User login
Minimally Invasive Nail Surgery: Techniques to Improve the Patient Experience
Nail surgical procedures including biopsies, correction of onychocryptosis and other deformities, and excision of tumors are essential for diagnosing and treating nail disorders. Nail surgery often is perceived by dermatologists as a difficult-to-perform, high-risk procedure associated with patient anxiety, pain, and permanent scarring, which may limit implementation. Misconceptions about nail surgical techniques, aftercare, and patient outcomes are prevalent, and a paucity of nail surgery randomized clinical trials hinder formulation of standardized guidelines.1 In a survey-based study of 95 dermatology residency programs (240 total respondents), 58% of residents said they performed 10 or fewer nail procedures, 10% performed more than 10 procedures, 25% only observed nail procedures, 4% were exposed by lecture only, and 1% had no exposure; 30% said they felt incompetent performing nail biopsies.2 In a retrospective study of nail biopsies performed from 2012 to 2017 in the Medicare Provider Utilization and Payment Database, only 0.28% and 1.01% of all general dermatologists and Mohs surgeons, respectively, performed nail biopsies annually.3 A minimally invasive nail surgery technique is essential to alleviating dermatologist and patient apprehension, which may lead to greater adoption and improved outcomes.
Reduce Patient Anxiety During Nail Surgery
The prospect of undergoing nail surgery can be psychologically distressing to patients because the nail unit is highly sensitive, intraoperative and postoperative pain are common concerns, patient education materials generally are scarce and inaccurate,4 and procedures are performed under local anesthesia with the patient fully awake. In a prospective study of 48 patients undergoing nail surgery, the median preoperative Spielberger State-Trait Anxiety Inventory level was 42.00 (IQR, 6.50).5 Patient distress may be minimized by providing verbal and written educational materials, discussing expectations, and preoperatively using fast-acting benzodiazepines when necessary.6 Utilizing a sleep mask,7 stress ball,8 music,9 and/or virtual reality10 also may reduce patient anxiety during nail surgery.
Use Proper Anesthetic Techniques
Proper anesthetic technique is crucial to achieve the optimal patient experience during nail surgery. With a wing block, the anesthetic is injected into 3 points: (1) the proximal nail fold, (2) the medial/lateral fold, and (3) the hyponychium. The wing block is the preferred technique by many nail surgeons because the second and third injections are given in skin that is already anesthetized, reducing patient discomfort to a single pinprick11; additionally, there is lower postoperative paresthesia risk with the wing block compared with other digital nerve blocks.12 Ropivacaine, a fast-acting and long-acting anesthetic, is preferred over lidocaine to minimize immediate postoperative pain. Buffering the anesthetic solution to physiologic pH and slow infiltration can reduce pain during infiltration.12 Distraction12 provided by ethyl chloride refrigerant spray, an air-cooling device,13 or vibration also can reduce pain during anesthesia.
Punch Biopsy and Excision Tips
The punch biopsy is a minimally invasive method for diagnosing various neoplastic and inflammatory nail unit conditions, except for pigmented lesions.12 For polydactylous nail conditions requiring biopsy, a digit on the nondominant hand should be selected if possible. The punch is applied directly to the nail plate and twisted with downward pressure until the bone is reached, with the instrument withdrawn slowly to prevent surrounding nail plate detachment. Hemostasis is easily achieved with direct pressure and/or use of epinephrine or ropivacaine during anesthesia, and a digital tourniquet generally is not required. Applying microporous polysaccharide hemospheres powder14 or kaolin-impregnated gauze15 with direct pressure is helpful in managing continued bleeding following nail surgery. Punching through the proximal nail matrix should be avoided to prevent permanent onychodystrophy.
A tangential matrix shave biopsy requires a more practiced technique and is preferred for sampling longitudinal melanonychia. A partial proximal nail plate avulsion adequately exposes the origin of pigment and avoids complete avulsion, which may cause more onychodystrophy.16 For broad erythronychia, a total nail avulsion may be necessary. For narrow, well-defined erythronychia, a less-invasive approach such as trap-door avulsion, longitudinal nail strip, or lateral nail plate curl, depending on the etiology, often is sufficient. Tissue excision should be tailored to the specific etiology, with localized excision sufficient for glomus tumors; onychopapillomas require tangential excision of the distal matrix, entire nail bed, and hyperkeratotic papule at the hyponychium. Pushing the cuticle with an elevator/spatula instead of making 2 tangential incisions on the proximal nail fold has been suggested to decrease postoperative paronychia risk.12 A Teflon-coated blade is used to achieve a smooth cut with minimal drag, enabling collection of specimens less than 1 mm thick, which provides sufficient nail matrix epithelium and dermis for histologic examination.16 After obtaining the specimen, the avulsed nail plate may be sutured back to the nail bed using a rapidly absorbable suture such as polyglactin 910, serving as a temporary biological dressing and splint for the nail unit during healing.12 In a retrospective study of 30 patients with longitudinal melanonychia undergoing tangential matrix excision, 27% (8/30) developed postoperative onychodystrophy.17 Although this technique carries relatively lower risk of permanent onychodystrophy compared to other methods, it still is important to acknowledge during the preoperative consent process.12
The lateral longitudinal excision is a valuable technique for diagnosing nail unit inflammatory conditions. Classically, a longitudinal sample including the proximal nail fold, complete matrix, lateral plate, lateral nail fold, hyponychium, and distal tip skin is obtained, with a 10% narrowing of the nail plate expected. If the lateral horn of the nail matrix is missed, permanent lateral malalignment and spicule formation are potential risks. To minimize narrowing of the nail plate and postoperative paronychia, a longitudinal nail strip—where the proximal nail fold and matrix are left intact—is an alternative technique.18
Pain Management Approaches
Appropriate postoperative pain management is crucial for optimizing patient outcomes. In a prospective study of 20 patients undergoing nail biopsy, the mean pain score 6 to 12 hours postprocedure was 5.7 on a scale of 0 to 10. Patients with presurgery pain vs those without experienced significantly higher pain levels both during anesthesia and after surgery (both P<.05).19 Therefore, a personalized approach to pain management based on presence of presurgical pain is warranted. In a randomized clinical trial of 16 patients anesthetized with lidocaine 2% and intraoperative infiltration with a combination of ropivacaine 0.5 mL and triamcinolone (10 mg/mL [0.5 mL]) vs lidocaine 2% alone, the intraoperative mixture reduced postoperative pain (mean pain score, 2 of 10 at 48 hours postprocedure vs 7.88 of 10 in the control group [P<.001]).20
A Cochrane review of 4 unpublished dental and orthopedic surgery studies showed that gabapentin is superior to placebo in the treatment of acute postoperative pain. Therefore, a single dose of gabapentin (250 mg) may be considered in patients at risk for high postoperative pain.21 In a randomized double-blind trial of 210 Mohs micrographic surgery patients, those receiving acetaminophen and ibuprofen reported lower pain scores at 2, 4, 8, and 12 hours postprocedure compared with patients taking acetaminophen and codeine or acetaminophen alone.22 However, the role of opioids in pain management following nail surgery has not been adequately studied.
Wound Care
An efficient dressing protects the surgical wound, facilitates healing, and provides comfort. In our experience, an initial layer of petrolatum-impregnated gauze followed by a pressure-padded bandage consisting of folded dry gauze secured in place with longitudinally applied tape to avoid a tourniquet effect is effective for nail surgical wounds. As the last step, self-adherent elastic wrap is applied around the digit and extended proximally to prevent a tourniquet effect.23
Final Thoughts
Due to the intricate anatomy of the nail unit, nail surgeries are inherently more invasive than most dermatologic surgical procedures. It is crucial to adopt a minimally invasive approach to reduce tissue damage and potential complications in both the short-term and long-term. Adopting this approach may substantially improve patient outcomes and enhance diagnostic and treatment efficacy.
- Ricardo JW, Lipner SR. Nail surgery myths and truths. J Drugs Dermatol. 2020;19:230-234.
- Lee EH, Nehal KS, Dusza SW, et al. Procedural dermatology training during dermatology residency: a survey of third-year dermatology residents. J Am Acad Dermatol. 2011;64:475-483.E4835. doi:10.1016/j.jaad.2010.05.044
- Wang Y, Lipner SR. Retrospective analysis of nail biopsies performed using the Medicare Provider Utilization and Payment Database 2012 to 2017. Dermatol Ther. 2021;34:E14928. doi:10.1111/dth.14928
- Ishack S, Lipner SR. Evaluating the impact and educational value of YouTube videos on nail biopsy procedures. Cutis. 2020;105:148-149, E1.
- Göktay F, Altan ZM, Talas A, et al. Anxiety among patients undergoing nail surgery and skin punch biopsy: effects of age, gender, educational status, and previous experience. J Cutan Med Surg. 2016;20:35-39. doi:10.1177/1203475415588645
- Lipner SR. Pain-minimizing strategies for nail surgery. Cutis. 2018;101:76-77.
- Ricardo JW, Lipner SR. Utilizing a sleep mask to reduce patient anxiety during nail surgery. Cutis. 2021;108:36. doi:10.12788/cutis.0285
- Ricardo JW, Lipner SR. Utilization of a stress ball to diminish anxiety during nail surgery. Cutis. 2020;105:294.
- Vachiramon V, Sobanko JF, Rattanaumpawan P, et al. Music reduces patient anxiety during Mohs surgery: an open-label randomized controlled trial. Dermatol Surg. 2013;39:298-305. doi:10.1111/dsu.12047
- Higgins S, Feinstein S, Hawkins M, et al. Virtual reality to improve the experience of the Mohs patient—a prospective interventional study. Dermatol Surg. 2019;45:1009-1018. doi:10.1097/DSS.0000000000001854
- Jellinek NJ, Vélez NF. Nail surgery: best way to obtain effective anesthesia. Dermatol Clin. 2015;33:265-271. doi:10.1016/j.det.2014.12.007
- Baltz JO, Jellinek NJ. Nail surgery: six essential techniques. Dermatol Clin. 2021;39:305-318. doi:10.1016/j.det.2020.12.015
- Ricardo JW, Lipner SR. Air cooling for improved analgesia during local anesthetic infiltration for nail surgery. J Am Acad Dermatol. 2021;84:E231-E232. doi:10.1016/j.jaad.2019.11.032
- Ricardo JW, Lipner SR. Microporous polysaccharide hemospheres powder for hemostasis following nail surgery [published online March 26, 2021]. J Am Acad Dermatol. doi:10.1016/j.jaad.2021.03.069
- Ricardo JW, Lipner SR. Kaolin-impregnated gauze for hemostasis following nail surgery. J Am Acad Dermatol. 2021;85:E13-E14. doi:10.1016/j.jaad.2020.02.008
- Jellinek N. Nail matrix biopsy of longitudinal melanonychia: diagnostic algorithm including the matrix shave biopsy. J Am Acad Dermatol. 2007;56:803-810. doi:10.1016/j.jaad.2006.12.001
- Richert B, Theunis A, Norrenberg S, et al. Tangential excision of pigmented nail matrix lesions responsible for longitudinal melanonychia: evaluation of the technique on a series of 30 patients. J Am Acad Dermatol. 2013;69:96-104. doi:10.1016/j.jaad.2013.01.029
- Godse R, Jariwala N, Rubin AI. How we do it: the longitudinal nail strip biopsy for nail unit inflammatory dermatoses. Dermatol Surg. 2023;49:311-313. doi:10.1097/DSS.0000000000003707
- Ricardo JW, Qiu Y, Lipner SR. Longitudinal perioperative pain assessment in nail surgery. J Am Acad Dermatol. 2022;87:874-876. doi:10.1016/j.jaad.2021.11.042
- Di Chiacchio N, Ocampo-Garza J, Villarreal-Villarreal CD, et al. Post-nail procedure analgesia: a randomized control pilot study. J Am Acad Dermatol. 2019;81:860-862. doi:10.1016/j.jaad.2019.05.015
- Straube S, Derry S, Moore RA, et al. Single dose oral gabapentin for established acute postoperative pain in adults [published online May 12, 2010]. Cochrane Database Syst Rev. 2010;2010:CD008183. doi:10.1002/14651858.CD008183.pub2
- Sniezek PJ, Brodland DG, Zitelli JA. A randomized controlled trial comparing acetaminophen, acetaminophen and ibuprofen, and acetaminophen and codeine for postoperative pain relief after Mohs surgery and cutaneous reconstruction. Dermatol Surg. 2011;37:1007-1013. doi:10.1111/j.1524-4725.2011.02022.x
- Ricardo JW, Lipner SR. How we do it: pressure-padded dressing with self-adherent elastic wrap for wound care after nail surgery. Dermatol Surg. 2021;47:442-444. doi:10.1097/DSS.0000000000002371
Nail surgical procedures including biopsies, correction of onychocryptosis and other deformities, and excision of tumors are essential for diagnosing and treating nail disorders. Nail surgery often is perceived by dermatologists as a difficult-to-perform, high-risk procedure associated with patient anxiety, pain, and permanent scarring, which may limit implementation. Misconceptions about nail surgical techniques, aftercare, and patient outcomes are prevalent, and a paucity of nail surgery randomized clinical trials hinder formulation of standardized guidelines.1 In a survey-based study of 95 dermatology residency programs (240 total respondents), 58% of residents said they performed 10 or fewer nail procedures, 10% performed more than 10 procedures, 25% only observed nail procedures, 4% were exposed by lecture only, and 1% had no exposure; 30% said they felt incompetent performing nail biopsies.2 In a retrospective study of nail biopsies performed from 2012 to 2017 in the Medicare Provider Utilization and Payment Database, only 0.28% and 1.01% of all general dermatologists and Mohs surgeons, respectively, performed nail biopsies annually.3 A minimally invasive nail surgery technique is essential to alleviating dermatologist and patient apprehension, which may lead to greater adoption and improved outcomes.
Reduce Patient Anxiety During Nail Surgery
The prospect of undergoing nail surgery can be psychologically distressing to patients because the nail unit is highly sensitive, intraoperative and postoperative pain are common concerns, patient education materials generally are scarce and inaccurate,4 and procedures are performed under local anesthesia with the patient fully awake. In a prospective study of 48 patients undergoing nail surgery, the median preoperative Spielberger State-Trait Anxiety Inventory level was 42.00 (IQR, 6.50).5 Patient distress may be minimized by providing verbal and written educational materials, discussing expectations, and preoperatively using fast-acting benzodiazepines when necessary.6 Utilizing a sleep mask,7 stress ball,8 music,9 and/or virtual reality10 also may reduce patient anxiety during nail surgery.
Use Proper Anesthetic Techniques
Proper anesthetic technique is crucial to achieve the optimal patient experience during nail surgery. With a wing block, the anesthetic is injected into 3 points: (1) the proximal nail fold, (2) the medial/lateral fold, and (3) the hyponychium. The wing block is the preferred technique by many nail surgeons because the second and third injections are given in skin that is already anesthetized, reducing patient discomfort to a single pinprick11; additionally, there is lower postoperative paresthesia risk with the wing block compared with other digital nerve blocks.12 Ropivacaine, a fast-acting and long-acting anesthetic, is preferred over lidocaine to minimize immediate postoperative pain. Buffering the anesthetic solution to physiologic pH and slow infiltration can reduce pain during infiltration.12 Distraction12 provided by ethyl chloride refrigerant spray, an air-cooling device,13 or vibration also can reduce pain during anesthesia.
Punch Biopsy and Excision Tips
The punch biopsy is a minimally invasive method for diagnosing various neoplastic and inflammatory nail unit conditions, except for pigmented lesions.12 For polydactylous nail conditions requiring biopsy, a digit on the nondominant hand should be selected if possible. The punch is applied directly to the nail plate and twisted with downward pressure until the bone is reached, with the instrument withdrawn slowly to prevent surrounding nail plate detachment. Hemostasis is easily achieved with direct pressure and/or use of epinephrine or ropivacaine during anesthesia, and a digital tourniquet generally is not required. Applying microporous polysaccharide hemospheres powder14 or kaolin-impregnated gauze15 with direct pressure is helpful in managing continued bleeding following nail surgery. Punching through the proximal nail matrix should be avoided to prevent permanent onychodystrophy.
A tangential matrix shave biopsy requires a more practiced technique and is preferred for sampling longitudinal melanonychia. A partial proximal nail plate avulsion adequately exposes the origin of pigment and avoids complete avulsion, which may cause more onychodystrophy.16 For broad erythronychia, a total nail avulsion may be necessary. For narrow, well-defined erythronychia, a less-invasive approach such as trap-door avulsion, longitudinal nail strip, or lateral nail plate curl, depending on the etiology, often is sufficient. Tissue excision should be tailored to the specific etiology, with localized excision sufficient for glomus tumors; onychopapillomas require tangential excision of the distal matrix, entire nail bed, and hyperkeratotic papule at the hyponychium. Pushing the cuticle with an elevator/spatula instead of making 2 tangential incisions on the proximal nail fold has been suggested to decrease postoperative paronychia risk.12 A Teflon-coated blade is used to achieve a smooth cut with minimal drag, enabling collection of specimens less than 1 mm thick, which provides sufficient nail matrix epithelium and dermis for histologic examination.16 After obtaining the specimen, the avulsed nail plate may be sutured back to the nail bed using a rapidly absorbable suture such as polyglactin 910, serving as a temporary biological dressing and splint for the nail unit during healing.12 In a retrospective study of 30 patients with longitudinal melanonychia undergoing tangential matrix excision, 27% (8/30) developed postoperative onychodystrophy.17 Although this technique carries relatively lower risk of permanent onychodystrophy compared to other methods, it still is important to acknowledge during the preoperative consent process.12
The lateral longitudinal excision is a valuable technique for diagnosing nail unit inflammatory conditions. Classically, a longitudinal sample including the proximal nail fold, complete matrix, lateral plate, lateral nail fold, hyponychium, and distal tip skin is obtained, with a 10% narrowing of the nail plate expected. If the lateral horn of the nail matrix is missed, permanent lateral malalignment and spicule formation are potential risks. To minimize narrowing of the nail plate and postoperative paronychia, a longitudinal nail strip—where the proximal nail fold and matrix are left intact—is an alternative technique.18
Pain Management Approaches
Appropriate postoperative pain management is crucial for optimizing patient outcomes. In a prospective study of 20 patients undergoing nail biopsy, the mean pain score 6 to 12 hours postprocedure was 5.7 on a scale of 0 to 10. Patients with presurgery pain vs those without experienced significantly higher pain levels both during anesthesia and after surgery (both P<.05).19 Therefore, a personalized approach to pain management based on presence of presurgical pain is warranted. In a randomized clinical trial of 16 patients anesthetized with lidocaine 2% and intraoperative infiltration with a combination of ropivacaine 0.5 mL and triamcinolone (10 mg/mL [0.5 mL]) vs lidocaine 2% alone, the intraoperative mixture reduced postoperative pain (mean pain score, 2 of 10 at 48 hours postprocedure vs 7.88 of 10 in the control group [P<.001]).20
A Cochrane review of 4 unpublished dental and orthopedic surgery studies showed that gabapentin is superior to placebo in the treatment of acute postoperative pain. Therefore, a single dose of gabapentin (250 mg) may be considered in patients at risk for high postoperative pain.21 In a randomized double-blind trial of 210 Mohs micrographic surgery patients, those receiving acetaminophen and ibuprofen reported lower pain scores at 2, 4, 8, and 12 hours postprocedure compared with patients taking acetaminophen and codeine or acetaminophen alone.22 However, the role of opioids in pain management following nail surgery has not been adequately studied.
Wound Care
An efficient dressing protects the surgical wound, facilitates healing, and provides comfort. In our experience, an initial layer of petrolatum-impregnated gauze followed by a pressure-padded bandage consisting of folded dry gauze secured in place with longitudinally applied tape to avoid a tourniquet effect is effective for nail surgical wounds. As the last step, self-adherent elastic wrap is applied around the digit and extended proximally to prevent a tourniquet effect.23
Final Thoughts
Due to the intricate anatomy of the nail unit, nail surgeries are inherently more invasive than most dermatologic surgical procedures. It is crucial to adopt a minimally invasive approach to reduce tissue damage and potential complications in both the short-term and long-term. Adopting this approach may substantially improve patient outcomes and enhance diagnostic and treatment efficacy.
Nail surgical procedures including biopsies, correction of onychocryptosis and other deformities, and excision of tumors are essential for diagnosing and treating nail disorders. Nail surgery often is perceived by dermatologists as a difficult-to-perform, high-risk procedure associated with patient anxiety, pain, and permanent scarring, which may limit implementation. Misconceptions about nail surgical techniques, aftercare, and patient outcomes are prevalent, and a paucity of nail surgery randomized clinical trials hinder formulation of standardized guidelines.1 In a survey-based study of 95 dermatology residency programs (240 total respondents), 58% of residents said they performed 10 or fewer nail procedures, 10% performed more than 10 procedures, 25% only observed nail procedures, 4% were exposed by lecture only, and 1% had no exposure; 30% said they felt incompetent performing nail biopsies.2 In a retrospective study of nail biopsies performed from 2012 to 2017 in the Medicare Provider Utilization and Payment Database, only 0.28% and 1.01% of all general dermatologists and Mohs surgeons, respectively, performed nail biopsies annually.3 A minimally invasive nail surgery technique is essential to alleviating dermatologist and patient apprehension, which may lead to greater adoption and improved outcomes.
Reduce Patient Anxiety During Nail Surgery
The prospect of undergoing nail surgery can be psychologically distressing to patients because the nail unit is highly sensitive, intraoperative and postoperative pain are common concerns, patient education materials generally are scarce and inaccurate,4 and procedures are performed under local anesthesia with the patient fully awake. In a prospective study of 48 patients undergoing nail surgery, the median preoperative Spielberger State-Trait Anxiety Inventory level was 42.00 (IQR, 6.50).5 Patient distress may be minimized by providing verbal and written educational materials, discussing expectations, and preoperatively using fast-acting benzodiazepines when necessary.6 Utilizing a sleep mask,7 stress ball,8 music,9 and/or virtual reality10 also may reduce patient anxiety during nail surgery.
Use Proper Anesthetic Techniques
Proper anesthetic technique is crucial to achieve the optimal patient experience during nail surgery. With a wing block, the anesthetic is injected into 3 points: (1) the proximal nail fold, (2) the medial/lateral fold, and (3) the hyponychium. The wing block is the preferred technique by many nail surgeons because the second and third injections are given in skin that is already anesthetized, reducing patient discomfort to a single pinprick11; additionally, there is lower postoperative paresthesia risk with the wing block compared with other digital nerve blocks.12 Ropivacaine, a fast-acting and long-acting anesthetic, is preferred over lidocaine to minimize immediate postoperative pain. Buffering the anesthetic solution to physiologic pH and slow infiltration can reduce pain during infiltration.12 Distraction12 provided by ethyl chloride refrigerant spray, an air-cooling device,13 or vibration also can reduce pain during anesthesia.
Punch Biopsy and Excision Tips
The punch biopsy is a minimally invasive method for diagnosing various neoplastic and inflammatory nail unit conditions, except for pigmented lesions.12 For polydactylous nail conditions requiring biopsy, a digit on the nondominant hand should be selected if possible. The punch is applied directly to the nail plate and twisted with downward pressure until the bone is reached, with the instrument withdrawn slowly to prevent surrounding nail plate detachment. Hemostasis is easily achieved with direct pressure and/or use of epinephrine or ropivacaine during anesthesia, and a digital tourniquet generally is not required. Applying microporous polysaccharide hemospheres powder14 or kaolin-impregnated gauze15 with direct pressure is helpful in managing continued bleeding following nail surgery. Punching through the proximal nail matrix should be avoided to prevent permanent onychodystrophy.
