User login
Myelin antibody predicts ADEM relapse
LOS ANGELES – There’s substantially higher risk of relapse and epilepsy after acute disseminated encephalomyelitis when children present with serum antibodies against myelin oligodendrocyte glycoprotein, according to British investigators.
“Traditionally, we told parents that ADEM [acute disseminated encephalomyelitis] is typically monophasic. I do tell parents now that the risk of relapse is higher if we see” myelin oligodendrocyte glycoprotein antibodies (MOG-Ab), said senior investigator Yael Hacohen, MBBS, DPhil, a pediatric neurology lecturer at University College London.
There was also a strong trend for relapsing disease when children presented with seizures, and an increased risk of post-ADEM epilepsy with oligoclonal bands on cerebrospinal fluid analysis, a marker of inflammation.
ADEM is an acute CNS demyelinating disorder primarily affecting young children, often after upper respiratory tract infections and occasionally after measles, mumps, and rubella vaccination. Signs can include limb weakness, stumbling, and coma. Many children recover without incident, but some don’t.
There’s been an increasing number of reports of children – and adults – presenting with antibodies against MOG, a glycoprotein on the outermost layer of the myelin sheath. Its exact function is unknown, but antibodies have been found in a number of inflammatory CNS conditions, and its role in pathogenesis is being explored. Testing is available for clinical use, but it isn’t standardized. For now, titer levels aren’t being used to guide treatment at University College London, Dr. Hacohen said at the American Academy of Neurology annual meeting.

The team reviewed 74 children with ADEM who presented at three pediatric neurology centers during 2005-2017, at a median age of 4.5 years. There were about equal numbers of boys and girls, and all had MRI abnormalities consistent with ADEM. Fifty children (68%) were MOG-ab positive.
Twenty-seven antibody-positive children (54%) relapsed, versus 3 of the 24 negative children (13%). Relapse was almost six times more likely with MOB-Ab (95% confidence interval [CI], 1.8-19.7; P = .002). The overall relapse rate of 42% (31/74) was higher than in previous studies, probably because of longer follow-up, lasting years in some cases.
Sixteen children (22%) presented with seizures, which nearly tripled the risk of relapse, although the finding wasn’t statistically significant (95% CI, 0.9-9.2; P = .06). There was a trend toward more seizures at onset in the MOG-Ab group.
Twelve children (16.2%) developed post-ADEM epilepsy, all but one MOG-Ab positive. The median time to seizure onset was 3 months. All of the children remained on antiepileptic medications at 2-year follow-up.
Oligoclonal bands were found in 8 of 37 children tested (22%), and also markedly increased the risk of post-ADEM seizures (odds ratio, 8.7; 95% CI, 1.5-54; P = .01).
“The majority of the children that we’ve looked at remain MOG-Ab positive. There may be a trend in antibody titers going down, but overall we didn’t find titers clinically useful. I know two children where titers went down. They relapsed,” and the titers went “up again, so we don’t’ really use them clinically for treatment,” Dr. Hacohen said.
“I think there is more to do” when it comes to optimizing ADEM management. “It’s a very heterogeneous [condition, and] I don’t want to put [everyone] on immunosuppression for years. I’ve got one patient who had an event, and 7 years later had a second event, and then was back to normal in a week.” On the other hand, “10%-20% of our patients do quite poorly and relapse on all treatments,” she said.
The investigators didn’t have any disclosures and there was no industry funding for the work.
SOURCE: Rossor T et al. Neurology. 2018 Apr 90(15 Suppl.):S35.004.
LOS ANGELES – There’s substantially higher risk of relapse and epilepsy after acute disseminated encephalomyelitis when children present with serum antibodies against myelin oligodendrocyte glycoprotein, according to British investigators.
“Traditionally, we told parents that ADEM [acute disseminated encephalomyelitis] is typically monophasic. I do tell parents now that the risk of relapse is higher if we see” myelin oligodendrocyte glycoprotein antibodies (MOG-Ab), said senior investigator Yael Hacohen, MBBS, DPhil, a pediatric neurology lecturer at University College London.
There was also a strong trend for relapsing disease when children presented with seizures, and an increased risk of post-ADEM epilepsy with oligoclonal bands on cerebrospinal fluid analysis, a marker of inflammation.
ADEM is an acute CNS demyelinating disorder primarily affecting young children, often after upper respiratory tract infections and occasionally after measles, mumps, and rubella vaccination. Signs can include limb weakness, stumbling, and coma. Many children recover without incident, but some don’t.
There’s been an increasing number of reports of children – and adults – presenting with antibodies against MOG, a glycoprotein on the outermost layer of the myelin sheath. Its exact function is unknown, but antibodies have been found in a number of inflammatory CNS conditions, and its role in pathogenesis is being explored. Testing is available for clinical use, but it isn’t standardized. For now, titer levels aren’t being used to guide treatment at University College London, Dr. Hacohen said at the American Academy of Neurology annual meeting.
The team reviewed 74 children with ADEM who presented at three pediatric neurology centers during 2005-2017, at a median age of 4.5 years. There were about equal numbers of boys and girls, and all had MRI abnormalities consistent with ADEM. Fifty children (68%) were MOG-ab positive.
Twenty-seven antibody-positive children (54%) relapsed, versus 3 of the 24 negative children (13%). Relapse was almost six times more likely with MOB-Ab (95% confidence interval [CI], 1.8-19.7; P = .002). The overall relapse rate of 42% (31/74) was higher than in previous studies, probably because of longer follow-up, lasting years in some cases.
Sixteen children (22%) presented with seizures, which nearly tripled the risk of relapse, although the finding wasn’t statistically significant (95% CI, 0.9-9.2; P = .06). There was a trend toward more seizures at onset in the MOG-Ab group.
Twelve children (16.2%) developed post-ADEM epilepsy, all but one MOG-Ab positive. The median time to seizure onset was 3 months. All of the children remained on antiepileptic medications at 2-year follow-up.
Oligoclonal bands were found in 8 of 37 children tested (22%), and also markedly increased the risk of post-ADEM seizures (odds ratio, 8.7; 95% CI, 1.5-54; P = .01).
“The majority of the children that we’ve looked at remain MOG-Ab positive. There may be a trend in antibody titers going down, but overall we didn’t find titers clinically useful. I know two children where titers went down. They relapsed,” and the titers went “up again, so we don’t’ really use them clinically for treatment,” Dr. Hacohen said.
“I think there is more to do” when it comes to optimizing ADEM management. “It’s a very heterogeneous [condition, and] I don’t want to put [everyone] on immunosuppression for years. I’ve got one patient who had an event, and 7 years later had a second event, and then was back to normal in a week.” On the other hand, “10%-20% of our patients do quite poorly and relapse on all treatments,” she said.
The investigators didn’t have any disclosures and there was no industry funding for the work.
SOURCE: Rossor T et al. Neurology. 2018 Apr 90(15 Suppl.):S35.004.
LOS ANGELES – There’s substantially higher risk of relapse and epilepsy after acute disseminated encephalomyelitis when children present with serum antibodies against myelin oligodendrocyte glycoprotein, according to British investigators.
“Traditionally, we told parents that ADEM [acute disseminated encephalomyelitis] is typically monophasic. I do tell parents now that the risk of relapse is higher if we see” myelin oligodendrocyte glycoprotein antibodies (MOG-Ab), said senior investigator Yael Hacohen, MBBS, DPhil, a pediatric neurology lecturer at University College London.
There was also a strong trend for relapsing disease when children presented with seizures, and an increased risk of post-ADEM epilepsy with oligoclonal bands on cerebrospinal fluid analysis, a marker of inflammation.
ADEM is an acute CNS demyelinating disorder primarily affecting young children, often after upper respiratory tract infections and occasionally after measles, mumps, and rubella vaccination. Signs can include limb weakness, stumbling, and coma. Many children recover without incident, but some don’t.
There’s been an increasing number of reports of children – and adults – presenting with antibodies against MOG, a glycoprotein on the outermost layer of the myelin sheath. Its exact function is unknown, but antibodies have been found in a number of inflammatory CNS conditions, and its role in pathogenesis is being explored. Testing is available for clinical use, but it isn’t standardized. For now, titer levels aren’t being used to guide treatment at University College London, Dr. Hacohen said at the American Academy of Neurology annual meeting.
The team reviewed 74 children with ADEM who presented at three pediatric neurology centers during 2005-2017, at a median age of 4.5 years. There were about equal numbers of boys and girls, and all had MRI abnormalities consistent with ADEM. Fifty children (68%) were MOG-ab positive.
Twenty-seven antibody-positive children (54%) relapsed, versus 3 of the 24 negative children (13%). Relapse was almost six times more likely with MOB-Ab (95% confidence interval [CI], 1.8-19.7; P = .002). The overall relapse rate of 42% (31/74) was higher than in previous studies, probably because of longer follow-up, lasting years in some cases.
Sixteen children (22%) presented with seizures, which nearly tripled the risk of relapse, although the finding wasn’t statistically significant (95% CI, 0.9-9.2; P = .06). There was a trend toward more seizures at onset in the MOG-Ab group.
Twelve children (16.2%) developed post-ADEM epilepsy, all but one MOG-Ab positive. The median time to seizure onset was 3 months. All of the children remained on antiepileptic medications at 2-year follow-up.
Oligoclonal bands were found in 8 of 37 children tested (22%), and also markedly increased the risk of post-ADEM seizures (odds ratio, 8.7; 95% CI, 1.5-54; P = .01).
“The majority of the children that we’ve looked at remain MOG-Ab positive. There may be a trend in antibody titers going down, but overall we didn’t find titers clinically useful. I know two children where titers went down. They relapsed,” and the titers went “up again, so we don’t’ really use them clinically for treatment,” Dr. Hacohen said.
“I think there is more to do” when it comes to optimizing ADEM management. “It’s a very heterogeneous [condition, and] I don’t want to put [everyone] on immunosuppression for years. I’ve got one patient who had an event, and 7 years later had a second event, and then was back to normal in a week.” On the other hand, “10%-20% of our patients do quite poorly and relapse on all treatments,” she said.
The investigators didn’t have any disclosures and there was no industry funding for the work.
SOURCE: Rossor T et al. Neurology. 2018 Apr 90(15 Suppl.):S35.004.
REPORTING FROM AAN 2018
Key clinical point: Myelin oligodendrocyte glycoprotein antibodies help to identify children who will have relapsing ADEM.
Major finding: Twenty-seven out of 50 antibody-positive children (54%) relapsed, versus 3 of 24 negative children (13%).
Study details: Review of 74 children with ADEM
Disclosures: There was no industry funding, and the investigators had no disclosures.
Source: Rossor T et al. Neurology. 2018 Apr 90(15 Suppl.):S35.004.
Diabetes spending topped $101 billion in 2013
according to investigators from the University of Washington, Seattle.
