User login
The economics of gynecologic surgery: 13 coding tips to ensure fair payment
The payment structure for physicians is changing. Our government, the American public, purchasers, and employers are unhappy with the fee-for-service system as it currently exists, and are pushing to drive the system into what is called “value-based purchasing.”
But what is value?
One way to define it is quality divided by cost—but how do we measure quality?
At present, insurers are measuring your quality based on some nebulous definition created at United Healthcare or Blue Cross Blue Shield—looking specifically at your “efficiency,” based on the costs attributed to you, as revealed in the codes you and others submit to payers.
Let’s say you perform minimally invasive surgery, and the referring physician ordered a lot of tests before sending the patient to you. Are you aware that all of those costs may be attributed to you in an administrative system?
ACOG is working hard to establish clinical systems rather than administrative ones to determine the true cost of care. We may want to think of obstetrics and gynecology as primary care and take advantage of advanced payment models and the opportunities afforded to accountable care organizations, but the truth is, insurers frequently do not consider us primary care. Although some of us may develop medical homes for women’s health care, we are unlikely to collect a per-patient, per-month income like primary care physicians do. That means that we need to be more assertive in negotiating contracts with insurers.
In this article, I offer recommendations for such negotiations and explain how to determine what you can and cannot accept in terms of payment.
You are the responsible party
Some of us do our own coding and some of us do not. However, if that coding is inaccurate, it is the physician who goes to jail, not the coder. You are personally responsible and liable for the coding submitted under your provider number.
Clearly, we need to do a better job of advocating for ourselves. We need to lobby. Legislators and bureaucrats are less likely to target people who have strong lobbyists working consistently on their behalf.
Accountable care organizations may have some leverage in negotiating lower prices, and some market forces may come into play in large systems. It remains to be seen which models will succeed as new payment structures develop. The overarching question: What can we do today to optimize our payments, given the system that we have? Here are 13 tactics that can enhance your bottom line.
1. Know the rules
To play the game, you must know the rules. You need to know what systems payers are using to determine your reimbursement—and you have to understand those systems as well as, or better than, the payers do. Then you’ll be able to use them to your advantage.
Payers are well aware that we don’t like to focus on this end of practice, that what we really want to do is spend the day practicing medicine. However, we need to learn these details because we’re leaving money on the table every single day.
2. Educate yourself
With the change to the International Classification of Diseases (ICD) scheduled to take effect on October 1, 2015, many of us are worried that payers are going to reject our claims because of our lack of familiarity with ICD-10.
Rest assured. There are crosswalks from ICD-9 to ICD-10. ACOG has published an information sheet for both obstetrics and gynecology that pairs typically used ICD-9 codes with their ICD-10 counterparts. And because it is published by ACOG, payers will find it hard to claim that it’s inaccurate.
ACOG also offers half-day courses on ICD-10 coding for both physicians and staff.
3. Record your decision-making process
When I audit medical charts, I often discover that this process has been neglected. Instead, the coder has relied on documentation from the electronic health record and a basic description of the treatment plan. But a plan is just that—what someone intends to do. It doesn’t convey the decision-making that underlies it. What was the differential diagnosis? What did you discuss with the patient? These details are critical for appropriate coding of the level of service—whether it’s high, intermediate, or low.
4. Refine your approach to coding
Recognize that the system is currently set up to pay physicians for the services we provide—and that service must be justified by the appropriate diagnosis code. Tougher cases, or high-risk patients, tend to have longer surgeries and hospital stays, and their outcomes often are not as good as those of more typical patients. They may have more complications because they’re obese or have severe diabetes, for example. If so, it is critical that these other conditions—obesity and severe diabetes—be included with the principal diagnosis code so that risk stratification is possible. Otherwise, we will be held to the same standard as someone treating a routine, low-risk case.
Risk stratification is being performed according to algorithms in the payers’ software—and payers are unlikely to share the details with us. However, the only real data payers have to run through these algorithms come from diagnosis coding. Even though you’re not required to code for variables such as obesity and diabetes in order to get paid for what you do, you do need to use those additional codes to make risk stratification possible—so that you don’t get inappropriately placed into a group of low-risk providers when you are treating a higher-risk cohort.
5. Develop an understanding of RVUs
Another variable that changes regularly is relative value units (RVUs) under Medicare rules. ACOG’s Committee on Health Economics and Coding—which enjoys the participation of AAGL, the American Urogynecologic Society (AUGS), the Society of Gynecologic Surgeons (SGS), and the Society of Gynecologic Oncology (SGO), as well as other organizations—tries to maintain the RVUs as up to date and appropriate as possible relative to other services in the fee schedule.
For example, about 10 years ago many urogynecologic procedures were getting bundled together when they were performed at the same time. We had only one or two ICD-9 codes to describe prolapse, with no separate codes to describe whether it affected the anterior, apical, or posterior compartment, even though we performed different procedures in the individual compartments. Payers were mapping all prolapse procedures to the same diagnosis code. So ACOG went to the National Center for Health Statistics, where ICD-9 coding was done—and developed a series of about 10 codes to describe the different areas that prolapse could affect.
That kind of nuanced coding is continuing today. In fact, we have a long list of areas to go forward with now that ICD-10 is scheduled to take effect. A good example involves new Pap smear guidelines, which recommend testing every 3 or 5 years except for patients who have undergone hysterectomy for benign disease. How do you code for a patient who has had a hysterectomy? There was no code for a woman with an absent cervix, so we created a “V-code,” a code classification for factors that influence health status, so that it is possible to explain why a Pap smear was not performed.
As we go forward into a value-based system, specialists like us likely will be negotiating contracts according to RVU-based payments. That’s why it’s important for you to understand the resource-based relative value scale (RBRVS). It has three components: a work component, which makes up about 52% of the total RVUs; a practice expense, which makes up more than 45% of total RVUS; and, finally, a malpractice component, a small percentage. There also is a geographic adjustment and a uniform conversion factor.
When you hear about the sustainable growth rate (SGR) fix, and the fact that we’re going to see a 20% or 24% reduction in payment, that talk is referring to a reduction in the conversion factor. Each component of the RVU is adjusted for geography and then multiplied by the dollar conversion factor to calculate the total RVUs. The work, practice, and malpractice components vary by where the service is provided.
Let’s use placement of Essure inserts as an example. If you perform the procedure in the hospital, then the hospital buys the equipment, including the hysteroscope and light source. The hospital also pays for the room and staff and manages equipment sterilization. If, on the other hand, you perform the procedure in your office, all those responsibilities are yours. If it’s done in your office, you get paid more but it also costs you more.
The Relative Value Update Committee, or RUC, plays a major role in determining RVUs. This committee is composed of 31 clinicians, including nonphysician providers, psychologists, and nurses who deliver services under the Medicare fee schedule. The RUC makes recommendations to the Centers for Medicare and Medicaid Services (CMS), but it is the Secretary of Health and Human Services who determines the final rule on RVUs.
Approximately 75% to 95% of the recommendations of the RUC are accepted by the Secretary and become law. So it’s not the RUC or the American Medical Association (AMA) that determines RVUs; in the long run, it is CMS and the Secretary of Health and Human Services. We are fortunate that, when CMS assigns RVUs we’re not happy with, we have an opportunity to appeal.
Under Medicare, all physician payments are based on the same conversion factor, regardless of specialty. That’s not necessarily true for other payers, who may, essentially, do whatever they wish. These other payers frequently will contract at higher or lower rates, depending on how prevalent a specialist is in the community. Sometimes they use a higher conversion factor for surgical specialists than they use for primary care.
6. Find out which RVUs the payer is using
When you negotiate contracts with payers, and you are in private practice or part of a medical practice, it’s important to know what year’s RVUs the payer is using, as RVUs vary from year to year. For example, if the payer is using the RBRVS from 2002, it is paying you less than you should be getting. So when you look at a contract, you should determine not only whether the payer is anchoring your payment to the RBRVS but also whether it is keeping up with current RVUs as well. What dollar conversion factor is the payer using? What global periods—the same as CMS, or something different?
7. Determine what global period is in play
Some private payers use 6 postoperative weeks as the global period for a surgical procedure, whereas Medicare uses 90 days. You need to know which period is in play so that you don’t leave money on the table if you see the patient within 90 days but more than 6 weeks postoperatively.
Current Procedural Terminology (CPT) has global surgical packages that include a 10-day or 90-day period. But those periods do not include services provided more than 24 hours before the procedure. They don’t include the administration of anesthesia or conscious sedation. And they don’t include management of complications, exacerbations, or recurrences. Nor do they include additional services that might be necessary due to the presence of another disease or injury.
Under Medicare, the rules are different. Medicare preoperative services begin 1 day before surgery. However, any preoperative intervention is included whether it’s performed 1 day or 1 week before surgery. If it’s simply a preoperative physical examination for the patient and you aren’t performing significant evaluation and management, it’s included in the global package, along with all the intraoperative work. In addition, under Medicare, you don’t get paid for the management of complications unless a return to the operating room is required.
8. Learn to use modifiers
As ObGyns, we often see patients for multiple conditions or problem reports, so you need to be aware that if a patient is within a global period and you do not submit a bill with a modifier to indicate special circumstances, the intervention will be bundled into the global and you will not get paid for it. Modifiers are two-digit codes that describe these separate services. They provide critical information to payers so that their computer programs separate these services out for payment.
Major surgical procedures don’t include unrelated procedures that are performed at the same time of surgery. Nor do they include visits that take place during the global period that are unrelated to the original surgery. For example, if a patient presents with a breast lump after you performed a hysterectomy, and you do a work-up, you deserve full payment for that evaluation and management service. If you don’t use a modifier, however, you won’t get that payment.
9. Don’t be passive when payers won’t pay
Let’s say you contract with HMOs or independent practice associations (IPAs), and they’re not compensating you for the extra things you’re doing and are failing to recognize surgical modifiers. What can you do about it?
You need to develop a profile of your typical patient. Because these organizations are individualizing it—they are saying that, in a typical scenario, this is the type of work you do. So these organizations offer a different kind of contract. Nevertheless, you can use your coding to help you determine what a fair payment should be, by going through your billing to determine what you’ve spent.
10. Analyze payer bundling
Medicare put in place a correct coding initiative (CCI) that lists services typically provided by the same person on the same day of service. The aim: to prevent separate payment for these services. These are “bundled” services. The CCI bundles are revised every quarter. They are listed on the ACOG Web site under “practice management.”
On October 1, 2014, the CCI inappropriately bundled pelvic organ prolapse repair procedures into the vaginal hysterectomy codes. ACOG, AUGS, SGS, and AAGL are arguing vehemently as this article is going to press to ensure that these damaging bundles are rescinded.
Private payers can bundle anything, and it may or may not make sense or be fair. One ACOG resource is the book Ob/Gyn Coding Manual: Components of Correct Procedural Coding, which is revised every year. It has a tear-out page for every procedure code and will help you determine whether or not a bundle is appropriate.
You need to know about bundling and dispute resolution. Why? Because it is possible to insert clauses into your contract that give you some rights. Insurers have all the clout and you have nothing unless you fight for it.
You may see clauses such as “the company reserves the right to re-bundle to the primary procedure....” You shouldn’t tolerate that. Rather, you want to say, “the company will use CCI bundled rules” so that you at least know what the rules are.
11. Don’t be afraid to revise a contract
If we have to hold a payer harmless, the payer should hold us harmless as well. If we consult an insurer’s Web site to confirm that a patient is covered, and we take her to surgery because we have evidence she has insurance, the insurer shouldn’t be able to rescind payment 6 months later because the patient didn’t pay for her insurance that month. That’s not fair. The company told you she was covered, and you deserve to get paid for that surgery because you are relying on information from the company itself. So when you sign a contract, you need to ensure that you are being held harmless as well as the insurer.
12. Calculate your own RVUs
Use your claims software for data. Consult the Federal Register or ACOG to determine the total number of RVUs for a given CPT code. Multiply the RVUs by the quantity for each code. Let’s say it’s an evaluation and management visit, code 99213, and you’ve done 50 this month. That’s 50 multiplied by 1.3 RVUs. Add all the codes together, then use your monthly profit and loss statement to determine what your expenses are. Divide your total expenses by the total number of RVUs to determine your practice cost per RVU. You then can decide on a conversion factor you can tolerate, and you can use this information when contracting with IPAs, HMOs, and other insurers.
13. Spend money to make money
There are many coding resources available to you. Coding is well worth what you spend on it because you can get it back in a heartbeat.
This information may not be easy to master, but it’s critically important for your economic survival—to get what’s rightfully yours and get paid fairly for what you do.
Share your thoughts on this article! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.

Barbara S. Levy, MD
Dr. Levy is Vice President for Health Policy at the American Congress of Obstetricians and Gynecologists. She also chairs the AMA Specialty Society Resource-Based Relative Value Update Committee, or RUC.
The author reports no financial relationships relevant to this article.
Barbara S. Levy, MD
Dr. Levy is Vice President for Health Policy at the American Congress of Obstetricians and Gynecologists. She also chairs the AMA Specialty Society Resource-Based Relative Value Update Committee, or RUC.
The author reports no financial relationships relevant to this article.
Barbara S. Levy, MD
Dr. Levy is Vice President for Health Policy at the American Congress of Obstetricians and Gynecologists. She also chairs the AMA Specialty Society Resource-Based Relative Value Update Committee, or RUC.
The author reports no financial relationships relevant to this article.
The payment structure for physicians is changing. Our government, the American public, purchasers, and employers are unhappy with the fee-for-service system as it currently exists, and are pushing to drive the system into what is called “value-based purchasing.”
But what is value?
One way to define it is quality divided by cost—but how do we measure quality?
At present, insurers are measuring your quality based on some nebulous definition created at United Healthcare or Blue Cross Blue Shield—looking specifically at your “efficiency,” based on the costs attributed to you, as revealed in the codes you and others submit to payers.
Let’s say you perform minimally invasive surgery, and the referring physician ordered a lot of tests before sending the patient to you. Are you aware that all of those costs may be attributed to you in an administrative system?
ACOG is working hard to establish clinical systems rather than administrative ones to determine the true cost of care. We may want to think of obstetrics and gynecology as primary care and take advantage of advanced payment models and the opportunities afforded to accountable care organizations, but the truth is, insurers frequently do not consider us primary care. Although some of us may develop medical homes for women’s health care, we are unlikely to collect a per-patient, per-month income like primary care physicians do. That means that we need to be more assertive in negotiating contracts with insurers.
In this article, I offer recommendations for such negotiations and explain how to determine what you can and cannot accept in terms of payment.
You are the responsible party
Some of us do our own coding and some of us do not. However, if that coding is inaccurate, it is the physician who goes to jail, not the coder. You are personally responsible and liable for the coding submitted under your provider number.
Clearly, we need to do a better job of advocating for ourselves. We need to lobby. Legislators and bureaucrats are less likely to target people who have strong lobbyists working consistently on their behalf.
Accountable care organizations may have some leverage in negotiating lower prices, and some market forces may come into play in large systems. It remains to be seen which models will succeed as new payment structures develop. The overarching question: What can we do today to optimize our payments, given the system that we have? Here are 13 tactics that can enhance your bottom line.
1. Know the rules
To play the game, you must know the rules. You need to know what systems payers are using to determine your reimbursement—and you have to understand those systems as well as, or better than, the payers do. Then you’ll be able to use them to your advantage.
Payers are well aware that we don’t like to focus on this end of practice, that what we really want to do is spend the day practicing medicine. However, we need to learn these details because we’re leaving money on the table every single day.
2. Educate yourself
With the change to the International Classification of Diseases (ICD) scheduled to take effect on October 1, 2015, many of us are worried that payers are going to reject our claims because of our lack of familiarity with ICD-10.
Rest assured. There are crosswalks from ICD-9 to ICD-10. ACOG has published an information sheet for both obstetrics and gynecology that pairs typically used ICD-9 codes with their ICD-10 counterparts. And because it is published by ACOG, payers will find it hard to claim that it’s inaccurate.
ACOG also offers half-day courses on ICD-10 coding for both physicians and staff.
3. Record your decision-making process
When I audit medical charts, I often discover that this process has been neglected. Instead, the coder has relied on documentation from the electronic health record and a basic description of the treatment plan. But a plan is just that—what someone intends to do. It doesn’t convey the decision-making that underlies it. What was the differential diagnosis? What did you discuss with the patient? These details are critical for appropriate coding of the level of service—whether it’s high, intermediate, or low.
4. Refine your approach to coding
Recognize that the system is currently set up to pay physicians for the services we provide—and that service must be justified by the appropriate diagnosis code. Tougher cases, or high-risk patients, tend to have longer surgeries and hospital stays, and their outcomes often are not as good as those of more typical patients. They may have more complications because they’re obese or have severe diabetes, for example. If so, it is critical that these other conditions—obesity and severe diabetes—be included with the principal diagnosis code so that risk stratification is possible. Otherwise, we will be held to the same standard as someone treating a routine, low-risk case.
Risk stratification is being performed according to algorithms in the payers’ software—and payers are unlikely to share the details with us. However, the only real data payers have to run through these algorithms come from diagnosis coding. Even though you’re not required to code for variables such as obesity and diabetes in order to get paid for what you do, you do need to use those additional codes to make risk stratification possible—so that you don’t get inappropriately placed into a group of low-risk providers when you are treating a higher-risk cohort.
5. Develop an understanding of RVUs
Another variable that changes regularly is relative value units (RVUs) under Medicare rules. ACOG’s Committee on Health Economics and Coding—which enjoys the participation of AAGL, the American Urogynecologic Society (AUGS), the Society of Gynecologic Surgeons (SGS), and the Society of Gynecologic Oncology (SGO), as well as other organizations—tries to maintain the RVUs as up to date and appropriate as possible relative to other services in the fee schedule.
