User login
Former UCLA Doctor Receives $14 Million in Gender Discrimination Retrial
A California jury has awarded $14 million to a former University of California, Los Angeles (UCLA) oncologist who claimed she was paid thousands less than her male colleagues and wrongfully terminated after her complaints of gender-based harassment and intimidation were ignored by program leadership.
The decision comes after a lengthy 8-year legal battle in which an appellate judge reversed a previous jury decision in her favor.
Lauren Pinter-Brown, MD, a hematologic oncologist, was hired in 2005 by the University of California, Los Angeles School of Medicine — now called UCLA’s David Geffen School of Medicine. As the school’s lymphoma program director, she conducted clinical research alongside other oncology doctors, including Sven de Vos, MD.
She claimed that her professional relationship with Dr. de Vos became contentious after he demonstrated “oppositional” and “disrespectful” behavior at team meetings, such as talking over her and turning his chair so Dr. Pinter-Brown faced his back. Court documents indicated that Dr. de Vos refused to use Dr. Pinter-Brown’s title in front of colleagues despite doing so for male counterparts.
Dr. Pinter-Brown argued that she was treated as the “butt of a joke” by Dr. de Vos and other male colleagues. In 2016, she sued Dr. de Vos, the university, and its governing body, the Board of Regents, for wrongful termination.
She was awarded a $13 million verdict in 2018. However, the California Court of Appeals overturned it in 2020 after concluding that several mistakes during the court proceedings impeded the school’s right to a fair and impartial trial. The case was retried, culminating in the even higher award of $14 million issued on May 9.
“Two juries have come to virtually identical findings showing multiple problems at UCLA involving gender discrimination,” Dr. Pinter-Brown’s attorney, Carney R. Shegerian, JD, told this news organization.
A spokesperson from UCLA’s David Geffen School of Medicine said administrators are carefully reviewing the new decision.
The spokesperson told this news organization that the medical school and its health system remain “deeply committed to maintaining a workplace free from discrimination, intimidation, retaliation, or harassment of any kind” and fostering a “respectful and inclusive environment ... in research, medical education, and patient care.”
Gender Pay Disparities Persist in Medicine
The gender pay gap in medicine is well documented. The 2024 Medscape Physician Compensation Report found that male doctors earn about 29% more than their female counterparts, with the disparity growing larger among specialists. In addition, a recent JAMA Health Forum study found that male physicians earned 21%-24% more per hour than female physicians.
Dr. Pinter-Brown, who now works at the University of California, Irvine, alleged that she was paid $200,000 less annually, on average, than her male colleagues.
That’s not surprising, says Martha Gulati, MD, professor and director of preventive cardiology at Cedars-Sinai Smidt Heart Institute, Los Angeles. She coauthored a commentary about gender disparities in JAMA Network Open. Dr. Gulati told this news organization that even a “small” pay disparity of $100,000 annually adds up.
“Let’s say the [male physician] invests it at 3% and adds to it yearly. Even without a raise, in 20 years, that is approximately $3 million,” Dr. Gulati explained. “Once you find out you are paid less than your male colleagues, you are upset. Your sense of value and self-worth disappears.”
Eileen Barrett, MD, MPH, president-elect of the American Medical Women’s Association, said that gender discrimination is likely more prevalent than research indicates. She told this news organization that self-doubt and fear of retaliation keep many from exposing the mistreatment.
Although more women are entering medicine, too few rise to the highest positions, Dr. Barrett said.
“Unfortunately, many are pulled and pushed into specialties and subspecialties that have lower compensation and are not promoted to leadership, so just having numbers isn’t enough to achieve equity,” Dr. Barrett said.
Dr. Pinter-Brown claimed she was repeatedly harassed and intimidated by Dr. de Vos from 2008 to 2015. Despite voicing concerns multiple times about the discriminatory behavior, the only resolutions offered by the male-dominated program leadership were for her to separate from the group and conduct lymphoma research independently or to avoid interacting with Dr. de Vos, court records said.
Even the school’s male Title IX officer, Jan Tillisch, MD, who handled gender-based discrimination complaints, reportedly made sexist comments. When Dr. Pinter-Brown sought his help, he allegedly told her that she had a reputation as an “angry woman” and “diva,” court records showed.
According to court documents, Dr. Pinter-Brown endured nitpicking and research audits as retaliation for speaking out, temporarily suspending her research privileges. She said she was subsequently removed from the director position and replaced by Dr. de Vos.
Female physicians who report discriminatory behavior often have unfavorable outcomes and risk future career prospects, Dr. Gulati said.
To shift this dynamic, she said institutions must increase transparency and practices that support female doctors receiving “equal pay for equal work.”
A version of this article appeared on Medscape.com.
A California jury has awarded $14 million to a former University of California, Los Angeles (UCLA) oncologist who claimed she was paid thousands less than her male colleagues and wrongfully terminated after her complaints of gender-based harassment and intimidation were ignored by program leadership.
The decision comes after a lengthy 8-year legal battle in which an appellate judge reversed a previous jury decision in her favor.
Lauren Pinter-Brown, MD, a hematologic oncologist, was hired in 2005 by the University of California, Los Angeles School of Medicine — now called UCLA’s David Geffen School of Medicine. As the school’s lymphoma program director, she conducted clinical research alongside other oncology doctors, including Sven de Vos, MD.
She claimed that her professional relationship with Dr. de Vos became contentious after he demonstrated “oppositional” and “disrespectful” behavior at team meetings, such as talking over her and turning his chair so Dr. Pinter-Brown faced his back. Court documents indicated that Dr. de Vos refused to use Dr. Pinter-Brown’s title in front of colleagues despite doing so for male counterparts.
Dr. Pinter-Brown argued that she was treated as the “butt of a joke” by Dr. de Vos and other male colleagues. In 2016, she sued Dr. de Vos, the university, and its governing body, the Board of Regents, for wrongful termination.
She was awarded a $13 million verdict in 2018. However, the California Court of Appeals overturned it in 2020 after concluding that several mistakes during the court proceedings impeded the school’s right to a fair and impartial trial. The case was retried, culminating in the even higher award of $14 million issued on May 9.
“Two juries have come to virtually identical findings showing multiple problems at UCLA involving gender discrimination,” Dr. Pinter-Brown’s attorney, Carney R. Shegerian, JD, told this news organization.
A spokesperson from UCLA’s David Geffen School of Medicine said administrators are carefully reviewing the new decision.
The spokesperson told this news organization that the medical school and its health system remain “deeply committed to maintaining a workplace free from discrimination, intimidation, retaliation, or harassment of any kind” and fostering a “respectful and inclusive environment ... in research, medical education, and patient care.”
Gender Pay Disparities Persist in Medicine
The gender pay gap in medicine is well documented. The 2024 Medscape Physician Compensation Report found that male doctors earn about 29% more than their female counterparts, with the disparity growing larger among specialists. In addition, a recent JAMA Health Forum study found that male physicians earned 21%-24% more per hour than female physicians.
Dr. Pinter-Brown, who now works at the University of California, Irvine, alleged that she was paid $200,000 less annually, on average, than her male colleagues.
That’s not surprising, says Martha Gulati, MD, professor and director of preventive cardiology at Cedars-Sinai Smidt Heart Institute, Los Angeles. She coauthored a commentary about gender disparities in JAMA Network Open. Dr. Gulati told this news organization that even a “small” pay disparity of $100,000 annually adds up.
“Let’s say the [male physician] invests it at 3% and adds to it yearly. Even without a raise, in 20 years, that is approximately $3 million,” Dr. Gulati explained. “Once you find out you are paid less than your male colleagues, you are upset. Your sense of value and self-worth disappears.”
Eileen Barrett, MD, MPH, president-elect of the American Medical Women’s Association, said that gender discrimination is likely more prevalent than research indicates. She told this news organization that self-doubt and fear of retaliation keep many from exposing the mistreatment.
Although more women are entering medicine, too few rise to the highest positions, Dr. Barrett said.
“Unfortunately, many are pulled and pushed into specialties and subspecialties that have lower compensation and are not promoted to leadership, so just having numbers isn’t enough to achieve equity,” Dr. Barrett said.
Dr. Pinter-Brown claimed she was repeatedly harassed and intimidated by Dr. de Vos from 2008 to 2015. Despite voicing concerns multiple times about the discriminatory behavior, the only resolutions offered by the male-dominated program leadership were for her to separate from the group and conduct lymphoma research independently or to avoid interacting with Dr. de Vos, court records said.
Even the school’s male Title IX officer, Jan Tillisch, MD, who handled gender-based discrimination complaints, reportedly made sexist comments. When Dr. Pinter-Brown sought his help, he allegedly told her that she had a reputation as an “angry woman” and “diva,” court records showed.
According to court documents, Dr. Pinter-Brown endured nitpicking and research audits as retaliation for speaking out, temporarily suspending her research privileges. She said she was subsequently removed from the director position and replaced by Dr. de Vos.
Female physicians who report discriminatory behavior often have unfavorable outcomes and risk future career prospects, Dr. Gulati said.
To shift this dynamic, she said institutions must increase transparency and practices that support female doctors receiving “equal pay for equal work.”
A version of this article appeared on Medscape.com.
A California jury has awarded $14 million to a former University of California, Los Angeles (UCLA) oncologist who claimed she was paid thousands less than her male colleagues and wrongfully terminated after her complaints of gender-based harassment and intimidation were ignored by program leadership.
The decision comes after a lengthy 8-year legal battle in which an appellate judge reversed a previous jury decision in her favor.
Lauren Pinter-Brown, MD, a hematologic oncologist, was hired in 2005 by the University of California, Los Angeles School of Medicine — now called UCLA’s David Geffen School of Medicine. As the school’s lymphoma program director, she conducted clinical research alongside other oncology doctors, including Sven de Vos, MD.
She claimed that her professional relationship with Dr. de Vos became contentious after he demonstrated “oppositional” and “disrespectful” behavior at team meetings, such as talking over her and turning his chair so Dr. Pinter-Brown faced his back. Court documents indicated that Dr. de Vos refused to use Dr. Pinter-Brown’s title in front of colleagues despite doing so for male counterparts.
Dr. Pinter-Brown argued that she was treated as the “butt of a joke” by Dr. de Vos and other male colleagues. In 2016, she sued Dr. de Vos, the university, and its governing body, the Board of Regents, for wrongful termination.
She was awarded a $13 million verdict in 2018. However, the California Court of Appeals overturned it in 2020 after concluding that several mistakes during the court proceedings impeded the school’s right to a fair and impartial trial. The case was retried, culminating in the even higher award of $14 million issued on May 9.
“Two juries have come to virtually identical findings showing multiple problems at UCLA involving gender discrimination,” Dr. Pinter-Brown’s attorney, Carney R. Shegerian, JD, told this news organization.
A spokesperson from UCLA’s David Geffen School of Medicine said administrators are carefully reviewing the new decision.
The spokesperson told this news organization that the medical school and its health system remain “deeply committed to maintaining a workplace free from discrimination, intimidation, retaliation, or harassment of any kind” and fostering a “respectful and inclusive environment ... in research, medical education, and patient care.”
Gender Pay Disparities Persist in Medicine
The gender pay gap in medicine is well documented. The 2024 Medscape Physician Compensation Report found that male doctors earn about 29% more than their female counterparts, with the disparity growing larger among specialists. In addition, a recent JAMA Health Forum study found that male physicians earned 21%-24% more per hour than female physicians.
Dr. Pinter-Brown, who now works at the University of California, Irvine, alleged that she was paid $200,000 less annually, on average, than her male colleagues.
That’s not surprising, says Martha Gulati, MD, professor and director of preventive cardiology at Cedars-Sinai Smidt Heart Institute, Los Angeles. She coauthored a commentary about gender disparities in JAMA Network Open. Dr. Gulati told this news organization that even a “small” pay disparity of $100,000 annually adds up.
“Let’s say the [male physician] invests it at 3% and adds to it yearly. Even without a raise, in 20 years, that is approximately $3 million,” Dr. Gulati explained. “Once you find out you are paid less than your male colleagues, you are upset. Your sense of value and self-worth disappears.”
Eileen Barrett, MD, MPH, president-elect of the American Medical Women’s Association, said that gender discrimination is likely more prevalent than research indicates. She told this news organization that self-doubt and fear of retaliation keep many from exposing the mistreatment.
Although more women are entering medicine, too few rise to the highest positions, Dr. Barrett said.
“Unfortunately, many are pulled and pushed into specialties and subspecialties that have lower compensation and are not promoted to leadership, so just having numbers isn’t enough to achieve equity,” Dr. Barrett said.
Dr. Pinter-Brown claimed she was repeatedly harassed and intimidated by Dr. de Vos from 2008 to 2015. Despite voicing concerns multiple times about the discriminatory behavior, the only resolutions offered by the male-dominated program leadership were for her to separate from the group and conduct lymphoma research independently or to avoid interacting with Dr. de Vos, court records said.
Even the school’s male Title IX officer, Jan Tillisch, MD, who handled gender-based discrimination complaints, reportedly made sexist comments. When Dr. Pinter-Brown sought his help, he allegedly told her that she had a reputation as an “angry woman” and “diva,” court records showed.
According to court documents, Dr. Pinter-Brown endured nitpicking and research audits as retaliation for speaking out, temporarily suspending her research privileges. She said she was subsequently removed from the director position and replaced by Dr. de Vos.
Female physicians who report discriminatory behavior often have unfavorable outcomes and risk future career prospects, Dr. Gulati said.
To shift this dynamic, she said institutions must increase transparency and practices that support female doctors receiving “equal pay for equal work.”
A version of this article appeared on Medscape.com.
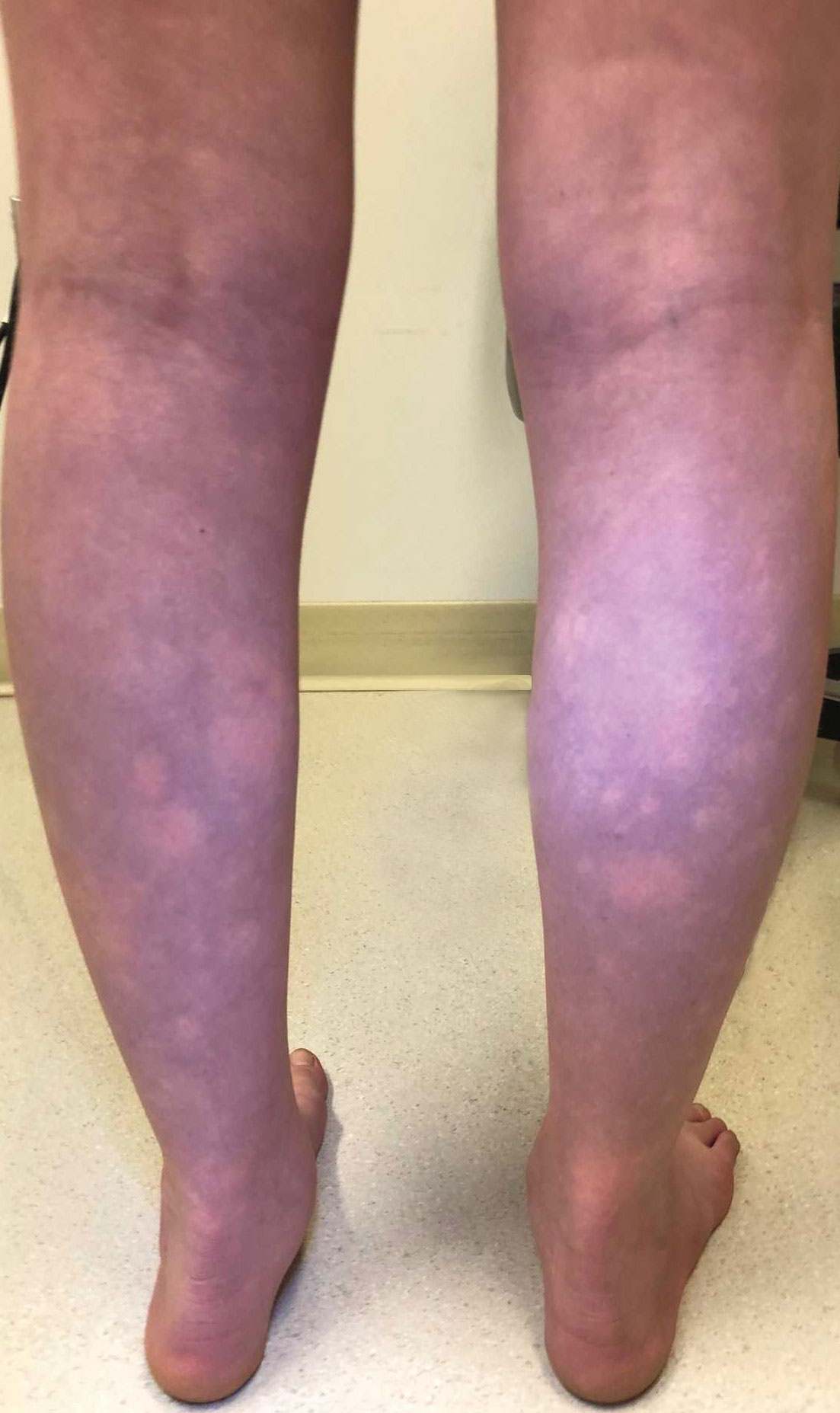
Transient Symmetric Blanching Macules on a Background of Reticulate Erythema
The Diagnosis: BASCULE Syndrome
The patient had previously been thought to have livedo reticularis by primary care. Repeat antinuclear antibody (ANA) testing was positive (1:1280 homogeneous [reflexive titers all negative]). However, upon dermatologic evaluation, the manifestation of the rash in addition to onset occurring with postural changes challenged the livedo reticularis diagnosis. Extensive research and consultation with dermatologic colleagues led to the diagnosis of the rare entity BASCULE syndrome. BASCULE (Bier anemic spots, cyanosis, and urticarialike eruption) syndrome was described by Bessis et al1 in 2016. It is a rare condition but may be underreported.2 It is a benign pediatric disorder in the vascular acrosyndrome family that is characterized by underlying vasomotor dysfunction in distal regions of the body. Raynaud phenomenon is a widely known member of this family. As seen in our patient, it typically presents on the distal legs and feet with numerous irregular hypopigmented macules on a cyanotic background. Red-orange papules may appear on the hypopigmented macules and often are pruritic. Lesions on the distal upper extremities are less common, and a case involving the trunk has been reported.3 Onset generally begins within a couple of minutes of standing or mechanical compression of the lower legs, with full reversal of symptoms occurring within minutes of laying down or walking. Commonly reported associated symptoms include tenderness, pruritus, edema, and pain; however, the cutaneous lesions may be asymptomatic. The condition tends to affect adolescents, as seen in our patient; however, there have been reports in infants as young as 3 months to adults aged 19 years.2
The pathophysiology behind BASCULE syndrome remains unclear but is believed to be centered around the role of physiologic venous stasis that occurs when standing. The hypoxia secondary to stasis is thought to induce amplified vasoconstriction of arterioles. These responses are further exaggerated due to absence of venoarteriolar reflexes in dermal ascending arterioles, leading to Bier spots.2 The role of mast cells and eosinophils remains unclear. It is a clinical diagnosis without clear histologic findings; therefore, biopsy was not pursued in our patient.
