User login
Beneath the Surface: Massive Retroperitoneal Liposarcoma Masquerading as Meralgia Paresthetica
In patients presenting with focal neurologic findings involving the lower extremities, a thorough abdominal examination should be considered an integral part of the full neurologic work up.
Meralgia paresthetica (MP) is a sensory mononeuropathy of the lateral femoral cutaneous nerve (LFCN), clinically characterized by numbness, pain, and paresthesias involving the anterolateral aspect of the thigh. Estimates of MP incidence are derived largely from observational studies and reported to be about 3.2 to 4.3 cases per 10,000 patient-years.1,2 Although typically arising during midlife and especially in the context of comorbid obesity, diabetes mellitus (DM), and excessive alcohol consumption, MP may occur at any age, and bears a slight predilection for males.2-4
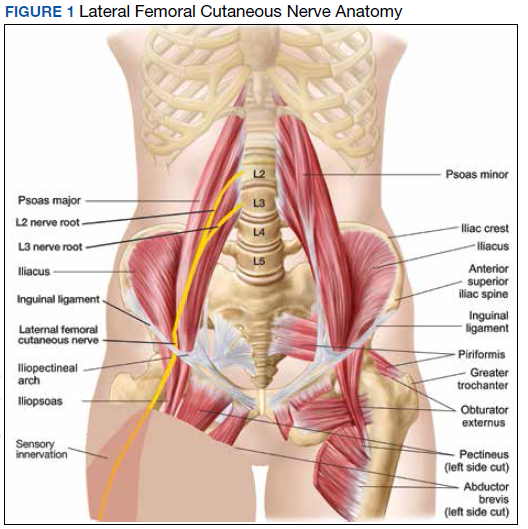
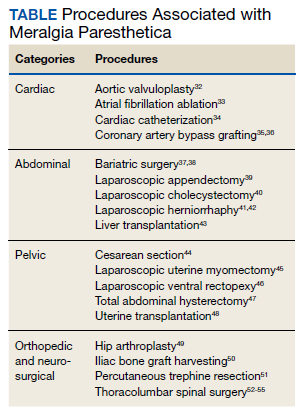
MP may be divided etiologically into iatrogenic and spontaneous subtypes.5 Iatrogenic cases generally are attributable to nerve injury in the setting of direct or indirect trauma (such as with patient malpositioning) arising in the context of multiple forms of procedural or surgical intervention (Table). Spontaneous MP is primarily thought to occur as a result of LFCN compression at the level of the inguinal ligament, wherein internal or external pressures may promote LFCN entrapment and resultant functional disruption (Figure 1).6,7
External forces, such as tight garments, wallets, or even elements of modern body armor, have been reported to provoke MP.8-11 Alternatively, states of increased intraabdominal pressure, such as obesity, ascites, and pregnancy may predispose to LFCN compression.2,12,13 Less commonly, lumbar radiculopathy, pelvic masses, and several forms of retroperitoneal pathology may present with clinical symptomatology indistinguishable from MP.14-17 Importantly, many of these represent must-not-miss diagnoses, and may be suggested via a focused history and physical examination.
Here, we present a case of MP secondary to a massive retroperitoneal sarcoma, ultimately drawing renewed attention to the known association of MP and retroperitoneal pathology, and therein highlighting the utility of a dedicated review of systems to identify red-flag features in patients who present with MP and a thorough abdominal examination in all patients presenting with focal neurologic deficits involving the lower extremities.
Case Presentation
A male Vietnam War veteran aged 69 years presented to a primary care clinic at West Roxbury Veterans Affairs Medical Center (WRVAMC) in Massachusetts with progressive right lower extremity numbness. Three months prior to this visit, he was evaluated in an urgent care clinic at WRVAMC for 6 months of numbness and increasingly painful nocturnal paresthesias involving the same extremity. A targeted physical examination at that visit revealed an obese male wearing tight suspenders, as well as focally diminished sensation to light touch involving the anterolateral aspect of the thigh, extending from just below the right hip to above the knee. Sensation in the medial thigh was spared. Strength and reflexes were normal in the bilateral lower extremities. An abdominal examination was not performed. He received a diagnosis of MP and counseled regarding weight loss, glycemic control, garment optimization, and conservative analgesia with as-needed nonsteroidal anti-inflammatory drugs. He was instructed to follow-up closely with his primary care physician for further monitoring.
During the current visit, the patient reported 2 atraumatic falls the prior 2 months, attributed to escalating right leg weakness. The patient reported that ascending stairs had become difficult, and he was unable to cross his right leg over his left while in a seated position. The territory of numbness expanded to his front and inner thigh. Although previously he was able to hike 4 miles, he now was unable to walk more than half of a mile without developing shortness of breath. He reported frequent urination without hematuria and a recent weight gain of 8 pounds despite early satiety.
His medical history included hypertension, hypercholesterolemia, truncal obesity, noninsulin dependent DM, coronary artery disease, atrial flutter, transient ischemic attack, and benign positional paroxysmal vertigo. He was exposed to Agent Orange during his service in Vietnam. Family history was notable for breast cancer (mother), lung cancer (father), and an unspecified form of lymphoma (brother). He had smoked approximately 2 packs of cigarettes daily for 15 years but quit 38 years prior. He reported consuming on average 3 alcohol-containing drinks per week and no illicit drug use. He was adherent with all medications, including furosemide 40 mg daily, losartan 25 mg daily, metoprolol succinate 50 mg daily, atorvastatin 80 mg daily, metformin 500 mg twice daily, and rivaroxaban 20 mg daily with dinner.
His vital signs included a blood pressure of 123/58 mmHg, a pulse of 74 beats per minute, a respiratory rate of 16 breaths per minute, and an oxygen saturation of 94% on ambient air. His temperature was recorded at 96.7°F, and his weight was 234 pounds with a body mass index (BMI) of 34. He was well groomed and in no acute distress. His cardiopulmonary examination was normal. Carotid, radial, and bilateral dorsalis pedis pulsations were 2+ bilaterally, and no jugular venous distension was observed at 30°. The abdomen was protuberant. Nonshifting dullness to percussion and firmness to palpation was observed throughout right upper and lower quadrants, with hyperactive bowel sounds primarily localized to the left upper and lower quadrants.
Neurologic examination revealed symmetric facies with normal phonation and diction. He was spontaneously moving all extremities, and his gait was normal. Sensation to light touch was severely diminished throughout the anterolateral and medial thigh, extending to the level of the knee, and otherwise reduced in a stocking-type pattern over the bilateral feet and toes. His right hip flexion, adduction, as well as internal and external rotation were focally diminished to 4- out of 5. Right knee extension was 4+ out of 5. Strength was otherwise 5 out of 5. The patient exhibited asymmetric Patellar reflexes—absent on the right and 2+ on the left. Achilles reflexes were absent bilaterally. Straight-leg raise test was negative bilaterally and did not clearly exacerbate his right leg numbness or paresthesias. There were no notable fasciculations. There was 2+ bilateral lower extremity pitting edema appreciated to the level of the midshin (right greater than left), without palpable cords or new skin lesions.
Upon referral to the neurology service, the patient underwent electromyography, which revealed complex repetitive discharges in the right tibialis anterior and pattern of reduced recruitment upon activation of the right vastus medialis, collectively suggestive of an L3-4 plexopathy. The patient was admitted for expedited workup.
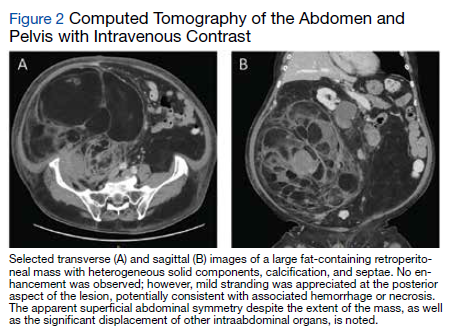
A complete blood count and metabolic panel that were taken in the emergency department were normal, save for a serum bicarbonate of 30 mEq/L. His hemoglobin A1c was 6.6%. Computed tomography (CT) of the abdomen and pelvis with IV contrast was obtained, and notable for a 30 cm fat-containing right-sided retroperitoneal mass with associated solid nodular components and calcification (Figure 2). No enhancement of the lesion was observed. There was significant associated mass effect, with superior displacement of the liver and right hemidiaphragm, as well as superomedial deflection of the right kidney, inferior vena cava, and other intraabdominal organs. Subsequent imaging with a CT of the chest, as well as magnetic resonance imaging of the brain, were without evidence of metastatic disease.
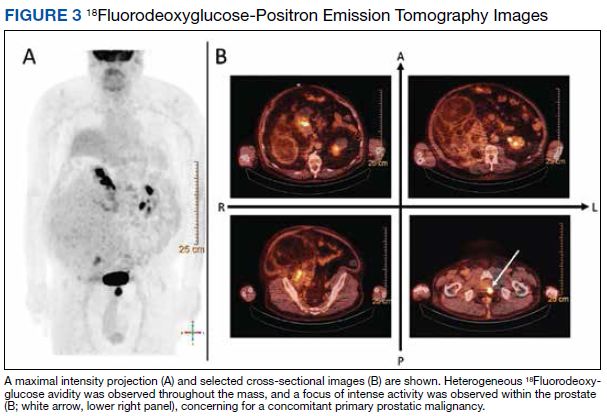
18Fluorodeoxyglucose-positron emission tomography (FDG-PET) was performed and demonstrated heterogeneous FDG avidity throughout the mass (SUVmax 5.9), as well as poor delineation of the boundary of the right psoas major, consistent with muscular invasion (Figure 3). The FDG-PET also revealed intense tracer uptake within the left prostate (SUVmax 26), concerning for a concomitant prostate malignancy.
To facilitate tissue diagnosis, the patient underwent a CT-guided biopsy of the retroperitoneal mass. Subsequent histopathologic analysis revealed a primarily well-differentiated spindle cell lesion with occasional adipocytic atypia, and a superimposed hypercellular element characterized by the presence of pleomorphic high-grade spindled cells. The neoplastic spindle cells were MDM2-positive by both immunohistochemistry and fluorescence in situ hybridization (FISH), and negative for pancytokeratin, smooth muscle myosin, and S100. The findings were collectively consistent with a dedifferentiated liposarcoma (DDLPS).
Given the focus of FDG avidity observed on the PET, the patient underwent a transrectal ultrasound-guided biopsy of the prostate, which yielded diagnosis of a concomitant high-risk (Gleason 4+4) prostate adenocarcinoma. A bone scan did not reveal evidence of osseous metastatic disease.
Outcome
The patient was treated with external beam radiotherapy (EBRT) delivered simultaneously to both the prostate and high-risk retroperitoneal margins of the DDLPS, as well as concurrent androgen deprivation therapy. Five months after completed radiotherapy, resection of the DDLPS was attempted. However, palliative tumor debulking was instead performed due to extensive locoregional invasion with involvement of the posterior peritoneum and ipsilateral quadratus, iliopsoas, and psoas muscles, as well as the adjacent lumbar nerve roots.
At present, the patient is undergoing surveillance imaging every 3 months to reevaluate his underlying disease burden, which has thus far been radiographically stable. Current management at the primary care level is focused on preserving quality of life, particularly maintaining mobility and functional independence.
Discussion
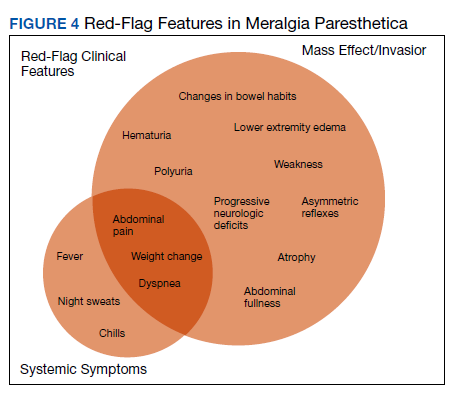
Although generally a benign entrapment neuropathy, MP bears well-established associations with multiple forms of must-not-miss pathology. Here, we present the case of a veteran in whom MP was the index presentation of a massive retroperitoneal liposarcoma, stressing the importance of a thorough history and physical examination in all patients presenting with MP. The case presented herein highlights many of the red-flag signs and symptoms that primary care physicians might encounter in patients with retroperitoneal pathology, including MP and MP-like syndromes (Figure 4).
In this case, the pretest probability of a spontaneous and uncomplicated MP was high given the patient’s sex, age, body habitus, and DM; however, there important atypia that emerged as the case evolved, including: (1) the progressive course; (2) proximal right lower extremity weakness; (3) asymmetric patellar reflexes; and (4) numerous clinical stigmata of intraabdominal mass effect. The patient exhibited abnormalities on abdominal examination that suggested the presence of an underlying intraabdominal mass, providing key diagnostic insight into this case. Given the slowly progressive nature of liposarcomas, we feel the abnormalities appreciated on abdominal examination were likely apparent during the initial presentation.18
There are numerous cognitive biases that may explain why an abdominal examination was not prioritized during the initial presentation. Namely, the patient’s numerous risk factors for spontaneous MP, as detailed above, may have contributed to framing bias that limited consideration of alternative diagnoses. In addition, the patient’s physical examination likely contributed to search satisfaction, whereby alternative diagnoses were not further entertained after discovery of findings consistent with spontaneous MP.19 Finally, it remains conceivable that an abdominal examination was not prioritized as it is often perceived as being distinct from, rather than an integral part of, the neurologic examination.20 Given that numerous neurologic disorders may present with abdominal pathology, we feel a thorough abdominal examination should be considered part of the full neurologic examination, especially in cases presenting with focal neurologic findings involving the lower extremities.21
Collectively, this case alludes to the importance of close clinical follow-up, as well as adequate anticipatory patient guidance in cases of suspected MP. In most patients, the clinical course of spontaneous MP is benign and favorable, with up to 85% of patients experiencing resolution within 4 to 6 months of the initial presentation.22 Common conservative measures include weight loss, garment optimization, and nonsteroidal anti-inflammatory drugs as needed for analgesia. In refractory cases, procedural interventions such as with neurolysis or resection of the lateral femoral cutaneous nerve, may be required after the ruling out of alternative diagnoses.23,24
Importantly, in even prolonged and resistant cases of MP, patient discomfort remains localized to the territory of the LFCN. Additional lower motor neuron signs, such as an expanding territory of sensory involvement, muscle weakness, or diminished reflexes, should prompt additional testing for alternative diagnoses. In addition, clinical findings concerning for intraabdominal mass effect, many of which were observed in this case, should lead to further evaluation and expeditious cross-sectional imaging. Although this patient’s early satiety, polyuria, bilateral lower extremity edema, weight gain, and lumbar plexopathy each may be explained by direct compression, invasion, or displacement, his report of progressive exertional dyspnea merits further discussion.
Exertional dyspnea is an uncommon complication of soft tissue sarcoma, reported almost exclusively in cases with cardiac, mediastinal, or other thoracic involvement.25-28 In this case, there was no evidence of thoracic involvement, either through direct extension or metastasis. Instead, the patient’s exertional dyspnea may have been attributable to increased intraabdominal pressure leading to compromised diaphragm excursion and reduced pulmonary reserve. In addition, the radiographic findings also raise the possibility of a potential contribution from preload failure due to IVC compression. Overall, dyspnea is a concerning feature that may suggest advanced disease.
Despite the value of a thorough history and physical examination in patients with MP, major clinical guidelines from neurologic, neurosurgical, and orthopedic organizations do not formally address MP evaluation and management. Further, proposed clinical practice algorithms are inconsistent in their recommendations regarding the identification of red-flag features and ruling out of alternative diagnoses.22,29,30 To supplement the abdominal examination, it would be reasonable to perform a pelvic compression test (PCT) in patients presenting with suspected MP. The PCT is a highly sensitive and specific provocative maneuver shown to enable reliable differentiation between MP and lumbar radiculopathy, and is performed by placing downward force on the anterior superior iliac spine of the affected extremity for 45 seconds with the patient in the lateral recumbent position.31 As this maneuver is intended to force relaxation of the inguinal ligament, thereby relieving pressure on the LFCN, improvement in the patient’s symptoms with the PCT is consistent with MP.
Conclusions
1. van Slobbe AM, Bohnen AM, Bernsen RM, Koes BW, Bierma-Zeinstra SM. Incidence rates and determinants in meralgia paresthetica in general practice. J Neurol. 2004;251(3):294-297. doi:10.1007/s00415-004-0310-x
2. Parisi TJ, Mandrekar J, Dyck PJ, Klein CJ. Meralgia paresthetica: relation to obesity, advanced age, and diabetes mellitus. Neurology. 2011;77(16):1538-1542. doi:10.1212/WNL.0b013e318233b356
3. Ecker AD. Diagnosis of meralgia paresthetica. JAMA. 1985;253(7):976.
4. Massey EW, Pellock JM. Meralgia paraesthetica in a child. J Pediatr. 1978;93(2):325-326. doi:10.1016/s0022-3476(78)80566-6
5. Harney D, Patijn J. Meralgia paresthetica: diagnosis and management strategies. Pain Med. 2007;8(8):669-677. doi:10.1111/j.1526-4637.2006.00227.x
6. Berini SE, Spinner RJ, Jentoft ME, et al. Chronic meralgia paresthetica and neurectomy: a clinical pathologic study. Neurology. 2014;82(17):1551-1555. doi:10.1212/WNL.0000000000000367
7. Payne RA, Harbaugh K, Specht CS, Rizk E. Correlation of histopathology and clinical symptoms in meralgia paresthetica. Cureus. 2017;9(10):e1789. Published 2017 Oct 20. doi:10.7759/cureus.1789
8. Boyce JR. Meralgia paresthetica and tight trousers. JAMA. 1984;251(12):1553.
9. Orton D. Meralgia paresthetica from a wallet. JAMA. 1984;252(24):3368.
10. Fargo MV, Konitzer LN. Meralgia paresthetica due to body armor wear in U.S. soldiers serving in Iraq: a case report and review of the literature. Mil Med. 2007;172(6):663-665. doi:10.7205/milmed.172.6.663
11. Korkmaz N, Ozçakar L. Meralgia paresthetica in a policeman: the belt or the gun. Plast Reconstr Surg. 2004;114(4):1012-1013. doi:10.1097/01.prs.0000138706.86633.01
12. Gooding MS, Evangelista V, Pereira L. Carpal Tunnel Syndrome and Meralgia Paresthetica in Pregnancy. Obstet Gynecol Surv. 2020;75(2):121-126. doi:10.1097/OGX.0000000000000745
13. Pauwels A, Amarenco P, Chazouillères O, Pigot F, Calmus Y, Lévy VG. Une complication rare et méconnue de l’ascite: la méralgie paresthésique [Unusual and unknown complication of ascites: meralgia paresthetica]. Gastroenterol Clin Biol. 1990;14(3):295.
14. Braddom RL. L2 rather than L1 radiculopathy mimics meralgia paresthetica. Muscle Nerve. 2010;42(5):842. doi:10.1002/mus.21826
15. Suber DA, Massey EW. Pelvic mass presenting as meralgia paresthetica. Obstet Gynecol. 1979;53(2):257-258.
16. Flowers RS. Meralgia paresthetica. A clue to retroperitoneal malignant tumor. Am J Surg. 1968;116(1):89-92. doi:10.1016/0002-9610(68)90423-6
17. Yi TI, Yoon TH, Kim JS, Lee GE, Kim BR. Femoral neuropathy and meralgia paresthetica secondary to an iliacus hematoma. Ann Rehabil Med. 2012;36(2):273-277. doi:10.5535/arm.2012.36.2.273
18. Lee ATJ, Thway K, Huang PH, Jones RL. Clinical and molecular spectrum of liposarcoma. J Clin Oncol. 2018;36(2):151-159. doi:10.1200/JCO.2017.74.9598
19. O’Sullivan ED, Schofield SJ. Cognitive bias in clinical medicine. J R Coll Physicians Edinb. 2018;48(3):225-232. doi:10.4997/JRCPE.2018.306
20. Bickley, LS. Bates’ Guide to Physical Examination and History Taking. 12th Edition. Wolters Kluwer Health/Lippincott Williams and Wilkins; 2016.
21. Bhavsar AS, Verma S, Lamba R, Lall CG, Koenigsknecht V, Rajesh A. Abdominal manifestations of neurologic disorders. Radiographics. 2013;33(1):135-153. doi:10.1148/rg.331125097
22. Dureja GP, Gulaya V, Jayalakshmi TS, Mandal P. Management of meralgia paresthetica: a multimodality regimen. Anesth Analg. 1995;80(5):1060-1061. doi:10.1097/00000539-199505000-00043
23. Patijn J, Mekhail N, Hayek S, Lataster A, van Kleef M, Van Zundert J. Meralgia paresthetica. Pain Pract. 2011;11(3):302-308. doi:10.1111/j.1533-2500.2011.00458.x24. Ivins GK. Meralgia paresthetica, the elusive diagnosis: clinical experience with 14 adult patients. Ann Surg. 2000;232(2):281-286. doi:10.1097/00000658-200008000-00019
25. Munin MA, Goerner MS, Raggio I, et al. A rare cause of dyspnea: undifferentiated pleomorphic sarcoma in the left atrium. Cardiol Res. 2017;8(5):241-245. doi:10.14740/cr590w
26. Nguyen A, Awad WI. Cardiac sarcoma arising from malignant transformation of a preexisting atrial myxoma. Ann Thorac Surg. 2016;101(4):1571-1573. doi:10.1016/j.athoracsur.2015.05.129
27. Jiang S, Li J, Zeng Q, Liang J. Pulmonary artery intimal sarcoma misdiagnosed as pulmonary embolism: a case report. Oncol Lett. 2017;13(4):2713-2716. doi:10.3892/ol.2017.5775
28. Cojocaru A, Oliveira PJ, Pellecchia C. A pleural presentation of a rare soft tissue sarcoma. Am J Resp Crit Care Med. 2012;185:A5201. doi:10.1164/ajrccm-conference.2012.185.1_MeetingAbstracts.A5201
29. Grossman MG, Ducey SA, Nadler SS, Levy AS. Meralgia paresthetica: diagnosis and treatment. J Am Acad Orthop Surg. 2001;9(5):336-344. doi:10.5435/00124635-200109000-00007
30. Cheatham SW, Kolber MJ, Salamh PA. Meralgia paresthetica: a review of the literature. Int J Sports Phys Ther. 2013;8(6):883-893.
31. Nouraei SA, Anand B, Spink G, O’Neill KS. A novel approach to the diagnosis and management of meralgia paresthetica. Neurosurgery. 2007;60(4):696-700. doi:10.1227/01.NEU.0000255392.69914.F7
32. Antunes PE, Antunes MJ. Meralgia paresthetica after aortic valve surgery. J Heart Valve Dis. 1997;6(6):589-590.
33. Reddy YM, Singh D, Chikkam V, et al. Postprocedural neuropathy after atrial fibrillation ablation. J Interv Card Electrophysiol. 2013;36(3):279-285. doi:10.1007/s10840-012-9724-z
34. Butler R, Webster MW. Meralgia paresthetica: an unusual complication of cardiac catheterization via the femoral artery. Catheter Cardiovasc Interv. 2002;56(1):69-71. doi:10.1002/ccd.10149
35. Jellish WS, Oftadeh M. Peripheral nerve injury in cardiac surgery. J Cardiothorac Vasc Anesth. 2018;32(1):495-511. doi:10.1053/j.jvca.2017.08.030
36. Parsonnet V, Karasakalides A, Gielchinsky I, Hochberg M, Hussain SM. Meralgia paresthetica after coronary bypass surgery. J Thorac Cardiovasc Surg. 1991;101(2):219-221.
37. Macgregor AM, Thoburn EK. Meralgia paresthetica following bariatric surgery. Obes Surg. 1999;9(4):364-368. doi:10.1381/096089299765552945
38. Grace DM. Meralgia paresthetica after gastroplasty for morbid obesity. Can J Surg. 1987;30(1):64-65.
39. Polidori L, Magarelli M, Tramutoli R. Meralgia paresthetica as a complication of laparoscopic appendectomy. Surg Endosc. 2003;17(5):832. doi:10.1007/s00464-002-4279-1
40. Yamout B, Tayyim A, Farhat W. Meralgia paresthetica as a complication of laparoscopic cholecystectomy. Clin Neurol Neurosurg. 1994;96(2):143-144. doi:10.1016/0303-8467(94)90048-5
41. Broin EO, Horner C, Mealy K, et al. Meralgia paraesthetica following laparoscopic inguinal hernia repair. an anatomical analysis. Surg Endosc. 1995;9(1):76-78. doi:10.1007/BF00187893
42. Eubanks S, Newman L 3rd, Goehring L, et al. Meralgia paresthetica: a complication of laparoscopic herniorrhaphy. Surg Laparosc Endosc. 1993;3(5):381-385.
43. Atamaz F, Hepgüler S, Karasu Z, Kilic M. Meralgia paresthetica after liver transplantation: a case report. Transplant Proc. 2005;37(10):4424-4425. doi:10.1016/j.transproceed.2005.11.047
44. Chung KH, Lee JY, Ko TK, et al. Meralgia paresthetica affecting parturient women who underwent cesarean section -a case report-. Korean J Anesthesiol. 2010;59 Suppl(Suppl):S86-S89. doi:10.4097/kjae.2010.59.S.S86
45. Hutchins FL Jr, Huggins J, Delaney ML. Laparoscopic myomectomy-an unusual cause of meralgia paresthetica. J Am Assoc Gynecol Laparosc. 1998;5(3):309-311. doi:10.1016/s1074-3804(98)80039-x
46. Jones CD, Guiot L, Portelli M, Bullen T, Skaife P. Two interesting cases of meralgia paraesthetica. Pain Physician. 2017;20(6):E987-E989.
