaking.
Helen T. Jackson, MD
Brookline, Massachusetts
Share your thoughts on this article! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
More questions than answers?
The data presented by Wright and colleagues on the prevalence of underlying cancer in women who undergo myomectomy is disturbing and thought-provoking.
Are those in the 50-and-older age group who undergo myomectomy different from their same-aged peers with fibroids who do not undergo myomectomy? If so, why? If not, then with a 1 in 154 to 1 in 31 risk of occult malignancy, should not all women 50 years and older with fibroids undergo hysterectomy for this occult risk? This certainly has not been the standard of care for women 50 and older with asymptomatic fibroids. Thoughts?
In conclusion, it appears that power morcellation, or should I say the morcellation issue, has brought forth more questions than answers.
Richard L. Myers, MD
Jacksonville, Florida
Dr. Barbieri responds
I agree with Dr. Myers: Women aged 50 and older who have fibroids and undergo myomectomy must be clinically different than women of the same age who have fibroids but do not undergo myomectomy. It is likely that the women who undergo myomectomy have larger pelvic tumors or are more symptomatic than those who do not undergo myomectomy. I think this demonstrates that gynecologists are successfully identifying those women with a pelvic mass thought to be due to fibroids with the greatest risk of occult cancer and recommending that those women undergo surgery, while simultaneously recommending expectant management for those at lowest risk of an occult cancer.
“UPDATE ON MINIMALLY INVASIVE gynecologic SURGERY”
AMY L. GARCIA, MD (APRIL 2015)
Additional tips for in-office hysteroscopy
Thank you for the excellent coverage of hysteroscopy in the April issue. For me, patient trust is extremely important. Before I begin in-office hysteroscopy, I explain how the procedure is performed and answer all questions. I reassure the patient that, if it is too painful, I will stop and we will move to the operating room. I find music to be distracting to me as I am talking and constantly reassuring her.
In addition, I don’t perform the procedure when the patient is menstruating as it decreases visibility and I don’t want the intrauterine lidocaine to enter open vessels. It is helpful to perform this procedure shortly after menses and prior to ovulation to avoid instrumenting a pregnant uterus. Even if the menses is normal in timing and flow, a pregnancy test is still performed prior to the procedure. Doing it in this time period also can offer better visibility, as the endometrium is thinner.
I prescribe oral misoprostol the night before (400 mg, or 200 mg if she has undergone a cesarean delivery). The patient also is instructed to take ibuprofen 800 mg 1 hour prior to the procedure.
I continuously tell the patient what to expect. First, I perform a bimanual exam to determine the uterine position. Then local anesthesia placed on the anterior lip of the cervix prevents pain when placing the tenaculum. A paracervical block is performed and lidocaine jelly is placed in the cervix. Using an angiocatheter, I inject 4 mL of 2% lidocaine into the uterus and then wait 3 minutes.
It is important to only use the amount of fluid necessary to avoid overdistending the uterus. I take care to avoid touching the fundus, as this increases pain. I use a 4-mm 30˚ scope. I agree that the pain is dependent on physician expertise and procedure length.
If the cavity is clean, I perform a thorough endometrial biopsy that causes minimal pain because of the intrauterine lidocaine. I recently started doing in-office diagnostic hysteroscopy again. When I did it years ago without intrauterine lidocaine, it was unacceptably painful. I have performed 25 cases, all of which were successful, including on postmenopausal patients. All of the patients reported being highly satisfied and glad to have had the procedure performed in the office.
Ray Wertheim, MD
Fairfax, Virginia
Would you approve this candidate for uterus transplantation?
Instant Poll
Dr. Barbieri presented 3 cases to readers in his recent editorial on uterus transplantation and asked, “Would you approve or disapprove of transplantation of the uterus in these cases?”
- 23-year-old Army sergeant (G0) injured by improvised explosive device. To save her life, military surgeons removed her uterus, which had been lacerated in the explosion. She requested uterus transplantation to pursue a pregnancy. The Department of Defense has approved her request.
- 30-year-old woman (G0) with congenital absence of the uterus who is a devout member of a religious community in which the tenets of faith prohibit gestational carriers. Rather than pursue adoption, she is seeking a uterus transplantation to pursue a pregnancy.
- 35-year-old woman (G1P1) who had her uterus removed to treat cervical cancer. She has been disease-free for 3 years. She would like a uterus transplant to pursue a pregnancy.
READERS WEIGH IN:
Concentrate on saving lives
We should be concentrating our resources on saving lives rather than on satisfying the wishes of some very genuine people.
Where will it end? Let us not compare uterine transplant with kidney, heart, and lung transplants.
Ram A. Singh, MD
Oklahoma City, Oklahoma
No to 35-year-old patient
Assuming, as stated, that the women are healthy and psychosocially approved, to which I would add, they are fully informed on the preparation, medications, procedure, postoperative recovery, and potential complications,I would approve the first 2 cases and disapprove of the last. My reasoning for denying a uterus transplant to the 35-year-old woman is that, after she goes through the process of screening and evaluation, she will be an “elderly gravida,” which in itself has risks. I would also be concerned that all the family members fully understand the potential risks of her undertaking.
Helen T. Jackson, MD
Brookline, Massachusetts
Share your thoughts on this article! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
More questions than answers?
The data presented by Wright and colleagues on the prevalence of underlying cancer in women who undergo myomectomy is disturbing and thought-provoking.
Are those in the 50-and-older age group who undergo myomectomy different from their same-aged peers with fibroids who do not undergo myomectomy? If so, why? If not, then with a 1 in 154 to 1 in 31 risk of occult malignancy, should not all women 50 years and older with fibroids undergo hysterectomy for this occult risk? This certainly has not been the standard of care for women 50 and older with asymptomatic fibroids. Thoughts?
In conclusion, it appears that power morcellation, or should I say the morcellation issue, has brought forth more questions than answers.
Richard L. Myers, MD
Jacksonville, Florida
Dr. Barbieri responds
I agree with Dr. Myers: Women aged 50 and older who have fibroids and undergo myomectomy must be clinically different than women of the same age who have fibroids but do not undergo myomectomy. It is likely that the women who undergo myomectomy have larger pelvic tumors or are more symptomatic than those who do not undergo myomectomy. I think this demonstrates that gynecologists are successfully identifying those women with a pelvic mass thought to be due to fibroids with the greatest risk of occult cancer and recommending that those women undergo surgery, while simultaneously recommending expectant management for those at lowest risk of an occult cancer.
“UPDATE ON MINIMALLY INVASIVE gynecologic SURGERY”
AMY L. GARCIA, MD (APRIL 2015)
Additional tips for in-office hysteroscopy
Thank you for the excellent coverage of hysteroscopy in the April issue. For me, patient trust is extremely important. Before I begin in-office hysteroscopy, I explain how the procedure is performed and answer all questions. I reassure the patient that, if it is too painful, I will stop and we will move to the operating room. I find music to be distracting to me as I am talking and constantly reassuring her.
In addition, I don’t perform the procedure when the patient is menstruating as it decreases visibility and I don’t want the intrauterine lidocaine to enter open vessels. It is helpful to perform this procedure shortly after menses and prior to ovulation to avoid instrumenting a pregnant uterus. Even if the menses is normal in timing and flow, a pregnancy test is still performed prior to the procedure. Doing it in this time period also can offer better visibility, as the endometrium is thinner.
I prescribe oral misoprostol the night before (400 mg, or 200 mg if she has undergone a cesarean delivery). The patient also is instructed to take ibuprofen 800 mg 1 hour prior to the procedure.
I continuously tell the patient what to expect. First, I perform a bimanual exam to determine the uterine position. Then local anesthesia placed on the anterior lip of the cervix prevents pain when placing the tenaculum. A paracervical block is performed and lidocaine jelly is placed in the cervix. Using an angiocatheter, I inject 4 mL of 2% lidocaine into the uterus and then wait 3 minutes.
It is important to only use the amount of fluid necessary to avoid overdistending the uterus. I take care to avoid touching the fundus, as this increases pain. I use a 4-mm 30˚ scope. I agree that the pain is dependent on physician expertise and procedure length.
If the cavity is clean, I perform a thorough endometrial biopsy that causes minimal pain because of the intrauterine lidocaine. I recently started doing in-office diagnostic hysteroscopy again. When I did it years ago without intrauterine lidocaine, it was unacceptably painful. I have performed 25 cases, all of which were successful, including on postmenopausal patients. All of the patients reported being highly satisfied and glad to have had the procedure performed in the office.
Ray Wertheim, MD
Fairfax, Virginia
Would you approve this candidate for uterus transplantation?
Instant Poll
Dr. Barbieri presented 3 cases to readers in his recent editorial on uterus transplantation and asked, “Would you approve or disapprove of transplantation of the uterus in these cases?”
- 23-year-old Army sergeant (G0) injured by improvised explosive device. To save her life, military surgeons removed her uterus, which had been lacerated in the explosion. She requested uterus transplantation to pursue a pregnancy. The Department of Defense has approved her request.
- 30-year-old woman (G0) with congenital absence of the uterus who is a devout member of a religious community in which the tenets of faith prohibit gestational carriers. Rather than pursue adoption, she is seeking a uterus transplantation to pursue a pregnancy.
- 35-year-old woman (G1P1) who had her uterus removed to treat cervical cancer. She has been disease-free for 3 years. She would like a uterus transplant to pursue a pregnancy.
READERS WEIGH IN:
Concentrate on saving lives
We should be concentrating our resources on saving lives rather than on satisfying the wishes of some very genuine people.
Where will it end? Let us not compare uterine transplant with kidney, heart, and lung transplants.
Ram A. Singh, MD
Oklahoma City, Oklahoma
No to 35-year-old patient
Assuming, as stated, that the women are healthy and psychosocially approved, to which I would add, they are fully informed on the preparation, medications, procedure, postoperative recovery, and potential complications,I would approve the first 2 cases and disapprove of the last. My reasoning for denying a uterus transplant to the 35-year-old woman is that, after she goes through the process of screening and evaluation, she will be an “elderly gravida,” which in itself has risks. I would also be concerned that all the family members fully understand the potential risks of her undertaking.
Helen T. Jackson, MD
Brookline, Massachusetts
Share your thoughts on this article! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
Computer Navigation and Robotics for Total Knee Arthroplasty
Total knee arthroplasty (TKA) is a good surgical option to relieve pain and improve function in patients with osteoarthritis. The goal of surgery is to achieve a well-aligned prosthesis with well-balanced ligaments in order to minimize wear and improve implant survival. Overall, 82% to 89% of patients are satisfied with their outcomes after TKA, with good 10- to 15-year implant survivorship; however, there is still a subset of patients that are unsatisfied. In many cases, patient dissatisfaction is attributed to improper component alignment.1-3 Over the past decade, computer navigation and robotics have been introduced to control surgical variables so as to gain greater consistency in implant placement and postoperative component alignment.
Computer-assisted navigation tools were introduced not only to improve implant alignment but, more importantly, to optimize clinical outcomes. Most studies have demonstrated that the use of navigation is associated with fewer radiographic outliers after TKA.4 Various studies have compared radiographic results of navigated TKA with results of TKA using standard instrumentation.4-7 While long-term studies are necessary, short-term follow-up has shown that computer-assisted TKA can improve alignment, especially in patients with severe deformity.8-10 Currently, there is no definitive consensus that computer-assisted TKA leads to significantly better component alignment or postoperative outcomes due to the fact that many studies are limited by study design or small cohorts. However, the currently published articles support better component alignment and clinical outcomes with computer-assisted TKA. While some argue that the use of computer-assisted surgery is dependent on the user’s experience, computer-assisted surgery can assist less-experienced surgeons to reliably achieve good midterm outcomes with a low complication rate.8,11 Various studies have looked at computer-assisted TKA at midterm follow-up, with no significant differences in clinical outcome between navigated and traditional techniques. However, long-term studies showing the benefits of computer navigation are beginning to emerge. For example, de Steiger and colleagues12 recently found that computer-assisted TKA reduced the overall revision rate for loosening after TKA in patients less than 65 years of age.
While surgical navigation helps improve implant planning, robotic tools have emerged as a tool to help refine surgical execution. Coupled with surgical navigation tools, robotic control of surgical gestures may further enhance precision in implant placement and/or enable novel implant design features. At present, robotic techniques are increasingly used in unicompartmental knee arthroplasty (UKA) and TKA.13 Studies have demonstrated that the robotic tool is 3 times more accurate with 3 times less variability than conventional techniques in UKA.14 The utility of robotic tools for TKA remains unclear. Robotic-driven automatic cutting guides have been shown to reduce time and improve accuracy compared with navigation guides in femoral TKA cutting procedures in a cadaveric model.15 However, robotic-enabled TKA procedures are poorly described at present, and the clinical implications of their proposed improved precision remain unclear.
