User login
Advocate for legislation to improve, protect LGBTQ lives
In January in many states, the start of a new year also means the start of a new legislative session. For LGBTQ youth and their families, these sessions can create a significant amount of anxiety, as legislators in several states introduce legislation to curtail the rights of this population. In some cases, legislators have attempted to criminalize the provision of gender-affirming medical care to the trans and gender-diverse adolescents that many of us provide care to on a daily basis. As pediatricians,
2020 started on a positive note for LGBTQ children and adolescents, with Virginia becoming the 20th state to ban conversion therapy for minors. Legislation was introduced in several other states to prohibit this practice, including Kentucky, Missouri, and Ohio, and but they ultimately died in committee or were never referred. While there is not yet a nationwide ban on conversion therapy, legislation was introduced in the last three U.S. Congress sessions to ban this harmful practice. In June 2020, the Supreme Court decision in Bostock vs. Clayton County stated that employers could not fire an employee solely because of that person’s sexual orientation and/or gender identity.
However, 19 separate bills were introduced in 2020 alone in states across the United States that would prohibit gender-affirming care for adolescents under age 18.1 Many of these bills also would make the provision of gender-affirming medical care codified as felony child abuse, with loss of licensure, fines and/or jail time a possibility for physicians who prescribe hormones or puberty blockers for gender-affirming care to minors. Fortunately, these bills either died in committee or never had a hearing. However, legislation has been prefiled in several states for their 2021 session to again attempt to prohibit minors from obtaining gender-affirming medical care and/or criminalizing the provision of this care by physicians. Other bills were filed or have been prefiled again to allow various medical and mental health providers to refuse to treat LGBTQ patients because of their personal religious beliefs and/or forcing these same providers to tell a parent if a minor reveals to that provider that they are LGBTQ.
Even if this legislation does not pass or get a hearing, the fact that the bills were introduced can have a profound impact on LGBTQ patients and their families. After a bill was introduced in Texas in their 2017 legislative session that would require trans and gender-diverse (TGD) people to use the bathroom based on their sex assigned at birth, the Trevor Project reported that it had an increase of 34% in crisis calls from trans youth who were in distress.2 This was similar, but slightly less, than was reported by the Trevor Project in September 2015 when in the run-up to a vote on Houston’s Equal Rights Ordinance, advertising was run equating trans women as predators who could be lying in wait in bathrooms. On the converse, when LGBTQ youth feel supported in the media, courts, and legislatures, this can have a positive impact on their mental health. A 2017 study found that, in states who enacted same-sex marriage laws prior to the 2015 Supreme Court decision in Obergefell, compared with those who did not, there was a 7% relative reduction in the proportion of high school students who attempted suicide.3
The American Academy of Pediatrics published its policy statement in September 2018 outlining suggestions for pediatricians to provide support to TGD youth.4 In this position statement, recommendation No. 7 states “that pediatricians have a role in advocating for policies and laws that protect youth who identify as TGD from discrimination and violence.” Therefore, it is incumbent upon us to use our voices to support our LGBTQ youth. In 2020, several pediatricians from the South Dakota chapter of the AAP provided testimony – and organized public rallies – against legislation in that state which would have made gender-affirming care to minors under age 16 punishable by a fine and/or up to 10 years in prison.5

So what can you do? First, get to know your local and state legislators. While it was difficult to meet them in person for much of 2020, you can always call their district and/or Capitol offices, email them, or fill out their constituent contact form typically found on their website. Let them know that you oppose bills which introduce discrimination against your LGBTQ patients or threaten to criminalize the care that you provide to these patients.
Second, work with your state medical association or state AAP chapter to encourage them to oppose these harmful laws and support laws that improve the lives of LGBTQ patients. Third, you can write op-eds to your local newspaper, expressing your support for your patients and outlining the detrimental effects that anti-LGBTQ laws have on your patients. Lastly, you can be active on Twitter, Facebook, or other social media platforms sharing stories of how harmful or helpful certain pieces of legislation can be for your patients.
Dr. Cooper is assistant professor of pediatrics at the University of Texas, Dallas, and an adolescent medicine specialist at Children’s Medical Center Dallas. He has no relevant financial disclosures. Email Dr. Cooper at [email protected].
References
1. “Leglislation affecting LGBT rights across country.” www.aclu.org.
2. “Bathroom Bills Fuel Spike In Calls From Trans Youth To Suicide Hotline.” www.outsmartmagazine.com. 2017 Aug.
3. JAMA Pediatr. 2017 Apr 1. doi: 10.1001/jamapediatrics.2016.4529.
4. Pediatrics. 2018 Oct. doi: 10.1542/peds.2018-2162.
5. Wyckoff AS. “State bills seek to place limits on transgender care, ‘punish’ physicians.” AAP News. 2020 Feb 18.
In January in many states, the start of a new year also means the start of a new legislative session. For LGBTQ youth and their families, these sessions can create a significant amount of anxiety, as legislators in several states introduce legislation to curtail the rights of this population. In some cases, legislators have attempted to criminalize the provision of gender-affirming medical care to the trans and gender-diverse adolescents that many of us provide care to on a daily basis. As pediatricians,
2020 started on a positive note for LGBTQ children and adolescents, with Virginia becoming the 20th state to ban conversion therapy for minors. Legislation was introduced in several other states to prohibit this practice, including Kentucky, Missouri, and Ohio, and but they ultimately died in committee or were never referred. While there is not yet a nationwide ban on conversion therapy, legislation was introduced in the last three U.S. Congress sessions to ban this harmful practice. In June 2020, the Supreme Court decision in Bostock vs. Clayton County stated that employers could not fire an employee solely because of that person’s sexual orientation and/or gender identity.
However, 19 separate bills were introduced in 2020 alone in states across the United States that would prohibit gender-affirming care for adolescents under age 18.1 Many of these bills also would make the provision of gender-affirming medical care codified as felony child abuse, with loss of licensure, fines and/or jail time a possibility for physicians who prescribe hormones or puberty blockers for gender-affirming care to minors. Fortunately, these bills either died in committee or never had a hearing. However, legislation has been prefiled in several states for their 2021 session to again attempt to prohibit minors from obtaining gender-affirming medical care and/or criminalizing the provision of this care by physicians. Other bills were filed or have been prefiled again to allow various medical and mental health providers to refuse to treat LGBTQ patients because of their personal religious beliefs and/or forcing these same providers to tell a parent if a minor reveals to that provider that they are LGBTQ.
Even if this legislation does not pass or get a hearing, the fact that the bills were introduced can have a profound impact on LGBTQ patients and their families. After a bill was introduced in Texas in their 2017 legislative session that would require trans and gender-diverse (TGD) people to use the bathroom based on their sex assigned at birth, the Trevor Project reported that it had an increase of 34% in crisis calls from trans youth who were in distress.2 This was similar, but slightly less, than was reported by the Trevor Project in September 2015 when in the run-up to a vote on Houston’s Equal Rights Ordinance, advertising was run equating trans women as predators who could be lying in wait in bathrooms. On the converse, when LGBTQ youth feel supported in the media, courts, and legislatures, this can have a positive impact on their mental health. A 2017 study found that, in states who enacted same-sex marriage laws prior to the 2015 Supreme Court decision in Obergefell, compared with those who did not, there was a 7% relative reduction in the proportion of high school students who attempted suicide.3
The American Academy of Pediatrics published its policy statement in September 2018 outlining suggestions for pediatricians to provide support to TGD youth.4 In this position statement, recommendation No. 7 states “that pediatricians have a role in advocating for policies and laws that protect youth who identify as TGD from discrimination and violence.” Therefore, it is incumbent upon us to use our voices to support our LGBTQ youth. In 2020, several pediatricians from the South Dakota chapter of the AAP provided testimony – and organized public rallies – against legislation in that state which would have made gender-affirming care to minors under age 16 punishable by a fine and/or up to 10 years in prison.5
So what can you do? First, get to know your local and state legislators. While it was difficult to meet them in person for much of 2020, you can always call their district and/or Capitol offices, email them, or fill out their constituent contact form typically found on their website. Let them know that you oppose bills which introduce discrimination against your LGBTQ patients or threaten to criminalize the care that you provide to these patients.
Second, work with your state medical association or state AAP chapter to encourage them to oppose these harmful laws and support laws that improve the lives of LGBTQ patients. Third, you can write op-eds to your local newspaper, expressing your support for your patients and outlining the detrimental effects that anti-LGBTQ laws have on your patients. Lastly, you can be active on Twitter, Facebook, or other social media platforms sharing stories of how harmful or helpful certain pieces of legislation can be for your patients.
Dr. Cooper is assistant professor of pediatrics at the University of Texas, Dallas, and an adolescent medicine specialist at Children’s Medical Center Dallas. He has no relevant financial disclosures. Email Dr. Cooper at [email protected].
References
1. “Leglislation affecting LGBT rights across country.” www.aclu.org.
2. “Bathroom Bills Fuel Spike In Calls From Trans Youth To Suicide Hotline.” www.outsmartmagazine.com. 2017 Aug.
3. JAMA Pediatr. 2017 Apr 1. doi: 10.1001/jamapediatrics.2016.4529.
4. Pediatrics. 2018 Oct. doi: 10.1542/peds.2018-2162.
5. Wyckoff AS. “State bills seek to place limits on transgender care, ‘punish’ physicians.” AAP News. 2020 Feb 18.
In January in many states, the start of a new year also means the start of a new legislative session. For LGBTQ youth and their families, these sessions can create a significant amount of anxiety, as legislators in several states introduce legislation to curtail the rights of this population. In some cases, legislators have attempted to criminalize the provision of gender-affirming medical care to the trans and gender-diverse adolescents that many of us provide care to on a daily basis. As pediatricians,
2020 started on a positive note for LGBTQ children and adolescents, with Virginia becoming the 20th state to ban conversion therapy for minors. Legislation was introduced in several other states to prohibit this practice, including Kentucky, Missouri, and Ohio, and but they ultimately died in committee or were never referred. While there is not yet a nationwide ban on conversion therapy, legislation was introduced in the last three U.S. Congress sessions to ban this harmful practice. In June 2020, the Supreme Court decision in Bostock vs. Clayton County stated that employers could not fire an employee solely because of that person’s sexual orientation and/or gender identity.
However, 19 separate bills were introduced in 2020 alone in states across the United States that would prohibit gender-affirming care for adolescents under age 18.1 Many of these bills also would make the provision of gender-affirming medical care codified as felony child abuse, with loss of licensure, fines and/or jail time a possibility for physicians who prescribe hormones or puberty blockers for gender-affirming care to minors. Fortunately, these bills either died in committee or never had a hearing. However, legislation has been prefiled in several states for their 2021 session to again attempt to prohibit minors from obtaining gender-affirming medical care and/or criminalizing the provision of this care by physicians. Other bills were filed or have been prefiled again to allow various medical and mental health providers to refuse to treat LGBTQ patients because of their personal religious beliefs and/or forcing these same providers to tell a parent if a minor reveals to that provider that they are LGBTQ.
Even if this legislation does not pass or get a hearing, the fact that the bills were introduced can have a profound impact on LGBTQ patients and their families. After a bill was introduced in Texas in their 2017 legislative session that would require trans and gender-diverse (TGD) people to use the bathroom based on their sex assigned at birth, the Trevor Project reported that it had an increase of 34% in crisis calls from trans youth who were in distress.2 This was similar, but slightly less, than was reported by the Trevor Project in September 2015 when in the run-up to a vote on Houston’s Equal Rights Ordinance, advertising was run equating trans women as predators who could be lying in wait in bathrooms. On the converse, when LGBTQ youth feel supported in the media, courts, and legislatures, this can have a positive impact on their mental health. A 2017 study found that, in states who enacted same-sex marriage laws prior to the 2015 Supreme Court decision in Obergefell, compared with those who did not, there was a 7% relative reduction in the proportion of high school students who attempted suicide.3
The American Academy of Pediatrics published its policy statement in September 2018 outlining suggestions for pediatricians to provide support to TGD youth.4 In this position statement, recommendation No. 7 states “that pediatricians have a role in advocating for policies and laws that protect youth who identify as TGD from discrimination and violence.” Therefore, it is incumbent upon us to use our voices to support our LGBTQ youth. In 2020, several pediatricians from the South Dakota chapter of the AAP provided testimony – and organized public rallies – against legislation in that state which would have made gender-affirming care to minors under age 16 punishable by a fine and/or up to 10 years in prison.5
So what can you do? First, get to know your local and state legislators. While it was difficult to meet them in person for much of 2020, you can always call their district and/or Capitol offices, email them, or fill out their constituent contact form typically found on their website. Let them know that you oppose bills which introduce discrimination against your LGBTQ patients or threaten to criminalize the care that you provide to these patients.
Second, work with your state medical association or state AAP chapter to encourage them to oppose these harmful laws and support laws that improve the lives of LGBTQ patients. Third, you can write op-eds to your local newspaper, expressing your support for your patients and outlining the detrimental effects that anti-LGBTQ laws have on your patients. Lastly, you can be active on Twitter, Facebook, or other social media platforms sharing stories of how harmful or helpful certain pieces of legislation can be for your patients.
Dr. Cooper is assistant professor of pediatrics at the University of Texas, Dallas, and an adolescent medicine specialist at Children’s Medical Center Dallas. He has no relevant financial disclosures. Email Dr. Cooper at [email protected].
References
1. “Leglislation affecting LGBT rights across country.” www.aclu.org.
2. “Bathroom Bills Fuel Spike In Calls From Trans Youth To Suicide Hotline.” www.outsmartmagazine.com. 2017 Aug.
3. JAMA Pediatr. 2017 Apr 1. doi: 10.1001/jamapediatrics.2016.4529.
4. Pediatrics. 2018 Oct. doi: 10.1542/peds.2018-2162.
5. Wyckoff AS. “State bills seek to place limits on transgender care, ‘punish’ physicians.” AAP News. 2020 Feb 18.

FDA approves liraglutide for adolescents with obesity
The Food and Drug Administration’s new indication for liraglutide (Saxenda) for weight loss in adolescents with obesity, announced on Dec. 4, received welcome as a milestone for advancing a field that’s seen no new drug options since 2003 and boosted by 50% the list of agents indicated for weight loss in this age group.

But liraglutide’s track record in adolescents in the key study published earlier in 2020 left some experts unconvinced that liraglutide’s modest effects would have much impact on blunting the expanding cohort of teens who are obese.
“Until now, we’ve had phentermine and orlistat with FDA approval” for adolescents with obesity, and phentermine’s label specifies only patients older than 16 years. “It’s important that the FDA deemed liraglutide’s benefits greater than its risks for adolescents,” said Aaron S. Kelly, PhD, leader of the 82-week, multicenter, randomized study of liraglutide in 251 adolescents with obesity that directly led to the FDA’s action.
“We have results from a strong, published randomized trial, and the green light from the FDA, and that should give clinicians reassurance and confidence to use liraglutide clinically,” said Dr. Kelly, professor of pediatrics and codirector of the Center for Pediatric Obesity Medicine at the University of Minnesota in Minneapolis.
An ‘unimpressive’ drop in BMI
Sonia Caprio, MD, had a more skeptical take on liraglutide’s role with its new indication: “Approval of higher-dose liraglutide is an improvement that reflects a willingness to accept adolescent obesity as a disease that needs treatment with pharmacological agents. However, the study, published in New England Journal of Medicine, was not impressive in terms of weight loss, and more importantly liraglutide was not associated with any significant changes in metabolic markers” such as insulin resistance, high-sensitivity C-reactive protein, lipoproteins and triglycerides, and hemoglobin A1c.
The observed average 5% drop in body mass index seen after a year on liraglutide treatment, compared with baseline and relative to no average change from baseline in the placebo arm, was “totally insufficient, and will not diminish any of the metabolic complications in youth with obesity,” commented Dr. Caprio, an endocrinologist and professor of pediatrics at Yale University in New Haven, Conn.
Results from the study led by Dr. Kelly also showed that liraglutide for 56 weeks cut BMI by 5% in 43% of patients, and by 10% in 26%, compared with respective rates of 19% and 8% among those in the placebo-control arm. He took a more expansive view of the potential benefits from weight loss of the caliber demonstrated by liraglutide in the study.
“In general, we wait too long with obesity in children; the earlier the intervention the better. A 3% or 4% reduction in BMI at 12 or 13 years old can pay big dividends down the road” when a typical adolescent trajectory of steadily rising weight can be flattened, he said in an interview.
Bariatric and metabolic surgery, although highly effective and usually safe, is seen by many clinicians, patients, and families as an “intervention of last resort,” and its very low level of uptake in adolescents bears witness to that reputation. It also creates an important niche for safe and effective drugs to fill as an adjunct to lifestyle changes, which are often ineffective when used by themselves. Liraglutide’s main mechanism for weight loss is depressing hunger, Dr. Kelly noted.
Existing meds have limitations
The existing medical treatments, orlistat and phentermine, both have significant drawbacks that limit their use. Orlistat (Xenical, Alli), FDA approved for adolescents 12-16 years old since 2003, limits intestinal fat absorption and as a result often produces unwanted GI effects. Phentermine’s approval for older adolescents dates from 1959 and has a weak evidence base, its label limits it to “short-term” use that’s generally taken to mean a maximum of 12 weeks. And, as a stimulant, phentermine has often been regarded as potentially dangerous, although Dr. Kelly noted that stimulants are well-accepted treatments for other disorders in children and adolescents.
“The earlier we treat obesity in youth, the better, given that it tends to track into adulthood,” agreed Dr. Caprio. “However, it remains to be seen whether weight reduction with a pharmacological agent is going to help prevent the intractable trajectories of weight and its complications. So far, it looks like surgery may be more efficacious,” she said in an interview.
Another drawback for the near future with liraglutide will likely be its cost for many patients, more than $10,000/year at full retail prices for the weight-loss formulation, given that insurers have had a poor record of covering the drug for this indication in adults, both Dr. Caprio and Dr. Kelly noted.
Compliance with liraglutide is also important. Dr. Kelly’s study followed patients for their first 26 weeks off treatment after 56 weeks on the drug, and showed that on average weights rebounded to virtually baseline levels by 6 months after treatment stopped.
Obesity treatment lasts a lifetime
“Obesity is a chronic disease, that requires chronic treatment, just like hypertension,” Dr. Kelly stressed, and cited the rebound seen in his study when liraglutide stopped as further proof of that concept. “All obesity treatment is lifelong,” he maintained.