47. Peters G, Larner AJ. Meralgia paresthetica following gynecologic and obstetric surgery. Int J Gynaecol Obstet. 2006;95(1):42-43. doi:10.1016/j.ijgo.2006.05.025
48. Kvarnström N, Järvholm S, Johannesson L, Dahm-Kähler P, Olausson M, Brännström M. Live donors of the initial observational study of uterus transplantation-psychological and medical follow-up until 1 year after surgery in the 9 cases. Transplantation. 2017;101(3):664-670. doi:10.1097/TP.0000000000001567
49. Goulding K, Beaulé PE, Kim PR, Fazekas A. Incidence of lateral femoral cutaneous nerve neuropraxia after anterior approach hip arthroplasty. Clin Orthop Relat Res. 2010;468(9):2397-2404. doi:10.1007/s11999-010-1406-5
50. Yamamoto T, Nagira K, Kurosaka M. Meralgia paresthetica occurring 40 years after iliac bone graft harvesting: case report. Neurosurgery. 2001;49(6):1455-1457. doi:10.1097/00006123-200112000-00028
51. Roqueplan F, Porcher R, Hamzé B, et al. Long-term results of percutaneous resection and interstitial laser ablation of osteoid osteomas. Eur Radiol. 2010;20(1):209-217. doi:10.1007/s00330-009-1537-9
52. Gupta A, Muzumdar D, Ramani PS. Meralgia paraesthetica following lumbar spine surgery: a study in 110 consecutive surgically treated cases. Neurol India. 2004;52(1):64-66.
53. Yang SH, Wu CC, Chen PQ. Postoperative meralgia paresthetica after posterior spine surgery: incidence, risk factors, and clinical outcomes. Spine (Phila Pa 1976). 2005;30(18):E547-E550. doi:10.1097/01.brs.0000178821.14102.9d
54. Tejwani SG, Scaduto AA, Bowen RE. Transient meralgia paresthetica after pediatric posterior spine fusion. J Pediatr Orthop. 2006;26(4):530-533. doi:10.1097/01.bpo.0000217721.95480.9e
55. Peker S, Ay B, Sun I, Ozgen S, Pamir M. Meralgia paraesthetica: complications of prone position during lumbar disc surgery. Internet J Anesthesiol. 2003;8(1):24-29.
In patients presenting with focal neurologic findings involving the lower extremities, a thorough abdominal examination should be considered an integral part of the full neurologic work up.
In patients presenting with focal neurologic findings involving the lower extremities, a thorough abdominal examination should be considered an integral part of the full neurologic work up.
Meralgia paresthetica (MP) is a sensory mononeuropathy of the lateral femoral cutaneous nerve (LFCN), clinically characterized by numbness, pain, and paresthesias involving the anterolateral aspect of the thigh. Estimates of MP incidence are derived largely from observational studies and reported to be about 3.2 to 4.3 cases per 10,000 patient-years.1,2 Although typically arising during midlife and especially in the context of comorbid obesity, diabetes mellitus (DM), and excessive alcohol consumption, MP may occur at any age, and bears a slight predilection for males.2-4
MP may be divided etiologically into iatrogenic and spontaneous subtypes.5 Iatrogenic cases generally are attributable to nerve injury in the setting of direct or indirect trauma (such as with patient malpositioning) arising in the context of multiple forms of procedural or surgical intervention (Table). Spontaneous MP is primarily thought to occur as a result of LFCN compression at the level of the inguinal ligament, wherein internal or external pressures may promote LFCN entrapment and resultant functional disruption (Figure 1).6,7
External forces, such as tight garments, wallets, or even elements of modern body armor, have been reported to provoke MP.8-11 Alternatively, states of increased intraabdominal pressure, such as obesity, ascites, and pregnancy may predispose to LFCN compression.2,12,13 Less commonly, lumbar radiculopathy, pelvic masses, and several forms of retroperitoneal pathology may present with clinical symptomatology indistinguishable from MP.14-17 Importantly, many of these represent must-not-miss diagnoses, and may be suggested via a focused history and physical examination.
Here, we present a case of MP secondary to a massive retroperitoneal sarcoma, ultimately drawing renewed attention to the known association of MP and retroperitoneal pathology, and therein highlighting the utility of a dedicated review of systems to identify red-flag features in patients who present with MP and a thorough abdominal examination in all patients presenting with focal neurologic deficits involving the lower extremities.
Case Presentation
A male Vietnam War veteran aged 69 years presented to a primary care clinic at West Roxbury Veterans Affairs Medical Center (WRVAMC) in Massachusetts with progressive right lower extremity numbness. Three months prior to this visit, he was evaluated in an urgent care clinic at WRVAMC for 6 months of numbness and increasingly painful nocturnal paresthesias involving the same extremity. A targeted physical examination at that visit revealed an obese male wearing tight suspenders, as well as focally diminished sensation to light touch involving the anterolateral aspect of the thigh, extending from just below the right hip to above the knee. Sensation in the medial thigh was spared. Strength and reflexes were normal in the bilateral lower extremities. An abdominal examination was not performed. He received a diagnosis of MP and counseled regarding weight loss, glycemic control, garment optimization, and conservative analgesia with as-needed nonsteroidal anti-inflammatory drugs. He was instructed to follow-up closely with his primary care physician for further monitoring.
During the current visit, the patient reported 2 atraumatic falls the prior 2 months, attributed to escalating right leg weakness. The patient reported that ascending stairs had become difficult, and he was unable to cross his right leg over his left while in a seated position. The territory of numbness expanded to his front and inner thigh. Although previously he was able to hike 4 miles, he now was unable to walk more than half of a mile without developing shortness of breath. He reported frequent urination without hematuria and a recent weight gain of 8 pounds despite early satiety.
His medical history included hypertension, hypercholesterolemia, truncal obesity, noninsulin dependent DM, coronary artery disease, atrial flutter, transient ischemic attack, and benign positional paroxysmal vertigo. He was exposed to Agent Orange during his service in Vietnam. Family history was notable for breast cancer (mother), lung cancer (father), and an unspecified form of lymphoma (brother). He had smoked approximately 2 packs of cigarettes daily for 15 years but quit 38 years prior. He reported consuming on average 3 alcohol-containing drinks per week and no illicit drug use. He was adherent with all medications, including furosemide 40 mg daily, losartan 25 mg daily, metoprolol succinate 50 mg daily, atorvastatin 80 mg daily, metformin 500 mg twice daily, and rivaroxaban 20 mg daily with dinner.
His vital signs included a blood pressure of 123/58 mmHg, a pulse of 74 beats per minute, a respiratory rate of 16 breaths per minute, and an oxygen saturation of 94% on ambient air. His temperature was recorded at 96.7°F, and his weight was 234 pounds with a body mass index (BMI) of 34. He was well groomed and in no acute distress. His cardiopulmonary examination was normal. Carotid, radial, and bilateral dorsalis pedis pulsations were 2+ bilaterally, and no jugular venous distension was observed at 30°. The abdomen was protuberant. Nonshifting dullness to percussion and firmness to palpation was observed throughout right upper and lower quadrants, with hyperactive bowel sounds primarily localized to the left upper and lower quadrants.
Neurologic examination revealed symmetric facies with normal phonation and diction. He was spontaneously moving all extremities, and his gait was normal. Sensation to light touch was severely diminished throughout the anterolateral and medial thigh, extending to the level of the knee, and otherwise reduced in a stocking-type pattern over the bilateral feet and toes. His right hip flexion, adduction, as well as internal and external rotation were focally diminished to 4- out of 5. Right knee extension was 4+ out of 5. Strength was otherwise 5 out of 5. The patient exhibited asymmetric Patellar reflexes—absent on the right and 2+ on the left. Achilles reflexes were absent bilaterally. Straight-leg raise test was negative bilaterally and did not clearly exacerbate his right leg numbness or paresthesias. There were no notable fasciculations. There was 2+ bilateral lower extremity pitting edema appreciated to the level of the midshin (right greater than left), without palpable cords or new skin lesions.
Upon referral to the neurology service, the patient underwent electromyography, which revealed complex repetitive discharges in the right tibialis anterior and pattern of reduced recruitment upon activation of the right vastus medialis, collectively suggestive of an L3-4 plexopathy. The patient was admitted for expedited workup.
A complete blood count and metabolic panel that were taken in the emergency department were normal, save for a serum bicarbonate of 30 mEq/L. His hemoglobin A1c was 6.6%. Computed tomography (CT) of the abdomen and pelvis with IV contrast was obtained, and notable for a 30 cm fat-containing right-sided retroperitoneal mass with associated solid nodular components and calcification (Figure 2). No enhancement of the lesion was observed. There was significant associated mass effect, with superior displacement of the liver and right hemidiaphragm, as well as superomedial deflection of the right kidney, inferior vena cava, and other intraabdominal organs. Subsequent imaging with a CT of the chest, as well as magnetic resonance imaging of the brain, were without evidence of metastatic disease.
18Fluorodeoxyglucose-positron emission tomography (FDG-PET) was performed and demonstrated heterogeneous FDG avidity throughout the mass (SUVmax 5.9), as well as poor delineation of the boundary of the right psoas major, consistent with muscular invasion (Figure 3). The FDG-PET also revealed intense tracer uptake within the left prostate (SUVmax 26), concerning for a concomitant prostate malignancy.
To facilitate tissue diagnosis, the patient underwent a CT-guided biopsy of the retroperitoneal mass. Subsequent histopathologic analysis revealed a primarily well-differentiated spindle cell lesion with occasional adipocytic atypia, and a superimposed hypercellular element characterized by the presence of pleomorphic high-grade spindled cells. The neoplastic spindle cells were MDM2-positive by both immunohistochemistry and fluorescence in situ hybridization (FISH), and negative for pancytokeratin, smooth muscle myosin, and S100. The findings were collectively consistent with a dedifferentiated liposarcoma (DDLPS).
Given the focus of FDG avidity observed on the PET, the patient underwent a transrectal ultrasound-guided biopsy of the prostate, which yielded diagnosis of a concomitant high-risk (Gleason 4+4) prostate adenocarcinoma. A bone scan did not reveal evidence of osseous metastatic disease.
Outcome
The patient was treated with external beam radiotherapy (EBRT) delivered simultaneously to both the prostate and high-risk retroperitoneal margins of the DDLPS, as well as concurrent androgen deprivation therapy. Five months after completed radiotherapy, resection of the DDLPS was attempted. However, palliative tumor debulking was instead performed due to extensive locoregional invasion with involvement of the posterior peritoneum and ipsilateral quadratus, iliopsoas, and psoas muscles, as well as the adjacent lumbar nerve roots.
At present, the patient is undergoing surveillance imaging every 3 months to reevaluate his underlying disease burden, which has thus far been radiographically stable. Current management at the primary care level is focused on preserving quality of life, particularly maintaining mobility and functional independence.
Discussion
Although generally a benign entrapment neuropathy, MP bears well-established associations with multiple forms of must-not-miss pathology. Here, we present the case of a veteran in whom MP was the index presentation of a massive retroperitoneal liposarcoma, stressing the importance of a thorough history and physical examination in all patients presenting with MP. The case presented herein highlights many of the red-flag signs and symptoms that primary care physicians might encounter in patients with retroperitoneal pathology, including MP and MP-like syndromes (Figure 4).
In this case, the pretest probability of a spontaneous and uncomplicated MP was high given the patient’s sex, age, body habitus, and DM; however, there important atypia that emerged as the case evolved, including: (1) the progressive course; (2) proximal right lower extremity weakness; (3) asymmetric patellar reflexes; and (4) numerous clinical stigmata of intraabdominal mass effect. The patient exhibited abnormalities on abdominal examination that suggested the presence of an underlying intraabdominal mass, providing key diagnostic insight into this case. Given the slowly progressive nature of liposarcomas, we feel the abnormalities appreciated on abdominal examination were likely apparent during the initial presentation.18
There are numerous cognitive biases that may explain why an abdominal examination was not prioritized during the initial presentation. Namely, the patient’s numerous risk factors for spontaneous MP, as detailed above, may have contributed to framing bias that limited consideration of alternative diagnoses. In addition, the patient’s physical examination likely contributed to search satisfaction, whereby alternative diagnoses were not further entertained after discovery of findings consistent with spontaneous MP.19 Finally, it remains conceivable that an abdominal examination was not prioritized as it is often perceived as being distinct from, rather than an integral part of, the neurologic examination.20 Given that numerous neurologic disorders may present with abdominal pathology, we feel a thorough abdominal examination should be considered part of the full neurologic examination, especially in cases presenting with focal neurologic findings involving the lower extremities.21
Collectively, this case alludes to the importance of close clinical follow-up, as well as adequate anticipatory patient guidance in cases of suspected MP. In most patients, the clinical course of spontaneous MP is benign and favorable, with up to 85% of patients experiencing resolution within 4 to 6 months of the initial presentation.22 Common conservative measures include weight loss, garment optimization, and nonsteroidal anti-inflammatory drugs as needed for analgesia. In refractory cases, procedural interventions such as with neurolysis or resection of the lateral femoral cutaneous nerve, may be required after the ruling out of alternative diagnoses.23,24
Importantly, in even prolonged and resistant cases of MP, patient discomfort remains localized to the territory of the LFCN. Additional lower motor neuron signs, such as an expanding territory of sensory involvement, muscle weakness, or diminished reflexes, should prompt additional testing for alternative diagnoses. In addition, clinical findings concerning for intraabdominal mass effect, many of which were observed in this case, should lead to further evaluation and expeditious cross-sectional imaging. Although this patient’s early satiety, polyuria, bilateral lower extremity edema, weight gain, and lumbar plexopathy each may be explained by direct compression, invasion, or displacement, his report of progressive exertional dyspnea merits further discussion.
Exertional dyspnea is an uncommon complication of soft tissue sarcoma, reported almost exclusively in cases with cardiac, mediastinal, or other thoracic involvement.25-28 In this case, there was no evidence of thoracic involvement, either through direct extension or metastasis. Instead, the patient’s exertional dyspnea may have been attributable to increased intraabdominal pressure leading to compromised diaphragm excursion and reduced pulmonary reserve. In addition, the radiographic findings also raise the possibility of a potential contribution from preload failure due to IVC compression. Overall, dyspnea is a concerning feature that may suggest advanced disease.
Despite the value of a thorough history and physical examination in patients with MP, major clinical guidelines from neurologic, neurosurgical, and orthopedic organizations do not formally address MP evaluation and management. Further, proposed clinical practice algorithms are inconsistent in their recommendations regarding the identification of red-flag features and ruling out of alternative diagnoses.22,29,30 To supplement the abdominal examination, it would be reasonable to perform a pelvic compression test (PCT) in patients presenting with suspected MP. The PCT is a highly sensitive and specific provocative maneuver shown to enable reliable differentiation between MP and lumbar radiculopathy, and is performed by placing downward force on the anterior superior iliac spine of the affected extremity for 45 seconds with the patient in the lateral recumbent position.31 As this maneuver is intended to force relaxation of the inguinal ligament, thereby relieving pressure on the LFCN, improvement in the patient’s symptoms with the PCT is consistent with MP.
Conclusions
Meralgia paresthetica (MP) is a sensory mononeuropathy of the lateral femoral cutaneous nerve (LFCN), clinically characterized by numbness, pain, and paresthesias involving the anterolateral aspect of the thigh. Estimates of MP incidence are derived largely from observational studies and reported to be about 3.2 to 4.3 cases per 10,000 patient-years.1,2 Although typically arising during midlife and especially in the context of comorbid obesity, diabetes mellitus (DM), and excessive alcohol consumption, MP may occur at any age, and bears a slight predilection for males.2-4
MP may be divided etiologically into iatrogenic and spontaneous subtypes.5 Iatrogenic cases generally are attributable to nerve injury in the setting of direct or indirect trauma (such as with patient malpositioning) arising in the context of multiple forms of procedural or surgical intervention (Table). Spontaneous MP is primarily thought to occur as a result of LFCN compression at the level of the inguinal ligament, wherein internal or external pressures may promote LFCN entrapment and resultant functional disruption (Figure 1).6,7
External forces, such as tight garments, wallets, or even elements of modern body armor, have been reported to provoke MP.8-11 Alternatively, states of increased intraabdominal pressure, such as obesity, ascites, and pregnancy may predispose to LFCN compression.2,12,13 Less commonly, lumbar radiculopathy, pelvic masses, and several forms of retroperitoneal pathology may present with clinical symptomatology indistinguishable from MP.14-17 Importantly, many of these represent must-not-miss diagnoses, and may be suggested via a focused history and physical examination.
Here, we present a case of MP secondary to a massive retroperitoneal sarcoma, ultimately drawing renewed attention to the known association of MP and retroperitoneal pathology, and therein highlighting the utility of a dedicated review of systems to identify red-flag features in patients who present with MP and a thorough abdominal examination in all patients presenting with focal neurologic deficits involving the lower extremities.
Case Presentation
A male Vietnam War veteran aged 69 years presented to a primary care clinic at West Roxbury Veterans Affairs Medical Center (WRVAMC) in Massachusetts with progressive right lower extremity numbness. Three months prior to this visit, he was evaluated in an urgent care clinic at WRVAMC for 6 months of numbness and increasingly painful nocturnal paresthesias involving the same extremity. A targeted physical examination at that visit revealed an obese male wearing tight suspenders, as well as focally diminished sensation to light touch involving the anterolateral aspect of the thigh, extending from just below the right hip to above the knee. Sensation in the medial thigh was spared. Strength and reflexes were normal in the bilateral lower extremities. An abdominal examination was not performed. He received a diagnosis of MP and counseled regarding weight loss, glycemic control, garment optimization, and conservative analgesia with as-needed nonsteroidal anti-inflammatory drugs. He was instructed to follow-up closely with his primary care physician for further monitoring.
During the current visit, the patient reported 2 atraumatic falls the prior 2 months, attributed to escalating right leg weakness. The patient reported that ascending stairs had become difficult, and he was unable to cross his right leg over his left while in a seated position. The territory of numbness expanded to his front and inner thigh. Although previously he was able to hike 4 miles, he now was unable to walk more than half of a mile without developing shortness of breath. He reported frequent urination without hematuria and a recent weight gain of 8 pounds despite early satiety.
His medical history included hypertension, hypercholesterolemia, truncal obesity, noninsulin dependent DM, coronary artery disease, atrial flutter, transient ischemic attack, and benign positional paroxysmal vertigo. He was exposed to Agent Orange during his service in Vietnam. Family history was notable for breast cancer (mother), lung cancer (father), and an unspecified form of lymphoma (brother). He had smoked approximately 2 packs of cigarettes daily for 15 years but quit 38 years prior. He reported consuming on average 3 alcohol-containing drinks per week and no illicit drug use. He was adherent with all medications, including furosemide 40 mg daily, losartan 25 mg daily, metoprolol succinate 50 mg daily, atorvastatin 80 mg daily, metformin 500 mg twice daily, and rivaroxaban 20 mg daily with dinner.
His vital signs included a blood pressure of 123/58 mmHg, a pulse of 74 beats per minute, a respiratory rate of 16 breaths per minute, and an oxygen saturation of 94% on ambient air. His temperature was recorded at 96.7°F, and his weight was 234 pounds with a body mass index (BMI) of 34. He was well groomed and in no acute distress. His cardiopulmonary examination was normal. Carotid, radial, and bilateral dorsalis pedis pulsations were 2+ bilaterally, and no jugular venous distension was observed at 30°. The abdomen was protuberant. Nonshifting dullness to percussion and firmness to palpation was observed throughout right upper and lower quadrants, with hyperactive bowel sounds primarily localized to the left upper and lower quadrants.
Neurologic examination revealed symmetric facies with normal phonation and diction. He was spontaneously moving all extremities, and his gait was normal. Sensation to light touch was severely diminished throughout the anterolateral and medial thigh, extending to the level of the knee, and otherwise reduced in a stocking-type pattern over the bilateral feet and toes. His right hip flexion, adduction, as well as internal and external rotation were focally diminished to 4- out of 5. Right knee extension was 4+ out of 5. Strength was otherwise 5 out of 5. The patient exhibited asymmetric Patellar reflexes—absent on the right and 2+ on the left. Achilles reflexes were absent bilaterally. Straight-leg raise test was negative bilaterally and did not clearly exacerbate his right leg numbness or paresthesias. There were no notable fasciculations. There was 2+ bilateral lower extremity pitting edema appreciated to the level of the midshin (right greater than left), without palpable cords or new skin lesions.
Upon referral to the neurology service, the patient underwent electromyography, which revealed complex repetitive discharges in the right tibialis anterior and pattern of reduced recruitment upon activation of the right vastus medialis, collectively suggestive of an L3-4 plexopathy. The patient was admitted for expedited workup.
A complete blood count and metabolic panel that were taken in the emergency department were normal, save for a serum bicarbonate of 30 mEq/L. His hemoglobin A1c was 6.6%. Computed tomography (CT) of the abdomen and pelvis with IV contrast was obtained, and notable for a 30 cm fat-containing right-sided retroperitoneal mass with associated solid nodular components and calcification (Figure 2). No enhancement of the lesion was observed. There was significant associated mass effect, with superior displacement of the liver and right hemidiaphragm, as well as superomedial deflection of the right kidney, inferior vena cava, and other intraabdominal organs. Subsequent imaging with a CT of the chest, as well as magnetic resonance imaging of the brain, were without evidence of metastatic disease.
18Fluorodeoxyglucose-positron emission tomography (FDG-PET) was performed and demonstrated heterogeneous FDG avidity throughout the mass (SUVmax 5.9), as well as poor delineation of the boundary of the right psoas major, consistent with muscular invasion (Figure 3). The FDG-PET also revealed intense tracer uptake within the left prostate (SUVmax 26), concerning for a concomitant prostate malignancy.
To facilitate tissue diagnosis, the patient underwent a CT-guided biopsy of the retroperitoneal mass. Subsequent histopathologic analysis revealed a primarily well-differentiated spindle cell lesion with occasional adipocytic atypia, and a superimposed hypercellular element characterized by the presence of pleomorphic high-grade spindled cells. The neoplastic spindle cells were MDM2-positive by both immunohistochemistry and fluorescence in situ hybridization (FISH), and negative for pancytokeratin, smooth muscle myosin, and S100. The findings were collectively consistent with a dedifferentiated liposarcoma (DDLPS).
Given the focus of FDG avidity observed on the PET, the patient underwent a transrectal ultrasound-guided biopsy of the prostate, which yielded diagnosis of a concomitant high-risk (Gleason 4+4) prostate adenocarcinoma. A bone scan did not reveal evidence of osseous metastatic disease.
Outcome
The patient was treated with external beam radiotherapy (EBRT) delivered simultaneously to both the prostate and high-risk retroperitoneal margins of the DDLPS, as well as concurrent androgen deprivation therapy. Five months after completed radiotherapy, resection of the DDLPS was attempted. However, palliative tumor debulking was instead performed due to extensive locoregional invasion with involvement of the posterior peritoneum and ipsilateral quadratus, iliopsoas, and psoas muscles, as well as the adjacent lumbar nerve roots.
At present, the patient is undergoing surveillance imaging every 3 months to reevaluate his underlying disease burden, which has thus far been radiographically stable. Current management at the primary care level is focused on preserving quality of life, particularly maintaining mobility and functional independence.
Discussion
Although generally a benign entrapment neuropathy, MP bears well-established associations with multiple forms of must-not-miss pathology. Here, we present the case of a veteran in whom MP was the index presentation of a massive retroperitoneal liposarcoma, stressing the importance of a thorough history and physical examination in all patients presenting with MP. The case presented herein highlights many of the red-flag signs and symptoms that primary care physicians might encounter in patients with retroperitoneal pathology, including MP and MP-like syndromes (Figure 4).
In this case, the pretest probability of a spontaneous and uncomplicated MP was high given the patient’s sex, age, body habitus, and DM; however, there important atypia that emerged as the case evolved, including: (1) the progressive course; (2) proximal right lower extremity weakness; (3) asymmetric patellar reflexes; and (4) numerous clinical stigmata of intraabdominal mass effect. The patient exhibited abnormalities on abdominal examination that suggested the presence of an underlying intraabdominal mass, providing key diagnostic insight into this case. Given the slowly progressive nature of liposarcomas, we feel the abnormalities appreciated on abdominal examination were likely apparent during the initial presentation.18
There are numerous cognitive biases that may explain why an abdominal examination was not prioritized during the initial presentation. Namely, the patient’s numerous risk factors for spontaneous MP, as detailed above, may have contributed to framing bias that limited consideration of alternative diagnoses. In addition, the patient’s physical examination likely contributed to search satisfaction, whereby alternative diagnoses were not further entertained after discovery of findings consistent with spontaneous MP.19 Finally, it remains conceivable that an abdominal examination was not prioritized as it is often perceived as being distinct from, rather than an integral part of, the neurologic examination.20 Given that numerous neurologic disorders may present with abdominal pathology, we feel a thorough abdominal examination should be considered part of the full neurologic examination, especially in cases presenting with focal neurologic findings involving the lower extremities.21
Collectively, this case alludes to the importance of close clinical follow-up, as well as adequate anticipatory patient guidance in cases of suspected MP. In most patients, the clinical course of spontaneous MP is benign and favorable, with up to 85% of patients experiencing resolution within 4 to 6 months of the initial presentation.22 Common conservative measures include weight loss, garment optimization, and nonsteroidal anti-inflammatory drugs as needed for analgesia. In refractory cases, procedural interventions such as with neurolysis or resection of the lateral femoral cutaneous nerve, may be required after the ruling out of alternative diagnoses.23,24
Importantly, in even prolonged and resistant cases of MP, patient discomfort remains localized to the territory of the LFCN. Additional lower motor neuron signs, such as an expanding territory of sensory involvement, muscle weakness, or diminished reflexes, should prompt additional testing for alternative diagnoses. In addition, clinical findings concerning for intraabdominal mass effect, many of which were observed in this case, should lead to further evaluation and expeditious cross-sectional imaging. Although this patient’s early satiety, polyuria, bilateral lower extremity edema, weight gain, and lumbar plexopathy each may be explained by direct compression, invasion, or displacement, his report of progressive exertional dyspnea merits further discussion.
