User login
Thelarche and menarche are associated with increased prevalence of migraine
PHILADELPHIA – , according to research presented at the annual meeting of the American Headache Society. The results suggest that earlier exposure to estrogen increases the risk for migraine in adolescent girls, said Vincent Martin, MD, director of the Headache and Facial Pain Center at the University of Cincinnati Gardner Neuroscience Institute.
Previous studies observed an association between earlier onset of menarche and greater prevalence of migraine in adolescent girls, but no investigators had examined the relationship between earlier stages of pubertal development, such as thelarche and pubarche, and migraine.
Dr. Martin and colleagues included participants in the Breast Cancer and Environment Research Program puberty cohort in their study. Physicians examined the girls every 6 to 12 months from the time that they were aged 6-8 years to the time of late adolescence. During the last examination, participants responded to a validated questionnaire to determine whether they met International Classification of Headache Disorders–3 criteria for a diagnosis of migraine. Dr. Martin and colleagues performed logistic regression to examine whether age at thelarche, pubarche, or menarche predicted migraine.
Of 761 girls included in this study, 85 (11.2%) received a diagnosis of migraine. The mean age at which the questionnaire was administered was 15.6 years. After adjusting the data for potential confounders, the researchers found that an earlier age of onset of thelarche and menarche was associated with a higher prevalence of migraine. A 1-year decrease in the age of onset of thelarche or menarche was associated with a 32.8% or 33.8% increase in the odds of migraine headache, respectively. Pubarche was not associated with migraine.
Dr. Martin had no relevant disclosures.
PHILADELPHIA – , according to research presented at the annual meeting of the American Headache Society. The results suggest that earlier exposure to estrogen increases the risk for migraine in adolescent girls, said Vincent Martin, MD, director of the Headache and Facial Pain Center at the University of Cincinnati Gardner Neuroscience Institute.
Previous studies observed an association between earlier onset of menarche and greater prevalence of migraine in adolescent girls, but no investigators had examined the relationship between earlier stages of pubertal development, such as thelarche and pubarche, and migraine.
Dr. Martin and colleagues included participants in the Breast Cancer and Environment Research Program puberty cohort in their study. Physicians examined the girls every 6 to 12 months from the time that they were aged 6-8 years to the time of late adolescence. During the last examination, participants responded to a validated questionnaire to determine whether they met International Classification of Headache Disorders–3 criteria for a diagnosis of migraine. Dr. Martin and colleagues performed logistic regression to examine whether age at thelarche, pubarche, or menarche predicted migraine.
Of 761 girls included in this study, 85 (11.2%) received a diagnosis of migraine. The mean age at which the questionnaire was administered was 15.6 years. After adjusting the data for potential confounders, the researchers found that an earlier age of onset of thelarche and menarche was associated with a higher prevalence of migraine. A 1-year decrease in the age of onset of thelarche or menarche was associated with a 32.8% or 33.8% increase in the odds of migraine headache, respectively. Pubarche was not associated with migraine.
Dr. Martin had no relevant disclosures.
PHILADELPHIA – , according to research presented at the annual meeting of the American Headache Society. The results suggest that earlier exposure to estrogen increases the risk for migraine in adolescent girls, said Vincent Martin, MD, director of the Headache and Facial Pain Center at the University of Cincinnati Gardner Neuroscience Institute.
Previous studies observed an association between earlier onset of menarche and greater prevalence of migraine in adolescent girls, but no investigators had examined the relationship between earlier stages of pubertal development, such as thelarche and pubarche, and migraine.
Dr. Martin and colleagues included participants in the Breast Cancer and Environment Research Program puberty cohort in their study. Physicians examined the girls every 6 to 12 months from the time that they were aged 6-8 years to the time of late adolescence. During the last examination, participants responded to a validated questionnaire to determine whether they met International Classification of Headache Disorders–3 criteria for a diagnosis of migraine. Dr. Martin and colleagues performed logistic regression to examine whether age at thelarche, pubarche, or menarche predicted migraine.
Of 761 girls included in this study, 85 (11.2%) received a diagnosis of migraine. The mean age at which the questionnaire was administered was 15.6 years. After adjusting the data for potential confounders, the researchers found that an earlier age of onset of thelarche and menarche was associated with a higher prevalence of migraine. A 1-year decrease in the age of onset of thelarche or menarche was associated with a 32.8% or 33.8% increase in the odds of migraine headache, respectively. Pubarche was not associated with migraine.
Dr. Martin had no relevant disclosures.
EXPERT ANALYSIS FROM AHS 2019

Maternal migraine is associated with infant colic
PHILADELPHIA – , according to research presented at the annual meeting of the American Headache Society. Fathers with migraine are not more likely to have children with colic, however. These findings may have implications for the care of mothers with migraine and their children, said Amy Gelfand, MD, associate professor of neurology at the University of California, San Francisco.
Smaller studies have suggested associations between migraine and colic. To examine this relationship in a large, national sample, Dr. Gelfand and her research colleagues conducted a cross-sectional survey of biological parents of 4- to 8-week-olds in the United States. The researchers analyzed data from 1,419 participants – 827 mothers and 592 fathers – who completed online surveys in 2017 and 2018.
Parents provided information about their and their infants’ health. The investigators identified migraineurs using modified International Classification of Headache Disorders 3rd edition criteria and determined infant colic by response to the question, “Has your baby cried for at least 3 hours on at least 3 days in the last week?”
In all, 33.5% of the mothers had migraine or probable migraine, and 20.8% of the fathers had migraine or probable migraine. Maternal migraine was associated with increased odds of infant colic (odds ratio, 1.7). Among mothers with migraine and headache frequency of 15 or more days per month, the likelihood of having an infant with colic was even greater (OR, 2.5).
“The cause of colic is unknown, yet colic is common, and these frequent bouts of intense crying or fussiness can be particularly frustrating for parents, creating family stress and anxiety,” Dr. Gelfand said in a news release. “New moms who are armed with knowledge of the connection between their own history of migraine and infant colic can be better prepared for these often difficult first months of a baby and new mother’s journey.”
PHILADELPHIA – , according to research presented at the annual meeting of the American Headache Society. Fathers with migraine are not more likely to have children with colic, however. These findings may have implications for the care of mothers with migraine and their children, said Amy Gelfand, MD, associate professor of neurology at the University of California, San Francisco.
Smaller studies have suggested associations between migraine and colic. To examine this relationship in a large, national sample, Dr. Gelfand and her research colleagues conducted a cross-sectional survey of biological parents of 4- to 8-week-olds in the United States. The researchers analyzed data from 1,419 participants – 827 mothers and 592 fathers – who completed online surveys in 2017 and 2018.
Parents provided information about their and their infants’ health. The investigators identified migraineurs using modified International Classification of Headache Disorders 3rd edition criteria and determined infant colic by response to the question, “Has your baby cried for at least 3 hours on at least 3 days in the last week?”
In all, 33.5% of the mothers had migraine or probable migraine, and 20.8% of the fathers had migraine or probable migraine. Maternal migraine was associated with increased odds of infant colic (odds ratio, 1.7). Among mothers with migraine and headache frequency of 15 or more days per month, the likelihood of having an infant with colic was even greater (OR, 2.5).
“The cause of colic is unknown, yet colic is common, and these frequent bouts of intense crying or fussiness can be particularly frustrating for parents, creating family stress and anxiety,” Dr. Gelfand said in a news release. “New moms who are armed with knowledge of the connection between their own history of migraine and infant colic can be better prepared for these often difficult first months of a baby and new mother’s journey.”
PHILADELPHIA – , according to research presented at the annual meeting of the American Headache Society. Fathers with migraine are not more likely to have children with colic, however. These findings may have implications for the care of mothers with migraine and their children, said Amy Gelfand, MD, associate professor of neurology at the University of California, San Francisco.
Smaller studies have suggested associations between migraine and colic. To examine this relationship in a large, national sample, Dr. Gelfand and her research colleagues conducted a cross-sectional survey of biological parents of 4- to 8-week-olds in the United States. The researchers analyzed data from 1,419 participants – 827 mothers and 592 fathers – who completed online surveys in 2017 and 2018.
Parents provided information about their and their infants’ health. The investigators identified migraineurs using modified International Classification of Headache Disorders 3rd edition criteria and determined infant colic by response to the question, “Has your baby cried for at least 3 hours on at least 3 days in the last week?”
In all, 33.5% of the mothers had migraine or probable migraine, and 20.8% of the fathers had migraine or probable migraine. Maternal migraine was associated with increased odds of infant colic (odds ratio, 1.7). Among mothers with migraine and headache frequency of 15 or more days per month, the likelihood of having an infant with colic was even greater (OR, 2.5).
“The cause of colic is unknown, yet colic is common, and these frequent bouts of intense crying or fussiness can be particularly frustrating for parents, creating family stress and anxiety,” Dr. Gelfand said in a news release. “New moms who are armed with knowledge of the connection between their own history of migraine and infant colic can be better prepared for these often difficult first months of a baby and new mother’s journey.”
EXPERT ANALYSIS FROM AHS 2019

Cellulitis ranks as top reason for skin-related pediatric inpatient admissions
AUSTIN, TEX. – showed.

“Skin conditions significantly affect pediatric inpatients, and dermatologists ought be accessible for consultation to enhance care and costs,” the study’s first author, Marcus L. Elias, said in an interview prior to the annual meeting of the Society for Pediatric Dermatology.
According to Mr. Elias, who is a 4th-year medical student at Rutgers New Jersey Medical School–Newark, few national studies on skin diseases for pediatric inpatients have been published in the medical literature. Earlier this year, researchers examined inpatient dermatologic conditions in patients aged 18 years and older (J Am Acad Dermatol 2019;80[2]:425-32), but Mr. Elias and associates set out to analyze the burden of inpatient pediatric dermatologic conditions on a national basis. “We wanted to see if the same conditions that were hospitalizing adults were also hospitalizing kids,” he said. “We found that this was indeed the case.”
The researchers queried the National Inpatient Sample database for all cases involving patients aged 18 years and younger during 2001-2013. The search yielded a sample of 16,837,857 patients. From this, the researchers analyzed diagnosis-related groups for dermatologic conditions denoting the principal diagnosis at discharge, which left a final sample of 84,090 patients. Frequency and chi-squared tests were used to analyze categorical variables.
More than half of patients (54%) were male, 36% were white, 48% had Medicaid insurance, and 43% had private insurance. Mr. Elias reported that the median length of stay for patients was 2 days and the median cost of care was $6,289.50 for each case. More than three-quarters of pediatric inpatients with dermatologic diagnoses were treated for “cellulitis” (66,147 cases, or 79%), with most cases involving the legs (16,875 cases, or 20%). Other pediatric inpatients were admitted for “minor skin disorder without complications” (5,458 cases, or 7%), and “minor skin disorder with complications” (2,822 cases, or 3%). A total of 64 patients died during the study period. Of these, 31 cases (50%) involved “skin graft and/or debridement of skin ulcer or cellulitis without complications,” the study found.
“We were surprised that the major cause of mortality for our patients was classified as ‘skin graft and/or debridement of skin ulcer or cellulitis without complications,’ as a similar diagnosis-related groupings exist denoting that complications did arise,” Mr. Elias said. “Still, it is not possible for us to determine if the mortality was from the skin graft/debridement or another cause entirely. It is possible that the procedure was without complications, only to have the patient succumb to an ancillary process.”
He acknowledged certain limitations of the study, including the fact that the function of dermatologic consults for hospitalized patients was not examined. “We also cannot draw conclusions as to whether improved outpatient therapy reduces the need for hospitalization,” he said. Mr. Elias reported having no financial disclosures.
AUSTIN, TEX. – showed.
“Skin conditions significantly affect pediatric inpatients, and dermatologists ought be accessible for consultation to enhance care and costs,” the study’s first author, Marcus L. Elias, said in an interview prior to the annual meeting of the Society for Pediatric Dermatology.
According to Mr. Elias, who is a 4th-year medical student at Rutgers New Jersey Medical School–Newark, few national studies on skin diseases for pediatric inpatients have been published in the medical literature. Earlier this year, researchers examined inpatient dermatologic conditions in patients aged 18 years and older (J Am Acad Dermatol 2019;80[2]:425-32), but Mr. Elias and associates set out to analyze the burden of inpatient pediatric dermatologic conditions on a national basis. “We wanted to see if the same conditions that were hospitalizing adults were also hospitalizing kids,” he said. “We found that this was indeed the case.”
The researchers queried the National Inpatient Sample database for all cases involving patients aged 18 years and younger during 2001-2013. The search yielded a sample of 16,837,857 patients. From this, the researchers analyzed diagnosis-related groups for dermatologic conditions denoting the principal diagnosis at discharge, which left a final sample of 84,090 patients. Frequency and chi-squared tests were used to analyze categorical variables.
