User login
AHA issues new scientific statement on heart health for LGBTQ adults
Cardiovascular health should be routinely assessed and addressed in LGBTQ adults, the American Heart Association concluded in a new scientific statement.
“Among the most important takeaways from this scientific statement is the need for health care providers in clinical settings to routinely assess sexual orientation and gender identity,” Billy A. Caceres, PhD, RN, chair of the statement writing group, said in an interview.
“This will help health care providers engage LGBTQ patients in discussions about their heart health that account for the unique experiences of this population,” said Dr. Caceres, assistant professor at Columbia University, New York.
The statement was published online Oct. 8 in Circulation.
‘Invisible’ population
There are roughly 11 million LGBTQ adults in the United States, yet they are often “invisible in health care settings and cardiovascular research,” Dr. Caceres noted. The AHA scientific statement is the first from a national organization in the United States to comprehensively summarize the evidence on cardiovascular (CV) research in LGBTQ adults.
There is mounting evidence that LGBTQ adults experience worse CV health relative to their cisgender heterosexual peers. Disparities in CV health may be driven by unique psychosocial stressors in the LGBTQ individuals such as family rejection and anxiety of concealment of their sexual orientation or gender identity.
While there is limited information on the CV health of LGBTQ people, the writing group said providers should be aware of the following:
- LGBTQ adults are more likely to use tobacco than their cisgender heterosexual peers.
- Transgender adults may be less physically active than their cisgender counterparts. Gender-affirming care might play a role in promoting physical activity among transgender people.
- Transgender women may be at increased risk for heart disease because of behavioral and clinical factors (such as the use of gender-affirming hormones like estrogen).
- Transgender women and nonbinary persons are more likely to binge drink.
- Lesbian and bisexual women have a higher prevalence of obesity than heterosexual women do.
“We need to better understand how to support LGBTQ adults in optimizing their CV health. To do this, we will need rigorous research that examines potential explanations for the CV health disparities that have been observed in LGBTQ adults,” Dr. Caceres said.
He noted that research is also needed within the LGBTQ population among groups that might be at greater risk for heart disease, including racial- and ethnic-minority and low-income LGBTQ adults.
“Researchers should also design and test evidence-based interventions to promote the heart health of LGBTQ adults. This is an area that is greatly lacking within CV health research,” said Dr. Caceres.
Discrimination in health care
Discrimination against LGBTQ adults in health care settings also remains a problem, the authors noted.
The writing group cites data showing that nearly 56% of sexual-minority and 70% of gender-minority adults report having experienced some form of discrimination from clinicians, including the use of harsh/abusive language.
“Perhaps most alarming,” roughly 8% of sexual-minority and 25% of transgender individuals have been denied health care by clinicians, they noted.
“LGBTQ individuals are delaying primary care and preventative visits because there is a great fear of being treated differently. Being treated differently often means receiving inadequate or inferior care because of sexual orientation or gender identity,” Dr. Caceres said in a news release.
The writing group calls for greater emphasis on LGBTQ health issues in the education of all health care providers. Dr. Caceres said it’s “paramount to include content about LGBTQ health in clinical training and licensure requirements in order to address these cardiovascular health disparities.”
Traditionally, there has been very little LGBTQ-related content in health care professional education training. A 2018 online survey of students at 10 medical schools found that approximately 80% of students did not feel competent to provide care for transgender patients.
But that may soon change. In September 2020, the Accreditation Review Commission on Education for the Physician Assistant began requiring LGBTQ curricular content, the writing group notes.
The AHA scientific statement on LGBTQ was developed by the writing group on behalf of the AHA Council on Cardiovascular and Stroke Nursing, the Council on Hypertension, the Council on Lifestyle and Cardiometabolic Health, the Council on Peripheral Vascular Disease, and the Stroke Council.
A version of this article originally appeared on Medscape.com.
Cardiovascular health should be routinely assessed and addressed in LGBTQ adults, the American Heart Association concluded in a new scientific statement.
“Among the most important takeaways from this scientific statement is the need for health care providers in clinical settings to routinely assess sexual orientation and gender identity,” Billy A. Caceres, PhD, RN, chair of the statement writing group, said in an interview.
“This will help health care providers engage LGBTQ patients in discussions about their heart health that account for the unique experiences of this population,” said Dr. Caceres, assistant professor at Columbia University, New York.
The statement was published online Oct. 8 in Circulation.
‘Invisible’ population
There are roughly 11 million LGBTQ adults in the United States, yet they are often “invisible in health care settings and cardiovascular research,” Dr. Caceres noted. The AHA scientific statement is the first from a national organization in the United States to comprehensively summarize the evidence on cardiovascular (CV) research in LGBTQ adults.
There is mounting evidence that LGBTQ adults experience worse CV health relative to their cisgender heterosexual peers. Disparities in CV health may be driven by unique psychosocial stressors in the LGBTQ individuals such as family rejection and anxiety of concealment of their sexual orientation or gender identity.
While there is limited information on the CV health of LGBTQ people, the writing group said providers should be aware of the following:
- LGBTQ adults are more likely to use tobacco than their cisgender heterosexual peers.
- Transgender adults may be less physically active than their cisgender counterparts. Gender-affirming care might play a role in promoting physical activity among transgender people.
- Transgender women may be at increased risk for heart disease because of behavioral and clinical factors (such as the use of gender-affirming hormones like estrogen).
- Transgender women and nonbinary persons are more likely to binge drink.
- Lesbian and bisexual women have a higher prevalence of obesity than heterosexual women do.
“We need to better understand how to support LGBTQ adults in optimizing their CV health. To do this, we will need rigorous research that examines potential explanations for the CV health disparities that have been observed in LGBTQ adults,” Dr. Caceres said.
He noted that research is also needed within the LGBTQ population among groups that might be at greater risk for heart disease, including racial- and ethnic-minority and low-income LGBTQ adults.
“Researchers should also design and test evidence-based interventions to promote the heart health of LGBTQ adults. This is an area that is greatly lacking within CV health research,” said Dr. Caceres.
Discrimination in health care
Discrimination against LGBTQ adults in health care settings also remains a problem, the authors noted.
The writing group cites data showing that nearly 56% of sexual-minority and 70% of gender-minority adults report having experienced some form of discrimination from clinicians, including the use of harsh/abusive language.
“Perhaps most alarming,” roughly 8% of sexual-minority and 25% of transgender individuals have been denied health care by clinicians, they noted.
“LGBTQ individuals are delaying primary care and preventative visits because there is a great fear of being treated differently. Being treated differently often means receiving inadequate or inferior care because of sexual orientation or gender identity,” Dr. Caceres said in a news release.
The writing group calls for greater emphasis on LGBTQ health issues in the education of all health care providers. Dr. Caceres said it’s “paramount to include content about LGBTQ health in clinical training and licensure requirements in order to address these cardiovascular health disparities.”
Traditionally, there has been very little LGBTQ-related content in health care professional education training. A 2018 online survey of students at 10 medical schools found that approximately 80% of students did not feel competent to provide care for transgender patients.
But that may soon change. In September 2020, the Accreditation Review Commission on Education for the Physician Assistant began requiring LGBTQ curricular content, the writing group notes.
The AHA scientific statement on LGBTQ was developed by the writing group on behalf of the AHA Council on Cardiovascular and Stroke Nursing, the Council on Hypertension, the Council on Lifestyle and Cardiometabolic Health, the Council on Peripheral Vascular Disease, and the Stroke Council.
A version of this article originally appeared on Medscape.com.
Cardiovascular health should be routinely assessed and addressed in LGBTQ adults, the American Heart Association concluded in a new scientific statement.
“Among the most important takeaways from this scientific statement is the need for health care providers in clinical settings to routinely assess sexual orientation and gender identity,” Billy A. Caceres, PhD, RN, chair of the statement writing group, said in an interview.
“This will help health care providers engage LGBTQ patients in discussions about their heart health that account for the unique experiences of this population,” said Dr. Caceres, assistant professor at Columbia University, New York.
The statement was published online Oct. 8 in Circulation.
‘Invisible’ population
There are roughly 11 million LGBTQ adults in the United States, yet they are often “invisible in health care settings and cardiovascular research,” Dr. Caceres noted. The AHA scientific statement is the first from a national organization in the United States to comprehensively summarize the evidence on cardiovascular (CV) research in LGBTQ adults.
There is mounting evidence that LGBTQ adults experience worse CV health relative to their cisgender heterosexual peers. Disparities in CV health may be driven by unique psychosocial stressors in the LGBTQ individuals such as family rejection and anxiety of concealment of their sexual orientation or gender identity.
While there is limited information on the CV health of LGBTQ people, the writing group said providers should be aware of the following:
- LGBTQ adults are more likely to use tobacco than their cisgender heterosexual peers.
- Transgender adults may be less physically active than their cisgender counterparts. Gender-affirming care might play a role in promoting physical activity among transgender people.
- Transgender women may be at increased risk for heart disease because of behavioral and clinical factors (such as the use of gender-affirming hormones like estrogen).
- Transgender women and nonbinary persons are more likely to binge drink.
- Lesbian and bisexual women have a higher prevalence of obesity than heterosexual women do.
“We need to better understand how to support LGBTQ adults in optimizing their CV health. To do this, we will need rigorous research that examines potential explanations for the CV health disparities that have been observed in LGBTQ adults,” Dr. Caceres said.
He noted that research is also needed within the LGBTQ population among groups that might be at greater risk for heart disease, including racial- and ethnic-minority and low-income LGBTQ adults.
“Researchers should also design and test evidence-based interventions to promote the heart health of LGBTQ adults. This is an area that is greatly lacking within CV health research,” said Dr. Caceres.
Discrimination in health care
Discrimination against LGBTQ adults in health care settings also remains a problem, the authors noted.
The writing group cites data showing that nearly 56% of sexual-minority and 70% of gender-minority adults report having experienced some form of discrimination from clinicians, including the use of harsh/abusive language.
“Perhaps most alarming,” roughly 8% of sexual-minority and 25% of transgender individuals have been denied health care by clinicians, they noted.
“LGBTQ individuals are delaying primary care and preventative visits because there is a great fear of being treated differently. Being treated differently often means receiving inadequate or inferior care because of sexual orientation or gender identity,” Dr. Caceres said in a news release.
The writing group calls for greater emphasis on LGBTQ health issues in the education of all health care providers. Dr. Caceres said it’s “paramount to include content about LGBTQ health in clinical training and licensure requirements in order to address these cardiovascular health disparities.”
Traditionally, there has been very little LGBTQ-related content in health care professional education training. A 2018 online survey of students at 10 medical schools found that approximately 80% of students did not feel competent to provide care for transgender patients.
But that may soon change. In September 2020, the Accreditation Review Commission on Education for the Physician Assistant began requiring LGBTQ curricular content, the writing group notes.
The AHA scientific statement on LGBTQ was developed by the writing group on behalf of the AHA Council on Cardiovascular and Stroke Nursing, the Council on Hypertension, the Council on Lifestyle and Cardiometabolic Health, the Council on Peripheral Vascular Disease, and the Stroke Council.
A version of this article originally appeared on Medscape.com.
Benefit of rivaroxaban after limb revascularization greatest in those with comorbid CAD
The absolute benefit of adding low-dose rivaroxaban to low-dose aspirin following revascularization for symptomatic lower-extremity peripheral artery disease (PAD) is significantly greater in patients with comorbid coronary artery disease (CAD), according to a new secondary analysis of the VOYAGER PAD trial.

“These findings suggest heterogeneity of prognostic risk for ischemic events in lower-extremity PAD patients, and may support shared decision-making with these patients,” William R. Hiatt, MD, observed in presenting the study results at the virtual annual congress of the European Society of Cardiology.
VOYAGER PAD was a 3-year, 34-country clinical trial in which 6,564 patients with symptomatic PAD who had recently undergone lower-limb revascularization were randomized in double-blind fashion to rivaroxaban (Xarelto) at 2.5 mg twice daily or placebo on top of background standard therapy with low-dose aspirin.
Among the 2,067 participants with baseline comorbid CAD, the primary outcome – a composite comprised of cardiovascular death, acute MI, ischemic stroke, acute limb ischemia, and major amputation – occurred in 18.9% of the rivaroxaban group at 3 years and 24.3% on placebo, for a highly significant 22% relative risk reduction.
In contrast, in the 4,497 patients with PAD only, the primary outcome occurred in 16.1% of those on rivaroxaban and 17.9% of controls, an 11% relative risk reduction which failed to reach statistical significance. The absolute risk reduction achieved with rivaroxaban was 5.4% in patients with PAD plus CAD versus 1.8% in those with PAD alone. Thus, the significant clinical benefit with rivaroxaban plus aspirin previously reported in the overall study population, with a number needed to treat for 3 years of 39 in order to prevent one primary outcome event, was largely driven by the superior outcomes in the dual-diagnosis subgroup, reported Dr. Hiatt, professor of medicine at the University of Colorado at Denver, Aurora.
“A strategy of rivaroxaban at 2.5 mg twice daily plus low-dose aspirin versus low-dose aspirin alone reduces ischemic events of the limb, brain, and heart, but also increases bleeding, with an overall net benefit,” the cardiologist said. “In particular, the benefits of this strategy for MI and ischemic stroke are robust, especially in patients with PAD and CAD.”
Indeed, the MI rate at 3 years in the dual diagnosis subgroup was 7.3% with rivaroxaban and 8.8% with placebo, for a 23% relative risk reduction, compared with rates of 3.3% and 3.7%, respectively, in patients with PAD only. Similarly, ischemic stroke occurred in 2.9% of patients with PAD and CAD in the rivaroxaban group, compared with 3.9% with placebo, whereas the rate in the PAD only group was identical at 2.6% regardless of whether patients were on rivaroxaban or placebo.
In patients without CAD, the clinical benefit of rivaroxaban was driven by reductions in severe limb events. Their rate of acute limb ischemia was 5.2% with rivaroxaban, compared with 8.3% with placebo, for a 37% relative risk reduction. In contrast, the reduction in acute limb ischemia with rivaroxaban in patients with PAD and CAD wasn’t significantly different from placebo.
Thrombolysis in Myocardial Infarction major bleeding occurred in 2.4% of patients with PAD and CAD on rivaroxaban, compared with 1.1% on placebo, and in 1.7% and 1.5% of patients with PAD alone. Of note, rates of ischemic stroke or fatal hemorrhage were low and similar at less than 1% in all four groups, Dr. Hiatt noted.
VOYAGER PAD was sponsored by Bayer and Janssen. Dr. Hiatt reported receiving research grant support from those two companies as well as Amgen.
The absolute benefit of adding low-dose rivaroxaban to low-dose aspirin following revascularization for symptomatic lower-extremity peripheral artery disease (PAD) is significantly greater in patients with comorbid coronary artery disease (CAD), according to a new secondary analysis of the VOYAGER PAD trial.
“These findings suggest heterogeneity of prognostic risk for ischemic events in lower-extremity PAD patients, and may support shared decision-making with these patients,” William R. Hiatt, MD, observed in presenting the study results at the virtual annual congress of the European Society of Cardiology.
VOYAGER PAD was a 3-year, 34-country clinical trial in which 6,564 patients with symptomatic PAD who had recently undergone lower-limb revascularization were randomized in double-blind fashion to rivaroxaban (Xarelto) at 2.5 mg twice daily or placebo on top of background standard therapy with low-dose aspirin.
Among the 2,067 participants with baseline comorbid CAD, the primary outcome – a composite comprised of cardiovascular death, acute MI, ischemic stroke, acute limb ischemia, and major amputation – occurred in 18.9% of the rivaroxaban group at 3 years and 24.3% on placebo, for a highly significant 22% relative risk reduction.
In contrast, in the 4,497 patients with PAD only, the primary outcome occurred in 16.1% of those on rivaroxaban and 17.9% of controls, an 11% relative risk reduction which failed to reach statistical significance. The absolute risk reduction achieved with rivaroxaban was 5.4% in patients with PAD plus CAD versus 1.8% in those with PAD alone. Thus, the significant clinical benefit with rivaroxaban plus aspirin previously reported in the overall study population, with a number needed to treat for 3 years of 39 in order to prevent one primary outcome event, was largely driven by the superior outcomes in the dual-diagnosis subgroup, reported Dr. Hiatt, professor of medicine at the University of Colorado at Denver, Aurora.
“A strategy of rivaroxaban at 2.5 mg twice daily plus low-dose aspirin versus low-dose aspirin alone reduces ischemic events of the limb, brain, and heart, but also increases bleeding, with an overall net benefit,” the cardiologist said. “In particular, the benefits of this strategy for MI and ischemic stroke are robust, especially in patients with PAD and CAD.”
Indeed, the MI rate at 3 years in the dual diagnosis subgroup was 7.3% with rivaroxaban and 8.8% with placebo, for a 23% relative risk reduction, compared with rates of 3.3% and 3.7%, respectively, in patients with PAD only. Similarly, ischemic stroke occurred in 2.9% of patients with PAD and CAD in the rivaroxaban group, compared with 3.9% with placebo, whereas the rate in the PAD only group was identical at 2.6% regardless of whether patients were on rivaroxaban or placebo.
In patients without CAD, the clinical benefit of rivaroxaban was driven by reductions in severe limb events. Their rate of acute limb ischemia was 5.2% with rivaroxaban, compared with 8.3% with placebo, for a 37% relative risk reduction. In contrast, the reduction in acute limb ischemia with rivaroxaban in patients with PAD and CAD wasn’t significantly different from placebo.
Thrombolysis in Myocardial Infarction major bleeding occurred in 2.4% of patients with PAD and CAD on rivaroxaban, compared with 1.1% on placebo, and in 1.7% and 1.5% of patients with PAD alone. Of note, rates of ischemic stroke or fatal hemorrhage were low and similar at less than 1% in all four groups, Dr. Hiatt noted.
VOYAGER PAD was sponsored by Bayer and Janssen. Dr. Hiatt reported receiving research grant support from those two companies as well as Amgen.
The absolute benefit of adding low-dose rivaroxaban to low-dose aspirin following revascularization for symptomatic lower-extremity peripheral artery disease (PAD) is significantly greater in patients with comorbid coronary artery disease (CAD), according to a new secondary analysis of the VOYAGER PAD trial.
“These findings suggest heterogeneity of prognostic risk for ischemic events in lower-extremity PAD patients, and may support shared decision-making with these patients,” William R. Hiatt, MD, observed in presenting the study results at the virtual annual congress of the European Society of Cardiology.
VOYAGER PAD was a 3-year, 34-country clinical trial in which 6,564 patients with symptomatic PAD who had recently undergone lower-limb revascularization were randomized in double-blind fashion to rivaroxaban (Xarelto) at 2.5 mg twice daily or placebo on top of background standard therapy with low-dose aspirin.
Among the 2,067 participants with baseline comorbid CAD, the primary outcome – a composite comprised of cardiovascular death, acute MI, ischemic stroke, acute limb ischemia, and major amputation – occurred in 18.9% of the rivaroxaban group at 3 years and 24.3% on placebo, for a highly significant 22% relative risk reduction.
In contrast, in the 4,497 patients with PAD only, the primary outcome occurred in 16.1% of those on rivaroxaban and 17.9% of controls, an 11% relative risk reduction which failed to reach statistical significance. The absolute risk reduction achieved with rivaroxaban was 5.4% in patients with PAD plus CAD versus 1.8% in those with PAD alone. Thus, the significant clinical benefit with rivaroxaban plus aspirin previously reported in the overall study population, with a number needed to treat for 3 years of 39 in order to prevent one primary outcome event, was largely driven by the superior outcomes in the dual-diagnosis subgroup, reported Dr. Hiatt, professor of medicine at the University of Colorado at Denver, Aurora.
“A strategy of rivaroxaban at 2.5 mg twice daily plus low-dose aspirin versus low-dose aspirin alone reduces ischemic events of the limb, brain, and heart, but also increases bleeding, with an overall net benefit,” the cardiologist said. “In particular, the benefits of this strategy for MI and ischemic stroke are robust, especially in patients with PAD and CAD.”
Indeed, the MI rate at 3 years in the dual diagnosis subgroup was 7.3% with rivaroxaban and 8.8% with placebo, for a 23% relative risk reduction, compared with rates of 3.3% and 3.7%, respectively, in patients with PAD only. Similarly, ischemic stroke occurred in 2.9% of patients with PAD and CAD in the rivaroxaban group, compared with 3.9% with placebo, whereas the rate in the PAD only group was identical at 2.6% regardless of whether patients were on rivaroxaban or placebo.
In patients without CAD, the clinical benefit of rivaroxaban was driven by reductions in severe limb events. Their rate of acute limb ischemia was 5.2% with rivaroxaban, compared with 8.3% with placebo, for a 37% relative risk reduction. In contrast, the reduction in acute limb ischemia with rivaroxaban in patients with PAD and CAD wasn’t significantly different from placebo.
Thrombolysis in Myocardial Infarction major bleeding occurred in 2.4% of patients with PAD and CAD on rivaroxaban, compared with 1.1% on placebo, and in 1.7% and 1.5% of patients with PAD alone. Of note, rates of ischemic stroke or fatal hemorrhage were low and similar at less than 1% in all four groups, Dr. Hiatt noted.
VOYAGER PAD was sponsored by Bayer and Janssen. Dr. Hiatt reported receiving research grant support from those two companies as well as Amgen.
FROM ESC CONGRESS 2020
Empagliflozin cut PA pressures in heart failure patients
Elevated pulmonary artery diastolic pressure is “perhaps the best predictor of bad outcomes in patients with heart failure, including hospitalization and death,” and new evidence clearly showed that the sodium-glucose cotransporter 2 (SGLT2) inhibitor empagliflozin cuts this metric in patients by a clinically significant amount, Mikhail Kosiborod, MD, said at the virtual annual scientific meeting of the Heart Failure Society of America.

The evidence he collected from a total of 65 heart failure patients with either reduced or preserved ejection fraction is the first documentation from a randomized, controlled study to show a direct effect by a SGLT2 inhibitor on pulmonary artery (PA) pressures.
Other key findings were that the drop in PA diastolic pressure with empagliflozin treatment compared with placebo became discernible early (within the first 4 weeks on treatment), that the pressure-lowering effect steadily grew over time, and that it showed no link to the intensity of loop diuretic treatment, which held steady during 12 weeks on treatment and 13 weeks of overall monitoring.
The study’s primary endpoint was the change from baseline in PA diastolic pressure after 12 weeks on treatment. The 31 patients who completed the full 12-week course had an average drop in their PA diastolic pressure of about 1.5 mm Hg, compared with 28 patients who completed 12 weeks on placebo. Average PA diastolic pressure at baseline was about 21 mm Hg in both treatment arms, and on treatment this fell by more than 0.5 mm Hg among those who received empagliflozin and rose by close to 1 mm Hg among control patients.
“There appears to be a direct effect of empagliflozin on pulmonary artery pressure that’s not been previously demonstrated” by an SGLT2 inhibitor, Dr. Kosiborod said. “I think this is one mechanism of action” for this drug class. “If you control pulmonary artery filling pressures you can prevent hospitalizations and deaths.”
Small reductions matter
“Small pressure differences are particularly important for pulmonary hypertension,” commented Lynne W. Stevenson, MD, professor of medicine at Vanderbilt University Medical Center in Nashville, Tenn., and the report’s designated discussant.
“In the Vanderbilt heart failure database, patients with a pulmonary artery mean pressure of 20-24 mm Hg had 30% higher mortality than patients with lower pressures,” Dr. Stevenson noted. “This has led to a new definition of pulmonary hypertension, a mean pulmonary artery pressure above at or above 20 mm Hg.”
In Dr. Kosiborod’s study, patients began with an average PA mean pressure of about 30 mm Hg, and empagliflozin treatment led to a reduction in this metric with about the same magnitude as its effect on PA diastolic pressure. Empagliflozin also produced a similar reduction in average PA systolic pressure.

A study built on ambulatory PA monitoring
The results “also provide more proof for the concept of ambulatory hemodynamic monitoring” in patients with heart failure to monitor their status, she added. The study enrolled only patients who had already received a CardioMEMS implant as part of their routine care. This device allows for frequent, noninvasive monitoring of PA pressures. Researchers collected PA pressure data from patients twice daily for the entire 13-week study.
The EMBRACE HF (Empagliflozin Impact on Hemodynamics in Patients With Heart Failure) study enrolled patients with established heart failure, a CardioMEMS implant, and New York Heart Association class II-IV symptoms at any of eight U.S. centers. Patients averaged about 65 years old, and slightly more than half had class III disease, which denotes marked limitation of physical activity.
Despite the brief treatment period, patients who received empagliflozin showed other evidence of benefit including a trend toward improved quality of life scores, reduced levels of two different forms of brain natriuretic peptide, and significant weight loss, compared with controls, that averaged 2.4 kg.
The mechanism by which empagliflozin and other drugs in its class might lower PA filling pressures is unclear, but Dr. Kosiborod stressed that the consistent level of loop diuretic use during the study seems to rule out a diuretic effect from the SGLT2 inhibitor as having a role. A pulmonary vasculature effect is “much more likely,” perhaps mediated through modified endothelial function and vasodilation, he suggested.
EMBRACE HF was funded by Boehringer Ingelheim, the company that markets empagliflozin (Jardiance) along with Eli Lilly. Dr. Kosiborod has received research support and honoraria from Boehringer Ingelheim, and he has received honoraria from several other companies. Dr. Stevenson had no disclosures.
Elevated pulmonary artery diastolic pressure is “perhaps the best predictor of bad outcomes in patients with heart failure, including hospitalization and death,” and new evidence clearly showed that the sodium-glucose cotransporter 2 (SGLT2) inhibitor empagliflozin cuts this metric in patients by a clinically significant amount, Mikhail Kosiborod, MD, said at the virtual annual scientific meeting of the Heart Failure Society of America.
The evidence he collected from a total of 65 heart failure patients with either reduced or preserved ejection fraction is the first documentation from a randomized, controlled study to show a direct effect by a SGLT2 inhibitor on pulmonary artery (PA) pressures.
Other key findings were that the drop in PA diastolic pressure with empagliflozin treatment compared with placebo became discernible early (within the first 4 weeks on treatment), that the pressure-lowering effect steadily grew over time, and that it showed no link to the intensity of loop diuretic treatment, which held steady during 12 weeks on treatment and 13 weeks of overall monitoring.
The study’s primary endpoint was the change from baseline in PA diastolic pressure after 12 weeks on treatment. The 31 patients who completed the full 12-week course had an average drop in their PA diastolic pressure of about 1.5 mm Hg, compared with 28 patients who completed 12 weeks on placebo. Average PA diastolic pressure at baseline was about 21 mm Hg in both treatment arms, and on treatment this fell by more than 0.5 mm Hg among those who received empagliflozin and rose by close to 1 mm Hg among control patients.
“There appears to be a direct effect of empagliflozin on pulmonary artery pressure that’s not been previously demonstrated” by an SGLT2 inhibitor, Dr. Kosiborod said. “I think this is one mechanism of action” for this drug class. “If you control pulmonary artery filling pressures you can prevent hospitalizations and deaths.”
Small reductions matter
“Small pressure differences are particularly important for pulmonary hypertension,” commented Lynne W. Stevenson, MD, professor of medicine at Vanderbilt University Medical Center in Nashville, Tenn., and the report’s designated discussant.
“In the Vanderbilt heart failure database, patients with a pulmonary artery mean pressure of 20-24 mm Hg had 30% higher mortality than patients with lower pressures,” Dr. Stevenson noted. “This has led to a new definition of pulmonary hypertension, a mean pulmonary artery pressure above at or above 20 mm Hg.”
In Dr. Kosiborod’s study, patients began with an average PA mean pressure of about 30 mm Hg, and empagliflozin treatment led to a reduction in this metric with about the same magnitude as its effect on PA diastolic pressure. Empagliflozin also produced a similar reduction in average PA systolic pressure.
A study built on ambulatory PA monitoring
The results “also provide more proof for the concept of ambulatory hemodynamic monitoring” in patients with heart failure to monitor their status, she added. The study enrolled only patients who had already received a CardioMEMS implant as part of their routine care. This device allows for frequent, noninvasive monitoring of PA pressures. Researchers collected PA pressure data from patients twice daily for the entire 13-week study.
The EMBRACE HF (Empagliflozin Impact on Hemodynamics in Patients With Heart Failure) study enrolled patients with established heart failure, a CardioMEMS implant, and New York Heart Association class II-IV symptoms at any of eight U.S. centers. Patients averaged about 65 years old, and slightly more than half had class III disease, which denotes marked limitation of physical activity.
Despite the brief treatment period, patients who received empagliflozin showed other evidence of benefit including a trend toward improved quality of life scores, reduced levels of two different forms of brain natriuretic peptide, and significant weight loss, compared with controls, that averaged 2.4 kg.
