User login
Topiramate Plus Metformin Effective for Weight Loss in PCOS
TOPLINE:
In women with polycystic ovary syndrome (PCOS) and with obesity or overweight, the combination of topiramate and metformin along with a low-calorie diet can result in effective weight loss and improve androgen levels, lipid levels, and psychosocial scores, without any serious adverse events.
METHODOLOGY:
- Topiramate is often used off-label for weight loss and may be a promising option added to a metformin regimen to improve cardiometabolic and reproductive health in women with PCOS and obesity or overweight when lifestyle changes alone fall short.
- This double-blind trial conducted at Hospital de Clínicas de Porto Alegre in Porto Alegre, Brazil, evaluated the effects of adding topiramate to metformin in 61 women aged 14-40 years with PCOS and body mass index (BMI) ≥ 30 or BMI ≥ 27 with concurrent hypertension, type 2 diabetes, or dyslipidemia.
- All participants were prescribed a 20 kcal/kg diet, as well as desogestrel for contraception during the study, and either started on 850 mg metformin or continued with their existing metformin regimen.
- They were randomly assigned to receive either topiramate or placebo (25 mg for 15 days and then 50 mg at night) along with metformin, with dose adjustments based on weight loss at 3 months.
- The primary outcome was the percent change in body weight from baseline, and the secondary outcomes included changes in clinical, cardiometabolic, and hormonal parameters and psychosocial features at 3 and 6 months.
TAKEAWAY:
- Topiramate combined with metformin resulted in greater mean weight loss at 3 months (−3.4% vs −1.6%; P = .03) and 6 months (−4.5% vs −1.4%; P = .03) than placebo plus metformin.
- Both treatment groups showed improvements in androgen and lipid levels and psychosocial scores, while the levels of C-reactive protein decreased only in the topiramate plus metformin group.
- Women who experienced ≥ 3% weight loss at 6 months showed a significant improvement in hirsutism scores (change in modified Ferriman-Gallwey scores, 8.4-6.5), unlike those who experienced < 3% weight loss (change in modified Ferriman-Gallwey scores, 8.02-8.78).
- Paresthesia was more common in the topiramate plus metformin group than in the metformin plus placebo group (23.3% vs 3.2%), but no serious adverse events were reported.
IN PRACTICE:
“In the era of new effective drugs for treating obesity, topiramate with metformin can be an option for women with obesity and PCOS, considering its low cost, reports of long-term experience with this medication, and ease to use,” the authors wrote.
SOURCE:
The study was led by Lucas Bandeira Marchesan, Gynecological Endocrinology Unit, Division of Endocrinology, Hospital de Clínicas de Porto Alegre, and was published online in The Journal of Clinical Endocrinology & Metabolism.
LIMITATIONS:
The small sample size and high attrition rates were major limitations of this study. Increasing the topiramate dose at 3 months in those with < 3% weight loss did not provide additional benefit, and this study did not test for a higher topiramate dose response from the beginning, which could have potentially provided a better response to the medication. The small sample size of the study also prevented the authors from conducting a subgroup analysis.
DISCLOSURES:
The study was supported by research grants from the Conselho Nacional de Desenvolvimento Científico e Tecnológico, Brazil, and Fundação de Amparo à Pesquisa do Estado do Rio Grande do Sul, Brazil. The authors declared no conflicts of interest.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
TOPLINE:
In women with polycystic ovary syndrome (PCOS) and with obesity or overweight, the combination of topiramate and metformin along with a low-calorie diet can result in effective weight loss and improve androgen levels, lipid levels, and psychosocial scores, without any serious adverse events.
METHODOLOGY:
- Topiramate is often used off-label for weight loss and may be a promising option added to a metformin regimen to improve cardiometabolic and reproductive health in women with PCOS and obesity or overweight when lifestyle changes alone fall short.
- This double-blind trial conducted at Hospital de Clínicas de Porto Alegre in Porto Alegre, Brazil, evaluated the effects of adding topiramate to metformin in 61 women aged 14-40 years with PCOS and body mass index (BMI) ≥ 30 or BMI ≥ 27 with concurrent hypertension, type 2 diabetes, or dyslipidemia.
- All participants were prescribed a 20 kcal/kg diet, as well as desogestrel for contraception during the study, and either started on 850 mg metformin or continued with their existing metformin regimen.
- They were randomly assigned to receive either topiramate or placebo (25 mg for 15 days and then 50 mg at night) along with metformin, with dose adjustments based on weight loss at 3 months.
- The primary outcome was the percent change in body weight from baseline, and the secondary outcomes included changes in clinical, cardiometabolic, and hormonal parameters and psychosocial features at 3 and 6 months.
TAKEAWAY:
- Topiramate combined with metformin resulted in greater mean weight loss at 3 months (−3.4% vs −1.6%; P = .03) and 6 months (−4.5% vs −1.4%; P = .03) than placebo plus metformin.
- Both treatment groups showed improvements in androgen and lipid levels and psychosocial scores, while the levels of C-reactive protein decreased only in the topiramate plus metformin group.
- Women who experienced ≥ 3% weight loss at 6 months showed a significant improvement in hirsutism scores (change in modified Ferriman-Gallwey scores, 8.4-6.5), unlike those who experienced < 3% weight loss (change in modified Ferriman-Gallwey scores, 8.02-8.78).
- Paresthesia was more common in the topiramate plus metformin group than in the metformin plus placebo group (23.3% vs 3.2%), but no serious adverse events were reported.
IN PRACTICE:
“In the era of new effective drugs for treating obesity, topiramate with metformin can be an option for women with obesity and PCOS, considering its low cost, reports of long-term experience with this medication, and ease to use,” the authors wrote.
SOURCE:
The study was led by Lucas Bandeira Marchesan, Gynecological Endocrinology Unit, Division of Endocrinology, Hospital de Clínicas de Porto Alegre, and was published online in The Journal of Clinical Endocrinology & Metabolism.
LIMITATIONS:
The small sample size and high attrition rates were major limitations of this study. Increasing the topiramate dose at 3 months in those with < 3% weight loss did not provide additional benefit, and this study did not test for a higher topiramate dose response from the beginning, which could have potentially provided a better response to the medication. The small sample size of the study also prevented the authors from conducting a subgroup analysis.
DISCLOSURES:
The study was supported by research grants from the Conselho Nacional de Desenvolvimento Científico e Tecnológico, Brazil, and Fundação de Amparo à Pesquisa do Estado do Rio Grande do Sul, Brazil. The authors declared no conflicts of interest.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
TOPLINE:
In women with polycystic ovary syndrome (PCOS) and with obesity or overweight, the combination of topiramate and metformin along with a low-calorie diet can result in effective weight loss and improve androgen levels, lipid levels, and psychosocial scores, without any serious adverse events.
METHODOLOGY:
- Topiramate is often used off-label for weight loss and may be a promising option added to a metformin regimen to improve cardiometabolic and reproductive health in women with PCOS and obesity or overweight when lifestyle changes alone fall short.
- This double-blind trial conducted at Hospital de Clínicas de Porto Alegre in Porto Alegre, Brazil, evaluated the effects of adding topiramate to metformin in 61 women aged 14-40 years with PCOS and body mass index (BMI) ≥ 30 or BMI ≥ 27 with concurrent hypertension, type 2 diabetes, or dyslipidemia.
- All participants were prescribed a 20 kcal/kg diet, as well as desogestrel for contraception during the study, and either started on 850 mg metformin or continued with their existing metformin regimen.
- They were randomly assigned to receive either topiramate or placebo (25 mg for 15 days and then 50 mg at night) along with metformin, with dose adjustments based on weight loss at 3 months.
- The primary outcome was the percent change in body weight from baseline, and the secondary outcomes included changes in clinical, cardiometabolic, and hormonal parameters and psychosocial features at 3 and 6 months.
TAKEAWAY:
- Topiramate combined with metformin resulted in greater mean weight loss at 3 months (−3.4% vs −1.6%; P = .03) and 6 months (−4.5% vs −1.4%; P = .03) than placebo plus metformin.
- Both treatment groups showed improvements in androgen and lipid levels and psychosocial scores, while the levels of C-reactive protein decreased only in the topiramate plus metformin group.
- Women who experienced ≥ 3% weight loss at 6 months showed a significant improvement in hirsutism scores (change in modified Ferriman-Gallwey scores, 8.4-6.5), unlike those who experienced < 3% weight loss (change in modified Ferriman-Gallwey scores, 8.02-8.78).
- Paresthesia was more common in the topiramate plus metformin group than in the metformin plus placebo group (23.3% vs 3.2%), but no serious adverse events were reported.
IN PRACTICE:
“In the era of new effective drugs for treating obesity, topiramate with metformin can be an option for women with obesity and PCOS, considering its low cost, reports of long-term experience with this medication, and ease to use,” the authors wrote.
SOURCE:
The study was led by Lucas Bandeira Marchesan, Gynecological Endocrinology Unit, Division of Endocrinology, Hospital de Clínicas de Porto Alegre, and was published online in The Journal of Clinical Endocrinology & Metabolism.
LIMITATIONS:
The small sample size and high attrition rates were major limitations of this study. Increasing the topiramate dose at 3 months in those with < 3% weight loss did not provide additional benefit, and this study did not test for a higher topiramate dose response from the beginning, which could have potentially provided a better response to the medication. The small sample size of the study also prevented the authors from conducting a subgroup analysis.
DISCLOSURES:
The study was supported by research grants from the Conselho Nacional de Desenvolvimento Científico e Tecnológico, Brazil, and Fundação de Amparo à Pesquisa do Estado do Rio Grande do Sul, Brazil. The authors declared no conflicts of interest.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
On Second Thought: Aspirin for Primary Prevention — What We Really Know
This transcript has been edited for clarity.
Our recommendations vis-à-vis aspirin have evolved at a dizzying pace. The young’uns watching us right now don’t know what things were like in the 1980s. The Reagan era was a wild, heady time where nuclear war was imminent and we didn’t prescribe aspirin to patients.
That only started in 1988, which was a banner year in human history. Not because a number of doves were incinerated by the lighting of the Olympic torch at the Seoul Olympics — look it up if you don’t know what I’m talking about — but because 1988 saw the publication of the ISIS-2 trial, which first showed a mortality benefit to prescribing aspirin post–myocardial infarction (MI).
Giving patients aspirin during or after a heart attack is not controversial. It’s one of the few things in this business that isn’t, but that’s secondary prevention — treating somebody after they develop a disease. Primary prevention, treating them before they have their incident event, is a very different ballgame. Here, things are messy.
For one thing, the doses used have been very inconsistent. We should point out that the reason for 81 mg of aspirin is very arbitrary and is rooted in the old apothecary system of weights and measurements. A standard dose of aspirin was 5 grains, where 20 grains made 1 scruple, 3 scruples made 1 dram, 8 drams made 1 oz, and 12 oz made 1 lb - because screw you, metric system. Therefore, 5 grains was 325 mg of aspirin, and 1 quarter of the standard dose became 81 mg if you rounded out the decimal.
People have tried all kinds of dosing structures with aspirin prophylaxis. The Physicians’ Health Study used a full-dose aspirin, 325 mg every 2 days, while the Hypertension Optimal Treatment (HOT) trial tested 75 mg daily and the Women’s Health Study tested 100 mg, but every other day.
Ironically, almost no one has studied 81 mg every day, which is weird if you think about it. The bigger problem here is not the variability of doses used, but the discrepancy when you look at older vs newer studies.
Older studies, like the Physicians’ Health Study, did show a benefit, at least in the subgroup of patients over age 50 years, which is probably where the “everybody over 50 should be taking an aspirin” idea comes from, at least as near as I can tell.
More recent studies, like the Women’s Health Study, ASPREE, or ASPIRE, didn’t show a benefit. I know what you’re thinking: Newer stuff is always better. That’s why you should never trust anybody over age 40 years. The context of primary prevention studies has changed. In the ‘80s and ‘90s, people smoked more and we didn’t have the same medications that we have today. We talked about all this in the beta-blocker video to explain why beta-blockers don’t seem to have a benefit post MI.
We have a similar issue here. The magnitude of the benefit with aspirin primary prevention has decreased because we’re all just healthier overall. So, yay! Progress! Here’s where the numbers matter. No one is saying that aspirin doesn’t help. It does.
If we look at the 2019 meta-analysis published in JAMA, there is a cardiovascular benefit. The numbers bear that out. I know you’re all here for the math, so here we go. Aspirin reduced the composite cardiovascular endpoint from 65.2 to 60.2 events per 10,000 patient-years; or to put it more meaningfully in absolute risk reduction terms, because that’s my jam, an absolute risk reduction of 0.41%, which means a number needed to treat of 241, which is okay-ish. It’s not super-great, but it may be justifiable for something that costs next to nothing.
The tradeoff is bleeding. Major bleeding increased from 16.4 to 23.1 bleeds per 10,000 patient-years, or an absolute risk increase of 0.47%, which is a number needed to harm of 210. That’s the problem. Aspirin does prevent heart disease. The benefit is small, for sure, but the real problem is that it’s outweighed by the risk of bleeding, so you’re not really coming out ahead.
The real tragedy here is that the public is locked into this idea of everyone over age 50 years should be taking an aspirin. Even today, even though guidelines have recommended against aspirin for primary prevention for some time, data from the National Health Interview Survey sample found that nearly one in three older adults take aspirin for primary prevention when they shouldn’t be. That’s a large number of people. That’s millions of Americans — and Canadians, but nobody cares about us. It’s fine.
That’s the point. We’re not debunking aspirin. It does work. The benefits are just really small in a primary prevention population and offset by the admittedly also really small risks of bleeding. It’s a tradeoff that doesn’t really work in your favor.
But that’s aspirin for cardiovascular disease. When it comes to cancer or DVT prophylaxis, that’s another really interesting story. We might have to save that for another time. Do I know how to tease a sequel or what?
Labos, a cardiologist at Kirkland Medical Center, Montreal, Quebec, Canada, has disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
This transcript has been edited for clarity.
Our recommendations vis-à-vis aspirin have evolved at a dizzying pace. The young’uns watching us right now don’t know what things were like in the 1980s. The Reagan era was a wild, heady time where nuclear war was imminent and we didn’t prescribe aspirin to patients.
That only started in 1988, which was a banner year in human history. Not because a number of doves were incinerated by the lighting of the Olympic torch at the Seoul Olympics — look it up if you don’t know what I’m talking about — but because 1988 saw the publication of the ISIS-2 trial, which first showed a mortality benefit to prescribing aspirin post–myocardial infarction (MI).
Giving patients aspirin during or after a heart attack is not controversial. It’s one of the few things in this business that isn’t, but that’s secondary prevention — treating somebody after they develop a disease. Primary prevention, treating them before they have their incident event, is a very different ballgame. Here, things are messy.
For one thing, the doses used have been very inconsistent. We should point out that the reason for 81 mg of aspirin is very arbitrary and is rooted in the old apothecary system of weights and measurements. A standard dose of aspirin was 5 grains, where 20 grains made 1 scruple, 3 scruples made 1 dram, 8 drams made 1 oz, and 12 oz made 1 lb - because screw you, metric system. Therefore, 5 grains was 325 mg of aspirin, and 1 quarter of the standard dose became 81 mg if you rounded out the decimal.
People have tried all kinds of dosing structures with aspirin prophylaxis. The Physicians’ Health Study used a full-dose aspirin, 325 mg every 2 days, while the Hypertension Optimal Treatment (HOT) trial tested 75 mg daily and the Women’s Health Study tested 100 mg, but every other day.
Ironically, almost no one has studied 81 mg every day, which is weird if you think about it. The bigger problem here is not the variability of doses used, but the discrepancy when you look at older vs newer studies.
Older studies, like the Physicians’ Health Study, did show a benefit, at least in the subgroup of patients over age 50 years, which is probably where the “everybody over 50 should be taking an aspirin” idea comes from, at least as near as I can tell.
More recent studies, like the Women’s Health Study, ASPREE, or ASPIRE, didn’t show a benefit. I know what you’re thinking: Newer stuff is always better. That’s why you should never trust anybody over age 40 years. The context of primary prevention studies has changed. In the ‘80s and ‘90s, people smoked more and we didn’t have the same medications that we have today. We talked about all this in the beta-blocker video to explain why beta-blockers don’t seem to have a benefit post MI.
We have a similar issue here. The magnitude of the benefit with aspirin primary prevention has decreased because we’re all just healthier overall. So, yay! Progress! Here’s where the numbers matter. No one is saying that aspirin doesn’t help. It does.
If we look at the 2019 meta-analysis published in JAMA, there is a cardiovascular benefit. The numbers bear that out. I know you’re all here for the math, so here we go. Aspirin reduced the composite cardiovascular endpoint from 65.2 to 60.2 events per 10,000 patient-years; or to put it more meaningfully in absolute risk reduction terms, because that’s my jam, an absolute risk reduction of 0.41%, which means a number needed to treat of 241, which is okay-ish. It’s not super-great, but it may be justifiable for something that costs next to nothing.
The tradeoff is bleeding. Major bleeding increased from 16.4 to 23.1 bleeds per 10,000 patient-years, or an absolute risk increase of 0.47%, which is a number needed to harm of 210. That’s the problem. Aspirin does prevent heart disease. The benefit is small, for sure, but the real problem is that it’s outweighed by the risk of bleeding, so you’re not really coming out ahead.
The real tragedy here is that the public is locked into this idea of everyone over age 50 years should be taking an aspirin. Even today, even though guidelines have recommended against aspirin for primary prevention for some time, data from the National Health Interview Survey sample found that nearly one in three older adults take aspirin for primary prevention when they shouldn’t be. That’s a large number of people. That’s millions of Americans — and Canadians, but nobody cares about us. It’s fine.
That’s the point. We’re not debunking aspirin. It does work. The benefits are just really small in a primary prevention population and offset by the admittedly also really small risks of bleeding. It’s a tradeoff that doesn’t really work in your favor.
But that’s aspirin for cardiovascular disease. When it comes to cancer or DVT prophylaxis, that’s another really interesting story. We might have to save that for another time. Do I know how to tease a sequel or what?
Labos, a cardiologist at Kirkland Medical Center, Montreal, Quebec, Canada, has disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
This transcript has been edited for clarity.
Our recommendations vis-à-vis aspirin have evolved at a dizzying pace. The young’uns watching us right now don’t know what things were like in the 1980s. The Reagan era was a wild, heady time where nuclear war was imminent and we didn’t prescribe aspirin to patients.
That only started in 1988, which was a banner year in human history. Not because a number of doves were incinerated by the lighting of the Olympic torch at the Seoul Olympics — look it up if you don’t know what I’m talking about — but because 1988 saw the publication of the ISIS-2 trial, which first showed a mortality benefit to prescribing aspirin post–myocardial infarction (MI).
Giving patients aspirin during or after a heart attack is not controversial. It’s one of the few things in this business that isn’t, but that’s secondary prevention — treating somebody after they develop a disease. Primary prevention, treating them before they have their incident event, is a very different ballgame. Here, things are messy.
For one thing, the doses used have been very inconsistent. We should point out that the reason for 81 mg of aspirin is very arbitrary and is rooted in the old apothecary system of weights and measurements. A standard dose of aspirin was 5 grains, where 20 grains made 1 scruple, 3 scruples made 1 dram, 8 drams made 1 oz, and 12 oz made 1 lb - because screw you, metric system. Therefore, 5 grains was 325 mg of aspirin, and 1 quarter of the standard dose became 81 mg if you rounded out the decimal.
People have tried all kinds of dosing structures with aspirin prophylaxis. The Physicians’ Health Study used a full-dose aspirin, 325 mg every 2 days, while the Hypertension Optimal Treatment (HOT) trial tested 75 mg daily and the Women’s Health Study tested 100 mg, but every other day.
Ironically, almost no one has studied 81 mg every day, which is weird if you think about it. The bigger problem here is not the variability of doses used, but the discrepancy when you look at older vs newer studies.
Older studies, like the Physicians’ Health Study, did show a benefit, at least in the subgroup of patients over age 50 years, which is probably where the “everybody over 50 should be taking an aspirin” idea comes from, at least as near as I can tell.
More recent studies, like the Women’s Health Study, ASPREE, or ASPIRE, didn’t show a benefit. I know what you’re thinking: Newer stuff is always better. That’s why you should never trust anybody over age 40 years. The context of primary prevention studies has changed. In the ‘80s and ‘90s, people smoked more and we didn’t have the same medications that we have today. We talked about all this in the beta-blocker video to explain why beta-blockers don’t seem to have a benefit post MI.
We have a similar issue here. The magnitude of the benefit with aspirin primary prevention has decreased because we’re all just healthier overall. So, yay! Progress! Here’s where the numbers matter. No one is saying that aspirin doesn’t help. It does.
If we look at the 2019 meta-analysis published in JAMA, there is a cardiovascular benefit. The numbers bear that out. I know you’re all here for the math, so here we go. Aspirin reduced the composite cardiovascular endpoint from 65.2 to 60.2 events per 10,000 patient-years; or to put it more meaningfully in absolute risk reduction terms, because that’s my jam, an absolute risk reduction of 0.41%, which means a number needed to treat of 241, which is okay-ish. It’s not super-great, but it may be justifiable for something that costs next to nothing.
The tradeoff is bleeding. Major bleeding increased from 16.4 to 23.1 bleeds per 10,000 patient-years, or an absolute risk increase of 0.47%, which is a number needed to harm of 210. That’s the problem. Aspirin does prevent heart disease. The benefit is small, for sure, but the real problem is that it’s outweighed by the risk of bleeding, so you’re not really coming out ahead.
The real tragedy here is that the public is locked into this idea of everyone over age 50 years should be taking an aspirin. Even today, even though guidelines have recommended against aspirin for primary prevention for some time, data from the National Health Interview Survey sample found that nearly one in three older adults take aspirin for primary prevention when they shouldn’t be. That’s a large number of people. That’s millions of Americans — and Canadians, but nobody cares about us. It’s fine.
