User login
New recommendations address ME/CFS diagnosis and management
New consensus recommendations address diagnosis and management of myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS), with advice that may also be helpful for patients with lingering symptoms following acute COVID-19 infection.

The document was published online Aug. 25, 2021, in the Mayo Clinic Proceedings by the 23-member U.S. ME/CFS Clinician Coalition, headed by Lucinda Bateman, MD, of the Bateman Horne Center of Excellence, Salt Lake City. The document is the culmination of work that began with a summit held at the center in March 2018.
The target audience is both generalist and specialist health care providers. While ME/CFS is estimated to affect up to 2.5 million Americans, more than 90% are either undiagnosed or misdiagnosed with other conditions such as depression. And those who are diagnosed often receive inappropriate, outdated treatments such as psychotherapy and exercise prescriptions.
“Despite myalgic encephalomyelitis/chronic fatigue syndrome affecting millions of people worldwide, many clinicians lack the knowledge to appropriately diagnose or manage ME/CFS. Unfortunately, clinical guidance has been scarce, obsolete, or potentially harmful,” Dr. Bateman and colleagues wrote.
The urgency of appropriate recognition and management of ME/CFS has increased as growing numbers of people are exhibiting signs and symptoms of ME/CFS following acute COVID-19 infection. This isn’t surprising because the illness has long been linked to other infections, including Epstein-Barr virus, the authors noted.
The document covers the epidemiology, impact, and prognosis of ME/CFS, as well as etiology and pathophysiology. “Scientific studies demonstrate multiple dysfunctional organ systems, including neuro, immune, and metabolic, in ME/CFS. These findings are not explained merely by deconditioning,” document coauthor Lily Chu, MD, an independent consultant in Burlingame, Calif., said in an interview.
The document reviews the 2015 U.S. Institute of Medicine (now Academy of Medicine) diagnostic criteria that are now also recommended by the Centers for Disease Control and Prevention. They are based on four main symptoms: substantial reduction or impairment in the ability to engage in preillness levels of occupational, educational, social or personal activities for longer than 6 months; postexertional malaise, a worsening of all current symptoms, that patients often describe as a “crash”; unrefreshing sleep; and cognitive impairment and/or orthostatic intolerance.
“The new diagnostic criteria focusing on the key symptom of postexertional malaise rather than chronic fatigue, which is common in many conditions, may make the diagnostic process quicker and more accurate. Diagnosis now is both an inclusionary and not just exclusionary process, so it’s not necessary to eliminate all causes of fatigue. Diagnose patients who fit the criteria and be alert for it in people with persistent symptoms post COVID,” Dr. Chu said.
The document provides advice for taking a clinical history to obtain the information necessary for making the diagnosis, including use of laboratory testing to rule out other conditions. Physical exams, while they may not reveal specific abnormalities, may help in identifying comorbidities and ruling out alternative diagnoses.
A long list of nonpharmacologic and pharmacologic treatment and management approaches is offered for each of the individual core and common ME/CFS symptoms, including postexertional malaise, orthostatic intolerance, sleep issues, cognitive dysfunction and fatigue, immune dysfunction, pain, and gastrointestinal issues.
The document recommends against using the “outdated standard of care” cognitive-behavioral therapy and graded exercise therapy as primary treatments for the illness. Instead, the authors recommend teaching patients “pacing,” an individualized approach to energy conservation aimed at minimizing the frequency, duration, and severity of postexertional malaise.
Clinicians are also advised to assess patients’ daily living needs and provide support, including acquiring handicap placards, work or school accommodations, and disability benefits.
“There are things clinicians can do now to help patients even without a disease-modifying treatment. These are actions they are already familiar with and carry out for people with other chronic diseases, which often have limited treatment options as well. Don’t underestimate the importance and value of supportive care for patients.” Dr. Chu said.
The recommendations are based primarily on clinical expertise because there are very few randomized trials, and much of the evidence from other types of trials has been flawed, document coauthor Anthony L. Komaroff, MD, of Brigham and Women’s Hospital and Harvard Medical School, both in Boston, said in an interview.
“The sad reality is there aren’t very many large randomized clinical trials with this illness and so what a group of very experienced clinicians did was to gather their collective experience and report it as that. It’s largely uncontrolled experience, but from people who have seen a lot of patients, for what it’s worth to the medical community.”
Dr. Komaroff also advised that clinicians watch out for ME/CFS in patients with long COVID. “If we find that those called long COVID meet ME/CFS criteria, the reason for knowing that is that there are already some treatments that according to experienced clinicians are helpful for ME/CFS, and it would be perfectly appropriate to try some of them in long COVID, particularly the ones that have minimal adverse reactions.”
The guidelines project was supported by the Open Medicine Foundation. Dr. Komaroff reported receiving personal fees from Serimmune outside the submitted work. Dr. Chu has no disclosures.
New consensus recommendations address diagnosis and management of myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS), with advice that may also be helpful for patients with lingering symptoms following acute COVID-19 infection.
The document was published online Aug. 25, 2021, in the Mayo Clinic Proceedings by the 23-member U.S. ME/CFS Clinician Coalition, headed by Lucinda Bateman, MD, of the Bateman Horne Center of Excellence, Salt Lake City. The document is the culmination of work that began with a summit held at the center in March 2018.
The target audience is both generalist and specialist health care providers. While ME/CFS is estimated to affect up to 2.5 million Americans, more than 90% are either undiagnosed or misdiagnosed with other conditions such as depression. And those who are diagnosed often receive inappropriate, outdated treatments such as psychotherapy and exercise prescriptions.
“Despite myalgic encephalomyelitis/chronic fatigue syndrome affecting millions of people worldwide, many clinicians lack the knowledge to appropriately diagnose or manage ME/CFS. Unfortunately, clinical guidance has been scarce, obsolete, or potentially harmful,” Dr. Bateman and colleagues wrote.
The urgency of appropriate recognition and management of ME/CFS has increased as growing numbers of people are exhibiting signs and symptoms of ME/CFS following acute COVID-19 infection. This isn’t surprising because the illness has long been linked to other infections, including Epstein-Barr virus, the authors noted.
The document covers the epidemiology, impact, and prognosis of ME/CFS, as well as etiology and pathophysiology. “Scientific studies demonstrate multiple dysfunctional organ systems, including neuro, immune, and metabolic, in ME/CFS. These findings are not explained merely by deconditioning,” document coauthor Lily Chu, MD, an independent consultant in Burlingame, Calif., said in an interview.
The document reviews the 2015 U.S. Institute of Medicine (now Academy of Medicine) diagnostic criteria that are now also recommended by the Centers for Disease Control and Prevention. They are based on four main symptoms: substantial reduction or impairment in the ability to engage in preillness levels of occupational, educational, social or personal activities for longer than 6 months; postexertional malaise, a worsening of all current symptoms, that patients often describe as a “crash”; unrefreshing sleep; and cognitive impairment and/or orthostatic intolerance.
“The new diagnostic criteria focusing on the key symptom of postexertional malaise rather than chronic fatigue, which is common in many conditions, may make the diagnostic process quicker and more accurate. Diagnosis now is both an inclusionary and not just exclusionary process, so it’s not necessary to eliminate all causes of fatigue. Diagnose patients who fit the criteria and be alert for it in people with persistent symptoms post COVID,” Dr. Chu said.
The document provides advice for taking a clinical history to obtain the information necessary for making the diagnosis, including use of laboratory testing to rule out other conditions. Physical exams, while they may not reveal specific abnormalities, may help in identifying comorbidities and ruling out alternative diagnoses.
A long list of nonpharmacologic and pharmacologic treatment and management approaches is offered for each of the individual core and common ME/CFS symptoms, including postexertional malaise, orthostatic intolerance, sleep issues, cognitive dysfunction and fatigue, immune dysfunction, pain, and gastrointestinal issues.
The document recommends against using the “outdated standard of care” cognitive-behavioral therapy and graded exercise therapy as primary treatments for the illness. Instead, the authors recommend teaching patients “pacing,” an individualized approach to energy conservation aimed at minimizing the frequency, duration, and severity of postexertional malaise.
Clinicians are also advised to assess patients’ daily living needs and provide support, including acquiring handicap placards, work or school accommodations, and disability benefits.
“There are things clinicians can do now to help patients even without a disease-modifying treatment. These are actions they are already familiar with and carry out for people with other chronic diseases, which often have limited treatment options as well. Don’t underestimate the importance and value of supportive care for patients.” Dr. Chu said.
The recommendations are based primarily on clinical expertise because there are very few randomized trials, and much of the evidence from other types of trials has been flawed, document coauthor Anthony L. Komaroff, MD, of Brigham and Women’s Hospital and Harvard Medical School, both in Boston, said in an interview.
“The sad reality is there aren’t very many large randomized clinical trials with this illness and so what a group of very experienced clinicians did was to gather their collective experience and report it as that. It’s largely uncontrolled experience, but from people who have seen a lot of patients, for what it’s worth to the medical community.”
Dr. Komaroff also advised that clinicians watch out for ME/CFS in patients with long COVID. “If we find that those called long COVID meet ME/CFS criteria, the reason for knowing that is that there are already some treatments that according to experienced clinicians are helpful for ME/CFS, and it would be perfectly appropriate to try some of them in long COVID, particularly the ones that have minimal adverse reactions.”
The guidelines project was supported by the Open Medicine Foundation. Dr. Komaroff reported receiving personal fees from Serimmune outside the submitted work. Dr. Chu has no disclosures.
New consensus recommendations address diagnosis and management of myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS), with advice that may also be helpful for patients with lingering symptoms following acute COVID-19 infection.
The document was published online Aug. 25, 2021, in the Mayo Clinic Proceedings by the 23-member U.S. ME/CFS Clinician Coalition, headed by Lucinda Bateman, MD, of the Bateman Horne Center of Excellence, Salt Lake City. The document is the culmination of work that began with a summit held at the center in March 2018.
The target audience is both generalist and specialist health care providers. While ME/CFS is estimated to affect up to 2.5 million Americans, more than 90% are either undiagnosed or misdiagnosed with other conditions such as depression. And those who are diagnosed often receive inappropriate, outdated treatments such as psychotherapy and exercise prescriptions.
“Despite myalgic encephalomyelitis/chronic fatigue syndrome affecting millions of people worldwide, many clinicians lack the knowledge to appropriately diagnose or manage ME/CFS. Unfortunately, clinical guidance has been scarce, obsolete, or potentially harmful,” Dr. Bateman and colleagues wrote.
The urgency of appropriate recognition and management of ME/CFS has increased as growing numbers of people are exhibiting signs and symptoms of ME/CFS following acute COVID-19 infection. This isn’t surprising because the illness has long been linked to other infections, including Epstein-Barr virus, the authors noted.
The document covers the epidemiology, impact, and prognosis of ME/CFS, as well as etiology and pathophysiology. “Scientific studies demonstrate multiple dysfunctional organ systems, including neuro, immune, and metabolic, in ME/CFS. These findings are not explained merely by deconditioning,” document coauthor Lily Chu, MD, an independent consultant in Burlingame, Calif., said in an interview.
The document reviews the 2015 U.S. Institute of Medicine (now Academy of Medicine) diagnostic criteria that are now also recommended by the Centers for Disease Control and Prevention. They are based on four main symptoms: substantial reduction or impairment in the ability to engage in preillness levels of occupational, educational, social or personal activities for longer than 6 months; postexertional malaise, a worsening of all current symptoms, that patients often describe as a “crash”; unrefreshing sleep; and cognitive impairment and/or orthostatic intolerance.
“The new diagnostic criteria focusing on the key symptom of postexertional malaise rather than chronic fatigue, which is common in many conditions, may make the diagnostic process quicker and more accurate. Diagnosis now is both an inclusionary and not just exclusionary process, so it’s not necessary to eliminate all causes of fatigue. Diagnose patients who fit the criteria and be alert for it in people with persistent symptoms post COVID,” Dr. Chu said.
The document provides advice for taking a clinical history to obtain the information necessary for making the diagnosis, including use of laboratory testing to rule out other conditions. Physical exams, while they may not reveal specific abnormalities, may help in identifying comorbidities and ruling out alternative diagnoses.
A long list of nonpharmacologic and pharmacologic treatment and management approaches is offered for each of the individual core and common ME/CFS symptoms, including postexertional malaise, orthostatic intolerance, sleep issues, cognitive dysfunction and fatigue, immune dysfunction, pain, and gastrointestinal issues.
The document recommends against using the “outdated standard of care” cognitive-behavioral therapy and graded exercise therapy as primary treatments for the illness. Instead, the authors recommend teaching patients “pacing,” an individualized approach to energy conservation aimed at minimizing the frequency, duration, and severity of postexertional malaise.
Clinicians are also advised to assess patients’ daily living needs and provide support, including acquiring handicap placards, work or school accommodations, and disability benefits.
“There are things clinicians can do now to help patients even without a disease-modifying treatment. These are actions they are already familiar with and carry out for people with other chronic diseases, which often have limited treatment options as well. Don’t underestimate the importance and value of supportive care for patients.” Dr. Chu said.
The recommendations are based primarily on clinical expertise because there are very few randomized trials, and much of the evidence from other types of trials has been flawed, document coauthor Anthony L. Komaroff, MD, of Brigham and Women’s Hospital and Harvard Medical School, both in Boston, said in an interview.
“The sad reality is there aren’t very many large randomized clinical trials with this illness and so what a group of very experienced clinicians did was to gather their collective experience and report it as that. It’s largely uncontrolled experience, but from people who have seen a lot of patients, for what it’s worth to the medical community.”
Dr. Komaroff also advised that clinicians watch out for ME/CFS in patients with long COVID. “If we find that those called long COVID meet ME/CFS criteria, the reason for knowing that is that there are already some treatments that according to experienced clinicians are helpful for ME/CFS, and it would be perfectly appropriate to try some of them in long COVID, particularly the ones that have minimal adverse reactions.”
The guidelines project was supported by the Open Medicine Foundation. Dr. Komaroff reported receiving personal fees from Serimmune outside the submitted work. Dr. Chu has no disclosures.
FROM THE MAYO CLINIC PROCEEDINGS
Anxiety, inactivity linked to cognitive impairment in Parkinson’s
Parkinson’s disease patients who develop anxiety early in their disease are at risk for reduced physical activity, which promotes further anxiety and cognitive decline, data from nearly 500 individuals show.
Anxiety occurs in 20%-60% of Parkinson’s disease (PD) patients but often goes undiagnosed, wrote Jacob D. Jones, PhD, of California State University, San Bernardino, and colleagues.
“Anxiety can attenuate motivation to engage in physical activity leading to more anxiety and other negative cognitive outcomes,” although physical activity has been shown to improve cognitive function in PD patients, they said. However, physical activity as a mediator between anxiety and cognitive function in PD has not been well studied, they noted.
In a study published in Mental Health and Physical Activity Participants were followed for up to 5 years and completed neuropsychological tests, tests of motor severity, and self-reports on anxiety and physical activity. Anxiety was assessed using the State-Trait Anxiety Inventory-Trait (STAI-T) subscale. Physical activity was assessed using the Physical Activity Scale for the Elderly (PASE). Motor severity was assessed using the Unified Parkinson’s Disease Rating Scale-Part III (UPDRS). The average age of the participants was 61 years, 65% were men, and 96% were White.
Using a direct-effect model, the researchers found that individuals whose anxiety increased during the study period also showed signs of cognitive decline. A significant between-person effect showed that individuals who were generally more anxious also scored lower on cognitive tests over the 5-year study period.
In a mediation model computed with structural equation modeling, physical activity mediated the link between anxiety and cognition, most notably household activity.
“There was a significant within-person association between anxiety and household activities, meaning that individuals who became more anxious over the 5-year study also became less active in the home,” reported Dr. Jones and colleagues.
However, no significant indirect effect was noted regarding the between-person findings of the impact of physical activity on anxiety and cognitive decline. Although more severe anxiety was associated with less activity, cognitive performance was not associated with either type of physical activity.
