User login
For psoriasis, review finds several biosimilars as safe and effective as biologics
The effectiveness and safety of biosimilars for psoriasis appear to be similar to the originator biologics, reported the authors of a review of studies comparing the two.
“This systematic review found that there was no clinically or statistically significant difference in the efficacy and safety between biosimilars and originators of adalimumab, etanercept, infliximab, and ustekinumab for the treatment of psoriasis,” senior study author and clinical lecturer Zenas Z. N. Yiu, MBChB, PhD, and his colleagues at the University of Manchester, England, wrote in JAMA Dermatology.“The biosimilars evaluated in this study could be considered alongside originators for biologic-naive patients to improve the accessibility of biological treatments,” they added. “Switching patients currently on originators to biosimilars could be considered where clinically appropriate to reduce treatment costs.”
Biologics versus biosimilars
In contrast to most chemically synthesized drugs, biologics are created from living organisms, and they have complex structures that can vary slightly from batch to batch, Luigi Naldi, MD, director of the department of dermatology of Ospedale San Bortolo, Vicenza, Italy, and Antonio Addis, PharmD, researcher in the department of epidemiology, Regione Lazio, in Rome, wrote in an accompanying editorial.
Once the patent on the “originator” biologic expires, U.S. and European regulators allow other manufacturers to develop similar molecules – biosimilars – through an abbreviated approval process. If the results of a limited number of equivalence or noninferiority clinical trials are acceptable, registration for all the indications of the originator is allowed for its biosimilars. Referring to the expense of biologics, Dr. Naldi and Dr. Addis noted that in the United States, “biologics comprise less than 3% of the volume of drugs on the market, but account for more than one-third of all drug spending.”
Systematic review
Dr. Yiu and his colleagues queried standard medical research databases in August 2022, and included 14 randomized clinical trials (10 adalimumab, 2 etanercept, 1 infliximab, and 1 ustekinumab) and 3 cohort studies (1 adalimumab, 1 etanercept, 1 infliximab and etanercept) in their review.
Twelve trials compared biosimilars vs. originators in originator-naive patients, and 11 trials compared switching from originators to biosimilars vs. continuous treatment with the originator.
The researchers found the following:
At week 16, mean PASI75 (Psoriasis Area and Severity Index) response rates ranges from 60.7% to 90.6% for adalimumab biosimilars, vs. 61.5% to 91.7% for the originator. Mean PASI75 responses for the two etanercept biosimilars were 56.1% and 76.7% vs. 55.5% and 73.4% for the originator. In the ustekinumab study, mean PASI75 responses were 86.1% for the biosimilar vs. 84.0% for the originator.
At week 52, mean PASI75 responses were between 86.3% and 92.8% for adalimumab biosimilars vs. 84.9% and 93.9% for the originator. In the one comparison of an etanercept biosimilar, mean PAS175 responses were 80.9% for the biosimilar vs. 82.9% for the originator.
In studies involving patients switching from the originator to a biosimilar vs. continuing treatment with the originator, 32-week response rates ranged from 87.0% to 91.3% for adalimumab biosimilars and from 88.2% to 93.2% for the originator. In the one ustekinumab study, the 32-week mean PASI75 response was 92.6% after switching from the originator to a biosimilar vs. 92.9% with continuous treatment with the originator.
At week 52, mean PASI75 responses to adalimumab were between 84.2% and 94.8% for patients who switched to biosimilars and between 88.1% and 93.9% for those who stayed on the originator.
At week 52, in all the randomized trials, the incidence of adverse events and serious adverse events among those who switched to the biosimilar and those who continued with the originator were similar. Two cohort studies showed similar safety outcomes between originators and biosimilars, but one reported more adverse events in patients who switched to adalimumab biosimilars (P = .04).
Three clinical trials showed low risk for bias, 11 had moderate risk, and all cohort studies had moderate to high risk for bias.
Experts weigh in
Asked to comment on the study, Steven R. Feldman, MD, PhD, professor of dermatology at Wake Forest University, Winston-Salem, N.C., told this news organization that he expects that the results will affect patient care.
However, he added, “I believe the decision of whether to use a biosimilar instead of the originator biologic may be more in the hands of the insurers than in the hands of physicians and patients.
“Biologics for psoriasis are so complicated that even the originator products vary from batch to batch. A biosimilar is basically like another batch of the innovative product,” explained Dr. Feldman, who was not involved in the study. “If we’re comfortable with patients being on different batches of the innovator product, we probably should be comfortable with them being on a biosimilar, as we have more evidence for the similarity of the biosimilar than we do for the current batch of the originator product.”
Aída Lugo-Somolinos, MD, professor of dermatology and director of the Contact Dermatitis Clinic at the University of North Carolina, Chapel Hill, said that “biologics have become the treatment of choice for moderate to severe psoriasis, and the use of biosimilars may be an alternative to reduce psoriasis treatment costs.
“Unfortunately, this study included a comparison of the existing biosimilars, which are drugs that are not the first line of treatment for psoriasis any longer,” added Dr. Lugo-Somolinos, who was not involved in the study.
Neil J. Korman, MD, PhD, professor of dermatology and codirector of the Skin Study Center at Case Western Reserve University, Cleveland, said the study was an important systematic review.
“This is a very timely publication because in the United States, several biosimilars are reaching the market in 2023,” he said. “The costs of the originator biologics are extraordinarily high, and the promise of biosimilars is that their costs will be significantly lower.”
Because all the studies were short term, Dr. Korman, who was not involved in the study, joins the study authors in recommending further related research into the long-term safety and efficacy of these agents.
Dr. Feldman, as well as one study author and one editorial author, reported relevant relationships with various pharmaceutical companies, including those that develop biosimilars. The remaining study authors, as well as Dr. Lugo-Somolinos and Dr. Korman, reported no relevant relationships. The study was funded by the Psoriasis Association and supported by the NIHR (National Institute for Health and Care Research) Manchester Biomedical Research Centre. All outside experts commented by email.
The effectiveness and safety of biosimilars for psoriasis appear to be similar to the originator biologics, reported the authors of a review of studies comparing the two.
“This systematic review found that there was no clinically or statistically significant difference in the efficacy and safety between biosimilars and originators of adalimumab, etanercept, infliximab, and ustekinumab for the treatment of psoriasis,” senior study author and clinical lecturer Zenas Z. N. Yiu, MBChB, PhD, and his colleagues at the University of Manchester, England, wrote in JAMA Dermatology.“The biosimilars evaluated in this study could be considered alongside originators for biologic-naive patients to improve the accessibility of biological treatments,” they added. “Switching patients currently on originators to biosimilars could be considered where clinically appropriate to reduce treatment costs.”
Biologics versus biosimilars
In contrast to most chemically synthesized drugs, biologics are created from living organisms, and they have complex structures that can vary slightly from batch to batch, Luigi Naldi, MD, director of the department of dermatology of Ospedale San Bortolo, Vicenza, Italy, and Antonio Addis, PharmD, researcher in the department of epidemiology, Regione Lazio, in Rome, wrote in an accompanying editorial.
Once the patent on the “originator” biologic expires, U.S. and European regulators allow other manufacturers to develop similar molecules – biosimilars – through an abbreviated approval process. If the results of a limited number of equivalence or noninferiority clinical trials are acceptable, registration for all the indications of the originator is allowed for its biosimilars. Referring to the expense of biologics, Dr. Naldi and Dr. Addis noted that in the United States, “biologics comprise less than 3% of the volume of drugs on the market, but account for more than one-third of all drug spending.”
Systematic review
Dr. Yiu and his colleagues queried standard medical research databases in August 2022, and included 14 randomized clinical trials (10 adalimumab, 2 etanercept, 1 infliximab, and 1 ustekinumab) and 3 cohort studies (1 adalimumab, 1 etanercept, 1 infliximab and etanercept) in their review.
Twelve trials compared biosimilars vs. originators in originator-naive patients, and 11 trials compared switching from originators to biosimilars vs. continuous treatment with the originator.
The researchers found the following:
At week 16, mean PASI75 (Psoriasis Area and Severity Index) response rates ranges from 60.7% to 90.6% for adalimumab biosimilars, vs. 61.5% to 91.7% for the originator. Mean PASI75 responses for the two etanercept biosimilars were 56.1% and 76.7% vs. 55.5% and 73.4% for the originator. In the ustekinumab study, mean PASI75 responses were 86.1% for the biosimilar vs. 84.0% for the originator.
At week 52, mean PASI75 responses were between 86.3% and 92.8% for adalimumab biosimilars vs. 84.9% and 93.9% for the originator. In the one comparison of an etanercept biosimilar, mean PAS175 responses were 80.9% for the biosimilar vs. 82.9% for the originator.
In studies involving patients switching from the originator to a biosimilar vs. continuing treatment with the originator, 32-week response rates ranged from 87.0% to 91.3% for adalimumab biosimilars and from 88.2% to 93.2% for the originator. In the one ustekinumab study, the 32-week mean PASI75 response was 92.6% after switching from the originator to a biosimilar vs. 92.9% with continuous treatment with the originator.
At week 52, mean PASI75 responses to adalimumab were between 84.2% and 94.8% for patients who switched to biosimilars and between 88.1% and 93.9% for those who stayed on the originator.
At week 52, in all the randomized trials, the incidence of adverse events and serious adverse events among those who switched to the biosimilar and those who continued with the originator were similar. Two cohort studies showed similar safety outcomes between originators and biosimilars, but one reported more adverse events in patients who switched to adalimumab biosimilars (P = .04).
Three clinical trials showed low risk for bias, 11 had moderate risk, and all cohort studies had moderate to high risk for bias.
Experts weigh in
Asked to comment on the study, Steven R. Feldman, MD, PhD, professor of dermatology at Wake Forest University, Winston-Salem, N.C., told this news organization that he expects that the results will affect patient care.
However, he added, “I believe the decision of whether to use a biosimilar instead of the originator biologic may be more in the hands of the insurers than in the hands of physicians and patients.
“Biologics for psoriasis are so complicated that even the originator products vary from batch to batch. A biosimilar is basically like another batch of the innovative product,” explained Dr. Feldman, who was not involved in the study. “If we’re comfortable with patients being on different batches of the innovator product, we probably should be comfortable with them being on a biosimilar, as we have more evidence for the similarity of the biosimilar than we do for the current batch of the originator product.”
Aída Lugo-Somolinos, MD, professor of dermatology and director of the Contact Dermatitis Clinic at the University of North Carolina, Chapel Hill, said that “biologics have become the treatment of choice for moderate to severe psoriasis, and the use of biosimilars may be an alternative to reduce psoriasis treatment costs.
“Unfortunately, this study included a comparison of the existing biosimilars, which are drugs that are not the first line of treatment for psoriasis any longer,” added Dr. Lugo-Somolinos, who was not involved in the study.
Neil J. Korman, MD, PhD, professor of dermatology and codirector of the Skin Study Center at Case Western Reserve University, Cleveland, said the study was an important systematic review.
“This is a very timely publication because in the United States, several biosimilars are reaching the market in 2023,” he said. “The costs of the originator biologics are extraordinarily high, and the promise of biosimilars is that their costs will be significantly lower.”
Because all the studies were short term, Dr. Korman, who was not involved in the study, joins the study authors in recommending further related research into the long-term safety and efficacy of these agents.
Dr. Feldman, as well as one study author and one editorial author, reported relevant relationships with various pharmaceutical companies, including those that develop biosimilars. The remaining study authors, as well as Dr. Lugo-Somolinos and Dr. Korman, reported no relevant relationships. The study was funded by the Psoriasis Association and supported by the NIHR (National Institute for Health and Care Research) Manchester Biomedical Research Centre. All outside experts commented by email.
The effectiveness and safety of biosimilars for psoriasis appear to be similar to the originator biologics, reported the authors of a review of studies comparing the two.
“This systematic review found that there was no clinically or statistically significant difference in the efficacy and safety between biosimilars and originators of adalimumab, etanercept, infliximab, and ustekinumab for the treatment of psoriasis,” senior study author and clinical lecturer Zenas Z. N. Yiu, MBChB, PhD, and his colleagues at the University of Manchester, England, wrote in JAMA Dermatology.“The biosimilars evaluated in this study could be considered alongside originators for biologic-naive patients to improve the accessibility of biological treatments,” they added. “Switching patients currently on originators to biosimilars could be considered where clinically appropriate to reduce treatment costs.”
Biologics versus biosimilars
In contrast to most chemically synthesized drugs, biologics are created from living organisms, and they have complex structures that can vary slightly from batch to batch, Luigi Naldi, MD, director of the department of dermatology of Ospedale San Bortolo, Vicenza, Italy, and Antonio Addis, PharmD, researcher in the department of epidemiology, Regione Lazio, in Rome, wrote in an accompanying editorial.
Once the patent on the “originator” biologic expires, U.S. and European regulators allow other manufacturers to develop similar molecules – biosimilars – through an abbreviated approval process. If the results of a limited number of equivalence or noninferiority clinical trials are acceptable, registration for all the indications of the originator is allowed for its biosimilars. Referring to the expense of biologics, Dr. Naldi and Dr. Addis noted that in the United States, “biologics comprise less than 3% of the volume of drugs on the market, but account for more than one-third of all drug spending.”
Systematic review
Dr. Yiu and his colleagues queried standard medical research databases in August 2022, and included 14 randomized clinical trials (10 adalimumab, 2 etanercept, 1 infliximab, and 1 ustekinumab) and 3 cohort studies (1 adalimumab, 1 etanercept, 1 infliximab and etanercept) in their review.
Twelve trials compared biosimilars vs. originators in originator-naive patients, and 11 trials compared switching from originators to biosimilars vs. continuous treatment with the originator.
The researchers found the following:
At week 16, mean PASI75 (Psoriasis Area and Severity Index) response rates ranges from 60.7% to 90.6% for adalimumab biosimilars, vs. 61.5% to 91.7% for the originator. Mean PASI75 responses for the two etanercept biosimilars were 56.1% and 76.7% vs. 55.5% and 73.4% for the originator. In the ustekinumab study, mean PASI75 responses were 86.1% for the biosimilar vs. 84.0% for the originator.
At week 52, mean PASI75 responses were between 86.3% and 92.8% for adalimumab biosimilars vs. 84.9% and 93.9% for the originator. In the one comparison of an etanercept biosimilar, mean PAS175 responses were 80.9% for the biosimilar vs. 82.9% for the originator.
In studies involving patients switching from the originator to a biosimilar vs. continuing treatment with the originator, 32-week response rates ranged from 87.0% to 91.3% for adalimumab biosimilars and from 88.2% to 93.2% for the originator. In the one ustekinumab study, the 32-week mean PASI75 response was 92.6% after switching from the originator to a biosimilar vs. 92.9% with continuous treatment with the originator.
At week 52, mean PASI75 responses to adalimumab were between 84.2% and 94.8% for patients who switched to biosimilars and between 88.1% and 93.9% for those who stayed on the originator.
At week 52, in all the randomized trials, the incidence of adverse events and serious adverse events among those who switched to the biosimilar and those who continued with the originator were similar. Two cohort studies showed similar safety outcomes between originators and biosimilars, but one reported more adverse events in patients who switched to adalimumab biosimilars (P = .04).
Three clinical trials showed low risk for bias, 11 had moderate risk, and all cohort studies had moderate to high risk for bias.
Experts weigh in
Asked to comment on the study, Steven R. Feldman, MD, PhD, professor of dermatology at Wake Forest University, Winston-Salem, N.C., told this news organization that he expects that the results will affect patient care.
However, he added, “I believe the decision of whether to use a biosimilar instead of the originator biologic may be more in the hands of the insurers than in the hands of physicians and patients.
“Biologics for psoriasis are so complicated that even the originator products vary from batch to batch. A biosimilar is basically like another batch of the innovative product,” explained Dr. Feldman, who was not involved in the study. “If we’re comfortable with patients being on different batches of the innovator product, we probably should be comfortable with them being on a biosimilar, as we have more evidence for the similarity of the biosimilar than we do for the current batch of the originator product.”
Aída Lugo-Somolinos, MD, professor of dermatology and director of the Contact Dermatitis Clinic at the University of North Carolina, Chapel Hill, said that “biologics have become the treatment of choice for moderate to severe psoriasis, and the use of biosimilars may be an alternative to reduce psoriasis treatment costs.
“Unfortunately, this study included a comparison of the existing biosimilars, which are drugs that are not the first line of treatment for psoriasis any longer,” added Dr. Lugo-Somolinos, who was not involved in the study.
Neil J. Korman, MD, PhD, professor of dermatology and codirector of the Skin Study Center at Case Western Reserve University, Cleveland, said the study was an important systematic review.
“This is a very timely publication because in the United States, several biosimilars are reaching the market in 2023,” he said. “The costs of the originator biologics are extraordinarily high, and the promise of biosimilars is that their costs will be significantly lower.”
Because all the studies were short term, Dr. Korman, who was not involved in the study, joins the study authors in recommending further related research into the long-term safety and efficacy of these agents.
Dr. Feldman, as well as one study author and one editorial author, reported relevant relationships with various pharmaceutical companies, including those that develop biosimilars. The remaining study authors, as well as Dr. Lugo-Somolinos and Dr. Korman, reported no relevant relationships. The study was funded by the Psoriasis Association and supported by the NIHR (National Institute for Health and Care Research) Manchester Biomedical Research Centre. All outside experts commented by email.
FROM JAMA DERMATOLOGY
WHO plans to declare common sweetener as possible carcinogen
The World Health Organization is set to list the artificial sweetener aspartame as a possible carcinogen.
The move, reported by multiple media sources, is expected during a July 14 meeting of WHO research experts – the International Agency for Research on Cancer. Reuters cited two unnamed sources “with knowledge of the process,” noting that aspartame is one of the world’s most commonly used sweeteners.
Aspartame is 200 times sweeter than sugar and was first approved by the Food and Drug Administration in 1974 for use as a tabletop sweetener and in chewing gum and cold breakfast cereals, as well as instant coffee, gelatins, puddings and fillings, and dairy products. Up to 95% of carbonated soft drinks that have a sweetener use aspartame, and the substance is often added by consumers to beverages (it’s the blue packet of sweetener in the array of packets that appear on diner and restaurant tables), The Washington Post reported.
The WHO currently lists 126 agents as known to be carcinogenic to humans, ranging from alcohol and tobacco to outdoor air pollution. The WHO also lists 94 agents as “probably” carcinogenic to humans and 322 agents as “possibly” carcinogenic to humans. Aspartame would join the “possibly” group, which includes gasoline engine exhaust and working as a dry cleaner.
Earlier this year, the WHO warned that people should not use nonsugar sweeteners to control their weight because of potential health risks.
A version of this article originally appeared on WebMD.com.
The World Health Organization is set to list the artificial sweetener aspartame as a possible carcinogen.
The move, reported by multiple media sources, is expected during a July 14 meeting of WHO research experts – the International Agency for Research on Cancer. Reuters cited two unnamed sources “with knowledge of the process,” noting that aspartame is one of the world’s most commonly used sweeteners.
