User login
AVAHO
div[contains(@class, 'header__large-screen')]
div[contains(@class, 'read-next-article')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
footer[@id='footer']
div[contains(@class, 'main-prefix')]
section[contains(@class, 'nav-hidden')]
div[contains(@class, 'ce-card-content')]
nav[contains(@class, 'nav-ce-stack')]
Strength Training Can Improve Lymphedema in Breast Cancer
TOPLINE:
A recent study found that 3 months of resistance training did not worsen lymphedema in breast cancer survivors and instead significantly improved fluid balance and increased upper extremity muscle mass. The edema index also improved, suggesting potential therapeutic benefits of intense resistance training for managing lymphedema.
METHODOLOGY:
- Lymphedema is a common adverse effect of breast cancer treatment that can limit mobility. Although strength training can have multiple benefits for breast cancer survivors, such as increased bone density and metabolism, data on whether more intense resistance training exacerbates lymphedema in this population are limited. Worries that more intense training will lead to or worsen lymphedema have typically led to cautious recommendations.
- Researchers conducted a cohort study involving 115 women with breast cancer (median age, 54 years; 96% White; 4% Black) between September 2022 and March 2024. Most (83%) underwent sentinel lymph node biopsy (SLNB), while 12% had axillary lymph node dissection (ALND). At baseline, 13% had clinical lymphedema, including 37% in the ALND group and 8% in the SLNB group.
- Participants attended resistance training sessions three times a week, with intensity escalation over 3 months. Exercises involved hand weights, resistance bands, and body weight (eg, pushups) to promote strength, mobility, and muscle hypertrophy.
- Bioimpedance analysis measured intracellular water, extracellular water, and total body water before and after exercise. Lymphedema was defined as more than a 3% increase in arm circumference discrepancy relative to preoperative ipsilateral arm measurements, along with an elevated edema index (extracellular water to total body water ratio).
TAKEAWAY:
- No participants experienced subjective or clinical worsening of lymphedema after completing the resistance training regimen.
- Lean mass in the affected arm increased from a median of 5.45 lb to 5.64 lb (P < .001), while lean mass in the unaffected arm rose from 5.51 lb to 5.53 lb (P < .001) after the resistance training.
- Overall, participants’ fluid balance improved. The edema index in both arms showed a significant reduction at training completion (mean, 0.383) vs baseline (mean, 0.385), indicating reduced lymphedema. Subgroup analysis of women who underwent SLNB showed similar improvements in the edema index.
IN PRACTICE:
“These findings highlight the safety of strength and resistance training in a large group of patients with breast cancer during and after treatment,” the authors wrote. Beyond that, the authors noted, the results point to a potential role for resistance training in reducing lymphedema.
SOURCE:
This study, led by Parisa Shamsesfandabadi, MD, Allegheny Health Network, Pittsburgh, was published online in JAMA Network Open.
LIMITATIONS:
A major limitation was the absence of a control group, which prevented a direct comparison between the effects of exercise and the natural progression of lymphedema. The 3-month intervention provided limited insight into the long-term sustainability of benefits. Patient-reported outcomes were not included. Additionally, potential confounding variables such as diet, medication use, and baseline physical activity levels were not controlled for in the analysis.
DISCLOSURES:
The authors did not disclose any funding information. Several authors reported having ties with various sources. Additional disclosures are noted in the original article.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
TOPLINE:
A recent study found that 3 months of resistance training did not worsen lymphedema in breast cancer survivors and instead significantly improved fluid balance and increased upper extremity muscle mass. The edema index also improved, suggesting potential therapeutic benefits of intense resistance training for managing lymphedema.
METHODOLOGY:
- Lymphedema is a common adverse effect of breast cancer treatment that can limit mobility. Although strength training can have multiple benefits for breast cancer survivors, such as increased bone density and metabolism, data on whether more intense resistance training exacerbates lymphedema in this population are limited. Worries that more intense training will lead to or worsen lymphedema have typically led to cautious recommendations.
- Researchers conducted a cohort study involving 115 women with breast cancer (median age, 54 years; 96% White; 4% Black) between September 2022 and March 2024. Most (83%) underwent sentinel lymph node biopsy (SLNB), while 12% had axillary lymph node dissection (ALND). At baseline, 13% had clinical lymphedema, including 37% in the ALND group and 8% in the SLNB group.
- Participants attended resistance training sessions three times a week, with intensity escalation over 3 months. Exercises involved hand weights, resistance bands, and body weight (eg, pushups) to promote strength, mobility, and muscle hypertrophy.
- Bioimpedance analysis measured intracellular water, extracellular water, and total body water before and after exercise. Lymphedema was defined as more than a 3% increase in arm circumference discrepancy relative to preoperative ipsilateral arm measurements, along with an elevated edema index (extracellular water to total body water ratio).
TAKEAWAY:
- No participants experienced subjective or clinical worsening of lymphedema after completing the resistance training regimen.
- Lean mass in the affected arm increased from a median of 5.45 lb to 5.64 lb (P < .001), while lean mass in the unaffected arm rose from 5.51 lb to 5.53 lb (P < .001) after the resistance training.
- Overall, participants’ fluid balance improved. The edema index in both arms showed a significant reduction at training completion (mean, 0.383) vs baseline (mean, 0.385), indicating reduced lymphedema. Subgroup analysis of women who underwent SLNB showed similar improvements in the edema index.
IN PRACTICE:
“These findings highlight the safety of strength and resistance training in a large group of patients with breast cancer during and after treatment,” the authors wrote. Beyond that, the authors noted, the results point to a potential role for resistance training in reducing lymphedema.
SOURCE:
This study, led by Parisa Shamsesfandabadi, MD, Allegheny Health Network, Pittsburgh, was published online in JAMA Network Open.
LIMITATIONS:
A major limitation was the absence of a control group, which prevented a direct comparison between the effects of exercise and the natural progression of lymphedema. The 3-month intervention provided limited insight into the long-term sustainability of benefits. Patient-reported outcomes were not included. Additionally, potential confounding variables such as diet, medication use, and baseline physical activity levels were not controlled for in the analysis.
DISCLOSURES:
The authors did not disclose any funding information. Several authors reported having ties with various sources. Additional disclosures are noted in the original article.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
TOPLINE:
A recent study found that 3 months of resistance training did not worsen lymphedema in breast cancer survivors and instead significantly improved fluid balance and increased upper extremity muscle mass. The edema index also improved, suggesting potential therapeutic benefits of intense resistance training for managing lymphedema.
METHODOLOGY:
- Lymphedema is a common adverse effect of breast cancer treatment that can limit mobility. Although strength training can have multiple benefits for breast cancer survivors, such as increased bone density and metabolism, data on whether more intense resistance training exacerbates lymphedema in this population are limited. Worries that more intense training will lead to or worsen lymphedema have typically led to cautious recommendations.
- Researchers conducted a cohort study involving 115 women with breast cancer (median age, 54 years; 96% White; 4% Black) between September 2022 and March 2024. Most (83%) underwent sentinel lymph node biopsy (SLNB), while 12% had axillary lymph node dissection (ALND). At baseline, 13% had clinical lymphedema, including 37% in the ALND group and 8% in the SLNB group.
- Participants attended resistance training sessions three times a week, with intensity escalation over 3 months. Exercises involved hand weights, resistance bands, and body weight (eg, pushups) to promote strength, mobility, and muscle hypertrophy.
- Bioimpedance analysis measured intracellular water, extracellular water, and total body water before and after exercise. Lymphedema was defined as more than a 3% increase in arm circumference discrepancy relative to preoperative ipsilateral arm measurements, along with an elevated edema index (extracellular water to total body water ratio).
TAKEAWAY:
- No participants experienced subjective or clinical worsening of lymphedema after completing the resistance training regimen.
- Lean mass in the affected arm increased from a median of 5.45 lb to 5.64 lb (P < .001), while lean mass in the unaffected arm rose from 5.51 lb to 5.53 lb (P < .001) after the resistance training.
- Overall, participants’ fluid balance improved. The edema index in both arms showed a significant reduction at training completion (mean, 0.383) vs baseline (mean, 0.385), indicating reduced lymphedema. Subgroup analysis of women who underwent SLNB showed similar improvements in the edema index.
IN PRACTICE:
“These findings highlight the safety of strength and resistance training in a large group of patients with breast cancer during and after treatment,” the authors wrote. Beyond that, the authors noted, the results point to a potential role for resistance training in reducing lymphedema.
SOURCE:
This study, led by Parisa Shamsesfandabadi, MD, Allegheny Health Network, Pittsburgh, was published online in JAMA Network Open.
LIMITATIONS:
A major limitation was the absence of a control group, which prevented a direct comparison between the effects of exercise and the natural progression of lymphedema. The 3-month intervention provided limited insight into the long-term sustainability of benefits. Patient-reported outcomes were not included. Additionally, potential confounding variables such as diet, medication use, and baseline physical activity levels were not controlled for in the analysis.
DISCLOSURES:
The authors did not disclose any funding information. Several authors reported having ties with various sources. Additional disclosures are noted in the original article.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
Ethnic Disparities in Cancer Reflect Disparities in HIV Care
While several cancers associated with immunosuppression are much more common in White men who have sex with men living with HIV (MSMWH) than in the male general population, they are even more frequently seen in Black and Hispanic MSMWH.
This suggests that racial and ethnic disparities in access to antiretroviral therapy and viral suppression are playing a role, said the authors of an analysis published last month in AIDS.
“Disparities in cancer risk may serve as an important proxy for disparities in HIV care,” they wrote.
The researchers at the National Cancer Institute leveraged data from the HIV/AIDS Cancer Match Study, which covers 13 US states and the District of Columbia. For this analysis, they examined cancer incidence in over 350,000 MSMWH followed for 3.2 million person years, between 2001 and 2019.
They focused on Kaposi sarcoma, non-Hodgkin lymphoma, Hodgkin lymphoma, anal cancer, and liver cancer — all malignancies that are associated with viral infections and immunosuppression. They restricted their analysis to MSM because behavioral factors (such as anal sex) contribute to increased exposure to viral infections in this population.
The study’s intersectional lens is valuable, Gita Suneja, MD, said in an interview. “It is looking at racial and ethnic disparities within an already minoritized group, which is men who have sex with men living with HIV,” said the professor of radiation oncology at the University of Utah, Salt Lake City, Utah, who was not involved in the study.
“It’s really profound to me to sit back and think about how these disparities intersect, and how somebody can be so marginalized: it’s not just race or ethnicity, it’s not just having a stigmatized medical condition, it’s the confluence of all of these factors that leads to exclusion from care and poor outcomes.”
Standardized incidence ratios (SIRs), using men of the same ethnicity and age in the general population as the comparator, were reported for MSMWH of different racial/ethnic groups. For non-Hodgkin lymphoma, the SIR was 3.11 for White MSMWH, rising to 4.84 for Black MSMWH and 5.46 for Hispanic MSMWH.
For Hodgkin lymphoma, the SIRs were 6.35, 7.69, and 11.5, respectively. For Kaposi sarcoma, they were many orders of magnitude higher, at 417 for White MSMWH, 772 for Black MSMWH, and 887 for Hispanic MSMWH.
In contrast, for anal cancer and liver cancer, the highest SIRs were among White MSMWH.
Given the role of immunosuppression, the researchers wanted to see whether cancer incidence differed according to prior AIDS diagnosis. However, they found that within each racial/ethnic group, there were no statistically significant differences in SIR according to AIDS status.
“There were disparities across the board for [racially minoritized] groups, regardless of immunosuppression status, which leads us to believe that it isn’t just about the diagnosis of AIDS, but about many other factors that we’re not capturing in the paper,” first author Benton Meldrum, MPH, told this news organization.
One study limitation is that AIDS diagnosis is an imprecise proxy for immunosuppression. It does not capture the duration and severity of immunosuppression, nor the extent of immune restoration. Many people with a previous AIDS diagnosis are now virally suppressed.
Database studies have inherent limitations in terms of the range of parameters recorded. In an ideal world, Meldrum said, they would have had access to information on CD4 count and viral suppression over time, as well as socioeconomic factors such as income and insurance status.
Differences in timely HIV diagnosis, viral suppression, and continued engagement in care are thought to drive the differences in cancer incidence. “HIV control today helps mitigate the risk of cancer development down the road,” Suneja said.
While not addressed by this study, there may be additional differences in cancer survival. Differences in cancer care, including prompt diagnosis and access to effective treatment, could play a role.
In terms of practical interventions to address these disparities, Suneja highlights the value of programs which help patients navigate a complex healthcare system. This may include care coordination navigation, peer navigation, and delivering services in community settings.
Such interventions don’t only benefit marginalized groups but help improve healthcare access and outcomes for everyone, she said. Even people with insurance and high health literacy often struggle to remain engaged.
“When we design healthcare systems to best serve those that have been left furthest behind, we all do better,” Suneja said.
The study was funded by the Intramural Research Program of the National Cancer Institute. Suneja and Meldrum reported having no relevant financial relationships.
A version of this article first appeared on Medscape.com.
While several cancers associated with immunosuppression are much more common in White men who have sex with men living with HIV (MSMWH) than in the male general population, they are even more frequently seen in Black and Hispanic MSMWH.
This suggests that racial and ethnic disparities in access to antiretroviral therapy and viral suppression are playing a role, said the authors of an analysis published last month in AIDS.
“Disparities in cancer risk may serve as an important proxy for disparities in HIV care,” they wrote.
The researchers at the National Cancer Institute leveraged data from the HIV/AIDS Cancer Match Study, which covers 13 US states and the District of Columbia. For this analysis, they examined cancer incidence in over 350,000 MSMWH followed for 3.2 million person years, between 2001 and 2019.
They focused on Kaposi sarcoma, non-Hodgkin lymphoma, Hodgkin lymphoma, anal cancer, and liver cancer — all malignancies that are associated with viral infections and immunosuppression. They restricted their analysis to MSM because behavioral factors (such as anal sex) contribute to increased exposure to viral infections in this population.
The study’s intersectional lens is valuable, Gita Suneja, MD, said in an interview. “It is looking at racial and ethnic disparities within an already minoritized group, which is men who have sex with men living with HIV,” said the professor of radiation oncology at the University of Utah, Salt Lake City, Utah, who was not involved in the study.
“It’s really profound to me to sit back and think about how these disparities intersect, and how somebody can be so marginalized: it’s not just race or ethnicity, it’s not just having a stigmatized medical condition, it’s the confluence of all of these factors that leads to exclusion from care and poor outcomes.”
Standardized incidence ratios (SIRs), using men of the same ethnicity and age in the general population as the comparator, were reported for MSMWH of different racial/ethnic groups. For non-Hodgkin lymphoma, the SIR was 3.11 for White MSMWH, rising to 4.84 for Black MSMWH and 5.46 for Hispanic MSMWH.
For Hodgkin lymphoma, the SIRs were 6.35, 7.69, and 11.5, respectively. For Kaposi sarcoma, they were many orders of magnitude higher, at 417 for White MSMWH, 772 for Black MSMWH, and 887 for Hispanic MSMWH.
In contrast, for anal cancer and liver cancer, the highest SIRs were among White MSMWH.
Given the role of immunosuppression, the researchers wanted to see whether cancer incidence differed according to prior AIDS diagnosis. However, they found that within each racial/ethnic group, there were no statistically significant differences in SIR according to AIDS status.
“There were disparities across the board for [racially minoritized] groups, regardless of immunosuppression status, which leads us to believe that it isn’t just about the diagnosis of AIDS, but about many other factors that we’re not capturing in the paper,” first author Benton Meldrum, MPH, told this news organization.
One study limitation is that AIDS diagnosis is an imprecise proxy for immunosuppression. It does not capture the duration and severity of immunosuppression, nor the extent of immune restoration. Many people with a previous AIDS diagnosis are now virally suppressed.
Database studies have inherent limitations in terms of the range of parameters recorded. In an ideal world, Meldrum said, they would have had access to information on CD4 count and viral suppression over time, as well as socioeconomic factors such as income and insurance status.
Differences in timely HIV diagnosis, viral suppression, and continued engagement in care are thought to drive the differences in cancer incidence. “HIV control today helps mitigate the risk of cancer development down the road,” Suneja said.
While not addressed by this study, there may be additional differences in cancer survival. Differences in cancer care, including prompt diagnosis and access to effective treatment, could play a role.
In terms of practical interventions to address these disparities, Suneja highlights the value of programs which help patients navigate a complex healthcare system. This may include care coordination navigation, peer navigation, and delivering services in community settings.
Such interventions don’t only benefit marginalized groups but help improve healthcare access and outcomes for everyone, she said. Even people with insurance and high health literacy often struggle to remain engaged.
“When we design healthcare systems to best serve those that have been left furthest behind, we all do better,” Suneja said.
The study was funded by the Intramural Research Program of the National Cancer Institute. Suneja and Meldrum reported having no relevant financial relationships.
A version of this article first appeared on Medscape.com.
While several cancers associated with immunosuppression are much more common in White men who have sex with men living with HIV (MSMWH) than in the male general population, they are even more frequently seen in Black and Hispanic MSMWH.
This suggests that racial and ethnic disparities in access to antiretroviral therapy and viral suppression are playing a role, said the authors of an analysis published last month in AIDS.
“Disparities in cancer risk may serve as an important proxy for disparities in HIV care,” they wrote.
The researchers at the National Cancer Institute leveraged data from the HIV/AIDS Cancer Match Study, which covers 13 US states and the District of Columbia. For this analysis, they examined cancer incidence in over 350,000 MSMWH followed for 3.2 million person years, between 2001 and 2019.
They focused on Kaposi sarcoma, non-Hodgkin lymphoma, Hodgkin lymphoma, anal cancer, and liver cancer — all malignancies that are associated with viral infections and immunosuppression. They restricted their analysis to MSM because behavioral factors (such as anal sex) contribute to increased exposure to viral infections in this population.
The study’s intersectional lens is valuable, Gita Suneja, MD, said in an interview. “It is looking at racial and ethnic disparities within an already minoritized group, which is men who have sex with men living with HIV,” said the professor of radiation oncology at the University of Utah, Salt Lake City, Utah, who was not involved in the study.
“It’s really profound to me to sit back and think about how these disparities intersect, and how somebody can be so marginalized: it’s not just race or ethnicity, it’s not just having a stigmatized medical condition, it’s the confluence of all of these factors that leads to exclusion from care and poor outcomes.”
Standardized incidence ratios (SIRs), using men of the same ethnicity and age in the general population as the comparator, were reported for MSMWH of different racial/ethnic groups. For non-Hodgkin lymphoma, the SIR was 3.11 for White MSMWH, rising to 4.84 for Black MSMWH and 5.46 for Hispanic MSMWH.
For Hodgkin lymphoma, the SIRs were 6.35, 7.69, and 11.5, respectively. For Kaposi sarcoma, they were many orders of magnitude higher, at 417 for White MSMWH, 772 for Black MSMWH, and 887 for Hispanic MSMWH.
In contrast, for anal cancer and liver cancer, the highest SIRs were among White MSMWH.
Given the role of immunosuppression, the researchers wanted to see whether cancer incidence differed according to prior AIDS diagnosis. However, they found that within each racial/ethnic group, there were no statistically significant differences in SIR according to AIDS status.
“There were disparities across the board for [racially minoritized] groups, regardless of immunosuppression status, which leads us to believe that it isn’t just about the diagnosis of AIDS, but about many other factors that we’re not capturing in the paper,” first author Benton Meldrum, MPH, told this news organization.
One study limitation is that AIDS diagnosis is an imprecise proxy for immunosuppression. It does not capture the duration and severity of immunosuppression, nor the extent of immune restoration. Many people with a previous AIDS diagnosis are now virally suppressed.
Database studies have inherent limitations in terms of the range of parameters recorded. In an ideal world, Meldrum said, they would have had access to information on CD4 count and viral suppression over time, as well as socioeconomic factors such as income and insurance status.
Differences in timely HIV diagnosis, viral suppression, and continued engagement in care are thought to drive the differences in cancer incidence. “HIV control today helps mitigate the risk of cancer development down the road,” Suneja said.
While not addressed by this study, there may be additional differences in cancer survival. Differences in cancer care, including prompt diagnosis and access to effective treatment, could play a role.
In terms of practical interventions to address these disparities, Suneja highlights the value of programs which help patients navigate a complex healthcare system. This may include care coordination navigation, peer navigation, and delivering services in community settings.
Such interventions don’t only benefit marginalized groups but help improve healthcare access and outcomes for everyone, she said. Even people with insurance and high health literacy often struggle to remain engaged.
“When we design healthcare systems to best serve those that have been left furthest behind, we all do better,” Suneja said.
The study was funded by the Intramural Research Program of the National Cancer Institute. Suneja and Meldrum reported having no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Landmark 20-Year Study Reshapes Understanding of PTSD
A large 20-year study — the longest and most detailed of its kind — shows that posttraumatic stress disorder (PTSD) symptoms can endure for decades, challenging conventional timelines for recovery and offering new insights to guide future treatment.
Researchers analyzed data from the World Trade Center Health Program (WTCHP), which is administered by the US CDC’s National Institute for Occupational Safety and Health (NIOSH), and found symptoms of PTSD persisted for as long as two decades in 10% of first responders involved in the World Trade Center disaster of September 2001.
Participation in the WTCHP is voluntary, but those who enroll receive free assessments, monitoring, and treatment, including psychiatric and behavioral healthcare. It is the longest and most detailed analysis of PTSD and includes 81,298 observations from 12,822 WTC responders.
Participants entered the WTCHP at different timepoints and were assessed annually. Not every enrollee was assessed every year, but the sheer number of participants and observations “just provides much greater density of data over that 20-year course than any previous study,” lead author Frank D. Mann, PhD, told this news organization.
The study was published online on May 27 in Nature Mental Health.
Filling the PTSD Knowledge Gap
Most PTSD research has focused on the short term, with limited insight into how symptoms evolve over the long haul. Without long-term data, it’s been difficult to understand whether PTSD resolves, persists, or worsens — hindering efforts to guide treatment and support. This study aimed to fill that gap by tracking symptom patterns over two decades.
Responders were assessed regularly using the PTSD Checklist for a Specific Stressor, a standardized tool that measures symptom severity on an 85-point scale. On average, each participant completed 6.3 assessments over the course of the study.
A score of ≥ 44 was considered indicative of clinically elevated PTSD symptoms. Between 2002 and 2022, the crude prevalence of elevated symptoms ranged from 8% to 15%. At the same time, 16% to 34% of responders each year reported little to no symptoms, scoring at or near the minimum on the scale.
The researchers found that symptom trajectories varied widely. Nearly as many participants experienced worsening symptoms as those who improved. As a result, the overall population average remained relatively flat over the 20-year period.
Among responders who met the threshold for PTSD, the median time to symptom improvement was 8.9 years — and by year 20, about 76% had shown improvement.
New Insights
Mann, a senior research scientist at Stony Brook University Renaissance School of Medicine, Stony Brook, New York, said the study not only reinforced existing knowledge about PTSD in responders but also uncovered new insights.
Most notably, it showed that PTSD symptoms tended to peak around a decade after 9/11 — significantly later than delayed-onset patterns reported in previous trauma studies.
He also noted a surprising outcome — the top 10% of responders who experienced worsening symptoms over the long term accounted for the majority of mental health costs. These individuals, Mann said, represent a critical gap in care, with current interventions proving largely ineffective for them.
Mann suggested that ongoing trauma exposure — especially for responders still in high-risk jobs — and potential genetic susceptibility may contribute to late-emerging or persistent symptoms.
“These individuals are an urgent priority for health systems, as available resources have not been effective for them,” the study authors wrote.
Mann and his colleagues also found that occupation offered the strongest protection against developing PTSD. Police officers and firefighters benefit from training designed to help them cope with trauma, and repeated exposure may build a degree of resilience.
In contrast, responders without such training — like construction workers — faced a 50% to 55% higher risk of developing PTSD symptoms. Mann emphasized that occupational status was a more powerful predictor of PTSD risk than the severity of the traumatic exposures themselves.
A Valuable Contribution
Commenting on the research for this news organization, Sandra Lowe, MD, medical director of the Mount Sinai WTCMH program, noted that while the study largely confirms what has been known about responders — such as the significant variability in symptom trajectories over time — it still makes a valuable contribution.
“Extending observations for up to 20 years is rare in any study, especially in a cohort this large,” said Lowe, an associate professor of psychiatry at the Icahn School of Medicine at Mount Sinai, New York City, who was not involved in the study.
Also commenting, James West, MD, chair of the American Psychiatric Association’s Committee on the Psychiatric Dimensions of Disaster, described the finding that 10% of responders continued to experience symptoms two decades after exposure as “sobering.”
However, he emphasized that it aligns with observations in the disaster recovery community, where the psychological impact “goes way beyond what most people see as the immediate aftermath and recovery.” West stressed the urgent need to develop effective treatments that enable those affected to live fuller, less impaired lives.
“We still need to be finding the effective treatments that can help these people live fuller lives without impairment from their trauma symptoms,” said West.
Lowe pointed out that the symptom peak around 10 years post-exposure is often linked to external factors. Some responders who had been managing symptoms might lose resilience due to major life changes such as retirement.
“One of the things that was able to keep them engaged is now lost,” she said. “They begin to spend more time reflecting on recollections, and symptoms can worsen.”
West agreed, adding that retirement or job loss often leads to symptom increases because it removes a primary coping mechanism. Both Lowe and Mann also highlighted that 9/11 memorial events can trigger new symptoms or exacerbate existing ones.
Lowe noted that responders with stronger coping skills tended to fare better over time. Effective coping strategies include maintaining regular schedules — especially for eating and sleeping — leading a structured life, and employing stress management techniques like meditation, yoga, or enjoyable hobbies. Social connection and being part of a community are also critical for resilience. She added that clinicians should always inquire about trauma history.
Lowe, West, and Mann all pointed out that PTSD is often accompanied by physical health issues, particularly cardiovascular problems, which tend to be worse in those with the disorder.
Responders with stronger coping skills tended to do better over time, said Lowe. Coping skills that can help make a difference include having a regular schedule, especially for eating and sleeping; having a structured life; and stress management tools, such as meditation or yoga or an enjoyable hobby. Social connection — being part of a community — is also critical, Lowe said.
Clinicians should always inquire about trauma, she said. Lowe, West, and Mann all noted that people with PTSD often have physical illness and that cardiovascular outcomes in particular are worse for those individuals.