The presence of a within-person effect “suggests that reductions in physical activity, specifically within the first 5 years of disease onset, may be detrimental to mental health,” the researchers emphasized. Given that the study population was newly diagnosed with PD “it is likely the within-person terms are more sensitive to changes in anxiety, physical activity, and cognition that are more directly the result of the PD process, as opposed to lifestyle/preexisting traits,” they said.
The study findings were limited by several factors, including the use of self-reports to measure physical activity, and the lack of granular information about the details of physical activity, the researchers noted. Another limitation was the inclusion of only newly diagnosed PD patients, which might limit generalizability.
“Future research is warranted to understand if other modes, intensities, or complexities of physical activity impact individuals with PD in a different manner in relation to cognition,” they said.
Dr. Jones and colleagues had no disclosures. The PPMI is supported by the Michael J. Fox Foundation for Parkinson’s Research and funding partners, including numerous pharmaceutical companies.
Parkinson’s disease patients who develop anxiety early in their disease are at risk for reduced physical activity, which promotes further anxiety and cognitive decline, data from nearly 500 individuals show.
Anxiety occurs in 20%-60% of Parkinson’s disease (PD) patients but often goes undiagnosed, wrote Jacob D. Jones, PhD, of California State University, San Bernardino, and colleagues.
“Anxiety can attenuate motivation to engage in physical activity leading to more anxiety and other negative cognitive outcomes,” although physical activity has been shown to improve cognitive function in PD patients, they said. However, physical activity as a mediator between anxiety and cognitive function in PD has not been well studied, they noted.
In a study published in Mental Health and Physical Activity Participants were followed for up to 5 years and completed neuropsychological tests, tests of motor severity, and self-reports on anxiety and physical activity. Anxiety was assessed using the State-Trait Anxiety Inventory-Trait (STAI-T) subscale. Physical activity was assessed using the Physical Activity Scale for the Elderly (PASE). Motor severity was assessed using the Unified Parkinson’s Disease Rating Scale-Part III (UPDRS). The average age of the participants was 61 years, 65% were men, and 96% were White.
Using a direct-effect model, the researchers found that individuals whose anxiety increased during the study period also showed signs of cognitive decline. A significant between-person effect showed that individuals who were generally more anxious also scored lower on cognitive tests over the 5-year study period.
In a mediation model computed with structural equation modeling, physical activity mediated the link between anxiety and cognition, most notably household activity.
“There was a significant within-person association between anxiety and household activities, meaning that individuals who became more anxious over the 5-year study also became less active in the home,” reported Dr. Jones and colleagues.
However, no significant indirect effect was noted regarding the between-person findings of the impact of physical activity on anxiety and cognitive decline. Although more severe anxiety was associated with less activity, cognitive performance was not associated with either type of physical activity.
The presence of a within-person effect “suggests that reductions in physical activity, specifically within the first 5 years of disease onset, may be detrimental to mental health,” the researchers emphasized. Given that the study population was newly diagnosed with PD “it is likely the within-person terms are more sensitive to changes in anxiety, physical activity, and cognition that are more directly the result of the PD process, as opposed to lifestyle/preexisting traits,” they said.
The study findings were limited by several factors, including the use of self-reports to measure physical activity, and the lack of granular information about the details of physical activity, the researchers noted. Another limitation was the inclusion of only newly diagnosed PD patients, which might limit generalizability.
“Future research is warranted to understand if other modes, intensities, or complexities of physical activity impact individuals with PD in a different manner in relation to cognition,” they said.
Dr. Jones and colleagues had no disclosures. The PPMI is supported by the Michael J. Fox Foundation for Parkinson’s Research and funding partners, including numerous pharmaceutical companies.
Parkinson’s disease patients who develop anxiety early in their disease are at risk for reduced physical activity, which promotes further anxiety and cognitive decline, data from nearly 500 individuals show.
Anxiety occurs in 20%-60% of Parkinson’s disease (PD) patients but often goes undiagnosed, wrote Jacob D. Jones, PhD, of California State University, San Bernardino, and colleagues.
“Anxiety can attenuate motivation to engage in physical activity leading to more anxiety and other negative cognitive outcomes,” although physical activity has been shown to improve cognitive function in PD patients, they said. However, physical activity as a mediator between anxiety and cognitive function in PD has not been well studied, they noted.
In a study published in Mental Health and Physical Activity Participants were followed for up to 5 years and completed neuropsychological tests, tests of motor severity, and self-reports on anxiety and physical activity. Anxiety was assessed using the State-Trait Anxiety Inventory-Trait (STAI-T) subscale. Physical activity was assessed using the Physical Activity Scale for the Elderly (PASE). Motor severity was assessed using the Unified Parkinson’s Disease Rating Scale-Part III (UPDRS). The average age of the participants was 61 years, 65% were men, and 96% were White.
Using a direct-effect model, the researchers found that individuals whose anxiety increased during the study period also showed signs of cognitive decline. A significant between-person effect showed that individuals who were generally more anxious also scored lower on cognitive tests over the 5-year study period.
In a mediation model computed with structural equation modeling, physical activity mediated the link between anxiety and cognition, most notably household activity.
“There was a significant within-person association between anxiety and household activities, meaning that individuals who became more anxious over the 5-year study also became less active in the home,” reported Dr. Jones and colleagues.
However, no significant indirect effect was noted regarding the between-person findings of the impact of physical activity on anxiety and cognitive decline. Although more severe anxiety was associated with less activity, cognitive performance was not associated with either type of physical activity.
The presence of a within-person effect “suggests that reductions in physical activity, specifically within the first 5 years of disease onset, may be detrimental to mental health,” the researchers emphasized. Given that the study population was newly diagnosed with PD “it is likely the within-person terms are more sensitive to changes in anxiety, physical activity, and cognition that are more directly the result of the PD process, as opposed to lifestyle/preexisting traits,” they said.
The study findings were limited by several factors, including the use of self-reports to measure physical activity, and the lack of granular information about the details of physical activity, the researchers noted. Another limitation was the inclusion of only newly diagnosed PD patients, which might limit generalizability.
“Future research is warranted to understand if other modes, intensities, or complexities of physical activity impact individuals with PD in a different manner in relation to cognition,” they said.
Dr. Jones and colleagues had no disclosures. The PPMI is supported by the Michael J. Fox Foundation for Parkinson’s Research and funding partners, including numerous pharmaceutical companies.
FROM MENTAL HEALTH AND PHYSICAL ACTIVITY
Stimulating jobs may help stave off dementia onset
Individuals with cognitively stimulating jobs are at a lower risk of developing dementia than their peers with less challenging employment, new research suggests.
Results from a large, multicohort study also showed an association between cognitive stimulation and lower levels of certain plasma proteins, providing possible clues on a protective biological mechanism.
“These new findings support the hypothesis that mental stimulation in adulthood may postpone the onset of dementia,” Mika Kivimäki, PhD, professor and director of the Whitehall II Study, department of epidemiology, University College London, said in an interview.
The results were published online Aug. 19, 2021, in the BMJ.
‘Work fast and hard’
Researchers assessed the association between workplace cognitive stimulation and dementia incidence in seven cohorts that included almost 108,000 men and women (mean age, 44.6 years). All were free of dementia at baseline.
Participants included civil servants, public sector employees, forestry workers, and others from the general working population.
Investigators separated the participants into three categories of workplace cognitive stimulation: “high,” which referred to both high job demand and high job control; “low,” which referred to low demands and low control; and “medium,” which referred to all other combinations of job demand and job control.
“Highly cognitively stimulating jobs require you to work fast and hard, learn new things, be creative, and have a high level of skill,” said Dr. Kivimäki.
The researchers controlled for low education, hypertension, smoking, obesity, depression, physical inactivity, diabetes, low social contact, excessive alcohol consumption, and traumatic brain injury. These represent 10 of the 12 dementia risk factors named by the 2020 Lancet Commission on Dementia Prevention as having convincing evidence, Dr. Kivimäki noted.
Although the investigators had no data on the other two risk factors of hearing loss and air pollution, these are unlikely to be confounding factors, he said.
Follow-up for incident dementia varied from 13.7 to 30.1 years, depending on the cohort, and was 16.7 years in the total patient population. The mean age at dementia onset was 71.2 years.
Benefits across the life course
Results showed that incident dementia per 10,000 person years was 7.3 in the low–cognitive stimulation group and 4.8 in the high-stimulation group, for a difference of 2.5.
“These differences were relatively small because the incidence of dementia in this relatively young population was low,” Dr. Kivimäki said.
Compared with those with low stimulation, the adjusted hazard ratio for dementia for this with high stimulation was 0.77 (95% CI, 0.65-0.92).
The results were similar for men and women, and for those younger and older than 60 years. However, the link between workplace cognitive stimulation appeared stronger for Alzheimer’s disease than for other dementias.
There also appeared to be additive effects of higher cognitive stimulation in both childhood, as indicated by higher educational attainment, and adulthood, based on work characteristics, said Dr. Kivimäki.
“These findings support the benefits of cognitive stimulation across the life course, with education leading to higher peak cognitive performance and cognitive stimulation at work lowering age-related cognitive decline,” he added.
The findings don’t seem to be the result of workers with cognitive impairment remaining in unchallenging jobs, he noted. Separate analyses showed lower dementia incidence even when 10 years or more separated the assessment of cognitive stimulation and the dementia diagnosis.
“This suggests that the findings are unlikely to be biased due to reverse causation,” Dr. Kivimäki said.
Possible mechanism
Findings were similar when the researchers assessed effect from job changes. “This is probably because people in highly stimulating jobs are more likely to change to another highly stimulating job than to a low-stimulating job,” said Dr. Kivimäki. “Similarly, people with less stimulating jobs are seldom able to change to a substantially more stimulating job.”
As a dementia risk factor, low workplace stimulation is comparable with high alcohol intake and physical inactivity, but is weaker than education, diabetes, smoking, hypertension, and obesity, Dr. Kivimäki noted.
When asked about individuals with less cognitively stimulating jobs who are enormously stimulated outside work, he said that “previous large-scale studies have failed to find evidence that leisure time cognitive activity would significantly reduce risk of dementia.”
To explore potential underlying mechanisms, the investigators examined almost 5,000 plasma proteins in more than 2,200 individuals from one cohort in the Whitehall II study. They found six proteins were significantly lower among participants with high versus low cognitive stimulation.
In another analysis that included more than 13,500 participants from the Whitehall and another cohort, higher levels of three of these plasma proteins were associated with increased dementia risk – or conversely, lower protein levels with lower dementia risk.
The findings suggest a “novel plausible explanation” for the link between workplace cognitive stimulation and dementia risk, said Dr. Kivimäki.
He noted that higher levels of certain proteins prevent brain cells from forming new connections.
‘Some of the most compelling evidence to date’
In an accompanying editorial, Serhiy Dekhtyar, PhD, assistant professor (Docent), Aging Research Center, Karolinska Institute, Stockholm, noted that the study is “an important piece of work” and “some of the most compelling evidence to date” on the role of occupational cognitive stimulation in dementia risk.
The large-scale investigation in multiple cohorts and contexts has “advanced the field” and could help “explain previously mixed findings in the literature,” Dekhtyar said in an interview.
Importantly, the researchers provide “an indication of biological mechanisms potentially connecting work mental stimulation and dementia,” he added.
However, Dr. Dekhtyar noted that the difference of 2.5 incident cases of dementia per 10,000 person years of follow-up between the low and high mental-stimulation groups “is not especially large” – although it is comparable with other established risk factors for dementia.
He suspects the effect size would have been larger had the follow-up for dementia been longer.
Dr. Dekhtyar also raised the possibility that “innate cognition” might affect both educational and occupational attainment, and the subsequent dementia risk.
“Without taking this into account, we may inadvertently conclude that education or occupational stimulation help differentially preserve cognition into late life – when in reality, it may be initial differences in cognitive ability that are preserved throughout life,” he concluded.
Funding sources for the study included Nordic Research Programme on Health and Welfare (NordForsk), Medical Research Council, Wellcome Trust, Academy of Finland, and Helsinki Institute of Life Science. Dr. Kivimäki has received support from NordForsk, the UK Medical Research Council, the Wellcome Trust, the Academy of Finland, and the Helsinki Institute of Life Science. Dr. Dekhtyar disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Individuals with cognitively stimulating jobs are at a lower risk of developing dementia than their peers with less challenging employment, new research suggests.
Results from a large, multicohort study also showed an association between cognitive stimulation and lower levels of certain plasma proteins, providing possible clues on a protective biological mechanism.
“These new findings support the hypothesis that mental stimulation in adulthood may postpone the onset of dementia,” Mika Kivimäki, PhD, professor and director of the Whitehall II Study, department of epidemiology, University College London, said in an interview.
The results were published online Aug. 19, 2021, in the BMJ.
‘Work fast and hard’
Researchers assessed the association between workplace cognitive stimulation and dementia incidence in seven cohorts that included almost 108,000 men and women (mean age, 44.6 years). All were free of dementia at baseline.
Participants included civil servants, public sector employees, forestry workers, and others from the general working population.
Investigators separated the participants into three categories of workplace cognitive stimulation: “high,” which referred to both high job demand and high job control; “low,” which referred to low demands and low control; and “medium,” which referred to all other combinations of job demand and job control.
“Highly cognitively stimulating jobs require you to work fast and hard, learn new things, be creative, and have a high level of skill,” said Dr. Kivimäki.
The researchers controlled for low education, hypertension, smoking, obesity, depression, physical inactivity, diabetes, low social contact, excessive alcohol consumption, and traumatic brain injury. These represent 10 of the 12 dementia risk factors named by the 2020 Lancet Commission on Dementia Prevention as having convincing evidence, Dr. Kivimäki noted.
Although the investigators had no data on the other two risk factors of hearing loss and air pollution, these are unlikely to be confounding factors, he said.
Follow-up for incident dementia varied from 13.7 to 30.1 years, depending on the cohort, and was 16.7 years in the total patient population. The mean age at dementia onset was 71.2 years.
Benefits across the life course
Results showed that incident dementia per 10,000 person years was 7.3 in the low–cognitive stimulation group and 4.8 in the high-stimulation group, for a difference of 2.5.
“These differences were relatively small because the incidence of dementia in this relatively young population was low,” Dr. Kivimäki said.
Compared with those with low stimulation, the adjusted hazard ratio for dementia for this with high stimulation was 0.77 (95% CI, 0.65-0.92).
The results were similar for men and women, and for those younger and older than 60 years. However, the link between workplace cognitive stimulation appeared stronger for Alzheimer’s disease than for other dementias.
There also appeared to be additive effects of higher cognitive stimulation in both childhood, as indicated by higher educational attainment, and adulthood, based on work characteristics, said Dr. Kivimäki.
“These findings support the benefits of cognitive stimulation across the life course, with education leading to higher peak cognitive performance and cognitive stimulation at work lowering age-related cognitive decline,” he added.
The findings don’t seem to be the result of workers with cognitive impairment remaining in unchallenging jobs, he noted. Separate analyses showed lower dementia incidence even when 10 years or more separated the assessment of cognitive stimulation and the dementia diagnosis.
“This suggests that the findings are unlikely to be biased due to reverse causation,” Dr. Kivimäki said.
Possible mechanism
Findings were similar when the researchers assessed effect from job changes. “This is probably because people in highly stimulating jobs are more likely to change to another highly stimulating job than to a low-stimulating job,” said Dr. Kivimäki. “Similarly, people with less stimulating jobs are seldom able to change to a substantially more stimulating job.”
As a dementia risk factor, low workplace stimulation is comparable with high alcohol intake and physical inactivity, but is weaker than education, diabetes, smoking, hypertension, and obesity, Dr. Kivimäki noted.
When asked about individuals with less cognitively stimulating jobs who are enormously stimulated outside work, he said that “previous large-scale studies have failed to find evidence that leisure time cognitive activity would significantly reduce risk of dementia.”