Aspartame is 200 times sweeter than sugar and was first approved by the Food and Drug Administration in 1974 for use as a tabletop sweetener and in chewing gum and cold breakfast cereals, as well as instant coffee, gelatins, puddings and fillings, and dairy products. Up to 95% of carbonated soft drinks that have a sweetener use aspartame, and the substance is often added by consumers to beverages (it’s the blue packet of sweetener in the array of packets that appear on diner and restaurant tables), The Washington Post reported.
The WHO currently lists 126 agents as known to be carcinogenic to humans, ranging from alcohol and tobacco to outdoor air pollution. The WHO also lists 94 agents as “probably” carcinogenic to humans and 322 agents as “possibly” carcinogenic to humans. Aspartame would join the “possibly” group, which includes gasoline engine exhaust and working as a dry cleaner.
Earlier this year, the WHO warned that people should not use nonsugar sweeteners to control their weight because of potential health risks.
A version of this article originally appeared on WebMD.com.
The World Health Organization is set to list the artificial sweetener aspartame as a possible carcinogen.
The move, reported by multiple media sources, is expected during a July 14 meeting of WHO research experts – the International Agency for Research on Cancer. Reuters cited two unnamed sources “with knowledge of the process,” noting that aspartame is one of the world’s most commonly used sweeteners.
Aspartame is 200 times sweeter than sugar and was first approved by the Food and Drug Administration in 1974 for use as a tabletop sweetener and in chewing gum and cold breakfast cereals, as well as instant coffee, gelatins, puddings and fillings, and dairy products. Up to 95% of carbonated soft drinks that have a sweetener use aspartame, and the substance is often added by consumers to beverages (it’s the blue packet of sweetener in the array of packets that appear on diner and restaurant tables), The Washington Post reported.
The WHO currently lists 126 agents as known to be carcinogenic to humans, ranging from alcohol and tobacco to outdoor air pollution. The WHO also lists 94 agents as “probably” carcinogenic to humans and 322 agents as “possibly” carcinogenic to humans. Aspartame would join the “possibly” group, which includes gasoline engine exhaust and working as a dry cleaner.
Earlier this year, the WHO warned that people should not use nonsugar sweeteners to control their weight because of potential health risks.
A version of this article originally appeared on WebMD.com.
Residency match process under scrutiny again, this time by AMA
The American Medical Association is considering whether to study alternatives to the current residency matching program in an effort to improve residents’ compensation and other job-related issues. A recent call-to-action resolution by the AMA’s House of Delegates is the latest in a long string of debates about whether to change the annual process that matches future doctors with compatible residency programs.
AMA’s Resident and Fellow Section introduced the resolution in March, and the delegates approved it earlier in June at AMA’s annual meeting. The resolution states that the match process of the National Resident Matching Program (NRMP) “poses significant anticompetition concerns.” Those include preventing residents from negotiating for higher wages, better benefits, and improved working conditions, according to the approved resolution.
The full AMA board still has to consider the resolution and hasn’t set a date for that review, though it’s expected to be in the next few months, according to Jennifer Sellers, AMA’s public information officer. She said in an interview that the organization declined to comment, wanting to hold off until the board decides how to proceed.
The NRMP, which oversees the matching process, told this news organization that the AMA doesn’t play a role in the Match.
The organization doesn’t believe studying alternative placement methods benefits applicants and residents, and returning to a pre-Match environment, would harm applicants and programs, according to Donna Lamb, DHSc, MBA, BSN, president and CEO.
“The NRMP has no role in determining, publishing, or setting resident salaries nor does the NRMP have a role in the contracting or employment of residents, and it never has.”
Dr. Lamb said changing the Match would “subject applicants to undue pressure and coercion to accept an offer of training. This will exacerbate disparities in candidate selection already evident in medical education and potentially result in salary reductions in more competitive specialties and in more desirable geographic locations.”
The latest push to reform the match process dates back two decades to a 2002 class action antitrust lawsuit by residents and doctors against the NRMP and other organizations involved in the Match.
The residents argued at that time that by restraining competition among teaching hospitals, the matching system allowed hospitals to keep residents’ wages artificially low. The defendants, which included large teaching hospitals, successfully lobbied Congress for an exemption to the antitrust laws, and the case was subsequently dismissed.
The AMA was one of the defendants, so if it moves forward to review the match process, it likely would pit the organization against the NRMP.
Sherman Marek, the attorney who represented the residents, said in an interview that he was not surprised by the latest AMA resolution. “Maybe the AMA leadership has come around to the idea that it’s better for young physicians to not have the match in place,” he says. “I would applaud that sort of evolution.”
Tyler Ramsey, DO, an internal medicine resident and AMA member, said he believes the group’s current president, Jesse Ehrenfeld, MD, MPH, empathizes with doctors in training. “I think he understands [our] views and is more progressive.”
The NRMP also has considered ways to improve the match process to make it easier and more equitable for applicants. In its latest effort, the organization is studying whether programs should certify their rank order list in advance of applicants. This change would give applicants more flexibility to visit residency locations before the programs consider changing their rankings, Dr. Lamb explained. The NRMP also is mulling the possibilities of a two-phase match after deciding in 2022 not to move forward with a previous version of the proposal.
The recent House of Delegates resolution states that “residents are using other means to obtain fair wages, safe working conditions, and other benefits that are unable to be negotiated within the current system.”
Dr. Ramsey, who trains in North Carolina, said the “other means” may include negotiating through a union. “The AMA realizes that there is a problem and that people are unionizing,” he said. “Obviously, as an organization, we’re not doing something correctly, to the point where people are feeling the need to get their rights a different way.”
The Committee of Interns and Residents, which represents 30,000 members, reported a rise in medical trainee unions across the country in 2022.
Not everyone believes that ditching the Match would benefit applicants and residents. Sam Payabvash, MD, assistant professor of radiology at Yale, New Haven, Conn., School of Medicine, tweeted about the resolution as part of a larger Twitter discussion that alternatives are likely to be “more onerous and expensive for applicants.”
An advantage of the match program, Dr. Lamb argued, is that it “improves the reach of applicants into medically underserved communities through widespread program participation.”
Dr. Ramsey agreed that the match program has benefits and drawbacks, but he believes it favors programs over residents. “It comes as no surprise that numerous residents suffer from depression and our suicide rates are the highest amongst all professions due to the lack of control or negotiation of fair salary and working conditions. Overall, the way things are now, residents just do not have a lot of rights.”
A version of this article originally appeared on Medscape.com.
The American Medical Association is considering whether to study alternatives to the current residency matching program in an effort to improve residents’ compensation and other job-related issues. A recent call-to-action resolution by the AMA’s House of Delegates is the latest in a long string of debates about whether to change the annual process that matches future doctors with compatible residency programs.
AMA’s Resident and Fellow Section introduced the resolution in March, and the delegates approved it earlier in June at AMA’s annual meeting. The resolution states that the match process of the National Resident Matching Program (NRMP) “poses significant anticompetition concerns.” Those include preventing residents from negotiating for higher wages, better benefits, and improved working conditions, according to the approved resolution.
The full AMA board still has to consider the resolution and hasn’t set a date for that review, though it’s expected to be in the next few months, according to Jennifer Sellers, AMA’s public information officer. She said in an interview that the organization declined to comment, wanting to hold off until the board decides how to proceed.
The NRMP, which oversees the matching process, told this news organization that the AMA doesn’t play a role in the Match.
The organization doesn’t believe studying alternative placement methods benefits applicants and residents, and returning to a pre-Match environment, would harm applicants and programs, according to Donna Lamb, DHSc, MBA, BSN, president and CEO.
“The NRMP has no role in determining, publishing, or setting resident salaries nor does the NRMP have a role in the contracting or employment of residents, and it never has.”
Dr. Lamb said changing the Match would “subject applicants to undue pressure and coercion to accept an offer of training. This will exacerbate disparities in candidate selection already evident in medical education and potentially result in salary reductions in more competitive specialties and in more desirable geographic locations.”
The latest push to reform the match process dates back two decades to a 2002 class action antitrust lawsuit by residents and doctors against the NRMP and other organizations involved in the Match.
The residents argued at that time that by restraining competition among teaching hospitals, the matching system allowed hospitals to keep residents’ wages artificially low. The defendants, which included large teaching hospitals, successfully lobbied Congress for an exemption to the antitrust laws, and the case was subsequently dismissed.
The AMA was one of the defendants, so if it moves forward to review the match process, it likely would pit the organization against the NRMP.
Sherman Marek, the attorney who represented the residents, said in an interview that he was not surprised by the latest AMA resolution. “Maybe the AMA leadership has come around to the idea that it’s better for young physicians to not have the match in place,” he says. “I would applaud that sort of evolution.”
Tyler Ramsey, DO, an internal medicine resident and AMA member, said he believes the group’s current president, Jesse Ehrenfeld, MD, MPH, empathizes with doctors in training. “I think he understands [our] views and is more progressive.”
The NRMP also has considered ways to improve the match process to make it easier and more equitable for applicants. In its latest effort, the organization is studying whether programs should certify their rank order list in advance of applicants. This change would give applicants more flexibility to visit residency locations before the programs consider changing their rankings, Dr. Lamb explained. The NRMP also is mulling the possibilities of a two-phase match after deciding in 2022 not to move forward with a previous version of the proposal.
The recent House of Delegates resolution states that “residents are using other means to obtain fair wages, safe working conditions, and other benefits that are unable to be negotiated within the current system.”
Dr. Ramsey, who trains in North Carolina, said the “other means” may include negotiating through a union. “The AMA realizes that there is a problem and that people are unionizing,” he said. “Obviously, as an organization, we’re not doing something correctly, to the point where people are feeling the need to get their rights a different way.”
The Committee of Interns and Residents, which represents 30,000 members, reported a rise in medical trainee unions across the country in 2022.
Not everyone believes that ditching the Match would benefit applicants and residents. Sam Payabvash, MD, assistant professor of radiology at Yale, New Haven, Conn., School of Medicine, tweeted about the resolution as part of a larger Twitter discussion that alternatives are likely to be “more onerous and expensive for applicants.”
An advantage of the match program, Dr. Lamb argued, is that it “improves the reach of applicants into medically underserved communities through widespread program participation.”
Dr. Ramsey agreed that the match program has benefits and drawbacks, but he believes it favors programs over residents. “It comes as no surprise that numerous residents suffer from depression and our suicide rates are the highest amongst all professions due to the lack of control or negotiation of fair salary and working conditions. Overall, the way things are now, residents just do not have a lot of rights.”
A version of this article originally appeared on Medscape.com.
The American Medical Association is considering whether to study alternatives to the current residency matching program in an effort to improve residents’ compensation and other job-related issues. A recent call-to-action resolution by the AMA’s House of Delegates is the latest in a long string of debates about whether to change the annual process that matches future doctors with compatible residency programs.
AMA’s Resident and Fellow Section introduced the resolution in March, and the delegates approved it earlier in June at AMA’s annual meeting. The resolution states that the match process of the National Resident Matching Program (NRMP) “poses significant anticompetition concerns.” Those include preventing residents from negotiating for higher wages, better benefits, and improved working conditions, according to the approved resolution.
The full AMA board still has to consider the resolution and hasn’t set a date for that review, though it’s expected to be in the next few months, according to Jennifer Sellers, AMA’s public information officer. She said in an interview that the organization declined to comment, wanting to hold off until the board decides how to proceed.
The NRMP, which oversees the matching process, told this news organization that the AMA doesn’t play a role in the Match.
The organization doesn’t believe studying alternative placement methods benefits applicants and residents, and returning to a pre-Match environment, would harm applicants and programs, according to Donna Lamb, DHSc, MBA, BSN, president and CEO.
“The NRMP has no role in determining, publishing, or setting resident salaries nor does the NRMP have a role in the contracting or employment of residents, and it never has.”
Dr. Lamb said changing the Match would “subject applicants to undue pressure and coercion to accept an offer of training. This will exacerbate disparities in candidate selection already evident in medical education and potentially result in salary reductions in more competitive specialties and in more desirable geographic locations.”
The latest push to reform the match process dates back two decades to a 2002 class action antitrust lawsuit by residents and doctors against the NRMP and other organizations involved in the Match.
The residents argued at that time that by restraining competition among teaching hospitals, the matching system allowed hospitals to keep residents’ wages artificially low. The defendants, which included large teaching hospitals, successfully lobbied Congress for an exemption to the antitrust laws, and the case was subsequently dismissed.
The AMA was one of the defendants, so if it moves forward to review the match process, it likely would pit the organization against the NRMP.
Sherman Marek, the attorney who represented the residents, said in an interview that he was not surprised by the latest AMA resolution. “Maybe the AMA leadership has come around to the idea that it’s better for young physicians to not have the match in place,” he says. “I would applaud that sort of evolution.”
Tyler Ramsey, DO, an internal medicine resident and AMA member, said he believes the group’s current president, Jesse Ehrenfeld, MD, MPH, empathizes with doctors in training. “I think he understands [our] views and is more progressive.”
The NRMP also has considered ways to improve the match process to make it easier and more equitable for applicants. In its latest effort, the organization is studying whether programs should certify their rank order list in advance of applicants. This change would give applicants more flexibility to visit residency locations before the programs consider changing their rankings, Dr. Lamb explained. The NRMP also is mulling the possibilities of a two-phase match after deciding in 2022 not to move forward with a previous version of the proposal.
The recent House of Delegates resolution states that “residents are using other means to obtain fair wages, safe working conditions, and other benefits that are unable to be negotiated within the current system.”
Dr. Ramsey, who trains in North Carolina, said the “other means” may include negotiating through a union. “The AMA realizes that there is a problem and that people are unionizing,” he said. “Obviously, as an organization, we’re not doing something correctly, to the point where people are feeling the need to get their rights a different way.”
The Committee of Interns and Residents, which represents 30,000 members, reported a rise in medical trainee unions across the country in 2022.
Not everyone believes that ditching the Match would benefit applicants and residents. Sam Payabvash, MD, assistant professor of radiology at Yale, New Haven, Conn., School of Medicine, tweeted about the resolution as part of a larger Twitter discussion that alternatives are likely to be “more onerous and expensive for applicants.”
An advantage of the match program, Dr. Lamb argued, is that it “improves the reach of applicants into medically underserved communities through widespread program participation.”
Dr. Ramsey agreed that the match program has benefits and drawbacks, but he believes it favors programs over residents. “It comes as no surprise that numerous residents suffer from depression and our suicide rates are the highest amongst all professions due to the lack of control or negotiation of fair salary and working conditions. Overall, the way things are now, residents just do not have a lot of rights.”
A version of this article originally appeared on Medscape.com.
Safety first: Regulations
The word “regulations” gets a mixed response.
This is common in all industries, and certainly pharmaceuticals. On any given day there are stories on industry news sites about disputes between companies and regulatory agencies.
I’d agree that some regulation is needed. The history of pharmacy has had both remarkable successes – and failures.

Let’s look at migraines, since that’s in my field. The calcitonin gene-related peptide (CGRP) drugs have been a remarkable breakthrough, certainly the biggest one since the triptans in 1992. There are currently seven on the market for both prevention and abortive use. They’re effective and (to date) pretty safe.
But it wasn’t always that way. Look back just 14 years ago to 2009, when the first promising CGRP agent (MK-3207) had its development halted because of hepatic abnormalities. It’s cousin telcagepant (MK-0974) came to a similar end 2 years later.
Without regulations in place (and the potential for lawsuits) these might have made it to market, bringing migraine relief to some and potentially serious liver damage to others. So Merck made the right decision to axe them. Researchers learned from the experience, went back to the drawing board, and developed the current generation of far-safer drugs.
This came into sharp focus in another industry recently, when the eyes of the world were on the north Atlantic. A small tourist submarine imploded and killed five people. During the inevitable media coverage it came out that the submarine hadn’t been certified for safety by any of the agencies that handle such things, falling into a gray area in international waters where inspections aren’t required.
This isn’t to say it wasn’t safe – it had made several dives before – but obviously not safe enough. While I didn’t know the late Stockton Rush (the owner/designer) it sounds like he viewed regulations as stifling innovation, and in one interview said “at some point, safety is just pure waste.” He ignored warnings from several sides about the submersible’s ability to handle deep ocean pressure and the inevitable wear and tear repeated dives will have on the hull.
I understand there’s a margin of luck, too. Bad things can happen to any of us – or any company. Some things can’t be clearly foreseen. Some drugs don’t start to show problems until they’re on the market and reach a certain number of prescriptions.
But there’s a reason we have regulations. Pretty much every government has, going back to the Roman Empire, covering numerous things. In a perfect world we wouldn’t need them.
But people are far from perfect. And the consequences can be terrible.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.
The word “regulations” gets a mixed response.
This is common in all industries, and certainly pharmaceuticals. On any given day there are stories on industry news sites about disputes between companies and regulatory agencies.
I’d agree that some regulation is needed. The history of pharmacy has had both remarkable successes – and failures.
Let’s look at migraines, since that’s in my field. The calcitonin gene-related peptide (CGRP) drugs have been a remarkable breakthrough, certainly the biggest one since the triptans in 1992. There are currently seven on the market for both prevention and abortive use. They’re effective and (to date) pretty safe.
But it wasn’t always that way. Look back just 14 years ago to 2009, when the first promising CGRP agent (MK-3207) had its development halted because of hepatic abnormalities. It’s cousin telcagepant (MK-0974) came to a similar end 2 years later.
Without regulations in place (and the potential for lawsuits) these might have made it to market, bringing migraine relief to some and potentially serious liver damage to others. So Merck made the right decision to axe them. Researchers learned from the experience, went back to the drawing board, and developed the current generation of far-safer drugs.
This came into sharp focus in another industry recently, when the eyes of the world were on the north Atlantic. A small tourist submarine imploded and killed five people. During the inevitable media coverage it came out that the submarine hadn’t been certified for safety by any of the agencies that handle such things, falling into a gray area in international waters where inspections aren’t required.
This isn’t to say it wasn’t safe – it had made several dives before – but obviously not safe enough. While I didn’t know the late Stockton Rush (the owner/designer) it sounds like he viewed regulations as stifling innovation, and in one interview said “at some point, safety is just pure waste.” He ignored warnings from several sides about the submersible’s ability to handle deep ocean pressure and the inevitable wear and tear repeated dives will have on the hull.
I understand there’s a margin of luck, too. Bad things can happen to any of us – or any company. Some things can’t be clearly foreseen. Some drugs don’t start to show problems until they’re on the market and reach a certain number of prescriptions.
But there’s a reason we have regulations. Pretty much every government has, going back to the Roman Empire, covering numerous things. In a perfect world we wouldn’t need them.
But people are far from perfect. And the consequences can be terrible.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.
The word “regulations” gets a mixed response.
This is common in all industries, and certainly pharmaceuticals. On any given day there are stories on industry news sites about disputes between companies and regulatory agencies.
I’d agree that some regulation is needed. The history of pharmacy has had both remarkable successes – and failures.
Let’s look at migraines, since that’s in my field. The calcitonin gene-related peptide (CGRP) drugs have been a remarkable breakthrough, certainly the biggest one since the triptans in 1992. There are currently seven on the market for both prevention and abortive use. They’re effective and (to date) pretty safe.