That’s the point. We’re not debunking aspirin. It does work. The benefits are just really small in a primary prevention population and offset by the admittedly also really small risks of bleeding. It’s a tradeoff that doesn’t really work in your favor.
But that’s aspirin for cardiovascular disease. When it comes to cancer or DVT prophylaxis, that’s another really interesting story. We might have to save that for another time. Do I know how to tease a sequel or what?
Labos, a cardiologist at Kirkland Medical Center, Montreal, Quebec, Canada, has disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
Skin Fungal Infections Increasing in the United States
TOPLINE:
. Tinea unguium, tinea pedis, and tinea corporis were among the most common infections.
METHODOLOGY:
- Researchers analyzed data from the National Ambulatory Medical Care Survey and National Hospital Ambulatory Medical Care Survey from 2005 to 2016, to evaluate trends in the prevalence of SCFIs during this period.
- The analysis included over 13 billion ambulatory visits to nonfederally funded community, office-based physician practices, and emergency or outpatient departments in the United States, with an estimated 1,104,258,333 annual average.
- The Jonckheere-Terpstra nonparametric test for trend was used to determine the pattern of SCFI prevalence over the 12-year period.
TAKEAWAY:
- SCFIs constituted approximately 0.54% of all annual ambulatory visits, with an estimated 6,001,852 visits for SCFIs per year and over 72 million total visits for the infections during the study period.
- Tinea unguium, tinea pedis, and tinea corporis were the most common infections, comprising 20.5%, 12.2%, and 12.0% of the total visits, respectively.
- Researchers noted an increasing trend in annual SCFIs (P = .03).
IN PRACTICE:
“We observed a high burden of SCFIs among outpatient visits in the United States and an increasing trend in their prevalence,” the authors wrote. These results, they added, “highlight the importance of healthcare providers being able to identify, treat, and, when necessary, refer patients with SCFIs, as a high burden of disease is associated with a significant negative impact on the individual and population levels.”
SOURCE:
The study was co-led by Sarah L. Spaulding, BS, and A. Mitchel Wride, BA, from the Yale School of Medicine, New Haven, Connecticut, and was published online October 30 in the Journal of the American Academy of Dermatology.
LIMITATIONS:
The authors did not list any study limitations.
DISCLOSURES:
The lead authors were supported by Yale School of Medicine Medical Student Research Fellowships. Two other authors declared receiving consulting fees, research funding, and licensing fees outside the submitted work and also served on a data and safety monitoring board for Advarra Inc.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
TOPLINE:
. Tinea unguium, tinea pedis, and tinea corporis were among the most common infections.
METHODOLOGY:
- Researchers analyzed data from the National Ambulatory Medical Care Survey and National Hospital Ambulatory Medical Care Survey from 2005 to 2016, to evaluate trends in the prevalence of SCFIs during this period.
- The analysis included over 13 billion ambulatory visits to nonfederally funded community, office-based physician practices, and emergency or outpatient departments in the United States, with an estimated 1,104,258,333 annual average.
- The Jonckheere-Terpstra nonparametric test for trend was used to determine the pattern of SCFI prevalence over the 12-year period.
TAKEAWAY:
- SCFIs constituted approximately 0.54% of all annual ambulatory visits, with an estimated 6,001,852 visits for SCFIs per year and over 72 million total visits for the infections during the study period.
- Tinea unguium, tinea pedis, and tinea corporis were the most common infections, comprising 20.5%, 12.2%, and 12.0% of the total visits, respectively.
- Researchers noted an increasing trend in annual SCFIs (P = .03).
IN PRACTICE:
“We observed a high burden of SCFIs among outpatient visits in the United States and an increasing trend in their prevalence,” the authors wrote. These results, they added, “highlight the importance of healthcare providers being able to identify, treat, and, when necessary, refer patients with SCFIs, as a high burden of disease is associated with a significant negative impact on the individual and population levels.”
SOURCE:
The study was co-led by Sarah L. Spaulding, BS, and A. Mitchel Wride, BA, from the Yale School of Medicine, New Haven, Connecticut, and was published online October 30 in the Journal of the American Academy of Dermatology.
LIMITATIONS:
The authors did not list any study limitations.
DISCLOSURES:
The lead authors were supported by Yale School of Medicine Medical Student Research Fellowships. Two other authors declared receiving consulting fees, research funding, and licensing fees outside the submitted work and also served on a data and safety monitoring board for Advarra Inc.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
TOPLINE:
. Tinea unguium, tinea pedis, and tinea corporis were among the most common infections.
METHODOLOGY:
- Researchers analyzed data from the National Ambulatory Medical Care Survey and National Hospital Ambulatory Medical Care Survey from 2005 to 2016, to evaluate trends in the prevalence of SCFIs during this period.
- The analysis included over 13 billion ambulatory visits to nonfederally funded community, office-based physician practices, and emergency or outpatient departments in the United States, with an estimated 1,104,258,333 annual average.
- The Jonckheere-Terpstra nonparametric test for trend was used to determine the pattern of SCFI prevalence over the 12-year period.
TAKEAWAY:
- SCFIs constituted approximately 0.54% of all annual ambulatory visits, with an estimated 6,001,852 visits for SCFIs per year and over 72 million total visits for the infections during the study period.
- Tinea unguium, tinea pedis, and tinea corporis were the most common infections, comprising 20.5%, 12.2%, and 12.0% of the total visits, respectively.
- Researchers noted an increasing trend in annual SCFIs (P = .03).
IN PRACTICE:
“We observed a high burden of SCFIs among outpatient visits in the United States and an increasing trend in their prevalence,” the authors wrote. These results, they added, “highlight the importance of healthcare providers being able to identify, treat, and, when necessary, refer patients with SCFIs, as a high burden of disease is associated with a significant negative impact on the individual and population levels.”
SOURCE:
The study was co-led by Sarah L. Spaulding, BS, and A. Mitchel Wride, BA, from the Yale School of Medicine, New Haven, Connecticut, and was published online October 30 in the Journal of the American Academy of Dermatology.
LIMITATIONS:
The authors did not list any study limitations.
DISCLOSURES:
The lead authors were supported by Yale School of Medicine Medical Student Research Fellowships. Two other authors declared receiving consulting fees, research funding, and licensing fees outside the submitted work and also served on a data and safety monitoring board for Advarra Inc.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
Study Finds Link to Increased Risk for Bulimia, Binge Eating and HS
“Clinicians should actively screen for eating disorders,” particularly bulimia nervosa and binge eating disorder, in patients with HS,” lead study author Christopher Guirguis, DMD, a student at Georgetown University School of Medicine, Washington, DC, told this news organization in advance of the annual Symposium on Hidradenitis Suppurative Advances, where the study was presented during an oral abstract session. “The significant psychological burden in these patients requires a holistic approach that integrates both dermatologic and psychosocial care. Addressing their mental health needs is essential for improving overall patient outcomes and quality of life,” he added.

In collaboration with fellow Georgetown medical student and first author Lauren Chin and Mikael Horissian, MD, a dermatologist and director of the HS Clinic at Gesinger Health System, Danville, Pennsylvania, Guirguis drew from the National Institutes of Health’s All of Us Research Program to identify 1653 individuals with a diagnosis of HS and a control group of 8265 individuals without a diagnosis of HS. They used the Observational Medical Outcomes Partnership to identify anorexia nervosa, bulimia nervosa, body dysmorphic disorder, binge eating disorder, and eating disorder, unspecified. Obsessive-compulsive disorder (OCD) was also included because of its association with bulimia. They used statistical models to compare cohorts and comorbidities. “What makes this work unique is its focus on the link between HS and eating disorders, a relationship previously underexplored,” he said.
The mean age of the overall study cohort was 46.8 years, and 78.6% were female. Univariate analysis revealed that, compared with controls, individuals in the HS cohort showed significantly increased diagnoses of bulimia, binge eating disorder, OCD, and eating disorder, unspecified, by 2.6, 5.48, 2.50, and 2.43 times, respectively (P < .05 for all associations). After adjusting for age, race, sex, and ethnicity, the researchers observed that patients with HS were 4.46 times as likely to have a diagnosis of binge eating disorder and 3.51 times as likely to have a diagnosis of bulimia as those who did not have HS (P < .05 for both associations).
Guirguis said that the absence of body dysmorphic disorder diagnoses in the HS cohort was unexpected. “Given HS’s known association with body image issues, we anticipated a higher prevalence of BDD,” he said. “This discrepancy may reflect underreporting or diagnostic overshadowing, where the physical symptoms of HS dominate clinical attention, potentially masking or complicating the identification of psychological conditions like BDD.”
He acknowledged certain limitations of the study, including the potential for variations in documentation practices in the database. “Additionally, there may be bias due to underrepresentation of certain demographic groups or underreporting of psychological comorbidities, which could influence the findings.”
Patricia M. Richey, MD, assistant professor of dermatology, at Boston University School of Medicine in Massachusetts, who was asked to comment on the study, said the results “should affect how physicians discuss lifestyle recommendations in those already at increased risk of psychiatric disease and disrupted body image.” The findings should also “prompt physicians to screen this patient population more thoroughly for eating disorders as we know they are an underrecognized and often undertreated entity,” she added.
Neither the study authors nor Richey reported having relevant disclosures.
A version of this article appeared on Medscape.com.
“Clinicians should actively screen for eating disorders,” particularly bulimia nervosa and binge eating disorder, in patients with HS,” lead study author Christopher Guirguis, DMD, a student at Georgetown University School of Medicine, Washington, DC, told this news organization in advance of the annual Symposium on Hidradenitis Suppurative Advances, where the study was presented during an oral abstract session. “The significant psychological burden in these patients requires a holistic approach that integrates both dermatologic and psychosocial care. Addressing their mental health needs is essential for improving overall patient outcomes and quality of life,” he added.
In collaboration with fellow Georgetown medical student and first author Lauren Chin and Mikael Horissian, MD, a dermatologist and director of the HS Clinic at Gesinger Health System, Danville, Pennsylvania, Guirguis drew from the National Institutes of Health’s All of Us Research Program to identify 1653 individuals with a diagnosis of HS and a control group of 8265 individuals without a diagnosis of HS. They used the Observational Medical Outcomes Partnership to identify anorexia nervosa, bulimia nervosa, body dysmorphic disorder, binge eating disorder, and eating disorder, unspecified. Obsessive-compulsive disorder (OCD) was also included because of its association with bulimia. They used statistical models to compare cohorts and comorbidities. “What makes this work unique is its focus on the link between HS and eating disorders, a relationship previously underexplored,” he said.
The mean age of the overall study cohort was 46.8 years, and 78.6% were female. Univariate analysis revealed that, compared with controls, individuals in the HS cohort showed significantly increased diagnoses of bulimia, binge eating disorder, OCD, and eating disorder, unspecified, by 2.6, 5.48, 2.50, and 2.43 times, respectively (P < .05 for all associations). After adjusting for age, race, sex, and ethnicity, the researchers observed that patients with HS were 4.46 times as likely to have a diagnosis of binge eating disorder and 3.51 times as likely to have a diagnosis of bulimia as those who did not have HS (P < .05 for both associations).
Guirguis said that the absence of body dysmorphic disorder diagnoses in the HS cohort was unexpected. “Given HS’s known association with body image issues, we anticipated a higher prevalence of BDD,” he said. “This discrepancy may reflect underreporting or diagnostic overshadowing, where the physical symptoms of HS dominate clinical attention, potentially masking or complicating the identification of psychological conditions like BDD.”
He acknowledged certain limitations of the study, including the potential for variations in documentation practices in the database. “Additionally, there may be bias due to underrepresentation of certain demographic groups or underreporting of psychological comorbidities, which could influence the findings.”
Patricia M. Richey, MD, assistant professor of dermatology, at Boston University School of Medicine in Massachusetts, who was asked to comment on the study, said the results “should affect how physicians discuss lifestyle recommendations in those already at increased risk of psychiatric disease and disrupted body image.” The findings should also “prompt physicians to screen this patient population more thoroughly for eating disorders as we know they are an underrecognized and often undertreated entity,” she added.
Neither the study authors nor Richey reported having relevant disclosures.
A version of this article appeared on Medscape.com.
“Clinicians should actively screen for eating disorders,” particularly bulimia nervosa and binge eating disorder, in patients with HS,” lead study author Christopher Guirguis, DMD, a student at Georgetown University School of Medicine, Washington, DC, told this news organization in advance of the annual Symposium on Hidradenitis Suppurative Advances, where the study was presented during an oral abstract session. “The significant psychological burden in these patients requires a holistic approach that integrates both dermatologic and psychosocial care. Addressing their mental health needs is essential for improving overall patient outcomes and quality of life,” he added.
In collaboration with fellow Georgetown medical student and first author Lauren Chin and Mikael Horissian, MD, a dermatologist and director of the HS Clinic at Gesinger Health System, Danville, Pennsylvania, Guirguis drew from the National Institutes of Health’s All of Us Research Program to identify 1653 individuals with a diagnosis of HS and a control group of 8265 individuals without a diagnosis of HS. They used the Observational Medical Outcomes Partnership to identify anorexia nervosa, bulimia nervosa, body dysmorphic disorder, binge eating disorder, and eating disorder, unspecified. Obsessive-compulsive disorder (OCD) was also included because of its association with bulimia. They used statistical models to compare cohorts and comorbidities. “What makes this work unique is its focus on the link between HS and eating disorders, a relationship previously underexplored,” he said.
The mean age of the overall study cohort was 46.8 years, and 78.6% were female. Univariate analysis revealed that, compared with controls, individuals in the HS cohort showed significantly increased diagnoses of bulimia, binge eating disorder, OCD, and eating disorder, unspecified, by 2.6, 5.48, 2.50, and 2.43 times, respectively (P < .05 for all associations). After adjusting for age, race, sex, and ethnicity, the researchers observed that patients with HS were 4.46 times as likely to have a diagnosis of binge eating disorder and 3.51 times as likely to have a diagnosis of bulimia as those who did not have HS (P < .05 for both associations).
Guirguis said that the absence of body dysmorphic disorder diagnoses in the HS cohort was unexpected. “Given HS’s known association with body image issues, we anticipated a higher prevalence of BDD,” he said. “This discrepancy may reflect underreporting or diagnostic overshadowing, where the physical symptoms of HS dominate clinical attention, potentially masking or complicating the identification of psychological conditions like BDD.”
He acknowledged certain limitations of the study, including the potential for variations in documentation practices in the database. “Additionally, there may be bias due to underrepresentation of certain demographic groups or underreporting of psychological comorbidities, which could influence the findings.”
Patricia M. Richey, MD, assistant professor of dermatology, at Boston University School of Medicine in Massachusetts, who was asked to comment on the study, said the results “should affect how physicians discuss lifestyle recommendations in those already at increased risk of psychiatric disease and disrupted body image.” The findings should also “prompt physicians to screen this patient population more thoroughly for eating disorders as we know they are an underrecognized and often undertreated entity,” she added.
Neither the study authors nor Richey reported having relevant disclosures.
A version of this article appeared on Medscape.com.
Brews, Bubbles, & Booze: Stroke Risk and Patients’ Favorite Drinks
This research roundup reviews the latest findings, highlighting both promising insights and remaining uncertainties to help guide discussions with your patients.
Coffee and Tea: Good or Bad?
In the INTERSTROKE study, high coffee consumption (> 4 cups daily) was associated with an significantly increased risk for all strokes (odds ratio [OR], 1.37) or ischemic stroke (OR, 1.31), while low to moderate coffee had no link to increased stroke risk. In contrast, tea consumption was associated with lower odds of all stroke (OR, 0.81 for highest intake) or ischemic stroke (OR, 0.81).
In a recent UK Biobank study, consumption of coffee or tea was associated with reduced risk for stroke and dementia, with the biggest benefit associated with consuming both beverages.
Specifically, the investigators found that individuals who drank two to three cups of coffee and two to three cups of tea per day had a 30% decrease in incidence of stroke and a 28% lower risk for dementia versus those who did not.
A recent systematic review and dose-response meta-analysis showed that each daily cup increase in tea was associated with an average 4% reduced risk for stroke and a 2% reduced risk for cardiovascular disease (CVD) events.
The protective effect of coffee and tea on stroke risk may be driven, in part, by flavonoids, which have antioxidant and anti-inflammatory properties, as well as positive effects on vascular function.
“The advice to patients should be that coffee and tea may protect against stroke, but that sweetening either beverage with sugar probably should be minimized,” said Cheryl Bushnell, MD, MHS, of Wake Forest University School of Medicine in Winston-Salem, North Carolina, and chair of the American Stroke Association (ASA) 2024 Guideline for the Primary Prevention of Stroke.
Taylor Wallace, PhD, a certified food scientist, said, “most people should consume a cup or two of unsweetened tea per day in moderation for cardiometabolic health. It is an easy step in the right direction for good health but not a cure-all.”
When it comes to coffee, adults who like it should drink it “in moderation — just lay off the cream and sugar,” said Wallace, adjunct associate professor at George Washington University, Washington, DC, and Tufts University, Boston, Massachusetts.
“A cup or two of black coffee with low-fat or nonfat milk with breakfast is a healthy way to start the day, especially when you’re like me and have an 8-year-old that is full of energy!” Wallace said.
The Skinny on Soda
When it comes to sugar-sweetened and diet beverages, data from the Nurses’ Health Study and Health Professionals Follow-Up Study, showed a 16% increased risk for stroke with one or more daily servings of sugar-sweetened or low-calorie soda per day (vs none), independent of established dietary and nondietary cardiovascular risk factors.
In the Women’s Health Initiative Observational Study of postmenopausal women, a higher intake of artificially sweetened beverages was associated with increased risk for all stroke (adjusted hazard ratio [aHR], 1.23), ischemic stroke (aHR, 1.31), coronary heart disease (aHR, 1.29) and all-cause mortality (aHR, 1.16).
In the Framingham Heart Study Offspring cohort, consumption of one can of diet soda or more each day (vs none) was associated with a nearly threefold increased risk for stroke and dementia over a 10-year follow-up period.
A separate French study showed that total artificial sweetener intake from all sources was associated with increased overall risk for cardiovascular and cerebrovascular disease.
However, given the limitations of these studies, it’s hard to draw any firm conclusions, Wallace cautioned.
“We know that sugar-sweetened beverages are correlated with weight gain and cardiometabolic dysfunction promotion in children and adults,” he said.
Yet, “there really isn’t any convincing evidence that diet soda has much impact on human health at all. Most observational studies are mixed and likely very confounded by other diet and lifestyle factors. That doesn’t mean go overboard; a daily diet soda is probably fine, but that doesn’t mean go drink 10 of them every day,” he added.
Alcohol: Moderation or Abstinence?
Evidence on alcohol use and stroke risk have been mixed over the years. For decades, the evidence was suggestive that a moderate amount of alcohol daily (one to two drinks in men and one drink in women) may be beneficial at reducing major vascular outcomes.
Yet, over the past few years, some research has found no evidence of benefit with moderate alcohol intake. And the detrimental effects of excessive alcohol use are clear.
A large meta-analysis showed that light to moderate alcohol consumption (up to one drink per day) was associated with a reduced risk for ischemic stroke. However, heavy drinking (more than two drinks per day) significantly increased the risk for both ischemic and hemorrhagic stroke.
A separate study showed young adults who are moderate to heavy drinkers are at increased risk for stroke — and the risk increases with more years of imbibing.
In the INTERSTROKE study, high to moderate alcohol consumption was associated with increased stroke risk, whereas low alcohol consumption conferred no increased risk.
However, Bushnell pointed out that the study data was derived from based on self-report, and that other healthy behaviors may counteract the risk for alcohol consumption.
“For alcohol, regardless of stroke risk, the most important data shows that any alcohol consumption is associated with worse cognitive function, so generally, the lower the alcohol consumption the better,” Bushnell said.
She noted that, currently, the American Heart Association (AHA)/ASA recommend a maximum of two drinks per day for men and one drink per day for women to reduce stroke risk.
“However, the data for the risk for cognitive impairment with any alcohol is convincing and should be kept in mind in addition to the maximum alcohol recommended by the AHA/ASA,” Bushnell advised.
“We know excessive intake puts you at major risk for CVD, cancer, cognitive decline, and a whole host of other health ailments — no question there,” said Wallace.
The impact of moderate intake, on the other hand, is less clear. “Alcohol is a highly biased and political issue and the evidence (or lack thereof) on both sides is shoddy at best,” Wallace added.
A key challenge is that accurate self-reporting of alcohol intake is difficult, even for scientists, and most studies rely on self-reported data from observational cohorts. These often include limited dietary assessments, which provide only a partial picture of long-term consumption patterns, Wallace noted.
“The short answer is we don’t know if moderation is beneficial, detrimental, or null with respect to health,” he said.
Bushnell reports no relevant disclosures. Wallace (www.drtaylorwallace.com) is CEO of Think Healthy Group; editor of The Journal of Dietary Supplements, deputy editor of The Journal of the American Nutrition Association (www.nutrition.org), nutrition section editor of Annals of Medicine, and an advisory board member with Forbes Health.
A version of this article appeared on Medscape.com.
This research roundup reviews the latest findings, highlighting both promising insights and remaining uncertainties to help guide discussions with your patients.
Coffee and Tea: Good or Bad?
In the INTERSTROKE study, high coffee consumption (> 4 cups daily) was associated with an significantly increased risk for all strokes (odds ratio [OR], 1.37) or ischemic stroke (OR, 1.31), while low to moderate coffee had no link to increased stroke risk. In contrast, tea consumption was associated with lower odds of all stroke (OR, 0.81 for highest intake) or ischemic stroke (OR, 0.81).
In a recent UK Biobank study, consumption of coffee or tea was associated with reduced risk for stroke and dementia, with the biggest benefit associated with consuming both beverages.
Specifically, the investigators found that individuals who drank two to three cups of coffee and two to three cups of tea per day had a 30% decrease in incidence of stroke and a 28% lower risk for dementia versus those who did not.