To explore potential underlying mechanisms, the investigators examined almost 5,000 plasma proteins in more than 2,200 individuals from one cohort in the Whitehall II study. They found six proteins were significantly lower among participants with high versus low cognitive stimulation.
In another analysis that included more than 13,500 participants from the Whitehall and another cohort, higher levels of three of these plasma proteins were associated with increased dementia risk – or conversely, lower protein levels with lower dementia risk.
The findings suggest a “novel plausible explanation” for the link between workplace cognitive stimulation and dementia risk, said Dr. Kivimäki.
He noted that higher levels of certain proteins prevent brain cells from forming new connections.
‘Some of the most compelling evidence to date’
In an accompanying editorial, Serhiy Dekhtyar, PhD, assistant professor (Docent), Aging Research Center, Karolinska Institute, Stockholm, noted that the study is “an important piece of work” and “some of the most compelling evidence to date” on the role of occupational cognitive stimulation in dementia risk.
The large-scale investigation in multiple cohorts and contexts has “advanced the field” and could help “explain previously mixed findings in the literature,” Dekhtyar said in an interview.
Importantly, the researchers provide “an indication of biological mechanisms potentially connecting work mental stimulation and dementia,” he added.
However, Dr. Dekhtyar noted that the difference of 2.5 incident cases of dementia per 10,000 person years of follow-up between the low and high mental-stimulation groups “is not especially large” – although it is comparable with other established risk factors for dementia.
He suspects the effect size would have been larger had the follow-up for dementia been longer.
Dr. Dekhtyar also raised the possibility that “innate cognition” might affect both educational and occupational attainment, and the subsequent dementia risk.
“Without taking this into account, we may inadvertently conclude that education or occupational stimulation help differentially preserve cognition into late life – when in reality, it may be initial differences in cognitive ability that are preserved throughout life,” he concluded.
Funding sources for the study included Nordic Research Programme on Health and Welfare (NordForsk), Medical Research Council, Wellcome Trust, Academy of Finland, and Helsinki Institute of Life Science. Dr. Kivimäki has received support from NordForsk, the UK Medical Research Council, the Wellcome Trust, the Academy of Finland, and the Helsinki Institute of Life Science. Dr. Dekhtyar disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Individuals with cognitively stimulating jobs are at a lower risk of developing dementia than their peers with less challenging employment, new research suggests.
Results from a large, multicohort study also showed an association between cognitive stimulation and lower levels of certain plasma proteins, providing possible clues on a protective biological mechanism.
“These new findings support the hypothesis that mental stimulation in adulthood may postpone the onset of dementia,” Mika Kivimäki, PhD, professor and director of the Whitehall II Study, department of epidemiology, University College London, said in an interview.
The results were published online Aug. 19, 2021, in the BMJ.
‘Work fast and hard’
Researchers assessed the association between workplace cognitive stimulation and dementia incidence in seven cohorts that included almost 108,000 men and women (mean age, 44.6 years). All were free of dementia at baseline.
Participants included civil servants, public sector employees, forestry workers, and others from the general working population.
Investigators separated the participants into three categories of workplace cognitive stimulation: “high,” which referred to both high job demand and high job control; “low,” which referred to low demands and low control; and “medium,” which referred to all other combinations of job demand and job control.
“Highly cognitively stimulating jobs require you to work fast and hard, learn new things, be creative, and have a high level of skill,” said Dr. Kivimäki.
The researchers controlled for low education, hypertension, smoking, obesity, depression, physical inactivity, diabetes, low social contact, excessive alcohol consumption, and traumatic brain injury. These represent 10 of the 12 dementia risk factors named by the 2020 Lancet Commission on Dementia Prevention as having convincing evidence, Dr. Kivimäki noted.
Although the investigators had no data on the other two risk factors of hearing loss and air pollution, these are unlikely to be confounding factors, he said.
Follow-up for incident dementia varied from 13.7 to 30.1 years, depending on the cohort, and was 16.7 years in the total patient population. The mean age at dementia onset was 71.2 years.
Benefits across the life course
Results showed that incident dementia per 10,000 person years was 7.3 in the low–cognitive stimulation group and 4.8 in the high-stimulation group, for a difference of 2.5.
“These differences were relatively small because the incidence of dementia in this relatively young population was low,” Dr. Kivimäki said.
Compared with those with low stimulation, the adjusted hazard ratio for dementia for this with high stimulation was 0.77 (95% CI, 0.65-0.92).
The results were similar for men and women, and for those younger and older than 60 years. However, the link between workplace cognitive stimulation appeared stronger for Alzheimer’s disease than for other dementias.
There also appeared to be additive effects of higher cognitive stimulation in both childhood, as indicated by higher educational attainment, and adulthood, based on work characteristics, said Dr. Kivimäki.
“These findings support the benefits of cognitive stimulation across the life course, with education leading to higher peak cognitive performance and cognitive stimulation at work lowering age-related cognitive decline,” he added.
The findings don’t seem to be the result of workers with cognitive impairment remaining in unchallenging jobs, he noted. Separate analyses showed lower dementia incidence even when 10 years or more separated the assessment of cognitive stimulation and the dementia diagnosis.
“This suggests that the findings are unlikely to be biased due to reverse causation,” Dr. Kivimäki said.
Possible mechanism
Findings were similar when the researchers assessed effect from job changes. “This is probably because people in highly stimulating jobs are more likely to change to another highly stimulating job than to a low-stimulating job,” said Dr. Kivimäki. “Similarly, people with less stimulating jobs are seldom able to change to a substantially more stimulating job.”
As a dementia risk factor, low workplace stimulation is comparable with high alcohol intake and physical inactivity, but is weaker than education, diabetes, smoking, hypertension, and obesity, Dr. Kivimäki noted.
When asked about individuals with less cognitively stimulating jobs who are enormously stimulated outside work, he said that “previous large-scale studies have failed to find evidence that leisure time cognitive activity would significantly reduce risk of dementia.”
To explore potential underlying mechanisms, the investigators examined almost 5,000 plasma proteins in more than 2,200 individuals from one cohort in the Whitehall II study. They found six proteins were significantly lower among participants with high versus low cognitive stimulation.
In another analysis that included more than 13,500 participants from the Whitehall and another cohort, higher levels of three of these plasma proteins were associated with increased dementia risk – or conversely, lower protein levels with lower dementia risk.
The findings suggest a “novel plausible explanation” for the link between workplace cognitive stimulation and dementia risk, said Dr. Kivimäki.
He noted that higher levels of certain proteins prevent brain cells from forming new connections.
‘Some of the most compelling evidence to date’
In an accompanying editorial, Serhiy Dekhtyar, PhD, assistant professor (Docent), Aging Research Center, Karolinska Institute, Stockholm, noted that the study is “an important piece of work” and “some of the most compelling evidence to date” on the role of occupational cognitive stimulation in dementia risk.
The large-scale investigation in multiple cohorts and contexts has “advanced the field” and could help “explain previously mixed findings in the literature,” Dekhtyar said in an interview.
Importantly, the researchers provide “an indication of biological mechanisms potentially connecting work mental stimulation and dementia,” he added.
However, Dr. Dekhtyar noted that the difference of 2.5 incident cases of dementia per 10,000 person years of follow-up between the low and high mental-stimulation groups “is not especially large” – although it is comparable with other established risk factors for dementia.
He suspects the effect size would have been larger had the follow-up for dementia been longer.
Dr. Dekhtyar also raised the possibility that “innate cognition” might affect both educational and occupational attainment, and the subsequent dementia risk.
“Without taking this into account, we may inadvertently conclude that education or occupational stimulation help differentially preserve cognition into late life – when in reality, it may be initial differences in cognitive ability that are preserved throughout life,” he concluded.
Funding sources for the study included Nordic Research Programme on Health and Welfare (NordForsk), Medical Research Council, Wellcome Trust, Academy of Finland, and Helsinki Institute of Life Science. Dr. Kivimäki has received support from NordForsk, the UK Medical Research Council, the Wellcome Trust, the Academy of Finland, and the Helsinki Institute of Life Science. Dr. Dekhtyar disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Headache seen affecting some pregnancy outcomes
, according to results from an observational study.
Migraine during pregnancy has been associated in previous studies with hypertensive pregnancy complications including preeclampsia; however, little is known about other headache types and their effects on pregnancy and birth outcomes.
For their research, published online July 20 in Cephalalgia, Isabella Neri, MD, PhD, and colleagues at Hospital Policlinico of Modena, Italy, looked at headache status for 515 consecutive pregnant women evaluated during their first trimester and followed through childbirth.
Altogether 224 women, or 43.5% of the cohort, were diagnosed with migraine without aura (n = 72), migraine with aura (n = 27), or tension-type headache (n = 125). The authors did not report on the severity or frequency of headaches.
Women with migraine with aura and tension-type headache saw higher rates of small-for-gestational-age infants (25.9% and 10.4% of births, respectively) compared with 5.5% for women without headache. Women presenting with tension-type headache saw elevated risk for small-for-gestational-age infants (odds ratio [OR] 4.19, P = .004) as did women with migraine with aura (OR 5.37, P = .02).
Admission to neonatal intensive care was significantly higher in all the headache groups. However, the authors found no statistically significant associations between headaches and any other perinatal outcome investigated in the study, including gestational diabetes, placental abruption, gestational hypertension, and preterm delivery.
A previous study conducted by the same research group had reported a relationship between migraine and gestational hypertension. The authors cited the small sample size of the migraine groups in the current study, “the diverse features of the population,” and the popularity of low-dose aspirin administration as potentially affecting that outcome.
Interpret findings with caution
Asked by this news organization to comment on the research, two headache neurologists praised Dr. Neri and colleagues’ research for focusing on an understudied topic – but also said that the results would not change their practice unless replicated in larger studies.
Elizabeth W. Loder, MD, MPH, chief emeritus of the division of headache at Brigham and Women’s Faulkner Hospital in Boston, urged caution in interpreting the findings, particularly with regard to tension-type headache. “This study adds to information suggesting that pregnancy complications probably are higher in women who have migraine with aura, and there’s biological plausibility for that,” Dr. Loder said. “Having aura means you may have some vascular abnormalities and things that logically might be associated with an increased risk of small-for-gestational age infants.” But the small size of the migraine-with-aura group in this study – 27 women – and the fact that other perinatal outcomes measured in the study did not reach significance, allows for the possibility that the small-for-gestational-age findings were due to chance, Dr. Loder noted.
With tension-type headache, a biological rationale for small-for-gestational-age risk is more elusive, Dr. Loder said. “I would want to see that association replicated in another study before I thought that I needed to warn women with tension-type headache about this potential outcome. There’s lot of uncertainty here about the magnitude of the risk.”
While Dr. Neri and colleagues described the instruments used in their study to diagnose migraine and migraine with aura, they did not explain how tension-type headache was diagnosed.
Tension-type headache, while common, is still not well characterized, Dr. Loder noted, and may represent a heterogeneous condition or the milder end of a biological continuum that includes migraine with aura. Also, the group in the study had a higher prevalence of smoking, and though the authors made statistical adjustments for smoking status, “smokers are systematically different than people who aren’t in other ways that could be associated with these outcomes,” Dr. Loder said.
While the authors of the study suggested that interventions might be indicated for women with tension-type headache in pregnancy, “showing an association doesn’t necessarily mean that intervening would make a difference” on pregnancy outcomes, Dr. Loder said.
Amaal J. Starling, MD, of the Mayo Clinic in Phoenix, Ariz., said in an interview that she, too, appreciated that this study looked at pregnancy outcomes in the setting of headache disorders. “Unfortunately even though headache disorders and especially migraine affect women so much, we still know very little about migraine in pregnancy,” she said.
Dr. Starling noted that many women with migraine are discouraged by their health care providers from becoming pregnant, because of the false belief that migraine cannot be managed in pregnancy. In her own practice, she said, she treats many patients with severe headache who become pregnant and who require pharmacological intervention during pregnancy.
This does not mean she regards headache in pregnancy as innocent. “I want patients to be on high alert for changes in headache symptoms in pregnancy. If someone has worsening of headache or migraine or aura in the setting of pregnancy, we consider that a red flag,” potentially indicating complications such as high blood pressure, gestational hypertension, or a blood clot.
Like Dr. Loder, Dr. Starling said she was not surprised by Dr. Neri and colleagues’ finding that migraine with aura might impact pregnancy outcomes. “We know that migraine with aura has a lot of vascular abnormalities that underlie the pathogenesis,” she said.
Dr. Starling found the findings related to tension-type headache less convincing, not least because the diagnostic criteria for tension-type headache was not made clear in the study. “I view this as an exploratory study that says maybe there’s a signal here. A larger epidemiological study would need to be done to confirm or refute this data,” Dr. Starling said. Until the findings can be replicated, “this study would not affect my clinical practice in any way.”
Dr. Neri and colleagues described no outside funding for their research or financial conflicts of interest. Dr. Starling has received consulting fees from pharmaceutical manufacturers but reported no disclosures relevant to the study discussed. Dr. Loder reported no financial conflicts of interest.
, according to results from an observational study.
Migraine during pregnancy has been associated in previous studies with hypertensive pregnancy complications including preeclampsia; however, little is known about other headache types and their effects on pregnancy and birth outcomes.
For their research, published online July 20 in Cephalalgia, Isabella Neri, MD, PhD, and colleagues at Hospital Policlinico of Modena, Italy, looked at headache status for 515 consecutive pregnant women evaluated during their first trimester and followed through childbirth.
Altogether 224 women, or 43.5% of the cohort, were diagnosed with migraine without aura (n = 72), migraine with aura (n = 27), or tension-type headache (n = 125). The authors did not report on the severity or frequency of headaches.
Women with migraine with aura and tension-type headache saw higher rates of small-for-gestational-age infants (25.9% and 10.4% of births, respectively) compared with 5.5% for women without headache. Women presenting with tension-type headache saw elevated risk for small-for-gestational-age infants (odds ratio [OR] 4.19, P = .004) as did women with migraine with aura (OR 5.37, P = .02).
Admission to neonatal intensive care was significantly higher in all the headache groups. However, the authors found no statistically significant associations between headaches and any other perinatal outcome investigated in the study, including gestational diabetes, placental abruption, gestational hypertension, and preterm delivery.
A previous study conducted by the same research group had reported a relationship between migraine and gestational hypertension. The authors cited the small sample size of the migraine groups in the current study, “the diverse features of the population,” and the popularity of low-dose aspirin administration as potentially affecting that outcome.
Interpret findings with caution
Asked by this news organization to comment on the research, two headache neurologists praised Dr. Neri and colleagues’ research for focusing on an understudied topic – but also said that the results would not change their practice unless replicated in larger studies.
Elizabeth W. Loder, MD, MPH, chief emeritus of the division of headache at Brigham and Women’s Faulkner Hospital in Boston, urged caution in interpreting the findings, particularly with regard to tension-type headache. “This study adds to information suggesting that pregnancy complications probably are higher in women who have migraine with aura, and there’s biological plausibility for that,” Dr. Loder said. “Having aura means you may have some vascular abnormalities and things that logically might be associated with an increased risk of small-for-gestational age infants.” But the small size of the migraine-with-aura group in this study – 27 women – and the fact that other perinatal outcomes measured in the study did not reach significance, allows for the possibility that the small-for-gestational-age findings were due to chance, Dr. Loder noted.
With tension-type headache, a biological rationale for small-for-gestational-age risk is more elusive, Dr. Loder said. “I would want to see that association replicated in another study before I thought that I needed to warn women with tension-type headache about this potential outcome. There’s lot of uncertainty here about the magnitude of the risk.”
While Dr. Neri and colleagues described the instruments used in their study to diagnose migraine and migraine with aura, they did not explain how tension-type headache was diagnosed.
