User login
Transdermal med may directly target hostility in schizophrenia
The results suggest that these effects are at least partially independent of general antipsychotic effects or effects on sedation or akathisia.
“It’s important not to assume that antipsychotics decrease hostility by having people feel more sedated and that the only way to treat someone hostile is by sedating them,” lead investigator Leslie Citrome, MD, MPH, clinical professor of psychiatry and behavioral sciences, New York Medical College, Valhalla, told this news organization.
“Our findings suggest that transdermal asenapine has a specific antihostility effect in patients with schizophrenia,” he added.

The study was published online in the Journal of Clinical Psychiatry.
A complex disorder
“Patients with schizophrenia are known to potentially exhibit aggressive, hostile behavior, especially during the acute phase of the illness, thus making effective management critical,” the authors write.
Dr. Citrome said schizophrenia is a complex condition that consists of five different symptom domains. These include positive (hallucinations, delusions), negative (amotivation, apathy), disorganization (cognitive symptoms), depression/anxiety, and excitability/hostility symptoms.
“These five domains are more or less independent of each other, in terms of treatment effects,” he noted.
Dr. Citrome has long been interested in the activity of antipsychotics and their impact on these various symptoms – particularly hostility – and recently published a review focusing on the impact of an array of antipsychotics on this symptom domain.
“What struck me here is that this is a transdermal system, a patch,” Dr. Citrome said. “None of the sedation that would ordinarily be associated with a sublingual asenapine would be present here.”
Dr. Citrome wanted to investigate whether the transdermal system would have an impact on hostility because, if so, “it would support the notion that hostility is an independent treatment target in schizophrenia.”
To investigate, Dr. Citrome and co-authors analyzed data from the pivotal HP-3070 phase 3 randomized, double-blind, placebo-controlled study of adults with schizophrenia who were randomly selected to receive either HP-3070 7.6 mg/24h, HP-3070 3.8 mg/24h, or placebo for 6 weeks.
The trial found that once-daily applications of HP-3070 demonstrated significant improvement in Positive and Negative Syndrome Scale (PANSS) total scores after 2-3 weeks of treatment, with the improvements sustained through week 6.
The current study was a post hoc analysis focusing specifically on 442 patients with hostility and agitation (defined as PANSS hostility item score > 1).
The outcome was the least-squares mean (LSM) changes in the PANSS hostility item. They also analyzed PANSS–Excited Component (PANSS-EC) from baseline to week 6 in all study participants. Findings were adjusted for the presence of somnolence or akathisia.
Demographic and baseline disease characteristics were “balanced” between the HP-3070–6.6-mg and the HP-3070–3.8-mg groups (n = 151 and n = 147, respectively) and the placebo group (n = 144) in the intent-to-treat analysis, with a mean (standard deviation) age of between 41.5 and 42.3 (11.6-11.9) years. Roughly three-quarters of participants were White, and most participants had a mean duration of between 15 and 16 years since diagnosis.
Independent effect
At week 6, the LSM mean change from baseline (CFB) in the PANSS hostility score was superior in both treatment groups at 6 weeks, compared with placebo (7.6 mg/24 hr: CFB, –0.4; 95% confidence interval, –0.6 to –0.2; P < .001; 3.8 mg/24 hr: CFB, –0.3; 95% CI, –0.6 to –0.1; P < .01).
The findings remained significant, even after the researchers adjusted for covariates.
For all patients, regardless of baseline PANSS hostility item score, PANSS-EC week 6 LSM CFB was greater in both treatment groups compared with placebo (7.6 mg/24 hr: CFB, –1.1; 95% CI, –1.9 to –0.4; P < .01; 3.8 mg/24 hr: CFB, –1.3; 95% CI, –2.0 to –0.6; P < .001).
Patients with a PANSS hostility score > 1 at baseline in both treatment groups also showed significant improvement in PANSS-EC score, compared with the placebo, beginning at week 2 and continuing through week 6.
“These effects of HP-3070 treatment on the PANSS hostility item score remained, even after adjustment for confounding variables, suggesting that the effect of HP-3070 on reducing symptoms of hostility may at be at least partially independent of general antipsychotic effects on hallucinations or delusions or the presence or absence of relevant medication-induced adverse effects, such as sedation or akathisia,” the authors comment.
They note that a limitation of the study is that it was conducted post hoc. In addition, the mean baseline PANSS hostility score was “low,” even among those with a score > 1, “translating to a severity level of minimal to mild,” which “limits the generalizability” of the analysis.
Important treatment target
Commenting on the study, Rifaat El-Mallakh, MD, MS, director of the Mood Disorders Research Program, department of psychiatry and behavioral sciences, University of Louisville (Ky.) School of Medicine, said, “aggression and hostility may exhibit themselves as symptoms of a psychotic illness or independent of psychosis and are an important treatment target.”
Dr. El-Mallakh, who was not involved with the study, said the “most effective anti-aggression medicine is clozapine.” He believes that it is this effect that “gives clozapine its stellar reputation,” rather than its antipsychotic effect.
“Of importance, the anti-aggression effect of clozapine is independent of its antipsychotic effect, which is an important point because if the behavior is rooted in psychosis, then successful treatment of psychosis with any agent should reduce aggression.”
The researchers “demonstrated that the effect was independent of psychosis” but because the study only recruited people with schizophrenia, the researchers “could not examine to see if the effect is independent of diagnosis,” Dr. El-Mallakh said.
“It is important to consider aggression/hostility as an independent behavior in pharmacologic studies, because it probably has its own biochemistry and neuroanatomy,” he added.
This study was funded by Hisamitsu Pharmaceutical. Dr. Citrome has received nonfinancial support from Hisamitsu Pharmaceutical and personal fees from Noven Pharmaceuticals during the conduct of the study; personal fees from numerous companies and organizations; and one-off ad hoc consulting for medical education companies such as Medscape, NACCME, NEI, Vindico, and universities and professional organizations/societies outside the submitted work. He has stocks and received royalties from numerous companies and organizations. Dr. El-Mallakh is a speaker for Noven, as well as Indivior, Intracellular, Janssen, Lundbeck, Otsuka, Sunovion, and Teva.
A version of this article first appeared on Medscape.com.
The results suggest that these effects are at least partially independent of general antipsychotic effects or effects on sedation or akathisia.
“It’s important not to assume that antipsychotics decrease hostility by having people feel more sedated and that the only way to treat someone hostile is by sedating them,” lead investigator Leslie Citrome, MD, MPH, clinical professor of psychiatry and behavioral sciences, New York Medical College, Valhalla, told this news organization.
“Our findings suggest that transdermal asenapine has a specific antihostility effect in patients with schizophrenia,” he added.
The study was published online in the Journal of Clinical Psychiatry.
A complex disorder
“Patients with schizophrenia are known to potentially exhibit aggressive, hostile behavior, especially during the acute phase of the illness, thus making effective management critical,” the authors write.
Dr. Citrome said schizophrenia is a complex condition that consists of five different symptom domains. These include positive (hallucinations, delusions), negative (amotivation, apathy), disorganization (cognitive symptoms), depression/anxiety, and excitability/hostility symptoms.
“These five domains are more or less independent of each other, in terms of treatment effects,” he noted.
Dr. Citrome has long been interested in the activity of antipsychotics and their impact on these various symptoms – particularly hostility – and recently published a review focusing on the impact of an array of antipsychotics on this symptom domain.
“What struck me here is that this is a transdermal system, a patch,” Dr. Citrome said. “None of the sedation that would ordinarily be associated with a sublingual asenapine would be present here.”
Dr. Citrome wanted to investigate whether the transdermal system would have an impact on hostility because, if so, “it would support the notion that hostility is an independent treatment target in schizophrenia.”
To investigate, Dr. Citrome and co-authors analyzed data from the pivotal HP-3070 phase 3 randomized, double-blind, placebo-controlled study of adults with schizophrenia who were randomly selected to receive either HP-3070 7.6 mg/24h, HP-3070 3.8 mg/24h, or placebo for 6 weeks.
The trial found that once-daily applications of HP-3070 demonstrated significant improvement in Positive and Negative Syndrome Scale (PANSS) total scores after 2-3 weeks of treatment, with the improvements sustained through week 6.
The current study was a post hoc analysis focusing specifically on 442 patients with hostility and agitation (defined as PANSS hostility item score > 1).
The outcome was the least-squares mean (LSM) changes in the PANSS hostility item. They also analyzed PANSS–Excited Component (PANSS-EC) from baseline to week 6 in all study participants. Findings were adjusted for the presence of somnolence or akathisia.
Demographic and baseline disease characteristics were “balanced” between the HP-3070–6.6-mg and the HP-3070–3.8-mg groups (n = 151 and n = 147, respectively) and the placebo group (n = 144) in the intent-to-treat analysis, with a mean (standard deviation) age of between 41.5 and 42.3 (11.6-11.9) years. Roughly three-quarters of participants were White, and most participants had a mean duration of between 15 and 16 years since diagnosis.
Independent effect
At week 6, the LSM mean change from baseline (CFB) in the PANSS hostility score was superior in both treatment groups at 6 weeks, compared with placebo (7.6 mg/24 hr: CFB, –0.4; 95% confidence interval, –0.6 to –0.2; P < .001; 3.8 mg/24 hr: CFB, –0.3; 95% CI, –0.6 to –0.1; P < .01).
The findings remained significant, even after the researchers adjusted for covariates.
For all patients, regardless of baseline PANSS hostility item score, PANSS-EC week 6 LSM CFB was greater in both treatment groups compared with placebo (7.6 mg/24 hr: CFB, –1.1; 95% CI, –1.9 to –0.4; P < .01; 3.8 mg/24 hr: CFB, –1.3; 95% CI, –2.0 to –0.6; P < .001).
Patients with a PANSS hostility score > 1 at baseline in both treatment groups also showed significant improvement in PANSS-EC score, compared with the placebo, beginning at week 2 and continuing through week 6.
“These effects of HP-3070 treatment on the PANSS hostility item score remained, even after adjustment for confounding variables, suggesting that the effect of HP-3070 on reducing symptoms of hostility may at be at least partially independent of general antipsychotic effects on hallucinations or delusions or the presence or absence of relevant medication-induced adverse effects, such as sedation or akathisia,” the authors comment.
They note that a limitation of the study is that it was conducted post hoc. In addition, the mean baseline PANSS hostility score was “low,” even among those with a score > 1, “translating to a severity level of minimal to mild,” which “limits the generalizability” of the analysis.
Important treatment target
Commenting on the study, Rifaat El-Mallakh, MD, MS, director of the Mood Disorders Research Program, department of psychiatry and behavioral sciences, University of Louisville (Ky.) School of Medicine, said, “aggression and hostility may exhibit themselves as symptoms of a psychotic illness or independent of psychosis and are an important treatment target.”
Dr. El-Mallakh, who was not involved with the study, said the “most effective anti-aggression medicine is clozapine.” He believes that it is this effect that “gives clozapine its stellar reputation,” rather than its antipsychotic effect.
“Of importance, the anti-aggression effect of clozapine is independent of its antipsychotic effect, which is an important point because if the behavior is rooted in psychosis, then successful treatment of psychosis with any agent should reduce aggression.”
The researchers “demonstrated that the effect was independent of psychosis” but because the study only recruited people with schizophrenia, the researchers “could not examine to see if the effect is independent of diagnosis,” Dr. El-Mallakh said.
“It is important to consider aggression/hostility as an independent behavior in pharmacologic studies, because it probably has its own biochemistry and neuroanatomy,” he added.
This study was funded by Hisamitsu Pharmaceutical. Dr. Citrome has received nonfinancial support from Hisamitsu Pharmaceutical and personal fees from Noven Pharmaceuticals during the conduct of the study; personal fees from numerous companies and organizations; and one-off ad hoc consulting for medical education companies such as Medscape, NACCME, NEI, Vindico, and universities and professional organizations/societies outside the submitted work. He has stocks and received royalties from numerous companies and organizations. Dr. El-Mallakh is a speaker for Noven, as well as Indivior, Intracellular, Janssen, Lundbeck, Otsuka, Sunovion, and Teva.
A version of this article first appeared on Medscape.com.
The results suggest that these effects are at least partially independent of general antipsychotic effects or effects on sedation or akathisia.
“It’s important not to assume that antipsychotics decrease hostility by having people feel more sedated and that the only way to treat someone hostile is by sedating them,” lead investigator Leslie Citrome, MD, MPH, clinical professor of psychiatry and behavioral sciences, New York Medical College, Valhalla, told this news organization.
“Our findings suggest that transdermal asenapine has a specific antihostility effect in patients with schizophrenia,” he added.
The study was published online in the Journal of Clinical Psychiatry.
A complex disorder
“Patients with schizophrenia are known to potentially exhibit aggressive, hostile behavior, especially during the acute phase of the illness, thus making effective management critical,” the authors write.
Dr. Citrome said schizophrenia is a complex condition that consists of five different symptom domains. These include positive (hallucinations, delusions), negative (amotivation, apathy), disorganization (cognitive symptoms), depression/anxiety, and excitability/hostility symptoms.
“These five domains are more or less independent of each other, in terms of treatment effects,” he noted.
Dr. Citrome has long been interested in the activity of antipsychotics and their impact on these various symptoms – particularly hostility – and recently published a review focusing on the impact of an array of antipsychotics on this symptom domain.
“What struck me here is that this is a transdermal system, a patch,” Dr. Citrome said. “None of the sedation that would ordinarily be associated with a sublingual asenapine would be present here.”
Dr. Citrome wanted to investigate whether the transdermal system would have an impact on hostility because, if so, “it would support the notion that hostility is an independent treatment target in schizophrenia.”
To investigate, Dr. Citrome and co-authors analyzed data from the pivotal HP-3070 phase 3 randomized, double-blind, placebo-controlled study of adults with schizophrenia who were randomly selected to receive either HP-3070 7.6 mg/24h, HP-3070 3.8 mg/24h, or placebo for 6 weeks.
The trial found that once-daily applications of HP-3070 demonstrated significant improvement in Positive and Negative Syndrome Scale (PANSS) total scores after 2-3 weeks of treatment, with the improvements sustained through week 6.
The current study was a post hoc analysis focusing specifically on 442 patients with hostility and agitation (defined as PANSS hostility item score > 1).
The outcome was the least-squares mean (LSM) changes in the PANSS hostility item. They also analyzed PANSS–Excited Component (PANSS-EC) from baseline to week 6 in all study participants. Findings were adjusted for the presence of somnolence or akathisia.
Demographic and baseline disease characteristics were “balanced” between the HP-3070–6.6-mg and the HP-3070–3.8-mg groups (n = 151 and n = 147, respectively) and the placebo group (n = 144) in the intent-to-treat analysis, with a mean (standard deviation) age of between 41.5 and 42.3 (11.6-11.9) years. Roughly three-quarters of participants were White, and most participants had a mean duration of between 15 and 16 years since diagnosis.
Independent effect
At week 6, the LSM mean change from baseline (CFB) in the PANSS hostility score was superior in both treatment groups at 6 weeks, compared with placebo (7.6 mg/24 hr: CFB, –0.4; 95% confidence interval, –0.6 to –0.2; P < .001; 3.8 mg/24 hr: CFB, –0.3; 95% CI, –0.6 to –0.1; P < .01).
The findings remained significant, even after the researchers adjusted for covariates.
For all patients, regardless of baseline PANSS hostility item score, PANSS-EC week 6 LSM CFB was greater in both treatment groups compared with placebo (7.6 mg/24 hr: CFB, –1.1; 95% CI, –1.9 to –0.4; P < .01; 3.8 mg/24 hr: CFB, –1.3; 95% CI, –2.0 to –0.6; P < .001).
Patients with a PANSS hostility score > 1 at baseline in both treatment groups also showed significant improvement in PANSS-EC score, compared with the placebo, beginning at week 2 and continuing through week 6.
“These effects of HP-3070 treatment on the PANSS hostility item score remained, even after adjustment for confounding variables, suggesting that the effect of HP-3070 on reducing symptoms of hostility may at be at least partially independent of general antipsychotic effects on hallucinations or delusions or the presence or absence of relevant medication-induced adverse effects, such as sedation or akathisia,” the authors comment.
They note that a limitation of the study is that it was conducted post hoc. In addition, the mean baseline PANSS hostility score was “low,” even among those with a score > 1, “translating to a severity level of minimal to mild,” which “limits the generalizability” of the analysis.
Important treatment target
Commenting on the study, Rifaat El-Mallakh, MD, MS, director of the Mood Disorders Research Program, department of psychiatry and behavioral sciences, University of Louisville (Ky.) School of Medicine, said, “aggression and hostility may exhibit themselves as symptoms of a psychotic illness or independent of psychosis and are an important treatment target.”
Dr. El-Mallakh, who was not involved with the study, said the “most effective anti-aggression medicine is clozapine.” He believes that it is this effect that “gives clozapine its stellar reputation,” rather than its antipsychotic effect.
“Of importance, the anti-aggression effect of clozapine is independent of its antipsychotic effect, which is an important point because if the behavior is rooted in psychosis, then successful treatment of psychosis with any agent should reduce aggression.”
The researchers “demonstrated that the effect was independent of psychosis” but because the study only recruited people with schizophrenia, the researchers “could not examine to see if the effect is independent of diagnosis,” Dr. El-Mallakh said.
“It is important to consider aggression/hostility as an independent behavior in pharmacologic studies, because it probably has its own biochemistry and neuroanatomy,” he added.
This study was funded by Hisamitsu Pharmaceutical. Dr. Citrome has received nonfinancial support from Hisamitsu Pharmaceutical and personal fees from Noven Pharmaceuticals during the conduct of the study; personal fees from numerous companies and organizations; and one-off ad hoc consulting for medical education companies such as Medscape, NACCME, NEI, Vindico, and universities and professional organizations/societies outside the submitted work. He has stocks and received royalties from numerous companies and organizations. Dr. El-Mallakh is a speaker for Noven, as well as Indivior, Intracellular, Janssen, Lundbeck, Otsuka, Sunovion, and Teva.
A version of this article first appeared on Medscape.com.
FROM THE JOURNAL OF CLINICAL PSYCHIATRY
Advance directives for psychiatric care reduce compulsory admissions
, new research shows.
Results of a randomized trial showed the peer worker PAD group had a 42% reduction in compulsory admission over the following 12 months. This study group also had lower symptom scores, greater rates of recovery, and increased empowerment, compared with patients assigned to usual care.
In addition to proving that PADs are effective in reducing compulsory admission, the results show that facilitation by peer workers is relevant, study investigator Aurélie Tinland, MD, PhD, Faculté de Médecine Timone, Aix-Marseille University, Marseille, France, told delegates attending the virtual European Psychiatric Association (EPA) 2022 Congress. The study was simultaneously published online in JAMA Psychiatry.
However, Dr. Tinland noted that more research that includes “harder to reach” populations is needed. In addition, greater use of PADs is also key to reducing compulsory admissions.
‘Most coercive’ country
The researchers note that respect for patient autonomy is a strong pillar of health care, such that “involuntary treatment should be unusual.” However, they point out that “compulsory psychiatric admissions are far too common in countries of all income levels.”
In France, said Dr. Tinland, 24% of psychiatric hospitalizations are compulsory. The country is ranked the sixth “most coercive” country in the world, and there are concerns about human rights in French psychiatric facilities.
She added that advance care statements are the most efficient tool for reducing coercion, with one study suggesting they could cut rates by 25%, compared with usual care.
However, she noted there is an “asymmetry” between medical professionals and patients and a risk of “undue influence” when clinicians facilitate the completion of care statements.
To examine the impact on clinical outcomes of peer-worker facilitated PADs, the researchers studied adults with a diagnosis of schizophrenia, bipolar I disorder, or schizoaffective disorder who were admitted to a psychiatric hospital within the previous 12 months. Peer workers are individuals who have lived experience with mental illness and help inform and guide current patients about care options in the event of a mental health crisis.
Study participants were randomly assigned 1:1 to an intervention group or a usual care control group. The intervention group received a PAD document and were assigned a peer worker while the usual care group received comprehensive information about the PAD concept at study entry and were free to complete it, but they were not connected with a peer worker.
The PAD document included information about future treatment and support preferences, early signs of relapse, and coping strategies. Participants could meet the peer worker in a place of their choice and be supported in drafting the document and in sharing it with health care professionals.