A recent systematic review and dose-response meta-analysis showed that each daily cup increase in tea was associated with an average 4% reduced risk for stroke and a 2% reduced risk for cardiovascular disease (CVD) events.
The protective effect of coffee and tea on stroke risk may be driven, in part, by flavonoids, which have antioxidant and anti-inflammatory properties, as well as positive effects on vascular function.
“The advice to patients should be that coffee and tea may protect against stroke, but that sweetening either beverage with sugar probably should be minimized,” said Cheryl Bushnell, MD, MHS, of Wake Forest University School of Medicine in Winston-Salem, North Carolina, and chair of the American Stroke Association (ASA) 2024 Guideline for the Primary Prevention of Stroke.
Taylor Wallace, PhD, a certified food scientist, said, “most people should consume a cup or two of unsweetened tea per day in moderation for cardiometabolic health. It is an easy step in the right direction for good health but not a cure-all.”
When it comes to coffee, adults who like it should drink it “in moderation — just lay off the cream and sugar,” said Wallace, adjunct associate professor at George Washington University, Washington, DC, and Tufts University, Boston, Massachusetts.
“A cup or two of black coffee with low-fat or nonfat milk with breakfast is a healthy way to start the day, especially when you’re like me and have an 8-year-old that is full of energy!” Wallace said.
The Skinny on Soda
When it comes to sugar-sweetened and diet beverages, data from the Nurses’ Health Study and Health Professionals Follow-Up Study, showed a 16% increased risk for stroke with one or more daily servings of sugar-sweetened or low-calorie soda per day (vs none), independent of established dietary and nondietary cardiovascular risk factors.
In the Women’s Health Initiative Observational Study of postmenopausal women, a higher intake of artificially sweetened beverages was associated with increased risk for all stroke (adjusted hazard ratio [aHR], 1.23), ischemic stroke (aHR, 1.31), coronary heart disease (aHR, 1.29) and all-cause mortality (aHR, 1.16).
In the Framingham Heart Study Offspring cohort, consumption of one can of diet soda or more each day (vs none) was associated with a nearly threefold increased risk for stroke and dementia over a 10-year follow-up period.
A separate French study showed that total artificial sweetener intake from all sources was associated with increased overall risk for cardiovascular and cerebrovascular disease.
However, given the limitations of these studies, it’s hard to draw any firm conclusions, Wallace cautioned.
“We know that sugar-sweetened beverages are correlated with weight gain and cardiometabolic dysfunction promotion in children and adults,” he said.
Yet, “there really isn’t any convincing evidence that diet soda has much impact on human health at all. Most observational studies are mixed and likely very confounded by other diet and lifestyle factors. That doesn’t mean go overboard; a daily diet soda is probably fine, but that doesn’t mean go drink 10 of them every day,” he added.
Alcohol: Moderation or Abstinence?
Evidence on alcohol use and stroke risk have been mixed over the years. For decades, the evidence was suggestive that a moderate amount of alcohol daily (one to two drinks in men and one drink in women) may be beneficial at reducing major vascular outcomes.
Yet, over the past few years, some research has found no evidence of benefit with moderate alcohol intake. And the detrimental effects of excessive alcohol use are clear.
A large meta-analysis showed that light to moderate alcohol consumption (up to one drink per day) was associated with a reduced risk for ischemic stroke. However, heavy drinking (more than two drinks per day) significantly increased the risk for both ischemic and hemorrhagic stroke.
A separate study showed young adults who are moderate to heavy drinkers are at increased risk for stroke — and the risk increases with more years of imbibing.
In the INTERSTROKE study, high to moderate alcohol consumption was associated with increased stroke risk, whereas low alcohol consumption conferred no increased risk.
However, Bushnell pointed out that the study data was derived from based on self-report, and that other healthy behaviors may counteract the risk for alcohol consumption.
“For alcohol, regardless of stroke risk, the most important data shows that any alcohol consumption is associated with worse cognitive function, so generally, the lower the alcohol consumption the better,” Bushnell said.
She noted that, currently, the American Heart Association (AHA)/ASA recommend a maximum of two drinks per day for men and one drink per day for women to reduce stroke risk.
“However, the data for the risk for cognitive impairment with any alcohol is convincing and should be kept in mind in addition to the maximum alcohol recommended by the AHA/ASA,” Bushnell advised.
“We know excessive intake puts you at major risk for CVD, cancer, cognitive decline, and a whole host of other health ailments — no question there,” said Wallace.
The impact of moderate intake, on the other hand, is less clear. “Alcohol is a highly biased and political issue and the evidence (or lack thereof) on both sides is shoddy at best,” Wallace added.
A key challenge is that accurate self-reporting of alcohol intake is difficult, even for scientists, and most studies rely on self-reported data from observational cohorts. These often include limited dietary assessments, which provide only a partial picture of long-term consumption patterns, Wallace noted.
“The short answer is we don’t know if moderation is beneficial, detrimental, or null with respect to health,” he said.
Bushnell reports no relevant disclosures. Wallace (www.drtaylorwallace.com) is CEO of Think Healthy Group; editor of The Journal of Dietary Supplements, deputy editor of The Journal of the American Nutrition Association (www.nutrition.org), nutrition section editor of Annals of Medicine, and an advisory board member with Forbes Health.
A version of this article appeared on Medscape.com.
This research roundup reviews the latest findings, highlighting both promising insights and remaining uncertainties to help guide discussions with your patients.
Coffee and Tea: Good or Bad?
In the INTERSTROKE study, high coffee consumption (> 4 cups daily) was associated with an significantly increased risk for all strokes (odds ratio [OR], 1.37) or ischemic stroke (OR, 1.31), while low to moderate coffee had no link to increased stroke risk. In contrast, tea consumption was associated with lower odds of all stroke (OR, 0.81 for highest intake) or ischemic stroke (OR, 0.81).
In a recent UK Biobank study, consumption of coffee or tea was associated with reduced risk for stroke and dementia, with the biggest benefit associated with consuming both beverages.
Specifically, the investigators found that individuals who drank two to three cups of coffee and two to three cups of tea per day had a 30% decrease in incidence of stroke and a 28% lower risk for dementia versus those who did not.
A recent systematic review and dose-response meta-analysis showed that each daily cup increase in tea was associated with an average 4% reduced risk for stroke and a 2% reduced risk for cardiovascular disease (CVD) events.
The protective effect of coffee and tea on stroke risk may be driven, in part, by flavonoids, which have antioxidant and anti-inflammatory properties, as well as positive effects on vascular function.
“The advice to patients should be that coffee and tea may protect against stroke, but that sweetening either beverage with sugar probably should be minimized,” said Cheryl Bushnell, MD, MHS, of Wake Forest University School of Medicine in Winston-Salem, North Carolina, and chair of the American Stroke Association (ASA) 2024 Guideline for the Primary Prevention of Stroke.
Taylor Wallace, PhD, a certified food scientist, said, “most people should consume a cup or two of unsweetened tea per day in moderation for cardiometabolic health. It is an easy step in the right direction for good health but not a cure-all.”
When it comes to coffee, adults who like it should drink it “in moderation — just lay off the cream and sugar,” said Wallace, adjunct associate professor at George Washington University, Washington, DC, and Tufts University, Boston, Massachusetts.
“A cup or two of black coffee with low-fat or nonfat milk with breakfast is a healthy way to start the day, especially when you’re like me and have an 8-year-old that is full of energy!” Wallace said.
The Skinny on Soda
When it comes to sugar-sweetened and diet beverages, data from the Nurses’ Health Study and Health Professionals Follow-Up Study, showed a 16% increased risk for stroke with one or more daily servings of sugar-sweetened or low-calorie soda per day (vs none), independent of established dietary and nondietary cardiovascular risk factors.
In the Women’s Health Initiative Observational Study of postmenopausal women, a higher intake of artificially sweetened beverages was associated with increased risk for all stroke (adjusted hazard ratio [aHR], 1.23), ischemic stroke (aHR, 1.31), coronary heart disease (aHR, 1.29) and all-cause mortality (aHR, 1.16).
In the Framingham Heart Study Offspring cohort, consumption of one can of diet soda or more each day (vs none) was associated with a nearly threefold increased risk for stroke and dementia over a 10-year follow-up period.
A separate French study showed that total artificial sweetener intake from all sources was associated with increased overall risk for cardiovascular and cerebrovascular disease.
However, given the limitations of these studies, it’s hard to draw any firm conclusions, Wallace cautioned.
“We know that sugar-sweetened beverages are correlated with weight gain and cardiometabolic dysfunction promotion in children and adults,” he said.
Yet, “there really isn’t any convincing evidence that diet soda has much impact on human health at all. Most observational studies are mixed and likely very confounded by other diet and lifestyle factors. That doesn’t mean go overboard; a daily diet soda is probably fine, but that doesn’t mean go drink 10 of them every day,” he added.
Alcohol: Moderation or Abstinence?
Evidence on alcohol use and stroke risk have been mixed over the years. For decades, the evidence was suggestive that a moderate amount of alcohol daily (one to two drinks in men and one drink in women) may be beneficial at reducing major vascular outcomes.
Yet, over the past few years, some research has found no evidence of benefit with moderate alcohol intake. And the detrimental effects of excessive alcohol use are clear.
A large meta-analysis showed that light to moderate alcohol consumption (up to one drink per day) was associated with a reduced risk for ischemic stroke. However, heavy drinking (more than two drinks per day) significantly increased the risk for both ischemic and hemorrhagic stroke.
A separate study showed young adults who are moderate to heavy drinkers are at increased risk for stroke — and the risk increases with more years of imbibing.
In the INTERSTROKE study, high to moderate alcohol consumption was associated with increased stroke risk, whereas low alcohol consumption conferred no increased risk.
However, Bushnell pointed out that the study data was derived from based on self-report, and that other healthy behaviors may counteract the risk for alcohol consumption.
“For alcohol, regardless of stroke risk, the most important data shows that any alcohol consumption is associated with worse cognitive function, so generally, the lower the alcohol consumption the better,” Bushnell said.
She noted that, currently, the American Heart Association (AHA)/ASA recommend a maximum of two drinks per day for men and one drink per day for women to reduce stroke risk.
“However, the data for the risk for cognitive impairment with any alcohol is convincing and should be kept in mind in addition to the maximum alcohol recommended by the AHA/ASA,” Bushnell advised.
“We know excessive intake puts you at major risk for CVD, cancer, cognitive decline, and a whole host of other health ailments — no question there,” said Wallace.
The impact of moderate intake, on the other hand, is less clear. “Alcohol is a highly biased and political issue and the evidence (or lack thereof) on both sides is shoddy at best,” Wallace added.
A key challenge is that accurate self-reporting of alcohol intake is difficult, even for scientists, and most studies rely on self-reported data from observational cohorts. These often include limited dietary assessments, which provide only a partial picture of long-term consumption patterns, Wallace noted.
“The short answer is we don’t know if moderation is beneficial, detrimental, or null with respect to health,” he said.
Bushnell reports no relevant disclosures. Wallace (www.drtaylorwallace.com) is CEO of Think Healthy Group; editor of The Journal of Dietary Supplements, deputy editor of The Journal of the American Nutrition Association (www.nutrition.org), nutrition section editor of Annals of Medicine, and an advisory board member with Forbes Health.
A version of this article appeared on Medscape.com.
Guselkumab Efficacy in Crohn’s Disease Unaffected by Prior Biologic Use
VIENNA — according to a pooled analysis of the two phase 3 double-blind GALAXI 2 and 3 studies.
“We found that guselkumab was effective in both biologic-naive and biologic-inadequate subpopulations,” said coinvestigator Bruce E. Sands, MD, AGAF, gastroenterologist from Icahn School of Medicine at Mount Sinai, New York City.
These latest results add to the primary results of these studies reported earlier in 2024 that guselkumab was shown to be superior to both placebo and ustekinumab in the same patient population with moderately to severely active CD.
Sands reported the new data in a presentation at the United European Gastroenterology (UEG) Week 2024.
Guselkumab potently blocks interleukin (IL)–23 and binds to CD64, a receptor on cells that produce IL-23. The dual-acting IL-23p19 subunit inhibitor agent is currently under review by the Food and Drug Administration (FDA) for moderately to severely active CD. In September, guselkumab (Tremfya, Johnson & Johnson) was approved for use in moderately to severely active ulcerative colitis.
GALAXI 2 and 3 Pooled Dataset
In the two independent, identically designed GALAXI 2 and 3 studies, patients were randomized to guselkumab treatment at either 200 mg intravenous (IV) induction at weeks 0, 4, and 8, followed by 200 mg subcutaneous maintenance every 4 weeks, starting at week 12, or 200 mg IV induction at weeks 0, 4, and 8, followed by 100 mg subcutaneous maintenance every 8 weeks, starting at week 16; or to ustekinumab; or to placebo.
Participants were required to remain on their treatment of initial randomization for a long-term extension study (up to 5 years) looking at clinical, endoscopic, and safety outcomes, except for participants on placebo who were allowed to switch to ustekinumab if clinical response was not met at week 12.
Inclusion criteria for the studies comprised a Crohn’s Disease Activity Index score between 220 and 450, a mean daily stool frequency count > 3 or an abdominal pain score > 1, and a simple endoscopic score for CD score ≥ 6. Participants were also required to have shown an inadequate response or intolerance to oral corticosteroids, 6-mercaptopurine/azathioprine/methotrexate, or biologic therapies.
The pooled dataset included patients on either dose of guselkumab and patients on placebo (total n = 730). Of these, 52% of participants had shown a prior inadequate response to a biologic, 42% were biologic naive, and 6% had prior exposure to biologics but no documented failure. Patients on ustekinumab were not included in this analysis.
Almost all patients (97%) in the biologic-inadequate response group had previously received at least one anti–tumor necrosis factor agent, and around 15% had received vedolizumab. As expected, the biologic-inadequate responders were a lot sicker than the biologic-naive patients, Sands reported.
The composite co–primary endpoints for each guselkumab regimen vs placebo were clinical response at week 12 plus clinical remission at week 48, and clinical response at week 12 plus endoscopic response at week 48.
The major secondary endpoints comprised clinical remission at week 12 and endoscopic response also at week 12.
Short- and Long-Term Endpoints in Both Subgroups
In the biologic-naive subgroup, 54.7% of patients receiving the 200-mg dose regimen of guselkumab and 51.7% of those receiving the 100-mg dose regimen showed a clinical response at week 12 plus clinical remission at week 48, compared with 11.5% in the placebo group (P < .001 for both compared with placebo).
In the biologic-inadequate response group, 49.7% of those receiving the 200-mg dose regimen of guselkumab and 45.8% on the 100-mg dose regimen reached the composite endpoint, compared with the placebo response of 12.8% (P < .001 for both compared with placebo).
“You can see a slight decrease in response in the biologic-inadequate responders, but on the whole, the confidence intervals are highly overlapping,” said Sands.
Turning to major secondary endpoints at week 12, clinical remission was reached by 49.6% of the biologic-naive group on the 200-mg guselkumab regimen vs 16.4% on placebo, and by 46.0% of the biologic-inadequate group on the 200-mg regimen vs 19.2% on placebo (P < .001 for both subgroups). Endoscopic response was achieved by 46.3% of patients in the biologic-naive group and 29.0% in the biologic-inadequate group on the 200-mg regimen vs 18.0% and 6.4%, respectively, on placebo (P < .001 for both subgroups).
Sands noted that the drug has an excellent safety profile.
“These data show the drug works for naive patients who have failed conventional therapies, as well as for those who have failed biologic therapies,” so it could be used as a first- or second-line biologic, he added.
Sands reported potential conflicts of interest with AbbVie, Abivax, Adiso Therapeutics, Agomab, Alimentiv, Amgen, AnaptysBio, Arena Pharmaceuticals, Artugen Therapeutics, AstraZeneca, Biora Therapeutics, Boehringer Ingelheim, Boston Pharmaceuticals, Bristol-Myers Squibb, Calibr, Celgene, Celltrion, ClostraBio, Equillium, Enthera, Evommune, Ferring, Fresenius Kabi, Galapagos, Genentech (Roche), Gilead Sciences, GlaxoSmithKline, Gossamer Bio, Index Pharmaceuticals, Innovation Pharmaceuticals, Inotrem, Janssen, Kaleido, Kallyope, Lilly, Merck, Microbiotica, Mobius Care, Morphic Therapeutic, MRM Health, Pfizer, Nexus Therapeutics, Nimbus Discovery, Odyssey Therapeutics, Progenity, Prometheus Biosciences, Prometheus Laboratories, Protagonist Therapeutics, Q32 Bio, Rasayana Therapeutics, Recludix Pharma, Reistone Biopharma, Sun Pharma, Surrozen, Target RWE, Takeda, Teva, Theravance Biopharma, TLL Pharmaceutical, Tr1X, UNION Therapeutics, and Ventyx Biosciences.
A version of this article appeared on Medscape.com.
VIENNA — according to a pooled analysis of the two phase 3 double-blind GALAXI 2 and 3 studies.
“We found that guselkumab was effective in both biologic-naive and biologic-inadequate subpopulations,” said coinvestigator Bruce E. Sands, MD, AGAF, gastroenterologist from Icahn School of Medicine at Mount Sinai, New York City.
These latest results add to the primary results of these studies reported earlier in 2024 that guselkumab was shown to be superior to both placebo and ustekinumab in the same patient population with moderately to severely active CD.
Sands reported the new data in a presentation at the United European Gastroenterology (UEG) Week 2024.
Guselkumab potently blocks interleukin (IL)–23 and binds to CD64, a receptor on cells that produce IL-23. The dual-acting IL-23p19 subunit inhibitor agent is currently under review by the Food and Drug Administration (FDA) for moderately to severely active CD. In September, guselkumab (Tremfya, Johnson & Johnson) was approved for use in moderately to severely active ulcerative colitis.
GALAXI 2 and 3 Pooled Dataset
In the two independent, identically designed GALAXI 2 and 3 studies, patients were randomized to guselkumab treatment at either 200 mg intravenous (IV) induction at weeks 0, 4, and 8, followed by 200 mg subcutaneous maintenance every 4 weeks, starting at week 12, or 200 mg IV induction at weeks 0, 4, and 8, followed by 100 mg subcutaneous maintenance every 8 weeks, starting at week 16; or to ustekinumab; or to placebo.
Participants were required to remain on their treatment of initial randomization for a long-term extension study (up to 5 years) looking at clinical, endoscopic, and safety outcomes, except for participants on placebo who were allowed to switch to ustekinumab if clinical response was not met at week 12.
Inclusion criteria for the studies comprised a Crohn’s Disease Activity Index score between 220 and 450, a mean daily stool frequency count > 3 or an abdominal pain score > 1, and a simple endoscopic score for CD score ≥ 6. Participants were also required to have shown an inadequate response or intolerance to oral corticosteroids, 6-mercaptopurine/azathioprine/methotrexate, or biologic therapies.
The pooled dataset included patients on either dose of guselkumab and patients on placebo (total n = 730). Of these, 52% of participants had shown a prior inadequate response to a biologic, 42% were biologic naive, and 6% had prior exposure to biologics but no documented failure. Patients on ustekinumab were not included in this analysis.
Almost all patients (97%) in the biologic-inadequate response group had previously received at least one anti–tumor necrosis factor agent, and around 15% had received vedolizumab. As expected, the biologic-inadequate responders were a lot sicker than the biologic-naive patients, Sands reported.
The composite co–primary endpoints for each guselkumab regimen vs placebo were clinical response at week 12 plus clinical remission at week 48, and clinical response at week 12 plus endoscopic response at week 48.
The major secondary endpoints comprised clinical remission at week 12 and endoscopic response also at week 12.
Short- and Long-Term Endpoints in Both Subgroups
In the biologic-naive subgroup, 54.7% of patients receiving the 200-mg dose regimen of guselkumab and 51.7% of those receiving the 100-mg dose regimen showed a clinical response at week 12 plus clinical remission at week 48, compared with 11.5% in the placebo group (P < .001 for both compared with placebo).
In the biologic-inadequate response group, 49.7% of those receiving the 200-mg dose regimen of guselkumab and 45.8% on the 100-mg dose regimen reached the composite endpoint, compared with the placebo response of 12.8% (P < .001 for both compared with placebo).
“You can see a slight decrease in response in the biologic-inadequate responders, but on the whole, the confidence intervals are highly overlapping,” said Sands.
Turning to major secondary endpoints at week 12, clinical remission was reached by 49.6% of the biologic-naive group on the 200-mg guselkumab regimen vs 16.4% on placebo, and by 46.0% of the biologic-inadequate group on the 200-mg regimen vs 19.2% on placebo (P < .001 for both subgroups). Endoscopic response was achieved by 46.3% of patients in the biologic-naive group and 29.0% in the biologic-inadequate group on the 200-mg regimen vs 18.0% and 6.4%, respectively, on placebo (P < .001 for both subgroups).
Sands noted that the drug has an excellent safety profile.
“These data show the drug works for naive patients who have failed conventional therapies, as well as for those who have failed biologic therapies,” so it could be used as a first- or second-line biologic, he added.
Sands reported potential conflicts of interest with AbbVie, Abivax, Adiso Therapeutics, Agomab, Alimentiv, Amgen, AnaptysBio, Arena Pharmaceuticals, Artugen Therapeutics, AstraZeneca, Biora Therapeutics, Boehringer Ingelheim, Boston Pharmaceuticals, Bristol-Myers Squibb, Calibr, Celgene, Celltrion, ClostraBio, Equillium, Enthera, Evommune, Ferring, Fresenius Kabi, Galapagos, Genentech (Roche), Gilead Sciences, GlaxoSmithKline, Gossamer Bio, Index Pharmaceuticals, Innovation Pharmaceuticals, Inotrem, Janssen, Kaleido, Kallyope, Lilly, Merck, Microbiotica, Mobius Care, Morphic Therapeutic, MRM Health, Pfizer, Nexus Therapeutics, Nimbus Discovery, Odyssey Therapeutics, Progenity, Prometheus Biosciences, Prometheus Laboratories, Protagonist Therapeutics, Q32 Bio, Rasayana Therapeutics, Recludix Pharma, Reistone Biopharma, Sun Pharma, Surrozen, Target RWE, Takeda, Teva, Theravance Biopharma, TLL Pharmaceutical, Tr1X, UNION Therapeutics, and Ventyx Biosciences.
