User login
One in three MS patients reports chronic itch
, according to investigators.
Itch is historically underrecognized as a symptom of MS, but physicians should know that it is common and may negatively impact quality of life, reported lead author Giuseppe Ingrasci, MD, a dermatology research fellow at the University of Miami, Miller School of Medicine, and colleagues.

While previous publications suggest that pruritus occurs in just 2%-6% of patients with MS, principal author Gil Yosipovitch, MD, professor, Stiefel Chair of Medical Dermatology, and director of the Miami Itch Center in the Dr. Phillip Frost department of dermatology and cutaneous surgery at the University of Miami Miller School of Medicine, encountered itch in enough patients with MS that he presented his observations to a group of neurologists.
Most of them dismissed him, he recalled in an interview: “The neurologists said, ‘Very interesting, but we don’t really see it.’ ”
One of those neurologists, however, decided to take a closer look.
Andrew Brown, MD, assistant professor of clinical neurology and chief of the general neurology division at the University of Miami, Miller School of Medicine, began asking his patients with MS if they were experiencing itch and soon found that it was “a very common problem,” according to Dr. Yosipovitch.
Dr. Yosipovitch, who was the first to report pruritus in patients with psoriasis, launched the present investigation with Dr. Brown to determine if itch is also a blind spot in the world of MS. Their results, and their uphill battle to publication, suggest that it very well could be.
After being rejected from six neurology journals, with one editor suggesting that itch is “not relevant at all to neurology,” their findings were published in the Journal of the European Academy of Dermatology & Venereology.
A common problem that may indicate more severe disease
At the Multiple Sclerosis Center of Excellence in Miami, 27 out of 79 outpatients with MS (35%) reported pruritus, with an average severity of 5.42 out of 10. Among those with itch, the extremities were affected in about half of the patients, while the face, scalp, and trunk were affected in about one-third of the patients. Many described paroxysmal itch that was aggravated by heat, and about half experienced itch on a weekly basis.
Further investigation showed that itch was associated with more severe MS. Compared with patients not experiencing itch, those with itch were significantly more likely to report fatigue (77% vs. 44%), anxiety or depression (48% vs. 16%), and cognitive impairment (62% vs. 26%).
MRI findings backed up these clinical results. Compared with patients not experiencing itch, patients with itch had significantly more T2 hyperintensities in the posterior cervical cord (74.1% vs. 46.0%) and anterior pons/ventromedial medulla (62% vs. 26%). These hyperintensities in the medulla were also associated with an 11-fold increased rate of itch on the face or scalp (odds ratio, 11.3; 95% confidence interval, 1.6-78.6, P = 0.025).
“Health care providers should be aware of episodes of localized, neuropathic itch in MS patients, as they appear to be more prevalent than previously thought and may impair these patients’ quality of life,” the investigators concluded.
Challenges with symptom characterization, management
“This is an important study for both patients and clinicians,” said Justin Abbatemarco, MD, of Cleveland Clinic’s Mellen Center for Multiple Sclerosis, in a written comment. “As the authors mention, many of our patients experience transient symptoms, including many different types of sensory disturbance (that is, pins & needles, burning, electrical shocks, and itching). These symptoms can be really distressing for patients and their caregivers.”
While Dr. Abbatemarco has encountered severe itching in “several patients” with MS, he maintained that it is “relatively uncommon” and noted that MS symptomatology is an inherently cloudy subject.

“I think it is difficult to be definite in any opinion on this topic,” Dr. Abbatemarco said. “How patients experience these symptoms is very subjective and can be difficult to describe/characterize.”
Dr. Abbatemarco emphasized that transient symptoms “do not usually represent MS relapse/flare or new inflammatory disease activity. Instead, we believe these symptoms are related to old areas of injury or demyelination.”
Symptom management can be challenging, he added. He recommended setting realistic expectations, and in the case of pruritus, asking dermatologists to rule out other causes of itch, and to offer “unique treatment approaches.”
Cool the itch?
Noting how heat appears to aggravate itch in patients with MS, Dr. Yosipovitch suggested that one of those unique – and simple – treatment approaches may be cooling itchy areas. Alternatively, clinicians may consider oral agents, like gabapentin to dampen neural transmission, or compounded formulations applied to the skin to reduce neural sensitivity, such as topical ketamine. Finally, Dr. Yosipovitch speculated that newer antibody agents for MS could potentially reduce itch.
All these treatment suggestions are purely hypothetical, he said, and require further investigation before they can be recommended with confidence.
The investigators disclosed relationships with Galderma, Pfizer, Novartis, and others. Dr. Abbatemarco disclosed no conflicts of interest.
Correction, 9/19/22: An earlier version of this article misidentified the photo of Dr. Justin Abbatemarco.
, according to investigators.
Itch is historically underrecognized as a symptom of MS, but physicians should know that it is common and may negatively impact quality of life, reported lead author Giuseppe Ingrasci, MD, a dermatology research fellow at the University of Miami, Miller School of Medicine, and colleagues.
While previous publications suggest that pruritus occurs in just 2%-6% of patients with MS, principal author Gil Yosipovitch, MD, professor, Stiefel Chair of Medical Dermatology, and director of the Miami Itch Center in the Dr. Phillip Frost department of dermatology and cutaneous surgery at the University of Miami Miller School of Medicine, encountered itch in enough patients with MS that he presented his observations to a group of neurologists.
Most of them dismissed him, he recalled in an interview: “The neurologists said, ‘Very interesting, but we don’t really see it.’ ”
One of those neurologists, however, decided to take a closer look.
Andrew Brown, MD, assistant professor of clinical neurology and chief of the general neurology division at the University of Miami, Miller School of Medicine, began asking his patients with MS if they were experiencing itch and soon found that it was “a very common problem,” according to Dr. Yosipovitch.
Dr. Yosipovitch, who was the first to report pruritus in patients with psoriasis, launched the present investigation with Dr. Brown to determine if itch is also a blind spot in the world of MS. Their results, and their uphill battle to publication, suggest that it very well could be.
After being rejected from six neurology journals, with one editor suggesting that itch is “not relevant at all to neurology,” their findings were published in the Journal of the European Academy of Dermatology & Venereology.
A common problem that may indicate more severe disease
At the Multiple Sclerosis Center of Excellence in Miami, 27 out of 79 outpatients with MS (35%) reported pruritus, with an average severity of 5.42 out of 10. Among those with itch, the extremities were affected in about half of the patients, while the face, scalp, and trunk were affected in about one-third of the patients. Many described paroxysmal itch that was aggravated by heat, and about half experienced itch on a weekly basis.
Further investigation showed that itch was associated with more severe MS. Compared with patients not experiencing itch, those with itch were significantly more likely to report fatigue (77% vs. 44%), anxiety or depression (48% vs. 16%), and cognitive impairment (62% vs. 26%).
MRI findings backed up these clinical results. Compared with patients not experiencing itch, patients with itch had significantly more T2 hyperintensities in the posterior cervical cord (74.1% vs. 46.0%) and anterior pons/ventromedial medulla (62% vs. 26%). These hyperintensities in the medulla were also associated with an 11-fold increased rate of itch on the face or scalp (odds ratio, 11.3; 95% confidence interval, 1.6-78.6, P = 0.025).
“Health care providers should be aware of episodes of localized, neuropathic itch in MS patients, as they appear to be more prevalent than previously thought and may impair these patients’ quality of life,” the investigators concluded.
Challenges with symptom characterization, management
“This is an important study for both patients and clinicians,” said Justin Abbatemarco, MD, of Cleveland Clinic’s Mellen Center for Multiple Sclerosis, in a written comment. “As the authors mention, many of our patients experience transient symptoms, including many different types of sensory disturbance (that is, pins & needles, burning, electrical shocks, and itching). These symptoms can be really distressing for patients and their caregivers.”
While Dr. Abbatemarco has encountered severe itching in “several patients” with MS, he maintained that it is “relatively uncommon” and noted that MS symptomatology is an inherently cloudy subject.
“I think it is difficult to be definite in any opinion on this topic,” Dr. Abbatemarco said. “How patients experience these symptoms is very subjective and can be difficult to describe/characterize.”
Dr. Abbatemarco emphasized that transient symptoms “do not usually represent MS relapse/flare or new inflammatory disease activity. Instead, we believe these symptoms are related to old areas of injury or demyelination.”
Symptom management can be challenging, he added. He recommended setting realistic expectations, and in the case of pruritus, asking dermatologists to rule out other causes of itch, and to offer “unique treatment approaches.”
Cool the itch?
Noting how heat appears to aggravate itch in patients with MS, Dr. Yosipovitch suggested that one of those unique – and simple – treatment approaches may be cooling itchy areas. Alternatively, clinicians may consider oral agents, like gabapentin to dampen neural transmission, or compounded formulations applied to the skin to reduce neural sensitivity, such as topical ketamine. Finally, Dr. Yosipovitch speculated that newer antibody agents for MS could potentially reduce itch.
All these treatment suggestions are purely hypothetical, he said, and require further investigation before they can be recommended with confidence.
The investigators disclosed relationships with Galderma, Pfizer, Novartis, and others. Dr. Abbatemarco disclosed no conflicts of interest.
Correction, 9/19/22: An earlier version of this article misidentified the photo of Dr. Justin Abbatemarco.
, according to investigators.
Itch is historically underrecognized as a symptom of MS, but physicians should know that it is common and may negatively impact quality of life, reported lead author Giuseppe Ingrasci, MD, a dermatology research fellow at the University of Miami, Miller School of Medicine, and colleagues.
While previous publications suggest that pruritus occurs in just 2%-6% of patients with MS, principal author Gil Yosipovitch, MD, professor, Stiefel Chair of Medical Dermatology, and director of the Miami Itch Center in the Dr. Phillip Frost department of dermatology and cutaneous surgery at the University of Miami Miller School of Medicine, encountered itch in enough patients with MS that he presented his observations to a group of neurologists.
Most of them dismissed him, he recalled in an interview: “The neurologists said, ‘Very interesting, but we don’t really see it.’ ”
One of those neurologists, however, decided to take a closer look.
Andrew Brown, MD, assistant professor of clinical neurology and chief of the general neurology division at the University of Miami, Miller School of Medicine, began asking his patients with MS if they were experiencing itch and soon found that it was “a very common problem,” according to Dr. Yosipovitch.
Dr. Yosipovitch, who was the first to report pruritus in patients with psoriasis, launched the present investigation with Dr. Brown to determine if itch is also a blind spot in the world of MS. Their results, and their uphill battle to publication, suggest that it very well could be.
After being rejected from six neurology journals, with one editor suggesting that itch is “not relevant at all to neurology,” their findings were published in the Journal of the European Academy of Dermatology & Venereology.
A common problem that may indicate more severe disease
At the Multiple Sclerosis Center of Excellence in Miami, 27 out of 79 outpatients with MS (35%) reported pruritus, with an average severity of 5.42 out of 10. Among those with itch, the extremities were affected in about half of the patients, while the face, scalp, and trunk were affected in about one-third of the patients. Many described paroxysmal itch that was aggravated by heat, and about half experienced itch on a weekly basis.
Further investigation showed that itch was associated with more severe MS. Compared with patients not experiencing itch, those with itch were significantly more likely to report fatigue (77% vs. 44%), anxiety or depression (48% vs. 16%), and cognitive impairment (62% vs. 26%).
MRI findings backed up these clinical results. Compared with patients not experiencing itch, patients with itch had significantly more T2 hyperintensities in the posterior cervical cord (74.1% vs. 46.0%) and anterior pons/ventromedial medulla (62% vs. 26%). These hyperintensities in the medulla were also associated with an 11-fold increased rate of itch on the face or scalp (odds ratio, 11.3; 95% confidence interval, 1.6-78.6, P = 0.025).
“Health care providers should be aware of episodes of localized, neuropathic itch in MS patients, as they appear to be more prevalent than previously thought and may impair these patients’ quality of life,” the investigators concluded.
Challenges with symptom characterization, management
“This is an important study for both patients and clinicians,” said Justin Abbatemarco, MD, of Cleveland Clinic’s Mellen Center for Multiple Sclerosis, in a written comment. “As the authors mention, many of our patients experience transient symptoms, including many different types of sensory disturbance (that is, pins & needles, burning, electrical shocks, and itching). These symptoms can be really distressing for patients and their caregivers.”
While Dr. Abbatemarco has encountered severe itching in “several patients” with MS, he maintained that it is “relatively uncommon” and noted that MS symptomatology is an inherently cloudy subject.
“I think it is difficult to be definite in any opinion on this topic,” Dr. Abbatemarco said. “How patients experience these symptoms is very subjective and can be difficult to describe/characterize.”
Dr. Abbatemarco emphasized that transient symptoms “do not usually represent MS relapse/flare or new inflammatory disease activity. Instead, we believe these symptoms are related to old areas of injury or demyelination.”
Symptom management can be challenging, he added. He recommended setting realistic expectations, and in the case of pruritus, asking dermatologists to rule out other causes of itch, and to offer “unique treatment approaches.”
Cool the itch?
Noting how heat appears to aggravate itch in patients with MS, Dr. Yosipovitch suggested that one of those unique – and simple – treatment approaches may be cooling itchy areas. Alternatively, clinicians may consider oral agents, like gabapentin to dampen neural transmission, or compounded formulations applied to the skin to reduce neural sensitivity, such as topical ketamine. Finally, Dr. Yosipovitch speculated that newer antibody agents for MS could potentially reduce itch.
All these treatment suggestions are purely hypothetical, he said, and require further investigation before they can be recommended with confidence.
The investigators disclosed relationships with Galderma, Pfizer, Novartis, and others. Dr. Abbatemarco disclosed no conflicts of interest.
Correction, 9/19/22: An earlier version of this article misidentified the photo of Dr. Justin Abbatemarco.
FROM THE JOURNAL OF THE EUROPEAN ACADEMY OF DERMATOLOGY & VENEREOLOGY
Not just what, but when: Neoadjuvant pembrolizumab in melanoma
PARIS – “It’s not just what you give, it’s when you give it,” said the investigator reporting “that the same treatment for resectable melanoma given in a different sequence can generate lower rates of melanoma recurrence.”
Sapna Patel, MD, associate professor of melanoma medical oncology at The University of Texas MD Anderson Cancer Center, Houston, reported the results from the SWOG S1801 trial, which showed that than patients who received pembrolizumab after surgery only.
At a median follow-up of almost 15 months, there was a 42% lower rate of recurrence or death.
“Compared to the same treatment given entirely in the adjuvant setting, neoadjuvant pembrolizumab followed by adjuvant pembrolizumab improves event-free survival in resectable melanoma,” Dr. Patel commented.
She suggested that the explanation for the findings was that “inhibiting the PD-1/PD-L1 immune checkpoints before surgery gives an antitumor response at local and distant sites, and this occurs before resection of the tumor bed. This approach tends to leave behind a larger number of anti-tumor T cells ... [and] these T cells can be activated and circulated systematically to recognize and attack micro-metastatic melanoma tumors.”
The findings were presented during a presidential symposium at the European Society for Medical Oncology (ESMO) Congress 2022, Paris.
“This trial provides us with more evidence of when one strategy may be preferred over the other,” commented Maya Dimitrova, MD, medical oncologist at NYU Langone Perlmutter Cancer Center. She was not involved with the trial.
“Neoadjuvant immunotherapy has elicited impressive complete pathologic responses, which thus far have proven to be associated with a durable response. Neoadjuvant therapy may help identify patients who will respond well to checkpoint inhibitors and allow for de-escalation of therapy,” she told this news organization when approached for comment.
“As with all neoadjuvant therapy, we don’t want the treatment to compromise the outcomes of surgery when the intent is curative, and we once again have evidence that this is not the case when it comes to immune therapy,” she said. However, she added that “we will need further survival data to really change the standard of practice in high-risk melanoma and demonstrate whether there is a superior sequence of therapy and surgery.”
Details of the new results
The S1801 clinical trial enrolled 345 participants with stage IIIB through stage IV melanoma considered resectable. The cohort was randomized to receive either upfront surgery followed by 18 doses of pembrolizumab 200 mg every 3 weeks for a total of 18 doses or neoadjuvant therapy with pembrolizumab 200 mg (3 doses) followed by 15 doses of adjuvant pembrolizumab.
The primary endpoint was event-free survival (EFS), defined as the time from randomization to the occurrence of one of the following: disease progression or toxicity that resulted in not receiving surgery, failure to begin adjuvant therapy within 84 days of surgery, melanoma recurrence after surgery, or death from any cause.
At a median follow-up of 14.7 months, EFS was significantly higher for patients in the neoadjuvant group, compared with those receiving adjuvant therapy only (HR, 0.58; one-sided log-rank P = .004). A total of 36 participants died in the neoadjuvant and adjuvant groups (14 and 22 patients, extrapolating to a hazard ratio of 0.63; one-sided P = .091).
“With a limited number of events, overall survival is not statistically different at this time,” Dr. Patel said. “Landmark 2-year survival was 72% in the neoadjuvant arm and 49% in the adjuvant arm.”
The authors note that the benefit of neoadjuvant therapy remained consistent across a range of factors, including patient age, sex, performance status, stage of disease, ulceration, and BRAF status. The same proportion of patients in both groups received adjuvant pembrolizumab following surgery.
Rates of adverse events were similar in both groups, and neoadjuvant pembrolizumab did not result in an increase in adverse events related to surgery. In the neoadjuvant group, 28 patients (21%) with submitted pathology reports were noted to have had a complete pathologic response (0% viable tumor) on local review.
Questions remain
Invited discussant James Larkin, PhD, FRCP, FMedSci, a clinical researcher at The Royal Marsden Hospital, London, noted that the study had “striking results” and was a landmark trial with a simple but powerful design.