More than half of patients (54%) were male, 36% were white, 48% had Medicaid insurance, and 43% had private insurance. Mr. Elias reported that the median length of stay for patients was 2 days and the median cost of care was $6,289.50 for each case. More than three-quarters of pediatric inpatients with dermatologic diagnoses were treated for “cellulitis” (66,147 cases, or 79%), with most cases involving the legs (16,875 cases, or 20%). Other pediatric inpatients were admitted for “minor skin disorder without complications” (5,458 cases, or 7%), and “minor skin disorder with complications” (2,822 cases, or 3%). A total of 64 patients died during the study period. Of these, 31 cases (50%) involved “skin graft and/or debridement of skin ulcer or cellulitis without complications,” the study found.
“We were surprised that the major cause of mortality for our patients was classified as ‘skin graft and/or debridement of skin ulcer or cellulitis without complications,’ as a similar diagnosis-related groupings exist denoting that complications did arise,” Mr. Elias said. “Still, it is not possible for us to determine if the mortality was from the skin graft/debridement or another cause entirely. It is possible that the procedure was without complications, only to have the patient succumb to an ancillary process.”
He acknowledged certain limitations of the study, including the fact that the function of dermatologic consults for hospitalized patients was not examined. “We also cannot draw conclusions as to whether improved outpatient therapy reduces the need for hospitalization,” he said. Mr. Elias reported having no financial disclosures.
AUSTIN, TEX. – showed.
“Skin conditions significantly affect pediatric inpatients, and dermatologists ought be accessible for consultation to enhance care and costs,” the study’s first author, Marcus L. Elias, said in an interview prior to the annual meeting of the Society for Pediatric Dermatology.
According to Mr. Elias, who is a 4th-year medical student at Rutgers New Jersey Medical School–Newark, few national studies on skin diseases for pediatric inpatients have been published in the medical literature. Earlier this year, researchers examined inpatient dermatologic conditions in patients aged 18 years and older (J Am Acad Dermatol 2019;80[2]:425-32), but Mr. Elias and associates set out to analyze the burden of inpatient pediatric dermatologic conditions on a national basis. “We wanted to see if the same conditions that were hospitalizing adults were also hospitalizing kids,” he said. “We found that this was indeed the case.”
The researchers queried the National Inpatient Sample database for all cases involving patients aged 18 years and younger during 2001-2013. The search yielded a sample of 16,837,857 patients. From this, the researchers analyzed diagnosis-related groups for dermatologic conditions denoting the principal diagnosis at discharge, which left a final sample of 84,090 patients. Frequency and chi-squared tests were used to analyze categorical variables.
More than half of patients (54%) were male, 36% were white, 48% had Medicaid insurance, and 43% had private insurance. Mr. Elias reported that the median length of stay for patients was 2 days and the median cost of care was $6,289.50 for each case. More than three-quarters of pediatric inpatients with dermatologic diagnoses were treated for “cellulitis” (66,147 cases, or 79%), with most cases involving the legs (16,875 cases, or 20%). Other pediatric inpatients were admitted for “minor skin disorder without complications” (5,458 cases, or 7%), and “minor skin disorder with complications” (2,822 cases, or 3%). A total of 64 patients died during the study period. Of these, 31 cases (50%) involved “skin graft and/or debridement of skin ulcer or cellulitis without complications,” the study found.
“We were surprised that the major cause of mortality for our patients was classified as ‘skin graft and/or debridement of skin ulcer or cellulitis without complications,’ as a similar diagnosis-related groupings exist denoting that complications did arise,” Mr. Elias said. “Still, it is not possible for us to determine if the mortality was from the skin graft/debridement or another cause entirely. It is possible that the procedure was without complications, only to have the patient succumb to an ancillary process.”
He acknowledged certain limitations of the study, including the fact that the function of dermatologic consults for hospitalized patients was not examined. “We also cannot draw conclusions as to whether improved outpatient therapy reduces the need for hospitalization,” he said. Mr. Elias reported having no financial disclosures.
REPORTING FROM SPD 2019
Key clinical point: Cellulitis is the cause of the majority of skin-related pediatric inpatient admissions in the United States.
Major finding: In all, 79% of pediatric inpatients with dermatologic diagnoses were treated for cellulitis.
Study details: An analysis of data from 84,090 patients younger than age 18 in the National Inpatient Sample.
Disclosures: The researchers reported having no financial disclosures.
Neonatal ICU stay found ‘protective’ against risk for developing atopic dermatitis
AUSTIN – The

“While more time in the NICU is associated with a lesser risk of developing atopic dermatitis, we certainly do not want to keep infants in the NICU longer in order to lower their risk of atopic dermatitis,” the study’s first author, Jennifer J. Schoch, MD, said in an interview prior to the annual meeting of the Society for Pediatric Dermatology. “Instead, we need to work on understanding the mechanisms behind this relationship. For example, are there certain exposures in the NICU that influence the cutaneous immunity to ultimately reduce the risk of atopic dermatitis?”
According to Dr. Schoch, a pediatric dermatologist at the University of Florida, Gainesville, the medical literature has been conflicted regarding the relationship between prematurity and eczema. A recent meta-analysis of 18 studies found an association between very preterm birth and a decreased risk of eczema, yet the risk became insignificant among children born moderately preterm (J Am Acad Dermatol. 2018;78[6]:1142-8). However, the factors contributing to this relationship are not well understood.
In an effort to explore the infant, maternal, and environmental factors of infants who developed AD, compared with infants who did not, Dr. Schoch and colleagues evaluated infants who were born at University of Florida Health from June 1, 2011, to April 30, 2017; had at least two well-child visits; and had at least one visit at 300 days old or later. The researchers included 4,016 mother-infant dyads in the study. Atopic dermatitis was diagnosed in 26.5% of the infants. Factors significantly associated with the incidence of AD were delivery mode (P = .0127), NICU stay (P = .0001), gestational age (P = .0006), and birth weight (P = .0020). Specifically, infants had a higher risk of developing AD if they were delivered vaginally, did not stay in the NICU, had a higher gestational age, or had a higher birth weight. Extremely preterm (less than 28 weeks’ gestation) and very preterm (28 to less than 32 weeks’ gestation) infants had the lowest rates of AD, at 10.9% and 19%, respectively.
When the researchers adjusted for other variables to their model, only length of stay in the NICU was related to the development of AD. Specifically, infants who spent more time in the NICU had a lower risk of developing atopic dermatitis (P = .0039).
“We were surprised to find that the length of stay in the neonatal intensive care unit was the strongest protective factor against the future development of eczema,” Dr. Schoch said. “Instead of this relationship being mediated by gestational age or birth weight, it was how much time the infants spent in the NICU that seemed to ‘protect’ from future eczema.”
She acknowledged certain limitations of the study, including its retrospective design with data gathered from electronic medical records. Also, “diagnosis was determined by ICD-9 or ICD-10 code, and not confirmed by dermatologists,” she said.
In their abstract, the researchers wrote that the finding highlights “the importance of early life interactions between the microbiome, developing cutaneous immunity, and the evolving skin barrier of the preterm infant. The skin microbiome of premature infants differs from full-term infants, in that the premature infant cutaneous microbiome is dominated by Staphylococcus species” (Microbiome. 2018;6[1]:98). They added that “the early presence of Staphylococcus on the skin may confer protection.”
Dr. Schoch reported having no relevant financial disclosures.
SOURCE: Schoch J et al. SPD 2019, Poster 2.
AUSTIN – The
“While more time in the NICU is associated with a lesser risk of developing atopic dermatitis, we certainly do not want to keep infants in the NICU longer in order to lower their risk of atopic dermatitis,” the study’s first author, Jennifer J. Schoch, MD, said in an interview prior to the annual meeting of the Society for Pediatric Dermatology. “Instead, we need to work on understanding the mechanisms behind this relationship. For example, are there certain exposures in the NICU that influence the cutaneous immunity to ultimately reduce the risk of atopic dermatitis?”
According to Dr. Schoch, a pediatric dermatologist at the University of Florida, Gainesville, the medical literature has been conflicted regarding the relationship between prematurity and eczema. A recent meta-analysis of 18 studies found an association between very preterm birth and a decreased risk of eczema, yet the risk became insignificant among children born moderately preterm (J Am Acad Dermatol. 2018;78[6]:1142-8). However, the factors contributing to this relationship are not well understood.
In an effort to explore the infant, maternal, and environmental factors of infants who developed AD, compared with infants who did not, Dr. Schoch and colleagues evaluated infants who were born at University of Florida Health from June 1, 2011, to April 30, 2017; had at least two well-child visits; and had at least one visit at 300 days old or later. The researchers included 4,016 mother-infant dyads in the study. Atopic dermatitis was diagnosed in 26.5% of the infants. Factors significantly associated with the incidence of AD were delivery mode (P = .0127), NICU stay (P = .0001), gestational age (P = .0006), and birth weight (P = .0020). Specifically, infants had a higher risk of developing AD if they were delivered vaginally, did not stay in the NICU, had a higher gestational age, or had a higher birth weight. Extremely preterm (less than 28 weeks’ gestation) and very preterm (28 to less than 32 weeks’ gestation) infants had the lowest rates of AD, at 10.9% and 19%, respectively.
When the researchers adjusted for other variables to their model, only length of stay in the NICU was related to the development of AD. Specifically, infants who spent more time in the NICU had a lower risk of developing atopic dermatitis (P = .0039).
“We were surprised to find that the length of stay in the neonatal intensive care unit was the strongest protective factor against the future development of eczema,” Dr. Schoch said. “Instead of this relationship being mediated by gestational age or birth weight, it was how much time the infants spent in the NICU that seemed to ‘protect’ from future eczema.”
She acknowledged certain limitations of the study, including its retrospective design with data gathered from electronic medical records. Also, “diagnosis was determined by ICD-9 or ICD-10 code, and not confirmed by dermatologists,” she said.
In their abstract, the researchers wrote that the finding highlights “the importance of early life interactions between the microbiome, developing cutaneous immunity, and the evolving skin barrier of the preterm infant. The skin microbiome of premature infants differs from full-term infants, in that the premature infant cutaneous microbiome is dominated by Staphylococcus species” (Microbiome. 2018;6[1]:98). They added that “the early presence of Staphylococcus on the skin may confer protection.”
Dr. Schoch reported having no relevant financial disclosures.
SOURCE: Schoch J et al. SPD 2019, Poster 2.
AUSTIN – The
“While more time in the NICU is associated with a lesser risk of developing atopic dermatitis, we certainly do not want to keep infants in the NICU longer in order to lower their risk of atopic dermatitis,” the study’s first author, Jennifer J. Schoch, MD, said in an interview prior to the annual meeting of the Society for Pediatric Dermatology. “Instead, we need to work on understanding the mechanisms behind this relationship. For example, are there certain exposures in the NICU that influence the cutaneous immunity to ultimately reduce the risk of atopic dermatitis?”
According to Dr. Schoch, a pediatric dermatologist at the University of Florida, Gainesville, the medical literature has been conflicted regarding the relationship between prematurity and eczema. A recent meta-analysis of 18 studies found an association between very preterm birth and a decreased risk of eczema, yet the risk became insignificant among children born moderately preterm (J Am Acad Dermatol. 2018;78[6]:1142-8). However, the factors contributing to this relationship are not well understood.
In an effort to explore the infant, maternal, and environmental factors of infants who developed AD, compared with infants who did not, Dr. Schoch and colleagues evaluated infants who were born at University of Florida Health from June 1, 2011, to April 30, 2017; had at least two well-child visits; and had at least one visit at 300 days old or later. The researchers included 4,016 mother-infant dyads in the study. Atopic dermatitis was diagnosed in 26.5% of the infants. Factors significantly associated with the incidence of AD were delivery mode (P = .0127), NICU stay (P = .0001), gestational age (P = .0006), and birth weight (P = .0020). Specifically, infants had a higher risk of developing AD if they were delivered vaginally, did not stay in the NICU, had a higher gestational age, or had a higher birth weight. Extremely preterm (less than 28 weeks’ gestation) and very preterm (28 to less than 32 weeks’ gestation) infants had the lowest rates of AD, at 10.9% and 19%, respectively.
When the researchers adjusted for other variables to their model, only length of stay in the NICU was related to the development of AD. Specifically, infants who spent more time in the NICU had a lower risk of developing atopic dermatitis (P = .0039).
“We were surprised to find that the length of stay in the neonatal intensive care unit was the strongest protective factor against the future development of eczema,” Dr. Schoch said. “Instead of this relationship being mediated by gestational age or birth weight, it was how much time the infants spent in the NICU that seemed to ‘protect’ from future eczema.”
She acknowledged certain limitations of the study, including its retrospective design with data gathered from electronic medical records. Also, “diagnosis was determined by ICD-9 or ICD-10 code, and not confirmed by dermatologists,” she said.
