User login
Marijuana: The good, the bad, and the ugly
With the recent legalization of marijuana in many states, marijuana and its uses are a hot topic in most social circles. As physicians, we see the full spectrum, from its healing properties to its destructive ones. The goal of this article is not to persuade you into changing positions on its legalization, but rather to stress the importance of remaining neutral and educating families on the facts and potential pros and cons as they relate to the health of their children.
On Jan. 26, 2015,* the American Academy of Pediatrics released its policy statement on marijuana and its use (Pediatrics 2014 [doi:10.1542/peds.2014-4146]). The AAP does not support the legalization of marijuana because of the harm that it poses to children and adolescents, nor does it support legalization of medical marijuana outside the regulatory process of the Food and Drug Administration. It does recognize that marijuana may be an option for children with life-threatening or debilitating illnesses. The AAP does support the decriminalization of marijuana use or possession and advocates for less-harsh criminal penalties. Many of the recommendations were made because of the current research on marijuana and its use.

According to 2014’s Monitoring the Future survey of drug use and attitudes among American 8th, 10th, and 12th graders, marijuana is the most common illegal drug used by adolescents. Among 8th graders, 6.5% reported use; among 10th graders, 16.6% reported use; and 21.2 % of 12th graders reported use. A total of 81% of 12th grade students stated it was easy to get. Marijuana use at all three grade levels was higher than cigarette use (National Institute on Drug Abuse. Drug Facts, 2014). Another study found that early initiation of marijuana use was 6.5 times more likely to result in addiction than if it was initiated after the age of 21 years (Adolescent substance use: America’s #1 public health problem. CASA Columbia, 2011).
One thing we can agree upon is that an adolescent using any substance to mask or lessen the pain of a situation is in trouble. Whether adolescents are overeating or denying themselves food, or using drugs to get high, or behaving promiscuously to get attention, overindulgence is never good. So when we evaluate the effects of marijuana use among teens, we have to separate out the underlying emotional issues from the effects related to the drug. Adolescents are at particular risk for overuse because most lack the experience or maturity to stop when things get out of hand. And they are at risk when using anything that will give them a “high.” Substances like glue, gasoline, and cold medicine can bring them that high, and marijuana is no different – except that it is illegal.

Alcohol, cigarettes, and prescription medications are also vehicles to that desired high. Each has greater addictive properties than marijuana does. According to the Monitoring the Future study, most high school seniors do not think occasional use of marijuana is harmful, with only 36% saying regular use puts you at greater risk, compared with 39.5% in 2013 and 52% in 2009. The perception that marijuana is harmful has definitely declined.
Cannabis smoke contains three times the amount of tar found in tobacco smoke and 50% more carcinogens (N. Engl. J. Med. 1988;318:347). It also can irritate the airways, causing exacerbations of asthma, cystic fibrosis, sputum production, and pharyngitis (Arch. Intern. Med. 2007;167:221). Long-term studies showed that extended use was associated with increased obstructive lung diseases.
There is substantial evidence that indicates that cannabis use can cause psychosis. One review noted evidence that genetic factors may influence the risk of psychosis in adults who used cannabis as adolescents (Biol. Psychiatry 2005;57:1117). Cannabis is believed to release dopamine in the body, which may lead to the psychosis. Another study found that the onset of psychotic illness occurred more than 2 years earlier in patients who were heavy cannabis users (Arch. Gen. Psychiatry 2011;68:555).
Another important finding is that marijuana can suppress testosterone secretion in men, which may result in decreased libido, impotence, and gynecomastia (N. Engl. J. Med. 1974;290:872). Many teens believe cannabis is safe because it’s a plant, and consequently, may not relate these symptoms to its use.
The research on cannabis smoke and its relationship to cancer are limited by inadequate sample sizes and confounding factors not taken into account, but there does seem to be a relationship between cannabis smoke and lung cancer and bladder cancer (J. Psychoactive Drugs 1994;26:285; Urology 2006;67:100). However, head and neck cancers have not shown a relationship to marijuana use (Cancer Epidemiol. Biomarkers Prev. 2009;18:1544-51). Cardiovascular effects have been related to the increased sympathetic activity and decreased parasympathetic activity that can result in bradycardia and hypotension with high doses. This may be of particular concern in older people with coronary artery disease (J. Clin. Pharmacol. 2002;42:58S).
The medicinal properties of marijuana are an important consideration. Marijuana has been shown to be particularly effective in controlling some forms of seizure, pain, nausea from chemotherapy, muscle spasms caused by multiple sclerosis, and Crohn’s disease. The FDA has approved tetrahydrocannabinol, or THC, a key ingredient in marijuana, to treat nausea and improve appetite. In states that have legalized cannabis, qualifying patients can get prescriptions from their physicians to use at authorized dispensaries. For some patients, the effects can be life changing; for others, it can help with pain management and the discomfort associated with certain illnesses.
Beyond the scope of medicine is the economics of the legalization of marijuana. States that have already legalized it have seen revenues in the billions. Marijuana cash crops are estimated at $14 billion in revenue. Jon Gettman’s 2007 study, “Lost Taxes and Other Costs of Marijuana,” states that the prohibition of marijuana costs the government $113 billion, while it costs taxpayers $31.1 billion each year. The study projects that legalization of cannabis may save the criminal justice system $10.7 billion and an additional $6.2 billion for taxpayers. That sort of money does talk: Regardless of current opposition to the legalization of marijuana, it is probably just a matter of time before marijuana is legalized in every state.
The scope of marijuana issues is broad and, for many, controversial. The drug can serve as a healer, create health challenges, lead to drug addiction, or even become a significant revenue source to a state’s coffers. As providers, we need to be able to provide our patients with research-based information and resources, and dispel myths, so that they can make informed decisions for themselves that are in the best interests of their children.
Dr. Pearce is a pediatrician in Frankfort, Ill. She had no relevant financial disclosures. E-mail her at [email protected].
*Correction, 1/29/2015: An earlier version of this story had the incorrect date of publication of the AAP's policy statement.
With the recent legalization of marijuana in many states, marijuana and its uses are a hot topic in most social circles. As physicians, we see the full spectrum, from its healing properties to its destructive ones. The goal of this article is not to persuade you into changing positions on its legalization, but rather to stress the importance of remaining neutral and educating families on the facts and potential pros and cons as they relate to the health of their children.
On Jan. 26, 2015,* the American Academy of Pediatrics released its policy statement on marijuana and its use (Pediatrics 2014 [doi:10.1542/peds.2014-4146]). The AAP does not support the legalization of marijuana because of the harm that it poses to children and adolescents, nor does it support legalization of medical marijuana outside the regulatory process of the Food and Drug Administration. It does recognize that marijuana may be an option for children with life-threatening or debilitating illnesses. The AAP does support the decriminalization of marijuana use or possession and advocates for less-harsh criminal penalties. Many of the recommendations were made because of the current research on marijuana and its use.
According to 2014’s Monitoring the Future survey of drug use and attitudes among American 8th, 10th, and 12th graders, marijuana is the most common illegal drug used by adolescents. Among 8th graders, 6.5% reported use; among 10th graders, 16.6% reported use; and 21.2 % of 12th graders reported use. A total of 81% of 12th grade students stated it was easy to get. Marijuana use at all three grade levels was higher than cigarette use (National Institute on Drug Abuse. Drug Facts, 2014). Another study found that early initiation of marijuana use was 6.5 times more likely to result in addiction than if it was initiated after the age of 21 years (Adolescent substance use: America’s #1 public health problem. CASA Columbia, 2011).
One thing we can agree upon is that an adolescent using any substance to mask or lessen the pain of a situation is in trouble. Whether adolescents are overeating or denying themselves food, or using drugs to get high, or behaving promiscuously to get attention, overindulgence is never good. So when we evaluate the effects of marijuana use among teens, we have to separate out the underlying emotional issues from the effects related to the drug. Adolescents are at particular risk for overuse because most lack the experience or maturity to stop when things get out of hand. And they are at risk when using anything that will give them a “high.” Substances like glue, gasoline, and cold medicine can bring them that high, and marijuana is no different – except that it is illegal.
Alcohol, cigarettes, and prescription medications are also vehicles to that desired high. Each has greater addictive properties than marijuana does. According to the Monitoring the Future study, most high school seniors do not think occasional use of marijuana is harmful, with only 36% saying regular use puts you at greater risk, compared with 39.5% in 2013 and 52% in 2009. The perception that marijuana is harmful has definitely declined.
Cannabis smoke contains three times the amount of tar found in tobacco smoke and 50% more carcinogens (N. Engl. J. Med. 1988;318:347). It also can irritate the airways, causing exacerbations of asthma, cystic fibrosis, sputum production, and pharyngitis (Arch. Intern. Med. 2007;167:221). Long-term studies showed that extended use was associated with increased obstructive lung diseases.
There is substantial evidence that indicates that cannabis use can cause psychosis. One review noted evidence that genetic factors may influence the risk of psychosis in adults who used cannabis as adolescents (Biol. Psychiatry 2005;57:1117). Cannabis is believed to release dopamine in the body, which may lead to the psychosis. Another study found that the onset of psychotic illness occurred more than 2 years earlier in patients who were heavy cannabis users (Arch. Gen. Psychiatry 2011;68:555).
Another important finding is that marijuana can suppress testosterone secretion in men, which may result in decreased libido, impotence, and gynecomastia (N. Engl. J. Med. 1974;290:872). Many teens believe cannabis is safe because it’s a plant, and consequently, may not relate these symptoms to its use.
The research on cannabis smoke and its relationship to cancer are limited by inadequate sample sizes and confounding factors not taken into account, but there does seem to be a relationship between cannabis smoke and lung cancer and bladder cancer (J. Psychoactive Drugs 1994;26:285; Urology 2006;67:100). However, head and neck cancers have not shown a relationship to marijuana use (Cancer Epidemiol. Biomarkers Prev. 2009;18:1544-51). Cardiovascular effects have been related to the increased sympathetic activity and decreased parasympathetic activity that can result in bradycardia and hypotension with high doses. This may be of particular concern in older people with coronary artery disease (J. Clin. Pharmacol. 2002;42:58S).
The medicinal properties of marijuana are an important consideration. Marijuana has been shown to be particularly effective in controlling some forms of seizure, pain, nausea from chemotherapy, muscle spasms caused by multiple sclerosis, and Crohn’s disease. The FDA has approved tetrahydrocannabinol, or THC, a key ingredient in marijuana, to treat nausea and improve appetite. In states that have legalized cannabis, qualifying patients can get prescriptions from their physicians to use at authorized dispensaries. For some patients, the effects can be life changing; for others, it can help with pain management and the discomfort associated with certain illnesses.
Beyond the scope of medicine is the economics of the legalization of marijuana. States that have already legalized it have seen revenues in the billions. Marijuana cash crops are estimated at $14 billion in revenue. Jon Gettman’s 2007 study, “Lost Taxes and Other Costs of Marijuana,” states that the prohibition of marijuana costs the government $113 billion, while it costs taxpayers $31.1 billion each year. The study projects that legalization of cannabis may save the criminal justice system $10.7 billion and an additional $6.2 billion for taxpayers. That sort of money does talk: Regardless of current opposition to the legalization of marijuana, it is probably just a matter of time before marijuana is legalized in every state.
The scope of marijuana issues is broad and, for many, controversial. The drug can serve as a healer, create health challenges, lead to drug addiction, or even become a significant revenue source to a state’s coffers. As providers, we need to be able to provide our patients with research-based information and resources, and dispel myths, so that they can make informed decisions for themselves that are in the best interests of their children.
Dr. Pearce is a pediatrician in Frankfort, Ill. She had no relevant financial disclosures. E-mail her at [email protected].
*Correction, 1/29/2015: An earlier version of this story had the incorrect date of publication of the AAP's policy statement.
With the recent legalization of marijuana in many states, marijuana and its uses are a hot topic in most social circles. As physicians, we see the full spectrum, from its healing properties to its destructive ones. The goal of this article is not to persuade you into changing positions on its legalization, but rather to stress the importance of remaining neutral and educating families on the facts and potential pros and cons as they relate to the health of their children.
On Jan. 26, 2015,* the American Academy of Pediatrics released its policy statement on marijuana and its use (Pediatrics 2014 [doi:10.1542/peds.2014-4146]). The AAP does not support the legalization of marijuana because of the harm that it poses to children and adolescents, nor does it support legalization of medical marijuana outside the regulatory process of the Food and Drug Administration. It does recognize that marijuana may be an option for children with life-threatening or debilitating illnesses. The AAP does support the decriminalization of marijuana use or possession and advocates for less-harsh criminal penalties. Many of the recommendations were made because of the current research on marijuana and its use.
According to 2014’s Monitoring the Future survey of drug use and attitudes among American 8th, 10th, and 12th graders, marijuana is the most common illegal drug used by adolescents. Among 8th graders, 6.5% reported use; among 10th graders, 16.6% reported use; and 21.2 % of 12th graders reported use. A total of 81% of 12th grade students stated it was easy to get. Marijuana use at all three grade levels was higher than cigarette use (National Institute on Drug Abuse. Drug Facts, 2014). Another study found that early initiation of marijuana use was 6.5 times more likely to result in addiction than if it was initiated after the age of 21 years (Adolescent substance use: America’s #1 public health problem. CASA Columbia, 2011).
One thing we can agree upon is that an adolescent using any substance to mask or lessen the pain of a situation is in trouble. Whether adolescents are overeating or denying themselves food, or using drugs to get high, or behaving promiscuously to get attention, overindulgence is never good. So when we evaluate the effects of marijuana use among teens, we have to separate out the underlying emotional issues from the effects related to the drug. Adolescents are at particular risk for overuse because most lack the experience or maturity to stop when things get out of hand. And they are at risk when using anything that will give them a “high.” Substances like glue, gasoline, and cold medicine can bring them that high, and marijuana is no different – except that it is illegal.
Alcohol, cigarettes, and prescription medications are also vehicles to that desired high. Each has greater addictive properties than marijuana does. According to the Monitoring the Future study, most high school seniors do not think occasional use of marijuana is harmful, with only 36% saying regular use puts you at greater risk, compared with 39.5% in 2013 and 52% in 2009. The perception that marijuana is harmful has definitely declined.
Cannabis smoke contains three times the amount of tar found in tobacco smoke and 50% more carcinogens (N. Engl. J. Med. 1988;318:347). It also can irritate the airways, causing exacerbations of asthma, cystic fibrosis, sputum production, and pharyngitis (Arch. Intern. Med. 2007;167:221). Long-term studies showed that extended use was associated with increased obstructive lung diseases.
There is substantial evidence that indicates that cannabis use can cause psychosis. One review noted evidence that genetic factors may influence the risk of psychosis in adults who used cannabis as adolescents (Biol. Psychiatry 2005;57:1117). Cannabis is believed to release dopamine in the body, which may lead to the psychosis. Another study found that the onset of psychotic illness occurred more than 2 years earlier in patients who were heavy cannabis users (Arch. Gen. Psychiatry 2011;68:555).
Another important finding is that marijuana can suppress testosterone secretion in men, which may result in decreased libido, impotence, and gynecomastia (N. Engl. J. Med. 1974;290:872). Many teens believe cannabis is safe because it’s a plant, and consequently, may not relate these symptoms to its use.
The research on cannabis smoke and its relationship to cancer are limited by inadequate sample sizes and confounding factors not taken into account, but there does seem to be a relationship between cannabis smoke and lung cancer and bladder cancer (J. Psychoactive Drugs 1994;26:285; Urology 2006;67:100). However, head and neck cancers have not shown a relationship to marijuana use (Cancer Epidemiol. Biomarkers Prev. 2009;18:1544-51). Cardiovascular effects have been related to the increased sympathetic activity and decreased parasympathetic activity that can result in bradycardia and hypotension with high doses. This may be of particular concern in older people with coronary artery disease (J. Clin. Pharmacol. 2002;42:58S).
The medicinal properties of marijuana are an important consideration. Marijuana has been shown to be particularly effective in controlling some forms of seizure, pain, nausea from chemotherapy, muscle spasms caused by multiple sclerosis, and Crohn’s disease. The FDA has approved tetrahydrocannabinol, or THC, a key ingredient in marijuana, to treat nausea and improve appetite. In states that have legalized cannabis, qualifying patients can get prescriptions from their physicians to use at authorized dispensaries. For some patients, the effects can be life changing; for others, it can help with pain management and the discomfort associated with certain illnesses.