A tangential matrix shave biopsy requires a more practiced technique and is preferred for sampling longitudinal melanonychia. A partial proximal nail plate avulsion adequately exposes the origin of pigment and avoids complete avulsion, which may cause more onychodystrophy.16 For broad erythronychia, a total nail avulsion may be necessary. For narrow, well-defined erythronychia, a less-invasive approach such as trap-door avulsion, longitudinal nail strip, or lateral nail plate curl, depending on the etiology, often is sufficient. Tissue excision should be tailored to the specific etiology, with localized excision sufficient for glomus tumors; onychopapillomas require tangential excision of the distal matrix, entire nail bed, and hyperkeratotic papule at the hyponychium. Pushing the cuticle with an elevator/spatula instead of making 2 tangential incisions on the proximal nail fold has been suggested to decrease postoperative paronychia risk.12 A Teflon-coated blade is used to achieve a smooth cut with minimal drag, enabling collection of specimens less than 1 mm thick, which provides sufficient nail matrix epithelium and dermis for histologic examination.16 After obtaining the specimen, the avulsed nail plate may be sutured back to the nail bed using a rapidly absorbable suture such as polyglactin 910, serving as a temporary biological dressing and splint for the nail unit during healing.12 In a retrospective study of 30 patients with longitudinal melanonychia undergoing tangential matrix excision, 27% (8/30) developed postoperative onychodystrophy.17 Although this technique carries relatively lower risk of permanent onychodystrophy compared to other methods, it still is important to acknowledge during the preoperative consent process.12
The lateral longitudinal excision is a valuable technique for diagnosing nail unit inflammatory conditions. Classically, a longitudinal sample including the proximal nail fold, complete matrix, lateral plate, lateral nail fold, hyponychium, and distal tip skin is obtained, with a 10% narrowing of the nail plate expected. If the lateral horn of the nail matrix is missed, permanent lateral malalignment and spicule formation are potential risks. To minimize narrowing of the nail plate and postoperative paronychia, a longitudinal nail strip—where the proximal nail fold and matrix are left intact—is an alternative technique.18
Pain Management Approaches
Appropriate postoperative pain management is crucial for optimizing patient outcomes. In a prospective study of 20 patients undergoing nail biopsy, the mean pain score 6 to 12 hours postprocedure was 5.7 on a scale of 0 to 10. Patients with presurgery pain vs those without experienced significantly higher pain levels both during anesthesia and after surgery (both P<.05).19 Therefore, a personalized approach to pain management based on presence of presurgical pain is warranted. In a randomized clinical trial of 16 patients anesthetized with lidocaine 2% and intraoperative infiltration with a combination of ropivacaine 0.5 mL and triamcinolone (10 mg/mL [0.5 mL]) vs lidocaine 2% alone, the intraoperative mixture reduced postoperative pain (mean pain score, 2 of 10 at 48 hours postprocedure vs 7.88 of 10 in the control group [P<.001]).20
A Cochrane review of 4 unpublished dental and orthopedic surgery studies showed that gabapentin is superior to placebo in the treatment of acute postoperative pain. Therefore, a single dose of gabapentin (250 mg) may be considered in patients at risk for high postoperative pain.21 In a randomized double-blind trial of 210 Mohs micrographic surgery patients, those receiving acetaminophen and ibuprofen reported lower pain scores at 2, 4, 8, and 12 hours postprocedure compared with patients taking acetaminophen and codeine or acetaminophen alone.22 However, the role of opioids in pain management following nail surgery has not been adequately studied.
Wound Care
An efficient dressing protects the surgical wound, facilitates healing, and provides comfort. In our experience, an initial layer of petrolatum-impregnated gauze followed by a pressure-padded bandage consisting of folded dry gauze secured in place with longitudinally applied tape to avoid a tourniquet effect is effective for nail surgical wounds. As the last step, self-adherent elastic wrap is applied around the digit and extended proximally to prevent a tourniquet effect.23
Final Thoughts
Due to the intricate anatomy of the nail unit, nail surgeries are inherently more invasive than most dermatologic surgical procedures. It is crucial to adopt a minimally invasive approach to reduce tissue damage and potential complications in both the short-term and long-term. Adopting this approach may substantially improve patient outcomes and enhance diagnostic and treatment efficacy.
- Ricardo JW, Lipner SR. Nail surgery myths and truths. J Drugs Dermatol. 2020;19:230-234.
- Lee EH, Nehal KS, Dusza SW, et al. Procedural dermatology training during dermatology residency: a survey of third-year dermatology residents. J Am Acad Dermatol. 2011;64:475-483.E4835. doi:10.1016/j.jaad.2010.05.044
- Wang Y, Lipner SR. Retrospective analysis of nail biopsies performed using the Medicare Provider Utilization and Payment Database 2012 to 2017. Dermatol Ther. 2021;34:E14928. doi:10.1111/dth.14928
- Ishack S, Lipner SR. Evaluating the impact and educational value of YouTube videos on nail biopsy procedures. Cutis. 2020;105:148-149, E1.
- Göktay F, Altan ZM, Talas A, et al. Anxiety among patients undergoing nail surgery and skin punch biopsy: effects of age, gender, educational status, and previous experience. J Cutan Med Surg. 2016;20:35-39. doi:10.1177/1203475415588645
- Lipner SR. Pain-minimizing strategies for nail surgery. Cutis. 2018;101:76-77.
- Ricardo JW, Lipner SR. Utilizing a sleep mask to reduce patient anxiety during nail surgery. Cutis. 2021;108:36. doi:10.12788/cutis.0285
- Ricardo JW, Lipner SR. Utilization of a stress ball to diminish anxiety during nail surgery. Cutis. 2020;105:294.
- Vachiramon V, Sobanko JF, Rattanaumpawan P, et al. Music reduces patient anxiety during Mohs surgery: an open-label randomized controlled trial. Dermatol Surg. 2013;39:298-305. doi:10.1111/dsu.12047
- Higgins S, Feinstein S, Hawkins M, et al. Virtual reality to improve the experience of the Mohs patient—a prospective interventional study. Dermatol Surg. 2019;45:1009-1018. doi:10.1097/DSS.0000000000001854
- Jellinek NJ, Vélez NF. Nail surgery: best way to obtain effective anesthesia. Dermatol Clin. 2015;33:265-271. doi:10.1016/j.det.2014.12.007
- Baltz JO, Jellinek NJ. Nail surgery: six essential techniques. Dermatol Clin. 2021;39:305-318. doi:10.1016/j.det.2020.12.015
- Ricardo JW, Lipner SR. Air cooling for improved analgesia during local anesthetic infiltration for nail surgery. J Am Acad Dermatol. 2021;84:E231-E232. doi:10.1016/j.jaad.2019.11.032
- Ricardo JW, Lipner SR. Microporous polysaccharide hemospheres powder for hemostasis following nail surgery [published online March 26, 2021]. J Am Acad Dermatol. doi:10.1016/j.jaad.2021.03.069
- Ricardo JW, Lipner SR. Kaolin-impregnated gauze for hemostasis following nail surgery. J Am Acad Dermatol. 2021;85:E13-E14. doi:10.1016/j.jaad.2020.02.008
- Jellinek N. Nail matrix biopsy of longitudinal melanonychia: diagnostic algorithm including the matrix shave biopsy. J Am Acad Dermatol. 2007;56:803-810. doi:10.1016/j.jaad.2006.12.001
- Richert B, Theunis A, Norrenberg S, et al. Tangential excision of pigmented nail matrix lesions responsible for longitudinal melanonychia: evaluation of the technique on a series of 30 patients. J Am Acad Dermatol. 2013;69:96-104. doi:10.1016/j.jaad.2013.01.029
- Godse R, Jariwala N, Rubin AI. How we do it: the longitudinal nail strip biopsy for nail unit inflammatory dermatoses. Dermatol Surg. 2023;49:311-313. doi:10.1097/DSS.0000000000003707
- Ricardo JW, Qiu Y, Lipner SR. Longitudinal perioperative pain assessment in nail surgery. J Am Acad Dermatol. 2022;87:874-876. doi:10.1016/j.jaad.2021.11.042
- Di Chiacchio N, Ocampo-Garza J, Villarreal-Villarreal CD, et al. Post-nail procedure analgesia: a randomized control pilot study. J Am Acad Dermatol. 2019;81:860-862. doi:10.1016/j.jaad.2019.05.015
- Straube S, Derry S, Moore RA, et al. Single dose oral gabapentin for established acute postoperative pain in adults [published online May 12, 2010]. Cochrane Database Syst Rev. 2010;2010:CD008183. doi:10.1002/14651858.CD008183.pub2
- Sniezek PJ, Brodland DG, Zitelli JA. A randomized controlled trial comparing acetaminophen, acetaminophen and ibuprofen, and acetaminophen and codeine for postoperative pain relief after Mohs surgery and cutaneous reconstruction. Dermatol Surg. 2011;37:1007-1013. doi:10.1111/j.1524-4725.2011.02022.x
- Ricardo JW, Lipner SR. How we do it: pressure-padded dressing with self-adherent elastic wrap for wound care after nail surgery. Dermatol Surg. 2021;47:442-444. doi:10.1097/DSS.0000000000002371
- Ricardo JW, Lipner SR. Nail surgery myths and truths. J Drugs Dermatol. 2020;19:230-234.
- Lee EH, Nehal KS, Dusza SW, et al. Procedural dermatology training during dermatology residency: a survey of third-year dermatology residents. J Am Acad Dermatol. 2011;64:475-483.E4835. doi:10.1016/j.jaad.2010.05.044
- Wang Y, Lipner SR. Retrospective analysis of nail biopsies performed using the Medicare Provider Utilization and Payment Database 2012 to 2017. Dermatol Ther. 2021;34:E14928. doi:10.1111/dth.14928
- Ishack S, Lipner SR. Evaluating the impact and educational value of YouTube videos on nail biopsy procedures. Cutis. 2020;105:148-149, E1.
- Göktay F, Altan ZM, Talas A, et al. Anxiety among patients undergoing nail surgery and skin punch biopsy: effects of age, gender, educational status, and previous experience. J Cutan Med Surg. 2016;20:35-39. doi:10.1177/1203475415588645
- Lipner SR. Pain-minimizing strategies for nail surgery. Cutis. 2018;101:76-77.
- Ricardo JW, Lipner SR. Utilizing a sleep mask to reduce patient anxiety during nail surgery. Cutis. 2021;108:36. doi:10.12788/cutis.0285
- Ricardo JW, Lipner SR. Utilization of a stress ball to diminish anxiety during nail surgery. Cutis. 2020;105:294.
- Vachiramon V, Sobanko JF, Rattanaumpawan P, et al. Music reduces patient anxiety during Mohs surgery: an open-label randomized controlled trial. Dermatol Surg. 2013;39:298-305. doi:10.1111/dsu.12047
- Higgins S, Feinstein S, Hawkins M, et al. Virtual reality to improve the experience of the Mohs patient—a prospective interventional study. Dermatol Surg. 2019;45:1009-1018. doi:10.1097/DSS.0000000000001854
- Jellinek NJ, Vélez NF. Nail surgery: best way to obtain effective anesthesia. Dermatol Clin. 2015;33:265-271. doi:10.1016/j.det.2014.12.007
- Baltz JO, Jellinek NJ. Nail surgery: six essential techniques. Dermatol Clin. 2021;39:305-318. doi:10.1016/j.det.2020.12.015
- Ricardo JW, Lipner SR. Air cooling for improved analgesia during local anesthetic infiltration for nail surgery. J Am Acad Dermatol. 2021;84:E231-E232. doi:10.1016/j.jaad.2019.11.032
- Ricardo JW, Lipner SR. Microporous polysaccharide hemospheres powder for hemostasis following nail surgery [published online March 26, 2021]. J Am Acad Dermatol. doi:10.1016/j.jaad.2021.03.069
- Ricardo JW, Lipner SR. Kaolin-impregnated gauze for hemostasis following nail surgery. J Am Acad Dermatol. 2021;85:E13-E14. doi:10.1016/j.jaad.2020.02.008
- Jellinek N. Nail matrix biopsy of longitudinal melanonychia: diagnostic algorithm including the matrix shave biopsy. J Am Acad Dermatol. 2007;56:803-810. doi:10.1016/j.jaad.2006.12.001
- Richert B, Theunis A, Norrenberg S, et al. Tangential excision of pigmented nail matrix lesions responsible for longitudinal melanonychia: evaluation of the technique on a series of 30 patients. J Am Acad Dermatol. 2013;69:96-104. doi:10.1016/j.jaad.2013.01.029
- Godse R, Jariwala N, Rubin AI. How we do it: the longitudinal nail strip biopsy for nail unit inflammatory dermatoses. Dermatol Surg. 2023;49:311-313. doi:10.1097/DSS.0000000000003707
- Ricardo JW, Qiu Y, Lipner SR. Longitudinal perioperative pain assessment in nail surgery. J Am Acad Dermatol. 2022;87:874-876. doi:10.1016/j.jaad.2021.11.042
- Di Chiacchio N, Ocampo-Garza J, Villarreal-Villarreal CD, et al. Post-nail procedure analgesia: a randomized control pilot study. J Am Acad Dermatol. 2019;81:860-862. doi:10.1016/j.jaad.2019.05.015
- Straube S, Derry S, Moore RA, et al. Single dose oral gabapentin for established acute postoperative pain in adults [published online May 12, 2010]. Cochrane Database Syst Rev. 2010;2010:CD008183. doi:10.1002/14651858.CD008183.pub2
- Sniezek PJ, Brodland DG, Zitelli JA. A randomized controlled trial comparing acetaminophen, acetaminophen and ibuprofen, and acetaminophen and codeine for postoperative pain relief after Mohs surgery and cutaneous reconstruction. Dermatol Surg. 2011;37:1007-1013. doi:10.1111/j.1524-4725.2011.02022.x
- Ricardo JW, Lipner SR. How we do it: pressure-padded dressing with self-adherent elastic wrap for wound care after nail surgery. Dermatol Surg. 2021;47:442-444. doi:10.1097/DSS.0000000000002371
A 45-year-old White woman with no significant medical history presented with a 1-month history of lesions on the nose and right cheek
Cultures for bacteria, varicella zoster virus, herpes simplex virus, and mpox virus were all negative. A biopsy revealed suprabasilar acantholysis with follicular involvement in association with blister formation and inflammation. Direct immunofluorescence was positive for suprabasilar IgG and C3 deposition, consistent with pemphigus vulgaris (PV).
. There is likely a genetic predisposition. Medications that may induce pemphigus include penicillamine, nifedipine, or captopril.
Clinically, flaccid blistering lesions are present that may be cutaneous and/or mucosal. Bullae can progress to erosions and crusting, which then heal with pigment alteration but not scarring. The most commonly affected sites are the mouth, intertriginous areas, face, and neck. Mucosal lesions may involve the lips, esophagus, conjunctiva, and genitals.

Biopsy for histology and direct immunofluorescence is important in distinguishing between PV and other blistering disorders. Up to 75% of patients with active disease also have a positive indirect immunofluorescence with circulating IgG.
Treatment is generally immunosuppressive. Systemic therapy usually begins with prednisone and then is transitioned to a steroid-sparing agent such as mycophenolate mofetil. Other steroid-sparing agents include azathioprine, methotrexate, cyclophosphamide, and intravenous immunoglobulin. Secondary infections are possible and should be treated. Topical therapies aimed at reducing pain, especially in mucosal lesions, can be beneficial.
This case and the photos are from Dr. Bilu Martin.
Dr. Bilu Martin is a board-certified dermatologist in private practice at Premier Dermatology, MD, in Aventura, Fla. More diagnostic cases are available at mdedge.com/dermatology. To submit a case for possible publication, send an email to [email protected].
Cultures for bacteria, varicella zoster virus, herpes simplex virus, and mpox virus were all negative. A biopsy revealed suprabasilar acantholysis with follicular involvement in association with blister formation and inflammation. Direct immunofluorescence was positive for suprabasilar IgG and C3 deposition, consistent with pemphigus vulgaris (PV).
. There is likely a genetic predisposition. Medications that may induce pemphigus include penicillamine, nifedipine, or captopril.
Clinically, flaccid blistering lesions are present that may be cutaneous and/or mucosal. Bullae can progress to erosions and crusting, which then heal with pigment alteration but not scarring. The most commonly affected sites are the mouth, intertriginous areas, face, and neck. Mucosal lesions may involve the lips, esophagus, conjunctiva, and genitals.
Biopsy for histology and direct immunofluorescence is important in distinguishing between PV and other blistering disorders. Up to 75% of patients with active disease also have a positive indirect immunofluorescence with circulating IgG.
Treatment is generally immunosuppressive. Systemic therapy usually begins with prednisone and then is transitioned to a steroid-sparing agent such as mycophenolate mofetil. Other steroid-sparing agents include azathioprine, methotrexate, cyclophosphamide, and intravenous immunoglobulin. Secondary infections are possible and should be treated. Topical therapies aimed at reducing pain, especially in mucosal lesions, can be beneficial.
This case and the photos are from Dr. Bilu Martin.
Dr. Bilu Martin is a board-certified dermatologist in private practice at Premier Dermatology, MD, in Aventura, Fla. More diagnostic cases are available at mdedge.com/dermatology. To submit a case for possible publication, send an email to [email protected].
Cultures for bacteria, varicella zoster virus, herpes simplex virus, and mpox virus were all negative. A biopsy revealed suprabasilar acantholysis with follicular involvement in association with blister formation and inflammation. Direct immunofluorescence was positive for suprabasilar IgG and C3 deposition, consistent with pemphigus vulgaris (PV).
. There is likely a genetic predisposition. Medications that may induce pemphigus include penicillamine, nifedipine, or captopril.
Clinically, flaccid blistering lesions are present that may be cutaneous and/or mucosal. Bullae can progress to erosions and crusting, which then heal with pigment alteration but not scarring. The most commonly affected sites are the mouth, intertriginous areas, face, and neck. Mucosal lesions may involve the lips, esophagus, conjunctiva, and genitals.
Biopsy for histology and direct immunofluorescence is important in distinguishing between PV and other blistering disorders. Up to 75% of patients with active disease also have a positive indirect immunofluorescence with circulating IgG.
Treatment is generally immunosuppressive. Systemic therapy usually begins with prednisone and then is transitioned to a steroid-sparing agent such as mycophenolate mofetil. Other steroid-sparing agents include azathioprine, methotrexate, cyclophosphamide, and intravenous immunoglobulin. Secondary infections are possible and should be treated. Topical therapies aimed at reducing pain, especially in mucosal lesions, can be beneficial.
This case and the photos are from Dr. Bilu Martin.
Dr. Bilu Martin is a board-certified dermatologist in private practice at Premier Dermatology, MD, in Aventura, Fla. More diagnostic cases are available at mdedge.com/dermatology. To submit a case for possible publication, send an email to [email protected].

For NSCLC, neoadjuvant, adjuvant, or both?
This transcript has been edited for clarity.
Dr. West: Here at ASCO 2023 [American Society of Clinical Oncology] in Chicago, we’ve seen some blockbuster presentations in thoracic oncology. Many of these have brought up some important questions about the clinical implications that we need to discuss further.
At ASCO, as well as in the couple or 3 months preceding ASCO, we’ve gotten more and more data on perioperative approaches. Of course, over the past couple of years, we’ve had some new options of postoperative immunotherapy for a year, say, after chemotherapy or possibly after chemotherapy.
We have also had very influential data, such as the CheckMate 816 trial that gave three cycles of chemotherapy with nivolumab vs. chemotherapy alone to patients with stage IB to IIIA disease, but largely, nearly two thirds, with IIIA disease. That showed a very clear improvement in the pathologic complete response (pCR) rate with nivolumab added to chemotherapy and also a highly significant improvement in event-free survival and a strong trend toward improved overall survival. This is FDA approved and has been increasingly adopted, I would say, maybe with some variability by geography and center, but really a good amount of enthusiasm.
Now, we have a bunch of trials that give chemotherapy with immunotherapy. We’ve got the AEGEAN trial with durvalumab. We have Neotorch with chemotherapy and toripalimab. At ASCO 2023, we had a highly prominent presentation of KEYNOTE-671, giving four cycles of chemotherapy with pembrolizumab vs. chemotherapy and placebo.
Then there’s the built-in postoperative component of a year of immunotherapy as well, in all these trials. The data for KEYNOTE-671 look quite good. Of course, the other trials also were significant. I would say the comparator now is not nothing or chemotherapy alone anymore; it’s really against what is the best current standard of care.
It certainly adds some cost, it adds some risk for toxicity, and it adds a year of a patient coming into the clinic and getting IV infusions all this time to get a treatment that the patient has already had for four cycles in most of these trials.
If your cancer is resistant, is there going to be an incremental benefit to giving more of it? What are your thoughts about the risk and benefit? Going to a patient in your own clinic, how are you going to counsel your patients? Will anything change after the presentation of all these data and how you approach preoperatively?
Dr. Rotow: I agree. In some sense, it’s an embarrassment of riches, right?
Dr. West: Yes.
Dr. Rotow: We have so many positive studies looking at perioperative immunotherapy for our patients. They all show improved outcomes, but of course, they all compare with the old control arm of chemotherapy alone in some form, and this is no longer a useful control in this space. The open question is, do you use neoadjuvant, do you use adjuvant, or do you use both?
My high-level takeaway from these data is that the neoadjuvant component appears to be important. I think the overall trend, comparing across studies, of course, is that outcomes seem to be better with the neoadjuvant component. You also get the advantage of potential downstaging and potential greater ease of surgical resection. We know they have lower morbidity resection and shorter surgeries. You can comment on that. You also get your pathologic response data.
Dr. West: You get the feedback.
Dr. Rotow: Exactly.
Dr. West: The deliverability is also a big issue. You know you can much more reliably deliver your intended treatment by doing neoadjuvant followed by surgery.
Dr. Rotow: Exactly.
Dr. West: We know there’s major drop-off if patients have surgery, and in the recovery room they hear you got it all, and then they need to come back and maybe get chemotherapy and immunotherapy for a year. They’d ask, “What for? I can’t see anything.”
Dr. Rotow: Exactly. I think there are many advantages to that neoadjuvant component. I think all or many of us now have integrated this into our routine practice. Now the question is, do you need the adjuvant element or not on top? That is challenging because no trial has compared adjuvant to nonadjuvant. I think we all advocate for the need for this trial to answer this in a more randomized, prospective fashion. Of course, that doesn’t help our clinic practice tomorrow when we see a patient.
Dr. West: Or for the next 4 years.
Dr. Rotow: Or for the next 4 years – exactly. There’s going to be the open question of who really needs this? In some sense, we may be guided by the path response during the surgery itself. I think there may be those who claim that if you have a pCR, do you really need additional therapy? We don’t know the answer, but it’s tempting to say we know the outcomes in event-free survival are extremely good with a pCR.
Dr. West: Which is only 20% or 25% of patients, so it’s not most.
Dr. Rotow: It’s not most, but it’s better than the 2% or so with chemotherapy alone. That’s real progress, and it’s nice to have that readout. For that 80% without a pCR, what to do? I suspect there will be variation from provider to provider and from patient to patient, depending on tolerability to prior therapy, the patient’s wishes around the goals of care, and the patient’s risk for autoimmune toxicities.
Maybe there’s a patient with underlying autoimmune disease who’s gotten their neoadjuvant therapy and done well. You don’t want to risk that ongoing risk of exposure. Perhaps a patient with no risk factors who desires very aggressive treatment might be interested in more treatment.
In KEYNOTE-671, I was interested in the PD-L1 subgroups. These did trend the way you expect, with better responses in PD-L1 high, but there were also good outcomes and benefit to immunotherapy with the perioperative strategy in PD-L1–negative patients.
Dr. West: That didn’t really exclude anybody.
Dr. Rotow: It didn’t exclude anybody. In CheckMate 816, everyone benefited, but the benefit was less with those PD-L1–negative patients.
Dr. West: True.
Dr. Rotow: Absent further data to guide me or any prospective data here comparing these strategies, I might lean toward a longer course of immunotherapy in that population in hopes of triggering a response. I suspect that there will be variation from clinician to clinician in that space.
Dr. West: This is a setting where I feel like I have equipoise. I really feel that the incremental benefit is pretty small.
Dr. Rotow: Small. I agree.
Dr. West: It’s, frankly, somewhat dubious. On the other hand, you’re in a situation where if you know that three of four patients will experience a relapse and less-than-amazing outcomes, it’s hard to leave something that’s FDA approved and studied and a well-sanctioned option on the table if this patient may have relapse later.
In the end, I feel like I’d like to offer this and discuss it with all my patients. I think it’s a great place for shared decision-making because if a patient hears about that and decides they’re not interested, I’ll be fine with that. I think that’s a very sensible approach, but I don’t want to make it unilaterally. Other patients may say they want every opportunity, and if it comes back, at least I’ll know I did everything we could.
Dr. Rotow: Exactly. I agree with your statement about equipoise. I truly think that this is present here in the situation, and that there’s room for discussion in both directions with patients.
Now, one caveat I’d like to add to all these data is that the data should not apply to patients with some of our classic nonsmoking-associated driver mutations. This is another piece to the neoadjuvant data that I think is worth commenting on – the need to get appropriate testing before initiation of therapy and the pitfalls of starting this kind of treatment without knowing full biomarker testing. I think that’s something we have to watch for in our clinical practice as well.
Dr. West: Perhaps especially if we’re talking about doing a year of postoperative and someone has an ALK rearrangement or an EGFR mutation and we didn’t know it. That is a group where we’re worried about a rapid transition and potentially prohibitive, even life-threatening, toxicities from not planning in advance for this. This is something you don’t want to give concurrently or one right on top of the other. You don’t want to give immunotherapy and then transition right to targeted therapy. It’s dangerous.
Dr. Rotow: Exactly. The stakes were already high with neoadjuvant alone, but at least you had that gap of the presurgical period, surgical recovery, and then initiation of adjuvant therapy, if needed, or at relapse. With a postoperative long adjuvant period, those stakes are elevated because the immunotherapy exposure continues, so it’s something to be mindful of.
Dr. West: We have a general sense that many, but not all, of the targets that we’re talking about are associated with low benefit from immunotherapy. It’s not that well studied. I think this is another place for individualized discussion of the pros and cons. They were included in the trial, but they probably benefit less.
Dr. Rotow: Exactly. I think with the best established, EGFR and ALK probably are not benefiting much. They were actually included in the trial. Many of the neoadjuvant studies do not allow them to enroll if they’re known. On the other end of that spectrum, I think KRAS is just fine to treat with immunotherapy.