A version of this article appeared on Medscape.com.
VIENNA — according to a pooled analysis of the two phase 3 double-blind GALAXI 2 and 3 studies.
“We found that guselkumab was effective in both biologic-naive and biologic-inadequate subpopulations,” said coinvestigator Bruce E. Sands, MD, AGAF, gastroenterologist from Icahn School of Medicine at Mount Sinai, New York City.
These latest results add to the primary results of these studies reported earlier in 2024 that guselkumab was shown to be superior to both placebo and ustekinumab in the same patient population with moderately to severely active CD.
Sands reported the new data in a presentation at the United European Gastroenterology (UEG) Week 2024.
Guselkumab potently blocks interleukin (IL)–23 and binds to CD64, a receptor on cells that produce IL-23. The dual-acting IL-23p19 subunit inhibitor agent is currently under review by the Food and Drug Administration (FDA) for moderately to severely active CD. In September, guselkumab (Tremfya, Johnson & Johnson) was approved for use in moderately to severely active ulcerative colitis.
GALAXI 2 and 3 Pooled Dataset
In the two independent, identically designed GALAXI 2 and 3 studies, patients were randomized to guselkumab treatment at either 200 mg intravenous (IV) induction at weeks 0, 4, and 8, followed by 200 mg subcutaneous maintenance every 4 weeks, starting at week 12, or 200 mg IV induction at weeks 0, 4, and 8, followed by 100 mg subcutaneous maintenance every 8 weeks, starting at week 16; or to ustekinumab; or to placebo.
Participants were required to remain on their treatment of initial randomization for a long-term extension study (up to 5 years) looking at clinical, endoscopic, and safety outcomes, except for participants on placebo who were allowed to switch to ustekinumab if clinical response was not met at week 12.
Inclusion criteria for the studies comprised a Crohn’s Disease Activity Index score between 220 and 450, a mean daily stool frequency count > 3 or an abdominal pain score > 1, and a simple endoscopic score for CD score ≥ 6. Participants were also required to have shown an inadequate response or intolerance to oral corticosteroids, 6-mercaptopurine/azathioprine/methotrexate, or biologic therapies.
The pooled dataset included patients on either dose of guselkumab and patients on placebo (total n = 730). Of these, 52% of participants had shown a prior inadequate response to a biologic, 42% were biologic naive, and 6% had prior exposure to biologics but no documented failure. Patients on ustekinumab were not included in this analysis.
Almost all patients (97%) in the biologic-inadequate response group had previously received at least one anti–tumor necrosis factor agent, and around 15% had received vedolizumab. As expected, the biologic-inadequate responders were a lot sicker than the biologic-naive patients, Sands reported.
The composite co–primary endpoints for each guselkumab regimen vs placebo were clinical response at week 12 plus clinical remission at week 48, and clinical response at week 12 plus endoscopic response at week 48.
The major secondary endpoints comprised clinical remission at week 12 and endoscopic response also at week 12.
Short- and Long-Term Endpoints in Both Subgroups
In the biologic-naive subgroup, 54.7% of patients receiving the 200-mg dose regimen of guselkumab and 51.7% of those receiving the 100-mg dose regimen showed a clinical response at week 12 plus clinical remission at week 48, compared with 11.5% in the placebo group (P < .001 for both compared with placebo).
In the biologic-inadequate response group, 49.7% of those receiving the 200-mg dose regimen of guselkumab and 45.8% on the 100-mg dose regimen reached the composite endpoint, compared with the placebo response of 12.8% (P < .001 for both compared with placebo).
“You can see a slight decrease in response in the biologic-inadequate responders, but on the whole, the confidence intervals are highly overlapping,” said Sands.
Turning to major secondary endpoints at week 12, clinical remission was reached by 49.6% of the biologic-naive group on the 200-mg guselkumab regimen vs 16.4% on placebo, and by 46.0% of the biologic-inadequate group on the 200-mg regimen vs 19.2% on placebo (P < .001 for both subgroups). Endoscopic response was achieved by 46.3% of patients in the biologic-naive group and 29.0% in the biologic-inadequate group on the 200-mg regimen vs 18.0% and 6.4%, respectively, on placebo (P < .001 for both subgroups).
Sands noted that the drug has an excellent safety profile.
“These data show the drug works for naive patients who have failed conventional therapies, as well as for those who have failed biologic therapies,” so it could be used as a first- or second-line biologic, he added.
Sands reported potential conflicts of interest with AbbVie, Abivax, Adiso Therapeutics, Agomab, Alimentiv, Amgen, AnaptysBio, Arena Pharmaceuticals, Artugen Therapeutics, AstraZeneca, Biora Therapeutics, Boehringer Ingelheim, Boston Pharmaceuticals, Bristol-Myers Squibb, Calibr, Celgene, Celltrion, ClostraBio, Equillium, Enthera, Evommune, Ferring, Fresenius Kabi, Galapagos, Genentech (Roche), Gilead Sciences, GlaxoSmithKline, Gossamer Bio, Index Pharmaceuticals, Innovation Pharmaceuticals, Inotrem, Janssen, Kaleido, Kallyope, Lilly, Merck, Microbiotica, Mobius Care, Morphic Therapeutic, MRM Health, Pfizer, Nexus Therapeutics, Nimbus Discovery, Odyssey Therapeutics, Progenity, Prometheus Biosciences, Prometheus Laboratories, Protagonist Therapeutics, Q32 Bio, Rasayana Therapeutics, Recludix Pharma, Reistone Biopharma, Sun Pharma, Surrozen, Target RWE, Takeda, Teva, Theravance Biopharma, TLL Pharmaceutical, Tr1X, UNION Therapeutics, and Ventyx Biosciences.
A version of this article appeared on Medscape.com.
FROM UEG 2024
Patients With IBD More Likely to Develop, or Have Prior, T1D
VIENNA —
Their findings showed that patients with IBD had a moderately increased risk for T1D and higher odds of having prior T1D than the general population. These bidirectional associations were partially independent of shared familial factors.
Although the absolute risk for T1D is low in patients with IBD, these findings suggest that if there are nonspecific symptoms, such as weight loss and fatigue, which are typical of T1D but not of IBD, then it might be reasonable to test for diabetes, lead researcher Jiangwei Sun, PhD, postdoctoral researcher at the Karolinska Institutet, Stockholm, Sweden, told this news organization.
“Patients with IBD and T1D also tend to have worse disease outcomes for both diseases, but these two diseases are not recognized as comorbidities in the clinical guidelines,” he said.
Anecdotally, “many clinicians believe there is a higher risk of autoimmune disease in patients with IBD but not much attention is paid to type 1 diabetes,” he added.
Sun presented the study at United European Gastroenterology (UEG) Week 2024. It was also published recently in The Lancet.
Exploring the Bidirectional Relationship
Prior research in the form of a systematic review found no association between IBD and T1D, which was surprising, Sun said. Further studies found an association between IBD and incident T1D; however, these studies did not explore bidirectionality between the two diseases.
These studies also did not take shared genetic and environmental factors into consideration, though “there is known to be familial co-aggregation of IBD and T1D based on previous findings,” he said.
In this current study, Sun and colleagues compared patients with IBD with the general population, as well as with siblings without IBD to consider the potential influence of shared genetics and earlier environmental factors.
The research used two approaches to look for a bidirectional association: A nationwide matched cohort study (IBD and incident T1D) and a case-control study (IBD and prior T1D).
The cohort study included 20,314 patients with IBD aged ≤ 28 years, who were identified between 1987 and 2017. Of these, 7277 had Crohn’s disease, 10,112 had ulcerative colitis, and 2925 had unclassified IBD. There were 99,200 individually matched reference individuals.
The case-control study included 87,001 patients with IBD (without age restriction) and 431,054 matched control individuals.
Risk ratios were calculated using an adjusted hazard ratio (aHR) of incident T1D in the cohort study and an adjusted odds ratio (aOR) of prior T1D in the case-control study.
In the cohort study, the median follow-up was 14 years. Over that time, 116 patients with IBD and 353 reference individuals developed T1D. The aHR for a patient with IBD developing T1D was 1.58 (95% CI, 1.27-1.95). For patients with ulcerative colitis, the aHR of developing T1D increased to 2.02 (95% CI, 1.51-2.70); however, the association was not found for Crohn’s disease or unclassified IBD possibly because of the sample size of these latter categories, noted Sun.
In the case-control study, Sun and colleagues identified 1018 (1.2%) patients with IBD and 3496 (0.8%) control individuals who had been previously diagnosed with T1D. Patients with IBD had higher odds of having prior T1D than those without IBD (aOR, 1.36; 95% CI, 1.26-1.46). This positive association was observed in all IBD subtypes, said Sun, who added that the sample size was larger in this analysis than in the cohort analysis.
Upon comparing patients with IBD with their siblings without IBD, analyses showed similar associations between IBD and T1D; the aHR was 1.44 (95% CI, 0.97-2.15) for developing T1D, and the aOR was 1.32 (95% CI, 1.18-1.49) for prior T1D.
That these positive associations between IBD and T1D exist even when comparing patients with IBD with their siblings without IBD suggests genetics and shared environmental factors do not fully explain the association, and that later environmental factors might play a role, said Sun.
“I’m not surprised with these results,” he added. “They make sense because we know that both IBD and T1D are immunity-related diseases and have some shared pathways.”
Commenting on the study, Tine Jess, MD, director, Center for Molecular Prediction of Inflammatory Bowel Disease, PREDICT, Aalborg University in Copenhagen, Denmark, said: “The really interesting finding here is that type 1 diabetes may precede IBD, which points toward common etiologies rather than one disease leading to the other.”
“This is in line with mounting evidence that IBD is measurable at the molecular level years prior to diagnosis,” she added.
Awareness of the bidirectional association may facilitate early detection of both conditions, Sun and his colleagues noted.
Sun reported no relevant financial relationships. Jess reported receiving consultancy fees from Ferring and Pfizer.
A version of this article appeared on Medscape.com.
VIENNA —
Their findings showed that patients with IBD had a moderately increased risk for T1D and higher odds of having prior T1D than the general population. These bidirectional associations were partially independent of shared familial factors.
Although the absolute risk for T1D is low in patients with IBD, these findings suggest that if there are nonspecific symptoms, such as weight loss and fatigue, which are typical of T1D but not of IBD, then it might be reasonable to test for diabetes, lead researcher Jiangwei Sun, PhD, postdoctoral researcher at the Karolinska Institutet, Stockholm, Sweden, told this news organization.
“Patients with IBD and T1D also tend to have worse disease outcomes for both diseases, but these two diseases are not recognized as comorbidities in the clinical guidelines,” he said.
Anecdotally, “many clinicians believe there is a higher risk of autoimmune disease in patients with IBD but not much attention is paid to type 1 diabetes,” he added.
Sun presented the study at United European Gastroenterology (UEG) Week 2024. It was also published recently in The Lancet.
Exploring the Bidirectional Relationship
Prior research in the form of a systematic review found no association between IBD and T1D, which was surprising, Sun said. Further studies found an association between IBD and incident T1D; however, these studies did not explore bidirectionality between the two diseases.
These studies also did not take shared genetic and environmental factors into consideration, though “there is known to be familial co-aggregation of IBD and T1D based on previous findings,” he said.
In this current study, Sun and colleagues compared patients with IBD with the general population, as well as with siblings without IBD to consider the potential influence of shared genetics and earlier environmental factors.
The research used two approaches to look for a bidirectional association: A nationwide matched cohort study (IBD and incident T1D) and a case-control study (IBD and prior T1D).
The cohort study included 20,314 patients with IBD aged ≤ 28 years, who were identified between 1987 and 2017. Of these, 7277 had Crohn’s disease, 10,112 had ulcerative colitis, and 2925 had unclassified IBD. There were 99,200 individually matched reference individuals.
The case-control study included 87,001 patients with IBD (without age restriction) and 431,054 matched control individuals.
Risk ratios were calculated using an adjusted hazard ratio (aHR) of incident T1D in the cohort study and an adjusted odds ratio (aOR) of prior T1D in the case-control study.
In the cohort study, the median follow-up was 14 years. Over that time, 116 patients with IBD and 353 reference individuals developed T1D. The aHR for a patient with IBD developing T1D was 1.58 (95% CI, 1.27-1.95). For patients with ulcerative colitis, the aHR of developing T1D increased to 2.02 (95% CI, 1.51-2.70); however, the association was not found for Crohn’s disease or unclassified IBD possibly because of the sample size of these latter categories, noted Sun.
In the case-control study, Sun and colleagues identified 1018 (1.2%) patients with IBD and 3496 (0.8%) control individuals who had been previously diagnosed with T1D. Patients with IBD had higher odds of having prior T1D than those without IBD (aOR, 1.36; 95% CI, 1.26-1.46). This positive association was observed in all IBD subtypes, said Sun, who added that the sample size was larger in this analysis than in the cohort analysis.
Upon comparing patients with IBD with their siblings without IBD, analyses showed similar associations between IBD and T1D; the aHR was 1.44 (95% CI, 0.97-2.15) for developing T1D, and the aOR was 1.32 (95% CI, 1.18-1.49) for prior T1D.
That these positive associations between IBD and T1D exist even when comparing patients with IBD with their siblings without IBD suggests genetics and shared environmental factors do not fully explain the association, and that later environmental factors might play a role, said Sun.
“I’m not surprised with these results,” he added. “They make sense because we know that both IBD and T1D are immunity-related diseases and have some shared pathways.”
Commenting on the study, Tine Jess, MD, director, Center for Molecular Prediction of Inflammatory Bowel Disease, PREDICT, Aalborg University in Copenhagen, Denmark, said: “The really interesting finding here is that type 1 diabetes may precede IBD, which points toward common etiologies rather than one disease leading to the other.”
“This is in line with mounting evidence that IBD is measurable at the molecular level years prior to diagnosis,” she added.
Awareness of the bidirectional association may facilitate early detection of both conditions, Sun and his colleagues noted.
Sun reported no relevant financial relationships. Jess reported receiving consultancy fees from Ferring and Pfizer.
A version of this article appeared on Medscape.com.
VIENNA —
Their findings showed that patients with IBD had a moderately increased risk for T1D and higher odds of having prior T1D than the general population. These bidirectional associations were partially independent of shared familial factors.
Although the absolute risk for T1D is low in patients with IBD, these findings suggest that if there are nonspecific symptoms, such as weight loss and fatigue, which are typical of T1D but not of IBD, then it might be reasonable to test for diabetes, lead researcher Jiangwei Sun, PhD, postdoctoral researcher at the Karolinska Institutet, Stockholm, Sweden, told this news organization.
“Patients with IBD and T1D also tend to have worse disease outcomes for both diseases, but these two diseases are not recognized as comorbidities in the clinical guidelines,” he said.
Anecdotally, “many clinicians believe there is a higher risk of autoimmune disease in patients with IBD but not much attention is paid to type 1 diabetes,” he added.
Sun presented the study at United European Gastroenterology (UEG) Week 2024. It was also published recently in The Lancet.
Exploring the Bidirectional Relationship
Prior research in the form of a systematic review found no association between IBD and T1D, which was surprising, Sun said. Further studies found an association between IBD and incident T1D; however, these studies did not explore bidirectionality between the two diseases.
These studies also did not take shared genetic and environmental factors into consideration, though “there is known to be familial co-aggregation of IBD and T1D based on previous findings,” he said.
In this current study, Sun and colleagues compared patients with IBD with the general population, as well as with siblings without IBD to consider the potential influence of shared genetics and earlier environmental factors.
The research used two approaches to look for a bidirectional association: A nationwide matched cohort study (IBD and incident T1D) and a case-control study (IBD and prior T1D).
The cohort study included 20,314 patients with IBD aged ≤ 28 years, who were identified between 1987 and 2017. Of these, 7277 had Crohn’s disease, 10,112 had ulcerative colitis, and 2925 had unclassified IBD. There were 99,200 individually matched reference individuals.
The case-control study included 87,001 patients with IBD (without age restriction) and 431,054 matched control individuals.
Risk ratios were calculated using an adjusted hazard ratio (aHR) of incident T1D in the cohort study and an adjusted odds ratio (aOR) of prior T1D in the case-control study.
In the cohort study, the median follow-up was 14 years. Over that time, 116 patients with IBD and 353 reference individuals developed T1D. The aHR for a patient with IBD developing T1D was 1.58 (95% CI, 1.27-1.95). For patients with ulcerative colitis, the aHR of developing T1D increased to 2.02 (95% CI, 1.51-2.70); however, the association was not found for Crohn’s disease or unclassified IBD possibly because of the sample size of these latter categories, noted Sun.
In the case-control study, Sun and colleagues identified 1018 (1.2%) patients with IBD and 3496 (0.8%) control individuals who had been previously diagnosed with T1D. Patients with IBD had higher odds of having prior T1D than those without IBD (aOR, 1.36; 95% CI, 1.26-1.46). This positive association was observed in all IBD subtypes, said Sun, who added that the sample size was larger in this analysis than in the cohort analysis.
Upon comparing patients with IBD with their siblings without IBD, analyses showed similar associations between IBD and T1D; the aHR was 1.44 (95% CI, 0.97-2.15) for developing T1D, and the aOR was 1.32 (95% CI, 1.18-1.49) for prior T1D.
That these positive associations between IBD and T1D exist even when comparing patients with IBD with their siblings without IBD suggests genetics and shared environmental factors do not fully explain the association, and that later environmental factors might play a role, said Sun.
“I’m not surprised with these results,” he added. “They make sense because we know that both IBD and T1D are immunity-related diseases and have some shared pathways.”
Commenting on the study, Tine Jess, MD, director, Center for Molecular Prediction of Inflammatory Bowel Disease, PREDICT, Aalborg University in Copenhagen, Denmark, said: “The really interesting finding here is that type 1 diabetes may precede IBD, which points toward common etiologies rather than one disease leading to the other.”
“This is in line with mounting evidence that IBD is measurable at the molecular level years prior to diagnosis,” she added.
Awareness of the bidirectional association may facilitate early detection of both conditions, Sun and his colleagues noted.
Sun reported no relevant financial relationships. Jess reported receiving consultancy fees from Ferring and Pfizer.
A version of this article appeared on Medscape.com.
FROM UEG 2024
Silent Epidemic: Loneliness a Serious Threat to Both Brain and Body
In a world that is more connected than ever, a silent epidemic is taking its toll. Overall, one in three US adults report chronic loneliness — a condition so detrimental that it rivals smoking and obesity with respect to its negative effect on health and well-being. From anxiety and depression to life-threatening conditions like cardiovascular disease, stroke, and Alzheimer’s and Parkinson’s diseases, loneliness is more than an emotion — it’s a serious threat to both the brain and body.
In 2023, a US Surgeon General advisory raised the alarm about the national problem of loneliness and isolation, describing it as an epidemic.
“Given the significant health consequences of loneliness and isolation, we must prioritize building social connection in the same way we have prioritized other critical public health issues such as tobacco, obesity, and substance use disorders. Together, we can build a country that’s healthier, more resilient, less lonely, and more connected,” the report concluded.
But how, exactly, does chronic loneliness affect the physiology and function of the brain? What does the latest research reveal about the link between loneliness and neurologic and psychiatric illness, and what can clinicians do to address the issue?
This news organization spoke to multiple experts in the field to explore these issues.
A Major Risk Factor
Anna Finley, PhD, assistant professor of psychology at North Dakota State University, Fargo, explained that loneliness and social isolation are different entities. Social isolation is an objective measure of the number of people someone interacts with on a regular basis, whereas loneliness is a subjective feeling that occurs when close connections are lacking.
“These two things are not actually as related as you think they would be. People can feel lonely in a crowd or feel well connected with only a few friendships. It’s more about the quality of the connection and the quality of your perception of it. So someone could be in some very supportive relationships but still feel that there’s something missing,” she said in an interview.
So what do we know about how loneliness affects health? Evidence supporting the hypothesis that loneliness is an emerging risk factor for many diseases is steadily building.
Recently, the American Heart Association published a statement summarizing the evidence for a direct association between social isolation and loneliness and coronary heart disease and stroke mortality.
In addition, many studies have shown that individuals experiencing social isolation or loneliness have an increased risk for anxiety and depression, dementia, infectious disease, hospitalization, and all-cause death, even after adjusting for age and many other traditional risk factors.
One study revealed that eliminating loneliness has the potential to prevent nearly 20% of cases of depression in adults aged 50 years or older.
Indu Subramanian, MD, professor of neurology at the University of California, Los Angeles, and colleagues conducted a study involving patients with Parkinson’s disease, which showed that the negative impact of loneliness on disease severity was as significant as the positive effects of 30 minutes of daily exercise.
“The importance of loneliness is under-recognized and undervalued, and it poses a major risk for health outcomes and quality of life,” said Subramanian.
Subramanian noted that loneliness is stigmatizing, causing people to feel unlikable and blame themselves, which prevents them from opening up to doctors or loved ones about their struggle. At the same time, healthcare providers may not think to ask about loneliness or know about potential interventions. She emphasized that much more work is needed to address this issue.
Early Mortality Risk
Julianne Holt-Lunstad, PhD, professor of psychology and neuroscience at Brigham Young University in Provo, Utah, is the author of two large meta-analyses that suggest loneliness, social isolation, or living alone are independent risk factors for early mortality, increasing this risk by about a third — the equivalent to the risk of smoking 15 cigarettes per day.
“We have quite robust evidence across a number of health outcomes implicating the harmful effects of loneliness and social isolation. While these are observational studies and show mainly associations, we do have evidence from longitudinal studies that show lacking social connection, whether that be loneliness or social isolation, predicts subsequent worse outcomes, and most of these studies have adjusted for alternative kinds of explanations, like age, initial health status, lifestyle factors,” Holt-Lunstad said.