However, he pointed to some questions which need to be addressed in the future. “One important question is what is the optimal duration of neoadjuvant treatment, and can we individualize it?”
Another question is just how much postoperative treatment is really needed and whether pathology help determine that. “Can surgery be safely avoided altogether?” he asked. “Another issue is the need for anti-CTL4 therapy – which patients might benefit from anti-CTL4, in addition to anti-PD-1?”
“And by extension, this paradigm provides a great platform for testing new agents, including combinations in cases where PD-1 is not sufficient to achieve a sufficient response,” said Dr. Larkin. “In the future, trials addressing these questions hand us a major opportunity to individualize and rationally de-escalate treatment.”
Also weighing in on the study, another expert pointed out that neoadjuvant therapy in this setting is already being considered as an option. “The use of immunotherapy before surgery has been reported in some trials such as the OPACIN-neo and PRADO trials,” said Anthony J. Olszanski, RPh, MD, Vice Chair of Research at the Fox Chase Cancer Center, Philadelphia. “Results have been quite exciting and have led the NCCN to list this as a potential option for some patients in the current melanoma guidelines.”
S1801 is funded by the NIH/NCI and in part by MSD through a Cooperative Research and Development Agreement with the NCI. Pembrolizumab (KEYTRUDA) is Merck’s anti-PD-1 therapy. Dr. Patel has declared multiple relationships with industry as noted in the abstract; several co-authors have also made disclosures. Dr. Olszanski has reported participating in advisory boards for BMS, Merck, and InstilBio and running trials for them.
A version of this article first appeared on Medscape.com.
PARIS – “It’s not just what you give, it’s when you give it,” said the investigator reporting “that the same treatment for resectable melanoma given in a different sequence can generate lower rates of melanoma recurrence.”
Sapna Patel, MD, associate professor of melanoma medical oncology at The University of Texas MD Anderson Cancer Center, Houston, reported the results from the SWOG S1801 trial, which showed that than patients who received pembrolizumab after surgery only.
At a median follow-up of almost 15 months, there was a 42% lower rate of recurrence or death.
“Compared to the same treatment given entirely in the adjuvant setting, neoadjuvant pembrolizumab followed by adjuvant pembrolizumab improves event-free survival in resectable melanoma,” Dr. Patel commented.
She suggested that the explanation for the findings was that “inhibiting the PD-1/PD-L1 immune checkpoints before surgery gives an antitumor response at local and distant sites, and this occurs before resection of the tumor bed. This approach tends to leave behind a larger number of anti-tumor T cells ... [and] these T cells can be activated and circulated systematically to recognize and attack micro-metastatic melanoma tumors.”
The findings were presented during a presidential symposium at the European Society for Medical Oncology (ESMO) Congress 2022, Paris.
“This trial provides us with more evidence of when one strategy may be preferred over the other,” commented Maya Dimitrova, MD, medical oncologist at NYU Langone Perlmutter Cancer Center. She was not involved with the trial.
“Neoadjuvant immunotherapy has elicited impressive complete pathologic responses, which thus far have proven to be associated with a durable response. Neoadjuvant therapy may help identify patients who will respond well to checkpoint inhibitors and allow for de-escalation of therapy,” she told this news organization when approached for comment.
“As with all neoadjuvant therapy, we don’t want the treatment to compromise the outcomes of surgery when the intent is curative, and we once again have evidence that this is not the case when it comes to immune therapy,” she said. However, she added that “we will need further survival data to really change the standard of practice in high-risk melanoma and demonstrate whether there is a superior sequence of therapy and surgery.”
Details of the new results
The S1801 clinical trial enrolled 345 participants with stage IIIB through stage IV melanoma considered resectable. The cohort was randomized to receive either upfront surgery followed by 18 doses of pembrolizumab 200 mg every 3 weeks for a total of 18 doses or neoadjuvant therapy with pembrolizumab 200 mg (3 doses) followed by 15 doses of adjuvant pembrolizumab.
The primary endpoint was event-free survival (EFS), defined as the time from randomization to the occurrence of one of the following: disease progression or toxicity that resulted in not receiving surgery, failure to begin adjuvant therapy within 84 days of surgery, melanoma recurrence after surgery, or death from any cause.
At a median follow-up of 14.7 months, EFS was significantly higher for patients in the neoadjuvant group, compared with those receiving adjuvant therapy only (HR, 0.58; one-sided log-rank P = .004). A total of 36 participants died in the neoadjuvant and adjuvant groups (14 and 22 patients, extrapolating to a hazard ratio of 0.63; one-sided P = .091).
“With a limited number of events, overall survival is not statistically different at this time,” Dr. Patel said. “Landmark 2-year survival was 72% in the neoadjuvant arm and 49% in the adjuvant arm.”
The authors note that the benefit of neoadjuvant therapy remained consistent across a range of factors, including patient age, sex, performance status, stage of disease, ulceration, and BRAF status. The same proportion of patients in both groups received adjuvant pembrolizumab following surgery.
Rates of adverse events were similar in both groups, and neoadjuvant pembrolizumab did not result in an increase in adverse events related to surgery. In the neoadjuvant group, 28 patients (21%) with submitted pathology reports were noted to have had a complete pathologic response (0% viable tumor) on local review.
Questions remain
Invited discussant James Larkin, PhD, FRCP, FMedSci, a clinical researcher at The Royal Marsden Hospital, London, noted that the study had “striking results” and was a landmark trial with a simple but powerful design.
However, he pointed to some questions which need to be addressed in the future. “One important question is what is the optimal duration of neoadjuvant treatment, and can we individualize it?”
Another question is just how much postoperative treatment is really needed and whether pathology help determine that. “Can surgery be safely avoided altogether?” he asked. “Another issue is the need for anti-CTL4 therapy – which patients might benefit from anti-CTL4, in addition to anti-PD-1?”
“And by extension, this paradigm provides a great platform for testing new agents, including combinations in cases where PD-1 is not sufficient to achieve a sufficient response,” said Dr. Larkin. “In the future, trials addressing these questions hand us a major opportunity to individualize and rationally de-escalate treatment.”
Also weighing in on the study, another expert pointed out that neoadjuvant therapy in this setting is already being considered as an option. “The use of immunotherapy before surgery has been reported in some trials such as the OPACIN-neo and PRADO trials,” said Anthony J. Olszanski, RPh, MD, Vice Chair of Research at the Fox Chase Cancer Center, Philadelphia. “Results have been quite exciting and have led the NCCN to list this as a potential option for some patients in the current melanoma guidelines.”
S1801 is funded by the NIH/NCI and in part by MSD through a Cooperative Research and Development Agreement with the NCI. Pembrolizumab (KEYTRUDA) is Merck’s anti-PD-1 therapy. Dr. Patel has declared multiple relationships with industry as noted in the abstract; several co-authors have also made disclosures. Dr. Olszanski has reported participating in advisory boards for BMS, Merck, and InstilBio and running trials for them.
A version of this article first appeared on Medscape.com.
PARIS – “It’s not just what you give, it’s when you give it,” said the investigator reporting “that the same treatment for resectable melanoma given in a different sequence can generate lower rates of melanoma recurrence.”
Sapna Patel, MD, associate professor of melanoma medical oncology at The University of Texas MD Anderson Cancer Center, Houston, reported the results from the SWOG S1801 trial, which showed that than patients who received pembrolizumab after surgery only.
At a median follow-up of almost 15 months, there was a 42% lower rate of recurrence or death.
“Compared to the same treatment given entirely in the adjuvant setting, neoadjuvant pembrolizumab followed by adjuvant pembrolizumab improves event-free survival in resectable melanoma,” Dr. Patel commented.
She suggested that the explanation for the findings was that “inhibiting the PD-1/PD-L1 immune checkpoints before surgery gives an antitumor response at local and distant sites, and this occurs before resection of the tumor bed. This approach tends to leave behind a larger number of anti-tumor T cells ... [and] these T cells can be activated and circulated systematically to recognize and attack micro-metastatic melanoma tumors.”
The findings were presented during a presidential symposium at the European Society for Medical Oncology (ESMO) Congress 2022, Paris.
“This trial provides us with more evidence of when one strategy may be preferred over the other,” commented Maya Dimitrova, MD, medical oncologist at NYU Langone Perlmutter Cancer Center. She was not involved with the trial.
“Neoadjuvant immunotherapy has elicited impressive complete pathologic responses, which thus far have proven to be associated with a durable response. Neoadjuvant therapy may help identify patients who will respond well to checkpoint inhibitors and allow for de-escalation of therapy,” she told this news organization when approached for comment.
“As with all neoadjuvant therapy, we don’t want the treatment to compromise the outcomes of surgery when the intent is curative, and we once again have evidence that this is not the case when it comes to immune therapy,” she said. However, she added that “we will need further survival data to really change the standard of practice in high-risk melanoma and demonstrate whether there is a superior sequence of therapy and surgery.”
Details of the new results
The S1801 clinical trial enrolled 345 participants with stage IIIB through stage IV melanoma considered resectable. The cohort was randomized to receive either upfront surgery followed by 18 doses of pembrolizumab 200 mg every 3 weeks for a total of 18 doses or neoadjuvant therapy with pembrolizumab 200 mg (3 doses) followed by 15 doses of adjuvant pembrolizumab.
The primary endpoint was event-free survival (EFS), defined as the time from randomization to the occurrence of one of the following: disease progression or toxicity that resulted in not receiving surgery, failure to begin adjuvant therapy within 84 days of surgery, melanoma recurrence after surgery, or death from any cause.
At a median follow-up of 14.7 months, EFS was significantly higher for patients in the neoadjuvant group, compared with those receiving adjuvant therapy only (HR, 0.58; one-sided log-rank P = .004). A total of 36 participants died in the neoadjuvant and adjuvant groups (14 and 22 patients, extrapolating to a hazard ratio of 0.63; one-sided P = .091).
“With a limited number of events, overall survival is not statistically different at this time,” Dr. Patel said. “Landmark 2-year survival was 72% in the neoadjuvant arm and 49% in the adjuvant arm.”
The authors note that the benefit of neoadjuvant therapy remained consistent across a range of factors, including patient age, sex, performance status, stage of disease, ulceration, and BRAF status. The same proportion of patients in both groups received adjuvant pembrolizumab following surgery.
Rates of adverse events were similar in both groups, and neoadjuvant pembrolizumab did not result in an increase in adverse events related to surgery. In the neoadjuvant group, 28 patients (21%) with submitted pathology reports were noted to have had a complete pathologic response (0% viable tumor) on local review.
Questions remain
Invited discussant James Larkin, PhD, FRCP, FMedSci, a clinical researcher at The Royal Marsden Hospital, London, noted that the study had “striking results” and was a landmark trial with a simple but powerful design.
However, he pointed to some questions which need to be addressed in the future. “One important question is what is the optimal duration of neoadjuvant treatment, and can we individualize it?”
Another question is just how much postoperative treatment is really needed and whether pathology help determine that. “Can surgery be safely avoided altogether?” he asked. “Another issue is the need for anti-CTL4 therapy – which patients might benefit from anti-CTL4, in addition to anti-PD-1?”
“And by extension, this paradigm provides a great platform for testing new agents, including combinations in cases where PD-1 is not sufficient to achieve a sufficient response,” said Dr. Larkin. “In the future, trials addressing these questions hand us a major opportunity to individualize and rationally de-escalate treatment.”
Also weighing in on the study, another expert pointed out that neoadjuvant therapy in this setting is already being considered as an option. “The use of immunotherapy before surgery has been reported in some trials such as the OPACIN-neo and PRADO trials,” said Anthony J. Olszanski, RPh, MD, Vice Chair of Research at the Fox Chase Cancer Center, Philadelphia. “Results have been quite exciting and have led the NCCN to list this as a potential option for some patients in the current melanoma guidelines.”
S1801 is funded by the NIH/NCI and in part by MSD through a Cooperative Research and Development Agreement with the NCI. Pembrolizumab (KEYTRUDA) is Merck’s anti-PD-1 therapy. Dr. Patel has declared multiple relationships with industry as noted in the abstract; several co-authors have also made disclosures. Dr. Olszanski has reported participating in advisory boards for BMS, Merck, and InstilBio and running trials for them.
A version of this article first appeared on Medscape.com.
Could nivolumab prevent oral cancer in high-risk patients?
(PL), a high-risk precancerous disease, into oral cancer, suggest the results from a phase 2 study.
“We think that immunotherapy as a preventative strategy, either as first-line or even secondary prevention, should be further explored,” said lead researcher Glenn J. Hanna, MD, director, Center for Salivary and Rare Head and Neck Cancers, Dana-Farber Cancer Institute, Boston.
The research was presented at the European Society for Medical Oncology Annual Congress in Paris.
Oral leukoplakia refers to a white plaque of “questionable cancer risk” that affects about 4% of the global population, Dr. Hanna explained. However, about 5% of leukoplakia cases develop into oral proliferative leukoplakia, an aggressive form of the disease characterized by multifocal lesions. It has a high risk of transformation to oral squamous cell carcinoma (OSCC), at approaching 10% per year, and the 5-year cancer-free survival rate is estimated to be 47%.
While there are no effective therapies to prevent progression to oral cancer, the condition does have a “rich immune microenvironment,” potentially making it amenable to programmed death (PD)-1 blockade, Dr. Hanna said.
His team conducted a single-arm, phase 2 trial involving 33 patients with proliferative leukoplakia with greater than or equal to 2 multifocal lesions, or contiguous lesions of greater than or equal to 3 cm, or a single lesion greater than or equal to 4 cm with any degree of epithelial dysplasia. The median age was 63.2 years, and 55% were women. Just over half (52%) were never smokers.
The main disease subsite was the oral tongue in 39% of participants, followed by the buccal gingiva in 30%, and 24% of patients had a prior diagnosis of OSCC.
Following a pretreatment biopsy at one to three sites, the patients received four doses of nivolumab every 28 days, followed by rebiopsy. At each visit, the patients had intraoral photographs taken of the lesions and measurements taken.
The median time from study registration to the first dose of nivolumab was 9 days. The majority (88%) of patients completed all four doses of nivolumab.
The median time from the first dose of nivolumab to the posttreatment biopsy was 115 days and ranged from 29 to 171 days.
The overall response rate, defined as a greater than or equal to 40% decrease in a composite score combining the size and degree of dysplasia between the pre- and posttreatment assessments, was observed in 36.4% of patients.
After a median follow-up of 14.7 months, the median cancer-free survival was not reached, with cancer events recorded in 21.2% of patients. The median time from the last dose of nivolumab to the first OSCC event was 3.7 months.
Cancer-free survival at 1 year was calculated to be 77.7%, which was unchanged at 2 years. At the final follow-up, all patients were still alive.
Additional analysis of the biopsies revealed that the lesions had programmed death ligand 1 (PD-L1) combined positive scores that ranged from 0 to 80, with 66.7% of patients having a score of greater than or equal to 1. A cutoff score of greater than or equal to 20 did not reveal any significant differences in cancer-free survival rates.
Turning to safety, Dr. Hanna said that nivolumab was associated with “acceptable toxicity” in this “non-cancer population,” with 21.2% of patients experiencing a grade 3-4 adverse event.
The most common adverse events of any grade were fatigue (55%), diarrhea (27%), elevated alanine transaminase levels (18%), elevated aspartate transaminase levels (18%), and other skin disorders (18%).
With a relatively low rate of adverse events and a “clinical benefit” in up to a third of patients, Dr. Hanna said that this was the “first study to our knowledge to demonstrate the potential efficacy of anti–PD-L1 blockade among patients with a high-risk oral precancerous disease.”
Discussing this study at the meeting, Amanda Psyrri, MD, PhD, professor of medical oncology, Attikon University Hospital, Athens, who was not involved in the research, said these data were “very interesting,” but she expressed some reservations over the way the study was conducted.
She said that the composite score to measure response rates was “defined arbitrarily,” its prognostic value “has not been demonstrated,” and also pointed out that mixed responses by lesions within the same patient led to changes in scores.
In addition, the time interval between the end of treatment and lesion rebiopsy was “highly variable,” and the follow-up period was short.
Consequently, Dr. Psyrri believes the importance of the findings is “unclear,” especially as several patients who responded to nivolumab went on to develop cancer anyway, a finding that needs further investigation.
The study was funded by Bristol Myers Squibb.
Dr. Hanna declared relationships with BMS, Bicara, Exicure, Gateway for Cancer Research, GSK, Kite, NantKwest, Regeneron, Sanofi Genzyme, Maverick, and Merck.
A version of this article first appeared on Medscape.com.
(PL), a high-risk precancerous disease, into oral cancer, suggest the results from a phase 2 study.
“We think that immunotherapy as a preventative strategy, either as first-line or even secondary prevention, should be further explored,” said lead researcher Glenn J. Hanna, MD, director, Center for Salivary and Rare Head and Neck Cancers, Dana-Farber Cancer Institute, Boston.
The research was presented at the European Society for Medical Oncology Annual Congress in Paris.
Oral leukoplakia refers to a white plaque of “questionable cancer risk” that affects about 4% of the global population, Dr. Hanna explained. However, about 5% of leukoplakia cases develop into oral proliferative leukoplakia, an aggressive form of the disease characterized by multifocal lesions. It has a high risk of transformation to oral squamous cell carcinoma (OSCC), at approaching 10% per year, and the 5-year cancer-free survival rate is estimated to be 47%.
While there are no effective therapies to prevent progression to oral cancer, the condition does have a “rich immune microenvironment,” potentially making it amenable to programmed death (PD)-1 blockade, Dr. Hanna said.