Dr. West: Sure.
Dr. Rotow: It’s an actionable driver. It’s not a traditional nonsmoking-associated driver, and those do just fine.
Dr. West: The studies show that these patients benefit just as much, at least, as the other patients.
Dr. Rotow: Exactly. I would never withhold this form of therapy for a KRAS driver mutation. The others, I think, are still in a gray zone. Depending on the patient demographics and tobacco use, I may elicit more or less caution in that space.
Dr. West: Well, I think we’re going to have much to still tease apart, with room for judgment here without a strong sense of the data telling us exactly what to do.
Dr. Rotow: Exactly.
Dr. West: There’s a large amount of excitement and interest in these new data, but there are still many open questions. I hope we continue to mull it over as we get more data and more insight to shape our plans.
Dr. West is an associate professor at City of Hope Comprehensive Cancer Center in Duarte, Calif., and vice president of network strategy at AccessHope in Los Angeles. Dr. Rotow is the clinical director of the Lowe Center for Thoracic Oncology at the Dana-Farber Cancer Institute in Boston. Dr. West reported conflicts of interest with Ariad/Takeda, Bristol Myers Squibb, Boehringer Ingelheim, Spectrum, AstraZeneca, Celgene, Genentech/Roche, Pfizer, Merck, and Eli Lilly. Dr. Rotow reported conflicts of interest with Genentech, AstraZeneca,Guardant, and Janssen.
A version of this article first appeared on Medscape.com.
This transcript has been edited for clarity.
Dr. West: Here at ASCO 2023 [American Society of Clinical Oncology] in Chicago, we’ve seen some blockbuster presentations in thoracic oncology. Many of these have brought up some important questions about the clinical implications that we need to discuss further.
At ASCO, as well as in the couple or 3 months preceding ASCO, we’ve gotten more and more data on perioperative approaches. Of course, over the past couple of years, we’ve had some new options of postoperative immunotherapy for a year, say, after chemotherapy or possibly after chemotherapy.
We have also had very influential data, such as the CheckMate 816 trial that gave three cycles of chemotherapy with nivolumab vs. chemotherapy alone to patients with stage IB to IIIA disease, but largely, nearly two thirds, with IIIA disease. That showed a very clear improvement in the pathologic complete response (pCR) rate with nivolumab added to chemotherapy and also a highly significant improvement in event-free survival and a strong trend toward improved overall survival. This is FDA approved and has been increasingly adopted, I would say, maybe with some variability by geography and center, but really a good amount of enthusiasm.
Now, we have a bunch of trials that give chemotherapy with immunotherapy. We’ve got the AEGEAN trial with durvalumab. We have Neotorch with chemotherapy and toripalimab. At ASCO 2023, we had a highly prominent presentation of KEYNOTE-671, giving four cycles of chemotherapy with pembrolizumab vs. chemotherapy and placebo.
Then there’s the built-in postoperative component of a year of immunotherapy as well, in all these trials. The data for KEYNOTE-671 look quite good. Of course, the other trials also were significant. I would say the comparator now is not nothing or chemotherapy alone anymore; it’s really against what is the best current standard of care.
It certainly adds some cost, it adds some risk for toxicity, and it adds a year of a patient coming into the clinic and getting IV infusions all this time to get a treatment that the patient has already had for four cycles in most of these trials.
If your cancer is resistant, is there going to be an incremental benefit to giving more of it? What are your thoughts about the risk and benefit? Going to a patient in your own clinic, how are you going to counsel your patients? Will anything change after the presentation of all these data and how you approach preoperatively?
Dr. Rotow: I agree. In some sense, it’s an embarrassment of riches, right?
Dr. West: Yes.
Dr. Rotow: We have so many positive studies looking at perioperative immunotherapy for our patients. They all show improved outcomes, but of course, they all compare with the old control arm of chemotherapy alone in some form, and this is no longer a useful control in this space. The open question is, do you use neoadjuvant, do you use adjuvant, or do you use both?
My high-level takeaway from these data is that the neoadjuvant component appears to be important. I think the overall trend, comparing across studies, of course, is that outcomes seem to be better with the neoadjuvant component. You also get the advantage of potential downstaging and potential greater ease of surgical resection. We know they have lower morbidity resection and shorter surgeries. You can comment on that. You also get your pathologic response data.
Dr. West: You get the feedback.
Dr. Rotow: Exactly.
Dr. West: The deliverability is also a big issue. You know you can much more reliably deliver your intended treatment by doing neoadjuvant followed by surgery.
Dr. Rotow: Exactly.
Dr. West: We know there’s major drop-off if patients have surgery, and in the recovery room they hear you got it all, and then they need to come back and maybe get chemotherapy and immunotherapy for a year. They’d ask, “What for? I can’t see anything.”
Dr. Rotow: Exactly. I think there are many advantages to that neoadjuvant component. I think all or many of us now have integrated this into our routine practice. Now the question is, do you need the adjuvant element or not on top? That is challenging because no trial has compared adjuvant to nonadjuvant. I think we all advocate for the need for this trial to answer this in a more randomized, prospective fashion. Of course, that doesn’t help our clinic practice tomorrow when we see a patient.
Dr. West: Or for the next 4 years.
Dr. Rotow: Or for the next 4 years – exactly. There’s going to be the open question of who really needs this? In some sense, we may be guided by the path response during the surgery itself. I think there may be those who claim that if you have a pCR, do you really need additional therapy? We don’t know the answer, but it’s tempting to say we know the outcomes in event-free survival are extremely good with a pCR.
Dr. West: Which is only 20% or 25% of patients, so it’s not most.
Dr. Rotow: It’s not most, but it’s better than the 2% or so with chemotherapy alone. That’s real progress, and it’s nice to have that readout. For that 80% without a pCR, what to do? I suspect there will be variation from provider to provider and from patient to patient, depending on tolerability to prior therapy, the patient’s wishes around the goals of care, and the patient’s risk for autoimmune toxicities.
Maybe there’s a patient with underlying autoimmune disease who’s gotten their neoadjuvant therapy and done well. You don’t want to risk that ongoing risk of exposure. Perhaps a patient with no risk factors who desires very aggressive treatment might be interested in more treatment.
In KEYNOTE-671, I was interested in the PD-L1 subgroups. These did trend the way you expect, with better responses in PD-L1 high, but there were also good outcomes and benefit to immunotherapy with the perioperative strategy in PD-L1–negative patients.
Dr. West: That didn’t really exclude anybody.
Dr. Rotow: It didn’t exclude anybody. In CheckMate 816, everyone benefited, but the benefit was less with those PD-L1–negative patients.
Dr. West: True.
Dr. Rotow: Absent further data to guide me or any prospective data here comparing these strategies, I might lean toward a longer course of immunotherapy in that population in hopes of triggering a response. I suspect that there will be variation from clinician to clinician in that space.
Dr. West: This is a setting where I feel like I have equipoise. I really feel that the incremental benefit is pretty small.
Dr. Rotow: Small. I agree.
Dr. West: It’s, frankly, somewhat dubious. On the other hand, you’re in a situation where if you know that three of four patients will experience a relapse and less-than-amazing outcomes, it’s hard to leave something that’s FDA approved and studied and a well-sanctioned option on the table if this patient may have relapse later.
In the end, I feel like I’d like to offer this and discuss it with all my patients. I think it’s a great place for shared decision-making because if a patient hears about that and decides they’re not interested, I’ll be fine with that. I think that’s a very sensible approach, but I don’t want to make it unilaterally. Other patients may say they want every opportunity, and if it comes back, at least I’ll know I did everything we could.
Dr. Rotow: Exactly. I agree with your statement about equipoise. I truly think that this is present here in the situation, and that there’s room for discussion in both directions with patients.
Now, one caveat I’d like to add to all these data is that the data should not apply to patients with some of our classic nonsmoking-associated driver mutations. This is another piece to the neoadjuvant data that I think is worth commenting on – the need to get appropriate testing before initiation of therapy and the pitfalls of starting this kind of treatment without knowing full biomarker testing. I think that’s something we have to watch for in our clinical practice as well.
Dr. West: Perhaps especially if we’re talking about doing a year of postoperative and someone has an ALK rearrangement or an EGFR mutation and we didn’t know it. That is a group where we’re worried about a rapid transition and potentially prohibitive, even life-threatening, toxicities from not planning in advance for this. This is something you don’t want to give concurrently or one right on top of the other. You don’t want to give immunotherapy and then transition right to targeted therapy. It’s dangerous.
Dr. Rotow: Exactly. The stakes were already high with neoadjuvant alone, but at least you had that gap of the presurgical period, surgical recovery, and then initiation of adjuvant therapy, if needed, or at relapse. With a postoperative long adjuvant period, those stakes are elevated because the immunotherapy exposure continues, so it’s something to be mindful of.
Dr. West: We have a general sense that many, but not all, of the targets that we’re talking about are associated with low benefit from immunotherapy. It’s not that well studied. I think this is another place for individualized discussion of the pros and cons. They were included in the trial, but they probably benefit less.
Dr. Rotow: Exactly. I think with the best established, EGFR and ALK probably are not benefiting much. They were actually included in the trial. Many of the neoadjuvant studies do not allow them to enroll if they’re known. On the other end of that spectrum, I think KRAS is just fine to treat with immunotherapy.
Dr. West: Sure.
Dr. Rotow: It’s an actionable driver. It’s not a traditional nonsmoking-associated driver, and those do just fine.
Dr. West: The studies show that these patients benefit just as much, at least, as the other patients.
Dr. Rotow: Exactly. I would never withhold this form of therapy for a KRAS driver mutation. The others, I think, are still in a gray zone. Depending on the patient demographics and tobacco use, I may elicit more or less caution in that space.
Dr. West: Well, I think we’re going to have much to still tease apart, with room for judgment here without a strong sense of the data telling us exactly what to do.
Dr. Rotow: Exactly.
Dr. West: There’s a large amount of excitement and interest in these new data, but there are still many open questions. I hope we continue to mull it over as we get more data and more insight to shape our plans.
Dr. West is an associate professor at City of Hope Comprehensive Cancer Center in Duarte, Calif., and vice president of network strategy at AccessHope in Los Angeles. Dr. Rotow is the clinical director of the Lowe Center for Thoracic Oncology at the Dana-Farber Cancer Institute in Boston. Dr. West reported conflicts of interest with Ariad/Takeda, Bristol Myers Squibb, Boehringer Ingelheim, Spectrum, AstraZeneca, Celgene, Genentech/Roche, Pfizer, Merck, and Eli Lilly. Dr. Rotow reported conflicts of interest with Genentech, AstraZeneca,Guardant, and Janssen.
A version of this article first appeared on Medscape.com.
This transcript has been edited for clarity.
Dr. West: Here at ASCO 2023 [American Society of Clinical Oncology] in Chicago, we’ve seen some blockbuster presentations in thoracic oncology. Many of these have brought up some important questions about the clinical implications that we need to discuss further.
At ASCO, as well as in the couple or 3 months preceding ASCO, we’ve gotten more and more data on perioperative approaches. Of course, over the past couple of years, we’ve had some new options of postoperative immunotherapy for a year, say, after chemotherapy or possibly after chemotherapy.
We have also had very influential data, such as the CheckMate 816 trial that gave three cycles of chemotherapy with nivolumab vs. chemotherapy alone to patients with stage IB to IIIA disease, but largely, nearly two thirds, with IIIA disease. That showed a very clear improvement in the pathologic complete response (pCR) rate with nivolumab added to chemotherapy and also a highly significant improvement in event-free survival and a strong trend toward improved overall survival. This is FDA approved and has been increasingly adopted, I would say, maybe with some variability by geography and center, but really a good amount of enthusiasm.
Now, we have a bunch of trials that give chemotherapy with immunotherapy. We’ve got the AEGEAN trial with durvalumab. We have Neotorch with chemotherapy and toripalimab. At ASCO 2023, we had a highly prominent presentation of KEYNOTE-671, giving four cycles of chemotherapy with pembrolizumab vs. chemotherapy and placebo.
Then there’s the built-in postoperative component of a year of immunotherapy as well, in all these trials. The data for KEYNOTE-671 look quite good. Of course, the other trials also were significant. I would say the comparator now is not nothing or chemotherapy alone anymore; it’s really against what is the best current standard of care.
It certainly adds some cost, it adds some risk for toxicity, and it adds a year of a patient coming into the clinic and getting IV infusions all this time to get a treatment that the patient has already had for four cycles in most of these trials.
If your cancer is resistant, is there going to be an incremental benefit to giving more of it? What are your thoughts about the risk and benefit? Going to a patient in your own clinic, how are you going to counsel your patients? Will anything change after the presentation of all these data and how you approach preoperatively?
Dr. Rotow: I agree. In some sense, it’s an embarrassment of riches, right?
Dr. West: Yes.
Dr. Rotow: We have so many positive studies looking at perioperative immunotherapy for our patients. They all show improved outcomes, but of course, they all compare with the old control arm of chemotherapy alone in some form, and this is no longer a useful control in this space. The open question is, do you use neoadjuvant, do you use adjuvant, or do you use both?
My high-level takeaway from these data is that the neoadjuvant component appears to be important. I think the overall trend, comparing across studies, of course, is that outcomes seem to be better with the neoadjuvant component. You also get the advantage of potential downstaging and potential greater ease of surgical resection. We know they have lower morbidity resection and shorter surgeries. You can comment on that. You also get your pathologic response data.
Dr. West: You get the feedback.
Dr. Rotow: Exactly.
Dr. West: The deliverability is also a big issue. You know you can much more reliably deliver your intended treatment by doing neoadjuvant followed by surgery.
Dr. Rotow: Exactly.
Dr. West: We know there’s major drop-off if patients have surgery, and in the recovery room they hear you got it all, and then they need to come back and maybe get chemotherapy and immunotherapy for a year. They’d ask, “What for? I can’t see anything.”
Dr. Rotow: Exactly. I think there are many advantages to that neoadjuvant component. I think all or many of us now have integrated this into our routine practice. Now the question is, do you need the adjuvant element or not on top? That is challenging because no trial has compared adjuvant to nonadjuvant. I think we all advocate for the need for this trial to answer this in a more randomized, prospective fashion. Of course, that doesn’t help our clinic practice tomorrow when we see a patient.
Dr. West: Or for the next 4 years.
Dr. Rotow: Or for the next 4 years – exactly. There’s going to be the open question of who really needs this? In some sense, we may be guided by the path response during the surgery itself. I think there may be those who claim that if you have a pCR, do you really need additional therapy? We don’t know the answer, but it’s tempting to say we know the outcomes in event-free survival are extremely good with a pCR.
Dr. West: Which is only 20% or 25% of patients, so it’s not most.
Dr. Rotow: It’s not most, but it’s better than the 2% or so with chemotherapy alone. That’s real progress, and it’s nice to have that readout. For that 80% without a pCR, what to do? I suspect there will be variation from provider to provider and from patient to patient, depending on tolerability to prior therapy, the patient’s wishes around the goals of care, and the patient’s risk for autoimmune toxicities.
Maybe there’s a patient with underlying autoimmune disease who’s gotten their neoadjuvant therapy and done well. You don’t want to risk that ongoing risk of exposure. Perhaps a patient with no risk factors who desires very aggressive treatment might be interested in more treatment.
In KEYNOTE-671, I was interested in the PD-L1 subgroups. These did trend the way you expect, with better responses in PD-L1 high, but there were also good outcomes and benefit to immunotherapy with the perioperative strategy in PD-L1–negative patients.
Dr. West: That didn’t really exclude anybody.
Dr. Rotow: It didn’t exclude anybody. In CheckMate 816, everyone benefited, but the benefit was less with those PD-L1–negative patients.
Dr. West: True.
Dr. Rotow: Absent further data to guide me or any prospective data here comparing these strategies, I might lean toward a longer course of immunotherapy in that population in hopes of triggering a response. I suspect that there will be variation from clinician to clinician in that space.
Dr. West: This is a setting where I feel like I have equipoise. I really feel that the incremental benefit is pretty small.
Dr. Rotow: Small. I agree.
Dr. West: It’s, frankly, somewhat dubious. On the other hand, you’re in a situation where if you know that three of four patients will experience a relapse and less-than-amazing outcomes, it’s hard to leave something that’s FDA approved and studied and a well-sanctioned option on the table if this patient may have relapse later.
In the end, I feel like I’d like to offer this and discuss it with all my patients. I think it’s a great place for shared decision-making because if a patient hears about that and decides they’re not interested, I’ll be fine with that. I think that’s a very sensible approach, but I don’t want to make it unilaterally. Other patients may say they want every opportunity, and if it comes back, at least I’ll know I did everything we could.
Dr. Rotow: Exactly. I agree with your statement about equipoise. I truly think that this is present here in the situation, and that there’s room for discussion in both directions with patients.
Now, one caveat I’d like to add to all these data is that the data should not apply to patients with some of our classic nonsmoking-associated driver mutations. This is another piece to the neoadjuvant data that I think is worth commenting on – the need to get appropriate testing before initiation of therapy and the pitfalls of starting this kind of treatment without knowing full biomarker testing. I think that’s something we have to watch for in our clinical practice as well.
Dr. West: Perhaps especially if we’re talking about doing a year of postoperative and someone has an ALK rearrangement or an EGFR mutation and we didn’t know it. That is a group where we’re worried about a rapid transition and potentially prohibitive, even life-threatening, toxicities from not planning in advance for this. This is something you don’t want to give concurrently or one right on top of the other. You don’t want to give immunotherapy and then transition right to targeted therapy. It’s dangerous.
Dr. Rotow: Exactly. The stakes were already high with neoadjuvant alone, but at least you had that gap of the presurgical period, surgical recovery, and then initiation of adjuvant therapy, if needed, or at relapse. With a postoperative long adjuvant period, those stakes are elevated because the immunotherapy exposure continues, so it’s something to be mindful of.
Dr. West: We have a general sense that many, but not all, of the targets that we’re talking about are associated with low benefit from immunotherapy. It’s not that well studied. I think this is another place for individualized discussion of the pros and cons. They were included in the trial, but they probably benefit less.
Dr. Rotow: Exactly. I think with the best established, EGFR and ALK probably are not benefiting much. They were actually included in the trial. Many of the neoadjuvant studies do not allow them to enroll if they’re known. On the other end of that spectrum, I think KRAS is just fine to treat with immunotherapy.
Dr. West: Sure.
Dr. Rotow: It’s an actionable driver. It’s not a traditional nonsmoking-associated driver, and those do just fine.
Dr. West: The studies show that these patients benefit just as much, at least, as the other patients.
Dr. Rotow: Exactly. I would never withhold this form of therapy for a KRAS driver mutation. The others, I think, are still in a gray zone. Depending on the patient demographics and tobacco use, I may elicit more or less caution in that space.
Dr. West: Well, I think we’re going to have much to still tease apart, with room for judgment here without a strong sense of the data telling us exactly what to do.
Dr. Rotow: Exactly.
Dr. West: There’s a large amount of excitement and interest in these new data, but there are still many open questions. I hope we continue to mull it over as we get more data and more insight to shape our plans.
Dr. West is an associate professor at City of Hope Comprehensive Cancer Center in Duarte, Calif., and vice president of network strategy at AccessHope in Los Angeles. Dr. Rotow is the clinical director of the Lowe Center for Thoracic Oncology at the Dana-Farber Cancer Institute in Boston. Dr. West reported conflicts of interest with Ariad/Takeda, Bristol Myers Squibb, Boehringer Ingelheim, Spectrum, AstraZeneca, Celgene, Genentech/Roche, Pfizer, Merck, and Eli Lilly. Dr. Rotow reported conflicts of interest with Genentech, AstraZeneca,Guardant, and Janssen.
A version of this article first appeared on Medscape.com.
FROM ASCO 2023
Prior auth is a self-inflicted wound; is there a way out?
A few months ago, a close friend called me in a panic.
Her mother had been on an oral treatment for relapsed multiple myeloma for nearly 1 year. Originally, she had been prescribed the oral pill pomalidomide as part of her regimen, but it had caused cytopenias, constipation, and nausea even at lower doses. Now, she was tolerating her new pill, ixazomib, quite well.
Then, without so much as a letter from her insurance company, the patient’s pharmacy called to tell her that ixazomib was no longer covered without a peer-to-peer conversation given its cost.
The peer to peer left the oncology team and patient even more frustrated. After leaving the team on hold for nearly an hour, the insurance company denied the request for ixazomib. The hematologist conducting the peer-to-peer did not seem to understand why the patient had discontinued her previous medication.
Ultimately, the patient was forced to return to the old, less expensive drug. Since going back to pomalidomide, she has needed multiple dosing changes to manage the intense drug side effects.
I wish that stories like this were uncommon. I am often reminded of the ongoing challenges related to prior authorization when I see colleagues regaling the Twitterverse with their latest horror stories about an insurance company rejecting standard of care treatment or imaging. The data confirm the frequency of these experiences. Among a general cohort of physicians, the American Medical Association has reported that most practices complete 29 prior authorizations per physician every week and spend on average 14.6 hours, or nearly 2 full business days, of staff time each week on these requirements.
Given the growing burden of prior authorization, reform has now become a major policy issue at the federal and state level. Within the past year, organizations like the American Society of Clinical Oncology have released policy positions on prior authorization and are devoting sizable advocacy dollars to fight payers’ ability to enact it. Entire sections of the ASCO education book are devoted to detailing the negative effects of prior authorization, and recent ASCO-commissioned surveys have highlighted alarming statistics about how prior authorization harms patient care.
As a practicing oncologist, I welcome increased attention to the burdens of prior authorization. This attention shows that our professional organizations care about one of the largest contributors to burnout.
But as a researcher who studies systems of care, I worry that focusing our collective ire on health insurance companies is somewhat misplaced or unlikely to succeed.
Why? Because policy statements, Tweets, and legislation ignore the fact that prior authorization is a self-inflicted wound caused by decades of pharmaceutical companies, health systems, oncologists, and guideline bodies failing to factor costs of care into clinical practice.
Making cost-conscious oncology care a priority would be ideal, but it is also a tall order.
But, as costs continue to rise uncontrollably, the prior authorization system has ballooned out of control and reining in this system will be quite a challenge. Perhaps, we can look to my oncology practice at a Veterans Affairs Medical Center as a guide.
A self-inflicted wound
In oncology, most medications and imaging are subject to prior authorization, particularly higher-cost items, and dealing with prior authorization typically requires an army of staff. As enrollment in commercial health plans or Medicare Advantage skyrockets, prior authorization will only become more prevalent in oncology.
Why is this happening?
The lazy answer to this question is because health insurance companies put profits over patients.
However, prior authorization is a symptom, not a disease. And that symptom is exploding cancer care costs. The causes of high costs are varied: Pharmaceutical companies and device manufacturers set ungodly prices for drugs; oncologists and other specialists are often reimbursed for volume of care, not quality; and hospitals and health systems charge incredible amounts for routine labs and imaging, amounts that are orders of magnitude higher than what these services actually cost.
There is no easy solution to fix the drivers of such costs. One approach to rein in drug costs would be to allow Medicare to negotiate drug prices and set site-neutral pricing.
Another would be to incentivize doctors or health systems to reduce the use of high-cost services. But physicians are often unaware of the costs of a given treatment to a system or patient, and practices reimbursed by volume of care typically have little incentive to curb overall spending.
We are then left with payers, the primary means of reimbursing care and, specifically, utilization management, such as prior authorization and restrictive formularies, as the major mechanism to reduce this spending.
Prior authorization is broken
Here’s the rub though: Although payers are incentivized to curb costs through prior authorization, the data that they have to adjudicate therapeutic appropriateness are often terrible.
Administrative claims contain no data on biomarkers or performance status and are notoriously bad at reflecting basic information, such as a patient’s stage of cancer. For instance, the positive predictive value of claims-based algorithms to identify stage IV breast cancer is well below 50%, meaning that a claims algorithm that classifies a patient as stage IV is wrong more often than right.
If payers had better data, they could be more selective in their prior-authorization requirements. In other words, if payers could reliably identify who has metastatic breast cancer, an aromatase inhibitor, a common, well-accepted adjuvant therapy in hormone-positive, late-stage breast cancer, wouldn’t need prior authorization. What we have now is an inefficient system that sets prior authorization as a guardrail for most oncology care and then forces doctors to submit all relevant information about a patient to justify their treatment choices.
Keeping up with oncology treatment advances is also a challenge and requires tremendous expertise. Many insurers delegate their prior-authorization responsibilities to medication management companies, such as Magellan Rx or New Century Health, who maintain proprietary treatment pathways.
These companies anchor their prior authorization requirements to common guidelines. That would be fine if guideline-producing bodies like the National Comprehensive Cancer Network provided more firm recommendations on high-value treatments.
The NCCN recommendations, however, are expert-driven more than evidence or value driven. Often, therapies with less evidence make it into recommended treatment guidelines, and in some cases, the NCCN will equally recommend five options for treating a certain cancer, even when there is an obvious lower-cost option.