Tension-type headache, while common, is still not well characterized, Dr. Loder noted, and may represent a heterogeneous condition or the milder end of a biological continuum that includes migraine with aura. Also, the group in the study had a higher prevalence of smoking, and though the authors made statistical adjustments for smoking status, “smokers are systematically different than people who aren’t in other ways that could be associated with these outcomes,” Dr. Loder said.
While the authors of the study suggested that interventions might be indicated for women with tension-type headache in pregnancy, “showing an association doesn’t necessarily mean that intervening would make a difference” on pregnancy outcomes, Dr. Loder said.
Amaal J. Starling, MD, of the Mayo Clinic in Phoenix, Ariz., said in an interview that she, too, appreciated that this study looked at pregnancy outcomes in the setting of headache disorders. “Unfortunately even though headache disorders and especially migraine affect women so much, we still know very little about migraine in pregnancy,” she said.
Dr. Starling noted that many women with migraine are discouraged by their health care providers from becoming pregnant, because of the false belief that migraine cannot be managed in pregnancy. In her own practice, she said, she treats many patients with severe headache who become pregnant and who require pharmacological intervention during pregnancy.
This does not mean she regards headache in pregnancy as innocent. “I want patients to be on high alert for changes in headache symptoms in pregnancy. If someone has worsening of headache or migraine or aura in the setting of pregnancy, we consider that a red flag,” potentially indicating complications such as high blood pressure, gestational hypertension, or a blood clot.
Like Dr. Loder, Dr. Starling said she was not surprised by Dr. Neri and colleagues’ finding that migraine with aura might impact pregnancy outcomes. “We know that migraine with aura has a lot of vascular abnormalities that underlie the pathogenesis,” she said.
Dr. Starling found the findings related to tension-type headache less convincing, not least because the diagnostic criteria for tension-type headache was not made clear in the study. “I view this as an exploratory study that says maybe there’s a signal here. A larger epidemiological study would need to be done to confirm or refute this data,” Dr. Starling said. Until the findings can be replicated, “this study would not affect my clinical practice in any way.”
Dr. Neri and colleagues described no outside funding for their research or financial conflicts of interest. Dr. Starling has received consulting fees from pharmaceutical manufacturers but reported no disclosures relevant to the study discussed. Dr. Loder reported no financial conflicts of interest.
, according to results from an observational study.
Migraine during pregnancy has been associated in previous studies with hypertensive pregnancy complications including preeclampsia; however, little is known about other headache types and their effects on pregnancy and birth outcomes.
For their research, published online July 20 in Cephalalgia, Isabella Neri, MD, PhD, and colleagues at Hospital Policlinico of Modena, Italy, looked at headache status for 515 consecutive pregnant women evaluated during their first trimester and followed through childbirth.
Altogether 224 women, or 43.5% of the cohort, were diagnosed with migraine without aura (n = 72), migraine with aura (n = 27), or tension-type headache (n = 125). The authors did not report on the severity or frequency of headaches.
Women with migraine with aura and tension-type headache saw higher rates of small-for-gestational-age infants (25.9% and 10.4% of births, respectively) compared with 5.5% for women without headache. Women presenting with tension-type headache saw elevated risk for small-for-gestational-age infants (odds ratio [OR] 4.19, P = .004) as did women with migraine with aura (OR 5.37, P = .02).
Admission to neonatal intensive care was significantly higher in all the headache groups. However, the authors found no statistically significant associations between headaches and any other perinatal outcome investigated in the study, including gestational diabetes, placental abruption, gestational hypertension, and preterm delivery.
A previous study conducted by the same research group had reported a relationship between migraine and gestational hypertension. The authors cited the small sample size of the migraine groups in the current study, “the diverse features of the population,” and the popularity of low-dose aspirin administration as potentially affecting that outcome.
Interpret findings with caution
Asked by this news organization to comment on the research, two headache neurologists praised Dr. Neri and colleagues’ research for focusing on an understudied topic – but also said that the results would not change their practice unless replicated in larger studies.
Elizabeth W. Loder, MD, MPH, chief emeritus of the division of headache at Brigham and Women’s Faulkner Hospital in Boston, urged caution in interpreting the findings, particularly with regard to tension-type headache. “This study adds to information suggesting that pregnancy complications probably are higher in women who have migraine with aura, and there’s biological plausibility for that,” Dr. Loder said. “Having aura means you may have some vascular abnormalities and things that logically might be associated with an increased risk of small-for-gestational age infants.” But the small size of the migraine-with-aura group in this study – 27 women – and the fact that other perinatal outcomes measured in the study did not reach significance, allows for the possibility that the small-for-gestational-age findings were due to chance, Dr. Loder noted.
With tension-type headache, a biological rationale for small-for-gestational-age risk is more elusive, Dr. Loder said. “I would want to see that association replicated in another study before I thought that I needed to warn women with tension-type headache about this potential outcome. There’s lot of uncertainty here about the magnitude of the risk.”
While Dr. Neri and colleagues described the instruments used in their study to diagnose migraine and migraine with aura, they did not explain how tension-type headache was diagnosed.
Tension-type headache, while common, is still not well characterized, Dr. Loder noted, and may represent a heterogeneous condition or the milder end of a biological continuum that includes migraine with aura. Also, the group in the study had a higher prevalence of smoking, and though the authors made statistical adjustments for smoking status, “smokers are systematically different than people who aren’t in other ways that could be associated with these outcomes,” Dr. Loder said.
While the authors of the study suggested that interventions might be indicated for women with tension-type headache in pregnancy, “showing an association doesn’t necessarily mean that intervening would make a difference” on pregnancy outcomes, Dr. Loder said.
Amaal J. Starling, MD, of the Mayo Clinic in Phoenix, Ariz., said in an interview that she, too, appreciated that this study looked at pregnancy outcomes in the setting of headache disorders. “Unfortunately even though headache disorders and especially migraine affect women so much, we still know very little about migraine in pregnancy,” she said.
Dr. Starling noted that many women with migraine are discouraged by their health care providers from becoming pregnant, because of the false belief that migraine cannot be managed in pregnancy. In her own practice, she said, she treats many patients with severe headache who become pregnant and who require pharmacological intervention during pregnancy.
This does not mean she regards headache in pregnancy as innocent. “I want patients to be on high alert for changes in headache symptoms in pregnancy. If someone has worsening of headache or migraine or aura in the setting of pregnancy, we consider that a red flag,” potentially indicating complications such as high blood pressure, gestational hypertension, or a blood clot.
Like Dr. Loder, Dr. Starling said she was not surprised by Dr. Neri and colleagues’ finding that migraine with aura might impact pregnancy outcomes. “We know that migraine with aura has a lot of vascular abnormalities that underlie the pathogenesis,” she said.
Dr. Starling found the findings related to tension-type headache less convincing, not least because the diagnostic criteria for tension-type headache was not made clear in the study. “I view this as an exploratory study that says maybe there’s a signal here. A larger epidemiological study would need to be done to confirm or refute this data,” Dr. Starling said. Until the findings can be replicated, “this study would not affect my clinical practice in any way.”
Dr. Neri and colleagues described no outside funding for their research or financial conflicts of interest. Dr. Starling has received consulting fees from pharmaceutical manufacturers but reported no disclosures relevant to the study discussed. Dr. Loder reported no financial conflicts of interest.
FROM CEPHALALGIA
Explosive aggression may be neurologic
Aggression is an underappreciated mental health issue, and biological mechanisms might help explain more extreme forms like intermittent explosive disorder (IED), which is characterized by episodes of sudden impulses and inappropriate aggression, violence, or even verbal outbursts. IED can lead to road rage, domestic abuse, in addition to throwing objects and engaging in other destructive behaviors.

Despite those consequences, aggression hasn’t gained the same level of attention as other psychiatric conditions, according to Emil F. Coccaro, MD, who spoke about the topic at a virtual meeting presented by Current Psychiatry and the American Academy of Clinical Psychiatrists.
“People seem to think that aggressive behavior is bad behavior, and therefore people just need an attitude adjustment. So there’s this sort of stigma, and there are no advocacy groups for it. There are no poster children for it. But there’s a whole lot of biology and neuroscience behind it,” said Dr. Coccaro, in an interview. He is a professor and vice chair of research in psychiatry and behavioral health at Ohio State University, Columbus.
, who spoke at the meeting presented by MedscapeLive. MedscapeLive and this news organization are owned by the same parent company.
There is a general view that psychiatric conditions may lead to increased aggression, but there is little evidence of that. “As a general statement, having a psychological [illness] in and of itself does not really increase the risk of being aggressive. What does is being aggressive in general, and substance use disorder. And the thing with [people who have] substance use disorders is that they only get aggressive when they are aggressive to begin with,” said Dr. Coccaro, noting that the strongest case for the relationship surrounds alcohol abuse.
The DSM-5 criteria for IED include: verbal or physical aggression without destruction, at least twice per week, or three or more episodes of assault or physical destruction within a year. The behavior must be out of proportion to the provocation, cause distress or impairment, and not be accountable by other diagnoses. “If they’re blowing up twice a week, for a few months, and usually they’re doing it for a long time, then that’s different than just blowing up very occasionally. Healthy people, nonaggressive people, maybe they blow up once a year, or even less frequently than that,” Dr. Coccaro said.
Functional magnetic resonance imaging and other imaging studies consistently show differences associated with aggression.
“The IEDs really do distinguish themselves from the psychiatric controls. They also have other stuff going on with them; they have a hostile attribution. And they’re kind of irritable at baseline. They’re not walking around irritable all the time, but the people around them may be walking on eggshells,” Dr. Coccaro said.
The results from these sorts of studies aren’t fully conclusive and can’t be used for diagnosis, in part because of a lack of power. “It’s hard to do these MRI studies and lots and lots of subjects, because they’re kind of expensive,” Dr. Coccaro said. “We’re just not there yet.”
Other, less expensive imaging techniques like near-infrared spectroscopy may improve matters. “That might be something down the road that could lead to something (diagnostic). Right now, most imaging studies are being done to really understand mechanisms,” said Dr. Coccaro.
Those mechanistic studies suggest that the culprit for IED may be a combination of too much drive from subcortical structures like the amygdala and insufficient inhibitor function in the frontal part of the brain. The frontal cortex may suffer a loss of gray matter, according to Dr. Coccaro, and there may be insufficient connectivity, which could weaken signals coming from the frontal areas that might otherwise inhibit lower centers of the brain.
Treatment for IED could be aimed at improving that connectivity and signaling. Ketamine and other anesthetic agents like nitrous oxide may increase connectivity to nerve cells by increasing branching at synaptic dendrites.
Selective serotonin reuptake inhibitors have the potential to treat IED, but their utility is limited because they bind to the presynaptic transporter for serotonin, and more aggressive people have fewer of those transporters. “You only get so much bang for your buck,” Dr. Coccaro said.
Cognitive-behavioral therapy that focuses on anger management and relaxation shows promise. “CBT does help people deal with what’s coming at them. So it’s like, ‘oh, I’m getting angry, I better start doing those relaxation (techniques).’ It teaches them to rethink things.”
During the Q&A session following the presentation, Henry A. Nasrallah, MD, who moderated the session, pointed out that misattribution can occur, leading an affected individual to misread someone’s facial expression and react aggressively, which is a problem also seen in psychosis.
“There are studies showing [that if] you show them a series of faces with different affects, many times paranoid patients read a normal facial expression as threatening. So it may be that it’s the same thing with aggression,” said Dr. Nasrallah, who is a professor of psychiatry, neurology, and neuroscience at the University of Cincinnati.
In the midst of the ongoing COVID-19 pandemic, it’s also possible that mask-wearing could improve or worsen such misunderstandings. “There is expression in the eyes that you can see, but you miss a lot,” Dr. Coccaro said.
For now, the effects of masks remain largely unknown. But that will change. “Sooner or later we will have a bunch of papers coming out about how masks have changed a lot of behaviors,” Dr. Nasrallah said.
Dr. Coccaro has consulted for Avanir, Azevan, and Brackett. Dr. Nasrallah has consulted for Acadia, Alkermes, Allergan Janssen, Otsuka, Indivior, IntraCellular, Neurocrine, Sunovion, Teva, and Boehringer-Ingelheim. Dr. Nasrallah has been on a speaker’s bureau for Acadia, Alkermes, Allergan, Janssen, Otsuka, Indivior, Intracellular, Neurocrine, Noven, Sunovion, and Teva.
Aggression is an underappreciated mental health issue, and biological mechanisms might help explain more extreme forms like intermittent explosive disorder (IED), which is characterized by episodes of sudden impulses and inappropriate aggression, violence, or even verbal outbursts. IED can lead to road rage, domestic abuse, in addition to throwing objects and engaging in other destructive behaviors.
Despite those consequences, aggression hasn’t gained the same level of attention as other psychiatric conditions, according to Emil F. Coccaro, MD, who spoke about the topic at a virtual meeting presented by Current Psychiatry and the American Academy of Clinical Psychiatrists.
“People seem to think that aggressive behavior is bad behavior, and therefore people just need an attitude adjustment. So there’s this sort of stigma, and there are no advocacy groups for it. There are no poster children for it. But there’s a whole lot of biology and neuroscience behind it,” said Dr. Coccaro, in an interview. He is a professor and vice chair of research in psychiatry and behavioral health at Ohio State University, Columbus.
, who spoke at the meeting presented by MedscapeLive. MedscapeLive and this news organization are owned by the same parent company.
There is a general view that psychiatric conditions may lead to increased aggression, but there is little evidence of that. “As a general statement, having a psychological [illness] in and of itself does not really increase the risk of being aggressive. What does is being aggressive in general, and substance use disorder. And the thing with [people who have] substance use disorders is that they only get aggressive when they are aggressive to begin with,” said Dr. Coccaro, noting that the strongest case for the relationship surrounds alcohol abuse.
The DSM-5 criteria for IED include: verbal or physical aggression without destruction, at least twice per week, or three or more episodes of assault or physical destruction within a year. The behavior must be out of proportion to the provocation, cause distress or impairment, and not be accountable by other diagnoses. “If they’re blowing up twice a week, for a few months, and usually they’re doing it for a long time, then that’s different than just blowing up very occasionally. Healthy people, nonaggressive people, maybe they blow up once a year, or even less frequently than that,” Dr. Coccaro said.
Functional magnetic resonance imaging and other imaging studies consistently show differences associated with aggression.
“The IEDs really do distinguish themselves from the psychiatric controls. They also have other stuff going on with them; they have a hostile attribution. And they’re kind of irritable at baseline. They’re not walking around irritable all the time, but the people around them may be walking on eggshells,” Dr. Coccaro said.
The results from these sorts of studies aren’t fully conclusive and can’t be used for diagnosis, in part because of a lack of power. “It’s hard to do these MRI studies and lots and lots of subjects, because they’re kind of expensive,” Dr. Coccaro said. “We’re just not there yet.”
Other, less expensive imaging techniques like near-infrared spectroscopy may improve matters. “That might be something down the road that could lead to something (diagnostic). Right now, most imaging studies are being done to really understand mechanisms,” said Dr. Coccaro.
Those mechanistic studies suggest that the culprit for IED may be a combination of too much drive from subcortical structures like the amygdala and insufficient inhibitor function in the frontal part of the brain. The frontal cortex may suffer a loss of gray matter, according to Dr. Coccaro, and there may be insufficient connectivity, which could weaken signals coming from the frontal areas that might otherwise inhibit lower centers of the brain.
Treatment for IED could be aimed at improving that connectivity and signaling. Ketamine and other anesthetic agents like nitrous oxide may increase connectivity to nerve cells by increasing branching at synaptic dendrites.
Selective serotonin reuptake inhibitors have the potential to treat IED, but their utility is limited because they bind to the presynaptic transporter for serotonin, and more aggressive people have fewer of those transporters. “You only get so much bang for your buck,” Dr. Coccaro said.
Cognitive-behavioral therapy that focuses on anger management and relaxation shows promise. “CBT does help people deal with what’s coming at them. So it’s like, ‘oh, I’m getting angry, I better start doing those relaxation (techniques).’ It teaches them to rethink things.”
