User login
Early psychosis: No need for antipsychotics to recover?
Two new studies highlight the importance of early intervention in first-episode psychosis (FEP).
In the first study, Australian investigators conclude that, for some FEP patients, early psychosocial interventions may fend off the need for immediate treatment with antipsychotic medications.
In the second study, UK researchers show that long duration of untreated psychosis (DUP) is linked to a significantly reduced treatment response.
For both studies, the findings highlight the importance of rapid access to a comprehensive range of treatments in the first weeks after FEP onset.
“In a select group of people with first-episode psychosis, we found there was no difference in symptoms and functioning between those who had antipsychotic medication and those who didn’t,” lead author Shona M. Francey, PhD, clinical psychologist at Orygen, the National Center of Excellence in Youth Mental Health, Parkville, Australia, told Medscape Medical News.
“These findings supported our idea that, in the early phases of psychosis, with close monitoring and good psychosocial intervention, antipsychotic medication can be delayed,” Francey said.
The Australian study was published in Schizophrenia Bulletin Open. The British study was published in Lancet Psychiatry.
Adverse effects
Francey and colleagues note that, in comparison with standard treatment, early interventions produce superior outcomes for patients with psychosis. Although there are a variety of treatment options, low-dose second-generation antipsychotics typically play a central role.
However, atypical antipsychotics have rapid metabolic side effects, including weight gain and altered glucose metabolism, that increase the risk for cardiovascular disease and premature mortality. Importantly, such adverse effects are amplified among patients with FEP, who tend to be younger and treatment naive.
On the other hand, a growing body of evidence shows the benefit of nonpharmacologic interventions for patients with FEP, the investigators note. In addition, clinical staging models appear to support the use of less aggressive treatment early in the disease course.
“We have been working in early intervention for psychosis for a number of years and have found it’s possible to intervene early with young people and either prevent the onset of psychosis or ameliorate its impact,” said Francey.
“Since we can see some improvement in people in the prepsychotic phase, we wanted to know if we can also see some benefit without medication after the onset of what we would call full-threshold psychosis,” she added.
Staged Treatment and Acceptability Guidelines in Early Psychosis (STAGES) was a 6-month, triple-blind, randomized controlled noninferiority study that included 90 participants between the ages of 15 and 25 years who had FEP.
To maximize safety, patients were required to have low levels of suicidality and aggression, a DUP of less than 6 months, and to be living in stable accommodation with social support.
Participants were randomly assigned to two groups – one in which patients underwent intensive psychosocial therapy and received low-dose antipsychotic medication (n = 44), and one in which patients underwent intensive psychosocial therapy and were given placebo (n = 46).
Depending on the timing of study enrollment, those in the medication group received risperidone 1 mg or paliperidone 3 mg.
that is strongly focused on therapeutic engagement.
CBCM delivers formulation-driven cognitive-behavioral therapy and psychoeducation within a therapeutic case management framework, Francey said.
The primary outcome was level of functioning at 6, 12, and 24 months, as measured by the Social and Occupational Functioning Scale (SOFAS). The primary prespecified endpoint was outcome at 6 months. A noninferiority margin of 10.5 on the SOFAS was used as the smallest value representing a clinically important effect.
Other assessment tools included the BPRS-4 to test for positive psychotic symptoms, the Scale for the Assessment of Negative Symptoms (SANS), the Hamilton Rating Scale for Depression, and the Hamilton Rating Scale for Anxiety.
At baseline, the two treatment groups were comparable with respect to all measures of functioning and psychopathology.
The study’s discontinuation rate was high. At 6 months, only 16 patients in the psychosocial group had completed therapy, compared with 11 in the antipsychotic group.
At this point, the two groups were comparable in terms of psychopathology and functioning ratings. Both groups had lower symptoms, higher functioning scores, and higher Quality of Life Scale (QLS) scores than at baseline.
SOFAS scores were not significantly different between the groups at this time point. The mean score was 61.7 ± 16.8 in the psychosocial group and 61.5 ± 13.4 in the medication group.
The researchers note that, because the upper limit of the confidence interval (CI) was less than the study’s a priori inferiority margin of 10.5, psychosocial therapy was not inferior to medication at the 6-month assessment point.
Antipsychotics: Use with caution
Although between-group differences in SOFAS scores were not significant at 12 and 24 months, noninferiority of psychosocial therapy alone could not be confirmed because the CIs included the inferiority margin at each time point.
The two groups were statistically comparable at 6 months with respect to all other measures of psychopathology and the QLS. Similar results were found at 12 and 24 months.
The lone exception was with SANS at 12 months, on which patients in the placebo group had significantly higher negative symptom scores than the patients in the medication group.
There were no significant differences between study groups with respect to the number of adverse events.
Francey noted that the findings are important because they suggest that some young people with early-stage FEP and short DUP may be able to achieve symptom remission and function better without antipsychotic medication, provided they receive psychological interventions and comprehensive case management.
This challenges conventional wisdom that antipsychotic medications should be used for all patients who experience psychosis, she added.
However, managing FEP with psychosocial interventions should only be considered when it is safe to do so, Francey noted. In addition, the benefits of psychosocial interventions in these patients are less clear at 12 and 24 months.
Given these caveats, she noted that antipsychotics still play an important role in the treatment of these patients.
“I think there is definitely a place for medications. But I think they should be used cautiously, and you need a good, strong relationship between your treating team and your [patient] to work out what is needed and when it’s needed,” said Francey.
In addition, “when we do use medications, we should use the smallest possible dose that we can and also incorporate psychological support. I think that’s a really important part of it as well,” she said.
Timing matters
In the Lancet Psychiatry study, the researchers note that prolonged DUP is associated with worse outcomes, including increased symptoms, diminished social functioning, and poorer quality of life. The mechanism by which delayed treatment causes more harm remains unclear.
It is possible that symptoms simply accumulate over time, thereby worsening presentation. Another possibility is that continued psychosis after an initial critical period may cause long-term harm, they write.
They hypothesize that untreated psychosis can cause general treatment resistance by exacerbating underlying disease processes and that such damage progresses faster in the early stages of illness and then slows over time.
In addition, socially disruptive symptoms that are evident prior to FEP presentation may have a confounding effect, thereby leading to earlier presentation.
The investigators used data from two longitudinal cohort studies – the National Evaluation of Development of Early Intervention Network (NEDEN) study and the Outlook study.
In the NEDEN trial, 290 of 901 FEP patients (32%) were assessed within 3 weeks of presentation. In Outlook, 69 of 332 patients (21%) were assessed within 3 weeks of presentation.
In both studies, patients were examined at baseline, 6 months, and 12 months using the Positive and Negative Syndrome Scale (PANSS), the Calgary Depression Scale for Schizophrenia, the Mania Rating Scale, the Insight Scale, and SOFAS. The latter two measures were used only at baseline and 12-month follow-up. Logistic regression analyses were used to determine the association between DUP and outcomes.
In the NEDEN study, 751 patients were assessed at 6 months, and 719 were assessed at 12 months. In the Outlook study, 238 and 220 were assessed at the same two time points, respectively.
Results showed a curvilinear relationship between DUP and symptom severity. Longer DUP was predictive of reduced treatment response. However, patient response worsened more slowly as DUP lengthened.
For example, increasing DUP by ten times was predictive of less improvement in PANSS total score by 7.34 (95% CI, 5.76 – 8.92; P < .0001) in NEDEN and by 3.85 (95% CI, 1.69 – 600; P =. 0005) in Outlook. Nevertheless, longer DUP was not associated with worse presentation for any symptoms except depression in NEDEN.
The findings seem to support that the potential harm incurred by delaying treatment among patients with FEP is greatest in the early weeks of psychosis and then levels off, the investigators note.
Given these insights, mental health professionals might consider focusing their efforts on the early detection and treatment of patients for whom DUP is short.
Similarly, because DUP was directly associated with all symptoms, early access to comprehensive treatment “might be preferable to early delivery of particular treatments with particular effects (eg, dopamine antagonists),” they write.
“A pragmatic call”
Commenting on the British study in an accompanying editorial, Lena K. Palaniyappan, MD, University of Western Ontario, London, Canada, and Rajeev Krishnadas, MD, University of Glasgow, Scotland, write that any illness left untreated can become more challenging to treat, including psychosis.
“This should make early intervention in psychosis a pragmatic call with no prima facie argument against it,” they write. A reduction in DUP “underpins the rationale behind early detection and intervention in psychosis.”
The editorialists note that the relationship between DUP and successful treatment in early psychosis “strengthens the argument for more proactive early assessment and intervention to shorten treatment delay.
“As we have learnt over the past two decades, even punctual treatment when symptoms first arise continues to be too late when it comes to psychosis,” they write.
Francey also recognizes the value of early intervention in FEP. However, she noted that comprehensive psychosocial therapy might well prove effective enough to stave off antipsychotic therapy in a certain subset of patients.
“For some people, antipsychotics may never need to be introduced,” she said. “Some people recover from their first episode of psychosis and don’t go on to have any more, while others have an episodic illness,” she said.
If another episode develops and the symptoms come back, further psychosocial interventions could then be tried “or you might want to move on” to psychotic medication “because trying to get people better and functioning as well as they can is our primary aim,” Francey said.
The STAGES study was supported by the Australian National Health and Medical Research Council. The British study was funded by the UK Department of Health, the National Institute of Health Research, and the Medical Research Council. Francey and Krishnadas have reported no relevant financial relationships. Palaniyappan has received grants and personal fees from Janssen Canada and Otsuka Canada, grants from Sunovion, and personal fees from SPMM Course UK and the Canadian Psychiatric Association.
This article first appeared on Medscape.com.
Two new studies highlight the importance of early intervention in first-episode psychosis (FEP).
In the first study, Australian investigators conclude that, for some FEP patients, early psychosocial interventions may fend off the need for immediate treatment with antipsychotic medications.
In the second study, UK researchers show that long duration of untreated psychosis (DUP) is linked to a significantly reduced treatment response.
For both studies, the findings highlight the importance of rapid access to a comprehensive range of treatments in the first weeks after FEP onset.
“In a select group of people with first-episode psychosis, we found there was no difference in symptoms and functioning between those who had antipsychotic medication and those who didn’t,” lead author Shona M. Francey, PhD, clinical psychologist at Orygen, the National Center of Excellence in Youth Mental Health, Parkville, Australia, told Medscape Medical News.
“These findings supported our idea that, in the early phases of psychosis, with close monitoring and good psychosocial intervention, antipsychotic medication can be delayed,” Francey said.
The Australian study was published in Schizophrenia Bulletin Open. The British study was published in Lancet Psychiatry.
Adverse effects
Francey and colleagues note that, in comparison with standard treatment, early interventions produce superior outcomes for patients with psychosis. Although there are a variety of treatment options, low-dose second-generation antipsychotics typically play a central role.
However, atypical antipsychotics have rapid metabolic side effects, including weight gain and altered glucose metabolism, that increase the risk for cardiovascular disease and premature mortality. Importantly, such adverse effects are amplified among patients with FEP, who tend to be younger and treatment naive.
On the other hand, a growing body of evidence shows the benefit of nonpharmacologic interventions for patients with FEP, the investigators note. In addition, clinical staging models appear to support the use of less aggressive treatment early in the disease course.
“We have been working in early intervention for psychosis for a number of years and have found it’s possible to intervene early with young people and either prevent the onset of psychosis or ameliorate its impact,” said Francey.
“Since we can see some improvement in people in the prepsychotic phase, we wanted to know if we can also see some benefit without medication after the onset of what we would call full-threshold psychosis,” she added.
Staged Treatment and Acceptability Guidelines in Early Psychosis (STAGES) was a 6-month, triple-blind, randomized controlled noninferiority study that included 90 participants between the ages of 15 and 25 years who had FEP.
To maximize safety, patients were required to have low levels of suicidality and aggression, a DUP of less than 6 months, and to be living in stable accommodation with social support.
Participants were randomly assigned to two groups – one in which patients underwent intensive psychosocial therapy and received low-dose antipsychotic medication (n = 44), and one in which patients underwent intensive psychosocial therapy and were given placebo (n = 46).
Depending on the timing of study enrollment, those in the medication group received risperidone 1 mg or paliperidone 3 mg.
that is strongly focused on therapeutic engagement.
CBCM delivers formulation-driven cognitive-behavioral therapy and psychoeducation within a therapeutic case management framework, Francey said.
The primary outcome was level of functioning at 6, 12, and 24 months, as measured by the Social and Occupational Functioning Scale (SOFAS). The primary prespecified endpoint was outcome at 6 months. A noninferiority margin of 10.5 on the SOFAS was used as the smallest value representing a clinically important effect.
Other assessment tools included the BPRS-4 to test for positive psychotic symptoms, the Scale for the Assessment of Negative Symptoms (SANS), the Hamilton Rating Scale for Depression, and the Hamilton Rating Scale for Anxiety.
At baseline, the two treatment groups were comparable with respect to all measures of functioning and psychopathology.
The study’s discontinuation rate was high. At 6 months, only 16 patients in the psychosocial group had completed therapy, compared with 11 in the antipsychotic group.
At this point, the two groups were comparable in terms of psychopathology and functioning ratings. Both groups had lower symptoms, higher functioning scores, and higher Quality of Life Scale (QLS) scores than at baseline.
SOFAS scores were not significantly different between the groups at this time point. The mean score was 61.7 ± 16.8 in the psychosocial group and 61.5 ± 13.4 in the medication group.
The researchers note that, because the upper limit of the confidence interval (CI) was less than the study’s a priori inferiority margin of 10.5, psychosocial therapy was not inferior to medication at the 6-month assessment point.
Antipsychotics: Use with caution
Although between-group differences in SOFAS scores were not significant at 12 and 24 months, noninferiority of psychosocial therapy alone could not be confirmed because the CIs included the inferiority margin at each time point.
The two groups were statistically comparable at 6 months with respect to all other measures of psychopathology and the QLS. Similar results were found at 12 and 24 months.
The lone exception was with SANS at 12 months, on which patients in the placebo group had significantly higher negative symptom scores than the patients in the medication group.
There were no significant differences between study groups with respect to the number of adverse events.
Francey noted that the findings are important because they suggest that some young people with early-stage FEP and short DUP may be able to achieve symptom remission and function better without antipsychotic medication, provided they receive psychological interventions and comprehensive case management.
This challenges conventional wisdom that antipsychotic medications should be used for all patients who experience psychosis, she added.
However, managing FEP with psychosocial interventions should only be considered when it is safe to do so, Francey noted. In addition, the benefits of psychosocial interventions in these patients are less clear at 12 and 24 months.
Given these caveats, she noted that antipsychotics still play an important role in the treatment of these patients.
“I think there is definitely a place for medications. But I think they should be used cautiously, and you need a good, strong relationship between your treating team and your [patient] to work out what is needed and when it’s needed,” said Francey.
In addition, “when we do use medications, we should use the smallest possible dose that we can and also incorporate psychological support. I think that’s a really important part of it as well,” she said.
Timing matters
In the Lancet Psychiatry study, the researchers note that prolonged DUP is associated with worse outcomes, including increased symptoms, diminished social functioning, and poorer quality of life. The mechanism by which delayed treatment causes more harm remains unclear.
It is possible that symptoms simply accumulate over time, thereby worsening presentation. Another possibility is that continued psychosis after an initial critical period may cause long-term harm, they write.
They hypothesize that untreated psychosis can cause general treatment resistance by exacerbating underlying disease processes and that such damage progresses faster in the early stages of illness and then slows over time.
In addition, socially disruptive symptoms that are evident prior to FEP presentation may have a confounding effect, thereby leading to earlier presentation.
The investigators used data from two longitudinal cohort studies – the National Evaluation of Development of Early Intervention Network (NEDEN) study and the Outlook study.
In the NEDEN trial, 290 of 901 FEP patients (32%) were assessed within 3 weeks of presentation. In Outlook, 69 of 332 patients (21%) were assessed within 3 weeks of presentation.
In both studies, patients were examined at baseline, 6 months, and 12 months using the Positive and Negative Syndrome Scale (PANSS), the Calgary Depression Scale for Schizophrenia, the Mania Rating Scale, the Insight Scale, and SOFAS. The latter two measures were used only at baseline and 12-month follow-up. Logistic regression analyses were used to determine the association between DUP and outcomes.