Beyond the scope of medicine is the economics of the legalization of marijuana. States that have already legalized it have seen revenues in the billions. Marijuana cash crops are estimated at $14 billion in revenue. Jon Gettman’s 2007 study, “Lost Taxes and Other Costs of Marijuana,” states that the prohibition of marijuana costs the government $113 billion, while it costs taxpayers $31.1 billion each year. The study projects that legalization of cannabis may save the criminal justice system $10.7 billion and an additional $6.2 billion for taxpayers. That sort of money does talk: Regardless of current opposition to the legalization of marijuana, it is probably just a matter of time before marijuana is legalized in every state.
The scope of marijuana issues is broad and, for many, controversial. The drug can serve as a healer, create health challenges, lead to drug addiction, or even become a significant revenue source to a state’s coffers. As providers, we need to be able to provide our patients with research-based information and resources, and dispel myths, so that they can make informed decisions for themselves that are in the best interests of their children.
Dr. Pearce is a pediatrician in Frankfort, Ill. She had no relevant financial disclosures. E-mail her at [email protected].
*Correction, 1/29/2015: An earlier version of this story had the incorrect date of publication of the AAP's policy statement.

Beware of methylmercury during pregnancy!
Dr. Henry A. Nasrallah is correct that wild salmon is a good choice for pregnant women who want to boost intake of omega-3 fatty acids (Current Psychiatry, Comments & Controversies, December 2014; pg 33 [http://bit.ly/1wQoXdP]). The main concern about fish intake during pregnancy is exposure to methylmercury, and much of this concern is derived from the tragic results of epic mercury poisonings of food sources in the past.
The FDA advises that pregnant women and children avoid eating shark, tilefish, king mackerel, and swordfish because these fish have a relatively high level of mercury.1 Fish that are low in methyl-mercury include salmon and canned light tuna. (More information is available at http://www.fda.gov/Food/ResourcesForYou/HealthEducators/ucm083324.htm.)
Although wild fish tend to be higher in omega-3 fatty acids than farm-raised fish, farmed fish can be an excellent source of omega-3 fatty acids. This is analogous to eating farm-produced livestock vs free-range, grass-fed livestock: Animals in their natural environment eat healthier and have more omega-3 fatty acids, whereas farmed livestock generally eat cheap and less healthy feed. Because wild fish can be pricey, it’s important that women understand that farm-raised fish are a good source of protein and other nutrients such as omega-3 fatty acids.
Research has been inconclusive regarding the antidepressant benefits of omega-3 fatty acids, with some, but not all, studies demonstrating an add-on benefit of omega-3 fatty acid supplements for mood disorders. However, several epidemiological studies have reported that the low quality of dietary intake of omega-3 fatty acids is associated with psychiatric illness, and fish and seafood are sources of essential fatty acids and other nutrients.2
1. Food safety for moms-to-be: while you’re pregnant–methylmercury. U.S. Food and Drug Administration. http://www.fda.gov/Food/ ResourcesForYou/HealthEducators/ucm083324. htm. Updated October 30, 2014. Accessed January 5, 2015.
2. Quirk SE, Williams LJ, O’Neil A, et al. The association between diet quality, dietary patterns and depression in adults: a systematic review. BMC Psychiatry. 2013;13:175.
Dr. Henry A. Nasrallah is correct that wild salmon is a good choice for pregnant women who want to boost intake of omega-3 fatty acids (Current Psychiatry, Comments & Controversies, December 2014; pg 33 [http://bit.ly/1wQoXdP]). The main concern about fish intake during pregnancy is exposure to methylmercury, and much of this concern is derived from the tragic results of epic mercury poisonings of food sources in the past.
The FDA advises that pregnant women and children avoid eating shark, tilefish, king mackerel, and swordfish because these fish have a relatively high level of mercury.1 Fish that are low in methyl-mercury include salmon and canned light tuna. (More information is available at http://www.fda.gov/Food/ResourcesForYou/HealthEducators/ucm083324.htm.)
Although wild fish tend to be higher in omega-3 fatty acids than farm-raised fish, farmed fish can be an excellent source of omega-3 fatty acids. This is analogous to eating farm-produced livestock vs free-range, grass-fed livestock: Animals in their natural environment eat healthier and have more omega-3 fatty acids, whereas farmed livestock generally eat cheap and less healthy feed. Because wild fish can be pricey, it’s important that women understand that farm-raised fish are a good source of protein and other nutrients such as omega-3 fatty acids.
Research has been inconclusive regarding the antidepressant benefits of omega-3 fatty acids, with some, but not all, studies demonstrating an add-on benefit of omega-3 fatty acid supplements for mood disorders. However, several epidemiological studies have reported that the low quality of dietary intake of omega-3 fatty acids is associated with psychiatric illness, and fish and seafood are sources of essential fatty acids and other nutrients.2
Dr. Henry A. Nasrallah is correct that wild salmon is a good choice for pregnant women who want to boost intake of omega-3 fatty acids (Current Psychiatry, Comments & Controversies, December 2014; pg 33 [http://bit.ly/1wQoXdP]). The main concern about fish intake during pregnancy is exposure to methylmercury, and much of this concern is derived from the tragic results of epic mercury poisonings of food sources in the past.
The FDA advises that pregnant women and children avoid eating shark, tilefish, king mackerel, and swordfish because these fish have a relatively high level of mercury.1 Fish that are low in methyl-mercury include salmon and canned light tuna. (More information is available at http://www.fda.gov/Food/ResourcesForYou/HealthEducators/ucm083324.htm.)
Although wild fish tend to be higher in omega-3 fatty acids than farm-raised fish, farmed fish can be an excellent source of omega-3 fatty acids. This is analogous to eating farm-produced livestock vs free-range, grass-fed livestock: Animals in their natural environment eat healthier and have more omega-3 fatty acids, whereas farmed livestock generally eat cheap and less healthy feed. Because wild fish can be pricey, it’s important that women understand that farm-raised fish are a good source of protein and other nutrients such as omega-3 fatty acids.
Research has been inconclusive regarding the antidepressant benefits of omega-3 fatty acids, with some, but not all, studies demonstrating an add-on benefit of omega-3 fatty acid supplements for mood disorders. However, several epidemiological studies have reported that the low quality of dietary intake of omega-3 fatty acids is associated with psychiatric illness, and fish and seafood are sources of essential fatty acids and other nutrients.2
1. Food safety for moms-to-be: while you’re pregnant–methylmercury. U.S. Food and Drug Administration. http://www.fda.gov/Food/ ResourcesForYou/HealthEducators/ucm083324. htm. Updated October 30, 2014. Accessed January 5, 2015.
2. Quirk SE, Williams LJ, O’Neil A, et al. The association between diet quality, dietary patterns and depression in adults: a systematic review. BMC Psychiatry. 2013;13:175.
1. Food safety for moms-to-be: while you’re pregnant–methylmercury. U.S. Food and Drug Administration. http://www.fda.gov/Food/ ResourcesForYou/HealthEducators/ucm083324. htm. Updated October 30, 2014. Accessed January 5, 2015.
2. Quirk SE, Williams LJ, O’Neil A, et al. The association between diet quality, dietary patterns and depression in adults: a systematic review. BMC Psychiatry. 2013;13:175.
More on insomnia disorders in older patients
Regarding Drs. Irene S. Hong’s and Jeffrey R. Bishop’s article, “Sedative-hypnotics for sleepless geriatric patients: Choose wisely” (Current Psychiatry, 2014;13(10):36-39, 46-50, 52 [http://bit.ly/1ApmcoO]), which undertook a comprehensive review of current therapies for insomnia in geriatric patients, here are 3 clarifications.
• I want to reinforce the latest thinking about the nature and pathophysiology of insomnia. DSM-5 classifies insomnia as a disorder, not as a symptom of other problems; the concept of “secondary insomnia” is rejected in DSM-5. Insomnia typically is seen as comorbid with other medical and psychiatric disorders. Often, insomnia predates the comorbid disorder (eg, depression), but rarely is it resolved by treating the comorbid condition.
• Good clinical practice, therefore, requires treating the comorbid condition and the insomnia each directly.
• The insomnia disorder manifests itself, in part, by a report of difficulty falling asleep or staying asleep. The authors use the example of sleep-onset insomnia as typical in older adults. However, sleep maintenance and early morning awakenings are the most common symptoms among geriatric insomnia patients.
• The authors mention only in passing an important medication for sleep maintenance in adults and in the geriatric patient specifically: doxepin. Low-dose doxepin, at 3 mg (for the geriatric patient) and 6 mg, is FDA-approved as a nonscheduled hypnotic for sleep maintenance insomnia. This formulationa is the only hypnotic classified as safe for geriatric patients in the 2012 Beers Criteria Update of the American Geriatrics Society.1 Unlike higher dosages of doxepin, the action of low-dose doxepin is, essentially, selective H1 antagonism.
aSold as Silenor.
Reference
1. American Geriatrics Society 2012 Beers Criteria Update Expert Panel. American Geriatrics Society updated Beers Criteria for potentially inappropriate medication use in older adults. J Am Geriatr Soc. 2012;60(4):616-631.
Regarding Drs. Irene S. Hong’s and Jeffrey R. Bishop’s article, “Sedative-hypnotics for sleepless geriatric patients: Choose wisely” (Current Psychiatry, 2014;13(10):36-39, 46-50, 52 [http://bit.ly/1ApmcoO]), which undertook a comprehensive review of current therapies for insomnia in geriatric patients, here are 3 clarifications.
• I want to reinforce the latest thinking about the nature and pathophysiology of insomnia. DSM-5 classifies insomnia as a disorder, not as a symptom of other problems; the concept of “secondary insomnia” is rejected in DSM-5. Insomnia typically is seen as comorbid with other medical and psychiatric disorders. Often, insomnia predates the comorbid disorder (eg, depression), but rarely is it resolved by treating the comorbid condition.
• Good clinical practice, therefore, requires treating the comorbid condition and the insomnia each directly.
• The insomnia disorder manifests itself, in part, by a report of difficulty falling asleep or staying asleep. The authors use the example of sleep-onset insomnia as typical in older adults. However, sleep maintenance and early morning awakenings are the most common symptoms among geriatric insomnia patients.
• The authors mention only in passing an important medication for sleep maintenance in adults and in the geriatric patient specifically: doxepin. Low-dose doxepin, at 3 mg (for the geriatric patient) and 6 mg, is FDA-approved as a nonscheduled hypnotic for sleep maintenance insomnia. This formulationa is the only hypnotic classified as safe for geriatric patients in the 2012 Beers Criteria Update of the American Geriatrics Society.1 Unlike higher dosages of doxepin, the action of low-dose doxepin is, essentially, selective H1 antagonism.
aSold as Silenor.
Regarding Drs. Irene S. Hong’s and Jeffrey R. Bishop’s article, “Sedative-hypnotics for sleepless geriatric patients: Choose wisely” (Current Psychiatry, 2014;13(10):36-39, 46-50, 52 [http://bit.ly/1ApmcoO]), which undertook a comprehensive review of current therapies for insomnia in geriatric patients, here are 3 clarifications.
• I want to reinforce the latest thinking about the nature and pathophysiology of insomnia. DSM-5 classifies insomnia as a disorder, not as a symptom of other problems; the concept of “secondary insomnia” is rejected in DSM-5. Insomnia typically is seen as comorbid with other medical and psychiatric disorders. Often, insomnia predates the comorbid disorder (eg, depression), but rarely is it resolved by treating the comorbid condition.
• Good clinical practice, therefore, requires treating the comorbid condition and the insomnia each directly.
• The insomnia disorder manifests itself, in part, by a report of difficulty falling asleep or staying asleep. The authors use the example of sleep-onset insomnia as typical in older adults. However, sleep maintenance and early morning awakenings are the most common symptoms among geriatric insomnia patients.
• The authors mention only in passing an important medication for sleep maintenance in adults and in the geriatric patient specifically: doxepin. Low-dose doxepin, at 3 mg (for the geriatric patient) and 6 mg, is FDA-approved as a nonscheduled hypnotic for sleep maintenance insomnia. This formulationa is the only hypnotic classified as safe for geriatric patients in the 2012 Beers Criteria Update of the American Geriatrics Society.1 Unlike higher dosages of doxepin, the action of low-dose doxepin is, essentially, selective H1 antagonism.
aSold as Silenor.
Reference
1. American Geriatrics Society 2012 Beers Criteria Update Expert Panel. American Geriatrics Society updated Beers Criteria for potentially inappropriate medication use in older adults. J Am Geriatr Soc. 2012;60(4):616-631.
Reference
1. American Geriatrics Society 2012 Beers Criteria Update Expert Panel. American Geriatrics Society updated Beers Criteria for potentially inappropriate medication use in older adults. J Am Geriatr Soc. 2012;60(4):616-631.
Sinus headaches
A 29-year-old woman presents for evaluation. She reports that she has had frequent headaches over the past 12 months that include pressure pain on her forehead, under her eyes, and over her cheeks. She usually has nasal congestion as well. She has not had any fevers or purulent nasal discharge. What is the most likely diagnosis?
A. Cluster headaches.
B. Migraine headaches.
C. Sinus headaches.
D. Tension headaches.
Myth: Recurrent sinus headaches are common.
Most physicians and patients would diagnose this case as sinus headache, but it is actually a common variant of migraine headache. Sinus headaches are rare, and when they do occur, they are almost always in the setting of acute sinusitis. Recurring headaches are rarely due to sinus problems.
In regard to sinus headache, the International Headache Society (IHS) classification states that chronic sinusitis is not a cause of headache and facial pain unless it relapses into an acute sinusitis (Expert Rev. Neurother. 2009;9:439-44). The recurrent nature of the headaches in this patient suggests a primary headache disorder, with migraine being the most likely.

In a study of 2,991 patients with self-diagnosed or physician-diagnosed “sinus headaches,” 88% of the patients met IHS criteria for migraine (Arch. Intern. Med. 2004;164:1769-72). In this study, most of the patients had symptoms suggesting sinus problems, with the most common symptoms being sinus pressure (84%), sinus pain (82%), and nasal congestion (63%).
The likely cause for these symptoms in migraine patients is vasodilation of the nasal mucosa that can be part of the migraine event (Expert Rev. Neurother. 2009;9:439-44).
In the Sinus, Allergy and Migraine Study, 100 patients who believed they had sinus headaches were recruited. All of the patients received a detailed history and physical exam, and all received a headache diagnosis based on IHS criteria (Headache 2007;47:213-24).
Final diagnoses were as follows: Migraine with or without aura, 52%; probable migraine, 23%; chronic migraine with medication overuse headache, 11%; nonclassifiable headache, 9%. A total of 76% of migraine patients reported pain in the distribution of the second division of the trigeminal nerve, and 62% experienced bilateral forehead and maxillary pain with their headaches.
It is interesting that both these studies showed the same thing: More than 85% of patients who think they have sinus headache actually meet criteria for migraine headache.
Two other articles also give strong evidence that patients with recurrent “sinus” headaches have causes other than sinus disease as the cause.
Dr. Mustafa Kaymakci and his colleagues studied 98 patients who had headaches diagnosed as “sinus” headaches (J. Int. Med. Res. 2013;41:218-23). All patients received a detailed history and physical, nasal endoscopy, and sinus CT scans. All patients who did not have findings that could be considered the cause of the headaches were diagnosed according to IHS criteria.
A total of 61 (62%) were diagnosed with migraine headache, 26 (27%) diagnosed with tension-type headache, and 11 (11%) had cluster headache. Seventy-seven percent of these patients had previously received at least one treatment for sinusitis.
Another study, by Dr. Mohsen Foroughipour and his colleagues, gave similar results (Eur. Arch. Otorhinolaryngol. 2011;268:1593-6). In this study, 58 patients with “sinus” headache were evaluated, with final diagnosis of migraine in 40 patients (69%), tension-type headache in 16 patients (27%), and chronic sinusitis with recurrent acute episodes in 2 patients (3%). Recurrent antibiotic therapy was given to 73% of the tension-type headache patients and 66% of the migraine patients.
In a study by Dr. Elina Kari and her colleagues, patients who had a history of “sinus headaches” were treated as though all these headaches were migraines (Laryngoscope 2008;118:2235-9). Fifty-four patients were enrolled, and 38 patients completed the study. All patients had nasal endoscopy and sinus CT scans that were negative. They were then given migraine-directed treatment to use for their headaches.
The majority of the patients who dropped out of the study did so because they did not believe their headaches could be due to migraines, and they did not want to take the migraine medications.
Of the 38 patient who completed the study, 31 patients (82%) had a significant reduction of headache pain with triptan use, and 35 patients (92%) had a significant response to migraine-directed therapy.