The mechanism by which empagliflozin and other drugs in its class might lower PA filling pressures is unclear, but Dr. Kosiborod stressed that the consistent level of loop diuretic use during the study seems to rule out a diuretic effect from the SGLT2 inhibitor as having a role. A pulmonary vasculature effect is “much more likely,” perhaps mediated through modified endothelial function and vasodilation, he suggested.
EMBRACE HF was funded by Boehringer Ingelheim, the company that markets empagliflozin (Jardiance) along with Eli Lilly. Dr. Kosiborod has received research support and honoraria from Boehringer Ingelheim, and he has received honoraria from several other companies. Dr. Stevenson had no disclosures.
Elevated pulmonary artery diastolic pressure is “perhaps the best predictor of bad outcomes in patients with heart failure, including hospitalization and death,” and new evidence clearly showed that the sodium-glucose cotransporter 2 (SGLT2) inhibitor empagliflozin cuts this metric in patients by a clinically significant amount, Mikhail Kosiborod, MD, said at the virtual annual scientific meeting of the Heart Failure Society of America.
The evidence he collected from a total of 65 heart failure patients with either reduced or preserved ejection fraction is the first documentation from a randomized, controlled study to show a direct effect by a SGLT2 inhibitor on pulmonary artery (PA) pressures.
Other key findings were that the drop in PA diastolic pressure with empagliflozin treatment compared with placebo became discernible early (within the first 4 weeks on treatment), that the pressure-lowering effect steadily grew over time, and that it showed no link to the intensity of loop diuretic treatment, which held steady during 12 weeks on treatment and 13 weeks of overall monitoring.
The study’s primary endpoint was the change from baseline in PA diastolic pressure after 12 weeks on treatment. The 31 patients who completed the full 12-week course had an average drop in their PA diastolic pressure of about 1.5 mm Hg, compared with 28 patients who completed 12 weeks on placebo. Average PA diastolic pressure at baseline was about 21 mm Hg in both treatment arms, and on treatment this fell by more than 0.5 mm Hg among those who received empagliflozin and rose by close to 1 mm Hg among control patients.
“There appears to be a direct effect of empagliflozin on pulmonary artery pressure that’s not been previously demonstrated” by an SGLT2 inhibitor, Dr. Kosiborod said. “I think this is one mechanism of action” for this drug class. “If you control pulmonary artery filling pressures you can prevent hospitalizations and deaths.”
Small reductions matter
“Small pressure differences are particularly important for pulmonary hypertension,” commented Lynne W. Stevenson, MD, professor of medicine at Vanderbilt University Medical Center in Nashville, Tenn., and the report’s designated discussant.
“In the Vanderbilt heart failure database, patients with a pulmonary artery mean pressure of 20-24 mm Hg had 30% higher mortality than patients with lower pressures,” Dr. Stevenson noted. “This has led to a new definition of pulmonary hypertension, a mean pulmonary artery pressure above at or above 20 mm Hg.”
In Dr. Kosiborod’s study, patients began with an average PA mean pressure of about 30 mm Hg, and empagliflozin treatment led to a reduction in this metric with about the same magnitude as its effect on PA diastolic pressure. Empagliflozin also produced a similar reduction in average PA systolic pressure.
A study built on ambulatory PA monitoring
The results “also provide more proof for the concept of ambulatory hemodynamic monitoring” in patients with heart failure to monitor their status, she added. The study enrolled only patients who had already received a CardioMEMS implant as part of their routine care. This device allows for frequent, noninvasive monitoring of PA pressures. Researchers collected PA pressure data from patients twice daily for the entire 13-week study.
The EMBRACE HF (Empagliflozin Impact on Hemodynamics in Patients With Heart Failure) study enrolled patients with established heart failure, a CardioMEMS implant, and New York Heart Association class II-IV symptoms at any of eight U.S. centers. Patients averaged about 65 years old, and slightly more than half had class III disease, which denotes marked limitation of physical activity.
Despite the brief treatment period, patients who received empagliflozin showed other evidence of benefit including a trend toward improved quality of life scores, reduced levels of two different forms of brain natriuretic peptide, and significant weight loss, compared with controls, that averaged 2.4 kg.
The mechanism by which empagliflozin and other drugs in its class might lower PA filling pressures is unclear, but Dr. Kosiborod stressed that the consistent level of loop diuretic use during the study seems to rule out a diuretic effect from the SGLT2 inhibitor as having a role. A pulmonary vasculature effect is “much more likely,” perhaps mediated through modified endothelial function and vasodilation, he suggested.
EMBRACE HF was funded by Boehringer Ingelheim, the company that markets empagliflozin (Jardiance) along with Eli Lilly. Dr. Kosiborod has received research support and honoraria from Boehringer Ingelheim, and he has received honoraria from several other companies. Dr. Stevenson had no disclosures.
FROM HFSA 2020
Choosing Wisely: 10 practices to stop—or adopt—to reduce overuse in health care
When medical care is based on consistent, good-quality evidence, most physicians adopt it. However, not all care is well supported by the literature and may, in fact, be overused without offering benefit to patients. Choosing Wisely, at www.choosingwisely.org, is a health care initiative that highlights screening and testing recommendations from specialty societies in an effort to encourage patients and clinicians to talk about how to make high-value, effective health care decisions and avoid overuse. (See “Test and Tx overutilization: A bigger problem than you might think"1-3).
SIDEBAR
Test and Tx overutilization: A bigger problem than you might think
Care that isn’t backed up by the medical literature is adopted by some physicians and not adopted by others, leading to practice variations. Some variation is to be expected, since no 2 patients require exactly the same care, but substantial variations may be a clue to overuse.
A 2006 analysis of inpatient lab studies found that doctors ordered an average of 2.96 studies per patient per day, but only 29% of these tests (0.95 test/patient/day) contributed to management.1 A 2016 systematic review found more than 800 studies on overuse were published in a single year.2 One study of thyroid nodules followed almost 1000 patients with nodules as they underwent routine follow-up imaging. At the end of the study, 7 were found to have cancer, but of those, only 3 had enlarging or changing nodules that would have been detected with the follow-up imaging being studied. Three of the cancers were stable in size and 1 was found incidentally.3
Enabling physician and patient dialogue. The initiative began in 2010 when the American Board of Internal Medicine convened a panel of experts to identify low-value tests and therapies. Their list took the form of a “Top Five Things” that may not be high value in patient care, and it used language tailored to patients and physicians so that they could converse meaningfully. Physicians could use the evidence to make a clinical decision, and patients could feel empowered to ask informed questions about recommendations they received. The initiative has now expanded to include ways that health care systems can reduce low-value interventions.

Scope of participation. Since the first Choosing Wisely recommendations were published in 2013, more than 80 professional associations have contributed lists of their own. Professional societies participate voluntarily. The American Academy of Family Physicians (AAFP), Society of General Internal Medicine, and American Academy of Pediatrics (AAP) have contributed lists relevant to primary care. All Choosing Wisely recommendations can be searched or sorted by specialty organization. Recommendations are reviewed and revised regularly. If the evidence becomes conflicted or contradictory, recommendations are withdrawn.
Making meaningful improvements by Choosing Wisely
Several studies have shown that health care systems can implement Choosing Wisely recommendations to reduce overuse of unnecessary tests. A 2015 study examined the effect of applying a Choosing Wisely recommendation to reduce the use of continuous pulse oximetry in pediatric inpatients with asthma, wheezing, or bronchiolitis. The recommendation, from the Society of Hospital Medicine–Pediatric Hospital Medicine, advises against continuous pulse oximetry in children with acute respiratory illnesses unless the child is using supplemental oxygen.4 This study, done at the Cincinnati Children’s Hospital Medical Center, found that within 3 months of initiating a protocol on all general pediatrics floors, the average time on pulse oximetry after meeting clinical goals decreased from 10.7 hours to 3.1 hours. In addition, the percentage of patients who had their continuous pulse oximetry stopped within 2 hours of clinical stability (a goal time) increased from 25% to 46%.5
Patients are important drivers of health care utilization. A 2003 study showed that physicians are more likely to order referrals, tests, and prescriptions when patients ask for them, and that nearly 1 in 4 patients did so.6 A 2002 study found that physicians granted all but 3% of patient’s requests for orders or tests, and that fulfilling requests correlated with patient satisfaction in the specialty office studied (cardiology) but not in the primary care (internal medicine) office.7
From its inception, Choosing Wisely has considered patients as full partners in conversations about health care utilization. Choosing Wisely partners with Consumer Reports to create and disseminate plain-language summaries of recommendations. Community groups and physician organizations have also participated in implementation efforts. In 2018, Choosing Wisely secured a grant to expand outreach to diverse or underserved communities.
Choosing Wisely recommendations are not guidelines or mandates. They are intended to be evidence-based advice from a specialty society to its members and to patients about care that is often unnecessary. The goal is to create a conversation and not to eliminate these services from ever being offered or used.
Continue to: Improve your practice with these 10 primary care recommendations
Improve your practice with these 10 primary care recommendations
1 Avoid imaging studies in early acute low back pain without red flags.
Both the AAFP and the American Society of Anesthesiologists recommend against routine X-rays, magnetic resonance imaging, and computed tomography (CT) scans in the first 6 weeks of acute low back pain (LBP).8,9 The American College of Emergency Physicians (ACEP) recommends against routine lumbar spine imaging for emergency department (ED) patients.10 In all cases, imaging is indicated if the patient has any signs or symptoms of neurologic deficits or other indications, such as signs of spinal infection or fracture. However, as ACEP notes, diagnostic imaging does not typically help identify the cause of acute LBP, and when it does, it does not reduce the time to symptom improvement.10
2 Prescribe oral contraceptives on the basis of a medical history and a blood pressure measurement. No routine pelvic exam or other physical exam is necessary.
This AAFP recommendation11 is based on clinical practice guidelines from the American College of Obstetricians and Gynecologists (ACOG) and other research.12 The ACOG practice guideline supports provision of hormonal contraception without a pelvic exam, cervical cancer (Pap) testing, urine pregnancy testing, or testing for sexually transmitted infections. ACOG guidelines also support over-the-counter provision of hormonal contraceptives, including combined oral contraceptives.12
3 Stop recommending daily self-glucose monitoring for patients with diabetes who are not using insulin.
Both the AAFP and the Society for General Internal Medicine recommend against daily blood sugar checks for people who do not use insulin.13,14 A Cochrane review of 9 trials (3300 patients) found that after 6 months, hemoglobin A1C was reduced by 0.3% in people who checked their sugar daily compared with those who did not, but this difference was not significant after a year.15 Hypoglycemic episodes were more common in the “checking” group, and there were no differences in quality of life. A qualitative study found that blood sugar results had little impact on patients’ motivation to change behavior.16
4 Don’t screen for herpes simplex virus (HSV) infection in asymptomatic adults, even those who are pregnant.
This AAFP recommendation17 comes from a US Preventive Services Task Force (USPSTF) Grade D recommendation.18 Most people with positive HSV-2 serology have had an outbreak; even those who do not think they have had one will realize that they had the symptoms once they hear them described.18 With available tests, 1 in 2 positive results for HSV-2 among asymptomatic people will be a false-positive.18
There is no known cure, intervention, or reduction in transmission for infected patients who do not have symptoms.18 Also, serologically detected HSV-2 does not reliably predict genital herpes; and HSV-1 has been found to cause an increasing percentage of genital infection cases.18
Continue to: 5 Don't screen for testicular cancer in asymptomatic individuals
5 Don’t screen for testicular cancer in asymptomatic individuals.
This AAFP recommendation19 also comes from a USPSTF Grade D recommendation.20 A 2010 systematic review found no evidence to support screening of asymptomatic people with a physical exam or ultrasound. All available studies involved symptomatic patients.20
6 Stop recommending cough and cold medicines for children younger than 4 years.
The AAP recommends that clinicians discourage the use of any cough or cold medicine for children in this age-group.21 A 2008 study found that more than 7000 children annually presented to EDs for adverse events from cough and cold medicines.22 Previous studies found no benefit in reducing symptoms.23 In children older than 12 months, a Cochrane review found that honey has a modest benefit for cough in single-night trials.24
7 Avoid performing serum allergy panels.
The American Academy of Allergy, Asthma, and Immunology discourages the use of serum panel testing when patients present with allergy symptoms.25 A patient can have a strong positive immunoglobulin E (IgE) serum result to an allergen and have no clinical allergic symptoms or can have a weak positive serum result and a strong clinical reaction. Targeted skin or serum IgE testing—for example, testing for cashew allergy in a patient known to have had a reaction after eating one—is reasonable.26
8 Avoid routine electroencephalography (EEG), head CT, and carotid ultrasound as initial work-up for simple syncope in adults.
These recommendations, from the American Epilepsy Society,27 ACEP,28 American College of Physicians,29 and American Academy of Neurology (AAN),30 emphasize the low yield of routine work-ups for patients with simple syncope. The AAN notes that 40% of people will experience syncope during adulthood and most will not have carotid disease, which generally manifests with stroke-like symptoms rather than syncope. One study found that approximately 1 in 8 patients referred to an epilepsy clinic had neurocardiogenic syncope rather than epilepsy.31
EEGs have high false-negative and false-positive rates, and history-taking is a better tool with which to make a diagnosis. CT scans performed in the ED were found to contribute to the diagnosis of simple syncope in fewer than 2% of cases of syncope, compared with orthostatic blood pressure (25% of cases).32
Continue to: 9 Wait to refer children with umbilical hernias to pediatric surgery until they are 4 to 5 years of age
9 Wait to refer children with umbilical hernias to pediatric surgery until they are 4 to 5 years of age.
The AAP Section on Surgery offers evidence that the risk-benefit analysis strongly favors waiting on intervention.33 About 1 in 4 children will have an umbilical hernia, and about 85% of cases will resolve by age 5. The strangulation rate with umbilical hernias is very low, and although the risk of infection with surgery is likewise low, the risk of recurrence following surgery before the age of 4 is as high as 2.4%.34 The AAP Section on Surgery recommends against strapping or restraining the hernia, as well.
10 Avoid using appetite stimulants, such as megesterol, and high-calorie nutritional supplements to treat anorexia and cachexia in older adults.
Instead, the American Geriatrics Society recommends that physicians encourage caregivers to serve appealing food, provide support with eating, and remove barriers to appetite and nutrition.35 A Cochrane review showed that high-calorie supplements, such as Boost or Ensure, are associated with very modest weight gain—about 2% of weight—but are not associated with an increased life expectancy or improved quality of life.36
Prescription appetite stimulants are associated with adverse effects and yield inconsistent benefits in older adults. Megesterol, for example, was associated with headache, gastrointestinal adverse effects, insomnia, weakness, and fatigue. Mirtazapine is associated with sedation and fatigue.37
CORRESPONDENCE
Kathleen Rowland, MD, MS, Rush Copley Family Medicine Residency, Rush Medical College, 600 South Paulina, Kidston House Room 605, Chicago IL 60612; [email protected].
1. Miyakis S, Karamanof G, Liontos M, et al. Factors contributing to inappropriate ordering of tests in an academic medical department and the effect of an educational feedback strategy. Postgrad Med J. 2006;82:823-829.
2. Morgan DJ, Dhruva SS, Wright SM, et al. Update on medical overuse: a systematic review. JAMA Intern Med. 2016;176:1687-1692.
3. Durante C, Costante G, Lucisano G, et al. The natural history of benign thyroid nodules. JAMA. 2015;313:926-935.
4. Choosing Wisely. Society of Hospital Medicine—Pediatric hospital medicine. Don’t use continuous pulse oximetry routinely in children with acute respiratory illness unless they are on supplemental oxygen. www.choosingwisely.org/clinician-lists/society-hospital-medicine-pediatric-continuous-pulse-oximetry-in-children-with-acute-respiratory-illness/. Accessed September 28, 2020.
5. Schondelmeyer AC, Simmons JM, Statile AM, et al. Using quality improvement to reduce continuous pulse oximetry use in children with wheezing. Pediatrics. 2015;135:e1044-e1051.
6. Kravitz RL, Bell RA, Azari R, et al. Direct observation of requests for clinical services in office practice: what do patients want and do they get it? Arch Intern Med. 2003;163:1673-1681.
7. Kravitz RL, Bell RA, Franz CE, et al. Characterizing patient requests and physician responses in office practice. Health Serv Res. 2002;37:217-238.
8. Choosing Wisely. American Academy of Family Physicians. Don’t do imaging for low back pain within the first six weeks, unless red flags are present. www.choosingwisely.org/clinician-lists/american-academy-family-physicians-imaging-low-back-pain/. Accessed September 28, 2020.
9. Choosing Wisely. American Society of Anesthesiologists–Pain Medicine. Avoid imaging studies (MRI, CT or X-rays) for acute low back pain without specific indications. www.choosingwisely.org/clinician-lists/american-society-anesthesiologists-imaging-studies-for-acute-low-back-pain/. Accessed September 28, 2020.
10. Choosing Wisely. American College of Emergency Physicians. Avoid lumbar spine imaging in the emergency department for adults with non-traumatic back pain unless the patient has severe or progressive neurologic deficits or is suspected of having a serious underlying condition (such as vertebral infection, cauda equina syndrome, or cancer with bony metastasis). www.choosingwisely.org/clinician-lists/acep-lumbar-spine-imaging-in-the-ed/. Accessed September 28, 2020.
11. Choosing Wisely. American Academy of Family Physicians. Don’t require a pelvic exam or other physical exam to prescribe oral contraceptive medications. www.choosingwisely.org/clinician-lists/american-academy-family-physicians-pelvic-or-physical-exams-to-prescribe-oral-contraceptives/. Accessed September 28, 2020.
12. Over-the-counter access to hormonal contraception. ACOG Committee Opinion, Number 788. Obstet Gynecol. 2019;134:e96-e105. https://journals.lww.com/greenjournal/Fulltext/2019/10000/Over_the_Counter_Access_to_Hormonal_Contraception_.46.aspx. Accessed September 28, 2020.
13. Choosing Wisely. American Academy of Family Physicians. Don’t routinely recommend daily home glucose monitoring for patients who have Type 2 diabetes mellitus and are not using insulin. www.choosingwisely.org/clinician-lists/aafp-daily-home-glucose-monitoring-for-patients-with-type-2-diabetes. Accessed September 28, 2020.
14. Choosing Wisely. Society of General Internal Medicine. Don’t recommend daily home finger glucose testing in patients with Type 2 diabetes mellitus not using insulin. www.choosingwisely.org/clinician-lists/society-general-internal-medicine-daily-home-finger-glucose-testing-type-2-diabetes-mellitus/. Accessed September 28, 2020.
15. Malanda UL, Welschen LM, Riphagen II, et al. Self‐monitoring of blood glucose in patients with type 2 diabetes mellitus who are not using insulin. Cochrane Database Syst Rev. 2012(1):CD005060.
16. Peel E, Douglas M, Lawton J. Self monitoring of blood glucose in type 2 diabetes: longitudinal qualitative study of patients’ perspectives. BMJ. 2007;335:493.
17. Choosing Wisely. American Academy of Family Physicians. Don’t screen for genital herpes simplex virus infection (HSV) in asymptomatic adults, including pregnant women. www.choosingwisely.org/clinician-lists/aafp-genital-herpes-screening-in-asymptomatic-adults/. Accessed September 28, 2020.
18. Bibbins-Domingo K, Grossman DC, Curry SJ, et al. Serologic screening for genital herpes infection: US Preventive Services Task Force recommendation statement. JAMA. 2016;316:2525-2530.
19. Choosing Wisely. American Academy of Family Physicians. Don’t screen for testicular cancer in asymptomatic adolescent and adult males. www.choosingwisely.org/clinician-lists/aafp-testicular-cancer-screening-in-asymptomatic-adolescent-and-adult-men/. Accessed September 28, 2020.
20. Lin K, Sharangpani R. Screening for testicular cancer: an evidence review for the U.S. Preventive Services Task Force. Ann Intern Med. 2010;153:396-399.
21. Choosing Wisely. American Academy of Pediatrics. Cough and cold medicines should not be prescribed, recommended or used for respiratory illnesses in young children. www.choosingwisely.org/clinician-lists/american-academy-pediatrics-cough-and-cold-medicines-for-children-under-four/. Accessed September 28, 2020.
22. Schaefer MK, Shehab N, Cohen AL, et al. Adverse events from cough and cold medications in children. Pediatrics. 2008;121:783-787.
23. Carr BC. Efficacy, abuse, and toxicity of over-the-counter cough and cold medicines in the pediatric population. Curr Opin Pediatr. 2006;18:184-188.
24. Oduwole O, Udoh EE, Oyo‐Ita A, et al. Honey for acute cough in children. Cochrane Database Syst Rev. 2018(4):CD007094.
25. Choosing Wisely. American Academy of Allergy, Asthma & Immunology. Don’t perform unproven diagnostic tests, such as immunoglobulin G(lgG) testing or an indiscriminate battery of immunoglobulin E(lgE) tests, in the evaluation of allergy. www.choosingwisely.org/clinician-lists/american-academy-allergy-asthma-immunology-diagnostic-tests-for-allergy-evaluation/. Accessed September 28, 2020.
26. Cox L, Williams B, Sicherer S, et al. Pearls and pitfalls of allergy diagnostic testing: report from the American College of Allergy, Asthma and Immunology Specific IgE Test Task Force. Ann Allergy Asthma Immunol. 2008;101:580-592.
27. Choosing Wisely. American Epilepsy Society. Do not routinely order electroencephalogram (EEG) as part of initial syncope work-up. www.choosingwisely.org/clinician-lists/aes-eeg-as-part-of-initial-syncope-work-up/. Accessed September 28, 2020.
28. Choosing Wisely. American College of Emergency Physicians. Avoid CT of the head in asymptomatic adult patients in the emergency department with syncope, insignificant trauma and a normal neurological evaluation. www.choosingwisely.org/clinician-lists/acep-avoid-head-ct-for-asymptomatic-adults-with-syncope/. Accessed September 28, 2020.
29. Choosing Wisely. American College of Physicians. In the evaluation of simple syncope and a normal neurological examination, don’t obtain brain imaging studies (CT or MRI). www.choosingwisely.org/clinician-lists/american-college-physicians-brain-imaging-to-evaluate-simple-syncope/. Accessed September 28, 2020.
30. Choosing Wisely. American Academy of Neurology. Don’t perform imaging of the carotid arteries for simple syncope without other neurologic symptoms. www.choosingwisely.org/clinician-lists/american-academy-neurology-carotid-artery-imaging-for-simple-syncope/. Accessed September 28, 2020.
31. Josephson CB, Rahey S, Sadler RM. Neurocardiogenic syncope: frequency and consequences of its misdiagnosis as epilepsy. Can J Neurol Sci. 2007;34:221-224.
32. Mendu ML, McAvay G, Lampert R, et al. Yield of diagnostic tests in evaluating syncopal episodes in older patients. Arch Intern Med. 2009;169:1299-1305.
33. Choosing Wisely. American Academy of Pediatrics–Section on Surgery. Avoid referring most children with umbilical hernias to a pediatric surgeon until around age 4-5 years. www.choosingwisely.org/clinician-lists/aap-sosu-avoid-surgery-referral-for-umbilical-hernias-until-age-4-5/. Accessed September 28, 2020.
34. Antonoff MB, Kreykes NS, Saltzman DA, et al. American Academy of Pediatrics Section on Surgery hernia survey revisited. J Pediatr Surg. 2005;40:1009-1014.
35. Choosing Wisely. American Geriatrics Society. Avoid using prescription appetite stimulants or high-calorie supplements for treatment of anorexia or cachexia in older adults; instead, optimize social supports, discontinue medications that may interfere with eating, provide appealing food and feeding assistance, and clarify patient goals and expectations. www.choosingwisely.org/clinician-lists/american-geriatrics-society-prescription-appetite-stimulants-to-treat-anorexia-cachexia-in-elderly/. Accessed September 28, 2020.
36. Milne AC, Potter J, Vivanti A, et al. Protein and energy supplementation in elderly people at risk from malnutrition. Cochrane Database Sys Rev. 2009(2):CD003288.
37. Fox CB, Treadway AK, Blaszczyk AT, et al. Megestrol acetate and mirtazapine for the treatment of unplanned weight loss in the elderly. Pharmacotherapy. 2009;29:383-397.
When medical care is based on consistent, good-quality evidence, most physicians adopt it. However, not all care is well supported by the literature and may, in fact, be overused without offering benefit to patients. Choosing Wisely, at www.choosingwisely.org, is a health care initiative that highlights screening and testing recommendations from specialty societies in an effort to encourage patients and clinicians to talk about how to make high-value, effective health care decisions and avoid overuse. (See “Test and Tx overutilization: A bigger problem than you might think"1-3).
SIDEBAR
Test and Tx overutilization: A bigger problem than you might think
Care that isn’t backed up by the medical literature is adopted by some physicians and not adopted by others, leading to practice variations. Some variation is to be expected, since no 2 patients require exactly the same care, but substantial variations may be a clue to overuse.
A 2006 analysis of inpatient lab studies found that doctors ordered an average of 2.96 studies per patient per day, but only 29% of these tests (0.95 test/patient/day) contributed to management.1 A 2016 systematic review found more than 800 studies on overuse were published in a single year.2 One study of thyroid nodules followed almost 1000 patients with nodules as they underwent routine follow-up imaging. At the end of the study, 7 were found to have cancer, but of those, only 3 had enlarging or changing nodules that would have been detected with the follow-up imaging being studied. Three of the cancers were stable in size and 1 was found incidentally.3
Enabling physician and patient dialogue. The initiative began in 2010 when the American Board of Internal Medicine convened a panel of experts to identify low-value tests and therapies. Their list took the form of a “Top Five Things” that may not be high value in patient care, and it used language tailored to patients and physicians so that they could converse meaningfully. Physicians could use the evidence to make a clinical decision, and patients could feel empowered to ask informed questions about recommendations they received. The initiative has now expanded to include ways that health care systems can reduce low-value interventions.
Scope of participation. Since the first Choosing Wisely recommendations were published in 2013, more than 80 professional associations have contributed lists of their own. Professional societies participate voluntarily. The American Academy of Family Physicians (AAFP), Society of General Internal Medicine, and American Academy of Pediatrics (AAP) have contributed lists relevant to primary care. All Choosing Wisely recommendations can be searched or sorted by specialty organization. Recommendations are reviewed and revised regularly. If the evidence becomes conflicted or contradictory, recommendations are withdrawn.
Making meaningful improvements by Choosing Wisely
Several studies have shown that health care systems can implement Choosing Wisely recommendations to reduce overuse of unnecessary tests. A 2015 study examined the effect of applying a Choosing Wisely recommendation to reduce the use of continuous pulse oximetry in pediatric inpatients with asthma, wheezing, or bronchiolitis. The recommendation, from the Society of Hospital Medicine–Pediatric Hospital Medicine, advises against continuous pulse oximetry in children with acute respiratory illnesses unless the child is using supplemental oxygen.4 This study, done at the Cincinnati Children’s Hospital Medical Center, found that within 3 months of initiating a protocol on all general pediatrics floors, the average time on pulse oximetry after meeting clinical goals decreased from 10.7 hours to 3.1 hours. In addition, the percentage of patients who had their continuous pulse oximetry stopped within 2 hours of clinical stability (a goal time) increased from 25% to 46%.5
Patients are important drivers of health care utilization. A 2003 study showed that physicians are more likely to order referrals, tests, and prescriptions when patients ask for them, and that nearly 1 in 4 patients did so.6 A 2002 study found that physicians granted all but 3% of patient’s requests for orders or tests, and that fulfilling requests correlated with patient satisfaction in the specialty office studied (cardiology) but not in the primary care (internal medicine) office.7
From its inception, Choosing Wisely has considered patients as full partners in conversations about health care utilization. Choosing Wisely partners with Consumer Reports to create and disseminate plain-language summaries of recommendations. Community groups and physician organizations have also participated in implementation efforts. In 2018, Choosing Wisely secured a grant to expand outreach to diverse or underserved communities.
Choosing Wisely recommendations are not guidelines or mandates. They are intended to be evidence-based advice from a specialty society to its members and to patients about care that is often unnecessary. The goal is to create a conversation and not to eliminate these services from ever being offered or used.
