User login
Tips on tics
As an experienced clinician who has seen tics and habits in your patients come and go, you may be surprised by the amount of concern parents express about them. At times, it seems, and may be, that the parent’s attention to the habit actually keeps it going! This does not always mean that the child keeps doing the habit to aggravate the parent, as parental correction may amp up the child’s anxiety, which may make the habit worse.
As with other parent concerns, both empathizing with their worry and providing evidence-based information is helpful in relieving their distress.

Habits are complex behaviors done the same way repeatedly. Habits can have a strong protective effect on our lives and be a foundation for success when they ensure that we wash our hands (protection from infection), help us know where the keys are (efficiency), or soothe us to sleep (bedtime routines).
Tics are “involuntary” (meaning often, but not always, suppressible), brief, abrupt, repeated movements usually of the face, head, or neck. More complex, apparently meaningless movements may fall into the category of stereotypies. If they last more than 4 weeks, are driven, and cause marked dysfunction or significant self-injury, they may even qualify as stereotypic movement disorder.
It is good to know that repeated behaviors such as thumb sucking, nail/lip biting, hair twirling, body rocking, self biting, and head banging are relatively common in childhood, and often (but not mostly) disappear after age 4. I like to set the expectation that one habit or tic often evolves to another to reduce panic when this happens. Thumb and hand sucking at a younger developmental age may be replaced by body rocking and head banging, and later by nail biting and finger and foot tapping.
Even in college, habits are common and stress-related such as touching the face; playing with hair, pens, or jewelry; shaking a leg; tapping fingers; or scratching the head. Parents may connect some of these to acne or poor hygiene (a good opening for coaching!) but more importantly they may be accompanied by general distress, anxiety, obsessive-compulsive symptoms, and impulsive aggressive symptoms, which need to be looked for and addressed.
Stereotypies occur in about 20% of typically developing children (called “primary”) and are classified into:
• Common behaviors (such as, rocking, head banging, finger drumming, pencil tapping, hair twisting),
• Head nodding.
• Complex motor movements (such as hand and arm flapping/waving).
Habits – including nail biting, lip chewing, and nose picking – also may be diagnosed as stereotypic movement disorders, although ICD-10 lists includes them as “other specified behavioral and emotional disorders.”
For both conditions, the behavior must not be better accounted for by a compulsion, a tic disorder, part of autism, hair pulling (trichotillomania), or paroxysmal dyskinesias.
So what is the difference between motor stereotypies and tics (and why do you care)? Motor stereotypies begin before 3 years in more than 60%, whereas tics appear later (mean 5-7 years). Stereotypies are more fixed in their pattern, compared with tics that keep shifting form, disappearing, and reappearing. Stereotypies frequently involve the arms, hands, or the entire body, while tics involve the eyes, face, head, and shoulders. Stereotypies are more fixed, rhythmic, and prolonged (most more than 10 seconds) than tics, which are mostly brief, rapid, random, and fluctuating.
One key distinguishing factor is that tics have a premonitory urge and result in a sense of relief after the tic is performed. This also means that they can be suppressed to some extent when the situation requires. While both may occur more during anxiety, excitement, or fatigue, stereotypic movements, unlike tics, also are common when the child is engrossed.
Tics can occur as a side effect of medications such as stimulants and may decrease by lowering the dose, but tics also come and go, so the impact of a medication can be hard to sort out.
One vocal or multiple motor tics occurring many times per day starting before age 18 years and lasting more than 1 year are considered chronic; those occurring less than 1 year are transient. Chronic multiple motor tics accompanied by vocalizations, even sniffing or throat clearing, qualify as Tourette syndrome. The feared component of Tourette of coprolalia (saying bad words or gestures) is fortunately rare. These diagnoses can only be made after ruling out the effects of medication or another neurological condition such as Sydenham’s chorea (resulting from infection via group A beta-hemolytic streptococcus, the bacterium that causes rheumatic fever) or PANDAS (pediatric autoimmune neuropsychiatric disorders associated with streptococcal infections).
The importance of distinguishing tics from stereotypies is in the treatment options, differential diagnosis, and prognosis. Some families (and certainly the kids themselves) do not even notice that they are moving abnormally even though 25% have at least one family member with a similar behavior. But many parents are upset about the potential for teasing and stigmatization. When you ask them directly what they are afraid of, they often admit fearing an underlying diagnosis such as intellectual disability, autism, or Tourette syndrome. The first two are straightforward to rule in or out, but Tourette can be subtle. If parents don’t bring up the possibilities, it is worth telling them directly which underlying conditions can be ruled out.
There are many conditions comorbid with tics including attention-deficit/hyperactivity disorder (ADHD), obsessive compulsive disorder (OCD), learning disorder (LD), behavioral, developmental or social problems, and mood or anxiety disorders. This clearly means that a comprehensive evaluation looking specifically for these conditions is needed when a child has chronic tics. Typically developing children with complex arm or hand movements also are more likely to have ADHD (30%), LD (20%), obsessive-compulsive behaviors (10%), or tics (18%).
Tics and stereotypies may be annoying, but generally are not harmful or progressive, although repeated movements such as skin or nose picking may result in scars or infections, and severe head banging can lead to eye injuries. Frequently repeated motor acts can cause significant muscle pain and fatigue. The most common problems are probably injury to self-esteem or oppositional behavior as a result of repeated (and fruitless) nagging or punishment by parents, even if well-meaning.
Since they occur so often along with comorbid conditions, our job includes determining the most problematic aspect before advising on a treatment. Both tics and stereotypies may be reduced by distraction, but the effect on stereotypies is faster and more certain. You can make this intervention in the office by simply asking how the child can tell when they make the movement and have them plan out what they could do instead. An example might be to shift a hand flapping movement (that makes peers think of autism) into more acceptable fist clenching. Habit reversal training or differential reinforcement based on a functional analysis can be taught by psychologists when this simple suggestion is not effective. When tics are severe, teacher education and school accommodations (504 Plan with extended time, scribe, private location for tic breaks) may be needed.
Medication is not indicated for most tics because most are mild. If ADHD is present, tics may actually be reduced by stimulants or atomoxetine rather than worsened. If the tic is severe and habit reversal training has not been successful, alpha agonists such as clonidine or guanfacine, or typical or atypical neuroleptics may be helpful. Even baclofen, benzodiazepines, anticonvulsants, nicotine, and Botox have been used. These require consultation with a specialist.
As for other chronic medical conditions, tics and persisting stereotypies deserve a comprehensive approach, including repeated education of the parent and child, evaluation for comorbidity, school accommodations, building other strengths and social support, and only rarely pulling out your prescription pad.
Dr. Howard is an assistant professor of pediatrics at The Johns Hopkins University, Baltimore, and creator of CHADIS (www.CHADIS.com). She has no other relevant disclosures. Dr. Howard’s contribution to this publication was as a paid expert to Frontline. E-mail her at [email protected].
As an experienced clinician who has seen tics and habits in your patients come and go, you may be surprised by the amount of concern parents express about them. At times, it seems, and may be, that the parent’s attention to the habit actually keeps it going! This does not always mean that the child keeps doing the habit to aggravate the parent, as parental correction may amp up the child’s anxiety, which may make the habit worse.
As with other parent concerns, both empathizing with their worry and providing evidence-based information is helpful in relieving their distress.
Habits are complex behaviors done the same way repeatedly. Habits can have a strong protective effect on our lives and be a foundation for success when they ensure that we wash our hands (protection from infection), help us know where the keys are (efficiency), or soothe us to sleep (bedtime routines).
Tics are “involuntary” (meaning often, but not always, suppressible), brief, abrupt, repeated movements usually of the face, head, or neck. More complex, apparently meaningless movements may fall into the category of stereotypies. If they last more than 4 weeks, are driven, and cause marked dysfunction or significant self-injury, they may even qualify as stereotypic movement disorder.
It is good to know that repeated behaviors such as thumb sucking, nail/lip biting, hair twirling, body rocking, self biting, and head banging are relatively common in childhood, and often (but not mostly) disappear after age 4. I like to set the expectation that one habit or tic often evolves to another to reduce panic when this happens. Thumb and hand sucking at a younger developmental age may be replaced by body rocking and head banging, and later by nail biting and finger and foot tapping.
Even in college, habits are common and stress-related such as touching the face; playing with hair, pens, or jewelry; shaking a leg; tapping fingers; or scratching the head. Parents may connect some of these to acne or poor hygiene (a good opening for coaching!) but more importantly they may be accompanied by general distress, anxiety, obsessive-compulsive symptoms, and impulsive aggressive symptoms, which need to be looked for and addressed.
Stereotypies occur in about 20% of typically developing children (called “primary”) and are classified into:
• Common behaviors (such as, rocking, head banging, finger drumming, pencil tapping, hair twisting),
• Head nodding.
• Complex motor movements (such as hand and arm flapping/waving).
Habits – including nail biting, lip chewing, and nose picking – also may be diagnosed as stereotypic movement disorders, although ICD-10 lists includes them as “other specified behavioral and emotional disorders.”
For both conditions, the behavior must not be better accounted for by a compulsion, a tic disorder, part of autism, hair pulling (trichotillomania), or paroxysmal dyskinesias.
So what is the difference between motor stereotypies and tics (and why do you care)? Motor stereotypies begin before 3 years in more than 60%, whereas tics appear later (mean 5-7 years). Stereotypies are more fixed in their pattern, compared with tics that keep shifting form, disappearing, and reappearing. Stereotypies frequently involve the arms, hands, or the entire body, while tics involve the eyes, face, head, and shoulders. Stereotypies are more fixed, rhythmic, and prolonged (most more than 10 seconds) than tics, which are mostly brief, rapid, random, and fluctuating.
One key distinguishing factor is that tics have a premonitory urge and result in a sense of relief after the tic is performed. This also means that they can be suppressed to some extent when the situation requires. While both may occur more during anxiety, excitement, or fatigue, stereotypic movements, unlike tics, also are common when the child is engrossed.
Tics can occur as a side effect of medications such as stimulants and may decrease by lowering the dose, but tics also come and go, so the impact of a medication can be hard to sort out.
One vocal or multiple motor tics occurring many times per day starting before age 18 years and lasting more than 1 year are considered chronic; those occurring less than 1 year are transient. Chronic multiple motor tics accompanied by vocalizations, even sniffing or throat clearing, qualify as Tourette syndrome. The feared component of Tourette of coprolalia (saying bad words or gestures) is fortunately rare. These diagnoses can only be made after ruling out the effects of medication or another neurological condition such as Sydenham’s chorea (resulting from infection via group A beta-hemolytic streptococcus, the bacterium that causes rheumatic fever) or PANDAS (pediatric autoimmune neuropsychiatric disorders associated with streptococcal infections).
The importance of distinguishing tics from stereotypies is in the treatment options, differential diagnosis, and prognosis. Some families (and certainly the kids themselves) do not even notice that they are moving abnormally even though 25% have at least one family member with a similar behavior. But many parents are upset about the potential for teasing and stigmatization. When you ask them directly what they are afraid of, they often admit fearing an underlying diagnosis such as intellectual disability, autism, or Tourette syndrome. The first two are straightforward to rule in or out, but Tourette can be subtle. If parents don’t bring up the possibilities, it is worth telling them directly which underlying conditions can be ruled out.
There are many conditions comorbid with tics including attention-deficit/hyperactivity disorder (ADHD), obsessive compulsive disorder (OCD), learning disorder (LD), behavioral, developmental or social problems, and mood or anxiety disorders. This clearly means that a comprehensive evaluation looking specifically for these conditions is needed when a child has chronic tics. Typically developing children with complex arm or hand movements also are more likely to have ADHD (30%), LD (20%), obsessive-compulsive behaviors (10%), or tics (18%).
Tics and stereotypies may be annoying, but generally are not harmful or progressive, although repeated movements such as skin or nose picking may result in scars or infections, and severe head banging can lead to eye injuries. Frequently repeated motor acts can cause significant muscle pain and fatigue. The most common problems are probably injury to self-esteem or oppositional behavior as a result of repeated (and fruitless) nagging or punishment by parents, even if well-meaning.
Since they occur so often along with comorbid conditions, our job includes determining the most problematic aspect before advising on a treatment. Both tics and stereotypies may be reduced by distraction, but the effect on stereotypies is faster and more certain. You can make this intervention in the office by simply asking how the child can tell when they make the movement and have them plan out what they could do instead. An example might be to shift a hand flapping movement (that makes peers think of autism) into more acceptable fist clenching. Habit reversal training or differential reinforcement based on a functional analysis can be taught by psychologists when this simple suggestion is not effective. When tics are severe, teacher education and school accommodations (504 Plan with extended time, scribe, private location for tic breaks) may be needed.
Medication is not indicated for most tics because most are mild. If ADHD is present, tics may actually be reduced by stimulants or atomoxetine rather than worsened. If the tic is severe and habit reversal training has not been successful, alpha agonists such as clonidine or guanfacine, or typical or atypical neuroleptics may be helpful. Even baclofen, benzodiazepines, anticonvulsants, nicotine, and Botox have been used. These require consultation with a specialist.
As for other chronic medical conditions, tics and persisting stereotypies deserve a comprehensive approach, including repeated education of the parent and child, evaluation for comorbidity, school accommodations, building other strengths and social support, and only rarely pulling out your prescription pad.
Dr. Howard is an assistant professor of pediatrics at The Johns Hopkins University, Baltimore, and creator of CHADIS (www.CHADIS.com). She has no other relevant disclosures. Dr. Howard’s contribution to this publication was as a paid expert to Frontline. E-mail her at [email protected].
As an experienced clinician who has seen tics and habits in your patients come and go, you may be surprised by the amount of concern parents express about them. At times, it seems, and may be, that the parent’s attention to the habit actually keeps it going! This does not always mean that the child keeps doing the habit to aggravate the parent, as parental correction may amp up the child’s anxiety, which may make the habit worse.
As with other parent concerns, both empathizing with their worry and providing evidence-based information is helpful in relieving their distress.
Habits are complex behaviors done the same way repeatedly. Habits can have a strong protective effect on our lives and be a foundation for success when they ensure that we wash our hands (protection from infection), help us know where the keys are (efficiency), or soothe us to sleep (bedtime routines).
Tics are “involuntary” (meaning often, but not always, suppressible), brief, abrupt, repeated movements usually of the face, head, or neck. More complex, apparently meaningless movements may fall into the category of stereotypies. If they last more than 4 weeks, are driven, and cause marked dysfunction or significant self-injury, they may even qualify as stereotypic movement disorder.
It is good to know that repeated behaviors such as thumb sucking, nail/lip biting, hair twirling, body rocking, self biting, and head banging are relatively common in childhood, and often (but not mostly) disappear after age 4. I like to set the expectation that one habit or tic often evolves to another to reduce panic when this happens. Thumb and hand sucking at a younger developmental age may be replaced by body rocking and head banging, and later by nail biting and finger and foot tapping.
Even in college, habits are common and stress-related such as touching the face; playing with hair, pens, or jewelry; shaking a leg; tapping fingers; or scratching the head. Parents may connect some of these to acne or poor hygiene (a good opening for coaching!) but more importantly they may be accompanied by general distress, anxiety, obsessive-compulsive symptoms, and impulsive aggressive symptoms, which need to be looked for and addressed.
Stereotypies occur in about 20% of typically developing children (called “primary”) and are classified into:
• Common behaviors (such as, rocking, head banging, finger drumming, pencil tapping, hair twisting),
• Head nodding.
• Complex motor movements (such as hand and arm flapping/waving).
Habits – including nail biting, lip chewing, and nose picking – also may be diagnosed as stereotypic movement disorders, although ICD-10 lists includes them as “other specified behavioral and emotional disorders.”
For both conditions, the behavior must not be better accounted for by a compulsion, a tic disorder, part of autism, hair pulling (trichotillomania), or paroxysmal dyskinesias.
So what is the difference between motor stereotypies and tics (and why do you care)? Motor stereotypies begin before 3 years in more than 60%, whereas tics appear later (mean 5-7 years). Stereotypies are more fixed in their pattern, compared with tics that keep shifting form, disappearing, and reappearing. Stereotypies frequently involve the arms, hands, or the entire body, while tics involve the eyes, face, head, and shoulders. Stereotypies are more fixed, rhythmic, and prolonged (most more than 10 seconds) than tics, which are mostly brief, rapid, random, and fluctuating.
One key distinguishing factor is that tics have a premonitory urge and result in a sense of relief after the tic is performed. This also means that they can be suppressed to some extent when the situation requires. While both may occur more during anxiety, excitement, or fatigue, stereotypic movements, unlike tics, also are common when the child is engrossed.
Tics can occur as a side effect of medications such as stimulants and may decrease by lowering the dose, but tics also come and go, so the impact of a medication can be hard to sort out.
One vocal or multiple motor tics occurring many times per day starting before age 18 years and lasting more than 1 year are considered chronic; those occurring less than 1 year are transient. Chronic multiple motor tics accompanied by vocalizations, even sniffing or throat clearing, qualify as Tourette syndrome. The feared component of Tourette of coprolalia (saying bad words or gestures) is fortunately rare. These diagnoses can only be made after ruling out the effects of medication or another neurological condition such as Sydenham’s chorea (resulting from infection via group A beta-hemolytic streptococcus, the bacterium that causes rheumatic fever) or PANDAS (pediatric autoimmune neuropsychiatric disorders associated with streptococcal infections).
The importance of distinguishing tics from stereotypies is in the treatment options, differential diagnosis, and prognosis. Some families (and certainly the kids themselves) do not even notice that they are moving abnormally even though 25% have at least one family member with a similar behavior. But many parents are upset about the potential for teasing and stigmatization. When you ask them directly what they are afraid of, they often admit fearing an underlying diagnosis such as intellectual disability, autism, or Tourette syndrome. The first two are straightforward to rule in or out, but Tourette can be subtle. If parents don’t bring up the possibilities, it is worth telling them directly which underlying conditions can be ruled out.
There are many conditions comorbid with tics including attention-deficit/hyperactivity disorder (ADHD), obsessive compulsive disorder (OCD), learning disorder (LD), behavioral, developmental or social problems, and mood or anxiety disorders. This clearly means that a comprehensive evaluation looking specifically for these conditions is needed when a child has chronic tics. Typically developing children with complex arm or hand movements also are more likely to have ADHD (30%), LD (20%), obsessive-compulsive behaviors (10%), or tics (18%).
Tics and stereotypies may be annoying, but generally are not harmful or progressive, although repeated movements such as skin or nose picking may result in scars or infections, and severe head banging can lead to eye injuries. Frequently repeated motor acts can cause significant muscle pain and fatigue. The most common problems are probably injury to self-esteem or oppositional behavior as a result of repeated (and fruitless) nagging or punishment by parents, even if well-meaning.
Since they occur so often along with comorbid conditions, our job includes determining the most problematic aspect before advising on a treatment. Both tics and stereotypies may be reduced by distraction, but the effect on stereotypies is faster and more certain. You can make this intervention in the office by simply asking how the child can tell when they make the movement and have them plan out what they could do instead. An example might be to shift a hand flapping movement (that makes peers think of autism) into more acceptable fist clenching. Habit reversal training or differential reinforcement based on a functional analysis can be taught by psychologists when this simple suggestion is not effective. When tics are severe, teacher education and school accommodations (504 Plan with extended time, scribe, private location for tic breaks) may be needed.
Medication is not indicated for most tics because most are mild. If ADHD is present, tics may actually be reduced by stimulants or atomoxetine rather than worsened. If the tic is severe and habit reversal training has not been successful, alpha agonists such as clonidine or guanfacine, or typical or atypical neuroleptics may be helpful. Even baclofen, benzodiazepines, anticonvulsants, nicotine, and Botox have been used. These require consultation with a specialist.
As for other chronic medical conditions, tics and persisting stereotypies deserve a comprehensive approach, including repeated education of the parent and child, evaluation for comorbidity, school accommodations, building other strengths and social support, and only rarely pulling out your prescription pad.
Dr. Howard is an assistant professor of pediatrics at The Johns Hopkins University, Baltimore, and creator of CHADIS (www.CHADIS.com). She has no other relevant disclosures. Dr. Howard’s contribution to this publication was as a paid expert to Frontline. E-mail her at [email protected].