There is some evidence to suggest that isolation is more predictive of physical health outcomes, whereas loneliness is more predictive of mental health outcomes. That said, both isolation and loneliness have significant effects on mental and physical health outcomes, she noted.
There is also the question of whether loneliness is causing poor health or whether people who are in poor health feel lonely because poor health can lead to social isolation.
Finley said there’s probably a bit of both going on, but longitudinal studies, where loneliness is measured at a fixed timepoint then health outcomes are reported a few years later, suggest that loneliness is contributing to these adverse outcomes.
She added that there is also some evidence in animal models to suggest that loneliness is a causal risk factor for adverse health outcomes. “But you can’t ask a mouse or rat how lonely they’re feeling. All you can do is house them individually — removing them from social connection. This isn’t necessarily the same thing as loneliness in humans.”
Finley is studying mechanisms in the brain that may be involved in mediating the adverse health consequences of loneliness.
“What I’ve been seeing in the data so far is that it tends to be the self-report of how lonely folks are feeling that has the associations with differences in the brain, as opposed to the number of social connections people have. It does seem to be the more subjective, emotional perception of loneliness that is important.”
In a review of potential mechanisms involved, she concluded that it is dysregulated emotions and altered perceptions of social interactions that has profound impacts on the brain, suggesting that people who are lonely may have a tendency to interpret social cues in a negative way, preventing them from forming productive positive relationships.
Lack of Trust
One researcher who has studied this phenomenon is Dirk Scheele, PhD, professor of social neuroscience at Ruhr University Bochum in Germany.
“We were interested to find out why people remained lonely,” he said in an interview. “Loneliness is an unpleasant experience, and there are so many opportunities for social contacts nowadays, it’s not really clear at first sight why people are chronically lonely.”
To examine this question, Scheele and his team conducted a study in which functional MRI was used to examine the brain in otherwise healthy individuals with high or low loneliness scores while they played a trust game.
They also simulated a positive social interaction between participants and researchers, in which they talked about plans for a fictitious lottery win, and about their hobbies and interests, during which mood was measured with questionnaires, and saliva samples were collected to measure hormone levels.
Results showed that the high-lonely individuals had reduced activation in the insula cortex during the trust decisions. “This area of the brain is involved in the processing of bodily signals, such as ‘gut feelings.’ So reduced activity here could be interpreted as fewer gut feelings on who can be trusted,” Scheele explained.
The high-lonely individuals also had reduced responsiveness to the positive social interaction with a lower release of oxytocin and a smaller elevation in mood compared with the control individuals.
Scheele pointed out that there is some evidence that oxytocin might increase trust, and there is reduced release of endogenous oxytocin in high loneliness.
“Our results are consistent with the idea that loneliness is associated with negative biases about other people. So if we expect negative things from other people — for instance, that they cannot be trusted — then that would hamper further social interactions and could lead to loneliness,” he added.
A Role for Oxytocin?
In another study, the same researchers tested short-term (five weekly sessions) group psychotherapy to reduce loneliness using established techniques to target these negative biases. They also investigated whether the effects of this group psychotherapy could be augmented by administering intranasal oxytocin (vs placebo) before the group psychotherapy sessions.
Results showed that the group psychotherapy intervention reduced trait loneliness (loneliness experienced over a prolonged period). The oxytocin did not show a significant effect on trait loneliness, but there was a suggestion that it may enhance the reduction in state loneliness (how someone is feeling at a specific time) brought about by the psychotherapy sessions.
“We found that bonding within the groups was experienced as more positive in the oxytocin treated groups. It is possible that a longer intervention would be helpful for longer-term results,” Scheele concluded. “It’s not going to be a quick fix for loneliness, but there may be a role for oxytocin as an adjunct to psychotherapy.”
A Basic Human Need
Another loneliness researcher, Livia Tomova, PhD, assistant professor of psychology at Cardiff University in Wales, has used social isolation to induce loneliness in young people and found that this intervention was linked to brain patterns similar to those associated with hunger.
“We know that the drive to eat food is a very basic human need. We know quite well how it is represented in the brain,” she explained.
The researchers tested how the brains of the participants responded to seeing pictures of social interactions after they underwent a prolonged period of social isolation. In a subsequent session, the same people were asked to undergo food fasting and then underwent brain scans when looking at pictures of food. Results showed that the neural patterns were similar in the two situations with increased activity in the substantia nigra area within the midbrain.
“This area of the brain processes rewards and motivation. It consists primarily of dopamine neurons and increased activity corresponds to a feeling of craving something. So this area of the brain that controls essential homeostatic needs is activated when people feel lonely, suggesting that our need for social contact with others is potentially a very basic need similar to eating,” Tomova said.
Lower Gray Matter Volumes in Key Brain Areas
And another group from Germany has found that higher loneliness scores are negatively associated with specific brain regions responsible for memory, emotion regulation, and social processing.
Sandra Düzel, PhD, and colleagues from the Max Planck Institute for Human Development and the Charité – Universitätsmedizin Berlin, both in Berlin, Germany, reported a study in which individuals who reported higher loneliness had smaller gray matter volumes in brain regions such as the left amygdala, anterior hippocampus, and cerebellum, regions which are crucial for both emotional regulation and higher-order cognitive processes, such as self-reflection and executive function.
Düzel believes that possible mechanisms behind the link between loneliness and brain volume differences could include stress-related damage, with prolonged loneliness associated with elevated levels of stress hormones, which can damage the hippocampus over time, and reduced cognitive and social stimulation, which may contribute to brain volume reductions in regions critical for memory and emotional processing.
“Loneliness is often characterized by reduced social and environmental diversity, leading to less engagement with novel experiences and potentially lower hippocampal-striatal connectivity.
Since novelty-seeking and environmental diversity are associated with positive emotional states, individuals experiencing loneliness might benefit from increased exposure to new environments which could stimulate the brain’s reward circuits, fostering positive affect and potentially mitigating the emotional burden of loneliness,” she said.
Is Social Prescribing the Answer?
So are there enough data now to act and attempt to develop interventions to reduce loneliness? Most of these researchers believe so.
“I think we have enough information to act on this now. There are a number of national academies consensus reports, which suggest that, while certainly there are still gaps in our evidence and more to be learned, there is sufficient evidence that a concerning portion of the population seems to lack connection, and that the consequences are serious enough that we need to do something about it,” said Holt-Lunstad.
Some countries have introduced social prescribing where doctors can prescribe a group activity or a regular visit or telephone conversation with a supportive person.
Subramanian pointed out that it’s easier to implement in countries with national health services and may be more difficult to embrace in the US healthcare system.
“We are not so encouraged from a financial perspective to think about preventive care in the US. We don’t have an easy way to recognize in any tangible way the downstream of such activities in terms of preventing future problems. That is something we need to work on,” she said.
Finley cautioned that to work well, social prescribing will require an understanding of each person’s individual situation.
“Some people may only receive benefit of interacting with others if they are also getting some sort of support to address the social and emotional concerns that are tagging along with loneliness. I’m not sure that just telling people to go join their local gardening club or whatever will be the correct answer for everyone.”
She pointed out that many people will have issues in their life that are making it hard for them to be social. These could be mobility or financial challenges, care responsibilities, or concerns about illnesses or life events. “We need to figure out what would have the most bang for the person’s buck, so to speak, as an intervention. That could mean connecting them to a group relevant to their individual situation.”
Opportunity to Connect Not Enough?
Tomova believes that training people in social skills may be a better option. “It appears that some people who are chronically lonely seem to struggle to make relationships with others. So just encouraging them to interact with others more will not necessarily help. We need to better understand the pathways involved and who are the people who become ill. We can then develop and target better interventions and teach people coping strategies for that situation.”
Scheele agreed. “While just giving people the opportunity to connect may work for some, others who are experiencing really chronic loneliness may not benefit very much from this unless their negative belief systems are addressed.” He suggested some sort of psychotherapy may be helpful in this situation.
But at least all seem to agree that healthcare providers need to be more aware of loneliness as a health risk factor, try to identify people at risk, and to think about how best to support them.
Holt-Lunstad noted that one of the recommendations in the US Surgeon General’s advisory was to increase the education, training, and resources on loneliness for healthcare providers.
“If we want this to be addressed, we need to give healthcare providers the time, resources, and training in order to do that, otherwise, we are adding one more thing to an already overburdened system. They need to understand how important it is, and how it might help them take care of the patient.”
“Our hope is that we can start to reverse some of the trends that we are seeing, both in terms of the prevalence rates of loneliness, but also that we could start seeing improvements in health and other kinds of outcomes,” she concluded.
Progress is being made in increasing awareness about the dangers of chronic loneliness. It’s now recognized as a serious health risk, but there are actionable steps that can help. Loneliness doesn’t have to be a permanent condition for anyone, said Scheele.
Holt-Lunstad served as an adviser for Foundation for Social Connection, Global Initiative on Loneliness and Connection, and Nextdoor Neighborhood Vitality Board and received research grants/income from Templeton Foundation, Eventbrite, Foundation for Social Connection, and Triple-S Foundation. Subramanian served as a speaker bureau for Acorda Pharma. The other researchers reported no disclosures.
A version of this article first appeared on Medscape.com.
In a world that is more connected than ever, a silent epidemic is taking its toll. Overall, one in three US adults report chronic loneliness — a condition so detrimental that it rivals smoking and obesity with respect to its negative effect on health and well-being. From anxiety and depression to life-threatening conditions like cardiovascular disease, stroke, and Alzheimer’s and Parkinson’s diseases, loneliness is more than an emotion — it’s a serious threat to both the brain and body.
In 2023, a US Surgeon General advisory raised the alarm about the national problem of loneliness and isolation, describing it as an epidemic.
“Given the significant health consequences of loneliness and isolation, we must prioritize building social connection in the same way we have prioritized other critical public health issues such as tobacco, obesity, and substance use disorders. Together, we can build a country that’s healthier, more resilient, less lonely, and more connected,” the report concluded.
But how, exactly, does chronic loneliness affect the physiology and function of the brain? What does the latest research reveal about the link between loneliness and neurologic and psychiatric illness, and what can clinicians do to address the issue?
This news organization spoke to multiple experts in the field to explore these issues.
A Major Risk Factor
Anna Finley, PhD, assistant professor of psychology at North Dakota State University, Fargo, explained that loneliness and social isolation are different entities. Social isolation is an objective measure of the number of people someone interacts with on a regular basis, whereas loneliness is a subjective feeling that occurs when close connections are lacking.
“These two things are not actually as related as you think they would be. People can feel lonely in a crowd or feel well connected with only a few friendships. It’s more about the quality of the connection and the quality of your perception of it. So someone could be in some very supportive relationships but still feel that there’s something missing,” she said in an interview.
So what do we know about how loneliness affects health? Evidence supporting the hypothesis that loneliness is an emerging risk factor for many diseases is steadily building.
Recently, the American Heart Association published a statement summarizing the evidence for a direct association between social isolation and loneliness and coronary heart disease and stroke mortality.
In addition, many studies have shown that individuals experiencing social isolation or loneliness have an increased risk for anxiety and depression, dementia, infectious disease, hospitalization, and all-cause death, even after adjusting for age and many other traditional risk factors.
One study revealed that eliminating loneliness has the potential to prevent nearly 20% of cases of depression in adults aged 50 years or older.
Indu Subramanian, MD, professor of neurology at the University of California, Los Angeles, and colleagues conducted a study involving patients with Parkinson’s disease, which showed that the negative impact of loneliness on disease severity was as significant as the positive effects of 30 minutes of daily exercise.
“The importance of loneliness is under-recognized and undervalued, and it poses a major risk for health outcomes and quality of life,” said Subramanian.
Subramanian noted that loneliness is stigmatizing, causing people to feel unlikable and blame themselves, which prevents them from opening up to doctors or loved ones about their struggle. At the same time, healthcare providers may not think to ask about loneliness or know about potential interventions. She emphasized that much more work is needed to address this issue.
Early Mortality Risk
Julianne Holt-Lunstad, PhD, professor of psychology and neuroscience at Brigham Young University in Provo, Utah, is the author of two large meta-analyses that suggest loneliness, social isolation, or living alone are independent risk factors for early mortality, increasing this risk by about a third — the equivalent to the risk of smoking 15 cigarettes per day.
“We have quite robust evidence across a number of health outcomes implicating the harmful effects of loneliness and social isolation. While these are observational studies and show mainly associations, we do have evidence from longitudinal studies that show lacking social connection, whether that be loneliness or social isolation, predicts subsequent worse outcomes, and most of these studies have adjusted for alternative kinds of explanations, like age, initial health status, lifestyle factors,” Holt-Lunstad said.
There is some evidence to suggest that isolation is more predictive of physical health outcomes, whereas loneliness is more predictive of mental health outcomes. That said, both isolation and loneliness have significant effects on mental and physical health outcomes, she noted.
There is also the question of whether loneliness is causing poor health or whether people who are in poor health feel lonely because poor health can lead to social isolation.
Finley said there’s probably a bit of both going on, but longitudinal studies, where loneliness is measured at a fixed timepoint then health outcomes are reported a few years later, suggest that loneliness is contributing to these adverse outcomes.
She added that there is also some evidence in animal models to suggest that loneliness is a causal risk factor for adverse health outcomes. “But you can’t ask a mouse or rat how lonely they’re feeling. All you can do is house them individually — removing them from social connection. This isn’t necessarily the same thing as loneliness in humans.”
Finley is studying mechanisms in the brain that may be involved in mediating the adverse health consequences of loneliness.
“What I’ve been seeing in the data so far is that it tends to be the self-report of how lonely folks are feeling that has the associations with differences in the brain, as opposed to the number of social connections people have. It does seem to be the more subjective, emotional perception of loneliness that is important.”
In a review of potential mechanisms involved, she concluded that it is dysregulated emotions and altered perceptions of social interactions that has profound impacts on the brain, suggesting that people who are lonely may have a tendency to interpret social cues in a negative way, preventing them from forming productive positive relationships.
Lack of Trust
One researcher who has studied this phenomenon is Dirk Scheele, PhD, professor of social neuroscience at Ruhr University Bochum in Germany.
“We were interested to find out why people remained lonely,” he said in an interview. “Loneliness is an unpleasant experience, and there are so many opportunities for social contacts nowadays, it’s not really clear at first sight why people are chronically lonely.”
To examine this question, Scheele and his team conducted a study in which functional MRI was used to examine the brain in otherwise healthy individuals with high or low loneliness scores while they played a trust game.
They also simulated a positive social interaction between participants and researchers, in which they talked about plans for a fictitious lottery win, and about their hobbies and interests, during which mood was measured with questionnaires, and saliva samples were collected to measure hormone levels.
Results showed that the high-lonely individuals had reduced activation in the insula cortex during the trust decisions. “This area of the brain is involved in the processing of bodily signals, such as ‘gut feelings.’ So reduced activity here could be interpreted as fewer gut feelings on who can be trusted,” Scheele explained.
The high-lonely individuals also had reduced responsiveness to the positive social interaction with a lower release of oxytocin and a smaller elevation in mood compared with the control individuals.
Scheele pointed out that there is some evidence that oxytocin might increase trust, and there is reduced release of endogenous oxytocin in high loneliness.
“Our results are consistent with the idea that loneliness is associated with negative biases about other people. So if we expect negative things from other people — for instance, that they cannot be trusted — then that would hamper further social interactions and could lead to loneliness,” he added.
A Role for Oxytocin?
In another study, the same researchers tested short-term (five weekly sessions) group psychotherapy to reduce loneliness using established techniques to target these negative biases. They also investigated whether the effects of this group psychotherapy could be augmented by administering intranasal oxytocin (vs placebo) before the group psychotherapy sessions.
Results showed that the group psychotherapy intervention reduced trait loneliness (loneliness experienced over a prolonged period). The oxytocin did not show a significant effect on trait loneliness, but there was a suggestion that it may enhance the reduction in state loneliness (how someone is feeling at a specific time) brought about by the psychotherapy sessions.
“We found that bonding within the groups was experienced as more positive in the oxytocin treated groups. It is possible that a longer intervention would be helpful for longer-term results,” Scheele concluded. “It’s not going to be a quick fix for loneliness, but there may be a role for oxytocin as an adjunct to psychotherapy.”
A Basic Human Need
Another loneliness researcher, Livia Tomova, PhD, assistant professor of psychology at Cardiff University in Wales, has used social isolation to induce loneliness in young people and found that this intervention was linked to brain patterns similar to those associated with hunger.
“We know that the drive to eat food is a very basic human need. We know quite well how it is represented in the brain,” she explained.
The researchers tested how the brains of the participants responded to seeing pictures of social interactions after they underwent a prolonged period of social isolation. In a subsequent session, the same people were asked to undergo food fasting and then underwent brain scans when looking at pictures of food. Results showed that the neural patterns were similar in the two situations with increased activity in the substantia nigra area within the midbrain.
“This area of the brain processes rewards and motivation. It consists primarily of dopamine neurons and increased activity corresponds to a feeling of craving something. So this area of the brain that controls essential homeostatic needs is activated when people feel lonely, suggesting that our need for social contact with others is potentially a very basic need similar to eating,” Tomova said.
Lower Gray Matter Volumes in Key Brain Areas
And another group from Germany has found that higher loneliness scores are negatively associated with specific brain regions responsible for memory, emotion regulation, and social processing.
Sandra Düzel, PhD, and colleagues from the Max Planck Institute for Human Development and the Charité – Universitätsmedizin Berlin, both in Berlin, Germany, reported a study in which individuals who reported higher loneliness had smaller gray matter volumes in brain regions such as the left amygdala, anterior hippocampus, and cerebellum, regions which are crucial for both emotional regulation and higher-order cognitive processes, such as self-reflection and executive function.
Düzel believes that possible mechanisms behind the link between loneliness and brain volume differences could include stress-related damage, with prolonged loneliness associated with elevated levels of stress hormones, which can damage the hippocampus over time, and reduced cognitive and social stimulation, which may contribute to brain volume reductions in regions critical for memory and emotional processing.
“Loneliness is often characterized by reduced social and environmental diversity, leading to less engagement with novel experiences and potentially lower hippocampal-striatal connectivity.
Since novelty-seeking and environmental diversity are associated with positive emotional states, individuals experiencing loneliness might benefit from increased exposure to new environments which could stimulate the brain’s reward circuits, fostering positive affect and potentially mitigating the emotional burden of loneliness,” she said.
Is Social Prescribing the Answer?
So are there enough data now to act and attempt to develop interventions to reduce loneliness? Most of these researchers believe so.
“I think we have enough information to act on this now. There are a number of national academies consensus reports, which suggest that, while certainly there are still gaps in our evidence and more to be learned, there is sufficient evidence that a concerning portion of the population seems to lack connection, and that the consequences are serious enough that we need to do something about it,” said Holt-Lunstad.
Some countries have introduced social prescribing where doctors can prescribe a group activity or a regular visit or telephone conversation with a supportive person.
Subramanian pointed out that it’s easier to implement in countries with national health services and may be more difficult to embrace in the US healthcare system.
“We are not so encouraged from a financial perspective to think about preventive care in the US. We don’t have an easy way to recognize in any tangible way the downstream of such activities in terms of preventing future problems. That is something we need to work on,” she said.
Finley cautioned that to work well, social prescribing will require an understanding of each person’s individual situation.
“Some people may only receive benefit of interacting with others if they are also getting some sort of support to address the social and emotional concerns that are tagging along with loneliness. I’m not sure that just telling people to go join their local gardening club or whatever will be the correct answer for everyone.”
She pointed out that many people will have issues in their life that are making it hard for them to be social. These could be mobility or financial challenges, care responsibilities, or concerns about illnesses or life events. “We need to figure out what would have the most bang for the person’s buck, so to speak, as an intervention. That could mean connecting them to a group relevant to their individual situation.”
Opportunity to Connect Not Enough?
Tomova believes that training people in social skills may be a better option. “It appears that some people who are chronically lonely seem to struggle to make relationships with others. So just encouraging them to interact with others more will not necessarily help. We need to better understand the pathways involved and who are the people who become ill. We can then develop and target better interventions and teach people coping strategies for that situation.”
Scheele agreed. “While just giving people the opportunity to connect may work for some, others who are experiencing really chronic loneliness may not benefit very much from this unless their negative belief systems are addressed.” He suggested some sort of psychotherapy may be helpful in this situation.
But at least all seem to agree that healthcare providers need to be more aware of loneliness as a health risk factor, try to identify people at risk, and to think about how best to support them.
Holt-Lunstad noted that one of the recommendations in the US Surgeon General’s advisory was to increase the education, training, and resources on loneliness for healthcare providers.
“If we want this to be addressed, we need to give healthcare providers the time, resources, and training in order to do that, otherwise, we are adding one more thing to an already overburdened system. They need to understand how important it is, and how it might help them take care of the patient.”
“Our hope is that we can start to reverse some of the trends that we are seeing, both in terms of the prevalence rates of loneliness, but also that we could start seeing improvements in health and other kinds of outcomes,” she concluded.
Progress is being made in increasing awareness about the dangers of chronic loneliness. It’s now recognized as a serious health risk, but there are actionable steps that can help. Loneliness doesn’t have to be a permanent condition for anyone, said Scheele.
Holt-Lunstad served as an adviser for Foundation for Social Connection, Global Initiative on Loneliness and Connection, and Nextdoor Neighborhood Vitality Board and received research grants/income from Templeton Foundation, Eventbrite, Foundation for Social Connection, and Triple-S Foundation. Subramanian served as a speaker bureau for Acorda Pharma. The other researchers reported no disclosures.
A version of this article first appeared on Medscape.com.
In a world that is more connected than ever, a silent epidemic is taking its toll. Overall, one in three US adults report chronic loneliness — a condition so detrimental that it rivals smoking and obesity with respect to its negative effect on health and well-being. From anxiety and depression to life-threatening conditions like cardiovascular disease, stroke, and Alzheimer’s and Parkinson’s diseases, loneliness is more than an emotion — it’s a serious threat to both the brain and body.