Continue to: Improve your practice with these 10 primary care recommendations
Improve your practice with these 10 primary care recommendations
1 Avoid imaging studies in early acute low back pain without red flags.
Both the AAFP and the American Society of Anesthesiologists recommend against routine X-rays, magnetic resonance imaging, and computed tomography (CT) scans in the first 6 weeks of acute low back pain (LBP).8,9 The American College of Emergency Physicians (ACEP) recommends against routine lumbar spine imaging for emergency department (ED) patients.10 In all cases, imaging is indicated if the patient has any signs or symptoms of neurologic deficits or other indications, such as signs of spinal infection or fracture. However, as ACEP notes, diagnostic imaging does not typically help identify the cause of acute LBP, and when it does, it does not reduce the time to symptom improvement.10
2 Prescribe oral contraceptives on the basis of a medical history and a blood pressure measurement. No routine pelvic exam or other physical exam is necessary.
This AAFP recommendation11 is based on clinical practice guidelines from the American College of Obstetricians and Gynecologists (ACOG) and other research.12 The ACOG practice guideline supports provision of hormonal contraception without a pelvic exam, cervical cancer (Pap) testing, urine pregnancy testing, or testing for sexually transmitted infections. ACOG guidelines also support over-the-counter provision of hormonal contraceptives, including combined oral contraceptives.12
3 Stop recommending daily self-glucose monitoring for patients with diabetes who are not using insulin.
Both the AAFP and the Society for General Internal Medicine recommend against daily blood sugar checks for people who do not use insulin.13,14 A Cochrane review of 9 trials (3300 patients) found that after 6 months, hemoglobin A1C was reduced by 0.3% in people who checked their sugar daily compared with those who did not, but this difference was not significant after a year.15 Hypoglycemic episodes were more common in the “checking” group, and there were no differences in quality of life. A qualitative study found that blood sugar results had little impact on patients’ motivation to change behavior.16
4 Don’t screen for herpes simplex virus (HSV) infection in asymptomatic adults, even those who are pregnant.
This AAFP recommendation17 comes from a US Preventive Services Task Force (USPSTF) Grade D recommendation.18 Most people with positive HSV-2 serology have had an outbreak; even those who do not think they have had one will realize that they had the symptoms once they hear them described.18 With available tests, 1 in 2 positive results for HSV-2 among asymptomatic people will be a false-positive.18
There is no known cure, intervention, or reduction in transmission for infected patients who do not have symptoms.18 Also, serologically detected HSV-2 does not reliably predict genital herpes; and HSV-1 has been found to cause an increasing percentage of genital infection cases.18
Continue to: 5 Don't screen for testicular cancer in asymptomatic individuals
5 Don’t screen for testicular cancer in asymptomatic individuals.
This AAFP recommendation19 also comes from a USPSTF Grade D recommendation.20 A 2010 systematic review found no evidence to support screening of asymptomatic people with a physical exam or ultrasound. All available studies involved symptomatic patients.20
6 Stop recommending cough and cold medicines for children younger than 4 years.
The AAP recommends that clinicians discourage the use of any cough or cold medicine for children in this age-group.21 A 2008 study found that more than 7000 children annually presented to EDs for adverse events from cough and cold medicines.22 Previous studies found no benefit in reducing symptoms.23 In children older than 12 months, a Cochrane review found that honey has a modest benefit for cough in single-night trials.24
7 Avoid performing serum allergy panels.
The American Academy of Allergy, Asthma, and Immunology discourages the use of serum panel testing when patients present with allergy symptoms.25 A patient can have a strong positive immunoglobulin E (IgE) serum result to an allergen and have no clinical allergic symptoms or can have a weak positive serum result and a strong clinical reaction. Targeted skin or serum IgE testing—for example, testing for cashew allergy in a patient known to have had a reaction after eating one—is reasonable.26
8 Avoid routine electroencephalography (EEG), head CT, and carotid ultrasound as initial work-up for simple syncope in adults.
These recommendations, from the American Epilepsy Society,27 ACEP,28 American College of Physicians,29 and American Academy of Neurology (AAN),30 emphasize the low yield of routine work-ups for patients with simple syncope. The AAN notes that 40% of people will experience syncope during adulthood and most will not have carotid disease, which generally manifests with stroke-like symptoms rather than syncope. One study found that approximately 1 in 8 patients referred to an epilepsy clinic had neurocardiogenic syncope rather than epilepsy.31
EEGs have high false-negative and false-positive rates, and history-taking is a better tool with which to make a diagnosis. CT scans performed in the ED were found to contribute to the diagnosis of simple syncope in fewer than 2% of cases of syncope, compared with orthostatic blood pressure (25% of cases).32
Continue to: 9 Wait to refer children with umbilical hernias to pediatric surgery until they are 4 to 5 years of age
9 Wait to refer children with umbilical hernias to pediatric surgery until they are 4 to 5 years of age.
The AAP Section on Surgery offers evidence that the risk-benefit analysis strongly favors waiting on intervention.33 About 1 in 4 children will have an umbilical hernia, and about 85% of cases will resolve by age 5. The strangulation rate with umbilical hernias is very low, and although the risk of infection with surgery is likewise low, the risk of recurrence following surgery before the age of 4 is as high as 2.4%.34 The AAP Section on Surgery recommends against strapping or restraining the hernia, as well.
10 Avoid using appetite stimulants, such as megesterol, and high-calorie nutritional supplements to treat anorexia and cachexia in older adults.
Instead, the American Geriatrics Society recommends that physicians encourage caregivers to serve appealing food, provide support with eating, and remove barriers to appetite and nutrition.35 A Cochrane review showed that high-calorie supplements, such as Boost or Ensure, are associated with very modest weight gain—about 2% of weight—but are not associated with an increased life expectancy or improved quality of life.36
Prescription appetite stimulants are associated with adverse effects and yield inconsistent benefits in older adults. Megesterol, for example, was associated with headache, gastrointestinal adverse effects, insomnia, weakness, and fatigue. Mirtazapine is associated with sedation and fatigue.37
CORRESPONDENCE
Kathleen Rowland, MD, MS, Rush Copley Family Medicine Residency, Rush Medical College, 600 South Paulina, Kidston House Room 605, Chicago IL 60612; [email protected].
When medical care is based on consistent, good-quality evidence, most physicians adopt it. However, not all care is well supported by the literature and may, in fact, be overused without offering benefit to patients. Choosing Wisely, at www.choosingwisely.org, is a health care initiative that highlights screening and testing recommendations from specialty societies in an effort to encourage patients and clinicians to talk about how to make high-value, effective health care decisions and avoid overuse. (See “Test and Tx overutilization: A bigger problem than you might think"1-3).
SIDEBAR
Test and Tx overutilization: A bigger problem than you might think
Care that isn’t backed up by the medical literature is adopted by some physicians and not adopted by others, leading to practice variations. Some variation is to be expected, since no 2 patients require exactly the same care, but substantial variations may be a clue to overuse.
A 2006 analysis of inpatient lab studies found that doctors ordered an average of 2.96 studies per patient per day, but only 29% of these tests (0.95 test/patient/day) contributed to management.1 A 2016 systematic review found more than 800 studies on overuse were published in a single year.2 One study of thyroid nodules followed almost 1000 patients with nodules as they underwent routine follow-up imaging. At the end of the study, 7 were found to have cancer, but of those, only 3 had enlarging or changing nodules that would have been detected with the follow-up imaging being studied. Three of the cancers were stable in size and 1 was found incidentally.3
Enabling physician and patient dialogue. The initiative began in 2010 when the American Board of Internal Medicine convened a panel of experts to identify low-value tests and therapies. Their list took the form of a “Top Five Things” that may not be high value in patient care, and it used language tailored to patients and physicians so that they could converse meaningfully. Physicians could use the evidence to make a clinical decision, and patients could feel empowered to ask informed questions about recommendations they received. The initiative has now expanded to include ways that health care systems can reduce low-value interventions.
Scope of participation. Since the first Choosing Wisely recommendations were published in 2013, more than 80 professional associations have contributed lists of their own. Professional societies participate voluntarily. The American Academy of Family Physicians (AAFP), Society of General Internal Medicine, and American Academy of Pediatrics (AAP) have contributed lists relevant to primary care. All Choosing Wisely recommendations can be searched or sorted by specialty organization. Recommendations are reviewed and revised regularly. If the evidence becomes conflicted or contradictory, recommendations are withdrawn.
Making meaningful improvements by Choosing Wisely
Several studies have shown that health care systems can implement Choosing Wisely recommendations to reduce overuse of unnecessary tests. A 2015 study examined the effect of applying a Choosing Wisely recommendation to reduce the use of continuous pulse oximetry in pediatric inpatients with asthma, wheezing, or bronchiolitis. The recommendation, from the Society of Hospital Medicine–Pediatric Hospital Medicine, advises against continuous pulse oximetry in children with acute respiratory illnesses unless the child is using supplemental oxygen.4 This study, done at the Cincinnati Children’s Hospital Medical Center, found that within 3 months of initiating a protocol on all general pediatrics floors, the average time on pulse oximetry after meeting clinical goals decreased from 10.7 hours to 3.1 hours. In addition, the percentage of patients who had their continuous pulse oximetry stopped within 2 hours of clinical stability (a goal time) increased from 25% to 46%.5
Patients are important drivers of health care utilization. A 2003 study showed that physicians are more likely to order referrals, tests, and prescriptions when patients ask for them, and that nearly 1 in 4 patients did so.6 A 2002 study found that physicians granted all but 3% of patient’s requests for orders or tests, and that fulfilling requests correlated with patient satisfaction in the specialty office studied (cardiology) but not in the primary care (internal medicine) office.7
From its inception, Choosing Wisely has considered patients as full partners in conversations about health care utilization. Choosing Wisely partners with Consumer Reports to create and disseminate plain-language summaries of recommendations. Community groups and physician organizations have also participated in implementation efforts. In 2018, Choosing Wisely secured a grant to expand outreach to diverse or underserved communities.
Choosing Wisely recommendations are not guidelines or mandates. They are intended to be evidence-based advice from a specialty society to its members and to patients about care that is often unnecessary. The goal is to create a conversation and not to eliminate these services from ever being offered or used.
Continue to: Improve your practice with these 10 primary care recommendations
Improve your practice with these 10 primary care recommendations
1 Avoid imaging studies in early acute low back pain without red flags.
Both the AAFP and the American Society of Anesthesiologists recommend against routine X-rays, magnetic resonance imaging, and computed tomography (CT) scans in the first 6 weeks of acute low back pain (LBP).8,9 The American College of Emergency Physicians (ACEP) recommends against routine lumbar spine imaging for emergency department (ED) patients.10 In all cases, imaging is indicated if the patient has any signs or symptoms of neurologic deficits or other indications, such as signs of spinal infection or fracture. However, as ACEP notes, diagnostic imaging does not typically help identify the cause of acute LBP, and when it does, it does not reduce the time to symptom improvement.10
2 Prescribe oral contraceptives on the basis of a medical history and a blood pressure measurement. No routine pelvic exam or other physical exam is necessary.
This AAFP recommendation11 is based on clinical practice guidelines from the American College of Obstetricians and Gynecologists (ACOG) and other research.12 The ACOG practice guideline supports provision of hormonal contraception without a pelvic exam, cervical cancer (Pap) testing, urine pregnancy testing, or testing for sexually transmitted infections. ACOG guidelines also support over-the-counter provision of hormonal contraceptives, including combined oral contraceptives.12
3 Stop recommending daily self-glucose monitoring for patients with diabetes who are not using insulin.
Both the AAFP and the Society for General Internal Medicine recommend against daily blood sugar checks for people who do not use insulin.13,14 A Cochrane review of 9 trials (3300 patients) found that after 6 months, hemoglobin A1C was reduced by 0.3% in people who checked their sugar daily compared with those who did not, but this difference was not significant after a year.15 Hypoglycemic episodes were more common in the “checking” group, and there were no differences in quality of life. A qualitative study found that blood sugar results had little impact on patients’ motivation to change behavior.16
4 Don’t screen for herpes simplex virus (HSV) infection in asymptomatic adults, even those who are pregnant.
This AAFP recommendation17 comes from a US Preventive Services Task Force (USPSTF) Grade D recommendation.18 Most people with positive HSV-2 serology have had an outbreak; even those who do not think they have had one will realize that they had the symptoms once they hear them described.18 With available tests, 1 in 2 positive results for HSV-2 among asymptomatic people will be a false-positive.18
There is no known cure, intervention, or reduction in transmission for infected patients who do not have symptoms.18 Also, serologically detected HSV-2 does not reliably predict genital herpes; and HSV-1 has been found to cause an increasing percentage of genital infection cases.18
Continue to: 5 Don't screen for testicular cancer in asymptomatic individuals
5 Don’t screen for testicular cancer in asymptomatic individuals.
This AAFP recommendation19 also comes from a USPSTF Grade D recommendation.20 A 2010 systematic review found no evidence to support screening of asymptomatic people with a physical exam or ultrasound. All available studies involved symptomatic patients.20
6 Stop recommending cough and cold medicines for children younger than 4 years.
The AAP recommends that clinicians discourage the use of any cough or cold medicine for children in this age-group.21 A 2008 study found that more than 7000 children annually presented to EDs for adverse events from cough and cold medicines.22 Previous studies found no benefit in reducing symptoms.23 In children older than 12 months, a Cochrane review found that honey has a modest benefit for cough in single-night trials.24
7 Avoid performing serum allergy panels.
The American Academy of Allergy, Asthma, and Immunology discourages the use of serum panel testing when patients present with allergy symptoms.25 A patient can have a strong positive immunoglobulin E (IgE) serum result to an allergen and have no clinical allergic symptoms or can have a weak positive serum result and a strong clinical reaction. Targeted skin or serum IgE testing—for example, testing for cashew allergy in a patient known to have had a reaction after eating one—is reasonable.26
8 Avoid routine electroencephalography (EEG), head CT, and carotid ultrasound as initial work-up for simple syncope in adults.
These recommendations, from the American Epilepsy Society,27 ACEP,28 American College of Physicians,29 and American Academy of Neurology (AAN),30 emphasize the low yield of routine work-ups for patients with simple syncope. The AAN notes that 40% of people will experience syncope during adulthood and most will not have carotid disease, which generally manifests with stroke-like symptoms rather than syncope. One study found that approximately 1 in 8 patients referred to an epilepsy clinic had neurocardiogenic syncope rather than epilepsy.31
EEGs have high false-negative and false-positive rates, and history-taking is a better tool with which to make a diagnosis. CT scans performed in the ED were found to contribute to the diagnosis of simple syncope in fewer than 2% of cases of syncope, compared with orthostatic blood pressure (25% of cases).32
Continue to: 9 Wait to refer children with umbilical hernias to pediatric surgery until they are 4 to 5 years of age
9 Wait to refer children with umbilical hernias to pediatric surgery until they are 4 to 5 years of age.
The AAP Section on Surgery offers evidence that the risk-benefit analysis strongly favors waiting on intervention.33 About 1 in 4 children will have an umbilical hernia, and about 85% of cases will resolve by age 5. The strangulation rate with umbilical hernias is very low, and although the risk of infection with surgery is likewise low, the risk of recurrence following surgery before the age of 4 is as high as 2.4%.34 The AAP Section on Surgery recommends against strapping or restraining the hernia, as well.
10 Avoid using appetite stimulants, such as megesterol, and high-calorie nutritional supplements to treat anorexia and cachexia in older adults.
Instead, the American Geriatrics Society recommends that physicians encourage caregivers to serve appealing food, provide support with eating, and remove barriers to appetite and nutrition.35 A Cochrane review showed that high-calorie supplements, such as Boost or Ensure, are associated with very modest weight gain—about 2% of weight—but are not associated with an increased life expectancy or improved quality of life.36
Prescription appetite stimulants are associated with adverse effects and yield inconsistent benefits in older adults. Megesterol, for example, was associated with headache, gastrointestinal adverse effects, insomnia, weakness, and fatigue. Mirtazapine is associated with sedation and fatigue.37
CORRESPONDENCE
Kathleen Rowland, MD, MS, Rush Copley Family Medicine Residency, Rush Medical College, 600 South Paulina, Kidston House Room 605, Chicago IL 60612; [email protected].
1. Miyakis S, Karamanof G, Liontos M, et al. Factors contributing to inappropriate ordering of tests in an academic medical department and the effect of an educational feedback strategy. Postgrad Med J. 2006;82:823-829.
2. Morgan DJ, Dhruva SS, Wright SM, et al. Update on medical overuse: a systematic review. JAMA Intern Med. 2016;176:1687-1692.
3. Durante C, Costante G, Lucisano G, et al. The natural history of benign thyroid nodules. JAMA. 2015;313:926-935.
4. Choosing Wisely. Society of Hospital Medicine—Pediatric hospital medicine. Don’t use continuous pulse oximetry routinely in children with acute respiratory illness unless they are on supplemental oxygen. www.choosingwisely.org/clinician-lists/society-hospital-medicine-pediatric-continuous-pulse-oximetry-in-children-with-acute-respiratory-illness/. Accessed September 28, 2020.
5. Schondelmeyer AC, Simmons JM, Statile AM, et al. Using quality improvement to reduce continuous pulse oximetry use in children with wheezing. Pediatrics. 2015;135:e1044-e1051.
6. Kravitz RL, Bell RA, Azari R, et al. Direct observation of requests for clinical services in office practice: what do patients want and do they get it? Arch Intern Med. 2003;163:1673-1681.
7. Kravitz RL, Bell RA, Franz CE, et al. Characterizing patient requests and physician responses in office practice. Health Serv Res. 2002;37:217-238.
8. Choosing Wisely. American Academy of Family Physicians. Don’t do imaging for low back pain within the first six weeks, unless red flags are present. www.choosingwisely.org/clinician-lists/american-academy-family-physicians-imaging-low-back-pain/. Accessed September 28, 2020.
9. Choosing Wisely. American Society of Anesthesiologists–Pain Medicine. Avoid imaging studies (MRI, CT or X-rays) for acute low back pain without specific indications. www.choosingwisely.org/clinician-lists/american-society-anesthesiologists-imaging-studies-for-acute-low-back-pain/. Accessed September 28, 2020.
10. Choosing Wisely. American College of Emergency Physicians. Avoid lumbar spine imaging in the emergency department for adults with non-traumatic back pain unless the patient has severe or progressive neurologic deficits or is suspected of having a serious underlying condition (such as vertebral infection, cauda equina syndrome, or cancer with bony metastasis). www.choosingwisely.org/clinician-lists/acep-lumbar-spine-imaging-in-the-ed/. Accessed September 28, 2020.
11. Choosing Wisely. American Academy of Family Physicians. Don’t require a pelvic exam or other physical exam to prescribe oral contraceptive medications. www.choosingwisely.org/clinician-lists/american-academy-family-physicians-pelvic-or-physical-exams-to-prescribe-oral-contraceptives/. Accessed September 28, 2020.
12. Over-the-counter access to hormonal contraception. ACOG Committee Opinion, Number 788. Obstet Gynecol. 2019;134:e96-e105. https://journals.lww.com/greenjournal/Fulltext/2019/10000/Over_the_Counter_Access_to_Hormonal_Contraception_.46.aspx. Accessed September 28, 2020.
13. Choosing Wisely. American Academy of Family Physicians. Don’t routinely recommend daily home glucose monitoring for patients who have Type 2 diabetes mellitus and are not using insulin. www.choosingwisely.org/clinician-lists/aafp-daily-home-glucose-monitoring-for-patients-with-type-2-diabetes. Accessed September 28, 2020.
14. Choosing Wisely. Society of General Internal Medicine. Don’t recommend daily home finger glucose testing in patients with Type 2 diabetes mellitus not using insulin. www.choosingwisely.org/clinician-lists/society-general-internal-medicine-daily-home-finger-glucose-testing-type-2-diabetes-mellitus/. Accessed September 28, 2020.
15. Malanda UL, Welschen LM, Riphagen II, et al. Self‐monitoring of blood glucose in patients with type 2 diabetes mellitus who are not using insulin. Cochrane Database Syst Rev. 2012(1):CD005060.
16. Peel E, Douglas M, Lawton J. Self monitoring of blood glucose in type 2 diabetes: longitudinal qualitative study of patients’ perspectives. BMJ. 2007;335:493.
17. Choosing Wisely. American Academy of Family Physicians. Don’t screen for genital herpes simplex virus infection (HSV) in asymptomatic adults, including pregnant women. www.choosingwisely.org/clinician-lists/aafp-genital-herpes-screening-in-asymptomatic-adults/. Accessed September 28, 2020.
18. Bibbins-Domingo K, Grossman DC, Curry SJ, et al. Serologic screening for genital herpes infection: US Preventive Services Task Force recommendation statement. JAMA. 2016;316:2525-2530.
19. Choosing Wisely. American Academy of Family Physicians. Don’t screen for testicular cancer in asymptomatic adolescent and adult males. www.choosingwisely.org/clinician-lists/aafp-testicular-cancer-screening-in-asymptomatic-adolescent-and-adult-men/. Accessed September 28, 2020.
20. Lin K, Sharangpani R. Screening for testicular cancer: an evidence review for the U.S. Preventive Services Task Force. Ann Intern Med. 2010;153:396-399.
21. Choosing Wisely. American Academy of Pediatrics. Cough and cold medicines should not be prescribed, recommended or used for respiratory illnesses in young children. www.choosingwisely.org/clinician-lists/american-academy-pediatrics-cough-and-cold-medicines-for-children-under-four/. Accessed September 28, 2020.
22. Schaefer MK, Shehab N, Cohen AL, et al. Adverse events from cough and cold medications in children. Pediatrics. 2008;121:783-787.
23. Carr BC. Efficacy, abuse, and toxicity of over-the-counter cough and cold medicines in the pediatric population. Curr Opin Pediatr. 2006;18:184-188.
24. Oduwole O, Udoh EE, Oyo‐Ita A, et al. Honey for acute cough in children. Cochrane Database Syst Rev. 2018(4):CD007094.
25. Choosing Wisely. American Academy of Allergy, Asthma & Immunology. Don’t perform unproven diagnostic tests, such as immunoglobulin G(lgG) testing or an indiscriminate battery of immunoglobulin E(lgE) tests, in the evaluation of allergy. www.choosingwisely.org/clinician-lists/american-academy-allergy-asthma-immunology-diagnostic-tests-for-allergy-evaluation/. Accessed September 28, 2020.
26. Cox L, Williams B, Sicherer S, et al. Pearls and pitfalls of allergy diagnostic testing: report from the American College of Allergy, Asthma and Immunology Specific IgE Test Task Force. Ann Allergy Asthma Immunol. 2008;101:580-592.
27. Choosing Wisely. American Epilepsy Society. Do not routinely order electroencephalogram (EEG) as part of initial syncope work-up. www.choosingwisely.org/clinician-lists/aes-eeg-as-part-of-initial-syncope-work-up/. Accessed September 28, 2020.
28. Choosing Wisely. American College of Emergency Physicians. Avoid CT of the head in asymptomatic adult patients in the emergency department with syncope, insignificant trauma and a normal neurological evaluation. www.choosingwisely.org/clinician-lists/acep-avoid-head-ct-for-asymptomatic-adults-with-syncope/. Accessed September 28, 2020.
29. Choosing Wisely. American College of Physicians. In the evaluation of simple syncope and a normal neurological examination, don’t obtain brain imaging studies (CT or MRI). www.choosingwisely.org/clinician-lists/american-college-physicians-brain-imaging-to-evaluate-simple-syncope/. Accessed September 28, 2020.
30. Choosing Wisely. American Academy of Neurology. Don’t perform imaging of the carotid arteries for simple syncope without other neurologic symptoms. www.choosingwisely.org/clinician-lists/american-academy-neurology-carotid-artery-imaging-for-simple-syncope/. Accessed September 28, 2020.
31. Josephson CB, Rahey S, Sadler RM. Neurocardiogenic syncope: frequency and consequences of its misdiagnosis as epilepsy. Can J Neurol Sci. 2007;34:221-224.
32. Mendu ML, McAvay G, Lampert R, et al. Yield of diagnostic tests in evaluating syncopal episodes in older patients. Arch Intern Med. 2009;169:1299-1305.
33. Choosing Wisely. American Academy of Pediatrics–Section on Surgery. Avoid referring most children with umbilical hernias to a pediatric surgeon until around age 4-5 years. www.choosingwisely.org/clinician-lists/aap-sosu-avoid-surgery-referral-for-umbilical-hernias-until-age-4-5/. Accessed September 28, 2020.
34. Antonoff MB, Kreykes NS, Saltzman DA, et al. American Academy of Pediatrics Section on Surgery hernia survey revisited. J Pediatr Surg. 2005;40:1009-1014.
35. Choosing Wisely. American Geriatrics Society. Avoid using prescription appetite stimulants or high-calorie supplements for treatment of anorexia or cachexia in older adults; instead, optimize social supports, discontinue medications that may interfere with eating, provide appealing food and feeding assistance, and clarify patient goals and expectations. www.choosingwisely.org/clinician-lists/american-geriatrics-society-prescription-appetite-stimulants-to-treat-anorexia-cachexia-in-elderly/. Accessed September 28, 2020.
36. Milne AC, Potter J, Vivanti A, et al. Protein and energy supplementation in elderly people at risk from malnutrition. Cochrane Database Sys Rev. 2009(2):CD003288.
37. Fox CB, Treadway AK, Blaszczyk AT, et al. Megestrol acetate and mirtazapine for the treatment of unplanned weight loss in the elderly. Pharmacotherapy. 2009;29:383-397.
1. Miyakis S, Karamanof G, Liontos M, et al. Factors contributing to inappropriate ordering of tests in an academic medical department and the effect of an educational feedback strategy. Postgrad Med J. 2006;82:823-829.
2. Morgan DJ, Dhruva SS, Wright SM, et al. Update on medical overuse: a systematic review. JAMA Intern Med. 2016;176:1687-1692.
3. Durante C, Costante G, Lucisano G, et al. The natural history of benign thyroid nodules. JAMA. 2015;313:926-935.
4. Choosing Wisely. Society of Hospital Medicine—Pediatric hospital medicine. Don’t use continuous pulse oximetry routinely in children with acute respiratory illness unless they are on supplemental oxygen. www.choosingwisely.org/clinician-lists/society-hospital-medicine-pediatric-continuous-pulse-oximetry-in-children-with-acute-respiratory-illness/. Accessed September 28, 2020.
5. Schondelmeyer AC, Simmons JM, Statile AM, et al. Using quality improvement to reduce continuous pulse oximetry use in children with wheezing. Pediatrics. 2015;135:e1044-e1051.
6. Kravitz RL, Bell RA, Azari R, et al. Direct observation of requests for clinical services in office practice: what do patients want and do they get it? Arch Intern Med. 2003;163:1673-1681.
7. Kravitz RL, Bell RA, Franz CE, et al. Characterizing patient requests and physician responses in office practice. Health Serv Res. 2002;37:217-238.
8. Choosing Wisely. American Academy of Family Physicians. Don’t do imaging for low back pain within the first six weeks, unless red flags are present. www.choosingwisely.org/clinician-lists/american-academy-family-physicians-imaging-low-back-pain/. Accessed September 28, 2020.
9. Choosing Wisely. American Society of Anesthesiologists–Pain Medicine. Avoid imaging studies (MRI, CT or X-rays) for acute low back pain without specific indications. www.choosingwisely.org/clinician-lists/american-society-anesthesiologists-imaging-studies-for-acute-low-back-pain/. Accessed September 28, 2020.
10. Choosing Wisely. American College of Emergency Physicians. Avoid lumbar spine imaging in the emergency department for adults with non-traumatic back pain unless the patient has severe or progressive neurologic deficits or is suspected of having a serious underlying condition (such as vertebral infection, cauda equina syndrome, or cancer with bony metastasis). www.choosingwisely.org/clinician-lists/acep-lumbar-spine-imaging-in-the-ed/. Accessed September 28, 2020.
11. Choosing Wisely. American Academy of Family Physicians. Don’t require a pelvic exam or other physical exam to prescribe oral contraceptive medications. www.choosingwisely.org/clinician-lists/american-academy-family-physicians-pelvic-or-physical-exams-to-prescribe-oral-contraceptives/. Accessed September 28, 2020.
12. Over-the-counter access to hormonal contraception. ACOG Committee Opinion, Number 788. Obstet Gynecol. 2019;134:e96-e105. https://journals.lww.com/greenjournal/Fulltext/2019/10000/Over_the_Counter_Access_to_Hormonal_Contraception_.46.aspx. Accessed September 28, 2020.
13. Choosing Wisely. American Academy of Family Physicians. Don’t routinely recommend daily home glucose monitoring for patients who have Type 2 diabetes mellitus and are not using insulin. www.choosingwisely.org/clinician-lists/aafp-daily-home-glucose-monitoring-for-patients-with-type-2-diabetes. Accessed September 28, 2020.