His team conducted a single-arm, phase 2 trial involving 33 patients with proliferative leukoplakia with greater than or equal to 2 multifocal lesions, or contiguous lesions of greater than or equal to 3 cm, or a single lesion greater than or equal to 4 cm with any degree of epithelial dysplasia. The median age was 63.2 years, and 55% were women. Just over half (52%) were never smokers.
The main disease subsite was the oral tongue in 39% of participants, followed by the buccal gingiva in 30%, and 24% of patients had a prior diagnosis of OSCC.
Following a pretreatment biopsy at one to three sites, the patients received four doses of nivolumab every 28 days, followed by rebiopsy. At each visit, the patients had intraoral photographs taken of the lesions and measurements taken.
The median time from study registration to the first dose of nivolumab was 9 days. The majority (88%) of patients completed all four doses of nivolumab.
The median time from the first dose of nivolumab to the posttreatment biopsy was 115 days and ranged from 29 to 171 days.
The overall response rate, defined as a greater than or equal to 40% decrease in a composite score combining the size and degree of dysplasia between the pre- and posttreatment assessments, was observed in 36.4% of patients.
After a median follow-up of 14.7 months, the median cancer-free survival was not reached, with cancer events recorded in 21.2% of patients. The median time from the last dose of nivolumab to the first OSCC event was 3.7 months.
Cancer-free survival at 1 year was calculated to be 77.7%, which was unchanged at 2 years. At the final follow-up, all patients were still alive.
Additional analysis of the biopsies revealed that the lesions had programmed death ligand 1 (PD-L1) combined positive scores that ranged from 0 to 80, with 66.7% of patients having a score of greater than or equal to 1. A cutoff score of greater than or equal to 20 did not reveal any significant differences in cancer-free survival rates.
Turning to safety, Dr. Hanna said that nivolumab was associated with “acceptable toxicity” in this “non-cancer population,” with 21.2% of patients experiencing a grade 3-4 adverse event.
The most common adverse events of any grade were fatigue (55%), diarrhea (27%), elevated alanine transaminase levels (18%), elevated aspartate transaminase levels (18%), and other skin disorders (18%).
With a relatively low rate of adverse events and a “clinical benefit” in up to a third of patients, Dr. Hanna said that this was the “first study to our knowledge to demonstrate the potential efficacy of anti–PD-L1 blockade among patients with a high-risk oral precancerous disease.”
Discussing this study at the meeting, Amanda Psyrri, MD, PhD, professor of medical oncology, Attikon University Hospital, Athens, who was not involved in the research, said these data were “very interesting,” but she expressed some reservations over the way the study was conducted.
She said that the composite score to measure response rates was “defined arbitrarily,” its prognostic value “has not been demonstrated,” and also pointed out that mixed responses by lesions within the same patient led to changes in scores.
In addition, the time interval between the end of treatment and lesion rebiopsy was “highly variable,” and the follow-up period was short.
Consequently, Dr. Psyrri believes the importance of the findings is “unclear,” especially as several patients who responded to nivolumab went on to develop cancer anyway, a finding that needs further investigation.
The study was funded by Bristol Myers Squibb.
Dr. Hanna declared relationships with BMS, Bicara, Exicure, Gateway for Cancer Research, GSK, Kite, NantKwest, Regeneron, Sanofi Genzyme, Maverick, and Merck.
A version of this article first appeared on Medscape.com.
(PL), a high-risk precancerous disease, into oral cancer, suggest the results from a phase 2 study.
“We think that immunotherapy as a preventative strategy, either as first-line or even secondary prevention, should be further explored,” said lead researcher Glenn J. Hanna, MD, director, Center for Salivary and Rare Head and Neck Cancers, Dana-Farber Cancer Institute, Boston.
The research was presented at the European Society for Medical Oncology Annual Congress in Paris.
Oral leukoplakia refers to a white plaque of “questionable cancer risk” that affects about 4% of the global population, Dr. Hanna explained. However, about 5% of leukoplakia cases develop into oral proliferative leukoplakia, an aggressive form of the disease characterized by multifocal lesions. It has a high risk of transformation to oral squamous cell carcinoma (OSCC), at approaching 10% per year, and the 5-year cancer-free survival rate is estimated to be 47%.
While there are no effective therapies to prevent progression to oral cancer, the condition does have a “rich immune microenvironment,” potentially making it amenable to programmed death (PD)-1 blockade, Dr. Hanna said.
His team conducted a single-arm, phase 2 trial involving 33 patients with proliferative leukoplakia with greater than or equal to 2 multifocal lesions, or contiguous lesions of greater than or equal to 3 cm, or a single lesion greater than or equal to 4 cm with any degree of epithelial dysplasia. The median age was 63.2 years, and 55% were women. Just over half (52%) were never smokers.
The main disease subsite was the oral tongue in 39% of participants, followed by the buccal gingiva in 30%, and 24% of patients had a prior diagnosis of OSCC.
Following a pretreatment biopsy at one to three sites, the patients received four doses of nivolumab every 28 days, followed by rebiopsy. At each visit, the patients had intraoral photographs taken of the lesions and measurements taken.
The median time from study registration to the first dose of nivolumab was 9 days. The majority (88%) of patients completed all four doses of nivolumab.
The median time from the first dose of nivolumab to the posttreatment biopsy was 115 days and ranged from 29 to 171 days.
The overall response rate, defined as a greater than or equal to 40% decrease in a composite score combining the size and degree of dysplasia between the pre- and posttreatment assessments, was observed in 36.4% of patients.
After a median follow-up of 14.7 months, the median cancer-free survival was not reached, with cancer events recorded in 21.2% of patients. The median time from the last dose of nivolumab to the first OSCC event was 3.7 months.
Cancer-free survival at 1 year was calculated to be 77.7%, which was unchanged at 2 years. At the final follow-up, all patients were still alive.
Additional analysis of the biopsies revealed that the lesions had programmed death ligand 1 (PD-L1) combined positive scores that ranged from 0 to 80, with 66.7% of patients having a score of greater than or equal to 1. A cutoff score of greater than or equal to 20 did not reveal any significant differences in cancer-free survival rates.
Turning to safety, Dr. Hanna said that nivolumab was associated with “acceptable toxicity” in this “non-cancer population,” with 21.2% of patients experiencing a grade 3-4 adverse event.
The most common adverse events of any grade were fatigue (55%), diarrhea (27%), elevated alanine transaminase levels (18%), elevated aspartate transaminase levels (18%), and other skin disorders (18%).
With a relatively low rate of adverse events and a “clinical benefit” in up to a third of patients, Dr. Hanna said that this was the “first study to our knowledge to demonstrate the potential efficacy of anti–PD-L1 blockade among patients with a high-risk oral precancerous disease.”
Discussing this study at the meeting, Amanda Psyrri, MD, PhD, professor of medical oncology, Attikon University Hospital, Athens, who was not involved in the research, said these data were “very interesting,” but she expressed some reservations over the way the study was conducted.
She said that the composite score to measure response rates was “defined arbitrarily,” its prognostic value “has not been demonstrated,” and also pointed out that mixed responses by lesions within the same patient led to changes in scores.
In addition, the time interval between the end of treatment and lesion rebiopsy was “highly variable,” and the follow-up period was short.
Consequently, Dr. Psyrri believes the importance of the findings is “unclear,” especially as several patients who responded to nivolumab went on to develop cancer anyway, a finding that needs further investigation.
The study was funded by Bristol Myers Squibb.
Dr. Hanna declared relationships with BMS, Bicara, Exicure, Gateway for Cancer Research, GSK, Kite, NantKwest, Regeneron, Sanofi Genzyme, Maverick, and Merck.
A version of this article first appeared on Medscape.com.
Novel cell therapy beats immunotherapy in melanoma
PARIS – Cell therapies have already had a huge impact on the treatment of blood cancers, but progress in solid tumors has proved more difficult. Now, in a first multicenter randomized trial to compare the two,
The cell therapy used in this trial was composed of adoptive tumor infiltrating lymphocytes (TIL), which were made individually for each patient, just as chimeric antigen receptor T cells (CAR T cells) are for patients with blood cancers. However, the process involved is somewhat different, as TILs are made from lymphocytes that have infiltrated the patient’s tumor and are obtained by surgery in the tumor, whereas CAR T cells are made from circulating blood cells.
The phase 3 trial involved 168 patients with unresectable stage IIIC-4 melanoma and showed that patients who were treated with TILs achieved a significantly improved progression-free survival (PFS) when compared with standard immunotherapy with ipilimumab (Yervoy).
The median PFS was more than doubled to 7.2 months with TILs versus 3.1 months with ipilimumab (hazard ratio, 0.50; P < .001).
“We do think that TIL could possibly become a new treatment option for patients with advanced stage melanoma,” commented lead author John Haanen, MD, PhD, research group leader at the Netherlands Cancer Institute in Amsterdam and a professor in translational immunotherapy of cancer at Leiden (the Netherlands) University Medical Center.
He presented the findings at a presidential symposium during the European Society for Medical Oncology Annual Congress, Paris.
“The results of this trial may fuel further research of TIL in other cancer types, potentially demonstrating benefit in many other solid tumors and expanding available treatments for patients,” said Maya Dimitrova, MD, medical oncologist at NYU Langone Perlmutter Cancer Center. She was approached for comment by this news organization and was not involved in the research.
Immune checkpoint inhibitors and targeted therapies have become the standard of care for advanced melanoma and greatly improved patient outcomes, she said. But as about half of patients treated with these agents will not achieve a durable benefit, there remains a need for new treatment options.
“Although immunotherapy can yield impressive long-term responses, a substantial percentage of patients will have no response, or no durable response, to checkpoint inhibitors,” said Dr. Dimitrova. “TIL therapy has proven effectiveness in melanoma. However, no phase III trials have been done to date to compare its effectiveness to a standard of care regimen.”
She noted that these results are consistent with past reports of an approximately 50% response rate with an impressive 20% complete response rate in the TIL group. Data from a phase 2 trial reported last year, for example, showed an objective response rate of 36.4%.
“It will be important to determine the persistence of antitumor activity and whether there are biomarkers that could help with patient selection given the resource intensity of the therapy,” Dr. Dimitrova said. “TIL therapy will likely become a new standard of care in metastatic melanoma refractory to immune checkpoint inhibitors.”
Superior to immunotherapy
In the current study, Dr. Haanen and colleagues randomly assigned 168 patients to TIL or ipilimumab (3 mg/kg every 3 weeks, maximum 4 doses). Patients were stratified for BRAFV600 mutation status, treatment line and center, and the majority (86%) were refractory to anti–PD-1 treatment.
Patients in the TIL group underwent resection of a melanoma lesion (2-3 cm) for the ex vivo outgrowth and expansion of tumor-resident T cells. Before the cultured TILs were infused back into the patients from which they were made, the patient underwent nonmyeloablative, lymphodepleting chemotherapy with cyclophosphamide plus fludarabine that was followed by high-dose interleukin-2.
The study’s primary endpoint was progression-free survival, and secondary endpoints included overall and complete response rate, overall survival, and safety.
At a median follow-up of 33 months, TIL significantly improved progression-free survival, compared with ipilimumab. The overall response rate also favored TIL, compared with ipilimumab (49% vs. 21%), with 20% versus 7% complete responses, respectively.
The median overall survival was 25.8 months for TIL and 18.9 months for ipilimumab (HR, 0.83; P = 0.39).
Grade 3 or higher treatment-related adverse events occurred in all TIL and 57% of ipilimumab patients, although Dr. Haanen noted they were manageable and, in most cases, resolved by the time patients were discharged from the hospital.
“There were no new safety concerns with TIL,” said Dr. Haanen, “And these toxicities are driven by the chemotherapy and interleukin-2 that are part of the TIL regimen. There were no long-term sequelae in patients treated with TIL, and health-related quality of life was higher in patients treated with TIL.”
Ultra-personalized
Also commenting on the study, Anthony J. Olszanski, MD, RPh, associate professor and vice chair of clinical research, department of hematology/oncology at Fox Chase Cancer Center, Philadelphia, agreed that the treatment of patients with melanoma who do not respond to or progress after receiving treatment with immunotherapy is “challenging and represents an unmet need.”
“TIL therapy is, in some ways, ultra-personalized therapy, because we harvest immune cells from the patient’s tumor, expand them outside of the body, and then re-infuse them,” he said. “This trial, which randomized patients between TIL versus the CTLA-4 inhibitor, ipilimumab, has shown an impressive progression-free survival and overall response rate benefit and will help establish TIL therapy as a viable treatment strategy for some patients.”
The study was supported by the Dutch Cancer Society, the Netherlands Organization for Health Research and Development, the Dutch Ministry of Health, Stichting Avento, Copenhagen University Hospital, Herlev, the Danish Cancer Society, and Capital Region of Denmark Research Foundation.
Dr. Haanen and several of the co-authors have declared multiple relationships with industry as noted in the abstract. Dr. Olszanski reports participation in advisory boards for BMS, Merck, and Instil Bio, and he reports running trials for them.
A version of this article first appeared on Medscape.com.
PARIS – Cell therapies have already had a huge impact on the treatment of blood cancers, but progress in solid tumors has proved more difficult. Now, in a first multicenter randomized trial to compare the two,
The cell therapy used in this trial was composed of adoptive tumor infiltrating lymphocytes (TIL), which were made individually for each patient, just as chimeric antigen receptor T cells (CAR T cells) are for patients with blood cancers. However, the process involved is somewhat different, as TILs are made from lymphocytes that have infiltrated the patient’s tumor and are obtained by surgery in the tumor, whereas CAR T cells are made from circulating blood cells.
The phase 3 trial involved 168 patients with unresectable stage IIIC-4 melanoma and showed that patients who were treated with TILs achieved a significantly improved progression-free survival (PFS) when compared with standard immunotherapy with ipilimumab (Yervoy).
The median PFS was more than doubled to 7.2 months with TILs versus 3.1 months with ipilimumab (hazard ratio, 0.50; P < .001).
“We do think that TIL could possibly become a new treatment option for patients with advanced stage melanoma,” commented lead author John Haanen, MD, PhD, research group leader at the Netherlands Cancer Institute in Amsterdam and a professor in translational immunotherapy of cancer at Leiden (the Netherlands) University Medical Center.
He presented the findings at a presidential symposium during the European Society for Medical Oncology Annual Congress, Paris.
“The results of this trial may fuel further research of TIL in other cancer types, potentially demonstrating benefit in many other solid tumors and expanding available treatments for patients,” said Maya Dimitrova, MD, medical oncologist at NYU Langone Perlmutter Cancer Center. She was approached for comment by this news organization and was not involved in the research.
Immune checkpoint inhibitors and targeted therapies have become the standard of care for advanced melanoma and greatly improved patient outcomes, she said. But as about half of patients treated with these agents will not achieve a durable benefit, there remains a need for new treatment options.
“Although immunotherapy can yield impressive long-term responses, a substantial percentage of patients will have no response, or no durable response, to checkpoint inhibitors,” said Dr. Dimitrova. “TIL therapy has proven effectiveness in melanoma. However, no phase III trials have been done to date to compare its effectiveness to a standard of care regimen.”
She noted that these results are consistent with past reports of an approximately 50% response rate with an impressive 20% complete response rate in the TIL group. Data from a phase 2 trial reported last year, for example, showed an objective response rate of 36.4%.
“It will be important to determine the persistence of antitumor activity and whether there are biomarkers that could help with patient selection given the resource intensity of the therapy,” Dr. Dimitrova said. “TIL therapy will likely become a new standard of care in metastatic melanoma refractory to immune checkpoint inhibitors.”
Superior to immunotherapy
In the current study, Dr. Haanen and colleagues randomly assigned 168 patients to TIL or ipilimumab (3 mg/kg every 3 weeks, maximum 4 doses). Patients were stratified for BRAFV600 mutation status, treatment line and center, and the majority (86%) were refractory to anti–PD-1 treatment.
Patients in the TIL group underwent resection of a melanoma lesion (2-3 cm) for the ex vivo outgrowth and expansion of tumor-resident T cells. Before the cultured TILs were infused back into the patients from which they were made, the patient underwent nonmyeloablative, lymphodepleting chemotherapy with cyclophosphamide plus fludarabine that was followed by high-dose interleukin-2.
The study’s primary endpoint was progression-free survival, and secondary endpoints included overall and complete response rate, overall survival, and safety.
At a median follow-up of 33 months, TIL significantly improved progression-free survival, compared with ipilimumab. The overall response rate also favored TIL, compared with ipilimumab (49% vs. 21%), with 20% versus 7% complete responses, respectively.
The median overall survival was 25.8 months for TIL and 18.9 months for ipilimumab (HR, 0.83; P = 0.39).
Grade 3 or higher treatment-related adverse events occurred in all TIL and 57% of ipilimumab patients, although Dr. Haanen noted they were manageable and, in most cases, resolved by the time patients were discharged from the hospital.
“There were no new safety concerns with TIL,” said Dr. Haanen, “And these toxicities are driven by the chemotherapy and interleukin-2 that are part of the TIL regimen. There were no long-term sequelae in patients treated with TIL, and health-related quality of life was higher in patients treated with TIL.”
Ultra-personalized
Also commenting on the study, Anthony J. Olszanski, MD, RPh, associate professor and vice chair of clinical research, department of hematology/oncology at Fox Chase Cancer Center, Philadelphia, agreed that the treatment of patients with melanoma who do not respond to or progress after receiving treatment with immunotherapy is “challenging and represents an unmet need.”