In 2023, a US Surgeon General advisory raised the alarm about the national problem of loneliness and isolation, describing it as an epidemic.
“Given the significant health consequences of loneliness and isolation, we must prioritize building social connection in the same way we have prioritized other critical public health issues such as tobacco, obesity, and substance use disorders. Together, we can build a country that’s healthier, more resilient, less lonely, and more connected,” the report concluded.
But how, exactly, does chronic loneliness affect the physiology and function of the brain? What does the latest research reveal about the link between loneliness and neurologic and psychiatric illness, and what can clinicians do to address the issue?
This news organization spoke to multiple experts in the field to explore these issues.
A Major Risk Factor
Anna Finley, PhD, assistant professor of psychology at North Dakota State University, Fargo, explained that loneliness and social isolation are different entities. Social isolation is an objective measure of the number of people someone interacts with on a regular basis, whereas loneliness is a subjective feeling that occurs when close connections are lacking.
“These two things are not actually as related as you think they would be. People can feel lonely in a crowd or feel well connected with only a few friendships. It’s more about the quality of the connection and the quality of your perception of it. So someone could be in some very supportive relationships but still feel that there’s something missing,” she said in an interview.
So what do we know about how loneliness affects health? Evidence supporting the hypothesis that loneliness is an emerging risk factor for many diseases is steadily building.
Recently, the American Heart Association published a statement summarizing the evidence for a direct association between social isolation and loneliness and coronary heart disease and stroke mortality.
In addition, many studies have shown that individuals experiencing social isolation or loneliness have an increased risk for anxiety and depression, dementia, infectious disease, hospitalization, and all-cause death, even after adjusting for age and many other traditional risk factors.
One study revealed that eliminating loneliness has the potential to prevent nearly 20% of cases of depression in adults aged 50 years or older.
Indu Subramanian, MD, professor of neurology at the University of California, Los Angeles, and colleagues conducted a study involving patients with Parkinson’s disease, which showed that the negative impact of loneliness on disease severity was as significant as the positive effects of 30 minutes of daily exercise.
“The importance of loneliness is under-recognized and undervalued, and it poses a major risk for health outcomes and quality of life,” said Subramanian.
Subramanian noted that loneliness is stigmatizing, causing people to feel unlikable and blame themselves, which prevents them from opening up to doctors or loved ones about their struggle. At the same time, healthcare providers may not think to ask about loneliness or know about potential interventions. She emphasized that much more work is needed to address this issue.
Early Mortality Risk
Julianne Holt-Lunstad, PhD, professor of psychology and neuroscience at Brigham Young University in Provo, Utah, is the author of two large meta-analyses that suggest loneliness, social isolation, or living alone are independent risk factors for early mortality, increasing this risk by about a third — the equivalent to the risk of smoking 15 cigarettes per day.
“We have quite robust evidence across a number of health outcomes implicating the harmful effects of loneliness and social isolation. While these are observational studies and show mainly associations, we do have evidence from longitudinal studies that show lacking social connection, whether that be loneliness or social isolation, predicts subsequent worse outcomes, and most of these studies have adjusted for alternative kinds of explanations, like age, initial health status, lifestyle factors,” Holt-Lunstad said.
There is some evidence to suggest that isolation is more predictive of physical health outcomes, whereas loneliness is more predictive of mental health outcomes. That said, both isolation and loneliness have significant effects on mental and physical health outcomes, she noted.
There is also the question of whether loneliness is causing poor health or whether people who are in poor health feel lonely because poor health can lead to social isolation.
Finley said there’s probably a bit of both going on, but longitudinal studies, where loneliness is measured at a fixed timepoint then health outcomes are reported a few years later, suggest that loneliness is contributing to these adverse outcomes.
She added that there is also some evidence in animal models to suggest that loneliness is a causal risk factor for adverse health outcomes. “But you can’t ask a mouse or rat how lonely they’re feeling. All you can do is house them individually — removing them from social connection. This isn’t necessarily the same thing as loneliness in humans.”
Finley is studying mechanisms in the brain that may be involved in mediating the adverse health consequences of loneliness.
“What I’ve been seeing in the data so far is that it tends to be the self-report of how lonely folks are feeling that has the associations with differences in the brain, as opposed to the number of social connections people have. It does seem to be the more subjective, emotional perception of loneliness that is important.”
In a review of potential mechanisms involved, she concluded that it is dysregulated emotions and altered perceptions of social interactions that has profound impacts on the brain, suggesting that people who are lonely may have a tendency to interpret social cues in a negative way, preventing them from forming productive positive relationships.
Lack of Trust
One researcher who has studied this phenomenon is Dirk Scheele, PhD, professor of social neuroscience at Ruhr University Bochum in Germany.
“We were interested to find out why people remained lonely,” he said in an interview. “Loneliness is an unpleasant experience, and there are so many opportunities for social contacts nowadays, it’s not really clear at first sight why people are chronically lonely.”
To examine this question, Scheele and his team conducted a study in which functional MRI was used to examine the brain in otherwise healthy individuals with high or low loneliness scores while they played a trust game.
They also simulated a positive social interaction between participants and researchers, in which they talked about plans for a fictitious lottery win, and about their hobbies and interests, during which mood was measured with questionnaires, and saliva samples were collected to measure hormone levels.
Results showed that the high-lonely individuals had reduced activation in the insula cortex during the trust decisions. “This area of the brain is involved in the processing of bodily signals, such as ‘gut feelings.’ So reduced activity here could be interpreted as fewer gut feelings on who can be trusted,” Scheele explained.
The high-lonely individuals also had reduced responsiveness to the positive social interaction with a lower release of oxytocin and a smaller elevation in mood compared with the control individuals.
Scheele pointed out that there is some evidence that oxytocin might increase trust, and there is reduced release of endogenous oxytocin in high loneliness.
“Our results are consistent with the idea that loneliness is associated with negative biases about other people. So if we expect negative things from other people — for instance, that they cannot be trusted — then that would hamper further social interactions and could lead to loneliness,” he added.
A Role for Oxytocin?
In another study, the same researchers tested short-term (five weekly sessions) group psychotherapy to reduce loneliness using established techniques to target these negative biases. They also investigated whether the effects of this group psychotherapy could be augmented by administering intranasal oxytocin (vs placebo) before the group psychotherapy sessions.
Results showed that the group psychotherapy intervention reduced trait loneliness (loneliness experienced over a prolonged period). The oxytocin did not show a significant effect on trait loneliness, but there was a suggestion that it may enhance the reduction in state loneliness (how someone is feeling at a specific time) brought about by the psychotherapy sessions.
“We found that bonding within the groups was experienced as more positive in the oxytocin treated groups. It is possible that a longer intervention would be helpful for longer-term results,” Scheele concluded. “It’s not going to be a quick fix for loneliness, but there may be a role for oxytocin as an adjunct to psychotherapy.”
A Basic Human Need
Another loneliness researcher, Livia Tomova, PhD, assistant professor of psychology at Cardiff University in Wales, has used social isolation to induce loneliness in young people and found that this intervention was linked to brain patterns similar to those associated with hunger.
“We know that the drive to eat food is a very basic human need. We know quite well how it is represented in the brain,” she explained.
The researchers tested how the brains of the participants responded to seeing pictures of social interactions after they underwent a prolonged period of social isolation. In a subsequent session, the same people were asked to undergo food fasting and then underwent brain scans when looking at pictures of food. Results showed that the neural patterns were similar in the two situations with increased activity in the substantia nigra area within the midbrain.
“This area of the brain processes rewards and motivation. It consists primarily of dopamine neurons and increased activity corresponds to a feeling of craving something. So this area of the brain that controls essential homeostatic needs is activated when people feel lonely, suggesting that our need for social contact with others is potentially a very basic need similar to eating,” Tomova said.
Lower Gray Matter Volumes in Key Brain Areas
And another group from Germany has found that higher loneliness scores are negatively associated with specific brain regions responsible for memory, emotion regulation, and social processing.
Sandra Düzel, PhD, and colleagues from the Max Planck Institute for Human Development and the Charité – Universitätsmedizin Berlin, both in Berlin, Germany, reported a study in which individuals who reported higher loneliness had smaller gray matter volumes in brain regions such as the left amygdala, anterior hippocampus, and cerebellum, regions which are crucial for both emotional regulation and higher-order cognitive processes, such as self-reflection and executive function.
Düzel believes that possible mechanisms behind the link between loneliness and brain volume differences could include stress-related damage, with prolonged loneliness associated with elevated levels of stress hormones, which can damage the hippocampus over time, and reduced cognitive and social stimulation, which may contribute to brain volume reductions in regions critical for memory and emotional processing.
“Loneliness is often characterized by reduced social and environmental diversity, leading to less engagement with novel experiences and potentially lower hippocampal-striatal connectivity.
Since novelty-seeking and environmental diversity are associated with positive emotional states, individuals experiencing loneliness might benefit from increased exposure to new environments which could stimulate the brain’s reward circuits, fostering positive affect and potentially mitigating the emotional burden of loneliness,” she said.
Is Social Prescribing the Answer?
So are there enough data now to act and attempt to develop interventions to reduce loneliness? Most of these researchers believe so.
“I think we have enough information to act on this now. There are a number of national academies consensus reports, which suggest that, while certainly there are still gaps in our evidence and more to be learned, there is sufficient evidence that a concerning portion of the population seems to lack connection, and that the consequences are serious enough that we need to do something about it,” said Holt-Lunstad.
Some countries have introduced social prescribing where doctors can prescribe a group activity or a regular visit or telephone conversation with a supportive person.
Subramanian pointed out that it’s easier to implement in countries with national health services and may be more difficult to embrace in the US healthcare system.
“We are not so encouraged from a financial perspective to think about preventive care in the US. We don’t have an easy way to recognize in any tangible way the downstream of such activities in terms of preventing future problems. That is something we need to work on,” she said.
Finley cautioned that to work well, social prescribing will require an understanding of each person’s individual situation.
“Some people may only receive benefit of interacting with others if they are also getting some sort of support to address the social and emotional concerns that are tagging along with loneliness. I’m not sure that just telling people to go join their local gardening club or whatever will be the correct answer for everyone.”
She pointed out that many people will have issues in their life that are making it hard for them to be social. These could be mobility or financial challenges, care responsibilities, or concerns about illnesses or life events. “We need to figure out what would have the most bang for the person’s buck, so to speak, as an intervention. That could mean connecting them to a group relevant to their individual situation.”
Opportunity to Connect Not Enough?
Tomova believes that training people in social skills may be a better option. “It appears that some people who are chronically lonely seem to struggle to make relationships with others. So just encouraging them to interact with others more will not necessarily help. We need to better understand the pathways involved and who are the people who become ill. We can then develop and target better interventions and teach people coping strategies for that situation.”
Scheele agreed. “While just giving people the opportunity to connect may work for some, others who are experiencing really chronic loneliness may not benefit very much from this unless their negative belief systems are addressed.” He suggested some sort of psychotherapy may be helpful in this situation.
But at least all seem to agree that healthcare providers need to be more aware of loneliness as a health risk factor, try to identify people at risk, and to think about how best to support them.
Holt-Lunstad noted that one of the recommendations in the US Surgeon General’s advisory was to increase the education, training, and resources on loneliness for healthcare providers.
“If we want this to be addressed, we need to give healthcare providers the time, resources, and training in order to do that, otherwise, we are adding one more thing to an already overburdened system. They need to understand how important it is, and how it might help them take care of the patient.”
“Our hope is that we can start to reverse some of the trends that we are seeing, both in terms of the prevalence rates of loneliness, but also that we could start seeing improvements in health and other kinds of outcomes,” she concluded.
Progress is being made in increasing awareness about the dangers of chronic loneliness. It’s now recognized as a serious health risk, but there are actionable steps that can help. Loneliness doesn’t have to be a permanent condition for anyone, said Scheele.
Holt-Lunstad served as an adviser for Foundation for Social Connection, Global Initiative on Loneliness and Connection, and Nextdoor Neighborhood Vitality Board and received research grants/income from Templeton Foundation, Eventbrite, Foundation for Social Connection, and Triple-S Foundation. Subramanian served as a speaker bureau for Acorda Pharma. The other researchers reported no disclosures.
A version of this article first appeared on Medscape.com.
Effects of Bimekizumab Durable for HS Through One Year
AMSTERDAM — The monoclonal antibody according to new data from an open-label extension period.
“Efficacy and health-related quality-of-life outcomes were maintained through 2 years of treatment,” study presenter Christos C. Zouboulis, MD, professor of dermatology, venereology, and allergology, Brandenburg Medical School Theodor Fontane, Dessau, Germany, said at the European Academy of Dermatology and Venereology (EADV) 2024 Congress.
“No new safety signals were observed,” he added. “These data highlight the durability and consistency of bimekizumab treatment in patients with moderate to severe hidradenitis suppurativa,” Zouboulis concluded.
Efficacy Maintained
“This is the type of long-term data that clinicians hope to see in large phase 3 trials for hidradenitis suppurativa medications,” commented Jennifer L. Hsiao, MD, clinical associate professor of dermatology, University of Southern California, Los Angeles, who was not involved in the study.
She told this news organization that, beyond maintained improvement of patient-reported quality of life, the results are “raising the bar in terms of measuring treatment success,” with over three quarters of patients achieving a high level of response on the Hidradenitis Suppurativa Clinical Response (HiSCR) scale at the final 96-week follow-up.
“Clinicians and patients have struggled with maintaining treatment efficacy over time with the first [Food and Drug Administration]–approved class of biologics for hidradenitis suppurativa — TNF [tumor necrosis factor]–alpha antagonists,” Hsiao said. She emphasized that sustained treatment efficacy will reduce the need for continued treatment switching and “hopefully improve treatment adherence.”
“It was also helpful to see that, consistent with studies of bimekizumab in psoriasis, rates of oral candidiasis appear to decrease with prolonged exposure over 2 years, though as with any open-label extension study, study dropout is a limitation,” she said.
“The availability of long-term efficacy and safety data, such as those shown in this study, will help guide shared decision-making discussions with our patients.” Overall, Hsiao believes there is “much to be excited about in the field of hidradenitis suppurativa, with a robust pipeline of potential treatments.”
One-Year Extension Study
HS is a “chronic and debilitating inflammatory skin disease,” Zouboulis told the audience. He noted that interleukin (IL)–17F and IL-17A are highly expressed in lesional skin and play a role in the disease immunopathogenesis.
Bimekizumab is a humanized immunoglobulin G1 monoclonal antibody that selectively inhibits both IL-17F and IL-17A. It has previously demonstrated clinically meaningful improvements in patients with moderate to severe HS in the phase 3 BE HEARD I and BE HEARD II trials evaluating several dosing regimens.
Zouboulis said the current analysis combines data from the two phase 3 studies with the BE HEARD EXT open-label extension study, in which patients from both trials were continued on bimekizumab 320 mg every 2 weeks.
Of the 1014 patients initially enrolled in the two trials, 556 continued into the open-label extension. Their average age was 36.6 years, and 53.8% were women. The majority (80.6%) were White. Of the 556 patients enrolled in the extension, 446 completed the 1-year extension study.
The average draining tunnel count at baseline was 3.8, and 54.5% had Hurley stage II disease; the remaining 45.5% had stage III disease. The mean total Dermatology Life Quality Index (DLQI) score at baseline was 11.0, indicating the HS was having a very large impact on the patients’ lives.
After the 16-week initial treatment period and the maintenance treatment period out to 48 weeks, 64.0% of patients achieved HiSCR75, indicating at least a 75% reduction from baseline in the total abscess and inflammatory nodule count, rising to 77.1% at the end of the open-label extension, after a total follow-up of 96 weeks.
HiSCR100 scores, indicating a 100% reduction in total abscess and inflammatory nodule counts, were achieved by 30.2% of 556 patients after 48 weeks and 44.2% of 446 at the 96-week follow-up.
These findings were mirrored by substantial reductions on the International HS Severity Score System, with a 70.3% reduction over baseline at 48 weeks and a 79.8% reduction at the final follow-up.
There were also “clinically meaningful” reductions in the total draining tunnel count at 1 year that were further reduced at 2 years, Zouboulis reported, at a 57.5% reduction over baseline, increasing to 73.7% by 96 weeks. The mean draining tunnel count at the end of follow-up was 1.1.
Over the full 96 weeks, the mean DLQI score reduced from 11.0 to 4.7, with 33.9% of patients achieving a score of 0 or 1 on the scale, which he said is basically patients saying: “I don’t have disease now.”
Finally, the safety data showed that there were “no differences compared to what we knew before,” Zouboulis said, with the most common treatment-related adverse events being hidradenitis, coronavirus infection, and oral candidiasis. There were few serious and severe treatment-related adverse events, and few that led to treatment discontinuation.
The study was funded by UCB.Zouboulis declared relationships with AstraZeneca, Boehringer Ingelheim, Brandenburg Medical School Theodor Fontane, EAD, European Union, German Federal Ministry of Education and Research, GSK, InflaRx, MSD, Novartis, Relaxera, UCB, Almirall, Boehringer Ingelheim, Eli Lilly, Idorsia, Incyte, L’Oréal, NAOS-BIODERMA, Pfizer, PM, Sanofi. Hsiao is on the board of directors for the Hidradenitis Suppurativa Foundation and has declared relationships with AbbVie, Aclaris Therapeutics, Amgen, Boehringer Ingelheim, Incyte, Novartis, Sanofi-Regeneron, and UCB.
A version of this article appeared on Medscape.com.
AMSTERDAM — The monoclonal antibody according to new data from an open-label extension period.
“Efficacy and health-related quality-of-life outcomes were maintained through 2 years of treatment,” study presenter Christos C. Zouboulis, MD, professor of dermatology, venereology, and allergology, Brandenburg Medical School Theodor Fontane, Dessau, Germany, said at the European Academy of Dermatology and Venereology (EADV) 2024 Congress.
“No new safety signals were observed,” he added. “These data highlight the durability and consistency of bimekizumab treatment in patients with moderate to severe hidradenitis suppurativa,” Zouboulis concluded.
Efficacy Maintained
“This is the type of long-term data that clinicians hope to see in large phase 3 trials for hidradenitis suppurativa medications,” commented Jennifer L. Hsiao, MD, clinical associate professor of dermatology, University of Southern California, Los Angeles, who was not involved in the study.
She told this news organization that, beyond maintained improvement of patient-reported quality of life, the results are “raising the bar in terms of measuring treatment success,” with over three quarters of patients achieving a high level of response on the Hidradenitis Suppurativa Clinical Response (HiSCR) scale at the final 96-week follow-up.
“Clinicians and patients have struggled with maintaining treatment efficacy over time with the first [Food and Drug Administration]–approved class of biologics for hidradenitis suppurativa — TNF [tumor necrosis factor]–alpha antagonists,” Hsiao said. She emphasized that sustained treatment efficacy will reduce the need for continued treatment switching and “hopefully improve treatment adherence.”
“It was also helpful to see that, consistent with studies of bimekizumab in psoriasis, rates of oral candidiasis appear to decrease with prolonged exposure over 2 years, though as with any open-label extension study, study dropout is a limitation,” she said.
“The availability of long-term efficacy and safety data, such as those shown in this study, will help guide shared decision-making discussions with our patients.” Overall, Hsiao believes there is “much to be excited about in the field of hidradenitis suppurativa, with a robust pipeline of potential treatments.”
One-Year Extension Study
HS is a “chronic and debilitating inflammatory skin disease,” Zouboulis told the audience. He noted that interleukin (IL)–17F and IL-17A are highly expressed in lesional skin and play a role in the disease immunopathogenesis.
Bimekizumab is a humanized immunoglobulin G1 monoclonal antibody that selectively inhibits both IL-17F and IL-17A. It has previously demonstrated clinically meaningful improvements in patients with moderate to severe HS in the phase 3 BE HEARD I and BE HEARD II trials evaluating several dosing regimens.
Zouboulis said the current analysis combines data from the two phase 3 studies with the BE HEARD EXT open-label extension study, in which patients from both trials were continued on bimekizumab 320 mg every 2 weeks.
Of the 1014 patients initially enrolled in the two trials, 556 continued into the open-label extension. Their average age was 36.6 years, and 53.8% were women. The majority (80.6%) were White. Of the 556 patients enrolled in the extension, 446 completed the 1-year extension study.
The average draining tunnel count at baseline was 3.8, and 54.5% had Hurley stage II disease; the remaining 45.5% had stage III disease. The mean total Dermatology Life Quality Index (DLQI) score at baseline was 11.0, indicating the HS was having a very large impact on the patients’ lives.
After the 16-week initial treatment period and the maintenance treatment period out to 48 weeks, 64.0% of patients achieved HiSCR75, indicating at least a 75% reduction from baseline in the total abscess and inflammatory nodule count, rising to 77.1% at the end of the open-label extension, after a total follow-up of 96 weeks.
HiSCR100 scores, indicating a 100% reduction in total abscess and inflammatory nodule counts, were achieved by 30.2% of 556 patients after 48 weeks and 44.2% of 446 at the 96-week follow-up.
These findings were mirrored by substantial reductions on the International HS Severity Score System, with a 70.3% reduction over baseline at 48 weeks and a 79.8% reduction at the final follow-up.
There were also “clinically meaningful” reductions in the total draining tunnel count at 1 year that were further reduced at 2 years, Zouboulis reported, at a 57.5% reduction over baseline, increasing to 73.7% by 96 weeks. The mean draining tunnel count at the end of follow-up was 1.1.
Over the full 96 weeks, the mean DLQI score reduced from 11.0 to 4.7, with 33.9% of patients achieving a score of 0 or 1 on the scale, which he said is basically patients saying: “I don’t have disease now.”
Finally, the safety data showed that there were “no differences compared to what we knew before,” Zouboulis said, with the most common treatment-related adverse events being hidradenitis, coronavirus infection, and oral candidiasis. There were few serious and severe treatment-related adverse events, and few that led to treatment discontinuation.