14. Choosing Wisely. Society of General Internal Medicine. Don’t recommend daily home finger glucose testing in patients with Type 2 diabetes mellitus not using insulin. www.choosingwisely.org/clinician-lists/society-general-internal-medicine-daily-home-finger-glucose-testing-type-2-diabetes-mellitus/. Accessed September 28, 2020.
15. Malanda UL, Welschen LM, Riphagen II, et al. Self‐monitoring of blood glucose in patients with type 2 diabetes mellitus who are not using insulin. Cochrane Database Syst Rev. 2012(1):CD005060.
16. Peel E, Douglas M, Lawton J. Self monitoring of blood glucose in type 2 diabetes: longitudinal qualitative study of patients’ perspectives. BMJ. 2007;335:493.
17. Choosing Wisely. American Academy of Family Physicians. Don’t screen for genital herpes simplex virus infection (HSV) in asymptomatic adults, including pregnant women. www.choosingwisely.org/clinician-lists/aafp-genital-herpes-screening-in-asymptomatic-adults/. Accessed September 28, 2020.
18. Bibbins-Domingo K, Grossman DC, Curry SJ, et al. Serologic screening for genital herpes infection: US Preventive Services Task Force recommendation statement. JAMA. 2016;316:2525-2530.
19. Choosing Wisely. American Academy of Family Physicians. Don’t screen for testicular cancer in asymptomatic adolescent and adult males. www.choosingwisely.org/clinician-lists/aafp-testicular-cancer-screening-in-asymptomatic-adolescent-and-adult-men/. Accessed September 28, 2020.
20. Lin K, Sharangpani R. Screening for testicular cancer: an evidence review for the U.S. Preventive Services Task Force. Ann Intern Med. 2010;153:396-399.
21. Choosing Wisely. American Academy of Pediatrics. Cough and cold medicines should not be prescribed, recommended or used for respiratory illnesses in young children. www.choosingwisely.org/clinician-lists/american-academy-pediatrics-cough-and-cold-medicines-for-children-under-four/. Accessed September 28, 2020.
22. Schaefer MK, Shehab N, Cohen AL, et al. Adverse events from cough and cold medications in children. Pediatrics. 2008;121:783-787.
23. Carr BC. Efficacy, abuse, and toxicity of over-the-counter cough and cold medicines in the pediatric population. Curr Opin Pediatr. 2006;18:184-188.
24. Oduwole O, Udoh EE, Oyo‐Ita A, et al. Honey for acute cough in children. Cochrane Database Syst Rev. 2018(4):CD007094.
25. Choosing Wisely. American Academy of Allergy, Asthma & Immunology. Don’t perform unproven diagnostic tests, such as immunoglobulin G(lgG) testing or an indiscriminate battery of immunoglobulin E(lgE) tests, in the evaluation of allergy. www.choosingwisely.org/clinician-lists/american-academy-allergy-asthma-immunology-diagnostic-tests-for-allergy-evaluation/. Accessed September 28, 2020.
26. Cox L, Williams B, Sicherer S, et al. Pearls and pitfalls of allergy diagnostic testing: report from the American College of Allergy, Asthma and Immunology Specific IgE Test Task Force. Ann Allergy Asthma Immunol. 2008;101:580-592.
27. Choosing Wisely. American Epilepsy Society. Do not routinely order electroencephalogram (EEG) as part of initial syncope work-up. www.choosingwisely.org/clinician-lists/aes-eeg-as-part-of-initial-syncope-work-up/. Accessed September 28, 2020.
28. Choosing Wisely. American College of Emergency Physicians. Avoid CT of the head in asymptomatic adult patients in the emergency department with syncope, insignificant trauma and a normal neurological evaluation. www.choosingwisely.org/clinician-lists/acep-avoid-head-ct-for-asymptomatic-adults-with-syncope/. Accessed September 28, 2020.
29. Choosing Wisely. American College of Physicians. In the evaluation of simple syncope and a normal neurological examination, don’t obtain brain imaging studies (CT or MRI). www.choosingwisely.org/clinician-lists/american-college-physicians-brain-imaging-to-evaluate-simple-syncope/. Accessed September 28, 2020.
30. Choosing Wisely. American Academy of Neurology. Don’t perform imaging of the carotid arteries for simple syncope without other neurologic symptoms. www.choosingwisely.org/clinician-lists/american-academy-neurology-carotid-artery-imaging-for-simple-syncope/. Accessed September 28, 2020.
31. Josephson CB, Rahey S, Sadler RM. Neurocardiogenic syncope: frequency and consequences of its misdiagnosis as epilepsy. Can J Neurol Sci. 2007;34:221-224.
32. Mendu ML, McAvay G, Lampert R, et al. Yield of diagnostic tests in evaluating syncopal episodes in older patients. Arch Intern Med. 2009;169:1299-1305.
33. Choosing Wisely. American Academy of Pediatrics–Section on Surgery. Avoid referring most children with umbilical hernias to a pediatric surgeon until around age 4-5 years. www.choosingwisely.org/clinician-lists/aap-sosu-avoid-surgery-referral-for-umbilical-hernias-until-age-4-5/. Accessed September 28, 2020.
34. Antonoff MB, Kreykes NS, Saltzman DA, et al. American Academy of Pediatrics Section on Surgery hernia survey revisited. J Pediatr Surg. 2005;40:1009-1014.
35. Choosing Wisely. American Geriatrics Society. Avoid using prescription appetite stimulants or high-calorie supplements for treatment of anorexia or cachexia in older adults; instead, optimize social supports, discontinue medications that may interfere with eating, provide appealing food and feeding assistance, and clarify patient goals and expectations. www.choosingwisely.org/clinician-lists/american-geriatrics-society-prescription-appetite-stimulants-to-treat-anorexia-cachexia-in-elderly/. Accessed September 28, 2020.
36. Milne AC, Potter J, Vivanti A, et al. Protein and energy supplementation in elderly people at risk from malnutrition. Cochrane Database Sys Rev. 2009(2):CD003288.
37. Fox CB, Treadway AK, Blaszczyk AT, et al. Megestrol acetate and mirtazapine for the treatment of unplanned weight loss in the elderly. Pharmacotherapy. 2009;29:383-397.

The socioeconomic revolving door of 30-day heart failure readmissions
Patients receiving even top-notch hospital care for heart failure (HF) are, once discharged to home, at higher short-term risk of another HF hospitalization if home is in a socioeconomically deprived neighborhood. That helps explain why Blacks in the United States have a much higher 30-day HF readmission risk than Whites, a disparity that only worsens with the level of neighborhood deprivation, a new analysis suggests.
Some systemic and entrenched socioeconomic inequities that health care providers have little sway over, and which disproportionately affect Black individuals, are independent and robust predictors of worsened HF outcomes, Alanna A. Morris, MD, MSc, Emory University, Atlanta, said during her presentation at the virtual annual scientific meeting of the Heart Failure Society of America.
In a retrospective cohort study, Blacks had a 45% higher risk of 30-day readmission than Whites (P < .001) independent of cardiovascular risk factors, clinical history, comorbidities, type and location of hospital, and type of third-party payer coverage. The analysis included more than 30,000 patients with at least one HF hospitalization at centers in a major metropolitan health system.
The racial disparity widened with worsening socioeconomic deprivation of patients’ residential neighborhoods, that is, with rising quartiles of neighborhood scores on the Social Deprivation Index (SDI).
The SDI, based on U.S. census data, incorporates seven socioeconomic criteria, including household income, education level, employment, and prevalence of rented housing and households that are without a car, single parent, or overcrowded.
There was a 4–percentage point gap in adjusted 30-day readmission rate between Blacks and Whites in the lowest quartile that widened to more than 8 points by the third quartile; the disparity in both the second and fourth quartiles was the same, at about 5.5 percentage points.
A remaining question, Dr. Morris said in an interview, is why the outcomes disparity between Blacks and Whites peaks in the third SDI quartile but drops a bit in the fourth quartile representing the most severe neighborhood deprivation.
“Our hypothesis is that when you look at patients who are the poorest, who live in the most deprived neighborhoods, race may be less of a factor,” she said. Socioeconomic deprivation may have similar consequences for everyone “regardless of race, ethnicity, gender, or other demographic characteristics if you live in a neighborhood that’s highly deprived.”

Based on the current study, “it does appear that increased heart failure incident rates are related to living in deprived neighborhoods, and it raises important clinical and public health concerns that must be addressed,” Keith C. Ferdinand, MD, Tulane University, New Orleans, said as invited discussant after the presentation from Dr. Morris.
“These findings could serve as an aid to policy makers, going forward, in terms of allocating resources for primary health care,” he said. “And it’s important looking at these data and other [data] that we target heart failure patients who reside in deprived neighborhoods before, during, and [after] hospitalization.”
Dr. Morris agreed that policy makers are in a better position to attack the racial disparity in HF readmission rates identified in the study. “This is not a problem that can be fixed within the health care system.”
If the reported interpretation is correct, it could add a twist to the public health care debate in the United States, observed session moderator Mandeep R. Mehra, MD, Brigham and Woman’s Hospital in Boston.
That debate, he noted, has often focused on insurability, access to coverage, and the merits or shortcomings of a single-payer system. Yet the study suggests outcomes disparities stemming from neighborhood deprivation will not be corrected by improved access to health insurance, a conclusion he finds “startling,” Dr. Mehra said in an interview.
Some proposed explanations for the disparities by race blame unequal access to health care and or variable health insurance coverage, Dr. Morris observed in an interview. But “that may not fully explain the increased risk that we see.”
Black patients followed at Emory University’s advanced HF clinic still have a higher risk of rehospitalization than Whites. “These are patients who have insurance, who are followed by advanced heart failure providers, who are on equal amounts of guideline-recommended medical therapy – and you still see about a 50% higher risk of rehospitalization,” Dr. Morris said, citing data that isn’t part of the current analysis.
“We can say that these patients are certainly able to access care, because they are able to access our emergency room and be taken care of within the hospital setting,” he said. The study controlled for whether health coverage was by private insurance, Medicare, or Medicaid.
Instead, the current analysis points to socioeconomic and environmental factors as a major source of the disparity in 30-day readmissions, Dr. Morris said.
“When patients are discharged from our healthcare systems, they still go back into environments where they don’t have the same resources as patients who live in higher-SDI neighborhoods,” she explained.
For example, “we tell them to eat low-sodium [foods], exercise, eat fresh fruits and vegetables, take their medicines, but the reality is that certain neighborhoods within the United States – and this is much more true for Blacks – make it very difficult to follow those self-care recommendations.”
The analysis included 16,147 Black patients and 14,483 White patients hospitalized with HF within the Emory Healthcare system at least once from 2010-2018, Dr. Morris reported. Compared with Whites, Blacks were younger (63.5 vs 69.1 years) and less likely to be 65 or older (48.9% vs. 66.5%); more likely to be women (53.5% vs. 42.2%), more likely to reside in deprived census tracts and to have diabetes, hypertension, or chronic kidney disease; and had higher comorbidity scores.
In all, 20.6% of Black and 13.5% of White patients were readmitted for HF within 30 days of discharge, for an unadjusted risk ratio of 1.52 (95% CI, 1.44-1.61).
The RR hardly budged, 1.45 (95% CI, 1.37-1.54, P < .001), after adjustment for age, sex, type of insurance, type of HF, vital signs and laboratory values, medical history (diabetes, hypertension, atrial fibrillation, coronary disease, chronic kidney disease, and chronic pulmonary disease), Charlson Comorbidity Index, discharging medical specialty, and hospital location.
The excess in 30-day HF readmissions for Black, compared with White patients climbed from the first to the third neighborhood SDI quartile, the disparity peaking at 8.2 absolute percentage points.
A major criticism of the Hospital Readmissions Reduction Program component of the Affordable Care Act, Dr. Morris said in a Q&A discussion after her presentation, is that it can hold hospitals “responsible for structural inequalities that exist beyond the health care system,” including neighborhood deprivation.
“But public policy makers have to realize that there are certain patients we take care of who don’t have the resources to carry out the therapeutic lifestyle changes that will allow them to live healthy.”
The HRRP’s 30-day HF readmission metric that steers reimbursement “is penalizing health care systems across the United States” with its premise that hospital performance can be measured by 30-day HF readmission rates, Dr. Morris said in an interview.
“The reality is that some of these patients are going to a postdischarge environment that is inherently high risk, and that many of them are going to come back to us within 30 days,” she said. “We would like to make sure that we don’t put excess penalties on health care systems that take care of disproportionate numbers of African Americans in neighborhoods that have fewer resources.”
Dr. Morris and Dr. Ferdinand have disclosed no relevant financial relationships. Dr. Mehra discloses consulting or serving on an advisory board for Abbott, Medtronic, Janssen, Leviticus, NupulseCV, FineHeart, Portola, Bayer, the Baim Institute for Clinical Research, and Mesoblast.
A version of this article originally appeared on Medscape.com.
Patients receiving even top-notch hospital care for heart failure (HF) are, once discharged to home, at higher short-term risk of another HF hospitalization if home is in a socioeconomically deprived neighborhood. That helps explain why Blacks in the United States have a much higher 30-day HF readmission risk than Whites, a disparity that only worsens with the level of neighborhood deprivation, a new analysis suggests.
Some systemic and entrenched socioeconomic inequities that health care providers have little sway over, and which disproportionately affect Black individuals, are independent and robust predictors of worsened HF outcomes, Alanna A. Morris, MD, MSc, Emory University, Atlanta, said during her presentation at the virtual annual scientific meeting of the Heart Failure Society of America.
In a retrospective cohort study, Blacks had a 45% higher risk of 30-day readmission than Whites (P < .001) independent of cardiovascular risk factors, clinical history, comorbidities, type and location of hospital, and type of third-party payer coverage. The analysis included more than 30,000 patients with at least one HF hospitalization at centers in a major metropolitan health system.
The racial disparity widened with worsening socioeconomic deprivation of patients’ residential neighborhoods, that is, with rising quartiles of neighborhood scores on the Social Deprivation Index (SDI).
The SDI, based on U.S. census data, incorporates seven socioeconomic criteria, including household income, education level, employment, and prevalence of rented housing and households that are without a car, single parent, or overcrowded.
There was a 4–percentage point gap in adjusted 30-day readmission rate between Blacks and Whites in the lowest quartile that widened to more than 8 points by the third quartile; the disparity in both the second and fourth quartiles was the same, at about 5.5 percentage points.
A remaining question, Dr. Morris said in an interview, is why the outcomes disparity between Blacks and Whites peaks in the third SDI quartile but drops a bit in the fourth quartile representing the most severe neighborhood deprivation.
“Our hypothesis is that when you look at patients who are the poorest, who live in the most deprived neighborhoods, race may be less of a factor,” she said. Socioeconomic deprivation may have similar consequences for everyone “regardless of race, ethnicity, gender, or other demographic characteristics if you live in a neighborhood that’s highly deprived.”
Based on the current study, “it does appear that increased heart failure incident rates are related to living in deprived neighborhoods, and it raises important clinical and public health concerns that must be addressed,” Keith C. Ferdinand, MD, Tulane University, New Orleans, said as invited discussant after the presentation from Dr. Morris.
“These findings could serve as an aid to policy makers, going forward, in terms of allocating resources for primary health care,” he said. “And it’s important looking at these data and other [data] that we target heart failure patients who reside in deprived neighborhoods before, during, and [after] hospitalization.”
Dr. Morris agreed that policy makers are in a better position to attack the racial disparity in HF readmission rates identified in the study. “This is not a problem that can be fixed within the health care system.”
If the reported interpretation is correct, it could add a twist to the public health care debate in the United States, observed session moderator Mandeep R. Mehra, MD, Brigham and Woman’s Hospital in Boston.
That debate, he noted, has often focused on insurability, access to coverage, and the merits or shortcomings of a single-payer system. Yet the study suggests outcomes disparities stemming from neighborhood deprivation will not be corrected by improved access to health insurance, a conclusion he finds “startling,” Dr. Mehra said in an interview.
Some proposed explanations for the disparities by race blame unequal access to health care and or variable health insurance coverage, Dr. Morris observed in an interview. But “that may not fully explain the increased risk that we see.”
Black patients followed at Emory University’s advanced HF clinic still have a higher risk of rehospitalization than Whites. “These are patients who have insurance, who are followed by advanced heart failure providers, who are on equal amounts of guideline-recommended medical therapy – and you still see about a 50% higher risk of rehospitalization,” Dr. Morris said, citing data that isn’t part of the current analysis.
“We can say that these patients are certainly able to access care, because they are able to access our emergency room and be taken care of within the hospital setting,” he said. The study controlled for whether health coverage was by private insurance, Medicare, or Medicaid.
Instead, the current analysis points to socioeconomic and environmental factors as a major source of the disparity in 30-day readmissions, Dr. Morris said.
“When patients are discharged from our healthcare systems, they still go back into environments where they don’t have the same resources as patients who live in higher-SDI neighborhoods,” she explained.
For example, “we tell them to eat low-sodium [foods], exercise, eat fresh fruits and vegetables, take their medicines, but the reality is that certain neighborhoods within the United States – and this is much more true for Blacks – make it very difficult to follow those self-care recommendations.”
The analysis included 16,147 Black patients and 14,483 White patients hospitalized with HF within the Emory Healthcare system at least once from 2010-2018, Dr. Morris reported. Compared with Whites, Blacks were younger (63.5 vs 69.1 years) and less likely to be 65 or older (48.9% vs. 66.5%); more likely to be women (53.5% vs. 42.2%), more likely to reside in deprived census tracts and to have diabetes, hypertension, or chronic kidney disease; and had higher comorbidity scores.
In all, 20.6% of Black and 13.5% of White patients were readmitted for HF within 30 days of discharge, for an unadjusted risk ratio of 1.52 (95% CI, 1.44-1.61).
The RR hardly budged, 1.45 (95% CI, 1.37-1.54, P < .001), after adjustment for age, sex, type of insurance, type of HF, vital signs and laboratory values, medical history (diabetes, hypertension, atrial fibrillation, coronary disease, chronic kidney disease, and chronic pulmonary disease), Charlson Comorbidity Index, discharging medical specialty, and hospital location.
The excess in 30-day HF readmissions for Black, compared with White patients climbed from the first to the third neighborhood SDI quartile, the disparity peaking at 8.2 absolute percentage points.
A major criticism of the Hospital Readmissions Reduction Program component of the Affordable Care Act, Dr. Morris said in a Q&A discussion after her presentation, is that it can hold hospitals “responsible for structural inequalities that exist beyond the health care system,” including neighborhood deprivation.
“But public policy makers have to realize that there are certain patients we take care of who don’t have the resources to carry out the therapeutic lifestyle changes that will allow them to live healthy.”
The HRRP’s 30-day HF readmission metric that steers reimbursement “is penalizing health care systems across the United States” with its premise that hospital performance can be measured by 30-day HF readmission rates, Dr. Morris said in an interview.
“The reality is that some of these patients are going to a postdischarge environment that is inherently high risk, and that many of them are going to come back to us within 30 days,” she said. “We would like to make sure that we don’t put excess penalties on health care systems that take care of disproportionate numbers of African Americans in neighborhoods that have fewer resources.”
Dr. Morris and Dr. Ferdinand have disclosed no relevant financial relationships. Dr. Mehra discloses consulting or serving on an advisory board for Abbott, Medtronic, Janssen, Leviticus, NupulseCV, FineHeart, Portola, Bayer, the Baim Institute for Clinical Research, and Mesoblast.
A version of this article originally appeared on Medscape.com.
Patients receiving even top-notch hospital care for heart failure (HF) are, once discharged to home, at higher short-term risk of another HF hospitalization if home is in a socioeconomically deprived neighborhood. That helps explain why Blacks in the United States have a much higher 30-day HF readmission risk than Whites, a disparity that only worsens with the level of neighborhood deprivation, a new analysis suggests.
Some systemic and entrenched socioeconomic inequities that health care providers have little sway over, and which disproportionately affect Black individuals, are independent and robust predictors of worsened HF outcomes, Alanna A. Morris, MD, MSc, Emory University, Atlanta, said during her presentation at the virtual annual scientific meeting of the Heart Failure Society of America.
In a retrospective cohort study, Blacks had a 45% higher risk of 30-day readmission than Whites (P < .001) independent of cardiovascular risk factors, clinical history, comorbidities, type and location of hospital, and type of third-party payer coverage. The analysis included more than 30,000 patients with at least one HF hospitalization at centers in a major metropolitan health system.
The racial disparity widened with worsening socioeconomic deprivation of patients’ residential neighborhoods, that is, with rising quartiles of neighborhood scores on the Social Deprivation Index (SDI).
The SDI, based on U.S. census data, incorporates seven socioeconomic criteria, including household income, education level, employment, and prevalence of rented housing and households that are without a car, single parent, or overcrowded.
There was a 4–percentage point gap in adjusted 30-day readmission rate between Blacks and Whites in the lowest quartile that widened to more than 8 points by the third quartile; the disparity in both the second and fourth quartiles was the same, at about 5.5 percentage points.
A remaining question, Dr. Morris said in an interview, is why the outcomes disparity between Blacks and Whites peaks in the third SDI quartile but drops a bit in the fourth quartile representing the most severe neighborhood deprivation.
“Our hypothesis is that when you look at patients who are the poorest, who live in the most deprived neighborhoods, race may be less of a factor,” she said. Socioeconomic deprivation may have similar consequences for everyone “regardless of race, ethnicity, gender, or other demographic characteristics if you live in a neighborhood that’s highly deprived.”
Based on the current study, “it does appear that increased heart failure incident rates are related to living in deprived neighborhoods, and it raises important clinical and public health concerns that must be addressed,” Keith C. Ferdinand, MD, Tulane University, New Orleans, said as invited discussant after the presentation from Dr. Morris.
“These findings could serve as an aid to policy makers, going forward, in terms of allocating resources for primary health care,” he said. “And it’s important looking at these data and other [data] that we target heart failure patients who reside in deprived neighborhoods before, during, and [after] hospitalization.”
Dr. Morris agreed that policy makers are in a better position to attack the racial disparity in HF readmission rates identified in the study. “This is not a problem that can be fixed within the health care system.”
If the reported interpretation is correct, it could add a twist to the public health care debate in the United States, observed session moderator Mandeep R. Mehra, MD, Brigham and Woman’s Hospital in Boston.
That debate, he noted, has often focused on insurability, access to coverage, and the merits or shortcomings of a single-payer system. Yet the study suggests outcomes disparities stemming from neighborhood deprivation will not be corrected by improved access to health insurance, a conclusion he finds “startling,” Dr. Mehra said in an interview.
Some proposed explanations for the disparities by race blame unequal access to health care and or variable health insurance coverage, Dr. Morris observed in an interview. But “that may not fully explain the increased risk that we see.”
Black patients followed at Emory University’s advanced HF clinic still have a higher risk of rehospitalization than Whites. “These are patients who have insurance, who are followed by advanced heart failure providers, who are on equal amounts of guideline-recommended medical therapy – and you still see about a 50% higher risk of rehospitalization,” Dr. Morris said, citing data that isn’t part of the current analysis.
“We can say that these patients are certainly able to access care, because they are able to access our emergency room and be taken care of within the hospital setting,” he said. The study controlled for whether health coverage was by private insurance, Medicare, or Medicaid.
Instead, the current analysis points to socioeconomic and environmental factors as a major source of the disparity in 30-day readmissions, Dr. Morris said.
“When patients are discharged from our healthcare systems, they still go back into environments where they don’t have the same resources as patients who live in higher-SDI neighborhoods,” she explained.
For example, “we tell them to eat low-sodium [foods], exercise, eat fresh fruits and vegetables, take their medicines, but the reality is that certain neighborhoods within the United States – and this is much more true for Blacks – make it very difficult to follow those self-care recommendations.”
The analysis included 16,147 Black patients and 14,483 White patients hospitalized with HF within the Emory Healthcare system at least once from 2010-2018, Dr. Morris reported. Compared with Whites, Blacks were younger (63.5 vs 69.1 years) and less likely to be 65 or older (48.9% vs. 66.5%); more likely to be women (53.5% vs. 42.2%), more likely to reside in deprived census tracts and to have diabetes, hypertension, or chronic kidney disease; and had higher comorbidity scores.
In all, 20.6% of Black and 13.5% of White patients were readmitted for HF within 30 days of discharge, for an unadjusted risk ratio of 1.52 (95% CI, 1.44-1.61).
The RR hardly budged, 1.45 (95% CI, 1.37-1.54, P < .001), after adjustment for age, sex, type of insurance, type of HF, vital signs and laboratory values, medical history (diabetes, hypertension, atrial fibrillation, coronary disease, chronic kidney disease, and chronic pulmonary disease), Charlson Comorbidity Index, discharging medical specialty, and hospital location.
The excess in 30-day HF readmissions for Black, compared with White patients climbed from the first to the third neighborhood SDI quartile, the disparity peaking at 8.2 absolute percentage points.
A major criticism of the Hospital Readmissions Reduction Program component of the Affordable Care Act, Dr. Morris said in a Q&A discussion after her presentation, is that it can hold hospitals “responsible for structural inequalities that exist beyond the health care system,” including neighborhood deprivation.
“But public policy makers have to realize that there are certain patients we take care of who don’t have the resources to carry out the therapeutic lifestyle changes that will allow them to live healthy.”
The HRRP’s 30-day HF readmission metric that steers reimbursement “is penalizing health care systems across the United States” with its premise that hospital performance can be measured by 30-day HF readmission rates, Dr. Morris said in an interview.
“The reality is that some of these patients are going to a postdischarge environment that is inherently high risk, and that many of them are going to come back to us within 30 days,” she said. “We would like to make sure that we don’t put excess penalties on health care systems that take care of disproportionate numbers of African Americans in neighborhoods that have fewer resources.”
Dr. Morris and Dr. Ferdinand have disclosed no relevant financial relationships. Dr. Mehra discloses consulting or serving on an advisory board for Abbott, Medtronic, Janssen, Leviticus, NupulseCV, FineHeart, Portola, Bayer, the Baim Institute for Clinical Research, and Mesoblast.
A version of this article originally appeared on Medscape.com.

Surgeon general pushes for improved hypertension control
Roughly half of American adults have hypertension, and about 71% of these cases are uncontrolled, according to data from the American Heart Association.
If left uncontrolled, hypertension can increase risk for conditions including heart disease, stroke, kidney disease, pregnancy complications, and cognitive decline, surgeon general Vice Adm. Jerome M. Adams, MD, said in a teleconference on Oct. 7. Hispanic and Black individuals are disproportionately affected, he added.
“We cannot wait to deal with this epidemic of uncontrolled high blood pressure,” even in the midst of the ongoing COVID-19 pandemic, said Dr. Adams. “We know what works” to help control hypertension, he added, citing his own use of a blood pressure monitoring device at home.
The Department of Health & Human Services has issued a Call to Action to Control Hypertension based on the latest science and research.
Dr. Adams outlined three goals to improve hypertension control, starting with making it a national priority. The Call to Action supports increasing awareness of the health risks associated with hypertension, recognizing the economic impact, overcoming barriers to controlling hypertension, and promoting health equity.
“In 2020, disparities in the burden of disease – especially among minority populations – have been recognized during the COVID-19 pandemic. A growing body of evidence has shown that people with underlying health conditions, including cardiovascular disease, are at increased risk of worse outcomes related to COVID-19 infection,” according to the Call to Action.
A second goal is to build and sustain communities that support individuals in taking responsibility for their health and blood pressure control, Dr. Adams said. He cited the need to create places for safe physical activity, access to healthy food, and opportunities to connect to resources to support lifestyle changes.
Finally, clinicians should continue to use standardized treatment approaches and promote team-based care to maximize outcomes for patients, Dr. Adams said.
Success starts with making hypertension control a priority across the leadership team, regardless of the size, location, or demographic population at a health care setting, he said. Dr. Adams cited the Million Hearts 2022 program, an ongoing initiative to prevent 1 million heart attacks in the United States over 5 years, as a way that HHS is recognizing and rewarding success stories in hypertension control from across the country.
Empowering patients and equipping them to take charge of their hypertension essential to reducing the epidemic of high blood pressure, especially during the ongoing pandemic, Dr. Adams said. His message to clinicians to extend to patients is that it is safe to visit their doctors. Hospitals have worked to create a safe environment, however, patients can and should monitor their blood pressure regularly at home, using a self-measured blood pressure monitoring (SMBP) device, which may be covered by some insurers.
“I would encourage people to know their numbers,” and that 130/80 mm Hg is considered high and a risk factor for poor health outcomes, Dr. Adams said. Clinicians also should continue to support patients in lifestyle changes such as healthy eating and exercising regularly to help control high blood pressure.