During the Q&A session following the presentation, Henry A. Nasrallah, MD, who moderated the session, pointed out that misattribution can occur, leading an affected individual to misread someone’s facial expression and react aggressively, which is a problem also seen in psychosis.
“There are studies showing [that if] you show them a series of faces with different affects, many times paranoid patients read a normal facial expression as threatening. So it may be that it’s the same thing with aggression,” said Dr. Nasrallah, who is a professor of psychiatry, neurology, and neuroscience at the University of Cincinnati.
In the midst of the ongoing COVID-19 pandemic, it’s also possible that mask-wearing could improve or worsen such misunderstandings. “There is expression in the eyes that you can see, but you miss a lot,” Dr. Coccaro said.
For now, the effects of masks remain largely unknown. But that will change. “Sooner or later we will have a bunch of papers coming out about how masks have changed a lot of behaviors,” Dr. Nasrallah said.
Dr. Coccaro has consulted for Avanir, Azevan, and Brackett. Dr. Nasrallah has consulted for Acadia, Alkermes, Allergan Janssen, Otsuka, Indivior, IntraCellular, Neurocrine, Sunovion, Teva, and Boehringer-Ingelheim. Dr. Nasrallah has been on a speaker’s bureau for Acadia, Alkermes, Allergan, Janssen, Otsuka, Indivior, Intracellular, Neurocrine, Noven, Sunovion, and Teva.
Aggression is an underappreciated mental health issue, and biological mechanisms might help explain more extreme forms like intermittent explosive disorder (IED), which is characterized by episodes of sudden impulses and inappropriate aggression, violence, or even verbal outbursts. IED can lead to road rage, domestic abuse, in addition to throwing objects and engaging in other destructive behaviors.
Despite those consequences, aggression hasn’t gained the same level of attention as other psychiatric conditions, according to Emil F. Coccaro, MD, who spoke about the topic at a virtual meeting presented by Current Psychiatry and the American Academy of Clinical Psychiatrists.
“People seem to think that aggressive behavior is bad behavior, and therefore people just need an attitude adjustment. So there’s this sort of stigma, and there are no advocacy groups for it. There are no poster children for it. But there’s a whole lot of biology and neuroscience behind it,” said Dr. Coccaro, in an interview. He is a professor and vice chair of research in psychiatry and behavioral health at Ohio State University, Columbus.
, who spoke at the meeting presented by MedscapeLive. MedscapeLive and this news organization are owned by the same parent company.
There is a general view that psychiatric conditions may lead to increased aggression, but there is little evidence of that. “As a general statement, having a psychological [illness] in and of itself does not really increase the risk of being aggressive. What does is being aggressive in general, and substance use disorder. And the thing with [people who have] substance use disorders is that they only get aggressive when they are aggressive to begin with,” said Dr. Coccaro, noting that the strongest case for the relationship surrounds alcohol abuse.
The DSM-5 criteria for IED include: verbal or physical aggression without destruction, at least twice per week, or three or more episodes of assault or physical destruction within a year. The behavior must be out of proportion to the provocation, cause distress or impairment, and not be accountable by other diagnoses. “If they’re blowing up twice a week, for a few months, and usually they’re doing it for a long time, then that’s different than just blowing up very occasionally. Healthy people, nonaggressive people, maybe they blow up once a year, or even less frequently than that,” Dr. Coccaro said.
Functional magnetic resonance imaging and other imaging studies consistently show differences associated with aggression.
“The IEDs really do distinguish themselves from the psychiatric controls. They also have other stuff going on with them; they have a hostile attribution. And they’re kind of irritable at baseline. They’re not walking around irritable all the time, but the people around them may be walking on eggshells,” Dr. Coccaro said.
The results from these sorts of studies aren’t fully conclusive and can’t be used for diagnosis, in part because of a lack of power. “It’s hard to do these MRI studies and lots and lots of subjects, because they’re kind of expensive,” Dr. Coccaro said. “We’re just not there yet.”
Other, less expensive imaging techniques like near-infrared spectroscopy may improve matters. “That might be something down the road that could lead to something (diagnostic). Right now, most imaging studies are being done to really understand mechanisms,” said Dr. Coccaro.
Those mechanistic studies suggest that the culprit for IED may be a combination of too much drive from subcortical structures like the amygdala and insufficient inhibitor function in the frontal part of the brain. The frontal cortex may suffer a loss of gray matter, according to Dr. Coccaro, and there may be insufficient connectivity, which could weaken signals coming from the frontal areas that might otherwise inhibit lower centers of the brain.
Treatment for IED could be aimed at improving that connectivity and signaling. Ketamine and other anesthetic agents like nitrous oxide may increase connectivity to nerve cells by increasing branching at synaptic dendrites.
Selective serotonin reuptake inhibitors have the potential to treat IED, but their utility is limited because they bind to the presynaptic transporter for serotonin, and more aggressive people have fewer of those transporters. “You only get so much bang for your buck,” Dr. Coccaro said.
Cognitive-behavioral therapy that focuses on anger management and relaxation shows promise. “CBT does help people deal with what’s coming at them. So it’s like, ‘oh, I’m getting angry, I better start doing those relaxation (techniques).’ It teaches them to rethink things.”
During the Q&A session following the presentation, Henry A. Nasrallah, MD, who moderated the session, pointed out that misattribution can occur, leading an affected individual to misread someone’s facial expression and react aggressively, which is a problem also seen in psychosis.
“There are studies showing [that if] you show them a series of faces with different affects, many times paranoid patients read a normal facial expression as threatening. So it may be that it’s the same thing with aggression,” said Dr. Nasrallah, who is a professor of psychiatry, neurology, and neuroscience at the University of Cincinnati.
In the midst of the ongoing COVID-19 pandemic, it’s also possible that mask-wearing could improve or worsen such misunderstandings. “There is expression in the eyes that you can see, but you miss a lot,” Dr. Coccaro said.
For now, the effects of masks remain largely unknown. But that will change. “Sooner or later we will have a bunch of papers coming out about how masks have changed a lot of behaviors,” Dr. Nasrallah said.
Dr. Coccaro has consulted for Avanir, Azevan, and Brackett. Dr. Nasrallah has consulted for Acadia, Alkermes, Allergan Janssen, Otsuka, Indivior, IntraCellular, Neurocrine, Sunovion, Teva, and Boehringer-Ingelheim. Dr. Nasrallah has been on a speaker’s bureau for Acadia, Alkermes, Allergan, Janssen, Otsuka, Indivior, Intracellular, Neurocrine, Noven, Sunovion, and Teva.
REPORTING FROM FOCUS ON NEUROPSYCHIATRY 2021
Guidance on additional COVID-19 vaccine dose for MS patients
Patients aged 12 years and older with multiple sclerosis (MS) who are fully immunized against COVID-19 with either the Pfizer-BioNTech or Moderna mRNA vaccine may be eligible to receive an additional dose now, the National Multiple Sclerosis Society has announced.
New guidance, which is “based on available data from studies and expert consensus opinion” by a panel of MS neurologists and experts, was published Aug. 19 on the organization’s website.
The Food and Drug Administration has authorized an additional dose of the coronavirus vaccine for patients who are expected to not have a normal or adequate immune response to the first two doses. Patients with MS who use certain treatments have a reduced or absent antibody response to the vaccine, according to recent data.
“We want people living with MS to be aware of this additional dose and discuss when they need an additional dose or booster dose with their health care provider,” Julie Fiol, RN, MSW, associate vice president of health care access, National MS Society, said in an interview.
Those who may benefit from an additional dose include patients with MS who use sphingosine 1-phosphate receptor modulators, anti-CD20 monoclonal antibodies, or alemtuzumab (Lemtrada), the National MS Society noted. These particular disease modifying therapies (DMTs) have a stronger effect on the immune system than do other treatments.
Protecting ‘the most vulnerable’
Sphingosine 1-phosphate receptor modulators include fingolimod (Gilenya), siponimod (Mayzent), ozanimod (Zeposia), and ponesimod (Ponvory).
Anti-CD20 monoclonal antibodies include ocrelizumab (Ocrevus), ofatumumab (Kesimpta), rituximab (Rituxan), and corresponding biosimilars.
Current data do not support an additional dose for immunocompromised patients who received the Johnson & Johnson vaccine. The FDA and the Centers for Disease Control and Prevention are developing recommendations for these patients, and the National MS Society will update its guidance as needed, the organization noted in its statement.
“Like other medical decisions, the decision to get an additional dose is best made in partnership with your health care provider,” said Ms. Fiol. “Talk to your MS health care provider to determine what is best for you.”
MS itself does not compromise the immune system, but some MS therapies alter the immune system and reduce the body’s response to vaccination. Patients with MS who use B cell-depleting therapies have a better antibody response when they receive the vaccine 3 months or more after the last dose of MS therapy, according to the National MS Society.
Data suggest that patients with MS are not more susceptible to COVID-19 infection, severe illness, or death than are patients without MS. However, certain groups of patients with MS, such as those who receive B cell-depleting treatments, are more susceptible to having a severe case of COVID-19.
That said, “everyone will need a booster at some point. Those who take DMTs that have greater impact on the immune system are the most urgent need now,” the organization noted.
“Vaccination against COVID-19 is critical for public safety and, especially, the safety of the most vulnerable among us,” said Ms. Fiol. “We encourage everyone with MS get vaccinated.”
A version of this article first appeared on Medscape.com.
Patients aged 12 years and older with multiple sclerosis (MS) who are fully immunized against COVID-19 with either the Pfizer-BioNTech or Moderna mRNA vaccine may be eligible to receive an additional dose now, the National Multiple Sclerosis Society has announced.
New guidance, which is “based on available data from studies and expert consensus opinion” by a panel of MS neurologists and experts, was published Aug. 19 on the organization’s website.
The Food and Drug Administration has authorized an additional dose of the coronavirus vaccine for patients who are expected to not have a normal or adequate immune response to the first two doses. Patients with MS who use certain treatments have a reduced or absent antibody response to the vaccine, according to recent data.
“We want people living with MS to be aware of this additional dose and discuss when they need an additional dose or booster dose with their health care provider,” Julie Fiol, RN, MSW, associate vice president of health care access, National MS Society, said in an interview.
Those who may benefit from an additional dose include patients with MS who use sphingosine 1-phosphate receptor modulators, anti-CD20 monoclonal antibodies, or alemtuzumab (Lemtrada), the National MS Society noted. These particular disease modifying therapies (DMTs) have a stronger effect on the immune system than do other treatments.
Protecting ‘the most vulnerable’
Sphingosine 1-phosphate receptor modulators include fingolimod (Gilenya), siponimod (Mayzent), ozanimod (Zeposia), and ponesimod (Ponvory).
Anti-CD20 monoclonal antibodies include ocrelizumab (Ocrevus), ofatumumab (Kesimpta), rituximab (Rituxan), and corresponding biosimilars.
Current data do not support an additional dose for immunocompromised patients who received the Johnson & Johnson vaccine. The FDA and the Centers for Disease Control and Prevention are developing recommendations for these patients, and the National MS Society will update its guidance as needed, the organization noted in its statement.
“Like other medical decisions, the decision to get an additional dose is best made in partnership with your health care provider,” said Ms. Fiol. “Talk to your MS health care provider to determine what is best for you.”
MS itself does not compromise the immune system, but some MS therapies alter the immune system and reduce the body’s response to vaccination. Patients with MS who use B cell-depleting therapies have a better antibody response when they receive the vaccine 3 months or more after the last dose of MS therapy, according to the National MS Society.
Data suggest that patients with MS are not more susceptible to COVID-19 infection, severe illness, or death than are patients without MS. However, certain groups of patients with MS, such as those who receive B cell-depleting treatments, are more susceptible to having a severe case of COVID-19.
That said, “everyone will need a booster at some point. Those who take DMTs that have greater impact on the immune system are the most urgent need now,” the organization noted.
“Vaccination against COVID-19 is critical for public safety and, especially, the safety of the most vulnerable among us,” said Ms. Fiol. “We encourage everyone with MS get vaccinated.”
A version of this article first appeared on Medscape.com.
Patients aged 12 years and older with multiple sclerosis (MS) who are fully immunized against COVID-19 with either the Pfizer-BioNTech or Moderna mRNA vaccine may be eligible to receive an additional dose now, the National Multiple Sclerosis Society has announced.
New guidance, which is “based on available data from studies and expert consensus opinion” by a panel of MS neurologists and experts, was published Aug. 19 on the organization’s website.
The Food and Drug Administration has authorized an additional dose of the coronavirus vaccine for patients who are expected to not have a normal or adequate immune response to the first two doses. Patients with MS who use certain treatments have a reduced or absent antibody response to the vaccine, according to recent data.
“We want people living with MS to be aware of this additional dose and discuss when they need an additional dose or booster dose with their health care provider,” Julie Fiol, RN, MSW, associate vice president of health care access, National MS Society, said in an interview.
Those who may benefit from an additional dose include patients with MS who use sphingosine 1-phosphate receptor modulators, anti-CD20 monoclonal antibodies, or alemtuzumab (Lemtrada), the National MS Society noted. These particular disease modifying therapies (DMTs) have a stronger effect on the immune system than do other treatments.
Protecting ‘the most vulnerable’
Sphingosine 1-phosphate receptor modulators include fingolimod (Gilenya), siponimod (Mayzent), ozanimod (Zeposia), and ponesimod (Ponvory).
Anti-CD20 monoclonal antibodies include ocrelizumab (Ocrevus), ofatumumab (Kesimpta), rituximab (Rituxan), and corresponding biosimilars.
Current data do not support an additional dose for immunocompromised patients who received the Johnson & Johnson vaccine. The FDA and the Centers for Disease Control and Prevention are developing recommendations for these patients, and the National MS Society will update its guidance as needed, the organization noted in its statement.
“Like other medical decisions, the decision to get an additional dose is best made in partnership with your health care provider,” said Ms. Fiol. “Talk to your MS health care provider to determine what is best for you.”
MS itself does not compromise the immune system, but some MS therapies alter the immune system and reduce the body’s response to vaccination. Patients with MS who use B cell-depleting therapies have a better antibody response when they receive the vaccine 3 months or more after the last dose of MS therapy, according to the National MS Society.
Data suggest that patients with MS are not more susceptible to COVID-19 infection, severe illness, or death than are patients without MS. However, certain groups of patients with MS, such as those who receive B cell-depleting treatments, are more susceptible to having a severe case of COVID-19.
That said, “everyone will need a booster at some point. Those who take DMTs that have greater impact on the immune system are the most urgent need now,” the organization noted.
“Vaccination against COVID-19 is critical for public safety and, especially, the safety of the most vulnerable among us,” said Ms. Fiol. “We encourage everyone with MS get vaccinated.”
A version of this article first appeared on Medscape.com.
Psychotic features among older adults tied to Parkinson’s
Adults aged 65 years and older who develop psychotic manifestations are significantly more likely than those without such manifestations to develop prodromal Parkinson’s disease, data from 925 individuals suggest.
“The presence of perceptual abnormalities and/or delusional ideation among community-dwelling elderly individuals is more widespread than considered in the past,” wrote Ioanna Pachi, MD, of National and Kapodistrian University of Athens Medical School and colleagues. However, those psychoses and their potential impact on prodromal Parkinson’s disease (PD) have not been well studied in community-dwelling populations, they noted in the study, published in Parkinsonism and Related Disorders.
In the study, Dr. Pachi and colleagues reviewed data from 914 participants in the Hellenic Longitudinal Investigation of Aging and Diet study (HELIAD), a cross-sectional, population-based cohort study of older adults in Greece. The average age of the participants was 76 years, and 41% were men. Participants had no delusional features at baseline; delusional features were assessed using the Neuropsychiatric Inventory scale and the Columbia University Scale for Psychopathology in Alzheimer’s disease. The researchers calculated the probability of prodromal PD (pPD) for each participant based on the 2019 International Parkinson and Movement Disorders Society research criteria for prodromal PD.