Solidarity II
In my last column, I wondered if the job satisfaction among American physicians had dipped so low that unionizing might have become a reasonable option. Much to my surprise when I opened the op-ed section of the Jan. 14, 2015, New York Times I discovered an article (Want to Be Happy? Join a Union) that added a bit of kindling to the spark I had hoped to ignite in my column.
Columnist John Guida interviewed two political scientists who had recently completed a study on labor union membership and life satisfaction in the United States (it appears to be unpublished at this point – but there is a link in the Times article to an October 2014 draft). Using data from a multiyear World Values Survey, these researchers discovered that union members are more satisfied than workers who were not in a union. This positive boost to life satisfaction was demonstrable across a broad selection of demographic groups: rich/poor, male/female, old/young, and disparate levels of education.
These political scientists found that being a union member generated a bigger boost of life satisfaction than that achieved by an increase in income. In an interview for the New York Times column, the authors postulated that the effect that they were observing could be occurring along four channels. One was a greater satisfaction in work experiences. The second was a feeling of greater job security. Do you think either of those benefits might sound appealing to some dissatisfied physicians? The other two were an increase in the number of opportunities for social intervention, and a positive feeling that can accompany participation in what they called democratic citizenship.
Although this study casts a warm glow over joining a union, unionization has an image problem here in the United States. Membership is down, and a study referred to in the Times article suggests that Americans have less confidence in unions than they do in banks.
As I suggested in my previous column, I sense that most physicians are not primarily troubled by their income. However, it is frustrating work environments and the lack of control or what these authors called “democratic citizenship” that is most frustrating. From a purely public relations standpoint, unionizing and going on strike for more money has the potential of creating a negative impression of the physicians who have organized. However, a work action with the aim of improving work conditions has a much more savory sound to it. And, as these political scientists have demonstrated, it is life satisfaction and not an increase in income that is the true benefit of unionization.
I have moved out of the workforce and am just sitting here on the sidelines watching with interest. But it seems to me that more of you who are still working should be looking outside the box for ways in which to improve your job (and life) satisfaction. If you are 50 years old and trying to calculate how many years it will be until you can retire, you have a problem. Unionization may be an answer. As the political scientists noted at the end of this column, their study “can give new meaning to the adage, ‘don’t mourn, organize.’ ”
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “Coping with a Picky Eater.” E-mail him at [email protected].
In my last column, I wondered if the job satisfaction among American physicians had dipped so low that unionizing might have become a reasonable option. Much to my surprise when I opened the op-ed section of the Jan. 14, 2015, New York Times I discovered an article (Want to Be Happy? Join a Union) that added a bit of kindling to the spark I had hoped to ignite in my column.
Columnist John Guida interviewed two political scientists who had recently completed a study on labor union membership and life satisfaction in the United States (it appears to be unpublished at this point – but there is a link in the Times article to an October 2014 draft). Using data from a multiyear World Values Survey, these researchers discovered that union members are more satisfied than workers who were not in a union. This positive boost to life satisfaction was demonstrable across a broad selection of demographic groups: rich/poor, male/female, old/young, and disparate levels of education.
These political scientists found that being a union member generated a bigger boost of life satisfaction than that achieved by an increase in income. In an interview for the New York Times column, the authors postulated that the effect that they were observing could be occurring along four channels. One was a greater satisfaction in work experiences. The second was a feeling of greater job security. Do you think either of those benefits might sound appealing to some dissatisfied physicians? The other two were an increase in the number of opportunities for social intervention, and a positive feeling that can accompany participation in what they called democratic citizenship.
Although this study casts a warm glow over joining a union, unionization has an image problem here in the United States. Membership is down, and a study referred to in the Times article suggests that Americans have less confidence in unions than they do in banks.
As I suggested in my previous column, I sense that most physicians are not primarily troubled by their income. However, it is frustrating work environments and the lack of control or what these authors called “democratic citizenship” that is most frustrating. From a purely public relations standpoint, unionizing and going on strike for more money has the potential of creating a negative impression of the physicians who have organized. However, a work action with the aim of improving work conditions has a much more savory sound to it. And, as these political scientists have demonstrated, it is life satisfaction and not an increase in income that is the true benefit of unionization.
I have moved out of the workforce and am just sitting here on the sidelines watching with interest. But it seems to me that more of you who are still working should be looking outside the box for ways in which to improve your job (and life) satisfaction. If you are 50 years old and trying to calculate how many years it will be until you can retire, you have a problem. Unionization may be an answer. As the political scientists noted at the end of this column, their study “can give new meaning to the adage, ‘don’t mourn, organize.’ ”
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “Coping with a Picky Eater.” E-mail him at [email protected].
In my last column, I wondered if the job satisfaction among American physicians had dipped so low that unionizing might have become a reasonable option. Much to my surprise when I opened the op-ed section of the Jan. 14, 2015, New York Times I discovered an article (Want to Be Happy? Join a Union) that added a bit of kindling to the spark I had hoped to ignite in my column.
Columnist John Guida interviewed two political scientists who had recently completed a study on labor union membership and life satisfaction in the United States (it appears to be unpublished at this point – but there is a link in the Times article to an October 2014 draft). Using data from a multiyear World Values Survey, these researchers discovered that union members are more satisfied than workers who were not in a union. This positive boost to life satisfaction was demonstrable across a broad selection of demographic groups: rich/poor, male/female, old/young, and disparate levels of education.
These political scientists found that being a union member generated a bigger boost of life satisfaction than that achieved by an increase in income. In an interview for the New York Times column, the authors postulated that the effect that they were observing could be occurring along four channels. One was a greater satisfaction in work experiences. The second was a feeling of greater job security. Do you think either of those benefits might sound appealing to some dissatisfied physicians? The other two were an increase in the number of opportunities for social intervention, and a positive feeling that can accompany participation in what they called democratic citizenship.
Although this study casts a warm glow over joining a union, unionization has an image problem here in the United States. Membership is down, and a study referred to in the Times article suggests that Americans have less confidence in unions than they do in banks.
As I suggested in my previous column, I sense that most physicians are not primarily troubled by their income. However, it is frustrating work environments and the lack of control or what these authors called “democratic citizenship” that is most frustrating. From a purely public relations standpoint, unionizing and going on strike for more money has the potential of creating a negative impression of the physicians who have organized. However, a work action with the aim of improving work conditions has a much more savory sound to it. And, as these political scientists have demonstrated, it is life satisfaction and not an increase in income that is the true benefit of unionization.
I have moved out of the workforce and am just sitting here on the sidelines watching with interest. But it seems to me that more of you who are still working should be looking outside the box for ways in which to improve your job (and life) satisfaction. If you are 50 years old and trying to calculate how many years it will be until you can retire, you have a problem. Unionization may be an answer. As the political scientists noted at the end of this column, their study “can give new meaning to the adage, ‘don’t mourn, organize.’ ”
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “Coping with a Picky Eater.” E-mail him at [email protected].

A generalist approach to fertility preservation
More than 500,000 women of reproductive age (20-49) are diagnosed with cancer each year. Fortunately, given advances in timely detection and effective therapy, more than 83% of these women will survive at least 5 years (SEER Cancer Statistics Review, 1975-2011). As a result, more women are concerned about their child-bearing potential after undergoing chemotherapy or radiation, and as reproductive technology advances, the issue of fertility preservation becomes even more salient.
Potential candidates for fertility preservation
The importance of considering fertility preservation for any reproductive-aged woman with a new cancer diagnosis cannot be overemphasized. This is especially true for women who may be receiving gonadotoxic therapies, such as alkylating agents or abdominal/pelvic radiation.

To assess the risk of various cancer treatments to fertility, patients and providers can access the Fertility Risk Tool at www.livestrong.org. The Fertility Risk Tool compiles known data about the risk of amenorrhea from specific cancers, chemotherapy agents, and radiation treatments, based on the woman’s age. The risk for infertility is likely higher than the stated incidence of amenorrhea, but the chart provides an initial counseling tool for health care providers and an overview for patients.
Discussions regarding fertility preservation are essential for any woman from menarche through mid-40s. However, as technological advances are rapidly occurring in reproductive medicine, options such as ovarian tissue cryopreservation are becoming available for prepubescent girls. Counseling these young patients with a new cancer diagnosis should not be overlooked.
Fertility preservation options
In vitro fertilization (IVF) with embryo banking is currently the most successful fertility preservation option and the standard of care. The process involves an IVF cycle, including monitored ovarian stimulation, transvaginal oocyte retrieval, fertilization of the oocytes, and cryopreservation of embryos.
The entire process takes a minimum of 12 days, and usually starts shortly after the onset of menses. The embryos can survive for years in liquid nitrogen and the survival rate of frozen embryos is greater than 95%. The pregnancy rate per embryo transfer cycle depends on the age of the woman when the embryos were created, with women under age 35 having higher live-birth rates compared with women older than 42 (live-birth rates 42.4% versus 17.8%, respectively, according to national summary data from the Society for Assisted Reproductive Technology).