Although BASCULE syndrome is a benign entity, it is imperative that it be recognized to avoid a time consuming, expensive, and anxiety-producing diagnostic workup, as occurred in our patient. Although not a manifestation of systemic disease, BASCULE syndrome may be associated with orthostatic hypotension in up to 20% of cases.2,4 Therefore, these patients should undergo orthostatic testing, including the tilt table test. In our patient, these manifestations were not appreciated.
There are no current guidelines for effective treatment of BASCULE syndrome. Given the possible role of mast cells in the condition, H1 antihistamines are proposed as first-line treatment. Desloratadine (10 mg/d for 7 days) has been found to be associated with improvement of pruritus. However, a recent literature review found little evidence to support the use of H1 antihistamines for resolution of other symptoms.2
The differential diagnosis includes livedo reticularis, Bier spots, Sneddon syndrome, and urticarial vasculitis. Livedo reticularis presents as distinct, netlike, blue-erythematousviolaceous discoloration, which differs from the distinct orange-red macules in BASCULE syndrome.5 In addition to distinct variances in dermatologic presentation, livedo reticularis typically is associated with cold exposure as a causative agent, with cold avoidance as the treatment for this benign and often transient condition.6 This phenomenon was not appreciated in our patient. Livedo reticularis commonly occurs with antiphospholipid syndrome.5 This association in combination with our patient's positive ANA findings and her mother's history of miscarriages resulted in the misdiagnosis as livedo reticularis.
Bier spots manifest as white macules with surrounding erythema and typically present in young adults. When first described in the literature, it was debated if BASCULE syndrome was simply another manifestation of Bier spots or postural orthostatic intolerance,4 as there was a large consensus that postural orthostatic intolerance was associated with BASCULE syndrome, with the majority of patients not meeting criteria for the condition. Heymann4 addressed the differences in BASCULE manifestations vs typical Bier spots. The author extended the syndrome to include cyanosis, an urticarialike eruption of red-orange macules with central papules located centrally, pruritus, tenderness, and partial or diffuse edema, in addition to Bier spots.4
Sneddon syndrome is a rare progressive disorder that affects small- to medium-sized blood vessels resulting in multiple episodes of ischemia in the brain. Skin manifestations of these repeated strokes are similar to livedo reticularis, typically manifesting as livedo racemosa—irregular reticular patterns of skin mottling with reddish-blue hues.6 However, Sneddon syndrome is more generalized and widespread and differs from BASCULE syndrome in shape and histologic findings. Our patient presented with findings on the legs, which is more characteristic of livedo reticularis vs livedo racemosa. Our patient experienced resolution upon laying down and sitting, and Sneddon syndrome persists beyond postural changes. Furthermore, patients with Sneddon syndrome present with neurologic symptoms such as prodromal headaches.6
Urticarial vasculitis was ruled out in our patient because of the duration of symptoms as well as the spatial changes. Urticarial vasculitis is a rare skin condition characterized by chronic recurring urticarial lesions that may persist for more than a day. This condition typically presents in middle-aged women and rarely in children. Urticarial vasculitis is thought to be immune-complex mediated, but its cause is largely unknown. It is a common manifestation of underlying conditions such as systemic lupus erythematosus.6 Our patient had a positive ANA and possible autoimmune history from her mother; however, urticarial vasculitis does not present transiently on the legs or in the rash pattern appreciated in our patient.
- Bessis D, Jeziorski E, Rigau V, et al. Bier anaemic spots, cyanosis with urticaria-like eruption (BASCULE) syndrome: a new entity? Br J Dermatol. 2016;175:218-220. doi:10.1111/bjd.14589
- Baurens N, Briand C, Giovannini-Chami L, et al. Case report, practices survey and literature review of an under-recognized pediatric vascular disorder: the BASCULE syndrome. Front Pediatr. 2022;10:849914. doi:10.3389/fped.2022.849914
- Jiménez-Gallo D, Collantes-Rodríguez C, Ossorio-García L, et al. Bier anaemic spots, cyanosis with urticaria-like eruption (BASCULE) syndrome on trunk and upper limbs. Pediatr Dermatol. 2018;35:E313-E315. doi:10.1111/pde.13558
- Heymann WR. BASCULE syndrome: is something brewing with Bier spots? Dermatology World Insights and Inquiries. September 7, 2022. https://www.aad.org/dw/dw-insights-and-inquiries/archive/2022/bascule-syndrome
- Sajjan VV, Lunge S, Swamy MB, et al. Livedo reticularis: a review of the literature. Indian Dermatol Online J. 2015;6:315-321. doi:10.4103/2229-5178.164493
- Gu SL, Jorizzo JL. Urticarial vasculitis. Int J Womens Dermatol. 2021;7:290-297. doi:10.1016/j.ijwd.2021.01.021
The Diagnosis: BASCULE Syndrome
The patient had previously been thought to have livedo reticularis by primary care. Repeat antinuclear antibody (ANA) testing was positive (1:1280 homogeneous [reflexive titers all negative]). However, upon dermatologic evaluation, the manifestation of the rash in addition to onset occurring with postural changes challenged the livedo reticularis diagnosis. Extensive research and consultation with dermatologic colleagues led to the diagnosis of the rare entity BASCULE syndrome. BASCULE (Bier anemic spots, cyanosis, and urticarialike eruption) syndrome was described by Bessis et al1 in 2016. It is a rare condition but may be underreported.2 It is a benign pediatric disorder in the vascular acrosyndrome family that is characterized by underlying vasomotor dysfunction in distal regions of the body. Raynaud phenomenon is a widely known member of this family. As seen in our patient, it typically presents on the distal legs and feet with numerous irregular hypopigmented macules on a cyanotic background. Red-orange papules may appear on the hypopigmented macules and often are pruritic. Lesions on the distal upper extremities are less common, and a case involving the trunk has been reported.3 Onset generally begins within a couple of minutes of standing or mechanical compression of the lower legs, with full reversal of symptoms occurring within minutes of laying down or walking. Commonly reported associated symptoms include tenderness, pruritus, edema, and pain; however, the cutaneous lesions may be asymptomatic. The condition tends to affect adolescents, as seen in our patient; however, there have been reports in infants as young as 3 months to adults aged 19 years.2
The pathophysiology behind BASCULE syndrome remains unclear but is believed to be centered around the role of physiologic venous stasis that occurs when standing. The hypoxia secondary to stasis is thought to induce amplified vasoconstriction of arterioles. These responses are further exaggerated due to absence of venoarteriolar reflexes in dermal ascending arterioles, leading to Bier spots.2 The role of mast cells and eosinophils remains unclear. It is a clinical diagnosis without clear histologic findings; therefore, biopsy was not pursued in our patient.
Although BASCULE syndrome is a benign entity, it is imperative that it be recognized to avoid a time consuming, expensive, and anxiety-producing diagnostic workup, as occurred in our patient. Although not a manifestation of systemic disease, BASCULE syndrome may be associated with orthostatic hypotension in up to 20% of cases.2,4 Therefore, these patients should undergo orthostatic testing, including the tilt table test. In our patient, these manifestations were not appreciated.
There are no current guidelines for effective treatment of BASCULE syndrome. Given the possible role of mast cells in the condition, H1 antihistamines are proposed as first-line treatment. Desloratadine (10 mg/d for 7 days) has been found to be associated with improvement of pruritus. However, a recent literature review found little evidence to support the use of H1 antihistamines for resolution of other symptoms.2
The differential diagnosis includes livedo reticularis, Bier spots, Sneddon syndrome, and urticarial vasculitis. Livedo reticularis presents as distinct, netlike, blue-erythematousviolaceous discoloration, which differs from the distinct orange-red macules in BASCULE syndrome.5 In addition to distinct variances in dermatologic presentation, livedo reticularis typically is associated with cold exposure as a causative agent, with cold avoidance as the treatment for this benign and often transient condition.6 This phenomenon was not appreciated in our patient. Livedo reticularis commonly occurs with antiphospholipid syndrome.5 This association in combination with our patient's positive ANA findings and her mother's history of miscarriages resulted in the misdiagnosis as livedo reticularis.
Bier spots manifest as white macules with surrounding erythema and typically present in young adults. When first described in the literature, it was debated if BASCULE syndrome was simply another manifestation of Bier spots or postural orthostatic intolerance,4 as there was a large consensus that postural orthostatic intolerance was associated with BASCULE syndrome, with the majority of patients not meeting criteria for the condition. Heymann4 addressed the differences in BASCULE manifestations vs typical Bier spots. The author extended the syndrome to include cyanosis, an urticarialike eruption of red-orange macules with central papules located centrally, pruritus, tenderness, and partial or diffuse edema, in addition to Bier spots.4
Sneddon syndrome is a rare progressive disorder that affects small- to medium-sized blood vessels resulting in multiple episodes of ischemia in the brain. Skin manifestations of these repeated strokes are similar to livedo reticularis, typically manifesting as livedo racemosa—irregular reticular patterns of skin mottling with reddish-blue hues.6 However, Sneddon syndrome is more generalized and widespread and differs from BASCULE syndrome in shape and histologic findings. Our patient presented with findings on the legs, which is more characteristic of livedo reticularis vs livedo racemosa. Our patient experienced resolution upon laying down and sitting, and Sneddon syndrome persists beyond postural changes. Furthermore, patients with Sneddon syndrome present with neurologic symptoms such as prodromal headaches.6
Urticarial vasculitis was ruled out in our patient because of the duration of symptoms as well as the spatial changes. Urticarial vasculitis is a rare skin condition characterized by chronic recurring urticarial lesions that may persist for more than a day. This condition typically presents in middle-aged women and rarely in children. Urticarial vasculitis is thought to be immune-complex mediated, but its cause is largely unknown. It is a common manifestation of underlying conditions such as systemic lupus erythematosus.6 Our patient had a positive ANA and possible autoimmune history from her mother; however, urticarial vasculitis does not present transiently on the legs or in the rash pattern appreciated in our patient.
The Diagnosis: BASCULE Syndrome
The patient had previously been thought to have livedo reticularis by primary care. Repeat antinuclear antibody (ANA) testing was positive (1:1280 homogeneous [reflexive titers all negative]). However, upon dermatologic evaluation, the manifestation of the rash in addition to onset occurring with postural changes challenged the livedo reticularis diagnosis. Extensive research and consultation with dermatologic colleagues led to the diagnosis of the rare entity BASCULE syndrome. BASCULE (Bier anemic spots, cyanosis, and urticarialike eruption) syndrome was described by Bessis et al1 in 2016. It is a rare condition but may be underreported.2 It is a benign pediatric disorder in the vascular acrosyndrome family that is characterized by underlying vasomotor dysfunction in distal regions of the body. Raynaud phenomenon is a widely known member of this family. As seen in our patient, it typically presents on the distal legs and feet with numerous irregular hypopigmented macules on a cyanotic background. Red-orange papules may appear on the hypopigmented macules and often are pruritic. Lesions on the distal upper extremities are less common, and a case involving the trunk has been reported.3 Onset generally begins within a couple of minutes of standing or mechanical compression of the lower legs, with full reversal of symptoms occurring within minutes of laying down or walking. Commonly reported associated symptoms include tenderness, pruritus, edema, and pain; however, the cutaneous lesions may be asymptomatic. The condition tends to affect adolescents, as seen in our patient; however, there have been reports in infants as young as 3 months to adults aged 19 years.2
The pathophysiology behind BASCULE syndrome remains unclear but is believed to be centered around the role of physiologic venous stasis that occurs when standing. The hypoxia secondary to stasis is thought to induce amplified vasoconstriction of arterioles. These responses are further exaggerated due to absence of venoarteriolar reflexes in dermal ascending arterioles, leading to Bier spots.2 The role of mast cells and eosinophils remains unclear. It is a clinical diagnosis without clear histologic findings; therefore, biopsy was not pursued in our patient.
Although BASCULE syndrome is a benign entity, it is imperative that it be recognized to avoid a time consuming, expensive, and anxiety-producing diagnostic workup, as occurred in our patient. Although not a manifestation of systemic disease, BASCULE syndrome may be associated with orthostatic hypotension in up to 20% of cases.2,4 Therefore, these patients should undergo orthostatic testing, including the tilt table test. In our patient, these manifestations were not appreciated.
There are no current guidelines for effective treatment of BASCULE syndrome. Given the possible role of mast cells in the condition, H1 antihistamines are proposed as first-line treatment. Desloratadine (10 mg/d for 7 days) has been found to be associated with improvement of pruritus. However, a recent literature review found little evidence to support the use of H1 antihistamines for resolution of other symptoms.2
The differential diagnosis includes livedo reticularis, Bier spots, Sneddon syndrome, and urticarial vasculitis. Livedo reticularis presents as distinct, netlike, blue-erythematousviolaceous discoloration, which differs from the distinct orange-red macules in BASCULE syndrome.5 In addition to distinct variances in dermatologic presentation, livedo reticularis typically is associated with cold exposure as a causative agent, with cold avoidance as the treatment for this benign and often transient condition.6 This phenomenon was not appreciated in our patient. Livedo reticularis commonly occurs with antiphospholipid syndrome.5 This association in combination with our patient's positive ANA findings and her mother's history of miscarriages resulted in the misdiagnosis as livedo reticularis.
Bier spots manifest as white macules with surrounding erythema and typically present in young adults. When first described in the literature, it was debated if BASCULE syndrome was simply another manifestation of Bier spots or postural orthostatic intolerance,4 as there was a large consensus that postural orthostatic intolerance was associated with BASCULE syndrome, with the majority of patients not meeting criteria for the condition. Heymann4 addressed the differences in BASCULE manifestations vs typical Bier spots. The author extended the syndrome to include cyanosis, an urticarialike eruption of red-orange macules with central papules located centrally, pruritus, tenderness, and partial or diffuse edema, in addition to Bier spots.4
Sneddon syndrome is a rare progressive disorder that affects small- to medium-sized blood vessels resulting in multiple episodes of ischemia in the brain. Skin manifestations of these repeated strokes are similar to livedo reticularis, typically manifesting as livedo racemosa—irregular reticular patterns of skin mottling with reddish-blue hues.6 However, Sneddon syndrome is more generalized and widespread and differs from BASCULE syndrome in shape and histologic findings. Our patient presented with findings on the legs, which is more characteristic of livedo reticularis vs livedo racemosa. Our patient experienced resolution upon laying down and sitting, and Sneddon syndrome persists beyond postural changes. Furthermore, patients with Sneddon syndrome present with neurologic symptoms such as prodromal headaches.6
Urticarial vasculitis was ruled out in our patient because of the duration of symptoms as well as the spatial changes. Urticarial vasculitis is a rare skin condition characterized by chronic recurring urticarial lesions that may persist for more than a day. This condition typically presents in middle-aged women and rarely in children. Urticarial vasculitis is thought to be immune-complex mediated, but its cause is largely unknown. It is a common manifestation of underlying conditions such as systemic lupus erythematosus.6 Our patient had a positive ANA and possible autoimmune history from her mother; however, urticarial vasculitis does not present transiently on the legs or in the rash pattern appreciated in our patient.