In their abstract, the researchers wrote that the finding highlights “the importance of early life interactions between the microbiome, developing cutaneous immunity, and the evolving skin barrier of the preterm infant. The skin microbiome of premature infants differs from full-term infants, in that the premature infant cutaneous microbiome is dominated by Staphylococcus species” (Microbiome. 2018;6[1]:98). They added that “the early presence of Staphylococcus on the skin may confer protection.”
Dr. Schoch reported having no relevant financial disclosures.
SOURCE: Schoch J et al. SPD 2019, Poster 2.
REPORTING FROM SPD 2019
Key clinical point: Preterm infants develop atopic dermatitis less often than full term infants.
Major finding: Infants that spent more time in the neonatal ICU had a lower risk of developing atopic dermatitis (P = .0039).
Study details: A single-center study of 4,016 mother-infant dyads.
Disclosures: Dr. Schoch reported having no relevant financial disclosures.
Source: Schoch J et al. SPD 2019, Poster 2.
Book Review: The hope that comes from ‘Growing Pains’
You might be surprised by child psychiatrist’s Mike Shooter’s response revealed in his book, “Growing Pains: Making Sense of Childhood: A Psychiatrist’s Story”(London: Hodder & Stoughton, 2018). Rather than hospitalizing this patient, as was done many times before, he makes a bold decision to listen to the group members, who help the patient develop a plan that ultimately leads to greater resiliency.
Dr. Shooter shares many stories about the power of therapy to heal, often visiting patients at their homes to better understand the dynamics of their distress. Stories themselves heal: “It is the job of the therapist to encourage them to reveal their story, to listen to it, and to help them find a better outcome.”
From these stories, we learn about Dr. Shooter’s passion and commitment to his relationship with the child – listening, fostering autonomy, recognizing the power of family systems, working with a multidisciplinary team, and using his own experiences with depression to better help his patients.
Dr. Shooter closes the distance between himself and readers by sharing his own story – his difficult relationship with his strict father, his own uncertainty about his future profession, the deep depression that could have derailed his family life and career, and the treatment that got him back on track.
This book is an excellent read for psychiatrists and other mental health professionals, whether they work with children or adults. It is especially valuable to psychiatrists like me who work with college students – transitional-age youth at the border between childhood and adulthood. Dr. Shooter beautifully describes the societal ills that have contributed to a global rise in child and adolescent mental health problems:
“We live in an ever-more competitive world. To the normal pressures of growing up are added the educational demands to pass more and more exams, a gloominess about the future, and a loss of faith in political processes to put it right; private catastrophes at home and global catastrophes beamed in from all over the world; and a media that’s in love with how to be popular, how to look attractive, and how to be a success.”

The general public would also find this book an interesting glimpse into the world of child psychiatry. The public as well as politicians would benefit from knowing the value child psychiatry can provide at a time when services are underfunded in many countries, including the United States.
This book uses the words of children to highlight the challenges young people face – from bereavement to bullying to abuse. He writes about children on the “margins of margins.” As I read the book, Dr. Shooter reminded me of psychiatrist and author Robert Coles, who taught my favorite college class and wrote about children in crisis from the Appalachians to Africa.
Not surprisingly, Dr. Shooter describes spending time with Dr. Coles at a conference on bereavement. He adheres to the advice Dr. Coles offered, which was to “Listen to what the children say, not what the adults say about them. ... Follow what your gut tells you, not your head.”
In addition to listening to the patient and your gut, Dr. Shooter describes offering hope as another essential element to treatment. He describes giving hope to children of parents who die by suicide, as these children often fear they will meet their parents’ fate. “And they need to know, too, that suicide is not inevitable. … Help is ready and available to stop the children and young people ever getting to that state.”
One element of treatment Dr. Shooter minimally addresses is psychopharmacology, and mostly in a negative way. While he acknowledges that some children genuinely do have attention-deficit/hyperactivity disorder or depression, he feels they are overdiagnosed and thus overtreated with medication. I would have liked to hear more about the times he prescribed medication and how it was integrated into comprehensive care that included therapy and lifestyle changes. I would not want parents reading this book to feel badly if they have supported having their child take medication for a mental health disorder.
Dr. Shooter does make the important point that therapy is often left on the sidelines in current medical systems. Therapy can benefit people of all ages as we face our own “growing pains.” He highlights the “opportunity for growth” that challenges provide, and indeed gives us a great sense of hope in our lives and our work as psychiatrists.
Dr. Morris is an associate professor of psychiatry and associate program director for student health psychiatry at the University of Florida, Gainesville. She is the author of “The Campus Cure: A Parent’s Guide to Mental Health and Wellness for College Students” (Lanham, Md.: Rowman & Littlefield of Lanham, 2018).
You might be surprised by child psychiatrist’s Mike Shooter’s response revealed in his book, “Growing Pains: Making Sense of Childhood: A Psychiatrist’s Story”(London: Hodder & Stoughton, 2018). Rather than hospitalizing this patient, as was done many times before, he makes a bold decision to listen to the group members, who help the patient develop a plan that ultimately leads to greater resiliency.
Dr. Shooter shares many stories about the power of therapy to heal, often visiting patients at their homes to better understand the dynamics of their distress. Stories themselves heal: “It is the job of the therapist to encourage them to reveal their story, to listen to it, and to help them find a better outcome.”
From these stories, we learn about Dr. Shooter’s passion and commitment to his relationship with the child – listening, fostering autonomy, recognizing the power of family systems, working with a multidisciplinary team, and using his own experiences with depression to better help his patients.
Dr. Shooter closes the distance between himself and readers by sharing his own story – his difficult relationship with his strict father, his own uncertainty about his future profession, the deep depression that could have derailed his family life and career, and the treatment that got him back on track.
This book is an excellent read for psychiatrists and other mental health professionals, whether they work with children or adults. It is especially valuable to psychiatrists like me who work with college students – transitional-age youth at the border between childhood and adulthood. Dr. Shooter beautifully describes the societal ills that have contributed to a global rise in child and adolescent mental health problems:
“We live in an ever-more competitive world. To the normal pressures of growing up are added the educational demands to pass more and more exams, a gloominess about the future, and a loss of faith in political processes to put it right; private catastrophes at home and global catastrophes beamed in from all over the world; and a media that’s in love with how to be popular, how to look attractive, and how to be a success.”
The general public would also find this book an interesting glimpse into the world of child psychiatry. The public as well as politicians would benefit from knowing the value child psychiatry can provide at a time when services are underfunded in many countries, including the United States.
This book uses the words of children to highlight the challenges young people face – from bereavement to bullying to abuse. He writes about children on the “margins of margins.” As I read the book, Dr. Shooter reminded me of psychiatrist and author Robert Coles, who taught my favorite college class and wrote about children in crisis from the Appalachians to Africa.
Not surprisingly, Dr. Shooter describes spending time with Dr. Coles at a conference on bereavement. He adheres to the advice Dr. Coles offered, which was to “Listen to what the children say, not what the adults say about them. ... Follow what your gut tells you, not your head.”
In addition to listening to the patient and your gut, Dr. Shooter describes offering hope as another essential element to treatment. He describes giving hope to children of parents who die by suicide, as these children often fear they will meet their parents’ fate. “And they need to know, too, that suicide is not inevitable. … Help is ready and available to stop the children and young people ever getting to that state.”
One element of treatment Dr. Shooter minimally addresses is psychopharmacology, and mostly in a negative way. While he acknowledges that some children genuinely do have attention-deficit/hyperactivity disorder or depression, he feels they are overdiagnosed and thus overtreated with medication. I would have liked to hear more about the times he prescribed medication and how it was integrated into comprehensive care that included therapy and lifestyle changes. I would not want parents reading this book to feel badly if they have supported having their child take medication for a mental health disorder.
Dr. Shooter does make the important point that therapy is often left on the sidelines in current medical systems. Therapy can benefit people of all ages as we face our own “growing pains.” He highlights the “opportunity for growth” that challenges provide, and indeed gives us a great sense of hope in our lives and our work as psychiatrists.
Dr. Morris is an associate professor of psychiatry and associate program director for student health psychiatry at the University of Florida, Gainesville. She is the author of “The Campus Cure: A Parent’s Guide to Mental Health and Wellness for College Students” (Lanham, Md.: Rowman & Littlefield of Lanham, 2018).
You might be surprised by child psychiatrist’s Mike Shooter’s response revealed in his book, “Growing Pains: Making Sense of Childhood: A Psychiatrist’s Story”(London: Hodder & Stoughton, 2018). Rather than hospitalizing this patient, as was done many times before, he makes a bold decision to listen to the group members, who help the patient develop a plan that ultimately leads to greater resiliency.
Dr. Shooter shares many stories about the power of therapy to heal, often visiting patients at their homes to better understand the dynamics of their distress. Stories themselves heal: “It is the job of the therapist to encourage them to reveal their story, to listen to it, and to help them find a better outcome.”
From these stories, we learn about Dr. Shooter’s passion and commitment to his relationship with the child – listening, fostering autonomy, recognizing the power of family systems, working with a multidisciplinary team, and using his own experiences with depression to better help his patients.
Dr. Shooter closes the distance between himself and readers by sharing his own story – his difficult relationship with his strict father, his own uncertainty about his future profession, the deep depression that could have derailed his family life and career, and the treatment that got him back on track.
This book is an excellent read for psychiatrists and other mental health professionals, whether they work with children or adults. It is especially valuable to psychiatrists like me who work with college students – transitional-age youth at the border between childhood and adulthood. Dr. Shooter beautifully describes the societal ills that have contributed to a global rise in child and adolescent mental health problems:
“We live in an ever-more competitive world. To the normal pressures of growing up are added the educational demands to pass more and more exams, a gloominess about the future, and a loss of faith in political processes to put it right; private catastrophes at home and global catastrophes beamed in from all over the world; and a media that’s in love with how to be popular, how to look attractive, and how to be a success.”
The general public would also find this book an interesting glimpse into the world of child psychiatry. The public as well as politicians would benefit from knowing the value child psychiatry can provide at a time when services are underfunded in many countries, including the United States.
This book uses the words of children to highlight the challenges young people face – from bereavement to bullying to abuse. He writes about children on the “margins of margins.” As I read the book, Dr. Shooter reminded me of psychiatrist and author Robert Coles, who taught my favorite college class and wrote about children in crisis from the Appalachians to Africa.
Not surprisingly, Dr. Shooter describes spending time with Dr. Coles at a conference on bereavement. He adheres to the advice Dr. Coles offered, which was to “Listen to what the children say, not what the adults say about them. ... Follow what your gut tells you, not your head.”
In addition to listening to the patient and your gut, Dr. Shooter describes offering hope as another essential element to treatment. He describes giving hope to children of parents who die by suicide, as these children often fear they will meet their parents’ fate. “And they need to know, too, that suicide is not inevitable. … Help is ready and available to stop the children and young people ever getting to that state.”
One element of treatment Dr. Shooter minimally addresses is psychopharmacology, and mostly in a negative way. While he acknowledges that some children genuinely do have attention-deficit/hyperactivity disorder or depression, he feels they are overdiagnosed and thus overtreated with medication. I would have liked to hear more about the times he prescribed medication and how it was integrated into comprehensive care that included therapy and lifestyle changes. I would not want parents reading this book to feel badly if they have supported having their child take medication for a mental health disorder.
Dr. Shooter does make the important point that therapy is often left on the sidelines in current medical systems. Therapy can benefit people of all ages as we face our own “growing pains.” He highlights the “opportunity for growth” that challenges provide, and indeed gives us a great sense of hope in our lives and our work as psychiatrists.
Dr. Morris is an associate professor of psychiatry and associate program director for student health psychiatry at the University of Florida, Gainesville. She is the author of “The Campus Cure: A Parent’s Guide to Mental Health and Wellness for College Students” (Lanham, Md.: Rowman & Littlefield of Lanham, 2018).
Comorbidities drive excess mortality after breast cancer diagnosis in childhood cancer survivors
Among women with breast cancer, risk of death is more than twice as high for those who are childhood cancer survivors than for those in whom this cancer is their first, found a retrospective cohort study. However, the excess deaths are mainly from comorbidities related to previous therapies.
Breast cancer is among the leading subsequent malignancies in adult survivors of pediatric cancers, note the investigators, who were led by Chaya S. Moskowitz, PhD, of the department of epidemiology and biostatistics at Memorial Sloan Kettering Cancer Center in New York. But outcomes after this diagnosis are not well characterized.
The investigators used the Childhood Cancer Survivor Study to identify 274 female 5-year survivors of cancer diagnosed before age 21 years who received a subsequent breast cancer diagnosis at a median age of 38 years. They then used Surveillance, Epidemiology, and End Results data to identify a control group of 1,095 female patients with de novo breast cancer matched on age, race, stage, and year of breast cancer diagnosis.
