User login
Responsive parenting intervention slows weight gain in infancy
TORONTO – Teaching parents of newborns to respond to eating and satiety cues in ways that promote self-regulation was associated with improvements in some weight outcomes at 3 years in a randomized clinical trial.
For the primary outcome of body mass index (BMI) z score at 3 years, a significant difference favoring the responsive parenting (RP) intervention was seen (–0.13 vs. 0.15 for controls; absolute difference, –0.28; P = .04). A longitudinal analysis examining the entire intervention period confirmed that the mean BMI group differences across seven study visits confirmed the effect of the RP intervention on BMI (P less than .001).
“We felt that the BMI z score and longitudinal growth analysis are probably the most sustained effects for an early-life intervention that have been recorded to date,” reported Ian M. Paul, MD, MSc, of Penn State University, Hershey. “While the differences between study groups were modest and not all achieved statistical significance, all favored the responsive-parenting intervention.”
Mean BMI percentile, a secondary outcome, was 47th for the RP group and 54th for controls, narrowly missing statistical significance (P = .07). Similarly, the percent of children deemed overweight at 3 years was 11.2% for the RP group and 19.8% for controls (P = .07), while 2.6% and 7.8%, respectively, were obese (P = .08).
No significant differences were seen in growth-related adverse events, such a weight-for-age less than the 5th percentile. The issue of “inducing” failure-to-thrive with a feeding intervention is a concern, said Dr. Paul, but there was no evidence for it in their study.
“One could question whether [the small differences seen between groups] are clinically significant, but if we look at how small differences have changed in the population over time and how those equate as far as longitudinal risk for cardiovascular outcomes and metabolic syndrome, etc., the small differences [we saw] might be important on a population level,” said Dr. Paul at the Pediatric Academic Societies meeting.
Study details
With upwards of one-quarter of U.S. children aged 2-5 years being overweight or obese, interventions to prevent rapid weight gain and reduce risk for overweight status in infancy are needed, noted Dr. Paul. Another reason to consider very early intervention, he added, is that infancy is a time of both “metabolic and behavioral plasticity.” However, most efforts to intervene early have, thus far, had limited success.
“Our responses to a baby crying are to feed that baby,” said Dr. Paul. This urge, along with others (such as “clear your plate”), evolved during times of food scarcity but persist now that we have inexpensive and palatable food, and promote rapid infant weight gain and increased obesity risk.
An alternative to those traditional parenting practices are responsive feeding and responsive parenting, he explained. “Responsive feeding and parenting requires prompt, developmentally appropriate responses to a child’s behaviors including hunger and satiety cues.”
In other studies, RP has been shown to foster cognitive, social, and emotional development. “The question we had was: Can responsive parenting reduce obesity risk?” he said.
The INSIGHT (Intervention Nurses Start Infants Growing on Healthy Trajectories) study is an ongoing, randomized clinical trial started in January 2012 comparing an RP intervention designed to prevent childhood obesity with a safety control, with the interventions matched on intensity and length.
Parent-child dyads were randomized 2 weeks after birth and were told that the purpose of the study was “to see if nurse visits to your home during your baby’s infancy can improve your ability to either respond to your child’s cues related to feeding and fussiness or improve your ability to provide a safe environment for your child and prevent injuries.”
A total of 279 primiparous mother-newborn dyads were studied. Most were white (89%) and non-Hispanic (94%), and the majority were married (75%). Mean prepregnancy BMI was 25.5 kg/m2.
“We chose first-time mothers because we thought they were more likely to listen to the parenting advice that we had to offer,” said Dr. Paul.
INSIGHT’s curriculum focused on RP in domains of infant feeding, sleep, interactive play, and emotion regulation. “We tried to promote self-regulation by setting limits but still being responsive in a variety of behavior domains,” Dr. Paul said. “So, for example…, for feeding we talked about exposure to healthy foods, shared feeding responsibility, for those that were bottle feeding we gave tips on size of bottle appropriate for the child and also not using bottle finishing practices. In the emotional and social regulation domain, we talked about alternatives to food to soothe, and emphasized embracing each child’s temperament and how to respond to different temperaments.”
Dr. Paul reported no conflicts of interest. INSIGHT is supported by National Institute of Diabetes and Digestive and Kidney Diseases research grants, with additional support from the Children’s Miracle Network at Penn State Children’s Hospital.
TORONTO – Teaching parents of newborns to respond to eating and satiety cues in ways that promote self-regulation was associated with improvements in some weight outcomes at 3 years in a randomized clinical trial.
For the primary outcome of body mass index (BMI) z score at 3 years, a significant difference favoring the responsive parenting (RP) intervention was seen (–0.13 vs. 0.15 for controls; absolute difference, –0.28; P = .04). A longitudinal analysis examining the entire intervention period confirmed that the mean BMI group differences across seven study visits confirmed the effect of the RP intervention on BMI (P less than .001).
“We felt that the BMI z score and longitudinal growth analysis are probably the most sustained effects for an early-life intervention that have been recorded to date,” reported Ian M. Paul, MD, MSc, of Penn State University, Hershey. “While the differences between study groups were modest and not all achieved statistical significance, all favored the responsive-parenting intervention.”
Mean BMI percentile, a secondary outcome, was 47th for the RP group and 54th for controls, narrowly missing statistical significance (P = .07). Similarly, the percent of children deemed overweight at 3 years was 11.2% for the RP group and 19.8% for controls (P = .07), while 2.6% and 7.8%, respectively, were obese (P = .08).
No significant differences were seen in growth-related adverse events, such a weight-for-age less than the 5th percentile. The issue of “inducing” failure-to-thrive with a feeding intervention is a concern, said Dr. Paul, but there was no evidence for it in their study.
“One could question whether [the small differences seen between groups] are clinically significant, but if we look at how small differences have changed in the population over time and how those equate as far as longitudinal risk for cardiovascular outcomes and metabolic syndrome, etc., the small differences [we saw] might be important on a population level,” said Dr. Paul at the Pediatric Academic Societies meeting.
Study details
With upwards of one-quarter of U.S. children aged 2-5 years being overweight or obese, interventions to prevent rapid weight gain and reduce risk for overweight status in infancy are needed, noted Dr. Paul. Another reason to consider very early intervention, he added, is that infancy is a time of both “metabolic and behavioral plasticity.” However, most efforts to intervene early have, thus far, had limited success.
“Our responses to a baby crying are to feed that baby,” said Dr. Paul. This urge, along with others (such as “clear your plate”), evolved during times of food scarcity but persist now that we have inexpensive and palatable food, and promote rapid infant weight gain and increased obesity risk.
An alternative to those traditional parenting practices are responsive feeding and responsive parenting, he explained. “Responsive feeding and parenting requires prompt, developmentally appropriate responses to a child’s behaviors including hunger and satiety cues.”
In other studies, RP has been shown to foster cognitive, social, and emotional development. “The question we had was: Can responsive parenting reduce obesity risk?” he said.
The INSIGHT (Intervention Nurses Start Infants Growing on Healthy Trajectories) study is an ongoing, randomized clinical trial started in January 2012 comparing an RP intervention designed to prevent childhood obesity with a safety control, with the interventions matched on intensity and length.
Parent-child dyads were randomized 2 weeks after birth and were told that the purpose of the study was “to see if nurse visits to your home during your baby’s infancy can improve your ability to either respond to your child’s cues related to feeding and fussiness or improve your ability to provide a safe environment for your child and prevent injuries.”
A total of 279 primiparous mother-newborn dyads were studied. Most were white (89%) and non-Hispanic (94%), and the majority were married (75%). Mean prepregnancy BMI was 25.5 kg/m2.
“We chose first-time mothers because we thought they were more likely to listen to the parenting advice that we had to offer,” said Dr. Paul.