He highlighted the importance of clinicians discussing with adolescent patients and their families the prospect of potentially remaining on liraglutide treatment for years to maintain weight loss. His experience with the randomized study convinced him that many adolescents with obesity are amenable to daily subcutaneous injection using the pen device that liraglutide comes in, but he acknowledged that some teens find this off-putting.
For the near term, Dr. Kelly foresaw liraglutide treatment of adolescents as something that will mostly be administered to patients who seek care at centers that specialize in obesity management. “I’ll think we’ll eventually see it move to more primary care settings, but that will be down the road.”
The study of liraglutide in adolescents was sponsored by Novo Nordisk, the company that markets liraglutide (Saxenda). Dr. Kelly has been a consultant to Novo Nordisk and also to Orexigen Therapeutics, Vivus, and WW, and he has received research funding from AstraZeneca. Dr. Caprio had no disclosures.
The Food and Drug Administration’s new indication for liraglutide (Saxenda) for weight loss in adolescents with obesity, announced on Dec. 4, received welcome as a milestone for advancing a field that’s seen no new drug options since 2003 and boosted by 50% the list of agents indicated for weight loss in this age group.
But liraglutide’s track record in adolescents in the key study published earlier in 2020 left some experts unconvinced that liraglutide’s modest effects would have much impact on blunting the expanding cohort of teens who are obese.
“Until now, we’ve had phentermine and orlistat with FDA approval” for adolescents with obesity, and phentermine’s label specifies only patients older than 16 years. “It’s important that the FDA deemed liraglutide’s benefits greater than its risks for adolescents,” said Aaron S. Kelly, PhD, leader of the 82-week, multicenter, randomized study of liraglutide in 251 adolescents with obesity that directly led to the FDA’s action.
“We have results from a strong, published randomized trial, and the green light from the FDA, and that should give clinicians reassurance and confidence to use liraglutide clinically,” said Dr. Kelly, professor of pediatrics and codirector of the Center for Pediatric Obesity Medicine at the University of Minnesota in Minneapolis.
An ‘unimpressive’ drop in BMI
Sonia Caprio, MD, had a more skeptical take on liraglutide’s role with its new indication: “Approval of higher-dose liraglutide is an improvement that reflects a willingness to accept adolescent obesity as a disease that needs treatment with pharmacological agents. However, the study, published in New England Journal of Medicine, was not impressive in terms of weight loss, and more importantly liraglutide was not associated with any significant changes in metabolic markers” such as insulin resistance, high-sensitivity C-reactive protein, lipoproteins and triglycerides, and hemoglobin A1c.
The observed average 5% drop in body mass index seen after a year on liraglutide treatment, compared with baseline and relative to no average change from baseline in the placebo arm, was “totally insufficient, and will not diminish any of the metabolic complications in youth with obesity,” commented Dr. Caprio, an endocrinologist and professor of pediatrics at Yale University in New Haven, Conn.
Results from the study led by Dr. Kelly also showed that liraglutide for 56 weeks cut BMI by 5% in 43% of patients, and by 10% in 26%, compared with respective rates of 19% and 8% among those in the placebo-control arm. He took a more expansive view of the potential benefits from weight loss of the caliber demonstrated by liraglutide in the study.
“In general, we wait too long with obesity in children; the earlier the intervention the better. A 3% or 4% reduction in BMI at 12 or 13 years old can pay big dividends down the road” when a typical adolescent trajectory of steadily rising weight can be flattened, he said in an interview.
Bariatric and metabolic surgery, although highly effective and usually safe, is seen by many clinicians, patients, and families as an “intervention of last resort,” and its very low level of uptake in adolescents bears witness to that reputation. It also creates an important niche for safe and effective drugs to fill as an adjunct to lifestyle changes, which are often ineffective when used by themselves. Liraglutide’s main mechanism for weight loss is depressing hunger, Dr. Kelly noted.
Existing meds have limitations
The existing medical treatments, orlistat and phentermine, both have significant drawbacks that limit their use. Orlistat (Xenical, Alli), FDA approved for adolescents 12-16 years old since 2003, limits intestinal fat absorption and as a result often produces unwanted GI effects. Phentermine’s approval for older adolescents dates from 1959 and has a weak evidence base, its label limits it to “short-term” use that’s generally taken to mean a maximum of 12 weeks. And, as a stimulant, phentermine has often been regarded as potentially dangerous, although Dr. Kelly noted that stimulants are well-accepted treatments for other disorders in children and adolescents.
“The earlier we treat obesity in youth, the better, given that it tends to track into adulthood,” agreed Dr. Caprio. “However, it remains to be seen whether weight reduction with a pharmacological agent is going to help prevent the intractable trajectories of weight and its complications. So far, it looks like surgery may be more efficacious,” she said in an interview.
Another drawback for the near future with liraglutide will likely be its cost for many patients, more than $10,000/year at full retail prices for the weight-loss formulation, given that insurers have had a poor record of covering the drug for this indication in adults, both Dr. Caprio and Dr. Kelly noted.
Compliance with liraglutide is also important. Dr. Kelly’s study followed patients for their first 26 weeks off treatment after 56 weeks on the drug, and showed that on average weights rebounded to virtually baseline levels by 6 months after treatment stopped.
Obesity treatment lasts a lifetime
“Obesity is a chronic disease, that requires chronic treatment, just like hypertension,” Dr. Kelly stressed, and cited the rebound seen in his study when liraglutide stopped as further proof of that concept. “All obesity treatment is lifelong,” he maintained.
He highlighted the importance of clinicians discussing with adolescent patients and their families the prospect of potentially remaining on liraglutide treatment for years to maintain weight loss. His experience with the randomized study convinced him that many adolescents with obesity are amenable to daily subcutaneous injection using the pen device that liraglutide comes in, but he acknowledged that some teens find this off-putting.
For the near term, Dr. Kelly foresaw liraglutide treatment of adolescents as something that will mostly be administered to patients who seek care at centers that specialize in obesity management. “I’ll think we’ll eventually see it move to more primary care settings, but that will be down the road.”
The study of liraglutide in adolescents was sponsored by Novo Nordisk, the company that markets liraglutide (Saxenda). Dr. Kelly has been a consultant to Novo Nordisk and also to Orexigen Therapeutics, Vivus, and WW, and he has received research funding from AstraZeneca. Dr. Caprio had no disclosures.
The Food and Drug Administration’s new indication for liraglutide (Saxenda) for weight loss in adolescents with obesity, announced on Dec. 4, received welcome as a milestone for advancing a field that’s seen no new drug options since 2003 and boosted by 50% the list of agents indicated for weight loss in this age group.
But liraglutide’s track record in adolescents in the key study published earlier in 2020 left some experts unconvinced that liraglutide’s modest effects would have much impact on blunting the expanding cohort of teens who are obese.
“Until now, we’ve had phentermine and orlistat with FDA approval” for adolescents with obesity, and phentermine’s label specifies only patients older than 16 years. “It’s important that the FDA deemed liraglutide’s benefits greater than its risks for adolescents,” said Aaron S. Kelly, PhD, leader of the 82-week, multicenter, randomized study of liraglutide in 251 adolescents with obesity that directly led to the FDA’s action.
“We have results from a strong, published randomized trial, and the green light from the FDA, and that should give clinicians reassurance and confidence to use liraglutide clinically,” said Dr. Kelly, professor of pediatrics and codirector of the Center for Pediatric Obesity Medicine at the University of Minnesota in Minneapolis.
An ‘unimpressive’ drop in BMI
Sonia Caprio, MD, had a more skeptical take on liraglutide’s role with its new indication: “Approval of higher-dose liraglutide is an improvement that reflects a willingness to accept adolescent obesity as a disease that needs treatment with pharmacological agents. However, the study, published in New England Journal of Medicine, was not impressive in terms of weight loss, and more importantly liraglutide was not associated with any significant changes in metabolic markers” such as insulin resistance, high-sensitivity C-reactive protein, lipoproteins and triglycerides, and hemoglobin A1c.
The observed average 5% drop in body mass index seen after a year on liraglutide treatment, compared with baseline and relative to no average change from baseline in the placebo arm, was “totally insufficient, and will not diminish any of the metabolic complications in youth with obesity,” commented Dr. Caprio, an endocrinologist and professor of pediatrics at Yale University in New Haven, Conn.
Results from the study led by Dr. Kelly also showed that liraglutide for 56 weeks cut BMI by 5% in 43% of patients, and by 10% in 26%, compared with respective rates of 19% and 8% among those in the placebo-control arm. He took a more expansive view of the potential benefits from weight loss of the caliber demonstrated by liraglutide in the study.
“In general, we wait too long with obesity in children; the earlier the intervention the better. A 3% or 4% reduction in BMI at 12 or 13 years old can pay big dividends down the road” when a typical adolescent trajectory of steadily rising weight can be flattened, he said in an interview.
Bariatric and metabolic surgery, although highly effective and usually safe, is seen by many clinicians, patients, and families as an “intervention of last resort,” and its very low level of uptake in adolescents bears witness to that reputation. It also creates an important niche for safe and effective drugs to fill as an adjunct to lifestyle changes, which are often ineffective when used by themselves. Liraglutide’s main mechanism for weight loss is depressing hunger, Dr. Kelly noted.
Existing meds have limitations
The existing medical treatments, orlistat and phentermine, both have significant drawbacks that limit their use. Orlistat (Xenical, Alli), FDA approved for adolescents 12-16 years old since 2003, limits intestinal fat absorption and as a result often produces unwanted GI effects. Phentermine’s approval for older adolescents dates from 1959 and has a weak evidence base, its label limits it to “short-term” use that’s generally taken to mean a maximum of 12 weeks. And, as a stimulant, phentermine has often been regarded as potentially dangerous, although Dr. Kelly noted that stimulants are well-accepted treatments for other disorders in children and adolescents.
“The earlier we treat obesity in youth, the better, given that it tends to track into adulthood,” agreed Dr. Caprio. “However, it remains to be seen whether weight reduction with a pharmacological agent is going to help prevent the intractable trajectories of weight and its complications. So far, it looks like surgery may be more efficacious,” she said in an interview.
Another drawback for the near future with liraglutide will likely be its cost for many patients, more than $10,000/year at full retail prices for the weight-loss formulation, given that insurers have had a poor record of covering the drug for this indication in adults, both Dr. Caprio and Dr. Kelly noted.
Compliance with liraglutide is also important. Dr. Kelly’s study followed patients for their first 26 weeks off treatment after 56 weeks on the drug, and showed that on average weights rebounded to virtually baseline levels by 6 months after treatment stopped.
Obesity treatment lasts a lifetime
“Obesity is a chronic disease, that requires chronic treatment, just like hypertension,” Dr. Kelly stressed, and cited the rebound seen in his study when liraglutide stopped as further proof of that concept. “All obesity treatment is lifelong,” he maintained.
He highlighted the importance of clinicians discussing with adolescent patients and their families the prospect of potentially remaining on liraglutide treatment for years to maintain weight loss. His experience with the randomized study convinced him that many adolescents with obesity are amenable to daily subcutaneous injection using the pen device that liraglutide comes in, but he acknowledged that some teens find this off-putting.
For the near term, Dr. Kelly foresaw liraglutide treatment of adolescents as something that will mostly be administered to patients who seek care at centers that specialize in obesity management. “I’ll think we’ll eventually see it move to more primary care settings, but that will be down the road.”
The study of liraglutide in adolescents was sponsored by Novo Nordisk, the company that markets liraglutide (Saxenda). Dr. Kelly has been a consultant to Novo Nordisk and also to Orexigen Therapeutics, Vivus, and WW, and he has received research funding from AstraZeneca. Dr. Caprio had no disclosures.

New tool may provide point-of-care differentiation between bacterial, viral infections
The World Health Organization estimates that 14.9 million of 57 million annual deaths worldwide (25%) are related directly to diseases caused by bacterial and/or viral infections.

The first crucial step in order to build a successful surveillance system is to accurately identify and diagnose disease, Ivana Pennisi reminded the audience at the annual meeting of the European Society for Paediatric Infectious Diseases, held virtually this year. A problem, particularly in primary care, is differentiating between patients with bacterial infections who might benefit from antibiotics and those with viral infections where supportive treatment is generally required. One solution might a rapid point-of-care tool.
Ms. Pennisi described early experiences of using microchip technology to detect RNA biomarkers in the blood rather than look for the pathogen itself. Early results suggest high diagnostic accuracy at low cost.
It is known that when a bacteria or virus enters the body, it stimulates the immune system in a unique way leading to the expression of different genes in the host blood. As part of the Personalized Management of Febrile Illnesses study, researchers have demonstrated a number of high correlated transcripts. Of current interest are two genes which are upregulated in childhood febrile illnesses.
Ms. Pennisi, a PhD student working as part of a multidisciplinary at the department of infectious disease and Centre for Bioinspired Technology at Imperial College, London, developed loop-mediated isothermal amplification (LAMP) assays to detect for the first time host RNA signatures on a nucleic acid–based point-of-care handheld system to discriminate bacterial from viral infection. The amplification reaction is then combined with microchip technology in the well of a portable point-of-care device named Lacewing. It translates the nucleic acid amplification signal into a quantitative electrochemical signal without the need for a thermal cycler.
The combination of genomic expertise in the section of paediatrics lead by Michael Levin, PhD, and microchip-based technologies in the department of electrical and electronic engineering under the guidance of Pantelis Georgiou, PhD, enabled the team overcome many clinical challenges.
Ms. Pennisi presented her team’s early experiences with clinical samples from 455 febrile children. First, transcription isothermal amplification techniques were employed to confirm bacterial and viral infections. Results were then validated using standard fluorescent-based quantitative polymerase chain reaction (PCR) instruments. In order to define a decision boundary between bacterial and viral patients, cutoff levels were determined using multivariate logistic regression analysis. Results then were evaluated using microarrays, reverse transcriptase PCR (RT-PCR), and the eLAMP to confirm comparability with preferred techniques.
In conclusion, Ms. Pennisi reported that the two-gene signature combined with the use of eLAMP technology in She outlined her vision for the future: “The patient sample and reagent are loaded into a disposable cartridge. This is then placed into a device to monitor in real time the reaction and share all the data via a Bluetooth to a dedicated app on a smart phone. All data and location of the outbreak are then stored in [the] cloud, making it easier for epidemiological studies and tracking of new outbreaks. We hope that by enhancing the capability of our platform, we contribute to better patient care.”
“Distinguishing between bacterial and viral infections remains one of the key questions in the daily pediatric acute care,” commented Lauri Ivaska, MD, from the department of pediatrics and adolescent medicine at Turku (Finland) University Hospital. “One of the most promising laboratory methods to do this is by measuring quantities of two specific host RNA transcripts from a blood sample. It would be of great importance if this could be done reliably by using a fast and cheap method as presented here by Ivana Pennisi.”
Ms. Pennisi had no relevant financial disclosures.
The World Health Organization estimates that 14.9 million of 57 million annual deaths worldwide (25%) are related directly to diseases caused by bacterial and/or viral infections.
The first crucial step in order to build a successful surveillance system is to accurately identify and diagnose disease, Ivana Pennisi reminded the audience at the annual meeting of the European Society for Paediatric Infectious Diseases, held virtually this year. A problem, particularly in primary care, is differentiating between patients with bacterial infections who might benefit from antibiotics and those with viral infections where supportive treatment is generally required. One solution might a rapid point-of-care tool.
Ms. Pennisi described early experiences of using microchip technology to detect RNA biomarkers in the blood rather than look for the pathogen itself. Early results suggest high diagnostic accuracy at low cost.
It is known that when a bacteria or virus enters the body, it stimulates the immune system in a unique way leading to the expression of different genes in the host blood. As part of the Personalized Management of Febrile Illnesses study, researchers have demonstrated a number of high correlated transcripts. Of current interest are two genes which are upregulated in childhood febrile illnesses.
Ms. Pennisi, a PhD student working as part of a multidisciplinary at the department of infectious disease and Centre for Bioinspired Technology at Imperial College, London, developed loop-mediated isothermal amplification (LAMP) assays to detect for the first time host RNA signatures on a nucleic acid–based point-of-care handheld system to discriminate bacterial from viral infection. The amplification reaction is then combined with microchip technology in the well of a portable point-of-care device named Lacewing. It translates the nucleic acid amplification signal into a quantitative electrochemical signal without the need for a thermal cycler.
The combination of genomic expertise in the section of paediatrics lead by Michael Levin, PhD, and microchip-based technologies in the department of electrical and electronic engineering under the guidance of Pantelis Georgiou, PhD, enabled the team overcome many clinical challenges.
Ms. Pennisi presented her team’s early experiences with clinical samples from 455 febrile children. First, transcription isothermal amplification techniques were employed to confirm bacterial and viral infections. Results were then validated using standard fluorescent-based quantitative polymerase chain reaction (PCR) instruments. In order to define a decision boundary between bacterial and viral patients, cutoff levels were determined using multivariate logistic regression analysis. Results then were evaluated using microarrays, reverse transcriptase PCR (RT-PCR), and the eLAMP to confirm comparability with preferred techniques.
In conclusion, Ms. Pennisi reported that the two-gene signature combined with the use of eLAMP technology in She outlined her vision for the future: “The patient sample and reagent are loaded into a disposable cartridge. This is then placed into a device to monitor in real time the reaction and share all the data via a Bluetooth to a dedicated app on a smart phone. All data and location of the outbreak are then stored in [the] cloud, making it easier for epidemiological studies and tracking of new outbreaks. We hope that by enhancing the capability of our platform, we contribute to better patient care.”
“Distinguishing between bacterial and viral infections remains one of the key questions in the daily pediatric acute care,” commented Lauri Ivaska, MD, from the department of pediatrics and adolescent medicine at Turku (Finland) University Hospital. “One of the most promising laboratory methods to do this is by measuring quantities of two specific host RNA transcripts from a blood sample. It would be of great importance if this could be done reliably by using a fast and cheap method as presented here by Ivana Pennisi.”
Ms. Pennisi had no relevant financial disclosures.
The World Health Organization estimates that 14.9 million of 57 million annual deaths worldwide (25%) are related directly to diseases caused by bacterial and/or viral infections.