In the NEDEN study, 751 patients were assessed at 6 months, and 719 were assessed at 12 months. In the Outlook study, 238 and 220 were assessed at the same two time points, respectively.
Results showed a curvilinear relationship between DUP and symptom severity. Longer DUP was predictive of reduced treatment response. However, patient response worsened more slowly as DUP lengthened.
For example, increasing DUP by ten times was predictive of less improvement in PANSS total score by 7.34 (95% CI, 5.76 – 8.92; P < .0001) in NEDEN and by 3.85 (95% CI, 1.69 – 600; P =. 0005) in Outlook. Nevertheless, longer DUP was not associated with worse presentation for any symptoms except depression in NEDEN.
The findings seem to support that the potential harm incurred by delaying treatment among patients with FEP is greatest in the early weeks of psychosis and then levels off, the investigators note.
Given these insights, mental health professionals might consider focusing their efforts on the early detection and treatment of patients for whom DUP is short.
Similarly, because DUP was directly associated with all symptoms, early access to comprehensive treatment “might be preferable to early delivery of particular treatments with particular effects (eg, dopamine antagonists),” they write.
“A pragmatic call”
Commenting on the British study in an accompanying editorial, Lena K. Palaniyappan, MD, University of Western Ontario, London, Canada, and Rajeev Krishnadas, MD, University of Glasgow, Scotland, write that any illness left untreated can become more challenging to treat, including psychosis.
“This should make early intervention in psychosis a pragmatic call with no prima facie argument against it,” they write. A reduction in DUP “underpins the rationale behind early detection and intervention in psychosis.”
The editorialists note that the relationship between DUP and successful treatment in early psychosis “strengthens the argument for more proactive early assessment and intervention to shorten treatment delay.
“As we have learnt over the past two decades, even punctual treatment when symptoms first arise continues to be too late when it comes to psychosis,” they write.
Francey also recognizes the value of early intervention in FEP. However, she noted that comprehensive psychosocial therapy might well prove effective enough to stave off antipsychotic therapy in a certain subset of patients.
“For some people, antipsychotics may never need to be introduced,” she said. “Some people recover from their first episode of psychosis and don’t go on to have any more, while others have an episodic illness,” she said.
If another episode develops and the symptoms come back, further psychosocial interventions could then be tried “or you might want to move on” to psychotic medication “because trying to get people better and functioning as well as they can is our primary aim,” Francey said.
The STAGES study was supported by the Australian National Health and Medical Research Council. The British study was funded by the UK Department of Health, the National Institute of Health Research, and the Medical Research Council. Francey and Krishnadas have reported no relevant financial relationships. Palaniyappan has received grants and personal fees from Janssen Canada and Otsuka Canada, grants from Sunovion, and personal fees from SPMM Course UK and the Canadian Psychiatric Association.
This article first appeared on Medscape.com.
Two new studies highlight the importance of early intervention in first-episode psychosis (FEP).
In the first study, Australian investigators conclude that, for some FEP patients, early psychosocial interventions may fend off the need for immediate treatment with antipsychotic medications.
In the second study, UK researchers show that long duration of untreated psychosis (DUP) is linked to a significantly reduced treatment response.
For both studies, the findings highlight the importance of rapid access to a comprehensive range of treatments in the first weeks after FEP onset.
“In a select group of people with first-episode psychosis, we found there was no difference in symptoms and functioning between those who had antipsychotic medication and those who didn’t,” lead author Shona M. Francey, PhD, clinical psychologist at Orygen, the National Center of Excellence in Youth Mental Health, Parkville, Australia, told Medscape Medical News.
“These findings supported our idea that, in the early phases of psychosis, with close monitoring and good psychosocial intervention, antipsychotic medication can be delayed,” Francey said.
The Australian study was published in Schizophrenia Bulletin Open. The British study was published in Lancet Psychiatry.
Adverse effects
Francey and colleagues note that, in comparison with standard treatment, early interventions produce superior outcomes for patients with psychosis. Although there are a variety of treatment options, low-dose second-generation antipsychotics typically play a central role.
However, atypical antipsychotics have rapid metabolic side effects, including weight gain and altered glucose metabolism, that increase the risk for cardiovascular disease and premature mortality. Importantly, such adverse effects are amplified among patients with FEP, who tend to be younger and treatment naive.
On the other hand, a growing body of evidence shows the benefit of nonpharmacologic interventions for patients with FEP, the investigators note. In addition, clinical staging models appear to support the use of less aggressive treatment early in the disease course.
“We have been working in early intervention for psychosis for a number of years and have found it’s possible to intervene early with young people and either prevent the onset of psychosis or ameliorate its impact,” said Francey.
“Since we can see some improvement in people in the prepsychotic phase, we wanted to know if we can also see some benefit without medication after the onset of what we would call full-threshold psychosis,” she added.
Staged Treatment and Acceptability Guidelines in Early Psychosis (STAGES) was a 6-month, triple-blind, randomized controlled noninferiority study that included 90 participants between the ages of 15 and 25 years who had FEP.
To maximize safety, patients were required to have low levels of suicidality and aggression, a DUP of less than 6 months, and to be living in stable accommodation with social support.
Participants were randomly assigned to two groups – one in which patients underwent intensive psychosocial therapy and received low-dose antipsychotic medication (n = 44), and one in which patients underwent intensive psychosocial therapy and were given placebo (n = 46).
Depending on the timing of study enrollment, those in the medication group received risperidone 1 mg or paliperidone 3 mg.
that is strongly focused on therapeutic engagement.
CBCM delivers formulation-driven cognitive-behavioral therapy and psychoeducation within a therapeutic case management framework, Francey said.
The primary outcome was level of functioning at 6, 12, and 24 months, as measured by the Social and Occupational Functioning Scale (SOFAS). The primary prespecified endpoint was outcome at 6 months. A noninferiority margin of 10.5 on the SOFAS was used as the smallest value representing a clinically important effect.
Other assessment tools included the BPRS-4 to test for positive psychotic symptoms, the Scale for the Assessment of Negative Symptoms (SANS), the Hamilton Rating Scale for Depression, and the Hamilton Rating Scale for Anxiety.
At baseline, the two treatment groups were comparable with respect to all measures of functioning and psychopathology.
The study’s discontinuation rate was high. At 6 months, only 16 patients in the psychosocial group had completed therapy, compared with 11 in the antipsychotic group.
At this point, the two groups were comparable in terms of psychopathology and functioning ratings. Both groups had lower symptoms, higher functioning scores, and higher Quality of Life Scale (QLS) scores than at baseline.
SOFAS scores were not significantly different between the groups at this time point. The mean score was 61.7 ± 16.8 in the psychosocial group and 61.5 ± 13.4 in the medication group.
The researchers note that, because the upper limit of the confidence interval (CI) was less than the study’s a priori inferiority margin of 10.5, psychosocial therapy was not inferior to medication at the 6-month assessment point.
Antipsychotics: Use with caution
Although between-group differences in SOFAS scores were not significant at 12 and 24 months, noninferiority of psychosocial therapy alone could not be confirmed because the CIs included the inferiority margin at each time point.
The two groups were statistically comparable at 6 months with respect to all other measures of psychopathology and the QLS. Similar results were found at 12 and 24 months.
The lone exception was with SANS at 12 months, on which patients in the placebo group had significantly higher negative symptom scores than the patients in the medication group.
There were no significant differences between study groups with respect to the number of adverse events.
Francey noted that the findings are important because they suggest that some young people with early-stage FEP and short DUP may be able to achieve symptom remission and function better without antipsychotic medication, provided they receive psychological interventions and comprehensive case management.
This challenges conventional wisdom that antipsychotic medications should be used for all patients who experience psychosis, she added.
However, managing FEP with psychosocial interventions should only be considered when it is safe to do so, Francey noted. In addition, the benefits of psychosocial interventions in these patients are less clear at 12 and 24 months.
Given these caveats, she noted that antipsychotics still play an important role in the treatment of these patients.
“I think there is definitely a place for medications. But I think they should be used cautiously, and you need a good, strong relationship between your treating team and your [patient] to work out what is needed and when it’s needed,” said Francey.
In addition, “when we do use medications, we should use the smallest possible dose that we can and also incorporate psychological support. I think that’s a really important part of it as well,” she said.
Timing matters
In the Lancet Psychiatry study, the researchers note that prolonged DUP is associated with worse outcomes, including increased symptoms, diminished social functioning, and poorer quality of life. The mechanism by which delayed treatment causes more harm remains unclear.
It is possible that symptoms simply accumulate over time, thereby worsening presentation. Another possibility is that continued psychosis after an initial critical period may cause long-term harm, they write.
They hypothesize that untreated psychosis can cause general treatment resistance by exacerbating underlying disease processes and that such damage progresses faster in the early stages of illness and then slows over time.
In addition, socially disruptive symptoms that are evident prior to FEP presentation may have a confounding effect, thereby leading to earlier presentation.
The investigators used data from two longitudinal cohort studies – the National Evaluation of Development of Early Intervention Network (NEDEN) study and the Outlook study.
In the NEDEN trial, 290 of 901 FEP patients (32%) were assessed within 3 weeks of presentation. In Outlook, 69 of 332 patients (21%) were assessed within 3 weeks of presentation.
In both studies, patients were examined at baseline, 6 months, and 12 months using the Positive and Negative Syndrome Scale (PANSS), the Calgary Depression Scale for Schizophrenia, the Mania Rating Scale, the Insight Scale, and SOFAS. The latter two measures were used only at baseline and 12-month follow-up. Logistic regression analyses were used to determine the association between DUP and outcomes.
In the NEDEN study, 751 patients were assessed at 6 months, and 719 were assessed at 12 months. In the Outlook study, 238 and 220 were assessed at the same two time points, respectively.
Results showed a curvilinear relationship between DUP and symptom severity. Longer DUP was predictive of reduced treatment response. However, patient response worsened more slowly as DUP lengthened.
For example, increasing DUP by ten times was predictive of less improvement in PANSS total score by 7.34 (95% CI, 5.76 – 8.92; P < .0001) in NEDEN and by 3.85 (95% CI, 1.69 – 600; P =. 0005) in Outlook. Nevertheless, longer DUP was not associated with worse presentation for any symptoms except depression in NEDEN.
The findings seem to support that the potential harm incurred by delaying treatment among patients with FEP is greatest in the early weeks of psychosis and then levels off, the investigators note.
Given these insights, mental health professionals might consider focusing their efforts on the early detection and treatment of patients for whom DUP is short.
Similarly, because DUP was directly associated with all symptoms, early access to comprehensive treatment “might be preferable to early delivery of particular treatments with particular effects (eg, dopamine antagonists),” they write.
“A pragmatic call”
Commenting on the British study in an accompanying editorial, Lena K. Palaniyappan, MD, University of Western Ontario, London, Canada, and Rajeev Krishnadas, MD, University of Glasgow, Scotland, write that any illness left untreated can become more challenging to treat, including psychosis.
“This should make early intervention in psychosis a pragmatic call with no prima facie argument against it,” they write. A reduction in DUP “underpins the rationale behind early detection and intervention in psychosis.”
The editorialists note that the relationship between DUP and successful treatment in early psychosis “strengthens the argument for more proactive early assessment and intervention to shorten treatment delay.
“As we have learnt over the past two decades, even punctual treatment when symptoms first arise continues to be too late when it comes to psychosis,” they write.
Francey also recognizes the value of early intervention in FEP. However, she noted that comprehensive psychosocial therapy might well prove effective enough to stave off antipsychotic therapy in a certain subset of patients.
“For some people, antipsychotics may never need to be introduced,” she said. “Some people recover from their first episode of psychosis and don’t go on to have any more, while others have an episodic illness,” she said.
If another episode develops and the symptoms come back, further psychosocial interventions could then be tried “or you might want to move on” to psychotic medication “because trying to get people better and functioning as well as they can is our primary aim,” Francey said.
The STAGES study was supported by the Australian National Health and Medical Research Council. The British study was funded by the UK Department of Health, the National Institute of Health Research, and the Medical Research Council. Francey and Krishnadas have reported no relevant financial relationships. Palaniyappan has received grants and personal fees from Janssen Canada and Otsuka Canada, grants from Sunovion, and personal fees from SPMM Course UK and the Canadian Psychiatric Association.
This article first appeared on Medscape.com.
Being a pediatric hospitalist during the COVID-19 pandemic
“Times of great calamity and confusion have been productive for the greatest minds. The purest ore is produced from the hottest furnace. The brightest thunderbolt is elicited from the darkest storm.” – Charles Caleb Colton
I walk inside the pediatric unit of our hospital, only to be welcomed by an eerie silence. There are a handful of nurses at the nursing station, faces covered with masks sitting 6 feet apart and quietly working on their computers. The resident work lounge also depicts a similar picture of emptiness. Just over a month ago, these halls were bustling with children, parents, consultants, and a host of ancillary staff. I recall times in which I was running around from one patient room to another talking to families and attending to patient needs. For the past 2 months I have often spent hours alone in my office waiting to see a patient. This is the new norm for many of us.
Across the board in hospitals, pediatric census has dropped since the start of the COVID-19 pandemic. Reasons for these are nonspecific but may include fear among parents of “exposure” to the virus by bringing their sick children to the hospital to get evaluated for other concerns. A few patients that we have seen in our hospital are sicker when they have arrived because their parents avoided seeking medical care earlier, plagued by the same fear. Social distancing and school closure have also limited the amount of infectious diseases going around, which are responsible for a bulk of pediatric admissions.

While many of us are still coming in to see the limited number of patients we have, we are not in the true sense frontline providers during this pandemic. There have been limited cases of COVID-19 in children, most of which – fortunately – present with mild symptoms. Although multisystem inflammatory syndrome in children (MIS-C) is a new disease that COVID-19 has brought us closer to, many of us have yet to see our first case because of its rarity.
I have read through the news daily in the past few months to find many adult provider physicians succumbing to COVID-19 and felt a pang of guilt. My social media is full of heartbreaking stories as adult hospitalists are having difficult conversations with families and supporting them through this unknown territory, often sacrificing their own safety. I feel so proud of them and my profession. My heart tells me, though, I personally may not be living up to the true calling I was expected to have as a physician.
As pediatric hospitalists, while we sit and wait for this pandemic to pass, we have been ruminating on and anxious about our future. As census drops, there is a financial strain that many of us are feeling. Job cuts and furloughing of health care workers in our surroundings leave us with a sense of insecurity and low morale. Many small inpatient pediatric units have had to be shut down temporarily either so they could be used for adult patients or because of lack of pediatric patients. Limiting staffing to avoid exposure and cohorting providers has also been a challenge.
A big question that has risen in these times is how to ensure productivity and stay useful while at the same time being prepared for the unknown that lies ahead. The economics of medicine is staring hard at our years of hard work, questioning the need for our specialty in the first place.
In smaller community settings, the closure of pediatric units has put an additional strain on the overall framework of the community, parents, and referring primary care providers. With the absence of local resources, children who have needed care have had to be transferred to bigger referral centers that are still taking care of pediatric patients. On one end of the spectrum there is concern for pediatric inpatient units not being productive enough for the hospital, but that coexists with a worry that, as we pass through this pandemic, we could see more hospitalizations for vaccine-preventable illnesses, child abuse/medical neglect, and respiratory syncytial virus plus COVID.
The question remains about how best to cope and use this time of uncertainty to be productive and prepare for the worst. A few solutions and suggestions are highlighted below.
- Helping adult providers: Many pediatric hospitalist colleagues in highly affected states have filled the increasing need for clinicians and taken care of adult patients. As pediatric units have closed, providers have continued to offer care where it is needed. Pediatric hospitalists have used this time to take urgent refresher courses in advanced cardiac life support and adult critical care. In states that are not as severely hit, many pediatric hospitalists have utilized this time to plan and prepare protocols for the future as information continues coming in regarding MIS-C and COVID-19 in pediatric patients.
- Use of telemedicine: With the ease in restrictions for use of telemedicine in many states, pediatric hospitalists can consider using it to restructure their staffing model whenever feasible. This can help in cohorting and allowing high risk and quarantined providers to work from home. This model simultaneously provides opportunities for pediatric hospitalists to continue providing their services, while at the same time decreasing financial burden on their institution.