INSIGHT’s curriculum focused on RP in domains of infant feeding, sleep, interactive play, and emotion regulation. “We tried to promote self-regulation by setting limits but still being responsive in a variety of behavior domains,” Dr. Paul said. “So, for example…, for feeding we talked about exposure to healthy foods, shared feeding responsibility, for those that were bottle feeding we gave tips on size of bottle appropriate for the child and also not using bottle finishing practices. In the emotional and social regulation domain, we talked about alternatives to food to soothe, and emphasized embracing each child’s temperament and how to respond to different temperaments.”
Dr. Paul reported no conflicts of interest. INSIGHT is supported by National Institute of Diabetes and Digestive and Kidney Diseases research grants, with additional support from the Children’s Miracle Network at Penn State Children’s Hospital.
TORONTO – Teaching parents of newborns to respond to eating and satiety cues in ways that promote self-regulation was associated with improvements in some weight outcomes at 3 years in a randomized clinical trial.
For the primary outcome of body mass index (BMI) z score at 3 years, a significant difference favoring the responsive parenting (RP) intervention was seen (–0.13 vs. 0.15 for controls; absolute difference, –0.28; P = .04). A longitudinal analysis examining the entire intervention period confirmed that the mean BMI group differences across seven study visits confirmed the effect of the RP intervention on BMI (P less than .001).
“We felt that the BMI z score and longitudinal growth analysis are probably the most sustained effects for an early-life intervention that have been recorded to date,” reported Ian M. Paul, MD, MSc, of Penn State University, Hershey. “While the differences between study groups were modest and not all achieved statistical significance, all favored the responsive-parenting intervention.”
Mean BMI percentile, a secondary outcome, was 47th for the RP group and 54th for controls, narrowly missing statistical significance (P = .07). Similarly, the percent of children deemed overweight at 3 years was 11.2% for the RP group and 19.8% for controls (P = .07), while 2.6% and 7.8%, respectively, were obese (P = .08).
No significant differences were seen in growth-related adverse events, such a weight-for-age less than the 5th percentile. The issue of “inducing” failure-to-thrive with a feeding intervention is a concern, said Dr. Paul, but there was no evidence for it in their study.
“One could question whether [the small differences seen between groups] are clinically significant, but if we look at how small differences have changed in the population over time and how those equate as far as longitudinal risk for cardiovascular outcomes and metabolic syndrome, etc., the small differences [we saw] might be important on a population level,” said Dr. Paul at the Pediatric Academic Societies meeting.
Study details
With upwards of one-quarter of U.S. children aged 2-5 years being overweight or obese, interventions to prevent rapid weight gain and reduce risk for overweight status in infancy are needed, noted Dr. Paul. Another reason to consider very early intervention, he added, is that infancy is a time of both “metabolic and behavioral plasticity.” However, most efforts to intervene early have, thus far, had limited success.
“Our responses to a baby crying are to feed that baby,” said Dr. Paul. This urge, along with others (such as “clear your plate”), evolved during times of food scarcity but persist now that we have inexpensive and palatable food, and promote rapid infant weight gain and increased obesity risk.
An alternative to those traditional parenting practices are responsive feeding and responsive parenting, he explained. “Responsive feeding and parenting requires prompt, developmentally appropriate responses to a child’s behaviors including hunger and satiety cues.”
In other studies, RP has been shown to foster cognitive, social, and emotional development. “The question we had was: Can responsive parenting reduce obesity risk?” he said.
The INSIGHT (Intervention Nurses Start Infants Growing on Healthy Trajectories) study is an ongoing, randomized clinical trial started in January 2012 comparing an RP intervention designed to prevent childhood obesity with a safety control, with the interventions matched on intensity and length.
Parent-child dyads were randomized 2 weeks after birth and were told that the purpose of the study was “to see if nurse visits to your home during your baby’s infancy can improve your ability to either respond to your child’s cues related to feeding and fussiness or improve your ability to provide a safe environment for your child and prevent injuries.”
A total of 279 primiparous mother-newborn dyads were studied. Most were white (89%) and non-Hispanic (94%), and the majority were married (75%). Mean prepregnancy BMI was 25.5 kg/m2.
“We chose first-time mothers because we thought they were more likely to listen to the parenting advice that we had to offer,” said Dr. Paul.
INSIGHT’s curriculum focused on RP in domains of infant feeding, sleep, interactive play, and emotion regulation. “We tried to promote self-regulation by setting limits but still being responsive in a variety of behavior domains,” Dr. Paul said. “So, for example…, for feeding we talked about exposure to healthy foods, shared feeding responsibility, for those that were bottle feeding we gave tips on size of bottle appropriate for the child and also not using bottle finishing practices. In the emotional and social regulation domain, we talked about alternatives to food to soothe, and emphasized embracing each child’s temperament and how to respond to different temperaments.”
Dr. Paul reported no conflicts of interest. INSIGHT is supported by National Institute of Diabetes and Digestive and Kidney Diseases research grants, with additional support from the Children’s Miracle Network at Penn State Children’s Hospital.
REPORTING FROM PAS 2018
Key clinical point:
Major finding: For the primary outcome of body mass index z score at 3 years, a significant difference favoring the responsive parenting intervention was seen (–0.13 vs. 0.15 for controls; absolute difference, –0.28; P = .04).
Study details: A randomized clinical trial including 279 mother-newborn dyads.
Disclosures: Dr. Paul reported no conflicts of interest. INSIGHT is supported by National Institute of Diabetes and Digestive and Kidney Diseases research grants, with additional support from the Children’s Miracle Network at Penn State Children’s Hospital.
IV superior to oral treatment for iron deficiency during pregnancy
AUSTIN, TEX. – Utilizing intravenous treatment for iron deficiency in anemic pregnant women was more efficacious than oral iron supplements, according to a study presented at the annual clinical and scientific meeting of the American College of Obstetricians and Gynecologists.
With 42% of pregnancies worldwide affected by anemia, according to the World Health Organization, improving treatment beyond the standard oral treatment could have a large effect on decreasing pregnancy complications.
“Women with bariatric surgery and inflammatory bowel disease are at higher risk of failure,” said Shravya Govindappagari, MD, a gynecologist affiliated with New York–Presbyterian Hospital. “Intravenous iron overcomes the limited intestinal absorption of oral formulations, and may increase iron stores more quickly.”
Dr. Govindappagari and her colleagues conducted a meta-analysis of 11 randomly controlled trials published between 2002 and 2017 to uncover the possible benefits of intravenous iron over oral treatment.
Studies were conducted in India, Egypt, France, and Turkey, with one additional multicenter study that gathered patients from seven different countries. Participants were given iron sucrose, ferric carboxymaltose, or low molecular weight iron dextran, according to Dr. Govindappagari.
In an overall assessment of subjects who achieved target hemoglobin levels, patients receiving intravenous iron were 2.66 times more likely to reach target levels than those given oral treatment (P less than .001). After 4 weeks of treatment, patients in the intravenous groups had a mean hemoglobin increase of 0.84 g/dl higher than those in the oral group (P less than .001).
Some clinicians may be wary about switching treatment modality from oral to intravenous; however, Dr. Govindappagari and fellow investigators found those taking oral treatment were 35% more likely to experience adverse effects than those receiving intravenous treatment.
While the analysis, according to Dr. Govindappagari, has merit, she and her team did not have access to relevant blinded, randomly controlled trials, which may have affected the findings. Maternal and neonatal outcomes were also not included in any of the studies analyzed, nor was a cost analysis of the financial burden of switching from oral to intravenous treatment.
Despite these limitations, Dr. Govindappagari and her colleagues assert the use of intravenous iron could have a significant effect on this problem.
“Intravenous iron compared to oral iron has a higher number reach target, a greater increase in hemoglobin, and has fewer side effects,” Dr. Govindappagari said to attendees. “This could be particularly useful in women in labor, during the third trimester, and women who are iron deficient and are at risk for postpartum hemorrhage.”
