User login
Bringing you the latest news, research and reviews, exclusive interviews, podcasts, quizzes, and more.
div[contains(@class, 'read-next-article')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
nav[contains(@class, 'nav-ce-stack nav-ce-stack__large-screen')]
header[@id='header']
div[contains(@class, 'header__large-screen')]
div[contains(@class, 'read-next-article')]
div[contains(@class, 'main-prefix')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
footer[@id='footer']
section[contains(@class, 'nav-hidden')]
div[contains(@class, 'ce-card-content')]
nav[contains(@class, 'nav-ce-stack')]
div[contains(@class, 'view-medstat-quiz-listing-panes')]
div[contains(@class, 'pane-article-sidebar-latest-news')]
No amount of alcohol safe for the heart: WHF
The widely held notion that consuming small to moderate amounts of alcohol is good for cardiovascular health is not supported by the data, the World Heart Federation says in a new policy brief.
In fact, the evidence is clear that any level of drinking can contribute to loss of a healthy life, the organization says.
“Over the past several decades, the prevalence of cardiovascular disease has nearly doubled, and alcohol has played a major role in the incidence of much of it,” the WHF said in the brief.
“The portrayal of alcohol as necessary for a vibrant social life has diverted attention from the harms of alcohol use, as have the frequent and widely publicized claims that moderate drinking, such as a glass of red wine a day, can offer protection against cardiovascular disease,” Monika Arora, PhD, member of the WHF advocacy committee and coauthor of the brief, said in a news release.
“These claims are at best misinformed and at worst an attempt by the alcohol industry to mislead the public about the danger of their product,” Dr. Arora added.
The WHF conclusions follow a report in the Lancet based on the Global Burden of Diseases, Injuries, and Risk Factors Study (GBD), which found that there is no safe level of alcohol consumption.
In 2019, nearly 2.4 million deaths were attributed to alcohol, accounting for 4.3% of all deaths globally and 12.6% of deaths in men 15 to 49 years of age.
Even small amounts of alcohol have been shown to raise the risk for cardiovascular disease, including coronary disease, stroke, heart failure, hypertensive heart disease, cardiomyopathy, atrial fibrillation, and aneurysm, the WHF notes.
Studies that claim otherwise are largely based on purely observational research, which fails to account for relevant cofactors, the organization writes.
Based on their summary of the evidence to date, there is no reliable correlation between moderate alcohol consumption and a lower risk for cardiovascular disease.
Alcohol use is also a “major avoidable risk factor” for cancer, digestive diseases, intentional and unintentional injuries, and several infectious diseases, the WHF says.
Alcohol use also has significant economic and social costs, which include costs to individuals and health systems, productivity losses, as well as the increased risk for violence, homelessness, and criminal activity.
The WHF policy brief calls for “urgent and decisive action” to tackle the unprecedented rise in alcohol-related death and disability worldwide.
Recommended actions include boosting restrictions on alcohol availability; advancing and enforcing drinking and driving countermeasures; increasing access to screening, brief interventions, and treatment for alcohol use disorder; enforcing bans on alcohol advertising; establishing a uniform minimum legal drinking age; and mandating health warnings on alcohol products.
A version of this article first appeared on Medscape.com.
The widely held notion that consuming small to moderate amounts of alcohol is good for cardiovascular health is not supported by the data, the World Heart Federation says in a new policy brief.
In fact, the evidence is clear that any level of drinking can contribute to loss of a healthy life, the organization says.
“Over the past several decades, the prevalence of cardiovascular disease has nearly doubled, and alcohol has played a major role in the incidence of much of it,” the WHF said in the brief.
“The portrayal of alcohol as necessary for a vibrant social life has diverted attention from the harms of alcohol use, as have the frequent and widely publicized claims that moderate drinking, such as a glass of red wine a day, can offer protection against cardiovascular disease,” Monika Arora, PhD, member of the WHF advocacy committee and coauthor of the brief, said in a news release.
“These claims are at best misinformed and at worst an attempt by the alcohol industry to mislead the public about the danger of their product,” Dr. Arora added.
The WHF conclusions follow a report in the Lancet based on the Global Burden of Diseases, Injuries, and Risk Factors Study (GBD), which found that there is no safe level of alcohol consumption.
In 2019, nearly 2.4 million deaths were attributed to alcohol, accounting for 4.3% of all deaths globally and 12.6% of deaths in men 15 to 49 years of age.
Even small amounts of alcohol have been shown to raise the risk for cardiovascular disease, including coronary disease, stroke, heart failure, hypertensive heart disease, cardiomyopathy, atrial fibrillation, and aneurysm, the WHF notes.
Studies that claim otherwise are largely based on purely observational research, which fails to account for relevant cofactors, the organization writes.
Based on their summary of the evidence to date, there is no reliable correlation between moderate alcohol consumption and a lower risk for cardiovascular disease.
Alcohol use is also a “major avoidable risk factor” for cancer, digestive diseases, intentional and unintentional injuries, and several infectious diseases, the WHF says.
Alcohol use also has significant economic and social costs, which include costs to individuals and health systems, productivity losses, as well as the increased risk for violence, homelessness, and criminal activity.
The WHF policy brief calls for “urgent and decisive action” to tackle the unprecedented rise in alcohol-related death and disability worldwide.
Recommended actions include boosting restrictions on alcohol availability; advancing and enforcing drinking and driving countermeasures; increasing access to screening, brief interventions, and treatment for alcohol use disorder; enforcing bans on alcohol advertising; establishing a uniform minimum legal drinking age; and mandating health warnings on alcohol products.
A version of this article first appeared on Medscape.com.
The widely held notion that consuming small to moderate amounts of alcohol is good for cardiovascular health is not supported by the data, the World Heart Federation says in a new policy brief.
In fact, the evidence is clear that any level of drinking can contribute to loss of a healthy life, the organization says.
“Over the past several decades, the prevalence of cardiovascular disease has nearly doubled, and alcohol has played a major role in the incidence of much of it,” the WHF said in the brief.
“The portrayal of alcohol as necessary for a vibrant social life has diverted attention from the harms of alcohol use, as have the frequent and widely publicized claims that moderate drinking, such as a glass of red wine a day, can offer protection against cardiovascular disease,” Monika Arora, PhD, member of the WHF advocacy committee and coauthor of the brief, said in a news release.
“These claims are at best misinformed and at worst an attempt by the alcohol industry to mislead the public about the danger of their product,” Dr. Arora added.
The WHF conclusions follow a report in the Lancet based on the Global Burden of Diseases, Injuries, and Risk Factors Study (GBD), which found that there is no safe level of alcohol consumption.
In 2019, nearly 2.4 million deaths were attributed to alcohol, accounting for 4.3% of all deaths globally and 12.6% of deaths in men 15 to 49 years of age.
Even small amounts of alcohol have been shown to raise the risk for cardiovascular disease, including coronary disease, stroke, heart failure, hypertensive heart disease, cardiomyopathy, atrial fibrillation, and aneurysm, the WHF notes.
Studies that claim otherwise are largely based on purely observational research, which fails to account for relevant cofactors, the organization writes.
Based on their summary of the evidence to date, there is no reliable correlation between moderate alcohol consumption and a lower risk for cardiovascular disease.
Alcohol use is also a “major avoidable risk factor” for cancer, digestive diseases, intentional and unintentional injuries, and several infectious diseases, the WHF says.
Alcohol use also has significant economic and social costs, which include costs to individuals and health systems, productivity losses, as well as the increased risk for violence, homelessness, and criminal activity.
The WHF policy brief calls for “urgent and decisive action” to tackle the unprecedented rise in alcohol-related death and disability worldwide.
Recommended actions include boosting restrictions on alcohol availability; advancing and enforcing drinking and driving countermeasures; increasing access to screening, brief interventions, and treatment for alcohol use disorder; enforcing bans on alcohol advertising; establishing a uniform minimum legal drinking age; and mandating health warnings on alcohol products.
A version of this article first appeared on Medscape.com.
Gut bacteria linked with long COVID
While links have been found between the gut’s microbiome and COVID-19, as well as other diseases, this is the first published research to show a link specifically to COVID’s long-term effects, the investigators, based at the Chinese University of Hong Kong, wrote in Gut.

“To our knowledge, this is the first study to show that altered gut microbiome composition is strongly associated with persistent symptoms in patients with COVID-19 up to 6 months after clearance of SARS-CoV-2 virus,” said Siew Ng, MBBS, PhD, associate director at the university’s Center for Gut Microbiota Research.
At three hospitals, the researchers enrolled 106 patients with COVID-19 from February to August 2020 with stool samples at admission and at 1 month and 6 months after discharge, and compared them with people who did not have COVID, recruited in 2019. The severity of COVID in the enrolled patients was mostly mild to moderate.
At 3 months, 86 of the patients with COVID had post–acute COVID-19 syndrome (PACS) – defined as at least one persistent, otherwise unexplained symptom 4 weeks after clearance of the virus. And 81 patients had PACS at 6 months, most commonly fatigue, poor memory, hair loss, anxiety, and trouble sleeping.
Using stool samples for their analysis, the researchers found that, broadly, the diversity of the types of bacteria, and the abundance of these bacteria, were significantly lower at 6 months for those with PACS, compared with those without PACS and with controls (P < .05 and P < .0001, respectively). Among those with PACS, 28 bacteria species were diminished and 14 were enriched, both at baseline and follow-up. Those patients who had COVID but not PACS showed just 25 alterations of bacteria species at the time of hospital admission, and they all normalized by 6 months.
Having respiratory symptoms at 6 months was linked with higher levels of opportunistic pathogens such as Streptococcus anginosus and S. vestibularis. Neuropsychiatric symptoms and fatigue were associated with nosocomial pathogens that are linked to opportunistic infections, such as Clostridium innocuum and Actinomyces naeslundii (P < .05).
Bacteria known for producing butyrate, a beneficial fatty acid, were significantly depleted in those patients with hair loss. And certain of these bacteria, including Bifidobacterium pseudocatenulatum and Faecalibacterium prausnitzii, had the largest inverse correlations with PACS at 6 months (P < .05), the researchers found.
“Particular gut microbial profiles may indicate heightened susceptibility,” Dr. Ng said.
Although the findings were drawn from patients with earlier strains of the COVID-19 virus, the findings still apply to new variants, including Omicron, since these pose the same problem of persistent disruption of the immune system, Dr. Ng said.
Her group is conducting trials to look at how modulating the microbiome might prevent long COVID and boost antibodies after vaccination in high-risk people, she said.
“Gut microbiota influences the health of the host,” Dr. Ng said. “It provides crucial benefits in the form of immune system development, prevention of infections, nutrient acquisition, and brain and nervous system functionality. Considering the millions of people infected during the ongoing pandemic, our findings are a strong impetus for consideration of microbiota modulation to facilitate timely recovery and reduce the burden of post–acute COVID-19 syndrome.”

John Haran, MD, PhD, associate professor of microbiology and physiological systems and emergency medicine at the University of Massachusetts, Worcester, said the research adds to the evidence base on the gut microbiome’s links to COVID, but there was likely be no clinical impact yet. Still, he said the findings linking specific species to specific symptoms was particularly interesting.
“Very early on during hospitalization, [the researchers] saw these differences and correlated out with people who have longer symptoms, and especially different groups of people that have longer symptoms, too,” said Dr. Haran, who has done research on the topic. “It’s very different if you have different symptoms, for example, you keep coughing for months versus you have brain fog and fatigue, or other debilitating symptoms.”
Dr. Haran noted that the findings didn’t identify bacteria types especially linked to COVID, but rather species that have already been found to be associated with a “bad” microbiome. He also pointed out that the patients enrolled in the study were not vaccinated, because vaccines weren’t available at the time. Still, further study to see whether modulation of gut bacteria can be a therapy seems worthwhile.
“Microbiome modulation is pretty safe, and that’s really the next big step that needs to be taken in this,” he said.
For now, the findings don’t give the clinician much new ammunition for treatment.
“We’re not there yet,” he added. “It’s not as if clinicians are going to tell their COVID patients: ‘Go out and buy some kale.’ ”
Eugene Chang, MD, professor of medicine at the University of Chicago, who has studied the gut microbiome and gastrointestinal disease, said it’s “too preliminary” to say whether the findings could lead to a clinical impact. The measures used merely identify the microbes present, but not what they are doing.
“These measures are unlikely to perform well enough to be useful for risk assessment or predicting clinical outcomes,” he said. “That being said, advances in technology are being made where next generations of metrics could be developed and useful as stratifiers and predictors of risk.”
Seeing shifting patterns associated with certain symptoms, he said, is “notable because it suggests that the disturbances of the gut microbiota in PACS are significant.”
But he said it’s important to know whether these changes are a cause of PACS in some way or just an effect of it.
“If causative or contributory – this has to be proven – then ‘microbiota modulation’ would make sense and could be a priority for development,” he said. “If merely an effect, these metrics and better ones to come could be useful as predictors or measures of the patient’s general state of health.”
As seen in his group’s work and other work, he said, “the gut microbiota is highly sensitive to changes in their ecosystem, which is influenced by the health state of the patient.”
Dr. Ng, Dr. Haran, and Dr. Chang reported no relevant disclosures.
This article was updated Jan. 27, 2022.
While links have been found between the gut’s microbiome and COVID-19, as well as other diseases, this is the first published research to show a link specifically to COVID’s long-term effects, the investigators, based at the Chinese University of Hong Kong, wrote in Gut.
“To our knowledge, this is the first study to show that altered gut microbiome composition is strongly associated with persistent symptoms in patients with COVID-19 up to 6 months after clearance of SARS-CoV-2 virus,” said Siew Ng, MBBS, PhD, associate director at the university’s Center for Gut Microbiota Research.
At three hospitals, the researchers enrolled 106 patients with COVID-19 from February to August 2020 with stool samples at admission and at 1 month and 6 months after discharge, and compared them with people who did not have COVID, recruited in 2019. The severity of COVID in the enrolled patients was mostly mild to moderate.
At 3 months, 86 of the patients with COVID had post–acute COVID-19 syndrome (PACS) – defined as at least one persistent, otherwise unexplained symptom 4 weeks after clearance of the virus. And 81 patients had PACS at 6 months, most commonly fatigue, poor memory, hair loss, anxiety, and trouble sleeping.
Using stool samples for their analysis, the researchers found that, broadly, the diversity of the types of bacteria, and the abundance of these bacteria, were significantly lower at 6 months for those with PACS, compared with those without PACS and with controls (P < .05 and P < .0001, respectively). Among those with PACS, 28 bacteria species were diminished and 14 were enriched, both at baseline and follow-up. Those patients who had COVID but not PACS showed just 25 alterations of bacteria species at the time of hospital admission, and they all normalized by 6 months.
Having respiratory symptoms at 6 months was linked with higher levels of opportunistic pathogens such as Streptococcus anginosus and S. vestibularis. Neuropsychiatric symptoms and fatigue were associated with nosocomial pathogens that are linked to opportunistic infections, such as Clostridium innocuum and Actinomyces naeslundii (P < .05).
Bacteria known for producing butyrate, a beneficial fatty acid, were significantly depleted in those patients with hair loss. And certain of these bacteria, including Bifidobacterium pseudocatenulatum and Faecalibacterium prausnitzii, had the largest inverse correlations with PACS at 6 months (P < .05), the researchers found.
“Particular gut microbial profiles may indicate heightened susceptibility,” Dr. Ng said.
Although the findings were drawn from patients with earlier strains of the COVID-19 virus, the findings still apply to new variants, including Omicron, since these pose the same problem of persistent disruption of the immune system, Dr. Ng said.
Her group is conducting trials to look at how modulating the microbiome might prevent long COVID and boost antibodies after vaccination in high-risk people, she said.
“Gut microbiota influences the health of the host,” Dr. Ng said. “It provides crucial benefits in the form of immune system development, prevention of infections, nutrient acquisition, and brain and nervous system functionality. Considering the millions of people infected during the ongoing pandemic, our findings are a strong impetus for consideration of microbiota modulation to facilitate timely recovery and reduce the burden of post–acute COVID-19 syndrome.”
John Haran, MD, PhD, associate professor of microbiology and physiological systems and emergency medicine at the University of Massachusetts, Worcester, said the research adds to the evidence base on the gut microbiome’s links to COVID, but there was likely be no clinical impact yet. Still, he said the findings linking specific species to specific symptoms was particularly interesting.
“Very early on during hospitalization, [the researchers] saw these differences and correlated out with people who have longer symptoms, and especially different groups of people that have longer symptoms, too,” said Dr. Haran, who has done research on the topic. “It’s very different if you have different symptoms, for example, you keep coughing for months versus you have brain fog and fatigue, or other debilitating symptoms.”
Dr. Haran noted that the findings didn’t identify bacteria types especially linked to COVID, but rather species that have already been found to be associated with a “bad” microbiome. He also pointed out that the patients enrolled in the study were not vaccinated, because vaccines weren’t available at the time. Still, further study to see whether modulation of gut bacteria can be a therapy seems worthwhile.
“Microbiome modulation is pretty safe, and that’s really the next big step that needs to be taken in this,” he said.
For now, the findings don’t give the clinician much new ammunition for treatment.
“We’re not there yet,” he added. “It’s not as if clinicians are going to tell their COVID patients: ‘Go out and buy some kale.’ ”
Eugene Chang, MD, professor of medicine at the University of Chicago, who has studied the gut microbiome and gastrointestinal disease, said it’s “too preliminary” to say whether the findings could lead to a clinical impact. The measures used merely identify the microbes present, but not what they are doing.
“These measures are unlikely to perform well enough to be useful for risk assessment or predicting clinical outcomes,” he said. “That being said, advances in technology are being made where next generations of metrics could be developed and useful as stratifiers and predictors of risk.”
Seeing shifting patterns associated with certain symptoms, he said, is “notable because it suggests that the disturbances of the gut microbiota in PACS are significant.”
But he said it’s important to know whether these changes are a cause of PACS in some way or just an effect of it.
“If causative or contributory – this has to be proven – then ‘microbiota modulation’ would make sense and could be a priority for development,” he said. “If merely an effect, these metrics and better ones to come could be useful as predictors or measures of the patient’s general state of health.”
As seen in his group’s work and other work, he said, “the gut microbiota is highly sensitive to changes in their ecosystem, which is influenced by the health state of the patient.”
Dr. Ng, Dr. Haran, and Dr. Chang reported no relevant disclosures.
This article was updated Jan. 27, 2022.
While links have been found between the gut’s microbiome and COVID-19, as well as other diseases, this is the first published research to show a link specifically to COVID’s long-term effects, the investigators, based at the Chinese University of Hong Kong, wrote in Gut.
“To our knowledge, this is the first study to show that altered gut microbiome composition is strongly associated with persistent symptoms in patients with COVID-19 up to 6 months after clearance of SARS-CoV-2 virus,” said Siew Ng, MBBS, PhD, associate director at the university’s Center for Gut Microbiota Research.
At three hospitals, the researchers enrolled 106 patients with COVID-19 from February to August 2020 with stool samples at admission and at 1 month and 6 months after discharge, and compared them with people who did not have COVID, recruited in 2019. The severity of COVID in the enrolled patients was mostly mild to moderate.
At 3 months, 86 of the patients with COVID had post–acute COVID-19 syndrome (PACS) – defined as at least one persistent, otherwise unexplained symptom 4 weeks after clearance of the virus. And 81 patients had PACS at 6 months, most commonly fatigue, poor memory, hair loss, anxiety, and trouble sleeping.
Using stool samples for their analysis, the researchers found that, broadly, the diversity of the types of bacteria, and the abundance of these bacteria, were significantly lower at 6 months for those with PACS, compared with those without PACS and with controls (P < .05 and P < .0001, respectively). Among those with PACS, 28 bacteria species were diminished and 14 were enriched, both at baseline and follow-up. Those patients who had COVID but not PACS showed just 25 alterations of bacteria species at the time of hospital admission, and they all normalized by 6 months.