- Reaching out to the community: Engaging with the community during these times can help ensure services and options remain available to our referral providers and patients for pediatric services. Information about COVID-19 can be widely disseminated. We can also play our part by continuing to encourage parents in our maximum capacity to obtain care for their children when needed and to not avoid the hospital because of fears of exposure.
- Supporting each other: There is no doubt that these times are unsettling for the pediatric hospitalist community, and the uncertainty that surrounds us can feel crippling. Strong team building is imperative in these times. While we may not be frequently meeting in work lounges and sharing meals, a good sense of support and camaraderie will go a long way in building morale for the future. Seeking mental health resources if needed is essential for us and should not be looked at with shame or guilt. This is something that many of us have never seen before, and it is okay to ask for help. Seeking help is and always will be a sign of strength.
Today, as I envision myself walking in the hospital on the other side of this pandemic I see a cheerful pediatric unit, smiling faces without masks, my 3-year-old patient cruising around the hallways in a toy car, our therapy dog walking around bringing joy to many, and many healthy patients feeling better and ready to go home. A time when we are not scared to hug each other, shake hands, or share emotion. When our teams are stronger and more well bonded. A time when parents are not scared to bring their sick children to the hospital. Will it be many months before this happens? I don’t know. But I do know that the children I take care of are known for their resilience. I will live up to them today by practicing the same.
Dr. Fatima is a pediatric hospitalist at Wesley Children’s Hospital and assistant professor of pediatrics at Kansas University School of Medicine, both in Wichita. Her research interests include medical errors, medical education, and high-value care.
“Times of great calamity and confusion have been productive for the greatest minds. The purest ore is produced from the hottest furnace. The brightest thunderbolt is elicited from the darkest storm.” – Charles Caleb Colton
I walk inside the pediatric unit of our hospital, only to be welcomed by an eerie silence. There are a handful of nurses at the nursing station, faces covered with masks sitting 6 feet apart and quietly working on their computers. The resident work lounge also depicts a similar picture of emptiness. Just over a month ago, these halls were bustling with children, parents, consultants, and a host of ancillary staff. I recall times in which I was running around from one patient room to another talking to families and attending to patient needs. For the past 2 months I have often spent hours alone in my office waiting to see a patient. This is the new norm for many of us.
Across the board in hospitals, pediatric census has dropped since the start of the COVID-19 pandemic. Reasons for these are nonspecific but may include fear among parents of “exposure” to the virus by bringing their sick children to the hospital to get evaluated for other concerns. A few patients that we have seen in our hospital are sicker when they have arrived because their parents avoided seeking medical care earlier, plagued by the same fear. Social distancing and school closure have also limited the amount of infectious diseases going around, which are responsible for a bulk of pediatric admissions.
While many of us are still coming in to see the limited number of patients we have, we are not in the true sense frontline providers during this pandemic. There have been limited cases of COVID-19 in children, most of which – fortunately – present with mild symptoms. Although multisystem inflammatory syndrome in children (MIS-C) is a new disease that COVID-19 has brought us closer to, many of us have yet to see our first case because of its rarity.
I have read through the news daily in the past few months to find many adult provider physicians succumbing to COVID-19 and felt a pang of guilt. My social media is full of heartbreaking stories as adult hospitalists are having difficult conversations with families and supporting them through this unknown territory, often sacrificing their own safety. I feel so proud of them and my profession. My heart tells me, though, I personally may not be living up to the true calling I was expected to have as a physician.
As pediatric hospitalists, while we sit and wait for this pandemic to pass, we have been ruminating on and anxious about our future. As census drops, there is a financial strain that many of us are feeling. Job cuts and furloughing of health care workers in our surroundings leave us with a sense of insecurity and low morale. Many small inpatient pediatric units have had to be shut down temporarily either so they could be used for adult patients or because of lack of pediatric patients. Limiting staffing to avoid exposure and cohorting providers has also been a challenge.
A big question that has risen in these times is how to ensure productivity and stay useful while at the same time being prepared for the unknown that lies ahead. The economics of medicine is staring hard at our years of hard work, questioning the need for our specialty in the first place.
In smaller community settings, the closure of pediatric units has put an additional strain on the overall framework of the community, parents, and referring primary care providers. With the absence of local resources, children who have needed care have had to be transferred to bigger referral centers that are still taking care of pediatric patients. On one end of the spectrum there is concern for pediatric inpatient units not being productive enough for the hospital, but that coexists with a worry that, as we pass through this pandemic, we could see more hospitalizations for vaccine-preventable illnesses, child abuse/medical neglect, and respiratory syncytial virus plus COVID.
The question remains about how best to cope and use this time of uncertainty to be productive and prepare for the worst. A few solutions and suggestions are highlighted below.
- Helping adult providers: Many pediatric hospitalist colleagues in highly affected states have filled the increasing need for clinicians and taken care of adult patients. As pediatric units have closed, providers have continued to offer care where it is needed. Pediatric hospitalists have used this time to take urgent refresher courses in advanced cardiac life support and adult critical care. In states that are not as severely hit, many pediatric hospitalists have utilized this time to plan and prepare protocols for the future as information continues coming in regarding MIS-C and COVID-19 in pediatric patients.
- Use of telemedicine: With the ease in restrictions for use of telemedicine in many states, pediatric hospitalists can consider using it to restructure their staffing model whenever feasible. This can help in cohorting and allowing high risk and quarantined providers to work from home. This model simultaneously provides opportunities for pediatric hospitalists to continue providing their services, while at the same time decreasing financial burden on their institution.
- Reaching out to the community: Engaging with the community during these times can help ensure services and options remain available to our referral providers and patients for pediatric services. Information about COVID-19 can be widely disseminated. We can also play our part by continuing to encourage parents in our maximum capacity to obtain care for their children when needed and to not avoid the hospital because of fears of exposure.
- Supporting each other: There is no doubt that these times are unsettling for the pediatric hospitalist community, and the uncertainty that surrounds us can feel crippling. Strong team building is imperative in these times. While we may not be frequently meeting in work lounges and sharing meals, a good sense of support and camaraderie will go a long way in building morale for the future. Seeking mental health resources if needed is essential for us and should not be looked at with shame or guilt. This is something that many of us have never seen before, and it is okay to ask for help. Seeking help is and always will be a sign of strength.
Today, as I envision myself walking in the hospital on the other side of this pandemic I see a cheerful pediatric unit, smiling faces without masks, my 3-year-old patient cruising around the hallways in a toy car, our therapy dog walking around bringing joy to many, and many healthy patients feeling better and ready to go home. A time when we are not scared to hug each other, shake hands, or share emotion. When our teams are stronger and more well bonded. A time when parents are not scared to bring their sick children to the hospital. Will it be many months before this happens? I don’t know. But I do know that the children I take care of are known for their resilience. I will live up to them today by practicing the same.
Dr. Fatima is a pediatric hospitalist at Wesley Children’s Hospital and assistant professor of pediatrics at Kansas University School of Medicine, both in Wichita. Her research interests include medical errors, medical education, and high-value care.
“Times of great calamity and confusion have been productive for the greatest minds. The purest ore is produced from the hottest furnace. The brightest thunderbolt is elicited from the darkest storm.” – Charles Caleb Colton
I walk inside the pediatric unit of our hospital, only to be welcomed by an eerie silence. There are a handful of nurses at the nursing station, faces covered with masks sitting 6 feet apart and quietly working on their computers. The resident work lounge also depicts a similar picture of emptiness. Just over a month ago, these halls were bustling with children, parents, consultants, and a host of ancillary staff. I recall times in which I was running around from one patient room to another talking to families and attending to patient needs. For the past 2 months I have often spent hours alone in my office waiting to see a patient. This is the new norm for many of us.
Across the board in hospitals, pediatric census has dropped since the start of the COVID-19 pandemic. Reasons for these are nonspecific but may include fear among parents of “exposure” to the virus by bringing their sick children to the hospital to get evaluated for other concerns. A few patients that we have seen in our hospital are sicker when they have arrived because their parents avoided seeking medical care earlier, plagued by the same fear. Social distancing and school closure have also limited the amount of infectious diseases going around, which are responsible for a bulk of pediatric admissions.
While many of us are still coming in to see the limited number of patients we have, we are not in the true sense frontline providers during this pandemic. There have been limited cases of COVID-19 in children, most of which – fortunately – present with mild symptoms. Although multisystem inflammatory syndrome in children (MIS-C) is a new disease that COVID-19 has brought us closer to, many of us have yet to see our first case because of its rarity.
I have read through the news daily in the past few months to find many adult provider physicians succumbing to COVID-19 and felt a pang of guilt. My social media is full of heartbreaking stories as adult hospitalists are having difficult conversations with families and supporting them through this unknown territory, often sacrificing their own safety. I feel so proud of them and my profession. My heart tells me, though, I personally may not be living up to the true calling I was expected to have as a physician.
As pediatric hospitalists, while we sit and wait for this pandemic to pass, we have been ruminating on and anxious about our future. As census drops, there is a financial strain that many of us are feeling. Job cuts and furloughing of health care workers in our surroundings leave us with a sense of insecurity and low morale. Many small inpatient pediatric units have had to be shut down temporarily either so they could be used for adult patients or because of lack of pediatric patients. Limiting staffing to avoid exposure and cohorting providers has also been a challenge.
A big question that has risen in these times is how to ensure productivity and stay useful while at the same time being prepared for the unknown that lies ahead. The economics of medicine is staring hard at our years of hard work, questioning the need for our specialty in the first place.
In smaller community settings, the closure of pediatric units has put an additional strain on the overall framework of the community, parents, and referring primary care providers. With the absence of local resources, children who have needed care have had to be transferred to bigger referral centers that are still taking care of pediatric patients. On one end of the spectrum there is concern for pediatric inpatient units not being productive enough for the hospital, but that coexists with a worry that, as we pass through this pandemic, we could see more hospitalizations for vaccine-preventable illnesses, child abuse/medical neglect, and respiratory syncytial virus plus COVID.
The question remains about how best to cope and use this time of uncertainty to be productive and prepare for the worst. A few solutions and suggestions are highlighted below.
- Helping adult providers: Many pediatric hospitalist colleagues in highly affected states have filled the increasing need for clinicians and taken care of adult patients. As pediatric units have closed, providers have continued to offer care where it is needed. Pediatric hospitalists have used this time to take urgent refresher courses in advanced cardiac life support and adult critical care. In states that are not as severely hit, many pediatric hospitalists have utilized this time to plan and prepare protocols for the future as information continues coming in regarding MIS-C and COVID-19 in pediatric patients.
- Use of telemedicine: With the ease in restrictions for use of telemedicine in many states, pediatric hospitalists can consider using it to restructure their staffing model whenever feasible. This can help in cohorting and allowing high risk and quarantined providers to work from home. This model simultaneously provides opportunities for pediatric hospitalists to continue providing their services, while at the same time decreasing financial burden on their institution.
- Reaching out to the community: Engaging with the community during these times can help ensure services and options remain available to our referral providers and patients for pediatric services. Information about COVID-19 can be widely disseminated. We can also play our part by continuing to encourage parents in our maximum capacity to obtain care for their children when needed and to not avoid the hospital because of fears of exposure.
- Supporting each other: There is no doubt that these times are unsettling for the pediatric hospitalist community, and the uncertainty that surrounds us can feel crippling. Strong team building is imperative in these times. While we may not be frequently meeting in work lounges and sharing meals, a good sense of support and camaraderie will go a long way in building morale for the future. Seeking mental health resources if needed is essential for us and should not be looked at with shame or guilt. This is something that many of us have never seen before, and it is okay to ask for help. Seeking help is and always will be a sign of strength.
Today, as I envision myself walking in the hospital on the other side of this pandemic I see a cheerful pediatric unit, smiling faces without masks, my 3-year-old patient cruising around the hallways in a toy car, our therapy dog walking around bringing joy to many, and many healthy patients feeling better and ready to go home. A time when we are not scared to hug each other, shake hands, or share emotion. When our teams are stronger and more well bonded. A time when parents are not scared to bring their sick children to the hospital. Will it be many months before this happens? I don’t know. But I do know that the children I take care of are known for their resilience. I will live up to them today by practicing the same.
Dr. Fatima is a pediatric hospitalist at Wesley Children’s Hospital and assistant professor of pediatrics at Kansas University School of Medicine, both in Wichita. Her research interests include medical errors, medical education, and high-value care.
As COVID-19 cases increase in children, deaths remain low
according to a report from the American Academy of Pediatrics and the Children’s Hospital Association.
The cumulative number of pediatric cases reported up to that date was 442,785, or 9.3% of the total COVID-19 case load of more than 4.76 million among all ages. There have been only 92 pediatric deaths, however, which works out to just 0.06% of the 154,279 reported for all ages, the AAP and the CHA said Aug. 24 in their most recent update.
Child hospitalizations also were on the low side, representing 1.7% (4,062) of the cumulative total of 234,810 admissions among all ages as of Aug. 20, based on data from 21 states and New York City.
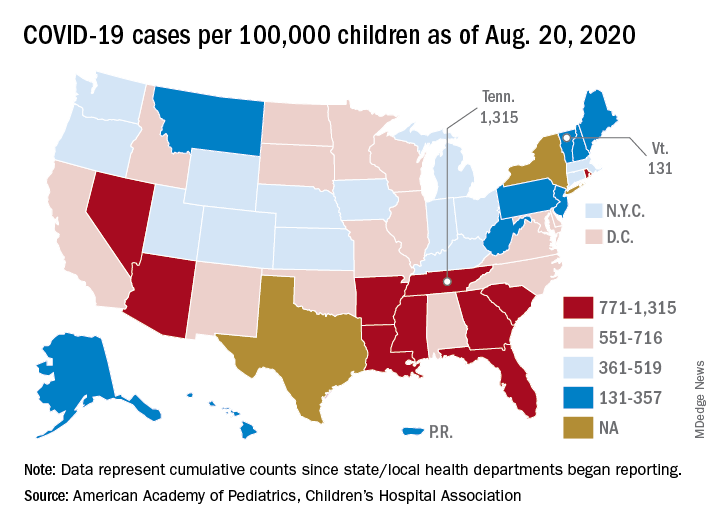
Nationally, the cumulative number of reported child cases is now up to 583 per 100,000 children, and that figure covers 49 states, Washington, D.C., Guam, New York City, and Puerto Rico.
There is some disagreement among the states, though, about the definition of “child.” Most states use an age range of 0-17, 0-18, or 0-19, but Florida and Utah go with a range of 0-14 years while South Carolina and Tennessee consider humans aged 0-20 years to be children. Other data limitations involve Texas, which has reported age distribution for only 8% of all cases, and New York, which is not reporting the age distribution of statewide cases, the AAP/CHA report noted.
The definition of child isn’t the only thing that varies between the states. The cumulative case rate for Tennessee, the highest in the country at 1,315 per 100,000 children, is 10 times that of Vermont, which is the lowest at 131 per 100,000, the AAP and CHA said. Vermont reports child COVID-19 cases using an age range of 0-19 years.
The other states with rates over 1,000 cases per 100,000 children are Arizona (1,300), which had the highest rate a week ago; South Carolina (1,214); Louisiana (1,127); Mississippi (1,120); and Nevada (1,068). Those with rates below 200 cases per 100,000 children are Maine (150), New Hampshire (175), and Hawaii (188), according to this week’s report.
according to a report from the American Academy of Pediatrics and the Children’s Hospital Association.
The cumulative number of pediatric cases reported up to that date was 442,785, or 9.3% of the total COVID-19 case load of more than 4.76 million among all ages. There have been only 92 pediatric deaths, however, which works out to just 0.06% of the 154,279 reported for all ages, the AAP and the CHA said Aug. 24 in their most recent update.
Child hospitalizations also were on the low side, representing 1.7% (4,062) of the cumulative total of 234,810 admissions among all ages as of Aug. 20, based on data from 21 states and New York City.
Nationally, the cumulative number of reported child cases is now up to 583 per 100,000 children, and that figure covers 49 states, Washington, D.C., Guam, New York City, and Puerto Rico.
There is some disagreement among the states, though, about the definition of “child.” Most states use an age range of 0-17, 0-18, or 0-19, but Florida and Utah go with a range of 0-14 years while South Carolina and Tennessee consider humans aged 0-20 years to be children. Other data limitations involve Texas, which has reported age distribution for only 8% of all cases, and New York, which is not reporting the age distribution of statewide cases, the AAP/CHA report noted.