In all, 394 individuals completed the study. The majority (61%) of participants were male and 66% had completed post-secondary education. Schizophrenia was diagnosed in 45%, bipolar I disorder in 36%, and schizoaffective disorder in 19%.
Participants in the intervention group were significantly younger than those in the control group, with a mean of 37.4 years versus 41 years (P = .003) and were less likely to have one or more somatic comorbidities, at 61.2% versus 69.2%.
A PAD was completed by 54.6% of individuals in the intervention group versus 7.1% of controls (P < .001). The PAD was written with peer worker support by 41.3% of those in the intervention and by 2% of controls. Of those who completed a PAD, 75.7% met care facilitators, and 27.1% used it during a crisis over the following 12 months.
Results showed that the rate of compulsory admissions was significantly lower in the peer worker PAD group, at 27% versus 39.9% in control participants, at an odds ratio of 0.58 (P = .007).
Participants in the intervention group had lower symptoms on the modified Colorado Symptom Score than usual care patients with an effect size of -0.20 (P = .03) and higher scores on the Empowerment Scale (effect size 0.30, P = .003).
Scores on the Recovery Assessment Scale were also significantly higher in the peer worker PAD group versus controls with an effect size of 0.44 (P < .001). There were no significant differences, however, in overall admission rates, the quality of the therapeutic alliance, or quality of life.
Putting patients in the driver’s seat
Commenting on the findings, Robert Dabney Jr., MA, MDiv, peer apprentice program manager at the Depression and Bipolar Support Alliance, Chicago, said the study “tells us there are many benefits to completing a psychiatric advance directive, but perhaps the most powerful one is putting the person receiving mental health care in the driver’s seat of their own recovery.”
However, he noted that “many people living with mental health conditions don’t know the option exists to decide on their treatment plan in advance of a crisis.”
“This is where peer support specialists can come in. Having a peer who has been through similar experiences and can guide you through the process is as comforting as it is empowering. I have witnessed and experienced firsthand the power of peer support,” he said.
“It’s my personal hope and the goal of the Depression and Bipolar Support Alliance to empower more people to either become peer support specialists or seek out peer support services, because we know it improves and even saves lives,” Mr. Dabney added.
Virginia A. Brown, PhD, department of psychiatry & behavioral sciences, University of Texas at Austin Dell Medical School, noted there are huge differences between the health care systems in France and the United States.
She explained that two of the greatest barriers to PADs in the United States is that until 2016, filling one out was not billable and that “practitioners don’t know anything about advanced care plans.”
Dr. Brown said her own work shows that individuals who support patients during a crisis believe it would be “really helpful if we had some kind of document that we could share with the health care system that says: ‘Hey, look, I’m the designated person to speak for this patient, they’ve identified me through a document.’ So, people were actually describing a need for this document but didn’t know that it existed.”
Another problem is that in the United States, hospitals operate in a “closed system” and cannot talk to an unrelated hospital or to the police department “to get information to those first responders during an emergency about who to talk to about their wishes and preferences.”
“There are a lot of hurdles that we’ve got to get over to make a more robust system that protects the autonomy of people who live with serious mental illness,” Dr. Brown said, as “losing capacity during a crisis is time-limited, and it requires us to respond to it as a medical emergency.”
The study was supported by an institutional grant from the French 2017 National Program of Health Services Research. The Clinical Research Direction of Assistance Publique Hôpitaux de Marseille sponsored the trial. Dr. Tinland declares grants from the French Ministry of Health Directorate General of Health Care Services during the conduct of the study.
A version of this article first appeared on Medscape.com.
, new research shows.
Results of a randomized trial showed the peer worker PAD group had a 42% reduction in compulsory admission over the following 12 months. This study group also had lower symptom scores, greater rates of recovery, and increased empowerment, compared with patients assigned to usual care.
In addition to proving that PADs are effective in reducing compulsory admission, the results show that facilitation by peer workers is relevant, study investigator Aurélie Tinland, MD, PhD, Faculté de Médecine Timone, Aix-Marseille University, Marseille, France, told delegates attending the virtual European Psychiatric Association (EPA) 2022 Congress. The study was simultaneously published online in JAMA Psychiatry.
However, Dr. Tinland noted that more research that includes “harder to reach” populations is needed. In addition, greater use of PADs is also key to reducing compulsory admissions.
‘Most coercive’ country
The researchers note that respect for patient autonomy is a strong pillar of health care, such that “involuntary treatment should be unusual.” However, they point out that “compulsory psychiatric admissions are far too common in countries of all income levels.”
In France, said Dr. Tinland, 24% of psychiatric hospitalizations are compulsory. The country is ranked the sixth “most coercive” country in the world, and there are concerns about human rights in French psychiatric facilities.
She added that advance care statements are the most efficient tool for reducing coercion, with one study suggesting they could cut rates by 25%, compared with usual care.
However, she noted there is an “asymmetry” between medical professionals and patients and a risk of “undue influence” when clinicians facilitate the completion of care statements.
To examine the impact on clinical outcomes of peer-worker facilitated PADs, the researchers studied adults with a diagnosis of schizophrenia, bipolar I disorder, or schizoaffective disorder who were admitted to a psychiatric hospital within the previous 12 months. Peer workers are individuals who have lived experience with mental illness and help inform and guide current patients about care options in the event of a mental health crisis.
Study participants were randomly assigned 1:1 to an intervention group or a usual care control group. The intervention group received a PAD document and were assigned a peer worker while the usual care group received comprehensive information about the PAD concept at study entry and were free to complete it, but they were not connected with a peer worker.
The PAD document included information about future treatment and support preferences, early signs of relapse, and coping strategies. Participants could meet the peer worker in a place of their choice and be supported in drafting the document and in sharing it with health care professionals.
In all, 394 individuals completed the study. The majority (61%) of participants were male and 66% had completed post-secondary education. Schizophrenia was diagnosed in 45%, bipolar I disorder in 36%, and schizoaffective disorder in 19%.
Participants in the intervention group were significantly younger than those in the control group, with a mean of 37.4 years versus 41 years (P = .003) and were less likely to have one or more somatic comorbidities, at 61.2% versus 69.2%.
A PAD was completed by 54.6% of individuals in the intervention group versus 7.1% of controls (P < .001). The PAD was written with peer worker support by 41.3% of those in the intervention and by 2% of controls. Of those who completed a PAD, 75.7% met care facilitators, and 27.1% used it during a crisis over the following 12 months.
Results showed that the rate of compulsory admissions was significantly lower in the peer worker PAD group, at 27% versus 39.9% in control participants, at an odds ratio of 0.58 (P = .007).
Participants in the intervention group had lower symptoms on the modified Colorado Symptom Score than usual care patients with an effect size of -0.20 (P = .03) and higher scores on the Empowerment Scale (effect size 0.30, P = .003).
Scores on the Recovery Assessment Scale were also significantly higher in the peer worker PAD group versus controls with an effect size of 0.44 (P < .001). There were no significant differences, however, in overall admission rates, the quality of the therapeutic alliance, or quality of life.
Putting patients in the driver’s seat
Commenting on the findings, Robert Dabney Jr., MA, MDiv, peer apprentice program manager at the Depression and Bipolar Support Alliance, Chicago, said the study “tells us there are many benefits to completing a psychiatric advance directive, but perhaps the most powerful one is putting the person receiving mental health care in the driver’s seat of their own recovery.”
However, he noted that “many people living with mental health conditions don’t know the option exists to decide on their treatment plan in advance of a crisis.”
“This is where peer support specialists can come in. Having a peer who has been through similar experiences and can guide you through the process is as comforting as it is empowering. I have witnessed and experienced firsthand the power of peer support,” he said.
“It’s my personal hope and the goal of the Depression and Bipolar Support Alliance to empower more people to either become peer support specialists or seek out peer support services, because we know it improves and even saves lives,” Mr. Dabney added.
Virginia A. Brown, PhD, department of psychiatry & behavioral sciences, University of Texas at Austin Dell Medical School, noted there are huge differences between the health care systems in France and the United States.
She explained that two of the greatest barriers to PADs in the United States is that until 2016, filling one out was not billable and that “practitioners don’t know anything about advanced care plans.”
Dr. Brown said her own work shows that individuals who support patients during a crisis believe it would be “really helpful if we had some kind of document that we could share with the health care system that says: ‘Hey, look, I’m the designated person to speak for this patient, they’ve identified me through a document.’ So, people were actually describing a need for this document but didn’t know that it existed.”
Another problem is that in the United States, hospitals operate in a “closed system” and cannot talk to an unrelated hospital or to the police department “to get information to those first responders during an emergency about who to talk to about their wishes and preferences.”
“There are a lot of hurdles that we’ve got to get over to make a more robust system that protects the autonomy of people who live with serious mental illness,” Dr. Brown said, as “losing capacity during a crisis is time-limited, and it requires us to respond to it as a medical emergency.”
The study was supported by an institutional grant from the French 2017 National Program of Health Services Research. The Clinical Research Direction of Assistance Publique Hôpitaux de Marseille sponsored the trial. Dr. Tinland declares grants from the French Ministry of Health Directorate General of Health Care Services during the conduct of the study.
A version of this article first appeared on Medscape.com.
, new research shows.
Results of a randomized trial showed the peer worker PAD group had a 42% reduction in compulsory admission over the following 12 months. This study group also had lower symptom scores, greater rates of recovery, and increased empowerment, compared with patients assigned to usual care.
In addition to proving that PADs are effective in reducing compulsory admission, the results show that facilitation by peer workers is relevant, study investigator Aurélie Tinland, MD, PhD, Faculté de Médecine Timone, Aix-Marseille University, Marseille, France, told delegates attending the virtual European Psychiatric Association (EPA) 2022 Congress. The study was simultaneously published online in JAMA Psychiatry.
However, Dr. Tinland noted that more research that includes “harder to reach” populations is needed. In addition, greater use of PADs is also key to reducing compulsory admissions.
‘Most coercive’ country
The researchers note that respect for patient autonomy is a strong pillar of health care, such that “involuntary treatment should be unusual.” However, they point out that “compulsory psychiatric admissions are far too common in countries of all income levels.”
In France, said Dr. Tinland, 24% of psychiatric hospitalizations are compulsory. The country is ranked the sixth “most coercive” country in the world, and there are concerns about human rights in French psychiatric facilities.
She added that advance care statements are the most efficient tool for reducing coercion, with one study suggesting they could cut rates by 25%, compared with usual care.
However, she noted there is an “asymmetry” between medical professionals and patients and a risk of “undue influence” when clinicians facilitate the completion of care statements.
To examine the impact on clinical outcomes of peer-worker facilitated PADs, the researchers studied adults with a diagnosis of schizophrenia, bipolar I disorder, or schizoaffective disorder who were admitted to a psychiatric hospital within the previous 12 months. Peer workers are individuals who have lived experience with mental illness and help inform and guide current patients about care options in the event of a mental health crisis.
Study participants were randomly assigned 1:1 to an intervention group or a usual care control group. The intervention group received a PAD document and were assigned a peer worker while the usual care group received comprehensive information about the PAD concept at study entry and were free to complete it, but they were not connected with a peer worker.
The PAD document included information about future treatment and support preferences, early signs of relapse, and coping strategies. Participants could meet the peer worker in a place of their choice and be supported in drafting the document and in sharing it with health care professionals.
In all, 394 individuals completed the study. The majority (61%) of participants were male and 66% had completed post-secondary education. Schizophrenia was diagnosed in 45%, bipolar I disorder in 36%, and schizoaffective disorder in 19%.
Participants in the intervention group were significantly younger than those in the control group, with a mean of 37.4 years versus 41 years (P = .003) and were less likely to have one or more somatic comorbidities, at 61.2% versus 69.2%.
A PAD was completed by 54.6% of individuals in the intervention group versus 7.1% of controls (P < .001). The PAD was written with peer worker support by 41.3% of those in the intervention and by 2% of controls. Of those who completed a PAD, 75.7% met care facilitators, and 27.1% used it during a crisis over the following 12 months.
Results showed that the rate of compulsory admissions was significantly lower in the peer worker PAD group, at 27% versus 39.9% in control participants, at an odds ratio of 0.58 (P = .007).
Participants in the intervention group had lower symptoms on the modified Colorado Symptom Score than usual care patients with an effect size of -0.20 (P = .03) and higher scores on the Empowerment Scale (effect size 0.30, P = .003).
Scores on the Recovery Assessment Scale were also significantly higher in the peer worker PAD group versus controls with an effect size of 0.44 (P < .001). There were no significant differences, however, in overall admission rates, the quality of the therapeutic alliance, or quality of life.
Putting patients in the driver’s seat
Commenting on the findings, Robert Dabney Jr., MA, MDiv, peer apprentice program manager at the Depression and Bipolar Support Alliance, Chicago, said the study “tells us there are many benefits to completing a psychiatric advance directive, but perhaps the most powerful one is putting the person receiving mental health care in the driver’s seat of their own recovery.”
However, he noted that “many people living with mental health conditions don’t know the option exists to decide on their treatment plan in advance of a crisis.”
“This is where peer support specialists can come in. Having a peer who has been through similar experiences and can guide you through the process is as comforting as it is empowering. I have witnessed and experienced firsthand the power of peer support,” he said.
“It’s my personal hope and the goal of the Depression and Bipolar Support Alliance to empower more people to either become peer support specialists or seek out peer support services, because we know it improves and even saves lives,” Mr. Dabney added.
Virginia A. Brown, PhD, department of psychiatry & behavioral sciences, University of Texas at Austin Dell Medical School, noted there are huge differences between the health care systems in France and the United States.
She explained that two of the greatest barriers to PADs in the United States is that until 2016, filling one out was not billable and that “practitioners don’t know anything about advanced care plans.”
Dr. Brown said her own work shows that individuals who support patients during a crisis believe it would be “really helpful if we had some kind of document that we could share with the health care system that says: ‘Hey, look, I’m the designated person to speak for this patient, they’ve identified me through a document.’ So, people were actually describing a need for this document but didn’t know that it existed.”
Another problem is that in the United States, hospitals operate in a “closed system” and cannot talk to an unrelated hospital or to the police department “to get information to those first responders during an emergency about who to talk to about their wishes and preferences.”
“There are a lot of hurdles that we’ve got to get over to make a more robust system that protects the autonomy of people who live with serious mental illness,” Dr. Brown said, as “losing capacity during a crisis is time-limited, and it requires us to respond to it as a medical emergency.”
The study was supported by an institutional grant from the French 2017 National Program of Health Services Research. The Clinical Research Direction of Assistance Publique Hôpitaux de Marseille sponsored the trial. Dr. Tinland declares grants from the French Ministry of Health Directorate General of Health Care Services during the conduct of the study.
A version of this article first appeared on Medscape.com.
FROM EPA 2022
FDA panel rejects pimavanserin for Alzheimer’s psychosis
In a 9-3 vote, the Psychopharmacologic Drugs Advisory Committee (PDAC) found that the drug’s manufacturer failed to offer convincing evidence of its efficacy in patients with ADP.
The June 17 rejection was the second rejection in as many years for a new indication for pimavanserin, which was approved in 2016 for Parkinson’s disease psychosis (PDP).
In April 2021, the FDA denied Acadia’s supplemental new drug application to expand the drug’s indication to include the treatment of all dementia-related psychosis, regardless of the underlying cause of dementia, citing issues with two studies the company presented as evidence of efficacy.

For the current application, Acadia submitted some new analysis of those studies but limited its application to ADP, which affects up to 30% of patients with Alzheimer’s disease (AD) and currently has no approved treatment.
Committee members who opposed the application were moved by testimony from caregivers and clinicians who treat patients with ADP but ultimately decided the evidence offered by Acadia once again failed to meet the threshold needed to demonstrate efficacy for an expanded indication.
“Sometimes I struggle with a decision on an advisory committee, but not today,” Dean Follmann, PhD, assistant director for biostatistics, National Institute of Allergy and Infectious Diseases, Bethesda, Md., said of his “no” vote.
Lack of efficacy
Pimavanserin is a selective serotonin inverse agonist and antagonist preferentially targeting 5-HT2A receptors, which are thought to play an important role in psychosis, schizophrenia, depression, and other neuropsychiatric disorders.
When it rejected Acadia’s original, broader application for pimavanserin for all dementia-related psychosis, the FDA found that the HARMONY phase 3 trial, previously covered by this news organization, was underpowered to assess efficacy in specific dementia patient subgroups and lacked statistical significance of efficacy in patients with AD. In addition, it noted that overall findings appeared to be driven by results in patients with Parkinson’s disease dementia, a condition already covered by the approved indication.
The FDA found that the second study, referred to in the June 17 hearing as Study 019, which was also previously reported by this news organization, was not “an adequate and well-controlled study.”
Specifically, the agency raised concerns about “protocol deviations,” such as the inclusion of patients who lacked clear documentation that psychotic symptoms developed after an AD diagnosis had been established and patients who received exclusionary medications at the time of randomization.
Discussions between Acadia and the FDA continued over the past year, with the company submitting new analyses and responses. An FDA briefing document published in advance of the committee meeting seemed to suggest the agency was satisfied with Acadia’s response.
Lack of diversity
The advisory committee disagreed, pointing to the same concerns raised last year. Members raised concerns about patient diversity in the HARMONY trial, which included an almost entirely White and mostly male study population.
In addition, although the findings at 26 weeks did demonstrate a marked improvement in psychosis symptoms overall, committee members noted that, again, those findings were largely driven by efficacy in patients with Parkinson’s disease dementia, for which the drug is already approved.
When discussing the phase 2 Study 019, the committee noted that while the study met the primary outcome of improvement in psychosis at 6 weeks, those positive responses were not found at any other timepoint in the 12-week study.
“While it might have had a positive numerical effect in the study, the evidence is really not there to support it,” Dr. Follmann said.
Dr. Follmann and other committee members called for additional trials that focus on patients with Alzheimer’s disease, have a longer follow-up, and include more gender and racial diversity in the study population. They also called for more information about any off-label use of pimavanserin for ADP since it was approved for PDP in 2016.
An unmet need
Most individuals who testified during the public comment period pleaded with the committee to vote in favor of the new indication, sharing stories of family members and patients with ADP.
“I have been caring for and studying patients with Alzheimer’s disease and other dementias for more than 30 years, and I can tell you very simply that if left untreated, psychosis has significant and sometimes devastating consequences for our patients,” said Pierre Tariot, MD, director of the Banner Alzheimer’s Institute and a research professor of psychiatry at the University of Arizona College of Medicine, Tucson, and an investigator on the HARMONY trial.
Those on the committee who voted against the application were quick to agree that lack of an approved treatment for ADP presents a hardship.
“I’m a neurologist who has cared for patients for more than 20 years,” said Madhav R. Thambisetty, MD, PhD, senior investigator for the National Institute on Aging and an adjunct professor of neurology at Johns Hopkins University School of Medicine, Baltimore. “I recognize the unmet need in the field, I just think that the unmet need should not be a justification to cut corners.”
The committee did not focus on drug safety or unmet need in its deliberations, although information on both were presented during the meeting.
Commenting on his “no” vote, PDAC member Walter S. Dunn, MD, PhD, assistant clinical professor of psychiatry at the University of California, Los Angeles, and director of Interventional Psychiatry Service at West Los Angeles Veterans Affairs Medical Center, said he hopes that the FDA will consider those issues more broadly as they complete their review.
“The questions before the committee have been narrow and precise, so I trust the agency will take a broader approach in their final decision about approval,” Dr. Dunn said.
Commenting on the decision, Howard Fillit, MD, cofounder and chief science officer, Alzheimer’s Drug Discovery Foundation, called the news disappointing, “but while the unmet need for a treatment for ADP is clear, it is vital that approved treatments meet stringent safety and efficacy criteria so we can offer patients medications with clear benefits.”
The FDA will make its final decision by August 4.
A version of this article first appeared on Medscape.com.
In a 9-3 vote, the Psychopharmacologic Drugs Advisory Committee (PDAC) found that the drug’s manufacturer failed to offer convincing evidence of its efficacy in patients with ADP.
The June 17 rejection was the second rejection in as many years for a new indication for pimavanserin, which was approved in 2016 for Parkinson’s disease psychosis (PDP).
In April 2021, the FDA denied Acadia’s supplemental new drug application to expand the drug’s indication to include the treatment of all dementia-related psychosis, regardless of the underlying cause of dementia, citing issues with two studies the company presented as evidence of efficacy.