Exertional dyspnea is an uncommon complication of soft tissue sarcoma, reported almost exclusively in cases with cardiac, mediastinal, or other thoracic involvement.25-28 In this case, there was no evidence of thoracic involvement, either through direct extension or metastasis. Instead, the patient’s exertional dyspnea may have been attributable to increased intraabdominal pressure leading to compromised diaphragm excursion and reduced pulmonary reserve. In addition, the radiographic findings also raise the possibility of a potential contribution from preload failure due to IVC compression. Overall, dyspnea is a concerning feature that may suggest advanced disease.
Despite the value of a thorough history and physical examination in patients with MP, major clinical guidelines from neurologic, neurosurgical, and orthopedic organizations do not formally address MP evaluation and management. Further, proposed clinical practice algorithms are inconsistent in their recommendations regarding the identification of red-flag features and ruling out of alternative diagnoses.22,29,30 To supplement the abdominal examination, it would be reasonable to perform a pelvic compression test (PCT) in patients presenting with suspected MP. The PCT is a highly sensitive and specific provocative maneuver shown to enable reliable differentiation between MP and lumbar radiculopathy, and is performed by placing downward force on the anterior superior iliac spine of the affected extremity for 45 seconds with the patient in the lateral recumbent position.31 As this maneuver is intended to force relaxation of the inguinal ligament, thereby relieving pressure on the LFCN, improvement in the patient’s symptoms with the PCT is consistent with MP.
Conclusions
1. van Slobbe AM, Bohnen AM, Bernsen RM, Koes BW, Bierma-Zeinstra SM. Incidence rates and determinants in meralgia paresthetica in general practice. J Neurol. 2004;251(3):294-297. doi:10.1007/s00415-004-0310-x
2. Parisi TJ, Mandrekar J, Dyck PJ, Klein CJ. Meralgia paresthetica: relation to obesity, advanced age, and diabetes mellitus. Neurology. 2011;77(16):1538-1542. doi:10.1212/WNL.0b013e318233b356
3. Ecker AD. Diagnosis of meralgia paresthetica. JAMA. 1985;253(7):976.
4. Massey EW, Pellock JM. Meralgia paraesthetica in a child. J Pediatr. 1978;93(2):325-326. doi:10.1016/s0022-3476(78)80566-6
5. Harney D, Patijn J. Meralgia paresthetica: diagnosis and management strategies. Pain Med. 2007;8(8):669-677. doi:10.1111/j.1526-4637.2006.00227.x
6. Berini SE, Spinner RJ, Jentoft ME, et al. Chronic meralgia paresthetica and neurectomy: a clinical pathologic study. Neurology. 2014;82(17):1551-1555. doi:10.1212/WNL.0000000000000367
7. Payne RA, Harbaugh K, Specht CS, Rizk E. Correlation of histopathology and clinical symptoms in meralgia paresthetica. Cureus. 2017;9(10):e1789. Published 2017 Oct 20. doi:10.7759/cureus.1789
8. Boyce JR. Meralgia paresthetica and tight trousers. JAMA. 1984;251(12):1553.
9. Orton D. Meralgia paresthetica from a wallet. JAMA. 1984;252(24):3368.
10. Fargo MV, Konitzer LN. Meralgia paresthetica due to body armor wear in U.S. soldiers serving in Iraq: a case report and review of the literature. Mil Med. 2007;172(6):663-665. doi:10.7205/milmed.172.6.663
11. Korkmaz N, Ozçakar L. Meralgia paresthetica in a policeman: the belt or the gun. Plast Reconstr Surg. 2004;114(4):1012-1013. doi:10.1097/01.prs.0000138706.86633.01
12. Gooding MS, Evangelista V, Pereira L. Carpal Tunnel Syndrome and Meralgia Paresthetica in Pregnancy. Obstet Gynecol Surv. 2020;75(2):121-126. doi:10.1097/OGX.0000000000000745
13. Pauwels A, Amarenco P, Chazouillères O, Pigot F, Calmus Y, Lévy VG. Une complication rare et méconnue de l’ascite: la méralgie paresthésique [Unusual and unknown complication of ascites: meralgia paresthetica]. Gastroenterol Clin Biol. 1990;14(3):295.
14. Braddom RL. L2 rather than L1 radiculopathy mimics meralgia paresthetica. Muscle Nerve. 2010;42(5):842. doi:10.1002/mus.21826
15. Suber DA, Massey EW. Pelvic mass presenting as meralgia paresthetica. Obstet Gynecol. 1979;53(2):257-258.
16. Flowers RS. Meralgia paresthetica. A clue to retroperitoneal malignant tumor. Am J Surg. 1968;116(1):89-92. doi:10.1016/0002-9610(68)90423-6
17. Yi TI, Yoon TH, Kim JS, Lee GE, Kim BR. Femoral neuropathy and meralgia paresthetica secondary to an iliacus hematoma. Ann Rehabil Med. 2012;36(2):273-277. doi:10.5535/arm.2012.36.2.273
18. Lee ATJ, Thway K, Huang PH, Jones RL. Clinical and molecular spectrum of liposarcoma. J Clin Oncol. 2018;36(2):151-159. doi:10.1200/JCO.2017.74.9598
19. O’Sullivan ED, Schofield SJ. Cognitive bias in clinical medicine. J R Coll Physicians Edinb. 2018;48(3):225-232. doi:10.4997/JRCPE.2018.306
20. Bickley, LS. Bates’ Guide to Physical Examination and History Taking. 12th Edition. Wolters Kluwer Health/Lippincott Williams and Wilkins; 2016.
21. Bhavsar AS, Verma S, Lamba R, Lall CG, Koenigsknecht V, Rajesh A. Abdominal manifestations of neurologic disorders. Radiographics. 2013;33(1):135-153. doi:10.1148/rg.331125097
22. Dureja GP, Gulaya V, Jayalakshmi TS, Mandal P. Management of meralgia paresthetica: a multimodality regimen. Anesth Analg. 1995;80(5):1060-1061. doi:10.1097/00000539-199505000-00043
23. Patijn J, Mekhail N, Hayek S, Lataster A, van Kleef M, Van Zundert J. Meralgia paresthetica. Pain Pract. 2011;11(3):302-308. doi:10.1111/j.1533-2500.2011.00458.x24. Ivins GK. Meralgia paresthetica, the elusive diagnosis: clinical experience with 14 adult patients. Ann Surg. 2000;232(2):281-286. doi:10.1097/00000658-200008000-00019
25. Munin MA, Goerner MS, Raggio I, et al. A rare cause of dyspnea: undifferentiated pleomorphic sarcoma in the left atrium. Cardiol Res. 2017;8(5):241-245. doi:10.14740/cr590w
26. Nguyen A, Awad WI. Cardiac sarcoma arising from malignant transformation of a preexisting atrial myxoma. Ann Thorac Surg. 2016;101(4):1571-1573. doi:10.1016/j.athoracsur.2015.05.129
27. Jiang S, Li J, Zeng Q, Liang J. Pulmonary artery intimal sarcoma misdiagnosed as pulmonary embolism: a case report. Oncol Lett. 2017;13(4):2713-2716. doi:10.3892/ol.2017.5775
28. Cojocaru A, Oliveira PJ, Pellecchia C. A pleural presentation of a rare soft tissue sarcoma. Am J Resp Crit Care Med. 2012;185:A5201. doi:10.1164/ajrccm-conference.2012.185.1_MeetingAbstracts.A5201
29. Grossman MG, Ducey SA, Nadler SS, Levy AS. Meralgia paresthetica: diagnosis and treatment. J Am Acad Orthop Surg. 2001;9(5):336-344. doi:10.5435/00124635-200109000-00007
30. Cheatham SW, Kolber MJ, Salamh PA. Meralgia paresthetica: a review of the literature. Int J Sports Phys Ther. 2013;8(6):883-893.
31. Nouraei SA, Anand B, Spink G, O’Neill KS. A novel approach to the diagnosis and management of meralgia paresthetica. Neurosurgery. 2007;60(4):696-700. doi:10.1227/01.NEU.0000255392.69914.F7
32. Antunes PE, Antunes MJ. Meralgia paresthetica after aortic valve surgery. J Heart Valve Dis. 1997;6(6):589-590.
33. Reddy YM, Singh D, Chikkam V, et al. Postprocedural neuropathy after atrial fibrillation ablation. J Interv Card Electrophysiol. 2013;36(3):279-285. doi:10.1007/s10840-012-9724-z
34. Butler R, Webster MW. Meralgia paresthetica: an unusual complication of cardiac catheterization via the femoral artery. Catheter Cardiovasc Interv. 2002;56(1):69-71. doi:10.1002/ccd.10149
35. Jellish WS, Oftadeh M. Peripheral nerve injury in cardiac surgery. J Cardiothorac Vasc Anesth. 2018;32(1):495-511. doi:10.1053/j.jvca.2017.08.030
36. Parsonnet V, Karasakalides A, Gielchinsky I, Hochberg M, Hussain SM. Meralgia paresthetica after coronary bypass surgery. J Thorac Cardiovasc Surg. 1991;101(2):219-221.
37. Macgregor AM, Thoburn EK. Meralgia paresthetica following bariatric surgery. Obes Surg. 1999;9(4):364-368. doi:10.1381/096089299765552945
38. Grace DM. Meralgia paresthetica after gastroplasty for morbid obesity. Can J Surg. 1987;30(1):64-65.
39. Polidori L, Magarelli M, Tramutoli R. Meralgia paresthetica as a complication of laparoscopic appendectomy. Surg Endosc. 2003;17(5):832. doi:10.1007/s00464-002-4279-1
40. Yamout B, Tayyim A, Farhat W. Meralgia paresthetica as a complication of laparoscopic cholecystectomy. Clin Neurol Neurosurg. 1994;96(2):143-144. doi:10.1016/0303-8467(94)90048-5
41. Broin EO, Horner C, Mealy K, et al. Meralgia paraesthetica following laparoscopic inguinal hernia repair. an anatomical analysis. Surg Endosc. 1995;9(1):76-78. doi:10.1007/BF00187893
42. Eubanks S, Newman L 3rd, Goehring L, et al. Meralgia paresthetica: a complication of laparoscopic herniorrhaphy. Surg Laparosc Endosc. 1993;3(5):381-385.
43. Atamaz F, Hepgüler S, Karasu Z, Kilic M. Meralgia paresthetica after liver transplantation: a case report. Transplant Proc. 2005;37(10):4424-4425. doi:10.1016/j.transproceed.2005.11.047
44. Chung KH, Lee JY, Ko TK, et al. Meralgia paresthetica affecting parturient women who underwent cesarean section -a case report-. Korean J Anesthesiol. 2010;59 Suppl(Suppl):S86-S89. doi:10.4097/kjae.2010.59.S.S86
45. Hutchins FL Jr, Huggins J, Delaney ML. Laparoscopic myomectomy-an unusual cause of meralgia paresthetica. J Am Assoc Gynecol Laparosc. 1998;5(3):309-311. doi:10.1016/s1074-3804(98)80039-x
46. Jones CD, Guiot L, Portelli M, Bullen T, Skaife P. Two interesting cases of meralgia paraesthetica. Pain Physician. 2017;20(6):E987-E989.
47. Peters G, Larner AJ. Meralgia paresthetica following gynecologic and obstetric surgery. Int J Gynaecol Obstet. 2006;95(1):42-43. doi:10.1016/j.ijgo.2006.05.025
48. Kvarnström N, Järvholm S, Johannesson L, Dahm-Kähler P, Olausson M, Brännström M. Live donors of the initial observational study of uterus transplantation-psychological and medical follow-up until 1 year after surgery in the 9 cases. Transplantation. 2017;101(3):664-670. doi:10.1097/TP.0000000000001567
49. Goulding K, Beaulé PE, Kim PR, Fazekas A. Incidence of lateral femoral cutaneous nerve neuropraxia after anterior approach hip arthroplasty. Clin Orthop Relat Res. 2010;468(9):2397-2404. doi:10.1007/s11999-010-1406-5
50. Yamamoto T, Nagira K, Kurosaka M. Meralgia paresthetica occurring 40 years after iliac bone graft harvesting: case report. Neurosurgery. 2001;49(6):1455-1457. doi:10.1097/00006123-200112000-00028
51. Roqueplan F, Porcher R, Hamzé B, et al. Long-term results of percutaneous resection and interstitial laser ablation of osteoid osteomas. Eur Radiol. 2010;20(1):209-217. doi:10.1007/s00330-009-1537-9
52. Gupta A, Muzumdar D, Ramani PS. Meralgia paraesthetica following lumbar spine surgery: a study in 110 consecutive surgically treated cases. Neurol India. 2004;52(1):64-66.
53. Yang SH, Wu CC, Chen PQ. Postoperative meralgia paresthetica after posterior spine surgery: incidence, risk factors, and clinical outcomes. Spine (Phila Pa 1976). 2005;30(18):E547-E550. doi:10.1097/01.brs.0000178821.14102.9d
54. Tejwani SG, Scaduto AA, Bowen RE. Transient meralgia paresthetica after pediatric posterior spine fusion. J Pediatr Orthop. 2006;26(4):530-533. doi:10.1097/01.bpo.0000217721.95480.9e
55. Peker S, Ay B, Sun I, Ozgen S, Pamir M. Meralgia paraesthetica: complications of prone position during lumbar disc surgery. Internet J Anesthesiol. 2003;8(1):24-29.
1. van Slobbe AM, Bohnen AM, Bernsen RM, Koes BW, Bierma-Zeinstra SM. Incidence rates and determinants in meralgia paresthetica in general practice. J Neurol. 2004;251(3):294-297. doi:10.1007/s00415-004-0310-x
2. Parisi TJ, Mandrekar J, Dyck PJ, Klein CJ. Meralgia paresthetica: relation to obesity, advanced age, and diabetes mellitus. Neurology. 2011;77(16):1538-1542. doi:10.1212/WNL.0b013e318233b356
3. Ecker AD. Diagnosis of meralgia paresthetica. JAMA. 1985;253(7):976.
4. Massey EW, Pellock JM. Meralgia paraesthetica in a child. J Pediatr. 1978;93(2):325-326. doi:10.1016/s0022-3476(78)80566-6
5. Harney D, Patijn J. Meralgia paresthetica: diagnosis and management strategies. Pain Med. 2007;8(8):669-677. doi:10.1111/j.1526-4637.2006.00227.x
6. Berini SE, Spinner RJ, Jentoft ME, et al. Chronic meralgia paresthetica and neurectomy: a clinical pathologic study. Neurology. 2014;82(17):1551-1555. doi:10.1212/WNL.0000000000000367
7. Payne RA, Harbaugh K, Specht CS, Rizk E. Correlation of histopathology and clinical symptoms in meralgia paresthetica. Cureus. 2017;9(10):e1789. Published 2017 Oct 20. doi:10.7759/cureus.1789
8. Boyce JR. Meralgia paresthetica and tight trousers. JAMA. 1984;251(12):1553.
9. Orton D. Meralgia paresthetica from a wallet. JAMA. 1984;252(24):3368.
10. Fargo MV, Konitzer LN. Meralgia paresthetica due to body armor wear in U.S. soldiers serving in Iraq: a case report and review of the literature. Mil Med. 2007;172(6):663-665. doi:10.7205/milmed.172.6.663
11. Korkmaz N, Ozçakar L. Meralgia paresthetica in a policeman: the belt or the gun. Plast Reconstr Surg. 2004;114(4):1012-1013. doi:10.1097/01.prs.0000138706.86633.01
12. Gooding MS, Evangelista V, Pereira L. Carpal Tunnel Syndrome and Meralgia Paresthetica in Pregnancy. Obstet Gynecol Surv. 2020;75(2):121-126. doi:10.1097/OGX.0000000000000745
13. Pauwels A, Amarenco P, Chazouillères O, Pigot F, Calmus Y, Lévy VG. Une complication rare et méconnue de l’ascite: la méralgie paresthésique [Unusual and unknown complication of ascites: meralgia paresthetica]. Gastroenterol Clin Biol. 1990;14(3):295.
14. Braddom RL. L2 rather than L1 radiculopathy mimics meralgia paresthetica. Muscle Nerve. 2010;42(5):842. doi:10.1002/mus.21826
15. Suber DA, Massey EW. Pelvic mass presenting as meralgia paresthetica. Obstet Gynecol. 1979;53(2):257-258.
16. Flowers RS. Meralgia paresthetica. A clue to retroperitoneal malignant tumor. Am J Surg. 1968;116(1):89-92. doi:10.1016/0002-9610(68)90423-6
17. Yi TI, Yoon TH, Kim JS, Lee GE, Kim BR. Femoral neuropathy and meralgia paresthetica secondary to an iliacus hematoma. Ann Rehabil Med. 2012;36(2):273-277. doi:10.5535/arm.2012.36.2.273
18. Lee ATJ, Thway K, Huang PH, Jones RL. Clinical and molecular spectrum of liposarcoma. J Clin Oncol. 2018;36(2):151-159. doi:10.1200/JCO.2017.74.9598
19. O’Sullivan ED, Schofield SJ. Cognitive bias in clinical medicine. J R Coll Physicians Edinb. 2018;48(3):225-232. doi:10.4997/JRCPE.2018.306
20. Bickley, LS. Bates’ Guide to Physical Examination and History Taking. 12th Edition. Wolters Kluwer Health/Lippincott Williams and Wilkins; 2016.
21. Bhavsar AS, Verma S, Lamba R, Lall CG, Koenigsknecht V, Rajesh A. Abdominal manifestations of neurologic disorders. Radiographics. 2013;33(1):135-153. doi:10.1148/rg.331125097
22. Dureja GP, Gulaya V, Jayalakshmi TS, Mandal P. Management of meralgia paresthetica: a multimodality regimen. Anesth Analg. 1995;80(5):1060-1061. doi:10.1097/00000539-199505000-00043
23. Patijn J, Mekhail N, Hayek S, Lataster A, van Kleef M, Van Zundert J. Meralgia paresthetica. Pain Pract. 2011;11(3):302-308. doi:10.1111/j.1533-2500.2011.00458.x24. Ivins GK. Meralgia paresthetica, the elusive diagnosis: clinical experience with 14 adult patients. Ann Surg. 2000;232(2):281-286. doi:10.1097/00000658-200008000-00019
25. Munin MA, Goerner MS, Raggio I, et al. A rare cause of dyspnea: undifferentiated pleomorphic sarcoma in the left atrium. Cardiol Res. 2017;8(5):241-245. doi:10.14740/cr590w
26. Nguyen A, Awad WI. Cardiac sarcoma arising from malignant transformation of a preexisting atrial myxoma. Ann Thorac Surg. 2016;101(4):1571-1573. doi:10.1016/j.athoracsur.2015.05.129
27. Jiang S, Li J, Zeng Q, Liang J. Pulmonary artery intimal sarcoma misdiagnosed as pulmonary embolism: a case report. Oncol Lett. 2017;13(4):2713-2716. doi:10.3892/ol.2017.5775
28. Cojocaru A, Oliveira PJ, Pellecchia C. A pleural presentation of a rare soft tissue sarcoma. Am J Resp Crit Care Med. 2012;185:A5201. doi:10.1164/ajrccm-conference.2012.185.1_MeetingAbstracts.A5201
29. Grossman MG, Ducey SA, Nadler SS, Levy AS. Meralgia paresthetica: diagnosis and treatment. J Am Acad Orthop Surg. 2001;9(5):336-344. doi:10.5435/00124635-200109000-00007
30. Cheatham SW, Kolber MJ, Salamh PA. Meralgia paresthetica: a review of the literature. Int J Sports Phys Ther. 2013;8(6):883-893.
31. Nouraei SA, Anand B, Spink G, O’Neill KS. A novel approach to the diagnosis and management of meralgia paresthetica. Neurosurgery. 2007;60(4):696-700. doi:10.1227/01.NEU.0000255392.69914.F7
32. Antunes PE, Antunes MJ. Meralgia paresthetica after aortic valve surgery. J Heart Valve Dis. 1997;6(6):589-590.
33. Reddy YM, Singh D, Chikkam V, et al. Postprocedural neuropathy after atrial fibrillation ablation. J Interv Card Electrophysiol. 2013;36(3):279-285. doi:10.1007/s10840-012-9724-z
34. Butler R, Webster MW. Meralgia paresthetica: an unusual complication of cardiac catheterization via the femoral artery. Catheter Cardiovasc Interv. 2002;56(1):69-71. doi:10.1002/ccd.10149
35. Jellish WS, Oftadeh M. Peripheral nerve injury in cardiac surgery. J Cardiothorac Vasc Anesth. 2018;32(1):495-511. doi:10.1053/j.jvca.2017.08.030
36. Parsonnet V, Karasakalides A, Gielchinsky I, Hochberg M, Hussain SM. Meralgia paresthetica after coronary bypass surgery. J Thorac Cardiovasc Surg. 1991;101(2):219-221.
37. Macgregor AM, Thoburn EK. Meralgia paresthetica following bariatric surgery. Obes Surg. 1999;9(4):364-368. doi:10.1381/096089299765552945
38. Grace DM. Meralgia paresthetica after gastroplasty for morbid obesity. Can J Surg. 1987;30(1):64-65.
39. Polidori L, Magarelli M, Tramutoli R. Meralgia paresthetica as a complication of laparoscopic appendectomy. Surg Endosc. 2003;17(5):832. doi:10.1007/s00464-002-4279-1
40. Yamout B, Tayyim A, Farhat W. Meralgia paresthetica as a complication of laparoscopic cholecystectomy. Clin Neurol Neurosurg. 1994;96(2):143-144. doi:10.1016/0303-8467(94)90048-5
41. Broin EO, Horner C, Mealy K, et al. Meralgia paraesthetica following laparoscopic inguinal hernia repair. an anatomical analysis. Surg Endosc. 1995;9(1):76-78. doi:10.1007/BF00187893
42. Eubanks S, Newman L 3rd, Goehring L, et al. Meralgia paresthetica: a complication of laparoscopic herniorrhaphy. Surg Laparosc Endosc. 1993;3(5):381-385.
43. Atamaz F, Hepgüler S, Karasu Z, Kilic M. Meralgia paresthetica after liver transplantation: a case report. Transplant Proc. 2005;37(10):4424-4425. doi:10.1016/j.transproceed.2005.11.047
44. Chung KH, Lee JY, Ko TK, et al. Meralgia paresthetica affecting parturient women who underwent cesarean section -a case report-. Korean J Anesthesiol. 2010;59 Suppl(Suppl):S86-S89. doi:10.4097/kjae.2010.59.S.S86
45. Hutchins FL Jr, Huggins J, Delaney ML. Laparoscopic myomectomy-an unusual cause of meralgia paresthetica. J Am Assoc Gynecol Laparosc. 1998;5(3):309-311. doi:10.1016/s1074-3804(98)80039-x
46. Jones CD, Guiot L, Portelli M, Bullen T, Skaife P. Two interesting cases of meralgia paraesthetica. Pain Physician. 2017;20(6):E987-E989.
47. Peters G, Larner AJ. Meralgia paresthetica following gynecologic and obstetric surgery. Int J Gynaecol Obstet. 2006;95(1):42-43. doi:10.1016/j.ijgo.2006.05.025
48. Kvarnström N, Järvholm S, Johannesson L, Dahm-Kähler P, Olausson M, Brännström M. Live donors of the initial observational study of uterus transplantation-psychological and medical follow-up until 1 year after surgery in the 9 cases. Transplantation. 2017;101(3):664-670. doi:10.1097/TP.0000000000001567
49. Goulding K, Beaulé PE, Kim PR, Fazekas A. Incidence of lateral femoral cutaneous nerve neuropraxia after anterior approach hip arthroplasty. Clin Orthop Relat Res. 2010;468(9):2397-2404. doi:10.1007/s11999-010-1406-5
50. Yamamoto T, Nagira K, Kurosaka M. Meralgia paresthetica occurring 40 years after iliac bone graft harvesting: case report. Neurosurgery. 2001;49(6):1455-1457. doi:10.1097/00006123-200112000-00028
51. Roqueplan F, Porcher R, Hamzé B, et al. Long-term results of percutaneous resection and interstitial laser ablation of osteoid osteomas. Eur Radiol. 2010;20(1):209-217. doi:10.1007/s00330-009-1537-9
52. Gupta A, Muzumdar D, Ramani PS. Meralgia paraesthetica following lumbar spine surgery: a study in 110 consecutive surgically treated cases. Neurol India. 2004;52(1):64-66.