Having respiratory symptoms at 6 months was linked with higher levels of opportunistic pathogens such as Streptococcus anginosus and S. vestibularis. Neuropsychiatric symptoms and fatigue were associated with nosocomial pathogens that are linked to opportunistic infections, such as Clostridium innocuum and Actinomyces naeslundii (P < .05).
Bacteria known for producing butyrate, a beneficial fatty acid, were significantly depleted in those patients with hair loss. And certain of these bacteria, including Bifidobacterium pseudocatenulatum and Faecalibacterium prausnitzii, had the largest inverse correlations with PACS at 6 months (P < .05), the researchers found.
“Particular gut microbial profiles may indicate heightened susceptibility,” Dr. Ng said.
Although the findings were drawn from patients with earlier strains of the COVID-19 virus, the findings still apply to new variants, including Omicron, since these pose the same problem of persistent disruption of the immune system, Dr. Ng said.
Her group is conducting trials to look at how modulating the microbiome might prevent long COVID and boost antibodies after vaccination in high-risk people, she said.
“Gut microbiota influences the health of the host,” Dr. Ng said. “It provides crucial benefits in the form of immune system development, prevention of infections, nutrient acquisition, and brain and nervous system functionality. Considering the millions of people infected during the ongoing pandemic, our findings are a strong impetus for consideration of microbiota modulation to facilitate timely recovery and reduce the burden of post–acute COVID-19 syndrome.”
John Haran, MD, PhD, associate professor of microbiology and physiological systems and emergency medicine at the University of Massachusetts, Worcester, said the research adds to the evidence base on the gut microbiome’s links to COVID, but there was likely be no clinical impact yet. Still, he said the findings linking specific species to specific symptoms was particularly interesting.
“Very early on during hospitalization, [the researchers] saw these differences and correlated out with people who have longer symptoms, and especially different groups of people that have longer symptoms, too,” said Dr. Haran, who has done research on the topic. “It’s very different if you have different symptoms, for example, you keep coughing for months versus you have brain fog and fatigue, or other debilitating symptoms.”
Dr. Haran noted that the findings didn’t identify bacteria types especially linked to COVID, but rather species that have already been found to be associated with a “bad” microbiome. He also pointed out that the patients enrolled in the study were not vaccinated, because vaccines weren’t available at the time. Still, further study to see whether modulation of gut bacteria can be a therapy seems worthwhile.
“Microbiome modulation is pretty safe, and that’s really the next big step that needs to be taken in this,” he said.
For now, the findings don’t give the clinician much new ammunition for treatment.
“We’re not there yet,” he added. “It’s not as if clinicians are going to tell their COVID patients: ‘Go out and buy some kale.’ ”
Eugene Chang, MD, professor of medicine at the University of Chicago, who has studied the gut microbiome and gastrointestinal disease, said it’s “too preliminary” to say whether the findings could lead to a clinical impact. The measures used merely identify the microbes present, but not what they are doing.
“These measures are unlikely to perform well enough to be useful for risk assessment or predicting clinical outcomes,” he said. “That being said, advances in technology are being made where next generations of metrics could be developed and useful as stratifiers and predictors of risk.”
Seeing shifting patterns associated with certain symptoms, he said, is “notable because it suggests that the disturbances of the gut microbiota in PACS are significant.”
But he said it’s important to know whether these changes are a cause of PACS in some way or just an effect of it.
“If causative or contributory – this has to be proven – then ‘microbiota modulation’ would make sense and could be a priority for development,” he said. “If merely an effect, these metrics and better ones to come could be useful as predictors or measures of the patient’s general state of health.”
As seen in his group’s work and other work, he said, “the gut microbiota is highly sensitive to changes in their ecosystem, which is influenced by the health state of the patient.”
Dr. Ng, Dr. Haran, and Dr. Chang reported no relevant disclosures.
This article was updated Jan. 27, 2022.
FROM GUT
‘Post-truth era’ hurts COVID-19 response, trust in science
Can you tell which of the following statements are true and which are false?
COVID-19 is not a threat to younger people, and only those who have other medical conditions are dying from it.
The mRNA vaccines developed to prevent the coronavirus alter your genes, can make your body “magnetic,” and are killing more people than the virus itself.
President Joe Biden’s climate change plan calls for a ban on meat consumption to cut greenhouse gas emissions.
The 2020 presidential election was rigged and stolen.
If you guessed that all of these claims are false, you’re right – take a bow. Not a single one of these statements has any factual support, according to scientific research, legal rulings, and legitimate government authorities.
And yet public opinion surveys show millions of Americans, and others around the world, believe some of these falsehoods are true and can’t be convinced otherwise.
Social media, politicians and partisan websites, TV programs, and commentators have widely circulated these and other unfounded claims so frequently that many people say they simply can’t tell what’s objectively true and not anymore.
So much so,
The new study – The Rise and Fall of Rationality in Language, published in the Proceedings of the National Academy of Sciences – found that facts have become less important in public discourse.
As a result, unsupported beliefs have taken precedent over readily identifiable truths in discussions of health, science, and politics. The upshot: “Feelings trump facts” in social media, news reports, books, and other sources of information.
And here’s the kicker: The trend did not begin with the rise of former President Donald Trump, the COVID-19 pandemic, or the advent of social media; in fact, it has been growing for much longer than you might think.
“While the current ‘post-truth era’ has taken many by surprise, the study shows that over the past 40 years, public interest has undergone an accelerating shift from the collective to the individual, and from rationality towards emotion,” concluded the researchers from Indiana University and Wageningen University & Research in the Netherlands.
“Our work suggests that the societal balance between emotion and reason has shifted back to what it used to be around 150 years ago,” says lead researcher Marten Scheffer, PhD, a professor in the department of environmental sciences at WUR. “This implies that scientists, experts, and policymakers will have to think about the best way to respond to that social change.”
Researchers surprised by findings
The findings are based on a very detailed analysis of language from millions of books, newspaper articles, Google searches, TV reports, social media posts, and other sources dating back to 1850.
The researchers analyzed how often the 5,000 most used words appeared over the past 170 years and found that the use of those having to do with facts and reasoning, such as “determine” and “conclusion,” has fallen dramatically since 1980. Meanwhile, the use of words related to human emotion, such as “feel” and “believe,” have skyrocketed.
Dr. Scheffer notes rapid developments in science and technology from 1850 to 1980 had profound social and economic benefits that helped boost the status of the scientific approach. That shift in public attitudes had ripple effects on culture, society, education, politics, and religion – and “the role of spiritualism dwindled” in the modern world, he says.
But since 1980, that trend has seen a major reversal, with beliefs becoming more important than facts to many people, he says. At the same time, trust in science and scientists has fallen.
Dr. Scheffer says the researchers expected to find some evidence of a swing toward more belief-based sentiments during the Trump era but were surprised to discover how strong it is and that the trend has actually been a long time coming.
“The shift in interest from rational to intuitive/emotional is pretty obvious now in the post-truth political and social media discussion,” he says. “However, our work shows that it already started in the 1980s. For me personally, that went under the radar, except perhaps for the rise of alternative (to religion) forms of spirituality.
“We were especially struck by how strong the patterns are and how universal they appear across languages, nonfiction and fiction, and even in The New York Times.”
In the political world, the implications are significant enough – impacting policies and politicians on both sides of the aisle and across the globe. Just look at the deepening political divisions during the Trump presidency.
But for health and science, the spread of misinformation and falsehoods can be matters of life or death, as we have seen in the politically charged debates over how best to combat COVID-19 and global climate change.
“Our public debate seems increasingly driven by what people want to be true rather than what is actually true. As a scientist, that worries me,” says study co-author Johan Bollen, PhD, a professor of informatics at Indiana University.
“As a society, we are now faced with major collective problems that we need to approach from a pragmatic, rational, and objective perspective to be successful,” he says. “After all, global warming doesn’t care about whether you believe in it or not … but we will all suffer as a society if we fail to take adequate measures.”
For WUR co-researcher Ingrid van de Leemput, the trend isn’t merely academic; she’s seen it play out in her personal life.
“I do speak to people that, for instance, think the vaccines are poison,” she says. “I’m also on Twitter, and there, I’m every day surprised about how easily many people form their opinions, based on feelings, on what others say, or on some unfounded source.”
Public health experts say the embrace of personal beliefs over facts is one reason only 63% of Americans have been vaccinated against COVID-19. The result: millions of preventable infections among those who downplay the risks of the virus and reject the strong scientific evidence of vaccine safety and effectiveness.
“None of this really surprises me,” Johns Hopkins University social and behavioral scientist Rupali Limaye, PhD, says of the new study findings. Dr. Limaye coauthored a paper in 2016 in JAMA Pediatrics about how to talk to parents about vaccine hesitancy and the fact that we’re living in what they called “this post-truth era.”
Dr. Limaye says the trend has made it difficult for doctors, scientists, and health authorities to make fact-based arguments for COVID-19 vaccination, mask-wearing, social distancing, and other measures to control the virus.
“It’s been really hard being a scientist to hear people say, ‘Well, that’s not true’ when we say something very basic that I think all of us can agree on – like the grass is green,” she says. “To be honest, I worry that a lot of scientists are going to quit being in science because they’re exhausted.”
What’s driving the trend?
So, what’s behind the embrace of “alternative facts,” as former White House counselor Kellyanne Conway put it so brazenly in 2017, in defending the White House’s false claims that Trump’s inauguration crowd was the largest ever?
Dr. Scheffer and colleagues identified a handful of things that have encouraged the embrace of falsehoods over facts in recent years.
- The Internet: Its rise in the late 1980s, and its growing role as a primary source of news and information, has allowed more belief-based misinformation to flourish and spread like wildfire.
- Social media: The new study found the use of sentiment- and intuition-related words accelerated around 2007, along with a global surge in social media that catapulted Facebook, Twitter, and others into the mainstream, replacing more traditional fact-based media (i.e., newspapers and magazines).
- The 2007 financial crisis: The downturn in the global economy meant more people were dealing with job stress, investment losses, and other problems that fed the interest in belief-based, anti-establishment social media posts.
- Conspiracy theories: Falsehoods involving hidden political agendas, shadow “elites,” and wealthy people with dark motives tend to thrive during times of crisis and societal anxiety. “Conspiracy theories originate particularly in times of uncertainty and crisis and generally depict established institutions as hiding the truth and sustaining an unfair situation,” the researchers noted. “As a result, they may find fertile grounds on social media platforms promulgating a sense of unfairness, subsequently feeding anti-system sentiments.”
Dr. Scheffer says that growing political divisions during the Trump era have widened the fact-vs.-fiction divide. The ex-president voiced many anti-science views on global climate change, for instance, and spread so many falsehoods about COVID-19 and the 2020 election that Facebook, Twitter, and YouTube suspended his accounts.
Yet Trump remains a popular figure among Republicans, with most saying in a December poll they believe his baseless claims that the 2020 election was “rigged” and “stolen,” despite all credible, easily accessible evidence that it was secure, according to a recent poll by the University of Massachusetts at Amherst.
More than 60 courts have rejected Trump’s lawsuits seeking to overturn the election results. All 50 states, the District of Columbia, and both branches of Congress have certified the election results, giving Biden the White House. Even Trump’s own Justice Department confirmed that the 2020 election was free and fair.
Nevertheless, the University of Massachusetts survey found that most Republicans believe one or more conspiracy theories floated by the former president and those pushing his “big lie” that Democrats rigged the election to elect Biden.
Ed Berliner, an Emmy Award-winning broadcast journalist and media consultant, suggests something else is driving the spread of misinformation: the pursuit of ratings by cable TV and media companies to boost ad and subscriber revenues.
As a former executive producer and syndicated cable TV show host, he says he has seen firsthand how facts are often lost in opinion-driven news programs, even on network programs claiming to offer “fair and balanced” journalism.
“Propaganda is the new currency in America, and those who do not fight back against it are doomed to be overrun by the misinformation,” says Mr. Berliner, host of The Man in the Arena and CEO of Entourage Media LLC.
“The broadcast news media has to stop this incessant ‘infotainment’ prattle, stop trying to nuzzle up to a soft side, and bear down on hard facts, exposing the lies and refusing to back down.”
Public health implications
Public health and media experts alike say the PNAS study findings are disheartening but underscore the need for doctors and scientists to do a better job of communicating about COVID-19 and other pressing issues.
Dr. Limaye, from Johns Hopkins, is particularly concerned about the rise in conspiracy theories that has led to COVID-19 vaccine hesitancy.
“When we speak to individuals about getting the COVID vaccine…the types of concerns that come up now are very different than they were 8 years ago,” she says. “The comments we used to hear were much more related to vaccine safety. [People] would say, ‘I’m worried about an ingredient in the vaccine’ or ‘I’m worried that my kiddo has to get three different shots within 6 months to have a series dose completed.’”
But now, a lot of comments they receive are about government and pharma conspiracies.
What that means is doctors and scientists must do more than simply say “here are the facts” and “trust me, I’m a doctor or a scientist,” she says. And these approaches don’t only apply to public health.
“It’s funny, because when we talk to climate change scientists, as vaccine [specialists], we’ll say we can’t believe that people think COVID is a hoax,” she says. “And they’re like, ‘Hold my beer, we’ve been dealing with this for 20 years. Hello, it’s just your guys’ turn to deal with this public denial of science.’”
Dr. Limaye is also concerned about the impacts on funding for scientific research.
“There’s always been a really strong bipartisan effort with regards to funding for science, when you look at Congress and when you look at appropriations,” she says. “But what ended up happening, especially with the Trump administration, was that there was a real shift in that. We’ve never really seen that before in past generations.”
So, what’s the big take-home message?
Dr. Limaye believes doctors and public health experts must show more empathy – and not be combative or arrogant – in communicating science in one-on-one conversations. This month, she’s launching a new course for parents, school administrators, and nurses on how to do precisely that.
“It’s really all about how to have hard conversations with people who might be anti-science,” she says. “It’s being empathetic and not being dismissive. But it’s hard work, and I think a lot of people are just not cut out for it and just don’t have the time for it…You can’t just say, ‘Well, this is science, and I’m a doctor’ – that doesn’t work anymore.”
Brendan Nyhan, PhD, a Dartmouth College political scientist, echoes those sentiments in a separate paper recently published in the Proceedings of the National Academy of Sciences. In fact, he suggests that providing accurate, fact-based information to counter false claims may actually backfire and reinforce some people’s unfounded beliefs.
“One response to the prevalence of mistaken beliefs is to try to set the record straight by providing accurate information – for instance, by providing evidence of the scientific consensus on climate change,” he writes. “The failures of this approach, which is sometimes referred to as the ‘deficit model’ in science communication, are well-known.”
Dr. Nyhan argues two things make some people more prone to believe falsehoods:
What scientists call “ingrouping,” a kind of tribal mentality that makes some people choose social identity or politics over truth-seeking and demonize others who don’t agree with their views
The rise of high-profile political figures, such as Trump, who encourage their followers to indulge in their desire for “identify-affirming misinformation”
Dr. Scheffer says the most important thing for doctors, health experts, and scientists to recognize is that it’s crucial to gain the trust of someone who may believe fictions over facts to make any persuasive argument on COVID-19 or any other issue.
He also has a standard response to those who present falsehoods to him as facts that he suggests anyone can use: “That is interesting. Would you mind helping me understand how you came to that opinion?”
A version of this article first appeared on WebMD.com.
Can you tell which of the following statements are true and which are false?
COVID-19 is not a threat to younger people, and only those who have other medical conditions are dying from it.
The mRNA vaccines developed to prevent the coronavirus alter your genes, can make your body “magnetic,” and are killing more people than the virus itself.
President Joe Biden’s climate change plan calls for a ban on meat consumption to cut greenhouse gas emissions.
The 2020 presidential election was rigged and stolen.
If you guessed that all of these claims are false, you’re right – take a bow. Not a single one of these statements has any factual support, according to scientific research, legal rulings, and legitimate government authorities.
And yet public opinion surveys show millions of Americans, and others around the world, believe some of these falsehoods are true and can’t be convinced otherwise.
Social media, politicians and partisan websites, TV programs, and commentators have widely circulated these and other unfounded claims so frequently that many people say they simply can’t tell what’s objectively true and not anymore.
So much so,
The new study – The Rise and Fall of Rationality in Language, published in the Proceedings of the National Academy of Sciences – found that facts have become less important in public discourse.
As a result, unsupported beliefs have taken precedent over readily identifiable truths in discussions of health, science, and politics. The upshot: “Feelings trump facts” in social media, news reports, books, and other sources of information.
And here’s the kicker: The trend did not begin with the rise of former President Donald Trump, the COVID-19 pandemic, or the advent of social media; in fact, it has been growing for much longer than you might think.
“While the current ‘post-truth era’ has taken many by surprise, the study shows that over the past 40 years, public interest has undergone an accelerating shift from the collective to the individual, and from rationality towards emotion,” concluded the researchers from Indiana University and Wageningen University & Research in the Netherlands.
“Our work suggests that the societal balance between emotion and reason has shifted back to what it used to be around 150 years ago,” says lead researcher Marten Scheffer, PhD, a professor in the department of environmental sciences at WUR. “This implies that scientists, experts, and policymakers will have to think about the best way to respond to that social change.”
Researchers surprised by findings
The findings are based on a very detailed analysis of language from millions of books, newspaper articles, Google searches, TV reports, social media posts, and other sources dating back to 1850.
The researchers analyzed how often the 5,000 most used words appeared over the past 170 years and found that the use of those having to do with facts and reasoning, such as “determine” and “conclusion,” has fallen dramatically since 1980. Meanwhile, the use of words related to human emotion, such as “feel” and “believe,” have skyrocketed.
Dr. Scheffer notes rapid developments in science and technology from 1850 to 1980 had profound social and economic benefits that helped boost the status of the scientific approach. That shift in public attitudes had ripple effects on culture, society, education, politics, and religion – and “the role of spiritualism dwindled” in the modern world, he says.
But since 1980, that trend has seen a major reversal, with beliefs becoming more important than facts to many people, he says. At the same time, trust in science and scientists has fallen.
Dr. Scheffer says the researchers expected to find some evidence of a swing toward more belief-based sentiments during the Trump era but were surprised to discover how strong it is and that the trend has actually been a long time coming.
“The shift in interest from rational to intuitive/emotional is pretty obvious now in the post-truth political and social media discussion,” he says. “However, our work shows that it already started in the 1980s. For me personally, that went under the radar, except perhaps for the rise of alternative (to religion) forms of spirituality.
“We were especially struck by how strong the patterns are and how universal they appear across languages, nonfiction and fiction, and even in The New York Times.”
In the political world, the implications are significant enough – impacting policies and politicians on both sides of the aisle and across the globe. Just look at the deepening political divisions during the Trump presidency.
But for health and science, the spread of misinformation and falsehoods can be matters of life or death, as we have seen in the politically charged debates over how best to combat COVID-19 and global climate change.
“Our public debate seems increasingly driven by what people want to be true rather than what is actually true. As a scientist, that worries me,” says study co-author Johan Bollen, PhD, a professor of informatics at Indiana University.
“As a society, we are now faced with major collective problems that we need to approach from a pragmatic, rational, and objective perspective to be successful,” he says. “After all, global warming doesn’t care about whether you believe in it or not … but we will all suffer as a society if we fail to take adequate measures.”
For WUR co-researcher Ingrid van de Leemput, the trend isn’t merely academic; she’s seen it play out in her personal life.
“I do speak to people that, for instance, think the vaccines are poison,” she says. “I’m also on Twitter, and there, I’m every day surprised about how easily many people form their opinions, based on feelings, on what others say, or on some unfounded source.”
Public health experts say the embrace of personal beliefs over facts is one reason only 63% of Americans have been vaccinated against COVID-19. The result: millions of preventable infections among those who downplay the risks of the virus and reject the strong scientific evidence of vaccine safety and effectiveness.