- Bessis D, Jeziorski E, Rigau V, et al. Bier anaemic spots, cyanosis with urticaria-like eruption (BASCULE) syndrome: a new entity? Br J Dermatol. 2016;175:218-220. doi:10.1111/bjd.14589
- Baurens N, Briand C, Giovannini-Chami L, et al. Case report, practices survey and literature review of an under-recognized pediatric vascular disorder: the BASCULE syndrome. Front Pediatr. 2022;10:849914. doi:10.3389/fped.2022.849914
- Jiménez-Gallo D, Collantes-Rodríguez C, Ossorio-García L, et al. Bier anaemic spots, cyanosis with urticaria-like eruption (BASCULE) syndrome on trunk and upper limbs. Pediatr Dermatol. 2018;35:E313-E315. doi:10.1111/pde.13558
- Heymann WR. BASCULE syndrome: is something brewing with Bier spots? Dermatology World Insights and Inquiries. September 7, 2022. https://www.aad.org/dw/dw-insights-and-inquiries/archive/2022/bascule-syndrome
- Sajjan VV, Lunge S, Swamy MB, et al. Livedo reticularis: a review of the literature. Indian Dermatol Online J. 2015;6:315-321. doi:10.4103/2229-5178.164493
- Gu SL, Jorizzo JL. Urticarial vasculitis. Int J Womens Dermatol. 2021;7:290-297. doi:10.1016/j.ijwd.2021.01.021
- Bessis D, Jeziorski E, Rigau V, et al. Bier anaemic spots, cyanosis with urticaria-like eruption (BASCULE) syndrome: a new entity? Br J Dermatol. 2016;175:218-220. doi:10.1111/bjd.14589
- Baurens N, Briand C, Giovannini-Chami L, et al. Case report, practices survey and literature review of an under-recognized pediatric vascular disorder: the BASCULE syndrome. Front Pediatr. 2022;10:849914. doi:10.3389/fped.2022.849914
- Jiménez-Gallo D, Collantes-Rodríguez C, Ossorio-García L, et al. Bier anaemic spots, cyanosis with urticaria-like eruption (BASCULE) syndrome on trunk and upper limbs. Pediatr Dermatol. 2018;35:E313-E315. doi:10.1111/pde.13558
- Heymann WR. BASCULE syndrome: is something brewing with Bier spots? Dermatology World Insights and Inquiries. September 7, 2022. https://www.aad.org/dw/dw-insights-and-inquiries/archive/2022/bascule-syndrome
- Sajjan VV, Lunge S, Swamy MB, et al. Livedo reticularis: a review of the literature. Indian Dermatol Online J. 2015;6:315-321. doi:10.4103/2229-5178.164493
- Gu SL, Jorizzo JL. Urticarial vasculitis. Int J Womens Dermatol. 2021;7:290-297. doi:10.1016/j.ijwd.2021.01.021
An 11-year-old girl was referred to the dermatology clinic for evaluation of a rash on the legs and feet of 1 year’s duration. The rash appeared every time she was standing for longer than 10 to 15 minutes and resolved when sitting or laying down. After the initial onset, the rash did not spread to other body areas but became more prominent in appearance. The patient endorsed intense pruritus associated with the rash. A review of systems was negative for fever, headaches, history of blood clots, and joint pain. She did not have any known medical conditions or take any medications. The patient’s mother reported that the patient experienced episodes of leg numbness while sitting in vehicles from 6 to 10 years of age. There was no family history of rheumatologic, hematologic, or cardiac conditions. The patient’s mother had experienced 2 miscarriages but denied any other obstetric complications. The patient had 1 sibling who was unaffected. Physical examination revealed reticulate erythema on the calves with scattered regions of blanching and evanescent pink macules as well as dermatographism.
One month prior to presenting to dermatology, the patient was evaluated by rheumatology, endocrinology, and hematology. Laboratory workup completed at age 3 years included antinuclear antibody, anticardiolipin antibody, and antithrombin III activity; factor V Leiden; cryoglobulins; quantitation (human chorionic gonadotropin); proteins S and C activity; antineutrophil cytoplasmic antibody screen; thyroid studies; prothrombin time; and partial thromboplastin time. All laboratory results were within reference range.

Does Eating Food With Emulsifiers Increase T2D Risk?
TOPLINE:
Various food additive emulsifiers, including total carrageenans, carrageenan gum, tripotassium phosphate, sodium citrate, and guar gum, can increase the risk for type 2 diabetes (T2D), showed a recent study.
METHODOLOGY:
- Food emulsifiers, which are extensively used to enhance the texture and improve the shelf life of various ultraprocessed food items, have been shown to increase the risk for cardiovascular disease and cancer.
- In this study, the dietary intake data of 104,139 adults (79.2% women; mean age, 42.7 years) enrolled in the French NutriNet-Santé prospective cohort study from May 2009 to April 2023 were assessed for 24 hours on 3 nonconsecutive days at inclusion and every 6 months thereafter to determine the risk for T2D.
- The dietary records of participants, which were linked to food composition databases, were used to quantify the food additive intake.
- T2D cases were identified using a multisource approach encompassing self-reports, health questionnaires, national health insurance system databases, and/or mortality registries.
TAKEAWAY:
- During a mean follow-up period of 6.8 years, 1056 incident cases of T2D were reported.
- Almost all (99.7%) participants were exposed to at least one food additive emulsifier, with the main contributors being ultraprocessed fruits and vegetables (18.5%), cakes and biscuits (14.7%), and dairy products (10.0%).
- The intake of the following emulsifiers increased the risk for T2D:
- Total carrageenans and carrageenan gum (3% increased risk per increment of 100 mg/d; P < .001)
- Tripotassium phosphate (15% increased risk per increment of 500 mg/d; P = .023)
- Acetyl tartaric acid esters of monoglycerides and diglycerides of fatty acids (4% increased risk per increment of 100 mg/d; P = .042)
- Sodium citrate (4% increased risk per increment of 500 mg/d; P = .008)
- Guar gum (11% increased risk per increment of 500 mg/d; P < .0001)
- Gum arabic (3% increased risk per increment of 1000 mg/d; P = .013)
- Xanthan gum (8% increased risk per increment of 500 mg/d; P = .013)
IN PRACTICE:
In an accompanying commentary, experts postulated that “findings from this and other studies could prompt regulatory agencies and policymakers to reconsider the rules governing the use of emulsifiers and other additives by the food industry such as setting limits and requiring better disclosure of food additive contents to help consumers make more informed choices.”
SOURCE:
Clara Salame, PhD, Université Sorbonne Paris Nord and Université Paris Cité, INSERM, INRAE, CNAM, Center of Research in Epidemiology and Statistics, Nutritional Epidemiology Research Team, Paris, France, led this study, which was published online in The Lancet Diabetes & Endocrinology.
LIMITATIONS:
The observational nature of this study is not sufficient to establish causality relationships. There may have been measurement errors in emulsifier exposure, particularly in products exempted from labeling requirements. This cohort’s demographics, which included a higher percentage of women and a health-conscious population, may affect the generalizability of the study’s findings.
DISCLOSURES:
This study received funding from the European Research Council, and the NutriNet-Santé study was supported by many public institutions such as the Ministère de la Santé, Santé publique France, Université Sorbonne Paris Nord, and others. The authors declared no conflicts of interest.
A version of this article appeared on Medscape.com.
TOPLINE:
Various food additive emulsifiers, including total carrageenans, carrageenan gum, tripotassium phosphate, sodium citrate, and guar gum, can increase the risk for type 2 diabetes (T2D), showed a recent study.
METHODOLOGY:
- Food emulsifiers, which are extensively used to enhance the texture and improve the shelf life of various ultraprocessed food items, have been shown to increase the risk for cardiovascular disease and cancer.
- In this study, the dietary intake data of 104,139 adults (79.2% women; mean age, 42.7 years) enrolled in the French NutriNet-Santé prospective cohort study from May 2009 to April 2023 were assessed for 24 hours on 3 nonconsecutive days at inclusion and every 6 months thereafter to determine the risk for T2D.
- The dietary records of participants, which were linked to food composition databases, were used to quantify the food additive intake.
- T2D cases were identified using a multisource approach encompassing self-reports, health questionnaires, national health insurance system databases, and/or mortality registries.
TAKEAWAY:
- During a mean follow-up period of 6.8 years, 1056 incident cases of T2D were reported.
- Almost all (99.7%) participants were exposed to at least one food additive emulsifier, with the main contributors being ultraprocessed fruits and vegetables (18.5%), cakes and biscuits (14.7%), and dairy products (10.0%).
- The intake of the following emulsifiers increased the risk for T2D:
- Total carrageenans and carrageenan gum (3% increased risk per increment of 100 mg/d; P < .001)
- Tripotassium phosphate (15% increased risk per increment of 500 mg/d; P = .023)
- Acetyl tartaric acid esters of monoglycerides and diglycerides of fatty acids (4% increased risk per increment of 100 mg/d; P = .042)
- Sodium citrate (4% increased risk per increment of 500 mg/d; P = .008)
- Guar gum (11% increased risk per increment of 500 mg/d; P < .0001)
- Gum arabic (3% increased risk per increment of 1000 mg/d; P = .013)
- Xanthan gum (8% increased risk per increment of 500 mg/d; P = .013)
IN PRACTICE:
In an accompanying commentary, experts postulated that “findings from this and other studies could prompt regulatory agencies and policymakers to reconsider the rules governing the use of emulsifiers and other additives by the food industry such as setting limits and requiring better disclosure of food additive contents to help consumers make more informed choices.”
SOURCE:
Clara Salame, PhD, Université Sorbonne Paris Nord and Université Paris Cité, INSERM, INRAE, CNAM, Center of Research in Epidemiology and Statistics, Nutritional Epidemiology Research Team, Paris, France, led this study, which was published online in The Lancet Diabetes & Endocrinology.
LIMITATIONS:
The observational nature of this study is not sufficient to establish causality relationships. There may have been measurement errors in emulsifier exposure, particularly in products exempted from labeling requirements. This cohort’s demographics, which included a higher percentage of women and a health-conscious population, may affect the generalizability of the study’s findings.
DISCLOSURES:
This study received funding from the European Research Council, and the NutriNet-Santé study was supported by many public institutions such as the Ministère de la Santé, Santé publique France, Université Sorbonne Paris Nord, and others. The authors declared no conflicts of interest.
A version of this article appeared on Medscape.com.
TOPLINE:
Various food additive emulsifiers, including total carrageenans, carrageenan gum, tripotassium phosphate, sodium citrate, and guar gum, can increase the risk for type 2 diabetes (T2D), showed a recent study.
METHODOLOGY:
- Food emulsifiers, which are extensively used to enhance the texture and improve the shelf life of various ultraprocessed food items, have been shown to increase the risk for cardiovascular disease and cancer.
- In this study, the dietary intake data of 104,139 adults (79.2% women; mean age, 42.7 years) enrolled in the French NutriNet-Santé prospective cohort study from May 2009 to April 2023 were assessed for 24 hours on 3 nonconsecutive days at inclusion and every 6 months thereafter to determine the risk for T2D.
- The dietary records of participants, which were linked to food composition databases, were used to quantify the food additive intake.
- T2D cases were identified using a multisource approach encompassing self-reports, health questionnaires, national health insurance system databases, and/or mortality registries.
TAKEAWAY:
- During a mean follow-up period of 6.8 years, 1056 incident cases of T2D were reported.
- Almost all (99.7%) participants were exposed to at least one food additive emulsifier, with the main contributors being ultraprocessed fruits and vegetables (18.5%), cakes and biscuits (14.7%), and dairy products (10.0%).
- The intake of the following emulsifiers increased the risk for T2D:
- Total carrageenans and carrageenan gum (3% increased risk per increment of 100 mg/d; P < .001)
- Tripotassium phosphate (15% increased risk per increment of 500 mg/d; P = .023)
- Acetyl tartaric acid esters of monoglycerides and diglycerides of fatty acids (4% increased risk per increment of 100 mg/d; P = .042)
- Sodium citrate (4% increased risk per increment of 500 mg/d; P = .008)
- Guar gum (11% increased risk per increment of 500 mg/d; P < .0001)
- Gum arabic (3% increased risk per increment of 1000 mg/d; P = .013)
- Xanthan gum (8% increased risk per increment of 500 mg/d; P = .013)
IN PRACTICE:
In an accompanying commentary, experts postulated that “findings from this and other studies could prompt regulatory agencies and policymakers to reconsider the rules governing the use of emulsifiers and other additives by the food industry such as setting limits and requiring better disclosure of food additive contents to help consumers make more informed choices.”
SOURCE:
Clara Salame, PhD, Université Sorbonne Paris Nord and Université Paris Cité, INSERM, INRAE, CNAM, Center of Research in Epidemiology and Statistics, Nutritional Epidemiology Research Team, Paris, France, led this study, which was published online in The Lancet Diabetes & Endocrinology.
LIMITATIONS:
The observational nature of this study is not sufficient to establish causality relationships. There may have been measurement errors in emulsifier exposure, particularly in products exempted from labeling requirements. This cohort’s demographics, which included a higher percentage of women and a health-conscious population, may affect the generalizability of the study’s findings.
DISCLOSURES:
This study received funding from the European Research Council, and the NutriNet-Santé study was supported by many public institutions such as the Ministère de la Santé, Santé publique France, Université Sorbonne Paris Nord, and others. The authors declared no conflicts of interest.
A version of this article appeared on Medscape.com.
Novel ENV-101 associated with improved lung function in IPF
SAN DIEGO —
Early efficacy data from a phase 2a safety trial suggest that the novel oral agent, dubbed ENV-101, is associated with improvements in forced vital capacity (FVC) and other measures of lung function, and may be a disease-modifying therapy for IPF, according to Toby M. Maher, MD, PhD, director of the interstitial lung disease program at Keck School of Medicine, University of Southern California, Los Angeles. Dr. Maher presented the results at the American Thoracic Society’s international conference.
“Historically we’ve not been seeing improvements in FVC, which is what we’ve been seeing [with ENV-101], and I think it’s conceivable that you can get remodeling of early areas of fibrosis in the lung,” Dr. Maher said in an interview with Chest Physician.
“We know from histology studies that if you look at IPF lungs you’ll see areas of end-stage fibrosis, but even in advanced disease you’ll see areas where the lung is relatively well preserved and there’s early fibrosis, so I think it’s conceivable that there is remodeling of some of those early areas of fibrosis,” he said.
Vital pathway
The Hedgehog pathway is highly conserved in evolution. The cell-signaling pathway is active embryogenesis, tissue proliferation, and organ development. There is also evidence to suggest that in adult the pathway becomes reactivated following tissue injury, as can occur in lung epithelia, Dr. Maher explained.
Although as the word “idiopathic” in IPF indicates the etiology of the disease is unknown, investigators have found that in IPF repetitive epithelial injury to lung tissue leads to activation of the Hedgehog pathway. Hedgehog signaling in turn induces formation and activation of myofibroblasts that lay down fibrotic matrix and contract lung tissue, leading to significant impairments in gas exchange, Dr. Maher said.
ENV-101 blocks Hedgehog from binding to the PTCH1 receptor, preventing release of the zinc-finger protein GLI1 from the kinase complex into the cell cytoplasm. With signaling blocked, myofibroblasts undergo apoptosis instead of initiating wound repair as they normally would, thereby eliminating an evident mechanism of IPF pathology, he explained.
Study details
In the phase 2a trial, investigators enrolled patients with IPF who were not taking antifibrotic agents and who had a percent predicted FVC greater than 50%, percent predicted diffusing capacity for carbon monoxide (DLCO) of at least 35%, and life expectancy of more than 1 year.
The patients were randomized to receive 200 mg oral ENV-101 daily (18 patients) or placebo (15 patients) for 12 weeks.
The primary endpoint of the trial was safety of the experimental agent. A previous phase 1b study of a different Hedgehog inhibitor — vismodegib (Erivedge), in combination with the antifibrotic agent pirfenidone (Pirespa) — in patients with IPF was discontinued because of poor tolerability.
In the current study, the most common treatment-related adverse events were dysgeusia in 57% of patients who received the drug, alopecia in 52%, and muscle spasms in 43%. The spasms were generally less severe than those seen in the vismodegib/pirfenidone trial mentioned above.
Seven patients (33%) had treatment-emergent events leading to dose interruption. Five patients discontinued treatment: one who withdrew because of taste alterations, one who was lost to follow-up after an IPF exacerbation, and three who withdrew consent.
There were no treatment-related deaths, and no clinically significant findings on labs, vital signs, electrocardiograms, or physical exam.
Efficacy endpoints
An analysis of the secondary efficacy endpoints showed a 1.9% mean improvement in FVC from baseline among patients assigned to ENV-101, compared with a mean decline of 1.3% of patients assigned to placebo (P = .035).
Patients on the active drug also had a 200-mL mean increase in total lung capacity, compared with a mean decline of 56 mL for patients on placebo (P = .005).
In addition, high-resolution CR studies showed a 9.4% absolute decrease from baseline in quantitative interstitial lung disease with ENV-101, vs. a 1.1% increase among controls, a 2% absolute decline from baseline in quantitative lung fibrosis compared with a 0.87% increase with placebo, and a 4.6% absolute decrease from baseline in quantitative ground glass, compared with an increase of 0.29% with placebo.
Bad taste a good sign?
Reinoud Gosens PhD, University of Groningen, the Netherlands, who co-moderated the session but was not involved in the study, questioned whether the dysgeusia seen in patients who received ENV-101 might be related to the dysgeusia seen in clinical trials of P2X3 receptor antagonists for cough.
“I was wondering if there would be a mechanistic overlap between Hedgehog inhibition and cough, which would be quite relevant for IPF,” he said in an interview.
The increase in FVC seen with ENV-101 and with the investigational agent buloxibutid, a novel angiotensin II type 2 receptor agonist described in a separate presentation by Dr. Maher, suggests that these drugs may have the ability to help remodel damaged lungs, Dr. Gosens said.
Investigators are currently planning a phase 2 dose-ranging trial (WHISTLE-PF) in patients with IPF or progressive pulmonary fibrosis.
The phase 2a trial was supported by Endeavor BioMedicines. Dr. Maher disclosed consultancy or speaker fees from Endeavor and others. Dr. Gosens had no relevant disclosures.
SAN DIEGO —
Early efficacy data from a phase 2a safety trial suggest that the novel oral agent, dubbed ENV-101, is associated with improvements in forced vital capacity (FVC) and other measures of lung function, and may be a disease-modifying therapy for IPF, according to Toby M. Maher, MD, PhD, director of the interstitial lung disease program at Keck School of Medicine, University of Southern California, Los Angeles. Dr. Maher presented the results at the American Thoracic Society’s international conference.