53. Yang SH, Wu CC, Chen PQ. Postoperative meralgia paresthetica after posterior spine surgery: incidence, risk factors, and clinical outcomes. Spine (Phila Pa 1976). 2005;30(18):E547-E550. doi:10.1097/01.brs.0000178821.14102.9d
54. Tejwani SG, Scaduto AA, Bowen RE. Transient meralgia paresthetica after pediatric posterior spine fusion. J Pediatr Orthop. 2006;26(4):530-533. doi:10.1097/01.bpo.0000217721.95480.9e
55. Peker S, Ay B, Sun I, Ozgen S, Pamir M. Meralgia paraesthetica: complications of prone position during lumbar disc surgery. Internet J Anesthesiol. 2003;8(1):24-29.
NSAIDs don’t make COVID-19 worse in hospitalized patients
NSAIDs don’t boost the risk of more severe disease or death in hospitalized patients with COVID-19, a new study finds.

“To our knowledge, our prospective study includes the largest number of patients admitted to hospital with COVID-19 to date, and adds to the literature on the safety of NSAIDs and in-hospital outcomes. NSAIDs do not appear to increase the risk of worse in-hospital outcomes ...” the study authors wrote. “NSAIDs are an important analgesic modality and have a vital opioid-sparing role in pain management. Patients and clinicians should be reassured by these findings that NSAIDs are safe in the context of the pandemic.”
The report was published online May 7 in The Lancet Rheumatology and led by clinical research fellow Thomas M. Drake, MBChB, of the University of Edinburgh’s Usher Institute.
For more than a year, researchers worldwide have debated about whether NSAIDs spell trouble for people at risk of COVID-19. In March 2020, French health officials announced that use of the painkillers such as NSAIDs may increase the severity of the disease, and they recommended that patients take acetaminophen instead. The National Health Service in the United Kingdom made a similar recommendation. But other agencies didn’t believe there was enough evidence to support ditching NSAIDs, and recent research studies published in Annals of the Rheumatic Diseases and PLoS Medicine suggested they may be right.
For the new study, researchers identified 72,179 patients who were treated for COVID-19 in British hospitals during January-August 2020. About 56% were men, 74% were White, and 6% took NSAIDs on a regular basis before they entered the hospital. The average age was 70.
The researchers examined whether the patients in either group were more or less likely to die in the hospital, be admitted into a critical care unit, need oxygen treatment, need a ventilator, or suffer kidney injury.
In terms of outcomes, there weren’t any major gaps between the groups overall. The differences in most comparisons were statistically insignificant. For example, 31% of those who didn’t take NSAIDs died vs. 30% of those who did (P = .227). In both groups, 14% required critical care admission (P = .476).
The researchers then focused on two matched groups of 4,205 patients: One group used NSAIDs regularly, and the other group didn’t. The difference in risk of death in those who took NSAIDs vs. those who didn’t was statistically insignificant (odds ratio, 0.95; 95% confidence interval, 0.84-1.07; P = .35). Other comparisons were also statistically insignificant.
The findings offer insight into whether the use of NSAIDs might actually be helpful for patients who develop COVID-19. Scientists believe that COVID-19 is linked to inflammation in the body, and NSAIDs, of course, reduce inflammation. But the researchers didn’t turn up any sign of a benefit.
The new study has some weaknesses: It doesn’t say anything about whether NSAIDs have an impact on whether people get COVID-19 in the first place. Researchers don’t know if high use of NSAIDs may affect the severity of the disease. And it doesn’t examine the potential effect of acetaminophen, although other research suggests the drug also may not cause harm in patients with COVID-19.
Still, the researchers say the study is the largest of its kind to look at the use of NSAIDs by patients who are admitted to the hospital with COVID-19. “Considering all the evidence, if there was an extreme effect of NSAIDs on COVID-19 outcomes or severity, this would have been observed in one or more of the studies that have been done, including the present study,” they wrote.
In a commentary that accompanied the study, three physicians from hospitals in Denmark, led by Kristian Kragholm, MD, of Aalborg University Hospital, praised the research and wrote that it adds to “a growing body of evidence” that NSAIDs don’t make things worse for patients with COVID-19.
The study was funded by the U.K. National Institute for Health Research and the U.K. Medical Research Council. The study and commentary authors reported no relevant disclosures.
NSAIDs don’t boost the risk of more severe disease or death in hospitalized patients with COVID-19, a new study finds.
“To our knowledge, our prospective study includes the largest number of patients admitted to hospital with COVID-19 to date, and adds to the literature on the safety of NSAIDs and in-hospital outcomes. NSAIDs do not appear to increase the risk of worse in-hospital outcomes ...” the study authors wrote. “NSAIDs are an important analgesic modality and have a vital opioid-sparing role in pain management. Patients and clinicians should be reassured by these findings that NSAIDs are safe in the context of the pandemic.”
The report was published online May 7 in The Lancet Rheumatology and led by clinical research fellow Thomas M. Drake, MBChB, of the University of Edinburgh’s Usher Institute.
For more than a year, researchers worldwide have debated about whether NSAIDs spell trouble for people at risk of COVID-19. In March 2020, French health officials announced that use of the painkillers such as NSAIDs may increase the severity of the disease, and they recommended that patients take acetaminophen instead. The National Health Service in the United Kingdom made a similar recommendation. But other agencies didn’t believe there was enough evidence to support ditching NSAIDs, and recent research studies published in Annals of the Rheumatic Diseases and PLoS Medicine suggested they may be right.
For the new study, researchers identified 72,179 patients who were treated for COVID-19 in British hospitals during January-August 2020. About 56% were men, 74% were White, and 6% took NSAIDs on a regular basis before they entered the hospital. The average age was 70.
The researchers examined whether the patients in either group were more or less likely to die in the hospital, be admitted into a critical care unit, need oxygen treatment, need a ventilator, or suffer kidney injury.
In terms of outcomes, there weren’t any major gaps between the groups overall. The differences in most comparisons were statistically insignificant. For example, 31% of those who didn’t take NSAIDs died vs. 30% of those who did (P = .227). In both groups, 14% required critical care admission (P = .476).
The researchers then focused on two matched groups of 4,205 patients: One group used NSAIDs regularly, and the other group didn’t. The difference in risk of death in those who took NSAIDs vs. those who didn’t was statistically insignificant (odds ratio, 0.95; 95% confidence interval, 0.84-1.07; P = .35). Other comparisons were also statistically insignificant.
The findings offer insight into whether the use of NSAIDs might actually be helpful for patients who develop COVID-19. Scientists believe that COVID-19 is linked to inflammation in the body, and NSAIDs, of course, reduce inflammation. But the researchers didn’t turn up any sign of a benefit.
The new study has some weaknesses: It doesn’t say anything about whether NSAIDs have an impact on whether people get COVID-19 in the first place. Researchers don’t know if high use of NSAIDs may affect the severity of the disease. And it doesn’t examine the potential effect of acetaminophen, although other research suggests the drug also may not cause harm in patients with COVID-19.
Still, the researchers say the study is the largest of its kind to look at the use of NSAIDs by patients who are admitted to the hospital with COVID-19. “Considering all the evidence, if there was an extreme effect of NSAIDs on COVID-19 outcomes or severity, this would have been observed in one or more of the studies that have been done, including the present study,” they wrote.
In a commentary that accompanied the study, three physicians from hospitals in Denmark, led by Kristian Kragholm, MD, of Aalborg University Hospital, praised the research and wrote that it adds to “a growing body of evidence” that NSAIDs don’t make things worse for patients with COVID-19.
The study was funded by the U.K. National Institute for Health Research and the U.K. Medical Research Council. The study and commentary authors reported no relevant disclosures.
NSAIDs don’t boost the risk of more severe disease or death in hospitalized patients with COVID-19, a new study finds.
“To our knowledge, our prospective study includes the largest number of patients admitted to hospital with COVID-19 to date, and adds to the literature on the safety of NSAIDs and in-hospital outcomes. NSAIDs do not appear to increase the risk of worse in-hospital outcomes ...” the study authors wrote. “NSAIDs are an important analgesic modality and have a vital opioid-sparing role in pain management. Patients and clinicians should be reassured by these findings that NSAIDs are safe in the context of the pandemic.”
The report was published online May 7 in The Lancet Rheumatology and led by clinical research fellow Thomas M. Drake, MBChB, of the University of Edinburgh’s Usher Institute.
For more than a year, researchers worldwide have debated about whether NSAIDs spell trouble for people at risk of COVID-19. In March 2020, French health officials announced that use of the painkillers such as NSAIDs may increase the severity of the disease, and they recommended that patients take acetaminophen instead. The National Health Service in the United Kingdom made a similar recommendation. But other agencies didn’t believe there was enough evidence to support ditching NSAIDs, and recent research studies published in Annals of the Rheumatic Diseases and PLoS Medicine suggested they may be right.
For the new study, researchers identified 72,179 patients who were treated for COVID-19 in British hospitals during January-August 2020. About 56% were men, 74% were White, and 6% took NSAIDs on a regular basis before they entered the hospital. The average age was 70.
The researchers examined whether the patients in either group were more or less likely to die in the hospital, be admitted into a critical care unit, need oxygen treatment, need a ventilator, or suffer kidney injury.
In terms of outcomes, there weren’t any major gaps between the groups overall. The differences in most comparisons were statistically insignificant. For example, 31% of those who didn’t take NSAIDs died vs. 30% of those who did (P = .227). In both groups, 14% required critical care admission (P = .476).
The researchers then focused on two matched groups of 4,205 patients: One group used NSAIDs regularly, and the other group didn’t. The difference in risk of death in those who took NSAIDs vs. those who didn’t was statistically insignificant (odds ratio, 0.95; 95% confidence interval, 0.84-1.07; P = .35). Other comparisons were also statistically insignificant.
The findings offer insight into whether the use of NSAIDs might actually be helpful for patients who develop COVID-19. Scientists believe that COVID-19 is linked to inflammation in the body, and NSAIDs, of course, reduce inflammation. But the researchers didn’t turn up any sign of a benefit.
The new study has some weaknesses: It doesn’t say anything about whether NSAIDs have an impact on whether people get COVID-19 in the first place. Researchers don’t know if high use of NSAIDs may affect the severity of the disease. And it doesn’t examine the potential effect of acetaminophen, although other research suggests the drug also may not cause harm in patients with COVID-19.
Still, the researchers say the study is the largest of its kind to look at the use of NSAIDs by patients who are admitted to the hospital with COVID-19. “Considering all the evidence, if there was an extreme effect of NSAIDs on COVID-19 outcomes or severity, this would have been observed in one or more of the studies that have been done, including the present study,” they wrote.
In a commentary that accompanied the study, three physicians from hospitals in Denmark, led by Kristian Kragholm, MD, of Aalborg University Hospital, praised the research and wrote that it adds to “a growing body of evidence” that NSAIDs don’t make things worse for patients with COVID-19.
The study was funded by the U.K. National Institute for Health Research and the U.K. Medical Research Council. The study and commentary authors reported no relevant disclosures.
FROM THE LANCET RHEUMATOLOGY
Transcranial brain stimulation can modulate placebo and nocebo experiences
, according to results of a new study published in the Proceedings of the National Academy of Sciences (PNAS).
“Placebo and nocebo effects are a critical component of clinical care and efficacy studies,” said senior author Jian Kong, MD, associate professor in the department of psychiatry at Massachusetts General Hospital, Charlestown campus. “Harnessing these effects in clinical practice and research could facilitate the development of new pain management methods,” he said. “Healing may involve multiple components: the self-healing properties of the body; the nonspecific effects of treatment (i.e., placebo effect); and the specific effect of a physical or pharmacologic intervention. Therefore, enhancing the placebo effect may ultimately boost the overall therapeutic effect of existing treatment,” he explained, emphasizing that the results are preliminary and should be interpreted with caution.
The authors noted that reducing nocebo effects could also be a major benefit “since patients discontinue prescribed medications, make unnecessary medical visits, and take additional medications to counteract adverse effects that are actually nocebo effects.”
Testing the hypothesis
The randomized, double-blind, sham-controlled study used transcranial direct current stimulation (tDCS), which delivers an electrical current to the brain via scalp electrodes. The aim was to see if stimulating the dorsolateral prefrontal cortex with tDCS could alter the brain’s perception of placebo and nocebo experiences.
The study included 81 participants (37 females, mean age: 27.4 years), who were randomized into one of three tDCS groups (anodal, cathodal, or sham).
All participants were first conditioned to believe that an inert cream was either lidocaine or capsaicin and that this cream could either dull the impact of a painful heat stimulus (placebo analgesia) or exacerbate it (nocebo hyperalgesia). Participants were then placed into a functional MRI scanner where tDCS was initiated. Painful stimuli were then applied to spots on their forearms where they believed they had either lidocaine, capsaicin, or a neutral control cream and they rated the pain using the Gracely Sensory Scale.
Placebo analgesia was defined as the difference between perceived pain intensity where participants believed they had lidocaine cream compared with where they believed they had control cream. Nocebo hyperalgesia was defined as the difference between perceived pain intensity where they believed they had capsaicin cream compared with where they believed they had control cream.
The researchers found that compared with sham tDCS, cathodal tDCS showed significant effects in increasing placebo analgesia and brain responses in the ventromedial prefrontal cortex (vmPFC), while anodal tDCS showed significant effects in inhibiting nocebo hyperalgesia and brain responses in the insula.
“The potential to enhance salubrious placebo effects and/or diminish treatment-interfering nocebo effects may have clinical significance,” the authors noted. “For example, clinical studies have suggested that expectancy is positively associated with chronic pain improvement, and using conditioning-like expectancy manipulation, we have shown that significantly boosting expectancy can improve treatment outcome.”
Proof of concept
Asked to comment on the study, Brian E. McGeeney, MD, of the John R. Graham Headache Center at Brigham and Women’s Faulkner Hospital in Boston, said “the findings are a proof of concept that it is possible to use noninvasive brain stimulation to modulate placebo and nocebo pain effects.”
Although the findings do not have immediate clinical application, they are “exciting” and “break new ground in expectancy research,” he said.
“It is important to recognize that the researchers are trying to utilize a purported expectancy mechanism rather than attempting to alter placebo/nocebo by verbal and other cues. It remains to be seen whether the manipulation of brief experimental pain like this can translate into altered chronic pain over time, the main clinical goal. Current tDCS therapy for various reasons is necessarily brief and one can ask whether there are meaningful changes from brief stimulation. Such results can foster speculation as to whether direct strategic placement of intracranial stimulation leads could result in more longstanding similar benefits.”
Dr. Kong holds equity in a startup company (MNT) and a pending patent to develop new peripheral neuromodulation tools, but declares no conflict of interest. All other authors declare no conflict of interest.
, according to results of a new study published in the Proceedings of the National Academy of Sciences (PNAS).
“Placebo and nocebo effects are a critical component of clinical care and efficacy studies,” said senior author Jian Kong, MD, associate professor in the department of psychiatry at Massachusetts General Hospital, Charlestown campus. “Harnessing these effects in clinical practice and research could facilitate the development of new pain management methods,” he said. “Healing may involve multiple components: the self-healing properties of the body; the nonspecific effects of treatment (i.e., placebo effect); and the specific effect of a physical or pharmacologic intervention. Therefore, enhancing the placebo effect may ultimately boost the overall therapeutic effect of existing treatment,” he explained, emphasizing that the results are preliminary and should be interpreted with caution.
The authors noted that reducing nocebo effects could also be a major benefit “since patients discontinue prescribed medications, make unnecessary medical visits, and take additional medications to counteract adverse effects that are actually nocebo effects.”
Testing the hypothesis
The randomized, double-blind, sham-controlled study used transcranial direct current stimulation (tDCS), which delivers an electrical current to the brain via scalp electrodes. The aim was to see if stimulating the dorsolateral prefrontal cortex with tDCS could alter the brain’s perception of placebo and nocebo experiences.
The study included 81 participants (37 females, mean age: 27.4 years), who were randomized into one of three tDCS groups (anodal, cathodal, or sham).
All participants were first conditioned to believe that an inert cream was either lidocaine or capsaicin and that this cream could either dull the impact of a painful heat stimulus (placebo analgesia) or exacerbate it (nocebo hyperalgesia). Participants were then placed into a functional MRI scanner where tDCS was initiated. Painful stimuli were then applied to spots on their forearms where they believed they had either lidocaine, capsaicin, or a neutral control cream and they rated the pain using the Gracely Sensory Scale.
Placebo analgesia was defined as the difference between perceived pain intensity where participants believed they had lidocaine cream compared with where they believed they had control cream. Nocebo hyperalgesia was defined as the difference between perceived pain intensity where they believed they had capsaicin cream compared with where they believed they had control cream.
The researchers found that compared with sham tDCS, cathodal tDCS showed significant effects in increasing placebo analgesia and brain responses in the ventromedial prefrontal cortex (vmPFC), while anodal tDCS showed significant effects in inhibiting nocebo hyperalgesia and brain responses in the insula.
“The potential to enhance salubrious placebo effects and/or diminish treatment-interfering nocebo effects may have clinical significance,” the authors noted. “For example, clinical studies have suggested that expectancy is positively associated with chronic pain improvement, and using conditioning-like expectancy manipulation, we have shown that significantly boosting expectancy can improve treatment outcome.”
Proof of concept
Asked to comment on the study, Brian E. McGeeney, MD, of the John R. Graham Headache Center at Brigham and Women’s Faulkner Hospital in Boston, said “the findings are a proof of concept that it is possible to use noninvasive brain stimulation to modulate placebo and nocebo pain effects.”
Although the findings do not have immediate clinical application, they are “exciting” and “break new ground in expectancy research,” he said.
“It is important to recognize that the researchers are trying to utilize a purported expectancy mechanism rather than attempting to alter placebo/nocebo by verbal and other cues. It remains to be seen whether the manipulation of brief experimental pain like this can translate into altered chronic pain over time, the main clinical goal. Current tDCS therapy for various reasons is necessarily brief and one can ask whether there are meaningful changes from brief stimulation. Such results can foster speculation as to whether direct strategic placement of intracranial stimulation leads could result in more longstanding similar benefits.”
Dr. Kong holds equity in a startup company (MNT) and a pending patent to develop new peripheral neuromodulation tools, but declares no conflict of interest. All other authors declare no conflict of interest.
, according to results of a new study published in the Proceedings of the National Academy of Sciences (PNAS).
“Placebo and nocebo effects are a critical component of clinical care and efficacy studies,” said senior author Jian Kong, MD, associate professor in the department of psychiatry at Massachusetts General Hospital, Charlestown campus. “Harnessing these effects in clinical practice and research could facilitate the development of new pain management methods,” he said. “Healing may involve multiple components: the self-healing properties of the body; the nonspecific effects of treatment (i.e., placebo effect); and the specific effect of a physical or pharmacologic intervention. Therefore, enhancing the placebo effect may ultimately boost the overall therapeutic effect of existing treatment,” he explained, emphasizing that the results are preliminary and should be interpreted with caution.
The authors noted that reducing nocebo effects could also be a major benefit “since patients discontinue prescribed medications, make unnecessary medical visits, and take additional medications to counteract adverse effects that are actually nocebo effects.”
Testing the hypothesis
The randomized, double-blind, sham-controlled study used transcranial direct current stimulation (tDCS), which delivers an electrical current to the brain via scalp electrodes. The aim was to see if stimulating the dorsolateral prefrontal cortex with tDCS could alter the brain’s perception of placebo and nocebo experiences.
The study included 81 participants (37 females, mean age: 27.4 years), who were randomized into one of three tDCS groups (anodal, cathodal, or sham).
All participants were first conditioned to believe that an inert cream was either lidocaine or capsaicin and that this cream could either dull the impact of a painful heat stimulus (placebo analgesia) or exacerbate it (nocebo hyperalgesia). Participants were then placed into a functional MRI scanner where tDCS was initiated. Painful stimuli were then applied to spots on their forearms where they believed they had either lidocaine, capsaicin, or a neutral control cream and they rated the pain using the Gracely Sensory Scale.
Placebo analgesia was defined as the difference between perceived pain intensity where participants believed they had lidocaine cream compared with where they believed they had control cream. Nocebo hyperalgesia was defined as the difference between perceived pain intensity where they believed they had capsaicin cream compared with where they believed they had control cream.
The researchers found that compared with sham tDCS, cathodal tDCS showed significant effects in increasing placebo analgesia and brain responses in the ventromedial prefrontal cortex (vmPFC), while anodal tDCS showed significant effects in inhibiting nocebo hyperalgesia and brain responses in the insula.
“The potential to enhance salubrious placebo effects and/or diminish treatment-interfering nocebo effects may have clinical significance,” the authors noted. “For example, clinical studies have suggested that expectancy is positively associated with chronic pain improvement, and using conditioning-like expectancy manipulation, we have shown that significantly boosting expectancy can improve treatment outcome.”
Proof of concept
Asked to comment on the study, Brian E. McGeeney, MD, of the John R. Graham Headache Center at Brigham and Women’s Faulkner Hospital in Boston, said “the findings are a proof of concept that it is possible to use noninvasive brain stimulation to modulate placebo and nocebo pain effects.”
Although the findings do not have immediate clinical application, they are “exciting” and “break new ground in expectancy research,” he said.
“It is important to recognize that the researchers are trying to utilize a purported expectancy mechanism rather than attempting to alter placebo/nocebo by verbal and other cues. It remains to be seen whether the manipulation of brief experimental pain like this can translate into altered chronic pain over time, the main clinical goal. Current tDCS therapy for various reasons is necessarily brief and one can ask whether there are meaningful changes from brief stimulation. Such results can foster speculation as to whether direct strategic placement of intracranial stimulation leads could result in more longstanding similar benefits.”
Dr. Kong holds equity in a startup company (MNT) and a pending patent to develop new peripheral neuromodulation tools, but declares no conflict of interest. All other authors declare no conflict of interest.
FROM PNAS
Insomnia? Referral, drugs not usually needed
Too often, medications are the treatment of choice, and when used long term they can perpetuate a problematic cycle, said Dr. Lettieri, professor in pulmonary, critical care, and sleep medicine at Johns Hopkins University, Baltimore.
However, medications alone won’t work without other behavior modifications and they come with potential side effects, he said in his talk. Prescription medications typically don’t treat the cause of the insomnia, just the symptoms.
“In the 15 years I’ve been practicing sleep medicine, I can honestly say I only have a handful of patients that I treat with long-term pharmacotherapy,” Dr. Lettieri said.
He said he typically uses pharmacotherapy only when conservative measures have failed or to help jump-start patients to behavior modifications.
Restricted sleep is a good place to start for chronic insomnia, he continued.
Physicians should ask patients the latest time they can wake up to make it to school, work, etc. If that time is 6 a.m., the goal is to move bedtime back to 10 p.m.–11 p.m. If the patient, however, is unable to sleep until 12:30 a.m., move bedtime there, he said.
Though the 5.5-hour window is not ideal, it’s better to get into bed when ready for sleep. From there, try to get the patient to move bedtime back 15 minutes each week as they train themselves to fall asleep earlier, he said.
“I promise you this works in the majority of patients and doesn’t require any medication. You can also accomplish this with one or two office visits, so it is not a huge drain on resources,” he said.
Sleep specialists in short supply
Cognitive-behavioral therapy (CBT) is “without question the best way to treat chronic insomnia and it’s recommended as first-line therapy by all published guidelines,” Dr. Lettieri said.
He defined chronic insomnia as happening most nights over at least 3 months. It affects twice as many women as men.
CBT offers a formalized way of changing sleep patterns with the help of an expert in sleep behavior disorders. It combines cognitive therapies with education about sleep and stimulus control and uses techniques such as mindfulness and relaxation.
However, most programs take 4-8 sessions with a sleep medicine provider and are usually not covered by insurance. In addition, the number of insomnia specialists is not nearly adequate to meet demand, he added.
Online and mobile-platform CBT programs are widely effective, Dr. Lettieri said. Many are free and all are convenient for patients to use. He said many of his patients use Sleepio, but many other online programs are effective.
“You can provide sufficient therapy for many of your patients and reserve CBT for patients who can’t be fixed with more conservative measures,” he said.
Insomnia among older patients
Interest in helping older patients with insomnia dominated the chat session associated with the talk.
Insomnia increases with age and older patients have often been using prescription or over-the-counter sleep aids for decades.
Additionally, “insomnia is the second-most common reason why people get admitted to long-term care facilities, second only to urinary incontinence,” Dr. Lettieri said.
If physicians use medications with older patients, he said, extra caution is needed. Older people have more neurocognitive impairments than younger adults and may already be taking several other medications. Sleep medications may come with longer elimination half-lives. Polypharmacy may increase risk for falls and have other consequences.
“If you have to go to a medication, try something simple like melatonin,” he said, adding that it should be pharmaceutical grade and extended release.
Also, bright lights during the day, movement throughout the day, and dim lights closer to bedtime are especially important for the elderly, Dr. Lettieri said.
Andrew Corr, MD, a geriatric specialist in primary care with the Riverside (Calif.) Medical Clinic, said in an interview the main message he will take back to his physician group is more CBT and less medication.
He said that, although he has long known CBT is the top first-line treatment, it is difficult to find experts in his area who are trained to do CBT for insomnia, so he was glad to hear online programs and self-directed reading are typically effective.
He also said there’s a common misperception that there’s no harm in prescribing medications such as trazodone (Desyrel), an antidepressant commonly used off label as a sleep aid.
Dr. Lettieri’s talk highlighted his recommendation against using trazodone for sleep. “Despite several recommendations against its use for insomnia, it is still commonly prescribed. You just shouldn’t use it for insomnia,” Dr. Lettieri said.
“It has no measurable effect in a third of patients and at least unacceptable side effects in another third. Right off the bat, it’s not efficacious in two thirds of patients.”