But it wasn’t always that way. Look back just 14 years ago to 2009, when the first promising CGRP agent (MK-3207) had its development halted because of hepatic abnormalities. It’s cousin telcagepant (MK-0974) came to a similar end 2 years later.
Without regulations in place (and the potential for lawsuits) these might have made it to market, bringing migraine relief to some and potentially serious liver damage to others. So Merck made the right decision to axe them. Researchers learned from the experience, went back to the drawing board, and developed the current generation of far-safer drugs.
This came into sharp focus in another industry recently, when the eyes of the world were on the north Atlantic. A small tourist submarine imploded and killed five people. During the inevitable media coverage it came out that the submarine hadn’t been certified for safety by any of the agencies that handle such things, falling into a gray area in international waters where inspections aren’t required.
This isn’t to say it wasn’t safe – it had made several dives before – but obviously not safe enough. While I didn’t know the late Stockton Rush (the owner/designer) it sounds like he viewed regulations as stifling innovation, and in one interview said “at some point, safety is just pure waste.” He ignored warnings from several sides about the submersible’s ability to handle deep ocean pressure and the inevitable wear and tear repeated dives will have on the hull.
I understand there’s a margin of luck, too. Bad things can happen to any of us – or any company. Some things can’t be clearly foreseen. Some drugs don’t start to show problems until they’re on the market and reach a certain number of prescriptions.
But there’s a reason we have regulations. Pretty much every government has, going back to the Roman Empire, covering numerous things. In a perfect world we wouldn’t need them.
But people are far from perfect. And the consequences can be terrible.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.
Interventional psychiatry: What are the next steps?
The explosion of interest in interventional psychiatry is highlighted by 2 recent reviews published in
Psychiatry’s failure to address these changes would be a dire error, as psychiatrists could lose control of our field’s advances and growth. But this creates an even larger question: what are the next steps we need to take? We believe interventional psychiatry must be recognized as its own psychiatric subspeciality, receive greater emphasis in psychiatry residency training, and be subject to standardization by professional organizations.
Psychiatry has incorporated procedures into patient care for almost 100 years, starting with electroconvulsive therapy (ECT) and insulin shock therapy in the 1930s.3,4 However, in the last 10 years, the rapid expansion of FDA approvals of neuromodulation procedures to treat psychiatric conditions (including vagus nerve stimulation in 2005, transcranial magnetic stimulation [TMS] in 2008, and the device exception granted for the use of deep brain stimulation in 2009) has produced the moniker “interventional psychiatry” for this unofficial psychiatric subspeciality.5,6
If we are to establish interventional psychiatry as a recognized subspeciality, it is important to create a universally accepted definition. We propose the term refer to therapeutic techniques or processes that may or may not be invasive but require special training to perform. Additionally, interventional psychiatry should include even minimally invasive procedures, such as ketamine infusions, medication implants, long-acting injectable (LAI) medications, and processes that require a Risk Evaluation and Mitigation Strategy (REMS), such as those utilized with clozapine, esketamine, or olanzapine for extended-release injectable suspension7 (see “Risk Evaluation and Mitigation Strategy programs: How they can be improved”). The proportions of clinicians who prescribe clozapine (7%)8 or LAIs (32.1% to 77.7%, depending on the patient population being treated)9,10 is evidence that the interventional nature of these treatments creates obstacles to their use.
This vacuum of adequate training among psychiatrists has caused interventional psychiatry to grow beyond the confines of the psychiatric field. In most metropolitan areas of the United States, there are clinicians who focus on a specific interventional treatment, such as ketamine infusions or TMS administration. The creation of these specialized clinics has frequently been pioneered by nonpsychiatrists, such as anesthesiologists. This may be attributed to these clinicians’ level of comfort with procedures, or because they possess an infrastructure within their practice that facilitates delivery of the services. In certain states with independent-practice laws, midlevel clinicians are granted permission to open these clinics. However, having nonpsychiatrists provide these treatments to patients with complex psychiatric disorders without psychiatrist involvement makes it less likely that the appropriateness of treatment will be determined, or that the treatment will be incorporated into the patient’s overall biopsychosocial treatment plan.
A gap in training
There is evidence the growth of interventional psychiatry has exceeded the capacity of the current training infrastructure to provide trainees with adequate exposure to these procedures. The Accreditation Council for Graduate Medical Education requires that psychiatry residents be trained in the indications for and use of ECT and neuromodulation therapies but does not provide any specifics about how this training should occur,11 and the Psychiatry Milestones do not indicate how competency in these therapies can be achieved.12 Most trainees have exposure to some interventional treatments, such as ECT or clozapine administration, during residency. However, in 1 survey, only 63% of residents had prescribed clozapine, and 83% indicated they wanted additional experience.13 In a survey of 91 training programs, 75% stated that ECT was required of residents, but 37% estimated that a typical resident would participate in <10 treatments.14 Even more surprising, 27% estimated that the typical resident would care for <5 patients receiving ECT.14
Addressing the changing role of interventional practices in our field must occur on multiple levels, starting with a core curriculum during residency training, expanded learning opportunities for residents with a specific interest in interventional psychiatry, and, most important, a formal interventional psychiatry fellowship leading to certification from the American Board of Medical Specialties.5,6 There are growing numbers of 1-year fellowship programs that offer extensive experiences in neuromodulation and novel pharmacologic treatment and may produce the next generation of leaders in this field. However, training in interventional psychiatry techniques for practicing psychiatrists wishing to expand their treatment offerings is generally quite limited.
Oversight of interventional psychiatry training should be performed by peers. Therefore, creation of an interventional psychiatry society, or a work group within a larger organization, is necessary. While much of this already exists, it is fragmented into associations focused on unique aspects of interventional psychiatry, such as just ECT (eg, International Society for ECT and Neurostimulation), just TMS (eg, Clinical TMS Society), or just ketamine (eg, the American Society of Ketamine Physicians). Despite disparate foci, the goal would be for all to unite into a parent interventional organization that can face these challenges. These organizations have already united a core of individual interventional psychiatrists who can lead psychiatry into the future. They can provide input into guidelines, minimal standards, procedures, protocols, and outcome measures. They also can address any ethical issues that may arise with the use of more invasive treatments.
Change, especially the monumental changes in practice that accompany interventional psychiatry, is both exciting and intimidating. However, certain “growing pains” along the way require urgent consideration. Ultimately, as a field, we either adapt to change or get left behind.
1. Arbuck D, Farooqui A, El-Mallakh RS. Interventional psychiatry (Part 1). Current Psychiatry. 2023;22(5):25-35. doi:10.12788/cp.0356
2. Arbuck D, Farooqui A, El-Mallakh RS. Interventional psychiatry (Part 2). Current Psychiatry. 2023;22(7):27-35. doi:10.12788/cp.0364
3. Jones K. Insulin coma therapy in schizophrenia. J R Soc Med. 2000;93(3):147-149. doi:10.1177/014107680009300313
4. Gazdag G, Ungvari GS. Electroconvulsive therapy: 80 years old and still going strong. World J Psychiatry. 2019;9(1):1-6. doi:10.5498/wjp.v9.i1.1
5. Williams NR, Taylor JJ, Snipes JM, et al. Interventional psychiatry: how should psychiatric educators incorporate neuromodulation into training? Acad Psychiatry. 2014;38(2):168-176. doi:10.1007/s40596-014-0050-x
6. Trapp NT, Williams NR. The future of training and practice in neuromodulation: an interventional psychiatry perspective. Front Psychiatry. 2021;12:734487. doi:10.3389/fpsyt.2021.734487
7. Vincent KM, Ryan M, Palmer E, et al. Interventional psychiatry. Postgrad Med. 2020;132(7):573-574. doi:10.1080/00325481.2020.1727671
8. Tang Y, Horvitz-Lennon M, Gellad WF, et al. Prescribing of clozapine and antipsychotic polypharmacy for schizophrenia in a large Medicaid program. Psychiatr Serv. 2017;68(6):579-586. doi:10.1176/appi.ps.201600041
9. Zhdanava M, Starr HL, Lefebvre P, et al. Understanding the health system conditions affecting the use of long-acting injectable antipsychotics in the treatment of schizophrenia in clinical practice: a US healthcare provider survey. Neuropsychiatr Dis Treat. 2022;18:1479-1493. doi:10.2147/NDT.S369494
10. Bunting SR, Chalmers K, Yohanna D, et al. Prescription of long-acting injectable antipsychotic medications among outpatient mental health care service providers. Psychiatr Serv. 2023:appips20220586. doi:10.1176/appi.ps.20220586
11. Accreditation Council for Graduate Medical Education. Common program requirements. July 2022. Accessed June 6, 2023. https://www.acgme.org/programs-and-institutions/programs/common-program-requirements
12. Kinzie JM, DeJong SM, Edgar L, et al. Psychiatry Milestones 2.0: using the supplemental guide to create a shared model of the development of professional identity and expertise. Acad Psychiatry. 2021;45(4):500-505. doi:10.1007/s40596-021-01455-6
13. Singh B, Hughes AJ, Roerig JL. Comfort level and barriers to the appropriate use of clozapine: a preliminary survey of US psychiatric residents. Acad Psychiatry. 2020;44(1):53-58 doi:10.1007/s40596-019-01134-7
14. Dinwiddie SH, Spitz D. Resident education in electroconvulsive therapy. J ECT. 2010;26(4):310-316. doi:10.1097/YCT.0b013e3181cb5f78
The explosion of interest in interventional psychiatry is highlighted by 2 recent reviews published in
Psychiatry’s failure to address these changes would be a dire error, as psychiatrists could lose control of our field’s advances and growth. But this creates an even larger question: what are the next steps we need to take? We believe interventional psychiatry must be recognized as its own psychiatric subspeciality, receive greater emphasis in psychiatry residency training, and be subject to standardization by professional organizations.
Psychiatry has incorporated procedures into patient care for almost 100 years, starting with electroconvulsive therapy (ECT) and insulin shock therapy in the 1930s.3,4 However, in the last 10 years, the rapid expansion of FDA approvals of neuromodulation procedures to treat psychiatric conditions (including vagus nerve stimulation in 2005, transcranial magnetic stimulation [TMS] in 2008, and the device exception granted for the use of deep brain stimulation in 2009) has produced the moniker “interventional psychiatry” for this unofficial psychiatric subspeciality.5,6
If we are to establish interventional psychiatry as a recognized subspeciality, it is important to create a universally accepted definition. We propose the term refer to therapeutic techniques or processes that may or may not be invasive but require special training to perform. Additionally, interventional psychiatry should include even minimally invasive procedures, such as ketamine infusions, medication implants, long-acting injectable (LAI) medications, and processes that require a Risk Evaluation and Mitigation Strategy (REMS), such as those utilized with clozapine, esketamine, or olanzapine for extended-release injectable suspension7 (see “Risk Evaluation and Mitigation Strategy programs: How they can be improved”). The proportions of clinicians who prescribe clozapine (7%)8 or LAIs (32.1% to 77.7%, depending on the patient population being treated)9,10 is evidence that the interventional nature of these treatments creates obstacles to their use.
This vacuum of adequate training among psychiatrists has caused interventional psychiatry to grow beyond the confines of the psychiatric field. In most metropolitan areas of the United States, there are clinicians who focus on a specific interventional treatment, such as ketamine infusions or TMS administration. The creation of these specialized clinics has frequently been pioneered by nonpsychiatrists, such as anesthesiologists. This may be attributed to these clinicians’ level of comfort with procedures, or because they possess an infrastructure within their practice that facilitates delivery of the services. In certain states with independent-practice laws, midlevel clinicians are granted permission to open these clinics. However, having nonpsychiatrists provide these treatments to patients with complex psychiatric disorders without psychiatrist involvement makes it less likely that the appropriateness of treatment will be determined, or that the treatment will be incorporated into the patient’s overall biopsychosocial treatment plan.
A gap in training
There is evidence the growth of interventional psychiatry has exceeded the capacity of the current training infrastructure to provide trainees with adequate exposure to these procedures. The Accreditation Council for Graduate Medical Education requires that psychiatry residents be trained in the indications for and use of ECT and neuromodulation therapies but does not provide any specifics about how this training should occur,11 and the Psychiatry Milestones do not indicate how competency in these therapies can be achieved.12 Most trainees have exposure to some interventional treatments, such as ECT or clozapine administration, during residency. However, in 1 survey, only 63% of residents had prescribed clozapine, and 83% indicated they wanted additional experience.13 In a survey of 91 training programs, 75% stated that ECT was required of residents, but 37% estimated that a typical resident would participate in <10 treatments.14 Even more surprising, 27% estimated that the typical resident would care for <5 patients receiving ECT.14
Addressing the changing role of interventional practices in our field must occur on multiple levels, starting with a core curriculum during residency training, expanded learning opportunities for residents with a specific interest in interventional psychiatry, and, most important, a formal interventional psychiatry fellowship leading to certification from the American Board of Medical Specialties.5,6 There are growing numbers of 1-year fellowship programs that offer extensive experiences in neuromodulation and novel pharmacologic treatment and may produce the next generation of leaders in this field. However, training in interventional psychiatry techniques for practicing psychiatrists wishing to expand their treatment offerings is generally quite limited.
Oversight of interventional psychiatry training should be performed by peers. Therefore, creation of an interventional psychiatry society, or a work group within a larger organization, is necessary. While much of this already exists, it is fragmented into associations focused on unique aspects of interventional psychiatry, such as just ECT (eg, International Society for ECT and Neurostimulation), just TMS (eg, Clinical TMS Society), or just ketamine (eg, the American Society of Ketamine Physicians). Despite disparate foci, the goal would be for all to unite into a parent interventional organization that can face these challenges. These organizations have already united a core of individual interventional psychiatrists who can lead psychiatry into the future. They can provide input into guidelines, minimal standards, procedures, protocols, and outcome measures. They also can address any ethical issues that may arise with the use of more invasive treatments.
Change, especially the monumental changes in practice that accompany interventional psychiatry, is both exciting and intimidating. However, certain “growing pains” along the way require urgent consideration. Ultimately, as a field, we either adapt to change or get left behind.
The explosion of interest in interventional psychiatry is highlighted by 2 recent reviews published in
Psychiatry’s failure to address these changes would be a dire error, as psychiatrists could lose control of our field’s advances and growth. But this creates an even larger question: what are the next steps we need to take? We believe interventional psychiatry must be recognized as its own psychiatric subspeciality, receive greater emphasis in psychiatry residency training, and be subject to standardization by professional organizations.
Psychiatry has incorporated procedures into patient care for almost 100 years, starting with electroconvulsive therapy (ECT) and insulin shock therapy in the 1930s.3,4 However, in the last 10 years, the rapid expansion of FDA approvals of neuromodulation procedures to treat psychiatric conditions (including vagus nerve stimulation in 2005, transcranial magnetic stimulation [TMS] in 2008, and the device exception granted for the use of deep brain stimulation in 2009) has produced the moniker “interventional psychiatry” for this unofficial psychiatric subspeciality.5,6
If we are to establish interventional psychiatry as a recognized subspeciality, it is important to create a universally accepted definition. We propose the term refer to therapeutic techniques or processes that may or may not be invasive but require special training to perform. Additionally, interventional psychiatry should include even minimally invasive procedures, such as ketamine infusions, medication implants, long-acting injectable (LAI) medications, and processes that require a Risk Evaluation and Mitigation Strategy (REMS), such as those utilized with clozapine, esketamine, or olanzapine for extended-release injectable suspension7 (see “Risk Evaluation and Mitigation Strategy programs: How they can be improved”). The proportions of clinicians who prescribe clozapine (7%)8 or LAIs (32.1% to 77.7%, depending on the patient population being treated)9,10 is evidence that the interventional nature of these treatments creates obstacles to their use.
This vacuum of adequate training among psychiatrists has caused interventional psychiatry to grow beyond the confines of the psychiatric field. In most metropolitan areas of the United States, there are clinicians who focus on a specific interventional treatment, such as ketamine infusions or TMS administration. The creation of these specialized clinics has frequently been pioneered by nonpsychiatrists, such as anesthesiologists. This may be attributed to these clinicians’ level of comfort with procedures, or because they possess an infrastructure within their practice that facilitates delivery of the services. In certain states with independent-practice laws, midlevel clinicians are granted permission to open these clinics. However, having nonpsychiatrists provide these treatments to patients with complex psychiatric disorders without psychiatrist involvement makes it less likely that the appropriateness of treatment will be determined, or that the treatment will be incorporated into the patient’s overall biopsychosocial treatment plan.
A gap in training
There is evidence the growth of interventional psychiatry has exceeded the capacity of the current training infrastructure to provide trainees with adequate exposure to these procedures. The Accreditation Council for Graduate Medical Education requires that psychiatry residents be trained in the indications for and use of ECT and neuromodulation therapies but does not provide any specifics about how this training should occur,11 and the Psychiatry Milestones do not indicate how competency in these therapies can be achieved.12 Most trainees have exposure to some interventional treatments, such as ECT or clozapine administration, during residency. However, in 1 survey, only 63% of residents had prescribed clozapine, and 83% indicated they wanted additional experience.13 In a survey of 91 training programs, 75% stated that ECT was required of residents, but 37% estimated that a typical resident would participate in <10 treatments.14 Even more surprising, 27% estimated that the typical resident would care for <5 patients receiving ECT.14
Addressing the changing role of interventional practices in our field must occur on multiple levels, starting with a core curriculum during residency training, expanded learning opportunities for residents with a specific interest in interventional psychiatry, and, most important, a formal interventional psychiatry fellowship leading to certification from the American Board of Medical Specialties.5,6 There are growing numbers of 1-year fellowship programs that offer extensive experiences in neuromodulation and novel pharmacologic treatment and may produce the next generation of leaders in this field. However, training in interventional psychiatry techniques for practicing psychiatrists wishing to expand their treatment offerings is generally quite limited.
Oversight of interventional psychiatry training should be performed by peers. Therefore, creation of an interventional psychiatry society, or a work group within a larger organization, is necessary. While much of this already exists, it is fragmented into associations focused on unique aspects of interventional psychiatry, such as just ECT (eg, International Society for ECT and Neurostimulation), just TMS (eg, Clinical TMS Society), or just ketamine (eg, the American Society of Ketamine Physicians). Despite disparate foci, the goal would be for all to unite into a parent interventional organization that can face these challenges. These organizations have already united a core of individual interventional psychiatrists who can lead psychiatry into the future. They can provide input into guidelines, minimal standards, procedures, protocols, and outcome measures. They also can address any ethical issues that may arise with the use of more invasive treatments.
Change, especially the monumental changes in practice that accompany interventional psychiatry, is both exciting and intimidating. However, certain “growing pains” along the way require urgent consideration. Ultimately, as a field, we either adapt to change or get left behind.
