User login
A Rare Delayed Presentation of Immune-Related Hepatitis in a Patient Treated With Pembrolizumab
Background
Immune checkpoint inhibitors, including pembrolizumab, are associated with a spectrum of immune-related adverse events (irAEs), including immune- mediated hepatitis. Typically, this toxicity manifests within the first 14 weeks of therapy. Delayed presentations beyond one year are exceedingly rare and pose diagnostic challenges.
Case Presentation
We report an elderly patient (over 90 years old) with stage IVa squamous cell carcinoma of the lung and high microsatellite instability (MSI) who had been receiving pembrolizumab since 2023. In 2024—13 months into therapy—he presented with subjective fevers, weakness, and altered mental status. Laboratory evaluation revealed cholestatic jaundice with AST 310 U/L, ALT 291 U/L, alkaline phosphatase 860 U/L, and total bilirubin 5.7 mg/dL. Infectious workup was negative. Imaging via MRCP showed multiple scattered hepatic cysts and a small pancreatic cyst, without biliary obstruction.
Further evaluation, including serologies for hepatitis B and C, CMV, HSV, autoimmune hepatitis panel, iron studies, and ceruloplasmin, was unremarkable except for mildly elevated alpha-1 antitrypsin. Scattered liver cysts were seen on an MRI. The overall findings were most consistent with immune-related hepatitis, as pembrolizumab is known to cause both hepatocellular and cholestatic patterns of liver injury.
The patient was started on high-dose prednisone, resulting in rapid clinical and biochemical improvement. Two weeks post-discharge, liver function tests (LFTs) had markedly improved (bilirubin 1.3, AST 19, ALT 40, ALP 193). Given the severity of transaminitis and hyperbilirubinemia (AST >8x ULN, bilirubin >3x ULN), pembrolizumab was permanently discontinued. LFTs normalized after completion of the steroid taper.
Conclusions
This case highlights a rare instance of delayed immune-related hepatitis occurring over a year after initiation of pembrolizumab, far beyond the typical window of onset. Clinicians should maintain a high index of suspicion for irAEs even in late stages of immunotherapy, particularly when common etiologies are excluded. Prompt recognition and corticosteroid treatment can lead to favorable outcomes, even in older patients.
Background
Immune checkpoint inhibitors, including pembrolizumab, are associated with a spectrum of immune-related adverse events (irAEs), including immune- mediated hepatitis. Typically, this toxicity manifests within the first 14 weeks of therapy. Delayed presentations beyond one year are exceedingly rare and pose diagnostic challenges.
Case Presentation
We report an elderly patient (over 90 years old) with stage IVa squamous cell carcinoma of the lung and high microsatellite instability (MSI) who had been receiving pembrolizumab since 2023. In 2024—13 months into therapy—he presented with subjective fevers, weakness, and altered mental status. Laboratory evaluation revealed cholestatic jaundice with AST 310 U/L, ALT 291 U/L, alkaline phosphatase 860 U/L, and total bilirubin 5.7 mg/dL. Infectious workup was negative. Imaging via MRCP showed multiple scattered hepatic cysts and a small pancreatic cyst, without biliary obstruction.
Further evaluation, including serologies for hepatitis B and C, CMV, HSV, autoimmune hepatitis panel, iron studies, and ceruloplasmin, was unremarkable except for mildly elevated alpha-1 antitrypsin. Scattered liver cysts were seen on an MRI. The overall findings were most consistent with immune-related hepatitis, as pembrolizumab is known to cause both hepatocellular and cholestatic patterns of liver injury.
The patient was started on high-dose prednisone, resulting in rapid clinical and biochemical improvement. Two weeks post-discharge, liver function tests (LFTs) had markedly improved (bilirubin 1.3, AST 19, ALT 40, ALP 193). Given the severity of transaminitis and hyperbilirubinemia (AST >8x ULN, bilirubin >3x ULN), pembrolizumab was permanently discontinued. LFTs normalized after completion of the steroid taper.
Conclusions
This case highlights a rare instance of delayed immune-related hepatitis occurring over a year after initiation of pembrolizumab, far beyond the typical window of onset. Clinicians should maintain a high index of suspicion for irAEs even in late stages of immunotherapy, particularly when common etiologies are excluded. Prompt recognition and corticosteroid treatment can lead to favorable outcomes, even in older patients.
Background
Immune checkpoint inhibitors, including pembrolizumab, are associated with a spectrum of immune-related adverse events (irAEs), including immune- mediated hepatitis. Typically, this toxicity manifests within the first 14 weeks of therapy. Delayed presentations beyond one year are exceedingly rare and pose diagnostic challenges.
Case Presentation
We report an elderly patient (over 90 years old) with stage IVa squamous cell carcinoma of the lung and high microsatellite instability (MSI) who had been receiving pembrolizumab since 2023. In 2024—13 months into therapy—he presented with subjective fevers, weakness, and altered mental status. Laboratory evaluation revealed cholestatic jaundice with AST 310 U/L, ALT 291 U/L, alkaline phosphatase 860 U/L, and total bilirubin 5.7 mg/dL. Infectious workup was negative. Imaging via MRCP showed multiple scattered hepatic cysts and a small pancreatic cyst, without biliary obstruction.
Further evaluation, including serologies for hepatitis B and C, CMV, HSV, autoimmune hepatitis panel, iron studies, and ceruloplasmin, was unremarkable except for mildly elevated alpha-1 antitrypsin. Scattered liver cysts were seen on an MRI. The overall findings were most consistent with immune-related hepatitis, as pembrolizumab is known to cause both hepatocellular and cholestatic patterns of liver injury.
The patient was started on high-dose prednisone, resulting in rapid clinical and biochemical improvement. Two weeks post-discharge, liver function tests (LFTs) had markedly improved (bilirubin 1.3, AST 19, ALT 40, ALP 193). Given the severity of transaminitis and hyperbilirubinemia (AST >8x ULN, bilirubin >3x ULN), pembrolizumab was permanently discontinued. LFTs normalized after completion of the steroid taper.
Conclusions
This case highlights a rare instance of delayed immune-related hepatitis occurring over a year after initiation of pembrolizumab, far beyond the typical window of onset. Clinicians should maintain a high index of suspicion for irAEs even in late stages of immunotherapy, particularly when common etiologies are excluded. Prompt recognition and corticosteroid treatment can lead to favorable outcomes, even in older patients.
Prognosis Paradox: Does HLA-B27 Improve the Prognosis of Immune-Related Pneumonitis in Metastatic Lung Cancer?
Background
Immune related adverse events (irAE) are a well-known complication in the treatment of nonsmall cell lung cancer (NSCLCA) with checkpoint inhibitors and have been shown to improve overall survival (OS) and progression free survival (PFS) across multiple studies. However, studies have shown that the prognosis of NSCLCA differs depending on the type of immune related adverse event and the grade of the irAE. For instance, patients who experienced endocrine irAEs like thyroid, or adrenal insufficiency tended to have an improved OS and PFS, whereas patients who developed pneumonitis that required discontinuation of checkpoint inhibitors had worse OS and PFS. While the literature describes the prognostic impacts of irAEs on NSCLCA, there is still a dearth of information on the implications of HLA supertypes on the prognosis of NSCLCA following irAEs.
Case Presentation
To address this point and to ask a question, we would like to share the case of a patient with a 10-year history of inflammatory arthropathy related to HLA-B27 antigen prior to his diagnosis of T2bN2M1b adenosquamous lung cancer with liver metastases. The tumor was 100% PD-L1 expressive and the patient was treated with pembrolizumab. The patient developed central adrenal insufficiency 10 months after pembrolizumab was initiated which was treated with physiologic dosing of hydrocortisone. The patient later developed a grade 3 pneumonitis 62 months after initiation of pembrolizumab and was treated with systemic glucocorticoids. Due to recurrent hospitalizations for pneumonitis, pembrolizumab was discontinued at 70 months post initiation. At the time of discontinuation PET was positive. However, there was a decrease in hyperactivity of the primary tumor at 4 months post discontinuation of pembrolizumab and there have been serial negative PETS from 7 months to 13 months post discontinuation. This led us to ask the question of whether HLA-B27 is protective of the poor prognostic immune related pneumonitis in this patient?
Background
Immune related adverse events (irAE) are a well-known complication in the treatment of nonsmall cell lung cancer (NSCLCA) with checkpoint inhibitors and have been shown to improve overall survival (OS) and progression free survival (PFS) across multiple studies. However, studies have shown that the prognosis of NSCLCA differs depending on the type of immune related adverse event and the grade of the irAE. For instance, patients who experienced endocrine irAEs like thyroid, or adrenal insufficiency tended to have an improved OS and PFS, whereas patients who developed pneumonitis that required discontinuation of checkpoint inhibitors had worse OS and PFS. While the literature describes the prognostic impacts of irAEs on NSCLCA, there is still a dearth of information on the implications of HLA supertypes on the prognosis of NSCLCA following irAEs.
Case Presentation
To address this point and to ask a question, we would like to share the case of a patient with a 10-year history of inflammatory arthropathy related to HLA-B27 antigen prior to his diagnosis of T2bN2M1b adenosquamous lung cancer with liver metastases. The tumor was 100% PD-L1 expressive and the patient was treated with pembrolizumab. The patient developed central adrenal insufficiency 10 months after pembrolizumab was initiated which was treated with physiologic dosing of hydrocortisone. The patient later developed a grade 3 pneumonitis 62 months after initiation of pembrolizumab and was treated with systemic glucocorticoids. Due to recurrent hospitalizations for pneumonitis, pembrolizumab was discontinued at 70 months post initiation. At the time of discontinuation PET was positive. However, there was a decrease in hyperactivity of the primary tumor at 4 months post discontinuation of pembrolizumab and there have been serial negative PETS from 7 months to 13 months post discontinuation. This led us to ask the question of whether HLA-B27 is protective of the poor prognostic immune related pneumonitis in this patient?
Background
Immune related adverse events (irAE) are a well-known complication in the treatment of nonsmall cell lung cancer (NSCLCA) with checkpoint inhibitors and have been shown to improve overall survival (OS) and progression free survival (PFS) across multiple studies. However, studies have shown that the prognosis of NSCLCA differs depending on the type of immune related adverse event and the grade of the irAE. For instance, patients who experienced endocrine irAEs like thyroid, or adrenal insufficiency tended to have an improved OS and PFS, whereas patients who developed pneumonitis that required discontinuation of checkpoint inhibitors had worse OS and PFS. While the literature describes the prognostic impacts of irAEs on NSCLCA, there is still a dearth of information on the implications of HLA supertypes on the prognosis of NSCLCA following irAEs.
Case Presentation
To address this point and to ask a question, we would like to share the case of a patient with a 10-year history of inflammatory arthropathy related to HLA-B27 antigen prior to his diagnosis of T2bN2M1b adenosquamous lung cancer with liver metastases. The tumor was 100% PD-L1 expressive and the patient was treated with pembrolizumab. The patient developed central adrenal insufficiency 10 months after pembrolizumab was initiated which was treated with physiologic dosing of hydrocortisone. The patient later developed a grade 3 pneumonitis 62 months after initiation of pembrolizumab and was treated with systemic glucocorticoids. Due to recurrent hospitalizations for pneumonitis, pembrolizumab was discontinued at 70 months post initiation. At the time of discontinuation PET was positive. However, there was a decrease in hyperactivity of the primary tumor at 4 months post discontinuation of pembrolizumab and there have been serial negative PETS from 7 months to 13 months post discontinuation. This led us to ask the question of whether HLA-B27 is protective of the poor prognostic immune related pneumonitis in this patient?
Metastatic Pulmonary LCNEC With Pancreatic Involvement in a Young Non-Smoker: An Unusual Presentation
Background
Pulmonary large-cell neuroendocrine carcinoma (LCNEC) is a rare, aggressive lung cancer subtype, comprising ~3% of lung malignancies. It commonly affects older, heavy smokers and presents at an advanced stage. Prognosis is poor, with a 5-year survival rate of 15–25% in metastatic disease.
Case Presentation
A 33-year-old previously healthy male presented with a month of abdominal and lower back pain, along with significant weight loss. Lab tests revealed elevated lipase (378), and he was initially treated for acute pancreatitis. Imaging revealed a 1.9 cm pancreatic head mass and three hypodense hepatic lesions. MRI confirmed these findings but remained inconclusive. An incidental 8 mm right lower lobe pulmonary nodule led to chest CT, identifying a dominant left lower lobe mass and mediastinal lymphadenopathy, raising suspicion for primary lung malignancy. The patient was discharged but returned three days later with worsening symptoms and a lipase of 754. Endoscopic biopsy of the pancreatic mass was deferred due to ongoing pancreatitis. A liver biopsy revealed neuroendocrine differentiation, positive for CK AE1/AE3, CK7, CK19, and synaptophysin. Molecular profiling showed PD-L1 (TPS 50%), low tumor mutational burden, microsatellite stability, and high loss of heterozygosity. Bronchoscopy revealed a left hilar mass, and lymph node biopsy confirmed LCNEC (CK7+, chromogranin+, TTF- 1+, synaptophysin+), establishing a diagnosis of stage IV pulmonary LCNEC with pancreatic and liver metastases. The patient began treatment with bevacizumab, paclitaxel, carboplatin, and atezolizumab, resulting in improvement in hilar, hepatic, and pancreatic lesions on further imagings. The patient was continued on chemoimmunotherapy.