The effect of this, however, is that payers may then cover these five options, despite a 40-fold price difference among them, but then lean on requiring prior authorization for everything rather than being selective. Broad rather than targeted use of prior authorization alongside well-known issue like uncertain time lines, huge numbers of forms, and nonexperts doing peer to peers make for a huge mess.
What can we do?
How can we begin to solve the prior authorization crisis? A first step would be for guideline bodies to have more teeth in their recommendations. If NCCN and other guideline bodies, for instance, incorporated cost into their recommendations and designated these as “preferred” regimens, then clinicians could have better direction on therapy selection and payers could align their prior authorization policies with those recommendations. If patients had adverse effects with low-cost drugs, then a preferred alternative could be specified in such guidelines rather than subject patients, like my friend’s mother, to a toxic drug.
Second, payers could tailor the intensity of prior authorization requirements to the type of physician and clinical scenario at hand. Payers have rich data on practice patterns of oncologists. Payers should incentivize oncologists who follow guideline-based, high-value treatment pathways by lowering the need for frequent peer-to-peers or other prior authorization for “good performers.” This strategy, often termed gold carding, would use relief from prior authorization as a carrot.
Similarly, payers could reward practices that implement clinical pathways that enforce high-value care. For example, a practice could develop a treatment pathway that emphasizes access to urgent care to avoid hospitalizations as well as prioritizes access to relatively lower cost but equally effective options for therapy. If a payer reviewed and approved the pathway, perhaps payers could propose relief of future prior authorizations for practices whose oncologist practice on this pathway.
Third, payers could step up the intensity of prior authorization for certain high-cost or low-value treatments and lessen requirements for more routine services. For example, if every initial staging PET-CT required a peer to peer, oncologists would spend most of the day on the phone. Rather, lower-level tasks such as imaging may require a simple electronic EHR message, whereas high-cost items such as indefinite systemic therapy may require more frequent peer to peers.
Fourth, health systems and real-world data companies should devise better data sharing partnerships with payers so that payers could automatically examine attributes that clarify the choice of therapy. For example, if a payer could view that a patient had estrogen receptor/progesterone receptor–positive early-stage breast cancer post surgery, perhaps that payer would not require a prior authorization for an aromatase inhibitor. These real-time data sharing partnerships could reduce friction points in the system.
Finally, researchers and other groups should partner with payers to continually examine the effectiveness of any prior-authorization program. If a prior-authorization policy is no longer effective because evidence changes and evolves, then payers should consider retiring it.
In my primary oncology practice at a VA Medical Center, none of my treatments require an external prior authorization. Why? Because our local practice agreed to an established formulary, and national treatment pathways firmly specify a recommended treatment course.
Do I sometimes go off pathway? Yes, when I feel there’s a compelling reason. But that requires a structured electronic form to a central pharmacy body. I get a response within 24 hours, with no onerous prior authorization form or lengthy peer to peer.
Though there are plenty of unique qualities about the VA, the fact is that health systems and guideline bodies assuming the burden of cost containment could reduce prior-authorization requirements from payers.
Ultimately, the goal should be for oncologists to choose the highest-value treatment possible. Perhaps then, when the end-goal of cost-conscious oncology care with payers maintain an arm’s length from the patient-doctor relationship, we could all stop shouting at the wind about the burden of prior authorization.
Dr. Parikh is a medical oncologist and faculty member at the University of Pennsylvania, Philadelphia, and the Philadelphia VA Medical Center, an adjunct fellow at the Leonard Davis Institute of Health Economics, and senior clinical advisor at the Coalition to Transform Advanced Care. He reported conflicts of interest with GNS Healthcare, Nanology, Cancer Study Group, Embedded Healthcare, Veterans Affairs, PCF, National Palliative Care Research Center, MUSC, and Flatiron Health.
A version of this article first appeared on Medscape.com.
A few months ago, a close friend called me in a panic.
Her mother had been on an oral treatment for relapsed multiple myeloma for nearly 1 year. Originally, she had been prescribed the oral pill pomalidomide as part of her regimen, but it had caused cytopenias, constipation, and nausea even at lower doses. Now, she was tolerating her new pill, ixazomib, quite well.
Then, without so much as a letter from her insurance company, the patient’s pharmacy called to tell her that ixazomib was no longer covered without a peer-to-peer conversation given its cost.
The peer to peer left the oncology team and patient even more frustrated. After leaving the team on hold for nearly an hour, the insurance company denied the request for ixazomib. The hematologist conducting the peer-to-peer did not seem to understand why the patient had discontinued her previous medication.
Ultimately, the patient was forced to return to the old, less expensive drug. Since going back to pomalidomide, she has needed multiple dosing changes to manage the intense drug side effects.
I wish that stories like this were uncommon. I am often reminded of the ongoing challenges related to prior authorization when I see colleagues regaling the Twitterverse with their latest horror stories about an insurance company rejecting standard of care treatment or imaging. The data confirm the frequency of these experiences. Among a general cohort of physicians, the American Medical Association has reported that most practices complete 29 prior authorizations per physician every week and spend on average 14.6 hours, or nearly 2 full business days, of staff time each week on these requirements.
Given the growing burden of prior authorization, reform has now become a major policy issue at the federal and state level. Within the past year, organizations like the American Society of Clinical Oncology have released policy positions on prior authorization and are devoting sizable advocacy dollars to fight payers’ ability to enact it. Entire sections of the ASCO education book are devoted to detailing the negative effects of prior authorization, and recent ASCO-commissioned surveys have highlighted alarming statistics about how prior authorization harms patient care.
As a practicing oncologist, I welcome increased attention to the burdens of prior authorization. This attention shows that our professional organizations care about one of the largest contributors to burnout.
But as a researcher who studies systems of care, I worry that focusing our collective ire on health insurance companies is somewhat misplaced or unlikely to succeed.
Why? Because policy statements, Tweets, and legislation ignore the fact that prior authorization is a self-inflicted wound caused by decades of pharmaceutical companies, health systems, oncologists, and guideline bodies failing to factor costs of care into clinical practice.
Making cost-conscious oncology care a priority would be ideal, but it is also a tall order.
But, as costs continue to rise uncontrollably, the prior authorization system has ballooned out of control and reining in this system will be quite a challenge. Perhaps, we can look to my oncology practice at a Veterans Affairs Medical Center as a guide.
A self-inflicted wound
In oncology, most medications and imaging are subject to prior authorization, particularly higher-cost items, and dealing with prior authorization typically requires an army of staff. As enrollment in commercial health plans or Medicare Advantage skyrockets, prior authorization will only become more prevalent in oncology.
Why is this happening?
The lazy answer to this question is because health insurance companies put profits over patients.
However, prior authorization is a symptom, not a disease. And that symptom is exploding cancer care costs. The causes of high costs are varied: Pharmaceutical companies and device manufacturers set ungodly prices for drugs; oncologists and other specialists are often reimbursed for volume of care, not quality; and hospitals and health systems charge incredible amounts for routine labs and imaging, amounts that are orders of magnitude higher than what these services actually cost.
There is no easy solution to fix the drivers of such costs. One approach to rein in drug costs would be to allow Medicare to negotiate drug prices and set site-neutral pricing.
Another would be to incentivize doctors or health systems to reduce the use of high-cost services. But physicians are often unaware of the costs of a given treatment to a system or patient, and practices reimbursed by volume of care typically have little incentive to curb overall spending.
We are then left with payers, the primary means of reimbursing care and, specifically, utilization management, such as prior authorization and restrictive formularies, as the major mechanism to reduce this spending.
Prior authorization is broken
Here’s the rub though: Although payers are incentivized to curb costs through prior authorization, the data that they have to adjudicate therapeutic appropriateness are often terrible.
Administrative claims contain no data on biomarkers or performance status and are notoriously bad at reflecting basic information, such as a patient’s stage of cancer. For instance, the positive predictive value of claims-based algorithms to identify stage IV breast cancer is well below 50%, meaning that a claims algorithm that classifies a patient as stage IV is wrong more often than right.
If payers had better data, they could be more selective in their prior-authorization requirements. In other words, if payers could reliably identify who has metastatic breast cancer, an aromatase inhibitor, a common, well-accepted adjuvant therapy in hormone-positive, late-stage breast cancer, wouldn’t need prior authorization. What we have now is an inefficient system that sets prior authorization as a guardrail for most oncology care and then forces doctors to submit all relevant information about a patient to justify their treatment choices.
Keeping up with oncology treatment advances is also a challenge and requires tremendous expertise. Many insurers delegate their prior-authorization responsibilities to medication management companies, such as Magellan Rx or New Century Health, who maintain proprietary treatment pathways.
These companies anchor their prior authorization requirements to common guidelines. That would be fine if guideline-producing bodies like the National Comprehensive Cancer Network provided more firm recommendations on high-value treatments.
The NCCN recommendations, however, are expert-driven more than evidence or value driven. Often, therapies with less evidence make it into recommended treatment guidelines, and in some cases, the NCCN will equally recommend five options for treating a certain cancer, even when there is an obvious lower-cost option.
The effect of this, however, is that payers may then cover these five options, despite a 40-fold price difference among them, but then lean on requiring prior authorization for everything rather than being selective. Broad rather than targeted use of prior authorization alongside well-known issue like uncertain time lines, huge numbers of forms, and nonexperts doing peer to peers make for a huge mess.
What can we do?
How can we begin to solve the prior authorization crisis? A first step would be for guideline bodies to have more teeth in their recommendations. If NCCN and other guideline bodies, for instance, incorporated cost into their recommendations and designated these as “preferred” regimens, then clinicians could have better direction on therapy selection and payers could align their prior authorization policies with those recommendations. If patients had adverse effects with low-cost drugs, then a preferred alternative could be specified in such guidelines rather than subject patients, like my friend’s mother, to a toxic drug.
Second, payers could tailor the intensity of prior authorization requirements to the type of physician and clinical scenario at hand. Payers have rich data on practice patterns of oncologists. Payers should incentivize oncologists who follow guideline-based, high-value treatment pathways by lowering the need for frequent peer-to-peers or other prior authorization for “good performers.” This strategy, often termed gold carding, would use relief from prior authorization as a carrot.
Similarly, payers could reward practices that implement clinical pathways that enforce high-value care. For example, a practice could develop a treatment pathway that emphasizes access to urgent care to avoid hospitalizations as well as prioritizes access to relatively lower cost but equally effective options for therapy. If a payer reviewed and approved the pathway, perhaps payers could propose relief of future prior authorizations for practices whose oncologist practice on this pathway.
Third, payers could step up the intensity of prior authorization for certain high-cost or low-value treatments and lessen requirements for more routine services. For example, if every initial staging PET-CT required a peer to peer, oncologists would spend most of the day on the phone. Rather, lower-level tasks such as imaging may require a simple electronic EHR message, whereas high-cost items such as indefinite systemic therapy may require more frequent peer to peers.
Fourth, health systems and real-world data companies should devise better data sharing partnerships with payers so that payers could automatically examine attributes that clarify the choice of therapy. For example, if a payer could view that a patient had estrogen receptor/progesterone receptor–positive early-stage breast cancer post surgery, perhaps that payer would not require a prior authorization for an aromatase inhibitor. These real-time data sharing partnerships could reduce friction points in the system.
Finally, researchers and other groups should partner with payers to continually examine the effectiveness of any prior-authorization program. If a prior-authorization policy is no longer effective because evidence changes and evolves, then payers should consider retiring it.
In my primary oncology practice at a VA Medical Center, none of my treatments require an external prior authorization. Why? Because our local practice agreed to an established formulary, and national treatment pathways firmly specify a recommended treatment course.
Do I sometimes go off pathway? Yes, when I feel there’s a compelling reason. But that requires a structured electronic form to a central pharmacy body. I get a response within 24 hours, with no onerous prior authorization form or lengthy peer to peer.
Though there are plenty of unique qualities about the VA, the fact is that health systems and guideline bodies assuming the burden of cost containment could reduce prior-authorization requirements from payers.
Ultimately, the goal should be for oncologists to choose the highest-value treatment possible. Perhaps then, when the end-goal of cost-conscious oncology care with payers maintain an arm’s length from the patient-doctor relationship, we could all stop shouting at the wind about the burden of prior authorization.
Dr. Parikh is a medical oncologist and faculty member at the University of Pennsylvania, Philadelphia, and the Philadelphia VA Medical Center, an adjunct fellow at the Leonard Davis Institute of Health Economics, and senior clinical advisor at the Coalition to Transform Advanced Care. He reported conflicts of interest with GNS Healthcare, Nanology, Cancer Study Group, Embedded Healthcare, Veterans Affairs, PCF, National Palliative Care Research Center, MUSC, and Flatiron Health.
A version of this article first appeared on Medscape.com.
A few months ago, a close friend called me in a panic.
Her mother had been on an oral treatment for relapsed multiple myeloma for nearly 1 year. Originally, she had been prescribed the oral pill pomalidomide as part of her regimen, but it had caused cytopenias, constipation, and nausea even at lower doses. Now, she was tolerating her new pill, ixazomib, quite well.
Then, without so much as a letter from her insurance company, the patient’s pharmacy called to tell her that ixazomib was no longer covered without a peer-to-peer conversation given its cost.
The peer to peer left the oncology team and patient even more frustrated. After leaving the team on hold for nearly an hour, the insurance company denied the request for ixazomib. The hematologist conducting the peer-to-peer did not seem to understand why the patient had discontinued her previous medication.
Ultimately, the patient was forced to return to the old, less expensive drug. Since going back to pomalidomide, she has needed multiple dosing changes to manage the intense drug side effects.
I wish that stories like this were uncommon. I am often reminded of the ongoing challenges related to prior authorization when I see colleagues regaling the Twitterverse with their latest horror stories about an insurance company rejecting standard of care treatment or imaging. The data confirm the frequency of these experiences. Among a general cohort of physicians, the American Medical Association has reported that most practices complete 29 prior authorizations per physician every week and spend on average 14.6 hours, or nearly 2 full business days, of staff time each week on these requirements.
Given the growing burden of prior authorization, reform has now become a major policy issue at the federal and state level. Within the past year, organizations like the American Society of Clinical Oncology have released policy positions on prior authorization and are devoting sizable advocacy dollars to fight payers’ ability to enact it. Entire sections of the ASCO education book are devoted to detailing the negative effects of prior authorization, and recent ASCO-commissioned surveys have highlighted alarming statistics about how prior authorization harms patient care.
As a practicing oncologist, I welcome increased attention to the burdens of prior authorization. This attention shows that our professional organizations care about one of the largest contributors to burnout.
But as a researcher who studies systems of care, I worry that focusing our collective ire on health insurance companies is somewhat misplaced or unlikely to succeed.
Why? Because policy statements, Tweets, and legislation ignore the fact that prior authorization is a self-inflicted wound caused by decades of pharmaceutical companies, health systems, oncologists, and guideline bodies failing to factor costs of care into clinical practice.
Making cost-conscious oncology care a priority would be ideal, but it is also a tall order.
But, as costs continue to rise uncontrollably, the prior authorization system has ballooned out of control and reining in this system will be quite a challenge. Perhaps, we can look to my oncology practice at a Veterans Affairs Medical Center as a guide.
A self-inflicted wound
In oncology, most medications and imaging are subject to prior authorization, particularly higher-cost items, and dealing with prior authorization typically requires an army of staff. As enrollment in commercial health plans or Medicare Advantage skyrockets, prior authorization will only become more prevalent in oncology.
Why is this happening?
The lazy answer to this question is because health insurance companies put profits over patients.
However, prior authorization is a symptom, not a disease. And that symptom is exploding cancer care costs. The causes of high costs are varied: Pharmaceutical companies and device manufacturers set ungodly prices for drugs; oncologists and other specialists are often reimbursed for volume of care, not quality; and hospitals and health systems charge incredible amounts for routine labs and imaging, amounts that are orders of magnitude higher than what these services actually cost.
There is no easy solution to fix the drivers of such costs. One approach to rein in drug costs would be to allow Medicare to negotiate drug prices and set site-neutral pricing.
Another would be to incentivize doctors or health systems to reduce the use of high-cost services. But physicians are often unaware of the costs of a given treatment to a system or patient, and practices reimbursed by volume of care typically have little incentive to curb overall spending.
We are then left with payers, the primary means of reimbursing care and, specifically, utilization management, such as prior authorization and restrictive formularies, as the major mechanism to reduce this spending.
Prior authorization is broken
Here’s the rub though: Although payers are incentivized to curb costs through prior authorization, the data that they have to adjudicate therapeutic appropriateness are often terrible.
Administrative claims contain no data on biomarkers or performance status and are notoriously bad at reflecting basic information, such as a patient’s stage of cancer. For instance, the positive predictive value of claims-based algorithms to identify stage IV breast cancer is well below 50%, meaning that a claims algorithm that classifies a patient as stage IV is wrong more often than right.
If payers had better data, they could be more selective in their prior-authorization requirements. In other words, if payers could reliably identify who has metastatic breast cancer, an aromatase inhibitor, a common, well-accepted adjuvant therapy in hormone-positive, late-stage breast cancer, wouldn’t need prior authorization. What we have now is an inefficient system that sets prior authorization as a guardrail for most oncology care and then forces doctors to submit all relevant information about a patient to justify their treatment choices.
Keeping up with oncology treatment advances is also a challenge and requires tremendous expertise. Many insurers delegate their prior-authorization responsibilities to medication management companies, such as Magellan Rx or New Century Health, who maintain proprietary treatment pathways.
These companies anchor their prior authorization requirements to common guidelines. That would be fine if guideline-producing bodies like the National Comprehensive Cancer Network provided more firm recommendations on high-value treatments.
The NCCN recommendations, however, are expert-driven more than evidence or value driven. Often, therapies with less evidence make it into recommended treatment guidelines, and in some cases, the NCCN will equally recommend five options for treating a certain cancer, even when there is an obvious lower-cost option.
The effect of this, however, is that payers may then cover these five options, despite a 40-fold price difference among them, but then lean on requiring prior authorization for everything rather than being selective. Broad rather than targeted use of prior authorization alongside well-known issue like uncertain time lines, huge numbers of forms, and nonexperts doing peer to peers make for a huge mess.
What can we do?
How can we begin to solve the prior authorization crisis? A first step would be for guideline bodies to have more teeth in their recommendations. If NCCN and other guideline bodies, for instance, incorporated cost into their recommendations and designated these as “preferred” regimens, then clinicians could have better direction on therapy selection and payers could align their prior authorization policies with those recommendations. If patients had adverse effects with low-cost drugs, then a preferred alternative could be specified in such guidelines rather than subject patients, like my friend’s mother, to a toxic drug.
Second, payers could tailor the intensity of prior authorization requirements to the type of physician and clinical scenario at hand. Payers have rich data on practice patterns of oncologists. Payers should incentivize oncologists who follow guideline-based, high-value treatment pathways by lowering the need for frequent peer-to-peers or other prior authorization for “good performers.” This strategy, often termed gold carding, would use relief from prior authorization as a carrot.
Similarly, payers could reward practices that implement clinical pathways that enforce high-value care. For example, a practice could develop a treatment pathway that emphasizes access to urgent care to avoid hospitalizations as well as prioritizes access to relatively lower cost but equally effective options for therapy. If a payer reviewed and approved the pathway, perhaps payers could propose relief of future prior authorizations for practices whose oncologist practice on this pathway.
Third, payers could step up the intensity of prior authorization for certain high-cost or low-value treatments and lessen requirements for more routine services. For example, if every initial staging PET-CT required a peer to peer, oncologists would spend most of the day on the phone. Rather, lower-level tasks such as imaging may require a simple electronic EHR message, whereas high-cost items such as indefinite systemic therapy may require more frequent peer to peers.
Fourth, health systems and real-world data companies should devise better data sharing partnerships with payers so that payers could automatically examine attributes that clarify the choice of therapy. For example, if a payer could view that a patient had estrogen receptor/progesterone receptor–positive early-stage breast cancer post surgery, perhaps that payer would not require a prior authorization for an aromatase inhibitor. These real-time data sharing partnerships could reduce friction points in the system.
Finally, researchers and other groups should partner with payers to continually examine the effectiveness of any prior-authorization program. If a prior-authorization policy is no longer effective because evidence changes and evolves, then payers should consider retiring it.
In my primary oncology practice at a VA Medical Center, none of my treatments require an external prior authorization. Why? Because our local practice agreed to an established formulary, and national treatment pathways firmly specify a recommended treatment course.
Do I sometimes go off pathway? Yes, when I feel there’s a compelling reason. But that requires a structured electronic form to a central pharmacy body. I get a response within 24 hours, with no onerous prior authorization form or lengthy peer to peer.
Though there are plenty of unique qualities about the VA, the fact is that health systems and guideline bodies assuming the burden of cost containment could reduce prior-authorization requirements from payers.
Ultimately, the goal should be for oncologists to choose the highest-value treatment possible. Perhaps then, when the end-goal of cost-conscious oncology care with payers maintain an arm’s length from the patient-doctor relationship, we could all stop shouting at the wind about the burden of prior authorization.
Dr. Parikh is a medical oncologist and faculty member at the University of Pennsylvania, Philadelphia, and the Philadelphia VA Medical Center, an adjunct fellow at the Leonard Davis Institute of Health Economics, and senior clinical advisor at the Coalition to Transform Advanced Care. He reported conflicts of interest with GNS Healthcare, Nanology, Cancer Study Group, Embedded Healthcare, Veterans Affairs, PCF, National Palliative Care Research Center, MUSC, and Flatiron Health.
A version of this article first appeared on Medscape.com.
Time-restricted eating gains for weight and glycemic control
Time-restricted eating (TRE) can be a practical, easy-to-follow way for some people to control their daily food intake and lose weight. It precludes a person’s need to pay close attention to how much they eat as long as they confine consumption to a limited time window. Plus, results from several recent studies show TRE can further benefit people with type 2 diabetes as well as obesity via mechanisms beyond weight loss.
The most tested and recommended eating window is 8 hours long, although periods up to roughly 10 hours may provide some benefits. Results from multiple studies document that TRE produces modest but consistent weight loss of less than 5% in many people. A recent meta-analysis of 17 randomized controlled studies involving 899 people showed an overall incremental weight loss, compared with controls of 1.60 kg on a TRE regimen.
The more limited data collected so far in people with type 2 diabetes show additional metabolic benefits from TRE, including improved beta-cell responsiveness, increased insulin sensitivity, nonoxidative glucose disposal, increased time in glycemic range, and virtually no hypoglycemic events, Courtney Peterson, PhD, said at the annual scientific sessions of the American Diabetes Association.

said Dr. Peterson, a researcher in the department of nutrition sciences at the University of Alabama, Birmingham.
‘Eating earlier is better’
An advantage of TRE is that it is “agnostic to food preferences and quality,” said Lisa S. Chow, MD, during a separate session at the meeting. TRE “may have benefits beyond calorie restriction” that appear related to “the timing of eating and the extent of the eating window restriction. Eating earlier [in the day] is better” for markers of metabolic health regardless of how much weight a person may lose on a TRE regimen, noted Dr. Chow, an endocrinologist and professor at the University of Minnesota Medical School, Minneapolis.

But the TRE paradigm seems amenable to some flexibility on the timing for the eating window while still having benefit.
“Self-selected eating windows are usually late,” Dr. Chow observed, and because compliance with a constrained eating window matters, it may be worth allowing people to choose whichever time window for eating works best for them.
“If you let people pick their eating window, they typically include dinner,” said Dr. Chow, who has run a small TRE study that showed this.
“To maximize the effects [of TRE] people should use the eating window that best fits their life,” agreed Kelsey Gabel, PhD, who also gave a TRE talk during the meeting. “Eating most of your [daily] calories first thing in the morning would have the best cardiometabolic benefit, but reduced adherence would mitigate the benefit,” said Dr. Gabel, a nutrition researcher at the University of Illinois.
‘Meeting people where they’re at’
“We can have a larger public health impact by meeting people where they’re at. People should position their eating window where it best fits so they can achieve calorie restriction without even knowing it,” Dr. Gabel advised.
She cited a report as evidence that most people prefer a later eating window. The report reviewed observational data from nearly 800,000 people who used either of two different TRE phone apps. The data showed that most people opted to start their daily eating during 11:00 AM-1:00 PM, and then stop during 6:00 PM-8:00 PM.
“TRE will not solve all of our obesity problems, but it’s a good place to start,” Dr. Gabel declared.
For people who include dinner at a typical evening time in their TRE window, a key message is that “dinner is your last food of the day. There’s no snacking later,” said Dr. Chow.
“The biggest challenge is adherence,” said Dr. Peterson. “Fewer people want to do TRE than you think. We know that calorie restriction works. We just need a way for people to do it,” and for at least some people, TRE is that way. While no evidence clearly shows that 8 hours is the best eating-window duration, “we think 8 hours is a good sweet-spot for motivated people,” she said.
Sparser data on TRE in people with T2D
Fewer studies have examined the impact of TRE on glycemic control, insulin sensitivity, and related effects in people with type 2 diabetes. According to Dr. Peterson, published reports currently include two randomized controlled studies and three single-arm studies in people with type 2 diabetes and an additional two studies in people with prediabetes.