Another option, which may be more attractive for women without a committed male partner, involves egg banking. This process also involves ovarian stimulation and egg retrieval, but fertilization is not performed. Instead the oocytes are cryopreserved, often by way of a vitrification technique shown to have a higher percentage of oocytes that survive the thaw (Fertil. Steril. 2011;96:277-85).
While the data regarding live birth after egg banking are limited, studies have shown reassuring birth outcomes for more than 900 babies from this technology (Reprod. Biomed. Online 2009;18:769-76).
Timing of treatment must be coordinated with the help of an oncologist. For example, many women with breast cancer opt to have their oncological surgery and undergo ovarian stimulation during the 4-6 week recovery period before initiating chemotherapy.
Ovarian tissue banking is considered experimental, but may be the only option available for women who must initiate treatment immediately, or for prepubescent girls. This technology involves surgical removal of part of an ovary, which is divided into small sections and frozen. The options for reproductive potential may include in vitro maturation of the immature oocytes in the strips of ovarian tissue with subsequent fertilization in the laboratory versus transplantation of the segments of ovarian tissue with the goal of some restoration of ovarian function (Hum. Reprod. 2014;29:1931-40).
Another option is the use of a gonadotropin-releasing hormone (GnRH) agonist during therapy to induce a prepubertal state, with the hypothetical goal to decrease damage to immature oocytes. A recent meta-analysis of randomized trials found that suppression with a GnRH agonist during chemotherapy significantly decreased premature ovarian failure in young women (Cancer Treat. Rev. 2014;40:675-83).
To date, the available literature does not address the effect of GnRH agonist use on rates of infertility in cancer survivors.
Special considerations for hormone sensitive cancers
Women with hormone sensitive cancers, such as breast cancer, often have understandable concerns about preserving their fertility and the impact that ovarian stimulation and future pregnancy may have on their prognosis.
For breast cancer patients, an effective adjuvant treatment during ovarian stimulation is an aromatase inhibitor, which lowers the peak estrogen levels compared to a standard ovarian stimulation cycle, with a similar oocyte yield (J. Clin. Endocrinol. Metab. 2006;91:3885-90).
There does not appear to be a difference in recurrence of breast cancer in women who pursued egg or embryo banking versus those who did not (J. Clin. Oncol. 2008;26:2630-5). Even after subsequent successful pregnancies, recurrence risk in hormone sensitive cancers, including breast cancer, is not increased (Cancer 2004;100:465-9). It is important to note that many women with breast cancer are placed on tamoxifen for many years. These women may consider a surrogate or a “tamoxifen break” after consultation with their oncologists.
When to refer
In any pediatric or reproductive-aged woman with a new cancer diagnosis, it is important to have a conversation exploring fertility options as soon as possible after the diagnosis is made. An early referral yields more options prior to initiating treatment and more time for the woman to discuss and consider all approaches to preserving her fertility.
Dr. Mersereau is an associate professor at the University of North Carolina at Chapel Hill, and director of UNC’s Fertility Preservation Program. Dr. Hoff is a clinical instructor and a fellow in reproductive endocrinology and infertility at UNC-Chapel Hill.
More than 500,000 women of reproductive age (20-49) are diagnosed with cancer each year. Fortunately, given advances in timely detection and effective therapy, more than 83% of these women will survive at least 5 years (SEER Cancer Statistics Review, 1975-2011). As a result, more women are concerned about their child-bearing potential after undergoing chemotherapy or radiation, and as reproductive technology advances, the issue of fertility preservation becomes even more salient.
Potential candidates for fertility preservation
The importance of considering fertility preservation for any reproductive-aged woman with a new cancer diagnosis cannot be overemphasized. This is especially true for women who may be receiving gonadotoxic therapies, such as alkylating agents or abdominal/pelvic radiation.
To assess the risk of various cancer treatments to fertility, patients and providers can access the Fertility Risk Tool at www.livestrong.org. The Fertility Risk Tool compiles known data about the risk of amenorrhea from specific cancers, chemotherapy agents, and radiation treatments, based on the woman’s age. The risk for infertility is likely higher than the stated incidence of amenorrhea, but the chart provides an initial counseling tool for health care providers and an overview for patients.
Discussions regarding fertility preservation are essential for any woman from menarche through mid-40s. However, as technological advances are rapidly occurring in reproductive medicine, options such as ovarian tissue cryopreservation are becoming available for prepubescent girls. Counseling these young patients with a new cancer diagnosis should not be overlooked.
Fertility preservation options
In vitro fertilization (IVF) with embryo banking is currently the most successful fertility preservation option and the standard of care. The process involves an IVF cycle, including monitored ovarian stimulation, transvaginal oocyte retrieval, fertilization of the oocytes, and cryopreservation of embryos.
The entire process takes a minimum of 12 days, and usually starts shortly after the onset of menses. The embryos can survive for years in liquid nitrogen and the survival rate of frozen embryos is greater than 95%. The pregnancy rate per embryo transfer cycle depends on the age of the woman when the embryos were created, with women under age 35 having higher live-birth rates compared with women older than 42 (live-birth rates 42.4% versus 17.8%, respectively, according to national summary data from the Society for Assisted Reproductive Technology).
Another option, which may be more attractive for women without a committed male partner, involves egg banking. This process also involves ovarian stimulation and egg retrieval, but fertilization is not performed. Instead the oocytes are cryopreserved, often by way of a vitrification technique shown to have a higher percentage of oocytes that survive the thaw (Fertil. Steril. 2011;96:277-85).
While the data regarding live birth after egg banking are limited, studies have shown reassuring birth outcomes for more than 900 babies from this technology (Reprod. Biomed. Online 2009;18:769-76).
Timing of treatment must be coordinated with the help of an oncologist. For example, many women with breast cancer opt to have their oncological surgery and undergo ovarian stimulation during the 4-6 week recovery period before initiating chemotherapy.
Ovarian tissue banking is considered experimental, but may be the only option available for women who must initiate treatment immediately, or for prepubescent girls. This technology involves surgical removal of part of an ovary, which is divided into small sections and frozen. The options for reproductive potential may include in vitro maturation of the immature oocytes in the strips of ovarian tissue with subsequent fertilization in the laboratory versus transplantation of the segments of ovarian tissue with the goal of some restoration of ovarian function (Hum. Reprod. 2014;29:1931-40).
Another option is the use of a gonadotropin-releasing hormone (GnRH) agonist during therapy to induce a prepubertal state, with the hypothetical goal to decrease damage to immature oocytes. A recent meta-analysis of randomized trials found that suppression with a GnRH agonist during chemotherapy significantly decreased premature ovarian failure in young women (Cancer Treat. Rev. 2014;40:675-83).
To date, the available literature does not address the effect of GnRH agonist use on rates of infertility in cancer survivors.
Special considerations for hormone sensitive cancers
Women with hormone sensitive cancers, such as breast cancer, often have understandable concerns about preserving their fertility and the impact that ovarian stimulation and future pregnancy may have on their prognosis.
For breast cancer patients, an effective adjuvant treatment during ovarian stimulation is an aromatase inhibitor, which lowers the peak estrogen levels compared to a standard ovarian stimulation cycle, with a similar oocyte yield (J. Clin. Endocrinol. Metab. 2006;91:3885-90).
There does not appear to be a difference in recurrence of breast cancer in women who pursued egg or embryo banking versus those who did not (J. Clin. Oncol. 2008;26:2630-5). Even after subsequent successful pregnancies, recurrence risk in hormone sensitive cancers, including breast cancer, is not increased (Cancer 2004;100:465-9). It is important to note that many women with breast cancer are placed on tamoxifen for many years. These women may consider a surrogate or a “tamoxifen break” after consultation with their oncologists.
When to refer
In any pediatric or reproductive-aged woman with a new cancer diagnosis, it is important to have a conversation exploring fertility options as soon as possible after the diagnosis is made. An early referral yields more options prior to initiating treatment and more time for the woman to discuss and consider all approaches to preserving her fertility.
Dr. Mersereau is an associate professor at the University of North Carolina at Chapel Hill, and director of UNC’s Fertility Preservation Program. Dr. Hoff is a clinical instructor and a fellow in reproductive endocrinology and infertility at UNC-Chapel Hill.
More than 500,000 women of reproductive age (20-49) are diagnosed with cancer each year. Fortunately, given advances in timely detection and effective therapy, more than 83% of these women will survive at least 5 years (SEER Cancer Statistics Review, 1975-2011). As a result, more women are concerned about their child-bearing potential after undergoing chemotherapy or radiation, and as reproductive technology advances, the issue of fertility preservation becomes even more salient.
Potential candidates for fertility preservation
The importance of considering fertility preservation for any reproductive-aged woman with a new cancer diagnosis cannot be overemphasized. This is especially true for women who may be receiving gonadotoxic therapies, such as alkylating agents or abdominal/pelvic radiation.
To assess the risk of various cancer treatments to fertility, patients and providers can access the Fertility Risk Tool at www.livestrong.org. The Fertility Risk Tool compiles known data about the risk of amenorrhea from specific cancers, chemotherapy agents, and radiation treatments, based on the woman’s age. The risk for infertility is likely higher than the stated incidence of amenorrhea, but the chart provides an initial counseling tool for health care providers and an overview for patients.
Discussions regarding fertility preservation are essential for any woman from menarche through mid-40s. However, as technological advances are rapidly occurring in reproductive medicine, options such as ovarian tissue cryopreservation are becoming available for prepubescent girls. Counseling these young patients with a new cancer diagnosis should not be overlooked.
Fertility preservation options
In vitro fertilization (IVF) with embryo banking is currently the most successful fertility preservation option and the standard of care. The process involves an IVF cycle, including monitored ovarian stimulation, transvaginal oocyte retrieval, fertilization of the oocytes, and cryopreservation of embryos.
The entire process takes a minimum of 12 days, and usually starts shortly after the onset of menses. The embryos can survive for years in liquid nitrogen and the survival rate of frozen embryos is greater than 95%. The pregnancy rate per embryo transfer cycle depends on the age of the woman when the embryos were created, with women under age 35 having higher live-birth rates compared with women older than 42 (live-birth rates 42.4% versus 17.8%, respectively, according to national summary data from the Society for Assisted Reproductive Technology).
Another option, which may be more attractive for women without a committed male partner, involves egg banking. This process also involves ovarian stimulation and egg retrieval, but fertilization is not performed. Instead the oocytes are cryopreserved, often by way of a vitrification technique shown to have a higher percentage of oocytes that survive the thaw (Fertil. Steril. 2011;96:277-85).
While the data regarding live birth after egg banking are limited, studies have shown reassuring birth outcomes for more than 900 babies from this technology (Reprod. Biomed. Online 2009;18:769-76).
Timing of treatment must be coordinated with the help of an oncologist. For example, many women with breast cancer opt to have their oncological surgery and undergo ovarian stimulation during the 4-6 week recovery period before initiating chemotherapy.
Ovarian tissue banking is considered experimental, but may be the only option available for women who must initiate treatment immediately, or for prepubescent girls. This technology involves surgical removal of part of an ovary, which is divided into small sections and frozen. The options for reproductive potential may include in vitro maturation of the immature oocytes in the strips of ovarian tissue with subsequent fertilization in the laboratory versus transplantation of the segments of ovarian tissue with the goal of some restoration of ovarian function (Hum. Reprod. 2014;29:1931-40).
Another option is the use of a gonadotropin-releasing hormone (GnRH) agonist during therapy to induce a prepubertal state, with the hypothetical goal to decrease damage to immature oocytes. A recent meta-analysis of randomized trials found that suppression with a GnRH agonist during chemotherapy significantly decreased premature ovarian failure in young women (Cancer Treat. Rev. 2014;40:675-83).
To date, the available literature does not address the effect of GnRH agonist use on rates of infertility in cancer survivors.
Special considerations for hormone sensitive cancers
Women with hormone sensitive cancers, such as breast cancer, often have understandable concerns about preserving their fertility and the impact that ovarian stimulation and future pregnancy may have on their prognosis.
For breast cancer patients, an effective adjuvant treatment during ovarian stimulation is an aromatase inhibitor, which lowers the peak estrogen levels compared to a standard ovarian stimulation cycle, with a similar oocyte yield (J. Clin. Endocrinol. Metab. 2006;91:3885-90).
There does not appear to be a difference in recurrence of breast cancer in women who pursued egg or embryo banking versus those who did not (J. Clin. Oncol. 2008;26:2630-5). Even after subsequent successful pregnancies, recurrence risk in hormone sensitive cancers, including breast cancer, is not increased (Cancer 2004;100:465-9). It is important to note that many women with breast cancer are placed on tamoxifen for many years. These women may consider a surrogate or a “tamoxifen break” after consultation with their oncologists.
When to refer
In any pediatric or reproductive-aged woman with a new cancer diagnosis, it is important to have a conversation exploring fertility options as soon as possible after the diagnosis is made. An early referral yields more options prior to initiating treatment and more time for the woman to discuss and consider all approaches to preserving her fertility.
Dr. Mersereau is an associate professor at the University of North Carolina at Chapel Hill, and director of UNC’s Fertility Preservation Program. Dr. Hoff is a clinical instructor and a fellow in reproductive endocrinology and infertility at UNC-Chapel Hill.

Doctors are easy targets for threats and attacks
Buried under news of the terrible Charlie Hebdo terrorism murders was another serious attack. A doctor was shot and killed by an angry patient at a Texas VA hospital, who then took his own life.
I’m not trying to belittle the tragedy in Paris, but instead point out that medicine can be more hazardous than many realize.
We don’t intentionally try to offend, but in a field like this, it’s impossible to please everyone. People get upset that I can’t cure them or find a cause for their (medically unexplainable) symptoms, or won’t give them as many narcotics as they want. The unhappy ones never come back, or post an angry review on Yelp, or send a nasty letter, or some combination of the above.

But, occasionally, we get threats. They’re rare in an office practice, though I suspect surprisingly common in emergency department work. Most are empty threats to sue, but occasionally my staff and I get threatened with physical harm. While most are simply words, there’s really no easy way of knowing who will or won’t actually snap and carry them out.
We live in a society where guns are common, easily obtained, and affordable. So anyone might have one. Unless your office has a metal detector or does pat downs, you’re at risk (at least hypothetically). Putting up a sign that says “no guns allowed” isn’t going to stop anyone. Neither do laws to protect health professionals. Those who have decided to harm others don’t worry about such things.
For that matter, I have several patients who usually have a gun on them. Sometimes concealed, sometimes obvious. Does it bother me? Not at all. They’re all polite and pleasant, and I understand their reason for keeping one on hand.
But doctors, unfortunately, are easy targets for the irrational and armed. The shooting in El Paso occurred in a government hospital with armed security, and that certainly didn’t make a difference. We generally keep predictable hours, park in the same spaces, and our offices aren’t locked up. We do a job where trust is assumed, because people are coming to us for help and we’re here for their benefit.
Is there an answer? I know doctors who keep a handgun under their coats, or in their desks. In a perfect world, they wouldn’t need it, but our world is far from it. Being a doctor, whether you’re on the front line in the emergency department or hidden in a nameless medical plaza, can still be a dangerous business.
Medicine is a surprising field to think of as a hazardous one, but these days, sadly, it is.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.
Buried under news of the terrible Charlie Hebdo terrorism murders was another serious attack. A doctor was shot and killed by an angry patient at a Texas VA hospital, who then took his own life.
I’m not trying to belittle the tragedy in Paris, but instead point out that medicine can be more hazardous than many realize.
We don’t intentionally try to offend, but in a field like this, it’s impossible to please everyone. People get upset that I can’t cure them or find a cause for their (medically unexplainable) symptoms, or won’t give them as many narcotics as they want. The unhappy ones never come back, or post an angry review on Yelp, or send a nasty letter, or some combination of the above.
But, occasionally, we get threats. They’re rare in an office practice, though I suspect surprisingly common in emergency department work. Most are empty threats to sue, but occasionally my staff and I get threatened with physical harm. While most are simply words, there’s really no easy way of knowing who will or won’t actually snap and carry them out.
We live in a society where guns are common, easily obtained, and affordable. So anyone might have one. Unless your office has a metal detector or does pat downs, you’re at risk (at least hypothetically). Putting up a sign that says “no guns allowed” isn’t going to stop anyone. Neither do laws to protect health professionals. Those who have decided to harm others don’t worry about such things.
For that matter, I have several patients who usually have a gun on them. Sometimes concealed, sometimes obvious. Does it bother me? Not at all. They’re all polite and pleasant, and I understand their reason for keeping one on hand.
But doctors, unfortunately, are easy targets for the irrational and armed. The shooting in El Paso occurred in a government hospital with armed security, and that certainly didn’t make a difference. We generally keep predictable hours, park in the same spaces, and our offices aren’t locked up. We do a job where trust is assumed, because people are coming to us for help and we’re here for their benefit.
Is there an answer? I know doctors who keep a handgun under their coats, or in their desks. In a perfect world, they wouldn’t need it, but our world is far from it. Being a doctor, whether you’re on the front line in the emergency department or hidden in a nameless medical plaza, can still be a dangerous business.
Medicine is a surprising field to think of as a hazardous one, but these days, sadly, it is.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.
Buried under news of the terrible Charlie Hebdo terrorism murders was another serious attack. A doctor was shot and killed by an angry patient at a Texas VA hospital, who then took his own life.
I’m not trying to belittle the tragedy in Paris, but instead point out that medicine can be more hazardous than many realize.
We don’t intentionally try to offend, but in a field like this, it’s impossible to please everyone. People get upset that I can’t cure them or find a cause for their (medically unexplainable) symptoms, or won’t give them as many narcotics as they want. The unhappy ones never come back, or post an angry review on Yelp, or send a nasty letter, or some combination of the above.
But, occasionally, we get threats. They’re rare in an office practice, though I suspect surprisingly common in emergency department work. Most are empty threats to sue, but occasionally my staff and I get threatened with physical harm. While most are simply words, there’s really no easy way of knowing who will or won’t actually snap and carry them out.
We live in a society where guns are common, easily obtained, and affordable. So anyone might have one. Unless your office has a metal detector or does pat downs, you’re at risk (at least hypothetically). Putting up a sign that says “no guns allowed” isn’t going to stop anyone. Neither do laws to protect health professionals. Those who have decided to harm others don’t worry about such things.
For that matter, I have several patients who usually have a gun on them. Sometimes concealed, sometimes obvious. Does it bother me? Not at all. They’re all polite and pleasant, and I understand their reason for keeping one on hand.
But doctors, unfortunately, are easy targets for the irrational and armed. The shooting in El Paso occurred in a government hospital with armed security, and that certainly didn’t make a difference. We generally keep predictable hours, park in the same spaces, and our offices aren’t locked up. We do a job where trust is assumed, because people are coming to us for help and we’re here for their benefit.
Is there an answer? I know doctors who keep a handgun under their coats, or in their desks. In a perfect world, they wouldn’t need it, but our world is far from it. Being a doctor, whether you’re on the front line in the emergency department or hidden in a nameless medical plaza, can still be a dangerous business.
Medicine is a surprising field to think of as a hazardous one, but these days, sadly, it is.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.