The 10-year overall survival was 73% among the childhood cancer survivors, investigators reported in the Journal of Clinical Oncology.
Compared with the control women whose breast cancer was their first cancer, the women with breast cancer who were childhood cancer survivors had an elevated risk of death from any cause (hazard ratio, 2.2) that persisted after analyses were adjusted for receipt of chemotherapy and radiation therapy (HR, 2.4). In addition, findings were similar in analyses restricted to women with ductal carcinoma in situ and women with stage 1-3 breast cancer.
The childhood cancer survivors had a modestly elevated risk of dying from breast cancer (HR, 1.3) but a sharply elevated risk of dying from other health-related causes, including other subsequent malignancies and cardiovascular or pulmonary disease often related to previous therapies (HR, 5.5).
In addition, the childhood cancer survivors had a higher cumulative incidence of diagnosis of second asynchronous breast cancers a year or more later, relative to the women in whom breast cancer was their first cancer (P less than .001). The 5-year cumulative incidence was 8.0% among the childhood cancer survivors and just 2.7% among the control women.
“Although BC [breast cancer]-specific mortality was modestly higher in childhood cancer survivors, deaths attributable to health conditions other than BC seem to be the driving force in the elevated all-cause mortality,” Dr. Moskowitz and colleagues wrote.
“To change the dismal outcomes of these women, our results suggest that it is imperative that at the time of a secondary BC diagnosis, they have a comprehensive evaluation that extends beyond a singular focus of the BC,” they concluded. “This should include an assessment of existing cardiopulmonary disease and a plan for future cancer screening to optimize the management of comorbidities and cardiopulmonary disease and prolong the lifespan of these survivors.”
Dr. Moskowitz reported that she has a consulting or advisory role with Bioclinica. The study was supported by the National Cancer Institute, a Memorial Sloan Kettering Cancer Center Core grant, the Meg Berté Owen Foundation, and the American Lebanese Syrian Associated Charities.
SOURCE: Moskowitz CS et al. J Clin Oncol. 2019 Jul 1. doi: 10.1200/JCO.18.02219.
Among women with breast cancer, risk of death is more than twice as high for those who are childhood cancer survivors than for those in whom this cancer is their first, found a retrospective cohort study. However, the excess deaths are mainly from comorbidities related to previous therapies.
Breast cancer is among the leading subsequent malignancies in adult survivors of pediatric cancers, note the investigators, who were led by Chaya S. Moskowitz, PhD, of the department of epidemiology and biostatistics at Memorial Sloan Kettering Cancer Center in New York. But outcomes after this diagnosis are not well characterized.
The investigators used the Childhood Cancer Survivor Study to identify 274 female 5-year survivors of cancer diagnosed before age 21 years who received a subsequent breast cancer diagnosis at a median age of 38 years. They then used Surveillance, Epidemiology, and End Results data to identify a control group of 1,095 female patients with de novo breast cancer matched on age, race, stage, and year of breast cancer diagnosis.
The 10-year overall survival was 73% among the childhood cancer survivors, investigators reported in the Journal of Clinical Oncology.
Compared with the control women whose breast cancer was their first cancer, the women with breast cancer who were childhood cancer survivors had an elevated risk of death from any cause (hazard ratio, 2.2) that persisted after analyses were adjusted for receipt of chemotherapy and radiation therapy (HR, 2.4). In addition, findings were similar in analyses restricted to women with ductal carcinoma in situ and women with stage 1-3 breast cancer.
The childhood cancer survivors had a modestly elevated risk of dying from breast cancer (HR, 1.3) but a sharply elevated risk of dying from other health-related causes, including other subsequent malignancies and cardiovascular or pulmonary disease often related to previous therapies (HR, 5.5).
In addition, the childhood cancer survivors had a higher cumulative incidence of diagnosis of second asynchronous breast cancers a year or more later, relative to the women in whom breast cancer was their first cancer (P less than .001). The 5-year cumulative incidence was 8.0% among the childhood cancer survivors and just 2.7% among the control women.
“Although BC [breast cancer]-specific mortality was modestly higher in childhood cancer survivors, deaths attributable to health conditions other than BC seem to be the driving force in the elevated all-cause mortality,” Dr. Moskowitz and colleagues wrote.
“To change the dismal outcomes of these women, our results suggest that it is imperative that at the time of a secondary BC diagnosis, they have a comprehensive evaluation that extends beyond a singular focus of the BC,” they concluded. “This should include an assessment of existing cardiopulmonary disease and a plan for future cancer screening to optimize the management of comorbidities and cardiopulmonary disease and prolong the lifespan of these survivors.”
Dr. Moskowitz reported that she has a consulting or advisory role with Bioclinica. The study was supported by the National Cancer Institute, a Memorial Sloan Kettering Cancer Center Core grant, the Meg Berté Owen Foundation, and the American Lebanese Syrian Associated Charities.
SOURCE: Moskowitz CS et al. J Clin Oncol. 2019 Jul 1. doi: 10.1200/JCO.18.02219.
Among women with breast cancer, risk of death is more than twice as high for those who are childhood cancer survivors than for those in whom this cancer is their first, found a retrospective cohort study. However, the excess deaths are mainly from comorbidities related to previous therapies.
Breast cancer is among the leading subsequent malignancies in adult survivors of pediatric cancers, note the investigators, who were led by Chaya S. Moskowitz, PhD, of the department of epidemiology and biostatistics at Memorial Sloan Kettering Cancer Center in New York. But outcomes after this diagnosis are not well characterized.
The investigators used the Childhood Cancer Survivor Study to identify 274 female 5-year survivors of cancer diagnosed before age 21 years who received a subsequent breast cancer diagnosis at a median age of 38 years. They then used Surveillance, Epidemiology, and End Results data to identify a control group of 1,095 female patients with de novo breast cancer matched on age, race, stage, and year of breast cancer diagnosis.
The 10-year overall survival was 73% among the childhood cancer survivors, investigators reported in the Journal of Clinical Oncology.
Compared with the control women whose breast cancer was their first cancer, the women with breast cancer who were childhood cancer survivors had an elevated risk of death from any cause (hazard ratio, 2.2) that persisted after analyses were adjusted for receipt of chemotherapy and radiation therapy (HR, 2.4). In addition, findings were similar in analyses restricted to women with ductal carcinoma in situ and women with stage 1-3 breast cancer.
The childhood cancer survivors had a modestly elevated risk of dying from breast cancer (HR, 1.3) but a sharply elevated risk of dying from other health-related causes, including other subsequent malignancies and cardiovascular or pulmonary disease often related to previous therapies (HR, 5.5).
In addition, the childhood cancer survivors had a higher cumulative incidence of diagnosis of second asynchronous breast cancers a year or more later, relative to the women in whom breast cancer was their first cancer (P less than .001). The 5-year cumulative incidence was 8.0% among the childhood cancer survivors and just 2.7% among the control women.
“Although BC [breast cancer]-specific mortality was modestly higher in childhood cancer survivors, deaths attributable to health conditions other than BC seem to be the driving force in the elevated all-cause mortality,” Dr. Moskowitz and colleagues wrote.
“To change the dismal outcomes of these women, our results suggest that it is imperative that at the time of a secondary BC diagnosis, they have a comprehensive evaluation that extends beyond a singular focus of the BC,” they concluded. “This should include an assessment of existing cardiopulmonary disease and a plan for future cancer screening to optimize the management of comorbidities and cardiopulmonary disease and prolong the lifespan of these survivors.”
Dr. Moskowitz reported that she has a consulting or advisory role with Bioclinica. The study was supported by the National Cancer Institute, a Memorial Sloan Kettering Cancer Center Core grant, the Meg Berté Owen Foundation, and the American Lebanese Syrian Associated Charities.
SOURCE: Moskowitz CS et al. J Clin Oncol. 2019 Jul 1. doi: 10.1200/JCO.18.02219.
FROM THE JOURNAL OF CLINICAL ONCOLOGY
Opioid exposure leads to poor perinatal and postnatal outcomes
according to data from more than 8,000 children.

Previous studies have shown the increased risk of a range of health problems associated with maternal opioid use, including neonatal abstinence syndrome (NAS), but data on the long-term consequences of in utero opioid exposure are limited, wrote Romuladus E. Azuine, DrPH, MPH, of the U.S. Department of Health and Human Services, Rockville, Md., and colleagues.
In a study published in JAMA Network Open, the researchers reviewed data from 8,509 mother/newborn pairs in the Boston Birth Cohort, a database that included a large urban, low-income, multiethnic population of women who had singleton births at the Boston Medical Center starting in 1998.
A total of 454 infants (5%) experienced prenatal opioid exposure. Mothers were interviewed 48-72 hours after delivery about sociodemographic factors, drug use, smoking, and alcohol use.
The risk of small for gestational age and preterm birth were significantly higher in babies exposed to opioids (OR 1.87 and OR 1.49, respectively), compared with unexposed newborns.
Children’s developmental outcomes were collected starting in 2003 based on electronic medical records. A total of 3,153 mother-newborn pairs were enrolled in a postnatal follow-up study. For preschoolers, prenatal opioid exposure was associated with increased risk of lack of expected physiological development and conduct disorder/emotional disturbance (OR 1.80 and OR 2.13, respectively), compared with unexposed children. School-aged children with prenatal opioid exposure had an increased risk of ADHD (OR 2.55).
The incidence of NAS in the study population was at least 24 per 1,000 hospital births starting in 2004, and peaked at 61 per 1,000 hospital births in 2008, but remained higher than 32 per 1,000 through 2016.
The study findings were limited by several factors including potential misclassification of opioid exposure, confounding from other pregnancy exposures, loss of many participants to follow-up, and a lack of generalizability, but the results support the need for additional research, and show that the prevalence of NAS was approximately 10 times the national average in a subset of low-income, urban, minority women, the researchers said.
“However, the effect of opioids is still difficult to disentangle from effects of other childhood exposures. Policy and programmatic efforts to prevent NAS and mitigate its health consequences require more comprehensive longitudinal and intergenerational research,” they concluded.
The study findings contribute to and support the evidence of poor neurodevelopmental and emotional/behavioral outcomes for children with prenatal exposure to opioids or a history of NAS, Susan Brogly, PhD, MSc, noted in an accompanying editorial. Other studies have shown increased risks for visual impairments including strabismus, reduced visual acuity, and delayed visual maturation.
Dr. Brogly, of Queen’s University, Kingston Health Science Center, Ontario, nonetheless noted that a child’s home environment may modify the impact of prenatal opioid exposure or NAS, as evidence has shown that children with in utero heroin exposure have improved outcomes in healthy home environments.
Although the mechanism for how opioid exposure affects development remains uncertain, she suggested that future research should address “interventions to improve health outcomes in this rapidly growing population of children, regardless of the causal mechanism of impairment.”
Dr. Brogly noted that most of the opioid-using mothers in the study by Azuine et al. were unmarried, non-Hispanic white, and multiparous, and had histories of other substance abuse. She emphasized the need for supportive communities for women at risk of opioid use, who also are more likely to have unstable housing situations and histories of sexual and physical abuse.
“The risks of poor pregnancy and child outcomes in cases of maternal opioid exposure are not because of prenatal opioid exposure alone; ongoing difficult social and environmental circumstances have an important role,” and future interventions should address these circumstances to improve long-term health of high-risk women and their children, she emphasized.
The Boston Birth Cohort study is supported in part by grants from the National Institutes of Health and the U.S. Department of Health and Human Services. None of the authors had financial conflicts to disclose.
Dr. Brogly disclosed grants from the Eunice Kennedy Shriver National Institute of Child Health and Human Development outside the submitted work.
SOURCE: Azuine RE et al. JAMA Network Open. 2019 Jun 28. doi: 10.1001/jamanetworkopen.2019.6405; Brogly S. JAMA Network Open. 2019 Jun 28. doi:10.1001/jamanetworkopen.2019.6428.
according to data from more than 8,000 children.
Previous studies have shown the increased risk of a range of health problems associated with maternal opioid use, including neonatal abstinence syndrome (NAS), but data on the long-term consequences of in utero opioid exposure are limited, wrote Romuladus E. Azuine, DrPH, MPH, of the U.S. Department of Health and Human Services, Rockville, Md., and colleagues.
In a study published in JAMA Network Open, the researchers reviewed data from 8,509 mother/newborn pairs in the Boston Birth Cohort, a database that included a large urban, low-income, multiethnic population of women who had singleton births at the Boston Medical Center starting in 1998.
A total of 454 infants (5%) experienced prenatal opioid exposure. Mothers were interviewed 48-72 hours after delivery about sociodemographic factors, drug use, smoking, and alcohol use.
The risk of small for gestational age and preterm birth were significantly higher in babies exposed to opioids (OR 1.87 and OR 1.49, respectively), compared with unexposed newborns.