Additionally, priapism, a prolonged erection, has been associated with trazodone, Dr. Lettieri said, “and I have literally never met a patient on trazodone who was counseled about this.”
Trazodone also has a black box warning from the Food and Drug Administration warning about increased risk for suicidal thoughts.
Dr. Lettieri and Dr. Corr disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Too often, medications are the treatment of choice, and when used long term they can perpetuate a problematic cycle, said Dr. Lettieri, professor in pulmonary, critical care, and sleep medicine at Johns Hopkins University, Baltimore.
However, medications alone won’t work without other behavior modifications and they come with potential side effects, he said in his talk. Prescription medications typically don’t treat the cause of the insomnia, just the symptoms.
“In the 15 years I’ve been practicing sleep medicine, I can honestly say I only have a handful of patients that I treat with long-term pharmacotherapy,” Dr. Lettieri said.
He said he typically uses pharmacotherapy only when conservative measures have failed or to help jump-start patients to behavior modifications.
Restricted sleep is a good place to start for chronic insomnia, he continued.
Physicians should ask patients the latest time they can wake up to make it to school, work, etc. If that time is 6 a.m., the goal is to move bedtime back to 10 p.m.–11 p.m. If the patient, however, is unable to sleep until 12:30 a.m., move bedtime there, he said.
Though the 5.5-hour window is not ideal, it’s better to get into bed when ready for sleep. From there, try to get the patient to move bedtime back 15 minutes each week as they train themselves to fall asleep earlier, he said.
“I promise you this works in the majority of patients and doesn’t require any medication. You can also accomplish this with one or two office visits, so it is not a huge drain on resources,” he said.
Sleep specialists in short supply
Cognitive-behavioral therapy (CBT) is “without question the best way to treat chronic insomnia and it’s recommended as first-line therapy by all published guidelines,” Dr. Lettieri said.
He defined chronic insomnia as happening most nights over at least 3 months. It affects twice as many women as men.
CBT offers a formalized way of changing sleep patterns with the help of an expert in sleep behavior disorders. It combines cognitive therapies with education about sleep and stimulus control and uses techniques such as mindfulness and relaxation.
However, most programs take 4-8 sessions with a sleep medicine provider and are usually not covered by insurance. In addition, the number of insomnia specialists is not nearly adequate to meet demand, he added.
Online and mobile-platform CBT programs are widely effective, Dr. Lettieri said. Many are free and all are convenient for patients to use. He said many of his patients use Sleepio, but many other online programs are effective.
“You can provide sufficient therapy for many of your patients and reserve CBT for patients who can’t be fixed with more conservative measures,” he said.
Insomnia among older patients
Interest in helping older patients with insomnia dominated the chat session associated with the talk.
Insomnia increases with age and older patients have often been using prescription or over-the-counter sleep aids for decades.
Additionally, “insomnia is the second-most common reason why people get admitted to long-term care facilities, second only to urinary incontinence,” Dr. Lettieri said.
If physicians use medications with older patients, he said, extra caution is needed. Older people have more neurocognitive impairments than younger adults and may already be taking several other medications. Sleep medications may come with longer elimination half-lives. Polypharmacy may increase risk for falls and have other consequences.
“If you have to go to a medication, try something simple like melatonin,” he said, adding that it should be pharmaceutical grade and extended release.
Also, bright lights during the day, movement throughout the day, and dim lights closer to bedtime are especially important for the elderly, Dr. Lettieri said.
Andrew Corr, MD, a geriatric specialist in primary care with the Riverside (Calif.) Medical Clinic, said in an interview the main message he will take back to his physician group is more CBT and less medication.
He said that, although he has long known CBT is the top first-line treatment, it is difficult to find experts in his area who are trained to do CBT for insomnia, so he was glad to hear online programs and self-directed reading are typically effective.
He also said there’s a common misperception that there’s no harm in prescribing medications such as trazodone (Desyrel), an antidepressant commonly used off label as a sleep aid.
Dr. Lettieri’s talk highlighted his recommendation against using trazodone for sleep. “Despite several recommendations against its use for insomnia, it is still commonly prescribed. You just shouldn’t use it for insomnia,” Dr. Lettieri said.
“It has no measurable effect in a third of patients and at least unacceptable side effects in another third. Right off the bat, it’s not efficacious in two thirds of patients.”
Additionally, priapism, a prolonged erection, has been associated with trazodone, Dr. Lettieri said, “and I have literally never met a patient on trazodone who was counseled about this.”
Trazodone also has a black box warning from the Food and Drug Administration warning about increased risk for suicidal thoughts.
Dr. Lettieri and Dr. Corr disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Too often, medications are the treatment of choice, and when used long term they can perpetuate a problematic cycle, said Dr. Lettieri, professor in pulmonary, critical care, and sleep medicine at Johns Hopkins University, Baltimore.
However, medications alone won’t work without other behavior modifications and they come with potential side effects, he said in his talk. Prescription medications typically don’t treat the cause of the insomnia, just the symptoms.
“In the 15 years I’ve been practicing sleep medicine, I can honestly say I only have a handful of patients that I treat with long-term pharmacotherapy,” Dr. Lettieri said.
He said he typically uses pharmacotherapy only when conservative measures have failed or to help jump-start patients to behavior modifications.
Restricted sleep is a good place to start for chronic insomnia, he continued.
Physicians should ask patients the latest time they can wake up to make it to school, work, etc. If that time is 6 a.m., the goal is to move bedtime back to 10 p.m.–11 p.m. If the patient, however, is unable to sleep until 12:30 a.m., move bedtime there, he said.
Though the 5.5-hour window is not ideal, it’s better to get into bed when ready for sleep. From there, try to get the patient to move bedtime back 15 minutes each week as they train themselves to fall asleep earlier, he said.
“I promise you this works in the majority of patients and doesn’t require any medication. You can also accomplish this with one or two office visits, so it is not a huge drain on resources,” he said.
Sleep specialists in short supply
Cognitive-behavioral therapy (CBT) is “without question the best way to treat chronic insomnia and it’s recommended as first-line therapy by all published guidelines,” Dr. Lettieri said.
He defined chronic insomnia as happening most nights over at least 3 months. It affects twice as many women as men.
CBT offers a formalized way of changing sleep patterns with the help of an expert in sleep behavior disorders. It combines cognitive therapies with education about sleep and stimulus control and uses techniques such as mindfulness and relaxation.
However, most programs take 4-8 sessions with a sleep medicine provider and are usually not covered by insurance. In addition, the number of insomnia specialists is not nearly adequate to meet demand, he added.
Online and mobile-platform CBT programs are widely effective, Dr. Lettieri said. Many are free and all are convenient for patients to use. He said many of his patients use Sleepio, but many other online programs are effective.
“You can provide sufficient therapy for many of your patients and reserve CBT for patients who can’t be fixed with more conservative measures,” he said.
Insomnia among older patients
Interest in helping older patients with insomnia dominated the chat session associated with the talk.
Insomnia increases with age and older patients have often been using prescription or over-the-counter sleep aids for decades.
Additionally, “insomnia is the second-most common reason why people get admitted to long-term care facilities, second only to urinary incontinence,” Dr. Lettieri said.
If physicians use medications with older patients, he said, extra caution is needed. Older people have more neurocognitive impairments than younger adults and may already be taking several other medications. Sleep medications may come with longer elimination half-lives. Polypharmacy may increase risk for falls and have other consequences.
“If you have to go to a medication, try something simple like melatonin,” he said, adding that it should be pharmaceutical grade and extended release.
Also, bright lights during the day, movement throughout the day, and dim lights closer to bedtime are especially important for the elderly, Dr. Lettieri said.
Andrew Corr, MD, a geriatric specialist in primary care with the Riverside (Calif.) Medical Clinic, said in an interview the main message he will take back to his physician group is more CBT and less medication.
He said that, although he has long known CBT is the top first-line treatment, it is difficult to find experts in his area who are trained to do CBT for insomnia, so he was glad to hear online programs and self-directed reading are typically effective.
He also said there’s a common misperception that there’s no harm in prescribing medications such as trazodone (Desyrel), an antidepressant commonly used off label as a sleep aid.
Dr. Lettieri’s talk highlighted his recommendation against using trazodone for sleep. “Despite several recommendations against its use for insomnia, it is still commonly prescribed. You just shouldn’t use it for insomnia,” Dr. Lettieri said.
“It has no measurable effect in a third of patients and at least unacceptable side effects in another third. Right off the bat, it’s not efficacious in two thirds of patients.”
Additionally, priapism, a prolonged erection, has been associated with trazodone, Dr. Lettieri said, “and I have literally never met a patient on trazodone who was counseled about this.”
Trazodone also has a black box warning from the Food and Drug Administration warning about increased risk for suicidal thoughts.
Dr. Lettieri and Dr. Corr disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM INTERNAL MEDICINE 2021
When to refer patients with new memory loss
Initial questions should zero in on what the patient is forgetting, said Megan Richie, MD, a neurohospitalist at the University of California, San Francisco, who spoke to a virtual audience at the American College of Physicians (ACP) annual Internal Medicine meeting.
Is the patient forgetting to buy things in a store, having trouble recalling events, forgetting important dates? How often do these incidents occur?
These questions “will help get at how pervasive and how likely the memory loss is affecting their lives, versus a subjective complaint that doesn’t have much impact on the day-to-day function,” she said.
It’s also important to ask whether other neurocognitive symptoms accompany the memory loss, Dr. Richie noted.
Does the patient search for words, struggle with attention, or have problems with executive function? Does the patient have psychiatric symptoms, such as hallucinations or delusions, or other neurologic complaints, including weakness, numbness, vision change, or movement disorders?
“When you know how many neurocognitive symptoms they have, think about how [those symptoms] are affecting their safety and functional status. How are they on their activities of daily living?” Dr. Richie suggests.
Also ask whether the patient is taking medications and whether they drive a vehicle. If they do drive, do they get lost?
“These are all going to help you determine the acuity of the workup,” she said.
After a thorough history, cognitive screening is the next consideration.
Cognitive screening can be performed in minutes
One of the tests Dr. Richie recommends is the Mini-Cog. It takes 3 minutes to administer and has been formally recommended by the Alzheimer’s Association because it can be completed in the time frame of a Medicare wellness visit, she said.
It entails a three-word recall and clock-drawing test.
Dr. Richie said it’s important to eliminate some key causes first: “Certainly if the patient has signs and symptoms of depression, pseudodementia is a very real and treatable disease you do not want to miss and should consider in these patients,” she pointed out.
Systemic medical conditions can also lead to memory loss.
If there’s an acute component to the complaint, a new infection or medication withdrawal or a side effect could be driving it, so that’s key in questioning.
Dr. Richie explained that the American Academy of Neurology recommends a very limited workup.
“It’s really just to check their thyroid, their vitamin B12 levels, and then a one-time picture of their brain, which can be either MRI or a CT, to look for structural problems or vascular dementia or hydrocephalus, etc.”
“You do not routinely need spinal fluid testing or an EEG,” she emphasized.
Signs that a neurologist should be involved include a rapid decline, signs of potential seizures, or that the patient doesn’t seem safe in their condition.
Neuropsychological testing is helpful, but it takes nearly 3 hours and may not be a good choice for restless or aggressive patients, Dr. Richie said.
Such testing is often not available, and if it is, insurance coverage is often a barrier because many plans don’t cover it.
Patients often ask about drugs and supplements they see advertised to help with memory loss. Medications are not helpful for mild cognitive impairment, although there is evidence that some are beneficial for patients with dementia, Dr. Richie said.
Celine Goetz, MD, assistant professor of internal medicine at Rush University Medical Center, Chicago, Illinois, told this news organization that it’s easy to relate to the fear that patients and families feel when cognitive impairment begins to emerge.
“[Dr.] Richie’s talk was right on point for internists like myself who see many patients with memory complaints, cognitive impairment, and dementia. I think we’re all terrified of losing our memory and the social and functional impairment that comes with that,” she said.
Although cognitive impairment and dementia aren’t curable or reversible, Dr. Goetz noted, internists can help patients optimize management of conditions such as diabetes and heart disease, which can affect cognitive function.
Dr. Richie pointed out that some interventions lack evidence for the treatment of mild cognitive impairment, but Dr. Goetz emphasized that resources are plentiful and can be effective in combination.
“Engaging social workers, pharmacists, nutritionists, physical and occupational therapists, and, on the inpatient side, delirium protocols, chaplains, and music therapists make a huge difference in patient care,” she said.
Dr. Richie and Dr. Goetz report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Initial questions should zero in on what the patient is forgetting, said Megan Richie, MD, a neurohospitalist at the University of California, San Francisco, who spoke to a virtual audience at the American College of Physicians (ACP) annual Internal Medicine meeting.
Is the patient forgetting to buy things in a store, having trouble recalling events, forgetting important dates? How often do these incidents occur?
These questions “will help get at how pervasive and how likely the memory loss is affecting their lives, versus a subjective complaint that doesn’t have much impact on the day-to-day function,” she said.
It’s also important to ask whether other neurocognitive symptoms accompany the memory loss, Dr. Richie noted.
Does the patient search for words, struggle with attention, or have problems with executive function? Does the patient have psychiatric symptoms, such as hallucinations or delusions, or other neurologic complaints, including weakness, numbness, vision change, or movement disorders?
“When you know how many neurocognitive symptoms they have, think about how [those symptoms] are affecting their safety and functional status. How are they on their activities of daily living?” Dr. Richie suggests.
Also ask whether the patient is taking medications and whether they drive a vehicle. If they do drive, do they get lost?
“These are all going to help you determine the acuity of the workup,” she said.
After a thorough history, cognitive screening is the next consideration.
Cognitive screening can be performed in minutes
One of the tests Dr. Richie recommends is the Mini-Cog. It takes 3 minutes to administer and has been formally recommended by the Alzheimer’s Association because it can be completed in the time frame of a Medicare wellness visit, she said.
It entails a three-word recall and clock-drawing test.
Dr. Richie said it’s important to eliminate some key causes first: “Certainly if the patient has signs and symptoms of depression, pseudodementia is a very real and treatable disease you do not want to miss and should consider in these patients,” she pointed out.
Systemic medical conditions can also lead to memory loss.
If there’s an acute component to the complaint, a new infection or medication withdrawal or a side effect could be driving it, so that’s key in questioning.
Dr. Richie explained that the American Academy of Neurology recommends a very limited workup.
“It’s really just to check their thyroid, their vitamin B12 levels, and then a one-time picture of their brain, which can be either MRI or a CT, to look for structural problems or vascular dementia or hydrocephalus, etc.”
“You do not routinely need spinal fluid testing or an EEG,” she emphasized.
Signs that a neurologist should be involved include a rapid decline, signs of potential seizures, or that the patient doesn’t seem safe in their condition.
Neuropsychological testing is helpful, but it takes nearly 3 hours and may not be a good choice for restless or aggressive patients, Dr. Richie said.
Such testing is often not available, and if it is, insurance coverage is often a barrier because many plans don’t cover it.
Patients often ask about drugs and supplements they see advertised to help with memory loss. Medications are not helpful for mild cognitive impairment, although there is evidence that some are beneficial for patients with dementia, Dr. Richie said.
Celine Goetz, MD, assistant professor of internal medicine at Rush University Medical Center, Chicago, Illinois, told this news organization that it’s easy to relate to the fear that patients and families feel when cognitive impairment begins to emerge.
“[Dr.] Richie’s talk was right on point for internists like myself who see many patients with memory complaints, cognitive impairment, and dementia. I think we’re all terrified of losing our memory and the social and functional impairment that comes with that,” she said.
Although cognitive impairment and dementia aren’t curable or reversible, Dr. Goetz noted, internists can help patients optimize management of conditions such as diabetes and heart disease, which can affect cognitive function.
Dr. Richie pointed out that some interventions lack evidence for the treatment of mild cognitive impairment, but Dr. Goetz emphasized that resources are plentiful and can be effective in combination.
“Engaging social workers, pharmacists, nutritionists, physical and occupational therapists, and, on the inpatient side, delirium protocols, chaplains, and music therapists make a huge difference in patient care,” she said.
Dr. Richie and Dr. Goetz report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Initial questions should zero in on what the patient is forgetting, said Megan Richie, MD, a neurohospitalist at the University of California, San Francisco, who spoke to a virtual audience at the American College of Physicians (ACP) annual Internal Medicine meeting.
Is the patient forgetting to buy things in a store, having trouble recalling events, forgetting important dates? How often do these incidents occur?
These questions “will help get at how pervasive and how likely the memory loss is affecting their lives, versus a subjective complaint that doesn’t have much impact on the day-to-day function,” she said.
It’s also important to ask whether other neurocognitive symptoms accompany the memory loss, Dr. Richie noted.
Does the patient search for words, struggle with attention, or have problems with executive function? Does the patient have psychiatric symptoms, such as hallucinations or delusions, or other neurologic complaints, including weakness, numbness, vision change, or movement disorders?
“When you know how many neurocognitive symptoms they have, think about how [those symptoms] are affecting their safety and functional status. How are they on their activities of daily living?” Dr. Richie suggests.
Also ask whether the patient is taking medications and whether they drive a vehicle. If they do drive, do they get lost?
“These are all going to help you determine the acuity of the workup,” she said.
After a thorough history, cognitive screening is the next consideration.
Cognitive screening can be performed in minutes
One of the tests Dr. Richie recommends is the Mini-Cog. It takes 3 minutes to administer and has been formally recommended by the Alzheimer’s Association because it can be completed in the time frame of a Medicare wellness visit, she said.
It entails a three-word recall and clock-drawing test.
Dr. Richie said it’s important to eliminate some key causes first: “Certainly if the patient has signs and symptoms of depression, pseudodementia is a very real and treatable disease you do not want to miss and should consider in these patients,” she pointed out.
Systemic medical conditions can also lead to memory loss.
If there’s an acute component to the complaint, a new infection or medication withdrawal or a side effect could be driving it, so that’s key in questioning.
Dr. Richie explained that the American Academy of Neurology recommends a very limited workup.
“It’s really just to check their thyroid, their vitamin B12 levels, and then a one-time picture of their brain, which can be either MRI or a CT, to look for structural problems or vascular dementia or hydrocephalus, etc.”
“You do not routinely need spinal fluid testing or an EEG,” she emphasized.
Signs that a neurologist should be involved include a rapid decline, signs of potential seizures, or that the patient doesn’t seem safe in their condition.
Neuropsychological testing is helpful, but it takes nearly 3 hours and may not be a good choice for restless or aggressive patients, Dr. Richie said.
Such testing is often not available, and if it is, insurance coverage is often a barrier because many plans don’t cover it.
Patients often ask about drugs and supplements they see advertised to help with memory loss. Medications are not helpful for mild cognitive impairment, although there is evidence that some are beneficial for patients with dementia, Dr. Richie said.
Celine Goetz, MD, assistant professor of internal medicine at Rush University Medical Center, Chicago, Illinois, told this news organization that it’s easy to relate to the fear that patients and families feel when cognitive impairment begins to emerge.
“[Dr.] Richie’s talk was right on point for internists like myself who see many patients with memory complaints, cognitive impairment, and dementia. I think we’re all terrified of losing our memory and the social and functional impairment that comes with that,” she said.
Although cognitive impairment and dementia aren’t curable or reversible, Dr. Goetz noted, internists can help patients optimize management of conditions such as diabetes and heart disease, which can affect cognitive function.
Dr. Richie pointed out that some interventions lack evidence for the treatment of mild cognitive impairment, but Dr. Goetz emphasized that resources are plentiful and can be effective in combination.
“Engaging social workers, pharmacists, nutritionists, physical and occupational therapists, and, on the inpatient side, delirium protocols, chaplains, and music therapists make a huge difference in patient care,” she said.
Dr. Richie and Dr. Goetz report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM INTERNAL MEDICINE 2021
Study calls for sex-specific concussion management in adolescent soccer players
A large study of adolescent soccer players in Michigan revealed key differences in concussion injury metrics among males and females, underscoring a need to develop sex-specific approaches to managing injury in the sport.

Sport-related concussion (SRC) is a specific concern in young female athletes, study authors Abigail C. Bretzin, PhD, and colleagues noted in their paper, which appears in JAMA Network Open. Previous surveillance studies on SRC at the high school and college level have reported higher rates of injury risk and longer recovery outcomes in female soccer athletes. Taking a deeper dive into these trends, the investigators explored whether sex-associated differences existed in SRC, addressing the mechanics, management, and recovery from SRC.
“This is an area that is remarkably underresearched,” William Stewart, MBChB, PhD, the study’s corresponding author, said in an interview. Prior studies of males and females have shown that female axons are thinner, with fewer microtubules or internal scaffolding than male axons. This potentially increases risk of shear injury in females. Limited research has also cited differences in concussion risk across the menstrual cycle in female athletes.
Reporting system targets four injury areas
The investigators conducted a high school injury surveillance project in 43,741 male and 39,637 female soccer athletes participating in the Michigan High School Athletic Association (MHSAA) Head Injury Reporting System. The study included students from 9th to 12th grade, spanning from the beginning of academic year 2016-2017 to the end of academic year 2018-2019. Since 2015, the state has mandated high schools to submit data to MHSAA.
MHSAA captures data on four categories: person-to-person contact, person-to-object contact, person-to-playing surface contact, or uncertain about cause of the event. Study outcomes included details regarding injury mechanism, immediate management, and return-to-play time for each documented SRC.
Investigators reported notable differences among male and female players. Documented SRC risk was 1.88 times higher among adolescent girls than boys across all academic years (RR, 1.88; 95% CI, 1.69-2.09; P < .001). They also cited inconsistencies in distribution of injury mechanisms among the sexes. Females were most likely to suffer injury from equipment contact such as heading a ball (41.9%), whereas male players commonly sustained SRC from contact with another player (48.4%). The authors suggested that “female soccer athletes have lower neck strength and girth, compared with male athletes, with these variables inversely associated with linear and rotational head acceleration after soccer ball heading.”
Boys had greater odds of immediate removal from play and but also returned to the sport 2 days sooner than girls. “The possibility exists, therefore, that this longer recovery time might, in part, be reflective of our observed differences in immediate care, in particular removal from play,” the authors wrote. Immediate removal from play was also more common in cases where an athletic trainer played a part in evaluating players for SRC.
Eliminating the one-size-fits-all approach
Current concussion management is based on a “one-size-fits-all” model, said Dr. Stewart. Male and female athletes are treated following a common concussion management protocol, covering concussion detection through to rehabilitation. “This model of management is based on research that is almost exclusively in male athletes.”
What the study showed is this one-size-fits-all approach may be flawed, letting down female athletes. “We should be pursuing more research in sex differences in concussion and, importantly, putting these into practice in sex-specific concussion management protocols,” he suggested.
Future studies should also look at the effects of athletic trainer employment on SRC metrics. “Although this was a large, statewide epidemiological study of reported SRC in adolescent soccer athletes, inclusive of high schools with and without access to athletic trainers, the Head Injury Reporting System did not include information on the whether there were athletic trainer services available at each school, including specific athletic training services for soccer,” wrote the investigators, in citing the study’s limitations.
Girls report symptoms more often
“The researchers are to be commended for taking a prospective approach to address this common observation in high school sports,” said Keith J. Loud, MD, MSc, FAAP, a sports pediatrician at Children’s Hospital at Dartmouth-Hitchcock in Manchester, N.H. The results are “entirely believable,” said Dr. Loud, who was not affiliated with the study. “We have long postulated differences in neurophysiology, neck strength, style of play, and tendency to report as explanations for the observation that girls in high school soccer are diagnosed with more concussions than boys.”
The findings suggest that boys play more aggressively, but sustain fewer concussions, he added. Girls in the meantime, are more likely to speak up about their injury.
“Concussion diagnosis still relies to a large degree on the athlete to report symptoms, which is one of our hypotheses as to why girls seem to sustain more concussions – they report symptoms more often. That could also be why they have a prolonged recovery,” offered Dr. Loud. A main limitation of this study is it can’t overcome this reporting bias.
Dr. Loud was also concerned that girls were less likely to be removed from game play, even though they apparently sustained more concussions. “Perhaps that is because their injuries are less obvious on the field, and they are diagnosed when reported after the games.”
Dr. Stewart reported receiving grants from The Football Association and National Health Service Research Scotland during the study. He also served as a nonremunerated member of the Fédération Internationale de Football Association Independent Football Concussion Advisory Group and the Football Association Expert Panel on Concussion and Head Injury in Football. None of the other authors had disclosures.
A large study of adolescent soccer players in Michigan revealed key differences in concussion injury metrics among males and females, underscoring a need to develop sex-specific approaches to managing injury in the sport.
Sport-related concussion (SRC) is a specific concern in young female athletes, study authors Abigail C. Bretzin, PhD, and colleagues noted in their paper, which appears in JAMA Network Open. Previous surveillance studies on SRC at the high school and college level have reported higher rates of injury risk and longer recovery outcomes in female soccer athletes. Taking a deeper dive into these trends, the investigators explored whether sex-associated differences existed in SRC, addressing the mechanics, management, and recovery from SRC.
“This is an area that is remarkably underresearched,” William Stewart, MBChB, PhD, the study’s corresponding author, said in an interview. Prior studies of males and females have shown that female axons are thinner, with fewer microtubules or internal scaffolding than male axons. This potentially increases risk of shear injury in females. Limited research has also cited differences in concussion risk across the menstrual cycle in female athletes.