“None of this really surprises me,” Johns Hopkins University social and behavioral scientist Rupali Limaye, PhD, says of the new study findings. Dr. Limaye coauthored a paper in 2016 in JAMA Pediatrics about how to talk to parents about vaccine hesitancy and the fact that we’re living in what they called “this post-truth era.”
Dr. Limaye says the trend has made it difficult for doctors, scientists, and health authorities to make fact-based arguments for COVID-19 vaccination, mask-wearing, social distancing, and other measures to control the virus.
“It’s been really hard being a scientist to hear people say, ‘Well, that’s not true’ when we say something very basic that I think all of us can agree on – like the grass is green,” she says. “To be honest, I worry that a lot of scientists are going to quit being in science because they’re exhausted.”
What’s driving the trend?
So, what’s behind the embrace of “alternative facts,” as former White House counselor Kellyanne Conway put it so brazenly in 2017, in defending the White House’s false claims that Trump’s inauguration crowd was the largest ever?
Dr. Scheffer and colleagues identified a handful of things that have encouraged the embrace of falsehoods over facts in recent years.
- The Internet: Its rise in the late 1980s, and its growing role as a primary source of news and information, has allowed more belief-based misinformation to flourish and spread like wildfire.
- Social media: The new study found the use of sentiment- and intuition-related words accelerated around 2007, along with a global surge in social media that catapulted Facebook, Twitter, and others into the mainstream, replacing more traditional fact-based media (i.e., newspapers and magazines).
- The 2007 financial crisis: The downturn in the global economy meant more people were dealing with job stress, investment losses, and other problems that fed the interest in belief-based, anti-establishment social media posts.
- Conspiracy theories: Falsehoods involving hidden political agendas, shadow “elites,” and wealthy people with dark motives tend to thrive during times of crisis and societal anxiety. “Conspiracy theories originate particularly in times of uncertainty and crisis and generally depict established institutions as hiding the truth and sustaining an unfair situation,” the researchers noted. “As a result, they may find fertile grounds on social media platforms promulgating a sense of unfairness, subsequently feeding anti-system sentiments.”
Dr. Scheffer says that growing political divisions during the Trump era have widened the fact-vs.-fiction divide. The ex-president voiced many anti-science views on global climate change, for instance, and spread so many falsehoods about COVID-19 and the 2020 election that Facebook, Twitter, and YouTube suspended his accounts.
Yet Trump remains a popular figure among Republicans, with most saying in a December poll they believe his baseless claims that the 2020 election was “rigged” and “stolen,” despite all credible, easily accessible evidence that it was secure, according to a recent poll by the University of Massachusetts at Amherst.
More than 60 courts have rejected Trump’s lawsuits seeking to overturn the election results. All 50 states, the District of Columbia, and both branches of Congress have certified the election results, giving Biden the White House. Even Trump’s own Justice Department confirmed that the 2020 election was free and fair.
Nevertheless, the University of Massachusetts survey found that most Republicans believe one or more conspiracy theories floated by the former president and those pushing his “big lie” that Democrats rigged the election to elect Biden.
Ed Berliner, an Emmy Award-winning broadcast journalist and media consultant, suggests something else is driving the spread of misinformation: the pursuit of ratings by cable TV and media companies to boost ad and subscriber revenues.
As a former executive producer and syndicated cable TV show host, he says he has seen firsthand how facts are often lost in opinion-driven news programs, even on network programs claiming to offer “fair and balanced” journalism.
“Propaganda is the new currency in America, and those who do not fight back against it are doomed to be overrun by the misinformation,” says Mr. Berliner, host of The Man in the Arena and CEO of Entourage Media LLC.
“The broadcast news media has to stop this incessant ‘infotainment’ prattle, stop trying to nuzzle up to a soft side, and bear down on hard facts, exposing the lies and refusing to back down.”
Public health implications
Public health and media experts alike say the PNAS study findings are disheartening but underscore the need for doctors and scientists to do a better job of communicating about COVID-19 and other pressing issues.
Dr. Limaye, from Johns Hopkins, is particularly concerned about the rise in conspiracy theories that has led to COVID-19 vaccine hesitancy.
“When we speak to individuals about getting the COVID vaccine…the types of concerns that come up now are very different than they were 8 years ago,” she says. “The comments we used to hear were much more related to vaccine safety. [People] would say, ‘I’m worried about an ingredient in the vaccine’ or ‘I’m worried that my kiddo has to get three different shots within 6 months to have a series dose completed.’”
But now, a lot of comments they receive are about government and pharma conspiracies.
What that means is doctors and scientists must do more than simply say “here are the facts” and “trust me, I’m a doctor or a scientist,” she says. And these approaches don’t only apply to public health.
“It’s funny, because when we talk to climate change scientists, as vaccine [specialists], we’ll say we can’t believe that people think COVID is a hoax,” she says. “And they’re like, ‘Hold my beer, we’ve been dealing with this for 20 years. Hello, it’s just your guys’ turn to deal with this public denial of science.’”
Dr. Limaye is also concerned about the impacts on funding for scientific research.
“There’s always been a really strong bipartisan effort with regards to funding for science, when you look at Congress and when you look at appropriations,” she says. “But what ended up happening, especially with the Trump administration, was that there was a real shift in that. We’ve never really seen that before in past generations.”
So, what’s the big take-home message?
Dr. Limaye believes doctors and public health experts must show more empathy – and not be combative or arrogant – in communicating science in one-on-one conversations. This month, she’s launching a new course for parents, school administrators, and nurses on how to do precisely that.
“It’s really all about how to have hard conversations with people who might be anti-science,” she says. “It’s being empathetic and not being dismissive. But it’s hard work, and I think a lot of people are just not cut out for it and just don’t have the time for it…You can’t just say, ‘Well, this is science, and I’m a doctor’ – that doesn’t work anymore.”
Brendan Nyhan, PhD, a Dartmouth College political scientist, echoes those sentiments in a separate paper recently published in the Proceedings of the National Academy of Sciences. In fact, he suggests that providing accurate, fact-based information to counter false claims may actually backfire and reinforce some people’s unfounded beliefs.
“One response to the prevalence of mistaken beliefs is to try to set the record straight by providing accurate information – for instance, by providing evidence of the scientific consensus on climate change,” he writes. “The failures of this approach, which is sometimes referred to as the ‘deficit model’ in science communication, are well-known.”
Dr. Nyhan argues two things make some people more prone to believe falsehoods:
What scientists call “ingrouping,” a kind of tribal mentality that makes some people choose social identity or politics over truth-seeking and demonize others who don’t agree with their views
The rise of high-profile political figures, such as Trump, who encourage their followers to indulge in their desire for “identify-affirming misinformation”
Dr. Scheffer says the most important thing for doctors, health experts, and scientists to recognize is that it’s crucial to gain the trust of someone who may believe fictions over facts to make any persuasive argument on COVID-19 or any other issue.
He also has a standard response to those who present falsehoods to him as facts that he suggests anyone can use: “That is interesting. Would you mind helping me understand how you came to that opinion?”
A version of this article first appeared on WebMD.com.
Can you tell which of the following statements are true and which are false?
COVID-19 is not a threat to younger people, and only those who have other medical conditions are dying from it.
The mRNA vaccines developed to prevent the coronavirus alter your genes, can make your body “magnetic,” and are killing more people than the virus itself.
President Joe Biden’s climate change plan calls for a ban on meat consumption to cut greenhouse gas emissions.
The 2020 presidential election was rigged and stolen.
If you guessed that all of these claims are false, you’re right – take a bow. Not a single one of these statements has any factual support, according to scientific research, legal rulings, and legitimate government authorities.
And yet public opinion surveys show millions of Americans, and others around the world, believe some of these falsehoods are true and can’t be convinced otherwise.
Social media, politicians and partisan websites, TV programs, and commentators have widely circulated these and other unfounded claims so frequently that many people say they simply can’t tell what’s objectively true and not anymore.
So much so,
The new study – The Rise and Fall of Rationality in Language, published in the Proceedings of the National Academy of Sciences – found that facts have become less important in public discourse.
As a result, unsupported beliefs have taken precedent over readily identifiable truths in discussions of health, science, and politics. The upshot: “Feelings trump facts” in social media, news reports, books, and other sources of information.
And here’s the kicker: The trend did not begin with the rise of former President Donald Trump, the COVID-19 pandemic, or the advent of social media; in fact, it has been growing for much longer than you might think.
“While the current ‘post-truth era’ has taken many by surprise, the study shows that over the past 40 years, public interest has undergone an accelerating shift from the collective to the individual, and from rationality towards emotion,” concluded the researchers from Indiana University and Wageningen University & Research in the Netherlands.
“Our work suggests that the societal balance between emotion and reason has shifted back to what it used to be around 150 years ago,” says lead researcher Marten Scheffer, PhD, a professor in the department of environmental sciences at WUR. “This implies that scientists, experts, and policymakers will have to think about the best way to respond to that social change.”
Researchers surprised by findings
The findings are based on a very detailed analysis of language from millions of books, newspaper articles, Google searches, TV reports, social media posts, and other sources dating back to 1850.
The researchers analyzed how often the 5,000 most used words appeared over the past 170 years and found that the use of those having to do with facts and reasoning, such as “determine” and “conclusion,” has fallen dramatically since 1980. Meanwhile, the use of words related to human emotion, such as “feel” and “believe,” have skyrocketed.
Dr. Scheffer notes rapid developments in science and technology from 1850 to 1980 had profound social and economic benefits that helped boost the status of the scientific approach. That shift in public attitudes had ripple effects on culture, society, education, politics, and religion – and “the role of spiritualism dwindled” in the modern world, he says.
But since 1980, that trend has seen a major reversal, with beliefs becoming more important than facts to many people, he says. At the same time, trust in science and scientists has fallen.
Dr. Scheffer says the researchers expected to find some evidence of a swing toward more belief-based sentiments during the Trump era but were surprised to discover how strong it is and that the trend has actually been a long time coming.
“The shift in interest from rational to intuitive/emotional is pretty obvious now in the post-truth political and social media discussion,” he says. “However, our work shows that it already started in the 1980s. For me personally, that went under the radar, except perhaps for the rise of alternative (to religion) forms of spirituality.
“We were especially struck by how strong the patterns are and how universal they appear across languages, nonfiction and fiction, and even in The New York Times.”
In the political world, the implications are significant enough – impacting policies and politicians on both sides of the aisle and across the globe. Just look at the deepening political divisions during the Trump presidency.
But for health and science, the spread of misinformation and falsehoods can be matters of life or death, as we have seen in the politically charged debates over how best to combat COVID-19 and global climate change.
“Our public debate seems increasingly driven by what people want to be true rather than what is actually true. As a scientist, that worries me,” says study co-author Johan Bollen, PhD, a professor of informatics at Indiana University.
“As a society, we are now faced with major collective problems that we need to approach from a pragmatic, rational, and objective perspective to be successful,” he says. “After all, global warming doesn’t care about whether you believe in it or not … but we will all suffer as a society if we fail to take adequate measures.”
For WUR co-researcher Ingrid van de Leemput, the trend isn’t merely academic; she’s seen it play out in her personal life.
“I do speak to people that, for instance, think the vaccines are poison,” she says. “I’m also on Twitter, and there, I’m every day surprised about how easily many people form their opinions, based on feelings, on what others say, or on some unfounded source.”
Public health experts say the embrace of personal beliefs over facts is one reason only 63% of Americans have been vaccinated against COVID-19. The result: millions of preventable infections among those who downplay the risks of the virus and reject the strong scientific evidence of vaccine safety and effectiveness.
“None of this really surprises me,” Johns Hopkins University social and behavioral scientist Rupali Limaye, PhD, says of the new study findings. Dr. Limaye coauthored a paper in 2016 in JAMA Pediatrics about how to talk to parents about vaccine hesitancy and the fact that we’re living in what they called “this post-truth era.”
Dr. Limaye says the trend has made it difficult for doctors, scientists, and health authorities to make fact-based arguments for COVID-19 vaccination, mask-wearing, social distancing, and other measures to control the virus.
“It’s been really hard being a scientist to hear people say, ‘Well, that’s not true’ when we say something very basic that I think all of us can agree on – like the grass is green,” she says. “To be honest, I worry that a lot of scientists are going to quit being in science because they’re exhausted.”
What’s driving the trend?
So, what’s behind the embrace of “alternative facts,” as former White House counselor Kellyanne Conway put it so brazenly in 2017, in defending the White House’s false claims that Trump’s inauguration crowd was the largest ever?
Dr. Scheffer and colleagues identified a handful of things that have encouraged the embrace of falsehoods over facts in recent years.
- The Internet: Its rise in the late 1980s, and its growing role as a primary source of news and information, has allowed more belief-based misinformation to flourish and spread like wildfire.
- Social media: The new study found the use of sentiment- and intuition-related words accelerated around 2007, along with a global surge in social media that catapulted Facebook, Twitter, and others into the mainstream, replacing more traditional fact-based media (i.e., newspapers and magazines).
- The 2007 financial crisis: The downturn in the global economy meant more people were dealing with job stress, investment losses, and other problems that fed the interest in belief-based, anti-establishment social media posts.
- Conspiracy theories: Falsehoods involving hidden political agendas, shadow “elites,” and wealthy people with dark motives tend to thrive during times of crisis and societal anxiety. “Conspiracy theories originate particularly in times of uncertainty and crisis and generally depict established institutions as hiding the truth and sustaining an unfair situation,” the researchers noted. “As a result, they may find fertile grounds on social media platforms promulgating a sense of unfairness, subsequently feeding anti-system sentiments.”
Dr. Scheffer says that growing political divisions during the Trump era have widened the fact-vs.-fiction divide. The ex-president voiced many anti-science views on global climate change, for instance, and spread so many falsehoods about COVID-19 and the 2020 election that Facebook, Twitter, and YouTube suspended his accounts.
Yet Trump remains a popular figure among Republicans, with most saying in a December poll they believe his baseless claims that the 2020 election was “rigged” and “stolen,” despite all credible, easily accessible evidence that it was secure, according to a recent poll by the University of Massachusetts at Amherst.
More than 60 courts have rejected Trump’s lawsuits seeking to overturn the election results. All 50 states, the District of Columbia, and both branches of Congress have certified the election results, giving Biden the White House. Even Trump’s own Justice Department confirmed that the 2020 election was free and fair.
Nevertheless, the University of Massachusetts survey found that most Republicans believe one or more conspiracy theories floated by the former president and those pushing his “big lie” that Democrats rigged the election to elect Biden.
Ed Berliner, an Emmy Award-winning broadcast journalist and media consultant, suggests something else is driving the spread of misinformation: the pursuit of ratings by cable TV and media companies to boost ad and subscriber revenues.
As a former executive producer and syndicated cable TV show host, he says he has seen firsthand how facts are often lost in opinion-driven news programs, even on network programs claiming to offer “fair and balanced” journalism.
“Propaganda is the new currency in America, and those who do not fight back against it are doomed to be overrun by the misinformation,” says Mr. Berliner, host of The Man in the Arena and CEO of Entourage Media LLC.
“The broadcast news media has to stop this incessant ‘infotainment’ prattle, stop trying to nuzzle up to a soft side, and bear down on hard facts, exposing the lies and refusing to back down.”
Public health implications
Public health and media experts alike say the PNAS study findings are disheartening but underscore the need for doctors and scientists to do a better job of communicating about COVID-19 and other pressing issues.
Dr. Limaye, from Johns Hopkins, is particularly concerned about the rise in conspiracy theories that has led to COVID-19 vaccine hesitancy.
“When we speak to individuals about getting the COVID vaccine…the types of concerns that come up now are very different than they were 8 years ago,” she says. “The comments we used to hear were much more related to vaccine safety. [People] would say, ‘I’m worried about an ingredient in the vaccine’ or ‘I’m worried that my kiddo has to get three different shots within 6 months to have a series dose completed.’”
But now, a lot of comments they receive are about government and pharma conspiracies.
What that means is doctors and scientists must do more than simply say “here are the facts” and “trust me, I’m a doctor or a scientist,” she says. And these approaches don’t only apply to public health.
“It’s funny, because when we talk to climate change scientists, as vaccine [specialists], we’ll say we can’t believe that people think COVID is a hoax,” she says. “And they’re like, ‘Hold my beer, we’ve been dealing with this for 20 years. Hello, it’s just your guys’ turn to deal with this public denial of science.’”
Dr. Limaye is also concerned about the impacts on funding for scientific research.
“There’s always been a really strong bipartisan effort with regards to funding for science, when you look at Congress and when you look at appropriations,” she says. “But what ended up happening, especially with the Trump administration, was that there was a real shift in that. We’ve never really seen that before in past generations.”
So, what’s the big take-home message?
Dr. Limaye believes doctors and public health experts must show more empathy – and not be combative or arrogant – in communicating science in one-on-one conversations. This month, she’s launching a new course for parents, school administrators, and nurses on how to do precisely that.
“It’s really all about how to have hard conversations with people who might be anti-science,” she says. “It’s being empathetic and not being dismissive. But it’s hard work, and I think a lot of people are just not cut out for it and just don’t have the time for it…You can’t just say, ‘Well, this is science, and I’m a doctor’ – that doesn’t work anymore.”
Brendan Nyhan, PhD, a Dartmouth College political scientist, echoes those sentiments in a separate paper recently published in the Proceedings of the National Academy of Sciences. In fact, he suggests that providing accurate, fact-based information to counter false claims may actually backfire and reinforce some people’s unfounded beliefs.
“One response to the prevalence of mistaken beliefs is to try to set the record straight by providing accurate information – for instance, by providing evidence of the scientific consensus on climate change,” he writes. “The failures of this approach, which is sometimes referred to as the ‘deficit model’ in science communication, are well-known.”
Dr. Nyhan argues two things make some people more prone to believe falsehoods:
What scientists call “ingrouping,” a kind of tribal mentality that makes some people choose social identity or politics over truth-seeking and demonize others who don’t agree with their views
The rise of high-profile political figures, such as Trump, who encourage their followers to indulge in their desire for “identify-affirming misinformation”
Dr. Scheffer says the most important thing for doctors, health experts, and scientists to recognize is that it’s crucial to gain the trust of someone who may believe fictions over facts to make any persuasive argument on COVID-19 or any other issue.
He also has a standard response to those who present falsehoods to him as facts that he suggests anyone can use: “That is interesting. Would you mind helping me understand how you came to that opinion?”
A version of this article first appeared on WebMD.com.
Physician burnout, depression compounded by COVID: Survey
In 2020, it was hard to imagine that the situation could get worse for doctors.
But 2021 presented a new set of challenges. As quarantines lifted and physicians tried to get back to work, they were forced to deal with reduced staff, continuing COVID stress, and pandemic-related anxieties about family and loved ones.
Medscape’s National Burnout and Depression Report 2022 asked more than 13,000 physicians from 29 specialties to share details about their lives and struggles with burnout and depression in 2021. The results paint a picture of physicians trying to fulfill their mission to care for patients, but struggling to maintain their own well-being amid a global pandemic.
Burnout bump
In 2021’s report, 42% of physicians said they were burned out. In 2022, that number increased to 47%. Perhaps not surprisingly, burnout among emergency physicians took the biggest leap, increasing from 43% to 60%. Critical care (56%), ob.gyn. (53%), and infectious disease and family medicine (both at 51%) rounded out the top five specialties with doctors experiencing burnout in 2021.
Burnout has typically been a greater problem for women than men physicians, and the pandemic hasn’t changed that. “There’s no question that women have reported far more role strain during the pandemic than men,” says Carol A. Bernstein, MD, psychiatrist at Montefiore Health System and professor and vice chair for faculty development and well-being at the Albert Einstein College of Medicine, both in New York. And indeed, 56% of women and 41% of men reported burnout in the 2022 survey.
