User login
Formerly Skin & Allergy News
ass lick
assault rifle
balls
ballsac
black jack
bleach
Boko Haram
bondage
causas
cheap
child abuse
cocaine
compulsive behaviors
cost of miracles
cunt
Daech
display network stats
drug paraphernalia
explosion
fart
fda and death
fda AND warn
fda AND warning
fda AND warns
feom
fuck
gambling
gfc
gun
human trafficking
humira AND expensive
illegal
ISIL
ISIS
Islamic caliphate
Islamic state
madvocate
masturbation
mixed martial arts
MMA
molestation
national rifle association
NRA
nsfw
nuccitelli
pedophile
pedophilia
poker
porn
porn
pornography
psychedelic drug
recreational drug
sex slave rings
shit
slot machine
snort
substance abuse
terrorism
terrorist
texarkana
Texas hold 'em
UFC
section[contains(@class, 'nav-hidden')]
section[contains(@class, 'nav-hidden active')]
The leading independent newspaper covering dermatology news and commentary.
75-year-old White male presenting with progressive pruritus and a worsening rash
, although it can also be contracted through contaminated bedding and clothing. It can affect all races and ages.
Patients typically present with extremely pruritic, symmetric papules and excoriations. In nodular scabies, nodules and large papules are seen on exam. Thin lines in the skin called burrows may be present, especially in the webs between fingers. Female mites create burrows as they tunnel through the epidermis and lay eggs. The wrists, areola, waistline, and groin may all be involved, creating an imaginary circle between the areas described as the “circle of Hebra.” Penile and scrotal lesions are common in men.
Patients usually experience worse pruritus at night, which disturbs sleep. Crusted scabies is a severe form of scabies more often seen in those with immunocompromised immune systems. Clinically, thick crusted and scaly patches are present that are teeming with mites.
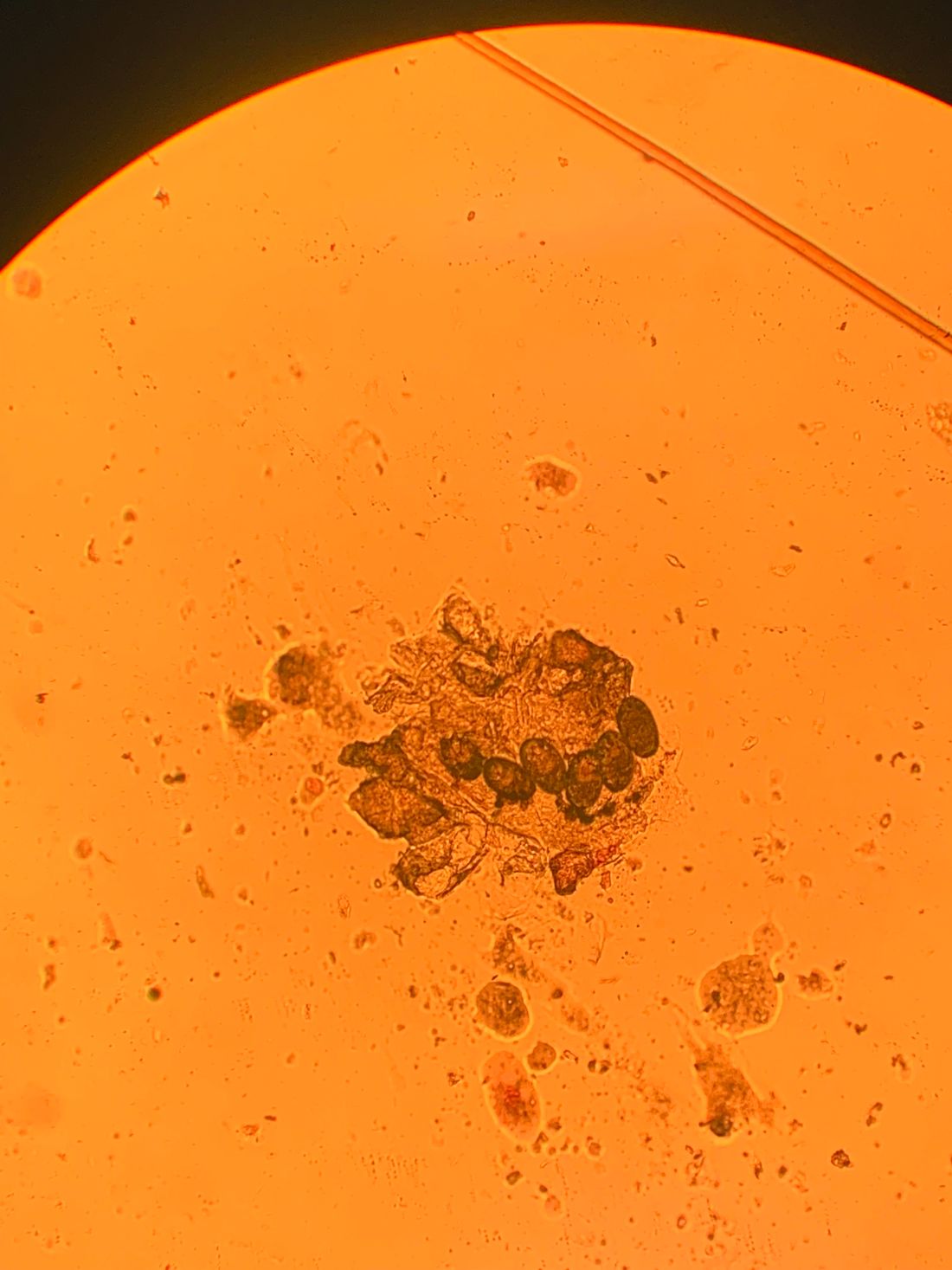
Diagnosis can be confirmed by performing a scabies prep, during which a burrow is scraped with a surgical blade. A drop of mineral oil is placed on the skin cells. The mite, ova, and feces can be visualized under the microscope. Wrists and hands usually have the highest yield for finding the parasites.

Topical treatments include permethrin 5% cream, lindane, benzyl benzoate, and crotamiton, and should be applied as two treatments a week apart. In the United States, permethrin is most commonly used. Ivermectin pills are used off label and are very effective and may be repeated for 1-2 weeks. All household contacts should be treated. Patients may still have pruritus for 2-4 weeks following treatment.
In this patient, a scabies prep was performed prior to performing repeat skin biopsies. Microscopic examination revealed ova, one mite, and feces. Treatment was initiated with ivermectin and permethrin.
Photos and case were submitted by Susannah Berke, MD, and Damon McClain, MD, Three Rivers Dermatology, Coraopolis, Pa.; and Dr. Bilu Martin.
Dr. Bilu Martin is a board-certified dermatologist in private practice at Premier Dermatology, MD, in Aventura, Fla. More diagnostic cases are available at mdedge.com/dermatology. To submit a case for possible publication, send an email to [email protected].
, although it can also be contracted through contaminated bedding and clothing. It can affect all races and ages.
Patients typically present with extremely pruritic, symmetric papules and excoriations. In nodular scabies, nodules and large papules are seen on exam. Thin lines in the skin called burrows may be present, especially in the webs between fingers. Female mites create burrows as they tunnel through the epidermis and lay eggs. The wrists, areola, waistline, and groin may all be involved, creating an imaginary circle between the areas described as the “circle of Hebra.” Penile and scrotal lesions are common in men.
Patients usually experience worse pruritus at night, which disturbs sleep. Crusted scabies is a severe form of scabies more often seen in those with immunocompromised immune systems. Clinically, thick crusted and scaly patches are present that are teeming with mites.
Diagnosis can be confirmed by performing a scabies prep, during which a burrow is scraped with a surgical blade. A drop of mineral oil is placed on the skin cells. The mite, ova, and feces can be visualized under the microscope. Wrists and hands usually have the highest yield for finding the parasites.
Topical treatments include permethrin 5% cream, lindane, benzyl benzoate, and crotamiton, and should be applied as two treatments a week apart. In the United States, permethrin is most commonly used. Ivermectin pills are used off label and are very effective and may be repeated for 1-2 weeks. All household contacts should be treated. Patients may still have pruritus for 2-4 weeks following treatment.
In this patient, a scabies prep was performed prior to performing repeat skin biopsies. Microscopic examination revealed ova, one mite, and feces. Treatment was initiated with ivermectin and permethrin.
Photos and case were submitted by Susannah Berke, MD, and Damon McClain, MD, Three Rivers Dermatology, Coraopolis, Pa.; and Dr. Bilu Martin.
Dr. Bilu Martin is a board-certified dermatologist in private practice at Premier Dermatology, MD, in Aventura, Fla. More diagnostic cases are available at mdedge.com/dermatology. To submit a case for possible publication, send an email to [email protected].
, although it can also be contracted through contaminated bedding and clothing. It can affect all races and ages.
Patients typically present with extremely pruritic, symmetric papules and excoriations. In nodular scabies, nodules and large papules are seen on exam. Thin lines in the skin called burrows may be present, especially in the webs between fingers. Female mites create burrows as they tunnel through the epidermis and lay eggs. The wrists, areola, waistline, and groin may all be involved, creating an imaginary circle between the areas described as the “circle of Hebra.” Penile and scrotal lesions are common in men.
Patients usually experience worse pruritus at night, which disturbs sleep. Crusted scabies is a severe form of scabies more often seen in those with immunocompromised immune systems. Clinically, thick crusted and scaly patches are present that are teeming with mites.
Diagnosis can be confirmed by performing a scabies prep, during which a burrow is scraped with a surgical blade. A drop of mineral oil is placed on the skin cells. The mite, ova, and feces can be visualized under the microscope. Wrists and hands usually have the highest yield for finding the parasites.
Topical treatments include permethrin 5% cream, lindane, benzyl benzoate, and crotamiton, and should be applied as two treatments a week apart. In the United States, permethrin is most commonly used. Ivermectin pills are used off label and are very effective and may be repeated for 1-2 weeks. All household contacts should be treated. Patients may still have pruritus for 2-4 weeks following treatment.
In this patient, a scabies prep was performed prior to performing repeat skin biopsies. Microscopic examination revealed ova, one mite, and feces. Treatment was initiated with ivermectin and permethrin.
Photos and case were submitted by Susannah Berke, MD, and Damon McClain, MD, Three Rivers Dermatology, Coraopolis, Pa.; and Dr. Bilu Martin.
Dr. Bilu Martin is a board-certified dermatologist in private practice at Premier Dermatology, MD, in Aventura, Fla. More diagnostic cases are available at mdedge.com/dermatology. To submit a case for possible publication, send an email to [email protected].

Hand eczema and atopic dermatitis closely linked
An estimated (AD), according to Jacob P. Thyssen, MD, PhD.
“If we look at individuals with AD, the lifetime prevalence of hand eczema reaches 50%, so we see a strong association between hand eczema and AD,” Dr. Thyssen, professor of dermatology at the University of Copenhagen, said at the Revolutionizing Atopic Dermatitis symposium.
Risk factors for hand eczema – defined as eczema on the hand and/or wrists – include AD, which increases the risk by two- to threefold, as well as genetic predisposition beyond AD, exposure to irritants and allergens, female gender, young age, low socioeconomic group, high risk occupations (including construction workers and hairdressers), and tobacco smoking.
“As clinicians, we sometimes need to rule out a few differentials, including psoriasis and T-cell lymphoma. As an example, 10% of T-cell lymphoma patients, a very rare condition, have first onset of the disease on their hands,” Dr. Thyssen said. “Once we see persistent hand eczema, we need to obtain a history of irritant exposure and allergen exposure, both at home and at work, perform a patch test, sometimes a skin prick test, and ask about personal and family history of AD and psoriasis.”
He noted that while formal classification of hand eczema has been a struggle for decades, he favors the “straightforward” clinical approach from the European Environmental and Contact Dermatitis Research Group. Atopic hand eczema, he said, “is very much characterized by dorsal involvement of the hands and fingers and sparse involvement of the palmar aspects of the hands.”
The cheeks and hands are predilection sites for AD in filaggrin mutation carriers (as they are sites of low filaggrin levels), and sometimes harsh environmental exposures, such as cold and dry air. In a study of 3,335 patients in Denmark, Dr. Thyssen and colleagues found that filaggrin mutations and AD were associated with early-onset and persistent hand eczema. In another study of 3,834 adults with AD or psoriasis, he and colleagues found that among those with AD, the wrists, back of the hands, and interdigital areas were often sites of severe eczema, while palmar involvement was more uncommon.
The same findings apply for the feet in filaggrin mutation carriers with AD; the dorsal aspect of the feet was more commonly affected, compared with plantar aspects of the feet.
Medical literature regarding foot eczema is scarce, but a retrospective cohort study from Germany found that foot eczema and hand eczema often co-occur. Among 723 hand eczema patients, 201 (28%) had concomitant foot eczema. The same morphological features were found on the hands and feet in 71% of patients. Foot eczema was significantly associated with male sex, atopic hand eczema, hyperhidrosis, wearing of safety shoes/boots at work, and tobacco smoking.
In addition, a systematic review and meta-analysis of studies of hand eczema and AD found that there was a 4.29-fold increased risk of hand eczema in individuals with AD, and the risk (lifetime prevalence) of occupational hand eczema was increased by more than twofold. “However, this study could not differentiate between irritant contact dermatitis on the hands and atopic dermatitis,” Dr. Thyssen said. “The studies were not accurate enough to allow for any conclusions.”
A multicenter study of adults with hand eczema in Italy found that the proportion of patients with AD was the highest among those with severe and refractory chronic hand eczema. In addition, certain professions, including those of hairdressers, health professionals, and those in trade work, such as plumbing, were more often associated with chronic hand eczema. “This teaches us that we should be very careful about steering these patients from at-risk occupations,” Dr. Thyssen said. “Also, we should remember to treat them aggressively in the beginning to reduce the risk of severe and refractory chronic hand eczema.”
Dr. Thyssen disclosed that he is a speaker, advisory board member, and/or investigator for Asian, Arena, Almirall, AbbVie, Eli Lilly, LEO Pharma, Pfizer, Regeneron, and Sanofi Genzyme.
An estimated (AD), according to Jacob P. Thyssen, MD, PhD.
“If we look at individuals with AD, the lifetime prevalence of hand eczema reaches 50%, so we see a strong association between hand eczema and AD,” Dr. Thyssen, professor of dermatology at the University of Copenhagen, said at the Revolutionizing Atopic Dermatitis symposium.
Risk factors for hand eczema – defined as eczema on the hand and/or wrists – include AD, which increases the risk by two- to threefold, as well as genetic predisposition beyond AD, exposure to irritants and allergens, female gender, young age, low socioeconomic group, high risk occupations (including construction workers and hairdressers), and tobacco smoking.