Dr. Govindappagari and her colleagues reported no relevant financial disclosures.
SOURCE: Govindappagari S et al. ACOG 2018, Abstract 10OP.
AUSTIN, TEX. – Utilizing intravenous treatment for iron deficiency in anemic pregnant women was more efficacious than oral iron supplements, according to a study presented at the annual clinical and scientific meeting of the American College of Obstetricians and Gynecologists.
With 42% of pregnancies worldwide affected by anemia, according to the World Health Organization, improving treatment beyond the standard oral treatment could have a large effect on decreasing pregnancy complications.
“Women with bariatric surgery and inflammatory bowel disease are at higher risk of failure,” said Shravya Govindappagari, MD, a gynecologist affiliated with New York–Presbyterian Hospital. “Intravenous iron overcomes the limited intestinal absorption of oral formulations, and may increase iron stores more quickly.”
Dr. Govindappagari and her colleagues conducted a meta-analysis of 11 randomly controlled trials published between 2002 and 2017 to uncover the possible benefits of intravenous iron over oral treatment.
Studies were conducted in India, Egypt, France, and Turkey, with one additional multicenter study that gathered patients from seven different countries. Participants were given iron sucrose, ferric carboxymaltose, or low molecular weight iron dextran, according to Dr. Govindappagari.
In an overall assessment of subjects who achieved target hemoglobin levels, patients receiving intravenous iron were 2.66 times more likely to reach target levels than those given oral treatment (P less than .001). After 4 weeks of treatment, patients in the intravenous groups had a mean hemoglobin increase of 0.84 g/dl higher than those in the oral group (P less than .001).
Some clinicians may be wary about switching treatment modality from oral to intravenous; however, Dr. Govindappagari and fellow investigators found those taking oral treatment were 35% more likely to experience adverse effects than those receiving intravenous treatment.
While the analysis, according to Dr. Govindappagari, has merit, she and her team did not have access to relevant blinded, randomly controlled trials, which may have affected the findings. Maternal and neonatal outcomes were also not included in any of the studies analyzed, nor was a cost analysis of the financial burden of switching from oral to intravenous treatment.
Despite these limitations, Dr. Govindappagari and her colleagues assert the use of intravenous iron could have a significant effect on this problem.
“Intravenous iron compared to oral iron has a higher number reach target, a greater increase in hemoglobin, and has fewer side effects,” Dr. Govindappagari said to attendees. “This could be particularly useful in women in labor, during the third trimester, and women who are iron deficient and are at risk for postpartum hemorrhage.”
Dr. Govindappagari and her colleagues reported no relevant financial disclosures.
SOURCE: Govindappagari S et al. ACOG 2018, Abstract 10OP.
AUSTIN, TEX. – Utilizing intravenous treatment for iron deficiency in anemic pregnant women was more efficacious than oral iron supplements, according to a study presented at the annual clinical and scientific meeting of the American College of Obstetricians and Gynecologists.
With 42% of pregnancies worldwide affected by anemia, according to the World Health Organization, improving treatment beyond the standard oral treatment could have a large effect on decreasing pregnancy complications.
“Women with bariatric surgery and inflammatory bowel disease are at higher risk of failure,” said Shravya Govindappagari, MD, a gynecologist affiliated with New York–Presbyterian Hospital. “Intravenous iron overcomes the limited intestinal absorption of oral formulations, and may increase iron stores more quickly.”
Dr. Govindappagari and her colleagues conducted a meta-analysis of 11 randomly controlled trials published between 2002 and 2017 to uncover the possible benefits of intravenous iron over oral treatment.
Studies were conducted in India, Egypt, France, and Turkey, with one additional multicenter study that gathered patients from seven different countries. Participants were given iron sucrose, ferric carboxymaltose, or low molecular weight iron dextran, according to Dr. Govindappagari.
In an overall assessment of subjects who achieved target hemoglobin levels, patients receiving intravenous iron were 2.66 times more likely to reach target levels than those given oral treatment (P less than .001). After 4 weeks of treatment, patients in the intravenous groups had a mean hemoglobin increase of 0.84 g/dl higher than those in the oral group (P less than .001).
Some clinicians may be wary about switching treatment modality from oral to intravenous; however, Dr. Govindappagari and fellow investigators found those taking oral treatment were 35% more likely to experience adverse effects than those receiving intravenous treatment.
While the analysis, according to Dr. Govindappagari, has merit, she and her team did not have access to relevant blinded, randomly controlled trials, which may have affected the findings. Maternal and neonatal outcomes were also not included in any of the studies analyzed, nor was a cost analysis of the financial burden of switching from oral to intravenous treatment.
Despite these limitations, Dr. Govindappagari and her colleagues assert the use of intravenous iron could have a significant effect on this problem.
“Intravenous iron compared to oral iron has a higher number reach target, a greater increase in hemoglobin, and has fewer side effects,” Dr. Govindappagari said to attendees. “This could be particularly useful in women in labor, during the third trimester, and women who are iron deficient and are at risk for postpartum hemorrhage.”
Dr. Govindappagari and her colleagues reported no relevant financial disclosures.
SOURCE: Govindappagari S et al. ACOG 2018, Abstract 10OP.
REPORTING FROM ACOG 2018
Key clinical point: Intravenous iron treatment is better for pregnant women with anemia.
Major finding: Hemoglobin levels in women with intravenous iron increased by 1.2 g/dl more than in those using oral supplements after 4 weeks (P less than .001).
Data source: A meta-analysis of 11 randomized, controlled trials comparing intravenous with oral iron treatment.
Disclosures: Dr. Govindappagari and her colleagues reported no relevant financial disclosures.
Source: Govindappagari S et al. ACOG 2018, Abstract 10OP.
SHM and Neurohospitalist Society partner on new program for stroke patients
The Society of Hospital Medicine recently partnered with the Neurohospitalist Society (NHS) to apply the neurology, stroke, and neurohospitalist expertise of NHS to the hospital and mentored implementation expertise of SHM for a uniquely positioned program for hospitals and health care systems: the Optimizing Neurovascular Intervention Care for Stroke Patients Mentored Implementation program.
This program aims to provide the resources and training to equip neurologists and hospitals with the skills to help assure continuous quality in the care of stroke patients with large vessel occlusion. The program will help neurohospitalists and other clinicians identify opportunities to engage multidisciplinary team members to implement evidence-based management practices in their hospital.
Reading Hospital – Tower Health, West Reading, Pa., was one of four hospitals selected to participate in the first wave of this program. Tower Health also recently became SHM’s first health system institutional partner. The Hospitalist spoke with a team from Reading Hospital about their participation in the new program and how they think it could affect their care. Interviewees included Sarah Keller, RN, nurse specialist; Deepam Gokal, MD, an associate director of hospitalist services; and Ruth Bailey, RN, stroke program manager.
What led you to partner with SHM for this program?
Dr. Gokal is an associate director of hospitalist services and comedical director of the stroke program, is a member of SHM, and was a former member of NHS; he received an email regarding the mentored implementation program for continuous quality monitoring and improvement in the care of stroke patients with large vessel occlusions. Karen Hoerst, MD, is a vascular neurologist and stroke program comedical director, and Ruth Bailey, RN, is the stroke program manager; together, we reviewed the introductory webinar with Dr. Gokal and felt this program would be beneficial for our organization, in particular because of Reading Hospital’s recent acquisition of five hospitals to form Tower Health – Brandywine Hospital, Coatesville, Pa.; Chestnut Hill Hospital, Philadelphia; Jennersville Hospital, West Grove, Pa.; Phoenixville (Pa.) Hospital; and Pottstown (Pa.) Hospital – and to help fulfill our vision to become the hub facility and a comprehensive stroke center.