Computer navigation and robotic tools in TKA hold the promise of enhanced control of surgical variables that influence clinical outcome. The variables that may be impacted by these advanced tools include implant positioning, lower limb alignment, soft-tissue balance, and, potentially, implant design and fixation. At present, these tools have primarily been shown to improve lower limb alignment in TKA. The clinical impact of the enhanced control of this single surgical variable (lower limb alignment) has been muted in short-term and midterm studies. Future studies should be directed at understanding which surgical variable, or combination of variables, it is most essential to precisely control so as to positively impact clinical outcomes. ◾
1. Bourne RB, Chesworth BM, Davis AM, Mahomed NN, Charron KD. Patient satisfaction after total knee arthroplasty: who is satisfied and who is not? Clin Orthop Relat Res. 2010;468(1):57-63.
2. Sharkey PF, Hozack WJ, Rothman RH, Shastri S, Jacoby SM. Insall Award paper. Why are total knee arthroplasties failing today? Clin Orthop Relat Res. 2002;(404):7-13.
3. Emmerson KP, Morgan CG, Pinder IM. Survivorship analysis of the Kinematic Stabilizer total knee replacement: a 10- to 14-year follow-up. J Bone Joint Surg Br. 1996;78(3):441-445.
4. Liow MH, Xia Z, Wong MK, Tay KJ, Yeo SJ, Chin PL. Robot-assisted total knee arthroplasty accurately restores the joint line and mechanical axis. A prospective randomized study. J Arthroplasty. 2014;29(12):2373-2377.
5. Sparmann M, Wolke B, Czupalla H, Banzer D, Zink A. Positioning of total knee arthroplasty with and without navigation support. A prospective, randomized study. J Bone Joint Surg Br. 2003;85(6):830-835.
6. Hoffart HE, Langenstein E, Vasak N. A prospective study comparing the functional outcome of computer-assisted and conventional total knee replacement. J Bone Joint Surg Br. 2012;94(2):194-199.
7. Cip J, Widemschek M, Luegmair M, Sheinkop MB, Benesch T, Martin A. Conventional versus computer-assisted technique for total knee arthroplasty: a minimum of 5-year follow-up of 200 patients in a prospective randomized comparative trial. J Arthroplasty. 2014;29(9):1795-1802.
8. Huang TW, Peng KT, Huang KC, Lee MS, Hsu RW. Differences in component and limb alignment between computer-assisted and conventional surgery total knee arthroplasty. Knee Surg Sports Traumatol Arthrosc. 2014;22(12):2954-2961.
9. Lee CY, Lin SJ, Kuo LT, et al. The benefits of computer-assisted total knee arthroplasty on coronal alignment with marked femoral bowing in Asian patients. J Orthop Surg Res. 2014;9:122.
10. Hernandez-Vaquero D, Noriega-Fernandez A, Fernandez-Carreira JM, Fernandez-Simon JM, Llorens de los Rios J. Computer-assisted surgery improves rotational positioning of the femoral component but not the tibial component in total knee arthroplasty. Knee Surg Sports Traumatol Arthrosc. 2014;22(12):3127-3134.
11. Khakha RS, Chowdhry M, Sivaprakasam M, Kheiran A, Chauhan SK. Radiological and functional outcomes in computer assisted total knee arthroplasty between consultants and trainees - a prospective randomized controlled trial [published online ahead of print March 14, 2015]. J Arthroplasty.
12. de Steiger RN, Liu YL, Graves SE. Computer navigation for total knee arthroplasty reduces revision rate for patients less than sixty-five years of age. J Bone Joint Surg Am. 2015;97(8):635-642.
13. Pearle AD, O’Loughlin PF, Kendoff DO. Robot-assisted unicompartmental knee arthroplasty. J Arthroplasty. 2010;25(2):230-237.
14. Citak M, Suero EM, Citak M, et al. Unicompartmental knee arthroplasty: is robotic technology more accurate than conventional technique? Knee. 2013;20(4):268-271.
15. Koulalis D, O’Loughlin PF, Plaskos C, Kendoff D, Cross MB, Pearle AD. Sequential versus automated cutting guides in computer-assisted total knee arthroplasty. Knee. 2011;18(6):436-442.
Total knee arthroplasty (TKA) is a good surgical option to relieve pain and improve function in patients with osteoarthritis. The goal of surgery is to achieve a well-aligned prosthesis with well-balanced ligaments in order to minimize wear and improve implant survival. Overall, 82% to 89% of patients are satisfied with their outcomes after TKA, with good 10- to 15-year implant survivorship; however, there is still a subset of patients that are unsatisfied. In many cases, patient dissatisfaction is attributed to improper component alignment.1-3 Over the past decade, computer navigation and robotics have been introduced to control surgical variables so as to gain greater consistency in implant placement and postoperative component alignment.
Computer-assisted navigation tools were introduced not only to improve implant alignment but, more importantly, to optimize clinical outcomes. Most studies have demonstrated that the use of navigation is associated with fewer radiographic outliers after TKA.4 Various studies have compared radiographic results of navigated TKA with results of TKA using standard instrumentation.4-7 While long-term studies are necessary, short-term follow-up has shown that computer-assisted TKA can improve alignment, especially in patients with severe deformity.8-10 Currently, there is no definitive consensus that computer-assisted TKA leads to significantly better component alignment or postoperative outcomes due to the fact that many studies are limited by study design or small cohorts. However, the currently published articles support better component alignment and clinical outcomes with computer-assisted TKA. While some argue that the use of computer-assisted surgery is dependent on the user’s experience, computer-assisted surgery can assist less-experienced surgeons to reliably achieve good midterm outcomes with a low complication rate.8,11 Various studies have looked at computer-assisted TKA at midterm follow-up, with no significant differences in clinical outcome between navigated and traditional techniques. However, long-term studies showing the benefits of computer navigation are beginning to emerge. For example, de Steiger and colleagues12 recently found that computer-assisted TKA reduced the overall revision rate for loosening after TKA in patients less than 65 years of age.
While surgical navigation helps improve implant planning, robotic tools have emerged as a tool to help refine surgical execution. Coupled with surgical navigation tools, robotic control of surgical gestures may further enhance precision in implant placement and/or enable novel implant design features. At present, robotic techniques are increasingly used in unicompartmental knee arthroplasty (UKA) and TKA.13 Studies have demonstrated that the robotic tool is 3 times more accurate with 3 times less variability than conventional techniques in UKA.14 The utility of robotic tools for TKA remains unclear. Robotic-driven automatic cutting guides have been shown to reduce time and improve accuracy compared with navigation guides in femoral TKA cutting procedures in a cadaveric model.15 However, robotic-enabled TKA procedures are poorly described at present, and the clinical implications of their proposed improved precision remain unclear.
Computer navigation and robotic tools in TKA hold the promise of enhanced control of surgical variables that influence clinical outcome. The variables that may be impacted by these advanced tools include implant positioning, lower limb alignment, soft-tissue balance, and, potentially, implant design and fixation. At present, these tools have primarily been shown to improve lower limb alignment in TKA. The clinical impact of the enhanced control of this single surgical variable (lower limb alignment) has been muted in short-term and midterm studies. Future studies should be directed at understanding which surgical variable, or combination of variables, it is most essential to precisely control so as to positively impact clinical outcomes. ◾
Total knee arthroplasty (TKA) is a good surgical option to relieve pain and improve function in patients with osteoarthritis. The goal of surgery is to achieve a well-aligned prosthesis with well-balanced ligaments in order to minimize wear and improve implant survival. Overall, 82% to 89% of patients are satisfied with their outcomes after TKA, with good 10- to 15-year implant survivorship; however, there is still a subset of patients that are unsatisfied. In many cases, patient dissatisfaction is attributed to improper component alignment.1-3 Over the past decade, computer navigation and robotics have been introduced to control surgical variables so as to gain greater consistency in implant placement and postoperative component alignment.
Computer-assisted navigation tools were introduced not only to improve implant alignment but, more importantly, to optimize clinical outcomes. Most studies have demonstrated that the use of navigation is associated with fewer radiographic outliers after TKA.4 Various studies have compared radiographic results of navigated TKA with results of TKA using standard instrumentation.4-7 While long-term studies are necessary, short-term follow-up has shown that computer-assisted TKA can improve alignment, especially in patients with severe deformity.8-10 Currently, there is no definitive consensus that computer-assisted TKA leads to significantly better component alignment or postoperative outcomes due to the fact that many studies are limited by study design or small cohorts. However, the currently published articles support better component alignment and clinical outcomes with computer-assisted TKA. While some argue that the use of computer-assisted surgery is dependent on the user’s experience, computer-assisted surgery can assist less-experienced surgeons to reliably achieve good midterm outcomes with a low complication rate.8,11 Various studies have looked at computer-assisted TKA at midterm follow-up, with no significant differences in clinical outcome between navigated and traditional techniques. However, long-term studies showing the benefits of computer navigation are beginning to emerge. For example, de Steiger and colleagues12 recently found that computer-assisted TKA reduced the overall revision rate for loosening after TKA in patients less than 65 years of age.
While surgical navigation helps improve implant planning, robotic tools have emerged as a tool to help refine surgical execution. Coupled with surgical navigation tools, robotic control of surgical gestures may further enhance precision in implant placement and/or enable novel implant design features. At present, robotic techniques are increasingly used in unicompartmental knee arthroplasty (UKA) and TKA.13 Studies have demonstrated that the robotic tool is 3 times more accurate with 3 times less variability than conventional techniques in UKA.14 The utility of robotic tools for TKA remains unclear. Robotic-driven automatic cutting guides have been shown to reduce time and improve accuracy compared with navigation guides in femoral TKA cutting procedures in a cadaveric model.15 However, robotic-enabled TKA procedures are poorly described at present, and the clinical implications of their proposed improved precision remain unclear.
Computer navigation and robotic tools in TKA hold the promise of enhanced control of surgical variables that influence clinical outcome. The variables that may be impacted by these advanced tools include implant positioning, lower limb alignment, soft-tissue balance, and, potentially, implant design and fixation. At present, these tools have primarily been shown to improve lower limb alignment in TKA. The clinical impact of the enhanced control of this single surgical variable (lower limb alignment) has been muted in short-term and midterm studies. Future studies should be directed at understanding which surgical variable, or combination of variables, it is most essential to precisely control so as to positively impact clinical outcomes. ◾
1. Bourne RB, Chesworth BM, Davis AM, Mahomed NN, Charron KD. Patient satisfaction after total knee arthroplasty: who is satisfied and who is not? Clin Orthop Relat Res. 2010;468(1):57-63.
2. Sharkey PF, Hozack WJ, Rothman RH, Shastri S, Jacoby SM. Insall Award paper. Why are total knee arthroplasties failing today? Clin Orthop Relat Res. 2002;(404):7-13.
3. Emmerson KP, Morgan CG, Pinder IM. Survivorship analysis of the Kinematic Stabilizer total knee replacement: a 10- to 14-year follow-up. J Bone Joint Surg Br. 1996;78(3):441-445.
4. Liow MH, Xia Z, Wong MK, Tay KJ, Yeo SJ, Chin PL. Robot-assisted total knee arthroplasty accurately restores the joint line and mechanical axis. A prospective randomized study. J Arthroplasty. 2014;29(12):2373-2377.
5. Sparmann M, Wolke B, Czupalla H, Banzer D, Zink A. Positioning of total knee arthroplasty with and without navigation support. A prospective, randomized study. J Bone Joint Surg Br. 2003;85(6):830-835.
6. Hoffart HE, Langenstein E, Vasak N. A prospective study comparing the functional outcome of computer-assisted and conventional total knee replacement. J Bone Joint Surg Br. 2012;94(2):194-199.
7. Cip J, Widemschek M, Luegmair M, Sheinkop MB, Benesch T, Martin A. Conventional versus computer-assisted technique for total knee arthroplasty: a minimum of 5-year follow-up of 200 patients in a prospective randomized comparative trial. J Arthroplasty. 2014;29(9):1795-1802.
8. Huang TW, Peng KT, Huang KC, Lee MS, Hsu RW. Differences in component and limb alignment between computer-assisted and conventional surgery total knee arthroplasty. Knee Surg Sports Traumatol Arthrosc. 2014;22(12):2954-2961.
9. Lee CY, Lin SJ, Kuo LT, et al. The benefits of computer-assisted total knee arthroplasty on coronal alignment with marked femoral bowing in Asian patients. J Orthop Surg Res. 2014;9:122.
10. Hernandez-Vaquero D, Noriega-Fernandez A, Fernandez-Carreira JM, Fernandez-Simon JM, Llorens de los Rios J. Computer-assisted surgery improves rotational positioning of the femoral component but not the tibial component in total knee arthroplasty. Knee Surg Sports Traumatol Arthrosc. 2014;22(12):3127-3134.
