User login
Bringing you the latest news, research and reviews, exclusive interviews, podcasts, quizzes, and more.
div[contains(@class, 'read-next-article')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
nav[contains(@class, 'nav-ce-stack nav-ce-stack__large-screen')]
header[@id='header']
div[contains(@class, 'header__large-screen')]
div[contains(@class, 'read-next-article')]
div[contains(@class, 'main-prefix')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
footer[@id='footer']
section[contains(@class, 'nav-hidden')]
div[contains(@class, 'ce-card-content')]
nav[contains(@class, 'nav-ce-stack')]
div[contains(@class, 'view-medstat-quiz-listing-panes')]
div[contains(@class, 'pane-article-sidebar-latest-news')]
FDA approves combo pill for severe, acute pain
enough to require an opioid analgesic and for which alternative treatments fail to provide adequate pain relief.

Celecoxib is a nonsteroidal anti-inflammatory drug and tramadol is an opioid agonist. Seglentis contains 56 mg of celecoxib and 44 mg of tramadol.
“The unique co-crystal formulation of Seglentis provides effective pain relief via a multimodal approach,” Craig A. Sponseller, MD, chief medical officer of Kowa Pharmaceuticals America, said in a news release.
Esteve Pharmaceuticals has entered into an agreement with Kowa Pharmaceuticals America to commercialize the pain medicine in the United States, with a launch planned for early 2022.
“Seglentis uses four different and complementary mechanisms of analgesia and offers healthcare providers an important option to treat acute pain in adults that is severe enough to require opioid treatment and for which alternative treatments are inadequate,” Dr. Sponseller said.
Because of the risks of addiction, abuse, and misuse with opioids, even at recommended doses, the FDA will require a Risk Evaluation and Mitigation Strategy (REMS) for Seglentis.
The label states that the drug should be initiated as two tablets every 12 hours as needed and should be prescribed for the shortest duration consistent with individual patient treatment goals.
Patients should be monitored for respiratory depression, especially within the first 24 to 72 hours of initiating therapy with Seglentis.
Prescribers should discuss naloxone (Narcan) with patients and consider prescribing the opioid antagonist naloxone based on the patient’s risk factors for overdose.
Full prescribing information is available online.
A version of this article was first published on Medscape.com.
enough to require an opioid analgesic and for which alternative treatments fail to provide adequate pain relief.
Celecoxib is a nonsteroidal anti-inflammatory drug and tramadol is an opioid agonist. Seglentis contains 56 mg of celecoxib and 44 mg of tramadol.
“The unique co-crystal formulation of Seglentis provides effective pain relief via a multimodal approach,” Craig A. Sponseller, MD, chief medical officer of Kowa Pharmaceuticals America, said in a news release.
Esteve Pharmaceuticals has entered into an agreement with Kowa Pharmaceuticals America to commercialize the pain medicine in the United States, with a launch planned for early 2022.
“Seglentis uses four different and complementary mechanisms of analgesia and offers healthcare providers an important option to treat acute pain in adults that is severe enough to require opioid treatment and for which alternative treatments are inadequate,” Dr. Sponseller said.
Because of the risks of addiction, abuse, and misuse with opioids, even at recommended doses, the FDA will require a Risk Evaluation and Mitigation Strategy (REMS) for Seglentis.
The label states that the drug should be initiated as two tablets every 12 hours as needed and should be prescribed for the shortest duration consistent with individual patient treatment goals.
Patients should be monitored for respiratory depression, especially within the first 24 to 72 hours of initiating therapy with Seglentis.
Prescribers should discuss naloxone (Narcan) with patients and consider prescribing the opioid antagonist naloxone based on the patient’s risk factors for overdose.
Full prescribing information is available online.
A version of this article was first published on Medscape.com.
enough to require an opioid analgesic and for which alternative treatments fail to provide adequate pain relief.
Celecoxib is a nonsteroidal anti-inflammatory drug and tramadol is an opioid agonist. Seglentis contains 56 mg of celecoxib and 44 mg of tramadol.
“The unique co-crystal formulation of Seglentis provides effective pain relief via a multimodal approach,” Craig A. Sponseller, MD, chief medical officer of Kowa Pharmaceuticals America, said in a news release.
Esteve Pharmaceuticals has entered into an agreement with Kowa Pharmaceuticals America to commercialize the pain medicine in the United States, with a launch planned for early 2022.
“Seglentis uses four different and complementary mechanisms of analgesia and offers healthcare providers an important option to treat acute pain in adults that is severe enough to require opioid treatment and for which alternative treatments are inadequate,” Dr. Sponseller said.
Because of the risks of addiction, abuse, and misuse with opioids, even at recommended doses, the FDA will require a Risk Evaluation and Mitigation Strategy (REMS) for Seglentis.
The label states that the drug should be initiated as two tablets every 12 hours as needed and should be prescribed for the shortest duration consistent with individual patient treatment goals.
Patients should be monitored for respiratory depression, especially within the first 24 to 72 hours of initiating therapy with Seglentis.
Prescribers should discuss naloxone (Narcan) with patients and consider prescribing the opioid antagonist naloxone based on the patient’s risk factors for overdose.
Full prescribing information is available online.
A version of this article was first published on Medscape.com.
Expensive insulins, pen devices dominate U.S. diabetes care
Despite the extensive recent focus on its cost, insulin use in the United States remains dominated by insulin glargine and other analogs, as well as pen devices for delivery, new research shows.

The findings come from a nationally representative audit of outpatient care with input from nearly 5,000 physicians who prescribed insulin to patients with type 2 diabetes in 2016-2020.
The dramatic rise in the price of insulin in the United States has been extensively discussed in recent years, particularly with the newer analogs as compared with older human insulins.
Few studies indicate analog insulins better than human insulins
“Our findings suggest that even with increased public scrutiny for insulin products ... [the market is] dominated by the use of insulin analogs and insulin pen delivery devices, with persistent uptake of newer products as they are approved,” lead author Rita R. Kalyani, MD, told this news organization.
“Though newer insulins offer potentially greater flexibility with reduced hypoglycemia for many patients, they are also much more costly, with minimal to no head-to-head studies suggesting significant differences in glucose-lowering efficacy when compared to human insulins,” she stressed.
“We found it surprising that, despite the much-publicized concerns regarding insulin costs, analog insulins continue to represent more than 80% of insulin visits in the U.S.” added Dr. Kalyani, of the Division of Endocrinology, Diabetes & Metabolism at Johns Hopkins University School of Medicine, Baltimore.
However, as expected, the study also revealed a gradual increased uptake in the use of biosimilar insulins as more have been introduced to the market.
Dr. Kalyani advised, “Clinicians should be aware of their individual prescribing patterns for insulin and consider the affordability of insulin for patients as part of shared decision-making during clinic visits, particularly given the greater financial strain that many patients have faced during the ongoing COVID-19 pandemic and the rising societal costs for diabetes care.”
The research was published online October 12 in JAMA Network Open by Dr. Kalyani and colleagues.
Analogs prevailed, while biosimilar use rose
The data come from the Health National Disease and Therapeutic Index, a quarterly sampling of approximately 4,800 physicians that provides nationally representative diagnostic and prescribing information on patients treated by office-based physicians in the United States.
Overall, there were 27,860,691 insulin treatment visits for type 2 diabetes in 2016-2020. Of those, long-acting analog insulins (glargine [Lantus], detemir [Levemir], and degludec [Tresiba]) accounted for 67.3% of treatment visits in 2016 and 74.8% of treatment visits in 2020.
Rapid-acting insulin analogs (lispro [Humalog], aspart [Novolog], faster aspart [Fiasp], and glulisine [Apidra]) accounted for about 21.2% of visits in 2016 and about 16.5% in 2020.
On the other hand, intermediate- and short-acting human insulins (NPH and regular) accounted for just 3.7% of visits in 2016 and 2.6% in 2020.
Grouped together, the long- and short-acting analogs accounted for 92.7% of visits in 2016 and 86.3% in 2020, while the human insulins represented just 7.3% of visits in 2016 and 5.5% in 2020.
The biosimilar analog insulins (glargine and lispro) first appeared in the database in 2017, accounting for 2.6% of visits that year and 8.2% by 2020.
Overall, the number of visits for insulin treatment declined by 18% between 2016 and 2020, from 6.0 million to 4.9 million. That drop may be due to multiple factors, Dr. Kalyani said.
“Recently updated clinical practice guidelines from professional societies such as the American Diabetes Association recommend the use of glucagon-like peptide-1 (GLP-1) receptor agonists prior to insulin when injectable medications are being considered [for type 2 diabetes],” she noted.
“In addition, during the pandemic, patients may not have been seeing their health care providers for routine diabetes care as often as before ... These and other factors may have contributed to the decrease in insulin visits that we observed.”
By specific insulins, glargine has topped the list all along, accounting for about half of all treatment visits, at 52.6% in 2020. Degludec came in second, at 17.4%, and lispro third, at 9.5%.
Use of pen devices also increased
The proportion of treatment visits for insulin vials/syringes declined from 63.9% in 2016 to 41.1% in 2020, while visits for insulin pens rose from 36.1% to 58.7%.
“Many pens are more costly compared to vials of the same insulin product. Interestingly, some studies have found that use of insulin pens may promote greater patient adherence to insulin and, as a result, more broadly decrease health care costs associated with diabetes. However, we did not specifically investigate the cost of insulin in our study,” Dr. Kalyani noted.
The proportion of visits for “newer” insulins, defined as those approved in 2010 or later, rose from 18.1% in 2016 to 40.9% in 2020, while the concurrent drop for insulins approved prior to 2010 was from 81.9% to 59.1%.
“The findings of our study provide insight into potential drivers of insulin costs in the U.S. and may inform health policy,” the researchers conclude.
Funded in part by the National Heart, Lung, and Blood Institute. Dr. Kalyani currently serves on the Endocrinologic and Metabolic Drugs Advisory Committee of the U.S. Food and Drug Administration.
A version of this article first appeared on Medscape.com.
Despite the extensive recent focus on its cost, insulin use in the United States remains dominated by insulin glargine and other analogs, as well as pen devices for delivery, new research shows.
The findings come from a nationally representative audit of outpatient care with input from nearly 5,000 physicians who prescribed insulin to patients with type 2 diabetes in 2016-2020.
The dramatic rise in the price of insulin in the United States has been extensively discussed in recent years, particularly with the newer analogs as compared with older human insulins.
Few studies indicate analog insulins better than human insulins
“Our findings suggest that even with increased public scrutiny for insulin products ... [the market is] dominated by the use of insulin analogs and insulin pen delivery devices, with persistent uptake of newer products as they are approved,” lead author Rita R. Kalyani, MD, told this news organization.
“Though newer insulins offer potentially greater flexibility with reduced hypoglycemia for many patients, they are also much more costly, with minimal to no head-to-head studies suggesting significant differences in glucose-lowering efficacy when compared to human insulins,” she stressed.
“We found it surprising that, despite the much-publicized concerns regarding insulin costs, analog insulins continue to represent more than 80% of insulin visits in the U.S.” added Dr. Kalyani, of the Division of Endocrinology, Diabetes & Metabolism at Johns Hopkins University School of Medicine, Baltimore.
However, as expected, the study also revealed a gradual increased uptake in the use of biosimilar insulins as more have been introduced to the market.
Dr. Kalyani advised, “Clinicians should be aware of their individual prescribing patterns for insulin and consider the affordability of insulin for patients as part of shared decision-making during clinic visits, particularly given the greater financial strain that many patients have faced during the ongoing COVID-19 pandemic and the rising societal costs for diabetes care.”
The research was published online October 12 in JAMA Network Open by Dr. Kalyani and colleagues.
Analogs prevailed, while biosimilar use rose
The data come from the Health National Disease and Therapeutic Index, a quarterly sampling of approximately 4,800 physicians that provides nationally representative diagnostic and prescribing information on patients treated by office-based physicians in the United States.
Overall, there were 27,860,691 insulin treatment visits for type 2 diabetes in 2016-2020. Of those, long-acting analog insulins (glargine [Lantus], detemir [Levemir], and degludec [Tresiba]) accounted for 67.3% of treatment visits in 2016 and 74.8% of treatment visits in 2020.
Rapid-acting insulin analogs (lispro [Humalog], aspart [Novolog], faster aspart [Fiasp], and glulisine [Apidra]) accounted for about 21.2% of visits in 2016 and about 16.5% in 2020.
On the other hand, intermediate- and short-acting human insulins (NPH and regular) accounted for just 3.7% of visits in 2016 and 2.6% in 2020.
Grouped together, the long- and short-acting analogs accounted for 92.7% of visits in 2016 and 86.3% in 2020, while the human insulins represented just 7.3% of visits in 2016 and 5.5% in 2020.
The biosimilar analog insulins (glargine and lispro) first appeared in the database in 2017, accounting for 2.6% of visits that year and 8.2% by 2020.
Overall, the number of visits for insulin treatment declined by 18% between 2016 and 2020, from 6.0 million to 4.9 million. That drop may be due to multiple factors, Dr. Kalyani said.
“Recently updated clinical practice guidelines from professional societies such as the American Diabetes Association recommend the use of glucagon-like peptide-1 (GLP-1) receptor agonists prior to insulin when injectable medications are being considered [for type 2 diabetes],” she noted.
“In addition, during the pandemic, patients may not have been seeing their health care providers for routine diabetes care as often as before ... These and other factors may have contributed to the decrease in insulin visits that we observed.”