These studies show us that recurrent “sinus headaches” are unlikely to be due to sinus disease. More likely, they represent migraine headache or, less likely, tension headache or cluster headache. Evaluation should include categorizing the headache by clinical features (IHS criteria) to make a diagnosis, followed by a trial of appropriate treatment for headache type. In patients who don’t meet criteria for a specific headache type, a trial of migraine-directed therapy is reasonable.
Dr. Paauw is a professor of medicine in the division of general internal medicine at the University of Washington, Seattle, and he serves as third-year medical student clerkship director at the University of Washington Medical School. He is the Rathmann Family Foundation Chair in Patient-Centered Clinical Education. Contact Dr. Paauw at [email protected].
A 29-year-old woman presents for evaluation. She reports that she has had frequent headaches over the past 12 months that include pressure pain on her forehead, under her eyes, and over her cheeks. She usually has nasal congestion as well. She has not had any fevers or purulent nasal discharge. What is the most likely diagnosis?
A. Cluster headaches.
B. Migraine headaches.
C. Sinus headaches.
D. Tension headaches.
Myth: Recurrent sinus headaches are common.
Most physicians and patients would diagnose this case as sinus headache, but it is actually a common variant of migraine headache. Sinus headaches are rare, and when they do occur, they are almost always in the setting of acute sinusitis. Recurring headaches are rarely due to sinus problems.
In regard to sinus headache, the International Headache Society (IHS) classification states that chronic sinusitis is not a cause of headache and facial pain unless it relapses into an acute sinusitis (Expert Rev. Neurother. 2009;9:439-44). The recurrent nature of the headaches in this patient suggests a primary headache disorder, with migraine being the most likely.
In a study of 2,991 patients with self-diagnosed or physician-diagnosed “sinus headaches,” 88% of the patients met IHS criteria for migraine (Arch. Intern. Med. 2004;164:1769-72). In this study, most of the patients had symptoms suggesting sinus problems, with the most common symptoms being sinus pressure (84%), sinus pain (82%), and nasal congestion (63%).
The likely cause for these symptoms in migraine patients is vasodilation of the nasal mucosa that can be part of the migraine event (Expert Rev. Neurother. 2009;9:439-44).
In the Sinus, Allergy and Migraine Study, 100 patients who believed they had sinus headaches were recruited. All of the patients received a detailed history and physical exam, and all received a headache diagnosis based on IHS criteria (Headache 2007;47:213-24).
Final diagnoses were as follows: Migraine with or without aura, 52%; probable migraine, 23%; chronic migraine with medication overuse headache, 11%; nonclassifiable headache, 9%. A total of 76% of migraine patients reported pain in the distribution of the second division of the trigeminal nerve, and 62% experienced bilateral forehead and maxillary pain with their headaches.
It is interesting that both these studies showed the same thing: More than 85% of patients who think they have sinus headache actually meet criteria for migraine headache.
Two other articles also give strong evidence that patients with recurrent “sinus” headaches have causes other than sinus disease as the cause.
Dr. Mustafa Kaymakci and his colleagues studied 98 patients who had headaches diagnosed as “sinus” headaches (J. Int. Med. Res. 2013;41:218-23). All patients received a detailed history and physical, nasal endoscopy, and sinus CT scans. All patients who did not have findings that could be considered the cause of the headaches were diagnosed according to IHS criteria.
A total of 61 (62%) were diagnosed with migraine headache, 26 (27%) diagnosed with tension-type headache, and 11 (11%) had cluster headache. Seventy-seven percent of these patients had previously received at least one treatment for sinusitis.
Another study, by Dr. Mohsen Foroughipour and his colleagues, gave similar results (Eur. Arch. Otorhinolaryngol. 2011;268:1593-6). In this study, 58 patients with “sinus” headache were evaluated, with final diagnosis of migraine in 40 patients (69%), tension-type headache in 16 patients (27%), and chronic sinusitis with recurrent acute episodes in 2 patients (3%). Recurrent antibiotic therapy was given to 73% of the tension-type headache patients and 66% of the migraine patients.
In a study by Dr. Elina Kari and her colleagues, patients who had a history of “sinus headaches” were treated as though all these headaches were migraines (Laryngoscope 2008;118:2235-9). Fifty-four patients were enrolled, and 38 patients completed the study. All patients had nasal endoscopy and sinus CT scans that were negative. They were then given migraine-directed treatment to use for their headaches.
The majority of the patients who dropped out of the study did so because they did not believe their headaches could be due to migraines, and they did not want to take the migraine medications.
Of the 38 patient who completed the study, 31 patients (82%) had a significant reduction of headache pain with triptan use, and 35 patients (92%) had a significant response to migraine-directed therapy.
These studies show us that recurrent “sinus headaches” are unlikely to be due to sinus disease. More likely, they represent migraine headache or, less likely, tension headache or cluster headache. Evaluation should include categorizing the headache by clinical features (IHS criteria) to make a diagnosis, followed by a trial of appropriate treatment for headache type. In patients who don’t meet criteria for a specific headache type, a trial of migraine-directed therapy is reasonable.
Dr. Paauw is a professor of medicine in the division of general internal medicine at the University of Washington, Seattle, and he serves as third-year medical student clerkship director at the University of Washington Medical School. He is the Rathmann Family Foundation Chair in Patient-Centered Clinical Education. Contact Dr. Paauw at [email protected].
A 29-year-old woman presents for evaluation. She reports that she has had frequent headaches over the past 12 months that include pressure pain on her forehead, under her eyes, and over her cheeks. She usually has nasal congestion as well. She has not had any fevers or purulent nasal discharge. What is the most likely diagnosis?
A. Cluster headaches.
B. Migraine headaches.
C. Sinus headaches.
D. Tension headaches.
Myth: Recurrent sinus headaches are common.
Most physicians and patients would diagnose this case as sinus headache, but it is actually a common variant of migraine headache. Sinus headaches are rare, and when they do occur, they are almost always in the setting of acute sinusitis. Recurring headaches are rarely due to sinus problems.
In regard to sinus headache, the International Headache Society (IHS) classification states that chronic sinusitis is not a cause of headache and facial pain unless it relapses into an acute sinusitis (Expert Rev. Neurother. 2009;9:439-44). The recurrent nature of the headaches in this patient suggests a primary headache disorder, with migraine being the most likely.
In a study of 2,991 patients with self-diagnosed or physician-diagnosed “sinus headaches,” 88% of the patients met IHS criteria for migraine (Arch. Intern. Med. 2004;164:1769-72). In this study, most of the patients had symptoms suggesting sinus problems, with the most common symptoms being sinus pressure (84%), sinus pain (82%), and nasal congestion (63%).
The likely cause for these symptoms in migraine patients is vasodilation of the nasal mucosa that can be part of the migraine event (Expert Rev. Neurother. 2009;9:439-44).
In the Sinus, Allergy and Migraine Study, 100 patients who believed they had sinus headaches were recruited. All of the patients received a detailed history and physical exam, and all received a headache diagnosis based on IHS criteria (Headache 2007;47:213-24).
Final diagnoses were as follows: Migraine with or without aura, 52%; probable migraine, 23%; chronic migraine with medication overuse headache, 11%; nonclassifiable headache, 9%. A total of 76% of migraine patients reported pain in the distribution of the second division of the trigeminal nerve, and 62% experienced bilateral forehead and maxillary pain with their headaches.
It is interesting that both these studies showed the same thing: More than 85% of patients who think they have sinus headache actually meet criteria for migraine headache.
Two other articles also give strong evidence that patients with recurrent “sinus” headaches have causes other than sinus disease as the cause.
Dr. Mustafa Kaymakci and his colleagues studied 98 patients who had headaches diagnosed as “sinus” headaches (J. Int. Med. Res. 2013;41:218-23). All patients received a detailed history and physical, nasal endoscopy, and sinus CT scans. All patients who did not have findings that could be considered the cause of the headaches were diagnosed according to IHS criteria.
A total of 61 (62%) were diagnosed with migraine headache, 26 (27%) diagnosed with tension-type headache, and 11 (11%) had cluster headache. Seventy-seven percent of these patients had previously received at least one treatment for sinusitis.
Another study, by Dr. Mohsen Foroughipour and his colleagues, gave similar results (Eur. Arch. Otorhinolaryngol. 2011;268:1593-6). In this study, 58 patients with “sinus” headache were evaluated, with final diagnosis of migraine in 40 patients (69%), tension-type headache in 16 patients (27%), and chronic sinusitis with recurrent acute episodes in 2 patients (3%). Recurrent antibiotic therapy was given to 73% of the tension-type headache patients and 66% of the migraine patients.
In a study by Dr. Elina Kari and her colleagues, patients who had a history of “sinus headaches” were treated as though all these headaches were migraines (Laryngoscope 2008;118:2235-9). Fifty-four patients were enrolled, and 38 patients completed the study. All patients had nasal endoscopy and sinus CT scans that were negative. They were then given migraine-directed treatment to use for their headaches.
The majority of the patients who dropped out of the study did so because they did not believe their headaches could be due to migraines, and they did not want to take the migraine medications.
Of the 38 patient who completed the study, 31 patients (82%) had a significant reduction of headache pain with triptan use, and 35 patients (92%) had a significant response to migraine-directed therapy.
These studies show us that recurrent “sinus headaches” are unlikely to be due to sinus disease. More likely, they represent migraine headache or, less likely, tension headache or cluster headache. Evaluation should include categorizing the headache by clinical features (IHS criteria) to make a diagnosis, followed by a trial of appropriate treatment for headache type. In patients who don’t meet criteria for a specific headache type, a trial of migraine-directed therapy is reasonable.
Dr. Paauw is a professor of medicine in the division of general internal medicine at the University of Washington, Seattle, and he serves as third-year medical student clerkship director at the University of Washington Medical School. He is the Rathmann Family Foundation Chair in Patient-Centered Clinical Education. Contact Dr. Paauw at [email protected].

Fetal alcohol spectrum disorder
Fetal alcohol spectrum disorders are a vibrant area of development and research. Awareness about this preventable group of conditions appears to be growing.
In fact, the Centers for Disease Control and Prevention has released an app that emphasizes how to recognize, prevent, and treat fetal alcohol spectrum disorders. Earlier rates of fetal alcohol syndrome were estimated at 1/1,000, but FASD is estimated to occur at rates of 1/100. However, as I will illustrate below, the rates of FASD are even higher – much higher among some populations than previously thought.

The DSM-5 included in its appendix the diagnostic category of neurobehavioral disorder associated with prenatal alcohol exposure (ND-PAE), which theoretically should help psychiatrists identify FASD. Of course, the DSM-5 also includes an official diagnosis of disruptive mood dysregulation disorder (DMDD), and for the life of me, I have a difficult time differentiating between the two clinically except that children and adults with ND-PAE, in contrast to patients with DMDD who are described as persistently irritable or angry most of the day, can be very amicable, naive, and overly friendly between outbursts. The other difference is that ND-PAE needs a history of the mother’s having more than minimal exposure to alcohol during gestation, including prior to pregnancy recognition, and DMDD does not have this criteria, although it may be present. And, lastly DMDD is official and ND-PAE not.
Last year, Philip A. May, Ph.D., and his associates published an important paper, “Prevalence and Characteristics of Fetal Alcohol Spectrum Disorders” (Pediatrics 2014 [doi.10.1542/peds.2013-3319]). The authors looked at a representative Midwestern U.S. community with a population base of 160,000, 87% of which were white. The per-capita income of the population was $28,000, the median household income was $51,800, and 11% were below the poverty line.
Dr. May and his associates examined 70.5% (1,433 of 2,033) of all first-graders. Using one method of prevalence estimation, they found that 28.6/1,000 had FASD. Using a second method of prevalence estimation calculated from cases of FASD, they found an FASD rate of 82/1,000. The take-home message is, regardless of the academic fine points of how prevalence is estimated, these prevalence rates are much higher than previously reported.
In a second paper by Dr. Ira J. Chasnoff and his associates – “Misdiagnosis and Missed Diagnosis in Foster Care and Adopted Children with Prenatal Alcohol Exposure” – also published in Pediatrics, the rates of FASD in foster care and adopted youth were estimated to be even higher.
This study looked at 547 youth (50.6% African American, 1.3% Asian, 32.2% white, 0.7% Native American, 12.2% biracial, and 3% other/unknown) referred for severe behavioral disorders. The researchers found that 28.5% of these youth had FASD, 86.5% of the youth had never been diagnosed or were misdiagnosed, and 26.4% of these youth were misdiagnosed as having ADHD (Pediatrics 2014 [doi:10.1542/peds.2014-2171]).
Radhika L. Chimata and I published the third paper of significance online in Psychiatric Services. This paper, which is also slated for publication in print, focused on our work in a family medicine clinic on Chicago’s South Side, serving a population of 143,000. We looked at 611 patients (96% African American with a median household income of $33,809 – only 21 were youth, the rest were adults) and found that 297 (49%) of the adults and youth had neurodevelopmental disorders with 237 (39%) having clinical profiles consistent with neurobehavioral disorders associated with prenatal alcohol exposure. Thus, this clinic population has a rate of 388/1,000.
Considering emerging research that suggests that this acquired biological disorder is being driven by the social determinants of health, for example, some low-income African Americans are living not only in food deserts but food swamps (where the liquid is alcohol; consider the plethora of liquor stores in low-income African American communities), we must recognize that FASD can be prevented prenatally and possibly improved postnatally by increasing the amount of choline in the diet. This is a potential prevention intervention issue that we cannot afford to overlook if psychiatry is going to maintain its relevance in the 21st century.
Dr. Bell is a retired professor of psychiatry and public health at the University of Illinois at Chicago and staff psychiatrist at Jackson Park Hospital’s Outpatient Family Practice Clinic in Chicago. Dr. Bell is the former president and CEO of the Community Mental Health Council and former director of the Institute for Juvenile Research (birthplace of child psychiatry) at the university.
Fetal alcohol spectrum disorders are a vibrant area of development and research. Awareness about this preventable group of conditions appears to be growing.
In fact, the Centers for Disease Control and Prevention has released an app that emphasizes how to recognize, prevent, and treat fetal alcohol spectrum disorders. Earlier rates of fetal alcohol syndrome were estimated at 1/1,000, but FASD is estimated to occur at rates of 1/100. However, as I will illustrate below, the rates of FASD are even higher – much higher among some populations than previously thought.
The DSM-5 included in its appendix the diagnostic category of neurobehavioral disorder associated with prenatal alcohol exposure (ND-PAE), which theoretically should help psychiatrists identify FASD. Of course, the DSM-5 also includes an official diagnosis of disruptive mood dysregulation disorder (DMDD), and for the life of me, I have a difficult time differentiating between the two clinically except that children and adults with ND-PAE, in contrast to patients with DMDD who are described as persistently irritable or angry most of the day, can be very amicable, naive, and overly friendly between outbursts. The other difference is that ND-PAE needs a history of the mother’s having more than minimal exposure to alcohol during gestation, including prior to pregnancy recognition, and DMDD does not have this criteria, although it may be present. And, lastly DMDD is official and ND-PAE not.
Last year, Philip A. May, Ph.D., and his associates published an important paper, “Prevalence and Characteristics of Fetal Alcohol Spectrum Disorders” (Pediatrics 2014 [doi.10.1542/peds.2013-3319]). The authors looked at a representative Midwestern U.S. community with a population base of 160,000, 87% of which were white. The per-capita income of the population was $28,000, the median household income was $51,800, and 11% were below the poverty line.
Dr. May and his associates examined 70.5% (1,433 of 2,033) of all first-graders. Using one method of prevalence estimation, they found that 28.6/1,000 had FASD. Using a second method of prevalence estimation calculated from cases of FASD, they found an FASD rate of 82/1,000. The take-home message is, regardless of the academic fine points of how prevalence is estimated, these prevalence rates are much higher than previously reported.
In a second paper by Dr. Ira J. Chasnoff and his associates – “Misdiagnosis and Missed Diagnosis in Foster Care and Adopted Children with Prenatal Alcohol Exposure” – also published in Pediatrics, the rates of FASD in foster care and adopted youth were estimated to be even higher.
This study looked at 547 youth (50.6% African American, 1.3% Asian, 32.2% white, 0.7% Native American, 12.2% biracial, and 3% other/unknown) referred for severe behavioral disorders. The researchers found that 28.5% of these youth had FASD, 86.5% of the youth had never been diagnosed or were misdiagnosed, and 26.4% of these youth were misdiagnosed as having ADHD (Pediatrics 2014 [doi:10.1542/peds.2014-2171]).
Radhika L. Chimata and I published the third paper of significance online in Psychiatric Services. This paper, which is also slated for publication in print, focused on our work in a family medicine clinic on Chicago’s South Side, serving a population of 143,000. We looked at 611 patients (96% African American with a median household income of $33,809 – only 21 were youth, the rest were adults) and found that 297 (49%) of the adults and youth had neurodevelopmental disorders with 237 (39%) having clinical profiles consistent with neurobehavioral disorders associated with prenatal alcohol exposure. Thus, this clinic population has a rate of 388/1,000.