Discussion
This case highlights an uncommon presentation of LCNEC in a young, non-smoking male, initially manifesting as pancreatitis due to pancreatic metastasis. The absence of pulmonary symptoms complicated the diagnosis. Histopathology and immunohistochemistry were essential. While no standardized treatment exists for LCNEC, platinum-based chemotherapy with immunotherapy remains the mainstay. PD-L1 expression may guide immunotherapy decisions.
Conclusions
Pulmonary LCNEC should be considered in metastatic neuroendocrine tumors, even in young, non-smoking patients without pulmonary symptoms. Early tissue diagnosis and molecular profiling are key to guiding management.
Background
Pulmonary large-cell neuroendocrine carcinoma (LCNEC) is a rare, aggressive lung cancer subtype, comprising ~3% of lung malignancies. It commonly affects older, heavy smokers and presents at an advanced stage. Prognosis is poor, with a 5-year survival rate of 15–25% in metastatic disease.
Case Presentation
A 33-year-old previously healthy male presented with a month of abdominal and lower back pain, along with significant weight loss. Lab tests revealed elevated lipase (378), and he was initially treated for acute pancreatitis. Imaging revealed a 1.9 cm pancreatic head mass and three hypodense hepatic lesions. MRI confirmed these findings but remained inconclusive. An incidental 8 mm right lower lobe pulmonary nodule led to chest CT, identifying a dominant left lower lobe mass and mediastinal lymphadenopathy, raising suspicion for primary lung malignancy. The patient was discharged but returned three days later with worsening symptoms and a lipase of 754. Endoscopic biopsy of the pancreatic mass was deferred due to ongoing pancreatitis. A liver biopsy revealed neuroendocrine differentiation, positive for CK AE1/AE3, CK7, CK19, and synaptophysin. Molecular profiling showed PD-L1 (TPS 50%), low tumor mutational burden, microsatellite stability, and high loss of heterozygosity. Bronchoscopy revealed a left hilar mass, and lymph node biopsy confirmed LCNEC (CK7+, chromogranin+, TTF- 1+, synaptophysin+), establishing a diagnosis of stage IV pulmonary LCNEC with pancreatic and liver metastases. The patient began treatment with bevacizumab, paclitaxel, carboplatin, and atezolizumab, resulting in improvement in hilar, hepatic, and pancreatic lesions on further imagings. The patient was continued on chemoimmunotherapy.
Discussion
This case highlights an uncommon presentation of LCNEC in a young, non-smoking male, initially manifesting as pancreatitis due to pancreatic metastasis. The absence of pulmonary symptoms complicated the diagnosis. Histopathology and immunohistochemistry were essential. While no standardized treatment exists for LCNEC, platinum-based chemotherapy with immunotherapy remains the mainstay. PD-L1 expression may guide immunotherapy decisions.
Conclusions
Pulmonary LCNEC should be considered in metastatic neuroendocrine tumors, even in young, non-smoking patients without pulmonary symptoms. Early tissue diagnosis and molecular profiling are key to guiding management.
Background
Pulmonary large-cell neuroendocrine carcinoma (LCNEC) is a rare, aggressive lung cancer subtype, comprising ~3% of lung malignancies. It commonly affects older, heavy smokers and presents at an advanced stage. Prognosis is poor, with a 5-year survival rate of 15–25% in metastatic disease.
Case Presentation
A 33-year-old previously healthy male presented with a month of abdominal and lower back pain, along with significant weight loss. Lab tests revealed elevated lipase (378), and he was initially treated for acute pancreatitis. Imaging revealed a 1.9 cm pancreatic head mass and three hypodense hepatic lesions. MRI confirmed these findings but remained inconclusive. An incidental 8 mm right lower lobe pulmonary nodule led to chest CT, identifying a dominant left lower lobe mass and mediastinal lymphadenopathy, raising suspicion for primary lung malignancy. The patient was discharged but returned three days later with worsening symptoms and a lipase of 754. Endoscopic biopsy of the pancreatic mass was deferred due to ongoing pancreatitis. A liver biopsy revealed neuroendocrine differentiation, positive for CK AE1/AE3, CK7, CK19, and synaptophysin. Molecular profiling showed PD-L1 (TPS 50%), low tumor mutational burden, microsatellite stability, and high loss of heterozygosity. Bronchoscopy revealed a left hilar mass, and lymph node biopsy confirmed LCNEC (CK7+, chromogranin+, TTF- 1+, synaptophysin+), establishing a diagnosis of stage IV pulmonary LCNEC with pancreatic and liver metastases. The patient began treatment with bevacizumab, paclitaxel, carboplatin, and atezolizumab, resulting in improvement in hilar, hepatic, and pancreatic lesions on further imagings. The patient was continued on chemoimmunotherapy.
Discussion
This case highlights an uncommon presentation of LCNEC in a young, non-smoking male, initially manifesting as pancreatitis due to pancreatic metastasis. The absence of pulmonary symptoms complicated the diagnosis. Histopathology and immunohistochemistry were essential. While no standardized treatment exists for LCNEC, platinum-based chemotherapy with immunotherapy remains the mainstay. PD-L1 expression may guide immunotherapy decisions.
Conclusions
Pulmonary LCNEC should be considered in metastatic neuroendocrine tumors, even in young, non-smoking patients without pulmonary symptoms. Early tissue diagnosis and molecular profiling are key to guiding management.
Brief Immunotherapy Yields Major Survival Benefits in Advanced NSCLC: A Case Report
Background
Lung cancer, primarily non-small cell lung cancer (NSCLC), typically presents at an advanced stage with a five-year survival rate below 5%. Treatment includes platinum-based chemotherapy and targeted therapies for specific mutations, with immunotherapy significantly improving outcomes for patients with high PD-L1 expression.
Case Presentation
A 72-year-old male, diagnosed with advanced lung adenocarcinoma in 2020 after showing symptoms of brain metastases, underwent successful surgical and CyberKnife treatments. Despite no actionable genetic targets and a high PD-L1 expression of 80%, his treatment with 3-cycles of Keytruda was cut short due to a psoriatic arthritis flare-up, though it initially decreased his CEA levels significantly. Over the following years, fluctuating CEA levels and various imaging studies indicated some concerning changes, such as potential radionecrosis or recurrence of cancer in the lung. His refusal of biopsy and a preference for avoiding invasive treatments led to only surveillance. Later, an MRI showed some metastasis, and the patient agreed to a lung biopsy, which showed poorly differentiated carcinoma of pulmonary origin. The patient only agreed to restart treatment with Keytruda 4-years later after his initial treatment with Keytruda, under close rheumatological care, and received only two doses. Afterward, the patient lost follow-ups. 3-months later, Repeated CT scans of the chest, abdomen, and pelvis showed no evidence of mass or pathological lymph nodes, and repeated CEA was 3.4.
Discussion
Managing advanced lung adenocarcinoma, especially with complications like brain metastases and psoriatic arthritis, is challenging. Pembrolizumab treatment showed promise by significantly reducing CEA levels despite early discontinuation due to autoimmune side effects, indicating effective tumor response in patients with high PD-L1 expression. The case underscores the need for balancing cancer treatment with autoimmune management and highlights the importance of patient preferences in treatment plans. Ongoing surveillance and genomic profiling remain crucial for guiding therapy.
Conclusions
This case of a 70-year-old male with advanced lung adenocarcinoma highlights the significant impact of immunotherapy, particularly PD-1/ PD-L1 inhibitors like pembrolizumab, in NSCLC. Despite a brief treatment period, the patient experienced extended disease control, demonstrating the potential of immunotherapy to enhance survival and its broad applicability in oncology.
Background
Lung cancer, primarily non-small cell lung cancer (NSCLC), typically presents at an advanced stage with a five-year survival rate below 5%. Treatment includes platinum-based chemotherapy and targeted therapies for specific mutations, with immunotherapy significantly improving outcomes for patients with high PD-L1 expression.
Case Presentation
A 72-year-old male, diagnosed with advanced lung adenocarcinoma in 2020 after showing symptoms of brain metastases, underwent successful surgical and CyberKnife treatments. Despite no actionable genetic targets and a high PD-L1 expression of 80%, his treatment with 3-cycles of Keytruda was cut short due to a psoriatic arthritis flare-up, though it initially decreased his CEA levels significantly. Over the following years, fluctuating CEA levels and various imaging studies indicated some concerning changes, such as potential radionecrosis or recurrence of cancer in the lung. His refusal of biopsy and a preference for avoiding invasive treatments led to only surveillance. Later, an MRI showed some metastasis, and the patient agreed to a lung biopsy, which showed poorly differentiated carcinoma of pulmonary origin. The patient only agreed to restart treatment with Keytruda 4-years later after his initial treatment with Keytruda, under close rheumatological care, and received only two doses. Afterward, the patient lost follow-ups. 3-months later, Repeated CT scans of the chest, abdomen, and pelvis showed no evidence of mass or pathological lymph nodes, and repeated CEA was 3.4.
Discussion
Managing advanced lung adenocarcinoma, especially with complications like brain metastases and psoriatic arthritis, is challenging. Pembrolizumab treatment showed promise by significantly reducing CEA levels despite early discontinuation due to autoimmune side effects, indicating effective tumor response in patients with high PD-L1 expression. The case underscores the need for balancing cancer treatment with autoimmune management and highlights the importance of patient preferences in treatment plans. Ongoing surveillance and genomic profiling remain crucial for guiding therapy.
Conclusions
This case of a 70-year-old male with advanced lung adenocarcinoma highlights the significant impact of immunotherapy, particularly PD-1/ PD-L1 inhibitors like pembrolizumab, in NSCLC. Despite a brief treatment period, the patient experienced extended disease control, demonstrating the potential of immunotherapy to enhance survival and its broad applicability in oncology.
Background
Lung cancer, primarily non-small cell lung cancer (NSCLC), typically presents at an advanced stage with a five-year survival rate below 5%. Treatment includes platinum-based chemotherapy and targeted therapies for specific mutations, with immunotherapy significantly improving outcomes for patients with high PD-L1 expression.
Case Presentation
A 72-year-old male, diagnosed with advanced lung adenocarcinoma in 2020 after showing symptoms of brain metastases, underwent successful surgical and CyberKnife treatments. Despite no actionable genetic targets and a high PD-L1 expression of 80%, his treatment with 3-cycles of Keytruda was cut short due to a psoriatic arthritis flare-up, though it initially decreased his CEA levels significantly. Over the following years, fluctuating CEA levels and various imaging studies indicated some concerning changes, such as potential radionecrosis or recurrence of cancer in the lung. His refusal of biopsy and a preference for avoiding invasive treatments led to only surveillance. Later, an MRI showed some metastasis, and the patient agreed to a lung biopsy, which showed poorly differentiated carcinoma of pulmonary origin. The patient only agreed to restart treatment with Keytruda 4-years later after his initial treatment with Keytruda, under close rheumatological care, and received only two doses. Afterward, the patient lost follow-ups. 3-months later, Repeated CT scans of the chest, abdomen, and pelvis showed no evidence of mass or pathological lymph nodes, and repeated CEA was 3.4.
Discussion
Managing advanced lung adenocarcinoma, especially with complications like brain metastases and psoriatic arthritis, is challenging. Pembrolizumab treatment showed promise by significantly reducing CEA levels despite early discontinuation due to autoimmune side effects, indicating effective tumor response in patients with high PD-L1 expression. The case underscores the need for balancing cancer treatment with autoimmune management and highlights the importance of patient preferences in treatment plans. Ongoing surveillance and genomic profiling remain crucial for guiding therapy.
Conclusions
This case of a 70-year-old male with advanced lung adenocarcinoma highlights the significant impact of immunotherapy, particularly PD-1/ PD-L1 inhibitors like pembrolizumab, in NSCLC. Despite a brief treatment period, the patient experienced extended disease control, demonstrating the potential of immunotherapy to enhance survival and its broad applicability in oncology.
Lung Cancer Exposome in U.S. Military Veterans: Study of Environment and Epigenetic Factors on Risk and Survival
Background
The Exposome—the comprehensive accumulation of environmental exposures from birth to death—provides a framework for linking external risk factors to cancer biology. In U.S. veterans, the exposome includes both military-specific exposures (e.g., asbestos, Agent Orange, burn pits) and postservice socioeconomic and environmental factors. These cumulative exposures may drive tumor development and progression via epigenetic mechanisms, though their impact on lung cancer outcomes remain poorly characterized.
Methods
This is a retrospective cohort study of 71 lung cancer subjects (NSCLC and SCLC) from the Jesse Brown VA Medical Center (IRB# 1586320). We assessed the Area Deprivation Index (ADI), Environmental Burden Index (EBI), and occupational exposure in relation to DNA methylation of CDO1, TAC1, SOX17, and HOXA7. Geospatial data were mapped to US census tracts, and standard statistical analysis were conducted.
Results
NSCLC patients exhibited significantly higher methylation levels across all genes. High EBI exposure was associated with lower SOX17 methylation (p = 0.064) and worse overall survival (p = 0.046). In NSCLC patients, occupational exposure predicted a 7.7-fold increased hazard of death (p = 0.027). SOX17 and TAC1 methylation were independently associated with reduced survival (p = 0.037 and 0.0058, respectively). While ADI did not independently predict survival, it correlated with late-stage presentation and reduced HOXA7 methylation.
Conclusions
Exposome factors such as environmental burden and occupational exposure are biologically embedded in lung cancer cell through gene-specific methylation and significantly impact survival. We posit that integrating exposomic and molecular data could enhance lung precision oncology approaches for high-risk veteran populations.