By specific insulins, glargine has topped the list all along, accounting for about half of all treatment visits, at 52.6% in 2020. Degludec came in second, at 17.4%, and lispro third, at 9.5%.
Use of pen devices also increased
The proportion of treatment visits for insulin vials/syringes declined from 63.9% in 2016 to 41.1% in 2020, while visits for insulin pens rose from 36.1% to 58.7%.
“Many pens are more costly compared to vials of the same insulin product. Interestingly, some studies have found that use of insulin pens may promote greater patient adherence to insulin and, as a result, more broadly decrease health care costs associated with diabetes. However, we did not specifically investigate the cost of insulin in our study,” Dr. Kalyani noted.
The proportion of visits for “newer” insulins, defined as those approved in 2010 or later, rose from 18.1% in 2016 to 40.9% in 2020, while the concurrent drop for insulins approved prior to 2010 was from 81.9% to 59.1%.
“The findings of our study provide insight into potential drivers of insulin costs in the U.S. and may inform health policy,” the researchers conclude.
Funded in part by the National Heart, Lung, and Blood Institute. Dr. Kalyani currently serves on the Endocrinologic and Metabolic Drugs Advisory Committee of the U.S. Food and Drug Administration.
A version of this article first appeared on Medscape.com.
Despite the extensive recent focus on its cost, insulin use in the United States remains dominated by insulin glargine and other analogs, as well as pen devices for delivery, new research shows.
The findings come from a nationally representative audit of outpatient care with input from nearly 5,000 physicians who prescribed insulin to patients with type 2 diabetes in 2016-2020.
The dramatic rise in the price of insulin in the United States has been extensively discussed in recent years, particularly with the newer analogs as compared with older human insulins.
Few studies indicate analog insulins better than human insulins
“Our findings suggest that even with increased public scrutiny for insulin products ... [the market is] dominated by the use of insulin analogs and insulin pen delivery devices, with persistent uptake of newer products as they are approved,” lead author Rita R. Kalyani, MD, told this news organization.
“Though newer insulins offer potentially greater flexibility with reduced hypoglycemia for many patients, they are also much more costly, with minimal to no head-to-head studies suggesting significant differences in glucose-lowering efficacy when compared to human insulins,” she stressed.
“We found it surprising that, despite the much-publicized concerns regarding insulin costs, analog insulins continue to represent more than 80% of insulin visits in the U.S.” added Dr. Kalyani, of the Division of Endocrinology, Diabetes & Metabolism at Johns Hopkins University School of Medicine, Baltimore.
However, as expected, the study also revealed a gradual increased uptake in the use of biosimilar insulins as more have been introduced to the market.
Dr. Kalyani advised, “Clinicians should be aware of their individual prescribing patterns for insulin and consider the affordability of insulin for patients as part of shared decision-making during clinic visits, particularly given the greater financial strain that many patients have faced during the ongoing COVID-19 pandemic and the rising societal costs for diabetes care.”
The research was published online October 12 in JAMA Network Open by Dr. Kalyani and colleagues.
Analogs prevailed, while biosimilar use rose
The data come from the Health National Disease and Therapeutic Index, a quarterly sampling of approximately 4,800 physicians that provides nationally representative diagnostic and prescribing information on patients treated by office-based physicians in the United States.
Overall, there were 27,860,691 insulin treatment visits for type 2 diabetes in 2016-2020. Of those, long-acting analog insulins (glargine [Lantus], detemir [Levemir], and degludec [Tresiba]) accounted for 67.3% of treatment visits in 2016 and 74.8% of treatment visits in 2020.
Rapid-acting insulin analogs (lispro [Humalog], aspart [Novolog], faster aspart [Fiasp], and glulisine [Apidra]) accounted for about 21.2% of visits in 2016 and about 16.5% in 2020.
On the other hand, intermediate- and short-acting human insulins (NPH and regular) accounted for just 3.7% of visits in 2016 and 2.6% in 2020.
Grouped together, the long- and short-acting analogs accounted for 92.7% of visits in 2016 and 86.3% in 2020, while the human insulins represented just 7.3% of visits in 2016 and 5.5% in 2020.
The biosimilar analog insulins (glargine and lispro) first appeared in the database in 2017, accounting for 2.6% of visits that year and 8.2% by 2020.
Overall, the number of visits for insulin treatment declined by 18% between 2016 and 2020, from 6.0 million to 4.9 million. That drop may be due to multiple factors, Dr. Kalyani said.
“Recently updated clinical practice guidelines from professional societies such as the American Diabetes Association recommend the use of glucagon-like peptide-1 (GLP-1) receptor agonists prior to insulin when injectable medications are being considered [for type 2 diabetes],” she noted.
“In addition, during the pandemic, patients may not have been seeing their health care providers for routine diabetes care as often as before ... These and other factors may have contributed to the decrease in insulin visits that we observed.”
By specific insulins, glargine has topped the list all along, accounting for about half of all treatment visits, at 52.6% in 2020. Degludec came in second, at 17.4%, and lispro third, at 9.5%.
Use of pen devices also increased
The proportion of treatment visits for insulin vials/syringes declined from 63.9% in 2016 to 41.1% in 2020, while visits for insulin pens rose from 36.1% to 58.7%.
“Many pens are more costly compared to vials of the same insulin product. Interestingly, some studies have found that use of insulin pens may promote greater patient adherence to insulin and, as a result, more broadly decrease health care costs associated with diabetes. However, we did not specifically investigate the cost of insulin in our study,” Dr. Kalyani noted.
The proportion of visits for “newer” insulins, defined as those approved in 2010 or later, rose from 18.1% in 2016 to 40.9% in 2020, while the concurrent drop for insulins approved prior to 2010 was from 81.9% to 59.1%.
“The findings of our study provide insight into potential drivers of insulin costs in the U.S. and may inform health policy,” the researchers conclude.
Funded in part by the National Heart, Lung, and Blood Institute. Dr. Kalyani currently serves on the Endocrinologic and Metabolic Drugs Advisory Committee of the U.S. Food and Drug Administration.
A version of this article first appeared on Medscape.com.
Children and COVID: Vaccinations lower than ever as cases continue to drop
As the COVID-19 vaccine heads toward approval for children under age 12 years, the number of older children receiving it dropped for the 10th consecutive week, based on data from the Centers for Disease Control and Prevention.
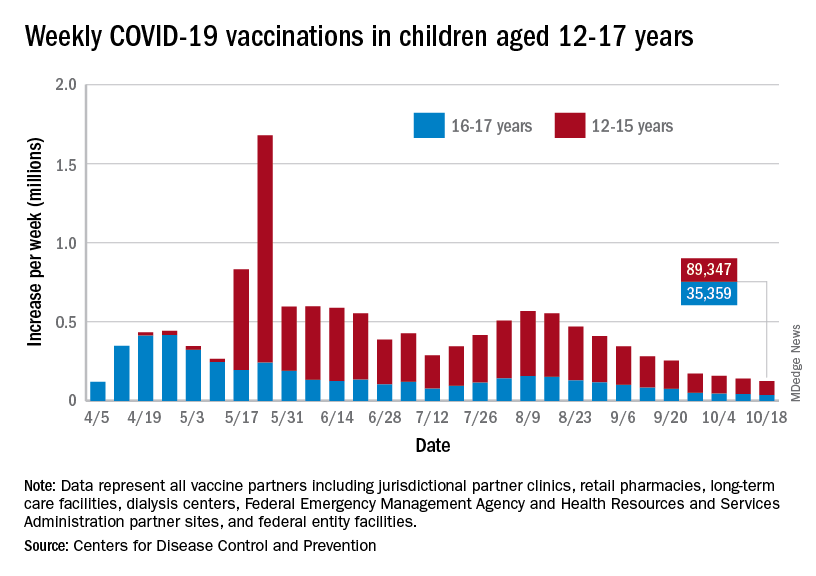
Over 47% of all children aged 12-17 years – that’s close to 12 million eligible individuals – have not received even one dose of COVID-19 vaccine, and less than 44% (about 11.1 million) were fully vaccinated as of Oct. 18, the CDC reported on its COVID Data Tracker.
, when eligibility expanded to include 12- to 15-year-olds, according to the CDC data, which also show that weekly vaccinations have never been lower.
Fortunately, the decline in new cases also continued, as the national total fell for a 6th straight week. There were more than 130,000 child cases reported during the week of Oct. 8-14, compared with 148,000 the previous week and the high of almost 252,000 in late August/early September, the American Academy of Pediatrics and the Children’s Hospital Association said in their weekly COVID-19 report.
That brings the cumulative count to 6.18 million, with children accounting for 16.4% of all cases reported since the start of the pandemic. For the week of Oct. 8-14, children represented 25.5% of all COVID-19 cases in the 46 states with up-to-date online dashboards, the AAP and CHA said, noting that New York has never reported age ranges for cases and that Alabama, Nebraska, and Texas stopped reporting over the summer.
Current data indicate that child cases in California now exceed 671,000, more than any other state, followed by Florida with 439,000 (the state defines a child as someone aged 0-14 years) and Illinois with 301,000. Vermont has the highest proportion of COVID-19 cases occurring in children (24.3%), with Alaska (24.1%) and South Carolina (23.2%) just behind. The highest rate of cases – 15,569 per 100,000 children – can be found in South Carolina, while the lowest is in Hawaii (4,838 per 100,000), the AAP and CHA reported.
The total number of COVID-related deaths in children is 681 as of Oct. 18, according to the CDC, with the AAP/CHA reporting 558 as of Oct. 14, based on data from 45 states, New York City, Puerto Rico, and Guam. The CDC reports 65,655 admissions since Aug. 1, 2020, in children aged 0-17 years, and the AAP/CHA tally 23,582 since May 5, 2020, among children in 24 states and New York City.
As the COVID-19 vaccine heads toward approval for children under age 12 years, the number of older children receiving it dropped for the 10th consecutive week, based on data from the Centers for Disease Control and Prevention.
Over 47% of all children aged 12-17 years – that’s close to 12 million eligible individuals – have not received even one dose of COVID-19 vaccine, and less than 44% (about 11.1 million) were fully vaccinated as of Oct. 18, the CDC reported on its COVID Data Tracker.
, when eligibility expanded to include 12- to 15-year-olds, according to the CDC data, which also show that weekly vaccinations have never been lower.
Fortunately, the decline in new cases also continued, as the national total fell for a 6th straight week. There were more than 130,000 child cases reported during the week of Oct. 8-14, compared with 148,000 the previous week and the high of almost 252,000 in late August/early September, the American Academy of Pediatrics and the Children’s Hospital Association said in their weekly COVID-19 report.
That brings the cumulative count to 6.18 million, with children accounting for 16.4% of all cases reported since the start of the pandemic. For the week of Oct. 8-14, children represented 25.5% of all COVID-19 cases in the 46 states with up-to-date online dashboards, the AAP and CHA said, noting that New York has never reported age ranges for cases and that Alabama, Nebraska, and Texas stopped reporting over the summer.
Current data indicate that child cases in California now exceed 671,000, more than any other state, followed by Florida with 439,000 (the state defines a child as someone aged 0-14 years) and Illinois with 301,000. Vermont has the highest proportion of COVID-19 cases occurring in children (24.3%), with Alaska (24.1%) and South Carolina (23.2%) just behind. The highest rate of cases – 15,569 per 100,000 children – can be found in South Carolina, while the lowest is in Hawaii (4,838 per 100,000), the AAP and CHA reported.
The total number of COVID-related deaths in children is 681 as of Oct. 18, according to the CDC, with the AAP/CHA reporting 558 as of Oct. 14, based on data from 45 states, New York City, Puerto Rico, and Guam. The CDC reports 65,655 admissions since Aug. 1, 2020, in children aged 0-17 years, and the AAP/CHA tally 23,582 since May 5, 2020, among children in 24 states and New York City.
As the COVID-19 vaccine heads toward approval for children under age 12 years, the number of older children receiving it dropped for the 10th consecutive week, based on data from the Centers for Disease Control and Prevention.
Over 47% of all children aged 12-17 years – that’s close to 12 million eligible individuals – have not received even one dose of COVID-19 vaccine, and less than 44% (about 11.1 million) were fully vaccinated as of Oct. 18, the CDC reported on its COVID Data Tracker.
, when eligibility expanded to include 12- to 15-year-olds, according to the CDC data, which also show that weekly vaccinations have never been lower.
Fortunately, the decline in new cases also continued, as the national total fell for a 6th straight week. There were more than 130,000 child cases reported during the week of Oct. 8-14, compared with 148,000 the previous week and the high of almost 252,000 in late August/early September, the American Academy of Pediatrics and the Children’s Hospital Association said in their weekly COVID-19 report.
That brings the cumulative count to 6.18 million, with children accounting for 16.4% of all cases reported since the start of the pandemic. For the week of Oct. 8-14, children represented 25.5% of all COVID-19 cases in the 46 states with up-to-date online dashboards, the AAP and CHA said, noting that New York has never reported age ranges for cases and that Alabama, Nebraska, and Texas stopped reporting over the summer.
Current data indicate that child cases in California now exceed 671,000, more than any other state, followed by Florida with 439,000 (the state defines a child as someone aged 0-14 years) and Illinois with 301,000. Vermont has the highest proportion of COVID-19 cases occurring in children (24.3%), with Alaska (24.1%) and South Carolina (23.2%) just behind. The highest rate of cases – 15,569 per 100,000 children – can be found in South Carolina, while the lowest is in Hawaii (4,838 per 100,000), the AAP and CHA reported.