For the current application, Acadia submitted some new analysis of those studies but limited its application to ADP, which affects up to 30% of patients with Alzheimer’s disease (AD) and currently has no approved treatment.
Committee members who opposed the application were moved by testimony from caregivers and clinicians who treat patients with ADP but ultimately decided the evidence offered by Acadia once again failed to meet the threshold needed to demonstrate efficacy for an expanded indication.
“Sometimes I struggle with a decision on an advisory committee, but not today,” Dean Follmann, PhD, assistant director for biostatistics, National Institute of Allergy and Infectious Diseases, Bethesda, Md., said of his “no” vote.
Lack of efficacy
Pimavanserin is a selective serotonin inverse agonist and antagonist preferentially targeting 5-HT2A receptors, which are thought to play an important role in psychosis, schizophrenia, depression, and other neuropsychiatric disorders.
When it rejected Acadia’s original, broader application for pimavanserin for all dementia-related psychosis, the FDA found that the HARMONY phase 3 trial, previously covered by this news organization, was underpowered to assess efficacy in specific dementia patient subgroups and lacked statistical significance of efficacy in patients with AD. In addition, it noted that overall findings appeared to be driven by results in patients with Parkinson’s disease dementia, a condition already covered by the approved indication.
The FDA found that the second study, referred to in the June 17 hearing as Study 019, which was also previously reported by this news organization, was not “an adequate and well-controlled study.”
Specifically, the agency raised concerns about “protocol deviations,” such as the inclusion of patients who lacked clear documentation that psychotic symptoms developed after an AD diagnosis had been established and patients who received exclusionary medications at the time of randomization.
Discussions between Acadia and the FDA continued over the past year, with the company submitting new analyses and responses. An FDA briefing document published in advance of the committee meeting seemed to suggest the agency was satisfied with Acadia’s response.
Lack of diversity
The advisory committee disagreed, pointing to the same concerns raised last year. Members raised concerns about patient diversity in the HARMONY trial, which included an almost entirely White and mostly male study population.
In addition, although the findings at 26 weeks did demonstrate a marked improvement in psychosis symptoms overall, committee members noted that, again, those findings were largely driven by efficacy in patients with Parkinson’s disease dementia, for which the drug is already approved.
When discussing the phase 2 Study 019, the committee noted that while the study met the primary outcome of improvement in psychosis at 6 weeks, those positive responses were not found at any other timepoint in the 12-week study.
“While it might have had a positive numerical effect in the study, the evidence is really not there to support it,” Dr. Follmann said.
Dr. Follmann and other committee members called for additional trials that focus on patients with Alzheimer’s disease, have a longer follow-up, and include more gender and racial diversity in the study population. They also called for more information about any off-label use of pimavanserin for ADP since it was approved for PDP in 2016.
An unmet need
Most individuals who testified during the public comment period pleaded with the committee to vote in favor of the new indication, sharing stories of family members and patients with ADP.
“I have been caring for and studying patients with Alzheimer’s disease and other dementias for more than 30 years, and I can tell you very simply that if left untreated, psychosis has significant and sometimes devastating consequences for our patients,” said Pierre Tariot, MD, director of the Banner Alzheimer’s Institute and a research professor of psychiatry at the University of Arizona College of Medicine, Tucson, and an investigator on the HARMONY trial.
Those on the committee who voted against the application were quick to agree that lack of an approved treatment for ADP presents a hardship.
“I’m a neurologist who has cared for patients for more than 20 years,” said Madhav R. Thambisetty, MD, PhD, senior investigator for the National Institute on Aging and an adjunct professor of neurology at Johns Hopkins University School of Medicine, Baltimore. “I recognize the unmet need in the field, I just think that the unmet need should not be a justification to cut corners.”
The committee did not focus on drug safety or unmet need in its deliberations, although information on both were presented during the meeting.
Commenting on his “no” vote, PDAC member Walter S. Dunn, MD, PhD, assistant clinical professor of psychiatry at the University of California, Los Angeles, and director of Interventional Psychiatry Service at West Los Angeles Veterans Affairs Medical Center, said he hopes that the FDA will consider those issues more broadly as they complete their review.
“The questions before the committee have been narrow and precise, so I trust the agency will take a broader approach in their final decision about approval,” Dr. Dunn said.
Commenting on the decision, Howard Fillit, MD, cofounder and chief science officer, Alzheimer’s Drug Discovery Foundation, called the news disappointing, “but while the unmet need for a treatment for ADP is clear, it is vital that approved treatments meet stringent safety and efficacy criteria so we can offer patients medications with clear benefits.”
The FDA will make its final decision by August 4.
A version of this article first appeared on Medscape.com.
In a 9-3 vote, the Psychopharmacologic Drugs Advisory Committee (PDAC) found that the drug’s manufacturer failed to offer convincing evidence of its efficacy in patients with ADP.
The June 17 rejection was the second rejection in as many years for a new indication for pimavanserin, which was approved in 2016 for Parkinson’s disease psychosis (PDP).
In April 2021, the FDA denied Acadia’s supplemental new drug application to expand the drug’s indication to include the treatment of all dementia-related psychosis, regardless of the underlying cause of dementia, citing issues with two studies the company presented as evidence of efficacy.
For the current application, Acadia submitted some new analysis of those studies but limited its application to ADP, which affects up to 30% of patients with Alzheimer’s disease (AD) and currently has no approved treatment.
Committee members who opposed the application were moved by testimony from caregivers and clinicians who treat patients with ADP but ultimately decided the evidence offered by Acadia once again failed to meet the threshold needed to demonstrate efficacy for an expanded indication.
“Sometimes I struggle with a decision on an advisory committee, but not today,” Dean Follmann, PhD, assistant director for biostatistics, National Institute of Allergy and Infectious Diseases, Bethesda, Md., said of his “no” vote.
Lack of efficacy
Pimavanserin is a selective serotonin inverse agonist and antagonist preferentially targeting 5-HT2A receptors, which are thought to play an important role in psychosis, schizophrenia, depression, and other neuropsychiatric disorders.
When it rejected Acadia’s original, broader application for pimavanserin for all dementia-related psychosis, the FDA found that the HARMONY phase 3 trial, previously covered by this news organization, was underpowered to assess efficacy in specific dementia patient subgroups and lacked statistical significance of efficacy in patients with AD. In addition, it noted that overall findings appeared to be driven by results in patients with Parkinson’s disease dementia, a condition already covered by the approved indication.
The FDA found that the second study, referred to in the June 17 hearing as Study 019, which was also previously reported by this news organization, was not “an adequate and well-controlled study.”
Specifically, the agency raised concerns about “protocol deviations,” such as the inclusion of patients who lacked clear documentation that psychotic symptoms developed after an AD diagnosis had been established and patients who received exclusionary medications at the time of randomization.
Discussions between Acadia and the FDA continued over the past year, with the company submitting new analyses and responses. An FDA briefing document published in advance of the committee meeting seemed to suggest the agency was satisfied with Acadia’s response.
Lack of diversity
The advisory committee disagreed, pointing to the same concerns raised last year. Members raised concerns about patient diversity in the HARMONY trial, which included an almost entirely White and mostly male study population.
In addition, although the findings at 26 weeks did demonstrate a marked improvement in psychosis symptoms overall, committee members noted that, again, those findings were largely driven by efficacy in patients with Parkinson’s disease dementia, for which the drug is already approved.
When discussing the phase 2 Study 019, the committee noted that while the study met the primary outcome of improvement in psychosis at 6 weeks, those positive responses were not found at any other timepoint in the 12-week study.
“While it might have had a positive numerical effect in the study, the evidence is really not there to support it,” Dr. Follmann said.
Dr. Follmann and other committee members called for additional trials that focus on patients with Alzheimer’s disease, have a longer follow-up, and include more gender and racial diversity in the study population. They also called for more information about any off-label use of pimavanserin for ADP since it was approved for PDP in 2016.
An unmet need
Most individuals who testified during the public comment period pleaded with the committee to vote in favor of the new indication, sharing stories of family members and patients with ADP.
“I have been caring for and studying patients with Alzheimer’s disease and other dementias for more than 30 years, and I can tell you very simply that if left untreated, psychosis has significant and sometimes devastating consequences for our patients,” said Pierre Tariot, MD, director of the Banner Alzheimer’s Institute and a research professor of psychiatry at the University of Arizona College of Medicine, Tucson, and an investigator on the HARMONY trial.
Those on the committee who voted against the application were quick to agree that lack of an approved treatment for ADP presents a hardship.
“I’m a neurologist who has cared for patients for more than 20 years,” said Madhav R. Thambisetty, MD, PhD, senior investigator for the National Institute on Aging and an adjunct professor of neurology at Johns Hopkins University School of Medicine, Baltimore. “I recognize the unmet need in the field, I just think that the unmet need should not be a justification to cut corners.”
The committee did not focus on drug safety or unmet need in its deliberations, although information on both were presented during the meeting.
Commenting on his “no” vote, PDAC member Walter S. Dunn, MD, PhD, assistant clinical professor of psychiatry at the University of California, Los Angeles, and director of Interventional Psychiatry Service at West Los Angeles Veterans Affairs Medical Center, said he hopes that the FDA will consider those issues more broadly as they complete their review.
“The questions before the committee have been narrow and precise, so I trust the agency will take a broader approach in their final decision about approval,” Dr. Dunn said.
Commenting on the decision, Howard Fillit, MD, cofounder and chief science officer, Alzheimer’s Drug Discovery Foundation, called the news disappointing, “but while the unmet need for a treatment for ADP is clear, it is vital that approved treatments meet stringent safety and efficacy criteria so we can offer patients medications with clear benefits.”
The FDA will make its final decision by August 4.
A version of this article first appeared on Medscape.com.

When suffering defies diagnosis
I still remember the woman who came to my office that day, years ago. She was struggling and uncomfortable, and she wanted “something” for stress. She described her life, and to me, it sounded stressful. She lived in a blended family and she described the chaos that one might expect to find in a household with four teens, their friends, their activities, and all it took to keep the household going. I spent 2 hours evaluating the patient, and I could not find a diagnosis that fit this problem nor – I believed – a pill that would fix it. She didn’t “meet criteria” for a psychiatric disorder, but she insisted she was uncomfortable and she wanted to try medication. I admit, I relented and I gave her a prescription for fluoxetine.
When she returned a few weeks later, my patient said she felt better, and what I remember decades later was her statement: “Now I can see dishes in the sink and be okay with it.” Perhaps she had downplayed her anxiety during our first meeting, but what I took from this was that some people are uncomfortable in ways that our lexicon does not capture, and sometimes medication helps with this discomfort.

The APA’s Diagnostic and Statistical Manual of Mental Disorders attempts to capture the problems of emotional and behavioral distress and classify them into discrete syndromes that can be validated and reliably diagnosed by different evaluators. Our disorders are syndromic; they are defined by clusters of symptoms that occur together, and not by a single symptom, lab value, or radiologic finding. The DSM is rewritten periodically so that what is or is not a disorder can bend with new discoveries and with a changing culture. And for better or for worse, when there is an available medication that can alleviate a problem, this may influence what once was a variant of normal into becoming a disorder.
Our illnesses often lie along a spectrum, so there is no precise point where someone who is easily distracted is a person with attention deficit disorder as opposed to being a mentally healthy person who is easily distracted, or a shy person is someone with social anxiety disorder. whether they want to address this with medications, and whether their distress warrants taking a chance that they might have side effects or an adverse reaction to a medication.
When we look at our criteria, sometimes we fall short. One needs to have at least five symptoms out of nine options, to be present for 2 weeks to be diagnosed with major depression, yet I don’t know a single psychiatrist who would not offer medication to a patient who ascribed to feeling profoundly sad with thoughts of suicide in the absence of other symptoms of depression. These issues have come to the forefront with the recent inclusion of prolonged grief in the DSM, as a disorder that is distinct from both normal grieving and from major depression.
In recent weeks, mass murder has been on everyone’s mind as we mourn those lost in Uvalde, Buffalo, and unfortunately, in so many other places. Absolutely no one thinks that someone who shoots strangers is “normal” or emotionally well. Yet psychiatry is often tasked with figuring out if someone is mad (mentally ill), bad (evil), or both. We don’t have a clear path for how to treat and manage people who commit horrendous acts of violence unless they meet criteria for another illness. Yet no one would argue that a person who informs others that he is thinking of killing strangers is in need of some type of intervention, regardless of his motive. We struggle too, with how to manage people who have more regular angry outbursts or emotional dysregulation. Perhaps we diagnose intermittent explosive disorder, or irritability caused by a mood disorder, but we don’t always know how to help people to control their tempers and modulate their emotions. And our semantics to describe psychic pain and anguish are surprisingly limited – sometimes we can only assume that someone who lashes out must be in turmoil.
Psychiatry continues to struggle with our relationship with human suffering. Suffering is part of life, not necessarily a sign of illness, and in his iconic memoir, “Man’s Search for Meaning,” psychiatrist Viktor Frankl, MD, wrote of the atrocities he endured in a Nazi concentration camp. It was through his suffering that Dr. Frankl found meaning and he used these harrowing experiences to fuel positive emotions later in life. Dr. Frankl wrote: “If there is a meaning in life at all, then there must be a meaning in suffering. Suffering is an ineradicable part of life, even as fate and death. Without suffering and death, human life cannot be complete.”
Suffering may be the kindling for acts of violence, or for profound creativity. Would we have music, art, cinema, poetry, or fiction if no one ever suffered? Yet suffering and emotional torment are often what leads people to seek treatment, and what leads us, as healers, to offer any range of therapies. For years, suicide rates have been rising, as have overdose death. And now, in addition to these “deaths of despair,” we are hearing about skyrocketing rates of depression and anxiety in our world that is so full of reasons to be sad and anxious. Access to treatment is limited by so many things, and it is not always clear when one needs psychiatric interventions or when problems will heal on their own, leaving scars or not.
I wrote this article in response to the hundreds of comments that were placed on an article I wrote after the horrors at Uvalde and Buffalo: “Don’t Equate Mass Shootings with Mental Illness.” Many of the commenters suggested I believe the shooter was perfectly sane, and that I am naive (or worse). Many wrote in with their own thoughts about what causes people to become mass murderers. One commenter wrote: “To suggest that random killers do not have mental health issues and their behavior is normal is ridiculous.” I don’t believe that I ever suggested that such behavior was normal, but – for many of these crimes – we as a society have decided to treat the behavior as criminal and not as the product of our current concept of mental disorders. Obviously, people who are well, who are emotionally at peace and comfortable in their own skin, don’t kill strangers.
Dr. Miller is a coauthor of “Committed: The Battle Over Involuntary Psychiatric Care” (Baltimore: Johns Hopkins University Press, 2016). She has a private practice and is assistant professor of psychiatry and behavioral sciences at Johns Hopkins in Baltimore.
I still remember the woman who came to my office that day, years ago. She was struggling and uncomfortable, and she wanted “something” for stress. She described her life, and to me, it sounded stressful. She lived in a blended family and she described the chaos that one might expect to find in a household with four teens, their friends, their activities, and all it took to keep the household going. I spent 2 hours evaluating the patient, and I could not find a diagnosis that fit this problem nor – I believed – a pill that would fix it. She didn’t “meet criteria” for a psychiatric disorder, but she insisted she was uncomfortable and she wanted to try medication. I admit, I relented and I gave her a prescription for fluoxetine.
When she returned a few weeks later, my patient said she felt better, and what I remember decades later was her statement: “Now I can see dishes in the sink and be okay with it.” Perhaps she had downplayed her anxiety during our first meeting, but what I took from this was that some people are uncomfortable in ways that our lexicon does not capture, and sometimes medication helps with this discomfort.
The APA’s Diagnostic and Statistical Manual of Mental Disorders attempts to capture the problems of emotional and behavioral distress and classify them into discrete syndromes that can be validated and reliably diagnosed by different evaluators. Our disorders are syndromic; they are defined by clusters of symptoms that occur together, and not by a single symptom, lab value, or radiologic finding. The DSM is rewritten periodically so that what is or is not a disorder can bend with new discoveries and with a changing culture. And for better or for worse, when there is an available medication that can alleviate a problem, this may influence what once was a variant of normal into becoming a disorder.
Our illnesses often lie along a spectrum, so there is no precise point where someone who is easily distracted is a person with attention deficit disorder as opposed to being a mentally healthy person who is easily distracted, or a shy person is someone with social anxiety disorder. whether they want to address this with medications, and whether their distress warrants taking a chance that they might have side effects or an adverse reaction to a medication.
When we look at our criteria, sometimes we fall short. One needs to have at least five symptoms out of nine options, to be present for 2 weeks to be diagnosed with major depression, yet I don’t know a single psychiatrist who would not offer medication to a patient who ascribed to feeling profoundly sad with thoughts of suicide in the absence of other symptoms of depression. These issues have come to the forefront with the recent inclusion of prolonged grief in the DSM, as a disorder that is distinct from both normal grieving and from major depression.
In recent weeks, mass murder has been on everyone’s mind as we mourn those lost in Uvalde, Buffalo, and unfortunately, in so many other places. Absolutely no one thinks that someone who shoots strangers is “normal” or emotionally well. Yet psychiatry is often tasked with figuring out if someone is mad (mentally ill), bad (evil), or both. We don’t have a clear path for how to treat and manage people who commit horrendous acts of violence unless they meet criteria for another illness. Yet no one would argue that a person who informs others that he is thinking of killing strangers is in need of some type of intervention, regardless of his motive. We struggle too, with how to manage people who have more regular angry outbursts or emotional dysregulation. Perhaps we diagnose intermittent explosive disorder, or irritability caused by a mood disorder, but we don’t always know how to help people to control their tempers and modulate their emotions. And our semantics to describe psychic pain and anguish are surprisingly limited – sometimes we can only assume that someone who lashes out must be in turmoil.
Psychiatry continues to struggle with our relationship with human suffering. Suffering is part of life, not necessarily a sign of illness, and in his iconic memoir, “Man’s Search for Meaning,” psychiatrist Viktor Frankl, MD, wrote of the atrocities he endured in a Nazi concentration camp. It was through his suffering that Dr. Frankl found meaning and he used these harrowing experiences to fuel positive emotions later in life. Dr. Frankl wrote: “If there is a meaning in life at all, then there must be a meaning in suffering. Suffering is an ineradicable part of life, even as fate and death. Without suffering and death, human life cannot be complete.”
Suffering may be the kindling for acts of violence, or for profound creativity. Would we have music, art, cinema, poetry, or fiction if no one ever suffered? Yet suffering and emotional torment are often what leads people to seek treatment, and what leads us, as healers, to offer any range of therapies. For years, suicide rates have been rising, as have overdose death. And now, in addition to these “deaths of despair,” we are hearing about skyrocketing rates of depression and anxiety in our world that is so full of reasons to be sad and anxious. Access to treatment is limited by so many things, and it is not always clear when one needs psychiatric interventions or when problems will heal on their own, leaving scars or not.
I wrote this article in response to the hundreds of comments that were placed on an article I wrote after the horrors at Uvalde and Buffalo: “Don’t Equate Mass Shootings with Mental Illness.” Many of the commenters suggested I believe the shooter was perfectly sane, and that I am naive (or worse). Many wrote in with their own thoughts about what causes people to become mass murderers. One commenter wrote: “To suggest that random killers do not have mental health issues and their behavior is normal is ridiculous.” I don’t believe that I ever suggested that such behavior was normal, but – for many of these crimes – we as a society have decided to treat the behavior as criminal and not as the product of our current concept of mental disorders. Obviously, people who are well, who are emotionally at peace and comfortable in their own skin, don’t kill strangers.
Dr. Miller is a coauthor of “Committed: The Battle Over Involuntary Psychiatric Care” (Baltimore: Johns Hopkins University Press, 2016). She has a private practice and is assistant professor of psychiatry and behavioral sciences at Johns Hopkins in Baltimore.
I still remember the woman who came to my office that day, years ago. She was struggling and uncomfortable, and she wanted “something” for stress. She described her life, and to me, it sounded stressful. She lived in a blended family and she described the chaos that one might expect to find in a household with four teens, their friends, their activities, and all it took to keep the household going. I spent 2 hours evaluating the patient, and I could not find a diagnosis that fit this problem nor – I believed – a pill that would fix it. She didn’t “meet criteria” for a psychiatric disorder, but she insisted she was uncomfortable and she wanted to try medication. I admit, I relented and I gave her a prescription for fluoxetine.