Did you have a history with SHM prior to this program and before Tower Health’s new institutional partnership with SHM?
Reading Hospital participated in Project BOOST, SHM’s care transitions mentored implementation program, from 2012 to 2013. The goal was to optimize the hospital discharge process and to mitigate and prevent known complications and errors that occur during transitions. This was championed by hospitalists Walter R. Bohnenblust Jr., MD, SFHM, former Director of Hospitalist Services, and Binu Pappachen, MD, FHM.
The pain management provider team at Reading Hospital also championed an opioid management mentored implementation program in 2016-2017 that sought to improve safety and reduce adverse events for patients receiving opioids.
How do you anticipate this program will affect outcomes?
Reading Hospital – Tower Health is committed to advancing health care and transforming lives. The aim is to provide better care for individuals, improve health strategies, and reduce health care costs. This mentorship program should support this commitment to value-based care and population health management. It should prove beneficial to Reading Hospital by optimizing neurovascular interventions, which will help it become the intended hub for the Tower Health Teleneurology Program.
What will success look like to you and to members of the hospitalist team?
Future success for hospitalist services at Reading Hospital will include the fruition of a neurohospitalist subspecialty. Participation in this mentored implementation program should provide valuable resources for the development of this subspecialty that are aligned with the vision of Reading Hospital’s Advanced Primary Stroke Center. This vision is to serve as the comprehensive stroke center of choice for the patients both in our community and the surrounding region and to provide them with 24/7 state-of-the-art complex stroke treatment with demonstrated optimization of quality patient outcomes throughout the continuum of care.
For more information about SHM’s mentored implementation programs, visit hospitalmedicine.org/qi.
The Society of Hospital Medicine recently partnered with the Neurohospitalist Society (NHS) to apply the neurology, stroke, and neurohospitalist expertise of NHS to the hospital and mentored implementation expertise of SHM for a uniquely positioned program for hospitals and health care systems: the Optimizing Neurovascular Intervention Care for Stroke Patients Mentored Implementation program.
This program aims to provide the resources and training to equip neurologists and hospitals with the skills to help assure continuous quality in the care of stroke patients with large vessel occlusion. The program will help neurohospitalists and other clinicians identify opportunities to engage multidisciplinary team members to implement evidence-based management practices in their hospital.
Reading Hospital – Tower Health, West Reading, Pa., was one of four hospitals selected to participate in the first wave of this program. Tower Health also recently became SHM’s first health system institutional partner. The Hospitalist spoke with a team from Reading Hospital about their participation in the new program and how they think it could affect their care. Interviewees included Sarah Keller, RN, nurse specialist; Deepam Gokal, MD, an associate director of hospitalist services; and Ruth Bailey, RN, stroke program manager.
What led you to partner with SHM for this program?
Dr. Gokal is an associate director of hospitalist services and comedical director of the stroke program, is a member of SHM, and was a former member of NHS; he received an email regarding the mentored implementation program for continuous quality monitoring and improvement in the care of stroke patients with large vessel occlusions. Karen Hoerst, MD, is a vascular neurologist and stroke program comedical director, and Ruth Bailey, RN, is the stroke program manager; together, we reviewed the introductory webinar with Dr. Gokal and felt this program would be beneficial for our organization, in particular because of Reading Hospital’s recent acquisition of five hospitals to form Tower Health – Brandywine Hospital, Coatesville, Pa.; Chestnut Hill Hospital, Philadelphia; Jennersville Hospital, West Grove, Pa.; Phoenixville (Pa.) Hospital; and Pottstown (Pa.) Hospital – and to help fulfill our vision to become the hub facility and a comprehensive stroke center.
Did you have a history with SHM prior to this program and before Tower Health’s new institutional partnership with SHM?
Reading Hospital participated in Project BOOST, SHM’s care transitions mentored implementation program, from 2012 to 2013. The goal was to optimize the hospital discharge process and to mitigate and prevent known complications and errors that occur during transitions. This was championed by hospitalists Walter R. Bohnenblust Jr., MD, SFHM, former Director of Hospitalist Services, and Binu Pappachen, MD, FHM.
The pain management provider team at Reading Hospital also championed an opioid management mentored implementation program in 2016-2017 that sought to improve safety and reduce adverse events for patients receiving opioids.
How do you anticipate this program will affect outcomes?
Reading Hospital – Tower Health is committed to advancing health care and transforming lives. The aim is to provide better care for individuals, improve health strategies, and reduce health care costs. This mentorship program should support this commitment to value-based care and population health management. It should prove beneficial to Reading Hospital by optimizing neurovascular interventions, which will help it become the intended hub for the Tower Health Teleneurology Program.
What will success look like to you and to members of the hospitalist team?
Future success for hospitalist services at Reading Hospital will include the fruition of a neurohospitalist subspecialty. Participation in this mentored implementation program should provide valuable resources for the development of this subspecialty that are aligned with the vision of Reading Hospital’s Advanced Primary Stroke Center. This vision is to serve as the comprehensive stroke center of choice for the patients both in our community and the surrounding region and to provide them with 24/7 state-of-the-art complex stroke treatment with demonstrated optimization of quality patient outcomes throughout the continuum of care.
For more information about SHM’s mentored implementation programs, visit hospitalmedicine.org/qi.
The Society of Hospital Medicine recently partnered with the Neurohospitalist Society (NHS) to apply the neurology, stroke, and neurohospitalist expertise of NHS to the hospital and mentored implementation expertise of SHM for a uniquely positioned program for hospitals and health care systems: the Optimizing Neurovascular Intervention Care for Stroke Patients Mentored Implementation program.
This program aims to provide the resources and training to equip neurologists and hospitals with the skills to help assure continuous quality in the care of stroke patients with large vessel occlusion. The program will help neurohospitalists and other clinicians identify opportunities to engage multidisciplinary team members to implement evidence-based management practices in their hospital.
Reading Hospital – Tower Health, West Reading, Pa., was one of four hospitals selected to participate in the first wave of this program. Tower Health also recently became SHM’s first health system institutional partner. The Hospitalist spoke with a team from Reading Hospital about their participation in the new program and how they think it could affect their care. Interviewees included Sarah Keller, RN, nurse specialist; Deepam Gokal, MD, an associate director of hospitalist services; and Ruth Bailey, RN, stroke program manager.
What led you to partner with SHM for this program?
Dr. Gokal is an associate director of hospitalist services and comedical director of the stroke program, is a member of SHM, and was a former member of NHS; he received an email regarding the mentored implementation program for continuous quality monitoring and improvement in the care of stroke patients with large vessel occlusions. Karen Hoerst, MD, is a vascular neurologist and stroke program comedical director, and Ruth Bailey, RN, is the stroke program manager; together, we reviewed the introductory webinar with Dr. Gokal and felt this program would be beneficial for our organization, in particular because of Reading Hospital’s recent acquisition of five hospitals to form Tower Health – Brandywine Hospital, Coatesville, Pa.; Chestnut Hill Hospital, Philadelphia; Jennersville Hospital, West Grove, Pa.; Phoenixville (Pa.) Hospital; and Pottstown (Pa.) Hospital – and to help fulfill our vision to become the hub facility and a comprehensive stroke center.
Did you have a history with SHM prior to this program and before Tower Health’s new institutional partnership with SHM?
Reading Hospital participated in Project BOOST, SHM’s care transitions mentored implementation program, from 2012 to 2013. The goal was to optimize the hospital discharge process and to mitigate and prevent known complications and errors that occur during transitions. This was championed by hospitalists Walter R. Bohnenblust Jr., MD, SFHM, former Director of Hospitalist Services, and Binu Pappachen, MD, FHM.
The pain management provider team at Reading Hospital also championed an opioid management mentored implementation program in 2016-2017 that sought to improve safety and reduce adverse events for patients receiving opioids.