The total number of COVID-related deaths in children is 681 as of Oct. 18, according to the CDC, with the AAP/CHA reporting 558 as of Oct. 14, based on data from 45 states, New York City, Puerto Rico, and Guam. The CDC reports 65,655 admissions since Aug. 1, 2020, in children aged 0-17 years, and the AAP/CHA tally 23,582 since May 5, 2020, among children in 24 states and New York City.
Tramadol linked to higher risk of mortality, compared with codeine
Tramadol is increasingly used to manage chronic noncancer pain, but as compared with opioids, it appears to be linked to a higher risk for adverse outcomes, according to new data.
Among a cohort of patients who received a prescription for either tramadol or codeine for orthopedic-related pain, tramadol was significantly associated with a higher risk of mortality, cardiovascular events, and fractures.

However, there was no significant difference in the risk of falls, delirium, constipation, opioid abuse/dependence, or sleep disorders between the two drugs.
“However, this is a retrospective cohort study, and despite it providing information that would otherwise be impossible to gather – such as from randomized controlled trials – clinicians should not solely base their decision on this study,” cautioned lead author Carlen Reyes, MD, PhD, of the Institut Universitari d’Investigació en Atenció Primària (IDIAP Jordi Gol), Barcelona.
Dr. Reyes noted that the intake of tramadol and codeine was analyzed using the number of “packages” that were dispensed, as an approximation of the real intake. “Logically we could think that the more packages dispensed of one drug, the more dose the patient is taking, but this is not always true given the availability of different doses commercialized of tramadol and different doses prescribed,” she said. “Given that we did not account for the real dose prescribed, we can only suspect an increased risk of these outcomes and reinforce the need for further prospective studies with more specific dose-response analysis comparing tramadol and codeine.”
The paper was published Oct. 19 in JAMA.
Tramadol has been considered to be a relatively safe opioid and was even strongly recommended by the American Academy of Orthopaedic Surgeons for patients experiencing symptomatic knee osteoarthritis. The authors point out that studies looking at opioid use from 2019 to 2020 show that tramadol was the most prescribed opioid in England, the Netherlands, and Spain.
In the United States, the age-adjusted rate of drug overdose deaths from synthetic opioids rose from 1.0 per 100 000 in 2013 to 11.4 in 2019. Most of these deaths were attributable to fentanyl but some were also related to tramadol.
But despite its wide use in managing chronic noncancer pain, results of recent studies suggest adverse outcomes as compared with other agents. Last year, one study found that older patients who received tramadol had a significant increase in the risk of hip fracture vs. those using NSAIDs or codeine. Another study, also published in 2020, showed that patients with osteoarthritis who were treated with tramadol had a 20%-50% higher risk of dying during the first year of treatment than did patients who were treated with NSAIDs.
In the current paper, Dr. Reyes and colleagues evaluated the association of tramadol with mortality and other adverse clinical outcomes in outpatient settings, compared with codeine.
They conducted a retrospective, population-based, propensity score–matched cohort study using a primary care database that routinely collects medical records and pharmacy dispensations for more than 80% of the population of Catalonia, Spain. The cohort included people 18 years or older who had been prescribed tramadol or codeine from 2007 to 2017 and were followed up to Dec. 31, 2017.
After propensity score matching, the final analysis included 368,960 participants: 184,480 in the tramadol arm and 184,480 in the codeine arm.
The mean age of patients was 52.7 years in the tramadol arm and 53.5 years in the codeine arm, and the prevalence of cancer was 3.2% and 3.3%, respectively. The most common diagnoses in this cohort were back pain (47.5% vs. 48.5%), neck/shoulder pain (28.6% vs. 29.5%), and osteoarthritis (15.3% vs. 15.5%). The most commonly used drugs were ibuprofen (34.4% vs. 34.3%) and paracetamol/acetaminophen (37.1% vs. 36.8%)
Higher risk of adverse outcomes
As compared with codeine, tramadol use was significantly associated with a higher risk of mortality (13.00 vs. 5.61 per 1,000 person-years; hazard ratio, 2.31; 95% confidence interval, 2.08-2.56); absolute rate differences (7.37 per 1,000 person-years; 95% CI, 6.09-8.78), cardiovascular events (10.03 vs. 8.67 per 1,000 person-years; HR, 1.15; 95% CI, 1.05-1.27; ARD, 1.36 per 1,000 person-years; 95% CI, 0.45-2.36), and fractures (12.26 vs. 8.13 per 1,000 person-years; HR, 1.50; 95% CI, 1.37-1.65; ARD, 4.10 per 1,000 person-years; 95% CI, 3.02-5.29).
A subgroup and sensitivity analysis showed that the increased mortality risk associated with tramadol was significantly higher in younger persons vs. older ones (HR, 3.14; 95% CI, 1.82-5.41 vs. 2.39; 95% CI, 2.20-2.60]; P < .001 for interaction). In addition, women had a significantly greater risk of cardiovascular events versus men (HR, 1.32; 95% CI, 1.19-1.46] vs. 1.03; 95% CI, 0.9-1.13]; P < .001 for interaction).
Potential for confounding
Weighing in on the data, Daniel Solomon, MD, MPH, chief of clinical sciences, division of rheumatology, Brigham and Women’s Hospital, and professor of medicine, Harvard Medical School, Boston, noted that because it is extremely unlikely that anyone will ever conduct a large, head-to-head safety trial comparing different opioids, the results of this paper are important to consider.
“However, as the authors appropriately caution, this type of analysis is limited by the strong potential for residual confounding,” he said. “In other words, even though the authors used state-of-the-art methods to limit imbalances between the patients initiating tramadol versus codeine, there is strong reason to believe that imbalances that may account for the differences in adverse events exist.”
For example, he noted that if one looks at the distribution of comorbid conditions in the before-matching group, tramadol initiators demonstrate a higher frequency of chronic kidney disease, diabetes, and overall chronic comorbid diseases. “This suggests to me that prescribers apply selection criteria when choosing who to prescribe which opioid,” Dr. Solomon explained.
“While the authors’ use of propensity score matching limits confounding, it only can improve balance for measured confounders,” he said. “Other factors not measured in this type of data set – blood pressure, pain, physical activity, tobacco use, body mass index – may still demonstrate imbalances even after matching.”
But after these limitations are taken into consideration, the results remain concerning, Dr. Solomon emphasized, particularly the all-cause mortality excess of tramadol versus codeine users. “This study did not include cause of death, which would help the reader understand why users of tramadol were dying more frequently,” he added. “It also might help in understanding whether this is a true biologic effect or residual confounding.”
Perceived safety
In an accompanying editorial, Howard S. Kim, MD, MS, and colleagues from Northwestern University, Chicago, write that the greatest risk of tramadol may involve the perception that it is “inherently safer than other opioids.”
“In actuality, the mechanisms of action and variable metabolism of tramadol in a given population create considerable therapeutic uncertainty and introduce additional risk exposure,” they say, as demonstrated in the current study.
Therefore, when clinicians determine that an opioid is needed for pain relief, it may be a better option to select a pure opioid agonist that has a more predictable therapeutic effect and known adverse effect profile, such as morphine or hydrocodone. “This would allow clinicians and patients to more properly weigh the risks and benefits of initiating opioid therapy through shared decision-making and prompt the level of counseling on safe use, storage, and disposal practices that all opioids deserve,” write the editorialists.
The study was funded by the Fundació Institut Universitari per a la recerca a l’Atenció Primària de Salut Jordi Gol i Gurina. The research was supported by the National Institute for Health Research Oxford Biomedical Research Centre. Dr. Reyes has disclosed no relevant financial relationships. Dr. Solomon disclosed salary support from research contracts to his hospital from Amgen, AbbVie, Moderna, the Rheumatology Research Foundation, and National Institutes of Health; and royalties from UpToDate. Dr. Kim reported unrelated grant support from the Agency for Healthcare Research and Quality.
A version of this article first appeared on Medscape.com.
Tramadol is increasingly used to manage chronic noncancer pain, but as compared with opioids, it appears to be linked to a higher risk for adverse outcomes, according to new data.
Among a cohort of patients who received a prescription for either tramadol or codeine for orthopedic-related pain, tramadol was significantly associated with a higher risk of mortality, cardiovascular events, and fractures.
However, there was no significant difference in the risk of falls, delirium, constipation, opioid abuse/dependence, or sleep disorders between the two drugs.
“However, this is a retrospective cohort study, and despite it providing information that would otherwise be impossible to gather – such as from randomized controlled trials – clinicians should not solely base their decision on this study,” cautioned lead author Carlen Reyes, MD, PhD, of the Institut Universitari d’Investigació en Atenció Primària (IDIAP Jordi Gol), Barcelona.
Dr. Reyes noted that the intake of tramadol and codeine was analyzed using the number of “packages” that were dispensed, as an approximation of the real intake. “Logically we could think that the more packages dispensed of one drug, the more dose the patient is taking, but this is not always true given the availability of different doses commercialized of tramadol and different doses prescribed,” she said. “Given that we did not account for the real dose prescribed, we can only suspect an increased risk of these outcomes and reinforce the need for further prospective studies with more specific dose-response analysis comparing tramadol and codeine.”
The paper was published Oct. 19 in JAMA.
Tramadol has been considered to be a relatively safe opioid and was even strongly recommended by the American Academy of Orthopaedic Surgeons for patients experiencing symptomatic knee osteoarthritis. The authors point out that studies looking at opioid use from 2019 to 2020 show that tramadol was the most prescribed opioid in England, the Netherlands, and Spain.
In the United States, the age-adjusted rate of drug overdose deaths from synthetic opioids rose from 1.0 per 100 000 in 2013 to 11.4 in 2019. Most of these deaths were attributable to fentanyl but some were also related to tramadol.
But despite its wide use in managing chronic noncancer pain, results of recent studies suggest adverse outcomes as compared with other agents. Last year, one study found that older patients who received tramadol had a significant increase in the risk of hip fracture vs. those using NSAIDs or codeine. Another study, also published in 2020, showed that patients with osteoarthritis who were treated with tramadol had a 20%-50% higher risk of dying during the first year of treatment than did patients who were treated with NSAIDs.
In the current paper, Dr. Reyes and colleagues evaluated the association of tramadol with mortality and other adverse clinical outcomes in outpatient settings, compared with codeine.
They conducted a retrospective, population-based, propensity score–matched cohort study using a primary care database that routinely collects medical records and pharmacy dispensations for more than 80% of the population of Catalonia, Spain. The cohort included people 18 years or older who had been prescribed tramadol or codeine from 2007 to 2017 and were followed up to Dec. 31, 2017.
After propensity score matching, the final analysis included 368,960 participants: 184,480 in the tramadol arm and 184,480 in the codeine arm.
The mean age of patients was 52.7 years in the tramadol arm and 53.5 years in the codeine arm, and the prevalence of cancer was 3.2% and 3.3%, respectively. The most common diagnoses in this cohort were back pain (47.5% vs. 48.5%), neck/shoulder pain (28.6% vs. 29.5%), and osteoarthritis (15.3% vs. 15.5%). The most commonly used drugs were ibuprofen (34.4% vs. 34.3%) and paracetamol/acetaminophen (37.1% vs. 36.8%)
Higher risk of adverse outcomes
As compared with codeine, tramadol use was significantly associated with a higher risk of mortality (13.00 vs. 5.61 per 1,000 person-years; hazard ratio, 2.31; 95% confidence interval, 2.08-2.56); absolute rate differences (7.37 per 1,000 person-years; 95% CI, 6.09-8.78), cardiovascular events (10.03 vs. 8.67 per 1,000 person-years; HR, 1.15; 95% CI, 1.05-1.27; ARD, 1.36 per 1,000 person-years; 95% CI, 0.45-2.36), and fractures (12.26 vs. 8.13 per 1,000 person-years; HR, 1.50; 95% CI, 1.37-1.65; ARD, 4.10 per 1,000 person-years; 95% CI, 3.02-5.29).
A subgroup and sensitivity analysis showed that the increased mortality risk associated with tramadol was significantly higher in younger persons vs. older ones (HR, 3.14; 95% CI, 1.82-5.41 vs. 2.39; 95% CI, 2.20-2.60]; P < .001 for interaction). In addition, women had a significantly greater risk of cardiovascular events versus men (HR, 1.32; 95% CI, 1.19-1.46] vs. 1.03; 95% CI, 0.9-1.13]; P < .001 for interaction).
Potential for confounding
Weighing in on the data, Daniel Solomon, MD, MPH, chief of clinical sciences, division of rheumatology, Brigham and Women’s Hospital, and professor of medicine, Harvard Medical School, Boston, noted that because it is extremely unlikely that anyone will ever conduct a large, head-to-head safety trial comparing different opioids, the results of this paper are important to consider.
“However, as the authors appropriately caution, this type of analysis is limited by the strong potential for residual confounding,” he said. “In other words, even though the authors used state-of-the-art methods to limit imbalances between the patients initiating tramadol versus codeine, there is strong reason to believe that imbalances that may account for the differences in adverse events exist.”
For example, he noted that if one looks at the distribution of comorbid conditions in the before-matching group, tramadol initiators demonstrate a higher frequency of chronic kidney disease, diabetes, and overall chronic comorbid diseases. “This suggests to me that prescribers apply selection criteria when choosing who to prescribe which opioid,” Dr. Solomon explained.
“While the authors’ use of propensity score matching limits confounding, it only can improve balance for measured confounders,” he said. “Other factors not measured in this type of data set – blood pressure, pain, physical activity, tobacco use, body mass index – may still demonstrate imbalances even after matching.”