Considering emerging research that suggests that this acquired biological disorder is being driven by the social determinants of health, for example, some low-income African Americans are living not only in food deserts but food swamps (where the liquid is alcohol; consider the plethora of liquor stores in low-income African American communities), we must recognize that FASD can be prevented prenatally and possibly improved postnatally by increasing the amount of choline in the diet. This is a potential prevention intervention issue that we cannot afford to overlook if psychiatry is going to maintain its relevance in the 21st century.
Dr. Bell is a retired professor of psychiatry and public health at the University of Illinois at Chicago and staff psychiatrist at Jackson Park Hospital’s Outpatient Family Practice Clinic in Chicago. Dr. Bell is the former president and CEO of the Community Mental Health Council and former director of the Institute for Juvenile Research (birthplace of child psychiatry) at the university.
Fetal alcohol spectrum disorders are a vibrant area of development and research. Awareness about this preventable group of conditions appears to be growing.
In fact, the Centers for Disease Control and Prevention has released an app that emphasizes how to recognize, prevent, and treat fetal alcohol spectrum disorders. Earlier rates of fetal alcohol syndrome were estimated at 1/1,000, but FASD is estimated to occur at rates of 1/100. However, as I will illustrate below, the rates of FASD are even higher – much higher among some populations than previously thought.
The DSM-5 included in its appendix the diagnostic category of neurobehavioral disorder associated with prenatal alcohol exposure (ND-PAE), which theoretically should help psychiatrists identify FASD. Of course, the DSM-5 also includes an official diagnosis of disruptive mood dysregulation disorder (DMDD), and for the life of me, I have a difficult time differentiating between the two clinically except that children and adults with ND-PAE, in contrast to patients with DMDD who are described as persistently irritable or angry most of the day, can be very amicable, naive, and overly friendly between outbursts. The other difference is that ND-PAE needs a history of the mother’s having more than minimal exposure to alcohol during gestation, including prior to pregnancy recognition, and DMDD does not have this criteria, although it may be present. And, lastly DMDD is official and ND-PAE not.
Last year, Philip A. May, Ph.D., and his associates published an important paper, “Prevalence and Characteristics of Fetal Alcohol Spectrum Disorders” (Pediatrics 2014 [doi.10.1542/peds.2013-3319]). The authors looked at a representative Midwestern U.S. community with a population base of 160,000, 87% of which were white. The per-capita income of the population was $28,000, the median household income was $51,800, and 11% were below the poverty line.
Dr. May and his associates examined 70.5% (1,433 of 2,033) of all first-graders. Using one method of prevalence estimation, they found that 28.6/1,000 had FASD. Using a second method of prevalence estimation calculated from cases of FASD, they found an FASD rate of 82/1,000. The take-home message is, regardless of the academic fine points of how prevalence is estimated, these prevalence rates are much higher than previously reported.
In a second paper by Dr. Ira J. Chasnoff and his associates – “Misdiagnosis and Missed Diagnosis in Foster Care and Adopted Children with Prenatal Alcohol Exposure” – also published in Pediatrics, the rates of FASD in foster care and adopted youth were estimated to be even higher.
This study looked at 547 youth (50.6% African American, 1.3% Asian, 32.2% white, 0.7% Native American, 12.2% biracial, and 3% other/unknown) referred for severe behavioral disorders. The researchers found that 28.5% of these youth had FASD, 86.5% of the youth had never been diagnosed or were misdiagnosed, and 26.4% of these youth were misdiagnosed as having ADHD (Pediatrics 2014 [doi:10.1542/peds.2014-2171]).
Radhika L. Chimata and I published the third paper of significance online in Psychiatric Services. This paper, which is also slated for publication in print, focused on our work in a family medicine clinic on Chicago’s South Side, serving a population of 143,000. We looked at 611 patients (96% African American with a median household income of $33,809 – only 21 were youth, the rest were adults) and found that 297 (49%) of the adults and youth had neurodevelopmental disorders with 237 (39%) having clinical profiles consistent with neurobehavioral disorders associated with prenatal alcohol exposure. Thus, this clinic population has a rate of 388/1,000.
Considering emerging research that suggests that this acquired biological disorder is being driven by the social determinants of health, for example, some low-income African Americans are living not only in food deserts but food swamps (where the liquid is alcohol; consider the plethora of liquor stores in low-income African American communities), we must recognize that FASD can be prevented prenatally and possibly improved postnatally by increasing the amount of choline in the diet. This is a potential prevention intervention issue that we cannot afford to overlook if psychiatry is going to maintain its relevance in the 21st century.
Dr. Bell is a retired professor of psychiatry and public health at the University of Illinois at Chicago and staff psychiatrist at Jackson Park Hospital’s Outpatient Family Practice Clinic in Chicago. Dr. Bell is the former president and CEO of the Community Mental Health Council and former director of the Institute for Juvenile Research (birthplace of child psychiatry) at the university.

Patient safety and tort reform
Question: Developments in medical tort reform include:
A. Continued constitutional challenges to caps on damages.
B. An emphasis on patient safety.
C. Hillary Clinton’s Senate bill.
D. Linking medical tort reform to error reduction.
E. All of the above.

Answer: E. Recent years have witnessed a stabilizing environment for medical liability, although insurance premiums continue to vary greatly by specialty and geographic location.
Recent statistics from the American Medical Association show that 2014 ob.gyn. insurance rates range from less than $50,000 in some areas of California to a high of $215,000 in Nassau and Suffolk counties in New York. The highest average expense in 2013, around a quarter of a million dollars, was for those claims that resulted in plaintiff verdicts, while defendant verdicts were substantially lower and averaged $140,000.
As in the past, most claims were dropped, dismissed, or withdrawn. About one-quarter of claims were settled, with only 2% decided by an alternative dispute resolution. Less than 8% were decided by trial verdict, with the vast majority won by the defendant.
The plaintiff bar continues to mount constitutional challenges to caps on damages. The California Supreme Court had previously ruled that reforms under California’s historic Medical Injury Compensation Reform Act (MICRA)1, which limits noneconomic recovery to $250,000, are constitutional, because they are rationally related to the legitimate legislative goal of reducing medical costs.
However, the statute has again come under challenge, only to be reaffirmed by a California state appeals court. In November 2014, California voters rejected Proposition 46, which sought to increase the cap from $250,000 to $1.1 million.
Texas, another pro-reform state, sides with California, and Mississippi also ruled that its damage cap is constitutional. However, Florida and Oklahoma recently joined jurisdictions such as Georgia, Illinois, and Missouri in ruling that damage caps are unconstitutional.
Asserting that the current health care liability system has been an inefficient and sometimes ineffective mechanism for initiating or resolving claims of medical error, medical negligence, or malpractice, then-U.S. senators Hillary Clinton (D-N.Y.) and Barack Obama (D-Ill.) in 2005 jointly sponsored legislation (S. 1784) to establish a National Medical Error Disclosure and Compensation Program (National MEDiC Act). Although the bill was killed in Senate committee, its key provisions were subsequently published in the New England Journal of Medicine (2006;354:2205-8).
The senators noted that the liability system has failed to the extent that only one medical malpractice claim is filed for every eight medical injuries, that it takes 4-8 years to resolve a claim, and that “solutions to the patient safety, litigation, and medical liability insurance problems have been elusive.”
Accordingly, the bill’s purpose was to promote the confidential disclosure to patients of medical errors in an effort to improve patient-safety systems. At the time of disclosure, there would be negotiations for compensation and proposals to prevent a recurrence of the problem that led to the patient’s injury. However, the patient would retain the right to counsel during negotiations, as well as access to the courts if no agreement were reached. The bill was entirely silent on traditional tort reform measures.
Nearly 4 decades earlier, a no-fault proposal by Professor Jeffrey O’Connell made some of these points, but with sharper focus and specificity, especially regarding damages.2
In marked contrast to the Clinton-Obama bill, his proposal gave the medical provider the exclusive option to tender payment, which would completely foreclose future tort action by the victim. Compensation benefits included net economic loss such as 100% of lost wages, replacement service loss, medical treatment expenses, and reasonable attorney’s fees. But noneconomic losses, such as pain and suffering, were not reimbursable, and payment was net of any benefits from collateral sources.
This proposal elegantly combined efficiency and fairness, and would have ameliorated the financial and emotional toll that comes with litigating injuries arising out of health care. Legislation in the House of Representatives, the Alternative Medical Liability Act (H.R. 5400), incorporated many of these features, and came before the 98th U.S. Congress in 1984. It, too, died in committee.
There may be something to the current trend toward pairing tort reform with error reduction. Thoughtful observers point to “disclosure and offer” programs such as the one at the Lexington (Ky.) Veterans Affairs Medical Center, which boasts average settlements of approximately $15,000 per claim – compared with more than $98,000 at other VA institutions. Its policy has also decreased the average duration of cases, previously 2-4 years, to 2-4 months, as well as reduced costs for legal defense.
Likewise, the program at the University of Michigan Health System has reduced both the frequency and severity of claims, duration of cases, and litigation costs. Aware of these developments, some private insurers, such as the COPIC Insurance Company in Colorado, are adopting a similar approach.
In its updated 2014 tort reform position paper, the American College of Physicians continues to endorse caps on noneconomic and punitive damages, as well as other tort reform measures.
However, it now acknowledges that “improving patient safety and preventing errors must be at the fore of the medical liability reform discussion.” The ACP correctly asserts that “emphasizing patient safety, promoting a culture of quality improvement and coordinated care, and training physicians in best practices to avoid errors and reduce risk will prevent harm and reduce the waste associated with defensive medicine.”
This hybrid approach combining traditional tort reforms with a renewed attention to patient safety through medical error reduction may yet yield additional practical benefits.
Here, the experience in anesthesiology bears recounting: Its dramatic progress in risk management has cut patient death rate from 1 in 5,000 to 1 in 200,000 to 300,000 in the space of 20 years, and this has been associated with a concurrent 37% fall in insurance premiums.
References
1. Medical Injury Compensation Reform Act of 1975, Cal. Civ. Proc. Code § 3333.2 (West 1982).
2. O’Connell, J. No-Fault Insurance for Injuries Arising from Medical Treatment: A Proposal for Elective Coverage. Emory L. J. 1975;24:21.
Dr. Tan is professor emeritus of medicine and former adjunct professor of law at the University of Hawaii. Currently, he directs the St. Francis International Center for Healthcare Ethics in Honolulu. This article is meant to be educational and does not constitute medical, ethical, or legal advice. Some of the articles in this series are adapted from the author’s 2006 book, “Medical Malpractice: Understanding the Law, Managing the Risk,” and his 2012 Halsbury treatise, “Medical Negligence and Professional Misconduct.” For additional information, readers may contact the author at [email protected].
Question: Developments in medical tort reform include:
A. Continued constitutional challenges to caps on damages.
B. An emphasis on patient safety.
C. Hillary Clinton’s Senate bill.
D. Linking medical tort reform to error reduction.
E. All of the above.
Answer: E. Recent years have witnessed a stabilizing environment for medical liability, although insurance premiums continue to vary greatly by specialty and geographic location.
Recent statistics from the American Medical Association show that 2014 ob.gyn. insurance rates range from less than $50,000 in some areas of California to a high of $215,000 in Nassau and Suffolk counties in New York. The highest average expense in 2013, around a quarter of a million dollars, was for those claims that resulted in plaintiff verdicts, while defendant verdicts were substantially lower and averaged $140,000.
As in the past, most claims were dropped, dismissed, or withdrawn. About one-quarter of claims were settled, with only 2% decided by an alternative dispute resolution. Less than 8% were decided by trial verdict, with the vast majority won by the defendant.
The plaintiff bar continues to mount constitutional challenges to caps on damages. The California Supreme Court had previously ruled that reforms under California’s historic Medical Injury Compensation Reform Act (MICRA)1, which limits noneconomic recovery to $250,000, are constitutional, because they are rationally related to the legitimate legislative goal of reducing medical costs.
However, the statute has again come under challenge, only to be reaffirmed by a California state appeals court. In November 2014, California voters rejected Proposition 46, which sought to increase the cap from $250,000 to $1.1 million.
Texas, another pro-reform state, sides with California, and Mississippi also ruled that its damage cap is constitutional. However, Florida and Oklahoma recently joined jurisdictions such as Georgia, Illinois, and Missouri in ruling that damage caps are unconstitutional.
Asserting that the current health care liability system has been an inefficient and sometimes ineffective mechanism for initiating or resolving claims of medical error, medical negligence, or malpractice, then-U.S. senators Hillary Clinton (D-N.Y.) and Barack Obama (D-Ill.) in 2005 jointly sponsored legislation (S. 1784) to establish a National Medical Error Disclosure and Compensation Program (National MEDiC Act). Although the bill was killed in Senate committee, its key provisions were subsequently published in the New England Journal of Medicine (2006;354:2205-8).
The senators noted that the liability system has failed to the extent that only one medical malpractice claim is filed for every eight medical injuries, that it takes 4-8 years to resolve a claim, and that “solutions to the patient safety, litigation, and medical liability insurance problems have been elusive.”
Accordingly, the bill’s purpose was to promote the confidential disclosure to patients of medical errors in an effort to improve patient-safety systems. At the time of disclosure, there would be negotiations for compensation and proposals to prevent a recurrence of the problem that led to the patient’s injury. However, the patient would retain the right to counsel during negotiations, as well as access to the courts if no agreement were reached. The bill was entirely silent on traditional tort reform measures.
Nearly 4 decades earlier, a no-fault proposal by Professor Jeffrey O’Connell made some of these points, but with sharper focus and specificity, especially regarding damages.2
In marked contrast to the Clinton-Obama bill, his proposal gave the medical provider the exclusive option to tender payment, which would completely foreclose future tort action by the victim. Compensation benefits included net economic loss such as 100% of lost wages, replacement service loss, medical treatment expenses, and reasonable attorney’s fees. But noneconomic losses, such as pain and suffering, were not reimbursable, and payment was net of any benefits from collateral sources.
This proposal elegantly combined efficiency and fairness, and would have ameliorated the financial and emotional toll that comes with litigating injuries arising out of health care. Legislation in the House of Representatives, the Alternative Medical Liability Act (H.R. 5400), incorporated many of these features, and came before the 98th U.S. Congress in 1984. It, too, died in committee.
There may be something to the current trend toward pairing tort reform with error reduction. Thoughtful observers point to “disclosure and offer” programs such as the one at the Lexington (Ky.) Veterans Affairs Medical Center, which boasts average settlements of approximately $15,000 per claim – compared with more than $98,000 at other VA institutions. Its policy has also decreased the average duration of cases, previously 2-4 years, to 2-4 months, as well as reduced costs for legal defense.
Likewise, the program at the University of Michigan Health System has reduced both the frequency and severity of claims, duration of cases, and litigation costs. Aware of these developments, some private insurers, such as the COPIC Insurance Company in Colorado, are adopting a similar approach.
In its updated 2014 tort reform position paper, the American College of Physicians continues to endorse caps on noneconomic and punitive damages, as well as other tort reform measures.
However, it now acknowledges that “improving patient safety and preventing errors must be at the fore of the medical liability reform discussion.” The ACP correctly asserts that “emphasizing patient safety, promoting a culture of quality improvement and coordinated care, and training physicians in best practices to avoid errors and reduce risk will prevent harm and reduce the waste associated with defensive medicine.”
This hybrid approach combining traditional tort reforms with a renewed attention to patient safety through medical error reduction may yet yield additional practical benefits.
Here, the experience in anesthesiology bears recounting: Its dramatic progress in risk management has cut patient death rate from 1 in 5,000 to 1 in 200,000 to 300,000 in the space of 20 years, and this has been associated with a concurrent 37% fall in insurance premiums.
References
1. Medical Injury Compensation Reform Act of 1975, Cal. Civ. Proc. Code § 3333.2 (West 1982).
2. O’Connell, J. No-Fault Insurance for Injuries Arising from Medical Treatment: A Proposal for Elective Coverage. Emory L. J. 1975;24:21.
Dr. Tan is professor emeritus of medicine and former adjunct professor of law at the University of Hawaii. Currently, he directs the St. Francis International Center for Healthcare Ethics in Honolulu. This article is meant to be educational and does not constitute medical, ethical, or legal advice. Some of the articles in this series are adapted from the author’s 2006 book, “Medical Malpractice: Understanding the Law, Managing the Risk,” and his 2012 Halsbury treatise, “Medical Negligence and Professional Misconduct.” For additional information, readers may contact the author at [email protected].