Reviewing 'Everyone’s a Critic'
Although I’m an avid reader, I don’t often review books. Yet, I recently read Bill Tancer’s latest book, “Everyone’s a Critic: Winning Customers in a Review Driven World,” and thought I needed to share it with you. Unlike many books about online reviews, Mr. Tancer dives deeply into this world, providing insightful and substantiated, real life examples that appeal to business owners, marketers, and consumers.
As physicians, we know only too well the importance of online reviews. Yet, online reviews affect all business owners. Some research has been conducted into the importance of online reviews (no doubt, with more to come), and many best practices have been developed to aid business owners who receive negative online reviews. Mr. Tancer draws on this research as well as his own to effectively dissect this “critic economy” we live in and offers practical advice on how to navigate these often murky and sometimes dangerous waters.
We live in a consumer-centric world that has been created in large part by online reviews. (Thanks, Amazon.) We know that 80% of consumers now consult online reviews before making a purchase. The same is true for selecting a new physician. A 2013 Industry View Report by Software Advice found that 62% of respondents said they read online reviews when seeking a new doctor. The most trusted site was Yelp.
If you don’t have time to read the book, here are four compelling takeaways that will help you in your quest to manage your online reputation:
• Many physicians feel they are being unfairly targeted in online reviews. They’re not. They just fall into the same behavioral trap that other conscientious business owners do. They think, I’m a good doctor providing high-quality care to my patients, so those patients posting negative reviews must be wrong. Turns out that restaurant, salon, and retail owners feel the same way. In fact, Mr. Tancer cited a compelling study from That’s Biz, a restaurant marketing firm, that shows 31% of restaurant owners feel that reviews on sites like Yelp, TripAdvisor, and Google are either “mostly inaccurate” or “not accurate at all,” while only 5% believe they are “very accurate” and 24% believe they are “mostly accurate.” We physicians are not alone. Many dermatologists, especially those whose practice is composed largely of cosmetic and elective services, need to understand that consumers view these practices as they do other consumer services, rather than as medicine.
• Mr. Tancer clearly and succinctly demystifies Yelp. We have all heard of business owners who accuse Yelp of unethical behavior at best and extortion at worst. Mr. Tancer cites several case studies, all of which end positively for Yelp. The bottom line: Freedom of speech on the consumer’s part wins virtually every time. To date, Yelp has not lost a legal challenge. I agree with many of Mr. Tancer’s tips that are relevant to physicians: Never incentivize consumers/patients for positive reviews. Decline offers from “freelance reviewers” who will write fake positive reviews on your site or fake negative reviews on competitors’ sites. Don’t ask patients to sign an online review gag order. Basically, it will just get you into more trouble. His advice for the best defense is a good offense, that is, to create as much positive content online about you and your practice as possible.
• Based upon research, Mr. Tancer defines four key online reviewer personalities (or in your case, patients) that help you as business owners gain a deeper understanding of why people post online reviews.
1. The Communitarian is the most predominant type of reviewer and one of the most important groups for businesses to reach because they’re motivated to build strong social connections and to be helpful to their community
2. The Benevolent Reviewer feels that the online review rewards businesses for exceptional service. They’re typically less prolific.
3. The Status Seeker is competitive and seeks status symbols such as becoming an “Elite Yelper.” Along with Communitarians, they tend to post unbiased reviews in their quest to rack up votes for the “most useful” reviews.
4. The One-Star Assassin, as the name suggests, uses online review sites to express grievances and attack businesses.
• Mr. Tancer encourages business owners to use negative online reviews as “data,” to be analyzed to improve their practice and ultimately their online reputation. You, your office manager, and your staff should regularly devote time to analyze your online reviews. Most important, take note of recurring criticisms, which will most likely be service related (long wait times, untidy office, abrasive bedside manner), and implement policies to change behaviors and services.
One thing I know for sure is that online ratings will continue to be an increasingly important player in how patients select health care providers and evaluate care delivered. The more we educate ourselves about the online world, the better care and service we will be able to deliver to our patients.
Dr. Benabio is a partner physician in the department of dermatology of the Southern California Permanente Group in San Diego, and volunteer clinical assistant professor at the University of California, San Diego. Dr. Benabio is @dermdoc on Twitter.
Although I’m an avid reader, I don’t often review books. Yet, I recently read Bill Tancer’s latest book, “Everyone’s a Critic: Winning Customers in a Review Driven World,” and thought I needed to share it with you. Unlike many books about online reviews, Mr. Tancer dives deeply into this world, providing insightful and substantiated, real life examples that appeal to business owners, marketers, and consumers.
As physicians, we know only too well the importance of online reviews. Yet, online reviews affect all business owners. Some research has been conducted into the importance of online reviews (no doubt, with more to come), and many best practices have been developed to aid business owners who receive negative online reviews. Mr. Tancer draws on this research as well as his own to effectively dissect this “critic economy” we live in and offers practical advice on how to navigate these often murky and sometimes dangerous waters.
We live in a consumer-centric world that has been created in large part by online reviews. (Thanks, Amazon.) We know that 80% of consumers now consult online reviews before making a purchase. The same is true for selecting a new physician. A 2013 Industry View Report by Software Advice found that 62% of respondents said they read online reviews when seeking a new doctor. The most trusted site was Yelp.
If you don’t have time to read the book, here are four compelling takeaways that will help you in your quest to manage your online reputation:
• Many physicians feel they are being unfairly targeted in online reviews. They’re not. They just fall into the same behavioral trap that other conscientious business owners do. They think, I’m a good doctor providing high-quality care to my patients, so those patients posting negative reviews must be wrong. Turns out that restaurant, salon, and retail owners feel the same way. In fact, Mr. Tancer cited a compelling study from That’s Biz, a restaurant marketing firm, that shows 31% of restaurant owners feel that reviews on sites like Yelp, TripAdvisor, and Google are either “mostly inaccurate” or “not accurate at all,” while only 5% believe they are “very accurate” and 24% believe they are “mostly accurate.” We physicians are not alone. Many dermatologists, especially those whose practice is composed largely of cosmetic and elective services, need to understand that consumers view these practices as they do other consumer services, rather than as medicine.
• Mr. Tancer clearly and succinctly demystifies Yelp. We have all heard of business owners who accuse Yelp of unethical behavior at best and extortion at worst. Mr. Tancer cites several case studies, all of which end positively for Yelp. The bottom line: Freedom of speech on the consumer’s part wins virtually every time. To date, Yelp has not lost a legal challenge. I agree with many of Mr. Tancer’s tips that are relevant to physicians: Never incentivize consumers/patients for positive reviews. Decline offers from “freelance reviewers” who will write fake positive reviews on your site or fake negative reviews on competitors’ sites. Don’t ask patients to sign an online review gag order. Basically, it will just get you into more trouble. His advice for the best defense is a good offense, that is, to create as much positive content online about you and your practice as possible.
• Based upon research, Mr. Tancer defines four key online reviewer personalities (or in your case, patients) that help you as business owners gain a deeper understanding of why people post online reviews.
1. The Communitarian is the most predominant type of reviewer and one of the most important groups for businesses to reach because they’re motivated to build strong social connections and to be helpful to their community
2. The Benevolent Reviewer feels that the online review rewards businesses for exceptional service. They’re typically less prolific.
3. The Status Seeker is competitive and seeks status symbols such as becoming an “Elite Yelper.” Along with Communitarians, they tend to post unbiased reviews in their quest to rack up votes for the “most useful” reviews.
4. The One-Star Assassin, as the name suggests, uses online review sites to express grievances and attack businesses.
• Mr. Tancer encourages business owners to use negative online reviews as “data,” to be analyzed to improve their practice and ultimately their online reputation. You, your office manager, and your staff should regularly devote time to analyze your online reviews. Most important, take note of recurring criticisms, which will most likely be service related (long wait times, untidy office, abrasive bedside manner), and implement policies to change behaviors and services.
One thing I know for sure is that online ratings will continue to be an increasingly important player in how patients select health care providers and evaluate care delivered. The more we educate ourselves about the online world, the better care and service we will be able to deliver to our patients.
Dr. Benabio is a partner physician in the department of dermatology of the Southern California Permanente Group in San Diego, and volunteer clinical assistant professor at the University of California, San Diego. Dr. Benabio is @dermdoc on Twitter.
Although I’m an avid reader, I don’t often review books. Yet, I recently read Bill Tancer’s latest book, “Everyone’s a Critic: Winning Customers in a Review Driven World,” and thought I needed to share it with you. Unlike many books about online reviews, Mr. Tancer dives deeply into this world, providing insightful and substantiated, real life examples that appeal to business owners, marketers, and consumers.
As physicians, we know only too well the importance of online reviews. Yet, online reviews affect all business owners. Some research has been conducted into the importance of online reviews (no doubt, with more to come), and many best practices have been developed to aid business owners who receive negative online reviews. Mr. Tancer draws on this research as well as his own to effectively dissect this “critic economy” we live in and offers practical advice on how to navigate these often murky and sometimes dangerous waters.
We live in a consumer-centric world that has been created in large part by online reviews. (Thanks, Amazon.) We know that 80% of consumers now consult online reviews before making a purchase. The same is true for selecting a new physician. A 2013 Industry View Report by Software Advice found that 62% of respondents said they read online reviews when seeking a new doctor. The most trusted site was Yelp.
If you don’t have time to read the book, here are four compelling takeaways that will help you in your quest to manage your online reputation:
• Many physicians feel they are being unfairly targeted in online reviews. They’re not. They just fall into the same behavioral trap that other conscientious business owners do. They think, I’m a good doctor providing high-quality care to my patients, so those patients posting negative reviews must be wrong. Turns out that restaurant, salon, and retail owners feel the same way. In fact, Mr. Tancer cited a compelling study from That’s Biz, a restaurant marketing firm, that shows 31% of restaurant owners feel that reviews on sites like Yelp, TripAdvisor, and Google are either “mostly inaccurate” or “not accurate at all,” while only 5% believe they are “very accurate” and 24% believe they are “mostly accurate.” We physicians are not alone. Many dermatologists, especially those whose practice is composed largely of cosmetic and elective services, need to understand that consumers view these practices as they do other consumer services, rather than as medicine.
• Mr. Tancer clearly and succinctly demystifies Yelp. We have all heard of business owners who accuse Yelp of unethical behavior at best and extortion at worst. Mr. Tancer cites several case studies, all of which end positively for Yelp. The bottom line: Freedom of speech on the consumer’s part wins virtually every time. To date, Yelp has not lost a legal challenge. I agree with many of Mr. Tancer’s tips that are relevant to physicians: Never incentivize consumers/patients for positive reviews. Decline offers from “freelance reviewers” who will write fake positive reviews on your site or fake negative reviews on competitors’ sites. Don’t ask patients to sign an online review gag order. Basically, it will just get you into more trouble. His advice for the best defense is a good offense, that is, to create as much positive content online about you and your practice as possible.
• Based upon research, Mr. Tancer defines four key online reviewer personalities (or in your case, patients) that help you as business owners gain a deeper understanding of why people post online reviews.
1. The Communitarian is the most predominant type of reviewer and one of the most important groups for businesses to reach because they’re motivated to build strong social connections and to be helpful to their community
2. The Benevolent Reviewer feels that the online review rewards businesses for exceptional service. They’re typically less prolific.
3. The Status Seeker is competitive and seeks status symbols such as becoming an “Elite Yelper.” Along with Communitarians, they tend to post unbiased reviews in their quest to rack up votes for the “most useful” reviews.
4. The One-Star Assassin, as the name suggests, uses online review sites to express grievances and attack businesses.
• Mr. Tancer encourages business owners to use negative online reviews as “data,” to be analyzed to improve their practice and ultimately their online reputation. You, your office manager, and your staff should regularly devote time to analyze your online reviews. Most important, take note of recurring criticisms, which will most likely be service related (long wait times, untidy office, abrasive bedside manner), and implement policies to change behaviors and services.
One thing I know for sure is that online ratings will continue to be an increasingly important player in how patients select health care providers and evaluate care delivered. The more we educate ourselves about the online world, the better care and service we will be able to deliver to our patients.
Dr. Benabio is a partner physician in the department of dermatology of the Southern California Permanente Group in San Diego, and volunteer clinical assistant professor at the University of California, San Diego. Dr. Benabio is @dermdoc on Twitter.

Mango
Mangifera indica (mango) is a member of the Anacardiaceae family with a tradition of use as a medicinal plant. Mango extracts have been characterized as exhibiting antioxidant, anti-inflammatory, analgesic, and immunomodulatory activities (Photodermatol. Photoimmunol. Photomed. 2013;29:84-9; Drug Chem. Toxicol. 2009;32:53-8). Mango is grown in more than 100 countries, primarily in Asia, in tropical as well as subtropical regions (Molecules 2014;19:17107-29). Mango stem bark and leaves have been used in traditional medicine to treat anemia, cutaneous infections, diabetes, diarrhea, scabies, syphilis, and malignant tumors (Pharmacol. Res. 2007;55:351-8). Polyphenols and carotenoids are among the phytonutrients identified as responsible for the biologic activity of mango (Photodermatol. Photoimmunol. Photomed. 2013;29:84-9).