“Historically we’ve not been seeing improvements in FVC, which is what we’ve been seeing [with ENV-101], and I think it’s conceivable that you can get remodeling of early areas of fibrosis in the lung,” Dr. Maher said in an interview with Chest Physician.
“We know from histology studies that if you look at IPF lungs you’ll see areas of end-stage fibrosis, but even in advanced disease you’ll see areas where the lung is relatively well preserved and there’s early fibrosis, so I think it’s conceivable that there is remodeling of some of those early areas of fibrosis,” he said.
Vital pathway
The Hedgehog pathway is highly conserved in evolution. The cell-signaling pathway is active embryogenesis, tissue proliferation, and organ development. There is also evidence to suggest that in adult the pathway becomes reactivated following tissue injury, as can occur in lung epithelia, Dr. Maher explained.
Although as the word “idiopathic” in IPF indicates the etiology of the disease is unknown, investigators have found that in IPF repetitive epithelial injury to lung tissue leads to activation of the Hedgehog pathway. Hedgehog signaling in turn induces formation and activation of myofibroblasts that lay down fibrotic matrix and contract lung tissue, leading to significant impairments in gas exchange, Dr. Maher said.
ENV-101 blocks Hedgehog from binding to the PTCH1 receptor, preventing release of the zinc-finger protein GLI1 from the kinase complex into the cell cytoplasm. With signaling blocked, myofibroblasts undergo apoptosis instead of initiating wound repair as they normally would, thereby eliminating an evident mechanism of IPF pathology, he explained.
Study details
In the phase 2a trial, investigators enrolled patients with IPF who were not taking antifibrotic agents and who had a percent predicted FVC greater than 50%, percent predicted diffusing capacity for carbon monoxide (DLCO) of at least 35%, and life expectancy of more than 1 year.
The patients were randomized to receive 200 mg oral ENV-101 daily (18 patients) or placebo (15 patients) for 12 weeks.
The primary endpoint of the trial was safety of the experimental agent. A previous phase 1b study of a different Hedgehog inhibitor — vismodegib (Erivedge), in combination with the antifibrotic agent pirfenidone (Pirespa) — in patients with IPF was discontinued because of poor tolerability.
In the current study, the most common treatment-related adverse events were dysgeusia in 57% of patients who received the drug, alopecia in 52%, and muscle spasms in 43%. The spasms were generally less severe than those seen in the vismodegib/pirfenidone trial mentioned above.
Seven patients (33%) had treatment-emergent events leading to dose interruption. Five patients discontinued treatment: one who withdrew because of taste alterations, one who was lost to follow-up after an IPF exacerbation, and three who withdrew consent.
There were no treatment-related deaths, and no clinically significant findings on labs, vital signs, electrocardiograms, or physical exam.
Efficacy endpoints
An analysis of the secondary efficacy endpoints showed a 1.9% mean improvement in FVC from baseline among patients assigned to ENV-101, compared with a mean decline of 1.3% of patients assigned to placebo (P = .035).
Patients on the active drug also had a 200-mL mean increase in total lung capacity, compared with a mean decline of 56 mL for patients on placebo (P = .005).
In addition, high-resolution CR studies showed a 9.4% absolute decrease from baseline in quantitative interstitial lung disease with ENV-101, vs. a 1.1% increase among controls, a 2% absolute decline from baseline in quantitative lung fibrosis compared with a 0.87% increase with placebo, and a 4.6% absolute decrease from baseline in quantitative ground glass, compared with an increase of 0.29% with placebo.
Bad taste a good sign?
Reinoud Gosens PhD, University of Groningen, the Netherlands, who co-moderated the session but was not involved in the study, questioned whether the dysgeusia seen in patients who received ENV-101 might be related to the dysgeusia seen in clinical trials of P2X3 receptor antagonists for cough.
“I was wondering if there would be a mechanistic overlap between Hedgehog inhibition and cough, which would be quite relevant for IPF,” he said in an interview.
The increase in FVC seen with ENV-101 and with the investigational agent buloxibutid, a novel angiotensin II type 2 receptor agonist described in a separate presentation by Dr. Maher, suggests that these drugs may have the ability to help remodel damaged lungs, Dr. Gosens said.
Investigators are currently planning a phase 2 dose-ranging trial (WHISTLE-PF) in patients with IPF or progressive pulmonary fibrosis.
The phase 2a trial was supported by Endeavor BioMedicines. Dr. Maher disclosed consultancy or speaker fees from Endeavor and others. Dr. Gosens had no relevant disclosures.
SAN DIEGO —
Early efficacy data from a phase 2a safety trial suggest that the novel oral agent, dubbed ENV-101, is associated with improvements in forced vital capacity (FVC) and other measures of lung function, and may be a disease-modifying therapy for IPF, according to Toby M. Maher, MD, PhD, director of the interstitial lung disease program at Keck School of Medicine, University of Southern California, Los Angeles. Dr. Maher presented the results at the American Thoracic Society’s international conference.
“Historically we’ve not been seeing improvements in FVC, which is what we’ve been seeing [with ENV-101], and I think it’s conceivable that you can get remodeling of early areas of fibrosis in the lung,” Dr. Maher said in an interview with Chest Physician.
“We know from histology studies that if you look at IPF lungs you’ll see areas of end-stage fibrosis, but even in advanced disease you’ll see areas where the lung is relatively well preserved and there’s early fibrosis, so I think it’s conceivable that there is remodeling of some of those early areas of fibrosis,” he said.
Vital pathway
The Hedgehog pathway is highly conserved in evolution. The cell-signaling pathway is active embryogenesis, tissue proliferation, and organ development. There is also evidence to suggest that in adult the pathway becomes reactivated following tissue injury, as can occur in lung epithelia, Dr. Maher explained.
Although as the word “idiopathic” in IPF indicates the etiology of the disease is unknown, investigators have found that in IPF repetitive epithelial injury to lung tissue leads to activation of the Hedgehog pathway. Hedgehog signaling in turn induces formation and activation of myofibroblasts that lay down fibrotic matrix and contract lung tissue, leading to significant impairments in gas exchange, Dr. Maher said.
ENV-101 blocks Hedgehog from binding to the PTCH1 receptor, preventing release of the zinc-finger protein GLI1 from the kinase complex into the cell cytoplasm. With signaling blocked, myofibroblasts undergo apoptosis instead of initiating wound repair as they normally would, thereby eliminating an evident mechanism of IPF pathology, he explained.
Study details
In the phase 2a trial, investigators enrolled patients with IPF who were not taking antifibrotic agents and who had a percent predicted FVC greater than 50%, percent predicted diffusing capacity for carbon monoxide (DLCO) of at least 35%, and life expectancy of more than 1 year.
The patients were randomized to receive 200 mg oral ENV-101 daily (18 patients) or placebo (15 patients) for 12 weeks.
The primary endpoint of the trial was safety of the experimental agent. A previous phase 1b study of a different Hedgehog inhibitor — vismodegib (Erivedge), in combination with the antifibrotic agent pirfenidone (Pirespa) — in patients with IPF was discontinued because of poor tolerability.
In the current study, the most common treatment-related adverse events were dysgeusia in 57% of patients who received the drug, alopecia in 52%, and muscle spasms in 43%. The spasms were generally less severe than those seen in the vismodegib/pirfenidone trial mentioned above.
Seven patients (33%) had treatment-emergent events leading to dose interruption. Five patients discontinued treatment: one who withdrew because of taste alterations, one who was lost to follow-up after an IPF exacerbation, and three who withdrew consent.
There were no treatment-related deaths, and no clinically significant findings on labs, vital signs, electrocardiograms, or physical exam.
Efficacy endpoints
An analysis of the secondary efficacy endpoints showed a 1.9% mean improvement in FVC from baseline among patients assigned to ENV-101, compared with a mean decline of 1.3% of patients assigned to placebo (P = .035).
Patients on the active drug also had a 200-mL mean increase in total lung capacity, compared with a mean decline of 56 mL for patients on placebo (P = .005).
In addition, high-resolution CR studies showed a 9.4% absolute decrease from baseline in quantitative interstitial lung disease with ENV-101, vs. a 1.1% increase among controls, a 2% absolute decline from baseline in quantitative lung fibrosis compared with a 0.87% increase with placebo, and a 4.6% absolute decrease from baseline in quantitative ground glass, compared with an increase of 0.29% with placebo.
Bad taste a good sign?
Reinoud Gosens PhD, University of Groningen, the Netherlands, who co-moderated the session but was not involved in the study, questioned whether the dysgeusia seen in patients who received ENV-101 might be related to the dysgeusia seen in clinical trials of P2X3 receptor antagonists for cough.
“I was wondering if there would be a mechanistic overlap between Hedgehog inhibition and cough, which would be quite relevant for IPF,” he said in an interview.
The increase in FVC seen with ENV-101 and with the investigational agent buloxibutid, a novel angiotensin II type 2 receptor agonist described in a separate presentation by Dr. Maher, suggests that these drugs may have the ability to help remodel damaged lungs, Dr. Gosens said.
Investigators are currently planning a phase 2 dose-ranging trial (WHISTLE-PF) in patients with IPF or progressive pulmonary fibrosis.
The phase 2a trial was supported by Endeavor BioMedicines. Dr. Maher disclosed consultancy or speaker fees from Endeavor and others. Dr. Gosens had no relevant disclosures.
FROM ATS 2024
Lilly’s Once-Weekly Insulin Top-Line Results Show Benefit
Eli Lilly has announced positive phase 3 top-line results for its once-weekly insulin efsitora alfa (efsitora) in insulin-naive adults with type 2 diabetes and those who require multiple daily insulin injections.
The new data come from the company’s QWINT-2 and QWINT-4 phase 3 clinical trials. In both, efsitora was noninferior to daily basal insulin in lowering A1c. The comparator was once-daily degludec in QUINT-2 and glargine in QUINT-4.
These results come days before the once-weekly competitor, Novo Nordisk’s insulin icodec, will be discussed by the US Food and Drug Administration’s Endocrinologic and Metabolic Drugs Advisory Committee. On May 24, 2024, the panel will review safety and efficacy of icodec for the proposed indication of improving glycemic control in adults with diabetes.
Hypoglycemia and Affordability Are Concerns
Asked to comment, Anne L. Peters, MD, director of the University of Southern California Westside Center for Diabetes, Los Angeles, told this news organization that she’s “cautiously optimistic” about once-weekly insulin. “I honestly think it’s going to have an important role in diabetes. … And I’m looking forward to learning how it’s going to help my patients.”
However, Dr. Peters also said she’s concerned about the possible risk for hypoglycemia with long-acting insulin, particularly in patients with variable schedules. “The real fear they have and I have is hypoglycemia. That being said, I think that it will be great for some patients where hypoglycemia is less of a concern, and they’re in a more stable environment. … I think there are patients who will really benefit but I have to figure out who those patients are.”
Dr. Peters, who takes care of many low-income patients, also pointed out that once approved, these newer insulins may not be affordable for those who could most benefit from them in terms of improved adherence. Insurance plans may not cover them initially, especially given that the data thus far show noninferiority, not superiority, to daily basal. “The patients in whom I would like to use it most are the patients who have the most trouble with social determinants of health and other issues. I really think it could really make a difference for them, but it won’t get there for a while.”
And, she noted, titrating doses of once-weekly insulin will likely come with a learning curve. “Having spent a lifetime adjusting basal insulin on a daily basis to suddenly do it on a weekly basis, as a diabetologist I’m going to have to get used to what that feels like.”
Topline Data Show Noninferiority to Daily Basal Insulin
In QWINT-2, efficacy and safety of once-weekly efsitora was compared with those of once-daily insulin degludec for 52 weeks. Study participants were all new to using insulin, but some were using glucagon-like peptide 1 receptor agonists.
The treat-to-target trial met its primary noninferiority endpoint for hemoglobin A1c reduction at week 52. A1c values were lowered by 1.34 percentage points with efsitora compared with 1.26 for insulin degludec, resulting in non–significantly different A1c values of 6.87% and 6.95%, respectively.
In QWINT-4, efficacy and safety of once-weekly efsitora was compared with those of daily insulin glargine for 26 weeks in adults with type 2 diabetes who had previously been treated with basal insulin and at least two injections of premeal insulin per day. Participants were randomized to receive efsitora once weekly or insulin glargine once daily, and both groups used lispro before meals.
This trial also met its primary endpoint, with both reducing A1c by 1.07 percentage points at 26 weeks, resulting in levels of 7.12% and 7.11%, respectively.
The full results for QWINT-2 will be presented at the European Association for the Study of Diabetes meeting this September.
Dr. Peters served on the advisory board for Abbott Diabetes Care; Becton Dickinson; Boehringer Ingelheim Pharmaceuticals, Inc.; Eli Lilly and Company; Lexicon Pharmaceuticals, Inc.; Livongo; Medscape Medical News; Merck & Co., Inc.; Novo Nordisk; Omada Health; OptumHealth; Sanofi; and Zafgen. She received research support from Dexcom, MannKind Corporation, and Astra Zeneca and served as a member of a speakers bureau for Novo Nordisk.
A version of this article first appeared on Medscape.com.
Eli Lilly has announced positive phase 3 top-line results for its once-weekly insulin efsitora alfa (efsitora) in insulin-naive adults with type 2 diabetes and those who require multiple daily insulin injections.
The new data come from the company’s QWINT-2 and QWINT-4 phase 3 clinical trials. In both, efsitora was noninferior to daily basal insulin in lowering A1c. The comparator was once-daily degludec in QUINT-2 and glargine in QUINT-4.
These results come days before the once-weekly competitor, Novo Nordisk’s insulin icodec, will be discussed by the US Food and Drug Administration’s Endocrinologic and Metabolic Drugs Advisory Committee. On May 24, 2024, the panel will review safety and efficacy of icodec for the proposed indication of improving glycemic control in adults with diabetes.
Hypoglycemia and Affordability Are Concerns
Asked to comment, Anne L. Peters, MD, director of the University of Southern California Westside Center for Diabetes, Los Angeles, told this news organization that she’s “cautiously optimistic” about once-weekly insulin. “I honestly think it’s going to have an important role in diabetes. … And I’m looking forward to learning how it’s going to help my patients.”
However, Dr. Peters also said she’s concerned about the possible risk for hypoglycemia with long-acting insulin, particularly in patients with variable schedules. “The real fear they have and I have is hypoglycemia. That being said, I think that it will be great for some patients where hypoglycemia is less of a concern, and they’re in a more stable environment. … I think there are patients who will really benefit but I have to figure out who those patients are.”
Dr. Peters, who takes care of many low-income patients, also pointed out that once approved, these newer insulins may not be affordable for those who could most benefit from them in terms of improved adherence. Insurance plans may not cover them initially, especially given that the data thus far show noninferiority, not superiority, to daily basal. “The patients in whom I would like to use it most are the patients who have the most trouble with social determinants of health and other issues. I really think it could really make a difference for them, but it won’t get there for a while.”
And, she noted, titrating doses of once-weekly insulin will likely come with a learning curve. “Having spent a lifetime adjusting basal insulin on a daily basis to suddenly do it on a weekly basis, as a diabetologist I’m going to have to get used to what that feels like.”
Topline Data Show Noninferiority to Daily Basal Insulin
In QWINT-2, efficacy and safety of once-weekly efsitora was compared with those of once-daily insulin degludec for 52 weeks. Study participants were all new to using insulin, but some were using glucagon-like peptide 1 receptor agonists.
The treat-to-target trial met its primary noninferiority endpoint for hemoglobin A1c reduction at week 52. A1c values were lowered by 1.34 percentage points with efsitora compared with 1.26 for insulin degludec, resulting in non–significantly different A1c values of 6.87% and 6.95%, respectively.
In QWINT-4, efficacy and safety of once-weekly efsitora was compared with those of daily insulin glargine for 26 weeks in adults with type 2 diabetes who had previously been treated with basal insulin and at least two injections of premeal insulin per day. Participants were randomized to receive efsitora once weekly or insulin glargine once daily, and both groups used lispro before meals.
This trial also met its primary endpoint, with both reducing A1c by 1.07 percentage points at 26 weeks, resulting in levels of 7.12% and 7.11%, respectively.
The full results for QWINT-2 will be presented at the European Association for the Study of Diabetes meeting this September.
Dr. Peters served on the advisory board for Abbott Diabetes Care; Becton Dickinson; Boehringer Ingelheim Pharmaceuticals, Inc.; Eli Lilly and Company; Lexicon Pharmaceuticals, Inc.; Livongo; Medscape Medical News; Merck & Co., Inc.; Novo Nordisk; Omada Health; OptumHealth; Sanofi; and Zafgen. She received research support from Dexcom, MannKind Corporation, and Astra Zeneca and served as a member of a speakers bureau for Novo Nordisk.
A version of this article first appeared on Medscape.com.
Eli Lilly has announced positive phase 3 top-line results for its once-weekly insulin efsitora alfa (efsitora) in insulin-naive adults with type 2 diabetes and those who require multiple daily insulin injections.
The new data come from the company’s QWINT-2 and QWINT-4 phase 3 clinical trials. In both, efsitora was noninferior to daily basal insulin in lowering A1c. The comparator was once-daily degludec in QUINT-2 and glargine in QUINT-4.
These results come days before the once-weekly competitor, Novo Nordisk’s insulin icodec, will be discussed by the US Food and Drug Administration’s Endocrinologic and Metabolic Drugs Advisory Committee. On May 24, 2024, the panel will review safety and efficacy of icodec for the proposed indication of improving glycemic control in adults with diabetes.