11. Khakha RS, Chowdhry M, Sivaprakasam M, Kheiran A, Chauhan SK. Radiological and functional outcomes in computer assisted total knee arthroplasty between consultants and trainees - a prospective randomized controlled trial [published online ahead of print March 14, 2015]. J Arthroplasty.
12. de Steiger RN, Liu YL, Graves SE. Computer navigation for total knee arthroplasty reduces revision rate for patients less than sixty-five years of age. J Bone Joint Surg Am. 2015;97(8):635-642.
13. Pearle AD, O’Loughlin PF, Kendoff DO. Robot-assisted unicompartmental knee arthroplasty. J Arthroplasty. 2010;25(2):230-237.
14. Citak M, Suero EM, Citak M, et al. Unicompartmental knee arthroplasty: is robotic technology more accurate than conventional technique? Knee. 2013;20(4):268-271.
15. Koulalis D, O’Loughlin PF, Plaskos C, Kendoff D, Cross MB, Pearle AD. Sequential versus automated cutting guides in computer-assisted total knee arthroplasty. Knee. 2011;18(6):436-442.
1. Bourne RB, Chesworth BM, Davis AM, Mahomed NN, Charron KD. Patient satisfaction after total knee arthroplasty: who is satisfied and who is not? Clin Orthop Relat Res. 2010;468(1):57-63.
2. Sharkey PF, Hozack WJ, Rothman RH, Shastri S, Jacoby SM. Insall Award paper. Why are total knee arthroplasties failing today? Clin Orthop Relat Res. 2002;(404):7-13.
3. Emmerson KP, Morgan CG, Pinder IM. Survivorship analysis of the Kinematic Stabilizer total knee replacement: a 10- to 14-year follow-up. J Bone Joint Surg Br. 1996;78(3):441-445.
4. Liow MH, Xia Z, Wong MK, Tay KJ, Yeo SJ, Chin PL. Robot-assisted total knee arthroplasty accurately restores the joint line and mechanical axis. A prospective randomized study. J Arthroplasty. 2014;29(12):2373-2377.
5. Sparmann M, Wolke B, Czupalla H, Banzer D, Zink A. Positioning of total knee arthroplasty with and without navigation support. A prospective, randomized study. J Bone Joint Surg Br. 2003;85(6):830-835.
6. Hoffart HE, Langenstein E, Vasak N. A prospective study comparing the functional outcome of computer-assisted and conventional total knee replacement. J Bone Joint Surg Br. 2012;94(2):194-199.
7. Cip J, Widemschek M, Luegmair M, Sheinkop MB, Benesch T, Martin A. Conventional versus computer-assisted technique for total knee arthroplasty: a minimum of 5-year follow-up of 200 patients in a prospective randomized comparative trial. J Arthroplasty. 2014;29(9):1795-1802.
8. Huang TW, Peng KT, Huang KC, Lee MS, Hsu RW. Differences in component and limb alignment between computer-assisted and conventional surgery total knee arthroplasty. Knee Surg Sports Traumatol Arthrosc. 2014;22(12):2954-2961.
9. Lee CY, Lin SJ, Kuo LT, et al. The benefits of computer-assisted total knee arthroplasty on coronal alignment with marked femoral bowing in Asian patients. J Orthop Surg Res. 2014;9:122.
10. Hernandez-Vaquero D, Noriega-Fernandez A, Fernandez-Carreira JM, Fernandez-Simon JM, Llorens de los Rios J. Computer-assisted surgery improves rotational positioning of the femoral component but not the tibial component in total knee arthroplasty. Knee Surg Sports Traumatol Arthrosc. 2014;22(12):3127-3134.
11. Khakha RS, Chowdhry M, Sivaprakasam M, Kheiran A, Chauhan SK. Radiological and functional outcomes in computer assisted total knee arthroplasty between consultants and trainees - a prospective randomized controlled trial [published online ahead of print March 14, 2015]. J Arthroplasty.
12. de Steiger RN, Liu YL, Graves SE. Computer navigation for total knee arthroplasty reduces revision rate for patients less than sixty-five years of age. J Bone Joint Surg Am. 2015;97(8):635-642.
13. Pearle AD, O’Loughlin PF, Kendoff DO. Robot-assisted unicompartmental knee arthroplasty. J Arthroplasty. 2010;25(2):230-237.
14. Citak M, Suero EM, Citak M, et al. Unicompartmental knee arthroplasty: is robotic technology more accurate than conventional technique? Knee. 2013;20(4):268-271.
15. Koulalis D, O’Loughlin PF, Plaskos C, Kendoff D, Cross MB, Pearle AD. Sequential versus automated cutting guides in computer-assisted total knee arthroplasty. Knee. 2011;18(6):436-442.
APA: Lay person’s guide to DSM-5 is good resource for primary care physicians
TORONTO – The American Psychiatric Association’s consumer guide to the DSM-5, “Understanding Mental Disorders,” debuted at the organization’s annual meeting this year.
Compared with the pricey clinical version of the manual, you get a lot for your $24.95 ($22.21 with an Amazon Prime account). At 370 pages, the guide is an easily digestible compendium; the diagnoses are grouped as they are in the primary manual, although without specifiers or subsets. Instead, there are bulleted lists of risk factors and symptoms. Treatment options are also bulleted, as are tips for remaining compliant with treatment regimens.
There are case histories written in lay person language and even blurbs that offer encouragement to those who might be, however slightly, alarmed to learn about various illnesses described. For example, in the chapter about “disorders that start in childhood” (neurodevelopmental disorders), the reader is advised that “treatment can lead to learning new ways to manage symptoms … and it can also offer hope.”
Although it’s the first book written and published by the APA specifically for the general public, when I asked the guide’s editorial adviser, Dr. Jeffrey Borenstein, if primary care doctors, who are very often the ones on the front lines of diagnosing and treating mental illness, would also benefit from having a copy at hand, he said yes. But primary care physicians apparently were not foremost in the minds of the editorial board that compiled this guide and planned its utility.
According to Dr. Borenstein, the guide is intended for the general public. In an interview, however, he singled out in particular, teachers, clergy, and others whose job it is to serve the community at large.
Now that the Medicare Access and CHIP Reauthorization Act means our health care system is moving inexorably toward value-based care and that physicians risk losing money if their overall patient panel outcomes – including mental health – are poor, understanding how to diagnose and appropriately treat mental and behavioral health issues is of growing concern, particularly in primary care.

Earlier this year, I spoke with Chet Burrell, CEO of CareFirst, the Patient-Centered Medical Home division of BlueCross BlueShield. He told me that since 1 in 10 hospital admissions out of the 10,000 admissions CareFirst covers annually are behavioral health and substance abuse related, not only does that mean primary care practices are coordinating complex, postdischarge psychiatric care on as much as 10% of their patient panels, it also means that these patients have been left untreated or undertreated long enough for their illnesses to lead to an acute crisis, which is costly in one way or another to the patient, the payer, and the physician practice. “To get admitted [to the hospital] for a behavioral health or substance abuse issue, you have to be pretty sick,” Mr. Burrell said.
By connecting primary care physicians with psychiatrists in the community, however, as well as adding other structural support such as social workers or nurse practitioners, Mr. Burrell said primary care physicians in his network were beginning to see better outcomes and less financial risk.
It’s not that the APA is unaware of the growing need in the primary care realm for psychiatric expertise: At its annual meeting, the APA held a session entitled, “Educating Psychiatrists for Work in Integrated Care: Focus on Interdisciplinary Collaboration.” (I attended and tweeted pearls from each speaker @whitneymcknight if you’d like to see highlights). While attending the session, I detected two salient themes across the four presentations and concluding panel discussion. The first was that for all the increased mental and behavioral health training various medical school programs have added in the last decade, newly graduated primary care physicians are still underprepared for the amount of mental health concerns with which they will be faced in practice. The second was that psychiatrists and primary care physicians don’t know how to talk to one another effectively; one reason is that primary care physicians often feel that psychiatrists patronize them.
Psychiatrists can’t necessarily do much about the former, at least not in short order, but they can certainly do something about the latter, particularly in light of the APA’s new, forward-thinking branding campaign: “medical leadership for mind, brain, and body.”
Even if psychiatrists, whom many in other specialties “forget” are actually medical doctors, now want to claim their place at the health care table in an era when the bidirectional nature of mental and physical health is increasingly substantiated in myriad studies and is emphasized in ever more health policy–related decisions, the fact is that, at least where nonserious mental illness is concerned, the gatekeepers of access to mental health in this country are not psychiatrists but primary care doctors. As we move toward a value-based accountable care system where mental health outcomes can mean the difference between a physician receiving an upgrade or a downgrade, the demand for psychiatrists and other mental health professionals who can help ensure good, efficient patient outcomes will only expand.
Which returns us to the lay person’s guide to the DSM-5: It’s well organized. It’s easy to understand. And while it is in hard copy only, it’s handy for primary care physicians who often use the same search criteria as their patients might when turning to Dr. Google to find a quick answer to something with which they are not that familiar. It’s a pretty good bridge between primary care and psychiatry.
Dr. Borenstein had no relevant financial disclosures. He is the editor-in-chief of the APA’s Psychiatric News.
On Twitter @whitneymcknight
TORONTO – The American Psychiatric Association’s consumer guide to the DSM-5, “Understanding Mental Disorders,” debuted at the organization’s annual meeting this year.
Compared with the pricey clinical version of the manual, you get a lot for your $24.95 ($22.21 with an Amazon Prime account). At 370 pages, the guide is an easily digestible compendium; the diagnoses are grouped as they are in the primary manual, although without specifiers or subsets. Instead, there are bulleted lists of risk factors and symptoms. Treatment options are also bulleted, as are tips for remaining compliant with treatment regimens.
There are case histories written in lay person language and even blurbs that offer encouragement to those who might be, however slightly, alarmed to learn about various illnesses described. For example, in the chapter about “disorders that start in childhood” (neurodevelopmental disorders), the reader is advised that “treatment can lead to learning new ways to manage symptoms … and it can also offer hope.”
Although it’s the first book written and published by the APA specifically for the general public, when I asked the guide’s editorial adviser, Dr. Jeffrey Borenstein, if primary care doctors, who are very often the ones on the front lines of diagnosing and treating mental illness, would also benefit from having a copy at hand, he said yes. But primary care physicians apparently were not foremost in the minds of the editorial board that compiled this guide and planned its utility.
According to Dr. Borenstein, the guide is intended for the general public. In an interview, however, he singled out in particular, teachers, clergy, and others whose job it is to serve the community at large.
Now that the Medicare Access and CHIP Reauthorization Act means our health care system is moving inexorably toward value-based care and that physicians risk losing money if their overall patient panel outcomes – including mental health – are poor, understanding how to diagnose and appropriately treat mental and behavioral health issues is of growing concern, particularly in primary care.
Earlier this year, I spoke with Chet Burrell, CEO of CareFirst, the Patient-Centered Medical Home division of BlueCross BlueShield. He told me that since 1 in 10 hospital admissions out of the 10,000 admissions CareFirst covers annually are behavioral health and substance abuse related, not only does that mean primary care practices are coordinating complex, postdischarge psychiatric care on as much as 10% of their patient panels, it also means that these patients have been left untreated or undertreated long enough for their illnesses to lead to an acute crisis, which is costly in one way or another to the patient, the payer, and the physician practice. “To get admitted [to the hospital] for a behavioral health or substance abuse issue, you have to be pretty sick,” Mr. Burrell said.
By connecting primary care physicians with psychiatrists in the community, however, as well as adding other structural support such as social workers or nurse practitioners, Mr. Burrell said primary care physicians in his network were beginning to see better outcomes and less financial risk.
It’s not that the APA is unaware of the growing need in the primary care realm for psychiatric expertise: At its annual meeting, the APA held a session entitled, “Educating Psychiatrists for Work in Integrated Care: Focus on Interdisciplinary Collaboration.” (I attended and tweeted pearls from each speaker @whitneymcknight if you’d like to see highlights). While attending the session, I detected two salient themes across the four presentations and concluding panel discussion. The first was that for all the increased mental and behavioral health training various medical school programs have added in the last decade, newly graduated primary care physicians are still underprepared for the amount of mental health concerns with which they will be faced in practice. The second was that psychiatrists and primary care physicians don’t know how to talk to one another effectively; one reason is that primary care physicians often feel that psychiatrists patronize them.
Psychiatrists can’t necessarily do much about the former, at least not in short order, but they can certainly do something about the latter, particularly in light of the APA’s new, forward-thinking branding campaign: “medical leadership for mind, brain, and body.”