Various biologic activities and traditional uses
Ojewole investigated the anti-inflammatory, analgesic, and antidiabetic activity of M. indica stem bark aqueous extract in rats and mice in 2005. In mice, mango extract dose-dependently delivered significant analgesic effects against thermally and chemically-generated pain. The investigators attributed the observed salutary effects of the plant to its constituent polyphenolics, flavonoids, triterpenoids, and mangiferin. They also noted that their findings support the folkloric uses of the plant for treating arthritic and other inflammatory conditions, as well as type 2 diabetes (Methods Find. Exp. Clin. Pharmacol. 2005;27:547-54).
Another important constituent of mango (also found in olive, strawberry, fig, and various medicinal herbs) is the triterpene lupeol, which has been characterized as exhibiting potent antioxidant, antimutagenic, anti-inflammatory, and antiarthritic activity (Oncogene 2004;23:5203-14). A 2014 study by Sahu et al. also showed that M. indica leaves display some antityrosinase activity, though not as strongly as other medicinal plants, such as Emblica officinalis (Pak. J. Biol. Sci. 2014;17:146-50).
Anticancer, antioxidant, and antiphotoaging activity
In 2004, Saleem et al. demonstrated that topically applied lupeol exhibited anti–tumor-promoting effects in a CD-1 mouse skin tumorigenesis model. Pretreatment with the mango constituent time- and dose-dependently inhibited multiple 12-O-tetradecanoyl-phorbol-13-acetate (TPA)-mediated increases in edema, hyperplasia, epidermal ornithine decarboxylase (ODC) activity, as well as protein expression of ODC, cyclooxygenase 2 (COX-2) and nitric oxide synthase. Pretreated animals also experienced significantly lower tumor incidence and tumor body burden as well as a significant delay in tumor latency period. The researchers concluded that lupeol exerts anti–skin tumor promoting effects on CD-1 mice (Oncogene 2004;23:5203-14).
Three years later, Núñez-Sellés et al. reported that a mango stem bark extract (Vimang) developed in Cuba exhibited antioxidant, analgesic, anti-inflammatory, and immunomodulating activity in basic, preclinical, and clinical studies (Pharmacol. Res. 2007;55:351-8).
A 2009 toxicological analysis of Vimang, which has been formulated into tablets, creams, capsules, syrup, vaginal oval, and suppositories for various applications, revealed via irritant tests conducted on rabbits that the topical formulation was not irritating to the skin, generally, with minimal irritancy noted after vaginal application. No adverse effects were reported (Drug Chem. Toxicol. 2009;32:53-8).
In 2012, Li et al. discovered norathyriol (1,3,6,7-tetrahydroxy-9H-xanthen-9-one), a plant-derived chemopreventive metabolite of mangiferin, found in mango, Hypericum elegans, and Tripterospermum lanceolatum. They found that norathyriol significantly inhibited solar UV-induced skin carcinogenesis in mouse models. In vitro investigations revealed that the compound suppressed cell growth in mouse skin epidermal JB6 P+ cells at the level of G2-M phase arrest. The investigators concluded that this newly identified substance appears to act as a safe chemopreventive agent against UV-induced skin cancer (Cancer Res. 2012;72:260-70).
A year later, Song et al. assessed the protective effects of orally administered mango extract against UVB-induced cutaneous aging in HR-1 hairless male mice. The animals were divided into control, UVB-treated vehicle, and UVB-treated mango extract groups. The researchers found that mango extract significantly suppressed the increase in epidermal thickness and hypertrophy indicative of UVB treatment, with mean length of wrinkles significantly lower in the mango group compared with the UVB-treated vehicle group. Treatment with mango extract also led to a significant increase in collagen bundles in animals treated with UVB. The authors concluded that mango extract displayed antiphotoaging properties in hairless mice exposed to UVB (Photodermatol. Photoimmunol. Photomed. 2013;29:84-9).
Further, a 2014 in vitro study revealed that extracts of Helicanthus elastica growing on M. indica exhibited antioxidant activity. H. elastica is a hemiparasite that often grows on mango trees in India and is known to be a rich source of phenolic substances (J. Tradit. Complement. Med. 2014;4:285-8).
Topical delivery
Mandawgade and Patravale developed a mango butter skin care formulation in 2008 that was used to test skin repair in rat excision and incision wound models. A healing response was noted in both animal models. The formulation also was found to be effective in achieving complete repair of worn and cracked skin on the feet of all human volunteers in the study. The investigators concluded that the mango butter preparation delivers superlative emolliency and warrants consideration as an excipient agent in cosmeceutical products (Indian J. Pharm. Sci. 2008;70:539-42).
It is worth noting that cases of “mango dermatitis” (allergic contact dermatitis to the sap or skin of M. indica), manifesting in urticaria and eczematous rashes, have been reported (Australas. J. Dermatol. 1996;37:59-60; Int. J. Dermatol. 2004;43:195-6).
In 2014, Leanpolchareanchai et al. developed a microemulsion system containing Thai mango seed kernel extract that displayed strong skin enhancement results in ex vivo skin permeation studies (penetrating skin layers up to 60-fold higher than controls) and physicochemical stability over 6 months (Drug Chem. Toxicol. 2009;32:53-8). Thai mango seed kernel extract had previously been shown to exhibit anti–methicillin-resistant Staphylococcus aureus and antityrosinase characteristics, as well as strong free radical scavenging, antioxidant, anti-inflammatory, and hepatoprotective activities.(Molecules 2014;19:17107-29).
Conclusion
Evidence on the cutaneous applications of mango is emerging, but does not have a significant track record. That said, this fruit has long been used in traditional medicine for a range of indications, including skin disorders. Much more research is necessary, however, to ascertain how beneficial this fruit and its extracts may be. At the very least, there are few reports of adverse events associated with topical application.
Dr. Baumann is chief executive officer of the Baumann Cosmetic & Research Institute in the Design District in Miami. She founded the Cosmetic Dermatology Center at the University of Miami in 1997. Dr. Baumann wrote the textbook “Cosmetic Dermatology: Principles and Practice” (New York: McGraw-Hill, 2002), and a book for consumers, “The Skin Type Solution” (New York: Bantam Dell, 2006). She has contributed to the Cosmeceutical Critique column in Dermatology News since January 2001. Her latest book, “Cosmeceuticals and Cosmetic Ingredients,” was published in November 2014. Dr. Baumann has received funding for clinical grants from Allergan, Aveeno, Avon Products, Evolus, Galderma, GlaxoSmithKline, Kythera, Mary Kay, Medicis Pharmaceuticals, Neutrogena, Philosophy, Topix Pharmaceuticals, and Unilever.
Mangifera indica (mango) is a member of the Anacardiaceae family with a tradition of use as a medicinal plant. Mango extracts have been characterized as exhibiting antioxidant, anti-inflammatory, analgesic, and immunomodulatory activities (Photodermatol. Photoimmunol. Photomed. 2013;29:84-9; Drug Chem. Toxicol. 2009;32:53-8). Mango is grown in more than 100 countries, primarily in Asia, in tropical as well as subtropical regions (Molecules 2014;19:17107-29). Mango stem bark and leaves have been used in traditional medicine to treat anemia, cutaneous infections, diabetes, diarrhea, scabies, syphilis, and malignant tumors (Pharmacol. Res. 2007;55:351-8). Polyphenols and carotenoids are among the phytonutrients identified as responsible for the biologic activity of mango (Photodermatol. Photoimmunol. Photomed. 2013;29:84-9).
Various biologic activities and traditional uses
Ojewole investigated the anti-inflammatory, analgesic, and antidiabetic activity of M. indica stem bark aqueous extract in rats and mice in 2005. In mice, mango extract dose-dependently delivered significant analgesic effects against thermally and chemically-generated pain. The investigators attributed the observed salutary effects of the plant to its constituent polyphenolics, flavonoids, triterpenoids, and mangiferin. They also noted that their findings support the folkloric uses of the plant for treating arthritic and other inflammatory conditions, as well as type 2 diabetes (Methods Find. Exp. Clin. Pharmacol. 2005;27:547-54).
Another important constituent of mango (also found in olive, strawberry, fig, and various medicinal herbs) is the triterpene lupeol, which has been characterized as exhibiting potent antioxidant, antimutagenic, anti-inflammatory, and antiarthritic activity (Oncogene 2004;23:5203-14). A 2014 study by Sahu et al. also showed that M. indica leaves display some antityrosinase activity, though not as strongly as other medicinal plants, such as Emblica officinalis (Pak. J. Biol. Sci. 2014;17:146-50).
Anticancer, antioxidant, and antiphotoaging activity
In 2004, Saleem et al. demonstrated that topically applied lupeol exhibited anti–tumor-promoting effects in a CD-1 mouse skin tumorigenesis model. Pretreatment with the mango constituent time- and dose-dependently inhibited multiple 12-O-tetradecanoyl-phorbol-13-acetate (TPA)-mediated increases in edema, hyperplasia, epidermal ornithine decarboxylase (ODC) activity, as well as protein expression of ODC, cyclooxygenase 2 (COX-2) and nitric oxide synthase. Pretreated animals also experienced significantly lower tumor incidence and tumor body burden as well as a significant delay in tumor latency period. The researchers concluded that lupeol exerts anti–skin tumor promoting effects on CD-1 mice (Oncogene 2004;23:5203-14).
Three years later, Núñez-Sellés et al. reported that a mango stem bark extract (Vimang) developed in Cuba exhibited antioxidant, analgesic, anti-inflammatory, and immunomodulating activity in basic, preclinical, and clinical studies (Pharmacol. Res. 2007;55:351-8).
A 2009 toxicological analysis of Vimang, which has been formulated into tablets, creams, capsules, syrup, vaginal oval, and suppositories for various applications, revealed via irritant tests conducted on rabbits that the topical formulation was not irritating to the skin, generally, with minimal irritancy noted after vaginal application. No adverse effects were reported (Drug Chem. Toxicol. 2009;32:53-8).
In 2012, Li et al. discovered norathyriol (1,3,6,7-tetrahydroxy-9H-xanthen-9-one), a plant-derived chemopreventive metabolite of mangiferin, found in mango, Hypericum elegans, and Tripterospermum lanceolatum. They found that norathyriol significantly inhibited solar UV-induced skin carcinogenesis in mouse models. In vitro investigations revealed that the compound suppressed cell growth in mouse skin epidermal JB6 P+ cells at the level of G2-M phase arrest. The investigators concluded that this newly identified substance appears to act as a safe chemopreventive agent against UV-induced skin cancer (Cancer Res. 2012;72:260-70).
A year later, Song et al. assessed the protective effects of orally administered mango extract against UVB-induced cutaneous aging in HR-1 hairless male mice. The animals were divided into control, UVB-treated vehicle, and UVB-treated mango extract groups. The researchers found that mango extract significantly suppressed the increase in epidermal thickness and hypertrophy indicative of UVB treatment, with mean length of wrinkles significantly lower in the mango group compared with the UVB-treated vehicle group. Treatment with mango extract also led to a significant increase in collagen bundles in animals treated with UVB. The authors concluded that mango extract displayed antiphotoaging properties in hairless mice exposed to UVB (Photodermatol. Photoimmunol. Photomed. 2013;29:84-9).
Further, a 2014 in vitro study revealed that extracts of Helicanthus elastica growing on M. indica exhibited antioxidant activity. H. elastica is a hemiparasite that often grows on mango trees in India and is known to be a rich source of phenolic substances (J. Tradit. Complement. Med. 2014;4:285-8).
Topical delivery
Mandawgade and Patravale developed a mango butter skin care formulation in 2008 that was used to test skin repair in rat excision and incision wound models. A healing response was noted in both animal models. The formulation also was found to be effective in achieving complete repair of worn and cracked skin on the feet of all human volunteers in the study. The investigators concluded that the mango butter preparation delivers superlative emolliency and warrants consideration as an excipient agent in cosmeceutical products (Indian J. Pharm. Sci. 2008;70:539-42).
It is worth noting that cases of “mango dermatitis” (allergic contact dermatitis to the sap or skin of M. indica), manifesting in urticaria and eczematous rashes, have been reported (Australas. J. Dermatol. 1996;37:59-60; Int. J. Dermatol. 2004;43:195-6).
In 2014, Leanpolchareanchai et al. developed a microemulsion system containing Thai mango seed kernel extract that displayed strong skin enhancement results in ex vivo skin permeation studies (penetrating skin layers up to 60-fold higher than controls) and physicochemical stability over 6 months (Drug Chem. Toxicol. 2009;32:53-8). Thai mango seed kernel extract had previously been shown to exhibit anti–methicillin-resistant Staphylococcus aureus and antityrosinase characteristics, as well as strong free radical scavenging, antioxidant, anti-inflammatory, and hepatoprotective activities.(Molecules 2014;19:17107-29).
Conclusion
Evidence on the cutaneous applications of mango is emerging, but does not have a significant track record. That said, this fruit has long been used in traditional medicine for a range of indications, including skin disorders. Much more research is necessary, however, to ascertain how beneficial this fruit and its extracts may be. At the very least, there are few reports of adverse events associated with topical application.
Dr. Baumann is chief executive officer of the Baumann Cosmetic & Research Institute in the Design District in Miami. She founded the Cosmetic Dermatology Center at the University of Miami in 1997. Dr. Baumann wrote the textbook “Cosmetic Dermatology: Principles and Practice” (New York: McGraw-Hill, 2002), and a book for consumers, “The Skin Type Solution” (New York: Bantam Dell, 2006). She has contributed to the Cosmeceutical Critique column in Dermatology News since January 2001. Her latest book, “Cosmeceuticals and Cosmetic Ingredients,” was published in November 2014. Dr. Baumann has received funding for clinical grants from Allergan, Aveeno, Avon Products, Evolus, Galderma, GlaxoSmithKline, Kythera, Mary Kay, Medicis Pharmaceuticals, Neutrogena, Philosophy, Topix Pharmaceuticals, and Unilever.
Mangifera indica (mango) is a member of the Anacardiaceae family with a tradition of use as a medicinal plant. Mango extracts have been characterized as exhibiting antioxidant, anti-inflammatory, analgesic, and immunomodulatory activities (Photodermatol. Photoimmunol. Photomed. 2013;29:84-9; Drug Chem. Toxicol. 2009;32:53-8). Mango is grown in more than 100 countries, primarily in Asia, in tropical as well as subtropical regions (Molecules 2014;19:17107-29). Mango stem bark and leaves have been used in traditional medicine to treat anemia, cutaneous infections, diabetes, diarrhea, scabies, syphilis, and malignant tumors (Pharmacol. Res. 2007;55:351-8). Polyphenols and carotenoids are among the phytonutrients identified as responsible for the biologic activity of mango (Photodermatol. Photoimmunol. Photomed. 2013;29:84-9).
Various biologic activities and traditional uses
Ojewole investigated the anti-inflammatory, analgesic, and antidiabetic activity of M. indica stem bark aqueous extract in rats and mice in 2005. In mice, mango extract dose-dependently delivered significant analgesic effects against thermally and chemically-generated pain. The investigators attributed the observed salutary effects of the plant to its constituent polyphenolics, flavonoids, triterpenoids, and mangiferin. They also noted that their findings support the folkloric uses of the plant for treating arthritic and other inflammatory conditions, as well as type 2 diabetes (Methods Find. Exp. Clin. Pharmacol. 2005;27:547-54).
Another important constituent of mango (also found in olive, strawberry, fig, and various medicinal herbs) is the triterpene lupeol, which has been characterized as exhibiting potent antioxidant, antimutagenic, anti-inflammatory, and antiarthritic activity (Oncogene 2004;23:5203-14). A 2014 study by Sahu et al. also showed that M. indica leaves display some antityrosinase activity, though not as strongly as other medicinal plants, such as Emblica officinalis (Pak. J. Biol. Sci. 2014;17:146-50).
Anticancer, antioxidant, and antiphotoaging activity
In 2004, Saleem et al. demonstrated that topically applied lupeol exhibited anti–tumor-promoting effects in a CD-1 mouse skin tumorigenesis model. Pretreatment with the mango constituent time- and dose-dependently inhibited multiple 12-O-tetradecanoyl-phorbol-13-acetate (TPA)-mediated increases in edema, hyperplasia, epidermal ornithine decarboxylase (ODC) activity, as well as protein expression of ODC, cyclooxygenase 2 (COX-2) and nitric oxide synthase. Pretreated animals also experienced significantly lower tumor incidence and tumor body burden as well as a significant delay in tumor latency period. The researchers concluded that lupeol exerts anti–skin tumor promoting effects on CD-1 mice (Oncogene 2004;23:5203-14).
Three years later, Núñez-Sellés et al. reported that a mango stem bark extract (Vimang) developed in Cuba exhibited antioxidant, analgesic, anti-inflammatory, and immunomodulating activity in basic, preclinical, and clinical studies (Pharmacol. Res. 2007;55:351-8).
A 2009 toxicological analysis of Vimang, which has been formulated into tablets, creams, capsules, syrup, vaginal oval, and suppositories for various applications, revealed via irritant tests conducted on rabbits that the topical formulation was not irritating to the skin, generally, with minimal irritancy noted after vaginal application. No adverse effects were reported (Drug Chem. Toxicol. 2009;32:53-8).
In 2012, Li et al. discovered norathyriol (1,3,6,7-tetrahydroxy-9H-xanthen-9-one), a plant-derived chemopreventive metabolite of mangiferin, found in mango, Hypericum elegans, and Tripterospermum lanceolatum. They found that norathyriol significantly inhibited solar UV-induced skin carcinogenesis in mouse models. In vitro investigations revealed that the compound suppressed cell growth in mouse skin epidermal JB6 P+ cells at the level of G2-M phase arrest. The investigators concluded that this newly identified substance appears to act as a safe chemopreventive agent against UV-induced skin cancer (Cancer Res. 2012;72:260-70).
A year later, Song et al. assessed the protective effects of orally administered mango extract against UVB-induced cutaneous aging in HR-1 hairless male mice. The animals were divided into control, UVB-treated vehicle, and UVB-treated mango extract groups. The researchers found that mango extract significantly suppressed the increase in epidermal thickness and hypertrophy indicative of UVB treatment, with mean length of wrinkles significantly lower in the mango group compared with the UVB-treated vehicle group. Treatment with mango extract also led to a significant increase in collagen bundles in animals treated with UVB. The authors concluded that mango extract displayed antiphotoaging properties in hairless mice exposed to UVB (Photodermatol. Photoimmunol. Photomed. 2013;29:84-9).
Further, a 2014 in vitro study revealed that extracts of Helicanthus elastica growing on M. indica exhibited antioxidant activity. H. elastica is a hemiparasite that often grows on mango trees in India and is known to be a rich source of phenolic substances (J. Tradit. Complement. Med. 2014;4:285-8).
Topical delivery
Mandawgade and Patravale developed a mango butter skin care formulation in 2008 that was used to test skin repair in rat excision and incision wound models. A healing response was noted in both animal models. The formulation also was found to be effective in achieving complete repair of worn and cracked skin on the feet of all human volunteers in the study. The investigators concluded that the mango butter preparation delivers superlative emolliency and warrants consideration as an excipient agent in cosmeceutical products (Indian J. Pharm. Sci. 2008;70:539-42).
It is worth noting that cases of “mango dermatitis” (allergic contact dermatitis to the sap or skin of M. indica), manifesting in urticaria and eczematous rashes, have been reported (Australas. J. Dermatol. 1996;37:59-60; Int. J. Dermatol. 2004;43:195-6).
In 2014, Leanpolchareanchai et al. developed a microemulsion system containing Thai mango seed kernel extract that displayed strong skin enhancement results in ex vivo skin permeation studies (penetrating skin layers up to 60-fold higher than controls) and physicochemical stability over 6 months (Drug Chem. Toxicol. 2009;32:53-8). Thai mango seed kernel extract had previously been shown to exhibit anti–methicillin-resistant Staphylococcus aureus and antityrosinase characteristics, as well as strong free radical scavenging, antioxidant, anti-inflammatory, and hepatoprotective activities.(Molecules 2014;19:17107-29).
Conclusion
Evidence on the cutaneous applications of mango is emerging, but does not have a significant track record. That said, this fruit has long been used in traditional medicine for a range of indications, including skin disorders. Much more research is necessary, however, to ascertain how beneficial this fruit and its extracts may be. At the very least, there are few reports of adverse events associated with topical application.
Dr. Baumann is chief executive officer of the Baumann Cosmetic & Research Institute in the Design District in Miami. She founded the Cosmetic Dermatology Center at the University of Miami in 1997. Dr. Baumann wrote the textbook “Cosmetic Dermatology: Principles and Practice” (New York: McGraw-Hill, 2002), and a book for consumers, “The Skin Type Solution” (New York: Bantam Dell, 2006). She has contributed to the Cosmeceutical Critique column in Dermatology News since January 2001. Her latest book, “Cosmeceuticals and Cosmetic Ingredients,” was published in November 2014. Dr. Baumann has received funding for clinical grants from Allergan, Aveeno, Avon Products, Evolus, Galderma, GlaxoSmithKline, Kythera, Mary Kay, Medicis Pharmaceuticals, Neutrogena, Philosophy, Topix Pharmaceuticals, and Unilever.

Microneedling
Microneedling, or skin needling, is an aesthetic technique used for decades prior to resurfacing lasers, but it has recently experienced a surge in popularity, particularly for ethnic skin. In 1995, subcision or dermal needling was identified as an effective treatment for scars. Since then, the technique initially referred to as collagen induction therapy has become a staple in the treatment of acne scars, surgical scars, photo aging, and stretch marks.
The skin needling technique involves using fine sterile needles 0.1mm-2.5 mm in length that repeatedly pierce the stratum corneum, producing microscopic “holes” in the dermis. These microscopic wounds lead to the release of growth factors stimulating the formation of new collagen, elastin, and neovascularization in the dermis. There are many brands and manufacturers of microneedling tools on the market, including dermarollers, Dermapen, Dermastamp, Cosmopen, and multiple other in-office and at-home devices. At-home devices usually have shorter needles and provide significantly less penetration and injury, and therefore may be less effective.

Prior to the procedure, patients are often anesthetized with topical anesthesia without vasoconstrictors for 1 hour. The area is cleaned with sterile gauze and alcohol or Hibiclens, and a microneedling device is used to either roll or prick the skin in multiple alternating passes. The depth of penetration, number of passes, and degree of overlap is highly dependent on the underlying condition, the area being treated, the brand of device used, and the length and frequency of the needle insertion. Petechiae and pinpoint bleeding occur during the treatment. Treatments are usually done 4-6 weeks apart. Post procedure, the patient often experiences mild erythema, bruising, and some mild edema.
This technique has been particularly beneficial to patients with skin of color who are not candidates for factional lasers because of the risks of hyperpigmentation and scarring. There is low risk of hyper- or hypopigmentation with microneedling, and multiple treatments can be performed in patients with types III-VI skin and those with a history of melasma.