The largest share of personal health spending on diabetes in 2013 went for prescribed retail pharmaceuticals, which tallied over $58 billion. That was followed by ambulatory care at $24 billion, inpatient care at just under $10 billion, nursing home care at $9 billion, and emergency department care at $0.4 billion, Ellen Squires and her associates said in Diabetes Care.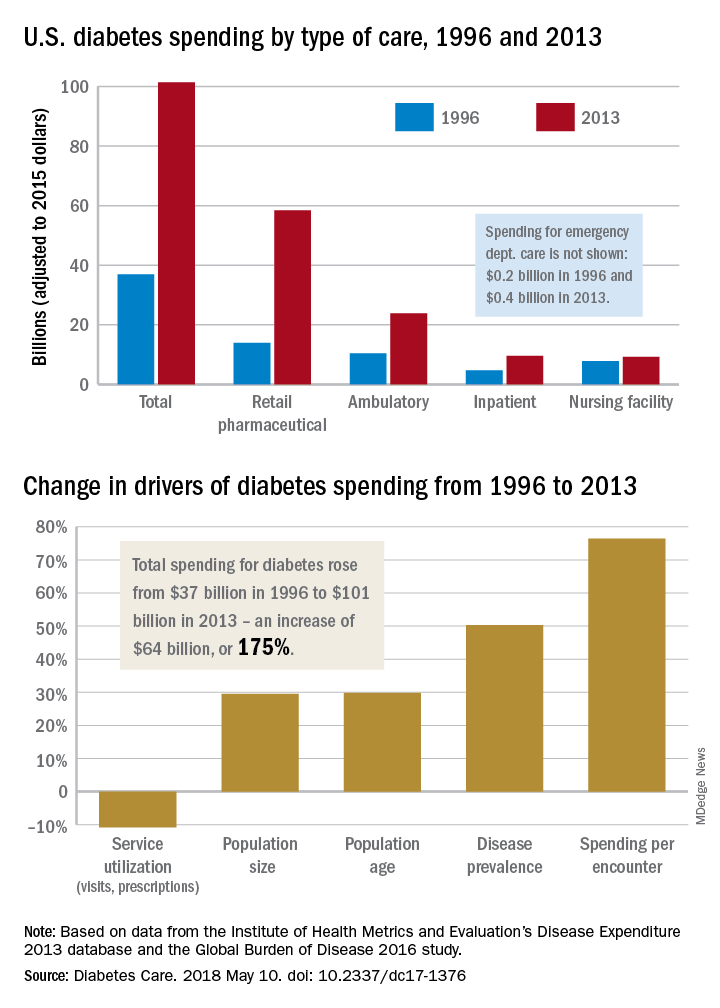
“The rate of increase in pharmaceutical spending was especially drastic from 2008 to 2013, and research suggests that these upward trends have continued in more recent years,” Ms. Squires and her associates wrote.
The analysis used data from the Institute for Health Metrics and Evaluation’s Disease Expenditure 2013 database and the Global Burden of Disease 2016 study. The current study was funded by the Peterson Center on Healthcare and the National Institute on Aging. One investigator receives research support from Medtronic Diabetes and is a consultant for Abbott Diabetes Care, Bigfoot Biomedical, Adocia, and Roche. No other relevant conflicts of interest were reported.
SOURCE: Squires E et al. Diabetes Care. 2018 May 10. doi: 10.2337/dc17-1376.
according to investigators from the University of Washington, Seattle.
The largest share of personal health spending on diabetes in 2013 went for prescribed retail pharmaceuticals, which tallied over $58 billion. That was followed by ambulatory care at $24 billion, inpatient care at just under $10 billion, nursing home care at $9 billion, and emergency department care at $0.4 billion, Ellen Squires and her associates said in Diabetes Care.
“The rate of increase in pharmaceutical spending was especially drastic from 2008 to 2013, and research suggests that these upward trends have continued in more recent years,” Ms. Squires and her associates wrote.
The analysis used data from the Institute for Health Metrics and Evaluation’s Disease Expenditure 2013 database and the Global Burden of Disease 2016 study. The current study was funded by the Peterson Center on Healthcare and the National Institute on Aging. One investigator receives research support from Medtronic Diabetes and is a consultant for Abbott Diabetes Care, Bigfoot Biomedical, Adocia, and Roche. No other relevant conflicts of interest were reported.
SOURCE: Squires E et al. Diabetes Care. 2018 May 10. doi: 10.2337/dc17-1376.
according to investigators from the University of Washington, Seattle.
The largest share of personal health spending on diabetes in 2013 went for prescribed retail pharmaceuticals, which tallied over $58 billion. That was followed by ambulatory care at $24 billion, inpatient care at just under $10 billion, nursing home care at $9 billion, and emergency department care at $0.4 billion, Ellen Squires and her associates said in Diabetes Care.
“The rate of increase in pharmaceutical spending was especially drastic from 2008 to 2013, and research suggests that these upward trends have continued in more recent years,” Ms. Squires and her associates wrote.
The analysis used data from the Institute for Health Metrics and Evaluation’s Disease Expenditure 2013 database and the Global Burden of Disease 2016 study. The current study was funded by the Peterson Center on Healthcare and the National Institute on Aging. One investigator receives research support from Medtronic Diabetes and is a consultant for Abbott Diabetes Care, Bigfoot Biomedical, Adocia, and Roche. No other relevant conflicts of interest were reported.
SOURCE: Squires E et al. Diabetes Care. 2018 May 10. doi: 10.2337/dc17-1376.
FROM DIABETES CARE
FDA: PrEP indication updated to include adolescents at risk of HIV infection
The following is the text of an announcement by the U.S. Food and Drug Administration regarding a revision in the Truvada label to expand the PrEP indication to include at-risk adolescents. The new label change has not yet been posted.
The Food and Drug Administration approved revisions to the Truvada (emtricitabine and tenofovir disoproxil fumarate) labeling to expand the Pre-Exposure Prophylaxis (PrEP) indication to include adolescents weighing at least 35 kg who are at risk of HIV-1 acquisition. The major labeling changes with respect to this expanded indication are summarized below. In addition, Section 8 was reformatted per the Pregnancy and Lactation Labeling Rule (PLLR) and includes updated information specific to the use of Truvada for PrEP during pregnancy and breastfeeding. Other sections of labeling were reformatted for consistency with current and best labeling practices, as well as with labeling for other HIV fixed-dose combination products. 
Indications and usage
1.2 HIV-1 pre-exposure prophylaxis (PrEP)
Truvada is indicated in combination with safer sex practices for pre-exposure prophylaxis (PrEP) to reduce the risk of sexually acquired HIV-1 in at-risk adults and adolescents weighing at least 35 kg. Individuals must have a negative HIV-1 test immediately prior to initiating Truvada for HIV-1 PrEP.
If clinical symptoms consistent with acute viral infection are present and recent (less than 1 month) exposures are suspected, delay starting PrEP for at least one month and reconfirm HIV-1 status or use a test cleared by the FDA as an aid in the diagnosis of HIV-1 infection, including acute or primary HIV-1 infection
When considering Truvada for HIV-1 PrEP, factors that help to identify individuals at risk may include:
– has partner(s) known to be HIV-1 infected, or
– engages in sexual activity within a high prevalence area or social network and has additional risk factors for HIV-1 acquisition, such as:
- inconsistent or no condom use.
- diagnosis of sexually transmitted infections.
- exchange of sex for commodities (such as money, food, shelter, or drugs).
- use of illicit drugs or alcohol dependence.
- incarceration.
- partner(s) of unknown HIV-1 status with any of the factors listed above.
Dosage and administration
2.1 Testing prior to initiation of Truvada for treatment of HIV-1 infection or for HIV-1 PrEP
Prior to or when initiating Truvada, test patients for hepatitis B virus infection [see Warnings and Precautions (5.1)].
Prior to initiation and during use of Truvada, on a clinically appropriate schedule, assess serum creatinine, estimated creatinine clearance, urine glucose and urine protein in all patients. In patients with chronic kidney disease, also assess serum phosphorus
2.2 HIV-1 screening for individuals receiving Truvada for HIV-1 PrEP
Screen all patients for HIV-1 infection before initiating Truvada for HIV-1 PrEP and at least once every 3 months while taking Truvada
2.5 Recommended dosage for HIV-1 PrEP
The dosage of Truvada in HIV-1 uninfected adults and adolescents weighing at least 35 kg is one tablet (containing 200 mg of FTC and 300 mg of TDF) once daily taken orally with or without food.
6.0 Adverse reactions
Clinical trials in adolescent subjects
In a single-arm, open-label clinical trial (ATN113), in which 67 HIV-1 uninfected adolescent (15 to 18 years of age) men who have sex with men received Truvada once daily for HIV-1 PrEP, the safety profile of Truvada was similar to that observed in adults. Median duration to exposure of Truvada was 47 weeks.
In the ATN113 trial, median BMD increased from baseline to Week 48, +2.58% for lumbar spine and +0.72% for total body. One subject had significant (greater than or equal to 4%) total body BMD loss at Week 24. Median changes from baseline BMD Z-scores were 0.0 for lumbar spine and −0.2 for total body at Week 48. Three subjects showed a worsening (change from greater than −2 to less than or equal to −2) from baseline in their lumbar spine or total body BMD Z-scores at Week 24 or 48. Interpretation of these data, however, may be limited by the low rate of adherence to Truvada by Week 48.
8.4 Pediatric use
HIV-1 PrEP
The safety and effectiveness of Truvada for HIV-1 PrEP in at-risk adolescents weighing at least 35 kg is supported by data from adequate and well-controlled studies of Truvada for HIV-1 PrEP in adults with additional data from safety and pharmacokinetic studies in previously conducted trials with the individual drug products, FTC and TDF, in HIV-1 infected adults and pediatric subjects.
Safety, adherence, and resistance were evaluated in a single-arm, open-label clinical trial (ATN113) in which 67 HIV-1 uninfected at-risk adolescent men who have sex with men received Truvada once daily for HIV-1 PrEP. The mean age of subjects was 17 years (range, 15-18 years); 46% were Hispanic, 52% black, and 37% white. The safety profile of Truvada in ATN113 was similar to that observed in the adult HIV-1 PrEP trials.
In the ATN113 trial, HIV-1 seroconversion occurred in three subjects. Tenofovir diphosphate levels in dried blood spot assays indicate that these subjects had poor adherence. No tenofovir- or FTC-associated HIV-1 resistance substitutions were detected in virus isolated from the three subjects who seroconverted.
Adherence to study drug, as demonstrated by tenofovir diphosphate levels in dried blood spot assays, declined markedly after Week 12 once subjects switched from monthly to quarterly visits, suggesting that adolescents may benefit from more frequent visits and counseling.
12.0 Clinical pharmacology
HIV-1 PrEP
The pharmacokinetic data for tenofovir and FTC following administration of Truvada in HIV-1 uninfected adolescents weighing 35 kg and above are not available. The dosage recommendations of Truvada for HIV-1 PrEP in this population are based on safety and adherence data from the ATN113 trial [see Use in Specific Populations (8.4)] and known pharmacokinetic information in HIV-infected adolescents taking TDF and FTC for treatment.
ResistanceATN113 Trial
In ATN113, a clinical trial of HIV-1 seronegative adolescent subjects [see Use in Specific Populations (8.4)], no amino acid substitutions associated with resistance to FTC or TDF were detected at the time of seroconversion from any of the 3 subjects who became infected with HIV-1 during the trial. All 3 subjects who seroconverted were nonadherent to the recommended Truvada dosage.
The updated label will soon be available at drugs@fda or DailyMed.
The following is the text of an announcement by the U.S. Food and Drug Administration regarding a revision in the Truvada label to expand the PrEP indication to include at-risk adolescents. The new label change has not yet been posted.
The Food and Drug Administration approved revisions to the Truvada (emtricitabine and tenofovir disoproxil fumarate) labeling to expand the Pre-Exposure Prophylaxis (PrEP) indication to include adolescents weighing at least 35 kg who are at risk of HIV-1 acquisition. The major labeling changes with respect to this expanded indication are summarized below. In addition, Section 8 was reformatted per the Pregnancy and Lactation Labeling Rule (PLLR) and includes updated information specific to the use of Truvada for PrEP during pregnancy and breastfeeding. Other sections of labeling were reformatted for consistency with current and best labeling practices, as well as with labeling for other HIV fixed-dose combination products.
Indications and usage
1.2 HIV-1 pre-exposure prophylaxis (PrEP)
Truvada is indicated in combination with safer sex practices for pre-exposure prophylaxis (PrEP) to reduce the risk of sexually acquired HIV-1 in at-risk adults and adolescents weighing at least 35 kg. Individuals must have a negative HIV-1 test immediately prior to initiating Truvada for HIV-1 PrEP.