The largest of these reports randomized 120 adults in China with type 2 diabetes and overweight to TRE using a 10-hour eating window (8:00 AM-6:00 PM) or unrestricted eating for 12 weeks. By the end of the study, those on the TRE regimen had an average reduction in their hemoglobin A1c from baseline that was 0.88 percentage points greater than among the controls, and the TRE arm had also lost an average of nearly 2.15 kg more from baseline than the controls.
Dr. Peterson highlighted the importance of expanding research using TRE in people with type 2 diabetes.
Dr. Peterson and Dr. Gabel report no relevant financial relationships. Dr. Chow has received research support from Dexcom.
A version of this article first appeared on Medscape.com.
Time-restricted eating (TRE) can be a practical, easy-to-follow way for some people to control their daily food intake and lose weight. It precludes a person’s need to pay close attention to how much they eat as long as they confine consumption to a limited time window. Plus, results from several recent studies show TRE can further benefit people with type 2 diabetes as well as obesity via mechanisms beyond weight loss.
The most tested and recommended eating window is 8 hours long, although periods up to roughly 10 hours may provide some benefits. Results from multiple studies document that TRE produces modest but consistent weight loss of less than 5% in many people. A recent meta-analysis of 17 randomized controlled studies involving 899 people showed an overall incremental weight loss, compared with controls of 1.60 kg on a TRE regimen.
The more limited data collected so far in people with type 2 diabetes show additional metabolic benefits from TRE, including improved beta-cell responsiveness, increased insulin sensitivity, nonoxidative glucose disposal, increased time in glycemic range, and virtually no hypoglycemic events, Courtney Peterson, PhD, said at the annual scientific sessions of the American Diabetes Association.
said Dr. Peterson, a researcher in the department of nutrition sciences at the University of Alabama, Birmingham.
‘Eating earlier is better’
An advantage of TRE is that it is “agnostic to food preferences and quality,” said Lisa S. Chow, MD, during a separate session at the meeting. TRE “may have benefits beyond calorie restriction” that appear related to “the timing of eating and the extent of the eating window restriction. Eating earlier [in the day] is better” for markers of metabolic health regardless of how much weight a person may lose on a TRE regimen, noted Dr. Chow, an endocrinologist and professor at the University of Minnesota Medical School, Minneapolis.
But the TRE paradigm seems amenable to some flexibility on the timing for the eating window while still having benefit.
“Self-selected eating windows are usually late,” Dr. Chow observed, and because compliance with a constrained eating window matters, it may be worth allowing people to choose whichever time window for eating works best for them.
“If you let people pick their eating window, they typically include dinner,” said Dr. Chow, who has run a small TRE study that showed this.
“To maximize the effects [of TRE] people should use the eating window that best fits their life,” agreed Kelsey Gabel, PhD, who also gave a TRE talk during the meeting. “Eating most of your [daily] calories first thing in the morning would have the best cardiometabolic benefit, but reduced adherence would mitigate the benefit,” said Dr. Gabel, a nutrition researcher at the University of Illinois.
‘Meeting people where they’re at’
“We can have a larger public health impact by meeting people where they’re at. People should position their eating window where it best fits so they can achieve calorie restriction without even knowing it,” Dr. Gabel advised.
She cited a report as evidence that most people prefer a later eating window. The report reviewed observational data from nearly 800,000 people who used either of two different TRE phone apps. The data showed that most people opted to start their daily eating during 11:00 AM-1:00 PM, and then stop during 6:00 PM-8:00 PM.
“TRE will not solve all of our obesity problems, but it’s a good place to start,” Dr. Gabel declared.
For people who include dinner at a typical evening time in their TRE window, a key message is that “dinner is your last food of the day. There’s no snacking later,” said Dr. Chow.
“The biggest challenge is adherence,” said Dr. Peterson. “Fewer people want to do TRE than you think. We know that calorie restriction works. We just need a way for people to do it,” and for at least some people, TRE is that way. While no evidence clearly shows that 8 hours is the best eating-window duration, “we think 8 hours is a good sweet-spot for motivated people,” she said.
Sparser data on TRE in people with T2D
Fewer studies have examined the impact of TRE on glycemic control, insulin sensitivity, and related effects in people with type 2 diabetes. According to Dr. Peterson, published reports currently include two randomized controlled studies and three single-arm studies in people with type 2 diabetes and an additional two studies in people with prediabetes.
The largest of these reports randomized 120 adults in China with type 2 diabetes and overweight to TRE using a 10-hour eating window (8:00 AM-6:00 PM) or unrestricted eating for 12 weeks. By the end of the study, those on the TRE regimen had an average reduction in their hemoglobin A1c from baseline that was 0.88 percentage points greater than among the controls, and the TRE arm had also lost an average of nearly 2.15 kg more from baseline than the controls.
Dr. Peterson highlighted the importance of expanding research using TRE in people with type 2 diabetes.
Dr. Peterson and Dr. Gabel report no relevant financial relationships. Dr. Chow has received research support from Dexcom.
A version of this article first appeared on Medscape.com.
Time-restricted eating (TRE) can be a practical, easy-to-follow way for some people to control their daily food intake and lose weight. It precludes a person’s need to pay close attention to how much they eat as long as they confine consumption to a limited time window. Plus, results from several recent studies show TRE can further benefit people with type 2 diabetes as well as obesity via mechanisms beyond weight loss.
The most tested and recommended eating window is 8 hours long, although periods up to roughly 10 hours may provide some benefits. Results from multiple studies document that TRE produces modest but consistent weight loss of less than 5% in many people. A recent meta-analysis of 17 randomized controlled studies involving 899 people showed an overall incremental weight loss, compared with controls of 1.60 kg on a TRE regimen.
The more limited data collected so far in people with type 2 diabetes show additional metabolic benefits from TRE, including improved beta-cell responsiveness, increased insulin sensitivity, nonoxidative glucose disposal, increased time in glycemic range, and virtually no hypoglycemic events, Courtney Peterson, PhD, said at the annual scientific sessions of the American Diabetes Association.
said Dr. Peterson, a researcher in the department of nutrition sciences at the University of Alabama, Birmingham.
‘Eating earlier is better’
An advantage of TRE is that it is “agnostic to food preferences and quality,” said Lisa S. Chow, MD, during a separate session at the meeting. TRE “may have benefits beyond calorie restriction” that appear related to “the timing of eating and the extent of the eating window restriction. Eating earlier [in the day] is better” for markers of metabolic health regardless of how much weight a person may lose on a TRE regimen, noted Dr. Chow, an endocrinologist and professor at the University of Minnesota Medical School, Minneapolis.
But the TRE paradigm seems amenable to some flexibility on the timing for the eating window while still having benefit.
“Self-selected eating windows are usually late,” Dr. Chow observed, and because compliance with a constrained eating window matters, it may be worth allowing people to choose whichever time window for eating works best for them.
“If you let people pick their eating window, they typically include dinner,” said Dr. Chow, who has run a small TRE study that showed this.
“To maximize the effects [of TRE] people should use the eating window that best fits their life,” agreed Kelsey Gabel, PhD, who also gave a TRE talk during the meeting. “Eating most of your [daily] calories first thing in the morning would have the best cardiometabolic benefit, but reduced adherence would mitigate the benefit,” said Dr. Gabel, a nutrition researcher at the University of Illinois.
‘Meeting people where they’re at’
“We can have a larger public health impact by meeting people where they’re at. People should position their eating window where it best fits so they can achieve calorie restriction without even knowing it,” Dr. Gabel advised.
She cited a report as evidence that most people prefer a later eating window. The report reviewed observational data from nearly 800,000 people who used either of two different TRE phone apps. The data showed that most people opted to start their daily eating during 11:00 AM-1:00 PM, and then stop during 6:00 PM-8:00 PM.
“TRE will not solve all of our obesity problems, but it’s a good place to start,” Dr. Gabel declared.
For people who include dinner at a typical evening time in their TRE window, a key message is that “dinner is your last food of the day. There’s no snacking later,” said Dr. Chow.
“The biggest challenge is adherence,” said Dr. Peterson. “Fewer people want to do TRE than you think. We know that calorie restriction works. We just need a way for people to do it,” and for at least some people, TRE is that way. While no evidence clearly shows that 8 hours is the best eating-window duration, “we think 8 hours is a good sweet-spot for motivated people,” she said.
Sparser data on TRE in people with T2D
Fewer studies have examined the impact of TRE on glycemic control, insulin sensitivity, and related effects in people with type 2 diabetes. According to Dr. Peterson, published reports currently include two randomized controlled studies and three single-arm studies in people with type 2 diabetes and an additional two studies in people with prediabetes.
The largest of these reports randomized 120 adults in China with type 2 diabetes and overweight to TRE using a 10-hour eating window (8:00 AM-6:00 PM) or unrestricted eating for 12 weeks. By the end of the study, those on the TRE regimen had an average reduction in their hemoglobin A1c from baseline that was 0.88 percentage points greater than among the controls, and the TRE arm had also lost an average of nearly 2.15 kg more from baseline than the controls.
Dr. Peterson highlighted the importance of expanding research using TRE in people with type 2 diabetes.
Dr. Peterson and Dr. Gabel report no relevant financial relationships. Dr. Chow has received research support from Dexcom.
A version of this article first appeared on Medscape.com.
FROM ADA 2023
A new and completely different pain medicine
This transcript has been edited for clarity.
When you stub your toe or get a paper cut on your finger, you feel the pain in that part of your body. It feels like the pain is coming from that place. But, of course, that’s not really what is happening. Pain doesn’t really happen in your toe or your finger. It happens in your brain.
It’s a game of telephone, really. The afferent nerve fiber detects the noxious stimulus, passing that signal to the second-order neuron in the dorsal root ganglia of the spinal cord, which runs it up to the thalamus to be passed to the third-order neuron which brings it to the cortex for localization and conscious perception. It’s not even a very good game of telephone. It takes about 100 ms for a pain signal to get from the hand to the brain – longer from the feet, given the greater distance. You see your foot hit the corner of the coffee table and have just enough time to think: “Oh no!” before the pain hits.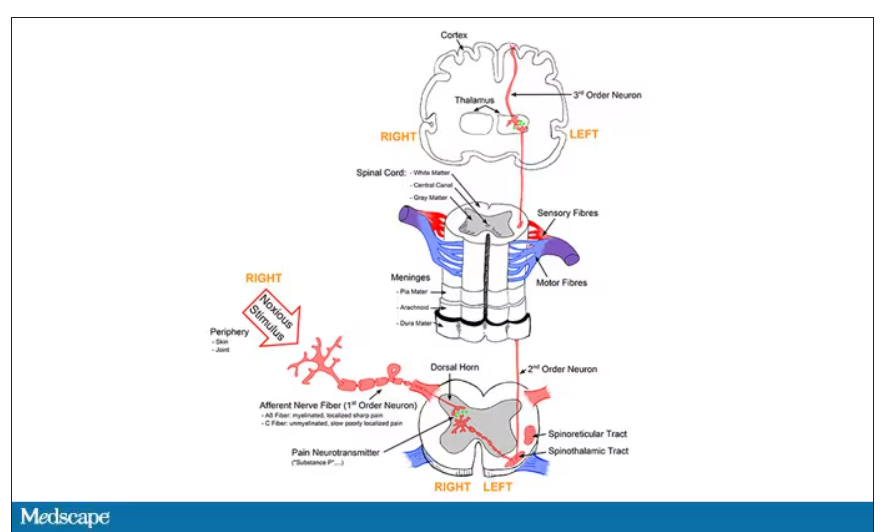
Given the Rube Goldberg nature of the process, it would seem like there are any number of places we could stop pain sensation. And sure, local anesthetics at the site of injury, or even spinal anesthetics, are powerful – if temporary and hard to administer – solutions to acute pain.
But in our everyday armamentarium, let’s be honest – we essentially have three options: opiates and opioids, which activate the mu-receptors in the brain to dull pain (and cause a host of other nasty side effects); NSAIDs, which block prostaglandin synthesis and thus limit the ability for pain-conducting neurons to get excited; and acetaminophen, which, despite being used for a century, is poorly understood.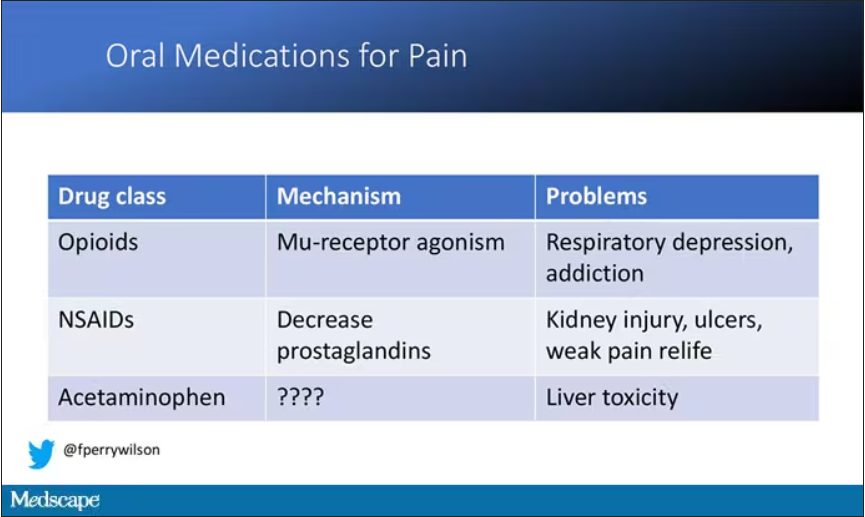
But
If you were to zoom in on the connection between that first afferent pain fiber and the secondary nerve in the spinal cord dorsal root ganglion, you would see a receptor called Nav1.8, a voltage-gated sodium channel.
This receptor is a key part of the apparatus that passes information from nerve 1 to nerve 2, but only for fibers that transmit pain signals. In fact, humans with mutations in this receptor that leave it always in the “open” state have a severe pain syndrome. Blocking the receptor, therefore, might reduce pain.
In preclinical work, researchers identified VX-548, which doesn’t have a brand name yet, as a potent blocker of that channel even in nanomolar concentrations. Importantly, the compound was highly selective for that particular channel – about 30,000 times more selective than it was for the other sodium channels in that family.
Of course, a highly selective and specific drug does not a blockbuster analgesic make. To determine how this drug would work on humans in pain, they turned to two populations: 303 individuals undergoing abdominoplasty and 274 undergoing bunionectomy, as reported in a new paper in the New England Journal of Medicine.
I know this seems a bit random, but abdominoplasty is quite painful and a good model for soft-tissue pain. Bunionectomy is also quite a painful procedure and a useful model of bone pain. After the surgeries, patients were randomized to several different doses of VX-548, hydrocodone plus acetaminophen, or placebo for 48 hours.
At 19 time points over that 48-hour period, participants were asked to rate their pain on a scale from 0 to 10. The primary outcome was the cumulative pain experienced over the 48 hours. So, higher pain would be worse here, but longer duration of pain would also be worse.
The story of the study is really told in this chart.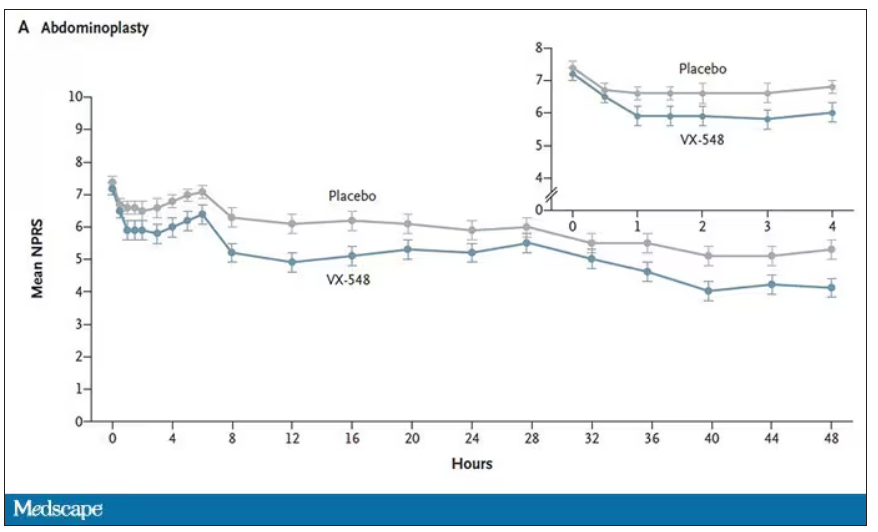
Yes, those assigned to the highest dose of VX-548 had a statistically significant lower cumulative amount of pain in the 48 hours after surgery. But the picture is really worth more than the stats here. You can see that the onset of pain relief was fairly quick, and that pain relief was sustained over time. You can also see that this is not a miracle drug. Pain scores were a bit better 48 hours out, but only by about a point and a half.
Placebo isn’t really the fair comparison here; few of us treat our postabdominoplasty patients with placebo, after all. The authors do not formally compare the effect of VX-548 with that of the opioid hydrocodone, for instance. But that doesn’t stop us.
This graph, which I put together from data in the paper, shows pain control across the four randomization categories, with higher numbers indicating more (cumulative) control. While all the active agents do a bit better than placebo, VX-548 at the higher dose appears to do the best. But I should note that 5 mg of hydrocodone may not be an adequate dose for most people.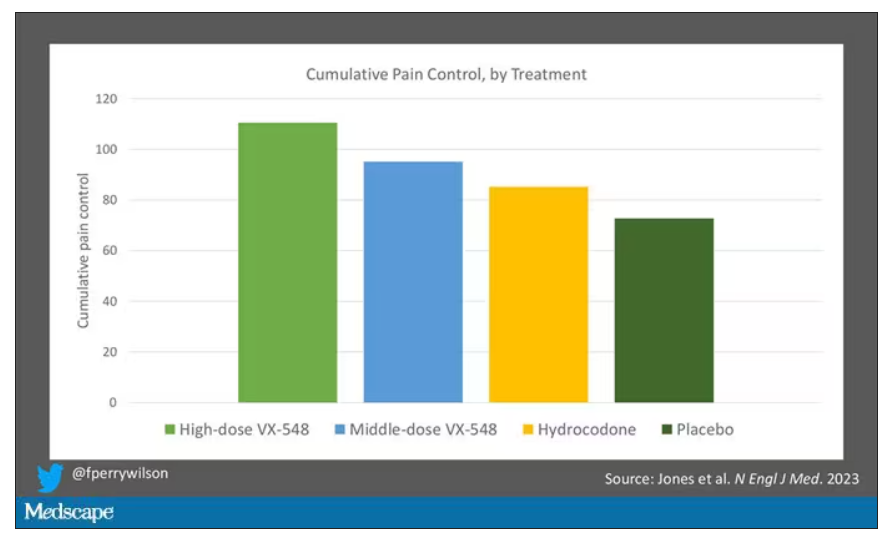
Yes, I would really have killed for an NSAID arm in this trial. Its absence, given that NSAIDs are a staple of postoperative care, is ... well, let’s just say, notable.
Although not a pain-destroying machine, VX-548 has some other things to recommend it. The receptor is really not found in the brain at all, which suggests that the drug should not carry much risk for dependency, though that has not been formally studied.
The side effects were generally mild – headache was the most common – and less prevalent than what you see even in the placebo arm.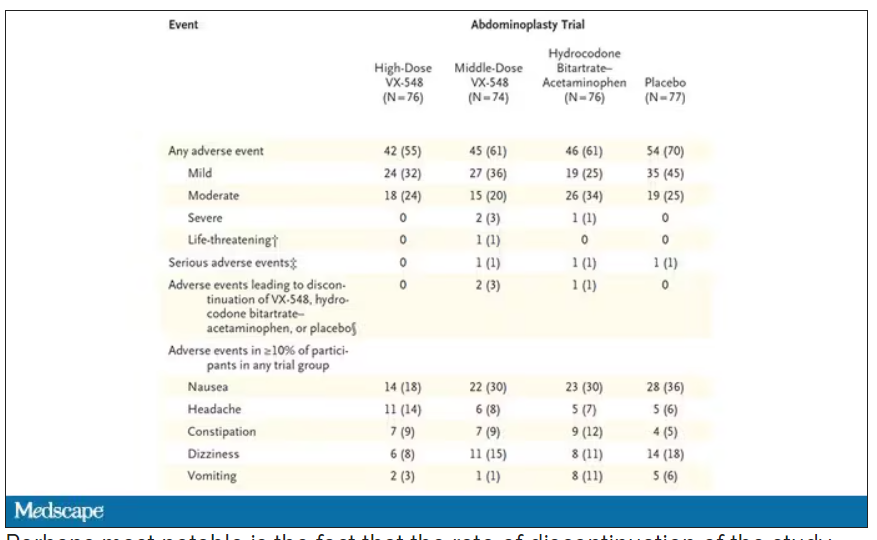
Perhaps most notable is the fact that the rate of discontinuation of the study drug was lowest in the VX-548 arm. Patients could stop taking the pill they were assigned for any reason, ranging from perceived lack of efficacy to side effects. A low discontinuation rate indicates to me a sort of “voting with your feet” that suggests this might be a well-tolerated and reasonably effective drug.
VX-548 isn’t on the market yet; phase 3 trials are ongoing. But whether it is this particular drug or another in this class, I’m happy to see researchers trying to find new ways to target that most primeval form of suffering: pain.
Dr. Wilson is an associate professor of medicine and public health and director of Yale’s Clinical and Translational Research Accelerator, New Haven, Conn. He disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
This transcript has been edited for clarity.
When you stub your toe or get a paper cut on your finger, you feel the pain in that part of your body. It feels like the pain is coming from that place. But, of course, that’s not really what is happening. Pain doesn’t really happen in your toe or your finger. It happens in your brain.
It’s a game of telephone, really. The afferent nerve fiber detects the noxious stimulus, passing that signal to the second-order neuron in the dorsal root ganglia of the spinal cord, which runs it up to the thalamus to be passed to the third-order neuron which brings it to the cortex for localization and conscious perception. It’s not even a very good game of telephone. It takes about 100 ms for a pain signal to get from the hand to the brain – longer from the feet, given the greater distance. You see your foot hit the corner of the coffee table and have just enough time to think: “Oh no!” before the pain hits.
Given the Rube Goldberg nature of the process, it would seem like there are any number of places we could stop pain sensation. And sure, local anesthetics at the site of injury, or even spinal anesthetics, are powerful – if temporary and hard to administer – solutions to acute pain.
But in our everyday armamentarium, let’s be honest – we essentially have three options: opiates and opioids, which activate the mu-receptors in the brain to dull pain (and cause a host of other nasty side effects); NSAIDs, which block prostaglandin synthesis and thus limit the ability for pain-conducting neurons to get excited; and acetaminophen, which, despite being used for a century, is poorly understood.
But
If you were to zoom in on the connection between that first afferent pain fiber and the secondary nerve in the spinal cord dorsal root ganglion, you would see a receptor called Nav1.8, a voltage-gated sodium channel.
This receptor is a key part of the apparatus that passes information from nerve 1 to nerve 2, but only for fibers that transmit pain signals. In fact, humans with mutations in this receptor that leave it always in the “open” state have a severe pain syndrome. Blocking the receptor, therefore, might reduce pain.
In preclinical work, researchers identified VX-548, which doesn’t have a brand name yet, as a potent blocker of that channel even in nanomolar concentrations. Importantly, the compound was highly selective for that particular channel – about 30,000 times more selective than it was for the other sodium channels in that family.
Of course, a highly selective and specific drug does not a blockbuster analgesic make. To determine how this drug would work on humans in pain, they turned to two populations: 303 individuals undergoing abdominoplasty and 274 undergoing bunionectomy, as reported in a new paper in the New England Journal of Medicine.
I know this seems a bit random, but abdominoplasty is quite painful and a good model for soft-tissue pain. Bunionectomy is also quite a painful procedure and a useful model of bone pain. After the surgeries, patients were randomized to several different doses of VX-548, hydrocodone plus acetaminophen, or placebo for 48 hours.
At 19 time points over that 48-hour period, participants were asked to rate their pain on a scale from 0 to 10. The primary outcome was the cumulative pain experienced over the 48 hours. So, higher pain would be worse here, but longer duration of pain would also be worse.
The story of the study is really told in this chart.
Yes, those assigned to the highest dose of VX-548 had a statistically significant lower cumulative amount of pain in the 48 hours after surgery. But the picture is really worth more than the stats here. You can see that the onset of pain relief was fairly quick, and that pain relief was sustained over time. You can also see that this is not a miracle drug. Pain scores were a bit better 48 hours out, but only by about a point and a half.
Placebo isn’t really the fair comparison here; few of us treat our postabdominoplasty patients with placebo, after all. The authors do not formally compare the effect of VX-548 with that of the opioid hydrocodone, for instance. But that doesn’t stop us.
This graph, which I put together from data in the paper, shows pain control across the four randomization categories, with higher numbers indicating more (cumulative) control. While all the active agents do a bit better than placebo, VX-548 at the higher dose appears to do the best. But I should note that 5 mg of hydrocodone may not be an adequate dose for most people.