Contraindications and precautions when considering microneedling include: history of keloid or hypertrophic scarring,recent skin rashes, history of herpes simplex infections if the perioral area is being treated, and the presence of raised moles, warts, or any raised lesions on the targeted area. Absolute contraindications include: scleroderma, collagen vascular diseases clotting problems, active bacterial or fungal infection, and immunosuppression.
Microneedling is a safe, effective, in-office procedure with a range of uses. Many new indications are currently being explored. In my practice, we have used microneedling for atrophic scars, repigmentation of depigmented scars and vitiligo, stimulation of hair regrowth in noninflammatory alopecias, and treatment of burn scars. Patients are generally very happy with the quick treatment time, minimal downtime, and overall long-term results.
References
1. Orentreich DS, Orentreich N. Subcutaneous incisionless (subcision) surgery for the correction of depressed scars and wrinkles. Dermatol. Surg. 1995;21:6543-9.
2. Camirand A, Doucet J. Needle dermabrasion. Aesthetic Plast. Surg. 1997;21:48-51.
3. Fernandes D. Minimally invasive percutaneous collagen induction. Oral Maxillofac. Surg. Clin. North Am. 2006;17:51-63.
4. Aust MC, Fernandes D, Kolokythas P, Kaplan HM, Vogt PM. Percutaneous collagen induction therapy: An alternative treatment for scars, wrinkles and skin laxity. Plast. Reconstr. Surg. 2008;21:1421-9.
5. Fernandes D, Signorini M. Combating photoaging with percutaneous collagen induction. Clin. Dermatol. 2008;26:192-9.
6. Aust MC, Reimers K, Repenning C, Stahl F, Jahn S, Guggenheim M et al. Percutaneous collagen induction: Minimally invasive skin rejuvenation without risk of hyperpigmentation – fact or fiction? Plast. Reconstr. Surg. 2008;122:1553-63.
7. Fabbrocini G, De Vita V, Pastore F, et al. Collagen induction therapy for the treatment of upper lip wrinkles. J. Dermatolog. Treat. 2012;23:144-52. 8. Majid I. Microneedling therapy in atrophic facial scars: an objective assessment. J. Cutan. Aesthet. Surg. 2009;2:26-30.
9. Doddaballapur S. Microneedling with dermaroller. J. Cutan. Aesthet. Surg 2009;2: 110-11.
10. Dogra S, Yadav S. Sarangal R. Microneedling for acne scars in Asian skin type: an effective low cost treatment modality. J. Cosmet. Dermatol. 2014;13:180-7.
Dr. Talakoub and Dr. Wesley are cocontributors to a monthly Aesthetic Dermatology column in Dermatology News. Dr. Talakoub is in private practice in McLean, Va. Dr. Wesley practices dermatology in Beverly Hills, Calif. This month’s column is by Dr. Talakoub.
Microneedling, or skin needling, is an aesthetic technique used for decades prior to resurfacing lasers, but it has recently experienced a surge in popularity, particularly for ethnic skin. In 1995, subcision or dermal needling was identified as an effective treatment for scars. Since then, the technique initially referred to as collagen induction therapy has become a staple in the treatment of acne scars, surgical scars, photo aging, and stretch marks.
The skin needling technique involves using fine sterile needles 0.1mm-2.5 mm in length that repeatedly pierce the stratum corneum, producing microscopic “holes” in the dermis. These microscopic wounds lead to the release of growth factors stimulating the formation of new collagen, elastin, and neovascularization in the dermis. There are many brands and manufacturers of microneedling tools on the market, including dermarollers, Dermapen, Dermastamp, Cosmopen, and multiple other in-office and at-home devices. At-home devices usually have shorter needles and provide significantly less penetration and injury, and therefore may be less effective.
Prior to the procedure, patients are often anesthetized with topical anesthesia without vasoconstrictors for 1 hour. The area is cleaned with sterile gauze and alcohol or Hibiclens, and a microneedling device is used to either roll or prick the skin in multiple alternating passes. The depth of penetration, number of passes, and degree of overlap is highly dependent on the underlying condition, the area being treated, the brand of device used, and the length and frequency of the needle insertion. Petechiae and pinpoint bleeding occur during the treatment. Treatments are usually done 4-6 weeks apart. Post procedure, the patient often experiences mild erythema, bruising, and some mild edema.
This technique has been particularly beneficial to patients with skin of color who are not candidates for factional lasers because of the risks of hyperpigmentation and scarring. There is low risk of hyper- or hypopigmentation with microneedling, and multiple treatments can be performed in patients with types III-VI skin and those with a history of melasma.
Contraindications and precautions when considering microneedling include: history of keloid or hypertrophic scarring,recent skin rashes, history of herpes simplex infections if the perioral area is being treated, and the presence of raised moles, warts, or any raised lesions on the targeted area. Absolute contraindications include: scleroderma, collagen vascular diseases clotting problems, active bacterial or fungal infection, and immunosuppression.
Microneedling is a safe, effective, in-office procedure with a range of uses. Many new indications are currently being explored. In my practice, we have used microneedling for atrophic scars, repigmentation of depigmented scars and vitiligo, stimulation of hair regrowth in noninflammatory alopecias, and treatment of burn scars. Patients are generally very happy with the quick treatment time, minimal downtime, and overall long-term results.
References
1. Orentreich DS, Orentreich N. Subcutaneous incisionless (subcision) surgery for the correction of depressed scars and wrinkles. Dermatol. Surg. 1995;21:6543-9.
2. Camirand A, Doucet J. Needle dermabrasion. Aesthetic Plast. Surg. 1997;21:48-51.
3. Fernandes D. Minimally invasive percutaneous collagen induction. Oral Maxillofac. Surg. Clin. North Am. 2006;17:51-63.
4. Aust MC, Fernandes D, Kolokythas P, Kaplan HM, Vogt PM. Percutaneous collagen induction therapy: An alternative treatment for scars, wrinkles and skin laxity. Plast. Reconstr. Surg. 2008;21:1421-9.
5. Fernandes D, Signorini M. Combating photoaging with percutaneous collagen induction. Clin. Dermatol. 2008;26:192-9.
6. Aust MC, Reimers K, Repenning C, Stahl F, Jahn S, Guggenheim M et al. Percutaneous collagen induction: Minimally invasive skin rejuvenation without risk of hyperpigmentation – fact or fiction? Plast. Reconstr. Surg. 2008;122:1553-63.
7. Fabbrocini G, De Vita V, Pastore F, et al. Collagen induction therapy for the treatment of upper lip wrinkles. J. Dermatolog. Treat. 2012;23:144-52. 8. Majid I. Microneedling therapy in atrophic facial scars: an objective assessment. J. Cutan. Aesthet. Surg. 2009;2:26-30.
9. Doddaballapur S. Microneedling with dermaroller. J. Cutan. Aesthet. Surg 2009;2: 110-11.
10. Dogra S, Yadav S. Sarangal R. Microneedling for acne scars in Asian skin type: an effective low cost treatment modality. J. Cosmet. Dermatol. 2014;13:180-7.
Dr. Talakoub and Dr. Wesley are cocontributors to a monthly Aesthetic Dermatology column in Dermatology News. Dr. Talakoub is in private practice in McLean, Va. Dr. Wesley practices dermatology in Beverly Hills, Calif. This month’s column is by Dr. Talakoub.
Microneedling, or skin needling, is an aesthetic technique used for decades prior to resurfacing lasers, but it has recently experienced a surge in popularity, particularly for ethnic skin. In 1995, subcision or dermal needling was identified as an effective treatment for scars. Since then, the technique initially referred to as collagen induction therapy has become a staple in the treatment of acne scars, surgical scars, photo aging, and stretch marks.
The skin needling technique involves using fine sterile needles 0.1mm-2.5 mm in length that repeatedly pierce the stratum corneum, producing microscopic “holes” in the dermis. These microscopic wounds lead to the release of growth factors stimulating the formation of new collagen, elastin, and neovascularization in the dermis. There are many brands and manufacturers of microneedling tools on the market, including dermarollers, Dermapen, Dermastamp, Cosmopen, and multiple other in-office and at-home devices. At-home devices usually have shorter needles and provide significantly less penetration and injury, and therefore may be less effective.
Prior to the procedure, patients are often anesthetized with topical anesthesia without vasoconstrictors for 1 hour. The area is cleaned with sterile gauze and alcohol or Hibiclens, and a microneedling device is used to either roll or prick the skin in multiple alternating passes. The depth of penetration, number of passes, and degree of overlap is highly dependent on the underlying condition, the area being treated, the brand of device used, and the length and frequency of the needle insertion. Petechiae and pinpoint bleeding occur during the treatment. Treatments are usually done 4-6 weeks apart. Post procedure, the patient often experiences mild erythema, bruising, and some mild edema.
This technique has been particularly beneficial to patients with skin of color who are not candidates for factional lasers because of the risks of hyperpigmentation and scarring. There is low risk of hyper- or hypopigmentation with microneedling, and multiple treatments can be performed in patients with types III-VI skin and those with a history of melasma.
Contraindications and precautions when considering microneedling include: history of keloid or hypertrophic scarring,recent skin rashes, history of herpes simplex infections if the perioral area is being treated, and the presence of raised moles, warts, or any raised lesions on the targeted area. Absolute contraindications include: scleroderma, collagen vascular diseases clotting problems, active bacterial or fungal infection, and immunosuppression.
Microneedling is a safe, effective, in-office procedure with a range of uses. Many new indications are currently being explored. In my practice, we have used microneedling for atrophic scars, repigmentation of depigmented scars and vitiligo, stimulation of hair regrowth in noninflammatory alopecias, and treatment of burn scars. Patients are generally very happy with the quick treatment time, minimal downtime, and overall long-term results.
References
1. Orentreich DS, Orentreich N. Subcutaneous incisionless (subcision) surgery for the correction of depressed scars and wrinkles. Dermatol. Surg. 1995;21:6543-9.
2. Camirand A, Doucet J. Needle dermabrasion. Aesthetic Plast. Surg. 1997;21:48-51.
3. Fernandes D. Minimally invasive percutaneous collagen induction. Oral Maxillofac. Surg. Clin. North Am. 2006;17:51-63.
4. Aust MC, Fernandes D, Kolokythas P, Kaplan HM, Vogt PM. Percutaneous collagen induction therapy: An alternative treatment for scars, wrinkles and skin laxity. Plast. Reconstr. Surg. 2008;21:1421-9.
5. Fernandes D, Signorini M. Combating photoaging with percutaneous collagen induction. Clin. Dermatol. 2008;26:192-9.
6. Aust MC, Reimers K, Repenning C, Stahl F, Jahn S, Guggenheim M et al. Percutaneous collagen induction: Minimally invasive skin rejuvenation without risk of hyperpigmentation – fact or fiction? Plast. Reconstr. Surg. 2008;122:1553-63.
7. Fabbrocini G, De Vita V, Pastore F, et al. Collagen induction therapy for the treatment of upper lip wrinkles. J. Dermatolog. Treat. 2012;23:144-52. 8. Majid I. Microneedling therapy in atrophic facial scars: an objective assessment. J. Cutan. Aesthet. Surg. 2009;2:26-30.
9. Doddaballapur S. Microneedling with dermaroller. J. Cutan. Aesthet. Surg 2009;2: 110-11.
10. Dogra S, Yadav S. Sarangal R. Microneedling for acne scars in Asian skin type: an effective low cost treatment modality. J. Cosmet. Dermatol. 2014;13:180-7.
Dr. Talakoub and Dr. Wesley are cocontributors to a monthly Aesthetic Dermatology column in Dermatology News. Dr. Talakoub is in private practice in McLean, Va. Dr. Wesley practices dermatology in Beverly Hills, Calif. This month’s column is by Dr. Talakoub.

Joining forces, Part 2
The ongoing sea change in medicine has led to a substantial erosion of physician autonomy, and to ever-increasing administrative burdens that hit small practices the hardest. Does this mean that the independent private physician practice model is doomed, as some predict? Absolutely not; but it will force many solo practitioners and small groups to join forces to protect themselves.
Those practices that offer unique services, or fill an unmet niche, may be able to remain small; but most smaller practices will need to consider a larger alternative. In a previous column, I outlined the basics of one such protective strategy – merging two or more small practices into a larger entity – but there are other options to consider.
One attractive and relatively straightforward strategy is the formation of a cooperative group. In most areas, there are very likely several small practices in similar predicaments that might be receptive to discussing a collaboration on billing and purchasing. This allows each participant to maintain independence as a private practice, while pooling resources to ease the administrative burdens of all. Once that arrangement is in place, the group can consider more ambitious projects, such as the joint purchase of an EHR system, sharing of personnel to lower staffing costs, and an integrated scheduling system. The latter will be particularly attractive to participants in later stages of their careers who are considering an intermediate option, somewhere between full-time work and complete retirement.
After a time, when the structure is stabilized and everyone agrees that his or her individual and shared interests and goals are being met, an outright merger can be contemplated. Projects of this scope require careful planning and implementation, and should not be undertaken without the help of competent legal counsel and an experienced business consultant.
A more complex but increasingly popular option is to join other small practices and providers in an independent practice association (IPA). An IPA is a legal entity organized and directed by physicians for the purpose of negotiating contracts with insurance companies on their behalf. Because of its structure, an IPA is better positioned to enter into such financial arrangements, and to counterbalance the leverage of insurers, but there are legal issues to consider. Many IPAs are vulnerable to antitrust charges because they include competing health care providers. You should check with legal counsel before signing on to an IPA, to make sure that it abides by antitrust and price fixing laws. IPAs have also been known to fail, particularly in states where they are not adequately regulated.
A possible successor to IPAs is the accountable care organization (ACO), an entity born as a component of the Affordable Care Act. While the official definition remains nebulous, an ACO is basically a network of doctors and hospitals that shares financial and medical responsibility for providing coordinated and efficient care to patients. The goal of ACO participants is to limit unnecessary spending, both individually and collectively, according to criteria established by the Centers for Medicare & Medicaid Services, without compromising quality of care in the process. More than 600 ACOs had been approved by the CMS as of the beginning of 2014.
It is important to remember that the ACO model remains very much a work in progress. ACOs make providers jointly accountable for the health of their patients. They offer financial incentives to cooperate, and to save money by avoiding unnecessary tests and procedures. A key component is the sharing of information. Providers who save money while also meeting quality targets are theoretically entitled to a portion of the savings.
As with IPAs, ACO ventures involve a measure of risk. ACOs that fail to meet the CMS performance and savings benchmarks can be stuck with the bill for investments made to improve care, such as equipment and computer purchases and the hiring of mid-level providers and managers, and they may be assessed monetary penalties as well. ACOs sponsored by physicians or rural providers, however, can apply to receive payments in advance to help finance infrastructure investments – a concession the Obama administration made after receiving complaints from rural hospitals.
Clearly, the price of remaining autonomous will be significant, and many private practitioners will be unwilling to pay it: Only 36% of physicians remained in independent practice at the end of the 2013, according to data from the American Medical Association – down from 57% in 2000 – but those of us who remain committed to independence will find ways to preserve it. In medicine, as in life, those most responsive to change will survive and flourish.
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, N.J. He is the author of numerous articles and textbook chapters, and is a longtime monthly columnist for Dermatology News.
The ongoing sea change in medicine has led to a substantial erosion of physician autonomy, and to ever-increasing administrative burdens that hit small practices the hardest. Does this mean that the independent private physician practice model is doomed, as some predict? Absolutely not; but it will force many solo practitioners and small groups to join forces to protect themselves.
Those practices that offer unique services, or fill an unmet niche, may be able to remain small; but most smaller practices will need to consider a larger alternative. In a previous column, I outlined the basics of one such protective strategy – merging two or more small practices into a larger entity – but there are other options to consider.
One attractive and relatively straightforward strategy is the formation of a cooperative group. In most areas, there are very likely several small practices in similar predicaments that might be receptive to discussing a collaboration on billing and purchasing. This allows each participant to maintain independence as a private practice, while pooling resources to ease the administrative burdens of all. Once that arrangement is in place, the group can consider more ambitious projects, such as the joint purchase of an EHR system, sharing of personnel to lower staffing costs, and an integrated scheduling system. The latter will be particularly attractive to participants in later stages of their careers who are considering an intermediate option, somewhere between full-time work and complete retirement.
After a time, when the structure is stabilized and everyone agrees that his or her individual and shared interests and goals are being met, an outright merger can be contemplated. Projects of this scope require careful planning and implementation, and should not be undertaken without the help of competent legal counsel and an experienced business consultant.
A more complex but increasingly popular option is to join other small practices and providers in an independent practice association (IPA). An IPA is a legal entity organized and directed by physicians for the purpose of negotiating contracts with insurance companies on their behalf. Because of its structure, an IPA is better positioned to enter into such financial arrangements, and to counterbalance the leverage of insurers, but there are legal issues to consider. Many IPAs are vulnerable to antitrust charges because they include competing health care providers. You should check with legal counsel before signing on to an IPA, to make sure that it abides by antitrust and price fixing laws. IPAs have also been known to fail, particularly in states where they are not adequately regulated.
A possible successor to IPAs is the accountable care organization (ACO), an entity born as a component of the Affordable Care Act. While the official definition remains nebulous, an ACO is basically a network of doctors and hospitals that shares financial and medical responsibility for providing coordinated and efficient care to patients. The goal of ACO participants is to limit unnecessary spending, both individually and collectively, according to criteria established by the Centers for Medicare & Medicaid Services, without compromising quality of care in the process. More than 600 ACOs had been approved by the CMS as of the beginning of 2014.
It is important to remember that the ACO model remains very much a work in progress. ACOs make providers jointly accountable for the health of their patients. They offer financial incentives to cooperate, and to save money by avoiding unnecessary tests and procedures. A key component is the sharing of information. Providers who save money while also meeting quality targets are theoretically entitled to a portion of the savings.
As with IPAs, ACO ventures involve a measure of risk. ACOs that fail to meet the CMS performance and savings benchmarks can be stuck with the bill for investments made to improve care, such as equipment and computer purchases and the hiring of mid-level providers and managers, and they may be assessed monetary penalties as well. ACOs sponsored by physicians or rural providers, however, can apply to receive payments in advance to help finance infrastructure investments – a concession the Obama administration made after receiving complaints from rural hospitals.
Clearly, the price of remaining autonomous will be significant, and many private practitioners will be unwilling to pay it: Only 36% of physicians remained in independent practice at the end of the 2013, according to data from the American Medical Association – down from 57% in 2000 – but those of us who remain committed to independence will find ways to preserve it. In medicine, as in life, those most responsive to change will survive and flourish.
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, N.J. He is the author of numerous articles and textbook chapters, and is a longtime monthly columnist for Dermatology News.
The ongoing sea change in medicine has led to a substantial erosion of physician autonomy, and to ever-increasing administrative burdens that hit small practices the hardest. Does this mean that the independent private physician practice model is doomed, as some predict? Absolutely not; but it will force many solo practitioners and small groups to join forces to protect themselves.
Those practices that offer unique services, or fill an unmet niche, may be able to remain small; but most smaller practices will need to consider a larger alternative. In a previous column, I outlined the basics of one such protective strategy – merging two or more small practices into a larger entity – but there are other options to consider.
One attractive and relatively straightforward strategy is the formation of a cooperative group. In most areas, there are very likely several small practices in similar predicaments that might be receptive to discussing a collaboration on billing and purchasing. This allows each participant to maintain independence as a private practice, while pooling resources to ease the administrative burdens of all. Once that arrangement is in place, the group can consider more ambitious projects, such as the joint purchase of an EHR system, sharing of personnel to lower staffing costs, and an integrated scheduling system. The latter will be particularly attractive to participants in later stages of their careers who are considering an intermediate option, somewhere between full-time work and complete retirement.
After a time, when the structure is stabilized and everyone agrees that his or her individual and shared interests and goals are being met, an outright merger can be contemplated. Projects of this scope require careful planning and implementation, and should not be undertaken without the help of competent legal counsel and an experienced business consultant.
A more complex but increasingly popular option is to join other small practices and providers in an independent practice association (IPA). An IPA is a legal entity organized and directed by physicians for the purpose of negotiating contracts with insurance companies on their behalf. Because of its structure, an IPA is better positioned to enter into such financial arrangements, and to counterbalance the leverage of insurers, but there are legal issues to consider. Many IPAs are vulnerable to antitrust charges because they include competing health care providers. You should check with legal counsel before signing on to an IPA, to make sure that it abides by antitrust and price fixing laws. IPAs have also been known to fail, particularly in states where they are not adequately regulated.
A possible successor to IPAs is the accountable care organization (ACO), an entity born as a component of the Affordable Care Act. While the official definition remains nebulous, an ACO is basically a network of doctors and hospitals that shares financial and medical responsibility for providing coordinated and efficient care to patients. The goal of ACO participants is to limit unnecessary spending, both individually and collectively, according to criteria established by the Centers for Medicare & Medicaid Services, without compromising quality of care in the process. More than 600 ACOs had been approved by the CMS as of the beginning of 2014.
It is important to remember that the ACO model remains very much a work in progress. ACOs make providers jointly accountable for the health of their patients. They offer financial incentives to cooperate, and to save money by avoiding unnecessary tests and procedures. A key component is the sharing of information. Providers who save money while also meeting quality targets are theoretically entitled to a portion of the savings.
As with IPAs, ACO ventures involve a measure of risk. ACOs that fail to meet the CMS performance and savings benchmarks can be stuck with the bill for investments made to improve care, such as equipment and computer purchases and the hiring of mid-level providers and managers, and they may be assessed monetary penalties as well. ACOs sponsored by physicians or rural providers, however, can apply to receive payments in advance to help finance infrastructure investments – a concession the Obama administration made after receiving complaints from rural hospitals.
Clearly, the price of remaining autonomous will be significant, and many private practitioners will be unwilling to pay it: Only 36% of physicians remained in independent practice at the end of the 2013, according to data from the American Medical Association – down from 57% in 2000 – but those of us who remain committed to independence will find ways to preserve it. In medicine, as in life, those most responsive to change will survive and flourish.
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, N.J. He is the author of numerous articles and textbook chapters, and is a longtime monthly columnist for Dermatology News.