Background
The Exposome—the comprehensive accumulation of environmental exposures from birth to death—provides a framework for linking external risk factors to cancer biology. In U.S. veterans, the exposome includes both military-specific exposures (e.g., asbestos, Agent Orange, burn pits) and postservice socioeconomic and environmental factors. These cumulative exposures may drive tumor development and progression via epigenetic mechanisms, though their impact on lung cancer outcomes remain poorly characterized.
Methods
This is a retrospective cohort study of 71 lung cancer subjects (NSCLC and SCLC) from the Jesse Brown VA Medical Center (IRB# 1586320). We assessed the Area Deprivation Index (ADI), Environmental Burden Index (EBI), and occupational exposure in relation to DNA methylation of CDO1, TAC1, SOX17, and HOXA7. Geospatial data were mapped to US census tracts, and standard statistical analysis were conducted.
Results
NSCLC patients exhibited significantly higher methylation levels across all genes. High EBI exposure was associated with lower SOX17 methylation (p = 0.064) and worse overall survival (p = 0.046). In NSCLC patients, occupational exposure predicted a 7.7-fold increased hazard of death (p = 0.027). SOX17 and TAC1 methylation were independently associated with reduced survival (p = 0.037 and 0.0058, respectively). While ADI did not independently predict survival, it correlated with late-stage presentation and reduced HOXA7 methylation.
Conclusions
Exposome factors such as environmental burden and occupational exposure are biologically embedded in lung cancer cell through gene-specific methylation and significantly impact survival. We posit that integrating exposomic and molecular data could enhance lung precision oncology approaches for high-risk veteran populations.
Background
The Exposome—the comprehensive accumulation of environmental exposures from birth to death—provides a framework for linking external risk factors to cancer biology. In U.S. veterans, the exposome includes both military-specific exposures (e.g., asbestos, Agent Orange, burn pits) and postservice socioeconomic and environmental factors. These cumulative exposures may drive tumor development and progression via epigenetic mechanisms, though their impact on lung cancer outcomes remain poorly characterized.
Methods
This is a retrospective cohort study of 71 lung cancer subjects (NSCLC and SCLC) from the Jesse Brown VA Medical Center (IRB# 1586320). We assessed the Area Deprivation Index (ADI), Environmental Burden Index (EBI), and occupational exposure in relation to DNA methylation of CDO1, TAC1, SOX17, and HOXA7. Geospatial data were mapped to US census tracts, and standard statistical analysis were conducted.
Results
NSCLC patients exhibited significantly higher methylation levels across all genes. High EBI exposure was associated with lower SOX17 methylation (p = 0.064) and worse overall survival (p = 0.046). In NSCLC patients, occupational exposure predicted a 7.7-fold increased hazard of death (p = 0.027). SOX17 and TAC1 methylation were independently associated with reduced survival (p = 0.037 and 0.0058, respectively). While ADI did not independently predict survival, it correlated with late-stage presentation and reduced HOXA7 methylation.
Conclusions
Exposome factors such as environmental burden and occupational exposure are biologically embedded in lung cancer cell through gene-specific methylation and significantly impact survival. We posit that integrating exposomic and molecular data could enhance lung precision oncology approaches for high-risk veteran populations.
A New ADC for Lung Cancer: Datopotamab Deruxtecan Now Approved by FDA
This transcript has been edited for clarity.
Hello. It’s Mark Kris, from Memorial Sloan Kettering, talking about a birthday gift I received on June 23 when the FDA approved the indication of datopotamab deruxtecan for people with lung cancers. We have another drug, our third ADC (antibody-drug conjugate) to fight lung cancer, so that’s a gift.
Let’s talk a little bit about that agent. It’s an interesting twist in our practice patterns. What can the drug do? It had a response rate of 45%, which is really important in patients that had EGFR mutations with progression on osimertinib. We really need drugs in that space. The duration of response was about 7 months, which is significant.
One interesting thing in the approval, [was] that the response rate of the blinded folks was greater than that in the investigator-assessed response by about 10%. It’s very interesting. Clearly, we have another drug, and we have it in a space where we need it.
Let’s talk a bit about the toxicity. I’m going to focus more on the paper by Bardia et al that compared datopotamab deruxtecan to various chemo drugs in breast cancer, not in lung cancer. You can take this a little bit with a grain of salt.
First, they saw a whole different array of side effects with datopotamab deruxtecan, things that we don’t normally deal with here. Nausea, stomatitis, alopecia, dry eye, and vomiting. All of those were more than 10% more common in patients that received datopotamab deruxtecan compared to the control. The only things that were more common with the control were neutropenia, leukopenia, and hand-foot syndrome in patients that had capecitabine.
One thing, though, is while you say, “Oh, these weren’t dangerous side effects,” they surely were lifestyle altering. Nobody wants to have these side effects on a daily basis. Again, there’s an increasing awareness about these kinds of lower-grade but still lifestyle-disrupting side effects. When it goes on day after day, you really have to balance that into the benefit you’re going to receive.
I think the second important point is how, when we use this drug, we’re going to have to go to another level to deal with the adverse effects that we are going to see. The first would be nausea and emesis. It is a highly emetogenic regimen based on the NCCN (National Comprehensive Cancer Network) guidelines, so you would need either 3 or 4 antiemetic drugs. That’s number one.
Number two, because of the potential eye problems, you need an eye exam before treatment — and the label says at least annually — with any symptoms. I think it’s very important that you give the patients eyedrops, and in general, the preservative-free eyedrops are the ones that are most effective.
Stomatitis is a very common side effect with that agent. It’s really not seen with the other drugs that even contain the same warhead. There, dexamethasone rinses are important. Now, this is a compounded medicine so you need to be very careful in making sure that you identify pharmacies that will prepare this and will have it available for the patients that need it.
Last, there is the risk of hypersensitivity reactions and there’s a recommendation for premedication for that. As you think about using datopotamab deruxtecan, you need to have all your ducks in a row to treat side effects. You need prophylaxis for hypersensitivity reactions, nausea, and emesis.
The patient will need an eye exam. You need to prepare the patient for possible dry eye and teach them which eyedrops are the best. You also need to ensure the availability of dexamethasone rinses and mouth washes. All that needs to be in place to make sure that the patient can safely use the drug.
I think it’s going to be a useful drug. We don’t yet have a uniformly available way to select patients for its use other than EGFR. I should note that the approval is for EGFR-mutated lung cancers. It doesn’t say which type of mutation, so that would give you some latitude in giving it for exon 20 atypicals as well as for the common sensitizing mutation.
We have another drug. It’s clearly going to be a useful one. It clearly comes with many adverse effects that we don’t normally treat on an everyday basis, we’re used to the diarrhea and skin changes that come on with the EGFR TKIs.
This pattern of side effects is different and requires some additional attention, but with it, the drug can be useful. I’m glad that we have yet another way to fight this disease.
Mark G. Kris, MD, Professor of Medicine, Weill Cornell Medical College; Attending Physician, Department of Medicine, Memorial Sloan Kettering Cancer Center, New York, New York , has disclosed the following relevant financial relationships:
Serve(d) as a director, officer, partner, employee, advisor, consultant, or trustee for: AstraZeneca; Bristol-Myers Squibb; Merck; Daiichi Sankyo; Received research grant from: National Institute of Health; Received income in an amount equal to or greater than $250 from: AstraZeneca; Bristol-Myers Squibb; Merck; Daiichi Sankyo Others: Editorial support from Genentech
A version of this article first appeared on Medscape.com.
This transcript has been edited for clarity.
Hello. It’s Mark Kris, from Memorial Sloan Kettering, talking about a birthday gift I received on June 23 when the FDA approved the indication of datopotamab deruxtecan for people with lung cancers. We have another drug, our third ADC (antibody-drug conjugate) to fight lung cancer, so that’s a gift.
Let’s talk a little bit about that agent. It’s an interesting twist in our practice patterns. What can the drug do? It had a response rate of 45%, which is really important in patients that had EGFR mutations with progression on osimertinib. We really need drugs in that space. The duration of response was about 7 months, which is significant.
One interesting thing in the approval, [was] that the response rate of the blinded folks was greater than that in the investigator-assessed response by about 10%. It’s very interesting. Clearly, we have another drug, and we have it in a space where we need it.
Let’s talk a bit about the toxicity. I’m going to focus more on the paper by Bardia et al that compared datopotamab deruxtecan to various chemo drugs in breast cancer, not in lung cancer. You can take this a little bit with a grain of salt.
First, they saw a whole different array of side effects with datopotamab deruxtecan, things that we don’t normally deal with here. Nausea, stomatitis, alopecia, dry eye, and vomiting. All of those were more than 10% more common in patients that received datopotamab deruxtecan compared to the control. The only things that were more common with the control were neutropenia, leukopenia, and hand-foot syndrome in patients that had capecitabine.
One thing, though, is while you say, “Oh, these weren’t dangerous side effects,” they surely were lifestyle altering. Nobody wants to have these side effects on a daily basis. Again, there’s an increasing awareness about these kinds of lower-grade but still lifestyle-disrupting side effects. When it goes on day after day, you really have to balance that into the benefit you’re going to receive.
I think the second important point is how, when we use this drug, we’re going to have to go to another level to deal with the adverse effects that we are going to see. The first would be nausea and emesis. It is a highly emetogenic regimen based on the NCCN (National Comprehensive Cancer Network) guidelines, so you would need either 3 or 4 antiemetic drugs. That’s number one.
Number two, because of the potential eye problems, you need an eye exam before treatment — and the label says at least annually — with any symptoms. I think it’s very important that you give the patients eyedrops, and in general, the preservative-free eyedrops are the ones that are most effective.
Stomatitis is a very common side effect with that agent. It’s really not seen with the other drugs that even contain the same warhead. There, dexamethasone rinses are important. Now, this is a compounded medicine so you need to be very careful in making sure that you identify pharmacies that will prepare this and will have it available for the patients that need it.
Last, there is the risk of hypersensitivity reactions and there’s a recommendation for premedication for that. As you think about using datopotamab deruxtecan, you need to have all your ducks in a row to treat side effects. You need prophylaxis for hypersensitivity reactions, nausea, and emesis.
The patient will need an eye exam. You need to prepare the patient for possible dry eye and teach them which eyedrops are the best. You also need to ensure the availability of dexamethasone rinses and mouth washes. All that needs to be in place to make sure that the patient can safely use the drug.
I think it’s going to be a useful drug. We don’t yet have a uniformly available way to select patients for its use other than EGFR. I should note that the approval is for EGFR-mutated lung cancers. It doesn’t say which type of mutation, so that would give you some latitude in giving it for exon 20 atypicals as well as for the common sensitizing mutation.
We have another drug. It’s clearly going to be a useful one. It clearly comes with many adverse effects that we don’t normally treat on an everyday basis, we’re used to the diarrhea and skin changes that come on with the EGFR TKIs.
This pattern of side effects is different and requires some additional attention, but with it, the drug can be useful. I’m glad that we have yet another way to fight this disease.
Mark G. Kris, MD, Professor of Medicine, Weill Cornell Medical College; Attending Physician, Department of Medicine, Memorial Sloan Kettering Cancer Center, New York, New York , has disclosed the following relevant financial relationships:
Serve(d) as a director, officer, partner, employee, advisor, consultant, or trustee for: AstraZeneca; Bristol-Myers Squibb; Merck; Daiichi Sankyo; Received research grant from: National Institute of Health; Received income in an amount equal to or greater than $250 from: AstraZeneca; Bristol-Myers Squibb; Merck; Daiichi Sankyo Others: Editorial support from Genentech
A version of this article first appeared on Medscape.com.
This transcript has been edited for clarity.
Hello. It’s Mark Kris, from Memorial Sloan Kettering, talking about a birthday gift I received on June 23 when the FDA approved the indication of datopotamab deruxtecan for people with lung cancers. We have another drug, our third ADC (antibody-drug conjugate) to fight lung cancer, so that’s a gift.
Let’s talk a little bit about that agent. It’s an interesting twist in our practice patterns. What can the drug do? It had a response rate of 45%, which is really important in patients that had EGFR mutations with progression on osimertinib. We really need drugs in that space. The duration of response was about 7 months, which is significant.
One interesting thing in the approval, [was] that the response rate of the blinded folks was greater than that in the investigator-assessed response by about 10%. It’s very interesting. Clearly, we have another drug, and we have it in a space where we need it.
Let’s talk a bit about the toxicity. I’m going to focus more on the paper by Bardia et al that compared datopotamab deruxtecan to various chemo drugs in breast cancer, not in lung cancer. You can take this a little bit with a grain of salt.
First, they saw a whole different array of side effects with datopotamab deruxtecan, things that we don’t normally deal with here. Nausea, stomatitis, alopecia, dry eye, and vomiting. All of those were more than 10% more common in patients that received datopotamab deruxtecan compared to the control. The only things that were more common with the control were neutropenia, leukopenia, and hand-foot syndrome in patients that had capecitabine.
One thing, though, is while you say, “Oh, these weren’t dangerous side effects,” they surely were lifestyle altering. Nobody wants to have these side effects on a daily basis. Again, there’s an increasing awareness about these kinds of lower-grade but still lifestyle-disrupting side effects. When it goes on day after day, you really have to balance that into the benefit you’re going to receive.
I think the second important point is how, when we use this drug, we’re going to have to go to another level to deal with the adverse effects that we are going to see. The first would be nausea and emesis. It is a highly emetogenic regimen based on the NCCN (National Comprehensive Cancer Network) guidelines, so you would need either 3 or 4 antiemetic drugs. That’s number one.
Number two, because of the potential eye problems, you need an eye exam before treatment — and the label says at least annually — with any symptoms. I think it’s very important that you give the patients eyedrops, and in general, the preservative-free eyedrops are the ones that are most effective.