Yes, I would really have killed for an NSAID arm in this trial. Its absence, given that NSAIDs are a staple of postoperative care, is ... well, let’s just say, notable.
Although not a pain-destroying machine, VX-548 has some other things to recommend it. The receptor is really not found in the brain at all, which suggests that the drug should not carry much risk for dependency, though that has not been formally studied.
The side effects were generally mild – headache was the most common – and less prevalent than what you see even in the placebo arm.
Perhaps most notable is the fact that the rate of discontinuation of the study drug was lowest in the VX-548 arm. Patients could stop taking the pill they were assigned for any reason, ranging from perceived lack of efficacy to side effects. A low discontinuation rate indicates to me a sort of “voting with your feet” that suggests this might be a well-tolerated and reasonably effective drug.
VX-548 isn’t on the market yet; phase 3 trials are ongoing. But whether it is this particular drug or another in this class, I’m happy to see researchers trying to find new ways to target that most primeval form of suffering: pain.
Dr. Wilson is an associate professor of medicine and public health and director of Yale’s Clinical and Translational Research Accelerator, New Haven, Conn. He disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
This transcript has been edited for clarity.
When you stub your toe or get a paper cut on your finger, you feel the pain in that part of your body. It feels like the pain is coming from that place. But, of course, that’s not really what is happening. Pain doesn’t really happen in your toe or your finger. It happens in your brain.
It’s a game of telephone, really. The afferent nerve fiber detects the noxious stimulus, passing that signal to the second-order neuron in the dorsal root ganglia of the spinal cord, which runs it up to the thalamus to be passed to the third-order neuron which brings it to the cortex for localization and conscious perception. It’s not even a very good game of telephone. It takes about 100 ms for a pain signal to get from the hand to the brain – longer from the feet, given the greater distance. You see your foot hit the corner of the coffee table and have just enough time to think: “Oh no!” before the pain hits.
Given the Rube Goldberg nature of the process, it would seem like there are any number of places we could stop pain sensation. And sure, local anesthetics at the site of injury, or even spinal anesthetics, are powerful – if temporary and hard to administer – solutions to acute pain.
But in our everyday armamentarium, let’s be honest – we essentially have three options: opiates and opioids, which activate the mu-receptors in the brain to dull pain (and cause a host of other nasty side effects); NSAIDs, which block prostaglandin synthesis and thus limit the ability for pain-conducting neurons to get excited; and acetaminophen, which, despite being used for a century, is poorly understood.
But
If you were to zoom in on the connection between that first afferent pain fiber and the secondary nerve in the spinal cord dorsal root ganglion, you would see a receptor called Nav1.8, a voltage-gated sodium channel.
This receptor is a key part of the apparatus that passes information from nerve 1 to nerve 2, but only for fibers that transmit pain signals. In fact, humans with mutations in this receptor that leave it always in the “open” state have a severe pain syndrome. Blocking the receptor, therefore, might reduce pain.
In preclinical work, researchers identified VX-548, which doesn’t have a brand name yet, as a potent blocker of that channel even in nanomolar concentrations. Importantly, the compound was highly selective for that particular channel – about 30,000 times more selective than it was for the other sodium channels in that family.
Of course, a highly selective and specific drug does not a blockbuster analgesic make. To determine how this drug would work on humans in pain, they turned to two populations: 303 individuals undergoing abdominoplasty and 274 undergoing bunionectomy, as reported in a new paper in the New England Journal of Medicine.
I know this seems a bit random, but abdominoplasty is quite painful and a good model for soft-tissue pain. Bunionectomy is also quite a painful procedure and a useful model of bone pain. After the surgeries, patients were randomized to several different doses of VX-548, hydrocodone plus acetaminophen, or placebo for 48 hours.
At 19 time points over that 48-hour period, participants were asked to rate their pain on a scale from 0 to 10. The primary outcome was the cumulative pain experienced over the 48 hours. So, higher pain would be worse here, but longer duration of pain would also be worse.
The story of the study is really told in this chart.
Yes, those assigned to the highest dose of VX-548 had a statistically significant lower cumulative amount of pain in the 48 hours after surgery. But the picture is really worth more than the stats here. You can see that the onset of pain relief was fairly quick, and that pain relief was sustained over time. You can also see that this is not a miracle drug. Pain scores were a bit better 48 hours out, but only by about a point and a half.
Placebo isn’t really the fair comparison here; few of us treat our postabdominoplasty patients with placebo, after all. The authors do not formally compare the effect of VX-548 with that of the opioid hydrocodone, for instance. But that doesn’t stop us.
This graph, which I put together from data in the paper, shows pain control across the four randomization categories, with higher numbers indicating more (cumulative) control. While all the active agents do a bit better than placebo, VX-548 at the higher dose appears to do the best. But I should note that 5 mg of hydrocodone may not be an adequate dose for most people.
Yes, I would really have killed for an NSAID arm in this trial. Its absence, given that NSAIDs are a staple of postoperative care, is ... well, let’s just say, notable.
Although not a pain-destroying machine, VX-548 has some other things to recommend it. The receptor is really not found in the brain at all, which suggests that the drug should not carry much risk for dependency, though that has not been formally studied.
The side effects were generally mild – headache was the most common – and less prevalent than what you see even in the placebo arm.
Perhaps most notable is the fact that the rate of discontinuation of the study drug was lowest in the VX-548 arm. Patients could stop taking the pill they were assigned for any reason, ranging from perceived lack of efficacy to side effects. A low discontinuation rate indicates to me a sort of “voting with your feet” that suggests this might be a well-tolerated and reasonably effective drug.
VX-548 isn’t on the market yet; phase 3 trials are ongoing. But whether it is this particular drug or another in this class, I’m happy to see researchers trying to find new ways to target that most primeval form of suffering: pain.
Dr. Wilson is an associate professor of medicine and public health and director of Yale’s Clinical and Translational Research Accelerator, New Haven, Conn. He disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
In 133-vehicle pileup, bleeding paramedic helps while hurt
It seemed like a typical kind of day. I was out the door by 6:00 a.m., heading into work for a shift on I-35 West, my daily commute. It was still dark out. A little bit colder that morning, but nothing us Texans aren’t used to.
I was cruising down the tollway, which is separated from the main highway by a barrier. That stretch has a slight hill and turns to the left. You can’t see anything beyond the hill when you’re at the bottom.
As I made my way up, I spotted brake lights about 400 yards ahead. I eased on my brake, and next thing I knew, I was sliding.
I realized, I’m on black ice.
I was driving a 2011 Toyota FJ Cruiser and I had it all beefed up – lift tires, winch bumpers front and back. I had never had any sort of issue like that.
My ABS brakes kicked in. I slowed, but not fast enough. I saw a wall of crashed cars in front of me.
I was in the left-hand lane, so I turned my steering wheel into the center median. I could hear the whole side of my vehicle scraping against it. I managed to slow down enough to just tap the vehicle in front of me.
I looked in my passenger side-view mirror and saw headlights coming in the right lane. But this car couldn’t slow down. It crashed into the wreckage to my right.
That’s when it sunk in: There was going to be a car coming in my lane, and it might not be able to stop.
I looked in my rear-view mirror and saw headlights. Sparks flying off that center median.
I didn’t know at the time, but it was a fully loaded semi-truck traveling about 60 miles an hour.
I had a split second to think: This is it. This is how it ends. I closed my eyes.
It was the most violent impact I’ve ever experienced in my life.
I had no idea until afterward, but I had slammed into the vehicle in front of me and my SUV did a kind of 360° barrel roll over the median into the northbound lanes, landing wheels down on top of my sheared off roof rack.
Everything stopped. I opened my eyes. All my airbags had deployed. I gently tried moving my arms and legs, and they worked. I couldn’t move my left foot. It was wedged underneath the brake pedal. But I wasn’t in any pain, just very confused and disoriented. I knew I needed to get out of the vehicle.
My door was wedged shut, so I crawled out of the broken window, slipping on the black ice. I realized I had hit a Fort Worth police cruiser, now all smashed up. The driver couldn’t open his door. So, I helped him force it open, got him out of the vehicle, and checked on him. He was fine.
I had no idea how many vehicles and people were involved. I was in so much shock that the only thing I could do was immediately revert back to my training. I was the only first responder there.
I was helping people with lacerations, back and neck issues from the violent impacts. When you’re involved in a mass casualty incident like that, you have to assess which patients will be the most viable and need the most immediate attention. You have greens, yellows, reds, and then blacks – the deceased. Someone who doesn’t have a pulse and isn’t breathing, you can’t necessarily do CPR because you don’t have enough resources. You have to use your best judgment.
Meanwhile, the crashes kept coming. I found out later I was roughly vehicle No. 50 in the pileup; 83 more would follow. I heard them over and over – a crash and then screams from people in their vehicles. Each time a car hit, the entire pileup would move a couple of inches, getting more and more compacted. With that going on, I couldn’t go in there to pull people out. That scene was absolutely unsafe.
It felt like forever, but about 10 minutes later, an ambulance showed up, and I walked over to them. Because I was in my work uniform, they thought I was there on a call.
A couple fire crews came, and a firefighter yelled, “Hey, we need a backboard!” So, I grabbed a backboard from their unit and helped load up a patient. Then I heard somebody screaming, “This patient needs a stretcher!” A woman was having lumbar pain that seemed excruciating. I helped move her from the wreckage and carry her over to the stretcher. I started trying to get as many people as I could out of their cars.
Around this time, one of my supervisors showed up. He thought I was there working. But then he asked me, “Why is your face bleeding? Why do you have blood coming from your nose?” I pointed to my vehicle, and his jaw just dropped. He said, “Okay, you’re done. Go sit in my vehicle over there.”
He put a stop to my helping out, which was probably for the best. Because I actually had a concussion, a bone contusion in my foot, and a severely sprained ankle. The next day, I felt like I had gotten hit by a truck. (I had!) But when you have so much adrenaline pumping, you don’t feel pain or emotion. You don’t really feel anything.
While I was sitting in that vehicle, I called my mom to let her know I was okay. My parents were watching the news, and there was an aerial view of the accident. It was massive – a giant pile of metal stretching 200 or 300 yards. Six people had perished, more than 60 were hurt.
That night, our public information officer reached out to me about doing an interview with NBC. So, I told my story about what happened. Because of the concussion, a lot of it was a blur.
A day later, I got a call on my cell phone and someone said, “This is Tyler from Toyota. We saw the NBC interview. We wanted to let you know, don’t worry about getting a new vehicle. Just tell us what color 4Runner you want.”
My first thought was: Okay, this can’t be real. This doesn’t happen to people like me. But it turned out that it was, and they put me in a brand new vehicle.
Toyota started sending me to events like NASCAR races, putting me up in VIP suites. It was a cool experience. But it’s just surface stuff – it’s never going to erase what happened. The experience left a mark. It took me 6 months to a year to get rid of that feeling of the impact. Every time I tried to fall asleep, the whole scenario would replay in my head.
In EMS, we have a saying: “Every patient is practice for the next one.” That pileup – you can’t train for something like that. We all learned from it, so we can better prepare if anything like that happens again.
Since then, I’ve seen people die in motor vehicle collisions from a lot less than what happened to me. I’m not religious or spiritual, but I believe there must be a reason why I’m still here.
Now I see patients in traffic accidents who are very distraught even though they’re going to be okay. I tell them, “I’m sorry this happened to you. But remember, this is not the end. You are alive. And I’m going to do everything I can to make sure that doesn’t change while you’re with me.”
Trey McDaniel is a paramedic with MedStar Mobile Healthcare in Fort Worth, Tex.
A version of this article first appeared on Medscape.com.
It seemed like a typical kind of day. I was out the door by 6:00 a.m., heading into work for a shift on I-35 West, my daily commute. It was still dark out. A little bit colder that morning, but nothing us Texans aren’t used to.
I was cruising down the tollway, which is separated from the main highway by a barrier. That stretch has a slight hill and turns to the left. You can’t see anything beyond the hill when you’re at the bottom.
As I made my way up, I spotted brake lights about 400 yards ahead. I eased on my brake, and next thing I knew, I was sliding.
I realized, I’m on black ice.
I was driving a 2011 Toyota FJ Cruiser and I had it all beefed up – lift tires, winch bumpers front and back. I had never had any sort of issue like that.
My ABS brakes kicked in. I slowed, but not fast enough. I saw a wall of crashed cars in front of me.
I was in the left-hand lane, so I turned my steering wheel into the center median. I could hear the whole side of my vehicle scraping against it. I managed to slow down enough to just tap the vehicle in front of me.
I looked in my passenger side-view mirror and saw headlights coming in the right lane. But this car couldn’t slow down. It crashed into the wreckage to my right.
That’s when it sunk in: There was going to be a car coming in my lane, and it might not be able to stop.
I looked in my rear-view mirror and saw headlights. Sparks flying off that center median.
I didn’t know at the time, but it was a fully loaded semi-truck traveling about 60 miles an hour.
I had a split second to think: This is it. This is how it ends. I closed my eyes.
It was the most violent impact I’ve ever experienced in my life.
I had no idea until afterward, but I had slammed into the vehicle in front of me and my SUV did a kind of 360° barrel roll over the median into the northbound lanes, landing wheels down on top of my sheared off roof rack.
Everything stopped. I opened my eyes. All my airbags had deployed. I gently tried moving my arms and legs, and they worked. I couldn’t move my left foot. It was wedged underneath the brake pedal. But I wasn’t in any pain, just very confused and disoriented. I knew I needed to get out of the vehicle.
My door was wedged shut, so I crawled out of the broken window, slipping on the black ice. I realized I had hit a Fort Worth police cruiser, now all smashed up. The driver couldn’t open his door. So, I helped him force it open, got him out of the vehicle, and checked on him. He was fine.
I had no idea how many vehicles and people were involved. I was in so much shock that the only thing I could do was immediately revert back to my training. I was the only first responder there.
I was helping people with lacerations, back and neck issues from the violent impacts. When you’re involved in a mass casualty incident like that, you have to assess which patients will be the most viable and need the most immediate attention. You have greens, yellows, reds, and then blacks – the deceased. Someone who doesn’t have a pulse and isn’t breathing, you can’t necessarily do CPR because you don’t have enough resources. You have to use your best judgment.
Meanwhile, the crashes kept coming. I found out later I was roughly vehicle No. 50 in the pileup; 83 more would follow. I heard them over and over – a crash and then screams from people in their vehicles. Each time a car hit, the entire pileup would move a couple of inches, getting more and more compacted. With that going on, I couldn’t go in there to pull people out. That scene was absolutely unsafe.
It felt like forever, but about 10 minutes later, an ambulance showed up, and I walked over to them. Because I was in my work uniform, they thought I was there on a call.
A couple fire crews came, and a firefighter yelled, “Hey, we need a backboard!” So, I grabbed a backboard from their unit and helped load up a patient. Then I heard somebody screaming, “This patient needs a stretcher!” A woman was having lumbar pain that seemed excruciating. I helped move her from the wreckage and carry her over to the stretcher. I started trying to get as many people as I could out of their cars.
Around this time, one of my supervisors showed up. He thought I was there working. But then he asked me, “Why is your face bleeding? Why do you have blood coming from your nose?” I pointed to my vehicle, and his jaw just dropped. He said, “Okay, you’re done. Go sit in my vehicle over there.”
He put a stop to my helping out, which was probably for the best. Because I actually had a concussion, a bone contusion in my foot, and a severely sprained ankle. The next day, I felt like I had gotten hit by a truck. (I had!) But when you have so much adrenaline pumping, you don’t feel pain or emotion. You don’t really feel anything.
While I was sitting in that vehicle, I called my mom to let her know I was okay. My parents were watching the news, and there was an aerial view of the accident. It was massive – a giant pile of metal stretching 200 or 300 yards. Six people had perished, more than 60 were hurt.
That night, our public information officer reached out to me about doing an interview with NBC. So, I told my story about what happened. Because of the concussion, a lot of it was a blur.
A day later, I got a call on my cell phone and someone said, “This is Tyler from Toyota. We saw the NBC interview. We wanted to let you know, don’t worry about getting a new vehicle. Just tell us what color 4Runner you want.”
My first thought was: Okay, this can’t be real. This doesn’t happen to people like me. But it turned out that it was, and they put me in a brand new vehicle.
Toyota started sending me to events like NASCAR races, putting me up in VIP suites. It was a cool experience. But it’s just surface stuff – it’s never going to erase what happened. The experience left a mark. It took me 6 months to a year to get rid of that feeling of the impact. Every time I tried to fall asleep, the whole scenario would replay in my head.
In EMS, we have a saying: “Every patient is practice for the next one.” That pileup – you can’t train for something like that. We all learned from it, so we can better prepare if anything like that happens again.
Since then, I’ve seen people die in motor vehicle collisions from a lot less than what happened to me. I’m not religious or spiritual, but I believe there must be a reason why I’m still here.
Now I see patients in traffic accidents who are very distraught even though they’re going to be okay. I tell them, “I’m sorry this happened to you. But remember, this is not the end. You are alive. And I’m going to do everything I can to make sure that doesn’t change while you’re with me.”
Trey McDaniel is a paramedic with MedStar Mobile Healthcare in Fort Worth, Tex.
A version of this article first appeared on Medscape.com.
It seemed like a typical kind of day. I was out the door by 6:00 a.m., heading into work for a shift on I-35 West, my daily commute. It was still dark out. A little bit colder that morning, but nothing us Texans aren’t used to.
I was cruising down the tollway, which is separated from the main highway by a barrier. That stretch has a slight hill and turns to the left. You can’t see anything beyond the hill when you’re at the bottom.
As I made my way up, I spotted brake lights about 400 yards ahead. I eased on my brake, and next thing I knew, I was sliding.
I realized, I’m on black ice.
I was driving a 2011 Toyota FJ Cruiser and I had it all beefed up – lift tires, winch bumpers front and back. I had never had any sort of issue like that.
My ABS brakes kicked in. I slowed, but not fast enough. I saw a wall of crashed cars in front of me.
I was in the left-hand lane, so I turned my steering wheel into the center median. I could hear the whole side of my vehicle scraping against it. I managed to slow down enough to just tap the vehicle in front of me.
I looked in my passenger side-view mirror and saw headlights coming in the right lane. But this car couldn’t slow down. It crashed into the wreckage to my right.
That’s when it sunk in: There was going to be a car coming in my lane, and it might not be able to stop.
I looked in my rear-view mirror and saw headlights. Sparks flying off that center median.
I didn’t know at the time, but it was a fully loaded semi-truck traveling about 60 miles an hour.
I had a split second to think: This is it. This is how it ends. I closed my eyes.
It was the most violent impact I’ve ever experienced in my life.
I had no idea until afterward, but I had slammed into the vehicle in front of me and my SUV did a kind of 360° barrel roll over the median into the northbound lanes, landing wheels down on top of my sheared off roof rack.
Everything stopped. I opened my eyes. All my airbags had deployed. I gently tried moving my arms and legs, and they worked. I couldn’t move my left foot. It was wedged underneath the brake pedal. But I wasn’t in any pain, just very confused and disoriented. I knew I needed to get out of the vehicle.
My door was wedged shut, so I crawled out of the broken window, slipping on the black ice. I realized I had hit a Fort Worth police cruiser, now all smashed up. The driver couldn’t open his door. So, I helped him force it open, got him out of the vehicle, and checked on him. He was fine.
I had no idea how many vehicles and people were involved. I was in so much shock that the only thing I could do was immediately revert back to my training. I was the only first responder there.
I was helping people with lacerations, back and neck issues from the violent impacts. When you’re involved in a mass casualty incident like that, you have to assess which patients will be the most viable and need the most immediate attention. You have greens, yellows, reds, and then blacks – the deceased. Someone who doesn’t have a pulse and isn’t breathing, you can’t necessarily do CPR because you don’t have enough resources. You have to use your best judgment.
Meanwhile, the crashes kept coming. I found out later I was roughly vehicle No. 50 in the pileup; 83 more would follow. I heard them over and over – a crash and then screams from people in their vehicles. Each time a car hit, the entire pileup would move a couple of inches, getting more and more compacted. With that going on, I couldn’t go in there to pull people out. That scene was absolutely unsafe.
It felt like forever, but about 10 minutes later, an ambulance showed up, and I walked over to them. Because I was in my work uniform, they thought I was there on a call.
A couple fire crews came, and a firefighter yelled, “Hey, we need a backboard!” So, I grabbed a backboard from their unit and helped load up a patient. Then I heard somebody screaming, “This patient needs a stretcher!” A woman was having lumbar pain that seemed excruciating. I helped move her from the wreckage and carry her over to the stretcher. I started trying to get as many people as I could out of their cars.
Around this time, one of my supervisors showed up. He thought I was there working. But then he asked me, “Why is your face bleeding? Why do you have blood coming from your nose?” I pointed to my vehicle, and his jaw just dropped. He said, “Okay, you’re done. Go sit in my vehicle over there.”
He put a stop to my helping out, which was probably for the best. Because I actually had a concussion, a bone contusion in my foot, and a severely sprained ankle. The next day, I felt like I had gotten hit by a truck. (I had!) But when you have so much adrenaline pumping, you don’t feel pain or emotion. You don’t really feel anything.
While I was sitting in that vehicle, I called my mom to let her know I was okay. My parents were watching the news, and there was an aerial view of the accident. It was massive – a giant pile of metal stretching 200 or 300 yards. Six people had perished, more than 60 were hurt.
That night, our public information officer reached out to me about doing an interview with NBC. So, I told my story about what happened. Because of the concussion, a lot of it was a blur.
A day later, I got a call on my cell phone and someone said, “This is Tyler from Toyota. We saw the NBC interview. We wanted to let you know, don’t worry about getting a new vehicle. Just tell us what color 4Runner you want.”
My first thought was: Okay, this can’t be real. This doesn’t happen to people like me. But it turned out that it was, and they put me in a brand new vehicle.
Toyota started sending me to events like NASCAR races, putting me up in VIP suites. It was a cool experience. But it’s just surface stuff – it’s never going to erase what happened. The experience left a mark. It took me 6 months to a year to get rid of that feeling of the impact. Every time I tried to fall asleep, the whole scenario would replay in my head.
In EMS, we have a saying: “Every patient is practice for the next one.” That pileup – you can’t train for something like that. We all learned from it, so we can better prepare if anything like that happens again.
Since then, I’ve seen people die in motor vehicle collisions from a lot less than what happened to me. I’m not religious or spiritual, but I believe there must be a reason why I’m still here.
Now I see patients in traffic accidents who are very distraught even though they’re going to be okay. I tell them, “I’m sorry this happened to you. But remember, this is not the end. You are alive. And I’m going to do everything I can to make sure that doesn’t change while you’re with me.”
Trey McDaniel is a paramedic with MedStar Mobile Healthcare in Fort Worth, Tex.
A version of this article first appeared on Medscape.com.
Obesity: Don’t separate mental health from physical health
“The patient is ready,” the medical assistant informs you while handing you the chart. The chart reads: “Chief complaint: Weight gain/Discuss weight loss options.” You note the normal vital signs other than an increased BMI to 34 from 4 months ago. You knock on the exam room door with your plan half-formulated.
“Come in,” the patient says, almost too softly for you to hear. Shock overtakes you as you enter the room and see something you never imagined. The patient is holding their disconnected head in their lap as they say, “Nice to see you, Doc. I want to do something about my weight.”
You’re baffled at how they are speaking with a disconnected head. Of course, this outlandish patient scenario isn’t real. Or is it?
Patients with mental health concerns don’t literally present with their head disconnected from their bodies. Too often, mental health is treated as separate from physical health, especially regarding weight management and obesity. However, studies have shown an association between mental health and obesity. In this pivotal time of pharmacologic innovation in obesity care, we must also ensure that we effectively address the mental health of our patients with obesity.
Screening
Mental health conditions can look different for everyone. It can be hard to diagnose a mental health condition without validated screening. For example, depression is one of the most common mental health disorders. The U.S. Preventive Services Task Force recommends depression screening in all adults.
The Patient Health Questionnaire-2 (PHQ-2) is one screening tool that can alert doctors and clinicians to potential depression. Patients with obesity have higher rates of depression and other mental health conditions. It’s even more critical to screen for depression and other mental health disorders when prescribing these new medications, given recent reports of suicidal ideation with certain antiobesity medications.
Stigma
Mental health–related stigma can trigger shame and prevent patients from seeking psychological help. Furthermore, compounded stigma in patients with larger bodies (weight bias) and from marginalized communities such as the Black community (racial discrimination) add more barriers to seeking mental health care. When patients seek care for mental health conditions, they may feel more comfortable seeing a primary care physician or other clinician than a mental health professional. Therefore, all physicians and clinicians are integral in normalizing mental health care. Instead of treating mental health as separate from physical health, discussing the bidirectional relationship between mental health conditions and physiologic diseases can help patients understand that having a mental health condition isn’t a choice and facilitate openness to multiple treatment options to improve their quality of life.