“TIL therapy is, in some ways, ultra-personalized therapy, because we harvest immune cells from the patient’s tumor, expand them outside of the body, and then re-infuse them,” he said. “This trial, which randomized patients between TIL versus the CTLA-4 inhibitor, ipilimumab, has shown an impressive progression-free survival and overall response rate benefit and will help establish TIL therapy as a viable treatment strategy for some patients.”
The study was supported by the Dutch Cancer Society, the Netherlands Organization for Health Research and Development, the Dutch Ministry of Health, Stichting Avento, Copenhagen University Hospital, Herlev, the Danish Cancer Society, and Capital Region of Denmark Research Foundation.
Dr. Haanen and several of the co-authors have declared multiple relationships with industry as noted in the abstract. Dr. Olszanski reports participation in advisory boards for BMS, Merck, and Instil Bio, and he reports running trials for them.
A version of this article first appeared on Medscape.com.
PARIS – Cell therapies have already had a huge impact on the treatment of blood cancers, but progress in solid tumors has proved more difficult. Now, in a first multicenter randomized trial to compare the two,
The cell therapy used in this trial was composed of adoptive tumor infiltrating lymphocytes (TIL), which were made individually for each patient, just as chimeric antigen receptor T cells (CAR T cells) are for patients with blood cancers. However, the process involved is somewhat different, as TILs are made from lymphocytes that have infiltrated the patient’s tumor and are obtained by surgery in the tumor, whereas CAR T cells are made from circulating blood cells.
The phase 3 trial involved 168 patients with unresectable stage IIIC-4 melanoma and showed that patients who were treated with TILs achieved a significantly improved progression-free survival (PFS) when compared with standard immunotherapy with ipilimumab (Yervoy).
The median PFS was more than doubled to 7.2 months with TILs versus 3.1 months with ipilimumab (hazard ratio, 0.50; P < .001).
“We do think that TIL could possibly become a new treatment option for patients with advanced stage melanoma,” commented lead author John Haanen, MD, PhD, research group leader at the Netherlands Cancer Institute in Amsterdam and a professor in translational immunotherapy of cancer at Leiden (the Netherlands) University Medical Center.
He presented the findings at a presidential symposium during the European Society for Medical Oncology Annual Congress, Paris.
“The results of this trial may fuel further research of TIL in other cancer types, potentially demonstrating benefit in many other solid tumors and expanding available treatments for patients,” said Maya Dimitrova, MD, medical oncologist at NYU Langone Perlmutter Cancer Center. She was approached for comment by this news organization and was not involved in the research.
Immune checkpoint inhibitors and targeted therapies have become the standard of care for advanced melanoma and greatly improved patient outcomes, she said. But as about half of patients treated with these agents will not achieve a durable benefit, there remains a need for new treatment options.
“Although immunotherapy can yield impressive long-term responses, a substantial percentage of patients will have no response, or no durable response, to checkpoint inhibitors,” said Dr. Dimitrova. “TIL therapy has proven effectiveness in melanoma. However, no phase III trials have been done to date to compare its effectiveness to a standard of care regimen.”
She noted that these results are consistent with past reports of an approximately 50% response rate with an impressive 20% complete response rate in the TIL group. Data from a phase 2 trial reported last year, for example, showed an objective response rate of 36.4%.
“It will be important to determine the persistence of antitumor activity and whether there are biomarkers that could help with patient selection given the resource intensity of the therapy,” Dr. Dimitrova said. “TIL therapy will likely become a new standard of care in metastatic melanoma refractory to immune checkpoint inhibitors.”
Superior to immunotherapy
In the current study, Dr. Haanen and colleagues randomly assigned 168 patients to TIL or ipilimumab (3 mg/kg every 3 weeks, maximum 4 doses). Patients were stratified for BRAFV600 mutation status, treatment line and center, and the majority (86%) were refractory to anti–PD-1 treatment.
Patients in the TIL group underwent resection of a melanoma lesion (2-3 cm) for the ex vivo outgrowth and expansion of tumor-resident T cells. Before the cultured TILs were infused back into the patients from which they were made, the patient underwent nonmyeloablative, lymphodepleting chemotherapy with cyclophosphamide plus fludarabine that was followed by high-dose interleukin-2.
The study’s primary endpoint was progression-free survival, and secondary endpoints included overall and complete response rate, overall survival, and safety.
At a median follow-up of 33 months, TIL significantly improved progression-free survival, compared with ipilimumab. The overall response rate also favored TIL, compared with ipilimumab (49% vs. 21%), with 20% versus 7% complete responses, respectively.
The median overall survival was 25.8 months for TIL and 18.9 months for ipilimumab (HR, 0.83; P = 0.39).
Grade 3 or higher treatment-related adverse events occurred in all TIL and 57% of ipilimumab patients, although Dr. Haanen noted they were manageable and, in most cases, resolved by the time patients were discharged from the hospital.
“There were no new safety concerns with TIL,” said Dr. Haanen, “And these toxicities are driven by the chemotherapy and interleukin-2 that are part of the TIL regimen. There were no long-term sequelae in patients treated with TIL, and health-related quality of life was higher in patients treated with TIL.”
Ultra-personalized
Also commenting on the study, Anthony J. Olszanski, MD, RPh, associate professor and vice chair of clinical research, department of hematology/oncology at Fox Chase Cancer Center, Philadelphia, agreed that the treatment of patients with melanoma who do not respond to or progress after receiving treatment with immunotherapy is “challenging and represents an unmet need.”
“TIL therapy is, in some ways, ultra-personalized therapy, because we harvest immune cells from the patient’s tumor, expand them outside of the body, and then re-infuse them,” he said. “This trial, which randomized patients between TIL versus the CTLA-4 inhibitor, ipilimumab, has shown an impressive progression-free survival and overall response rate benefit and will help establish TIL therapy as a viable treatment strategy for some patients.”
The study was supported by the Dutch Cancer Society, the Netherlands Organization for Health Research and Development, the Dutch Ministry of Health, Stichting Avento, Copenhagen University Hospital, Herlev, the Danish Cancer Society, and Capital Region of Denmark Research Foundation.
Dr. Haanen and several of the co-authors have declared multiple relationships with industry as noted in the abstract. Dr. Olszanski reports participation in advisory boards for BMS, Merck, and Instil Bio, and he reports running trials for them.
A version of this article first appeared on Medscape.com.
‘Unprecedented’ responses to neoadjuvant treatment in dMMR colon cancer
PARIS – was given before surgery to patients with DNA mismatch repair deficient (dMMR) colon cancer, say researchers reporting new results from the NICHE-2 trial.
The trial involved 112 patients with dMMR colon cancer who were given one cycle of low-dose ipilimumab and two cycles of nivolumab followed by surgery.
The results show that 95% of patients had a major pathologic response (MPR), and 67% had a pathologic complete response (pCR) to immunotherapy.
To date, none of these patients have had disease recurrence after a median follow-up of 13.1 months.
Study presenter Myriam Chalabi, MD, an oncologist at the Netherlands Cancer Institute, Amsterdam, described the findings as “unprecedented,” especially as many of the patients had stage 3 and high-risk disease, and the expected disease recurrence rate with standard-of-care adjuvant chemotherapy in these patients would usually have been around 15%.
“Importantly, this treatment was very well-tolerated,” she added.
Dr. Chalabi presented the new results during a presidential session at the European Society for Medical Oncology Congress 2022, held in Paris.
Neoadjuvant immunotherapy “has the potential to become standard of care” in these patients, she said, adding that the “future has never been brighter” for dMMR colon cancer.
Around 10%-15% of colon cancers are dMMR, and around 33% of these are associated with Lynch syndrome, she noted.
She also urged pharmaceutical companies to seek approval for immunotherapy in this patient population, to warm applause from the audience.
Commenting on the results, Andrés Cervantes, MD, PhD, professor of medicine at the University of Valencia, Spain, said in an ESMO press release that the “innovative” study “questions the need for surgery and postoperative chemotherapy in all patients in whom the primary tumor has disappeared.”
He observed that adjuvant chemotherapy has remained standard of care, “despite the fact that chemotherapy is not so active, and a complete disappearance of the tumor in the surgical specimen is not observed.”
Overall, Dr. Cervantes said that dMMR status is a “strong predictor of the positive effect observed with this short-course immunotherapy,” adding that “determining dMMR can be easily done by immunohistochemistry in the conventional pathology lab, without the need for complex molecular testing.”
The “minimal toxicity” seen in the study “may also facilitate the implementation of this strategy, potentially sparing patients from surgery.”
Details of the new results
For the NICHE-2 study, patients with stage cT3 dMMR colon cancer and/or nodal involvement but without metastases and no signs of obstruction received one dose of ipilimumab 1 mg/kg and two doses of nivolumab 3 mg/kg before undergoing surgery within 6 weeks of enrollment.
The 112 participants were a median age of 60 years, and just over half were women. High-risk stage 3 disease was present in 74% of patients, which included 64% of patients with clinical T4a or T4b tumors and 62% with radiologic N2 stage cancer.
Median time from the first immunotherapy dose to surgery was 5.4 weeks.
Immune-related adverse events were seen in 61% of patients, but just 4% of patients experienced grade 3-4 immune-related adverse events, and 2% consequently had a delay in surgery, meaning the study met its primary safety endpoint.
In the end, all patients underwent surgery, with 100% having R0 resections.
A pathologic response was seen in 99% of patients, with 95% having an MPR, defined as less than or equal to 10% residual viable tumor, and 4% a partial response, defined as 10% to less than or equal to 50% residual viable tumor. A pCR, which included both the tumor bed and lymph nodes, was seen in 67% of participants.
There was a borderline significant difference in pCR patients between the 66 patients with sporadic tumors and the 32 with Lynch syndrome, at 58% versus 78% (P = .056).
At the meeting, discussant James Larkin, MD, PhD, consultant medical oncologist, The Royal Marsden, London, who was not involved with the study, agreed that the results were “striking,” with “brief treatment ... [showing] a major effect.”
However, he emphasized that it will be “important” to see the prespecified 3-year disease-free survival data, and he questioned whether the single low dose of ipilimumab was, in fact, necessary.
Dr. Larkin also emphasized that organ-sparing strategies in colon cancer are less “clear cut” than they are in rectal cancer and would require ongoing follow-up with colonoscopies and, potentially, biopsies. He also said it is “critical” to get patients’ views on the desirability of organ sparing.
The study was funded by Bristol Myers Squibb. Dr. Chalabi has reported no financial interests. Disclosures for the other authors are listed with the abstract. Dr. Larkin has declared relationships with Eisai, Novartis, Merck, Pfizer, BMS, iOnctura, Debiopharm, Incyte, MSD, Pierre Fabre, Ibsen, Roche, EUSA Pharma, AstraZeneca, GSK, Calithera, Ultimovacs, Seagen, and Nektar Therapeutics.
A version of this article first appeared on Medscape.com.
PARIS – was given before surgery to patients with DNA mismatch repair deficient (dMMR) colon cancer, say researchers reporting new results from the NICHE-2 trial.
The trial involved 112 patients with dMMR colon cancer who were given one cycle of low-dose ipilimumab and two cycles of nivolumab followed by surgery.
The results show that 95% of patients had a major pathologic response (MPR), and 67% had a pathologic complete response (pCR) to immunotherapy.
To date, none of these patients have had disease recurrence after a median follow-up of 13.1 months.
Study presenter Myriam Chalabi, MD, an oncologist at the Netherlands Cancer Institute, Amsterdam, described the findings as “unprecedented,” especially as many of the patients had stage 3 and high-risk disease, and the expected disease recurrence rate with standard-of-care adjuvant chemotherapy in these patients would usually have been around 15%.
“Importantly, this treatment was very well-tolerated,” she added.
Dr. Chalabi presented the new results during a presidential session at the European Society for Medical Oncology Congress 2022, held in Paris.
Neoadjuvant immunotherapy “has the potential to become standard of care” in these patients, she said, adding that the “future has never been brighter” for dMMR colon cancer.
Around 10%-15% of colon cancers are dMMR, and around 33% of these are associated with Lynch syndrome, she noted.
She also urged pharmaceutical companies to seek approval for immunotherapy in this patient population, to warm applause from the audience.
Commenting on the results, Andrés Cervantes, MD, PhD, professor of medicine at the University of Valencia, Spain, said in an ESMO press release that the “innovative” study “questions the need for surgery and postoperative chemotherapy in all patients in whom the primary tumor has disappeared.”
He observed that adjuvant chemotherapy has remained standard of care, “despite the fact that chemotherapy is not so active, and a complete disappearance of the tumor in the surgical specimen is not observed.”
Overall, Dr. Cervantes said that dMMR status is a “strong predictor of the positive effect observed with this short-course immunotherapy,” adding that “determining dMMR can be easily done by immunohistochemistry in the conventional pathology lab, without the need for complex molecular testing.”
The “minimal toxicity” seen in the study “may also facilitate the implementation of this strategy, potentially sparing patients from surgery.”
Details of the new results
For the NICHE-2 study, patients with stage cT3 dMMR colon cancer and/or nodal involvement but without metastases and no signs of obstruction received one dose of ipilimumab 1 mg/kg and two doses of nivolumab 3 mg/kg before undergoing surgery within 6 weeks of enrollment.
The 112 participants were a median age of 60 years, and just over half were women. High-risk stage 3 disease was present in 74% of patients, which included 64% of patients with clinical T4a or T4b tumors and 62% with radiologic N2 stage cancer.
Median time from the first immunotherapy dose to surgery was 5.4 weeks.
Immune-related adverse events were seen in 61% of patients, but just 4% of patients experienced grade 3-4 immune-related adverse events, and 2% consequently had a delay in surgery, meaning the study met its primary safety endpoint.
In the end, all patients underwent surgery, with 100% having R0 resections.
A pathologic response was seen in 99% of patients, with 95% having an MPR, defined as less than or equal to 10% residual viable tumor, and 4% a partial response, defined as 10% to less than or equal to 50% residual viable tumor. A pCR, which included both the tumor bed and lymph nodes, was seen in 67% of participants.
There was a borderline significant difference in pCR patients between the 66 patients with sporadic tumors and the 32 with Lynch syndrome, at 58% versus 78% (P = .056).
At the meeting, discussant James Larkin, MD, PhD, consultant medical oncologist, The Royal Marsden, London, who was not involved with the study, agreed that the results were “striking,” with “brief treatment ... [showing] a major effect.”
However, he emphasized that it will be “important” to see the prespecified 3-year disease-free survival data, and he questioned whether the single low dose of ipilimumab was, in fact, necessary.
Dr. Larkin also emphasized that organ-sparing strategies in colon cancer are less “clear cut” than they are in rectal cancer and would require ongoing follow-up with colonoscopies and, potentially, biopsies. He also said it is “critical” to get patients’ views on the desirability of organ sparing.
The study was funded by Bristol Myers Squibb. Dr. Chalabi has reported no financial interests. Disclosures for the other authors are listed with the abstract. Dr. Larkin has declared relationships with Eisai, Novartis, Merck, Pfizer, BMS, iOnctura, Debiopharm, Incyte, MSD, Pierre Fabre, Ibsen, Roche, EUSA Pharma, AstraZeneca, GSK, Calithera, Ultimovacs, Seagen, and Nektar Therapeutics.
A version of this article first appeared on Medscape.com.
PARIS – was given before surgery to patients with DNA mismatch repair deficient (dMMR) colon cancer, say researchers reporting new results from the NICHE-2 trial.
The trial involved 112 patients with dMMR colon cancer who were given one cycle of low-dose ipilimumab and two cycles of nivolumab followed by surgery.
The results show that 95% of patients had a major pathologic response (MPR), and 67% had a pathologic complete response (pCR) to immunotherapy.
To date, none of these patients have had disease recurrence after a median follow-up of 13.1 months.
Study presenter Myriam Chalabi, MD, an oncologist at the Netherlands Cancer Institute, Amsterdam, described the findings as “unprecedented,” especially as many of the patients had stage 3 and high-risk disease, and the expected disease recurrence rate with standard-of-care adjuvant chemotherapy in these patients would usually have been around 15%.
“Importantly, this treatment was very well-tolerated,” she added.
Dr. Chalabi presented the new results during a presidential session at the European Society for Medical Oncology Congress 2022, held in Paris.
Neoadjuvant immunotherapy “has the potential to become standard of care” in these patients, she said, adding that the “future has never been brighter” for dMMR colon cancer.
Around 10%-15% of colon cancers are dMMR, and around 33% of these are associated with Lynch syndrome, she noted.
She also urged pharmaceutical companies to seek approval for immunotherapy in this patient population, to warm applause from the audience.
Commenting on the results, Andrés Cervantes, MD, PhD, professor of medicine at the University of Valencia, Spain, said in an ESMO press release that the “innovative” study “questions the need for surgery and postoperative chemotherapy in all patients in whom the primary tumor has disappeared.”
He observed that adjuvant chemotherapy has remained standard of care, “despite the fact that chemotherapy is not so active, and a complete disappearance of the tumor in the surgical specimen is not observed.”
Overall, Dr. Cervantes said that dMMR status is a “strong predictor of the positive effect observed with this short-course immunotherapy,” adding that “determining dMMR can be easily done by immunohistochemistry in the conventional pathology lab, without the need for complex molecular testing.”
The “minimal toxicity” seen in the study “may also facilitate the implementation of this strategy, potentially sparing patients from surgery.”
Details of the new results
For the NICHE-2 study, patients with stage cT3 dMMR colon cancer and/or nodal involvement but without metastases and no signs of obstruction received one dose of ipilimumab 1 mg/kg and two doses of nivolumab 3 mg/kg before undergoing surgery within 6 weeks of enrollment.
The 112 participants were a median age of 60 years, and just over half were women. High-risk stage 3 disease was present in 74% of patients, which included 64% of patients with clinical T4a or T4b tumors and 62% with radiologic N2 stage cancer.