1. Arbuck D, Farooqui A, El-Mallakh RS. Interventional psychiatry (Part 1). Current Psychiatry. 2023;22(5):25-35. doi:10.12788/cp.0356
2. Arbuck D, Farooqui A, El-Mallakh RS. Interventional psychiatry (Part 2). Current Psychiatry. 2023;22(7):27-35. doi:10.12788/cp.0364
3. Jones K. Insulin coma therapy in schizophrenia. J R Soc Med. 2000;93(3):147-149. doi:10.1177/014107680009300313
4. Gazdag G, Ungvari GS. Electroconvulsive therapy: 80 years old and still going strong. World J Psychiatry. 2019;9(1):1-6. doi:10.5498/wjp.v9.i1.1
5. Williams NR, Taylor JJ, Snipes JM, et al. Interventional psychiatry: how should psychiatric educators incorporate neuromodulation into training? Acad Psychiatry. 2014;38(2):168-176. doi:10.1007/s40596-014-0050-x
6. Trapp NT, Williams NR. The future of training and practice in neuromodulation: an interventional psychiatry perspective. Front Psychiatry. 2021;12:734487. doi:10.3389/fpsyt.2021.734487
7. Vincent KM, Ryan M, Palmer E, et al. Interventional psychiatry. Postgrad Med. 2020;132(7):573-574. doi:10.1080/00325481.2020.1727671
8. Tang Y, Horvitz-Lennon M, Gellad WF, et al. Prescribing of clozapine and antipsychotic polypharmacy for schizophrenia in a large Medicaid program. Psychiatr Serv. 2017;68(6):579-586. doi:10.1176/appi.ps.201600041
9. Zhdanava M, Starr HL, Lefebvre P, et al. Understanding the health system conditions affecting the use of long-acting injectable antipsychotics in the treatment of schizophrenia in clinical practice: a US healthcare provider survey. Neuropsychiatr Dis Treat. 2022;18:1479-1493. doi:10.2147/NDT.S369494
10. Bunting SR, Chalmers K, Yohanna D, et al. Prescription of long-acting injectable antipsychotic medications among outpatient mental health care service providers. Psychiatr Serv. 2023:appips20220586. doi:10.1176/appi.ps.20220586
11. Accreditation Council for Graduate Medical Education. Common program requirements. July 2022. Accessed June 6, 2023. https://www.acgme.org/programs-and-institutions/programs/common-program-requirements
12. Kinzie JM, DeJong SM, Edgar L, et al. Psychiatry Milestones 2.0: using the supplemental guide to create a shared model of the development of professional identity and expertise. Acad Psychiatry. 2021;45(4):500-505. doi:10.1007/s40596-021-01455-6
13. Singh B, Hughes AJ, Roerig JL. Comfort level and barriers to the appropriate use of clozapine: a preliminary survey of US psychiatric residents. Acad Psychiatry. 2020;44(1):53-58 doi:10.1007/s40596-019-01134-7
14. Dinwiddie SH, Spitz D. Resident education in electroconvulsive therapy. J ECT. 2010;26(4):310-316. doi:10.1097/YCT.0b013e3181cb5f78
1. Arbuck D, Farooqui A, El-Mallakh RS. Interventional psychiatry (Part 1). Current Psychiatry. 2023;22(5):25-35. doi:10.12788/cp.0356
2. Arbuck D, Farooqui A, El-Mallakh RS. Interventional psychiatry (Part 2). Current Psychiatry. 2023;22(7):27-35. doi:10.12788/cp.0364
3. Jones K. Insulin coma therapy in schizophrenia. J R Soc Med. 2000;93(3):147-149. doi:10.1177/014107680009300313
4. Gazdag G, Ungvari GS. Electroconvulsive therapy: 80 years old and still going strong. World J Psychiatry. 2019;9(1):1-6. doi:10.5498/wjp.v9.i1.1
5. Williams NR, Taylor JJ, Snipes JM, et al. Interventional psychiatry: how should psychiatric educators incorporate neuromodulation into training? Acad Psychiatry. 2014;38(2):168-176. doi:10.1007/s40596-014-0050-x
6. Trapp NT, Williams NR. The future of training and practice in neuromodulation: an interventional psychiatry perspective. Front Psychiatry. 2021;12:734487. doi:10.3389/fpsyt.2021.734487
7. Vincent KM, Ryan M, Palmer E, et al. Interventional psychiatry. Postgrad Med. 2020;132(7):573-574. doi:10.1080/00325481.2020.1727671
8. Tang Y, Horvitz-Lennon M, Gellad WF, et al. Prescribing of clozapine and antipsychotic polypharmacy for schizophrenia in a large Medicaid program. Psychiatr Serv. 2017;68(6):579-586. doi:10.1176/appi.ps.201600041
9. Zhdanava M, Starr HL, Lefebvre P, et al. Understanding the health system conditions affecting the use of long-acting injectable antipsychotics in the treatment of schizophrenia in clinical practice: a US healthcare provider survey. Neuropsychiatr Dis Treat. 2022;18:1479-1493. doi:10.2147/NDT.S369494
10. Bunting SR, Chalmers K, Yohanna D, et al. Prescription of long-acting injectable antipsychotic medications among outpatient mental health care service providers. Psychiatr Serv. 2023:appips20220586. doi:10.1176/appi.ps.20220586
11. Accreditation Council for Graduate Medical Education. Common program requirements. July 2022. Accessed June 6, 2023. https://www.acgme.org/programs-and-institutions/programs/common-program-requirements
12. Kinzie JM, DeJong SM, Edgar L, et al. Psychiatry Milestones 2.0: using the supplemental guide to create a shared model of the development of professional identity and expertise. Acad Psychiatry. 2021;45(4):500-505. doi:10.1007/s40596-021-01455-6
13. Singh B, Hughes AJ, Roerig JL. Comfort level and barriers to the appropriate use of clozapine: a preliminary survey of US psychiatric residents. Acad Psychiatry. 2020;44(1):53-58 doi:10.1007/s40596-019-01134-7
14. Dinwiddie SH, Spitz D. Resident education in electroconvulsive therapy. J ECT. 2010;26(4):310-316. doi:10.1097/YCT.0b013e3181cb5f78

Will the doctor see you now? The health system’s changing landscape
Lucia Agajanian, a 25-year-old freelance film producer in Chicago, doesn’t have a specific primary care doctor, preferring the convenience of visiting a local clinic for flu shots or going online for video visits. “You say what you need, and there’s a 15-minute wait time,” she said, explaining how her appointments usually work. “I really liked that.”
But Olga Lucia Torres, a 52-year-old who teaches narrative medicine classes at Columbia University in New York, misses her longtime primary care doctor, who kept tabs for two decades on her conditions, including lupus and rheumatoid arthritis, and made sure she was up to date on vaccines and screening tests. Two years ago, Torres received a letter informing her that he was changing to a “boutique practice” and would charge a retainer fee of $10,000 for her to stay on as a patient.
“I felt really sad and abandoned,” Ms. Torres said. “This was my PCP. I was like, ‘Dude, I thought we were in this together!’ ”
The two women reflect an ongoing reality: The primary care landscape is changing in ways that could shape patients’ access and quality of care now and for decades to come. A solid and enduring relationship with a primary care doctor – who knows a patient’s history and can monitor new problems – has long been regarded as the bedrock of a quality health care system. But investment in primary care in the U.S. lags behind that of other high-income countries, and America has a smaller share of primary care physicians than most of its European counterparts.
An estimated one-third of all physicians in the U.S. are primary care doctors – who include family medicine physicians, general internists, and pediatricians – according to the Robert Graham Center, a research and analysis organization that studies primary care. Other researchers say the numbers are lower, with the Peterson-KFF Health System Tracker reporting only 12% of U.S. doctors are generalists, compared with 23% in Germany and as many as 45% in the Netherlands.
That means it’s often hard to find a doctor and make an appointment that’s not weeks or months away.
“This is a problem that has been simmering and now beginning to erupt in some communities at a boil. It’s hard to find that front door of the health system,” said Ann Greiner, president and CEO of the Primary Care Collaborative, a nonprofit membership organization.
Today, a smaller percentage of physicians are entering the field than are practicing, suggesting that shortages will worsen over time.
Interest has waned partly because, in the U.S., primary care yields lower salaries than other medical and surgical specialties.
Some doctors now in practice also say they are burned out, facing cumbersome electronic health record systems and limits on appointment times, making it harder to get to know a patient and establish a relationship.
Others are retiring or selling their practices. Hospitals, insurers like Aetna-CVS Health, and other corporate entities like Amazon are on a buying spree, snapping up primary care practices, furthering a move away from the “Marcus Welby, M.D.”-style neighborhood doctor. About 48% of primary care physicians currently work in practices they do not own. Two-thirds of those doctors don’t work for other physicians but are employed by private equity investors or other corporate entities, according to data in the “Primary Care Chartbook,” which is collected and published by the Graham Center.
Patients who seek care at these offices may not be seen by the same doctor at every visit. Indeed, they may not be seen by a doctor at all but by a paraprofessional – a nurse practitioner or a physician assistant, for instance – who works under the doctor’s license. That trend has been accelerated by new state laws – as well as changes in Medicare policy – that loosen the requirements for physician supervisors and billing. And these jobs are expected to be among the decade’s fastest-growing in the health sector.
Overall, demand for primary care is up, spurred partly by record enrollment in Affordable Care Act plans. All those new patients, combined with the low supply of doctors, are contributing to a years-long downward trend in the number of people reporting they have a usual source of care, be it an individual doctor or a specific clinic or practice.
Researchers say that raises questions, including whether people can’t find a primary care doctor, can’t afford one, or simply no longer want an established relationship.
“Is it poor access or problems with the supply of providers? Does it reflect a societal disconnection, a go-it-alone phenomenon?” asked Christopher F. Koller, president of the Milbank Memorial Fund, a foundation whose nonpartisan analyses focus on state health policy.
For patients, frustrating wait times are one result. A recent survey by a physician staffing firm found it now takes an average of 21 days just to get in to see a doctor of family medicine, defined as a subgroup of primary care, which includes general internists and pediatricians. Those physicians are many patients’ first stop for health care. That runs counter to the trend in other countries, where patients complain of months- or years-long waits for elective procedures like hip replacements but generally experience short waits for primary care visits.
Another complication: All these factors are adding urgency to ongoing concerns about attracting new primary care physicians to the specialty.
When she was in medical school, Natalie A. Cameron, MD, specifically chose primary care because she enjoyed forming relationships with patients and because “I’m specifically interested in prevention and women’s health, and you do a lot of that in primary care.” The 33-year-old is currently an instructor of medicine at Northwestern University, Chicago, where she also sees patients at a primary care practice.
Still, she understands why many of her colleagues chose something else. For some, it’s the pay differential. For others, it’s because of primary care’s reputation for involving “a lot of care and paperwork and coordinating a lot of issues that may not just be medical,” Dr. Cameron said.
The million-dollar question, then, is how much does having a usual source of care influence medical outcomes and cost? And for which kinds of patients is having a close relationship with a doctor important? While studies show that many young people value the convenience of visiting urgent care – especially when it takes so long to see a primary care doctor – will their long-term health suffer because of that strategy?
Many patients – particularly the young and generally healthy ones – shrug at the new normal, embracing alternatives that require less waiting. These options are particularly attractive to millennials, who tell focus groups that the convenience of a one-off video call or visit to a big-box store clinic trumps a long-standing relationship with a doctor, especially if they have to wait days, weeks, or longer for a traditional appointment.
“The doctor I have is a family friend, but definitely I would take access and ease over a relationship,” said Matt Degn, 24, who says it can take two to three months to book a routine appointment in Salt Lake City, where he lives.
Patients are increasingly turning to what are dubbed “retail clinics,” such as CVS’ Minute Clinics, which tout “in-person and virtual care 7 days a week.” CVS Health’s more than 1,000 clinics inside stores across the U.S. treated more than 5 million people last year, Creagh Milford, a physician and the company’s senior vice president of retail health, said in a written statement. He cited a recent study by a data products firm showing the use of retail clinics has grown 200% over the past five years.
Health policy experts say increased access to alternatives can be good, but forgoing an ongoing relationship to a regular provider is not, especially as people get older and are more likely to develop chronic conditions or other medical problems.
“There’s a lot of data that show communities with a lot of primary care have better health,” said Mr. Koller.
People with a regular primary care doctor or practice are more likely to get preventive care, such as cancer screenings or flu shots, studies show, and are less likely to die if they do suffer a heart attack.
Physicians who see patients regularly are better able to spot patterns of seemingly minor concerns that could add up to a serious health issue.
“What happens when you go to four different providers on four platforms for urinary tract infections because, well, they are just UTIs,” posed Yalda Jabbarpour, MD, a family physician practicing in Washington, and the director of the Robert Graham Center for Policy Studies. “But actually, you have a large kidney stone that’s causing your UTI or have some sort of immune deficiency like diabetes that’s causing frequent UTIs. But no one tested you.”
Most experts agree that figuring out how to coordinate care amid this changing landscape and make it more accessible without undermining quality – even when different doctors, locations, health systems, and electronic health records are involved – will be as complex as the pressures causing long waits and less interest in today’s primary care market.
And experiences sometimes lead patients to change their minds.
There’s something to be said for establishing a relationship, said Ms. Agajanian, in Chicago. She’s rethinking her decision to cobble together care, rather than have a specific primary care doctor or clinic, following an injury at work last year that led to shoulder surgery.
“As I’m getting older, even though I’m still young,” she said, “I have all these problems with my body, and it would be nice to have a consistent person who knows all my problems to talk with.”
KFF Health News’ Colleen DeGuzman contributed to this report.
KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF – an independent source of health policy research, polling, and journalism. Learn more about KFF.
Lucia Agajanian, a 25-year-old freelance film producer in Chicago, doesn’t have a specific primary care doctor, preferring the convenience of visiting a local clinic for flu shots or going online for video visits. “You say what you need, and there’s a 15-minute wait time,” she said, explaining how her appointments usually work. “I really liked that.”
But Olga Lucia Torres, a 52-year-old who teaches narrative medicine classes at Columbia University in New York, misses her longtime primary care doctor, who kept tabs for two decades on her conditions, including lupus and rheumatoid arthritis, and made sure she was up to date on vaccines and screening tests. Two years ago, Torres received a letter informing her that he was changing to a “boutique practice” and would charge a retainer fee of $10,000 for her to stay on as a patient.
“I felt really sad and abandoned,” Ms. Torres said. “This was my PCP. I was like, ‘Dude, I thought we were in this together!’ ”
The two women reflect an ongoing reality: The primary care landscape is changing in ways that could shape patients’ access and quality of care now and for decades to come. A solid and enduring relationship with a primary care doctor – who knows a patient’s history and can monitor new problems – has long been regarded as the bedrock of a quality health care system. But investment in primary care in the U.S. lags behind that of other high-income countries, and America has a smaller share of primary care physicians than most of its European counterparts.
An estimated one-third of all physicians in the U.S. are primary care doctors – who include family medicine physicians, general internists, and pediatricians – according to the Robert Graham Center, a research and analysis organization that studies primary care. Other researchers say the numbers are lower, with the Peterson-KFF Health System Tracker reporting only 12% of U.S. doctors are generalists, compared with 23% in Germany and as many as 45% in the Netherlands.
That means it’s often hard to find a doctor and make an appointment that’s not weeks or months away.
“This is a problem that has been simmering and now beginning to erupt in some communities at a boil. It’s hard to find that front door of the health system,” said Ann Greiner, president and CEO of the Primary Care Collaborative, a nonprofit membership organization.
Today, a smaller percentage of physicians are entering the field than are practicing, suggesting that shortages will worsen over time.
Interest has waned partly because, in the U.S., primary care yields lower salaries than other medical and surgical specialties.
Some doctors now in practice also say they are burned out, facing cumbersome electronic health record systems and limits on appointment times, making it harder to get to know a patient and establish a relationship.
Others are retiring or selling their practices. Hospitals, insurers like Aetna-CVS Health, and other corporate entities like Amazon are on a buying spree, snapping up primary care practices, furthering a move away from the “Marcus Welby, M.D.”-style neighborhood doctor. About 48% of primary care physicians currently work in practices they do not own. Two-thirds of those doctors don’t work for other physicians but are employed by private equity investors or other corporate entities, according to data in the “Primary Care Chartbook,” which is collected and published by the Graham Center.
Patients who seek care at these offices may not be seen by the same doctor at every visit. Indeed, they may not be seen by a doctor at all but by a paraprofessional – a nurse practitioner or a physician assistant, for instance – who works under the doctor’s license. That trend has been accelerated by new state laws – as well as changes in Medicare policy – that loosen the requirements for physician supervisors and billing. And these jobs are expected to be among the decade’s fastest-growing in the health sector.
Overall, demand for primary care is up, spurred partly by record enrollment in Affordable Care Act plans. All those new patients, combined with the low supply of doctors, are contributing to a years-long downward trend in the number of people reporting they have a usual source of care, be it an individual doctor or a specific clinic or practice.
Researchers say that raises questions, including whether people can’t find a primary care doctor, can’t afford one, or simply no longer want an established relationship.
“Is it poor access or problems with the supply of providers? Does it reflect a societal disconnection, a go-it-alone phenomenon?” asked Christopher F. Koller, president of the Milbank Memorial Fund, a foundation whose nonpartisan analyses focus on state health policy.
For patients, frustrating wait times are one result. A recent survey by a physician staffing firm found it now takes an average of 21 days just to get in to see a doctor of family medicine, defined as a subgroup of primary care, which includes general internists and pediatricians. Those physicians are many patients’ first stop for health care. That runs counter to the trend in other countries, where patients complain of months- or years-long waits for elective procedures like hip replacements but generally experience short waits for primary care visits.
Another complication: All these factors are adding urgency to ongoing concerns about attracting new primary care physicians to the specialty.
When she was in medical school, Natalie A. Cameron, MD, specifically chose primary care because she enjoyed forming relationships with patients and because “I’m specifically interested in prevention and women’s health, and you do a lot of that in primary care.” The 33-year-old is currently an instructor of medicine at Northwestern University, Chicago, where she also sees patients at a primary care practice.
Still, she understands why many of her colleagues chose something else. For some, it’s the pay differential. For others, it’s because of primary care’s reputation for involving “a lot of care and paperwork and coordinating a lot of issues that may not just be medical,” Dr. Cameron said.
The million-dollar question, then, is how much does having a usual source of care influence medical outcomes and cost? And for which kinds of patients is having a close relationship with a doctor important? While studies show that many young people value the convenience of visiting urgent care – especially when it takes so long to see a primary care doctor – will their long-term health suffer because of that strategy?
Many patients – particularly the young and generally healthy ones – shrug at the new normal, embracing alternatives that require less waiting. These options are particularly attractive to millennials, who tell focus groups that the convenience of a one-off video call or visit to a big-box store clinic trumps a long-standing relationship with a doctor, especially if they have to wait days, weeks, or longer for a traditional appointment.
“The doctor I have is a family friend, but definitely I would take access and ease over a relationship,” said Matt Degn, 24, who says it can take two to three months to book a routine appointment in Salt Lake City, where he lives.
Patients are increasingly turning to what are dubbed “retail clinics,” such as CVS’ Minute Clinics, which tout “in-person and virtual care 7 days a week.” CVS Health’s more than 1,000 clinics inside stores across the U.S. treated more than 5 million people last year, Creagh Milford, a physician and the company’s senior vice president of retail health, said in a written statement. He cited a recent study by a data products firm showing the use of retail clinics has grown 200% over the past five years.