The definition of child isn’t the only thing that varies between the states. The cumulative case rate for Tennessee, the highest in the country at 1,315 per 100,000 children, is 10 times that of Vermont, which is the lowest at 131 per 100,000, the AAP and CHA said. Vermont reports child COVID-19 cases using an age range of 0-19 years.
The other states with rates over 1,000 cases per 100,000 children are Arizona (1,300), which had the highest rate a week ago; South Carolina (1,214); Louisiana (1,127); Mississippi (1,120); and Nevada (1,068). Those with rates below 200 cases per 100,000 children are Maine (150), New Hampshire (175), and Hawaii (188), according to this week’s report.
according to a report from the American Academy of Pediatrics and the Children’s Hospital Association.
The cumulative number of pediatric cases reported up to that date was 442,785, or 9.3% of the total COVID-19 case load of more than 4.76 million among all ages. There have been only 92 pediatric deaths, however, which works out to just 0.06% of the 154,279 reported for all ages, the AAP and the CHA said Aug. 24 in their most recent update.
Child hospitalizations also were on the low side, representing 1.7% (4,062) of the cumulative total of 234,810 admissions among all ages as of Aug. 20, based on data from 21 states and New York City.
Nationally, the cumulative number of reported child cases is now up to 583 per 100,000 children, and that figure covers 49 states, Washington, D.C., Guam, New York City, and Puerto Rico.
There is some disagreement among the states, though, about the definition of “child.” Most states use an age range of 0-17, 0-18, or 0-19, but Florida and Utah go with a range of 0-14 years while South Carolina and Tennessee consider humans aged 0-20 years to be children. Other data limitations involve Texas, which has reported age distribution for only 8% of all cases, and New York, which is not reporting the age distribution of statewide cases, the AAP/CHA report noted.
The definition of child isn’t the only thing that varies between the states. The cumulative case rate for Tennessee, the highest in the country at 1,315 per 100,000 children, is 10 times that of Vermont, which is the lowest at 131 per 100,000, the AAP and CHA said. Vermont reports child COVID-19 cases using an age range of 0-19 years.
The other states with rates over 1,000 cases per 100,000 children are Arizona (1,300), which had the highest rate a week ago; South Carolina (1,214); Louisiana (1,127); Mississippi (1,120); and Nevada (1,068). Those with rates below 200 cases per 100,000 children are Maine (150), New Hampshire (175), and Hawaii (188), according to this week’s report.
Weighing children in school: No good can come of it
The United Kingdom’s National Obesity Forum has apparently decided that returning to school this fall in the middle of a pandemic isn’t stressful enough for kids, and is recommending that its National Child Measurement Programme be expanded to have 4- to 5-year-old and 10- to 11-year-old children weighed when they return to the classroom – and then weighed again in the spring – in a bid to tackle COVID-19–related gains.
It’s difficult to conceive a single plausible mechanism by which this recommendation could be helpful. Given that weight is, by a substantial margin, the No. 1 reported cause of schoolyard bullying, it’s certainly unlikely that children with obesity don’t already know that they have it. It’s also unlikely that they don’t know that obesity confers risks to health, given the near constant drumbeats of concern percussed by the media and public health authorities, and the fact that watching people with obesity be blamed, shamed, and berated for their condition has in the past 2 decades become a regularly repeated prime-time reality show spectacle.
It’s also unlikely, especially in younger grades, to be something within a child’s direct control.
What about the parents? Well, given that they dress their children and that changes in weight affect clothing sizes and fit, they’re already aware if their kids are gaining weight. And like their children, they have been exposed to constant public health alarms around obesity.
Many parents will have seen their time and resources, both real and mental, become significantly impaired during the time of COVID-19, which in turn understandably challenges change. Simply put, permanent intentional behavior change in the name of health requires tremendous privilege and is elusive for many people even during easier times. For non–evidence-based proof of this assertion, simply reflect on all of your own best-laid intentions and plans that might have been good for your health (fitness, relationships, CME, etc.) that you let slide despite probably having far more privilege than the average person.
Then, of course, there is the hugely inconvenient truth that we have yet to see the development of a parent- or child-based educational intervention or directive for weight gain that has shown itself to be beneficial on a population level.
Can something else be done instead?
At this point, we can only speculate about the potential risks associated with school room weigh-ins because randomized controlled trials, thankfully, have not been conducted to explore this area. But I can certainly tell you that I have met many adult patients in my office who traced their lifetime of yo-yo dieting – along with a history of teenage eating disorders, at times – to their well-intentioned physician, school nurse, gym teacher, or parent using a scale to measure their weights. And in doing so, they were teaching that scales measure health, happiness, success, self-worth, and effort.
If governments are concerned about weight gain in children, they need to look to initiatives that will help all children and parents. Weighing them will not somehow inspire parents or kids to discover an as-yet unknown effective childhood obesity treatment. Changes that would be helpful may include:
- Banning food advertisements to children.
- Reforming school cafeteria meals and then ensuring that school meals are made available to children during COVID-19–related school shutdowns.
- Bringing back home economics classes to teach children how to cook (and perhaps doing the same for parents during school off-hours or in community centers).
- Enacting sugar-sweetened beverage taxes and using revenues to fund aforementioned reforms and programs, along with others, which might include the subsidization of fresh produce.
- Reforming front-of-package health claims for foods with questionable nutritional quality.
Given that there is literally no age category in any country on the planet that hasn’t seen rising weights, this is clearly not a disease reflecting a pandemic loss of willpower. Rather, this is a disease of the world’s changing food environments and culture, and until we address both through systemic changes, schemes such as the one being proposed by the UK National Obesity Forum are far more likely to do harm than good.
Yoni Freedhoff is associate professor of family medicine at the University of Ottawa and medical director of the Bariatric Medical Institute, a nonsurgical weight management center. He is one of Canada’s most outspoken obesity experts and the author of “The Diet Fix: Why Diets Fail and How to Make Yours Work.” A version of this article originally appeared on Medscape.com.
The United Kingdom’s National Obesity Forum has apparently decided that returning to school this fall in the middle of a pandemic isn’t stressful enough for kids, and is recommending that its National Child Measurement Programme be expanded to have 4- to 5-year-old and 10- to 11-year-old children weighed when they return to the classroom – and then weighed again in the spring – in a bid to tackle COVID-19–related gains.
It’s difficult to conceive a single plausible mechanism by which this recommendation could be helpful. Given that weight is, by a substantial margin, the No. 1 reported cause of schoolyard bullying, it’s certainly unlikely that children with obesity don’t already know that they have it. It’s also unlikely that they don’t know that obesity confers risks to health, given the near constant drumbeats of concern percussed by the media and public health authorities, and the fact that watching people with obesity be blamed, shamed, and berated for their condition has in the past 2 decades become a regularly repeated prime-time reality show spectacle.
It’s also unlikely, especially in younger grades, to be something within a child’s direct control.
What about the parents? Well, given that they dress their children and that changes in weight affect clothing sizes and fit, they’re already aware if their kids are gaining weight. And like their children, they have been exposed to constant public health alarms around obesity.
Many parents will have seen their time and resources, both real and mental, become significantly impaired during the time of COVID-19, which in turn understandably challenges change. Simply put, permanent intentional behavior change in the name of health requires tremendous privilege and is elusive for many people even during easier times. For non–evidence-based proof of this assertion, simply reflect on all of your own best-laid intentions and plans that might have been good for your health (fitness, relationships, CME, etc.) that you let slide despite probably having far more privilege than the average person.
Then, of course, there is the hugely inconvenient truth that we have yet to see the development of a parent- or child-based educational intervention or directive for weight gain that has shown itself to be beneficial on a population level.
Can something else be done instead?
At this point, we can only speculate about the potential risks associated with school room weigh-ins because randomized controlled trials, thankfully, have not been conducted to explore this area. But I can certainly tell you that I have met many adult patients in my office who traced their lifetime of yo-yo dieting – along with a history of teenage eating disorders, at times – to their well-intentioned physician, school nurse, gym teacher, or parent using a scale to measure their weights. And in doing so, they were teaching that scales measure health, happiness, success, self-worth, and effort.
If governments are concerned about weight gain in children, they need to look to initiatives that will help all children and parents. Weighing them will not somehow inspire parents or kids to discover an as-yet unknown effective childhood obesity treatment. Changes that would be helpful may include:
- Banning food advertisements to children.
- Reforming school cafeteria meals and then ensuring that school meals are made available to children during COVID-19–related school shutdowns.
- Bringing back home economics classes to teach children how to cook (and perhaps doing the same for parents during school off-hours or in community centers).
- Enacting sugar-sweetened beverage taxes and using revenues to fund aforementioned reforms and programs, along with others, which might include the subsidization of fresh produce.
- Reforming front-of-package health claims for foods with questionable nutritional quality.
Given that there is literally no age category in any country on the planet that hasn’t seen rising weights, this is clearly not a disease reflecting a pandemic loss of willpower. Rather, this is a disease of the world’s changing food environments and culture, and until we address both through systemic changes, schemes such as the one being proposed by the UK National Obesity Forum are far more likely to do harm than good.
Yoni Freedhoff is associate professor of family medicine at the University of Ottawa and medical director of the Bariatric Medical Institute, a nonsurgical weight management center. He is one of Canada’s most outspoken obesity experts and the author of “The Diet Fix: Why Diets Fail and How to Make Yours Work.” A version of this article originally appeared on Medscape.com.
The United Kingdom’s National Obesity Forum has apparently decided that returning to school this fall in the middle of a pandemic isn’t stressful enough for kids, and is recommending that its National Child Measurement Programme be expanded to have 4- to 5-year-old and 10- to 11-year-old children weighed when they return to the classroom – and then weighed again in the spring – in a bid to tackle COVID-19–related gains.
It’s difficult to conceive a single plausible mechanism by which this recommendation could be helpful. Given that weight is, by a substantial margin, the No. 1 reported cause of schoolyard bullying, it’s certainly unlikely that children with obesity don’t already know that they have it. It’s also unlikely that they don’t know that obesity confers risks to health, given the near constant drumbeats of concern percussed by the media and public health authorities, and the fact that watching people with obesity be blamed, shamed, and berated for their condition has in the past 2 decades become a regularly repeated prime-time reality show spectacle.
It’s also unlikely, especially in younger grades, to be something within a child’s direct control.
What about the parents? Well, given that they dress their children and that changes in weight affect clothing sizes and fit, they’re already aware if their kids are gaining weight. And like their children, they have been exposed to constant public health alarms around obesity.
Many parents will have seen their time and resources, both real and mental, become significantly impaired during the time of COVID-19, which in turn understandably challenges change. Simply put, permanent intentional behavior change in the name of health requires tremendous privilege and is elusive for many people even during easier times. For non–evidence-based proof of this assertion, simply reflect on all of your own best-laid intentions and plans that might have been good for your health (fitness, relationships, CME, etc.) that you let slide despite probably having far more privilege than the average person.
Then, of course, there is the hugely inconvenient truth that we have yet to see the development of a parent- or child-based educational intervention or directive for weight gain that has shown itself to be beneficial on a population level.
Can something else be done instead?
At this point, we can only speculate about the potential risks associated with school room weigh-ins because randomized controlled trials, thankfully, have not been conducted to explore this area. But I can certainly tell you that I have met many adult patients in my office who traced their lifetime of yo-yo dieting – along with a history of teenage eating disorders, at times – to their well-intentioned physician, school nurse, gym teacher, or parent using a scale to measure their weights. And in doing so, they were teaching that scales measure health, happiness, success, self-worth, and effort.
If governments are concerned about weight gain in children, they need to look to initiatives that will help all children and parents. Weighing them will not somehow inspire parents or kids to discover an as-yet unknown effective childhood obesity treatment. Changes that would be helpful may include:
- Banning food advertisements to children.
- Reforming school cafeteria meals and then ensuring that school meals are made available to children during COVID-19–related school shutdowns.
- Bringing back home economics classes to teach children how to cook (and perhaps doing the same for parents during school off-hours or in community centers).
- Enacting sugar-sweetened beverage taxes and using revenues to fund aforementioned reforms and programs, along with others, which might include the subsidization of fresh produce.
- Reforming front-of-package health claims for foods with questionable nutritional quality.
Given that there is literally no age category in any country on the planet that hasn’t seen rising weights, this is clearly not a disease reflecting a pandemic loss of willpower. Rather, this is a disease of the world’s changing food environments and culture, and until we address both through systemic changes, schemes such as the one being proposed by the UK National Obesity Forum are far more likely to do harm than good.
Yoni Freedhoff is associate professor of family medicine at the University of Ottawa and medical director of the Bariatric Medical Institute, a nonsurgical weight management center. He is one of Canada’s most outspoken obesity experts and the author of “The Diet Fix: Why Diets Fail and How to Make Yours Work.” A version of this article originally appeared on Medscape.com.
ADHD and dyslexia may affect evaluation of concussion
, a new study shows.
“Our results suggest kids with certain learning disorders may respond differently to concussion tests, and this needs to be taken into account when advising on recovery times and when they can return to sport,” said lead author Mathew Stokes, MD. Dr. Stokes is assistant professor of pediatrics and neurology/neurotherapeutics at the University of Texas–Southwestern Medical Center, Dallas.
The study was presented at the American Academy of Neurology Sports Concussion Virtual Conference, held online July 31 to Aug. 1.
Learning disorders affected scores
The researchers analyzed data from participants aged 10-18 years who were enrolled in the North Texas Concussion Registry (ConTex). Participants had been diagnosed with a concussion that was sustained within 30 days of enrollment. The researchers investigated whether there were differences between patients who had no history of learning disorders and those with a history of dyslexia and/or ADD/ADHD with regard to results of clinical testing following concussion.
Of the 1,298 individuals in the study, 58 had been diagnosed with dyslexia, 158 had been diagnosed with ADD/ADHD, and 35 had been diagnosed with both conditions. There was no difference in age, time since injury, or history of concussion between those with learning disorders and those without, but there were more male patients in the ADD/ADHD group.
Results showed that in the dyslexia group, mean time was slower (P = .011), and there was an increase in error scores on the King-Devick (KD) test (P = .028). That test assesses eye movements and involves the rapid naming of numbers that are spaced differently. In addition, those with ADD/ADHD had significantly higher impulse control scores (P = .007) on the ImPACT series of tests, which are commonly used in the evaluation of concussion. Participants with both dyslexia and ADHD demonstrated slower KD times (P = .009) and had higher depression scores and anxiety scores.
Dr. Stokes noted that a limiting factor of the study was that baseline scores were not available. “It is possible that kids with ADD have less impulse control even at baseline, and this would need to be taken into account,” he said. “You may perhaps also expect someone with dyslexia to have a worse score on the KD tests, so we need more data on how these scores are affected from baseline in these individuals. But our results show that when evaluating kids pre- or post concussion, it is important to know about learning disorders, as this will affect how we interpret the data.”
At 3-month follow-up, there were no longer significant differences in anxiety and depression scores for those with and those without learning disorders. “This suggests anxiety and depression may well be worse temporarily after concussion for those with ADD/ADHD but gets better with time,” Dr. Stokes said.
Follow-up data were not available for the other cognitive tests.
Are recovery times longer?
Asked whether young people with these learning disorders needed a longer time to recover after concussion, Dr. Stokes said: “That is a million-dollar question. Studies so far on this have shown conflicting results. Our results add to a growing body of literature on this.” He stressed that it is important to include anxiety and depression scores on both baseline and postconcussion tests. “People don’t tend to think of these symptoms as being associated with concussion, but they are actually very prominent in this situation,” he noted. “Our results suggest that individuals with ADHD may be more prone to anxiety and depression, and a blow to the head may tip them more into these symptoms.”
Discussing the study at a virtual press conference as part of the AAN Sports Concussion meeting, the codirector of the meeting, David Dodick, MD, Mayo Clinic, Scottsdale, Ariz., said: “This is a very interesting and important study which suggests there are differences between adolescents with a history of dyslexia/ADHD and those without these conditions in performance in concussion tests. Understanding the differences in these groups will help health care providers in evaluating these athletes and assisting in counseling them and their families with regard to their risk of injury.
“It is important to recognize that athletes with ADHD, whether or not they are on medication, may take longer to recover from a concussion,” Dr. Dodick added. They also exhibit greater reductions in cognitive skills and visual motor speed regarding hand-eye coordination, he said. There is an increase in the severity of symptoms. “Symptoms that exist in both groups tend to more severe in those individuals with ADHD,” he noted.