“As clinicians, we sometimes need to rule out a few differentials, including psoriasis and T-cell lymphoma. As an example, 10% of T-cell lymphoma patients, a very rare condition, have first onset of the disease on their hands,” Dr. Thyssen said. “Once we see persistent hand eczema, we need to obtain a history of irritant exposure and allergen exposure, both at home and at work, perform a patch test, sometimes a skin prick test, and ask about personal and family history of AD and psoriasis.”
He noted that while formal classification of hand eczema has been a struggle for decades, he favors the “straightforward” clinical approach from the European Environmental and Contact Dermatitis Research Group. Atopic hand eczema, he said, “is very much characterized by dorsal involvement of the hands and fingers and sparse involvement of the palmar aspects of the hands.”
The cheeks and hands are predilection sites for AD in filaggrin mutation carriers (as they are sites of low filaggrin levels), and sometimes harsh environmental exposures, such as cold and dry air. In a study of 3,335 patients in Denmark, Dr. Thyssen and colleagues found that filaggrin mutations and AD were associated with early-onset and persistent hand eczema. In another study of 3,834 adults with AD or psoriasis, he and colleagues found that among those with AD, the wrists, back of the hands, and interdigital areas were often sites of severe eczema, while palmar involvement was more uncommon.
The same findings apply for the feet in filaggrin mutation carriers with AD; the dorsal aspect of the feet was more commonly affected, compared with plantar aspects of the feet.
Medical literature regarding foot eczema is scarce, but a retrospective cohort study from Germany found that foot eczema and hand eczema often co-occur. Among 723 hand eczema patients, 201 (28%) had concomitant foot eczema. The same morphological features were found on the hands and feet in 71% of patients. Foot eczema was significantly associated with male sex, atopic hand eczema, hyperhidrosis, wearing of safety shoes/boots at work, and tobacco smoking.
In addition, a systematic review and meta-analysis of studies of hand eczema and AD found that there was a 4.29-fold increased risk of hand eczema in individuals with AD, and the risk (lifetime prevalence) of occupational hand eczema was increased by more than twofold. “However, this study could not differentiate between irritant contact dermatitis on the hands and atopic dermatitis,” Dr. Thyssen said. “The studies were not accurate enough to allow for any conclusions.”
A multicenter study of adults with hand eczema in Italy found that the proportion of patients with AD was the highest among those with severe and refractory chronic hand eczema. In addition, certain professions, including those of hairdressers, health professionals, and those in trade work, such as plumbing, were more often associated with chronic hand eczema. “This teaches us that we should be very careful about steering these patients from at-risk occupations,” Dr. Thyssen said. “Also, we should remember to treat them aggressively in the beginning to reduce the risk of severe and refractory chronic hand eczema.”
Dr. Thyssen disclosed that he is a speaker, advisory board member, and/or investigator for Asian, Arena, Almirall, AbbVie, Eli Lilly, LEO Pharma, Pfizer, Regeneron, and Sanofi Genzyme.
An estimated (AD), according to Jacob P. Thyssen, MD, PhD.
“If we look at individuals with AD, the lifetime prevalence of hand eczema reaches 50%, so we see a strong association between hand eczema and AD,” Dr. Thyssen, professor of dermatology at the University of Copenhagen, said at the Revolutionizing Atopic Dermatitis symposium.
Risk factors for hand eczema – defined as eczema on the hand and/or wrists – include AD, which increases the risk by two- to threefold, as well as genetic predisposition beyond AD, exposure to irritants and allergens, female gender, young age, low socioeconomic group, high risk occupations (including construction workers and hairdressers), and tobacco smoking.
“As clinicians, we sometimes need to rule out a few differentials, including psoriasis and T-cell lymphoma. As an example, 10% of T-cell lymphoma patients, a very rare condition, have first onset of the disease on their hands,” Dr. Thyssen said. “Once we see persistent hand eczema, we need to obtain a history of irritant exposure and allergen exposure, both at home and at work, perform a patch test, sometimes a skin prick test, and ask about personal and family history of AD and psoriasis.”
He noted that while formal classification of hand eczema has been a struggle for decades, he favors the “straightforward” clinical approach from the European Environmental and Contact Dermatitis Research Group. Atopic hand eczema, he said, “is very much characterized by dorsal involvement of the hands and fingers and sparse involvement of the palmar aspects of the hands.”
The cheeks and hands are predilection sites for AD in filaggrin mutation carriers (as they are sites of low filaggrin levels), and sometimes harsh environmental exposures, such as cold and dry air. In a study of 3,335 patients in Denmark, Dr. Thyssen and colleagues found that filaggrin mutations and AD were associated with early-onset and persistent hand eczema. In another study of 3,834 adults with AD or psoriasis, he and colleagues found that among those with AD, the wrists, back of the hands, and interdigital areas were often sites of severe eczema, while palmar involvement was more uncommon.
The same findings apply for the feet in filaggrin mutation carriers with AD; the dorsal aspect of the feet was more commonly affected, compared with plantar aspects of the feet.
Medical literature regarding foot eczema is scarce, but a retrospective cohort study from Germany found that foot eczema and hand eczema often co-occur. Among 723 hand eczema patients, 201 (28%) had concomitant foot eczema. The same morphological features were found on the hands and feet in 71% of patients. Foot eczema was significantly associated with male sex, atopic hand eczema, hyperhidrosis, wearing of safety shoes/boots at work, and tobacco smoking.
In addition, a systematic review and meta-analysis of studies of hand eczema and AD found that there was a 4.29-fold increased risk of hand eczema in individuals with AD, and the risk (lifetime prevalence) of occupational hand eczema was increased by more than twofold. “However, this study could not differentiate between irritant contact dermatitis on the hands and atopic dermatitis,” Dr. Thyssen said. “The studies were not accurate enough to allow for any conclusions.”
A multicenter study of adults with hand eczema in Italy found that the proportion of patients with AD was the highest among those with severe and refractory chronic hand eczema. In addition, certain professions, including those of hairdressers, health professionals, and those in trade work, such as plumbing, were more often associated with chronic hand eczema. “This teaches us that we should be very careful about steering these patients from at-risk occupations,” Dr. Thyssen said. “Also, we should remember to treat them aggressively in the beginning to reduce the risk of severe and refractory chronic hand eczema.”
Dr. Thyssen disclosed that he is a speaker, advisory board member, and/or investigator for Asian, Arena, Almirall, AbbVie, Eli Lilly, LEO Pharma, Pfizer, Regeneron, and Sanofi Genzyme.
FROM REVOLUTIONIZING AD 2021
Wilderness Medical Society issues clinical guidelines for tick-borne illness
The recently published “Clinical Practice Guidelines for the Prevention and Management of Tick-Borne Illness,” from the Wilderness Medical Society, are a good compilation of treatment suggestions but are not, in fact, new recommendations, lead author Benjamin Ho, MD, of Southern Wisconsin Emergency Associates in Janesville, acknowledged in an interview.
Dr. Ho emphasized that the focus of the report was on “practitioners who practice in resource-limited settings” and are “the group’s way of solidifying a ... standard of practice” for such physicians. Dr. Ho also said that, while “a lot of the recommendations aren’t well supported, the risk-benefit ratio, we believe, supports the recommendations.”
The article first reviewed the different types of ticks and their distribution in the United States, the specific pathogen associated with each, the disease it causes, and comments about seasonal variations in biting behavior. Another table outlines the most common clinical syndromes, typical lab findings, recommended diagnostic testing, and antibiotic treatments. A third section contains images of different types of ticks and photos of ticks in various life-cycle stages and different levels of engorgement.
The authors were careful to note: “Several tick species are able to carry multiple pathogens. In one study, nearly 25% of Ixodes were coinfected with some combination of the bacteria or parasites causing Lyme disease, anaplasmosis, or babesiosis. Although TBI [tick-borne illness] diagnosis is not the focus of this [clinical practice guideline], providers should be aware of high rates of coinfection; the presence of one TBI should in many instances prompt testing for others.”
In terms of recommendations for preventing TBIs, the authors challenge the suggestion of wearing light-colored clothing. For repellents, they recommend DEET, picaridin, and permethrin. And they also give instructions for laundering clothing and removing ticks.
One recommendation is controversial: that of providing single-dose doxycycline as prophylaxis against Lyme disease. Dr. Ho stresses that this was only for “high-risk” tick bites, defined as a tick bite from an identified Ixodes vector species in which the tick was attached for at least 36 hours and that occurred in an endemic area.
The recommendation for prophylactic doxycycline originated with an article by Robert Nadelman and colleagues in the New England Journal of Medicine and has been strongly challenged by ILADS (International Lyme and Associated Diseases Society) physicians, including Daniel Cameron, MD, and others.
Sam Donta, MD, a recent member of the Department of Health & Human Services Tick-borne Working Group and a member of the Infectious Disease Society of America, said in an interview: “The problem with the one-dose doxycycline is you may not begin to develop symptoms until 2 months later.” It might mask the early symptoms of Lyme. “My impression is that the doxycycline – even the single dose – might have abrogated the ability to see an immune response. The idea, though, if you’ve had a tick bite, is to do nothing and to wait for symptoms to develop. That becomes a little bit more complex. But even then, you could choose to follow the patient and see the patient in 2 weeks and then get blood testing.”
Dr. Donta added: “I think the screening test is inadequate. So you have to go directly to the Western blot. And you have to do both the IgM and IgG” and look for specific bands.
Dr. Donta emphasized that patients should be encouraged to save any ticks that were attached and that, if at all possible, ticks should be sent to a reference lab for testing before committing a patient to a course of antibiotics. There is no harm in that brief delay, he said, and most labs can identify an array of pathogens.
The Wilderness Society guidelines on TBIs provide a good overview for clinicians practicing in limited resource settings and mirror those from the IDSA.
Dr. Ho and Dr. Donta reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
The recently published “Clinical Practice Guidelines for the Prevention and Management of Tick-Borne Illness,” from the Wilderness Medical Society, are a good compilation of treatment suggestions but are not, in fact, new recommendations, lead author Benjamin Ho, MD, of Southern Wisconsin Emergency Associates in Janesville, acknowledged in an interview.
Dr. Ho emphasized that the focus of the report was on “practitioners who practice in resource-limited settings” and are “the group’s way of solidifying a ... standard of practice” for such physicians. Dr. Ho also said that, while “a lot of the recommendations aren’t well supported, the risk-benefit ratio, we believe, supports the recommendations.”
The article first reviewed the different types of ticks and their distribution in the United States, the specific pathogen associated with each, the disease it causes, and comments about seasonal variations in biting behavior. Another table outlines the most common clinical syndromes, typical lab findings, recommended diagnostic testing, and antibiotic treatments. A third section contains images of different types of ticks and photos of ticks in various life-cycle stages and different levels of engorgement.
The authors were careful to note: “Several tick species are able to carry multiple pathogens. In one study, nearly 25% of Ixodes were coinfected with some combination of the bacteria or parasites causing Lyme disease, anaplasmosis, or babesiosis. Although TBI [tick-borne illness] diagnosis is not the focus of this [clinical practice guideline], providers should be aware of high rates of coinfection; the presence of one TBI should in many instances prompt testing for others.”
In terms of recommendations for preventing TBIs, the authors challenge the suggestion of wearing light-colored clothing. For repellents, they recommend DEET, picaridin, and permethrin. And they also give instructions for laundering clothing and removing ticks.
One recommendation is controversial: that of providing single-dose doxycycline as prophylaxis against Lyme disease. Dr. Ho stresses that this was only for “high-risk” tick bites, defined as a tick bite from an identified Ixodes vector species in which the tick was attached for at least 36 hours and that occurred in an endemic area.
The recommendation for prophylactic doxycycline originated with an article by Robert Nadelman and colleagues in the New England Journal of Medicine and has been strongly challenged by ILADS (International Lyme and Associated Diseases Society) physicians, including Daniel Cameron, MD, and others.
Sam Donta, MD, a recent member of the Department of Health & Human Services Tick-borne Working Group and a member of the Infectious Disease Society of America, said in an interview: “The problem with the one-dose doxycycline is you may not begin to develop symptoms until 2 months later.” It might mask the early symptoms of Lyme. “My impression is that the doxycycline – even the single dose – might have abrogated the ability to see an immune response. The idea, though, if you’ve had a tick bite, is to do nothing and to wait for symptoms to develop. That becomes a little bit more complex. But even then, you could choose to follow the patient and see the patient in 2 weeks and then get blood testing.”
Dr. Donta added: “I think the screening test is inadequate. So you have to go directly to the Western blot. And you have to do both the IgM and IgG” and look for specific bands.
Dr. Donta emphasized that patients should be encouraged to save any ticks that were attached and that, if at all possible, ticks should be sent to a reference lab for testing before committing a patient to a course of antibiotics. There is no harm in that brief delay, he said, and most labs can identify an array of pathogens.
The Wilderness Society guidelines on TBIs provide a good overview for clinicians practicing in limited resource settings and mirror those from the IDSA.
Dr. Ho and Dr. Donta reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
The recently published “Clinical Practice Guidelines for the Prevention and Management of Tick-Borne Illness,” from the Wilderness Medical Society, are a good compilation of treatment suggestions but are not, in fact, new recommendations, lead author Benjamin Ho, MD, of Southern Wisconsin Emergency Associates in Janesville, acknowledged in an interview.
Dr. Ho emphasized that the focus of the report was on “practitioners who practice in resource-limited settings” and are “the group’s way of solidifying a ... standard of practice” for such physicians. Dr. Ho also said that, while “a lot of the recommendations aren’t well supported, the risk-benefit ratio, we believe, supports the recommendations.”
The article first reviewed the different types of ticks and their distribution in the United States, the specific pathogen associated with each, the disease it causes, and comments about seasonal variations in biting behavior. Another table outlines the most common clinical syndromes, typical lab findings, recommended diagnostic testing, and antibiotic treatments. A third section contains images of different types of ticks and photos of ticks in various life-cycle stages and different levels of engorgement.
The authors were careful to note: “Several tick species are able to carry multiple pathogens. In one study, nearly 25% of Ixodes were coinfected with some combination of the bacteria or parasites causing Lyme disease, anaplasmosis, or babesiosis. Although TBI [tick-borne illness] diagnosis is not the focus of this [clinical practice guideline], providers should be aware of high rates of coinfection; the presence of one TBI should in many instances prompt testing for others.”
In terms of recommendations for preventing TBIs, the authors challenge the suggestion of wearing light-colored clothing. For repellents, they recommend DEET, picaridin, and permethrin. And they also give instructions for laundering clothing and removing ticks.
One recommendation is controversial: that of providing single-dose doxycycline as prophylaxis against Lyme disease. Dr. Ho stresses that this was only for “high-risk” tick bites, defined as a tick bite from an identified Ixodes vector species in which the tick was attached for at least 36 hours and that occurred in an endemic area.