The first crucial step in order to build a successful surveillance system is to accurately identify and diagnose disease, Ivana Pennisi reminded the audience at the annual meeting of the European Society for Paediatric Infectious Diseases, held virtually this year. A problem, particularly in primary care, is differentiating between patients with bacterial infections who might benefit from antibiotics and those with viral infections where supportive treatment is generally required. One solution might a rapid point-of-care tool.
Ms. Pennisi described early experiences of using microchip technology to detect RNA biomarkers in the blood rather than look for the pathogen itself. Early results suggest high diagnostic accuracy at low cost.
It is known that when a bacteria or virus enters the body, it stimulates the immune system in a unique way leading to the expression of different genes in the host blood. As part of the Personalized Management of Febrile Illnesses study, researchers have demonstrated a number of high correlated transcripts. Of current interest are two genes which are upregulated in childhood febrile illnesses.
Ms. Pennisi, a PhD student working as part of a multidisciplinary at the department of infectious disease and Centre for Bioinspired Technology at Imperial College, London, developed loop-mediated isothermal amplification (LAMP) assays to detect for the first time host RNA signatures on a nucleic acid–based point-of-care handheld system to discriminate bacterial from viral infection. The amplification reaction is then combined with microchip technology in the well of a portable point-of-care device named Lacewing. It translates the nucleic acid amplification signal into a quantitative electrochemical signal without the need for a thermal cycler.
The combination of genomic expertise in the section of paediatrics lead by Michael Levin, PhD, and microchip-based technologies in the department of electrical and electronic engineering under the guidance of Pantelis Georgiou, PhD, enabled the team overcome many clinical challenges.
Ms. Pennisi presented her team’s early experiences with clinical samples from 455 febrile children. First, transcription isothermal amplification techniques were employed to confirm bacterial and viral infections. Results were then validated using standard fluorescent-based quantitative polymerase chain reaction (PCR) instruments. In order to define a decision boundary between bacterial and viral patients, cutoff levels were determined using multivariate logistic regression analysis. Results then were evaluated using microarrays, reverse transcriptase PCR (RT-PCR), and the eLAMP to confirm comparability with preferred techniques.
In conclusion, Ms. Pennisi reported that the two-gene signature combined with the use of eLAMP technology in She outlined her vision for the future: “The patient sample and reagent are loaded into a disposable cartridge. This is then placed into a device to monitor in real time the reaction and share all the data via a Bluetooth to a dedicated app on a smart phone. All data and location of the outbreak are then stored in [the] cloud, making it easier for epidemiological studies and tracking of new outbreaks. We hope that by enhancing the capability of our platform, we contribute to better patient care.”
“Distinguishing between bacterial and viral infections remains one of the key questions in the daily pediatric acute care,” commented Lauri Ivaska, MD, from the department of pediatrics and adolescent medicine at Turku (Finland) University Hospital. “One of the most promising laboratory methods to do this is by measuring quantities of two specific host RNA transcripts from a blood sample. It would be of great importance if this could be done reliably by using a fast and cheap method as presented here by Ivana Pennisi.”
Ms. Pennisi had no relevant financial disclosures.
FROM ESPID 2020
Three genes could predict congenital Zika infection susceptibility
Dr. Irene Rivero-Calle, MD, shared at the annual meeting of the European Society for Paediatric Infectious Diseases, held virtually this year.
ZIKV, an emerging flavivirus, is responsible for one the most critical pandemic emergencies of the last decade and has been associated with severe neonatal brain disabilities, declared Dr. Rivero-Calle, of the Hospital Clínico Universitario de Santiago de Compostela in Santiago de Compostela, Spain. “We think that understanding the genomic background could explain some of the most relevant symptoms of congenital Zika syndrome (CZS) and could be essential to better comprehend this disease.”
To achieve this understanding, Dr. Rivero-Calle and her colleagues conducted a study aiming to analyze any genetic factors that could explain the variation in phenotypes in newborns from mothers who had a Zika infection during their pregnancy. Additionally, they strove to “elucidate if the possible genetic association is specific to mothers or their newborns, and to check if this genomic background or any genomic ancestry pattern could be related with the phenotype,” she explained.
In their study, Dr. Rivero-Calle and her team analyzed 80 samples, comprising 40 samples from mothers who had been infected by ZIKV during their pregnancy and 40 from their newborns. Of those descendants, 20 were asymptomatic and 20 were symptomatic (13 had CZS, 3 had microcephaly, 2 had a pathologic MRI, 1 had hearing loss, and 1 was born preterm).
Population stratification, which Dr. Rivero-Calle explained “lets us know if the population is African, European, or Native American looking at the genes,” did not show any relation with the phenotype. We had a mixture of population genomics among all samples.”
Dr. Rivero-Calle and her team then performed three analyses: genotype analysis, an allelic test, and gene analysis. The allelic test and gene-collapsing method highlighted three genes (PANO1, PIDD1, and SLC25A22) as potential determinants of the varying phenotypes in the newborns from ZIKV-infected mothers. Overrepresentation analysis of gene ontology terms shows that PIDD1 and PANO1 are related to apoptosis and cell death, which is closely related to early infantile epilepsy. This could explain the most severe complications of CZS: seizures, brain damage, microcephaly, and detrimental neurodevelopmental growth. Regarding reactome and KEGG analysis, gene PIID1 is related with p53 pathway, which correlates with cell’s death and apoptosis, and with microcephaly, a typical phenotypic feature of CZS.
“So, in conclusion, we found three genes which could predict susceptibility to congenital Zika infection; we saw that the functionality of these genes seems to be deeply related with mechanisms which could explain the different phenotypes; and we saw that these three genes only appear in the children’s cohort, so there is no candidate gene in the mother’s genomic background which can help predict the phenotype of the newborn,” Dr. Rivero-Calle declared. “Finally, there is no ancestry pattern associated with disabilities caused by Zika infection.”
Dr. Rivero-Calle reported that this project (ZikAction) has received funding from the European Union’s Horizon 2020 research and innovation program, under grant agreement 734857.
Dr. Irene Rivero-Calle, MD, shared at the annual meeting of the European Society for Paediatric Infectious Diseases, held virtually this year.
ZIKV, an emerging flavivirus, is responsible for one the most critical pandemic emergencies of the last decade and has been associated with severe neonatal brain disabilities, declared Dr. Rivero-Calle, of the Hospital Clínico Universitario de Santiago de Compostela in Santiago de Compostela, Spain. “We think that understanding the genomic background could explain some of the most relevant symptoms of congenital Zika syndrome (CZS) and could be essential to better comprehend this disease.”
To achieve this understanding, Dr. Rivero-Calle and her colleagues conducted a study aiming to analyze any genetic factors that could explain the variation in phenotypes in newborns from mothers who had a Zika infection during their pregnancy. Additionally, they strove to “elucidate if the possible genetic association is specific to mothers or their newborns, and to check if this genomic background or any genomic ancestry pattern could be related with the phenotype,” she explained.
In their study, Dr. Rivero-Calle and her team analyzed 80 samples, comprising 40 samples from mothers who had been infected by ZIKV during their pregnancy and 40 from their newborns. Of those descendants, 20 were asymptomatic and 20 were symptomatic (13 had CZS, 3 had microcephaly, 2 had a pathologic MRI, 1 had hearing loss, and 1 was born preterm).
Population stratification, which Dr. Rivero-Calle explained “lets us know if the population is African, European, or Native American looking at the genes,” did not show any relation with the phenotype. We had a mixture of population genomics among all samples.”
Dr. Rivero-Calle and her team then performed three analyses: genotype analysis, an allelic test, and gene analysis. The allelic test and gene-collapsing method highlighted three genes (PANO1, PIDD1, and SLC25A22) as potential determinants of the varying phenotypes in the newborns from ZIKV-infected mothers. Overrepresentation analysis of gene ontology terms shows that PIDD1 and PANO1 are related to apoptosis and cell death, which is closely related to early infantile epilepsy. This could explain the most severe complications of CZS: seizures, brain damage, microcephaly, and detrimental neurodevelopmental growth. Regarding reactome and KEGG analysis, gene PIID1 is related with p53 pathway, which correlates with cell’s death and apoptosis, and with microcephaly, a typical phenotypic feature of CZS.
“So, in conclusion, we found three genes which could predict susceptibility to congenital Zika infection; we saw that the functionality of these genes seems to be deeply related with mechanisms which could explain the different phenotypes; and we saw that these three genes only appear in the children’s cohort, so there is no candidate gene in the mother’s genomic background which can help predict the phenotype of the newborn,” Dr. Rivero-Calle declared. “Finally, there is no ancestry pattern associated with disabilities caused by Zika infection.”
Dr. Rivero-Calle reported that this project (ZikAction) has received funding from the European Union’s Horizon 2020 research and innovation program, under grant agreement 734857.
Dr. Irene Rivero-Calle, MD, shared at the annual meeting of the European Society for Paediatric Infectious Diseases, held virtually this year.
ZIKV, an emerging flavivirus, is responsible for one the most critical pandemic emergencies of the last decade and has been associated with severe neonatal brain disabilities, declared Dr. Rivero-Calle, of the Hospital Clínico Universitario de Santiago de Compostela in Santiago de Compostela, Spain. “We think that understanding the genomic background could explain some of the most relevant symptoms of congenital Zika syndrome (CZS) and could be essential to better comprehend this disease.”
To achieve this understanding, Dr. Rivero-Calle and her colleagues conducted a study aiming to analyze any genetic factors that could explain the variation in phenotypes in newborns from mothers who had a Zika infection during their pregnancy. Additionally, they strove to “elucidate if the possible genetic association is specific to mothers or their newborns, and to check if this genomic background or any genomic ancestry pattern could be related with the phenotype,” she explained.
In their study, Dr. Rivero-Calle and her team analyzed 80 samples, comprising 40 samples from mothers who had been infected by ZIKV during their pregnancy and 40 from their newborns. Of those descendants, 20 were asymptomatic and 20 were symptomatic (13 had CZS, 3 had microcephaly, 2 had a pathologic MRI, 1 had hearing loss, and 1 was born preterm).
Population stratification, which Dr. Rivero-Calle explained “lets us know if the population is African, European, or Native American looking at the genes,” did not show any relation with the phenotype. We had a mixture of population genomics among all samples.”
Dr. Rivero-Calle and her team then performed three analyses: genotype analysis, an allelic test, and gene analysis. The allelic test and gene-collapsing method highlighted three genes (PANO1, PIDD1, and SLC25A22) as potential determinants of the varying phenotypes in the newborns from ZIKV-infected mothers. Overrepresentation analysis of gene ontology terms shows that PIDD1 and PANO1 are related to apoptosis and cell death, which is closely related to early infantile epilepsy. This could explain the most severe complications of CZS: seizures, brain damage, microcephaly, and detrimental neurodevelopmental growth. Regarding reactome and KEGG analysis, gene PIID1 is related with p53 pathway, which correlates with cell’s death and apoptosis, and with microcephaly, a typical phenotypic feature of CZS.
“So, in conclusion, we found three genes which could predict susceptibility to congenital Zika infection; we saw that the functionality of these genes seems to be deeply related with mechanisms which could explain the different phenotypes; and we saw that these three genes only appear in the children’s cohort, so there is no candidate gene in the mother’s genomic background which can help predict the phenotype of the newborn,” Dr. Rivero-Calle declared. “Finally, there is no ancestry pattern associated with disabilities caused by Zika infection.”
Dr. Rivero-Calle reported that this project (ZikAction) has received funding from the European Union’s Horizon 2020 research and innovation program, under grant agreement 734857.
FROM ESPID 2020
Children and school during the pandemic: What’s the answer?
Countries across the world are in the process of closing and reopening schools to contain the spread of COVID-19. Should there be universal testing and quarantining of sick school children and their classmates?
In a lively debate at the annual meeting of the European Society for Paediatric Infectious Diseases, held virtually this year, Andreea M. Panciu, MD, from the National Institute of Infectious Diseases in Bucharest, argued for routine testing and quarantining of all school children. Her opposite number, Danilo Buonsenso, MD, from the Centre for Global Health Research and Studies, Fondazione Policlinico Universitario Agostino Gemelli Istituto di Ricovero e Cura a Carattere Scientifico, Rome, made the case for a more selective approach.
Should children be sent to school?
stated Dr. Panciu as she started the debate by explaining the challenges faced by schools in adhering to key mitigation strategies. The U.S. Centers for Disease Control and Prevention recommends that students keep 1.8 m (6 feet) distance from one another. “In many school settings this is not feasible without drastically limiting the number of students,” she explained. “This is a massive challenge for many schools that are already overcrowded.”
The use of facemasks also is a challenge in classrooms. Children have a lower tolerance or may not be able to use the mask properly. There also are concerns regarding impaired learning, speech development, social development, and facial recognition. “We need to look at the evidence; preventive measures work,” responded Dr. Buonsenso. If distance can be implemented, the more distance the lower the transmission of infection, with 1.5-2 meters having the best effects. “Distance can be difficult when school buildings do not allow it, however, governments have had time to plan, and this should not be a limitation to education for kids.”
A recent review clearly showed that children and adolescents aged under 20 years have a much lower risk of susceptibility to COVID-19 infection, compared with adults. This is especially the case for children younger than 14 years. “There is no excuse, let’s bring the children back to school,” argued Dr. Buonsenso.
Dr. Panciu responded with several studies that have tried to quantify the amount of SARS-CoV-2 virus that is carried by infected children. Viral load in the nasopharynx in children under 5 years with mild to moderate COVID-19 symptoms was higher than that of both children over 5 as well as adults. The viral load in young children did not seem to differ by age or symptom severity. “There doesn’t appear to be a significant difference in viral load between symptomatic children and symptomatic adults,” she stated.
“But the question is: ‘How infectious are children?’ ” reacted Dr. Buonsenso. Data from South Korea showed that, for children, particularly those under 10 years, the number of secondary cases of contacts was very low, suggesting that children are rarely spreading the virus.
Dr. Buonsenso and colleagues assessed 30 households containing children aged under 18 years where an adult had been infected with COVID-19 in Rome during the peak of the pandemic. In no cases was it found that a child was the index case. This was supported by data from China, also obtained during the peak of the pandemic, which showed that the number of children infected was very low, but more importantly the number of secondary attacks from contact with children was also very low.
What about children who are sick at school?
The debate moved to discussing what should be done when a child is sick at school. Dr. Panciu clarified recommendations by the CDC regarding what steps to take if a student displays signs of infection consistent with COVID-19: Should they test positive, they are to stay at home for 10 days from the time signs and symptoms first appeared. Further, any teachers or students identified as close contacts are advised to stay at home for 14 days. (Since the ESPID meeting, the CDC has made changes in quarantine times for COVID-19. People can now quarantine for 10 days without a COVID-19 test if they have no symptoms. Alternatively, a quarantine can end after 7 days for someone with a negative test and no symptoms. The agency recommends a polymerase chain reaction test or an antigen assay within 48 hours before the end of a quarantine.)
A significant problem is the overlap between COVID-19 symptoms and those associated with other common illnesses because of a range of viruses. This is particularly true in younger children who often suffer from viral infections. “It is common for children to have up to eight respiratory illnesses a year,” explained Dr. Panciu, “and some may have symptoms so mild that they don’t notice them.”
“We need to be a little bit more children focused, otherwise we are going to be isolating children all the time,” said Dr. Buonsenso. The Royal College of Paediatrics and Child Health state that a child with a simple runny nose or sporadic cough without a fever, who would have attended school in other times, should not be tested for COVID-19. He moved on to then cite several studies that show little or no evidence of COVID-19 transmission between school children. This included a prospective cohort study in Australia showing that child-to-child transmission occurred in 0.3%. “To date, the advantages from routine quarantine and over testing seem too low to balance the social consequences on children and families,” he concluded.
As the debate drew to a close, Dr. Panciu reported several studies that did demonstrate transmission between school-age children. Data from an overnight camp in Georgia where the median age was 12 years showed the attack rate was 44% for ages 11-17 years and 51% for ages 6-10 years. Similar conclusions were reached in an Israeli study looking at a large COVID-19 outbreak in a school. This occurred 10 days after reopening, in spite of preventive measures being in place. “Opening safely isn’t just about the adjustments a school makes,” she said, “it’s also about how much of the virus is circulating in the community, which affects the likelihood that students and staff will bring COVID-19 into their classrooms.”
Damian Roland, consultant and honorary associate professor in pediatric emergency medicine at the University of Leicester (England), commented: “Maximizing educational potential while reducing the spread of COVID19 is a challenge laden with scientific equipoise while simultaneously infused with emotion. The evidence of transmission between, and infectivity from, children is not complete, as this debate has demonstrated. It is important scientists, clinicians, educators, and policy makers make collaborative decisions, aware there is not one perfect answer, and willing to understand and incorporate others views and objectives rather than holding onto single beliefs or approaches.”
No financial conflicts of interest were declared.
Countries across the world are in the process of closing and reopening schools to contain the spread of COVID-19. Should there be universal testing and quarantining of sick school children and their classmates?
In a lively debate at the annual meeting of the European Society for Paediatric Infectious Diseases, held virtually this year, Andreea M. Panciu, MD, from the National Institute of Infectious Diseases in Bucharest, argued for routine testing and quarantining of all school children. Her opposite number, Danilo Buonsenso, MD, from the Centre for Global Health Research and Studies, Fondazione Policlinico Universitario Agostino Gemelli Istituto di Ricovero e Cura a Carattere Scientifico, Rome, made the case for a more selective approach.
Should children be sent to school?
stated Dr. Panciu as she started the debate by explaining the challenges faced by schools in adhering to key mitigation strategies. The U.S. Centers for Disease Control and Prevention recommends that students keep 1.8 m (6 feet) distance from one another. “In many school settings this is not feasible without drastically limiting the number of students,” she explained. “This is a massive challenge for many schools that are already overcrowded.”
The use of facemasks also is a challenge in classrooms. Children have a lower tolerance or may not be able to use the mask properly. There also are concerns regarding impaired learning, speech development, social development, and facial recognition. “We need to look at the evidence; preventive measures work,” responded Dr. Buonsenso. If distance can be implemented, the more distance the lower the transmission of infection, with 1.5-2 meters having the best effects. “Distance can be difficult when school buildings do not allow it, however, governments have had time to plan, and this should not be a limitation to education for kids.”