How do you anticipate this program will affect outcomes?
Reading Hospital – Tower Health is committed to advancing health care and transforming lives. The aim is to provide better care for individuals, improve health strategies, and reduce health care costs. This mentorship program should support this commitment to value-based care and population health management. It should prove beneficial to Reading Hospital by optimizing neurovascular interventions, which will help it become the intended hub for the Tower Health Teleneurology Program.
What will success look like to you and to members of the hospitalist team?
Future success for hospitalist services at Reading Hospital will include the fruition of a neurohospitalist subspecialty. Participation in this mentored implementation program should provide valuable resources for the development of this subspecialty that are aligned with the vision of Reading Hospital’s Advanced Primary Stroke Center. This vision is to serve as the comprehensive stroke center of choice for the patients both in our community and the surrounding region and to provide them with 24/7 state-of-the-art complex stroke treatment with demonstrated optimization of quality patient outcomes throughout the continuum of care.
For more information about SHM’s mentored implementation programs, visit hospitalmedicine.org/qi.
A Novel Technique for the Treatment of Jersey Fingers
ABSTRACT
The avulsion of the flexor digitorum profundus from its insertion, or “jersey finger,” is a relatively common injury. Numerous modifications have been made to the classification and treatment of this injury since its initial description. We describe a novel variation of the surgical management of jersey finger.
The avulsion-type injury of the flexor digitorum profundus (FDP) from its insertion on the distal phalanx is relatively common. FDP avulsions are seen in athletes and nonathletes, and are the result of the sudden hyperextension of the distal interphalangeal joint during active flexion. These injuries usually occur while grasping the jersey of an opposing player and are thus commonly referred to as “jersey finger.” Initially described in 1977 by Leddy and Packer1, FDP avulsions are classified on the basis of the proximal extent of the retraction of the FDP and the presence or absence of a bony avulsion fracture fragment. Type I injuries are defined by tendon retraction to the level of the palm, where it is tethered by the lumbricals. At this level, the vinculum longus profundus (VLP) and vinculum brevis profundus (VBP) are ruptured, resulting in the substantial loss of intrinsic and extrinsic vascular supply to the tendon. In type II injuries, which are the most common type of FDP avulsions, the FDP tendon retracts to the level of the proximal interphalangeal (PIP) joint. Although the VBP is disrupted in this scenario, the VLP remains preserved because it arises at the level of the volar plate of the PIP joint. Type III lesions involve tendon avulsions with an associated bony fragment that is typically sufficiently large to not pass through the flexor sheath, thus limiting retraction to the level of the A4 pulley. Both vincula remain intact, given that the VBP originates at the distal portion of the middle phalanx. The Leddy and Packer classification was later expanded to include type IV and V injury patterns, which are less common than other injury patterns. Similar to type III injuries, type IV injuries involve a bony avulsion; however, the FDP subsequently ruptures from this fragment and the tendon subsequently retracts into the finger or palm.2,3 Type V injuries are more complex than other injury types because they involve a concomitant distal phalanx fracture with the FDP avulsion.4 Al-Qattan5 subclassified type V injuries into extra-articular (type Va) and intra-articular (type Vb) distal phalanx fractures on the basis of the distinct management of these 2 entities.
Numerous techniques have been proposed and described for the repair of FDP avulsion injuries. The pullout suture-dorsal button combination is the most widely described technique and was initially described by Bunnell.6 Unfortunately, this technique is accompanied by numerous potential postoperative complications.6 Nail plate deformity is the most commonly described complication. Other complications include local wound irritation, pain, button snagging, and repair failure. Additionally, the presence of external sutures creates a potential route of ingress for bacterial infection.
Continue to: Bone suture anchor techniques...
Bone suture anchor techniques were later utilized to repair FDP avulsions in an attempt to decrease complications associated with the external suture-button construct.7 The use of a transosseous suture without external button fixation has also been proposed. Sood and Elliot8 described a technique where the suture is passed through a hole, drilled transversely through the tuft of the distal phalanx, and affixed to the other limb. In 1999, Schultz and colleagues9 described a technique where transosseous tunnels are placed in the distal phalanx in a dorsal-to-volar direction. The suture is then passed through and tied on the dorsal surface. In this article, we propose a transosseous suture technique that may provide advantages over previously described methods.
SURGICAL TECHNIQUE
TYPES I, II, AND III
A Bruner incision is performed on the volar aspect of the affected finger, and full thickness flaps are elevated off the flexor sheath (Figures 1A-1C). 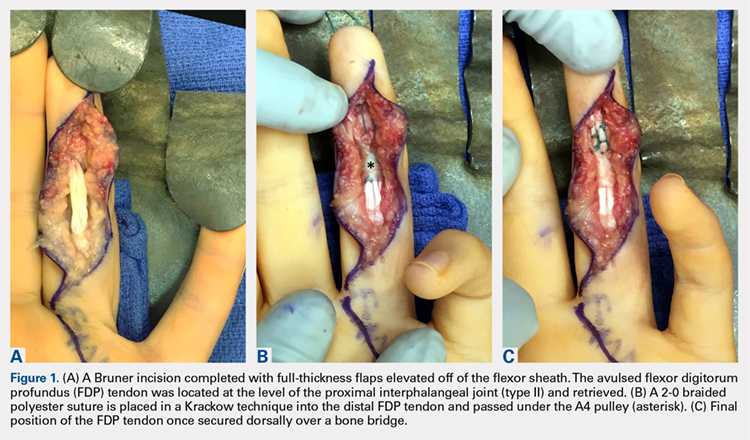
TYPES IV AND V
In cases of type IV or V injury (Figure 4A), a screw or plate construct is first used to allow for the successful reduction and fixation of the fracture (Figure 4B). 
DISCUSSION
The avulsion of the FDP tendon from its insertion (zone I) on the distal phalanx is commonly called “jersey finger” and is a well-described injury that occurs most commonly in the ring finger.10 These injuries can be difficult to treat and are associated with a complication rate of as high as 60%.11,12 Bunnell’s initial description of a suture passed through the fingernail and then tied over a polypropylene button has been associated with multiple complications. Kang and colleagues13 reported abnormal nail growth, nail fold necrosis, fingertip deformity, stiffness, infection, and amputation, 43% of all complications were directly related to the button. As an alternative to the button, sutures may be tied directly over the nail plate itself via 2 separate holes.14 While this technique eliminates the complications directly associated with the button, the potential for infection remains. Additionally, increased direct pressure is placed on the nail plate and nail bed, thus potentially increasing the risk of nail deformity.
In 1994, Hallock7 initially described the use of bone anchors as an “internal fixation” alternative and cited the “expense of the apparatus” as the major drawback of this technique. McCallister and colleagues15 compared the clinical outcome of suture anchor fixation with that of the button-over-nail technique. Although they ultimately demonstrated that the clinical outcomes of the 2 techniques are not significantly different, they noted that suture anchor fixation is associated with decreased infection rate (7% vs 0%) and time to return to work. Poor bone mineral density and low cortical thickness are correlated with anchor pull-out, thus limiting its universal use.16 Furthermore, the universal use of many commonly available anchors is limited given that they are too large to be accommodated within many phalanges, particularly in women and in the small and ring fingers.17 The use of microanchors rather than mini anchors not only decreases this risk but also decreases construct strength, thus necessitating the use of 2 anchors to restore adequate fixation strength. Anchor use is associated with specific risks, including the dorsal migration of the anchor, the osteolysis of the surrounding bone, as well as the perforation of the dorsal cortex and the possible extrusion of the anchor through the phalanx and into the nail bed.18,19 Additionally, in the wake of a changing healthcare system, the cost of suture anchors, as initially noted by Hallock,7 must be considered. This consideration is particularly relevant to the use of a 2 microanchor construct, which has been advocated given its biomechanical advantage.20,21
Continue to: Transosseous tendon repair...