Children’s developmental outcomes were collected starting in 2003 based on electronic medical records. A total of 3,153 mother-newborn pairs were enrolled in a postnatal follow-up study. For preschoolers, prenatal opioid exposure was associated with increased risk of lack of expected physiological development and conduct disorder/emotional disturbance (OR 1.80 and OR 2.13, respectively), compared with unexposed children. School-aged children with prenatal opioid exposure had an increased risk of ADHD (OR 2.55).
The incidence of NAS in the study population was at least 24 per 1,000 hospital births starting in 2004, and peaked at 61 per 1,000 hospital births in 2008, but remained higher than 32 per 1,000 through 2016.
The study findings were limited by several factors including potential misclassification of opioid exposure, confounding from other pregnancy exposures, loss of many participants to follow-up, and a lack of generalizability, but the results support the need for additional research, and show that the prevalence of NAS was approximately 10 times the national average in a subset of low-income, urban, minority women, the researchers said.
“However, the effect of opioids is still difficult to disentangle from effects of other childhood exposures. Policy and programmatic efforts to prevent NAS and mitigate its health consequences require more comprehensive longitudinal and intergenerational research,” they concluded.
The study findings contribute to and support the evidence of poor neurodevelopmental and emotional/behavioral outcomes for children with prenatal exposure to opioids or a history of NAS, Susan Brogly, PhD, MSc, noted in an accompanying editorial. Other studies have shown increased risks for visual impairments including strabismus, reduced visual acuity, and delayed visual maturation.
Dr. Brogly, of Queen’s University, Kingston Health Science Center, Ontario, nonetheless noted that a child’s home environment may modify the impact of prenatal opioid exposure or NAS, as evidence has shown that children with in utero heroin exposure have improved outcomes in healthy home environments.
Although the mechanism for how opioid exposure affects development remains uncertain, she suggested that future research should address “interventions to improve health outcomes in this rapidly growing population of children, regardless of the causal mechanism of impairment.”
Dr. Brogly noted that most of the opioid-using mothers in the study by Azuine et al. were unmarried, non-Hispanic white, and multiparous, and had histories of other substance abuse. She emphasized the need for supportive communities for women at risk of opioid use, who also are more likely to have unstable housing situations and histories of sexual and physical abuse.
“The risks of poor pregnancy and child outcomes in cases of maternal opioid exposure are not because of prenatal opioid exposure alone; ongoing difficult social and environmental circumstances have an important role,” and future interventions should address these circumstances to improve long-term health of high-risk women and their children, she emphasized.
The Boston Birth Cohort study is supported in part by grants from the National Institutes of Health and the U.S. Department of Health and Human Services. None of the authors had financial conflicts to disclose.
Dr. Brogly disclosed grants from the Eunice Kennedy Shriver National Institute of Child Health and Human Development outside the submitted work.
SOURCE: Azuine RE et al. JAMA Network Open. 2019 Jun 28. doi: 10.1001/jamanetworkopen.2019.6405; Brogly S. JAMA Network Open. 2019 Jun 28. doi:10.1001/jamanetworkopen.2019.6428.
according to data from more than 8,000 children.
Previous studies have shown the increased risk of a range of health problems associated with maternal opioid use, including neonatal abstinence syndrome (NAS), but data on the long-term consequences of in utero opioid exposure are limited, wrote Romuladus E. Azuine, DrPH, MPH, of the U.S. Department of Health and Human Services, Rockville, Md., and colleagues.
In a study published in JAMA Network Open, the researchers reviewed data from 8,509 mother/newborn pairs in the Boston Birth Cohort, a database that included a large urban, low-income, multiethnic population of women who had singleton births at the Boston Medical Center starting in 1998.
A total of 454 infants (5%) experienced prenatal opioid exposure. Mothers were interviewed 48-72 hours after delivery about sociodemographic factors, drug use, smoking, and alcohol use.
The risk of small for gestational age and preterm birth were significantly higher in babies exposed to opioids (OR 1.87 and OR 1.49, respectively), compared with unexposed newborns.
Children’s developmental outcomes were collected starting in 2003 based on electronic medical records. A total of 3,153 mother-newborn pairs were enrolled in a postnatal follow-up study. For preschoolers, prenatal opioid exposure was associated with increased risk of lack of expected physiological development and conduct disorder/emotional disturbance (OR 1.80 and OR 2.13, respectively), compared with unexposed children. School-aged children with prenatal opioid exposure had an increased risk of ADHD (OR 2.55).
The incidence of NAS in the study population was at least 24 per 1,000 hospital births starting in 2004, and peaked at 61 per 1,000 hospital births in 2008, but remained higher than 32 per 1,000 through 2016.
The study findings were limited by several factors including potential misclassification of opioid exposure, confounding from other pregnancy exposures, loss of many participants to follow-up, and a lack of generalizability, but the results support the need for additional research, and show that the prevalence of NAS was approximately 10 times the national average in a subset of low-income, urban, minority women, the researchers said.
“However, the effect of opioids is still difficult to disentangle from effects of other childhood exposures. Policy and programmatic efforts to prevent NAS and mitigate its health consequences require more comprehensive longitudinal and intergenerational research,” they concluded.
The study findings contribute to and support the evidence of poor neurodevelopmental and emotional/behavioral outcomes for children with prenatal exposure to opioids or a history of NAS, Susan Brogly, PhD, MSc, noted in an accompanying editorial. Other studies have shown increased risks for visual impairments including strabismus, reduced visual acuity, and delayed visual maturation.
Dr. Brogly, of Queen’s University, Kingston Health Science Center, Ontario, nonetheless noted that a child’s home environment may modify the impact of prenatal opioid exposure or NAS, as evidence has shown that children with in utero heroin exposure have improved outcomes in healthy home environments.
Although the mechanism for how opioid exposure affects development remains uncertain, she suggested that future research should address “interventions to improve health outcomes in this rapidly growing population of children, regardless of the causal mechanism of impairment.”
Dr. Brogly noted that most of the opioid-using mothers in the study by Azuine et al. were unmarried, non-Hispanic white, and multiparous, and had histories of other substance abuse. She emphasized the need for supportive communities for women at risk of opioid use, who also are more likely to have unstable housing situations and histories of sexual and physical abuse.
“The risks of poor pregnancy and child outcomes in cases of maternal opioid exposure are not because of prenatal opioid exposure alone; ongoing difficult social and environmental circumstances have an important role,” and future interventions should address these circumstances to improve long-term health of high-risk women and their children, she emphasized.
The Boston Birth Cohort study is supported in part by grants from the National Institutes of Health and the U.S. Department of Health and Human Services. None of the authors had financial conflicts to disclose.
Dr. Brogly disclosed grants from the Eunice Kennedy Shriver National Institute of Child Health and Human Development outside the submitted work.
SOURCE: Azuine RE et al. JAMA Network Open. 2019 Jun 28. doi: 10.1001/jamanetworkopen.2019.6405; Brogly S. JAMA Network Open. 2019 Jun 28. doi:10.1001/jamanetworkopen.2019.6428.
FROM JAMA NETWORK OPEN
Type 2 diabetes is particularly devastating in adolescents
SAN FRANCISCO – and by the time those with youth-onset diabetes reach their early 20s, they are beset with disease-related complications usually seen in older populations, findings from the RISE and TODAY2 studies have demonstrated.
“Additional research is urgently needed to better understand the reasons for this more serious trajectory,” Philip Zeitler, MD, PhD, of Children’s Hospital Colorado, Aurora, said at the annual scientific sessions of the American Diabetes Association. The hope is to identify at-risk children and prevent the disease, but at this point “we don’t know the answer.”
In the meantime, “we are getting more aggressive with bariatric surgery at our center, because nothing else is working as well. It would be nice to move away from that, but these kids are going to die,” he added.
Steven Kahn, MD, of the diabetes Research Center at the University of Washington, Seattle, presented the findings from a comparison of outcomes from the Restoring Insulin Secretion (RISE) studies in adolescents aged 10-19 years and in adults. The RISE Pediatric Medication Study (Diabetes Care. 2018; 41[8]:1717-25) and RISE Adult Medication Study were parallel investigations treatments to preserve or improve beta-cell function.
“This is the first-ever true comparison of outcomes in youth versus adults,” he said. Both arms had the same design and lab measurements, but the differences in outcomes were “very scary,” he added. “The disease is much more aggressive in youth than in adults.”
Among other things, the RISE youth-versus-adult study compared the outcomes after 3 months of insulin glargine followed by 9 months of metformin, or 12 months of metformin in 132 obese adults and 91 obese adolescents with impaired glucose tolerance or recently diagnosed type 2 diabetes. The treatments were stopped after 12 months, and the participants were reevaluated at 15 months. Hyperglycemic clamps were conducted at baseline, 12 months, and 3 months after treatment cessation (Diabetes. 2019 Jun 9. doi: 10.2337/db19-0299).
In adults, treatment improved insulin sensitivity and beta-cell response, but after treatment cessation, they reverted to baseline by the 15-month evaluation. However, there was no improvement in insulin sensitivity and beta-cell response in adolescents, either during treatment or after cessation, and in fact, they were worse off at 15 months than they had been at baseline, with lower insulin secretion and higher hemoglobin A1c.
Those stark differences in outcomes between the adolescents and adults were indicative of a more aggressive disease trajectory for younger patients.
Compliance was not the issue, with more than 80% of both adults and children taking more than 80% of their medications, Dr. Kahn said.
He suggested that adolescents might have a different underlying pathology that makes it worse to develop diabetes during puberty, which is already an insulin-resistant state. But, whatever the case, there is an “urgent need” to better understand the differences between adolescents and adults and to find better treatments for younger patients with diabetes, he said.
In regard to using weight loss as a means of treatment or prevention, Dr. Zeitler emphasized that type 2 diabetes in younger patients “occurs in a context of very low socioeconomic status, family dysfunction, and a great deal of stress and [family] illness. It’s often a complex situation and it’s difficult to accomplish effective lifestyle change when families are struggling to have afford quality food, facing challenges of family and neighborhood violence, and working multiple jobs.”
The RISE findings of a more aggressive deterioration in beta-cell function for younger patients were reflected in outcomes in the TODAY2 study, which found that adolescents who are diagnosed with type 2 diabetes face severe renal, cardiovascular, eye, and nerve complications by the time they reach their early 20s.
TODAY2 was an 8-year follow-up to the Treatment Options for Type 2 Diabetes in Adolescents and Youth (TODAY) trial published in 2012 (N Engl J Med. 2012;366:2247-56). Data from the original study of patients aged 10-17 years with type 2 diabetes showed that after a roughly 4-year follow-up, almost half of all participants had experienced loss of glycemic control on their original treatment assignment, a rate much higher than that reported in adults. Metformin plus rosiglitazone was superior to metformin alone in maintaining durable glycemic control and metformin plus an intensive lifestyle intervention was intermediate to the other groups, but not significantly different from them. In addition, metformin alone was found to be least effective in non-Hispanic black patients, metformin and rosiglitazone was most effective in girls.
Overall, 517 participants of the original study’s 669 participants are still being followed as part of the TODAY2 trial. They are managed in community practices now and are in their early 20s, on average.
But, less than 10 years down the road from TODAY, the young adults “have problems you’d expect in your grandparents. Target-organ damage is already evident, and serious cardiovascular events are occurring,” Dr. Zeitler said.
Cardiovascular complications
The cardiovascular event rate in TODAY 2 was about the same as is seen in older adults with type 1 diabetes. Overall, there were 38 cardiovascular events in 19 patients for an event rate of 6.4/1,000 patients per year. Those events included heart failure, arrhythmia, coronary artery disease or myocardial infarction, deep venous thrombosis, stroke or transient ischemic attack, and vascular insufficiency.
Over that time, the cumulative incidence of elevated LDL cholesterol increased from 3% in the TODAY report to 26% for TODAY2, and for triglycerides, it went from 18% to 35%. The cumulative incidence of hypertension increased from 19% to 55%.
Decline renal function
In regard to renal complications, the cumulative incident curve for microalbuminuria went from 8% at baseline to 40% at 12 years, while macroalbuminuria prevalence increased from 1.5% to 11% during the same time. The cumulative incidence of hyperfiltration increased from 12% to 48%. Risk factors for hyperfiltration included female sex, Hispanic ethnicity, loss of glycemic control, and hypertension, although body mass index was actually associated with lower risk.
So far, there have been four renal events in two patients, who both had chronic kidney disease and end-stage renal failure, for an event rate of 0.7/1,000 patients per year.
Pregnancy outcomes
Women in the cohort – about two-thirds of the study population – have had high rates of maternal complications, and their offspring also face complications after birth.