The recommendation for prophylactic doxycycline originated with an article by Robert Nadelman and colleagues in the New England Journal of Medicine and has been strongly challenged by ILADS (International Lyme and Associated Diseases Society) physicians, including Daniel Cameron, MD, and others.
Sam Donta, MD, a recent member of the Department of Health & Human Services Tick-borne Working Group and a member of the Infectious Disease Society of America, said in an interview: “The problem with the one-dose doxycycline is you may not begin to develop symptoms until 2 months later.” It might mask the early symptoms of Lyme. “My impression is that the doxycycline – even the single dose – might have abrogated the ability to see an immune response. The idea, though, if you’ve had a tick bite, is to do nothing and to wait for symptoms to develop. That becomes a little bit more complex. But even then, you could choose to follow the patient and see the patient in 2 weeks and then get blood testing.”
Dr. Donta added: “I think the screening test is inadequate. So you have to go directly to the Western blot. And you have to do both the IgM and IgG” and look for specific bands.
Dr. Donta emphasized that patients should be encouraged to save any ticks that were attached and that, if at all possible, ticks should be sent to a reference lab for testing before committing a patient to a course of antibiotics. There is no harm in that brief delay, he said, and most labs can identify an array of pathogens.
The Wilderness Society guidelines on TBIs provide a good overview for clinicians practicing in limited resource settings and mirror those from the IDSA.
Dr. Ho and Dr. Donta reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM WILDERNESS ENVIRONMENTAL MEDICINE
U.S. cancer deaths continue to fall, especially lung cancer
There has been an overall decline of 32% in cancer deaths as of 2019, or approximately 3.5 million cancer deaths averted, the report noted.
“This success is largely because of reductions in smoking that resulted in downstream declines in lung and other smoking-related cancers,” lead author Rebecca L. Siegel of the ACS, and colleagues, noted in the latest edition of the society’s annual report on cancer rates and trends.
The paper was published online Jan. 12 in CA: A Cancer Journal for Clinicians.
In particular, there has been a fall in both the incidence of and mortality from lung cancer, largely due to successful efforts to get people to quit smoking, but also from earlier diagnosis at a stage when the disease is far more amenable to treatment, noted the authors.
For example, the incidence of lung cancer declined by almost 3% per year in men between the years 2009 and 2018 and by 1% a year in women. Currently, the historically large gender gap in lung cancer incidence is disappearing such that in 2018, lung cancer rates were 24% higher in men than they were in women, and rates in women were actually higher in some younger age groups than they were in men.
Moreover, 28% of lung cancers detected in 2018 were found at a localized stage of disease compared with 17% in 2004.
Patients diagnosed with lung cancer are also living longer, with almost one-third of lung cancer patients still alive 3 years after their diagnosis compared with 21% a decade ago.
However, lung cancer is still the biggest contributor to cancer-related mortality overall, at a death toll of 350 per day – more than breast, prostate, and pancreatic cancer combined, the authors wrote.
This is 2.5 times higher than the death rate from colorectal cancer (CRC), the second leading cause of cancer death in the United States, they added.
Nevertheless, the decrease in lung cancer mortality accelerated from 3.1% per year between 2010 and 2014 to 5.4% per year during 2015 to 2019 in men and from 1.8% to 4.3% in women. “Overall, the lung cancer death rate has dropped by 56% from 1990 to 2019 in men and by 32% from 2002 to 2019 in women,” Ms. Siegel and colleagues emphasized.
Overall, the ACS projects there will be over 1.9 million new cancer cases and over 600,000 cancer deaths across the United States in 2022.
Patterns are changing
With prostate cancer now accounting for some 27% of all cancer diagnoses in men, recent trends in the incidence of prostate cancer are somewhat worrisome, the authors wrote. While the incidence for local-stage disease remained stable from 2014 through to 2018, the incidence of advanced-stage disease has increased by 6% a year since 2011. “Consequently, the proportion of distant-stage diagnoses has more than doubled,” the authors noted, “from a low of 3.9% in 2007 to 8.2% in 2018.”
The incidence of breast cancer among women has been slowly increasing by 0.5% per year since about the mid-2000s. This increase is due at least in part to declines in fertility and increases in body weight among women, the authors suggested. Declines in breast cancer mortality have slowed in recent years, dropping from 1% per year from 2013 to 2019 from 2%-3% per year seen during the 1990s and the early 2000s.
As for CRC, incidence patterns are similar by sex but differ by age. For example, incidence rates of CRC declined by about 2% per year between 2014 and 2018 in individuals 50 years and older, but they increased by 1.5% per year in adults under the age of 50. Overall, however, mortality from CRC decreased by about 2% per year between 2010 and 2019, although this trend again masks increasing mortality from CRC among younger adults, where death rates rose by 1.2% per year from 2005 through 2019 in patients under the age of 50.
The third leading cause of death in men and women combined is pancreatic cancer. Here again, mortality rates slowly increased in men between 2000 and 2013 but have remained relatively stable in women.
Between 2010 and 2019, cancers of the tongue, tonsils, and oropharynx caused by human papilloma virus (HPV) increased by about 2% per year in men and by 1% per year in women.
Death from cervical cancer – despite its being one of the most preventable cancers overall – is still the second leading cause of cancer death in women between 20 and 39 years of age. “Most of these women have never been screened so this is low-hanging fruit easily addressed by increasing access to screening and [HPV] vaccination among underserved women,” Ms. Siegel said in a statement.
On the other hand, mortality from liver cancer – having increased rapidly over the past number of decades – appears to have stabilized in more recent years.
Survival at 5 years
For all cancers combined, survival at 5 years between the mid-1970s and 2011 through 2017 increased from 50% to 68% for White patients and by 39% to 63% for Black patients. “For all stages combined, survival is highest for prostate cancer (98%), melanoma of the skin (93%) and female breast cancer (90%),” the authors pointed out.
In contrast, survival at 5 years is lowest, at 11% for pancreatic cancer, 20% for cancers of the liver and esophagus, and 22% for lung cancer.
Indeed, for most of the common cancers, cancer survival has improved since the mid-1970s with the exception or uterine and cervical cancer, the latter because there have been few advancements in treatment.
Even among the more rare blood and lymphoid malignancies, improvements in treatment strategies, including the use of targeted therapies, have resulted in major survival gains from around 20% in the mid-1970s for chronic myeloid leukemia (CML) patients to over 70% for CML patients diagnosed between 2011 and 2017.
Similarly, the discovery and use of immunotherapy has doubled 5-year survival rates to 30% for patients with metastatic melanoma from 15% in 2004. On the other hand, racial disparities in survival odds continue to persist. For every cancer type except for cancer of the pancreas and kidney, survival rates were lower for Black patients than for White patients, the researchers pointed out.
“Black individuals also have lower stage-specific survival for most cancer types,” the report authors noted. Indeed, after adjustment for sex, age, and stage at diagnosis, the risk of death is 33% higher in Black patients than White patients and 51% higher in American Indian/Alaska Natives compared to White patients.
That said, the overall incidence of cancer is still highest among White individuals, in part because of high rates of breast cancer in White women, which may in part reflect overdiagnosis of breast cancer in this patient population, as the authors suggested.
“However, Black women have the highest cancer mortality rates – 12% higher than White women,” they observed. Even more striking, Black women have a 4% lower incidence of breast cancer than White women but a 41% higher mortality risk from it.
As for pediatric and adolescent cancers, incidence rates may be increasing slightly among both age groups, but dramatic reductions in death by 71% among children and by 61% among adolescents from the mid-70s until now continue as a singular success story in the treatment of cancer overall.
All the authors are employed by the ACS.
A version of this article first appeared on Medscape.com.
There has been an overall decline of 32% in cancer deaths as of 2019, or approximately 3.5 million cancer deaths averted, the report noted.
“This success is largely because of reductions in smoking that resulted in downstream declines in lung and other smoking-related cancers,” lead author Rebecca L. Siegel of the ACS, and colleagues, noted in the latest edition of the society’s annual report on cancer rates and trends.
The paper was published online Jan. 12 in CA: A Cancer Journal for Clinicians.
In particular, there has been a fall in both the incidence of and mortality from lung cancer, largely due to successful efforts to get people to quit smoking, but also from earlier diagnosis at a stage when the disease is far more amenable to treatment, noted the authors.
For example, the incidence of lung cancer declined by almost 3% per year in men between the years 2009 and 2018 and by 1% a year in women. Currently, the historically large gender gap in lung cancer incidence is disappearing such that in 2018, lung cancer rates were 24% higher in men than they were in women, and rates in women were actually higher in some younger age groups than they were in men.
Moreover, 28% of lung cancers detected in 2018 were found at a localized stage of disease compared with 17% in 2004.
Patients diagnosed with lung cancer are also living longer, with almost one-third of lung cancer patients still alive 3 years after their diagnosis compared with 21% a decade ago.
However, lung cancer is still the biggest contributor to cancer-related mortality overall, at a death toll of 350 per day – more than breast, prostate, and pancreatic cancer combined, the authors wrote.
This is 2.5 times higher than the death rate from colorectal cancer (CRC), the second leading cause of cancer death in the United States, they added.
Nevertheless, the decrease in lung cancer mortality accelerated from 3.1% per year between 2010 and 2014 to 5.4% per year during 2015 to 2019 in men and from 1.8% to 4.3% in women. “Overall, the lung cancer death rate has dropped by 56% from 1990 to 2019 in men and by 32% from 2002 to 2019 in women,” Ms. Siegel and colleagues emphasized.
Overall, the ACS projects there will be over 1.9 million new cancer cases and over 600,000 cancer deaths across the United States in 2022.
Patterns are changing
With prostate cancer now accounting for some 27% of all cancer diagnoses in men, recent trends in the incidence of prostate cancer are somewhat worrisome, the authors wrote. While the incidence for local-stage disease remained stable from 2014 through to 2018, the incidence of advanced-stage disease has increased by 6% a year since 2011. “Consequently, the proportion of distant-stage diagnoses has more than doubled,” the authors noted, “from a low of 3.9% in 2007 to 8.2% in 2018.”
The incidence of breast cancer among women has been slowly increasing by 0.5% per year since about the mid-2000s. This increase is due at least in part to declines in fertility and increases in body weight among women, the authors suggested. Declines in breast cancer mortality have slowed in recent years, dropping from 1% per year from 2013 to 2019 from 2%-3% per year seen during the 1990s and the early 2000s.
As for CRC, incidence patterns are similar by sex but differ by age. For example, incidence rates of CRC declined by about 2% per year between 2014 and 2018 in individuals 50 years and older, but they increased by 1.5% per year in adults under the age of 50. Overall, however, mortality from CRC decreased by about 2% per year between 2010 and 2019, although this trend again masks increasing mortality from CRC among younger adults, where death rates rose by 1.2% per year from 2005 through 2019 in patients under the age of 50.
The third leading cause of death in men and women combined is pancreatic cancer. Here again, mortality rates slowly increased in men between 2000 and 2013 but have remained relatively stable in women.
Between 2010 and 2019, cancers of the tongue, tonsils, and oropharynx caused by human papilloma virus (HPV) increased by about 2% per year in men and by 1% per year in women.
Death from cervical cancer – despite its being one of the most preventable cancers overall – is still the second leading cause of cancer death in women between 20 and 39 years of age. “Most of these women have never been screened so this is low-hanging fruit easily addressed by increasing access to screening and [HPV] vaccination among underserved women,” Ms. Siegel said in a statement.
On the other hand, mortality from liver cancer – having increased rapidly over the past number of decades – appears to have stabilized in more recent years.
Survival at 5 years
For all cancers combined, survival at 5 years between the mid-1970s and 2011 through 2017 increased from 50% to 68% for White patients and by 39% to 63% for Black patients. “For all stages combined, survival is highest for prostate cancer (98%), melanoma of the skin (93%) and female breast cancer (90%),” the authors pointed out.
In contrast, survival at 5 years is lowest, at 11% for pancreatic cancer, 20% for cancers of the liver and esophagus, and 22% for lung cancer.
Indeed, for most of the common cancers, cancer survival has improved since the mid-1970s with the exception or uterine and cervical cancer, the latter because there have been few advancements in treatment.
Even among the more rare blood and lymphoid malignancies, improvements in treatment strategies, including the use of targeted therapies, have resulted in major survival gains from around 20% in the mid-1970s for chronic myeloid leukemia (CML) patients to over 70% for CML patients diagnosed between 2011 and 2017.
Similarly, the discovery and use of immunotherapy has doubled 5-year survival rates to 30% for patients with metastatic melanoma from 15% in 2004. On the other hand, racial disparities in survival odds continue to persist. For every cancer type except for cancer of the pancreas and kidney, survival rates were lower for Black patients than for White patients, the researchers pointed out.
“Black individuals also have lower stage-specific survival for most cancer types,” the report authors noted. Indeed, after adjustment for sex, age, and stage at diagnosis, the risk of death is 33% higher in Black patients than White patients and 51% higher in American Indian/Alaska Natives compared to White patients.
That said, the overall incidence of cancer is still highest among White individuals, in part because of high rates of breast cancer in White women, which may in part reflect overdiagnosis of breast cancer in this patient population, as the authors suggested.
“However, Black women have the highest cancer mortality rates – 12% higher than White women,” they observed. Even more striking, Black women have a 4% lower incidence of breast cancer than White women but a 41% higher mortality risk from it.
As for pediatric and adolescent cancers, incidence rates may be increasing slightly among both age groups, but dramatic reductions in death by 71% among children and by 61% among adolescents from the mid-70s until now continue as a singular success story in the treatment of cancer overall.
All the authors are employed by the ACS.
A version of this article first appeared on Medscape.com.
There has been an overall decline of 32% in cancer deaths as of 2019, or approximately 3.5 million cancer deaths averted, the report noted.
“This success is largely because of reductions in smoking that resulted in downstream declines in lung and other smoking-related cancers,” lead author Rebecca L. Siegel of the ACS, and colleagues, noted in the latest edition of the society’s annual report on cancer rates and trends.
The paper was published online Jan. 12 in CA: A Cancer Journal for Clinicians.
In particular, there has been a fall in both the incidence of and mortality from lung cancer, largely due to successful efforts to get people to quit smoking, but also from earlier diagnosis at a stage when the disease is far more amenable to treatment, noted the authors.
For example, the incidence of lung cancer declined by almost 3% per year in men between the years 2009 and 2018 and by 1% a year in women. Currently, the historically large gender gap in lung cancer incidence is disappearing such that in 2018, lung cancer rates were 24% higher in men than they were in women, and rates in women were actually higher in some younger age groups than they were in men.
Moreover, 28% of lung cancers detected in 2018 were found at a localized stage of disease compared with 17% in 2004.