Question: Developments in medical tort reform include:
A. Continued constitutional challenges to caps on damages.
B. An emphasis on patient safety.
C. Hillary Clinton’s Senate bill.
D. Linking medical tort reform to error reduction.
E. All of the above.
Answer: E. Recent years have witnessed a stabilizing environment for medical liability, although insurance premiums continue to vary greatly by specialty and geographic location.
Recent statistics from the American Medical Association show that 2014 ob.gyn. insurance rates range from less than $50,000 in some areas of California to a high of $215,000 in Nassau and Suffolk counties in New York. The highest average expense in 2013, around a quarter of a million dollars, was for those claims that resulted in plaintiff verdicts, while defendant verdicts were substantially lower and averaged $140,000.
As in the past, most claims were dropped, dismissed, or withdrawn. About one-quarter of claims were settled, with only 2% decided by an alternative dispute resolution. Less than 8% were decided by trial verdict, with the vast majority won by the defendant.
The plaintiff bar continues to mount constitutional challenges to caps on damages. The California Supreme Court had previously ruled that reforms under California’s historic Medical Injury Compensation Reform Act (MICRA)1, which limits noneconomic recovery to $250,000, are constitutional, because they are rationally related to the legitimate legislative goal of reducing medical costs.
However, the statute has again come under challenge, only to be reaffirmed by a California state appeals court. In November 2014, California voters rejected Proposition 46, which sought to increase the cap from $250,000 to $1.1 million.
Texas, another pro-reform state, sides with California, and Mississippi also ruled that its damage cap is constitutional. However, Florida and Oklahoma recently joined jurisdictions such as Georgia, Illinois, and Missouri in ruling that damage caps are unconstitutional.
Asserting that the current health care liability system has been an inefficient and sometimes ineffective mechanism for initiating or resolving claims of medical error, medical negligence, or malpractice, then-U.S. senators Hillary Clinton (D-N.Y.) and Barack Obama (D-Ill.) in 2005 jointly sponsored legislation (S. 1784) to establish a National Medical Error Disclosure and Compensation Program (National MEDiC Act). Although the bill was killed in Senate committee, its key provisions were subsequently published in the New England Journal of Medicine (2006;354:2205-8).
The senators noted that the liability system has failed to the extent that only one medical malpractice claim is filed for every eight medical injuries, that it takes 4-8 years to resolve a claim, and that “solutions to the patient safety, litigation, and medical liability insurance problems have been elusive.”
Accordingly, the bill’s purpose was to promote the confidential disclosure to patients of medical errors in an effort to improve patient-safety systems. At the time of disclosure, there would be negotiations for compensation and proposals to prevent a recurrence of the problem that led to the patient’s injury. However, the patient would retain the right to counsel during negotiations, as well as access to the courts if no agreement were reached. The bill was entirely silent on traditional tort reform measures.
Nearly 4 decades earlier, a no-fault proposal by Professor Jeffrey O’Connell made some of these points, but with sharper focus and specificity, especially regarding damages.2
In marked contrast to the Clinton-Obama bill, his proposal gave the medical provider the exclusive option to tender payment, which would completely foreclose future tort action by the victim. Compensation benefits included net economic loss such as 100% of lost wages, replacement service loss, medical treatment expenses, and reasonable attorney’s fees. But noneconomic losses, such as pain and suffering, were not reimbursable, and payment was net of any benefits from collateral sources.
This proposal elegantly combined efficiency and fairness, and would have ameliorated the financial and emotional toll that comes with litigating injuries arising out of health care. Legislation in the House of Representatives, the Alternative Medical Liability Act (H.R. 5400), incorporated many of these features, and came before the 98th U.S. Congress in 1984. It, too, died in committee.
There may be something to the current trend toward pairing tort reform with error reduction. Thoughtful observers point to “disclosure and offer” programs such as the one at the Lexington (Ky.) Veterans Affairs Medical Center, which boasts average settlements of approximately $15,000 per claim – compared with more than $98,000 at other VA institutions. Its policy has also decreased the average duration of cases, previously 2-4 years, to 2-4 months, as well as reduced costs for legal defense.
Likewise, the program at the University of Michigan Health System has reduced both the frequency and severity of claims, duration of cases, and litigation costs. Aware of these developments, some private insurers, such as the COPIC Insurance Company in Colorado, are adopting a similar approach.
In its updated 2014 tort reform position paper, the American College of Physicians continues to endorse caps on noneconomic and punitive damages, as well as other tort reform measures.
However, it now acknowledges that “improving patient safety and preventing errors must be at the fore of the medical liability reform discussion.” The ACP correctly asserts that “emphasizing patient safety, promoting a culture of quality improvement and coordinated care, and training physicians in best practices to avoid errors and reduce risk will prevent harm and reduce the waste associated with defensive medicine.”
This hybrid approach combining traditional tort reforms with a renewed attention to patient safety through medical error reduction may yet yield additional practical benefits.
Here, the experience in anesthesiology bears recounting: Its dramatic progress in risk management has cut patient death rate from 1 in 5,000 to 1 in 200,000 to 300,000 in the space of 20 years, and this has been associated with a concurrent 37% fall in insurance premiums.
References
1. Medical Injury Compensation Reform Act of 1975, Cal. Civ. Proc. Code § 3333.2 (West 1982).
2. O’Connell, J. No-Fault Insurance for Injuries Arising from Medical Treatment: A Proposal for Elective Coverage. Emory L. J. 1975;24:21.
Dr. Tan is professor emeritus of medicine and former adjunct professor of law at the University of Hawaii. Currently, he directs the St. Francis International Center for Healthcare Ethics in Honolulu. This article is meant to be educational and does not constitute medical, ethical, or legal advice. Some of the articles in this series are adapted from the author’s 2006 book, “Medical Malpractice: Understanding the Law, Managing the Risk,” and his 2012 Halsbury treatise, “Medical Negligence and Professional Misconduct.” For additional information, readers may contact the author at [email protected].

Going for the Gold
As we enter 2015 and approach the golden (50th) anniversary of both the NP and PA professions, dating back to Dr. Loretta Ford1 at the University of Colorado and Dr. Eugene Stead2 at Duke University (circa 1965), it is important to reflect on not only where we have been but also where we want our professions to go in the next half-century.
Since I am a PA, some may suggest that it is dangerous and ambitious for me to speak/project for both professions. They may also note that the professions are distinct and my suggestions and reflections do not apply to NPs. Well, I guess I am willing to take that risk. As a colleague, friend, and co-Editor-in-Chief of Marie-Eileen Onieal, I have found that we agree much more often on issues (both political and practical) than we disagree.
NPs and PAs have worked diligently over the past half-century to develop our individual professions, in terms of reimbursement, prescribing privileges, state licensure, commissioning in the uniformed services, and expansion of scope of practice. Studies continue to show that we provide quality health care with similar outcomes as physicians, thus making us cost-effective members of the health care team.3-7
So, here we are in 2015. While it is difficult to get accurate data, Table 1 shows the number of clinicians reported in the most recent US Health Workforce Chartbook.8 As we well know, our professions have grown exponentially from our humble beginnings in the mid-1960s. (The first class of PAs comprised four students, if you recall.)
At the risk of sounding like a fossil (Oh never mind—I am a fossil!), let me be presumptuous and share with you six areas in which I think both professions can “do more” through the second half-century of our existence. In my opinion, we should focus on:
1. Diversity. As presented in Table 2, the majority of PAs and NPs are (non-Hispanic) white. Our efforts, should you agree with me, must start at the educational program level, through recruitment and retention of students from unrepresented and underrepresented groups. Another focal point should be the recruitment and retention of faculty and staff in these programs who reflect the diversity of our nation.
When I consider the origins of my profession, the key point is opportunity. Dr. Stead and other pioneers sought to fill a serious need for health care providers while also creating opportunities for military medics who were highly skilled but who did not meet requirements for many jobs within the medical community. Now it is time for us to ensure that other groups have similar opportunities to advance themselves and also fill gaps in the health care system.
Continue for more areas to focus on >>
2. Workforce planning and policy. This requires better data collection and an improved information infrastructure. In a 2014 editorial, Rod Hooker suggested that this is the golden age for PAs (about whom he was writing, although the same holds true for NPs) because US health care reform has identified our contributions to society and new policies place us upfront and center stage in producing labor solutions.9
It is time for our professions to do a better job in studying and reporting the important contributions we make in health care delivery. We need to have a place at the table—be it within a facility or at the state or federal level—whenever policy, utilization, and roles are discussed. Even if we as employees are subordinate to management in a particular setting, we should have a voice in how we are utilized in the workplace; we should ensure that those who make decisions—if we are not them—have the fullest picture of who we are and what we can do. It is not enough to use anecdotal evidence; we need to have data readily at hand that unequivocally support our assertions of value to patient care.

Hooker went so far as to call for the creation of a “physician assistant institute” to assist in the development and dissemination of reliable information about the profession. I think this is an idea whose time has come, but who will step up to the plate? If you are an NP, you may say, “What about us?” I would suggest this issue pertains to both of our professions—and in fact, this is an area in which I would encourage a collaborative effort. What a concept!
3. Ethics. In the past decade, there has been a renewed focus on maintaining an ethical culture in health care. As clinicians, we practice in an environment that affects the lives of everyone. Our patients and their family members expect high-quality care, patient safety, and use of the latest and most appropriate technology.
In the middle of this climate, we find a health care system that is probably the most entrepreneurial, corporatized, and profit-driven health system in the world. Most of our practice settings (outside the federal government) are for-profit entities. It is easy in this environment to fall victim to conflicts of interest and to acquire an economically oriented practice attitude.
If our first priority is the best possible health care for our patients, then integrity and ethical behavior naturally follow. Professionalism at its very heart places the patient’s interests ahead of our own. We must keep this in mind as we navigate the ever-changing health system.
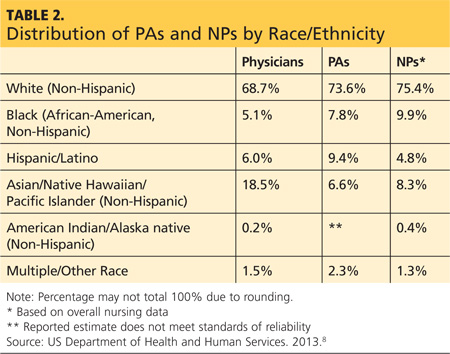
Next page: Key area number four >>
4. Humanitarianism. I would encourage us to be actively engaged in promoting human welfare and social reforms with no prejudice on grounds of gender, sexual orientation, or religious or ethnic differences. Our goal should be to save lives, relieve suffering, and maintain human dignity.
How do we do this? Many of us have at some point in our careers volunteered our professional services at free clinics or other venues that provide health care to those who otherwise have difficulty accessing it. Some of us take that spirit a step further, traveling abroad on medical missions or responding to natural disasters or civil disturbances.
While using our medical and nursing skills for the good of society is ideal, we can also represent ourselves and our professions well by being good members of the community—not just the “medical” community. Perhaps we provide food and shelter to the homeless in our area or mentor young people.
Anything we do to help not only benefits us and the recipient; it also shows the community that our concept of “care” extends beyond the confines of the clinic or emergency department or operating theater in which we work. We have a very special calling, and I’m always pleased when our professional journals highlight the efforts of our colleagues to “help out”; their stories should inspire us all.
5. Appreciation. As NPs and PAs, we provide health care (whether from a medical or nursing standpoint), a revered calling since the days of Hippocrates. This privilege allows us to enter into a bond with our patients and assist them in a personal and fundamental way. It is no small thing to be involved in curing illness and promoting well-being. We should always remember that our role carries responsibility as well as provides rewards.
Despite the greater availability of diagnostic technologies and advancements in therapeutic abilities, we continue to see increasing disparities in the delivery of health care. Our professions must work diligently to find ways to address the issues of quality, accessibility, and cost of health care in the US. What kind of “stewards” will we be? That is our heritage!
Continue for the last area PAs and NPs need to grow in >>
6. Action. At the risk of sounding like a cheerleader, being part of the NP or PA profession is something special; it always has been and always will be. Our professions have grown impressively in numbers, utilization, and stature. We need to cultivate and support our professions and their representative organizations (ie, AANP and AAPA).
In the early decades of each profession, individuals with a great deal of passion and dedication created, advanced, and led these organizations on both state and national levels—and even an international level. You know who they are! Without them, we would not have made the strides that we have as professionals—the attainment of licensure, authority, and reimbursement.
Now that we are being truly recognized for our role in the health care team and our contributions to patient care, some of us may become complacent with regard to our professional organizations. But there will always be legislative and regulatory gains to make, and strong representation (and “strength in numbers”) is the best way to achieve our professional goals. Please, let’s continue to support our organizations not only via membership (which provides funding for initiatives) but also by participating in whatever ways we can to further our professions.
If we are going to fully cement our place in America’s health care system, NPs and PAs must strive to keep up the national dialogue about our patients, their needs, and how our contributions address those needs. I hope you agree. Please share your thoughts with me at PAEditor@frontline medcom.com.
REFERENCES
1. Ridgway S. Loretta Ford, founded nurse practitioner movement. Working Nurse. www.workingnurse.com/articles/loretta-ford-founded-nurse-practitioner-movement. Accessed January 16, 2015.
2. Physician Assistant History Society. Eugene A. Stead Jr, MD. http://pahx.org/stead-jr-eugene. Accessed January 16, 2015.
3. Kartha A, Restuccia J, Burgess J, et al. Nurse practitioner and physician assistant scope of practice in 118 acute care hospitals. J Hosp Med. 2014:9(10); 615-620.
4. Naylor MD, Kurtzman ET. The role of nurse practitioners in reinventing primary care. Health Affairs. 2010;29(5):893-899.
5. Horrocks S, Anderson E, Salisbury C. Systematic review of whether nurse practitioners working in primary care can provide equivalent care to doctors. BMJ. 2002;324:819-823.
6. Halter M, Drennan V, Chattopadhyay K, et al. The contribution of physician assistants in primary care: a systematic review. BMC Health Services Research. 2013;13:223-236.
7. Hooker RS, Everett CM. The contributions of physician assistants in primary care systems. Health Social Care Commun. 2012;20(1):20-31.
8. US Department of Health and Human Services, Health Resources and Services Administration, National Center for Health Workforce Analysis. The US Health Workforce Chartbook. Part 1: Clinicians. Rockville, MD; 2013.
9. Hooker R. A physician assistant institute [editorial]. J Phys Assist Ed. 2014;25(3):5-6.
As we enter 2015 and approach the golden (50th) anniversary of both the NP and PA professions, dating back to Dr. Loretta Ford1 at the University of Colorado and Dr. Eugene Stead2 at Duke University (circa 1965), it is important to reflect on not only where we have been but also where we want our professions to go in the next half-century.
Since I am a PA, some may suggest that it is dangerous and ambitious for me to speak/project for both professions. They may also note that the professions are distinct and my suggestions and reflections do not apply to NPs. Well, I guess I am willing to take that risk. As a colleague, friend, and co-Editor-in-Chief of Marie-Eileen Onieal, I have found that we agree much more often on issues (both political and practical) than we disagree.
NPs and PAs have worked diligently over the past half-century to develop our individual professions, in terms of reimbursement, prescribing privileges, state licensure, commissioning in the uniformed services, and expansion of scope of practice. Studies continue to show that we provide quality health care with similar outcomes as physicians, thus making us cost-effective members of the health care team.3-7
So, here we are in 2015. While it is difficult to get accurate data, Table 1 shows the number of clinicians reported in the most recent US Health Workforce Chartbook.8 As we well know, our professions have grown exponentially from our humble beginnings in the mid-1960s. (The first class of PAs comprised four students, if you recall.)
At the risk of sounding like a fossil (Oh never mind—I am a fossil!), let me be presumptuous and share with you six areas in which I think both professions can “do more” through the second half-century of our existence. In my opinion, we should focus on:
1. Diversity. As presented in Table 2, the majority of PAs and NPs are (non-Hispanic) white. Our efforts, should you agree with me, must start at the educational program level, through recruitment and retention of students from unrepresented and underrepresented groups. Another focal point should be the recruitment and retention of faculty and staff in these programs who reflect the diversity of our nation.
When I consider the origins of my profession, the key point is opportunity. Dr. Stead and other pioneers sought to fill a serious need for health care providers while also creating opportunities for military medics who were highly skilled but who did not meet requirements for many jobs within the medical community. Now it is time for us to ensure that other groups have similar opportunities to advance themselves and also fill gaps in the health care system.