The AHA expressed support for the surgeon general’s Call to Action. “Today’s call to action references updated hypertension guidelines the AHA and the American College of Cardiology issued in 2017 that apply the latest science to help clinicians work with patients to control their blood pressure,” the AHA said in a statement. The AHA also called on the Centers for Medicare & Medicaid Services and other insurance providers “to include coverage of SMBP devices for treatment and management of hypertension.”
The Call to Action was accompanied by a Viewpoint from Dr. Adams and Janet S. Wright, MD, also of the HHS, published in JAMA. Dr. Adams and Dr. Wright emphasized that the timing of the Call to Action recognizes that many of the same social factors that support or impede successful high blood pressure control are factors in worse outcomes from COVID-19 infections as well.
“When coupled with widespread implementation of best practices in clinical settings and empowering individuals to actively manage their blood pressure, acknowledging and addressing a community’s social conditions may generate sustained improvements in control of both hypertension and COVID-19,” they said.
Read and download the full Call to Action here, and read the Executive Summary at hhs.gov.
Roughly half of American adults have hypertension, and about 71% of these cases are uncontrolled, according to data from the American Heart Association.
If left uncontrolled, hypertension can increase risk for conditions including heart disease, stroke, kidney disease, pregnancy complications, and cognitive decline, surgeon general Vice Adm. Jerome M. Adams, MD, said in a teleconference on Oct. 7. Hispanic and Black individuals are disproportionately affected, he added.
“We cannot wait to deal with this epidemic of uncontrolled high blood pressure,” even in the midst of the ongoing COVID-19 pandemic, said Dr. Adams. “We know what works” to help control hypertension, he added, citing his own use of a blood pressure monitoring device at home.
The Department of Health & Human Services has issued a Call to Action to Control Hypertension based on the latest science and research.
Dr. Adams outlined three goals to improve hypertension control, starting with making it a national priority. The Call to Action supports increasing awareness of the health risks associated with hypertension, recognizing the economic impact, overcoming barriers to controlling hypertension, and promoting health equity.
“In 2020, disparities in the burden of disease – especially among minority populations – have been recognized during the COVID-19 pandemic. A growing body of evidence has shown that people with underlying health conditions, including cardiovascular disease, are at increased risk of worse outcomes related to COVID-19 infection,” according to the Call to Action.
A second goal is to build and sustain communities that support individuals in taking responsibility for their health and blood pressure control, Dr. Adams said. He cited the need to create places for safe physical activity, access to healthy food, and opportunities to connect to resources to support lifestyle changes.
Finally, clinicians should continue to use standardized treatment approaches and promote team-based care to maximize outcomes for patients, Dr. Adams said.
Success starts with making hypertension control a priority across the leadership team, regardless of the size, location, or demographic population at a health care setting, he said. Dr. Adams cited the Million Hearts 2022 program, an ongoing initiative to prevent 1 million heart attacks in the United States over 5 years, as a way that HHS is recognizing and rewarding success stories in hypertension control from across the country.
Empowering patients and equipping them to take charge of their hypertension essential to reducing the epidemic of high blood pressure, especially during the ongoing pandemic, Dr. Adams said. His message to clinicians to extend to patients is that it is safe to visit their doctors. Hospitals have worked to create a safe environment, however, patients can and should monitor their blood pressure regularly at home, using a self-measured blood pressure monitoring (SMBP) device, which may be covered by some insurers.
“I would encourage people to know their numbers,” and that 130/80 mm Hg is considered high and a risk factor for poor health outcomes, Dr. Adams said. Clinicians also should continue to support patients in lifestyle changes such as healthy eating and exercising regularly to help control high blood pressure.
The AHA expressed support for the surgeon general’s Call to Action. “Today’s call to action references updated hypertension guidelines the AHA and the American College of Cardiology issued in 2017 that apply the latest science to help clinicians work with patients to control their blood pressure,” the AHA said in a statement. The AHA also called on the Centers for Medicare & Medicaid Services and other insurance providers “to include coverage of SMBP devices for treatment and management of hypertension.”
The Call to Action was accompanied by a Viewpoint from Dr. Adams and Janet S. Wright, MD, also of the HHS, published in JAMA. Dr. Adams and Dr. Wright emphasized that the timing of the Call to Action recognizes that many of the same social factors that support or impede successful high blood pressure control are factors in worse outcomes from COVID-19 infections as well.
“When coupled with widespread implementation of best practices in clinical settings and empowering individuals to actively manage their blood pressure, acknowledging and addressing a community’s social conditions may generate sustained improvements in control of both hypertension and COVID-19,” they said.
Read and download the full Call to Action here, and read the Executive Summary at hhs.gov.
Roughly half of American adults have hypertension, and about 71% of these cases are uncontrolled, according to data from the American Heart Association.
If left uncontrolled, hypertension can increase risk for conditions including heart disease, stroke, kidney disease, pregnancy complications, and cognitive decline, surgeon general Vice Adm. Jerome M. Adams, MD, said in a teleconference on Oct. 7. Hispanic and Black individuals are disproportionately affected, he added.
“We cannot wait to deal with this epidemic of uncontrolled high blood pressure,” even in the midst of the ongoing COVID-19 pandemic, said Dr. Adams. “We know what works” to help control hypertension, he added, citing his own use of a blood pressure monitoring device at home.
The Department of Health & Human Services has issued a Call to Action to Control Hypertension based on the latest science and research.
Dr. Adams outlined three goals to improve hypertension control, starting with making it a national priority. The Call to Action supports increasing awareness of the health risks associated with hypertension, recognizing the economic impact, overcoming barriers to controlling hypertension, and promoting health equity.
“In 2020, disparities in the burden of disease – especially among minority populations – have been recognized during the COVID-19 pandemic. A growing body of evidence has shown that people with underlying health conditions, including cardiovascular disease, are at increased risk of worse outcomes related to COVID-19 infection,” according to the Call to Action.
A second goal is to build and sustain communities that support individuals in taking responsibility for their health and blood pressure control, Dr. Adams said. He cited the need to create places for safe physical activity, access to healthy food, and opportunities to connect to resources to support lifestyle changes.
Finally, clinicians should continue to use standardized treatment approaches and promote team-based care to maximize outcomes for patients, Dr. Adams said.
Success starts with making hypertension control a priority across the leadership team, regardless of the size, location, or demographic population at a health care setting, he said. Dr. Adams cited the Million Hearts 2022 program, an ongoing initiative to prevent 1 million heart attacks in the United States over 5 years, as a way that HHS is recognizing and rewarding success stories in hypertension control from across the country.
Empowering patients and equipping them to take charge of their hypertension essential to reducing the epidemic of high blood pressure, especially during the ongoing pandemic, Dr. Adams said. His message to clinicians to extend to patients is that it is safe to visit their doctors. Hospitals have worked to create a safe environment, however, patients can and should monitor their blood pressure regularly at home, using a self-measured blood pressure monitoring (SMBP) device, which may be covered by some insurers.
“I would encourage people to know their numbers,” and that 130/80 mm Hg is considered high and a risk factor for poor health outcomes, Dr. Adams said. Clinicians also should continue to support patients in lifestyle changes such as healthy eating and exercising regularly to help control high blood pressure.
The AHA expressed support for the surgeon general’s Call to Action. “Today’s call to action references updated hypertension guidelines the AHA and the American College of Cardiology issued in 2017 that apply the latest science to help clinicians work with patients to control their blood pressure,” the AHA said in a statement. The AHA also called on the Centers for Medicare & Medicaid Services and other insurance providers “to include coverage of SMBP devices for treatment and management of hypertension.”
The Call to Action was accompanied by a Viewpoint from Dr. Adams and Janet S. Wright, MD, also of the HHS, published in JAMA. Dr. Adams and Dr. Wright emphasized that the timing of the Call to Action recognizes that many of the same social factors that support or impede successful high blood pressure control are factors in worse outcomes from COVID-19 infections as well.
“When coupled with widespread implementation of best practices in clinical settings and empowering individuals to actively manage their blood pressure, acknowledging and addressing a community’s social conditions may generate sustained improvements in control of both hypertension and COVID-19,” they said.
Read and download the full Call to Action here, and read the Executive Summary at hhs.gov.
Teen affective disorders raise risk for midlife acute MI
in a Swedish national registry study presented at the virtual annual congress of the European Society of Cardiology.

The association was mediated in part by poor stress resilience and lack of physical fitness among these teenagers with an affective disorder, reported Cecilia Bergh, PhD, of Obrero (Sweden) University.
Her study was made possible by Sweden’s comprehensive national health care registries coupled with the Nordic nation’s compulsory conscription for military service. The mandatory conscription evaluation during the study years included a semistructured interview with a psychologist to assess stress resilience through questions about coping with everyday life, a medical history and physical examination, and a cardiovascular fitness test using a bicycle ergometer.
The study included 238,013 males born in 1952-1956. They were aged 18-19 years when they underwent their conscription examination, at which time 34,503 of them either received or already had a diagnosis of depression or anxiety. During follow-up from 1987 to 2010, a first acute MI occurred in 5,891 of the men. The risk was increased 51% among those with an earlier teen diagnosis of depression or anxiety.
In a Cox regression analysis adjusted for levels of adolescent cardiovascular risk factors, including blood pressure, body mass index, and systemic inflammation, as well as additional potential confounders, such as cognitive function, parental socioeconomic index, and a summary disease score, the midlife MI risk associated with adolescent depression or anxiety was attenuated, but still significant, with a 24% increase. Upon further statistical adjustment incorporating adolescent stress resilience and cardiovascular fitness, the increased risk of acute MI in midlife associated with adolescent depression or anxiety was further attenuated yet remained significant, at 18%.
Dr. Bergh shared her thoughts on preventing this increased risk of acute MI at a relatively young age: “Effective prevention might focus on behavior, lifestyle, and psychosocial stress in early life. If a healthy lifestyle is encouraged as early as possible in childhood and adolescence, it is more likely to persist into adulthood and to improve longterm health. So look for signs of stress, depression, or anxiety that is beyond normal teenager behavior and a persistent problem. Teenagers with poor well-being could benefit from additional support to encourage exercise and also to develop strategies to deal with stress.”
She reported having no financial conflicts regarding her study, conducted free of commercial support.
SOURCE: Bergh C et al. ESC 2020, Abstract 90524.
in a Swedish national registry study presented at the virtual annual congress of the European Society of Cardiology.
The association was mediated in part by poor stress resilience and lack of physical fitness among these teenagers with an affective disorder, reported Cecilia Bergh, PhD, of Obrero (Sweden) University.
Her study was made possible by Sweden’s comprehensive national health care registries coupled with the Nordic nation’s compulsory conscription for military service. The mandatory conscription evaluation during the study years included a semistructured interview with a psychologist to assess stress resilience through questions about coping with everyday life, a medical history and physical examination, and a cardiovascular fitness test using a bicycle ergometer.
The study included 238,013 males born in 1952-1956. They were aged 18-19 years when they underwent their conscription examination, at which time 34,503 of them either received or already had a diagnosis of depression or anxiety. During follow-up from 1987 to 2010, a first acute MI occurred in 5,891 of the men. The risk was increased 51% among those with an earlier teen diagnosis of depression or anxiety.
In a Cox regression analysis adjusted for levels of adolescent cardiovascular risk factors, including blood pressure, body mass index, and systemic inflammation, as well as additional potential confounders, such as cognitive function, parental socioeconomic index, and a summary disease score, the midlife MI risk associated with adolescent depression or anxiety was attenuated, but still significant, with a 24% increase. Upon further statistical adjustment incorporating adolescent stress resilience and cardiovascular fitness, the increased risk of acute MI in midlife associated with adolescent depression or anxiety was further attenuated yet remained significant, at 18%.
Dr. Bergh shared her thoughts on preventing this increased risk of acute MI at a relatively young age: “Effective prevention might focus on behavior, lifestyle, and psychosocial stress in early life. If a healthy lifestyle is encouraged as early as possible in childhood and adolescence, it is more likely to persist into adulthood and to improve longterm health. So look for signs of stress, depression, or anxiety that is beyond normal teenager behavior and a persistent problem. Teenagers with poor well-being could benefit from additional support to encourage exercise and also to develop strategies to deal with stress.”
She reported having no financial conflicts regarding her study, conducted free of commercial support.
SOURCE: Bergh C et al. ESC 2020, Abstract 90524.
in a Swedish national registry study presented at the virtual annual congress of the European Society of Cardiology.
The association was mediated in part by poor stress resilience and lack of physical fitness among these teenagers with an affective disorder, reported Cecilia Bergh, PhD, of Obrero (Sweden) University.
Her study was made possible by Sweden’s comprehensive national health care registries coupled with the Nordic nation’s compulsory conscription for military service. The mandatory conscription evaluation during the study years included a semistructured interview with a psychologist to assess stress resilience through questions about coping with everyday life, a medical history and physical examination, and a cardiovascular fitness test using a bicycle ergometer.
The study included 238,013 males born in 1952-1956. They were aged 18-19 years when they underwent their conscription examination, at which time 34,503 of them either received or already had a diagnosis of depression or anxiety. During follow-up from 1987 to 2010, a first acute MI occurred in 5,891 of the men. The risk was increased 51% among those with an earlier teen diagnosis of depression or anxiety.
In a Cox regression analysis adjusted for levels of adolescent cardiovascular risk factors, including blood pressure, body mass index, and systemic inflammation, as well as additional potential confounders, such as cognitive function, parental socioeconomic index, and a summary disease score, the midlife MI risk associated with adolescent depression or anxiety was attenuated, but still significant, with a 24% increase. Upon further statistical adjustment incorporating adolescent stress resilience and cardiovascular fitness, the increased risk of acute MI in midlife associated with adolescent depression or anxiety was further attenuated yet remained significant, at 18%.
Dr. Bergh shared her thoughts on preventing this increased risk of acute MI at a relatively young age: “Effective prevention might focus on behavior, lifestyle, and psychosocial stress in early life. If a healthy lifestyle is encouraged as early as possible in childhood and adolescence, it is more likely to persist into adulthood and to improve longterm health. So look for signs of stress, depression, or anxiety that is beyond normal teenager behavior and a persistent problem. Teenagers with poor well-being could benefit from additional support to encourage exercise and also to develop strategies to deal with stress.”
She reported having no financial conflicts regarding her study, conducted free of commercial support.
SOURCE: Bergh C et al. ESC 2020, Abstract 90524.
FROM ESC CONGRESS 2020
Retrospective Review on the Safety and Efficacy of Direct Oral Anticoagulants Compared With Warfarin in Patients With Cirrhosis
Coagulation in patients with cirrhosis is a complicated area of evolving research. Patients with cirrhosis were originally thought to be naturally anticoagulated due to the decreased production of clotting factors and platelets, combined with an increased international normalized ratio (INR).1 New data have shown that patients with cirrhosis are at a concomitant risk of bleeding and thrombosis due to increased platelet aggregation, decreased fibrinolysis, and decreased production of natural anticoagulants such as protein C and antithrombin.1 Traditionally, patients with cirrhosis needing anticoagulation therapy for comorbid conditions, such as nonvalvular atrial fibrillation (NVAF) or venous thromboembolism (VTE) were placed on warfarin therapy. Managing warfarin in patients with cirrhosis poses a challenge to clinicians due to the many food and drug interactions, narrow therapeutic index, and complications with maintaining a therapeutic INR.1
Direct oral anticoagulants (DOACs) have several benefits over warfarin therapy, including convenience, decreased monitoring, decreased drug and dietary restrictions, and faster onset of action.2 Conversely, DOACs undergo extensive hepatic metabolism giving rise to concerns about supratherapeutic drug levels and increased bleeding rates in patients with liver dysfunction.1 Consequently, patients with cirrhosis were excluded from the pivotal trials establishing DOACs for NVAF and VTE treatment. Exclusion of these patients in major clinical trials alongside the challenges of managing warfarin warrant an evaluation of the efficacy and safety of DOACs in patients with cirrhosis.
Recent retrospective studies have examined the use of DOACs in patients with cirrhosis and found favorable results. A retrospective chart review by Intagliata and colleagues consisting of 39 patients with cirrhosis using either a DOAC or warfarin found similar rates of all-cause bleeding and major bleeding between the 2 groups.3 A retrospective cohort study by Hum and colleagues consisting of 45 patients with cirrhosis compared the use of DOACs with warfarin or low-molecular weight heparin (LMWH).4 Hum and colleagues found patients prescribed a DOAC had significantly fewer major bleeding events than did patients using warfarin or LMWH.4 The largest retrospective cohort study consisted of 233 patients with chronic liver disease and found no differences among all-cause bleeding and major bleeding rates between patients using DOACs compared with those of patients using warfarin.5
The purpose of this research is to evaluate the safety and efficacy of DOACs in veteran patients with cirrhosis compared with patients using warfarin.
Methods
A retrospective single-center chart review was conducted at the Michael E. DeBakey Veterans Affairs Medical Center (MEDVAMC) in Houston, Texas, between October 31, 2014 and October 31, 2018. Patients included in the study were adults aged ≥ 18 years with a diagnosis of cirrhosis and prescribed any of the following oral anticoagulants: apixaban, dabigatran, edoxaban, rivaroxaban, or warfarin. Patients prescribed apixaban, dabigatran, edoxaban, or rivaroxaban were collectively grouped into the DOAC group, while patients prescribed warfarin were classified as the standard of care comparator group.
A diagnosis of cirrhosis was confirmed using a combination of the codes from the ninth and tenth editions of the International Classification of Diseases (ICD) for cirrhosis, documentation of diagnostic confirmation by clinicians from the gastroenterology or hepatology services, and positive liver biopsy result. Liver function tests, liver ultrasound results, and FibroSure biomarker assays were used to aid in confirming the diagnosis of cirrhosis but were not considered definitive. Patients were excluded from the trial if they had indications for anticoagulation other than NVAF and VTE and/or were prescribed triple antithrombotic therapy (dual antiplatelet therapy plus an anticoagulant). Patients who switched anticoagulant therapy during the trial period (ie, switched from warfarin to a DOAC) were also excluded from the analysis.
Patient demographic characteristics that were collected included weight; body mass index (BMI); etiology of cirrhosis; Child-Turcotte-Pugh, Model for End-Stage Liver Disease (MELD), and CHA2DS2-VASc score; concomitant antiplatelet, nonsteroidal anti-inflammatory drug (NSAID), proton pump inhibitor (PPI), and histamine-2 receptor antagonist
Two patient lists were used to identify patients for inclusion in the warfarin arm. The first patient list was generated using the US Department of Veterans Affairs (VA) Cirrhosis Tracker, which identified patients with an ICD-9/10 code for cirrhosis and an INR laboratory value. Patients generated from the VA Cirrhosis Tracker with an INR > 1.5 were screened for a warfarin prescription and then evaluated for full study inclusion. The second patient list was generated using the VA Advanced Liver Disease Dashboard which identified patients with ICD-9/10 codes for advanced liver disease and an active warfarin prescription. Patients with an active warfarin prescription were then evaluated for full study inclusion. A single patient list was generated to identify patients for inclusion in the DOAC arm. This patient list was generated using the VA DOAC dashboard, which identified patients with an active DOAC prescription and an ICD-9/10 code for cirrhosis. Patients with an ICD-9/10 code for cirrhosis and prescribed a DOAC were screened for full study inclusion. Patient data were collected from the MEDVAMC Computerized Patient Record System (CPRS) electronic health record (EHR). The research study was approved by the Baylor College of Medicine Institutional Review Board and the VA Office of Research and Development.
Outcomes
The primary endpoint for the study was all-cause bleeding. The secondary endpoints for the study were major bleeding and failed efficacy. Major bleeding was defined using the International Society on Thrombosis and Haemostasis (ISTH) 2005 definition: fatal bleeding, symptomatic bleeding in a critical organ area (ie, intracranial, intraspinal, intraocular, retroperitoneal, intraarticular, pericardial, or intramuscular with compartment syndrome), or bleeding causing a fall in hemoglobin level of > 2 g/dL or leading to the transfusion of ≥ 2 units of red cells.6 Failed efficacy was a combination endpoint that included development of VTE, stroke, myocardial infarction (MI), and/or death. A prespecified subgroup analysis was conducted at the end of the study period to analyze trends in the DOAC and warfarin groups with respect to all-cause bleeding. All-cause bleeding risk was stratified by weight, BMI, Child-Turcotte-Pugh score, MELD score, presence of gastric and/or esophageal varices, active malignancies, percentage of time within therapeutic INR range in the warfarin group, indications for anticoagulation, and antiplatelet, NSAID, PPI, and H2RA therapy.
Statistical Analysis
Data were analyzed using descriptive and inferential statistics. Continuous data were analyzed using the Student t test, and categorical data were analyzed using the Fisher exact test. Previous studies determined an all-cause bleeding rate of 10 to 17% for warfarin compared with 5% for DOACs.7,8 To detect a 12% difference in the all-cause bleeding rate between DOACs and warfarin, 212 patients would be needed to achieve 80% power at an α level of 0.05.
Results
A total of 170 patients were screened, and after applying inclusion and exclusion criteria, 79 patients were enrolled in the study (Figure). The DOAC group included 42 patients, and the warfarin group included 37 patients. In the DOAC group, 69.1% (n = 29) of patients were taking apixaban, 21.4% (n = 9) rivaroxaban, and 9.5% (n = 4) dabigatran. There were no patients prescribed edoxaban during the study period.
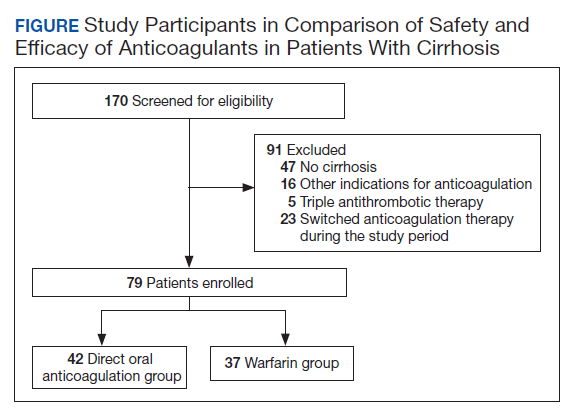
Baseline characteristics were similar between the 2 groups except for Child-Turcotte-Pugh score, MELD score, mean INR, and number of days on anticoagulation therapy (Table 1). Most of the patients were male (98.7%), and the mean age was 71 years. The most common causes of cirrhosis were viral (29.1%), nonalcoholic fatty liver disease (NAFLD) (24.1%), multiple causes (22.8%), and alcohol (21.5%). Sixty-two patients (78.5%) had a NVAF indication for anticoagulation. The average CHA2DS2-VASc score was 3.7. Aspirin was prescribed in 51.9% (n = 41) of patients, and PPIs were prescribed in 48.1% (n = 38) of patients. At inclusion, esophageal varices were present in 13 patients and active malignancies were present in 6 patients.
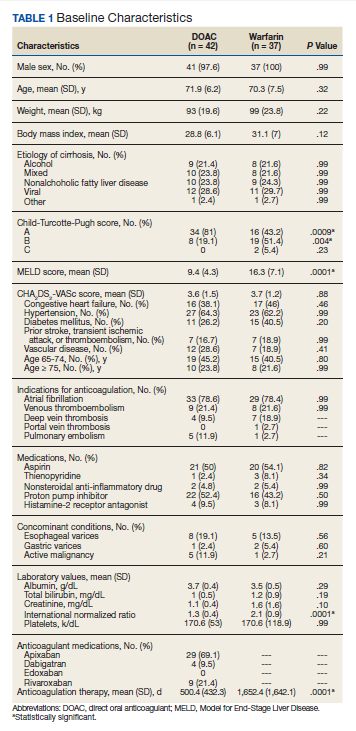
Statistically significant differences in baseline characteristics were found between mean INR, Child-Turcotte-Pugh scores, MELD scores, and number of days on anticoagulant therapy. The mean INR was 1.3 in the DOAC group compared with 2.1 in the warfarin group (P = .0001). Eighty-one percent (n = 34) of patients in the DOAC group had a Child-Turcotte-Pugh score of A compared with 43.2% (n = 16) of patients in the warfarin group (P = .0009). Eight patients in the DOAC group had a Child-Turcotte-Pugh score of B compared with 19 patients in the warfarin group (P = .004). The mean MELD score was 9.4 in the DOAC group compared with 16.3 in the warfarin group (P = .0001). The mean days on anticoagulant therapy was 500.4 days for the DOAC group compared with 1,652.4 days for the warfarin group (P = .0001).
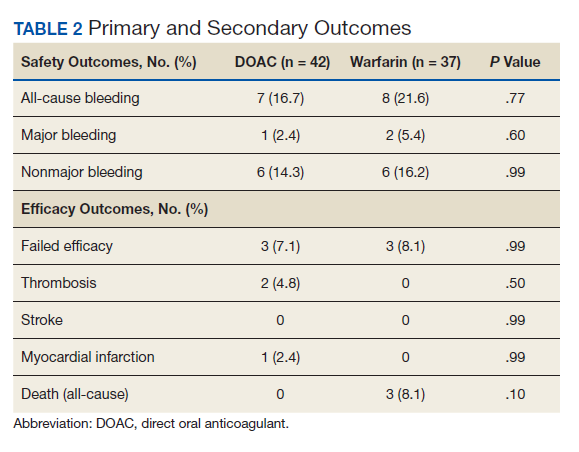
Safety Outcome
The primary outcome comparing all-cause bleeding rates between patients on DOACs compared with warfarin are listed in Table 2. With respect to the primary outcome, 7 (16.7%) patients on DOACs experienced a bleeding event compared with 8 (21.6%) patients on warfarin (P = .77). No statistically significant differences were detected between the DOAC and warfarin groups with respect to all-cause bleeding. Seven bleeding events occurred in the DOAC group; 1 met the qualification for major bleeding with a suspected gastrointestinal (GI) bleed.6 The other 6 bleeding episodes in the DOAC group consisted of hematoma, epistaxis, hematuria, and hematochezia. Eight bleeding events occurred in the warfarin group; 2 met the qualification for major bleeding with an intracranial hemorrhage and upper GI bleed.6 The other 6 bleeding episodes in the warfarin group consisted of epistaxis, bleeding gums, hematuria, and hematochezia. There were no statistically significant differences between the rates of major bleeding and nonmajor bleeding between the DOAC and warfarin groups.
Efficacy Outcomes
There were 3 events in the DOAC group and 3 events in the warfarin group (P = .99). In the DOAC group, 2 patients experienced a pulmonary embolism, and 1 patient experienced a MI. In the warfarin group, 3 patients died (end-stage heart failure, unknown cause due to death at an outside hospital, and sepsis/organ failure). There were no statistically significant differences between the composite endpoint of failed efficacy or the individual endpoints of VTE, stroke, MI, and death.
Subgroup Analysis
A prespecified subgroup analysis was conducted to determine risk factors for all-cause bleeding within each treatment group (Table 3). No significant trends were observed in the following risk factors: Child-Turcotte-Pugh score, indication for anticoagulation, use of NSAIDs, PPIs or H2RAs, presence of gastric or esophageal varices, active malignancies, and time within therapeutic INR range in the warfarin group. Patients with bleeding events had slightly increased weight and BMI vs patients without bleeding events. Within the warfarin group, patients with bleeding events had slightly elevated MELD scores compared to patients without bleeding events. There was an equal balance of patients prescribed aspirin therapy between the groups with and without bleeding events. Overall, no significant risk factors were identified for all-cause bleeding.
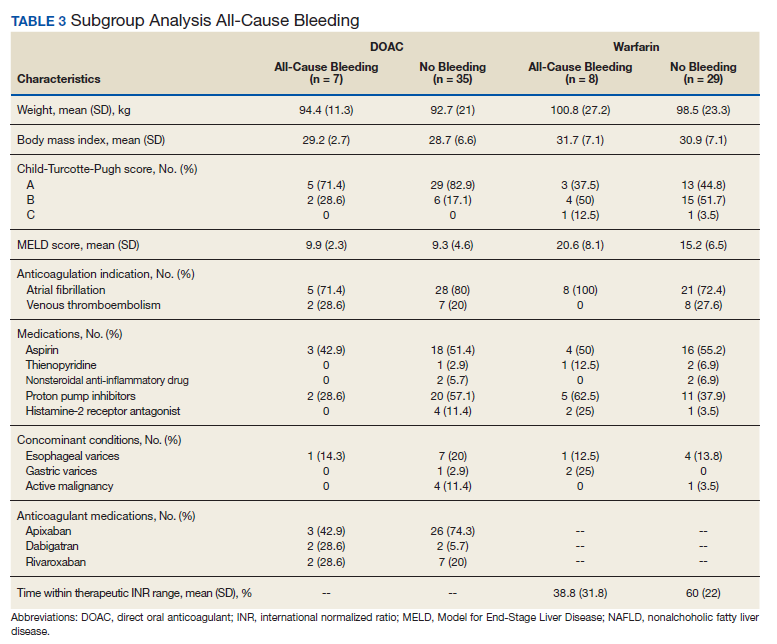
Discussion
Initially, patients with cirrhosis were excluded from DOAC trials due to concerns for increased bleeding risk with hepatically eliminated medications. New retrospective research has concluded that in patients with cirrhosis, DOACs have similar or lower bleeding rates when compared directly to warfarin.9,10
In this study, no statistically significant differences were detected between the primary and secondary outcomes of all-cause bleeding, major bleeding, or failed efficacy. Subgroup analysis did not identify any significant risk factors with respect to all-cause bleeding among patients in the DOAC and warfarin groups. To meet 80% power, 212 patients needed to be enrolled in the study; however, only 79 patients were enrolled, and power was not met. The results of this study should be interpreted cautiously as hypothesis-generating due to the small sample size. Strengths of this study include similar baseline characteristics between the DOAC and warfarin groups, 4-year length of retrospective data review, and availability of both inpatient and outpatient EHR limiting the amount of missing data points.