For example, about 10 years ago many urogynecologic procedures were getting bundled together when they were performed at the same time. We had only one or two ICD-9 codes to describe prolapse, with no separate codes to describe whether it affected the anterior, apical, or posterior compartment, even though we performed different procedures in the individual compartments. Payers were mapping all prolapse procedures to the same diagnosis code. So ACOG went to the National Center for Health Statistics, where ICD-9 coding was done—and developed a series of about 10 codes to describe the different areas that prolapse could affect.
That kind of nuanced coding is continuing today. In fact, we have a long list of areas to go forward with now that ICD-10 is scheduled to take effect. A good example involves new Pap smear guidelines, which recommend testing every 3 or 5 years except for patients who have undergone hysterectomy for benign disease. How do you code for a patient who has had a hysterectomy? There was no code for a woman with an absent cervix, so we created a “V-code,” a code classification for factors that influence health status, so that it is possible to explain why a Pap smear was not performed.
As we go forward into a value-based system, specialists like us likely will be negotiating contracts according to RVU-based payments. That’s why it’s important for you to understand the resource-based relative value scale (RBRVS). It has three components: a work component, which makes up about 52% of the total RVUs; a practice expense, which makes up more than 45% of total RVUS; and, finally, a malpractice component, a small percentage. There also is a geographic adjustment and a uniform conversion factor.
When you hear about the sustainable growth rate (SGR) fix, and the fact that we’re going to see a 20% or 24% reduction in payment, that talk is referring to a reduction in the conversion factor. Each component of the RVU is adjusted for geography and then multiplied by the dollar conversion factor to calculate the total RVUs. The work, practice, and malpractice components vary by where the service is provided.
Let’s use placement of Essure inserts as an example. If you perform the procedure in the hospital, then the hospital buys the equipment, including the hysteroscope and light source. The hospital also pays for the room and staff and manages equipment sterilization. If, on the other hand, you perform the procedure in your office, all those responsibilities are yours. If it’s done in your office, you get paid more but it also costs you more.
The Relative Value Update Committee, or RUC, plays a major role in determining RVUs. This committee is composed of 31 clinicians, including nonphysician providers, psychologists, and nurses who deliver services under the Medicare fee schedule. The RUC makes recommendations to the Centers for Medicare and Medicaid Services (CMS), but it is the Secretary of Health and Human Services who determines the final rule on RVUs.
Approximately 75% to 95% of the recommendations of the RUC are accepted by the Secretary and become law. So it’s not the RUC or the American Medical Association (AMA) that determines RVUs; in the long run, it is CMS and the Secretary of Health and Human Services. We are fortunate that, when CMS assigns RVUs we’re not happy with, we have an opportunity to appeal.
Under Medicare, all physician payments are based on the same conversion factor, regardless of specialty. That’s not necessarily true for other payers, who may, essentially, do whatever they wish. These other payers frequently will contract at higher or lower rates, depending on how prevalent a specialist is in the community. Sometimes they use a higher conversion factor for surgical specialists than they use for primary care.
6. Find out which RVUs the payer is using
When you negotiate contracts with payers, and you are in private practice or part of a medical practice, it’s important to know what year’s RVUs the payer is using, as RVUs vary from year to year. For example, if the payer is using the RBRVS from 2002, it is paying you less than you should be getting. So when you look at a contract, you should determine not only whether the payer is anchoring your payment to the RBRVS but also whether it is keeping up with current RVUs as well. What dollar conversion factor is the payer using? What global periods—the same as CMS, or something different?
7. Determine what global period is in play
Some private payers use 6 postoperative weeks as the global period for a surgical procedure, whereas Medicare uses 90 days. You need to know which period is in play so that you don’t leave money on the table if you see the patient within 90 days but more than 6 weeks postoperatively.
Current Procedural Terminology (CPT) has global surgical packages that include a 10-day or 90-day period. But those periods do not include services provided more than 24 hours before the procedure. They don’t include the administration of anesthesia or conscious sedation. And they don’t include management of complications, exacerbations, or recurrences. Nor do they include additional services that might be necessary due to the presence of another disease or injury.
Under Medicare, the rules are different. Medicare preoperative services begin 1 day before surgery. However, any preoperative intervention is included whether it’s performed 1 day or 1 week before surgery. If it’s simply a preoperative physical examination for the patient and you aren’t performing significant evaluation and management, it’s included in the global package, along with all the intraoperative work. In addition, under Medicare, you don’t get paid for the management of complications unless a return to the operating room is required.
8. Learn to use modifiers
As ObGyns, we often see patients for multiple conditions or problem reports, so you need to be aware that if a patient is within a global period and you do not submit a bill with a modifier to indicate special circumstances, the intervention will be bundled into the global and you will not get paid for it. Modifiers are two-digit codes that describe these separate services. They provide critical information to payers so that their computer programs separate these services out for payment.
Major surgical procedures don’t include unrelated procedures that are performed at the same time of surgery. Nor do they include visits that take place during the global period that are unrelated to the original surgery. For example, if a patient presents with a breast lump after you performed a hysterectomy, and you do a work-up, you deserve full payment for that evaluation and management service. If you don’t use a modifier, however, you won’t get that payment.
9. Don’t be passive when payers won’t pay
Let’s say you contract with HMOs or independent practice associations (IPAs), and they’re not compensating you for the extra things you’re doing and are failing to recognize surgical modifiers. What can you do about it?
You need to develop a profile of your typical patient. Because these organizations are individualizing it—they are saying that, in a typical scenario, this is the type of work you do. So these organizations offer a different kind of contract. Nevertheless, you can use your coding to help you determine what a fair payment should be, by going through your billing to determine what you’ve spent.
10. Analyze payer bundling
Medicare put in place a correct coding initiative (CCI) that lists services typically provided by the same person on the same day of service. The aim: to prevent separate payment for these services. These are “bundled” services. The CCI bundles are revised every quarter. They are listed on the ACOG Web site under “practice management.”
On October 1, 2014, the CCI inappropriately bundled pelvic organ prolapse repair procedures into the vaginal hysterectomy codes. ACOG, AUGS, SGS, and AAGL are arguing vehemently as this article is going to press to ensure that these damaging bundles are rescinded.
Private payers can bundle anything, and it may or may not make sense or be fair. One ACOG resource is the book Ob/Gyn Coding Manual: Components of Correct Procedural Coding, which is revised every year. It has a tear-out page for every procedure code and will help you determine whether or not a bundle is appropriate.
You need to know about bundling and dispute resolution. Why? Because it is possible to insert clauses into your contract that give you some rights. Insurers have all the clout and you have nothing unless you fight for it.
You may see clauses such as “the company reserves the right to re-bundle to the primary procedure....” You shouldn’t tolerate that. Rather, you want to say, “the company will use CCI bundled rules” so that you at least know what the rules are.
11. Don’t be afraid to revise a contract
If we have to hold a payer harmless, the payer should hold us harmless as well. If we consult an insurer’s Web site to confirm that a patient is covered, and we take her to surgery because we have evidence she has insurance, the insurer shouldn’t be able to rescind payment 6 months later because the patient didn’t pay for her insurance that month. That’s not fair. The company told you she was covered, and you deserve to get paid for that surgery because you are relying on information from the company itself. So when you sign a contract, you need to ensure that you are being held harmless as well as the insurer.
12. Calculate your own RVUs
Use your claims software for data. Consult the Federal Register or ACOG to determine the total number of RVUs for a given CPT code. Multiply the RVUs by the quantity for each code. Let’s say it’s an evaluation and management visit, code 99213, and you’ve done 50 this month. That’s 50 multiplied by 1.3 RVUs. Add all the codes together, then use your monthly profit and loss statement to determine what your expenses are. Divide your total expenses by the total number of RVUs to determine your practice cost per RVU. You then can decide on a conversion factor you can tolerate, and you can use this information when contracting with IPAs, HMOs, and other insurers.
13. Spend money to make money
There are many coding resources available to you. Coding is well worth what you spend on it because you can get it back in a heartbeat.
This information may not be easy to master, but it’s critically important for your economic survival—to get what’s rightfully yours and get paid fairly for what you do.
Share your thoughts on this article! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
The payment structure for physicians is changing. Our government, the American public, purchasers, and employers are unhappy with the fee-for-service system as it currently exists, and are pushing to drive the system into what is called “value-based purchasing.”
But what is value?
One way to define it is quality divided by cost—but how do we measure quality?
At present, insurers are measuring your quality based on some nebulous definition created at United Healthcare or Blue Cross Blue Shield—looking specifically at your “efficiency,” based on the costs attributed to you, as revealed in the codes you and others submit to payers.
Let’s say you perform minimally invasive surgery, and the referring physician ordered a lot of tests before sending the patient to you. Are you aware that all of those costs may be attributed to you in an administrative system?
ACOG is working hard to establish clinical systems rather than administrative ones to determine the true cost of care. We may want to think of obstetrics and gynecology as primary care and take advantage of advanced payment models and the opportunities afforded to accountable care organizations, but the truth is, insurers frequently do not consider us primary care. Although some of us may develop medical homes for women’s health care, we are unlikely to collect a per-patient, per-month income like primary care physicians do. That means that we need to be more assertive in negotiating contracts with insurers.
In this article, I offer recommendations for such negotiations and explain how to determine what you can and cannot accept in terms of payment.
You are the responsible party
Some of us do our own coding and some of us do not. However, if that coding is inaccurate, it is the physician who goes to jail, not the coder. You are personally responsible and liable for the coding submitted under your provider number.
Clearly, we need to do a better job of advocating for ourselves. We need to lobby. Legislators and bureaucrats are less likely to target people who have strong lobbyists working consistently on their behalf.
Accountable care organizations may have some leverage in negotiating lower prices, and some market forces may come into play in large systems. It remains to be seen which models will succeed as new payment structures develop. The overarching question: What can we do today to optimize our payments, given the system that we have? Here are 13 tactics that can enhance your bottom line.
1. Know the rules
To play the game, you must know the rules. You need to know what systems payers are using to determine your reimbursement—and you have to understand those systems as well as, or better than, the payers do. Then you’ll be able to use them to your advantage.
Payers are well aware that we don’t like to focus on this end of practice, that what we really want to do is spend the day practicing medicine. However, we need to learn these details because we’re leaving money on the table every single day.
2. Educate yourself
With the change to the International Classification of Diseases (ICD) scheduled to take effect on October 1, 2015, many of us are worried that payers are going to reject our claims because of our lack of familiarity with ICD-10.
Rest assured. There are crosswalks from ICD-9 to ICD-10. ACOG has published an information sheet for both obstetrics and gynecology that pairs typically used ICD-9 codes with their ICD-10 counterparts. And because it is published by ACOG, payers will find it hard to claim that it’s inaccurate.
ACOG also offers half-day courses on ICD-10 coding for both physicians and staff.
3. Record your decision-making process
When I audit medical charts, I often discover that this process has been neglected. Instead, the coder has relied on documentation from the electronic health record and a basic description of the treatment plan. But a plan is just that—what someone intends to do. It doesn’t convey the decision-making that underlies it. What was the differential diagnosis? What did you discuss with the patient? These details are critical for appropriate coding of the level of service—whether it’s high, intermediate, or low.
4. Refine your approach to coding
Recognize that the system is currently set up to pay physicians for the services we provide—and that service must be justified by the appropriate diagnosis code. Tougher cases, or high-risk patients, tend to have longer surgeries and hospital stays, and their outcomes often are not as good as those of more typical patients. They may have more complications because they’re obese or have severe diabetes, for example. If so, it is critical that these other conditions—obesity and severe diabetes—be included with the principal diagnosis code so that risk stratification is possible. Otherwise, we will be held to the same standard as someone treating a routine, low-risk case.
Risk stratification is being performed according to algorithms in the payers’ software—and payers are unlikely to share the details with us. However, the only real data payers have to run through these algorithms come from diagnosis coding. Even though you’re not required to code for variables such as obesity and diabetes in order to get paid for what you do, you do need to use those additional codes to make risk stratification possible—so that you don’t get inappropriately placed into a group of low-risk providers when you are treating a higher-risk cohort.
5. Develop an understanding of RVUs
Another variable that changes regularly is relative value units (RVUs) under Medicare rules. ACOG’s Committee on Health Economics and Coding—which enjoys the participation of AAGL, the American Urogynecologic Society (AUGS), the Society of Gynecologic Surgeons (SGS), and the Society of Gynecologic Oncology (SGO), as well as other organizations—tries to maintain the RVUs as up to date and appropriate as possible relative to other services in the fee schedule.
For example, about 10 years ago many urogynecologic procedures were getting bundled together when they were performed at the same time. We had only one or two ICD-9 codes to describe prolapse, with no separate codes to describe whether it affected the anterior, apical, or posterior compartment, even though we performed different procedures in the individual compartments. Payers were mapping all prolapse procedures to the same diagnosis code. So ACOG went to the National Center for Health Statistics, where ICD-9 coding was done—and developed a series of about 10 codes to describe the different areas that prolapse could affect.
That kind of nuanced coding is continuing today. In fact, we have a long list of areas to go forward with now that ICD-10 is scheduled to take effect. A good example involves new Pap smear guidelines, which recommend testing every 3 or 5 years except for patients who have undergone hysterectomy for benign disease. How do you code for a patient who has had a hysterectomy? There was no code for a woman with an absent cervix, so we created a “V-code,” a code classification for factors that influence health status, so that it is possible to explain why a Pap smear was not performed.
As we go forward into a value-based system, specialists like us likely will be negotiating contracts according to RVU-based payments. That’s why it’s important for you to understand the resource-based relative value scale (RBRVS). It has three components: a work component, which makes up about 52% of the total RVUs; a practice expense, which makes up more than 45% of total RVUS; and, finally, a malpractice component, a small percentage. There also is a geographic adjustment and a uniform conversion factor.
When you hear about the sustainable growth rate (SGR) fix, and the fact that we’re going to see a 20% or 24% reduction in payment, that talk is referring to a reduction in the conversion factor. Each component of the RVU is adjusted for geography and then multiplied by the dollar conversion factor to calculate the total RVUs. The work, practice, and malpractice components vary by where the service is provided.
Let’s use placement of Essure inserts as an example. If you perform the procedure in the hospital, then the hospital buys the equipment, including the hysteroscope and light source. The hospital also pays for the room and staff and manages equipment sterilization. If, on the other hand, you perform the procedure in your office, all those responsibilities are yours. If it’s done in your office, you get paid more but it also costs you more.
The Relative Value Update Committee, or RUC, plays a major role in determining RVUs. This committee is composed of 31 clinicians, including nonphysician providers, psychologists, and nurses who deliver services under the Medicare fee schedule. The RUC makes recommendations to the Centers for Medicare and Medicaid Services (CMS), but it is the Secretary of Health and Human Services who determines the final rule on RVUs.
Approximately 75% to 95% of the recommendations of the RUC are accepted by the Secretary and become law. So it’s not the RUC or the American Medical Association (AMA) that determines RVUs; in the long run, it is CMS and the Secretary of Health and Human Services. We are fortunate that, when CMS assigns RVUs we’re not happy with, we have an opportunity to appeal.
Under Medicare, all physician payments are based on the same conversion factor, regardless of specialty. That’s not necessarily true for other payers, who may, essentially, do whatever they wish. These other payers frequently will contract at higher or lower rates, depending on how prevalent a specialist is in the community. Sometimes they use a higher conversion factor for surgical specialists than they use for primary care.
6. Find out which RVUs the payer is using
When you negotiate contracts with payers, and you are in private practice or part of a medical practice, it’s important to know what year’s RVUs the payer is using, as RVUs vary from year to year. For example, if the payer is using the RBRVS from 2002, it is paying you less than you should be getting. So when you look at a contract, you should determine not only whether the payer is anchoring your payment to the RBRVS but also whether it is keeping up with current RVUs as well. What dollar conversion factor is the payer using? What global periods—the same as CMS, or something different?
7. Determine what global period is in play
Some private payers use 6 postoperative weeks as the global period for a surgical procedure, whereas Medicare uses 90 days. You need to know which period is in play so that you don’t leave money on the table if you see the patient within 90 days but more than 6 weeks postoperatively.
Current Procedural Terminology (CPT) has global surgical packages that include a 10-day or 90-day period. But those periods do not include services provided more than 24 hours before the procedure. They don’t include the administration of anesthesia or conscious sedation. And they don’t include management of complications, exacerbations, or recurrences. Nor do they include additional services that might be necessary due to the presence of another disease or injury.
Under Medicare, the rules are different. Medicare preoperative services begin 1 day before surgery. However, any preoperative intervention is included whether it’s performed 1 day or 1 week before surgery. If it’s simply a preoperative physical examination for the patient and you aren’t performing significant evaluation and management, it’s included in the global package, along with all the intraoperative work. In addition, under Medicare, you don’t get paid for the management of complications unless a return to the operating room is required.
8. Learn to use modifiers
As ObGyns, we often see patients for multiple conditions or problem reports, so you need to be aware that if a patient is within a global period and you do not submit a bill with a modifier to indicate special circumstances, the intervention will be bundled into the global and you will not get paid for it. Modifiers are two-digit codes that describe these separate services. They provide critical information to payers so that their computer programs separate these services out for payment.
Major surgical procedures don’t include unrelated procedures that are performed at the same time of surgery. Nor do they include visits that take place during the global period that are unrelated to the original surgery. For example, if a patient presents with a breast lump after you performed a hysterectomy, and you do a work-up, you deserve full payment for that evaluation and management service. If you don’t use a modifier, however, you won’t get that payment.
9. Don’t be passive when payers won’t pay
Let’s say you contract with HMOs or independent practice associations (IPAs), and they’re not compensating you for the extra things you’re doing and are failing to recognize surgical modifiers. What can you do about it?
You need to develop a profile of your typical patient. Because these organizations are individualizing it—they are saying that, in a typical scenario, this is the type of work you do. So these organizations offer a different kind of contract. Nevertheless, you can use your coding to help you determine what a fair payment should be, by going through your billing to determine what you’ve spent.