The causes, however, weren’t especially pandemic related – or at least not directly. As in previous surveys, the major contributing factor to burnout was too much paperwork (60%), such as charting and other bureaucratic tasks. Treating COVID-19 patients was cited as the major source of stress by 10% of respondents. About 34% said too many hours at work was the biggest contributing factor to burnout.
The nature of the beast
What is burnout like for these doctors? One described the conditions that lead to burnout like this: “I barely spend enough time with most patients, just running from one to the next; and then after work, I spend hours documenting, charting, dealing with reports. I feel like an overpaid clerk.” Another said: “Where’s the relationships with patients that used to make this worthwhile?” Others fingered staffing shortages at work or an overwhelming home life: “Staff calls in sick; we’re all running around trying to find things and get things done. It never ends.”
Of those who do experience burnout, the problem reaches beyond the workplace, with 54% saying that their burnout has a strong/severe impact on life and 68% reporting that burnout affects their relationships. One respondent said: “I’m always tired; I have trouble concentrating, no time for the children, more arguments with my hubby.” Another put it this way: “Home is just as busy and chaotic as work. I can never relax.”
It doesn’t help matters that physicians are likely to think they’re the only professionals experiencing job burnout. For example, only 36% of respondents believe teachers experience comparable burnout, yet more than 41% of teachers leave the profession within 5 years of starting – often because of burnout.
When it comes to methods for coping with burnout, exercise is the clear favorite, with 63% of respondents saying exercise helps maintain their mental health. About 41% talk with family members or close friends. However, less healthy coping mechanisms were cited as well, such as isolating themselves from others (45%), sleeping (41%), and eating junk food (35%) or drinking alcohol (24%).
When it comes to trying to alleviate burnout, 29% have tried meditation or similar stress-reduction techniques, while others have reduced their work hours (29%) or changed their work settings (19%).
‘Now I feel like there’s no hope’
About a fifth of physicians (21%) said they suffered from clinical depression, and 64% reported feeling “blue, down, or sad.” One physician characterized their depression this way: “I used to think my life would be great. Now I feel like there’s no hope, this will never get better, I’ll never be happy.”
Of doctors reporting depression, 53% said their illness did not affect their interactions with patients, while 34% said depression caused them to be more easily exasperated by patients.
When asked about seeking help for depression, about half (49%) said they believed they could deal with emotional stress on their own. Unfortunately, fear of medical boards finding out keeps 43% of physicians from reaching out for help, according to the survey.
A version of this article first appeared on Medscape.com.
In 2020, it was hard to imagine that the situation could get worse for doctors.
But 2021 presented a new set of challenges. As quarantines lifted and physicians tried to get back to work, they were forced to deal with reduced staff, continuing COVID stress, and pandemic-related anxieties about family and loved ones.
Medscape’s National Burnout and Depression Report 2022 asked more than 13,000 physicians from 29 specialties to share details about their lives and struggles with burnout and depression in 2021. The results paint a picture of physicians trying to fulfill their mission to care for patients, but struggling to maintain their own well-being amid a global pandemic.
Burnout bump
In 2021’s report, 42% of physicians said they were burned out. In 2022, that number increased to 47%. Perhaps not surprisingly, burnout among emergency physicians took the biggest leap, increasing from 43% to 60%. Critical care (56%), ob.gyn. (53%), and infectious disease and family medicine (both at 51%) rounded out the top five specialties with doctors experiencing burnout in 2021.
Burnout has typically been a greater problem for women than men physicians, and the pandemic hasn’t changed that. “There’s no question that women have reported far more role strain during the pandemic than men,” says Carol A. Bernstein, MD, psychiatrist at Montefiore Health System and professor and vice chair for faculty development and well-being at the Albert Einstein College of Medicine, both in New York. And indeed, 56% of women and 41% of men reported burnout in the 2022 survey.
The causes, however, weren’t especially pandemic related – or at least not directly. As in previous surveys, the major contributing factor to burnout was too much paperwork (60%), such as charting and other bureaucratic tasks. Treating COVID-19 patients was cited as the major source of stress by 10% of respondents. About 34% said too many hours at work was the biggest contributing factor to burnout.
The nature of the beast
What is burnout like for these doctors? One described the conditions that lead to burnout like this: “I barely spend enough time with most patients, just running from one to the next; and then after work, I spend hours documenting, charting, dealing with reports. I feel like an overpaid clerk.” Another said: “Where’s the relationships with patients that used to make this worthwhile?” Others fingered staffing shortages at work or an overwhelming home life: “Staff calls in sick; we’re all running around trying to find things and get things done. It never ends.”
Of those who do experience burnout, the problem reaches beyond the workplace, with 54% saying that their burnout has a strong/severe impact on life and 68% reporting that burnout affects their relationships. One respondent said: “I’m always tired; I have trouble concentrating, no time for the children, more arguments with my hubby.” Another put it this way: “Home is just as busy and chaotic as work. I can never relax.”
It doesn’t help matters that physicians are likely to think they’re the only professionals experiencing job burnout. For example, only 36% of respondents believe teachers experience comparable burnout, yet more than 41% of teachers leave the profession within 5 years of starting – often because of burnout.
When it comes to methods for coping with burnout, exercise is the clear favorite, with 63% of respondents saying exercise helps maintain their mental health. About 41% talk with family members or close friends. However, less healthy coping mechanisms were cited as well, such as isolating themselves from others (45%), sleeping (41%), and eating junk food (35%) or drinking alcohol (24%).
When it comes to trying to alleviate burnout, 29% have tried meditation or similar stress-reduction techniques, while others have reduced their work hours (29%) or changed their work settings (19%).
‘Now I feel like there’s no hope’
About a fifth of physicians (21%) said they suffered from clinical depression, and 64% reported feeling “blue, down, or sad.” One physician characterized their depression this way: “I used to think my life would be great. Now I feel like there’s no hope, this will never get better, I’ll never be happy.”
Of doctors reporting depression, 53% said their illness did not affect their interactions with patients, while 34% said depression caused them to be more easily exasperated by patients.
When asked about seeking help for depression, about half (49%) said they believed they could deal with emotional stress on their own. Unfortunately, fear of medical boards finding out keeps 43% of physicians from reaching out for help, according to the survey.
A version of this article first appeared on Medscape.com.
In 2020, it was hard to imagine that the situation could get worse for doctors.
But 2021 presented a new set of challenges. As quarantines lifted and physicians tried to get back to work, they were forced to deal with reduced staff, continuing COVID stress, and pandemic-related anxieties about family and loved ones.
Medscape’s National Burnout and Depression Report 2022 asked more than 13,000 physicians from 29 specialties to share details about their lives and struggles with burnout and depression in 2021. The results paint a picture of physicians trying to fulfill their mission to care for patients, but struggling to maintain their own well-being amid a global pandemic.
Burnout bump
In 2021’s report, 42% of physicians said they were burned out. In 2022, that number increased to 47%. Perhaps not surprisingly, burnout among emergency physicians took the biggest leap, increasing from 43% to 60%. Critical care (56%), ob.gyn. (53%), and infectious disease and family medicine (both at 51%) rounded out the top five specialties with doctors experiencing burnout in 2021.
Burnout has typically been a greater problem for women than men physicians, and the pandemic hasn’t changed that. “There’s no question that women have reported far more role strain during the pandemic than men,” says Carol A. Bernstein, MD, psychiatrist at Montefiore Health System and professor and vice chair for faculty development and well-being at the Albert Einstein College of Medicine, both in New York. And indeed, 56% of women and 41% of men reported burnout in the 2022 survey.
The causes, however, weren’t especially pandemic related – or at least not directly. As in previous surveys, the major contributing factor to burnout was too much paperwork (60%), such as charting and other bureaucratic tasks. Treating COVID-19 patients was cited as the major source of stress by 10% of respondents. About 34% said too many hours at work was the biggest contributing factor to burnout.
The nature of the beast
What is burnout like for these doctors? One described the conditions that lead to burnout like this: “I barely spend enough time with most patients, just running from one to the next; and then after work, I spend hours documenting, charting, dealing with reports. I feel like an overpaid clerk.” Another said: “Where’s the relationships with patients that used to make this worthwhile?” Others fingered staffing shortages at work or an overwhelming home life: “Staff calls in sick; we’re all running around trying to find things and get things done. It never ends.”
Of those who do experience burnout, the problem reaches beyond the workplace, with 54% saying that their burnout has a strong/severe impact on life and 68% reporting that burnout affects their relationships. One respondent said: “I’m always tired; I have trouble concentrating, no time for the children, more arguments with my hubby.” Another put it this way: “Home is just as busy and chaotic as work. I can never relax.”
It doesn’t help matters that physicians are likely to think they’re the only professionals experiencing job burnout. For example, only 36% of respondents believe teachers experience comparable burnout, yet more than 41% of teachers leave the profession within 5 years of starting – often because of burnout.
When it comes to methods for coping with burnout, exercise is the clear favorite, with 63% of respondents saying exercise helps maintain their mental health. About 41% talk with family members or close friends. However, less healthy coping mechanisms were cited as well, such as isolating themselves from others (45%), sleeping (41%), and eating junk food (35%) or drinking alcohol (24%).
When it comes to trying to alleviate burnout, 29% have tried meditation or similar stress-reduction techniques, while others have reduced their work hours (29%) or changed their work settings (19%).
‘Now I feel like there’s no hope’
About a fifth of physicians (21%) said they suffered from clinical depression, and 64% reported feeling “blue, down, or sad.” One physician characterized their depression this way: “I used to think my life would be great. Now I feel like there’s no hope, this will never get better, I’ll never be happy.”
Of doctors reporting depression, 53% said their illness did not affect their interactions with patients, while 34% said depression caused them to be more easily exasperated by patients.
When asked about seeking help for depression, about half (49%) said they believed they could deal with emotional stress on their own. Unfortunately, fear of medical boards finding out keeps 43% of physicians from reaching out for help, according to the survey.
A version of this article first appeared on Medscape.com.
Celebratory binge drinking a potential trigger for new-onset AFib
Emergency department visits for atrial fibrillation (AFib) appear to go up on days around some annual events in the United States that many people commemorate by consuming alcohol in excess – think Christmas, New Year’s Day, and Super Bowl Sunday.
The novel finding seemed especially true for people without a previous AFib diagnosis, suggesting that alcohol intake, and especially binge drinking, “may acutely enhance the risk” of new-onset AFib, propose researchers in their Jan. 12 report for the inaugural issue of Nature Cardiovascular Research.
Leveraging an international database of breathalyzer test results, the group saw jumps in alcohol intake across several days surrounding eight “recurrent, nationally recognized events,” which also included U.S. Independence Day and the FIFA World Cup.
They then compared the timing of those events to ED visits linked to acute alcohol ingestion and, separately, to ED visits coded for AFib in 10 years of data that cover all of California.
Collectively, the eight annual occasions for heavy alcohol use corresponded to spikes in both kinds of ED visit. Their relationship to AFib-related visits overall grew in strength when the analysis was restricted to new AFib diagnoses.
The researchers acknowledge the limitations of their observational study. Still, the findings represent “the first evidence that acute exposure to alcohol can lead to a given atrial fib episode in a short period of time, even among those without an established AFib diagnosis,” senior author Gregory M. Marcus, MD, MAS, University of California, San Francisco, told this news organization.
“The observation that this was detectable in the general population is a warning to those who drink heavily that any one episode of excessive alcohol consumption could land them in the ED with atrial fibrillation,” he said.
It’s “definitely speculation,” but such ED visits could represent an opportunity for individuals to link their new arrhythmia with a specific episode of excessive drinking, strengthening the message that the two are likely connected, Dr. Marcus observed. The experience could potentially inspire some to “reduce or eliminate” their alcohol intake in an effort to avoid future AFib.
The group obtained data from 2014 to 2016 on more than 1.2 million breath alcohol measurements from about 36,000 people in 59 countries, half residing in the United States, who used commercially available breathalyzer devices from one manufacturer (BACtrack).
The 8 days marking recurrent nationally recognized events, and the days before and after them, were associated with mean blood-alcohol concentrations in the top fifth percentile for the year.
The same eight occasions marked significant bumps in ED visits related to acute alcohol ingestion in records from the California Office of Statewide Health Planning and Development (OSHPD), which documented almost 1.2 million such visits from 2005 to 2015.
Collectively in adjusted analysis, the eight nationally recognized events, compared with other days of the year, accounted for 2,640 excess alcohol-related ED visits per 100,000 person-years across all of California (P < .001).
Separately, ED visits coded for a diagnosis of AFib concentrated significantly around those same 8 days, on which there was an excess of 719 such AFib-related visits per 100,000 person-years (P = .008).
The analysis was replicated after exclusion of OSHPD records from anyone with a previous AFib-related ED visit or hospitalization, or previous outpatient procedure related to AFib, such as ablation or cardioversion. It saw 1,757 excess ED visits per 100,000 person-years (P < .001) for what was considered new-onset AFib in association with the eight nationally recognized events, compared with the rest of the year.
The implication, that a bout of alcohol use leading to an ED visit can acutely raise the risk for a first episode of AFib, was subjected to a “negative control analysis” that focused on ED visits for supraventricular tachycardia. It showed no significant relationships with the eight nationally recognized events.
“We think that helps demonstrate that it’s not just more ED visits, more palpitations, or more heart-related visits per se” associated with acute alcohol use, Dr. Marcus said, “but that it’s something fairly specific to AFib.”
The authors declare no competing interests. Dr. Marcus has previously reported research with Medtronic, Eight Sleep, and Baylis; consulting for InCarda Therapeutics and Johnson & Johnson; and equity in InCarda Therapeutics as cofounder.
A version of this article first appeared on Medscape.com.
Emergency department visits for atrial fibrillation (AFib) appear to go up on days around some annual events in the United States that many people commemorate by consuming alcohol in excess – think Christmas, New Year’s Day, and Super Bowl Sunday.
The novel finding seemed especially true for people without a previous AFib diagnosis, suggesting that alcohol intake, and especially binge drinking, “may acutely enhance the risk” of new-onset AFib, propose researchers in their Jan. 12 report for the inaugural issue of Nature Cardiovascular Research.
Leveraging an international database of breathalyzer test results, the group saw jumps in alcohol intake across several days surrounding eight “recurrent, nationally recognized events,” which also included U.S. Independence Day and the FIFA World Cup.
They then compared the timing of those events to ED visits linked to acute alcohol ingestion and, separately, to ED visits coded for AFib in 10 years of data that cover all of California.
Collectively, the eight annual occasions for heavy alcohol use corresponded to spikes in both kinds of ED visit. Their relationship to AFib-related visits overall grew in strength when the analysis was restricted to new AFib diagnoses.
The researchers acknowledge the limitations of their observational study. Still, the findings represent “the first evidence that acute exposure to alcohol can lead to a given atrial fib episode in a short period of time, even among those without an established AFib diagnosis,” senior author Gregory M. Marcus, MD, MAS, University of California, San Francisco, told this news organization.
“The observation that this was detectable in the general population is a warning to those who drink heavily that any one episode of excessive alcohol consumption could land them in the ED with atrial fibrillation,” he said.
It’s “definitely speculation,” but such ED visits could represent an opportunity for individuals to link their new arrhythmia with a specific episode of excessive drinking, strengthening the message that the two are likely connected, Dr. Marcus observed. The experience could potentially inspire some to “reduce or eliminate” their alcohol intake in an effort to avoid future AFib.
The group obtained data from 2014 to 2016 on more than 1.2 million breath alcohol measurements from about 36,000 people in 59 countries, half residing in the United States, who used commercially available breathalyzer devices from one manufacturer (BACtrack).
The 8 days marking recurrent nationally recognized events, and the days before and after them, were associated with mean blood-alcohol concentrations in the top fifth percentile for the year.
The same eight occasions marked significant bumps in ED visits related to acute alcohol ingestion in records from the California Office of Statewide Health Planning and Development (OSHPD), which documented almost 1.2 million such visits from 2005 to 2015.
Collectively in adjusted analysis, the eight nationally recognized events, compared with other days of the year, accounted for 2,640 excess alcohol-related ED visits per 100,000 person-years across all of California (P < .001).
Separately, ED visits coded for a diagnosis of AFib concentrated significantly around those same 8 days, on which there was an excess of 719 such AFib-related visits per 100,000 person-years (P = .008).
The analysis was replicated after exclusion of OSHPD records from anyone with a previous AFib-related ED visit or hospitalization, or previous outpatient procedure related to AFib, such as ablation or cardioversion. It saw 1,757 excess ED visits per 100,000 person-years (P < .001) for what was considered new-onset AFib in association with the eight nationally recognized events, compared with the rest of the year.
The implication, that a bout of alcohol use leading to an ED visit can acutely raise the risk for a first episode of AFib, was subjected to a “negative control analysis” that focused on ED visits for supraventricular tachycardia. It showed no significant relationships with the eight nationally recognized events.
“We think that helps demonstrate that it’s not just more ED visits, more palpitations, or more heart-related visits per se” associated with acute alcohol use, Dr. Marcus said, “but that it’s something fairly specific to AFib.”
The authors declare no competing interests. Dr. Marcus has previously reported research with Medtronic, Eight Sleep, and Baylis; consulting for InCarda Therapeutics and Johnson & Johnson; and equity in InCarda Therapeutics as cofounder.
A version of this article first appeared on Medscape.com.
Emergency department visits for atrial fibrillation (AFib) appear to go up on days around some annual events in the United States that many people commemorate by consuming alcohol in excess – think Christmas, New Year’s Day, and Super Bowl Sunday.
The novel finding seemed especially true for people without a previous AFib diagnosis, suggesting that alcohol intake, and especially binge drinking, “may acutely enhance the risk” of new-onset AFib, propose researchers in their Jan. 12 report for the inaugural issue of Nature Cardiovascular Research.
Leveraging an international database of breathalyzer test results, the group saw jumps in alcohol intake across several days surrounding eight “recurrent, nationally recognized events,” which also included U.S. Independence Day and the FIFA World Cup.
They then compared the timing of those events to ED visits linked to acute alcohol ingestion and, separately, to ED visits coded for AFib in 10 years of data that cover all of California.
Collectively, the eight annual occasions for heavy alcohol use corresponded to spikes in both kinds of ED visit. Their relationship to AFib-related visits overall grew in strength when the analysis was restricted to new AFib diagnoses.
The researchers acknowledge the limitations of their observational study. Still, the findings represent “the first evidence that acute exposure to alcohol can lead to a given atrial fib episode in a short period of time, even among those without an established AFib diagnosis,” senior author Gregory M. Marcus, MD, MAS, University of California, San Francisco, told this news organization.
“The observation that this was detectable in the general population is a warning to those who drink heavily that any one episode of excessive alcohol consumption could land them in the ED with atrial fibrillation,” he said.
It’s “definitely speculation,” but such ED visits could represent an opportunity for individuals to link their new arrhythmia with a specific episode of excessive drinking, strengthening the message that the two are likely connected, Dr. Marcus observed. The experience could potentially inspire some to “reduce or eliminate” their alcohol intake in an effort to avoid future AFib.
The group obtained data from 2014 to 2016 on more than 1.2 million breath alcohol measurements from about 36,000 people in 59 countries, half residing in the United States, who used commercially available breathalyzer devices from one manufacturer (BACtrack).
The 8 days marking recurrent nationally recognized events, and the days before and after them, were associated with mean blood-alcohol concentrations in the top fifth percentile for the year.
The same eight occasions marked significant bumps in ED visits related to acute alcohol ingestion in records from the California Office of Statewide Health Planning and Development (OSHPD), which documented almost 1.2 million such visits from 2005 to 2015.
Collectively in adjusted analysis, the eight nationally recognized events, compared with other days of the year, accounted for 2,640 excess alcohol-related ED visits per 100,000 person-years across all of California (P < .001).
Separately, ED visits coded for a diagnosis of AFib concentrated significantly around those same 8 days, on which there was an excess of 719 such AFib-related visits per 100,000 person-years (P = .008).