There were 306 pregnancies reported, of which there are known outcomes for 53 (TODAY) and 236 (TODAY2). In all, 5% of the total cohort had voluntary elective termination; 9% and 12% of patients, respectively, suffered a miscarriage before 20 weeks; and 4% of pregnancies in the total cohort ended in stillbirth.
Preterm live births more than doubled from 11% to 24%, and full-term deliveries decreased from 62% to 46% in the TODAY2 patients.
In regard to offspring characteristics, average birth weight in the total cohort was just over 4.5 pounds (national average, 7.3 pounds), and the prevalence of very low birth weight more than doubled from 8% to 16% at the 12-year mark. The prevalence of macrosomia was 19% for the cohort, more than double the national average of 8%. In all, 5% and 7% of offspring were small for gestational age, whereas 22% and 26% of offspring were large for gestational age.
Among other complications, respiratory distress occurred in 8% and 14% of offspring, and cardiac anomalies occurred in 10% and 9%, which, although they held steady across the cohorts, were significantly higher than the national average of 1%. Similarly, neonatal hypoglycemia occurred in 17% and 29% of offspring, again, notably higher than the national average of 2%. Offspring outcomes were worse in mothers with loss of glycemic control.
In regard to maternal pregnancy complications, the rate of hospitalization before delivery increased from 25% to 36%; hypertension increased in prevalence from 19% to 36%; and while macroalbuminuria held steady at 9.4%, microalbuminuria increased from 6% to 8%. Thirty-three percent of the TODAY2 cohort had a hemoglobin A1c level of more than 8%.
Retinopathy
Serious eye problems were common, with notable progression seen in diabetic retinopathy in patients who had fundus photos taken in 2011 (TODAY) and 2018 (TODAY2). Among the patients, 86% and 51%, respectively, of 371 patients had no definitive diabetic retinopathy; 14% and 22% of patients had very mild nonproliferative diabetic retinopathy (NPDR); and 0% and 16% of patients had mild NPDR. None of the TODAY patients had early or high-risk proliferative diabetic retinopathy, compared with 3% and 1%, respectively, in TODAY2. Risk factors included loss of glycemic control (hazard ratio, 19.23; 95% confidence interval, 4.62-80.07).
None of the TODAY patients had macular edema, whereas it occurred in 4% of TODAY2 patients. In all, there were 142 adjudicated eye-related events reported for 92 patients, for an event rate of 15.5/1,000 patients per year. The events included NPDR, proliferative diabetic retinopathy, macular edema, cataracts, glaucoma, and vitreous hemorrhage).
Neuropathy
The prevalence of diabetic neuropathy also increased over the duration of follow-up, rising to 28%-33% based on Michigan Neuropathy Screening Instrument scores. There were 14 adjudicated events reported for 12 patients (2.4 events/1,000 patients per year), including peripheral diabetic neuropathy, autonomic neuropathy, and diabetic mononeuropathy.
“We’ve had a number of amputations; quite a number of toes are now missing in this group of kids,” Dr. Zeitler said.
There have been five deaths so far: one heart attack, one renal failure, one overwhelming sepsis, one postop cardiac arrest, and a drug overdose.
Dr. Zeitler was the senior author on 2018 updated ADA guidelines for managing youth-onset type 2 diabetes. The recommendations where extensively shaped by the TODAY findings and were more aggressive than those previously put forward, suggesting, among other things, hemoglobin A1c targets of 6.5%-7%; earlier treatment with insulin; and stricter management of hypertension, dyslipidemia, and proteinuria (Diabetes Care. 2018;41[12]:2648-68).
The National Institute of Diabetes & Kidney disease funded the studies. The presenters reported no relevant disclosures or conflicts of interest.
This article was updated 7/22/19.
SAN FRANCISCO – and by the time those with youth-onset diabetes reach their early 20s, they are beset with disease-related complications usually seen in older populations, findings from the RISE and TODAY2 studies have demonstrated.
“Additional research is urgently needed to better understand the reasons for this more serious trajectory,” Philip Zeitler, MD, PhD, of Children’s Hospital Colorado, Aurora, said at the annual scientific sessions of the American Diabetes Association. The hope is to identify at-risk children and prevent the disease, but at this point “we don’t know the answer.”
In the meantime, “we are getting more aggressive with bariatric surgery at our center, because nothing else is working as well. It would be nice to move away from that, but these kids are going to die,” he added.
Steven Kahn, MD, of the diabetes Research Center at the University of Washington, Seattle, presented the findings from a comparison of outcomes from the Restoring Insulin Secretion (RISE) studies in adolescents aged 10-19 years and in adults. The RISE Pediatric Medication Study (Diabetes Care. 2018; 41[8]:1717-25) and RISE Adult Medication Study were parallel investigations treatments to preserve or improve beta-cell function.
“This is the first-ever true comparison of outcomes in youth versus adults,” he said. Both arms had the same design and lab measurements, but the differences in outcomes were “very scary,” he added. “The disease is much more aggressive in youth than in adults.”
Among other things, the RISE youth-versus-adult study compared the outcomes after 3 months of insulin glargine followed by 9 months of metformin, or 12 months of metformin in 132 obese adults and 91 obese adolescents with impaired glucose tolerance or recently diagnosed type 2 diabetes. The treatments were stopped after 12 months, and the participants were reevaluated at 15 months. Hyperglycemic clamps were conducted at baseline, 12 months, and 3 months after treatment cessation (Diabetes. 2019 Jun 9. doi: 10.2337/db19-0299).
In adults, treatment improved insulin sensitivity and beta-cell response, but after treatment cessation, they reverted to baseline by the 15-month evaluation. However, there was no improvement in insulin sensitivity and beta-cell response in adolescents, either during treatment or after cessation, and in fact, they were worse off at 15 months than they had been at baseline, with lower insulin secretion and higher hemoglobin A1c.
Those stark differences in outcomes between the adolescents and adults were indicative of a more aggressive disease trajectory for younger patients.
Compliance was not the issue, with more than 80% of both adults and children taking more than 80% of their medications, Dr. Kahn said.
He suggested that adolescents might have a different underlying pathology that makes it worse to develop diabetes during puberty, which is already an insulin-resistant state. But, whatever the case, there is an “urgent need” to better understand the differences between adolescents and adults and to find better treatments for younger patients with diabetes, he said.
In regard to using weight loss as a means of treatment or prevention, Dr. Zeitler emphasized that type 2 diabetes in younger patients “occurs in a context of very low socioeconomic status, family dysfunction, and a great deal of stress and [family] illness. It’s often a complex situation and it’s difficult to accomplish effective lifestyle change when families are struggling to have afford quality food, facing challenges of family and neighborhood violence, and working multiple jobs.”
The RISE findings of a more aggressive deterioration in beta-cell function for younger patients were reflected in outcomes in the TODAY2 study, which found that adolescents who are diagnosed with type 2 diabetes face severe renal, cardiovascular, eye, and nerve complications by the time they reach their early 20s.
TODAY2 was an 8-year follow-up to the Treatment Options for Type 2 Diabetes in Adolescents and Youth (TODAY) trial published in 2012 (N Engl J Med. 2012;366:2247-56). Data from the original study of patients aged 10-17 years with type 2 diabetes showed that after a roughly 4-year follow-up, almost half of all participants had experienced loss of glycemic control on their original treatment assignment, a rate much higher than that reported in adults. Metformin plus rosiglitazone was superior to metformin alone in maintaining durable glycemic control and metformin plus an intensive lifestyle intervention was intermediate to the other groups, but not significantly different from them. In addition, metformin alone was found to be least effective in non-Hispanic black patients, metformin and rosiglitazone was most effective in girls.
Overall, 517 participants of the original study’s 669 participants are still being followed as part of the TODAY2 trial. They are managed in community practices now and are in their early 20s, on average.
But, less than 10 years down the road from TODAY, the young adults “have problems you’d expect in your grandparents. Target-organ damage is already evident, and serious cardiovascular events are occurring,” Dr. Zeitler said.
Cardiovascular complications
The cardiovascular event rate in TODAY 2 was about the same as is seen in older adults with type 1 diabetes. Overall, there were 38 cardiovascular events in 19 patients for an event rate of 6.4/1,000 patients per year. Those events included heart failure, arrhythmia, coronary artery disease or myocardial infarction, deep venous thrombosis, stroke or transient ischemic attack, and vascular insufficiency.
Over that time, the cumulative incidence of elevated LDL cholesterol increased from 3% in the TODAY report to 26% for TODAY2, and for triglycerides, it went from 18% to 35%. The cumulative incidence of hypertension increased from 19% to 55%.
Decline renal function
In regard to renal complications, the cumulative incident curve for microalbuminuria went from 8% at baseline to 40% at 12 years, while macroalbuminuria prevalence increased from 1.5% to 11% during the same time. The cumulative incidence of hyperfiltration increased from 12% to 48%. Risk factors for hyperfiltration included female sex, Hispanic ethnicity, loss of glycemic control, and hypertension, although body mass index was actually associated with lower risk.
So far, there have been four renal events in two patients, who both had chronic kidney disease and end-stage renal failure, for an event rate of 0.7/1,000 patients per year.
Pregnancy outcomes
Women in the cohort – about two-thirds of the study population – have had high rates of maternal complications, and their offspring also face complications after birth.
There were 306 pregnancies reported, of which there are known outcomes for 53 (TODAY) and 236 (TODAY2). In all, 5% of the total cohort had voluntary elective termination; 9% and 12% of patients, respectively, suffered a miscarriage before 20 weeks; and 4% of pregnancies in the total cohort ended in stillbirth.
Preterm live births more than doubled from 11% to 24%, and full-term deliveries decreased from 62% to 46% in the TODAY2 patients.
In regard to offspring characteristics, average birth weight in the total cohort was just over 4.5 pounds (national average, 7.3 pounds), and the prevalence of very low birth weight more than doubled from 8% to 16% at the 12-year mark. The prevalence of macrosomia was 19% for the cohort, more than double the national average of 8%. In all, 5% and 7% of offspring were small for gestational age, whereas 22% and 26% of offspring were large for gestational age.
Among other complications, respiratory distress occurred in 8% and 14% of offspring, and cardiac anomalies occurred in 10% and 9%, which, although they held steady across the cohorts, were significantly higher than the national average of 1%. Similarly, neonatal hypoglycemia occurred in 17% and 29% of offspring, again, notably higher than the national average of 2%. Offspring outcomes were worse in mothers with loss of glycemic control.
In regard to maternal pregnancy complications, the rate of hospitalization before delivery increased from 25% to 36%; hypertension increased in prevalence from 19% to 36%; and while macroalbuminuria held steady at 9.4%, microalbuminuria increased from 6% to 8%. Thirty-three percent of the TODAY2 cohort had a hemoglobin A1c level of more than 8%.
Retinopathy
Serious eye problems were common, with notable progression seen in diabetic retinopathy in patients who had fundus photos taken in 2011 (TODAY) and 2018 (TODAY2). Among the patients, 86% and 51%, respectively, of 371 patients had no definitive diabetic retinopathy; 14% and 22% of patients had very mild nonproliferative diabetic retinopathy (NPDR); and 0% and 16% of patients had mild NPDR. None of the TODAY patients had early or high-risk proliferative diabetic retinopathy, compared with 3% and 1%, respectively, in TODAY2. Risk factors included loss of glycemic control (hazard ratio, 19.23; 95% confidence interval, 4.62-80.07).
None of the TODAY patients had macular edema, whereas it occurred in 4% of TODAY2 patients. In all, there were 142 adjudicated eye-related events reported for 92 patients, for an event rate of 15.5/1,000 patients per year. The events included NPDR, proliferative diabetic retinopathy, macular edema, cataracts, glaucoma, and vitreous hemorrhage).
Neuropathy
The prevalence of diabetic neuropathy also increased over the duration of follow-up, rising to 28%-33% based on Michigan Neuropathy Screening Instrument scores. There were 14 adjudicated events reported for 12 patients (2.4 events/1,000 patients per year), including peripheral diabetic neuropathy, autonomic neuropathy, and diabetic mononeuropathy.
“We’ve had a number of amputations; quite a number of toes are now missing in this group of kids,” Dr. Zeitler said.
There have been five deaths so far: one heart attack, one renal failure, one overwhelming sepsis, one postop cardiac arrest, and a drug overdose.
Dr. Zeitler was the senior author on 2018 updated ADA guidelines for managing youth-onset type 2 diabetes. The recommendations where extensively shaped by the TODAY findings and were more aggressive than those previously put forward, suggesting, among other things, hemoglobin A1c targets of 6.5%-7%; earlier treatment with insulin; and stricter management of hypertension, dyslipidemia, and proteinuria (Diabetes Care. 2018;41[12]:2648-68).
The National Institute of Diabetes & Kidney disease funded the studies. The presenters reported no relevant disclosures or conflicts of interest.
This article was updated 7/22/19.