10. Analyze payer bundling
Medicare put in place a correct coding initiative (CCI) that lists services typically provided by the same person on the same day of service. The aim: to prevent separate payment for these services. These are “bundled” services. The CCI bundles are revised every quarter. They are listed on the ACOG Web site under “practice management.”
On October 1, 2014, the CCI inappropriately bundled pelvic organ prolapse repair procedures into the vaginal hysterectomy codes. ACOG, AUGS, SGS, and AAGL are arguing vehemently as this article is going to press to ensure that these damaging bundles are rescinded.
Private payers can bundle anything, and it may or may not make sense or be fair. One ACOG resource is the book Ob/Gyn Coding Manual: Components of Correct Procedural Coding, which is revised every year. It has a tear-out page for every procedure code and will help you determine whether or not a bundle is appropriate.
You need to know about bundling and dispute resolution. Why? Because it is possible to insert clauses into your contract that give you some rights. Insurers have all the clout and you have nothing unless you fight for it.
You may see clauses such as “the company reserves the right to re-bundle to the primary procedure....” You shouldn’t tolerate that. Rather, you want to say, “the company will use CCI bundled rules” so that you at least know what the rules are.
11. Don’t be afraid to revise a contract
If we have to hold a payer harmless, the payer should hold us harmless as well. If we consult an insurer’s Web site to confirm that a patient is covered, and we take her to surgery because we have evidence she has insurance, the insurer shouldn’t be able to rescind payment 6 months later because the patient didn’t pay for her insurance that month. That’s not fair. The company told you she was covered, and you deserve to get paid for that surgery because you are relying on information from the company itself. So when you sign a contract, you need to ensure that you are being held harmless as well as the insurer.
12. Calculate your own RVUs
Use your claims software for data. Consult the Federal Register or ACOG to determine the total number of RVUs for a given CPT code. Multiply the RVUs by the quantity for each code. Let’s say it’s an evaluation and management visit, code 99213, and you’ve done 50 this month. That’s 50 multiplied by 1.3 RVUs. Add all the codes together, then use your monthly profit and loss statement to determine what your expenses are. Divide your total expenses by the total number of RVUs to determine your practice cost per RVU. You then can decide on a conversion factor you can tolerate, and you can use this information when contracting with IPAs, HMOs, and other insurers.
13. Spend money to make money
There are many coding resources available to you. Coding is well worth what you spend on it because you can get it back in a heartbeat.
This information may not be easy to master, but it’s critically important for your economic survival—to get what’s rightfully yours and get paid fairly for what you do.
Share your thoughts on this article! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.

Avoid Billing, Coding Discrepancies When Documenting Patient History

- Continue to educate physicians on proper billing for E/M services;
- Encourage its contractors to review physicians’ billing for E/M services; and
- Review physicians who bill higher level E/M codes for appropriate action.1
When documenting patient history, physicians must be aware of the common discrepancies that occur. Although the physician becomes familiar with the patient as he/she provides care throughout the hospitalization, the auditor must acquaint himself or herself with the patient using only the limited information provided in the progress note.
When documentation is requested by the payer for a specific service date, only the documentation from that service date is considered. Be sure that the information is adequate to support both clinical care and the reported service level.
Patient History Requirements
Chief complaint. The chief complaint (CC) is the reason for the visit as stated in the patient’s own words. Every encounter, regardless of visit type, must include a CC. The physician must personally document and/or validate the CC with reference to a specific condition or symptom (e.g. patient complains of abdominal pain).
- Incomplete CC example: “Follow-up”;
- Better CC example: “Follow-up for severe abdominal cramping.”
History of present illness. The history of present illness (HPI) describes the development or progression of the patient’s current problem(s). The traditional HPI elements recognized in the 1995 documentation guidelines are location, quality, severity, duration, timing, context, modifying factors, and associated signs/symptoms.2,3
The physician must obtain and personally document the HPI. He/she also has the option to link to the HPI documented by residents (i.e., residents, fellows, interns) in compliance with the teaching physician rules or nonphysician practitioners (i.e., nurse practitioners and physician assistants) as defined by the split-shared billing rules. An auditor will not accept HPI information if the physician attempts to link to any other individual, even if that person may be qualified to obtain this (e.g. registered nurse, medical assistant) or is a student (e.g. medical students, nurse practitioner students).
Because auditors recognize both 1995 and 1997 documentation guidelines, they must also recognize the HPI differences. The 1997 HPI format promotes the status of the patient’s chronic or inactive conditions.4 The physician receives one credit for each chronic condition that is noted, along with documentation of what has occurred since the last physician encounter as it relates to the chronic condition (e.g. “patient has a history of chronic obstructive bronchitis without acute exacerbation in past six months”).
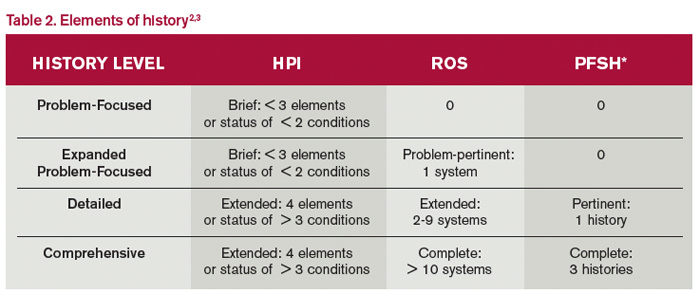
Physicians may utilize either style of HPI documentation, and auditors must review provider records against each set of guidelines. The final audited result reflects the highest visit level supported by either set of guidelines. For example, if physician documentation yields an “extended” HPI when 1995 guidelines are used but only a “brief” HPI (see Table 2) when 1997 guidelines are reviewed, the auditor awards the physician credit for the “extended” HPI.
- 1995 example: “The patient has intermittent (duration), sharp (quality) pain in the right upper quadrant (location) without associated nausea, vomiting, or diarrhea (associated signs/symptoms).”
- 1997 example: “Diabetes controlled by oral medication; hyperlipidemia stable on simvastatin with increased dietary efforts; hypertension stable with pressures ranging from 130-140/80-90 overnight” (status of three chronic conditions).
Review of systems. A review of systems (ROS) is a series of questions inquiring about additional signs, symptoms, or problems currently or previously experienced by the patient as related to the CC or presenting problem. The recognized systems are constitutional; eyes; ears, nose, mouth, throat; cardiovascular; respiratory; gastrointestinal; genitourinary; musculoskeletal; integumentary (including skin and/or breast); neurological; psychiatric; endocrine; hematologic/lymphatic; and allergic/immunologic.2,3
The physician may choose to document the ROS by making a notation for individual systems: “no fever/chills (constitutional) or blurred vision (eyes); no chest pain (cardiovascular) or shortness of breath (respiratory); intermittent nausea (gastrointestinal) and occasional runny nose (ears, nose, mouth, throat).” Alternatively, the physician may inquire about all of the systems but only document the positive and pertinent negative findings related to the CC, along with an additional comment that “all other systems are negative.” Most Medicare audit contractors currently accept this method as long as all systems were reviewed.5,6,7,8,9
Be advised that ROS information can be documented by anyone, including the patient. The physician must remember to reference ROS information that is completed by individuals other than residents or nonphysician practitioners (the physician is already required to reference the documentation of the latter individuals under the Teaching Physician Rules or Split-Shared Billing Rules).
Past, family, and social histories. Documentation of past, family, and social histories (PFSH) involves data obtained about the patient’s previous illness or medical conditions/therapies, family occurrences with illness, and relevant patient activities. An auditor credits the physician for a single comment correlated to each history for the PFSH. Using the term “noncontributory” (N/C) with any of the histories can result in downcoding. Many contractors do not allow this statement due to previous misunderstandings over its use.
- Incomplete PFSH example: “Patient is status-post cholecystectomy in August 2013; family history N/C; patient is former smoker” (Note: “family history N/C” is not accepted by most contractors).
- Better PFSH example: “Patient currently on Prilosec 20 mg daily; family history of Barrett’s Esophagus; no tobacco or alcohol use.”
PFSH data can also be documented by anyone, including the patient, and the physician must reference the PFSH information in his own progress note. Re-documenting the PFSH is not necessary unless a revision is required. PFSH documentation is only required for initial care services (i.e., initial hospital care, initial observation care, consultations). It is not required for subsequent care services, unless additional pertinent information that impacts care is obtained during the hospital stay.
Common Problems to Avoid
Information cannot be obtained. Some contractors will not penalize the physician for the inability to ascertain complete historical information as long as there is evidenced documentation of an attempt to obtain the information. When the physician cannot extract historical information from the patient directly and no other source is available, the physician documents that he is “unable to obtain” the history. Additionally, the physician must provide a comment to explain why the information is unobtainable (e.g. patient confused, no caregiver present) along with the available information from the limited resources (e.g. emergency medical technicians, records from previous hospitalizations at the same facility).
Previous information referenced. When referencing items from a previous encounter, be sure to include the referenced information when documentation is requested by the payer. Per CMS guidelines, the ROS and/or PFSH obtained during an earlier encounter does not need to be re-recorded if there is evidence that the physician reviewed and updated the previous information. The review and update may be documented by either describing any new ROS and/or PFSH information or noting that there has been no change in the information and noting the date and location of the earlier ROS and/or PFSH.2
Pre-op clearance and HPI deficiencies. HPI is typically not as deficient as the ROS or family history elements; however, HPI underdocumentation is mostly associated with encounters for pre-op clearance. The physician may state that “patient requires pre-op clearance for left knee repair.” In the absence of any comorbidities or acute illness, HPI documentation may be missing. The physician should remember to identify the details of the presenting problem: “Patient runs five miles daily. Knee felt unstable after running two weeks ago. Swelling and intermittent sharp pain 7/10. Patient has been taking ibuprofen daily without relief.”
Not medically necessary. Remember not to document any elements for the purpose of “getting paid.” Only document information that is clinically relevant, lends to the quality of care provided, or demonstrates the delivery of healthcare services. This prevents accusations of fraud and abuse, promotes billing compliance, and supports medical necessity for the services provided.
Varying levels of history. E/M services are selected based on the content of the three “key” components: history, exam, and decision-making (or visit time). If counseling and/or coordination of care does not encompass >50% of the physician’s total visit time or the service is not exclusively designated as a time-based service (e.g. critical care and discharge day management), the physician’s service time is not considered.
Documentation for each of the three key components must support the reported visit level when reporting initial hospital care and consultations (for those payers who still recognize consultation codes). Subsequent hospital care (e.g. 99233) only requires supportive documentation from two key components. Medical decision-making should be one of the two supporting components in order to demonstrate the medical necessity and nature of the presenting problem; the other supporting component can be history or exam.
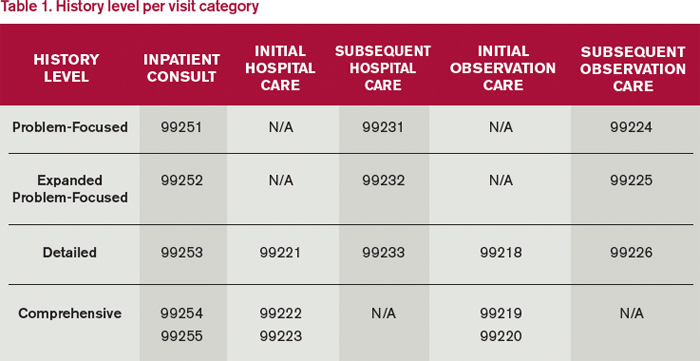
Each visit category (e.g. initial hospital care or subsequent hospital care) and service level (e.g. 99221-99233) identifies corresponding documentation requirements. Failure to document any essential element in a given visit level (e.g. family history required for a comprehensive history when billing for 99222 and 99223) may result in service denial or downcoding (e.g. 99221). Be aware of what an auditor expects when reviewing patient history (see Table 1).
There are four levels of history: problem-focused, expanded problem-focused, detailed, and comprehensive. An auditor determines the number of history elements documented in the progress note (see Table 2). The history level corresponds to the lowest documented element. For example, if physician documentation includes four HPI elements, eight ROS, and a comment in each of the PFSHs, the history level is equivalent to “detailed.” The history would support initial hospital care 99221 or subsequent hospital care 99233.
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center, Philadelphia. She is also on the faculty of SHM’s inpatient coding course.
References
- Levinson DR. Department of Health and Human Services, Office of Inspector General: Coding Trends of Medicare Evaluation and Management Services. May 2012. Available at: oig.hhs.gov/oei/reports/oei-04-10-00180.pdf. Accessed October 4, 2014.
- Centers for Medicare and Medicaid Services. 1995 Documentation Guidelines for Evaluation and Management Services. Available at: www.cms.gov/Outreach-and-Education/Medicare-Learning-Network-MLN/MLNEdWebGuide/Downloads/95Docguidelines.pdf. Accessed October 4, 2014.
- Abraham M, Ahlman J, Boudreau A, Connelly J, Levreau-Davis L. CPT 2013 Professional Edition (Current Procedural Terminology). Chicago: American Medical Association Press; 2012:4-10.
- Centers for Medicare and Medicaid Services. 1997 Documentation Guidelines for Evaluation and Management Services. Available at: www.cms.gov/Outreach-and-Education/Medicare-Learning-Network-MLN/MLNEdWebGuide/Downloads/97Docguidelines.pdf. Accessed October 4, 2014.
- Noridian Healthcare Solutions. Medicare Part B: Evaluation and Management Workshop Questions and Answers. Available at: www.noridianmedicare.com/cgi-bin/coranto/viewnews.cgi?id=EkZpEVAyylqZyOfqel&tmpl=part_b_viewnews&style=part_ab_viewnews Accessed on October 4, 2014.
- WPS Medicare Health Insurance. J5 MAC Part B: Documentation (Q&As). Available at: www.wpsmedicare.com/j5macpartb/resources/provider_types/evalmngmntqa.shtml. Accessed October 4, 2014.
- NHIC, Corp. Building Your Medicare Knowledge: Advanced Building Blocks. Available at: www.medicarenhic.com/providers/pubs/AdvdBuildBlocks061212.pdf.
- Palmetto GBA. Jurisdiction 11 Part B: History Component. Available at: www.palmettogba.com/Palmetto/Providers.nsf/docsCat/Jurisdiction%2011%20Part%20B~EM%20Help%20Center~General%20Articles~History%20Component?open&Expand=1. Accessed October 4, 2014.
- Novitas Solutions. Frequently Asked Questions: Evaluation and Management Services (Part B). Available at: https://www.novitas-solutions.com/faq/partb/pet/lpet-evaluation_management_services.html. Accessed October 4, 2014.
- Continue to educate physicians on proper billing for E/M services;
- Encourage its contractors to review physicians’ billing for E/M services; and
- Review physicians who bill higher level E/M codes for appropriate action.1
When documenting patient history, physicians must be aware of the common discrepancies that occur. Although the physician becomes familiar with the patient as he/she provides care throughout the hospitalization, the auditor must acquaint himself or herself with the patient using only the limited information provided in the progress note.
When documentation is requested by the payer for a specific service date, only the documentation from that service date is considered. Be sure that the information is adequate to support both clinical care and the reported service level.
Patient History Requirements
Chief complaint. The chief complaint (CC) is the reason for the visit as stated in the patient’s own words. Every encounter, regardless of visit type, must include a CC. The physician must personally document and/or validate the CC with reference to a specific condition or symptom (e.g. patient complains of abdominal pain).
- Incomplete CC example: “Follow-up”;
- Better CC example: “Follow-up for severe abdominal cramping.”
History of present illness. The history of present illness (HPI) describes the development or progression of the patient’s current problem(s). The traditional HPI elements recognized in the 1995 documentation guidelines are location, quality, severity, duration, timing, context, modifying factors, and associated signs/symptoms.2,3
The physician must obtain and personally document the HPI. He/she also has the option to link to the HPI documented by residents (i.e., residents, fellows, interns) in compliance with the teaching physician rules or nonphysician practitioners (i.e., nurse practitioners and physician assistants) as defined by the split-shared billing rules. An auditor will not accept HPI information if the physician attempts to link to any other individual, even if that person may be qualified to obtain this (e.g. registered nurse, medical assistant) or is a student (e.g. medical students, nurse practitioner students).
Because auditors recognize both 1995 and 1997 documentation guidelines, they must also recognize the HPI differences. The 1997 HPI format promotes the status of the patient’s chronic or inactive conditions.4 The physician receives one credit for each chronic condition that is noted, along with documentation of what has occurred since the last physician encounter as it relates to the chronic condition (e.g. “patient has a history of chronic obstructive bronchitis without acute exacerbation in past six months”).
Physicians may utilize either style of HPI documentation, and auditors must review provider records against each set of guidelines. The final audited result reflects the highest visit level supported by either set of guidelines. For example, if physician documentation yields an “extended” HPI when 1995 guidelines are used but only a “brief” HPI (see Table 2) when 1997 guidelines are reviewed, the auditor awards the physician credit for the “extended” HPI.
- 1995 example: “The patient has intermittent (duration), sharp (quality) pain in the right upper quadrant (location) without associated nausea, vomiting, or diarrhea (associated signs/symptoms).”
- 1997 example: “Diabetes controlled by oral medication; hyperlipidemia stable on simvastatin with increased dietary efforts; hypertension stable with pressures ranging from 130-140/80-90 overnight” (status of three chronic conditions).