Transosseous tendon repair is a cost-effective option that obviates many complications commonly observed with other fixation methods. By keeping the suture within the body, the complications inherent in external sutures and buttons are eliminated, including the loss of fixation as a result of button or suture damage and facilitating hand hygiene maintenance. The rate of infection is also reduced. Moreover, the risk of nail deformities is decreased because the suture is not passed through the nail bed and nail plate in the described technique. Occasionally, some patients do note irritation from the dorsal suture knot under the thin skin proximal to the germinal matrix. This can be easily addressed in the clinic by removing the knot under local anesthesia following sufficient tendon healing. Additionally, the described technique can be used safely in pediatric patients with open physes because the needles can be placed to prevent violating the physis. This technique can be performed in conjunction with the skeletal fixation of type III, IV, and V jersey fingers. In our experience, the transosseous suture repair is more secure than the limited screw fixation, which can be accomplished in many type III jersey fingers, and in at least 1 case, has maintained flexor function when the skeletal fixation of the jersey finger has failed (Figures 5A, 5B).

All internal fixation techniques have been described previously by Sood and Elliot8 and, later, by Schultz and colleagues.9 In contrast to Sood and Elliott’s8 technique, which requires the creation of transverse tunnels, a volar-to-dorsal tunnel is technically easy to create and creates a direct repair to tendon insertion. Our technique is similar to that of Schultz and colleagues'9 but has the following differences and potential improvements:
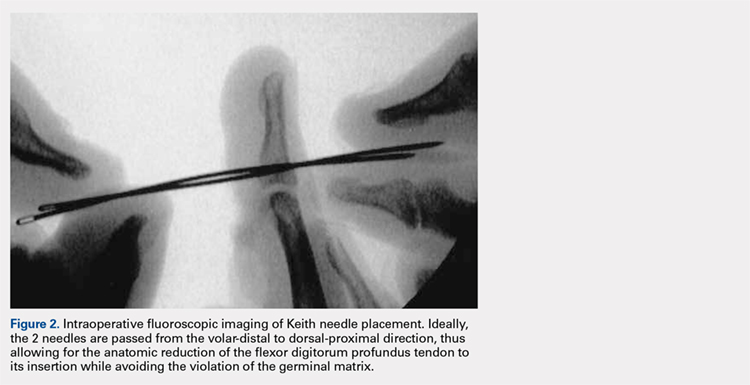
- Keith needles are passed in a volar-to-dorsal fashion, thus allowing for the direct visualization of the transosseous tunnel origin, minimizing the size of the transosseous tunnels, and allowing for the anatomic reduction of the tendon.
- Fluoroscopy is used to confirm wire placement prior to skin incision, thus enabling precise placement and potentially allowing the needles to be placed so as to avoid physeal injury in pediatric jersey fingers.
- By using Keith needles, sutures can be passed with the same instrument that created the tunnel, thus simplifying surgical technique.
- A Krakow suture technique is used. This technique results in less gapping and higher load-to-failure than other suturing techniques.22
- A 2-0 braided suture is used, therefore strengthening repair.
This paper will be judged for the Resident Writer’s Award.
1. Leddy JP, Packer JW. Avulsion of the profundus tendon insertion in athletes. J Hand Surg Am. 1977;2(1):66-69. doi:https://doi.org/10.1016/S0363-5023(77)80012-9.
2. Langa V, Posner MA. Unusual rupture of a flexor profundus tendon. J Hand Surg Am. 1986;11(2):227-229. doi:https://doi.org/10.1016/S0363-5023(86)80056-9.
3. Ehlert KJ, Gould JS, Black KP. A simultaneous distal phalanx avulsion fracture with profundus tendon avulsion: A case report and review of the literature. Clin Orthop Relat Res. 1992;(283):265-269.
4. Smith JH. Avulsion of a profundus tendon with simultaneous intraarticular fracture of the distal phalanx–case report. J Hand Surg Am. 1981;6(6):600-601. doi:10.1097/00006534-198305000-00081.
5. Al-Qattan MM. Type 5 avulsion of the insertion of the flexor digitorum profundus tendon. J Hand Surg Br. 2001;26(5):427-431. doi:10.1054/jhsb.2001.0619.
6. Bunnell S. Surgery of the hand, 2nd edition. Philadelphia, PA: JB Lippincott; 1948:381-466.
7. Hallock GG. The Mitek Mini GII anchor introduced for tendon reinsertion in the hand. Ann Plast Surg. 1994;33(2):211-213.
8. Sood MK, Elliot D. A new technique of attachment of flexor tendons to the distal phalanx without a button tie-over. J Hand Surg Br. 1996;21(5):629-632. doi:https://doi.org/10.1016/S0266-7681(96)80146-X.
9. Schultz RO, Drake DB, Morgan RF. A new technique for the treatment of flexor digitorum profundus tendon avulsion. Ann Plast Surg. 1999;42(1):46-48. doi:10.1097/00000637-199901000-00008.
10. Manske PR, Lesker PA. Avulsion of the ring finger flexor digitorum profundus tendon: An experimental study. Hand 1978;10(1):52-55. doi:https://doi.org/10.1016/S0072-968X(78)80025-4.
11. Gerbino PG, Saldana MJ, Westerbeck P, Schacherer TG. Complications experienced in the rehabilitation of zone I flexor tendon injuries with dynamic traction splinting. J Hand Surg Am. 1991;16(4):680-686. doi:https://doi.org/10.1016/0363-5023(91)90194-G
12. Evans RB. Zone I flexor tendon rehabilitation with limited extension and active flexion. J Hand Ther. 2005;18(2):128-140. doi:10.1197/j.jht.2005.02.001
13. Kang N, Marsh D, Dewar D. The morbidity of the button-over-nail technique for zone 1 flexor tendon repairs. Should we still be using this technique? J Hand Surg Eur Vol. 2008;33(5):566-570. doi:10.1177/1753193408090118
14. Taras JS. Flexor tendon reconstruction: Single stage flexor tendon grafting: FDP, FDS disrupted. In: Green DP, Hotchkiss RN, Pederson WL, Wolfe SW, eds. Green’s Operative Hand Surgery. 5th ed. Philadelphia, PA: Elsevier Health Sciences; 2005:248-249.
15. McCallister WV, Ambrose HC, Katolik LI, Trumble TE. Comparison of pullout button versus suture anchor for zone I flexor tendon repair. J Hand Surg Am. 2006;31:246-251. doi:10.1016/j.jhsa.2005.10.020
16. Matzsuzaki H, Zaegel MA, Gelberman RH, Silva MJ. Effect of suture material and bone quality on the mechanical properties of zone 1 flexor tendon-bone reattachment with bone anchors. J Hand Surg Am. 2008;33(5):709-717. doi:10.1016/j.jhsa.2008.01.025
17. Singh R, Kakarala G, Persaud I, Roberts M, Strandring S, Compson J. The optimal length of tissue anchors for distal phalanges. A study in 395 cadaver digits. J Bone Joint Surg Br. 2006;88-B(SUPP I):37.