“Ascertaining the presence or absence of ADHD or dyslexia in those who are participating in sport is important, especially when trying to interpret the results of baseline testing, the results of postinjury testing, decisions on when to return to play, and assessing for individuals and their families the risk of long-term repeat concussions and adverse outcomes,” he concluded.
The other codirector of the AAN meeting, Brian Hainline, MD, chief medical officer of the National Collegiate Athletic Association, added: “It appears that athletes with ADHD may suffer more with concussion and have a longer recovery time. This can inform our decision making and help these individuals to understand that they are at higher risk.”
Dr. Hainline said this raises another important point: “Concussion is not a homogeneous entity. It is a brain injury that can manifest in multiple parts of the brain, and the way the brain is from a premorbid or comorbid point of view can influence the manifestation of concussion as well,” he said. “All these things need to be taken into account.”
Attentional deficit may itself make an individual more susceptible to sustaining an injury in the first place, he said. “All of this is an evolving body of research which is helping clinicians to make better-informed decisions for athletes who may manifest differently.”
A version of this article originally appeared on Medscape.com.
, a new study shows.
“Our results suggest kids with certain learning disorders may respond differently to concussion tests, and this needs to be taken into account when advising on recovery times and when they can return to sport,” said lead author Mathew Stokes, MD. Dr. Stokes is assistant professor of pediatrics and neurology/neurotherapeutics at the University of Texas–Southwestern Medical Center, Dallas.
The study was presented at the American Academy of Neurology Sports Concussion Virtual Conference, held online July 31 to Aug. 1.
Learning disorders affected scores
The researchers analyzed data from participants aged 10-18 years who were enrolled in the North Texas Concussion Registry (ConTex). Participants had been diagnosed with a concussion that was sustained within 30 days of enrollment. The researchers investigated whether there were differences between patients who had no history of learning disorders and those with a history of dyslexia and/or ADD/ADHD with regard to results of clinical testing following concussion.
Of the 1,298 individuals in the study, 58 had been diagnosed with dyslexia, 158 had been diagnosed with ADD/ADHD, and 35 had been diagnosed with both conditions. There was no difference in age, time since injury, or history of concussion between those with learning disorders and those without, but there were more male patients in the ADD/ADHD group.
Results showed that in the dyslexia group, mean time was slower (P = .011), and there was an increase in error scores on the King-Devick (KD) test (P = .028). That test assesses eye movements and involves the rapid naming of numbers that are spaced differently. In addition, those with ADD/ADHD had significantly higher impulse control scores (P = .007) on the ImPACT series of tests, which are commonly used in the evaluation of concussion. Participants with both dyslexia and ADHD demonstrated slower KD times (P = .009) and had higher depression scores and anxiety scores.
Dr. Stokes noted that a limiting factor of the study was that baseline scores were not available. “It is possible that kids with ADD have less impulse control even at baseline, and this would need to be taken into account,” he said. “You may perhaps also expect someone with dyslexia to have a worse score on the KD tests, so we need more data on how these scores are affected from baseline in these individuals. But our results show that when evaluating kids pre- or post concussion, it is important to know about learning disorders, as this will affect how we interpret the data.”
At 3-month follow-up, there were no longer significant differences in anxiety and depression scores for those with and those without learning disorders. “This suggests anxiety and depression may well be worse temporarily after concussion for those with ADD/ADHD but gets better with time,” Dr. Stokes said.
Follow-up data were not available for the other cognitive tests.
Are recovery times longer?
Asked whether young people with these learning disorders needed a longer time to recover after concussion, Dr. Stokes said: “That is a million-dollar question. Studies so far on this have shown conflicting results. Our results add to a growing body of literature on this.” He stressed that it is important to include anxiety and depression scores on both baseline and postconcussion tests. “People don’t tend to think of these symptoms as being associated with concussion, but they are actually very prominent in this situation,” he noted. “Our results suggest that individuals with ADHD may be more prone to anxiety and depression, and a blow to the head may tip them more into these symptoms.”
Discussing the study at a virtual press conference as part of the AAN Sports Concussion meeting, the codirector of the meeting, David Dodick, MD, Mayo Clinic, Scottsdale, Ariz., said: “This is a very interesting and important study which suggests there are differences between adolescents with a history of dyslexia/ADHD and those without these conditions in performance in concussion tests. Understanding the differences in these groups will help health care providers in evaluating these athletes and assisting in counseling them and their families with regard to their risk of injury.
“It is important to recognize that athletes with ADHD, whether or not they are on medication, may take longer to recover from a concussion,” Dr. Dodick added. They also exhibit greater reductions in cognitive skills and visual motor speed regarding hand-eye coordination, he said. There is an increase in the severity of symptoms. “Symptoms that exist in both groups tend to more severe in those individuals with ADHD,” he noted.
“Ascertaining the presence or absence of ADHD or dyslexia in those who are participating in sport is important, especially when trying to interpret the results of baseline testing, the results of postinjury testing, decisions on when to return to play, and assessing for individuals and their families the risk of long-term repeat concussions and adverse outcomes,” he concluded.
The other codirector of the AAN meeting, Brian Hainline, MD, chief medical officer of the National Collegiate Athletic Association, added: “It appears that athletes with ADHD may suffer more with concussion and have a longer recovery time. This can inform our decision making and help these individuals to understand that they are at higher risk.”
Dr. Hainline said this raises another important point: “Concussion is not a homogeneous entity. It is a brain injury that can manifest in multiple parts of the brain, and the way the brain is from a premorbid or comorbid point of view can influence the manifestation of concussion as well,” he said. “All these things need to be taken into account.”
Attentional deficit may itself make an individual more susceptible to sustaining an injury in the first place, he said. “All of this is an evolving body of research which is helping clinicians to make better-informed decisions for athletes who may manifest differently.”
A version of this article originally appeared on Medscape.com.
, a new study shows.
“Our results suggest kids with certain learning disorders may respond differently to concussion tests, and this needs to be taken into account when advising on recovery times and when they can return to sport,” said lead author Mathew Stokes, MD. Dr. Stokes is assistant professor of pediatrics and neurology/neurotherapeutics at the University of Texas–Southwestern Medical Center, Dallas.
The study was presented at the American Academy of Neurology Sports Concussion Virtual Conference, held online July 31 to Aug. 1.
Learning disorders affected scores
The researchers analyzed data from participants aged 10-18 years who were enrolled in the North Texas Concussion Registry (ConTex). Participants had been diagnosed with a concussion that was sustained within 30 days of enrollment. The researchers investigated whether there were differences between patients who had no history of learning disorders and those with a history of dyslexia and/or ADD/ADHD with regard to results of clinical testing following concussion.
Of the 1,298 individuals in the study, 58 had been diagnosed with dyslexia, 158 had been diagnosed with ADD/ADHD, and 35 had been diagnosed with both conditions. There was no difference in age, time since injury, or history of concussion between those with learning disorders and those without, but there were more male patients in the ADD/ADHD group.
Results showed that in the dyslexia group, mean time was slower (P = .011), and there was an increase in error scores on the King-Devick (KD) test (P = .028). That test assesses eye movements and involves the rapid naming of numbers that are spaced differently. In addition, those with ADD/ADHD had significantly higher impulse control scores (P = .007) on the ImPACT series of tests, which are commonly used in the evaluation of concussion. Participants with both dyslexia and ADHD demonstrated slower KD times (P = .009) and had higher depression scores and anxiety scores.
Dr. Stokes noted that a limiting factor of the study was that baseline scores were not available. “It is possible that kids with ADD have less impulse control even at baseline, and this would need to be taken into account,” he said. “You may perhaps also expect someone with dyslexia to have a worse score on the KD tests, so we need more data on how these scores are affected from baseline in these individuals. But our results show that when evaluating kids pre- or post concussion, it is important to know about learning disorders, as this will affect how we interpret the data.”
At 3-month follow-up, there were no longer significant differences in anxiety and depression scores for those with and those without learning disorders. “This suggests anxiety and depression may well be worse temporarily after concussion for those with ADD/ADHD but gets better with time,” Dr. Stokes said.
Follow-up data were not available for the other cognitive tests.
Are recovery times longer?
Asked whether young people with these learning disorders needed a longer time to recover after concussion, Dr. Stokes said: “That is a million-dollar question. Studies so far on this have shown conflicting results. Our results add to a growing body of literature on this.” He stressed that it is important to include anxiety and depression scores on both baseline and postconcussion tests. “People don’t tend to think of these symptoms as being associated with concussion, but they are actually very prominent in this situation,” he noted. “Our results suggest that individuals with ADHD may be more prone to anxiety and depression, and a blow to the head may tip them more into these symptoms.”
Discussing the study at a virtual press conference as part of the AAN Sports Concussion meeting, the codirector of the meeting, David Dodick, MD, Mayo Clinic, Scottsdale, Ariz., said: “This is a very interesting and important study which suggests there are differences between adolescents with a history of dyslexia/ADHD and those without these conditions in performance in concussion tests. Understanding the differences in these groups will help health care providers in evaluating these athletes and assisting in counseling them and their families with regard to their risk of injury.
“It is important to recognize that athletes with ADHD, whether or not they are on medication, may take longer to recover from a concussion,” Dr. Dodick added. They also exhibit greater reductions in cognitive skills and visual motor speed regarding hand-eye coordination, he said. There is an increase in the severity of symptoms. “Symptoms that exist in both groups tend to more severe in those individuals with ADHD,” he noted.
“Ascertaining the presence or absence of ADHD or dyslexia in those who are participating in sport is important, especially when trying to interpret the results of baseline testing, the results of postinjury testing, decisions on when to return to play, and assessing for individuals and their families the risk of long-term repeat concussions and adverse outcomes,” he concluded.
The other codirector of the AAN meeting, Brian Hainline, MD, chief medical officer of the National Collegiate Athletic Association, added: “It appears that athletes with ADHD may suffer more with concussion and have a longer recovery time. This can inform our decision making and help these individuals to understand that they are at higher risk.”
Dr. Hainline said this raises another important point: “Concussion is not a homogeneous entity. It is a brain injury that can manifest in multiple parts of the brain, and the way the brain is from a premorbid or comorbid point of view can influence the manifestation of concussion as well,” he said. “All these things need to be taken into account.”
Attentional deficit may itself make an individual more susceptible to sustaining an injury in the first place, he said. “All of this is an evolving body of research which is helping clinicians to make better-informed decisions for athletes who may manifest differently.”
A version of this article originally appeared on Medscape.com.
From AAN Sports Concussion Conference
Canakinumab (Ilaris) tapering tested in systemic JIA trial
A trial that tested two ways of tapering canakinumab (Ilaris) monotherapy in children with systemic juvenile idiopathic arthritis (sJIA) showed that both approaches might be feasible, but the lack of a control arm means that more data are needed before putting either into routine clinical practice.

Pierre Quartier, MD, and associates reported in Arthritis & Rheumatology. That’s with the proviso that children are taking canakinumab at the recommended dose of 4 mg/kg every 4 weeks and achieve clinical remission before any tapering is started.
The researchers found that 70%-80% of children who were in complete clinical remission (CR) maintained this for 6 months after the first dose-tapering step had been taken. However, at least one-fifth of study participants experienced a disease flare during treatment withdrawal, and only one-third were able to discontinue treatment altogether, which suggests continued treatment is needed.
“The results are a step in the right direction,” commented Athimaleipet Ramanan, MBBS, a consultant pediatric rheumatologist who was not involved in the study. They “offer the first vision of whether we can actually taper a medication” in sJIA because “until now we have not had any evidence for this,” he added.
“What we really need to know, which the study doesn’t tell you, is: Is decreasing the dose better than stopping?” said Dr. Ramanan, of the Bristol (England) Royal Hospital for Children.
Another thing that is important to know is: Does reducing the dose lead to the development of anti-drug antibodies? he said.

“There were some concerns that, when you give less of a monoclonal antibody, you might get more neutralizing anti-drug antibodies or you might make a drug more immunogenic,” he said. These data perhaps suggest that this isn’t the case because only one child on one occasion had detectable non-neutralizing anti-drug antibodies during the entire study, and that was 11 weeks after the last dose of canakinumab had been given.
Study results and design
Canakinumab is a monoclonal antibody that inhibits interleukin-1 (IL-1) that has been approved in the United States and Europe for the treatment of sJIA since 2013. Reducing a child’s exposure to canakinumab once their disease is under control is an attractive proposition given the treat-to-target approach used increasingly throughout modern rheumatologic practice. It could also help reduce the cost of what is an expensive treatment, compared with other available options for sJIA such as the interleukin-6 inhibitor tocilizumab (Actemra) or another IL-1 inhibitor anakinra (Kineret), which is not FDA-approved for use in sJIA and requires weekly injections.
“We don’t want to the disease to reappear, to flare, but we also don’t want to overuse treatments in these patients,” explained Dr. Quartier of Hôpital Necker-Enfants Malades, Assistance Publique-Hôpitaux de Paris in an interview.
The study he coconducted, given the acronym B-SPECIFIC-4 Patients, was an open-label study that consisted of two parts. In part 1, 182 children were given subcutaneous canakinumab 4 mg/kg every 4 weeks. In part 2, 76 children who were in complete CR after canakinumab treatment were randomized to one of two tapering strategies. In one arm, the dose of canakinumab was reduced from 4 mg/kg to 2 mg/kg given every 4 weeks before eventually discontinuing treatment, and in other arm the duration between dosing was increased by 4-week intervals, from 4 to 8 weeks, then 12 weeks, then discontinuation.
If children were taking glucocorticoids or methotrexate, the treating physicians were encouraged to stop these medications if possible, with 34%-39% and 42%-59% of children, respectively, being able to do so. The rate depended on whether children had received canakinumab before entering the study because some had been recruited from a long-term extension study while others were naive to the biologic; all had inactive disease at study entry.
This was the first study to evaluate the effectiveness of canakinumab in enabling the discontinuation of methotrexate, but the primary objective was to assess whether more than 40% of randomized patients in either discontinuation arm remained in CR for 24 weeks after the first step of discontinuation. This was achieved in 71% of children who were in the dose-reduction arm and in 84% of children in the dose-prolongation arm (P ≤ .0001 for each arm vs. 40%).
Prior exposure to canakinumab did not seem to affect the maintenance of CR, but it was also found that more children who maintained CR at their second but not their first attempt at tapering were in CR than those who were still in CR at the first step (76% and 89% in the dose-reduction and dose-prolongation arms, respectively).
Among the two dosing regimens, failure occurred in 18% of children in the dose-reduction arm at the first step, 10% at the second, and 8% at the third, whereas 2.7% of children in the dose-prolongation arm experienced regimen failure at the first step, 6.1% at the second, and 15% at the third.
No substantial difference between the two tapering approaches was observed because the study was not powered to look at this. There was also no control arm, such as a group continuing treatment while the other groups tapered, or as Dr. Ramanan had pointed out, stopping canakinumab altogether.
“As long as the treatment was continued, even at very low dosage, most patients remained in inactive disease,” Dr. Quartier said. He added, however, that only a minority of patients could stop treatment completely. Treatment should not be stopped abruptly, he advised, because this was associated with a substantial number of disease flares that needed treatment to be reinstated.
These findings suggest that “a certain level of sustained inhibition of the IL-1 pathway seems important for the maintenance of CR in most sJIA patients,” Dr. Quartier and coinvestigators wrote in their article.
They added: “We believe that these results are relevant for clinical practice, particularly for designing personalized tapering strategies that can allow an adequate control of disease while minimizing the side effects of certain medications, notably glucocorticoids.”
The study was funded by Novartis in collaboration with the Pediatric Rheumatology International Trials Organization and the Pediatric Rheumatology Collaborative Study Group. Dr. Quartier was an investigator for the trial and has received research and consultancy fees from Novartis, among other pharmaceutical companies. Two of his coauthors are employees of Novartis. Dr. Ramanan has acted as an investigator in prior canakinumab trials and has received consultancy fees from Novartis and multiple other companies.
SOURCE: Quartier P et al. Arthritis Rheumatol. 2020 Aug 11. doi: 10.1002/art.41488.
A trial that tested two ways of tapering canakinumab (Ilaris) monotherapy in children with systemic juvenile idiopathic arthritis (sJIA) showed that both approaches might be feasible, but the lack of a control arm means that more data are needed before putting either into routine clinical practice.