A recent review clearly showed that children and adolescents aged under 20 years have a much lower risk of susceptibility to COVID-19 infection, compared with adults. This is especially the case for children younger than 14 years. “There is no excuse, let’s bring the children back to school,” argued Dr. Buonsenso.
Dr. Panciu responded with several studies that have tried to quantify the amount of SARS-CoV-2 virus that is carried by infected children. Viral load in the nasopharynx in children under 5 years with mild to moderate COVID-19 symptoms was higher than that of both children over 5 as well as adults. The viral load in young children did not seem to differ by age or symptom severity. “There doesn’t appear to be a significant difference in viral load between symptomatic children and symptomatic adults,” she stated.
“But the question is: ‘How infectious are children?’ ” reacted Dr. Buonsenso. Data from South Korea showed that, for children, particularly those under 10 years, the number of secondary cases of contacts was very low, suggesting that children are rarely spreading the virus.
Dr. Buonsenso and colleagues assessed 30 households containing children aged under 18 years where an adult had been infected with COVID-19 in Rome during the peak of the pandemic. In no cases was it found that a child was the index case. This was supported by data from China, also obtained during the peak of the pandemic, which showed that the number of children infected was very low, but more importantly the number of secondary attacks from contact with children was also very low.
What about children who are sick at school?
The debate moved to discussing what should be done when a child is sick at school. Dr. Panciu clarified recommendations by the CDC regarding what steps to take if a student displays signs of infection consistent with COVID-19: Should they test positive, they are to stay at home for 10 days from the time signs and symptoms first appeared. Further, any teachers or students identified as close contacts are advised to stay at home for 14 days. (Since the ESPID meeting, the CDC has made changes in quarantine times for COVID-19. People can now quarantine for 10 days without a COVID-19 test if they have no symptoms. Alternatively, a quarantine can end after 7 days for someone with a negative test and no symptoms. The agency recommends a polymerase chain reaction test or an antigen assay within 48 hours before the end of a quarantine.)
A significant problem is the overlap between COVID-19 symptoms and those associated with other common illnesses because of a range of viruses. This is particularly true in younger children who often suffer from viral infections. “It is common for children to have up to eight respiratory illnesses a year,” explained Dr. Panciu, “and some may have symptoms so mild that they don’t notice them.”
“We need to be a little bit more children focused, otherwise we are going to be isolating children all the time,” said Dr. Buonsenso. The Royal College of Paediatrics and Child Health state that a child with a simple runny nose or sporadic cough without a fever, who would have attended school in other times, should not be tested for COVID-19. He moved on to then cite several studies that show little or no evidence of COVID-19 transmission between school children. This included a prospective cohort study in Australia showing that child-to-child transmission occurred in 0.3%. “To date, the advantages from routine quarantine and over testing seem too low to balance the social consequences on children and families,” he concluded.
As the debate drew to a close, Dr. Panciu reported several studies that did demonstrate transmission between school-age children. Data from an overnight camp in Georgia where the median age was 12 years showed the attack rate was 44% for ages 11-17 years and 51% for ages 6-10 years. Similar conclusions were reached in an Israeli study looking at a large COVID-19 outbreak in a school. This occurred 10 days after reopening, in spite of preventive measures being in place. “Opening safely isn’t just about the adjustments a school makes,” she said, “it’s also about how much of the virus is circulating in the community, which affects the likelihood that students and staff will bring COVID-19 into their classrooms.”
Damian Roland, consultant and honorary associate professor in pediatric emergency medicine at the University of Leicester (England), commented: “Maximizing educational potential while reducing the spread of COVID19 is a challenge laden with scientific equipoise while simultaneously infused with emotion. The evidence of transmission between, and infectivity from, children is not complete, as this debate has demonstrated. It is important scientists, clinicians, educators, and policy makers make collaborative decisions, aware there is not one perfect answer, and willing to understand and incorporate others views and objectives rather than holding onto single beliefs or approaches.”
No financial conflicts of interest were declared.
Countries across the world are in the process of closing and reopening schools to contain the spread of COVID-19. Should there be universal testing and quarantining of sick school children and their classmates?
In a lively debate at the annual meeting of the European Society for Paediatric Infectious Diseases, held virtually this year, Andreea M. Panciu, MD, from the National Institute of Infectious Diseases in Bucharest, argued for routine testing and quarantining of all school children. Her opposite number, Danilo Buonsenso, MD, from the Centre for Global Health Research and Studies, Fondazione Policlinico Universitario Agostino Gemelli Istituto di Ricovero e Cura a Carattere Scientifico, Rome, made the case for a more selective approach.
Should children be sent to school?
stated Dr. Panciu as she started the debate by explaining the challenges faced by schools in adhering to key mitigation strategies. The U.S. Centers for Disease Control and Prevention recommends that students keep 1.8 m (6 feet) distance from one another. “In many school settings this is not feasible without drastically limiting the number of students,” she explained. “This is a massive challenge for many schools that are already overcrowded.”
The use of facemasks also is a challenge in classrooms. Children have a lower tolerance or may not be able to use the mask properly. There also are concerns regarding impaired learning, speech development, social development, and facial recognition. “We need to look at the evidence; preventive measures work,” responded Dr. Buonsenso. If distance can be implemented, the more distance the lower the transmission of infection, with 1.5-2 meters having the best effects. “Distance can be difficult when school buildings do not allow it, however, governments have had time to plan, and this should not be a limitation to education for kids.”
A recent review clearly showed that children and adolescents aged under 20 years have a much lower risk of susceptibility to COVID-19 infection, compared with adults. This is especially the case for children younger than 14 years. “There is no excuse, let’s bring the children back to school,” argued Dr. Buonsenso.
Dr. Panciu responded with several studies that have tried to quantify the amount of SARS-CoV-2 virus that is carried by infected children. Viral load in the nasopharynx in children under 5 years with mild to moderate COVID-19 symptoms was higher than that of both children over 5 as well as adults. The viral load in young children did not seem to differ by age or symptom severity. “There doesn’t appear to be a significant difference in viral load between symptomatic children and symptomatic adults,” she stated.
“But the question is: ‘How infectious are children?’ ” reacted Dr. Buonsenso. Data from South Korea showed that, for children, particularly those under 10 years, the number of secondary cases of contacts was very low, suggesting that children are rarely spreading the virus.
Dr. Buonsenso and colleagues assessed 30 households containing children aged under 18 years where an adult had been infected with COVID-19 in Rome during the peak of the pandemic. In no cases was it found that a child was the index case. This was supported by data from China, also obtained during the peak of the pandemic, which showed that the number of children infected was very low, but more importantly the number of secondary attacks from contact with children was also very low.
What about children who are sick at school?
The debate moved to discussing what should be done when a child is sick at school. Dr. Panciu clarified recommendations by the CDC regarding what steps to take if a student displays signs of infection consistent with COVID-19: Should they test positive, they are to stay at home for 10 days from the time signs and symptoms first appeared. Further, any teachers or students identified as close contacts are advised to stay at home for 14 days. (Since the ESPID meeting, the CDC has made changes in quarantine times for COVID-19. People can now quarantine for 10 days without a COVID-19 test if they have no symptoms. Alternatively, a quarantine can end after 7 days for someone with a negative test and no symptoms. The agency recommends a polymerase chain reaction test or an antigen assay within 48 hours before the end of a quarantine.)
A significant problem is the overlap between COVID-19 symptoms and those associated with other common illnesses because of a range of viruses. This is particularly true in younger children who often suffer from viral infections. “It is common for children to have up to eight respiratory illnesses a year,” explained Dr. Panciu, “and some may have symptoms so mild that they don’t notice them.”
“We need to be a little bit more children focused, otherwise we are going to be isolating children all the time,” said Dr. Buonsenso. The Royal College of Paediatrics and Child Health state that a child with a simple runny nose or sporadic cough without a fever, who would have attended school in other times, should not be tested for COVID-19. He moved on to then cite several studies that show little or no evidence of COVID-19 transmission between school children. This included a prospective cohort study in Australia showing that child-to-child transmission occurred in 0.3%. “To date, the advantages from routine quarantine and over testing seem too low to balance the social consequences on children and families,” he concluded.
As the debate drew to a close, Dr. Panciu reported several studies that did demonstrate transmission between school-age children. Data from an overnight camp in Georgia where the median age was 12 years showed the attack rate was 44% for ages 11-17 years and 51% for ages 6-10 years. Similar conclusions were reached in an Israeli study looking at a large COVID-19 outbreak in a school. This occurred 10 days after reopening, in spite of preventive measures being in place. “Opening safely isn’t just about the adjustments a school makes,” she said, “it’s also about how much of the virus is circulating in the community, which affects the likelihood that students and staff will bring COVID-19 into their classrooms.”
Damian Roland, consultant and honorary associate professor in pediatric emergency medicine at the University of Leicester (England), commented: “Maximizing educational potential while reducing the spread of COVID19 is a challenge laden with scientific equipoise while simultaneously infused with emotion. The evidence of transmission between, and infectivity from, children is not complete, as this debate has demonstrated. It is important scientists, clinicians, educators, and policy makers make collaborative decisions, aware there is not one perfect answer, and willing to understand and incorporate others views and objectives rather than holding onto single beliefs or approaches.”
No financial conflicts of interest were declared.
FROM ESPID 2020
Rap music mention of mental health topics more than doubles

Mental health distress is rising but often is undertreated among children and young adults in the United States, wrote Alex Kresovich, MA, of the University of North Carolina, Chapel Hill, and colleagues.
“Mental health risk especially is increasing among young Black/ African American male individuals (YBAAM), who are often disproportionately exposed to environmental, economic, and family stressors linked with depression and anxiety,” they said. Adolescents and young adults, especially YBAAM, make up a large part of the audience for rap music.
In recent years, more rap artists have disclosed mental health issues, and they have included mental health topics such as depression and suicidal thoughts into their music, the researchers said.
In a study published in JAMA Pediatrics, the researchers identified 125 songs from the period between 1998 and 2018, then assessed them for references to mental health. The song selections included the top 25 rap songs in 1998, 2003, 2008, 2013, and 2018, based on the Billboard music charts.
The majority of the songs (123) featured lead artists from North America, and 97 of them were Black/African American males. The average age of the artists was 28 years. “Prominent artists captured in the sample included 50 Cent, Drake, Eminem, Kanye West, Jay-Z, and Lil’Wayne, among others,” they said. The researchers divided mental health issues into four categories: anxiety or anxious thinking; depression or depressive thinking; metaphors (such as struggling with mental stability); and suicide or suicidal ideation.
Mental health references rise
Across the study period, 35 songs (28%) mentioned anxiety, 28 (22%) mentioned depression, 8 (6%) mentioned suicide, and 26 (21%) mentioned a mental health metaphor. The proportion of songs with a mental health reference increased in a significant linear trend across the study period for suicide (0%-12%), depression (16%-32%), and mental health metaphors (8%-44%).
All references to suicide or suicidal ideation were found in songs that were popular between 2013 and 2018, the researchers noted.
“This increase is important, given that rap artists serve as role models to their audience, which extends beyond YBAAM to include U.S. young people across strata, constituting a large group with increased risk of mental health issues and underuse of mental health services,” Mr. Kresovich and associates said.
In addition, the researchers found that stressors related to environmental conditions and love were significantly more likely to co-occur with mental health references (adjusted odds ratios 8.1 and 4.8, respectively).
The study findings were limited by several factors including the selection of songs only from the Billboard hot rap songs year-end charts, which “does not fully represent the population of rap music between 1998 and 2018,” the researchers said. In addition, they could not address causation or motivations for the increased mental health references over the study period. “We are also unable to ascertain how U.S. youth interact with this music or are positively or negatively affected by its messages.”
“For example, positively framed references to mental health awareness, treatment, or support may lead to reduced stigma and increased willingness to seek treatment,” Mr. Kresovich and associates wrote. “However, negatively framed references to mental health struggles might lead to negative outcomes, including copycat behavior in which listeners model harmful behavior, such as suicide attempts, if those behaviors are described in lyrics (i.e., the Werther effect),” they added.
Despite these limitations, the results support the need for more research on the impact of rap music as a way to reduce stigma and potentially reduce mental health risk in adolescents and young adults, Mr. Kresovich and associates concluded.
Music may help raise tough topics
The study is important because children and adolescents have more control than ever over the media they consume, Sarah Vinson, MD, founder of the Lorio Psych Group in Atlanta, said in an interview.
“With more and more children with access to their own devices, they spend a great amount of time consuming content, including music,” Dr. Vinson said. “The norms reflected in the lyrics they hear have an impact on their emerging view of themselves, others, and the world.”
The increased recognition of mental health issues by rap musicians as a topic “certainly has the potential to have a positive impact; however, the way that it is discussed can influence [the] nature of that impact,” she explained.
“It is important for people who are dealing with the normal range of human emotions to know that they are not alone. It is even more important for people dealing with suicidality or mental illness to know that,” Dr. Vinson said.
“Validation and sense of connection are human needs, and stigma related to mental illness can be isolating,” she emphasized. “Rappers have a platform and are often people that children and adolescents look up to, for better or for worse.” Through their music, “the rappers are signaling that these topics are worthy of our attention and okay to talk about.”
Unfortunately, many barriers persist for adolescents in need of mental health treatment, said Dr. Vinson. “The children’s mental health workforce, quantitatively, is not enough to meet the current needs,” she said. “Mental health is not reimbursed at the same rate as other kinds of health care, which contributes to healthy systems not prioritizing these services. Additionally, the racial, ethnic, and socioeconomic background of those who are mental health providers is not reflective of the larger population, and mental health training insufficiently incorporates the cultural and structural humility needed to help professionals navigate those differences,” she explained.
“Children at increased risk are those who face many of those environmental barriers that the rappers reference in those lyrics. They are likely to have even poorer access because they are disproportionately impacted by residential segregation, transportation challenges, financial barriers, and structural racism in mental health care,” Dr. Vinson added. A take-home message for clinicians is to find out what their patients are listening to. “One way to understand what is on the hearts and minds of children is to ask them what’s in their playlist,” she said.
Additional research is needed to examine “moderating factors for the impact, good or bad, of increased mental health content in hip hop for young listeners’ mental health awareness, symptoms and/or interest in seeking treatment,” Dr. Vinson concluded.
The study received no outside funding. The researchers had no financial conflicts to disclose.
Dr. Vinson served as chair for a workshop on mental health and hip-hop at the American Psychiatric Association annual meeting. She had no financial conflicts to disclose.
SOURCE: Kresovich A et al. JAMA Pediatr. 2020 Dec 7. doi: 10.1001/jamapediatrics.2020.5155.
This article was updated on December 21, 2020.
Mental health distress is rising but often is undertreated among children and young adults in the United States, wrote Alex Kresovich, MA, of the University of North Carolina, Chapel Hill, and colleagues.
“Mental health risk especially is increasing among young Black/ African American male individuals (YBAAM), who are often disproportionately exposed to environmental, economic, and family stressors linked with depression and anxiety,” they said. Adolescents and young adults, especially YBAAM, make up a large part of the audience for rap music.
In recent years, more rap artists have disclosed mental health issues, and they have included mental health topics such as depression and suicidal thoughts into their music, the researchers said.
In a study published in JAMA Pediatrics, the researchers identified 125 songs from the period between 1998 and 2018, then assessed them for references to mental health. The song selections included the top 25 rap songs in 1998, 2003, 2008, 2013, and 2018, based on the Billboard music charts.
The majority of the songs (123) featured lead artists from North America, and 97 of them were Black/African American males. The average age of the artists was 28 years. “Prominent artists captured in the sample included 50 Cent, Drake, Eminem, Kanye West, Jay-Z, and Lil’Wayne, among others,” they said. The researchers divided mental health issues into four categories: anxiety or anxious thinking; depression or depressive thinking; metaphors (such as struggling with mental stability); and suicide or suicidal ideation.
Mental health references rise
Across the study period, 35 songs (28%) mentioned anxiety, 28 (22%) mentioned depression, 8 (6%) mentioned suicide, and 26 (21%) mentioned a mental health metaphor. The proportion of songs with a mental health reference increased in a significant linear trend across the study period for suicide (0%-12%), depression (16%-32%), and mental health metaphors (8%-44%).
All references to suicide or suicidal ideation were found in songs that were popular between 2013 and 2018, the researchers noted.
“This increase is important, given that rap artists serve as role models to their audience, which extends beyond YBAAM to include U.S. young people across strata, constituting a large group with increased risk of mental health issues and underuse of mental health services,” Mr. Kresovich and associates said.
In addition, the researchers found that stressors related to environmental conditions and love were significantly more likely to co-occur with mental health references (adjusted odds ratios 8.1 and 4.8, respectively).
The study findings were limited by several factors including the selection of songs only from the Billboard hot rap songs year-end charts, which “does not fully represent the population of rap music between 1998 and 2018,” the researchers said. In addition, they could not address causation or motivations for the increased mental health references over the study period. “We are also unable to ascertain how U.S. youth interact with this music or are positively or negatively affected by its messages.”
“For example, positively framed references to mental health awareness, treatment, or support may lead to reduced stigma and increased willingness to seek treatment,” Mr. Kresovich and associates wrote. “However, negatively framed references to mental health struggles might lead to negative outcomes, including copycat behavior in which listeners model harmful behavior, such as suicide attempts, if those behaviors are described in lyrics (i.e., the Werther effect),” they added.
Despite these limitations, the results support the need for more research on the impact of rap music as a way to reduce stigma and potentially reduce mental health risk in adolescents and young adults, Mr. Kresovich and associates concluded.
Music may help raise tough topics
The study is important because children and adolescents have more control than ever over the media they consume, Sarah Vinson, MD, founder of the Lorio Psych Group in Atlanta, said in an interview.
“With more and more children with access to their own devices, they spend a great amount of time consuming content, including music,” Dr. Vinson said. “The norms reflected in the lyrics they hear have an impact on their emerging view of themselves, others, and the world.”
The increased recognition of mental health issues by rap musicians as a topic “certainly has the potential to have a positive impact; however, the way that it is discussed can influence [the] nature of that impact,” she explained.
“It is important for people who are dealing with the normal range of human emotions to know that they are not alone. It is even more important for people dealing with suicidality or mental illness to know that,” Dr. Vinson said.
“Validation and sense of connection are human needs, and stigma related to mental illness can be isolating,” she emphasized. “Rappers have a platform and are often people that children and adolescents look up to, for better or for worse.” Through their music, “the rappers are signaling that these topics are worthy of our attention and okay to talk about.”