WTCHP Future Uncertain
However, despite advances in understanding PTSD and the importance of ongoing care, the future of the program supporting World Trade Center responders remains uncertain.
Some 140,000 people are now enrolled in the WTCHP, which was established as a federal program in 2010. Congress has generally reauthorized the program whenever its funding came up for renewal.
However, earlier this year, the Trump administration dismissed two thirds of the NIOSH workforce, including John Howard, MD, the administrator of the WTCHP.
In response, members of Congress and advocates for 9/11 survivors urged the US Department of Health and Human Services (HHS) to reinstate Howard and the affected employees. Howard is listed as back on the job has since returned to his position, and HHS reportedly reinstated hundreds of NIOSH workers in May.
An HHS spokesperson told this news organization that the WTCHP continues to provide services and is actively “accepting, reviewing, and processing new enrollment applications and certification requests.”
Meanwhile, the Trump administration’s fiscal year 2026 budget proposal seeks to reduce CDC funding by $3.5 billion — approximately 40% — with a shift in focus toward infectious diseases. It remains unclear how the WTCHP will be affected by this new direction.
Mann said he is not involved in the program’s funding details but added, “Presumably, as long as some funding continues to keep the program alive, we will continue monitoring responders and providing free treatment until the very last World Trade Center responder passes.”
The study was partially funded through National Institutes of Health and CDC grants, the SUNY Research Foundation, and the CDC’s World Trade Center Health Program. Mann, Lowe, and West reported having no relevant financial relationships.
A version of this article first appeared on Medscape.com.
A large 20-year study — the longest and most detailed of its kind — shows that posttraumatic stress disorder (PTSD) symptoms can endure for decades, challenging conventional timelines for recovery and offering new insights to guide future treatment.
Researchers analyzed data from the World Trade Center Health Program (WTCHP), which is administered by the US CDC’s National Institute for Occupational Safety and Health (NIOSH), and found symptoms of PTSD persisted for as long as two decades in 10% of first responders involved in the World Trade Center disaster of September 2001.
Participation in the WTCHP is voluntary, but those who enroll receive free assessments, monitoring, and treatment, including psychiatric and behavioral healthcare. It is the longest and most detailed analysis of PTSD and includes 81,298 observations from 12,822 WTC responders.
Participants entered the WTCHP at different timepoints and were assessed annually. Not every enrollee was assessed every year, but the sheer number of participants and observations “just provides much greater density of data over that 20-year course than any previous study,” lead author Frank D. Mann, PhD, told this news organization.
The study was published online on May 27 in Nature Mental Health.
Filling the PTSD Knowledge Gap
Most PTSD research has focused on the short term, with limited insight into how symptoms evolve over the long haul. Without long-term data, it’s been difficult to understand whether PTSD resolves, persists, or worsens — hindering efforts to guide treatment and support. This study aimed to fill that gap by tracking symptom patterns over two decades.
Responders were assessed regularly using the PTSD Checklist for a Specific Stressor, a standardized tool that measures symptom severity on an 85-point scale. On average, each participant completed 6.3 assessments over the course of the study.
A score of ≥ 44 was considered indicative of clinically elevated PTSD symptoms. Between 2002 and 2022, the crude prevalence of elevated symptoms ranged from 8% to 15%. At the same time, 16% to 34% of responders each year reported little to no symptoms, scoring at or near the minimum on the scale.
The researchers found that symptom trajectories varied widely. Nearly as many participants experienced worsening symptoms as those who improved. As a result, the overall population average remained relatively flat over the 20-year period.
Among responders who met the threshold for PTSD, the median time to symptom improvement was 8.9 years — and by year 20, about 76% had shown improvement.
New Insights
Mann, a senior research scientist at Stony Brook University Renaissance School of Medicine, Stony Brook, New York, said the study not only reinforced existing knowledge about PTSD in responders but also uncovered new insights.
Most notably, it showed that PTSD symptoms tended to peak around a decade after 9/11 — significantly later than delayed-onset patterns reported in previous trauma studies.
He also noted a surprising outcome — the top 10% of responders who experienced worsening symptoms over the long term accounted for the majority of mental health costs. These individuals, Mann said, represent a critical gap in care, with current interventions proving largely ineffective for them.
Mann suggested that ongoing trauma exposure — especially for responders still in high-risk jobs — and potential genetic susceptibility may contribute to late-emerging or persistent symptoms.
“These individuals are an urgent priority for health systems, as available resources have not been effective for them,” the study authors wrote.
Mann and his colleagues also found that occupation offered the strongest protection against developing PTSD. Police officers and firefighters benefit from training designed to help them cope with trauma, and repeated exposure may build a degree of resilience.
In contrast, responders without such training — like construction workers — faced a 50% to 55% higher risk of developing PTSD symptoms. Mann emphasized that occupational status was a more powerful predictor of PTSD risk than the severity of the traumatic exposures themselves.
A Valuable Contribution
Commenting on the research for this news organization, Sandra Lowe, MD, medical director of the Mount Sinai WTCMH program, noted that while the study largely confirms what has been known about responders — such as the significant variability in symptom trajectories over time — it still makes a valuable contribution.
“Extending observations for up to 20 years is rare in any study, especially in a cohort this large,” said Lowe, an associate professor of psychiatry at the Icahn School of Medicine at Mount Sinai, New York City, who was not involved in the study.
Also commenting, James West, MD, chair of the American Psychiatric Association’s Committee on the Psychiatric Dimensions of Disaster, described the finding that 10% of responders continued to experience symptoms two decades after exposure as “sobering.”
However, he emphasized that it aligns with observations in the disaster recovery community, where the psychological impact “goes way beyond what most people see as the immediate aftermath and recovery.” West stressed the urgent need to develop effective treatments that enable those affected to live fuller, less impaired lives.
“We still need to be finding the effective treatments that can help these people live fuller lives without impairment from their trauma symptoms,” said West.
Lowe pointed out that the symptom peak around 10 years post-exposure is often linked to external factors. Some responders who had been managing symptoms might lose resilience due to major life changes such as retirement.
“One of the things that was able to keep them engaged is now lost,” she said. “They begin to spend more time reflecting on recollections, and symptoms can worsen.”
West agreed, adding that retirement or job loss often leads to symptom increases because it removes a primary coping mechanism. Both Lowe and Mann also highlighted that 9/11 memorial events can trigger new symptoms or exacerbate existing ones.
Lowe noted that responders with stronger coping skills tended to fare better over time. Effective coping strategies include maintaining regular schedules — especially for eating and sleeping — leading a structured life, and employing stress management techniques like meditation, yoga, or enjoyable hobbies. Social connection and being part of a community are also critical for resilience. She added that clinicians should always inquire about trauma history.
Lowe, West, and Mann all pointed out that PTSD is often accompanied by physical health issues, particularly cardiovascular problems, which tend to be worse in those with the disorder.
Responders with stronger coping skills tended to do better over time, said Lowe. Coping skills that can help make a difference include having a regular schedule, especially for eating and sleeping; having a structured life; and stress management tools, such as meditation or yoga or an enjoyable hobby. Social connection — being part of a community — is also critical, Lowe said.
Clinicians should always inquire about trauma, she said. Lowe, West, and Mann all noted that people with PTSD often have physical illness and that cardiovascular outcomes in particular are worse for those individuals.
WTCHP Future Uncertain
However, despite advances in understanding PTSD and the importance of ongoing care, the future of the program supporting World Trade Center responders remains uncertain.
Some 140,000 people are now enrolled in the WTCHP, which was established as a federal program in 2010. Congress has generally reauthorized the program whenever its funding came up for renewal.
However, earlier this year, the Trump administration dismissed two thirds of the NIOSH workforce, including John Howard, MD, the administrator of the WTCHP.
In response, members of Congress and advocates for 9/11 survivors urged the US Department of Health and Human Services (HHS) to reinstate Howard and the affected employees. Howard is listed as back on the job has since returned to his position, and HHS reportedly reinstated hundreds of NIOSH workers in May.
An HHS spokesperson told this news organization that the WTCHP continues to provide services and is actively “accepting, reviewing, and processing new enrollment applications and certification requests.”
Meanwhile, the Trump administration’s fiscal year 2026 budget proposal seeks to reduce CDC funding by $3.5 billion — approximately 40% — with a shift in focus toward infectious diseases. It remains unclear how the WTCHP will be affected by this new direction.
Mann said he is not involved in the program’s funding details but added, “Presumably, as long as some funding continues to keep the program alive, we will continue monitoring responders and providing free treatment until the very last World Trade Center responder passes.”
The study was partially funded through National Institutes of Health and CDC grants, the SUNY Research Foundation, and the CDC’s World Trade Center Health Program. Mann, Lowe, and West reported having no relevant financial relationships.
A version of this article first appeared on Medscape.com.
A large 20-year study — the longest and most detailed of its kind — shows that posttraumatic stress disorder (PTSD) symptoms can endure for decades, challenging conventional timelines for recovery and offering new insights to guide future treatment.
Researchers analyzed data from the World Trade Center Health Program (WTCHP), which is administered by the US CDC’s National Institute for Occupational Safety and Health (NIOSH), and found symptoms of PTSD persisted for as long as two decades in 10% of first responders involved in the World Trade Center disaster of September 2001.
Participation in the WTCHP is voluntary, but those who enroll receive free assessments, monitoring, and treatment, including psychiatric and behavioral healthcare. It is the longest and most detailed analysis of PTSD and includes 81,298 observations from 12,822 WTC responders.
Participants entered the WTCHP at different timepoints and were assessed annually. Not every enrollee was assessed every year, but the sheer number of participants and observations “just provides much greater density of data over that 20-year course than any previous study,” lead author Frank D. Mann, PhD, told this news organization.
The study was published online on May 27 in Nature Mental Health.
Filling the PTSD Knowledge Gap
Most PTSD research has focused on the short term, with limited insight into how symptoms evolve over the long haul. Without long-term data, it’s been difficult to understand whether PTSD resolves, persists, or worsens — hindering efforts to guide treatment and support. This study aimed to fill that gap by tracking symptom patterns over two decades.
Responders were assessed regularly using the PTSD Checklist for a Specific Stressor, a standardized tool that measures symptom severity on an 85-point scale. On average, each participant completed 6.3 assessments over the course of the study.
A score of ≥ 44 was considered indicative of clinically elevated PTSD symptoms. Between 2002 and 2022, the crude prevalence of elevated symptoms ranged from 8% to 15%. At the same time, 16% to 34% of responders each year reported little to no symptoms, scoring at or near the minimum on the scale.
The researchers found that symptom trajectories varied widely. Nearly as many participants experienced worsening symptoms as those who improved. As a result, the overall population average remained relatively flat over the 20-year period.
Among responders who met the threshold for PTSD, the median time to symptom improvement was 8.9 years — and by year 20, about 76% had shown improvement.
New Insights
Mann, a senior research scientist at Stony Brook University Renaissance School of Medicine, Stony Brook, New York, said the study not only reinforced existing knowledge about PTSD in responders but also uncovered new insights.
Most notably, it showed that PTSD symptoms tended to peak around a decade after 9/11 — significantly later than delayed-onset patterns reported in previous trauma studies.
He also noted a surprising outcome — the top 10% of responders who experienced worsening symptoms over the long term accounted for the majority of mental health costs. These individuals, Mann said, represent a critical gap in care, with current interventions proving largely ineffective for them.
Mann suggested that ongoing trauma exposure — especially for responders still in high-risk jobs — and potential genetic susceptibility may contribute to late-emerging or persistent symptoms.
“These individuals are an urgent priority for health systems, as available resources have not been effective for them,” the study authors wrote.
Mann and his colleagues also found that occupation offered the strongest protection against developing PTSD. Police officers and firefighters benefit from training designed to help them cope with trauma, and repeated exposure may build a degree of resilience.
In contrast, responders without such training — like construction workers — faced a 50% to 55% higher risk of developing PTSD symptoms. Mann emphasized that occupational status was a more powerful predictor of PTSD risk than the severity of the traumatic exposures themselves.
A Valuable Contribution
Commenting on the research for this news organization, Sandra Lowe, MD, medical director of the Mount Sinai WTCMH program, noted that while the study largely confirms what has been known about responders — such as the significant variability in symptom trajectories over time — it still makes a valuable contribution.
“Extending observations for up to 20 years is rare in any study, especially in a cohort this large,” said Lowe, an associate professor of psychiatry at the Icahn School of Medicine at Mount Sinai, New York City, who was not involved in the study.
Also commenting, James West, MD, chair of the American Psychiatric Association’s Committee on the Psychiatric Dimensions of Disaster, described the finding that 10% of responders continued to experience symptoms two decades after exposure as “sobering.”
However, he emphasized that it aligns with observations in the disaster recovery community, where the psychological impact “goes way beyond what most people see as the immediate aftermath and recovery.” West stressed the urgent need to develop effective treatments that enable those affected to live fuller, less impaired lives.
“We still need to be finding the effective treatments that can help these people live fuller lives without impairment from their trauma symptoms,” said West.
Lowe pointed out that the symptom peak around 10 years post-exposure is often linked to external factors. Some responders who had been managing symptoms might lose resilience due to major life changes such as retirement.
“One of the things that was able to keep them engaged is now lost,” she said. “They begin to spend more time reflecting on recollections, and symptoms can worsen.”
West agreed, adding that retirement or job loss often leads to symptom increases because it removes a primary coping mechanism. Both Lowe and Mann also highlighted that 9/11 memorial events can trigger new symptoms or exacerbate existing ones.
Lowe noted that responders with stronger coping skills tended to fare better over time. Effective coping strategies include maintaining regular schedules — especially for eating and sleeping — leading a structured life, and employing stress management techniques like meditation, yoga, or enjoyable hobbies. Social connection and being part of a community are also critical for resilience. She added that clinicians should always inquire about trauma history.
Lowe, West, and Mann all pointed out that PTSD is often accompanied by physical health issues, particularly cardiovascular problems, which tend to be worse in those with the disorder.
Responders with stronger coping skills tended to do better over time, said Lowe. Coping skills that can help make a difference include having a regular schedule, especially for eating and sleeping; having a structured life; and stress management tools, such as meditation or yoga or an enjoyable hobby. Social connection — being part of a community — is also critical, Lowe said.
Clinicians should always inquire about trauma, she said. Lowe, West, and Mann all noted that people with PTSD often have physical illness and that cardiovascular outcomes in particular are worse for those individuals.
WTCHP Future Uncertain
However, despite advances in understanding PTSD and the importance of ongoing care, the future of the program supporting World Trade Center responders remains uncertain.
Some 140,000 people are now enrolled in the WTCHP, which was established as a federal program in 2010. Congress has generally reauthorized the program whenever its funding came up for renewal.
However, earlier this year, the Trump administration dismissed two thirds of the NIOSH workforce, including John Howard, MD, the administrator of the WTCHP.
In response, members of Congress and advocates for 9/11 survivors urged the US Department of Health and Human Services (HHS) to reinstate Howard and the affected employees. Howard is listed as back on the job has since returned to his position, and HHS reportedly reinstated hundreds of NIOSH workers in May.
An HHS spokesperson told this news organization that the WTCHP continues to provide services and is actively “accepting, reviewing, and processing new enrollment applications and certification requests.”
Meanwhile, the Trump administration’s fiscal year 2026 budget proposal seeks to reduce CDC funding by $3.5 billion — approximately 40% — with a shift in focus toward infectious diseases. It remains unclear how the WTCHP will be affected by this new direction.
Mann said he is not involved in the program’s funding details but added, “Presumably, as long as some funding continues to keep the program alive, we will continue monitoring responders and providing free treatment until the very last World Trade Center responder passes.”
The study was partially funded through National Institutes of Health and CDC grants, the SUNY Research Foundation, and the CDC’s World Trade Center Health Program. Mann, Lowe, and West reported having no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM NATURE MENTAL HEALTH

Posttraumatic Stress Disorder May Increase Morbidity Risk in Veterans With HIV
TOPLINE:
Posttraumatic stress disorder (PTSD) among veterans living with HIV significantly increased the risk for AIDS and multiple comorbidities, particularly arthritis, cardiovascular disease (CVD), chronic obstructive pulmonary disease (COPD), chronic kidney disease (CKD), and multimorbidity — with the greatest impact seen in the first decade after diagnosis.
METHODOLOGY:
- Researchers conducted a prospective cohort study to assess whether PTSD is associated with increased risk for adverse clinical outcomes in veterans with HIV who received care at the Department of Veterans Affairs.
- They included 3206 veterans (97.4% men; median age at HIV diagnosis, 31.7 years; 42.1% with PTSD) who were deployed in Iraq and Afghanistan while serving in the military and initiated antiretroviral therapy before December 31, 2020.
- Participants were followed-up until December 2022, with censoring at death, the last health care visit, or study termination. The association between PTSD with morbidity and mortality, considering the number of deployments and levels of combat exposure were determined.
TAKEAWAY:
- PTSD significantly increased the overall risks for AIDS by 11% (adjusted hazard ratio [aHR], 1.11), CKD by 21% (aHR, 1.21), COPD by 46% (aHR, 1.46), multimorbidity by 49% (aHR, 1.49), CVD by 57% (aHR, 1.57), and arthritis by two folds (aHR, 1.95; P <.05 for all).
- Among veterans with a single deployment, those with PTSD had 92%, 87%, 80%, 53%, 44%, 32%, and 27% higher risks for asthma, CVD, arthritis, multimorbidity, COPD, liver disease, and AIDS, respectively, than those without PTSD.
- Veterans with PTSD and combat exposure had a lower risk for AIDS but higher risks for multimorbidity, asthma, CVD, and arthritis than those never diagnosed with PTSD and unexposed to combat.
- The associations of PTSD with mortality and morbidity appeared most pronounced in the first decade post-diagnosis, followed by a gradual decline in association strength; however, risks remained elevated.
IN PRACTICE:
“It is recommended that providers who work with VWH [veterans with HIV] consider adopting a trauma-informed model of HIV care and that providers screen veterans for PTSD, so that their unique trauma history can help guide medical decisions and treatment,” the authors wrote.
SOURCE:
This study was led by Kartavya J. Vyas, PhD, Department of Epidemiology, Rollins School of Public Health, Emory University, Atlanta. It was published online in AIDS .
LIMITATIONS:
The data could not capture each individual’s true index trauma or the severity of their PTSD. Additionally, the study was limited by considerable loss to follow-up, potential uncontrolled confounding related to homelessness, and a lack of generalizability to veterans with HIV who were not receiving antiretroviral therapy.
DISCLOSURES:
The study did not receive any specific funding. Two authors reported receiving federal research support — one from the Emory Center for AIDS Research and the National Institute of Allergy and Infectious Diseases, and the other from the National Institutes of Health and the CDC — in addition to investigator-initiated grants and consulting fees from various pharmaceutical companies.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
TOPLINE:
Posttraumatic stress disorder (PTSD) among veterans living with HIV significantly increased the risk for AIDS and multiple comorbidities, particularly arthritis, cardiovascular disease (CVD), chronic obstructive pulmonary disease (COPD), chronic kidney disease (CKD), and multimorbidity — with the greatest impact seen in the first decade after diagnosis.
METHODOLOGY:
- Researchers conducted a prospective cohort study to assess whether PTSD is associated with increased risk for adverse clinical outcomes in veterans with HIV who received care at the Department of Veterans Affairs.
- They included 3206 veterans (97.4% men; median age at HIV diagnosis, 31.7 years; 42.1% with PTSD) who were deployed in Iraq and Afghanistan while serving in the military and initiated antiretroviral therapy before December 31, 2020.
- Participants were followed-up until December 2022, with censoring at death, the last health care visit, or study termination. The association between PTSD with morbidity and mortality, considering the number of deployments and levels of combat exposure were determined.
TAKEAWAY:
- PTSD significantly increased the overall risks for AIDS by 11% (adjusted hazard ratio [aHR], 1.11), CKD by 21% (aHR, 1.21), COPD by 46% (aHR, 1.46), multimorbidity by 49% (aHR, 1.49), CVD by 57% (aHR, 1.57), and arthritis by two folds (aHR, 1.95; P <.05 for all).
- Among veterans with a single deployment, those with PTSD had 92%, 87%, 80%, 53%, 44%, 32%, and 27% higher risks for asthma, CVD, arthritis, multimorbidity, COPD, liver disease, and AIDS, respectively, than those without PTSD.
- Veterans with PTSD and combat exposure had a lower risk for AIDS but higher risks for multimorbidity, asthma, CVD, and arthritis than those never diagnosed with PTSD and unexposed to combat.
- The associations of PTSD with mortality and morbidity appeared most pronounced in the first decade post-diagnosis, followed by a gradual decline in association strength; however, risks remained elevated.
IN PRACTICE:
“It is recommended that providers who work with VWH [veterans with HIV] consider adopting a trauma-informed model of HIV care and that providers screen veterans for PTSD, so that their unique trauma history can help guide medical decisions and treatment,” the authors wrote.
SOURCE:
This study was led by Kartavya J. Vyas, PhD, Department of Epidemiology, Rollins School of Public Health, Emory University, Atlanta. It was published online in AIDS .
LIMITATIONS:
The data could not capture each individual’s true index trauma or the severity of their PTSD. Additionally, the study was limited by considerable loss to follow-up, potential uncontrolled confounding related to homelessness, and a lack of generalizability to veterans with HIV who were not receiving antiretroviral therapy.
DISCLOSURES:
The study did not receive any specific funding. Two authors reported receiving federal research support — one from the Emory Center for AIDS Research and the National Institute of Allergy and Infectious Diseases, and the other from the National Institutes of Health and the CDC — in addition to investigator-initiated grants and consulting fees from various pharmaceutical companies.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
TOPLINE:
Posttraumatic stress disorder (PTSD) among veterans living with HIV significantly increased the risk for AIDS and multiple comorbidities, particularly arthritis, cardiovascular disease (CVD), chronic obstructive pulmonary disease (COPD), chronic kidney disease (CKD), and multimorbidity — with the greatest impact seen in the first decade after diagnosis.
METHODOLOGY:
- Researchers conducted a prospective cohort study to assess whether PTSD is associated with increased risk for adverse clinical outcomes in veterans with HIV who received care at the Department of Veterans Affairs.
- They included 3206 veterans (97.4% men; median age at HIV diagnosis, 31.7 years; 42.1% with PTSD) who were deployed in Iraq and Afghanistan while serving in the military and initiated antiretroviral therapy before December 31, 2020.
- Participants were followed-up until December 2022, with censoring at death, the last health care visit, or study termination. The association between PTSD with morbidity and mortality, considering the number of deployments and levels of combat exposure were determined.
TAKEAWAY:
- PTSD significantly increased the overall risks for AIDS by 11% (adjusted hazard ratio [aHR], 1.11), CKD by 21% (aHR, 1.21), COPD by 46% (aHR, 1.46), multimorbidity by 49% (aHR, 1.49), CVD by 57% (aHR, 1.57), and arthritis by two folds (aHR, 1.95; P <.05 for all).
- Among veterans with a single deployment, those with PTSD had 92%, 87%, 80%, 53%, 44%, 32%, and 27% higher risks for asthma, CVD, arthritis, multimorbidity, COPD, liver disease, and AIDS, respectively, than those without PTSD.
- Veterans with PTSD and combat exposure had a lower risk for AIDS but higher risks for multimorbidity, asthma, CVD, and arthritis than those never diagnosed with PTSD and unexposed to combat.
- The associations of PTSD with mortality and morbidity appeared most pronounced in the first decade post-diagnosis, followed by a gradual decline in association strength; however, risks remained elevated.
IN PRACTICE:
“It is recommended that providers who work with VWH [veterans with HIV] consider adopting a trauma-informed model of HIV care and that providers screen veterans for PTSD, so that their unique trauma history can help guide medical decisions and treatment,” the authors wrote.
SOURCE:
This study was led by Kartavya J. Vyas, PhD, Department of Epidemiology, Rollins School of Public Health, Emory University, Atlanta. It was published online in AIDS .
LIMITATIONS:
The data could not capture each individual’s true index trauma or the severity of their PTSD. Additionally, the study was limited by considerable loss to follow-up, potential uncontrolled confounding related to homelessness, and a lack of generalizability to veterans with HIV who were not receiving antiretroviral therapy.
DISCLOSURES:
The study did not receive any specific funding. Two authors reported receiving federal research support — one from the Emory Center for AIDS Research and the National Institute of Allergy and Infectious Diseases, and the other from the National Institutes of Health and the CDC — in addition to investigator-initiated grants and consulting fees from various pharmaceutical companies.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
Can Patients Really Say No to Life-Saving Cancer Care?
Mrs G.O. is an 80-year-old retired teacher who was widowed a decade ago. With no close relatives, she lives alone, accompanied by only two cats and a dog that she has rescued. “I am alone,” she told Gustavo Kusminsky, MD, consultant in Hematology and Hematopoietic Transplant Service at Austral University Hospital and lecturer in medicine at the Hospital Universitario Austral, Buenos Aires, Argentina. She said this calmly while refusing treatment for life-threatening multiple myeloma. “Doctor, I would rather not,” she added — her words lingering in the quiet consulting room. That moment is now the focus of a recent article in the journal Medicina.
In the article, Kusminsky described how he made an effort to clarify to the patient that she needed cancer treatment. He explained that the treatment was mostly oral, required no initial hospitalization, and that consultations could be spaced out. However, Mrs G.O. maintained her position.
“The patient had no signs of depression, and her argument was logical. Mrs G.O. was already receiving several medications for high blood pressure, was on anticoagulation therapy for atrial fibrillation, and managed dyslipidemia with fenofibrate. But she preferred not to receive treatment for her multiple myeloma.” Kusminsky noted.
“Doctor, I have lived my life. I am old. I am already taking too many medications. I do not have a family, and it would be very difficult to deal with the side effects and be dependent on the hospital. As long as I can take care of myself, I do not want any more treatment, at least not for now. We will talk in a few months if I am still here,” she told him before leaving.
The article mentioned that responses such as Mrs G.O. spark perplexity in modern medicine to the extent that clinicians initiate protocols to rule out depression or other psychological factors when a patient rejects treatments that could prolong their life. On the contrary, no such checks are made when patients agree to treatment, because acceptance is deemed “normal.”
Because of collective assumptions and the war metaphors often used in oncology, Mrs G.O. risked being labeled a “deserter from the battalion” of patients with cancer.
In truth, her decision invites reflection on the doctor-patient relationship, respect for autonomy, and the benefits of modern cancer care offered today, Kusminsky said.
This provides an opportunity to consider the patient’s perspective rather than a purely medical perspective.