Continue for more areas to focus on >>
2. Workforce planning and policy. This requires better data collection and an improved information infrastructure. In a 2014 editorial, Rod Hooker suggested that this is the golden age for PAs (about whom he was writing, although the same holds true for NPs) because US health care reform has identified our contributions to society and new policies place us upfront and center stage in producing labor solutions.9
It is time for our professions to do a better job in studying and reporting the important contributions we make in health care delivery. We need to have a place at the table—be it within a facility or at the state or federal level—whenever policy, utilization, and roles are discussed. Even if we as employees are subordinate to management in a particular setting, we should have a voice in how we are utilized in the workplace; we should ensure that those who make decisions—if we are not them—have the fullest picture of who we are and what we can do. It is not enough to use anecdotal evidence; we need to have data readily at hand that unequivocally support our assertions of value to patient care.
Hooker went so far as to call for the creation of a “physician assistant institute” to assist in the development and dissemination of reliable information about the profession. I think this is an idea whose time has come, but who will step up to the plate? If you are an NP, you may say, “What about us?” I would suggest this issue pertains to both of our professions—and in fact, this is an area in which I would encourage a collaborative effort. What a concept!
3. Ethics. In the past decade, there has been a renewed focus on maintaining an ethical culture in health care. As clinicians, we practice in an environment that affects the lives of everyone. Our patients and their family members expect high-quality care, patient safety, and use of the latest and most appropriate technology.
In the middle of this climate, we find a health care system that is probably the most entrepreneurial, corporatized, and profit-driven health system in the world. Most of our practice settings (outside the federal government) are for-profit entities. It is easy in this environment to fall victim to conflicts of interest and to acquire an economically oriented practice attitude.
If our first priority is the best possible health care for our patients, then integrity and ethical behavior naturally follow. Professionalism at its very heart places the patient’s interests ahead of our own. We must keep this in mind as we navigate the ever-changing health system.
Next page: Key area number four >>
4. Humanitarianism. I would encourage us to be actively engaged in promoting human welfare and social reforms with no prejudice on grounds of gender, sexual orientation, or religious or ethnic differences. Our goal should be to save lives, relieve suffering, and maintain human dignity.
How do we do this? Many of us have at some point in our careers volunteered our professional services at free clinics or other venues that provide health care to those who otherwise have difficulty accessing it. Some of us take that spirit a step further, traveling abroad on medical missions or responding to natural disasters or civil disturbances.
While using our medical and nursing skills for the good of society is ideal, we can also represent ourselves and our professions well by being good members of the community—not just the “medical” community. Perhaps we provide food and shelter to the homeless in our area or mentor young people.
Anything we do to help not only benefits us and the recipient; it also shows the community that our concept of “care” extends beyond the confines of the clinic or emergency department or operating theater in which we work. We have a very special calling, and I’m always pleased when our professional journals highlight the efforts of our colleagues to “help out”; their stories should inspire us all.
5. Appreciation. As NPs and PAs, we provide health care (whether from a medical or nursing standpoint), a revered calling since the days of Hippocrates. This privilege allows us to enter into a bond with our patients and assist them in a personal and fundamental way. It is no small thing to be involved in curing illness and promoting well-being. We should always remember that our role carries responsibility as well as provides rewards.
Despite the greater availability of diagnostic technologies and advancements in therapeutic abilities, we continue to see increasing disparities in the delivery of health care. Our professions must work diligently to find ways to address the issues of quality, accessibility, and cost of health care in the US. What kind of “stewards” will we be? That is our heritage!
Continue for the last area PAs and NPs need to grow in >>
6. Action. At the risk of sounding like a cheerleader, being part of the NP or PA profession is something special; it always has been and always will be. Our professions have grown impressively in numbers, utilization, and stature. We need to cultivate and support our professions and their representative organizations (ie, AANP and AAPA).
In the early decades of each profession, individuals with a great deal of passion and dedication created, advanced, and led these organizations on both state and national levels—and even an international level. You know who they are! Without them, we would not have made the strides that we have as professionals—the attainment of licensure, authority, and reimbursement.
Now that we are being truly recognized for our role in the health care team and our contributions to patient care, some of us may become complacent with regard to our professional organizations. But there will always be legislative and regulatory gains to make, and strong representation (and “strength in numbers”) is the best way to achieve our professional goals. Please, let’s continue to support our organizations not only via membership (which provides funding for initiatives) but also by participating in whatever ways we can to further our professions.
If we are going to fully cement our place in America’s health care system, NPs and PAs must strive to keep up the national dialogue about our patients, their needs, and how our contributions address those needs. I hope you agree. Please share your thoughts with me at PAEditor@frontline medcom.com.
REFERENCES
1. Ridgway S. Loretta Ford, founded nurse practitioner movement. Working Nurse. www.workingnurse.com/articles/loretta-ford-founded-nurse-practitioner-movement. Accessed January 16, 2015.
2. Physician Assistant History Society. Eugene A. Stead Jr, MD. http://pahx.org/stead-jr-eugene. Accessed January 16, 2015.
3. Kartha A, Restuccia J, Burgess J, et al. Nurse practitioner and physician assistant scope of practice in 118 acute care hospitals. J Hosp Med. 2014:9(10); 615-620.
4. Naylor MD, Kurtzman ET. The role of nurse practitioners in reinventing primary care. Health Affairs. 2010;29(5):893-899.
5. Horrocks S, Anderson E, Salisbury C. Systematic review of whether nurse practitioners working in primary care can provide equivalent care to doctors. BMJ. 2002;324:819-823.
6. Halter M, Drennan V, Chattopadhyay K, et al. The contribution of physician assistants in primary care: a systematic review. BMC Health Services Research. 2013;13:223-236.
7. Hooker RS, Everett CM. The contributions of physician assistants in primary care systems. Health Social Care Commun. 2012;20(1):20-31.
8. US Department of Health and Human Services, Health Resources and Services Administration, National Center for Health Workforce Analysis. The US Health Workforce Chartbook. Part 1: Clinicians. Rockville, MD; 2013.
9. Hooker R. A physician assistant institute [editorial]. J Phys Assist Ed. 2014;25(3):5-6.
As we enter 2015 and approach the golden (50th) anniversary of both the NP and PA professions, dating back to Dr. Loretta Ford1 at the University of Colorado and Dr. Eugene Stead2 at Duke University (circa 1965), it is important to reflect on not only where we have been but also where we want our professions to go in the next half-century.
Since I am a PA, some may suggest that it is dangerous and ambitious for me to speak/project for both professions. They may also note that the professions are distinct and my suggestions and reflections do not apply to NPs. Well, I guess I am willing to take that risk. As a colleague, friend, and co-Editor-in-Chief of Marie-Eileen Onieal, I have found that we agree much more often on issues (both political and practical) than we disagree.
NPs and PAs have worked diligently over the past half-century to develop our individual professions, in terms of reimbursement, prescribing privileges, state licensure, commissioning in the uniformed services, and expansion of scope of practice. Studies continue to show that we provide quality health care with similar outcomes as physicians, thus making us cost-effective members of the health care team.3-7
So, here we are in 2015. While it is difficult to get accurate data, Table 1 shows the number of clinicians reported in the most recent US Health Workforce Chartbook.8 As we well know, our professions have grown exponentially from our humble beginnings in the mid-1960s. (The first class of PAs comprised four students, if you recall.)
At the risk of sounding like a fossil (Oh never mind—I am a fossil!), let me be presumptuous and share with you six areas in which I think both professions can “do more” through the second half-century of our existence. In my opinion, we should focus on:
1. Diversity. As presented in Table 2, the majority of PAs and NPs are (non-Hispanic) white. Our efforts, should you agree with me, must start at the educational program level, through recruitment and retention of students from unrepresented and underrepresented groups. Another focal point should be the recruitment and retention of faculty and staff in these programs who reflect the diversity of our nation.
When I consider the origins of my profession, the key point is opportunity. Dr. Stead and other pioneers sought to fill a serious need for health care providers while also creating opportunities for military medics who were highly skilled but who did not meet requirements for many jobs within the medical community. Now it is time for us to ensure that other groups have similar opportunities to advance themselves and also fill gaps in the health care system.
Continue for more areas to focus on >>
2. Workforce planning and policy. This requires better data collection and an improved information infrastructure. In a 2014 editorial, Rod Hooker suggested that this is the golden age for PAs (about whom he was writing, although the same holds true for NPs) because US health care reform has identified our contributions to society and new policies place us upfront and center stage in producing labor solutions.9
It is time for our professions to do a better job in studying and reporting the important contributions we make in health care delivery. We need to have a place at the table—be it within a facility or at the state or federal level—whenever policy, utilization, and roles are discussed. Even if we as employees are subordinate to management in a particular setting, we should have a voice in how we are utilized in the workplace; we should ensure that those who make decisions—if we are not them—have the fullest picture of who we are and what we can do. It is not enough to use anecdotal evidence; we need to have data readily at hand that unequivocally support our assertions of value to patient care.
Hooker went so far as to call for the creation of a “physician assistant institute” to assist in the development and dissemination of reliable information about the profession. I think this is an idea whose time has come, but who will step up to the plate? If you are an NP, you may say, “What about us?” I would suggest this issue pertains to both of our professions—and in fact, this is an area in which I would encourage a collaborative effort. What a concept!
3. Ethics. In the past decade, there has been a renewed focus on maintaining an ethical culture in health care. As clinicians, we practice in an environment that affects the lives of everyone. Our patients and their family members expect high-quality care, patient safety, and use of the latest and most appropriate technology.
In the middle of this climate, we find a health care system that is probably the most entrepreneurial, corporatized, and profit-driven health system in the world. Most of our practice settings (outside the federal government) are for-profit entities. It is easy in this environment to fall victim to conflicts of interest and to acquire an economically oriented practice attitude.
If our first priority is the best possible health care for our patients, then integrity and ethical behavior naturally follow. Professionalism at its very heart places the patient’s interests ahead of our own. We must keep this in mind as we navigate the ever-changing health system.
Next page: Key area number four >>
4. Humanitarianism. I would encourage us to be actively engaged in promoting human welfare and social reforms with no prejudice on grounds of gender, sexual orientation, or religious or ethnic differences. Our goal should be to save lives, relieve suffering, and maintain human dignity.
How do we do this? Many of us have at some point in our careers volunteered our professional services at free clinics or other venues that provide health care to those who otherwise have difficulty accessing it. Some of us take that spirit a step further, traveling abroad on medical missions or responding to natural disasters or civil disturbances.
While using our medical and nursing skills for the good of society is ideal, we can also represent ourselves and our professions well by being good members of the community—not just the “medical” community. Perhaps we provide food and shelter to the homeless in our area or mentor young people.
Anything we do to help not only benefits us and the recipient; it also shows the community that our concept of “care” extends beyond the confines of the clinic or emergency department or operating theater in which we work. We have a very special calling, and I’m always pleased when our professional journals highlight the efforts of our colleagues to “help out”; their stories should inspire us all.
5. Appreciation. As NPs and PAs, we provide health care (whether from a medical or nursing standpoint), a revered calling since the days of Hippocrates. This privilege allows us to enter into a bond with our patients and assist them in a personal and fundamental way. It is no small thing to be involved in curing illness and promoting well-being. We should always remember that our role carries responsibility as well as provides rewards.
Despite the greater availability of diagnostic technologies and advancements in therapeutic abilities, we continue to see increasing disparities in the delivery of health care. Our professions must work diligently to find ways to address the issues of quality, accessibility, and cost of health care in the US. What kind of “stewards” will we be? That is our heritage!
Continue for the last area PAs and NPs need to grow in >>
6. Action. At the risk of sounding like a cheerleader, being part of the NP or PA profession is something special; it always has been and always will be. Our professions have grown impressively in numbers, utilization, and stature. We need to cultivate and support our professions and their representative organizations (ie, AANP and AAPA).
In the early decades of each profession, individuals with a great deal of passion and dedication created, advanced, and led these organizations on both state and national levels—and even an international level. You know who they are! Without them, we would not have made the strides that we have as professionals—the attainment of licensure, authority, and reimbursement.
Now that we are being truly recognized for our role in the health care team and our contributions to patient care, some of us may become complacent with regard to our professional organizations. But there will always be legislative and regulatory gains to make, and strong representation (and “strength in numbers”) is the best way to achieve our professional goals. Please, let’s continue to support our organizations not only via membership (which provides funding for initiatives) but also by participating in whatever ways we can to further our professions.
If we are going to fully cement our place in America’s health care system, NPs and PAs must strive to keep up the national dialogue about our patients, their needs, and how our contributions address those needs. I hope you agree. Please share your thoughts with me at PAEditor@frontline medcom.com.
REFERENCES
1. Ridgway S. Loretta Ford, founded nurse practitioner movement. Working Nurse. www.workingnurse.com/articles/loretta-ford-founded-nurse-practitioner-movement. Accessed January 16, 2015.
2. Physician Assistant History Society. Eugene A. Stead Jr, MD. http://pahx.org/stead-jr-eugene. Accessed January 16, 2015.
3. Kartha A, Restuccia J, Burgess J, et al. Nurse practitioner and physician assistant scope of practice in 118 acute care hospitals. J Hosp Med. 2014:9(10); 615-620.
4. Naylor MD, Kurtzman ET. The role of nurse practitioners in reinventing primary care. Health Affairs. 2010;29(5):893-899.
5. Horrocks S, Anderson E, Salisbury C. Systematic review of whether nurse practitioners working in primary care can provide equivalent care to doctors. BMJ. 2002;324:819-823.
6. Halter M, Drennan V, Chattopadhyay K, et al. The contribution of physician assistants in primary care: a systematic review. BMC Health Services Research. 2013;13:223-236.
7. Hooker RS, Everett CM. The contributions of physician assistants in primary care systems. Health Social Care Commun. 2012;20(1):20-31.
8. US Department of Health and Human Services, Health Resources and Services Administration, National Center for Health Workforce Analysis. The US Health Workforce Chartbook. Part 1: Clinicians. Rockville, MD; 2013.
9. Hooker R. A physician assistant institute [editorial]. J Phys Assist Ed. 2014;25(3):5-6.
Mother knew better
Like most pediatricians, I often think about parenting. It’s hard to ignore when your days and some nights are surrounded by it in a variety of forms ... the good the bad, and the ugly. Recently, I was trying to recall my own parents’ (mostly my Mom’s) style of parenting and discovered that I was having trouble remembering many of the specifics of how my sister and I were raised.
The haziness of that recollection could simply reflect my aging memory, but I prefer to interpret it as a sign that our parents consciously avoided being heavy handed in their approach. Granted, my sister and I have grown up to be reasonably agreeable adults and were relatively unadventurous children. But, we were far from angelic.
My mother was a quiet person. In fact, I have trouble recalling much about the sound of her voice. She was not one to debate or argue. Although my parents had their disagreements, my mother would refuse to argue, which infuriated my father. Instead she would state her position once and wait for the issue to play out. The result usually vindicated her softly stated position.
But, my mother wasn’t perfect, and it is those few parenting missteps that I remember ... most of them fondly. For example, when she first heard me swear (I don’t even remember the word), she said that I was to have my mouth washed out with soap. I assume she had heard this advice from my grandmother. However, she wasn’t quite clear on the technique. The result was a lot of fumbling around with a large bar of soap and a very small mouth. It certainly wasn’t a deterrent in large part, because I sensed she was giggling during the ordeal.
I don’t recall being spanked, but my mother was not adverse to physical deterrent. After years of reminding me to sit up straight at the dinner table, she took to nonchalantly – and without a word – poking me between the shoulder blades with a fork as she passed behind me while serving supper. No more idle threats, just a sharp reminder. Of course, it was no more effective than the soap, and I am still a sloucher.
My mother occasionally made attempts at anticipatory guidance with mixed results. One cold December morning as I was heading off to school, she took me aside and cautioned, “Now Willy, don’t ever stick your tongue on a cold pipe.” I’m not sure what prompted this warning because it was decades before this foolishness made it to the silver screen in Jean Shepherd’s “A Christmas Story.” Up to that point, putting my tongue on a cold pipe was an activity that had never crossed my little mind. But now she had planted the seed and for many winters I couldn’t pass a parking meter without the little devil on my shoulder whispering in my ear, “Go try it.”
The only parenting misstep for which I still hold a grudge is one in which my mother ignored her ample storehouse of good sense and floated with the mainstream of bad parental advice. Those of you born prior to 1965 probably share my painful memories of having to sit on the edge of the pond or lake until it had been exactly an hour since you had last eaten – eaten anything! A thoughtlessly nibbled cookie could result in a stomach cramp that could send you to the bottom, never to take another breath of air. It is unclear which medical genius came up with this idea, but I hope he is rotting in hell, doubled over with unremitting abdominal cramps. A rough calculation reveals that between the ages of 7 and 14 years, I wasted nearly 1,000 child-hours sitting on the edge of the town pool, impatiently waiting for peanut butter sandwiches to digest. I know my mother knew that the whole stomach cramp thing was bogus. But, she wasn’t strong enough to swim against the terrible tide of old wives’ tales.