When she returned a few weeks later, my patient said she felt better, and what I remember decades later was her statement: “Now I can see dishes in the sink and be okay with it.” Perhaps she had downplayed her anxiety during our first meeting, but what I took from this was that some people are uncomfortable in ways that our lexicon does not capture, and sometimes medication helps with this discomfort.
The APA’s Diagnostic and Statistical Manual of Mental Disorders attempts to capture the problems of emotional and behavioral distress and classify them into discrete syndromes that can be validated and reliably diagnosed by different evaluators. Our disorders are syndromic; they are defined by clusters of symptoms that occur together, and not by a single symptom, lab value, or radiologic finding. The DSM is rewritten periodically so that what is or is not a disorder can bend with new discoveries and with a changing culture. And for better or for worse, when there is an available medication that can alleviate a problem, this may influence what once was a variant of normal into becoming a disorder.
Our illnesses often lie along a spectrum, so there is no precise point where someone who is easily distracted is a person with attention deficit disorder as opposed to being a mentally healthy person who is easily distracted, or a shy person is someone with social anxiety disorder. whether they want to address this with medications, and whether their distress warrants taking a chance that they might have side effects or an adverse reaction to a medication.
When we look at our criteria, sometimes we fall short. One needs to have at least five symptoms out of nine options, to be present for 2 weeks to be diagnosed with major depression, yet I don’t know a single psychiatrist who would not offer medication to a patient who ascribed to feeling profoundly sad with thoughts of suicide in the absence of other symptoms of depression. These issues have come to the forefront with the recent inclusion of prolonged grief in the DSM, as a disorder that is distinct from both normal grieving and from major depression.
In recent weeks, mass murder has been on everyone’s mind as we mourn those lost in Uvalde, Buffalo, and unfortunately, in so many other places. Absolutely no one thinks that someone who shoots strangers is “normal” or emotionally well. Yet psychiatry is often tasked with figuring out if someone is mad (mentally ill), bad (evil), or both. We don’t have a clear path for how to treat and manage people who commit horrendous acts of violence unless they meet criteria for another illness. Yet no one would argue that a person who informs others that he is thinking of killing strangers is in need of some type of intervention, regardless of his motive. We struggle too, with how to manage people who have more regular angry outbursts or emotional dysregulation. Perhaps we diagnose intermittent explosive disorder, or irritability caused by a mood disorder, but we don’t always know how to help people to control their tempers and modulate their emotions. And our semantics to describe psychic pain and anguish are surprisingly limited – sometimes we can only assume that someone who lashes out must be in turmoil.
Psychiatry continues to struggle with our relationship with human suffering. Suffering is part of life, not necessarily a sign of illness, and in his iconic memoir, “Man’s Search for Meaning,” psychiatrist Viktor Frankl, MD, wrote of the atrocities he endured in a Nazi concentration camp. It was through his suffering that Dr. Frankl found meaning and he used these harrowing experiences to fuel positive emotions later in life. Dr. Frankl wrote: “If there is a meaning in life at all, then there must be a meaning in suffering. Suffering is an ineradicable part of life, even as fate and death. Without suffering and death, human life cannot be complete.”
Suffering may be the kindling for acts of violence, or for profound creativity. Would we have music, art, cinema, poetry, or fiction if no one ever suffered? Yet suffering and emotional torment are often what leads people to seek treatment, and what leads us, as healers, to offer any range of therapies. For years, suicide rates have been rising, as have overdose death. And now, in addition to these “deaths of despair,” we are hearing about skyrocketing rates of depression and anxiety in our world that is so full of reasons to be sad and anxious. Access to treatment is limited by so many things, and it is not always clear when one needs psychiatric interventions or when problems will heal on their own, leaving scars or not.
I wrote this article in response to the hundreds of comments that were placed on an article I wrote after the horrors at Uvalde and Buffalo: “Don’t Equate Mass Shootings with Mental Illness.” Many of the commenters suggested I believe the shooter was perfectly sane, and that I am naive (or worse). Many wrote in with their own thoughts about what causes people to become mass murderers. One commenter wrote: “To suggest that random killers do not have mental health issues and their behavior is normal is ridiculous.” I don’t believe that I ever suggested that such behavior was normal, but – for many of these crimes – we as a society have decided to treat the behavior as criminal and not as the product of our current concept of mental disorders. Obviously, people who are well, who are emotionally at peace and comfortable in their own skin, don’t kill strangers.
Dr. Miller is a coauthor of “Committed: The Battle Over Involuntary Psychiatric Care” (Baltimore: Johns Hopkins University Press, 2016). She has a private practice and is assistant professor of psychiatry and behavioral sciences at Johns Hopkins in Baltimore.
A prescription for de-diagnosing
In 2016, Gupta and Cahill challenged the field of psychiatry to reexamine prescribing patterns.1 They warned against the use of polypharmacy when not attached to improved patient functioning. They were concerned with the limited evidence for polypharmacy as well as DSM diagnostic criteria. In their inspiring article, they described a process of deprescribing.
In an effort to study and practice their recommendations, we have noticed a lack of literature examining the elimination of diagnostic labels. While there have been some studies looking at comorbidity, especially with substance use disorders,2 there is a paucity of scientific evidence on patients with numerous diagnoses. Yet our practices are filled with patients who have been labeled with multiple conflicting or redundant diagnoses throughout their lives depending on the setting or the orientation of the practitioner.

The DSM-5 warns against diagnosing disorders when “the occurrence … is not better explained by” another disorder.3 A mix of diagnoses creates confusion for patients as well as clinicians trying to sort through their reported psychiatric histories.
A routine example would include a patient presenting for an initial evaluation and stating “I’ve been diagnosed as manic-depressive, high anxiety, split personality, posttraumatic stress, insomnia, ADD, and depression.” A review of the medical record will reveal a list of diagnoses, including bipolar II, generalized anxiety disorder, borderline personality disorder, posttraumatic stress disorder, unspecified insomnia, attention-deficit/hyperactivity disorder, and major depressive disorder. The medication list includes lamotrigine, valproic acid, citalopram, bupropion, buspirone, prazosin, methylphenidate, clonazepam, hydroxyzine, and low-dose quetiapine at night as needed.
This is an example of polypharmacy treating multiple, and at times conflicting, diagnoses. While an extreme case, in our experience, cases like this are not uncommon. It was actually in our efforts to examine deprescribing that we noticed this quandary. When inquiring about patients on many psychotropic medications, we often receive this retort: the patient is only prescribed one medication per disorder. Some providers have the belief that multiple disorders justify multiple medications, and that this tautological thinking legitimizes polypharmacy.
A patient who has varying moods, some fears, a fluctuating temperament, past traumas, occasional difficulty sleeping, intermittent inattention, and some sadness may be given all the diagnoses listed above and the resulting medication list. The multiplication of diagnoses, “polydiagnosing,” is a convenient justification for future polypharmacy. A lack of careful assessment and thinking in the application of new diagnoses permits the use of increasing numbers of pharmacological agents. A constellation of symptoms of anxiety, concentration deficits, affective dysregulation, and psychosis may justify the combination of benzodiazepines, stimulants, mood stabilizers, and antipsychotics, while a patient with “just” schizophrenia who is sometimes sad, scared, or distracted is more likely to be kept on just one medication, likely an antipsychotic.
Contrary to most medical disorders (for example, tuberculosis) but similar to others (for example, chronic pain), psychiatric disorders are based on the opinion of a “modest number of ‘expert’ classifications.”4 While the broad categories of disorders are justifiable, individual diagnoses are burdened with high rates of comorbidity; lack of treatment specificity; and evidence that distinct syndromes share a genetic basis. Those concerns were exemplified in the study examining the inter-rater reliability of DSM-5 diagnoses, where many disorders were found to have questionable validity.5
A psychiatric diagnosis should be based on biological, psychological, and social factors, which align with our understanding of the natural course of an illness. A patient presenting with transient symptoms of sadness in the context of significant social factors like homelessness and/or significant biological factors associated with schizophrenia should not reflexively receive an additional diagnosis of a depressive disorder. A patient reporting poor concentration in the context of a manic episode should not receive an additional diagnosis of attention-deficit disorder. An older patient with depression on multiple antipsychotics for adjunctive treatment should not necessarily receive a diagnosis of cognitive disorder at the first sign of memory problems.
The cavalier and inconsistent use of diagnoses renders the patients with no clear narrative of who they are. They end up integrating the varying providers’ opinions as a cacophony of labels of unclear significance. Many patients have contradictory diagnoses like major depressive disorder and bipolar disorder, or schizophrenia and schizoaffective disorder. Those inaccurate diagnoses could not only lead to treatment mistakes, but also psychological harm.6

A clearer diagnostic picture is not only more scientifically sound but also more coherent to the patient. This in turn can lead to an improved treatment alliance and buy-in from the patient.
How should a provider practice de-diagnosing? Based on the work of Reeve, et al.,7 on the principles crucial to deprescribing, and subsequent research by Gupta and Cahill,8 we compiled a list of considerations for practitioners wishing to engage in this type of work with their patients.
Choose the right time. While insurance companies require diagnostic findings from the first visit, abrupt de-diagnosing for the sake of simplifying the record from that first visit could be detrimental. Patients can become attached to and find meaning in their diagnostic labels. This was exemplified with the removal of Asperger’s syndrome from the DSM-5.9 Acute symptomatology may be an opportune time to revisit the core pathology of a patient, or a poor time for a patient to have this discussion.
Compile a list of all the patient’s diagnoses. Our initial visits are often illuminated when patients enumerate the vast number of diagnoses they have been given by different providers. Patients will often list half a dozen diagnoses. The patterns often follow life courses with ADHD, conduct disorder, and learning disability in childhood; with anxiety, depression, and/or bipolar disorder in early adulthood; to complicated grief, depression with pseudodementia, and neurocognitive disorders in older adults. Yet patients rarely appreciate the temporary or episodic nature of mental disorders and instead accumulate diagnoses at each change of provider.
Initiate discussion with the patient. It is meaningful to see if patients resonate with the question, “Do you ever feel like every psychiatrist you have seen has given you a different diagnosis?” In our experience, patients’ reactions to this question usually exemplify the problematic nature of the vast array of diagnoses our patients are given. The majority of them are unable to confidently explain the meaning of those diagnoses, the context in which they were given, or their significance. This simple exercise has a powerful effect on raising awareness to patients of the problematic nature of polydiagnosing.
Introduce de-diagnosing. The engagement of patients in the diagnostic process has a significant effect. Reviewing not only diagnostic criteria but also nosology and debates in our understanding of diagnoses can provide patients with further engagement in their care. A simple review of the debate of the bereavement exclusion may permit a patient to not only understand the complexity, but also the changing nature of diagnoses. Suddenly, they are no longer bystanders, but informed participants in their care.
Identify diagnoses most appropriate for removal. Contradictory diagnoses are common in the clinical settings we work in. We routinely see patients carrying multiple mood diagnoses, despite our diagnostic systems not permitting one to have both unipolar and bipolar depression. Superfluous diagnoses are also frequent, with patients receiving depressive, or anxious labels when in an acute state of psychosis or mania. This is exemplified by patients suffering from thought blocking and receiving cognitive or attention-related diagnoses. Concurrent yet different diagnoses are also common in patients with a different list of diagnoses by their primary care provider, their therapist, and their psychiatrist. This is particularly problematic as it forces the patient to alternate their thinking or choose between their providers.
Create a new narrative for the patient. Once diagnoses are explained, clarified, and understood, patients with the help of their providers can reexamine their life story under a new and simplified construct. This process often leads to a less confusing sense of self, an increased dedication to the treatment process, whether behavioral, social, psychological, or pharmacologic.
Consider deprescribing. With a more straightforward and more grounded list of diagnoses (or simply one diagnosis), we find the process of deprescribing to be simpler and more engaging for patients. For example, patients can clearly understand the lack of necessity of an antipsychotic prescription for a resolved substance-induced psychosis. Patients are more engaged in their care, leading to improved medication compliance and less attachment to discontinued medications.
Monitor and adapt. One should of course reevaluate diagnoses as the course of illness provides us with additional information. However, we suggest waiting for a manic episode to emerge prior to diagnosing bipolar rather than suggesting the diagnosis because a patient was wearing red shoes, spoke multiple languages, had multiple degrees and was creative.10 The contextual basis and progression of the symptoms should lead to continual reassessment of diagnoses.
Physicians are aware of the balance between Occam’s razor, which promotes the simplest single explanation for a problem, versus Hickam’s dictum that reminds us that patients can have as many diseases as they please. However, similarly to polypharmacy, “polydiagnosing” has negative effects. While the field of psychiatry’s advancing knowledge may encourage providers to diagnose their patients with the growing number of diagnoses, patients still need and benefit from a coherent and clear medical narrative. Psychiatry would be wise to recognize this concerning trend, in its attempt at rectifying polypharmacy.
Dr. Badre is a clinical and forensic psychiatrist in San Diego. He holds teaching positions at the University of California, San Diego, and the University of San Diego. He teaches medical education, psychopharmacology, ethics in psychiatry, and correctional care. Dr. Badre can be reached at his website, BadreMD.com. He has no conflicts of interest. Dr. Lehman is a professor of psychiatry at the University of California, San Diego. He is codirector of all acute and intensive psychiatric treatment at the Veterans Affairs Medical Center in San Diego, where he practices clinical psychiatry. He has no conflicts of interest.
References
1. Gupta S & Cahill JD. A prescription for “deprescribing” in psychiatry. Psychiatr Serv. 2016 Aug 1;67(8):904-7. doi: 10.1176/appi.ps.201500359.
2. Schuckit MA. Comorbidity between substance use disorders and psychiatric conditions. Addiction. 2006 Sep;101 Suppl 1:76-88. doi: 10.1111/j.1360-0443.2006.01592.x.
3. The Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, Text Revision (DSM-5-TR). American Psychiatric Association, 2022. https://psychiatry.org/psychiatrists/practice/dsm.
4. Kendler KS. An historical framework for psychiatric nosology. Psychol Med. 2009 Dec;39(12):1935-41. doi: 10.1017/S0033291709005753.
5. Regier DA et al. DSM-5 field trials in the United States and Canada. Am J Psychiatry. 2013 Jan;170(1):59-70. doi: 10.1176/appi.ajp.2012.12070999.
6. Bhattacharya R et al. When good news is bad news: psychological impact of false-positive diagnosis of HIV. AIDS Care. 2008 May;20(5):560-4. doi: 10.1080/09540120701867206.
7. Reeve E et al. Review of deprescribing processes and development of an evidence‐based, patient‐centred deprescribing process. Br J Clin Pharmacol. 2014 Oct;78(4):738-47. doi: 10.1111/bcp.12386.
8. Gupta S and Cahill JD. A prescription for “deprescribing” in psychiatry.
9. Solomon M. “On the appearance and disappearance of Asperger’s syndrome” in Kendler and Parnas (eds.) Philosophical Issues in Psychiatry IV: Classification of Psychiatric Illness. Oxford University Press, 2017. doi: 10.1093/med/9780198796022.003.0023.
10. Akiskal HS. Searching for behavioral indicators of bipolar II in patients presenting with major depressive episodes: The “red sign,” the “rule of three,” and other biographic signs of temperamental extravagance, activation, and hypomania. J Affect Disord. 2005 Feb;84(2-3):279-90. doi: 10.1016/j.jad.2004.06.002.
In 2016, Gupta and Cahill challenged the field of psychiatry to reexamine prescribing patterns.1 They warned against the use of polypharmacy when not attached to improved patient functioning. They were concerned with the limited evidence for polypharmacy as well as DSM diagnostic criteria. In their inspiring article, they described a process of deprescribing.
In an effort to study and practice their recommendations, we have noticed a lack of literature examining the elimination of diagnostic labels. While there have been some studies looking at comorbidity, especially with substance use disorders,2 there is a paucity of scientific evidence on patients with numerous diagnoses. Yet our practices are filled with patients who have been labeled with multiple conflicting or redundant diagnoses throughout their lives depending on the setting or the orientation of the practitioner.
The DSM-5 warns against diagnosing disorders when “the occurrence … is not better explained by” another disorder.3 A mix of diagnoses creates confusion for patients as well as clinicians trying to sort through their reported psychiatric histories.
A routine example would include a patient presenting for an initial evaluation and stating “I’ve been diagnosed as manic-depressive, high anxiety, split personality, posttraumatic stress, insomnia, ADD, and depression.” A review of the medical record will reveal a list of diagnoses, including bipolar II, generalized anxiety disorder, borderline personality disorder, posttraumatic stress disorder, unspecified insomnia, attention-deficit/hyperactivity disorder, and major depressive disorder. The medication list includes lamotrigine, valproic acid, citalopram, bupropion, buspirone, prazosin, methylphenidate, clonazepam, hydroxyzine, and low-dose quetiapine at night as needed.
This is an example of polypharmacy treating multiple, and at times conflicting, diagnoses. While an extreme case, in our experience, cases like this are not uncommon. It was actually in our efforts to examine deprescribing that we noticed this quandary. When inquiring about patients on many psychotropic medications, we often receive this retort: the patient is only prescribed one medication per disorder. Some providers have the belief that multiple disorders justify multiple medications, and that this tautological thinking legitimizes polypharmacy.
A patient who has varying moods, some fears, a fluctuating temperament, past traumas, occasional difficulty sleeping, intermittent inattention, and some sadness may be given all the diagnoses listed above and the resulting medication list. The multiplication of diagnoses, “polydiagnosing,” is a convenient justification for future polypharmacy. A lack of careful assessment and thinking in the application of new diagnoses permits the use of increasing numbers of pharmacological agents. A constellation of symptoms of anxiety, concentration deficits, affective dysregulation, and psychosis may justify the combination of benzodiazepines, stimulants, mood stabilizers, and antipsychotics, while a patient with “just” schizophrenia who is sometimes sad, scared, or distracted is more likely to be kept on just one medication, likely an antipsychotic.
Contrary to most medical disorders (for example, tuberculosis) but similar to others (for example, chronic pain), psychiatric disorders are based on the opinion of a “modest number of ‘expert’ classifications.”4 While the broad categories of disorders are justifiable, individual diagnoses are burdened with high rates of comorbidity; lack of treatment specificity; and evidence that distinct syndromes share a genetic basis. Those concerns were exemplified in the study examining the inter-rater reliability of DSM-5 diagnoses, where many disorders were found to have questionable validity.5
A psychiatric diagnosis should be based on biological, psychological, and social factors, which align with our understanding of the natural course of an illness. A patient presenting with transient symptoms of sadness in the context of significant social factors like homelessness and/or significant biological factors associated with schizophrenia should not reflexively receive an additional diagnosis of a depressive disorder. A patient reporting poor concentration in the context of a manic episode should not receive an additional diagnosis of attention-deficit disorder. An older patient with depression on multiple antipsychotics for adjunctive treatment should not necessarily receive a diagnosis of cognitive disorder at the first sign of memory problems.
The cavalier and inconsistent use of diagnoses renders the patients with no clear narrative of who they are. They end up integrating the varying providers’ opinions as a cacophony of labels of unclear significance. Many patients have contradictory diagnoses like major depressive disorder and bipolar disorder, or schizophrenia and schizoaffective disorder. Those inaccurate diagnoses could not only lead to treatment mistakes, but also psychological harm.6
A clearer diagnostic picture is not only more scientifically sound but also more coherent to the patient. This in turn can lead to an improved treatment alliance and buy-in from the patient.
How should a provider practice de-diagnosing? Based on the work of Reeve, et al.,7 on the principles crucial to deprescribing, and subsequent research by Gupta and Cahill,8 we compiled a list of considerations for practitioners wishing to engage in this type of work with their patients.
Choose the right time. While insurance companies require diagnostic findings from the first visit, abrupt de-diagnosing for the sake of simplifying the record from that first visit could be detrimental. Patients can become attached to and find meaning in their diagnostic labels. This was exemplified with the removal of Asperger’s syndrome from the DSM-5.9 Acute symptomatology may be an opportune time to revisit the core pathology of a patient, or a poor time for a patient to have this discussion.