Health policy experts say increased access to alternatives can be good, but forgoing an ongoing relationship to a regular provider is not, especially as people get older and are more likely to develop chronic conditions or other medical problems.
“There’s a lot of data that show communities with a lot of primary care have better health,” said Mr. Koller.
People with a regular primary care doctor or practice are more likely to get preventive care, such as cancer screenings or flu shots, studies show, and are less likely to die if they do suffer a heart attack.
Physicians who see patients regularly are better able to spot patterns of seemingly minor concerns that could add up to a serious health issue.
“What happens when you go to four different providers on four platforms for urinary tract infections because, well, they are just UTIs,” posed Yalda Jabbarpour, MD, a family physician practicing in Washington, and the director of the Robert Graham Center for Policy Studies. “But actually, you have a large kidney stone that’s causing your UTI or have some sort of immune deficiency like diabetes that’s causing frequent UTIs. But no one tested you.”
Most experts agree that figuring out how to coordinate care amid this changing landscape and make it more accessible without undermining quality – even when different doctors, locations, health systems, and electronic health records are involved – will be as complex as the pressures causing long waits and less interest in today’s primary care market.
And experiences sometimes lead patients to change their minds.
There’s something to be said for establishing a relationship, said Ms. Agajanian, in Chicago. She’s rethinking her decision to cobble together care, rather than have a specific primary care doctor or clinic, following an injury at work last year that led to shoulder surgery.
“As I’m getting older, even though I’m still young,” she said, “I have all these problems with my body, and it would be nice to have a consistent person who knows all my problems to talk with.”
KFF Health News’ Colleen DeGuzman contributed to this report.
KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF – an independent source of health policy research, polling, and journalism. Learn more about KFF.
Lucia Agajanian, a 25-year-old freelance film producer in Chicago, doesn’t have a specific primary care doctor, preferring the convenience of visiting a local clinic for flu shots or going online for video visits. “You say what you need, and there’s a 15-minute wait time,” she said, explaining how her appointments usually work. “I really liked that.”
But Olga Lucia Torres, a 52-year-old who teaches narrative medicine classes at Columbia University in New York, misses her longtime primary care doctor, who kept tabs for two decades on her conditions, including lupus and rheumatoid arthritis, and made sure she was up to date on vaccines and screening tests. Two years ago, Torres received a letter informing her that he was changing to a “boutique practice” and would charge a retainer fee of $10,000 for her to stay on as a patient.
“I felt really sad and abandoned,” Ms. Torres said. “This was my PCP. I was like, ‘Dude, I thought we were in this together!’ ”
The two women reflect an ongoing reality: The primary care landscape is changing in ways that could shape patients’ access and quality of care now and for decades to come. A solid and enduring relationship with a primary care doctor – who knows a patient’s history and can monitor new problems – has long been regarded as the bedrock of a quality health care system. But investment in primary care in the U.S. lags behind that of other high-income countries, and America has a smaller share of primary care physicians than most of its European counterparts.
An estimated one-third of all physicians in the U.S. are primary care doctors – who include family medicine physicians, general internists, and pediatricians – according to the Robert Graham Center, a research and analysis organization that studies primary care. Other researchers say the numbers are lower, with the Peterson-KFF Health System Tracker reporting only 12% of U.S. doctors are generalists, compared with 23% in Germany and as many as 45% in the Netherlands.
That means it’s often hard to find a doctor and make an appointment that’s not weeks or months away.
“This is a problem that has been simmering and now beginning to erupt in some communities at a boil. It’s hard to find that front door of the health system,” said Ann Greiner, president and CEO of the Primary Care Collaborative, a nonprofit membership organization.
Today, a smaller percentage of physicians are entering the field than are practicing, suggesting that shortages will worsen over time.
Interest has waned partly because, in the U.S., primary care yields lower salaries than other medical and surgical specialties.
Some doctors now in practice also say they are burned out, facing cumbersome electronic health record systems and limits on appointment times, making it harder to get to know a patient and establish a relationship.
Others are retiring or selling their practices. Hospitals, insurers like Aetna-CVS Health, and other corporate entities like Amazon are on a buying spree, snapping up primary care practices, furthering a move away from the “Marcus Welby, M.D.”-style neighborhood doctor. About 48% of primary care physicians currently work in practices they do not own. Two-thirds of those doctors don’t work for other physicians but are employed by private equity investors or other corporate entities, according to data in the “Primary Care Chartbook,” which is collected and published by the Graham Center.
Patients who seek care at these offices may not be seen by the same doctor at every visit. Indeed, they may not be seen by a doctor at all but by a paraprofessional – a nurse practitioner or a physician assistant, for instance – who works under the doctor’s license. That trend has been accelerated by new state laws – as well as changes in Medicare policy – that loosen the requirements for physician supervisors and billing. And these jobs are expected to be among the decade’s fastest-growing in the health sector.
Overall, demand for primary care is up, spurred partly by record enrollment in Affordable Care Act plans. All those new patients, combined with the low supply of doctors, are contributing to a years-long downward trend in the number of people reporting they have a usual source of care, be it an individual doctor or a specific clinic or practice.
Researchers say that raises questions, including whether people can’t find a primary care doctor, can’t afford one, or simply no longer want an established relationship.
“Is it poor access or problems with the supply of providers? Does it reflect a societal disconnection, a go-it-alone phenomenon?” asked Christopher F. Koller, president of the Milbank Memorial Fund, a foundation whose nonpartisan analyses focus on state health policy.
For patients, frustrating wait times are one result. A recent survey by a physician staffing firm found it now takes an average of 21 days just to get in to see a doctor of family medicine, defined as a subgroup of primary care, which includes general internists and pediatricians. Those physicians are many patients’ first stop for health care. That runs counter to the trend in other countries, where patients complain of months- or years-long waits for elective procedures like hip replacements but generally experience short waits for primary care visits.
Another complication: All these factors are adding urgency to ongoing concerns about attracting new primary care physicians to the specialty.
When she was in medical school, Natalie A. Cameron, MD, specifically chose primary care because she enjoyed forming relationships with patients and because “I’m specifically interested in prevention and women’s health, and you do a lot of that in primary care.” The 33-year-old is currently an instructor of medicine at Northwestern University, Chicago, where she also sees patients at a primary care practice.
Still, she understands why many of her colleagues chose something else. For some, it’s the pay differential. For others, it’s because of primary care’s reputation for involving “a lot of care and paperwork and coordinating a lot of issues that may not just be medical,” Dr. Cameron said.
The million-dollar question, then, is how much does having a usual source of care influence medical outcomes and cost? And for which kinds of patients is having a close relationship with a doctor important? While studies show that many young people value the convenience of visiting urgent care – especially when it takes so long to see a primary care doctor – will their long-term health suffer because of that strategy?
Many patients – particularly the young and generally healthy ones – shrug at the new normal, embracing alternatives that require less waiting. These options are particularly attractive to millennials, who tell focus groups that the convenience of a one-off video call or visit to a big-box store clinic trumps a long-standing relationship with a doctor, especially if they have to wait days, weeks, or longer for a traditional appointment.
“The doctor I have is a family friend, but definitely I would take access and ease over a relationship,” said Matt Degn, 24, who says it can take two to three months to book a routine appointment in Salt Lake City, where he lives.
Patients are increasingly turning to what are dubbed “retail clinics,” such as CVS’ Minute Clinics, which tout “in-person and virtual care 7 days a week.” CVS Health’s more than 1,000 clinics inside stores across the U.S. treated more than 5 million people last year, Creagh Milford, a physician and the company’s senior vice president of retail health, said in a written statement. He cited a recent study by a data products firm showing the use of retail clinics has grown 200% over the past five years.
Health policy experts say increased access to alternatives can be good, but forgoing an ongoing relationship to a regular provider is not, especially as people get older and are more likely to develop chronic conditions or other medical problems.
“There’s a lot of data that show communities with a lot of primary care have better health,” said Mr. Koller.
People with a regular primary care doctor or practice are more likely to get preventive care, such as cancer screenings or flu shots, studies show, and are less likely to die if they do suffer a heart attack.
Physicians who see patients regularly are better able to spot patterns of seemingly minor concerns that could add up to a serious health issue.
“What happens when you go to four different providers on four platforms for urinary tract infections because, well, they are just UTIs,” posed Yalda Jabbarpour, MD, a family physician practicing in Washington, and the director of the Robert Graham Center for Policy Studies. “But actually, you have a large kidney stone that’s causing your UTI or have some sort of immune deficiency like diabetes that’s causing frequent UTIs. But no one tested you.”
Most experts agree that figuring out how to coordinate care amid this changing landscape and make it more accessible without undermining quality – even when different doctors, locations, health systems, and electronic health records are involved – will be as complex as the pressures causing long waits and less interest in today’s primary care market.
And experiences sometimes lead patients to change their minds.
There’s something to be said for establishing a relationship, said Ms. Agajanian, in Chicago. She’s rethinking her decision to cobble together care, rather than have a specific primary care doctor or clinic, following an injury at work last year that led to shoulder surgery.
“As I’m getting older, even though I’m still young,” she said, “I have all these problems with my body, and it would be nice to have a consistent person who knows all my problems to talk with.”
KFF Health News’ Colleen DeGuzman contributed to this report.
KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF – an independent source of health policy research, polling, and journalism. Learn more about KFF.
New DEA CME mandate affects 2 million prescribers
The Consolidated Appropriations Act of 2023 mandates that all Drug Enforcement Administration–registered physicians and health care providers complete a one-time, 8-hour CME training on managing and treating opioid and other substance abuse disorders. This requirement goes into effect on June 27, 2023. New DEA registrants must also comply. Veterinarians are exempt.
A DEA registration is required to prescribe any controlled substance. The DEA categorizes these as Schedule I-V, with V being the least likely to be abused (Table 1). For example, opioids like fentanyl, oxycodone, and morphine are Schedule II. Medications without abuse potential are not scheduled.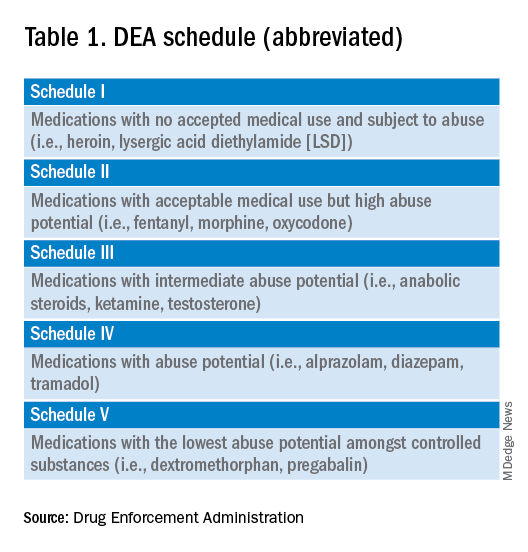
Will 16 million hours of opioid education save lives?
One should not underestimate the sweeping scope of this new federal requirement. DEA registrants include physicians and other health care providers such as nurse practitioners, physician assistants, and dentists. That is 8 hours per provider x 2 million providers: 16 million hours of CME!
Many states already require 1 or more hours of opioid training and pain management as part of their relicensure requirements (Table 2). To avoid redundancy, the DEA-mandated 8-hour training satisfies the various states’ requirements. 
An uncompensated mandate
Physicians are no strangers to lifelong learning and most eagerly pursue educational opportunities. Though some physicians may have CME time and stipends allocated by their employers, many others, such as the approximately 50,000 locum tenens doctors, do not. However, as enthusiastic as these physicians may be about this new CME course, they will likely lose a day of seeing patients (and income) to comply with this new obligation.
Not just pain doctors
The mandate’s broad brush includes many health care providers who hold DEA certificates but do not prescribe opioids. For example, as a general neurologist and epileptologist, I do not treat patients with chronic pain and cannot remember the last time I wrote an opioid prescription. However, I frequently prescribe lacosamide, a Schedule V drug. A surprisingly large number of antiseizure drugs are Schedule III, IV, or V drugs (Table 3).
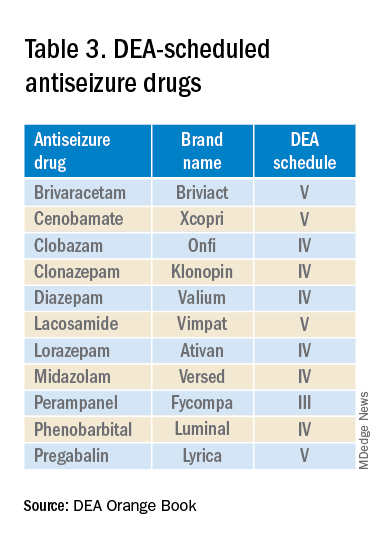
Real-world abuse?
How often scheduled antiseizure drugs are diverted or abused in an epilepsy population is unknown but appears to be infrequent. For example, perampanel abuse has not been reported despite its classification as a Schedule III drug. Anecdotally, in more than 40 years of clinical practice, I have never known a patient with epilepsy to abuse their antiseizure medications.
Take the course
Many organizations are happy to charge for the new 8-hour course. For example, the Tennessee Medical Association offers the training for $299 online or $400 in person. Materials from Elite Learning satisfy the 8-hour requirement for $80. However, NEJM Knowledge+ provides a complimentary 10-hour DEA-compliant course.
I recently completed the NEJM course. The information was thorough and took the whole 10 hours to finish. As excellent as it was, the content was only tangentially relevant to my clinical practice.
Conclusions
To obtain or renew a DEA certificate, neurologists, epilepsy specialists, and many other health care providers must comply with the new 8-hour CME opioid training mandate. Because the course requires 1 day to complete, health care providers would be prudent to obtain their CME well before their DEA certificate expires.
Though efforts to control the morbidity and mortality of the opioid epidemic are laudatory, perhaps the training should be more targeted to physicians who actually prescribe opioids rather than every DEA registrant. In the meantime, whether 16 million CME hours will save lives remains to be seen.
Dr. Wilner is professor of neurology at the University of Tennessee Health Science Center, Memphis. He reported a conflict of interest with Accordant Health Services.
A version of this article first appeared on Medscape.com.
The Consolidated Appropriations Act of 2023 mandates that all Drug Enforcement Administration–registered physicians and health care providers complete a one-time, 8-hour CME training on managing and treating opioid and other substance abuse disorders. This requirement goes into effect on June 27, 2023. New DEA registrants must also comply. Veterinarians are exempt.
A DEA registration is required to prescribe any controlled substance. The DEA categorizes these as Schedule I-V, with V being the least likely to be abused (Table 1). For example, opioids like fentanyl, oxycodone, and morphine are Schedule II. Medications without abuse potential are not scheduled.
Will 16 million hours of opioid education save lives?
One should not underestimate the sweeping scope of this new federal requirement. DEA registrants include physicians and other health care providers such as nurse practitioners, physician assistants, and dentists. That is 8 hours per provider x 2 million providers: 16 million hours of CME!
Many states already require 1 or more hours of opioid training and pain management as part of their relicensure requirements (Table 2). To avoid redundancy, the DEA-mandated 8-hour training satisfies the various states’ requirements.
An uncompensated mandate
Physicians are no strangers to lifelong learning and most eagerly pursue educational opportunities. Though some physicians may have CME time and stipends allocated by their employers, many others, such as the approximately 50,000 locum tenens doctors, do not. However, as enthusiastic as these physicians may be about this new CME course, they will likely lose a day of seeing patients (and income) to comply with this new obligation.
Not just pain doctors
The mandate’s broad brush includes many health care providers who hold DEA certificates but do not prescribe opioids. For example, as a general neurologist and epileptologist, I do not treat patients with chronic pain and cannot remember the last time I wrote an opioid prescription. However, I frequently prescribe lacosamide, a Schedule V drug. A surprisingly large number of antiseizure drugs are Schedule III, IV, or V drugs (Table 3).
Real-world abuse?
How often scheduled antiseizure drugs are diverted or abused in an epilepsy population is unknown but appears to be infrequent. For example, perampanel abuse has not been reported despite its classification as a Schedule III drug. Anecdotally, in more than 40 years of clinical practice, I have never known a patient with epilepsy to abuse their antiseizure medications.
Take the course
Many organizations are happy to charge for the new 8-hour course. For example, the Tennessee Medical Association offers the training for $299 online or $400 in person. Materials from Elite Learning satisfy the 8-hour requirement for $80. However, NEJM Knowledge+ provides a complimentary 10-hour DEA-compliant course.
I recently completed the NEJM course. The information was thorough and took the whole 10 hours to finish. As excellent as it was, the content was only tangentially relevant to my clinical practice.
Conclusions
To obtain or renew a DEA certificate, neurologists, epilepsy specialists, and many other health care providers must comply with the new 8-hour CME opioid training mandate. Because the course requires 1 day to complete, health care providers would be prudent to obtain their CME well before their DEA certificate expires.
Though efforts to control the morbidity and mortality of the opioid epidemic are laudatory, perhaps the training should be more targeted to physicians who actually prescribe opioids rather than every DEA registrant. In the meantime, whether 16 million CME hours will save lives remains to be seen.
Dr. Wilner is professor of neurology at the University of Tennessee Health Science Center, Memphis. He reported a conflict of interest with Accordant Health Services.
A version of this article first appeared on Medscape.com.
The Consolidated Appropriations Act of 2023 mandates that all Drug Enforcement Administration–registered physicians and health care providers complete a one-time, 8-hour CME training on managing and treating opioid and other substance abuse disorders. This requirement goes into effect on June 27, 2023. New DEA registrants must also comply. Veterinarians are exempt.
A DEA registration is required to prescribe any controlled substance. The DEA categorizes these as Schedule I-V, with V being the least likely to be abused (Table 1). For example, opioids like fentanyl, oxycodone, and morphine are Schedule II. Medications without abuse potential are not scheduled.
Will 16 million hours of opioid education save lives?
One should not underestimate the sweeping scope of this new federal requirement. DEA registrants include physicians and other health care providers such as nurse practitioners, physician assistants, and dentists. That is 8 hours per provider x 2 million providers: 16 million hours of CME!
Many states already require 1 or more hours of opioid training and pain management as part of their relicensure requirements (Table 2). To avoid redundancy, the DEA-mandated 8-hour training satisfies the various states’ requirements.
An uncompensated mandate
Physicians are no strangers to lifelong learning and most eagerly pursue educational opportunities. Though some physicians may have CME time and stipends allocated by their employers, many others, such as the approximately 50,000 locum tenens doctors, do not. However, as enthusiastic as these physicians may be about this new CME course, they will likely lose a day of seeing patients (and income) to comply with this new obligation.
Not just pain doctors
The mandate’s broad brush includes many health care providers who hold DEA certificates but do not prescribe opioids. For example, as a general neurologist and epileptologist, I do not treat patients with chronic pain and cannot remember the last time I wrote an opioid prescription. However, I frequently prescribe lacosamide, a Schedule V drug. A surprisingly large number of antiseizure drugs are Schedule III, IV, or V drugs (Table 3).