Jennifer Hincapié Sánchez, PhD, professor in the Faculty of Medicine at the National Autonomous University of Mexico (UNAM). She is the director of the UNAM University Bioethics Program and coordinates its Institutional Ethics and Bioethics Program for the Faculty of Medicine in Mexico. Although not involved in the article, she regards it as vital. “It’s crucial to remind medical staff that their role is to promote patients’ well-being and that this is related to the life plan that patients have set for themselves, even though this vision is sometimes not aligned with biomedical progress,” she said.
Patient Autonomy
Science-guided medicine aims to prolong life, improve quality, and relieve suffering. However, acceptance or refusal of treatment remains a personal choice for anyone with cancer.
Some evidence showed that patients who decline treatment do not always experience rapid decline. Many can live acceptable, even fulfilling, lives on their own for varying periods, even though they know that there is a possibility of shorter survival. Valuing fewer side effects and better quality of life. This suggested that quality of life is subjective and cannot be measured solely by biomedical standards but also by the meaning each person finds in their existence, even in the face of serious illness.
“There is a myth that quality of life is only valid when defined by objective success. Our task is to explain that it is subjective, and life can be meaningful despite limitations.” Kusminsky said.
Mrs G.O. knew her prognosis and treatment options but chose not to pursue treatment, which, while medically advisable, did not align with her values or vision of life.
Hincapié Sánchez stated that the priority is always to honor the patient’s choice. Clinicians must ensure that the patient has all necessary information that is always appropriate to their sociocultural context before making the decision.
“If the decision persists despite being informed and aware of the effects of the patient’s choice, all we can do is provide support, manage the pain, and seek the patient’s comfort,” she emphasized.
Medical Omnipotence
Physicians should not view the refusal of treatment as an abandonment of the fundamental principles of the profession. Rather, it means respecting patient priorities and recognizing medicine as a dialogue between science and humanity, not as an exercise of control.
However, many clinicians struggle with such decisions because they conflict with their impulse to act and a sense of medical omnipotence. Hincapié Sánchez attributed these difficulties to medical training.
“We are taught to preserve life at all costs. If treatment even slightly prolongs life, many doctors continue to recommend it. The question becomes: Is it valid to extend life when its quality is in doubt?” she asked.
“Medicine is more than a science; it is an art. It is the most human in the sciences and the most scientific in the humanities. Let us not lose sight of the human element that allows us to see the patient as a person, not just a disease to be treated,” Hincapié Sánchez urges.
Kusminsky describes a common therapeutic obstinacy — doctors’ reluctance to stop “doing something,” to avoid “throwing in the towel,” or to uphold “hope is the last thing to be lost.”
“But physicians are growing more aware of these situations, and change is slowly coming,” he said. However, he added: “Of course, there is the issue of the perceived omnipotence of doctors — their words descending with authority to ‘prescribe’ treatment, issue ‘medical orders,’ or dictate ‘pharmacological’ therapy.
For the specialist, such terminology reflects a view of the doctor-patient relationship not as a mutual, two-way exchange, but as a vertical, paternalistic dynamic.
He suggested looking at ancient Greece for perspective. “Hippocrates, or rather the Hippocratic school, taught that the doctor-patient encounter is inherently one of compassion. We must approach this in that way. Reflecting on that bond, improving communication, humanizing relationships, and, above all, being available to listen are key,” Kusminsky said.
Another intersection that has long fascinated Kusminsky is between literature and medicine. This interest led him to explore the field of narrative medicine, serve on the board of directors of the Argentine Society of Narrative Medicine (SAMEN), and join the roster of speakers at the upcoming second SAMEN Conference in Buenos Aires on July 10 and 11, 2025.
“Narrative medicine uses storytelling tools to absorb, process, acknowledge, and empathize with patients’ illness narratives, aiming to restore humanism to practice,” he explained.
According to Kusminsky, the circumstances under which Mrs G.O. expressed her wish not to begin treatment immediately reminded him of a text by Melville’s famous “I would prefer not to” from Bartleby, the Scrivener.
This reflection inspired him to publish an article cited at its beginning. At the same time, it reinforced his belief that what patients say can itself be a form of narrative that extends beyond the confines of clinical history.
Mrs G.O. chose not to pursue treatment for multiple myeloma. However, she returned to Kusminsky’s office approximately 2 months ago. She felt well, and her disease slowly progressed; however, she still had no clinical signs or symptoms.
Kusminsky and Hincapié Sánchez have declared no relevant financial conflicts of interest.
This story was translated from Medscape’s Portuguese edition using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication.
A version of this article first appeared on Medscape.com.
Mrs G.O. is an 80-year-old retired teacher who was widowed a decade ago. With no close relatives, she lives alone, accompanied by only two cats and a dog that she has rescued. “I am alone,” she told Gustavo Kusminsky, MD, consultant in Hematology and Hematopoietic Transplant Service at Austral University Hospital and lecturer in medicine at the Hospital Universitario Austral, Buenos Aires, Argentina. She said this calmly while refusing treatment for life-threatening multiple myeloma. “Doctor, I would rather not,” she added — her words lingering in the quiet consulting room. That moment is now the focus of a recent article in the journal Medicina.
In the article, Kusminsky described how he made an effort to clarify to the patient that she needed cancer treatment. He explained that the treatment was mostly oral, required no initial hospitalization, and that consultations could be spaced out. However, Mrs G.O. maintained her position.
“The patient had no signs of depression, and her argument was logical. Mrs G.O. was already receiving several medications for high blood pressure, was on anticoagulation therapy for atrial fibrillation, and managed dyslipidemia with fenofibrate. But she preferred not to receive treatment for her multiple myeloma.” Kusminsky noted.
“Doctor, I have lived my life. I am old. I am already taking too many medications. I do not have a family, and it would be very difficult to deal with the side effects and be dependent on the hospital. As long as I can take care of myself, I do not want any more treatment, at least not for now. We will talk in a few months if I am still here,” she told him before leaving.
The article mentioned that responses such as Mrs G.O. spark perplexity in modern medicine to the extent that clinicians initiate protocols to rule out depression or other psychological factors when a patient rejects treatments that could prolong their life. On the contrary, no such checks are made when patients agree to treatment, because acceptance is deemed “normal.”
Because of collective assumptions and the war metaphors often used in oncology, Mrs G.O. risked being labeled a “deserter from the battalion” of patients with cancer.
In truth, her decision invites reflection on the doctor-patient relationship, respect for autonomy, and the benefits of modern cancer care offered today, Kusminsky said.
This provides an opportunity to consider the patient’s perspective rather than a purely medical perspective.
Jennifer Hincapié Sánchez, PhD, professor in the Faculty of Medicine at the National Autonomous University of Mexico (UNAM). She is the director of the UNAM University Bioethics Program and coordinates its Institutional Ethics and Bioethics Program for the Faculty of Medicine in Mexico. Although not involved in the article, she regards it as vital. “It’s crucial to remind medical staff that their role is to promote patients’ well-being and that this is related to the life plan that patients have set for themselves, even though this vision is sometimes not aligned with biomedical progress,” she said.
Patient Autonomy
Science-guided medicine aims to prolong life, improve quality, and relieve suffering. However, acceptance or refusal of treatment remains a personal choice for anyone with cancer.
Some evidence showed that patients who decline treatment do not always experience rapid decline. Many can live acceptable, even fulfilling, lives on their own for varying periods, even though they know that there is a possibility of shorter survival. Valuing fewer side effects and better quality of life. This suggested that quality of life is subjective and cannot be measured solely by biomedical standards but also by the meaning each person finds in their existence, even in the face of serious illness.
“There is a myth that quality of life is only valid when defined by objective success. Our task is to explain that it is subjective, and life can be meaningful despite limitations.” Kusminsky said.
Mrs G.O. knew her prognosis and treatment options but chose not to pursue treatment, which, while medically advisable, did not align with her values or vision of life.
Hincapié Sánchez stated that the priority is always to honor the patient’s choice. Clinicians must ensure that the patient has all necessary information that is always appropriate to their sociocultural context before making the decision.
“If the decision persists despite being informed and aware of the effects of the patient’s choice, all we can do is provide support, manage the pain, and seek the patient’s comfort,” she emphasized.
Medical Omnipotence
Physicians should not view the refusal of treatment as an abandonment of the fundamental principles of the profession. Rather, it means respecting patient priorities and recognizing medicine as a dialogue between science and humanity, not as an exercise of control.
However, many clinicians struggle with such decisions because they conflict with their impulse to act and a sense of medical omnipotence. Hincapié Sánchez attributed these difficulties to medical training.
“We are taught to preserve life at all costs. If treatment even slightly prolongs life, many doctors continue to recommend it. The question becomes: Is it valid to extend life when its quality is in doubt?” she asked.
“Medicine is more than a science; it is an art. It is the most human in the sciences and the most scientific in the humanities. Let us not lose sight of the human element that allows us to see the patient as a person, not just a disease to be treated,” Hincapié Sánchez urges.
Kusminsky describes a common therapeutic obstinacy — doctors’ reluctance to stop “doing something,” to avoid “throwing in the towel,” or to uphold “hope is the last thing to be lost.”
“But physicians are growing more aware of these situations, and change is slowly coming,” he said. However, he added: “Of course, there is the issue of the perceived omnipotence of doctors — their words descending with authority to ‘prescribe’ treatment, issue ‘medical orders,’ or dictate ‘pharmacological’ therapy.
For the specialist, such terminology reflects a view of the doctor-patient relationship not as a mutual, two-way exchange, but as a vertical, paternalistic dynamic.
He suggested looking at ancient Greece for perspective. “Hippocrates, or rather the Hippocratic school, taught that the doctor-patient encounter is inherently one of compassion. We must approach this in that way. Reflecting on that bond, improving communication, humanizing relationships, and, above all, being available to listen are key,” Kusminsky said.
Another intersection that has long fascinated Kusminsky is between literature and medicine. This interest led him to explore the field of narrative medicine, serve on the board of directors of the Argentine Society of Narrative Medicine (SAMEN), and join the roster of speakers at the upcoming second SAMEN Conference in Buenos Aires on July 10 and 11, 2025.
“Narrative medicine uses storytelling tools to absorb, process, acknowledge, and empathize with patients’ illness narratives, aiming to restore humanism to practice,” he explained.
According to Kusminsky, the circumstances under which Mrs G.O. expressed her wish not to begin treatment immediately reminded him of a text by Melville’s famous “I would prefer not to” from Bartleby, the Scrivener.
This reflection inspired him to publish an article cited at its beginning. At the same time, it reinforced his belief that what patients say can itself be a form of narrative that extends beyond the confines of clinical history.
Mrs G.O. chose not to pursue treatment for multiple myeloma. However, she returned to Kusminsky’s office approximately 2 months ago. She felt well, and her disease slowly progressed; however, she still had no clinical signs or symptoms.
Kusminsky and Hincapié Sánchez have declared no relevant financial conflicts of interest.
This story was translated from Medscape’s Portuguese edition using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication.
A version of this article first appeared on Medscape.com.
Mrs G.O. is an 80-year-old retired teacher who was widowed a decade ago. With no close relatives, she lives alone, accompanied by only two cats and a dog that she has rescued. “I am alone,” she told Gustavo Kusminsky, MD, consultant in Hematology and Hematopoietic Transplant Service at Austral University Hospital and lecturer in medicine at the Hospital Universitario Austral, Buenos Aires, Argentina. She said this calmly while refusing treatment for life-threatening multiple myeloma. “Doctor, I would rather not,” she added — her words lingering in the quiet consulting room. That moment is now the focus of a recent article in the journal Medicina.
In the article, Kusminsky described how he made an effort to clarify to the patient that she needed cancer treatment. He explained that the treatment was mostly oral, required no initial hospitalization, and that consultations could be spaced out. However, Mrs G.O. maintained her position.
“The patient had no signs of depression, and her argument was logical. Mrs G.O. was already receiving several medications for high blood pressure, was on anticoagulation therapy for atrial fibrillation, and managed dyslipidemia with fenofibrate. But she preferred not to receive treatment for her multiple myeloma.” Kusminsky noted.
“Doctor, I have lived my life. I am old. I am already taking too many medications. I do not have a family, and it would be very difficult to deal with the side effects and be dependent on the hospital. As long as I can take care of myself, I do not want any more treatment, at least not for now. We will talk in a few months if I am still here,” she told him before leaving.
The article mentioned that responses such as Mrs G.O. spark perplexity in modern medicine to the extent that clinicians initiate protocols to rule out depression or other psychological factors when a patient rejects treatments that could prolong their life. On the contrary, no such checks are made when patients agree to treatment, because acceptance is deemed “normal.”
Because of collective assumptions and the war metaphors often used in oncology, Mrs G.O. risked being labeled a “deserter from the battalion” of patients with cancer.
In truth, her decision invites reflection on the doctor-patient relationship, respect for autonomy, and the benefits of modern cancer care offered today, Kusminsky said.
This provides an opportunity to consider the patient’s perspective rather than a purely medical perspective.
Jennifer Hincapié Sánchez, PhD, professor in the Faculty of Medicine at the National Autonomous University of Mexico (UNAM). She is the director of the UNAM University Bioethics Program and coordinates its Institutional Ethics and Bioethics Program for the Faculty of Medicine in Mexico. Although not involved in the article, she regards it as vital. “It’s crucial to remind medical staff that their role is to promote patients’ well-being and that this is related to the life plan that patients have set for themselves, even though this vision is sometimes not aligned with biomedical progress,” she said.
Patient Autonomy
Science-guided medicine aims to prolong life, improve quality, and relieve suffering. However, acceptance or refusal of treatment remains a personal choice for anyone with cancer.
Some evidence showed that patients who decline treatment do not always experience rapid decline. Many can live acceptable, even fulfilling, lives on their own for varying periods, even though they know that there is a possibility of shorter survival. Valuing fewer side effects and better quality of life. This suggested that quality of life is subjective and cannot be measured solely by biomedical standards but also by the meaning each person finds in their existence, even in the face of serious illness.
“There is a myth that quality of life is only valid when defined by objective success. Our task is to explain that it is subjective, and life can be meaningful despite limitations.” Kusminsky said.
Mrs G.O. knew her prognosis and treatment options but chose not to pursue treatment, which, while medically advisable, did not align with her values or vision of life.
Hincapié Sánchez stated that the priority is always to honor the patient’s choice. Clinicians must ensure that the patient has all necessary information that is always appropriate to their sociocultural context before making the decision.
“If the decision persists despite being informed and aware of the effects of the patient’s choice, all we can do is provide support, manage the pain, and seek the patient’s comfort,” she emphasized.
Medical Omnipotence
Physicians should not view the refusal of treatment as an abandonment of the fundamental principles of the profession. Rather, it means respecting patient priorities and recognizing medicine as a dialogue between science and humanity, not as an exercise of control.
However, many clinicians struggle with such decisions because they conflict with their impulse to act and a sense of medical omnipotence. Hincapié Sánchez attributed these difficulties to medical training.
“We are taught to preserve life at all costs. If treatment even slightly prolongs life, many doctors continue to recommend it. The question becomes: Is it valid to extend life when its quality is in doubt?” she asked.
“Medicine is more than a science; it is an art. It is the most human in the sciences and the most scientific in the humanities. Let us not lose sight of the human element that allows us to see the patient as a person, not just a disease to be treated,” Hincapié Sánchez urges.
Kusminsky describes a common therapeutic obstinacy — doctors’ reluctance to stop “doing something,” to avoid “throwing in the towel,” or to uphold “hope is the last thing to be lost.”
“But physicians are growing more aware of these situations, and change is slowly coming,” he said. However, he added: “Of course, there is the issue of the perceived omnipotence of doctors — their words descending with authority to ‘prescribe’ treatment, issue ‘medical orders,’ or dictate ‘pharmacological’ therapy.
For the specialist, such terminology reflects a view of the doctor-patient relationship not as a mutual, two-way exchange, but as a vertical, paternalistic dynamic.
He suggested looking at ancient Greece for perspective. “Hippocrates, or rather the Hippocratic school, taught that the doctor-patient encounter is inherently one of compassion. We must approach this in that way. Reflecting on that bond, improving communication, humanizing relationships, and, above all, being available to listen are key,” Kusminsky said.
Another intersection that has long fascinated Kusminsky is between literature and medicine. This interest led him to explore the field of narrative medicine, serve on the board of directors of the Argentine Society of Narrative Medicine (SAMEN), and join the roster of speakers at the upcoming second SAMEN Conference in Buenos Aires on July 10 and 11, 2025.
“Narrative medicine uses storytelling tools to absorb, process, acknowledge, and empathize with patients’ illness narratives, aiming to restore humanism to practice,” he explained.
According to Kusminsky, the circumstances under which Mrs G.O. expressed her wish not to begin treatment immediately reminded him of a text by Melville’s famous “I would prefer not to” from Bartleby, the Scrivener.
This reflection inspired him to publish an article cited at its beginning. At the same time, it reinforced his belief that what patients say can itself be a form of narrative that extends beyond the confines of clinical history.
Mrs G.O. chose not to pursue treatment for multiple myeloma. However, she returned to Kusminsky’s office approximately 2 months ago. She felt well, and her disease slowly progressed; however, she still had no clinical signs or symptoms.
Kusminsky and Hincapié Sánchez have declared no relevant financial conflicts of interest.
This story was translated from Medscape’s Portuguese edition using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication.
A version of this article first appeared on Medscape.com.

Add-On Niraparib May Slow Hormone-Sensitive Metastatic Prostate Cancer
Adding the poly (ADP-ribose) polymerase (PARP) inhibitor niraparib to abiraterone acetate plus prednisone delayed disease progression and postponed the onset of symptoms in patients with metastatic castration-sensitive prostate cancer with homologous recombination repair (HRR) genetic alterations, according to findings from the AMPLITUDE trial.
An interim analysis also demonstrated an early trend toward improved overall survival in patients who received niraparib.
These findings support adding niraparib to abiraterone acetate plus prednisone “as a new treatment option” in patients with HRR alterations, said Study Chief Gerhardt Attard, MD, PhD, chair of medical oncology, University College London Cancer Institute, London, England, speaking at the American Society of Clinical Oncology (ASCO) 2025 annual meeting.
The findings also highlight that “it’s going to be incredibly important that patients who get diagnosed with hormone-sensitive prostate cancer are tested to see if they have these mutations, so they can be offered the right therapy at the right time,” Outside Expert Bradley McGregor, MD, with Dana-Farber Cancer Institute in Boston, said during a press briefing.
Ultimately, “you don’t know if you don’t test,” McGregor added.
About one quarter of patients with metastatic castration-sensitive prostate cancer have alterations in HRR genes, about half of which are BRCA mutations. These patients typically experience faster disease progression and worse outcomes. An androgen receptor pathway inhibitor, such as abiraterone, alongside androgen deprivation therapy with or without docetaxel, is standard therapy for these patients, but “there is still a need for treatments that are tailored to patients whose tumors harbor HRR alterations,” Attard said in a press release.
Adding niraparib to this standard regimen could help improve survival in these patients.
In 2023, the FDA approved niraparib and abiraterone acetate to treat BRCA-mutated metastatic castration-resistant prostate cancer, after findings from the MAGNITUDE study demonstrated improved progression-free survival (PFS).
The phase 3 AMPLITUDE trial set out to evaluate whether this combination would yield similar survival benefits in metastatic castration-sensitive prostate cancer with HRR mutations.
In the study, 696 patients (median age, 68 years) with metastatic castration-sensitive prostate cancer and one or more HRR gene alterations were randomly allocated (1:1) to niraparib with abiraterone acetate plus prednisone or placebo with abiraterone acetate plus prednisone.
Exclusion criteria included any prior PARP inhibitor therapy or androgen receptor pathway inhibitor other than abiraterone. Eligible patients could have received at most 6 months of androgen deprivation therapy, ≤ 6 cycles of docetaxel, ≤ 45 days of abiraterone acetate plus prednisone and palliative radiation.
Baseline characteristics were well balanced between the groups. Just over half the patients in each group had BRCA1 or BRCA2 alterations. The majority had an electrocorticogram performance status of 0, but high-risk features with a predominance for synchronous metastatic disease and metastatic high volume. About 16% had received prior docetaxel, in keeping with real world data, Attard noted.
At a median follow-up of 30.8 months, niraparib plus standard therapy led to a significant 37% reduction in the risk for radiographic progression or death. The median radiographic PFS (rPFS) was not reached in the niraparib group vs 29.5 months in the placebo group (hazard ratio [HR], 0.63; P = .0001).
Patients with BRCA alterations, in particular, showed the greatest benefit, with niraparib reducing the risk for radiographic progression or death by 48% compared to placebo (median rPFS not reached vs 26 months; HR, 0.52; P < .0001).
On the key secondary endpoint of time to symptomatic progression, adding niraparib led to a “statistically and clinically” significant benefit — a 50% lower in the risk for symptomatic progression in the full population (HR, 0.50), and a 56% lower risk in BRCA-mutant group (HR, 0.44).
The first interim analysis also showed an early trend toward improved overall survival favoring the niraparib combination, with a reduction in the risk for death of 21% in the HRR-mutant population (HR, 0.79; P = .10) and 25% (HR, 0.75; P = .15) in the BRCA-mutant population.
Grade 3/4 adverse events were more common with the niraparib combination group compared to the placebo group (75% vs 59%), with anemia and hypertension being the most common. However, treatment discontinuations due to adverse remained low (15% with niraparib vs 10% with placebo).
Attard noted, however, that half the target number of patients required for the final analysis died. Still, “in my view, there’s a clear trend for favoring survival in the patients randomized to niraparib,” he told attendees.
‘Exciting News’ for Patients
The AMPLITUDE results are “really exciting news for our patients,” McGregor said.
Considering the poor prognosis of patients with metastatic castration-sensitive prostate cancer, “it is reasonable to prioritize early access to PARP inhibitors for these men, at least for the ones with BRCA mutations,” added ASCO discussant Joaquin Mateo, MD, PhD, with Vall d’Hebron Institute of Oncology, Barcelona, Spain.
However, Mateo explained, “I think that for patients with mutations in the other genes, I will be more prudent, and I’ll be on the lookout for the overall survival data to mature.”
The other key conclusion, Mateo said, is that genomic profiling “should be moved earlier into the patient course, and I am confident that embedding genomic profiling into the diagnostic evaluations of metastatic prostate cancer is also going to result in better quality of testing, more efficacious testing, and also a more equitable framework of access to testing for patients.”
This study was funded by Janssen Research & Development, LLC. Attard and Mateo disclosed relationships with Janssen and other pharmaceutical companies. McGregor disclosed relationships with Arcus Biosciences, Astellas, AVEO, Bristol Myers Squibb, Daiichi Sankyo, AstraZeneca, and other companies.
A version of this article first appeared on Medscape.com.
Adding the poly (ADP-ribose) polymerase (PARP) inhibitor niraparib to abiraterone acetate plus prednisone delayed disease progression and postponed the onset of symptoms in patients with metastatic castration-sensitive prostate cancer with homologous recombination repair (HRR) genetic alterations, according to findings from the AMPLITUDE trial.
An interim analysis also demonstrated an early trend toward improved overall survival in patients who received niraparib.
These findings support adding niraparib to abiraterone acetate plus prednisone “as a new treatment option” in patients with HRR alterations, said Study Chief Gerhardt Attard, MD, PhD, chair of medical oncology, University College London Cancer Institute, London, England, speaking at the American Society of Clinical Oncology (ASCO) 2025 annual meeting.
The findings also highlight that “it’s going to be incredibly important that patients who get diagnosed with hormone-sensitive prostate cancer are tested to see if they have these mutations, so they can be offered the right therapy at the right time,” Outside Expert Bradley McGregor, MD, with Dana-Farber Cancer Institute in Boston, said during a press briefing.
Ultimately, “you don’t know if you don’t test,” McGregor added.
About one quarter of patients with metastatic castration-sensitive prostate cancer have alterations in HRR genes, about half of which are BRCA mutations. These patients typically experience faster disease progression and worse outcomes. An androgen receptor pathway inhibitor, such as abiraterone, alongside androgen deprivation therapy with or without docetaxel, is standard therapy for these patients, but “there is still a need for treatments that are tailored to patients whose tumors harbor HRR alterations,” Attard said in a press release.
Adding niraparib to this standard regimen could help improve survival in these patients.
In 2023, the FDA approved niraparib and abiraterone acetate to treat BRCA-mutated metastatic castration-resistant prostate cancer, after findings from the MAGNITUDE study demonstrated improved progression-free survival (PFS).
The phase 3 AMPLITUDE trial set out to evaluate whether this combination would yield similar survival benefits in metastatic castration-sensitive prostate cancer with HRR mutations.
In the study, 696 patients (median age, 68 years) with metastatic castration-sensitive prostate cancer and one or more HRR gene alterations were randomly allocated (1:1) to niraparib with abiraterone acetate plus prednisone or placebo with abiraterone acetate plus prednisone.
Exclusion criteria included any prior PARP inhibitor therapy or androgen receptor pathway inhibitor other than abiraterone. Eligible patients could have received at most 6 months of androgen deprivation therapy, ≤ 6 cycles of docetaxel, ≤ 45 days of abiraterone acetate plus prednisone and palliative radiation.
Baseline characteristics were well balanced between the groups. Just over half the patients in each group had BRCA1 or BRCA2 alterations. The majority had an electrocorticogram performance status of 0, but high-risk features with a predominance for synchronous metastatic disease and metastatic high volume. About 16% had received prior docetaxel, in keeping with real world data, Attard noted.
At a median follow-up of 30.8 months, niraparib plus standard therapy led to a significant 37% reduction in the risk for radiographic progression or death. The median radiographic PFS (rPFS) was not reached in the niraparib group vs 29.5 months in the placebo group (hazard ratio [HR], 0.63; P = .0001).
Patients with BRCA alterations, in particular, showed the greatest benefit, with niraparib reducing the risk for radiographic progression or death by 48% compared to placebo (median rPFS not reached vs 26 months; HR, 0.52; P < .0001).
On the key secondary endpoint of time to symptomatic progression, adding niraparib led to a “statistically and clinically” significant benefit — a 50% lower in the risk for symptomatic progression in the full population (HR, 0.50), and a 56% lower risk in BRCA-mutant group (HR, 0.44).
The first interim analysis also showed an early trend toward improved overall survival favoring the niraparib combination, with a reduction in the risk for death of 21% in the HRR-mutant population (HR, 0.79; P = .10) and 25% (HR, 0.75; P = .15) in the BRCA-mutant population.