If clinical symptoms consistent with acute viral infection are present and recent (less than 1 month) exposures are suspected, delay starting PrEP for at least one month and reconfirm HIV-1 status or use a test cleared by the FDA as an aid in the diagnosis of HIV-1 infection, including acute or primary HIV-1 infection
When considering Truvada for HIV-1 PrEP, factors that help to identify individuals at risk may include:
– has partner(s) known to be HIV-1 infected, or
– engages in sexual activity within a high prevalence area or social network and has additional risk factors for HIV-1 acquisition, such as:
- inconsistent or no condom use.
- diagnosis of sexually transmitted infections.
- exchange of sex for commodities (such as money, food, shelter, or drugs).
- use of illicit drugs or alcohol dependence.
- incarceration.
- partner(s) of unknown HIV-1 status with any of the factors listed above.
Dosage and administration
2.1 Testing prior to initiation of Truvada for treatment of HIV-1 infection or for HIV-1 PrEP
Prior to or when initiating Truvada, test patients for hepatitis B virus infection [see Warnings and Precautions (5.1)].
Prior to initiation and during use of Truvada, on a clinically appropriate schedule, assess serum creatinine, estimated creatinine clearance, urine glucose and urine protein in all patients. In patients with chronic kidney disease, also assess serum phosphorus
2.2 HIV-1 screening for individuals receiving Truvada for HIV-1 PrEP
Screen all patients for HIV-1 infection before initiating Truvada for HIV-1 PrEP and at least once every 3 months while taking Truvada
2.5 Recommended dosage for HIV-1 PrEP
The dosage of Truvada in HIV-1 uninfected adults and adolescents weighing at least 35 kg is one tablet (containing 200 mg of FTC and 300 mg of TDF) once daily taken orally with or without food.
6.0 Adverse reactions
Clinical trials in adolescent subjects
In a single-arm, open-label clinical trial (ATN113), in which 67 HIV-1 uninfected adolescent (15 to 18 years of age) men who have sex with men received Truvada once daily for HIV-1 PrEP, the safety profile of Truvada was similar to that observed in adults. Median duration to exposure of Truvada was 47 weeks.
In the ATN113 trial, median BMD increased from baseline to Week 48, +2.58% for lumbar spine and +0.72% for total body. One subject had significant (greater than or equal to 4%) total body BMD loss at Week 24. Median changes from baseline BMD Z-scores were 0.0 for lumbar spine and −0.2 for total body at Week 48. Three subjects showed a worsening (change from greater than −2 to less than or equal to −2) from baseline in their lumbar spine or total body BMD Z-scores at Week 24 or 48. Interpretation of these data, however, may be limited by the low rate of adherence to Truvada by Week 48.
8.4 Pediatric use
HIV-1 PrEP
The safety and effectiveness of Truvada for HIV-1 PrEP in at-risk adolescents weighing at least 35 kg is supported by data from adequate and well-controlled studies of Truvada for HIV-1 PrEP in adults with additional data from safety and pharmacokinetic studies in previously conducted trials with the individual drug products, FTC and TDF, in HIV-1 infected adults and pediatric subjects.
Safety, adherence, and resistance were evaluated in a single-arm, open-label clinical trial (ATN113) in which 67 HIV-1 uninfected at-risk adolescent men who have sex with men received Truvada once daily for HIV-1 PrEP. The mean age of subjects was 17 years (range, 15-18 years); 46% were Hispanic, 52% black, and 37% white. The safety profile of Truvada in ATN113 was similar to that observed in the adult HIV-1 PrEP trials.
In the ATN113 trial, HIV-1 seroconversion occurred in three subjects. Tenofovir diphosphate levels in dried blood spot assays indicate that these subjects had poor adherence. No tenofovir- or FTC-associated HIV-1 resistance substitutions were detected in virus isolated from the three subjects who seroconverted.
Adherence to study drug, as demonstrated by tenofovir diphosphate levels in dried blood spot assays, declined markedly after Week 12 once subjects switched from monthly to quarterly visits, suggesting that adolescents may benefit from more frequent visits and counseling.
12.0 Clinical pharmacology
HIV-1 PrEP
The pharmacokinetic data for tenofovir and FTC following administration of Truvada in HIV-1 uninfected adolescents weighing 35 kg and above are not available. The dosage recommendations of Truvada for HIV-1 PrEP in this population are based on safety and adherence data from the ATN113 trial [see Use in Specific Populations (8.4)] and known pharmacokinetic information in HIV-infected adolescents taking TDF and FTC for treatment.
ResistanceATN113 Trial
In ATN113, a clinical trial of HIV-1 seronegative adolescent subjects [see Use in Specific Populations (8.4)], no amino acid substitutions associated with resistance to FTC or TDF were detected at the time of seroconversion from any of the 3 subjects who became infected with HIV-1 during the trial. All 3 subjects who seroconverted were nonadherent to the recommended Truvada dosage.
The updated label will soon be available at drugs@fda or DailyMed.
The following is the text of an announcement by the U.S. Food and Drug Administration regarding a revision in the Truvada label to expand the PrEP indication to include at-risk adolescents. The new label change has not yet been posted.
The Food and Drug Administration approved revisions to the Truvada (emtricitabine and tenofovir disoproxil fumarate) labeling to expand the Pre-Exposure Prophylaxis (PrEP) indication to include adolescents weighing at least 35 kg who are at risk of HIV-1 acquisition. The major labeling changes with respect to this expanded indication are summarized below. In addition, Section 8 was reformatted per the Pregnancy and Lactation Labeling Rule (PLLR) and includes updated information specific to the use of Truvada for PrEP during pregnancy and breastfeeding. Other sections of labeling were reformatted for consistency with current and best labeling practices, as well as with labeling for other HIV fixed-dose combination products.
Indications and usage
1.2 HIV-1 pre-exposure prophylaxis (PrEP)
Truvada is indicated in combination with safer sex practices for pre-exposure prophylaxis (PrEP) to reduce the risk of sexually acquired HIV-1 in at-risk adults and adolescents weighing at least 35 kg. Individuals must have a negative HIV-1 test immediately prior to initiating Truvada for HIV-1 PrEP.
If clinical symptoms consistent with acute viral infection are present and recent (less than 1 month) exposures are suspected, delay starting PrEP for at least one month and reconfirm HIV-1 status or use a test cleared by the FDA as an aid in the diagnosis of HIV-1 infection, including acute or primary HIV-1 infection
When considering Truvada for HIV-1 PrEP, factors that help to identify individuals at risk may include:
– has partner(s) known to be HIV-1 infected, or
– engages in sexual activity within a high prevalence area or social network and has additional risk factors for HIV-1 acquisition, such as:
- inconsistent or no condom use.
- diagnosis of sexually transmitted infections.
- exchange of sex for commodities (such as money, food, shelter, or drugs).
- use of illicit drugs or alcohol dependence.
- incarceration.
- partner(s) of unknown HIV-1 status with any of the factors listed above.
Dosage and administration
2.1 Testing prior to initiation of Truvada for treatment of HIV-1 infection or for HIV-1 PrEP
Prior to or when initiating Truvada, test patients for hepatitis B virus infection [see Warnings and Precautions (5.1)].
Prior to initiation and during use of Truvada, on a clinically appropriate schedule, assess serum creatinine, estimated creatinine clearance, urine glucose and urine protein in all patients. In patients with chronic kidney disease, also assess serum phosphorus
2.2 HIV-1 screening for individuals receiving Truvada for HIV-1 PrEP
Screen all patients for HIV-1 infection before initiating Truvada for HIV-1 PrEP and at least once every 3 months while taking Truvada
2.5 Recommended dosage for HIV-1 PrEP
The dosage of Truvada in HIV-1 uninfected adults and adolescents weighing at least 35 kg is one tablet (containing 200 mg of FTC and 300 mg of TDF) once daily taken orally with or without food.
6.0 Adverse reactions
Clinical trials in adolescent subjects
In a single-arm, open-label clinical trial (ATN113), in which 67 HIV-1 uninfected adolescent (15 to 18 years of age) men who have sex with men received Truvada once daily for HIV-1 PrEP, the safety profile of Truvada was similar to that observed in adults. Median duration to exposure of Truvada was 47 weeks.
In the ATN113 trial, median BMD increased from baseline to Week 48, +2.58% for lumbar spine and +0.72% for total body. One subject had significant (greater than or equal to 4%) total body BMD loss at Week 24. Median changes from baseline BMD Z-scores were 0.0 for lumbar spine and −0.2 for total body at Week 48. Three subjects showed a worsening (change from greater than −2 to less than or equal to −2) from baseline in their lumbar spine or total body BMD Z-scores at Week 24 or 48. Interpretation of these data, however, may be limited by the low rate of adherence to Truvada by Week 48.
8.4 Pediatric use
HIV-1 PrEP
The safety and effectiveness of Truvada for HIV-1 PrEP in at-risk adolescents weighing at least 35 kg is supported by data from adequate and well-controlled studies of Truvada for HIV-1 PrEP in adults with additional data from safety and pharmacokinetic studies in previously conducted trials with the individual drug products, FTC and TDF, in HIV-1 infected adults and pediatric subjects.
Safety, adherence, and resistance were evaluated in a single-arm, open-label clinical trial (ATN113) in which 67 HIV-1 uninfected at-risk adolescent men who have sex with men received Truvada once daily for HIV-1 PrEP. The mean age of subjects was 17 years (range, 15-18 years); 46% were Hispanic, 52% black, and 37% white. The safety profile of Truvada in ATN113 was similar to that observed in the adult HIV-1 PrEP trials.
In the ATN113 trial, HIV-1 seroconversion occurred in three subjects. Tenofovir diphosphate levels in dried blood spot assays indicate that these subjects had poor adherence. No tenofovir- or FTC-associated HIV-1 resistance substitutions were detected in virus isolated from the three subjects who seroconverted.
Adherence to study drug, as demonstrated by tenofovir diphosphate levels in dried blood spot assays, declined markedly after Week 12 once subjects switched from monthly to quarterly visits, suggesting that adolescents may benefit from more frequent visits and counseling.
12.0 Clinical pharmacology
HIV-1 PrEP
The pharmacokinetic data for tenofovir and FTC following administration of Truvada in HIV-1 uninfected adolescents weighing 35 kg and above are not available. The dosage recommendations of Truvada for HIV-1 PrEP in this population are based on safety and adherence data from the ATN113 trial [see Use in Specific Populations (8.4)] and known pharmacokinetic information in HIV-infected adolescents taking TDF and FTC for treatment.
ResistanceATN113 Trial
In ATN113, a clinical trial of HIV-1 seronegative adolescent subjects [see Use in Specific Populations (8.4)], no amino acid substitutions associated with resistance to FTC or TDF were detected at the time of seroconversion from any of the 3 subjects who became infected with HIV-1 during the trial. All 3 subjects who seroconverted were nonadherent to the recommended Truvada dosage.
The updated label will soon be available at drugs@fda or DailyMed.
Study supports observation for select cases of porcelain gallbladder
Some adults with porcelain gallbladder may be eligible to forgo prophylactic cholecystectomy, suggest the results of a single-center retrospective study.
Over 1.7 years of median follow-up (range, 0 to 12.7 years), the observational group had no detected gallbladder malignancies and 4% developed adverse events versus 13% in the prophylactic cholecystectomy group (P = .15), wrote Haley DesJardins and her associates at Tufts University, Boston. The report was published in the Journal of the American College of Surgery.
The findings “still raise concern about an association between gallbladder wall calcifications and gallbladder malignancies, and therefore still suggest the need for cholecystectomy in the young, healthy, or symptomatic patient,” the researchers wrote. Nonetheless, surveillance for patients “who are poor surgical candidates is a reasonable approach, with a low risk of malignancy over a limited time frame.”