Even if psychiatrists, whom many in other specialties “forget” are actually medical doctors, now want to claim their place at the health care table in an era when the bidirectional nature of mental and physical health is increasingly substantiated in myriad studies and is emphasized in ever more health policy–related decisions, the fact is that, at least where nonserious mental illness is concerned, the gatekeepers of access to mental health in this country are not psychiatrists but primary care doctors. As we move toward a value-based accountable care system where mental health outcomes can mean the difference between a physician receiving an upgrade or a downgrade, the demand for psychiatrists and other mental health professionals who can help ensure good, efficient patient outcomes will only expand.
Which returns us to the lay person’s guide to the DSM-5: It’s well organized. It’s easy to understand. And while it is in hard copy only, it’s handy for primary care physicians who often use the same search criteria as their patients might when turning to Dr. Google to find a quick answer to something with which they are not that familiar. It’s a pretty good bridge between primary care and psychiatry.
Dr. Borenstein had no relevant financial disclosures. He is the editor-in-chief of the APA’s Psychiatric News.
On Twitter @whitneymcknight
TORONTO – The American Psychiatric Association’s consumer guide to the DSM-5, “Understanding Mental Disorders,” debuted at the organization’s annual meeting this year.
Compared with the pricey clinical version of the manual, you get a lot for your $24.95 ($22.21 with an Amazon Prime account). At 370 pages, the guide is an easily digestible compendium; the diagnoses are grouped as they are in the primary manual, although without specifiers or subsets. Instead, there are bulleted lists of risk factors and symptoms. Treatment options are also bulleted, as are tips for remaining compliant with treatment regimens.
There are case histories written in lay person language and even blurbs that offer encouragement to those who might be, however slightly, alarmed to learn about various illnesses described. For example, in the chapter about “disorders that start in childhood” (neurodevelopmental disorders), the reader is advised that “treatment can lead to learning new ways to manage symptoms … and it can also offer hope.”
Although it’s the first book written and published by the APA specifically for the general public, when I asked the guide’s editorial adviser, Dr. Jeffrey Borenstein, if primary care doctors, who are very often the ones on the front lines of diagnosing and treating mental illness, would also benefit from having a copy at hand, he said yes. But primary care physicians apparently were not foremost in the minds of the editorial board that compiled this guide and planned its utility.
According to Dr. Borenstein, the guide is intended for the general public. In an interview, however, he singled out in particular, teachers, clergy, and others whose job it is to serve the community at large.
Now that the Medicare Access and CHIP Reauthorization Act means our health care system is moving inexorably toward value-based care and that physicians risk losing money if their overall patient panel outcomes – including mental health – are poor, understanding how to diagnose and appropriately treat mental and behavioral health issues is of growing concern, particularly in primary care.
Earlier this year, I spoke with Chet Burrell, CEO of CareFirst, the Patient-Centered Medical Home division of BlueCross BlueShield. He told me that since 1 in 10 hospital admissions out of the 10,000 admissions CareFirst covers annually are behavioral health and substance abuse related, not only does that mean primary care practices are coordinating complex, postdischarge psychiatric care on as much as 10% of their patient panels, it also means that these patients have been left untreated or undertreated long enough for their illnesses to lead to an acute crisis, which is costly in one way or another to the patient, the payer, and the physician practice. “To get admitted [to the hospital] for a behavioral health or substance abuse issue, you have to be pretty sick,” Mr. Burrell said.
By connecting primary care physicians with psychiatrists in the community, however, as well as adding other structural support such as social workers or nurse practitioners, Mr. Burrell said primary care physicians in his network were beginning to see better outcomes and less financial risk.
It’s not that the APA is unaware of the growing need in the primary care realm for psychiatric expertise: At its annual meeting, the APA held a session entitled, “Educating Psychiatrists for Work in Integrated Care: Focus on Interdisciplinary Collaboration.” (I attended and tweeted pearls from each speaker @whitneymcknight if you’d like to see highlights). While attending the session, I detected two salient themes across the four presentations and concluding panel discussion. The first was that for all the increased mental and behavioral health training various medical school programs have added in the last decade, newly graduated primary care physicians are still underprepared for the amount of mental health concerns with which they will be faced in practice. The second was that psychiatrists and primary care physicians don’t know how to talk to one another effectively; one reason is that primary care physicians often feel that psychiatrists patronize them.
Psychiatrists can’t necessarily do much about the former, at least not in short order, but they can certainly do something about the latter, particularly in light of the APA’s new, forward-thinking branding campaign: “medical leadership for mind, brain, and body.”
Even if psychiatrists, whom many in other specialties “forget” are actually medical doctors, now want to claim their place at the health care table in an era when the bidirectional nature of mental and physical health is increasingly substantiated in myriad studies and is emphasized in ever more health policy–related decisions, the fact is that, at least where nonserious mental illness is concerned, the gatekeepers of access to mental health in this country are not psychiatrists but primary care doctors. As we move toward a value-based accountable care system where mental health outcomes can mean the difference between a physician receiving an upgrade or a downgrade, the demand for psychiatrists and other mental health professionals who can help ensure good, efficient patient outcomes will only expand.
Which returns us to the lay person’s guide to the DSM-5: It’s well organized. It’s easy to understand. And while it is in hard copy only, it’s handy for primary care physicians who often use the same search criteria as their patients might when turning to Dr. Google to find a quick answer to something with which they are not that familiar. It’s a pretty good bridge between primary care and psychiatry.
Dr. Borenstein had no relevant financial disclosures. He is the editor-in-chief of the APA’s Psychiatric News.
On Twitter @whitneymcknight
AT THE APA ANNUAL MEETING
Exercise-induced anaphylaxis
Anaphylaxis is a relatively common occurrence for many adolescents. As primary care doctors, we normally see the patient after the acute phase, and then are required to do the detective work to figure out the causes of the episode. The cause may be obvious, but many times we have to hope for another occurrence with similar circumstances to identify it. Surprisingly, the cause may not be what you think. Factors that contribute to an anaphylaxis response may be related to activity, timing of food ingestion, an environmental factor, or medication.
Let’s look at just one type, exercise-induced anaphylaxis. It’s divided into two categories: food dependent and nonfood dependent. Both are described as an induction of itching, urticaria, and fatigue, with progression to angioedema and hypotension, associated with exercise (J. Allergy Clin. Immunol. 1980;66:106-11).
Food-dependent exercise-induced anaphylaxis occurs when exercise is started 30 minutes after ingesting food. This may be difficult to identify because patients react to the food only if they exercise, so food is usually eliminated as a cause. Wheat and wheat flour are common culprits for this type of reaction because of the omega-5 gliadin, which is the protein in gluten (J. Allergy Clin. Immunol. 1991;87:34-40). In one study, larger amounts of the suspected agent were given; hives and angioedema did start to occur in 20% of patients challenged, which suggested that there was likely a baseline allergy to the food, and exercise itself might be a cofactor in augmentation of the allergic reaction.
In nonfood-dependent exercise-induced anaphylaxis, symptoms of itching, urticaria, and fatigue can occur 5-30 minutes after the start of exercise. Although bronchospasm is rare, it can occur along with angioedema, nausea, vomiting, and hypotension, and can even be fatal if exercise continues. If exercise is stopped, it usually resolves. However, many people try to push through it, which only worsens the symptoms.
Cofactors associated with nonfood-dependent exercise-induced anaphylaxis are ingestion of alcohol and an NSAID several hours beforehand. These agents also might be overlooked if well tolerated independently (Br. J. Dermatol. 2001;145:336-9).
Timing of the episode also plays a role. Premenstrual syndrome can be a factor in augmentation of anaphylaxis, so it also should be considered. Knowing the date of the last menstrual cycle and identifying if the anaphylaxis is episodic will identify premenstrual syndrome as a cause.
The work-up should include standard allergy testing and determination of tryptase levels. Skin testing is essential to identify offending agents, and is rarely negative. If a food is suspected and skin testing is negative, repeat the skin testing in 6 months. In one study, wheat extract was found to be positive in only 29% of persons suspected of having a wheat allergy, but when the paste of wheat flour was tested, 80% were identified. The ImmunoCAP Test also was found to have a sensitivity of 80%, so it is a valuable test to try along with the skin prick.
Tryptase levels should be evaluated because in nonfood-dependent exercise-induced anaphylaxis, these levels are slightly elevated at the time of the anaphylaxis, but return to normal. A patient with mastocytosis, a group of disorders characterized by pathologic mast cells infiltrating the skin, will consistently have elevated tryptase levels. Seasonal allergies associated with pollen, and asthma bronchospasm also should be considered as causes.
Although these exercise-induced anaphylaxis episodes can occur at any age, they are most frequent in the adolescent age group, probably because that’s the time most of this population are involved in organized sports. Upon presentation, a careful detailed history will help to identify the cause of anaphylaxis and result in quicker resolution.
Treatment includes avoidance of the offending agent if identified and an antihistamine, and if symptoms do occur, ceasing exercise immediately to avoid a full-blown anaphylactic reaction.
Dr. Pearce is a pediatrician in Frankfort, Ill. E-mail her at [email protected].
Anaphylaxis is a relatively common occurrence for many adolescents. As primary care doctors, we normally see the patient after the acute phase, and then are required to do the detective work to figure out the causes of the episode. The cause may be obvious, but many times we have to hope for another occurrence with similar circumstances to identify it. Surprisingly, the cause may not be what you think. Factors that contribute to an anaphylaxis response may be related to activity, timing of food ingestion, an environmental factor, or medication.
Let’s look at just one type, exercise-induced anaphylaxis. It’s divided into two categories: food dependent and nonfood dependent. Both are described as an induction of itching, urticaria, and fatigue, with progression to angioedema and hypotension, associated with exercise (J. Allergy Clin. Immunol. 1980;66:106-11).
Food-dependent exercise-induced anaphylaxis occurs when exercise is started 30 minutes after ingesting food. This may be difficult to identify because patients react to the food only if they exercise, so food is usually eliminated as a cause. Wheat and wheat flour are common culprits for this type of reaction because of the omega-5 gliadin, which is the protein in gluten (J. Allergy Clin. Immunol. 1991;87:34-40). In one study, larger amounts of the suspected agent were given; hives and angioedema did start to occur in 20% of patients challenged, which suggested that there was likely a baseline allergy to the food, and exercise itself might be a cofactor in augmentation of the allergic reaction.
In nonfood-dependent exercise-induced anaphylaxis, symptoms of itching, urticaria, and fatigue can occur 5-30 minutes after the start of exercise. Although bronchospasm is rare, it can occur along with angioedema, nausea, vomiting, and hypotension, and can even be fatal if exercise continues. If exercise is stopped, it usually resolves. However, many people try to push through it, which only worsens the symptoms.
Cofactors associated with nonfood-dependent exercise-induced anaphylaxis are ingestion of alcohol and an NSAID several hours beforehand. These agents also might be overlooked if well tolerated independently (Br. J. Dermatol. 2001;145:336-9).
Timing of the episode also plays a role. Premenstrual syndrome can be a factor in augmentation of anaphylaxis, so it also should be considered. Knowing the date of the last menstrual cycle and identifying if the anaphylaxis is episodic will identify premenstrual syndrome as a cause.
The work-up should include standard allergy testing and determination of tryptase levels. Skin testing is essential to identify offending agents, and is rarely negative. If a food is suspected and skin testing is negative, repeat the skin testing in 6 months. In one study, wheat extract was found to be positive in only 29% of persons suspected of having a wheat allergy, but when the paste of wheat flour was tested, 80% were identified. The ImmunoCAP Test also was found to have a sensitivity of 80%, so it is a valuable test to try along with the skin prick.
Tryptase levels should be evaluated because in nonfood-dependent exercise-induced anaphylaxis, these levels are slightly elevated at the time of the anaphylaxis, but return to normal. A patient with mastocytosis, a group of disorders characterized by pathologic mast cells infiltrating the skin, will consistently have elevated tryptase levels. Seasonal allergies associated with pollen, and asthma bronchospasm also should be considered as causes.
Although these exercise-induced anaphylaxis episodes can occur at any age, they are most frequent in the adolescent age group, probably because that’s the time most of this population are involved in organized sports. Upon presentation, a careful detailed history will help to identify the cause of anaphylaxis and result in quicker resolution.
Treatment includes avoidance of the offending agent if identified and an antihistamine, and if symptoms do occur, ceasing exercise immediately to avoid a full-blown anaphylactic reaction.
Dr. Pearce is a pediatrician in Frankfort, Ill. E-mail her at [email protected].
Anaphylaxis is a relatively common occurrence for many adolescents. As primary care doctors, we normally see the patient after the acute phase, and then are required to do the detective work to figure out the causes of the episode. The cause may be obvious, but many times we have to hope for another occurrence with similar circumstances to identify it. Surprisingly, the cause may not be what you think. Factors that contribute to an anaphylaxis response may be related to activity, timing of food ingestion, an environmental factor, or medication.