Stomatitis is a very common side effect with that agent. It’s really not seen with the other drugs that even contain the same warhead. There, dexamethasone rinses are important. Now, this is a compounded medicine so you need to be very careful in making sure that you identify pharmacies that will prepare this and will have it available for the patients that need it.
Last, there is the risk of hypersensitivity reactions and there’s a recommendation for premedication for that. As you think about using datopotamab deruxtecan, you need to have all your ducks in a row to treat side effects. You need prophylaxis for hypersensitivity reactions, nausea, and emesis.
The patient will need an eye exam. You need to prepare the patient for possible dry eye and teach them which eyedrops are the best. You also need to ensure the availability of dexamethasone rinses and mouth washes. All that needs to be in place to make sure that the patient can safely use the drug.
I think it’s going to be a useful drug. We don’t yet have a uniformly available way to select patients for its use other than EGFR. I should note that the approval is for EGFR-mutated lung cancers. It doesn’t say which type of mutation, so that would give you some latitude in giving it for exon 20 atypicals as well as for the common sensitizing mutation.
We have another drug. It’s clearly going to be a useful one. It clearly comes with many adverse effects that we don’t normally treat on an everyday basis, we’re used to the diarrhea and skin changes that come on with the EGFR TKIs.
This pattern of side effects is different and requires some additional attention, but with it, the drug can be useful. I’m glad that we have yet another way to fight this disease.
Mark G. Kris, MD, Professor of Medicine, Weill Cornell Medical College; Attending Physician, Department of Medicine, Memorial Sloan Kettering Cancer Center, New York, New York , has disclosed the following relevant financial relationships:
Serve(d) as a director, officer, partner, employee, advisor, consultant, or trustee for: AstraZeneca; Bristol-Myers Squibb; Merck; Daiichi Sankyo; Received research grant from: National Institute of Health; Received income in an amount equal to or greater than $250 from: AstraZeneca; Bristol-Myers Squibb; Merck; Daiichi Sankyo Others: Editorial support from Genentech
A version of this article first appeared on Medscape.com.
Lung Cancer: Mortality Trends in Veterans and New Treatments
Lung Cancer: Mortality Trends in Veterans and New Treatments
Click to view more from Cancer Data Trends 2025.
- Tehzeeb J, Mahmood F, Gemoets D, Azem A, Mehdi SA. Epidemiology and survival
trends of lung carcinoids in the veteran population. J Clin Oncol. 2023;41:e21049.
doi:10.1200/JCO.2023.41.16_suppl.e21049 - Moghanaki D, Taylor J, Bryant AK, et al. Lung Cancer Survival Trends in the Veterans
Health Administration. Clin Lung Cancer. 2024;25(3):225-232. doi:10.1016/j.
cllc.2024.02.009 - Jalal SI, Guo A, Ahmed S, Kelley MJ. Analysis of actionable genetic alterations in
lung carcinoma from the VA National Precision Oncology Program. Semin Oncol.
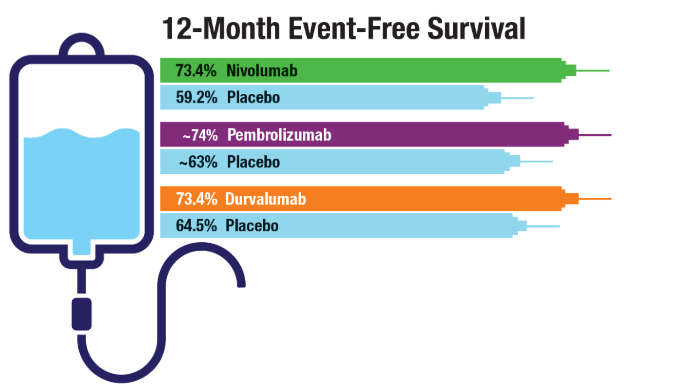
2022;49(3-4):265-274. doi:10.1053/j.seminoncol.2022.06.014 - Cascone T, Awad MM, Spicer JD, et al; for the CheckMate 77T Investigators.
Perioperative Nivolumab in Resectable Lung Cancer. N Engl J Med.
2024;390(19):1756-1769. doi:10.1056/NEJMoa2311926 - Wakelee H, Liberman M, Kato T, et al; for the KEYNOTE-671 Investigators.
Perioperative Pembrolizumab for Early-Stage Non-Small-Cell Lung Cancer. N Engl J
Med. 2023;389(6):491-503. doi:10.1056/NEJMoa2302983 - Heymach JV, Harpole D, Mitsudomi T, et al; for the AEGEAN Investigators.
Perioperative Durvalumab for Resectable Non-Small-Cell Lung Cancer. N Engl J
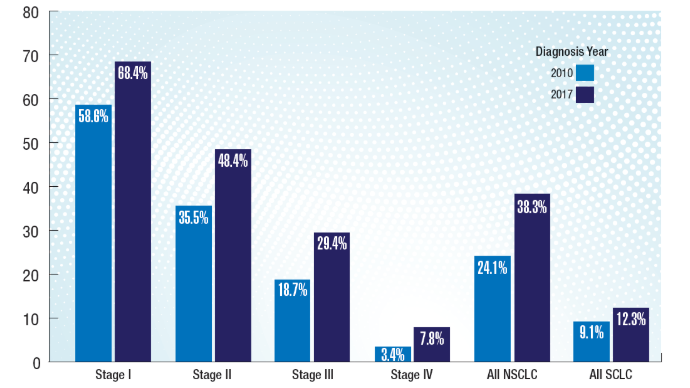
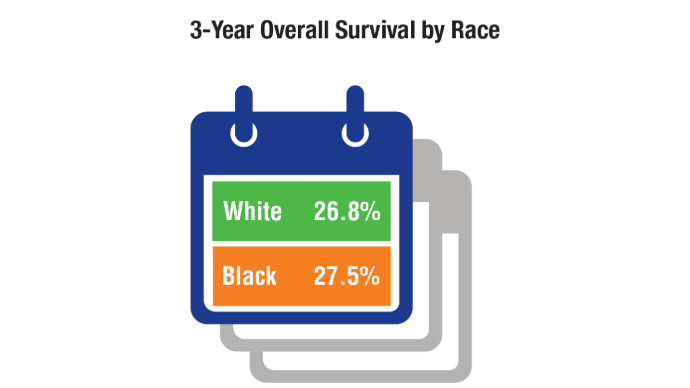
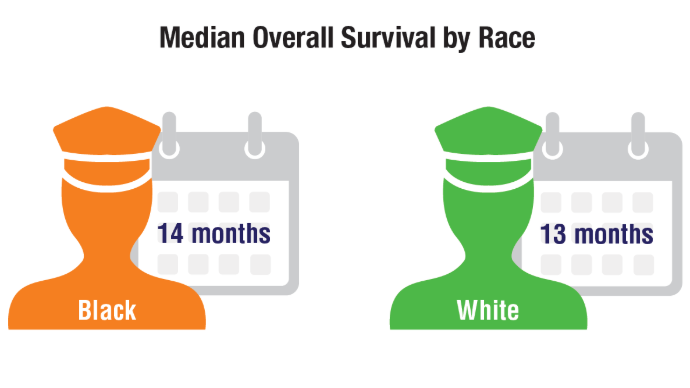
Med. 2023;389(18):1672-1684. doi:10.1056/NEJMoa2304875 - Duncan FC, Al Nasrallah N, Nephew L, et al. Racial disparities in staging, treatment,
and mortality in non-small cell lung cancer. Transl Lung Cancer Res. 2024;13(1):76-
94. doi:10.21037/tlcr-23-407
Click to view more from Cancer Data Trends 2025.
Click to view more from Cancer Data Trends 2025.
- Tehzeeb J, Mahmood F, Gemoets D, Azem A, Mehdi SA. Epidemiology and survival
trends of lung carcinoids in the veteran population. J Clin Oncol. 2023;41:e21049.
doi:10.1200/JCO.2023.41.16_suppl.e21049 - Moghanaki D, Taylor J, Bryant AK, et al. Lung Cancer Survival Trends in the Veterans
Health Administration. Clin Lung Cancer. 2024;25(3):225-232. doi:10.1016/j.
cllc.2024.02.009 - Jalal SI, Guo A, Ahmed S, Kelley MJ. Analysis of actionable genetic alterations in
lung carcinoma from the VA National Precision Oncology Program. Semin Oncol.
2022;49(3-4):265-274. doi:10.1053/j.seminoncol.2022.06.014 - Cascone T, Awad MM, Spicer JD, et al; for the CheckMate 77T Investigators.
Perioperative Nivolumab in Resectable Lung Cancer. N Engl J Med.
2024;390(19):1756-1769. doi:10.1056/NEJMoa2311926 - Wakelee H, Liberman M, Kato T, et al; for the KEYNOTE-671 Investigators.
Perioperative Pembrolizumab for Early-Stage Non-Small-Cell Lung Cancer. N Engl J
Med. 2023;389(6):491-503. doi:10.1056/NEJMoa2302983 - Heymach JV, Harpole D, Mitsudomi T, et al; for the AEGEAN Investigators.
Perioperative Durvalumab for Resectable Non-Small-Cell Lung Cancer. N Engl J
Med. 2023;389(18):1672-1684. doi:10.1056/NEJMoa2304875 - Duncan FC, Al Nasrallah N, Nephew L, et al. Racial disparities in staging, treatment,
and mortality in non-small cell lung cancer. Transl Lung Cancer Res. 2024;13(1):76-
94. doi:10.21037/tlcr-23-407
- Tehzeeb J, Mahmood F, Gemoets D, Azem A, Mehdi SA. Epidemiology and survival
trends of lung carcinoids in the veteran population. J Clin Oncol. 2023;41:e21049.
doi:10.1200/JCO.2023.41.16_suppl.e21049 - Moghanaki D, Taylor J, Bryant AK, et al. Lung Cancer Survival Trends in the Veterans
Health Administration. Clin Lung Cancer. 2024;25(3):225-232. doi:10.1016/j.
cllc.2024.02.009 - Jalal SI, Guo A, Ahmed S, Kelley MJ. Analysis of actionable genetic alterations in
lung carcinoma from the VA National Precision Oncology Program. Semin Oncol.
2022;49(3-4):265-274. doi:10.1053/j.seminoncol.2022.06.014 - Cascone T, Awad MM, Spicer JD, et al; for the CheckMate 77T Investigators.
Perioperative Nivolumab in Resectable Lung Cancer. N Engl J Med.
2024;390(19):1756-1769. doi:10.1056/NEJMoa2311926 - Wakelee H, Liberman M, Kato T, et al; for the KEYNOTE-671 Investigators.
Perioperative Pembrolizumab for Early-Stage Non-Small-Cell Lung Cancer. N Engl J
Med. 2023;389(6):491-503. doi:10.1056/NEJMoa2302983 - Heymach JV, Harpole D, Mitsudomi T, et al; for the AEGEAN Investigators.
Perioperative Durvalumab for Resectable Non-Small-Cell Lung Cancer. N Engl J
Med. 2023;389(18):1672-1684. doi:10.1056/NEJMoa2304875 - Duncan FC, Al Nasrallah N, Nephew L, et al. Racial disparities in staging, treatment,
and mortality in non-small cell lung cancer. Transl Lung Cancer Res. 2024;13(1):76-
94. doi:10.21037/tlcr-23-407
Lung Cancer: Mortality Trends in Veterans and New Treatments
Lung Cancer: Mortality Trends in Veterans and New Treatments
Lung Cancer Screening Is the Push Smokers Need to Quit
Quitting smoking is challenging, particularly when resources are limited. A recent study in the United States confirmed that an intensive program combining behavioral therapy and medication, linked to a lung cancer screening program, offers the highest success rate. However, its long-term success was similar to that of telephone counseling and drug therapy.
Pulmonologist and experienced smoking cessation specialist from Stuttgart, Germany, Alexander Rupp, MD, emphasized the importance of leveraging routine healthcare interactions to encourage smoking cessation. “Although every doctor-patient contact offers the opportunity to discuss the risks of smoking and the opportunities for smoking cessation, the ‘window of opportunity’ is very wide, especially during lung cancer screening,” he said.
Germany is preparing to launch a lung cancer screening program for high-risk individuals, primarily current smokers and former smokers. Following the establishment of radiation protection regulations for such a program last year, the German Federal Joint Committee is currently working on its design. The initiative could be a game-changer for smoking cessation.
Lung cancer screening has been available for smokers in the United States for some time. Paul M. Cinciripini, PhD, and colleagues from the University of Texas MD Anderson Cancer Center, Houston, examined three smoking cessation strategies with decreasing treatment intensity among screening participants.
Unique Opportunity
Previous studies have shown that participation in a lung cancer screening program — typically offered only to high-risk individuals — significantly increases motivation to quit smoking.
“Repeated contact with doctors, repeated CT scans, and especially the findings that require monitoring all contribute to this effect,” explained Rupp, who regularly offers smoking cessation courses.
It has long been known how smoking cessation works best. “The gold standard is a combination of behavioral therapy support and drug treatment — if there is an addiction and withdrawal symptoms occur after quitting, which is the case for the majority of smokers,” Rupp explained.
The US study reinforced what is already well known: More intensive treatment approaches lead to higher quit rates.
“We know that the more intensively we look after smokers, the higher the quit rate. This applies in both areas: The more therapy sessions we do and the more often we prescribe medication, the more likely the patients are to succeed in remaining abstinent,” Rupp said.