The analysis was replicated after exclusion of OSHPD records from anyone with a previous AFib-related ED visit or hospitalization, or previous outpatient procedure related to AFib, such as ablation or cardioversion. It saw 1,757 excess ED visits per 100,000 person-years (P < .001) for what was considered new-onset AFib in association with the eight nationally recognized events, compared with the rest of the year.
The implication, that a bout of alcohol use leading to an ED visit can acutely raise the risk for a first episode of AFib, was subjected to a “negative control analysis” that focused on ED visits for supraventricular tachycardia. It showed no significant relationships with the eight nationally recognized events.
“We think that helps demonstrate that it’s not just more ED visits, more palpitations, or more heart-related visits per se” associated with acute alcohol use, Dr. Marcus said, “but that it’s something fairly specific to AFib.”
The authors declare no competing interests. Dr. Marcus has previously reported research with Medtronic, Eight Sleep, and Baylis; consulting for InCarda Therapeutics and Johnson & Johnson; and equity in InCarda Therapeutics as cofounder.
A version of this article first appeared on Medscape.com.
Long COVID associated with risk of metabolic liver disease
Postacute COVID syndrome (PACS), an ongoing inflammatory state following infection with SARS-CoV-2, is associated with greater risk of metabolic-associated fatty liver disease (MAFLD), according to an analysis of patients at a single clinic in Canada published in Open Forum Infectious Diseases.
MAFLD, also known as nonalcoholic fatty liver disease (NAFLD), is considered an indicator of general health and is in turn linked to greater risk of cardiovascular complications and mortality. It may be a multisystem disorder with various underlying causes.
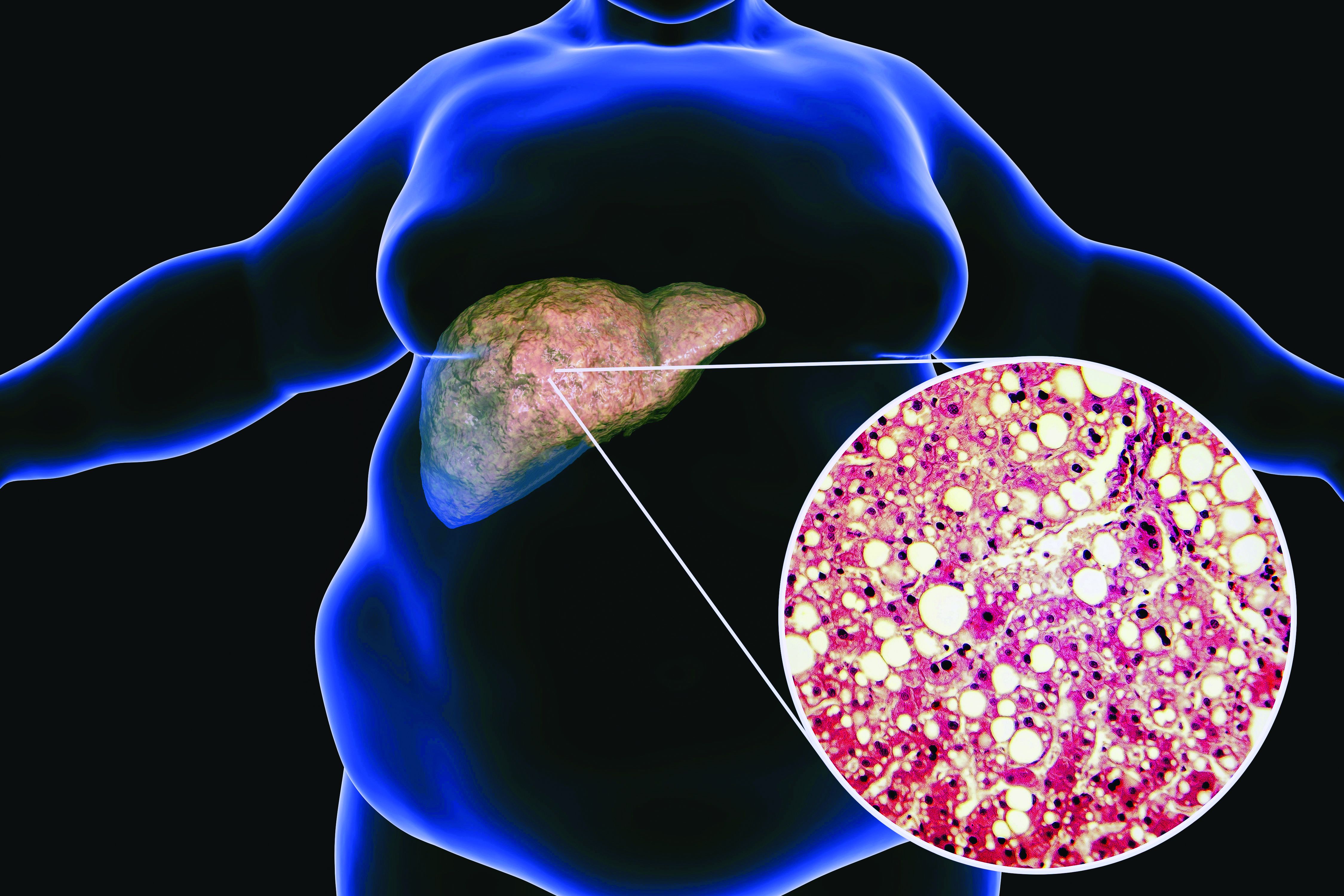
PACS includes symptoms that affect various organ systems, with neurocognitive, autonomic, gastrointestinal, respiratory, musculoskeletal, psychological, sensory, and dermatologic clusters. An estimated 50%-80% of COVID-19 patients experience one or more clusters of symptoms 3 months after leaving the hospital.
But liver problems also appear in the acute phase, said Paul Martin, MD, who was asked to comment on the study. “Up to about half the patients during the acute illness may have elevated liver tests, but there seems to be a subset of patients in whom the abnormality persists. And then there are some reports in the literature of patients developing injury to their bile ducts in the liver over the long term, apparently as a consequence of COVID infection. What this paper suggests is that there may be some metabolic derangements associated with COVID infection, which in turn can accentuate or possibly cause fatty liver,” said Dr. Martin in an interview. He is chief of digestive health and liver diseases and a professor of medicine at the University of Miami.
“It highlights the need to get vaccinated against COVID and to take appropriate precautions because contracting the infection may lead to all sorts of consequences quite apart from having a respiratory illness,” said Dr. Martin.
The researchers retrospectively identified 235 patients hospitalized with COVID-19 between July 2020 and April 2021. Overall, 69% were men, and the median age was 61 years; 19.2% underwent mechanical ventilation and the mean duration of hospitalization was 11.7 days. They were seen for PACS symptoms a median 143 days after COVID-19 symptoms began, with 77.5% having symptoms of at least one PACS cluster. Of these clusters, 34.9% were neurocognitive, 53.2% were respiratory, 26.4% were musculoskeletal, 29.4% were psychological, 25.1% were dermatologic, and 17.5% were sensory.
At the later clinical visit for PACS symptoms, all patients underwent screening for MAFLD, which was defined as the presence of liver steatosis plus overweight/obesity or type 2 diabetes. Hepatic steatosis was determined from controlled attenuation parameter using transient elastrography. The analysis excluded patients with significant alcohol intake or hepatitis B or C. All patients with liver steatosis also had MAFLD, and this included 55.3% of the study population.
The hospital was able to obtain hepatic steatosis index (HSI) scores for 103 of 235 patients. Of these, 50% had MAFLD on admission for acute COVID-19, and 48.1% had MAFLD upon discharge based on this criterion. At the PACS follow-up visit, 71.3% were diagnosed with MAFLD. There was no statistically significant difference in the use of glucocorticoids or tocilizumab during hospitalization between those with and without MAFLD, and remdesivir use was insignificant in the patient population.
Given that the prevalence of MAFLD among the study population is more than double that in the general population, the authors suggest that MAFLD may be a new PACS cluster phenotype that could lead to long-term metabolic and cardiovascular complications. A potential explanation is loss of lean body mass during COVID-19 hospitalization followed by liver fat accumulation during recovery.
Other infections have also shown an association with increased MAFLD incidence, including HIV, Heliobacter pylori, and viral hepatitis. The authors worry that COVID-19 infection could exacerbate underlying conditions to a more severe MAFLD disease state.
The study is limited by a small sample size, limited follow-up, and the lack of a control group. Its retrospective nature leaves it vulnerable to biases.
“The natural history of MAFLD in the context of PACS is unknown at this time, and careful follow-up of these patients is needed to understand the clinical implications of this syndrome in the context of long COVID,” the authors wrote. “We speculate that [MAFLD] may be considered as an independent PACS-cluster phenotype, potentially affecting the metabolic and cardiovascular health of patients with PACS.”
One author has relationships with several pharmaceutical companies, but the remaining authors reported no conflicts of interest. Dr. Martin has no relevant financial disclosures.
Postacute COVID syndrome (PACS), an ongoing inflammatory state following infection with SARS-CoV-2, is associated with greater risk of metabolic-associated fatty liver disease (MAFLD), according to an analysis of patients at a single clinic in Canada published in Open Forum Infectious Diseases.
MAFLD, also known as nonalcoholic fatty liver disease (NAFLD), is considered an indicator of general health and is in turn linked to greater risk of cardiovascular complications and mortality. It may be a multisystem disorder with various underlying causes.
PACS includes symptoms that affect various organ systems, with neurocognitive, autonomic, gastrointestinal, respiratory, musculoskeletal, psychological, sensory, and dermatologic clusters. An estimated 50%-80% of COVID-19 patients experience one or more clusters of symptoms 3 months after leaving the hospital.
But liver problems also appear in the acute phase, said Paul Martin, MD, who was asked to comment on the study. “Up to about half the patients during the acute illness may have elevated liver tests, but there seems to be a subset of patients in whom the abnormality persists. And then there are some reports in the literature of patients developing injury to their bile ducts in the liver over the long term, apparently as a consequence of COVID infection. What this paper suggests is that there may be some metabolic derangements associated with COVID infection, which in turn can accentuate or possibly cause fatty liver,” said Dr. Martin in an interview. He is chief of digestive health and liver diseases and a professor of medicine at the University of Miami.
“It highlights the need to get vaccinated against COVID and to take appropriate precautions because contracting the infection may lead to all sorts of consequences quite apart from having a respiratory illness,” said Dr. Martin.
The researchers retrospectively identified 235 patients hospitalized with COVID-19 between July 2020 and April 2021. Overall, 69% were men, and the median age was 61 years; 19.2% underwent mechanical ventilation and the mean duration of hospitalization was 11.7 days. They were seen for PACS symptoms a median 143 days after COVID-19 symptoms began, with 77.5% having symptoms of at least one PACS cluster. Of these clusters, 34.9% were neurocognitive, 53.2% were respiratory, 26.4% were musculoskeletal, 29.4% were psychological, 25.1% were dermatologic, and 17.5% were sensory.
At the later clinical visit for PACS symptoms, all patients underwent screening for MAFLD, which was defined as the presence of liver steatosis plus overweight/obesity or type 2 diabetes. Hepatic steatosis was determined from controlled attenuation parameter using transient elastrography. The analysis excluded patients with significant alcohol intake or hepatitis B or C. All patients with liver steatosis also had MAFLD, and this included 55.3% of the study population.
The hospital was able to obtain hepatic steatosis index (HSI) scores for 103 of 235 patients. Of these, 50% had MAFLD on admission for acute COVID-19, and 48.1% had MAFLD upon discharge based on this criterion. At the PACS follow-up visit, 71.3% were diagnosed with MAFLD. There was no statistically significant difference in the use of glucocorticoids or tocilizumab during hospitalization between those with and without MAFLD, and remdesivir use was insignificant in the patient population.
Given that the prevalence of MAFLD among the study population is more than double that in the general population, the authors suggest that MAFLD may be a new PACS cluster phenotype that could lead to long-term metabolic and cardiovascular complications. A potential explanation is loss of lean body mass during COVID-19 hospitalization followed by liver fat accumulation during recovery.
Other infections have also shown an association with increased MAFLD incidence, including HIV, Heliobacter pylori, and viral hepatitis. The authors worry that COVID-19 infection could exacerbate underlying conditions to a more severe MAFLD disease state.
The study is limited by a small sample size, limited follow-up, and the lack of a control group. Its retrospective nature leaves it vulnerable to biases.
“The natural history of MAFLD in the context of PACS is unknown at this time, and careful follow-up of these patients is needed to understand the clinical implications of this syndrome in the context of long COVID,” the authors wrote. “We speculate that [MAFLD] may be considered as an independent PACS-cluster phenotype, potentially affecting the metabolic and cardiovascular health of patients with PACS.”
One author has relationships with several pharmaceutical companies, but the remaining authors reported no conflicts of interest. Dr. Martin has no relevant financial disclosures.
Postacute COVID syndrome (PACS), an ongoing inflammatory state following infection with SARS-CoV-2, is associated with greater risk of metabolic-associated fatty liver disease (MAFLD), according to an analysis of patients at a single clinic in Canada published in Open Forum Infectious Diseases.
MAFLD, also known as nonalcoholic fatty liver disease (NAFLD), is considered an indicator of general health and is in turn linked to greater risk of cardiovascular complications and mortality. It may be a multisystem disorder with various underlying causes.
PACS includes symptoms that affect various organ systems, with neurocognitive, autonomic, gastrointestinal, respiratory, musculoskeletal, psychological, sensory, and dermatologic clusters. An estimated 50%-80% of COVID-19 patients experience one or more clusters of symptoms 3 months after leaving the hospital.
But liver problems also appear in the acute phase, said Paul Martin, MD, who was asked to comment on the study. “Up to about half the patients during the acute illness may have elevated liver tests, but there seems to be a subset of patients in whom the abnormality persists. And then there are some reports in the literature of patients developing injury to their bile ducts in the liver over the long term, apparently as a consequence of COVID infection. What this paper suggests is that there may be some metabolic derangements associated with COVID infection, which in turn can accentuate or possibly cause fatty liver,” said Dr. Martin in an interview. He is chief of digestive health and liver diseases and a professor of medicine at the University of Miami.
“It highlights the need to get vaccinated against COVID and to take appropriate precautions because contracting the infection may lead to all sorts of consequences quite apart from having a respiratory illness,” said Dr. Martin.
The researchers retrospectively identified 235 patients hospitalized with COVID-19 between July 2020 and April 2021. Overall, 69% were men, and the median age was 61 years; 19.2% underwent mechanical ventilation and the mean duration of hospitalization was 11.7 days. They were seen for PACS symptoms a median 143 days after COVID-19 symptoms began, with 77.5% having symptoms of at least one PACS cluster. Of these clusters, 34.9% were neurocognitive, 53.2% were respiratory, 26.4% were musculoskeletal, 29.4% were psychological, 25.1% were dermatologic, and 17.5% were sensory.
At the later clinical visit for PACS symptoms, all patients underwent screening for MAFLD, which was defined as the presence of liver steatosis plus overweight/obesity or type 2 diabetes. Hepatic steatosis was determined from controlled attenuation parameter using transient elastrography. The analysis excluded patients with significant alcohol intake or hepatitis B or C. All patients with liver steatosis also had MAFLD, and this included 55.3% of the study population.
The hospital was able to obtain hepatic steatosis index (HSI) scores for 103 of 235 patients. Of these, 50% had MAFLD on admission for acute COVID-19, and 48.1% had MAFLD upon discharge based on this criterion. At the PACS follow-up visit, 71.3% were diagnosed with MAFLD. There was no statistically significant difference in the use of glucocorticoids or tocilizumab during hospitalization between those with and without MAFLD, and remdesivir use was insignificant in the patient population.
Given that the prevalence of MAFLD among the study population is more than double that in the general population, the authors suggest that MAFLD may be a new PACS cluster phenotype that could lead to long-term metabolic and cardiovascular complications. A potential explanation is loss of lean body mass during COVID-19 hospitalization followed by liver fat accumulation during recovery.
Other infections have also shown an association with increased MAFLD incidence, including HIV, Heliobacter pylori, and viral hepatitis. The authors worry that COVID-19 infection could exacerbate underlying conditions to a more severe MAFLD disease state.
The study is limited by a small sample size, limited follow-up, and the lack of a control group. Its retrospective nature leaves it vulnerable to biases.
“The natural history of MAFLD in the context of PACS is unknown at this time, and careful follow-up of these patients is needed to understand the clinical implications of this syndrome in the context of long COVID,” the authors wrote. “We speculate that [MAFLD] may be considered as an independent PACS-cluster phenotype, potentially affecting the metabolic and cardiovascular health of patients with PACS.”
One author has relationships with several pharmaceutical companies, but the remaining authors reported no conflicts of interest. Dr. Martin has no relevant financial disclosures.
FROM OPEN FORUM INFECTIOUS DISEASES
Intensive weight loss fails to help women with obesity and infertility
An intensive weight-loss intervention prior to conception had no effect on birth rates in women with obesity and unexplained infertility, compared with a standard weight-maintenance program, based on data from nearly 400 women.
Obese women experiencing infertility are often counseled to lose weight before attempting fertility treatments in order to improve outcomes based on epidemiologic evidence of an association between obesity and infertility, but data to support this advice are limited, wrote Richard S. Legro, MD, of Penn State University, Hershey, and colleagues.
The researchers proposed that a more intensive preconception weight loss intervention followed by infertility treatment would be more likely to yield a healthy live birth, compared with a standard weight maintenance intervention.
In an open-label study published in PLOS Medicine, the researchers randomized 379 women at nine academic centers to a standard lifestyle group that followed a weight-maintenance plan focused on physical activity, but not weight loss; or an intensive intervention of diet and medication with a target weight loss of 7%. Both interventions lasted for 16 weeks between July 2015 and July 2018. After the interventions, patients in both groups underwent standardized empiric fertility treatment with three cycles of ovarian stimulation and intrauterine insemination.
The primary outcome was a live birth at 37 weeks’ gestation or later, with no congenital abnormalities and a birth weight between 2,500 g and 4,000 g. Baseline characteristics including age, education level, race, and body mass index (BMI) were similar between the groups.
The incidence of healthy live births was not significantly different between the standard treatment and intensive treatment groups (15.2% vs. 12.2%; P = 0.40) by the final follow-up time of September 2019. However, women in the intensive group had significantly greater weight loss, compared with the standard group (–6.6% vs. –0.3%; P < .001). Women in the intensive group also showed improvements in metabolic health. Notably, the incidence of metabolic syndrome dropped from 53.6% to 49.4% in the standard group, compared with a decrease from 52.8% to 32.2% in the intensive group over the 16-week study period, the researchers wrote.
Gastrointestinal side effects were significantly more common in the intensive group, but these were consistent with documented side effects of the weight loss medication used (Orlistat).
First-trimester pregnancy loss was higher in the intensive group, compared with the standard group (33.3% vs. 23.7%), but the difference was not significant. Most pregnancy complications, including preterm labor, premature rupture of membranes, preeclampsia, and gestational diabetes had nonsignificant improvements in the intensive group, compared with the standard group. Similarly, nonsignificant improvements were noted in the intervention group for intrauterine growth restriction and admission to the neonatal ICU.
Limitations of the study included the relatively small number of pregnancies, which prevented assessment of rare complications in subgroups, and the challenge of matching control interventions, the researchers noted.
However, the results were strengthened by the focus on women with unexplained infertility, the inclusion of a comparison group, and the collection of data on complications after conception, they wrote.
Avenues for future research include interventions of different duration and intensity prior to conception, which may improve outcomes, the researchers said in their discussion of the findings. “A period of weight stabilization and maintenance after a weight-loss intervention prior to commencing infertility therapy is worth exploring,” they noted, but couples eager to conceive may be reluctant to wait for a weight-loss intervention, they added.
“Our findings directly impact current standards of clinical care, where women who are obese with unexplained infertility are to our knowledge routinely counseled to lose weight prior to initiation of infertility treatment,” they concluded.