The investigators suggest that surgeons consider intervention when symptoms and workup points to gallbladder malignancy. But consider avoiding prophylactic cholecystectomy in patients with “limited life expectancy and significant comorbidities,” they emphasized. “Based on the results of this study, the act of prophylactic cholecystectomy for every single patient with gallbladder wall calcifications seems obsolete.”
The study comprised 113 patients with porcelain gallbladder diagnosed between 2004 and 2016. Radiographic reviews identified 70 definite cases and 43 “highly probable” cases. In all, 90 patients started out with observation only, of whom 26% with abdominal pain did not have cholecystectomy because of “significant comorbidities.” Four patients (4.4%) in the observational group subsequently underwent cholecystectomy for biliary colic, as part of liver transplantation, or for prophylactic reasons. None developed complications. In all, 11% developed new gallstones on follow-up imaging and 8% showed progression from focal to diffuse porcelain bladder, the researchers said. None developed gallbladder malignancy during 1.7 years of median follow-up.
Histopathologies of the operative group identified two cases of gallbladder malignancy, of which one was detected on initial imaging. “This patient had a mass at the gallbladder infundibulum extending into the hepatic duct bifurcation,” the researchers explained. “It was not entirely evident whether the resected adenocarcinoma was originating from the gallbladder or from the bile duct. For the purpose of this study, this patient was listed as [having] gallbladder cancer.” The second case consisted of metastatic squamous cell gallbladder carcinoma.
The investigators concluded that “while it is seemingly very reasonable to observe asymptomatic patients with limited life expectancy and significant comorbidities, the decision to proceed with prophylactic cholecystectomy versus observation remains in the hands of the treating physician and patient; especially since absolute criteria or cut-offs cannot be defined at this point.”
No external funding sources were reported. The researchers reported having no conflicts of interest.
SOURCE: DesJardins H et al. J Am Coll Surg. 2018 Apr 22. doi: 10.1016/j.jamcollsurg.2017.11.026.
Some adults with porcelain gallbladder may be eligible to forgo prophylactic cholecystectomy, suggest the results of a single-center retrospective study.
Over 1.7 years of median follow-up (range, 0 to 12.7 years), the observational group had no detected gallbladder malignancies and 4% developed adverse events versus 13% in the prophylactic cholecystectomy group (P = .15), wrote Haley DesJardins and her associates at Tufts University, Boston. The report was published in the Journal of the American College of Surgery.
The findings “still raise concern about an association between gallbladder wall calcifications and gallbladder malignancies, and therefore still suggest the need for cholecystectomy in the young, healthy, or symptomatic patient,” the researchers wrote. Nonetheless, surveillance for patients “who are poor surgical candidates is a reasonable approach, with a low risk of malignancy over a limited time frame.”
The investigators suggest that surgeons consider intervention when symptoms and workup points to gallbladder malignancy. But consider avoiding prophylactic cholecystectomy in patients with “limited life expectancy and significant comorbidities,” they emphasized. “Based on the results of this study, the act of prophylactic cholecystectomy for every single patient with gallbladder wall calcifications seems obsolete.”
The study comprised 113 patients with porcelain gallbladder diagnosed between 2004 and 2016. Radiographic reviews identified 70 definite cases and 43 “highly probable” cases. In all, 90 patients started out with observation only, of whom 26% with abdominal pain did not have cholecystectomy because of “significant comorbidities.” Four patients (4.4%) in the observational group subsequently underwent cholecystectomy for biliary colic, as part of liver transplantation, or for prophylactic reasons. None developed complications. In all, 11% developed new gallstones on follow-up imaging and 8% showed progression from focal to diffuse porcelain bladder, the researchers said. None developed gallbladder malignancy during 1.7 years of median follow-up.
Histopathologies of the operative group identified two cases of gallbladder malignancy, of which one was detected on initial imaging. “This patient had a mass at the gallbladder infundibulum extending into the hepatic duct bifurcation,” the researchers explained. “It was not entirely evident whether the resected adenocarcinoma was originating from the gallbladder or from the bile duct. For the purpose of this study, this patient was listed as [having] gallbladder cancer.” The second case consisted of metastatic squamous cell gallbladder carcinoma.
The investigators concluded that “while it is seemingly very reasonable to observe asymptomatic patients with limited life expectancy and significant comorbidities, the decision to proceed with prophylactic cholecystectomy versus observation remains in the hands of the treating physician and patient; especially since absolute criteria or cut-offs cannot be defined at this point.”
No external funding sources were reported. The researchers reported having no conflicts of interest.
SOURCE: DesJardins H et al. J Am Coll Surg. 2018 Apr 22. doi: 10.1016/j.jamcollsurg.2017.11.026.
Some adults with porcelain gallbladder may be eligible to forgo prophylactic cholecystectomy, suggest the results of a single-center retrospective study.
Over 1.7 years of median follow-up (range, 0 to 12.7 years), the observational group had no detected gallbladder malignancies and 4% developed adverse events versus 13% in the prophylactic cholecystectomy group (P = .15), wrote Haley DesJardins and her associates at Tufts University, Boston. The report was published in the Journal of the American College of Surgery.
The findings “still raise concern about an association between gallbladder wall calcifications and gallbladder malignancies, and therefore still suggest the need for cholecystectomy in the young, healthy, or symptomatic patient,” the researchers wrote. Nonetheless, surveillance for patients “who are poor surgical candidates is a reasonable approach, with a low risk of malignancy over a limited time frame.”
The investigators suggest that surgeons consider intervention when symptoms and workup points to gallbladder malignancy. But consider avoiding prophylactic cholecystectomy in patients with “limited life expectancy and significant comorbidities,” they emphasized. “Based on the results of this study, the act of prophylactic cholecystectomy for every single patient with gallbladder wall calcifications seems obsolete.”
The study comprised 113 patients with porcelain gallbladder diagnosed between 2004 and 2016. Radiographic reviews identified 70 definite cases and 43 “highly probable” cases. In all, 90 patients started out with observation only, of whom 26% with abdominal pain did not have cholecystectomy because of “significant comorbidities.” Four patients (4.4%) in the observational group subsequently underwent cholecystectomy for biliary colic, as part of liver transplantation, or for prophylactic reasons. None developed complications. In all, 11% developed new gallstones on follow-up imaging and 8% showed progression from focal to diffuse porcelain bladder, the researchers said. None developed gallbladder malignancy during 1.7 years of median follow-up.
Histopathologies of the operative group identified two cases of gallbladder malignancy, of which one was detected on initial imaging. “This patient had a mass at the gallbladder infundibulum extending into the hepatic duct bifurcation,” the researchers explained. “It was not entirely evident whether the resected adenocarcinoma was originating from the gallbladder or from the bile duct. For the purpose of this study, this patient was listed as [having] gallbladder cancer.” The second case consisted of metastatic squamous cell gallbladder carcinoma.
The investigators concluded that “while it is seemingly very reasonable to observe asymptomatic patients with limited life expectancy and significant comorbidities, the decision to proceed with prophylactic cholecystectomy versus observation remains in the hands of the treating physician and patient; especially since absolute criteria or cut-offs cannot be defined at this point.”
No external funding sources were reported. The researchers reported having no conflicts of interest.
SOURCE: DesJardins H et al. J Am Coll Surg. 2018 Apr 22. doi: 10.1016/j.jamcollsurg.2017.11.026.
FROM JOURNAL OF THE AMERICAN COLLEGE OF SURGERY
Key clinical point: Observation is an option for select patients with porcelain gallbladder .
Major finding: Rates of adverse events were 4% with observation and 13% with surgery (P = .15).
Study details: Single-center retrospective cohort study of 113 patients.
Disclosures: No external funding sources were reported. The researchers reported having no conflicts of interest.
Source: DesJardins H et al. J Am Coll Surg. 2018 Apr 22. doi: 10.1016/j.jamcollsurg.2017.11.026.
Guidance coming for mTOR inhibitors in infantile TSC
LOS ANGELES – Someday soon, physicians will probably have solid, evidence-based guidelines on how to use mTOR inhibitors in infants with tuberous sclerosis complex.
They couldn’t come soon enough. Everolimus (Afinitor) is being used off label more and more often in children under 2 years old for seizures and other manifestations of the genetic disorder, often with a decent response.

“I get emails all the time saying ‘how would you start treatment at this age?’ and we say there are no data,” he said at the American Academy of Neurology annual meeting.
Dr. Krueger presented a survey of 19 TSC centers to get the ball rolling. They reported on treating 45 children under 2 years old, at least one child at each center. The goal of the survey was to establish a baseline “to allow us to move forward with what proper studies would look like, and what needs to be done. Two-thirds of patients have seizures before their first birthday; we need to establish a safety [and efficacy] profile well before 2 years of age,” and evidence-based guidelines, he said.
On average, everolimus treatment started at 11.7 months, and continued for 27 months. Sirolimus treatment started at a mean of 16 months and continued for 16 months. Dosing ranged from once a week to daily. In contrast to case reports that skew heavily toward rhabdomyomas, most of the children were treated for epilepsy and subependymal giant cell astrocytoma (SEGA). Almost all the centers had participated in a clinical evaluation of everolimus for TSC epilepsy and SEGAs in older children, “so there was familiarity and a comfort level” for those indications, Dr. Krueger said.
Everolimus was used much more often than was sirolimus, which probably reflects ongoing clinical development of the drug. A handful of children switched between the two, probably because of side effects. Most centers reported a favorable response. The average initial daily dose of everolimus was 1.05 mg/m2; the average initial daily dose of sirolimus was 0.42 mg/m2.
Thirty-five children (78%) had an adverse event (AE), usually infections or lipid problems. Most were mild or moderate and didn’t affect treatment. Seven children (16%) had severe grade 3 events.
“The frequency of these AEs and the severity and type were not different from the earlier trials,” but almost 40% of the children discontinued treatment due to AEs, which was “much higher” than in past trials. “I think this represents the lack of real data with which to guide clinical judgment. There was a high tendency with any AE for discontinuation,” Dr. Krueger said.
There were more boys than girls among the 45 children. The majority were from the United States, and predominantly Cincinnati Children’s Hospital. Most had TSC2 mutations, which are associated with worse disease than TSC1 mutations.
Dr. Krueger reported research funding and personal compensation from Novartis, maker of everolimus. Almost all of his coinvestigators reported ties to the company. The work was supported by the Tuberous Sclerosis Alliance, which is funded in part by Novartis.
SOURCE: Krueger D et al. Neurology. 2018 Apr 90(15 Suppl.):S35.003.
LOS ANGELES – Someday soon, physicians will probably have solid, evidence-based guidelines on how to use mTOR inhibitors in infants with tuberous sclerosis complex.
They couldn’t come soon enough. Everolimus (Afinitor) is being used off label more and more often in children under 2 years old for seizures and other manifestations of the genetic disorder, often with a decent response.
“I get emails all the time saying ‘how would you start treatment at this age?’ and we say there are no data,” he said at the American Academy of Neurology annual meeting.
Dr. Krueger presented a survey of 19 TSC centers to get the ball rolling. They reported on treating 45 children under 2 years old, at least one child at each center. The goal of the survey was to establish a baseline “to allow us to move forward with what proper studies would look like, and what needs to be done. Two-thirds of patients have seizures before their first birthday; we need to establish a safety [and efficacy] profile well before 2 years of age,” and evidence-based guidelines, he said.
On average, everolimus treatment started at 11.7 months, and continued for 27 months. Sirolimus treatment started at a mean of 16 months and continued for 16 months. Dosing ranged from once a week to daily. In contrast to case reports that skew heavily toward rhabdomyomas, most of the children were treated for epilepsy and subependymal giant cell astrocytoma (SEGA). Almost all the centers had participated in a clinical evaluation of everolimus for TSC epilepsy and SEGAs in older children, “so there was familiarity and a comfort level” for those indications, Dr. Krueger said.