The study was funded by UCB.Zouboulis declared relationships with AstraZeneca, Boehringer Ingelheim, Brandenburg Medical School Theodor Fontane, EAD, European Union, German Federal Ministry of Education and Research, GSK, InflaRx, MSD, Novartis, Relaxera, UCB, Almirall, Boehringer Ingelheim, Eli Lilly, Idorsia, Incyte, L’Oréal, NAOS-BIODERMA, Pfizer, PM, Sanofi. Hsiao is on the board of directors for the Hidradenitis Suppurativa Foundation and has declared relationships with AbbVie, Aclaris Therapeutics, Amgen, Boehringer Ingelheim, Incyte, Novartis, Sanofi-Regeneron, and UCB.
A version of this article appeared on Medscape.com.
AMSTERDAM — The monoclonal antibody according to new data from an open-label extension period.
“Efficacy and health-related quality-of-life outcomes were maintained through 2 years of treatment,” study presenter Christos C. Zouboulis, MD, professor of dermatology, venereology, and allergology, Brandenburg Medical School Theodor Fontane, Dessau, Germany, said at the European Academy of Dermatology and Venereology (EADV) 2024 Congress.
“No new safety signals were observed,” he added. “These data highlight the durability and consistency of bimekizumab treatment in patients with moderate to severe hidradenitis suppurativa,” Zouboulis concluded.
Efficacy Maintained
“This is the type of long-term data that clinicians hope to see in large phase 3 trials for hidradenitis suppurativa medications,” commented Jennifer L. Hsiao, MD, clinical associate professor of dermatology, University of Southern California, Los Angeles, who was not involved in the study.
She told this news organization that, beyond maintained improvement of patient-reported quality of life, the results are “raising the bar in terms of measuring treatment success,” with over three quarters of patients achieving a high level of response on the Hidradenitis Suppurativa Clinical Response (HiSCR) scale at the final 96-week follow-up.
“Clinicians and patients have struggled with maintaining treatment efficacy over time with the first [Food and Drug Administration]–approved class of biologics for hidradenitis suppurativa — TNF [tumor necrosis factor]–alpha antagonists,” Hsiao said. She emphasized that sustained treatment efficacy will reduce the need for continued treatment switching and “hopefully improve treatment adherence.”
“It was also helpful to see that, consistent with studies of bimekizumab in psoriasis, rates of oral candidiasis appear to decrease with prolonged exposure over 2 years, though as with any open-label extension study, study dropout is a limitation,” she said.
“The availability of long-term efficacy and safety data, such as those shown in this study, will help guide shared decision-making discussions with our patients.” Overall, Hsiao believes there is “much to be excited about in the field of hidradenitis suppurativa, with a robust pipeline of potential treatments.”
One-Year Extension Study
HS is a “chronic and debilitating inflammatory skin disease,” Zouboulis told the audience. He noted that interleukin (IL)–17F and IL-17A are highly expressed in lesional skin and play a role in the disease immunopathogenesis.
Bimekizumab is a humanized immunoglobulin G1 monoclonal antibody that selectively inhibits both IL-17F and IL-17A. It has previously demonstrated clinically meaningful improvements in patients with moderate to severe HS in the phase 3 BE HEARD I and BE HEARD II trials evaluating several dosing regimens.
Zouboulis said the current analysis combines data from the two phase 3 studies with the BE HEARD EXT open-label extension study, in which patients from both trials were continued on bimekizumab 320 mg every 2 weeks.
Of the 1014 patients initially enrolled in the two trials, 556 continued into the open-label extension. Their average age was 36.6 years, and 53.8% were women. The majority (80.6%) were White. Of the 556 patients enrolled in the extension, 446 completed the 1-year extension study.
The average draining tunnel count at baseline was 3.8, and 54.5% had Hurley stage II disease; the remaining 45.5% had stage III disease. The mean total Dermatology Life Quality Index (DLQI) score at baseline was 11.0, indicating the HS was having a very large impact on the patients’ lives.
After the 16-week initial treatment period and the maintenance treatment period out to 48 weeks, 64.0% of patients achieved HiSCR75, indicating at least a 75% reduction from baseline in the total abscess and inflammatory nodule count, rising to 77.1% at the end of the open-label extension, after a total follow-up of 96 weeks.
HiSCR100 scores, indicating a 100% reduction in total abscess and inflammatory nodule counts, were achieved by 30.2% of 556 patients after 48 weeks and 44.2% of 446 at the 96-week follow-up.
These findings were mirrored by substantial reductions on the International HS Severity Score System, with a 70.3% reduction over baseline at 48 weeks and a 79.8% reduction at the final follow-up.
There were also “clinically meaningful” reductions in the total draining tunnel count at 1 year that were further reduced at 2 years, Zouboulis reported, at a 57.5% reduction over baseline, increasing to 73.7% by 96 weeks. The mean draining tunnel count at the end of follow-up was 1.1.
Over the full 96 weeks, the mean DLQI score reduced from 11.0 to 4.7, with 33.9% of patients achieving a score of 0 or 1 on the scale, which he said is basically patients saying: “I don’t have disease now.”
Finally, the safety data showed that there were “no differences compared to what we knew before,” Zouboulis said, with the most common treatment-related adverse events being hidradenitis, coronavirus infection, and oral candidiasis. There were few serious and severe treatment-related adverse events, and few that led to treatment discontinuation.
The study was funded by UCB.Zouboulis declared relationships with AstraZeneca, Boehringer Ingelheim, Brandenburg Medical School Theodor Fontane, EAD, European Union, German Federal Ministry of Education and Research, GSK, InflaRx, MSD, Novartis, Relaxera, UCB, Almirall, Boehringer Ingelheim, Eli Lilly, Idorsia, Incyte, L’Oréal, NAOS-BIODERMA, Pfizer, PM, Sanofi. Hsiao is on the board of directors for the Hidradenitis Suppurativa Foundation and has declared relationships with AbbVie, Aclaris Therapeutics, Amgen, Boehringer Ingelheim, Incyte, Novartis, Sanofi-Regeneron, and UCB.
A version of this article appeared on Medscape.com.
FROM EADV 2024
IBS: Understanding a Common Yet Misunderstood Condition
Irritable bowel syndrome (IBS) is one of the most common conditions encountered by both primary care providers and gastroenterologists, with a pooled global prevalence of 11.2%. This functional bowel disorder is characterized by abdominal pain or discomfort, diarrhea and/or constipation, and bloating.
Unfortunately, , according to Alan Desmond, MB, consultant in gastroenterology and general internal medicine, Torbay Hospital, UK National Health Service.
Desmond regularly sees patients who either haven’t been accurately diagnosed or have been told, “Don’t worry, it’s ‘just’ irritable bowel syndrome,” he said at the recent International Conference on Nutrition in Medicine.
A 2017 study involving nearly 2000 patients with a history of gastrointestinal (GI) symptoms found that 43.1% of those who met the criteria for IBS were undiagnosed, and among those who were diagnosed, 26% were not receiving treatment.
“Many clinicians vastly underestimate the impact functional GI symptoms have on our patients in lack of productivity, becoming homebound or losing employment, the inability to enjoy a meal with friends or family, and always needing to know where the nearest bathroom is, for example,” Desmond said in an interview.
IBS can profoundly affect patients’ mental health. One study found that 38% of patients with IBS attending a tertiary care clinic contemplated suicide because they felt hopeless about ever achieving symptom relief.
Today, several dietary, pharmacologic, and psychological/behavioral approaches are available to treat patients with IBS, noted William D. Chey, MD, AGAF, chief of the Division of Gastroenterology and Hepatology, University of Michigan, Ann Arbor, Michigan.
“Each individual patient may need a different combination of these foundational treatments,” he said. “One size doesn’t fit all.”
Diagnostic Pathway
One reason IBS is so hard to diagnose is that it’s a “symptom-based disorder, with identification of the condition predicated upon certain key characteristics that are heterogeneous,” Chey said in an interview. “IBS in patient ‘A’ may not present the same way as IBS in patient ‘B,’ although there are certain foundational common characteristics.”
IBS involves “abnormalities in the motility and contractility of the GI tract,” he said. It can present with diarrhea (IBS-D), constipation (IBS-C), or a mixture or alternation of diarrhea and constipation (IBS-M).
Patients with IBS-D often have an exaggerated gastro-colonic response, while those with IBS-C often have a blunted response.
Beyond stool abnormalities and abdominal pain/discomfort, patients often report bloating/distension, low backache, lethargy, nausea, thigh pain, and urinary and gynecologic symptoms.
Historically, IBS has been regarded as a “diagnosis of exclusion” because classic diagnostic tests typically yield no concrete findings. Desmond noted that several blood tests, procedures, imaging studies, and other tests are available to rule out other organic GI conditions, as outlined in the Table.
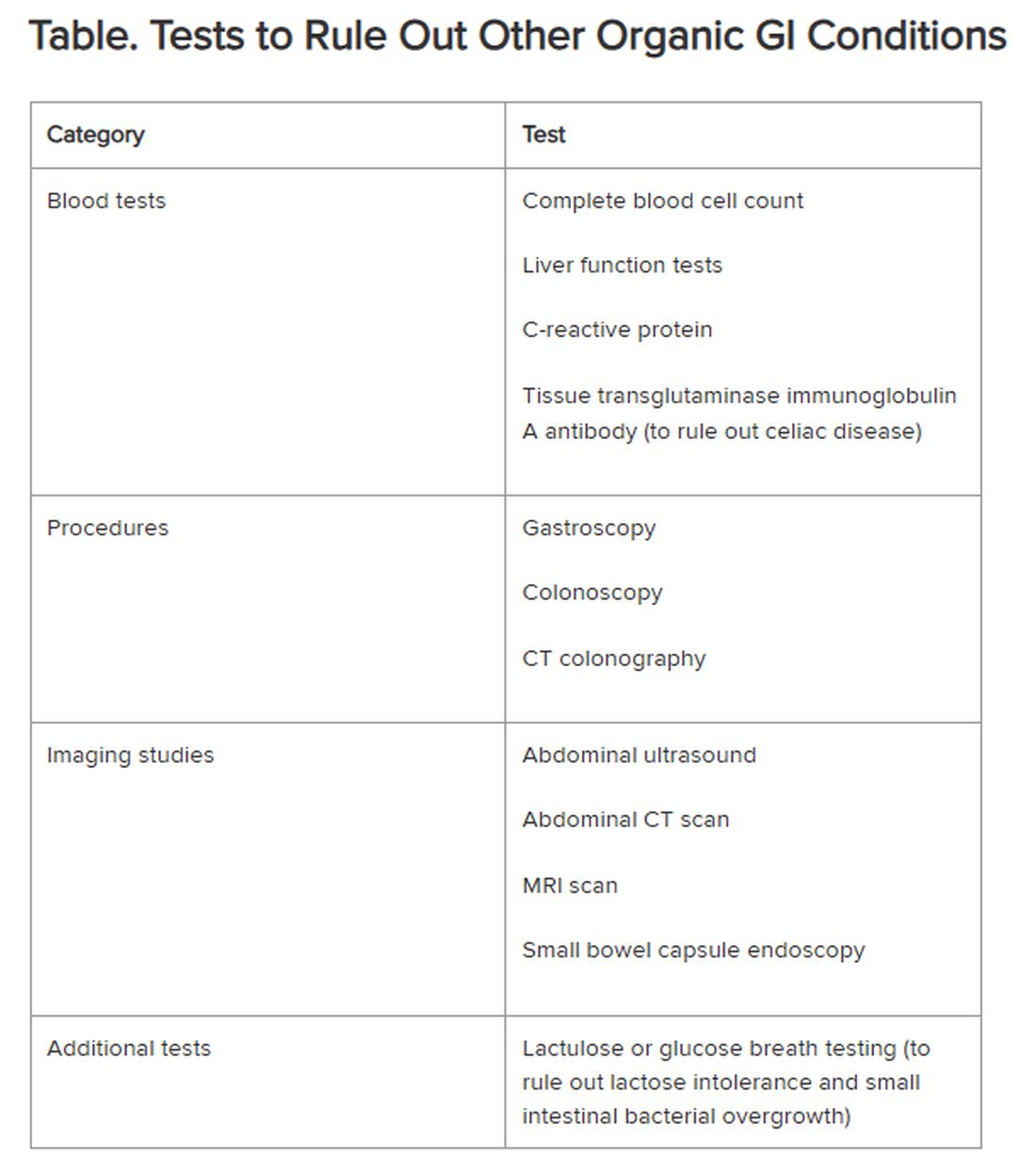
If the patient comes from a geographical region where giardia is endemic, clinicians also should consider testing for the parasite, Chey said.
New Understanding of IBS Etiology
Now, advances in the understanding of IBS are changing the approach to the disease.
“The field is moving away from seeing IBS as a ‘wastebasket diagnosis,’ recognizing that there are other causes of a patient’s symptoms,” Mark Pimentel, MD, associate professor of medicine and gastroenterology, Cedars-Sinai, Los Angeles, said in an interview. “What’s made IBS so difficult to diagnose has been the absence of biological markers and hallmark findings on endoscopy.”
Recent research points to novel bacterial causes as culprits in the development of IBS. In particular, altered small bowel microbiota can be triggered by acute gastroenteritis.
Food poisoning can trigger the onset of IBS — a phenomenon called “postinfectious IBS (PI-IBS),” said Pimentel, who is also executive director of the Medically Associated Science and Technology Program at Cedars-Sinai. PI-IBS almost always takes the form of IBS-D, with up to 60% of patients with IBS-D suffering the long-term sequelae of food poisoning.
The types of bacteria most commonly associated with gastroenteritis are Shigella, Campylobacter, Salmonella, and Escherichia coli, Pimentel said. All of them release cytolethal distending toxin B (CdtB), causing the body to produce antibodies to the toxin.
CdtB resembles vinculin, a naturally occurring protein critical for healthy gut function. “Because of this molecular resemblance, the immune system often mistakes one for the other, producing anti-vinculin,” Pimentel explained.
This autoimmune response leads to disruptions in the gut microbiome, ultimately resulting in PI-IBS. The chain of events “doesn’t necessarily happen immediately,” Pimentel said. “You might have developed food poisoning at a party weeks or months ago.”
Acute gastroenteritis is common, affecting as many as 179 million people in the United States annually. A meta-analysis of 47 studies, incorporating 28,270 patients, found that those who had experienced acute gastroenteritis had a fourfold higher risk of developing IBS compared with nonexposed controls.
“The problem isn’t only the IBS itself, but the fact that people with PI-IBS are four times as likely to contract food poisoning again, which can further exacerbate IBS symptoms,” Pimentel said.
Diarrhea-predominant IBS can be detected through the presence of two blood biomarkers — anti-CdtB and anti-vinculin — in a blood test developed by Pimentel and his group.
“Elevation in either of these biomarkers establishes the diagnosis,” Pimentel said. “This is a breakthrough because it represents the first test that can make IBS a ‘diagnosis of inclusion.’”
The blood test also can identify IBS-M but not IBS-C.
Pimentel said that IBS-C is associated with increased levels of methanogenic archaea, which can be diagnosed by a positive methane breath test. “Methane gas slows intestinal contractility, which might result in constipation,” he said.
Diet as a Treatment Option
Diet is usually the starting point for IBS treatment, Chey said. “The standard dietary recommendations, as defined by the National Institute for Health and Care Excellence Guidance for managing IBS, are reasonable and common sense — eating three meals a day, avoiding carbonated beverages, excess alcohol, and excess caffeine, and avoiding hard-to-digest foods that can be gas producing.”
A diet low in fermentable oligosaccharides, disaccharides, monosaccharides and polyols (FODMAPs), which are carbohydrates that aren’t completely absorbed in the intestines, has been shown to be effective in alleviating GI distress in as many as 86% of patients with IBS, leading to improvements in overall GI symptoms as well as individual symptoms (eg, abdominal pain, bloating, constipation, diarrhea, and flatulence).
Desmond recommends the low FODMAP program delineated by Monash University in Australia. The diet should be undertaken only under the supervision of a dietitian, he warned. Moreover, following it on a long-term basis can have an adverse impact on dietary quality and the gut microbiome. Therefore, “it’s important to embark on stepwise reintroduction of FODMAPS under supervision to find acceptable thresholds that don’t cause a return of symptoms.”
A growing body of research suggests that following the Mediterranean diet can be helpful in reducing IBS symptoms. Chey said that some patients who tend to over-restrict their eating might benefit from a less restrictive diet than the typical low FODMAPs diet. For them, the Mediterranean diet may be a good option.
Pharmacotherapy for IBS
Nutritional approaches aren’t for everyone, Chey noted. “Some people don’t want to be on a highly restricted diet.” For them, medications addressing symptoms might be a better option.
Antispasmodics — either anticholinergics (hyoscine and dicyclomine) or smooth muscle relaxants (alverine, mebeverine, and peppermint oil) — can be helpful, although they can worsen constipation in a dose-dependent manner. It is advisable to use them on an as-needed rather than long-term basis.
Antidiarrheal agents include loperamide and diphenoxylate.
For constipation, laxatives (eg, senna, bisacodyl, polyethylene glycol, and sodium picosulfate) can be helpful.
Desmond noted that the American Gastroenterological Association does not recommend routine use of probiotics for most GI disorders, including IBS. Exceptions include prevention of Clostridioides difficile, ulcerative colitis, and pouchitis.
Targeting the Gut-Brain Relationship
Stress plays a role in exacerbating symptoms in patients with IBS and is an important target for intervention.
“If patients are living with a level of stress that’s impairing, we won’t be able to solve their gut issues until we resolve their stress issues,” Desmond said. “We need to calm the gut-microbiome-brain axis, which is multidimensional and bidirectional.”
Many people — even those without IBS — experience queasiness or diarrhea prior to a major event they’re nervous about, Chey noted. These events activate the brain, which activates the nervous system, which interacts with the GI tract. Indeed, IBS is now recognized as a disorder of gut-brain interaction, he said.
“We now know that the microbiome in the GI tract influences cognition and emotional function, depression, and anxiety. One might say that the gut is the ‘center of the universe’ to human beings,” Chey said.
Evidence-based psychological approaches for stress reduction in patients with IBS include cognitive behavioral therapy, specifically tailored to helping the patient identify associations between IBS symptoms and thoughts, emotions, and actions, as well as learning new behaviors and engaging in stress management. Psychodynamic (interpersonal) therapy enables patients to understand the connection between GI symptoms and interpersonal conflicts, emotional factors, or relationship difficulties.
Gut-directed hypnotherapy (GDH) is a “proven modality for IBS,” Desmond said. Unlike other forms of hypnotherapy, GDH focuses specifically on controlling and normalizing GI function. Studies have shown a reduction of ≥ 30% in abdominal pain in two thirds of participants, with overall response rates up to 85%. It can be delivered in an individual or group setting or via a smartphone.
Desmond recommends mindfulness-based therapy (MBT) for IBS. MBT focuses on the “cultivation of mindfulness, defined as intentional, nonjudgmental, present-focused awareness.” It has been found effective in reducing flares and the markers of gut inflammation in ulcerative colitis, as well as reducing symptoms of IBS.
Chey noted that an emerging body of literature supports the potential role of acupuncture in treating IBS, and his clinic employs it. “I would like to see further research into other areas of CAM [complementary and alternative medicine], including herbal approaches to IBS symptoms as well as stress.”
Finally, all the experts agree that more research is needed.
“The real tragedy is that the NIH invests next to nothing in IBS, in contrast to inflammatory bowel disease and many other conditions,” Pimentel said. “Yet IBS is 45 times more common than inflammatory bowel disease.”
Pimentel hopes that with enough advocacy and recognition that IBS isn’t “just stress-related,” more resources will be devoted to understanding this debilitating condition.
Desmond is the author of a book on the benefits of a plant-based diet. He has also received honoraria, speaking, and consultancy fees from the European Space Agency, Dyson Institute of Engineering and Technology, Riverford Organic Farmers, Ltd., Salesforce Inc., Sentara Healthcare, Saudi Sports for All Federation, the Physicians Committee for Responsible Medicine, The Plantrician Project, Doctors for Nutrition, and The Happy Pear.
Pimentel is a consultant for Bausch Health, Ferring Pharmaceuticals, and Ardelyx. He holds equity in and is also a consultant for Dieta Health, Salvo Health, Cylinder Health, and Gemelli Biotech. Cedars-Sinai has a licensing agreement with Gemelli Biotech and Hobbs Medical.
Chey is a consultant to AbbVie, Ardelyx, Atmo, Biomerica, Gemelli Biotech, Ironwood Pharmaceuticals, Nestlé, QOL Medical, Phathom Pharmaceuticals, Redhill, Salix/Valeant, Takeda, and Vibrant. He receives grant/research funding from Commonwealth Diagnostics International, Inc., US Food and Drug Administration, National Institutes of Health, QOL Medical, and Salix/Valeant. He holds stock options in Coprata, Dieta Health, Evinature, FoodMarble, Kiwi Biosciences, and ModifyHealth. He is a board or advisory panel member of the American College of Gastroenterology, GI Health Foundation, International Foundation for Gastrointestinal Disorders, Rome. He holds patents on My Nutrition Health, Digital Manometry, and Rectal Expulsion Device.
A version of this article appeared on Medscape.com.
Irritable bowel syndrome (IBS) is one of the most common conditions encountered by both primary care providers and gastroenterologists, with a pooled global prevalence of 11.2%. This functional bowel disorder is characterized by abdominal pain or discomfort, diarrhea and/or constipation, and bloating.
Unfortunately, , according to Alan Desmond, MB, consultant in gastroenterology and general internal medicine, Torbay Hospital, UK National Health Service.
Desmond regularly sees patients who either haven’t been accurately diagnosed or have been told, “Don’t worry, it’s ‘just’ irritable bowel syndrome,” he said at the recent International Conference on Nutrition in Medicine.
A 2017 study involving nearly 2000 patients with a history of gastrointestinal (GI) symptoms found that 43.1% of those who met the criteria for IBS were undiagnosed, and among those who were diagnosed, 26% were not receiving treatment.