Grade 3/4 adverse events were more common with the niraparib combination group compared to the placebo group (75% vs 59%), with anemia and hypertension being the most common. However, treatment discontinuations due to adverse remained low (15% with niraparib vs 10% with placebo).
Attard noted, however, that half the target number of patients required for the final analysis died. Still, “in my view, there’s a clear trend for favoring survival in the patients randomized to niraparib,” he told attendees.
‘Exciting News’ for Patients
The AMPLITUDE results are “really exciting news for our patients,” McGregor said.
Considering the poor prognosis of patients with metastatic castration-sensitive prostate cancer, “it is reasonable to prioritize early access to PARP inhibitors for these men, at least for the ones with BRCA mutations,” added ASCO discussant Joaquin Mateo, MD, PhD, with Vall d’Hebron Institute of Oncology, Barcelona, Spain.
However, Mateo explained, “I think that for patients with mutations in the other genes, I will be more prudent, and I’ll be on the lookout for the overall survival data to mature.”
The other key conclusion, Mateo said, is that genomic profiling “should be moved earlier into the patient course, and I am confident that embedding genomic profiling into the diagnostic evaluations of metastatic prostate cancer is also going to result in better quality of testing, more efficacious testing, and also a more equitable framework of access to testing for patients.”
This study was funded by Janssen Research & Development, LLC. Attard and Mateo disclosed relationships with Janssen and other pharmaceutical companies. McGregor disclosed relationships with Arcus Biosciences, Astellas, AVEO, Bristol Myers Squibb, Daiichi Sankyo, AstraZeneca, and other companies.
A version of this article first appeared on Medscape.com.
Adding the poly (ADP-ribose) polymerase (PARP) inhibitor niraparib to abiraterone acetate plus prednisone delayed disease progression and postponed the onset of symptoms in patients with metastatic castration-sensitive prostate cancer with homologous recombination repair (HRR) genetic alterations, according to findings from the AMPLITUDE trial.
An interim analysis also demonstrated an early trend toward improved overall survival in patients who received niraparib.
These findings support adding niraparib to abiraterone acetate plus prednisone “as a new treatment option” in patients with HRR alterations, said Study Chief Gerhardt Attard, MD, PhD, chair of medical oncology, University College London Cancer Institute, London, England, speaking at the American Society of Clinical Oncology (ASCO) 2025 annual meeting.
The findings also highlight that “it’s going to be incredibly important that patients who get diagnosed with hormone-sensitive prostate cancer are tested to see if they have these mutations, so they can be offered the right therapy at the right time,” Outside Expert Bradley McGregor, MD, with Dana-Farber Cancer Institute in Boston, said during a press briefing.
Ultimately, “you don’t know if you don’t test,” McGregor added.
About one quarter of patients with metastatic castration-sensitive prostate cancer have alterations in HRR genes, about half of which are BRCA mutations. These patients typically experience faster disease progression and worse outcomes. An androgen receptor pathway inhibitor, such as abiraterone, alongside androgen deprivation therapy with or without docetaxel, is standard therapy for these patients, but “there is still a need for treatments that are tailored to patients whose tumors harbor HRR alterations,” Attard said in a press release.
Adding niraparib to this standard regimen could help improve survival in these patients.
In 2023, the FDA approved niraparib and abiraterone acetate to treat BRCA-mutated metastatic castration-resistant prostate cancer, after findings from the MAGNITUDE study demonstrated improved progression-free survival (PFS).
The phase 3 AMPLITUDE trial set out to evaluate whether this combination would yield similar survival benefits in metastatic castration-sensitive prostate cancer with HRR mutations.
In the study, 696 patients (median age, 68 years) with metastatic castration-sensitive prostate cancer and one or more HRR gene alterations were randomly allocated (1:1) to niraparib with abiraterone acetate plus prednisone or placebo with abiraterone acetate plus prednisone.
Exclusion criteria included any prior PARP inhibitor therapy or androgen receptor pathway inhibitor other than abiraterone. Eligible patients could have received at most 6 months of androgen deprivation therapy, ≤ 6 cycles of docetaxel, ≤ 45 days of abiraterone acetate plus prednisone and palliative radiation.
Baseline characteristics were well balanced between the groups. Just over half the patients in each group had BRCA1 or BRCA2 alterations. The majority had an electrocorticogram performance status of 0, but high-risk features with a predominance for synchronous metastatic disease and metastatic high volume. About 16% had received prior docetaxel, in keeping with real world data, Attard noted.
At a median follow-up of 30.8 months, niraparib plus standard therapy led to a significant 37% reduction in the risk for radiographic progression or death. The median radiographic PFS (rPFS) was not reached in the niraparib group vs 29.5 months in the placebo group (hazard ratio [HR], 0.63; P = .0001).
Patients with BRCA alterations, in particular, showed the greatest benefit, with niraparib reducing the risk for radiographic progression or death by 48% compared to placebo (median rPFS not reached vs 26 months; HR, 0.52; P < .0001).
On the key secondary endpoint of time to symptomatic progression, adding niraparib led to a “statistically and clinically” significant benefit — a 50% lower in the risk for symptomatic progression in the full population (HR, 0.50), and a 56% lower risk in BRCA-mutant group (HR, 0.44).
The first interim analysis also showed an early trend toward improved overall survival favoring the niraparib combination, with a reduction in the risk for death of 21% in the HRR-mutant population (HR, 0.79; P = .10) and 25% (HR, 0.75; P = .15) in the BRCA-mutant population.
Grade 3/4 adverse events were more common with the niraparib combination group compared to the placebo group (75% vs 59%), with anemia and hypertension being the most common. However, treatment discontinuations due to adverse remained low (15% with niraparib vs 10% with placebo).
Attard noted, however, that half the target number of patients required for the final analysis died. Still, “in my view, there’s a clear trend for favoring survival in the patients randomized to niraparib,” he told attendees.
‘Exciting News’ for Patients
The AMPLITUDE results are “really exciting news for our patients,” McGregor said.
Considering the poor prognosis of patients with metastatic castration-sensitive prostate cancer, “it is reasonable to prioritize early access to PARP inhibitors for these men, at least for the ones with BRCA mutations,” added ASCO discussant Joaquin Mateo, MD, PhD, with Vall d’Hebron Institute of Oncology, Barcelona, Spain.
However, Mateo explained, “I think that for patients with mutations in the other genes, I will be more prudent, and I’ll be on the lookout for the overall survival data to mature.”
The other key conclusion, Mateo said, is that genomic profiling “should be moved earlier into the patient course, and I am confident that embedding genomic profiling into the diagnostic evaluations of metastatic prostate cancer is also going to result in better quality of testing, more efficacious testing, and also a more equitable framework of access to testing for patients.”
This study was funded by Janssen Research & Development, LLC. Attard and Mateo disclosed relationships with Janssen and other pharmaceutical companies. McGregor disclosed relationships with Arcus Biosciences, Astellas, AVEO, Bristol Myers Squibb, Daiichi Sankyo, AstraZeneca, and other companies.
A version of this article first appeared on Medscape.com.
FROM ASCO 2025
Less Invasive Screening May Identify Barrett’s Esophagus Earlier
A new combination modality demonstrated excellent sensitivity and negative predictive value compared with endoscopy in a prospective study of at-risk veterans screened for Barrett’s esophagus (BE) and esophageal adenocarcinoma (EAC), a small comparative study in US veterans found.
BE is up to three times more prevalent in veterans than in the general population.
This and other minimally invasive approaches may reduce patient anxiety and increase screening rates, according to investigators led by Katarina B. Greer, MD, MS, of the VA Northeast Ohio Healthcare System and Case Western University in Cleveland. Such screening platforms are expected to open a window on improved prognosis for EAC by offering well-tolerated, office-based testing, the authors wrote in The American Journal of Gastroenterology.
Greer and colleagues compared standard upper endoscopy with EsoCheck (EC), a nonendoscopic esophageal balloon cell-sampling device coupled with EsoGuard (EG), a DNA-based precancer screening assay, with standard upper endoscopy, an FDA-approved minimally invasive alternative.
Sensitivity and specificity of combined EC/EG for esophagogastroduodenoscopy (EGD)-detected BE/EAC were 92.9% (95% CI, 66.1-99.8) and 72.2% (95% CI, 62.1-80.8), respectively. Positive and negative predictive values were 32.5% (95% CI, 18.6-49.1) and 98.6% (95% CI, 92.4-100), respectively.
“With its strong negative predictive power, this screening modality could be a first-line tool available to a greater number of patients,” Greer and associates wrote. “Data from this test support the notion that EC could be performed as a triaging test to increase the yield of diagnostic upper endoscopy 2.5-fold.”
The US rates of EAC have increased more than six-fold in the past four decades and continue to rise. In 2023, 21,560 cases of EAC were diagnosed here. The prognosis for EAC is still poor, with fewer than 22% of patients surviving beyond 5 years.
Current guidelines recommend sedated EGD for patients with chronic gastroesophageal reflux disease (GERD) and additional BE risk factors such as smoking, obesity, and family history. This strategy, however, often fails to detect BE when symptoms are well controlled with over-the-counter or physician-prescribed therapies, Greer and colleagues noted. It also fails to detect BE in individuals without GERD, who comprise 40% of those who develop EAC.
Fewer than 5% of EACs are diagnosed as early-stage lesions caught by surveillance of patients with previously detected BE.
Study Details
The researchers recruited veterans meeting American College of Gastroenterology criteria for endoscopic BE and EAC screening at the Louis Stokes Cleveland Veterans Affairs Medical Center.
Of 782 eligible veterans, 130 (16.6%) entered the study and 124 completed screening. Common reasons for nonparticipation included completion of upper endoscopy outside of the VA healthcare system, lack of interest in joining a research study, and no recommendation for screening from referring gastroenterology or primary care providers. Eligible candidates had gastroesophageal reflux disorder plus three additional risk factors, such as smoking, higher BMI, male sex, age 50 years or older, and family history. The mean number of risk factors was 4.1.
“Available data suggest that family history is the strongest predictor of BE diagnosis, as prevalence of BE among those with family history was 23%,” Greer’s group wrote. “This points to high priority of pursuing screening in patients with family history of the condition, followed by patients who share multiple risk factors.”
All participants completed unsedated EC-guided distal esophageal sampling followed by a sedated EGD on the same day. The prevalence of BE/EAC was 12.9% (n = 14/2), based on standard EGD.
“The study was not powered to prospectively determine EC diagnostic accuracy for subgroups of nondysplastic and dysplastic BE and EAC. These data are reported for this device in development studies but not available for our study population,” the authors wrote. In comparison, they noted, the Cytosponge-TFF3, another nonendoscopic screening device for EAC and BE, exhibited lower sensitivity of 79.5%-87.2%, depending on lesion length, but higher specificity of 92.4%.
Procedural Anxiety
Baseline scores on the short-form six-item Spielberger State-Trait Anxiety Inventory-6 (STAI-6) revealed notable levels of periprocedural anxiety. STAI-6 scores range from 20 to 80, with higher scores indicating more severe anxiety. In the VA study, scores ranged from 20 to 60, and most domains constituting the scores were the same before and after the procedure. Participants did, however, report a statistically significant decrease in sense of worry after EC and reported good tolerability for both EC and EG.
Offering an outsider’s perspective on the study, Joshua Sloan, DO, an esophageal gastroenterologist at University of Minnesota Medical Center in Minneapolis, said that with the acceleration of US rates of EAC, developing a nonendoscopic screening tool to improve identification of Barrett’s and perhaps early EAC is important. “The study by Greer et al helps support the use of nonendoscopic screening with EsoCheck and EsoGuard to identify these conditions,” he told this news organization. “It will be interesting to see similar studies in the non-VA population as well. As the study notes, veterans are an enriched population with a higher prevalence of Barrett’s esophagus.”
Ultimately, Sloan added, “the hope is to increase our ability to identify and manage BE before it becomes EAC. Nonendoscopic screening tools have the potential to increase diagnosis and funnel the appropriate patients for endoscopic surveillance.”
The Bottom Line
“Calculations regarding effectiveness of the two-step screening strategy afforded by EC indicate that the burden of screening would be reduced by at least half (53%),” the authors wrote. Since the estimated size of the US screen-eligible population ranges from 19.7 million to 120.1 million, noninvasive tools could significantly decrease EGD procedures. A formal cost effectiveness analysis is being conducted and will be published separately.
This study was funded by a Department of Defense award.
Co-Author Chak reported device patents assigned to Case Western Reserve University and licensed to Lucid Diagnostics. The other authors had no competing interests to declare. Sloan disclosed speaking and/or advisory work for Sanofi-Regeneron, Phathom Pharmaceuticals, and Takeda Pharmaceuticals unrelated to his comments.
A version of this article first appeared on Medscape.com.
A new combination modality demonstrated excellent sensitivity and negative predictive value compared with endoscopy in a prospective study of at-risk veterans screened for Barrett’s esophagus (BE) and esophageal adenocarcinoma (EAC), a small comparative study in US veterans found.
BE is up to three times more prevalent in veterans than in the general population.
This and other minimally invasive approaches may reduce patient anxiety and increase screening rates, according to investigators led by Katarina B. Greer, MD, MS, of the VA Northeast Ohio Healthcare System and Case Western University in Cleveland. Such screening platforms are expected to open a window on improved prognosis for EAC by offering well-tolerated, office-based testing, the authors wrote in The American Journal of Gastroenterology.
Greer and colleagues compared standard upper endoscopy with EsoCheck (EC), a nonendoscopic esophageal balloon cell-sampling device coupled with EsoGuard (EG), a DNA-based precancer screening assay, with standard upper endoscopy, an FDA-approved minimally invasive alternative.
Sensitivity and specificity of combined EC/EG for esophagogastroduodenoscopy (EGD)-detected BE/EAC were 92.9% (95% CI, 66.1-99.8) and 72.2% (95% CI, 62.1-80.8), respectively. Positive and negative predictive values were 32.5% (95% CI, 18.6-49.1) and 98.6% (95% CI, 92.4-100), respectively.
“With its strong negative predictive power, this screening modality could be a first-line tool available to a greater number of patients,” Greer and associates wrote. “Data from this test support the notion that EC could be performed as a triaging test to increase the yield of diagnostic upper endoscopy 2.5-fold.”
The US rates of EAC have increased more than six-fold in the past four decades and continue to rise. In 2023, 21,560 cases of EAC were diagnosed here. The prognosis for EAC is still poor, with fewer than 22% of patients surviving beyond 5 years.
Current guidelines recommend sedated EGD for patients with chronic gastroesophageal reflux disease (GERD) and additional BE risk factors such as smoking, obesity, and family history. This strategy, however, often fails to detect BE when symptoms are well controlled with over-the-counter or physician-prescribed therapies, Greer and colleagues noted. It also fails to detect BE in individuals without GERD, who comprise 40% of those who develop EAC.
Fewer than 5% of EACs are diagnosed as early-stage lesions caught by surveillance of patients with previously detected BE.
Study Details
The researchers recruited veterans meeting American College of Gastroenterology criteria for endoscopic BE and EAC screening at the Louis Stokes Cleveland Veterans Affairs Medical Center.
Of 782 eligible veterans, 130 (16.6%) entered the study and 124 completed screening. Common reasons for nonparticipation included completion of upper endoscopy outside of the VA healthcare system, lack of interest in joining a research study, and no recommendation for screening from referring gastroenterology or primary care providers. Eligible candidates had gastroesophageal reflux disorder plus three additional risk factors, such as smoking, higher BMI, male sex, age 50 years or older, and family history. The mean number of risk factors was 4.1.
“Available data suggest that family history is the strongest predictor of BE diagnosis, as prevalence of BE among those with family history was 23%,” Greer’s group wrote. “This points to high priority of pursuing screening in patients with family history of the condition, followed by patients who share multiple risk factors.”
All participants completed unsedated EC-guided distal esophageal sampling followed by a sedated EGD on the same day. The prevalence of BE/EAC was 12.9% (n = 14/2), based on standard EGD.
“The study was not powered to prospectively determine EC diagnostic accuracy for subgroups of nondysplastic and dysplastic BE and EAC. These data are reported for this device in development studies but not available for our study population,” the authors wrote. In comparison, they noted, the Cytosponge-TFF3, another nonendoscopic screening device for EAC and BE, exhibited lower sensitivity of 79.5%-87.2%, depending on lesion length, but higher specificity of 92.4%.
Procedural Anxiety
Baseline scores on the short-form six-item Spielberger State-Trait Anxiety Inventory-6 (STAI-6) revealed notable levels of periprocedural anxiety. STAI-6 scores range from 20 to 80, with higher scores indicating more severe anxiety. In the VA study, scores ranged from 20 to 60, and most domains constituting the scores were the same before and after the procedure. Participants did, however, report a statistically significant decrease in sense of worry after EC and reported good tolerability for both EC and EG.
Offering an outsider’s perspective on the study, Joshua Sloan, DO, an esophageal gastroenterologist at University of Minnesota Medical Center in Minneapolis, said that with the acceleration of US rates of EAC, developing a nonendoscopic screening tool to improve identification of Barrett’s and perhaps early EAC is important. “The study by Greer et al helps support the use of nonendoscopic screening with EsoCheck and EsoGuard to identify these conditions,” he told this news organization. “It will be interesting to see similar studies in the non-VA population as well. As the study notes, veterans are an enriched population with a higher prevalence of Barrett’s esophagus.”
Ultimately, Sloan added, “the hope is to increase our ability to identify and manage BE before it becomes EAC. Nonendoscopic screening tools have the potential to increase diagnosis and funnel the appropriate patients for endoscopic surveillance.”
The Bottom Line
“Calculations regarding effectiveness of the two-step screening strategy afforded by EC indicate that the burden of screening would be reduced by at least half (53%),” the authors wrote. Since the estimated size of the US screen-eligible population ranges from 19.7 million to 120.1 million, noninvasive tools could significantly decrease EGD procedures. A formal cost effectiveness analysis is being conducted and will be published separately.
This study was funded by a Department of Defense award.
Co-Author Chak reported device patents assigned to Case Western Reserve University and licensed to Lucid Diagnostics. The other authors had no competing interests to declare. Sloan disclosed speaking and/or advisory work for Sanofi-Regeneron, Phathom Pharmaceuticals, and Takeda Pharmaceuticals unrelated to his comments.
A version of this article first appeared on Medscape.com.
A new combination modality demonstrated excellent sensitivity and negative predictive value compared with endoscopy in a prospective study of at-risk veterans screened for Barrett’s esophagus (BE) and esophageal adenocarcinoma (EAC), a small comparative study in US veterans found.
BE is up to three times more prevalent in veterans than in the general population.
This and other minimally invasive approaches may reduce patient anxiety and increase screening rates, according to investigators led by Katarina B. Greer, MD, MS, of the VA Northeast Ohio Healthcare System and Case Western University in Cleveland. Such screening platforms are expected to open a window on improved prognosis for EAC by offering well-tolerated, office-based testing, the authors wrote in The American Journal of Gastroenterology.
Greer and colleagues compared standard upper endoscopy with EsoCheck (EC), a nonendoscopic esophageal balloon cell-sampling device coupled with EsoGuard (EG), a DNA-based precancer screening assay, with standard upper endoscopy, an FDA-approved minimally invasive alternative.
Sensitivity and specificity of combined EC/EG for esophagogastroduodenoscopy (EGD)-detected BE/EAC were 92.9% (95% CI, 66.1-99.8) and 72.2% (95% CI, 62.1-80.8), respectively. Positive and negative predictive values were 32.5% (95% CI, 18.6-49.1) and 98.6% (95% CI, 92.4-100), respectively.
“With its strong negative predictive power, this screening modality could be a first-line tool available to a greater number of patients,” Greer and associates wrote. “Data from this test support the notion that EC could be performed as a triaging test to increase the yield of diagnostic upper endoscopy 2.5-fold.”
The US rates of EAC have increased more than six-fold in the past four decades and continue to rise. In 2023, 21,560 cases of EAC were diagnosed here. The prognosis for EAC is still poor, with fewer than 22% of patients surviving beyond 5 years.
Current guidelines recommend sedated EGD for patients with chronic gastroesophageal reflux disease (GERD) and additional BE risk factors such as smoking, obesity, and family history. This strategy, however, often fails to detect BE when symptoms are well controlled with over-the-counter or physician-prescribed therapies, Greer and colleagues noted. It also fails to detect BE in individuals without GERD, who comprise 40% of those who develop EAC.
Fewer than 5% of EACs are diagnosed as early-stage lesions caught by surveillance of patients with previously detected BE.
Study Details
The researchers recruited veterans meeting American College of Gastroenterology criteria for endoscopic BE and EAC screening at the Louis Stokes Cleveland Veterans Affairs Medical Center.
Of 782 eligible veterans, 130 (16.6%) entered the study and 124 completed screening. Common reasons for nonparticipation included completion of upper endoscopy outside of the VA healthcare system, lack of interest in joining a research study, and no recommendation for screening from referring gastroenterology or primary care providers. Eligible candidates had gastroesophageal reflux disorder plus three additional risk factors, such as smoking, higher BMI, male sex, age 50 years or older, and family history. The mean number of risk factors was 4.1.
“Available data suggest that family history is the strongest predictor of BE diagnosis, as prevalence of BE among those with family history was 23%,” Greer’s group wrote. “This points to high priority of pursuing screening in patients with family history of the condition, followed by patients who share multiple risk factors.”
All participants completed unsedated EC-guided distal esophageal sampling followed by a sedated EGD on the same day. The prevalence of BE/EAC was 12.9% (n = 14/2), based on standard EGD.
“The study was not powered to prospectively determine EC diagnostic accuracy for subgroups of nondysplastic and dysplastic BE and EAC. These data are reported for this device in development studies but not available for our study population,” the authors wrote. In comparison, they noted, the Cytosponge-TFF3, another nonendoscopic screening device for EAC and BE, exhibited lower sensitivity of 79.5%-87.2%, depending on lesion length, but higher specificity of 92.4%.
Procedural Anxiety
Baseline scores on the short-form six-item Spielberger State-Trait Anxiety Inventory-6 (STAI-6) revealed notable levels of periprocedural anxiety. STAI-6 scores range from 20 to 80, with higher scores indicating more severe anxiety. In the VA study, scores ranged from 20 to 60, and most domains constituting the scores were the same before and after the procedure. Participants did, however, report a statistically significant decrease in sense of worry after EC and reported good tolerability for both EC and EG.
Offering an outsider’s perspective on the study, Joshua Sloan, DO, an esophageal gastroenterologist at University of Minnesota Medical Center in Minneapolis, said that with the acceleration of US rates of EAC, developing a nonendoscopic screening tool to improve identification of Barrett’s and perhaps early EAC is important. “The study by Greer et al helps support the use of nonendoscopic screening with EsoCheck and EsoGuard to identify these conditions,” he told this news organization. “It will be interesting to see similar studies in the non-VA population as well. As the study notes, veterans are an enriched population with a higher prevalence of Barrett’s esophagus.”
Ultimately, Sloan added, “the hope is to increase our ability to identify and manage BE before it becomes EAC. Nonendoscopic screening tools have the potential to increase diagnosis and funnel the appropriate patients for endoscopic surveillance.”
The Bottom Line
“Calculations regarding effectiveness of the two-step screening strategy afforded by EC indicate that the burden of screening would be reduced by at least half (53%),” the authors wrote. Since the estimated size of the US screen-eligible population ranges from 19.7 million to 120.1 million, noninvasive tools could significantly decrease EGD procedures. A formal cost effectiveness analysis is being conducted and will be published separately.
This study was funded by a Department of Defense award.
Co-Author Chak reported device patents assigned to Case Western Reserve University and licensed to Lucid Diagnostics. The other authors had no competing interests to declare. Sloan disclosed speaking and/or advisory work for Sanofi-Regeneron, Phathom Pharmaceuticals, and Takeda Pharmaceuticals unrelated to his comments.
A version of this article first appeared on Medscape.com.
FROM AMERICAN JOURNAL OF GASTROENTEROLOGY
The Use of Lung Cancer Screening to Increase Chronic Obstructive Pulmonary Disease Diagnosis in Veterans Affairs Primary Care
The Use of Lung Cancer Screening to Increase Chronic Obstructive Pulmonary Disease Diagnosis in Veterans Affairs Primary Care
Primary care practitioners (PCPs) in the US Department of Veterans Affairs (VA) provide care for patients with higher rates of many diseases—diabetes, heart disease, cancer, chronic obstructive pulmonary disease (COPD), and stroke—compared to the nonveteran population. 1 Due to the medical complexities of these diseases, they are often misdiagnosed or not diagnosed at all.
COPD is hiding in plain sight, impacting quality of life and burdening US health care systems.2 Research has yielded new treatments and evidence-based guidelines; however, COPD remains underdiagnosed. Only 13 million of the estimated 79 million US adults with COPD aged 20 to 79 years have been formally diagnosed.3 By the time patients are diagnosed, the disease is often advanced, and therapies are less effective. In 2 large studies of patients with COPD symptoms, later diagnosis was associated with worse outcomes.4,5
Veterans have a higher prevalence of COPD (8%-19%) than nonveterans (6%), likely due to higher rates of smoking and service-related exposures, especially among veterans of post-9/11 conflicts.6,7 Veterans do not always report symptoms and PCPs may not ask about symptoms, leading to underdiagnosis.8 The combination of high likelihood and underdetection of COPD presents a challenge and a target for VA quality improvement (QI).
The US Preventive Services Task Force (USPSTF) recommends against screening asymptomatic patients for COPD. However, both the USPSTF and the Global Initiative for Chronic Obstructive Lung Disease Report advocate for active case finding in primary care clinics to determine whether high-risk patients, such as smokers, experience COPD symptoms and warrant spirometry. 9,10 To make early COPD diagnoses, clinicians may use questionnaires alone or in combination with handheld peak expiratory flow rate measurements.11,12 Formal spirometry, considered the gold standard for COPD diagnosis, is ordered for patients who report COPD symptoms (ie, shortness of breath with exertion) or who have both COPD symptoms and reduced peak flow rates.
A systematic review and meta-analysis found that while the combination of questionnaires and peak flows was the more effective strategy overall, questionnaires alone were also valuable for identifying patients with possible COPD.13 Implementation of either screening method in primary care practices would be challenging. In a simulation study that applied chronic disease and preventive care guidelines to hypothetical patient panels, the time required for PCPs to provide guideline-recommended chronic and preventive care in addition to acute care far exceeded 8 hours per day, even in team-based settings.14 Overburdened PCPs are therefore unlikely to accept additional tasks like COPD case finding.