Review of systems. A review of systems (ROS) is a series of questions inquiring about additional signs, symptoms, or problems currently or previously experienced by the patient as related to the CC or presenting problem. The recognized systems are constitutional; eyes; ears, nose, mouth, throat; cardiovascular; respiratory; gastrointestinal; genitourinary; musculoskeletal; integumentary (including skin and/or breast); neurological; psychiatric; endocrine; hematologic/lymphatic; and allergic/immunologic.2,3
The physician may choose to document the ROS by making a notation for individual systems: “no fever/chills (constitutional) or blurred vision (eyes); no chest pain (cardiovascular) or shortness of breath (respiratory); intermittent nausea (gastrointestinal) and occasional runny nose (ears, nose, mouth, throat).” Alternatively, the physician may inquire about all of the systems but only document the positive and pertinent negative findings related to the CC, along with an additional comment that “all other systems are negative.” Most Medicare audit contractors currently accept this method as long as all systems were reviewed.5,6,7,8,9
Be advised that ROS information can be documented by anyone, including the patient. The physician must remember to reference ROS information that is completed by individuals other than residents or nonphysician practitioners (the physician is already required to reference the documentation of the latter individuals under the Teaching Physician Rules or Split-Shared Billing Rules).
Past, family, and social histories. Documentation of past, family, and social histories (PFSH) involves data obtained about the patient’s previous illness or medical conditions/therapies, family occurrences with illness, and relevant patient activities. An auditor credits the physician for a single comment correlated to each history for the PFSH. Using the term “noncontributory” (N/C) with any of the histories can result in downcoding. Many contractors do not allow this statement due to previous misunderstandings over its use.
- Incomplete PFSH example: “Patient is status-post cholecystectomy in August 2013; family history N/C; patient is former smoker” (Note: “family history N/C” is not accepted by most contractors).
- Better PFSH example: “Patient currently on Prilosec 20 mg daily; family history of Barrett’s Esophagus; no tobacco or alcohol use.”
PFSH data can also be documented by anyone, including the patient, and the physician must reference the PFSH information in his own progress note. Re-documenting the PFSH is not necessary unless a revision is required. PFSH documentation is only required for initial care services (i.e., initial hospital care, initial observation care, consultations). It is not required for subsequent care services, unless additional pertinent information that impacts care is obtained during the hospital stay.
Common Problems to Avoid
Information cannot be obtained. Some contractors will not penalize the physician for the inability to ascertain complete historical information as long as there is evidenced documentation of an attempt to obtain the information. When the physician cannot extract historical information from the patient directly and no other source is available, the physician documents that he is “unable to obtain” the history. Additionally, the physician must provide a comment to explain why the information is unobtainable (e.g. patient confused, no caregiver present) along with the available information from the limited resources (e.g. emergency medical technicians, records from previous hospitalizations at the same facility).
Previous information referenced. When referencing items from a previous encounter, be sure to include the referenced information when documentation is requested by the payer. Per CMS guidelines, the ROS and/or PFSH obtained during an earlier encounter does not need to be re-recorded if there is evidence that the physician reviewed and updated the previous information. The review and update may be documented by either describing any new ROS and/or PFSH information or noting that there has been no change in the information and noting the date and location of the earlier ROS and/or PFSH.2
Pre-op clearance and HPI deficiencies. HPI is typically not as deficient as the ROS or family history elements; however, HPI underdocumentation is mostly associated with encounters for pre-op clearance. The physician may state that “patient requires pre-op clearance for left knee repair.” In the absence of any comorbidities or acute illness, HPI documentation may be missing. The physician should remember to identify the details of the presenting problem: “Patient runs five miles daily. Knee felt unstable after running two weeks ago. Swelling and intermittent sharp pain 7/10. Patient has been taking ibuprofen daily without relief.”
Not medically necessary. Remember not to document any elements for the purpose of “getting paid.” Only document information that is clinically relevant, lends to the quality of care provided, or demonstrates the delivery of healthcare services. This prevents accusations of fraud and abuse, promotes billing compliance, and supports medical necessity for the services provided.
Varying levels of history. E/M services are selected based on the content of the three “key” components: history, exam, and decision-making (or visit time). If counseling and/or coordination of care does not encompass >50% of the physician’s total visit time or the service is not exclusively designated as a time-based service (e.g. critical care and discharge day management), the physician’s service time is not considered.
Documentation for each of the three key components must support the reported visit level when reporting initial hospital care and consultations (for those payers who still recognize consultation codes). Subsequent hospital care (e.g. 99233) only requires supportive documentation from two key components. Medical decision-making should be one of the two supporting components in order to demonstrate the medical necessity and nature of the presenting problem; the other supporting component can be history or exam.
Each visit category (e.g. initial hospital care or subsequent hospital care) and service level (e.g. 99221-99233) identifies corresponding documentation requirements. Failure to document any essential element in a given visit level (e.g. family history required for a comprehensive history when billing for 99222 and 99223) may result in service denial or downcoding (e.g. 99221). Be aware of what an auditor expects when reviewing patient history (see Table 1).
There are four levels of history: problem-focused, expanded problem-focused, detailed, and comprehensive. An auditor determines the number of history elements documented in the progress note (see Table 2). The history level corresponds to the lowest documented element. For example, if physician documentation includes four HPI elements, eight ROS, and a comment in each of the PFSHs, the history level is equivalent to “detailed.” The history would support initial hospital care 99221 or subsequent hospital care 99233.
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center, Philadelphia. She is also on the faculty of SHM’s inpatient coding course.
References
- Levinson DR. Department of Health and Human Services, Office of Inspector General: Coding Trends of Medicare Evaluation and Management Services. May 2012. Available at: oig.hhs.gov/oei/reports/oei-04-10-00180.pdf. Accessed October 4, 2014.
- Centers for Medicare and Medicaid Services. 1995 Documentation Guidelines for Evaluation and Management Services. Available at: www.cms.gov/Outreach-and-Education/Medicare-Learning-Network-MLN/MLNEdWebGuide/Downloads/95Docguidelines.pdf. Accessed October 4, 2014.
- Abraham M, Ahlman J, Boudreau A, Connelly J, Levreau-Davis L. CPT 2013 Professional Edition (Current Procedural Terminology). Chicago: American Medical Association Press; 2012:4-10.
- Centers for Medicare and Medicaid Services. 1997 Documentation Guidelines for Evaluation and Management Services. Available at: www.cms.gov/Outreach-and-Education/Medicare-Learning-Network-MLN/MLNEdWebGuide/Downloads/97Docguidelines.pdf. Accessed October 4, 2014.
- Noridian Healthcare Solutions. Medicare Part B: Evaluation and Management Workshop Questions and Answers. Available at: www.noridianmedicare.com/cgi-bin/coranto/viewnews.cgi?id=EkZpEVAyylqZyOfqel&tmpl=part_b_viewnews&style=part_ab_viewnews Accessed on October 4, 2014.
- WPS Medicare Health Insurance. J5 MAC Part B: Documentation (Q&As). Available at: www.wpsmedicare.com/j5macpartb/resources/provider_types/evalmngmntqa.shtml. Accessed October 4, 2014.
- NHIC, Corp. Building Your Medicare Knowledge: Advanced Building Blocks. Available at: www.medicarenhic.com/providers/pubs/AdvdBuildBlocks061212.pdf.
- Palmetto GBA. Jurisdiction 11 Part B: History Component. Available at: www.palmettogba.com/Palmetto/Providers.nsf/docsCat/Jurisdiction%2011%20Part%20B~EM%20Help%20Center~General%20Articles~History%20Component?open&Expand=1. Accessed October 4, 2014.
- Novitas Solutions. Frequently Asked Questions: Evaluation and Management Services (Part B). Available at: https://www.novitas-solutions.com/faq/partb/pet/lpet-evaluation_management_services.html. Accessed October 4, 2014.
- Continue to educate physicians on proper billing for E/M services;
- Encourage its contractors to review physicians’ billing for E/M services; and
- Review physicians who bill higher level E/M codes for appropriate action.1
When documenting patient history, physicians must be aware of the common discrepancies that occur. Although the physician becomes familiar with the patient as he/she provides care throughout the hospitalization, the auditor must acquaint himself or herself with the patient using only the limited information provided in the progress note.
When documentation is requested by the payer for a specific service date, only the documentation from that service date is considered. Be sure that the information is adequate to support both clinical care and the reported service level.
Patient History Requirements
Chief complaint. The chief complaint (CC) is the reason for the visit as stated in the patient’s own words. Every encounter, regardless of visit type, must include a CC. The physician must personally document and/or validate the CC with reference to a specific condition or symptom (e.g. patient complains of abdominal pain).
- Incomplete CC example: “Follow-up”;
- Better CC example: “Follow-up for severe abdominal cramping.”
History of present illness. The history of present illness (HPI) describes the development or progression of the patient’s current problem(s). The traditional HPI elements recognized in the 1995 documentation guidelines are location, quality, severity, duration, timing, context, modifying factors, and associated signs/symptoms.2,3
The physician must obtain and personally document the HPI. He/she also has the option to link to the HPI documented by residents (i.e., residents, fellows, interns) in compliance with the teaching physician rules or nonphysician practitioners (i.e., nurse practitioners and physician assistants) as defined by the split-shared billing rules. An auditor will not accept HPI information if the physician attempts to link to any other individual, even if that person may be qualified to obtain this (e.g. registered nurse, medical assistant) or is a student (e.g. medical students, nurse practitioner students).
Because auditors recognize both 1995 and 1997 documentation guidelines, they must also recognize the HPI differences. The 1997 HPI format promotes the status of the patient’s chronic or inactive conditions.4 The physician receives one credit for each chronic condition that is noted, along with documentation of what has occurred since the last physician encounter as it relates to the chronic condition (e.g. “patient has a history of chronic obstructive bronchitis without acute exacerbation in past six months”).
Physicians may utilize either style of HPI documentation, and auditors must review provider records against each set of guidelines. The final audited result reflects the highest visit level supported by either set of guidelines. For example, if physician documentation yields an “extended” HPI when 1995 guidelines are used but only a “brief” HPI (see Table 2) when 1997 guidelines are reviewed, the auditor awards the physician credit for the “extended” HPI.
- 1995 example: “The patient has intermittent (duration), sharp (quality) pain in the right upper quadrant (location) without associated nausea, vomiting, or diarrhea (associated signs/symptoms).”
- 1997 example: “Diabetes controlled by oral medication; hyperlipidemia stable on simvastatin with increased dietary efforts; hypertension stable with pressures ranging from 130-140/80-90 overnight” (status of three chronic conditions).
Review of systems. A review of systems (ROS) is a series of questions inquiring about additional signs, symptoms, or problems currently or previously experienced by the patient as related to the CC or presenting problem. The recognized systems are constitutional; eyes; ears, nose, mouth, throat; cardiovascular; respiratory; gastrointestinal; genitourinary; musculoskeletal; integumentary (including skin and/or breast); neurological; psychiatric; endocrine; hematologic/lymphatic; and allergic/immunologic.2,3
The physician may choose to document the ROS by making a notation for individual systems: “no fever/chills (constitutional) or blurred vision (eyes); no chest pain (cardiovascular) or shortness of breath (respiratory); intermittent nausea (gastrointestinal) and occasional runny nose (ears, nose, mouth, throat).” Alternatively, the physician may inquire about all of the systems but only document the positive and pertinent negative findings related to the CC, along with an additional comment that “all other systems are negative.” Most Medicare audit contractors currently accept this method as long as all systems were reviewed.5,6,7,8,9
Be advised that ROS information can be documented by anyone, including the patient. The physician must remember to reference ROS information that is completed by individuals other than residents or nonphysician practitioners (the physician is already required to reference the documentation of the latter individuals under the Teaching Physician Rules or Split-Shared Billing Rules).
Past, family, and social histories. Documentation of past, family, and social histories (PFSH) involves data obtained about the patient’s previous illness or medical conditions/therapies, family occurrences with illness, and relevant patient activities. An auditor credits the physician for a single comment correlated to each history for the PFSH. Using the term “noncontributory” (N/C) with any of the histories can result in downcoding. Many contractors do not allow this statement due to previous misunderstandings over its use.
- Incomplete PFSH example: “Patient is status-post cholecystectomy in August 2013; family history N/C; patient is former smoker” (Note: “family history N/C” is not accepted by most contractors).
- Better PFSH example: “Patient currently on Prilosec 20 mg daily; family history of Barrett’s Esophagus; no tobacco or alcohol use.”
PFSH data can also be documented by anyone, including the patient, and the physician must reference the PFSH information in his own progress note. Re-documenting the PFSH is not necessary unless a revision is required. PFSH documentation is only required for initial care services (i.e., initial hospital care, initial observation care, consultations). It is not required for subsequent care services, unless additional pertinent information that impacts care is obtained during the hospital stay.
Common Problems to Avoid
Information cannot be obtained. Some contractors will not penalize the physician for the inability to ascertain complete historical information as long as there is evidenced documentation of an attempt to obtain the information. When the physician cannot extract historical information from the patient directly and no other source is available, the physician documents that he is “unable to obtain” the history. Additionally, the physician must provide a comment to explain why the information is unobtainable (e.g. patient confused, no caregiver present) along with the available information from the limited resources (e.g. emergency medical technicians, records from previous hospitalizations at the same facility).
Previous information referenced. When referencing items from a previous encounter, be sure to include the referenced information when documentation is requested by the payer. Per CMS guidelines, the ROS and/or PFSH obtained during an earlier encounter does not need to be re-recorded if there is evidence that the physician reviewed and updated the previous information. The review and update may be documented by either describing any new ROS and/or PFSH information or noting that there has been no change in the information and noting the date and location of the earlier ROS and/or PFSH.2
Pre-op clearance and HPI deficiencies. HPI is typically not as deficient as the ROS or family history elements; however, HPI underdocumentation is mostly associated with encounters for pre-op clearance. The physician may state that “patient requires pre-op clearance for left knee repair.” In the absence of any comorbidities or acute illness, HPI documentation may be missing. The physician should remember to identify the details of the presenting problem: “Patient runs five miles daily. Knee felt unstable after running two weeks ago. Swelling and intermittent sharp pain 7/10. Patient has been taking ibuprofen daily without relief.”
Not medically necessary. Remember not to document any elements for the purpose of “getting paid.” Only document information that is clinically relevant, lends to the quality of care provided, or demonstrates the delivery of healthcare services. This prevents accusations of fraud and abuse, promotes billing compliance, and supports medical necessity for the services provided.
Varying levels of history. E/M services are selected based on the content of the three “key” components: history, exam, and decision-making (or visit time). If counseling and/or coordination of care does not encompass >50% of the physician’s total visit time or the service is not exclusively designated as a time-based service (e.g. critical care and discharge day management), the physician’s service time is not considered.
Documentation for each of the three key components must support the reported visit level when reporting initial hospital care and consultations (for those payers who still recognize consultation codes). Subsequent hospital care (e.g. 99233) only requires supportive documentation from two key components. Medical decision-making should be one of the two supporting components in order to demonstrate the medical necessity and nature of the presenting problem; the other supporting component can be history or exam.
Each visit category (e.g. initial hospital care or subsequent hospital care) and service level (e.g. 99221-99233) identifies corresponding documentation requirements. Failure to document any essential element in a given visit level (e.g. family history required for a comprehensive history when billing for 99222 and 99223) may result in service denial or downcoding (e.g. 99221). Be aware of what an auditor expects when reviewing patient history (see Table 1).
There are four levels of history: problem-focused, expanded problem-focused, detailed, and comprehensive. An auditor determines the number of history elements documented in the progress note (see Table 2). The history level corresponds to the lowest documented element. For example, if physician documentation includes four HPI elements, eight ROS, and a comment in each of the PFSHs, the history level is equivalent to “detailed.” The history would support initial hospital care 99221 or subsequent hospital care 99233.
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center, Philadelphia. She is also on the faculty of SHM’s inpatient coding course.
References
- Levinson DR. Department of Health and Human Services, Office of Inspector General: Coding Trends of Medicare Evaluation and Management Services. May 2012. Available at: oig.hhs.gov/oei/reports/oei-04-10-00180.pdf. Accessed October 4, 2014.
- Centers for Medicare and Medicaid Services. 1995 Documentation Guidelines for Evaluation and Management Services. Available at: www.cms.gov/Outreach-and-Education/Medicare-Learning-Network-MLN/MLNEdWebGuide/Downloads/95Docguidelines.pdf. Accessed October 4, 2014.
- Abraham M, Ahlman J, Boudreau A, Connelly J, Levreau-Davis L. CPT 2013 Professional Edition (Current Procedural Terminology). Chicago: American Medical Association Press; 2012:4-10.
- Centers for Medicare and Medicaid Services. 1997 Documentation Guidelines for Evaluation and Management Services. Available at: www.cms.gov/Outreach-and-Education/Medicare-Learning-Network-MLN/MLNEdWebGuide/Downloads/97Docguidelines.pdf. Accessed October 4, 2014.
- Noridian Healthcare Solutions. Medicare Part B: Evaluation and Management Workshop Questions and Answers. Available at: www.noridianmedicare.com/cgi-bin/coranto/viewnews.cgi?id=EkZpEVAyylqZyOfqel&tmpl=part_b_viewnews&style=part_ab_viewnews Accessed on October 4, 2014.
- WPS Medicare Health Insurance. J5 MAC Part B: Documentation (Q&As). Available at: www.wpsmedicare.com/j5macpartb/resources/provider_types/evalmngmntqa.shtml. Accessed October 4, 2014.
- NHIC, Corp. Building Your Medicare Knowledge: Advanced Building Blocks. Available at: www.medicarenhic.com/providers/pubs/AdvdBuildBlocks061212.pdf.
- Palmetto GBA. Jurisdiction 11 Part B: History Component. Available at: www.palmettogba.com/Palmetto/Providers.nsf/docsCat/Jurisdiction%2011%20Part%20B~EM%20Help%20Center~General%20Articles~History%20Component?open&Expand=1. Accessed October 4, 2014.
- Novitas Solutions. Frequently Asked Questions: Evaluation and Management Services (Part B). Available at: https://www.novitas-solutions.com/faq/partb/pet/lpet-evaluation_management_services.html. Accessed October 4, 2014.