“Many clinicians vastly underestimate the impact functional GI symptoms have on our patients in lack of productivity, becoming homebound or losing employment, the inability to enjoy a meal with friends or family, and always needing to know where the nearest bathroom is, for example,” Desmond said in an interview.
IBS can profoundly affect patients’ mental health. One study found that 38% of patients with IBS attending a tertiary care clinic contemplated suicide because they felt hopeless about ever achieving symptom relief.
Today, several dietary, pharmacologic, and psychological/behavioral approaches are available to treat patients with IBS, noted William D. Chey, MD, AGAF, chief of the Division of Gastroenterology and Hepatology, University of Michigan, Ann Arbor, Michigan.
“Each individual patient may need a different combination of these foundational treatments,” he said. “One size doesn’t fit all.”
Diagnostic Pathway
One reason IBS is so hard to diagnose is that it’s a “symptom-based disorder, with identification of the condition predicated upon certain key characteristics that are heterogeneous,” Chey said in an interview. “IBS in patient ‘A’ may not present the same way as IBS in patient ‘B,’ although there are certain foundational common characteristics.”
IBS involves “abnormalities in the motility and contractility of the GI tract,” he said. It can present with diarrhea (IBS-D), constipation (IBS-C), or a mixture or alternation of diarrhea and constipation (IBS-M).
Patients with IBS-D often have an exaggerated gastro-colonic response, while those with IBS-C often have a blunted response.
Beyond stool abnormalities and abdominal pain/discomfort, patients often report bloating/distension, low backache, lethargy, nausea, thigh pain, and urinary and gynecologic symptoms.
Historically, IBS has been regarded as a “diagnosis of exclusion” because classic diagnostic tests typically yield no concrete findings. Desmond noted that several blood tests, procedures, imaging studies, and other tests are available to rule out other organic GI conditions, as outlined in the Table.
If the patient comes from a geographical region where giardia is endemic, clinicians also should consider testing for the parasite, Chey said.
New Understanding of IBS Etiology
Now, advances in the understanding of IBS are changing the approach to the disease.
“The field is moving away from seeing IBS as a ‘wastebasket diagnosis,’ recognizing that there are other causes of a patient’s symptoms,” Mark Pimentel, MD, associate professor of medicine and gastroenterology, Cedars-Sinai, Los Angeles, said in an interview. “What’s made IBS so difficult to diagnose has been the absence of biological markers and hallmark findings on endoscopy.”
Recent research points to novel bacterial causes as culprits in the development of IBS. In particular, altered small bowel microbiota can be triggered by acute gastroenteritis.
Food poisoning can trigger the onset of IBS — a phenomenon called “postinfectious IBS (PI-IBS),” said Pimentel, who is also executive director of the Medically Associated Science and Technology Program at Cedars-Sinai. PI-IBS almost always takes the form of IBS-D, with up to 60% of patients with IBS-D suffering the long-term sequelae of food poisoning.
The types of bacteria most commonly associated with gastroenteritis are Shigella, Campylobacter, Salmonella, and Escherichia coli, Pimentel said. All of them release cytolethal distending toxin B (CdtB), causing the body to produce antibodies to the toxin.
CdtB resembles vinculin, a naturally occurring protein critical for healthy gut function. “Because of this molecular resemblance, the immune system often mistakes one for the other, producing anti-vinculin,” Pimentel explained.
This autoimmune response leads to disruptions in the gut microbiome, ultimately resulting in PI-IBS. The chain of events “doesn’t necessarily happen immediately,” Pimentel said. “You might have developed food poisoning at a party weeks or months ago.”
Acute gastroenteritis is common, affecting as many as 179 million people in the United States annually. A meta-analysis of 47 studies, incorporating 28,270 patients, found that those who had experienced acute gastroenteritis had a fourfold higher risk of developing IBS compared with nonexposed controls.
“The problem isn’t only the IBS itself, but the fact that people with PI-IBS are four times as likely to contract food poisoning again, which can further exacerbate IBS symptoms,” Pimentel said.
Diarrhea-predominant IBS can be detected through the presence of two blood biomarkers — anti-CdtB and anti-vinculin — in a blood test developed by Pimentel and his group.
“Elevation in either of these biomarkers establishes the diagnosis,” Pimentel said. “This is a breakthrough because it represents the first test that can make IBS a ‘diagnosis of inclusion.’”
The blood test also can identify IBS-M but not IBS-C.
Pimentel said that IBS-C is associated with increased levels of methanogenic archaea, which can be diagnosed by a positive methane breath test. “Methane gas slows intestinal contractility, which might result in constipation,” he said.
Diet as a Treatment Option
Diet is usually the starting point for IBS treatment, Chey said. “The standard dietary recommendations, as defined by the National Institute for Health and Care Excellence Guidance for managing IBS, are reasonable and common sense — eating three meals a day, avoiding carbonated beverages, excess alcohol, and excess caffeine, and avoiding hard-to-digest foods that can be gas producing.”
A diet low in fermentable oligosaccharides, disaccharides, monosaccharides and polyols (FODMAPs), which are carbohydrates that aren’t completely absorbed in the intestines, has been shown to be effective in alleviating GI distress in as many as 86% of patients with IBS, leading to improvements in overall GI symptoms as well as individual symptoms (eg, abdominal pain, bloating, constipation, diarrhea, and flatulence).
Desmond recommends the low FODMAP program delineated by Monash University in Australia. The diet should be undertaken only under the supervision of a dietitian, he warned. Moreover, following it on a long-term basis can have an adverse impact on dietary quality and the gut microbiome. Therefore, “it’s important to embark on stepwise reintroduction of FODMAPS under supervision to find acceptable thresholds that don’t cause a return of symptoms.”
A growing body of research suggests that following the Mediterranean diet can be helpful in reducing IBS symptoms. Chey said that some patients who tend to over-restrict their eating might benefit from a less restrictive diet than the typical low FODMAPs diet. For them, the Mediterranean diet may be a good option.
Pharmacotherapy for IBS
Nutritional approaches aren’t for everyone, Chey noted. “Some people don’t want to be on a highly restricted diet.” For them, medications addressing symptoms might be a better option.
Antispasmodics — either anticholinergics (hyoscine and dicyclomine) or smooth muscle relaxants (alverine, mebeverine, and peppermint oil) — can be helpful, although they can worsen constipation in a dose-dependent manner. It is advisable to use them on an as-needed rather than long-term basis.
Antidiarrheal agents include loperamide and diphenoxylate.
For constipation, laxatives (eg, senna, bisacodyl, polyethylene glycol, and sodium picosulfate) can be helpful.
Desmond noted that the American Gastroenterological Association does not recommend routine use of probiotics for most GI disorders, including IBS. Exceptions include prevention of Clostridioides difficile, ulcerative colitis, and pouchitis.
Targeting the Gut-Brain Relationship
Stress plays a role in exacerbating symptoms in patients with IBS and is an important target for intervention.
“If patients are living with a level of stress that’s impairing, we won’t be able to solve their gut issues until we resolve their stress issues,” Desmond said. “We need to calm the gut-microbiome-brain axis, which is multidimensional and bidirectional.”
Many people — even those without IBS — experience queasiness or diarrhea prior to a major event they’re nervous about, Chey noted. These events activate the brain, which activates the nervous system, which interacts with the GI tract. Indeed, IBS is now recognized as a disorder of gut-brain interaction, he said.
“We now know that the microbiome in the GI tract influences cognition and emotional function, depression, and anxiety. One might say that the gut is the ‘center of the universe’ to human beings,” Chey said.
Evidence-based psychological approaches for stress reduction in patients with IBS include cognitive behavioral therapy, specifically tailored to helping the patient identify associations between IBS symptoms and thoughts, emotions, and actions, as well as learning new behaviors and engaging in stress management. Psychodynamic (interpersonal) therapy enables patients to understand the connection between GI symptoms and interpersonal conflicts, emotional factors, or relationship difficulties.
Gut-directed hypnotherapy (GDH) is a “proven modality for IBS,” Desmond said. Unlike other forms of hypnotherapy, GDH focuses specifically on controlling and normalizing GI function. Studies have shown a reduction of ≥ 30% in abdominal pain in two thirds of participants, with overall response rates up to 85%. It can be delivered in an individual or group setting or via a smartphone.
Desmond recommends mindfulness-based therapy (MBT) for IBS. MBT focuses on the “cultivation of mindfulness, defined as intentional, nonjudgmental, present-focused awareness.” It has been found effective in reducing flares and the markers of gut inflammation in ulcerative colitis, as well as reducing symptoms of IBS.
Chey noted that an emerging body of literature supports the potential role of acupuncture in treating IBS, and his clinic employs it. “I would like to see further research into other areas of CAM [complementary and alternative medicine], including herbal approaches to IBS symptoms as well as stress.”
Finally, all the experts agree that more research is needed.
“The real tragedy is that the NIH invests next to nothing in IBS, in contrast to inflammatory bowel disease and many other conditions,” Pimentel said. “Yet IBS is 45 times more common than inflammatory bowel disease.”
Pimentel hopes that with enough advocacy and recognition that IBS isn’t “just stress-related,” more resources will be devoted to understanding this debilitating condition.
Desmond is the author of a book on the benefits of a plant-based diet. He has also received honoraria, speaking, and consultancy fees from the European Space Agency, Dyson Institute of Engineering and Technology, Riverford Organic Farmers, Ltd., Salesforce Inc., Sentara Healthcare, Saudi Sports for All Federation, the Physicians Committee for Responsible Medicine, The Plantrician Project, Doctors for Nutrition, and The Happy Pear.
Pimentel is a consultant for Bausch Health, Ferring Pharmaceuticals, and Ardelyx. He holds equity in and is also a consultant for Dieta Health, Salvo Health, Cylinder Health, and Gemelli Biotech. Cedars-Sinai has a licensing agreement with Gemelli Biotech and Hobbs Medical.
Chey is a consultant to AbbVie, Ardelyx, Atmo, Biomerica, Gemelli Biotech, Ironwood Pharmaceuticals, Nestlé, QOL Medical, Phathom Pharmaceuticals, Redhill, Salix/Valeant, Takeda, and Vibrant. He receives grant/research funding from Commonwealth Diagnostics International, Inc., US Food and Drug Administration, National Institutes of Health, QOL Medical, and Salix/Valeant. He holds stock options in Coprata, Dieta Health, Evinature, FoodMarble, Kiwi Biosciences, and ModifyHealth. He is a board or advisory panel member of the American College of Gastroenterology, GI Health Foundation, International Foundation for Gastrointestinal Disorders, Rome. He holds patents on My Nutrition Health, Digital Manometry, and Rectal Expulsion Device.
A version of this article appeared on Medscape.com.
Irritable bowel syndrome (IBS) is one of the most common conditions encountered by both primary care providers and gastroenterologists, with a pooled global prevalence of 11.2%. This functional bowel disorder is characterized by abdominal pain or discomfort, diarrhea and/or constipation, and bloating.
Unfortunately, , according to Alan Desmond, MB, consultant in gastroenterology and general internal medicine, Torbay Hospital, UK National Health Service.
Desmond regularly sees patients who either haven’t been accurately diagnosed or have been told, “Don’t worry, it’s ‘just’ irritable bowel syndrome,” he said at the recent International Conference on Nutrition in Medicine.
A 2017 study involving nearly 2000 patients with a history of gastrointestinal (GI) symptoms found that 43.1% of those who met the criteria for IBS were undiagnosed, and among those who were diagnosed, 26% were not receiving treatment.
“Many clinicians vastly underestimate the impact functional GI symptoms have on our patients in lack of productivity, becoming homebound or losing employment, the inability to enjoy a meal with friends or family, and always needing to know where the nearest bathroom is, for example,” Desmond said in an interview.
IBS can profoundly affect patients’ mental health. One study found that 38% of patients with IBS attending a tertiary care clinic contemplated suicide because they felt hopeless about ever achieving symptom relief.
Today, several dietary, pharmacologic, and psychological/behavioral approaches are available to treat patients with IBS, noted William D. Chey, MD, AGAF, chief of the Division of Gastroenterology and Hepatology, University of Michigan, Ann Arbor, Michigan.
“Each individual patient may need a different combination of these foundational treatments,” he said. “One size doesn’t fit all.”
Diagnostic Pathway
One reason IBS is so hard to diagnose is that it’s a “symptom-based disorder, with identification of the condition predicated upon certain key characteristics that are heterogeneous,” Chey said in an interview. “IBS in patient ‘A’ may not present the same way as IBS in patient ‘B,’ although there are certain foundational common characteristics.”
IBS involves “abnormalities in the motility and contractility of the GI tract,” he said. It can present with diarrhea (IBS-D), constipation (IBS-C), or a mixture or alternation of diarrhea and constipation (IBS-M).
Patients with IBS-D often have an exaggerated gastro-colonic response, while those with IBS-C often have a blunted response.
Beyond stool abnormalities and abdominal pain/discomfort, patients often report bloating/distension, low backache, lethargy, nausea, thigh pain, and urinary and gynecologic symptoms.
Historically, IBS has been regarded as a “diagnosis of exclusion” because classic diagnostic tests typically yield no concrete findings. Desmond noted that several blood tests, procedures, imaging studies, and other tests are available to rule out other organic GI conditions, as outlined in the Table.
If the patient comes from a geographical region where giardia is endemic, clinicians also should consider testing for the parasite, Chey said.
New Understanding of IBS Etiology
Now, advances in the understanding of IBS are changing the approach to the disease.
“The field is moving away from seeing IBS as a ‘wastebasket diagnosis,’ recognizing that there are other causes of a patient’s symptoms,” Mark Pimentel, MD, associate professor of medicine and gastroenterology, Cedars-Sinai, Los Angeles, said in an interview. “What’s made IBS so difficult to diagnose has been the absence of biological markers and hallmark findings on endoscopy.”
Recent research points to novel bacterial causes as culprits in the development of IBS. In particular, altered small bowel microbiota can be triggered by acute gastroenteritis.
Food poisoning can trigger the onset of IBS — a phenomenon called “postinfectious IBS (PI-IBS),” said Pimentel, who is also executive director of the Medically Associated Science and Technology Program at Cedars-Sinai. PI-IBS almost always takes the form of IBS-D, with up to 60% of patients with IBS-D suffering the long-term sequelae of food poisoning.
The types of bacteria most commonly associated with gastroenteritis are Shigella, Campylobacter, Salmonella, and Escherichia coli, Pimentel said. All of them release cytolethal distending toxin B (CdtB), causing the body to produce antibodies to the toxin.
CdtB resembles vinculin, a naturally occurring protein critical for healthy gut function. “Because of this molecular resemblance, the immune system often mistakes one for the other, producing anti-vinculin,” Pimentel explained.
This autoimmune response leads to disruptions in the gut microbiome, ultimately resulting in PI-IBS. The chain of events “doesn’t necessarily happen immediately,” Pimentel said. “You might have developed food poisoning at a party weeks or months ago.”
Acute gastroenteritis is common, affecting as many as 179 million people in the United States annually. A meta-analysis of 47 studies, incorporating 28,270 patients, found that those who had experienced acute gastroenteritis had a fourfold higher risk of developing IBS compared with nonexposed controls.
“The problem isn’t only the IBS itself, but the fact that people with PI-IBS are four times as likely to contract food poisoning again, which can further exacerbate IBS symptoms,” Pimentel said.
Diarrhea-predominant IBS can be detected through the presence of two blood biomarkers — anti-CdtB and anti-vinculin — in a blood test developed by Pimentel and his group.
“Elevation in either of these biomarkers establishes the diagnosis,” Pimentel said. “This is a breakthrough because it represents the first test that can make IBS a ‘diagnosis of inclusion.’”
The blood test also can identify IBS-M but not IBS-C.
Pimentel said that IBS-C is associated with increased levels of methanogenic archaea, which can be diagnosed by a positive methane breath test. “Methane gas slows intestinal contractility, which might result in constipation,” he said.
Diet as a Treatment Option
Diet is usually the starting point for IBS treatment, Chey said. “The standard dietary recommendations, as defined by the National Institute for Health and Care Excellence Guidance for managing IBS, are reasonable and common sense — eating three meals a day, avoiding carbonated beverages, excess alcohol, and excess caffeine, and avoiding hard-to-digest foods that can be gas producing.”
A diet low in fermentable oligosaccharides, disaccharides, monosaccharides and polyols (FODMAPs), which are carbohydrates that aren’t completely absorbed in the intestines, has been shown to be effective in alleviating GI distress in as many as 86% of patients with IBS, leading to improvements in overall GI symptoms as well as individual symptoms (eg, abdominal pain, bloating, constipation, diarrhea, and flatulence).
Desmond recommends the low FODMAP program delineated by Monash University in Australia. The diet should be undertaken only under the supervision of a dietitian, he warned. Moreover, following it on a long-term basis can have an adverse impact on dietary quality and the gut microbiome. Therefore, “it’s important to embark on stepwise reintroduction of FODMAPS under supervision to find acceptable thresholds that don’t cause a return of symptoms.”
A growing body of research suggests that following the Mediterranean diet can be helpful in reducing IBS symptoms. Chey said that some patients who tend to over-restrict their eating might benefit from a less restrictive diet than the typical low FODMAPs diet. For them, the Mediterranean diet may be a good option.
Pharmacotherapy for IBS
Nutritional approaches aren’t for everyone, Chey noted. “Some people don’t want to be on a highly restricted diet.” For them, medications addressing symptoms might be a better option.
Antispasmodics — either anticholinergics (hyoscine and dicyclomine) or smooth muscle relaxants (alverine, mebeverine, and peppermint oil) — can be helpful, although they can worsen constipation in a dose-dependent manner. It is advisable to use them on an as-needed rather than long-term basis.
Antidiarrheal agents include loperamide and diphenoxylate.
For constipation, laxatives (eg, senna, bisacodyl, polyethylene glycol, and sodium picosulfate) can be helpful.
Desmond noted that the American Gastroenterological Association does not recommend routine use of probiotics for most GI disorders, including IBS. Exceptions include prevention of Clostridioides difficile, ulcerative colitis, and pouchitis.
Targeting the Gut-Brain Relationship
Stress plays a role in exacerbating symptoms in patients with IBS and is an important target for intervention.
“If patients are living with a level of stress that’s impairing, we won’t be able to solve their gut issues until we resolve their stress issues,” Desmond said. “We need to calm the gut-microbiome-brain axis, which is multidimensional and bidirectional.”
Many people — even those without IBS — experience queasiness or diarrhea prior to a major event they’re nervous about, Chey noted. These events activate the brain, which activates the nervous system, which interacts with the GI tract. Indeed, IBS is now recognized as a disorder of gut-brain interaction, he said.
“We now know that the microbiome in the GI tract influences cognition and emotional function, depression, and anxiety. One might say that the gut is the ‘center of the universe’ to human beings,” Chey said.
Evidence-based psychological approaches for stress reduction in patients with IBS include cognitive behavioral therapy, specifically tailored to helping the patient identify associations between IBS symptoms and thoughts, emotions, and actions, as well as learning new behaviors and engaging in stress management. Psychodynamic (interpersonal) therapy enables patients to understand the connection between GI symptoms and interpersonal conflicts, emotional factors, or relationship difficulties.
Gut-directed hypnotherapy (GDH) is a “proven modality for IBS,” Desmond said. Unlike other forms of hypnotherapy, GDH focuses specifically on controlling and normalizing GI function. Studies have shown a reduction of ≥ 30% in abdominal pain in two thirds of participants, with overall response rates up to 85%. It can be delivered in an individual or group setting or via a smartphone.
Desmond recommends mindfulness-based therapy (MBT) for IBS. MBT focuses on the “cultivation of mindfulness, defined as intentional, nonjudgmental, present-focused awareness.” It has been found effective in reducing flares and the markers of gut inflammation in ulcerative colitis, as well as reducing symptoms of IBS.
Chey noted that an emerging body of literature supports the potential role of acupuncture in treating IBS, and his clinic employs it. “I would like to see further research into other areas of CAM [complementary and alternative medicine], including herbal approaches to IBS symptoms as well as stress.”
Finally, all the experts agree that more research is needed.
“The real tragedy is that the NIH invests next to nothing in IBS, in contrast to inflammatory bowel disease and many other conditions,” Pimentel said. “Yet IBS is 45 times more common than inflammatory bowel disease.”
Pimentel hopes that with enough advocacy and recognition that IBS isn’t “just stress-related,” more resources will be devoted to understanding this debilitating condition.
Desmond is the author of a book on the benefits of a plant-based diet. He has also received honoraria, speaking, and consultancy fees from the European Space Agency, Dyson Institute of Engineering and Technology, Riverford Organic Farmers, Ltd., Salesforce Inc., Sentara Healthcare, Saudi Sports for All Federation, the Physicians Committee for Responsible Medicine, The Plantrician Project, Doctors for Nutrition, and The Happy Pear.
Pimentel is a consultant for Bausch Health, Ferring Pharmaceuticals, and Ardelyx. He holds equity in and is also a consultant for Dieta Health, Salvo Health, Cylinder Health, and Gemelli Biotech. Cedars-Sinai has a licensing agreement with Gemelli Biotech and Hobbs Medical.
Chey is a consultant to AbbVie, Ardelyx, Atmo, Biomerica, Gemelli Biotech, Ironwood Pharmaceuticals, Nestlé, QOL Medical, Phathom Pharmaceuticals, Redhill, Salix/Valeant, Takeda, and Vibrant. He receives grant/research funding from Commonwealth Diagnostics International, Inc., US Food and Drug Administration, National Institutes of Health, QOL Medical, and Salix/Valeant. He holds stock options in Coprata, Dieta Health, Evinature, FoodMarble, Kiwi Biosciences, and ModifyHealth. He is a board or advisory panel member of the American College of Gastroenterology, GI Health Foundation, International Foundation for Gastrointestinal Disorders, Rome. He holds patents on My Nutrition Health, Digital Manometry, and Rectal Expulsion Device.
A version of this article appeared on Medscape.com.