Support
Addressing mental health effectively often requires multiple layers of patient support. Support can come from loved ones or community groups. But for severe stress and other mental health conditions, treatment with psychotherapy or psychiatric medications is essential. Unfortunately, even if a patient is willing to see a mental health professional, availability or access may be a challenge. Therefore, other clinicians may have to step in and serve as a bridge to mental health care. It’s also essential to ensure that patients are aware of crisis support lines and online resources for mental health care.
Stress
Having a high level of stress can be harmful physically and can also worsen mental health conditions. Additionally, it can contribute to a higher risk for obesity and can trigger emotional eating. Chronic stress has become so common in society that patients often underestimate how much stress they are under. Assessments like the Holmes-Rahe Stress Inventory can help patients identify and quantify potential stressors. While some stressors are uncontrollable, such as social determinants of health (SDOH), addressing controllable stressors and improving coping mechanisms is possible. For instance, mindfulness and breathwork are easy to follow and relatively accessible for most patients.
Social determinants of health
For a treatment plan to be maximally impactful, we must incorporate SDOH in clinical care. SDOH includes financial instability, safe neighborhoods, and more, and can significantly influence an ideal treatment plan. Furthermore, a high SDOH burden can negatively affect mental health and obesity rates. It’s helpful to incorporate patients’ SDOH burden into treatment planning. Learn how to take action on SDOH.
Empowerment
Patients who address their mental health have taken a courageous step toward health and healing. As mentioned, they may experience gaps in care while awaiting connection to the next steps of their journey, such as starting care with a mental health professional or waiting for a medication to take effect. All clinicians can empower patients about their weight by informing them that:
Food may affect their mood. Studies show that certain foods and eating patterns are associated with high levels of depression and anxiety. Limiting processed foods and increasing fruits, vegetables, and foods high in vitamin D, C, and other nutrients is helpful. Everyone is different, so encourage patients to pay attention to how food uniquely affects their mood by keeping a food/feeling log for 1-3 days.
Move more. Increased physical activity can improve mental health.
Get outdoors. Time in nature is associated with better mental health. Spending as little as 10 minutes outside can be beneficial. It’s important to be aware that SDOH factors such as unsafe environments or limited outdoor access may make this difficult for some patients.
Positive stress-relieving activities. Each person has their own way of reducing stress. It is helpful to remind patients of unhealthy stress relievers such as overeating, drinking alcohol, and smoking, and encourage them to replace those with positive stress relievers.
Spiritual well-being. Spirituality is often overlooked in health care. But studies have shown that incorporating a person’s spirituality may have positive health benefits.
It’s time to stop disconnecting mental health from physical health. Each clinician plays a vital role in treating the whole person. Just as you wouldn’t let a patient with a disconnected head leave the office without addressing it, let’s not leave mental health out when addressing our patients’ weight concerns.
Dr. Gonsahn-Bollie is an integrative obesity specialist focused on individualized solutions for emotional and biological overeating. Connect with her at www.embraceyouweightloss.com or on Instagram @embraceyoumd. Her bestselling book, “Embrace You: Your Guide to Transforming Weight Loss Misconceptions Into Lifelong Wellness,” (Baltimore: Purposely Created Publishing Group, 2019) was Healthline.com’s Best Overall Weight Loss Book of 2022 and one of Livestrong.com’s 8 Best Weight-Loss Books to Read in 2022.
Dr. Gonsahn-Bollie is CEO and Lead Physician, Embrace You Weight and Wellness, Telehealth & Virtual Counseling. She has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
“The patient is ready,” the medical assistant informs you while handing you the chart. The chart reads: “Chief complaint: Weight gain/Discuss weight loss options.” You note the normal vital signs other than an increased BMI to 34 from 4 months ago. You knock on the exam room door with your plan half-formulated.
“Come in,” the patient says, almost too softly for you to hear. Shock overtakes you as you enter the room and see something you never imagined. The patient is holding their disconnected head in their lap as they say, “Nice to see you, Doc. I want to do something about my weight.”
You’re baffled at how they are speaking with a disconnected head. Of course, this outlandish patient scenario isn’t real. Or is it?
Patients with mental health concerns don’t literally present with their head disconnected from their bodies. Too often, mental health is treated as separate from physical health, especially regarding weight management and obesity. However, studies have shown an association between mental health and obesity. In this pivotal time of pharmacologic innovation in obesity care, we must also ensure that we effectively address the mental health of our patients with obesity.
Screening
Mental health conditions can look different for everyone. It can be hard to diagnose a mental health condition without validated screening. For example, depression is one of the most common mental health disorders. The U.S. Preventive Services Task Force recommends depression screening in all adults.
The Patient Health Questionnaire-2 (PHQ-2) is one screening tool that can alert doctors and clinicians to potential depression. Patients with obesity have higher rates of depression and other mental health conditions. It’s even more critical to screen for depression and other mental health disorders when prescribing these new medications, given recent reports of suicidal ideation with certain antiobesity medications.
Stigma
Mental health–related stigma can trigger shame and prevent patients from seeking psychological help. Furthermore, compounded stigma in patients with larger bodies (weight bias) and from marginalized communities such as the Black community (racial discrimination) add more barriers to seeking mental health care. When patients seek care for mental health conditions, they may feel more comfortable seeing a primary care physician or other clinician than a mental health professional. Therefore, all physicians and clinicians are integral in normalizing mental health care. Instead of treating mental health as separate from physical health, discussing the bidirectional relationship between mental health conditions and physiologic diseases can help patients understand that having a mental health condition isn’t a choice and facilitate openness to multiple treatment options to improve their quality of life.
Support
Addressing mental health effectively often requires multiple layers of patient support. Support can come from loved ones or community groups. But for severe stress and other mental health conditions, treatment with psychotherapy or psychiatric medications is essential. Unfortunately, even if a patient is willing to see a mental health professional, availability or access may be a challenge. Therefore, other clinicians may have to step in and serve as a bridge to mental health care. It’s also essential to ensure that patients are aware of crisis support lines and online resources for mental health care.
Stress
Having a high level of stress can be harmful physically and can also worsen mental health conditions. Additionally, it can contribute to a higher risk for obesity and can trigger emotional eating. Chronic stress has become so common in society that patients often underestimate how much stress they are under. Assessments like the Holmes-Rahe Stress Inventory can help patients identify and quantify potential stressors. While some stressors are uncontrollable, such as social determinants of health (SDOH), addressing controllable stressors and improving coping mechanisms is possible. For instance, mindfulness and breathwork are easy to follow and relatively accessible for most patients.
Social determinants of health
For a treatment plan to be maximally impactful, we must incorporate SDOH in clinical care. SDOH includes financial instability, safe neighborhoods, and more, and can significantly influence an ideal treatment plan. Furthermore, a high SDOH burden can negatively affect mental health and obesity rates. It’s helpful to incorporate patients’ SDOH burden into treatment planning. Learn how to take action on SDOH.
Empowerment
Patients who address their mental health have taken a courageous step toward health and healing. As mentioned, they may experience gaps in care while awaiting connection to the next steps of their journey, such as starting care with a mental health professional or waiting for a medication to take effect. All clinicians can empower patients about their weight by informing them that:
Food may affect their mood. Studies show that certain foods and eating patterns are associated with high levels of depression and anxiety. Limiting processed foods and increasing fruits, vegetables, and foods high in vitamin D, C, and other nutrients is helpful. Everyone is different, so encourage patients to pay attention to how food uniquely affects their mood by keeping a food/feeling log for 1-3 days.
Move more. Increased physical activity can improve mental health.
Get outdoors. Time in nature is associated with better mental health. Spending as little as 10 minutes outside can be beneficial. It’s important to be aware that SDOH factors such as unsafe environments or limited outdoor access may make this difficult for some patients.
Positive stress-relieving activities. Each person has their own way of reducing stress. It is helpful to remind patients of unhealthy stress relievers such as overeating, drinking alcohol, and smoking, and encourage them to replace those with positive stress relievers.
Spiritual well-being. Spirituality is often overlooked in health care. But studies have shown that incorporating a person’s spirituality may have positive health benefits.
It’s time to stop disconnecting mental health from physical health. Each clinician plays a vital role in treating the whole person. Just as you wouldn’t let a patient with a disconnected head leave the office without addressing it, let’s not leave mental health out when addressing our patients’ weight concerns.
Dr. Gonsahn-Bollie is an integrative obesity specialist focused on individualized solutions for emotional and biological overeating. Connect with her at www.embraceyouweightloss.com or on Instagram @embraceyoumd. Her bestselling book, “Embrace You: Your Guide to Transforming Weight Loss Misconceptions Into Lifelong Wellness,” (Baltimore: Purposely Created Publishing Group, 2019) was Healthline.com’s Best Overall Weight Loss Book of 2022 and one of Livestrong.com’s 8 Best Weight-Loss Books to Read in 2022.
Dr. Gonsahn-Bollie is CEO and Lead Physician, Embrace You Weight and Wellness, Telehealth & Virtual Counseling. She has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
“The patient is ready,” the medical assistant informs you while handing you the chart. The chart reads: “Chief complaint: Weight gain/Discuss weight loss options.” You note the normal vital signs other than an increased BMI to 34 from 4 months ago. You knock on the exam room door with your plan half-formulated.
“Come in,” the patient says, almost too softly for you to hear. Shock overtakes you as you enter the room and see something you never imagined. The patient is holding their disconnected head in their lap as they say, “Nice to see you, Doc. I want to do something about my weight.”
You’re baffled at how they are speaking with a disconnected head. Of course, this outlandish patient scenario isn’t real. Or is it?
Patients with mental health concerns don’t literally present with their head disconnected from their bodies. Too often, mental health is treated as separate from physical health, especially regarding weight management and obesity. However, studies have shown an association between mental health and obesity. In this pivotal time of pharmacologic innovation in obesity care, we must also ensure that we effectively address the mental health of our patients with obesity.
Screening
Mental health conditions can look different for everyone. It can be hard to diagnose a mental health condition without validated screening. For example, depression is one of the most common mental health disorders. The U.S. Preventive Services Task Force recommends depression screening in all adults.
The Patient Health Questionnaire-2 (PHQ-2) is one screening tool that can alert doctors and clinicians to potential depression. Patients with obesity have higher rates of depression and other mental health conditions. It’s even more critical to screen for depression and other mental health disorders when prescribing these new medications, given recent reports of suicidal ideation with certain antiobesity medications.
Stigma
Mental health–related stigma can trigger shame and prevent patients from seeking psychological help. Furthermore, compounded stigma in patients with larger bodies (weight bias) and from marginalized communities such as the Black community (racial discrimination) add more barriers to seeking mental health care. When patients seek care for mental health conditions, they may feel more comfortable seeing a primary care physician or other clinician than a mental health professional. Therefore, all physicians and clinicians are integral in normalizing mental health care. Instead of treating mental health as separate from physical health, discussing the bidirectional relationship between mental health conditions and physiologic diseases can help patients understand that having a mental health condition isn’t a choice and facilitate openness to multiple treatment options to improve their quality of life.
Support
Addressing mental health effectively often requires multiple layers of patient support. Support can come from loved ones or community groups. But for severe stress and other mental health conditions, treatment with psychotherapy or psychiatric medications is essential. Unfortunately, even if a patient is willing to see a mental health professional, availability or access may be a challenge. Therefore, other clinicians may have to step in and serve as a bridge to mental health care. It’s also essential to ensure that patients are aware of crisis support lines and online resources for mental health care.
Stress
Having a high level of stress can be harmful physically and can also worsen mental health conditions. Additionally, it can contribute to a higher risk for obesity and can trigger emotional eating. Chronic stress has become so common in society that patients often underestimate how much stress they are under. Assessments like the Holmes-Rahe Stress Inventory can help patients identify and quantify potential stressors. While some stressors are uncontrollable, such as social determinants of health (SDOH), addressing controllable stressors and improving coping mechanisms is possible. For instance, mindfulness and breathwork are easy to follow and relatively accessible for most patients.
Social determinants of health
For a treatment plan to be maximally impactful, we must incorporate SDOH in clinical care. SDOH includes financial instability, safe neighborhoods, and more, and can significantly influence an ideal treatment plan. Furthermore, a high SDOH burden can negatively affect mental health and obesity rates. It’s helpful to incorporate patients’ SDOH burden into treatment planning. Learn how to take action on SDOH.
Empowerment
Patients who address their mental health have taken a courageous step toward health and healing. As mentioned, they may experience gaps in care while awaiting connection to the next steps of their journey, such as starting care with a mental health professional or waiting for a medication to take effect. All clinicians can empower patients about their weight by informing them that:
Food may affect their mood. Studies show that certain foods and eating patterns are associated with high levels of depression and anxiety. Limiting processed foods and increasing fruits, vegetables, and foods high in vitamin D, C, and other nutrients is helpful. Everyone is different, so encourage patients to pay attention to how food uniquely affects their mood by keeping a food/feeling log for 1-3 days.
Move more. Increased physical activity can improve mental health.
Get outdoors. Time in nature is associated with better mental health. Spending as little as 10 minutes outside can be beneficial. It’s important to be aware that SDOH factors such as unsafe environments or limited outdoor access may make this difficult for some patients.
Positive stress-relieving activities. Each person has their own way of reducing stress. It is helpful to remind patients of unhealthy stress relievers such as overeating, drinking alcohol, and smoking, and encourage them to replace those with positive stress relievers.
Spiritual well-being. Spirituality is often overlooked in health care. But studies have shown that incorporating a person’s spirituality may have positive health benefits.
It’s time to stop disconnecting mental health from physical health. Each clinician plays a vital role in treating the whole person. Just as you wouldn’t let a patient with a disconnected head leave the office without addressing it, let’s not leave mental health out when addressing our patients’ weight concerns.
Dr. Gonsahn-Bollie is an integrative obesity specialist focused on individualized solutions for emotional and biological overeating. Connect with her at www.embraceyouweightloss.com or on Instagram @embraceyoumd. Her bestselling book, “Embrace You: Your Guide to Transforming Weight Loss Misconceptions Into Lifelong Wellness,” (Baltimore: Purposely Created Publishing Group, 2019) was Healthline.com’s Best Overall Weight Loss Book of 2022 and one of Livestrong.com’s 8 Best Weight-Loss Books to Read in 2022.
Dr. Gonsahn-Bollie is CEO and Lead Physician, Embrace You Weight and Wellness, Telehealth & Virtual Counseling. She has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Prescribing lifestyle changes: When medicine isn’t enough
In psychiatry, patients come to us with their list of symptoms, often a diagnosis they’ve made themselves, and the expectation that they will be given medication to fix their problem. Their diagnoses are often right on target – people often know if they are depressed or anxious, and Doctor Google may provide useful information.

Sometimes they want a specific medication, one they saw in a TV ad, or one that helped them in the past or has helped someone they know. As psychiatrists have focused more on their strengths as psychopharmacologists and less on psychotherapy, it gets easy for both the patient and the doctor to look to medication, cocktails, and titration as the only thing we do.
“My medicine stopped working,” is a line I commonly hear. Often the patient is on a complicated regimen that has been serving them well, and it seems unlikely that the five psychotropic medications they are taking have suddenly “stopped working.” An obvious exception is the SSRI “poop out” that can occur 6-12 months or more after beginning treatment. In addition, it’s important to make sure patients are taking their medications as prescribed, and that the generic formulations have not changed.
But as rates of mental illness increase, some of it spurred on by difficult times,
This is not to devalue our medications, but to help the patient see symptoms as having multiple factors and give them some means to intervene, in addition to medications. At the beginning of therapy, it is important to “prescribe” lifestyle changes that will facilitate the best possible outcomes.
Nonpharmaceutical prescriptions
Early in my career, people with alcohol use problems were told they needed to be substance free before they were candidates for antidepressants. While we no longer do that, it is still important to emphasize abstinence from addictive substances, and to recommend specific treatment when necessary.
Patients are often reluctant to see their use of alcohol, marijuana (it’s medical! It’s part of wellness!), or their pain medications as part of the problem, and this can be difficult. There have been times, after multiple medications have failed to help their symptoms, when I have said, “If you don’t get treatment for this problem, I am not going to be able to help you feel better” and that has been motivating for the patient.
There are other “prescriptions” to write. Regular sleep is essential for people with mood disorders, and this can be difficult for many patients, especially those who do shift work, or who have regular disruptions to their sleep from noise, pets, and children. Exercise is wonderful for the cardiovascular system, calms anxiety, and maintains strength, endurance, mobility, and quality of life as people age. But it can be a hard sell to people in a mental health crisis.
Nature is healing, and sunshine helps with maintaining circadian rhythms. For those who don’t exercise, I often “prescribe” 20 to 30 minutes a day of walking, preferably outside, during daylight hours, in a park or natural setting. For people with anxiety, it is important to check their caffeine consumption and to suggest ways to moderate it – moving to decaffeinated beverages or titrating down by mixing decaf with caffeinated.
Meditation is something that many people find helpful. For anxious people, it can be very difficult, and I will prescribe a specific instructional video course that I like on the well-being app InsightTimer – Sarah Blondin’s Learn How to Meditate in Seven Days. The sessions are approximately 10 minutes long, and that seems like the right amount of time for a beginner.
When people are very ill and don’t want to go into the hospital, I talk with them about things that happen in the hospital that are helpful, things they can try to mimic at home. In the hospital, patients don’t go to work, they don’t spend hours a day on the computer, and they are given a pass from dealing with the routine stresses of daily life.
I ask them to take time off work, to avoid as much stress as possible, to spend time with loved ones who give them comfort, and to avoid the people who leave them feeling drained or distressed. I ask them to engage in activities they find healing, to eat well, exercise, and avoid social media. In the hospital, I emphasize, they wake patients up in the morning, ask them to get out of bed and engage in therapeutic activities. They are fed and kept from intoxicants.
When it comes to nutrition, we know so little about how food affects mental health. I feel like it can’t hurt to ask people to avoid fast foods, soft drinks, and processed foods, and so I do.
And what about compliance? Of course, not everyone complies; not everyone is interested in making changes and these can be hard changes. I’ve recently started to recommend the book Atomic Habits by James Clear. Sometimes a bit of motivational interviewing can also be helpful in getting people to look at slowly moving toward making changes.
In prescribing lifestyle changes, it is important to offer most of these changes as suggestions, not as things we insist on, or that will leave the patient feeling ashamed if he doesn’t follow through. They should be discussed early in treatment so that patients don’t feel blamed for their illness or relapses. As with all the things we prescribe, some of these behavior changes help some of the people some of the time. Suggesting them, however, makes the strong statement that treating psychiatric disorders can be about more than passively swallowing a pill.
Dr. Miller is a coauthor of “Committed: The Battle Over Involuntary Psychiatric Care” (Baltimore: Johns Hopkins University Press, 2016). She has a private practice and is an assistant professor of psychiatry and behavioral sciences at Johns Hopkins University, Baltimore. She disclosed no relevant conflicts of interest.
In psychiatry, patients come to us with their list of symptoms, often a diagnosis they’ve made themselves, and the expectation that they will be given medication to fix their problem. Their diagnoses are often right on target – people often know if they are depressed or anxious, and Doctor Google may provide useful information.
Sometimes they want a specific medication, one they saw in a TV ad, or one that helped them in the past or has helped someone they know. As psychiatrists have focused more on their strengths as psychopharmacologists and less on psychotherapy, it gets easy for both the patient and the doctor to look to medication, cocktails, and titration as the only thing we do.
“My medicine stopped working,” is a line I commonly hear. Often the patient is on a complicated regimen that has been serving them well, and it seems unlikely that the five psychotropic medications they are taking have suddenly “stopped working.” An obvious exception is the SSRI “poop out” that can occur 6-12 months or more after beginning treatment. In addition, it’s important to make sure patients are taking their medications as prescribed, and that the generic formulations have not changed.
But as rates of mental illness increase, some of it spurred on by difficult times,
This is not to devalue our medications, but to help the patient see symptoms as having multiple factors and give them some means to intervene, in addition to medications. At the beginning of therapy, it is important to “prescribe” lifestyle changes that will facilitate the best possible outcomes.
Nonpharmaceutical prescriptions
Early in my career, people with alcohol use problems were told they needed to be substance free before they were candidates for antidepressants. While we no longer do that, it is still important to emphasize abstinence from addictive substances, and to recommend specific treatment when necessary.
Patients are often reluctant to see their use of alcohol, marijuana (it’s medical! It’s part of wellness!), or their pain medications as part of the problem, and this can be difficult. There have been times, after multiple medications have failed to help their symptoms, when I have said, “If you don’t get treatment for this problem, I am not going to be able to help you feel better” and that has been motivating for the patient.
There are other “prescriptions” to write. Regular sleep is essential for people with mood disorders, and this can be difficult for many patients, especially those who do shift work, or who have regular disruptions to their sleep from noise, pets, and children. Exercise is wonderful for the cardiovascular system, calms anxiety, and maintains strength, endurance, mobility, and quality of life as people age. But it can be a hard sell to people in a mental health crisis.
Nature is healing, and sunshine helps with maintaining circadian rhythms. For those who don’t exercise, I often “prescribe” 20 to 30 minutes a day of walking, preferably outside, during daylight hours, in a park or natural setting. For people with anxiety, it is important to check their caffeine consumption and to suggest ways to moderate it – moving to decaffeinated beverages or titrating down by mixing decaf with caffeinated.
Meditation is something that many people find helpful. For anxious people, it can be very difficult, and I will prescribe a specific instructional video course that I like on the well-being app InsightTimer – Sarah Blondin’s Learn How to Meditate in Seven Days. The sessions are approximately 10 minutes long, and that seems like the right amount of time for a beginner.
When people are very ill and don’t want to go into the hospital, I talk with them about things that happen in the hospital that are helpful, things they can try to mimic at home. In the hospital, patients don’t go to work, they don’t spend hours a day on the computer, and they are given a pass from dealing with the routine stresses of daily life.
I ask them to take time off work, to avoid as much stress as possible, to spend time with loved ones who give them comfort, and to avoid the people who leave them feeling drained or distressed. I ask them to engage in activities they find healing, to eat well, exercise, and avoid social media. In the hospital, I emphasize, they wake patients up in the morning, ask them to get out of bed and engage in therapeutic activities. They are fed and kept from intoxicants.
When it comes to nutrition, we know so little about how food affects mental health. I feel like it can’t hurt to ask people to avoid fast foods, soft drinks, and processed foods, and so I do.
And what about compliance? Of course, not everyone complies; not everyone is interested in making changes and these can be hard changes. I’ve recently started to recommend the book Atomic Habits by James Clear. Sometimes a bit of motivational interviewing can also be helpful in getting people to look at slowly moving toward making changes.
In prescribing lifestyle changes, it is important to offer most of these changes as suggestions, not as things we insist on, or that will leave the patient feeling ashamed if he doesn’t follow through. They should be discussed early in treatment so that patients don’t feel blamed for their illness or relapses. As with all the things we prescribe, some of these behavior changes help some of the people some of the time. Suggesting them, however, makes the strong statement that treating psychiatric disorders can be about more than passively swallowing a pill.
Dr. Miller is a coauthor of “Committed: The Battle Over Involuntary Psychiatric Care” (Baltimore: Johns Hopkins University Press, 2016). She has a private practice and is an assistant professor of psychiatry and behavioral sciences at Johns Hopkins University, Baltimore. She disclosed no relevant conflicts of interest.
In psychiatry, patients come to us with their list of symptoms, often a diagnosis they’ve made themselves, and the expectation that they will be given medication to fix their problem. Their diagnoses are often right on target – people often know if they are depressed or anxious, and Doctor Google may provide useful information.
Sometimes they want a specific medication, one they saw in a TV ad, or one that helped them in the past or has helped someone they know. As psychiatrists have focused more on their strengths as psychopharmacologists and less on psychotherapy, it gets easy for both the patient and the doctor to look to medication, cocktails, and titration as the only thing we do.
“My medicine stopped working,” is a line I commonly hear. Often the patient is on a complicated regimen that has been serving them well, and it seems unlikely that the five psychotropic medications they are taking have suddenly “stopped working.” An obvious exception is the SSRI “poop out” that can occur 6-12 months or more after beginning treatment. In addition, it’s important to make sure patients are taking their medications as prescribed, and that the generic formulations have not changed.
But as rates of mental illness increase, some of it spurred on by difficult times,
This is not to devalue our medications, but to help the patient see symptoms as having multiple factors and give them some means to intervene, in addition to medications. At the beginning of therapy, it is important to “prescribe” lifestyle changes that will facilitate the best possible outcomes.
Nonpharmaceutical prescriptions
Early in my career, people with alcohol use problems were told they needed to be substance free before they were candidates for antidepressants. While we no longer do that, it is still important to emphasize abstinence from addictive substances, and to recommend specific treatment when necessary.
Patients are often reluctant to see their use of alcohol, marijuana (it’s medical! It’s part of wellness!), or their pain medications as part of the problem, and this can be difficult. There have been times, after multiple medications have failed to help their symptoms, when I have said, “If you don’t get treatment for this problem, I am not going to be able to help you feel better” and that has been motivating for the patient.
There are other “prescriptions” to write. Regular sleep is essential for people with mood disorders, and this can be difficult for many patients, especially those who do shift work, or who have regular disruptions to their sleep from noise, pets, and children. Exercise is wonderful for the cardiovascular system, calms anxiety, and maintains strength, endurance, mobility, and quality of life as people age. But it can be a hard sell to people in a mental health crisis.