Despite these trivial errors when I was a young child, my mother did her best parenting when I reached adolescence. Pleasantville, N.Y., was a small town of 5,000, and my mother seemed to know two-thirds of them by their first name. Or, at least I thought she did. Her web of contacts covered the town like a blanket. I was convinced that, like Santa Claus, she knew when I was sleeping, she knew when I was awake, she knew if I’d been bad or good. You get the picture. It was only many years later that I realized I had been buffaloed. Her omniscience had been a masterful act ... but it had worked.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “Coping with a Picky Eater.” E-mail him at [email protected].
Like most pediatricians, I often think about parenting. It’s hard to ignore when your days and some nights are surrounded by it in a variety of forms ... the good the bad, and the ugly. Recently, I was trying to recall my own parents’ (mostly my Mom’s) style of parenting and discovered that I was having trouble remembering many of the specifics of how my sister and I were raised.
The haziness of that recollection could simply reflect my aging memory, but I prefer to interpret it as a sign that our parents consciously avoided being heavy handed in their approach. Granted, my sister and I have grown up to be reasonably agreeable adults and were relatively unadventurous children. But, we were far from angelic.
My mother was a quiet person. In fact, I have trouble recalling much about the sound of her voice. She was not one to debate or argue. Although my parents had their disagreements, my mother would refuse to argue, which infuriated my father. Instead she would state her position once and wait for the issue to play out. The result usually vindicated her softly stated position.
But, my mother wasn’t perfect, and it is those few parenting missteps that I remember ... most of them fondly. For example, when she first heard me swear (I don’t even remember the word), she said that I was to have my mouth washed out with soap. I assume she had heard this advice from my grandmother. However, she wasn’t quite clear on the technique. The result was a lot of fumbling around with a large bar of soap and a very small mouth. It certainly wasn’t a deterrent in large part, because I sensed she was giggling during the ordeal.
I don’t recall being spanked, but my mother was not adverse to physical deterrent. After years of reminding me to sit up straight at the dinner table, she took to nonchalantly – and without a word – poking me between the shoulder blades with a fork as she passed behind me while serving supper. No more idle threats, just a sharp reminder. Of course, it was no more effective than the soap, and I am still a sloucher.
My mother occasionally made attempts at anticipatory guidance with mixed results. One cold December morning as I was heading off to school, she took me aside and cautioned, “Now Willy, don’t ever stick your tongue on a cold pipe.” I’m not sure what prompted this warning because it was decades before this foolishness made it to the silver screen in Jean Shepherd’s “A Christmas Story.” Up to that point, putting my tongue on a cold pipe was an activity that had never crossed my little mind. But now she had planted the seed and for many winters I couldn’t pass a parking meter without the little devil on my shoulder whispering in my ear, “Go try it.”
The only parenting misstep for which I still hold a grudge is one in which my mother ignored her ample storehouse of good sense and floated with the mainstream of bad parental advice. Those of you born prior to 1965 probably share my painful memories of having to sit on the edge of the pond or lake until it had been exactly an hour since you had last eaten – eaten anything! A thoughtlessly nibbled cookie could result in a stomach cramp that could send you to the bottom, never to take another breath of air. It is unclear which medical genius came up with this idea, but I hope he is rotting in hell, doubled over with unremitting abdominal cramps. A rough calculation reveals that between the ages of 7 and 14 years, I wasted nearly 1,000 child-hours sitting on the edge of the town pool, impatiently waiting for peanut butter sandwiches to digest. I know my mother knew that the whole stomach cramp thing was bogus. But, she wasn’t strong enough to swim against the terrible tide of old wives’ tales.
Despite these trivial errors when I was a young child, my mother did her best parenting when I reached adolescence. Pleasantville, N.Y., was a small town of 5,000, and my mother seemed to know two-thirds of them by their first name. Or, at least I thought she did. Her web of contacts covered the town like a blanket. I was convinced that, like Santa Claus, she knew when I was sleeping, she knew when I was awake, she knew if I’d been bad or good. You get the picture. It was only many years later that I realized I had been buffaloed. Her omniscience had been a masterful act ... but it had worked.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “Coping with a Picky Eater.” E-mail him at [email protected].
Like most pediatricians, I often think about parenting. It’s hard to ignore when your days and some nights are surrounded by it in a variety of forms ... the good the bad, and the ugly. Recently, I was trying to recall my own parents’ (mostly my Mom’s) style of parenting and discovered that I was having trouble remembering many of the specifics of how my sister and I were raised.
The haziness of that recollection could simply reflect my aging memory, but I prefer to interpret it as a sign that our parents consciously avoided being heavy handed in their approach. Granted, my sister and I have grown up to be reasonably agreeable adults and were relatively unadventurous children. But, we were far from angelic.
My mother was a quiet person. In fact, I have trouble recalling much about the sound of her voice. She was not one to debate or argue. Although my parents had their disagreements, my mother would refuse to argue, which infuriated my father. Instead she would state her position once and wait for the issue to play out. The result usually vindicated her softly stated position.
But, my mother wasn’t perfect, and it is those few parenting missteps that I remember ... most of them fondly. For example, when she first heard me swear (I don’t even remember the word), she said that I was to have my mouth washed out with soap. I assume she had heard this advice from my grandmother. However, she wasn’t quite clear on the technique. The result was a lot of fumbling around with a large bar of soap and a very small mouth. It certainly wasn’t a deterrent in large part, because I sensed she was giggling during the ordeal.
I don’t recall being spanked, but my mother was not adverse to physical deterrent. After years of reminding me to sit up straight at the dinner table, she took to nonchalantly – and without a word – poking me between the shoulder blades with a fork as she passed behind me while serving supper. No more idle threats, just a sharp reminder. Of course, it was no more effective than the soap, and I am still a sloucher.
My mother occasionally made attempts at anticipatory guidance with mixed results. One cold December morning as I was heading off to school, she took me aside and cautioned, “Now Willy, don’t ever stick your tongue on a cold pipe.” I’m not sure what prompted this warning because it was decades before this foolishness made it to the silver screen in Jean Shepherd’s “A Christmas Story.” Up to that point, putting my tongue on a cold pipe was an activity that had never crossed my little mind. But now she had planted the seed and for many winters I couldn’t pass a parking meter without the little devil on my shoulder whispering in my ear, “Go try it.”
The only parenting misstep for which I still hold a grudge is one in which my mother ignored her ample storehouse of good sense and floated with the mainstream of bad parental advice. Those of you born prior to 1965 probably share my painful memories of having to sit on the edge of the pond or lake until it had been exactly an hour since you had last eaten – eaten anything! A thoughtlessly nibbled cookie could result in a stomach cramp that could send you to the bottom, never to take another breath of air. It is unclear which medical genius came up with this idea, but I hope he is rotting in hell, doubled over with unremitting abdominal cramps. A rough calculation reveals that between the ages of 7 and 14 years, I wasted nearly 1,000 child-hours sitting on the edge of the town pool, impatiently waiting for peanut butter sandwiches to digest. I know my mother knew that the whole stomach cramp thing was bogus. But, she wasn’t strong enough to swim against the terrible tide of old wives’ tales.
Despite these trivial errors when I was a young child, my mother did her best parenting when I reached adolescence. Pleasantville, N.Y., was a small town of 5,000, and my mother seemed to know two-thirds of them by their first name. Or, at least I thought she did. Her web of contacts covered the town like a blanket. I was convinced that, like Santa Claus, she knew when I was sleeping, she knew when I was awake, she knew if I’d been bad or good. You get the picture. It was only many years later that I realized I had been buffaloed. Her omniscience had been a masterful act ... but it had worked.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “Coping with a Picky Eater.” E-mail him at [email protected].

TLR - Target lesion recurrence
In November I attended the VEITHsymposium in New York. Almost 600 experts from around the world gave lectures on every aspect of vascular surgery. Given 5 minutes per talk, the presenters had to carefully select data they believed would bolster their viewpoint. So will someone please explain to me why some speakers still feel obliged to include target lesion revascularization (TLR) in their presentations? Furthermore, it’s not just in talks but also in peer-reviewed journals that we seem to be bombarded with this useless and often deceiving piece of information. I know that many feel the same way about TLR. However, for those not yet convinced, let me outline why I think TLR should rather stand for “The Least Relevant.”
The concept of TLR materialized during the early days of coronary balloon angioplasty and stenting. In the coronary arteries it is difficult to determine the restenosis rate of a treated lesion without repeating another coronary arteriogram. Accordingly, researchers resorted to TLR as an alternative method of evaluating whether a new treatment worked. However, in the peripheral circulation we have other methods of evaluating the lesion such as duplex scanning, CTA and MRA. This allows us minimally invasive and noninvasive means to evaluate the fate of the lesion itself. Thus, we are able to evaluate TLR as target lesion recurrence rather than target lesion revascularization.

Subsequently, companies and researchers have developed new devices such as balloons, stents, atherectomy devices, and drug-eluting variations that directly target peripheral vascular lesions. Despite the availability of noninvasive techniques to evaluate the target lesion itself, they use TLR data to convince physicians and purchasing entities to buy and use their device. The implication is that avoidance of another procedure to achieve the desired clinical endpoint proves that the new instrument works. However, as I have mentioned in previous editorials, semantics can have negative consequences. Here the problem arises when we attempt to define “works.” The inventor of a device that opens a narrowed or blocked artery wants to make sure that the device indeed does just that. In that case it would be appropriate to claim that it “works.”
If the lesion remains open and does not re-narrow we may conclude the device not only works but is also “effective.” The manufacturer and the FDA will want to make sure that it also does no harm and is “safe.” All are hopeful that it will improve the patient’s condition and have “clinical utility.” Certainly, success can be defined in many ways and clinical benefit must reign supreme. Accordingly, a device that is effective, safe and has clinical utility may be considered “successful” and, if cost effective, worth using. However, we are all aware that some procedures can improve a patient’s condition through a placebo effect. Therefore, it is incorrect for researchers to suggest that low TLR rates equate with clinical success. The most reliable judge of the efficacy of the procedure will be what happens to the targeted lesion and not what happens to the patient. It is more salient that we are assured that the device provides persistent improvement in luminal diameter at the site of the treated lesion.
It may help to further define the problem with TLR if we use a hypothetical example of a new medicated stent inserted to open a single SFA lesion responsible for toe gangrene. If that stent keeps the stenotic lesion widely patent, it should be considered effective even if the patient ultimately requires an above-knee amputation. On the other hand if the stent occludes in the recovery room, yet the toe subsequently heals without any further intervention, that stent did not work. In the latter scenario the patient will not have had a revascularization and so will not be included with the patients requiring TLR. Thus the stent would appear to have had more clinical utility or to have been more”successful” than it really was. Similarly, TLR will not be negatively impacted when, as in some circumstances of stent occlusion, a patient decides to live with discomfort rather than consent to another procedure. Furthermore, investigators of that stent may have a perverse incentive after occlusion to minimize TLR by not performing another procedure. On the other hand a bypass of an artery with an open and functional stent would negatively impact TLR statistics for that type of stent. This may occur if the stented lesion was not the only cause of distal ischemia.What concerns me most about TLR, even more than its limited relevance, is that this statistic is used to support data that otherwise would not stand up to scrutiny. It is often included in trials where numbers are small or where Industry bias is obvious. Accordingly, I am hopeful that researchers seriously consider describing TLR as target lesion recurrence rates omitting target lesion revascularization from their presentations and manuscripts. If they insist on using this irrelevant statistic then they should provide information as to why the revascularization was performed.
Was it for lesion recurrence or failure to improve the indicated condition? If the lesion recurred but TLR was not performed, was that because recovery had been achieved despite restenosis of the target lesion? Was it because the patient was not offered further treatment? Perhaps the patient succumbed before TLR could have been provided?
I may be accused of being overly cynical, but it may have been because the patient had decided that the better part of valor would be to run away and join a witness protection program rather than take part in that clinical trial.
In November I attended the VEITHsymposium in New York. Almost 600 experts from around the world gave lectures on every aspect of vascular surgery. Given 5 minutes per talk, the presenters had to carefully select data they believed would bolster their viewpoint. So will someone please explain to me why some speakers still feel obliged to include target lesion revascularization (TLR) in their presentations? Furthermore, it’s not just in talks but also in peer-reviewed journals that we seem to be bombarded with this useless and often deceiving piece of information. I know that many feel the same way about TLR. However, for those not yet convinced, let me outline why I think TLR should rather stand for “The Least Relevant.”
The concept of TLR materialized during the early days of coronary balloon angioplasty and stenting. In the coronary arteries it is difficult to determine the restenosis rate of a treated lesion without repeating another coronary arteriogram. Accordingly, researchers resorted to TLR as an alternative method of evaluating whether a new treatment worked. However, in the peripheral circulation we have other methods of evaluating the lesion such as duplex scanning, CTA and MRA. This allows us minimally invasive and noninvasive means to evaluate the fate of the lesion itself. Thus, we are able to evaluate TLR as target lesion recurrence rather than target lesion revascularization.
Subsequently, companies and researchers have developed new devices such as balloons, stents, atherectomy devices, and drug-eluting variations that directly target peripheral vascular lesions. Despite the availability of noninvasive techniques to evaluate the target lesion itself, they use TLR data to convince physicians and purchasing entities to buy and use their device. The implication is that avoidance of another procedure to achieve the desired clinical endpoint proves that the new instrument works. However, as I have mentioned in previous editorials, semantics can have negative consequences. Here the problem arises when we attempt to define “works.” The inventor of a device that opens a narrowed or blocked artery wants to make sure that the device indeed does just that. In that case it would be appropriate to claim that it “works.”
If the lesion remains open and does not re-narrow we may conclude the device not only works but is also “effective.” The manufacturer and the FDA will want to make sure that it also does no harm and is “safe.” All are hopeful that it will improve the patient’s condition and have “clinical utility.” Certainly, success can be defined in many ways and clinical benefit must reign supreme. Accordingly, a device that is effective, safe and has clinical utility may be considered “successful” and, if cost effective, worth using. However, we are all aware that some procedures can improve a patient’s condition through a placebo effect. Therefore, it is incorrect for researchers to suggest that low TLR rates equate with clinical success. The most reliable judge of the efficacy of the procedure will be what happens to the targeted lesion and not what happens to the patient. It is more salient that we are assured that the device provides persistent improvement in luminal diameter at the site of the treated lesion.
It may help to further define the problem with TLR if we use a hypothetical example of a new medicated stent inserted to open a single SFA lesion responsible for toe gangrene. If that stent keeps the stenotic lesion widely patent, it should be considered effective even if the patient ultimately requires an above-knee amputation. On the other hand if the stent occludes in the recovery room, yet the toe subsequently heals without any further intervention, that stent did not work. In the latter scenario the patient will not have had a revascularization and so will not be included with the patients requiring TLR. Thus the stent would appear to have had more clinical utility or to have been more”successful” than it really was. Similarly, TLR will not be negatively impacted when, as in some circumstances of stent occlusion, a patient decides to live with discomfort rather than consent to another procedure. Furthermore, investigators of that stent may have a perverse incentive after occlusion to minimize TLR by not performing another procedure. On the other hand a bypass of an artery with an open and functional stent would negatively impact TLR statistics for that type of stent. This may occur if the stented lesion was not the only cause of distal ischemia.What concerns me most about TLR, even more than its limited relevance, is that this statistic is used to support data that otherwise would not stand up to scrutiny. It is often included in trials where numbers are small or where Industry bias is obvious. Accordingly, I am hopeful that researchers seriously consider describing TLR as target lesion recurrence rates omitting target lesion revascularization from their presentations and manuscripts. If they insist on using this irrelevant statistic then they should provide information as to why the revascularization was performed.
Was it for lesion recurrence or failure to improve the indicated condition? If the lesion recurred but TLR was not performed, was that because recovery had been achieved despite restenosis of the target lesion? Was it because the patient was not offered further treatment? Perhaps the patient succumbed before TLR could have been provided?
I may be accused of being overly cynical, but it may have been because the patient had decided that the better part of valor would be to run away and join a witness protection program rather than take part in that clinical trial.