Unfortunately, many barriers persist for adolescents in need of mental health treatment, said Dr. Vinson. “The children’s mental health workforce, quantitatively, is not enough to meet the current needs,” she said. “Mental health is not reimbursed at the same rate as other kinds of health care, which contributes to healthy systems not prioritizing these services. Additionally, the racial, ethnic, and socioeconomic background of those who are mental health providers is not reflective of the larger population, and mental health training insufficiently incorporates the cultural and structural humility needed to help professionals navigate those differences,” she explained.
“Children at increased risk are those who face many of those environmental barriers that the rappers reference in those lyrics. They are likely to have even poorer access because they are disproportionately impacted by residential segregation, transportation challenges, financial barriers, and structural racism in mental health care,” Dr. Vinson added. A take-home message for clinicians is to find out what their patients are listening to. “One way to understand what is on the hearts and minds of children is to ask them what’s in their playlist,” she said.
Additional research is needed to examine “moderating factors for the impact, good or bad, of increased mental health content in hip hop for young listeners’ mental health awareness, symptoms and/or interest in seeking treatment,” Dr. Vinson concluded.
The study received no outside funding. The researchers had no financial conflicts to disclose.
Dr. Vinson served as chair for a workshop on mental health and hip-hop at the American Psychiatric Association annual meeting. She had no financial conflicts to disclose.
SOURCE: Kresovich A et al. JAMA Pediatr. 2020 Dec 7. doi: 10.1001/jamapediatrics.2020.5155.
This article was updated on December 21, 2020.
Mental health distress is rising but often is undertreated among children and young adults in the United States, wrote Alex Kresovich, MA, of the University of North Carolina, Chapel Hill, and colleagues.
“Mental health risk especially is increasing among young Black/ African American male individuals (YBAAM), who are often disproportionately exposed to environmental, economic, and family stressors linked with depression and anxiety,” they said. Adolescents and young adults, especially YBAAM, make up a large part of the audience for rap music.
In recent years, more rap artists have disclosed mental health issues, and they have included mental health topics such as depression and suicidal thoughts into their music, the researchers said.
In a study published in JAMA Pediatrics, the researchers identified 125 songs from the period between 1998 and 2018, then assessed them for references to mental health. The song selections included the top 25 rap songs in 1998, 2003, 2008, 2013, and 2018, based on the Billboard music charts.
The majority of the songs (123) featured lead artists from North America, and 97 of them were Black/African American males. The average age of the artists was 28 years. “Prominent artists captured in the sample included 50 Cent, Drake, Eminem, Kanye West, Jay-Z, and Lil’Wayne, among others,” they said. The researchers divided mental health issues into four categories: anxiety or anxious thinking; depression or depressive thinking; metaphors (such as struggling with mental stability); and suicide or suicidal ideation.
Mental health references rise
Across the study period, 35 songs (28%) mentioned anxiety, 28 (22%) mentioned depression, 8 (6%) mentioned suicide, and 26 (21%) mentioned a mental health metaphor. The proportion of songs with a mental health reference increased in a significant linear trend across the study period for suicide (0%-12%), depression (16%-32%), and mental health metaphors (8%-44%).
All references to suicide or suicidal ideation were found in songs that were popular between 2013 and 2018, the researchers noted.
“This increase is important, given that rap artists serve as role models to their audience, which extends beyond YBAAM to include U.S. young people across strata, constituting a large group with increased risk of mental health issues and underuse of mental health services,” Mr. Kresovich and associates said.
In addition, the researchers found that stressors related to environmental conditions and love were significantly more likely to co-occur with mental health references (adjusted odds ratios 8.1 and 4.8, respectively).
The study findings were limited by several factors including the selection of songs only from the Billboard hot rap songs year-end charts, which “does not fully represent the population of rap music between 1998 and 2018,” the researchers said. In addition, they could not address causation or motivations for the increased mental health references over the study period. “We are also unable to ascertain how U.S. youth interact with this music or are positively or negatively affected by its messages.”
“For example, positively framed references to mental health awareness, treatment, or support may lead to reduced stigma and increased willingness to seek treatment,” Mr. Kresovich and associates wrote. “However, negatively framed references to mental health struggles might lead to negative outcomes, including copycat behavior in which listeners model harmful behavior, such as suicide attempts, if those behaviors are described in lyrics (i.e., the Werther effect),” they added.
Despite these limitations, the results support the need for more research on the impact of rap music as a way to reduce stigma and potentially reduce mental health risk in adolescents and young adults, Mr. Kresovich and associates concluded.
Music may help raise tough topics
The study is important because children and adolescents have more control than ever over the media they consume, Sarah Vinson, MD, founder of the Lorio Psych Group in Atlanta, said in an interview.
“With more and more children with access to their own devices, they spend a great amount of time consuming content, including music,” Dr. Vinson said. “The norms reflected in the lyrics they hear have an impact on their emerging view of themselves, others, and the world.”
The increased recognition of mental health issues by rap musicians as a topic “certainly has the potential to have a positive impact; however, the way that it is discussed can influence [the] nature of that impact,” she explained.
“It is important for people who are dealing with the normal range of human emotions to know that they are not alone. It is even more important for people dealing with suicidality or mental illness to know that,” Dr. Vinson said.
“Validation and sense of connection are human needs, and stigma related to mental illness can be isolating,” she emphasized. “Rappers have a platform and are often people that children and adolescents look up to, for better or for worse.” Through their music, “the rappers are signaling that these topics are worthy of our attention and okay to talk about.”
Unfortunately, many barriers persist for adolescents in need of mental health treatment, said Dr. Vinson. “The children’s mental health workforce, quantitatively, is not enough to meet the current needs,” she said. “Mental health is not reimbursed at the same rate as other kinds of health care, which contributes to healthy systems not prioritizing these services. Additionally, the racial, ethnic, and socioeconomic background of those who are mental health providers is not reflective of the larger population, and mental health training insufficiently incorporates the cultural and structural humility needed to help professionals navigate those differences,” she explained.
“Children at increased risk are those who face many of those environmental barriers that the rappers reference in those lyrics. They are likely to have even poorer access because they are disproportionately impacted by residential segregation, transportation challenges, financial barriers, and structural racism in mental health care,” Dr. Vinson added. A take-home message for clinicians is to find out what their patients are listening to. “One way to understand what is on the hearts and minds of children is to ask them what’s in their playlist,” she said.
Additional research is needed to examine “moderating factors for the impact, good or bad, of increased mental health content in hip hop for young listeners’ mental health awareness, symptoms and/or interest in seeking treatment,” Dr. Vinson concluded.
The study received no outside funding. The researchers had no financial conflicts to disclose.
Dr. Vinson served as chair for a workshop on mental health and hip-hop at the American Psychiatric Association annual meeting. She had no financial conflicts to disclose.
SOURCE: Kresovich A et al. JAMA Pediatr. 2020 Dec 7. doi: 10.1001/jamapediatrics.2020.5155.
This article was updated on December 21, 2020.
FROM JAMA PEDIATRICS
New child COVID-19 cases down in last weekly count
A tiny bit of light may have broken though the COVID-19 storm clouds.
The number of new cases in children in the United States did not set a new weekly high for the first time in months and the cumulative proportion of COVID-19 cases occurring in children did not go up for the first time since the pandemic started, according to a report from the American Academy of Pediatrics and the Children’s Hospital Association. 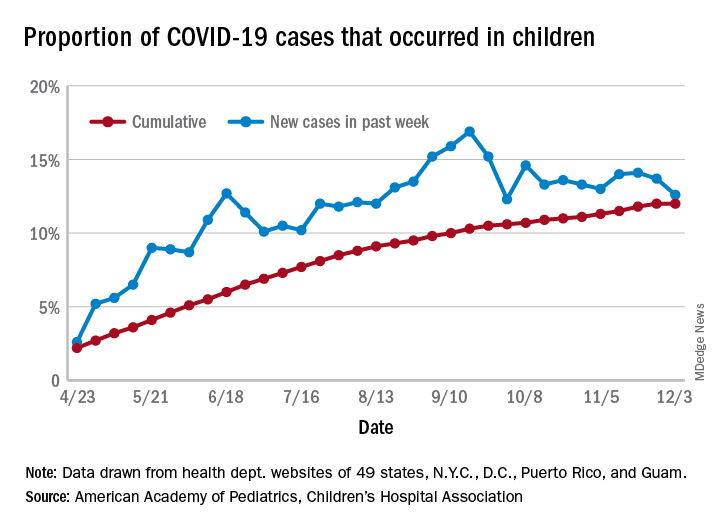
which is the first time since late September that the weekly total has fallen in the United States, the AAP/CHA data show.
Another measure, the cumulative proportion of infected children among all COVID-19 cases, stayed at 12.0% for the second week in a row, and that is the first time there was no increase since the AAP and CHA started tracking health department websites in 49 states (not New York), the District of Columbia, New York City, Puerto Rico, and Guam in April.
For the week ending Dec. 3, those 123,688 children represented 12.6% of all U.S. COVID-19 cases, marking the second consecutive weekly drop in that figure, which has been as high as 16.9% in the previous 3 months, based on data in the AAP/CHA weekly report.
The total number of reported COVID-19 cases in children is now up to 1.46 million, and the overall rate is 1,941 per 100,000 children. Comparable figures for states show that California has the most cumulative cases at over 139,000 and that North Dakota has the highest rate at over 6,800 per 100,000 children. Vermont, the state with the smallest child population, has the fewest cases (687) and the lowest rate (511 per 100,000), the report said.
The total number of COVID-19–related deaths in children has reached 154 in the 44 jurisdictions (43 states and New York City) reporting such data. That number represents 0.06% of all coronavirus deaths, a proportion that has changed little – ranging from 0.04% to 0.07% – over the course of the pandemic, the AAP and CHA said.
A tiny bit of light may have broken though the COVID-19 storm clouds.
The number of new cases in children in the United States did not set a new weekly high for the first time in months and the cumulative proportion of COVID-19 cases occurring in children did not go up for the first time since the pandemic started, according to a report from the American Academy of Pediatrics and the Children’s Hospital Association.
which is the first time since late September that the weekly total has fallen in the United States, the AAP/CHA data show.
Another measure, the cumulative proportion of infected children among all COVID-19 cases, stayed at 12.0% for the second week in a row, and that is the first time there was no increase since the AAP and CHA started tracking health department websites in 49 states (not New York), the District of Columbia, New York City, Puerto Rico, and Guam in April.
For the week ending Dec. 3, those 123,688 children represented 12.6% of all U.S. COVID-19 cases, marking the second consecutive weekly drop in that figure, which has been as high as 16.9% in the previous 3 months, based on data in the AAP/CHA weekly report.
The total number of reported COVID-19 cases in children is now up to 1.46 million, and the overall rate is 1,941 per 100,000 children. Comparable figures for states show that California has the most cumulative cases at over 139,000 and that North Dakota has the highest rate at over 6,800 per 100,000 children. Vermont, the state with the smallest child population, has the fewest cases (687) and the lowest rate (511 per 100,000), the report said.
The total number of COVID-19–related deaths in children has reached 154 in the 44 jurisdictions (43 states and New York City) reporting such data. That number represents 0.06% of all coronavirus deaths, a proportion that has changed little – ranging from 0.04% to 0.07% – over the course of the pandemic, the AAP and CHA said.
A tiny bit of light may have broken though the COVID-19 storm clouds.
The number of new cases in children in the United States did not set a new weekly high for the first time in months and the cumulative proportion of COVID-19 cases occurring in children did not go up for the first time since the pandemic started, according to a report from the American Academy of Pediatrics and the Children’s Hospital Association.
which is the first time since late September that the weekly total has fallen in the United States, the AAP/CHA data show.
Another measure, the cumulative proportion of infected children among all COVID-19 cases, stayed at 12.0% for the second week in a row, and that is the first time there was no increase since the AAP and CHA started tracking health department websites in 49 states (not New York), the District of Columbia, New York City, Puerto Rico, and Guam in April.
For the week ending Dec. 3, those 123,688 children represented 12.6% of all U.S. COVID-19 cases, marking the second consecutive weekly drop in that figure, which has been as high as 16.9% in the previous 3 months, based on data in the AAP/CHA weekly report.
The total number of reported COVID-19 cases in children is now up to 1.46 million, and the overall rate is 1,941 per 100,000 children. Comparable figures for states show that California has the most cumulative cases at over 139,000 and that North Dakota has the highest rate at over 6,800 per 100,000 children. Vermont, the state with the smallest child population, has the fewest cases (687) and the lowest rate (511 per 100,000), the report said.
The total number of COVID-19–related deaths in children has reached 154 in the 44 jurisdictions (43 states and New York City) reporting such data. That number represents 0.06% of all coronavirus deaths, a proportion that has changed little – ranging from 0.04% to 0.07% – over the course of the pandemic, the AAP and CHA said.
Combined Treatment of Disfiguring Facial Angiofibromas in Tuberous Sclerosis Complex With Surgical Debulking and Topical Sirolimus
Practice Gap
Tuberous sclerosis complex (TSC) is an autosomal-dominant genetic disorder resulting in loss-of-function mutations in the TSC1 and TSC2 genes. These mutations lead to constitutive activation of the mitogenic mTOR pathway and release of lymphangiogenic growth factors, causing the formation of hamartomatous tumors throughout multiple organ systems.1 Facial angiofibromas (FAs) are a common cutaneous manifestation of TSC, affecting up to 80% of patients worldwide.2 Aesthetic disfigurement, vision obstruction, and breathing impairment often are associated with FAs. They frequently arise in children with TSC and impose a psychosocial burden that can affect the patient’s overall quality of life.
Cutaneous stigmata of TSC pose a significant therapeutic challenge. Topical sirolimus has become a first-line treatment of FAs by inhibiting the mitogenic mTOR pathway1; however, thicker, more extensive lesions are less responsive to topical therapy. The entire dermis is involved in TSC, and topical sirolimus alone often is ineffective for large fibrous FAs.3 Likewise, oral mTOR inhibition has shown only 25% to 50% improvement in FAs and has potential side effects that can limit patients’ tolerance and compliance.4
The Technique
A 46-year-old man with TSC was referred to dermatology for treatment of numerous facial papules and plaques that had been present since childhood and were consistent with FAs (Figure 1A). The lesions were tender, impaired the patient’s breathing, and caused emotional distress. Dermabrasion was attempted 20 years prior with minimal improvement and subsequent progression of the FAs. Other stigmata of TSC were present, including cutaneous hypopigmented macules and shagreen patches as well as seizures and renal angiomyolipomas. Due to multiorgan involvement, the patient was started on once-daily oral everolimus 2.5 mg; however, the FAs were progressive despite the systemic mTOR inhibition. Furthermore, it was presumed that topical sirolimus monotherapy would be ineffective due to thickness and extent of FAs; therefore, we proposed a novel treatment approach combining initial surgical debulking with subsequent longitudinal use of topical sirolimus to reduce the risk of recurrence.
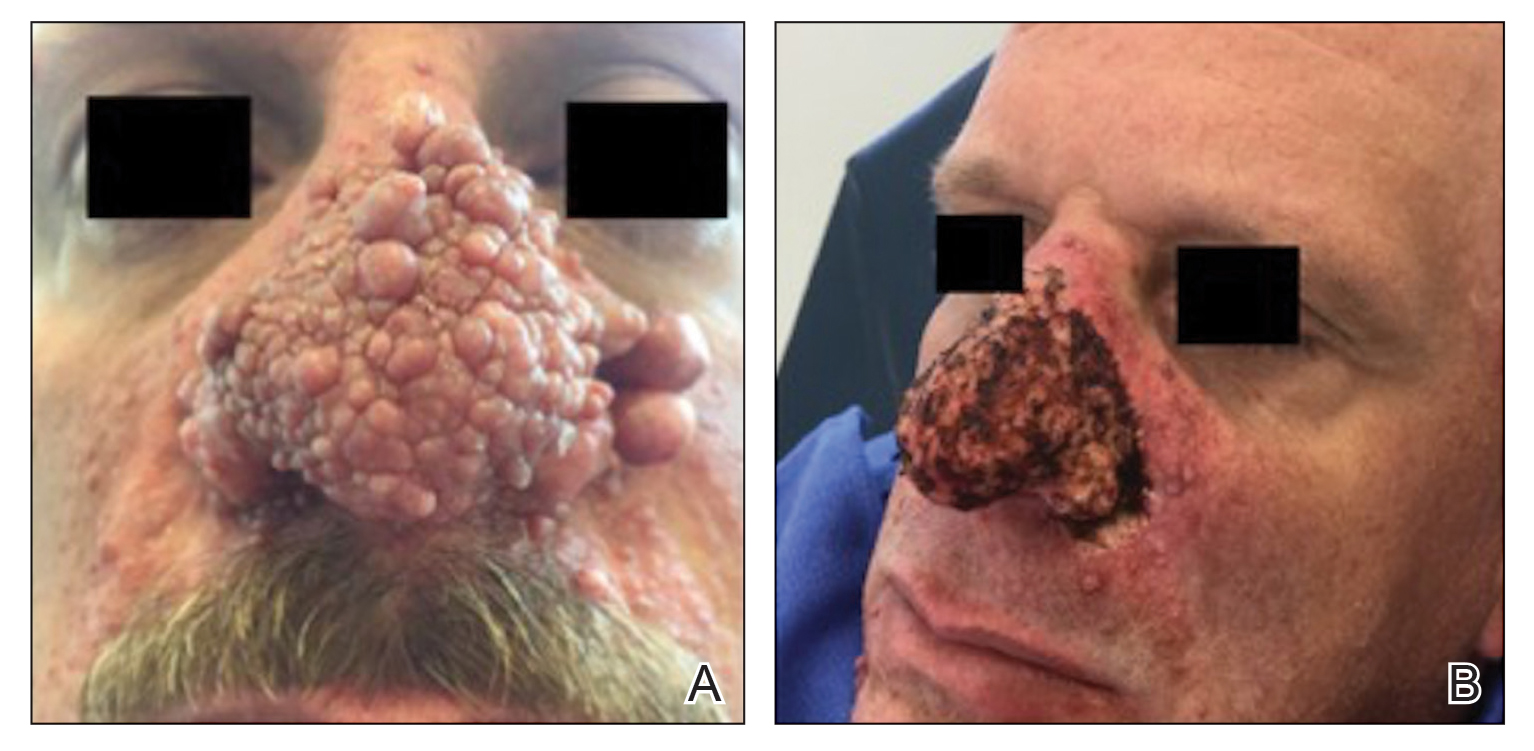
Local anesthesia with lidocaine 1% and epinephrine 1:100,000 was administered. Larger FAs were removed at the base with a sterile surgical blade. Nasal recontouring subsequently was performed using a combination of shave biopsy and curettage. Extensive electrocautery was performed for hemostasis and destruction of residual FAs. Figure 1B shows the immediate postoperative result.