Patients diagnosed with lung cancer are also living longer, with almost one-third of lung cancer patients still alive 3 years after their diagnosis compared with 21% a decade ago.
However, lung cancer is still the biggest contributor to cancer-related mortality overall, at a death toll of 350 per day – more than breast, prostate, and pancreatic cancer combined, the authors wrote.
This is 2.5 times higher than the death rate from colorectal cancer (CRC), the second leading cause of cancer death in the United States, they added.
Nevertheless, the decrease in lung cancer mortality accelerated from 3.1% per year between 2010 and 2014 to 5.4% per year during 2015 to 2019 in men and from 1.8% to 4.3% in women. “Overall, the lung cancer death rate has dropped by 56% from 1990 to 2019 in men and by 32% from 2002 to 2019 in women,” Ms. Siegel and colleagues emphasized.
Overall, the ACS projects there will be over 1.9 million new cancer cases and over 600,000 cancer deaths across the United States in 2022.
Patterns are changing
With prostate cancer now accounting for some 27% of all cancer diagnoses in men, recent trends in the incidence of prostate cancer are somewhat worrisome, the authors wrote. While the incidence for local-stage disease remained stable from 2014 through to 2018, the incidence of advanced-stage disease has increased by 6% a year since 2011. “Consequently, the proportion of distant-stage diagnoses has more than doubled,” the authors noted, “from a low of 3.9% in 2007 to 8.2% in 2018.”
The incidence of breast cancer among women has been slowly increasing by 0.5% per year since about the mid-2000s. This increase is due at least in part to declines in fertility and increases in body weight among women, the authors suggested. Declines in breast cancer mortality have slowed in recent years, dropping from 1% per year from 2013 to 2019 from 2%-3% per year seen during the 1990s and the early 2000s.
As for CRC, incidence patterns are similar by sex but differ by age. For example, incidence rates of CRC declined by about 2% per year between 2014 and 2018 in individuals 50 years and older, but they increased by 1.5% per year in adults under the age of 50. Overall, however, mortality from CRC decreased by about 2% per year between 2010 and 2019, although this trend again masks increasing mortality from CRC among younger adults, where death rates rose by 1.2% per year from 2005 through 2019 in patients under the age of 50.
The third leading cause of death in men and women combined is pancreatic cancer. Here again, mortality rates slowly increased in men between 2000 and 2013 but have remained relatively stable in women.
Between 2010 and 2019, cancers of the tongue, tonsils, and oropharynx caused by human papilloma virus (HPV) increased by about 2% per year in men and by 1% per year in women.
Death from cervical cancer – despite its being one of the most preventable cancers overall – is still the second leading cause of cancer death in women between 20 and 39 years of age. “Most of these women have never been screened so this is low-hanging fruit easily addressed by increasing access to screening and [HPV] vaccination among underserved women,” Ms. Siegel said in a statement.
On the other hand, mortality from liver cancer – having increased rapidly over the past number of decades – appears to have stabilized in more recent years.
Survival at 5 years
For all cancers combined, survival at 5 years between the mid-1970s and 2011 through 2017 increased from 50% to 68% for White patients and by 39% to 63% for Black patients. “For all stages combined, survival is highest for prostate cancer (98%), melanoma of the skin (93%) and female breast cancer (90%),” the authors pointed out.
In contrast, survival at 5 years is lowest, at 11% for pancreatic cancer, 20% for cancers of the liver and esophagus, and 22% for lung cancer.
Indeed, for most of the common cancers, cancer survival has improved since the mid-1970s with the exception or uterine and cervical cancer, the latter because there have been few advancements in treatment.
Even among the more rare blood and lymphoid malignancies, improvements in treatment strategies, including the use of targeted therapies, have resulted in major survival gains from around 20% in the mid-1970s for chronic myeloid leukemia (CML) patients to over 70% for CML patients diagnosed between 2011 and 2017.
Similarly, the discovery and use of immunotherapy has doubled 5-year survival rates to 30% for patients with metastatic melanoma from 15% in 2004. On the other hand, racial disparities in survival odds continue to persist. For every cancer type except for cancer of the pancreas and kidney, survival rates were lower for Black patients than for White patients, the researchers pointed out.
“Black individuals also have lower stage-specific survival for most cancer types,” the report authors noted. Indeed, after adjustment for sex, age, and stage at diagnosis, the risk of death is 33% higher in Black patients than White patients and 51% higher in American Indian/Alaska Natives compared to White patients.
That said, the overall incidence of cancer is still highest among White individuals, in part because of high rates of breast cancer in White women, which may in part reflect overdiagnosis of breast cancer in this patient population, as the authors suggested.
“However, Black women have the highest cancer mortality rates – 12% higher than White women,” they observed. Even more striking, Black women have a 4% lower incidence of breast cancer than White women but a 41% higher mortality risk from it.
As for pediatric and adolescent cancers, incidence rates may be increasing slightly among both age groups, but dramatic reductions in death by 71% among children and by 61% among adolescents from the mid-70s until now continue as a singular success story in the treatment of cancer overall.
All the authors are employed by the ACS.
A version of this article first appeared on Medscape.com.
FROM CA: A CANCER JOURNAL FOR CLINICIANS
Quebec plans to fine unvaccinated adults
The amount hasn’t been decided yet, but it will be “significant” and more than $100. More details will be released at a later date, The Associated Press reported.
“Those who refuse to get their first doses in the coming weeks will have to pay a new health contribution,” Premier Francois Legault said during a news conference.
Not getting vaccinated burdens the health care system, and not all residents should pay for it, he said. About 10% of adults in Quebec are unvaccinated, but they represent about 50% of intensive care patients.
“I think it’s reasonable a majority of the population is asking that there be consequences,” he said. “It’s a question of fairness for the 90% of the population that have made some sacrifices. We owe them.”
The fine will apply to those who don’t qualify for a medical exemption, Mr. Legault said.
Provinces across Canada have reported a surge in COVID-19 cases due to the Omicron variant, with Quebec being one of the hardest-hit, according to Reuters. The province is regularly recording the highest daily case count across the country.
Quebec also has announced a 10 p.m. to 5 a.m. curfew, the AP reported. Starting Jan. 18, liquor and cannabis stores in the province will require proof of vaccination, and shopping malls and hair salons could soon require them as well.
About a quarter of all Canadians live in Quebec, according to CNN. The province was one of the first in Canada to require proof of vaccination for residents to eat in restaurants, go to the gym, or attend sporting events.
Some European countries have announced fees for unvaccinated residents, the AP reported, but Quebec is the first in Canada to announce a financial penalty for those who don’t get a shot.
In Greece, people older than 60 have until Jan. 16 to receive the first dose, or they will be fined 100 euros for every month they remain unvaccinated, the AP reported.
Austria will impose fines up to 3,600 euros for those who don’t follow the vaccine mandate for ages 14 and older, which is slated to start in February.
In Italy, residents who are 50 and older are required to be vaccinated. In mid-February, those who are unvaccinated could be fined up to 1,600 euros if they enter their workplaces, the AP reported.
A version of this article first appeared on WebMD.com.
The amount hasn’t been decided yet, but it will be “significant” and more than $100. More details will be released at a later date, The Associated Press reported.
“Those who refuse to get their first doses in the coming weeks will have to pay a new health contribution,” Premier Francois Legault said during a news conference.
Not getting vaccinated burdens the health care system, and not all residents should pay for it, he said. About 10% of adults in Quebec are unvaccinated, but they represent about 50% of intensive care patients.
“I think it’s reasonable a majority of the population is asking that there be consequences,” he said. “It’s a question of fairness for the 90% of the population that have made some sacrifices. We owe them.”
The fine will apply to those who don’t qualify for a medical exemption, Mr. Legault said.
Provinces across Canada have reported a surge in COVID-19 cases due to the Omicron variant, with Quebec being one of the hardest-hit, according to Reuters. The province is regularly recording the highest daily case count across the country.
Quebec also has announced a 10 p.m. to 5 a.m. curfew, the AP reported. Starting Jan. 18, liquor and cannabis stores in the province will require proof of vaccination, and shopping malls and hair salons could soon require them as well.
About a quarter of all Canadians live in Quebec, according to CNN. The province was one of the first in Canada to require proof of vaccination for residents to eat in restaurants, go to the gym, or attend sporting events.
Some European countries have announced fees for unvaccinated residents, the AP reported, but Quebec is the first in Canada to announce a financial penalty for those who don’t get a shot.
In Greece, people older than 60 have until Jan. 16 to receive the first dose, or they will be fined 100 euros for every month they remain unvaccinated, the AP reported.
Austria will impose fines up to 3,600 euros for those who don’t follow the vaccine mandate for ages 14 and older, which is slated to start in February.
In Italy, residents who are 50 and older are required to be vaccinated. In mid-February, those who are unvaccinated could be fined up to 1,600 euros if they enter their workplaces, the AP reported.
A version of this article first appeared on WebMD.com.
The amount hasn’t been decided yet, but it will be “significant” and more than $100. More details will be released at a later date, The Associated Press reported.
“Those who refuse to get their first doses in the coming weeks will have to pay a new health contribution,” Premier Francois Legault said during a news conference.
Not getting vaccinated burdens the health care system, and not all residents should pay for it, he said. About 10% of adults in Quebec are unvaccinated, but they represent about 50% of intensive care patients.
“I think it’s reasonable a majority of the population is asking that there be consequences,” he said. “It’s a question of fairness for the 90% of the population that have made some sacrifices. We owe them.”
The fine will apply to those who don’t qualify for a medical exemption, Mr. Legault said.
Provinces across Canada have reported a surge in COVID-19 cases due to the Omicron variant, with Quebec being one of the hardest-hit, according to Reuters. The province is regularly recording the highest daily case count across the country.
Quebec also has announced a 10 p.m. to 5 a.m. curfew, the AP reported. Starting Jan. 18, liquor and cannabis stores in the province will require proof of vaccination, and shopping malls and hair salons could soon require them as well.
About a quarter of all Canadians live in Quebec, according to CNN. The province was one of the first in Canada to require proof of vaccination for residents to eat in restaurants, go to the gym, or attend sporting events.
Some European countries have announced fees for unvaccinated residents, the AP reported, but Quebec is the first in Canada to announce a financial penalty for those who don’t get a shot.
In Greece, people older than 60 have until Jan. 16 to receive the first dose, or they will be fined 100 euros for every month they remain unvaccinated, the AP reported.
Austria will impose fines up to 3,600 euros for those who don’t follow the vaccine mandate for ages 14 and older, which is slated to start in February.
In Italy, residents who are 50 and older are required to be vaccinated. In mid-February, those who are unvaccinated could be fined up to 1,600 euros if they enter their workplaces, the AP reported.
A version of this article first appeared on WebMD.com.
CDC to update mask recommendations as Omicron spreads
Director Rochelle Walensky, MD, said on Jan. 12.
“We are preparing an update to the info on our mask website to best reflect the options that are available to people and the different levels of protection different masks provide, and we want to provide Americans the best and most updated information to choose what mask is going to be right for them,” she said at a White House news briefing.
While the higher-quality masks provide better protection, they can be uncomfortable to wear, expensive, and harder to find. That’s why Dr. Walensky added an important caveat.
“Any mask is better than no mask, and we do encourage all Americans to wear a well-fitting mask to protect themselves and prevent the spread of COVID-19. That recommendation is not going to change,” she said.
“Most importantly, the best mask that you wear is the one you will wear and the one you can keep on all day long and tolerate in public indoor settings.”
Meanwhile, the World Health Organization was more focused on vaccines.
WHO officials stressed on Jan. 12 that global vaccine distribution is first priority in defeating the highly contagious Omicron variant, as well as other variants that may evolve.
The WHO’s Technical Advisory Group on COVID-19 Vaccine Composition – a group of experts assessing how COVID-19 vaccines perform against Omicron and other emerging variants – says there is an “urgent need” for broader access to vaccines, along with reviewing and updating current vaccines as needed to ensure protection.
The WHO also disputed the idea that COVID-19 could become endemic in one largely vaccinated nation, while the rest of the world remains unprotected.
“It is up to us how this pandemic unfolds,” Maria Van Kerkhove, PhD, the WHO’s technical lead on COVID-19 response, said at a news briefing.
The WHO has a goal of vaccinating 70% of the population of every country by the middle of the year.
But right now, 90 countries have yet to reach 40% vaccination rates, and 36 of those countries have less than 10% of their populations vaccinated, according to WHO Director General Tedros Adhanom Ghebreyesus, PhD.
A staggering 85% of the African population has not received a first dose.
But progress is being made, Dr. Ghebreyesus said at the briefing.
The WHO said there were over 15 million COVID-19 cases reported last week – the most ever in a single week – and this is likely an underestimate.
The Omicron variant, first identified in South Africa 2 months ago and now found on all seven continents, is “rapidly replacing Delta in almost all countries,” Dr. Ghebreyesus said.
Dr. Walensky said this week’s U.S. daily average COVID-19 case count was 751,000, an increase of 47% from last week. The average daily hospital admissions this week is 19,800, an increase of 33%. Deaths are up 40%, reaching 1,600 per day.
But she also reported new data that supports other research showing Omicron may produce less severe disease. Kaiser Permanente Southern California released a study on Jan. 11 showing that, compared with Delta infections, Omicron was associated with a 53% reduction in hospitalizations, a 74% reduction in intensive care unit admissions, and a 91% lower risk of death.
In the study, no patients with Omicron required mechanical ventilation. The strain now accounts for 98% of cases nationwide.
But Dr. Walensky warned the lower disease severity is not enough to make up for the sheer number of cases that continue to overwhelm hospital systems.
“While we are seeing early evidence that Omicron is less severe than Delta and that those infected are less likely to require hospitalization, it’s important to note that Omicron continues to be much more transmissible than Delta,” she said. “The sudden rise in cases due to Omicron is resulting in unprecedented daily case counts, sickness, absenteeism, and strains on our health care system.”
A version of this article first appeared on WebMD.com.
Director Rochelle Walensky, MD, said on Jan. 12.
“We are preparing an update to the info on our mask website to best reflect the options that are available to people and the different levels of protection different masks provide, and we want to provide Americans the best and most updated information to choose what mask is going to be right for them,” she said at a White House news briefing.
While the higher-quality masks provide better protection, they can be uncomfortable to wear, expensive, and harder to find. That’s why Dr. Walensky added an important caveat.
“Any mask is better than no mask, and we do encourage all Americans to wear a well-fitting mask to protect themselves and prevent the spread of COVID-19. That recommendation is not going to change,” she said.
“Most importantly, the best mask that you wear is the one you will wear and the one you can keep on all day long and tolerate in public indoor settings.”
Meanwhile, the World Health Organization was more focused on vaccines.
WHO officials stressed on Jan. 12 that global vaccine distribution is first priority in defeating the highly contagious Omicron variant, as well as other variants that may evolve.