Let’s look at just one type, exercise-induced anaphylaxis. It’s divided into two categories: food dependent and nonfood dependent. Both are described as an induction of itching, urticaria, and fatigue, with progression to angioedema and hypotension, associated with exercise (J. Allergy Clin. Immunol. 1980;66:106-11).
Food-dependent exercise-induced anaphylaxis occurs when exercise is started 30 minutes after ingesting food. This may be difficult to identify because patients react to the food only if they exercise, so food is usually eliminated as a cause. Wheat and wheat flour are common culprits for this type of reaction because of the omega-5 gliadin, which is the protein in gluten (J. Allergy Clin. Immunol. 1991;87:34-40). In one study, larger amounts of the suspected agent were given; hives and angioedema did start to occur in 20% of patients challenged, which suggested that there was likely a baseline allergy to the food, and exercise itself might be a cofactor in augmentation of the allergic reaction.
In nonfood-dependent exercise-induced anaphylaxis, symptoms of itching, urticaria, and fatigue can occur 5-30 minutes after the start of exercise. Although bronchospasm is rare, it can occur along with angioedema, nausea, vomiting, and hypotension, and can even be fatal if exercise continues. If exercise is stopped, it usually resolves. However, many people try to push through it, which only worsens the symptoms.
Cofactors associated with nonfood-dependent exercise-induced anaphylaxis are ingestion of alcohol and an NSAID several hours beforehand. These agents also might be overlooked if well tolerated independently (Br. J. Dermatol. 2001;145:336-9).
Timing of the episode also plays a role. Premenstrual syndrome can be a factor in augmentation of anaphylaxis, so it also should be considered. Knowing the date of the last menstrual cycle and identifying if the anaphylaxis is episodic will identify premenstrual syndrome as a cause.
The work-up should include standard allergy testing and determination of tryptase levels. Skin testing is essential to identify offending agents, and is rarely negative. If a food is suspected and skin testing is negative, repeat the skin testing in 6 months. In one study, wheat extract was found to be positive in only 29% of persons suspected of having a wheat allergy, but when the paste of wheat flour was tested, 80% were identified. The ImmunoCAP Test also was found to have a sensitivity of 80%, so it is a valuable test to try along with the skin prick.
Tryptase levels should be evaluated because in nonfood-dependent exercise-induced anaphylaxis, these levels are slightly elevated at the time of the anaphylaxis, but return to normal. A patient with mastocytosis, a group of disorders characterized by pathologic mast cells infiltrating the skin, will consistently have elevated tryptase levels. Seasonal allergies associated with pollen, and asthma bronchospasm also should be considered as causes.
Although these exercise-induced anaphylaxis episodes can occur at any age, they are most frequent in the adolescent age group, probably because that’s the time most of this population are involved in organized sports. Upon presentation, a careful detailed history will help to identify the cause of anaphylaxis and result in quicker resolution.
Treatment includes avoidance of the offending agent if identified and an antihistamine, and if symptoms do occur, ceasing exercise immediately to avoid a full-blown anaphylactic reaction.
Dr. Pearce is a pediatrician in Frankfort, Ill. E-mail her at [email protected].

Treatment of preschool ADHD
Attention deficit/hyperactivity disorder (ADHD) has been identified in children, and appropriate treatments studied now for over half a century. The vast majority of cases that present for treatment do so after the child starts school and concerns are raised about ability to manage academics. Yet, when asked when the symptoms first began, many parents will describe onset prior to the school years – in the preschool period. But identification of ADHD in preschoolers can be difficult because of the developmental changes that are ongoing during the period from 3 to 5 years. Many of the symptoms that one would attribute to ADHD, such as increased motor activity, inattention, and distractibility are commonplace in this age group. Furthermore, some behaviors commonly associated with ADHD, such as emotional lability and obstinacy, are nearly synonymous with being a preschooler. So, how is the diagnosis made? When is it appropriate to treat? And what would that treatment look like? The following case, where symptoms of preschool ADHD go beyond typical development, provides some guides for treatment based on the evolving literature regarding preschool ADHD.
Case Summary
Johnny is a 4-year-old boy who was the product of a complicated pregnancy and delivery. Born at 35 weeks to a 17-year-old mother with a history of tobacco use disorder and depression, he spent several weeks in the special care nursery before leaving the hospital with his mother. His early temperament was described as being “difficult” with frequent episodes of colic and trouble establishing a sleep routine. His father had a history of conduct problems and school failure, and would come in and out of the family for the first 3 years. Lately, he had moved in with Johnny and his mother, and they were trying to “make a go of it.” Johnny had been slightly behind in his developmental milestones – particularly his language – but by 4 years he was able to speak in simple sentences, was able to name his colors, and had started copying circles and squares.

His parents bring Johnny in for an appointment that they made specifically to discuss his activity level and the question of ADHD, which has been brought up by multiple family members and his preschool teacher. They describe some behaviors that you have not heard about previously because they had assumed that “this is what boys did.” At age 3 years, he impulsively ran into the road after being told “no” and was nearly struck by a car. He continually tries to put things into the toaster, and they have had to get “industrial strength” plug covers because he tries to pry them off with a kitchen knife. On multiple occasions, his mother has locked herself in her bedroom because he wouldn’t stop talking to her and she couldn’t stand it anymore. When this happens, she checks often to make sure Johnny is safe, but then calls Johnny’s father home from his job as a delivery driver because she’s at her limit. In fact, Johnny’s father has been called to the preschool to bring Johnny home so many times that his father is in danger of losing his job. While Johnny appears to be a good athlete, he is often picked last for teams because he doesn’t pay attention in the game and likes to “play his own game” of tackling the other children. The stress of raising Johnny is weighing on the parents’ relationship, and Johnny’s father is considering moving out again. The parents ask for an assessment and treatment, preferably with medication.
Case Discussion
Johnny very likely has ADHD. However, to take appropriate caution in the diagnosis, one would consider that he needs to have six of nine criteria of inattention (being careless, difficulty sustaining attention, not listening, not following through, avoiding hard mental tasks, not organizing, losing important items, being easily distractible, and being forgetful) and/or six of nine criteria of hyperactivity/impulsivity (squirming/fidgeting, can’t stay seated, running or climbing excessively, can’t play quietly, “driven by a motor,” talking excessively, blurting out answers, not waiting his turn, and interrupting/intruding on others). As with school-aged ADHD, there need to be symptoms that are frequent (“often”) and that interfere with home, academic, or occupational function. One must take into account the base rate for these symptoms in preschoolers. For example, Willoughby and colleagues (J. Abnorm. Child Psychol. 2012;40:1301-12) demonstrated that at age 4 years, 26.3% of children fidget or squirm, 39.5% act as if “driven by a motor,” 46.3% talk excessively, 28.8% are easily distracted, and 25.4% have difficult waiting their turn. In fact, on average, a 4-year-old will have 1.3 inattentive items and 2.4 hyperactive-impulsive items. Still, Johnny seems to have more than his fair share. This can be validated by a) doing a careful evaluation over time using multiple informants, b) taking a family history, c) looking at developmental signs and ruling out other developmental disorders, d) making physical observations in the office (although these can be deceiving) and e) having the parents and others complete parent and caregiver checklists.
When asking parents and caregivers to complete checklists, it is crucial to make sure that these checklists look for symptoms other than just ADHD, because there are often co-occurring symptoms and disorders. These include oppositional defiant disorder, anxiety, obsessive compulsive disorder, depressive disorders, autism spectrum disorders, trauma, and learning/communication disorders. In fact, the Preschool ADHD Treatment Study (PATS) demonstrated that 71.5% of children with preschool ADHD had at least one other diagnosis and 29.7% had two or more (J. Child Adolesc. Psychopharmacol. 2007;17:563-80). Use of a broad-based instrument that captures all of these domains, in addition to attention, is warranted. In our clinic, we also assess the parents for psychopathology using the same instruments. The reason for this is, first, that family history increases the likelihood of an ADHD diagnosis and, perhaps more importantly, presence of family psychopathology makes treatment more difficult. This is because the treatment you will prescribe is going to actively involve the parents.
The treatment of choice for preschool ADHD, based on practice parameters and expert opinion, is to start with family-based behavioral treatments. There are now several empirically-based treatments that have shown efficacy for the symptoms of inattention and hyperactivity-impulsivity in preschoolers. These include Triple P (“Practitioner’s Manual for Enhanced Triple P” [Brisbane: Families International Publishing, 1998]), The Incredible Years (Webster-Stratton & Hancock, 1998), and the Revised New Forest Parent Program (Daley & Thompson, 2007), among others. If these are not available in your community, other options would be “Helping the noncompliant child: A clinician’s guide to effective parent training,” 2nd ed. (The Guilford Press: New York, 2003) or any other empirically-based parent training program. This is why it is critical to engage the parents in treatment and to refer them for treatment for their own psychopathology, if present. Furthermore, engaging the family in a program of wellness (freedom from substances, enhanced nutrition, avoidance of artificial food coloring, increased exercise), has less of a research base, but the available evidence is that it is helpful.
If medications become necessary because of safety concerns, there are few options that have a Food and Drug Administration indication. Those that do have an indication for disruptive behavior below the age of 5 years (haloperidol, dextroamphetamine, chlorpromazine, and risperidone) should not be considered as first line. The PATS study demonstrated the safety and efficacy of methylphenidate, but with optimal doses lower than those seen in school-aged children (0.7 mg/kg per day) and with increased numbers of adverse effects (11% discontinuing) (J. Am. Acad. Child Adolesc. Psychiatry 2006;45:1284-93; J. Am. Acad. Child Adolesc. Psychiatry 2006;45:1294-303).
Because of the increased amount of side effects, medication treatment cannot be considered as the first treatment. Treatment with nonstimulants is poorly studied. Any treatment with methylphenidate would be considered off-label prescribing, which must be done with great caution and, preferably, in consultation with a child and adolescent psychiatrist.
The diagnosis and management of ADHD in the very young is tricky, but possible. Doing a comprehensive evaluation with information from multiple informants, assessing and treating the parents for psychopathology, engaging the family in wellness, and starting with behavioral management is the way to go. If you feel that medication treatment is necessary for safety of the little ones, it’s best to consult, because none of the medications with FDA indication are likely to be the answer.
Dr. Althoff is associate professor of psychiatry, psychology, and pediatrics at the University of Vermont, Burlington. He is director of the division of behavioral genetics and conducts research on the development of self-regulation in children. Dr. Althoff receives no funding from pharmaceutical companies or industry. He has grant funding from the National Institute of General Medical Sciences and the Klingenstein Third Generation Foundation, and is employed, in part, by the nonprofit Research Center for Children, Youth, and Families that develops the Child Behavior Checklist and associated instruments. E-mail him at [email protected].
Attention deficit/hyperactivity disorder (ADHD) has been identified in children, and appropriate treatments studied now for over half a century. The vast majority of cases that present for treatment do so after the child starts school and concerns are raised about ability to manage academics. Yet, when asked when the symptoms first began, many parents will describe onset prior to the school years – in the preschool period. But identification of ADHD in preschoolers can be difficult because of the developmental changes that are ongoing during the period from 3 to 5 years. Many of the symptoms that one would attribute to ADHD, such as increased motor activity, inattention, and distractibility are commonplace in this age group. Furthermore, some behaviors commonly associated with ADHD, such as emotional lability and obstinacy, are nearly synonymous with being a preschooler. So, how is the diagnosis made? When is it appropriate to treat? And what would that treatment look like? The following case, where symptoms of preschool ADHD go beyond typical development, provides some guides for treatment based on the evolving literature regarding preschool ADHD.
Case Summary
Johnny is a 4-year-old boy who was the product of a complicated pregnancy and delivery. Born at 35 weeks to a 17-year-old mother with a history of tobacco use disorder and depression, he spent several weeks in the special care nursery before leaving the hospital with his mother. His early temperament was described as being “difficult” with frequent episodes of colic and trouble establishing a sleep routine. His father had a history of conduct problems and school failure, and would come in and out of the family for the first 3 years. Lately, he had moved in with Johnny and his mother, and they were trying to “make a go of it.” Johnny had been slightly behind in his developmental milestones – particularly his language – but by 4 years he was able to speak in simple sentences, was able to name his colors, and had started copying circles and squares.
His parents bring Johnny in for an appointment that they made specifically to discuss his activity level and the question of ADHD, which has been brought up by multiple family members and his preschool teacher. They describe some behaviors that you have not heard about previously because they had assumed that “this is what boys did.” At age 3 years, he impulsively ran into the road after being told “no” and was nearly struck by a car. He continually tries to put things into the toaster, and they have had to get “industrial strength” plug covers because he tries to pry them off with a kitchen knife. On multiple occasions, his mother has locked herself in her bedroom because he wouldn’t stop talking to her and she couldn’t stand it anymore. When this happens, she checks often to make sure Johnny is safe, but then calls Johnny’s father home from his job as a delivery driver because she’s at her limit. In fact, Johnny’s father has been called to the preschool to bring Johnny home so many times that his father is in danger of losing his job. While Johnny appears to be a good athlete, he is often picked last for teams because he doesn’t pay attention in the game and likes to “play his own game” of tackling the other children. The stress of raising Johnny is weighing on the parents’ relationship, and Johnny’s father is considering moving out again. The parents ask for an assessment and treatment, preferably with medication.