Everolimus was used much more often than was sirolimus, which probably reflects ongoing clinical development of the drug. A handful of children switched between the two, probably because of side effects. Most centers reported a favorable response. The average initial daily dose of everolimus was 1.05 mg/m2; the average initial daily dose of sirolimus was 0.42 mg/m2.
Thirty-five children (78%) had an adverse event (AE), usually infections or lipid problems. Most were mild or moderate and didn’t affect treatment. Seven children (16%) had severe grade 3 events.
“The frequency of these AEs and the severity and type were not different from the earlier trials,” but almost 40% of the children discontinued treatment due to AEs, which was “much higher” than in past trials. “I think this represents the lack of real data with which to guide clinical judgment. There was a high tendency with any AE for discontinuation,” Dr. Krueger said.
There were more boys than girls among the 45 children. The majority were from the United States, and predominantly Cincinnati Children’s Hospital. Most had TSC2 mutations, which are associated with worse disease than TSC1 mutations.
Dr. Krueger reported research funding and personal compensation from Novartis, maker of everolimus. Almost all of his coinvestigators reported ties to the company. The work was supported by the Tuberous Sclerosis Alliance, which is funded in part by Novartis.
SOURCE: Krueger D et al. Neurology. 2018 Apr 90(15 Suppl.):S35.003.
LOS ANGELES – Someday soon, physicians will probably have solid, evidence-based guidelines on how to use mTOR inhibitors in infants with tuberous sclerosis complex.
They couldn’t come soon enough. Everolimus (Afinitor) is being used off label more and more often in children under 2 years old for seizures and other manifestations of the genetic disorder, often with a decent response.
“I get emails all the time saying ‘how would you start treatment at this age?’ and we say there are no data,” he said at the American Academy of Neurology annual meeting.
Dr. Krueger presented a survey of 19 TSC centers to get the ball rolling. They reported on treating 45 children under 2 years old, at least one child at each center. The goal of the survey was to establish a baseline “to allow us to move forward with what proper studies would look like, and what needs to be done. Two-thirds of patients have seizures before their first birthday; we need to establish a safety [and efficacy] profile well before 2 years of age,” and evidence-based guidelines, he said.
On average, everolimus treatment started at 11.7 months, and continued for 27 months. Sirolimus treatment started at a mean of 16 months and continued for 16 months. Dosing ranged from once a week to daily. In contrast to case reports that skew heavily toward rhabdomyomas, most of the children were treated for epilepsy and subependymal giant cell astrocytoma (SEGA). Almost all the centers had participated in a clinical evaluation of everolimus for TSC epilepsy and SEGAs in older children, “so there was familiarity and a comfort level” for those indications, Dr. Krueger said.
Everolimus was used much more often than was sirolimus, which probably reflects ongoing clinical development of the drug. A handful of children switched between the two, probably because of side effects. Most centers reported a favorable response. The average initial daily dose of everolimus was 1.05 mg/m2; the average initial daily dose of sirolimus was 0.42 mg/m2.
Thirty-five children (78%) had an adverse event (AE), usually infections or lipid problems. Most were mild or moderate and didn’t affect treatment. Seven children (16%) had severe grade 3 events.
“The frequency of these AEs and the severity and type were not different from the earlier trials,” but almost 40% of the children discontinued treatment due to AEs, which was “much higher” than in past trials. “I think this represents the lack of real data with which to guide clinical judgment. There was a high tendency with any AE for discontinuation,” Dr. Krueger said.
There were more boys than girls among the 45 children. The majority were from the United States, and predominantly Cincinnati Children’s Hospital. Most had TSC2 mutations, which are associated with worse disease than TSC1 mutations.
Dr. Krueger reported research funding and personal compensation from Novartis, maker of everolimus. Almost all of his coinvestigators reported ties to the company. The work was supported by the Tuberous Sclerosis Alliance, which is funded in part by Novartis.
SOURCE: Krueger D et al. Neurology. 2018 Apr 90(15 Suppl.):S35.003.
REPORTING FROM AAN 2018
Key clinical point: A survey of treatment centers has begun to plug the evidence gap for using mTOR inhibitors in infants with tuberous sclerosis.
Major finding: Adverse events don’t seem more common than in trials of adults and older children, but the discontinuation rate is much higher, at about 40%.
Study details: Review of 45 children under 2 years old.
Disclosures: The lead investigator reported research funding and personal compensation from Novartis, maker of everolimus.
Source: Krueger D et al. Neurology. 2018 Apr 90(15 Suppl.):S35.003.
Long-acting bronchodilators increase CVD risk in certain COPD patients
Background: Long-acting inhaled bronchodilator use (LABA or LAMA) in patients with COPD is the mainstay of treatment. Prior studies have reported a possible interaction between LABA or LAMA use and increased rates of cardiovascular events; however, the results have been variable. The findings have been confounded by incomplete medical records, exclusion of patients with CVD in bronchodilator trials, and high patient drop out rates. This study aims to assess the association between LABA or LAMA use in patients with COPD and the risk of CVD.
Study design: Nested case control study.
Setting: Taiwanese national database.
Synopsis: This study included 284,200 LABA and LAMA naive patients who were aged 40 years or older and had COPD (mean age, 71.4 years); it retrieved health care claims data from 2007 through 2011 for these patients from the Taiwan National Health Insurance Research Database. During a mean follow-up of 2.0 years, 37,719 patients experienced a cardiovascular event, and 146,139 matched controls were identified. LABA or LAMA use was measured in the year preceding the cardiovascular event and stratified by duration since initiation of LABA or LAMA treatment. Logistical regression was performed to estimate the odds ratios of CVD from LABA and LAMA treatment. New LABA use was associated with a 1.50-fold (95% confidence interval, 1.35-1.67; P less than .001) increased cardiovascular risk within 30 days of initiation, and new LAMA use was associated with a 1.52 fold (95% CI, 1.28-1.80; P less than .001) increased risk. In patients with prevalent LABA or LAMA use, the risk of CVD was absent or reduced.
Key limitations included the omission of contributors to cardiovascular disease, including smoking status and alcohol consumption, in the final analysis. Also, the contribution of worsening COPD to cardiovascular events was not accounted for.
Bottom line: Initiation of inhaled LABAs or LAMAs in patients with COPD is associated with a 1.5-fold increased risk of cardiovascular disease – including emergency or inpatient care for coronary artery disease, heart failure, ischemic stroke, or arrhythmia – in the first 30 days.
Citation: Wang MT et al. Association of cardiovascular risk with inhaled long-acting bronchodilators in patients with chronic obstructive pulmonary disease. JAMA Intern Med. 2018; 178(2):229-38.

Dr. Skinner is a hospitalist at Denver Health Medical Center and an assistant professor of medicine at the University of Colorado at Denver, Aurora.
Background: Long-acting inhaled bronchodilator use (LABA or LAMA) in patients with COPD is the mainstay of treatment. Prior studies have reported a possible interaction between LABA or LAMA use and increased rates of cardiovascular events; however, the results have been variable. The findings have been confounded by incomplete medical records, exclusion of patients with CVD in bronchodilator trials, and high patient drop out rates. This study aims to assess the association between LABA or LAMA use in patients with COPD and the risk of CVD.
Study design: Nested case control study.
Setting: Taiwanese national database.
Synopsis: This study included 284,200 LABA and LAMA naive patients who were aged 40 years or older and had COPD (mean age, 71.4 years); it retrieved health care claims data from 2007 through 2011 for these patients from the Taiwan National Health Insurance Research Database. During a mean follow-up of 2.0 years, 37,719 patients experienced a cardiovascular event, and 146,139 matched controls were identified. LABA or LAMA use was measured in the year preceding the cardiovascular event and stratified by duration since initiation of LABA or LAMA treatment. Logistical regression was performed to estimate the odds ratios of CVD from LABA and LAMA treatment. New LABA use was associated with a 1.50-fold (95% confidence interval, 1.35-1.67; P less than .001) increased cardiovascular risk within 30 days of initiation, and new LAMA use was associated with a 1.52 fold (95% CI, 1.28-1.80; P less than .001) increased risk. In patients with prevalent LABA or LAMA use, the risk of CVD was absent or reduced.
Key limitations included the omission of contributors to cardiovascular disease, including smoking status and alcohol consumption, in the final analysis. Also, the contribution of worsening COPD to cardiovascular events was not accounted for.
Bottom line: Initiation of inhaled LABAs or LAMAs in patients with COPD is associated with a 1.5-fold increased risk of cardiovascular disease – including emergency or inpatient care for coronary artery disease, heart failure, ischemic stroke, or arrhythmia – in the first 30 days.
Citation: Wang MT et al. Association of cardiovascular risk with inhaled long-acting bronchodilators in patients with chronic obstructive pulmonary disease. JAMA Intern Med. 2018; 178(2):229-38.
Dr. Skinner is a hospitalist at Denver Health Medical Center and an assistant professor of medicine at the University of Colorado at Denver, Aurora.
Background: Long-acting inhaled bronchodilator use (LABA or LAMA) in patients with COPD is the mainstay of treatment. Prior studies have reported a possible interaction between LABA or LAMA use and increased rates of cardiovascular events; however, the results have been variable. The findings have been confounded by incomplete medical records, exclusion of patients with CVD in bronchodilator trials, and high patient drop out rates. This study aims to assess the association between LABA or LAMA use in patients with COPD and the risk of CVD.
Study design: Nested case control study.
Setting: Taiwanese national database.
Synopsis: This study included 284,200 LABA and LAMA naive patients who were aged 40 years or older and had COPD (mean age, 71.4 years); it retrieved health care claims data from 2007 through 2011 for these patients from the Taiwan National Health Insurance Research Database. During a mean follow-up of 2.0 years, 37,719 patients experienced a cardiovascular event, and 146,139 matched controls were identified. LABA or LAMA use was measured in the year preceding the cardiovascular event and stratified by duration since initiation of LABA or LAMA treatment. Logistical regression was performed to estimate the odds ratios of CVD from LABA and LAMA treatment. New LABA use was associated with a 1.50-fold (95% confidence interval, 1.35-1.67; P less than .001) increased cardiovascular risk within 30 days of initiation, and new LAMA use was associated with a 1.52 fold (95% CI, 1.28-1.80; P less than .001) increased risk. In patients with prevalent LABA or LAMA use, the risk of CVD was absent or reduced.
Key limitations included the omission of contributors to cardiovascular disease, including smoking status and alcohol consumption, in the final analysis. Also, the contribution of worsening COPD to cardiovascular events was not accounted for.
Bottom line: Initiation of inhaled LABAs or LAMAs in patients with COPD is associated with a 1.5-fold increased risk of cardiovascular disease – including emergency or inpatient care for coronary artery disease, heart failure, ischemic stroke, or arrhythmia – in the first 30 days.
Citation: Wang MT et al. Association of cardiovascular risk with inhaled long-acting bronchodilators in patients with chronic obstructive pulmonary disease. JAMA Intern Med. 2018; 178(2):229-38.
Dr. Skinner is a hospitalist at Denver Health Medical Center and an assistant professor of medicine at the University of Colorado at Denver, Aurora.
ESBL-B before colorectal surgery ups risk of surgical site infection
MADRID – Patients who are carriers of , despite a standard prophylactic antibiotic regimen.
Surgical site infections (SSIs) occurred in 23% of those who tested positive for the pathogens preoperatively, compared with 10.5% of ESBL-B–negative patients – a significant increased risk of 2.25, Yehuda Carmeli, MD, said at the European Congress of Clinical Microbiology and Infectious Diseases annual congress.