State of Hospital Medicine Report an Evaluation Tool for Hospital Medicine Groups
I think my team of hospitalists is probably tired of hearing my sports analogies. But as I look at the State of Hospital Medicine 2014 report (SOHM), I cannot help but see relationships to athletics.
When you think about football, you automatically contemplate the scope of a particular team and the context of the upcoming season. What are the strengths of the team—do we emphasize offense or defense or special teams? How about the variety of formations or the scheduling and strength of opponents? How about the depth of our roster—what is the talent level available? How do we compare to other teams?
How in the world does this relate to the SOHM? It gives us a chance to evaluate our own hospital medicine groups (HMGs) in the context of the other HMGs across the country. When I look at scope of services and, particularly, the data from Figure 3.1, I am struck with the breadth of the range of services in which HMGs engage. Certainly, our core identity as hospitalists includes admitting referral patients and unassigned patients, but, as of 2014, nearly 90% of hospitalist groups are also managing and co-managing surgical and medical subspecialty patients. To my eyes, the big change since 2012 is the 20% increase in the number of HMGs medically co-managing medical subspecialty patients.
There are some newcomers to our roster, as well—the palliative care and post-acute care work being done by 15% and 25% of our groups, respectively. Particularly striking is the fact that one quarter of HMGs are involved in post-acute care, follow-up clinics, nursing homes, and the like.
My take on this is that factors such as increased complexity of hospitalized patients with lean length of stay and higher acuity needs at discharge transition are driving the need for a measure of continuity and expertise post discharge that may best be provided by HMGs. The trending of the post-acute care challenges/opportunities will certainly be worth watching—sort of like a rookie player who is having a big impact.

As hospitalists may become focused on throughput (admissions discharges and transfers), the interruption to perform procedures may decrease the net value of the hospitalist to the institution.
—William A. Landis, MD, FHM
Not surprisingly, nighttime admissions work continues to gain traction. Nearly 60% of HMGs are performing nighttime admissions.
In my regional chapter, we recently heard a presentation on “nocturnists.” An interesting contention that caught my attention was that the nocturnist viewed herself as providing expert clinical care during off-hours—particularly at night—and that she was looking to increase the value and not just “put her finger in the dike,” so to speak, until the cavalry arrived at daybreak. As HMG responsibilities increase during the off-hours, I am thinking that my colleague is right: We are going to have to increase our depth and strength at this particular position so that we might actually become known as the “nighttime experts.” I look for this trend to continue.
Finally, I am drawn to the data on care of patients in the ICU, a number that continues to rise—almost 70% of HMGs now. Meanwhile, procedures have dipped to 33% from 53% in the last report. At first, it seemed a little bit puzzling to me that as involvement in the ICUs seemed to increase, procedures diminished. My anecdotal experience is that most of my procedures occurred on patients who had intensive care requirements. Nonetheless, many hospitalists I have talked to seem to believe that the requirement/expectation of imaging in the performance of more and more invasive procedures—now a standard of care— has increasingly driven procedures to specialized areas of the hospital such as imaging/radiology departments. There may also be a net decrease in the number of procedures performed as more noninvasive diagnostic modalities provide satisfactory information.
As hospitalists may become focused on throughput (admissions discharges and transfers), the interruption to perform procedures may decrease the net value of the hospitalist to the institution. It may make sense for others to be doing procedures. Whatever the cause, my guess is these two trends may continue.
Diving deeper into the granularity of the report will lead the reader to discover subtle differences and trends. Academics, pediatric hospitalists, and independent HMGs all have some nuances, not to mention regional variation. You will have to dig into the report yourself to explore.
Just as there is a freshness to every new sports season, there is a freshness to reviewing the information from the SOHM reports, and evaluating the scope of service is always an exciting moment.
Dr. Landis is medical director of Wellspan Hospitalists in York, Pa., and a member of SHM’s Practice Analysis Committee.
I think my team of hospitalists is probably tired of hearing my sports analogies. But as I look at the State of Hospital Medicine 2014 report (SOHM), I cannot help but see relationships to athletics.
When you think about football, you automatically contemplate the scope of a particular team and the context of the upcoming season. What are the strengths of the team—do we emphasize offense or defense or special teams? How about the variety of formations or the scheduling and strength of opponents? How about the depth of our roster—what is the talent level available? How do we compare to other teams?
How in the world does this relate to the SOHM? It gives us a chance to evaluate our own hospital medicine groups (HMGs) in the context of the other HMGs across the country. When I look at scope of services and, particularly, the data from Figure 3.1, I am struck with the breadth of the range of services in which HMGs engage. Certainly, our core identity as hospitalists includes admitting referral patients and unassigned patients, but, as of 2014, nearly 90% of hospitalist groups are also managing and co-managing surgical and medical subspecialty patients. To my eyes, the big change since 2012 is the 20% increase in the number of HMGs medically co-managing medical subspecialty patients.
There are some newcomers to our roster, as well—the palliative care and post-acute care work being done by 15% and 25% of our groups, respectively. Particularly striking is the fact that one quarter of HMGs are involved in post-acute care, follow-up clinics, nursing homes, and the like.
My take on this is that factors such as increased complexity of hospitalized patients with lean length of stay and higher acuity needs at discharge transition are driving the need for a measure of continuity and expertise post discharge that may best be provided by HMGs. The trending of the post-acute care challenges/opportunities will certainly be worth watching—sort of like a rookie player who is having a big impact.
As hospitalists may become focused on throughput (admissions discharges and transfers), the interruption to perform procedures may decrease the net value of the hospitalist to the institution.
—William A. Landis, MD, FHM
Not surprisingly, nighttime admissions work continues to gain traction. Nearly 60% of HMGs are performing nighttime admissions.
In my regional chapter, we recently heard a presentation on “nocturnists.” An interesting contention that caught my attention was that the nocturnist viewed herself as providing expert clinical care during off-hours—particularly at night—and that she was looking to increase the value and not just “put her finger in the dike,” so to speak, until the cavalry arrived at daybreak. As HMG responsibilities increase during the off-hours, I am thinking that my colleague is right: We are going to have to increase our depth and strength at this particular position so that we might actually become known as the “nighttime experts.” I look for this trend to continue.
Finally, I am drawn to the data on care of patients in the ICU, a number that continues to rise—almost 70% of HMGs now. Meanwhile, procedures have dipped to 33% from 53% in the last report. At first, it seemed a little bit puzzling to me that as involvement in the ICUs seemed to increase, procedures diminished. My anecdotal experience is that most of my procedures occurred on patients who had intensive care requirements. Nonetheless, many hospitalists I have talked to seem to believe that the requirement/expectation of imaging in the performance of more and more invasive procedures—now a standard of care— has increasingly driven procedures to specialized areas of the hospital such as imaging/radiology departments. There may also be a net decrease in the number of procedures performed as more noninvasive diagnostic modalities provide satisfactory information.
As hospitalists may become focused on throughput (admissions discharges and transfers), the interruption to perform procedures may decrease the net value of the hospitalist to the institution. It may make sense for others to be doing procedures. Whatever the cause, my guess is these two trends may continue.
Diving deeper into the granularity of the report will lead the reader to discover subtle differences and trends. Academics, pediatric hospitalists, and independent HMGs all have some nuances, not to mention regional variation. You will have to dig into the report yourself to explore.
Just as there is a freshness to every new sports season, there is a freshness to reviewing the information from the SOHM reports, and evaluating the scope of service is always an exciting moment.
Dr. Landis is medical director of Wellspan Hospitalists in York, Pa., and a member of SHM’s Practice Analysis Committee.
I think my team of hospitalists is probably tired of hearing my sports analogies. But as I look at the State of Hospital Medicine 2014 report (SOHM), I cannot help but see relationships to athletics.
When you think about football, you automatically contemplate the scope of a particular team and the context of the upcoming season. What are the strengths of the team—do we emphasize offense or defense or special teams? How about the variety of formations or the scheduling and strength of opponents? How about the depth of our roster—what is the talent level available? How do we compare to other teams?
How in the world does this relate to the SOHM? It gives us a chance to evaluate our own hospital medicine groups (HMGs) in the context of the other HMGs across the country. When I look at scope of services and, particularly, the data from Figure 3.1, I am struck with the breadth of the range of services in which HMGs engage. Certainly, our core identity as hospitalists includes admitting referral patients and unassigned patients, but, as of 2014, nearly 90% of hospitalist groups are also managing and co-managing surgical and medical subspecialty patients. To my eyes, the big change since 2012 is the 20% increase in the number of HMGs medically co-managing medical subspecialty patients.
There are some newcomers to our roster, as well—the palliative care and post-acute care work being done by 15% and 25% of our groups, respectively. Particularly striking is the fact that one quarter of HMGs are involved in post-acute care, follow-up clinics, nursing homes, and the like.
My take on this is that factors such as increased complexity of hospitalized patients with lean length of stay and higher acuity needs at discharge transition are driving the need for a measure of continuity and expertise post discharge that may best be provided by HMGs. The trending of the post-acute care challenges/opportunities will certainly be worth watching—sort of like a rookie player who is having a big impact.
As hospitalists may become focused on throughput (admissions discharges and transfers), the interruption to perform procedures may decrease the net value of the hospitalist to the institution.
—William A. Landis, MD, FHM
Not surprisingly, nighttime admissions work continues to gain traction. Nearly 60% of HMGs are performing nighttime admissions.
In my regional chapter, we recently heard a presentation on “nocturnists.” An interesting contention that caught my attention was that the nocturnist viewed herself as providing expert clinical care during off-hours—particularly at night—and that she was looking to increase the value and not just “put her finger in the dike,” so to speak, until the cavalry arrived at daybreak. As HMG responsibilities increase during the off-hours, I am thinking that my colleague is right: We are going to have to increase our depth and strength at this particular position so that we might actually become known as the “nighttime experts.” I look for this trend to continue.
Finally, I am drawn to the data on care of patients in the ICU, a number that continues to rise—almost 70% of HMGs now. Meanwhile, procedures have dipped to 33% from 53% in the last report. At first, it seemed a little bit puzzling to me that as involvement in the ICUs seemed to increase, procedures diminished. My anecdotal experience is that most of my procedures occurred on patients who had intensive care requirements. Nonetheless, many hospitalists I have talked to seem to believe that the requirement/expectation of imaging in the performance of more and more invasive procedures—now a standard of care— has increasingly driven procedures to specialized areas of the hospital such as imaging/radiology departments. There may also be a net decrease in the number of procedures performed as more noninvasive diagnostic modalities provide satisfactory information.
As hospitalists may become focused on throughput (admissions discharges and transfers), the interruption to perform procedures may decrease the net value of the hospitalist to the institution. It may make sense for others to be doing procedures. Whatever the cause, my guess is these two trends may continue.
Diving deeper into the granularity of the report will lead the reader to discover subtle differences and trends. Academics, pediatric hospitalists, and independent HMGs all have some nuances, not to mention regional variation. You will have to dig into the report yourself to explore.
Just as there is a freshness to every new sports season, there is a freshness to reviewing the information from the SOHM reports, and evaluating the scope of service is always an exciting moment.
Dr. Landis is medical director of Wellspan Hospitalists in York, Pa., and a member of SHM’s Practice Analysis Committee.
To Outsource or Not to Outsource Your Physical Therapy Service Line Management?
You currently offer a physical therapy (PT) service line but feel like it could be doing better, or you are thinking of adding PT services and are not sure where to begin. Either way, the thought of your patients and bottom line benefiting from PT services within your practice but without you having to manage another service line is appealing. Although related to orthopedic surgery and an obvious ancillary service, PT is a different type of practice that requires active management of the professionals, revenue cycle, operations, regulatory requirements, and changing coding and reimbursement protocols. There are more and more companies nationwide that claim a mastery of the PT management niche and would be more than happy to shoulder your burden and share in your profits. Whether you already have PT services in your practice or are looking to add them, proceed with care and caution as you consider partnering with a PT management company.
Drawing on my involvement with both successful PT management–orthopedic practice partnerships and the arduous, expensive demise of one, this article offers my recommendations for determining if a PT management partnership is best for your practice. Many of the contracts last for several years and include clauses that are extremely binding even after the contract conclusion. As with any decision to outsource, the decision to outsource PT services deserves a comprehensive request for proposal (RFP) to multiple candidate companies, a thorough vetting and decision process that includes all partners or an executive committee/board, and legal review of the contract by an experienced health care attorney representing the practice.
Request for Proposal
Begin the RFP with a reference to your website and a brief description of the practice and current PT services. For example, state that you don’t have PT and are looking to start it, or, if your practice offers PT, include a description of the number of locations, square footage allocation, and number of full-time equivalent (FTE) physical therapists, occupational therapists, physical therapy assistants, and support staff of the existing program. Also mention whether the billing is done within the practice or is outsourced.
Next, you want to learn about the company. Ask about its number of years in PT management and the history of the company. Ask them to provide the previous business names and an overview of the history of ownership. You want to know this because the national PT management community is relatively small and includes frequent acquisitions and mergers. Just as important as the company’s history is any future plans it has to acquire or be acquired. This is all part of knowing who you may be partnering with.
You will want to know how many other practices the company provides PT/occupational therapy (OT) management services for, in what states those practices are located, and a breakdown of specialties. The number of physician providers the company represents along with the answers to the other questions will give you an idea of its size, experience, location, alignment, and focus. Some of these companies manage PT in family practices. You will want to know how many orthopedic practices the company partners with. If your practice has subspecialties, ask about its experience with subspecialty orthopedics.
Ask for the company’s website so that you can get an idea of the company and its mission, vision, and values. Even though you will likely be interacting with regional representatives, you will be signing the contract with the company leadership, so be sure to learn—either from the company’s website or its response to the RFP—about the individuals leading the organization and any parent company. Ask for a list of officers, board of directors, managers, and perhaps an organization chart with titles and names. Because you are looking to partner with the company, it might be good to ask for managerial turnover rates in the last few years. PT is a professional health care service, so take note of the number of licensed therapists the company has in leadership positions. If you were partnering with a medical organization, you would certainly want physicians in leadership positions, and this is no different. Determine if the company is publicly traded or privately held. You may also consider requesting the company’s last few annual reports to learn more.
Exclusivity
Some PT management companies have their own facilities and are partnering with practices in the same market despite the seemingly inherent conflict. As part of your RFP, ask the company to include the names of practices, their specialties, and site locations where it already has a presence as well as a list of its own (independent of a physician practice) locations in the state or region. Future plans are important here too; if the company does not currently have a presence in the region, what commitment will it make to exclusivity or noncompete?
Human Resources
In many cases, the PT management company actually employs the entire staff for the service line. If you already have PT in your practice, this means the employees will transition from your employment to another company. After the contract is signed, some of the employees will get paychecks and benefits from your practice and be subject to your practice’s policies, while others will not. Having 2 different employers in the same practice can have an impact on employee morale and satisfaction. Find out during the proposal process if the company’s typical model is based on the company’s or the practice’s employment of the professional and support staff.
Obtain the following information from the management company if it is to be the employer:
1. Titles and compensation ranges for each position
2. Description of all bonuses and incentive structures
3. Paid time off (PTO) policies and accrual rates
4. Paid holidays
5. Details of employee benefits, such as employee out-of-pocket premiums for individual and family health care coverage, availability of vision and dental coverage, and investment and match for retirement or 401(k) plans.
6. Human resources (HR) support. Describe how employees get needed support from human resources, such as questions about benefits, FMLA (Family Medical Leave Act), HR policies, and other issues.
7. Results of any employee satisfaction surveys completed in the last 2 years
8. Nonrecruitment. In what ways will the professional staff’s careers be affected by this partnership? Will the professional staff have to sign employment agreements? If so, please provide a sample. Will there be covenants not to compete for the professional staff?
9. Provide a schematic on how you typically cover professional staff vacation and family leave.
10. Does your organization provide accredited continuing education for professional staff or do you send staff to state and national meetings and courses to maintain their CEU (continuing education units) requirement?
11. Do you provide annual regulatory training, such as HIPAA (Health Insurance Portability and Accountability Act) training, for all staff or is the practice responsible for that?
12. Professional liability coverage for the therapists.
Initially, the company may say they are open to doing it either way and you may proceed with the process without answers to these questions. If at any point, you explore a situation in which the employer is not the practice, you must get answers to these questions before agreeing to anything. Number 8 above is extremely important. Many PT management companies will include a nonrecruitment clause in their contracts so that neither party can recruit therapists from the engagement. Depending on how the clause is written, you may not be able to legally hire therapists who were with you for years before the management agreement at the conclusion of the contract. Individual therapists can find themselves very limited in where they can work in the community depending on a covenant not to compete. And while covenants not to compete and nonrecruitment clauses may be generalized as “indefensible,” it is expensive, time-consuming, and exhausting to get one rendered as such after the fact.
Operations
Operational compatibility is essential to a smooth transition or start-up. As part of your RFP, let the candidate companies know which electronic medical record (EMR) and electronic practice management (EPM) systems you use and ask about their experience level with those. Ask if it is expected that PT will operate on the practice’s EMR and EPM systems or if the company will be having PT operate on separate systems. If the company will be implementing different systems, find out which one and then do an accounting of the costs for interface, training, and other compatibility elements.
Inquire as to each candidate company’s standard operations policies and procedures as well as the operational and productivity standards the company maintains. For example, ask for a range of how many patients a physical therapist should be able to see (including documentation) in an 8-hour day? If you already have a PT service line, compare the company’s productivity standards to what your therapists are currently doing. Of the many enhancements a therapy management company can bring, an increase in productivity is essential. Request a description of productivity incentive programs for the professional staff so that you can determine if you are comfortable with them. By the same token, ask if the company has a comprehensive compliance program including procedures and policies.
Any outsourcing agreements will be subject to operational and contractual compliance elements such as HIPAA, business associates agreement, and all other applicable regulations through state, federal, and payor entities. Ask each candidate company about its compliance program.