However, resources for intensive smoking cessation programs are limited. A database maintained by the German Cancer Research Center and the German Federal Center for Health Education lists only 455 providers of smoking cessation courses in Germany, “not all of which even work on an evidence-based basis,” Rupp emphasized. Given that there are around 16 million smokers in Germany, there is an urgent need for smoking cessation programs that are less resource-intensive.
Intensity Variations
The US study compared three smoking cessation strategies of varying intensities, integrating behavioral counseling and medication.
Group 1: An integrated program with eight behavioral therapy sessions and 10-12 weeks of nicotine replacement therapy or medication (bupropion or varenicline).
Group 2: Lighter version of the integrated program. It consisted of four telephone consultations, written materials, online support, and 12 weeks of nicotine replacement therapy or medication prescribed by a radiologist.
Group 3: The least intensive approach, with 12 weeks of nicotine replacement therapy alone.
Each strategy was evaluated in 210 lung cancer screening participants aged 55-64 years who smoked an average of 15-20 cigarettes per day.
After 3 months, significantly more participants in the most intensive program (Group 1, 37.1%) had quit smoking than those in the other two groups (Group 2, 27.1%; Group 3, 25.2%).
But after 6 months, the difference between Groups 1 and 2 was not significant. The quit rates were as follows: Group 1, 32.4%; Group 2, 27.6%; and Group 3, 20.5%.
“It can be concluded from these results that the intensity of smoking cessation can be reduced to a certain extent as long as the combination of behavioral counseling and medication is given,” Rupp concluded.
Digital Solutions
Another new possibility, which was not examined in the US study, is digital health applications.
Smoke Free is a digital health application that provides behavioral therapy support for smoking cessation and is available in both German and English. Designed to replicate structured smoking cessation programs and offers an accessible alternative for individuals seeking to quit smoking.
Rupp emphasized the potential of digital tools like Smoke Free to expand access to effective smoking cessation strategies, particularly for those unable to attend in-person programs. While traditional cessation programs are limited in availability, digital apps can increase engagement in and adherence to smoking cessation efforts.
However, the biggest hurdle is smokers’ procrastination: “If you make smokers an offer, they usually do not take action afterward because they are caught in their ambivalence about whether they should quit or not.”
Policy Implications
This makes smoking cessation a mandatory component of lung cancer screening in the future. “It’s about cancer, and patients are really afraid of that,” Rupp advocated.
In a position paper, the German Respiratory Society, supported by multiple medical societies, has called for smoking cessation to be integrated into lung cancer screening protocols, with full coverage of counseling and medication by health insurance.
“Smoking cessation must be a mandatory component. If a participant in the lung cancer screening does not want this, then he or she must actively object,” stressed Rupp, lead author of the position paper. Also, the costs of smoking cessation, including those of withdrawal-inhibiting medication, must be fully covered by statutory health insurance, which has not been the case to date.
“That’s the only thing that makes sense. You can’t deny an addict access to proven treatments, especially when we know that a smoker who quits spontaneously without support has a relapse rate of 95%-97%, and the medication per se increases the quit rate by a factor of two or three,” Rupp concluded.
This story was translated and adapted from Medscape’s German edition using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
Quitting smoking is challenging, particularly when resources are limited. A recent study in the United States confirmed that an intensive program combining behavioral therapy and medication, linked to a lung cancer screening program, offers the highest success rate. However, its long-term success was similar to that of telephone counseling and drug therapy.
Pulmonologist and experienced smoking cessation specialist from Stuttgart, Germany, Alexander Rupp, MD, emphasized the importance of leveraging routine healthcare interactions to encourage smoking cessation. “Although every doctor-patient contact offers the opportunity to discuss the risks of smoking and the opportunities for smoking cessation, the ‘window of opportunity’ is very wide, especially during lung cancer screening,” he said.
Germany is preparing to launch a lung cancer screening program for high-risk individuals, primarily current smokers and former smokers. Following the establishment of radiation protection regulations for such a program last year, the German Federal Joint Committee is currently working on its design. The initiative could be a game-changer for smoking cessation.
Lung cancer screening has been available for smokers in the United States for some time. Paul M. Cinciripini, PhD, and colleagues from the University of Texas MD Anderson Cancer Center, Houston, examined three smoking cessation strategies with decreasing treatment intensity among screening participants.
Unique Opportunity
Previous studies have shown that participation in a lung cancer screening program — typically offered only to high-risk individuals — significantly increases motivation to quit smoking.
“Repeated contact with doctors, repeated CT scans, and especially the findings that require monitoring all contribute to this effect,” explained Rupp, who regularly offers smoking cessation courses.
It has long been known how smoking cessation works best. “The gold standard is a combination of behavioral therapy support and drug treatment — if there is an addiction and withdrawal symptoms occur after quitting, which is the case for the majority of smokers,” Rupp explained.
The US study reinforced what is already well known: More intensive treatment approaches lead to higher quit rates.
“We know that the more intensively we look after smokers, the higher the quit rate. This applies in both areas: The more therapy sessions we do and the more often we prescribe medication, the more likely the patients are to succeed in remaining abstinent,” Rupp said.
However, resources for intensive smoking cessation programs are limited. A database maintained by the German Cancer Research Center and the German Federal Center for Health Education lists only 455 providers of smoking cessation courses in Germany, “not all of which even work on an evidence-based basis,” Rupp emphasized. Given that there are around 16 million smokers in Germany, there is an urgent need for smoking cessation programs that are less resource-intensive.
Intensity Variations
The US study compared three smoking cessation strategies of varying intensities, integrating behavioral counseling and medication.
Group 1: An integrated program with eight behavioral therapy sessions and 10-12 weeks of nicotine replacement therapy or medication (bupropion or varenicline).
Group 2: Lighter version of the integrated program. It consisted of four telephone consultations, written materials, online support, and 12 weeks of nicotine replacement therapy or medication prescribed by a radiologist.
Group 3: The least intensive approach, with 12 weeks of nicotine replacement therapy alone.
Each strategy was evaluated in 210 lung cancer screening participants aged 55-64 years who smoked an average of 15-20 cigarettes per day.
After 3 months, significantly more participants in the most intensive program (Group 1, 37.1%) had quit smoking than those in the other two groups (Group 2, 27.1%; Group 3, 25.2%).
But after 6 months, the difference between Groups 1 and 2 was not significant. The quit rates were as follows: Group 1, 32.4%; Group 2, 27.6%; and Group 3, 20.5%.
“It can be concluded from these results that the intensity of smoking cessation can be reduced to a certain extent as long as the combination of behavioral counseling and medication is given,” Rupp concluded.
Digital Solutions
Another new possibility, which was not examined in the US study, is digital health applications.
Smoke Free is a digital health application that provides behavioral therapy support for smoking cessation and is available in both German and English. Designed to replicate structured smoking cessation programs and offers an accessible alternative for individuals seeking to quit smoking.
Rupp emphasized the potential of digital tools like Smoke Free to expand access to effective smoking cessation strategies, particularly for those unable to attend in-person programs. While traditional cessation programs are limited in availability, digital apps can increase engagement in and adherence to smoking cessation efforts.
However, the biggest hurdle is smokers’ procrastination: “If you make smokers an offer, they usually do not take action afterward because they are caught in their ambivalence about whether they should quit or not.”
Policy Implications
This makes smoking cessation a mandatory component of lung cancer screening in the future. “It’s about cancer, and patients are really afraid of that,” Rupp advocated.
In a position paper, the German Respiratory Society, supported by multiple medical societies, has called for smoking cessation to be integrated into lung cancer screening protocols, with full coverage of counseling and medication by health insurance.
“Smoking cessation must be a mandatory component. If a participant in the lung cancer screening does not want this, then he or she must actively object,” stressed Rupp, lead author of the position paper. Also, the costs of smoking cessation, including those of withdrawal-inhibiting medication, must be fully covered by statutory health insurance, which has not been the case to date.
“That’s the only thing that makes sense. You can’t deny an addict access to proven treatments, especially when we know that a smoker who quits spontaneously without support has a relapse rate of 95%-97%, and the medication per se increases the quit rate by a factor of two or three,” Rupp concluded.
This story was translated and adapted from Medscape’s German edition using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
Quitting smoking is challenging, particularly when resources are limited. A recent study in the United States confirmed that an intensive program combining behavioral therapy and medication, linked to a lung cancer screening program, offers the highest success rate. However, its long-term success was similar to that of telephone counseling and drug therapy.
Pulmonologist and experienced smoking cessation specialist from Stuttgart, Germany, Alexander Rupp, MD, emphasized the importance of leveraging routine healthcare interactions to encourage smoking cessation. “Although every doctor-patient contact offers the opportunity to discuss the risks of smoking and the opportunities for smoking cessation, the ‘window of opportunity’ is very wide, especially during lung cancer screening,” he said.
Germany is preparing to launch a lung cancer screening program for high-risk individuals, primarily current smokers and former smokers. Following the establishment of radiation protection regulations for such a program last year, the German Federal Joint Committee is currently working on its design. The initiative could be a game-changer for smoking cessation.
Lung cancer screening has been available for smokers in the United States for some time. Paul M. Cinciripini, PhD, and colleagues from the University of Texas MD Anderson Cancer Center, Houston, examined three smoking cessation strategies with decreasing treatment intensity among screening participants.
Unique Opportunity
Previous studies have shown that participation in a lung cancer screening program — typically offered only to high-risk individuals — significantly increases motivation to quit smoking.
“Repeated contact with doctors, repeated CT scans, and especially the findings that require monitoring all contribute to this effect,” explained Rupp, who regularly offers smoking cessation courses.
It has long been known how smoking cessation works best. “The gold standard is a combination of behavioral therapy support and drug treatment — if there is an addiction and withdrawal symptoms occur after quitting, which is the case for the majority of smokers,” Rupp explained.
The US study reinforced what is already well known: More intensive treatment approaches lead to higher quit rates.
“We know that the more intensively we look after smokers, the higher the quit rate. This applies in both areas: The more therapy sessions we do and the more often we prescribe medication, the more likely the patients are to succeed in remaining abstinent,” Rupp said.
However, resources for intensive smoking cessation programs are limited. A database maintained by the German Cancer Research Center and the German Federal Center for Health Education lists only 455 providers of smoking cessation courses in Germany, “not all of which even work on an evidence-based basis,” Rupp emphasized. Given that there are around 16 million smokers in Germany, there is an urgent need for smoking cessation programs that are less resource-intensive.
Intensity Variations
The US study compared three smoking cessation strategies of varying intensities, integrating behavioral counseling and medication.
Group 1: An integrated program with eight behavioral therapy sessions and 10-12 weeks of nicotine replacement therapy or medication (bupropion or varenicline).
Group 2: Lighter version of the integrated program. It consisted of four telephone consultations, written materials, online support, and 12 weeks of nicotine replacement therapy or medication prescribed by a radiologist.
Group 3: The least intensive approach, with 12 weeks of nicotine replacement therapy alone.
Each strategy was evaluated in 210 lung cancer screening participants aged 55-64 years who smoked an average of 15-20 cigarettes per day.
After 3 months, significantly more participants in the most intensive program (Group 1, 37.1%) had quit smoking than those in the other two groups (Group 2, 27.1%; Group 3, 25.2%).
But after 6 months, the difference between Groups 1 and 2 was not significant. The quit rates were as follows: Group 1, 32.4%; Group 2, 27.6%; and Group 3, 20.5%.
“It can be concluded from these results that the intensity of smoking cessation can be reduced to a certain extent as long as the combination of behavioral counseling and medication is given,” Rupp concluded.
Digital Solutions
Another new possibility, which was not examined in the US study, is digital health applications.
Smoke Free is a digital health application that provides behavioral therapy support for smoking cessation and is available in both German and English. Designed to replicate structured smoking cessation programs and offers an accessible alternative for individuals seeking to quit smoking.
Rupp emphasized the potential of digital tools like Smoke Free to expand access to effective smoking cessation strategies, particularly for those unable to attend in-person programs. While traditional cessation programs are limited in availability, digital apps can increase engagement in and adherence to smoking cessation efforts.
However, the biggest hurdle is smokers’ procrastination: “If you make smokers an offer, they usually do not take action afterward because they are caught in their ambivalence about whether they should quit or not.”
Policy Implications
This makes smoking cessation a mandatory component of lung cancer screening in the future. “It’s about cancer, and patients are really afraid of that,” Rupp advocated.
In a position paper, the German Respiratory Society, supported by multiple medical societies, has called for smoking cessation to be integrated into lung cancer screening protocols, with full coverage of counseling and medication by health insurance.
“Smoking cessation must be a mandatory component. If a participant in the lung cancer screening does not want this, then he or she must actively object,” stressed Rupp, lead author of the position paper. Also, the costs of smoking cessation, including those of withdrawal-inhibiting medication, must be fully covered by statutory health insurance, which has not been the case to date.
“That’s the only thing that makes sense. You can’t deny an addict access to proven treatments, especially when we know that a smoker who quits spontaneously without support has a relapse rate of 95%-97%, and the medication per se increases the quit rate by a factor of two or three,” Rupp concluded.
This story was translated and adapted from Medscape’s German edition using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.

MRI-Invisible Prostate Lesions: Are They Dangerous?
MRI-invisible prostate lesions. It sounds like the stuff of science fiction and fantasy, a creation from the minds of H.G. Wells, who wrote The Invisible Man, or J.K. Rowling, who authored the Harry Potter series.
But MRI-invisible prostate lesions are real. And what these lesions may, or may not, indicate is the subject of intense debate.