In November I attended the VEITHsymposium in New York. Almost 600 experts from around the world gave lectures on every aspect of vascular surgery. Given 5 minutes per talk, the presenters had to carefully select data they believed would bolster their viewpoint. So will someone please explain to me why some speakers still feel obliged to include target lesion revascularization (TLR) in their presentations? Furthermore, it’s not just in talks but also in peer-reviewed journals that we seem to be bombarded with this useless and often deceiving piece of information. I know that many feel the same way about TLR. However, for those not yet convinced, let me outline why I think TLR should rather stand for “The Least Relevant.”
The concept of TLR materialized during the early days of coronary balloon angioplasty and stenting. In the coronary arteries it is difficult to determine the restenosis rate of a treated lesion without repeating another coronary arteriogram. Accordingly, researchers resorted to TLR as an alternative method of evaluating whether a new treatment worked. However, in the peripheral circulation we have other methods of evaluating the lesion such as duplex scanning, CTA and MRA. This allows us minimally invasive and noninvasive means to evaluate the fate of the lesion itself. Thus, we are able to evaluate TLR as target lesion recurrence rather than target lesion revascularization.
Subsequently, companies and researchers have developed new devices such as balloons, stents, atherectomy devices, and drug-eluting variations that directly target peripheral vascular lesions. Despite the availability of noninvasive techniques to evaluate the target lesion itself, they use TLR data to convince physicians and purchasing entities to buy and use their device. The implication is that avoidance of another procedure to achieve the desired clinical endpoint proves that the new instrument works. However, as I have mentioned in previous editorials, semantics can have negative consequences. Here the problem arises when we attempt to define “works.” The inventor of a device that opens a narrowed or blocked artery wants to make sure that the device indeed does just that. In that case it would be appropriate to claim that it “works.”
If the lesion remains open and does not re-narrow we may conclude the device not only works but is also “effective.” The manufacturer and the FDA will want to make sure that it also does no harm and is “safe.” All are hopeful that it will improve the patient’s condition and have “clinical utility.” Certainly, success can be defined in many ways and clinical benefit must reign supreme. Accordingly, a device that is effective, safe and has clinical utility may be considered “successful” and, if cost effective, worth using. However, we are all aware that some procedures can improve a patient’s condition through a placebo effect. Therefore, it is incorrect for researchers to suggest that low TLR rates equate with clinical success. The most reliable judge of the efficacy of the procedure will be what happens to the targeted lesion and not what happens to the patient. It is more salient that we are assured that the device provides persistent improvement in luminal diameter at the site of the treated lesion.
It may help to further define the problem with TLR if we use a hypothetical example of a new medicated stent inserted to open a single SFA lesion responsible for toe gangrene. If that stent keeps the stenotic lesion widely patent, it should be considered effective even if the patient ultimately requires an above-knee amputation. On the other hand if the stent occludes in the recovery room, yet the toe subsequently heals without any further intervention, that stent did not work. In the latter scenario the patient will not have had a revascularization and so will not be included with the patients requiring TLR. Thus the stent would appear to have had more clinical utility or to have been more”successful” than it really was. Similarly, TLR will not be negatively impacted when, as in some circumstances of stent occlusion, a patient decides to live with discomfort rather than consent to another procedure. Furthermore, investigators of that stent may have a perverse incentive after occlusion to minimize TLR by not performing another procedure. On the other hand a bypass of an artery with an open and functional stent would negatively impact TLR statistics for that type of stent. This may occur if the stented lesion was not the only cause of distal ischemia.What concerns me most about TLR, even more than its limited relevance, is that this statistic is used to support data that otherwise would not stand up to scrutiny. It is often included in trials where numbers are small or where Industry bias is obvious. Accordingly, I am hopeful that researchers seriously consider describing TLR as target lesion recurrence rates omitting target lesion revascularization from their presentations and manuscripts. If they insist on using this irrelevant statistic then they should provide information as to why the revascularization was performed.
Was it for lesion recurrence or failure to improve the indicated condition? If the lesion recurred but TLR was not performed, was that because recovery had been achieved despite restenosis of the target lesion? Was it because the patient was not offered further treatment? Perhaps the patient succumbed before TLR could have been provided?
I may be accused of being overly cynical, but it may have been because the patient had decided that the better part of valor would be to run away and join a witness protection program rather than take part in that clinical trial.

From the Washington Office
Shortly after passage of the $1.1 trillion “Cromnibus,” the House and Senate concluded their legislative business for the 113th Congress and adjourned. Many issues of importance to surgeons and our patients remain unresolved and are expected to be high on the legislative agenda of the 114th Congress in the first quarter of 2015.
Returning as Members of Congress in January will be two physicians whose campaigns were assisted by the active participation of SurgeonsPAC. They are Dr. Ami Bera, an emergency physician from the 7th District of California (Sacramento area) and Dr. Dan Benishek, a general surgeon and fellow of the American College of Surgeons from the 1st District of Michigan (Upper Peninsula). Both Dr. Bera and Dr. Benishek have served as champions for the cause of the legislative agenda supported by the College.

One of the ways by which SurgeonsPAC participated in the re-election campaign of both Members is known as an independent expenditure (IE). The Code of Federal Regulations defines and independent expenditure as an expenditure for a communication that expressly advocates for “the election or defeat of a clearly identified candidate that is not made in cooperation, consultation, or concert with, or at the request or suggestion of, a candidate, a candidate’s authorized committee, or their agents, or a political party committee or its agents.” [11 CFR 100.16(a)]
In August, the Board of Directors of SurgeonsPAC unanimously voted to direct staff of the Division of Advocacy and Health Policy to develop recommendations for independent expenditures for a bipartisan slate of candidates who had a record of being supportive of the College’s legislative agenda and whose election was enough at risk that an independent expenditure by the College would potentially be of significant benefit for their race. In October, the PAC Board considered those recommendations and voted to support the expenditure of $100,000 each for IEs for Dr. Bera, a Democrat, and Dr. Benishek, a Republican. Both have been champions on issues such as repeal and replacement of the Sustainable Growth Rate (SGR), medical liability reform, and repeal of the 96-hour rule.
For Dr. Bera, the SurgeonsPAC dollars were utilized for a radio and direct mail campaign that was part of a larger effort in which other physician political action committees participated similarly. For Dr. Benishek, a television ad was produced and run through local cable providers.
On election night, Dr. Benishek was declared the winner, receiving 52.1% of the vote compared with his opponent’s 45.3%. As one of four fellows of the American College of Surgeons in Congress, we look forward to continuing to work with “Dr. Dan” and his excellent staff in his upcoming third term.
Dr. Bera’s race was much closer, as he actually trailed his opponent when election night closed with 49.8% of the vote. Subsequently, with the counting and inclusion of the mail-in ballots specifically targeted by the physician community’s IE effort, Dr. Bera overtook his opponent’s slim margin. Two weeks later, on 19 Nov. 2014, the Associated Press called the election for Dr. Bera, whose 1,400-vote lead at that time was felt to be substantial enough to preclude his opponent making up the difference with the remaining 4,300 provisional ballots that had yet to be counted. Dr. Bera’s CA-7 district race proved to be the most expensive in the nation with an estimated $19.6 million in total expenditures. Despite representing only 0.51% of that total, SurgeonsPAC’s contribution, in the collective with that of other physician organizations, no doubt played a significant role in returning a physician to Congress to continue to champion our causes.
In my opinion, these examples of careful candidate selection and subsequent support of Drs. Benishek and Bera exemplify the importance of a strong political action committee. The ultimate goal of SurgeonsPAC is the election to Congress and retention in Congress of those who support our policy positions and legislative agenda. Though SurgeonsPAC is one of nine physician PACs that can be accurately labeled as “million dollar” (per election cycle) PACs, our relative size and, thus, the number of candidates like Drs. Bera and Benishek we could support would be much greater if the Fellow participation rate more closely resembled that of our colleagues in other physician organizations. However, year after year, only 3%-4% of Fellows contribute, as compared with participation rates of 10%-25% in those physician PACs larger than SurgeonsPAC.
Recently, all Fellows received an e-mail from Dr. Andrew Warshaw, founding SurgeonsPAC Board Chairman and current President of the ACS, urging Fellows to make a $25 donation to SurgeonsPAC. Those wishing to learn more about the critical role SurgeonsPAC plays in our advocacy efforts can log on to www.surgeonspac.org.
Until next month...
Dr. Bailey is a pediatric surgeon and Medical Director, Advocacy for the Division of Advocacy and Health Policy in the ACS offices in Washington, DC.
Shortly after passage of the $1.1 trillion “Cromnibus,” the House and Senate concluded their legislative business for the 113th Congress and adjourned. Many issues of importance to surgeons and our patients remain unresolved and are expected to be high on the legislative agenda of the 114th Congress in the first quarter of 2015.
Returning as Members of Congress in January will be two physicians whose campaigns were assisted by the active participation of SurgeonsPAC. They are Dr. Ami Bera, an emergency physician from the 7th District of California (Sacramento area) and Dr. Dan Benishek, a general surgeon and fellow of the American College of Surgeons from the 1st District of Michigan (Upper Peninsula). Both Dr. Bera and Dr. Benishek have served as champions for the cause of the legislative agenda supported by the College.
One of the ways by which SurgeonsPAC participated in the re-election campaign of both Members is known as an independent expenditure (IE). The Code of Federal Regulations defines and independent expenditure as an expenditure for a communication that expressly advocates for “the election or defeat of a clearly identified candidate that is not made in cooperation, consultation, or concert with, or at the request or suggestion of, a candidate, a candidate’s authorized committee, or their agents, or a political party committee or its agents.” [11 CFR 100.16(a)]
In August, the Board of Directors of SurgeonsPAC unanimously voted to direct staff of the Division of Advocacy and Health Policy to develop recommendations for independent expenditures for a bipartisan slate of candidates who had a record of being supportive of the College’s legislative agenda and whose election was enough at risk that an independent expenditure by the College would potentially be of significant benefit for their race. In October, the PAC Board considered those recommendations and voted to support the expenditure of $100,000 each for IEs for Dr. Bera, a Democrat, and Dr. Benishek, a Republican. Both have been champions on issues such as repeal and replacement of the Sustainable Growth Rate (SGR), medical liability reform, and repeal of the 96-hour rule.
For Dr. Bera, the SurgeonsPAC dollars were utilized for a radio and direct mail campaign that was part of a larger effort in which other physician political action committees participated similarly. For Dr. Benishek, a television ad was produced and run through local cable providers.
On election night, Dr. Benishek was declared the winner, receiving 52.1% of the vote compared with his opponent’s 45.3%. As one of four fellows of the American College of Surgeons in Congress, we look forward to continuing to work with “Dr. Dan” and his excellent staff in his upcoming third term.
Dr. Bera’s race was much closer, as he actually trailed his opponent when election night closed with 49.8% of the vote. Subsequently, with the counting and inclusion of the mail-in ballots specifically targeted by the physician community’s IE effort, Dr. Bera overtook his opponent’s slim margin. Two weeks later, on 19 Nov. 2014, the Associated Press called the election for Dr. Bera, whose 1,400-vote lead at that time was felt to be substantial enough to preclude his opponent making up the difference with the remaining 4,300 provisional ballots that had yet to be counted. Dr. Bera’s CA-7 district race proved to be the most expensive in the nation with an estimated $19.6 million in total expenditures. Despite representing only 0.51% of that total, SurgeonsPAC’s contribution, in the collective with that of other physician organizations, no doubt played a significant role in returning a physician to Congress to continue to champion our causes.
In my opinion, these examples of careful candidate selection and subsequent support of Drs. Benishek and Bera exemplify the importance of a strong political action committee. The ultimate goal of SurgeonsPAC is the election to Congress and retention in Congress of those who support our policy positions and legislative agenda. Though SurgeonsPAC is one of nine physician PACs that can be accurately labeled as “million dollar” (per election cycle) PACs, our relative size and, thus, the number of candidates like Drs. Bera and Benishek we could support would be much greater if the Fellow participation rate more closely resembled that of our colleagues in other physician organizations. However, year after year, only 3%-4% of Fellows contribute, as compared with participation rates of 10%-25% in those physician PACs larger than SurgeonsPAC.
Recently, all Fellows received an e-mail from Dr. Andrew Warshaw, founding SurgeonsPAC Board Chairman and current President of the ACS, urging Fellows to make a $25 donation to SurgeonsPAC. Those wishing to learn more about the critical role SurgeonsPAC plays in our advocacy efforts can log on to www.surgeonspac.org.
Until next month...
Dr. Bailey is a pediatric surgeon and Medical Director, Advocacy for the Division of Advocacy and Health Policy in the ACS offices in Washington, DC.
Shortly after passage of the $1.1 trillion “Cromnibus,” the House and Senate concluded their legislative business for the 113th Congress and adjourned. Many issues of importance to surgeons and our patients remain unresolved and are expected to be high on the legislative agenda of the 114th Congress in the first quarter of 2015.
Returning as Members of Congress in January will be two physicians whose campaigns were assisted by the active participation of SurgeonsPAC. They are Dr. Ami Bera, an emergency physician from the 7th District of California (Sacramento area) and Dr. Dan Benishek, a general surgeon and fellow of the American College of Surgeons from the 1st District of Michigan (Upper Peninsula). Both Dr. Bera and Dr. Benishek have served as champions for the cause of the legislative agenda supported by the College.
One of the ways by which SurgeonsPAC participated in the re-election campaign of both Members is known as an independent expenditure (IE). The Code of Federal Regulations defines and independent expenditure as an expenditure for a communication that expressly advocates for “the election or defeat of a clearly identified candidate that is not made in cooperation, consultation, or concert with, or at the request or suggestion of, a candidate, a candidate’s authorized committee, or their agents, or a political party committee or its agents.” [11 CFR 100.16(a)]
In August, the Board of Directors of SurgeonsPAC unanimously voted to direct staff of the Division of Advocacy and Health Policy to develop recommendations for independent expenditures for a bipartisan slate of candidates who had a record of being supportive of the College’s legislative agenda and whose election was enough at risk that an independent expenditure by the College would potentially be of significant benefit for their race. In October, the PAC Board considered those recommendations and voted to support the expenditure of $100,000 each for IEs for Dr. Bera, a Democrat, and Dr. Benishek, a Republican. Both have been champions on issues such as repeal and replacement of the Sustainable Growth Rate (SGR), medical liability reform, and repeal of the 96-hour rule.
For Dr. Bera, the SurgeonsPAC dollars were utilized for a radio and direct mail campaign that was part of a larger effort in which other physician political action committees participated similarly. For Dr. Benishek, a television ad was produced and run through local cable providers.
On election night, Dr. Benishek was declared the winner, receiving 52.1% of the vote compared with his opponent’s 45.3%. As one of four fellows of the American College of Surgeons in Congress, we look forward to continuing to work with “Dr. Dan” and his excellent staff in his upcoming third term.
Dr. Bera’s race was much closer, as he actually trailed his opponent when election night closed with 49.8% of the vote. Subsequently, with the counting and inclusion of the mail-in ballots specifically targeted by the physician community’s IE effort, Dr. Bera overtook his opponent’s slim margin. Two weeks later, on 19 Nov. 2014, the Associated Press called the election for Dr. Bera, whose 1,400-vote lead at that time was felt to be substantial enough to preclude his opponent making up the difference with the remaining 4,300 provisional ballots that had yet to be counted. Dr. Bera’s CA-7 district race proved to be the most expensive in the nation with an estimated $19.6 million in total expenditures. Despite representing only 0.51% of that total, SurgeonsPAC’s contribution, in the collective with that of other physician organizations, no doubt played a significant role in returning a physician to Congress to continue to champion our causes.
In my opinion, these examples of careful candidate selection and subsequent support of Drs. Benishek and Bera exemplify the importance of a strong political action committee. The ultimate goal of SurgeonsPAC is the election to Congress and retention in Congress of those who support our policy positions and legislative agenda. Though SurgeonsPAC is one of nine physician PACs that can be accurately labeled as “million dollar” (per election cycle) PACs, our relative size and, thus, the number of candidates like Drs. Bera and Benishek we could support would be much greater if the Fellow participation rate more closely resembled that of our colleagues in other physician organizations. However, year after year, only 3%-4% of Fellows contribute, as compared with participation rates of 10%-25% in those physician PACs larger than SurgeonsPAC.
Recently, all Fellows received an e-mail from Dr. Andrew Warshaw, founding SurgeonsPAC Board Chairman and current President of the ACS, urging Fellows to make a $25 donation to SurgeonsPAC. Those wishing to learn more about the critical role SurgeonsPAC plays in our advocacy efforts can log on to www.surgeonspac.org.
Until next month...
Dr. Bailey is a pediatric surgeon and Medical Director, Advocacy for the Division of Advocacy and Health Policy in the ACS offices in Washington, DC.