Compile a list of all the patient’s diagnoses. Our initial visits are often illuminated when patients enumerate the vast number of diagnoses they have been given by different providers. Patients will often list half a dozen diagnoses. The patterns often follow life courses with ADHD, conduct disorder, and learning disability in childhood; with anxiety, depression, and/or bipolar disorder in early adulthood; to complicated grief, depression with pseudodementia, and neurocognitive disorders in older adults. Yet patients rarely appreciate the temporary or episodic nature of mental disorders and instead accumulate diagnoses at each change of provider.
Initiate discussion with the patient. It is meaningful to see if patients resonate with the question, “Do you ever feel like every psychiatrist you have seen has given you a different diagnosis?” In our experience, patients’ reactions to this question usually exemplify the problematic nature of the vast array of diagnoses our patients are given. The majority of them are unable to confidently explain the meaning of those diagnoses, the context in which they were given, or their significance. This simple exercise has a powerful effect on raising awareness to patients of the problematic nature of polydiagnosing.
Introduce de-diagnosing. The engagement of patients in the diagnostic process has a significant effect. Reviewing not only diagnostic criteria but also nosology and debates in our understanding of diagnoses can provide patients with further engagement in their care. A simple review of the debate of the bereavement exclusion may permit a patient to not only understand the complexity, but also the changing nature of diagnoses. Suddenly, they are no longer bystanders, but informed participants in their care.
Identify diagnoses most appropriate for removal. Contradictory diagnoses are common in the clinical settings we work in. We routinely see patients carrying multiple mood diagnoses, despite our diagnostic systems not permitting one to have both unipolar and bipolar depression. Superfluous diagnoses are also frequent, with patients receiving depressive, or anxious labels when in an acute state of psychosis or mania. This is exemplified by patients suffering from thought blocking and receiving cognitive or attention-related diagnoses. Concurrent yet different diagnoses are also common in patients with a different list of diagnoses by their primary care provider, their therapist, and their psychiatrist. This is particularly problematic as it forces the patient to alternate their thinking or choose between their providers.
Create a new narrative for the patient. Once diagnoses are explained, clarified, and understood, patients with the help of their providers can reexamine their life story under a new and simplified construct. This process often leads to a less confusing sense of self, an increased dedication to the treatment process, whether behavioral, social, psychological, or pharmacologic.
Consider deprescribing. With a more straightforward and more grounded list of diagnoses (or simply one diagnosis), we find the process of deprescribing to be simpler and more engaging for patients. For example, patients can clearly understand the lack of necessity of an antipsychotic prescription for a resolved substance-induced psychosis. Patients are more engaged in their care, leading to improved medication compliance and less attachment to discontinued medications.
Monitor and adapt. One should of course reevaluate diagnoses as the course of illness provides us with additional information. However, we suggest waiting for a manic episode to emerge prior to diagnosing bipolar rather than suggesting the diagnosis because a patient was wearing red shoes, spoke multiple languages, had multiple degrees and was creative.10 The contextual basis and progression of the symptoms should lead to continual reassessment of diagnoses.
Physicians are aware of the balance between Occam’s razor, which promotes the simplest single explanation for a problem, versus Hickam’s dictum that reminds us that patients can have as many diseases as they please. However, similarly to polypharmacy, “polydiagnosing” has negative effects. While the field of psychiatry’s advancing knowledge may encourage providers to diagnose their patients with the growing number of diagnoses, patients still need and benefit from a coherent and clear medical narrative. Psychiatry would be wise to recognize this concerning trend, in its attempt at rectifying polypharmacy.
Dr. Badre is a clinical and forensic psychiatrist in San Diego. He holds teaching positions at the University of California, San Diego, and the University of San Diego. He teaches medical education, psychopharmacology, ethics in psychiatry, and correctional care. Dr. Badre can be reached at his website, BadreMD.com. He has no conflicts of interest. Dr. Lehman is a professor of psychiatry at the University of California, San Diego. He is codirector of all acute and intensive psychiatric treatment at the Veterans Affairs Medical Center in San Diego, where he practices clinical psychiatry. He has no conflicts of interest.
References
1. Gupta S & Cahill JD. A prescription for “deprescribing” in psychiatry. Psychiatr Serv. 2016 Aug 1;67(8):904-7. doi: 10.1176/appi.ps.201500359.
2. Schuckit MA. Comorbidity between substance use disorders and psychiatric conditions. Addiction. 2006 Sep;101 Suppl 1:76-88. doi: 10.1111/j.1360-0443.2006.01592.x.
3. The Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, Text Revision (DSM-5-TR). American Psychiatric Association, 2022. https://psychiatry.org/psychiatrists/practice/dsm.
4. Kendler KS. An historical framework for psychiatric nosology. Psychol Med. 2009 Dec;39(12):1935-41. doi: 10.1017/S0033291709005753.
5. Regier DA et al. DSM-5 field trials in the United States and Canada. Am J Psychiatry. 2013 Jan;170(1):59-70. doi: 10.1176/appi.ajp.2012.12070999.
6. Bhattacharya R et al. When good news is bad news: psychological impact of false-positive diagnosis of HIV. AIDS Care. 2008 May;20(5):560-4. doi: 10.1080/09540120701867206.
7. Reeve E et al. Review of deprescribing processes and development of an evidence‐based, patient‐centred deprescribing process. Br J Clin Pharmacol. 2014 Oct;78(4):738-47. doi: 10.1111/bcp.12386.
8. Gupta S and Cahill JD. A prescription for “deprescribing” in psychiatry.
9. Solomon M. “On the appearance and disappearance of Asperger’s syndrome” in Kendler and Parnas (eds.) Philosophical Issues in Psychiatry IV: Classification of Psychiatric Illness. Oxford University Press, 2017. doi: 10.1093/med/9780198796022.003.0023.
10. Akiskal HS. Searching for behavioral indicators of bipolar II in patients presenting with major depressive episodes: The “red sign,” the “rule of three,” and other biographic signs of temperamental extravagance, activation, and hypomania. J Affect Disord. 2005 Feb;84(2-3):279-90. doi: 10.1016/j.jad.2004.06.002.
In 2016, Gupta and Cahill challenged the field of psychiatry to reexamine prescribing patterns.1 They warned against the use of polypharmacy when not attached to improved patient functioning. They were concerned with the limited evidence for polypharmacy as well as DSM diagnostic criteria. In their inspiring article, they described a process of deprescribing.
In an effort to study and practice their recommendations, we have noticed a lack of literature examining the elimination of diagnostic labels. While there have been some studies looking at comorbidity, especially with substance use disorders,2 there is a paucity of scientific evidence on patients with numerous diagnoses. Yet our practices are filled with patients who have been labeled with multiple conflicting or redundant diagnoses throughout their lives depending on the setting or the orientation of the practitioner.
The DSM-5 warns against diagnosing disorders when “the occurrence … is not better explained by” another disorder.3 A mix of diagnoses creates confusion for patients as well as clinicians trying to sort through their reported psychiatric histories.
A routine example would include a patient presenting for an initial evaluation and stating “I’ve been diagnosed as manic-depressive, high anxiety, split personality, posttraumatic stress, insomnia, ADD, and depression.” A review of the medical record will reveal a list of diagnoses, including bipolar II, generalized anxiety disorder, borderline personality disorder, posttraumatic stress disorder, unspecified insomnia, attention-deficit/hyperactivity disorder, and major depressive disorder. The medication list includes lamotrigine, valproic acid, citalopram, bupropion, buspirone, prazosin, methylphenidate, clonazepam, hydroxyzine, and low-dose quetiapine at night as needed.
This is an example of polypharmacy treating multiple, and at times conflicting, diagnoses. While an extreme case, in our experience, cases like this are not uncommon. It was actually in our efforts to examine deprescribing that we noticed this quandary. When inquiring about patients on many psychotropic medications, we often receive this retort: the patient is only prescribed one medication per disorder. Some providers have the belief that multiple disorders justify multiple medications, and that this tautological thinking legitimizes polypharmacy.
A patient who has varying moods, some fears, a fluctuating temperament, past traumas, occasional difficulty sleeping, intermittent inattention, and some sadness may be given all the diagnoses listed above and the resulting medication list. The multiplication of diagnoses, “polydiagnosing,” is a convenient justification for future polypharmacy. A lack of careful assessment and thinking in the application of new diagnoses permits the use of increasing numbers of pharmacological agents. A constellation of symptoms of anxiety, concentration deficits, affective dysregulation, and psychosis may justify the combination of benzodiazepines, stimulants, mood stabilizers, and antipsychotics, while a patient with “just” schizophrenia who is sometimes sad, scared, or distracted is more likely to be kept on just one medication, likely an antipsychotic.
Contrary to most medical disorders (for example, tuberculosis) but similar to others (for example, chronic pain), psychiatric disorders are based on the opinion of a “modest number of ‘expert’ classifications.”4 While the broad categories of disorders are justifiable, individual diagnoses are burdened with high rates of comorbidity; lack of treatment specificity; and evidence that distinct syndromes share a genetic basis. Those concerns were exemplified in the study examining the inter-rater reliability of DSM-5 diagnoses, where many disorders were found to have questionable validity.5
A psychiatric diagnosis should be based on biological, psychological, and social factors, which align with our understanding of the natural course of an illness. A patient presenting with transient symptoms of sadness in the context of significant social factors like homelessness and/or significant biological factors associated with schizophrenia should not reflexively receive an additional diagnosis of a depressive disorder. A patient reporting poor concentration in the context of a manic episode should not receive an additional diagnosis of attention-deficit disorder. An older patient with depression on multiple antipsychotics for adjunctive treatment should not necessarily receive a diagnosis of cognitive disorder at the first sign of memory problems.
The cavalier and inconsistent use of diagnoses renders the patients with no clear narrative of who they are. They end up integrating the varying providers’ opinions as a cacophony of labels of unclear significance. Many patients have contradictory diagnoses like major depressive disorder and bipolar disorder, or schizophrenia and schizoaffective disorder. Those inaccurate diagnoses could not only lead to treatment mistakes, but also psychological harm.6
A clearer diagnostic picture is not only more scientifically sound but also more coherent to the patient. This in turn can lead to an improved treatment alliance and buy-in from the patient.
How should a provider practice de-diagnosing? Based on the work of Reeve, et al.,7 on the principles crucial to deprescribing, and subsequent research by Gupta and Cahill,8 we compiled a list of considerations for practitioners wishing to engage in this type of work with their patients.
Choose the right time. While insurance companies require diagnostic findings from the first visit, abrupt de-diagnosing for the sake of simplifying the record from that first visit could be detrimental. Patients can become attached to and find meaning in their diagnostic labels. This was exemplified with the removal of Asperger’s syndrome from the DSM-5.9 Acute symptomatology may be an opportune time to revisit the core pathology of a patient, or a poor time for a patient to have this discussion.
Compile a list of all the patient’s diagnoses. Our initial visits are often illuminated when patients enumerate the vast number of diagnoses they have been given by different providers. Patients will often list half a dozen diagnoses. The patterns often follow life courses with ADHD, conduct disorder, and learning disability in childhood; with anxiety, depression, and/or bipolar disorder in early adulthood; to complicated grief, depression with pseudodementia, and neurocognitive disorders in older adults. Yet patients rarely appreciate the temporary or episodic nature of mental disorders and instead accumulate diagnoses at each change of provider.
Initiate discussion with the patient. It is meaningful to see if patients resonate with the question, “Do you ever feel like every psychiatrist you have seen has given you a different diagnosis?” In our experience, patients’ reactions to this question usually exemplify the problematic nature of the vast array of diagnoses our patients are given. The majority of them are unable to confidently explain the meaning of those diagnoses, the context in which they were given, or their significance. This simple exercise has a powerful effect on raising awareness to patients of the problematic nature of polydiagnosing.
Introduce de-diagnosing. The engagement of patients in the diagnostic process has a significant effect. Reviewing not only diagnostic criteria but also nosology and debates in our understanding of diagnoses can provide patients with further engagement in their care. A simple review of the debate of the bereavement exclusion may permit a patient to not only understand the complexity, but also the changing nature of diagnoses. Suddenly, they are no longer bystanders, but informed participants in their care.
Identify diagnoses most appropriate for removal. Contradictory diagnoses are common in the clinical settings we work in. We routinely see patients carrying multiple mood diagnoses, despite our diagnostic systems not permitting one to have both unipolar and bipolar depression. Superfluous diagnoses are also frequent, with patients receiving depressive, or anxious labels when in an acute state of psychosis or mania. This is exemplified by patients suffering from thought blocking and receiving cognitive or attention-related diagnoses. Concurrent yet different diagnoses are also common in patients with a different list of diagnoses by their primary care provider, their therapist, and their psychiatrist. This is particularly problematic as it forces the patient to alternate their thinking or choose between their providers.
Create a new narrative for the patient. Once diagnoses are explained, clarified, and understood, patients with the help of their providers can reexamine their life story under a new and simplified construct. This process often leads to a less confusing sense of self, an increased dedication to the treatment process, whether behavioral, social, psychological, or pharmacologic.
Consider deprescribing. With a more straightforward and more grounded list of diagnoses (or simply one diagnosis), we find the process of deprescribing to be simpler and more engaging for patients. For example, patients can clearly understand the lack of necessity of an antipsychotic prescription for a resolved substance-induced psychosis. Patients are more engaged in their care, leading to improved medication compliance and less attachment to discontinued medications.
Monitor and adapt. One should of course reevaluate diagnoses as the course of illness provides us with additional information. However, we suggest waiting for a manic episode to emerge prior to diagnosing bipolar rather than suggesting the diagnosis because a patient was wearing red shoes, spoke multiple languages, had multiple degrees and was creative.10 The contextual basis and progression of the symptoms should lead to continual reassessment of diagnoses.
Physicians are aware of the balance between Occam’s razor, which promotes the simplest single explanation for a problem, versus Hickam’s dictum that reminds us that patients can have as many diseases as they please. However, similarly to polypharmacy, “polydiagnosing” has negative effects. While the field of psychiatry’s advancing knowledge may encourage providers to diagnose their patients with the growing number of diagnoses, patients still need and benefit from a coherent and clear medical narrative. Psychiatry would be wise to recognize this concerning trend, in its attempt at rectifying polypharmacy.
Dr. Badre is a clinical and forensic psychiatrist in San Diego. He holds teaching positions at the University of California, San Diego, and the University of San Diego. He teaches medical education, psychopharmacology, ethics in psychiatry, and correctional care. Dr. Badre can be reached at his website, BadreMD.com. He has no conflicts of interest. Dr. Lehman is a professor of psychiatry at the University of California, San Diego. He is codirector of all acute and intensive psychiatric treatment at the Veterans Affairs Medical Center in San Diego, where he practices clinical psychiatry. He has no conflicts of interest.
References
1. Gupta S & Cahill JD. A prescription for “deprescribing” in psychiatry. Psychiatr Serv. 2016 Aug 1;67(8):904-7. doi: 10.1176/appi.ps.201500359.
2. Schuckit MA. Comorbidity between substance use disorders and psychiatric conditions. Addiction. 2006 Sep;101 Suppl 1:76-88. doi: 10.1111/j.1360-0443.2006.01592.x.
3. The Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, Text Revision (DSM-5-TR). American Psychiatric Association, 2022. https://psychiatry.org/psychiatrists/practice/dsm.
4. Kendler KS. An historical framework for psychiatric nosology. Psychol Med. 2009 Dec;39(12):1935-41. doi: 10.1017/S0033291709005753.
5. Regier DA et al. DSM-5 field trials in the United States and Canada. Am J Psychiatry. 2013 Jan;170(1):59-70. doi: 10.1176/appi.ajp.2012.12070999.
6. Bhattacharya R et al. When good news is bad news: psychological impact of false-positive diagnosis of HIV. AIDS Care. 2008 May;20(5):560-4. doi: 10.1080/09540120701867206.
7. Reeve E et al. Review of deprescribing processes and development of an evidence‐based, patient‐centred deprescribing process. Br J Clin Pharmacol. 2014 Oct;78(4):738-47. doi: 10.1111/bcp.12386.
8. Gupta S and Cahill JD. A prescription for “deprescribing” in psychiatry.
9. Solomon M. “On the appearance and disappearance of Asperger’s syndrome” in Kendler and Parnas (eds.) Philosophical Issues in Psychiatry IV: Classification of Psychiatric Illness. Oxford University Press, 2017. doi: 10.1093/med/9780198796022.003.0023.
10. Akiskal HS. Searching for behavioral indicators of bipolar II in patients presenting with major depressive episodes: The “red sign,” the “rule of three,” and other biographic signs of temperamental extravagance, activation, and hypomania. J Affect Disord. 2005 Feb;84(2-3):279-90. doi: 10.1016/j.jad.2004.06.002.
Schizophrenia patients in long-term facilities benefit from lower-dose antipsychotics
NEW ORLEANS –
“There is an argument by some experts in the field that state hospital populations represent a different set of patients who require higher antipsychotic dosages, with no alternative, but I don’t agree with that,” study lead author Mujeeb U. Shad, MD, GME-psychiatry program director and adjunct professor at the University of Nevada, Las Vegas, said in an interview.
In reducing doses, “patients appeared to blossom, becoming more active and less ‘zombie-like’; they started taking more interest in activities and their social [involvement] increased,” he said.

The study was among several presenting pros and cons of high antipsychotic doses at the 2022 annual meeting of the American Psychiatric Association.
Higher doses of antipsychotics are often relied upon when patients with acute psychosis fail to respond to standard treatment, however evidence supporting the approach is lacking.
And while some studies in fact show no benefit from the higher-dose maintenance therapy over conventional or even lower doses of antipsychotics, evidence regarding forensic patients hospitalized in long-term psychiatric facilities is also scant.
Meanwhile, the need to restore competency among those patients can be more pressing than normal.
“In a forensic population where executive cognitive function is one of the key elements to restore competency to stand trial, the continuation of high-dose therapy with excessive dopamine blockade may further compromise preexisting executive dysfunction to delay competency restoration,” Dr. Shad notes in the study.
The study describes a case series in which antipsychotic doses were lowered among 22 of Dr. Shad’s patients who had been determined to be incompetent to stand trial and referred to a state hospital to restore their competency.
With the objective of regaining the mental fitness to stand trial and being discharged from the facility, those on high doses of therapy, defined as a dose greater than 50% of the average package-insert dose, had their doses reduced to conventional dosages.
The approach led to as many as 68% of the patients being stabilized and discharged after having their competency restored, without symptom relapse, following an average antipsychotic dose reduction of 44%.
The average time to discharge following the dose reduction was just 2.3 months, after an average total hospitalization time of 11 months.
The shortest hospitalization durations (less than 7 months) were observed among those who did not receive changes in doses as they were already achieving efficacy with standard dosages.
Among two patients who were treated subtherapeutically, dose increases were required and they had the longest overall hospitalization (14.5 months)
Additional benefits of reduced dosages
Dr. Shad noted that, in addition to the earlier discharges, patients also had reductions in their polypharmacy, and in prolactin.
“We know that high prolactin level is such a huge problem, especially for female patients because it can cause osteoporosis, infertility, and abnormal menstruation, and the reductions in hyperprolactinemia can help reduce weight gain,” he said.
Dr. Shad added that he let some of those effects be his guide in making dose reductions.
“I was trying to gradually minimize the dose while monitoring the patients for relapse, and I used extrapyramidal symptoms and prolactin levels as my guide, looking for a sweet spot with the dosing,” he said.
“For example, if patients were taking an average of about 40-60 mg of a drug, I brought it down close to 20 mg, or close to the average package insert,” Dr. Shad said.
Key concerns among clinicians about reducing antipsychotic doses include the emergence of discontinuation or rebound symptoms, including psychosis, akathisia, or Parkinsonian symptoms, and studies, including a recent meta-analysis have supported those concerns, urging caution in reducing doses below standard levels.
However, Dr. Shad said his series suggests that reducing doses gradually while carefully monitoring extrapyramidal symptoms and prolactin levels may indeed pay off.
“They’re not the perfect guides, but they’re good guides, and with the right approach, [some] may be able to do this,” Dr. Shad said.
“However, the key to a successful dose reduction or discontinuation of an [antipsychotic medication] is to avoid abrupt discontinuation and follow a gradual dose reduction while monitoring symptoms and tolerability,” he said.

Commenting on the research, T. Scott Stroup, MD, a professor of psychiatry at Columbia University, New York, chimed in on the side of urging caution with higher doses and supporting possible benefits with the lower-dose approach.