The WHO’s Technical Advisory Group on COVID-19 Vaccine Composition – a group of experts assessing how COVID-19 vaccines perform against Omicron and other emerging variants – says there is an “urgent need” for broader access to vaccines, along with reviewing and updating current vaccines as needed to ensure protection.
The WHO also disputed the idea that COVID-19 could become endemic in one largely vaccinated nation, while the rest of the world remains unprotected.
“It is up to us how this pandemic unfolds,” Maria Van Kerkhove, PhD, the WHO’s technical lead on COVID-19 response, said at a news briefing.
The WHO has a goal of vaccinating 70% of the population of every country by the middle of the year.
But right now, 90 countries have yet to reach 40% vaccination rates, and 36 of those countries have less than 10% of their populations vaccinated, according to WHO Director General Tedros Adhanom Ghebreyesus, PhD.
A staggering 85% of the African population has not received a first dose.
But progress is being made, Dr. Ghebreyesus said at the briefing.
The WHO said there were over 15 million COVID-19 cases reported last week – the most ever in a single week – and this is likely an underestimate.
The Omicron variant, first identified in South Africa 2 months ago and now found on all seven continents, is “rapidly replacing Delta in almost all countries,” Dr. Ghebreyesus said.
Dr. Walensky said this week’s U.S. daily average COVID-19 case count was 751,000, an increase of 47% from last week. The average daily hospital admissions this week is 19,800, an increase of 33%. Deaths are up 40%, reaching 1,600 per day.
But she also reported new data that supports other research showing Omicron may produce less severe disease. Kaiser Permanente Southern California released a study on Jan. 11 showing that, compared with Delta infections, Omicron was associated with a 53% reduction in hospitalizations, a 74% reduction in intensive care unit admissions, and a 91% lower risk of death.
In the study, no patients with Omicron required mechanical ventilation. The strain now accounts for 98% of cases nationwide.
But Dr. Walensky warned the lower disease severity is not enough to make up for the sheer number of cases that continue to overwhelm hospital systems.
“While we are seeing early evidence that Omicron is less severe than Delta and that those infected are less likely to require hospitalization, it’s important to note that Omicron continues to be much more transmissible than Delta,” she said. “The sudden rise in cases due to Omicron is resulting in unprecedented daily case counts, sickness, absenteeism, and strains on our health care system.”
A version of this article first appeared on WebMD.com.
Director Rochelle Walensky, MD, said on Jan. 12.
“We are preparing an update to the info on our mask website to best reflect the options that are available to people and the different levels of protection different masks provide, and we want to provide Americans the best and most updated information to choose what mask is going to be right for them,” she said at a White House news briefing.
While the higher-quality masks provide better protection, they can be uncomfortable to wear, expensive, and harder to find. That’s why Dr. Walensky added an important caveat.
“Any mask is better than no mask, and we do encourage all Americans to wear a well-fitting mask to protect themselves and prevent the spread of COVID-19. That recommendation is not going to change,” she said.
“Most importantly, the best mask that you wear is the one you will wear and the one you can keep on all day long and tolerate in public indoor settings.”
Meanwhile, the World Health Organization was more focused on vaccines.
WHO officials stressed on Jan. 12 that global vaccine distribution is first priority in defeating the highly contagious Omicron variant, as well as other variants that may evolve.
The WHO’s Technical Advisory Group on COVID-19 Vaccine Composition – a group of experts assessing how COVID-19 vaccines perform against Omicron and other emerging variants – says there is an “urgent need” for broader access to vaccines, along with reviewing and updating current vaccines as needed to ensure protection.
The WHO also disputed the idea that COVID-19 could become endemic in one largely vaccinated nation, while the rest of the world remains unprotected.
“It is up to us how this pandemic unfolds,” Maria Van Kerkhove, PhD, the WHO’s technical lead on COVID-19 response, said at a news briefing.
The WHO has a goal of vaccinating 70% of the population of every country by the middle of the year.
But right now, 90 countries have yet to reach 40% vaccination rates, and 36 of those countries have less than 10% of their populations vaccinated, according to WHO Director General Tedros Adhanom Ghebreyesus, PhD.
A staggering 85% of the African population has not received a first dose.
But progress is being made, Dr. Ghebreyesus said at the briefing.
The WHO said there were over 15 million COVID-19 cases reported last week – the most ever in a single week – and this is likely an underestimate.
The Omicron variant, first identified in South Africa 2 months ago and now found on all seven continents, is “rapidly replacing Delta in almost all countries,” Dr. Ghebreyesus said.
Dr. Walensky said this week’s U.S. daily average COVID-19 case count was 751,000, an increase of 47% from last week. The average daily hospital admissions this week is 19,800, an increase of 33%. Deaths are up 40%, reaching 1,600 per day.
But she also reported new data that supports other research showing Omicron may produce less severe disease. Kaiser Permanente Southern California released a study on Jan. 11 showing that, compared with Delta infections, Omicron was associated with a 53% reduction in hospitalizations, a 74% reduction in intensive care unit admissions, and a 91% lower risk of death.
In the study, no patients with Omicron required mechanical ventilation. The strain now accounts for 98% of cases nationwide.
But Dr. Walensky warned the lower disease severity is not enough to make up for the sheer number of cases that continue to overwhelm hospital systems.
“While we are seeing early evidence that Omicron is less severe than Delta and that those infected are less likely to require hospitalization, it’s important to note that Omicron continues to be much more transmissible than Delta,” she said. “The sudden rise in cases due to Omicron is resulting in unprecedented daily case counts, sickness, absenteeism, and strains on our health care system.”
A version of this article first appeared on WebMD.com.
Urine for a new vaccine alternative
Urine for a new vaccine alternative
Yep, you read that right: Another vaccine alternative. Urine sounds disgusting, but you’ve got to admit, it’s resourceful at least.
Christopher Key, the leader of a group of antivaxxers known as the “Vaccine Police,” is now claiming that you should do “urine therapy,” when means drinking your own pee to ward off COVID-19. According to My. Key, “tons and tons of research” shows the benefits of drinking urine to fight COVID-19, the Guardian reported.

He doesn’t seem like the best source of information, especially since he’s been arrested in the past for refusing to wear a mask in a store. Not wanting to wear a mask in a store doesn’t seem like much, but he also believes that those who administer the COVID-19 vaccine should be “executed” and he tried to impersonate a law official toattempt to arrest a Democratic governor for vaccine mandates.
The overwhelming amount of COVID-19 misinformation has been stressful, yet sometimes laugh-worthy. Urine is not the first “cure” and probably won’t be the last. If you heard something works in a sketchy group on Facebook, it’s probably safe to assume that it absolutely does not. Please don’t recycle your urine.
Vaccine or beer? You must now choose
As the COVID-19 pandemic drags on toward its third year, the large subset of the population who refuse to get vaccinated has proved nearly intractable. Governments have tried numerous incentives to boost vaccination rates, ranging from free beer to million dollar lotteries. Needless to say, beyond their ability to generate LOTME stories, these incentives have been less than effective.
As the frankly unfairly contagious Omicron variant makes it way through the world, our friends in the Great White North have decided enough is enough. If the carrot doesn’t work, the people of Quebec are going to get the stick. Starting on Jan. 18, vaccination cards will be required to enter stores that sell alcohol or cannabis, better known as the things that have gotten us all through this pandemic.
And you know what? Cutting off the booze supply seems to be working. Christian Dubé, Quebec’s health minister, said that the number of vaccination appointments had quadrupled in the new year, rising from 1,500 per day to 6,000 per day, according to the CTV News report. Now, those aren’t massive numbers, but this is big empty Canada we’re talking about, and the unvaccinated make up about 10% of Quebec’s population, so 6,000 a day is quite impressive.
Mr. Dubé added that additional nonessential businesses could be added to the restriction list in the coming weeks, but we’re not sure it’ll be necessary. Those middle-aged soccer moms will do anything to secure their daily merlot. Also, alcohol and cannabis nonessential? The LOTME staff is appalled and offended at this insinuation.
All I need is the polyester that I breathe
When you do laundry, you’re probably thinking more of how to get that ketchup stain out of your white shirt than the effect it has on the environment. Well, research shows it actually has some significance.

That significance comes in the form of microfibers, which are released from natural fabrics such as cotton and from synthetic fabrics such as polyester, which are also considered to be microplastics.
The microfibers that get released in the water when we wash clothes are filtered out eventually, but the dryer is the real culprit, according to a study in Environmental Science & Technology Letters. We’re talking a discharge of up to 120 million microfiber fragments directly into the air annually from just one dryer!
Dryers, they found, emitted between 1.4-40 times more microfibers than did washing machines in previous studies. And polyester fabrics produced more fragments when load sizes increased, while fragment production from cotton fabrics remained constant.
Recent findings suggest that inhaling these microfibers can cause lung inflammation, increase cancer risk, and induce asthma attacks. The authors of the current study suggested additional filtration should be done on dryer vents to reduce the amount of pollutants emitted into the air.
Who would have thought just drying your sheets could be such a dangerous act?
It’s always in the last place you look
At least a million times every morning in this country, a million children yell something like this as they get ready for school: “Mom, have you seen my ...?”
Well, thanks to Defector.com, now we know what Mom should yell back: “Look in your weird cousin Mortimer!”
We will explain ... again.
When they’re not dealing with COVID-19, the folks who work in emergency departments spend a lot of their time removing things that are stuck in people’s bodily orifices. The U.S. Consumer Product Safety Commission even keeps track of them.
So if you’re looking for the number 8 button from the TV remote, or maybe a bullet, check Mortimer’s nose. Maybe you’re missing a lollipop, a hairpin, or some espresso beans. Mortimer’s friend Beulah might have put them in her ear.
Has an earbud gone missing? Another friend of Mortimer’s went to the ED with something stuck in his throat and said that he had a “pill in one hand and his earbud in the other hand, got distracted and took the earbud instead.” Yes, that is an actual quote (via Defector) from the CPSC database.
What about that old saying that someone’s lost his marbles? Well, the ED found one of Mortimer’s marbles ... in his penis. Also a spork, and a bread twist tie, and a chopstick. No, not all at the same time. As for Beulah, a barbell and a Spider-Man action figure somehow found their way – not at the same time, thank goodness – into her vagina.
And have you ever heard someone say that they’re “not going to stand for this”? Mortimer has, so he sat down ... on a light bulb, and a rolling pin, and a billiard ball. Yup, the ED had to remove these items from his rectum.
But not all at the same time, thank goodness.
Urine for a new vaccine alternative
Yep, you read that right: Another vaccine alternative. Urine sounds disgusting, but you’ve got to admit, it’s resourceful at least.
Christopher Key, the leader of a group of antivaxxers known as the “Vaccine Police,” is now claiming that you should do “urine therapy,” when means drinking your own pee to ward off COVID-19. According to My. Key, “tons and tons of research” shows the benefits of drinking urine to fight COVID-19, the Guardian reported.
He doesn’t seem like the best source of information, especially since he’s been arrested in the past for refusing to wear a mask in a store. Not wanting to wear a mask in a store doesn’t seem like much, but he also believes that those who administer the COVID-19 vaccine should be “executed” and he tried to impersonate a law official toattempt to arrest a Democratic governor for vaccine mandates.
The overwhelming amount of COVID-19 misinformation has been stressful, yet sometimes laugh-worthy. Urine is not the first “cure” and probably won’t be the last. If you heard something works in a sketchy group on Facebook, it’s probably safe to assume that it absolutely does not. Please don’t recycle your urine.
Vaccine or beer? You must now choose
As the COVID-19 pandemic drags on toward its third year, the large subset of the population who refuse to get vaccinated has proved nearly intractable. Governments have tried numerous incentives to boost vaccination rates, ranging from free beer to million dollar lotteries. Needless to say, beyond their ability to generate LOTME stories, these incentives have been less than effective.
As the frankly unfairly contagious Omicron variant makes it way through the world, our friends in the Great White North have decided enough is enough. If the carrot doesn’t work, the people of Quebec are going to get the stick. Starting on Jan. 18, vaccination cards will be required to enter stores that sell alcohol or cannabis, better known as the things that have gotten us all through this pandemic.
And you know what? Cutting off the booze supply seems to be working. Christian Dubé, Quebec’s health minister, said that the number of vaccination appointments had quadrupled in the new year, rising from 1,500 per day to 6,000 per day, according to the CTV News report. Now, those aren’t massive numbers, but this is big empty Canada we’re talking about, and the unvaccinated make up about 10% of Quebec’s population, so 6,000 a day is quite impressive.
Mr. Dubé added that additional nonessential businesses could be added to the restriction list in the coming weeks, but we’re not sure it’ll be necessary. Those middle-aged soccer moms will do anything to secure their daily merlot. Also, alcohol and cannabis nonessential? The LOTME staff is appalled and offended at this insinuation.
All I need is the polyester that I breathe
When you do laundry, you’re probably thinking more of how to get that ketchup stain out of your white shirt than the effect it has on the environment. Well, research shows it actually has some significance.
That significance comes in the form of microfibers, which are released from natural fabrics such as cotton and from synthetic fabrics such as polyester, which are also considered to be microplastics.
The microfibers that get released in the water when we wash clothes are filtered out eventually, but the dryer is the real culprit, according to a study in Environmental Science & Technology Letters. We’re talking a discharge of up to 120 million microfiber fragments directly into the air annually from just one dryer!
Dryers, they found, emitted between 1.4-40 times more microfibers than did washing machines in previous studies. And polyester fabrics produced more fragments when load sizes increased, while fragment production from cotton fabrics remained constant.
Recent findings suggest that inhaling these microfibers can cause lung inflammation, increase cancer risk, and induce asthma attacks. The authors of the current study suggested additional filtration should be done on dryer vents to reduce the amount of pollutants emitted into the air.
Who would have thought just drying your sheets could be such a dangerous act?
It’s always in the last place you look
At least a million times every morning in this country, a million children yell something like this as they get ready for school: “Mom, have you seen my ...?”
Well, thanks to Defector.com, now we know what Mom should yell back: “Look in your weird cousin Mortimer!”
We will explain ... again.
When they’re not dealing with COVID-19, the folks who work in emergency departments spend a lot of their time removing things that are stuck in people’s bodily orifices. The U.S. Consumer Product Safety Commission even keeps track of them.
So if you’re looking for the number 8 button from the TV remote, or maybe a bullet, check Mortimer’s nose. Maybe you’re missing a lollipop, a hairpin, or some espresso beans. Mortimer’s friend Beulah might have put them in her ear.
Has an earbud gone missing? Another friend of Mortimer’s went to the ED with something stuck in his throat and said that he had a “pill in one hand and his earbud in the other hand, got distracted and took the earbud instead.” Yes, that is an actual quote (via Defector) from the CPSC database.