ESBL-B was not the infective pathogen in most infection cases, but being a carrier increased the likelihood of an ESBL-B SSI. ESBL-B was the pathogen in 7.2% of the carriers and 1.6% of the noncarriers. However, investigators are still working to determine if the species present in the wound infection are the same as the ones present at baseline, said Dr. Carmeli of Tel Aviv Medical Center.
All of these results are emerging from the WP4 study, which was carried out in three hospitals in Serbia, Switzerland, and Israel. Designed as a before-and-after trial, it tested the theory that identifying ESBL carriers and targeting presurgical antibiotic prophylaxis could improve their surgical outcomes.
WP4 was one of five studies in the multinational R-GNOSIS project. “Resistance in Gram-Negative Organisms: Studying Intervention Strategies” is a 12-million-euro, 5-year European collaborative research project designed to identify effective interventions for reducing the carriage, infection, and spread of multi-drug resistant Gram-negative bacteria. From 2012 to 2017, WP4 enrolled almost 4,000 adults scheduled to undergo colorectal surgery (excluding appendectomy or minor anorectal procedures).
Several of the studies were reported at ECCMID 2018.
This portion of R-GNOSIS was intended to investigate the relationship between ESBL-B carriage and postoperative surgical site infections among colorectal surgery patients.
The study comprised 3,626 patients who were preoperatively screened for ESBL-B within 2 weeks of colorectal surgery. The ESBL-B carriage rate was 15.3% overall, but ranged from 12% to 20% by site. Of the carriers, 222 were included in this study sample. They were randomly matched with 444 noncarriers.
Anywhere from 2 weeks to 2 days before surgery, all of the patients received a standard prophylactic antibiotic. This was most often an infusion of 1.5 g cefuroxime plus 500 mg metronidazole. Other cephalosporins were allowed at the clinician’s discretion.
Patients were a mean of 62 years old. Nearly half (48%) had cardiovascular disease and about a third had undergone a prior colorectal surgical procedure. Cancer was the surgical indication in about 70%. Other indications were inflammatory bowel disease and diverticular disease.
A multivariate analysis controlled for age, cardiovascular disease, indication for surgery, and whether the procedure included a rectal resection, retention of drain at the surgical site, or stoma. The model also controlled for National Nosocomial Infection Surveillance score, a three-point scale that estimates surgical infection risk. Among this cohort, 48% were at low risk, 43% at moderate risk, and 10% at high risk.
Dr. Carmeli made no financial disclosures.
SOURCE: Carmeli et al, ECCMID 2018, Oral Abstract O1133.
MADRID – Patients who are carriers of , despite a standard prophylactic antibiotic regimen.
Surgical site infections (SSIs) occurred in 23% of those who tested positive for the pathogens preoperatively, compared with 10.5% of ESBL-B–negative patients – a significant increased risk of 2.25, Yehuda Carmeli, MD, said at the European Congress of Clinical Microbiology and Infectious Diseases annual congress.
ESBL-B was not the infective pathogen in most infection cases, but being a carrier increased the likelihood of an ESBL-B SSI. ESBL-B was the pathogen in 7.2% of the carriers and 1.6% of the noncarriers. However, investigators are still working to determine if the species present in the wound infection are the same as the ones present at baseline, said Dr. Carmeli of Tel Aviv Medical Center.
All of these results are emerging from the WP4 study, which was carried out in three hospitals in Serbia, Switzerland, and Israel. Designed as a before-and-after trial, it tested the theory that identifying ESBL carriers and targeting presurgical antibiotic prophylaxis could improve their surgical outcomes.
WP4 was one of five studies in the multinational R-GNOSIS project. “Resistance in Gram-Negative Organisms: Studying Intervention Strategies” is a 12-million-euro, 5-year European collaborative research project designed to identify effective interventions for reducing the carriage, infection, and spread of multi-drug resistant Gram-negative bacteria. From 2012 to 2017, WP4 enrolled almost 4,000 adults scheduled to undergo colorectal surgery (excluding appendectomy or minor anorectal procedures).
Several of the studies were reported at ECCMID 2018.
This portion of R-GNOSIS was intended to investigate the relationship between ESBL-B carriage and postoperative surgical site infections among colorectal surgery patients.
The study comprised 3,626 patients who were preoperatively screened for ESBL-B within 2 weeks of colorectal surgery. The ESBL-B carriage rate was 15.3% overall, but ranged from 12% to 20% by site. Of the carriers, 222 were included in this study sample. They were randomly matched with 444 noncarriers.
Anywhere from 2 weeks to 2 days before surgery, all of the patients received a standard prophylactic antibiotic. This was most often an infusion of 1.5 g cefuroxime plus 500 mg metronidazole. Other cephalosporins were allowed at the clinician’s discretion.
Patients were a mean of 62 years old. Nearly half (48%) had cardiovascular disease and about a third had undergone a prior colorectal surgical procedure. Cancer was the surgical indication in about 70%. Other indications were inflammatory bowel disease and diverticular disease.
A multivariate analysis controlled for age, cardiovascular disease, indication for surgery, and whether the procedure included a rectal resection, retention of drain at the surgical site, or stoma. The model also controlled for National Nosocomial Infection Surveillance score, a three-point scale that estimates surgical infection risk. Among this cohort, 48% were at low risk, 43% at moderate risk, and 10% at high risk.
Dr. Carmeli made no financial disclosures.
SOURCE: Carmeli et al, ECCMID 2018, Oral Abstract O1133.
MADRID – Patients who are carriers of , despite a standard prophylactic antibiotic regimen.
Surgical site infections (SSIs) occurred in 23% of those who tested positive for the pathogens preoperatively, compared with 10.5% of ESBL-B–negative patients – a significant increased risk of 2.25, Yehuda Carmeli, MD, said at the European Congress of Clinical Microbiology and Infectious Diseases annual congress.
ESBL-B was not the infective pathogen in most infection cases, but being a carrier increased the likelihood of an ESBL-B SSI. ESBL-B was the pathogen in 7.2% of the carriers and 1.6% of the noncarriers. However, investigators are still working to determine if the species present in the wound infection are the same as the ones present at baseline, said Dr. Carmeli of Tel Aviv Medical Center.
All of these results are emerging from the WP4 study, which was carried out in three hospitals in Serbia, Switzerland, and Israel. Designed as a before-and-after trial, it tested the theory that identifying ESBL carriers and targeting presurgical antibiotic prophylaxis could improve their surgical outcomes.
WP4 was one of five studies in the multinational R-GNOSIS project. “Resistance in Gram-Negative Organisms: Studying Intervention Strategies” is a 12-million-euro, 5-year European collaborative research project designed to identify effective interventions for reducing the carriage, infection, and spread of multi-drug resistant Gram-negative bacteria. From 2012 to 2017, WP4 enrolled almost 4,000 adults scheduled to undergo colorectal surgery (excluding appendectomy or minor anorectal procedures).
Several of the studies were reported at ECCMID 2018.
This portion of R-GNOSIS was intended to investigate the relationship between ESBL-B carriage and postoperative surgical site infections among colorectal surgery patients.
The study comprised 3,626 patients who were preoperatively screened for ESBL-B within 2 weeks of colorectal surgery. The ESBL-B carriage rate was 15.3% overall, but ranged from 12% to 20% by site. Of the carriers, 222 were included in this study sample. They were randomly matched with 444 noncarriers.
Anywhere from 2 weeks to 2 days before surgery, all of the patients received a standard prophylactic antibiotic. This was most often an infusion of 1.5 g cefuroxime plus 500 mg metronidazole. Other cephalosporins were allowed at the clinician’s discretion.
Patients were a mean of 62 years old. Nearly half (48%) had cardiovascular disease and about a third had undergone a prior colorectal surgical procedure. Cancer was the surgical indication in about 70%. Other indications were inflammatory bowel disease and diverticular disease.
A multivariate analysis controlled for age, cardiovascular disease, indication for surgery, and whether the procedure included a rectal resection, retention of drain at the surgical site, or stoma. The model also controlled for National Nosocomial Infection Surveillance score, a three-point scale that estimates surgical infection risk. Among this cohort, 48% were at low risk, 43% at moderate risk, and 10% at high risk.
Dr. Carmeli made no financial disclosures.
SOURCE: Carmeli et al, ECCMID 2018, Oral Abstract O1133.
REPORTING FROM ECCMID 2018
Key clinical point: ESBL-B colonization increased the risk of surgical site infections after colorectal surgery, despite use of standard preoperative antibiotics.
Major finding: ESBL-B carriage more than doubled the risk of a colorectal surgical site infection by (OR 2.25).
Study details: The prospective study comprised 222 carriers and 444 noncarriers.
Disclosures: The study is part of the R-GNOSIS project, a 12-million-euro, 5-year European collaborative research project designed to identify effective interventions for reducing the carriage, infection, and spread of multi-drug resistant Gram-negative bacteria.
Source: Carmeli Y et al. ECCMID 2018, Oral Abstract O1130.
Simple QI intervention helped improve HPV vaccination rates
TORONTO – Teaching simple quality improvement principles to individual pediatric practices can improve adolescent human papillomavirus (HPV) vaccination rates, results from a multicenter study showed.
“We know that HPV vaccination rates are low, and there have been many efforts to improve the vaccination rates nationwide,” one of the study authors, Manika Suryadevara, MD, said in an interview at the Pediatric Academic Societies meeting. “One reason that vaccine rates are low in adolescents is missed opportunities. Adolescents don’t always show up for routine well-child visits where immunization records are reviewed, but they may show up with a cold, a sprained ankle, or a hospital follow-up. Providers do not routinely check immunizations at these visits, then don’t recommend vaccine to those who need it. These are the missed opportunities we need to act upon.”

Data were entered into the AAP Quality Improvement Data Aggregator and run charts were printed. Next, each practice held monthly team meetings for 5 months to discuss chart review data, run chart results, and to determine intervention change for the next cycle. “Most of the interventions included standing orders, optimizing nurse’s visits, using electronic medical reminders to review immunization records, and having immunization records pulled for all adolescents who show up in their practice,” Dr. Suryadevara said. “The goal of these systematic changes is to make the work flow seamless.”
Analysis of run chart data revealed that over the five monthly cycles, the HPV vaccine completion rate improved from 45% to 65%, while the overall HPV vaccine missed opportunities was reduced from 45% to 19%. Specifically, reductions in missed opportunities fell from 9% to 0% during well-child visits, from 80% to 61% during acute visits, from 25% to 0% during follow-up visits, and from 11% to 0% during nurse-only visits. “We did see missed opportunities for acute visits – those who come in sick, but even these missed opportunities decreased over the 6-month study period,” Dr. Suryadevara said.
During follow-up teleconference calls, practice representatives reported positive experiences about the QI process and outcome improvements. “Once the practices were able to pull everyone on board and develop practice changes, I wasn’t surprised that the interventions worked,” she said. “They were able to develop systematic interventions, change the work flow in their practice, and get the results we anticipated.”
The study was funded by the AAP Hub and Spoke Initiative. Dr. Suryadevara reported having no financial disclosures.
[email protected]
TORONTO – Teaching simple quality improvement principles to individual pediatric practices can improve adolescent human papillomavirus (HPV) vaccination rates, results from a multicenter study showed.
“We know that HPV vaccination rates are low, and there have been many efforts to improve the vaccination rates nationwide,” one of the study authors, Manika Suryadevara, MD, said in an interview at the Pediatric Academic Societies meeting. “One reason that vaccine rates are low in adolescents is missed opportunities. Adolescents don’t always show up for routine well-child visits where immunization records are reviewed, but they may show up with a cold, a sprained ankle, or a hospital follow-up. Providers do not routinely check immunizations at these visits, then don’t recommend vaccine to those who need it. These are the missed opportunities we need to act upon.”