Median time from the first immunotherapy dose to surgery was 5.4 weeks.
Immune-related adverse events were seen in 61% of patients, but just 4% of patients experienced grade 3-4 immune-related adverse events, and 2% consequently had a delay in surgery, meaning the study met its primary safety endpoint.
In the end, all patients underwent surgery, with 100% having R0 resections.
A pathologic response was seen in 99% of patients, with 95% having an MPR, defined as less than or equal to 10% residual viable tumor, and 4% a partial response, defined as 10% to less than or equal to 50% residual viable tumor. A pCR, which included both the tumor bed and lymph nodes, was seen in 67% of participants.
There was a borderline significant difference in pCR patients between the 66 patients with sporadic tumors and the 32 with Lynch syndrome, at 58% versus 78% (P = .056).
At the meeting, discussant James Larkin, MD, PhD, consultant medical oncologist, The Royal Marsden, London, who was not involved with the study, agreed that the results were “striking,” with “brief treatment ... [showing] a major effect.”
However, he emphasized that it will be “important” to see the prespecified 3-year disease-free survival data, and he questioned whether the single low dose of ipilimumab was, in fact, necessary.
Dr. Larkin also emphasized that organ-sparing strategies in colon cancer are less “clear cut” than they are in rectal cancer and would require ongoing follow-up with colonoscopies and, potentially, biopsies. He also said it is “critical” to get patients’ views on the desirability of organ sparing.
The study was funded by Bristol Myers Squibb. Dr. Chalabi has reported no financial interests. Disclosures for the other authors are listed with the abstract. Dr. Larkin has declared relationships with Eisai, Novartis, Merck, Pfizer, BMS, iOnctura, Debiopharm, Incyte, MSD, Pierre Fabre, Ibsen, Roche, EUSA Pharma, AstraZeneca, GSK, Calithera, Ultimovacs, Seagen, and Nektar Therapeutics.
A version of this article first appeared on Medscape.com.
TBI is an unrecognized risk factor for cardiovascular disease
(CVD). More severe TBI is associated with higher risk of CVD, new research shows.
Given the relatively young age of post-9/11–era veterans with TBI, there may be an increased burden of heart disease in the future as these veterans age and develop traditional risk factors for CVD, the investigators, led by Ian J. Stewart, MD, with Uniformed Services University, Bethesda, Md., wrote.
The study was published online in JAMA Neurology.
Novel data
Since Sept. 11, 2001, 4.5 million people have served in the U.S. military, with their time in service defined by the long-running wars in Iraq and Afghanistan. Estimates suggest that up to 20% of post-9/11 veterans sustained a TBI.
While some evidence suggests that TBI increases the risk of CVD, prior reports have focused mainly on cerebrovascular outcomes. Until now, the potential association of TBI with CVD has not been comprehensively examined in post-9/11–era veterans.
The retrospective cohort study included 1,559,928 predominantly male post-9/11 veterans, including 301,169 (19.3%) with a history of TBI and 1,258,759 (81%) with no TBI history.
In fully adjusted models, compared with veterans with no TBI history, a history of mild, moderate/severe, or penetrating TBI was associated with increased risk of developing the composite CVD endpoint (coronary artery disease, stroke, peripheral artery disease, and CVD death).
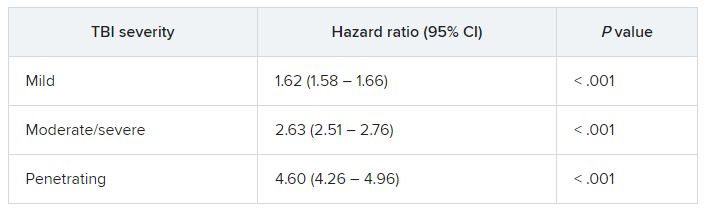
TBIs of all severities were associated with the individual components of the composite outcome, except penetrating TBI and CVD death.
“The association of TBI with subsequent CVD was not attenuated in multivariable models, suggesting that TBI may be accounting for risk that is independent from the other variables,” Dr. Stewart and colleagues wrote.
They noted that the risk was highest shortly after injury, but TBI remained significantly associated with CVD for years after the initial insult.
Why TBI may raise the risk of subsequent CVD remains unclear.
It’s possible that patients with TBI develop more traditional risk factors for CVD through time than do patients without TBI. A study in mice found that TBI led to increased rates of atherosclerosis, the researchers said.
An additional mechanism may be disruption of autonomic regulation, which has been known to occur after TBI.
Another potential pathway is through mental health diagnoses, such as posttraumatic stress disorder; a large body of work has identified associations between PTSD and CVD, including among post-9/11 veterans.
Further work is needed to determine how this risk can be modified to improve outcomes for post-9/11–era veterans, the researchers write.
Unrecognized CVD risk factor?
Reached for comment, Shaheen E. Lakhan, MD, PhD, a neurologist and researcher from Boston who wasn’t involved in the study, said the effects of TBI on heart health are “very underreported, and most clinicians would not make the link.”
“When the brain suffers a traumatic injury, it activates a cascade of neuro-inflammation that goes haywire in an attempt to protect further brain damage. Oftentimes, these inflammatory by-products leak into the body, especially in trauma, when the barriers are broken between brain and body, and can cause systemic body inflammation, which is well associated with heart disease,” Dr. Lakhan said.
In addition, Dr. Lakhan said, “TBI itself localized to just the brain can negatively affect good health habits, leading to worsening heart health, too.”
“Research like this brings light where not much exists and underscores the importance of protecting our brains from physical trauma,” he said.
The study was supported by the assistant secretary of defense for health affairs, endorsed by the Department of Defense through the Psychological Health/Traumatic Brain Injury Research Program Long-Term Impact of Military-Relevant Brain Injury Consortium, and by the U.S. Department of Veterans Affairs. Dr. Stewart and Dr. Lakhan have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
(CVD). More severe TBI is associated with higher risk of CVD, new research shows.
Given the relatively young age of post-9/11–era veterans with TBI, there may be an increased burden of heart disease in the future as these veterans age and develop traditional risk factors for CVD, the investigators, led by Ian J. Stewart, MD, with Uniformed Services University, Bethesda, Md., wrote.
The study was published online in JAMA Neurology.
Novel data
Since Sept. 11, 2001, 4.5 million people have served in the U.S. military, with their time in service defined by the long-running wars in Iraq and Afghanistan. Estimates suggest that up to 20% of post-9/11 veterans sustained a TBI.
While some evidence suggests that TBI increases the risk of CVD, prior reports have focused mainly on cerebrovascular outcomes. Until now, the potential association of TBI with CVD has not been comprehensively examined in post-9/11–era veterans.
The retrospective cohort study included 1,559,928 predominantly male post-9/11 veterans, including 301,169 (19.3%) with a history of TBI and 1,258,759 (81%) with no TBI history.
In fully adjusted models, compared with veterans with no TBI history, a history of mild, moderate/severe, or penetrating TBI was associated with increased risk of developing the composite CVD endpoint (coronary artery disease, stroke, peripheral artery disease, and CVD death).
TBIs of all severities were associated with the individual components of the composite outcome, except penetrating TBI and CVD death.
“The association of TBI with subsequent CVD was not attenuated in multivariable models, suggesting that TBI may be accounting for risk that is independent from the other variables,” Dr. Stewart and colleagues wrote.
They noted that the risk was highest shortly after injury, but TBI remained significantly associated with CVD for years after the initial insult.
Why TBI may raise the risk of subsequent CVD remains unclear.
It’s possible that patients with TBI develop more traditional risk factors for CVD through time than do patients without TBI. A study in mice found that TBI led to increased rates of atherosclerosis, the researchers said.
An additional mechanism may be disruption of autonomic regulation, which has been known to occur after TBI.
Another potential pathway is through mental health diagnoses, such as posttraumatic stress disorder; a large body of work has identified associations between PTSD and CVD, including among post-9/11 veterans.
Further work is needed to determine how this risk can be modified to improve outcomes for post-9/11–era veterans, the researchers write.
Unrecognized CVD risk factor?
Reached for comment, Shaheen E. Lakhan, MD, PhD, a neurologist and researcher from Boston who wasn’t involved in the study, said the effects of TBI on heart health are “very underreported, and most clinicians would not make the link.”
“When the brain suffers a traumatic injury, it activates a cascade of neuro-inflammation that goes haywire in an attempt to protect further brain damage. Oftentimes, these inflammatory by-products leak into the body, especially in trauma, when the barriers are broken between brain and body, and can cause systemic body inflammation, which is well associated with heart disease,” Dr. Lakhan said.
In addition, Dr. Lakhan said, “TBI itself localized to just the brain can negatively affect good health habits, leading to worsening heart health, too.”
“Research like this brings light where not much exists and underscores the importance of protecting our brains from physical trauma,” he said.
The study was supported by the assistant secretary of defense for health affairs, endorsed by the Department of Defense through the Psychological Health/Traumatic Brain Injury Research Program Long-Term Impact of Military-Relevant Brain Injury Consortium, and by the U.S. Department of Veterans Affairs. Dr. Stewart and Dr. Lakhan have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
(CVD). More severe TBI is associated with higher risk of CVD, new research shows.
Given the relatively young age of post-9/11–era veterans with TBI, there may be an increased burden of heart disease in the future as these veterans age and develop traditional risk factors for CVD, the investigators, led by Ian J. Stewart, MD, with Uniformed Services University, Bethesda, Md., wrote.
The study was published online in JAMA Neurology.
Novel data
Since Sept. 11, 2001, 4.5 million people have served in the U.S. military, with their time in service defined by the long-running wars in Iraq and Afghanistan. Estimates suggest that up to 20% of post-9/11 veterans sustained a TBI.
While some evidence suggests that TBI increases the risk of CVD, prior reports have focused mainly on cerebrovascular outcomes. Until now, the potential association of TBI with CVD has not been comprehensively examined in post-9/11–era veterans.
The retrospective cohort study included 1,559,928 predominantly male post-9/11 veterans, including 301,169 (19.3%) with a history of TBI and 1,258,759 (81%) with no TBI history.
In fully adjusted models, compared with veterans with no TBI history, a history of mild, moderate/severe, or penetrating TBI was associated with increased risk of developing the composite CVD endpoint (coronary artery disease, stroke, peripheral artery disease, and CVD death).
TBIs of all severities were associated with the individual components of the composite outcome, except penetrating TBI and CVD death.
“The association of TBI with subsequent CVD was not attenuated in multivariable models, suggesting that TBI may be accounting for risk that is independent from the other variables,” Dr. Stewart and colleagues wrote.
They noted that the risk was highest shortly after injury, but TBI remained significantly associated with CVD for years after the initial insult.
Why TBI may raise the risk of subsequent CVD remains unclear.
It’s possible that patients with TBI develop more traditional risk factors for CVD through time than do patients without TBI. A study in mice found that TBI led to increased rates of atherosclerosis, the researchers said.
An additional mechanism may be disruption of autonomic regulation, which has been known to occur after TBI.
Another potential pathway is through mental health diagnoses, such as posttraumatic stress disorder; a large body of work has identified associations between PTSD and CVD, including among post-9/11 veterans.
Further work is needed to determine how this risk can be modified to improve outcomes for post-9/11–era veterans, the researchers write.
Unrecognized CVD risk factor?
Reached for comment, Shaheen E. Lakhan, MD, PhD, a neurologist and researcher from Boston who wasn’t involved in the study, said the effects of TBI on heart health are “very underreported, and most clinicians would not make the link.”
“When the brain suffers a traumatic injury, it activates a cascade of neuro-inflammation that goes haywire in an attempt to protect further brain damage. Oftentimes, these inflammatory by-products leak into the body, especially in trauma, when the barriers are broken between brain and body, and can cause systemic body inflammation, which is well associated with heart disease,” Dr. Lakhan said.
In addition, Dr. Lakhan said, “TBI itself localized to just the brain can negatively affect good health habits, leading to worsening heart health, too.”
“Research like this brings light where not much exists and underscores the importance of protecting our brains from physical trauma,” he said.
The study was supported by the assistant secretary of defense for health affairs, endorsed by the Department of Defense through the Psychological Health/Traumatic Brain Injury Research Program Long-Term Impact of Military-Relevant Brain Injury Consortium, and by the U.S. Department of Veterans Affairs. Dr. Stewart and Dr. Lakhan have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Pembro/chemo combo fails to improve event-free survival in head and neck cancer
PARIS – compared with CRT plus placebo as first-line therapy for patients with locally advanced head and neck squamous cell cancers (HNSCC), reported investigators of the KEYNOTE-412 trial.
Among 804 patients with newly diagnosed, pathologically proven, unresected locally advanced head and neck squamous cell carcinomas who were followed for a median of 47.7 months, the event-free survival (EFS) rate with the pembrolizumab/CRT combination followed by maintenance pembrolizumab was 63.2%, compared with 56.2% for CRT plus placebo. This translated into a nonsignificant hazard ratio of 0.83, said Jean-Pascal Machiels, MD, PhD, at the annual meeting of the European Society for Medical Oncology.
Despite the trial failing to meet its primary endpoint, Dr. Machiels expressed optimism about the results.
“Pembrolizumab with chemoradiation was associated with a favorable trend toward improved event-free survival versus placebo plus chemoradiation in patients with locally advanced head and neck cancer,” he said.
He noted that the 2-year EFS rate was 63% with pembrolizumab, compared with 56% with placebo.
The data also support the hypothesis that programmed death–ligand 1 (PD-L1) expression as measured by a combined positive score (CPS) could be a predictive biomarker for identifying those patients most likely to respond to the immune checkpoint inhibitor, he added.
KEYNOTE-412 details
The rationale for combining the checkpoint inhibitors pembrolizumab with chemoradiotherapy comes from the KEYNOTE-048 trial results of which showed a survival improvement for the use of pembrolizumab plus a platinum-containing regimen as a first-line therapy for recurrent or metastatic HNSCC, as well as pembrolizumab monotherapy for patients with PD-L1 CPS of 1 or greater.
In the current study, Dr. Machiels and colleagues studied whether adding pembrolizumab to CRT could benefit patients with treatment-naive unresected, locally advanced HNSCC.
Eligible patients included those with stage T3 or T4, N0-N3 or any N2a-3 (T1-T4) cancers of the larynx, hypopharynx, or oral cavity, and either p16-negative oropharynx cancers or T4 or N3 p16-positive oropharynx cancer. Patients were required to be eligible for high-dose cisplatin-based CRT.
A total of 804 patients were randomized, 402 in each arm, to receive either pembrolizumab 200 mg intravenously every 3 weeks for 3 cycles plus CRT followed by maintenance pembrolizumab for 14 cycles, or to placebo plus CRT followed by placebo maintenance.
As noted before, there was no significant difference between the study arms for the primary endpoint of EFS. The 24-month EFS rate was 63.2% for the pembrolizumab group, compared with 56.2% for controls. The respective 6-month EFS rates were 57.4% versus 52.1%.
In a post hoc analysis, both EFS and overall survival were numerically with pembrolizumab among patients with PD-L1 CPS of 20 or greater. The respective 2- and 3-year EFS rates were 71.2% versus 62.6%, and 66.7% versus 57.2%.
The 24-months overall survival rates were 83.3% with pembrolizumab and 79.9% with placebo, and 36-month rates were 79.1% and 73%, respectively.
Neither EFS rates nor OS rates among patients in this subgroup differed significantly; however, there were no new safety signals with the combination, Dr. Machiels said. The incidence of grade 3 or greater adverse events was 92.2% in the pembrolizumab arm versus 88.4% in the placebo arm. Four patients in the pembrolizumab arm and six in the control arm died from treatment-related causes.
Benefit still to be proven
In a media briefing held prior to his presentation, Dr. Machiels was asked how he could justify his conclusions about a benefit for adding pembrolizumab given that there was no difference between the treatment groups for the primary endpoint.
He said that when the investigators designed the trial 7 years ago, the CPS score for PD-L1 expression had not yet been developed, and that if it had been they might have designed the trial to explore the effect of the pembrolizumab chemoradiation combination according to CPS subgroups.
He also pointed to the numerically superior 2-year EFS and overall rates.
In the presidential symposium, James Larkin, MD, PhD, an invited discussant from the Royal Marsden Hospital, London, said that chemotherapy and anti–PD-1 therapies are known to offer benefit in advanced cancers despite the trial’s failure.
“There is a signal, particularly as we’ve seen in the high PD-L1 group,” he said, noting that the signal was consistent with that seen in the JAVELIN 100 study, which was also a negative trial. He cautioned against relying too heavily on the comparison, however, as JAVELIN 100 was conducted with avelumab, a PD-L1 inhibitor, whereas pembrolizumab is a PD-1 inhibitor.
“Could there be an issue here with treatment schedule? An example and a comparison might be the PACIFIC study in non–small cell lung cancer, which is a positive trial, where actually the checkpoint inhibit with durvalumab was given immediately after the chemoradiotherapy, leading to benefit, rather than being concurrent,” he said.
Dr. Larkin also questioned whether, as codiscussant Sherene Loi, MD, PhD, from the Peter MacCallum Cancer Center, Melbourne, suggested radiotherapy to lymph nodes might alter the immune response to checkpoint inhibitors.
“Clearly radiotherapy is the central component of treatment in this setting, so it would be quite difficult to scale too much on that, but the question is: ‘Could it be modified?’ For example, just to irradiate the primary tumor and involved lymph nodes and potentially spare noninvolved lymph nodes,” he said.
The KEYNOTE-412 study was funded by Merck Sharp & Dohme. Dr. Machiels reported uncompensated consulting to the company. Dr. Larkin reported consulting for and receiving honoraria from Merck and others. Dr. Loi reported uncompensated advisory board activity for Merck and others.