What about that old saying that someone’s lost his marbles? Well, the ED found one of Mortimer’s marbles ... in his penis. Also a spork, and a bread twist tie, and a chopstick. No, not all at the same time. As for Beulah, a barbell and a Spider-Man action figure somehow found their way – not at the same time, thank goodness – into her vagina.
And have you ever heard someone say that they’re “not going to stand for this”? Mortimer has, so he sat down ... on a light bulb, and a rolling pin, and a billiard ball. Yup, the ED had to remove these items from his rectum.
But not all at the same time, thank goodness.
Urine for a new vaccine alternative
Yep, you read that right: Another vaccine alternative. Urine sounds disgusting, but you’ve got to admit, it’s resourceful at least.
Christopher Key, the leader of a group of antivaxxers known as the “Vaccine Police,” is now claiming that you should do “urine therapy,” when means drinking your own pee to ward off COVID-19. According to My. Key, “tons and tons of research” shows the benefits of drinking urine to fight COVID-19, the Guardian reported.
He doesn’t seem like the best source of information, especially since he’s been arrested in the past for refusing to wear a mask in a store. Not wanting to wear a mask in a store doesn’t seem like much, but he also believes that those who administer the COVID-19 vaccine should be “executed” and he tried to impersonate a law official toattempt to arrest a Democratic governor for vaccine mandates.
The overwhelming amount of COVID-19 misinformation has been stressful, yet sometimes laugh-worthy. Urine is not the first “cure” and probably won’t be the last. If you heard something works in a sketchy group on Facebook, it’s probably safe to assume that it absolutely does not. Please don’t recycle your urine.
Vaccine or beer? You must now choose
As the COVID-19 pandemic drags on toward its third year, the large subset of the population who refuse to get vaccinated has proved nearly intractable. Governments have tried numerous incentives to boost vaccination rates, ranging from free beer to million dollar lotteries. Needless to say, beyond their ability to generate LOTME stories, these incentives have been less than effective.
As the frankly unfairly contagious Omicron variant makes it way through the world, our friends in the Great White North have decided enough is enough. If the carrot doesn’t work, the people of Quebec are going to get the stick. Starting on Jan. 18, vaccination cards will be required to enter stores that sell alcohol or cannabis, better known as the things that have gotten us all through this pandemic.
And you know what? Cutting off the booze supply seems to be working. Christian Dubé, Quebec’s health minister, said that the number of vaccination appointments had quadrupled in the new year, rising from 1,500 per day to 6,000 per day, according to the CTV News report. Now, those aren’t massive numbers, but this is big empty Canada we’re talking about, and the unvaccinated make up about 10% of Quebec’s population, so 6,000 a day is quite impressive.
Mr. Dubé added that additional nonessential businesses could be added to the restriction list in the coming weeks, but we’re not sure it’ll be necessary. Those middle-aged soccer moms will do anything to secure their daily merlot. Also, alcohol and cannabis nonessential? The LOTME staff is appalled and offended at this insinuation.
All I need is the polyester that I breathe
When you do laundry, you’re probably thinking more of how to get that ketchup stain out of your white shirt than the effect it has on the environment. Well, research shows it actually has some significance.
That significance comes in the form of microfibers, which are released from natural fabrics such as cotton and from synthetic fabrics such as polyester, which are also considered to be microplastics.
The microfibers that get released in the water when we wash clothes are filtered out eventually, but the dryer is the real culprit, according to a study in Environmental Science & Technology Letters. We’re talking a discharge of up to 120 million microfiber fragments directly into the air annually from just one dryer!
Dryers, they found, emitted between 1.4-40 times more microfibers than did washing machines in previous studies. And polyester fabrics produced more fragments when load sizes increased, while fragment production from cotton fabrics remained constant.
Recent findings suggest that inhaling these microfibers can cause lung inflammation, increase cancer risk, and induce asthma attacks. The authors of the current study suggested additional filtration should be done on dryer vents to reduce the amount of pollutants emitted into the air.
Who would have thought just drying your sheets could be such a dangerous act?
It’s always in the last place you look
At least a million times every morning in this country, a million children yell something like this as they get ready for school: “Mom, have you seen my ...?”
Well, thanks to Defector.com, now we know what Mom should yell back: “Look in your weird cousin Mortimer!”
We will explain ... again.
When they’re not dealing with COVID-19, the folks who work in emergency departments spend a lot of their time removing things that are stuck in people’s bodily orifices. The U.S. Consumer Product Safety Commission even keeps track of them.
So if you’re looking for the number 8 button from the TV remote, or maybe a bullet, check Mortimer’s nose. Maybe you’re missing a lollipop, a hairpin, or some espresso beans. Mortimer’s friend Beulah might have put them in her ear.
Has an earbud gone missing? Another friend of Mortimer’s went to the ED with something stuck in his throat and said that he had a “pill in one hand and his earbud in the other hand, got distracted and took the earbud instead.” Yes, that is an actual quote (via Defector) from the CPSC database.
What about that old saying that someone’s lost his marbles? Well, the ED found one of Mortimer’s marbles ... in his penis. Also a spork, and a bread twist tie, and a chopstick. No, not all at the same time. As for Beulah, a barbell and a Spider-Man action figure somehow found their way – not at the same time, thank goodness – into her vagina.
And have you ever heard someone say that they’re “not going to stand for this”? Mortimer has, so he sat down ... on a light bulb, and a rolling pin, and a billiard ball. Yup, the ED had to remove these items from his rectum.
But not all at the same time, thank goodness.
What is the diagnosis?
Hidradenitis suppurativa (HS) is a chronic inflammatory skin condition that is becoming more recognized in children. It has a variable presentation, most commonly presenting as painful, recurrent cysts, abscesses, nodules, and/or pustules in classic locations with associated scarring and sinus tract formation.
The majority of patients present with bilateral lesions found most commonly in the axillae and inguinal folds.1 There are myriad other potential sites of involvement including the inframammary folds, inner thighs, buttocks, and groin.1 Diagnosis is made based on history and physical exam. There is a standard severity classification scheme called the Hurley score, which stratifies disease severity based on the presence of sinus tracts and extent of disease.1 HS is associated with comorbid conditions such as obesity, overweight, acne, and inflammatory bowel and joint disease.2 This painful, persistent condition is well documented to have a negative impact on quality of life in adult patients, and similar impairment has been found in pediatric patients.3,4
HS may be increasing in pediatric and adolescent patients, with recent studies showing onset coinciding most commonly with the onset of puberty.1,2 There is often a period of several years between symptom onset and diagnosis.1 A recent editorial highlighted the disparities that exist in HS, with disease more common in Black children and limited information about disease prevalence in Hispanic children.5
What’s the treatment plan?
HS is a difficult disease to treat, with few patients achieving remission and a significant proportion of patients with treatment-refractory disease.1 There are limited studies of HS treatment in pediatric patients. Topical and systemic antibiotic therapy are mainstays of HS treatment, with tetracyclines and a combination of clindamycin plus rifampin commonly used in adults and children alike. Topical therapies including topical antibiotics and antibacterial solutions are frequently used as adjunctive therapy.6 Adalimumab, a tumor necrosis factor receptor blocker, has been Food and Drug Administration approved for HS for ages 12 and up and is currently the only FDA-approved medication for HS in pediatric patients. Our patient was started on 100 mg doxycycline twice daily, with short-dose topical corticosteroids for symptom management of the most inflamed lesions.
What’s on the differential?
Acne conglobata
Acne conglobata is an uncommon, severe variant of acne vulgaris which arise in patients with a history of acne vulgaris and presents with comedones, cysts, abscesses, and scarring with possible drainage of pus. Lesions can present diffusely on the face, back, and body, including in the axillae, groin, and buttocks, and as such can be confused with HS.7
However, in contrast with HS, patients with acne conglobata will also develop disease in non–apocrine gland–bearing skin. This patient’s lack of preceding acne and restriction of lesions to the axillae, inguinal folds, and buttocks makes acne conglobata less likely.
Epidermal inclusion cyst
Epidermal inclusion cyst (EIC) is a common cutaneous cyst, presenting as a well-circumscribed nodule(s) with a central punctum. If not excised, lesions can sometimes become infected and painful.8 In contrast with HS, EIC presents only uncommonly as multiple lesions arising in different areas, and spontaneous drainage is uncommon. Our patient’s development of multiple draining lesions makes this diagnosis unlikely.
Furunculosis
Furunculosis is a common bacterial infection of the skin, presenting with inflammatory nodules or pustules centered around the hair follicle. Lesions may commonly present at sites of skin trauma and are found most frequently on the extremities.9 Though furunculosis lesions may drain pus and can coalesce to form larger “carbuncles,” our patient’s presence of significant scarring and lack of extremity involvement makes HS more likely.
Recurrent MRSA abscesses
Methicillin-resistant Staphylococcus aureus skin and soft-tissue infections are not uncommon in the pediatric population, with presentation of infection ranging from cellulitis to fluid-containing abscesses.10 Recurrent abscesses may be seen in MRSA infection, however in this patient the presence of draining, scarring lesions in multiple locations typical for HS over time is more consistent with a diagnosis of HS.
Dr. Eichenfield is vice chair of the department of dermatology and professor of dermatology and pediatrics at the University of California, San Diego, and Rady Children’s Hospital, San Diego. Ms. Appiah is a pediatric dermatology research associate in the division of pediatric and adolescent dermatology at the University of California, San Diego, and Rady Children’s Hospital. Dr. Eichenfield and Ms. Appiah have no relevant financial disclosures.
References
1. Liy-Wong C et al. JAMA Dermatol. 2021;157(4):385-91.
2. Choi E et al. J Am Acad Dermatol. 2022;86(1):140-7.
3. Machado MO et al. JAMA Dermatol. 2019;155(8):939-45.
4. McAndrew R et al. J Am Acad Dermatol. 2021;84(3):829-30.
5. Kirby JS and Zaenglein AL. JAMA Dermatol. 2021;157(4):379-80.
6. Alikhan A et al. J Am Acad Dermatol. 2019;81(1):91-101.
7. Greydanus DE et al. Dis Mon. 2021;67(4):101103.
8. Weir CB, St. Hilaire NJ. Epidermal Inclusion Cyst, in “StatPearls.” Treasure Island, Fla: StatPearls Publishing, 2021.
9. Atanaskova N and Tomecki KJ. Dermatol Clin. 2010;28(3):479-87.
10. Papastefan ST et al. J Surg Res. 2019;242:70-7.
Hidradenitis suppurativa (HS) is a chronic inflammatory skin condition that is becoming more recognized in children. It has a variable presentation, most commonly presenting as painful, recurrent cysts, abscesses, nodules, and/or pustules in classic locations with associated scarring and sinus tract formation.
The majority of patients present with bilateral lesions found most commonly in the axillae and inguinal folds.1 There are myriad other potential sites of involvement including the inframammary folds, inner thighs, buttocks, and groin.1 Diagnosis is made based on history and physical exam. There is a standard severity classification scheme called the Hurley score, which stratifies disease severity based on the presence of sinus tracts and extent of disease.1 HS is associated with comorbid conditions such as obesity, overweight, acne, and inflammatory bowel and joint disease.2 This painful, persistent condition is well documented to have a negative impact on quality of life in adult patients, and similar impairment has been found in pediatric patients.3,4
HS may be increasing in pediatric and adolescent patients, with recent studies showing onset coinciding most commonly with the onset of puberty.1,2 There is often a period of several years between symptom onset and diagnosis.1 A recent editorial highlighted the disparities that exist in HS, with disease more common in Black children and limited information about disease prevalence in Hispanic children.5
What’s the treatment plan?
HS is a difficult disease to treat, with few patients achieving remission and a significant proportion of patients with treatment-refractory disease.1 There are limited studies of HS treatment in pediatric patients. Topical and systemic antibiotic therapy are mainstays of HS treatment, with tetracyclines and a combination of clindamycin plus rifampin commonly used in adults and children alike. Topical therapies including topical antibiotics and antibacterial solutions are frequently used as adjunctive therapy.6 Adalimumab, a tumor necrosis factor receptor blocker, has been Food and Drug Administration approved for HS for ages 12 and up and is currently the only FDA-approved medication for HS in pediatric patients. Our patient was started on 100 mg doxycycline twice daily, with short-dose topical corticosteroids for symptom management of the most inflamed lesions.
What’s on the differential?
Acne conglobata
Acne conglobata is an uncommon, severe variant of acne vulgaris which arise in patients with a history of acne vulgaris and presents with comedones, cysts, abscesses, and scarring with possible drainage of pus. Lesions can present diffusely on the face, back, and body, including in the axillae, groin, and buttocks, and as such can be confused with HS.7
However, in contrast with HS, patients with acne conglobata will also develop disease in non–apocrine gland–bearing skin. This patient’s lack of preceding acne and restriction of lesions to the axillae, inguinal folds, and buttocks makes acne conglobata less likely.
Epidermal inclusion cyst
Epidermal inclusion cyst (EIC) is a common cutaneous cyst, presenting as a well-circumscribed nodule(s) with a central punctum. If not excised, lesions can sometimes become infected and painful.8 In contrast with HS, EIC presents only uncommonly as multiple lesions arising in different areas, and spontaneous drainage is uncommon. Our patient’s development of multiple draining lesions makes this diagnosis unlikely.
Furunculosis
Furunculosis is a common bacterial infection of the skin, presenting with inflammatory nodules or pustules centered around the hair follicle. Lesions may commonly present at sites of skin trauma and are found most frequently on the extremities.9 Though furunculosis lesions may drain pus and can coalesce to form larger “carbuncles,” our patient’s presence of significant scarring and lack of extremity involvement makes HS more likely.
Recurrent MRSA abscesses
Methicillin-resistant Staphylococcus aureus skin and soft-tissue infections are not uncommon in the pediatric population, with presentation of infection ranging from cellulitis to fluid-containing abscesses.10 Recurrent abscesses may be seen in MRSA infection, however in this patient the presence of draining, scarring lesions in multiple locations typical for HS over time is more consistent with a diagnosis of HS.
Dr. Eichenfield is vice chair of the department of dermatology and professor of dermatology and pediatrics at the University of California, San Diego, and Rady Children’s Hospital, San Diego. Ms. Appiah is a pediatric dermatology research associate in the division of pediatric and adolescent dermatology at the University of California, San Diego, and Rady Children’s Hospital. Dr. Eichenfield and Ms. Appiah have no relevant financial disclosures.