Revenue Cycle
Some therapy management companies will leave the billing and collections to the practice, while others have their own operations. As part of the RFP, ask the company which way it is done in its standard model. If the company manages the revenue cycle, ask which key revenue cycle performance indicators it monitors, how it calculates them, and with what frequency it tracks and reports them. Ask how the company has approached a revenue cycle performance improvement effort and what successes it has had. And definitely ask about the emphasis, training, and performance standards on point-of-service (POS) collections. In PT, successful, service-oriented POS collections are essential to cash flow and patient satisfaction. Typically, there is a copayment for each visit, and patients come 3 times or more per week. When patients pay the copayment before each visit, it feels manageable to them. If they get a bill for 6 copayments 2 weeks into PT, they often get angry and do not see the value of the therapy.
Seek specifics on the elements of the company’s performance improvement. A number of companies will default to providing incentive bonuses for POS collections and other revenue cycle improvements. Incentive bonuses for collections can compromise the coding and billing integrity of the practice and are guaranteed to cause discontent among support staff. Everyone who works hard should be recognized, not just the staff in a position to collect money. On top of this, if the PT reception staff are getting paid POS collections bonuses and the practice reception staff are not, a managerial dichotomy ensues.
Accounting and Financial Reporting
In your RFP, ask about the accounting and financial model that each candidate company most often uses. Inquire as to which—the practice or the management company—is responsible for monthly, quarterly, and annual accounting and financial reporting and what typical monthly reconcilement process the company recommends. Include the following requests in your RFP:
1. Please provide samples of the monthly financials produced or preferred.
2. Describe your annual expense and revenue budgeting and approval processes.
3. Please address how you recommend handling the purchase of new equipment and supplies as well as the handling of existing equipment and supplies.
4. Will you rent our current space? Will you look to move the PT department into an alternate space in the future? If so, where?
General
Make some general inquiries that will help you get to know each organization and determine which one may be the best fit for a long, committed relationship with your practice. Find out how often the organization will have corporate representatives in the practice and at physician board meetings. Inquire as to the types of referral reports they generate and share with the practice. Request the names and contact information of 3 to 5 orthopedic surgery practice managers or physician leaders whom you can contact as references for the company.
If you have an existing PT service line, ask the company how it proposes to enhance the services, quality, and bottom line. What value will the company’s management services add to an existing program?
Get to know the organization by asking how many of its partnering practices have terminated their agreements with the management company and if it has any current or past litigation with partner practices. These are detailed, binding contracts with the potential for a lot of money. When the relationships or even the local markets change, suits are filed.
As part of the RFP, inquire as to the standard proposed model for income distribution between the practice and the management company.
Conclusion
If your RFP covers all of the inquiries discussed in this article, it will be necessarily comprehensive. Send it to several companies with a clear indication of the response deadline and the contact person for the response and for any questions they may have. The contact person is typically the practice manager or executive administrator. Individual physicians in your group may have relationships with local representatives of a PT management company, and it can put them in an awkward position during the proposal submission and evaluation process.
Some companies may not respond to an RFP this comprehensive, which provides an unequivocal answer that they are not qualified to be your practice’s partner. Compare the responses you receive and set up presentations or conference calls for those companies whose proposals warrant it.
Hire your own health care attorney to review any and all contracts before signing. The HR support, exclusivity, income distribution models, compliance, and duration of these contracts must be approved by an experienced attorney that advocates for the practice alone.
You currently offer a physical therapy (PT) service line but feel like it could be doing better, or you are thinking of adding PT services and are not sure where to begin. Either way, the thought of your patients and bottom line benefiting from PT services within your practice but without you having to manage another service line is appealing. Although related to orthopedic surgery and an obvious ancillary service, PT is a different type of practice that requires active management of the professionals, revenue cycle, operations, regulatory requirements, and changing coding and reimbursement protocols. There are more and more companies nationwide that claim a mastery of the PT management niche and would be more than happy to shoulder your burden and share in your profits. Whether you already have PT services in your practice or are looking to add them, proceed with care and caution as you consider partnering with a PT management company.
Drawing on my involvement with both successful PT management–orthopedic practice partnerships and the arduous, expensive demise of one, this article offers my recommendations for determining if a PT management partnership is best for your practice. Many of the contracts last for several years and include clauses that are extremely binding even after the contract conclusion. As with any decision to outsource, the decision to outsource PT services deserves a comprehensive request for proposal (RFP) to multiple candidate companies, a thorough vetting and decision process that includes all partners or an executive committee/board, and legal review of the contract by an experienced health care attorney representing the practice.
Request for Proposal
Begin the RFP with a reference to your website and a brief description of the practice and current PT services. For example, state that you don’t have PT and are looking to start it, or, if your practice offers PT, include a description of the number of locations, square footage allocation, and number of full-time equivalent (FTE) physical therapists, occupational therapists, physical therapy assistants, and support staff of the existing program. Also mention whether the billing is done within the practice or is outsourced.
Next, you want to learn about the company. Ask about its number of years in PT management and the history of the company. Ask them to provide the previous business names and an overview of the history of ownership. You want to know this because the national PT management community is relatively small and includes frequent acquisitions and mergers. Just as important as the company’s history is any future plans it has to acquire or be acquired. This is all part of knowing who you may be partnering with.
You will want to know how many other practices the company provides PT/occupational therapy (OT) management services for, in what states those practices are located, and a breakdown of specialties. The number of physician providers the company represents along with the answers to the other questions will give you an idea of its size, experience, location, alignment, and focus. Some of these companies manage PT in family practices. You will want to know how many orthopedic practices the company partners with. If your practice has subspecialties, ask about its experience with subspecialty orthopedics.
Ask for the company’s website so that you can get an idea of the company and its mission, vision, and values. Even though you will likely be interacting with regional representatives, you will be signing the contract with the company leadership, so be sure to learn—either from the company’s website or its response to the RFP—about the individuals leading the organization and any parent company. Ask for a list of officers, board of directors, managers, and perhaps an organization chart with titles and names. Because you are looking to partner with the company, it might be good to ask for managerial turnover rates in the last few years. PT is a professional health care service, so take note of the number of licensed therapists the company has in leadership positions. If you were partnering with a medical organization, you would certainly want physicians in leadership positions, and this is no different. Determine if the company is publicly traded or privately held. You may also consider requesting the company’s last few annual reports to learn more.
Exclusivity
Some PT management companies have their own facilities and are partnering with practices in the same market despite the seemingly inherent conflict. As part of your RFP, ask the company to include the names of practices, their specialties, and site locations where it already has a presence as well as a list of its own (independent of a physician practice) locations in the state or region. Future plans are important here too; if the company does not currently have a presence in the region, what commitment will it make to exclusivity or noncompete?
Human Resources
In many cases, the PT management company actually employs the entire staff for the service line. If you already have PT in your practice, this means the employees will transition from your employment to another company. After the contract is signed, some of the employees will get paychecks and benefits from your practice and be subject to your practice’s policies, while others will not. Having 2 different employers in the same practice can have an impact on employee morale and satisfaction. Find out during the proposal process if the company’s typical model is based on the company’s or the practice’s employment of the professional and support staff.
Obtain the following information from the management company if it is to be the employer:
1. Titles and compensation ranges for each position
2. Description of all bonuses and incentive structures
3. Paid time off (PTO) policies and accrual rates
4. Paid holidays
5. Details of employee benefits, such as employee out-of-pocket premiums for individual and family health care coverage, availability of vision and dental coverage, and investment and match for retirement or 401(k) plans.
6. Human resources (HR) support. Describe how employees get needed support from human resources, such as questions about benefits, FMLA (Family Medical Leave Act), HR policies, and other issues.
7. Results of any employee satisfaction surveys completed in the last 2 years
8. Nonrecruitment. In what ways will the professional staff’s careers be affected by this partnership? Will the professional staff have to sign employment agreements? If so, please provide a sample. Will there be covenants not to compete for the professional staff?
9. Provide a schematic on how you typically cover professional staff vacation and family leave.
10. Does your organization provide accredited continuing education for professional staff or do you send staff to state and national meetings and courses to maintain their CEU (continuing education units) requirement?
11. Do you provide annual regulatory training, such as HIPAA (Health Insurance Portability and Accountability Act) training, for all staff or is the practice responsible for that?
12. Professional liability coverage for the therapists.
Initially, the company may say they are open to doing it either way and you may proceed with the process without answers to these questions. If at any point, you explore a situation in which the employer is not the practice, you must get answers to these questions before agreeing to anything. Number 8 above is extremely important. Many PT management companies will include a nonrecruitment clause in their contracts so that neither party can recruit therapists from the engagement. Depending on how the clause is written, you may not be able to legally hire therapists who were with you for years before the management agreement at the conclusion of the contract. Individual therapists can find themselves very limited in where they can work in the community depending on a covenant not to compete. And while covenants not to compete and nonrecruitment clauses may be generalized as “indefensible,” it is expensive, time-consuming, and exhausting to get one rendered as such after the fact.
Operations
Operational compatibility is essential to a smooth transition or start-up. As part of your RFP, let the candidate companies know which electronic medical record (EMR) and electronic practice management (EPM) systems you use and ask about their experience level with those. Ask if it is expected that PT will operate on the practice’s EMR and EPM systems or if the company will be having PT operate on separate systems. If the company will be implementing different systems, find out which one and then do an accounting of the costs for interface, training, and other compatibility elements.
Inquire as to each candidate company’s standard operations policies and procedures as well as the operational and productivity standards the company maintains. For example, ask for a range of how many patients a physical therapist should be able to see (including documentation) in an 8-hour day? If you already have a PT service line, compare the company’s productivity standards to what your therapists are currently doing. Of the many enhancements a therapy management company can bring, an increase in productivity is essential. Request a description of productivity incentive programs for the professional staff so that you can determine if you are comfortable with them. By the same token, ask if the company has a comprehensive compliance program including procedures and policies.
Any outsourcing agreements will be subject to operational and contractual compliance elements such as HIPAA, business associates agreement, and all other applicable regulations through state, federal, and payor entities. Ask each candidate company about its compliance program.
Revenue Cycle
Some therapy management companies will leave the billing and collections to the practice, while others have their own operations. As part of the RFP, ask the company which way it is done in its standard model. If the company manages the revenue cycle, ask which key revenue cycle performance indicators it monitors, how it calculates them, and with what frequency it tracks and reports them. Ask how the company has approached a revenue cycle performance improvement effort and what successes it has had. And definitely ask about the emphasis, training, and performance standards on point-of-service (POS) collections. In PT, successful, service-oriented POS collections are essential to cash flow and patient satisfaction. Typically, there is a copayment for each visit, and patients come 3 times or more per week. When patients pay the copayment before each visit, it feels manageable to them. If they get a bill for 6 copayments 2 weeks into PT, they often get angry and do not see the value of the therapy.
Seek specifics on the elements of the company’s performance improvement. A number of companies will default to providing incentive bonuses for POS collections and other revenue cycle improvements. Incentive bonuses for collections can compromise the coding and billing integrity of the practice and are guaranteed to cause discontent among support staff. Everyone who works hard should be recognized, not just the staff in a position to collect money. On top of this, if the PT reception staff are getting paid POS collections bonuses and the practice reception staff are not, a managerial dichotomy ensues.
Accounting and Financial Reporting
In your RFP, ask about the accounting and financial model that each candidate company most often uses. Inquire as to which—the practice or the management company—is responsible for monthly, quarterly, and annual accounting and financial reporting and what typical monthly reconcilement process the company recommends. Include the following requests in your RFP:
1. Please provide samples of the monthly financials produced or preferred.
2. Describe your annual expense and revenue budgeting and approval processes.
3. Please address how you recommend handling the purchase of new equipment and supplies as well as the handling of existing equipment and supplies.
4. Will you rent our current space? Will you look to move the PT department into an alternate space in the future? If so, where?
General
Make some general inquiries that will help you get to know each organization and determine which one may be the best fit for a long, committed relationship with your practice. Find out how often the organization will have corporate representatives in the practice and at physician board meetings. Inquire as to the types of referral reports they generate and share with the practice. Request the names and contact information of 3 to 5 orthopedic surgery practice managers or physician leaders whom you can contact as references for the company.
If you have an existing PT service line, ask the company how it proposes to enhance the services, quality, and bottom line. What value will the company’s management services add to an existing program?
Get to know the organization by asking how many of its partnering practices have terminated their agreements with the management company and if it has any current or past litigation with partner practices. These are detailed, binding contracts with the potential for a lot of money. When the relationships or even the local markets change, suits are filed.
As part of the RFP, inquire as to the standard proposed model for income distribution between the practice and the management company.
Conclusion
If your RFP covers all of the inquiries discussed in this article, it will be necessarily comprehensive. Send it to several companies with a clear indication of the response deadline and the contact person for the response and for any questions they may have. The contact person is typically the practice manager or executive administrator. Individual physicians in your group may have relationships with local representatives of a PT management company, and it can put them in an awkward position during the proposal submission and evaluation process.
Some companies may not respond to an RFP this comprehensive, which provides an unequivocal answer that they are not qualified to be your practice’s partner. Compare the responses you receive and set up presentations or conference calls for those companies whose proposals warrant it.
Hire your own health care attorney to review any and all contracts before signing. The HR support, exclusivity, income distribution models, compliance, and duration of these contracts must be approved by an experienced attorney that advocates for the practice alone.
You currently offer a physical therapy (PT) service line but feel like it could be doing better, or you are thinking of adding PT services and are not sure where to begin. Either way, the thought of your patients and bottom line benefiting from PT services within your practice but without you having to manage another service line is appealing. Although related to orthopedic surgery and an obvious ancillary service, PT is a different type of practice that requires active management of the professionals, revenue cycle, operations, regulatory requirements, and changing coding and reimbursement protocols. There are more and more companies nationwide that claim a mastery of the PT management niche and would be more than happy to shoulder your burden and share in your profits. Whether you already have PT services in your practice or are looking to add them, proceed with care and caution as you consider partnering with a PT management company.
Drawing on my involvement with both successful PT management–orthopedic practice partnerships and the arduous, expensive demise of one, this article offers my recommendations for determining if a PT management partnership is best for your practice. Many of the contracts last for several years and include clauses that are extremely binding even after the contract conclusion. As with any decision to outsource, the decision to outsource PT services deserves a comprehensive request for proposal (RFP) to multiple candidate companies, a thorough vetting and decision process that includes all partners or an executive committee/board, and legal review of the contract by an experienced health care attorney representing the practice.
Request for Proposal
Begin the RFP with a reference to your website and a brief description of the practice and current PT services. For example, state that you don’t have PT and are looking to start it, or, if your practice offers PT, include a description of the number of locations, square footage allocation, and number of full-time equivalent (FTE) physical therapists, occupational therapists, physical therapy assistants, and support staff of the existing program. Also mention whether the billing is done within the practice or is outsourced.
Next, you want to learn about the company. Ask about its number of years in PT management and the history of the company. Ask them to provide the previous business names and an overview of the history of ownership. You want to know this because the national PT management community is relatively small and includes frequent acquisitions and mergers. Just as important as the company’s history is any future plans it has to acquire or be acquired. This is all part of knowing who you may be partnering with.
You will want to know how many other practices the company provides PT/occupational therapy (OT) management services for, in what states those practices are located, and a breakdown of specialties. The number of physician providers the company represents along with the answers to the other questions will give you an idea of its size, experience, location, alignment, and focus. Some of these companies manage PT in family practices. You will want to know how many orthopedic practices the company partners with. If your practice has subspecialties, ask about its experience with subspecialty orthopedics.
Ask for the company’s website so that you can get an idea of the company and its mission, vision, and values. Even though you will likely be interacting with regional representatives, you will be signing the contract with the company leadership, so be sure to learn—either from the company’s website or its response to the RFP—about the individuals leading the organization and any parent company. Ask for a list of officers, board of directors, managers, and perhaps an organization chart with titles and names. Because you are looking to partner with the company, it might be good to ask for managerial turnover rates in the last few years. PT is a professional health care service, so take note of the number of licensed therapists the company has in leadership positions. If you were partnering with a medical organization, you would certainly want physicians in leadership positions, and this is no different. Determine if the company is publicly traded or privately held. You may also consider requesting the company’s last few annual reports to learn more.
Exclusivity
Some PT management companies have their own facilities and are partnering with practices in the same market despite the seemingly inherent conflict. As part of your RFP, ask the company to include the names of practices, their specialties, and site locations where it already has a presence as well as a list of its own (independent of a physician practice) locations in the state or region. Future plans are important here too; if the company does not currently have a presence in the region, what commitment will it make to exclusivity or noncompete?
Human Resources
In many cases, the PT management company actually employs the entire staff for the service line. If you already have PT in your practice, this means the employees will transition from your employment to another company. After the contract is signed, some of the employees will get paychecks and benefits from your practice and be subject to your practice’s policies, while others will not. Having 2 different employers in the same practice can have an impact on employee morale and satisfaction. Find out during the proposal process if the company’s typical model is based on the company’s or the practice’s employment of the professional and support staff.
Obtain the following information from the management company if it is to be the employer:
1. Titles and compensation ranges for each position
2. Description of all bonuses and incentive structures
3. Paid time off (PTO) policies and accrual rates
4. Paid holidays
5. Details of employee benefits, such as employee out-of-pocket premiums for individual and family health care coverage, availability of vision and dental coverage, and investment and match for retirement or 401(k) plans.
6. Human resources (HR) support. Describe how employees get needed support from human resources, such as questions about benefits, FMLA (Family Medical Leave Act), HR policies, and other issues.
7. Results of any employee satisfaction surveys completed in the last 2 years
8. Nonrecruitment. In what ways will the professional staff’s careers be affected by this partnership? Will the professional staff have to sign employment agreements? If so, please provide a sample. Will there be covenants not to compete for the professional staff?