When those genes no longer fit
If you ask most folks why some of us are obese, they will answer that it’s because overweight people have eaten too much of the wrong foods and not exercised enough. If prompted, they might expand their response by saying that people who come from families with overweight members will usually have more trouble maintaining a healthy weight. It seems to me that just about covers our state-of-the-art understanding of obesity.
You can argue that there is always new information coming out from experiments on genetically altered mice. And, the recently appreciated relationship between sleep deprivation and being overweight sounds interesting. But it still boils down to the simple equation of too much energy in and too little burned.
In 2007, it was discovered that a variant of a gene known as FTO was closely linked to excess weight gain in humans. Individuals with one copy of the gene were on average 3.5 pounds heavier than were those without the gene. Those people with a double copy of the variant gene were 7 pounds heavier and 50% more likely to be obese than was the general population.
It looked like the FTO gene might be one of the answers beyond the simplicity of too much consumption and too little expenditure. But why would the gene suddenly become more prevalent over the last 5 or 6 decades that obesity has become epidemic in America? It seemed unlikely that this shift could occur in such a short time frame.
A recently published study in Proceedings of the National Academy of Sciences (PNAS 2014 [doi: 10.1073/pnas.1411893111]) suggests another more plausible explanation. Using data from the venerable and ongoing Framingham Heart Study, the researchers found that the FTO variant became a risk factor only after World War II. In other words, people with the FTO variant born prior to 1942 weren’t any more likely to be overweight than the rest of the population.
What has changed since the 1940s? Our diet has shifted toward more processed and fried foods. And, our lives and our jobs have become more sedentary. Television crept into our living rooms in the 1950s and into our bedrooms in the 1970s.
The FTO gene variant may have been advantageous to humans in lean times when the heavier of us were more likely to survive long periods of starvation. But now here in the land of fries and soft drinks, the gene has become hazardous to our health. We now look (and are) fat wearing the same genes that seemed to fit us so well a century ago.
We must have sympathy for those of us who have a gene that makes us more vulnerable when food is plentiful, and technology has made it easier to survive with very little energy expenditure. It is tempting to hope that someday scientists will find a way to alter the offending genes to help those cursed to carry them. But this kind of manipulation must be considered cautiously because a natural or man-made catastrophe on a global scale could once again make this gene advantageous.
We must face the fact that it is the environment in which we live – an environment that we have altered and can continue to alter – that is the primary driver of the obesity epidemic. One wonders whether we are experiencing other epidemics analogous to the FTO/obesity story.
Attention-deficit/hyperactivity disorder (ADHD) comes to mind. Some observers feel that a short attention span and impulsivity may have been advantageous when we were hunter-gatherers. The disadvantages of those traits were just a nuisance when having a formal education was merely optional for success. However, we have now trapped those who carry these traits in a one-size-fits-all educational system and sleep deprived them with a combination of electric lights and electronic distractions, to name just a few of the environmental changes that we have imposed.
Maybe it’s not the genes, but the environment that is the issue. The problem is that we haven’t found the genetic variant(s) that might allow us to answer these kinds of questions about ADHD.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “Coping with a Picky Eater.” E-mail him at [email protected].
If you ask most folks why some of us are obese, they will answer that it’s because overweight people have eaten too much of the wrong foods and not exercised enough. If prompted, they might expand their response by saying that people who come from families with overweight members will usually have more trouble maintaining a healthy weight. It seems to me that just about covers our state-of-the-art understanding of obesity.
You can argue that there is always new information coming out from experiments on genetically altered mice. And, the recently appreciated relationship between sleep deprivation and being overweight sounds interesting. But it still boils down to the simple equation of too much energy in and too little burned.
In 2007, it was discovered that a variant of a gene known as FTO was closely linked to excess weight gain in humans. Individuals with one copy of the gene were on average 3.5 pounds heavier than were those without the gene. Those people with a double copy of the variant gene were 7 pounds heavier and 50% more likely to be obese than was the general population.
It looked like the FTO gene might be one of the answers beyond the simplicity of too much consumption and too little expenditure. But why would the gene suddenly become more prevalent over the last 5 or 6 decades that obesity has become epidemic in America? It seemed unlikely that this shift could occur in such a short time frame.
A recently published study in Proceedings of the National Academy of Sciences (PNAS 2014 [doi: 10.1073/pnas.1411893111]) suggests another more plausible explanation. Using data from the venerable and ongoing Framingham Heart Study, the researchers found that the FTO variant became a risk factor only after World War II. In other words, people with the FTO variant born prior to 1942 weren’t any more likely to be overweight than the rest of the population.
What has changed since the 1940s? Our diet has shifted toward more processed and fried foods. And, our lives and our jobs have become more sedentary. Television crept into our living rooms in the 1950s and into our bedrooms in the 1970s.
The FTO gene variant may have been advantageous to humans in lean times when the heavier of us were more likely to survive long periods of starvation. But now here in the land of fries and soft drinks, the gene has become hazardous to our health. We now look (and are) fat wearing the same genes that seemed to fit us so well a century ago.
We must have sympathy for those of us who have a gene that makes us more vulnerable when food is plentiful, and technology has made it easier to survive with very little energy expenditure. It is tempting to hope that someday scientists will find a way to alter the offending genes to help those cursed to carry them. But this kind of manipulation must be considered cautiously because a natural or man-made catastrophe on a global scale could once again make this gene advantageous.
We must face the fact that it is the environment in which we live – an environment that we have altered and can continue to alter – that is the primary driver of the obesity epidemic. One wonders whether we are experiencing other epidemics analogous to the FTO/obesity story.
Attention-deficit/hyperactivity disorder (ADHD) comes to mind. Some observers feel that a short attention span and impulsivity may have been advantageous when we were hunter-gatherers. The disadvantages of those traits were just a nuisance when having a formal education was merely optional for success. However, we have now trapped those who carry these traits in a one-size-fits-all educational system and sleep deprived them with a combination of electric lights and electronic distractions, to name just a few of the environmental changes that we have imposed.
Maybe it’s not the genes, but the environment that is the issue. The problem is that we haven’t found the genetic variant(s) that might allow us to answer these kinds of questions about ADHD.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “Coping with a Picky Eater.” E-mail him at [email protected].
If you ask most folks why some of us are obese, they will answer that it’s because overweight people have eaten too much of the wrong foods and not exercised enough. If prompted, they might expand their response by saying that people who come from families with overweight members will usually have more trouble maintaining a healthy weight. It seems to me that just about covers our state-of-the-art understanding of obesity.
You can argue that there is always new information coming out from experiments on genetically altered mice. And, the recently appreciated relationship between sleep deprivation and being overweight sounds interesting. But it still boils down to the simple equation of too much energy in and too little burned.
In 2007, it was discovered that a variant of a gene known as FTO was closely linked to excess weight gain in humans. Individuals with one copy of the gene were on average 3.5 pounds heavier than were those without the gene. Those people with a double copy of the variant gene were 7 pounds heavier and 50% more likely to be obese than was the general population.
It looked like the FTO gene might be one of the answers beyond the simplicity of too much consumption and too little expenditure. But why would the gene suddenly become more prevalent over the last 5 or 6 decades that obesity has become epidemic in America? It seemed unlikely that this shift could occur in such a short time frame.
A recently published study in Proceedings of the National Academy of Sciences (PNAS 2014 [doi: 10.1073/pnas.1411893111]) suggests another more plausible explanation. Using data from the venerable and ongoing Framingham Heart Study, the researchers found that the FTO variant became a risk factor only after World War II. In other words, people with the FTO variant born prior to 1942 weren’t any more likely to be overweight than the rest of the population.
What has changed since the 1940s? Our diet has shifted toward more processed and fried foods. And, our lives and our jobs have become more sedentary. Television crept into our living rooms in the 1950s and into our bedrooms in the 1970s.
The FTO gene variant may have been advantageous to humans in lean times when the heavier of us were more likely to survive long periods of starvation. But now here in the land of fries and soft drinks, the gene has become hazardous to our health. We now look (and are) fat wearing the same genes that seemed to fit us so well a century ago.
We must have sympathy for those of us who have a gene that makes us more vulnerable when food is plentiful, and technology has made it easier to survive with very little energy expenditure. It is tempting to hope that someday scientists will find a way to alter the offending genes to help those cursed to carry them. But this kind of manipulation must be considered cautiously because a natural or man-made catastrophe on a global scale could once again make this gene advantageous.
We must face the fact that it is the environment in which we live – an environment that we have altered and can continue to alter – that is the primary driver of the obesity epidemic. One wonders whether we are experiencing other epidemics analogous to the FTO/obesity story.
Attention-deficit/hyperactivity disorder (ADHD) comes to mind. Some observers feel that a short attention span and impulsivity may have been advantageous when we were hunter-gatherers. The disadvantages of those traits were just a nuisance when having a formal education was merely optional for success. However, we have now trapped those who carry these traits in a one-size-fits-all educational system and sleep deprived them with a combination of electric lights and electronic distractions, to name just a few of the environmental changes that we have imposed.
Maybe it’s not the genes, but the environment that is the issue. The problem is that we haven’t found the genetic variant(s) that might allow us to answer these kinds of questions about ADHD.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “Coping with a Picky Eater.” E-mail him at [email protected].