Real-world abuse?
How often scheduled antiseizure drugs are diverted or abused in an epilepsy population is unknown but appears to be infrequent. For example, perampanel abuse has not been reported despite its classification as a Schedule III drug. Anecdotally, in more than 40 years of clinical practice, I have never known a patient with epilepsy to abuse their antiseizure medications.
Take the course
Many organizations are happy to charge for the new 8-hour course. For example, the Tennessee Medical Association offers the training for $299 online or $400 in person. Materials from Elite Learning satisfy the 8-hour requirement for $80. However, NEJM Knowledge+ provides a complimentary 10-hour DEA-compliant course.
I recently completed the NEJM course. The information was thorough and took the whole 10 hours to finish. As excellent as it was, the content was only tangentially relevant to my clinical practice.
Conclusions
To obtain or renew a DEA certificate, neurologists, epilepsy specialists, and many other health care providers must comply with the new 8-hour CME opioid training mandate. Because the course requires 1 day to complete, health care providers would be prudent to obtain their CME well before their DEA certificate expires.
Though efforts to control the morbidity and mortality of the opioid epidemic are laudatory, perhaps the training should be more targeted to physicians who actually prescribe opioids rather than every DEA registrant. In the meantime, whether 16 million CME hours will save lives remains to be seen.
Dr. Wilner is professor of neurology at the University of Tennessee Health Science Center, Memphis. He reported a conflict of interest with Accordant Health Services.
A version of this article first appeared on Medscape.com.
New law allows international medical graduates to bypass U.S. residency
Pediatric nephrologist Bryan Carmody, MD, recalls working alongside an extremely experienced neonatologist during his residency. She had managed a neonatal intensive care unit in her home country of Lithuania, but because she wanted to practice in the United States, it took years of repeat training before she was eligible for a medical license.
“She was very accomplished, and she was wonderful to have as a coresident at the time,” Dr. Carmody said in an interview.
The neonatologist now practices at a U.S. academic medical center, but to obtain that position, she had to complete 3 years of pediatric residency and 3 years of fellowship in the United States, Dr. Carmody said.
Such training for international medical graduates (IMGs) is a routine part of obtaining a U.S. medical license, but
The American Medical Association took similar measures at its recent annual meeting, making it easier for IMGs to gain licensure. Because the pandemic and Russia’s invasion of Ukraine disrupted the process by which some IMGs had their licenses verified, the AMA is now encouraging state licensing boards and other credentialing institutions to accept certification from the Educational Commission for Foreign Medical Graduates as verification, rather than requiring documents directly from international medical schools.
When it comes to Tennessee’s new law, signed by Gov. Bill Lee in April, experienced IMGs who have received medical training abroad can skip U.S. residency requirements and obtain a temporary license to practice medicine in Tennessee if they meet certain qualifications.
The international doctors must demonstrate competency, as determined by the state medical board. In addition, they must have completed a 3-year postgraduate training program in the graduate’s licensing country or otherwise have practiced as a medical professional in which they performed the duties of a physician for at least 3 of the past 5 years outside the United States, according to the new law.
To be approved, IMGs must also have received an employment offer from a Tennessee health care provider that has a residency program accredited by the Accreditation Council for Graduate Medical Education.
If physicians remain in good standing for 2 years, the board will grant them a full and unrestricted license to practice in Tennessee.
“The new legislation opens up a lot of doors for international medical graduates and is also a lifeline for a lot of underserved areas in Tennessee,” said Asim Ansari, MD, a Canadian who attended medical school in the Caribbean and is an advocate for IMGs.
Dr. Ansari is participating in a child and adolescent psychiatry fellowship at the University of Kansas Medical Center, Kansas City, until he can apply for the sixth time to a residency program. “This could possibly be a model that other states may want to implement in a few years.”
What’s behind the law?
A predicted physician shortage in Tennessee drove the legislation, said Rep. Sabi “Doc” Kumar, MD, vice chair for the Tennessee House Health Committee and a cosponsor of the legislation. Legislators hope the law will mitigate that shortage and boost the number of physicians practicing in underserved areas of the state.
“Considering that one in four physicians in the U.S. are international medical gradates, it was important for us to be able to attract those physicians to Tennessee,” he said.
The Tennessee Board of Medical Examiners will develop administrative rules for the law, which may take up to a year, Rep. Kumar said. He expects the program to be available to IMGs beginning in mid-2024.
Upon completion of the program, IMGs will be able to practice general medicine in Tennessee, not a specialty. Requirements for specialty certification would have to be met through the specialties’ respective boards.
Dr. Carmody, who blogs about medical education, including the new legislation, said in an interview the law will greatly benefit experienced IMGs, who often are bypassed as residency candidates because they graduated years ago. Hospitals also win because they can fill positions that otherwise might sit vacant, he said.
Family physician Sahil Bawa, MD, an IMG from India who recently matched into his specialty, said the Tennessee legislation will help fellow IMGs find U.S. medical jobs.
“It’s very difficult for IMGs to get into residency in the U.S.,” he said. “I’ve seen people with medical degrees from other countries drive Uber or do odd jobs to sustain themselves here. I’ve known a few people who have left and gone back to their home country because they were not accepted into a residency.”
Who benefits most?
Dr. Bawa noted that the legislation would not have helped him, as he needed a visa to practice in the United States and the law does not include the sponsoring of visas. The legislation requires IMGs to show evidence of citizenship or evidence that they are legally entitled to live or work in the United States.
U.S. citizen IMGs who haven’t completed residency or who practiced in another country also are left out of the law, Dr. Carmody said.
“This law is designed to take the most accomplished cream of the crop international medical graduates with the most experience and the most sophisticated skill set and send them to Tennessee. I think that’s the intent,” he said. “But many international medical graduates are U.S. citizens who don’t have the opportunity to practice in countries other than United States or do residencies. A lot of these people are sitting on the sidelines, unable to secure residency positions. I’m sure they would be desperate for a program like this.”
Questions remain
“Just because the doctor can get a [temporary] license without the training doesn’t mean employers are going to be interested in sponsoring those doctors,” said Adam Cohen, an immigration attorney who practices in Memphis. “What is the inclination of these employers to hire these physicians who have undergone training outside the U.S.? And will there be skepticism on the part of employers about the competence of these doctors?”
“Hospital systems will be able to hire experienced practitioners for a very low cost,” Dr. Ansari said. “So now you have these additional bodies who can do the work of a physician, but you don’t have to pay them as much as a physician for 2 years. And because some are desperate to work, they will take lower pay as long as they have a pathway to full licensure in Tennessee. What are the protections for these physicians? Who will cover their insurance? Who will be responsible for them, the attendees? And will the attendees be willing to put their license on the line for them?”
In addition, Dr. Carmody questions what, if anything, will encourage IMGs to work in underserved areas in Tennessee after their 2 years are up and whether there will be any incentives to guide them. He wonders, too, whether the physicians will be stuck practicing in Tennessee following completion of the program.
“Will these physicians only be able to work in Tennessee?” he asked. “I think that’s probably going to be the case, because they’ll be licensed in Tennessee, but to go to another state, they would be missing the required residency training. So it might be these folks are stuck in Tennessee unless other states develop reciprocal arrangements.”
Other states would have to decide whether to recognize the Tennessee license acquired through this pathway, Rep. Kumar said.
He explained that the sponsoring sites would be responsible for providing work-hour restrictions and liability protections. There are currently no incentives in the legislation for IMGs to practice in rural, underserved areas, but the hospitals and communities there generally offer incentives when recruiting, Rep. Kumar said.
“The law definitely has the potential to be helpful,” Mr. Cohen said, “because there’s an ability to place providers in the state without having to go through the bottleneck of limited residency slots. If other states see a positive effect on Tennessee or are exploring ways to alleviate their own shortages, it’s possible [they] might follow suit.”
Rep. Kumar agreed that other states will be watching Tennessee to weigh the law’s success.
“I think the law will have to prove itself and show that Tennessee has benefited from it and that the results have been good,” he said. “We are providing a pioneering way for attracting medical graduates and making it easier for them to obtain a license. I would think other states would want to do that.”
A version of this article first appeared on Medscape.com.
Pediatric nephrologist Bryan Carmody, MD, recalls working alongside an extremely experienced neonatologist during his residency. She had managed a neonatal intensive care unit in her home country of Lithuania, but because she wanted to practice in the United States, it took years of repeat training before she was eligible for a medical license.
“She was very accomplished, and she was wonderful to have as a coresident at the time,” Dr. Carmody said in an interview.
The neonatologist now practices at a U.S. academic medical center, but to obtain that position, she had to complete 3 years of pediatric residency and 3 years of fellowship in the United States, Dr. Carmody said.
Such training for international medical graduates (IMGs) is a routine part of obtaining a U.S. medical license, but
The American Medical Association took similar measures at its recent annual meeting, making it easier for IMGs to gain licensure. Because the pandemic and Russia’s invasion of Ukraine disrupted the process by which some IMGs had their licenses verified, the AMA is now encouraging state licensing boards and other credentialing institutions to accept certification from the Educational Commission for Foreign Medical Graduates as verification, rather than requiring documents directly from international medical schools.
When it comes to Tennessee’s new law, signed by Gov. Bill Lee in April, experienced IMGs who have received medical training abroad can skip U.S. residency requirements and obtain a temporary license to practice medicine in Tennessee if they meet certain qualifications.
The international doctors must demonstrate competency, as determined by the state medical board. In addition, they must have completed a 3-year postgraduate training program in the graduate’s licensing country or otherwise have practiced as a medical professional in which they performed the duties of a physician for at least 3 of the past 5 years outside the United States, according to the new law.
To be approved, IMGs must also have received an employment offer from a Tennessee health care provider that has a residency program accredited by the Accreditation Council for Graduate Medical Education.
If physicians remain in good standing for 2 years, the board will grant them a full and unrestricted license to practice in Tennessee.
“The new legislation opens up a lot of doors for international medical graduates and is also a lifeline for a lot of underserved areas in Tennessee,” said Asim Ansari, MD, a Canadian who attended medical school in the Caribbean and is an advocate for IMGs.
Dr. Ansari is participating in a child and adolescent psychiatry fellowship at the University of Kansas Medical Center, Kansas City, until he can apply for the sixth time to a residency program. “This could possibly be a model that other states may want to implement in a few years.”
What’s behind the law?
A predicted physician shortage in Tennessee drove the legislation, said Rep. Sabi “Doc” Kumar, MD, vice chair for the Tennessee House Health Committee and a cosponsor of the legislation. Legislators hope the law will mitigate that shortage and boost the number of physicians practicing in underserved areas of the state.
“Considering that one in four physicians in the U.S. are international medical gradates, it was important for us to be able to attract those physicians to Tennessee,” he said.
The Tennessee Board of Medical Examiners will develop administrative rules for the law, which may take up to a year, Rep. Kumar said. He expects the program to be available to IMGs beginning in mid-2024.
Upon completion of the program, IMGs will be able to practice general medicine in Tennessee, not a specialty. Requirements for specialty certification would have to be met through the specialties’ respective boards.
Dr. Carmody, who blogs about medical education, including the new legislation, said in an interview the law will greatly benefit experienced IMGs, who often are bypassed as residency candidates because they graduated years ago. Hospitals also win because they can fill positions that otherwise might sit vacant, he said.
Family physician Sahil Bawa, MD, an IMG from India who recently matched into his specialty, said the Tennessee legislation will help fellow IMGs find U.S. medical jobs.
“It’s very difficult for IMGs to get into residency in the U.S.,” he said. “I’ve seen people with medical degrees from other countries drive Uber or do odd jobs to sustain themselves here. I’ve known a few people who have left and gone back to their home country because they were not accepted into a residency.”
Who benefits most?
Dr. Bawa noted that the legislation would not have helped him, as he needed a visa to practice in the United States and the law does not include the sponsoring of visas. The legislation requires IMGs to show evidence of citizenship or evidence that they are legally entitled to live or work in the United States.
U.S. citizen IMGs who haven’t completed residency or who practiced in another country also are left out of the law, Dr. Carmody said.
“This law is designed to take the most accomplished cream of the crop international medical graduates with the most experience and the most sophisticated skill set and send them to Tennessee. I think that’s the intent,” he said. “But many international medical graduates are U.S. citizens who don’t have the opportunity to practice in countries other than United States or do residencies. A lot of these people are sitting on the sidelines, unable to secure residency positions. I’m sure they would be desperate for a program like this.”
Questions remain
“Just because the doctor can get a [temporary] license without the training doesn’t mean employers are going to be interested in sponsoring those doctors,” said Adam Cohen, an immigration attorney who practices in Memphis. “What is the inclination of these employers to hire these physicians who have undergone training outside the U.S.? And will there be skepticism on the part of employers about the competence of these doctors?”
“Hospital systems will be able to hire experienced practitioners for a very low cost,” Dr. Ansari said. “So now you have these additional bodies who can do the work of a physician, but you don’t have to pay them as much as a physician for 2 years. And because some are desperate to work, they will take lower pay as long as they have a pathway to full licensure in Tennessee. What are the protections for these physicians? Who will cover their insurance? Who will be responsible for them, the attendees? And will the attendees be willing to put their license on the line for them?”
In addition, Dr. Carmody questions what, if anything, will encourage IMGs to work in underserved areas in Tennessee after their 2 years are up and whether there will be any incentives to guide them. He wonders, too, whether the physicians will be stuck practicing in Tennessee following completion of the program.
“Will these physicians only be able to work in Tennessee?” he asked. “I think that’s probably going to be the case, because they’ll be licensed in Tennessee, but to go to another state, they would be missing the required residency training. So it might be these folks are stuck in Tennessee unless other states develop reciprocal arrangements.”
Other states would have to decide whether to recognize the Tennessee license acquired through this pathway, Rep. Kumar said.
He explained that the sponsoring sites would be responsible for providing work-hour restrictions and liability protections. There are currently no incentives in the legislation for IMGs to practice in rural, underserved areas, but the hospitals and communities there generally offer incentives when recruiting, Rep. Kumar said.
“The law definitely has the potential to be helpful,” Mr. Cohen said, “because there’s an ability to place providers in the state without having to go through the bottleneck of limited residency slots. If other states see a positive effect on Tennessee or are exploring ways to alleviate their own shortages, it’s possible [they] might follow suit.”
Rep. Kumar agreed that other states will be watching Tennessee to weigh the law’s success.
“I think the law will have to prove itself and show that Tennessee has benefited from it and that the results have been good,” he said. “We are providing a pioneering way for attracting medical graduates and making it easier for them to obtain a license. I would think other states would want to do that.”
A version of this article first appeared on Medscape.com.
Pediatric nephrologist Bryan Carmody, MD, recalls working alongside an extremely experienced neonatologist during his residency. She had managed a neonatal intensive care unit in her home country of Lithuania, but because she wanted to practice in the United States, it took years of repeat training before she was eligible for a medical license.
“She was very accomplished, and she was wonderful to have as a coresident at the time,” Dr. Carmody said in an interview.
The neonatologist now practices at a U.S. academic medical center, but to obtain that position, she had to complete 3 years of pediatric residency and 3 years of fellowship in the United States, Dr. Carmody said.
Such training for international medical graduates (IMGs) is a routine part of obtaining a U.S. medical license, but
The American Medical Association took similar measures at its recent annual meeting, making it easier for IMGs to gain licensure. Because the pandemic and Russia’s invasion of Ukraine disrupted the process by which some IMGs had their licenses verified, the AMA is now encouraging state licensing boards and other credentialing institutions to accept certification from the Educational Commission for Foreign Medical Graduates as verification, rather than requiring documents directly from international medical schools.
When it comes to Tennessee’s new law, signed by Gov. Bill Lee in April, experienced IMGs who have received medical training abroad can skip U.S. residency requirements and obtain a temporary license to practice medicine in Tennessee if they meet certain qualifications.
The international doctors must demonstrate competency, as determined by the state medical board. In addition, they must have completed a 3-year postgraduate training program in the graduate’s licensing country or otherwise have practiced as a medical professional in which they performed the duties of a physician for at least 3 of the past 5 years outside the United States, according to the new law.
To be approved, IMGs must also have received an employment offer from a Tennessee health care provider that has a residency program accredited by the Accreditation Council for Graduate Medical Education.
If physicians remain in good standing for 2 years, the board will grant them a full and unrestricted license to practice in Tennessee.
“The new legislation opens up a lot of doors for international medical graduates and is also a lifeline for a lot of underserved areas in Tennessee,” said Asim Ansari, MD, a Canadian who attended medical school in the Caribbean and is an advocate for IMGs.
Dr. Ansari is participating in a child and adolescent psychiatry fellowship at the University of Kansas Medical Center, Kansas City, until he can apply for the sixth time to a residency program. “This could possibly be a model that other states may want to implement in a few years.”
What’s behind the law?
A predicted physician shortage in Tennessee drove the legislation, said Rep. Sabi “Doc” Kumar, MD, vice chair for the Tennessee House Health Committee and a cosponsor of the legislation. Legislators hope the law will mitigate that shortage and boost the number of physicians practicing in underserved areas of the state.
“Considering that one in four physicians in the U.S. are international medical gradates, it was important for us to be able to attract those physicians to Tennessee,” he said.
The Tennessee Board of Medical Examiners will develop administrative rules for the law, which may take up to a year, Rep. Kumar said. He expects the program to be available to IMGs beginning in mid-2024.
Upon completion of the program, IMGs will be able to practice general medicine in Tennessee, not a specialty. Requirements for specialty certification would have to be met through the specialties’ respective boards.
Dr. Carmody, who blogs about medical education, including the new legislation, said in an interview the law will greatly benefit experienced IMGs, who often are bypassed as residency candidates because they graduated years ago. Hospitals also win because they can fill positions that otherwise might sit vacant, he said.
Family physician Sahil Bawa, MD, an IMG from India who recently matched into his specialty, said the Tennessee legislation will help fellow IMGs find U.S. medical jobs.
“It’s very difficult for IMGs to get into residency in the U.S.,” he said. “I’ve seen people with medical degrees from other countries drive Uber or do odd jobs to sustain themselves here. I’ve known a few people who have left and gone back to their home country because they were not accepted into a residency.”
Who benefits most?
Dr. Bawa noted that the legislation would not have helped him, as he needed a visa to practice in the United States and the law does not include the sponsoring of visas. The legislation requires IMGs to show evidence of citizenship or evidence that they are legally entitled to live or work in the United States.
U.S. citizen IMGs who haven’t completed residency or who practiced in another country also are left out of the law, Dr. Carmody said.
“This law is designed to take the most accomplished cream of the crop international medical graduates with the most experience and the most sophisticated skill set and send them to Tennessee. I think that’s the intent,” he said. “But many international medical graduates are U.S. citizens who don’t have the opportunity to practice in countries other than United States or do residencies. A lot of these people are sitting on the sidelines, unable to secure residency positions. I’m sure they would be desperate for a program like this.”