Reporting system targets four injury areas
The investigators conducted a high school injury surveillance project in 43,741 male and 39,637 female soccer athletes participating in the Michigan High School Athletic Association (MHSAA) Head Injury Reporting System. The study included students from 9th to 12th grade, spanning from the beginning of academic year 2016-2017 to the end of academic year 2018-2019. Since 2015, the state has mandated high schools to submit data to MHSAA.
MHSAA captures data on four categories: person-to-person contact, person-to-object contact, person-to-playing surface contact, or uncertain about cause of the event. Study outcomes included details regarding injury mechanism, immediate management, and return-to-play time for each documented SRC.
Investigators reported notable differences among male and female players. Documented SRC risk was 1.88 times higher among adolescent girls than boys across all academic years (RR, 1.88; 95% CI, 1.69-2.09; P < .001). They also cited inconsistencies in distribution of injury mechanisms among the sexes. Females were most likely to suffer injury from equipment contact such as heading a ball (41.9%), whereas male players commonly sustained SRC from contact with another player (48.4%). The authors suggested that “female soccer athletes have lower neck strength and girth, compared with male athletes, with these variables inversely associated with linear and rotational head acceleration after soccer ball heading.”
Boys had greater odds of immediate removal from play and but also returned to the sport 2 days sooner than girls. “The possibility exists, therefore, that this longer recovery time might, in part, be reflective of our observed differences in immediate care, in particular removal from play,” the authors wrote. Immediate removal from play was also more common in cases where an athletic trainer played a part in evaluating players for SRC.
Eliminating the one-size-fits-all approach
Current concussion management is based on a “one-size-fits-all” model, said Dr. Stewart. Male and female athletes are treated following a common concussion management protocol, covering concussion detection through to rehabilitation. “This model of management is based on research that is almost exclusively in male athletes.”
What the study showed is this one-size-fits-all approach may be flawed, letting down female athletes. “We should be pursuing more research in sex differences in concussion and, importantly, putting these into practice in sex-specific concussion management protocols,” he suggested.
Future studies should also look at the effects of athletic trainer employment on SRC metrics. “Although this was a large, statewide epidemiological study of reported SRC in adolescent soccer athletes, inclusive of high schools with and without access to athletic trainers, the Head Injury Reporting System did not include information on the whether there were athletic trainer services available at each school, including specific athletic training services for soccer,” wrote the investigators, in citing the study’s limitations.
Girls report symptoms more often
“The researchers are to be commended for taking a prospective approach to address this common observation in high school sports,” said Keith J. Loud, MD, MSc, FAAP, a sports pediatrician at Children’s Hospital at Dartmouth-Hitchcock in Manchester, N.H. The results are “entirely believable,” said Dr. Loud, who was not affiliated with the study. “We have long postulated differences in neurophysiology, neck strength, style of play, and tendency to report as explanations for the observation that girls in high school soccer are diagnosed with more concussions than boys.”
The findings suggest that boys play more aggressively, but sustain fewer concussions, he added. Girls in the meantime, are more likely to speak up about their injury.
“Concussion diagnosis still relies to a large degree on the athlete to report symptoms, which is one of our hypotheses as to why girls seem to sustain more concussions – they report symptoms more often. That could also be why they have a prolonged recovery,” offered Dr. Loud. A main limitation of this study is it can’t overcome this reporting bias.
Dr. Loud was also concerned that girls were less likely to be removed from game play, even though they apparently sustained more concussions. “Perhaps that is because their injuries are less obvious on the field, and they are diagnosed when reported after the games.”
Dr. Stewart reported receiving grants from The Football Association and National Health Service Research Scotland during the study. He also served as a nonremunerated member of the Fédération Internationale de Football Association Independent Football Concussion Advisory Group and the Football Association Expert Panel on Concussion and Head Injury in Football. None of the other authors had disclosures.
A large study of adolescent soccer players in Michigan revealed key differences in concussion injury metrics among males and females, underscoring a need to develop sex-specific approaches to managing injury in the sport.
Sport-related concussion (SRC) is a specific concern in young female athletes, study authors Abigail C. Bretzin, PhD, and colleagues noted in their paper, which appears in JAMA Network Open. Previous surveillance studies on SRC at the high school and college level have reported higher rates of injury risk and longer recovery outcomes in female soccer athletes. Taking a deeper dive into these trends, the investigators explored whether sex-associated differences existed in SRC, addressing the mechanics, management, and recovery from SRC.
“This is an area that is remarkably underresearched,” William Stewart, MBChB, PhD, the study’s corresponding author, said in an interview. Prior studies of males and females have shown that female axons are thinner, with fewer microtubules or internal scaffolding than male axons. This potentially increases risk of shear injury in females. Limited research has also cited differences in concussion risk across the menstrual cycle in female athletes.
Reporting system targets four injury areas
The investigators conducted a high school injury surveillance project in 43,741 male and 39,637 female soccer athletes participating in the Michigan High School Athletic Association (MHSAA) Head Injury Reporting System. The study included students from 9th to 12th grade, spanning from the beginning of academic year 2016-2017 to the end of academic year 2018-2019. Since 2015, the state has mandated high schools to submit data to MHSAA.
MHSAA captures data on four categories: person-to-person contact, person-to-object contact, person-to-playing surface contact, or uncertain about cause of the event. Study outcomes included details regarding injury mechanism, immediate management, and return-to-play time for each documented SRC.
Investigators reported notable differences among male and female players. Documented SRC risk was 1.88 times higher among adolescent girls than boys across all academic years (RR, 1.88; 95% CI, 1.69-2.09; P < .001). They also cited inconsistencies in distribution of injury mechanisms among the sexes. Females were most likely to suffer injury from equipment contact such as heading a ball (41.9%), whereas male players commonly sustained SRC from contact with another player (48.4%). The authors suggested that “female soccer athletes have lower neck strength and girth, compared with male athletes, with these variables inversely associated with linear and rotational head acceleration after soccer ball heading.”
Boys had greater odds of immediate removal from play and but also returned to the sport 2 days sooner than girls. “The possibility exists, therefore, that this longer recovery time might, in part, be reflective of our observed differences in immediate care, in particular removal from play,” the authors wrote. Immediate removal from play was also more common in cases where an athletic trainer played a part in evaluating players for SRC.
Eliminating the one-size-fits-all approach
Current concussion management is based on a “one-size-fits-all” model, said Dr. Stewart. Male and female athletes are treated following a common concussion management protocol, covering concussion detection through to rehabilitation. “This model of management is based on research that is almost exclusively in male athletes.”
What the study showed is this one-size-fits-all approach may be flawed, letting down female athletes. “We should be pursuing more research in sex differences in concussion and, importantly, putting these into practice in sex-specific concussion management protocols,” he suggested.
Future studies should also look at the effects of athletic trainer employment on SRC metrics. “Although this was a large, statewide epidemiological study of reported SRC in adolescent soccer athletes, inclusive of high schools with and without access to athletic trainers, the Head Injury Reporting System did not include information on the whether there were athletic trainer services available at each school, including specific athletic training services for soccer,” wrote the investigators, in citing the study’s limitations.
Girls report symptoms more often
“The researchers are to be commended for taking a prospective approach to address this common observation in high school sports,” said Keith J. Loud, MD, MSc, FAAP, a sports pediatrician at Children’s Hospital at Dartmouth-Hitchcock in Manchester, N.H. The results are “entirely believable,” said Dr. Loud, who was not affiliated with the study. “We have long postulated differences in neurophysiology, neck strength, style of play, and tendency to report as explanations for the observation that girls in high school soccer are diagnosed with more concussions than boys.”
The findings suggest that boys play more aggressively, but sustain fewer concussions, he added. Girls in the meantime, are more likely to speak up about their injury.
“Concussion diagnosis still relies to a large degree on the athlete to report symptoms, which is one of our hypotheses as to why girls seem to sustain more concussions – they report symptoms more often. That could also be why they have a prolonged recovery,” offered Dr. Loud. A main limitation of this study is it can’t overcome this reporting bias.
Dr. Loud was also concerned that girls were less likely to be removed from game play, even though they apparently sustained more concussions. “Perhaps that is because their injuries are less obvious on the field, and they are diagnosed when reported after the games.”
Dr. Stewart reported receiving grants from The Football Association and National Health Service Research Scotland during the study. He also served as a nonremunerated member of the Fédération Internationale de Football Association Independent Football Concussion Advisory Group and the Football Association Expert Panel on Concussion and Head Injury in Football. None of the other authors had disclosures.
FROM JAMA NETWORK OPEN
Modest clinical gain for AF screening of asymptomatic elderly: STROKESTOP
Some, perhaps many, previously unrecognized cases of atrial fibrillation (AF) will come to light in a screening program aimed at older asymptomatic adults. The key question is whether the challenges of such systematic but age-restricted AF screening in the community, with oral anticoagulation (OAC) offered to those found to have the arrhythmia, is worthwhile in preventing events such as death or stroke.
Now there is evidence supporting such a clinical benefit from a large, prospective, randomized trial. A screening program restricted to people 75 or 76 years of age in two Swedish communities, which called on them to use a handheld single-lead ECG system at home intermittently for 2 weeks, was followed by a slight drop in clinical events over about 7 years.
The 4% decline in risk (P = .045) in the STROKESTOP trial’s “intention-to-treat” (ITT) analysis yielded a number needed to treat of 91; that is, that many people had to be targeted by the screening program to prevent one primary-endpoint clinical event.
Those included ischemic stroke, systemic thromboembolism, hospitalization for severe bleeding, and death from any cause, investigators reported April 23 during the virtual European Heart Rhythm Association (EHRA) 2021 Congress.
If that benefit and its significance seem marginal, some secondary findings might be reassuring. Half the population of the target age in the two communities – 13,979 randomly selected people – were invited to join the trial and follow the screening protocol, comprising the ITT cohort. The other half, numbering 13,996, was not invited and served as control subjects.
However, only 51% of the ITT cohort accepted the invitation and participated in the trial; they represented the “as-treated” cohort, observed Emma Svennberg, MD, PhD, Karolinska Institute, Danderyd Hospital, Stockholm, who presented the analysis at the EHRA sessions.
The screening protocol identified untreated AF, whether previously known or unknown, in about 5% of the 7,165 as-treated screening participants; OAC was initiated in about three-fourths of those cases.
The as-treated group, on their own, benefited with a 24% drop in the prospectively defined secondary endpoint of ischemic stroke, compared with the entire control group.
The clinical benefit in the ITT population was “small but significant,” but over the same period in the as-treated cohort, there was a highly significant drop in risk for ischemic stroke, Dr. Svennberg said in an interview.
The trial’s lead message, she said, is that “screening for atrial fibrillation in an elderly population reduces the risk of death and ischemic stroke without increasing the risk of bleeding.”
Caveats: As-treated vs. ITT
But there are caveats that complicate interpretation of the trial and, Dr. Svennberg proposed, point to the importance of that interpretation of both the ITT and as-treated analyses.
“We detected significantly more atrial fibrillation in the group that was randomized to screening. A major strength of our study was that we referred all of those individuals for a structured follow-up within the study,” she said. “Although the focus of the follow-up was oral anticoagulant therapy, other risk factors were also assessed and managed, such as hypertension and diabetes.”
It’s possible that increased detection of AF followed by such structured management contributed to the observed benefit, Dr. Svennberg proposed.
However, the exclusion of those in the prespecified ITT population who declined to be screened or otherwise didn’t participate left an as-treated cohort that was healthier than the ITT population or the control group.
Indeed, the nonparticipating invitees were sicker, with significantly more diabetes, vascular disease, hypertension, and heart failure, and higher CHA2DS2VASc stroke risk scores than those who agreed to participate.
“We took a more difficult route in setting up this study, in that we identified all individuals aged 75 to 76 residing in our two regions and excluded no one,” Dr. Svennberg said in an interview. “That means even individuals with end-stage disease, severe dementia, bedridden in nursing homes, et cetera, were also randomized but perhaps not likely or eligible to participate.”
Therefore, some invitees were unable to join the study even as others might have declined “out of low interest” or other personal reasons, she said. “We believe that this mimics how a population-based screening program would be performed if done in our country.”
In the ITT analysis, screening successfully identified previously unknown or untreated cases of AF, which led to expanded OAC use and intensified risk-factor management, “which was key to a successful outcome.”
In the as-treated analysis, Dr. Svennberg said, “I think a combination of the intervention and the population being overall more healthy was driving the secondary endpoint.”
Systematic vs. opportunistic screening
Although “opportunistic screening in individuals aged 65 and older” is recommended by current European Society of Cardiology guidelines, systematic screening, such as that used in STROKESTOP, has a much weaker evidence base, observed Renate B. Schnabel, MD, PhD, University Heart & Vascular Center, Hamburg, Germany, as the invited discussant after the STROKESTOP presentation.
STROKESTOP “is one of the first studies, if not the first study,” to show a clinical benefit from screening for AF, Dr. Schnabel said.
Fewer-than-projected primary outcome events were seen during the trial, and event curves for screened and control participants didn’t start to separate until about 4 years into the study, she said. It therefore might take a long time for the screened elderly to realize the clinical benefits of screening.
Studies such as the recent SCREEN-AF and mSTOPS have amply shown that AF screening in the asymptomatic elderly can reveal previously unrecognized AF far more often than would be detected in routine practice, allowing them the opportunity to go on OAC. But the trials weren’t able to show whether the benefits of such management outweigh the risks or costs.
Indeed, on April 20, the U.S. Preventive Services Task Force (USPSTF) released a draft recommendation statement concluding that “the current evidence is insufficient to assess the balance of benefits and harms” associated with AF screening in asymptomatic people at least 50 years of age.
In STROKESTOP, however, benefit for the primary outcome reached significance in the prespecified ITT analysis and “appeared to be driven by the reduction in ischemic stroke incidence,” Dr. Schnabel said.
“The future guidelines have gained strong evidence to judge on systematic atrial fibrillation screening” as it was performed in the trial, she said. “How to implement atrial fibrillation screening, including systematic screening in health care systems across Europe and beyond, remains an open question.”
A randomized population
STROKESTOP considered all 75- and 76-year-olds living in Sweden’s Stockholm County (n = 23,888) and the Halland region (n = 4,880) and randomly assigned them to the ITT group or a control group, with stratification by sex, birth year, and geographic region. In both groups, 54.6% were female and the mean CHA2DS2VASc score was 3.5.
People assigned to the ITT cohort were invited to be screened and followed. Those who agreed to participate underwent a baseline ECG assessment to detect or rule out permanent AF. Guideline-based OAC and follow-up was offered to those found with the arrhythmia. Those in sinus rhythm with no history of AF used a handheld single-lead ECG recorder (Zenicor) for 30 seconds twice daily for 14 days.
Structured management, including OAC, was offered to anyone demonstrating sufficient AF, that is, at least one bout without p waves in one 30-second recording or at least two such episodes lasting 10-29 seconds during the 2-week screening period.
In the ITT analysis, the hazard ratio (HR) for the composite clinical primary endpoint was 0.96 (95% confidence interval, 0.920-0.999; P = .045), but in the as-treated analysis, the HR for ischemic stroke was 0.76 (95% CI, 0.68-0.87; P < .001).
“I believe that this will likely be generalizable to most countries’ elderly residents,” Dr. Svennberg said. “I think if we can find a significant difference in our elderly population in Sweden, most countries will be able to do so, or find even more significant results.”
That’s because “baseline detection of AF in Sweden is high,” she said, “so new detection is likely more difficult.” Also, in Sweden, “care can be sought without monetary concern, and prescriptions are provided at low costs to the patients.” Therefore, patients newly identified with AF, whether in studies or not, “would likely be started on therapy.”
It will be important to know whether the screening strategy is cost-effective, Dr. Schnabel said, because “the overall effect, with a hazard ratio of 0.96, is not too big, and costs incurred by systematic screening are comparatively high.”
STROKESTOP “now provides sound information for cost-effectiveness analyses, which to date have largely relied on assumptions.”
STROKESTOP was partially supported by Carl Bennet AB, Boehringer-Ingelheim, Bayer, Bristol-Meyers Squibb, and Pfizer. Dr. Svennberg disclosed receiving fees for lectures or consulting from Bayer, Bristol-Meyers Squibb, Pfizer, Boehringer-Ingelheim, Merck Sharp & Dohme, and Sanofi; and institutional grants from Roche Diagnostics and Carl Bennett Ltd.
A version of this article first appeared on Medscape.com.
Some, perhaps many, previously unrecognized cases of atrial fibrillation (AF) will come to light in a screening program aimed at older asymptomatic adults. The key question is whether the challenges of such systematic but age-restricted AF screening in the community, with oral anticoagulation (OAC) offered to those found to have the arrhythmia, is worthwhile in preventing events such as death or stroke.
Now there is evidence supporting such a clinical benefit from a large, prospective, randomized trial. A screening program restricted to people 75 or 76 years of age in two Swedish communities, which called on them to use a handheld single-lead ECG system at home intermittently for 2 weeks, was followed by a slight drop in clinical events over about 7 years.
The 4% decline in risk (P = .045) in the STROKESTOP trial’s “intention-to-treat” (ITT) analysis yielded a number needed to treat of 91; that is, that many people had to be targeted by the screening program to prevent one primary-endpoint clinical event.
Those included ischemic stroke, systemic thromboembolism, hospitalization for severe bleeding, and death from any cause, investigators reported April 23 during the virtual European Heart Rhythm Association (EHRA) 2021 Congress.
If that benefit and its significance seem marginal, some secondary findings might be reassuring. Half the population of the target age in the two communities – 13,979 randomly selected people – were invited to join the trial and follow the screening protocol, comprising the ITT cohort. The other half, numbering 13,996, was not invited and served as control subjects.
However, only 51% of the ITT cohort accepted the invitation and participated in the trial; they represented the “as-treated” cohort, observed Emma Svennberg, MD, PhD, Karolinska Institute, Danderyd Hospital, Stockholm, who presented the analysis at the EHRA sessions.
The screening protocol identified untreated AF, whether previously known or unknown, in about 5% of the 7,165 as-treated screening participants; OAC was initiated in about three-fourths of those cases.
The as-treated group, on their own, benefited with a 24% drop in the prospectively defined secondary endpoint of ischemic stroke, compared with the entire control group.
The clinical benefit in the ITT population was “small but significant,” but over the same period in the as-treated cohort, there was a highly significant drop in risk for ischemic stroke, Dr. Svennberg said in an interview.
The trial’s lead message, she said, is that “screening for atrial fibrillation in an elderly population reduces the risk of death and ischemic stroke without increasing the risk of bleeding.”
Caveats: As-treated vs. ITT
But there are caveats that complicate interpretation of the trial and, Dr. Svennberg proposed, point to the importance of that interpretation of both the ITT and as-treated analyses.
“We detected significantly more atrial fibrillation in the group that was randomized to screening. A major strength of our study was that we referred all of those individuals for a structured follow-up within the study,” she said. “Although the focus of the follow-up was oral anticoagulant therapy, other risk factors were also assessed and managed, such as hypertension and diabetes.”
It’s possible that increased detection of AF followed by such structured management contributed to the observed benefit, Dr. Svennberg proposed.
However, the exclusion of those in the prespecified ITT population who declined to be screened or otherwise didn’t participate left an as-treated cohort that was healthier than the ITT population or the control group.
Indeed, the nonparticipating invitees were sicker, with significantly more diabetes, vascular disease, hypertension, and heart failure, and higher CHA2DS2VASc stroke risk scores than those who agreed to participate.
“We took a more difficult route in setting up this study, in that we identified all individuals aged 75 to 76 residing in our two regions and excluded no one,” Dr. Svennberg said in an interview. “That means even individuals with end-stage disease, severe dementia, bedridden in nursing homes, et cetera, were also randomized but perhaps not likely or eligible to participate.”
Therefore, some invitees were unable to join the study even as others might have declined “out of low interest” or other personal reasons, she said. “We believe that this mimics how a population-based screening program would be performed if done in our country.”
In the ITT analysis, screening successfully identified previously unknown or untreated cases of AF, which led to expanded OAC use and intensified risk-factor management, “which was key to a successful outcome.”
In the as-treated analysis, Dr. Svennberg said, “I think a combination of the intervention and the population being overall more healthy was driving the secondary endpoint.”
Systematic vs. opportunistic screening
Although “opportunistic screening in individuals aged 65 and older” is recommended by current European Society of Cardiology guidelines, systematic screening, such as that used in STROKESTOP, has a much weaker evidence base, observed Renate B. Schnabel, MD, PhD, University Heart & Vascular Center, Hamburg, Germany, as the invited discussant after the STROKESTOP presentation.
STROKESTOP “is one of the first studies, if not the first study,” to show a clinical benefit from screening for AF, Dr. Schnabel said.
Fewer-than-projected primary outcome events were seen during the trial, and event curves for screened and control participants didn’t start to separate until about 4 years into the study, she said. It therefore might take a long time for the screened elderly to realize the clinical benefits of screening.
Studies such as the recent SCREEN-AF and mSTOPS have amply shown that AF screening in the asymptomatic elderly can reveal previously unrecognized AF far more often than would be detected in routine practice, allowing them the opportunity to go on OAC. But the trials weren’t able to show whether the benefits of such management outweigh the risks or costs.
Indeed, on April 20, the U.S. Preventive Services Task Force (USPSTF) released a draft recommendation statement concluding that “the current evidence is insufficient to assess the balance of benefits and harms” associated with AF screening in asymptomatic people at least 50 years of age.
In STROKESTOP, however, benefit for the primary outcome reached significance in the prespecified ITT analysis and “appeared to be driven by the reduction in ischemic stroke incidence,” Dr. Schnabel said.
“The future guidelines have gained strong evidence to judge on systematic atrial fibrillation screening” as it was performed in the trial, she said. “How to implement atrial fibrillation screening, including systematic screening in health care systems across Europe and beyond, remains an open question.”
A randomized population
STROKESTOP considered all 75- and 76-year-olds living in Sweden’s Stockholm County (n = 23,888) and the Halland region (n = 4,880) and randomly assigned them to the ITT group or a control group, with stratification by sex, birth year, and geographic region. In both groups, 54.6% were female and the mean CHA2DS2VASc score was 3.5.
People assigned to the ITT cohort were invited to be screened and followed. Those who agreed to participate underwent a baseline ECG assessment to detect or rule out permanent AF. Guideline-based OAC and follow-up was offered to those found with the arrhythmia. Those in sinus rhythm with no history of AF used a handheld single-lead ECG recorder (Zenicor) for 30 seconds twice daily for 14 days.
Structured management, including OAC, was offered to anyone demonstrating sufficient AF, that is, at least one bout without p waves in one 30-second recording or at least two such episodes lasting 10-29 seconds during the 2-week screening period.
In the ITT analysis, the hazard ratio (HR) for the composite clinical primary endpoint was 0.96 (95% confidence interval, 0.920-0.999; P = .045), but in the as-treated analysis, the HR for ischemic stroke was 0.76 (95% CI, 0.68-0.87; P < .001).
“I believe that this will likely be generalizable to most countries’ elderly residents,” Dr. Svennberg said. “I think if we can find a significant difference in our elderly population in Sweden, most countries will be able to do so, or find even more significant results.”
That’s because “baseline detection of AF in Sweden is high,” she said, “so new detection is likely more difficult.” Also, in Sweden, “care can be sought without monetary concern, and prescriptions are provided at low costs to the patients.” Therefore, patients newly identified with AF, whether in studies or not, “would likely be started on therapy.”
It will be important to know whether the screening strategy is cost-effective, Dr. Schnabel said, because “the overall effect, with a hazard ratio of 0.96, is not too big, and costs incurred by systematic screening are comparatively high.”
STROKESTOP “now provides sound information for cost-effectiveness analyses, which to date have largely relied on assumptions.”
STROKESTOP was partially supported by Carl Bennet AB, Boehringer-Ingelheim, Bayer, Bristol-Meyers Squibb, and Pfizer. Dr. Svennberg disclosed receiving fees for lectures or consulting from Bayer, Bristol-Meyers Squibb, Pfizer, Boehringer-Ingelheim, Merck Sharp & Dohme, and Sanofi; and institutional grants from Roche Diagnostics and Carl Bennett Ltd.
A version of this article first appeared on Medscape.com.
Some, perhaps many, previously unrecognized cases of atrial fibrillation (AF) will come to light in a screening program aimed at older asymptomatic adults. The key question is whether the challenges of such systematic but age-restricted AF screening in the community, with oral anticoagulation (OAC) offered to those found to have the arrhythmia, is worthwhile in preventing events such as death or stroke.
Now there is evidence supporting such a clinical benefit from a large, prospective, randomized trial. A screening program restricted to people 75 or 76 years of age in two Swedish communities, which called on them to use a handheld single-lead ECG system at home intermittently for 2 weeks, was followed by a slight drop in clinical events over about 7 years.
The 4% decline in risk (P = .045) in the STROKESTOP trial’s “intention-to-treat” (ITT) analysis yielded a number needed to treat of 91; that is, that many people had to be targeted by the screening program to prevent one primary-endpoint clinical event.
Those included ischemic stroke, systemic thromboembolism, hospitalization for severe bleeding, and death from any cause, investigators reported April 23 during the virtual European Heart Rhythm Association (EHRA) 2021 Congress.
If that benefit and its significance seem marginal, some secondary findings might be reassuring. Half the population of the target age in the two communities – 13,979 randomly selected people – were invited to join the trial and follow the screening protocol, comprising the ITT cohort. The other half, numbering 13,996, was not invited and served as control subjects.
However, only 51% of the ITT cohort accepted the invitation and participated in the trial; they represented the “as-treated” cohort, observed Emma Svennberg, MD, PhD, Karolinska Institute, Danderyd Hospital, Stockholm, who presented the analysis at the EHRA sessions.