Data may inform patient discussions
The current study is important because a large amount of previous research has shown an association between obesity and decreased fecundity in women and men, Mark P. Trolice, MD, of the University of Central Florida, Orlando, and director of the IVF Center in Winter Park, Fla., said in an interview.
According to the Centers for Disease Control and Prevention, the prevalence of obesity in the United States remains more than 40%, said Dr. Trolice. “Patients and physicians would benefit from clarity of obesity’s effect, if any, on reproduction,” he noted.
In contrast to the authors’ hypothesis, “the study did not find a difference in the live birth rate following up to three cycles of intrauterine insemination (IUI) between an intensive weight loss group [and] women who exercised without weight loss,” said Dr. Trolice. “Prior to this study, many reports suggested a decline in fertility with elevations in BMI, particularly during fertility treatment,” he added.
The take-home message from the current study is a that an elevated BMI, while possibly increasing the risks of metabolic disorders, did not appear to impact fecundity, he said.
The authors therefore concluded, “There is not strong evidence to recommend weight loss prior to conception in women who are obese with unexplained infertility,” Dr. Trolice said.
Regardless of the potential effect of preconception weight loss on fertility, barriers to starting a weight loss program include a woman’s eagerness to move forward with fertility treatments without waiting for weight loss, Dr. Trolice noted. “By the time a woman reaches an infertility specialist, she has been trying to conceive for at least 1 year,” he said. “At the initial consultation, these patients are anxious to undergo necessary additional diagnostic testing followed by treatment. Consequently, initiation of a weight-loss program is viewed as a delay toward the goal of family building,” he explained.
“More research is needed to demonstrate the safety of intensive weight loss preconception,” said Dr. Trolice. However, he said, “the issue of elevated BMI and increased risk of pregnancy complications remains, but this study provides important information for providers regarding counseling their patients desiring pregnancy.”
The study was supported by multiple grants from the National Institutes of Health through the Eunice Kennedy Shriver National Institute of Child Health and Human Development and the National Center for Advancing Translational Sciences. Nutrisystem provided discounted coupons for food allotments in the standardized treatment group, and FitBit provided the study organizers with discounted Fitbits for activity monitoring. Lead author Dr. Legro disclosed consulting fees from InSupp, Ferring, Bayer, Abbvie and Fractyl, and research sponsorship from Guerbet and the National Institutes of Health. Dr. Trolice had no financial conflicts to disclose and serves on the Editorial Advisory Board of Ob.Gyn News.
An intensive weight-loss intervention prior to conception had no effect on birth rates in women with obesity and unexplained infertility, compared with a standard weight-maintenance program, based on data from nearly 400 women.
Obese women experiencing infertility are often counseled to lose weight before attempting fertility treatments in order to improve outcomes based on epidemiologic evidence of an association between obesity and infertility, but data to support this advice are limited, wrote Richard S. Legro, MD, of Penn State University, Hershey, and colleagues.
The researchers proposed that a more intensive preconception weight loss intervention followed by infertility treatment would be more likely to yield a healthy live birth, compared with a standard weight maintenance intervention.
In an open-label study published in PLOS Medicine, the researchers randomized 379 women at nine academic centers to a standard lifestyle group that followed a weight-maintenance plan focused on physical activity, but not weight loss; or an intensive intervention of diet and medication with a target weight loss of 7%. Both interventions lasted for 16 weeks between July 2015 and July 2018. After the interventions, patients in both groups underwent standardized empiric fertility treatment with three cycles of ovarian stimulation and intrauterine insemination.
The primary outcome was a live birth at 37 weeks’ gestation or later, with no congenital abnormalities and a birth weight between 2,500 g and 4,000 g. Baseline characteristics including age, education level, race, and body mass index (BMI) were similar between the groups.
The incidence of healthy live births was not significantly different between the standard treatment and intensive treatment groups (15.2% vs. 12.2%; P = 0.40) by the final follow-up time of September 2019. However, women in the intensive group had significantly greater weight loss, compared with the standard group (–6.6% vs. –0.3%; P < .001). Women in the intensive group also showed improvements in metabolic health. Notably, the incidence of metabolic syndrome dropped from 53.6% to 49.4% in the standard group, compared with a decrease from 52.8% to 32.2% in the intensive group over the 16-week study period, the researchers wrote.
Gastrointestinal side effects were significantly more common in the intensive group, but these were consistent with documented side effects of the weight loss medication used (Orlistat).
First-trimester pregnancy loss was higher in the intensive group, compared with the standard group (33.3% vs. 23.7%), but the difference was not significant. Most pregnancy complications, including preterm labor, premature rupture of membranes, preeclampsia, and gestational diabetes had nonsignificant improvements in the intensive group, compared with the standard group. Similarly, nonsignificant improvements were noted in the intervention group for intrauterine growth restriction and admission to the neonatal ICU.
Limitations of the study included the relatively small number of pregnancies, which prevented assessment of rare complications in subgroups, and the challenge of matching control interventions, the researchers noted.
However, the results were strengthened by the focus on women with unexplained infertility, the inclusion of a comparison group, and the collection of data on complications after conception, they wrote.
Avenues for future research include interventions of different duration and intensity prior to conception, which may improve outcomes, the researchers said in their discussion of the findings. “A period of weight stabilization and maintenance after a weight-loss intervention prior to commencing infertility therapy is worth exploring,” they noted, but couples eager to conceive may be reluctant to wait for a weight-loss intervention, they added.
“Our findings directly impact current standards of clinical care, where women who are obese with unexplained infertility are to our knowledge routinely counseled to lose weight prior to initiation of infertility treatment,” they concluded.
Data may inform patient discussions
The current study is important because a large amount of previous research has shown an association between obesity and decreased fecundity in women and men, Mark P. Trolice, MD, of the University of Central Florida, Orlando, and director of the IVF Center in Winter Park, Fla., said in an interview.
According to the Centers for Disease Control and Prevention, the prevalence of obesity in the United States remains more than 40%, said Dr. Trolice. “Patients and physicians would benefit from clarity of obesity’s effect, if any, on reproduction,” he noted.
In contrast to the authors’ hypothesis, “the study did not find a difference in the live birth rate following up to three cycles of intrauterine insemination (IUI) between an intensive weight loss group [and] women who exercised without weight loss,” said Dr. Trolice. “Prior to this study, many reports suggested a decline in fertility with elevations in BMI, particularly during fertility treatment,” he added.
The take-home message from the current study is a that an elevated BMI, while possibly increasing the risks of metabolic disorders, did not appear to impact fecundity, he said.
The authors therefore concluded, “There is not strong evidence to recommend weight loss prior to conception in women who are obese with unexplained infertility,” Dr. Trolice said.
Regardless of the potential effect of preconception weight loss on fertility, barriers to starting a weight loss program include a woman’s eagerness to move forward with fertility treatments without waiting for weight loss, Dr. Trolice noted. “By the time a woman reaches an infertility specialist, she has been trying to conceive for at least 1 year,” he said. “At the initial consultation, these patients are anxious to undergo necessary additional diagnostic testing followed by treatment. Consequently, initiation of a weight-loss program is viewed as a delay toward the goal of family building,” he explained.
“More research is needed to demonstrate the safety of intensive weight loss preconception,” said Dr. Trolice. However, he said, “the issue of elevated BMI and increased risk of pregnancy complications remains, but this study provides important information for providers regarding counseling their patients desiring pregnancy.”
The study was supported by multiple grants from the National Institutes of Health through the Eunice Kennedy Shriver National Institute of Child Health and Human Development and the National Center for Advancing Translational Sciences. Nutrisystem provided discounted coupons for food allotments in the standardized treatment group, and FitBit provided the study organizers with discounted Fitbits for activity monitoring. Lead author Dr. Legro disclosed consulting fees from InSupp, Ferring, Bayer, Abbvie and Fractyl, and research sponsorship from Guerbet and the National Institutes of Health. Dr. Trolice had no financial conflicts to disclose and serves on the Editorial Advisory Board of Ob.Gyn News.
An intensive weight-loss intervention prior to conception had no effect on birth rates in women with obesity and unexplained infertility, compared with a standard weight-maintenance program, based on data from nearly 400 women.
Obese women experiencing infertility are often counseled to lose weight before attempting fertility treatments in order to improve outcomes based on epidemiologic evidence of an association between obesity and infertility, but data to support this advice are limited, wrote Richard S. Legro, MD, of Penn State University, Hershey, and colleagues.
The researchers proposed that a more intensive preconception weight loss intervention followed by infertility treatment would be more likely to yield a healthy live birth, compared with a standard weight maintenance intervention.
In an open-label study published in PLOS Medicine, the researchers randomized 379 women at nine academic centers to a standard lifestyle group that followed a weight-maintenance plan focused on physical activity, but not weight loss; or an intensive intervention of diet and medication with a target weight loss of 7%. Both interventions lasted for 16 weeks between July 2015 and July 2018. After the interventions, patients in both groups underwent standardized empiric fertility treatment with three cycles of ovarian stimulation and intrauterine insemination.
The primary outcome was a live birth at 37 weeks’ gestation or later, with no congenital abnormalities and a birth weight between 2,500 g and 4,000 g. Baseline characteristics including age, education level, race, and body mass index (BMI) were similar between the groups.
The incidence of healthy live births was not significantly different between the standard treatment and intensive treatment groups (15.2% vs. 12.2%; P = 0.40) by the final follow-up time of September 2019. However, women in the intensive group had significantly greater weight loss, compared with the standard group (–6.6% vs. –0.3%; P < .001). Women in the intensive group also showed improvements in metabolic health. Notably, the incidence of metabolic syndrome dropped from 53.6% to 49.4% in the standard group, compared with a decrease from 52.8% to 32.2% in the intensive group over the 16-week study period, the researchers wrote.
Gastrointestinal side effects were significantly more common in the intensive group, but these were consistent with documented side effects of the weight loss medication used (Orlistat).
First-trimester pregnancy loss was higher in the intensive group, compared with the standard group (33.3% vs. 23.7%), but the difference was not significant. Most pregnancy complications, including preterm labor, premature rupture of membranes, preeclampsia, and gestational diabetes had nonsignificant improvements in the intensive group, compared with the standard group. Similarly, nonsignificant improvements were noted in the intervention group for intrauterine growth restriction and admission to the neonatal ICU.
Limitations of the study included the relatively small number of pregnancies, which prevented assessment of rare complications in subgroups, and the challenge of matching control interventions, the researchers noted.
However, the results were strengthened by the focus on women with unexplained infertility, the inclusion of a comparison group, and the collection of data on complications after conception, they wrote.
Avenues for future research include interventions of different duration and intensity prior to conception, which may improve outcomes, the researchers said in their discussion of the findings. “A period of weight stabilization and maintenance after a weight-loss intervention prior to commencing infertility therapy is worth exploring,” they noted, but couples eager to conceive may be reluctant to wait for a weight-loss intervention, they added.
“Our findings directly impact current standards of clinical care, where women who are obese with unexplained infertility are to our knowledge routinely counseled to lose weight prior to initiation of infertility treatment,” they concluded.
Data may inform patient discussions
The current study is important because a large amount of previous research has shown an association between obesity and decreased fecundity in women and men, Mark P. Trolice, MD, of the University of Central Florida, Orlando, and director of the IVF Center in Winter Park, Fla., said in an interview.
According to the Centers for Disease Control and Prevention, the prevalence of obesity in the United States remains more than 40%, said Dr. Trolice. “Patients and physicians would benefit from clarity of obesity’s effect, if any, on reproduction,” he noted.
In contrast to the authors’ hypothesis, “the study did not find a difference in the live birth rate following up to three cycles of intrauterine insemination (IUI) between an intensive weight loss group [and] women who exercised without weight loss,” said Dr. Trolice. “Prior to this study, many reports suggested a decline in fertility with elevations in BMI, particularly during fertility treatment,” he added.
The take-home message from the current study is a that an elevated BMI, while possibly increasing the risks of metabolic disorders, did not appear to impact fecundity, he said.
The authors therefore concluded, “There is not strong evidence to recommend weight loss prior to conception in women who are obese with unexplained infertility,” Dr. Trolice said.
Regardless of the potential effect of preconception weight loss on fertility, barriers to starting a weight loss program include a woman’s eagerness to move forward with fertility treatments without waiting for weight loss, Dr. Trolice noted. “By the time a woman reaches an infertility specialist, she has been trying to conceive for at least 1 year,” he said. “At the initial consultation, these patients are anxious to undergo necessary additional diagnostic testing followed by treatment. Consequently, initiation of a weight-loss program is viewed as a delay toward the goal of family building,” he explained.
“More research is needed to demonstrate the safety of intensive weight loss preconception,” said Dr. Trolice. However, he said, “the issue of elevated BMI and increased risk of pregnancy complications remains, but this study provides important information for providers regarding counseling their patients desiring pregnancy.”
The study was supported by multiple grants from the National Institutes of Health through the Eunice Kennedy Shriver National Institute of Child Health and Human Development and the National Center for Advancing Translational Sciences. Nutrisystem provided discounted coupons for food allotments in the standardized treatment group, and FitBit provided the study organizers with discounted Fitbits for activity monitoring. Lead author Dr. Legro disclosed consulting fees from InSupp, Ferring, Bayer, Abbvie and Fractyl, and research sponsorship from Guerbet and the National Institutes of Health. Dr. Trolice had no financial conflicts to disclose and serves on the Editorial Advisory Board of Ob.Gyn News.
FROM PLOS MEDICINE
Nodule on the left cheek
An 85-year-old man with a history of skin cancer presented to my dermatology practice (NT) for evaluation of a “pimple” on his left cheek that failed to resolve after 2 months (FIGURE). The patient noted that the lesion had grown, but that he otherwise felt well.

On examination, the lesion was plum colored, and the area was firm and nontender to palpation. The patient was referred to a plastic surgeon for an excisional biopsy to clarify the nature of the lesion.
WHAT IS YOUR DIAGNOSIS?
HOW WOULD YOU TREAT THIS PATIENT?
Diagnosis: Merkel cell carcinoma
A biopsy performed 2 weeks after the initial visit confirmed the clinical suspicion for Merkel cell carcinoma (MCC).
MCC is a cutaneous neuroendocrine malignancy. Although its name acknowledges similarities between the tumor cells and Merkel cells, it is now considered unlikely that Merkel cells are the actual cells of origin.1
The majority of MCCs are asymptomatic despite rapid growth and are typically red or pink and occur on UV-exposed areas, as in our patient.2 A cyst or acneiform lesion is the single most common diagnosis given at the time of biopsy.2
The incidence of MCC is greatest in people of advanced age and in those who are immunosuppressed. In the United States, the estimated annual incidence rate rose from 0.5 cases per 100,000 people in 2000 to 0.7 cases per 100,000 people in 2013.3 MCC increases exponentially with advancing age, from 0.1 (per 100,000) in those ages 40 to 44 years to 9.8 in those older than 85 years.3 The growing cohort of ageing baby boomers and the increased number of immunosuppressed individuals in the community suggest that clinicians are now more likely to encounter MCC than in the past.
While UV radiation is highly associated with MCC, the major causative factor is considered to be Merkel cell polyomavirus (MCPyV).1 In fact, MCPyV has been linked to 80% of MCC cases.1,3 Most people have positive serology for MCPyV in early childhood, but the association between MCC and old age highlights the impact of immunosuppression on MCPyV activity and MCC development.1
Clinical suspicion is the first step in diagnosing MCC
The mnemonic AEIOU highlights the key clinical features of this aggressive tumor2,4:
- Asymptomatic
- Expanding rapidly (often grows in less than 3 months)
- Immune suppression (eg, chronic lymphocytic leukemia, solid organ transplant patient)
- Older than 50
- UV exposure on fair skin.
If a lesion is suspected to be MCC, the next step includes biopsy so that a definitive diagnosis can be made. A firm, nontender nodule that lacks fluctuance should raise suspicion for a neoplastic process.
Continue to: The differential is broad, ranging from cysts to melanoma
The differential is broad, ranging from cysts to melanoma
The differential diagnosis for an enlarging, plum-colored nodule on sun-exposed skin includes an abscess, a ruptured or inflamed epidermoid cyst, basal cell carcinoma, squamous cell carcinoma, and malignant melanoma.
An abscess is typically tender and expands within a matter of days rather than months.
A cyst can be ruled out by the clinical appearance and lack of an overlying pore.
Basal cell carcinoma can be characterized by a rolled border and central ulceration.
Squamous cell carcinomas often exhibit a verrucous surface with marked hyperkeratosis.
Continue to: Melanoma
Melanoma manifests with brown or irregular pigmentation and may be associated with a precursor lesion.
Tx includes excision and consistent follow-up
Complete excision is the critical first step to successful therapy. Sentinel lymph node studies are typically performed because of the high incidence of lymph node metastasis. Frequent follow-up is required because of the high risk of recurrent or persistent disease.
Local recurrence usually occurs within 1 year of diagnosis in more than 40% of patients.5 Distant metastasis can be treated with a programmed cell death ligand 1 blocking agent (avelumab) or a programmed cell death protein 1 inhibitor (nivolumab or pembrolizumab).6
Our patient was referred to a regional cancer center for sentinel lymph node evaluation, where he was found to have nodal disease. The patient was put on pembrolizumab and received radiation therapy but showed only limited response. Seven months after diagnosis, he passed away from metastatic MCC.
1. Pietropaolo V, Prezioso C, Moens U. Merkel cell polyomavirus and Merkel cell carcinoma. Cancers (Basel). 2020;12:1774. doi: 10.3390/cancers12071774
2. Heath M, Jaimes N, Lemos B, et al. Clinical characteristics of Merkel cell carcinoma at diagnosis in 195 patients: the AEIOU features. J Am Acad Dermatol. 2008;58:375-381. doi: 10.1016/j.jaad.2007.11.020
3. Paulson KG, Park SY, Vandeven NA, et al. Merkel cell carcinoma: current US incidence and projected increases based on changing demographics. J Am Acad Dermatol. 2018;78:457-463.e2. doi: 10.1016/j.jaad.2017.10.028
4. Voelker R. Why Merkel cell cancer is garnering more attention. JAMA. 2018;320:18-20. doi: 10.1001/jama.2018.7042
5. Allen PJ, Browne WB, Jacques DP, et al. Merkel cell carcinoma: prognosis and treatment of patients from a single institution. J Clin Oncol. 2005;23:2300-2309. doi: 10.1200/JCO.2005.02.329
6. D’Angelo SP, Russell J, Lebbé C, et al. Efficacy and safety of first-line avelumab treatment in patients with stage IV metastatic Merkel cell carcinoma: a preplanned interim analysis of a clinical trial. JAMA Oncol. 2018;4:e180077. doi: 10.1001/jamaoncol.2018.0077
An 85-year-old man with a history of skin cancer presented to my dermatology practice (NT) for evaluation of a “pimple” on his left cheek that failed to resolve after 2 months (FIGURE). The patient noted that the lesion had grown, but that he otherwise felt well.
On examination, the lesion was plum colored, and the area was firm and nontender to palpation. The patient was referred to a plastic surgeon for an excisional biopsy to clarify the nature of the lesion.
WHAT IS YOUR DIAGNOSIS?
HOW WOULD YOU TREAT THIS PATIENT?
Diagnosis: Merkel cell carcinoma
A biopsy performed 2 weeks after the initial visit confirmed the clinical suspicion for Merkel cell carcinoma (MCC).
MCC is a cutaneous neuroendocrine malignancy. Although its name acknowledges similarities between the tumor cells and Merkel cells, it is now considered unlikely that Merkel cells are the actual cells of origin.1
The majority of MCCs are asymptomatic despite rapid growth and are typically red or pink and occur on UV-exposed areas, as in our patient.2 A cyst or acneiform lesion is the single most common diagnosis given at the time of biopsy.2
The incidence of MCC is greatest in people of advanced age and in those who are immunosuppressed. In the United States, the estimated annual incidence rate rose from 0.5 cases per 100,000 people in 2000 to 0.7 cases per 100,000 people in 2013.3 MCC increases exponentially with advancing age, from 0.1 (per 100,000) in those ages 40 to 44 years to 9.8 in those older than 85 years.3 The growing cohort of ageing baby boomers and the increased number of immunosuppressed individuals in the community suggest that clinicians are now more likely to encounter MCC than in the past.