Why don’t patients report their pulmonary symptoms? Patients may not recognize the symptoms as evidence of COPD. Others may be afraid of a COPD diagnosis or the stigma that is associated with it.15 Perhaps they believe COPD treatment is ineffective because of lung damage from smoking. Some patients may not want to know if they have COPD, while others reduce activity levels to avoid symptoms.16
QUALITY IMPROVEMENT PROJECT
Given the high prevalence of COPD among veterans and the potential for underdiagnosis, VA Northeast Ohio Healthcare System (VANEOHS) internal medicine residents and faculty assessed the state of COPD diagnosis in its primary care clinic with a QI project in 2022. Patients in the clinic between August 1, 2015, and November 30, 2022, with an International Classification of Diseases-10 (ICD-10) COPD diagnosis code (J44) in the electronic health record were included. Of 157 included patients, 105 patients who had prior spirometry testing were excluded. Of the 52 patients with diagnosed COPD and no spirometry testing, 30 patients had computed tomography (CT) findings consistent with COPD (ie, airway thickening, emphysema, air trapping) that was performed for CT lung cancer screening (LCS).17 Twenty-three of these 30 patients were contacted by phone. All 23 were ever smokers and 13 reported COPD symptoms. The PCPs of the symptomatic patients were then contacted. Spirometry was ordered for all 13 patients and completed by 7. Three spirometry tests confirmed the COPD diagnosis. One PCP initiated inhaler therapy for a patient with newly diagnosed COPD.
All 11 PCPs of symptomatic patients were interviewed (many had > 1 symptomatic patient). They reported being unaware of patients’ COPD symptoms because the patients did not mention them, noting that screening for COPD was not a priority.
Role of Lung Cancer Screening
VA PCPs use electronic health record clinical reminders to track tests, consults, chronic disease education, cancer screenings, and routine health maintenance. A clinical reminder already exists (based on USPSTF recommendations) for LCS for patients aged 50 to 80 years who have a smoking history of 20 pack years. Patients who meet these criteria would also be considered high risk for COPD.
The VANEOHS QI project suggests that previously undiagnosed patients with findings of COPD on LCS may also have symptoms of COPD. Therefore, we wondered whether the LCS clinical reminder could serve a second purpose by prompting PCPs to ask veterans who meet LCS criteria about their COPD symptoms.
In 2022, about 13 million patients were eligible for LCS.18 Patients who qualify for LCS are at high risk for other cardiopulmonary disorders, such as COPD and coronary artery disease. Lung cancer is detected in only 1% of patients screened with CT at baseline. However, more often LCS yields evidence of additional cardiopulmonary disorders, such as emphysema or coronary artery calcifications. The International Early Lung Cancer Program (I-ELCAP) and the National Lung Cancer Screening Trial (NLST), which included > 79,000 patients, found evidence of emphysema on CT imaging in 24% and 31% of cases, respectively.19,20 In both cohorts, > 80% of patients with emphysema on CT imaging had no prior history of COPD.
In a 2022 article summarizing the potential impact of CT LCS on COPD diagnosis, Mulshine et al suggest that detection of emphysema on CT LCS provides “earlier recognition for PCPs to identify patients who would benefit from detailed symptom screening to prompt spirometry for COPD detection” and additional motivation for tobacco cessation.21 The VANEOHS QI project was developed and implemented prior to I-ELCAP or NLST reporting results but reinforces the value of CT LCS for COPD diagnosis.
Early diagnosis of COPD remains challenging because PCPs do not ask, patients do not tell, and symptoms can easily be dismissed. However, earlier diagnosis of COPD in symptomatic patients improves outcomes.3,4 To bridge this gap, VA PCPs and primary care patient aligned care teams (PACTs) need to commit to probing high-risk patients for COPD symptoms and ordering spirometry for those who are symptomatic. To accomplish this task, primary care teams need help.
The VANEOHS QI project confirmed that some patients with evidence of COPD on CT have symptoms of COPD that they did not share with their PCPs and suggests that LCS can be used as a dual action case finding method to screen both for lung cancer and COPD. We propose that patients who are eligible for LCS should also be probed for COPD symptoms at their clinic visits; for symptomatic patients, spirometry should be ordered, and COPD evidence-based management should be initiated when spirometry results are consistent with COPD. Annual probing for COPD symptoms could be considered in asymptomatic patients with ongoing tobacco use or emphysema on CT, since they may develop symptoms in the future. This new case-finding method bypasses the need for time-prohibitive questionnaires or peak flow measurements.
Future Opportunities
VA PCPs juggle many priorities and despite the simplicity of this new case finding COPD method, it may be unintentionally overlooked. PCPs often run out of time or may forget to ask patients about COPD symptoms when ordering LCS.
Future innovations to increase COPD diagnosis could include the creation of a yearly VA clinical reminder linked to the tobacco use reminder that has check boxes asking about symptoms of COPD in current and prior smokers. If patients have COPD symptoms, the reminder can prompt the ordering of spirometry. Similar reminders could be implemented to identify veterans with exposures to burn pits or other military environmental exposures who may have COPD symptoms. Another possible way to increase COPD diagnosis would be a partnership between primary care and the VA LCS program where patients receiving screening are asked about COPD symptoms during their LCS interviews and PACTs are alerted to order spirometry for symptomatic patients.
Elusive no longer! We can pull the veil back on COPD diagnosis and identify patients with possible COPD earlier in their course using their eligibility for LCS as a yearly reminder to probe them for symptoms. While not all patients who undergo LCS—even those with evidence of COPD on CT—will have COPD symptoms, symptoms may develop over time. LCS provides the possibility of 2 diagnoses from 1 test. This is an opportunity we cannot afford to miss.
- Betancourt JA, Granados PS, Pacheco GJ, et al. Exploring health outcomes for U.S. veterans compared to non-veterans from 2003 to 2019. Healthcare (Basel). 2021;9(5):604. doi:10.3390/healthcare90506064
- Bamonti PM, Fischer I, Moye J, Poghosyan H, Pietrzak RH. Obstructive respiratory disease in U.S. veterans: prevalence, characteristics, and health burden. J Psychiatr Res. 2024;176:140-147. doi:10.1016/j.jpsychires.2024.05.053
- Criner RN, Han MK. COPD care in the 21st century: a public health priority. Respir Care. 2018;63(5):591-600. doi:10.4187/respcare.06276
- Larsson K, Janson C, Ställberg B, et al. Impact of COPD diagnosis timing on clinical and economic outcomes: the ARCTIC observational cohort study. Int J Chron Obstruct Pulmon Dis. 2019;14:995-1008. doi:10.2147/COPD.S195382
- Kostikas K, Price D, Gutzwiller FS, et al. Clinical impact and healthcare resource utilization associated with early versus late COPD diagnosis in patients from UK CPRD Database. Int J Chron Obstruct Pulmon Dis. 2020;15:1729- 1738. doi:10.2147/COPD.S255414
- Bamonti PM, Robinson SA, Wan ES, Moy ML. Improving physiological, physical, and psychological health outcomes: a narrative review in US veterans with COPD. Int J Chron Obstruct Pulmon Dis. 2022;17:1269-1283. doi:10.2147/COPD.S339323
- Savitz DA, Woskie SR, Bello A, et al. Deployment to military bases with open burn pits and respiratory and cardiovascular disease. JAMA Netw Open. 2024;7(4):e247629. doi:10.1001/jamanetworkopen.2024.7629
- Murphy DE, Chaudhry Z, Almoosa KF, Panos RJ. High prevalence of chronic obstructive pulmonary disease among veterans in the urban midwest. Mil Med. 2011;176(5):552-560. doi:10.7205/milmed-d-10-00377
- Guirguis-Blake JM, Senger CA, Webber EM, Mularski RA, Whitlock EP. Screening for chronic obstructive pulmonary disease: evidence report and systematic review for the US Preventive Services Task Force. JAMA. 2016;315(13):1378-1393. doi:10.1001/jama.2016.2654
- Capriotti T, Tomy R, Morales M. COPD updates: 2023 GOLD Report for primary care providers. Clinical Advisor. May 9, 2023. Accessed May 14, 2025. https://www.clinicaladvisor.com/features/copd-updates-2023-gold-report-primary-care/
- Leidy NK, Martinez FJ, Malley KG, et al. Can CAPTURE be used to identify undiagnosed patients with mild- to- moderate COPD likely to benefit from treatment? Int J Chron Obstruct Pulmon Dis. 2018;13:1901-1912. doi:10.2147/COPD.S152226
- Jithoo A, Enright PL, Burney P, et al. Case-finding options for COPD: results from the burden of obstructive lung disease study. Eur Respir J. 2013;41(3):548-555. doi:10.1183/09031936.00132011
- Haroon SM, Jordan RE, O’Beirne-Elliman J, Adab P. Effectiveness of case finding strategies for COPD in primary care: a systematic review and meta-analysis. NPJ Prim Care Respir Med. 2015;25:15056. doi:10.1038/npjpcrm.2015.56
- Porter J, Boyd C, Skandari MR, Laiteerapong N. Revisiting the time needed to provide adult primary care. J Gen Intern Med. 2023;38(1)147-155. doi:10.1007/s11606-022-07707-x
- Woo S, Zhou W, Larson JL. Stigma experiences in people with chronic obstructive pulmonary disease: an integrative review. Int J Chron Obstruct Pulmon Dis. 2021;16:1647- 1659. doi:10.2147/COPD.S306874
- Aaron SD, Montes de Oca M, Celli B, et al. Early diagnosis and treatment of COPD: the costs and benefits of case finding. Am J Respir Crit Care Med. 2024;209(8):928-937. doi:10.1164/rccm.202311-2120PP
- Kwon A, Lee C, Arafah A, Klein M, Namboodiri S, Lee C. Increasing chronic obstructive pulmonary disease (COPD) diagnosis with pulmonary function testing for patients with chest imaging evidence of COPD. Poster presented at: Society of General Internal Medicine Midwest Regional Meeting; October 19-20, 2023; Chicago, IL.
- Henderson LM, Su I, Rivera MP, et al. Prevalence of lung cancer screening in the US, 2022. JAMA Netw Open. 2024;7(3):e243190. doi:10.1001/jamanetworkopen.2024.3190
- Steiger D, Siddiqi MF, Yip R, Yankelevitz DF, Henschke CI; I-ELCAP investigators. The importance of low-dose CT screening to identify emphysema in asymptomatic participants with and without a prior diagnosis of COPD. Clin Imaging. 2021;78:136-141. doi:10.1016/j.clinimag.2021.03.012
- Pinsky PF, Lynch DA, Gierada DS. Incidental findings on low-dose CT scan lung cancer screenings and deaths from respiratory diseases. Chest. 2022;161(4):1092-1100. doi:10.1016/j.chest.2021.11.015
- Mulshine JL, Aldigé CR, Ambrose LF, et al. Emphysema detection in the course of lung cancer screening: optimizing a rare opportunity to impact population health. Ann Am Thorac Soc. 2023;20(4):499- 503. doi:10.1513/AnnalsATS.202207-631PS
Primary care practitioners (PCPs) in the US Department of Veterans Affairs (VA) provide care for patients with higher rates of many diseases—diabetes, heart disease, cancer, chronic obstructive pulmonary disease (COPD), and stroke—compared to the nonveteran population. 1 Due to the medical complexities of these diseases, they are often misdiagnosed or not diagnosed at all.
COPD is hiding in plain sight, impacting quality of life and burdening US health care systems.2 Research has yielded new treatments and evidence-based guidelines; however, COPD remains underdiagnosed. Only 13 million of the estimated 79 million US adults with COPD aged 20 to 79 years have been formally diagnosed.3 By the time patients are diagnosed, the disease is often advanced, and therapies are less effective. In 2 large studies of patients with COPD symptoms, later diagnosis was associated with worse outcomes.4,5
Veterans have a higher prevalence of COPD (8%-19%) than nonveterans (6%), likely due to higher rates of smoking and service-related exposures, especially among veterans of post-9/11 conflicts.6,7 Veterans do not always report symptoms and PCPs may not ask about symptoms, leading to underdiagnosis.8 The combination of high likelihood and underdetection of COPD presents a challenge and a target for VA quality improvement (QI).
The US Preventive Services Task Force (USPSTF) recommends against screening asymptomatic patients for COPD. However, both the USPSTF and the Global Initiative for Chronic Obstructive Lung Disease Report advocate for active case finding in primary care clinics to determine whether high-risk patients, such as smokers, experience COPD symptoms and warrant spirometry. 9,10 To make early COPD diagnoses, clinicians may use questionnaires alone or in combination with handheld peak expiratory flow rate measurements.11,12 Formal spirometry, considered the gold standard for COPD diagnosis, is ordered for patients who report COPD symptoms (ie, shortness of breath with exertion) or who have both COPD symptoms and reduced peak flow rates.
A systematic review and meta-analysis found that while the combination of questionnaires and peak flows was the more effective strategy overall, questionnaires alone were also valuable for identifying patients with possible COPD.13 Implementation of either screening method in primary care practices would be challenging. In a simulation study that applied chronic disease and preventive care guidelines to hypothetical patient panels, the time required for PCPs to provide guideline-recommended chronic and preventive care in addition to acute care far exceeded 8 hours per day, even in team-based settings.14 Overburdened PCPs are therefore unlikely to accept additional tasks like COPD case finding.
Why don’t patients report their pulmonary symptoms? Patients may not recognize the symptoms as evidence of COPD. Others may be afraid of a COPD diagnosis or the stigma that is associated with it.15 Perhaps they believe COPD treatment is ineffective because of lung damage from smoking. Some patients may not want to know if they have COPD, while others reduce activity levels to avoid symptoms.16
QUALITY IMPROVEMENT PROJECT
Given the high prevalence of COPD among veterans and the potential for underdiagnosis, VA Northeast Ohio Healthcare System (VANEOHS) internal medicine residents and faculty assessed the state of COPD diagnosis in its primary care clinic with a QI project in 2022. Patients in the clinic between August 1, 2015, and November 30, 2022, with an International Classification of Diseases-10 (ICD-10) COPD diagnosis code (J44) in the electronic health record were included. Of 157 included patients, 105 patients who had prior spirometry testing were excluded. Of the 52 patients with diagnosed COPD and no spirometry testing, 30 patients had computed tomography (CT) findings consistent with COPD (ie, airway thickening, emphysema, air trapping) that was performed for CT lung cancer screening (LCS).17 Twenty-three of these 30 patients were contacted by phone. All 23 were ever smokers and 13 reported COPD symptoms. The PCPs of the symptomatic patients were then contacted. Spirometry was ordered for all 13 patients and completed by 7. Three spirometry tests confirmed the COPD diagnosis. One PCP initiated inhaler therapy for a patient with newly diagnosed COPD.
All 11 PCPs of symptomatic patients were interviewed (many had > 1 symptomatic patient). They reported being unaware of patients’ COPD symptoms because the patients did not mention them, noting that screening for COPD was not a priority.
Role of Lung Cancer Screening
VA PCPs use electronic health record clinical reminders to track tests, consults, chronic disease education, cancer screenings, and routine health maintenance. A clinical reminder already exists (based on USPSTF recommendations) for LCS for patients aged 50 to 80 years who have a smoking history of 20 pack years. Patients who meet these criteria would also be considered high risk for COPD.
The VANEOHS QI project suggests that previously undiagnosed patients with findings of COPD on LCS may also have symptoms of COPD. Therefore, we wondered whether the LCS clinical reminder could serve a second purpose by prompting PCPs to ask veterans who meet LCS criteria about their COPD symptoms.
In 2022, about 13 million patients were eligible for LCS.18 Patients who qualify for LCS are at high risk for other cardiopulmonary disorders, such as COPD and coronary artery disease. Lung cancer is detected in only 1% of patients screened with CT at baseline. However, more often LCS yields evidence of additional cardiopulmonary disorders, such as emphysema or coronary artery calcifications. The International Early Lung Cancer Program (I-ELCAP) and the National Lung Cancer Screening Trial (NLST), which included > 79,000 patients, found evidence of emphysema on CT imaging in 24% and 31% of cases, respectively.19,20 In both cohorts, > 80% of patients with emphysema on CT imaging had no prior history of COPD.
In a 2022 article summarizing the potential impact of CT LCS on COPD diagnosis, Mulshine et al suggest that detection of emphysema on CT LCS provides “earlier recognition for PCPs to identify patients who would benefit from detailed symptom screening to prompt spirometry for COPD detection” and additional motivation for tobacco cessation.21 The VANEOHS QI project was developed and implemented prior to I-ELCAP or NLST reporting results but reinforces the value of CT LCS for COPD diagnosis.
Early diagnosis of COPD remains challenging because PCPs do not ask, patients do not tell, and symptoms can easily be dismissed. However, earlier diagnosis of COPD in symptomatic patients improves outcomes.3,4 To bridge this gap, VA PCPs and primary care patient aligned care teams (PACTs) need to commit to probing high-risk patients for COPD symptoms and ordering spirometry for those who are symptomatic. To accomplish this task, primary care teams need help.
The VANEOHS QI project confirmed that some patients with evidence of COPD on CT have symptoms of COPD that they did not share with their PCPs and suggests that LCS can be used as a dual action case finding method to screen both for lung cancer and COPD. We propose that patients who are eligible for LCS should also be probed for COPD symptoms at their clinic visits; for symptomatic patients, spirometry should be ordered, and COPD evidence-based management should be initiated when spirometry results are consistent with COPD. Annual probing for COPD symptoms could be considered in asymptomatic patients with ongoing tobacco use or emphysema on CT, since they may develop symptoms in the future. This new case-finding method bypasses the need for time-prohibitive questionnaires or peak flow measurements.
Future Opportunities
VA PCPs juggle many priorities and despite the simplicity of this new case finding COPD method, it may be unintentionally overlooked. PCPs often run out of time or may forget to ask patients about COPD symptoms when ordering LCS.
Future innovations to increase COPD diagnosis could include the creation of a yearly VA clinical reminder linked to the tobacco use reminder that has check boxes asking about symptoms of COPD in current and prior smokers. If patients have COPD symptoms, the reminder can prompt the ordering of spirometry. Similar reminders could be implemented to identify veterans with exposures to burn pits or other military environmental exposures who may have COPD symptoms. Another possible way to increase COPD diagnosis would be a partnership between primary care and the VA LCS program where patients receiving screening are asked about COPD symptoms during their LCS interviews and PACTs are alerted to order spirometry for symptomatic patients.
Elusive no longer! We can pull the veil back on COPD diagnosis and identify patients with possible COPD earlier in their course using their eligibility for LCS as a yearly reminder to probe them for symptoms. While not all patients who undergo LCS—even those with evidence of COPD on CT—will have COPD symptoms, symptoms may develop over time. LCS provides the possibility of 2 diagnoses from 1 test. This is an opportunity we cannot afford to miss.
Primary care practitioners (PCPs) in the US Department of Veterans Affairs (VA) provide care for patients with higher rates of many diseases—diabetes, heart disease, cancer, chronic obstructive pulmonary disease (COPD), and stroke—compared to the nonveteran population. 1 Due to the medical complexities of these diseases, they are often misdiagnosed or not diagnosed at all.
COPD is hiding in plain sight, impacting quality of life and burdening US health care systems.2 Research has yielded new treatments and evidence-based guidelines; however, COPD remains underdiagnosed. Only 13 million of the estimated 79 million US adults with COPD aged 20 to 79 years have been formally diagnosed.3 By the time patients are diagnosed, the disease is often advanced, and therapies are less effective. In 2 large studies of patients with COPD symptoms, later diagnosis was associated with worse outcomes.4,5
Veterans have a higher prevalence of COPD (8%-19%) than nonveterans (6%), likely due to higher rates of smoking and service-related exposures, especially among veterans of post-9/11 conflicts.6,7 Veterans do not always report symptoms and PCPs may not ask about symptoms, leading to underdiagnosis.8 The combination of high likelihood and underdetection of COPD presents a challenge and a target for VA quality improvement (QI).
The US Preventive Services Task Force (USPSTF) recommends against screening asymptomatic patients for COPD. However, both the USPSTF and the Global Initiative for Chronic Obstructive Lung Disease Report advocate for active case finding in primary care clinics to determine whether high-risk patients, such as smokers, experience COPD symptoms and warrant spirometry. 9,10 To make early COPD diagnoses, clinicians may use questionnaires alone or in combination with handheld peak expiratory flow rate measurements.11,12 Formal spirometry, considered the gold standard for COPD diagnosis, is ordered for patients who report COPD symptoms (ie, shortness of breath with exertion) or who have both COPD symptoms and reduced peak flow rates.
A systematic review and meta-analysis found that while the combination of questionnaires and peak flows was the more effective strategy overall, questionnaires alone were also valuable for identifying patients with possible COPD.13 Implementation of either screening method in primary care practices would be challenging. In a simulation study that applied chronic disease and preventive care guidelines to hypothetical patient panels, the time required for PCPs to provide guideline-recommended chronic and preventive care in addition to acute care far exceeded 8 hours per day, even in team-based settings.14 Overburdened PCPs are therefore unlikely to accept additional tasks like COPD case finding.
Why don’t patients report their pulmonary symptoms? Patients may not recognize the symptoms as evidence of COPD. Others may be afraid of a COPD diagnosis or the stigma that is associated with it.15 Perhaps they believe COPD treatment is ineffective because of lung damage from smoking. Some patients may not want to know if they have COPD, while others reduce activity levels to avoid symptoms.16
QUALITY IMPROVEMENT PROJECT
Given the high prevalence of COPD among veterans and the potential for underdiagnosis, VA Northeast Ohio Healthcare System (VANEOHS) internal medicine residents and faculty assessed the state of COPD diagnosis in its primary care clinic with a QI project in 2022. Patients in the clinic between August 1, 2015, and November 30, 2022, with an International Classification of Diseases-10 (ICD-10) COPD diagnosis code (J44) in the electronic health record were included. Of 157 included patients, 105 patients who had prior spirometry testing were excluded. Of the 52 patients with diagnosed COPD and no spirometry testing, 30 patients had computed tomography (CT) findings consistent with COPD (ie, airway thickening, emphysema, air trapping) that was performed for CT lung cancer screening (LCS).17 Twenty-three of these 30 patients were contacted by phone. All 23 were ever smokers and 13 reported COPD symptoms. The PCPs of the symptomatic patients were then contacted. Spirometry was ordered for all 13 patients and completed by 7. Three spirometry tests confirmed the COPD diagnosis. One PCP initiated inhaler therapy for a patient with newly diagnosed COPD.
All 11 PCPs of symptomatic patients were interviewed (many had > 1 symptomatic patient). They reported being unaware of patients’ COPD symptoms because the patients did not mention them, noting that screening for COPD was not a priority.
Role of Lung Cancer Screening
VA PCPs use electronic health record clinical reminders to track tests, consults, chronic disease education, cancer screenings, and routine health maintenance. A clinical reminder already exists (based on USPSTF recommendations) for LCS for patients aged 50 to 80 years who have a smoking history of 20 pack years. Patients who meet these criteria would also be considered high risk for COPD.
The VANEOHS QI project suggests that previously undiagnosed patients with findings of COPD on LCS may also have symptoms of COPD. Therefore, we wondered whether the LCS clinical reminder could serve a second purpose by prompting PCPs to ask veterans who meet LCS criteria about their COPD symptoms.
In 2022, about 13 million patients were eligible for LCS.18 Patients who qualify for LCS are at high risk for other cardiopulmonary disorders, such as COPD and coronary artery disease. Lung cancer is detected in only 1% of patients screened with CT at baseline. However, more often LCS yields evidence of additional cardiopulmonary disorders, such as emphysema or coronary artery calcifications. The International Early Lung Cancer Program (I-ELCAP) and the National Lung Cancer Screening Trial (NLST), which included > 79,000 patients, found evidence of emphysema on CT imaging in 24% and 31% of cases, respectively.19,20 In both cohorts, > 80% of patients with emphysema on CT imaging had no prior history of COPD.
In a 2022 article summarizing the potential impact of CT LCS on COPD diagnosis, Mulshine et al suggest that detection of emphysema on CT LCS provides “earlier recognition for PCPs to identify patients who would benefit from detailed symptom screening to prompt spirometry for COPD detection” and additional motivation for tobacco cessation.21 The VANEOHS QI project was developed and implemented prior to I-ELCAP or NLST reporting results but reinforces the value of CT LCS for COPD diagnosis.
Early diagnosis of COPD remains challenging because PCPs do not ask, patients do not tell, and symptoms can easily be dismissed. However, earlier diagnosis of COPD in symptomatic patients improves outcomes.3,4 To bridge this gap, VA PCPs and primary care patient aligned care teams (PACTs) need to commit to probing high-risk patients for COPD symptoms and ordering spirometry for those who are symptomatic. To accomplish this task, primary care teams need help.
The VANEOHS QI project confirmed that some patients with evidence of COPD on CT have symptoms of COPD that they did not share with their PCPs and suggests that LCS can be used as a dual action case finding method to screen both for lung cancer and COPD. We propose that patients who are eligible for LCS should also be probed for COPD symptoms at their clinic visits; for symptomatic patients, spirometry should be ordered, and COPD evidence-based management should be initiated when spirometry results are consistent with COPD. Annual probing for COPD symptoms could be considered in asymptomatic patients with ongoing tobacco use or emphysema on CT, since they may develop symptoms in the future. This new case-finding method bypasses the need for time-prohibitive questionnaires or peak flow measurements.
Future Opportunities
VA PCPs juggle many priorities and despite the simplicity of this new case finding COPD method, it may be unintentionally overlooked. PCPs often run out of time or may forget to ask patients about COPD symptoms when ordering LCS.
Future innovations to increase COPD diagnosis could include the creation of a yearly VA clinical reminder linked to the tobacco use reminder that has check boxes asking about symptoms of COPD in current and prior smokers. If patients have COPD symptoms, the reminder can prompt the ordering of spirometry. Similar reminders could be implemented to identify veterans with exposures to burn pits or other military environmental exposures who may have COPD symptoms. Another possible way to increase COPD diagnosis would be a partnership between primary care and the VA LCS program where patients receiving screening are asked about COPD symptoms during their LCS interviews and PACTs are alerted to order spirometry for symptomatic patients.