The screening protocol identified untreated AF, whether previously known or unknown, in about 5% of the 7,165 as-treated screening participants; OAC was initiated in about three-fourths of those cases.
The as-treated group, on their own, benefited with a 24% drop in the prospectively defined secondary endpoint of ischemic stroke, compared with the entire control group.
The clinical benefit in the ITT population was “small but significant,” but over the same period in the as-treated cohort, there was a highly significant drop in risk for ischemic stroke, Dr. Svennberg said in an interview.
The trial’s lead message, she said, is that “screening for atrial fibrillation in an elderly population reduces the risk of death and ischemic stroke without increasing the risk of bleeding.”
Caveats: As-treated vs. ITT
But there are caveats that complicate interpretation of the trial and, Dr. Svennberg proposed, point to the importance of that interpretation of both the ITT and as-treated analyses.
“We detected significantly more atrial fibrillation in the group that was randomized to screening. A major strength of our study was that we referred all of those individuals for a structured follow-up within the study,” she said. “Although the focus of the follow-up was oral anticoagulant therapy, other risk factors were also assessed and managed, such as hypertension and diabetes.”
It’s possible that increased detection of AF followed by such structured management contributed to the observed benefit, Dr. Svennberg proposed.
However, the exclusion of those in the prespecified ITT population who declined to be screened or otherwise didn’t participate left an as-treated cohort that was healthier than the ITT population or the control group.
Indeed, the nonparticipating invitees were sicker, with significantly more diabetes, vascular disease, hypertension, and heart failure, and higher CHA2DS2VASc stroke risk scores than those who agreed to participate.
“We took a more difficult route in setting up this study, in that we identified all individuals aged 75 to 76 residing in our two regions and excluded no one,” Dr. Svennberg said in an interview. “That means even individuals with end-stage disease, severe dementia, bedridden in nursing homes, et cetera, were also randomized but perhaps not likely or eligible to participate.”
Therefore, some invitees were unable to join the study even as others might have declined “out of low interest” or other personal reasons, she said. “We believe that this mimics how a population-based screening program would be performed if done in our country.”
In the ITT analysis, screening successfully identified previously unknown or untreated cases of AF, which led to expanded OAC use and intensified risk-factor management, “which was key to a successful outcome.”
In the as-treated analysis, Dr. Svennberg said, “I think a combination of the intervention and the population being overall more healthy was driving the secondary endpoint.”
Systematic vs. opportunistic screening
Although “opportunistic screening in individuals aged 65 and older” is recommended by current European Society of Cardiology guidelines, systematic screening, such as that used in STROKESTOP, has a much weaker evidence base, observed Renate B. Schnabel, MD, PhD, University Heart & Vascular Center, Hamburg, Germany, as the invited discussant after the STROKESTOP presentation.
STROKESTOP “is one of the first studies, if not the first study,” to show a clinical benefit from screening for AF, Dr. Schnabel said.
Fewer-than-projected primary outcome events were seen during the trial, and event curves for screened and control participants didn’t start to separate until about 4 years into the study, she said. It therefore might take a long time for the screened elderly to realize the clinical benefits of screening.
Studies such as the recent SCREEN-AF and mSTOPS have amply shown that AF screening in the asymptomatic elderly can reveal previously unrecognized AF far more often than would be detected in routine practice, allowing them the opportunity to go on OAC. But the trials weren’t able to show whether the benefits of such management outweigh the risks or costs.
Indeed, on April 20, the U.S. Preventive Services Task Force (USPSTF) released a draft recommendation statement concluding that “the current evidence is insufficient to assess the balance of benefits and harms” associated with AF screening in asymptomatic people at least 50 years of age.
In STROKESTOP, however, benefit for the primary outcome reached significance in the prespecified ITT analysis and “appeared to be driven by the reduction in ischemic stroke incidence,” Dr. Schnabel said.
“The future guidelines have gained strong evidence to judge on systematic atrial fibrillation screening” as it was performed in the trial, she said. “How to implement atrial fibrillation screening, including systematic screening in health care systems across Europe and beyond, remains an open question.”
A randomized population
STROKESTOP considered all 75- and 76-year-olds living in Sweden’s Stockholm County (n = 23,888) and the Halland region (n = 4,880) and randomly assigned them to the ITT group or a control group, with stratification by sex, birth year, and geographic region. In both groups, 54.6% were female and the mean CHA2DS2VASc score was 3.5.
People assigned to the ITT cohort were invited to be screened and followed. Those who agreed to participate underwent a baseline ECG assessment to detect or rule out permanent AF. Guideline-based OAC and follow-up was offered to those found with the arrhythmia. Those in sinus rhythm with no history of AF used a handheld single-lead ECG recorder (Zenicor) for 30 seconds twice daily for 14 days.
Structured management, including OAC, was offered to anyone demonstrating sufficient AF, that is, at least one bout without p waves in one 30-second recording or at least two such episodes lasting 10-29 seconds during the 2-week screening period.
In the ITT analysis, the hazard ratio (HR) for the composite clinical primary endpoint was 0.96 (95% confidence interval, 0.920-0.999; P = .045), but in the as-treated analysis, the HR for ischemic stroke was 0.76 (95% CI, 0.68-0.87; P < .001).
“I believe that this will likely be generalizable to most countries’ elderly residents,” Dr. Svennberg said. “I think if we can find a significant difference in our elderly population in Sweden, most countries will be able to do so, or find even more significant results.”
That’s because “baseline detection of AF in Sweden is high,” she said, “so new detection is likely more difficult.” Also, in Sweden, “care can be sought without monetary concern, and prescriptions are provided at low costs to the patients.” Therefore, patients newly identified with AF, whether in studies or not, “would likely be started on therapy.”
It will be important to know whether the screening strategy is cost-effective, Dr. Schnabel said, because “the overall effect, with a hazard ratio of 0.96, is not too big, and costs incurred by systematic screening are comparatively high.”
STROKESTOP “now provides sound information for cost-effectiveness analyses, which to date have largely relied on assumptions.”
STROKESTOP was partially supported by Carl Bennet AB, Boehringer-Ingelheim, Bayer, Bristol-Meyers Squibb, and Pfizer. Dr. Svennberg disclosed receiving fees for lectures or consulting from Bayer, Bristol-Meyers Squibb, Pfizer, Boehringer-Ingelheim, Merck Sharp & Dohme, and Sanofi; and institutional grants from Roche Diagnostics and Carl Bennett Ltd.
A version of this article first appeared on Medscape.com.
Rituximab benefits seen in neuropsychiatric lupus
Patients with neuropsychiatric manifestations of systemic lupus erythematosus (NPSLE) seem to benefit from rituximab (Rituxan) therapy, according to data from the British Isles Lupus Assessment Group Biologics Register (BILAG-BR).
Indeed, the percentage of patients with active disease, as scored by the BILAG-2004 index or SLEDAI-2K (SLE Disease Activity Index 2000), fell significantly (P < .0001) when comparing pre- and postrituximab treatment scores. There was also a reduction in the dose of oral steroids used.
Interestingly, the use of concomitant cyclophosphamide might enhance the level of improvement seen in some patients, Trixy David, MBBS, reported during an abstract session at the British Society for Rheumatology annual conference.
“Larger-scale studies are warranted to establish the effectiveness of rituximab alone, or in combination with cyclophosphamide, in the treatment neuropsychiatric lupus,” said Dr. David, a clinical research fellow at the University of Manchester (England) and specialist registrar in rheumatology at the Manchester University National Health Service Foundation Trust.
Neil Basu, MBChB, PhD, who chaired the virtual session, called the findings “enlightening” and “descriptive.”
The study “provides some interesting data, which should be tested in a robust, randomized clinical trial,” he agreed, and not that clinicians should now start using rituximab for their NPSLE cases.
Dr. Basu, who is a clinical senior lecturer in rheumatology and honorary consultant rheumatologist at the Institute of Infection, Immunity and Inflammation at the University of Glasgow, added: “It is really important that we do these studies to help support a rationale for such a trial, which are obviously very expensive and require strong evidence before we go down that track. I think these data have really been quite enlightening in that respect.”
Rationale for rituximab in neuropsychiatric lupus
Managing patients with NPSLE remains an area of substantial unmet need. According to a recent review in Rheumatology, “there is a dearth of controlled clinical trials to guide management” and “therapeutic options include symptomatic, antithrombotic, and immunosuppressive agents that are supported by observational cohort studies.”
Despite being seen in at least half of all patients with SLE, neuropsychiatric disease “is not very well studied in patients with lupus, as a lot of large-scale trials tend to exclude patients with active neurological disease,” Dr. David said.
Although it is unclear why neuropsychiatric disease occurs in SLE, it could be “as a result of vascular injury or disruption of the blood brain barrier, thereby allowing the passive diffusion of autoantibodies and cytokines across through the cerebral spinal fluid, thereby generating a proinflammatory response,” Dr. David suggested.
“We know B cells are involved in the pathogenesis of lupus, and rituximab is a chimeric monoclonal antibody that selectively targets CD20-positive B cells and mediates transient B-cell depletion,” she said. Notably, there have been some small studies suggesting that rituximab may be effective in neuropsychiatric lupus, and it is currently widely used to treat refractory lupus in the United Kingdom.
About the BILAG-BR and results
“Our aim was to describe the baseline characteristics and short-term effectiveness of rituximab in patients treated for neuropsychiatric lupus within the BILAG-BR,” Dr. David explained.
Started in 2009, the BILAG-BR now contains information on more than 1,400 individuals with SLE who have been recruited at 62 centers in the United Kingdom. Its purpose is to evaluate the long-term safety and effectiveness of biologic drugs versus standard immunosuppressive therapy such as azathioprine, mycophenolate mofetil, cyclophosphamide, and cyclosporine. To date, 1,229 patients have been treated with biologics, of whom 1,056 have received rituximab.
A total of 74 rituximab-treated patients were identified as having active neuropsychiatric disease, making this “the largest prospective observational cohort to date, to our knowledge,” Dr. David said.
The median age of patients was 45.5 years, the majority was female (82%) and White (74%). The median disease duration was 11.5 years.
A total of 96% had multiple organ involvement and not just neuropsychiatric disease, and 91% were positive for antineutrophil antibodies.
The top six neuropsychiatric manifestations were cognitive dysfunction and lupus headache (both affecting 27.5% of patients); acute confessional state or mononeuropathy (each seen in 10% of patients); and seizure disorder and polyneuropathy, seen in a respective 8.6% and 8.7% of patients. These findings are in line with a 2011 meta-analysis, Dr. David pointed out.
BILAG-2004 scores before and after rituximab treatment were available for 50 patients. The number of patients with a BILAG A score dropped from 24 (48%) at baseline to 7 (14%) after treatment with rituximab, and the number with a BILAG B score declined from 26 (52%) at baseline to 4 (8%) after rituximab (both P < .0001).
There was also a reduction following rituximab treatment in the percentage of patients categorized as having mainly central nervous system disease (70% vs. 11%), peripheral nervous system disease (19% vs. 6%), or both (11% vs. 8%).
Total SLEDAI-2K scores were also reduced following rituximab treatment, from a median of 12 at baseline to 2 (P < .0001).
Pre- and postrituximab oral prednisolone doses were a median of 15 mg and 10 mg (P = .009).
Limitations
“Our data are from a real-world setting of patients who had active neuropsychiatric disease and were treated with rituximab,” Dr. David said. There are of course many limitations that go hand in hand with observational studies.
“There was the issue of missing data,” Dr. David said. It was difficult or not possible to determine what doses of steroids patients were taking after rituximab therapy, particularly in terms of intravenous steroids, and what doses of any other concomitant disease-modifying therapy might have been around the time that patients initiated or stopped rituximab treatment.
“These could have acted as potential confounders,” she acknowledged.
Dr. Basu noted: “My major haziness from it is the uncertainty of knowing why these patients improved. Yes, they had rituximab, but I’m sure also that they probably received high doses of steroids if they had quite severe CNS lupus which was categorized as a BILAG-A or a B.”
Patients may also be given methylprednisolone when clinicians are really concerned, he continued, and “as was quite clearly pointed out,” there was quite a lot of missing data from a steroid perspective.
Dr. David and coinvestigators reported having no conflicts of interest. The BILAG-BR is supported by funding from Lupus UK, GlaxoSmithKline, and Roche. Dr. Basu did not state having any disclosures.
Patients with neuropsychiatric manifestations of systemic lupus erythematosus (NPSLE) seem to benefit from rituximab (Rituxan) therapy, according to data from the British Isles Lupus Assessment Group Biologics Register (BILAG-BR).
Indeed, the percentage of patients with active disease, as scored by the BILAG-2004 index or SLEDAI-2K (SLE Disease Activity Index 2000), fell significantly (P < .0001) when comparing pre- and postrituximab treatment scores. There was also a reduction in the dose of oral steroids used.
Interestingly, the use of concomitant cyclophosphamide might enhance the level of improvement seen in some patients, Trixy David, MBBS, reported during an abstract session at the British Society for Rheumatology annual conference.
“Larger-scale studies are warranted to establish the effectiveness of rituximab alone, or in combination with cyclophosphamide, in the treatment neuropsychiatric lupus,” said Dr. David, a clinical research fellow at the University of Manchester (England) and specialist registrar in rheumatology at the Manchester University National Health Service Foundation Trust.
Neil Basu, MBChB, PhD, who chaired the virtual session, called the findings “enlightening” and “descriptive.”
The study “provides some interesting data, which should be tested in a robust, randomized clinical trial,” he agreed, and not that clinicians should now start using rituximab for their NPSLE cases.
Dr. Basu, who is a clinical senior lecturer in rheumatology and honorary consultant rheumatologist at the Institute of Infection, Immunity and Inflammation at the University of Glasgow, added: “It is really important that we do these studies to help support a rationale for such a trial, which are obviously very expensive and require strong evidence before we go down that track. I think these data have really been quite enlightening in that respect.”
Rationale for rituximab in neuropsychiatric lupus
Managing patients with NPSLE remains an area of substantial unmet need. According to a recent review in Rheumatology, “there is a dearth of controlled clinical trials to guide management” and “therapeutic options include symptomatic, antithrombotic, and immunosuppressive agents that are supported by observational cohort studies.”
Despite being seen in at least half of all patients with SLE, neuropsychiatric disease “is not very well studied in patients with lupus, as a lot of large-scale trials tend to exclude patients with active neurological disease,” Dr. David said.
Although it is unclear why neuropsychiatric disease occurs in SLE, it could be “as a result of vascular injury or disruption of the blood brain barrier, thereby allowing the passive diffusion of autoantibodies and cytokines across through the cerebral spinal fluid, thereby generating a proinflammatory response,” Dr. David suggested.
“We know B cells are involved in the pathogenesis of lupus, and rituximab is a chimeric monoclonal antibody that selectively targets CD20-positive B cells and mediates transient B-cell depletion,” she said. Notably, there have been some small studies suggesting that rituximab may be effective in neuropsychiatric lupus, and it is currently widely used to treat refractory lupus in the United Kingdom.
About the BILAG-BR and results
“Our aim was to describe the baseline characteristics and short-term effectiveness of rituximab in patients treated for neuropsychiatric lupus within the BILAG-BR,” Dr. David explained.
Started in 2009, the BILAG-BR now contains information on more than 1,400 individuals with SLE who have been recruited at 62 centers in the United Kingdom. Its purpose is to evaluate the long-term safety and effectiveness of biologic drugs versus standard immunosuppressive therapy such as azathioprine, mycophenolate mofetil, cyclophosphamide, and cyclosporine. To date, 1,229 patients have been treated with biologics, of whom 1,056 have received rituximab.
A total of 74 rituximab-treated patients were identified as having active neuropsychiatric disease, making this “the largest prospective observational cohort to date, to our knowledge,” Dr. David said.
The median age of patients was 45.5 years, the majority was female (82%) and White (74%). The median disease duration was 11.5 years.
A total of 96% had multiple organ involvement and not just neuropsychiatric disease, and 91% were positive for antineutrophil antibodies.
The top six neuropsychiatric manifestations were cognitive dysfunction and lupus headache (both affecting 27.5% of patients); acute confessional state or mononeuropathy (each seen in 10% of patients); and seizure disorder and polyneuropathy, seen in a respective 8.6% and 8.7% of patients. These findings are in line with a 2011 meta-analysis, Dr. David pointed out.
BILAG-2004 scores before and after rituximab treatment were available for 50 patients. The number of patients with a BILAG A score dropped from 24 (48%) at baseline to 7 (14%) after treatment with rituximab, and the number with a BILAG B score declined from 26 (52%) at baseline to 4 (8%) after rituximab (both P < .0001).
There was also a reduction following rituximab treatment in the percentage of patients categorized as having mainly central nervous system disease (70% vs. 11%), peripheral nervous system disease (19% vs. 6%), or both (11% vs. 8%).
Total SLEDAI-2K scores were also reduced following rituximab treatment, from a median of 12 at baseline to 2 (P < .0001).
Pre- and postrituximab oral prednisolone doses were a median of 15 mg and 10 mg (P = .009).
Limitations
“Our data are from a real-world setting of patients who had active neuropsychiatric disease and were treated with rituximab,” Dr. David said. There are of course many limitations that go hand in hand with observational studies.
“There was the issue of missing data,” Dr. David said. It was difficult or not possible to determine what doses of steroids patients were taking after rituximab therapy, particularly in terms of intravenous steroids, and what doses of any other concomitant disease-modifying therapy might have been around the time that patients initiated or stopped rituximab treatment.
“These could have acted as potential confounders,” she acknowledged.
Dr. Basu noted: “My major haziness from it is the uncertainty of knowing why these patients improved. Yes, they had rituximab, but I’m sure also that they probably received high doses of steroids if they had quite severe CNS lupus which was categorized as a BILAG-A or a B.”
Patients may also be given methylprednisolone when clinicians are really concerned, he continued, and “as was quite clearly pointed out,” there was quite a lot of missing data from a steroid perspective.
Dr. David and coinvestigators reported having no conflicts of interest. The BILAG-BR is supported by funding from Lupus UK, GlaxoSmithKline, and Roche. Dr. Basu did not state having any disclosures.
Patients with neuropsychiatric manifestations of systemic lupus erythematosus (NPSLE) seem to benefit from rituximab (Rituxan) therapy, according to data from the British Isles Lupus Assessment Group Biologics Register (BILAG-BR).
Indeed, the percentage of patients with active disease, as scored by the BILAG-2004 index or SLEDAI-2K (SLE Disease Activity Index 2000), fell significantly (P < .0001) when comparing pre- and postrituximab treatment scores. There was also a reduction in the dose of oral steroids used.
Interestingly, the use of concomitant cyclophosphamide might enhance the level of improvement seen in some patients, Trixy David, MBBS, reported during an abstract session at the British Society for Rheumatology annual conference.
“Larger-scale studies are warranted to establish the effectiveness of rituximab alone, or in combination with cyclophosphamide, in the treatment neuropsychiatric lupus,” said Dr. David, a clinical research fellow at the University of Manchester (England) and specialist registrar in rheumatology at the Manchester University National Health Service Foundation Trust.
Neil Basu, MBChB, PhD, who chaired the virtual session, called the findings “enlightening” and “descriptive.”
The study “provides some interesting data, which should be tested in a robust, randomized clinical trial,” he agreed, and not that clinicians should now start using rituximab for their NPSLE cases.
Dr. Basu, who is a clinical senior lecturer in rheumatology and honorary consultant rheumatologist at the Institute of Infection, Immunity and Inflammation at the University of Glasgow, added: “It is really important that we do these studies to help support a rationale for such a trial, which are obviously very expensive and require strong evidence before we go down that track. I think these data have really been quite enlightening in that respect.”
Rationale for rituximab in neuropsychiatric lupus
Managing patients with NPSLE remains an area of substantial unmet need. According to a recent review in Rheumatology, “there is a dearth of controlled clinical trials to guide management” and “therapeutic options include symptomatic, antithrombotic, and immunosuppressive agents that are supported by observational cohort studies.”
Despite being seen in at least half of all patients with SLE, neuropsychiatric disease “is not very well studied in patients with lupus, as a lot of large-scale trials tend to exclude patients with active neurological disease,” Dr. David said.
Although it is unclear why neuropsychiatric disease occurs in SLE, it could be “as a result of vascular injury or disruption of the blood brain barrier, thereby allowing the passive diffusion of autoantibodies and cytokines across through the cerebral spinal fluid, thereby generating a proinflammatory response,” Dr. David suggested.
“We know B cells are involved in the pathogenesis of lupus, and rituximab is a chimeric monoclonal antibody that selectively targets CD20-positive B cells and mediates transient B-cell depletion,” she said. Notably, there have been some small studies suggesting that rituximab may be effective in neuropsychiatric lupus, and it is currently widely used to treat refractory lupus in the United Kingdom.
About the BILAG-BR and results
“Our aim was to describe the baseline characteristics and short-term effectiveness of rituximab in patients treated for neuropsychiatric lupus within the BILAG-BR,” Dr. David explained.
Started in 2009, the BILAG-BR now contains information on more than 1,400 individuals with SLE who have been recruited at 62 centers in the United Kingdom. Its purpose is to evaluate the long-term safety and effectiveness of biologic drugs versus standard immunosuppressive therapy such as azathioprine, mycophenolate mofetil, cyclophosphamide, and cyclosporine. To date, 1,229 patients have been treated with biologics, of whom 1,056 have received rituximab.
A total of 74 rituximab-treated patients were identified as having active neuropsychiatric disease, making this “the largest prospective observational cohort to date, to our knowledge,” Dr. David said.
The median age of patients was 45.5 years, the majority was female (82%) and White (74%). The median disease duration was 11.5 years.
A total of 96% had multiple organ involvement and not just neuropsychiatric disease, and 91% were positive for antineutrophil antibodies.
The top six neuropsychiatric manifestations were cognitive dysfunction and lupus headache (both affecting 27.5% of patients); acute confessional state or mononeuropathy (each seen in 10% of patients); and seizure disorder and polyneuropathy, seen in a respective 8.6% and 8.7% of patients. These findings are in line with a 2011 meta-analysis, Dr. David pointed out.
BILAG-2004 scores before and after rituximab treatment were available for 50 patients. The number of patients with a BILAG A score dropped from 24 (48%) at baseline to 7 (14%) after treatment with rituximab, and the number with a BILAG B score declined from 26 (52%) at baseline to 4 (8%) after rituximab (both P < .0001).
There was also a reduction following rituximab treatment in the percentage of patients categorized as having mainly central nervous system disease (70% vs. 11%), peripheral nervous system disease (19% vs. 6%), or both (11% vs. 8%).
Total SLEDAI-2K scores were also reduced following rituximab treatment, from a median of 12 at baseline to 2 (P < .0001).
Pre- and postrituximab oral prednisolone doses were a median of 15 mg and 10 mg (P = .009).
Limitations
“Our data are from a real-world setting of patients who had active neuropsychiatric disease and were treated with rituximab,” Dr. David said. There are of course many limitations that go hand in hand with observational studies.
“There was the issue of missing data,” Dr. David said. It was difficult or not possible to determine what doses of steroids patients were taking after rituximab therapy, particularly in terms of intravenous steroids, and what doses of any other concomitant disease-modifying therapy might have been around the time that patients initiated or stopped rituximab treatment.
“These could have acted as potential confounders,” she acknowledged.
Dr. Basu noted: “My major haziness from it is the uncertainty of knowing why these patients improved. Yes, they had rituximab, but I’m sure also that they probably received high doses of steroids if they had quite severe CNS lupus which was categorized as a BILAG-A or a B.”
Patients may also be given methylprednisolone when clinicians are really concerned, he continued, and “as was quite clearly pointed out,” there was quite a lot of missing data from a steroid perspective.
Dr. David and coinvestigators reported having no conflicts of interest. The BILAG-BR is supported by funding from Lupus UK, GlaxoSmithKline, and Roche. Dr. Basu did not state having any disclosures.
FROM BSR 2021
Some MS treatments may heighten COVID risk
, according to a new analysis of an Italian cohort of patients with MS. The study confirmed that steroid exposure in the month before COVID-19 symptom onset is tied to more severe disease, and anti-CD20 therapy poses similar risks. But the researchers noted that interferon and possibly teriflunomide were associated with a protective effect in the multivariate analysis.

Maria Pia Sormani, PhD, who is a professor of biostatistics at the University of Genoa, presented the study at the 2021 annual meeting of the American Academy of Neurology.
The results confirm some previous analyses, and add to the body of evidence clinicians rely on, according to Jiwon Oh, MD, PhD, who moderated the session. “These data about the risk with the anti-CD20 therapies have been around for a while, but it seems that risk is pretty apparent, with this registry and other registries around the world. It affects counseling to patients on anti-CD20 therapies. We would counsel them to be cautious, obviously, follow public health precautions, but maybe be even more cautious. It affects our recommendations about the urgency of vaccination in these folks, how high priority they should be,” Dr. Oh said in an interview. She is the clinical director of the Barlo MS Center at St. Michael’s Unity Health in Toronto.
The analysis also hinted at complexities within demographics that might help explain some of the differing outcomes of infections. “We have learned that the course of the viral infection per se may not be the cause of severe outcomes, but the exaggerated inflammatory response to the virus is mainly responsible for intubations and deaths. The hypothesis we are investigating is whether anti-CD20 therapies can cause a more severe viral infection (that is something already known for other viral infections) but do not play a crucial role in causing the explosion of the inflammatory process,” said Dr. Sormani in an email.