Pierre Quartier, MD, and associates reported in Arthritis & Rheumatology. That’s with the proviso that children are taking canakinumab at the recommended dose of 4 mg/kg every 4 weeks and achieve clinical remission before any tapering is started.
The researchers found that 70%-80% of children who were in complete clinical remission (CR) maintained this for 6 months after the first dose-tapering step had been taken. However, at least one-fifth of study participants experienced a disease flare during treatment withdrawal, and only one-third were able to discontinue treatment altogether, which suggests continued treatment is needed.
“The results are a step in the right direction,” commented Athimaleipet Ramanan, MBBS, a consultant pediatric rheumatologist who was not involved in the study. They “offer the first vision of whether we can actually taper a medication” in sJIA because “until now we have not had any evidence for this,” he added.
“What we really need to know, which the study doesn’t tell you, is: Is decreasing the dose better than stopping?” said Dr. Ramanan, of the Bristol (England) Royal Hospital for Children.
Another thing that is important to know is: Does reducing the dose lead to the development of anti-drug antibodies? he said.
“There were some concerns that, when you give less of a monoclonal antibody, you might get more neutralizing anti-drug antibodies or you might make a drug more immunogenic,” he said. These data perhaps suggest that this isn’t the case because only one child on one occasion had detectable non-neutralizing anti-drug antibodies during the entire study, and that was 11 weeks after the last dose of canakinumab had been given.
Study results and design
Canakinumab is a monoclonal antibody that inhibits interleukin-1 (IL-1) that has been approved in the United States and Europe for the treatment of sJIA since 2013. Reducing a child’s exposure to canakinumab once their disease is under control is an attractive proposition given the treat-to-target approach used increasingly throughout modern rheumatologic practice. It could also help reduce the cost of what is an expensive treatment, compared with other available options for sJIA such as the interleukin-6 inhibitor tocilizumab (Actemra) or another IL-1 inhibitor anakinra (Kineret), which is not FDA-approved for use in sJIA and requires weekly injections.
“We don’t want to the disease to reappear, to flare, but we also don’t want to overuse treatments in these patients,” explained Dr. Quartier of Hôpital Necker-Enfants Malades, Assistance Publique-Hôpitaux de Paris in an interview.
The study he coconducted, given the acronym B-SPECIFIC-4 Patients, was an open-label study that consisted of two parts. In part 1, 182 children were given subcutaneous canakinumab 4 mg/kg every 4 weeks. In part 2, 76 children who were in complete CR after canakinumab treatment were randomized to one of two tapering strategies. In one arm, the dose of canakinumab was reduced from 4 mg/kg to 2 mg/kg given every 4 weeks before eventually discontinuing treatment, and in other arm the duration between dosing was increased by 4-week intervals, from 4 to 8 weeks, then 12 weeks, then discontinuation.
If children were taking glucocorticoids or methotrexate, the treating physicians were encouraged to stop these medications if possible, with 34%-39% and 42%-59% of children, respectively, being able to do so. The rate depended on whether children had received canakinumab before entering the study because some had been recruited from a long-term extension study while others were naive to the biologic; all had inactive disease at study entry.
This was the first study to evaluate the effectiveness of canakinumab in enabling the discontinuation of methotrexate, but the primary objective was to assess whether more than 40% of randomized patients in either discontinuation arm remained in CR for 24 weeks after the first step of discontinuation. This was achieved in 71% of children who were in the dose-reduction arm and in 84% of children in the dose-prolongation arm (P ≤ .0001 for each arm vs. 40%).
Prior exposure to canakinumab did not seem to affect the maintenance of CR, but it was also found that more children who maintained CR at their second but not their first attempt at tapering were in CR than those who were still in CR at the first step (76% and 89% in the dose-reduction and dose-prolongation arms, respectively).
Among the two dosing regimens, failure occurred in 18% of children in the dose-reduction arm at the first step, 10% at the second, and 8% at the third, whereas 2.7% of children in the dose-prolongation arm experienced regimen failure at the first step, 6.1% at the second, and 15% at the third.
No substantial difference between the two tapering approaches was observed because the study was not powered to look at this. There was also no control arm, such as a group continuing treatment while the other groups tapered, or as Dr. Ramanan had pointed out, stopping canakinumab altogether.
“As long as the treatment was continued, even at very low dosage, most patients remained in inactive disease,” Dr. Quartier said. He added, however, that only a minority of patients could stop treatment completely. Treatment should not be stopped abruptly, he advised, because this was associated with a substantial number of disease flares that needed treatment to be reinstated.
These findings suggest that “a certain level of sustained inhibition of the IL-1 pathway seems important for the maintenance of CR in most sJIA patients,” Dr. Quartier and coinvestigators wrote in their article.
They added: “We believe that these results are relevant for clinical practice, particularly for designing personalized tapering strategies that can allow an adequate control of disease while minimizing the side effects of certain medications, notably glucocorticoids.”
The study was funded by Novartis in collaboration with the Pediatric Rheumatology International Trials Organization and the Pediatric Rheumatology Collaborative Study Group. Dr. Quartier was an investigator for the trial and has received research and consultancy fees from Novartis, among other pharmaceutical companies. Two of his coauthors are employees of Novartis. Dr. Ramanan has acted as an investigator in prior canakinumab trials and has received consultancy fees from Novartis and multiple other companies.
SOURCE: Quartier P et al. Arthritis Rheumatol. 2020 Aug 11. doi: 10.1002/art.41488.
A trial that tested two ways of tapering canakinumab (Ilaris) monotherapy in children with systemic juvenile idiopathic arthritis (sJIA) showed that both approaches might be feasible, but the lack of a control arm means that more data are needed before putting either into routine clinical practice.
Pierre Quartier, MD, and associates reported in Arthritis & Rheumatology. That’s with the proviso that children are taking canakinumab at the recommended dose of 4 mg/kg every 4 weeks and achieve clinical remission before any tapering is started.
The researchers found that 70%-80% of children who were in complete clinical remission (CR) maintained this for 6 months after the first dose-tapering step had been taken. However, at least one-fifth of study participants experienced a disease flare during treatment withdrawal, and only one-third were able to discontinue treatment altogether, which suggests continued treatment is needed.
“The results are a step in the right direction,” commented Athimaleipet Ramanan, MBBS, a consultant pediatric rheumatologist who was not involved in the study. They “offer the first vision of whether we can actually taper a medication” in sJIA because “until now we have not had any evidence for this,” he added.
“What we really need to know, which the study doesn’t tell you, is: Is decreasing the dose better than stopping?” said Dr. Ramanan, of the Bristol (England) Royal Hospital for Children.
Another thing that is important to know is: Does reducing the dose lead to the development of anti-drug antibodies? he said.
“There were some concerns that, when you give less of a monoclonal antibody, you might get more neutralizing anti-drug antibodies or you might make a drug more immunogenic,” he said. These data perhaps suggest that this isn’t the case because only one child on one occasion had detectable non-neutralizing anti-drug antibodies during the entire study, and that was 11 weeks after the last dose of canakinumab had been given.
Study results and design
Canakinumab is a monoclonal antibody that inhibits interleukin-1 (IL-1) that has been approved in the United States and Europe for the treatment of sJIA since 2013. Reducing a child’s exposure to canakinumab once their disease is under control is an attractive proposition given the treat-to-target approach used increasingly throughout modern rheumatologic practice. It could also help reduce the cost of what is an expensive treatment, compared with other available options for sJIA such as the interleukin-6 inhibitor tocilizumab (Actemra) or another IL-1 inhibitor anakinra (Kineret), which is not FDA-approved for use in sJIA and requires weekly injections.
“We don’t want to the disease to reappear, to flare, but we also don’t want to overuse treatments in these patients,” explained Dr. Quartier of Hôpital Necker-Enfants Malades, Assistance Publique-Hôpitaux de Paris in an interview.
The study he coconducted, given the acronym B-SPECIFIC-4 Patients, was an open-label study that consisted of two parts. In part 1, 182 children were given subcutaneous canakinumab 4 mg/kg every 4 weeks. In part 2, 76 children who were in complete CR after canakinumab treatment were randomized to one of two tapering strategies. In one arm, the dose of canakinumab was reduced from 4 mg/kg to 2 mg/kg given every 4 weeks before eventually discontinuing treatment, and in other arm the duration between dosing was increased by 4-week intervals, from 4 to 8 weeks, then 12 weeks, then discontinuation.
If children were taking glucocorticoids or methotrexate, the treating physicians were encouraged to stop these medications if possible, with 34%-39% and 42%-59% of children, respectively, being able to do so. The rate depended on whether children had received canakinumab before entering the study because some had been recruited from a long-term extension study while others were naive to the biologic; all had inactive disease at study entry.
This was the first study to evaluate the effectiveness of canakinumab in enabling the discontinuation of methotrexate, but the primary objective was to assess whether more than 40% of randomized patients in either discontinuation arm remained in CR for 24 weeks after the first step of discontinuation. This was achieved in 71% of children who were in the dose-reduction arm and in 84% of children in the dose-prolongation arm (P ≤ .0001 for each arm vs. 40%).
Prior exposure to canakinumab did not seem to affect the maintenance of CR, but it was also found that more children who maintained CR at their second but not their first attempt at tapering were in CR than those who were still in CR at the first step (76% and 89% in the dose-reduction and dose-prolongation arms, respectively).
Among the two dosing regimens, failure occurred in 18% of children in the dose-reduction arm at the first step, 10% at the second, and 8% at the third, whereas 2.7% of children in the dose-prolongation arm experienced regimen failure at the first step, 6.1% at the second, and 15% at the third.
No substantial difference between the two tapering approaches was observed because the study was not powered to look at this. There was also no control arm, such as a group continuing treatment while the other groups tapered, or as Dr. Ramanan had pointed out, stopping canakinumab altogether.
“As long as the treatment was continued, even at very low dosage, most patients remained in inactive disease,” Dr. Quartier said. He added, however, that only a minority of patients could stop treatment completely. Treatment should not be stopped abruptly, he advised, because this was associated with a substantial number of disease flares that needed treatment to be reinstated.
These findings suggest that “a certain level of sustained inhibition of the IL-1 pathway seems important for the maintenance of CR in most sJIA patients,” Dr. Quartier and coinvestigators wrote in their article.
They added: “We believe that these results are relevant for clinical practice, particularly for designing personalized tapering strategies that can allow an adequate control of disease while minimizing the side effects of certain medications, notably glucocorticoids.”
The study was funded by Novartis in collaboration with the Pediatric Rheumatology International Trials Organization and the Pediatric Rheumatology Collaborative Study Group. Dr. Quartier was an investigator for the trial and has received research and consultancy fees from Novartis, among other pharmaceutical companies. Two of his coauthors are employees of Novartis. Dr. Ramanan has acted as an investigator in prior canakinumab trials and has received consultancy fees from Novartis and multiple other companies.
SOURCE: Quartier P et al. Arthritis Rheumatol. 2020 Aug 11. doi: 10.1002/art.41488.
FROM ARTHRITIS & RHEUMATOLOGY
Maternal depression may derail children’s school readiness
based on data from a cohort study of more than 50,000 children.

Previous research supports a link between maternal depression and poor cognitive development in children, but the effect of children’s age when exposed to depression on their development has not been well studied, wrote Elizabeth Wall-Wieler, PhD, of Stanford (Calif.) University, and colleagues.
In a population-based cohort study published in Pediatrics, the researchers examined data from 52,103 children born in Manitoba, Canada who completed the Early Development Instrument (EDI) between 2005 and 2016. The EDI is a 103-item questionnaire given to kindergarteners in a classroom setting during the second half of the school year. The EDI is designed to assess five domains: physical health and well-being, social competence, emotional maturity, language and cognitive development, and communication skills and general knowledge. The researchers assessed maternal depression using a combination of physician visits, hospitalizations, and pharmaceutical data; 19% of the children had a mother diagnosed with depression during the study.
Difficulties emerged in social functioning, emotion regulation
Children whose mothers had a diagnosis of depression before they reached age 5 years had a 1.17 times increased risk of having a problem in one or more of the developmental domains at school entry, compared with those whose mothers had no such diagnosis. Overall, exposure to maternal depression was significantly associated with problems in the areas of social competence (adjusted risk ratio 1.28), physical health and well-being (aRR 1.28), and emotional maturity (aRR 1.27) in kindergarten. For these three domains, children exposed to maternal depression between the ages of 4 and 5 years showed the greatest risk of developmental vulnerability, the researchers said.
“It is noteworthy that these difficulties were reported by the children’s teachers, avoiding negative biases inherent in having mothers with depression serve as informants,” Dr. Wall-Wieler and associates wrote.
The study findings were limited by several factors related to the observational design, including incomplete data on maternal depression prevalence and severity, the researchers said. In addition, the study did not account for confounding variables related to parenting style and information on the presence and psychiatric profiles of fathers.
The results support previous studies by identifying the impact of exposure to maternal depression on particular developmental domains, the researchers concluded. However, more research is needed to extend their findings.
“In particular, investigators should work to elucidate the mechanisms that underlie this intergenerational transmission to young children of mothers with depression at risk for social and emotional difficulties, focusing on aspects of the caregiving environments and behaviors to which these children are exposed,” Dr. Wall-Wieler and associates concluded.
Approximately 70% of the children exposed to maternal depression did not test as vulnerable in any of the developmental domains. Factors that promoted resilience in the children exposed to maternal depression who did not experience developmental vulnerability should be identified, they noted.
Maternal depression is a public health crisis
“The widespread prevalence of maternal depression in the United States and worldwide, with estimates ranging from 3% to 60%, constitutes a public health crisis, particularly one affecting low-income women and their children,” Stephanie Klees Goeglein, MD, and Yvette E. Yatchmink, MD, PhD, of Brown University, Providence, R.I., wrote in an accompanying editorial (Pediatrics. 2020 Aug 17. doi: 10.1542/peds.2020-010413). The study adds to the research and understanding of the negative impact of maternal depression on child development, but also raises questions because some key confounders were not addressed, mainly “the presence of prenatal depression, severity and chronicity of maternal depression, comorbidities, and parenting practices including the involvement of fathers or partners,” they noted.
Don’t discount the impact of prenatal depression, the editorialists stressed. “Surprising to some, prenatal depression is more common than postpartum depression and may be a major, unexplored contributor to the developmental vulnerability of the children in the sample,” Dr. Goeglein and Dr. Yatchmink said.
However, the fact that approximately 70% of the children exposed to maternal depression did not have developmental vulnerability in any domain is encouraging, and speaks to the resiliency of children to overcome adverse conditions, they added.
Pediatricians can play a role in reducing maternal depression by screening mothers starting at a prenatal visit and continuing through post partum, infancy, and beyond. In addition, actions to improve access to mental health care for mothers and to develop culturally-sensitive positive parenting programs may help reduce the effects of depression on mothers and children, Dr. Goeglein and Dr. Yatchmink emphasized.
Empower depressed mothers to seek assistance
The results were not surprising, but a study that “validates that which we feel we know is clinically significant,” Lillian M. Beard, MD, of Children’s National in Washington, said in an interview.

“This study restates why it is so important for us to evaluate and recognize maternal depression,” she said. “As a busy pediatrician, once I recognize a problem, I struggle with how to provide viable professional and valuable community resources for these mothers.
“My take-home message from the study is that we must screen for maternal depression. When we suspect maternal depression, it is usually present,” Dr. Beard said. “While we cannot change all the factors that contribute to this condition, to help the children we serve to be physically and emotionally sound, we must help empower their mothers to seek assistance, when needed, to be emotionally healthy,” she emphasized.
“More research is needed to recognize the efficacy and value of community-based assistance for maternal and family depression,” said Dr. Beard, who was not involved with the study and was asked to comment on the findings.
The study was supported by the Canadian Institutes of Health Research, the National Institute of Mental Health, and the National Institutes of Health. The researchers and editorialists had no financial conflicts to disclose. Dr. Beard, a member of the Pediatric News editorial advisory board, had no relevant financial disclosures.
SOURCE: Wall-Wieler E et al. Pediatrics. 2020 Aug 17. doi: 10.1542/peds.2020-0794.
based on data from a cohort study of more than 50,000 children.