Baseline characteristics were similar between the groups except for mean INR, Child-Turcotte-Pugh score, MELD score, and number of days on anticoagulation therapy. The difference in mean INR between groups is expected as patients in the warfarin group have a goal INR of 2 to 3 to maintain therapeutic efficacy and safety. INR is not used as a marker of efficacy or safety with DOACs; therefore, a consistent elevation in INR is not expected. Child- Turcotte-Pugh scores are calculated using INR levels.11 When calculating the score, patients with an INR < 1.7 receive 1 point; patients with an INR between 1.7 and 2.3 receive 2 points.11 Therefore, patients in the warfarin group will have artificially inflated Child-Turcotte-Pugh scores as this group has goal INR levels of 2 to 3. This makes Child-Turcotte-Pugh scores unreliable markers of disease severity in patients using warfarin therapy. When the INR scores for patients prescribed warfarin were replaced with values < 1.7, the statistical difference disappeared between the warfarin and DOAC groups. The same effect is seen on MELD scores for patients prescribed warfarin therapy. The MELD score is calculated using INR levels.12 MELD scores also will be artificially elevated in patients prescribed warfarin therapy due to the INR elevation to between 2 and 3. When MELD scores for patients prescribed warfarin were replaced with values similar to those in the DOAC group, the statistical difference disappeared between the warfarin and DOAC groups.
The last statistically significant difference was found in number of days on anticoagulant therapy. This difference was expected as warfarin is the standard of care for anticoagulation treatment in patients with cirrhosis. The first DOAC, dabigatran, was not approved by the US Food and Drug Administration until 2010.13 DOACs have only recently been used in patients with cirrhosis accounting for the statistically significant difference in days on anticoagulation therapy between the warfarin and DOAC groups.
Limitations
The inability to meet power or evaluate adherence and appropriate renal dose adjustments for DOACs limited this study. This study was conducted at a single center in a predominantly male veteran population and therefore may not be generalizable to other populations. A majority of patients in the DOAC group were prescribed apixaban (69.1%), which may have affected the overall rate of major bleeding in the DOAC group. Pivotal trials of apixaban have shown a consistent decreased risk of major bleeding in patients with NVAF or VTE when compared with warfarin.14,15 Therefore, the results of this study may not be generalizable to all DOACs.
An inherent limitation of this study was the inability to collect data verifying adherence in the DOAC group. However, in the warfarin group, percentage of time within the therapeutic INR range of 2 to 3 was collected. While not a direct marker of adherence, this does allow for limited evaluation of therapeutic efficacy and safety within the warfarin group. Last, proper dosing of DOACs in patients with and without adequate renal function was not evaluated in this study.
Conclusions
The results of this study are consistent with other retrospective research and literature reviews. There were no statistically significant differences identified between the rates of all-cause bleeding, major bleeding, and failed efficacy between the DOAC and warfarin groups. DOACs may be a safe alternative to warfarin in patients with cirrhosis requiring anticoagulation for NVAF or VTE, but large randomized trials are required to confirm these results.
1. Qamar A, Vaduganathan M, Greenberger NJ, Giugliano RP. Oral anticoagulation in patients with liver disease. J Am Coll Cardiol. 2018;71(19):2162-2175. doi:10.1016/j.jacc.2018.03.023
2. Priyanka P, Kupec JT, Krafft M, Shah NA, Reynolds GJ. Newer oral anticoagulants in the treatment of acute portal vein thrombosis in patients with and without cirrhosis. Int J Hepatol. 2018;2018:8432781. Published 2018 Jun 5. doi:10.1155/2018/8432781
3. Intagliata NM, Henry ZH, Maitland H, et al. Direct oral anticoagulants in cirrhosis patients pose similar risks of bleeding when compared to traditional anticoagulation. Dig Dis Sci. 2016;61(6):1721-1727. doi:10.1007/s10620-015-4012-2
4. Hum J, Shatzel JJ, Jou JH, Deloughery TG. The efficacy and safety of direct oral anticoagulants vs traditional anticoagulants in cirrhosis. Eur J Haematol. 2017;98(4):393-397. doi:10.1111/ejh.12844
5. Goriacko P, Veltri KT. Safety of direct oral anticoagulants vs warfarin in patients with chronic liver disease and atrial fibrillation. Eur J Haematol. 2018;100(5):488-493. doi:10.1111/ejh.13045
6. Schulman S, Kearon C; Subcommittee on Control of Anticoagulation of the Scientific and Standardization Committee of the International Society on Thrombosis and Haemostasis. Definition of major bleeding in clinical investigations of antihemostatic medicinal products in non-surgical patients. J Thromb Haemost. 2005;3(4):692-694. doi:10.1111/j.1538-7836.2005.01204.x
7. Rubboli A, Becattini C, Verheugt FW. Incidence, clinical impact and risk of bleeding during oral anticoagulation therapy. World J Cardiol. 2011;3(11):351-358. doi:10.4330/wjc.v3.i11.351
8. Ruff CT, Giugliano RP, Braunwald E, et al. Comparison of the efficacy and safety of new oral anticoagulants with warfarin in patients with atrial fibrillation: a meta-analysis of randomised trials. Lancet. 2014;383(9921):955-962. doi:10.1016/S0140-6736(13)62343-0
9. Hoolwerf EW, Kraaijpoel N, Büller HR, van Es N. Direct oral anticoagulants in patients with liver cirrhosis: A systematic review. Thromb Res. 2018;170:102-108. doi:10.1016/j.thromres.2018.08.011
10. Steuber TD, Howard ML, Nisly SA. Direct oral anticoagulants in chronic liver disease. Ann Pharmacother. 2019;53(10):1042-1049. doi:10.1177/1060028019841582
11. Janevska D, Chaloska-Ivanova V, Janevski V. Hepatocellular carcinoma: risk factors, diagnosis and treatment. Open Access Maced J Med Sci. 2015;3(4):732-736. doi:10.3889/oamjms.2015.111
12. Singal AK, Kamath PS. Model for End-Stage Liver Disease. J Clin Exp Hepatol. 2013;3(1):50-60. doi:10.1016/j.jceh.2012.11.002
13. Joppa SA, Salciccioli J, Adamski J, et al. A practical review of the emerging direct anticoagulants, laboratory monitoring, and reversal agents. J Clin Med. 2018;7(2):29. Published 2018 Feb 11. doi:10.3390/jcm7020029
14. Granger CB, Alexander JH, McMurray JJ, et al. Apixaban versus warfarin in patients with atrial fibrillation. N Engl J Med. 2011;365(11):981-992. doi:10.1056/NEJMoa1107039
15. Agnelli G, Buller HR, Cohen A, et al. Oral apixaban for the treatment of acute venous thromboembolism. N Engl J Med. 2013;369(9):799-808. doi:10.1056/NEJMoa1302507
Coagulation in patients with cirrhosis is a complicated area of evolving research. Patients with cirrhosis were originally thought to be naturally anticoagulated due to the decreased production of clotting factors and platelets, combined with an increased international normalized ratio (INR).1 New data have shown that patients with cirrhosis are at a concomitant risk of bleeding and thrombosis due to increased platelet aggregation, decreased fibrinolysis, and decreased production of natural anticoagulants such as protein C and antithrombin.1 Traditionally, patients with cirrhosis needing anticoagulation therapy for comorbid conditions, such as nonvalvular atrial fibrillation (NVAF) or venous thromboembolism (VTE) were placed on warfarin therapy. Managing warfarin in patients with cirrhosis poses a challenge to clinicians due to the many food and drug interactions, narrow therapeutic index, and complications with maintaining a therapeutic INR.1
Direct oral anticoagulants (DOACs) have several benefits over warfarin therapy, including convenience, decreased monitoring, decreased drug and dietary restrictions, and faster onset of action.2 Conversely, DOACs undergo extensive hepatic metabolism giving rise to concerns about supratherapeutic drug levels and increased bleeding rates in patients with liver dysfunction.1 Consequently, patients with cirrhosis were excluded from the pivotal trials establishing DOACs for NVAF and VTE treatment. Exclusion of these patients in major clinical trials alongside the challenges of managing warfarin warrant an evaluation of the efficacy and safety of DOACs in patients with cirrhosis.
Recent retrospective studies have examined the use of DOACs in patients with cirrhosis and found favorable results. A retrospective chart review by Intagliata and colleagues consisting of 39 patients with cirrhosis using either a DOAC or warfarin found similar rates of all-cause bleeding and major bleeding between the 2 groups.3 A retrospective cohort study by Hum and colleagues consisting of 45 patients with cirrhosis compared the use of DOACs with warfarin or low-molecular weight heparin (LMWH).4 Hum and colleagues found patients prescribed a DOAC had significantly fewer major bleeding events than did patients using warfarin or LMWH.4 The largest retrospective cohort study consisted of 233 patients with chronic liver disease and found no differences among all-cause bleeding and major bleeding rates between patients using DOACs compared with those of patients using warfarin.5
The purpose of this research is to evaluate the safety and efficacy of DOACs in veteran patients with cirrhosis compared with patients using warfarin.
Methods
A retrospective single-center chart review was conducted at the Michael E. DeBakey Veterans Affairs Medical Center (MEDVAMC) in Houston, Texas, between October 31, 2014 and October 31, 2018. Patients included in the study were adults aged ≥ 18 years with a diagnosis of cirrhosis and prescribed any of the following oral anticoagulants: apixaban, dabigatran, edoxaban, rivaroxaban, or warfarin. Patients prescribed apixaban, dabigatran, edoxaban, or rivaroxaban were collectively grouped into the DOAC group, while patients prescribed warfarin were classified as the standard of care comparator group.
A diagnosis of cirrhosis was confirmed using a combination of the codes from the ninth and tenth editions of the International Classification of Diseases (ICD) for cirrhosis, documentation of diagnostic confirmation by clinicians from the gastroenterology or hepatology services, and positive liver biopsy result. Liver function tests, liver ultrasound results, and FibroSure biomarker assays were used to aid in confirming the diagnosis of cirrhosis but were not considered definitive. Patients were excluded from the trial if they had indications for anticoagulation other than NVAF and VTE and/or were prescribed triple antithrombotic therapy (dual antiplatelet therapy plus an anticoagulant). Patients who switched anticoagulant therapy during the trial period (ie, switched from warfarin to a DOAC) were also excluded from the analysis.
Patient demographic characteristics that were collected included weight; body mass index (BMI); etiology of cirrhosis; Child-Turcotte-Pugh, Model for End-Stage Liver Disease (MELD), and CHA2DS2-VASc score; concomitant antiplatelet, nonsteroidal anti-inflammatory drug (NSAID), proton pump inhibitor (PPI), and histamine-2 receptor antagonist
Two patient lists were used to identify patients for inclusion in the warfarin arm. The first patient list was generated using the US Department of Veterans Affairs (VA) Cirrhosis Tracker, which identified patients with an ICD-9/10 code for cirrhosis and an INR laboratory value. Patients generated from the VA Cirrhosis Tracker with an INR > 1.5 were screened for a warfarin prescription and then evaluated for full study inclusion. The second patient list was generated using the VA Advanced Liver Disease Dashboard which identified patients with ICD-9/10 codes for advanced liver disease and an active warfarin prescription. Patients with an active warfarin prescription were then evaluated for full study inclusion. A single patient list was generated to identify patients for inclusion in the DOAC arm. This patient list was generated using the VA DOAC dashboard, which identified patients with an active DOAC prescription and an ICD-9/10 code for cirrhosis. Patients with an ICD-9/10 code for cirrhosis and prescribed a DOAC were screened for full study inclusion. Patient data were collected from the MEDVAMC Computerized Patient Record System (CPRS) electronic health record (EHR). The research study was approved by the Baylor College of Medicine Institutional Review Board and the VA Office of Research and Development.
Outcomes
The primary endpoint for the study was all-cause bleeding. The secondary endpoints for the study were major bleeding and failed efficacy. Major bleeding was defined using the International Society on Thrombosis and Haemostasis (ISTH) 2005 definition: fatal bleeding, symptomatic bleeding in a critical organ area (ie, intracranial, intraspinal, intraocular, retroperitoneal, intraarticular, pericardial, or intramuscular with compartment syndrome), or bleeding causing a fall in hemoglobin level of > 2 g/dL or leading to the transfusion of ≥ 2 units of red cells.6 Failed efficacy was a combination endpoint that included development of VTE, stroke, myocardial infarction (MI), and/or death. A prespecified subgroup analysis was conducted at the end of the study period to analyze trends in the DOAC and warfarin groups with respect to all-cause bleeding. All-cause bleeding risk was stratified by weight, BMI, Child-Turcotte-Pugh score, MELD score, presence of gastric and/or esophageal varices, active malignancies, percentage of time within therapeutic INR range in the warfarin group, indications for anticoagulation, and antiplatelet, NSAID, PPI, and H2RA therapy.
Statistical Analysis
Data were analyzed using descriptive and inferential statistics. Continuous data were analyzed using the Student t test, and categorical data were analyzed using the Fisher exact test. Previous studies determined an all-cause bleeding rate of 10 to 17% for warfarin compared with 5% for DOACs.7,8 To detect a 12% difference in the all-cause bleeding rate between DOACs and warfarin, 212 patients would be needed to achieve 80% power at an α level of 0.05.
Results
A total of 170 patients were screened, and after applying inclusion and exclusion criteria, 79 patients were enrolled in the study (Figure). The DOAC group included 42 patients, and the warfarin group included 37 patients. In the DOAC group, 69.1% (n = 29) of patients were taking apixaban, 21.4% (n = 9) rivaroxaban, and 9.5% (n = 4) dabigatran. There were no patients prescribed edoxaban during the study period.
Baseline characteristics were similar between the 2 groups except for Child-Turcotte-Pugh score, MELD score, mean INR, and number of days on anticoagulation therapy (Table 1). Most of the patients were male (98.7%), and the mean age was 71 years. The most common causes of cirrhosis were viral (29.1%), nonalcoholic fatty liver disease (NAFLD) (24.1%), multiple causes (22.8%), and alcohol (21.5%). Sixty-two patients (78.5%) had a NVAF indication for anticoagulation. The average CHA2DS2-VASc score was 3.7. Aspirin was prescribed in 51.9% (n = 41) of patients, and PPIs were prescribed in 48.1% (n = 38) of patients. At inclusion, esophageal varices were present in 13 patients and active malignancies were present in 6 patients.
Statistically significant differences in baseline characteristics were found between mean INR, Child-Turcotte-Pugh scores, MELD scores, and number of days on anticoagulant therapy. The mean INR was 1.3 in the DOAC group compared with 2.1 in the warfarin group (P = .0001). Eighty-one percent (n = 34) of patients in the DOAC group had a Child-Turcotte-Pugh score of A compared with 43.2% (n = 16) of patients in the warfarin group (P = .0009). Eight patients in the DOAC group had a Child-Turcotte-Pugh score of B compared with 19 patients in the warfarin group (P = .004). The mean MELD score was 9.4 in the DOAC group compared with 16.3 in the warfarin group (P = .0001). The mean days on anticoagulant therapy was 500.4 days for the DOAC group compared with 1,652.4 days for the warfarin group (P = .0001).
Safety Outcome
The primary outcome comparing all-cause bleeding rates between patients on DOACs compared with warfarin are listed in Table 2. With respect to the primary outcome, 7 (16.7%) patients on DOACs experienced a bleeding event compared with 8 (21.6%) patients on warfarin (P = .77). No statistically significant differences were detected between the DOAC and warfarin groups with respect to all-cause bleeding. Seven bleeding events occurred in the DOAC group; 1 met the qualification for major bleeding with a suspected gastrointestinal (GI) bleed.6 The other 6 bleeding episodes in the DOAC group consisted of hematoma, epistaxis, hematuria, and hematochezia. Eight bleeding events occurred in the warfarin group; 2 met the qualification for major bleeding with an intracranial hemorrhage and upper GI bleed.6 The other 6 bleeding episodes in the warfarin group consisted of epistaxis, bleeding gums, hematuria, and hematochezia. There were no statistically significant differences between the rates of major bleeding and nonmajor bleeding between the DOAC and warfarin groups.
Efficacy Outcomes
There were 3 events in the DOAC group and 3 events in the warfarin group (P = .99). In the DOAC group, 2 patients experienced a pulmonary embolism, and 1 patient experienced a MI. In the warfarin group, 3 patients died (end-stage heart failure, unknown cause due to death at an outside hospital, and sepsis/organ failure). There were no statistically significant differences between the composite endpoint of failed efficacy or the individual endpoints of VTE, stroke, MI, and death.
Subgroup Analysis
A prespecified subgroup analysis was conducted to determine risk factors for all-cause bleeding within each treatment group (Table 3). No significant trends were observed in the following risk factors: Child-Turcotte-Pugh score, indication for anticoagulation, use of NSAIDs, PPIs or H2RAs, presence of gastric or esophageal varices, active malignancies, and time within therapeutic INR range in the warfarin group. Patients with bleeding events had slightly increased weight and BMI vs patients without bleeding events. Within the warfarin group, patients with bleeding events had slightly elevated MELD scores compared to patients without bleeding events. There was an equal balance of patients prescribed aspirin therapy between the groups with and without bleeding events. Overall, no significant risk factors were identified for all-cause bleeding.
Discussion
Initially, patients with cirrhosis were excluded from DOAC trials due to concerns for increased bleeding risk with hepatically eliminated medications. New retrospective research has concluded that in patients with cirrhosis, DOACs have similar or lower bleeding rates when compared directly to warfarin.9,10
In this study, no statistically significant differences were detected between the primary and secondary outcomes of all-cause bleeding, major bleeding, or failed efficacy. Subgroup analysis did not identify any significant risk factors with respect to all-cause bleeding among patients in the DOAC and warfarin groups. To meet 80% power, 212 patients needed to be enrolled in the study; however, only 79 patients were enrolled, and power was not met. The results of this study should be interpreted cautiously as hypothesis-generating due to the small sample size. Strengths of this study include similar baseline characteristics between the DOAC and warfarin groups, 4-year length of retrospective data review, and availability of both inpatient and outpatient EHR limiting the amount of missing data points.
Baseline characteristics were similar between the groups except for mean INR, Child-Turcotte-Pugh score, MELD score, and number of days on anticoagulation therapy. The difference in mean INR between groups is expected as patients in the warfarin group have a goal INR of 2 to 3 to maintain therapeutic efficacy and safety. INR is not used as a marker of efficacy or safety with DOACs; therefore, a consistent elevation in INR is not expected. Child- Turcotte-Pugh scores are calculated using INR levels.11 When calculating the score, patients with an INR < 1.7 receive 1 point; patients with an INR between 1.7 and 2.3 receive 2 points.11 Therefore, patients in the warfarin group will have artificially inflated Child-Turcotte-Pugh scores as this group has goal INR levels of 2 to 3. This makes Child-Turcotte-Pugh scores unreliable markers of disease severity in patients using warfarin therapy. When the INR scores for patients prescribed warfarin were replaced with values < 1.7, the statistical difference disappeared between the warfarin and DOAC groups. The same effect is seen on MELD scores for patients prescribed warfarin therapy. The MELD score is calculated using INR levels.12 MELD scores also will be artificially elevated in patients prescribed warfarin therapy due to the INR elevation to between 2 and 3. When MELD scores for patients prescribed warfarin were replaced with values similar to those in the DOAC group, the statistical difference disappeared between the warfarin and DOAC groups.
The last statistically significant difference was found in number of days on anticoagulant therapy. This difference was expected as warfarin is the standard of care for anticoagulation treatment in patients with cirrhosis. The first DOAC, dabigatran, was not approved by the US Food and Drug Administration until 2010.13 DOACs have only recently been used in patients with cirrhosis accounting for the statistically significant difference in days on anticoagulation therapy between the warfarin and DOAC groups.
Limitations
The inability to meet power or evaluate adherence and appropriate renal dose adjustments for DOACs limited this study. This study was conducted at a single center in a predominantly male veteran population and therefore may not be generalizable to other populations. A majority of patients in the DOAC group were prescribed apixaban (69.1%), which may have affected the overall rate of major bleeding in the DOAC group. Pivotal trials of apixaban have shown a consistent decreased risk of major bleeding in patients with NVAF or VTE when compared with warfarin.14,15 Therefore, the results of this study may not be generalizable to all DOACs.
An inherent limitation of this study was the inability to collect data verifying adherence in the DOAC group. However, in the warfarin group, percentage of time within the therapeutic INR range of 2 to 3 was collected. While not a direct marker of adherence, this does allow for limited evaluation of therapeutic efficacy and safety within the warfarin group. Last, proper dosing of DOACs in patients with and without adequate renal function was not evaluated in this study.
Conclusions
The results of this study are consistent with other retrospective research and literature reviews. There were no statistically significant differences identified between the rates of all-cause bleeding, major bleeding, and failed efficacy between the DOAC and warfarin groups. DOACs may be a safe alternative to warfarin in patients with cirrhosis requiring anticoagulation for NVAF or VTE, but large randomized trials are required to confirm these results.
Coagulation in patients with cirrhosis is a complicated area of evolving research. Patients with cirrhosis were originally thought to be naturally anticoagulated due to the decreased production of clotting factors and platelets, combined with an increased international normalized ratio (INR).1 New data have shown that patients with cirrhosis are at a concomitant risk of bleeding and thrombosis due to increased platelet aggregation, decreased fibrinolysis, and decreased production of natural anticoagulants such as protein C and antithrombin.1 Traditionally, patients with cirrhosis needing anticoagulation therapy for comorbid conditions, such as nonvalvular atrial fibrillation (NVAF) or venous thromboembolism (VTE) were placed on warfarin therapy. Managing warfarin in patients with cirrhosis poses a challenge to clinicians due to the many food and drug interactions, narrow therapeutic index, and complications with maintaining a therapeutic INR.1
Direct oral anticoagulants (DOACs) have several benefits over warfarin therapy, including convenience, decreased monitoring, decreased drug and dietary restrictions, and faster onset of action.2 Conversely, DOACs undergo extensive hepatic metabolism giving rise to concerns about supratherapeutic drug levels and increased bleeding rates in patients with liver dysfunction.1 Consequently, patients with cirrhosis were excluded from the pivotal trials establishing DOACs for NVAF and VTE treatment. Exclusion of these patients in major clinical trials alongside the challenges of managing warfarin warrant an evaluation of the efficacy and safety of DOACs in patients with cirrhosis.
Recent retrospective studies have examined the use of DOACs in patients with cirrhosis and found favorable results. A retrospective chart review by Intagliata and colleagues consisting of 39 patients with cirrhosis using either a DOAC or warfarin found similar rates of all-cause bleeding and major bleeding between the 2 groups.3 A retrospective cohort study by Hum and colleagues consisting of 45 patients with cirrhosis compared the use of DOACs with warfarin or low-molecular weight heparin (LMWH).4 Hum and colleagues found patients prescribed a DOAC had significantly fewer major bleeding events than did patients using warfarin or LMWH.4 The largest retrospective cohort study consisted of 233 patients with chronic liver disease and found no differences among all-cause bleeding and major bleeding rates between patients using DOACs compared with those of patients using warfarin.5
The purpose of this research is to evaluate the safety and efficacy of DOACs in veteran patients with cirrhosis compared with patients using warfarin.
Methods
A retrospective single-center chart review was conducted at the Michael E. DeBakey Veterans Affairs Medical Center (MEDVAMC) in Houston, Texas, between October 31, 2014 and October 31, 2018. Patients included in the study were adults aged ≥ 18 years with a diagnosis of cirrhosis and prescribed any of the following oral anticoagulants: apixaban, dabigatran, edoxaban, rivaroxaban, or warfarin. Patients prescribed apixaban, dabigatran, edoxaban, or rivaroxaban were collectively grouped into the DOAC group, while patients prescribed warfarin were classified as the standard of care comparator group.
A diagnosis of cirrhosis was confirmed using a combination of the codes from the ninth and tenth editions of the International Classification of Diseases (ICD) for cirrhosis, documentation of diagnostic confirmation by clinicians from the gastroenterology or hepatology services, and positive liver biopsy result. Liver function tests, liver ultrasound results, and FibroSure biomarker assays were used to aid in confirming the diagnosis of cirrhosis but were not considered definitive. Patients were excluded from the trial if they had indications for anticoagulation other than NVAF and VTE and/or were prescribed triple antithrombotic therapy (dual antiplatelet therapy plus an anticoagulant). Patients who switched anticoagulant therapy during the trial period (ie, switched from warfarin to a DOAC) were also excluded from the analysis.
Patient demographic characteristics that were collected included weight; body mass index (BMI); etiology of cirrhosis; Child-Turcotte-Pugh, Model for End-Stage Liver Disease (MELD), and CHA2DS2-VASc score; concomitant antiplatelet, nonsteroidal anti-inflammatory drug (NSAID), proton pump inhibitor (PPI), and histamine-2 receptor antagonist
Two patient lists were used to identify patients for inclusion in the warfarin arm. The first patient list was generated using the US Department of Veterans Affairs (VA) Cirrhosis Tracker, which identified patients with an ICD-9/10 code for cirrhosis and an INR laboratory value. Patients generated from the VA Cirrhosis Tracker with an INR > 1.5 were screened for a warfarin prescription and then evaluated for full study inclusion. The second patient list was generated using the VA Advanced Liver Disease Dashboard which identified patients with ICD-9/10 codes for advanced liver disease and an active warfarin prescription. Patients with an active warfarin prescription were then evaluated for full study inclusion. A single patient list was generated to identify patients for inclusion in the DOAC arm. This patient list was generated using the VA DOAC dashboard, which identified patients with an active DOAC prescription and an ICD-9/10 code for cirrhosis. Patients with an ICD-9/10 code for cirrhosis and prescribed a DOAC were screened for full study inclusion. Patient data were collected from the MEDVAMC Computerized Patient Record System (CPRS) electronic health record (EHR). The research study was approved by the Baylor College of Medicine Institutional Review Board and the VA Office of Research and Development.
Outcomes
The primary endpoint for the study was all-cause bleeding. The secondary endpoints for the study were major bleeding and failed efficacy. Major bleeding was defined using the International Society on Thrombosis and Haemostasis (ISTH) 2005 definition: fatal bleeding, symptomatic bleeding in a critical organ area (ie, intracranial, intraspinal, intraocular, retroperitoneal, intraarticular, pericardial, or intramuscular with compartment syndrome), or bleeding causing a fall in hemoglobin level of > 2 g/dL or leading to the transfusion of ≥ 2 units of red cells.6 Failed efficacy was a combination endpoint that included development of VTE, stroke, myocardial infarction (MI), and/or death. A prespecified subgroup analysis was conducted at the end of the study period to analyze trends in the DOAC and warfarin groups with respect to all-cause bleeding. All-cause bleeding risk was stratified by weight, BMI, Child-Turcotte-Pugh score, MELD score, presence of gastric and/or esophageal varices, active malignancies, percentage of time within therapeutic INR range in the warfarin group, indications for anticoagulation, and antiplatelet, NSAID, PPI, and H2RA therapy.
Statistical Analysis
Data were analyzed using descriptive and inferential statistics. Continuous data were analyzed using the Student t test, and categorical data were analyzed using the Fisher exact test. Previous studies determined an all-cause bleeding rate of 10 to 17% for warfarin compared with 5% for DOACs.7,8 To detect a 12% difference in the all-cause bleeding rate between DOACs and warfarin, 212 patients would be needed to achieve 80% power at an α level of 0.05.