Elusive no longer! We can pull the veil back on COPD diagnosis and identify patients with possible COPD earlier in their course using their eligibility for LCS as a yearly reminder to probe them for symptoms. While not all patients who undergo LCS—even those with evidence of COPD on CT—will have COPD symptoms, symptoms may develop over time. LCS provides the possibility of 2 diagnoses from 1 test. This is an opportunity we cannot afford to miss.
- Betancourt JA, Granados PS, Pacheco GJ, et al. Exploring health outcomes for U.S. veterans compared to non-veterans from 2003 to 2019. Healthcare (Basel). 2021;9(5):604. doi:10.3390/healthcare90506064
- Bamonti PM, Fischer I, Moye J, Poghosyan H, Pietrzak RH. Obstructive respiratory disease in U.S. veterans: prevalence, characteristics, and health burden. J Psychiatr Res. 2024;176:140-147. doi:10.1016/j.jpsychires.2024.05.053
- Criner RN, Han MK. COPD care in the 21st century: a public health priority. Respir Care. 2018;63(5):591-600. doi:10.4187/respcare.06276
- Larsson K, Janson C, Ställberg B, et al. Impact of COPD diagnosis timing on clinical and economic outcomes: the ARCTIC observational cohort study. Int J Chron Obstruct Pulmon Dis. 2019;14:995-1008. doi:10.2147/COPD.S195382
- Kostikas K, Price D, Gutzwiller FS, et al. Clinical impact and healthcare resource utilization associated with early versus late COPD diagnosis in patients from UK CPRD Database. Int J Chron Obstruct Pulmon Dis. 2020;15:1729- 1738. doi:10.2147/COPD.S255414
- Bamonti PM, Robinson SA, Wan ES, Moy ML. Improving physiological, physical, and psychological health outcomes: a narrative review in US veterans with COPD. Int J Chron Obstruct Pulmon Dis. 2022;17:1269-1283. doi:10.2147/COPD.S339323
- Savitz DA, Woskie SR, Bello A, et al. Deployment to military bases with open burn pits and respiratory and cardiovascular disease. JAMA Netw Open. 2024;7(4):e247629. doi:10.1001/jamanetworkopen.2024.7629
- Murphy DE, Chaudhry Z, Almoosa KF, Panos RJ. High prevalence of chronic obstructive pulmonary disease among veterans in the urban midwest. Mil Med. 2011;176(5):552-560. doi:10.7205/milmed-d-10-00377
- Guirguis-Blake JM, Senger CA, Webber EM, Mularski RA, Whitlock EP. Screening for chronic obstructive pulmonary disease: evidence report and systematic review for the US Preventive Services Task Force. JAMA. 2016;315(13):1378-1393. doi:10.1001/jama.2016.2654
- Capriotti T, Tomy R, Morales M. COPD updates: 2023 GOLD Report for primary care providers. Clinical Advisor. May 9, 2023. Accessed May 14, 2025. https://www.clinicaladvisor.com/features/copd-updates-2023-gold-report-primary-care/
- Leidy NK, Martinez FJ, Malley KG, et al. Can CAPTURE be used to identify undiagnosed patients with mild- to- moderate COPD likely to benefit from treatment? Int J Chron Obstruct Pulmon Dis. 2018;13:1901-1912. doi:10.2147/COPD.S152226
- Jithoo A, Enright PL, Burney P, et al. Case-finding options for COPD: results from the burden of obstructive lung disease study. Eur Respir J. 2013;41(3):548-555. doi:10.1183/09031936.00132011
- Haroon SM, Jordan RE, O’Beirne-Elliman J, Adab P. Effectiveness of case finding strategies for COPD in primary care: a systematic review and meta-analysis. NPJ Prim Care Respir Med. 2015;25:15056. doi:10.1038/npjpcrm.2015.56
- Porter J, Boyd C, Skandari MR, Laiteerapong N. Revisiting the time needed to provide adult primary care. J Gen Intern Med. 2023;38(1)147-155. doi:10.1007/s11606-022-07707-x
- Woo S, Zhou W, Larson JL. Stigma experiences in people with chronic obstructive pulmonary disease: an integrative review. Int J Chron Obstruct Pulmon Dis. 2021;16:1647- 1659. doi:10.2147/COPD.S306874
- Aaron SD, Montes de Oca M, Celli B, et al. Early diagnosis and treatment of COPD: the costs and benefits of case finding. Am J Respir Crit Care Med. 2024;209(8):928-937. doi:10.1164/rccm.202311-2120PP
- Kwon A, Lee C, Arafah A, Klein M, Namboodiri S, Lee C. Increasing chronic obstructive pulmonary disease (COPD) diagnosis with pulmonary function testing for patients with chest imaging evidence of COPD. Poster presented at: Society of General Internal Medicine Midwest Regional Meeting; October 19-20, 2023; Chicago, IL.
- Henderson LM, Su I, Rivera MP, et al. Prevalence of lung cancer screening in the US, 2022. JAMA Netw Open. 2024;7(3):e243190. doi:10.1001/jamanetworkopen.2024.3190
- Steiger D, Siddiqi MF, Yip R, Yankelevitz DF, Henschke CI; I-ELCAP investigators. The importance of low-dose CT screening to identify emphysema in asymptomatic participants with and without a prior diagnosis of COPD. Clin Imaging. 2021;78:136-141. doi:10.1016/j.clinimag.2021.03.012
- Pinsky PF, Lynch DA, Gierada DS. Incidental findings on low-dose CT scan lung cancer screenings and deaths from respiratory diseases. Chest. 2022;161(4):1092-1100. doi:10.1016/j.chest.2021.11.015
- Mulshine JL, Aldigé CR, Ambrose LF, et al. Emphysema detection in the course of lung cancer screening: optimizing a rare opportunity to impact population health. Ann Am Thorac Soc. 2023;20(4):499- 503. doi:10.1513/AnnalsATS.202207-631PS
- Betancourt JA, Granados PS, Pacheco GJ, et al. Exploring health outcomes for U.S. veterans compared to non-veterans from 2003 to 2019. Healthcare (Basel). 2021;9(5):604. doi:10.3390/healthcare90506064
- Bamonti PM, Fischer I, Moye J, Poghosyan H, Pietrzak RH. Obstructive respiratory disease in U.S. veterans: prevalence, characteristics, and health burden. J Psychiatr Res. 2024;176:140-147. doi:10.1016/j.jpsychires.2024.05.053
- Criner RN, Han MK. COPD care in the 21st century: a public health priority. Respir Care. 2018;63(5):591-600. doi:10.4187/respcare.06276
- Larsson K, Janson C, Ställberg B, et al. Impact of COPD diagnosis timing on clinical and economic outcomes: the ARCTIC observational cohort study. Int J Chron Obstruct Pulmon Dis. 2019;14:995-1008. doi:10.2147/COPD.S195382
- Kostikas K, Price D, Gutzwiller FS, et al. Clinical impact and healthcare resource utilization associated with early versus late COPD diagnosis in patients from UK CPRD Database. Int J Chron Obstruct Pulmon Dis. 2020;15:1729- 1738. doi:10.2147/COPD.S255414
- Bamonti PM, Robinson SA, Wan ES, Moy ML. Improving physiological, physical, and psychological health outcomes: a narrative review in US veterans with COPD. Int J Chron Obstruct Pulmon Dis. 2022;17:1269-1283. doi:10.2147/COPD.S339323
- Savitz DA, Woskie SR, Bello A, et al. Deployment to military bases with open burn pits and respiratory and cardiovascular disease. JAMA Netw Open. 2024;7(4):e247629. doi:10.1001/jamanetworkopen.2024.7629
- Murphy DE, Chaudhry Z, Almoosa KF, Panos RJ. High prevalence of chronic obstructive pulmonary disease among veterans in the urban midwest. Mil Med. 2011;176(5):552-560. doi:10.7205/milmed-d-10-00377
- Guirguis-Blake JM, Senger CA, Webber EM, Mularski RA, Whitlock EP. Screening for chronic obstructive pulmonary disease: evidence report and systematic review for the US Preventive Services Task Force. JAMA. 2016;315(13):1378-1393. doi:10.1001/jama.2016.2654
- Capriotti T, Tomy R, Morales M. COPD updates: 2023 GOLD Report for primary care providers. Clinical Advisor. May 9, 2023. Accessed May 14, 2025. https://www.clinicaladvisor.com/features/copd-updates-2023-gold-report-primary-care/
- Leidy NK, Martinez FJ, Malley KG, et al. Can CAPTURE be used to identify undiagnosed patients with mild- to- moderate COPD likely to benefit from treatment? Int J Chron Obstruct Pulmon Dis. 2018;13:1901-1912. doi:10.2147/COPD.S152226
- Jithoo A, Enright PL, Burney P, et al. Case-finding options for COPD: results from the burden of obstructive lung disease study. Eur Respir J. 2013;41(3):548-555. doi:10.1183/09031936.00132011
- Haroon SM, Jordan RE, O’Beirne-Elliman J, Adab P. Effectiveness of case finding strategies for COPD in primary care: a systematic review and meta-analysis. NPJ Prim Care Respir Med. 2015;25:15056. doi:10.1038/npjpcrm.2015.56
- Porter J, Boyd C, Skandari MR, Laiteerapong N. Revisiting the time needed to provide adult primary care. J Gen Intern Med. 2023;38(1)147-155. doi:10.1007/s11606-022-07707-x
- Woo S, Zhou W, Larson JL. Stigma experiences in people with chronic obstructive pulmonary disease: an integrative review. Int J Chron Obstruct Pulmon Dis. 2021;16:1647- 1659. doi:10.2147/COPD.S306874
- Aaron SD, Montes de Oca M, Celli B, et al. Early diagnosis and treatment of COPD: the costs and benefits of case finding. Am J Respir Crit Care Med. 2024;209(8):928-937. doi:10.1164/rccm.202311-2120PP
- Kwon A, Lee C, Arafah A, Klein M, Namboodiri S, Lee C. Increasing chronic obstructive pulmonary disease (COPD) diagnosis with pulmonary function testing for patients with chest imaging evidence of COPD. Poster presented at: Society of General Internal Medicine Midwest Regional Meeting; October 19-20, 2023; Chicago, IL.
- Henderson LM, Su I, Rivera MP, et al. Prevalence of lung cancer screening in the US, 2022. JAMA Netw Open. 2024;7(3):e243190. doi:10.1001/jamanetworkopen.2024.3190
- Steiger D, Siddiqi MF, Yip R, Yankelevitz DF, Henschke CI; I-ELCAP investigators. The importance of low-dose CT screening to identify emphysema in asymptomatic participants with and without a prior diagnosis of COPD. Clin Imaging. 2021;78:136-141. doi:10.1016/j.clinimag.2021.03.012
- Pinsky PF, Lynch DA, Gierada DS. Incidental findings on low-dose CT scan lung cancer screenings and deaths from respiratory diseases. Chest. 2022;161(4):1092-1100. doi:10.1016/j.chest.2021.11.015
- Mulshine JL, Aldigé CR, Ambrose LF, et al. Emphysema detection in the course of lung cancer screening: optimizing a rare opportunity to impact population health. Ann Am Thorac Soc. 2023;20(4):499- 503. doi:10.1513/AnnalsATS.202207-631PS
The Use of Lung Cancer Screening to Increase Chronic Obstructive Pulmonary Disease Diagnosis in Veterans Affairs Primary Care
The Use of Lung Cancer Screening to Increase Chronic Obstructive Pulmonary Disease Diagnosis in Veterans Affairs Primary Care
When Patient-Centered Care Initiatives Align: Integrating VA Whole Health and Shared Decision-Making for Lung Cancer Screening
When Patient-Centered Care Initiatives Align: Integrating VA Whole Health and Shared Decision-Making for Lung Cancer Screening
The landmark Crossing the Quality Chasm report from the National Academy of Medicine identified patient- centered care as essential to health care quality. The report defines patientcentered care as “respectful of and responsive to individual patient preferences, needs, and values.”1 Many health care systems, including the Veterans Health Administration, are transforming to a patient-centered model of care.2 The US Department of Veterans Affairs (VA) Whole Health System of Care initiative is a system-wide, cultural transformation. Within whole health, what matters most to the patient—including their preferences, needs, and values—is foundational to health care and meant to be essential in every clinical encounter. Whole health implementation includes a progressive rollout with health care practitioner (HCP) trainings across the VA.2
Shared decision-making (SDM) is a different but aligned patient-centered care concept. SDM is a process through which a decision or care plan, based on patients’ preferences, needs, and values, is made or developed.3-5 SDM is ideal in situations with equipoise (decisions with equivalent choices), individualized risks, and/or greater uncertainty of the net benefit, such as with lung cancer screening (LCS).3 SDM for LCS is required by the US Centers for Medicare and Medicaid Services and has been adopted by many US health care systems, including the VA.6,7 Early detection of lung cancer can reduce death by 20% at the population level.8 However, at the patient level there is wide variation in the risk of developing lung cancer and a range of potential harms.8 LCS follow-up procedures may be more invasive than with other cancer screenings. Thus, there is concern about the risk of false-positive results leading to unnecessary care or complications.8 Given this balance between benefit and harm and the differing patient value on the trade-offs of LCS, an individualized, patient-centered approach is essential when deciding whether LCS is the right choice for a specific patient.
Despite the importance of LCS SDM, observational studies have shown poor implementation in clinical encounters.9,10 HCP barriers include competing demands, limited time, lack of familiarity with and training in SDM, and beliefs biasing screening over no screening.11-13 Additionally, HCPs may assume that patients want them to make the decision. However, research has shown that patients actually want to be more involved in their health care decisions.14 One suggested strategy to overcome these barriers is aligning SDM for LCS within an organization’s broader patient-centered initiatives.15
This project sought to align the need for SDM for LCS and the broader VA whole health initiative as part of a multilevel strategy to implement SDM for LCS across Veterans Integrated Service Network (VISN) 1.16
This article addresses HCP-level barriers. HCPs targeted are those typically involved in LCS. The VA utilizes LCS coordinators (LCSCs) in both centralized or consult models (in which LCSCs are involved in all aspects of screening) and hybrid models (in which primary care practitioners and LCSCs are both engaged in LCS tasks). The goal of this program was to generate areas of conceptual alignment between SDM and whole health as a first step in integrating these VA initiatives. This work was conducted as a foundation for an SDM for lung cancer HCP training and consultation initiative.
ALIGNMENT PROCESS
We reviewed relevant literature and resources for SDM and whole health. In reviewing the SDM literature, we included a sample of the most widely cited literature on the topic, and focused primarily on the systematic review by Bomhof-Roordink et al.4,5,17,18 This review provided a synthesis of SDM elements across SDM models and identified 53 different elements clustered into 24 components.4 The most common components were present in at least half of all SDM published models, including: make the decision, patient preferences, tailor information, deliberate, create choice awareness, and learn about the patient. Bomhof-Roordink et al provided the guiding framework for this conceptualization of SDM because that study included the available recent published SDM models.4
Second, published literature on VA whole health along with supplemental promotional and training materials were reviewed. The whole health materials included 2 sets of training slides developed for VA HCPs (available to VA employees): Implementing Whole Health in Clinical Care, which is focused on HCPs’ work with patients, and Whole Health for You and Me, which is about HCPs’ personal well-being.19 We also reviewed a publication describing the history of whole health and patient-facing online whole health tools.2,19
Each document was reviewed for key elements related to SDM, patient-centered care, and whole health. Using the 53 elements identified by Bomhof-Roordink et al, we reviewed and compared each element to the whole health materials to create the integrated model of SDM and whole health. We iteratively discussed and organized the elements until we reached consensus.
SDM and Whole Health Alignment
We created an integrated model of SDM for LCS within the context of the VA whole health initiative. This integrated model is directed at HCPs who would likely engage patients in discussions of LCS, including primary care practitioners and nurse coordinators. The model includes 3 steps for HCPs to follow that align SDM within whole health: (1) frame the conversation and partner with the patient; (2) share clinical perspective and elicit patient values; and (3) deliberate and decide together. For each step, the SDM elements, whole health elements, and integration of SDM and whole health are provided. Table 1 provides an overview of the similarities and differences between SDM and whole health. Example phrases that merge SDM and whole health for HCPs to use in patient conversations about LCS are included in Table 2.
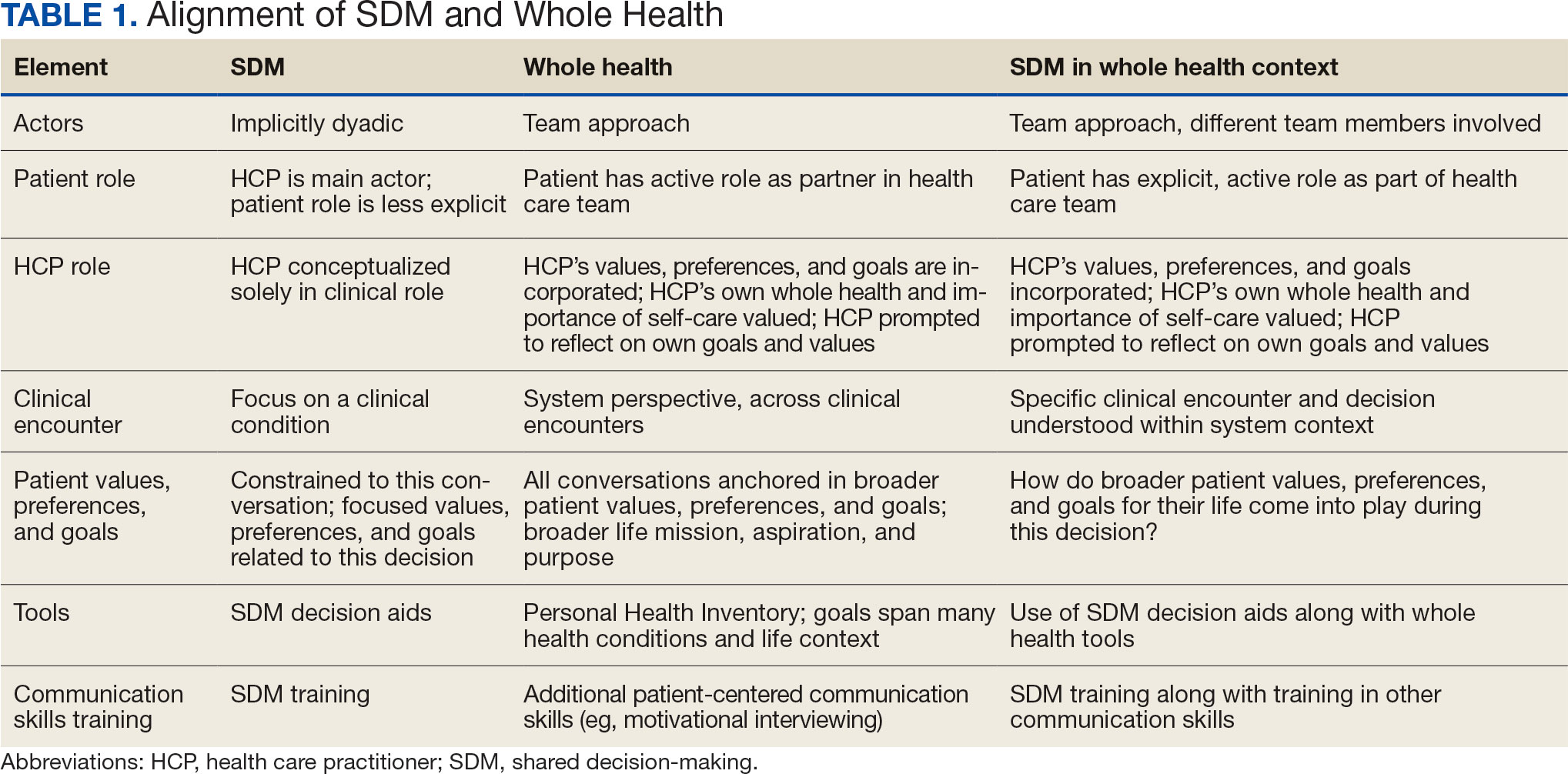
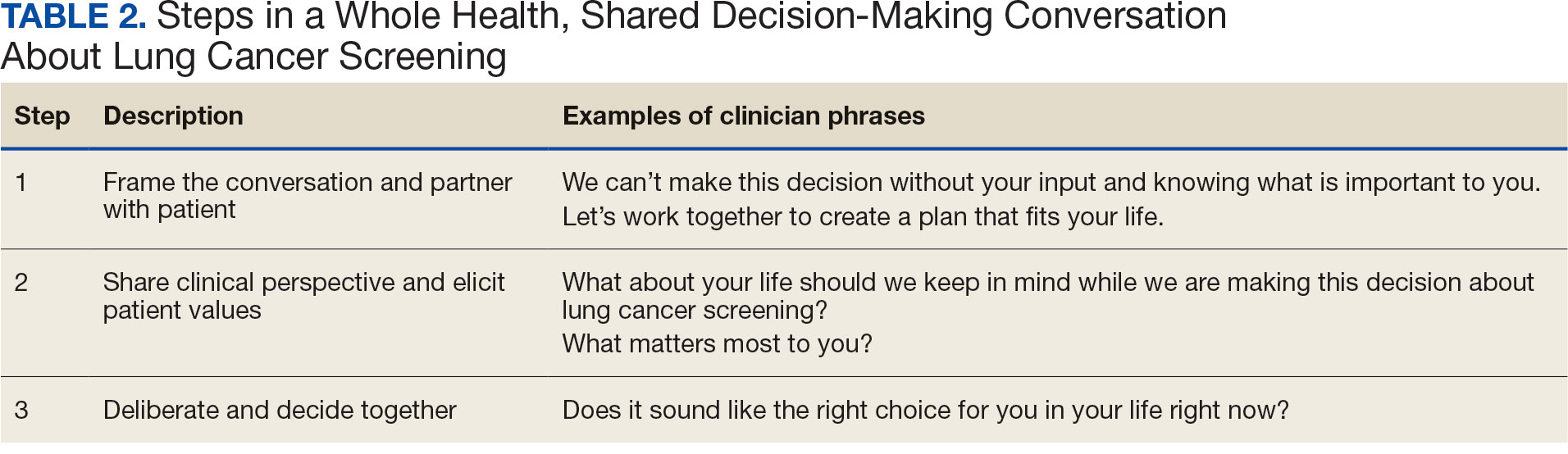
STEP 1. FRAME THE CONVERSATION AND PARTNER WITH THE PATIENT
Shared decision-making. Traditional SDM literature includes an initial step of letting patients know that there is a choice to be made between ≥ 2 clinical options.4 Ancillary elements of this first step include asking patients their preferences about the degree to which they want to be involved in SDM and about how they like to receive information (eg, verbal, written, video). These steps open the SDM conversation and ensure the patient and HCP are on the same page before moving forward. For example, the US Agency for Healthcare Research and Quality SHARE model’s first step is for HCPs to communicate that choices exist and to invite the patient to be involved in decisions.20 Similarly, Elwyn’s 3-step SDM model begins with establishing that a choice exists and inviting patient input on making that choice.17
Whole health. Patients are encouraged to play an active role in their health care. Through whole health programs such as Taking Charge of My Life and Health, patients explore their values and set self-care goals.21 HCP whole health trainings teach and reinforce communication skills, including SDM, listening skills, and motivational interviewing.19
Shared decision-making/whole health integration. SDM and whole health both prioritize respect, compassion, and patients’ expertise. They focus on the patient-HCP relationship with an emphasis on fostering egalitarian interactions. HCPs frame the SDM conversation and partner with the patient so they know what to expect and who will be involved. This conversation is framed from the outset as a collaborative discussion. HCPs empower the patient to play an active role in decision-making and help them understand why their engagement is critical.
STEP 2. SHARE CLINICAL PERSPECTIVE AND ELICIT PATIENT VALUES
Shared decision-making. HCPs share clinical perspective on LCS tailored to individual patients while explicitly inviting the patient to share their preferences and values when thinking about whether to undergo LCS. HCPs give a balanced description of LCS, including the benefits and harms, tailored to the patient’s unique information needs and questions. Sharing clinical perspective also includes describing treatment options, the most common element across SDM models.4 Decision aids, which provide unbiased information and include a values clarification exercise, may be helpful in sharing clinical perspectives and clarifying patient values related to the trade-offs of LCS.22 For example, the VA National Center for Health Promotion and Disease Prevention developed a LCS decision aid to be used for SDM for LCS.
Whole health. The conversation shifts from “What is the matter with you?” to “What matters to you?” starting with the patient’s goals and priorities rather than disease prevention, diagnosis, and treatment.2 Several whole health tools exist, including the Personal Health Inventory, used to identify what matters most to patients and understand their current well-being and self-care.23 Using the inventory, the patient and their health care team develop the patient’s personal health plan.24 Additionally, whole health trains HCPs to reflect on their own attitudes and biases when providing clinical care.
Shared decision-making/whole health integration. The LCS conversation can build on other whole health-related conversations with a HCP or other team members. HCPs can reference the patient’s personal health plan for documentation of the patient’s preferences, values, and goals in the electronic medical record. During this process, HCPs can give space for patients to discuss factors in their life and experiences that impact their perspective and decision-making. For example, patient concerns could be explored here, including fear of a cancer diagnosis, stigma around smoking, and fears around the screening and/or treatment process. HCPs may ask, “What matters most to you when making this decision?” Finally, by sharing clinical information, HCPs will focus on patient values to help overcome their own biases toward a desire for LCS. HCPs, similar to the rest of the US public, tend to hold highly favorable attitudes toward cancer screening as well as misconceptions about the magnitude of benefits from screening.13
STEP 3. DELIBERATE AND DECIDE TOGETHER
Shared decision-making. Decision-making is almost always considered the last SDM step.4 In the final step, the patient and HCP discuss the options (ie, to screen or not to screen) considering the patient’s values and preferences, and patients decide with their HCP whether they will undergo LCS. Patients may decide they need more time to think about these options. As part of deliberation, HCPs assess what other information patients may need to arrive at a decision. Family members, friends, or peers may be included in making the final decision.
Whole health. In Whole health, decisions also may include the entire health care team and other individuals important to the patient (eg, family, friends). Integration across different health care settings is also considered a key whole health element. Finally, whole health focuses on long-term relationships with patients; thus, the LCS SDM process is situated within longer term relationship building and patient empowerment, both of which will facilitate partnering with the patient in future conversations about other decisions.
Shared decision-making/whole health integration. Both SDM and whole health emphasize partnership with the patient in making a final decision. There is also focus on decision-making as an ongoing process. Deciding whether LCS is the best choice might include naming and addressing emotions, voicing questions not raised, and exploring whether screening fits the patient’s goals, values, and life context. HCPs may give guidance, but patients retain the authority to make decisions. The goal is to empower patients to know that the only right decision is the one right for them and they will be supported.