Previous research supports a link between maternal depression and poor cognitive development in children, but the effect of children’s age when exposed to depression on their development has not been well studied, wrote Elizabeth Wall-Wieler, PhD, of Stanford (Calif.) University, and colleagues.
In a population-based cohort study published in Pediatrics, the researchers examined data from 52,103 children born in Manitoba, Canada who completed the Early Development Instrument (EDI) between 2005 and 2016. The EDI is a 103-item questionnaire given to kindergarteners in a classroom setting during the second half of the school year. The EDI is designed to assess five domains: physical health and well-being, social competence, emotional maturity, language and cognitive development, and communication skills and general knowledge. The researchers assessed maternal depression using a combination of physician visits, hospitalizations, and pharmaceutical data; 19% of the children had a mother diagnosed with depression during the study.
Difficulties emerged in social functioning, emotion regulation
Children whose mothers had a diagnosis of depression before they reached age 5 years had a 1.17 times increased risk of having a problem in one or more of the developmental domains at school entry, compared with those whose mothers had no such diagnosis. Overall, exposure to maternal depression was significantly associated with problems in the areas of social competence (adjusted risk ratio 1.28), physical health and well-being (aRR 1.28), and emotional maturity (aRR 1.27) in kindergarten. For these three domains, children exposed to maternal depression between the ages of 4 and 5 years showed the greatest risk of developmental vulnerability, the researchers said.
“It is noteworthy that these difficulties were reported by the children’s teachers, avoiding negative biases inherent in having mothers with depression serve as informants,” Dr. Wall-Wieler and associates wrote.
The study findings were limited by several factors related to the observational design, including incomplete data on maternal depression prevalence and severity, the researchers said. In addition, the study did not account for confounding variables related to parenting style and information on the presence and psychiatric profiles of fathers.
The results support previous studies by identifying the impact of exposure to maternal depression on particular developmental domains, the researchers concluded. However, more research is needed to extend their findings.
“In particular, investigators should work to elucidate the mechanisms that underlie this intergenerational transmission to young children of mothers with depression at risk for social and emotional difficulties, focusing on aspects of the caregiving environments and behaviors to which these children are exposed,” Dr. Wall-Wieler and associates concluded.
Approximately 70% of the children exposed to maternal depression did not test as vulnerable in any of the developmental domains. Factors that promoted resilience in the children exposed to maternal depression who did not experience developmental vulnerability should be identified, they noted.
Maternal depression is a public health crisis
“The widespread prevalence of maternal depression in the United States and worldwide, with estimates ranging from 3% to 60%, constitutes a public health crisis, particularly one affecting low-income women and their children,” Stephanie Klees Goeglein, MD, and Yvette E. Yatchmink, MD, PhD, of Brown University, Providence, R.I., wrote in an accompanying editorial (Pediatrics. 2020 Aug 17. doi: 10.1542/peds.2020-010413). The study adds to the research and understanding of the negative impact of maternal depression on child development, but also raises questions because some key confounders were not addressed, mainly “the presence of prenatal depression, severity and chronicity of maternal depression, comorbidities, and parenting practices including the involvement of fathers or partners,” they noted.
Don’t discount the impact of prenatal depression, the editorialists stressed. “Surprising to some, prenatal depression is more common than postpartum depression and may be a major, unexplored contributor to the developmental vulnerability of the children in the sample,” Dr. Goeglein and Dr. Yatchmink said.
However, the fact that approximately 70% of the children exposed to maternal depression did not have developmental vulnerability in any domain is encouraging, and speaks to the resiliency of children to overcome adverse conditions, they added.
Pediatricians can play a role in reducing maternal depression by screening mothers starting at a prenatal visit and continuing through post partum, infancy, and beyond. In addition, actions to improve access to mental health care for mothers and to develop culturally-sensitive positive parenting programs may help reduce the effects of depression on mothers and children, Dr. Goeglein and Dr. Yatchmink emphasized.
Empower depressed mothers to seek assistance
The results were not surprising, but a study that “validates that which we feel we know is clinically significant,” Lillian M. Beard, MD, of Children’s National in Washington, said in an interview.
“This study restates why it is so important for us to evaluate and recognize maternal depression,” she said. “As a busy pediatrician, once I recognize a problem, I struggle with how to provide viable professional and valuable community resources for these mothers.
“My take-home message from the study is that we must screen for maternal depression. When we suspect maternal depression, it is usually present,” Dr. Beard said. “While we cannot change all the factors that contribute to this condition, to help the children we serve to be physically and emotionally sound, we must help empower their mothers to seek assistance, when needed, to be emotionally healthy,” she emphasized.
“More research is needed to recognize the efficacy and value of community-based assistance for maternal and family depression,” said Dr. Beard, who was not involved with the study and was asked to comment on the findings.
The study was supported by the Canadian Institutes of Health Research, the National Institute of Mental Health, and the National Institutes of Health. The researchers and editorialists had no financial conflicts to disclose. Dr. Beard, a member of the Pediatric News editorial advisory board, had no relevant financial disclosures.
SOURCE: Wall-Wieler E et al. Pediatrics. 2020 Aug 17. doi: 10.1542/peds.2020-0794.
based on data from a cohort study of more than 50,000 children.
Previous research supports a link between maternal depression and poor cognitive development in children, but the effect of children’s age when exposed to depression on their development has not been well studied, wrote Elizabeth Wall-Wieler, PhD, of Stanford (Calif.) University, and colleagues.
In a population-based cohort study published in Pediatrics, the researchers examined data from 52,103 children born in Manitoba, Canada who completed the Early Development Instrument (EDI) between 2005 and 2016. The EDI is a 103-item questionnaire given to kindergarteners in a classroom setting during the second half of the school year. The EDI is designed to assess five domains: physical health and well-being, social competence, emotional maturity, language and cognitive development, and communication skills and general knowledge. The researchers assessed maternal depression using a combination of physician visits, hospitalizations, and pharmaceutical data; 19% of the children had a mother diagnosed with depression during the study.
Difficulties emerged in social functioning, emotion regulation
Children whose mothers had a diagnosis of depression before they reached age 5 years had a 1.17 times increased risk of having a problem in one or more of the developmental domains at school entry, compared with those whose mothers had no such diagnosis. Overall, exposure to maternal depression was significantly associated with problems in the areas of social competence (adjusted risk ratio 1.28), physical health and well-being (aRR 1.28), and emotional maturity (aRR 1.27) in kindergarten. For these three domains, children exposed to maternal depression between the ages of 4 and 5 years showed the greatest risk of developmental vulnerability, the researchers said.
“It is noteworthy that these difficulties were reported by the children’s teachers, avoiding negative biases inherent in having mothers with depression serve as informants,” Dr. Wall-Wieler and associates wrote.
The study findings were limited by several factors related to the observational design, including incomplete data on maternal depression prevalence and severity, the researchers said. In addition, the study did not account for confounding variables related to parenting style and information on the presence and psychiatric profiles of fathers.
The results support previous studies by identifying the impact of exposure to maternal depression on particular developmental domains, the researchers concluded. However, more research is needed to extend their findings.
“In particular, investigators should work to elucidate the mechanisms that underlie this intergenerational transmission to young children of mothers with depression at risk for social and emotional difficulties, focusing on aspects of the caregiving environments and behaviors to which these children are exposed,” Dr. Wall-Wieler and associates concluded.
Approximately 70% of the children exposed to maternal depression did not test as vulnerable in any of the developmental domains. Factors that promoted resilience in the children exposed to maternal depression who did not experience developmental vulnerability should be identified, they noted.
Maternal depression is a public health crisis
“The widespread prevalence of maternal depression in the United States and worldwide, with estimates ranging from 3% to 60%, constitutes a public health crisis, particularly one affecting low-income women and their children,” Stephanie Klees Goeglein, MD, and Yvette E. Yatchmink, MD, PhD, of Brown University, Providence, R.I., wrote in an accompanying editorial (Pediatrics. 2020 Aug 17. doi: 10.1542/peds.2020-010413). The study adds to the research and understanding of the negative impact of maternal depression on child development, but also raises questions because some key confounders were not addressed, mainly “the presence of prenatal depression, severity and chronicity of maternal depression, comorbidities, and parenting practices including the involvement of fathers or partners,” they noted.
Don’t discount the impact of prenatal depression, the editorialists stressed. “Surprising to some, prenatal depression is more common than postpartum depression and may be a major, unexplored contributor to the developmental vulnerability of the children in the sample,” Dr. Goeglein and Dr. Yatchmink said.
However, the fact that approximately 70% of the children exposed to maternal depression did not have developmental vulnerability in any domain is encouraging, and speaks to the resiliency of children to overcome adverse conditions, they added.
Pediatricians can play a role in reducing maternal depression by screening mothers starting at a prenatal visit and continuing through post partum, infancy, and beyond. In addition, actions to improve access to mental health care for mothers and to develop culturally-sensitive positive parenting programs may help reduce the effects of depression on mothers and children, Dr. Goeglein and Dr. Yatchmink emphasized.
Empower depressed mothers to seek assistance
The results were not surprising, but a study that “validates that which we feel we know is clinically significant,” Lillian M. Beard, MD, of Children’s National in Washington, said in an interview.
“This study restates why it is so important for us to evaluate and recognize maternal depression,” she said. “As a busy pediatrician, once I recognize a problem, I struggle with how to provide viable professional and valuable community resources for these mothers.
“My take-home message from the study is that we must screen for maternal depression. When we suspect maternal depression, it is usually present,” Dr. Beard said. “While we cannot change all the factors that contribute to this condition, to help the children we serve to be physically and emotionally sound, we must help empower their mothers to seek assistance, when needed, to be emotionally healthy,” she emphasized.
“More research is needed to recognize the efficacy and value of community-based assistance for maternal and family depression,” said Dr. Beard, who was not involved with the study and was asked to comment on the findings.
The study was supported by the Canadian Institutes of Health Research, the National Institute of Mental Health, and the National Institutes of Health. The researchers and editorialists had no financial conflicts to disclose. Dr. Beard, a member of the Pediatric News editorial advisory board, had no relevant financial disclosures.
SOURCE: Wall-Wieler E et al. Pediatrics. 2020 Aug 17. doi: 10.1542/peds.2020-0794.
FROM PEDIATRICS
A 4-year-old with a lesion on her cheek, which grew and became firmer over two months
The patient was diagnosed with idiopathic facial aseptic granuloma (IFAG) based on the clinical findings, as well as the associated history of chalazia and erythematous papules seen in childhood rosacea.

She was treated with several months of azithromycin, sulfur wash, and metronidazole cream with improvement of some of the smaller lesions but no change on the larger nodules. Later she was treated with oral and topical ivermectin with no improvement. Some of the nodules slowly resolved except for the larger lesion on the right cheek. She was later treated with a 6-week course of clarithromycin with partial improvement of the nodule. The lesion resolved after 2 months of stopping clarithromycin.
IFAG is a rare condition seen in prepubescent children. The etiology of this condition is not well understood and is thought to be on the spectrum of childhood rosacea.1 From several recent reports, IFAG usually is seen in children with associated conditions including chalazia, conjunctivitis, blepharitis, and telangiectasias, which can be seen in patients with rosacea. These associated findings suggest the possibility of IFAG being a form of granulomatous rosacea in children.
This condition presents in childhood between the ages of 8 months and 13 years. Most of the cases occur in toddlers, and girls appear to be more affected than boys. The lesions appear as pink, rubbery, nontender, nonfluctuant nodules on the cheeks, which can be single or multiple. A large prospective study in 30 children demonstrated that more 70% of the lesions cultured were negative for bacteria. Histologic analysis of some of the lesions showed a chronic dermal lymphohistiocytic granulomatous perifollicular infiltrate with numerous foreign body–type giant cells.2
The differential diagnosis of these lesions should include infectious pyodermas such as mycobacterial infections, cutaneous leishmaniasis, and botryomycosis; deep fungal infections such as sporotrichosis, coccidioidomycosis, and cryptococcosis; childhood nodulocystic acne; pilomatrixoma; epidermoid cyst; vascular tumors or malformations; and leukemia cutis.3
The diagnosis is usually clinical but in atypical cases a skin biopsy with tissue cultures should be performed. The decision to biopsy these lesions will need to be done in a one by one basis, as a biopsy may leave scaring on the area affected.
It has been postulated that a color Doppler ultrasound of the lesion may be a helpful ancillary study. Echographic findings show a well demarcated solid-cystic, hypoechoic dermal lesion, the largest axis of which lies parallel to the skin surface. The lesion lacks calcium deposits. Other findings include increased echogenicity of the underlaying hypodermis. The findings may vary depending on the stage of the lesion.4
The course of the condition may last on average months to years. Some lesions resolve spontaneously and others may respond to courses of oral antibiotics such as clarithromycin, azithromycin, or ivermectin. In our patient, several lesions improved with oral antibiotics, but the larger lesions were more persistent and resolved after a year.
The lesions usually resolve without scarring. In those patients with associated rosacea, maintenance topical treatments may be warranted and also may need follow-up with ophthalmology because they tend to commonly have ocular rosacea as well.
Dr. Matiz is a pediatric dermatologist at Southern California Permanente Medical Group, San Diego. She said she had no relevant financial disclosures. Email her at [email protected].
References
1. Pediatr Dermatol. 2013 Jan-Feb;30(1):109-11.
2. Br J Dermatol. 2007 Apr;156(4):705-8.
3. Pediatr Dermatol. 2018 Jul;35(4):490-3.
4. Actas Dermosifiliogr. 2019 Oct;110(8):637-41.
The patient was diagnosed with idiopathic facial aseptic granuloma (IFAG) based on the clinical findings, as well as the associated history of chalazia and erythematous papules seen in childhood rosacea.
She was treated with several months of azithromycin, sulfur wash, and metronidazole cream with improvement of some of the smaller lesions but no change on the larger nodules. Later she was treated with oral and topical ivermectin with no improvement. Some of the nodules slowly resolved except for the larger lesion on the right cheek. She was later treated with a 6-week course of clarithromycin with partial improvement of the nodule. The lesion resolved after 2 months of stopping clarithromycin.
IFAG is a rare condition seen in prepubescent children. The etiology of this condition is not well understood and is thought to be on the spectrum of childhood rosacea.1 From several recent reports, IFAG usually is seen in children with associated conditions including chalazia, conjunctivitis, blepharitis, and telangiectasias, which can be seen in patients with rosacea. These associated findings suggest the possibility of IFAG being a form of granulomatous rosacea in children.
This condition presents in childhood between the ages of 8 months and 13 years. Most of the cases occur in toddlers, and girls appear to be more affected than boys. The lesions appear as pink, rubbery, nontender, nonfluctuant nodules on the cheeks, which can be single or multiple. A large prospective study in 30 children demonstrated that more 70% of the lesions cultured were negative for bacteria. Histologic analysis of some of the lesions showed a chronic dermal lymphohistiocytic granulomatous perifollicular infiltrate with numerous foreign body–type giant cells.2
The differential diagnosis of these lesions should include infectious pyodermas such as mycobacterial infections, cutaneous leishmaniasis, and botryomycosis; deep fungal infections such as sporotrichosis, coccidioidomycosis, and cryptococcosis; childhood nodulocystic acne; pilomatrixoma; epidermoid cyst; vascular tumors or malformations; and leukemia cutis.3
The diagnosis is usually clinical but in atypical cases a skin biopsy with tissue cultures should be performed. The decision to biopsy these lesions will need to be done in a one by one basis, as a biopsy may leave scaring on the area affected.
It has been postulated that a color Doppler ultrasound of the lesion may be a helpful ancillary study. Echographic findings show a well demarcated solid-cystic, hypoechoic dermal lesion, the largest axis of which lies parallel to the skin surface. The lesion lacks calcium deposits. Other findings include increased echogenicity of the underlaying hypodermis. The findings may vary depending on the stage of the lesion.4
The course of the condition may last on average months to years. Some lesions resolve spontaneously and others may respond to courses of oral antibiotics such as clarithromycin, azithromycin, or ivermectin. In our patient, several lesions improved with oral antibiotics, but the larger lesions were more persistent and resolved after a year.
The lesions usually resolve without scarring. In those patients with associated rosacea, maintenance topical treatments may be warranted and also may need follow-up with ophthalmology because they tend to commonly have ocular rosacea as well.
Dr. Matiz is a pediatric dermatologist at Southern California Permanente Medical Group, San Diego. She said she had no relevant financial disclosures. Email her at [email protected].