Data were entered into the AAP Quality Improvement Data Aggregator and run charts were printed. Next, each practice held monthly team meetings for 5 months to discuss chart review data, run chart results, and to determine intervention change for the next cycle. “Most of the interventions included standing orders, optimizing nurse’s visits, using electronic medical reminders to review immunization records, and having immunization records pulled for all adolescents who show up in their practice,” Dr. Suryadevara said. “The goal of these systematic changes is to make the work flow seamless.”
Analysis of run chart data revealed that over the five monthly cycles, the HPV vaccine completion rate improved from 45% to 65%, while the overall HPV vaccine missed opportunities was reduced from 45% to 19%. Specifically, reductions in missed opportunities fell from 9% to 0% during well-child visits, from 80% to 61% during acute visits, from 25% to 0% during follow-up visits, and from 11% to 0% during nurse-only visits. “We did see missed opportunities for acute visits – those who come in sick, but even these missed opportunities decreased over the 6-month study period,” Dr. Suryadevara said.
During follow-up teleconference calls, practice representatives reported positive experiences about the QI process and outcome improvements. “Once the practices were able to pull everyone on board and develop practice changes, I wasn’t surprised that the interventions worked,” she said. “They were able to develop systematic interventions, change the work flow in their practice, and get the results we anticipated.”
The study was funded by the AAP Hub and Spoke Initiative. Dr. Suryadevara reported having no financial disclosures.
[email protected]
TORONTO – Teaching simple quality improvement principles to individual pediatric practices can improve adolescent human papillomavirus (HPV) vaccination rates, results from a multicenter study showed.
“We know that HPV vaccination rates are low, and there have been many efforts to improve the vaccination rates nationwide,” one of the study authors, Manika Suryadevara, MD, said in an interview at the Pediatric Academic Societies meeting. “One reason that vaccine rates are low in adolescents is missed opportunities. Adolescents don’t always show up for routine well-child visits where immunization records are reviewed, but they may show up with a cold, a sprained ankle, or a hospital follow-up. Providers do not routinely check immunizations at these visits, then don’t recommend vaccine to those who need it. These are the missed opportunities we need to act upon.”
Data were entered into the AAP Quality Improvement Data Aggregator and run charts were printed. Next, each practice held monthly team meetings for 5 months to discuss chart review data, run chart results, and to determine intervention change for the next cycle. “Most of the interventions included standing orders, optimizing nurse’s visits, using electronic medical reminders to review immunization records, and having immunization records pulled for all adolescents who show up in their practice,” Dr. Suryadevara said. “The goal of these systematic changes is to make the work flow seamless.”
Analysis of run chart data revealed that over the five monthly cycles, the HPV vaccine completion rate improved from 45% to 65%, while the overall HPV vaccine missed opportunities was reduced from 45% to 19%. Specifically, reductions in missed opportunities fell from 9% to 0% during well-child visits, from 80% to 61% during acute visits, from 25% to 0% during follow-up visits, and from 11% to 0% during nurse-only visits. “We did see missed opportunities for acute visits – those who come in sick, but even these missed opportunities decreased over the 6-month study period,” Dr. Suryadevara said.
During follow-up teleconference calls, practice representatives reported positive experiences about the QI process and outcome improvements. “Once the practices were able to pull everyone on board and develop practice changes, I wasn’t surprised that the interventions worked,” she said. “They were able to develop systematic interventions, change the work flow in their practice, and get the results we anticipated.”
The study was funded by the AAP Hub and Spoke Initiative. Dr. Suryadevara reported having no financial disclosures.
[email protected]
REPORTING FROM PAS 2018
Key clinical point: Teaching quality improvement to pediatric practices can improve adolescent human papillomavirus (HPV) vaccine completion rates.
Major finding:
Study details: A quality improvement project conducted at five large pediatric practices in New York state aimed at reducing missed vaccination opportunities in an effort to improve HPV vaccination completion rates.
Disclosures: The study was funded by the American Academy of Pediatrics Hub and Spoke Initiative. Dr. Suryadevara reported having no financial disclosures.
Upfront NGS testing of metastatic NSCLC saves money, time
Comprehensive testing of newly diagnosed metastatic non–small cell lung cancer (NSCLC) with next-generation sequencing (NGS) for known lung cancer–related genomic alterations is cost-saving relative to single-gene testing strategies and often faster, a new study finds.
“We know now that genomic testing for all patients with advanced NSCLC is the standard of care to help detect oncogenic drivers, to inform treatment decisions,” lead study author Nathan A. Pennell, MD, PhD, codirector of the Cleveland Clinic lung cancer program, said in a press briefing leading up to the ASCO annual meeting. But the optimal strategy for this testing is unclear.
He and his colleagues conducted a decision analytic modeling study among hypothetical insurance plans having 1 million enrollees. Outcomes were compared between NGS testing and three single-gene testing strategies.
Data indicated that compared with exclusionary, sequential, or hot-spot panel testing approaches, NGS testing simultaneously for eight genomic alterations having Food and Drug Administration–approved or investigational targeted therapies could save up to $2.1 million among Medicare beneficiaries and up to $250,842 among patients covered by commercial insurance. The costs to payers decreased as the percentage of patients receiving NGS testing increased. Moreover, the wait time for results was similar or roughly half as long with NGS.
“Our results showed that there were substantial cost savings associated with upfront NGS testing compared to all other strategies,” Dr. Pennell said. “In addition, NGS had a faster turnaround time than either sequential or exclusionary testing, which is critically important for sick lung cancer patients, to make sure they get their treatment as quickly as possible. Waiting a month or longer is simply no longer viable for patients because they get sick very quickly and these treatments work very well.”
Of note, the model indicated that some patients undergoing initial single-gene testing strategies never had their genomic alterations detected because tissue for testing ran out and they were too sick to undergo another biopsy.
“The bottom line is, ultimately, using the best single test upfront results in the fastest turnaround time, the highest percentage of patients with targetable alterations identified, and overall the lowest cost to payers,” he summarized.
A major challenge in this population is going back and retesting for known or new genomic alterations, agreed ASCO President Bruce E. Johnson, MD, FASCO. “At our upcoming meeting, we are going to hear about RET, which may end up as a target and may therefore need to be tested for.”
Recently, oncologists have a new attractive option of billing for NGS panels rather than for single gene tests, he noted.
“This study really shows that by doing all the testing at the same time, you can both get results back more quickly as well as get information,” said Dr. Johnson, professor of medicine at the Dana-Farber Cancer Institute and a leader of the Dana-Farber/Harvard Cancer Center Lung Cancer Program, Boston. “This study looked at an NGS panel of eight genes, but most of the NGS panels contain somewhere between 50 and 400 genes, so you get a lot more information with this at a cost that’s competitive or less. So this will be welcome news to people who are ordering these gene panels.”
Study details
For NSCLC, there are currently approved treatments that target alterations in EGFR, ALK, ROS1, and BRAF, and investigational treatments in clinical trials that target alterations in MET, HER2, RET, and NTRK1.
In the model Dr. Pennell and his colleagues developed, patients with newly diagnosed metastatic NSCLC received testing for programmed death ligand 1 (PD-L1) plus testing for the above known lung cancer–related genes using one of four strategies:
- NGS testing (testing of all eight genes plus KRAS simultaneously).
- Sequential testing (testing one gene at a time starting with EGFR).
- Exclusionary testing (testing for KRAS mutation, the most common genomic alteration, followed by sequential testing for changes in other genes only if KRAS was not mutated).
- Hot-spot panel testing (combined testing for EGFR, ALK, ROS1, and BRAF), followed by either single-gene or NGS testing for alterations in other genes.
Model results indicated that among 1 million hypothetical plan enrollees, 2,066 patients covered by the Centers for Medicare & Medicaid Services and 156 covered by U.S. commercial insurers would have newly diagnosed metastatic NSCLC and therefore be eligible for testing.
Estimated time to receive test results was 2 weeks for NGS testing and for panel testing, compared with 4.7 weeks for exclusionary testing and 4.8 weeks for sequential testing.
In the CMS population, NGS testing would save about $1.4 million compared with exclusionary testing, more than $1.5 million compared with sequential testing, and about $2.1 million compared with panel testing. In the commercial health plan cohort, NGS would save $3,809 compared with exclusionary testing, $127,402 compared with sequential testing, and $250,842 compared with panel testing.
Dr. Pennell disclosed that he has a consulting or advisory role with AstraZeneca, Lilly, and Regeneron, and that his institution receives research funding from Genentech, NewLink Genetics, Clovis Oncology, Astex Pharmaceuticals, Celgene, AstraZeneca, Pfizer, and Merck. The study received funding from Novartis.
SOURCE: Pennell et al., ASCO Annual Meeting Abstract 9031.
Comprehensive testing of newly diagnosed metastatic non–small cell lung cancer (NSCLC) with next-generation sequencing (NGS) for known lung cancer–related genomic alterations is cost-saving relative to single-gene testing strategies and often faster, a new study finds.
“We know now that genomic testing for all patients with advanced NSCLC is the standard of care to help detect oncogenic drivers, to inform treatment decisions,” lead study author Nathan A. Pennell, MD, PhD, codirector of the Cleveland Clinic lung cancer program, said in a press briefing leading up to the ASCO annual meeting. But the optimal strategy for this testing is unclear.
He and his colleagues conducted a decision analytic modeling study among hypothetical insurance plans having 1 million enrollees. Outcomes were compared between NGS testing and three single-gene testing strategies.
Data indicated that compared with exclusionary, sequential, or hot-spot panel testing approaches, NGS testing simultaneously for eight genomic alterations having Food and Drug Administration–approved or investigational targeted therapies could save up to $2.1 million among Medicare beneficiaries and up to $250,842 among patients covered by commercial insurance. The costs to payers decreased as the percentage of patients receiving NGS testing increased. Moreover, the wait time for results was similar or roughly half as long with NGS.
“Our results showed that there were substantial cost savings associated with upfront NGS testing compared to all other strategies,” Dr. Pennell said. “In addition, NGS had a faster turnaround time than either sequential or exclusionary testing, which is critically important for sick lung cancer patients, to make sure they get their treatment as quickly as possible. Waiting a month or longer is simply no longer viable for patients because they get sick very quickly and these treatments work very well.”
Of note, the model indicated that some patients undergoing initial single-gene testing strategies never had their genomic alterations detected because tissue for testing ran out and they were too sick to undergo another biopsy.
“The bottom line is, ultimately, using the best single test upfront results in the fastest turnaround time, the highest percentage of patients with targetable alterations identified, and overall the lowest cost to payers,” he summarized.
A major challenge in this population is going back and retesting for known or new genomic alterations, agreed ASCO President Bruce E. Johnson, MD, FASCO. “At our upcoming meeting, we are going to hear about RET, which may end up as a target and may therefore need to be tested for.”
Recently, oncologists have a new attractive option of billing for NGS panels rather than for single gene tests, he noted.
“This study really shows that by doing all the testing at the same time, you can both get results back more quickly as well as get information,” said Dr. Johnson, professor of medicine at the Dana-Farber Cancer Institute and a leader of the Dana-Farber/Harvard Cancer Center Lung Cancer Program, Boston. “This study looked at an NGS panel of eight genes, but most of the NGS panels contain somewhere between 50 and 400 genes, so you get a lot more information with this at a cost that’s competitive or less. So this will be welcome news to people who are ordering these gene panels.”
Study details
For NSCLC, there are currently approved treatments that target alterations in EGFR, ALK, ROS1, and BRAF, and investigational treatments in clinical trials that target alterations in MET, HER2, RET, and NTRK1.
In the model Dr. Pennell and his colleagues developed, patients with newly diagnosed metastatic NSCLC received testing for programmed death ligand 1 (PD-L1) plus testing for the above known lung cancer–related genes using one of four strategies:
- NGS testing (testing of all eight genes plus KRAS simultaneously).
- Sequential testing (testing one gene at a time starting with EGFR).