Case Discussion
Johnny very likely has ADHD. However, to take appropriate caution in the diagnosis, one would consider that he needs to have six of nine criteria of inattention (being careless, difficulty sustaining attention, not listening, not following through, avoiding hard mental tasks, not organizing, losing important items, being easily distractible, and being forgetful) and/or six of nine criteria of hyperactivity/impulsivity (squirming/fidgeting, can’t stay seated, running or climbing excessively, can’t play quietly, “driven by a motor,” talking excessively, blurting out answers, not waiting his turn, and interrupting/intruding on others). As with school-aged ADHD, there need to be symptoms that are frequent (“often”) and that interfere with home, academic, or occupational function. One must take into account the base rate for these symptoms in preschoolers. For example, Willoughby and colleagues (J. Abnorm. Child Psychol. 2012;40:1301-12) demonstrated that at age 4 years, 26.3% of children fidget or squirm, 39.5% act as if “driven by a motor,” 46.3% talk excessively, 28.8% are easily distracted, and 25.4% have difficult waiting their turn. In fact, on average, a 4-year-old will have 1.3 inattentive items and 2.4 hyperactive-impulsive items. Still, Johnny seems to have more than his fair share. This can be validated by a) doing a careful evaluation over time using multiple informants, b) taking a family history, c) looking at developmental signs and ruling out other developmental disorders, d) making physical observations in the office (although these can be deceiving) and e) having the parents and others complete parent and caregiver checklists.
When asking parents and caregivers to complete checklists, it is crucial to make sure that these checklists look for symptoms other than just ADHD, because there are often co-occurring symptoms and disorders. These include oppositional defiant disorder, anxiety, obsessive compulsive disorder, depressive disorders, autism spectrum disorders, trauma, and learning/communication disorders. In fact, the Preschool ADHD Treatment Study (PATS) demonstrated that 71.5% of children with preschool ADHD had at least one other diagnosis and 29.7% had two or more (J. Child Adolesc. Psychopharmacol. 2007;17:563-80). Use of a broad-based instrument that captures all of these domains, in addition to attention, is warranted. In our clinic, we also assess the parents for psychopathology using the same instruments. The reason for this is, first, that family history increases the likelihood of an ADHD diagnosis and, perhaps more importantly, presence of family psychopathology makes treatment more difficult. This is because the treatment you will prescribe is going to actively involve the parents.
The treatment of choice for preschool ADHD, based on practice parameters and expert opinion, is to start with family-based behavioral treatments. There are now several empirically-based treatments that have shown efficacy for the symptoms of inattention and hyperactivity-impulsivity in preschoolers. These include Triple P (“Practitioner’s Manual for Enhanced Triple P” [Brisbane: Families International Publishing, 1998]), The Incredible Years (Webster-Stratton & Hancock, 1998), and the Revised New Forest Parent Program (Daley & Thompson, 2007), among others. If these are not available in your community, other options would be “Helping the noncompliant child: A clinician’s guide to effective parent training,” 2nd ed. (The Guilford Press: New York, 2003) or any other empirically-based parent training program. This is why it is critical to engage the parents in treatment and to refer them for treatment for their own psychopathology, if present. Furthermore, engaging the family in a program of wellness (freedom from substances, enhanced nutrition, avoidance of artificial food coloring, increased exercise), has less of a research base, but the available evidence is that it is helpful.
If medications become necessary because of safety concerns, there are few options that have a Food and Drug Administration indication. Those that do have an indication for disruptive behavior below the age of 5 years (haloperidol, dextroamphetamine, chlorpromazine, and risperidone) should not be considered as first line. The PATS study demonstrated the safety and efficacy of methylphenidate, but with optimal doses lower than those seen in school-aged children (0.7 mg/kg per day) and with increased numbers of adverse effects (11% discontinuing) (J. Am. Acad. Child Adolesc. Psychiatry 2006;45:1284-93; J. Am. Acad. Child Adolesc. Psychiatry 2006;45:1294-303).
Because of the increased amount of side effects, medication treatment cannot be considered as the first treatment. Treatment with nonstimulants is poorly studied. Any treatment with methylphenidate would be considered off-label prescribing, which must be done with great caution and, preferably, in consultation with a child and adolescent psychiatrist.
The diagnosis and management of ADHD in the very young is tricky, but possible. Doing a comprehensive evaluation with information from multiple informants, assessing and treating the parents for psychopathology, engaging the family in wellness, and starting with behavioral management is the way to go. If you feel that medication treatment is necessary for safety of the little ones, it’s best to consult, because none of the medications with FDA indication are likely to be the answer.
Dr. Althoff is associate professor of psychiatry, psychology, and pediatrics at the University of Vermont, Burlington. He is director of the division of behavioral genetics and conducts research on the development of self-regulation in children. Dr. Althoff receives no funding from pharmaceutical companies or industry. He has grant funding from the National Institute of General Medical Sciences and the Klingenstein Third Generation Foundation, and is employed, in part, by the nonprofit Research Center for Children, Youth, and Families that develops the Child Behavior Checklist and associated instruments. E-mail him at [email protected].
Attention deficit/hyperactivity disorder (ADHD) has been identified in children, and appropriate treatments studied now for over half a century. The vast majority of cases that present for treatment do so after the child starts school and concerns are raised about ability to manage academics. Yet, when asked when the symptoms first began, many parents will describe onset prior to the school years – in the preschool period. But identification of ADHD in preschoolers can be difficult because of the developmental changes that are ongoing during the period from 3 to 5 years. Many of the symptoms that one would attribute to ADHD, such as increased motor activity, inattention, and distractibility are commonplace in this age group. Furthermore, some behaviors commonly associated with ADHD, such as emotional lability and obstinacy, are nearly synonymous with being a preschooler. So, how is the diagnosis made? When is it appropriate to treat? And what would that treatment look like? The following case, where symptoms of preschool ADHD go beyond typical development, provides some guides for treatment based on the evolving literature regarding preschool ADHD.
Case Summary
Johnny is a 4-year-old boy who was the product of a complicated pregnancy and delivery. Born at 35 weeks to a 17-year-old mother with a history of tobacco use disorder and depression, he spent several weeks in the special care nursery before leaving the hospital with his mother. His early temperament was described as being “difficult” with frequent episodes of colic and trouble establishing a sleep routine. His father had a history of conduct problems and school failure, and would come in and out of the family for the first 3 years. Lately, he had moved in with Johnny and his mother, and they were trying to “make a go of it.” Johnny had been slightly behind in his developmental milestones – particularly his language – but by 4 years he was able to speak in simple sentences, was able to name his colors, and had started copying circles and squares.
His parents bring Johnny in for an appointment that they made specifically to discuss his activity level and the question of ADHD, which has been brought up by multiple family members and his preschool teacher. They describe some behaviors that you have not heard about previously because they had assumed that “this is what boys did.” At age 3 years, he impulsively ran into the road after being told “no” and was nearly struck by a car. He continually tries to put things into the toaster, and they have had to get “industrial strength” plug covers because he tries to pry them off with a kitchen knife. On multiple occasions, his mother has locked herself in her bedroom because he wouldn’t stop talking to her and she couldn’t stand it anymore. When this happens, she checks often to make sure Johnny is safe, but then calls Johnny’s father home from his job as a delivery driver because she’s at her limit. In fact, Johnny’s father has been called to the preschool to bring Johnny home so many times that his father is in danger of losing his job. While Johnny appears to be a good athlete, he is often picked last for teams because he doesn’t pay attention in the game and likes to “play his own game” of tackling the other children. The stress of raising Johnny is weighing on the parents’ relationship, and Johnny’s father is considering moving out again. The parents ask for an assessment and treatment, preferably with medication.
Case Discussion
Johnny very likely has ADHD. However, to take appropriate caution in the diagnosis, one would consider that he needs to have six of nine criteria of inattention (being careless, difficulty sustaining attention, not listening, not following through, avoiding hard mental tasks, not organizing, losing important items, being easily distractible, and being forgetful) and/or six of nine criteria of hyperactivity/impulsivity (squirming/fidgeting, can’t stay seated, running or climbing excessively, can’t play quietly, “driven by a motor,” talking excessively, blurting out answers, not waiting his turn, and interrupting/intruding on others). As with school-aged ADHD, there need to be symptoms that are frequent (“often”) and that interfere with home, academic, or occupational function. One must take into account the base rate for these symptoms in preschoolers. For example, Willoughby and colleagues (J. Abnorm. Child Psychol. 2012;40:1301-12) demonstrated that at age 4 years, 26.3% of children fidget or squirm, 39.5% act as if “driven by a motor,” 46.3% talk excessively, 28.8% are easily distracted, and 25.4% have difficult waiting their turn. In fact, on average, a 4-year-old will have 1.3 inattentive items and 2.4 hyperactive-impulsive items. Still, Johnny seems to have more than his fair share. This can be validated by a) doing a careful evaluation over time using multiple informants, b) taking a family history, c) looking at developmental signs and ruling out other developmental disorders, d) making physical observations in the office (although these can be deceiving) and e) having the parents and others complete parent and caregiver checklists.
When asking parents and caregivers to complete checklists, it is crucial to make sure that these checklists look for symptoms other than just ADHD, because there are often co-occurring symptoms and disorders. These include oppositional defiant disorder, anxiety, obsessive compulsive disorder, depressive disorders, autism spectrum disorders, trauma, and learning/communication disorders. In fact, the Preschool ADHD Treatment Study (PATS) demonstrated that 71.5% of children with preschool ADHD had at least one other diagnosis and 29.7% had two or more (J. Child Adolesc. Psychopharmacol. 2007;17:563-80). Use of a broad-based instrument that captures all of these domains, in addition to attention, is warranted. In our clinic, we also assess the parents for psychopathology using the same instruments. The reason for this is, first, that family history increases the likelihood of an ADHD diagnosis and, perhaps more importantly, presence of family psychopathology makes treatment more difficult. This is because the treatment you will prescribe is going to actively involve the parents.
The treatment of choice for preschool ADHD, based on practice parameters and expert opinion, is to start with family-based behavioral treatments. There are now several empirically-based treatments that have shown efficacy for the symptoms of inattention and hyperactivity-impulsivity in preschoolers. These include Triple P (“Practitioner’s Manual for Enhanced Triple P” [Brisbane: Families International Publishing, 1998]), The Incredible Years (Webster-Stratton & Hancock, 1998), and the Revised New Forest Parent Program (Daley & Thompson, 2007), among others. If these are not available in your community, other options would be “Helping the noncompliant child: A clinician’s guide to effective parent training,” 2nd ed. (The Guilford Press: New York, 2003) or any other empirically-based parent training program. This is why it is critical to engage the parents in treatment and to refer them for treatment for their own psychopathology, if present. Furthermore, engaging the family in a program of wellness (freedom from substances, enhanced nutrition, avoidance of artificial food coloring, increased exercise), has less of a research base, but the available evidence is that it is helpful.
If medications become necessary because of safety concerns, there are few options that have a Food and Drug Administration indication. Those that do have an indication for disruptive behavior below the age of 5 years (haloperidol, dextroamphetamine, chlorpromazine, and risperidone) should not be considered as first line. The PATS study demonstrated the safety and efficacy of methylphenidate, but with optimal doses lower than those seen in school-aged children (0.7 mg/kg per day) and with increased numbers of adverse effects (11% discontinuing) (J. Am. Acad. Child Adolesc. Psychiatry 2006;45:1284-93; J. Am. Acad. Child Adolesc. Psychiatry 2006;45:1294-303).
Because of the increased amount of side effects, medication treatment cannot be considered as the first treatment. Treatment with nonstimulants is poorly studied. Any treatment with methylphenidate would be considered off-label prescribing, which must be done with great caution and, preferably, in consultation with a child and adolescent psychiatrist.
The diagnosis and management of ADHD in the very young is tricky, but possible. Doing a comprehensive evaluation with information from multiple informants, assessing and treating the parents for psychopathology, engaging the family in wellness, and starting with behavioral management is the way to go. If you feel that medication treatment is necessary for safety of the little ones, it’s best to consult, because none of the medications with FDA indication are likely to be the answer.
Dr. Althoff is associate professor of psychiatry, psychology, and pediatrics at the University of Vermont, Burlington. He is director of the division of behavioral genetics and conducts research on the development of self-regulation in children. Dr. Althoff receives no funding from pharmaceutical companies or industry. He has grant funding from the National Institute of General Medical Sciences and the Klingenstein Third Generation Foundation, and is employed, in part, by the nonprofit Research Center for Children, Youth, and Families that develops the Child Behavior Checklist and associated instruments. E-mail him at [email protected].