Questions remain
“Just because the doctor can get a [temporary] license without the training doesn’t mean employers are going to be interested in sponsoring those doctors,” said Adam Cohen, an immigration attorney who practices in Memphis. “What is the inclination of these employers to hire these physicians who have undergone training outside the U.S.? And will there be skepticism on the part of employers about the competence of these doctors?”
“Hospital systems will be able to hire experienced practitioners for a very low cost,” Dr. Ansari said. “So now you have these additional bodies who can do the work of a physician, but you don’t have to pay them as much as a physician for 2 years. And because some are desperate to work, they will take lower pay as long as they have a pathway to full licensure in Tennessee. What are the protections for these physicians? Who will cover their insurance? Who will be responsible for them, the attendees? And will the attendees be willing to put their license on the line for them?”
In addition, Dr. Carmody questions what, if anything, will encourage IMGs to work in underserved areas in Tennessee after their 2 years are up and whether there will be any incentives to guide them. He wonders, too, whether the physicians will be stuck practicing in Tennessee following completion of the program.
“Will these physicians only be able to work in Tennessee?” he asked. “I think that’s probably going to be the case, because they’ll be licensed in Tennessee, but to go to another state, they would be missing the required residency training. So it might be these folks are stuck in Tennessee unless other states develop reciprocal arrangements.”
Other states would have to decide whether to recognize the Tennessee license acquired through this pathway, Rep. Kumar said.
He explained that the sponsoring sites would be responsible for providing work-hour restrictions and liability protections. There are currently no incentives in the legislation for IMGs to practice in rural, underserved areas, but the hospitals and communities there generally offer incentives when recruiting, Rep. Kumar said.
“The law definitely has the potential to be helpful,” Mr. Cohen said, “because there’s an ability to place providers in the state without having to go through the bottleneck of limited residency slots. If other states see a positive effect on Tennessee or are exploring ways to alleviate their own shortages, it’s possible [they] might follow suit.”
Rep. Kumar agreed that other states will be watching Tennessee to weigh the law’s success.
“I think the law will have to prove itself and show that Tennessee has benefited from it and that the results have been good,” he said. “We are providing a pioneering way for attracting medical graduates and making it easier for them to obtain a license. I would think other states would want to do that.”
A version of this article first appeared on Medscape.com.
The metaverse is the dermatologist’s ally
MADRID – There are endless possibilities within the dermoverse (a term coined by joining “dermatology” and “metaverse”), from a robot office assistant to the brand new world it offers for virtual training and simulation.
A group of dermatologists expert in new technologies came together at the 50th National Congress of the Spanish Academy for Dermatology and Venereology to discuss the metaverse: that sum of all virtual spaces that bridges physical and digital reality, where users interact through their avatars and where these experts are discovering new opportunities for treating their patients. The metaverse and AI offer a massive opportunity for improving telehealth visits, immersive surgical planning, or virtual training using 3-D skin models. These are just a few examples of what this technology may eventually provide.
“The possibilities offered by the metaverse in the field of dermatology could be endless,” explained Miriam Fernández-Parrado, MD, dermatologist at Navarre Hospital, Pamplona, Spain. To her, “the metaverse could mean a step forward in teledermatology, which has come of age as a result of the pandemic.” These past few years have shown that it’s possible to perform some screenings online. This, in turn, has produced significant time and cost savings, along with greater efficacy in initial screening and early detection of serious diseases.
The overall percentage of cases that are potentially treatable in absentia is estimated to exceed 70%. “This isn’t a matter of replacing in-person visits but of finding a quality alternative that, far from dehumanizing the doctor-patient relationship, helps to satisfy the growing need for this relationship,” said Dr. Fernández-Parrado.
Always on duty
Julián Conejo-Mir, MD, PhD, professor and head of dermatology at the Virgen del Rocío Hospital in Seville, Spain, told this news organization that AI will help with day-to-day interactions with patients. It’s already a reality. “But to say that with a simple photo, we can address 70% of dermatology cases without being physically present with our patients – I don’t think that will become a reality in the next 20 years.”
Currently, algorithms can identify tumors with high success rates (80%-90%) using photographs and dermoscopic images; rates increase significantly when both kinds of images are available. These high success rates are possible because tumor morphology is stationary. “However, for inflammatory conditions, accurate diagnosis generally doesn’t exceed 60%, since these are conditions in which morphology can change a lot from one day to the next and can vary significantly, depending on their anatomic location or the patient’s age.”
Maybe once metaclinics, with 3-D virtual reality, have been established and clinicians can see the patient in real time from their offices, the rate of accurate diagnosis will reach 70%, especially with patients who have limited mobility or who live at a distance from the hospital. “But that’s still 10-15 years away, since more powerful computers are needed, most likely quantum computers,” cautioned Dr. Conejo-Mir.
The patient’s ally
In clinical practice, facilitating access to the dermoverse may help reduce pain and divert the patient’s attention, especially during in-person visits that require bothersome or uncomfortable interventions. “This is especially effective in pediatric dermatology, since settings of immersive virtual reality may contribute to relaxation among children,” explained Dr. Fernández-Parrado. She also sees potential applications among patients who need surgery. The metaverse would allow them to preview a simulation of their operation before undergoing it, thus reducing their anxiety and allaying their fears about these procedures.
Two lines are being pursued: automated diagnosis for telehealth consultations, which are primarily for tumors, and robotic office assistants.
“We have been using the first one in clinical practice, and we can achieve a success rate of 85%-90%.” The second one is much more complex, “and we’re having a hard time moving it forward within our research team, since it doesn’t involve only one algorithm. Instead, it requires five algorithms working together simultaneously (chatbot, automatic writing, image analysis, selecting the most appropriate treatment, ability to make recommendations, and even an additional one involving feelings),” explained Dr. Conejo-Mir.
A wise consultant
Dr. Conejo-Mir offered examples of how this might work in the near future. “In under 5 years, you’ll be able to sit in front of a computer or your smartphone, talk to an avatar that we’re able to select (sex, appearance, age, kind/serious), show the avatar your lesions, and it will tell us a basic diagnostic impression and even the treatment.”
With virtual learning, physicians can also gather knowledge or take refresher courses, using skin models in augmented reality with tumors and other skin lesions, or using immersive simulation courses that aid learning. Digital models that replicate the anatomy and elasticity of the skin or other characteristics unique to the patient can be used to reach decisions regarding surgeries and to practice interventions before entering the operating room, explained Dr. Fernández-Parrado.
Optimal virtual training
Virtual reality and simulation will doubtless play a major role in this promising field of using these devices for training purposes. “There will be virtual dermatology clinics or metaclinics, where you can do everything with virtual simulated patients, from gaining experience in interviews or health histories (even with patients who are difficult to deal with), to taking biopsies and performing interventions,” said Dr. Conejo-Mir.
A recent study titled “How the World Sees the Metaverse and Extended Reality” gathered data from 29 countries regarding the next 10 years. One of the greatest benefits of this technology is expected in health resources (59%), even more than in the trading of digital assets. While it is difficult to predict when the dermoverse will be in operation, Dr. Fernández-Parrado says she’s a techno-optimist. Together with Dr. Héctor Perandones, MD, a dermatologist at the University Healthcare Complex in León, Spain, and coauthor with Dr. Fernández-Parrado of the article, “A New Universe in Dermatology: From Metaverse to Dermoverse,” she’s convinced that “if we can imagine it, we can create it.”
A differential diagnostician
Over the past 10 years, AI has become a major ally of dermatology, providing new techniques that simplify the diagnosis and treatment of patients. There are many applications for which it adds tremendous value in dermatology: establishing precise differential diagnoses for common diseases, such as psoriasis, atopic dermatitis, or acne; eveloping personalized therapeutic protocols; and predicting medium- and long-term outcomes.
Furthermore, in onco-dermatology, AI has helped to automate the diagnosis of skin tumors by making it possible to differentiate between melanocytic and nonmelanocytic lesions. This distinction promotes early diagnosis and helps produce screening systems that are capable of prioritizing cases on the basis of their seriousness.
When asked whether any group has published any promising tools with good preliminary results, Dr. Conejo-Mir stated that his group has produced three articles that have been published in top-ranking journals. In these articles, “we explain our experience with artificial intelligence in Mohs surgery, in automated diagnosis, and for calculating the thickness of melanomas.” The eight-person research team, which comprises dermatologists and software engineers, has been working together in this area for the past 4 years.
Aesthetic dermatology
Unlike other specialists, dermatologists have 4-D vision when it comes to aesthetics, since they are also skin experts. AI plays a major role in aesthetic dermatology. It supports this specialty by providing a greater analytic capacity and by evaluating the procedure and technique to be used. “It’s going to help us think and make decisions. It has taken great strides in aesthetic dermatology, especially when it comes to techniques and products. There have been products like collagen, hyaluronic acid, then thread lifts ... Also, different techniques have been developed, like Botox, for example. Before, Botox was given following one method. Now, there are other methods,” explained Dr. Conejo-Mir.
He explained, “We have analyzed the facial image to detect wrinkles, spots, enlarged pores, et cetera, to see whether there are any lesions, and, depending on what the machine says you have, it provides you with a personalized treatment. It tells you the pattern of care that the patient should follow. It also tells you what you’re going to do, whether or not there is any problem, depending on the location and on what the person is like, et cetera. Then, for follow-up, you’re given an AI program that tells you if you’re doing well or not. Lastly, it gives you product recommendations.
“We are among the specialties that are going through the most change,” said Dr. Conejo-Mir.
An intrusive technology?
AI will be a tremendous help in decision-making, to the point where “in 4 or 5 years, it will become indispensable, just like the loupe in years past, and then the dermatoscope.” However, the machine will have to depend on human beings. “They won’t replace us, but they will become unavoidable assistants in our day-to-day medical practice.”
Questions have arisen regarding the potential dangers of these new technologies, like that of reducing the number of dermatologists within the population, and whether they might encourage intrusiveness. Dr. Conejo-Mir made no bones about it. “AI will never cut back the number of specialists. That is false. When AI supports us in teledermatology, even currently on our team, it spits out information, but the one making the decision is the practitioner, not the machine.”
AI is a tool but is not in itself something that treats patients. It is akin to the dermatoscope. Dermatologists use these tools every day, and they help arrive at diagnoses in difficult cases, but they are not a replacement for humans. “At least for the next 50 years, then we’ll see. In 2050 is when they say AI will surpass humans in its intelligence and reasoning capacity,” said Dr. Conejo-Mir.
Dr. Conejo-Mir has disclosed no relevant financial relationships.
This article was translated from the Medscape Spanish Edition. A version of this article appeared on Medscape.com.
MADRID – There are endless possibilities within the dermoverse (a term coined by joining “dermatology” and “metaverse”), from a robot office assistant to the brand new world it offers for virtual training and simulation.
A group of dermatologists expert in new technologies came together at the 50th National Congress of the Spanish Academy for Dermatology and Venereology to discuss the metaverse: that sum of all virtual spaces that bridges physical and digital reality, where users interact through their avatars and where these experts are discovering new opportunities for treating their patients. The metaverse and AI offer a massive opportunity for improving telehealth visits, immersive surgical planning, or virtual training using 3-D skin models. These are just a few examples of what this technology may eventually provide.
“The possibilities offered by the metaverse in the field of dermatology could be endless,” explained Miriam Fernández-Parrado, MD, dermatologist at Navarre Hospital, Pamplona, Spain. To her, “the metaverse could mean a step forward in teledermatology, which has come of age as a result of the pandemic.” These past few years have shown that it’s possible to perform some screenings online. This, in turn, has produced significant time and cost savings, along with greater efficacy in initial screening and early detection of serious diseases.
The overall percentage of cases that are potentially treatable in absentia is estimated to exceed 70%. “This isn’t a matter of replacing in-person visits but of finding a quality alternative that, far from dehumanizing the doctor-patient relationship, helps to satisfy the growing need for this relationship,” said Dr. Fernández-Parrado.
Always on duty
Julián Conejo-Mir, MD, PhD, professor and head of dermatology at the Virgen del Rocío Hospital in Seville, Spain, told this news organization that AI will help with day-to-day interactions with patients. It’s already a reality. “But to say that with a simple photo, we can address 70% of dermatology cases without being physically present with our patients – I don’t think that will become a reality in the next 20 years.”
Currently, algorithms can identify tumors with high success rates (80%-90%) using photographs and dermoscopic images; rates increase significantly when both kinds of images are available. These high success rates are possible because tumor morphology is stationary. “However, for inflammatory conditions, accurate diagnosis generally doesn’t exceed 60%, since these are conditions in which morphology can change a lot from one day to the next and can vary significantly, depending on their anatomic location or the patient’s age.”
Maybe once metaclinics, with 3-D virtual reality, have been established and clinicians can see the patient in real time from their offices, the rate of accurate diagnosis will reach 70%, especially with patients who have limited mobility or who live at a distance from the hospital. “But that’s still 10-15 years away, since more powerful computers are needed, most likely quantum computers,” cautioned Dr. Conejo-Mir.
The patient’s ally
In clinical practice, facilitating access to the dermoverse may help reduce pain and divert the patient’s attention, especially during in-person visits that require bothersome or uncomfortable interventions. “This is especially effective in pediatric dermatology, since settings of immersive virtual reality may contribute to relaxation among children,” explained Dr. Fernández-Parrado. She also sees potential applications among patients who need surgery. The metaverse would allow them to preview a simulation of their operation before undergoing it, thus reducing their anxiety and allaying their fears about these procedures.
Two lines are being pursued: automated diagnosis for telehealth consultations, which are primarily for tumors, and robotic office assistants.
“We have been using the first one in clinical practice, and we can achieve a success rate of 85%-90%.” The second one is much more complex, “and we’re having a hard time moving it forward within our research team, since it doesn’t involve only one algorithm. Instead, it requires five algorithms working together simultaneously (chatbot, automatic writing, image analysis, selecting the most appropriate treatment, ability to make recommendations, and even an additional one involving feelings),” explained Dr. Conejo-Mir.
A wise consultant
Dr. Conejo-Mir offered examples of how this might work in the near future. “In under 5 years, you’ll be able to sit in front of a computer or your smartphone, talk to an avatar that we’re able to select (sex, appearance, age, kind/serious), show the avatar your lesions, and it will tell us a basic diagnostic impression and even the treatment.”
With virtual learning, physicians can also gather knowledge or take refresher courses, using skin models in augmented reality with tumors and other skin lesions, or using immersive simulation courses that aid learning. Digital models that replicate the anatomy and elasticity of the skin or other characteristics unique to the patient can be used to reach decisions regarding surgeries and to practice interventions before entering the operating room, explained Dr. Fernández-Parrado.
Optimal virtual training
Virtual reality and simulation will doubtless play a major role in this promising field of using these devices for training purposes. “There will be virtual dermatology clinics or metaclinics, where you can do everything with virtual simulated patients, from gaining experience in interviews or health histories (even with patients who are difficult to deal with), to taking biopsies and performing interventions,” said Dr. Conejo-Mir.
A recent study titled “How the World Sees the Metaverse and Extended Reality” gathered data from 29 countries regarding the next 10 years. One of the greatest benefits of this technology is expected in health resources (59%), even more than in the trading of digital assets. While it is difficult to predict when the dermoverse will be in operation, Dr. Fernández-Parrado says she’s a techno-optimist. Together with Dr. Héctor Perandones, MD, a dermatologist at the University Healthcare Complex in León, Spain, and coauthor with Dr. Fernández-Parrado of the article, “A New Universe in Dermatology: From Metaverse to Dermoverse,” she’s convinced that “if we can imagine it, we can create it.”
A differential diagnostician
Over the past 10 years, AI has become a major ally of dermatology, providing new techniques that simplify the diagnosis and treatment of patients. There are many applications for which it adds tremendous value in dermatology: establishing precise differential diagnoses for common diseases, such as psoriasis, atopic dermatitis, or acne; eveloping personalized therapeutic protocols; and predicting medium- and long-term outcomes.
Furthermore, in onco-dermatology, AI has helped to automate the diagnosis of skin tumors by making it possible to differentiate between melanocytic and nonmelanocytic lesions. This distinction promotes early diagnosis and helps produce screening systems that are capable of prioritizing cases on the basis of their seriousness.
When asked whether any group has published any promising tools with good preliminary results, Dr. Conejo-Mir stated that his group has produced three articles that have been published in top-ranking journals. In these articles, “we explain our experience with artificial intelligence in Mohs surgery, in automated diagnosis, and for calculating the thickness of melanomas.” The eight-person research team, which comprises dermatologists and software engineers, has been working together in this area for the past 4 years.
Aesthetic dermatology
Unlike other specialists, dermatologists have 4-D vision when it comes to aesthetics, since they are also skin experts. AI plays a major role in aesthetic dermatology. It supports this specialty by providing a greater analytic capacity and by evaluating the procedure and technique to be used. “It’s going to help us think and make decisions. It has taken great strides in aesthetic dermatology, especially when it comes to techniques and products. There have been products like collagen, hyaluronic acid, then thread lifts ... Also, different techniques have been developed, like Botox, for example. Before, Botox was given following one method. Now, there are other methods,” explained Dr. Conejo-Mir.
He explained, “We have analyzed the facial image to detect wrinkles, spots, enlarged pores, et cetera, to see whether there are any lesions, and, depending on what the machine says you have, it provides you with a personalized treatment. It tells you the pattern of care that the patient should follow. It also tells you what you’re going to do, whether or not there is any problem, depending on the location and on what the person is like, et cetera. Then, for follow-up, you’re given an AI program that tells you if you’re doing well or not. Lastly, it gives you product recommendations.
“We are among the specialties that are going through the most change,” said Dr. Conejo-Mir.
An intrusive technology?
AI will be a tremendous help in decision-making, to the point where “in 4 or 5 years, it will become indispensable, just like the loupe in years past, and then the dermatoscope.” However, the machine will have to depend on human beings. “They won’t replace us, but they will become unavoidable assistants in our day-to-day medical practice.”
Questions have arisen regarding the potential dangers of these new technologies, like that of reducing the number of dermatologists within the population, and whether they might encourage intrusiveness. Dr. Conejo-Mir made no bones about it. “AI will never cut back the number of specialists. That is false. When AI supports us in teledermatology, even currently on our team, it spits out information, but the one making the decision is the practitioner, not the machine.”
AI is a tool but is not in itself something that treats patients. It is akin to the dermatoscope. Dermatologists use these tools every day, and they help arrive at diagnoses in difficult cases, but they are not a replacement for humans. “At least for the next 50 years, then we’ll see. In 2050 is when they say AI will surpass humans in its intelligence and reasoning capacity,” said Dr. Conejo-Mir.
Dr. Conejo-Mir has disclosed no relevant financial relationships.
This article was translated from the Medscape Spanish Edition. A version of this article appeared on Medscape.com.
MADRID – There are endless possibilities within the dermoverse (a term coined by joining “dermatology” and “metaverse”), from a robot office assistant to the brand new world it offers for virtual training and simulation.
A group of dermatologists expert in new technologies came together at the 50th National Congress of the Spanish Academy for Dermatology and Venereology to discuss the metaverse: that sum of all virtual spaces that bridges physical and digital reality, where users interact through their avatars and where these experts are discovering new opportunities for treating their patients. The metaverse and AI offer a massive opportunity for improving telehealth visits, immersive surgical planning, or virtual training using 3-D skin models. These are just a few examples of what this technology may eventually provide.