MRI plays an increasingly important role in detecting and diagnosing prostate cancer, staging prostate cancer as well as monitoring disease progression. However, on occasion, a puzzling phenomenon arises. Certain prostate lesions that appear when pathologists examine biopsied tissue samples under a microscope are not visible on MRI. The prostate tissue will, instead, appear normal to a radiologist’s eye.
Some experts believe these MRI-invisible lesions are nothing to worry about.
If the clinician can’t see the cancer on MRI, then it simply isn’t a threat, according to Mark Emberton, MD, a pioneer in prostate MRIs and director of interventional oncology at University College London, England.
Laurence Klotz, MD, of the University of Toronto, Ontario, Canada, agreed, noting that “invisible cancers are clinically insignificant and don’t require systematic biopsies.”
Emberton and Klotz compared MRI-invisible lesions to grade group 1 prostate cancer (Gleason score ≤ 6) — the least aggressive category that indicates the cancer that is not likely to spread or kill. For patients on active surveillance, those with MRI-invisible cancers do drastically better than those with visible cancers, Klotz explained.
But other experts in the field are skeptical that MRI-invisible lesions are truly innocuous.
Although statistically an MRI-visible prostate lesion indicates a more aggressive tumor, that is not always the case for every individual, said Brian Helfand, MD, PhD, chief of urology at NorthShore University Health System, Evanston, Illinois.
MRIs can lead to false negatives in about 10%-20% of patients who have clinically significant prostate cancer, though estimates vary.
In one analysis, 16% of men with no suspicious lesions on MRI had clinically significant prostate cancer identified after undergoing a systematic biopsy. Another analysis found that about 35% of MRI-invisible prostate cancers identified via biopsy were clinically significant.
Other studies, however, have indicated that negative MRI results accurately indicate patients at low risk of developing clinically significant cancers. A recent JAMA Oncology analysis, for instance, found that only seven of 233 men (3%) with negative MRI results at baseline who completed 3 years of monitoring were diagnosed with clinically significant prostate cancer.
When a patient has an MRI-invisible prostate tumor, there are a couple of reasons the MRI may not be picking it up, said urologic oncologist Alexander Putnam Cole, MD, assistant professor of surgery, Harvard Medical School, Boston, Massachusetts. “One is that the cancer is aggressive but just very small,” said Cole.
“Another possibility is that the cancer looks very similar to background prostate tissue, which is something that you might expect if you think about more of a low-grade cancer,” he explained.
The experience level of the radiologist interpreting the MRI can also play into the accuracy of the reading.
But Cole agreed that “in general, MRI visibility is associated with molecular and histologic features of progression and aggressiveness and non-visible cancers are less likely to have aggressive features.”
The genomic profiles of MRI-visible and -invisible cancers bear this out.
According to Todd Morgan, MD, chief of urologic oncology at Michigan Medicine, University of Michigan, Ann Arbor, the gene expression in visible disease tends to be linked to more aggressive prostate tumors whereas gene expression in invisible disease does not.
In one analysis, for instance, researchers found that four genes — PHYHD1, CENPF, ALDH2, and GDF15 — associated with worse progression-free survival and metastasis-free survival in prostate cancer also predicted MRI visibility.
“Genes that are associated with visibility are essentially the same genes that are associated with aggressive cancers,” Klotz said.
Next Steps After Negative MRI Result
What do MRI-invisible lesions mean for patient care? If, for instance, a patient has elevated PSA levels but a normal MRI, is a targeted or systematic biopsy warranted?
The overarching message, according to Klotz, is that “you don’t need to find them.” Klotz noted, however, that patients with a negative MRI result should still be followed with periodic repeat imaging.
Several trials support this approach of using MRI to decide who needs a biopsy and delaying a biopsy in men with normal MRIs.
The recent JAMA Oncology analysis found that, among men with negative MRI results, 86% avoided a biopsy over 3 years, with clinically significant prostate cancer detected in only 4% of men across the study period — four in the initial diagnostic phase and seven in the 3-year monitoring phase. However, during the initial diagnostic phase, more than half the men with positive MRI findings had clinically significant prostate cancer detected.
Another recent study found that patients with negative MRI results were much less likely to upgrade to higher Gleason scores over time. Among 522 patients who underwent a systematic and targeted biopsy within 18 months of their grade group 1 designation, 9.2% with negative MRI findings had tumors reclassified as grade group 2 or higher vs 27% with positive MRI findings, and 2.3% with negative MRI findings had tumors reclassified as grade group 3 or higher vs 7.8% with positive MRI findings.
These data suggest that men with grade group 1 cancer and negative MRI result “may be able to avoid confirmatory biopsies until a routine surveillance biopsy in 2-3 years,” according to study author Christian Pavlovich, MD, professor of urologic oncology at the Johns Hopkins University School of Medicine, Baltimore.
Cole used MRI findings to triage who gets a biopsy. When a biopsy is warranted, “I usually recommend adding in some systematic sampling of the other side to assess for nonvisible cancers,” he noted.
Sampling prostate tissue outside the target area “adds maybe 1-2 minutes to the procedure and doesn’t drastically increase the morbidity or risks,” Cole said. It also can help “confirm there is cancer in the MRI target and also confirm there is no cancer in the nonvisible areas.”
According to Klotz, if imaging demonstrates progression, patients should receive a biopsy — in most cases, a targeted biopsy only. And, Klotz noted, skipping routine prostate biopsies in men with negative MRI results can save thousands of men from these procedures, which carry risks for infections and sepsis.
Looking beyond Gleason scores for risk prediction, MRI “visibility is a very powerful risk stratifier,” he said.
A version of this article appeared on Medscape.com.
MRI-invisible prostate lesions. It sounds like the stuff of science fiction and fantasy, a creation from the minds of H.G. Wells, who wrote The Invisible Man, or J.K. Rowling, who authored the Harry Potter series.
But MRI-invisible prostate lesions are real. And what these lesions may, or may not, indicate is the subject of intense debate.
MRI plays an increasingly important role in detecting and diagnosing prostate cancer, staging prostate cancer as well as monitoring disease progression. However, on occasion, a puzzling phenomenon arises. Certain prostate lesions that appear when pathologists examine biopsied tissue samples under a microscope are not visible on MRI. The prostate tissue will, instead, appear normal to a radiologist’s eye.
Some experts believe these MRI-invisible lesions are nothing to worry about.
If the clinician can’t see the cancer on MRI, then it simply isn’t a threat, according to Mark Emberton, MD, a pioneer in prostate MRIs and director of interventional oncology at University College London, England.
Laurence Klotz, MD, of the University of Toronto, Ontario, Canada, agreed, noting that “invisible cancers are clinically insignificant and don’t require systematic biopsies.”
Emberton and Klotz compared MRI-invisible lesions to grade group 1 prostate cancer (Gleason score ≤ 6) — the least aggressive category that indicates the cancer that is not likely to spread or kill. For patients on active surveillance, those with MRI-invisible cancers do drastically better than those with visible cancers, Klotz explained.
But other experts in the field are skeptical that MRI-invisible lesions are truly innocuous.
Although statistically an MRI-visible prostate lesion indicates a more aggressive tumor, that is not always the case for every individual, said Brian Helfand, MD, PhD, chief of urology at NorthShore University Health System, Evanston, Illinois.
MRIs can lead to false negatives in about 10%-20% of patients who have clinically significant prostate cancer, though estimates vary.
In one analysis, 16% of men with no suspicious lesions on MRI had clinically significant prostate cancer identified after undergoing a systematic biopsy. Another analysis found that about 35% of MRI-invisible prostate cancers identified via biopsy were clinically significant.
Other studies, however, have indicated that negative MRI results accurately indicate patients at low risk of developing clinically significant cancers. A recent JAMA Oncology analysis, for instance, found that only seven of 233 men (3%) with negative MRI results at baseline who completed 3 years of monitoring were diagnosed with clinically significant prostate cancer.
When a patient has an MRI-invisible prostate tumor, there are a couple of reasons the MRI may not be picking it up, said urologic oncologist Alexander Putnam Cole, MD, assistant professor of surgery, Harvard Medical School, Boston, Massachusetts. “One is that the cancer is aggressive but just very small,” said Cole.
“Another possibility is that the cancer looks very similar to background prostate tissue, which is something that you might expect if you think about more of a low-grade cancer,” he explained.
The experience level of the radiologist interpreting the MRI can also play into the accuracy of the reading.
But Cole agreed that “in general, MRI visibility is associated with molecular and histologic features of progression and aggressiveness and non-visible cancers are less likely to have aggressive features.”
The genomic profiles of MRI-visible and -invisible cancers bear this out.
According to Todd Morgan, MD, chief of urologic oncology at Michigan Medicine, University of Michigan, Ann Arbor, the gene expression in visible disease tends to be linked to more aggressive prostate tumors whereas gene expression in invisible disease does not.
In one analysis, for instance, researchers found that four genes — PHYHD1, CENPF, ALDH2, and GDF15 — associated with worse progression-free survival and metastasis-free survival in prostate cancer also predicted MRI visibility.
“Genes that are associated with visibility are essentially the same genes that are associated with aggressive cancers,” Klotz said.
Next Steps After Negative MRI Result
What do MRI-invisible lesions mean for patient care? If, for instance, a patient has elevated PSA levels but a normal MRI, is a targeted or systematic biopsy warranted?
The overarching message, according to Klotz, is that “you don’t need to find them.” Klotz noted, however, that patients with a negative MRI result should still be followed with periodic repeat imaging.
Several trials support this approach of using MRI to decide who needs a biopsy and delaying a biopsy in men with normal MRIs.
The recent JAMA Oncology analysis found that, among men with negative MRI results, 86% avoided a biopsy over 3 years, with clinically significant prostate cancer detected in only 4% of men across the study period — four in the initial diagnostic phase and seven in the 3-year monitoring phase. However, during the initial diagnostic phase, more than half the men with positive MRI findings had clinically significant prostate cancer detected.
Another recent study found that patients with negative MRI results were much less likely to upgrade to higher Gleason scores over time. Among 522 patients who underwent a systematic and targeted biopsy within 18 months of their grade group 1 designation, 9.2% with negative MRI findings had tumors reclassified as grade group 2 or higher vs 27% with positive MRI findings, and 2.3% with negative MRI findings had tumors reclassified as grade group 3 or higher vs 7.8% with positive MRI findings.
These data suggest that men with grade group 1 cancer and negative MRI result “may be able to avoid confirmatory biopsies until a routine surveillance biopsy in 2-3 years,” according to study author Christian Pavlovich, MD, professor of urologic oncology at the Johns Hopkins University School of Medicine, Baltimore.
Cole used MRI findings to triage who gets a biopsy. When a biopsy is warranted, “I usually recommend adding in some systematic sampling of the other side to assess for nonvisible cancers,” he noted.
Sampling prostate tissue outside the target area “adds maybe 1-2 minutes to the procedure and doesn’t drastically increase the morbidity or risks,” Cole said. It also can help “confirm there is cancer in the MRI target and also confirm there is no cancer in the nonvisible areas.”
According to Klotz, if imaging demonstrates progression, patients should receive a biopsy — in most cases, a targeted biopsy only. And, Klotz noted, skipping routine prostate biopsies in men with negative MRI results can save thousands of men from these procedures, which carry risks for infections and sepsis.
Looking beyond Gleason scores for risk prediction, MRI “visibility is a very powerful risk stratifier,” he said.
A version of this article appeared on Medscape.com.
MRI-invisible prostate lesions. It sounds like the stuff of science fiction and fantasy, a creation from the minds of H.G. Wells, who wrote The Invisible Man, or J.K. Rowling, who authored the Harry Potter series.
But MRI-invisible prostate lesions are real. And what these lesions may, or may not, indicate is the subject of intense debate.
MRI plays an increasingly important role in detecting and diagnosing prostate cancer, staging prostate cancer as well as monitoring disease progression. However, on occasion, a puzzling phenomenon arises. Certain prostate lesions that appear when pathologists examine biopsied tissue samples under a microscope are not visible on MRI. The prostate tissue will, instead, appear normal to a radiologist’s eye.
Some experts believe these MRI-invisible lesions are nothing to worry about.
If the clinician can’t see the cancer on MRI, then it simply isn’t a threat, according to Mark Emberton, MD, a pioneer in prostate MRIs and director of interventional oncology at University College London, England.
Laurence Klotz, MD, of the University of Toronto, Ontario, Canada, agreed, noting that “invisible cancers are clinically insignificant and don’t require systematic biopsies.”
Emberton and Klotz compared MRI-invisible lesions to grade group 1 prostate cancer (Gleason score ≤ 6) — the least aggressive category that indicates the cancer that is not likely to spread or kill. For patients on active surveillance, those with MRI-invisible cancers do drastically better than those with visible cancers, Klotz explained.
But other experts in the field are skeptical that MRI-invisible lesions are truly innocuous.
Although statistically an MRI-visible prostate lesion indicates a more aggressive tumor, that is not always the case for every individual, said Brian Helfand, MD, PhD, chief of urology at NorthShore University Health System, Evanston, Illinois.
MRIs can lead to false negatives in about 10%-20% of patients who have clinically significant prostate cancer, though estimates vary.
In one analysis, 16% of men with no suspicious lesions on MRI had clinically significant prostate cancer identified after undergoing a systematic biopsy. Another analysis found that about 35% of MRI-invisible prostate cancers identified via biopsy were clinically significant.
Other studies, however, have indicated that negative MRI results accurately indicate patients at low risk of developing clinically significant cancers. A recent JAMA Oncology analysis, for instance, found that only seven of 233 men (3%) with negative MRI results at baseline who completed 3 years of monitoring were diagnosed with clinically significant prostate cancer.