PARIS – compared with CRT plus placebo as first-line therapy for patients with locally advanced head and neck squamous cell cancers (HNSCC), reported investigators of the KEYNOTE-412 trial.
Among 804 patients with newly diagnosed, pathologically proven, unresected locally advanced head and neck squamous cell carcinomas who were followed for a median of 47.7 months, the event-free survival (EFS) rate with the pembrolizumab/CRT combination followed by maintenance pembrolizumab was 63.2%, compared with 56.2% for CRT plus placebo. This translated into a nonsignificant hazard ratio of 0.83, said Jean-Pascal Machiels, MD, PhD, at the annual meeting of the European Society for Medical Oncology.
Despite the trial failing to meet its primary endpoint, Dr. Machiels expressed optimism about the results.
“Pembrolizumab with chemoradiation was associated with a favorable trend toward improved event-free survival versus placebo plus chemoradiation in patients with locally advanced head and neck cancer,” he said.
He noted that the 2-year EFS rate was 63% with pembrolizumab, compared with 56% with placebo.
The data also support the hypothesis that programmed death–ligand 1 (PD-L1) expression as measured by a combined positive score (CPS) could be a predictive biomarker for identifying those patients most likely to respond to the immune checkpoint inhibitor, he added.
KEYNOTE-412 details
The rationale for combining the checkpoint inhibitors pembrolizumab with chemoradiotherapy comes from the KEYNOTE-048 trial results of which showed a survival improvement for the use of pembrolizumab plus a platinum-containing regimen as a first-line therapy for recurrent or metastatic HNSCC, as well as pembrolizumab monotherapy for patients with PD-L1 CPS of 1 or greater.
In the current study, Dr. Machiels and colleagues studied whether adding pembrolizumab to CRT could benefit patients with treatment-naive unresected, locally advanced HNSCC.
Eligible patients included those with stage T3 or T4, N0-N3 or any N2a-3 (T1-T4) cancers of the larynx, hypopharynx, or oral cavity, and either p16-negative oropharynx cancers or T4 or N3 p16-positive oropharynx cancer. Patients were required to be eligible for high-dose cisplatin-based CRT.
A total of 804 patients were randomized, 402 in each arm, to receive either pembrolizumab 200 mg intravenously every 3 weeks for 3 cycles plus CRT followed by maintenance pembrolizumab for 14 cycles, or to placebo plus CRT followed by placebo maintenance.
As noted before, there was no significant difference between the study arms for the primary endpoint of EFS. The 24-month EFS rate was 63.2% for the pembrolizumab group, compared with 56.2% for controls. The respective 6-month EFS rates were 57.4% versus 52.1%.
In a post hoc analysis, both EFS and overall survival were numerically with pembrolizumab among patients with PD-L1 CPS of 20 or greater. The respective 2- and 3-year EFS rates were 71.2% versus 62.6%, and 66.7% versus 57.2%.
The 24-months overall survival rates were 83.3% with pembrolizumab and 79.9% with placebo, and 36-month rates were 79.1% and 73%, respectively.
Neither EFS rates nor OS rates among patients in this subgroup differed significantly; however, there were no new safety signals with the combination, Dr. Machiels said. The incidence of grade 3 or greater adverse events was 92.2% in the pembrolizumab arm versus 88.4% in the placebo arm. Four patients in the pembrolizumab arm and six in the control arm died from treatment-related causes.
Benefit still to be proven
In a media briefing held prior to his presentation, Dr. Machiels was asked how he could justify his conclusions about a benefit for adding pembrolizumab given that there was no difference between the treatment groups for the primary endpoint.
He said that when the investigators designed the trial 7 years ago, the CPS score for PD-L1 expression had not yet been developed, and that if it had been they might have designed the trial to explore the effect of the pembrolizumab chemoradiation combination according to CPS subgroups.
He also pointed to the numerically superior 2-year EFS and overall rates.
In the presidential symposium, James Larkin, MD, PhD, an invited discussant from the Royal Marsden Hospital, London, said that chemotherapy and anti–PD-1 therapies are known to offer benefit in advanced cancers despite the trial’s failure.
“There is a signal, particularly as we’ve seen in the high PD-L1 group,” he said, noting that the signal was consistent with that seen in the JAVELIN 100 study, which was also a negative trial. He cautioned against relying too heavily on the comparison, however, as JAVELIN 100 was conducted with avelumab, a PD-L1 inhibitor, whereas pembrolizumab is a PD-1 inhibitor.
“Could there be an issue here with treatment schedule? An example and a comparison might be the PACIFIC study in non–small cell lung cancer, which is a positive trial, where actually the checkpoint inhibit with durvalumab was given immediately after the chemoradiotherapy, leading to benefit, rather than being concurrent,” he said.
Dr. Larkin also questioned whether, as codiscussant Sherene Loi, MD, PhD, from the Peter MacCallum Cancer Center, Melbourne, suggested radiotherapy to lymph nodes might alter the immune response to checkpoint inhibitors.
“Clearly radiotherapy is the central component of treatment in this setting, so it would be quite difficult to scale too much on that, but the question is: ‘Could it be modified?’ For example, just to irradiate the primary tumor and involved lymph nodes and potentially spare noninvolved lymph nodes,” he said.
The KEYNOTE-412 study was funded by Merck Sharp & Dohme. Dr. Machiels reported uncompensated consulting to the company. Dr. Larkin reported consulting for and receiving honoraria from Merck and others. Dr. Loi reported uncompensated advisory board activity for Merck and others.
PARIS – compared with CRT plus placebo as first-line therapy for patients with locally advanced head and neck squamous cell cancers (HNSCC), reported investigators of the KEYNOTE-412 trial.
Among 804 patients with newly diagnosed, pathologically proven, unresected locally advanced head and neck squamous cell carcinomas who were followed for a median of 47.7 months, the event-free survival (EFS) rate with the pembrolizumab/CRT combination followed by maintenance pembrolizumab was 63.2%, compared with 56.2% for CRT plus placebo. This translated into a nonsignificant hazard ratio of 0.83, said Jean-Pascal Machiels, MD, PhD, at the annual meeting of the European Society for Medical Oncology.
Despite the trial failing to meet its primary endpoint, Dr. Machiels expressed optimism about the results.
“Pembrolizumab with chemoradiation was associated with a favorable trend toward improved event-free survival versus placebo plus chemoradiation in patients with locally advanced head and neck cancer,” he said.
He noted that the 2-year EFS rate was 63% with pembrolizumab, compared with 56% with placebo.
The data also support the hypothesis that programmed death–ligand 1 (PD-L1) expression as measured by a combined positive score (CPS) could be a predictive biomarker for identifying those patients most likely to respond to the immune checkpoint inhibitor, he added.
KEYNOTE-412 details
The rationale for combining the checkpoint inhibitors pembrolizumab with chemoradiotherapy comes from the KEYNOTE-048 trial results of which showed a survival improvement for the use of pembrolizumab plus a platinum-containing regimen as a first-line therapy for recurrent or metastatic HNSCC, as well as pembrolizumab monotherapy for patients with PD-L1 CPS of 1 or greater.
In the current study, Dr. Machiels and colleagues studied whether adding pembrolizumab to CRT could benefit patients with treatment-naive unresected, locally advanced HNSCC.
Eligible patients included those with stage T3 or T4, N0-N3 or any N2a-3 (T1-T4) cancers of the larynx, hypopharynx, or oral cavity, and either p16-negative oropharynx cancers or T4 or N3 p16-positive oropharynx cancer. Patients were required to be eligible for high-dose cisplatin-based CRT.
A total of 804 patients were randomized, 402 in each arm, to receive either pembrolizumab 200 mg intravenously every 3 weeks for 3 cycles plus CRT followed by maintenance pembrolizumab for 14 cycles, or to placebo plus CRT followed by placebo maintenance.
As noted before, there was no significant difference between the study arms for the primary endpoint of EFS. The 24-month EFS rate was 63.2% for the pembrolizumab group, compared with 56.2% for controls. The respective 6-month EFS rates were 57.4% versus 52.1%.
In a post hoc analysis, both EFS and overall survival were numerically with pembrolizumab among patients with PD-L1 CPS of 20 or greater. The respective 2- and 3-year EFS rates were 71.2% versus 62.6%, and 66.7% versus 57.2%.
The 24-months overall survival rates were 83.3% with pembrolizumab and 79.9% with placebo, and 36-month rates were 79.1% and 73%, respectively.
Neither EFS rates nor OS rates among patients in this subgroup differed significantly; however, there were no new safety signals with the combination, Dr. Machiels said. The incidence of grade 3 or greater adverse events was 92.2% in the pembrolizumab arm versus 88.4% in the placebo arm. Four patients in the pembrolizumab arm and six in the control arm died from treatment-related causes.
Benefit still to be proven
In a media briefing held prior to his presentation, Dr. Machiels was asked how he could justify his conclusions about a benefit for adding pembrolizumab given that there was no difference between the treatment groups for the primary endpoint.
He said that when the investigators designed the trial 7 years ago, the CPS score for PD-L1 expression had not yet been developed, and that if it had been they might have designed the trial to explore the effect of the pembrolizumab chemoradiation combination according to CPS subgroups.
He also pointed to the numerically superior 2-year EFS and overall rates.
In the presidential symposium, James Larkin, MD, PhD, an invited discussant from the Royal Marsden Hospital, London, said that chemotherapy and anti–PD-1 therapies are known to offer benefit in advanced cancers despite the trial’s failure.
“There is a signal, particularly as we’ve seen in the high PD-L1 group,” he said, noting that the signal was consistent with that seen in the JAVELIN 100 study, which was also a negative trial. He cautioned against relying too heavily on the comparison, however, as JAVELIN 100 was conducted with avelumab, a PD-L1 inhibitor, whereas pembrolizumab is a PD-1 inhibitor.
“Could there be an issue here with treatment schedule? An example and a comparison might be the PACIFIC study in non–small cell lung cancer, which is a positive trial, where actually the checkpoint inhibit with durvalumab was given immediately after the chemoradiotherapy, leading to benefit, rather than being concurrent,” he said.
Dr. Larkin also questioned whether, as codiscussant Sherene Loi, MD, PhD, from the Peter MacCallum Cancer Center, Melbourne, suggested radiotherapy to lymph nodes might alter the immune response to checkpoint inhibitors.
“Clearly radiotherapy is the central component of treatment in this setting, so it would be quite difficult to scale too much on that, but the question is: ‘Could it be modified?’ For example, just to irradiate the primary tumor and involved lymph nodes and potentially spare noninvolved lymph nodes,” he said.
The KEYNOTE-412 study was funded by Merck Sharp & Dohme. Dr. Machiels reported uncompensated consulting to the company. Dr. Larkin reported consulting for and receiving honoraria from Merck and others. Dr. Loi reported uncompensated advisory board activity for Merck and others.
AT ESMO CONGRESS 2022
In NSCLC, not all EGFR mutations are the same
In non–small cell lung cancer (NSCLC), . However, there is a range of different EGFR mutations, and different mutation combinations can lead to different tumor characteristics that might in turn affect response to therapy.
A new real-world analysis of 159 NSCLC patients found that a combination of a mutation of the TP53 tumor suppressor gene and the EGFR Ex20 mutation is associated with worse disease outcomes, compared to patients with the EGFR Ex20 mutation alone. But the news wasn’t all bad. The same group of patients also responded better to ICB (immune checkpoint blockade) therapy than did the broader population of EGFR Ex20 patients.
The EGFR Ex20 mutation occurs in about 4% of NSCLC cases, while TP53 is quite common: The new study found a frequency of 43.9%. “We first have to mention that the findings regarding TP53 do not reach statistical significance; however, the trend is very strong, and results might be hampered due to small sample sizes. We think it is [appropriate] to exhaust more treatment options for these patients, especially targeted approaches with newer drugs that specifically target exon 20 insertions, as these drugs were not applied in our cohort,” Anna Kron, Dr. rer. medic., said in an email exchange. Dr. Kron presented the results at a poster session in Paris at the ESMO Congress. She is a researcher at University Hospital of Cologne, Germany.
The ImmunoTarget study, published in 2019, examined over 500 NSCLC patients with a range of driver mutations including EGFR and found that they responded poorly to ICIs in comparison to KRAS mutations.
But Dr. Kron’s group was not convinced. “Ex20 mutations differ clinically from other tyrosine kinase mutations in EGFR. We set out this study to rechallenge the paradigm of impaired benefit from ICI in EGFR-mutated patients, as we consider these mutations not interchangeable with other EGFR mutations,” Dr. Kron said.
“We would postulate that in EGFR Exon 20 mutations, ICI and specific inhibitors should be part of the therapeutic course. In patients with co-occurring TP53 mutations, treatment escalation could be considered,” Dr. Kron said.
The study included 159 patients with advanced NSCLC with the EGFR exon 20 insertion, who were treated between 2014 and 2020 at German hospitals. Among the patients, 37.7% were female; mean age at diagnosis was 65.87 years; 50.3% had a smoking history and 38.4% did not (data were unavailable for the rest); and 9.4% of tumors were stage I, 4.4% stage II, 8.2% stage IIIA, 3.8% stage IIIB, and 74.2% stage IV.
Over a follow-up of 4.1 years, there was a trend toward longer survival among patients with TP53 wild type (OS, 20 versus 12 months; P = .092). Sixty-six patients who received ICI therapy had better OS compared with those who did not (22 versus 10 months; P = .018). Among patients with co-occurring TP53 mutations, receipt of ICI therapy was associated with longer OS (16 versus 8 months; P = .048). There was a trend toward patients with TP53 wild type treated with ICI faring better than those who didn’t receive ICI (27.0 months versus 11.0 months; P = .109).
The researchers are continuing to study patients with EGFR Ex20 to better understand the role of TP53 and ICI therapy in these patients.
The study received no funding. Dr. Kron has no relevant financial disclosures.
In non–small cell lung cancer (NSCLC), . However, there is a range of different EGFR mutations, and different mutation combinations can lead to different tumor characteristics that might in turn affect response to therapy.
A new real-world analysis of 159 NSCLC patients found that a combination of a mutation of the TP53 tumor suppressor gene and the EGFR Ex20 mutation is associated with worse disease outcomes, compared to patients with the EGFR Ex20 mutation alone. But the news wasn’t all bad. The same group of patients also responded better to ICB (immune checkpoint blockade) therapy than did the broader population of EGFR Ex20 patients.
The EGFR Ex20 mutation occurs in about 4% of NSCLC cases, while TP53 is quite common: The new study found a frequency of 43.9%. “We first have to mention that the findings regarding TP53 do not reach statistical significance; however, the trend is very strong, and results might be hampered due to small sample sizes. We think it is [appropriate] to exhaust more treatment options for these patients, especially targeted approaches with newer drugs that specifically target exon 20 insertions, as these drugs were not applied in our cohort,” Anna Kron, Dr. rer. medic., said in an email exchange. Dr. Kron presented the results at a poster session in Paris at the ESMO Congress. She is a researcher at University Hospital of Cologne, Germany.
The ImmunoTarget study, published in 2019, examined over 500 NSCLC patients with a range of driver mutations including EGFR and found that they responded poorly to ICIs in comparison to KRAS mutations.
But Dr. Kron’s group was not convinced. “Ex20 mutations differ clinically from other tyrosine kinase mutations in EGFR. We set out this study to rechallenge the paradigm of impaired benefit from ICI in EGFR-mutated patients, as we consider these mutations not interchangeable with other EGFR mutations,” Dr. Kron said.
“We would postulate that in EGFR Exon 20 mutations, ICI and specific inhibitors should be part of the therapeutic course. In patients with co-occurring TP53 mutations, treatment escalation could be considered,” Dr. Kron said.
The study included 159 patients with advanced NSCLC with the EGFR exon 20 insertion, who were treated between 2014 and 2020 at German hospitals. Among the patients, 37.7% were female; mean age at diagnosis was 65.87 years; 50.3% had a smoking history and 38.4% did not (data were unavailable for the rest); and 9.4% of tumors were stage I, 4.4% stage II, 8.2% stage IIIA, 3.8% stage IIIB, and 74.2% stage IV.
Over a follow-up of 4.1 years, there was a trend toward longer survival among patients with TP53 wild type (OS, 20 versus 12 months; P = .092). Sixty-six patients who received ICI therapy had better OS compared with those who did not (22 versus 10 months; P = .018). Among patients with co-occurring TP53 mutations, receipt of ICI therapy was associated with longer OS (16 versus 8 months; P = .048). There was a trend toward patients with TP53 wild type treated with ICI faring better than those who didn’t receive ICI (27.0 months versus 11.0 months; P = .109).
The researchers are continuing to study patients with EGFR Ex20 to better understand the role of TP53 and ICI therapy in these patients.
The study received no funding. Dr. Kron has no relevant financial disclosures.
In non–small cell lung cancer (NSCLC), . However, there is a range of different EGFR mutations, and different mutation combinations can lead to different tumor characteristics that might in turn affect response to therapy.
A new real-world analysis of 159 NSCLC patients found that a combination of a mutation of the TP53 tumor suppressor gene and the EGFR Ex20 mutation is associated with worse disease outcomes, compared to patients with the EGFR Ex20 mutation alone. But the news wasn’t all bad. The same group of patients also responded better to ICB (immune checkpoint blockade) therapy than did the broader population of EGFR Ex20 patients.