18. Giannikas D, Athanaselis E, Matzaroglou C, Saridis A, Tyllianakis M. An unusual complication of Mitek suture anchor use in primary treatment of flexor digitorum profundus tendon laceration: a case report. Cases J. 2009;2:9319. doi:10.1186/1757-1626-2-9319
19. Tiong WH, O'Sullivan ST. Extrusion of bone anchor suture following flexor digitorum profundus tendon avulsion injury repair. J Plast Reconstr Aesthet Surg. 2011;64(9):1242-1244. doi:10.1016/j.bjps.2011.01.016
20. Silva MJ, Hollstien SB, Brodt MD, Boyer MI, Tetro AM, Gelberman RH. Flexor digitorum profundus tendon-to-bone repair: An ex vivo biomechanical analysis of 3 pullout suture techniques. J Hand Surg Am. 1998;23(1):120-126. doi:10.1016/S0363-5023(98)80099-3
21. Latendresse K, Dona E, Scougall PJ, Schreuder FB, Puchert E, Walsh WR. Cyclic testing of pullout sutures and micro-mitek suture anchors in flexor digitorum profundus tendon distal fixation. J Hand Surg Am. 2005;30(3):471-478. doi:10.1016/j.jhsa.2004.10.014
22. Lee SK, Fajardo M, Kardashian G, Klein J, Tsai P, Christoforou D. Repair of flexor digitorum profundus to distal phalanx: a biomechanical evaluation of four techniques. J Hand Surg Am. 2011;36(10):1604-1609. doi:10.1016/j.jhsa.2011.07.017
ABSTRACT
The avulsion of the flexor digitorum profundus from its insertion, or “jersey finger,” is a relatively common injury. Numerous modifications have been made to the classification and treatment of this injury since its initial description. We describe a novel variation of the surgical management of jersey finger.
The avulsion-type injury of the flexor digitorum profundus (FDP) from its insertion on the distal phalanx is relatively common. FDP avulsions are seen in athletes and nonathletes, and are the result of the sudden hyperextension of the distal interphalangeal joint during active flexion. These injuries usually occur while grasping the jersey of an opposing player and are thus commonly referred to as “jersey finger.” Initially described in 1977 by Leddy and Packer1, FDP avulsions are classified on the basis of the proximal extent of the retraction of the FDP and the presence or absence of a bony avulsion fracture fragment. Type I injuries are defined by tendon retraction to the level of the palm, where it is tethered by the lumbricals. At this level, the vinculum longus profundus (VLP) and vinculum brevis profundus (VBP) are ruptured, resulting in the substantial loss of intrinsic and extrinsic vascular supply to the tendon. In type II injuries, which are the most common type of FDP avulsions, the FDP tendon retracts to the level of the proximal interphalangeal (PIP) joint. Although the VBP is disrupted in this scenario, the VLP remains preserved because it arises at the level of the volar plate of the PIP joint. Type III lesions involve tendon avulsions with an associated bony fragment that is typically sufficiently large to not pass through the flexor sheath, thus limiting retraction to the level of the A4 pulley. Both vincula remain intact, given that the VBP originates at the distal portion of the middle phalanx. The Leddy and Packer classification was later expanded to include type IV and V injury patterns, which are less common than other injury patterns. Similar to type III injuries, type IV injuries involve a bony avulsion; however, the FDP subsequently ruptures from this fragment and the tendon subsequently retracts into the finger or palm.2,3 Type V injuries are more complex than other injury types because they involve a concomitant distal phalanx fracture with the FDP avulsion.4 Al-Qattan5 subclassified type V injuries into extra-articular (type Va) and intra-articular (type Vb) distal phalanx fractures on the basis of the distinct management of these 2 entities.
Numerous techniques have been proposed and described for the repair of FDP avulsion injuries. The pullout suture-dorsal button combination is the most widely described technique and was initially described by Bunnell.6 Unfortunately, this technique is accompanied by numerous potential postoperative complications.6 Nail plate deformity is the most commonly described complication. Other complications include local wound irritation, pain, button snagging, and repair failure. Additionally, the presence of external sutures creates a potential route of ingress for bacterial infection.
Continue to: Bone suture anchor techniques...
Bone suture anchor techniques were later utilized to repair FDP avulsions in an attempt to decrease complications associated with the external suture-button construct.7 The use of a transosseous suture without external button fixation has also been proposed. Sood and Elliot8 described a technique where the suture is passed through a hole, drilled transversely through the tuft of the distal phalanx, and affixed to the other limb. In 1999, Schultz and colleagues9 described a technique where transosseous tunnels are placed in the distal phalanx in a dorsal-to-volar direction. The suture is then passed through and tied on the dorsal surface. In this article, we propose a transosseous suture technique that may provide advantages over previously described methods.
SURGICAL TECHNIQUE
TYPES I, II, AND III
A Bruner incision is performed on the volar aspect of the affected finger, and full thickness flaps are elevated off the flexor sheath (Figures 1A-1C).
TYPES IV AND V
In cases of type IV or V injury (Figure 4A), a screw or plate construct is first used to allow for the successful reduction and fixation of the fracture (Figure 4B).
DISCUSSION
The avulsion of the FDP tendon from its insertion (zone I) on the distal phalanx is commonly called “jersey finger” and is a well-described injury that occurs most commonly in the ring finger.10 These injuries can be difficult to treat and are associated with a complication rate of as high as 60%.11,12 Bunnell’s initial description of a suture passed through the fingernail and then tied over a polypropylene button has been associated with multiple complications. Kang and colleagues13 reported abnormal nail growth, nail fold necrosis, fingertip deformity, stiffness, infection, and amputation, 43% of all complications were directly related to the button. As an alternative to the button, sutures may be tied directly over the nail plate itself via 2 separate holes.14 While this technique eliminates the complications directly associated with the button, the potential for infection remains. Additionally, increased direct pressure is placed on the nail plate and nail bed, thus potentially increasing the risk of nail deformity.
In 1994, Hallock7 initially described the use of bone anchors as an “internal fixation” alternative and cited the “expense of the apparatus” as the major drawback of this technique. McCallister and colleagues15 compared the clinical outcome of suture anchor fixation with that of the button-over-nail technique. Although they ultimately demonstrated that the clinical outcomes of the 2 techniques are not significantly different, they noted that suture anchor fixation is associated with decreased infection rate (7% vs 0%) and time to return to work. Poor bone mineral density and low cortical thickness are correlated with anchor pull-out, thus limiting its universal use.16 Furthermore, the universal use of many commonly available anchors is limited given that they are too large to be accommodated within many phalanges, particularly in women and in the small and ring fingers.17 The use of microanchors rather than mini anchors not only decreases this risk but also decreases construct strength, thus necessitating the use of 2 anchors to restore adequate fixation strength. Anchor use is associated with specific risks, including the dorsal migration of the anchor, the osteolysis of the surrounding bone, as well as the perforation of the dorsal cortex and the possible extrusion of the anchor through the phalanx and into the nail bed.18,19 Additionally, in the wake of a changing healthcare system, the cost of suture anchors, as initially noted by Hallock,7 must be considered. This consideration is particularly relevant to the use of a 2 microanchor construct, which has been advocated given its biomechanical advantage.20,21
Continue to: Transosseous tendon repair...
Transosseous tendon repair is a cost-effective option that obviates many complications commonly observed with other fixation methods. By keeping the suture within the body, the complications inherent in external sutures and buttons are eliminated, including the loss of fixation as a result of button or suture damage and facilitating hand hygiene maintenance. The rate of infection is also reduced. Moreover, the risk of nail deformities is decreased because the suture is not passed through the nail bed and nail plate in the described technique. Occasionally, some patients do note irritation from the dorsal suture knot under the thin skin proximal to the germinal matrix. This can be easily addressed in the clinic by removing the knot under local anesthesia following sufficient tendon healing. Additionally, the described technique can be used safely in pediatric patients with open physes because the needles can be placed to prevent violating the physis. This technique can be performed in conjunction with the skeletal fixation of type III, IV, and V jersey fingers. In our experience, the transosseous suture repair is more secure than the limited screw fixation, which can be accomplished in many type III jersey fingers, and in at least 1 case, has maintained flexor function when the skeletal fixation of the jersey finger has failed (Figures 5A, 5B).