One month postoperatively, the patient stopped the oral everolimus at his oncologist’s recommendation due to abdominal pain and peripheral edema. Once the abraded skin showed evidence of wound healing, the patient was instructed to initiate sirolimus ointment 1% twice daily to reduce the risk of recurrence.1,5,6 At 8-week follow-up, the patient was noted to have cosmetic improvement and resolution of breathing impairment (Figure 2A). He continued to show excellent cosmetic results at 1-year follow-up using topical sirolimus monotherapy (Figure 2B).
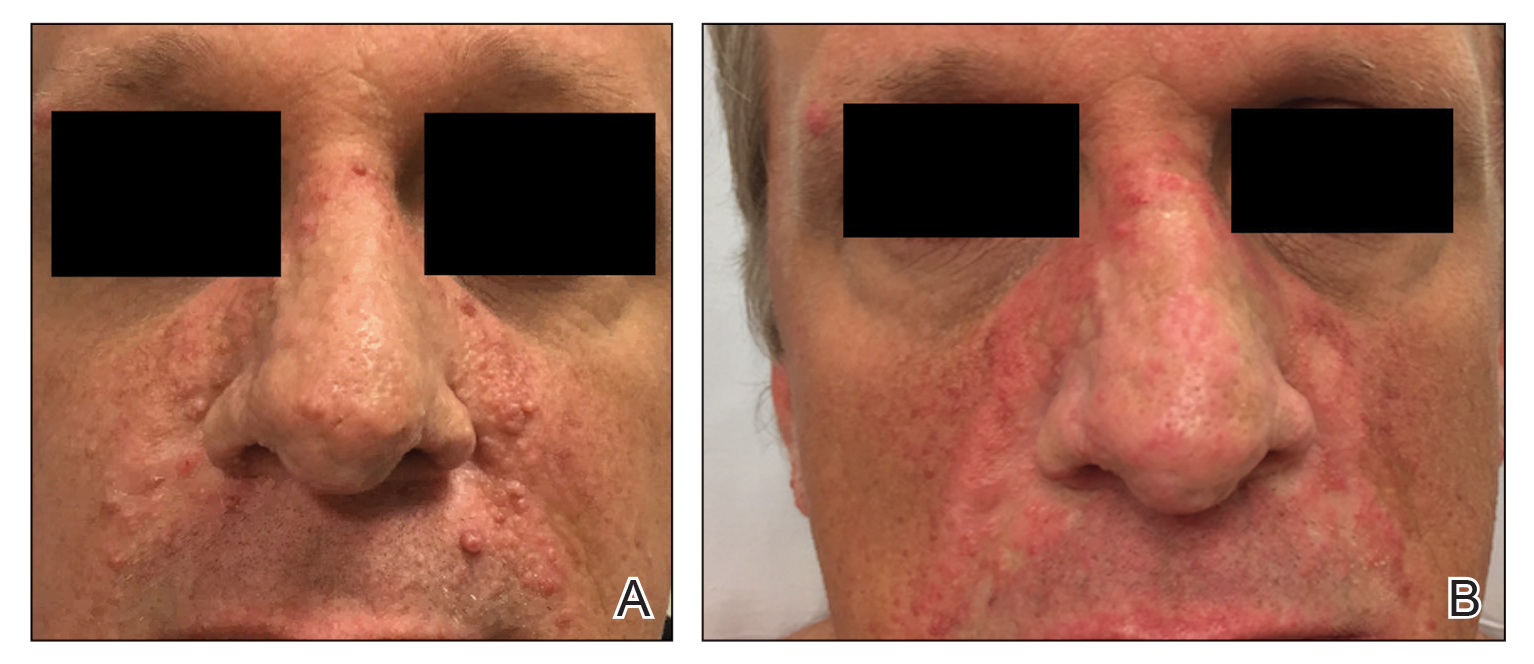
Practical Implications
Surgical debulking combined with longitudinal use of sirolimus ointment 1% can achieve an optimal therapeutic response for disfiguring phymatous presentation of FAs in the setting of TSC. We believe it is an effective approach for thick disfiguring FAs that are unlikely to respond to mTOR inhibition alone.
- Wataya-Kaneda M, Nakamura A, Tanaka M, et al. Efficacy and safety of topical sirolimus therapy for facial angiofibromas in the tuberous sclerosis complex: a randomized clinical trial. JAMA Dermatol. 2017;153:39‐48.
- Koenig MK, Hebert AA, Roberson J, et al. Topical rapamycin therapy to alleviate the cutaneous manifestations of tuberous sclerosis complex. Drugs R D. 2012;12:121-126.
- Wataya-Kaneda M, Ohno Y, Fujita Y, et al. Sirolimus gel treatment vs placebo for facial angiofibromas in patients with tuberous sclerosis complex: a randomized clinical trial. JAMA Dermatol. 2018;154:781-788.
- Nathan N, Wang JA, Li S, et al. Improvement of tuberous sclerosis complex (TSC) skin tumors during long-term treatment with oral sirolimus. J Am Acad Dermatol. 2015;73:802-808.
- Kaplan B, Qazi Y, Wellen JR. Strategies for the management of adverse events associated with mTOR inhibitors. Transplant Rev (Orlando). 2014;28:126-133.
- Haemel AK, O’Brian AL, Teng JM. Topical rapamycin therapy to alleviate the cutaneous manifestations of tuberous sclerosis complex. Arch Dermatol. 2010;146:1538-3652.
Practice Gap
Tuberous sclerosis complex (TSC) is an autosomal-dominant genetic disorder resulting in loss-of-function mutations in the TSC1 and TSC2 genes. These mutations lead to constitutive activation of the mitogenic mTOR pathway and release of lymphangiogenic growth factors, causing the formation of hamartomatous tumors throughout multiple organ systems.1 Facial angiofibromas (FAs) are a common cutaneous manifestation of TSC, affecting up to 80% of patients worldwide.2 Aesthetic disfigurement, vision obstruction, and breathing impairment often are associated with FAs. They frequently arise in children with TSC and impose a psychosocial burden that can affect the patient’s overall quality of life.
Cutaneous stigmata of TSC pose a significant therapeutic challenge. Topical sirolimus has become a first-line treatment of FAs by inhibiting the mitogenic mTOR pathway1; however, thicker, more extensive lesions are less responsive to topical therapy. The entire dermis is involved in TSC, and topical sirolimus alone often is ineffective for large fibrous FAs.3 Likewise, oral mTOR inhibition has shown only 25% to 50% improvement in FAs and has potential side effects that can limit patients’ tolerance and compliance.4
The Technique
A 46-year-old man with TSC was referred to dermatology for treatment of numerous facial papules and plaques that had been present since childhood and were consistent with FAs (Figure 1A). The lesions were tender, impaired the patient’s breathing, and caused emotional distress. Dermabrasion was attempted 20 years prior with minimal improvement and subsequent progression of the FAs. Other stigmata of TSC were present, including cutaneous hypopigmented macules and shagreen patches as well as seizures and renal angiomyolipomas. Due to multiorgan involvement, the patient was started on once-daily oral everolimus 2.5 mg; however, the FAs were progressive despite the systemic mTOR inhibition. Furthermore, it was presumed that topical sirolimus monotherapy would be ineffective due to thickness and extent of FAs; therefore, we proposed a novel treatment approach combining initial surgical debulking with subsequent longitudinal use of topical sirolimus to reduce the risk of recurrence.
Local anesthesia with lidocaine 1% and epinephrine 1:100,000 was administered. Larger FAs were removed at the base with a sterile surgical blade. Nasal recontouring subsequently was performed using a combination of shave biopsy and curettage. Extensive electrocautery was performed for hemostasis and destruction of residual FAs. Figure 1B shows the immediate postoperative result.
One month postoperatively, the patient stopped the oral everolimus at his oncologist’s recommendation due to abdominal pain and peripheral edema. Once the abraded skin showed evidence of wound healing, the patient was instructed to initiate sirolimus ointment 1% twice daily to reduce the risk of recurrence.1,5,6 At 8-week follow-up, the patient was noted to have cosmetic improvement and resolution of breathing impairment (Figure 2A). He continued to show excellent cosmetic results at 1-year follow-up using topical sirolimus monotherapy (Figure 2B).
Practical Implications
Surgical debulking combined with longitudinal use of sirolimus ointment 1% can achieve an optimal therapeutic response for disfiguring phymatous presentation of FAs in the setting of TSC. We believe it is an effective approach for thick disfiguring FAs that are unlikely to respond to mTOR inhibition alone.
Practice Gap
Tuberous sclerosis complex (TSC) is an autosomal-dominant genetic disorder resulting in loss-of-function mutations in the TSC1 and TSC2 genes. These mutations lead to constitutive activation of the mitogenic mTOR pathway and release of lymphangiogenic growth factors, causing the formation of hamartomatous tumors throughout multiple organ systems.1 Facial angiofibromas (FAs) are a common cutaneous manifestation of TSC, affecting up to 80% of patients worldwide.2 Aesthetic disfigurement, vision obstruction, and breathing impairment often are associated with FAs. They frequently arise in children with TSC and impose a psychosocial burden that can affect the patient’s overall quality of life.
Cutaneous stigmata of TSC pose a significant therapeutic challenge. Topical sirolimus has become a first-line treatment of FAs by inhibiting the mitogenic mTOR pathway1; however, thicker, more extensive lesions are less responsive to topical therapy. The entire dermis is involved in TSC, and topical sirolimus alone often is ineffective for large fibrous FAs.3 Likewise, oral mTOR inhibition has shown only 25% to 50% improvement in FAs and has potential side effects that can limit patients’ tolerance and compliance.4
The Technique
A 46-year-old man with TSC was referred to dermatology for treatment of numerous facial papules and plaques that had been present since childhood and were consistent with FAs (Figure 1A). The lesions were tender, impaired the patient’s breathing, and caused emotional distress. Dermabrasion was attempted 20 years prior with minimal improvement and subsequent progression of the FAs. Other stigmata of TSC were present, including cutaneous hypopigmented macules and shagreen patches as well as seizures and renal angiomyolipomas. Due to multiorgan involvement, the patient was started on once-daily oral everolimus 2.5 mg; however, the FAs were progressive despite the systemic mTOR inhibition. Furthermore, it was presumed that topical sirolimus monotherapy would be ineffective due to thickness and extent of FAs; therefore, we proposed a novel treatment approach combining initial surgical debulking with subsequent longitudinal use of topical sirolimus to reduce the risk of recurrence.
Local anesthesia with lidocaine 1% and epinephrine 1:100,000 was administered. Larger FAs were removed at the base with a sterile surgical blade. Nasal recontouring subsequently was performed using a combination of shave biopsy and curettage. Extensive electrocautery was performed for hemostasis and destruction of residual FAs. Figure 1B shows the immediate postoperative result.
One month postoperatively, the patient stopped the oral everolimus at his oncologist’s recommendation due to abdominal pain and peripheral edema. Once the abraded skin showed evidence of wound healing, the patient was instructed to initiate sirolimus ointment 1% twice daily to reduce the risk of recurrence.1,5,6 At 8-week follow-up, the patient was noted to have cosmetic improvement and resolution of breathing impairment (Figure 2A). He continued to show excellent cosmetic results at 1-year follow-up using topical sirolimus monotherapy (Figure 2B).
Practical Implications
Surgical debulking combined with longitudinal use of sirolimus ointment 1% can achieve an optimal therapeutic response for disfiguring phymatous presentation of FAs in the setting of TSC. We believe it is an effective approach for thick disfiguring FAs that are unlikely to respond to mTOR inhibition alone.
- Wataya-Kaneda M, Nakamura A, Tanaka M, et al. Efficacy and safety of topical sirolimus therapy for facial angiofibromas in the tuberous sclerosis complex: a randomized clinical trial. JAMA Dermatol. 2017;153:39‐48.
- Koenig MK, Hebert AA, Roberson J, et al. Topical rapamycin therapy to alleviate the cutaneous manifestations of tuberous sclerosis complex. Drugs R D. 2012;12:121-126.
- Wataya-Kaneda M, Ohno Y, Fujita Y, et al. Sirolimus gel treatment vs placebo for facial angiofibromas in patients with tuberous sclerosis complex: a randomized clinical trial. JAMA Dermatol. 2018;154:781-788.
- Nathan N, Wang JA, Li S, et al. Improvement of tuberous sclerosis complex (TSC) skin tumors during long-term treatment with oral sirolimus. J Am Acad Dermatol. 2015;73:802-808.
- Kaplan B, Qazi Y, Wellen JR. Strategies for the management of adverse events associated with mTOR inhibitors. Transplant Rev (Orlando). 2014;28:126-133.
- Haemel AK, O’Brian AL, Teng JM. Topical rapamycin therapy to alleviate the cutaneous manifestations of tuberous sclerosis complex. Arch Dermatol. 2010;146:1538-3652.
- Wataya-Kaneda M, Nakamura A, Tanaka M, et al. Efficacy and safety of topical sirolimus therapy for facial angiofibromas in the tuberous sclerosis complex: a randomized clinical trial. JAMA Dermatol. 2017;153:39‐48.
- Koenig MK, Hebert AA, Roberson J, et al. Topical rapamycin therapy to alleviate the cutaneous manifestations of tuberous sclerosis complex. Drugs R D. 2012;12:121-126.
- Wataya-Kaneda M, Ohno Y, Fujita Y, et al. Sirolimus gel treatment vs placebo for facial angiofibromas in patients with tuberous sclerosis complex: a randomized clinical trial. JAMA Dermatol. 2018;154:781-788.
- Nathan N, Wang JA, Li S, et al. Improvement of tuberous sclerosis complex (TSC) skin tumors during long-term treatment with oral sirolimus. J Am Acad Dermatol. 2015;73:802-808.
- Kaplan B, Qazi Y, Wellen JR. Strategies for the management of adverse events associated with mTOR inhibitors. Transplant Rev (Orlando). 2014;28:126-133.
- Haemel AK, O’Brian AL, Teng JM. Topical rapamycin therapy to alleviate the cutaneous manifestations of tuberous sclerosis complex. Arch Dermatol. 2010;146:1538-3652.

Infant’s COVID-19–related myocardial injury reversed
Reports of signs of heart failure in adults with COVID-19 have been rare – just four such cases have been published since the outbreak started in China – and now a team of pediatric cardiologists in New York have reported a case of acute but reversible myocardial injury in an infant with COVID-19.

and right upper lobe atelectasis.
The 2-month-old infant went home after more than 2 weeks in the hospital with no apparent lingering cardiac effects of the illness and not needing any oral heart failure medications, Madhu Sharma, MD, of the Children’s Hospital and Montefiore in New York and colleagues reported in JACC Case Reports. With close follow-up, the child’s left ventricle size and systolic function have remained normal and mitral regurgitation resolved. The case report didn’t mention the infant’s gender.
But before the straightforward postdischarge course emerged, the infant was in a precarious state, and Dr. Sharma and her team were challenged to diagnose the underlying causes.
The child, who was born about 7 weeks premature, first came to the hospital having turned blue after choking on food. Nonrebreather mask ventilation was initiated in the ED, and an examination detected a holosystolic murmur. A test for COVID-19 was negative, but a later test was positive, and a chest x-ray exhibited cardiomegaly and signs of fluid and inflammation in the lungs.
An electrocardiogram detected sinus tachycardia, ST-segment depression and other anomalies in cardiac function. Further investigation with a transthoracic ECG showed severely depressed left ventricle systolic function with an ejection fraction of 30%, severe mitral regurgitation, and normal right ventricular systolic function.
Treatment included remdesivir and intravenous antibiotics. Through the hospital course, the patient was extubated to noninvasive ventilation, reintubated, put on intravenous steroid (methylprednisolone) and low-molecular-weight heparin, extubated, and tested throughout for cardiac function.
By day 14, left ventricle size and function normalized, and while the mitral regurgitation remained severe, it improved later without HF therapies. Left ventricle ejection fraction had recovered to 60%, and key cardiac biomarkers had normalized. On day 16, milrinone was discontinued, and the care team determined the patient no longer needed oral heart failure therapies.
“Most children with COVID-19 are either asymptomatic or have mild symptoms, but our case shows the potential for reversible myocardial injury in infants with COVID-19,” said Dr. Sharma. “Testing for COVID-19 in children presenting with signs and symptoms of heart failure is very important as we learn more about the impact of this virus.”
Dr. Sharma and coauthors have no relevant financial relationships to disclose.
SOURCE: Sharma M et al. JACC Case Rep. 2020. doi: 10.1016/j.jaccas.2020.09.031.
Reports of signs of heart failure in adults with COVID-19 have been rare – just four such cases have been published since the outbreak started in China – and now a team of pediatric cardiologists in New York have reported a case of acute but reversible myocardial injury in an infant with COVID-19.
and right upper lobe atelectasis.
The 2-month-old infant went home after more than 2 weeks in the hospital with no apparent lingering cardiac effects of the illness and not needing any oral heart failure medications, Madhu Sharma, MD, of the Children’s Hospital and Montefiore in New York and colleagues reported in JACC Case Reports. With close follow-up, the child’s left ventricle size and systolic function have remained normal and mitral regurgitation resolved. The case report didn’t mention the infant’s gender.
But before the straightforward postdischarge course emerged, the infant was in a precarious state, and Dr. Sharma and her team were challenged to diagnose the underlying causes.
The child, who was born about 7 weeks premature, first came to the hospital having turned blue after choking on food. Nonrebreather mask ventilation was initiated in the ED, and an examination detected a holosystolic murmur. A test for COVID-19 was negative, but a later test was positive, and a chest x-ray exhibited cardiomegaly and signs of fluid and inflammation in the lungs.