Youth sports
As my children grow older, our family is increasingly drawn into the world of preteen youth sports. As both kids love playing, and have significantly more athleticism and coordination than I ever did, we – and many of the families around us – are being faced with the question: How much is too much? Especially during this season of travel team tryouts and summer training camps, parents may seek your guidance as they try to navigate an increasingly competitive and intense environment.
While there are no easy answers to many of these questions, which are in many ways highly individualized, there are a few guiding principles that I have applied with my own family, and when giving advice to parents.
First and foremost, sports should be fun. Whether your child is an aspiring Olympic athlete or the clumsiest recreational player, they should be having fun. Sports are a wonderful way to teach children the rewards of hard work, physical exercise, teamwork, and perseverance, but it will all be lost on them if they are miserable and dread going to practice. Likewise, even the most talented athlete will burn out and move on to other things if it is not intrinsically enjoyable and rewarding to play. Every child has moments of whining or complaining, but if they are consistently telling you they don’t want to go to practice or seem unhappy, you should listen. On the flip side, if you have a child who seems to love training, who looks forward to practice, and who asks to play more and more competitively, then a more intense environment may be suitable. Just be sure it is really the child, and not the parent, who is having the most fun!
Second, the coaches (and the parents) should be encouraging, positive, and train their athletes in age- and developmentally appropriate ways. It is absolutely reasonable for coaches to require the team to come to practice reliably, pay attention, work hard, and push themselves to do their best. What is not developmentally appropriate – or even productive or motivating in the long term – is for coaches to yell, criticize, or make demeaning comments. After one game where the opposing coach continuously shouted statements to the players such as “What were you thinking?” and “Listen to what I tell you to do, not to the little voice in your head!” my daughter commented, “I don’t think I could play for that team. It would make me too nervous with the coach yelling like that all the time.”Even for the very best and most talented players, the goals of youth sports (in addition to having fun!) should be to develop skills, good sportsmanship, and the ability to understand and implement the strategy of the game. These are the core skills you need whether you ultimately become a professional athlete or a weekend warrior, but they are not things children can learn if they are afraid of being yelled at for making a wrong move, or losing a game or race. On the contrary, it may decrease a child’s confidence and even reinforce opposite behaviors. When considering where and when a child should play, parents should carefully assess the coaching and league environment. Kids should feel more confident as a result of their involvement in sports, not less. The most elite teams may actually have an environment that can do more harm than good in the long run – not only for a child’s skills, but for their self-esteem and character. On the flip side, a less intense team with good and positive coaching may develop a child’s skills in a way that leads to greater long-term success in sports and in life!
Lastly, for children of all ages, but especially prepubertal children, be alert to the dangers of over training. Every child develops differently and can tolerate different levels and amounts of training, but be sure to advise parents on what activities (for example, weight lifting) are and aren’t appropriate for kids of different ages. Children should increase their level of training gradually, be monitored carefully for signs of overuse injuries, and they, their parents, and their coaches need to be willing to back off if injuries begin recurring. Parents should be very wary of teams and coaches who push children through injuries or who are not patient about letting children take time to recover before they return to play. These are the bodies children will have for their whole lives; repeated and chronic injuries at young ages ultimately can be quite harmful.
Youth sports can be an incredibly positive experience for many children, with lifelong benefits. Unfortunately, it sometimes also can be overly competitive and frankly a little crazy! Like anything, our role as pediatricians is to provide the guidance and information to help parents and their children make both physically and emotionally healthy decisions every step of the way.
Dr. Beers is assistant professor of pediatrics at Children’s National Medical Center and the George Washington University Medical Center, Washington.
As my children grow older, our family is increasingly drawn into the world of preteen youth sports. As both kids love playing, and have significantly more athleticism and coordination than I ever did, we – and many of the families around us – are being faced with the question: How much is too much? Especially during this season of travel team tryouts and summer training camps, parents may seek your guidance as they try to navigate an increasingly competitive and intense environment.
While there are no easy answers to many of these questions, which are in many ways highly individualized, there are a few guiding principles that I have applied with my own family, and when giving advice to parents.
First and foremost, sports should be fun. Whether your child is an aspiring Olympic athlete or the clumsiest recreational player, they should be having fun. Sports are a wonderful way to teach children the rewards of hard work, physical exercise, teamwork, and perseverance, but it will all be lost on them if they are miserable and dread going to practice. Likewise, even the most talented athlete will burn out and move on to other things if it is not intrinsically enjoyable and rewarding to play. Every child has moments of whining or complaining, but if they are consistently telling you they don’t want to go to practice or seem unhappy, you should listen. On the flip side, if you have a child who seems to love training, who looks forward to practice, and who asks to play more and more competitively, then a more intense environment may be suitable. Just be sure it is really the child, and not the parent, who is having the most fun!
Second, the coaches (and the parents) should be encouraging, positive, and train their athletes in age- and developmentally appropriate ways. It is absolutely reasonable for coaches to require the team to come to practice reliably, pay attention, work hard, and push themselves to do their best. What is not developmentally appropriate – or even productive or motivating in the long term – is for coaches to yell, criticize, or make demeaning comments. After one game where the opposing coach continuously shouted statements to the players such as “What were you thinking?” and “Listen to what I tell you to do, not to the little voice in your head!” my daughter commented, “I don’t think I could play for that team. It would make me too nervous with the coach yelling like that all the time.”Even for the very best and most talented players, the goals of youth sports (in addition to having fun!) should be to develop skills, good sportsmanship, and the ability to understand and implement the strategy of the game. These are the core skills you need whether you ultimately become a professional athlete or a weekend warrior, but they are not things children can learn if they are afraid of being yelled at for making a wrong move, or losing a game or race. On the contrary, it may decrease a child’s confidence and even reinforce opposite behaviors. When considering where and when a child should play, parents should carefully assess the coaching and league environment. Kids should feel more confident as a result of their involvement in sports, not less. The most elite teams may actually have an environment that can do more harm than good in the long run – not only for a child’s skills, but for their self-esteem and character. On the flip side, a less intense team with good and positive coaching may develop a child’s skills in a way that leads to greater long-term success in sports and in life!
Lastly, for children of all ages, but especially prepubertal children, be alert to the dangers of over training. Every child develops differently and can tolerate different levels and amounts of training, but be sure to advise parents on what activities (for example, weight lifting) are and aren’t appropriate for kids of different ages. Children should increase their level of training gradually, be monitored carefully for signs of overuse injuries, and they, their parents, and their coaches need to be willing to back off if injuries begin recurring. Parents should be very wary of teams and coaches who push children through injuries or who are not patient about letting children take time to recover before they return to play. These are the bodies children will have for their whole lives; repeated and chronic injuries at young ages ultimately can be quite harmful.
Youth sports can be an incredibly positive experience for many children, with lifelong benefits. Unfortunately, it sometimes also can be overly competitive and frankly a little crazy! Like anything, our role as pediatricians is to provide the guidance and information to help parents and their children make both physically and emotionally healthy decisions every step of the way.
Dr. Beers is assistant professor of pediatrics at Children’s National Medical Center and the George Washington University Medical Center, Washington.
As my children grow older, our family is increasingly drawn into the world of preteen youth sports. As both kids love playing, and have significantly more athleticism and coordination than I ever did, we – and many of the families around us – are being faced with the question: How much is too much? Especially during this season of travel team tryouts and summer training camps, parents may seek your guidance as they try to navigate an increasingly competitive and intense environment.
While there are no easy answers to many of these questions, which are in many ways highly individualized, there are a few guiding principles that I have applied with my own family, and when giving advice to parents.
First and foremost, sports should be fun. Whether your child is an aspiring Olympic athlete or the clumsiest recreational player, they should be having fun. Sports are a wonderful way to teach children the rewards of hard work, physical exercise, teamwork, and perseverance, but it will all be lost on them if they are miserable and dread going to practice. Likewise, even the most talented athlete will burn out and move on to other things if it is not intrinsically enjoyable and rewarding to play. Every child has moments of whining or complaining, but if they are consistently telling you they don’t want to go to practice or seem unhappy, you should listen. On the flip side, if you have a child who seems to love training, who looks forward to practice, and who asks to play more and more competitively, then a more intense environment may be suitable. Just be sure it is really the child, and not the parent, who is having the most fun!
Second, the coaches (and the parents) should be encouraging, positive, and train their athletes in age- and developmentally appropriate ways. It is absolutely reasonable for coaches to require the team to come to practice reliably, pay attention, work hard, and push themselves to do their best. What is not developmentally appropriate – or even productive or motivating in the long term – is for coaches to yell, criticize, or make demeaning comments. After one game where the opposing coach continuously shouted statements to the players such as “What were you thinking?” and “Listen to what I tell you to do, not to the little voice in your head!” my daughter commented, “I don’t think I could play for that team. It would make me too nervous with the coach yelling like that all the time.”Even for the very best and most talented players, the goals of youth sports (in addition to having fun!) should be to develop skills, good sportsmanship, and the ability to understand and implement the strategy of the game. These are the core skills you need whether you ultimately become a professional athlete or a weekend warrior, but they are not things children can learn if they are afraid of being yelled at for making a wrong move, or losing a game or race. On the contrary, it may decrease a child’s confidence and even reinforce opposite behaviors. When considering where and when a child should play, parents should carefully assess the coaching and league environment. Kids should feel more confident as a result of their involvement in sports, not less. The most elite teams may actually have an environment that can do more harm than good in the long run – not only for a child’s skills, but for their self-esteem and character. On the flip side, a less intense team with good and positive coaching may develop a child’s skills in a way that leads to greater long-term success in sports and in life!
Lastly, for children of all ages, but especially prepubertal children, be alert to the dangers of over training. Every child develops differently and can tolerate different levels and amounts of training, but be sure to advise parents on what activities (for example, weight lifting) are and aren’t appropriate for kids of different ages. Children should increase their level of training gradually, be monitored carefully for signs of overuse injuries, and they, their parents, and their coaches need to be willing to back off if injuries begin recurring. Parents should be very wary of teams and coaches who push children through injuries or who are not patient about letting children take time to recover before they return to play. These are the bodies children will have for their whole lives; repeated and chronic injuries at young ages ultimately can be quite harmful.
Youth sports can be an incredibly positive experience for many children, with lifelong benefits. Unfortunately, it sometimes also can be overly competitive and frankly a little crazy! Like anything, our role as pediatricians is to provide the guidance and information to help parents and their children make both physically and emotionally healthy decisions every step of the way.
Dr. Beers is assistant professor of pediatrics at Children’s National Medical Center and the George Washington University Medical Center, Washington.

Patient satisfaction doesn’t equal better hospital care
What happens when you give children everything they ask for? They get spoiled, of course. Any parent can tell you that.
The problem is that you’re trying to raise children to (eventually) be responsible adults. Part of this is teaching them that you can’t always win, you should always share, and you can’t always get what you want.
Most kids don’t like it. (I know I didn’t.) They only see that the candy or toy they want is being refused and don’t grasp the long-term plan of growing up to be a decent person. Across a thousand human cultures, any parent would agree.
But the same principle doesn’t seem to apply in modern health care. What would you think is more important in a hospital: competent staff or having a beverage offered to you after being checked into the emergency department?
Sadly, things like the latter seem to be winning because of the recent emphasis on patient satisfaction scores. In today’s world, 30% of a hospital’s Medicare reimbursement is based on these scores. That’s a lot of money.
Unfortunately, quality of care doesn’t necessarily have the same meaning between doctors and patients. The former will say it means you left the hospital with a good outcome. The latter will agree but also will throw in things like whether they got enough pain meds or their call light answered fast enough. If you’re having chest pain or severe dyspnea, getting that call light answered quickly is pretty important. But if all you want is a soda or for someone to hand you the TV remote … not so much.
The problem is that the patient satisfaction surveys (and yes, speed of call-light response is on there) don’t take that key point into account. What might make some patients happy isn’t necessarily in their best interest. The post-CABG patient who wants a double cheeseburger won’t be thrilled if he gets a salad instead. Another patient in for detox won’t be pleased if she doesn’t get Dilaudid on demand. A third will be angry that he’s not allowed to smoke. Those refusals are an integral part of their successful treatment and recovery plan, but they may not see it that way. And they’ll be sure to mark it on the survey.
As a result, the hospital gets penalized in spite of the fact that they’re doing their best to provide quality care. And the business-minded CEOs, who generally have no medical background, only care about this part of it.
Measuring what counts is important. But the idea that hospital care should be held to the same standards as Burger King and Walmart is fundamentally flawed. The things that are done in hospitals – cut people open, draw blood, biopsy bone marrow, put in endotracheal and feeding tubes – aren’t intended as recreational experiences. We try to make them as painless as possible, but in health care “do no harm” often means doing some harm in order to prevent a catastrophe.