References
1. Liy-Wong C et al. JAMA Dermatol. 2021;157(4):385-91.
2. Choi E et al. J Am Acad Dermatol. 2022;86(1):140-7.
3. Machado MO et al. JAMA Dermatol. 2019;155(8):939-45.
4. McAndrew R et al. J Am Acad Dermatol. 2021;84(3):829-30.
5. Kirby JS and Zaenglein AL. JAMA Dermatol. 2021;157(4):379-80.
6. Alikhan A et al. J Am Acad Dermatol. 2019;81(1):91-101.
7. Greydanus DE et al. Dis Mon. 2021;67(4):101103.
8. Weir CB, St. Hilaire NJ. Epidermal Inclusion Cyst, in “StatPearls.” Treasure Island, Fla: StatPearls Publishing, 2021.
9. Atanaskova N and Tomecki KJ. Dermatol Clin. 2010;28(3):479-87.
10. Papastefan ST et al. J Surg Res. 2019;242:70-7.
Hidradenitis suppurativa (HS) is a chronic inflammatory skin condition that is becoming more recognized in children. It has a variable presentation, most commonly presenting as painful, recurrent cysts, abscesses, nodules, and/or pustules in classic locations with associated scarring and sinus tract formation.
The majority of patients present with bilateral lesions found most commonly in the axillae and inguinal folds.1 There are myriad other potential sites of involvement including the inframammary folds, inner thighs, buttocks, and groin.1 Diagnosis is made based on history and physical exam. There is a standard severity classification scheme called the Hurley score, which stratifies disease severity based on the presence of sinus tracts and extent of disease.1 HS is associated with comorbid conditions such as obesity, overweight, acne, and inflammatory bowel and joint disease.2 This painful, persistent condition is well documented to have a negative impact on quality of life in adult patients, and similar impairment has been found in pediatric patients.3,4
HS may be increasing in pediatric and adolescent patients, with recent studies showing onset coinciding most commonly with the onset of puberty.1,2 There is often a period of several years between symptom onset and diagnosis.1 A recent editorial highlighted the disparities that exist in HS, with disease more common in Black children and limited information about disease prevalence in Hispanic children.5
What’s the treatment plan?
HS is a difficult disease to treat, with few patients achieving remission and a significant proportion of patients with treatment-refractory disease.1 There are limited studies of HS treatment in pediatric patients. Topical and systemic antibiotic therapy are mainstays of HS treatment, with tetracyclines and a combination of clindamycin plus rifampin commonly used in adults and children alike. Topical therapies including topical antibiotics and antibacterial solutions are frequently used as adjunctive therapy.6 Adalimumab, a tumor necrosis factor receptor blocker, has been Food and Drug Administration approved for HS for ages 12 and up and is currently the only FDA-approved medication for HS in pediatric patients. Our patient was started on 100 mg doxycycline twice daily, with short-dose topical corticosteroids for symptom management of the most inflamed lesions.
What’s on the differential?
Acne conglobata
Acne conglobata is an uncommon, severe variant of acne vulgaris which arise in patients with a history of acne vulgaris and presents with comedones, cysts, abscesses, and scarring with possible drainage of pus. Lesions can present diffusely on the face, back, and body, including in the axillae, groin, and buttocks, and as such can be confused with HS.7
However, in contrast with HS, patients with acne conglobata will also develop disease in non–apocrine gland–bearing skin. This patient’s lack of preceding acne and restriction of lesions to the axillae, inguinal folds, and buttocks makes acne conglobata less likely.
Epidermal inclusion cyst
Epidermal inclusion cyst (EIC) is a common cutaneous cyst, presenting as a well-circumscribed nodule(s) with a central punctum. If not excised, lesions can sometimes become infected and painful.8 In contrast with HS, EIC presents only uncommonly as multiple lesions arising in different areas, and spontaneous drainage is uncommon. Our patient’s development of multiple draining lesions makes this diagnosis unlikely.
Furunculosis
Furunculosis is a common bacterial infection of the skin, presenting with inflammatory nodules or pustules centered around the hair follicle. Lesions may commonly present at sites of skin trauma and are found most frequently on the extremities.9 Though furunculosis lesions may drain pus and can coalesce to form larger “carbuncles,” our patient’s presence of significant scarring and lack of extremity involvement makes HS more likely.
Recurrent MRSA abscesses
Methicillin-resistant Staphylococcus aureus skin and soft-tissue infections are not uncommon in the pediatric population, with presentation of infection ranging from cellulitis to fluid-containing abscesses.10 Recurrent abscesses may be seen in MRSA infection, however in this patient the presence of draining, scarring lesions in multiple locations typical for HS over time is more consistent with a diagnosis of HS.
Dr. Eichenfield is vice chair of the department of dermatology and professor of dermatology and pediatrics at the University of California, San Diego, and Rady Children’s Hospital, San Diego. Ms. Appiah is a pediatric dermatology research associate in the division of pediatric and adolescent dermatology at the University of California, San Diego, and Rady Children’s Hospital. Dr. Eichenfield and Ms. Appiah have no relevant financial disclosures.
References
1. Liy-Wong C et al. JAMA Dermatol. 2021;157(4):385-91.
2. Choi E et al. J Am Acad Dermatol. 2022;86(1):140-7.
3. Machado MO et al. JAMA Dermatol. 2019;155(8):939-45.
4. McAndrew R et al. J Am Acad Dermatol. 2021;84(3):829-30.
5. Kirby JS and Zaenglein AL. JAMA Dermatol. 2021;157(4):379-80.
6. Alikhan A et al. J Am Acad Dermatol. 2019;81(1):91-101.
7. Greydanus DE et al. Dis Mon. 2021;67(4):101103.
8. Weir CB, St. Hilaire NJ. Epidermal Inclusion Cyst, in “StatPearls.” Treasure Island, Fla: StatPearls Publishing, 2021.
9. Atanaskova N and Tomecki KJ. Dermatol Clin. 2010;28(3):479-87.
10. Papastefan ST et al. J Surg Res. 2019;242:70-7.


Common cold could protect against COVID-19, study says
, according to a small study published Jan. 10 in Nature Communications.
Previous studies have shown that T cells created from other coronaviruses can recognize SARS-CoV-2, the virus that causes COVID-19. In the new study, researchers at Imperial College London found that the presence of these T cells at the time of COVID-19 exposure could reduce the chance of getting infected.
The findings could provide a blueprint for a second-generation, universal vaccine to prevent infection from COVID-19 variants, including Omicron and ones that crop up later.
“Being exposed to SARS-CoV-2 virus doesn’t always result in infection, and we’ve been keen to understand why,” Rhia Kundu, PhD, the lead study author from Imperial’s National Heart and Lung Institute, said in a statement.
People with higher levels of T cells from the common cold were less likely to become infected with COVID-19, the researchers found.
“While this is an important discovery, it is only one form of protection, and I would stress that no one should rely on this alone,” Dr. Kundu said. “Instead, the best way to protect yourself against COVID-19 is to be fully vaccinated, including getting your booster dose.”
For the study, Dr. Kundu and colleagues analyzed blood samples from 52 people who lived with someone with confirmed COVID-19 in September 2020. Among the 26 people who didn’t contract COVID-19, there were “significantly higher levels” of preexisting T cells from common cold coronaviruses, as compared with the 26 people who did become infected.
The T cells researched in the study are considered “cross-reactive” and can recognize the proteins of SARS-CoV-2. They offer protection by targeting proteins inside the SARS-CoV-2 virus, rather than the spike proteins on the surface that allow the virus to invade cells.
The current COVID-19 vaccines target the spike proteins, which are more likely to mutate than internal proteins, the researchers wrote. The Omicron variant, for instance, has numerous mutations on spike proteins that may allow it to evade vaccines.
The data suggest that the next step of COVID-19 vaccine development could focus on internal proteins, the researchers said, which could provide lasting protection because T-cell responses persist longer than antibody responses that fade within a few months of vaccination.
“New vaccines that include these conserved, internal proteins would therefore induce broadly protective T-cell responses that should protect against current and future SARS-CoV-2 variants,” Ajit Lalvani, MD, the senior study author and director of Imperial’s respiratory infections health protection research unit, said in the statement.
But more research is needed, the authors said, noting that the study had a small sample size and lacked ethnic diversity, which puts limits on the research.
A version of this article first appeared on WebMD.com
, according to a small study published Jan. 10 in Nature Communications.
Previous studies have shown that T cells created from other coronaviruses can recognize SARS-CoV-2, the virus that causes COVID-19. In the new study, researchers at Imperial College London found that the presence of these T cells at the time of COVID-19 exposure could reduce the chance of getting infected.
The findings could provide a blueprint for a second-generation, universal vaccine to prevent infection from COVID-19 variants, including Omicron and ones that crop up later.
“Being exposed to SARS-CoV-2 virus doesn’t always result in infection, and we’ve been keen to understand why,” Rhia Kundu, PhD, the lead study author from Imperial’s National Heart and Lung Institute, said in a statement.
People with higher levels of T cells from the common cold were less likely to become infected with COVID-19, the researchers found.
“While this is an important discovery, it is only one form of protection, and I would stress that no one should rely on this alone,” Dr. Kundu said. “Instead, the best way to protect yourself against COVID-19 is to be fully vaccinated, including getting your booster dose.”
For the study, Dr. Kundu and colleagues analyzed blood samples from 52 people who lived with someone with confirmed COVID-19 in September 2020. Among the 26 people who didn’t contract COVID-19, there were “significantly higher levels” of preexisting T cells from common cold coronaviruses, as compared with the 26 people who did become infected.
The T cells researched in the study are considered “cross-reactive” and can recognize the proteins of SARS-CoV-2. They offer protection by targeting proteins inside the SARS-CoV-2 virus, rather than the spike proteins on the surface that allow the virus to invade cells.
The current COVID-19 vaccines target the spike proteins, which are more likely to mutate than internal proteins, the researchers wrote. The Omicron variant, for instance, has numerous mutations on spike proteins that may allow it to evade vaccines.
The data suggest that the next step of COVID-19 vaccine development could focus on internal proteins, the researchers said, which could provide lasting protection because T-cell responses persist longer than antibody responses that fade within a few months of vaccination.
“New vaccines that include these conserved, internal proteins would therefore induce broadly protective T-cell responses that should protect against current and future SARS-CoV-2 variants,” Ajit Lalvani, MD, the senior study author and director of Imperial’s respiratory infections health protection research unit, said in the statement.
But more research is needed, the authors said, noting that the study had a small sample size and lacked ethnic diversity, which puts limits on the research.
A version of this article first appeared on WebMD.com
, according to a small study published Jan. 10 in Nature Communications.
Previous studies have shown that T cells created from other coronaviruses can recognize SARS-CoV-2, the virus that causes COVID-19. In the new study, researchers at Imperial College London found that the presence of these T cells at the time of COVID-19 exposure could reduce the chance of getting infected.
The findings could provide a blueprint for a second-generation, universal vaccine to prevent infection from COVID-19 variants, including Omicron and ones that crop up later.
“Being exposed to SARS-CoV-2 virus doesn’t always result in infection, and we’ve been keen to understand why,” Rhia Kundu, PhD, the lead study author from Imperial’s National Heart and Lung Institute, said in a statement.
People with higher levels of T cells from the common cold were less likely to become infected with COVID-19, the researchers found.
“While this is an important discovery, it is only one form of protection, and I would stress that no one should rely on this alone,” Dr. Kundu said. “Instead, the best way to protect yourself against COVID-19 is to be fully vaccinated, including getting your booster dose.”
For the study, Dr. Kundu and colleagues analyzed blood samples from 52 people who lived with someone with confirmed COVID-19 in September 2020. Among the 26 people who didn’t contract COVID-19, there were “significantly higher levels” of preexisting T cells from common cold coronaviruses, as compared with the 26 people who did become infected.
The T cells researched in the study are considered “cross-reactive” and can recognize the proteins of SARS-CoV-2. They offer protection by targeting proteins inside the SARS-CoV-2 virus, rather than the spike proteins on the surface that allow the virus to invade cells.
The current COVID-19 vaccines target the spike proteins, which are more likely to mutate than internal proteins, the researchers wrote. The Omicron variant, for instance, has numerous mutations on spike proteins that may allow it to evade vaccines.
The data suggest that the next step of COVID-19 vaccine development could focus on internal proteins, the researchers said, which could provide lasting protection because T-cell responses persist longer than antibody responses that fade within a few months of vaccination.
“New vaccines that include these conserved, internal proteins would therefore induce broadly protective T-cell responses that should protect against current and future SARS-CoV-2 variants,” Ajit Lalvani, MD, the senior study author and director of Imperial’s respiratory infections health protection research unit, said in the statement.
But more research is needed, the authors said, noting that the study had a small sample size and lacked ethnic diversity, which puts limits on the research.
A version of this article first appeared on WebMD.com
Physicians react: Should docs lose their licenses for spreading false COVID information?
Doctors providing “fraudulent” COVID-19 information became a hot-button issue for physicians responding to Medscape’s recent article, "Shouldn’t Doctors Who Spread False COVID-19 Information Lose Their Licenses?”
COVID-19 safety recommendations are set by mainstream medical organizations as new information becomes available, but some doctors consistently oppose advice from the Centers for Disease Control and Prevention and other medical authorities. These physicians often promote off-label, unapproved use of medications for COVID-19 and/or contradict mainstream safety guidelines such as vaccines, masks, and social distancing.
Some medical organizations are concerned that these doctors are hampering efforts to control the highly contagious coronavirus and are, at worst, placing lives in danger with their contrarian views that can spread like wildfire on social media sites. Their words are often used by those who refuse to be vaccinated or wear masks.
State licensing boards have mostly refused to discipline these doctors for making false and/or misleading claims, but as the virus spreads, there are calls to take action against them. However, others worry that such actions would violate free speech and critical thought.
Yes, those doctors are doing wrong
Several physicians took a strong stand against their fellow doctors who are spreading misinformation about COVID-19.
One doctor endorsed the idea of removing licenses for spreading misinformation and called for criminal prosecution: “It should certainly be grounds for cancellation of all licensing (after appropriate examination to rule out acute psychotic episodes, dementia, tumor, etc.) and very likely [include] a charge of manslaughter.”
Another health care provider said, “A person who does not accept science should not, of course, be allowed to practice medicine. One who argues publicly that vaccines and masks don’t work should be prosecuted for crimes ranging from reckless endangerment to attempted murder.”
One reader framed COVID-19 misinformers in stark terms: “These men and women are medical prostitutes. Their medical and surgical colleges [should] have a panel to track in-court testimony and the disinformation they spread ...”
“This is malpractice of the worst kind,” said a clinician. “Public health officials and science are quite clear on [the] best practices for safety during a pandemic, which is killing millions. This is a standard of care.”
“Medical Boards should suspend licenses and give the physician a chance to testify [about] the scientific basis for his comments,” added a health care provider. “Boards involve themselves in all kinds of perceived disciplinary infractions. We are in the midst of a lethal pandemic. I would think that would take precedence over many other issues?”