An electrocardiogram detected sinus tachycardia, ST-segment depression and other anomalies in cardiac function. Further investigation with a transthoracic ECG showed severely depressed left ventricle systolic function with an ejection fraction of 30%, severe mitral regurgitation, and normal right ventricular systolic function.
Treatment included remdesivir and intravenous antibiotics. Through the hospital course, the patient was extubated to noninvasive ventilation, reintubated, put on intravenous steroid (methylprednisolone) and low-molecular-weight heparin, extubated, and tested throughout for cardiac function.
By day 14, left ventricle size and function normalized, and while the mitral regurgitation remained severe, it improved later without HF therapies. Left ventricle ejection fraction had recovered to 60%, and key cardiac biomarkers had normalized. On day 16, milrinone was discontinued, and the care team determined the patient no longer needed oral heart failure therapies.
“Most children with COVID-19 are either asymptomatic or have mild symptoms, but our case shows the potential for reversible myocardial injury in infants with COVID-19,” said Dr. Sharma. “Testing for COVID-19 in children presenting with signs and symptoms of heart failure is very important as we learn more about the impact of this virus.”
Dr. Sharma and coauthors have no relevant financial relationships to disclose.
SOURCE: Sharma M et al. JACC Case Rep. 2020. doi: 10.1016/j.jaccas.2020.09.031.
Reports of signs of heart failure in adults with COVID-19 have been rare – just four such cases have been published since the outbreak started in China – and now a team of pediatric cardiologists in New York have reported a case of acute but reversible myocardial injury in an infant with COVID-19.
and right upper lobe atelectasis.
The 2-month-old infant went home after more than 2 weeks in the hospital with no apparent lingering cardiac effects of the illness and not needing any oral heart failure medications, Madhu Sharma, MD, of the Children’s Hospital and Montefiore in New York and colleagues reported in JACC Case Reports. With close follow-up, the child’s left ventricle size and systolic function have remained normal and mitral regurgitation resolved. The case report didn’t mention the infant’s gender.
But before the straightforward postdischarge course emerged, the infant was in a precarious state, and Dr. Sharma and her team were challenged to diagnose the underlying causes.
The child, who was born about 7 weeks premature, first came to the hospital having turned blue after choking on food. Nonrebreather mask ventilation was initiated in the ED, and an examination detected a holosystolic murmur. A test for COVID-19 was negative, but a later test was positive, and a chest x-ray exhibited cardiomegaly and signs of fluid and inflammation in the lungs.
An electrocardiogram detected sinus tachycardia, ST-segment depression and other anomalies in cardiac function. Further investigation with a transthoracic ECG showed severely depressed left ventricle systolic function with an ejection fraction of 30%, severe mitral regurgitation, and normal right ventricular systolic function.
Treatment included remdesivir and intravenous antibiotics. Through the hospital course, the patient was extubated to noninvasive ventilation, reintubated, put on intravenous steroid (methylprednisolone) and low-molecular-weight heparin, extubated, and tested throughout for cardiac function.
By day 14, left ventricle size and function normalized, and while the mitral regurgitation remained severe, it improved later without HF therapies. Left ventricle ejection fraction had recovered to 60%, and key cardiac biomarkers had normalized. On day 16, milrinone was discontinued, and the care team determined the patient no longer needed oral heart failure therapies.
“Most children with COVID-19 are either asymptomatic or have mild symptoms, but our case shows the potential for reversible myocardial injury in infants with COVID-19,” said Dr. Sharma. “Testing for COVID-19 in children presenting with signs and symptoms of heart failure is very important as we learn more about the impact of this virus.”
Dr. Sharma and coauthors have no relevant financial relationships to disclose.
SOURCE: Sharma M et al. JACC Case Rep. 2020. doi: 10.1016/j.jaccas.2020.09.031.
FROM JACC CASE REPORTS
Key clinical point: Children presenting with COVID-19 should be tested for heart failure.
Major finding: A 2-month-old infant with COVID-19 had acute but reversible myocardial injury.
Study details: Single case report.
Disclosures: Dr. Sharma, MD, has no relevant financial relationships to disclose.
Source: Sharma M et al. JACC Case Rep. 2020. doi: 10.1016/j.jaccas.2020.09.031.
Watch for cognitive traps that lead diagnostics astray
While it’s important not to think immediately of zebras when hearing hoofbeats, it’s just as important not to assume it’s always a horse. The delicate balance between not jumping to the seemingly obvious diagnosis without overanalyzing and overtesting is familiar to all physicians, and

“When these errors are made, it’s not because physicians lack knowledge, but they go down a wrong path in their thinking process,” Richard Scarfone, MD, a pediatric emergency medicine physician at the Children’s Hospital of Philadelphia, told attendees at the annual meeting of the American Academy of Pediatrics, held virtually this year. “An important point to be made here is that how physicians think seems to be much more important than what physicians know.”
Dr. Scarfone and Joshua Nagler, MD, MHPEd, director, pediatric emergency medicine fellowship program at Children’s Hospital Boston, presented a session on the cognitive biases that can trip up clinicians when making diagnoses and how to avoid them. Research shows that the rate of diagnostic error is approximately 15%. Although those findings come from studies in adults, the rates are likely similar in pediatrics, Dr. Scarfone said.
A wide range of clinical factors contribute to diagnostic errors: limited information, vague or undifferentiated symptoms, incomplete history, multiple transitions of care, diagnostic uncertainty, daily decision density, and reliance on pattern recognition, among others. Personal contributing factors can play a role as well, such as atypical work hours, fatigue, one’s emotional or affective state, a high cognitive load, and others. On top of all that, medical decision-making can be really complex on its own, Dr. Scarfone said. He compared differential diagnosis with a tree where a single leaf is the correct diagnosis.
System 1 thinking: Pros and cons
Dr. Scarfone and Dr. Nagler explained system 1 and system 2 thinking, two different ways of thinking that can influence decision-making that Daniel Kahneman explained in his book “Thinking, Fast and Slow.” System 1 refers to the snap judgments that rely on heuristics while system 2 refers to a more analytic, slower process.

Neither system 1 nor 2 is inherently “right or wrong,” Dr. Scarfone said. “The diagnostic sweet spot is to try to apply the correct system to the correct patient.”
Heuristics are the mental shortcuts people use to make decisions based on past experience. They exist because they’re useful, enabling people to focus only on what they need to accomplish everyday tasks, such as driving or brushing teeth. But heuristics can also lead to predictable cognitive errors.
“The good news about heuristics and system 1 thinking is that it’s efficient and simple, and we desire that in a busy practice or ED setting, but we should recognize that the trade-off is that it may be at the expense of accuracy,” Dr. Scarfone said.
The advantage to system 1 thinking is easy, simple, rapid, and efficient decision-making that rejects ambiguity. It’s also usually accurate, which rewards the approach, and accuracy increases with time based on memory, experience, and pattern recognition. Doctors develop “illness scripts” that help in identifying diagnoses.
“Illness scripts are common patterns of clinical presentations that usually lead us to a diagnostic possibility,” Dr. Scarfone said. “A classic illness script might be a 4-week-old firstborn male with forceful vomiting, and immediately your mind may go to pyloric stenosis as a likely diagnosis.” But the patient may have a different diagnosis than the initial impression your system 1 thinking leads you to believe.
“Generally, the more experience a clinician has, the more accurate they’ll be in using system 1,” he said. “Seasoned physicians are much more likely to employ system 1 than a newer physician or trainee,” which is why heuristics shouldn’t be thought of as hindrances. Dr. Scarfone quoted Kevin Eva in a 2005 review on clinical reasoning: “Successful heuristics should be embraced rather than overcome.”
A drawback to system 1 thinking, however, is thinking that “what you see is all there is,” which can lead to cognitive errors. Feeling wrong feels the same as feeling right, so you may not realize when you’re off target and therefore neglect to consider alternatives.
“When we learn a little about our patient’s complaint, it’s easier to fit everything into a coherent explanation,” Dr. Scarfone said, but “don’t ask, don’t tell doesn’t work in medicine.”
Another challenge with system 1 thinking is that pattern recognition can be unreliable because it’s dependent on context. For example, consider the difference in assessing a patient’s sore throat in a primary care office versus a resuscitation bay. “Clearly our consideration of what may be going on with the patient and what the diagnosis may be is likely to vary in those two settings,” he said.
System 2 thinking: Of zebras and horses
System 2 is the analytic thinking that involves pondering and seek out the optimal answer rather than the “good-enough” answer.
“The good news about system 2 is that it really can monitor system 1,” said Dr. Nagler, who has a master’s degree in health professions education. “If you spend the time to do analytic reasoning, you can actually mitigate some of those errors that may occur from intuitive judgments from system 1 thinking. System 2 spends the time to say ‘let’s make sure we’re doing this right.’ ” In multiple-choice tests, for example, people are twice as likely to change a wrong answer to a right one than a right one to a wrong one.
System 2 thinking allows for the reasoning to assess questions in the gray zone. It’s vigilant, it’s reliable, it’s effective, it acknowledges uncertainty and doubt, it can be safe in terms of providing care, and it has high scientific rigor. But it also has disadvantages, starting with the fact that it’s slower and more time-consuming. System 2 thinking is resource intensive, requiring a higher cognitive demand and more time and effort.
“Sometimes the quick judgment is the best judgment,” Dr. Nagler said. System 2 thinking also is sometimes unnecessary and counter to value-based care. “If you start to think about all the possibilities of what a presentation may be, all of a sudden you might find yourself wanting to do all kinds of tests and all kinds of referrals and other things, which is not necessarily value-based care.” When system 2 thinking goes astray, it makes us think everything we see is a zebra rather than a horse.
Sonia Khan, MD, a pediatrician in Fremont, Calif., found this session particularly worthwhile.
“It really tries to explain the difference between leaping to conclusions and learning how to hold your horses and do a bit more, to double check that you’re not locking everything into a horse stall and missing a zebra, and avoiding go too far with system 2 and thinking that everything’s a zebra,” Dr. Khan said. “It’s a difficult talk to have because you’re asking pediatricians to look in the mirror and own up, to learn to step back and reconsider the picture, and consider the biases that may come into your decision-making; then learn to extrude them, and rethink the case to be sure your knee-jerk diagnostic response is correct.”
Types of cognitive errors
The presenters listed some of the most common cognitive errors, although their list is far from exhaustive.
- Affective error. Avoiding unpleasant but necessary tests or examinations because of sympathy for the patient, such as avoiding blood work to spare a needle stick in a cancer patient with abdominal pain because the mother is convinced it’s constipation from opioids. This is similar to omission bias, which places excessive concern on avoiding a therapy’s adverse effects when the therapy could be highly effective.
- Anchoring. Clinging to an initial impression or salient features of initial presentation, even as conflicting and contradictory data accumulate, such as diagnosing a patient with fever and vomiting with gastroenteritis even when the patient has an oxygen saturation of 94% and tachypnea.
- Attribution errors. Negative stereotypes lead clinicians to ignore or minimize the possibility of serious disease, such as evaluating a confused teen covered in piercings and tattoos for drug ingestion when the actual diagnosis is new-onset diabetic ketoacidosis.
- Availability bias. Overestimating or underestimating the probability of disease because of recent experience, what was most recently “available” to your brain cognitively, such as getting head imaging on several vomiting patients in a row because you recently had one with a new brain tumor diagnosis.
- Bandwagon effect. Accepting the group’s opinion without assessing a clinical situation yourself, such as sending home a crying, vomiting infant with a presumed viral infection only to see the infant return later with intussusception.
- Base rate neglect. Ignoring the true prevalence of disease by either inflating it or reducing it, such as searching for cardiac disease in all pediatric patients with chest pain.
- Commission. A tendency toward action with the belief that harm may only be prevented by action, such as ordering every possible test for a patient with fever to “rule everything out.”
- Confirmation bias. Subconscious cherry-picking: A tendency to look for, notice, and remember information that fits with preexisting expectations while disregarding information that contradicts those expectations.
- Diagnostic momentum. Clinging to that initial diagnostic impression that may have been generated by others, which is particularly common during transitions of care.
- Premature closure. Narrowing down to a diagnosis without thinking about other diagnoses or asking enough questions about other symptoms that may have opened up other diagnostic possibilities.
- Representation bias. Making a decision in the absence of appropriate context by incorrectly comparing two situations because of a perceived similarity between them, or on the flip side, evaluating a situation without comparing it with other situations.
- Overconfidence. Making a decision without enough supportive evidence yet feeling confident about the diagnosis.
- Search satisfying. Stopping the search for additional diagnoses after the anticipated diagnosis has been made.
Cognitive pills for cognitive ills
Being aware of the pitfalls of cognitive errors is the first step to avoiding and mitigating them. “It really does start with preparation and awareness,” Dr. Scarfone said before presenting strategies to build a cognitive “firewall” that can help physicians practice reflectively instead of reflexively.
First, be aware of your cognitive style. People usually have the same thinking pattern in everyday life as in the clinical setting, so determine whether you’re more of a system 1 or system 2 thinker. System 1 thinkers need to watch out for framing (relying too heavily on context), premature closure, diagnostic momentum, anchoring, and confirmation bias. System 2 thinkers need to watch out for commission, availability bias, and base rate neglect.
“Neither system is inherently right or wrong,” Dr. Scarfone reiterated. “In the perfect world, you may use system 1 to form an initial impression, but then system 2 should really act as a check and balance system to cause you to reflect on your initial diagnostic impressions.”
Additional strategies include being a good history taker and performing a meticulous physical exam: be a good listener, clarify unclear aspects of the history, and identify and address the main concern.
“Remember children and families have a story to tell, and if we listen carefully enough, the diagnostic clues are there,” Dr. Scarfone said. “Sometimes they may be quite subtle.” He recommended doctors perform each part of the physical exam as if expecting an abnormality.
Another strategy is using meta-cognition, a forced analysis of the thinking that led to a diagnosis. It involves asking: “If I had to explain my medical decision-making to others, would this make inherent sense?” Dr. Scarfone said. “If you’re testing, try to avoid anchoring and confirmation biases.”
Finally, take a diagnostic time-out with a checklist that asks these questions:
- Does my presumptive diagnosis make sense?
- What evidence supports or refutes it?
- Did I arrive at it via cognitive biases?
- Are there other diagnostic possibilities that should be considered?
One way to do this is creating a table listing the complaint/finding, diagnostic possibilities with system 1 thinking, diagnostic possibilities with system 2 thinking, and then going beyond system 2 – the potential zebras – when even system 2 diagnostic possibilities don’t account for what the patient is saying or what the exam shows.
Enough overlap exists between these cognitive biases and the intrinsic bias related to individual characteristics that Dr. Khan appreciated the talk on another level as well.
“For me, as a brown Muslim immigrant woman of color, I can sometimes see cognitive biases in action with my colleagues and realize that they are oblivious to it,” Dr. Khan said. “It’s really refreshing to see this issue come up and being discussed at the [AAP] National Conference and Exhibition.”
Dr. Scarfone, Dr. Nagler and Dr. Khan have no relevant financial disclosures.
This article was updated 12/8/2020.
While it’s important not to think immediately of zebras when hearing hoofbeats, it’s just as important not to assume it’s always a horse. The delicate balance between not jumping to the seemingly obvious diagnosis without overanalyzing and overtesting is familiar to all physicians, and
“When these errors are made, it’s not because physicians lack knowledge, but they go down a wrong path in their thinking process,” Richard Scarfone, MD, a pediatric emergency medicine physician at the Children’s Hospital of Philadelphia, told attendees at the annual meeting of the American Academy of Pediatrics, held virtually this year. “An important point to be made here is that how physicians think seems to be much more important than what physicians know.”
Dr. Scarfone and Joshua Nagler, MD, MHPEd, director, pediatric emergency medicine fellowship program at Children’s Hospital Boston, presented a session on the cognitive biases that can trip up clinicians when making diagnoses and how to avoid them. Research shows that the rate of diagnostic error is approximately 15%. Although those findings come from studies in adults, the rates are likely similar in pediatrics, Dr. Scarfone said.
A wide range of clinical factors contribute to diagnostic errors: limited information, vague or undifferentiated symptoms, incomplete history, multiple transitions of care, diagnostic uncertainty, daily decision density, and reliance on pattern recognition, among others. Personal contributing factors can play a role as well, such as atypical work hours, fatigue, one’s emotional or affective state, a high cognitive load, and others. On top of all that, medical decision-making can be really complex on its own, Dr. Scarfone said. He compared differential diagnosis with a tree where a single leaf is the correct diagnosis.
System 1 thinking: Pros and cons
Dr. Scarfone and Dr. Nagler explained system 1 and system 2 thinking, two different ways of thinking that can influence decision-making that Daniel Kahneman explained in his book “Thinking, Fast and Slow.” System 1 refers to the snap judgments that rely on heuristics while system 2 refers to a more analytic, slower process.
Neither system 1 nor 2 is inherently “right or wrong,” Dr. Scarfone said. “The diagnostic sweet spot is to try to apply the correct system to the correct patient.”
Heuristics are the mental shortcuts people use to make decisions based on past experience. They exist because they’re useful, enabling people to focus only on what they need to accomplish everyday tasks, such as driving or brushing teeth. But heuristics can also lead to predictable cognitive errors.
“The good news about heuristics and system 1 thinking is that it’s efficient and simple, and we desire that in a busy practice or ED setting, but we should recognize that the trade-off is that it may be at the expense of accuracy,” Dr. Scarfone said.
The advantage to system 1 thinking is easy, simple, rapid, and efficient decision-making that rejects ambiguity. It’s also usually accurate, which rewards the approach, and accuracy increases with time based on memory, experience, and pattern recognition. Doctors develop “illness scripts” that help in identifying diagnoses.
“Illness scripts are common patterns of clinical presentations that usually lead us to a diagnostic possibility,” Dr. Scarfone said. “A classic illness script might be a 4-week-old firstborn male with forceful vomiting, and immediately your mind may go to pyloric stenosis as a likely diagnosis.” But the patient may have a different diagnosis than the initial impression your system 1 thinking leads you to believe.
“Generally, the more experience a clinician has, the more accurate they’ll be in using system 1,” he said. “Seasoned physicians are much more likely to employ system 1 than a newer physician or trainee,” which is why heuristics shouldn’t be thought of as hindrances. Dr. Scarfone quoted Kevin Eva in a 2005 review on clinical reasoning: “Successful heuristics should be embraced rather than overcome.”