Limitations
This article describes a VA practice program and was not a formal research study. Further work is needed to evaluate the presented strategies. Additionally, we did not conduct a systematic literature review and thus elements of SDM and whole health may not be exhaustive.
CONCLUSIONS
This article describes the alignment of 2 distinct VA initiatives, whole health and SDM for LCS. The goal was to reduce known barriers to SDM, such as competing demands, limited time, and lack of familiarity with and training in SDM.11-13 These concepts are well aligned. This integrated model is the first step in informing the development of a HCP training program and materials as part of a multilevel strategy that our team is using to implement SDM for LCS in VISN 1.16 The final training and materials resulting from this work were delivered to LCSCs in 3 ways: (1) a series of 3 interactive group training sessions, including didactic elements, role play, and time for open discussion; (2) 1-on-1 academic detailing; and (3) educational handouts. In academic detailing, a member of the research team trained in academic detailing met virtually with each nurse coordinator, identified that individual’s barriers to SDM, and used the training materials to highlight messages to overcome those barriers; follow-up calls provided a forum for discussing progress and overcoming additional challenges. Although this article focused specifically on whole health and SDM, the conceptual alignment process strategy can be applied to other implementations of multiple initiatives.
- Institute of Medicine (US) Committee on Quality of Health Care in America. Crossing the Quality Chasm: A New Health System for the 21st Century. The National Academies Press; 2001. doi:10.17226/10027
- Bokhour BG, Haun JN, Hyde J, Charns M, Kligler B. Transforming the Veterans Affairs to a whole health system of care: time for action and research. Med Care. 2020;58:295- 300. doi:10.1097/MLR.0000000000001316
- Elwyn G, Frosch D, Rollnick S. Dual equipoise shared decision making: definitions for decision and behaviour support interventions. Implement Sci. 2009;4:75. doi:7510.1186/1748-5908-4-75
- Bomhof-Roordink H, Gärtner FR, Stiggelbout AM, Pieterse AH. Key components of shared decision making models: a systematic review. BMJ Open. 2019;9:e031763. doi:10.1136/bmjopen-2019-031763
- Charles C, Gafni A, Whelan T. Decision-making in the physician- patient encounter: revisiting the shared treatment decision-making model. Soc Sci Med. 1999;49:651-661. doi:10.1016/s0277-9536(99)00145-8
- Moyer VA; US Preventive Services Task Force. Screening for lung cancer: U.S. Preventive Services Task Force recommendation statement. Ann Intern Med. 2014;160:330- 338. doi:10.7326/m13-2771
- Centers for Medicare & Medicaid Services. Screening for lung cancer with low dose computed tomography (LDCT). February 10, 2022. Accessed February 7, 2025. https://www.cms.gov/medicare-coverage-database/view/ncacal-decision-memo.aspx?proposed=N&ncaid=304
- Aberle DR, Adams AM, Berg CD, et al. Reduced lung-cancer mortality with low-dose computed tomographic screening. N Engl J Med. 2011;365:395-409. doi:10.1056/NEJMoa1102873
- Slatore CG, Wiener RS. Pulmonary nodules: a small problem for many, severe distress for some, and how to communicate about it. Chest. 2018;153:1004-1015. doi:10.1016/j.chest.2017.10.013
- Nishi SPE, Lowenstein LM, Mendoza TR, et al. Shared decision-making for lung cancer screening: how well are we “sharing”? Chest. 2021;160:330-340. doi:10.1016/j.chest.2021.01.041
- Wiener RS, Koppelman E, Bolton R, et al. Patient and clinician perspectives on shared decision-making in early adopting lung cancer screening programs: a qualitative study. J Gen Intern Med. 2018;33:1035-1042. doi:10.1007/s11606-018-4350-9
- Melzer AC, Golden SE, Ono SS, Datta S, Triplette M, Slatore CG. “We just never have enough time”: clinician views of lung cancer screening processes and implementation. Ann Am Thorac Soc. 2020. doi:10.1513/AnnalsATS.202003-262OC
- Schwartz LM, Woloshin S, Fowler FJ Jr, Welch HG. Enthusiasm for cancer screening in the United States. JAMA. 2004;291:71-78. doi:10.1001/jama.291.1.71
- Lown BA, Rosen J, Marttila J. An agenda for improving compassionate care: a survey shows about half of patients say such care is missing. Health Aff (Millwood). 2011;30:1772-1778. doi:10.1377/hlthaff.2011.0539
- Scholl I, LaRussa A, Hahlweg P, Kobrin S, Elwyn G. Organizational- and system-level characteristics that influence implementation of shared decision-making and strategies to address them - a scoping review. Implement Sci. 2018;13:40. doi:10.1186/s13012-018-0731-z
- Khanna A, Fix GM, Anderson E, et al. Towards a framework for patient-centred care coordination: a scoping review protocol. BMJ Open. 2022;12:e066808. doi:10.1136/bmjopen-2022-066808
- Elwyn G, Durand MA, Song J, et al. A three-talk model for shared decision making: multistage consultation process. BMJ. 2017;359:j4891. doi:10.1136/bmj.j4891
- Makoul G, Clayman ML. An integrative model of shared decision making in medical encounters. Patient Educ Couns. 2006;60:301-312. doi:10.1016/j.pec.2005.06.010
- Whole Health. US Department of Veterans Affairs. Accessed April 14, 2025. https://www.va.gov/wholehealth/
- Agency for Healthcare Research and Quality. The SHARE approach. Accessed April 14, 2025. https://www.ahrq.gov/health-literacy/professional-training/shared-decision/index.html
- Abadi MH, Barker AM, Rao SR, Orner M, Rychener D, Bokhour BG. Examining the impact of a peer-led group program for veteran engagement and well-being. J Altern Complement Med. 2021;27:S37-S44. doi:10.1089/acm.2020.0124
- Stacey D, Lewis KB, Smith M, et al. Decision aids for people facing health treatment or screening decisions. Cochrane Database Syst Rev. 2024;1:CD001431. doi:10.1002/14651858.CD001431.pub6
- US Department of Veterans Affairs, Veterans Health Administration, Office of Patient Centered Care and Cultural Transformation. Personal health inventory. Revised April 2019. Accessed April 14, 2025. https://www.va.gov/wholehealth/docs/10-773_PHI_July2019_508.pdf
- US Department of Veterans Affairs. Build your personal health plan. Updated July 24, 2024. Accessed April 14, 2025. https://www.va.gov/wholehealth/phi.asp
The landmark Crossing the Quality Chasm report from the National Academy of Medicine identified patient- centered care as essential to health care quality. The report defines patientcentered care as “respectful of and responsive to individual patient preferences, needs, and values.”1 Many health care systems, including the Veterans Health Administration, are transforming to a patient-centered model of care.2 The US Department of Veterans Affairs (VA) Whole Health System of Care initiative is a system-wide, cultural transformation. Within whole health, what matters most to the patient—including their preferences, needs, and values—is foundational to health care and meant to be essential in every clinical encounter. Whole health implementation includes a progressive rollout with health care practitioner (HCP) trainings across the VA.2
Shared decision-making (SDM) is a different but aligned patient-centered care concept. SDM is a process through which a decision or care plan, based on patients’ preferences, needs, and values, is made or developed.3-5 SDM is ideal in situations with equipoise (decisions with equivalent choices), individualized risks, and/or greater uncertainty of the net benefit, such as with lung cancer screening (LCS).3 SDM for LCS is required by the US Centers for Medicare and Medicaid Services and has been adopted by many US health care systems, including the VA.6,7 Early detection of lung cancer can reduce death by 20% at the population level.8 However, at the patient level there is wide variation in the risk of developing lung cancer and a range of potential harms.8 LCS follow-up procedures may be more invasive than with other cancer screenings. Thus, there is concern about the risk of false-positive results leading to unnecessary care or complications.8 Given this balance between benefit and harm and the differing patient value on the trade-offs of LCS, an individualized, patient-centered approach is essential when deciding whether LCS is the right choice for a specific patient.
Despite the importance of LCS SDM, observational studies have shown poor implementation in clinical encounters.9,10 HCP barriers include competing demands, limited time, lack of familiarity with and training in SDM, and beliefs biasing screening over no screening.11-13 Additionally, HCPs may assume that patients want them to make the decision. However, research has shown that patients actually want to be more involved in their health care decisions.14 One suggested strategy to overcome these barriers is aligning SDM for LCS within an organization’s broader patient-centered initiatives.15
This project sought to align the need for SDM for LCS and the broader VA whole health initiative as part of a multilevel strategy to implement SDM for LCS across Veterans Integrated Service Network (VISN) 1.16
This article addresses HCP-level barriers. HCPs targeted are those typically involved in LCS. The VA utilizes LCS coordinators (LCSCs) in both centralized or consult models (in which LCSCs are involved in all aspects of screening) and hybrid models (in which primary care practitioners and LCSCs are both engaged in LCS tasks). The goal of this program was to generate areas of conceptual alignment between SDM and whole health as a first step in integrating these VA initiatives. This work was conducted as a foundation for an SDM for lung cancer HCP training and consultation initiative.
ALIGNMENT PROCESS
We reviewed relevant literature and resources for SDM and whole health. In reviewing the SDM literature, we included a sample of the most widely cited literature on the topic, and focused primarily on the systematic review by Bomhof-Roordink et al.4,5,17,18 This review provided a synthesis of SDM elements across SDM models and identified 53 different elements clustered into 24 components.4 The most common components were present in at least half of all SDM published models, including: make the decision, patient preferences, tailor information, deliberate, create choice awareness, and learn about the patient. Bomhof-Roordink et al provided the guiding framework for this conceptualization of SDM because that study included the available recent published SDM models.4
Second, published literature on VA whole health along with supplemental promotional and training materials were reviewed. The whole health materials included 2 sets of training slides developed for VA HCPs (available to VA employees): Implementing Whole Health in Clinical Care, which is focused on HCPs’ work with patients, and Whole Health for You and Me, which is about HCPs’ personal well-being.19 We also reviewed a publication describing the history of whole health and patient-facing online whole health tools.2,19
Each document was reviewed for key elements related to SDM, patient-centered care, and whole health. Using the 53 elements identified by Bomhof-Roordink et al, we reviewed and compared each element to the whole health materials to create the integrated model of SDM and whole health. We iteratively discussed and organized the elements until we reached consensus.
SDM and Whole Health Alignment
We created an integrated model of SDM for LCS within the context of the VA whole health initiative. This integrated model is directed at HCPs who would likely engage patients in discussions of LCS, including primary care practitioners and nurse coordinators. The model includes 3 steps for HCPs to follow that align SDM within whole health: (1) frame the conversation and partner with the patient; (2) share clinical perspective and elicit patient values; and (3) deliberate and decide together. For each step, the SDM elements, whole health elements, and integration of SDM and whole health are provided. Table 1 provides an overview of the similarities and differences between SDM and whole health. Example phrases that merge SDM and whole health for HCPs to use in patient conversations about LCS are included in Table 2.
STEP 1. FRAME THE CONVERSATION AND PARTNER WITH THE PATIENT
Shared decision-making. Traditional SDM literature includes an initial step of letting patients know that there is a choice to be made between ≥ 2 clinical options.4 Ancillary elements of this first step include asking patients their preferences about the degree to which they want to be involved in SDM and about how they like to receive information (eg, verbal, written, video). These steps open the SDM conversation and ensure the patient and HCP are on the same page before moving forward. For example, the US Agency for Healthcare Research and Quality SHARE model’s first step is for HCPs to communicate that choices exist and to invite the patient to be involved in decisions.20 Similarly, Elwyn’s 3-step SDM model begins with establishing that a choice exists and inviting patient input on making that choice.17
Whole health. Patients are encouraged to play an active role in their health care. Through whole health programs such as Taking Charge of My Life and Health, patients explore their values and set self-care goals.21 HCP whole health trainings teach and reinforce communication skills, including SDM, listening skills, and motivational interviewing.19
Shared decision-making/whole health integration. SDM and whole health both prioritize respect, compassion, and patients’ expertise. They focus on the patient-HCP relationship with an emphasis on fostering egalitarian interactions. HCPs frame the SDM conversation and partner with the patient so they know what to expect and who will be involved. This conversation is framed from the outset as a collaborative discussion. HCPs empower the patient to play an active role in decision-making and help them understand why their engagement is critical.
STEP 2. SHARE CLINICAL PERSPECTIVE AND ELICIT PATIENT VALUES
Shared decision-making. HCPs share clinical perspective on LCS tailored to individual patients while explicitly inviting the patient to share their preferences and values when thinking about whether to undergo LCS. HCPs give a balanced description of LCS, including the benefits and harms, tailored to the patient’s unique information needs and questions. Sharing clinical perspective also includes describing treatment options, the most common element across SDM models.4 Decision aids, which provide unbiased information and include a values clarification exercise, may be helpful in sharing clinical perspectives and clarifying patient values related to the trade-offs of LCS.22 For example, the VA National Center for Health Promotion and Disease Prevention developed a LCS decision aid to be used for SDM for LCS.
Whole health. The conversation shifts from “What is the matter with you?” to “What matters to you?” starting with the patient’s goals and priorities rather than disease prevention, diagnosis, and treatment.2 Several whole health tools exist, including the Personal Health Inventory, used to identify what matters most to patients and understand their current well-being and self-care.23 Using the inventory, the patient and their health care team develop the patient’s personal health plan.24 Additionally, whole health trains HCPs to reflect on their own attitudes and biases when providing clinical care.
Shared decision-making/whole health integration. The LCS conversation can build on other whole health-related conversations with a HCP or other team members. HCPs can reference the patient’s personal health plan for documentation of the patient’s preferences, values, and goals in the electronic medical record. During this process, HCPs can give space for patients to discuss factors in their life and experiences that impact their perspective and decision-making. For example, patient concerns could be explored here, including fear of a cancer diagnosis, stigma around smoking, and fears around the screening and/or treatment process. HCPs may ask, “What matters most to you when making this decision?” Finally, by sharing clinical information, HCPs will focus on patient values to help overcome their own biases toward a desire for LCS. HCPs, similar to the rest of the US public, tend to hold highly favorable attitudes toward cancer screening as well as misconceptions about the magnitude of benefits from screening.13
STEP 3. DELIBERATE AND DECIDE TOGETHER
Shared decision-making. Decision-making is almost always considered the last SDM step.4 In the final step, the patient and HCP discuss the options (ie, to screen or not to screen) considering the patient’s values and preferences, and patients decide with their HCP whether they will undergo LCS. Patients may decide they need more time to think about these options. As part of deliberation, HCPs assess what other information patients may need to arrive at a decision. Family members, friends, or peers may be included in making the final decision.
Whole health. In Whole health, decisions also may include the entire health care team and other individuals important to the patient (eg, family, friends). Integration across different health care settings is also considered a key whole health element. Finally, whole health focuses on long-term relationships with patients; thus, the LCS SDM process is situated within longer term relationship building and patient empowerment, both of which will facilitate partnering with the patient in future conversations about other decisions.
Shared decision-making/whole health integration. Both SDM and whole health emphasize partnership with the patient in making a final decision. There is also focus on decision-making as an ongoing process. Deciding whether LCS is the best choice might include naming and addressing emotions, voicing questions not raised, and exploring whether screening fits the patient’s goals, values, and life context. HCPs may give guidance, but patients retain the authority to make decisions. The goal is to empower patients to know that the only right decision is the one right for them and they will be supported.
Limitations
This article describes a VA practice program and was not a formal research study. Further work is needed to evaluate the presented strategies. Additionally, we did not conduct a systematic literature review and thus elements of SDM and whole health may not be exhaustive.
CONCLUSIONS
This article describes the alignment of 2 distinct VA initiatives, whole health and SDM for LCS. The goal was to reduce known barriers to SDM, such as competing demands, limited time, and lack of familiarity with and training in SDM.11-13 These concepts are well aligned. This integrated model is the first step in informing the development of a HCP training program and materials as part of a multilevel strategy that our team is using to implement SDM for LCS in VISN 1.16 The final training and materials resulting from this work were delivered to LCSCs in 3 ways: (1) a series of 3 interactive group training sessions, including didactic elements, role play, and time for open discussion; (2) 1-on-1 academic detailing; and (3) educational handouts. In academic detailing, a member of the research team trained in academic detailing met virtually with each nurse coordinator, identified that individual’s barriers to SDM, and used the training materials to highlight messages to overcome those barriers; follow-up calls provided a forum for discussing progress and overcoming additional challenges. Although this article focused specifically on whole health and SDM, the conceptual alignment process strategy can be applied to other implementations of multiple initiatives.
The landmark Crossing the Quality Chasm report from the National Academy of Medicine identified patient- centered care as essential to health care quality. The report defines patientcentered care as “respectful of and responsive to individual patient preferences, needs, and values.”1 Many health care systems, including the Veterans Health Administration, are transforming to a patient-centered model of care.2 The US Department of Veterans Affairs (VA) Whole Health System of Care initiative is a system-wide, cultural transformation. Within whole health, what matters most to the patient—including their preferences, needs, and values—is foundational to health care and meant to be essential in every clinical encounter. Whole health implementation includes a progressive rollout with health care practitioner (HCP) trainings across the VA.2
Shared decision-making (SDM) is a different but aligned patient-centered care concept. SDM is a process through which a decision or care plan, based on patients’ preferences, needs, and values, is made or developed.3-5 SDM is ideal in situations with equipoise (decisions with equivalent choices), individualized risks, and/or greater uncertainty of the net benefit, such as with lung cancer screening (LCS).3 SDM for LCS is required by the US Centers for Medicare and Medicaid Services and has been adopted by many US health care systems, including the VA.6,7 Early detection of lung cancer can reduce death by 20% at the population level.8 However, at the patient level there is wide variation in the risk of developing lung cancer and a range of potential harms.8 LCS follow-up procedures may be more invasive than with other cancer screenings. Thus, there is concern about the risk of false-positive results leading to unnecessary care or complications.8 Given this balance between benefit and harm and the differing patient value on the trade-offs of LCS, an individualized, patient-centered approach is essential when deciding whether LCS is the right choice for a specific patient.
Despite the importance of LCS SDM, observational studies have shown poor implementation in clinical encounters.9,10 HCP barriers include competing demands, limited time, lack of familiarity with and training in SDM, and beliefs biasing screening over no screening.11-13 Additionally, HCPs may assume that patients want them to make the decision. However, research has shown that patients actually want to be more involved in their health care decisions.14 One suggested strategy to overcome these barriers is aligning SDM for LCS within an organization’s broader patient-centered initiatives.15
This project sought to align the need for SDM for LCS and the broader VA whole health initiative as part of a multilevel strategy to implement SDM for LCS across Veterans Integrated Service Network (VISN) 1.16
This article addresses HCP-level barriers. HCPs targeted are those typically involved in LCS. The VA utilizes LCS coordinators (LCSCs) in both centralized or consult models (in which LCSCs are involved in all aspects of screening) and hybrid models (in which primary care practitioners and LCSCs are both engaged in LCS tasks). The goal of this program was to generate areas of conceptual alignment between SDM and whole health as a first step in integrating these VA initiatives. This work was conducted as a foundation for an SDM for lung cancer HCP training and consultation initiative.
ALIGNMENT PROCESS
We reviewed relevant literature and resources for SDM and whole health. In reviewing the SDM literature, we included a sample of the most widely cited literature on the topic, and focused primarily on the systematic review by Bomhof-Roordink et al.4,5,17,18 This review provided a synthesis of SDM elements across SDM models and identified 53 different elements clustered into 24 components.4 The most common components were present in at least half of all SDM published models, including: make the decision, patient preferences, tailor information, deliberate, create choice awareness, and learn about the patient. Bomhof-Roordink et al provided the guiding framework for this conceptualization of SDM because that study included the available recent published SDM models.4
Second, published literature on VA whole health along with supplemental promotional and training materials were reviewed. The whole health materials included 2 sets of training slides developed for VA HCPs (available to VA employees): Implementing Whole Health in Clinical Care, which is focused on HCPs’ work with patients, and Whole Health for You and Me, which is about HCPs’ personal well-being.19 We also reviewed a publication describing the history of whole health and patient-facing online whole health tools.2,19
Each document was reviewed for key elements related to SDM, patient-centered care, and whole health. Using the 53 elements identified by Bomhof-Roordink et al, we reviewed and compared each element to the whole health materials to create the integrated model of SDM and whole health. We iteratively discussed and organized the elements until we reached consensus.
SDM and Whole Health Alignment
We created an integrated model of SDM for LCS within the context of the VA whole health initiative. This integrated model is directed at HCPs who would likely engage patients in discussions of LCS, including primary care practitioners and nurse coordinators. The model includes 3 steps for HCPs to follow that align SDM within whole health: (1) frame the conversation and partner with the patient; (2) share clinical perspective and elicit patient values; and (3) deliberate and decide together. For each step, the SDM elements, whole health elements, and integration of SDM and whole health are provided. Table 1 provides an overview of the similarities and differences between SDM and whole health. Example phrases that merge SDM and whole health for HCPs to use in patient conversations about LCS are included in Table 2.
STEP 1. FRAME THE CONVERSATION AND PARTNER WITH THE PATIENT
Shared decision-making. Traditional SDM literature includes an initial step of letting patients know that there is a choice to be made between ≥ 2 clinical options.4 Ancillary elements of this first step include asking patients their preferences about the degree to which they want to be involved in SDM and about how they like to receive information (eg, verbal, written, video). These steps open the SDM conversation and ensure the patient and HCP are on the same page before moving forward. For example, the US Agency for Healthcare Research and Quality SHARE model’s first step is for HCPs to communicate that choices exist and to invite the patient to be involved in decisions.20 Similarly, Elwyn’s 3-step SDM model begins with establishing that a choice exists and inviting patient input on making that choice.17
Whole health. Patients are encouraged to play an active role in their health care. Through whole health programs such as Taking Charge of My Life and Health, patients explore their values and set self-care goals.21 HCP whole health trainings teach and reinforce communication skills, including SDM, listening skills, and motivational interviewing.19
Shared decision-making/whole health integration. SDM and whole health both prioritize respect, compassion, and patients’ expertise. They focus on the patient-HCP relationship with an emphasis on fostering egalitarian interactions. HCPs frame the SDM conversation and partner with the patient so they know what to expect and who will be involved. This conversation is framed from the outset as a collaborative discussion. HCPs empower the patient to play an active role in decision-making and help them understand why their engagement is critical.
STEP 2. SHARE CLINICAL PERSPECTIVE AND ELICIT PATIENT VALUES
Shared decision-making. HCPs share clinical perspective on LCS tailored to individual patients while explicitly inviting the patient to share their preferences and values when thinking about whether to undergo LCS. HCPs give a balanced description of LCS, including the benefits and harms, tailored to the patient’s unique information needs and questions. Sharing clinical perspective also includes describing treatment options, the most common element across SDM models.4 Decision aids, which provide unbiased information and include a values clarification exercise, may be helpful in sharing clinical perspectives and clarifying patient values related to the trade-offs of LCS.22 For example, the VA National Center for Health Promotion and Disease Prevention developed a LCS decision aid to be used for SDM for LCS.
Whole health. The conversation shifts from “What is the matter with you?” to “What matters to you?” starting with the patient’s goals and priorities rather than disease prevention, diagnosis, and treatment.2 Several whole health tools exist, including the Personal Health Inventory, used to identify what matters most to patients and understand their current well-being and self-care.23 Using the inventory, the patient and their health care team develop the patient’s personal health plan.24 Additionally, whole health trains HCPs to reflect on their own attitudes and biases when providing clinical care.
Shared decision-making/whole health integration. The LCS conversation can build on other whole health-related conversations with a HCP or other team members. HCPs can reference the patient’s personal health plan for documentation of the patient’s preferences, values, and goals in the electronic medical record. During this process, HCPs can give space for patients to discuss factors in their life and experiences that impact their perspective and decision-making. For example, patient concerns could be explored here, including fear of a cancer diagnosis, stigma around smoking, and fears around the screening and/or treatment process. HCPs may ask, “What matters most to you when making this decision?” Finally, by sharing clinical information, HCPs will focus on patient values to help overcome their own biases toward a desire for LCS. HCPs, similar to the rest of the US public, tend to hold highly favorable attitudes toward cancer screening as well as misconceptions about the magnitude of benefits from screening.13
STEP 3. DELIBERATE AND DECIDE TOGETHER
Shared decision-making. Decision-making is almost always considered the last SDM step.4 In the final step, the patient and HCP discuss the options (ie, to screen or not to screen) considering the patient’s values and preferences, and patients decide with their HCP whether they will undergo LCS. Patients may decide they need more time to think about these options. As part of deliberation, HCPs assess what other information patients may need to arrive at a decision. Family members, friends, or peers may be included in making the final decision.
Whole health. In Whole health, decisions also may include the entire health care team and other individuals important to the patient (eg, family, friends). Integration across different health care settings is also considered a key whole health element. Finally, whole health focuses on long-term relationships with patients; thus, the LCS SDM process is situated within longer term relationship building and patient empowerment, both of which will facilitate partnering with the patient in future conversations about other decisions.
Shared decision-making/whole health integration. Both SDM and whole health emphasize partnership with the patient in making a final decision. There is also focus on decision-making as an ongoing process. Deciding whether LCS is the best choice might include naming and addressing emotions, voicing questions not raised, and exploring whether screening fits the patient’s goals, values, and life context. HCPs may give guidance, but patients retain the authority to make decisions. The goal is to empower patients to know that the only right decision is the one right for them and they will be supported.
Limitations
This article describes a VA practice program and was not a formal research study. Further work is needed to evaluate the presented strategies. Additionally, we did not conduct a systematic literature review and thus elements of SDM and whole health may not be exhaustive.
CONCLUSIONS
This article describes the alignment of 2 distinct VA initiatives, whole health and SDM for LCS. The goal was to reduce known barriers to SDM, such as competing demands, limited time, and lack of familiarity with and training in SDM.11-13 These concepts are well aligned. This integrated model is the first step in informing the development of a HCP training program and materials as part of a multilevel strategy that our team is using to implement SDM for LCS in VISN 1.16 The final training and materials resulting from this work were delivered to LCSCs in 3 ways: (1) a series of 3 interactive group training sessions, including didactic elements, role play, and time for open discussion; (2) 1-on-1 academic detailing; and (3) educational handouts. In academic detailing, a member of the research team trained in academic detailing met virtually with each nurse coordinator, identified that individual’s barriers to SDM, and used the training materials to highlight messages to overcome those barriers; follow-up calls provided a forum for discussing progress and overcoming additional challenges. Although this article focused specifically on whole health and SDM, the conceptual alignment process strategy can be applied to other implementations of multiple initiatives.