Results
A total of 170 patients were screened, and after applying inclusion and exclusion criteria, 79 patients were enrolled in the study (Figure). The DOAC group included 42 patients, and the warfarin group included 37 patients. In the DOAC group, 69.1% (n = 29) of patients were taking apixaban, 21.4% (n = 9) rivaroxaban, and 9.5% (n = 4) dabigatran. There were no patients prescribed edoxaban during the study period.
Baseline characteristics were similar between the 2 groups except for Child-Turcotte-Pugh score, MELD score, mean INR, and number of days on anticoagulation therapy (Table 1). Most of the patients were male (98.7%), and the mean age was 71 years. The most common causes of cirrhosis were viral (29.1%), nonalcoholic fatty liver disease (NAFLD) (24.1%), multiple causes (22.8%), and alcohol (21.5%). Sixty-two patients (78.5%) had a NVAF indication for anticoagulation. The average CHA2DS2-VASc score was 3.7. Aspirin was prescribed in 51.9% (n = 41) of patients, and PPIs were prescribed in 48.1% (n = 38) of patients. At inclusion, esophageal varices were present in 13 patients and active malignancies were present in 6 patients.
Statistically significant differences in baseline characteristics were found between mean INR, Child-Turcotte-Pugh scores, MELD scores, and number of days on anticoagulant therapy. The mean INR was 1.3 in the DOAC group compared with 2.1 in the warfarin group (P = .0001). Eighty-one percent (n = 34) of patients in the DOAC group had a Child-Turcotte-Pugh score of A compared with 43.2% (n = 16) of patients in the warfarin group (P = .0009). Eight patients in the DOAC group had a Child-Turcotte-Pugh score of B compared with 19 patients in the warfarin group (P = .004). The mean MELD score was 9.4 in the DOAC group compared with 16.3 in the warfarin group (P = .0001). The mean days on anticoagulant therapy was 500.4 days for the DOAC group compared with 1,652.4 days for the warfarin group (P = .0001).
Safety Outcome
The primary outcome comparing all-cause bleeding rates between patients on DOACs compared with warfarin are listed in Table 2. With respect to the primary outcome, 7 (16.7%) patients on DOACs experienced a bleeding event compared with 8 (21.6%) patients on warfarin (P = .77). No statistically significant differences were detected between the DOAC and warfarin groups with respect to all-cause bleeding. Seven bleeding events occurred in the DOAC group; 1 met the qualification for major bleeding with a suspected gastrointestinal (GI) bleed.6 The other 6 bleeding episodes in the DOAC group consisted of hematoma, epistaxis, hematuria, and hematochezia. Eight bleeding events occurred in the warfarin group; 2 met the qualification for major bleeding with an intracranial hemorrhage and upper GI bleed.6 The other 6 bleeding episodes in the warfarin group consisted of epistaxis, bleeding gums, hematuria, and hematochezia. There were no statistically significant differences between the rates of major bleeding and nonmajor bleeding between the DOAC and warfarin groups.
Efficacy Outcomes
There were 3 events in the DOAC group and 3 events in the warfarin group (P = .99). In the DOAC group, 2 patients experienced a pulmonary embolism, and 1 patient experienced a MI. In the warfarin group, 3 patients died (end-stage heart failure, unknown cause due to death at an outside hospital, and sepsis/organ failure). There were no statistically significant differences between the composite endpoint of failed efficacy or the individual endpoints of VTE, stroke, MI, and death.
Subgroup Analysis
A prespecified subgroup analysis was conducted to determine risk factors for all-cause bleeding within each treatment group (Table 3). No significant trends were observed in the following risk factors: Child-Turcotte-Pugh score, indication for anticoagulation, use of NSAIDs, PPIs or H2RAs, presence of gastric or esophageal varices, active malignancies, and time within therapeutic INR range in the warfarin group. Patients with bleeding events had slightly increased weight and BMI vs patients without bleeding events. Within the warfarin group, patients with bleeding events had slightly elevated MELD scores compared to patients without bleeding events. There was an equal balance of patients prescribed aspirin therapy between the groups with and without bleeding events. Overall, no significant risk factors were identified for all-cause bleeding.
Discussion
Initially, patients with cirrhosis were excluded from DOAC trials due to concerns for increased bleeding risk with hepatically eliminated medications. New retrospective research has concluded that in patients with cirrhosis, DOACs have similar or lower bleeding rates when compared directly to warfarin.9,10
In this study, no statistically significant differences were detected between the primary and secondary outcomes of all-cause bleeding, major bleeding, or failed efficacy. Subgroup analysis did not identify any significant risk factors with respect to all-cause bleeding among patients in the DOAC and warfarin groups. To meet 80% power, 212 patients needed to be enrolled in the study; however, only 79 patients were enrolled, and power was not met. The results of this study should be interpreted cautiously as hypothesis-generating due to the small sample size. Strengths of this study include similar baseline characteristics between the DOAC and warfarin groups, 4-year length of retrospective data review, and availability of both inpatient and outpatient EHR limiting the amount of missing data points.
Baseline characteristics were similar between the groups except for mean INR, Child-Turcotte-Pugh score, MELD score, and number of days on anticoagulation therapy. The difference in mean INR between groups is expected as patients in the warfarin group have a goal INR of 2 to 3 to maintain therapeutic efficacy and safety. INR is not used as a marker of efficacy or safety with DOACs; therefore, a consistent elevation in INR is not expected. Child- Turcotte-Pugh scores are calculated using INR levels.11 When calculating the score, patients with an INR < 1.7 receive 1 point; patients with an INR between 1.7 and 2.3 receive 2 points.11 Therefore, patients in the warfarin group will have artificially inflated Child-Turcotte-Pugh scores as this group has goal INR levels of 2 to 3. This makes Child-Turcotte-Pugh scores unreliable markers of disease severity in patients using warfarin therapy. When the INR scores for patients prescribed warfarin were replaced with values < 1.7, the statistical difference disappeared between the warfarin and DOAC groups. The same effect is seen on MELD scores for patients prescribed warfarin therapy. The MELD score is calculated using INR levels.12 MELD scores also will be artificially elevated in patients prescribed warfarin therapy due to the INR elevation to between 2 and 3. When MELD scores for patients prescribed warfarin were replaced with values similar to those in the DOAC group, the statistical difference disappeared between the warfarin and DOAC groups.
The last statistically significant difference was found in number of days on anticoagulant therapy. This difference was expected as warfarin is the standard of care for anticoagulation treatment in patients with cirrhosis. The first DOAC, dabigatran, was not approved by the US Food and Drug Administration until 2010.13 DOACs have only recently been used in patients with cirrhosis accounting for the statistically significant difference in days on anticoagulation therapy between the warfarin and DOAC groups.
Limitations
The inability to meet power or evaluate adherence and appropriate renal dose adjustments for DOACs limited this study. This study was conducted at a single center in a predominantly male veteran population and therefore may not be generalizable to other populations. A majority of patients in the DOAC group were prescribed apixaban (69.1%), which may have affected the overall rate of major bleeding in the DOAC group. Pivotal trials of apixaban have shown a consistent decreased risk of major bleeding in patients with NVAF or VTE when compared with warfarin.14,15 Therefore, the results of this study may not be generalizable to all DOACs.
An inherent limitation of this study was the inability to collect data verifying adherence in the DOAC group. However, in the warfarin group, percentage of time within the therapeutic INR range of 2 to 3 was collected. While not a direct marker of adherence, this does allow for limited evaluation of therapeutic efficacy and safety within the warfarin group. Last, proper dosing of DOACs in patients with and without adequate renal function was not evaluated in this study.
Conclusions
The results of this study are consistent with other retrospective research and literature reviews. There were no statistically significant differences identified between the rates of all-cause bleeding, major bleeding, and failed efficacy between the DOAC and warfarin groups. DOACs may be a safe alternative to warfarin in patients with cirrhosis requiring anticoagulation for NVAF or VTE, but large randomized trials are required to confirm these results.
1. Qamar A, Vaduganathan M, Greenberger NJ, Giugliano RP. Oral anticoagulation in patients with liver disease. J Am Coll Cardiol. 2018;71(19):2162-2175. doi:10.1016/j.jacc.2018.03.023
2. Priyanka P, Kupec JT, Krafft M, Shah NA, Reynolds GJ. Newer oral anticoagulants in the treatment of acute portal vein thrombosis in patients with and without cirrhosis. Int J Hepatol. 2018;2018:8432781. Published 2018 Jun 5. doi:10.1155/2018/8432781
3. Intagliata NM, Henry ZH, Maitland H, et al. Direct oral anticoagulants in cirrhosis patients pose similar risks of bleeding when compared to traditional anticoagulation. Dig Dis Sci. 2016;61(6):1721-1727. doi:10.1007/s10620-015-4012-2
4. Hum J, Shatzel JJ, Jou JH, Deloughery TG. The efficacy and safety of direct oral anticoagulants vs traditional anticoagulants in cirrhosis. Eur J Haematol. 2017;98(4):393-397. doi:10.1111/ejh.12844
5. Goriacko P, Veltri KT. Safety of direct oral anticoagulants vs warfarin in patients with chronic liver disease and atrial fibrillation. Eur J Haematol. 2018;100(5):488-493. doi:10.1111/ejh.13045
6. Schulman S, Kearon C; Subcommittee on Control of Anticoagulation of the Scientific and Standardization Committee of the International Society on Thrombosis and Haemostasis. Definition of major bleeding in clinical investigations of antihemostatic medicinal products in non-surgical patients. J Thromb Haemost. 2005;3(4):692-694. doi:10.1111/j.1538-7836.2005.01204.x
7. Rubboli A, Becattini C, Verheugt FW. Incidence, clinical impact and risk of bleeding during oral anticoagulation therapy. World J Cardiol. 2011;3(11):351-358. doi:10.4330/wjc.v3.i11.351
8. Ruff CT, Giugliano RP, Braunwald E, et al. Comparison of the efficacy and safety of new oral anticoagulants with warfarin in patients with atrial fibrillation: a meta-analysis of randomised trials. Lancet. 2014;383(9921):955-962. doi:10.1016/S0140-6736(13)62343-0
9. Hoolwerf EW, Kraaijpoel N, Büller HR, van Es N. Direct oral anticoagulants in patients with liver cirrhosis: A systematic review. Thromb Res. 2018;170:102-108. doi:10.1016/j.thromres.2018.08.011
10. Steuber TD, Howard ML, Nisly SA. Direct oral anticoagulants in chronic liver disease. Ann Pharmacother. 2019;53(10):1042-1049. doi:10.1177/1060028019841582
11. Janevska D, Chaloska-Ivanova V, Janevski V. Hepatocellular carcinoma: risk factors, diagnosis and treatment. Open Access Maced J Med Sci. 2015;3(4):732-736. doi:10.3889/oamjms.2015.111
12. Singal AK, Kamath PS. Model for End-Stage Liver Disease. J Clin Exp Hepatol. 2013;3(1):50-60. doi:10.1016/j.jceh.2012.11.002
13. Joppa SA, Salciccioli J, Adamski J, et al. A practical review of the emerging direct anticoagulants, laboratory monitoring, and reversal agents. J Clin Med. 2018;7(2):29. Published 2018 Feb 11. doi:10.3390/jcm7020029
14. Granger CB, Alexander JH, McMurray JJ, et al. Apixaban versus warfarin in patients with atrial fibrillation. N Engl J Med. 2011;365(11):981-992. doi:10.1056/NEJMoa1107039
15. Agnelli G, Buller HR, Cohen A, et al. Oral apixaban for the treatment of acute venous thromboembolism. N Engl J Med. 2013;369(9):799-808. doi:10.1056/NEJMoa1302507
1. Qamar A, Vaduganathan M, Greenberger NJ, Giugliano RP. Oral anticoagulation in patients with liver disease. J Am Coll Cardiol. 2018;71(19):2162-2175. doi:10.1016/j.jacc.2018.03.023
2. Priyanka P, Kupec JT, Krafft M, Shah NA, Reynolds GJ. Newer oral anticoagulants in the treatment of acute portal vein thrombosis in patients with and without cirrhosis. Int J Hepatol. 2018;2018:8432781. Published 2018 Jun 5. doi:10.1155/2018/8432781
3. Intagliata NM, Henry ZH, Maitland H, et al. Direct oral anticoagulants in cirrhosis patients pose similar risks of bleeding when compared to traditional anticoagulation. Dig Dis Sci. 2016;61(6):1721-1727. doi:10.1007/s10620-015-4012-2
4. Hum J, Shatzel JJ, Jou JH, Deloughery TG. The efficacy and safety of direct oral anticoagulants vs traditional anticoagulants in cirrhosis. Eur J Haematol. 2017;98(4):393-397. doi:10.1111/ejh.12844
5. Goriacko P, Veltri KT. Safety of direct oral anticoagulants vs warfarin in patients with chronic liver disease and atrial fibrillation. Eur J Haematol. 2018;100(5):488-493. doi:10.1111/ejh.13045
6. Schulman S, Kearon C; Subcommittee on Control of Anticoagulation of the Scientific and Standardization Committee of the International Society on Thrombosis and Haemostasis. Definition of major bleeding in clinical investigations of antihemostatic medicinal products in non-surgical patients. J Thromb Haemost. 2005;3(4):692-694. doi:10.1111/j.1538-7836.2005.01204.x
7. Rubboli A, Becattini C, Verheugt FW. Incidence, clinical impact and risk of bleeding during oral anticoagulation therapy. World J Cardiol. 2011;3(11):351-358. doi:10.4330/wjc.v3.i11.351
8. Ruff CT, Giugliano RP, Braunwald E, et al. Comparison of the efficacy and safety of new oral anticoagulants with warfarin in patients with atrial fibrillation: a meta-analysis of randomised trials. Lancet. 2014;383(9921):955-962. doi:10.1016/S0140-6736(13)62343-0
9. Hoolwerf EW, Kraaijpoel N, Büller HR, van Es N. Direct oral anticoagulants in patients with liver cirrhosis: A systematic review. Thromb Res. 2018;170:102-108. doi:10.1016/j.thromres.2018.08.011
10. Steuber TD, Howard ML, Nisly SA. Direct oral anticoagulants in chronic liver disease. Ann Pharmacother. 2019;53(10):1042-1049. doi:10.1177/1060028019841582
11. Janevska D, Chaloska-Ivanova V, Janevski V. Hepatocellular carcinoma: risk factors, diagnosis and treatment. Open Access Maced J Med Sci. 2015;3(4):732-736. doi:10.3889/oamjms.2015.111
12. Singal AK, Kamath PS. Model for End-Stage Liver Disease. J Clin Exp Hepatol. 2013;3(1):50-60. doi:10.1016/j.jceh.2012.11.002
13. Joppa SA, Salciccioli J, Adamski J, et al. A practical review of the emerging direct anticoagulants, laboratory monitoring, and reversal agents. J Clin Med. 2018;7(2):29. Published 2018 Feb 11. doi:10.3390/jcm7020029
14. Granger CB, Alexander JH, McMurray JJ, et al. Apixaban versus warfarin in patients with atrial fibrillation. N Engl J Med. 2011;365(11):981-992. doi:10.1056/NEJMoa1107039
15. Agnelli G, Buller HR, Cohen A, et al. Oral apixaban for the treatment of acute venous thromboembolism. N Engl J Med. 2013;369(9):799-808. doi:10.1056/NEJMoa1302507
MI recurrences drop, but women underestimate disease risk
The number of heart attack survivors in the United States who experienced repeat attacks within a year decreased between 2008 and 2017, especially among women, yet women’s awareness of their risk of death from heart disease also decreased, according to data from a pair of studies published in Circulation.
Recurrent MI rates drop, but not enough
Although the overall morbidity and mortality from coronary heart disease (CHD) in the United States has been on the decline for decades, CHD remains the leading cause of death and disability in both sexes, wrote Sanne A.E. Peters, PhD, of Imperial College London, and colleagues.
To better assess the rates of recurrent CHD by sex, the researchers reviewed data from 770,408 women and 700,477 men younger than 65 years with commercial health insurance or aged 66 years and older with Medicare who were hospitalized for myocardial infarction between 2008 and 2017. The patients were followed for 1 year for recurrent MIs, recurrent CHD events, heart failure hospitalization, and all-cause mortality.
In the study of recurrent heart disease, the rate of recurrent heart attacks per 1,000 person-years declined from 89.2 to 72.3 in women and from 94.2 to 81.3 in men. In addition, the rate of recurrent heart disease events (defined as either an MI or an artery-opening procedure), dropped per 1,000 person-years from 166.3 to 133.3 in women and from 198.1 to 176.8 in men. The reduction was significantly greater among women compared with men (P < .001 for both recurrent MIs and recurrent CHD events) and the differences by sex were consistent throughout the study period.
However, no significant difference occurred in recurrent MI rates among younger women (aged 21-54 years), or men aged 55-79 years, the researchers noted.
Heart failure rates per 1,000 person-years decreased from 177.4 to 158.1 in women and from 162.9 to 156.1 in men during the study period, and all-cause mortality decreased per 1,000 person-years from 403.2 to 389.5 for women and from 436.1 to 417.9 in men.
Potential contributing factors to the reductions in rates of recurrent events after a heart attack may include improved acute cardiac procedures, in-hospital therapy, and secondary prevention, the researchers noted. In addition, “changes in the type and definition of MI may also have contributed to the decline in recurrent events,” they said. “Also, the introduction and increasing sensitivity of cardiac biomarkers assays, especially cardiac troponin, may have contributed to an increased detection of less severe MIs over time, which, in turn, could have resulted in artifactual reductions in the consequences of MI,” they said.
The study findings were limited by several factors including the use of claims data, lack of information on the severity of heart attacks, and inability to analyze population subgroups, but the results were strengthened by the use of a large, multicultural database.
Despite the decline seen in this study, overall rates of recurrent MI, recurrent CHD events, heart failure hospitalization, and mortality remain high, the researchers said, and the results “highlight the need for interventions to ensure men and women receive guideline recommended treatment to lower the risk for recurrent MI, recurrent CHD, heart failure, and mortality after hospital discharge for MI,” they concluded.
Many women don’t recognize heart disease risk
Although women showed a greater reduction in recurrent MI and recurrent CHD events compared with men, the awareness of heart disease as the No. 1 killer of women has declined, according to a special report from the American Heart Association.
Based on survey data from 2009, 65% of women were aware that heart disease was their leading cause of death (LCOD); by 2019 the number dropped to 44%. The 10-year decline occurred across all races and ethnicities, as well as ages, with the exception of women aged 65 years and older.
The American Heart Association has conducted national surveys since 1997 to monitor awareness of cardiovascular disease among U.S. women. Data from earlier surveys showed increased awareness of heart disease as LCOD and increased awareness of heart attack symptoms between 1997 and 2012, wrote Mary Cushman, MD, of the University of Vermont, Burlington, chair of the writing group for the statement, and colleagues.

However, overall awareness and knowledge of heart disease among women remains poor, they wrote.
“Awareness programs designed to educate the public about CVD among women in the United States include Go Red for Women by the American Heart Association; The Heart Truth by the National Heart, Lung, and Blood Institute; and Make the Call, Don’t Miss a Beat by the U.S. Department of Health and Human Services,” the researchers noted. To determine the change in awareness of heart disease as the LCOD among women, the researchers conducted a multivariate analysis of 1,158 women who completed the 2009 survey and 1,345 who completed the 2019 survey. The average age was 50 years; roughly 70% of the participants in the 2009 survey and 62% in the 2019 survey were non-Hispanic White.
The greatest declines in awareness of heart disease as LCOD occurred among Hispanics and non-Hispanic Blacks and among all respondents aged 25-34 years.
Awareness of heart disease as LCOD was 30% lower among women with high blood pressure compared with women overall, the researchers noted.
“In both surveys, higher educational attainment was strongly related to awareness that heart disease is the LCOD,” the researchers said. However, the results highlight the need for renewed efforts to educate younger women, Hispanic women, and non-Hispanic Black women, they emphasized. Unpublished data from the AHA survey showed that “younger women were less likely to report leading a heart-healthy lifestyle and were more likely to identify multiple barriers to leading a heart-healthy lifestyle, including lack of time, stress, and lack of confidence,” they wrote.
In addition, awareness of heart attack warning signs declined overall and within each ethnic group between 2009 and 2019.
The survey results were limited by several factors including the use of an online-only model that might limit generalizability to populations without online access, and was conducted only in English, the researchers wrote.
Heart disease needs new PR plan
The study of heart disease risk awareness among women was an important update to understand how well the message about women’s risk is getting out, said Martha Gulati, MD, president-elect of the American Society of Preventive Cardiology, in an interview.
The issue remains that heart disease is the No. 1 killer of women, and the decrease in awareness “means we need to amplify our message,” she said.
“I also question whether the symbol of the red dress [for women’s heart disease] is working, and it seems that now is the time to change this symbol,” she emphasized. “I wear a red dress pin on my lab coat and every day someone asks what it means, and no one recognizes it,” she said. “I think ‘Go Red for Women’ is great and part of our outward campaign, but our symbol needs to change to increase the connection and awareness in women,” she said.
What might be a better symbol? Simply, a heart, said Dr. Gulati. But “we need to study whatever is next to really connect with women and make them understand their risk for heart disease,” she added.
“Additionally, we really need to get to minority women,” she said. “We are lagging there, and the survey was conducted in English so it missed many people,” she noted.
Dr. Gulati said she was shocked at how much awareness of heart disease risk has fallen among women, even in those with risk factors such as hypertension, who were 30% less likely to be aware that heart disease remains their leading cause of death. “Younger women as well as very unaware; what this means to me is that our public education efforts need to be amplified,” Dr. Gulati said.
Barriers to educating women about heart disease risk include language and access to affordable screening, Dr. Gulati emphasized. “We need to ensure screening for heart disease is always included as a covered cost for a preventive service,” she said.
“Research needs to be done to identify what works toward educating women about cardiac risk. We need to identify a marketing tool to increase awareness in women. It might be something different for one race versus another,” Dr. Gulati said. “Our messaging needs to improve, but how we improve it needs more than just health care professionals,” she said.
Focus on prevention to reduce MI recurrence
“The study regarding recurrent events after MI is important because we really don’t know much about recurrent coronary heart disease after a MI over time,” said Dr. Gulati. These data can be helpful in managing surviving patients and understanding future risk, she said. “But I was surprised to see fewer recurrent events in women, as women still have more heart failure than men even if it has declined with time,” she noted.
Dr. Gulati questioned several aspects of the study and highlighted some of the limitations. “These are claims data, so do they accurately reflect the U.S. population?” she asked. “Remember, this is a study of people who survived a heart attack; those who didn’t survive aren’t included, and that group is more likely to be women, especially women younger than 55 years,” she said.
In addition, Dr. Gulati noted the lack of data on type of heart attack and on treatment adherence or referral to cardiac rehab, as well as lack of data on long-term medication adherence or follow-up care.
Prevention is the key take-home message from both studies, “whether we are talking primary prevention for the heart disease awareness study or secondary prevention for the recurrent heart attack study,” Dr. Gulati said.
The recurrent heart disease study was supported in part by Amgen and the University of Alabama at Birmingham. Lead author Dr. Peters disclosed support from a UK Medical Research Council Skills Development Fellowship with no financial conflicts. Dr. Cushman had no financial conflicts to disclose; several coauthors on the writing committee disclosed relationships with companies including Amarin and Boehringer Ingelheim. Dr. Gulati had no financial conflicts to disclose.
SOURCE: Peters SAE et al. Circulation. 2020 Sep 21. doi: 10.1161/CIRCULATIONAHA.120.047065; Cushman M et al. Circulation. 2020 Sep 21. doi: 10.1161/CIR.0000000000000907.
The number of heart attack survivors in the United States who experienced repeat attacks within a year decreased between 2008 and 2017, especially among women, yet women’s awareness of their risk of death from heart disease also decreased, according to data from a pair of studies published in Circulation.
Recurrent MI rates drop, but not enough
Although the overall morbidity and mortality from coronary heart disease (CHD) in the United States has been on the decline for decades, CHD remains the leading cause of death and disability in both sexes, wrote Sanne A.E. Peters, PhD, of Imperial College London, and colleagues.
To better assess the rates of recurrent CHD by sex, the researchers reviewed data from 770,408 women and 700,477 men younger than 65 years with commercial health insurance or aged 66 years and older with Medicare who were hospitalized for myocardial infarction between 2008 and 2017. The patients were followed for 1 year for recurrent MIs, recurrent CHD events, heart failure hospitalization, and all-cause mortality.
In the study of recurrent heart disease, the rate of recurrent heart attacks per 1,000 person-years declined from 89.2 to 72.3 in women and from 94.2 to 81.3 in men. In addition, the rate of recurrent heart disease events (defined as either an MI or an artery-opening procedure), dropped per 1,000 person-years from 166.3 to 133.3 in women and from 198.1 to 176.8 in men. The reduction was significantly greater among women compared with men (P < .001 for both recurrent MIs and recurrent CHD events) and the differences by sex were consistent throughout the study period.
However, no significant difference occurred in recurrent MI rates among younger women (aged 21-54 years), or men aged 55-79 years, the researchers noted.
Heart failure rates per 1,000 person-years decreased from 177.4 to 158.1 in women and from 162.9 to 156.1 in men during the study period, and all-cause mortality decreased per 1,000 person-years from 403.2 to 389.5 for women and from 436.1 to 417.9 in men.
Potential contributing factors to the reductions in rates of recurrent events after a heart attack may include improved acute cardiac procedures, in-hospital therapy, and secondary prevention, the researchers noted. In addition, “changes in the type and definition of MI may also have contributed to the decline in recurrent events,” they said. “Also, the introduction and increasing sensitivity of cardiac biomarkers assays, especially cardiac troponin, may have contributed to an increased detection of less severe MIs over time, which, in turn, could have resulted in artifactual reductions in the consequences of MI,” they said.
The study findings were limited by several factors including the use of claims data, lack of information on the severity of heart attacks, and inability to analyze population subgroups, but the results were strengthened by the use of a large, multicultural database.
Despite the decline seen in this study, overall rates of recurrent MI, recurrent CHD events, heart failure hospitalization, and mortality remain high, the researchers said, and the results “highlight the need for interventions to ensure men and women receive guideline recommended treatment to lower the risk for recurrent MI, recurrent CHD, heart failure, and mortality after hospital discharge for MI,” they concluded.
Many women don’t recognize heart disease risk
Although women showed a greater reduction in recurrent MI and recurrent CHD events compared with men, the awareness of heart disease as the No. 1 killer of women has declined, according to a special report from the American Heart Association.
Based on survey data from 2009, 65% of women were aware that heart disease was their leading cause of death (LCOD); by 2019 the number dropped to 44%. The 10-year decline occurred across all races and ethnicities, as well as ages, with the exception of women aged 65 years and older.
The American Heart Association has conducted national surveys since 1997 to monitor awareness of cardiovascular disease among U.S. women. Data from earlier surveys showed increased awareness of heart disease as LCOD and increased awareness of heart attack symptoms between 1997 and 2012, wrote Mary Cushman, MD, of the University of Vermont, Burlington, chair of the writing group for the statement, and colleagues.
However, overall awareness and knowledge of heart disease among women remains poor, they wrote.
“Awareness programs designed to educate the public about CVD among women in the United States include Go Red for Women by the American Heart Association; The Heart Truth by the National Heart, Lung, and Blood Institute; and Make the Call, Don’t Miss a Beat by the U.S. Department of Health and Human Services,” the researchers noted. To determine the change in awareness of heart disease as the LCOD among women, the researchers conducted a multivariate analysis of 1,158 women who completed the 2009 survey and 1,345 who completed the 2019 survey. The average age was 50 years; roughly 70% of the participants in the 2009 survey and 62% in the 2019 survey were non-Hispanic White.
The greatest declines in awareness of heart disease as LCOD occurred among Hispanics and non-Hispanic Blacks and among all respondents aged 25-34 years.
Awareness of heart disease as LCOD was 30% lower among women with high blood pressure compared with women overall, the researchers noted.
“In both surveys, higher educational attainment was strongly related to awareness that heart disease is the LCOD,” the researchers said. However, the results highlight the need for renewed efforts to educate younger women, Hispanic women, and non-Hispanic Black women, they emphasized. Unpublished data from the AHA survey showed that “younger women were less likely to report leading a heart-healthy lifestyle and were more likely to identify multiple barriers to leading a heart-healthy lifestyle, including lack of time, stress, and lack of confidence,” they wrote.
In addition, awareness of heart attack warning signs declined overall and within each ethnic group between 2009 and 2019.
The survey results were limited by several factors including the use of an online-only model that might limit generalizability to populations without online access, and was conducted only in English, the researchers wrote.
Heart disease needs new PR plan
The study of heart disease risk awareness among women was an important update to understand how well the message about women’s risk is getting out, said Martha Gulati, MD, president-elect of the American Society of Preventive Cardiology, in an interview.