- Exclusionary testing (testing for KRAS mutation, the most common genomic alteration, followed by sequential testing for changes in other genes only if KRAS was not mutated).
- Hot-spot panel testing (combined testing for EGFR, ALK, ROS1, and BRAF), followed by either single-gene or NGS testing for alterations in other genes.
Model results indicated that among 1 million hypothetical plan enrollees, 2,066 patients covered by the Centers for Medicare & Medicaid Services and 156 covered by U.S. commercial insurers would have newly diagnosed metastatic NSCLC and therefore be eligible for testing.
Estimated time to receive test results was 2 weeks for NGS testing and for panel testing, compared with 4.7 weeks for exclusionary testing and 4.8 weeks for sequential testing.
In the CMS population, NGS testing would save about $1.4 million compared with exclusionary testing, more than $1.5 million compared with sequential testing, and about $2.1 million compared with panel testing. In the commercial health plan cohort, NGS would save $3,809 compared with exclusionary testing, $127,402 compared with sequential testing, and $250,842 compared with panel testing.
Dr. Pennell disclosed that he has a consulting or advisory role with AstraZeneca, Lilly, and Regeneron, and that his institution receives research funding from Genentech, NewLink Genetics, Clovis Oncology, Astex Pharmaceuticals, Celgene, AstraZeneca, Pfizer, and Merck. The study received funding from Novartis.
SOURCE: Pennell et al., ASCO Annual Meeting Abstract 9031.
Comprehensive testing of newly diagnosed metastatic non–small cell lung cancer (NSCLC) with next-generation sequencing (NGS) for known lung cancer–related genomic alterations is cost-saving relative to single-gene testing strategies and often faster, a new study finds.
“We know now that genomic testing for all patients with advanced NSCLC is the standard of care to help detect oncogenic drivers, to inform treatment decisions,” lead study author Nathan A. Pennell, MD, PhD, codirector of the Cleveland Clinic lung cancer program, said in a press briefing leading up to the ASCO annual meeting. But the optimal strategy for this testing is unclear.
He and his colleagues conducted a decision analytic modeling study among hypothetical insurance plans having 1 million enrollees. Outcomes were compared between NGS testing and three single-gene testing strategies.
Data indicated that compared with exclusionary, sequential, or hot-spot panel testing approaches, NGS testing simultaneously for eight genomic alterations having Food and Drug Administration–approved or investigational targeted therapies could save up to $2.1 million among Medicare beneficiaries and up to $250,842 among patients covered by commercial insurance. The costs to payers decreased as the percentage of patients receiving NGS testing increased. Moreover, the wait time for results was similar or roughly half as long with NGS.
“Our results showed that there were substantial cost savings associated with upfront NGS testing compared to all other strategies,” Dr. Pennell said. “In addition, NGS had a faster turnaround time than either sequential or exclusionary testing, which is critically important for sick lung cancer patients, to make sure they get their treatment as quickly as possible. Waiting a month or longer is simply no longer viable for patients because they get sick very quickly and these treatments work very well.”
Of note, the model indicated that some patients undergoing initial single-gene testing strategies never had their genomic alterations detected because tissue for testing ran out and they were too sick to undergo another biopsy.
“The bottom line is, ultimately, using the best single test upfront results in the fastest turnaround time, the highest percentage of patients with targetable alterations identified, and overall the lowest cost to payers,” he summarized.
A major challenge in this population is going back and retesting for known or new genomic alterations, agreed ASCO President Bruce E. Johnson, MD, FASCO. “At our upcoming meeting, we are going to hear about RET, which may end up as a target and may therefore need to be tested for.”
Recently, oncologists have a new attractive option of billing for NGS panels rather than for single gene tests, he noted.
“This study really shows that by doing all the testing at the same time, you can both get results back more quickly as well as get information,” said Dr. Johnson, professor of medicine at the Dana-Farber Cancer Institute and a leader of the Dana-Farber/Harvard Cancer Center Lung Cancer Program, Boston. “This study looked at an NGS panel of eight genes, but most of the NGS panels contain somewhere between 50 and 400 genes, so you get a lot more information with this at a cost that’s competitive or less. So this will be welcome news to people who are ordering these gene panels.”
Study details
For NSCLC, there are currently approved treatments that target alterations in EGFR, ALK, ROS1, and BRAF, and investigational treatments in clinical trials that target alterations in MET, HER2, RET, and NTRK1.
In the model Dr. Pennell and his colleagues developed, patients with newly diagnosed metastatic NSCLC received testing for programmed death ligand 1 (PD-L1) plus testing for the above known lung cancer–related genes using one of four strategies:
- NGS testing (testing of all eight genes plus KRAS simultaneously).
- Sequential testing (testing one gene at a time starting with EGFR).
- Exclusionary testing (testing for KRAS mutation, the most common genomic alteration, followed by sequential testing for changes in other genes only if KRAS was not mutated).
- Hot-spot panel testing (combined testing for EGFR, ALK, ROS1, and BRAF), followed by either single-gene or NGS testing for alterations in other genes.
Model results indicated that among 1 million hypothetical plan enrollees, 2,066 patients covered by the Centers for Medicare & Medicaid Services and 156 covered by U.S. commercial insurers would have newly diagnosed metastatic NSCLC and therefore be eligible for testing.
Estimated time to receive test results was 2 weeks for NGS testing and for panel testing, compared with 4.7 weeks for exclusionary testing and 4.8 weeks for sequential testing.
In the CMS population, NGS testing would save about $1.4 million compared with exclusionary testing, more than $1.5 million compared with sequential testing, and about $2.1 million compared with panel testing. In the commercial health plan cohort, NGS would save $3,809 compared with exclusionary testing, $127,402 compared with sequential testing, and $250,842 compared with panel testing.
Dr. Pennell disclosed that he has a consulting or advisory role with AstraZeneca, Lilly, and Regeneron, and that his institution receives research funding from Genentech, NewLink Genetics, Clovis Oncology, Astex Pharmaceuticals, Celgene, AstraZeneca, Pfizer, and Merck. The study received funding from Novartis.
SOURCE: Pennell et al., ASCO Annual Meeting Abstract 9031.
REPORTING FROM THE ASCO ANNUAL MEETING
Key clinical point:
Major finding: Relative to exclusionary, sequential, or panel testing, NGS testing could save up to $2.1 million among CMS beneficiaries and up to $250,842 among patients covered by commercial insurance.
Study details: A decision analytic modeling study in hypothetical cohorts of 1 million insurance plan enrollees.
Disclosures: Dr. Pennell disclosed that he has a consulting or advisory role with AstraZeneca, Lilly, and Regeneron, and that his institution receives research funding from Genentech, NewLink Genetics, Clovis Oncology, Astex Pharmaceuticals, Celgene, AstraZeneca, Pfizer, and Merck. The study received funding from Novartis.
Source: Pennell et al. ASCO Annual Meeting, Abstract 9031.
FDA’s Gottlieb floats ideas on Medicare drug coverage
When the current Part B drug reimbursement scheme – average sales price plus an additional 6% to cover administration and storage – was developed, there was little competition in most of the covered therapeutic categories, Scott Gottlieb, MD, Food and Drug Administration commissioner, said May 15 at an event hosted by the Alliance for Health Policy.

The situation is different now. “Not only are these product categories multisource and in some cases quite crowded, but there is also a lot of therapeutic equivalence,” Dr. Gottlieb said. “There are a lot of other types of drugs [physicians] might use to try to address the same clinical condition.”
He specifically noted that autoimmune and inflammatory conditions have a wealth of products that address them in different ways, with the opportunity for therapeutic substitutions. He also mentioned drugs that are delivered through durable medical equipment as another area open to being moved into a more price-competitive space.
“I don’t think anyone envisioned how competitive these categories would become,” he said.
Switching drug coverage from Medicare Part B to Part D is just one of more than 50 proposals contained in a broad package introduced by the White House on May 11 to address the rising prices of prescription drugs.
“In situations where you have a lot of therapeutic variety ... you have [insurance] plans negotiating pricing using formularies and using things like step therapy, putting drugs on preferred tiers relative to the price concessions they are able to extract,” Dr. Gottlieb said.
In contrast, the current Part B [program], “looks like the small molecule world with respect to how much competition we see within some of these categories, but you don’t have the same structure. Times have changed, and I think that is why you see Secretary [Alex Azar of the Health & Human Services department] rethinking how we bid out those Part B drugs into a competitive scheme.”
Dr. Gottlieb suggested that more competition could come from the moving coverage to Medicare Part D or possibly through a reinvigorated competitive acquisition program for Part B.
When the current Part B drug reimbursement scheme – average sales price plus an additional 6% to cover administration and storage – was developed, there was little competition in most of the covered therapeutic categories, Scott Gottlieb, MD, Food and Drug Administration commissioner, said May 15 at an event hosted by the Alliance for Health Policy.
The situation is different now. “Not only are these product categories multisource and in some cases quite crowded, but there is also a lot of therapeutic equivalence,” Dr. Gottlieb said. “There are a lot of other types of drugs [physicians] might use to try to address the same clinical condition.”
He specifically noted that autoimmune and inflammatory conditions have a wealth of products that address them in different ways, with the opportunity for therapeutic substitutions. He also mentioned drugs that are delivered through durable medical equipment as another area open to being moved into a more price-competitive space.
“I don’t think anyone envisioned how competitive these categories would become,” he said.
Switching drug coverage from Medicare Part B to Part D is just one of more than 50 proposals contained in a broad package introduced by the White House on May 11 to address the rising prices of prescription drugs.
“In situations where you have a lot of therapeutic variety ... you have [insurance] plans negotiating pricing using formularies and using things like step therapy, putting drugs on preferred tiers relative to the price concessions they are able to extract,” Dr. Gottlieb said.
In contrast, the current Part B [program], “looks like the small molecule world with respect to how much competition we see within some of these categories, but you don’t have the same structure. Times have changed, and I think that is why you see Secretary [Alex Azar of the Health & Human Services department] rethinking how we bid out those Part B drugs into a competitive scheme.”
Dr. Gottlieb suggested that more competition could come from the moving coverage to Medicare Part D or possibly through a reinvigorated competitive acquisition program for Part B.
When the current Part B drug reimbursement scheme – average sales price plus an additional 6% to cover administration and storage – was developed, there was little competition in most of the covered therapeutic categories, Scott Gottlieb, MD, Food and Drug Administration commissioner, said May 15 at an event hosted by the Alliance for Health Policy.
The situation is different now. “Not only are these product categories multisource and in some cases quite crowded, but there is also a lot of therapeutic equivalence,” Dr. Gottlieb said. “There are a lot of other types of drugs [physicians] might use to try to address the same clinical condition.”
He specifically noted that autoimmune and inflammatory conditions have a wealth of products that address them in different ways, with the opportunity for therapeutic substitutions. He also mentioned drugs that are delivered through durable medical equipment as another area open to being moved into a more price-competitive space.
“I don’t think anyone envisioned how competitive these categories would become,” he said.
Switching drug coverage from Medicare Part B to Part D is just one of more than 50 proposals contained in a broad package introduced by the White House on May 11 to address the rising prices of prescription drugs.
“In situations where you have a lot of therapeutic variety ... you have [insurance] plans negotiating pricing using formularies and using things like step therapy, putting drugs on preferred tiers relative to the price concessions they are able to extract,” Dr. Gottlieb said.
In contrast, the current Part B [program], “looks like the small molecule world with respect to how much competition we see within some of these categories, but you don’t have the same structure. Times have changed, and I think that is why you see Secretary [Alex Azar of the Health & Human Services department] rethinking how we bid out those Part B drugs into a competitive scheme.”
Dr. Gottlieb suggested that more competition could come from the moving coverage to Medicare Part D or possibly through a reinvigorated competitive acquisition program for Part B.