But after these limitations are taken into consideration, the results remain concerning, Dr. Solomon emphasized, particularly the all-cause mortality excess of tramadol versus codeine users. “This study did not include cause of death, which would help the reader understand why users of tramadol were dying more frequently,” he added. “It also might help in understanding whether this is a true biologic effect or residual confounding.”
Perceived safety
In an accompanying editorial, Howard S. Kim, MD, MS, and colleagues from Northwestern University, Chicago, write that the greatest risk of tramadol may involve the perception that it is “inherently safer than other opioids.”
“In actuality, the mechanisms of action and variable metabolism of tramadol in a given population create considerable therapeutic uncertainty and introduce additional risk exposure,” they say, as demonstrated in the current study.
Therefore, when clinicians determine that an opioid is needed for pain relief, it may be a better option to select a pure opioid agonist that has a more predictable therapeutic effect and known adverse effect profile, such as morphine or hydrocodone. “This would allow clinicians and patients to more properly weigh the risks and benefits of initiating opioid therapy through shared decision-making and prompt the level of counseling on safe use, storage, and disposal practices that all opioids deserve,” write the editorialists.
The study was funded by the Fundació Institut Universitari per a la recerca a l’Atenció Primària de Salut Jordi Gol i Gurina. The research was supported by the National Institute for Health Research Oxford Biomedical Research Centre. Dr. Reyes has disclosed no relevant financial relationships. Dr. Solomon disclosed salary support from research contracts to his hospital from Amgen, AbbVie, Moderna, the Rheumatology Research Foundation, and National Institutes of Health; and royalties from UpToDate. Dr. Kim reported unrelated grant support from the Agency for Healthcare Research and Quality.
A version of this article first appeared on Medscape.com.
Tramadol is increasingly used to manage chronic noncancer pain, but as compared with opioids, it appears to be linked to a higher risk for adverse outcomes, according to new data.
Among a cohort of patients who received a prescription for either tramadol or codeine for orthopedic-related pain, tramadol was significantly associated with a higher risk of mortality, cardiovascular events, and fractures.
However, there was no significant difference in the risk of falls, delirium, constipation, opioid abuse/dependence, or sleep disorders between the two drugs.
“However, this is a retrospective cohort study, and despite it providing information that would otherwise be impossible to gather – such as from randomized controlled trials – clinicians should not solely base their decision on this study,” cautioned lead author Carlen Reyes, MD, PhD, of the Institut Universitari d’Investigació en Atenció Primària (IDIAP Jordi Gol), Barcelona.
Dr. Reyes noted that the intake of tramadol and codeine was analyzed using the number of “packages” that were dispensed, as an approximation of the real intake. “Logically we could think that the more packages dispensed of one drug, the more dose the patient is taking, but this is not always true given the availability of different doses commercialized of tramadol and different doses prescribed,” she said. “Given that we did not account for the real dose prescribed, we can only suspect an increased risk of these outcomes and reinforce the need for further prospective studies with more specific dose-response analysis comparing tramadol and codeine.”
The paper was published Oct. 19 in JAMA.
Tramadol has been considered to be a relatively safe opioid and was even strongly recommended by the American Academy of Orthopaedic Surgeons for patients experiencing symptomatic knee osteoarthritis. The authors point out that studies looking at opioid use from 2019 to 2020 show that tramadol was the most prescribed opioid in England, the Netherlands, and Spain.
In the United States, the age-adjusted rate of drug overdose deaths from synthetic opioids rose from 1.0 per 100 000 in 2013 to 11.4 in 2019. Most of these deaths were attributable to fentanyl but some were also related to tramadol.
But despite its wide use in managing chronic noncancer pain, results of recent studies suggest adverse outcomes as compared with other agents. Last year, one study found that older patients who received tramadol had a significant increase in the risk of hip fracture vs. those using NSAIDs or codeine. Another study, also published in 2020, showed that patients with osteoarthritis who were treated with tramadol had a 20%-50% higher risk of dying during the first year of treatment than did patients who were treated with NSAIDs.
In the current paper, Dr. Reyes and colleagues evaluated the association of tramadol with mortality and other adverse clinical outcomes in outpatient settings, compared with codeine.
They conducted a retrospective, population-based, propensity score–matched cohort study using a primary care database that routinely collects medical records and pharmacy dispensations for more than 80% of the population of Catalonia, Spain. The cohort included people 18 years or older who had been prescribed tramadol or codeine from 2007 to 2017 and were followed up to Dec. 31, 2017.
After propensity score matching, the final analysis included 368,960 participants: 184,480 in the tramadol arm and 184,480 in the codeine arm.
The mean age of patients was 52.7 years in the tramadol arm and 53.5 years in the codeine arm, and the prevalence of cancer was 3.2% and 3.3%, respectively. The most common diagnoses in this cohort were back pain (47.5% vs. 48.5%), neck/shoulder pain (28.6% vs. 29.5%), and osteoarthritis (15.3% vs. 15.5%). The most commonly used drugs were ibuprofen (34.4% vs. 34.3%) and paracetamol/acetaminophen (37.1% vs. 36.8%)
Higher risk of adverse outcomes
As compared with codeine, tramadol use was significantly associated with a higher risk of mortality (13.00 vs. 5.61 per 1,000 person-years; hazard ratio, 2.31; 95% confidence interval, 2.08-2.56); absolute rate differences (7.37 per 1,000 person-years; 95% CI, 6.09-8.78), cardiovascular events (10.03 vs. 8.67 per 1,000 person-years; HR, 1.15; 95% CI, 1.05-1.27; ARD, 1.36 per 1,000 person-years; 95% CI, 0.45-2.36), and fractures (12.26 vs. 8.13 per 1,000 person-years; HR, 1.50; 95% CI, 1.37-1.65; ARD, 4.10 per 1,000 person-years; 95% CI, 3.02-5.29).
A subgroup and sensitivity analysis showed that the increased mortality risk associated with tramadol was significantly higher in younger persons vs. older ones (HR, 3.14; 95% CI, 1.82-5.41 vs. 2.39; 95% CI, 2.20-2.60]; P < .001 for interaction). In addition, women had a significantly greater risk of cardiovascular events versus men (HR, 1.32; 95% CI, 1.19-1.46] vs. 1.03; 95% CI, 0.9-1.13]; P < .001 for interaction).
Potential for confounding
Weighing in on the data, Daniel Solomon, MD, MPH, chief of clinical sciences, division of rheumatology, Brigham and Women’s Hospital, and professor of medicine, Harvard Medical School, Boston, noted that because it is extremely unlikely that anyone will ever conduct a large, head-to-head safety trial comparing different opioids, the results of this paper are important to consider.
“However, as the authors appropriately caution, this type of analysis is limited by the strong potential for residual confounding,” he said. “In other words, even though the authors used state-of-the-art methods to limit imbalances between the patients initiating tramadol versus codeine, there is strong reason to believe that imbalances that may account for the differences in adverse events exist.”
For example, he noted that if one looks at the distribution of comorbid conditions in the before-matching group, tramadol initiators demonstrate a higher frequency of chronic kidney disease, diabetes, and overall chronic comorbid diseases. “This suggests to me that prescribers apply selection criteria when choosing who to prescribe which opioid,” Dr. Solomon explained.
“While the authors’ use of propensity score matching limits confounding, it only can improve balance for measured confounders,” he said. “Other factors not measured in this type of data set – blood pressure, pain, physical activity, tobacco use, body mass index – may still demonstrate imbalances even after matching.”
But after these limitations are taken into consideration, the results remain concerning, Dr. Solomon emphasized, particularly the all-cause mortality excess of tramadol versus codeine users. “This study did not include cause of death, which would help the reader understand why users of tramadol were dying more frequently,” he added. “It also might help in understanding whether this is a true biologic effect or residual confounding.”
Perceived safety
In an accompanying editorial, Howard S. Kim, MD, MS, and colleagues from Northwestern University, Chicago, write that the greatest risk of tramadol may involve the perception that it is “inherently safer than other opioids.”
“In actuality, the mechanisms of action and variable metabolism of tramadol in a given population create considerable therapeutic uncertainty and introduce additional risk exposure,” they say, as demonstrated in the current study.
Therefore, when clinicians determine that an opioid is needed for pain relief, it may be a better option to select a pure opioid agonist that has a more predictable therapeutic effect and known adverse effect profile, such as morphine or hydrocodone. “This would allow clinicians and patients to more properly weigh the risks and benefits of initiating opioid therapy through shared decision-making and prompt the level of counseling on safe use, storage, and disposal practices that all opioids deserve,” write the editorialists.
The study was funded by the Fundació Institut Universitari per a la recerca a l’Atenció Primària de Salut Jordi Gol i Gurina. The research was supported by the National Institute for Health Research Oxford Biomedical Research Centre. Dr. Reyes has disclosed no relevant financial relationships. Dr. Solomon disclosed salary support from research contracts to his hospital from Amgen, AbbVie, Moderna, the Rheumatology Research Foundation, and National Institutes of Health; and royalties from UpToDate. Dr. Kim reported unrelated grant support from the Agency for Healthcare Research and Quality.
A version of this article first appeared on Medscape.com.
National Academies issue guidance for childhood COVID-19 vaccines
While the U.S. Food and Drug Administration has yet to give the green light to COVID-19 vaccination for children who are under age 12, it is expected that approval will be granted. In anticipation of the FDA’s go-ahead, which is expected in the coming weeks, a new “rapid expert consultation” has identified “actionable guidance” that state and local decision-makers can use to communicate with the public. The goal is to build confidence in and promote the uptake of COVID-19 vaccines, especially for parents who are contemplating vaccinating their children.
They note that key factors in decision-making concern vaccine side effects, the efficacy of the vaccine in children, availability of research in their child’s age group, research conducted by the parents themselves, and recommendations by the child’s health care provider.
“One of the reasons that the COVID vaccine only became available for children 12 and over months after it was approved for adults is that it takes time and many, many trial participants who are closely monitored before the vaccine ever reaches the general public,” said Nusheen Ameenuddin, MD, MPH, MPA, an assistant professor of pediatrics at the Mayo Clinic, Rochester, Minn. “We continue to talk to parents about the fact that the vaccines have been very safe and effective in this group, and even though people are concerned about side effects, they are much milder and less frequent than the effects of the disease itself.”
Dr. Ameenuddin noted that the lack of data in this age group can be concerning for parents. “It’s not like other vaccines which have been available for a long time, and the clinical trial data are still limited for this age group,” she said. “But I think the main point that practitioners need to emphasize is that, even though the vaccine is new, the science for this vaccine has been around for about a decade.”
The unique circumstances of a pandemic, she pointed out, allowed for important information about effectiveness, safety, and side effects to be obtained more quickly from clinical trial data.
“We have really good evidence for kids 12 and over, about safety and effectiveness, and even though children are not small adults and have their own unique physiology, this has provided a good starting point to suggest that kids slightly younger will also respond well to the vaccines,” said Dr. Ameenuddin, who is also chair of the American Academy of Pediatrics Council on Communications and Media. “As we learn more, we can start gathering more information about even younger kids to ensure that the right dosage and spacing of vaccines can provide maximum vaccine effectiveness and protection from disease.”
The guidance was published Oct. 13 by the National Academies of Sciences, Engineering, and Medicine.
The rapid expert consultation was produced through the Societal Experts Action Network, an activity of the National Academies that is sponsored by the NASEM and the Alfred P. Sloan Foundation. The goal of SEAN is to connect researchers in the social, behavioral, and economic sciences with decision-makers to respond to policy questions related to the COVID-19 pandemic.
In their expert consultation, the authors emphasize that vaccination is critical for decreasing transmission and controlling infection, as well as limiting the emergence of future serious variants. As of Oct. 3, 2021, about 65% of the U.S. population had received at least one dose of the vaccine, and the rate has begun to lag in many areas of the country. There are a variety of reasons for vaccine hesitancy, they note, including perception of low risks from COVID-19 or of high risks from COVID-19 vaccines, exposure to media, political agendas, lack of confidence in science, and distrust of the medical establishment. The Pfizer/BioNTech vaccine is currently authorized for emergency use for individuals 12 years of age and older and fully approved for those aged 16 and older, while the Moderna and the Johnson & Johnson vaccines are authorized for emergency use for those 18 years of age and older.
Many children between the ages of 12 and 17 have not been vaccinated, and the major concerns reported by parents include not knowing enough about the long-term effects of the COVID-19 vaccine in children (88%), concerns about children experiencing serious side effects (79%), and concerns that the COVID-19 vaccine might negatively affect future fertility (73%).
The National Academies have previously released two other “rapid expert consultations” which have addressed building vaccine confidence, and both reports provide key strategies for communicating information about COVID-19 vaccines. In this paper, the focus was on communicating with parents to gain confidence in the vaccine and address concerns.
Key points
The key strategies highlighted for communicating with parents include the following:
- Emphasizing safety and efficacy: Parents should be informed about the ongoing research and clinical trials that will answer more questions about the vaccine and that there is continued monitoring for any safety risks. Pointing to the safety data from the clinical trials for 12- to 17-year-olds, and the lack of serious adverse events from the vaccine in this age group may help alleviate concerns.
- CalibriEncouraging parents to talk with a primary care provider: Research shows that parents trust family physicians and other health care practitioners to provide them with accurate information about vaccines. Local, state, and national leaders can provide messaging templates and other resources to health care professionals who are engaged in these conversations.
- Leveraging social networks to influence parents’ vaccination decisions: Parents are influenced by their social network connections. It is important to engage these networks, especially with members of their community who are considered trustworthy and influential. Social networks may also be very diverse, and include family members, friends, coworkers, social media, and members of their religious community.