9. Provide a schematic on how you typically cover professional staff vacation and family leave.
10. Does your organization provide accredited continuing education for professional staff or do you send staff to state and national meetings and courses to maintain their CEU (continuing education units) requirement?
11. Do you provide annual regulatory training, such as HIPAA (Health Insurance Portability and Accountability Act) training, for all staff or is the practice responsible for that?
12. Professional liability coverage for the therapists.
Initially, the company may say they are open to doing it either way and you may proceed with the process without answers to these questions. If at any point, you explore a situation in which the employer is not the practice, you must get answers to these questions before agreeing to anything. Number 8 above is extremely important. Many PT management companies will include a nonrecruitment clause in their contracts so that neither party can recruit therapists from the engagement. Depending on how the clause is written, you may not be able to legally hire therapists who were with you for years before the management agreement at the conclusion of the contract. Individual therapists can find themselves very limited in where they can work in the community depending on a covenant not to compete. And while covenants not to compete and nonrecruitment clauses may be generalized as “indefensible,” it is expensive, time-consuming, and exhausting to get one rendered as such after the fact.
Operations
Operational compatibility is essential to a smooth transition or start-up. As part of your RFP, let the candidate companies know which electronic medical record (EMR) and electronic practice management (EPM) systems you use and ask about their experience level with those. Ask if it is expected that PT will operate on the practice’s EMR and EPM systems or if the company will be having PT operate on separate systems. If the company will be implementing different systems, find out which one and then do an accounting of the costs for interface, training, and other compatibility elements.
Inquire as to each candidate company’s standard operations policies and procedures as well as the operational and productivity standards the company maintains. For example, ask for a range of how many patients a physical therapist should be able to see (including documentation) in an 8-hour day? If you already have a PT service line, compare the company’s productivity standards to what your therapists are currently doing. Of the many enhancements a therapy management company can bring, an increase in productivity is essential. Request a description of productivity incentive programs for the professional staff so that you can determine if you are comfortable with them. By the same token, ask if the company has a comprehensive compliance program including procedures and policies.
Any outsourcing agreements will be subject to operational and contractual compliance elements such as HIPAA, business associates agreement, and all other applicable regulations through state, federal, and payor entities. Ask each candidate company about its compliance program.
Revenue Cycle
Some therapy management companies will leave the billing and collections to the practice, while others have their own operations. As part of the RFP, ask the company which way it is done in its standard model. If the company manages the revenue cycle, ask which key revenue cycle performance indicators it monitors, how it calculates them, and with what frequency it tracks and reports them. Ask how the company has approached a revenue cycle performance improvement effort and what successes it has had. And definitely ask about the emphasis, training, and performance standards on point-of-service (POS) collections. In PT, successful, service-oriented POS collections are essential to cash flow and patient satisfaction. Typically, there is a copayment for each visit, and patients come 3 times or more per week. When patients pay the copayment before each visit, it feels manageable to them. If they get a bill for 6 copayments 2 weeks into PT, they often get angry and do not see the value of the therapy.
Seek specifics on the elements of the company’s performance improvement. A number of companies will default to providing incentive bonuses for POS collections and other revenue cycle improvements. Incentive bonuses for collections can compromise the coding and billing integrity of the practice and are guaranteed to cause discontent among support staff. Everyone who works hard should be recognized, not just the staff in a position to collect money. On top of this, if the PT reception staff are getting paid POS collections bonuses and the practice reception staff are not, a managerial dichotomy ensues.
Accounting and Financial Reporting
In your RFP, ask about the accounting and financial model that each candidate company most often uses. Inquire as to which—the practice or the management company—is responsible for monthly, quarterly, and annual accounting and financial reporting and what typical monthly reconcilement process the company recommends. Include the following requests in your RFP:
1. Please provide samples of the monthly financials produced or preferred.
2. Describe your annual expense and revenue budgeting and approval processes.
3. Please address how you recommend handling the purchase of new equipment and supplies as well as the handling of existing equipment and supplies.
4. Will you rent our current space? Will you look to move the PT department into an alternate space in the future? If so, where?
General
Make some general inquiries that will help you get to know each organization and determine which one may be the best fit for a long, committed relationship with your practice. Find out how often the organization will have corporate representatives in the practice and at physician board meetings. Inquire as to the types of referral reports they generate and share with the practice. Request the names and contact information of 3 to 5 orthopedic surgery practice managers or physician leaders whom you can contact as references for the company.
If you have an existing PT service line, ask the company how it proposes to enhance the services, quality, and bottom line. What value will the company’s management services add to an existing program?
Get to know the organization by asking how many of its partnering practices have terminated their agreements with the management company and if it has any current or past litigation with partner practices. These are detailed, binding contracts with the potential for a lot of money. When the relationships or even the local markets change, suits are filed.
As part of the RFP, inquire as to the standard proposed model for income distribution between the practice and the management company.
Conclusion
If your RFP covers all of the inquiries discussed in this article, it will be necessarily comprehensive. Send it to several companies with a clear indication of the response deadline and the contact person for the response and for any questions they may have. The contact person is typically the practice manager or executive administrator. Individual physicians in your group may have relationships with local representatives of a PT management company, and it can put them in an awkward position during the proposal submission and evaluation process.
Some companies may not respond to an RFP this comprehensive, which provides an unequivocal answer that they are not qualified to be your practice’s partner. Compare the responses you receive and set up presentations or conference calls for those companies whose proposals warrant it.
Hire your own health care attorney to review any and all contracts before signing. The HR support, exclusivity, income distribution models, compliance, and duration of these contracts must be approved by an experienced attorney that advocates for the practice alone.
Eliminating Adverse Events and Redundant Tests Could Generate U.S. Healthcare Savings
Clinical question: Using available data, what is the estimated cost savings of eliminating adverse events and avoiding redundant tests?
Background: Reimbursement schemes are changing such that hospitals are reimbursed less for some adverse events. This financial disincentive is expected to spark interest in improved patient safety. The authors sought to model the cost savings generated by eliminating redundant testing and adverse events from literature-based estimates.
Study design: Development of conceptual model to identify common or costly adverse events, redundant tests, and simulated costs.
Setting: Literature review, expert opinion, data from safety organizations and epidemiologic studies, and patient data from the 2004 National Inpatient Data Sample.
Synopsis: The conceptual model identified 5.7 million adverse events in U.S. hospitals, of which 3 million were considered preventable. The most common events included hospital-acquired infections (82% preventable), adverse drug events (26%), falls (33%), and iatrogenic thromboembolic events (62%). The calculated cost savings totaled $16.6 billion (5.5% of total inpatient costs) for adverse events and $8.2 billion for the elimination of redundant tests. When looking at hospital subtypes, the greatest savings would come from major teaching hospitals.
This study is limited by its use of published and heterogeneous data spanning a 15-year period. The authors did not include events for which there was no epidemiologic or cost data. As hospital-care changes and technology is adopted, it is uncertain how this changes the costs, prevalence, and the preventable nature of these events. The model was not consistently able to identifying high- and low-risk patients. For instance, in some models, all patients were considered at risk for events.
Bottom line: Based on a conceptual model of 2004 hospitalized patients, eliminating preventable adverse events could have saved $16.6 billion, while eliminating redundant tests could have saved another $8 billion.
Citation: Jha AK, Chan DC, Ridgway AB, Franz C, Bates DW. Improving safety and eliminating redundant tests: cutting costs in U.S. hospitals. Health Aff (Millwood). 2009;28(5):1475-1484.
Clinical question: Using available data, what is the estimated cost savings of eliminating adverse events and avoiding redundant tests?
Background: Reimbursement schemes are changing such that hospitals are reimbursed less for some adverse events. This financial disincentive is expected to spark interest in improved patient safety. The authors sought to model the cost savings generated by eliminating redundant testing and adverse events from literature-based estimates.
Study design: Development of conceptual model to identify common or costly adverse events, redundant tests, and simulated costs.
Setting: Literature review, expert opinion, data from safety organizations and epidemiologic studies, and patient data from the 2004 National Inpatient Data Sample.
Synopsis: The conceptual model identified 5.7 million adverse events in U.S. hospitals, of which 3 million were considered preventable. The most common events included hospital-acquired infections (82% preventable), adverse drug events (26%), falls (33%), and iatrogenic thromboembolic events (62%). The calculated cost savings totaled $16.6 billion (5.5% of total inpatient costs) for adverse events and $8.2 billion for the elimination of redundant tests. When looking at hospital subtypes, the greatest savings would come from major teaching hospitals.
This study is limited by its use of published and heterogeneous data spanning a 15-year period. The authors did not include events for which there was no epidemiologic or cost data. As hospital-care changes and technology is adopted, it is uncertain how this changes the costs, prevalence, and the preventable nature of these events. The model was not consistently able to identifying high- and low-risk patients. For instance, in some models, all patients were considered at risk for events.
Bottom line: Based on a conceptual model of 2004 hospitalized patients, eliminating preventable adverse events could have saved $16.6 billion, while eliminating redundant tests could have saved another $8 billion.
Citation: Jha AK, Chan DC, Ridgway AB, Franz C, Bates DW. Improving safety and eliminating redundant tests: cutting costs in U.S. hospitals. Health Aff (Millwood). 2009;28(5):1475-1484.
Clinical question: Using available data, what is the estimated cost savings of eliminating adverse events and avoiding redundant tests?
Background: Reimbursement schemes are changing such that hospitals are reimbursed less for some adverse events. This financial disincentive is expected to spark interest in improved patient safety. The authors sought to model the cost savings generated by eliminating redundant testing and adverse events from literature-based estimates.
Study design: Development of conceptual model to identify common or costly adverse events, redundant tests, and simulated costs.
Setting: Literature review, expert opinion, data from safety organizations and epidemiologic studies, and patient data from the 2004 National Inpatient Data Sample.
Synopsis: The conceptual model identified 5.7 million adverse events in U.S. hospitals, of which 3 million were considered preventable. The most common events included hospital-acquired infections (82% preventable), adverse drug events (26%), falls (33%), and iatrogenic thromboembolic events (62%). The calculated cost savings totaled $16.6 billion (5.5% of total inpatient costs) for adverse events and $8.2 billion for the elimination of redundant tests. When looking at hospital subtypes, the greatest savings would come from major teaching hospitals.
This study is limited by its use of published and heterogeneous data spanning a 15-year period. The authors did not include events for which there was no epidemiologic or cost data. As hospital-care changes and technology is adopted, it is uncertain how this changes the costs, prevalence, and the preventable nature of these events. The model was not consistently able to identifying high- and low-risk patients. For instance, in some models, all patients were considered at risk for events.
Bottom line: Based on a conceptual model of 2004 hospitalized patients, eliminating preventable adverse events could have saved $16.6 billion, while eliminating redundant tests could have saved another $8 billion.
Citation: Jha AK, Chan DC, Ridgway AB, Franz C, Bates DW. Improving safety and eliminating redundant tests: cutting costs in U.S. hospitals. Health Aff (Millwood). 2009;28(5):1475-1484.
Patient Signout Is Not Uniformly Comprehensive and Often Lacks Critical Information
Clinical question: Do signouts vary in the quality and quantity of information, and what are the various factors affecting signout quality?
Background: Miscommunication during transfers of responsibility for hospitalized patients is common and can result in harm. Recommendations for safe and effective handoffs emphasize key content, clear communication, senior staff supervision, and adequate time for questions. Still, little is known about adherence to these recommendations in clinical practice.
Study design: Prospective, observational cohort.
Setting: Medical unit of an acute-care teaching hospital.
Synopsis: Oral signouts were audiotaped among IM house staff teams and the accompanying written signouts were collected for review of content. Signout sessions (n=88) included eight IM teams at one hospital and contained 503 patient signouts.
The median signout duration was 35 seconds (IQR 19-62) per patient. Key clinical information was present in just 62% of combined written or oral signouts. Most signouts included no questions from the recipient. Factors associated with higher rate of content inclusion included: familiarity with the patient, sense of responsibility (primary team vs. covering team), only one signout per day (as compared to sequential signout), presence of a senior resident, and comprehensive, written signouts.
Study limitations include the Hawthorne effect, as several participants mentioned that the presence of audiotape led to more comprehensive signouts than are typical. Also, the signout quality assessment in this study has not been validated with patient-safety outcomes.
Bottom line: Signouts among internal-medicine residents at this one hospital showed variability in terms of quantitative and qualitative information and often missed crucial information about patient care.
Citation: Horwitz LI, Moin T, Krumholz HM, Wang L, Bradley EH. What are covering doctors told about their patients? Analysis of sign-out among internal medicine house staff. Qual Saf Health Care. 2009;18(4):248-255.
Clinical question: Do signouts vary in the quality and quantity of information, and what are the various factors affecting signout quality?
Background: Miscommunication during transfers of responsibility for hospitalized patients is common and can result in harm. Recommendations for safe and effective handoffs emphasize key content, clear communication, senior staff supervision, and adequate time for questions. Still, little is known about adherence to these recommendations in clinical practice.
Study design: Prospective, observational cohort.
Setting: Medical unit of an acute-care teaching hospital.
Synopsis: Oral signouts were audiotaped among IM house staff teams and the accompanying written signouts were collected for review of content. Signout sessions (n=88) included eight IM teams at one hospital and contained 503 patient signouts.
The median signout duration was 35 seconds (IQR 19-62) per patient. Key clinical information was present in just 62% of combined written or oral signouts. Most signouts included no questions from the recipient. Factors associated with higher rate of content inclusion included: familiarity with the patient, sense of responsibility (primary team vs. covering team), only one signout per day (as compared to sequential signout), presence of a senior resident, and comprehensive, written signouts.
Study limitations include the Hawthorne effect, as several participants mentioned that the presence of audiotape led to more comprehensive signouts than are typical. Also, the signout quality assessment in this study has not been validated with patient-safety outcomes.
Bottom line: Signouts among internal-medicine residents at this one hospital showed variability in terms of quantitative and qualitative information and often missed crucial information about patient care.
Citation: Horwitz LI, Moin T, Krumholz HM, Wang L, Bradley EH. What are covering doctors told about their patients? Analysis of sign-out among internal medicine house staff. Qual Saf Health Care. 2009;18(4):248-255.
Clinical question: Do signouts vary in the quality and quantity of information, and what are the various factors affecting signout quality?
Background: Miscommunication during transfers of responsibility for hospitalized patients is common and can result in harm. Recommendations for safe and effective handoffs emphasize key content, clear communication, senior staff supervision, and adequate time for questions. Still, little is known about adherence to these recommendations in clinical practice.
Study design: Prospective, observational cohort.
Setting: Medical unit of an acute-care teaching hospital.
Synopsis: Oral signouts were audiotaped among IM house staff teams and the accompanying written signouts were collected for review of content. Signout sessions (n=88) included eight IM teams at one hospital and contained 503 patient signouts.
The median signout duration was 35 seconds (IQR 19-62) per patient. Key clinical information was present in just 62% of combined written or oral signouts. Most signouts included no questions from the recipient. Factors associated with higher rate of content inclusion included: familiarity with the patient, sense of responsibility (primary team vs. covering team), only one signout per day (as compared to sequential signout), presence of a senior resident, and comprehensive, written signouts.
Study limitations include the Hawthorne effect, as several participants mentioned that the presence of audiotape led to more comprehensive signouts than are typical. Also, the signout quality assessment in this study has not been validated with patient-safety outcomes.
Bottom line: Signouts among internal-medicine residents at this one hospital showed variability in terms of quantitative and qualitative information and often missed crucial information about patient care.
Citation: Horwitz LI, Moin T, Krumholz HM, Wang L, Bradley EH. What are covering doctors told about their patients? Analysis of sign-out among internal medicine house staff. Qual Saf Health Care. 2009;18(4):248-255.
Emergency Department Signout via Voicemail Yields Mixed Reviews
Clinical question: How does traditional, oral signout from emergency providers to inpatient medicine physicians compare to dictated, voicemail signout?
Background: Communication failures contribute to errors in care transition from ED to inpatient medicine units. Signout between ED providers and internal medicine (IM) physicians is typically oral (“synchronous communication”). It is not known how dictated signout to a voicemail system (“asynchronous communication”) affects the quality and safety of handoff communications.
Study design: Prospective, pre-post analysis.
Setting: A 944-bed urban academic medical center in Connecticut.
Synopsis: Surveys were administered to all IM and ED providers before and after the implementation of a voicemail signout system. In the new system, ED providers dictated signout for stable patients, rather than giving traditional synchronous telephone signout. It was the responsibility of the admitting IM physician to listen to the voicemail after receiving a text notification that a patient was being admitted.
ED providers recorded signouts in 89.5% of medicine admissions. However, voicemails were accessed only 58.5% of the time by receiving physicians. All ED providers and 56% of IM physicians believed signout was easier following the voicemail intervention. Overall, ED providers gave the quality, content, and accuracy of their signout communication higher ratings than IM physicians did; 69% of all providers felt the interaction among participants was worse following the intervention. There was no change in the rate of perceived adverse events or ICU transfers within 24 hours after admission.
This intervention was a QI initiative at a single center. Mixed results and small sample size limit generalizability of the study.
Bottom line: Asynchronous signout by voicemail increased efficiency, particularly among ED providers but decreased perceived quality of interaction between medical providers without obviously affecting patient safety.
Citation: Horwitz LI, Parwani V, Shah NR, et al. Evaluation of an asynchronous physician voicemail sign-out for emergency department admissions. Ann Emerg Med. 2009;54:368-378.
Clinical question: How does traditional, oral signout from emergency providers to inpatient medicine physicians compare to dictated, voicemail signout?
Background: Communication failures contribute to errors in care transition from ED to inpatient medicine units. Signout between ED providers and internal medicine (IM) physicians is typically oral (“synchronous communication”). It is not known how dictated signout to a voicemail system (“asynchronous communication”) affects the quality and safety of handoff communications.