While UV radiation is highly associated with MCC, the major causative factor is considered to be Merkel cell polyomavirus (MCPyV).1 In fact, MCPyV has been linked to 80% of MCC cases.1,3 Most people have positive serology for MCPyV in early childhood, but the association between MCC and old age highlights the impact of immunosuppression on MCPyV activity and MCC development.1
Clinical suspicion is the first step in diagnosing MCC
The mnemonic AEIOU highlights the key clinical features of this aggressive tumor2,4:
- Asymptomatic
- Expanding rapidly (often grows in less than 3 months)
- Immune suppression (eg, chronic lymphocytic leukemia, solid organ transplant patient)
- Older than 50
- UV exposure on fair skin.
If a lesion is suspected to be MCC, the next step includes biopsy so that a definitive diagnosis can be made. A firm, nontender nodule that lacks fluctuance should raise suspicion for a neoplastic process.
Continue to: The differential is broad, ranging from cysts to melanoma
The differential is broad, ranging from cysts to melanoma
The differential diagnosis for an enlarging, plum-colored nodule on sun-exposed skin includes an abscess, a ruptured or inflamed epidermoid cyst, basal cell carcinoma, squamous cell carcinoma, and malignant melanoma.
An abscess is typically tender and expands within a matter of days rather than months.
A cyst can be ruled out by the clinical appearance and lack of an overlying pore.
Basal cell carcinoma can be characterized by a rolled border and central ulceration.
Squamous cell carcinomas often exhibit a verrucous surface with marked hyperkeratosis.
Continue to: Melanoma
Melanoma manifests with brown or irregular pigmentation and may be associated with a precursor lesion.
Tx includes excision and consistent follow-up
Complete excision is the critical first step to successful therapy. Sentinel lymph node studies are typically performed because of the high incidence of lymph node metastasis. Frequent follow-up is required because of the high risk of recurrent or persistent disease.
Local recurrence usually occurs within 1 year of diagnosis in more than 40% of patients.5 Distant metastasis can be treated with a programmed cell death ligand 1 blocking agent (avelumab) or a programmed cell death protein 1 inhibitor (nivolumab or pembrolizumab).6
Our patient was referred to a regional cancer center for sentinel lymph node evaluation, where he was found to have nodal disease. The patient was put on pembrolizumab and received radiation therapy but showed only limited response. Seven months after diagnosis, he passed away from metastatic MCC.
An 85-year-old man with a history of skin cancer presented to my dermatology practice (NT) for evaluation of a “pimple” on his left cheek that failed to resolve after 2 months (FIGURE). The patient noted that the lesion had grown, but that he otherwise felt well.
On examination, the lesion was plum colored, and the area was firm and nontender to palpation. The patient was referred to a plastic surgeon for an excisional biopsy to clarify the nature of the lesion.
WHAT IS YOUR DIAGNOSIS?
HOW WOULD YOU TREAT THIS PATIENT?
Diagnosis: Merkel cell carcinoma
A biopsy performed 2 weeks after the initial visit confirmed the clinical suspicion for Merkel cell carcinoma (MCC).
MCC is a cutaneous neuroendocrine malignancy. Although its name acknowledges similarities between the tumor cells and Merkel cells, it is now considered unlikely that Merkel cells are the actual cells of origin.1
The majority of MCCs are asymptomatic despite rapid growth and are typically red or pink and occur on UV-exposed areas, as in our patient.2 A cyst or acneiform lesion is the single most common diagnosis given at the time of biopsy.2
The incidence of MCC is greatest in people of advanced age and in those who are immunosuppressed. In the United States, the estimated annual incidence rate rose from 0.5 cases per 100,000 people in 2000 to 0.7 cases per 100,000 people in 2013.3 MCC increases exponentially with advancing age, from 0.1 (per 100,000) in those ages 40 to 44 years to 9.8 in those older than 85 years.3 The growing cohort of ageing baby boomers and the increased number of immunosuppressed individuals in the community suggest that clinicians are now more likely to encounter MCC than in the past.
While UV radiation is highly associated with MCC, the major causative factor is considered to be Merkel cell polyomavirus (MCPyV).1 In fact, MCPyV has been linked to 80% of MCC cases.1,3 Most people have positive serology for MCPyV in early childhood, but the association between MCC and old age highlights the impact of immunosuppression on MCPyV activity and MCC development.1
Clinical suspicion is the first step in diagnosing MCC
The mnemonic AEIOU highlights the key clinical features of this aggressive tumor2,4:
- Asymptomatic
- Expanding rapidly (often grows in less than 3 months)
- Immune suppression (eg, chronic lymphocytic leukemia, solid organ transplant patient)
- Older than 50
- UV exposure on fair skin.
If a lesion is suspected to be MCC, the next step includes biopsy so that a definitive diagnosis can be made. A firm, nontender nodule that lacks fluctuance should raise suspicion for a neoplastic process.
Continue to: The differential is broad, ranging from cysts to melanoma
The differential is broad, ranging from cysts to melanoma
The differential diagnosis for an enlarging, plum-colored nodule on sun-exposed skin includes an abscess, a ruptured or inflamed epidermoid cyst, basal cell carcinoma, squamous cell carcinoma, and malignant melanoma.
An abscess is typically tender and expands within a matter of days rather than months.
A cyst can be ruled out by the clinical appearance and lack of an overlying pore.
Basal cell carcinoma can be characterized by a rolled border and central ulceration.
Squamous cell carcinomas often exhibit a verrucous surface with marked hyperkeratosis.
Continue to: Melanoma
Melanoma manifests with brown or irregular pigmentation and may be associated with a precursor lesion.
Tx includes excision and consistent follow-up
Complete excision is the critical first step to successful therapy. Sentinel lymph node studies are typically performed because of the high incidence of lymph node metastasis. Frequent follow-up is required because of the high risk of recurrent or persistent disease.
Local recurrence usually occurs within 1 year of diagnosis in more than 40% of patients.5 Distant metastasis can be treated with a programmed cell death ligand 1 blocking agent (avelumab) or a programmed cell death protein 1 inhibitor (nivolumab or pembrolizumab).6
Our patient was referred to a regional cancer center for sentinel lymph node evaluation, where he was found to have nodal disease. The patient was put on pembrolizumab and received radiation therapy but showed only limited response. Seven months after diagnosis, he passed away from metastatic MCC.
1. Pietropaolo V, Prezioso C, Moens U. Merkel cell polyomavirus and Merkel cell carcinoma. Cancers (Basel). 2020;12:1774. doi: 10.3390/cancers12071774
2. Heath M, Jaimes N, Lemos B, et al. Clinical characteristics of Merkel cell carcinoma at diagnosis in 195 patients: the AEIOU features. J Am Acad Dermatol. 2008;58:375-381. doi: 10.1016/j.jaad.2007.11.020
3. Paulson KG, Park SY, Vandeven NA, et al. Merkel cell carcinoma: current US incidence and projected increases based on changing demographics. J Am Acad Dermatol. 2018;78:457-463.e2. doi: 10.1016/j.jaad.2017.10.028
4. Voelker R. Why Merkel cell cancer is garnering more attention. JAMA. 2018;320:18-20. doi: 10.1001/jama.2018.7042
5. Allen PJ, Browne WB, Jacques DP, et al. Merkel cell carcinoma: prognosis and treatment of patients from a single institution. J Clin Oncol. 2005;23:2300-2309. doi: 10.1200/JCO.2005.02.329
6. D’Angelo SP, Russell J, Lebbé C, et al. Efficacy and safety of first-line avelumab treatment in patients with stage IV metastatic Merkel cell carcinoma: a preplanned interim analysis of a clinical trial. JAMA Oncol. 2018;4:e180077. doi: 10.1001/jamaoncol.2018.0077
1. Pietropaolo V, Prezioso C, Moens U. Merkel cell polyomavirus and Merkel cell carcinoma. Cancers (Basel). 2020;12:1774. doi: 10.3390/cancers12071774
2. Heath M, Jaimes N, Lemos B, et al. Clinical characteristics of Merkel cell carcinoma at diagnosis in 195 patients: the AEIOU features. J Am Acad Dermatol. 2008;58:375-381. doi: 10.1016/j.jaad.2007.11.020
3. Paulson KG, Park SY, Vandeven NA, et al. Merkel cell carcinoma: current US incidence and projected increases based on changing demographics. J Am Acad Dermatol. 2018;78:457-463.e2. doi: 10.1016/j.jaad.2017.10.028
4. Voelker R. Why Merkel cell cancer is garnering more attention. JAMA. 2018;320:18-20. doi: 10.1001/jama.2018.7042
5. Allen PJ, Browne WB, Jacques DP, et al. Merkel cell carcinoma: prognosis and treatment of patients from a single institution. J Clin Oncol. 2005;23:2300-2309. doi: 10.1200/JCO.2005.02.329
6. D’Angelo SP, Russell J, Lebbé C, et al. Efficacy and safety of first-line avelumab treatment in patients with stage IV metastatic Merkel cell carcinoma: a preplanned interim analysis of a clinical trial. JAMA Oncol. 2018;4:e180077. doi: 10.1001/jamaoncol.2018.0077

Five things you should know about ‘free’ at-home COVID tests
Americans keep hearing that it is important to test frequently for COVID-19 at home. But just try to find an “at-home” rapid COVID test in a store and at a price that makes frequent tests affordable.
Testing, as well as mask-wearing, is an important measure if the country ever hopes to beat COVID, restore normal routines and get the economy running efficiently. To get Americans cheaper tests, the federal government now plans to have insurance companies pay for them.
You can either get one without any out-of-pocket expense from retail pharmacies that are part of an insurance company’s network or buy it at any store and get reimbursed by the insurer.
Congress said private insurers must cover all COVID testing and any associated medical services when it passed the Families First Coronavirus Response Act and the Coronavirus Aid, Relief and Economic Security, or CARES, Act. The have-insurance-pay-for-it solution has been used frequently through the pandemic. Insurance companies have been told to pay for polymerase chain reaction tests, COVID treatments and the administration of vaccines. (Taxpayers are paying for the cost of the vaccines themselves.) It appears to be an elegant solution for a politician because it looks free and isn’t using taxpayer money.
1. Are the tests really free?
Well, no. As many an economist will tell you, there ain’t no such thing as a free lunch. Someone has to pick up the tab. Initially, the insurance companies bear the cost. Cynthia Cox, a vice president at KFF who studies the Affordable Care Act and private insurers, said the total bill could amount to billions of dollars. Exactly how much depends on “how easy it is to get them, and how many will be reimbursed,” she said.
2. Will the insurance company just swallow those imposed costs?
If companies draw from the time-tested insurance giants’ playbook, they’ll pass along those costs to customers. “This will put upward pressure on premiums,” said Emily Gee, vice president and coordinator for health policy at the Center for American Progress.
Major insurance companies like Cigna, Anthem, UnitedHealthcare, and Aetna did not respond to requests to discuss this issue.
3. If that’s the case, why haven’t I been hit with higher premiums already?
Insurance companies had the chance last year to raise premiums but, mostly, they did not.
Why? Perhaps because insurers have so far made so much money during the pandemic they didn’t need to. For example, the industry’s profits in 2020 increased 41% to $31 billion from $22 billion, according to the National Association of Insurance Commissioners. The NAIC said the industry has continued its “tremendous growth trend” that started before COVID emerged. Companies will be reporting 2021 results soon.
The reason behind these profits is clear. You were paying premiums based on projections your insurance company made about how much health care consumers would use that year. Because people stayed home, had fewer accidents, postponed surgeries and often avoided going to visit the doctor or the hospital, insurers paid out less. They rebated some of their earnings back to customers, but they pocketed a lot more.
As the companies’ actuaries work on predicting 2023 expenditures, premiums could go up if they foresee more claims and expenses. Paying for millions of rapid tests is something they would include in their calculations.
4. Regardless of my premiums, will the tests cost me money directly?
It’s quite possible. If your insurance company doesn’t have an arrangement with a retailer where you can simply pick up your allotted tests, you’ll have to pay for them – at whatever price the store sets. If that’s the case, you’ll need to fill out a form to request a reimbursement from the insurance company. How many times have you lost receipts or just plain neglected to mail in for rebates on something you bought? A lot, right?
Here’s another thing: The reimbursement is set at $12 per test. If you pay $30 for a test – and that is not unheard of – your insurer is only on the hook for $12. You eat the $18.
And by the way, people on Medicare will have to pay for their tests themselves. People who get their health care covered by Medicaid can obtain free test kits at community centers.
A few free tests are supposed to arrive at every American home via the U.S. Postal Service. And the Biden administration has activated a website where Americans can order free tests from a cache of a billion the federal government ordered.
5. Will this help bring down the costs of at-home tests and make them easier to find?
The free COVID tests are unlikely to have much immediate impact on general cost and availability. You will still need to search for them. The federal measures likely will stimulate the demand for tests, which in the short term may make them harder to find.
But the demand, and some government guarantees to manufacturers, may induce test makers to make more of them faster. The increased competition and supply theoretically could bring down the price. There is certainly room for prices to decline since the wholesale cost of the test is between $5 and $7, analysts estimate. “It’s a big step in the right direction,” Ms. Gee said.
KHN (Kaiser Health News) is a national newsroom that produces in-depth journalism about health issues. Together with Policy Analysis and Polling, KHN is one of the three major operating programs at KFF (Kaiser Family Foundation). KFF is an endowed nonprofit organization providing information on health issues to the nation.
Americans keep hearing that it is important to test frequently for COVID-19 at home. But just try to find an “at-home” rapid COVID test in a store and at a price that makes frequent tests affordable.
Testing, as well as mask-wearing, is an important measure if the country ever hopes to beat COVID, restore normal routines and get the economy running efficiently. To get Americans cheaper tests, the federal government now plans to have insurance companies pay for them.
You can either get one without any out-of-pocket expense from retail pharmacies that are part of an insurance company’s network or buy it at any store and get reimbursed by the insurer.
Congress said private insurers must cover all COVID testing and any associated medical services when it passed the Families First Coronavirus Response Act and the Coronavirus Aid, Relief and Economic Security, or CARES, Act. The have-insurance-pay-for-it solution has been used frequently through the pandemic. Insurance companies have been told to pay for polymerase chain reaction tests, COVID treatments and the administration of vaccines. (Taxpayers are paying for the cost of the vaccines themselves.) It appears to be an elegant solution for a politician because it looks free and isn’t using taxpayer money.
1. Are the tests really free?
Well, no. As many an economist will tell you, there ain’t no such thing as a free lunch. Someone has to pick up the tab. Initially, the insurance companies bear the cost. Cynthia Cox, a vice president at KFF who studies the Affordable Care Act and private insurers, said the total bill could amount to billions of dollars. Exactly how much depends on “how easy it is to get them, and how many will be reimbursed,” she said.
2. Will the insurance company just swallow those imposed costs?
If companies draw from the time-tested insurance giants’ playbook, they’ll pass along those costs to customers. “This will put upward pressure on premiums,” said Emily Gee, vice president and coordinator for health policy at the Center for American Progress.
Major insurance companies like Cigna, Anthem, UnitedHealthcare, and Aetna did not respond to requests to discuss this issue.
3. If that’s the case, why haven’t I been hit with higher premiums already?
Insurance companies had the chance last year to raise premiums but, mostly, they did not.
Why? Perhaps because insurers have so far made so much money during the pandemic they didn’t need to. For example, the industry’s profits in 2020 increased 41% to $31 billion from $22 billion, according to the National Association of Insurance Commissioners. The NAIC said the industry has continued its “tremendous growth trend” that started before COVID emerged. Companies will be reporting 2021 results soon.
The reason behind these profits is clear. You were paying premiums based on projections your insurance company made about how much health care consumers would use that year. Because people stayed home, had fewer accidents, postponed surgeries and often avoided going to visit the doctor or the hospital, insurers paid out less. They rebated some of their earnings back to customers, but they pocketed a lot more.
As the companies’ actuaries work on predicting 2023 expenditures, premiums could go up if they foresee more claims and expenses. Paying for millions of rapid tests is something they would include in their calculations.
4. Regardless of my premiums, will the tests cost me money directly?
It’s quite possible. If your insurance company doesn’t have an arrangement with a retailer where you can simply pick up your allotted tests, you’ll have to pay for them – at whatever price the store sets. If that’s the case, you’ll need to fill out a form to request a reimbursement from the insurance company. How many times have you lost receipts or just plain neglected to mail in for rebates on something you bought? A lot, right?
Here’s another thing: The reimbursement is set at $12 per test. If you pay $30 for a test – and that is not unheard of – your insurer is only on the hook for $12. You eat the $18.
And by the way, people on Medicare will have to pay for their tests themselves. People who get their health care covered by Medicaid can obtain free test kits at community centers.
A few free tests are supposed to arrive at every American home via the U.S. Postal Service. And the Biden administration has activated a website where Americans can order free tests from a cache of a billion the federal government ordered.
5. Will this help bring down the costs of at-home tests and make them easier to find?
The free COVID tests are unlikely to have much immediate impact on general cost and availability. You will still need to search for them. The federal measures likely will stimulate the demand for tests, which in the short term may make them harder to find.
But the demand, and some government guarantees to manufacturers, may induce test makers to make more of them faster. The increased competition and supply theoretically could bring down the price. There is certainly room for prices to decline since the wholesale cost of the test is between $5 and $7, analysts estimate. “It’s a big step in the right direction,” Ms. Gee said.
KHN (Kaiser Health News) is a national newsroom that produces in-depth journalism about health issues. Together with Policy Analysis and Polling, KHN is one of the three major operating programs at KFF (Kaiser Family Foundation). KFF is an endowed nonprofit organization providing information on health issues to the nation.
Americans keep hearing that it is important to test frequently for COVID-19 at home. But just try to find an “at-home” rapid COVID test in a store and at a price that makes frequent tests affordable.
Testing, as well as mask-wearing, is an important measure if the country ever hopes to beat COVID, restore normal routines and get the economy running efficiently. To get Americans cheaper tests, the federal government now plans to have insurance companies pay for them.
You can either get one without any out-of-pocket expense from retail pharmacies that are part of an insurance company’s network or buy it at any store and get reimbursed by the insurer.
Congress said private insurers must cover all COVID testing and any associated medical services when it passed the Families First Coronavirus Response Act and the Coronavirus Aid, Relief and Economic Security, or CARES, Act. The have-insurance-pay-for-it solution has been used frequently through the pandemic. Insurance companies have been told to pay for polymerase chain reaction tests, COVID treatments and the administration of vaccines. (Taxpayers are paying for the cost of the vaccines themselves.) It appears to be an elegant solution for a politician because it looks free and isn’t using taxpayer money.
1. Are the tests really free?
Well, no. As many an economist will tell you, there ain’t no such thing as a free lunch. Someone has to pick up the tab. Initially, the insurance companies bear the cost. Cynthia Cox, a vice president at KFF who studies the Affordable Care Act and private insurers, said the total bill could amount to billions of dollars. Exactly how much depends on “how easy it is to get them, and how many will be reimbursed,” she said.
2. Will the insurance company just swallow those imposed costs?
If companies draw from the time-tested insurance giants’ playbook, they’ll pass along those costs to customers. “This will put upward pressure on premiums,” said Emily Gee, vice president and coordinator for health policy at the Center for American Progress.
Major insurance companies like Cigna, Anthem, UnitedHealthcare, and Aetna did not respond to requests to discuss this issue.
3. If that’s the case, why haven’t I been hit with higher premiums already?
Insurance companies had the chance last year to raise premiums but, mostly, they did not.