“I do believe that physicians have the responsibility to speak the truth and have scientifically displayed minds,” said a reader. “Not [to] promulgate misleading, false, and/or unverified information.”
“Any physician, who holds a license, should abide [by] government and state regulation,” asserted a doctor. “He should be disciplined by the board for spreading medical/public misinformation since he is creating potential harm to the population.”
One specialist insisted that “state boards do not do enough to restrict/limit the practice of physicians touting questionable therapies.”
“Any doctor who spreads false information about Covid is hurting our country, our individuals, and our economy and leading to needless deaths,” asserted a physician. “However, there are uncertainties, and where those exist, physicians [should] simply say ‘it is unknown.’”
No, those physicians have a right to speak their beliefs
However, many physicians worried that science and controversial thought were being muzzled.
“Absolutely no,” a doctor stated. “Who judges what is misinformation in this age where debate is canceled? Science advances with challenge, and it’s not about an authority dictating the allowable opinion.”
Another clinician claimed the “truth is very difficult to discern from less-than-truth in a country running on a profit-oriented economic ideology.”
One specialist warned that if disinformation doctors are held responsible, then “that means a lot of doctors” will be “gone” because “almost anything that is written or said about COVID can be contested.”
Another physician warned his colleagues about suppressing new ideas: “To condemn what we didn’t try, or purposefully ignore a different approach because [it] doesn’t agree with our opinion is suppression of information.”
Some doctors insisted the issue extended beyond medicine and into Constitutional freedoms. They also expressed their mistrust in the government to regulate physicians.
“There is a First Amendment in this country,” said one reader. “What you think is false may not be so. The people can listen to whoever they want to and make their own medical decisions. We do not need one iota more of politicizing medicine. Having an MD or DO does not mean you relinquish your First Amendment rights.”
“One of the fundamental problems with a system that allows government to ‘license’ physicians, or any other profession, is that politics inevitably turn to cronyism, and big businesses and wealthy people start controlling the government,” argued a doctor.
One clinician suggested enforcement against health food, drug company commercials, and talk shows: “What about all the [misinformation] at the health food stores and the like. Doctors of natural-whatever? Those info-commercials on tv. How many faxes do I get to ‘approve’ because ‘patients request’ braces and pain-treating expensive compounds advertised on TV? We tolerate those ... What about Dr. Oz and the docs on talk shows claiming BS?”
And the debate goes even further
Some physicians questioned the very notion of claiming “truth.”
“Nobody should be certain that they have the ‘absolute truth,’” said one reader. “In fact, the best clinical insights exceed so-called knowledge by at least one step.”
“Who can determine exactly what is truth?” asked another clinician. “For sure, the ‘Federal Government,’ who ‘is here to help you,’ is not qualified to make such determinations, and who are you to make such a suggestion as to remove someone’s license because they disagree with you? Give me a break!”
Another physician echoed that sentiment: “What’s true and false is often and certainly currently debatable. There are well-qualified physicians (with credentials such as the development of mRNA technology), virologists, and biostatisticians that have valid thoughts on this but do not necessarily agree with the drug company-sponsored journals and news channels (most of them). Their voices should be heard, and they should not lose their licenses. They are doing their work in good conscience.”
One reader commented that he wanted his “freedom of speech,” and offered this defiant advice: “You can take this license and shove it.”
Finally, a physician noted that the political climate has influenced medical directives: “If someone in a leadership role knowingly, and with intent, spread false information, that is wrong. However, during this global pandemic the active and the politics have combined. Red state no mandate, blue state mandate – what does that tell you about American leadership?”
A version of this article first appeared on Medscape.com.
Doctors providing “fraudulent” COVID-19 information became a hot-button issue for physicians responding to Medscape’s recent article, "Shouldn’t Doctors Who Spread False COVID-19 Information Lose Their Licenses?”
COVID-19 safety recommendations are set by mainstream medical organizations as new information becomes available, but some doctors consistently oppose advice from the Centers for Disease Control and Prevention and other medical authorities. These physicians often promote off-label, unapproved use of medications for COVID-19 and/or contradict mainstream safety guidelines such as vaccines, masks, and social distancing.
Some medical organizations are concerned that these doctors are hampering efforts to control the highly contagious coronavirus and are, at worst, placing lives in danger with their contrarian views that can spread like wildfire on social media sites. Their words are often used by those who refuse to be vaccinated or wear masks.
State licensing boards have mostly refused to discipline these doctors for making false and/or misleading claims, but as the virus spreads, there are calls to take action against them. However, others worry that such actions would violate free speech and critical thought.
Yes, those doctors are doing wrong
Several physicians took a strong stand against their fellow doctors who are spreading misinformation about COVID-19.
One doctor endorsed the idea of removing licenses for spreading misinformation and called for criminal prosecution: “It should certainly be grounds for cancellation of all licensing (after appropriate examination to rule out acute psychotic episodes, dementia, tumor, etc.) and very likely [include] a charge of manslaughter.”
Another health care provider said, “A person who does not accept science should not, of course, be allowed to practice medicine. One who argues publicly that vaccines and masks don’t work should be prosecuted for crimes ranging from reckless endangerment to attempted murder.”
One reader framed COVID-19 misinformers in stark terms: “These men and women are medical prostitutes. Their medical and surgical colleges [should] have a panel to track in-court testimony and the disinformation they spread ...”
“This is malpractice of the worst kind,” said a clinician. “Public health officials and science are quite clear on [the] best practices for safety during a pandemic, which is killing millions. This is a standard of care.”
“Medical Boards should suspend licenses and give the physician a chance to testify [about] the scientific basis for his comments,” added a health care provider. “Boards involve themselves in all kinds of perceived disciplinary infractions. We are in the midst of a lethal pandemic. I would think that would take precedence over many other issues?”
“I do believe that physicians have the responsibility to speak the truth and have scientifically displayed minds,” said a reader. “Not [to] promulgate misleading, false, and/or unverified information.”
“Any physician, who holds a license, should abide [by] government and state regulation,” asserted a doctor. “He should be disciplined by the board for spreading medical/public misinformation since he is creating potential harm to the population.”
One specialist insisted that “state boards do not do enough to restrict/limit the practice of physicians touting questionable therapies.”
“Any doctor who spreads false information about Covid is hurting our country, our individuals, and our economy and leading to needless deaths,” asserted a physician. “However, there are uncertainties, and where those exist, physicians [should] simply say ‘it is unknown.’”
No, those physicians have a right to speak their beliefs
However, many physicians worried that science and controversial thought were being muzzled.
“Absolutely no,” a doctor stated. “Who judges what is misinformation in this age where debate is canceled? Science advances with challenge, and it’s not about an authority dictating the allowable opinion.”
Another clinician claimed the “truth is very difficult to discern from less-than-truth in a country running on a profit-oriented economic ideology.”
One specialist warned that if disinformation doctors are held responsible, then “that means a lot of doctors” will be “gone” because “almost anything that is written or said about COVID can be contested.”
Another physician warned his colleagues about suppressing new ideas: “To condemn what we didn’t try, or purposefully ignore a different approach because [it] doesn’t agree with our opinion is suppression of information.”
Some doctors insisted the issue extended beyond medicine and into Constitutional freedoms. They also expressed their mistrust in the government to regulate physicians.
“There is a First Amendment in this country,” said one reader. “What you think is false may not be so. The people can listen to whoever they want to and make their own medical decisions. We do not need one iota more of politicizing medicine. Having an MD or DO does not mean you relinquish your First Amendment rights.”
“One of the fundamental problems with a system that allows government to ‘license’ physicians, or any other profession, is that politics inevitably turn to cronyism, and big businesses and wealthy people start controlling the government,” argued a doctor.
One clinician suggested enforcement against health food, drug company commercials, and talk shows: “What about all the [misinformation] at the health food stores and the like. Doctors of natural-whatever? Those info-commercials on tv. How many faxes do I get to ‘approve’ because ‘patients request’ braces and pain-treating expensive compounds advertised on TV? We tolerate those ... What about Dr. Oz and the docs on talk shows claiming BS?”
And the debate goes even further
Some physicians questioned the very notion of claiming “truth.”
“Nobody should be certain that they have the ‘absolute truth,’” said one reader. “In fact, the best clinical insights exceed so-called knowledge by at least one step.”
“Who can determine exactly what is truth?” asked another clinician. “For sure, the ‘Federal Government,’ who ‘is here to help you,’ is not qualified to make such determinations, and who are you to make such a suggestion as to remove someone’s license because they disagree with you? Give me a break!”
Another physician echoed that sentiment: “What’s true and false is often and certainly currently debatable. There are well-qualified physicians (with credentials such as the development of mRNA technology), virologists, and biostatisticians that have valid thoughts on this but do not necessarily agree with the drug company-sponsored journals and news channels (most of them). Their voices should be heard, and they should not lose their licenses. They are doing their work in good conscience.”
One reader commented that he wanted his “freedom of speech,” and offered this defiant advice: “You can take this license and shove it.”
Finally, a physician noted that the political climate has influenced medical directives: “If someone in a leadership role knowingly, and with intent, spread false information, that is wrong. However, during this global pandemic the active and the politics have combined. Red state no mandate, blue state mandate – what does that tell you about American leadership?”
A version of this article first appeared on Medscape.com.
Doctors providing “fraudulent” COVID-19 information became a hot-button issue for physicians responding to Medscape’s recent article, "Shouldn’t Doctors Who Spread False COVID-19 Information Lose Their Licenses?”
COVID-19 safety recommendations are set by mainstream medical organizations as new information becomes available, but some doctors consistently oppose advice from the Centers for Disease Control and Prevention and other medical authorities. These physicians often promote off-label, unapproved use of medications for COVID-19 and/or contradict mainstream safety guidelines such as vaccines, masks, and social distancing.
Some medical organizations are concerned that these doctors are hampering efforts to control the highly contagious coronavirus and are, at worst, placing lives in danger with their contrarian views that can spread like wildfire on social media sites. Their words are often used by those who refuse to be vaccinated or wear masks.
State licensing boards have mostly refused to discipline these doctors for making false and/or misleading claims, but as the virus spreads, there are calls to take action against them. However, others worry that such actions would violate free speech and critical thought.
Yes, those doctors are doing wrong
Several physicians took a strong stand against their fellow doctors who are spreading misinformation about COVID-19.
One doctor endorsed the idea of removing licenses for spreading misinformation and called for criminal prosecution: “It should certainly be grounds for cancellation of all licensing (after appropriate examination to rule out acute psychotic episodes, dementia, tumor, etc.) and very likely [include] a charge of manslaughter.”
Another health care provider said, “A person who does not accept science should not, of course, be allowed to practice medicine. One who argues publicly that vaccines and masks don’t work should be prosecuted for crimes ranging from reckless endangerment to attempted murder.”
One reader framed COVID-19 misinformers in stark terms: “These men and women are medical prostitutes. Their medical and surgical colleges [should] have a panel to track in-court testimony and the disinformation they spread ...”
“This is malpractice of the worst kind,” said a clinician. “Public health officials and science are quite clear on [the] best practices for safety during a pandemic, which is killing millions. This is a standard of care.”
“Medical Boards should suspend licenses and give the physician a chance to testify [about] the scientific basis for his comments,” added a health care provider. “Boards involve themselves in all kinds of perceived disciplinary infractions. We are in the midst of a lethal pandemic. I would think that would take precedence over many other issues?”
“I do believe that physicians have the responsibility to speak the truth and have scientifically displayed minds,” said a reader. “Not [to] promulgate misleading, false, and/or unverified information.”
“Any physician, who holds a license, should abide [by] government and state regulation,” asserted a doctor. “He should be disciplined by the board for spreading medical/public misinformation since he is creating potential harm to the population.”
One specialist insisted that “state boards do not do enough to restrict/limit the practice of physicians touting questionable therapies.”
“Any doctor who spreads false information about Covid is hurting our country, our individuals, and our economy and leading to needless deaths,” asserted a physician. “However, there are uncertainties, and where those exist, physicians [should] simply say ‘it is unknown.’”
No, those physicians have a right to speak their beliefs
However, many physicians worried that science and controversial thought were being muzzled.
“Absolutely no,” a doctor stated. “Who judges what is misinformation in this age where debate is canceled? Science advances with challenge, and it’s not about an authority dictating the allowable opinion.”
Another clinician claimed the “truth is very difficult to discern from less-than-truth in a country running on a profit-oriented economic ideology.”
One specialist warned that if disinformation doctors are held responsible, then “that means a lot of doctors” will be “gone” because “almost anything that is written or said about COVID can be contested.”
Another physician warned his colleagues about suppressing new ideas: “To condemn what we didn’t try, or purposefully ignore a different approach because [it] doesn’t agree with our opinion is suppression of information.”
Some doctors insisted the issue extended beyond medicine and into Constitutional freedoms. They also expressed their mistrust in the government to regulate physicians.
“There is a First Amendment in this country,” said one reader. “What you think is false may not be so. The people can listen to whoever they want to and make their own medical decisions. We do not need one iota more of politicizing medicine. Having an MD or DO does not mean you relinquish your First Amendment rights.”
“One of the fundamental problems with a system that allows government to ‘license’ physicians, or any other profession, is that politics inevitably turn to cronyism, and big businesses and wealthy people start controlling the government,” argued a doctor.
One clinician suggested enforcement against health food, drug company commercials, and talk shows: “What about all the [misinformation] at the health food stores and the like. Doctors of natural-whatever? Those info-commercials on tv. How many faxes do I get to ‘approve’ because ‘patients request’ braces and pain-treating expensive compounds advertised on TV? We tolerate those ... What about Dr. Oz and the docs on talk shows claiming BS?”
And the debate goes even further
Some physicians questioned the very notion of claiming “truth.”
“Nobody should be certain that they have the ‘absolute truth,’” said one reader. “In fact, the best clinical insights exceed so-called knowledge by at least one step.”
“Who can determine exactly what is truth?” asked another clinician. “For sure, the ‘Federal Government,’ who ‘is here to help you,’ is not qualified to make such determinations, and who are you to make such a suggestion as to remove someone’s license because they disagree with you? Give me a break!”
Another physician echoed that sentiment: “What’s true and false is often and certainly currently debatable. There are well-qualified physicians (with credentials such as the development of mRNA technology), virologists, and biostatisticians that have valid thoughts on this but do not necessarily agree with the drug company-sponsored journals and news channels (most of them). Their voices should be heard, and they should not lose their licenses. They are doing their work in good conscience.”
One reader commented that he wanted his “freedom of speech,” and offered this defiant advice: “You can take this license and shove it.”
Finally, a physician noted that the political climate has influenced medical directives: “If someone in a leadership role knowingly, and with intent, spread false information, that is wrong. However, during this global pandemic the active and the politics have combined. Red state no mandate, blue state mandate – what does that tell you about American leadership?”
A version of this article first appeared on Medscape.com.