Over a 3-year follow-up period, 20 participants developed psychotic manifestations and were 1.3 times more likely to have pPD, compared with those without psychoses (P = .006). Those with new-onset psychotic features were categorized together as the NPSY group, regardless of symptom severity or frequency; those with no symptoms at either baseline or during follow-up were categorized as unaffected (UPSY). Most of the NPSY participants showed isolated delusional features, although some expressed hallucinations. Most symptoms were mild.
New-onset psychosis was associated with a fivefold increased risk of both subthreshold parkinsonism and depression (adjusted odds ratios, 4.5 and 5.0, respectively) and with a threefold increased risk of constipation (aOR 2.6). Other factors, including nonsmoking, global cognitive deficit, and anxiety were not significantly associated with new-onset psychotic symptoms after adjusting for confounding factors.
Although the mechanism behind the association remains unclear,
The study findings were limited by several factors, including the administration of neuropsychiatric questionnaires by nonpsychiatrists, and lack of detailed psychiatric history, including complete information on medication use, the researchers noted. The small size of the NPSY group also prevented evaluation of the potential associations between pPD and different modalities of hallucinations, they said.
However, the results were strengthened by the overall large and population-based sample size, and the comprehensive evaluation of psychotic features, they wrote. More follow-up evaluations in the HELIAD cohort are planned to further explore the underlying mechanism of the association between late-life psychosis and pPD.
“Provided that these results are confirmed in other community cohorts of elderly subjects, psychotic features may be added to the list of manifestations of pPD,” they concluded.
The study was supported in part by grants from the Alzheimer’s Association, ARISTEIA, and the ESPA-EU program Excellence Grant. It was cofunded by the European Social Fund and Greek National resources, the Ministry for Health and Social Solidarity, Greece, and the Greek State Scholarships Foundation. Dr. Pachi had no disclosures.
Adults aged 65 years and older who develop psychotic manifestations are significantly more likely than those without such manifestations to develop prodromal Parkinson’s disease, data from 925 individuals suggest.
“The presence of perceptual abnormalities and/or delusional ideation among community-dwelling elderly individuals is more widespread than considered in the past,” wrote Ioanna Pachi, MD, of National and Kapodistrian University of Athens Medical School and colleagues. However, those psychoses and their potential impact on prodromal Parkinson’s disease (PD) have not been well studied in community-dwelling populations, they noted in the study, published in Parkinsonism and Related Disorders.
In the study, Dr. Pachi and colleagues reviewed data from 914 participants in the Hellenic Longitudinal Investigation of Aging and Diet study (HELIAD), a cross-sectional, population-based cohort study of older adults in Greece. The average age of the participants was 76 years, and 41% were men. Participants had no delusional features at baseline; delusional features were assessed using the Neuropsychiatric Inventory scale and the Columbia University Scale for Psychopathology in Alzheimer’s disease. The researchers calculated the probability of prodromal PD (pPD) for each participant based on the 2019 International Parkinson and Movement Disorders Society research criteria for prodromal PD.
Over a 3-year follow-up period, 20 participants developed psychotic manifestations and were 1.3 times more likely to have pPD, compared with those without psychoses (P = .006). Those with new-onset psychotic features were categorized together as the NPSY group, regardless of symptom severity or frequency; those with no symptoms at either baseline or during follow-up were categorized as unaffected (UPSY). Most of the NPSY participants showed isolated delusional features, although some expressed hallucinations. Most symptoms were mild.
New-onset psychosis was associated with a fivefold increased risk of both subthreshold parkinsonism and depression (adjusted odds ratios, 4.5 and 5.0, respectively) and with a threefold increased risk of constipation (aOR 2.6). Other factors, including nonsmoking, global cognitive deficit, and anxiety were not significantly associated with new-onset psychotic symptoms after adjusting for confounding factors.
Although the mechanism behind the association remains unclear,
The study findings were limited by several factors, including the administration of neuropsychiatric questionnaires by nonpsychiatrists, and lack of detailed psychiatric history, including complete information on medication use, the researchers noted. The small size of the NPSY group also prevented evaluation of the potential associations between pPD and different modalities of hallucinations, they said.
However, the results were strengthened by the overall large and population-based sample size, and the comprehensive evaluation of psychotic features, they wrote. More follow-up evaluations in the HELIAD cohort are planned to further explore the underlying mechanism of the association between late-life psychosis and pPD.
“Provided that these results are confirmed in other community cohorts of elderly subjects, psychotic features may be added to the list of manifestations of pPD,” they concluded.
The study was supported in part by grants from the Alzheimer’s Association, ARISTEIA, and the ESPA-EU program Excellence Grant. It was cofunded by the European Social Fund and Greek National resources, the Ministry for Health and Social Solidarity, Greece, and the Greek State Scholarships Foundation. Dr. Pachi had no disclosures.
Adults aged 65 years and older who develop psychotic manifestations are significantly more likely than those without such manifestations to develop prodromal Parkinson’s disease, data from 925 individuals suggest.
“The presence of perceptual abnormalities and/or delusional ideation among community-dwelling elderly individuals is more widespread than considered in the past,” wrote Ioanna Pachi, MD, of National and Kapodistrian University of Athens Medical School and colleagues. However, those psychoses and their potential impact on prodromal Parkinson’s disease (PD) have not been well studied in community-dwelling populations, they noted in the study, published in Parkinsonism and Related Disorders.
In the study, Dr. Pachi and colleagues reviewed data from 914 participants in the Hellenic Longitudinal Investigation of Aging and Diet study (HELIAD), a cross-sectional, population-based cohort study of older adults in Greece. The average age of the participants was 76 years, and 41% were men. Participants had no delusional features at baseline; delusional features were assessed using the Neuropsychiatric Inventory scale and the Columbia University Scale for Psychopathology in Alzheimer’s disease. The researchers calculated the probability of prodromal PD (pPD) for each participant based on the 2019 International Parkinson and Movement Disorders Society research criteria for prodromal PD.
Over a 3-year follow-up period, 20 participants developed psychotic manifestations and were 1.3 times more likely to have pPD, compared with those without psychoses (P = .006). Those with new-onset psychotic features were categorized together as the NPSY group, regardless of symptom severity or frequency; those with no symptoms at either baseline or during follow-up were categorized as unaffected (UPSY). Most of the NPSY participants showed isolated delusional features, although some expressed hallucinations. Most symptoms were mild.
New-onset psychosis was associated with a fivefold increased risk of both subthreshold parkinsonism and depression (adjusted odds ratios, 4.5 and 5.0, respectively) and with a threefold increased risk of constipation (aOR 2.6). Other factors, including nonsmoking, global cognitive deficit, and anxiety were not significantly associated with new-onset psychotic symptoms after adjusting for confounding factors.
Although the mechanism behind the association remains unclear,
The study findings were limited by several factors, including the administration of neuropsychiatric questionnaires by nonpsychiatrists, and lack of detailed psychiatric history, including complete information on medication use, the researchers noted. The small size of the NPSY group also prevented evaluation of the potential associations between pPD and different modalities of hallucinations, they said.
However, the results were strengthened by the overall large and population-based sample size, and the comprehensive evaluation of psychotic features, they wrote. More follow-up evaluations in the HELIAD cohort are planned to further explore the underlying mechanism of the association between late-life psychosis and pPD.
“Provided that these results are confirmed in other community cohorts of elderly subjects, psychotic features may be added to the list of manifestations of pPD,” they concluded.
The study was supported in part by grants from the Alzheimer’s Association, ARISTEIA, and the ESPA-EU program Excellence Grant. It was cofunded by the European Social Fund and Greek National resources, the Ministry for Health and Social Solidarity, Greece, and the Greek State Scholarships Foundation. Dr. Pachi had no disclosures.
FROM PARKINSONISM AND RELATED DISORDERS
Increased risk of hospitalization and death with Parkinson’s drug
, according to a new study.
A retrospective cohort study of elderly patients with Parkinson’s disease who were in long-term care facilities found that the use of pimavanserin (Nuplazid) was associated with an increased risk of 30-day hospitalization and mortality for up to a year.
“Given that a previous study showed typical and atypical antipsychotics more than doubled mortality risk in patients with Parkinson’s disease, we aimed to assess the risk of hospitalization and death associated with pimavanserin,” wrote lead author Y. Joseph Hwang, MD, Johns Hopkins University, Baltimore, and colleagues in the paper. “These findings, in a large real-world cohort within long-term care facilities, may help to inform decisions regarding its risk-benefit balance among patients with Parkinson’s disease.”
The findings were published online Aug. 13 in Neurology.
The researchers enrolled 2,186 patients with Parkinson’s disease aged 65 years and older in Medicare-certified long-term care facilities who also had a pimavanserin prescription and 18,212 nonusers of pimavanserin between Nov. 1, 2015, and December 31, 2018. Patients in the pimavanserin group used the drug over the course of the entire study period. Hospitalization and mortality were calculated from the date of pimavanserin prescription. Propensity score–based inverse probability of treatment weighting (IPTW) was used to balance the two groups on 24 baseline characteristics such as age, sex, and comorbidities.
Pimavanserin use was associated with a 24% higher risk of 30-day hospitalization (adjusted hazard ratio, 1.24; 95% confidence interval, 1.06-1.43). However, “the association did not reach statistical significance in a smaller subcohort of propensity score-matched users and nonusers,” Dr. Hwang and colleagues wrote.
Pimavanserin use was also linked to higher mortality at:
- 90 days (aHR, 1.20; 95% CI, 1.02-1.41).
- 180 days (aHR, 1.28; 95% CI, 1.13-1.45).
- 365 days (aHR, 1.56; 95% CI, 1.42-1.72).
No associations were found between pimavanserin use and 90-day hospitalization (aHR, 1.10; 95% CI, 0.99-1.24) nor with 30-day mortality (aHR, 0.76; 95% CI, 0.56-1.03).
Important considerations
“This study raises three important points to consider for any practicing neurology provider: 1) how to address and interpret risks associated with pimavanserin use in this patient population 2) utility of pimavanserin 3) interpretation of data showing increased mortality in patients being treated for Parkinson’s disease psychosis,” wrote Farwa Ali, MBBS, of the Mayo Clinic, Rochester, Minn., in an accompanying editorial published in Neurology.
Hallucinations and delusions are highly prevalent in Parkinson’s disease; as many as 60% of patients will develop psychosis over the course of their illness. Pimavanserin is a selective serotonin inverse agonist which targets 5-HT2A serotonin receptors in the brain, decreasing their activity in order to attenuate hallucinations and delusions.
“Pimavanserin has been approved by the FDA [Food and Drug Administration] for Parkinson’s disease psychosis, but its safety has been called into question based on previous reports of increased mortality risk, compared with a rather modest benefit seen in a 6-week clinical trial, the duration of which limits determination of long-term safety,” wrote Dr. Ali.
Pimavanserin carries a boxed warning that elderly patients with dementia may be at an increased risk of death. After its approval in 2016, the U.S. FDA later reviewed 893 deaths in association with pimavanserin during the postmarketing surveillance period – “an unexpected number in a new drug,” Dr. Hwang and colleagues noted. “It [the FDA] noted that most reports occurred in a population with high underlying death rates and did not signal any additional risk beyond the current warning for all antipsychotics, which could have resulted in annual mortality rates of up to 60%.”
As the first cohort study to examine hospitalization and death between pimavanserin users and nonusers, “the study confirms previous concerns regarding safety of pimavanserin and more importantly brings to attention the importance of carefully considering risks and benefits of pharmacotherapy in Parkinson’s disease psychosis, clear communication with patients and families, and close observation to ensure safety,” wrote Dr. Ali.
The study limitations include its observational design, which subjected the findings to residual confounding.
“While we developed models to maximize the strength of causal inference, our comparison group was pimavanserin nonusers and the very reason for prescription of pimavanserin could have predisposed its users to the outcomes of hospitalization and death, introducing confounding by indication,” Dr. Hwang and colleagues wrote in the paper.
Additionally, “while robust analyses were conducted to ensure pimavanserin users and nonusers were comparable, Dr. Hwang et al. did find that pimavanserin users were more likely to concomitantly use other antipsychotic drugs which has been demonstrated as increasing the mortality risk,” Dr. Ali pointed out.
Since patients living in long-term care facilities may have a higher risk of mortality because of more severe or later-stage Parkinson’s disease, the study results “may not be generalizable to community-dwelling PD patients,” Dr. Ali wrote. “These factors are important to consider while making individual management decisions.”
Dr. Hwang and Dr. Ali disclosed no relevant financial relationships. The study authors reported no targeted funding.
, according to a new study.
A retrospective cohort study of elderly patients with Parkinson’s disease who were in long-term care facilities found that the use of pimavanserin (Nuplazid) was associated with an increased risk of 30-day hospitalization and mortality for up to a year.
“Given that a previous study showed typical and atypical antipsychotics more than doubled mortality risk in patients with Parkinson’s disease, we aimed to assess the risk of hospitalization and death associated with pimavanserin,” wrote lead author Y. Joseph Hwang, MD, Johns Hopkins University, Baltimore, and colleagues in the paper. “These findings, in a large real-world cohort within long-term care facilities, may help to inform decisions regarding its risk-benefit balance among patients with Parkinson’s disease.”
The findings were published online Aug. 13 in Neurology.
The researchers enrolled 2,186 patients with Parkinson’s disease aged 65 years and older in Medicare-certified long-term care facilities who also had a pimavanserin prescription and 18,212 nonusers of pimavanserin between Nov. 1, 2015, and December 31, 2018. Patients in the pimavanserin group used the drug over the course of the entire study period. Hospitalization and mortality were calculated from the date of pimavanserin prescription. Propensity score–based inverse probability of treatment weighting (IPTW) was used to balance the two groups on 24 baseline characteristics such as age, sex, and comorbidities.
Pimavanserin use was associated with a 24% higher risk of 30-day hospitalization (adjusted hazard ratio, 1.24; 95% confidence interval, 1.06-1.43). However, “the association did not reach statistical significance in a smaller subcohort of propensity score-matched users and nonusers,” Dr. Hwang and colleagues wrote.
Pimavanserin use was also linked to higher mortality at:
- 90 days (aHR, 1.20; 95% CI, 1.02-1.41).
- 180 days (aHR, 1.28; 95% CI, 1.13-1.45).
- 365 days (aHR, 1.56; 95% CI, 1.42-1.72).
No associations were found between pimavanserin use and 90-day hospitalization (aHR, 1.10; 95% CI, 0.99-1.24) nor with 30-day mortality (aHR, 0.76; 95% CI, 0.56-1.03).
Important considerations
“This study raises three important points to consider for any practicing neurology provider: 1) how to address and interpret risks associated with pimavanserin use in this patient population 2) utility of pimavanserin 3) interpretation of data showing increased mortality in patients being treated for Parkinson’s disease psychosis,” wrote Farwa Ali, MBBS, of the Mayo Clinic, Rochester, Minn., in an accompanying editorial published in Neurology.
Hallucinations and delusions are highly prevalent in Parkinson’s disease; as many as 60% of patients will develop psychosis over the course of their illness. Pimavanserin is a selective serotonin inverse agonist which targets 5-HT2A serotonin receptors in the brain, decreasing their activity in order to attenuate hallucinations and delusions.
“Pimavanserin has been approved by the FDA [Food and Drug Administration] for Parkinson’s disease psychosis, but its safety has been called into question based on previous reports of increased mortality risk, compared with a rather modest benefit seen in a 6-week clinical trial, the duration of which limits determination of long-term safety,” wrote Dr. Ali.
Pimavanserin carries a boxed warning that elderly patients with dementia may be at an increased risk of death. After its approval in 2016, the U.S. FDA later reviewed 893 deaths in association with pimavanserin during the postmarketing surveillance period – “an unexpected number in a new drug,” Dr. Hwang and colleagues noted. “It [the FDA] noted that most reports occurred in a population with high underlying death rates and did not signal any additional risk beyond the current warning for all antipsychotics, which could have resulted in annual mortality rates of up to 60%.”