“I agree that people who need antipsychotic medications should receive the lowest effective dose and that often this is identified by careful dose reduction,” he said in an interview.
Dr. Shad and Stroup had no disclosures to report.
NEW ORLEANS –
“There is an argument by some experts in the field that state hospital populations represent a different set of patients who require higher antipsychotic dosages, with no alternative, but I don’t agree with that,” study lead author Mujeeb U. Shad, MD, GME-psychiatry program director and adjunct professor at the University of Nevada, Las Vegas, said in an interview.
In reducing doses, “patients appeared to blossom, becoming more active and less ‘zombie-like’; they started taking more interest in activities and their social [involvement] increased,” he said.
The study was among several presenting pros and cons of high antipsychotic doses at the 2022 annual meeting of the American Psychiatric Association.
Higher doses of antipsychotics are often relied upon when patients with acute psychosis fail to respond to standard treatment, however evidence supporting the approach is lacking.
And while some studies in fact show no benefit from the higher-dose maintenance therapy over conventional or even lower doses of antipsychotics, evidence regarding forensic patients hospitalized in long-term psychiatric facilities is also scant.
Meanwhile, the need to restore competency among those patients can be more pressing than normal.
“In a forensic population where executive cognitive function is one of the key elements to restore competency to stand trial, the continuation of high-dose therapy with excessive dopamine blockade may further compromise preexisting executive dysfunction to delay competency restoration,” Dr. Shad notes in the study.
The study describes a case series in which antipsychotic doses were lowered among 22 of Dr. Shad’s patients who had been determined to be incompetent to stand trial and referred to a state hospital to restore their competency.
With the objective of regaining the mental fitness to stand trial and being discharged from the facility, those on high doses of therapy, defined as a dose greater than 50% of the average package-insert dose, had their doses reduced to conventional dosages.
The approach led to as many as 68% of the patients being stabilized and discharged after having their competency restored, without symptom relapse, following an average antipsychotic dose reduction of 44%.
The average time to discharge following the dose reduction was just 2.3 months, after an average total hospitalization time of 11 months.
The shortest hospitalization durations (less than 7 months) were observed among those who did not receive changes in doses as they were already achieving efficacy with standard dosages.
Among two patients who were treated subtherapeutically, dose increases were required and they had the longest overall hospitalization (14.5 months)
Additional benefits of reduced dosages
Dr. Shad noted that, in addition to the earlier discharges, patients also had reductions in their polypharmacy, and in prolactin.
“We know that high prolactin level is such a huge problem, especially for female patients because it can cause osteoporosis, infertility, and abnormal menstruation, and the reductions in hyperprolactinemia can help reduce weight gain,” he said.
Dr. Shad added that he let some of those effects be his guide in making dose reductions.
“I was trying to gradually minimize the dose while monitoring the patients for relapse, and I used extrapyramidal symptoms and prolactin levels as my guide, looking for a sweet spot with the dosing,” he said.
“For example, if patients were taking an average of about 40-60 mg of a drug, I brought it down close to 20 mg, or close to the average package insert,” Dr. Shad said.
Key concerns among clinicians about reducing antipsychotic doses include the emergence of discontinuation or rebound symptoms, including psychosis, akathisia, or Parkinsonian symptoms, and studies, including a recent meta-analysis have supported those concerns, urging caution in reducing doses below standard levels.
However, Dr. Shad said his series suggests that reducing doses gradually while carefully monitoring extrapyramidal symptoms and prolactin levels may indeed pay off.
“They’re not the perfect guides, but they’re good guides, and with the right approach, [some] may be able to do this,” Dr. Shad said.
“However, the key to a successful dose reduction or discontinuation of an [antipsychotic medication] is to avoid abrupt discontinuation and follow a gradual dose reduction while monitoring symptoms and tolerability,” he said.
Commenting on the research, T. Scott Stroup, MD, a professor of psychiatry at Columbia University, New York, chimed in on the side of urging caution with higher doses and supporting possible benefits with the lower-dose approach.
“I agree that people who need antipsychotic medications should receive the lowest effective dose and that often this is identified by careful dose reduction,” he said in an interview.
Dr. Shad and Stroup had no disclosures to report.
NEW ORLEANS –
“There is an argument by some experts in the field that state hospital populations represent a different set of patients who require higher antipsychotic dosages, with no alternative, but I don’t agree with that,” study lead author Mujeeb U. Shad, MD, GME-psychiatry program director and adjunct professor at the University of Nevada, Las Vegas, said in an interview.
In reducing doses, “patients appeared to blossom, becoming more active and less ‘zombie-like’; they started taking more interest in activities and their social [involvement] increased,” he said.
The study was among several presenting pros and cons of high antipsychotic doses at the 2022 annual meeting of the American Psychiatric Association.
Higher doses of antipsychotics are often relied upon when patients with acute psychosis fail to respond to standard treatment, however evidence supporting the approach is lacking.
And while some studies in fact show no benefit from the higher-dose maintenance therapy over conventional or even lower doses of antipsychotics, evidence regarding forensic patients hospitalized in long-term psychiatric facilities is also scant.
Meanwhile, the need to restore competency among those patients can be more pressing than normal.
“In a forensic population where executive cognitive function is one of the key elements to restore competency to stand trial, the continuation of high-dose therapy with excessive dopamine blockade may further compromise preexisting executive dysfunction to delay competency restoration,” Dr. Shad notes in the study.
The study describes a case series in which antipsychotic doses were lowered among 22 of Dr. Shad’s patients who had been determined to be incompetent to stand trial and referred to a state hospital to restore their competency.
With the objective of regaining the mental fitness to stand trial and being discharged from the facility, those on high doses of therapy, defined as a dose greater than 50% of the average package-insert dose, had their doses reduced to conventional dosages.
The approach led to as many as 68% of the patients being stabilized and discharged after having their competency restored, without symptom relapse, following an average antipsychotic dose reduction of 44%.
The average time to discharge following the dose reduction was just 2.3 months, after an average total hospitalization time of 11 months.
The shortest hospitalization durations (less than 7 months) were observed among those who did not receive changes in doses as they were already achieving efficacy with standard dosages.
Among two patients who were treated subtherapeutically, dose increases were required and they had the longest overall hospitalization (14.5 months)
Additional benefits of reduced dosages
Dr. Shad noted that, in addition to the earlier discharges, patients also had reductions in their polypharmacy, and in prolactin.
“We know that high prolactin level is such a huge problem, especially for female patients because it can cause osteoporosis, infertility, and abnormal menstruation, and the reductions in hyperprolactinemia can help reduce weight gain,” he said.
Dr. Shad added that he let some of those effects be his guide in making dose reductions.
“I was trying to gradually minimize the dose while monitoring the patients for relapse, and I used extrapyramidal symptoms and prolactin levels as my guide, looking for a sweet spot with the dosing,” he said.
“For example, if patients were taking an average of about 40-60 mg of a drug, I brought it down close to 20 mg, or close to the average package insert,” Dr. Shad said.
Key concerns among clinicians about reducing antipsychotic doses include the emergence of discontinuation or rebound symptoms, including psychosis, akathisia, or Parkinsonian symptoms, and studies, including a recent meta-analysis have supported those concerns, urging caution in reducing doses below standard levels.
However, Dr. Shad said his series suggests that reducing doses gradually while carefully monitoring extrapyramidal symptoms and prolactin levels may indeed pay off.
“They’re not the perfect guides, but they’re good guides, and with the right approach, [some] may be able to do this,” Dr. Shad said.
“However, the key to a successful dose reduction or discontinuation of an [antipsychotic medication] is to avoid abrupt discontinuation and follow a gradual dose reduction while monitoring symptoms and tolerability,” he said.
Commenting on the research, T. Scott Stroup, MD, a professor of psychiatry at Columbia University, New York, chimed in on the side of urging caution with higher doses and supporting possible benefits with the lower-dose approach.
“I agree that people who need antipsychotic medications should receive the lowest effective dose and that often this is identified by careful dose reduction,” he said in an interview.
Dr. Shad and Stroup had no disclosures to report.
FROM APA 2022
Motor abnormalities drive decreased function in schizophrenia
Approximately half of adults with schizophrenia suffer from motor abnormalities that may impair their ability to work and decrease their quality of life, wrote Niluja Nadesalingam, MD, of the University of Bern, Switzerland, and colleagues. “Although previous reports show strong associations between single movement abnormalities and global as well as social functioning, we still struggle to understand the contribution of various motor domains,” they said.

The impact of these abnormalities on social and global functioning and on functional capacity remains unclear, but the researchers proposed that motor abnormalities would be associated with worse functional outcomes in schizophrenia patients.
In a study published in Comprehensive Psychiatry, the researchers identified patients with diagnosed schizophrenia spectrum disorders who were treated on an inpatient or outpatient basis at a single center. They collected data on five motor abnormalities: parkinsonism, catatonia, dyskinesia, neurological soft signs (NSS), and psychomotor slowing (PS). They assessed functional outcomes using the Global Assessment of Functioning (GAF), the Social and Occupational Functioning Assessment Scale (SOFAS), and the UCSD Performance-Based Skills Assessment (UPSA-B). The average age of the participants was 37.9 years and 88 of the 156 were male. The average duration of illness was 12.5 years.
Overall, patients with catatonia and parkinsonism scored significantly lower on GAF and SOFAS scale compared to those without catatonia and parkinsonism (P < .035 and P < .027, respectively).
No significant differences in functional outcomes appeared between patients with and without dyskinesia.
However, significant negative correlations were identified for parkinsonism and PS with GAF, SOFAS, and UPSA-B (P < .036 for all). “Our study further found that parkinsonism and psychomotor slowing also impair the functional capacity of patients,” which may be influenced by factors including deficits in social interaction and cognitive impairment, the researchers said.
Overall, the study findings demonstrate that motor abnormalities in patients with schizophrenia are strongly associated with poor functional outcomes, and the stronger the motor impairment, the worse the global and social functioning, the researchers said.
As for potential pathways, “motor abnormalities are readily observable signs, allowing laypersons to perceive subjects with schizophrenia as somebody with severe mental illness. Thus, motor abnormalities might lead to stigmatization of patients suffering from schizophrenia,” they wrote in their discussion.
The researchers emphasized the need to explore alternative treatment options that might improve motor abnormalities, such as transcranial magnetic stimulation, given the potential of antipsychotic medications to introduce additional motor abnormalities.
The study findings were limited by several factors including the potential for missed confounding variables, the small number of patients with dyskinesia, and the inability to deduce the course of illness because most of the patients were in psychotic episodes, the researchers noted.
However, the results suggest that specific motor abnormalities are associated with poor global and social functioning, and with reduced functional capacity, in adults with schizophrenia, the researchers said. “Future studies need to test whether amelioration of motor abnormalities may improve community functioning,” they concluded.
The study was supported by the Swiss National Science Foundation, the Bangerter Rhyner Foundation, and the Adrian and Simone Frutiger Foundation. Lead author Dr. Nadesalingam had no financial conflicts to disclose.
Approximately half of adults with schizophrenia suffer from motor abnormalities that may impair their ability to work and decrease their quality of life, wrote Niluja Nadesalingam, MD, of the University of Bern, Switzerland, and colleagues. “Although previous reports show strong associations between single movement abnormalities and global as well as social functioning, we still struggle to understand the contribution of various motor domains,” they said.
The impact of these abnormalities on social and global functioning and on functional capacity remains unclear, but the researchers proposed that motor abnormalities would be associated with worse functional outcomes in schizophrenia patients.
In a study published in Comprehensive Psychiatry, the researchers identified patients with diagnosed schizophrenia spectrum disorders who were treated on an inpatient or outpatient basis at a single center. They collected data on five motor abnormalities: parkinsonism, catatonia, dyskinesia, neurological soft signs (NSS), and psychomotor slowing (PS). They assessed functional outcomes using the Global Assessment of Functioning (GAF), the Social and Occupational Functioning Assessment Scale (SOFAS), and the UCSD Performance-Based Skills Assessment (UPSA-B). The average age of the participants was 37.9 years and 88 of the 156 were male. The average duration of illness was 12.5 years.
Overall, patients with catatonia and parkinsonism scored significantly lower on GAF and SOFAS scale compared to those without catatonia and parkinsonism (P < .035 and P < .027, respectively).
No significant differences in functional outcomes appeared between patients with and without dyskinesia.
However, significant negative correlations were identified for parkinsonism and PS with GAF, SOFAS, and UPSA-B (P < .036 for all). “Our study further found that parkinsonism and psychomotor slowing also impair the functional capacity of patients,” which may be influenced by factors including deficits in social interaction and cognitive impairment, the researchers said.
Overall, the study findings demonstrate that motor abnormalities in patients with schizophrenia are strongly associated with poor functional outcomes, and the stronger the motor impairment, the worse the global and social functioning, the researchers said.
As for potential pathways, “motor abnormalities are readily observable signs, allowing laypersons to perceive subjects with schizophrenia as somebody with severe mental illness. Thus, motor abnormalities might lead to stigmatization of patients suffering from schizophrenia,” they wrote in their discussion.
The researchers emphasized the need to explore alternative treatment options that might improve motor abnormalities, such as transcranial magnetic stimulation, given the potential of antipsychotic medications to introduce additional motor abnormalities.
The study findings were limited by several factors including the potential for missed confounding variables, the small number of patients with dyskinesia, and the inability to deduce the course of illness because most of the patients were in psychotic episodes, the researchers noted.
However, the results suggest that specific motor abnormalities are associated with poor global and social functioning, and with reduced functional capacity, in adults with schizophrenia, the researchers said. “Future studies need to test whether amelioration of motor abnormalities may improve community functioning,” they concluded.
The study was supported by the Swiss National Science Foundation, the Bangerter Rhyner Foundation, and the Adrian and Simone Frutiger Foundation. Lead author Dr. Nadesalingam had no financial conflicts to disclose.
Approximately half of adults with schizophrenia suffer from motor abnormalities that may impair their ability to work and decrease their quality of life, wrote Niluja Nadesalingam, MD, of the University of Bern, Switzerland, and colleagues. “Although previous reports show strong associations between single movement abnormalities and global as well as social functioning, we still struggle to understand the contribution of various motor domains,” they said.
The impact of these abnormalities on social and global functioning and on functional capacity remains unclear, but the researchers proposed that motor abnormalities would be associated with worse functional outcomes in schizophrenia patients.
In a study published in Comprehensive Psychiatry, the researchers identified patients with diagnosed schizophrenia spectrum disorders who were treated on an inpatient or outpatient basis at a single center. They collected data on five motor abnormalities: parkinsonism, catatonia, dyskinesia, neurological soft signs (NSS), and psychomotor slowing (PS). They assessed functional outcomes using the Global Assessment of Functioning (GAF), the Social and Occupational Functioning Assessment Scale (SOFAS), and the UCSD Performance-Based Skills Assessment (UPSA-B). The average age of the participants was 37.9 years and 88 of the 156 were male. The average duration of illness was 12.5 years.
Overall, patients with catatonia and parkinsonism scored significantly lower on GAF and SOFAS scale compared to those without catatonia and parkinsonism (P < .035 and P < .027, respectively).
No significant differences in functional outcomes appeared between patients with and without dyskinesia.
However, significant negative correlations were identified for parkinsonism and PS with GAF, SOFAS, and UPSA-B (P < .036 for all). “Our study further found that parkinsonism and psychomotor slowing also impair the functional capacity of patients,” which may be influenced by factors including deficits in social interaction and cognitive impairment, the researchers said.
Overall, the study findings demonstrate that motor abnormalities in patients with schizophrenia are strongly associated with poor functional outcomes, and the stronger the motor impairment, the worse the global and social functioning, the researchers said.
As for potential pathways, “motor abnormalities are readily observable signs, allowing laypersons to perceive subjects with schizophrenia as somebody with severe mental illness. Thus, motor abnormalities might lead to stigmatization of patients suffering from schizophrenia,” they wrote in their discussion.
The researchers emphasized the need to explore alternative treatment options that might improve motor abnormalities, such as transcranial magnetic stimulation, given the potential of antipsychotic medications to introduce additional motor abnormalities.
The study findings were limited by several factors including the potential for missed confounding variables, the small number of patients with dyskinesia, and the inability to deduce the course of illness because most of the patients were in psychotic episodes, the researchers noted.
However, the results suggest that specific motor abnormalities are associated with poor global and social functioning, and with reduced functional capacity, in adults with schizophrenia, the researchers said. “Future studies need to test whether amelioration of motor abnormalities may improve community functioning,” they concluded.
The study was supported by the Swiss National Science Foundation, the Bangerter Rhyner Foundation, and the Adrian and Simone Frutiger Foundation. Lead author Dr. Nadesalingam had no financial conflicts to disclose.
FROM COMPREHENSIVE PSYCHIATRY
Social activities may offset psychosis risk in poor communities
, new research suggests.
A study of more than 170 young participants showed reduced hippocampal volume in those living in poor neighborhoods who had low social engagement versus their peers with greater community engagement.
“These findings demonstrate the importance of considering broader environmental influences and indices of social engagement when conceptualizing adversity and potential interventions for individuals at clinical high risk for psychosis,” co-investigator Benson Ku, MD, a postdoctoral fellow and psychiatry resident at Emory University School of Medicine, Atlanta, told this news organization.

The results were presented at the virtual American Society of Clinical Psychopharmacology annual meeting.
A personal connection
It’s well known that growing up in low-income housing is associated with lower hippocampal volume and an increased risk for schizophrenia, said Dr. Ku.
“The inverse relationship between poverty and hippocampal gray matter volume has [also] been shown to be mediated by social stress, which can include things like lack of parental caregiving and stressful life events,” he added.
Dr. Ku himself grew up in a socioeconomically disadvantaged family in Queens, New York, and he said he had initially performed poorly in school. His early experiences have helped inform his clinical and research interests in the social determinants of mental health.
“I found community support in the Boys’ Club of New York and a local Magic Shop near where I lived, which helped me thrive and become the successful man I am today. I have also heard from my patients how their living conditions and neighborhood have significantly impacted their mental health,” Dr. Ku said.
“A more in-depth understanding of the social determinants of mental health has helped build rapport and empathy with my patients,” he added.
To explore the association between neighborhood poverty, social engagement, and hippocampal volume in youth at high risk for psychosis, the researchers analyzed data from the North American Prodrome Longitudinal Study Phase 2, a multisite consortium.
The researchers recruited and followed up with help-seeking adolescents and young adults from diverse neighborhoods. The analysis included 174 youth, ages 12-33 years, at high clinical risk for psychosis.
Hippocampal volume was assessed using structural MRI. Neighborhood poverty was defined as the percentage of residents with an annual income below the poverty level in the past year.
Social engagement was derived from the desirable events subscale items of the Life Events Scale. These activities included involvement in a church or synagogue; participation in a club, neighborhood, or other organization; taking a vacation; engaging in a hobby, sport, craft, or recreational activity; acquiring a pet; or making new friends.
Lower hippocampal volume
Results showed neighborhood poverty was associated with reduced hippocampal volume, even after controlling for several confounders, including race/ethnicity, family history of mental illnesses, household poverty, educational level, and stressful life events.
Among the 77 participants with lower social engagement, which was defined as three or fewer social activities, neighborhood poverty was associated with reduced hippocampal volume.
However, in the 97 participants who reported greater social engagement, which was defined as four or more social activities, neighborhood poverty was not significantly associated with hippocampal volume.
“It is possible that social engagement may mitigate the deleterious effects of neighborhood poverty on brain morphology, which may inform interventions offered to individuals from disadvantaged neighborhoods,” Dr. Ku said.
“If replication of the relationships between neighborhood poverty, hippocampal volume, and social engagement is established in other populations in longitudinal studies, then targeted interventions at the community level and increased social engagement may potentially play a major role in disease prevention among at-risk youth,” he said.
Dr. Ku noted social engagement might look different in urban versus rural settings.
“In urban areas, it might mean friends, clubs, neighborhood organizations, etc. In rural areas, it might mean family, pets, crafts, etc. The level of social engagement may also depend on neighborhood characteristics, and more research would be needed to better understand how geographic area characteristics – remote, rural, urban – affects social engagement,” he said.
Interesting, innovative
Nagy Youssef, MD, PhD, director of clinical research and professor of psychiatry, Ohio State University College of Medicine, Columbus, said the study suggests “social engagement may reduce the negative effect of poverty in this population, and if replicated in a larger study, could assist and be a part of the early intervention and prevention in psychosis.”