While the guidance states that different groups of parents will require different messaging, they suggest that communication can begin with a focus on the things that vaccination can accomplish. In addition to preventing infection with COVID-19, it will allow children to attend school in person and participate in extracurricular activities such as sports, without risking their health. “One thing I’ve learned over several years of working with vaccine-hesitant parents is that you have to tailor each approach to the individual,” said Dr. Ameenuddin. “Different people have different concerns, and first and foremost, it’s important to listen.”
For some parents, emphasizing that the more people that can be vaccinated and the sooner it can be done, the sooner everyone can return to a normal life is a good approach, she added. “I think it’s important to emphasize both the individual and communal benefits of vaccines, but that won’t necessarily reach every person with concerns. I think it’s important to find out what is most important to individuals and work from there to find a way to connect with that family to encourage vaccination.”
Dr. Ameenuddin has no disclosures.
While the U.S. Food and Drug Administration has yet to give the green light to COVID-19 vaccination for children who are under age 12, it is expected that approval will be granted. In anticipation of the FDA’s go-ahead, which is expected in the coming weeks, a new “rapid expert consultation” has identified “actionable guidance” that state and local decision-makers can use to communicate with the public. The goal is to build confidence in and promote the uptake of COVID-19 vaccines, especially for parents who are contemplating vaccinating their children.
They note that key factors in decision-making concern vaccine side effects, the efficacy of the vaccine in children, availability of research in their child’s age group, research conducted by the parents themselves, and recommendations by the child’s health care provider.
“One of the reasons that the COVID vaccine only became available for children 12 and over months after it was approved for adults is that it takes time and many, many trial participants who are closely monitored before the vaccine ever reaches the general public,” said Nusheen Ameenuddin, MD, MPH, MPA, an assistant professor of pediatrics at the Mayo Clinic, Rochester, Minn. “We continue to talk to parents about the fact that the vaccines have been very safe and effective in this group, and even though people are concerned about side effects, they are much milder and less frequent than the effects of the disease itself.”
Dr. Ameenuddin noted that the lack of data in this age group can be concerning for parents. “It’s not like other vaccines which have been available for a long time, and the clinical trial data are still limited for this age group,” she said. “But I think the main point that practitioners need to emphasize is that, even though the vaccine is new, the science for this vaccine has been around for about a decade.”
The unique circumstances of a pandemic, she pointed out, allowed for important information about effectiveness, safety, and side effects to be obtained more quickly from clinical trial data.
“We have really good evidence for kids 12 and over, about safety and effectiveness, and even though children are not small adults and have their own unique physiology, this has provided a good starting point to suggest that kids slightly younger will also respond well to the vaccines,” said Dr. Ameenuddin, who is also chair of the American Academy of Pediatrics Council on Communications and Media. “As we learn more, we can start gathering more information about even younger kids to ensure that the right dosage and spacing of vaccines can provide maximum vaccine effectiveness and protection from disease.”
The guidance was published Oct. 13 by the National Academies of Sciences, Engineering, and Medicine.
The rapid expert consultation was produced through the Societal Experts Action Network, an activity of the National Academies that is sponsored by the NASEM and the Alfred P. Sloan Foundation. The goal of SEAN is to connect researchers in the social, behavioral, and economic sciences with decision-makers to respond to policy questions related to the COVID-19 pandemic.
In their expert consultation, the authors emphasize that vaccination is critical for decreasing transmission and controlling infection, as well as limiting the emergence of future serious variants. As of Oct. 3, 2021, about 65% of the U.S. population had received at least one dose of the vaccine, and the rate has begun to lag in many areas of the country. There are a variety of reasons for vaccine hesitancy, they note, including perception of low risks from COVID-19 or of high risks from COVID-19 vaccines, exposure to media, political agendas, lack of confidence in science, and distrust of the medical establishment. The Pfizer/BioNTech vaccine is currently authorized for emergency use for individuals 12 years of age and older and fully approved for those aged 16 and older, while the Moderna and the Johnson & Johnson vaccines are authorized for emergency use for those 18 years of age and older.
Many children between the ages of 12 and 17 have not been vaccinated, and the major concerns reported by parents include not knowing enough about the long-term effects of the COVID-19 vaccine in children (88%), concerns about children experiencing serious side effects (79%), and concerns that the COVID-19 vaccine might negatively affect future fertility (73%).
The National Academies have previously released two other “rapid expert consultations” which have addressed building vaccine confidence, and both reports provide key strategies for communicating information about COVID-19 vaccines. In this paper, the focus was on communicating with parents to gain confidence in the vaccine and address concerns.
Key points
The key strategies highlighted for communicating with parents include the following:
- Emphasizing safety and efficacy: Parents should be informed about the ongoing research and clinical trials that will answer more questions about the vaccine and that there is continued monitoring for any safety risks. Pointing to the safety data from the clinical trials for 12- to 17-year-olds, and the lack of serious adverse events from the vaccine in this age group may help alleviate concerns.
- CalibriEncouraging parents to talk with a primary care provider: Research shows that parents trust family physicians and other health care practitioners to provide them with accurate information about vaccines. Local, state, and national leaders can provide messaging templates and other resources to health care professionals who are engaged in these conversations.
- Leveraging social networks to influence parents’ vaccination decisions: Parents are influenced by their social network connections. It is important to engage these networks, especially with members of their community who are considered trustworthy and influential. Social networks may also be very diverse, and include family members, friends, coworkers, social media, and members of their religious community.
While the guidance states that different groups of parents will require different messaging, they suggest that communication can begin with a focus on the things that vaccination can accomplish. In addition to preventing infection with COVID-19, it will allow children to attend school in person and participate in extracurricular activities such as sports, without risking their health. “One thing I’ve learned over several years of working with vaccine-hesitant parents is that you have to tailor each approach to the individual,” said Dr. Ameenuddin. “Different people have different concerns, and first and foremost, it’s important to listen.”
For some parents, emphasizing that the more people that can be vaccinated and the sooner it can be done, the sooner everyone can return to a normal life is a good approach, she added. “I think it’s important to emphasize both the individual and communal benefits of vaccines, but that won’t necessarily reach every person with concerns. I think it’s important to find out what is most important to individuals and work from there to find a way to connect with that family to encourage vaccination.”
Dr. Ameenuddin has no disclosures.
While the U.S. Food and Drug Administration has yet to give the green light to COVID-19 vaccination for children who are under age 12, it is expected that approval will be granted. In anticipation of the FDA’s go-ahead, which is expected in the coming weeks, a new “rapid expert consultation” has identified “actionable guidance” that state and local decision-makers can use to communicate with the public. The goal is to build confidence in and promote the uptake of COVID-19 vaccines, especially for parents who are contemplating vaccinating their children.
They note that key factors in decision-making concern vaccine side effects, the efficacy of the vaccine in children, availability of research in their child’s age group, research conducted by the parents themselves, and recommendations by the child’s health care provider.
“One of the reasons that the COVID vaccine only became available for children 12 and over months after it was approved for adults is that it takes time and many, many trial participants who are closely monitored before the vaccine ever reaches the general public,” said Nusheen Ameenuddin, MD, MPH, MPA, an assistant professor of pediatrics at the Mayo Clinic, Rochester, Minn. “We continue to talk to parents about the fact that the vaccines have been very safe and effective in this group, and even though people are concerned about side effects, they are much milder and less frequent than the effects of the disease itself.”
Dr. Ameenuddin noted that the lack of data in this age group can be concerning for parents. “It’s not like other vaccines which have been available for a long time, and the clinical trial data are still limited for this age group,” she said. “But I think the main point that practitioners need to emphasize is that, even though the vaccine is new, the science for this vaccine has been around for about a decade.”
The unique circumstances of a pandemic, she pointed out, allowed for important information about effectiveness, safety, and side effects to be obtained more quickly from clinical trial data.
“We have really good evidence for kids 12 and over, about safety and effectiveness, and even though children are not small adults and have their own unique physiology, this has provided a good starting point to suggest that kids slightly younger will also respond well to the vaccines,” said Dr. Ameenuddin, who is also chair of the American Academy of Pediatrics Council on Communications and Media. “As we learn more, we can start gathering more information about even younger kids to ensure that the right dosage and spacing of vaccines can provide maximum vaccine effectiveness and protection from disease.”
The guidance was published Oct. 13 by the National Academies of Sciences, Engineering, and Medicine.
The rapid expert consultation was produced through the Societal Experts Action Network, an activity of the National Academies that is sponsored by the NASEM and the Alfred P. Sloan Foundation. The goal of SEAN is to connect researchers in the social, behavioral, and economic sciences with decision-makers to respond to policy questions related to the COVID-19 pandemic.
In their expert consultation, the authors emphasize that vaccination is critical for decreasing transmission and controlling infection, as well as limiting the emergence of future serious variants. As of Oct. 3, 2021, about 65% of the U.S. population had received at least one dose of the vaccine, and the rate has begun to lag in many areas of the country. There are a variety of reasons for vaccine hesitancy, they note, including perception of low risks from COVID-19 or of high risks from COVID-19 vaccines, exposure to media, political agendas, lack of confidence in science, and distrust of the medical establishment. The Pfizer/BioNTech vaccine is currently authorized for emergency use for individuals 12 years of age and older and fully approved for those aged 16 and older, while the Moderna and the Johnson & Johnson vaccines are authorized for emergency use for those 18 years of age and older.
Many children between the ages of 12 and 17 have not been vaccinated, and the major concerns reported by parents include not knowing enough about the long-term effects of the COVID-19 vaccine in children (88%), concerns about children experiencing serious side effects (79%), and concerns that the COVID-19 vaccine might negatively affect future fertility (73%).
The National Academies have previously released two other “rapid expert consultations” which have addressed building vaccine confidence, and both reports provide key strategies for communicating information about COVID-19 vaccines. In this paper, the focus was on communicating with parents to gain confidence in the vaccine and address concerns.
Key points
The key strategies highlighted for communicating with parents include the following:
- Emphasizing safety and efficacy: Parents should be informed about the ongoing research and clinical trials that will answer more questions about the vaccine and that there is continued monitoring for any safety risks. Pointing to the safety data from the clinical trials for 12- to 17-year-olds, and the lack of serious adverse events from the vaccine in this age group may help alleviate concerns.
- CalibriEncouraging parents to talk with a primary care provider: Research shows that parents trust family physicians and other health care practitioners to provide them with accurate information about vaccines. Local, state, and national leaders can provide messaging templates and other resources to health care professionals who are engaged in these conversations.
- Leveraging social networks to influence parents’ vaccination decisions: Parents are influenced by their social network connections. It is important to engage these networks, especially with members of their community who are considered trustworthy and influential. Social networks may also be very diverse, and include family members, friends, coworkers, social media, and members of their religious community.
While the guidance states that different groups of parents will require different messaging, they suggest that communication can begin with a focus on the things that vaccination can accomplish. In addition to preventing infection with COVID-19, it will allow children to attend school in person and participate in extracurricular activities such as sports, without risking their health. “One thing I’ve learned over several years of working with vaccine-hesitant parents is that you have to tailor each approach to the individual,” said Dr. Ameenuddin. “Different people have different concerns, and first and foremost, it’s important to listen.”
For some parents, emphasizing that the more people that can be vaccinated and the sooner it can be done, the sooner everyone can return to a normal life is a good approach, she added. “I think it’s important to emphasize both the individual and communal benefits of vaccines, but that won’t necessarily reach every person with concerns. I think it’s important to find out what is most important to individuals and work from there to find a way to connect with that family to encourage vaccination.”
Dr. Ameenuddin has no disclosures.
PA defends against license suspension for COVID treatment
The suspension stemmed from allegations against Scott C. Miller, PA-C, by at least six COVID patients, including some who weren’t his patients or whom he never examined and a few who later died from the virus, according to the Washington Medical Commission.
“Miller’s treatment of COVID-19 patients fell below the standard of care,” the suspension report states. “Miller began a public campaign promoting ivermectin as a curative for COVID-19, and prescribing it without adequate examination to at least one person, with no reliable clinical studies that establish its efficacy in preventing or treating COVID-19.”
Mr. Miller has until early November to respond to the allegations. On his clinic’s website, Mr. Miller stated, “In response to the charges, I want to reassure all of you that the initial attacks against me have been brought on by a small handful of people that have no ties to our medical practice, and by pharmacies and hospitals that have a zero tolerance policy on family members asking that I help them advocate for loved ones that have been admitted and written off in our current system of dismissiveness and neglect.”
Mr. Miller also expressed gratitude for the support he has received recently. A GoFundMe campaign to raise money for Mr. Miller’s legal fund had raised more than $59,000 at press time. His GoFundMe page had been shared 2,400 times. He has more than 550 followers and more than 400 donors.
“I don’t know that I have the words to adequately describe the deep sense of love and connection I have received from you, the families I serve, and those that have reached out to me in this deeply challenging time,” he wrote on the clinic website.
Mr. Miller has spoken publicly about his anti-mask views and his support for ivermectin, according to the commission report. As part of the suspension, he was charged with making “misleading representations regarding the efficacy of non-FDA approved treatment and mask use.”
In one case that was cited in the report, a 39-year-old patient contacted the pediatric clinic, and Mr. Miller spoke with the patient by phone. The patient reported that he had tested positive for COVID. Mr. Miller advised the patient to take supplements, including vitamin D and C, zinc, and melatonin, and he prescribed ivermectin, dexamethasone, and azithromycin. He did not perform an exam, verify the information that the patient had provided, advise the patient regarding interactions, or order follow-up testing, the report states.