References
1. Pediatr Dermatol. 2013 Jan-Feb;30(1):109-11.
2. Br J Dermatol. 2007 Apr;156(4):705-8.
3. Pediatr Dermatol. 2018 Jul;35(4):490-3.
4. Actas Dermosifiliogr. 2019 Oct;110(8):637-41.
The patient was diagnosed with idiopathic facial aseptic granuloma (IFAG) based on the clinical findings, as well as the associated history of chalazia and erythematous papules seen in childhood rosacea.
She was treated with several months of azithromycin, sulfur wash, and metronidazole cream with improvement of some of the smaller lesions but no change on the larger nodules. Later she was treated with oral and topical ivermectin with no improvement. Some of the nodules slowly resolved except for the larger lesion on the right cheek. She was later treated with a 6-week course of clarithromycin with partial improvement of the nodule. The lesion resolved after 2 months of stopping clarithromycin.
IFAG is a rare condition seen in prepubescent children. The etiology of this condition is not well understood and is thought to be on the spectrum of childhood rosacea.1 From several recent reports, IFAG usually is seen in children with associated conditions including chalazia, conjunctivitis, blepharitis, and telangiectasias, which can be seen in patients with rosacea. These associated findings suggest the possibility of IFAG being a form of granulomatous rosacea in children.
This condition presents in childhood between the ages of 8 months and 13 years. Most of the cases occur in toddlers, and girls appear to be more affected than boys. The lesions appear as pink, rubbery, nontender, nonfluctuant nodules on the cheeks, which can be single or multiple. A large prospective study in 30 children demonstrated that more 70% of the lesions cultured were negative for bacteria. Histologic analysis of some of the lesions showed a chronic dermal lymphohistiocytic granulomatous perifollicular infiltrate with numerous foreign body–type giant cells.2
The differential diagnosis of these lesions should include infectious pyodermas such as mycobacterial infections, cutaneous leishmaniasis, and botryomycosis; deep fungal infections such as sporotrichosis, coccidioidomycosis, and cryptococcosis; childhood nodulocystic acne; pilomatrixoma; epidermoid cyst; vascular tumors or malformations; and leukemia cutis.3
The diagnosis is usually clinical but in atypical cases a skin biopsy with tissue cultures should be performed. The decision to biopsy these lesions will need to be done in a one by one basis, as a biopsy may leave scaring on the area affected.
It has been postulated that a color Doppler ultrasound of the lesion may be a helpful ancillary study. Echographic findings show a well demarcated solid-cystic, hypoechoic dermal lesion, the largest axis of which lies parallel to the skin surface. The lesion lacks calcium deposits. Other findings include increased echogenicity of the underlaying hypodermis. The findings may vary depending on the stage of the lesion.4
The course of the condition may last on average months to years. Some lesions resolve spontaneously and others may respond to courses of oral antibiotics such as clarithromycin, azithromycin, or ivermectin. In our patient, several lesions improved with oral antibiotics, but the larger lesions were more persistent and resolved after a year.
The lesions usually resolve without scarring. In those patients with associated rosacea, maintenance topical treatments may be warranted and also may need follow-up with ophthalmology because they tend to commonly have ocular rosacea as well.
Dr. Matiz is a pediatric dermatologist at Southern California Permanente Medical Group, San Diego. She said she had no relevant financial disclosures. Email her at [email protected].
References
1. Pediatr Dermatol. 2013 Jan-Feb;30(1):109-11.
2. Br J Dermatol. 2007 Apr;156(4):705-8.
3. Pediatr Dermatol. 2018 Jul;35(4):490-3.
4. Actas Dermosifiliogr. 2019 Oct;110(8):637-41.
A 4-year-old female is brought to our pediatric dermatology clinic for evaluation of a persistent lesion on the cheek.

The mother of the child reports that the lesion started as a small "bug bite" and then started growing and getting firmer for the past 2 months. The girl has developed other smaller red, pimple-like lesions on the cheeks and one of them is starting to increase in size.
She denies any tenderness on the area or any purulent discharge. She has had no fevers, chills, weight loss, nose bleeds, fatigue, or any other symptoms. The mother has not noted any changes on the child's body odor, any rapid growth, or hair on her axillary or pubic area. She was treated with three different courses of oral antibiotics including cephalexin, trimethoprim/sulfamethoxazole, and clindamycin, as well as topical mupirocin, with no improvement.
Her past medical history is significant for several episodes of eyelid cysts that were treated with warm compresses and topical erythromycin ointment. The family history is significant for the father having severe acne as a teenager. She has two cats, she has not traveled, and she has an older sister who has no lesions.
On physical examination she is a lovely 4-year-old female in no acute distress. Her height is on the 70th percentile and weight on the 40th percentile for her age. Her blood pressure is 95/84 with a heart rate of 96. On skin examination she has several pink macules and papules on her bilateral cheeks. On the left cheek there are two pink nodules: One is 1 cm, and the other is 7 mm. The nodules are not tender. There is no warmth, fluctuance, or discharge from the lesions.
She has no cervical lymphadenopathy. She has no axillary or pubic hair. She is Tanner stage I.
PHM20 Virtual: Can’t miss heart disease for hospitalists
PHM20 Virtual session title
Can’t Miss Heart Disease for Hospitalists
Presenter
Erich Maul, DO, MPH, FAAP, SFHM
Session summary
Dr. Erich Maul, professor of pediatrics, medical director for progressive care and acute care, and chief of hospital pediatrics at Kentucky Children’s Hospital, Lexington, presented an engaging, case-based approach to evaluate heart disease when “on call.” He iterated the importance of recognizing congenital heart disease, especially since 25% of these patients usually need surgical intervention within the first month of diagnosis and about 50% of congenital heart disease patients do not have a murmur.
Presenting cases seen during a busy hospitalist call night, Dr. Maul highlighted that patients can present with signs of heart failure, cyanosis, sepsis or hypoperfusion, failure to thrive, and respiratory distress or failure. He discussed the presentation, epidemiology, diagnosis, treatment, and prognosis. He also provided examples of common arrhythmias and provided refreshers on management using basic life support (BLS) and pediatric advanced life support.
Key takeaways
- Always start with the nine steps to resuscitation: ABC (airway, breathing, circulation), ABC, oxygen, access, monitoring.
- Early BLS is important.
- Congenital heart disease often presents with either cyanosis, hypoperfusion, failure to thrive, or respiratory distress.
Dr. Tantoco is an academic med-peds hospitalist practicing at Northwestern Memorial Hospital and Ann & Robert H. Lurie Children’s Hospital of Chicago. She is an instructor of medicine (hospital medicine) and pediatrics at Northwestern University, Chicago.
PHM20 Virtual session title
Can’t Miss Heart Disease for Hospitalists
Presenter
Erich Maul, DO, MPH, FAAP, SFHM
Session summary
Dr. Erich Maul, professor of pediatrics, medical director for progressive care and acute care, and chief of hospital pediatrics at Kentucky Children’s Hospital, Lexington, presented an engaging, case-based approach to evaluate heart disease when “on call.” He iterated the importance of recognizing congenital heart disease, especially since 25% of these patients usually need surgical intervention within the first month of diagnosis and about 50% of congenital heart disease patients do not have a murmur.
Presenting cases seen during a busy hospitalist call night, Dr. Maul highlighted that patients can present with signs of heart failure, cyanosis, sepsis or hypoperfusion, failure to thrive, and respiratory distress or failure. He discussed the presentation, epidemiology, diagnosis, treatment, and prognosis. He also provided examples of common arrhythmias and provided refreshers on management using basic life support (BLS) and pediatric advanced life support.
Key takeaways
- Always start with the nine steps to resuscitation: ABC (airway, breathing, circulation), ABC, oxygen, access, monitoring.
- Early BLS is important.
- Congenital heart disease often presents with either cyanosis, hypoperfusion, failure to thrive, or respiratory distress.
Dr. Tantoco is an academic med-peds hospitalist practicing at Northwestern Memorial Hospital and Ann & Robert H. Lurie Children’s Hospital of Chicago. She is an instructor of medicine (hospital medicine) and pediatrics at Northwestern University, Chicago.
PHM20 Virtual session title
Can’t Miss Heart Disease for Hospitalists
Presenter
Erich Maul, DO, MPH, FAAP, SFHM
Session summary
Dr. Erich Maul, professor of pediatrics, medical director for progressive care and acute care, and chief of hospital pediatrics at Kentucky Children’s Hospital, Lexington, presented an engaging, case-based approach to evaluate heart disease when “on call.” He iterated the importance of recognizing congenital heart disease, especially since 25% of these patients usually need surgical intervention within the first month of diagnosis and about 50% of congenital heart disease patients do not have a murmur.
Presenting cases seen during a busy hospitalist call night, Dr. Maul highlighted that patients can present with signs of heart failure, cyanosis, sepsis or hypoperfusion, failure to thrive, and respiratory distress or failure. He discussed the presentation, epidemiology, diagnosis, treatment, and prognosis. He also provided examples of common arrhythmias and provided refreshers on management using basic life support (BLS) and pediatric advanced life support.
Key takeaways
- Always start with the nine steps to resuscitation: ABC (airway, breathing, circulation), ABC, oxygen, access, monitoring.
- Early BLS is important.
- Congenital heart disease often presents with either cyanosis, hypoperfusion, failure to thrive, or respiratory distress.
Dr. Tantoco is an academic med-peds hospitalist practicing at Northwestern Memorial Hospital and Ann & Robert H. Lurie Children’s Hospital of Chicago. She is an instructor of medicine (hospital medicine) and pediatrics at Northwestern University, Chicago.
COVID-19 child case count now over 400,000
according to a new report from the American Academy of Pediatrics and the Children’s Hospital Association.
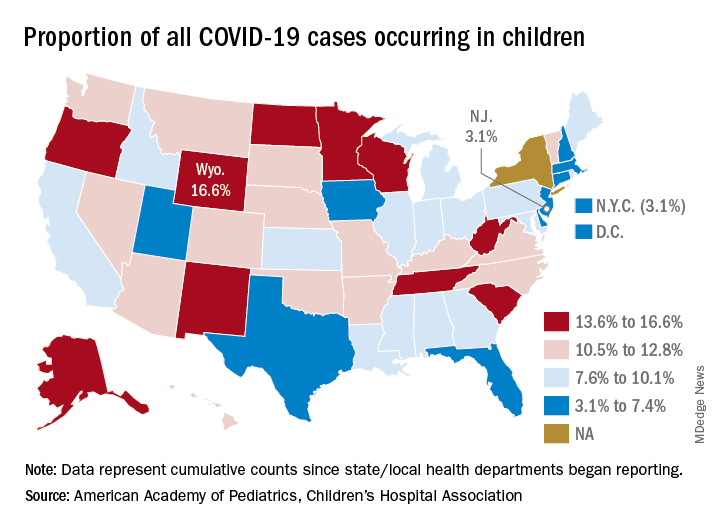
The 406,000 children who have tested positive for COVID-19 represent 9.1% of all cases reported so far by 49 states (New York does not provide age distribution), New York City, the District of Columbia, Puerto Rico, and Guam. Since the proportion of child cases also was 9.1% on Aug. 6, the most recent week is the first without an increase since tracking began in mid-April, the report shows.
State-level data show that Wyoming has the highest percentage of child cases (16.6%) after Alabama changed its “definition of child case from 0-24 to 0-17 years, resulting in a downward revision of cumulative child cases,” the AAP and the CHA said. Alabama’s proportion of such cases dropped from 22.5% to 9.0%.
New Jersey had the lowest rate (3.1%) again this week, along with New York City, but both were up slightly from the week before, when New Jersey was at 2.9% and N.Y.C. was 3.0%. The only states, other than Alabama, that saw declines over the last week were Arkansas, Massachusetts, Mississippi, South Dakota, Texas, and West Virginia. Texas, however, has reported age for only 8% of its confirmed cases, the report noted.
The overall rate of child COVID-19 cases as of Aug. 13 was 538 per 100,000 children, up from 500.7 per 100,000 a week earlier. Arizona was again highest among the states with a rate of 1,254 per 100,000 (up from 1,206) and Vermont was lowest at 121, although Puerto Rico (114) and Guam (88) were lower still, the AAP/CHA data indicate.
For the nine states that report testing information for children, Arizona has the highest positivity rate at 18.3% and West Virginia has the lowest at 3.6%. Data on hospitalizations – available from 21 states and N.Y.C. – show that 3,849 children have been admitted, with rates varying from 0.2% of children in Hawaii to 8.8% in the Big Apple, according to the report.
More specific information on child cases, such as symptoms or underlying conditions, is not being provided by states at this time, the AAP and CHA pointed out.
according to a new report from the American Academy of Pediatrics and the Children’s Hospital Association.
The 406,000 children who have tested positive for COVID-19 represent 9.1% of all cases reported so far by 49 states (New York does not provide age distribution), New York City, the District of Columbia, Puerto Rico, and Guam. Since the proportion of child cases also was 9.1% on Aug. 6, the most recent week is the first without an increase since tracking began in mid-April, the report shows.
State-level data show that Wyoming has the highest percentage of child cases (16.6%) after Alabama changed its “definition of child case from 0-24 to 0-17 years, resulting in a downward revision of cumulative child cases,” the AAP and the CHA said. Alabama’s proportion of such cases dropped from 22.5% to 9.0%.
New Jersey had the lowest rate (3.1%) again this week, along with New York City, but both were up slightly from the week before, when New Jersey was at 2.9% and N.Y.C. was 3.0%. The only states, other than Alabama, that saw declines over the last week were Arkansas, Massachusetts, Mississippi, South Dakota, Texas, and West Virginia. Texas, however, has reported age for only 8% of its confirmed cases, the report noted.
The overall rate of child COVID-19 cases as of Aug. 13 was 538 per 100,000 children, up from 500.7 per 100,000 a week earlier. Arizona was again highest among the states with a rate of 1,254 per 100,000 (up from 1,206) and Vermont was lowest at 121, although Puerto Rico (114) and Guam (88) were lower still, the AAP/CHA data indicate.
For the nine states that report testing information for children, Arizona has the highest positivity rate at 18.3% and West Virginia has the lowest at 3.6%. Data on hospitalizations – available from 21 states and N.Y.C. – show that 3,849 children have been admitted, with rates varying from 0.2% of children in Hawaii to 8.8% in the Big Apple, according to the report.
More specific information on child cases, such as symptoms or underlying conditions, is not being provided by states at this time, the AAP and CHA pointed out.
according to a new report from the American Academy of Pediatrics and the Children’s Hospital Association.
The 406,000 children who have tested positive for COVID-19 represent 9.1% of all cases reported so far by 49 states (New York does not provide age distribution), New York City, the District of Columbia, Puerto Rico, and Guam. Since the proportion of child cases also was 9.1% on Aug. 6, the most recent week is the first without an increase since tracking began in mid-April, the report shows.
State-level data show that Wyoming has the highest percentage of child cases (16.6%) after Alabama changed its “definition of child case from 0-24 to 0-17 years, resulting in a downward revision of cumulative child cases,” the AAP and the CHA said. Alabama’s proportion of such cases dropped from 22.5% to 9.0%.
New Jersey had the lowest rate (3.1%) again this week, along with New York City, but both were up slightly from the week before, when New Jersey was at 2.9% and N.Y.C. was 3.0%. The only states, other than Alabama, that saw declines over the last week were Arkansas, Massachusetts, Mississippi, South Dakota, Texas, and West Virginia. Texas, however, has reported age for only 8% of its confirmed cases, the report noted.
The overall rate of child COVID-19 cases as of Aug. 13 was 538 per 100,000 children, up from 500.7 per 100,000 a week earlier. Arizona was again highest among the states with a rate of 1,254 per 100,000 (up from 1,206) and Vermont was lowest at 121, although Puerto Rico (114) and Guam (88) were lower still, the AAP/CHA data indicate.
For the nine states that report testing information for children, Arizona has the highest positivity rate at 18.3% and West Virginia has the lowest at 3.6%. Data on hospitalizations – available from 21 states and N.Y.C. – show that 3,849 children have been admitted, with rates varying from 0.2% of children in Hawaii to 8.8% in the Big Apple, according to the report.
More specific information on child cases, such as symptoms or underlying conditions, is not being provided by states at this time, the AAP and CHA pointed out.