When a patient has an MRI-invisible prostate tumor, there are a couple of reasons the MRI may not be picking it up, said urologic oncologist Alexander Putnam Cole, MD, assistant professor of surgery, Harvard Medical School, Boston, Massachusetts. “One is that the cancer is aggressive but just very small,” said Cole.
“Another possibility is that the cancer looks very similar to background prostate tissue, which is something that you might expect if you think about more of a low-grade cancer,” he explained.
The experience level of the radiologist interpreting the MRI can also play into the accuracy of the reading.
But Cole agreed that “in general, MRI visibility is associated with molecular and histologic features of progression and aggressiveness and non-visible cancers are less likely to have aggressive features.”
The genomic profiles of MRI-visible and -invisible cancers bear this out.
According to Todd Morgan, MD, chief of urologic oncology at Michigan Medicine, University of Michigan, Ann Arbor, the gene expression in visible disease tends to be linked to more aggressive prostate tumors whereas gene expression in invisible disease does not.
In one analysis, for instance, researchers found that four genes — PHYHD1, CENPF, ALDH2, and GDF15 — associated with worse progression-free survival and metastasis-free survival in prostate cancer also predicted MRI visibility.
“Genes that are associated with visibility are essentially the same genes that are associated with aggressive cancers,” Klotz said.
Next Steps After Negative MRI Result
What do MRI-invisible lesions mean for patient care? If, for instance, a patient has elevated PSA levels but a normal MRI, is a targeted or systematic biopsy warranted?
The overarching message, according to Klotz, is that “you don’t need to find them.” Klotz noted, however, that patients with a negative MRI result should still be followed with periodic repeat imaging.
Several trials support this approach of using MRI to decide who needs a biopsy and delaying a biopsy in men with normal MRIs.
The recent JAMA Oncology analysis found that, among men with negative MRI results, 86% avoided a biopsy over 3 years, with clinically significant prostate cancer detected in only 4% of men across the study period — four in the initial diagnostic phase and seven in the 3-year monitoring phase. However, during the initial diagnostic phase, more than half the men with positive MRI findings had clinically significant prostate cancer detected.
Another recent study found that patients with negative MRI results were much less likely to upgrade to higher Gleason scores over time. Among 522 patients who underwent a systematic and targeted biopsy within 18 months of their grade group 1 designation, 9.2% with negative MRI findings had tumors reclassified as grade group 2 or higher vs 27% with positive MRI findings, and 2.3% with negative MRI findings had tumors reclassified as grade group 3 or higher vs 7.8% with positive MRI findings.
These data suggest that men with grade group 1 cancer and negative MRI result “may be able to avoid confirmatory biopsies until a routine surveillance biopsy in 2-3 years,” according to study author Christian Pavlovich, MD, professor of urologic oncology at the Johns Hopkins University School of Medicine, Baltimore.
Cole used MRI findings to triage who gets a biopsy. When a biopsy is warranted, “I usually recommend adding in some systematic sampling of the other side to assess for nonvisible cancers,” he noted.
Sampling prostate tissue outside the target area “adds maybe 1-2 minutes to the procedure and doesn’t drastically increase the morbidity or risks,” Cole said. It also can help “confirm there is cancer in the MRI target and also confirm there is no cancer in the nonvisible areas.”
According to Klotz, if imaging demonstrates progression, patients should receive a biopsy — in most cases, a targeted biopsy only. And, Klotz noted, skipping routine prostate biopsies in men with negative MRI results can save thousands of men from these procedures, which carry risks for infections and sepsis.
Looking beyond Gleason scores for risk prediction, MRI “visibility is a very powerful risk stratifier,” he said.
A version of this article appeared on Medscape.com.
The Evidence Gap: Immunotherapy Timing in Early-Stage NSCLC?
Since October 2023, the US Food and Drug Administration (FDA) has approved three checkpoint inhibitors — pembrolizumab (Keytruda), durvalumab (Imfinzi), and most recently nivolumab (Opdivo) — alongside platinum-containing chemotherapy before surgery and as monotherapy after surgery to treat resectable NSCLC.
But the trials leading to each approval had a major design flaw. The studies failed to distinguish when patients with resectable NSCLC benefited from immunotherapy — before surgery, after surgery, or at both points.
That missing piece has left oncologists without definitive guidance on how best to treat their patients with resectable disease.
Jamie E. Chaft, MD, a thoracic medical oncologist and attending physician at Memorial Sloan Kettering Cancer Center in New York City, was “surprised” that the FDA had approved the three immunotherapy combination regimens without this clarity. Clinicians are now left with studies that can’t evaluate the contribution of the neoadjuvant and adjuvant phases, she said.
But that may soon change.
In July, an FDA advisory committee met to discuss the pending approval of durvalumab.
During this July meeting, the FDA’s Oncologic Drugs Advisory Committee (ODAC) called out issues with AstraZeneca’s design of the trial, expressing concern that AstraZeneca had not followed the agency’s advice to compare patient outcomes with durvalumab in the neoadjuvant and adjuvant phases.
The ODAC panel ultimately voted unanimously in favor of requiring drug companies to demonstrate that patients need immunotherapy both before and after surgery in resectable NSCLC. Several panelists said this requirement should extend beyond NSCLC to other tumor types.
“We need to understand who needs what therapy when,” Daniel Spratt, MD, chairman of the FDA’s ODAC, told Medscape Medical News.
But even if the FDA does require drug companies to assess the benefit of immunotherapy pre- and post-surgery, will oncologists get the answers they need for their patients with resectable NSCLC? Or will the new costly trial design requirements dead-end progress in this space?
Treating Patients Without Clear Evidence
Despite the ODAC’s strong urging to require — not simply request — that drug companies show patients with resectable NSCLC benefit from immunotherapy in both the neoadjuvant and adjuvant settings, the advisory panel did not think durvalumab’s approval should be delayed until the neoadjuvant vs adjuvant question is answered.
A month later, in August, the FDA approved durvalumab for this indication.
Pembrolizumab (Keytruda, Merck) had already been approved 10 months earlier in the neoadjuvant and adjuvant settings in this setting. And most recently, in October, the FDA added nivolumab (Opdivo, Bristol Myers Squibb) to these approvals.
No trial, however, identified when patients benefited from the drug.
Without this understanding, patients may be taking immunotherapy unnecessarily, at significant expense and toxicity risk.
“Toxicities from immunotherapy can occur at any time after initiation,” said Joshua Eric Reuss, MD, a thoracic medical oncologist at Georgetown University’s Lombardi Comprehensive Cancer Center in Washington, DC. And these “risks definitely continue into the adjuvant period.”
So far, the available evidence does suggest that the neoadjuvant phase of immunotherapy confers the greatest benefit, while adjuvant immunotherapy — which can last a year or longer — may expose patients to more costs and toxicities, with no clear benefit.
A 2024 meta-analysis, which included four trials of neoadjuvant-adjuvant immunotherapy and one trial of neoadjuvant immunotherapy in resectable NSCLC, suggested that the addition of adjuvant immunotherapy did not improve event-free survival (hazard ratio [HR], 0.90; P = .59) or overall survival (HR, 1.18; P = .51) compared with neoadjuvant immunotherapy alone.
According to Spratt, “It’s very clear that the neoadjuvant phase is the more important of the two phases.” Given that, “we’re probably overtreating some patients,” said Spratt, also chairman of Radiation Oncology at University Hospitals Seidman Cancer Center and Case Western Reserve University in Cleveland.
Chaft agreed that “there’s very little data that we need the postoperative phase, and what data we do have is post hoc and limited.”
This evidence gap “has created considerable dilemmas” for oncologists and patients who are faced with “the challenge of deciding which therapeutic options or approach are best suited for each individual,” experts wrote in recent consensus recommendations from the International Association for the Study of Lung Cancer.
Clinicians may ultimately be left to make decisions about prescribing postoperative immunotherapy based on their experience and comfort level.
When Chaft’s patients have a pathologic complete response with immunotherapy and chemotherapy in the neoadjuvant phase, “I’m comfortable stopping because the data would suggest they’re almost certainly cured,” she said.
For patients who have viable disease after neoadjuvant therapy, continuing an immunotherapy postoperatively when it didn’t work preoperatively “is not going to make a difference,” Chaft explained. In these cases, Chaft would look to enroll them in a clinical trial evaluating a different regimen because of the risk for relapse.
With patients who did well preoperatively but still have tumor left at the time of surgery, she would discuss continuing the immunotherapy or participating in a trial, she said.
All the FDA-approved regimens are covered by insurance, said Chaft. Clinicians are most comfortable with pembrolizumab because it is the most widely used immunotherapy in advanced NSCLC, she said. But, she added, “there’s really no strong differentiating data between any of the studies; all the results look very comparable.”
When assessing whether a patient may benefit from immunotherapy after surgery, Reuss looks at a range of factors, including disease stage, histology, gene mutations, and pathologic response. Reuss also weighs patient preferences. A patient coming from another country might only want a neoadjuvant regimen, for instance, he said.
That “isn’t exactly the kind of the level one evidence that one likes to see when making treatment decisions,” said Reuss. “Without prospective data, all we can do is cross-trial comparisons and assessment of subgroups.”
If a new regimen comes along that improves outcomes or decision-making, “I think we would pivot to that in a heartbeat,” he said.
But Will FDA Follow ODAC’s Recommendation?
“ODAC has made their point clear,” said Chaft. “Our patients deserve to know that whatever added risk and cost they’re incurring is merited by a clinical outcome.”
Despite the ODAC’s recommendation, it’s not guaranteed that the FDA will follow it.
An FDA spokesperson did not confirm the agency’s decision on the matter but noted that the FDA is “incorporating the panel’s advice.”
Spratt thinks that, going forward, companies will be held to “a higher bar,” but it’s unclear what that bar will look like.
“Whether this is a mandate or a strong recommendation, I think industry is definitely paying attention,” Spratt said. Companies that do not follow the guidance may risk not having their drug approved, “unless it’s just an absolute huge slam dunk of a major benefit to patients.”
In fact, according to Chaft, drug makers seeking approvals of novel entities in this space “won’t have a choice” but to follow any new trial design requirements from the FDA.
Still, getting answers may be a challenge.
Drug companies with immunotherapies already on the market are unlikely to invest the resources to conduct trials comparing the neoadjuvant and adjuvant settings, said Chaft. “It will take too long and cost too much,” she said.
And it remains unclear whether drug companies will decide to stop pursuing novel agents if approvals will ultimately require more expensive and time-consuming trials.
According to Chaft, oncologists have been discussing protocols that could help fill the knowledge gaps. Such trials will be conducted by the National Cancer Institute’s Cooperative Groups, she noted. But it’s early days.
For the time being, with comparative data from phase 3 trials years away, oncologists will have to work with the limited evidence and individual patients in front of them.
Chaft disclosed ties with AstraZeneca, Boehringer Ingelheim, Bristol Myers Squibb, Genentech/Roche, Guardant Health, Janssen Pharmaceuticals, Eli Lilly, and Merck. Reuss disclosed ties with AstraZeneca, Arcus, AbbVie, Bristol Myers Squibb, CatalYm, Daiichi Sankyo, and Eli Lilly, and that Georgetown has received research funding from Genentech/Roche, Verastem, Nuvalent, LUNGevity Foundation, Exelixis, Arcus, and Revolution Medicines. Spratt disclosed ties with Astellas, AstraZeneca, Bayer, Boston Scientific, Janssen Pharmaceuticals, Novartis, and Pfizer.
A version of this article appeared on Medscape.com.
Since October 2023, the US Food and Drug Administration (FDA) has approved three checkpoint inhibitors — pembrolizumab (Keytruda), durvalumab (Imfinzi), and most recently nivolumab (Opdivo) — alongside platinum-containing chemotherapy before surgery and as monotherapy after surgery to treat resectable NSCLC.
But the trials leading to each approval had a major design flaw. The studies failed to distinguish when patients with resectable NSCLC benefited from immunotherapy — before surgery, after surgery, or at both points.
That missing piece has left oncologists without definitive guidance on how best to treat their patients with resectable disease.
Jamie E. Chaft, MD, a thoracic medical oncologist and attending physician at Memorial Sloan Kettering Cancer Center in New York City, was “surprised” that the FDA had approved the three immunotherapy combination regimens without this clarity. Clinicians are now left with studies that can’t evaluate the contribution of the neoadjuvant and adjuvant phases, she said.
But that may soon change.
In July, an FDA advisory committee met to discuss the pending approval of durvalumab.
During this July meeting, the FDA’s Oncologic Drugs Advisory Committee (ODAC) called out issues with AstraZeneca’s design of the trial, expressing concern that AstraZeneca had not followed the agency’s advice to compare patient outcomes with durvalumab in the neoadjuvant and adjuvant phases.
The ODAC panel ultimately voted unanimously in favor of requiring drug companies to demonstrate that patients need immunotherapy both before and after surgery in resectable NSCLC. Several panelists said this requirement should extend beyond NSCLC to other tumor types.
“We need to understand who needs what therapy when,” Daniel Spratt, MD, chairman of the FDA’s ODAC, told Medscape Medical News.
But even if the FDA does require drug companies to assess the benefit of immunotherapy pre- and post-surgery, will oncologists get the answers they need for their patients with resectable NSCLC? Or will the new costly trial design requirements dead-end progress in this space?
Treating Patients Without Clear Evidence
Despite the ODAC’s strong urging to require — not simply request — that drug companies show patients with resectable NSCLC benefit from immunotherapy in both the neoadjuvant and adjuvant settings, the advisory panel did not think durvalumab’s approval should be delayed until the neoadjuvant vs adjuvant question is answered.