Other charges against Mr. Miller include harassing hospital staff by making threatening statements about hospitals and doctors who treat COVID-19 patients and misrepresenting his original 2013 license application. He denied on the application that he was being investigated by another licensing board. At the time, the California Physician Assistant Board was investigating him for providing medical care and prescribing without a supervising doctor’s authorization and without conducting physical exams, among other charges.
A version of this article first appeared on Medscape.com.
The suspension stemmed from allegations against Scott C. Miller, PA-C, by at least six COVID patients, including some who weren’t his patients or whom he never examined and a few who later died from the virus, according to the Washington Medical Commission.
“Miller’s treatment of COVID-19 patients fell below the standard of care,” the suspension report states. “Miller began a public campaign promoting ivermectin as a curative for COVID-19, and prescribing it without adequate examination to at least one person, with no reliable clinical studies that establish its efficacy in preventing or treating COVID-19.”
Mr. Miller has until early November to respond to the allegations. On his clinic’s website, Mr. Miller stated, “In response to the charges, I want to reassure all of you that the initial attacks against me have been brought on by a small handful of people that have no ties to our medical practice, and by pharmacies and hospitals that have a zero tolerance policy on family members asking that I help them advocate for loved ones that have been admitted and written off in our current system of dismissiveness and neglect.”
Mr. Miller also expressed gratitude for the support he has received recently. A GoFundMe campaign to raise money for Mr. Miller’s legal fund had raised more than $59,000 at press time. His GoFundMe page had been shared 2,400 times. He has more than 550 followers and more than 400 donors.
“I don’t know that I have the words to adequately describe the deep sense of love and connection I have received from you, the families I serve, and those that have reached out to me in this deeply challenging time,” he wrote on the clinic website.
Mr. Miller has spoken publicly about his anti-mask views and his support for ivermectin, according to the commission report. As part of the suspension, he was charged with making “misleading representations regarding the efficacy of non-FDA approved treatment and mask use.”
In one case that was cited in the report, a 39-year-old patient contacted the pediatric clinic, and Mr. Miller spoke with the patient by phone. The patient reported that he had tested positive for COVID. Mr. Miller advised the patient to take supplements, including vitamin D and C, zinc, and melatonin, and he prescribed ivermectin, dexamethasone, and azithromycin. He did not perform an exam, verify the information that the patient had provided, advise the patient regarding interactions, or order follow-up testing, the report states.
Other charges against Mr. Miller include harassing hospital staff by making threatening statements about hospitals and doctors who treat COVID-19 patients and misrepresenting his original 2013 license application. He denied on the application that he was being investigated by another licensing board. At the time, the California Physician Assistant Board was investigating him for providing medical care and prescribing without a supervising doctor’s authorization and without conducting physical exams, among other charges.
A version of this article first appeared on Medscape.com.
The suspension stemmed from allegations against Scott C. Miller, PA-C, by at least six COVID patients, including some who weren’t his patients or whom he never examined and a few who later died from the virus, according to the Washington Medical Commission.
“Miller’s treatment of COVID-19 patients fell below the standard of care,” the suspension report states. “Miller began a public campaign promoting ivermectin as a curative for COVID-19, and prescribing it without adequate examination to at least one person, with no reliable clinical studies that establish its efficacy in preventing or treating COVID-19.”
Mr. Miller has until early November to respond to the allegations. On his clinic’s website, Mr. Miller stated, “In response to the charges, I want to reassure all of you that the initial attacks against me have been brought on by a small handful of people that have no ties to our medical practice, and by pharmacies and hospitals that have a zero tolerance policy on family members asking that I help them advocate for loved ones that have been admitted and written off in our current system of dismissiveness and neglect.”
Mr. Miller also expressed gratitude for the support he has received recently. A GoFundMe campaign to raise money for Mr. Miller’s legal fund had raised more than $59,000 at press time. His GoFundMe page had been shared 2,400 times. He has more than 550 followers and more than 400 donors.
“I don’t know that I have the words to adequately describe the deep sense of love and connection I have received from you, the families I serve, and those that have reached out to me in this deeply challenging time,” he wrote on the clinic website.
Mr. Miller has spoken publicly about his anti-mask views and his support for ivermectin, according to the commission report. As part of the suspension, he was charged with making “misleading representations regarding the efficacy of non-FDA approved treatment and mask use.”
In one case that was cited in the report, a 39-year-old patient contacted the pediatric clinic, and Mr. Miller spoke with the patient by phone. The patient reported that he had tested positive for COVID. Mr. Miller advised the patient to take supplements, including vitamin D and C, zinc, and melatonin, and he prescribed ivermectin, dexamethasone, and azithromycin. He did not perform an exam, verify the information that the patient had provided, advise the patient regarding interactions, or order follow-up testing, the report states.
Other charges against Mr. Miller include harassing hospital staff by making threatening statements about hospitals and doctors who treat COVID-19 patients and misrepresenting his original 2013 license application. He denied on the application that he was being investigated by another licensing board. At the time, the California Physician Assistant Board was investigating him for providing medical care and prescribing without a supervising doctor’s authorization and without conducting physical exams, among other charges.
A version of this article first appeared on Medscape.com.
Facing Up to the Diagnosis
ANSWER
All of these items were rightly considered to be in the differential for this lesion, so the answer is choice “f.”
DISCUSSION
Individuals with type IV skin are less likely than those with types II and III to develop skin cancer. So, although cancer was definitely in the differential, the other items were considered just as, if not more, likely in this case.
The only way to sort through these diagnostic possibilities was to perform a biopsy. In this case, the entire lesion was removed by saucerization technique, under local anesthesia. The specimen provided would be adequate to detect any cancer, which a smaller specimen could easily miss.
The pathology results showed pigmented basal cell carcinoma. Given the patient’s extensive history of sun exposure, and the steady growth of the lesion, this was hardly a surprise. But prior to the biopsy, one could just as easily imagine the lesion to be, for example, a wart.
The take-home message is obvious: Nothing can take the place of biopsy in establishing a precise diagnosis. With that information in hand, the patient was referred for consultation with a Mohs surgeon. Surgical removal and closure would likely set him back several thousand dollars and leave a considerable scar.
ANSWER
All of these items were rightly considered to be in the differential for this lesion, so the answer is choice “f.”
DISCUSSION
Individuals with type IV skin are less likely than those with types II and III to develop skin cancer. So, although cancer was definitely in the differential, the other items were considered just as, if not more, likely in this case.
The only way to sort through these diagnostic possibilities was to perform a biopsy. In this case, the entire lesion was removed by saucerization technique, under local anesthesia. The specimen provided would be adequate to detect any cancer, which a smaller specimen could easily miss.
The pathology results showed pigmented basal cell carcinoma. Given the patient’s extensive history of sun exposure, and the steady growth of the lesion, this was hardly a surprise. But prior to the biopsy, one could just as easily imagine the lesion to be, for example, a wart.
The take-home message is obvious: Nothing can take the place of biopsy in establishing a precise diagnosis. With that information in hand, the patient was referred for consultation with a Mohs surgeon. Surgical removal and closure would likely set him back several thousand dollars and leave a considerable scar.
ANSWER
All of these items were rightly considered to be in the differential for this lesion, so the answer is choice “f.”
DISCUSSION
Individuals with type IV skin are less likely than those with types II and III to develop skin cancer. So, although cancer was definitely in the differential, the other items were considered just as, if not more, likely in this case.
The only way to sort through these diagnostic possibilities was to perform a biopsy. In this case, the entire lesion was removed by saucerization technique, under local anesthesia. The specimen provided would be adequate to detect any cancer, which a smaller specimen could easily miss.
The pathology results showed pigmented basal cell carcinoma. Given the patient’s extensive history of sun exposure, and the steady growth of the lesion, this was hardly a surprise. But prior to the biopsy, one could just as easily imagine the lesion to be, for example, a wart.
The take-home message is obvious: Nothing can take the place of biopsy in establishing a precise diagnosis. With that information in hand, the patient was referred for consultation with a Mohs surgeon. Surgical removal and closure would likely set him back several thousand dollars and leave a considerable scar.

“Like a berry,” was how a 38-year-old Hispanic man described the lesion that had been slowly growing on his face for 4 years. His family was alarmed by it, but he reasoned that since it didn’t hurt and the surrounding area wasn’t especially red, it likely wasn’t much of a problem.
The patient worked as roofer up to 7 days per week when the weather was good and had been doing so since he was old enough to work. He had no insurance and was not inclined to spend money on a health care visit. When his wife finally convinced him to go to the urgent care clinic, he paid $100 just to be told he needed to see a dermatologist. He was so disgusted he almost refused to wait the 6 weeks it took to get into the dermatology office.
The patient, who had type IV skin with little evidence of sun damage, had an obvious, large, coarsely mamillated nodule on the left upper nasolabial area. The lesion measured 1.8 cm and was reddish blue. It was moderately firm, but no increased warmth could be detected. No nodes could be felt in the area. His skin elsewhere was free of any notable changes.

Mortality in 2nd wave higher with ECMO for COVID-ARDS
For patients with refractory acute respiratory distress syndrome (ARDS) caused by COVID-19 infections, extracorporeal membrane oxygenation (ECMO) may be the treatment of last resort.
But for reasons that aren’t clear, in the second wave of the COVID-19 pandemic at a major teaching hospital, the mortality rate of patients on ECMO for COVID-induced ARDS was significantly higher than it was during the first wave, despite changes in drug therapy and clinical management, reported Rohit Reddy, BS, a second-year medical student, and colleagues at Thomas Jefferson University Hospital in Philadelphia.
During the first wave, from April to September 2020, the survival rate of patients while on ECMO in their ICUs was 67%. In contrast, for patients treated during the second wave, from November 2020 to March 2021, the ECMO survival rate was 31% (P = .003).
The 30-day survival rates were also higher in the first wave compared with the second, at 54% versus 31%, but this difference was not statistically significant.
“More research is required to develop stricter inclusion/exclusion criteria and to improve pre-ECMO management in order to improve outcomes,” Mr. Reddy said in a narrated poster presented at the annual meeting of the American College of Chest Physicians, held virtually this year.
ARDS severity higher
ARDS is a major complication of COVID-19 infections, and there is evidence to suggest that COVID-associated ARDS is more severe than ARDS caused by other causes, the investigators noted.
“ECMO, which has been used as a rescue therapy in prior viral outbreaks, has been used to support certain patients with refractory ARDS due to COVID-19, but evidence for its efficacy is limited. Respiratory failure remained a highly concerning complication in the second wave of the COVID-19 pandemic, but it is unclear how the evolution of the disease and pharmacologic utility has affected the clinical utility of ECMO,” Mr. Reddy said.
To see whether changes in disease course or in treatment could explain changes in outcomes for patients with COVID-related ARDS, the investigators compared characteristics and outcomes for patients treated in the first versus second waves of the pandemic. Their study did not include data from patients infected with the Delta variant of the SARS-CoV-2 virus, which became the predominant viral strain later in 2021.
The study included data on 28 patients treated during the first wave, and 13 during the second. The sample included 28 men and 13 women with a mean age of 51 years.
All patients had venovenous ECMO, with cannulation in the femoral or internal jugular veins; some patients received ECMO via a single double-lumen cannula.
There were no significant differences between the two time periods in patient comorbidities prior to initiation of ECMO.
Patients in the second wave were significantly more likely to receive steroids (54% vs. 100%; P = .003) and remdesivir (39% vs. 85%; P = .007). Prone positioning before ECMO was also significantly more frequent in the second wave (11% vs. 85%; P < .001).
Patients in the second wave stayed on ECMO longer – median 20 days versus 14 days for first-wave patients – but as noted before, ECMO mortality rates were significantly higher during the second wave. During the first wave, 33% of patients died while on ECMO, compared with 69% in the second wave (P = .03). Respective 30-day mortality rates were 46% versus 69% (ns).
Rates of complications during ECMO were generally comparable between the groups, including acute renal failure (39% in the first wave vs 38% in the second), sepsis (32% vs. 23%), bacterial pneumonia (11% vs. 8%), and gastrointestinal bleeding (21% vs. 15%). However, significantly more patients in the second wave had cerebral vascular accidents (4% vs. 23%; P = .050).
Senior author Hitoshi Hirose, MD, PhD, professor of surgery at Thomas Jefferson University, said in an interview that the difference in outcomes was likely caused by changes in pre-ECMO therapy between the first and second waves.
“Our study showed the incidence of sepsis had a large impact on the patient outcomes,” he wrote. “We speculate that sepsis was attributed to use of immune modulation therapy. The prevention of the sepsis would be key to improve survival of ECMO for COVID 19.”
“It’s possible that the explanation for this is that patients in the second wave were sicker in a way that wasn’t adequately measured in the first wave,” CHEST 2021 program cochair Christopher Carroll, MD, FCCP, from Connecticut Children’s Medical Center in Hartford, said in an interview.
The differences may also have been attributable to changes in virulence, or to clinical decisions to put sicker patients on ECMO, he said.
Casey Cable, MD, MSc, a pulmonary disease and critical care specialist at Virginia Commonwealth Medical Center in Richmond, also speculated in an interview that second-wave patients may have been sicker.
“One interesting piece of this story is that we now know a lot more – we know about the use of steroids plus or minus remdesivir and proning, and patients received a large majority of those treatments but still got put on ECMO,” she said. “I wonder if there is a subset of really sick patients, and no matter what we treat with – steroids, proning – whatever we do they’re just not going to do well.”