The side effects of chemotherapy are (hopefully) offset by the successful treatment of cancer. But that doesn’t mean hair loss, nausea, vomiting, diarrhea, and other toxic symptoms are part of “customer satisfaction.” One study even found that the most satisfied patients had the highest mortality.
We owe patients the very best care we can give them, but they also need to understand that “best care” doesn’t always mean what they want in the short term. We’re focused on a goal that’s beyond the immediate horizon.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.
What happens when you give children everything they ask for? They get spoiled, of course. Any parent can tell you that.
The problem is that you’re trying to raise children to (eventually) be responsible adults. Part of this is teaching them that you can’t always win, you should always share, and you can’t always get what you want.
Most kids don’t like it. (I know I didn’t.) They only see that the candy or toy they want is being refused and don’t grasp the long-term plan of growing up to be a decent person. Across a thousand human cultures, any parent would agree.
But the same principle doesn’t seem to apply in modern health care. What would you think is more important in a hospital: competent staff or having a beverage offered to you after being checked into the emergency department?
Sadly, things like the latter seem to be winning because of the recent emphasis on patient satisfaction scores. In today’s world, 30% of a hospital’s Medicare reimbursement is based on these scores. That’s a lot of money.
Unfortunately, quality of care doesn’t necessarily have the same meaning between doctors and patients. The former will say it means you left the hospital with a good outcome. The latter will agree but also will throw in things like whether they got enough pain meds or their call light answered fast enough. If you’re having chest pain or severe dyspnea, getting that call light answered quickly is pretty important. But if all you want is a soda or for someone to hand you the TV remote … not so much.
The problem is that the patient satisfaction surveys (and yes, speed of call-light response is on there) don’t take that key point into account. What might make some patients happy isn’t necessarily in their best interest. The post-CABG patient who wants a double cheeseburger won’t be thrilled if he gets a salad instead. Another patient in for detox won’t be pleased if she doesn’t get Dilaudid on demand. A third will be angry that he’s not allowed to smoke. Those refusals are an integral part of their successful treatment and recovery plan, but they may not see it that way. And they’ll be sure to mark it on the survey.
As a result, the hospital gets penalized in spite of the fact that they’re doing their best to provide quality care. And the business-minded CEOs, who generally have no medical background, only care about this part of it.
Measuring what counts is important. But the idea that hospital care should be held to the same standards as Burger King and Walmart is fundamentally flawed. The things that are done in hospitals – cut people open, draw blood, biopsy bone marrow, put in endotracheal and feeding tubes – aren’t intended as recreational experiences. We try to make them as painless as possible, but in health care “do no harm” often means doing some harm in order to prevent a catastrophe.
The side effects of chemotherapy are (hopefully) offset by the successful treatment of cancer. But that doesn’t mean hair loss, nausea, vomiting, diarrhea, and other toxic symptoms are part of “customer satisfaction.” One study even found that the most satisfied patients had the highest mortality.
We owe patients the very best care we can give them, but they also need to understand that “best care” doesn’t always mean what they want in the short term. We’re focused on a goal that’s beyond the immediate horizon.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.
What happens when you give children everything they ask for? They get spoiled, of course. Any parent can tell you that.
The problem is that you’re trying to raise children to (eventually) be responsible adults. Part of this is teaching them that you can’t always win, you should always share, and you can’t always get what you want.
Most kids don’t like it. (I know I didn’t.) They only see that the candy or toy they want is being refused and don’t grasp the long-term plan of growing up to be a decent person. Across a thousand human cultures, any parent would agree.
But the same principle doesn’t seem to apply in modern health care. What would you think is more important in a hospital: competent staff or having a beverage offered to you after being checked into the emergency department?
Sadly, things like the latter seem to be winning because of the recent emphasis on patient satisfaction scores. In today’s world, 30% of a hospital’s Medicare reimbursement is based on these scores. That’s a lot of money.
Unfortunately, quality of care doesn’t necessarily have the same meaning between doctors and patients. The former will say it means you left the hospital with a good outcome. The latter will agree but also will throw in things like whether they got enough pain meds or their call light answered fast enough. If you’re having chest pain or severe dyspnea, getting that call light answered quickly is pretty important. But if all you want is a soda or for someone to hand you the TV remote … not so much.
The problem is that the patient satisfaction surveys (and yes, speed of call-light response is on there) don’t take that key point into account. What might make some patients happy isn’t necessarily in their best interest. The post-CABG patient who wants a double cheeseburger won’t be thrilled if he gets a salad instead. Another patient in for detox won’t be pleased if she doesn’t get Dilaudid on demand. A third will be angry that he’s not allowed to smoke. Those refusals are an integral part of their successful treatment and recovery plan, but they may not see it that way. And they’ll be sure to mark it on the survey.
As a result, the hospital gets penalized in spite of the fact that they’re doing their best to provide quality care. And the business-minded CEOs, who generally have no medical background, only care about this part of it.
Measuring what counts is important. But the idea that hospital care should be held to the same standards as Burger King and Walmart is fundamentally flawed. The things that are done in hospitals – cut people open, draw blood, biopsy bone marrow, put in endotracheal and feeding tubes – aren’t intended as recreational experiences. We try to make them as painless as possible, but in health care “do no harm” often means doing some harm in order to prevent a catastrophe.
The side effects of chemotherapy are (hopefully) offset by the successful treatment of cancer. But that doesn’t mean hair loss, nausea, vomiting, diarrhea, and other toxic symptoms are part of “customer satisfaction.” One study even found that the most satisfied patients had the highest mortality.
We owe patients the very best care we can give them, but they also need to understand that “best care” doesn’t always mean what they want in the short term. We’re focused on a goal that’s beyond the immediate horizon.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.

Putting isthmocele into perspective
With the increase in cesarean sections worldwide, it is imperative that physicians properly inform their patients as to potential procedure risks. One potential postcesarean section problem that is receiving increasing attention is the isthmocele or niche.
Defined as an anechoic area in the cesarean section scar, it has been noted to occur in 24%-69% of women undergoing transvaginal sonography, and 56%-78% of women evaluated with transvaginal saline infused sonogram. While most cesarean section defects are asymptomatic, the isthmocele has been noted to be associated with abnormal uterine bleeding, including prolonged menstruation or postmenopausal spotting, and fertility concerns (BJOG. 2014;121:145-56).

Interestingly, it has been 40 years since Stewart, et al. first reported the relationship of abnormal uterine bleeding and cesarean section (Br. J. Gynaecol. 1975;82:682-6). Bloody fluid can be generated at the isthmocele site, which travels up the endometrial canal, thus impacting implantation. The niche can also be the site of ectopic pregnancy implantation.
In this edition of Master Class in gynecologic surgery, I have asked my newest partner, Dr. Kirsten Sasaki, to share our views on this increasingly important subject. Dr. Sasaki completed her internship and residency at Tufts Medical Center, Boston, where she was awarded the Outstanding Chief Resident Clinician Award. Dr. Sasaki then went on to become our second fellow in the Fellowship in Minimally Invasive Gynecologic Surgery in affiliation with AAGL and SRS at Advocate Lutheran General Hospital, Park Ridge, Ill. Once again, Dr. Sasaki was singled out for her excellent teaching and research capabilities. Ultimately however, it was her tremendous surgical skills and surgical sense that led Dr. Aarathi Cholkeri-Singh and I to invite her into our practice.
Dr. Miller is clinical associate professor at the University of Illinois at Chicago, immediate past president of the International Society for Gynecologic Endoscopy (ISGE), and a past president of the AAGL. He is a reproductive endocrinologist and minimally invasive gynecologic surgeon in private practice in Naperville, Ill., and Schaumburg, Ill.; the director of minimally invasive gynecologic surgery and the director of the AAGL/SRS fellowship in minimally invasive gynecologic surgery at Advocate Lutheran General Hospital, Park Ridge, Ill.; and the medical editor of this column, Master Class. Dr. Miller is a consultant and on the speakers bureau for Ethicon. He is also a consultant, on the speakers bureau, and has received grant and research support from Intuitive Surgical.
With the increase in cesarean sections worldwide, it is imperative that physicians properly inform their patients as to potential procedure risks. One potential postcesarean section problem that is receiving increasing attention is the isthmocele or niche.
Defined as an anechoic area in the cesarean section scar, it has been noted to occur in 24%-69% of women undergoing transvaginal sonography, and 56%-78% of women evaluated with transvaginal saline infused sonogram. While most cesarean section defects are asymptomatic, the isthmocele has been noted to be associated with abnormal uterine bleeding, including prolonged menstruation or postmenopausal spotting, and fertility concerns (BJOG. 2014;121:145-56).
Interestingly, it has been 40 years since Stewart, et al. first reported the relationship of abnormal uterine bleeding and cesarean section (Br. J. Gynaecol. 1975;82:682-6). Bloody fluid can be generated at the isthmocele site, which travels up the endometrial canal, thus impacting implantation. The niche can also be the site of ectopic pregnancy implantation.
In this edition of Master Class in gynecologic surgery, I have asked my newest partner, Dr. Kirsten Sasaki, to share our views on this increasingly important subject. Dr. Sasaki completed her internship and residency at Tufts Medical Center, Boston, where she was awarded the Outstanding Chief Resident Clinician Award. Dr. Sasaki then went on to become our second fellow in the Fellowship in Minimally Invasive Gynecologic Surgery in affiliation with AAGL and SRS at Advocate Lutheran General Hospital, Park Ridge, Ill. Once again, Dr. Sasaki was singled out for her excellent teaching and research capabilities. Ultimately however, it was her tremendous surgical skills and surgical sense that led Dr. Aarathi Cholkeri-Singh and I to invite her into our practice.
Dr. Miller is clinical associate professor at the University of Illinois at Chicago, immediate past president of the International Society for Gynecologic Endoscopy (ISGE), and a past president of the AAGL. He is a reproductive endocrinologist and minimally invasive gynecologic surgeon in private practice in Naperville, Ill., and Schaumburg, Ill.; the director of minimally invasive gynecologic surgery and the director of the AAGL/SRS fellowship in minimally invasive gynecologic surgery at Advocate Lutheran General Hospital, Park Ridge, Ill.; and the medical editor of this column, Master Class. Dr. Miller is a consultant and on the speakers bureau for Ethicon. He is also a consultant, on the speakers bureau, and has received grant and research support from Intuitive Surgical.
With the increase in cesarean sections worldwide, it is imperative that physicians properly inform their patients as to potential procedure risks. One potential postcesarean section problem that is receiving increasing attention is the isthmocele or niche.
Defined as an anechoic area in the cesarean section scar, it has been noted to occur in 24%-69% of women undergoing transvaginal sonography, and 56%-78% of women evaluated with transvaginal saline infused sonogram. While most cesarean section defects are asymptomatic, the isthmocele has been noted to be associated with abnormal uterine bleeding, including prolonged menstruation or postmenopausal spotting, and fertility concerns (BJOG. 2014;121:145-56).
Interestingly, it has been 40 years since Stewart, et al. first reported the relationship of abnormal uterine bleeding and cesarean section (Br. J. Gynaecol. 1975;82:682-6). Bloody fluid can be generated at the isthmocele site, which travels up the endometrial canal, thus impacting implantation. The niche can also be the site of ectopic pregnancy implantation.
In this edition of Master Class in gynecologic surgery, I have asked my newest partner, Dr. Kirsten Sasaki, to share our views on this increasingly important subject. Dr. Sasaki completed her internship and residency at Tufts Medical Center, Boston, where she was awarded the Outstanding Chief Resident Clinician Award. Dr. Sasaki then went on to become our second fellow in the Fellowship in Minimally Invasive Gynecologic Surgery in affiliation with AAGL and SRS at Advocate Lutheran General Hospital, Park Ridge, Ill. Once again, Dr. Sasaki was singled out for her excellent teaching and research capabilities. Ultimately however, it was her tremendous surgical skills and surgical sense that led Dr. Aarathi Cholkeri-Singh and I to invite her into our practice.
Dr. Miller is clinical associate professor at the University of Illinois at Chicago, immediate past president of the International Society for Gynecologic Endoscopy (ISGE), and a past president of the AAGL. He is a reproductive endocrinologist and minimally invasive gynecologic surgeon in private practice in Naperville, Ill., and Schaumburg, Ill.; the director of minimally invasive gynecologic surgery and the director of the AAGL/SRS fellowship in minimally invasive gynecologic surgery at Advocate Lutheran General Hospital, Park Ridge, Ill.; and the medical editor of this column, Master Class. Dr. Miller is a consultant and on the speakers bureau for Ethicon. He is also a consultant, on the speakers bureau, and has received grant and research support from Intuitive Surgical.