A drawback to system 1 thinking, however, is thinking that “what you see is all there is,” which can lead to cognitive errors. Feeling wrong feels the same as feeling right, so you may not realize when you’re off target and therefore neglect to consider alternatives.
“When we learn a little about our patient’s complaint, it’s easier to fit everything into a coherent explanation,” Dr. Scarfone said, but “don’t ask, don’t tell doesn’t work in medicine.”
Another challenge with system 1 thinking is that pattern recognition can be unreliable because it’s dependent on context. For example, consider the difference in assessing a patient’s sore throat in a primary care office versus a resuscitation bay. “Clearly our consideration of what may be going on with the patient and what the diagnosis may be is likely to vary in those two settings,” he said.
System 2 thinking: Of zebras and horses
System 2 is the analytic thinking that involves pondering and seek out the optimal answer rather than the “good-enough” answer.
“The good news about system 2 is that it really can monitor system 1,” said Dr. Nagler, who has a master’s degree in health professions education. “If you spend the time to do analytic reasoning, you can actually mitigate some of those errors that may occur from intuitive judgments from system 1 thinking. System 2 spends the time to say ‘let’s make sure we’re doing this right.’ ” In multiple-choice tests, for example, people are twice as likely to change a wrong answer to a right one than a right one to a wrong one.
System 2 thinking allows for the reasoning to assess questions in the gray zone. It’s vigilant, it’s reliable, it’s effective, it acknowledges uncertainty and doubt, it can be safe in terms of providing care, and it has high scientific rigor. But it also has disadvantages, starting with the fact that it’s slower and more time-consuming. System 2 thinking is resource intensive, requiring a higher cognitive demand and more time and effort.
“Sometimes the quick judgment is the best judgment,” Dr. Nagler said. System 2 thinking also is sometimes unnecessary and counter to value-based care. “If you start to think about all the possibilities of what a presentation may be, all of a sudden you might find yourself wanting to do all kinds of tests and all kinds of referrals and other things, which is not necessarily value-based care.” When system 2 thinking goes astray, it makes us think everything we see is a zebra rather than a horse.
Sonia Khan, MD, a pediatrician in Fremont, Calif., found this session particularly worthwhile.
“It really tries to explain the difference between leaping to conclusions and learning how to hold your horses and do a bit more, to double check that you’re not locking everything into a horse stall and missing a zebra, and avoiding go too far with system 2 and thinking that everything’s a zebra,” Dr. Khan said. “It’s a difficult talk to have because you’re asking pediatricians to look in the mirror and own up, to learn to step back and reconsider the picture, and consider the biases that may come into your decision-making; then learn to extrude them, and rethink the case to be sure your knee-jerk diagnostic response is correct.”
Types of cognitive errors
The presenters listed some of the most common cognitive errors, although their list is far from exhaustive.
- Affective error. Avoiding unpleasant but necessary tests or examinations because of sympathy for the patient, such as avoiding blood work to spare a needle stick in a cancer patient with abdominal pain because the mother is convinced it’s constipation from opioids. This is similar to omission bias, which places excessive concern on avoiding a therapy’s adverse effects when the therapy could be highly effective.
- Anchoring. Clinging to an initial impression or salient features of initial presentation, even as conflicting and contradictory data accumulate, such as diagnosing a patient with fever and vomiting with gastroenteritis even when the patient has an oxygen saturation of 94% and tachypnea.
- Attribution errors. Negative stereotypes lead clinicians to ignore or minimize the possibility of serious disease, such as evaluating a confused teen covered in piercings and tattoos for drug ingestion when the actual diagnosis is new-onset diabetic ketoacidosis.
- Availability bias. Overestimating or underestimating the probability of disease because of recent experience, what was most recently “available” to your brain cognitively, such as getting head imaging on several vomiting patients in a row because you recently had one with a new brain tumor diagnosis.
- Bandwagon effect. Accepting the group’s opinion without assessing a clinical situation yourself, such as sending home a crying, vomiting infant with a presumed viral infection only to see the infant return later with intussusception.
- Base rate neglect. Ignoring the true prevalence of disease by either inflating it or reducing it, such as searching for cardiac disease in all pediatric patients with chest pain.
- Commission. A tendency toward action with the belief that harm may only be prevented by action, such as ordering every possible test for a patient with fever to “rule everything out.”
- Confirmation bias. Subconscious cherry-picking: A tendency to look for, notice, and remember information that fits with preexisting expectations while disregarding information that contradicts those expectations.
- Diagnostic momentum. Clinging to that initial diagnostic impression that may have been generated by others, which is particularly common during transitions of care.
- Premature closure. Narrowing down to a diagnosis without thinking about other diagnoses or asking enough questions about other symptoms that may have opened up other diagnostic possibilities.
- Representation bias. Making a decision in the absence of appropriate context by incorrectly comparing two situations because of a perceived similarity between them, or on the flip side, evaluating a situation without comparing it with other situations.
- Overconfidence. Making a decision without enough supportive evidence yet feeling confident about the diagnosis.
- Search satisfying. Stopping the search for additional diagnoses after the anticipated diagnosis has been made.
Cognitive pills for cognitive ills
Being aware of the pitfalls of cognitive errors is the first step to avoiding and mitigating them. “It really does start with preparation and awareness,” Dr. Scarfone said before presenting strategies to build a cognitive “firewall” that can help physicians practice reflectively instead of reflexively.
First, be aware of your cognitive style. People usually have the same thinking pattern in everyday life as in the clinical setting, so determine whether you’re more of a system 1 or system 2 thinker. System 1 thinkers need to watch out for framing (relying too heavily on context), premature closure, diagnostic momentum, anchoring, and confirmation bias. System 2 thinkers need to watch out for commission, availability bias, and base rate neglect.
“Neither system is inherently right or wrong,” Dr. Scarfone reiterated. “In the perfect world, you may use system 1 to form an initial impression, but then system 2 should really act as a check and balance system to cause you to reflect on your initial diagnostic impressions.”
Additional strategies include being a good history taker and performing a meticulous physical exam: be a good listener, clarify unclear aspects of the history, and identify and address the main concern.
“Remember children and families have a story to tell, and if we listen carefully enough, the diagnostic clues are there,” Dr. Scarfone said. “Sometimes they may be quite subtle.” He recommended doctors perform each part of the physical exam as if expecting an abnormality.
Another strategy is using meta-cognition, a forced analysis of the thinking that led to a diagnosis. It involves asking: “If I had to explain my medical decision-making to others, would this make inherent sense?” Dr. Scarfone said. “If you’re testing, try to avoid anchoring and confirmation biases.”
Finally, take a diagnostic time-out with a checklist that asks these questions:
- Does my presumptive diagnosis make sense?
- What evidence supports or refutes it?
- Did I arrive at it via cognitive biases?
- Are there other diagnostic possibilities that should be considered?
One way to do this is creating a table listing the complaint/finding, diagnostic possibilities with system 1 thinking, diagnostic possibilities with system 2 thinking, and then going beyond system 2 – the potential zebras – when even system 2 diagnostic possibilities don’t account for what the patient is saying or what the exam shows.
Enough overlap exists between these cognitive biases and the intrinsic bias related to individual characteristics that Dr. Khan appreciated the talk on another level as well.
“For me, as a brown Muslim immigrant woman of color, I can sometimes see cognitive biases in action with my colleagues and realize that they are oblivious to it,” Dr. Khan said. “It’s really refreshing to see this issue come up and being discussed at the [AAP] National Conference and Exhibition.”
Dr. Scarfone, Dr. Nagler and Dr. Khan have no relevant financial disclosures.
This article was updated 12/8/2020.
While it’s important not to think immediately of zebras when hearing hoofbeats, it’s just as important not to assume it’s always a horse. The delicate balance between not jumping to the seemingly obvious diagnosis without overanalyzing and overtesting is familiar to all physicians, and
“When these errors are made, it’s not because physicians lack knowledge, but they go down a wrong path in their thinking process,” Richard Scarfone, MD, a pediatric emergency medicine physician at the Children’s Hospital of Philadelphia, told attendees at the annual meeting of the American Academy of Pediatrics, held virtually this year. “An important point to be made here is that how physicians think seems to be much more important than what physicians know.”
Dr. Scarfone and Joshua Nagler, MD, MHPEd, director, pediatric emergency medicine fellowship program at Children’s Hospital Boston, presented a session on the cognitive biases that can trip up clinicians when making diagnoses and how to avoid them. Research shows that the rate of diagnostic error is approximately 15%. Although those findings come from studies in adults, the rates are likely similar in pediatrics, Dr. Scarfone said.
A wide range of clinical factors contribute to diagnostic errors: limited information, vague or undifferentiated symptoms, incomplete history, multiple transitions of care, diagnostic uncertainty, daily decision density, and reliance on pattern recognition, among others. Personal contributing factors can play a role as well, such as atypical work hours, fatigue, one’s emotional or affective state, a high cognitive load, and others. On top of all that, medical decision-making can be really complex on its own, Dr. Scarfone said. He compared differential diagnosis with a tree where a single leaf is the correct diagnosis.
System 1 thinking: Pros and cons
Dr. Scarfone and Dr. Nagler explained system 1 and system 2 thinking, two different ways of thinking that can influence decision-making that Daniel Kahneman explained in his book “Thinking, Fast and Slow.” System 1 refers to the snap judgments that rely on heuristics while system 2 refers to a more analytic, slower process.
Neither system 1 nor 2 is inherently “right or wrong,” Dr. Scarfone said. “The diagnostic sweet spot is to try to apply the correct system to the correct patient.”
Heuristics are the mental shortcuts people use to make decisions based on past experience. They exist because they’re useful, enabling people to focus only on what they need to accomplish everyday tasks, such as driving or brushing teeth. But heuristics can also lead to predictable cognitive errors.
“The good news about heuristics and system 1 thinking is that it’s efficient and simple, and we desire that in a busy practice or ED setting, but we should recognize that the trade-off is that it may be at the expense of accuracy,” Dr. Scarfone said.
The advantage to system 1 thinking is easy, simple, rapid, and efficient decision-making that rejects ambiguity. It’s also usually accurate, which rewards the approach, and accuracy increases with time based on memory, experience, and pattern recognition. Doctors develop “illness scripts” that help in identifying diagnoses.
“Illness scripts are common patterns of clinical presentations that usually lead us to a diagnostic possibility,” Dr. Scarfone said. “A classic illness script might be a 4-week-old firstborn male with forceful vomiting, and immediately your mind may go to pyloric stenosis as a likely diagnosis.” But the patient may have a different diagnosis than the initial impression your system 1 thinking leads you to believe.
“Generally, the more experience a clinician has, the more accurate they’ll be in using system 1,” he said. “Seasoned physicians are much more likely to employ system 1 than a newer physician or trainee,” which is why heuristics shouldn’t be thought of as hindrances. Dr. Scarfone quoted Kevin Eva in a 2005 review on clinical reasoning: “Successful heuristics should be embraced rather than overcome.”
A drawback to system 1 thinking, however, is thinking that “what you see is all there is,” which can lead to cognitive errors. Feeling wrong feels the same as feeling right, so you may not realize when you’re off target and therefore neglect to consider alternatives.
“When we learn a little about our patient’s complaint, it’s easier to fit everything into a coherent explanation,” Dr. Scarfone said, but “don’t ask, don’t tell doesn’t work in medicine.”
Another challenge with system 1 thinking is that pattern recognition can be unreliable because it’s dependent on context. For example, consider the difference in assessing a patient’s sore throat in a primary care office versus a resuscitation bay. “Clearly our consideration of what may be going on with the patient and what the diagnosis may be is likely to vary in those two settings,” he said.
System 2 thinking: Of zebras and horses
System 2 is the analytic thinking that involves pondering and seek out the optimal answer rather than the “good-enough” answer.
“The good news about system 2 is that it really can monitor system 1,” said Dr. Nagler, who has a master’s degree in health professions education. “If you spend the time to do analytic reasoning, you can actually mitigate some of those errors that may occur from intuitive judgments from system 1 thinking. System 2 spends the time to say ‘let’s make sure we’re doing this right.’ ” In multiple-choice tests, for example, people are twice as likely to change a wrong answer to a right one than a right one to a wrong one.
System 2 thinking allows for the reasoning to assess questions in the gray zone. It’s vigilant, it’s reliable, it’s effective, it acknowledges uncertainty and doubt, it can be safe in terms of providing care, and it has high scientific rigor. But it also has disadvantages, starting with the fact that it’s slower and more time-consuming. System 2 thinking is resource intensive, requiring a higher cognitive demand and more time and effort.
“Sometimes the quick judgment is the best judgment,” Dr. Nagler said. System 2 thinking also is sometimes unnecessary and counter to value-based care. “If you start to think about all the possibilities of what a presentation may be, all of a sudden you might find yourself wanting to do all kinds of tests and all kinds of referrals and other things, which is not necessarily value-based care.” When system 2 thinking goes astray, it makes us think everything we see is a zebra rather than a horse.
Sonia Khan, MD, a pediatrician in Fremont, Calif., found this session particularly worthwhile.
“It really tries to explain the difference between leaping to conclusions and learning how to hold your horses and do a bit more, to double check that you’re not locking everything into a horse stall and missing a zebra, and avoiding go too far with system 2 and thinking that everything’s a zebra,” Dr. Khan said. “It’s a difficult talk to have because you’re asking pediatricians to look in the mirror and own up, to learn to step back and reconsider the picture, and consider the biases that may come into your decision-making; then learn to extrude them, and rethink the case to be sure your knee-jerk diagnostic response is correct.”
Types of cognitive errors
The presenters listed some of the most common cognitive errors, although their list is far from exhaustive.
- Affective error. Avoiding unpleasant but necessary tests or examinations because of sympathy for the patient, such as avoiding blood work to spare a needle stick in a cancer patient with abdominal pain because the mother is convinced it’s constipation from opioids. This is similar to omission bias, which places excessive concern on avoiding a therapy’s adverse effects when the therapy could be highly effective.
- Anchoring. Clinging to an initial impression or salient features of initial presentation, even as conflicting and contradictory data accumulate, such as diagnosing a patient with fever and vomiting with gastroenteritis even when the patient has an oxygen saturation of 94% and tachypnea.
- Attribution errors. Negative stereotypes lead clinicians to ignore or minimize the possibility of serious disease, such as evaluating a confused teen covered in piercings and tattoos for drug ingestion when the actual diagnosis is new-onset diabetic ketoacidosis.
- Availability bias. Overestimating or underestimating the probability of disease because of recent experience, what was most recently “available” to your brain cognitively, such as getting head imaging on several vomiting patients in a row because you recently had one with a new brain tumor diagnosis.
- Bandwagon effect. Accepting the group’s opinion without assessing a clinical situation yourself, such as sending home a crying, vomiting infant with a presumed viral infection only to see the infant return later with intussusception.
- Base rate neglect. Ignoring the true prevalence of disease by either inflating it or reducing it, such as searching for cardiac disease in all pediatric patients with chest pain.
- Commission. A tendency toward action with the belief that harm may only be prevented by action, such as ordering every possible test for a patient with fever to “rule everything out.”
- Confirmation bias. Subconscious cherry-picking: A tendency to look for, notice, and remember information that fits with preexisting expectations while disregarding information that contradicts those expectations.
- Diagnostic momentum. Clinging to that initial diagnostic impression that may have been generated by others, which is particularly common during transitions of care.
- Premature closure. Narrowing down to a diagnosis without thinking about other diagnoses or asking enough questions about other symptoms that may have opened up other diagnostic possibilities.
- Representation bias. Making a decision in the absence of appropriate context by incorrectly comparing two situations because of a perceived similarity between them, or on the flip side, evaluating a situation without comparing it with other situations.
- Overconfidence. Making a decision without enough supportive evidence yet feeling confident about the diagnosis.
- Search satisfying. Stopping the search for additional diagnoses after the anticipated diagnosis has been made.
Cognitive pills for cognitive ills
Being aware of the pitfalls of cognitive errors is the first step to avoiding and mitigating them. “It really does start with preparation and awareness,” Dr. Scarfone said before presenting strategies to build a cognitive “firewall” that can help physicians practice reflectively instead of reflexively.
First, be aware of your cognitive style. People usually have the same thinking pattern in everyday life as in the clinical setting, so determine whether you’re more of a system 1 or system 2 thinker. System 1 thinkers need to watch out for framing (relying too heavily on context), premature closure, diagnostic momentum, anchoring, and confirmation bias. System 2 thinkers need to watch out for commission, availability bias, and base rate neglect.
“Neither system is inherently right or wrong,” Dr. Scarfone reiterated. “In the perfect world, you may use system 1 to form an initial impression, but then system 2 should really act as a check and balance system to cause you to reflect on your initial diagnostic impressions.”
Additional strategies include being a good history taker and performing a meticulous physical exam: be a good listener, clarify unclear aspects of the history, and identify and address the main concern.
“Remember children and families have a story to tell, and if we listen carefully enough, the diagnostic clues are there,” Dr. Scarfone said. “Sometimes they may be quite subtle.” He recommended doctors perform each part of the physical exam as if expecting an abnormality.
Another strategy is using meta-cognition, a forced analysis of the thinking that led to a diagnosis. It involves asking: “If I had to explain my medical decision-making to others, would this make inherent sense?” Dr. Scarfone said. “If you’re testing, try to avoid anchoring and confirmation biases.”
Finally, take a diagnostic time-out with a checklist that asks these questions:
- Does my presumptive diagnosis make sense?
- What evidence supports or refutes it?
- Did I arrive at it via cognitive biases?
- Are there other diagnostic possibilities that should be considered?
One way to do this is creating a table listing the complaint/finding, diagnostic possibilities with system 1 thinking, diagnostic possibilities with system 2 thinking, and then going beyond system 2 – the potential zebras – when even system 2 diagnostic possibilities don’t account for what the patient is saying or what the exam shows.
Enough overlap exists between these cognitive biases and the intrinsic bias related to individual characteristics that Dr. Khan appreciated the talk on another level as well.
“For me, as a brown Muslim immigrant woman of color, I can sometimes see cognitive biases in action with my colleagues and realize that they are oblivious to it,” Dr. Khan said. “It’s really refreshing to see this issue come up and being discussed at the [AAP] National Conference and Exhibition.”
Dr. Scarfone, Dr. Nagler and Dr. Khan have no relevant financial disclosures.
This article was updated 12/8/2020.
FROM AAP 2020