Hypoglycemia and Affordability Are Concerns
Asked to comment, Anne L. Peters, MD, director of the University of Southern California Westside Center for Diabetes, Los Angeles, told this news organization that she’s “cautiously optimistic” about once-weekly insulin. “I honestly think it’s going to have an important role in diabetes. … And I’m looking forward to learning how it’s going to help my patients.”
However, Dr. Peters also said she’s concerned about the possible risk for hypoglycemia with long-acting insulin, particularly in patients with variable schedules. “The real fear they have and I have is hypoglycemia. That being said, I think that it will be great for some patients where hypoglycemia is less of a concern, and they’re in a more stable environment. … I think there are patients who will really benefit but I have to figure out who those patients are.”
Dr. Peters, who takes care of many low-income patients, also pointed out that once approved, these newer insulins may not be affordable for those who could most benefit from them in terms of improved adherence. Insurance plans may not cover them initially, especially given that the data thus far show noninferiority, not superiority, to daily basal. “The patients in whom I would like to use it most are the patients who have the most trouble with social determinants of health and other issues. I really think it could really make a difference for them, but it won’t get there for a while.”
And, she noted, titrating doses of once-weekly insulin will likely come with a learning curve. “Having spent a lifetime adjusting basal insulin on a daily basis to suddenly do it on a weekly basis, as a diabetologist I’m going to have to get used to what that feels like.”
Topline Data Show Noninferiority to Daily Basal Insulin
In QWINT-2, efficacy and safety of once-weekly efsitora was compared with those of once-daily insulin degludec for 52 weeks. Study participants were all new to using insulin, but some were using glucagon-like peptide 1 receptor agonists.
The treat-to-target trial met its primary noninferiority endpoint for hemoglobin A1c reduction at week 52. A1c values were lowered by 1.34 percentage points with efsitora compared with 1.26 for insulin degludec, resulting in non–significantly different A1c values of 6.87% and 6.95%, respectively.
In QWINT-4, efficacy and safety of once-weekly efsitora was compared with those of daily insulin glargine for 26 weeks in adults with type 2 diabetes who had previously been treated with basal insulin and at least two injections of premeal insulin per day. Participants were randomized to receive efsitora once weekly or insulin glargine once daily, and both groups used lispro before meals.
This trial also met its primary endpoint, with both reducing A1c by 1.07 percentage points at 26 weeks, resulting in levels of 7.12% and 7.11%, respectively.
The full results for QWINT-2 will be presented at the European Association for the Study of Diabetes meeting this September.
Dr. Peters served on the advisory board for Abbott Diabetes Care; Becton Dickinson; Boehringer Ingelheim Pharmaceuticals, Inc.; Eli Lilly and Company; Lexicon Pharmaceuticals, Inc.; Livongo; Medscape Medical News; Merck & Co., Inc.; Novo Nordisk; Omada Health; OptumHealth; Sanofi; and Zafgen. She received research support from Dexcom, MannKind Corporation, and Astra Zeneca and served as a member of a speakers bureau for Novo Nordisk.
A version of this article first appeared on Medscape.com.
How Physician Mortgage Loans Work for Doctors With Debt
Tell someone you’re a doctor, and the reaction is often: “You must be rich.” But physicians who are just finishing medical school or are in their early careers might feel far from it. The average medical school debt is more than $200,000, with total debts including undergrad climbing well north of $250,000.
That leaves house-hunting physicians in a predicament. A key factor for lending institutions is the “debt to income” ratio, a calculation which indicates if you already have too much debt to pay your mortgage. That single equation could eliminate you from lenders’ mortgage requirements.
But young doctors are also in a unique situation. Yes, they carry above-average levels of debt, but they are on a path to substantial income in future years. That’s where the physician mortgage loan (PML) becomes a useful option.
What Is a Physician Mortgage Loan?
, according to Stephen Chang, MD, a radiologist, and a managing director at Acts Financial Advisors in McLean, Virginia.
The key features, according to James M. Dahle, MD, an emergency physician and founder of The White Coat Investor, include:
- No required down payment, which is typically 20% with a conventional loan.
- No private mortgage insurance (PMI). This is often a requirement of traditional loans, designed to protect the lender if the buyer misses payments. PMLs don’t involve PMI even if you don’t put down 20%.
- No pay stubs. With a conventional loan, pay stubs are often required to prove income level and reliability. PMLs will often allow an employment contract in place of those.
- Different consideration of the student loan burden.
Those are the upsides, of course, but there may be downsides. Dr. Dahle said a PML might involve slightly higher rates and fees than a conventional mortgage does but not always.
Who Is Best Suited for a Physician Mortgage Loan?
Financial advisers caution that everyone should first consider their full financial picture before applying for a mortgage, PML or otherwise. “If you don’t have the money saved for a down payment, one can ask if you are financially prepared to purchase a home,” says Cobin Soelberg, MD, an anesthesiologist and owner of Greeley Wealth Management, a financial planning firm serving physician families in Bend, Oregon.
If your savings are slim, you might need to build those accounts further before pursuing home ownership and the expenses that come along with it.
Your credit score can contribute to the equation. “With any loan product, we always recommend working to optimize your personal credit score as soon as possible before applying for a loan,” said Mark P. Eid, MD, a dermatologist and co–managing director (with Dr. Chang) at Act Financial Advisors. “Once you get into the high 700s, you’ve typically qualified for the best interest rates, so while that perfect 850 is nice to achieve, it’s by no means necessary.”
Also, assess your reasons for purchasing a home and whether it will fit your lifestyle in the coming years. “The main reason that [my wife and I] wanted to buy a home was for stability,” said Jordan Frey, MD, founder of The Prudent Plastic Surgeon. “After living in apartments for years, we wanted a place that was truly our own. We definitely felt disappointed and frustrated when worrying that our student debt may limit our ability to do this.”
Like many physicians, Dr. Frey had taken on a huge amount of debt, to the tune of half a million dollars in student loans and credit card debt when he finished training in 2020. The question Dr. Frey and his wife wrestled with was: “How much debt should we take on in addition to what we already have?”
What Are the Risks? What’s in the Fine Print?
The eased limitations of PMLs come with potential pitfalls, and physicians should not imagine that they have unlimited buying power.
“Many physicians buy more expensive or bigger houses than they need simply because banks are willing to lend physicians money,” Dr. Soelberg warns. “So, the doctor gets locked into a large mortgage and cannot build wealth, save for retirement, and repay their student loans.”
As you shop around, beware of omissions and scams. When meeting with lenders, Dr. Frey recalled that some didn’t even present PMLs as an option, and others presented them with unfavorable terms. He was careful to look for disadvantages hidden in the fine print, such as a potential “big hike in the rate a year later.”
But sometimes, a scam is not outright deception but is more like temptation. So it’s important to have your own best interests in mind without relying on lenders’ advice.
“When we were shopping around, some mortgage lenders would [offer] $1.5 million, and we thought ‘that makes no sense,’ ” said Dr. Frey. “[Physicians] have big future income, which makes us attractive to these lenders. No one in their right mind would give a mortgage like this to anyone else. They aren’t worried about whether it’s a smart decision for you or not.”
What Other Red Flags Should You Look Out for?
Dr. Frey recommends medical professionals beware of these red flags when shopping for PMLs:
- A request for any type of collateral, including your medical practice
- A rate that is much higher than others
- A lender is pushing you to borrow a higher amount than you’re comfortable with
- A lender attempts to influence your decision about the size of your down payment
Remember, if you are choosing an adjustable-rate mortgage (ARM), your rate will recalibrate on the basis of the market’s rates — for better or worse. This means that your payment might be higher or lower, taking current interest rates into account, based on the market.
Looking back, Dr. Frey said he might reconsider his decision to use a 10-year ARM. He and his wife chose it because the rate was low at the time, and they planned to pay off the mortgage quickly or move before it went up. But the uncertainty added an element of pressure.
How Can PMLs Contribute to Overall Financial Health?
Dr. Frey says his physician mortgage was “a huge advantage,” allowing him and his wife to put 0% down on their home without PMI. But most importantly, it fit within their overall financial plan, which included investing. “The money that we would have potentially used for a down payment, we used to buy a rental property, which then got us more income,” he says.
Of course, buying a rental property is not the only path to financial health and freedom. Many people approach a home as an investment that will eventually become fully their own. Others might put that down payment toward building a safety net of savings accounts.
Used strategically and intentionally, PMLs can put you on a more predictable financial path. And with less money stress, buying a home can be an exciting milestone as you plan your future and put down roots in a community.
A version of this article appeared on Medscape.com.
Tell someone you’re a doctor, and the reaction is often: “You must be rich.” But physicians who are just finishing medical school or are in their early careers might feel far from it. The average medical school debt is more than $200,000, with total debts including undergrad climbing well north of $250,000.
That leaves house-hunting physicians in a predicament. A key factor for lending institutions is the “debt to income” ratio, a calculation which indicates if you already have too much debt to pay your mortgage. That single equation could eliminate you from lenders’ mortgage requirements.
But young doctors are also in a unique situation. Yes, they carry above-average levels of debt, but they are on a path to substantial income in future years. That’s where the physician mortgage loan (PML) becomes a useful option.
What Is a Physician Mortgage Loan?
, according to Stephen Chang, MD, a radiologist, and a managing director at Acts Financial Advisors in McLean, Virginia.
The key features, according to James M. Dahle, MD, an emergency physician and founder of The White Coat Investor, include:
- No required down payment, which is typically 20% with a conventional loan.
- No private mortgage insurance (PMI). This is often a requirement of traditional loans, designed to protect the lender if the buyer misses payments. PMLs don’t involve PMI even if you don’t put down 20%.
- No pay stubs. With a conventional loan, pay stubs are often required to prove income level and reliability. PMLs will often allow an employment contract in place of those.
- Different consideration of the student loan burden.
Those are the upsides, of course, but there may be downsides. Dr. Dahle said a PML might involve slightly higher rates and fees than a conventional mortgage does but not always.
Who Is Best Suited for a Physician Mortgage Loan?
Financial advisers caution that everyone should first consider their full financial picture before applying for a mortgage, PML or otherwise. “If you don’t have the money saved for a down payment, one can ask if you are financially prepared to purchase a home,” says Cobin Soelberg, MD, an anesthesiologist and owner of Greeley Wealth Management, a financial planning firm serving physician families in Bend, Oregon.
If your savings are slim, you might need to build those accounts further before pursuing home ownership and the expenses that come along with it.
Your credit score can contribute to the equation. “With any loan product, we always recommend working to optimize your personal credit score as soon as possible before applying for a loan,” said Mark P. Eid, MD, a dermatologist and co–managing director (with Dr. Chang) at Act Financial Advisors. “Once you get into the high 700s, you’ve typically qualified for the best interest rates, so while that perfect 850 is nice to achieve, it’s by no means necessary.”
Also, assess your reasons for purchasing a home and whether it will fit your lifestyle in the coming years. “The main reason that [my wife and I] wanted to buy a home was for stability,” said Jordan Frey, MD, founder of The Prudent Plastic Surgeon. “After living in apartments for years, we wanted a place that was truly our own. We definitely felt disappointed and frustrated when worrying that our student debt may limit our ability to do this.”
Like many physicians, Dr. Frey had taken on a huge amount of debt, to the tune of half a million dollars in student loans and credit card debt when he finished training in 2020. The question Dr. Frey and his wife wrestled with was: “How much debt should we take on in addition to what we already have?”
What Are the Risks? What’s in the Fine Print?
The eased limitations of PMLs come with potential pitfalls, and physicians should not imagine that they have unlimited buying power.
“Many physicians buy more expensive or bigger houses than they need simply because banks are willing to lend physicians money,” Dr. Soelberg warns. “So, the doctor gets locked into a large mortgage and cannot build wealth, save for retirement, and repay their student loans.”
As you shop around, beware of omissions and scams. When meeting with lenders, Dr. Frey recalled that some didn’t even present PMLs as an option, and others presented them with unfavorable terms. He was careful to look for disadvantages hidden in the fine print, such as a potential “big hike in the rate a year later.”
But sometimes, a scam is not outright deception but is more like temptation. So it’s important to have your own best interests in mind without relying on lenders’ advice.
“When we were shopping around, some mortgage lenders would [offer] $1.5 million, and we thought ‘that makes no sense,’ ” said Dr. Frey. “[Physicians] have big future income, which makes us attractive to these lenders. No one in their right mind would give a mortgage like this to anyone else. They aren’t worried about whether it’s a smart decision for you or not.”
What Other Red Flags Should You Look Out for?
Dr. Frey recommends medical professionals beware of these red flags when shopping for PMLs:
- A request for any type of collateral, including your medical practice
- A rate that is much higher than others
- A lender is pushing you to borrow a higher amount than you’re comfortable with
- A lender attempts to influence your decision about the size of your down payment
Remember, if you are choosing an adjustable-rate mortgage (ARM), your rate will recalibrate on the basis of the market’s rates — for better or worse. This means that your payment might be higher or lower, taking current interest rates into account, based on the market.
Looking back, Dr. Frey said he might reconsider his decision to use a 10-year ARM. He and his wife chose it because the rate was low at the time, and they planned to pay off the mortgage quickly or move before it went up. But the uncertainty added an element of pressure.
How Can PMLs Contribute to Overall Financial Health?
Dr. Frey says his physician mortgage was “a huge advantage,” allowing him and his wife to put 0% down on their home without PMI. But most importantly, it fit within their overall financial plan, which included investing. “The money that we would have potentially used for a down payment, we used to buy a rental property, which then got us more income,” he says.
Of course, buying a rental property is not the only path to financial health and freedom. Many people approach a home as an investment that will eventually become fully their own. Others might put that down payment toward building a safety net of savings accounts.
Used strategically and intentionally, PMLs can put you on a more predictable financial path. And with less money stress, buying a home can be an exciting milestone as you plan your future and put down roots in a community.
A version of this article appeared on Medscape.com.
Tell someone you’re a doctor, and the reaction is often: “You must be rich.” But physicians who are just finishing medical school or are in their early careers might feel far from it. The average medical school debt is more than $200,000, with total debts including undergrad climbing well north of $250,000.
That leaves house-hunting physicians in a predicament. A key factor for lending institutions is the “debt to income” ratio, a calculation which indicates if you already have too much debt to pay your mortgage. That single equation could eliminate you from lenders’ mortgage requirements.
But young doctors are also in a unique situation. Yes, they carry above-average levels of debt, but they are on a path to substantial income in future years. That’s where the physician mortgage loan (PML) becomes a useful option.
What Is a Physician Mortgage Loan?
, according to Stephen Chang, MD, a radiologist, and a managing director at Acts Financial Advisors in McLean, Virginia.
The key features, according to James M. Dahle, MD, an emergency physician and founder of The White Coat Investor, include:
- No required down payment, which is typically 20% with a conventional loan.
- No private mortgage insurance (PMI). This is often a requirement of traditional loans, designed to protect the lender if the buyer misses payments. PMLs don’t involve PMI even if you don’t put down 20%.
- No pay stubs. With a conventional loan, pay stubs are often required to prove income level and reliability. PMLs will often allow an employment contract in place of those.
- Different consideration of the student loan burden.
Those are the upsides, of course, but there may be downsides. Dr. Dahle said a PML might involve slightly higher rates and fees than a conventional mortgage does but not always.
Who Is Best Suited for a Physician Mortgage Loan?
Financial advisers caution that everyone should first consider their full financial picture before applying for a mortgage, PML or otherwise. “If you don’t have the money saved for a down payment, one can ask if you are financially prepared to purchase a home,” says Cobin Soelberg, MD, an anesthesiologist and owner of Greeley Wealth Management, a financial planning firm serving physician families in Bend, Oregon.
If your savings are slim, you might need to build those accounts further before pursuing home ownership and the expenses that come along with it.
Your credit score can contribute to the equation. “With any loan product, we always recommend working to optimize your personal credit score as soon as possible before applying for a loan,” said Mark P. Eid, MD, a dermatologist and co–managing director (with Dr. Chang) at Act Financial Advisors. “Once you get into the high 700s, you’ve typically qualified for the best interest rates, so while that perfect 850 is nice to achieve, it’s by no means necessary.”
Also, assess your reasons for purchasing a home and whether it will fit your lifestyle in the coming years. “The main reason that [my wife and I] wanted to buy a home was for stability,” said Jordan Frey, MD, founder of The Prudent Plastic Surgeon. “After living in apartments for years, we wanted a place that was truly our own. We definitely felt disappointed and frustrated when worrying that our student debt may limit our ability to do this.”
Like many physicians, Dr. Frey had taken on a huge amount of debt, to the tune of half a million dollars in student loans and credit card debt when he finished training in 2020. The question Dr. Frey and his wife wrestled with was: “How much debt should we take on in addition to what we already have?”
What Are the Risks? What’s in the Fine Print?
The eased limitations of PMLs come with potential pitfalls, and physicians should not imagine that they have unlimited buying power.
“Many physicians buy more expensive or bigger houses than they need simply because banks are willing to lend physicians money,” Dr. Soelberg warns. “So, the doctor gets locked into a large mortgage and cannot build wealth, save for retirement, and repay their student loans.”
As you shop around, beware of omissions and scams. When meeting with lenders, Dr. Frey recalled that some didn’t even present PMLs as an option, and others presented them with unfavorable terms. He was careful to look for disadvantages hidden in the fine print, such as a potential “big hike in the rate a year later.”
But sometimes, a scam is not outright deception but is more like temptation. So it’s important to have your own best interests in mind without relying on lenders’ advice.