Both Dr. Carroll and Dr. Cable emphasized the importance of ECMO as a rescue therapy for patients with severe, refractory ARDS associated with COVID-19 or other diseases.
Neither Dr. Carroll nor Dr. Cable were involved in the study.
No study funding was reported. Mr. Reddy, Dr. Hirose, Dr. Carroll, and Dr. Cable disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
For patients with refractory acute respiratory distress syndrome (ARDS) caused by COVID-19 infections, extracorporeal membrane oxygenation (ECMO) may be the treatment of last resort.
But for reasons that aren’t clear, in the second wave of the COVID-19 pandemic at a major teaching hospital, the mortality rate of patients on ECMO for COVID-induced ARDS was significantly higher than it was during the first wave, despite changes in drug therapy and clinical management, reported Rohit Reddy, BS, a second-year medical student, and colleagues at Thomas Jefferson University Hospital in Philadelphia.
During the first wave, from April to September 2020, the survival rate of patients while on ECMO in their ICUs was 67%. In contrast, for patients treated during the second wave, from November 2020 to March 2021, the ECMO survival rate was 31% (P = .003).
The 30-day survival rates were also higher in the first wave compared with the second, at 54% versus 31%, but this difference was not statistically significant.
“More research is required to develop stricter inclusion/exclusion criteria and to improve pre-ECMO management in order to improve outcomes,” Mr. Reddy said in a narrated poster presented at the annual meeting of the American College of Chest Physicians, held virtually this year.
ARDS severity higher
ARDS is a major complication of COVID-19 infections, and there is evidence to suggest that COVID-associated ARDS is more severe than ARDS caused by other causes, the investigators noted.
“ECMO, which has been used as a rescue therapy in prior viral outbreaks, has been used to support certain patients with refractory ARDS due to COVID-19, but evidence for its efficacy is limited. Respiratory failure remained a highly concerning complication in the second wave of the COVID-19 pandemic, but it is unclear how the evolution of the disease and pharmacologic utility has affected the clinical utility of ECMO,” Mr. Reddy said.
To see whether changes in disease course or in treatment could explain changes in outcomes for patients with COVID-related ARDS, the investigators compared characteristics and outcomes for patients treated in the first versus second waves of the pandemic. Their study did not include data from patients infected with the Delta variant of the SARS-CoV-2 virus, which became the predominant viral strain later in 2021.
The study included data on 28 patients treated during the first wave, and 13 during the second. The sample included 28 men and 13 women with a mean age of 51 years.
All patients had venovenous ECMO, with cannulation in the femoral or internal jugular veins; some patients received ECMO via a single double-lumen cannula.
There were no significant differences between the two time periods in patient comorbidities prior to initiation of ECMO.
Patients in the second wave were significantly more likely to receive steroids (54% vs. 100%; P = .003) and remdesivir (39% vs. 85%; P = .007). Prone positioning before ECMO was also significantly more frequent in the second wave (11% vs. 85%; P < .001).
Patients in the second wave stayed on ECMO longer – median 20 days versus 14 days for first-wave patients – but as noted before, ECMO mortality rates were significantly higher during the second wave. During the first wave, 33% of patients died while on ECMO, compared with 69% in the second wave (P = .03). Respective 30-day mortality rates were 46% versus 69% (ns).
Rates of complications during ECMO were generally comparable between the groups, including acute renal failure (39% in the first wave vs 38% in the second), sepsis (32% vs. 23%), bacterial pneumonia (11% vs. 8%), and gastrointestinal bleeding (21% vs. 15%). However, significantly more patients in the second wave had cerebral vascular accidents (4% vs. 23%; P = .050).
Senior author Hitoshi Hirose, MD, PhD, professor of surgery at Thomas Jefferson University, said in an interview that the difference in outcomes was likely caused by changes in pre-ECMO therapy between the first and second waves.
“Our study showed the incidence of sepsis had a large impact on the patient outcomes,” he wrote. “We speculate that sepsis was attributed to use of immune modulation therapy. The prevention of the sepsis would be key to improve survival of ECMO for COVID 19.”
“It’s possible that the explanation for this is that patients in the second wave were sicker in a way that wasn’t adequately measured in the first wave,” CHEST 2021 program cochair Christopher Carroll, MD, FCCP, from Connecticut Children’s Medical Center in Hartford, said in an interview.
The differences may also have been attributable to changes in virulence, or to clinical decisions to put sicker patients on ECMO, he said.
Casey Cable, MD, MSc, a pulmonary disease and critical care specialist at Virginia Commonwealth Medical Center in Richmond, also speculated in an interview that second-wave patients may have been sicker.
“One interesting piece of this story is that we now know a lot more – we know about the use of steroids plus or minus remdesivir and proning, and patients received a large majority of those treatments but still got put on ECMO,” she said. “I wonder if there is a subset of really sick patients, and no matter what we treat with – steroids, proning – whatever we do they’re just not going to do well.”
Both Dr. Carroll and Dr. Cable emphasized the importance of ECMO as a rescue therapy for patients with severe, refractory ARDS associated with COVID-19 or other diseases.
Neither Dr. Carroll nor Dr. Cable were involved in the study.
No study funding was reported. Mr. Reddy, Dr. Hirose, Dr. Carroll, and Dr. Cable disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
For patients with refractory acute respiratory distress syndrome (ARDS) caused by COVID-19 infections, extracorporeal membrane oxygenation (ECMO) may be the treatment of last resort.
But for reasons that aren’t clear, in the second wave of the COVID-19 pandemic at a major teaching hospital, the mortality rate of patients on ECMO for COVID-induced ARDS was significantly higher than it was during the first wave, despite changes in drug therapy and clinical management, reported Rohit Reddy, BS, a second-year medical student, and colleagues at Thomas Jefferson University Hospital in Philadelphia.
During the first wave, from April to September 2020, the survival rate of patients while on ECMO in their ICUs was 67%. In contrast, for patients treated during the second wave, from November 2020 to March 2021, the ECMO survival rate was 31% (P = .003).
The 30-day survival rates were also higher in the first wave compared with the second, at 54% versus 31%, but this difference was not statistically significant.
“More research is required to develop stricter inclusion/exclusion criteria and to improve pre-ECMO management in order to improve outcomes,” Mr. Reddy said in a narrated poster presented at the annual meeting of the American College of Chest Physicians, held virtually this year.
ARDS severity higher
ARDS is a major complication of COVID-19 infections, and there is evidence to suggest that COVID-associated ARDS is more severe than ARDS caused by other causes, the investigators noted.
“ECMO, which has been used as a rescue therapy in prior viral outbreaks, has been used to support certain patients with refractory ARDS due to COVID-19, but evidence for its efficacy is limited. Respiratory failure remained a highly concerning complication in the second wave of the COVID-19 pandemic, but it is unclear how the evolution of the disease and pharmacologic utility has affected the clinical utility of ECMO,” Mr. Reddy said.
To see whether changes in disease course or in treatment could explain changes in outcomes for patients with COVID-related ARDS, the investigators compared characteristics and outcomes for patients treated in the first versus second waves of the pandemic. Their study did not include data from patients infected with the Delta variant of the SARS-CoV-2 virus, which became the predominant viral strain later in 2021.
The study included data on 28 patients treated during the first wave, and 13 during the second. The sample included 28 men and 13 women with a mean age of 51 years.
All patients had venovenous ECMO, with cannulation in the femoral or internal jugular veins; some patients received ECMO via a single double-lumen cannula.
There were no significant differences between the two time periods in patient comorbidities prior to initiation of ECMO.
Patients in the second wave were significantly more likely to receive steroids (54% vs. 100%; P = .003) and remdesivir (39% vs. 85%; P = .007). Prone positioning before ECMO was also significantly more frequent in the second wave (11% vs. 85%; P < .001).
Patients in the second wave stayed on ECMO longer – median 20 days versus 14 days for first-wave patients – but as noted before, ECMO mortality rates were significantly higher during the second wave. During the first wave, 33% of patients died while on ECMO, compared with 69% in the second wave (P = .03). Respective 30-day mortality rates were 46% versus 69% (ns).
Rates of complications during ECMO were generally comparable between the groups, including acute renal failure (39% in the first wave vs 38% in the second), sepsis (32% vs. 23%), bacterial pneumonia (11% vs. 8%), and gastrointestinal bleeding (21% vs. 15%). However, significantly more patients in the second wave had cerebral vascular accidents (4% vs. 23%; P = .050).
Senior author Hitoshi Hirose, MD, PhD, professor of surgery at Thomas Jefferson University, said in an interview that the difference in outcomes was likely caused by changes in pre-ECMO therapy between the first and second waves.
“Our study showed the incidence of sepsis had a large impact on the patient outcomes,” he wrote. “We speculate that sepsis was attributed to use of immune modulation therapy. The prevention of the sepsis would be key to improve survival of ECMO for COVID 19.”
“It’s possible that the explanation for this is that patients in the second wave were sicker in a way that wasn’t adequately measured in the first wave,” CHEST 2021 program cochair Christopher Carroll, MD, FCCP, from Connecticut Children’s Medical Center in Hartford, said in an interview.
The differences may also have been attributable to changes in virulence, or to clinical decisions to put sicker patients on ECMO, he said.
Casey Cable, MD, MSc, a pulmonary disease and critical care specialist at Virginia Commonwealth Medical Center in Richmond, also speculated in an interview that second-wave patients may have been sicker.
“One interesting piece of this story is that we now know a lot more – we know about the use of steroids plus or minus remdesivir and proning, and patients received a large majority of those treatments but still got put on ECMO,” she said. “I wonder if there is a subset of really sick patients, and no matter what we treat with – steroids, proning – whatever we do they’re just not going to do well.”
Both Dr. Carroll and Dr. Cable emphasized the importance of ECMO as a rescue therapy for patients with severe, refractory ARDS associated with COVID-19 or other diseases.
Neither Dr. Carroll nor Dr. Cable were involved in the study.
No study funding was reported. Mr. Reddy, Dr. Hirose, Dr. Carroll, and Dr. Cable disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
States can reserve COVID shots for kids 5-11 this week
States can preorder COVID-19 vaccine doses for younger children this week as they begin to set up vaccination campaigns for ages 5-11.
Vaccine advisory groups for the FDA and CDC are scheduled to discuss and approve the Pfizer shot for kids in the next three weeks. To help states and cities prepare for the rollout, the CDC issued guidance on how to set up expanded vaccination programs.
Immunization program managers can begin ordering doses on Wednesday, according to the guidance. The vials won’t be delivered until the FDA and CDC authorize the shot, but registering now will help federal officials ship doses quickly once they’re available.
Pharmacies in every state will be able to give COVID-19 shots to children, but they can only use doses that are prepared specifically for children. Ages 5-11 will need a 10-microgram dose, which is one-third of the dose administered to ages 12 and older. The guidance warns that doctors should not try to split up or fraction the adult doses.
The CDC guidance also recommends that pediatricians and family practice doctors should serve as primary places to give shots to kids. The document mentions other options, such as vaccination clinics at schools, but doesn’t endorse them as the first choice for vaccinating kids.
The CDC hasn’t yet addressed questions around whether kids should be required to get vaccinated to attend school. The decision will likely be left to state and city officials.
Federal health officials aren’t yet sure how many parents and guardians will seek shots for their younger kids right away, the AP reported. Demand may be high at first for some families, but it may not be as high as when shots first became available for adults, Marcus Plescia, MD, chief medical officer of the Association of State and Territorial Health Officials, told The Associated Press.
“We’re going to have potentially a very busy, and perhaps modestly chaotic time,” he said.
When vaccines were first authorized for adults, hospitals and pharmacies received priority for ordering shots. Some doctors felt left out. This time, however, the CDC has said that pediatricians will receive higher priority and be able to receive shipments quickly.
As the vaccine rollout begins, health officials should consider logistical concerns to address racial and economic disparities for younger kids, Richard Besser, MD, president and CEO of the Robert Wood Johnson Foundation and a former acting director of the CDC, told the AP.
If parents or guardians can’t leave work to take their kids to a pharmacy or doctor’s office, for instance, their kids may not receive a shot quickly – or at all.
“It’s really important that we recognize the barriers to vaccinations,” he said.
A version of this article first appeared on WebMD.com.
States can preorder COVID-19 vaccine doses for younger children this week as they begin to set up vaccination campaigns for ages 5-11.
Vaccine advisory groups for the FDA and CDC are scheduled to discuss and approve the Pfizer shot for kids in the next three weeks. To help states and cities prepare for the rollout, the CDC issued guidance on how to set up expanded vaccination programs.
Immunization program managers can begin ordering doses on Wednesday, according to the guidance. The vials won’t be delivered until the FDA and CDC authorize the shot, but registering now will help federal officials ship doses quickly once they’re available.
Pharmacies in every state will be able to give COVID-19 shots to children, but they can only use doses that are prepared specifically for children. Ages 5-11 will need a 10-microgram dose, which is one-third of the dose administered to ages 12 and older. The guidance warns that doctors should not try to split up or fraction the adult doses.
The CDC guidance also recommends that pediatricians and family practice doctors should serve as primary places to give shots to kids. The document mentions other options, such as vaccination clinics at schools, but doesn’t endorse them as the first choice for vaccinating kids.
The CDC hasn’t yet addressed questions around whether kids should be required to get vaccinated to attend school. The decision will likely be left to state and city officials.
Federal health officials aren’t yet sure how many parents and guardians will seek shots for their younger kids right away, the AP reported. Demand may be high at first for some families, but it may not be as high as when shots first became available for adults, Marcus Plescia, MD, chief medical officer of the Association of State and Territorial Health Officials, told The Associated Press.