The EGFR Ex20 mutation occurs in about 4% of NSCLC cases, while TP53 is quite common: The new study found a frequency of 43.9%. “We first have to mention that the findings regarding TP53 do not reach statistical significance; however, the trend is very strong, and results might be hampered due to small sample sizes. We think it is [appropriate] to exhaust more treatment options for these patients, especially targeted approaches with newer drugs that specifically target exon 20 insertions, as these drugs were not applied in our cohort,” Anna Kron, Dr. rer. medic., said in an email exchange. Dr. Kron presented the results at a poster session in Paris at the ESMO Congress. She is a researcher at University Hospital of Cologne, Germany.
The ImmunoTarget study, published in 2019, examined over 500 NSCLC patients with a range of driver mutations including EGFR and found that they responded poorly to ICIs in comparison to KRAS mutations.
But Dr. Kron’s group was not convinced. “Ex20 mutations differ clinically from other tyrosine kinase mutations in EGFR. We set out this study to rechallenge the paradigm of impaired benefit from ICI in EGFR-mutated patients, as we consider these mutations not interchangeable with other EGFR mutations,” Dr. Kron said.
“We would postulate that in EGFR Exon 20 mutations, ICI and specific inhibitors should be part of the therapeutic course. In patients with co-occurring TP53 mutations, treatment escalation could be considered,” Dr. Kron said.
The study included 159 patients with advanced NSCLC with the EGFR exon 20 insertion, who were treated between 2014 and 2020 at German hospitals. Among the patients, 37.7% were female; mean age at diagnosis was 65.87 years; 50.3% had a smoking history and 38.4% did not (data were unavailable for the rest); and 9.4% of tumors were stage I, 4.4% stage II, 8.2% stage IIIA, 3.8% stage IIIB, and 74.2% stage IV.
Over a follow-up of 4.1 years, there was a trend toward longer survival among patients with TP53 wild type (OS, 20 versus 12 months; P = .092). Sixty-six patients who received ICI therapy had better OS compared with those who did not (22 versus 10 months; P = .018). Among patients with co-occurring TP53 mutations, receipt of ICI therapy was associated with longer OS (16 versus 8 months; P = .048). There was a trend toward patients with TP53 wild type treated with ICI faring better than those who didn’t receive ICI (27.0 months versus 11.0 months; P = .109).
The researchers are continuing to study patients with EGFR Ex20 to better understand the role of TP53 and ICI therapy in these patients.
The study received no funding. Dr. Kron has no relevant financial disclosures.
FROM ESMO CONGRESS 2022
Spondyloarthritis disease activity measurement with ASDAS not influenced by gender
GHENT, BELGIUM – The Ankylosing Spondylitis Disease Activity Score (ASDAS) should be the preferred tool for disease activity assessment in patients with axial spondyloarthritis (axSpA) because it is not influenced by gender, according to new data on gender and patient outcomes as assessed by commonly used scoring methods and indices across the spectrum of SpA disease subtypes.
In contrast, researchers led by Diego Benavent, MD, a rheumatologist at La Paz University Hospital, Madrid, found that gender influenced the Bath Ankylosing Spondylitis Disease Activity Index (BASDAI) in all three disease subtypes: axSpA, peripheral SpA (pSpA), and psoriatic arthritis (PsA).
In addition, data show that women with axSpA, pSpA, or PsA reported higher disease activity, functional limitation, and poorer overall health.
Dr. Benavent presented the results at the 13th International Congress on Spondyloarthritides. The study was also published online Sept. 12 in RMD Open.
“The ASDAS is more likely to be the activity score used because we are reassured that it performs well in both men and women. However, there is a need for more appropriate validated indices that are not affected by gender in peripheral spondyloarthropathies and psoriatic arthritis,” Dr. Benavent said.
So far, most data concerning gender differences have been described in patients with axSpA, and with various measurement instruments available to assess disease activity, function, and overall health. Dr. Benavent and his colleagues wanted to investigate the influence of gender on disease outcomes across not only axSpA but pSpA and PsA, too, to see if there were differences in the relationship between gender and these other disease subtypes.
In previous studies, ASDAS has shown better psychometric properties than the BASDAI for disease activity in axSpA. “But there is little validation in pSpA and PsA, and the influence of gender in the outcomes assessed by these instruments is unknown.
“Compared with men, women with an axSpA diagnosis tend to have more frequent peripheral and extramusculoskeletal manifestations, such as enthesitis and inflammatory bowel disease,” Dr. Benavent said in an interview. “However, males with axSpA present more radiographic damage and objective signs of inflammation.”
Martin Rudwaleit, MD, head of the department of internal medicine and rheumatology at Klinikum Bielefeld (Germany), who attended the talk, reflected on the findings.
“Decades ago, ankylosing spondylitis was largely considered a male disease as found in 80%-90% of cases. Later, with MRI, we started to diagnose patients earlier and learned that more females have the disease and that females have less structural damage in the spine than men. As such, male gender is a predictor for worse radiographic progression,” Dr. Rudwaleit said.
“The question is whether the female patients who are considered to have axSpA really have axSpA, or do they have other origins of their back pain?” he continued.
“Also, this study shows us that females report a wider spectrum of symptoms than males. For example, headache, general discomfort, and overall, a broader spectrum of symptoms than men. This might have contributed to the fact that, previously, diagnoses of axSpA might have been made later in females than males.”
Large study across SpA phenotypes and disease-scoring methods
A total of 4,185 patients from 24 countries participated, with 65% having axSpA, 10% pSpA, and 25% PsA. Females totaled 38.8% of patients across all three types of spondyloarthritis. The researchers drew the data from the Assessment of SpondyloArthritis International Society (ASAS)-perSpA study.
The researchers looked for associations between gender and disease activity as measured by ASDAS and BASDAI, C-reactive protein (CRP), physical function with the Bath Ankylosing Spondylitis Functional Index (BASFI), overall health with the ASAS Health Index (ASAS HI), and European Quality of Life Five Dimensions (EQ-5D) outcomes.
In axSpA, there was a split of 68% men vs. 32% women. The researchers observed certain factors that were more common among men: smoking (49% vs. 32%), HLA-B27 positivity (83% vs. 70%), and elevated CRP (75% vs. 66%). Women more often had enthesitis (45% vs. 39%) and fibromyalgia (17% vs. 3%).
In pSpA, the gender split was approximately equal at 47% men and 53% women. But compared with women, men had more inflammatory back pain (62% vs. 50%), HLA-B27 positivity (70% vs. 54%), and elevated CRP (75% vs. 66%). Women more frequently had inflammatory bowel disease (IBD, 8% vs. 3%) and fibromyalgia (18% vs. 3%).
An approximately equal gender split was also found with PsA (48.5% men vs. 51.5% women). Men more frequently reported ever drinking alcohol than did women (63% vs. 26%), whereas women had a greater family history of both spondyloarthritis (41% vs. 32%) and psoriasis (41% vs. 31%). Women also more often reported enthesitis (49% vs. 42%) and fibromyalgia (19% vs. 3%) than men.
“These data strongly suggest that female patients showed significantly more fibromyalgia across all disease subtypes, and the magnitude of the difference with men is notable,” Dr. Benavent said.”Fibromyalgia is associated with pain and worse patient-reported outcomes, which may bias outcomes with disease activity scores.”
When the researchers analyzed outcomes by the different scores and indices for each disease subtype, they found that females had worse scores for most indices (ASDAS, BASDAI, patient’s global assessment (PtGA), BASFI, ASAS HI, and EQ-5D). “However, for CRP, men presented worse scores across axSpA and pSpA, and no differences were found with women in PsA,” Dr. Benavent added.
Although there are differences between the genders according to the scores, these differences may be confounded and this will affect the score outcome: for example, confounding by fibromyalgia in women, he explained.
To avoid the confounding effect, multivariable regression models were used, including the dependent variable as the explored outcome: for example, with BASDAI or ASDAS serving as the dependent variable and gender as the main independent variable, along with adjustments for potential confounders. When the influence of gender on BASDAI was considered, Dr. Benavent and colleagues found that being female increased all scores across the spectrum: axSpA (0.39 units; 95% confidence interval, 0.2-0.58), pSpA (1.22 units; 95% CI, 0.77-1.69), and PsA (0.88 units; 95% CI, 0.59-1.19). When the influence of gender on ASDAS was considered, the researchers found that being female had no effect on axSpA (0.02 units; 95% CI, –0.07 to 0.11), but did for pSpA (0.36 units; 95% CI, 0.15-0.58) and PsA (0.25 units; 95% CI, 0.12-0.38).
“ASDAS is better than BASDAI because it is similar in males and females, but this only holds true in axSpA, not in pSpA or PsA,” Dr. Benavent concluded.
Dr. Benavent declared serving on speakers bureaus for Janssen, Galapagos, and AbbVie, and receiving grant or research support from Novartis outside the submitted work. Dr. Rudwaleit declared financial relationships with AbbVie, UCB, and Lilly.
GHENT, BELGIUM – The Ankylosing Spondylitis Disease Activity Score (ASDAS) should be the preferred tool for disease activity assessment in patients with axial spondyloarthritis (axSpA) because it is not influenced by gender, according to new data on gender and patient outcomes as assessed by commonly used scoring methods and indices across the spectrum of SpA disease subtypes.
In contrast, researchers led by Diego Benavent, MD, a rheumatologist at La Paz University Hospital, Madrid, found that gender influenced the Bath Ankylosing Spondylitis Disease Activity Index (BASDAI) in all three disease subtypes: axSpA, peripheral SpA (pSpA), and psoriatic arthritis (PsA).
In addition, data show that women with axSpA, pSpA, or PsA reported higher disease activity, functional limitation, and poorer overall health.
Dr. Benavent presented the results at the 13th International Congress on Spondyloarthritides. The study was also published online Sept. 12 in RMD Open.
“The ASDAS is more likely to be the activity score used because we are reassured that it performs well in both men and women. However, there is a need for more appropriate validated indices that are not affected by gender in peripheral spondyloarthropathies and psoriatic arthritis,” Dr. Benavent said.
So far, most data concerning gender differences have been described in patients with axSpA, and with various measurement instruments available to assess disease activity, function, and overall health. Dr. Benavent and his colleagues wanted to investigate the influence of gender on disease outcomes across not only axSpA but pSpA and PsA, too, to see if there were differences in the relationship between gender and these other disease subtypes.
In previous studies, ASDAS has shown better psychometric properties than the BASDAI for disease activity in axSpA. “But there is little validation in pSpA and PsA, and the influence of gender in the outcomes assessed by these instruments is unknown.
“Compared with men, women with an axSpA diagnosis tend to have more frequent peripheral and extramusculoskeletal manifestations, such as enthesitis and inflammatory bowel disease,” Dr. Benavent said in an interview. “However, males with axSpA present more radiographic damage and objective signs of inflammation.”
Martin Rudwaleit, MD, head of the department of internal medicine and rheumatology at Klinikum Bielefeld (Germany), who attended the talk, reflected on the findings.
“Decades ago, ankylosing spondylitis was largely considered a male disease as found in 80%-90% of cases. Later, with MRI, we started to diagnose patients earlier and learned that more females have the disease and that females have less structural damage in the spine than men. As such, male gender is a predictor for worse radiographic progression,” Dr. Rudwaleit said.
“The question is whether the female patients who are considered to have axSpA really have axSpA, or do they have other origins of their back pain?” he continued.
“Also, this study shows us that females report a wider spectrum of symptoms than males. For example, headache, general discomfort, and overall, a broader spectrum of symptoms than men. This might have contributed to the fact that, previously, diagnoses of axSpA might have been made later in females than males.”
Large study across SpA phenotypes and disease-scoring methods
A total of 4,185 patients from 24 countries participated, with 65% having axSpA, 10% pSpA, and 25% PsA. Females totaled 38.8% of patients across all three types of spondyloarthritis. The researchers drew the data from the Assessment of SpondyloArthritis International Society (ASAS)-perSpA study.
The researchers looked for associations between gender and disease activity as measured by ASDAS and BASDAI, C-reactive protein (CRP), physical function with the Bath Ankylosing Spondylitis Functional Index (BASFI), overall health with the ASAS Health Index (ASAS HI), and European Quality of Life Five Dimensions (EQ-5D) outcomes.
In axSpA, there was a split of 68% men vs. 32% women. The researchers observed certain factors that were more common among men: smoking (49% vs. 32%), HLA-B27 positivity (83% vs. 70%), and elevated CRP (75% vs. 66%). Women more often had enthesitis (45% vs. 39%) and fibromyalgia (17% vs. 3%).
In pSpA, the gender split was approximately equal at 47% men and 53% women. But compared with women, men had more inflammatory back pain (62% vs. 50%), HLA-B27 positivity (70% vs. 54%), and elevated CRP (75% vs. 66%). Women more frequently had inflammatory bowel disease (IBD, 8% vs. 3%) and fibromyalgia (18% vs. 3%).
An approximately equal gender split was also found with PsA (48.5% men vs. 51.5% women). Men more frequently reported ever drinking alcohol than did women (63% vs. 26%), whereas women had a greater family history of both spondyloarthritis (41% vs. 32%) and psoriasis (41% vs. 31%). Women also more often reported enthesitis (49% vs. 42%) and fibromyalgia (19% vs. 3%) than men.
“These data strongly suggest that female patients showed significantly more fibromyalgia across all disease subtypes, and the magnitude of the difference with men is notable,” Dr. Benavent said.”Fibromyalgia is associated with pain and worse patient-reported outcomes, which may bias outcomes with disease activity scores.”
When the researchers analyzed outcomes by the different scores and indices for each disease subtype, they found that females had worse scores for most indices (ASDAS, BASDAI, patient’s global assessment (PtGA), BASFI, ASAS HI, and EQ-5D). “However, for CRP, men presented worse scores across axSpA and pSpA, and no differences were found with women in PsA,” Dr. Benavent added.
Although there are differences between the genders according to the scores, these differences may be confounded and this will affect the score outcome: for example, confounding by fibromyalgia in women, he explained.
To avoid the confounding effect, multivariable regression models were used, including the dependent variable as the explored outcome: for example, with BASDAI or ASDAS serving as the dependent variable and gender as the main independent variable, along with adjustments for potential confounders. When the influence of gender on BASDAI was considered, Dr. Benavent and colleagues found that being female increased all scores across the spectrum: axSpA (0.39 units; 95% confidence interval, 0.2-0.58), pSpA (1.22 units; 95% CI, 0.77-1.69), and PsA (0.88 units; 95% CI, 0.59-1.19). When the influence of gender on ASDAS was considered, the researchers found that being female had no effect on axSpA (0.02 units; 95% CI, –0.07 to 0.11), but did for pSpA (0.36 units; 95% CI, 0.15-0.58) and PsA (0.25 units; 95% CI, 0.12-0.38).
“ASDAS is better than BASDAI because it is similar in males and females, but this only holds true in axSpA, not in pSpA or PsA,” Dr. Benavent concluded.
Dr. Benavent declared serving on speakers bureaus for Janssen, Galapagos, and AbbVie, and receiving grant or research support from Novartis outside the submitted work. Dr. Rudwaleit declared financial relationships with AbbVie, UCB, and Lilly.
GHENT, BELGIUM – The Ankylosing Spondylitis Disease Activity Score (ASDAS) should be the preferred tool for disease activity assessment in patients with axial spondyloarthritis (axSpA) because it is not influenced by gender, according to new data on gender and patient outcomes as assessed by commonly used scoring methods and indices across the spectrum of SpA disease subtypes.
In contrast, researchers led by Diego Benavent, MD, a rheumatologist at La Paz University Hospital, Madrid, found that gender influenced the Bath Ankylosing Spondylitis Disease Activity Index (BASDAI) in all three disease subtypes: axSpA, peripheral SpA (pSpA), and psoriatic arthritis (PsA).
In addition, data show that women with axSpA, pSpA, or PsA reported higher disease activity, functional limitation, and poorer overall health.
Dr. Benavent presented the results at the 13th International Congress on Spondyloarthritides. The study was also published online Sept. 12 in RMD Open.
“The ASDAS is more likely to be the activity score used because we are reassured that it performs well in both men and women. However, there is a need for more appropriate validated indices that are not affected by gender in peripheral spondyloarthropathies and psoriatic arthritis,” Dr. Benavent said.
So far, most data concerning gender differences have been described in patients with axSpA, and with various measurement instruments available to assess disease activity, function, and overall health. Dr. Benavent and his colleagues wanted to investigate the influence of gender on disease outcomes across not only axSpA but pSpA and PsA, too, to see if there were differences in the relationship between gender and these other disease subtypes.
In previous studies, ASDAS has shown better psychometric properties than the BASDAI for disease activity in axSpA. “But there is little validation in pSpA and PsA, and the influence of gender in the outcomes assessed by these instruments is unknown.
“Compared with men, women with an axSpA diagnosis tend to have more frequent peripheral and extramusculoskeletal manifestations, such as enthesitis and inflammatory bowel disease,” Dr. Benavent said in an interview. “However, males with axSpA present more radiographic damage and objective signs of inflammation.”
Martin Rudwaleit, MD, head of the department of internal medicine and rheumatology at Klinikum Bielefeld (Germany), who attended the talk, reflected on the findings.
“Decades ago, ankylosing spondylitis was largely considered a male disease as found in 80%-90% of cases. Later, with MRI, we started to diagnose patients earlier and learned that more females have the disease and that females have less structural damage in the spine than men. As such, male gender is a predictor for worse radiographic progression,” Dr. Rudwaleit said.
“The question is whether the female patients who are considered to have axSpA really have axSpA, or do they have other origins of their back pain?” he continued.
“Also, this study shows us that females report a wider spectrum of symptoms than males. For example, headache, general discomfort, and overall, a broader spectrum of symptoms than men. This might have contributed to the fact that, previously, diagnoses of axSpA might have been made later in females than males.”