Why? Perhaps because insurers have so far made so much money during the pandemic they didn’t need to. For example, the industry’s profits in 2020 increased 41% to $31 billion from $22 billion, according to the National Association of Insurance Commissioners. The NAIC said the industry has continued its “tremendous growth trend” that started before COVID emerged. Companies will be reporting 2021 results soon.
The reason behind these profits is clear. You were paying premiums based on projections your insurance company made about how much health care consumers would use that year. Because people stayed home, had fewer accidents, postponed surgeries and often avoided going to visit the doctor or the hospital, insurers paid out less. They rebated some of their earnings back to customers, but they pocketed a lot more.
As the companies’ actuaries work on predicting 2023 expenditures, premiums could go up if they foresee more claims and expenses. Paying for millions of rapid tests is something they would include in their calculations.
4. Regardless of my premiums, will the tests cost me money directly?
It’s quite possible. If your insurance company doesn’t have an arrangement with a retailer where you can simply pick up your allotted tests, you’ll have to pay for them – at whatever price the store sets. If that’s the case, you’ll need to fill out a form to request a reimbursement from the insurance company. How many times have you lost receipts or just plain neglected to mail in for rebates on something you bought? A lot, right?
Here’s another thing: The reimbursement is set at $12 per test. If you pay $30 for a test – and that is not unheard of – your insurer is only on the hook for $12. You eat the $18.
And by the way, people on Medicare will have to pay for their tests themselves. People who get their health care covered by Medicaid can obtain free test kits at community centers.
A few free tests are supposed to arrive at every American home via the U.S. Postal Service. And the Biden administration has activated a website where Americans can order free tests from a cache of a billion the federal government ordered.
5. Will this help bring down the costs of at-home tests and make them easier to find?
The free COVID tests are unlikely to have much immediate impact on general cost and availability. You will still need to search for them. The federal measures likely will stimulate the demand for tests, which in the short term may make them harder to find.
But the demand, and some government guarantees to manufacturers, may induce test makers to make more of them faster. The increased competition and supply theoretically could bring down the price. There is certainly room for prices to decline since the wholesale cost of the test is between $5 and $7, analysts estimate. “It’s a big step in the right direction,” Ms. Gee said.
KHN (Kaiser Health News) is a national newsroom that produces in-depth journalism about health issues. Together with Policy Analysis and Polling, KHN is one of the three major operating programs at KFF (Kaiser Family Foundation). KFF is an endowed nonprofit organization providing information on health issues to the nation.
‘Artificial pancreas’ life-changing in kids with type 1 diabetes
A semiautomated insulin delivery system improved glycemic control in young children with type 1 diabetes aged 1-7 years without increasing hypoglycemia.
“Hybrid closed-loop” systems – comprising an insulin pump, a continuous glucose monitor (CGM), and software enabling communication that semiautomates insulin delivery based on glucose levels – have been shown to improve glucose control in older children and adults.
The technology, also known as an artificial pancreas, has been less studied in very young children even though it may uniquely benefit them, said the authors of the new study, led by Julia Ware, MD, of the Wellcome Trust–Medical Research Council Institute of Metabolic Science and the University of Cambridge (England). The findings were published online Jan. 19, 2022, in the New England Journal of Medicine.
“Very young children are extremely vulnerable to changes in their blood sugar levels. High levels in particular can have potentially lasting consequences to their brain development. On top of that, diabetes is very challenging to manage in this age group, creating a huge burden for families,” she said in a University of Cambridge statement.
There is “high variability of insulin requirements, marked insulin sensitivity, and unpredictable eating and activity patterns,” Dr. Ware and colleagues noted.
“Caregiver fear of hypoglycemia, particularly overnight, is common and, coupled with young children’s unawareness that hypoglycemia is occurring, contributes to children not meeting the recommended glycemic targets or having difficulty maintaining recommended glycemic control unless caregivers can provide constant monitoring. These issues often lead to ... reduced quality of life for the whole family,” they added.
Except for mealtimes, device is fully automated
The new multicenter, randomized, crossover trial was conducted at seven centers across Austria, Germany, Luxembourg, and the United Kingdom in 2019-2020.
The trial compared the safety and efficacy of hybrid closed-loop therapy with sensor-augmented pump therapy (that is, without the device communication, as a control). All 74 children used the CamAPS FX hybrid closed-loop system for 16 weeks, and then used the control treatment for 16 weeks. The children were a mean age of 5.6 years and had a baseline hemoglobin A1c of 7.3% (56.6 mmol/mol).
The hybrid closed-loop system consisted of components that are commercially available in Europe: the Sooil insulin pump (Dana Diabecare RS) and the Dexcom G6 CGM, along with an unlocked Samsung Galaxy 8 smartphone housing an app (CamAPS FX, CamDiab) that runs the Cambridge proprietary model predictive control algorithm.
The smartphone communicates wirelessly with both the pump and the CGM transmitter and automatically adjusts the pump’s insulin delivery based on real-time sensor glucose readings. It also issues alarms if glucose levels fall below or rise above user-specified thresholds. This functionality was disabled during the study control periods.
Senior investigator Roman Hovorka, PhD, who developed the CamAPS FX app, explained in the University of Cambridge statement that the app “makes predictions about what it thinks is likely to happen next based on past experience. It learns how much insulin the child needs per day and how this changes at different times of the day.
“It then uses this [information] to adjust insulin levels to help achieve ideal blood sugar levels. Other than at mealtimes, it is fully automated, so parents do not need to continually monitor their child’s blood sugar levels.”
Indeed, the time spent in target glucose range (70-180 mg/dL) during the 16-week closed-loop period was 8.7 percentage points higher than during the control period (P < .001).
That difference translates to “a clinically meaningful 125 minutes per day,” and represented around three-quarters of their day (71.6%) in the target range, the investigators wrote.
The mean adjusted difference in time spent above 180 mg/dL was 8.5 percentage points lower with the closed-loop, also a significant difference (P < .001). Time spent below 70 mg/dL did not differ significantly between the two interventions (P = .74).
At the end of the study periods, the mean adjusted between-treatment difference in A1c was –0.4 percentage points, significantly lower following the closed-loop, compared with the control period (P < .001).
That percentage point difference (equivalent to 3.9 mmol/mol) “is important in a population of patients who had tight glycemic control at baseline. This result was observed without an increase in the time spent in a hypoglycemic state,” Dr. Ware and colleagues noted.
Median glucose sensor use was 99% during the closed-loop period and 96% during the control periods. During the closed-loop periods, the system was in closed-loop mode 95% of the time.
This finding supports longer-term usability in this age group and compares well with use in older children, they said.
One serious hypoglycemic episode, attributed to parental error rather than system malfunction, occurred during the closed-loop period. There were no episodes of diabetic ketoacidosis. Rates of other adverse events didn’t differ between the two periods.
“CamAPS FX led to improvements in several measures, including hyperglycemia and average blood sugar levels, without increasing the risk of hypos. This is likely to have important benefits for those children who use it,” Dr. Ware summarized.
Sleep quality could improve for children and caregivers
Reductions in time spent in hyperglycemia without increasing hypoglycemia could minimize the risk for neurocognitive deficits that have been reported among young children with type 1 diabetes, the authors speculated.
In addition, they noted that because 80% of overnight sensor readings were within target range and less than 3% were below 70 mg/dL, sleep quality could improve for both the children and their parents. This, in turn, “would confer associated quality of life benefits.”
“Parents have described our artificial pancreas as ‘life changing’ as it meant they were able to relax and spend less time worrying about their child’s blood sugar levels, particularly at nighttime. They tell us it gives them more time to do what any ‘normal’ family can do, to play and do fun things with their children,” observed Dr. Ware.
The CamAPS FX has been commercialized by CamDiab, a spin-out company set up by Dr. Hovorka. It is currently available through several NHS trusts across the United Kingdom, including Cambridge University Hospitals NHS Foundation Trust, and is expected to be more widely available soon.
The study was supported by the European Commission within the Horizon 2020 Framework Program, the NIHR Cambridge Biomedical Research Centre, and JDRF. Dr. Ware had no further disclosures. Dr. Hovorka has reported acting as consultant for Abbott Diabetes Care, BD, Dexcom, being a speaker for Novo Nordisk and Eli Lilly, and receiving royalty payments from B. Braun for software. He is director of CamDiab.
A version of this article first appeared on Medscape.com.
A semiautomated insulin delivery system improved glycemic control in young children with type 1 diabetes aged 1-7 years without increasing hypoglycemia.
“Hybrid closed-loop” systems – comprising an insulin pump, a continuous glucose monitor (CGM), and software enabling communication that semiautomates insulin delivery based on glucose levels – have been shown to improve glucose control in older children and adults.
The technology, also known as an artificial pancreas, has been less studied in very young children even though it may uniquely benefit them, said the authors of the new study, led by Julia Ware, MD, of the Wellcome Trust–Medical Research Council Institute of Metabolic Science and the University of Cambridge (England). The findings were published online Jan. 19, 2022, in the New England Journal of Medicine.
“Very young children are extremely vulnerable to changes in their blood sugar levels. High levels in particular can have potentially lasting consequences to their brain development. On top of that, diabetes is very challenging to manage in this age group, creating a huge burden for families,” she said in a University of Cambridge statement.
There is “high variability of insulin requirements, marked insulin sensitivity, and unpredictable eating and activity patterns,” Dr. Ware and colleagues noted.
“Caregiver fear of hypoglycemia, particularly overnight, is common and, coupled with young children’s unawareness that hypoglycemia is occurring, contributes to children not meeting the recommended glycemic targets or having difficulty maintaining recommended glycemic control unless caregivers can provide constant monitoring. These issues often lead to ... reduced quality of life for the whole family,” they added.
Except for mealtimes, device is fully automated
The new multicenter, randomized, crossover trial was conducted at seven centers across Austria, Germany, Luxembourg, and the United Kingdom in 2019-2020.
The trial compared the safety and efficacy of hybrid closed-loop therapy with sensor-augmented pump therapy (that is, without the device communication, as a control). All 74 children used the CamAPS FX hybrid closed-loop system for 16 weeks, and then used the control treatment for 16 weeks. The children were a mean age of 5.6 years and had a baseline hemoglobin A1c of 7.3% (56.6 mmol/mol).
The hybrid closed-loop system consisted of components that are commercially available in Europe: the Sooil insulin pump (Dana Diabecare RS) and the Dexcom G6 CGM, along with an unlocked Samsung Galaxy 8 smartphone housing an app (CamAPS FX, CamDiab) that runs the Cambridge proprietary model predictive control algorithm.
The smartphone communicates wirelessly with both the pump and the CGM transmitter and automatically adjusts the pump’s insulin delivery based on real-time sensor glucose readings. It also issues alarms if glucose levels fall below or rise above user-specified thresholds. This functionality was disabled during the study control periods.
Senior investigator Roman Hovorka, PhD, who developed the CamAPS FX app, explained in the University of Cambridge statement that the app “makes predictions about what it thinks is likely to happen next based on past experience. It learns how much insulin the child needs per day and how this changes at different times of the day.
“It then uses this [information] to adjust insulin levels to help achieve ideal blood sugar levels. Other than at mealtimes, it is fully automated, so parents do not need to continually monitor their child’s blood sugar levels.”
Indeed, the time spent in target glucose range (70-180 mg/dL) during the 16-week closed-loop period was 8.7 percentage points higher than during the control period (P < .001).
That difference translates to “a clinically meaningful 125 minutes per day,” and represented around three-quarters of their day (71.6%) in the target range, the investigators wrote.
The mean adjusted difference in time spent above 180 mg/dL was 8.5 percentage points lower with the closed-loop, also a significant difference (P < .001). Time spent below 70 mg/dL did not differ significantly between the two interventions (P = .74).
At the end of the study periods, the mean adjusted between-treatment difference in A1c was –0.4 percentage points, significantly lower following the closed-loop, compared with the control period (P < .001).
That percentage point difference (equivalent to 3.9 mmol/mol) “is important in a population of patients who had tight glycemic control at baseline. This result was observed without an increase in the time spent in a hypoglycemic state,” Dr. Ware and colleagues noted.
Median glucose sensor use was 99% during the closed-loop period and 96% during the control periods. During the closed-loop periods, the system was in closed-loop mode 95% of the time.
This finding supports longer-term usability in this age group and compares well with use in older children, they said.
One serious hypoglycemic episode, attributed to parental error rather than system malfunction, occurred during the closed-loop period. There were no episodes of diabetic ketoacidosis. Rates of other adverse events didn’t differ between the two periods.
“CamAPS FX led to improvements in several measures, including hyperglycemia and average blood sugar levels, without increasing the risk of hypos. This is likely to have important benefits for those children who use it,” Dr. Ware summarized.
Sleep quality could improve for children and caregivers
Reductions in time spent in hyperglycemia without increasing hypoglycemia could minimize the risk for neurocognitive deficits that have been reported among young children with type 1 diabetes, the authors speculated.
In addition, they noted that because 80% of overnight sensor readings were within target range and less than 3% were below 70 mg/dL, sleep quality could improve for both the children and their parents. This, in turn, “would confer associated quality of life benefits.”
“Parents have described our artificial pancreas as ‘life changing’ as it meant they were able to relax and spend less time worrying about their child’s blood sugar levels, particularly at nighttime. They tell us it gives them more time to do what any ‘normal’ family can do, to play and do fun things with their children,” observed Dr. Ware.
The CamAPS FX has been commercialized by CamDiab, a spin-out company set up by Dr. Hovorka. It is currently available through several NHS trusts across the United Kingdom, including Cambridge University Hospitals NHS Foundation Trust, and is expected to be more widely available soon.
The study was supported by the European Commission within the Horizon 2020 Framework Program, the NIHR Cambridge Biomedical Research Centre, and JDRF. Dr. Ware had no further disclosures. Dr. Hovorka has reported acting as consultant for Abbott Diabetes Care, BD, Dexcom, being a speaker for Novo Nordisk and Eli Lilly, and receiving royalty payments from B. Braun for software. He is director of CamDiab.
A version of this article first appeared on Medscape.com.
A semiautomated insulin delivery system improved glycemic control in young children with type 1 diabetes aged 1-7 years without increasing hypoglycemia.
“Hybrid closed-loop” systems – comprising an insulin pump, a continuous glucose monitor (CGM), and software enabling communication that semiautomates insulin delivery based on glucose levels – have been shown to improve glucose control in older children and adults.
The technology, also known as an artificial pancreas, has been less studied in very young children even though it may uniquely benefit them, said the authors of the new study, led by Julia Ware, MD, of the Wellcome Trust–Medical Research Council Institute of Metabolic Science and the University of Cambridge (England). The findings were published online Jan. 19, 2022, in the New England Journal of Medicine.
“Very young children are extremely vulnerable to changes in their blood sugar levels. High levels in particular can have potentially lasting consequences to their brain development. On top of that, diabetes is very challenging to manage in this age group, creating a huge burden for families,” she said in a University of Cambridge statement.
There is “high variability of insulin requirements, marked insulin sensitivity, and unpredictable eating and activity patterns,” Dr. Ware and colleagues noted.
“Caregiver fear of hypoglycemia, particularly overnight, is common and, coupled with young children’s unawareness that hypoglycemia is occurring, contributes to children not meeting the recommended glycemic targets or having difficulty maintaining recommended glycemic control unless caregivers can provide constant monitoring. These issues often lead to ... reduced quality of life for the whole family,” they added.
Except for mealtimes, device is fully automated
The new multicenter, randomized, crossover trial was conducted at seven centers across Austria, Germany, Luxembourg, and the United Kingdom in 2019-2020.
The trial compared the safety and efficacy of hybrid closed-loop therapy with sensor-augmented pump therapy (that is, without the device communication, as a control). All 74 children used the CamAPS FX hybrid closed-loop system for 16 weeks, and then used the control treatment for 16 weeks. The children were a mean age of 5.6 years and had a baseline hemoglobin A1c of 7.3% (56.6 mmol/mol).
The hybrid closed-loop system consisted of components that are commercially available in Europe: the Sooil insulin pump (Dana Diabecare RS) and the Dexcom G6 CGM, along with an unlocked Samsung Galaxy 8 smartphone housing an app (CamAPS FX, CamDiab) that runs the Cambridge proprietary model predictive control algorithm.
The smartphone communicates wirelessly with both the pump and the CGM transmitter and automatically adjusts the pump’s insulin delivery based on real-time sensor glucose readings. It also issues alarms if glucose levels fall below or rise above user-specified thresholds. This functionality was disabled during the study control periods.
Senior investigator Roman Hovorka, PhD, who developed the CamAPS FX app, explained in the University of Cambridge statement that the app “makes predictions about what it thinks is likely to happen next based on past experience. It learns how much insulin the child needs per day and how this changes at different times of the day.
“It then uses this [information] to adjust insulin levels to help achieve ideal blood sugar levels. Other than at mealtimes, it is fully automated, so parents do not need to continually monitor their child’s blood sugar levels.”
Indeed, the time spent in target glucose range (70-180 mg/dL) during the 16-week closed-loop period was 8.7 percentage points higher than during the control period (P < .001).
That difference translates to “a clinically meaningful 125 minutes per day,” and represented around three-quarters of their day (71.6%) in the target range, the investigators wrote.
The mean adjusted difference in time spent above 180 mg/dL was 8.5 percentage points lower with the closed-loop, also a significant difference (P < .001). Time spent below 70 mg/dL did not differ significantly between the two interventions (P = .74).
At the end of the study periods, the mean adjusted between-treatment difference in A1c was –0.4 percentage points, significantly lower following the closed-loop, compared with the control period (P < .001).
That percentage point difference (equivalent to 3.9 mmol/mol) “is important in a population of patients who had tight glycemic control at baseline. This result was observed without an increase in the time spent in a hypoglycemic state,” Dr. Ware and colleagues noted.
Median glucose sensor use was 99% during the closed-loop period and 96% during the control periods. During the closed-loop periods, the system was in closed-loop mode 95% of the time.
This finding supports longer-term usability in this age group and compares well with use in older children, they said.
One serious hypoglycemic episode, attributed to parental error rather than system malfunction, occurred during the closed-loop period. There were no episodes of diabetic ketoacidosis. Rates of other adverse events didn’t differ between the two periods.
“CamAPS FX led to improvements in several measures, including hyperglycemia and average blood sugar levels, without increasing the risk of hypos. This is likely to have important benefits for those children who use it,” Dr. Ware summarized.
Sleep quality could improve for children and caregivers
Reductions in time spent in hyperglycemia without increasing hypoglycemia could minimize the risk for neurocognitive deficits that have been reported among young children with type 1 diabetes, the authors speculated.
In addition, they noted that because 80% of overnight sensor readings were within target range and less than 3% were below 70 mg/dL, sleep quality could improve for both the children and their parents. This, in turn, “would confer associated quality of life benefits.”
“Parents have described our artificial pancreas as ‘life changing’ as it meant they were able to relax and spend less time worrying about their child’s blood sugar levels, particularly at nighttime. They tell us it gives them more time to do what any ‘normal’ family can do, to play and do fun things with their children,” observed Dr. Ware.
The CamAPS FX has been commercialized by CamDiab, a spin-out company set up by Dr. Hovorka. It is currently available through several NHS trusts across the United Kingdom, including Cambridge University Hospitals NHS Foundation Trust, and is expected to be more widely available soon.
The study was supported by the European Commission within the Horizon 2020 Framework Program, the NIHR Cambridge Biomedical Research Centre, and JDRF. Dr. Ware had no further disclosures. Dr. Hovorka has reported acting as consultant for Abbott Diabetes Care, BD, Dexcom, being a speaker for Novo Nordisk and Eli Lilly, and receiving royalty payments from B. Braun for software. He is director of CamDiab.
A version of this article first appeared on Medscape.com.
FROM THE NEW ENGLAND JOURNAL OF MEDICINE