“We’re going to have potentially a very busy, and perhaps modestly chaotic time,” he said.
When vaccines were first authorized for adults, hospitals and pharmacies received priority for ordering shots. Some doctors felt left out. This time, however, the CDC has said that pediatricians will receive higher priority and be able to receive shipments quickly.
As the vaccine rollout begins, health officials should consider logistical concerns to address racial and economic disparities for younger kids, Richard Besser, MD, president and CEO of the Robert Wood Johnson Foundation and a former acting director of the CDC, told the AP.
If parents or guardians can’t leave work to take their kids to a pharmacy or doctor’s office, for instance, their kids may not receive a shot quickly – or at all.
“It’s really important that we recognize the barriers to vaccinations,” he said.
A version of this article first appeared on WebMD.com.
States can preorder COVID-19 vaccine doses for younger children this week as they begin to set up vaccination campaigns for ages 5-11.
Vaccine advisory groups for the FDA and CDC are scheduled to discuss and approve the Pfizer shot for kids in the next three weeks. To help states and cities prepare for the rollout, the CDC issued guidance on how to set up expanded vaccination programs.
Immunization program managers can begin ordering doses on Wednesday, according to the guidance. The vials won’t be delivered until the FDA and CDC authorize the shot, but registering now will help federal officials ship doses quickly once they’re available.
Pharmacies in every state will be able to give COVID-19 shots to children, but they can only use doses that are prepared specifically for children. Ages 5-11 will need a 10-microgram dose, which is one-third of the dose administered to ages 12 and older. The guidance warns that doctors should not try to split up or fraction the adult doses.
The CDC guidance also recommends that pediatricians and family practice doctors should serve as primary places to give shots to kids. The document mentions other options, such as vaccination clinics at schools, but doesn’t endorse them as the first choice for vaccinating kids.
The CDC hasn’t yet addressed questions around whether kids should be required to get vaccinated to attend school. The decision will likely be left to state and city officials.
Federal health officials aren’t yet sure how many parents and guardians will seek shots for their younger kids right away, the AP reported. Demand may be high at first for some families, but it may not be as high as when shots first became available for adults, Marcus Plescia, MD, chief medical officer of the Association of State and Territorial Health Officials, told The Associated Press.
“We’re going to have potentially a very busy, and perhaps modestly chaotic time,” he said.
When vaccines were first authorized for adults, hospitals and pharmacies received priority for ordering shots. Some doctors felt left out. This time, however, the CDC has said that pediatricians will receive higher priority and be able to receive shipments quickly.
As the vaccine rollout begins, health officials should consider logistical concerns to address racial and economic disparities for younger kids, Richard Besser, MD, president and CEO of the Robert Wood Johnson Foundation and a former acting director of the CDC, told the AP.
If parents or guardians can’t leave work to take their kids to a pharmacy or doctor’s office, for instance, their kids may not receive a shot quickly – or at all.
“It’s really important that we recognize the barriers to vaccinations,” he said.
A version of this article first appeared on WebMD.com.
COVID-19: Can doctors refuse to see unvaccinated patients?
In June, Gerald Bock, MD, a dermatologist in central California, instituted a new office policy: He would not be seeing any more patients who remain unvaccinated against COVID-19 in his practice.

“[It is] the height of self-centered and irresponsible behavior,” he told me. “People who come in unvaccinated, when vaccination is widely available, are stating that their personal preferences are more important than their health, and are more important than any risk that they may expose their friends and family to, and also to any risk they might present to my staff and me. We have gone to considerable effort and expense to diminish any risk that visiting our office might entail. I see no reason why we should tolerate this.”
Other doctors appear to be following in his footsteps. There is no question that physicians have the right to choose their patients, just as patients are free to choose their doctors, but That is a complicated question without a clear answer. In a statement on whether physicians can decline unvaccinated patients, the American Medical Association continues to maintain that “in general” a physician may not “ethically turn a patient away based solely on the individual’s infectious disease status,” but does concede that “the decision to accept or decline a patient must balance the urgency of the individual patient’s need; the risk the patient may pose to other patients in the physician’s practice; and the need for the physician and staff, to be available to provide care in the future.”
Medical ethics experts have offered varying opinions. Daniel Wikler, PhD, professor of ethics and population health at the Harvard School of Public Health, Boston, wrote in an op-ed in the Washington Post that “ignorance or other personal failing” should not be factors in the evaluation of patients for health care. He argues that “doctors and hospitals are not in the blame and punishment business. Nor should they be. That doctors treat sinners and responsible citizens alike is a noble tradition.”

Timothy Hoff, professor of management, healthcare systems, and health policy at Northeastern University, Boston, maintains that, in nonemergency situations, physicians are legally able to refuse patients for a variety of reasons, provided they are not doing so because of some aspect of the patient’s race, gender, sexuality, or religion. However, in the same Northeastern University news release,Robert Baginski, MD, the director of interdisciplinary affairs for the department of medical sciences at Northeastern, cautions that it is vital for health authorities to continue urging the public to get vaccinated, but not at the expense of care.
Arthur L. Caplan, PhD, the head of the division of medical ethics at New York University, said in a Medscape commentary, that the decision to refuse to see patients who can vaccinate, but choose not to, is justifiable. “If you’re trying to protect yourself, your staff, or other patients, I think you do have the right to not take on somebody who won’t vaccinate,” he writes. “This is somewhat similar to when pediatricians do not accept a family if they won’t give their kids the state-required shots to go to school. That’s been happening for many years now.
“I also think it is morally justified if they won’t take your advice,” he continues. “If they won’t follow what you think is the best healthcare for them [such as getting vaccinated], there’s not much point in building that relationship.”
The situation is different in ED and hospital settings, however. “It’s a little harder to use unvaccinated status when someone really is at death’s door,” Dr. Caplan pointed out. “When someone comes in very sick, or whatever the reason, I think we have to take care of them ethically, and legally we’re bound to get them stable in the emergency room. I do think different rules apply there.”
In the end, every private practitioner will have to make his or her own decision on this question. Dr. Bock feels he made the right one. “Since instituting the policy, we have written 55 refund checks for people who had paid for a series of cosmetic procedures. We have no idea how many people were deterred from making appointments. We’ve had several negative online reviews and one woman who wrote a letter to the Medical Board of California complaining that we were discriminating against her,” he said. He added, however, that “we’ve also had several patients who commented favorably about the policy. I have no regrets about instituting the policy, and would do it again.”
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, N.J. He is the author of numerous articles and textbook chapters, and is a longtime monthly columnist for Dermatology News. Write to him at [email protected].
In June, Gerald Bock, MD, a dermatologist in central California, instituted a new office policy: He would not be seeing any more patients who remain unvaccinated against COVID-19 in his practice.
“[It is] the height of self-centered and irresponsible behavior,” he told me. “People who come in unvaccinated, when vaccination is widely available, are stating that their personal preferences are more important than their health, and are more important than any risk that they may expose their friends and family to, and also to any risk they might present to my staff and me. We have gone to considerable effort and expense to diminish any risk that visiting our office might entail. I see no reason why we should tolerate this.”
Other doctors appear to be following in his footsteps. There is no question that physicians have the right to choose their patients, just as patients are free to choose their doctors, but That is a complicated question without a clear answer. In a statement on whether physicians can decline unvaccinated patients, the American Medical Association continues to maintain that “in general” a physician may not “ethically turn a patient away based solely on the individual’s infectious disease status,” but does concede that “the decision to accept or decline a patient must balance the urgency of the individual patient’s need; the risk the patient may pose to other patients in the physician’s practice; and the need for the physician and staff, to be available to provide care in the future.”
Medical ethics experts have offered varying opinions. Daniel Wikler, PhD, professor of ethics and population health at the Harvard School of Public Health, Boston, wrote in an op-ed in the Washington Post that “ignorance or other personal failing” should not be factors in the evaluation of patients for health care. He argues that “doctors and hospitals are not in the blame and punishment business. Nor should they be. That doctors treat sinners and responsible citizens alike is a noble tradition.”
Timothy Hoff, professor of management, healthcare systems, and health policy at Northeastern University, Boston, maintains that, in nonemergency situations, physicians are legally able to refuse patients for a variety of reasons, provided they are not doing so because of some aspect of the patient’s race, gender, sexuality, or religion. However, in the same Northeastern University news release,Robert Baginski, MD, the director of interdisciplinary affairs for the department of medical sciences at Northeastern, cautions that it is vital for health authorities to continue urging the public to get vaccinated, but not at the expense of care.
Arthur L. Caplan, PhD, the head of the division of medical ethics at New York University, said in a Medscape commentary, that the decision to refuse to see patients who can vaccinate, but choose not to, is justifiable. “If you’re trying to protect yourself, your staff, or other patients, I think you do have the right to not take on somebody who won’t vaccinate,” he writes. “This is somewhat similar to when pediatricians do not accept a family if they won’t give their kids the state-required shots to go to school. That’s been happening for many years now.
“I also think it is morally justified if they won’t take your advice,” he continues. “If they won’t follow what you think is the best healthcare for them [such as getting vaccinated], there’s not much point in building that relationship.”
The situation is different in ED and hospital settings, however. “It’s a little harder to use unvaccinated status when someone really is at death’s door,” Dr. Caplan pointed out. “When someone comes in very sick, or whatever the reason, I think we have to take care of them ethically, and legally we’re bound to get them stable in the emergency room. I do think different rules apply there.”
In the end, every private practitioner will have to make his or her own decision on this question. Dr. Bock feels he made the right one. “Since instituting the policy, we have written 55 refund checks for people who had paid for a series of cosmetic procedures. We have no idea how many people were deterred from making appointments. We’ve had several negative online reviews and one woman who wrote a letter to the Medical Board of California complaining that we were discriminating against her,” he said. He added, however, that “we’ve also had several patients who commented favorably about the policy. I have no regrets about instituting the policy, and would do it again.”
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, N.J. He is the author of numerous articles and textbook chapters, and is a longtime monthly columnist for Dermatology News. Write to him at [email protected].
In June, Gerald Bock, MD, a dermatologist in central California, instituted a new office policy: He would not be seeing any more patients who remain unvaccinated against COVID-19 in his practice.
“[It is] the height of self-centered and irresponsible behavior,” he told me. “People who come in unvaccinated, when vaccination is widely available, are stating that their personal preferences are more important than their health, and are more important than any risk that they may expose their friends and family to, and also to any risk they might present to my staff and me. We have gone to considerable effort and expense to diminish any risk that visiting our office might entail. I see no reason why we should tolerate this.”
Other doctors appear to be following in his footsteps. There is no question that physicians have the right to choose their patients, just as patients are free to choose their doctors, but That is a complicated question without a clear answer. In a statement on whether physicians can decline unvaccinated patients, the American Medical Association continues to maintain that “in general” a physician may not “ethically turn a patient away based solely on the individual’s infectious disease status,” but does concede that “the decision to accept or decline a patient must balance the urgency of the individual patient’s need; the risk the patient may pose to other patients in the physician’s practice; and the need for the physician and staff, to be available to provide care in the future.”
Medical ethics experts have offered varying opinions. Daniel Wikler, PhD, professor of ethics and population health at the Harvard School of Public Health, Boston, wrote in an op-ed in the Washington Post that “ignorance or other personal failing” should not be factors in the evaluation of patients for health care. He argues that “doctors and hospitals are not in the blame and punishment business. Nor should they be. That doctors treat sinners and responsible citizens alike is a noble tradition.”
Timothy Hoff, professor of management, healthcare systems, and health policy at Northeastern University, Boston, maintains that, in nonemergency situations, physicians are legally able to refuse patients for a variety of reasons, provided they are not doing so because of some aspect of the patient’s race, gender, sexuality, or religion. However, in the same Northeastern University news release,Robert Baginski, MD, the director of interdisciplinary affairs for the department of medical sciences at Northeastern, cautions that it is vital for health authorities to continue urging the public to get vaccinated, but not at the expense of care.
Arthur L. Caplan, PhD, the head of the division of medical ethics at New York University, said in a Medscape commentary, that the decision to refuse to see patients who can vaccinate, but choose not to, is justifiable. “If you’re trying to protect yourself, your staff, or other patients, I think you do have the right to not take on somebody who won’t vaccinate,” he writes. “This is somewhat similar to when pediatricians do not accept a family if they won’t give their kids the state-required shots to go to school. That’s been happening for many years now.
“I also think it is morally justified if they won’t take your advice,” he continues. “If they won’t follow what you think is the best healthcare for them [such as getting vaccinated], there’s not much point in building that relationship.”
The situation is different in ED and hospital settings, however. “It’s a little harder to use unvaccinated status when someone really is at death’s door,” Dr. Caplan pointed out. “When someone comes in very sick, or whatever the reason, I think we have to take care of them ethically, and legally we’re bound to get them stable in the emergency room. I do think different rules apply there.”
In the end, every private practitioner will have to make his or her own decision on this question. Dr. Bock feels he made the right one. “Since instituting the policy, we have written 55 refund checks for people who had paid for a series of cosmetic procedures. We have no idea how many people were deterred from making appointments. We’ve had several negative online reviews and one woman who wrote a letter to the Medical Board of California complaining that we were discriminating against her,” he said. He added, however, that “we’ve also had several patients who commented favorably about the policy. I have no regrets about instituting the policy, and would do it again.”
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, N.J. He is the author of numerous articles and textbook chapters, and is a longtime monthly columnist for Dermatology News. Write to him at [email protected].