The group plans to look at the risk of anti-CD20 therapies in different age groups, “to try to understand the underlying mechanism through which anti-CD20 increases the risk of more severe outcome,” she said.
Dr. Sormani presented an analysis of 3,274 patients with MS who contracted COVID-19 in Italy. The mean age was 44, the median Expanded Disability Status Scale (EDSS) score was 2, Among the study cohort, 68.6% were female; 14% had progressive MS and 26 patients died. Patients who died had a mean age of 63, 48% were female, 73% had progressive MS, and 50% were not on any DMT.
The researchers used ordinal logistic regression that “orders” outcome on a severity scale of 0 (mild disease, no pneumonia or hospitalization), 1 (pneumonia or hospitalization, n = 184), or 2 (ICU admission or death, n = 36). They calculated the odds ratio of moving from 0 to 1, or 1 to 2, and carried the assumption that the risk is the same. For example, an odds ratio of 2 for males versus females would mean that males are twice as likely to be hospitalized and twice as likely to go from being hospitalized to going to the ICU or dying.
The researchers found that older age, male sex, and comorbidities increase risk of worse COVID-19 outcomes. Exposure to methylprednisolone 1 month before COVID-19 symptom onset carried an increased risk (OR, 2.33; P = .03). Compared with no therapy, receiving interferon was associated with lower risk (OR, 0.34; P = .009) and teriflunomide trended towards an association with better outcomes (OR, 0.49; P = .054). Anti-CD20 treatment (ocrelizumab or rituximab) was linked to worse outcomes (OR, 1.89; P = .012) overall, which held up when ocrelizumab (OR, 1.71; P = .04) and rituximab (OR, 2.77; P = .03) were considered separately.
To understand why the risk of ocrelizumab might be lower, the researchers examined risk by duration of anti-CD20 treatment, and found that risk increased with increased duration of treatment, with the lowest risk at treatment duration less than 6 months (OR, 1.56; 95% CI, 0.65-3.77; not significant), followed by 6 months to 1 year (OR, 1.68; 95% CI, 0.69-4.03; P < .001), 1-2 years (OR, 1.74; 95% CI, 0.83-3.64; trend), and the highest risk at more than 2 years (OR, 2.75; 95% CI, 1.28-5.88).
Dr. Sormani suggested that the greater risk associated with rituximab may be because of a tendency towards longer treatment length, since patients treated with rituximab were more often treated for greater lengths of time; 11% had been treated for 6 months or less (vs. 24% of ocrelizumab patients); 26%, 6-12 months (vs. 18% ocrelizumab); 19%, 1-2 years (vs. 37% ocrelizumab); and 44%, 2 years or longer (vs. 21% ocrelizumab).
Dr. Sormani has received consulting fees from Biogen, GeNeuro, Genzyme, MedDay, Merck KGaA, Novartis, Roche, and Immunic. The platform for data collection was donated by Merck. Dr. Oh has consulted for Roche, Celgene, Biogen-Idec, EMD-Serono, Sanofi-Genzyme, Novartis, Alexion. She has been on a scientific advisory or data safety monitoring board for Roche, Biogen-Idec, and Sanofi-Genzyme.
, according to a new analysis of an Italian cohort of patients with MS. The study confirmed that steroid exposure in the month before COVID-19 symptom onset is tied to more severe disease, and anti-CD20 therapy poses similar risks. But the researchers noted that interferon and possibly teriflunomide were associated with a protective effect in the multivariate analysis.
Maria Pia Sormani, PhD, who is a professor of biostatistics at the University of Genoa, presented the study at the 2021 annual meeting of the American Academy of Neurology.
The results confirm some previous analyses, and add to the body of evidence clinicians rely on, according to Jiwon Oh, MD, PhD, who moderated the session. “These data about the risk with the anti-CD20 therapies have been around for a while, but it seems that risk is pretty apparent, with this registry and other registries around the world. It affects counseling to patients on anti-CD20 therapies. We would counsel them to be cautious, obviously, follow public health precautions, but maybe be even more cautious. It affects our recommendations about the urgency of vaccination in these folks, how high priority they should be,” Dr. Oh said in an interview. She is the clinical director of the Barlo MS Center at St. Michael’s Unity Health in Toronto.
The analysis also hinted at complexities within demographics that might help explain some of the differing outcomes of infections. “We have learned that the course of the viral infection per se may not be the cause of severe outcomes, but the exaggerated inflammatory response to the virus is mainly responsible for intubations and deaths. The hypothesis we are investigating is whether anti-CD20 therapies can cause a more severe viral infection (that is something already known for other viral infections) but do not play a crucial role in causing the explosion of the inflammatory process,” said Dr. Sormani in an email.
The group plans to look at the risk of anti-CD20 therapies in different age groups, “to try to understand the underlying mechanism through which anti-CD20 increases the risk of more severe outcome,” she said.
Dr. Sormani presented an analysis of 3,274 patients with MS who contracted COVID-19 in Italy. The mean age was 44, the median Expanded Disability Status Scale (EDSS) score was 2, Among the study cohort, 68.6% were female; 14% had progressive MS and 26 patients died. Patients who died had a mean age of 63, 48% were female, 73% had progressive MS, and 50% were not on any DMT.
The researchers used ordinal logistic regression that “orders” outcome on a severity scale of 0 (mild disease, no pneumonia or hospitalization), 1 (pneumonia or hospitalization, n = 184), or 2 (ICU admission or death, n = 36). They calculated the odds ratio of moving from 0 to 1, or 1 to 2, and carried the assumption that the risk is the same. For example, an odds ratio of 2 for males versus females would mean that males are twice as likely to be hospitalized and twice as likely to go from being hospitalized to going to the ICU or dying.
The researchers found that older age, male sex, and comorbidities increase risk of worse COVID-19 outcomes. Exposure to methylprednisolone 1 month before COVID-19 symptom onset carried an increased risk (OR, 2.33; P = .03). Compared with no therapy, receiving interferon was associated with lower risk (OR, 0.34; P = .009) and teriflunomide trended towards an association with better outcomes (OR, 0.49; P = .054). Anti-CD20 treatment (ocrelizumab or rituximab) was linked to worse outcomes (OR, 1.89; P = .012) overall, which held up when ocrelizumab (OR, 1.71; P = .04) and rituximab (OR, 2.77; P = .03) were considered separately.
To understand why the risk of ocrelizumab might be lower, the researchers examined risk by duration of anti-CD20 treatment, and found that risk increased with increased duration of treatment, with the lowest risk at treatment duration less than 6 months (OR, 1.56; 95% CI, 0.65-3.77; not significant), followed by 6 months to 1 year (OR, 1.68; 95% CI, 0.69-4.03; P < .001), 1-2 years (OR, 1.74; 95% CI, 0.83-3.64; trend), and the highest risk at more than 2 years (OR, 2.75; 95% CI, 1.28-5.88).
Dr. Sormani suggested that the greater risk associated with rituximab may be because of a tendency towards longer treatment length, since patients treated with rituximab were more often treated for greater lengths of time; 11% had been treated for 6 months or less (vs. 24% of ocrelizumab patients); 26%, 6-12 months (vs. 18% ocrelizumab); 19%, 1-2 years (vs. 37% ocrelizumab); and 44%, 2 years or longer (vs. 21% ocrelizumab).
Dr. Sormani has received consulting fees from Biogen, GeNeuro, Genzyme, MedDay, Merck KGaA, Novartis, Roche, and Immunic. The platform for data collection was donated by Merck. Dr. Oh has consulted for Roche, Celgene, Biogen-Idec, EMD-Serono, Sanofi-Genzyme, Novartis, Alexion. She has been on a scientific advisory or data safety monitoring board for Roche, Biogen-Idec, and Sanofi-Genzyme.
, according to a new analysis of an Italian cohort of patients with MS. The study confirmed that steroid exposure in the month before COVID-19 symptom onset is tied to more severe disease, and anti-CD20 therapy poses similar risks. But the researchers noted that interferon and possibly teriflunomide were associated with a protective effect in the multivariate analysis.
Maria Pia Sormani, PhD, who is a professor of biostatistics at the University of Genoa, presented the study at the 2021 annual meeting of the American Academy of Neurology.
The results confirm some previous analyses, and add to the body of evidence clinicians rely on, according to Jiwon Oh, MD, PhD, who moderated the session. “These data about the risk with the anti-CD20 therapies have been around for a while, but it seems that risk is pretty apparent, with this registry and other registries around the world. It affects counseling to patients on anti-CD20 therapies. We would counsel them to be cautious, obviously, follow public health precautions, but maybe be even more cautious. It affects our recommendations about the urgency of vaccination in these folks, how high priority they should be,” Dr. Oh said in an interview. She is the clinical director of the Barlo MS Center at St. Michael’s Unity Health in Toronto.
The analysis also hinted at complexities within demographics that might help explain some of the differing outcomes of infections. “We have learned that the course of the viral infection per se may not be the cause of severe outcomes, but the exaggerated inflammatory response to the virus is mainly responsible for intubations and deaths. The hypothesis we are investigating is whether anti-CD20 therapies can cause a more severe viral infection (that is something already known for other viral infections) but do not play a crucial role in causing the explosion of the inflammatory process,” said Dr. Sormani in an email.
The group plans to look at the risk of anti-CD20 therapies in different age groups, “to try to understand the underlying mechanism through which anti-CD20 increases the risk of more severe outcome,” she said.
Dr. Sormani presented an analysis of 3,274 patients with MS who contracted COVID-19 in Italy. The mean age was 44, the median Expanded Disability Status Scale (EDSS) score was 2, Among the study cohort, 68.6% were female; 14% had progressive MS and 26 patients died. Patients who died had a mean age of 63, 48% were female, 73% had progressive MS, and 50% were not on any DMT.
The researchers used ordinal logistic regression that “orders” outcome on a severity scale of 0 (mild disease, no pneumonia or hospitalization), 1 (pneumonia or hospitalization, n = 184), or 2 (ICU admission or death, n = 36). They calculated the odds ratio of moving from 0 to 1, or 1 to 2, and carried the assumption that the risk is the same. For example, an odds ratio of 2 for males versus females would mean that males are twice as likely to be hospitalized and twice as likely to go from being hospitalized to going to the ICU or dying.
The researchers found that older age, male sex, and comorbidities increase risk of worse COVID-19 outcomes. Exposure to methylprednisolone 1 month before COVID-19 symptom onset carried an increased risk (OR, 2.33; P = .03). Compared with no therapy, receiving interferon was associated with lower risk (OR, 0.34; P = .009) and teriflunomide trended towards an association with better outcomes (OR, 0.49; P = .054). Anti-CD20 treatment (ocrelizumab or rituximab) was linked to worse outcomes (OR, 1.89; P = .012) overall, which held up when ocrelizumab (OR, 1.71; P = .04) and rituximab (OR, 2.77; P = .03) were considered separately.
To understand why the risk of ocrelizumab might be lower, the researchers examined risk by duration of anti-CD20 treatment, and found that risk increased with increased duration of treatment, with the lowest risk at treatment duration less than 6 months (OR, 1.56; 95% CI, 0.65-3.77; not significant), followed by 6 months to 1 year (OR, 1.68; 95% CI, 0.69-4.03; P < .001), 1-2 years (OR, 1.74; 95% CI, 0.83-3.64; trend), and the highest risk at more than 2 years (OR, 2.75; 95% CI, 1.28-5.88).
Dr. Sormani suggested that the greater risk associated with rituximab may be because of a tendency towards longer treatment length, since patients treated with rituximab were more often treated for greater lengths of time; 11% had been treated for 6 months or less (vs. 24% of ocrelizumab patients); 26%, 6-12 months (vs. 18% ocrelizumab); 19%, 1-2 years (vs. 37% ocrelizumab); and 44%, 2 years or longer (vs. 21% ocrelizumab).
Dr. Sormani has received consulting fees from Biogen, GeNeuro, Genzyme, MedDay, Merck KGaA, Novartis, Roche, and Immunic. The platform for data collection was donated by Merck. Dr. Oh has consulted for Roche, Celgene, Biogen-Idec, EMD-Serono, Sanofi-Genzyme, Novartis, Alexion. She has been on a scientific advisory or data safety monitoring board for Roche, Biogen-Idec, and Sanofi-Genzyme.
FROM AAN 2021

Infective endocarditis from IV drug use tied to hemorrhagic stroke
One consequence of the ongoing opioid epidemic in the United States may be an increase in the number of hemorrhagic strokes caused by infective endocarditis, research suggests.
Intravenous drug use (IVDU) can cause this bacterial infection of the heart. In a single-center study, infective endocarditis was associated with an increase in the risk for hemorrhagic stroke as well as an increase in health care use and costs.
“Patients who are known IV drug users who have endocarditis should be more carefully screened for symptoms of cardiovascular disease,” Shahid M. Nimjee, MD, PhD, associate professor of neurosurgery and surgical director of the Comprehensive Stroke Center at the Ohio State University Wexner Medical Center, Columbus, said in a press release.
The findings were presented at the International Stroke Conference sponsored by the American Heart Association.
In the United States, 47,000 patients are treated in the hospital for endocarditis each year. Endocarditis increases the risk for stroke, which can entail significant morbidity and mortality, the authors noted.
IVDU is a risk factor for endocarditis. In the context of the opioid epidemic, Dr. Nimjee and colleagues sought to compare the risk for stroke among patients with endocarditis from IVDU with the risk among patients with endocarditis from other causes.
They retrospectively studied patients who had undergone treatment for infective endocarditis at Wexner Medical Center between Jan. 1, 2014, and July 1, 2018. They examined patients’ concomitant intravenous drug abuse and evaluated demographics, risk factors, and associated costs.
Dramatic increase
In all, 351 patients met the study’s inclusion criteria, and 170 (48%) had a history of IVDU-associated endocarditis. The incidence of patients with IVDU-associated endocarditis increased 630% from 2014 to 2018.
The prevalence of overall intracranial hemorrhage was increased among patients with IVDU, compared with those without (25.9% vs. 13.9%; P = .005).
This increase in prevalence included increases in intraparenchymal hemorrhage (12.4% vs. 5.1%; P = .012), subarachnoid hemorrhage (17.6% vs. 4.4%; P = .0001), and cerebral microbleeds (14.1% vs. 7.2%; P = .022).
IVDU also was associated with an increase in prevalence of infectious intracranial aneurysm (10.6% vs. 1.8%; P = .0001) and brain abscess (4.7% vs. 1.1%; P = .025).
Compared with patients with endocarditis from other causes, significantly higher numbers of patients with IVDU-associated endocarditis were homeless (5.9% vs. 1.1%; P = .014), uninsured (10.0% vs. 2.8%; P = .005), and unemployed (75.9% vs. 31.7%; P = .0001).
Medical costs were more than twice as high among patients with endocarditis from IVDU than among those with endocarditis from other causes. The difference in health care costs during admission per patient was more than $100,000.
“The wider societal impact of the opioid epidemic is not well understood,” Dr. Nimjee said in the press release. “Our research suggests that the impact of the opioid epidemic is far-reaching and contributes to increased costs in the criminal justice, health care systems, and the workplace. The increased costs can be particularly substantial for stroke care.”
Nationwide data desirable
“Past publications from the U.S. have shown an increase in incidence of IVDU-related endocarditis, and the current publication emphasizes this worrying trend,” Manuel Bolognese, MD, head of the stroke center at the Lucerne (Switzerland) Cantonal Hospital, said in an interview. “The higher degree of hemorrhagic strokes and brain abscesses as further complications is alarming as well and shows that IVDU-related endocarditis is becoming a more and more relevant medical problem in the U.S., with high morbidity and mortality.”
The study period is long enough to show a clear trend of increasing incidence of IVDU-related endocarditis, Dr. Bolognese said. The study’s biggest weaknesses are its retrospective design and restriction to a single center.
“Without knowing the prevalence of drug abuse and the socioeconomical situation in Columbus, it is difficult to generalize these findings to other regions in the U.S.A. or even abroad,” he said.
Also, the abstract does not provide some essential information, said Dr. Bolognese. It would be important to know which valve was affected in each patient, which bacteria were identified, whether patients also used nonopioid drugs, and what each patient’s immune status was.
A lack of sterile material such as syringes could explain the apparent association between IVDU-associated endocarditis and low socioeconomic status, said Dr. Bolognese. Delayed presentation to medical institutions because of a lack of insurance could have led to a more complicated course.
“It would be interesting to see numbers from a broader spectrum in a nationwide registry,” said Dr. Bolognese. “It might be worth studying interventions to improve the hygienic aspects (like supply of sterile material, especially in the most vulnerable groups, like homeless people) or to provide easier access to emergency health care despite lack of insurance, which could decrease the incidence of IVDU.”
Dr. Nimjee and Dr. Bolognese disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
One consequence of the ongoing opioid epidemic in the United States may be an increase in the number of hemorrhagic strokes caused by infective endocarditis, research suggests.
Intravenous drug use (IVDU) can cause this bacterial infection of the heart. In a single-center study, infective endocarditis was associated with an increase in the risk for hemorrhagic stroke as well as an increase in health care use and costs.
“Patients who are known IV drug users who have endocarditis should be more carefully screened for symptoms of cardiovascular disease,” Shahid M. Nimjee, MD, PhD, associate professor of neurosurgery and surgical director of the Comprehensive Stroke Center at the Ohio State University Wexner Medical Center, Columbus, said in a press release.
The findings were presented at the International Stroke Conference sponsored by the American Heart Association.
In the United States, 47,000 patients are treated in the hospital for endocarditis each year. Endocarditis increases the risk for stroke, which can entail significant morbidity and mortality, the authors noted.
IVDU is a risk factor for endocarditis. In the context of the opioid epidemic, Dr. Nimjee and colleagues sought to compare the risk for stroke among patients with endocarditis from IVDU with the risk among patients with endocarditis from other causes.
They retrospectively studied patients who had undergone treatment for infective endocarditis at Wexner Medical Center between Jan. 1, 2014, and July 1, 2018. They examined patients’ concomitant intravenous drug abuse and evaluated demographics, risk factors, and associated costs.
Dramatic increase
In all, 351 patients met the study’s inclusion criteria, and 170 (48%) had a history of IVDU-associated endocarditis. The incidence of patients with IVDU-associated endocarditis increased 630% from 2014 to 2018.
The prevalence of overall intracranial hemorrhage was increased among patients with IVDU, compared with those without (25.9% vs. 13.9%; P = .005).
This increase in prevalence included increases in intraparenchymal hemorrhage (12.4% vs. 5.1%; P = .012), subarachnoid hemorrhage (17.6% vs. 4.4%; P = .0001), and cerebral microbleeds (14.1% vs. 7.2%; P = .022).
IVDU also was associated with an increase in prevalence of infectious intracranial aneurysm (10.6% vs. 1.8%; P = .0001) and brain abscess (4.7% vs. 1.1%; P = .025).
Compared with patients with endocarditis from other causes, significantly higher numbers of patients with IVDU-associated endocarditis were homeless (5.9% vs. 1.1%; P = .014), uninsured (10.0% vs. 2.8%; P = .005), and unemployed (75.9% vs. 31.7%; P = .0001).
Medical costs were more than twice as high among patients with endocarditis from IVDU than among those with endocarditis from other causes. The difference in health care costs during admission per patient was more than $100,000.
“The wider societal impact of the opioid epidemic is not well understood,” Dr. Nimjee said in the press release. “Our research suggests that the impact of the opioid epidemic is far-reaching and contributes to increased costs in the criminal justice, health care systems, and the workplace. The increased costs can be particularly substantial for stroke care.”
Nationwide data desirable
“Past publications from the U.S. have shown an increase in incidence of IVDU-related endocarditis, and the current publication emphasizes this worrying trend,” Manuel Bolognese, MD, head of the stroke center at the Lucerne (Switzerland) Cantonal Hospital, said in an interview. “The higher degree of hemorrhagic strokes and brain abscesses as further complications is alarming as well and shows that IVDU-related endocarditis is becoming a more and more relevant medical problem in the U.S., with high morbidity and mortality.”
The study period is long enough to show a clear trend of increasing incidence of IVDU-related endocarditis, Dr. Bolognese said. The study’s biggest weaknesses are its retrospective design and restriction to a single center.
“Without knowing the prevalence of drug abuse and the socioeconomical situation in Columbus, it is difficult to generalize these findings to other regions in the U.S.A. or even abroad,” he said.
Also, the abstract does not provide some essential information, said Dr. Bolognese. It would be important to know which valve was affected in each patient, which bacteria were identified, whether patients also used nonopioid drugs, and what each patient’s immune status was.
A lack of sterile material such as syringes could explain the apparent association between IVDU-associated endocarditis and low socioeconomic status, said Dr. Bolognese. Delayed presentation to medical institutions because of a lack of insurance could have led to a more complicated course.
“It would be interesting to see numbers from a broader spectrum in a nationwide registry,” said Dr. Bolognese. “It might be worth studying interventions to improve the hygienic aspects (like supply of sterile material, especially in the most vulnerable groups, like homeless people) or to provide easier access to emergency health care despite lack of insurance, which could decrease the incidence of IVDU.”
Dr. Nimjee and Dr. Bolognese disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
One consequence of the ongoing opioid epidemic in the United States may be an increase in the number of hemorrhagic strokes caused by infective endocarditis, research suggests.
Intravenous drug use (IVDU) can cause this bacterial infection of the heart. In a single-center study, infective endocarditis was associated with an increase in the risk for hemorrhagic stroke as well as an increase in health care use and costs.
“Patients who are known IV drug users who have endocarditis should be more carefully screened for symptoms of cardiovascular disease,” Shahid M. Nimjee, MD, PhD, associate professor of neurosurgery and surgical director of the Comprehensive Stroke Center at the Ohio State University Wexner Medical Center, Columbus, said in a press release.
The findings were presented at the International Stroke Conference sponsored by the American Heart Association.
In the United States, 47,000 patients are treated in the hospital for endocarditis each year. Endocarditis increases the risk for stroke, which can entail significant morbidity and mortality, the authors noted.
IVDU is a risk factor for endocarditis. In the context of the opioid epidemic, Dr. Nimjee and colleagues sought to compare the risk for stroke among patients with endocarditis from IVDU with the risk among patients with endocarditis from other causes.
They retrospectively studied patients who had undergone treatment for infective endocarditis at Wexner Medical Center between Jan. 1, 2014, and July 1, 2018. They examined patients’ concomitant intravenous drug abuse and evaluated demographics, risk factors, and associated costs.
Dramatic increase
In all, 351 patients met the study’s inclusion criteria, and 170 (48%) had a history of IVDU-associated endocarditis. The incidence of patients with IVDU-associated endocarditis increased 630% from 2014 to 2018.
The prevalence of overall intracranial hemorrhage was increased among patients with IVDU, compared with those without (25.9% vs. 13.9%; P = .005).
This increase in prevalence included increases in intraparenchymal hemorrhage (12.4% vs. 5.1%; P = .012), subarachnoid hemorrhage (17.6% vs. 4.4%; P = .0001), and cerebral microbleeds (14.1% vs. 7.2%; P = .022).
IVDU also was associated with an increase in prevalence of infectious intracranial aneurysm (10.6% vs. 1.8%; P = .0001) and brain abscess (4.7% vs. 1.1%; P = .025).
Compared with patients with endocarditis from other causes, significantly higher numbers of patients with IVDU-associated endocarditis were homeless (5.9% vs. 1.1%; P = .014), uninsured (10.0% vs. 2.8%; P = .005), and unemployed (75.9% vs. 31.7%; P = .0001).
Medical costs were more than twice as high among patients with endocarditis from IVDU than among those with endocarditis from other causes. The difference in health care costs during admission per patient was more than $100,000.
“The wider societal impact of the opioid epidemic is not well understood,” Dr. Nimjee said in the press release. “Our research suggests that the impact of the opioid epidemic is far-reaching and contributes to increased costs in the criminal justice, health care systems, and the workplace. The increased costs can be particularly substantial for stroke care.”
Nationwide data desirable
“Past publications from the U.S. have shown an increase in incidence of IVDU-related endocarditis, and the current publication emphasizes this worrying trend,” Manuel Bolognese, MD, head of the stroke center at the Lucerne (Switzerland) Cantonal Hospital, said in an interview. “The higher degree of hemorrhagic strokes and brain abscesses as further complications is alarming as well and shows that IVDU-related endocarditis is becoming a more and more relevant medical problem in the U.S., with high morbidity and mortality.”
The study period is long enough to show a clear trend of increasing incidence of IVDU-related endocarditis, Dr. Bolognese said. The study’s biggest weaknesses are its retrospective design and restriction to a single center.
“Without knowing the prevalence of drug abuse and the socioeconomical situation in Columbus, it is difficult to generalize these findings to other regions in the U.S.A. or even abroad,” he said.
Also, the abstract does not provide some essential information, said Dr. Bolognese. It would be important to know which valve was affected in each patient, which bacteria were identified, whether patients also used nonopioid drugs, and what each patient’s immune status was.
A lack of sterile material such as syringes could explain the apparent association between IVDU-associated endocarditis and low socioeconomic status, said Dr. Bolognese. Delayed presentation to medical institutions because of a lack of insurance could have led to a more complicated course.
“It would be interesting to see numbers from a broader spectrum in a nationwide registry,” said Dr. Bolognese. “It might be worth studying interventions to improve the hygienic aspects (like supply of sterile material, especially in the most vulnerable groups, like homeless people) or to provide easier access to emergency health care despite lack of insurance, which could decrease the incidence of IVDU.”
Dr. Nimjee and Dr. Bolognese disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.