- Institute of Medicine (US) Committee on Quality of Health Care in America. Crossing the Quality Chasm: A New Health System for the 21st Century. The National Academies Press; 2001. doi:10.17226/10027
- Bokhour BG, Haun JN, Hyde J, Charns M, Kligler B. Transforming the Veterans Affairs to a whole health system of care: time for action and research. Med Care. 2020;58:295- 300. doi:10.1097/MLR.0000000000001316
- Elwyn G, Frosch D, Rollnick S. Dual equipoise shared decision making: definitions for decision and behaviour support interventions. Implement Sci. 2009;4:75. doi:7510.1186/1748-5908-4-75
- Bomhof-Roordink H, Gärtner FR, Stiggelbout AM, Pieterse AH. Key components of shared decision making models: a systematic review. BMJ Open. 2019;9:e031763. doi:10.1136/bmjopen-2019-031763
- Charles C, Gafni A, Whelan T. Decision-making in the physician- patient encounter: revisiting the shared treatment decision-making model. Soc Sci Med. 1999;49:651-661. doi:10.1016/s0277-9536(99)00145-8
- Moyer VA; US Preventive Services Task Force. Screening for lung cancer: U.S. Preventive Services Task Force recommendation statement. Ann Intern Med. 2014;160:330- 338. doi:10.7326/m13-2771
- Centers for Medicare & Medicaid Services. Screening for lung cancer with low dose computed tomography (LDCT). February 10, 2022. Accessed February 7, 2025. https://www.cms.gov/medicare-coverage-database/view/ncacal-decision-memo.aspx?proposed=N&ncaid=304
- Aberle DR, Adams AM, Berg CD, et al. Reduced lung-cancer mortality with low-dose computed tomographic screening. N Engl J Med. 2011;365:395-409. doi:10.1056/NEJMoa1102873
- Slatore CG, Wiener RS. Pulmonary nodules: a small problem for many, severe distress for some, and how to communicate about it. Chest. 2018;153:1004-1015. doi:10.1016/j.chest.2017.10.013
- Nishi SPE, Lowenstein LM, Mendoza TR, et al. Shared decision-making for lung cancer screening: how well are we “sharing”? Chest. 2021;160:330-340. doi:10.1016/j.chest.2021.01.041
- Wiener RS, Koppelman E, Bolton R, et al. Patient and clinician perspectives on shared decision-making in early adopting lung cancer screening programs: a qualitative study. J Gen Intern Med. 2018;33:1035-1042. doi:10.1007/s11606-018-4350-9
- Melzer AC, Golden SE, Ono SS, Datta S, Triplette M, Slatore CG. “We just never have enough time”: clinician views of lung cancer screening processes and implementation. Ann Am Thorac Soc. 2020. doi:10.1513/AnnalsATS.202003-262OC
- Schwartz LM, Woloshin S, Fowler FJ Jr, Welch HG. Enthusiasm for cancer screening in the United States. JAMA. 2004;291:71-78. doi:10.1001/jama.291.1.71
- Lown BA, Rosen J, Marttila J. An agenda for improving compassionate care: a survey shows about half of patients say such care is missing. Health Aff (Millwood). 2011;30:1772-1778. doi:10.1377/hlthaff.2011.0539
- Scholl I, LaRussa A, Hahlweg P, Kobrin S, Elwyn G. Organizational- and system-level characteristics that influence implementation of shared decision-making and strategies to address them - a scoping review. Implement Sci. 2018;13:40. doi:10.1186/s13012-018-0731-z
- Khanna A, Fix GM, Anderson E, et al. Towards a framework for patient-centred care coordination: a scoping review protocol. BMJ Open. 2022;12:e066808. doi:10.1136/bmjopen-2022-066808
- Elwyn G, Durand MA, Song J, et al. A three-talk model for shared decision making: multistage consultation process. BMJ. 2017;359:j4891. doi:10.1136/bmj.j4891
- Makoul G, Clayman ML. An integrative model of shared decision making in medical encounters. Patient Educ Couns. 2006;60:301-312. doi:10.1016/j.pec.2005.06.010
- Whole Health. US Department of Veterans Affairs. Accessed April 14, 2025. https://www.va.gov/wholehealth/
- Agency for Healthcare Research and Quality. The SHARE approach. Accessed April 14, 2025. https://www.ahrq.gov/health-literacy/professional-training/shared-decision/index.html
- Abadi MH, Barker AM, Rao SR, Orner M, Rychener D, Bokhour BG. Examining the impact of a peer-led group program for veteran engagement and well-being. J Altern Complement Med. 2021;27:S37-S44. doi:10.1089/acm.2020.0124
- Stacey D, Lewis KB, Smith M, et al. Decision aids for people facing health treatment or screening decisions. Cochrane Database Syst Rev. 2024;1:CD001431. doi:10.1002/14651858.CD001431.pub6
- US Department of Veterans Affairs, Veterans Health Administration, Office of Patient Centered Care and Cultural Transformation. Personal health inventory. Revised April 2019. Accessed April 14, 2025. https://www.va.gov/wholehealth/docs/10-773_PHI_July2019_508.pdf
- US Department of Veterans Affairs. Build your personal health plan. Updated July 24, 2024. Accessed April 14, 2025. https://www.va.gov/wholehealth/phi.asp
- Institute of Medicine (US) Committee on Quality of Health Care in America. Crossing the Quality Chasm: A New Health System for the 21st Century. The National Academies Press; 2001. doi:10.17226/10027
- Bokhour BG, Haun JN, Hyde J, Charns M, Kligler B. Transforming the Veterans Affairs to a whole health system of care: time for action and research. Med Care. 2020;58:295- 300. doi:10.1097/MLR.0000000000001316
- Elwyn G, Frosch D, Rollnick S. Dual equipoise shared decision making: definitions for decision and behaviour support interventions. Implement Sci. 2009;4:75. doi:7510.1186/1748-5908-4-75
- Bomhof-Roordink H, Gärtner FR, Stiggelbout AM, Pieterse AH. Key components of shared decision making models: a systematic review. BMJ Open. 2019;9:e031763. doi:10.1136/bmjopen-2019-031763
- Charles C, Gafni A, Whelan T. Decision-making in the physician- patient encounter: revisiting the shared treatment decision-making model. Soc Sci Med. 1999;49:651-661. doi:10.1016/s0277-9536(99)00145-8
- Moyer VA; US Preventive Services Task Force. Screening for lung cancer: U.S. Preventive Services Task Force recommendation statement. Ann Intern Med. 2014;160:330- 338. doi:10.7326/m13-2771
- Centers for Medicare & Medicaid Services. Screening for lung cancer with low dose computed tomography (LDCT). February 10, 2022. Accessed February 7, 2025. https://www.cms.gov/medicare-coverage-database/view/ncacal-decision-memo.aspx?proposed=N&ncaid=304
- Aberle DR, Adams AM, Berg CD, et al. Reduced lung-cancer mortality with low-dose computed tomographic screening. N Engl J Med. 2011;365:395-409. doi:10.1056/NEJMoa1102873
- Slatore CG, Wiener RS. Pulmonary nodules: a small problem for many, severe distress for some, and how to communicate about it. Chest. 2018;153:1004-1015. doi:10.1016/j.chest.2017.10.013
- Nishi SPE, Lowenstein LM, Mendoza TR, et al. Shared decision-making for lung cancer screening: how well are we “sharing”? Chest. 2021;160:330-340. doi:10.1016/j.chest.2021.01.041
- Wiener RS, Koppelman E, Bolton R, et al. Patient and clinician perspectives on shared decision-making in early adopting lung cancer screening programs: a qualitative study. J Gen Intern Med. 2018;33:1035-1042. doi:10.1007/s11606-018-4350-9
- Melzer AC, Golden SE, Ono SS, Datta S, Triplette M, Slatore CG. “We just never have enough time”: clinician views of lung cancer screening processes and implementation. Ann Am Thorac Soc. 2020. doi:10.1513/AnnalsATS.202003-262OC
- Schwartz LM, Woloshin S, Fowler FJ Jr, Welch HG. Enthusiasm for cancer screening in the United States. JAMA. 2004;291:71-78. doi:10.1001/jama.291.1.71
- Lown BA, Rosen J, Marttila J. An agenda for improving compassionate care: a survey shows about half of patients say such care is missing. Health Aff (Millwood). 2011;30:1772-1778. doi:10.1377/hlthaff.2011.0539
- Scholl I, LaRussa A, Hahlweg P, Kobrin S, Elwyn G. Organizational- and system-level characteristics that influence implementation of shared decision-making and strategies to address them - a scoping review. Implement Sci. 2018;13:40. doi:10.1186/s13012-018-0731-z
- Khanna A, Fix GM, Anderson E, et al. Towards a framework for patient-centred care coordination: a scoping review protocol. BMJ Open. 2022;12:e066808. doi:10.1136/bmjopen-2022-066808
- Elwyn G, Durand MA, Song J, et al. A three-talk model for shared decision making: multistage consultation process. BMJ. 2017;359:j4891. doi:10.1136/bmj.j4891
- Makoul G, Clayman ML. An integrative model of shared decision making in medical encounters. Patient Educ Couns. 2006;60:301-312. doi:10.1016/j.pec.2005.06.010
- Whole Health. US Department of Veterans Affairs. Accessed April 14, 2025. https://www.va.gov/wholehealth/
- Agency for Healthcare Research and Quality. The SHARE approach. Accessed April 14, 2025. https://www.ahrq.gov/health-literacy/professional-training/shared-decision/index.html
- Abadi MH, Barker AM, Rao SR, Orner M, Rychener D, Bokhour BG. Examining the impact of a peer-led group program for veteran engagement and well-being. J Altern Complement Med. 2021;27:S37-S44. doi:10.1089/acm.2020.0124
- Stacey D, Lewis KB, Smith M, et al. Decision aids for people facing health treatment or screening decisions. Cochrane Database Syst Rev. 2024;1:CD001431. doi:10.1002/14651858.CD001431.pub6
- US Department of Veterans Affairs, Veterans Health Administration, Office of Patient Centered Care and Cultural Transformation. Personal health inventory. Revised April 2019. Accessed April 14, 2025. https://www.va.gov/wholehealth/docs/10-773_PHI_July2019_508.pdf
- US Department of Veterans Affairs. Build your personal health plan. Updated July 24, 2024. Accessed April 14, 2025. https://www.va.gov/wholehealth/phi.asp
When Patient-Centered Care Initiatives Align: Integrating VA Whole Health and Shared Decision-Making for Lung Cancer Screening
When Patient-Centered Care Initiatives Align: Integrating VA Whole Health and Shared Decision-Making for Lung Cancer Screening
Can Popular Weight-Loss Drugs Protect Against Obesity-Related Cancers?
Can Popular Weight-Loss Drugs Protect Against Obesity-Related Cancers?
New data suggest that glucagon-like peptide 1 (GLP-1) receptor agonists, used to treat diabetes and obesity, may also help guard against obesity-related cancers.
In a large observational study, new GLP-1 agonist users with obesity and diabetes had a significantly lower risk for 14 obesity-related cancers than similar individuals who received dipeptidyl peptidase-4 (DPP-4) inhibitors, which are weight-neutral.
This study provides a “reassuring safety signal” showing that GLP-1 drugs are linked to a modest drop in obesity-related cancer risk, and not a higher risk for these cancers, said lead investigator Lucas Mavromatis, medical student at NYU Grossman School of Medicine in New York City, during a press conference at American Society of Clinical Oncology (ASCO) 2025 annual meeting.
However, there were some nuances to the findings. The protective effect of GLP-1 agonists was only significant for colon and rectal cancers and for women, Mavromatis reported. And although GLP-1 users had an 8% lower risk of dying from any cause, the survival benefit was also only significant for women.
Still, the overall “message to patients is GLP-1 receptor treatments remain a strong option for patients with diabetes and obesity and may have an additional, small favorable benefit in cancer,” Mavromatis explained at the press briefing.
'Intriguing Hypothesis'
Obesity is linked to an increased risk of developing more than a dozen cancer types, including esophageal, colon, rectal, stomach, liver, gallbladder, pancreatic, kidney, postmenopausal breast, ovarian, endometrial and thyroid, as well as multiple myeloma and meningiomas.
About 12% of Americans have been prescribed a GLP-1 medication to treat diabetes and/or obesity. However, little is known about how these drugs affect cancer risk.
To investigate, Mavromatis and colleagues used the Optum healthcare database to identify 170,030 adults with obesity and type 2 diabetes from 43 health systems in the United States.
Between 2013 and 2023, half started a GLP-1 agonist and half started a DPP-4 inhibitor, with propensity score matching used to balance characteristics of the two cohorts.
Participants were a mean age of 56.8 years, with an average body mass index of 38.5; more than 70% were White individuals and more than 14% were Black individuals.
During a mean follow-up of 3.9 years, 2501 new obesity-related cancers were identified in the GLP-1 group and 2671 in the DPP-4 group — representing a 7% overall reduced risk for any obesity-related cancer in the GLP-1 group (hazard ratio [HR], 0.93).
When analyzing each of the 14 obesity-related cancers separately, the protective link between GLP-1 use and cancer was primarily driven by colon and rectal cancers. GLP-1 users had a 16% lower risk for colon cancer (HR, 0.84) and a 28% lower risk for rectal cancer (HR, 0.72).
“No other cancers had statistically significant associations with GLP-1 use,” Mavromatis told briefing attendees. But “importantly, no cancers had statistically significant adverse associations with GLP-1 use,” he added.
Experts have expressed some concern about a possible link between GLP-1 use and pancreatic cancer given that pancreatitis is a known side effect of GLP-1 use. However, “this is not borne out by epidemiological data,” Mavromatis said.
“Additionally, we were not able to specifically assess medullary thyroid cancer, which is on the warning label for several GLP-1 medications, but we did see a reassuring lack of association between GLP-1 use and thyroid cancer as a whole,” he added.
During follow-up, there were 2783 deaths in the GLP-1 group and 2961 deaths in the DPP-4 group — translating to an 8% lower risk for death due to any cause among GLP-1 users (HR, 0.92; P = .001).
Mavromatis and colleagues observed sex differences as well. Women taking a GLP-1 had an 8% lower risk for obesity-related cancers (HR, 0.92; P = .01) and a 20% lower risk for death from any cause (HR, 0.80; P < .001) compared with women taking a DPP-4 inhibitor.
Among men, researchers found no statistically significant difference between GLP-1 and DPP-4 use for obesity-related cancer risk (HR, 0.95; P = .29) or all-cause mortality (HR, 1.04; P = .34).
Overall, Mavromatis said, it’s important to note that the absolute risk reduction seen in the study is “small and the number of patients that would need to be given one of these medications to prevent an obesity-related cancer, based on our data, would be very large.”
Mavromatis also noted that the length of follow-up was short, and the study assessed primarily older and weaker GLP-1 agonists compared with newer agents on the market. Therefore, longer-term studies with newer GLP-1s are needed to confirm the effects seen as well as safety.
In a statement, ASCO President Robin Zon, MD, said this trial raises the “intriguing hypothesis” that the increasingly popular GLP-1 medications might offer some benefit in reducing the risk of developing cancer.
Zon said she sees many patients with obesity, and given the clear link between cancer and obesity, defining the clinical role of GLP-1 medications in cancer prevention is “important.”
This study “leads us in the direction” of a potential protective effect of GLP-1s on cancer, but “there are a lot of questions that are generated by this particular study, especially as we move forward and we think about prevention of cancers,” Zon told the briefing.
This study was funded by the National Institute of Diabetes and Digestive and Kidney Diseases of the National Institutes of Health. Mavromatis reported no relevant disclosures. Zon reported stock or ownership interests in Oncolytics Biotech, TG Therapeutics, Select Sector SPDR Health Care, AstraZeneca, CRISPR, McKesson, and Berkshire Hathaway.
A version of this article first appeared on Medscape.com.
New data suggest that glucagon-like peptide 1 (GLP-1) receptor agonists, used to treat diabetes and obesity, may also help guard against obesity-related cancers.
In a large observational study, new GLP-1 agonist users with obesity and diabetes had a significantly lower risk for 14 obesity-related cancers than similar individuals who received dipeptidyl peptidase-4 (DPP-4) inhibitors, which are weight-neutral.
This study provides a “reassuring safety signal” showing that GLP-1 drugs are linked to a modest drop in obesity-related cancer risk, and not a higher risk for these cancers, said lead investigator Lucas Mavromatis, medical student at NYU Grossman School of Medicine in New York City, during a press conference at American Society of Clinical Oncology (ASCO) 2025 annual meeting.
However, there were some nuances to the findings. The protective effect of GLP-1 agonists was only significant for colon and rectal cancers and for women, Mavromatis reported. And although GLP-1 users had an 8% lower risk of dying from any cause, the survival benefit was also only significant for women.
Still, the overall “message to patients is GLP-1 receptor treatments remain a strong option for patients with diabetes and obesity and may have an additional, small favorable benefit in cancer,” Mavromatis explained at the press briefing.
'Intriguing Hypothesis'
Obesity is linked to an increased risk of developing more than a dozen cancer types, including esophageal, colon, rectal, stomach, liver, gallbladder, pancreatic, kidney, postmenopausal breast, ovarian, endometrial and thyroid, as well as multiple myeloma and meningiomas.
About 12% of Americans have been prescribed a GLP-1 medication to treat diabetes and/or obesity. However, little is known about how these drugs affect cancer risk.
To investigate, Mavromatis and colleagues used the Optum healthcare database to identify 170,030 adults with obesity and type 2 diabetes from 43 health systems in the United States.
Between 2013 and 2023, half started a GLP-1 agonist and half started a DPP-4 inhibitor, with propensity score matching used to balance characteristics of the two cohorts.
Participants were a mean age of 56.8 years, with an average body mass index of 38.5; more than 70% were White individuals and more than 14% were Black individuals.
During a mean follow-up of 3.9 years, 2501 new obesity-related cancers were identified in the GLP-1 group and 2671 in the DPP-4 group — representing a 7% overall reduced risk for any obesity-related cancer in the GLP-1 group (hazard ratio [HR], 0.93).
When analyzing each of the 14 obesity-related cancers separately, the protective link between GLP-1 use and cancer was primarily driven by colon and rectal cancers. GLP-1 users had a 16% lower risk for colon cancer (HR, 0.84) and a 28% lower risk for rectal cancer (HR, 0.72).
“No other cancers had statistically significant associations with GLP-1 use,” Mavromatis told briefing attendees. But “importantly, no cancers had statistically significant adverse associations with GLP-1 use,” he added.
Experts have expressed some concern about a possible link between GLP-1 use and pancreatic cancer given that pancreatitis is a known side effect of GLP-1 use. However, “this is not borne out by epidemiological data,” Mavromatis said.
“Additionally, we were not able to specifically assess medullary thyroid cancer, which is on the warning label for several GLP-1 medications, but we did see a reassuring lack of association between GLP-1 use and thyroid cancer as a whole,” he added.
During follow-up, there were 2783 deaths in the GLP-1 group and 2961 deaths in the DPP-4 group — translating to an 8% lower risk for death due to any cause among GLP-1 users (HR, 0.92; P = .001).
Mavromatis and colleagues observed sex differences as well. Women taking a GLP-1 had an 8% lower risk for obesity-related cancers (HR, 0.92; P = .01) and a 20% lower risk for death from any cause (HR, 0.80; P < .001) compared with women taking a DPP-4 inhibitor.
Among men, researchers found no statistically significant difference between GLP-1 and DPP-4 use for obesity-related cancer risk (HR, 0.95; P = .29) or all-cause mortality (HR, 1.04; P = .34).
Overall, Mavromatis said, it’s important to note that the absolute risk reduction seen in the study is “small and the number of patients that would need to be given one of these medications to prevent an obesity-related cancer, based on our data, would be very large.”
Mavromatis also noted that the length of follow-up was short, and the study assessed primarily older and weaker GLP-1 agonists compared with newer agents on the market. Therefore, longer-term studies with newer GLP-1s are needed to confirm the effects seen as well as safety.
In a statement, ASCO President Robin Zon, MD, said this trial raises the “intriguing hypothesis” that the increasingly popular GLP-1 medications might offer some benefit in reducing the risk of developing cancer.
Zon said she sees many patients with obesity, and given the clear link between cancer and obesity, defining the clinical role of GLP-1 medications in cancer prevention is “important.”
This study “leads us in the direction” of a potential protective effect of GLP-1s on cancer, but “there are a lot of questions that are generated by this particular study, especially as we move forward and we think about prevention of cancers,” Zon told the briefing.
This study was funded by the National Institute of Diabetes and Digestive and Kidney Diseases of the National Institutes of Health. Mavromatis reported no relevant disclosures. Zon reported stock or ownership interests in Oncolytics Biotech, TG Therapeutics, Select Sector SPDR Health Care, AstraZeneca, CRISPR, McKesson, and Berkshire Hathaway.
A version of this article first appeared on Medscape.com.
New data suggest that glucagon-like peptide 1 (GLP-1) receptor agonists, used to treat diabetes and obesity, may also help guard against obesity-related cancers.
In a large observational study, new GLP-1 agonist users with obesity and diabetes had a significantly lower risk for 14 obesity-related cancers than similar individuals who received dipeptidyl peptidase-4 (DPP-4) inhibitors, which are weight-neutral.
This study provides a “reassuring safety signal” showing that GLP-1 drugs are linked to a modest drop in obesity-related cancer risk, and not a higher risk for these cancers, said lead investigator Lucas Mavromatis, medical student at NYU Grossman School of Medicine in New York City, during a press conference at American Society of Clinical Oncology (ASCO) 2025 annual meeting.
However, there were some nuances to the findings. The protective effect of GLP-1 agonists was only significant for colon and rectal cancers and for women, Mavromatis reported. And although GLP-1 users had an 8% lower risk of dying from any cause, the survival benefit was also only significant for women.
Still, the overall “message to patients is GLP-1 receptor treatments remain a strong option for patients with diabetes and obesity and may have an additional, small favorable benefit in cancer,” Mavromatis explained at the press briefing.
'Intriguing Hypothesis'
Obesity is linked to an increased risk of developing more than a dozen cancer types, including esophageal, colon, rectal, stomach, liver, gallbladder, pancreatic, kidney, postmenopausal breast, ovarian, endometrial and thyroid, as well as multiple myeloma and meningiomas.
About 12% of Americans have been prescribed a GLP-1 medication to treat diabetes and/or obesity. However, little is known about how these drugs affect cancer risk.
To investigate, Mavromatis and colleagues used the Optum healthcare database to identify 170,030 adults with obesity and type 2 diabetes from 43 health systems in the United States.
Between 2013 and 2023, half started a GLP-1 agonist and half started a DPP-4 inhibitor, with propensity score matching used to balance characteristics of the two cohorts.
Participants were a mean age of 56.8 years, with an average body mass index of 38.5; more than 70% were White individuals and more than 14% were Black individuals.
During a mean follow-up of 3.9 years, 2501 new obesity-related cancers were identified in the GLP-1 group and 2671 in the DPP-4 group — representing a 7% overall reduced risk for any obesity-related cancer in the GLP-1 group (hazard ratio [HR], 0.93).
When analyzing each of the 14 obesity-related cancers separately, the protective link between GLP-1 use and cancer was primarily driven by colon and rectal cancers. GLP-1 users had a 16% lower risk for colon cancer (HR, 0.84) and a 28% lower risk for rectal cancer (HR, 0.72).
“No other cancers had statistically significant associations with GLP-1 use,” Mavromatis told briefing attendees. But “importantly, no cancers had statistically significant adverse associations with GLP-1 use,” he added.
Experts have expressed some concern about a possible link between GLP-1 use and pancreatic cancer given that pancreatitis is a known side effect of GLP-1 use. However, “this is not borne out by epidemiological data,” Mavromatis said.
“Additionally, we were not able to specifically assess medullary thyroid cancer, which is on the warning label for several GLP-1 medications, but we did see a reassuring lack of association between GLP-1 use and thyroid cancer as a whole,” he added.
During follow-up, there were 2783 deaths in the GLP-1 group and 2961 deaths in the DPP-4 group — translating to an 8% lower risk for death due to any cause among GLP-1 users (HR, 0.92; P = .001).
Mavromatis and colleagues observed sex differences as well. Women taking a GLP-1 had an 8% lower risk for obesity-related cancers (HR, 0.92; P = .01) and a 20% lower risk for death from any cause (HR, 0.80; P < .001) compared with women taking a DPP-4 inhibitor.
Among men, researchers found no statistically significant difference between GLP-1 and DPP-4 use for obesity-related cancer risk (HR, 0.95; P = .29) or all-cause mortality (HR, 1.04; P = .34).
Overall, Mavromatis said, it’s important to note that the absolute risk reduction seen in the study is “small and the number of patients that would need to be given one of these medications to prevent an obesity-related cancer, based on our data, would be very large.”
Mavromatis also noted that the length of follow-up was short, and the study assessed primarily older and weaker GLP-1 agonists compared with newer agents on the market. Therefore, longer-term studies with newer GLP-1s are needed to confirm the effects seen as well as safety.
In a statement, ASCO President Robin Zon, MD, said this trial raises the “intriguing hypothesis” that the increasingly popular GLP-1 medications might offer some benefit in reducing the risk of developing cancer.
Zon said she sees many patients with obesity, and given the clear link between cancer and obesity, defining the clinical role of GLP-1 medications in cancer prevention is “important.”
This study “leads us in the direction” of a potential protective effect of GLP-1s on cancer, but “there are a lot of questions that are generated by this particular study, especially as we move forward and we think about prevention of cancers,” Zon told the briefing.
This study was funded by the National Institute of Diabetes and Digestive and Kidney Diseases of the National Institutes of Health. Mavromatis reported no relevant disclosures. Zon reported stock or ownership interests in Oncolytics Biotech, TG Therapeutics, Select Sector SPDR Health Care, AstraZeneca, CRISPR, McKesson, and Berkshire Hathaway.
A version of this article first appeared on Medscape.com.
Can Popular Weight-Loss Drugs Protect Against Obesity-Related Cancers?
Can Popular Weight-Loss Drugs Protect Against Obesity-Related Cancers?