The issue remains that heart disease is the No. 1 killer of women, and the decrease in awareness “means we need to amplify our message,” she said.
“I also question whether the symbol of the red dress [for women’s heart disease] is working, and it seems that now is the time to change this symbol,” she emphasized. “I wear a red dress pin on my lab coat and every day someone asks what it means, and no one recognizes it,” she said. “I think ‘Go Red for Women’ is great and part of our outward campaign, but our symbol needs to change to increase the connection and awareness in women,” she said.
What might be a better symbol? Simply, a heart, said Dr. Gulati. But “we need to study whatever is next to really connect with women and make them understand their risk for heart disease,” she added.
“Additionally, we really need to get to minority women,” she said. “We are lagging there, and the survey was conducted in English so it missed many people,” she noted.
Dr. Gulati said she was shocked at how much awareness of heart disease risk has fallen among women, even in those with risk factors such as hypertension, who were 30% less likely to be aware that heart disease remains their leading cause of death. “Younger women as well as very unaware; what this means to me is that our public education efforts need to be amplified,” Dr. Gulati said.
Barriers to educating women about heart disease risk include language and access to affordable screening, Dr. Gulati emphasized. “We need to ensure screening for heart disease is always included as a covered cost for a preventive service,” she said.
“Research needs to be done to identify what works toward educating women about cardiac risk. We need to identify a marketing tool to increase awareness in women. It might be something different for one race versus another,” Dr. Gulati said. “Our messaging needs to improve, but how we improve it needs more than just health care professionals,” she said.
Focus on prevention to reduce MI recurrence
“The study regarding recurrent events after MI is important because we really don’t know much about recurrent coronary heart disease after a MI over time,” said Dr. Gulati. These data can be helpful in managing surviving patients and understanding future risk, she said. “But I was surprised to see fewer recurrent events in women, as women still have more heart failure than men even if it has declined with time,” she noted.
Dr. Gulati questioned several aspects of the study and highlighted some of the limitations. “These are claims data, so do they accurately reflect the U.S. population?” she asked. “Remember, this is a study of people who survived a heart attack; those who didn’t survive aren’t included, and that group is more likely to be women, especially women younger than 55 years,” she said.
In addition, Dr. Gulati noted the lack of data on type of heart attack and on treatment adherence or referral to cardiac rehab, as well as lack of data on long-term medication adherence or follow-up care.
Prevention is the key take-home message from both studies, “whether we are talking primary prevention for the heart disease awareness study or secondary prevention for the recurrent heart attack study,” Dr. Gulati said.
The recurrent heart disease study was supported in part by Amgen and the University of Alabama at Birmingham. Lead author Dr. Peters disclosed support from a UK Medical Research Council Skills Development Fellowship with no financial conflicts. Dr. Cushman had no financial conflicts to disclose; several coauthors on the writing committee disclosed relationships with companies including Amarin and Boehringer Ingelheim. Dr. Gulati had no financial conflicts to disclose.
SOURCE: Peters SAE et al. Circulation. 2020 Sep 21. doi: 10.1161/CIRCULATIONAHA.120.047065; Cushman M et al. Circulation. 2020 Sep 21. doi: 10.1161/CIR.0000000000000907.
The number of heart attack survivors in the United States who experienced repeat attacks within a year decreased between 2008 and 2017, especially among women, yet women’s awareness of their risk of death from heart disease also decreased, according to data from a pair of studies published in Circulation.
Recurrent MI rates drop, but not enough
Although the overall morbidity and mortality from coronary heart disease (CHD) in the United States has been on the decline for decades, CHD remains the leading cause of death and disability in both sexes, wrote Sanne A.E. Peters, PhD, of Imperial College London, and colleagues.
To better assess the rates of recurrent CHD by sex, the researchers reviewed data from 770,408 women and 700,477 men younger than 65 years with commercial health insurance or aged 66 years and older with Medicare who were hospitalized for myocardial infarction between 2008 and 2017. The patients were followed for 1 year for recurrent MIs, recurrent CHD events, heart failure hospitalization, and all-cause mortality.
In the study of recurrent heart disease, the rate of recurrent heart attacks per 1,000 person-years declined from 89.2 to 72.3 in women and from 94.2 to 81.3 in men. In addition, the rate of recurrent heart disease events (defined as either an MI or an artery-opening procedure), dropped per 1,000 person-years from 166.3 to 133.3 in women and from 198.1 to 176.8 in men. The reduction was significantly greater among women compared with men (P < .001 for both recurrent MIs and recurrent CHD events) and the differences by sex were consistent throughout the study period.
However, no significant difference occurred in recurrent MI rates among younger women (aged 21-54 years), or men aged 55-79 years, the researchers noted.
Heart failure rates per 1,000 person-years decreased from 177.4 to 158.1 in women and from 162.9 to 156.1 in men during the study period, and all-cause mortality decreased per 1,000 person-years from 403.2 to 389.5 for women and from 436.1 to 417.9 in men.
Potential contributing factors to the reductions in rates of recurrent events after a heart attack may include improved acute cardiac procedures, in-hospital therapy, and secondary prevention, the researchers noted. In addition, “changes in the type and definition of MI may also have contributed to the decline in recurrent events,” they said. “Also, the introduction and increasing sensitivity of cardiac biomarkers assays, especially cardiac troponin, may have contributed to an increased detection of less severe MIs over time, which, in turn, could have resulted in artifactual reductions in the consequences of MI,” they said.
The study findings were limited by several factors including the use of claims data, lack of information on the severity of heart attacks, and inability to analyze population subgroups, but the results were strengthened by the use of a large, multicultural database.
Despite the decline seen in this study, overall rates of recurrent MI, recurrent CHD events, heart failure hospitalization, and mortality remain high, the researchers said, and the results “highlight the need for interventions to ensure men and women receive guideline recommended treatment to lower the risk for recurrent MI, recurrent CHD, heart failure, and mortality after hospital discharge for MI,” they concluded.
Many women don’t recognize heart disease risk
Although women showed a greater reduction in recurrent MI and recurrent CHD events compared with men, the awareness of heart disease as the No. 1 killer of women has declined, according to a special report from the American Heart Association.
Based on survey data from 2009, 65% of women were aware that heart disease was their leading cause of death (LCOD); by 2019 the number dropped to 44%. The 10-year decline occurred across all races and ethnicities, as well as ages, with the exception of women aged 65 years and older.
The American Heart Association has conducted national surveys since 1997 to monitor awareness of cardiovascular disease among U.S. women. Data from earlier surveys showed increased awareness of heart disease as LCOD and increased awareness of heart attack symptoms between 1997 and 2012, wrote Mary Cushman, MD, of the University of Vermont, Burlington, chair of the writing group for the statement, and colleagues.
However, overall awareness and knowledge of heart disease among women remains poor, they wrote.
“Awareness programs designed to educate the public about CVD among women in the United States include Go Red for Women by the American Heart Association; The Heart Truth by the National Heart, Lung, and Blood Institute; and Make the Call, Don’t Miss a Beat by the U.S. Department of Health and Human Services,” the researchers noted. To determine the change in awareness of heart disease as the LCOD among women, the researchers conducted a multivariate analysis of 1,158 women who completed the 2009 survey and 1,345 who completed the 2019 survey. The average age was 50 years; roughly 70% of the participants in the 2009 survey and 62% in the 2019 survey were non-Hispanic White.
The greatest declines in awareness of heart disease as LCOD occurred among Hispanics and non-Hispanic Blacks and among all respondents aged 25-34 years.
Awareness of heart disease as LCOD was 30% lower among women with high blood pressure compared with women overall, the researchers noted.
“In both surveys, higher educational attainment was strongly related to awareness that heart disease is the LCOD,” the researchers said. However, the results highlight the need for renewed efforts to educate younger women, Hispanic women, and non-Hispanic Black women, they emphasized. Unpublished data from the AHA survey showed that “younger women were less likely to report leading a heart-healthy lifestyle and were more likely to identify multiple barriers to leading a heart-healthy lifestyle, including lack of time, stress, and lack of confidence,” they wrote.
In addition, awareness of heart attack warning signs declined overall and within each ethnic group between 2009 and 2019.
The survey results were limited by several factors including the use of an online-only model that might limit generalizability to populations without online access, and was conducted only in English, the researchers wrote.
Heart disease needs new PR plan
The study of heart disease risk awareness among women was an important update to understand how well the message about women’s risk is getting out, said Martha Gulati, MD, president-elect of the American Society of Preventive Cardiology, in an interview.
The issue remains that heart disease is the No. 1 killer of women, and the decrease in awareness “means we need to amplify our message,” she said.
“I also question whether the symbol of the red dress [for women’s heart disease] is working, and it seems that now is the time to change this symbol,” she emphasized. “I wear a red dress pin on my lab coat and every day someone asks what it means, and no one recognizes it,” she said. “I think ‘Go Red for Women’ is great and part of our outward campaign, but our symbol needs to change to increase the connection and awareness in women,” she said.
What might be a better symbol? Simply, a heart, said Dr. Gulati. But “we need to study whatever is next to really connect with women and make them understand their risk for heart disease,” she added.
“Additionally, we really need to get to minority women,” she said. “We are lagging there, and the survey was conducted in English so it missed many people,” she noted.
Dr. Gulati said she was shocked at how much awareness of heart disease risk has fallen among women, even in those with risk factors such as hypertension, who were 30% less likely to be aware that heart disease remains their leading cause of death. “Younger women as well as very unaware; what this means to me is that our public education efforts need to be amplified,” Dr. Gulati said.
Barriers to educating women about heart disease risk include language and access to affordable screening, Dr. Gulati emphasized. “We need to ensure screening for heart disease is always included as a covered cost for a preventive service,” she said.
“Research needs to be done to identify what works toward educating women about cardiac risk. We need to identify a marketing tool to increase awareness in women. It might be something different for one race versus another,” Dr. Gulati said. “Our messaging needs to improve, but how we improve it needs more than just health care professionals,” she said.
Focus on prevention to reduce MI recurrence
“The study regarding recurrent events after MI is important because we really don’t know much about recurrent coronary heart disease after a MI over time,” said Dr. Gulati. These data can be helpful in managing surviving patients and understanding future risk, she said. “But I was surprised to see fewer recurrent events in women, as women still have more heart failure than men even if it has declined with time,” she noted.
Dr. Gulati questioned several aspects of the study and highlighted some of the limitations. “These are claims data, so do they accurately reflect the U.S. population?” she asked. “Remember, this is a study of people who survived a heart attack; those who didn’t survive aren’t included, and that group is more likely to be women, especially women younger than 55 years,” she said.
In addition, Dr. Gulati noted the lack of data on type of heart attack and on treatment adherence or referral to cardiac rehab, as well as lack of data on long-term medication adherence or follow-up care.
Prevention is the key take-home message from both studies, “whether we are talking primary prevention for the heart disease awareness study or secondary prevention for the recurrent heart attack study,” Dr. Gulati said.
The recurrent heart disease study was supported in part by Amgen and the University of Alabama at Birmingham. Lead author Dr. Peters disclosed support from a UK Medical Research Council Skills Development Fellowship with no financial conflicts. Dr. Cushman had no financial conflicts to disclose; several coauthors on the writing committee disclosed relationships with companies including Amarin and Boehringer Ingelheim. Dr. Gulati had no financial conflicts to disclose.
SOURCE: Peters SAE et al. Circulation. 2020 Sep 21. doi: 10.1161/CIRCULATIONAHA.120.047065; Cushman M et al. Circulation. 2020 Sep 21. doi: 10.1161/CIR.0000000000000907.
FROM CIRCULATION
Time-restricted eating shows no weight-loss benefit in RCT
The popular new weight-loss approach of eating within a restricted window of time during the day, allowing for an extended period of fasting – also known as intermittent fasting – does not result in greater weight loss, compared with nonrestricted meal timing, results from a randomized clinical trial show.
“I was very surprised by all of [the results],” senior author Ethan J. Weiss, MD, said in an interview.
“Part of the reason we did the study was because I had been doing time-restricted eating myself for years and even recommending it to friends and patients as an effective weight-loss tool,” said Dr. Weiss, of the Cardiovascular Research Institute, University of California, San Francisco.
“But no matter how you slice it, prescription of time-restricted eating – at least this version –is not a very effective weight-loss strategy,” Dr. Weiss said.
The study, published online in JAMA Internal Medicine by Dylan A. Lowe, PhD, also of the University of California, San Francisco, involved 116 participants who were randomized to a 12-week regimen of either three structured meals per day or time-restricted eating, with instructions to eat only between 12:00 p.m. and 8:00 p.m. and to completely abstain from eating at other times.
The participants were not given any specific instructions regarding caloric or macronutrient intake “so as to offer a simple, real-world recommendation to free-living individuals,” the authors wrote.
Although some prior research has shown improvements in measures such as glucose tolerance with time-restricted eating, studies showing weight loss with the approach, including one recently reported by Medscape Medical News, have been small and lacked control groups.
“To my knowledge this is the first randomized, controlled trial and definitely the biggest,” Dr. Weiss. “I think it is the most comprehensive dataset available in people, at least for this intervention.”
Participants used app to log details
At baseline, participants had a mean weight of 99.2 kg (approximately 219 lb). Their mean age was 46.5 years and 60.3% were men. They were drawn from anywhere in the United States and received study surveys through a custom mobile study application on the Eureka Research Platform. They were given a Bluetooth weight scale to use daily, which was connected with the app, and randomized to one of the two interventions. A subset of 50 participants living near San Francisco underwent in-person testing.
At the end of the 12 weeks, those in the time-restricted eating group (n = 59) did have a significant decrease in weight, compared with baseline (−0.94 kg; P = .01), while weight loss in the consistent-meal group (n = 57) was not significant (−0.68 kg; P = .07).
But importantly, the difference in weight loss between the groups was not significant (−0.26 kg; P = .63).
There were no significant differences in secondary outcomes of fasting insulin, glucose, hemoglobin A1c, or blood lipids within or between the time-restricted eating and consistent-meal group either. Nor were there any significant differences in resting metabolic rate.
Although participants did not self-report their caloric intake, the authors estimated that the differences were not significant using mathematical modeling developed at the National Institutes of Health.
Rates of adherence to the diets were 92.1% in the consistent-meal group versus 83.5% in the time-restricted group.
Not all diets are equal: Time-restricted eating group lost more lean mass
In a subset analysis, loss of lean mass was significantly greater in the time-restricted eating group, compared with the consistent-meals group, in terms of both appendicular lean mass (P = .009) and the appendicular lean mass index (P = .005).
In fact, as much as 65% of the weight lost (1.10 kg of the average 1.70 kg) in the time-restricted eating group consisted of lean mass, while much less was fat mass (0.51 kg).
“The proportion of lean mass loss in this study (approximately 65%) far exceeds the normal range of 20%-30%,” the authors wrote. “In addition, there was a highly significant between-group difference in appendicular lean mass.”
Appendicular lean mass correlates with nutritional and physical status, and its reduction can lead to weakness, disability, and impaired quality of life.
“This serves as a caution for patient populations at risk for sarcopenia because time-restricted eating could exacerbate muscle loss,” the authors asserted.
Furthermore, previous studies suggest that the loss of lean mass in such studies is positively linked with weight regain.
While a limitation of the work is that self-reported measures of energy or macronutrient or protein intake were not obtained, the authors speculated that the role of protein intake could be linked to the greater loss of lean mass.
“Given the loss of appendicular lean mass in participants in the time-restricted eating arm and previous reports of decreased protein consumption from time-restricted eating, it is possible that protein intake was altered by time-restricted eating in this cohort, and this clearly warrants future study,” they wrote.
Dr. Weiss said the findings underscore that not all weight loss in dieting is beneficial.
“Losing 1 kg of lean mass (is not equal) to a kilogram of fat,” he said. “Indeed, if one loses 0.65 kg of lean mass and only 0.35 kg of fat mass, that is an intervention I’d probably pass on.”
Time-restricted eating is popular, perhaps because it’s easy?
Time-restricted eating has gained popularity in recent years.
The approach “is attractive as a weight-loss option in that it does not require tedious and time-consuming methods such as calorie counting or adherence to complicated diets,” the authors noted. “Indeed, we found that self-reported adherence to the time-restricted eating schedule was high; however, in contrast to our hypothesis, there was no greater weight loss with time-restricted eating compared with the consistent meal timing.”
They explain that the 12 p.m. to 8 p.m. window for eating was chosen because they thought people might find it easier culturally to skip breakfast than dinner, the more social meal.
However, an 8 p.m. cutoff is somewhat late given there is some suggestion that fasting several hours before bedtime is most beneficial, Dr. Weiss noted. So it may be worth examining different time windows.
“I am very intrigued about looking at early time-restricted eating – 6 a.m. to 2 p.m.,” for example, he said. “It is on our list.”
Meanwhile, the study results support previous research showing no effect on weight outcomes in relation to skipping breakfast.
The study received funding from the UCSF cardiology division’s Cardiology Innovations Award Program and the National Institute of Diabetes and Digestive and Kidney Diseases, with additional support from the James Peter Read Foundation. Dr. Weiss has reported nonfinancial support from Mocacare and nonfinancial support from iHealth Labs during the conduct of the study. He also is a cofounder and equity stakeholder of Keyto, and owns stock and was formerly on the board of Virta.
A version of this article originally appeared on Medscape.com.
The popular new weight-loss approach of eating within a restricted window of time during the day, allowing for an extended period of fasting – also known as intermittent fasting – does not result in greater weight loss, compared with nonrestricted meal timing, results from a randomized clinical trial show.
“I was very surprised by all of [the results],” senior author Ethan J. Weiss, MD, said in an interview.
“Part of the reason we did the study was because I had been doing time-restricted eating myself for years and even recommending it to friends and patients as an effective weight-loss tool,” said Dr. Weiss, of the Cardiovascular Research Institute, University of California, San Francisco.
“But no matter how you slice it, prescription of time-restricted eating – at least this version –is not a very effective weight-loss strategy,” Dr. Weiss said.
The study, published online in JAMA Internal Medicine by Dylan A. Lowe, PhD, also of the University of California, San Francisco, involved 116 participants who were randomized to a 12-week regimen of either three structured meals per day or time-restricted eating, with instructions to eat only between 12:00 p.m. and 8:00 p.m. and to completely abstain from eating at other times.
The participants were not given any specific instructions regarding caloric or macronutrient intake “so as to offer a simple, real-world recommendation to free-living individuals,” the authors wrote.
Although some prior research has shown improvements in measures such as glucose tolerance with time-restricted eating, studies showing weight loss with the approach, including one recently reported by Medscape Medical News, have been small and lacked control groups.
“To my knowledge this is the first randomized, controlled trial and definitely the biggest,” Dr. Weiss. “I think it is the most comprehensive dataset available in people, at least for this intervention.”
Participants used app to log details
At baseline, participants had a mean weight of 99.2 kg (approximately 219 lb). Their mean age was 46.5 years and 60.3% were men. They were drawn from anywhere in the United States and received study surveys through a custom mobile study application on the Eureka Research Platform. They were given a Bluetooth weight scale to use daily, which was connected with the app, and randomized to one of the two interventions. A subset of 50 participants living near San Francisco underwent in-person testing.
At the end of the 12 weeks, those in the time-restricted eating group (n = 59) did have a significant decrease in weight, compared with baseline (−0.94 kg; P = .01), while weight loss in the consistent-meal group (n = 57) was not significant (−0.68 kg; P = .07).
But importantly, the difference in weight loss between the groups was not significant (−0.26 kg; P = .63).
There were no significant differences in secondary outcomes of fasting insulin, glucose, hemoglobin A1c, or blood lipids within or between the time-restricted eating and consistent-meal group either. Nor were there any significant differences in resting metabolic rate.
Although participants did not self-report their caloric intake, the authors estimated that the differences were not significant using mathematical modeling developed at the National Institutes of Health.
Rates of adherence to the diets were 92.1% in the consistent-meal group versus 83.5% in the time-restricted group.
Not all diets are equal: Time-restricted eating group lost more lean mass
In a subset analysis, loss of lean mass was significantly greater in the time-restricted eating group, compared with the consistent-meals group, in terms of both appendicular lean mass (P = .009) and the appendicular lean mass index (P = .005).
In fact, as much as 65% of the weight lost (1.10 kg of the average 1.70 kg) in the time-restricted eating group consisted of lean mass, while much less was fat mass (0.51 kg).
“The proportion of lean mass loss in this study (approximately 65%) far exceeds the normal range of 20%-30%,” the authors wrote. “In addition, there was a highly significant between-group difference in appendicular lean mass.”
Appendicular lean mass correlates with nutritional and physical status, and its reduction can lead to weakness, disability, and impaired quality of life.
“This serves as a caution for patient populations at risk for sarcopenia because time-restricted eating could exacerbate muscle loss,” the authors asserted.
Furthermore, previous studies suggest that the loss of lean mass in such studies is positively linked with weight regain.
While a limitation of the work is that self-reported measures of energy or macronutrient or protein intake were not obtained, the authors speculated that the role of protein intake could be linked to the greater loss of lean mass.
“Given the loss of appendicular lean mass in participants in the time-restricted eating arm and previous reports of decreased protein consumption from time-restricted eating, it is possible that protein intake was altered by time-restricted eating in this cohort, and this clearly warrants future study,” they wrote.
Dr. Weiss said the findings underscore that not all weight loss in dieting is beneficial.
“Losing 1 kg of lean mass (is not equal) to a kilogram of fat,” he said. “Indeed, if one loses 0.65 kg of lean mass and only 0.35 kg of fat mass, that is an intervention I’d probably pass on.”
Time-restricted eating is popular, perhaps because it’s easy?
Time-restricted eating has gained popularity in recent years.
The approach “is attractive as a weight-loss option in that it does not require tedious and time-consuming methods such as calorie counting or adherence to complicated diets,” the authors noted. “Indeed, we found that self-reported adherence to the time-restricted eating schedule was high; however, in contrast to our hypothesis, there was no greater weight loss with time-restricted eating compared with the consistent meal timing.”
They explain that the 12 p.m. to 8 p.m. window for eating was chosen because they thought people might find it easier culturally to skip breakfast than dinner, the more social meal.
However, an 8 p.m. cutoff is somewhat late given there is some suggestion that fasting several hours before bedtime is most beneficial, Dr. Weiss noted. So it may be worth examining different time windows.
“I am very intrigued about looking at early time-restricted eating – 6 a.m. to 2 p.m.,” for example, he said. “It is on our list.”
Meanwhile, the study results support previous research showing no effect on weight outcomes in relation to skipping breakfast.
The study received funding from the UCSF cardiology division’s Cardiology Innovations Award Program and the National Institute of Diabetes and Digestive and Kidney Diseases, with additional support from the James Peter Read Foundation. Dr. Weiss has reported nonfinancial support from Mocacare and nonfinancial support from iHealth Labs during the conduct of the study. He also is a cofounder and equity stakeholder of Keyto, and owns stock and was formerly on the board of Virta.
A version of this article originally appeared on Medscape.com.
The popular new weight-loss approach of eating within a restricted window of time during the day, allowing for an extended period of fasting – also known as intermittent fasting – does not result in greater weight loss, compared with nonrestricted meal timing, results from a randomized clinical trial show.
“I was very surprised by all of [the results],” senior author Ethan J. Weiss, MD, said in an interview.
“Part of the reason we did the study was because I had been doing time-restricted eating myself for years and even recommending it to friends and patients as an effective weight-loss tool,” said Dr. Weiss, of the Cardiovascular Research Institute, University of California, San Francisco.
“But no matter how you slice it, prescription of time-restricted eating – at least this version –is not a very effective weight-loss strategy,” Dr. Weiss said.
The study, published online in JAMA Internal Medicine by Dylan A. Lowe, PhD, also of the University of California, San Francisco, involved 116 participants who were randomized to a 12-week regimen of either three structured meals per day or time-restricted eating, with instructions to eat only between 12:00 p.m. and 8:00 p.m. and to completely abstain from eating at other times.
The participants were not given any specific instructions regarding caloric or macronutrient intake “so as to offer a simple, real-world recommendation to free-living individuals,” the authors wrote.
Although some prior research has shown improvements in measures such as glucose tolerance with time-restricted eating, studies showing weight loss with the approach, including one recently reported by Medscape Medical News, have been small and lacked control groups.
“To my knowledge this is the first randomized, controlled trial and definitely the biggest,” Dr. Weiss. “I think it is the most comprehensive dataset available in people, at least for this intervention.”
Participants used app to log details
At baseline, participants had a mean weight of 99.2 kg (approximately 219 lb). Their mean age was 46.5 years and 60.3% were men. They were drawn from anywhere in the United States and received study surveys through a custom mobile study application on the Eureka Research Platform. They were given a Bluetooth weight scale to use daily, which was connected with the app, and randomized to one of the two interventions. A subset of 50 participants living near San Francisco underwent in-person testing.
At the end of the 12 weeks, those in the time-restricted eating group (n = 59) did have a significant decrease in weight, compared with baseline (−0.94 kg; P = .01), while weight loss in the consistent-meal group (n = 57) was not significant (−0.68 kg; P = .07).
But importantly, the difference in weight loss between the groups was not significant (−0.26 kg; P = .63).
There were no significant differences in secondary outcomes of fasting insulin, glucose, hemoglobin A1c, or blood lipids within or between the time-restricted eating and consistent-meal group either. Nor were there any significant differences in resting metabolic rate.
Although participants did not self-report their caloric intake, the authors estimated that the differences were not significant using mathematical modeling developed at the National Institutes of Health.
Rates of adherence to the diets were 92.1% in the consistent-meal group versus 83.5% in the time-restricted group.
Not all diets are equal: Time-restricted eating group lost more lean mass
In a subset analysis, loss of lean mass was significantly greater in the time-restricted eating group, compared with the consistent-meals group, in terms of both appendicular lean mass (P = .009) and the appendicular lean mass index (P = .005).
In fact, as much as 65% of the weight lost (1.10 kg of the average 1.70 kg) in the time-restricted eating group consisted of lean mass, while much less was fat mass (0.51 kg).
“The proportion of lean mass loss in this study (approximately 65%) far exceeds the normal range of 20%-30%,” the authors wrote. “In addition, there was a highly significant between-group difference in appendicular lean mass.”
Appendicular lean mass correlates with nutritional and physical status, and its reduction can lead to weakness, disability, and impaired quality of life.
“This serves as a caution for patient populations at risk for sarcopenia because time-restricted eating could exacerbate muscle loss,” the authors asserted.
Furthermore, previous studies suggest that the loss of lean mass in such studies is positively linked with weight regain.
While a limitation of the work is that self-reported measures of energy or macronutrient or protein intake were not obtained, the authors speculated that the role of protein intake could be linked to the greater loss of lean mass.
“Given the loss of appendicular lean mass in participants in the time-restricted eating arm and previous reports of decreased protein consumption from time-restricted eating, it is possible that protein intake was altered by time-restricted eating in this cohort, and this clearly warrants future study,” they wrote.
Dr. Weiss said the findings underscore that not all weight loss in dieting is beneficial.
“Losing 1 kg of lean mass (is not equal) to a kilogram of fat,” he said. “Indeed, if one loses 0.65 kg of lean mass and only 0.35 kg of fat mass, that is an intervention I’d probably pass on.”
Time-restricted eating is popular, perhaps because it’s easy?
Time-restricted eating has gained popularity in recent years.
The approach “is attractive as a weight-loss option in that it does not require tedious and time-consuming methods such as calorie counting or adherence to complicated diets,” the authors noted. “Indeed, we found that self-reported adherence to the time-restricted eating schedule was high; however, in contrast to our hypothesis, there was no greater weight loss with time-restricted eating compared with the consistent meal timing.”
They explain that the 12 p.m. to 8 p.m. window for eating was chosen because they thought people might find it easier culturally to skip breakfast than dinner, the more social meal.
However, an 8 p.m. cutoff is somewhat late given there is some suggestion that fasting several hours before bedtime is most beneficial, Dr. Weiss noted. So it may be worth examining different time windows.
“I am very intrigued about looking at early time-restricted eating – 6 a.m. to 2 p.m.,” for example, he said. “It is on our list.”
Meanwhile, the study results support previous research showing no effect on weight outcomes in relation to skipping breakfast.
The study received funding from the UCSF cardiology division’s Cardiology Innovations Award Program and the National Institute of Diabetes and Digestive and Kidney Diseases, with additional support from the James Peter Read Foundation. Dr. Weiss has reported nonfinancial support from Mocacare and nonfinancial support from iHealth Labs during the conduct of the study. He also is a cofounder and equity stakeholder of Keyto, and owns stock and was formerly on the board of Virta.
A version of this article originally appeared on Medscape.com.