“When we were shopping around, some mortgage lenders would [offer] $1.5 million, and we thought ‘that makes no sense,’ ” said Dr. Frey. “[Physicians] have big future income, which makes us attractive to these lenders. No one in their right mind would give a mortgage like this to anyone else. They aren’t worried about whether it’s a smart decision for you or not.”
What Other Red Flags Should You Look Out for?
Dr. Frey recommends medical professionals beware of these red flags when shopping for PMLs:
- A request for any type of collateral, including your medical practice
- A rate that is much higher than others
- A lender is pushing you to borrow a higher amount than you’re comfortable with
- A lender attempts to influence your decision about the size of your down payment
Remember, if you are choosing an adjustable-rate mortgage (ARM), your rate will recalibrate on the basis of the market’s rates — for better or worse. This means that your payment might be higher or lower, taking current interest rates into account, based on the market.
Looking back, Dr. Frey said he might reconsider his decision to use a 10-year ARM. He and his wife chose it because the rate was low at the time, and they planned to pay off the mortgage quickly or move before it went up. But the uncertainty added an element of pressure.
How Can PMLs Contribute to Overall Financial Health?
Dr. Frey says his physician mortgage was “a huge advantage,” allowing him and his wife to put 0% down on their home without PMI. But most importantly, it fit within their overall financial plan, which included investing. “The money that we would have potentially used for a down payment, we used to buy a rental property, which then got us more income,” he says.
Of course, buying a rental property is not the only path to financial health and freedom. Many people approach a home as an investment that will eventually become fully their own. Others might put that down payment toward building a safety net of savings accounts.
Used strategically and intentionally, PMLs can put you on a more predictable financial path. And with less money stress, buying a home can be an exciting milestone as you plan your future and put down roots in a community.
A version of this article appeared on Medscape.com.
New Data to Change Practice on BP Control in Acute Stroke: INTERACT4
BASEL, SWITZERLAND — Early reduction of blood pressure has a beneficial effect in hemorrhagic stroke but a detrimental effect in ischemic stroke, new trial data show. The findings could shake up recommendations on control of blood pressure in acute stroke patients.
“This is the first time that we have randomized evidence of blood pressure control prior to reperfusion in ischemic stroke patients, and our data will challenge the current guidelines that recommend lowering blood pressure to below 180 mm Hg systolic in these patients,” said study coauthor Craig Anderson, MD, George Institute for Global Health, Sydney, Australia.
“And this study also clearly shows for the first time that getting blood pressure under control in hemorrhagic stroke patients in the first couple of hours has definitive benefits,” he added.
The findings were presented on May 16 at the European Stroke Organization Conference (ESOC) annual meeting and published online simultaneously in The New England Journal of Medicine.
A Test of Early BP Control
The trial was conducted to test the strategy of very early blood pressure control during patient transport in an ambulance after acute stroke, which investigators suspected could benefit patients with both types of stroke.
The hypothesis was that this would reduce bleeding in the brain for those with hemorrhagic stroke. For ischemic stroke patients, it was thought this strategy would speed up administration of thrombolysis, because guidelines recommend bringing blood pressure under control before thrombolysis.
For the INTERACT4 trial, which was conducted in China, 2404 patients with suspected acute stroke and elevated systolic blood pressure (≥ 150 mm Hg) who were assessed in the ambulance within 2 hours after symptom onset were randomized to receive immediate treatment with intravenous urapidil to lower the systolic blood pressure or usual blood pressure management (usual care group).
The median time between symptom onset and randomization was 61 minutes, and the mean blood pressure at randomization was 178/98 mm Hg.
Stroke was subsequently confirmed by imaging in 2240 patients, of whom 46% had a hemorrhagic stroke and 54% an ischemic stroke.
At the time of arrival at the hospital, the mean systolic blood pressure in the intervention group was 158 mm Hg, compared with 170 mm Hg in the usual care group.
The primary efficacy outcome was functional status as assessed by modified Rankin scale score at 90 days.
Overall, there was no difference between the two groups in terms of functional outcome scores (common odds ratio [OR], 1.00; 95% CI, 0.87-1.15), and the incidence of serious adverse events was similar.
But the study showed very different results in patients with hemorrhagic stroke vs those with ischemic stroke.
‘Slam-Dunk’ Effect
Anderson has led several previous trials of blood pressure control in stroke patients, some of which have suggested benefit of lowering blood pressure in those with hemorrhagic stroke, but he says the results of the current trial are more clear-cut.
“We have never seen such a slam-dunk effect as there was in INTERACT4,” Dr. Anderson said. “Not only did we show that early reduction of blood pressure in hemorrhagic stroke patients improved functional outcome, it also reduced bleeding in the brain, improved survival and quality of life, and reduced surgery and infection complications. That’s quite remarkable.”
The findings offer “clear evidence that for patients with hemorrhagic stroke, we must get the blood pressure under control as soon as possible and introduce systems of care to ensure this happens,” he added.
The reason for the clear findings in the current trial is probably the treatment time, Dr. Anderson said.
“This is the first trial in which blood pressure has been controlled in the ambulance and occurred much earlier than in the previous trials.”
Challenging Ischemic Stroke Guidelines
The INTERACT4 results in ischemic stroke patients are likely to be more controversial.
“Our results are clearly challenging longstanding beliefs around blood pressure control in ischemic stroke prior to thrombolysis,” Dr. Anderson said.
Current guidelines recommend a blood pressure < 185 mm Hg systolic before initiation of thrombolysis because of concerns about intracerebral hemorrhage, he noted. Often, blood pressure is lowered rapidly down to much lower levels in order give thrombolysis quickly.
“Our results suggest this may not be a good idea,” Dr. Anderson said. “I think these data will shake us up a bit and make us more cautious about reducing blood pressure in these patients. Personally, I wouldn’t touch the blood pressure at all in ischemic stroke patients after these results.”
He said the mechanisms behind the different stroke types would explain the results.
“If a patient is bleeding, it makes sense that higher blood pressure would make that worse,” Dr. Anderson said. “But when a patient has a blocked artery and ischemia in the brain, it seems likely that the extra pressure is needed to keep oxygen delivery to the ischemic tissue.”
Accurate Diagnosis Necessary
Because it is not possible to make an accurate diagnosis between ischemic and hemorrhagic stroke without a CT scan, Dr. Anderson stressed that at the present time, no action on blood pressure can be taken in the ambulance.
“There is a lot of interest in developing a lightweight brain scanner to be used in ambulances, but this won’t be routinely available for several years,” he said. “So for now, quick diagnosis of the type of stroke that is occurring on the patient’s arrival at the emergency department and, for hemorrhagic stroke patients, swift action to control blood pressure at this point is critical to preserving brain function.”
Commenting on the INTERACT4 results at the ESOC meeting, Simona Sacco, MD, professor of neurology at the University of L’Aquila, Italy, said this was a very important trial that would impact clinical practice.
“The data really reinforce that hemorrhagic stroke patients must have their blood pressure reduced as soon as possible,” she stated.
Dr. Sacco said the trial emphasizes the need to be able to distinguish between a hemorrhagic and ischemic stroke in a prehospital setting and supports the introduction of more mobile stroke units carrying CT scanners and calls for the development of biomarkers that can allow rapid differentiation between the two conditions.
In an accompanying editorial, Jonathan Edlow, MD, Department of Emergency Medicine, Beth Israel Deaconess Medical Center, Boston, points out several aspects of the trial that may potentially limit the generalizability of the findings. These include use of urapidil as the antihypertensive agent, which is unavailable in the United States; all patients being of Han Chinese ethnicity; and an unusually high sensitivity of initial CT scans in detecting visible signs of ischemia or infarction in patients in acute ischemic stroke.
“These findings should be considered hypothesis-generating, and they make the case for validation of the trial results in other settings,” Dr. Edlow wrote.
The INTERACT4 trial was funded by the National Health and Medical Research Council of Australia, the George Institute for Global Health, several Chinese healthcare institutions, and Takeda Pharmaceuticals China. Disclosures for study and editorial authors are provided in the original articles.
A version of this article appeared on Medscape.com.
BASEL, SWITZERLAND — Early reduction of blood pressure has a beneficial effect in hemorrhagic stroke but a detrimental effect in ischemic stroke, new trial data show. The findings could shake up recommendations on control of blood pressure in acute stroke patients.
“This is the first time that we have randomized evidence of blood pressure control prior to reperfusion in ischemic stroke patients, and our data will challenge the current guidelines that recommend lowering blood pressure to below 180 mm Hg systolic in these patients,” said study coauthor Craig Anderson, MD, George Institute for Global Health, Sydney, Australia.
“And this study also clearly shows for the first time that getting blood pressure under control in hemorrhagic stroke patients in the first couple of hours has definitive benefits,” he added.
The findings were presented on May 16 at the European Stroke Organization Conference (ESOC) annual meeting and published online simultaneously in The New England Journal of Medicine.
A Test of Early BP Control
The trial was conducted to test the strategy of very early blood pressure control during patient transport in an ambulance after acute stroke, which investigators suspected could benefit patients with both types of stroke.
The hypothesis was that this would reduce bleeding in the brain for those with hemorrhagic stroke. For ischemic stroke patients, it was thought this strategy would speed up administration of thrombolysis, because guidelines recommend bringing blood pressure under control before thrombolysis.
For the INTERACT4 trial, which was conducted in China, 2404 patients with suspected acute stroke and elevated systolic blood pressure (≥ 150 mm Hg) who were assessed in the ambulance within 2 hours after symptom onset were randomized to receive immediate treatment with intravenous urapidil to lower the systolic blood pressure or usual blood pressure management (usual care group).
The median time between symptom onset and randomization was 61 minutes, and the mean blood pressure at randomization was 178/98 mm Hg.
Stroke was subsequently confirmed by imaging in 2240 patients, of whom 46% had a hemorrhagic stroke and 54% an ischemic stroke.
At the time of arrival at the hospital, the mean systolic blood pressure in the intervention group was 158 mm Hg, compared with 170 mm Hg in the usual care group.
The primary efficacy outcome was functional status as assessed by modified Rankin scale score at 90 days.
Overall, there was no difference between the two groups in terms of functional outcome scores (common odds ratio [OR], 1.00; 95% CI, 0.87-1.15), and the incidence of serious adverse events was similar.
But the study showed very different results in patients with hemorrhagic stroke vs those with ischemic stroke.
‘Slam-Dunk’ Effect
Anderson has led several previous trials of blood pressure control in stroke patients, some of which have suggested benefit of lowering blood pressure in those with hemorrhagic stroke, but he says the results of the current trial are more clear-cut.
“We have never seen such a slam-dunk effect as there was in INTERACT4,” Dr. Anderson said. “Not only did we show that early reduction of blood pressure in hemorrhagic stroke patients improved functional outcome, it also reduced bleeding in the brain, improved survival and quality of life, and reduced surgery and infection complications. That’s quite remarkable.”
The findings offer “clear evidence that for patients with hemorrhagic stroke, we must get the blood pressure under control as soon as possible and introduce systems of care to ensure this happens,” he added.
The reason for the clear findings in the current trial is probably the treatment time, Dr. Anderson said.
“This is the first trial in which blood pressure has been controlled in the ambulance and occurred much earlier than in the previous trials.”
Challenging Ischemic Stroke Guidelines
The INTERACT4 results in ischemic stroke patients are likely to be more controversial.
“Our results are clearly challenging longstanding beliefs around blood pressure control in ischemic stroke prior to thrombolysis,” Dr. Anderson said.
Current guidelines recommend a blood pressure < 185 mm Hg systolic before initiation of thrombolysis because of concerns about intracerebral hemorrhage, he noted. Often, blood pressure is lowered rapidly down to much lower levels in order give thrombolysis quickly.
“Our results suggest this may not be a good idea,” Dr. Anderson said. “I think these data will shake us up a bit and make us more cautious about reducing blood pressure in these patients. Personally, I wouldn’t touch the blood pressure at all in ischemic stroke patients after these results.”
He said the mechanisms behind the different stroke types would explain the results.
“If a patient is bleeding, it makes sense that higher blood pressure would make that worse,” Dr. Anderson said. “But when a patient has a blocked artery and ischemia in the brain, it seems likely that the extra pressure is needed to keep oxygen delivery to the ischemic tissue.”
Accurate Diagnosis Necessary
Because it is not possible to make an accurate diagnosis between ischemic and hemorrhagic stroke without a CT scan, Dr. Anderson stressed that at the present time, no action on blood pressure can be taken in the ambulance.
“There is a lot of interest in developing a lightweight brain scanner to be used in ambulances, but this won’t be routinely available for several years,” he said. “So for now, quick diagnosis of the type of stroke that is occurring on the patient’s arrival at the emergency department and, for hemorrhagic stroke patients, swift action to control blood pressure at this point is critical to preserving brain function.”
Commenting on the INTERACT4 results at the ESOC meeting, Simona Sacco, MD, professor of neurology at the University of L’Aquila, Italy, said this was a very important trial that would impact clinical practice.
“The data really reinforce that hemorrhagic stroke patients must have their blood pressure reduced as soon as possible,” she stated.
Dr. Sacco said the trial emphasizes the need to be able to distinguish between a hemorrhagic and ischemic stroke in a prehospital setting and supports the introduction of more mobile stroke units carrying CT scanners and calls for the development of biomarkers that can allow rapid differentiation between the two conditions.
In an accompanying editorial, Jonathan Edlow, MD, Department of Emergency Medicine, Beth Israel Deaconess Medical Center, Boston, points out several aspects of the trial that may potentially limit the generalizability of the findings. These include use of urapidil as the antihypertensive agent, which is unavailable in the United States; all patients being of Han Chinese ethnicity; and an unusually high sensitivity of initial CT scans in detecting visible signs of ischemia or infarction in patients in acute ischemic stroke.
“These findings should be considered hypothesis-generating, and they make the case for validation of the trial results in other settings,” Dr. Edlow wrote.
The INTERACT4 trial was funded by the National Health and Medical Research Council of Australia, the George Institute for Global Health, several Chinese healthcare institutions, and Takeda Pharmaceuticals China. Disclosures for study and editorial authors are provided in the original articles.
A version of this article appeared on Medscape.com.
BASEL, SWITZERLAND — Early reduction of blood pressure has a beneficial effect in hemorrhagic stroke but a detrimental effect in ischemic stroke, new trial data show. The findings could shake up recommendations on control of blood pressure in acute stroke patients.
“This is the first time that we have randomized evidence of blood pressure control prior to reperfusion in ischemic stroke patients, and our data will challenge the current guidelines that recommend lowering blood pressure to below 180 mm Hg systolic in these patients,” said study coauthor Craig Anderson, MD, George Institute for Global Health, Sydney, Australia.
“And this study also clearly shows for the first time that getting blood pressure under control in hemorrhagic stroke patients in the first couple of hours has definitive benefits,” he added.
The findings were presented on May 16 at the European Stroke Organization Conference (ESOC) annual meeting and published online simultaneously in The New England Journal of Medicine.
A Test of Early BP Control
The trial was conducted to test the strategy of very early blood pressure control during patient transport in an ambulance after acute stroke, which investigators suspected could benefit patients with both types of stroke.
The hypothesis was that this would reduce bleeding in the brain for those with hemorrhagic stroke. For ischemic stroke patients, it was thought this strategy would speed up administration of thrombolysis, because guidelines recommend bringing blood pressure under control before thrombolysis.
For the INTERACT4 trial, which was conducted in China, 2404 patients with suspected acute stroke and elevated systolic blood pressure (≥ 150 mm Hg) who were assessed in the ambulance within 2 hours after symptom onset were randomized to receive immediate treatment with intravenous urapidil to lower the systolic blood pressure or usual blood pressure management (usual care group).
The median time between symptom onset and randomization was 61 minutes, and the mean blood pressure at randomization was 178/98 mm Hg.
Stroke was subsequently confirmed by imaging in 2240 patients, of whom 46% had a hemorrhagic stroke and 54% an ischemic stroke.
At the time of arrival at the hospital, the mean systolic blood pressure in the intervention group was 158 mm Hg, compared with 170 mm Hg in the usual care group.
The primary efficacy outcome was functional status as assessed by modified Rankin scale score at 90 days.
Overall, there was no difference between the two groups in terms of functional outcome scores (common odds ratio [OR], 1.00; 95% CI, 0.87-1.15), and the incidence of serious adverse events was similar.
But the study showed very different results in patients with hemorrhagic stroke vs those with ischemic stroke.
‘Slam-Dunk’ Effect
Anderson has led several previous trials of blood pressure control in stroke patients, some of which have suggested benefit of lowering blood pressure in those with hemorrhagic stroke, but he says the results of the current trial are more clear-cut.
“We have never seen such a slam-dunk effect as there was in INTERACT4,” Dr. Anderson said. “Not only did we show that early reduction of blood pressure in hemorrhagic stroke patients improved functional outcome, it also reduced bleeding in the brain, improved survival and quality of life, and reduced surgery and infection complications. That’s quite remarkable.”
The findings offer “clear evidence that for patients with hemorrhagic stroke, we must get the blood pressure under control as soon as possible and introduce systems of care to ensure this happens,” he added.
The reason for the clear findings in the current trial is probably the treatment time, Dr. Anderson said.
“This is the first trial in which blood pressure has been controlled in the ambulance and occurred much earlier than in the previous trials.”
Challenging Ischemic Stroke Guidelines
The INTERACT4 results in ischemic stroke patients are likely to be more controversial.
“Our results are clearly challenging longstanding beliefs around blood pressure control in ischemic stroke prior to thrombolysis,” Dr. Anderson said.
Current guidelines recommend a blood pressure < 185 mm Hg systolic before initiation of thrombolysis because of concerns about intracerebral hemorrhage, he noted. Often, blood pressure is lowered rapidly down to much lower levels in order give thrombolysis quickly.