Overall, “this is an interesting and innovative study that has important medical and social implications and is a good step toward helping us understand these relationships and mitigate and prevent negative consequences, as best as possible, in this population,” said Dr. Youssef, who was not part of the research.
The analysis was supported by a grant from the National Institute of Mental Health to the North American Prodrome Longitudinal Study. Dr. Ku and Dr. Youssef report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
, new research suggests.
A study of more than 170 young participants showed reduced hippocampal volume in those living in poor neighborhoods who had low social engagement versus their peers with greater community engagement.
“These findings demonstrate the importance of considering broader environmental influences and indices of social engagement when conceptualizing adversity and potential interventions for individuals at clinical high risk for psychosis,” co-investigator Benson Ku, MD, a postdoctoral fellow and psychiatry resident at Emory University School of Medicine, Atlanta, told this news organization.
The results were presented at the virtual American Society of Clinical Psychopharmacology annual meeting.
A personal connection
It’s well known that growing up in low-income housing is associated with lower hippocampal volume and an increased risk for schizophrenia, said Dr. Ku.
“The inverse relationship between poverty and hippocampal gray matter volume has [also] been shown to be mediated by social stress, which can include things like lack of parental caregiving and stressful life events,” he added.
Dr. Ku himself grew up in a socioeconomically disadvantaged family in Queens, New York, and he said he had initially performed poorly in school. His early experiences have helped inform his clinical and research interests in the social determinants of mental health.
“I found community support in the Boys’ Club of New York and a local Magic Shop near where I lived, which helped me thrive and become the successful man I am today. I have also heard from my patients how their living conditions and neighborhood have significantly impacted their mental health,” Dr. Ku said.
“A more in-depth understanding of the social determinants of mental health has helped build rapport and empathy with my patients,” he added.
To explore the association between neighborhood poverty, social engagement, and hippocampal volume in youth at high risk for psychosis, the researchers analyzed data from the North American Prodrome Longitudinal Study Phase 2, a multisite consortium.
The researchers recruited and followed up with help-seeking adolescents and young adults from diverse neighborhoods. The analysis included 174 youth, ages 12-33 years, at high clinical risk for psychosis.
Hippocampal volume was assessed using structural MRI. Neighborhood poverty was defined as the percentage of residents with an annual income below the poverty level in the past year.
Social engagement was derived from the desirable events subscale items of the Life Events Scale. These activities included involvement in a church or synagogue; participation in a club, neighborhood, or other organization; taking a vacation; engaging in a hobby, sport, craft, or recreational activity; acquiring a pet; or making new friends.
Lower hippocampal volume
Results showed neighborhood poverty was associated with reduced hippocampal volume, even after controlling for several confounders, including race/ethnicity, family history of mental illnesses, household poverty, educational level, and stressful life events.
Among the 77 participants with lower social engagement, which was defined as three or fewer social activities, neighborhood poverty was associated with reduced hippocampal volume.
However, in the 97 participants who reported greater social engagement, which was defined as four or more social activities, neighborhood poverty was not significantly associated with hippocampal volume.
“It is possible that social engagement may mitigate the deleterious effects of neighborhood poverty on brain morphology, which may inform interventions offered to individuals from disadvantaged neighborhoods,” Dr. Ku said.
“If replication of the relationships between neighborhood poverty, hippocampal volume, and social engagement is established in other populations in longitudinal studies, then targeted interventions at the community level and increased social engagement may potentially play a major role in disease prevention among at-risk youth,” he said.
Dr. Ku noted social engagement might look different in urban versus rural settings.
“In urban areas, it might mean friends, clubs, neighborhood organizations, etc. In rural areas, it might mean family, pets, crafts, etc. The level of social engagement may also depend on neighborhood characteristics, and more research would be needed to better understand how geographic area characteristics – remote, rural, urban – affects social engagement,” he said.
Interesting, innovative
Nagy Youssef, MD, PhD, director of clinical research and professor of psychiatry, Ohio State University College of Medicine, Columbus, said the study suggests “social engagement may reduce the negative effect of poverty in this population, and if replicated in a larger study, could assist and be a part of the early intervention and prevention in psychosis.”
Overall, “this is an interesting and innovative study that has important medical and social implications and is a good step toward helping us understand these relationships and mitigate and prevent negative consequences, as best as possible, in this population,” said Dr. Youssef, who was not part of the research.
The analysis was supported by a grant from the National Institute of Mental Health to the North American Prodrome Longitudinal Study. Dr. Ku and Dr. Youssef report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
, new research suggests.
A study of more than 170 young participants showed reduced hippocampal volume in those living in poor neighborhoods who had low social engagement versus their peers with greater community engagement.
“These findings demonstrate the importance of considering broader environmental influences and indices of social engagement when conceptualizing adversity and potential interventions for individuals at clinical high risk for psychosis,” co-investigator Benson Ku, MD, a postdoctoral fellow and psychiatry resident at Emory University School of Medicine, Atlanta, told this news organization.
The results were presented at the virtual American Society of Clinical Psychopharmacology annual meeting.
A personal connection
It’s well known that growing up in low-income housing is associated with lower hippocampal volume and an increased risk for schizophrenia, said Dr. Ku.
“The inverse relationship between poverty and hippocampal gray matter volume has [also] been shown to be mediated by social stress, which can include things like lack of parental caregiving and stressful life events,” he added.
Dr. Ku himself grew up in a socioeconomically disadvantaged family in Queens, New York, and he said he had initially performed poorly in school. His early experiences have helped inform his clinical and research interests in the social determinants of mental health.
“I found community support in the Boys’ Club of New York and a local Magic Shop near where I lived, which helped me thrive and become the successful man I am today. I have also heard from my patients how their living conditions and neighborhood have significantly impacted their mental health,” Dr. Ku said.
“A more in-depth understanding of the social determinants of mental health has helped build rapport and empathy with my patients,” he added.
To explore the association between neighborhood poverty, social engagement, and hippocampal volume in youth at high risk for psychosis, the researchers analyzed data from the North American Prodrome Longitudinal Study Phase 2, a multisite consortium.
The researchers recruited and followed up with help-seeking adolescents and young adults from diverse neighborhoods. The analysis included 174 youth, ages 12-33 years, at high clinical risk for psychosis.
Hippocampal volume was assessed using structural MRI. Neighborhood poverty was defined as the percentage of residents with an annual income below the poverty level in the past year.
Social engagement was derived from the desirable events subscale items of the Life Events Scale. These activities included involvement in a church or synagogue; participation in a club, neighborhood, or other organization; taking a vacation; engaging in a hobby, sport, craft, or recreational activity; acquiring a pet; or making new friends.
Lower hippocampal volume
Results showed neighborhood poverty was associated with reduced hippocampal volume, even after controlling for several confounders, including race/ethnicity, family history of mental illnesses, household poverty, educational level, and stressful life events.
Among the 77 participants with lower social engagement, which was defined as three or fewer social activities, neighborhood poverty was associated with reduced hippocampal volume.
However, in the 97 participants who reported greater social engagement, which was defined as four or more social activities, neighborhood poverty was not significantly associated with hippocampal volume.
“It is possible that social engagement may mitigate the deleterious effects of neighborhood poverty on brain morphology, which may inform interventions offered to individuals from disadvantaged neighborhoods,” Dr. Ku said.
“If replication of the relationships between neighborhood poverty, hippocampal volume, and social engagement is established in other populations in longitudinal studies, then targeted interventions at the community level and increased social engagement may potentially play a major role in disease prevention among at-risk youth,” he said.
Dr. Ku noted social engagement might look different in urban versus rural settings.
“In urban areas, it might mean friends, clubs, neighborhood organizations, etc. In rural areas, it might mean family, pets, crafts, etc. The level of social engagement may also depend on neighborhood characteristics, and more research would be needed to better understand how geographic area characteristics – remote, rural, urban – affects social engagement,” he said.
Interesting, innovative
Nagy Youssef, MD, PhD, director of clinical research and professor of psychiatry, Ohio State University College of Medicine, Columbus, said the study suggests “social engagement may reduce the negative effect of poverty in this population, and if replicated in a larger study, could assist and be a part of the early intervention and prevention in psychosis.”
Overall, “this is an interesting and innovative study that has important medical and social implications and is a good step toward helping us understand these relationships and mitigate and prevent negative consequences, as best as possible, in this population,” said Dr. Youssef, who was not part of the research.
The analysis was supported by a grant from the National Institute of Mental Health to the North American Prodrome Longitudinal Study. Dr. Ku and Dr. Youssef report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM ASCP 2022
Antipsychotic tied to dose-related weight gain, higher cholesterol
new research suggests.
Investigators analyzed 1-year data for more than 400 patients who were taking risperidone and/or its metabolite paliperidone (Invega). Results showed increments of 1 mg of risperidone-equivalent doses were associated with an increase of 0.25% of weight within a year of follow-up.
“Although our findings report a positive and statistically significant dose-dependence of weight gain and cholesterol, both total and LDL [cholesterol], the size of the predicted changes of metabolic effects is clinically nonrelevant,” lead author Marianna Piras, PharmD, Centre for Psychiatric Neuroscience, Lausanne (Switzerland) University Hospital, said in an interview.
“Therefore, dose lowering would not have a beneficial effect on attenuating weight gain or cholesterol increases and could lead to psychiatric decompensation,” said Ms. Piras, who is also a PhD candidate in the unit of pharmacogenetics and clinical psychopharmacology at the University of Lausanne.
However, she added that because dose increments could increase risk for significant weight gain in the first month of treatment – the dose can be increased typically in a range of 1-10 grams – and strong dose increments could contribute to metabolic worsening over time, “risperidone minimum effective doses should be preferred.”
The findings were published online in the Journal of Clinical Psychiatry.
‘Serious public health issue’
Compared with the general population, patients with mental illness present with a greater prevalence of metabolic disorders. In addition, several psychotropic medications, including antipsychotics, can induce metabolic alterations such as weight gain, the investigators noted.
Antipsychotic-induced metabolic adverse effects “constitute a serious public health issue” because they are risk factors for cardiovascular diseases such as obesity and/or dyslipidemia, “which have been associated with a 10-year reduced life expectancy in the psychiatric population,” Ms. Piras said.
“The dose-dependence of metabolic adverse effects is a debated subject that needs to be assessed for each psychotropic drug known to induce weight gain,” she added.
Several previous studies have examined whether there is a dose-related effect of antipsychotics on metabolic parameters, “with some results suggesting that [weight gain] seems to develop even when low off-label doses are prescribed,” Ms. Piras noted.
She and her colleagues had already studied dose-related metabolic effects of quetiapine (Seroquel) and olanzapine (Zyprexa).
Risperidone is an antipsychotic with a “medium to high metabolic risk profile,” the researchers note, and few studies have examined the impact of risperidone on metabolic parameters other than weight gain.
For the current analysis, they analyzed data from a longitudinal study that included 438 patients (mean age, 40.7 years; 50.7% men) who started treatment with risperidone and/or paliperidone between 2007 and 2018.
The participants had diagnoses of schizophrenia, schizoaffective disorder, bipolar disorder, depression, “other,” or “unknown.”
Clinical follow-up periods were up to a year, but were no shorter than 3 weeks. The investigators also assessed the data at different time intervals at 1, 3, 6, and 12 months “to appreciate the evolution of the metabolic parameters.”
In addition, they collected demographic and clinical information, such as comorbidities, and measured patients’ weight, height, waist circumference, blood pressure, plasma glucose, and lipids at baseline and at 1, 3, and 12 months and then annually. Weight, waist circumference, and BP were also assessed at 2 and 6 months.
Doses of paliperidone were converted into risperidone-equivalent doses.
Significant weight gain over time
The mean duration of follow-up for the participants, of whom 374 were being treated with risperidone and 64 with paliperidone, was 153 days. Close to half (48.2%) were taking other psychotropic medications known to be associated with some degree of metabolic risk.
Patients were divided into two cohorts based on their daily dose intake (DDI): less than 3 mg/day (n = 201) and at least 3 mg/day (n = 237).
In the overall cohort, a “significant effect of time on weight change was found for each time point,” the investigators reported.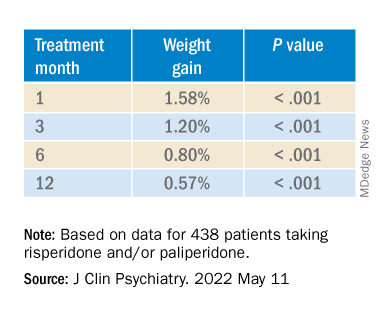
When the researchers looked at the changes according to DDI, they found that each 1-mg dose increase was associated with incremental weight gain at each time point.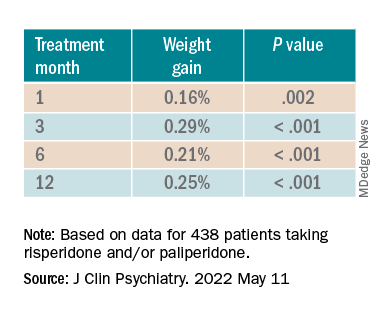
Patients who had 5% or greater weight gain in the first month continued to gain weight more than patients who did not reach that threshold, leading the researchers to call that early threshold a “strong predictor of important weight gain in the long term.” There was a weight gain of 6.68% at 3 months, of 7.36% at 6 months, and of 7.7% at 12 months.
After the patients were stratified by age, there were differences in the effect of DDI on various age groups at different time points.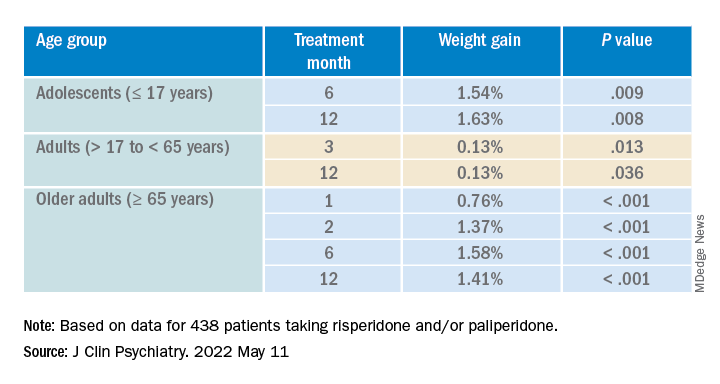
Dose was shown to have a significant effect on weight gain for women at all four time points (P ≥ .001), but for men only at 3 months (P = .003).
For each additional 1-mg dose, there was a 0.05 mmol/L (1.93 mg/dL) increase in total cholesterol (P = .018) after 1 year and a 0.04 mmol/L (1.54 mg/dL) increase in LDL cholesterol (P = .011).
There were no significant effects of time or DDI on triglycerides, HDL cholesterol, glucose levels, and systolic BP, and there was a negative effect of DDI on diastolic BP (P = .001).
The findings “provide evidence for a small dose effect of risperidone” on weight gain and total and LDL cholesterol levels, the investigators note.
Ms. Piras added that because each antipsychotic differs in its metabolic risk profile, “further analyses on other antipsychotics are ongoing in our laboratory, so far confirming our findings.”
Small increases, big changes
Commenting on the study, Erika Nurmi, MD, PhD, associate professor in the department of psychiatry and biobehavioral sciences at the Semel Institute for Neuroscience, University of California, Los Angeles, said the study is “unique in the field.”

It “leverages real-world data from a large patient registry to ask a long-unanswered question: Are weight and metabolic adverse effects proportional to dose? Big data approaches like these are very powerful, given the large number of participants that can be included,” said Dr. Nurmi, who was not involved with the research.
However, she cautioned, the “biggest drawback [is that] these data are by nature much more complex and prone to confounding effects.”
In this case, a “critical confounder” for the study was that the majority of individuals taking higher risperidone doses were also taking other drugs known to cause weight gain, whereas the majority of those on lower risperidone doses were not. “This difference may explain the dose relationship observed,” she said.
Because real-world, big data are “valuable but also messy, conclusions drawn from them must be interpreted with caution,” Dr. Nurmi said.
She added that it is generally wise to use the lowest effective dose possible.
“Clinicians should appreciate that even small doses of antipsychotics can cause big changes in weight. Risks and benefits of medications must be carefully considered in clinical practice,” Dr. Nurmi said.
The research was funded in part by the Swiss National Research Foundation. Piras reports no relevant financial relationships. The other investigators’ disclosures are listed in the original article. Dr. Nurmi reported no relevant financial relationships, but she is an unpaid member of the Tourette Association of America’s medical advisory board and of the Myriad Genetics scientific advisory board.
A version of this article first appeared on Medscape.com.
new research suggests.
Investigators analyzed 1-year data for more than 400 patients who were taking risperidone and/or its metabolite paliperidone (Invega). Results showed increments of 1 mg of risperidone-equivalent doses were associated with an increase of 0.25% of weight within a year of follow-up.
“Although our findings report a positive and statistically significant dose-dependence of weight gain and cholesterol, both total and LDL [cholesterol], the size of the predicted changes of metabolic effects is clinically nonrelevant,” lead author Marianna Piras, PharmD, Centre for Psychiatric Neuroscience, Lausanne (Switzerland) University Hospital, said in an interview.
“Therefore, dose lowering would not have a beneficial effect on attenuating weight gain or cholesterol increases and could lead to psychiatric decompensation,” said Ms. Piras, who is also a PhD candidate in the unit of pharmacogenetics and clinical psychopharmacology at the University of Lausanne.
However, she added that because dose increments could increase risk for significant weight gain in the first month of treatment – the dose can be increased typically in a range of 1-10 grams – and strong dose increments could contribute to metabolic worsening over time, “risperidone minimum effective doses should be preferred.”
The findings were published online in the Journal of Clinical Psychiatry.
‘Serious public health issue’
Compared with the general population, patients with mental illness present with a greater prevalence of metabolic disorders. In addition, several psychotropic medications, including antipsychotics, can induce metabolic alterations such as weight gain, the investigators noted.
Antipsychotic-induced metabolic adverse effects “constitute a serious public health issue” because they are risk factors for cardiovascular diseases such as obesity and/or dyslipidemia, “which have been associated with a 10-year reduced life expectancy in the psychiatric population,” Ms. Piras said.
“The dose-dependence of metabolic adverse effects is a debated subject that needs to be assessed for each psychotropic drug known to induce weight gain,” she added.
Several previous studies have examined whether there is a dose-related effect of antipsychotics on metabolic parameters, “with some results suggesting that [weight gain] seems to develop even when low off-label doses are prescribed,” Ms. Piras noted.
She and her colleagues had already studied dose-related metabolic effects of quetiapine (Seroquel) and olanzapine (Zyprexa).
Risperidone is an antipsychotic with a “medium to high metabolic risk profile,” the researchers note, and few studies have examined the impact of risperidone on metabolic parameters other than weight gain.
For the current analysis, they analyzed data from a longitudinal study that included 438 patients (mean age, 40.7 years; 50.7% men) who started treatment with risperidone and/or paliperidone between 2007 and 2018.
The participants had diagnoses of schizophrenia, schizoaffective disorder, bipolar disorder, depression, “other,” or “unknown.”
Clinical follow-up periods were up to a year, but were no shorter than 3 weeks. The investigators also assessed the data at different time intervals at 1, 3, 6, and 12 months “to appreciate the evolution of the metabolic parameters.”
In addition, they collected demographic and clinical information, such as comorbidities, and measured patients’ weight, height, waist circumference, blood pressure, plasma glucose, and lipids at baseline and at 1, 3, and 12 months and then annually. Weight, waist circumference, and BP were also assessed at 2 and 6 months.
Doses of paliperidone were converted into risperidone-equivalent doses.
Significant weight gain over time
The mean duration of follow-up for the participants, of whom 374 were being treated with risperidone and 64 with paliperidone, was 153 days. Close to half (48.2%) were taking other psychotropic medications known to be associated with some degree of metabolic risk.
Patients were divided into two cohorts based on their daily dose intake (DDI): less than 3 mg/day (n = 201) and at least 3 mg/day (n = 237).
In the overall cohort, a “significant effect of time on weight change was found for each time point,” the investigators reported.
When the researchers looked at the changes according to DDI, they found that each 1-mg dose increase was associated with incremental weight gain at each time point.