A month later, in August, the FDA approved durvalumab for this indication.
Pembrolizumab (Keytruda, Merck) had already been approved 10 months earlier in the neoadjuvant and adjuvant settings in this setting. And most recently, in October, the FDA added nivolumab (Opdivo, Bristol Myers Squibb) to these approvals.
No trial, however, identified when patients benefited from the drug.
Without this understanding, patients may be taking immunotherapy unnecessarily, at significant expense and toxicity risk.
“Toxicities from immunotherapy can occur at any time after initiation,” said Joshua Eric Reuss, MD, a thoracic medical oncologist at Georgetown University’s Lombardi Comprehensive Cancer Center in Washington, DC. And these “risks definitely continue into the adjuvant period.”
So far, the available evidence does suggest that the neoadjuvant phase of immunotherapy confers the greatest benefit, while adjuvant immunotherapy — which can last a year or longer — may expose patients to more costs and toxicities, with no clear benefit.
A 2024 meta-analysis, which included four trials of neoadjuvant-adjuvant immunotherapy and one trial of neoadjuvant immunotherapy in resectable NSCLC, suggested that the addition of adjuvant immunotherapy did not improve event-free survival (hazard ratio [HR], 0.90; P = .59) or overall survival (HR, 1.18; P = .51) compared with neoadjuvant immunotherapy alone.
According to Spratt, “It’s very clear that the neoadjuvant phase is the more important of the two phases.” Given that, “we’re probably overtreating some patients,” said Spratt, also chairman of Radiation Oncology at University Hospitals Seidman Cancer Center and Case Western Reserve University in Cleveland.
Chaft agreed that “there’s very little data that we need the postoperative phase, and what data we do have is post hoc and limited.”
This evidence gap “has created considerable dilemmas” for oncologists and patients who are faced with “the challenge of deciding which therapeutic options or approach are best suited for each individual,” experts wrote in recent consensus recommendations from the International Association for the Study of Lung Cancer.
Clinicians may ultimately be left to make decisions about prescribing postoperative immunotherapy based on their experience and comfort level.
When Chaft’s patients have a pathologic complete response with immunotherapy and chemotherapy in the neoadjuvant phase, “I’m comfortable stopping because the data would suggest they’re almost certainly cured,” she said.
For patients who have viable disease after neoadjuvant therapy, continuing an immunotherapy postoperatively when it didn’t work preoperatively “is not going to make a difference,” Chaft explained. In these cases, Chaft would look to enroll them in a clinical trial evaluating a different regimen because of the risk for relapse.
With patients who did well preoperatively but still have tumor left at the time of surgery, she would discuss continuing the immunotherapy or participating in a trial, she said.
All the FDA-approved regimens are covered by insurance, said Chaft. Clinicians are most comfortable with pembrolizumab because it is the most widely used immunotherapy in advanced NSCLC, she said. But, she added, “there’s really no strong differentiating data between any of the studies; all the results look very comparable.”
When assessing whether a patient may benefit from immunotherapy after surgery, Reuss looks at a range of factors, including disease stage, histology, gene mutations, and pathologic response. Reuss also weighs patient preferences. A patient coming from another country might only want a neoadjuvant regimen, for instance, he said.
That “isn’t exactly the kind of the level one evidence that one likes to see when making treatment decisions,” said Reuss. “Without prospective data, all we can do is cross-trial comparisons and assessment of subgroups.”
If a new regimen comes along that improves outcomes or decision-making, “I think we would pivot to that in a heartbeat,” he said.
But Will FDA Follow ODAC’s Recommendation?
“ODAC has made their point clear,” said Chaft. “Our patients deserve to know that whatever added risk and cost they’re incurring is merited by a clinical outcome.”
Despite the ODAC’s recommendation, it’s not guaranteed that the FDA will follow it.
An FDA spokesperson did not confirm the agency’s decision on the matter but noted that the FDA is “incorporating the panel’s advice.”
Spratt thinks that, going forward, companies will be held to “a higher bar,” but it’s unclear what that bar will look like.
“Whether this is a mandate or a strong recommendation, I think industry is definitely paying attention,” Spratt said. Companies that do not follow the guidance may risk not having their drug approved, “unless it’s just an absolute huge slam dunk of a major benefit to patients.”
In fact, according to Chaft, drug makers seeking approvals of novel entities in this space “won’t have a choice” but to follow any new trial design requirements from the FDA.
Still, getting answers may be a challenge.
Drug companies with immunotherapies already on the market are unlikely to invest the resources to conduct trials comparing the neoadjuvant and adjuvant settings, said Chaft. “It will take too long and cost too much,” she said.
And it remains unclear whether drug companies will decide to stop pursuing novel agents if approvals will ultimately require more expensive and time-consuming trials.
According to Chaft, oncologists have been discussing protocols that could help fill the knowledge gaps. Such trials will be conducted by the National Cancer Institute’s Cooperative Groups, she noted. But it’s early days.
For the time being, with comparative data from phase 3 trials years away, oncologists will have to work with the limited evidence and individual patients in front of them.
Chaft disclosed ties with AstraZeneca, Boehringer Ingelheim, Bristol Myers Squibb, Genentech/Roche, Guardant Health, Janssen Pharmaceuticals, Eli Lilly, and Merck. Reuss disclosed ties with AstraZeneca, Arcus, AbbVie, Bristol Myers Squibb, CatalYm, Daiichi Sankyo, and Eli Lilly, and that Georgetown has received research funding from Genentech/Roche, Verastem, Nuvalent, LUNGevity Foundation, Exelixis, Arcus, and Revolution Medicines. Spratt disclosed ties with Astellas, AstraZeneca, Bayer, Boston Scientific, Janssen Pharmaceuticals, Novartis, and Pfizer.
A version of this article appeared on Medscape.com.
Since October 2023, the US Food and Drug Administration (FDA) has approved three checkpoint inhibitors — pembrolizumab (Keytruda), durvalumab (Imfinzi), and most recently nivolumab (Opdivo) — alongside platinum-containing chemotherapy before surgery and as monotherapy after surgery to treat resectable NSCLC.
But the trials leading to each approval had a major design flaw. The studies failed to distinguish when patients with resectable NSCLC benefited from immunotherapy — before surgery, after surgery, or at both points.
That missing piece has left oncologists without definitive guidance on how best to treat their patients with resectable disease.
Jamie E. Chaft, MD, a thoracic medical oncologist and attending physician at Memorial Sloan Kettering Cancer Center in New York City, was “surprised” that the FDA had approved the three immunotherapy combination regimens without this clarity. Clinicians are now left with studies that can’t evaluate the contribution of the neoadjuvant and adjuvant phases, she said.
But that may soon change.
In July, an FDA advisory committee met to discuss the pending approval of durvalumab.
During this July meeting, the FDA’s Oncologic Drugs Advisory Committee (ODAC) called out issues with AstraZeneca’s design of the trial, expressing concern that AstraZeneca had not followed the agency’s advice to compare patient outcomes with durvalumab in the neoadjuvant and adjuvant phases.
The ODAC panel ultimately voted unanimously in favor of requiring drug companies to demonstrate that patients need immunotherapy both before and after surgery in resectable NSCLC. Several panelists said this requirement should extend beyond NSCLC to other tumor types.
“We need to understand who needs what therapy when,” Daniel Spratt, MD, chairman of the FDA’s ODAC, told Medscape Medical News.
But even if the FDA does require drug companies to assess the benefit of immunotherapy pre- and post-surgery, will oncologists get the answers they need for their patients with resectable NSCLC? Or will the new costly trial design requirements dead-end progress in this space?
Treating Patients Without Clear Evidence
Despite the ODAC’s strong urging to require — not simply request — that drug companies show patients with resectable NSCLC benefit from immunotherapy in both the neoadjuvant and adjuvant settings, the advisory panel did not think durvalumab’s approval should be delayed until the neoadjuvant vs adjuvant question is answered.
A month later, in August, the FDA approved durvalumab for this indication.
Pembrolizumab (Keytruda, Merck) had already been approved 10 months earlier in the neoadjuvant and adjuvant settings in this setting. And most recently, in October, the FDA added nivolumab (Opdivo, Bristol Myers Squibb) to these approvals.
No trial, however, identified when patients benefited from the drug.
Without this understanding, patients may be taking immunotherapy unnecessarily, at significant expense and toxicity risk.
“Toxicities from immunotherapy can occur at any time after initiation,” said Joshua Eric Reuss, MD, a thoracic medical oncologist at Georgetown University’s Lombardi Comprehensive Cancer Center in Washington, DC. And these “risks definitely continue into the adjuvant period.”
So far, the available evidence does suggest that the neoadjuvant phase of immunotherapy confers the greatest benefit, while adjuvant immunotherapy — which can last a year or longer — may expose patients to more costs and toxicities, with no clear benefit.
A 2024 meta-analysis, which included four trials of neoadjuvant-adjuvant immunotherapy and one trial of neoadjuvant immunotherapy in resectable NSCLC, suggested that the addition of adjuvant immunotherapy did not improve event-free survival (hazard ratio [HR], 0.90; P = .59) or overall survival (HR, 1.18; P = .51) compared with neoadjuvant immunotherapy alone.
According to Spratt, “It’s very clear that the neoadjuvant phase is the more important of the two phases.” Given that, “we’re probably overtreating some patients,” said Spratt, also chairman of Radiation Oncology at University Hospitals Seidman Cancer Center and Case Western Reserve University in Cleveland.
Chaft agreed that “there’s very little data that we need the postoperative phase, and what data we do have is post hoc and limited.”
This evidence gap “has created considerable dilemmas” for oncologists and patients who are faced with “the challenge of deciding which therapeutic options or approach are best suited for each individual,” experts wrote in recent consensus recommendations from the International Association for the Study of Lung Cancer.
Clinicians may ultimately be left to make decisions about prescribing postoperative immunotherapy based on their experience and comfort level.
When Chaft’s patients have a pathologic complete response with immunotherapy and chemotherapy in the neoadjuvant phase, “I’m comfortable stopping because the data would suggest they’re almost certainly cured,” she said.
For patients who have viable disease after neoadjuvant therapy, continuing an immunotherapy postoperatively when it didn’t work preoperatively “is not going to make a difference,” Chaft explained. In these cases, Chaft would look to enroll them in a clinical trial evaluating a different regimen because of the risk for relapse.
With patients who did well preoperatively but still have tumor left at the time of surgery, she would discuss continuing the immunotherapy or participating in a trial, she said.
All the FDA-approved regimens are covered by insurance, said Chaft. Clinicians are most comfortable with pembrolizumab because it is the most widely used immunotherapy in advanced NSCLC, she said. But, she added, “there’s really no strong differentiating data between any of the studies; all the results look very comparable.”
When assessing whether a patient may benefit from immunotherapy after surgery, Reuss looks at a range of factors, including disease stage, histology, gene mutations, and pathologic response. Reuss also weighs patient preferences. A patient coming from another country might only want a neoadjuvant regimen, for instance, he said.
That “isn’t exactly the kind of the level one evidence that one likes to see when making treatment decisions,” said Reuss. “Without prospective data, all we can do is cross-trial comparisons and assessment of subgroups.”
If a new regimen comes along that improves outcomes or decision-making, “I think we would pivot to that in a heartbeat,” he said.
But Will FDA Follow ODAC’s Recommendation?
“ODAC has made their point clear,” said Chaft. “Our patients deserve to know that whatever added risk and cost they’re incurring is merited by a clinical outcome.”
Despite the ODAC’s recommendation, it’s not guaranteed that the FDA will follow it.
An FDA spokesperson did not confirm the agency’s decision on the matter but noted that the FDA is “incorporating the panel’s advice.”
Spratt thinks that, going forward, companies will be held to “a higher bar,” but it’s unclear what that bar will look like.
“Whether this is a mandate or a strong recommendation, I think industry is definitely paying attention,” Spratt said. Companies that do not follow the guidance may risk not having their drug approved, “unless it’s just an absolute huge slam dunk of a major benefit to patients.”
In fact, according to Chaft, drug makers seeking approvals of novel entities in this space “won’t have a choice” but to follow any new trial design requirements from the FDA.
Still, getting answers may be a challenge.
Drug companies with immunotherapies already on the market are unlikely to invest the resources to conduct trials comparing the neoadjuvant and adjuvant settings, said Chaft. “It will take too long and cost too much,” she said.
And it remains unclear whether drug companies will decide to stop pursuing novel agents if approvals will ultimately require more expensive and time-consuming trials.
According to Chaft, oncologists have been discussing protocols that could help fill the knowledge gaps. Such trials will be conducted by the National Cancer Institute’s Cooperative Groups, she noted. But it’s early days.
For the time being, with comparative data from phase 3 trials years away, oncologists will have to work with the limited evidence and individual patients in front of them.
Chaft disclosed ties with AstraZeneca, Boehringer Ingelheim, Bristol Myers Squibb, Genentech/Roche, Guardant Health, Janssen Pharmaceuticals, Eli Lilly, and Merck. Reuss disclosed ties with AstraZeneca, Arcus, AbbVie, Bristol Myers Squibb, CatalYm, Daiichi Sankyo, and Eli Lilly, and that Georgetown has received research funding from Genentech/Roche, Verastem, Nuvalent, LUNGevity Foundation, Exelixis, Arcus, and Revolution Medicines. Spratt disclosed ties with Astellas, AstraZeneca, Bayer, Boston Scientific, Janssen Pharmaceuticals, Novartis, and Pfizer.
A version of this article appeared on Medscape.com.