Preparing the Military Health System for the 21st Century
Assistant Secretary of Defense for Health Affairs Dr. Jonathan Woodson sits atop a massively complex health care system. With an annual budget of > $50 billion and 133,000 military and civilian health care providers, allied health professionals, and health administrators spread around the globe, the Military Health System (MHS) is exceedingly complex. Keeping the system running is challenging enough, but Woodson is focused on transforming it into a more nimble, efficient, proactive and cost-effective health care system.
Federal Practitioner recently talked with Dr. Woodson about the challenges of transforming the MHS. We also discussed the Defense Health Agency and how global health threats like Ebola fit in to the MHS mission. The following is condensed and edited, but the complete interview can be heard here: Jonathan Woodson on Military Health Readiness.
The Military Health System Mission
Assistant Secretary of Defense for Health Affairs Jonathan Woodson. The Department of Defense has a unique mission. So yes, we do deliver health care; but we deliver health care on a global basis. And in fact, we are the ones who are asked anytime there is a crisis to set up health care systems in austere places as a key enabler to those who would go in harm’s way and defend our nation.
That is a sober undertaking, and we undertake it with the full understanding that in today’s world, the American leadership and the American public expect us to not only deliver the standard of care, but really go above the standard of care and advance care anywhere in the world....If you look at the experience of the last 12 plus years of war, and you look at what has been accomplished in terms of combat casualty care, we have advanced that strategy for care.
At the beginning of the war, it was clear that we were operating from a traditional platform but a number of experts recognized that what we needed to develop was a system that could drive change based upon data. The Joint Trauma System was born, which analyzed the outcomes of just about every case that was treated. But more importantly, [it] mined the data and rapidly changed the strategies for care as we found optimal ways of delivering care.
This included everything from our strategy for evacuation and the development of critical care air medical transplant units that provided prompt evacuation from the battlefield and echelons of care so those service members would receive very sophisticated advanced care, to strategies for employing new drugs, new techniques, new training strategies for medics and bringing critical care skills closer to the point of injury. Across a wide swath of strategies for delivering care, the system has been constantly improved.
And now we see from the data that despite the fact that we’re taking care of more severely injured individuals, the fatality rates have dropped. An individual who makes it to a role 3 facility—whatever the injury severity—has a 98% chance of surviving.
This has culminated most recently in terms of this transfer of knowledge with us signing a partnership agreement with the American College of Surgeons, which will allow us to further interact with the civilian communities in terms of trying to define optimal ways for caring for injured patients. This will be good not only for us, but it will be good for the civilian communities as well.
Research and Sharing Advances
Dr. Woodson. We have outlined 6 strategic lines of effort to help modernize the military health system, and they include modernizing our management with an enterprise focus, defining our 21st century capabilities that are necessary to make us better, stronger, and more relevant for the future. [We are also] looking at the medical force structure, particularly since today we have to ensure that we understand and employ subspecialists in the right way.
In addition, we are looking at defining and investing in strategic partners. Our strategic partners are like the American College of Surgeons but represent a wide range of potential academic and research institutions that can collaborate with us to ensure that we achieve results in our research portfolio, particularly against the priorities that are very important to military medicine.
The other areas that we need to concentrate on is reforming TRICARE and defining our requirements and competencies in global health engagement. The issue is investing in and defining our strategic partners, which is what I think is going to make us extraordinarily strong, because realistically we need to approach this as the whole-of-society investment in our national defense. Our strategic partners, of course, include our other federal partners, such as the Veterans Administration.
Continuity of Care
Dr. Woodson. We are committed to serving the needs of servicemen and women who might be injured or become ill as a result of their service for decades to come. That is, we understand that they may, in fact, require care for decades. And as a result, we, of course, have several ways of ensuring that they do receive that care. We have a defined sort of insurance benefit called TRICARE; a vehicle that allows separating servicemen and women who qualify to receive care in the civilian sector.
But beyond that, we have strengthened our partnership and our collaboration with the Veterans Administration to break down barriers so that we can transition servicemen and women more effectively and easily. [For] things like transferring critical medical information, we’ve developed an integrative mental health strategy so that we have common evidence-based strategies for mental health care.
We’ve recently concluded an agreement to reform the way the 2 departments reimburse each other so that the whole issue of billing doesn’t become an encumbrance to delivery of care. We’ve agreed to a common credentialing system so that our providers can more easily serve in either system, which leads to more effective, efficient care and use of our human resources.
Across many lines—the ones I’ve mentioned, and many others—we are ensuring that we can care for the servicemen and women who might become ill or injured and require care going on into the decades to ensure that they have high-quality lives and they’re kept healthy.
The Global Response to Ebola
Dr. Woodson. We have subject matter experts that have worked in infectious diseases for some time. You know, the United States Army Institute of Infectious Diseases is a well-recognized, longstanding organization that has helped produce vaccines and strategies to care for infectious diseases and has contributed very substantially to the biosecurity not only of this nation, but of the world.
We’ve got really the indomitable spirit of the average serviceman and woman who, when given a complex job, know how to meet the mission. And so we have superb leaders, and we have become a key enabler.
When the U.S. shows up, then other countries rally. It provides a platform in which other countries can now commit to the effort. And that’s probably as important as anything else, because this needs to be a worldwide effort to stem this epidemic that is occurring in West Africa.
The Defense Health Agency
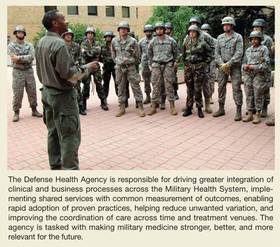
The Defense Health Agency has as its mission to put in effect common clinical and business processes to achieve those economies of scale and allow us to use our dollars and other resources more wisely. The Defense Health Agency was charged with initially standing up 10 shared services to include facilities planning, medical logistics, health information technology, managing the TRICARE health plan, pharmacy programs, the Public Health System, acquisitions, budget and resources, management systems, medical education and training, and medical research and development.
As such, we’ve achieved great results over the first year, saving about $248 million. But more importantly, we set the foundation for 21st century systems that will allow us to manage the Military Health System much more effectively, such as establishing a foundation for a common cost accounting system and the development of an enterprise performance management system.
The Military Health System added what we call the Quadruple Aim, which is providing better outcomes, better patient care experience, managing costs, and meeting our readiness mission. We have also established a solid strategic plan and framework in which to ensure that we will meet that end. We’ve had tremendous progress over the first year.
I just want to remind you and everyone of what a heavy lift this was. This is a major reorganization where thousands of people have been reassigned and reorganized to produce a more effective management system. This was no easy lift, but it has been tremendously successful to date.
You don’t necessarily flip the switch and everything is mature and working optimally overnight. The intent was to ensure that it was fully operational and capable by 1 October 2015. What we have seen to date is that it’s ahead of schedule, and that’s good news.
It represents major transformational change. Many people have to be moved. We had to build a new leadership team that, in fact, was heavily invested and contributed to by the uniformed services, the Army, Navy, and Air Force. So they’re deeply invested in the leadership and the governance of the Defense Health Agency.
The Military’s Health Care Challenges
Dr. Woodson. Our central guiding principle is the Quadruple Aim. And at the center, as I mentioned before, is this issue of readiness; and readiness is about ensuring that we have a healthy force to do the nation’s bidding in terms of defense. Not only do we have a healthy force, but we keep them healthy. So we commit to looking at environmental concerns wherever they are deployed. Of course, we provide force protection measures such as vaccines and medicines to prevent infectious diseases, such as malaria if they’re working in a part of the world where that’s endemic.
This is all part of the responsibilities of the military health system. But also, the second part of the readiness responsibility is ensuring that we have a ready medical force. A group of superbly trained providers from the embedded combat medic up to the super subspecialist neurosurgeon, nurses of all specialties and varieties, and other allied health professionals that can create a robust Military Health System and provide above the standard of care anywhere in the world where our sailors, marines, airmen, and soldiers may be operating.
We also have to deal with the issue of chronic problems, health problems that afflict our society. We have started initiatives to address obesity and fitness across a broad spectrum. As a strategy for the military health system, we’re moving from the system of health care, which is just providing treatment after an established disease has occurred, to one of health, which is looking at the whole paradigm of wellness and preventing disease from occurring. It is about reaching into that white space where people learn, work, and play to ensure that they can make healthy choices....We’re deeply invested in the health of the beneficiaries that we serve across a broad spectrum, and we’re deeply invested in the issue of prevention, not only the treatment of disease.
The issue that I would want everyone to understand is that health care and health care delivery in the 21st century is very complex. It’s about not only the actual technology, advances in medical science, but it’s also about addressing where medical science hits human systems and how do you make the system work so that you achieve the best outcomes? And in that mix are the issues of cost and ensuring that you have the ability to deliver that care wherever it’s needed. We’ve mapped out with the leadership of the Military Health System, the surgeons general, and all of their leaders a pathway forward that, in fact, will ensure that the Military Health System will be strong, better, and relevant going into the 21st century and will continue to be a key enabler for the national security, national defense, and the national military strategies.
As a designated Combat Support Agency, the Defense Health Agency is also responsible for meeting the medical needs of the combatant commanders. Central to this role is to ensure our service members are medically ready to perform their mission, and our military medical personnel are ready to perform their mission—“Medically Ready Force…Ready Medical Force.”
Assistant Secretary of Defense for Health Affairs Dr. Jonathan Woodson sits atop a massively complex health care system. With an annual budget of > $50 billion and 133,000 military and civilian health care providers, allied health professionals, and health administrators spread around the globe, the Military Health System (MHS) is exceedingly complex. Keeping the system running is challenging enough, but Woodson is focused on transforming it into a more nimble, efficient, proactive and cost-effective health care system.
Federal Practitioner recently talked with Dr. Woodson about the challenges of transforming the MHS. We also discussed the Defense Health Agency and how global health threats like Ebola fit in to the MHS mission. The following is condensed and edited, but the complete interview can be heard here: Jonathan Woodson on Military Health Readiness.
The Military Health System Mission
Assistant Secretary of Defense for Health Affairs Jonathan Woodson. The Department of Defense has a unique mission. So yes, we do deliver health care; but we deliver health care on a global basis. And in fact, we are the ones who are asked anytime there is a crisis to set up health care systems in austere places as a key enabler to those who would go in harm’s way and defend our nation.
That is a sober undertaking, and we undertake it with the full understanding that in today’s world, the American leadership and the American public expect us to not only deliver the standard of care, but really go above the standard of care and advance care anywhere in the world....If you look at the experience of the last 12 plus years of war, and you look at what has been accomplished in terms of combat casualty care, we have advanced that strategy for care.
At the beginning of the war, it was clear that we were operating from a traditional platform but a number of experts recognized that what we needed to develop was a system that could drive change based upon data. The Joint Trauma System was born, which analyzed the outcomes of just about every case that was treated. But more importantly, [it] mined the data and rapidly changed the strategies for care as we found optimal ways of delivering care.
This included everything from our strategy for evacuation and the development of critical care air medical transplant units that provided prompt evacuation from the battlefield and echelons of care so those service members would receive very sophisticated advanced care, to strategies for employing new drugs, new techniques, new training strategies for medics and bringing critical care skills closer to the point of injury. Across a wide swath of strategies for delivering care, the system has been constantly improved.
And now we see from the data that despite the fact that we’re taking care of more severely injured individuals, the fatality rates have dropped. An individual who makes it to a role 3 facility—whatever the injury severity—has a 98% chance of surviving.
This has culminated most recently in terms of this transfer of knowledge with us signing a partnership agreement with the American College of Surgeons, which will allow us to further interact with the civilian communities in terms of trying to define optimal ways for caring for injured patients. This will be good not only for us, but it will be good for the civilian communities as well.
Research and Sharing Advances
Dr. Woodson. We have outlined 6 strategic lines of effort to help modernize the military health system, and they include modernizing our management with an enterprise focus, defining our 21st century capabilities that are necessary to make us better, stronger, and more relevant for the future. [We are also] looking at the medical force structure, particularly since today we have to ensure that we understand and employ subspecialists in the right way.
In addition, we are looking at defining and investing in strategic partners. Our strategic partners are like the American College of Surgeons but represent a wide range of potential academic and research institutions that can collaborate with us to ensure that we achieve results in our research portfolio, particularly against the priorities that are very important to military medicine.
The other areas that we need to concentrate on is reforming TRICARE and defining our requirements and competencies in global health engagement. The issue is investing in and defining our strategic partners, which is what I think is going to make us extraordinarily strong, because realistically we need to approach this as the whole-of-society investment in our national defense. Our strategic partners, of course, include our other federal partners, such as the Veterans Administration.
Continuity of Care
Dr. Woodson. We are committed to serving the needs of servicemen and women who might be injured or become ill as a result of their service for decades to come. That is, we understand that they may, in fact, require care for decades. And as a result, we, of course, have several ways of ensuring that they do receive that care. We have a defined sort of insurance benefit called TRICARE; a vehicle that allows separating servicemen and women who qualify to receive care in the civilian sector.
But beyond that, we have strengthened our partnership and our collaboration with the Veterans Administration to break down barriers so that we can transition servicemen and women more effectively and easily. [For] things like transferring critical medical information, we’ve developed an integrative mental health strategy so that we have common evidence-based strategies for mental health care.
We’ve recently concluded an agreement to reform the way the 2 departments reimburse each other so that the whole issue of billing doesn’t become an encumbrance to delivery of care. We’ve agreed to a common credentialing system so that our providers can more easily serve in either system, which leads to more effective, efficient care and use of our human resources.
Across many lines—the ones I’ve mentioned, and many others—we are ensuring that we can care for the servicemen and women who might become ill or injured and require care going on into the decades to ensure that they have high-quality lives and they’re kept healthy.
The Global Response to Ebola
Dr. Woodson. We have subject matter experts that have worked in infectious diseases for some time. You know, the United States Army Institute of Infectious Diseases is a well-recognized, longstanding organization that has helped produce vaccines and strategies to care for infectious diseases and has contributed very substantially to the biosecurity not only of this nation, but of the world.
We’ve got really the indomitable spirit of the average serviceman and woman who, when given a complex job, know how to meet the mission. And so we have superb leaders, and we have become a key enabler.
When the U.S. shows up, then other countries rally. It provides a platform in which other countries can now commit to the effort. And that’s probably as important as anything else, because this needs to be a worldwide effort to stem this epidemic that is occurring in West Africa.
The Defense Health Agency
The Defense Health Agency has as its mission to put in effect common clinical and business processes to achieve those economies of scale and allow us to use our dollars and other resources more wisely. The Defense Health Agency was charged with initially standing up 10 shared services to include facilities planning, medical logistics, health information technology, managing the TRICARE health plan, pharmacy programs, the Public Health System, acquisitions, budget and resources, management systems, medical education and training, and medical research and development.
As such, we’ve achieved great results over the first year, saving about $248 million. But more importantly, we set the foundation for 21st century systems that will allow us to manage the Military Health System much more effectively, such as establishing a foundation for a common cost accounting system and the development of an enterprise performance management system.
The Military Health System added what we call the Quadruple Aim, which is providing better outcomes, better patient care experience, managing costs, and meeting our readiness mission. We have also established a solid strategic plan and framework in which to ensure that we will meet that end. We’ve had tremendous progress over the first year.
I just want to remind you and everyone of what a heavy lift this was. This is a major reorganization where thousands of people have been reassigned and reorganized to produce a more effective management system. This was no easy lift, but it has been tremendously successful to date.
You don’t necessarily flip the switch and everything is mature and working optimally overnight. The intent was to ensure that it was fully operational and capable by 1 October 2015. What we have seen to date is that it’s ahead of schedule, and that’s good news.
It represents major transformational change. Many people have to be moved. We had to build a new leadership team that, in fact, was heavily invested and contributed to by the uniformed services, the Army, Navy, and Air Force. So they’re deeply invested in the leadership and the governance of the Defense Health Agency.
The Military’s Health Care Challenges
Dr. Woodson. Our central guiding principle is the Quadruple Aim. And at the center, as I mentioned before, is this issue of readiness; and readiness is about ensuring that we have a healthy force to do the nation’s bidding in terms of defense. Not only do we have a healthy force, but we keep them healthy. So we commit to looking at environmental concerns wherever they are deployed. Of course, we provide force protection measures such as vaccines and medicines to prevent infectious diseases, such as malaria if they’re working in a part of the world where that’s endemic.
This is all part of the responsibilities of the military health system. But also, the second part of the readiness responsibility is ensuring that we have a ready medical force. A group of superbly trained providers from the embedded combat medic up to the super subspecialist neurosurgeon, nurses of all specialties and varieties, and other allied health professionals that can create a robust Military Health System and provide above the standard of care anywhere in the world where our sailors, marines, airmen, and soldiers may be operating.
We also have to deal with the issue of chronic problems, health problems that afflict our society. We have started initiatives to address obesity and fitness across a broad spectrum. As a strategy for the military health system, we’re moving from the system of health care, which is just providing treatment after an established disease has occurred, to one of health, which is looking at the whole paradigm of wellness and preventing disease from occurring. It is about reaching into that white space where people learn, work, and play to ensure that they can make healthy choices....We’re deeply invested in the health of the beneficiaries that we serve across a broad spectrum, and we’re deeply invested in the issue of prevention, not only the treatment of disease.
The issue that I would want everyone to understand is that health care and health care delivery in the 21st century is very complex. It’s about not only the actual technology, advances in medical science, but it’s also about addressing where medical science hits human systems and how do you make the system work so that you achieve the best outcomes? And in that mix are the issues of cost and ensuring that you have the ability to deliver that care wherever it’s needed. We’ve mapped out with the leadership of the Military Health System, the surgeons general, and all of their leaders a pathway forward that, in fact, will ensure that the Military Health System will be strong, better, and relevant going into the 21st century and will continue to be a key enabler for the national security, national defense, and the national military strategies.
As a designated Combat Support Agency, the Defense Health Agency is also responsible for meeting the medical needs of the combatant commanders. Central to this role is to ensure our service members are medically ready to perform their mission, and our military medical personnel are ready to perform their mission—“Medically Ready Force…Ready Medical Force.”
Assistant Secretary of Defense for Health Affairs Dr. Jonathan Woodson sits atop a massively complex health care system. With an annual budget of > $50 billion and 133,000 military and civilian health care providers, allied health professionals, and health administrators spread around the globe, the Military Health System (MHS) is exceedingly complex. Keeping the system running is challenging enough, but Woodson is focused on transforming it into a more nimble, efficient, proactive and cost-effective health care system.
Federal Practitioner recently talked with Dr. Woodson about the challenges of transforming the MHS. We also discussed the Defense Health Agency and how global health threats like Ebola fit in to the MHS mission. The following is condensed and edited, but the complete interview can be heard here: Jonathan Woodson on Military Health Readiness.
The Military Health System Mission
Assistant Secretary of Defense for Health Affairs Jonathan Woodson. The Department of Defense has a unique mission. So yes, we do deliver health care; but we deliver health care on a global basis. And in fact, we are the ones who are asked anytime there is a crisis to set up health care systems in austere places as a key enabler to those who would go in harm’s way and defend our nation.
That is a sober undertaking, and we undertake it with the full understanding that in today’s world, the American leadership and the American public expect us to not only deliver the standard of care, but really go above the standard of care and advance care anywhere in the world....If you look at the experience of the last 12 plus years of war, and you look at what has been accomplished in terms of combat casualty care, we have advanced that strategy for care.
At the beginning of the war, it was clear that we were operating from a traditional platform but a number of experts recognized that what we needed to develop was a system that could drive change based upon data. The Joint Trauma System was born, which analyzed the outcomes of just about every case that was treated. But more importantly, [it] mined the data and rapidly changed the strategies for care as we found optimal ways of delivering care.
This included everything from our strategy for evacuation and the development of critical care air medical transplant units that provided prompt evacuation from the battlefield and echelons of care so those service members would receive very sophisticated advanced care, to strategies for employing new drugs, new techniques, new training strategies for medics and bringing critical care skills closer to the point of injury. Across a wide swath of strategies for delivering care, the system has been constantly improved.
And now we see from the data that despite the fact that we’re taking care of more severely injured individuals, the fatality rates have dropped. An individual who makes it to a role 3 facility—whatever the injury severity—has a 98% chance of surviving.
This has culminated most recently in terms of this transfer of knowledge with us signing a partnership agreement with the American College of Surgeons, which will allow us to further interact with the civilian communities in terms of trying to define optimal ways for caring for injured patients. This will be good not only for us, but it will be good for the civilian communities as well.
Research and Sharing Advances
Dr. Woodson. We have outlined 6 strategic lines of effort to help modernize the military health system, and they include modernizing our management with an enterprise focus, defining our 21st century capabilities that are necessary to make us better, stronger, and more relevant for the future. [We are also] looking at the medical force structure, particularly since today we have to ensure that we understand and employ subspecialists in the right way.
In addition, we are looking at defining and investing in strategic partners. Our strategic partners are like the American College of Surgeons but represent a wide range of potential academic and research institutions that can collaborate with us to ensure that we achieve results in our research portfolio, particularly against the priorities that are very important to military medicine.
The other areas that we need to concentrate on is reforming TRICARE and defining our requirements and competencies in global health engagement. The issue is investing in and defining our strategic partners, which is what I think is going to make us extraordinarily strong, because realistically we need to approach this as the whole-of-society investment in our national defense. Our strategic partners, of course, include our other federal partners, such as the Veterans Administration.
Continuity of Care
Dr. Woodson. We are committed to serving the needs of servicemen and women who might be injured or become ill as a result of their service for decades to come. That is, we understand that they may, in fact, require care for decades. And as a result, we, of course, have several ways of ensuring that they do receive that care. We have a defined sort of insurance benefit called TRICARE; a vehicle that allows separating servicemen and women who qualify to receive care in the civilian sector.
But beyond that, we have strengthened our partnership and our collaboration with the Veterans Administration to break down barriers so that we can transition servicemen and women more effectively and easily. [For] things like transferring critical medical information, we’ve developed an integrative mental health strategy so that we have common evidence-based strategies for mental health care.
We’ve recently concluded an agreement to reform the way the 2 departments reimburse each other so that the whole issue of billing doesn’t become an encumbrance to delivery of care. We’ve agreed to a common credentialing system so that our providers can more easily serve in either system, which leads to more effective, efficient care and use of our human resources.
Across many lines—the ones I’ve mentioned, and many others—we are ensuring that we can care for the servicemen and women who might become ill or injured and require care going on into the decades to ensure that they have high-quality lives and they’re kept healthy.
The Global Response to Ebola
Dr. Woodson. We have subject matter experts that have worked in infectious diseases for some time. You know, the United States Army Institute of Infectious Diseases is a well-recognized, longstanding organization that has helped produce vaccines and strategies to care for infectious diseases and has contributed very substantially to the biosecurity not only of this nation, but of the world.
We’ve got really the indomitable spirit of the average serviceman and woman who, when given a complex job, know how to meet the mission. And so we have superb leaders, and we have become a key enabler.
When the U.S. shows up, then other countries rally. It provides a platform in which other countries can now commit to the effort. And that’s probably as important as anything else, because this needs to be a worldwide effort to stem this epidemic that is occurring in West Africa.
The Defense Health Agency
The Defense Health Agency has as its mission to put in effect common clinical and business processes to achieve those economies of scale and allow us to use our dollars and other resources more wisely. The Defense Health Agency was charged with initially standing up 10 shared services to include facilities planning, medical logistics, health information technology, managing the TRICARE health plan, pharmacy programs, the Public Health System, acquisitions, budget and resources, management systems, medical education and training, and medical research and development.
As such, we’ve achieved great results over the first year, saving about $248 million. But more importantly, we set the foundation for 21st century systems that will allow us to manage the Military Health System much more effectively, such as establishing a foundation for a common cost accounting system and the development of an enterprise performance management system.
The Military Health System added what we call the Quadruple Aim, which is providing better outcomes, better patient care experience, managing costs, and meeting our readiness mission. We have also established a solid strategic plan and framework in which to ensure that we will meet that end. We’ve had tremendous progress over the first year.
I just want to remind you and everyone of what a heavy lift this was. This is a major reorganization where thousands of people have been reassigned and reorganized to produce a more effective management system. This was no easy lift, but it has been tremendously successful to date.
You don’t necessarily flip the switch and everything is mature and working optimally overnight. The intent was to ensure that it was fully operational and capable by 1 October 2015. What we have seen to date is that it’s ahead of schedule, and that’s good news.
It represents major transformational change. Many people have to be moved. We had to build a new leadership team that, in fact, was heavily invested and contributed to by the uniformed services, the Army, Navy, and Air Force. So they’re deeply invested in the leadership and the governance of the Defense Health Agency.
The Military’s Health Care Challenges
Dr. Woodson. Our central guiding principle is the Quadruple Aim. And at the center, as I mentioned before, is this issue of readiness; and readiness is about ensuring that we have a healthy force to do the nation’s bidding in terms of defense. Not only do we have a healthy force, but we keep them healthy. So we commit to looking at environmental concerns wherever they are deployed. Of course, we provide force protection measures such as vaccines and medicines to prevent infectious diseases, such as malaria if they’re working in a part of the world where that’s endemic.
This is all part of the responsibilities of the military health system. But also, the second part of the readiness responsibility is ensuring that we have a ready medical force. A group of superbly trained providers from the embedded combat medic up to the super subspecialist neurosurgeon, nurses of all specialties and varieties, and other allied health professionals that can create a robust Military Health System and provide above the standard of care anywhere in the world where our sailors, marines, airmen, and soldiers may be operating.
We also have to deal with the issue of chronic problems, health problems that afflict our society. We have started initiatives to address obesity and fitness across a broad spectrum. As a strategy for the military health system, we’re moving from the system of health care, which is just providing treatment after an established disease has occurred, to one of health, which is looking at the whole paradigm of wellness and preventing disease from occurring. It is about reaching into that white space where people learn, work, and play to ensure that they can make healthy choices....We’re deeply invested in the health of the beneficiaries that we serve across a broad spectrum, and we’re deeply invested in the issue of prevention, not only the treatment of disease.
The issue that I would want everyone to understand is that health care and health care delivery in the 21st century is very complex. It’s about not only the actual technology, advances in medical science, but it’s also about addressing where medical science hits human systems and how do you make the system work so that you achieve the best outcomes? And in that mix are the issues of cost and ensuring that you have the ability to deliver that care wherever it’s needed. We’ve mapped out with the leadership of the Military Health System, the surgeons general, and all of their leaders a pathway forward that, in fact, will ensure that the Military Health System will be strong, better, and relevant going into the 21st century and will continue to be a key enabler for the national security, national defense, and the national military strategies.
As a designated Combat Support Agency, the Defense Health Agency is also responsible for meeting the medical needs of the combatant commanders. Central to this role is to ensure our service members are medically ready to perform their mission, and our military medical personnel are ready to perform their mission—“Medically Ready Force…Ready Medical Force.”