“Our results suggest this may not be a good idea,” Dr. Anderson said. “I think these data will shake us up a bit and make us more cautious about reducing blood pressure in these patients. Personally, I wouldn’t touch the blood pressure at all in ischemic stroke patients after these results.”
He said the mechanisms behind the different stroke types would explain the results.
“If a patient is bleeding, it makes sense that higher blood pressure would make that worse,” Dr. Anderson said. “But when a patient has a blocked artery and ischemia in the brain, it seems likely that the extra pressure is needed to keep oxygen delivery to the ischemic tissue.”
Accurate Diagnosis Necessary
Because it is not possible to make an accurate diagnosis between ischemic and hemorrhagic stroke without a CT scan, Dr. Anderson stressed that at the present time, no action on blood pressure can be taken in the ambulance.
“There is a lot of interest in developing a lightweight brain scanner to be used in ambulances, but this won’t be routinely available for several years,” he said. “So for now, quick diagnosis of the type of stroke that is occurring on the patient’s arrival at the emergency department and, for hemorrhagic stroke patients, swift action to control blood pressure at this point is critical to preserving brain function.”
Commenting on the INTERACT4 results at the ESOC meeting, Simona Sacco, MD, professor of neurology at the University of L’Aquila, Italy, said this was a very important trial that would impact clinical practice.
“The data really reinforce that hemorrhagic stroke patients must have their blood pressure reduced as soon as possible,” she stated.
Dr. Sacco said the trial emphasizes the need to be able to distinguish between a hemorrhagic and ischemic stroke in a prehospital setting and supports the introduction of more mobile stroke units carrying CT scanners and calls for the development of biomarkers that can allow rapid differentiation between the two conditions.
In an accompanying editorial, Jonathan Edlow, MD, Department of Emergency Medicine, Beth Israel Deaconess Medical Center, Boston, points out several aspects of the trial that may potentially limit the generalizability of the findings. These include use of urapidil as the antihypertensive agent, which is unavailable in the United States; all patients being of Han Chinese ethnicity; and an unusually high sensitivity of initial CT scans in detecting visible signs of ischemia or infarction in patients in acute ischemic stroke.
“These findings should be considered hypothesis-generating, and they make the case for validation of the trial results in other settings,” Dr. Edlow wrote.
The INTERACT4 trial was funded by the National Health and Medical Research Council of Australia, the George Institute for Global Health, several Chinese healthcare institutions, and Takeda Pharmaceuticals China. Disclosures for study and editorial authors are provided in the original articles.
A version of this article appeared on Medscape.com.
‘Big Breakthrough’: New Low-Field MRI Is Safer and Easier
For years, researchers and medical companies have explored low-field MRI systems (those with a magnetic field strength of less than 1 T) — searching for a feasible alternative to the loud, expensive machines requiring special rooms with shielding to block their powerful magnetic field.
Most low-field scanners in development are for brain scans only. In 2022, the US Food and Drug Administration (FDA) cleared the first portable MRI system — Hyperfine’s Swoop, designed for use at a patient’s bedside — for head and brain scans. But the technology has not been applied to whole-body MRI — until now.
In a new study published in Science, researchers from Hong Kong described a whole-body, ultra low–field MRI.
The device uses a 0.05 T magnet — one sixtieth the magnetic field strength of the standard 3 T MRI model common in hospitals today, said lead author Ed Wu, PhD, professor of biomedical engineering at The University of Hong Kong.
Because the field strength is so low, no protective shielding is needed. Patients and bystanders can safely use smart phones . And the scanner is safe for patients with implanted devices, like a cochlear implant or pacemaker, or any metal on their body or clothes. No hearing protection is required, either, because the machine is so quiet.
If all goes well, the technology could be commercially available in as little as a few years, Dr. Wu said.
But first, funding and FDA approval would be needed. “A company is going to have to come along and say, ‘This looks fantastic. We’re going to commercialize this, and we’re going to go through this certification process,’ ” said Andrew Webb, PhD, professor of radiology and the founding director of the C.J. Gorter MRI Center at the Leiden University Medical Center, Leiden, the Netherlands. (Dr. Webb was not involved in the study.)
Improving Access to MRI
One hope for this technology is to bring MRI to more people worldwide. Africa has less than one MRI scanner per million residents, whereas the United States has about 40.
While a new 3 T machine can cost about $1 million, the low-field version is much cheaper — only about $22,000 in materials cost per scanner, according to Dr. Wu.
A low magnetic field means less electricity, too — the machine can be plugged into a standard wall outlet. And because a fully shielded room isn’t needed, that could save another $100,000 in materials, Dr. Webb said.
Its ease of use could improve accessibility in countries with limited training, Dr. Webb pointed out.
“To be a technician is 2-3 years training for a regular MRI machine, a lot of it to do safety, a lot of it to do very subtle planning,” said Webb. “These [low-field] systems are much simpler.”
Challenges and the Future
The prototype weighs about 1.5 tons or 3000 lb. (A 3 T MRI can weigh between 6 and 13 tons or 12,000 and 26,000 lb.) That might sound like a lot, but it’s comparable to a mobile CT scanner, which is designed to be moved from room to room. Plus, “its weight can be substantially reduced if further optimized,” Dr. Wu said.
One challenge with low-field MRIs is image quality, which tends to be not as clear and detailed as those from high-power machines. To address this, the research team used deep learning (artificial intelligence) to enhance the image quality. “Computing power and large-scale data underpin our success, which tackles the physics and math problems that are traditionally considered intractable in existing MRI methodology,” Dr. Wu said.
Dr. Webb said he was impressed by the image quality shown in the study. They “look much higher quality than you would expect from such a low-field system,” he said. Still, only healthy volunteers were scanned. The true test will be using it to view subtle pathologies, Dr. Webb said.
That’s what Dr. Wu and his team are working on now — taking scans to diagnose various medical conditions. His group’s brain-only version of the low-field MRI has been used for diagnosis, he noted.
A version of this article appeared on Medscape.com.
For years, researchers and medical companies have explored low-field MRI systems (those with a magnetic field strength of less than 1 T) — searching for a feasible alternative to the loud, expensive machines requiring special rooms with shielding to block their powerful magnetic field.
Most low-field scanners in development are for brain scans only. In 2022, the US Food and Drug Administration (FDA) cleared the first portable MRI system — Hyperfine’s Swoop, designed for use at a patient’s bedside — for head and brain scans. But the technology has not been applied to whole-body MRI — until now.
In a new study published in Science, researchers from Hong Kong described a whole-body, ultra low–field MRI.
The device uses a 0.05 T magnet — one sixtieth the magnetic field strength of the standard 3 T MRI model common in hospitals today, said lead author Ed Wu, PhD, professor of biomedical engineering at The University of Hong Kong.
Because the field strength is so low, no protective shielding is needed. Patients and bystanders can safely use smart phones . And the scanner is safe for patients with implanted devices, like a cochlear implant or pacemaker, or any metal on their body or clothes. No hearing protection is required, either, because the machine is so quiet.
If all goes well, the technology could be commercially available in as little as a few years, Dr. Wu said.
But first, funding and FDA approval would be needed. “A company is going to have to come along and say, ‘This looks fantastic. We’re going to commercialize this, and we’re going to go through this certification process,’ ” said Andrew Webb, PhD, professor of radiology and the founding director of the C.J. Gorter MRI Center at the Leiden University Medical Center, Leiden, the Netherlands. (Dr. Webb was not involved in the study.)
Improving Access to MRI
One hope for this technology is to bring MRI to more people worldwide. Africa has less than one MRI scanner per million residents, whereas the United States has about 40.
While a new 3 T machine can cost about $1 million, the low-field version is much cheaper — only about $22,000 in materials cost per scanner, according to Dr. Wu.
A low magnetic field means less electricity, too — the machine can be plugged into a standard wall outlet. And because a fully shielded room isn’t needed, that could save another $100,000 in materials, Dr. Webb said.
Its ease of use could improve accessibility in countries with limited training, Dr. Webb pointed out.
“To be a technician is 2-3 years training for a regular MRI machine, a lot of it to do safety, a lot of it to do very subtle planning,” said Webb. “These [low-field] systems are much simpler.”
Challenges and the Future
The prototype weighs about 1.5 tons or 3000 lb. (A 3 T MRI can weigh between 6 and 13 tons or 12,000 and 26,000 lb.) That might sound like a lot, but it’s comparable to a mobile CT scanner, which is designed to be moved from room to room. Plus, “its weight can be substantially reduced if further optimized,” Dr. Wu said.
One challenge with low-field MRIs is image quality, which tends to be not as clear and detailed as those from high-power machines. To address this, the research team used deep learning (artificial intelligence) to enhance the image quality. “Computing power and large-scale data underpin our success, which tackles the physics and math problems that are traditionally considered intractable in existing MRI methodology,” Dr. Wu said.
Dr. Webb said he was impressed by the image quality shown in the study. They “look much higher quality than you would expect from such a low-field system,” he said. Still, only healthy volunteers were scanned. The true test will be using it to view subtle pathologies, Dr. Webb said.
That’s what Dr. Wu and his team are working on now — taking scans to diagnose various medical conditions. His group’s brain-only version of the low-field MRI has been used for diagnosis, he noted.
A version of this article appeared on Medscape.com.
For years, researchers and medical companies have explored low-field MRI systems (those with a magnetic field strength of less than 1 T) — searching for a feasible alternative to the loud, expensive machines requiring special rooms with shielding to block their powerful magnetic field.
Most low-field scanners in development are for brain scans only. In 2022, the US Food and Drug Administration (FDA) cleared the first portable MRI system — Hyperfine’s Swoop, designed for use at a patient’s bedside — for head and brain scans. But the technology has not been applied to whole-body MRI — until now.
In a new study published in Science, researchers from Hong Kong described a whole-body, ultra low–field MRI.
The device uses a 0.05 T magnet — one sixtieth the magnetic field strength of the standard 3 T MRI model common in hospitals today, said lead author Ed Wu, PhD, professor of biomedical engineering at The University of Hong Kong.
Because the field strength is so low, no protective shielding is needed. Patients and bystanders can safely use smart phones . And the scanner is safe for patients with implanted devices, like a cochlear implant or pacemaker, or any metal on their body or clothes. No hearing protection is required, either, because the machine is so quiet.
If all goes well, the technology could be commercially available in as little as a few years, Dr. Wu said.
But first, funding and FDA approval would be needed. “A company is going to have to come along and say, ‘This looks fantastic. We’re going to commercialize this, and we’re going to go through this certification process,’ ” said Andrew Webb, PhD, professor of radiology and the founding director of the C.J. Gorter MRI Center at the Leiden University Medical Center, Leiden, the Netherlands. (Dr. Webb was not involved in the study.)
Improving Access to MRI
One hope for this technology is to bring MRI to more people worldwide. Africa has less than one MRI scanner per million residents, whereas the United States has about 40.
While a new 3 T machine can cost about $1 million, the low-field version is much cheaper — only about $22,000 in materials cost per scanner, according to Dr. Wu.
A low magnetic field means less electricity, too — the machine can be plugged into a standard wall outlet. And because a fully shielded room isn’t needed, that could save another $100,000 in materials, Dr. Webb said.
Its ease of use could improve accessibility in countries with limited training, Dr. Webb pointed out.
“To be a technician is 2-3 years training for a regular MRI machine, a lot of it to do safety, a lot of it to do very subtle planning,” said Webb. “These [low-field] systems are much simpler.”
Challenges and the Future
The prototype weighs about 1.5 tons or 3000 lb. (A 3 T MRI can weigh between 6 and 13 tons or 12,000 and 26,000 lb.) That might sound like a lot, but it’s comparable to a mobile CT scanner, which is designed to be moved from room to room. Plus, “its weight can be substantially reduced if further optimized,” Dr. Wu said.
One challenge with low-field MRIs is image quality, which tends to be not as clear and detailed as those from high-power machines. To address this, the research team used deep learning (artificial intelligence) to enhance the image quality. “Computing power and large-scale data underpin our success, which tackles the physics and math problems that are traditionally considered intractable in existing MRI methodology,” Dr. Wu said.
Dr. Webb said he was impressed by the image quality shown in the study. They “look much higher quality than you would expect from such a low-field system,” he said. Still, only healthy volunteers were scanned. The true test will be using it to view subtle pathologies, Dr. Webb said.
That’s what Dr. Wu and his team are working on now — taking scans to diagnose various medical conditions. His group’s brain-only version of the low-field MRI has been used for diagnosis, he noted.
A version of this article appeared on Medscape.com.
Crossing State Lines: PA Licensure Compact Coming Soon
For decades, physicians and nurses who ventured across state lines to practice, particularly in locum tenens roles, have reaped the benefits of medical licensure compacts. Yet, the same courtesy has eluded physician assistants (PAs), until now.
In April, Virginia Governor Glenn Youngkin signed the bill enacting the PA Compact making Virginia the seventh state to join. The legislation opens a cross-state agreement with seven states and finally allows locum tenens PAs to practice across these state’s borders.
How the PA Compact Works
The interstate arrangement recognizes valid, unencumbered PA licenses issued by other states in the compact. PAs working within the seven states won’t need a separate license from any of those states to practice.
The states include Delaware, Nebraska, Utah, Washington, West Virginia, Wisconsin, and Virginia. While the compact has been approved, the American Academy of Physician Associates said it could take an additional 18-24 months for the states to execute it, giving PAs the access they need to work in the compact states.
How the PA Compact Helps
The PA Compact holds the promise of alleviating some of the travel barriers that PAs often encounter, especially when they work locum tenens or in telehealth and must traverse state lines to deliver essential healthcare. This agreement not only enhances healthcare access but also empowers facilities to recruit new PAs, thereby bridging gaps in their healthcare staffing and addressing public health emergencies more effectively.
PAs will also gain increased flexibility and additional opportunities to earn and benefit from the right to practice in more states without requiring a time-consuming and expensive licensure from each state.
One motivating factor behind developing an interstate compact for physician assistants is that the same types of compacts for physicians and nurses are highly successful. The Nurse Licensure Compact and the Interstate Medical Licensure Compact for physicians encompass 37 and 41 states, respectively. While the seven-state PA Compact is in its earliest stages, it will likely be equally beneficial for PAs.
A survey by Barton Associates found that 95% of PAs said they would be more likely to consider working in a different state if the PA Compact made it more accessible.
Other states have begun legislation to enact a PA Compact, including Colorado, New Hampshire, Maine, Michigan New York, Ohio, Oklahoma, Rhode Island, Tennessee, and Vermont.
If your state still needs to enact a compact or file for compact legislation, let your elected officials know that the PAs in your state want to join a compact.
A version of this article appeared on Medscape.com .
For decades, physicians and nurses who ventured across state lines to practice, particularly in locum tenens roles, have reaped the benefits of medical licensure compacts. Yet, the same courtesy has eluded physician assistants (PAs), until now.
In April, Virginia Governor Glenn Youngkin signed the bill enacting the PA Compact making Virginia the seventh state to join. The legislation opens a cross-state agreement with seven states and finally allows locum tenens PAs to practice across these state’s borders.
How the PA Compact Works
The interstate arrangement recognizes valid, unencumbered PA licenses issued by other states in the compact. PAs working within the seven states won’t need a separate license from any of those states to practice.
The states include Delaware, Nebraska, Utah, Washington, West Virginia, Wisconsin, and Virginia. While the compact has been approved, the American Academy of Physician Associates said it could take an additional 18-24 months for the states to execute it, giving PAs the access they need to work in the compact states.
How the PA Compact Helps
The PA Compact holds the promise of alleviating some of the travel barriers that PAs often encounter, especially when they work locum tenens or in telehealth and must traverse state lines to deliver essential healthcare. This agreement not only enhances healthcare access but also empowers facilities to recruit new PAs, thereby bridging gaps in their healthcare staffing and addressing public health emergencies more effectively.
PAs will also gain increased flexibility and additional opportunities to earn and benefit from the right to practice in more states without requiring a time-consuming and expensive licensure from each state.
One motivating factor behind developing an interstate compact for physician assistants is that the same types of compacts for physicians and nurses are highly successful. The Nurse Licensure Compact and the Interstate Medical Licensure Compact for physicians encompass 37 and 41 states, respectively. While the seven-state PA Compact is in its earliest stages, it will likely be equally beneficial for PAs.
A survey by Barton Associates found that 95% of PAs said they would be more likely to consider working in a different state if the PA Compact made it more accessible.
Other states have begun legislation to enact a PA Compact, including Colorado, New Hampshire, Maine, Michigan New York, Ohio, Oklahoma, Rhode Island, Tennessee, and Vermont.
If your state still needs to enact a compact or file for compact legislation, let your elected officials know that the PAs in your state want to join a compact.
A version of this article appeared on Medscape.com .
For decades, physicians and nurses who ventured across state lines to practice, particularly in locum tenens roles, have reaped the benefits of medical licensure compacts. Yet, the same courtesy has eluded physician assistants (PAs), until now.
In April, Virginia Governor Glenn Youngkin signed the bill enacting the PA Compact making Virginia the seventh state to join. The legislation opens a cross-state agreement with seven states and finally allows locum tenens PAs to practice across these state’s borders.
How the PA Compact Works
The interstate arrangement recognizes valid, unencumbered PA licenses issued by other states in the compact. PAs working within the seven states won’t need a separate license from any of those states to practice.
The states include Delaware, Nebraska, Utah, Washington, West Virginia, Wisconsin, and Virginia. While the compact has been approved, the American Academy of Physician Associates said it could take an additional 18-24 months for the states to execute it, giving PAs the access they need to work in the compact states.