Study design: Prospective, pre-post analysis.
Setting: A 944-bed urban academic medical center in Connecticut.
Synopsis: Surveys were administered to all IM and ED providers before and after the implementation of a voicemail signout system. In the new system, ED providers dictated signout for stable patients, rather than giving traditional synchronous telephone signout. It was the responsibility of the admitting IM physician to listen to the voicemail after receiving a text notification that a patient was being admitted.
ED providers recorded signouts in 89.5% of medicine admissions. However, voicemails were accessed only 58.5% of the time by receiving physicians. All ED providers and 56% of IM physicians believed signout was easier following the voicemail intervention. Overall, ED providers gave the quality, content, and accuracy of their signout communication higher ratings than IM physicians did; 69% of all providers felt the interaction among participants was worse following the intervention. There was no change in the rate of perceived adverse events or ICU transfers within 24 hours after admission.
This intervention was a QI initiative at a single center. Mixed results and small sample size limit generalizability of the study.
Bottom line: Asynchronous signout by voicemail increased efficiency, particularly among ED providers but decreased perceived quality of interaction between medical providers without obviously affecting patient safety.
Citation: Horwitz LI, Parwani V, Shah NR, et al. Evaluation of an asynchronous physician voicemail sign-out for emergency department admissions. Ann Emerg Med. 2009;54:368-378.
Clinical question: How does traditional, oral signout from emergency providers to inpatient medicine physicians compare to dictated, voicemail signout?
Background: Communication failures contribute to errors in care transition from ED to inpatient medicine units. Signout between ED providers and internal medicine (IM) physicians is typically oral (“synchronous communication”). It is not known how dictated signout to a voicemail system (“asynchronous communication”) affects the quality and safety of handoff communications.
Study design: Prospective, pre-post analysis.
Setting: A 944-bed urban academic medical center in Connecticut.
Synopsis: Surveys were administered to all IM and ED providers before and after the implementation of a voicemail signout system. In the new system, ED providers dictated signout for stable patients, rather than giving traditional synchronous telephone signout. It was the responsibility of the admitting IM physician to listen to the voicemail after receiving a text notification that a patient was being admitted.
ED providers recorded signouts in 89.5% of medicine admissions. However, voicemails were accessed only 58.5% of the time by receiving physicians. All ED providers and 56% of IM physicians believed signout was easier following the voicemail intervention. Overall, ED providers gave the quality, content, and accuracy of their signout communication higher ratings than IM physicians did; 69% of all providers felt the interaction among participants was worse following the intervention. There was no change in the rate of perceived adverse events or ICU transfers within 24 hours after admission.
This intervention was a QI initiative at a single center. Mixed results and small sample size limit generalizability of the study.
Bottom line: Asynchronous signout by voicemail increased efficiency, particularly among ED providers but decreased perceived quality of interaction between medical providers without obviously affecting patient safety.
Citation: Horwitz LI, Parwani V, Shah NR, et al. Evaluation of an asynchronous physician voicemail sign-out for emergency department admissions. Ann Emerg Med. 2009;54:368-378.
Decreased ICU Duty Hours Does Not Affect Patient Mortality
Clinical question: Does the reduction in work hours for residents affect mortality in medical and surgical ICUs?
Background: A reduction in work hours for residents was enforced in July 2003. Several prior studies using administrative or claims data did not show an association of the reduced work hours for residents with mortality in teaching hospitals when compared with nonteaching hospitals.
Study design: Observational retrospective registry cohort.
Setting: Twelve academic, 12 community, and 16 nonteaching hospitals in the U.S.
Synopsis: Data from 230,151 patients were extracted as post-hoc analysis from a voluntary clinical registry that uses a well-validated severity-of-illness scoring system. The exposure was defined as date of admission to ICU within two years before and after the reform. Hospitals were categorized as academic, community with residents, or nonteaching. Sophisticated statistical analyses were performed, including interaction terms for teaching status and time. To test the effect the reduced work hours had on mortality, the mortality trends of academic hospitals and community hospitals with residents were compared with the baseline trend of nonteaching hospitals. After risk adjustments, all hospitals had improved in-hospital and ICU mortality after the reform. None of the statistical improvements were significantly different.
Study limitations include the selection bias, as only highly motivated hospitals participating in the registry were included, and misclassification bias, as not all hospitals implemented the reform at the same time. Nevertheless, this study supports the consistent literature on the topic and adds a more robust assessment of severity of illness.
Bottom line: The restriction on resident duty hours does not appear to affect patient mortality.
Citation: Prasad M, Iwashyna TJ, Christie JD, et al. Effect of work-hours regulations on intensive care unit mortality in United States teaching hospitals. Crit Care Med. 2009;37(9):2564-2569.
Clinical question: Does the reduction in work hours for residents affect mortality in medical and surgical ICUs?
Background: A reduction in work hours for residents was enforced in July 2003. Several prior studies using administrative or claims data did not show an association of the reduced work hours for residents with mortality in teaching hospitals when compared with nonteaching hospitals.
Study design: Observational retrospective registry cohort.
Setting: Twelve academic, 12 community, and 16 nonteaching hospitals in the U.S.
Synopsis: Data from 230,151 patients were extracted as post-hoc analysis from a voluntary clinical registry that uses a well-validated severity-of-illness scoring system. The exposure was defined as date of admission to ICU within two years before and after the reform. Hospitals were categorized as academic, community with residents, or nonteaching. Sophisticated statistical analyses were performed, including interaction terms for teaching status and time. To test the effect the reduced work hours had on mortality, the mortality trends of academic hospitals and community hospitals with residents were compared with the baseline trend of nonteaching hospitals. After risk adjustments, all hospitals had improved in-hospital and ICU mortality after the reform. None of the statistical improvements were significantly different.
Study limitations include the selection bias, as only highly motivated hospitals participating in the registry were included, and misclassification bias, as not all hospitals implemented the reform at the same time. Nevertheless, this study supports the consistent literature on the topic and adds a more robust assessment of severity of illness.
Bottom line: The restriction on resident duty hours does not appear to affect patient mortality.
Citation: Prasad M, Iwashyna TJ, Christie JD, et al. Effect of work-hours regulations on intensive care unit mortality in United States teaching hospitals. Crit Care Med. 2009;37(9):2564-2569.
Clinical question: Does the reduction in work hours for residents affect mortality in medical and surgical ICUs?
Background: A reduction in work hours for residents was enforced in July 2003. Several prior studies using administrative or claims data did not show an association of the reduced work hours for residents with mortality in teaching hospitals when compared with nonteaching hospitals.
Study design: Observational retrospective registry cohort.
Setting: Twelve academic, 12 community, and 16 nonteaching hospitals in the U.S.
Synopsis: Data from 230,151 patients were extracted as post-hoc analysis from a voluntary clinical registry that uses a well-validated severity-of-illness scoring system. The exposure was defined as date of admission to ICU within two years before and after the reform. Hospitals were categorized as academic, community with residents, or nonteaching. Sophisticated statistical analyses were performed, including interaction terms for teaching status and time. To test the effect the reduced work hours had on mortality, the mortality trends of academic hospitals and community hospitals with residents were compared with the baseline trend of nonteaching hospitals. After risk adjustments, all hospitals had improved in-hospital and ICU mortality after the reform. None of the statistical improvements were significantly different.
Study limitations include the selection bias, as only highly motivated hospitals participating in the registry were included, and misclassification bias, as not all hospitals implemented the reform at the same time. Nevertheless, this study supports the consistent literature on the topic and adds a more robust assessment of severity of illness.
Bottom line: The restriction on resident duty hours does not appear to affect patient mortality.
Citation: Prasad M, Iwashyna TJ, Christie JD, et al. Effect of work-hours regulations on intensive care unit mortality in United States teaching hospitals. Crit Care Med. 2009;37(9):2564-2569.
Baystate Medical Center's Unit-Based, Multidisciplinary Rounding Enhances Inpatient Care
The hospitalist-led Broder Service empowers all care-team members to focus on patient quality, satisfaction. Get an up-close look at the service with our 6-minute feature video:
The hospitalist-led Broder Service empowers all care-team members to focus on patient quality, satisfaction. Get an up-close look at the service with our 6-minute feature video:
The hospitalist-led Broder Service empowers all care-team members to focus on patient quality, satisfaction. Get an up-close look at the service with our 6-minute feature video:
Selling your practice
A generation ago, the sale of a medical practice was much like the sale of any other business: A retiring physician would sell his or her practice to a young doctor, and the practice would continue on as before. Occasionally that still happens, but changes in the business of medicine – most significantly the growth of managed care – have had a big impact on the way medical practices are bought and sold.
For one thing, there are far fewer solo practitioners these days, and polls indicate that most young physicians intend to continue that trend. The buyer of a medical practice today is more likely to be an institution, such as a hospital, an HMO, or a large practice group, rather than an individual physician.
Also, because the rules governing such sales have become so numbingly complex, the services of expert (and expensive) third parties are essential.
While these issues may complicate matters, there is still a market for the sale of medical practices. However, you must do everything possible to ensure you identify the best possible buyer and structure the best deal.
The first hurdle is the accurate valuation of your practice, which was covered in some detail last month. For the protection of both parties, it is important that the appraisal be done by an experienced and neutral financial consultant, that all techniques used in the valuation be divulged and explained, and that documentation be supplied to support the conclusions reached.
Keep in mind that the valuation will not necessarily equal the purchase price; other factors may need to be considered before a final price can be agreed upon. Keep in mind, too, that there may be legal constraints on the purchase price. For example, if the buyer is a nonprofit corporation, such as a hospital or HMO, by law it cannot pay in excess of fair market value for the practice – which may rule out any valuation of “good will.” In some states, such as mine (New Jersey), the purchase of private practices by hospitals is prohibited altogether – so you might need to consider a long-term lease rather than a sale.
Once a value has been agreed upon, you must consider how the transaction will be structured. The most popular structures include purchase of assets, purchase of corporate stock, or merger.
Buyers, especially institutional buyers, prefer to purchase assets, because it allows them to pick and choose only those items that have value to them. This can leave the seller with a bunch of “odd lots” to dispose of. But depending on the circumstances, an asset sale may be to the advantage of both parties.
Sellers typically prefer to sell stock because it allows them to sell their entire practice, which is often worth more than the sum of its parts, and often provides tax advantages.
The third option, merger, continues to grow in popularity. I’ll cover some of the more common merger variants in a future column.
Tax issues must always be considered. Most private practices are corporations, and the sale of corporate stock will result in a long-term capital gain which will be taxed (under current law) at 28%. As the saying goes, it’s not what you earn, it’s what you keep; so it may benefit the seller to accept a slightly lower price if the sale can be structured to provide significantly lower tax treatment. However, any gain that does not qualify as a long-term capital gain will be taxed as regular income – currently around 40% – plus a social security tax of about 15%.
Payment in installments is a popular way to defer taxes, since they are incurred on each installment as it is paid. However, such payments may be mistaken by the Internal Revenue Service for payments for referrals, which is illegal. And there is always the problem of making certain all the payments are made.
The seller may wish to continue working at the practice as an employee, and this is often to the buyer’s advantage as well. Transitioning to new ownership in stages often maximizes the value of the business by improving patient retention, and allows patients to become accustomed to the transition. However, care must be taken, with the aid of good legal advice, to structure such an arrangement in a way that minimizes concerns of fraud and abuse.
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, N.J. He is the author of numerous articles and textbook chapters, and is a longtime monthly columnist for Skin & Allergy News. Additional columns are available online at edermatologynews.com.
A generation ago, the sale of a medical practice was much like the sale of any other business: A retiring physician would sell his or her practice to a young doctor, and the practice would continue on as before. Occasionally that still happens, but changes in the business of medicine – most significantly the growth of managed care – have had a big impact on the way medical practices are bought and sold.
For one thing, there are far fewer solo practitioners these days, and polls indicate that most young physicians intend to continue that trend. The buyer of a medical practice today is more likely to be an institution, such as a hospital, an HMO, or a large practice group, rather than an individual physician.
Also, because the rules governing such sales have become so numbingly complex, the services of expert (and expensive) third parties are essential.
While these issues may complicate matters, there is still a market for the sale of medical practices. However, you must do everything possible to ensure you identify the best possible buyer and structure the best deal.
The first hurdle is the accurate valuation of your practice, which was covered in some detail last month. For the protection of both parties, it is important that the appraisal be done by an experienced and neutral financial consultant, that all techniques used in the valuation be divulged and explained, and that documentation be supplied to support the conclusions reached.
Keep in mind that the valuation will not necessarily equal the purchase price; other factors may need to be considered before a final price can be agreed upon. Keep in mind, too, that there may be legal constraints on the purchase price. For example, if the buyer is a nonprofit corporation, such as a hospital or HMO, by law it cannot pay in excess of fair market value for the practice – which may rule out any valuation of “good will.” In some states, such as mine (New Jersey), the purchase of private practices by hospitals is prohibited altogether – so you might need to consider a long-term lease rather than a sale.
Once a value has been agreed upon, you must consider how the transaction will be structured. The most popular structures include purchase of assets, purchase of corporate stock, or merger.
Buyers, especially institutional buyers, prefer to purchase assets, because it allows them to pick and choose only those items that have value to them. This can leave the seller with a bunch of “odd lots” to dispose of. But depending on the circumstances, an asset sale may be to the advantage of both parties.
Sellers typically prefer to sell stock because it allows them to sell their entire practice, which is often worth more than the sum of its parts, and often provides tax advantages.
The third option, merger, continues to grow in popularity. I’ll cover some of the more common merger variants in a future column.
Tax issues must always be considered. Most private practices are corporations, and the sale of corporate stock will result in a long-term capital gain which will be taxed (under current law) at 28%. As the saying goes, it’s not what you earn, it’s what you keep; so it may benefit the seller to accept a slightly lower price if the sale can be structured to provide significantly lower tax treatment. However, any gain that does not qualify as a long-term capital gain will be taxed as regular income – currently around 40% – plus a social security tax of about 15%.
Payment in installments is a popular way to defer taxes, since they are incurred on each installment as it is paid. However, such payments may be mistaken by the Internal Revenue Service for payments for referrals, which is illegal. And there is always the problem of making certain all the payments are made.
The seller may wish to continue working at the practice as an employee, and this is often to the buyer’s advantage as well. Transitioning to new ownership in stages often maximizes the value of the business by improving patient retention, and allows patients to become accustomed to the transition. However, care must be taken, with the aid of good legal advice, to structure such an arrangement in a way that minimizes concerns of fraud and abuse.
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, N.J. He is the author of numerous articles and textbook chapters, and is a longtime monthly columnist for Skin & Allergy News. Additional columns are available online at edermatologynews.com.
A generation ago, the sale of a medical practice was much like the sale of any other business: A retiring physician would sell his or her practice to a young doctor, and the practice would continue on as before. Occasionally that still happens, but changes in the business of medicine – most significantly the growth of managed care – have had a big impact on the way medical practices are bought and sold.
For one thing, there are far fewer solo practitioners these days, and polls indicate that most young physicians intend to continue that trend. The buyer of a medical practice today is more likely to be an institution, such as a hospital, an HMO, or a large practice group, rather than an individual physician.
Also, because the rules governing such sales have become so numbingly complex, the services of expert (and expensive) third parties are essential.
While these issues may complicate matters, there is still a market for the sale of medical practices. However, you must do everything possible to ensure you identify the best possible buyer and structure the best deal.
The first hurdle is the accurate valuation of your practice, which was covered in some detail last month. For the protection of both parties, it is important that the appraisal be done by an experienced and neutral financial consultant, that all techniques used in the valuation be divulged and explained, and that documentation be supplied to support the conclusions reached.
Keep in mind that the valuation will not necessarily equal the purchase price; other factors may need to be considered before a final price can be agreed upon. Keep in mind, too, that there may be legal constraints on the purchase price. For example, if the buyer is a nonprofit corporation, such as a hospital or HMO, by law it cannot pay in excess of fair market value for the practice – which may rule out any valuation of “good will.” In some states, such as mine (New Jersey), the purchase of private practices by hospitals is prohibited altogether – so you might need to consider a long-term lease rather than a sale.
Once a value has been agreed upon, you must consider how the transaction will be structured. The most popular structures include purchase of assets, purchase of corporate stock, or merger.
Buyers, especially institutional buyers, prefer to purchase assets, because it allows them to pick and choose only those items that have value to them. This can leave the seller with a bunch of “odd lots” to dispose of. But depending on the circumstances, an asset sale may be to the advantage of both parties.
Sellers typically prefer to sell stock because it allows them to sell their entire practice, which is often worth more than the sum of its parts, and often provides tax advantages.
The third option, merger, continues to grow in popularity. I’ll cover some of the more common merger variants in a future column.
Tax issues must always be considered. Most private practices are corporations, and the sale of corporate stock will result in a long-term capital gain which will be taxed (under current law) at 28%. As the saying goes, it’s not what you earn, it’s what you keep; so it may benefit the seller to accept a slightly lower price if the sale can be structured to provide significantly lower tax treatment. However, any gain that does not qualify as a long-term capital gain will be taxed as regular income – currently around 40% – plus a social security tax of about 15%.
Payment in installments is a popular way to defer taxes, since they are incurred on each installment as it is paid. However, such payments may be mistaken by the Internal Revenue Service for payments for referrals, which is illegal. And there is always the problem of making certain all the payments are made.
The seller may wish to continue working at the practice as an employee, and this is often to the buyer’s advantage as well. Transitioning to new ownership in stages often maximizes the value of the business by improving patient retention, and allows patients to become accustomed to the transition. However, care must be taken, with the aid of good legal advice, to structure such an arrangement in a way that minimizes concerns of fraud and abuse.
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, N.J. He is the author of numerous articles and textbook chapters, and is a longtime monthly columnist for Skin & Allergy News. Additional columns are available online at edermatologynews.com.