“The possibilities offered by the metaverse in the field of dermatology could be endless,” explained Miriam Fernández-Parrado, MD, dermatologist at Navarre Hospital, Pamplona, Spain. To her, “the metaverse could mean a step forward in teledermatology, which has come of age as a result of the pandemic.” These past few years have shown that it’s possible to perform some screenings online. This, in turn, has produced significant time and cost savings, along with greater efficacy in initial screening and early detection of serious diseases.
The overall percentage of cases that are potentially treatable in absentia is estimated to exceed 70%. “This isn’t a matter of replacing in-person visits but of finding a quality alternative that, far from dehumanizing the doctor-patient relationship, helps to satisfy the growing need for this relationship,” said Dr. Fernández-Parrado.
Always on duty
Julián Conejo-Mir, MD, PhD, professor and head of dermatology at the Virgen del Rocío Hospital in Seville, Spain, told this news organization that AI will help with day-to-day interactions with patients. It’s already a reality. “But to say that with a simple photo, we can address 70% of dermatology cases without being physically present with our patients – I don’t think that will become a reality in the next 20 years.”
Currently, algorithms can identify tumors with high success rates (80%-90%) using photographs and dermoscopic images; rates increase significantly when both kinds of images are available. These high success rates are possible because tumor morphology is stationary. “However, for inflammatory conditions, accurate diagnosis generally doesn’t exceed 60%, since these are conditions in which morphology can change a lot from one day to the next and can vary significantly, depending on their anatomic location or the patient’s age.”
Maybe once metaclinics, with 3-D virtual reality, have been established and clinicians can see the patient in real time from their offices, the rate of accurate diagnosis will reach 70%, especially with patients who have limited mobility or who live at a distance from the hospital. “But that’s still 10-15 years away, since more powerful computers are needed, most likely quantum computers,” cautioned Dr. Conejo-Mir.
The patient’s ally
In clinical practice, facilitating access to the dermoverse may help reduce pain and divert the patient’s attention, especially during in-person visits that require bothersome or uncomfortable interventions. “This is especially effective in pediatric dermatology, since settings of immersive virtual reality may contribute to relaxation among children,” explained Dr. Fernández-Parrado. She also sees potential applications among patients who need surgery. The metaverse would allow them to preview a simulation of their operation before undergoing it, thus reducing their anxiety and allaying their fears about these procedures.
Two lines are being pursued: automated diagnosis for telehealth consultations, which are primarily for tumors, and robotic office assistants.
“We have been using the first one in clinical practice, and we can achieve a success rate of 85%-90%.” The second one is much more complex, “and we’re having a hard time moving it forward within our research team, since it doesn’t involve only one algorithm. Instead, it requires five algorithms working together simultaneously (chatbot, automatic writing, image analysis, selecting the most appropriate treatment, ability to make recommendations, and even an additional one involving feelings),” explained Dr. Conejo-Mir.
A wise consultant
Dr. Conejo-Mir offered examples of how this might work in the near future. “In under 5 years, you’ll be able to sit in front of a computer or your smartphone, talk to an avatar that we’re able to select (sex, appearance, age, kind/serious), show the avatar your lesions, and it will tell us a basic diagnostic impression and even the treatment.”
With virtual learning, physicians can also gather knowledge or take refresher courses, using skin models in augmented reality with tumors and other skin lesions, or using immersive simulation courses that aid learning. Digital models that replicate the anatomy and elasticity of the skin or other characteristics unique to the patient can be used to reach decisions regarding surgeries and to practice interventions before entering the operating room, explained Dr. Fernández-Parrado.
Optimal virtual training
Virtual reality and simulation will doubtless play a major role in this promising field of using these devices for training purposes. “There will be virtual dermatology clinics or metaclinics, where you can do everything with virtual simulated patients, from gaining experience in interviews or health histories (even with patients who are difficult to deal with), to taking biopsies and performing interventions,” said Dr. Conejo-Mir.
A recent study titled “How the World Sees the Metaverse and Extended Reality” gathered data from 29 countries regarding the next 10 years. One of the greatest benefits of this technology is expected in health resources (59%), even more than in the trading of digital assets. While it is difficult to predict when the dermoverse will be in operation, Dr. Fernández-Parrado says she’s a techno-optimist. Together with Dr. Héctor Perandones, MD, a dermatologist at the University Healthcare Complex in León, Spain, and coauthor with Dr. Fernández-Parrado of the article, “A New Universe in Dermatology: From Metaverse to Dermoverse,” she’s convinced that “if we can imagine it, we can create it.”
A differential diagnostician
Over the past 10 years, AI has become a major ally of dermatology, providing new techniques that simplify the diagnosis and treatment of patients. There are many applications for which it adds tremendous value in dermatology: establishing precise differential diagnoses for common diseases, such as psoriasis, atopic dermatitis, or acne; eveloping personalized therapeutic protocols; and predicting medium- and long-term outcomes.
Furthermore, in onco-dermatology, AI has helped to automate the diagnosis of skin tumors by making it possible to differentiate between melanocytic and nonmelanocytic lesions. This distinction promotes early diagnosis and helps produce screening systems that are capable of prioritizing cases on the basis of their seriousness.
When asked whether any group has published any promising tools with good preliminary results, Dr. Conejo-Mir stated that his group has produced three articles that have been published in top-ranking journals. In these articles, “we explain our experience with artificial intelligence in Mohs surgery, in automated diagnosis, and for calculating the thickness of melanomas.” The eight-person research team, which comprises dermatologists and software engineers, has been working together in this area for the past 4 years.
Aesthetic dermatology
Unlike other specialists, dermatologists have 4-D vision when it comes to aesthetics, since they are also skin experts. AI plays a major role in aesthetic dermatology. It supports this specialty by providing a greater analytic capacity and by evaluating the procedure and technique to be used. “It’s going to help us think and make decisions. It has taken great strides in aesthetic dermatology, especially when it comes to techniques and products. There have been products like collagen, hyaluronic acid, then thread lifts ... Also, different techniques have been developed, like Botox, for example. Before, Botox was given following one method. Now, there are other methods,” explained Dr. Conejo-Mir.
He explained, “We have analyzed the facial image to detect wrinkles, spots, enlarged pores, et cetera, to see whether there are any lesions, and, depending on what the machine says you have, it provides you with a personalized treatment. It tells you the pattern of care that the patient should follow. It also tells you what you’re going to do, whether or not there is any problem, depending on the location and on what the person is like, et cetera. Then, for follow-up, you’re given an AI program that tells you if you’re doing well or not. Lastly, it gives you product recommendations.
“We are among the specialties that are going through the most change,” said Dr. Conejo-Mir.
An intrusive technology?
AI will be a tremendous help in decision-making, to the point where “in 4 or 5 years, it will become indispensable, just like the loupe in years past, and then the dermatoscope.” However, the machine will have to depend on human beings. “They won’t replace us, but they will become unavoidable assistants in our day-to-day medical practice.”
Questions have arisen regarding the potential dangers of these new technologies, like that of reducing the number of dermatologists within the population, and whether they might encourage intrusiveness. Dr. Conejo-Mir made no bones about it. “AI will never cut back the number of specialists. That is false. When AI supports us in teledermatology, even currently on our team, it spits out information, but the one making the decision is the practitioner, not the machine.”
AI is a tool but is not in itself something that treats patients. It is akin to the dermatoscope. Dermatologists use these tools every day, and they help arrive at diagnoses in difficult cases, but they are not a replacement for humans. “At least for the next 50 years, then we’ll see. In 2050 is when they say AI will surpass humans in its intelligence and reasoning capacity,” said Dr. Conejo-Mir.
Dr. Conejo-Mir has disclosed no relevant financial relationships.
This article was translated from the Medscape Spanish Edition. A version of this article appeared on Medscape.com.
Multiprong strategy makes clinical trials less White
CHICAGO – Clinical trials are so White. Only a small percentage of eligible patients participate in clinical trials in the first place, and very few come from racial and ethnic minority groups.
For example, according to the Food and Drug Administration, in trials that resulted in drug approvals from 2017 to 2020, only 2%-5% of participants were Black patients.
When clinical trials lack diverse patient populations, those who are left out have fewer opportunities to get new therapies. Moreover, the scope of the research is limited by smaller phenotypic and genotypic samples, and the trial results are applicable only to more homogeneous patient groups.
There has been a push to include more underrepresented patients in clinical trials. One group reported its success in doing so here at the annual meeting of the American Society of Clinical Oncology.
a period that included a pandemic-induced hiatus in clinical trials in general.
Alliance member Electra D. Paskett, PhD, from the College of Public Health at the Ohio State University in Columbus, presented accrual data from 117 trials led by the Alliance from 2014 to 2022.
During this period, accrual of racial and ethnic minority patients increased from 13.6% to 25.3% for cancer treatment trials and from 13% to 21.5% for cancer control trials.
Overall, the recruitment program resulted in an absolute increase from 13.5 % to 23.6% of underrepresented populations, which translated into a relative 74.8% improvement.
“We’re focusing now on monitoring accrual of women, rural populations, younger AYAs [adolescents and young adults] and older patients, and we’ll see what strategies we need to implement,” Dr. Packett told this news organization.
The Alliance has implemented a real-time accrual dashboard on its website that allows individual sites to review accrual by trial and overall for all of the identified underrepresented populations, she noted.
Program to increase underrepresented patient accrual
The impetus for the program to increase enrollment of underrepresented patients came from the goal set by Monica M. Bertagnolli, MD, group chair of the Alliance from 2011 to 2022 and currently the director of the U.S. National Cancer Institute.
“Our leader, Dr. Bertagnolli, set out a group-wide goal for accrual of underrepresented minorities to our trials of 20%, and that gave us permission to implement a whole host of new strategies,” Dr. Paskett said in an interview.
“These strategies follow the Accrual of Clinical Trials framework, which essentially says that the interaction between the patient and the provider for going on a clinical trial is not just an interaction between the patient and provider but recognizes, for example, that the provider has coworkers and they have norms and beliefs and attitudes, and the patient comes from a family with their own values. And then there are system-level barriers, and there are community barriers that all relate to this interaction about going on a trial,” Dr. Packett said.
What works?
The study was presented as a poster at the meeting. During the poster discussion session, comoderator Victoria S. Blinder, MD, from Memorial Sloan Kettering Cancer Center in New York, asked Dr. Paskett, “If you had a certain amount of money and you really wanted to use that resource to focus on one area, where would you put that resource?”
“I’m going to violate the rules of your question,” Dr. Paskett replied.
“You cannot change this problem by focusing on one thing, and that’s what we showed in our Alliance poster, and what I’ve said is based on over 30 years of work in this area,” she said.
She cited what she considered as the two most important components for improving accrual of underrepresented populations: a commitment by leadership to a recruitment goal, and the development of protocols with specific accrual goals for minority populations.
Still, those are only two components of a comprehensive program that includes the aforementioned accrual goal set by Dr. Bertagnolli, as well as the following:
- Funding of minority junior investigators and research that focuses on issues of concern to underrepresented populations.
- Establishment of work groups that focus on specific populations with the Alliance health disparities committee.
- Translation of informational materials for patients.
- Opening studies at National Cancer Institute Community. Oncology Research Program–designated minority underserved sites.
- Real-time monitoring of accrual demographics by the Alliance and at the trial site.
- Closing protocol enrollment to majority populations.
- Increasing the study sample sizes to enroll additional minority participants and to allow for subgroup analyses.
The study was funded by the National Institutes of Health. Dr. Packett and Dr. Blinder reported no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
CHICAGO – Clinical trials are so White. Only a small percentage of eligible patients participate in clinical trials in the first place, and very few come from racial and ethnic minority groups.
For example, according to the Food and Drug Administration, in trials that resulted in drug approvals from 2017 to 2020, only 2%-5% of participants were Black patients.
When clinical trials lack diverse patient populations, those who are left out have fewer opportunities to get new therapies. Moreover, the scope of the research is limited by smaller phenotypic and genotypic samples, and the trial results are applicable only to more homogeneous patient groups.
There has been a push to include more underrepresented patients in clinical trials. One group reported its success in doing so here at the annual meeting of the American Society of Clinical Oncology.
a period that included a pandemic-induced hiatus in clinical trials in general.
Alliance member Electra D. Paskett, PhD, from the College of Public Health at the Ohio State University in Columbus, presented accrual data from 117 trials led by the Alliance from 2014 to 2022.
During this period, accrual of racial and ethnic minority patients increased from 13.6% to 25.3% for cancer treatment trials and from 13% to 21.5% for cancer control trials.
Overall, the recruitment program resulted in an absolute increase from 13.5 % to 23.6% of underrepresented populations, which translated into a relative 74.8% improvement.
“We’re focusing now on monitoring accrual of women, rural populations, younger AYAs [adolescents and young adults] and older patients, and we’ll see what strategies we need to implement,” Dr. Packett told this news organization.
The Alliance has implemented a real-time accrual dashboard on its website that allows individual sites to review accrual by trial and overall for all of the identified underrepresented populations, she noted.
Program to increase underrepresented patient accrual
The impetus for the program to increase enrollment of underrepresented patients came from the goal set by Monica M. Bertagnolli, MD, group chair of the Alliance from 2011 to 2022 and currently the director of the U.S. National Cancer Institute.
“Our leader, Dr. Bertagnolli, set out a group-wide goal for accrual of underrepresented minorities to our trials of 20%, and that gave us permission to implement a whole host of new strategies,” Dr. Paskett said in an interview.
“These strategies follow the Accrual of Clinical Trials framework, which essentially says that the interaction between the patient and the provider for going on a clinical trial is not just an interaction between the patient and provider but recognizes, for example, that the provider has coworkers and they have norms and beliefs and attitudes, and the patient comes from a family with their own values. And then there are system-level barriers, and there are community barriers that all relate to this interaction about going on a trial,” Dr. Packett said.
What works?
The study was presented as a poster at the meeting. During the poster discussion session, comoderator Victoria S. Blinder, MD, from Memorial Sloan Kettering Cancer Center in New York, asked Dr. Paskett, “If you had a certain amount of money and you really wanted to use that resource to focus on one area, where would you put that resource?”
“I’m going to violate the rules of your question,” Dr. Paskett replied.
“You cannot change this problem by focusing on one thing, and that’s what we showed in our Alliance poster, and what I’ve said is based on over 30 years of work in this area,” she said.
She cited what she considered as the two most important components for improving accrual of underrepresented populations: a commitment by leadership to a recruitment goal, and the development of protocols with specific accrual goals for minority populations.
Still, those are only two components of a comprehensive program that includes the aforementioned accrual goal set by Dr. Bertagnolli, as well as the following:
- Funding of minority junior investigators and research that focuses on issues of concern to underrepresented populations.
- Establishment of work groups that focus on specific populations with the Alliance health disparities committee.
- Translation of informational materials for patients.
- Opening studies at National Cancer Institute Community. Oncology Research Program–designated minority underserved sites.
- Real-time monitoring of accrual demographics by the Alliance and at the trial site.
- Closing protocol enrollment to majority populations.
- Increasing the study sample sizes to enroll additional minority participants and to allow for subgroup analyses.
The study was funded by the National Institutes of Health. Dr. Packett and Dr. Blinder reported no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
CHICAGO – Clinical trials are so White. Only a small percentage of eligible patients participate in clinical trials in the first place, and very few come from racial and ethnic minority groups.
For example, according to the Food and Drug Administration, in trials that resulted in drug approvals from 2017 to 2020, only 2%-5% of participants were Black patients.
When clinical trials lack diverse patient populations, those who are left out have fewer opportunities to get new therapies. Moreover, the scope of the research is limited by smaller phenotypic and genotypic samples, and the trial results are applicable only to more homogeneous patient groups.
There has been a push to include more underrepresented patients in clinical trials. One group reported its success in doing so here at the annual meeting of the American Society of Clinical Oncology.
a period that included a pandemic-induced hiatus in clinical trials in general.
Alliance member Electra D. Paskett, PhD, from the College of Public Health at the Ohio State University in Columbus, presented accrual data from 117 trials led by the Alliance from 2014 to 2022.
During this period, accrual of racial and ethnic minority patients increased from 13.6% to 25.3% for cancer treatment trials and from 13% to 21.5% for cancer control trials.
Overall, the recruitment program resulted in an absolute increase from 13.5 % to 23.6% of underrepresented populations, which translated into a relative 74.8% improvement.
“We’re focusing now on monitoring accrual of women, rural populations, younger AYAs [adolescents and young adults] and older patients, and we’ll see what strategies we need to implement,” Dr. Packett told this news organization.
The Alliance has implemented a real-time accrual dashboard on its website that allows individual sites to review accrual by trial and overall for all of the identified underrepresented populations, she noted.
Program to increase underrepresented patient accrual
The impetus for the program to increase enrollment of underrepresented patients came from the goal set by Monica M. Bertagnolli, MD, group chair of the Alliance from 2011 to 2022 and currently the director of the U.S. National Cancer Institute.
“Our leader, Dr. Bertagnolli, set out a group-wide goal for accrual of underrepresented minorities to our trials of 20%, and that gave us permission to implement a whole host of new strategies,” Dr. Paskett said in an interview.
“These strategies follow the Accrual of Clinical Trials framework, which essentially says that the interaction between the patient and the provider for going on a clinical trial is not just an interaction between the patient and provider but recognizes, for example, that the provider has coworkers and they have norms and beliefs and attitudes, and the patient comes from a family with their own values. And then there are system-level barriers, and there are community barriers that all relate to this interaction about going on a trial,” Dr. Packett said.
What works?
The study was presented as a poster at the meeting. During the poster discussion session, comoderator Victoria S. Blinder, MD, from Memorial Sloan Kettering Cancer Center in New York, asked Dr. Paskett, “If you had a certain amount of money and you really wanted to use that resource to focus on one area, where would you put that resource?”
“I’m going to violate the rules of your question,” Dr. Paskett replied.
“You cannot change this problem by focusing on one thing, and that’s what we showed in our Alliance poster, and what I’ve said is based on over 30 years of work in this area,” she said.
She cited what she considered as the two most important components for improving accrual of underrepresented populations: a commitment by leadership to a recruitment goal, and the development of protocols with specific accrual goals for minority populations.
Still, those are only two components of a comprehensive program that includes the aforementioned accrual goal set by Dr. Bertagnolli, as well as the following:
- Funding of minority junior investigators and research that focuses on issues of concern to underrepresented populations.
- Establishment of work groups that focus on specific populations with the Alliance health disparities committee.
- Translation of informational materials for patients.
- Opening studies at National Cancer Institute Community. Oncology Research Program–designated minority underserved sites.
- Real-time monitoring of accrual demographics by the Alliance and at the trial site.
- Closing protocol enrollment to majority populations.
- Increasing the study sample sizes to enroll additional minority participants and to allow for subgroup analyses.
The study was funded by the National Institutes of Health. Dr. Packett and Dr. Blinder reported no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
AT ASCO 2023