SAN FRANCISCO – and by the time those with youth-onset diabetes reach their early 20s, they are beset with disease-related complications usually seen in older populations, findings from the RISE and TODAY2 studies have demonstrated.
“Additional research is urgently needed to better understand the reasons for this more serious trajectory,” Philip Zeitler, MD, PhD, of Children’s Hospital Colorado, Aurora, said at the annual scientific sessions of the American Diabetes Association. The hope is to identify at-risk children and prevent the disease, but at this point “we don’t know the answer.”
In the meantime, “we are getting more aggressive with bariatric surgery at our center, because nothing else is working as well. It would be nice to move away from that, but these kids are going to die,” he added.
Steven Kahn, MD, of the diabetes Research Center at the University of Washington, Seattle, presented the findings from a comparison of outcomes from the Restoring Insulin Secretion (RISE) studies in adolescents aged 10-19 years and in adults. The RISE Pediatric Medication Study (Diabetes Care. 2018; 41[8]:1717-25) and RISE Adult Medication Study were parallel investigations treatments to preserve or improve beta-cell function.
“This is the first-ever true comparison of outcomes in youth versus adults,” he said. Both arms had the same design and lab measurements, but the differences in outcomes were “very scary,” he added. “The disease is much more aggressive in youth than in adults.”
Among other things, the RISE youth-versus-adult study compared the outcomes after 3 months of insulin glargine followed by 9 months of metformin, or 12 months of metformin in 132 obese adults and 91 obese adolescents with impaired glucose tolerance or recently diagnosed type 2 diabetes. The treatments were stopped after 12 months, and the participants were reevaluated at 15 months. Hyperglycemic clamps were conducted at baseline, 12 months, and 3 months after treatment cessation (Diabetes. 2019 Jun 9. doi: 10.2337/db19-0299).
In adults, treatment improved insulin sensitivity and beta-cell response, but after treatment cessation, they reverted to baseline by the 15-month evaluation. However, there was no improvement in insulin sensitivity and beta-cell response in adolescents, either during treatment or after cessation, and in fact, they were worse off at 15 months than they had been at baseline, with lower insulin secretion and higher hemoglobin A1c.
Those stark differences in outcomes between the adolescents and adults were indicative of a more aggressive disease trajectory for younger patients.
Compliance was not the issue, with more than 80% of both adults and children taking more than 80% of their medications, Dr. Kahn said.
He suggested that adolescents might have a different underlying pathology that makes it worse to develop diabetes during puberty, which is already an insulin-resistant state. But, whatever the case, there is an “urgent need” to better understand the differences between adolescents and adults and to find better treatments for younger patients with diabetes, he said.
In regard to using weight loss as a means of treatment or prevention, Dr. Zeitler emphasized that type 2 diabetes in younger patients “occurs in a context of very low socioeconomic status, family dysfunction, and a great deal of stress and [family] illness. It’s often a complex situation and it’s difficult to accomplish effective lifestyle change when families are struggling to have afford quality food, facing challenges of family and neighborhood violence, and working multiple jobs.”
The RISE findings of a more aggressive deterioration in beta-cell function for younger patients were reflected in outcomes in the TODAY2 study, which found that adolescents who are diagnosed with type 2 diabetes face severe renal, cardiovascular, eye, and nerve complications by the time they reach their early 20s.
TODAY2 was an 8-year follow-up to the Treatment Options for Type 2 Diabetes in Adolescents and Youth (TODAY) trial published in 2012 (N Engl J Med. 2012;366:2247-56). Data from the original study of patients aged 10-17 years with type 2 diabetes showed that after a roughly 4-year follow-up, almost half of all participants had experienced loss of glycemic control on their original treatment assignment, a rate much higher than that reported in adults. Metformin plus rosiglitazone was superior to metformin alone in maintaining durable glycemic control and metformin plus an intensive lifestyle intervention was intermediate to the other groups, but not significantly different from them. In addition, metformin alone was found to be least effective in non-Hispanic black patients, metformin and rosiglitazone was most effective in girls.
Overall, 517 participants of the original study’s 669 participants are still being followed as part of the TODAY2 trial. They are managed in community practices now and are in their early 20s, on average.
But, less than 10 years down the road from TODAY, the young adults “have problems you’d expect in your grandparents. Target-organ damage is already evident, and serious cardiovascular events are occurring,” Dr. Zeitler said.
Cardiovascular complications
The cardiovascular event rate in TODAY 2 was about the same as is seen in older adults with type 1 diabetes. Overall, there were 38 cardiovascular events in 19 patients for an event rate of 6.4/1,000 patients per year. Those events included heart failure, arrhythmia, coronary artery disease or myocardial infarction, deep venous thrombosis, stroke or transient ischemic attack, and vascular insufficiency.
Over that time, the cumulative incidence of elevated LDL cholesterol increased from 3% in the TODAY report to 26% for TODAY2, and for triglycerides, it went from 18% to 35%. The cumulative incidence of hypertension increased from 19% to 55%.
Decline renal function
In regard to renal complications, the cumulative incident curve for microalbuminuria went from 8% at baseline to 40% at 12 years, while macroalbuminuria prevalence increased from 1.5% to 11% during the same time. The cumulative incidence of hyperfiltration increased from 12% to 48%. Risk factors for hyperfiltration included female sex, Hispanic ethnicity, loss of glycemic control, and hypertension, although body mass index was actually associated with lower risk.
So far, there have been four renal events in two patients, who both had chronic kidney disease and end-stage renal failure, for an event rate of 0.7/1,000 patients per year.
Pregnancy outcomes
Women in the cohort – about two-thirds of the study population – have had high rates of maternal complications, and their offspring also face complications after birth.
There were 306 pregnancies reported, of which there are known outcomes for 53 (TODAY) and 236 (TODAY2). In all, 5% of the total cohort had voluntary elective termination; 9% and 12% of patients, respectively, suffered a miscarriage before 20 weeks; and 4% of pregnancies in the total cohort ended in stillbirth.
Preterm live births more than doubled from 11% to 24%, and full-term deliveries decreased from 62% to 46% in the TODAY2 patients.
In regard to offspring characteristics, average birth weight in the total cohort was just over 4.5 pounds (national average, 7.3 pounds), and the prevalence of very low birth weight more than doubled from 8% to 16% at the 12-year mark. The prevalence of macrosomia was 19% for the cohort, more than double the national average of 8%. In all, 5% and 7% of offspring were small for gestational age, whereas 22% and 26% of offspring were large for gestational age.
Among other complications, respiratory distress occurred in 8% and 14% of offspring, and cardiac anomalies occurred in 10% and 9%, which, although they held steady across the cohorts, were significantly higher than the national average of 1%. Similarly, neonatal hypoglycemia occurred in 17% and 29% of offspring, again, notably higher than the national average of 2%. Offspring outcomes were worse in mothers with loss of glycemic control.
In regard to maternal pregnancy complications, the rate of hospitalization before delivery increased from 25% to 36%; hypertension increased in prevalence from 19% to 36%; and while macroalbuminuria held steady at 9.4%, microalbuminuria increased from 6% to 8%. Thirty-three percent of the TODAY2 cohort had a hemoglobin A1c level of more than 8%.
Retinopathy
Serious eye problems were common, with notable progression seen in diabetic retinopathy in patients who had fundus photos taken in 2011 (TODAY) and 2018 (TODAY2). Among the patients, 86% and 51%, respectively, of 371 patients had no definitive diabetic retinopathy; 14% and 22% of patients had very mild nonproliferative diabetic retinopathy (NPDR); and 0% and 16% of patients had mild NPDR. None of the TODAY patients had early or high-risk proliferative diabetic retinopathy, compared with 3% and 1%, respectively, in TODAY2. Risk factors included loss of glycemic control (hazard ratio, 19.23; 95% confidence interval, 4.62-80.07).
None of the TODAY patients had macular edema, whereas it occurred in 4% of TODAY2 patients. In all, there were 142 adjudicated eye-related events reported for 92 patients, for an event rate of 15.5/1,000 patients per year. The events included NPDR, proliferative diabetic retinopathy, macular edema, cataracts, glaucoma, and vitreous hemorrhage).
Neuropathy
The prevalence of diabetic neuropathy also increased over the duration of follow-up, rising to 28%-33% based on Michigan Neuropathy Screening Instrument scores. There were 14 adjudicated events reported for 12 patients (2.4 events/1,000 patients per year), including peripheral diabetic neuropathy, autonomic neuropathy, and diabetic mononeuropathy.
“We’ve had a number of amputations; quite a number of toes are now missing in this group of kids,” Dr. Zeitler said.
There have been five deaths so far: one heart attack, one renal failure, one overwhelming sepsis, one postop cardiac arrest, and a drug overdose.
Dr. Zeitler was the senior author on 2018 updated ADA guidelines for managing youth-onset type 2 diabetes. The recommendations where extensively shaped by the TODAY findings and were more aggressive than those previously put forward, suggesting, among other things, hemoglobin A1c targets of 6.5%-7%; earlier treatment with insulin; and stricter management of hypertension, dyslipidemia, and proteinuria (Diabetes Care. 2018;41[12]:2648-68).
The National Institute of Diabetes & Kidney disease funded the studies. The presenters reported no relevant disclosures or conflicts of interest.
This article was updated 7/22/19.
EXPERT ANALYSIS FROM ADA 2019
Parent education improves pediatric influenza vaccination rates
according to a randomized clinical trial published in Pediatrics.

Vanessa P. Scott, MD, MS, of Columbia University, New York, and colleagues randomized 400 parent-child dyads into any of three arms: receiving a handout based on national data, receiving a handout based on local data, or receiving usual care. This convenience sample was drawn from two pediatric clinics in New York between August 2016 and March 2017.
After adjustment for parents’ education level, the trial found that parents who received either handout were significantly more likely than were those receiving usual care to vaccinate their children by the end of season (75% and 65%, respectively; adjusted odds ratio, 1.68; 95% confidence interval, 1.06-2.67), but the effects of any intervention versus those of usual care on vaccination on day of visit were not statistically significant (59% vs. 53%; aOR, 1.36; 95% CI, 0.89-2.09).The researchers had hoped that using a targeted approach based on local data would increase vaccine receipt, but that was not seen in the results.
They did find that, across all three arms in the trial, baseline parental intent to vaccinate (likely versus unlikely) was associated with vaccination rates: Both vaccination on clinic visit day (70% vs. 22%; aOR, 8.38; 95% CI, 4.85-14.34) and vaccination by end of season (87% vs. 29%; aOR, 18.26; 95% CI, 9.94-33.52) were affected.
Strengths of the study included the randomized, controlled design and assessment of baseline factors, such as intention to vaccinate, to reduce confounding effects. Limitations included use of a convenience sample, which could have introduced selection bias.
One author was an unremunerated coinvestigator of an unrelated trial that received an investigator-initiated grant from the Pfizer Medical Education Group. Two authors were funded by other grants, but no potential conflicts of interests to disclose were indicated by any of the authors in this study.
SOURCE: Scott VP et al. Pediatrics. 2019. doi: 10.1542/peds.2018-2580.
according to a randomized clinical trial published in Pediatrics.
Vanessa P. Scott, MD, MS, of Columbia University, New York, and colleagues randomized 400 parent-child dyads into any of three arms: receiving a handout based on national data, receiving a handout based on local data, or receiving usual care. This convenience sample was drawn from two pediatric clinics in New York between August 2016 and March 2017.
After adjustment for parents’ education level, the trial found that parents who received either handout were significantly more likely than were those receiving usual care to vaccinate their children by the end of season (75% and 65%, respectively; adjusted odds ratio, 1.68; 95% confidence interval, 1.06-2.67), but the effects of any intervention versus those of usual care on vaccination on day of visit were not statistically significant (59% vs. 53%; aOR, 1.36; 95% CI, 0.89-2.09).The researchers had hoped that using a targeted approach based on local data would increase vaccine receipt, but that was not seen in the results.
They did find that, across all three arms in the trial, baseline parental intent to vaccinate (likely versus unlikely) was associated with vaccination rates: Both vaccination on clinic visit day (70% vs. 22%; aOR, 8.38; 95% CI, 4.85-14.34) and vaccination by end of season (87% vs. 29%; aOR, 18.26; 95% CI, 9.94-33.52) were affected.
Strengths of the study included the randomized, controlled design and assessment of baseline factors, such as intention to vaccinate, to reduce confounding effects. Limitations included use of a convenience sample, which could have introduced selection bias.
One author was an unremunerated coinvestigator of an unrelated trial that received an investigator-initiated grant from the Pfizer Medical Education Group. Two authors were funded by other grants, but no potential conflicts of interests to disclose were indicated by any of the authors in this study.
SOURCE: Scott VP et al. Pediatrics. 2019. doi: 10.1542/peds.2018-2580.
according to a randomized clinical trial published in Pediatrics.