As the first cohort study to examine hospitalization and death between pimavanserin users and nonusers, “the study confirms previous concerns regarding safety of pimavanserin and more importantly brings to attention the importance of carefully considering risks and benefits of pharmacotherapy in Parkinson’s disease psychosis, clear communication with patients and families, and close observation to ensure safety,” wrote Dr. Ali.
The study limitations include its observational design, which subjected the findings to residual confounding.
“While we developed models to maximize the strength of causal inference, our comparison group was pimavanserin nonusers and the very reason for prescription of pimavanserin could have predisposed its users to the outcomes of hospitalization and death, introducing confounding by indication,” Dr. Hwang and colleagues wrote in the paper.
Additionally, “while robust analyses were conducted to ensure pimavanserin users and nonusers were comparable, Dr. Hwang et al. did find that pimavanserin users were more likely to concomitantly use other antipsychotic drugs which has been demonstrated as increasing the mortality risk,” Dr. Ali pointed out.
Since patients living in long-term care facilities may have a higher risk of mortality because of more severe or later-stage Parkinson’s disease, the study results “may not be generalizable to community-dwelling PD patients,” Dr. Ali wrote. “These factors are important to consider while making individual management decisions.”
Dr. Hwang and Dr. Ali disclosed no relevant financial relationships. The study authors reported no targeted funding.
, according to a new study.
A retrospective cohort study of elderly patients with Parkinson’s disease who were in long-term care facilities found that the use of pimavanserin (Nuplazid) was associated with an increased risk of 30-day hospitalization and mortality for up to a year.
“Given that a previous study showed typical and atypical antipsychotics more than doubled mortality risk in patients with Parkinson’s disease, we aimed to assess the risk of hospitalization and death associated with pimavanserin,” wrote lead author Y. Joseph Hwang, MD, Johns Hopkins University, Baltimore, and colleagues in the paper. “These findings, in a large real-world cohort within long-term care facilities, may help to inform decisions regarding its risk-benefit balance among patients with Parkinson’s disease.”
The findings were published online Aug. 13 in Neurology.
The researchers enrolled 2,186 patients with Parkinson’s disease aged 65 years and older in Medicare-certified long-term care facilities who also had a pimavanserin prescription and 18,212 nonusers of pimavanserin between Nov. 1, 2015, and December 31, 2018. Patients in the pimavanserin group used the drug over the course of the entire study period. Hospitalization and mortality were calculated from the date of pimavanserin prescription. Propensity score–based inverse probability of treatment weighting (IPTW) was used to balance the two groups on 24 baseline characteristics such as age, sex, and comorbidities.
Pimavanserin use was associated with a 24% higher risk of 30-day hospitalization (adjusted hazard ratio, 1.24; 95% confidence interval, 1.06-1.43). However, “the association did not reach statistical significance in a smaller subcohort of propensity score-matched users and nonusers,” Dr. Hwang and colleagues wrote.
Pimavanserin use was also linked to higher mortality at:
- 90 days (aHR, 1.20; 95% CI, 1.02-1.41).
- 180 days (aHR, 1.28; 95% CI, 1.13-1.45).
- 365 days (aHR, 1.56; 95% CI, 1.42-1.72).
No associations were found between pimavanserin use and 90-day hospitalization (aHR, 1.10; 95% CI, 0.99-1.24) nor with 30-day mortality (aHR, 0.76; 95% CI, 0.56-1.03).
Important considerations
“This study raises three important points to consider for any practicing neurology provider: 1) how to address and interpret risks associated with pimavanserin use in this patient population 2) utility of pimavanserin 3) interpretation of data showing increased mortality in patients being treated for Parkinson’s disease psychosis,” wrote Farwa Ali, MBBS, of the Mayo Clinic, Rochester, Minn., in an accompanying editorial published in Neurology.
Hallucinations and delusions are highly prevalent in Parkinson’s disease; as many as 60% of patients will develop psychosis over the course of their illness. Pimavanserin is a selective serotonin inverse agonist which targets 5-HT2A serotonin receptors in the brain, decreasing their activity in order to attenuate hallucinations and delusions.
“Pimavanserin has been approved by the FDA [Food and Drug Administration] for Parkinson’s disease psychosis, but its safety has been called into question based on previous reports of increased mortality risk, compared with a rather modest benefit seen in a 6-week clinical trial, the duration of which limits determination of long-term safety,” wrote Dr. Ali.
Pimavanserin carries a boxed warning that elderly patients with dementia may be at an increased risk of death. After its approval in 2016, the U.S. FDA later reviewed 893 deaths in association with pimavanserin during the postmarketing surveillance period – “an unexpected number in a new drug,” Dr. Hwang and colleagues noted. “It [the FDA] noted that most reports occurred in a population with high underlying death rates and did not signal any additional risk beyond the current warning for all antipsychotics, which could have resulted in annual mortality rates of up to 60%.”
As the first cohort study to examine hospitalization and death between pimavanserin users and nonusers, “the study confirms previous concerns regarding safety of pimavanserin and more importantly brings to attention the importance of carefully considering risks and benefits of pharmacotherapy in Parkinson’s disease psychosis, clear communication with patients and families, and close observation to ensure safety,” wrote Dr. Ali.
The study limitations include its observational design, which subjected the findings to residual confounding.
“While we developed models to maximize the strength of causal inference, our comparison group was pimavanserin nonusers and the very reason for prescription of pimavanserin could have predisposed its users to the outcomes of hospitalization and death, introducing confounding by indication,” Dr. Hwang and colleagues wrote in the paper.
Additionally, “while robust analyses were conducted to ensure pimavanserin users and nonusers were comparable, Dr. Hwang et al. did find that pimavanserin users were more likely to concomitantly use other antipsychotic drugs which has been demonstrated as increasing the mortality risk,” Dr. Ali pointed out.
Since patients living in long-term care facilities may have a higher risk of mortality because of more severe or later-stage Parkinson’s disease, the study results “may not be generalizable to community-dwelling PD patients,” Dr. Ali wrote. “These factors are important to consider while making individual management decisions.”
Dr. Hwang and Dr. Ali disclosed no relevant financial relationships. The study authors reported no targeted funding.
FROM NEUROLOGY
Pandemic derails small success in lowering diabetes-related amputations
Rates of minor diabetes-related lower extremity amputations (LEAs) in hospitalized patients increased between 2009 and 2017 in all racial and ethnic groups, in both rural and urban areas, and in all geographic regions across the United States, a new retrospective, observational study indicates.
In contrast, major lower extremity amputation rates held steady during the study period with a few exceptions.
There was also a decline in major-to-minor amputation ratios, especially among Native Americans – a sign that diabetes was being better managed and foot ulcers were being caught earlier, preventing the need for a major amputation above the foot or below or above the knee.
Minor LEAs include the loss of a toe, toes, or a foot.
“While I know an amputation is devastating either way, having a minor amputation is better than having a major amputation, and trends [at least to 2017] show that comprehensive foot examinations are paying off,” lead author Marvellous Akinlotan, PhD, MPH, a research associate at the Southwest Rural Health Research Center in Bryan, Texas, said in an interview.
Asked to comment, Marcia Ory, PhD, MPH, director of the Center for Population Health & Aging, Texas A&M School of Public Health, College Station, who was not involved in the study, said: “It points to some successes, but it also points to the need for continued education and preventive care to reduce all types of amputations.”
The study was published online in Diabetes Care.
Amputations increased during COVID-19
However, the study was conducted prior to the COVID-19 pandemic, and amputation rates appear to have significantly worsened during the past 18 months.
In a summary of recent evidence collated by the Amputee Coalition, the authors point out that not only does COVID-19 itself put patients at higher risk for limb loss because severe infection increases the risk of blood clots, but patients with diabetes appear to have been far more likely to undergo any level of amputation during the pandemic than before it began.
In a study of patients with diabetes attending a foot and ankle surgery service in Ohio, the risk of having any level of amputation was 10.8 times higher during compared with before the pandemic. And of patients undergoing any amputation, the odds for receiving a major amputation was 3.1 times higher than before the pandemic.
Telehealth and web-based options for diabetes care and education could help improve health outcomes, particularly during lockdowns.
“Having a diabetes-related amputation is life-changing – it brings disability and functional limitations to the individual – and within the health care system, it reflects the failure of secondary prevention efforts, which ideally should slow the progression of diabetic complications,” noted Dr. Akinlotan.
Race and geography affect risk of amputation
In their study, Dr. Akinlotan and colleagues used data from the National Inpatient Sample to identify trends in LEAs among patients primarily hospitalized for diabetes in the United States between 2009 and 2017.
“The primary outcome variable was documentation of either minor or major LEA during a diabetes-related admission,” they explain.
Minor LEAs increased significantly across all ethnic groups.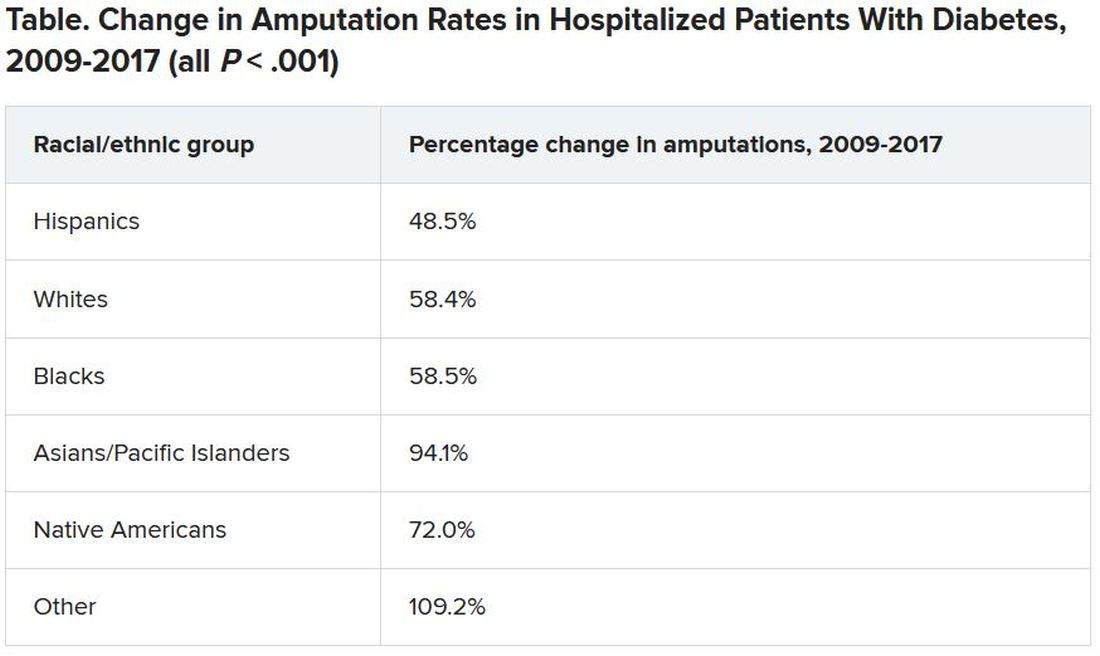
Although major amputation rates remained steady, “we did find that some groups remained at risk for having a major amputation,” Dr. Akinlotan noted.
White populations, people in the Midwest, and rural areas saw notable increases in major LEAs, as did “... Blacks, Hispanics, [and] those living in the South,” she said.
Patients need to be encouraged to monitor and control their blood glucose, to offset modifiable risk factors, and to seek regular medical attention to prevent an insidious diabetic complication from developing further, she said.
“It’s important for patients to know that continuing care is necessary,” Dr. Akinlotan stressed. “Diabetes is chronic and complex, but it can be managed, so that’s the good news.”
Dr. Ory agrees: “Effective management will require an all-in approach, with doctors and patients working together.
“Given the limited time in doctor-patient encounters, physicians can benefit patients by referring them to evidence-based, self-management education programs, which are proliferating around in the county,” she added.
The authors and Dr. Ory have reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Rates of minor diabetes-related lower extremity amputations (LEAs) in hospitalized patients increased between 2009 and 2017 in all racial and ethnic groups, in both rural and urban areas, and in all geographic regions across the United States, a new retrospective, observational study indicates.
In contrast, major lower extremity amputation rates held steady during the study period with a few exceptions.
There was also a decline in major-to-minor amputation ratios, especially among Native Americans – a sign that diabetes was being better managed and foot ulcers were being caught earlier, preventing the need for a major amputation above the foot or below or above the knee.
Minor LEAs include the loss of a toe, toes, or a foot.
“While I know an amputation is devastating either way, having a minor amputation is better than having a major amputation, and trends [at least to 2017] show that comprehensive foot examinations are paying off,” lead author Marvellous Akinlotan, PhD, MPH, a research associate at the Southwest Rural Health Research Center in Bryan, Texas, said in an interview.
Asked to comment, Marcia Ory, PhD, MPH, director of the Center for Population Health & Aging, Texas A&M School of Public Health, College Station, who was not involved in the study, said: “It points to some successes, but it also points to the need for continued education and preventive care to reduce all types of amputations.”
The study was published online in Diabetes Care.
Amputations increased during COVID-19
However, the study was conducted prior to the COVID-19 pandemic, and amputation rates appear to have significantly worsened during the past 18 months.
In a summary of recent evidence collated by the Amputee Coalition, the authors point out that not only does COVID-19 itself put patients at higher risk for limb loss because severe infection increases the risk of blood clots, but patients with diabetes appear to have been far more likely to undergo any level of amputation during the pandemic than before it began.
In a study of patients with diabetes attending a foot and ankle surgery service in Ohio, the risk of having any level of amputation was 10.8 times higher during compared with before the pandemic. And of patients undergoing any amputation, the odds for receiving a major amputation was 3.1 times higher than before the pandemic.
Telehealth and web-based options for diabetes care and education could help improve health outcomes, particularly during lockdowns.
“Having a diabetes-related amputation is life-changing – it brings disability and functional limitations to the individual – and within the health care system, it reflects the failure of secondary prevention efforts, which ideally should slow the progression of diabetic complications,” noted Dr. Akinlotan.
Race and geography affect risk of amputation
In their study, Dr. Akinlotan and colleagues used data from the National Inpatient Sample to identify trends in LEAs among patients primarily hospitalized for diabetes in the United States between 2009 and 2017.
“The primary outcome variable was documentation of either minor or major LEA during a diabetes-related admission,” they explain.
Minor LEAs increased significantly across all ethnic groups.
Although major amputation rates remained steady, “we did find that some groups remained at risk for having a major amputation,” Dr. Akinlotan noted.
White populations, people in the Midwest, and rural areas saw notable increases in major LEAs, as did “... Blacks, Hispanics, [and] those living in the South,” she said.
Patients need to be encouraged to monitor and control their blood glucose, to offset modifiable risk factors, and to seek regular medical attention to prevent an insidious diabetic complication from developing further, she said.
“It’s important for patients to know that continuing care is necessary,” Dr. Akinlotan stressed. “Diabetes is chronic and complex, but it can be managed, so that’s the good news.”
Dr. Ory agrees: “Effective management will require an all-in approach, with doctors and patients working together.
“Given the limited time in doctor-patient encounters, physicians can benefit patients by referring them to evidence-based, self-management education programs, which are proliferating around in the county,” she added.
The authors and Dr. Ory have reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Rates of minor diabetes-related lower extremity amputations (LEAs) in hospitalized patients increased between 2009 and 2017 in all racial and ethnic groups, in both rural and urban areas, and in all geographic regions across the United States, a new retrospective, observational study indicates.
In contrast, major lower extremity amputation rates held steady during the study period with a few exceptions.
There was also a decline in major-to-minor amputation ratios, especially among Native Americans – a sign that diabetes was being better managed and foot ulcers were being caught earlier, preventing the need for a major amputation above the foot or below or above the knee.