Patients who had 5% or greater weight gain in the first month continued to gain weight more than patients who did not reach that threshold, leading the researchers to call that early threshold a “strong predictor of important weight gain in the long term.” There was a weight gain of 6.68% at 3 months, of 7.36% at 6 months, and of 7.7% at 12 months.
After the patients were stratified by age, there were differences in the effect of DDI on various age groups at different time points.
Dose was shown to have a significant effect on weight gain for women at all four time points (P ≥ .001), but for men only at 3 months (P = .003).
For each additional 1-mg dose, there was a 0.05 mmol/L (1.93 mg/dL) increase in total cholesterol (P = .018) after 1 year and a 0.04 mmol/L (1.54 mg/dL) increase in LDL cholesterol (P = .011).
There were no significant effects of time or DDI on triglycerides, HDL cholesterol, glucose levels, and systolic BP, and there was a negative effect of DDI on diastolic BP (P = .001).
The findings “provide evidence for a small dose effect of risperidone” on weight gain and total and LDL cholesterol levels, the investigators note.
Ms. Piras added that because each antipsychotic differs in its metabolic risk profile, “further analyses on other antipsychotics are ongoing in our laboratory, so far confirming our findings.”
Small increases, big changes
Commenting on the study, Erika Nurmi, MD, PhD, associate professor in the department of psychiatry and biobehavioral sciences at the Semel Institute for Neuroscience, University of California, Los Angeles, said the study is “unique in the field.”
It “leverages real-world data from a large patient registry to ask a long-unanswered question: Are weight and metabolic adverse effects proportional to dose? Big data approaches like these are very powerful, given the large number of participants that can be included,” said Dr. Nurmi, who was not involved with the research.
However, she cautioned, the “biggest drawback [is that] these data are by nature much more complex and prone to confounding effects.”
In this case, a “critical confounder” for the study was that the majority of individuals taking higher risperidone doses were also taking other drugs known to cause weight gain, whereas the majority of those on lower risperidone doses were not. “This difference may explain the dose relationship observed,” she said.
Because real-world, big data are “valuable but also messy, conclusions drawn from them must be interpreted with caution,” Dr. Nurmi said.
She added that it is generally wise to use the lowest effective dose possible.
“Clinicians should appreciate that even small doses of antipsychotics can cause big changes in weight. Risks and benefits of medications must be carefully considered in clinical practice,” Dr. Nurmi said.
The research was funded in part by the Swiss National Research Foundation. Piras reports no relevant financial relationships. The other investigators’ disclosures are listed in the original article. Dr. Nurmi reported no relevant financial relationships, but she is an unpaid member of the Tourette Association of America’s medical advisory board and of the Myriad Genetics scientific advisory board.
A version of this article first appeared on Medscape.com.
new research suggests.
Investigators analyzed 1-year data for more than 400 patients who were taking risperidone and/or its metabolite paliperidone (Invega). Results showed increments of 1 mg of risperidone-equivalent doses were associated with an increase of 0.25% of weight within a year of follow-up.
“Although our findings report a positive and statistically significant dose-dependence of weight gain and cholesterol, both total and LDL [cholesterol], the size of the predicted changes of metabolic effects is clinically nonrelevant,” lead author Marianna Piras, PharmD, Centre for Psychiatric Neuroscience, Lausanne (Switzerland) University Hospital, said in an interview.
“Therefore, dose lowering would not have a beneficial effect on attenuating weight gain or cholesterol increases and could lead to psychiatric decompensation,” said Ms. Piras, who is also a PhD candidate in the unit of pharmacogenetics and clinical psychopharmacology at the University of Lausanne.
However, she added that because dose increments could increase risk for significant weight gain in the first month of treatment – the dose can be increased typically in a range of 1-10 grams – and strong dose increments could contribute to metabolic worsening over time, “risperidone minimum effective doses should be preferred.”
The findings were published online in the Journal of Clinical Psychiatry.
‘Serious public health issue’
Compared with the general population, patients with mental illness present with a greater prevalence of metabolic disorders. In addition, several psychotropic medications, including antipsychotics, can induce metabolic alterations such as weight gain, the investigators noted.
Antipsychotic-induced metabolic adverse effects “constitute a serious public health issue” because they are risk factors for cardiovascular diseases such as obesity and/or dyslipidemia, “which have been associated with a 10-year reduced life expectancy in the psychiatric population,” Ms. Piras said.
“The dose-dependence of metabolic adverse effects is a debated subject that needs to be assessed for each psychotropic drug known to induce weight gain,” she added.
Several previous studies have examined whether there is a dose-related effect of antipsychotics on metabolic parameters, “with some results suggesting that [weight gain] seems to develop even when low off-label doses are prescribed,” Ms. Piras noted.
She and her colleagues had already studied dose-related metabolic effects of quetiapine (Seroquel) and olanzapine (Zyprexa).
Risperidone is an antipsychotic with a “medium to high metabolic risk profile,” the researchers note, and few studies have examined the impact of risperidone on metabolic parameters other than weight gain.
For the current analysis, they analyzed data from a longitudinal study that included 438 patients (mean age, 40.7 years; 50.7% men) who started treatment with risperidone and/or paliperidone between 2007 and 2018.
The participants had diagnoses of schizophrenia, schizoaffective disorder, bipolar disorder, depression, “other,” or “unknown.”
Clinical follow-up periods were up to a year, but were no shorter than 3 weeks. The investigators also assessed the data at different time intervals at 1, 3, 6, and 12 months “to appreciate the evolution of the metabolic parameters.”
In addition, they collected demographic and clinical information, such as comorbidities, and measured patients’ weight, height, waist circumference, blood pressure, plasma glucose, and lipids at baseline and at 1, 3, and 12 months and then annually. Weight, waist circumference, and BP were also assessed at 2 and 6 months.
Doses of paliperidone were converted into risperidone-equivalent doses.
Significant weight gain over time
The mean duration of follow-up for the participants, of whom 374 were being treated with risperidone and 64 with paliperidone, was 153 days. Close to half (48.2%) were taking other psychotropic medications known to be associated with some degree of metabolic risk.
Patients were divided into two cohorts based on their daily dose intake (DDI): less than 3 mg/day (n = 201) and at least 3 mg/day (n = 237).
In the overall cohort, a “significant effect of time on weight change was found for each time point,” the investigators reported.
When the researchers looked at the changes according to DDI, they found that each 1-mg dose increase was associated with incremental weight gain at each time point.
Patients who had 5% or greater weight gain in the first month continued to gain weight more than patients who did not reach that threshold, leading the researchers to call that early threshold a “strong predictor of important weight gain in the long term.” There was a weight gain of 6.68% at 3 months, of 7.36% at 6 months, and of 7.7% at 12 months.
After the patients were stratified by age, there were differences in the effect of DDI on various age groups at different time points.
Dose was shown to have a significant effect on weight gain for women at all four time points (P ≥ .001), but for men only at 3 months (P = .003).
For each additional 1-mg dose, there was a 0.05 mmol/L (1.93 mg/dL) increase in total cholesterol (P = .018) after 1 year and a 0.04 mmol/L (1.54 mg/dL) increase in LDL cholesterol (P = .011).
There were no significant effects of time or DDI on triglycerides, HDL cholesterol, glucose levels, and systolic BP, and there was a negative effect of DDI on diastolic BP (P = .001).
The findings “provide evidence for a small dose effect of risperidone” on weight gain and total and LDL cholesterol levels, the investigators note.
Ms. Piras added that because each antipsychotic differs in its metabolic risk profile, “further analyses on other antipsychotics are ongoing in our laboratory, so far confirming our findings.”
Small increases, big changes
Commenting on the study, Erika Nurmi, MD, PhD, associate professor in the department of psychiatry and biobehavioral sciences at the Semel Institute for Neuroscience, University of California, Los Angeles, said the study is “unique in the field.”
It “leverages real-world data from a large patient registry to ask a long-unanswered question: Are weight and metabolic adverse effects proportional to dose? Big data approaches like these are very powerful, given the large number of participants that can be included,” said Dr. Nurmi, who was not involved with the research.
However, she cautioned, the “biggest drawback [is that] these data are by nature much more complex and prone to confounding effects.”
In this case, a “critical confounder” for the study was that the majority of individuals taking higher risperidone doses were also taking other drugs known to cause weight gain, whereas the majority of those on lower risperidone doses were not. “This difference may explain the dose relationship observed,” she said.
Because real-world, big data are “valuable but also messy, conclusions drawn from them must be interpreted with caution,” Dr. Nurmi said.
She added that it is generally wise to use the lowest effective dose possible.
“Clinicians should appreciate that even small doses of antipsychotics can cause big changes in weight. Risks and benefits of medications must be carefully considered in clinical practice,” Dr. Nurmi said.
The research was funded in part by the Swiss National Research Foundation. Piras reports no relevant financial relationships. The other investigators’ disclosures are listed in the original article. Dr. Nurmi reported no relevant financial relationships, but she is an unpaid member of the Tourette Association of America’s medical advisory board and of the Myriad Genetics scientific advisory board.
A version of this article first appeared on Medscape.com.
FROM THE JOURNAL OF CLINICAL PSYCHIATRY
Long-term schizophrenia treatment may not always be necessary
NEW ORLEANS – Patients with new-onset schizophrenia often ask psychiatrist Stephen R. Marder, MD, whether they’ll need to be on medications forever to treat the disorder. Now, he said, research is showing that the answer isn’t always yes.
In many cases, “it’s an open question” whether lifelong medical treatment is needed, said Dr. Marder, a professor at the Semel Institute for Neuroscience and Human Behavior at the University of California, Los Angeles, who spoke in a presentation about schizophrenia treatment at the annual meeting of the American Psychiatric Association.

According to Dr. Marder, research about relapses suggests that there may be a subpopulation of patients who can come off antipsychotics and remain in remission or partial remission. “The problem,” he said, “is that group is very hard to identify.”
Indeed, he highlighted a 2017 study that suggested The study noted choosing the best candidates isn’t simple, as “we do not have clinical measures or biomarkers that allow us to identify them prospectively. Because relapses and delays in the treatment of psychosis have been associated with poorer outcomes, there may be risk associated with withholding or discontinuing medication.”
There are more complications. There’s some evidence that antipsychotic drugs reduce brain volume, Dr. Marder said. But on the other hand, each psychotic episode can itself be harmful. “There is clear evidence that for each psychotic episode, they can take longer to improve, and they need higher doses.”
What to do? “My suggestion for most patients is to keep them on a relatively mild dose of an antipsychotic,” Dr. Marder said, “then to have a gradual decrease in the dose. I’ve done it in many patients.”
Which drug is best over the long term – oral or long-acting injectable antipsychotics? “It’s a hard question to answer because if you rely on randomized clinical trials – with patients who signed consent and are willing to be in a study like that – the subjects are sometimes not the ones who benefit the most from the long-acting drugs. So for many of the randomized clinical trials, the data was incomplete, and it was hard to make the case.”
But if you combine meta-analyses and cohort studies, as a 2021 study did, “you come up with a really clear answer: LAIs [long-acting injectables] are superior. They lead to a superior outcomes when it comes to rehospitalization and psychotic relapse,” Dr. Marder said.
That study reported that “LAIs were more beneficial than oral antipsychotics in 60 [18.3%] of 328 comparisons, not different in 252 [76.8%] comparisons, and less beneficial in 16 [4.9%] comparisons.”
More schizophrenia treatment pearls
People with schizophrenia – including those who aren’t on medication – face three times the risk of developing type 2 diabetes as the general population, “maybe because there’s a shared genetic risk for both disorders,” Dr. Marder said. “Those of you who have a lot of schizophrenia patients, I suspect you’re monitoring if they’re treating their type 2 diabetes and their obesity.”
Which antipsychotics are the best option for these patients? He highlighted a 2020 systematic review and meta-analysis that offers helpful insight into connections between 18 drugs and factors like weight and cholesterol.
Dr. Marder added that “if somebody has an elevation in their triglycerides or [hemoglobin] A1c in one single fasting blood glucose during the first 6 weeks of treatment, even if they haven’t been rated, it suggests that they’re developing insulin resistance.” At that point, he said, it’s a good idea to reconsider the medication choice.
Also, he said, keep in mind that “there’s substantial evidence that metformin is the appropriate treatment for patients who begin to demonstrate insulin resistance. It also works sometimes for weight loss.”
Exercise in people with schizophrenia can pay important dividends. A 2016 meta-analysis suggests that “not only does exercise for people with schizophrenia lead to better cardiovascular health, it’s good for the brain and improves cognitive functioning,” Dr. Marder said. “It’s not easy sometimes to get people with schizophrenia to exercise, but it’s many times worth the effort.”
Dr. Marder reported consulting for Boehringer Ingelheim, Lundbeck, Otsuka, Roche, Neurocrine, Sunovion, Newron, Merck, and Biogen; editor of UptoDate and Schizophrenia Bulletin Open; and research support from Boehringer Ingelheim.
NEW ORLEANS – Patients with new-onset schizophrenia often ask psychiatrist Stephen R. Marder, MD, whether they’ll need to be on medications forever to treat the disorder. Now, he said, research is showing that the answer isn’t always yes.
In many cases, “it’s an open question” whether lifelong medical treatment is needed, said Dr. Marder, a professor at the Semel Institute for Neuroscience and Human Behavior at the University of California, Los Angeles, who spoke in a presentation about schizophrenia treatment at the annual meeting of the American Psychiatric Association.
According to Dr. Marder, research about relapses suggests that there may be a subpopulation of patients who can come off antipsychotics and remain in remission or partial remission. “The problem,” he said, “is that group is very hard to identify.”
Indeed, he highlighted a 2017 study that suggested The study noted choosing the best candidates isn’t simple, as “we do not have clinical measures or biomarkers that allow us to identify them prospectively. Because relapses and delays in the treatment of psychosis have been associated with poorer outcomes, there may be risk associated with withholding or discontinuing medication.”
There are more complications. There’s some evidence that antipsychotic drugs reduce brain volume, Dr. Marder said. But on the other hand, each psychotic episode can itself be harmful. “There is clear evidence that for each psychotic episode, they can take longer to improve, and they need higher doses.”
What to do? “My suggestion for most patients is to keep them on a relatively mild dose of an antipsychotic,” Dr. Marder said, “then to have a gradual decrease in the dose. I’ve done it in many patients.”
Which drug is best over the long term – oral or long-acting injectable antipsychotics? “It’s a hard question to answer because if you rely on randomized clinical trials – with patients who signed consent and are willing to be in a study like that – the subjects are sometimes not the ones who benefit the most from the long-acting drugs. So for many of the randomized clinical trials, the data was incomplete, and it was hard to make the case.”
But if you combine meta-analyses and cohort studies, as a 2021 study did, “you come up with a really clear answer: LAIs [long-acting injectables] are superior. They lead to a superior outcomes when it comes to rehospitalization and psychotic relapse,” Dr. Marder said.
That study reported that “LAIs were more beneficial than oral antipsychotics in 60 [18.3%] of 328 comparisons, not different in 252 [76.8%] comparisons, and less beneficial in 16 [4.9%] comparisons.”
More schizophrenia treatment pearls
People with schizophrenia – including those who aren’t on medication – face three times the risk of developing type 2 diabetes as the general population, “maybe because there’s a shared genetic risk for both disorders,” Dr. Marder said. “Those of you who have a lot of schizophrenia patients, I suspect you’re monitoring if they’re treating their type 2 diabetes and their obesity.”
Which antipsychotics are the best option for these patients? He highlighted a 2020 systematic review and meta-analysis that offers helpful insight into connections between 18 drugs and factors like weight and cholesterol.
Dr. Marder added that “if somebody has an elevation in their triglycerides or [hemoglobin] A1c in one single fasting blood glucose during the first 6 weeks of treatment, even if they haven’t been rated, it suggests that they’re developing insulin resistance.” At that point, he said, it’s a good idea to reconsider the medication choice.
Also, he said, keep in mind that “there’s substantial evidence that metformin is the appropriate treatment for patients who begin to demonstrate insulin resistance. It also works sometimes for weight loss.”
Exercise in people with schizophrenia can pay important dividends. A 2016 meta-analysis suggests that “not only does exercise for people with schizophrenia lead to better cardiovascular health, it’s good for the brain and improves cognitive functioning,” Dr. Marder said. “It’s not easy sometimes to get people with schizophrenia to exercise, but it’s many times worth the effort.”
Dr. Marder reported consulting for Boehringer Ingelheim, Lundbeck, Otsuka, Roche, Neurocrine, Sunovion, Newron, Merck, and Biogen; editor of UptoDate and Schizophrenia Bulletin Open; and research support from Boehringer Ingelheim.
NEW ORLEANS – Patients with new-onset schizophrenia often ask psychiatrist Stephen R. Marder, MD, whether they’ll need to be on medications forever to treat the disorder. Now, he said, research is showing that the answer isn’t always yes.
In many cases, “it’s an open question” whether lifelong medical treatment is needed, said Dr. Marder, a professor at the Semel Institute for Neuroscience and Human Behavior at the University of California, Los Angeles, who spoke in a presentation about schizophrenia treatment at the annual meeting of the American Psychiatric Association.
According to Dr. Marder, research about relapses suggests that there may be a subpopulation of patients who can come off antipsychotics and remain in remission or partial remission. “The problem,” he said, “is that group is very hard to identify.”
Indeed, he highlighted a 2017 study that suggested The study noted choosing the best candidates isn’t simple, as “we do not have clinical measures or biomarkers that allow us to identify them prospectively. Because relapses and delays in the treatment of psychosis have been associated with poorer outcomes, there may be risk associated with withholding or discontinuing medication.”
There are more complications. There’s some evidence that antipsychotic drugs reduce brain volume, Dr. Marder said. But on the other hand, each psychotic episode can itself be harmful. “There is clear evidence that for each psychotic episode, they can take longer to improve, and they need higher doses.”
What to do? “My suggestion for most patients is to keep them on a relatively mild dose of an antipsychotic,” Dr. Marder said, “then to have a gradual decrease in the dose. I’ve done it in many patients.”
Which drug is best over the long term – oral or long-acting injectable antipsychotics? “It’s a hard question to answer because if you rely on randomized clinical trials – with patients who signed consent and are willing to be in a study like that – the subjects are sometimes not the ones who benefit the most from the long-acting drugs. So for many of the randomized clinical trials, the data was incomplete, and it was hard to make the case.”
But if you combine meta-analyses and cohort studies, as a 2021 study did, “you come up with a really clear answer: LAIs [long-acting injectables] are superior. They lead to a superior outcomes when it comes to rehospitalization and psychotic relapse,” Dr. Marder said.
That study reported that “LAIs were more beneficial than oral antipsychotics in 60 [18.3%] of 328 comparisons, not different in 252 [76.8%] comparisons, and less beneficial in 16 [4.9%] comparisons.”
More schizophrenia treatment pearls
People with schizophrenia – including those who aren’t on medication – face three times the risk of developing type 2 diabetes as the general population, “maybe because there’s a shared genetic risk for both disorders,” Dr. Marder said. “Those of you who have a lot of schizophrenia patients, I suspect you’re monitoring if they’re treating their type 2 diabetes and their obesity.”
Which antipsychotics are the best option for these patients? He highlighted a 2020 systematic review and meta-analysis that offers helpful insight into connections between 18 drugs and factors like weight and cholesterol.
Dr. Marder added that “if somebody has an elevation in their triglycerides or [hemoglobin] A1c in one single fasting blood glucose during the first 6 weeks of treatment, even if they haven’t been rated, it suggests that they’re developing insulin resistance.” At that point, he said, it’s a good idea to reconsider the medication choice.
Also, he said, keep in mind that “there’s substantial evidence that metformin is the appropriate treatment for patients who begin to demonstrate insulin resistance. It also works sometimes for weight loss.”
Exercise in people with schizophrenia can pay important dividends. A 2016 meta-analysis suggests that “not only does exercise for people with schizophrenia lead to better cardiovascular health, it’s good for the brain and improves cognitive functioning,” Dr. Marder said. “It’s not easy sometimes to get people with schizophrenia to exercise, but it’s many times worth the effort.”
Dr. Marder reported consulting for Boehringer Ingelheim, Lundbeck, Otsuka, Roche, Neurocrine, Sunovion, Newron, Merck, and Biogen; editor of UptoDate and Schizophrenia Bulletin Open; and research support from Boehringer Ingelheim.
AT APA 2022