Vanessa P. Scott, MD, MS, of Columbia University, New York, and colleagues randomized 400 parent-child dyads into any of three arms: receiving a handout based on national data, receiving a handout based on local data, or receiving usual care. This convenience sample was drawn from two pediatric clinics in New York between August 2016 and March 2017.
After adjustment for parents’ education level, the trial found that parents who received either handout were significantly more likely than were those receiving usual care to vaccinate their children by the end of season (75% and 65%, respectively; adjusted odds ratio, 1.68; 95% confidence interval, 1.06-2.67), but the effects of any intervention versus those of usual care on vaccination on day of visit were not statistically significant (59% vs. 53%; aOR, 1.36; 95% CI, 0.89-2.09).The researchers had hoped that using a targeted approach based on local data would increase vaccine receipt, but that was not seen in the results.
They did find that, across all three arms in the trial, baseline parental intent to vaccinate (likely versus unlikely) was associated with vaccination rates: Both vaccination on clinic visit day (70% vs. 22%; aOR, 8.38; 95% CI, 4.85-14.34) and vaccination by end of season (87% vs. 29%; aOR, 18.26; 95% CI, 9.94-33.52) were affected.
Strengths of the study included the randomized, controlled design and assessment of baseline factors, such as intention to vaccinate, to reduce confounding effects. Limitations included use of a convenience sample, which could have introduced selection bias.
One author was an unremunerated coinvestigator of an unrelated trial that received an investigator-initiated grant from the Pfizer Medical Education Group. Two authors were funded by other grants, but no potential conflicts of interests to disclose were indicated by any of the authors in this study.
SOURCE: Scott VP et al. Pediatrics. 2019. doi: 10.1542/peds.2018-2580.
FROM PEDIATRICS
CDC: Look for early symptoms of acute flaccid myelitis, report suspected cases
the CDC said in a telebriefing.
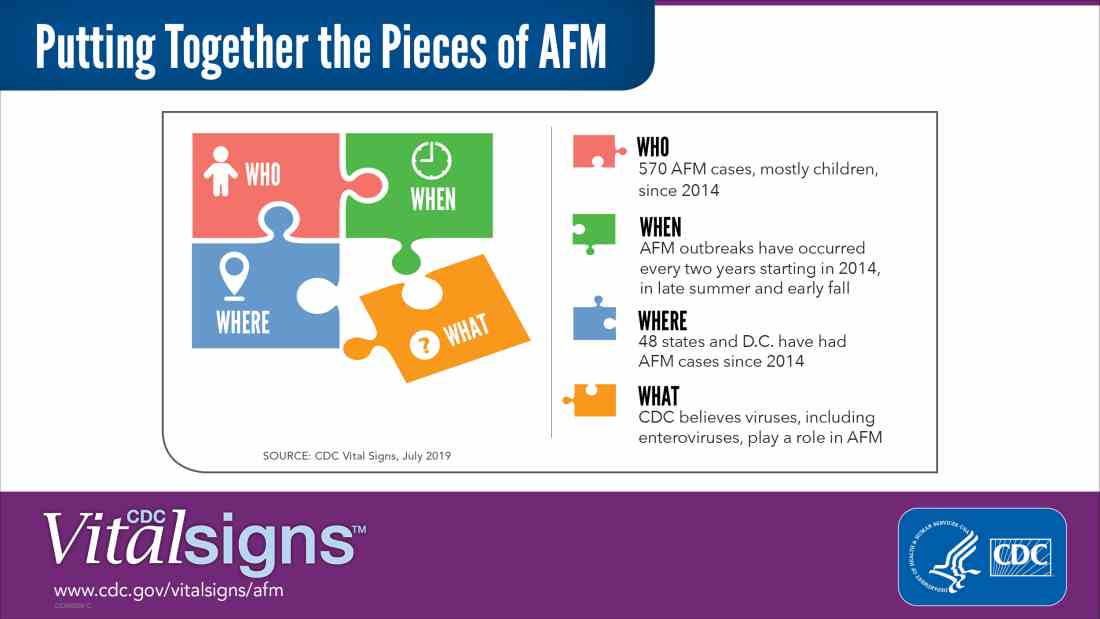
Acute flaccid myelitis (AFM) is defined as acute, flaccid muscle weakness that occurs less than 1 week after a fever or respiratory illness. Viruses, including enterovirus, are believed to play a role in AFM, but the cause still is unknown. The disease appears mostly in children, and the average age of a patient diagnosed with AFM is 5 years.
“Doctors and other clinicians in the United States play a critical role,” Anne Schuchat, MD, principal deputy director of the Centers for Disease Control and Prevention, said in the telebriefing. “We ask for your help with early recognition of patients with AFM symptoms, prompt specimen collection for testing, and immediate reporting of suspected AFM cases to health departments.”
While there is no proven treatment for AFM, early diagnosis is critical to getting patients the best care possible, according to a Vital Signs report released today. This means that clinicians should not wait for the CDC’s case definition before diagnosis, the CDC said.
“When specimens are collected as soon as possible after symptom onset, we have a better chance of understanding the causes of AFM, these recurrent outbreaks, and developing a diagnostic test,” Dr. Schuchat said. “Rapid reporting also helps us to identify and respond to outbreaks early and alert other clinicians and the public.”
AFM appears to follow a seasonal and biennial pattern, with the number of cases increasing mainly in the late summer and early fall. As the season approaches where AFM cases increase, CDC is asking clinicians to look out for patients with suspected AFM so cases can be reported as early as possible.
Since the CDC began tracking AFM, the number of cases has risen every 2 years. In 2018, there were 233 cases in 41 states, the highest number of reported cases since the CDC began tracking AFM following an outbreak in 2014, according to a Vital Signs report. Overall, there have been 570 cases of AFM reported in 48 states and the District of Columbia since 2014.
There is yet to be a confirmatory test for AFM, but clinicians should obtain cerebrospinal fluid, serum, stool and nasopharyngeal swab from patients with suspected AFM as soon as possible, followed by an MRI. AFM has unique MRI features , such as gray matter involvement, that can help distinguish it from other diseases characterized by acute weakness.
In the Vital Signs report, which examined AFM in 2018, 92% of confirmed cases had respiratory symptoms or fever, and 42% of confirmed cases had upper limb involvement. The median time from limb weakness to hospitalization was 1 day, and time from weakness to MRI was 2 days. Cases were reported to the CDC a median of 18 days from onset of limb weakness, but time to reporting ranged between 18 days and 36 days, said Tom Clark, MD, MPH, deputy director of the division of viral diseases at CDC.
“This delay hampers our ability to understand the causes AFM,” he said. “We believe that recognizing AFM early is critical and can lead to better patient management.”
In lieu of a diagnostic test for AFM, clinicians should make management decisions through review of patient symptoms, exam findings, MRI, other test results, and in consulting with neurology experts. The Transverse Myelitis Association also has created a support portal for 24/7 physician consultation in AFM cases.
SOURCE: Lopez A et al. MMWR Morb Mortal Wkly Rep. 2019;68:1-7 .
the CDC said in a telebriefing.
Acute flaccid myelitis (AFM) is defined as acute, flaccid muscle weakness that occurs less than 1 week after a fever or respiratory illness. Viruses, including enterovirus, are believed to play a role in AFM, but the cause still is unknown. The disease appears mostly in children, and the average age of a patient diagnosed with AFM is 5 years.
“Doctors and other clinicians in the United States play a critical role,” Anne Schuchat, MD, principal deputy director of the Centers for Disease Control and Prevention, said in the telebriefing. “We ask for your help with early recognition of patients with AFM symptoms, prompt specimen collection for testing, and immediate reporting of suspected AFM cases to health departments.”
While there is no proven treatment for AFM, early diagnosis is critical to getting patients the best care possible, according to a Vital Signs report released today. This means that clinicians should not wait for the CDC’s case definition before diagnosis, the CDC said.
“When specimens are collected as soon as possible after symptom onset, we have a better chance of understanding the causes of AFM, these recurrent outbreaks, and developing a diagnostic test,” Dr. Schuchat said. “Rapid reporting also helps us to identify and respond to outbreaks early and alert other clinicians and the public.”
AFM appears to follow a seasonal and biennial pattern, with the number of cases increasing mainly in the late summer and early fall. As the season approaches where AFM cases increase, CDC is asking clinicians to look out for patients with suspected AFM so cases can be reported as early as possible.
Since the CDC began tracking AFM, the number of cases has risen every 2 years. In 2018, there were 233 cases in 41 states, the highest number of reported cases since the CDC began tracking AFM following an outbreak in 2014, according to a Vital Signs report. Overall, there have been 570 cases of AFM reported in 48 states and the District of Columbia since 2014.
There is yet to be a confirmatory test for AFM, but clinicians should obtain cerebrospinal fluid, serum, stool and nasopharyngeal swab from patients with suspected AFM as soon as possible, followed by an MRI. AFM has unique MRI features , such as gray matter involvement, that can help distinguish it from other diseases characterized by acute weakness.
In the Vital Signs report, which examined AFM in 2018, 92% of confirmed cases had respiratory symptoms or fever, and 42% of confirmed cases had upper limb involvement. The median time from limb weakness to hospitalization was 1 day, and time from weakness to MRI was 2 days. Cases were reported to the CDC a median of 18 days from onset of limb weakness, but time to reporting ranged between 18 days and 36 days, said Tom Clark, MD, MPH, deputy director of the division of viral diseases at CDC.
“This delay hampers our ability to understand the causes AFM,” he said. “We believe that recognizing AFM early is critical and can lead to better patient management.”
In lieu of a diagnostic test for AFM, clinicians should make management decisions through review of patient symptoms, exam findings, MRI, other test results, and in consulting with neurology experts. The Transverse Myelitis Association also has created a support portal for 24/7 physician consultation in AFM cases.
SOURCE: Lopez A et al. MMWR Morb Mortal Wkly Rep. 2019;68:1-7 .
the CDC said in a telebriefing.
Acute flaccid myelitis (AFM) is defined as acute, flaccid muscle weakness that occurs less than 1 week after a fever or respiratory illness. Viruses, including enterovirus, are believed to play a role in AFM, but the cause still is unknown. The disease appears mostly in children, and the average age of a patient diagnosed with AFM is 5 years.
“Doctors and other clinicians in the United States play a critical role,” Anne Schuchat, MD, principal deputy director of the Centers for Disease Control and Prevention, said in the telebriefing. “We ask for your help with early recognition of patients with AFM symptoms, prompt specimen collection for testing, and immediate reporting of suspected AFM cases to health departments.”
While there is no proven treatment for AFM, early diagnosis is critical to getting patients the best care possible, according to a Vital Signs report released today. This means that clinicians should not wait for the CDC’s case definition before diagnosis, the CDC said.
“When specimens are collected as soon as possible after symptom onset, we have a better chance of understanding the causes of AFM, these recurrent outbreaks, and developing a diagnostic test,” Dr. Schuchat said. “Rapid reporting also helps us to identify and respond to outbreaks early and alert other clinicians and the public.”
AFM appears to follow a seasonal and biennial pattern, with the number of cases increasing mainly in the late summer and early fall. As the season approaches where AFM cases increase, CDC is asking clinicians to look out for patients with suspected AFM so cases can be reported as early as possible.
Since the CDC began tracking AFM, the number of cases has risen every 2 years. In 2018, there were 233 cases in 41 states, the highest number of reported cases since the CDC began tracking AFM following an outbreak in 2014, according to a Vital Signs report. Overall, there have been 570 cases of AFM reported in 48 states and the District of Columbia since 2014.
There is yet to be a confirmatory test for AFM, but clinicians should obtain cerebrospinal fluid, serum, stool and nasopharyngeal swab from patients with suspected AFM as soon as possible, followed by an MRI. AFM has unique MRI features , such as gray matter involvement, that can help distinguish it from other diseases characterized by acute weakness.
In the Vital Signs report, which examined AFM in 2018, 92% of confirmed cases had respiratory symptoms or fever, and 42% of confirmed cases had upper limb involvement. The median time from limb weakness to hospitalization was 1 day, and time from weakness to MRI was 2 days. Cases were reported to the CDC a median of 18 days from onset of limb weakness, but time to reporting ranged between 18 days and 36 days, said Tom Clark, MD, MPH, deputy director of the division of viral diseases at CDC.
“This delay hampers our ability to understand the causes AFM,” he said. “We believe that recognizing AFM early is critical and can lead to better patient management.”
In lieu of a diagnostic test for AFM, clinicians should make management decisions through review of patient symptoms, exam findings, MRI, other test results, and in consulting with neurology experts. The Transverse Myelitis Association also has created a support portal for 24/7 physician consultation in AFM cases.
SOURCE: Lopez A et al. MMWR Morb Mortal Wkly Rep. 2019;68:1-7 .
NEWS FROM THE FDA/CDC