Large study across SpA phenotypes and disease-scoring methods
A total of 4,185 patients from 24 countries participated, with 65% having axSpA, 10% pSpA, and 25% PsA. Females totaled 38.8% of patients across all three types of spondyloarthritis. The researchers drew the data from the Assessment of SpondyloArthritis International Society (ASAS)-perSpA study.
The researchers looked for associations between gender and disease activity as measured by ASDAS and BASDAI, C-reactive protein (CRP), physical function with the Bath Ankylosing Spondylitis Functional Index (BASFI), overall health with the ASAS Health Index (ASAS HI), and European Quality of Life Five Dimensions (EQ-5D) outcomes.
In axSpA, there was a split of 68% men vs. 32% women. The researchers observed certain factors that were more common among men: smoking (49% vs. 32%), HLA-B27 positivity (83% vs. 70%), and elevated CRP (75% vs. 66%). Women more often had enthesitis (45% vs. 39%) and fibromyalgia (17% vs. 3%).
In pSpA, the gender split was approximately equal at 47% men and 53% women. But compared with women, men had more inflammatory back pain (62% vs. 50%), HLA-B27 positivity (70% vs. 54%), and elevated CRP (75% vs. 66%). Women more frequently had inflammatory bowel disease (IBD, 8% vs. 3%) and fibromyalgia (18% vs. 3%).
An approximately equal gender split was also found with PsA (48.5% men vs. 51.5% women). Men more frequently reported ever drinking alcohol than did women (63% vs. 26%), whereas women had a greater family history of both spondyloarthritis (41% vs. 32%) and psoriasis (41% vs. 31%). Women also more often reported enthesitis (49% vs. 42%) and fibromyalgia (19% vs. 3%) than men.
“These data strongly suggest that female patients showed significantly more fibromyalgia across all disease subtypes, and the magnitude of the difference with men is notable,” Dr. Benavent said.”Fibromyalgia is associated with pain and worse patient-reported outcomes, which may bias outcomes with disease activity scores.”
When the researchers analyzed outcomes by the different scores and indices for each disease subtype, they found that females had worse scores for most indices (ASDAS, BASDAI, patient’s global assessment (PtGA), BASFI, ASAS HI, and EQ-5D). “However, for CRP, men presented worse scores across axSpA and pSpA, and no differences were found with women in PsA,” Dr. Benavent added.
Although there are differences between the genders according to the scores, these differences may be confounded and this will affect the score outcome: for example, confounding by fibromyalgia in women, he explained.
To avoid the confounding effect, multivariable regression models were used, including the dependent variable as the explored outcome: for example, with BASDAI or ASDAS serving as the dependent variable and gender as the main independent variable, along with adjustments for potential confounders. When the influence of gender on BASDAI was considered, Dr. Benavent and colleagues found that being female increased all scores across the spectrum: axSpA (0.39 units; 95% confidence interval, 0.2-0.58), pSpA (1.22 units; 95% CI, 0.77-1.69), and PsA (0.88 units; 95% CI, 0.59-1.19). When the influence of gender on ASDAS was considered, the researchers found that being female had no effect on axSpA (0.02 units; 95% CI, –0.07 to 0.11), but did for pSpA (0.36 units; 95% CI, 0.15-0.58) and PsA (0.25 units; 95% CI, 0.12-0.38).
“ASDAS is better than BASDAI because it is similar in males and females, but this only holds true in axSpA, not in pSpA or PsA,” Dr. Benavent concluded.
Dr. Benavent declared serving on speakers bureaus for Janssen, Galapagos, and AbbVie, and receiving grant or research support from Novartis outside the submitted work. Dr. Rudwaleit declared financial relationships with AbbVie, UCB, and Lilly.
AT THE 2022 SPA CONGRESS
In early NSCLC, comorbidities linked to survival
Cardiometabolic and respiratory comorbidities are associated with worse survival in patients with non–small cell lung cancer (NSCLC), and new research suggests a potential mechanism.
Prior studies had shown mixed results when it came to these comorbidities and survival, according to study coauthor author Geoffrey Liu, MD, who is an epidemiology researcher at the University of Toronto Princess Margaret Cancer Centre. The new work represents data from multiple continents, from various ethnicities and cultures.
“We found that comorbidities had much greater impact on earlier than later stages of lung cancer, consistent with this previous study,” said Dr. Liu in an email. The study was presented by Miguel Garcia-Pardo, who is a researcher at University of Toronto Princess Margaret Cancer Centre, during a poster session at the annual meeting of the European Society for Medical Oncology.
“Deaths from [cardiometabolic] comorbidities were mainly from non–lung cancer competing causes, whereas the deaths from respiratory comorbidities were primarily driven by lung cancer specific survival, i.e., deaths from lung cancer itself. We conclude that Dr. Liu said.
Dr. Liu noted that controlling cardiometabolic risk factors like diabetes and hypertension is typically de-emphasized after diagnosis with early-stage lung cancer. The rationale is often that the lung cancer is a more acute concern than longer-term cardiometabolic risks. “The data from our analyses suggest a rethinking of this strategy. We need to pay more attention to controlling cardiovascular risk factors in early-stage lung cancer,” Dr. Liu said.
The findings also suggest that respiratory comorbidities should be managed more aggressively. That would allow more patients to undergo treatments like surgery and stereotactic radiation.
The Clinical Outcome Studies of the International Lung Cancer Consortium drew from two dozen studies conducted across five continents. It examined clinical, epidemiologic, genetic, and genomic factors and their potential influence on NSCLC outcomes. Cardiometabolic comorbidities included coronary artery disease, diabetes, vascular related diseases, and other heart diseases. Respiratory comorbidities included chronic obstructive pulmonary disease and asthma.
The analysis included 16,354 patients. Among patients with stage I NSCLC, there was an association between reduced overall survival (OS) and cardiometabolic comorbidity (adjusted hazard ratio, 1.17; P = .01) and respiratory comorbidity (aHR, 1.36; P < .001). For stage II/III patients, there was no significant association between OS and cardiometabolic comorbidities, but respiratory comorbidity was associated with worse OS (aHR, 1.15; P < .001). In stage 4, worse OS was associated with both cardiometabolic health comorbidity (aHR, 1.11; P = .03), but not respiratory comorbidity.
Among patients with stage IV NSCLC, there were no associations between overall survival or lung cancer–specific survival (LCSS) and respiratory or cardiometabolic risk factors. However, an examination of cause of death found a different pattern in patients with stage IB-IIIA disease: LCSS was worse among patients with respiratory comorbidities (aHR, 1.21; 95% CI, 1.09-1.34). Among those with cardiovascular comorbidities, the risk of non-NSCLC mortality was higher (aHR, 1.36; 95% CI, 1.15-1.63). The presence of respiratory comorbidity was associated with a reduced probability of undergoing surgical resection for both stage I (adjusted odds ratio, 0.45; 95% CI, 0.35-0.59) and stage II/III patients (aOR, 0.66; 95% CI, 0.53-0.80).
There was an association between non-NSCLC mortality and cardiometabolic comorbidities in stage IA (aHR, 1.37; 95% CI, 1.06-1.77) and in stages IB-IIIA (aHR, 1.32; 95% CI, 1.03-1.71) NSCLC. There were also associations between NSCLC mortality and respiratory comorbidity among stage IA (aHR, 1.51; 95% CI, 1.17-1.95) and stages IB-IIIA (aHR, 1.20; 95% CI, 1.06-1.36) NSCLC. There were no associations between respiratory comorbidity and non-NSCLC mortality.
Respiratory comorbidity was associated with a lower chance of undergoing surgical resection in stage IA (aHR, 0.54; 95% CI, 0.35-0.83) and stage IB-IIIA (aHR, 0.57; 95% CI, 0.46-0.70) cancers. Cardiometabolic comorbidity was associated with a lower rate of surgical resection only in stage 1B-3A patients (aHR, 0.73; 95% CI, 0.56-0.96). Among those who underwent resection, stage IA patients were less likely to die of lung cancer (aHR, 0.38; 95% CI, 0.28-0.52) but more likely to die of other causes (aHR, 1.73; 95% CI, 1.07-1.78). Stage IB-IIIA patients who underwent resection were less likely to die of lung cancer (aHR, 0.37; 95%, 0.32-0.42), but there was no significant association with non–lung cancer mortality.
The study was funded by the Lusi Wong Family Fund and the Alan Brown Chair. Dr. Liu has no relevant financial disclosures.
Cardiometabolic and respiratory comorbidities are associated with worse survival in patients with non–small cell lung cancer (NSCLC), and new research suggests a potential mechanism.
Prior studies had shown mixed results when it came to these comorbidities and survival, according to study coauthor author Geoffrey Liu, MD, who is an epidemiology researcher at the University of Toronto Princess Margaret Cancer Centre. The new work represents data from multiple continents, from various ethnicities and cultures.
“We found that comorbidities had much greater impact on earlier than later stages of lung cancer, consistent with this previous study,” said Dr. Liu in an email. The study was presented by Miguel Garcia-Pardo, who is a researcher at University of Toronto Princess Margaret Cancer Centre, during a poster session at the annual meeting of the European Society for Medical Oncology.
“Deaths from [cardiometabolic] comorbidities were mainly from non–lung cancer competing causes, whereas the deaths from respiratory comorbidities were primarily driven by lung cancer specific survival, i.e., deaths from lung cancer itself. We conclude that Dr. Liu said.
Dr. Liu noted that controlling cardiometabolic risk factors like diabetes and hypertension is typically de-emphasized after diagnosis with early-stage lung cancer. The rationale is often that the lung cancer is a more acute concern than longer-term cardiometabolic risks. “The data from our analyses suggest a rethinking of this strategy. We need to pay more attention to controlling cardiovascular risk factors in early-stage lung cancer,” Dr. Liu said.
The findings also suggest that respiratory comorbidities should be managed more aggressively. That would allow more patients to undergo treatments like surgery and stereotactic radiation.
The Clinical Outcome Studies of the International Lung Cancer Consortium drew from two dozen studies conducted across five continents. It examined clinical, epidemiologic, genetic, and genomic factors and their potential influence on NSCLC outcomes. Cardiometabolic comorbidities included coronary artery disease, diabetes, vascular related diseases, and other heart diseases. Respiratory comorbidities included chronic obstructive pulmonary disease and asthma.
The analysis included 16,354 patients. Among patients with stage I NSCLC, there was an association between reduced overall survival (OS) and cardiometabolic comorbidity (adjusted hazard ratio, 1.17; P = .01) and respiratory comorbidity (aHR, 1.36; P < .001). For stage II/III patients, there was no significant association between OS and cardiometabolic comorbidities, but respiratory comorbidity was associated with worse OS (aHR, 1.15; P < .001). In stage 4, worse OS was associated with both cardiometabolic health comorbidity (aHR, 1.11; P = .03), but not respiratory comorbidity.
Among patients with stage IV NSCLC, there were no associations between overall survival or lung cancer–specific survival (LCSS) and respiratory or cardiometabolic risk factors. However, an examination of cause of death found a different pattern in patients with stage IB-IIIA disease: LCSS was worse among patients with respiratory comorbidities (aHR, 1.21; 95% CI, 1.09-1.34). Among those with cardiovascular comorbidities, the risk of non-NSCLC mortality was higher (aHR, 1.36; 95% CI, 1.15-1.63). The presence of respiratory comorbidity was associated with a reduced probability of undergoing surgical resection for both stage I (adjusted odds ratio, 0.45; 95% CI, 0.35-0.59) and stage II/III patients (aOR, 0.66; 95% CI, 0.53-0.80).
There was an association between non-NSCLC mortality and cardiometabolic comorbidities in stage IA (aHR, 1.37; 95% CI, 1.06-1.77) and in stages IB-IIIA (aHR, 1.32; 95% CI, 1.03-1.71) NSCLC. There were also associations between NSCLC mortality and respiratory comorbidity among stage IA (aHR, 1.51; 95% CI, 1.17-1.95) and stages IB-IIIA (aHR, 1.20; 95% CI, 1.06-1.36) NSCLC. There were no associations between respiratory comorbidity and non-NSCLC mortality.
Respiratory comorbidity was associated with a lower chance of undergoing surgical resection in stage IA (aHR, 0.54; 95% CI, 0.35-0.83) and stage IB-IIIA (aHR, 0.57; 95% CI, 0.46-0.70) cancers. Cardiometabolic comorbidity was associated with a lower rate of surgical resection only in stage 1B-3A patients (aHR, 0.73; 95% CI, 0.56-0.96). Among those who underwent resection, stage IA patients were less likely to die of lung cancer (aHR, 0.38; 95% CI, 0.28-0.52) but more likely to die of other causes (aHR, 1.73; 95% CI, 1.07-1.78). Stage IB-IIIA patients who underwent resection were less likely to die of lung cancer (aHR, 0.37; 95%, 0.32-0.42), but there was no significant association with non–lung cancer mortality.
The study was funded by the Lusi Wong Family Fund and the Alan Brown Chair. Dr. Liu has no relevant financial disclosures.
Cardiometabolic and respiratory comorbidities are associated with worse survival in patients with non–small cell lung cancer (NSCLC), and new research suggests a potential mechanism.
Prior studies had shown mixed results when it came to these comorbidities and survival, according to study coauthor author Geoffrey Liu, MD, who is an epidemiology researcher at the University of Toronto Princess Margaret Cancer Centre. The new work represents data from multiple continents, from various ethnicities and cultures.
“We found that comorbidities had much greater impact on earlier than later stages of lung cancer, consistent with this previous study,” said Dr. Liu in an email. The study was presented by Miguel Garcia-Pardo, who is a researcher at University of Toronto Princess Margaret Cancer Centre, during a poster session at the annual meeting of the European Society for Medical Oncology.
“Deaths from [cardiometabolic] comorbidities were mainly from non–lung cancer competing causes, whereas the deaths from respiratory comorbidities were primarily driven by lung cancer specific survival, i.e., deaths from lung cancer itself. We conclude that Dr. Liu said.
Dr. Liu noted that controlling cardiometabolic risk factors like diabetes and hypertension is typically de-emphasized after diagnosis with early-stage lung cancer. The rationale is often that the lung cancer is a more acute concern than longer-term cardiometabolic risks. “The data from our analyses suggest a rethinking of this strategy. We need to pay more attention to controlling cardiovascular risk factors in early-stage lung cancer,” Dr. Liu said.
The findings also suggest that respiratory comorbidities should be managed more aggressively. That would allow more patients to undergo treatments like surgery and stereotactic radiation.
The Clinical Outcome Studies of the International Lung Cancer Consortium drew from two dozen studies conducted across five continents. It examined clinical, epidemiologic, genetic, and genomic factors and their potential influence on NSCLC outcomes. Cardiometabolic comorbidities included coronary artery disease, diabetes, vascular related diseases, and other heart diseases. Respiratory comorbidities included chronic obstructive pulmonary disease and asthma.
The analysis included 16,354 patients. Among patients with stage I NSCLC, there was an association between reduced overall survival (OS) and cardiometabolic comorbidity (adjusted hazard ratio, 1.17; P = .01) and respiratory comorbidity (aHR, 1.36; P < .001). For stage II/III patients, there was no significant association between OS and cardiometabolic comorbidities, but respiratory comorbidity was associated with worse OS (aHR, 1.15; P < .001). In stage 4, worse OS was associated with both cardiometabolic health comorbidity (aHR, 1.11; P = .03), but not respiratory comorbidity.
Among patients with stage IV NSCLC, there were no associations between overall survival or lung cancer–specific survival (LCSS) and respiratory or cardiometabolic risk factors. However, an examination of cause of death found a different pattern in patients with stage IB-IIIA disease: LCSS was worse among patients with respiratory comorbidities (aHR, 1.21; 95% CI, 1.09-1.34). Among those with cardiovascular comorbidities, the risk of non-NSCLC mortality was higher (aHR, 1.36; 95% CI, 1.15-1.63). The presence of respiratory comorbidity was associated with a reduced probability of undergoing surgical resection for both stage I (adjusted odds ratio, 0.45; 95% CI, 0.35-0.59) and stage II/III patients (aOR, 0.66; 95% CI, 0.53-0.80).
There was an association between non-NSCLC mortality and cardiometabolic comorbidities in stage IA (aHR, 1.37; 95% CI, 1.06-1.77) and in stages IB-IIIA (aHR, 1.32; 95% CI, 1.03-1.71) NSCLC. There were also associations between NSCLC mortality and respiratory comorbidity among stage IA (aHR, 1.51; 95% CI, 1.17-1.95) and stages IB-IIIA (aHR, 1.20; 95% CI, 1.06-1.36) NSCLC. There were no associations between respiratory comorbidity and non-NSCLC mortality.
Respiratory comorbidity was associated with a lower chance of undergoing surgical resection in stage IA (aHR, 0.54; 95% CI, 0.35-0.83) and stage IB-IIIA (aHR, 0.57; 95% CI, 0.46-0.70) cancers. Cardiometabolic comorbidity was associated with a lower rate of surgical resection only in stage 1B-3A patients (aHR, 0.73; 95% CI, 0.56-0.96). Among those who underwent resection, stage IA patients were less likely to die of lung cancer (aHR, 0.38; 95% CI, 0.28-0.52) but more likely to die of other causes (aHR, 1.73; 95% CI, 1.07-1.78). Stage IB-IIIA patients who underwent resection were less likely to die of lung cancer (aHR, 0.37; 95%, 0.32-0.42), but there was no significant association with non–lung cancer mortality.
The study was funded by the Lusi Wong Family Fund and the Alan Brown Chair. Dr. Liu has no relevant financial disclosures.
FROM ESMO CONGRESS 2022