Nature is healing, and sunshine helps with maintaining circadian rhythms. For those who don’t exercise, I often “prescribe” 20 to 30 minutes a day of walking, preferably outside, during daylight hours, in a park or natural setting. For people with anxiety, it is important to check their caffeine consumption and to suggest ways to moderate it – moving to decaffeinated beverages or titrating down by mixing decaf with caffeinated.
Meditation is something that many people find helpful. For anxious people, it can be very difficult, and I will prescribe a specific instructional video course that I like on the well-being app InsightTimer – Sarah Blondin’s Learn How to Meditate in Seven Days. The sessions are approximately 10 minutes long, and that seems like the right amount of time for a beginner.
When people are very ill and don’t want to go into the hospital, I talk with them about things that happen in the hospital that are helpful, things they can try to mimic at home. In the hospital, patients don’t go to work, they don’t spend hours a day on the computer, and they are given a pass from dealing with the routine stresses of daily life.
I ask them to take time off work, to avoid as much stress as possible, to spend time with loved ones who give them comfort, and to avoid the people who leave them feeling drained or distressed. I ask them to engage in activities they find healing, to eat well, exercise, and avoid social media. In the hospital, I emphasize, they wake patients up in the morning, ask them to get out of bed and engage in therapeutic activities. They are fed and kept from intoxicants.
When it comes to nutrition, we know so little about how food affects mental health. I feel like it can’t hurt to ask people to avoid fast foods, soft drinks, and processed foods, and so I do.
And what about compliance? Of course, not everyone complies; not everyone is interested in making changes and these can be hard changes. I’ve recently started to recommend the book Atomic Habits by James Clear. Sometimes a bit of motivational interviewing can also be helpful in getting people to look at slowly moving toward making changes.
In prescribing lifestyle changes, it is important to offer most of these changes as suggestions, not as things we insist on, or that will leave the patient feeling ashamed if he doesn’t follow through. They should be discussed early in treatment so that patients don’t feel blamed for their illness or relapses. As with all the things we prescribe, some of these behavior changes help some of the people some of the time. Suggesting them, however, makes the strong statement that treating psychiatric disorders can be about more than passively swallowing a pill.
Dr. Miller is a coauthor of “Committed: The Battle Over Involuntary Psychiatric Care” (Baltimore: Johns Hopkins University Press, 2016). She has a private practice and is an assistant professor of psychiatry and behavioral sciences at Johns Hopkins University, Baltimore. She disclosed no relevant conflicts of interest.
Will this trial help solve chronic back pain?
Chronic pain, and back pain in particular, is among the most frequent concerns for patients in the primary care setting. Roughly 8% of adults in the United States say they suffer from chronic low back pain, and many of them say the pain is significant enough to impair their ability to move, work, and otherwise enjoy life. All this, despite decades of research and countless millions in funding to find the optimal approach to treating chronic pain.
As the United States crawls out of the opioid epidemic, a group of pain specialists is hoping to identify effective, personalized approaches to managing back pain. Daniel Clauw, MD, professor of anesthesiology, internal medicine, and psychiatry at the University of Michigan, Ann Arbor, is helping lead the BEST trial. With projected enrollment of nearly 800 patients, BEST will be the largest federally funded clinical trial of interventions to treat chronic low back pain.
In an interview, The interview has been edited for length and clarity.
What are your thoughts on the current state of primary care physicians’ understanding and management of pain?
Primary care physicians need a lot of help in demystifying the diagnosis and treatment of any kind of pain, but back pain is a really good place to start. When it comes to back pain, most primary care physicians are not any more knowledgeable than a layperson.
What has the opioid debacle-cum-tragedy taught you about pain management, particular as regards people with chronic pain?
I don’t feel opioids should ever be used to treat chronic low back pain. The few long-term studies that have been performed using opioids for longer than 3 months suggest that they often make pain worse rather than just failing to make pain better – and we know they are associated with a significantly increased all-cause mortality with increased deaths from myocardial infarction, accidents, and suicides, in addition to overdose.
Given how many patients experience back pain, how did we come to the point at which primary care physicians are so ill equipped?
We’ve had terrible pain curricula in medical schools. To give you an example: I’m one of the leading pain experts in the world and I’m not allowed to teach our medical students their pain curriculum. The students learn about neurophysiology and the anatomy of the nerves, not what’s relevant in pain.
This is notorious in medical school: Curricula are almost impossible to modify and change. So it starts with poor training in medical school. And then, regardless of what education they do or don’t get in medical school, a lot of their education about pain management is through our residencies – mainly in inpatient settings, where you’re really seeing the management of acute pain and not the management of chronic pain.
People get more accustomed to managing acute pain, where opioids are a reasonable option. It’s just that when you start managing subacute or chronic pain, opioids don’t work as well.
The other big problem is that historically, most people trained in medicine think that if you have pain in your elbow, there’s got to be something wrong in your elbow. This third mechanism of pain, central sensitization – or nociplastic pain – the kind of pain that we see in fibromyalgia, headache, and low back pain, where the pain is coming from the brain – that’s confusing to people. People can have pain without any damage or inflammation to that region of the body.
Physicians are trained that if there’s pain, there’s something wrong and we have to do surgery or there’s been some trauma. Most chronic pain is none of that. There’s a big disconnect between how people are trained, and then when they go out and are seeing a tremendous number of people with chronic pain.
What are the different types of pain, and how should they inform clinicians’ understanding about what approaches might work for managing their patients in pain?
The way the central nervous system responds to pain is analogous to the loudness of an electric guitar. You can make an electric guitar louder either by strumming the strings harder or by turning up the amplifier. For many people with fibromyalgia, low back pain, and endometriosis, for example, the problem is really more that the amplifier is turned up too high rather than its being that the guitar is strummed too strongly. That kind of pain where the pain is not due to anatomic damage or inflammation is particularly flummoxing for providers.
Can you explain the design of the new study?
It’s a 13-site study looking at four treatments: enhanced self-care, cognitive-behavioral therapy, physical therapy, and duloxetine. It’s a big precision medicine trial, trying to take everything we’ve learned and putting it all into one big study.
We’re using a SMART design, which randomizes people to two of those treatments, unless they are very much improved from the first treatment. To be eligible for the trial, you have to be able to be randomized to three of the four treatments, and people can’t choose which of the four they get.
We give them one of those treatments for 12 weeks, and at the end of 12 weeks we make the call – “Did you respond or not respond?” – and then we go back to the phenotypic data we collected at the beginning of that trial and say, “What information at baseline that we collected predicts that someone is going to respond better to duloxetine or worse to duloxetine?” And then we create the phenotype that responds best to each of those four treatments.
None of our treatments works so well that someone doesn’t end up getting randomized to a second treatment. About 85% of people so far need a second treatment because they still have enough pain that they want more relief. But the nice thing about that is we’ve already done all the functional brain imaging and all these really expensive and time-consuming things.
We’re hoping to have around 700-800 people total in this trial, which means that around 170 people will get randomized to each of the four initial treatments. No one’s ever done a study that has functional brain imaging and all these other things in it with more than 80 or 100 people. The scale of this is totally unprecedented.
Given that the individual therapies don’t appear to be all that successful on their own, what is your goal?
The primary aim is to match the phenotypic characteristics of a patient with chronic low back pain with treatment response to each of these four treatments. So at the end, we can give clinicians information on which of the patients is going to respond to physical therapy, for instance.
Right now, about one out of three people respond to most treatments for pain. We think by doing a trial like this, we can take treatments that work in one out of three people and make them work in one out of two or two out of three people just by using them in the right people.
How do you differentiate between these types of pain in your study?
We phenotype people by asking them a number of questions. We also do brain imaging, look at their back with MRI, test biomechanics, and then give them four different treatments that we know work in groups of people with low back pain.
We think one of the first parts of the phenotype is, do they have pain just in their back? Or do they have pain in their back plus a lot of other body regions? Because the more body regions that people have pain in, the more likely it is that this is an amplifier problem rather than a guitar problem.
Treatments like physical therapy, surgery, and injections are going to work better for people in whom the pain is a guitar problem rather than an amplifier problem. And drugs like duloxetine, which works in the brain, and cognitive-behavioral therapy are going to work a lot better in the people with pain in multiple sites besides the back.
To pick up on your metaphor, do any symptoms help clinicians differentiate between the guitar and the amplifier?
Sleep problems, fatigue, memory problems, and mood problems are common in patients with chronic pain and are more common with amplifier pain. Because again, those are all central nervous system problems. And so we see that the people that have anxiety, depression, and a lot of distress are more likely to have this kind of pain.
Does medical imaging help?
There’s a terrible relationship between what you see on an MRI of the back and whether someone has pain or how severe the pain is going to be. There’s always going to be individuals that have a lot of anatomic damage who don’t have any pain because they happen to be on the other end of the continuum from fibromyalgia; they’re actually pain-insensitive people.
What are your thoughts about ketamine as a possible treatment for chronic pain?
I have a mentee who’s doing a ketamine trial. We’re doing psilocybin trials in patients with fibromyalgia. Ketamine is such a dirty drug; it has so many different mechanisms of action. It does have some psychedelic effects, but it also is an NMDA blocker. It really has so many different effects.
I think it’s being thrown around like water in settings where we don’t yet know it to be efficacious. Even the data in treatment-refractory depression are pretty weak, but we’re so desperate to do something for those patients. If you’re trying to harness the psychedelic properties of ketamine, I think there’s other psychedelics that are a lot more interesting, which is why we’re using psilocybin for a subset of patients. Most of us in the pain field think that the psychedelics will work best for the people with chronic pain who have a lot of comorbid psychiatric illness, especially the ones with a lot of trauma. These drugs will allow us therapeutically to get at a lot of these patients with the side-by-side psychotherapy that’s being done as people are getting care in the medicalized setting.
Dr. Clauw reported conflicts of interest with Pfizer, Tonix, Theravance, Zynerba, Samumed, Aptinyx, Daiichi Sankyo, Intec, Regeneron, Teva, Lundbeck, Virios, and Cerephex.
A version of this article first appeared on Medscape.com.
Chronic pain, and back pain in particular, is among the most frequent concerns for patients in the primary care setting. Roughly 8% of adults in the United States say they suffer from chronic low back pain, and many of them say the pain is significant enough to impair their ability to move, work, and otherwise enjoy life. All this, despite decades of research and countless millions in funding to find the optimal approach to treating chronic pain.
As the United States crawls out of the opioid epidemic, a group of pain specialists is hoping to identify effective, personalized approaches to managing back pain. Daniel Clauw, MD, professor of anesthesiology, internal medicine, and psychiatry at the University of Michigan, Ann Arbor, is helping lead the BEST trial. With projected enrollment of nearly 800 patients, BEST will be the largest federally funded clinical trial of interventions to treat chronic low back pain.
In an interview, The interview has been edited for length and clarity.
What are your thoughts on the current state of primary care physicians’ understanding and management of pain?
Primary care physicians need a lot of help in demystifying the diagnosis and treatment of any kind of pain, but back pain is a really good place to start. When it comes to back pain, most primary care physicians are not any more knowledgeable than a layperson.
What has the opioid debacle-cum-tragedy taught you about pain management, particular as regards people with chronic pain?
I don’t feel opioids should ever be used to treat chronic low back pain. The few long-term studies that have been performed using opioids for longer than 3 months suggest that they often make pain worse rather than just failing to make pain better – and we know they are associated with a significantly increased all-cause mortality with increased deaths from myocardial infarction, accidents, and suicides, in addition to overdose.
Given how many patients experience back pain, how did we come to the point at which primary care physicians are so ill equipped?
We’ve had terrible pain curricula in medical schools. To give you an example: I’m one of the leading pain experts in the world and I’m not allowed to teach our medical students their pain curriculum. The students learn about neurophysiology and the anatomy of the nerves, not what’s relevant in pain.
This is notorious in medical school: Curricula are almost impossible to modify and change. So it starts with poor training in medical school. And then, regardless of what education they do or don’t get in medical school, a lot of their education about pain management is through our residencies – mainly in inpatient settings, where you’re really seeing the management of acute pain and not the management of chronic pain.
People get more accustomed to managing acute pain, where opioids are a reasonable option. It’s just that when you start managing subacute or chronic pain, opioids don’t work as well.
The other big problem is that historically, most people trained in medicine think that if you have pain in your elbow, there’s got to be something wrong in your elbow. This third mechanism of pain, central sensitization – or nociplastic pain – the kind of pain that we see in fibromyalgia, headache, and low back pain, where the pain is coming from the brain – that’s confusing to people. People can have pain without any damage or inflammation to that region of the body.
Physicians are trained that if there’s pain, there’s something wrong and we have to do surgery or there’s been some trauma. Most chronic pain is none of that. There’s a big disconnect between how people are trained, and then when they go out and are seeing a tremendous number of people with chronic pain.
What are the different types of pain, and how should they inform clinicians’ understanding about what approaches might work for managing their patients in pain?
The way the central nervous system responds to pain is analogous to the loudness of an electric guitar. You can make an electric guitar louder either by strumming the strings harder or by turning up the amplifier. For many people with fibromyalgia, low back pain, and endometriosis, for example, the problem is really more that the amplifier is turned up too high rather than its being that the guitar is strummed too strongly. That kind of pain where the pain is not due to anatomic damage or inflammation is particularly flummoxing for providers.
Can you explain the design of the new study?
It’s a 13-site study looking at four treatments: enhanced self-care, cognitive-behavioral therapy, physical therapy, and duloxetine. It’s a big precision medicine trial, trying to take everything we’ve learned and putting it all into one big study.
We’re using a SMART design, which randomizes people to two of those treatments, unless they are very much improved from the first treatment. To be eligible for the trial, you have to be able to be randomized to three of the four treatments, and people can’t choose which of the four they get.
We give them one of those treatments for 12 weeks, and at the end of 12 weeks we make the call – “Did you respond or not respond?” – and then we go back to the phenotypic data we collected at the beginning of that trial and say, “What information at baseline that we collected predicts that someone is going to respond better to duloxetine or worse to duloxetine?” And then we create the phenotype that responds best to each of those four treatments.
None of our treatments works so well that someone doesn’t end up getting randomized to a second treatment. About 85% of people so far need a second treatment because they still have enough pain that they want more relief. But the nice thing about that is we’ve already done all the functional brain imaging and all these really expensive and time-consuming things.
We’re hoping to have around 700-800 people total in this trial, which means that around 170 people will get randomized to each of the four initial treatments. No one’s ever done a study that has functional brain imaging and all these other things in it with more than 80 or 100 people. The scale of this is totally unprecedented.
Given that the individual therapies don’t appear to be all that successful on their own, what is your goal?
The primary aim is to match the phenotypic characteristics of a patient with chronic low back pain with treatment response to each of these four treatments. So at the end, we can give clinicians information on which of the patients is going to respond to physical therapy, for instance.
Right now, about one out of three people respond to most treatments for pain. We think by doing a trial like this, we can take treatments that work in one out of three people and make them work in one out of two or two out of three people just by using them in the right people.
How do you differentiate between these types of pain in your study?
We phenotype people by asking them a number of questions. We also do brain imaging, look at their back with MRI, test biomechanics, and then give them four different treatments that we know work in groups of people with low back pain.
We think one of the first parts of the phenotype is, do they have pain just in their back? Or do they have pain in their back plus a lot of other body regions? Because the more body regions that people have pain in, the more likely it is that this is an amplifier problem rather than a guitar problem.
Treatments like physical therapy, surgery, and injections are going to work better for people in whom the pain is a guitar problem rather than an amplifier problem. And drugs like duloxetine, which works in the brain, and cognitive-behavioral therapy are going to work a lot better in the people with pain in multiple sites besides the back.
To pick up on your metaphor, do any symptoms help clinicians differentiate between the guitar and the amplifier?
Sleep problems, fatigue, memory problems, and mood problems are common in patients with chronic pain and are more common with amplifier pain. Because again, those are all central nervous system problems. And so we see that the people that have anxiety, depression, and a lot of distress are more likely to have this kind of pain.
Does medical imaging help?
There’s a terrible relationship between what you see on an MRI of the back and whether someone has pain or how severe the pain is going to be. There’s always going to be individuals that have a lot of anatomic damage who don’t have any pain because they happen to be on the other end of the continuum from fibromyalgia; they’re actually pain-insensitive people.
What are your thoughts about ketamine as a possible treatment for chronic pain?
I have a mentee who’s doing a ketamine trial. We’re doing psilocybin trials in patients with fibromyalgia. Ketamine is such a dirty drug; it has so many different mechanisms of action. It does have some psychedelic effects, but it also is an NMDA blocker. It really has so many different effects.
I think it’s being thrown around like water in settings where we don’t yet know it to be efficacious. Even the data in treatment-refractory depression are pretty weak, but we’re so desperate to do something for those patients. If you’re trying to harness the psychedelic properties of ketamine, I think there’s other psychedelics that are a lot more interesting, which is why we’re using psilocybin for a subset of patients. Most of us in the pain field think that the psychedelics will work best for the people with chronic pain who have a lot of comorbid psychiatric illness, especially the ones with a lot of trauma. These drugs will allow us therapeutically to get at a lot of these patients with the side-by-side psychotherapy that’s being done as people are getting care in the medicalized setting.
Dr. Clauw reported conflicts of interest with Pfizer, Tonix, Theravance, Zynerba, Samumed, Aptinyx, Daiichi Sankyo, Intec, Regeneron, Teva, Lundbeck, Virios, and Cerephex.
A version of this article first appeared on Medscape.com.
Chronic pain, and back pain in particular, is among the most frequent concerns for patients in the primary care setting. Roughly 8% of adults in the United States say they suffer from chronic low back pain, and many of them say the pain is significant enough to impair their ability to move, work, and otherwise enjoy life. All this, despite decades of research and countless millions in funding to find the optimal approach to treating chronic pain.
As the United States crawls out of the opioid epidemic, a group of pain specialists is hoping to identify effective, personalized approaches to managing back pain. Daniel Clauw, MD, professor of anesthesiology, internal medicine, and psychiatry at the University of Michigan, Ann Arbor, is helping lead the BEST trial. With projected enrollment of nearly 800 patients, BEST will be the largest federally funded clinical trial of interventions to treat chronic low back pain.
In an interview, The interview has been edited for length and clarity.
What are your thoughts on the current state of primary care physicians’ understanding and management of pain?
Primary care physicians need a lot of help in demystifying the diagnosis and treatment of any kind of pain, but back pain is a really good place to start. When it comes to back pain, most primary care physicians are not any more knowledgeable than a layperson.
What has the opioid debacle-cum-tragedy taught you about pain management, particular as regards people with chronic pain?
I don’t feel opioids should ever be used to treat chronic low back pain. The few long-term studies that have been performed using opioids for longer than 3 months suggest that they often make pain worse rather than just failing to make pain better – and we know they are associated with a significantly increased all-cause mortality with increased deaths from myocardial infarction, accidents, and suicides, in addition to overdose.
Given how many patients experience back pain, how did we come to the point at which primary care physicians are so ill equipped?
We’ve had terrible pain curricula in medical schools. To give you an example: I’m one of the leading pain experts in the world and I’m not allowed to teach our medical students their pain curriculum. The students learn about neurophysiology and the anatomy of the nerves, not what’s relevant in pain.
This is notorious in medical school: Curricula are almost impossible to modify and change. So it starts with poor training in medical school. And then, regardless of what education they do or don’t get in medical school, a lot of their education about pain management is through our residencies – mainly in inpatient settings, where you’re really seeing the management of acute pain and not the management of chronic pain.
People get more accustomed to managing acute pain, where opioids are a reasonable option. It’s just that when you start managing subacute or chronic pain, opioids don’t work as well.
The other big problem is that historically, most people trained in medicine think that if you have pain in your elbow, there’s got to be something wrong in your elbow. This third mechanism of pain, central sensitization – or nociplastic pain – the kind of pain that we see in fibromyalgia, headache, and low back pain, where the pain is coming from the brain – that’s confusing to people. People can have pain without any damage or inflammation to that region of the body.
Physicians are trained that if there’s pain, there’s something wrong and we have to do surgery or there’s been some trauma. Most chronic pain is none of that. There’s a big disconnect between how people are trained, and then when they go out and are seeing a tremendous number of people with chronic pain.
What are the different types of pain, and how should they inform clinicians’ understanding about what approaches might work for managing their patients in pain?
The way the central nervous system responds to pain is analogous to the loudness of an electric guitar. You can make an electric guitar louder either by strumming the strings harder or by turning up the amplifier. For many people with fibromyalgia, low back pain, and endometriosis, for example, the problem is really more that the amplifier is turned up too high rather than its being that the guitar is strummed too strongly. That kind of pain where the pain is not due to anatomic damage or inflammation is particularly flummoxing for providers.
Can you explain the design of the new study?
It’s a 13-site study looking at four treatments: enhanced self-care, cognitive-behavioral therapy, physical therapy, and duloxetine. It’s a big precision medicine trial, trying to take everything we’ve learned and putting it all into one big study.
We’re using a SMART design, which randomizes people to two of those treatments, unless they are very much improved from the first treatment. To be eligible for the trial, you have to be able to be randomized to three of the four treatments, and people can’t choose which of the four they get.
We give them one of those treatments for 12 weeks, and at the end of 12 weeks we make the call – “Did you respond or not respond?” – and then we go back to the phenotypic data we collected at the beginning of that trial and say, “What information at baseline that we collected predicts that someone is going to respond better to duloxetine or worse to duloxetine?” And then we create the phenotype that responds best to each of those four treatments.
None of our treatments works so well that someone doesn’t end up getting randomized to a second treatment. About 85% of people so far need a second treatment because they still have enough pain that they want more relief. But the nice thing about that is we’ve already done all the functional brain imaging and all these really expensive and time-consuming things.
We’re hoping to have around 700-800 people total in this trial, which means that around 170 people will get randomized to each of the four initial treatments. No one’s ever done a study that has functional brain imaging and all these other things in it with more than 80 or 100 people. The scale of this is totally unprecedented.
Given that the individual therapies don’t appear to be all that successful on their own, what is your goal?
The primary aim is to match the phenotypic characteristics of a patient with chronic low back pain with treatment response to each of these four treatments. So at the end, we can give clinicians information on which of the patients is going to respond to physical therapy, for instance.
Right now, about one out of three people respond to most treatments for pain. We think by doing a trial like this, we can take treatments that work in one out of three people and make them work in one out of two or two out of three people just by using them in the right people.
How do you differentiate between these types of pain in your study?
We phenotype people by asking them a number of questions. We also do brain imaging, look at their back with MRI, test biomechanics, and then give them four different treatments that we know work in groups of people with low back pain.
We think one of the first parts of the phenotype is, do they have pain just in their back? Or do they have pain in their back plus a lot of other body regions? Because the more body regions that people have pain in, the more likely it is that this is an amplifier problem rather than a guitar problem.
Treatments like physical therapy, surgery, and injections are going to work better for people in whom the pain is a guitar problem rather than an amplifier problem. And drugs like duloxetine, which works in the brain, and cognitive-behavioral therapy are going to work a lot better in the people with pain in multiple sites besides the back.
To pick up on your metaphor, do any symptoms help clinicians differentiate between the guitar and the amplifier?
Sleep problems, fatigue, memory problems, and mood problems are common in patients with chronic pain and are more common with amplifier pain. Because again, those are all central nervous system problems. And so we see that the people that have anxiety, depression, and a lot of distress are more likely to have this kind of pain.
Does medical imaging help?
There’s a terrible relationship between what you see on an MRI of the back and whether someone has pain or how severe the pain is going to be. There’s always going to be individuals that have a lot of anatomic damage who don’t have any pain because they happen to be on the other end of the continuum from fibromyalgia; they’re actually pain-insensitive people.
What are your thoughts about ketamine as a possible treatment for chronic pain?
I have a mentee who’s doing a ketamine trial. We’re doing psilocybin trials in patients with fibromyalgia. Ketamine is such a dirty drug; it has so many different mechanisms of action. It does have some psychedelic effects, but it also is an NMDA blocker. It really has so many different effects.
I think it’s being thrown around like water in settings where we don’t yet know it to be efficacious. Even the data in treatment-refractory depression are pretty weak, but we’re so desperate to do something for those patients. If you’re trying to harness the psychedelic properties of ketamine, I think there’s other psychedelics that are a lot more interesting, which is why we’re using psilocybin for a subset of patients. Most of us in the pain field think that the psychedelics will work best for the people with chronic pain who have a lot of comorbid psychiatric illness, especially the ones with a lot of trauma. These drugs will allow us therapeutically to get at a lot of these patients with the side-by-side psychotherapy that’s being done as people are getting care in the medicalized setting.
Dr. Clauw reported conflicts of interest with Pfizer, Tonix, Theravance, Zynerba, Samumed, Aptinyx, Daiichi Sankyo, Intec, Regeneron, Teva, Lundbeck, Virios, and Cerephex.
A version of this article first appeared on Medscape.com.