How the PA Compact Helps
The PA Compact holds the promise of alleviating some of the travel barriers that PAs often encounter, especially when they work locum tenens or in telehealth and must traverse state lines to deliver essential healthcare. This agreement not only enhances healthcare access but also empowers facilities to recruit new PAs, thereby bridging gaps in their healthcare staffing and addressing public health emergencies more effectively.
PAs will also gain increased flexibility and additional opportunities to earn and benefit from the right to practice in more states without requiring a time-consuming and expensive licensure from each state.
One motivating factor behind developing an interstate compact for physician assistants is that the same types of compacts for physicians and nurses are highly successful. The Nurse Licensure Compact and the Interstate Medical Licensure Compact for physicians encompass 37 and 41 states, respectively. While the seven-state PA Compact is in its earliest stages, it will likely be equally beneficial for PAs.
A survey by Barton Associates found that 95% of PAs said they would be more likely to consider working in a different state if the PA Compact made it more accessible.
Other states have begun legislation to enact a PA Compact, including Colorado, New Hampshire, Maine, Michigan New York, Ohio, Oklahoma, Rhode Island, Tennessee, and Vermont.
If your state still needs to enact a compact or file for compact legislation, let your elected officials know that the PAs in your state want to join a compact.
A version of this article appeared on Medscape.com .
Is Body Fat a Better Measure of Obesity in Midlife Than BMI?
VENICE, ITALY — Obesity as defined by adiposity measures corresponds to a lower body mass index (BMI) cutoff (≥ 27) in men and women of middle age or older than does the widely used conventional obesity threshold of ≥ 30, shows a study performed in Italy.
Presenting at this year’s European Congress on Obesity (ECO), researchers from the University of Rome Tor Vergata and University of Modena and Reggio Emilia, Italy, and Beirut Arab University, Lebanon, conducted the study to compare the validity of the traditional World Health Organization (WHO) BMI threshold for obesity classification (≥ 30) vs adiposity levels as an alternative measure in middle-aged and older Italians.
Marwan El Ghoch, PhD, a professor in the Department of Biomedical, Metabolic and Neuroscience, University of Modena and Reggio Emilia, presented the findings as a poster (GC4.152). “If you classify obesity with only BMI and without consideration of body composition, then this will not be enough. I believe BMI can be considered as a screening starting point, but we need to understand the body composition of fat and muscle too,” he said.
“We recommend this new cutoff point be applied in clinical settings when screening individuals for obesity in Italy,” El Ghoch asserted.
BMI Limitations Misses Body Composition
If obesity is a chronic disease defined as excessive accumulation of body fat and leading to increased risk for disease, disability, and mortality, then “the identification of obesity based on body fat measurements is the most reliable method,” but he acknowledged that measuring this is not readily available in most clinical settings, and as such, “simple BMI has a place,” Dr. El Ghoch said.
[for example, the shift to more fat and less muscle with age] and it varies by ethnicity,” he pointed out.
This led El Ghoch to ask whether using BMI as a threshold for obesity was suitable for all age groups.
The researchers included 4800 participants of mixed gender aged 40-80 years of age. Based on the WHO’s BMI classification, 1087 people had normal body weight, 1826 had overweight, and 1887 had obesity. The participants were then categorized by adiposity status on the basis of the total body fat percentage as measured by dual-energy x-ray absorptiometry (DXA), and obesity was predicted by statistical analysis.
The analysis found that around 38% of men and 41% of women had a BMI ≥ 30 based on conventional BMI criteria, indicating obesity. However, when assessed according to body fat percentage, around 71% of the men and 64% of the women were determined to have obesity.
Dr. El Ghoch and his colleagues calculated that a lower BMI cutoff of around 27 for obesity in people older than 40 years may be more appropriate than the existing BMI threshold of 30.
The researchers noted some limitations of their work, including that it was a single-center, cross-sectional observational study conducted in one area of Italy. In addition, they did not account for possible confounders, such as dietary habits, and physical activity patterns, and sleep health, all of which can increase the likelihood of obesity and may interact with age-related differences.
Missing a Significant Proportion of the Population at Risk for Obesity-Related Diseases
In an interview, Luca Busetto, MD, obesity specialist and research assistant at the Center for the Study and the Integrated Treatment of the Obesity, University of Padova, Italy, and local ECO president, commented on the study and the issue of BMI as a measure and threshold. “I think the problem we face with a classic cutoff using BMI is that we miss a significant group of people who have BMI less than 30 but have a high fat mass,” he said, adding, “but these people have the same risk of developing chronic diseases as those people with higher BMI. If they have a bad fat distribution, then their risk of complications is even higher.
“Dr El Ghoch’s study underlines the lack of treatment for this significant part of the population,” he remarked. “We also need to use waist circumference and waist-to-height [ratio] as additional measures in this population.”
Dr. Busetto also presented a population-based study at ECO that included over 400,000 people with a follow-up of 8 years. “We found the risk of developing obesity complications, including type 2 diabetes, hypertension, osteoarthritis, and cardiovascular disease, is not only dependent on BMI but [also] dependent on your waist-to-height ratio,” he said, highlighting that “some of these complications are only predicted by the waist-to-height ratio and not by your BMI — in particular cardiovascular diseases.
“I honestly think any screening process today needs to include both BMI and waist-to-height ratio. Having a DXA scan is great in a specialist setting, but routinely we need a measure that is valid in every office in every country and small town.”
Francesco Rubino, MD, chair of metabolic and bariatric surgery at King›s College London, United Kingdom, also remarked that understanding the changes in fat and lean mass proportions and distribution in middle years will affect health in later life, and importantly from a clinical perspective, it is a time where there is still some opportunity to intervene.
Reflecting further on how it underscores the limitations of BMI in misclassifying people as having obesity or not, Rubino asked, “Importantly, does this make a difference to health and longevity? Really, we need an active measure of adiposity first, and then even if we do say someone has obesity — so excess adiposity — then does this translate into illness, because [excess adiposity] does not translate into disease for every individual?
“Any measure we use as a diagnostic criterion needs to reflect the ongoing disease in an individual, not only the risk of future disease — because not every person experiences this. As a doctor, we deal with the individual and how the diagnosis of disease relates to the individual in a clinic now, as well as the risk of tomorrow,” he concluded.
Dr. El Ghoch declares no conflicts of interest. Dr. Rubino disclosed that he has received research grants from Novo Nordisk, Medtronic, and Johnson & Johnson. He has undertaken paid consultancy work for GI Dynamics and received honoraria for lectures from Medtronic, Novo Nordisk, and Johnson & Johnson. He is a member of the data safety monitoring board for GT Metabolic Solutions and has provided scientific advice to Keyron, MetaDeq, GHP Scientific, and ViBo Health for no remuneration. Dr. Busetto discloses relationships with Burno Farmaceutici, Novo Nordisk, PronoKal, Rhythm, and Therascience.
A version of this article appeared on Medscape.com.
VENICE, ITALY — Obesity as defined by adiposity measures corresponds to a lower body mass index (BMI) cutoff (≥ 27) in men and women of middle age or older than does the widely used conventional obesity threshold of ≥ 30, shows a study performed in Italy.
Presenting at this year’s European Congress on Obesity (ECO), researchers from the University of Rome Tor Vergata and University of Modena and Reggio Emilia, Italy, and Beirut Arab University, Lebanon, conducted the study to compare the validity of the traditional World Health Organization (WHO) BMI threshold for obesity classification (≥ 30) vs adiposity levels as an alternative measure in middle-aged and older Italians.
Marwan El Ghoch, PhD, a professor in the Department of Biomedical, Metabolic and Neuroscience, University of Modena and Reggio Emilia, presented the findings as a poster (GC4.152). “If you classify obesity with only BMI and without consideration of body composition, then this will not be enough. I believe BMI can be considered as a screening starting point, but we need to understand the body composition of fat and muscle too,” he said.
“We recommend this new cutoff point be applied in clinical settings when screening individuals for obesity in Italy,” El Ghoch asserted.
BMI Limitations Misses Body Composition
If obesity is a chronic disease defined as excessive accumulation of body fat and leading to increased risk for disease, disability, and mortality, then “the identification of obesity based on body fat measurements is the most reliable method,” but he acknowledged that measuring this is not readily available in most clinical settings, and as such, “simple BMI has a place,” Dr. El Ghoch said.
[for example, the shift to more fat and less muscle with age] and it varies by ethnicity,” he pointed out.
This led El Ghoch to ask whether using BMI as a threshold for obesity was suitable for all age groups.
The researchers included 4800 participants of mixed gender aged 40-80 years of age. Based on the WHO’s BMI classification, 1087 people had normal body weight, 1826 had overweight, and 1887 had obesity. The participants were then categorized by adiposity status on the basis of the total body fat percentage as measured by dual-energy x-ray absorptiometry (DXA), and obesity was predicted by statistical analysis.
The analysis found that around 38% of men and 41% of women had a BMI ≥ 30 based on conventional BMI criteria, indicating obesity. However, when assessed according to body fat percentage, around 71% of the men and 64% of the women were determined to have obesity.
Dr. El Ghoch and his colleagues calculated that a lower BMI cutoff of around 27 for obesity in people older than 40 years may be more appropriate than the existing BMI threshold of 30.
The researchers noted some limitations of their work, including that it was a single-center, cross-sectional observational study conducted in one area of Italy. In addition, they did not account for possible confounders, such as dietary habits, and physical activity patterns, and sleep health, all of which can increase the likelihood of obesity and may interact with age-related differences.
Missing a Significant Proportion of the Population at Risk for Obesity-Related Diseases
In an interview, Luca Busetto, MD, obesity specialist and research assistant at the Center for the Study and the Integrated Treatment of the Obesity, University of Padova, Italy, and local ECO president, commented on the study and the issue of BMI as a measure and threshold. “I think the problem we face with a classic cutoff using BMI is that we miss a significant group of people who have BMI less than 30 but have a high fat mass,” he said, adding, “but these people have the same risk of developing chronic diseases as those people with higher BMI. If they have a bad fat distribution, then their risk of complications is even higher.
“Dr El Ghoch’s study underlines the lack of treatment for this significant part of the population,” he remarked. “We also need to use waist circumference and waist-to-height [ratio] as additional measures in this population.”
Dr. Busetto also presented a population-based study at ECO that included over 400,000 people with a follow-up of 8 years. “We found the risk of developing obesity complications, including type 2 diabetes, hypertension, osteoarthritis, and cardiovascular disease, is not only dependent on BMI but [also] dependent on your waist-to-height ratio,” he said, highlighting that “some of these complications are only predicted by the waist-to-height ratio and not by your BMI — in particular cardiovascular diseases.
“I honestly think any screening process today needs to include both BMI and waist-to-height ratio. Having a DXA scan is great in a specialist setting, but routinely we need a measure that is valid in every office in every country and small town.”
Francesco Rubino, MD, chair of metabolic and bariatric surgery at King›s College London, United Kingdom, also remarked that understanding the changes in fat and lean mass proportions and distribution in middle years will affect health in later life, and importantly from a clinical perspective, it is a time where there is still some opportunity to intervene.
Reflecting further on how it underscores the limitations of BMI in misclassifying people as having obesity or not, Rubino asked, “Importantly, does this make a difference to health and longevity? Really, we need an active measure of adiposity first, and then even if we do say someone has obesity — so excess adiposity — then does this translate into illness, because [excess adiposity] does not translate into disease for every individual?
“Any measure we use as a diagnostic criterion needs to reflect the ongoing disease in an individual, not only the risk of future disease — because not every person experiences this. As a doctor, we deal with the individual and how the diagnosis of disease relates to the individual in a clinic now, as well as the risk of tomorrow,” he concluded.
Dr. El Ghoch declares no conflicts of interest. Dr. Rubino disclosed that he has received research grants from Novo Nordisk, Medtronic, and Johnson & Johnson. He has undertaken paid consultancy work for GI Dynamics and received honoraria for lectures from Medtronic, Novo Nordisk, and Johnson & Johnson. He is a member of the data safety monitoring board for GT Metabolic Solutions and has provided scientific advice to Keyron, MetaDeq, GHP Scientific, and ViBo Health for no remuneration. Dr. Busetto discloses relationships with Burno Farmaceutici, Novo Nordisk, PronoKal, Rhythm, and Therascience.
A version of this article appeared on Medscape.com.
VENICE, ITALY — Obesity as defined by adiposity measures corresponds to a lower body mass index (BMI) cutoff (≥ 27) in men and women of middle age or older than does the widely used conventional obesity threshold of ≥ 30, shows a study performed in Italy.
Presenting at this year’s European Congress on Obesity (ECO), researchers from the University of Rome Tor Vergata and University of Modena and Reggio Emilia, Italy, and Beirut Arab University, Lebanon, conducted the study to compare the validity of the traditional World Health Organization (WHO) BMI threshold for obesity classification (≥ 30) vs adiposity levels as an alternative measure in middle-aged and older Italians.
Marwan El Ghoch, PhD, a professor in the Department of Biomedical, Metabolic and Neuroscience, University of Modena and Reggio Emilia, presented the findings as a poster (GC4.152). “If you classify obesity with only BMI and without consideration of body composition, then this will not be enough. I believe BMI can be considered as a screening starting point, but we need to understand the body composition of fat and muscle too,” he said.
“We recommend this new cutoff point be applied in clinical settings when screening individuals for obesity in Italy,” El Ghoch asserted.
BMI Limitations Misses Body Composition
If obesity is a chronic disease defined as excessive accumulation of body fat and leading to increased risk for disease, disability, and mortality, then “the identification of obesity based on body fat measurements is the most reliable method,” but he acknowledged that measuring this is not readily available in most clinical settings, and as such, “simple BMI has a place,” Dr. El Ghoch said.
[for example, the shift to more fat and less muscle with age] and it varies by ethnicity,” he pointed out.
This led El Ghoch to ask whether using BMI as a threshold for obesity was suitable for all age groups.
The researchers included 4800 participants of mixed gender aged 40-80 years of age. Based on the WHO’s BMI classification, 1087 people had normal body weight, 1826 had overweight, and 1887 had obesity. The participants were then categorized by adiposity status on the basis of the total body fat percentage as measured by dual-energy x-ray absorptiometry (DXA), and obesity was predicted by statistical analysis.
The analysis found that around 38% of men and 41% of women had a BMI ≥ 30 based on conventional BMI criteria, indicating obesity. However, when assessed according to body fat percentage, around 71% of the men and 64% of the women were determined to have obesity.
Dr. El Ghoch and his colleagues calculated that a lower BMI cutoff of around 27 for obesity in people older than 40 years may be more appropriate than the existing BMI threshold of 30.
The researchers noted some limitations of their work, including that it was a single-center, cross-sectional observational study conducted in one area of Italy. In addition, they did not account for possible confounders, such as dietary habits, and physical activity patterns, and sleep health, all of which can increase the likelihood of obesity and may interact with age-related differences.
Missing a Significant Proportion of the Population at Risk for Obesity-Related Diseases
In an interview, Luca Busetto, MD, obesity specialist and research assistant at the Center for the Study and the Integrated Treatment of the Obesity, University of Padova, Italy, and local ECO president, commented on the study and the issue of BMI as a measure and threshold. “I think the problem we face with a classic cutoff using BMI is that we miss a significant group of people who have BMI less than 30 but have a high fat mass,” he said, adding, “but these people have the same risk of developing chronic diseases as those people with higher BMI. If they have a bad fat distribution, then their risk of complications is even higher.
“Dr El Ghoch’s study underlines the lack of treatment for this significant part of the population,” he remarked. “We also need to use waist circumference and waist-to-height [ratio] as additional measures in this population.”
Dr. Busetto also presented a population-based study at ECO that included over 400,000 people with a follow-up of 8 years. “We found the risk of developing obesity complications, including type 2 diabetes, hypertension, osteoarthritis, and cardiovascular disease, is not only dependent on BMI but [also] dependent on your waist-to-height ratio,” he said, highlighting that “some of these complications are only predicted by the waist-to-height ratio and not by your BMI — in particular cardiovascular diseases.
“I honestly think any screening process today needs to include both BMI and waist-to-height ratio. Having a DXA scan is great in a specialist setting, but routinely we need a measure that is valid in every office in every country and small town.”
Francesco Rubino, MD, chair of metabolic and bariatric surgery at King›s College London, United Kingdom, also remarked that understanding the changes in fat and lean mass proportions and distribution in middle years will affect health in later life, and importantly from a clinical perspective, it is a time where there is still some opportunity to intervene.
Reflecting further on how it underscores the limitations of BMI in misclassifying people as having obesity or not, Rubino asked, “Importantly, does this make a difference to health and longevity? Really, we need an active measure of adiposity first, and then even if we do say someone has obesity — so excess adiposity — then does this translate into illness, because [excess adiposity] does not translate into disease for every individual?
“Any measure we use as a diagnostic criterion needs to reflect the ongoing disease in an individual, not only the risk of future disease — because not every person experiences this. As a doctor, we deal with the individual and how the diagnosis of disease relates to the individual in a clinic now, as well as the risk of tomorrow,” he concluded.
Dr. El Ghoch declares no conflicts of interest. Dr. Rubino disclosed that he has received research grants from Novo Nordisk, Medtronic, and Johnson & Johnson. He has undertaken paid consultancy work for GI Dynamics and received honoraria for lectures from Medtronic, Novo Nordisk, and Johnson & Johnson. He is a member of the data safety monitoring board for GT Metabolic Solutions and has provided scientific advice to Keyron, MetaDeq, GHP Scientific, and ViBo Health for no remuneration. Dr. Busetto discloses relationships with Burno Farmaceutici, Novo Nordisk, PronoKal, Rhythm, and Therascience.
A version of this article appeared on Medscape.com.