Minor LEAs include the loss of a toe, toes, or a foot.
“While I know an amputation is devastating either way, having a minor amputation is better than having a major amputation, and trends [at least to 2017] show that comprehensive foot examinations are paying off,” lead author Marvellous Akinlotan, PhD, MPH, a research associate at the Southwest Rural Health Research Center in Bryan, Texas, said in an interview.
Asked to comment, Marcia Ory, PhD, MPH, director of the Center for Population Health & Aging, Texas A&M School of Public Health, College Station, who was not involved in the study, said: “It points to some successes, but it also points to the need for continued education and preventive care to reduce all types of amputations.”
The study was published online in Diabetes Care.
Amputations increased during COVID-19
However, the study was conducted prior to the COVID-19 pandemic, and amputation rates appear to have significantly worsened during the past 18 months.
In a summary of recent evidence collated by the Amputee Coalition, the authors point out that not only does COVID-19 itself put patients at higher risk for limb loss because severe infection increases the risk of blood clots, but patients with diabetes appear to have been far more likely to undergo any level of amputation during the pandemic than before it began.
In a study of patients with diabetes attending a foot and ankle surgery service in Ohio, the risk of having any level of amputation was 10.8 times higher during compared with before the pandemic. And of patients undergoing any amputation, the odds for receiving a major amputation was 3.1 times higher than before the pandemic.
Telehealth and web-based options for diabetes care and education could help improve health outcomes, particularly during lockdowns.
“Having a diabetes-related amputation is life-changing – it brings disability and functional limitations to the individual – and within the health care system, it reflects the failure of secondary prevention efforts, which ideally should slow the progression of diabetic complications,” noted Dr. Akinlotan.
Race and geography affect risk of amputation
In their study, Dr. Akinlotan and colleagues used data from the National Inpatient Sample to identify trends in LEAs among patients primarily hospitalized for diabetes in the United States between 2009 and 2017.
“The primary outcome variable was documentation of either minor or major LEA during a diabetes-related admission,” they explain.
Minor LEAs increased significantly across all ethnic groups.
Although major amputation rates remained steady, “we did find that some groups remained at risk for having a major amputation,” Dr. Akinlotan noted.
White populations, people in the Midwest, and rural areas saw notable increases in major LEAs, as did “... Blacks, Hispanics, [and] those living in the South,” she said.
Patients need to be encouraged to monitor and control their blood glucose, to offset modifiable risk factors, and to seek regular medical attention to prevent an insidious diabetic complication from developing further, she said.
“It’s important for patients to know that continuing care is necessary,” Dr. Akinlotan stressed. “Diabetes is chronic and complex, but it can be managed, so that’s the good news.”
Dr. Ory agrees: “Effective management will require an all-in approach, with doctors and patients working together.
“Given the limited time in doctor-patient encounters, physicians can benefit patients by referring them to evidence-based, self-management education programs, which are proliferating around in the county,” she added.
The authors and Dr. Ory have reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Increased stroke risk linked with excess sitting in those under 60
While the risk of stroke increased more than fourfold among sedentary people under the age of 60, no significant increase in risk was observed among older individuals, according to the study based on self-reported data from more than 140,000 people. This highlights the need for relevant public health messaging directed at younger people, reported lead author, Raed A. Joundi, MD, DPhil, a stroke fellow at the University of Calgary (Alta.), and colleagues, in the paper published in Stroke.
“Sedentary time has increased over the past 2 decades in the United States and Canada, particularly in the young, raising the importance of characterizing its effect on long-term health , ” the investigators wrote. “A better understanding of the risk of sedentary time specific to stroke may be important for public health campaigns to reduce sedentary behavior.” Dr. Joundi and colleagues reviewed data from the Canadian Community Health Survey, including 143,180 healthy individuals without baseline history of cancer, heart disease, or stroke. Those under the age of 40 years were also excluded from the analysis.
Excess sedentary leisure time was defined as 8 or more hours of sedentary leisure time per day, whereas low physical activity was defined as less than 3.5 metabolic equivalent hours per week. The analysis also included a range of demographic and medical covariates, such as age, sex, marital status, smoking status, presence of hypertension, and others.
After a median follow-up of 9.4 years, 2,965 stroke events occurred, with a median time from survey response of 5.6 years. Risk of stroke among individuals aged younger than 60 years who engaged in low physical activity and excess sedentary leisure time was increased 4.5-fold, compared with individuals with low physical activity who were sedentary less than 4 hours per day (fully adjusted hazard ratio, 4.50; 95% confidence interval, 1.64-12.3).
Findings highlight benefits of physical activity
Similar risk elevations were not observed among individuals aged 60-79 years, or those older than 80. And among people younger than 60, high physical activity appeared to eliminate the additional risk imposed by excess sedentary leisure time.
“Sedentary time is associated with higher risk of stroke in inactive individuals, but not an active individual, ” Dr. Joundi said in an interview. “So it suggests that there’s two ways to lower risk: One would be to lower your sedentary time, and the other would be to engage in physical activity.”
These interpretations are speculative, Dr. Joundi cautioned, as the study was not interventional. Even so, he said that the findings “bring the spotlight back on physical activity,” thereby aligning with previous research.
“The more you exercise, the more that relationship between sedentary time and poor health outcomes is blunted, and in fact, can be completely negated with enough physical activity,” he said.
How exactly physical activity offers such protection remains unclear, Dr. Joundi added. He speculated that regularity of exercise may be key, with each session counteracting the adverse effects of prolonged sedentary time, which may include reduced blood flow, increased insulin resistance, and inflammatory changes that can affect blood vessels.
“This study is particularly a message for younger individuals,” Dr. Joundi said, suggesting that the findings may alter behavior, as many people have witnessed, or are aware of, the long-term impacts of stroke.
“There’s a sort of social or cognitive aversion to stroke, I think, in the general population, because of how disabling it can be, and how it can lower your quality of life,” he said.
Subtle lifestyle changes may be enough.
For those aiming to lower their risk of stroke, Dr. Joundi suggested that subtle lifestyle changes may be enough.
“Ultimately, what we saw is that even minimal amounts of physical activity – walking 3 hours a week, for example – could blunt the impact of sedentary time,” he said. “Doing what you can, even if it’s a small amount, tends to be quite meaningful over a long period of time.”
Daniel T. Lackland, DrPH, professor of epidemiology in the department of neurology at the Medical University of South Carolina, Charleston, offered a similar takeaway, noting that small efforts can lead to great benefits.
“Less intense activity is still better than being sedentary,” he said in an interview. “For many people, if you do get up and you just walk around, move your arms around – do any kind of movement – that’s better than being sedentary.”
Dr. Lackland applauded the practicality of studying sedentary leisure time, versus overall leisure time, as many people can’t control their work environment.
“You can’t do very much about how you work your job,” Dr. Lackland said. “Sometimes we have to sit, and I guess there are things you can do – you can put a treadmill instead of a chair and that kind of thing – but more often than not, you don’t really have that choice to do something. With leisure time, though, you’re in full control. And so what do you do with your leisure time? Do you sit and watch TV, or do you engage in some type of activity? Not necessarily aerobic activity, but some type of activity that would not let you be sedentary. You want to be active as much as you possibly can.”
Dr. Joundi disclosed grant support from the Canadian Institutes of Health Research. The other investigators and Dr. Lackland reported no relevant disclosures.
While the risk of stroke increased more than fourfold among sedentary people under the age of 60, no significant increase in risk was observed among older individuals, according to the study based on self-reported data from more than 140,000 people. This highlights the need for relevant public health messaging directed at younger people, reported lead author, Raed A. Joundi, MD, DPhil, a stroke fellow at the University of Calgary (Alta.), and colleagues, in the paper published in Stroke.
“Sedentary time has increased over the past 2 decades in the United States and Canada, particularly in the young, raising the importance of characterizing its effect on long-term health , ” the investigators wrote. “A better understanding of the risk of sedentary time specific to stroke may be important for public health campaigns to reduce sedentary behavior.” Dr. Joundi and colleagues reviewed data from the Canadian Community Health Survey, including 143,180 healthy individuals without baseline history of cancer, heart disease, or stroke. Those under the age of 40 years were also excluded from the analysis.
Excess sedentary leisure time was defined as 8 or more hours of sedentary leisure time per day, whereas low physical activity was defined as less than 3.5 metabolic equivalent hours per week. The analysis also included a range of demographic and medical covariates, such as age, sex, marital status, smoking status, presence of hypertension, and others.
After a median follow-up of 9.4 years, 2,965 stroke events occurred, with a median time from survey response of 5.6 years. Risk of stroke among individuals aged younger than 60 years who engaged in low physical activity and excess sedentary leisure time was increased 4.5-fold, compared with individuals with low physical activity who were sedentary less than 4 hours per day (fully adjusted hazard ratio, 4.50; 95% confidence interval, 1.64-12.3).
Findings highlight benefits of physical activity
Similar risk elevations were not observed among individuals aged 60-79 years, or those older than 80. And among people younger than 60, high physical activity appeared to eliminate the additional risk imposed by excess sedentary leisure time.
“Sedentary time is associated with higher risk of stroke in inactive individuals, but not an active individual, ” Dr. Joundi said in an interview. “So it suggests that there’s two ways to lower risk: One would be to lower your sedentary time, and the other would be to engage in physical activity.”
These interpretations are speculative, Dr. Joundi cautioned, as the study was not interventional. Even so, he said that the findings “bring the spotlight back on physical activity,” thereby aligning with previous research.
“The more you exercise, the more that relationship between sedentary time and poor health outcomes is blunted, and in fact, can be completely negated with enough physical activity,” he said.
How exactly physical activity offers such protection remains unclear, Dr. Joundi added. He speculated that regularity of exercise may be key, with each session counteracting the adverse effects of prolonged sedentary time, which may include reduced blood flow, increased insulin resistance, and inflammatory changes that can affect blood vessels.
“This study is particularly a message for younger individuals,” Dr. Joundi said, suggesting that the findings may alter behavior, as many people have witnessed, or are aware of, the long-term impacts of stroke.
“There’s a sort of social or cognitive aversion to stroke, I think, in the general population, because of how disabling it can be, and how it can lower your quality of life,” he said.
Subtle lifestyle changes may be enough.
For those aiming to lower their risk of stroke, Dr. Joundi suggested that subtle lifestyle changes may be enough.
“Ultimately, what we saw is that even minimal amounts of physical activity – walking 3 hours a week, for example – could blunt the impact of sedentary time,” he said. “Doing what you can, even if it’s a small amount, tends to be quite meaningful over a long period of time.”
Daniel T. Lackland, DrPH, professor of epidemiology in the department of neurology at the Medical University of South Carolina, Charleston, offered a similar takeaway, noting that small efforts can lead to great benefits.
“Less intense activity is still better than being sedentary,” he said in an interview. “For many people, if you do get up and you just walk around, move your arms around – do any kind of movement – that’s better than being sedentary.”
Dr. Lackland applauded the practicality of studying sedentary leisure time, versus overall leisure time, as many people can’t control their work environment.
“You can’t do very much about how you work your job,” Dr. Lackland said. “Sometimes we have to sit, and I guess there are things you can do – you can put a treadmill instead of a chair and that kind of thing – but more often than not, you don’t really have that choice to do something. With leisure time, though, you’re in full control. And so what do you do with your leisure time? Do you sit and watch TV, or do you engage in some type of activity? Not necessarily aerobic activity, but some type of activity that would not let you be sedentary. You want to be active as much as you possibly can.”
Dr. Joundi disclosed grant support from the Canadian Institutes of Health Research. The other investigators and Dr. Lackland reported no relevant disclosures.
While the risk of stroke increased more than fourfold among sedentary people under the age of 60, no significant increase in risk was observed among older individuals, according to the study based on self-reported data from more than 140,000 people. This highlights the need for relevant public health messaging directed at younger people, reported lead author, Raed A. Joundi, MD, DPhil, a stroke fellow at the University of Calgary (Alta.), and colleagues, in the paper published in Stroke.
“Sedentary time has increased over the past 2 decades in the United States and Canada, particularly in the young, raising the importance of characterizing its effect on long-term health , ” the investigators wrote. “A better understanding of the risk of sedentary time specific to stroke may be important for public health campaigns to reduce sedentary behavior.” Dr. Joundi and colleagues reviewed data from the Canadian Community Health Survey, including 143,180 healthy individuals without baseline history of cancer, heart disease, or stroke. Those under the age of 40 years were also excluded from the analysis.
Excess sedentary leisure time was defined as 8 or more hours of sedentary leisure time per day, whereas low physical activity was defined as less than 3.5 metabolic equivalent hours per week. The analysis also included a range of demographic and medical covariates, such as age, sex, marital status, smoking status, presence of hypertension, and others.
After a median follow-up of 9.4 years, 2,965 stroke events occurred, with a median time from survey response of 5.6 years. Risk of stroke among individuals aged younger than 60 years who engaged in low physical activity and excess sedentary leisure time was increased 4.5-fold, compared with individuals with low physical activity who were sedentary less than 4 hours per day (fully adjusted hazard ratio, 4.50; 95% confidence interval, 1.64-12.3).
Findings highlight benefits of physical activity
Similar risk elevations were not observed among individuals aged 60-79 years, or those older than 80. And among people younger than 60, high physical activity appeared to eliminate the additional risk imposed by excess sedentary leisure time.
“Sedentary time is associated with higher risk of stroke in inactive individuals, but not an active individual, ” Dr. Joundi said in an interview. “So it suggests that there’s two ways to lower risk: One would be to lower your sedentary time, and the other would be to engage in physical activity.”
These interpretations are speculative, Dr. Joundi cautioned, as the study was not interventional. Even so, he said that the findings “bring the spotlight back on physical activity,” thereby aligning with previous research.
“The more you exercise, the more that relationship between sedentary time and poor health outcomes is blunted, and in fact, can be completely negated with enough physical activity,” he said.
How exactly physical activity offers such protection remains unclear, Dr. Joundi added. He speculated that regularity of exercise may be key, with each session counteracting the adverse effects of prolonged sedentary time, which may include reduced blood flow, increased insulin resistance, and inflammatory changes that can affect blood vessels.
“This study is particularly a message for younger individuals,” Dr. Joundi said, suggesting that the findings may alter behavior, as many people have witnessed, or are aware of, the long-term impacts of stroke.
“There’s a sort of social or cognitive aversion to stroke, I think, in the general population, because of how disabling it can be, and how it can lower your quality of life,” he said.
Subtle lifestyle changes may be enough.
For those aiming to lower their risk of stroke, Dr. Joundi suggested that subtle lifestyle changes may be enough.
“Ultimately, what we saw is that even minimal amounts of physical activity – walking 3 hours a week, for example – could blunt the impact of sedentary time,” he said. “Doing what you can, even if it’s a small amount, tends to be quite meaningful over a long period of time.”
Daniel T. Lackland, DrPH, professor of epidemiology in the department of neurology at the Medical University of South Carolina, Charleston, offered a similar takeaway, noting that small efforts can lead to great benefits.
“Less intense activity is still better than being sedentary,” he said in an interview. “For many people, if you do get up and you just walk around, move your arms around – do any kind of movement – that’s better than being sedentary.”
Dr. Lackland applauded the practicality of studying sedentary leisure time, versus overall leisure time, as many people can’t control their work environment.
“You can’t do very much about how you work your job,” Dr. Lackland said. “Sometimes we have to sit, and I guess there are things you can do – you can put a treadmill instead of a chair and that kind of thing – but more often than not, you don’t really have that choice to do something. With leisure time, though, you’re in full control. And so what do you do with your leisure time? Do you sit and watch TV, or do you engage in some type of activity? Not necessarily aerobic activity, but some type of activity that would not let you be sedentary. You want to be active as much as you possibly can.”
Dr. Joundi disclosed grant support from the Canadian Institutes of Health Research. The other investigators and Dr. Lackland reported no relevant disclosures.
FROM STROKE