All internal fixation techniques have been described previously by Sood and Elliot8 and, later, by Schultz and colleagues.9 In contrast to Sood and Elliott’s8 technique, which requires the creation of transverse tunnels, a volar-to-dorsal tunnel is technically easy to create and creates a direct repair to tendon insertion. Our technique is similar to that of Schultz and colleagues'9 but has the following differences and potential improvements:
- Keith needles are passed in a volar-to-dorsal fashion, thus allowing for the direct visualization of the transosseous tunnel origin, minimizing the size of the transosseous tunnels, and allowing for the anatomic reduction of the tendon.
- Fluoroscopy is used to confirm wire placement prior to skin incision, thus enabling precise placement and potentially allowing the needles to be placed so as to avoid physeal injury in pediatric jersey fingers.
- By using Keith needles, sutures can be passed with the same instrument that created the tunnel, thus simplifying surgical technique.
- A Krakow suture technique is used. This technique results in less gapping and higher load-to-failure than other suturing techniques.22
- A 2-0 braided suture is used, therefore strengthening repair.
This paper will be judged for the Resident Writer’s Award.
ABSTRACT
The avulsion of the flexor digitorum profundus from its insertion, or “jersey finger,” is a relatively common injury. Numerous modifications have been made to the classification and treatment of this injury since its initial description. We describe a novel variation of the surgical management of jersey finger.
The avulsion-type injury of the flexor digitorum profundus (FDP) from its insertion on the distal phalanx is relatively common. FDP avulsions are seen in athletes and nonathletes, and are the result of the sudden hyperextension of the distal interphalangeal joint during active flexion. These injuries usually occur while grasping the jersey of an opposing player and are thus commonly referred to as “jersey finger.” Initially described in 1977 by Leddy and Packer1, FDP avulsions are classified on the basis of the proximal extent of the retraction of the FDP and the presence or absence of a bony avulsion fracture fragment. Type I injuries are defined by tendon retraction to the level of the palm, where it is tethered by the lumbricals. At this level, the vinculum longus profundus (VLP) and vinculum brevis profundus (VBP) are ruptured, resulting in the substantial loss of intrinsic and extrinsic vascular supply to the tendon. In type II injuries, which are the most common type of FDP avulsions, the FDP tendon retracts to the level of the proximal interphalangeal (PIP) joint. Although the VBP is disrupted in this scenario, the VLP remains preserved because it arises at the level of the volar plate of the PIP joint. Type III lesions involve tendon avulsions with an associated bony fragment that is typically sufficiently large to not pass through the flexor sheath, thus limiting retraction to the level of the A4 pulley. Both vincula remain intact, given that the VBP originates at the distal portion of the middle phalanx. The Leddy and Packer classification was later expanded to include type IV and V injury patterns, which are less common than other injury patterns. Similar to type III injuries, type IV injuries involve a bony avulsion; however, the FDP subsequently ruptures from this fragment and the tendon subsequently retracts into the finger or palm.2,3 Type V injuries are more complex than other injury types because they involve a concomitant distal phalanx fracture with the FDP avulsion.4 Al-Qattan5 subclassified type V injuries into extra-articular (type Va) and intra-articular (type Vb) distal phalanx fractures on the basis of the distinct management of these 2 entities.
Numerous techniques have been proposed and described for the repair of FDP avulsion injuries. The pullout suture-dorsal button combination is the most widely described technique and was initially described by Bunnell.6 Unfortunately, this technique is accompanied by numerous potential postoperative complications.6 Nail plate deformity is the most commonly described complication. Other complications include local wound irritation, pain, button snagging, and repair failure. Additionally, the presence of external sutures creates a potential route of ingress for bacterial infection.
Continue to: Bone suture anchor techniques...
Bone suture anchor techniques were later utilized to repair FDP avulsions in an attempt to decrease complications associated with the external suture-button construct.7 The use of a transosseous suture without external button fixation has also been proposed. Sood and Elliot8 described a technique where the suture is passed through a hole, drilled transversely through the tuft of the distal phalanx, and affixed to the other limb. In 1999, Schultz and colleagues9 described a technique where transosseous tunnels are placed in the distal phalanx in a dorsal-to-volar direction. The suture is then passed through and tied on the dorsal surface. In this article, we propose a transosseous suture technique that may provide advantages over previously described methods.
SURGICAL TECHNIQUE
TYPES I, II, AND III
A Bruner incision is performed on the volar aspect of the affected finger, and full thickness flaps are elevated off the flexor sheath (Figures 1A-1C).
TYPES IV AND V
In cases of type IV or V injury (Figure 4A), a screw or plate construct is first used to allow for the successful reduction and fixation of the fracture (Figure 4B).
DISCUSSION
The avulsion of the FDP tendon from its insertion (zone I) on the distal phalanx is commonly called “jersey finger” and is a well-described injury that occurs most commonly in the ring finger.10 These injuries can be difficult to treat and are associated with a complication rate of as high as 60%.11,12 Bunnell’s initial description of a suture passed through the fingernail and then tied over a polypropylene button has been associated with multiple complications. Kang and colleagues13 reported abnormal nail growth, nail fold necrosis, fingertip deformity, stiffness, infection, and amputation, 43% of all complications were directly related to the button. As an alternative to the button, sutures may be tied directly over the nail plate itself via 2 separate holes.14 While this technique eliminates the complications directly associated with the button, the potential for infection remains. Additionally, increased direct pressure is placed on the nail plate and nail bed, thus potentially increasing the risk of nail deformity.
In 1994, Hallock7 initially described the use of bone anchors as an “internal fixation” alternative and cited the “expense of the apparatus” as the major drawback of this technique. McCallister and colleagues15 compared the clinical outcome of suture anchor fixation with that of the button-over-nail technique. Although they ultimately demonstrated that the clinical outcomes of the 2 techniques are not significantly different, they noted that suture anchor fixation is associated with decreased infection rate (7% vs 0%) and time to return to work. Poor bone mineral density and low cortical thickness are correlated with anchor pull-out, thus limiting its universal use.16 Furthermore, the universal use of many commonly available anchors is limited given that they are too large to be accommodated within many phalanges, particularly in women and in the small and ring fingers.17 The use of microanchors rather than mini anchors not only decreases this risk but also decreases construct strength, thus necessitating the use of 2 anchors to restore adequate fixation strength. Anchor use is associated with specific risks, including the dorsal migration of the anchor, the osteolysis of the surrounding bone, as well as the perforation of the dorsal cortex and the possible extrusion of the anchor through the phalanx and into the nail bed.18,19 Additionally, in the wake of a changing healthcare system, the cost of suture anchors, as initially noted by Hallock,7 must be considered. This consideration is particularly relevant to the use of a 2 microanchor construct, which has been advocated given its biomechanical advantage.20,21
Continue to: Transosseous tendon repair...
Transosseous tendon repair is a cost-effective option that obviates many complications commonly observed with other fixation methods. By keeping the suture within the body, the complications inherent in external sutures and buttons are eliminated, including the loss of fixation as a result of button or suture damage and facilitating hand hygiene maintenance. The rate of infection is also reduced. Moreover, the risk of nail deformities is decreased because the suture is not passed through the nail bed and nail plate in the described technique. Occasionally, some patients do note irritation from the dorsal suture knot under the thin skin proximal to the germinal matrix. This can be easily addressed in the clinic by removing the knot under local anesthesia following sufficient tendon healing. Additionally, the described technique can be used safely in pediatric patients with open physes because the needles can be placed to prevent violating the physis. This technique can be performed in conjunction with the skeletal fixation of type III, IV, and V jersey fingers. In our experience, the transosseous suture repair is more secure than the limited screw fixation, which can be accomplished in many type III jersey fingers, and in at least 1 case, has maintained flexor function when the skeletal fixation of the jersey finger has failed (Figures 5A, 5B).
All internal fixation techniques have been described previously by Sood and Elliot8 and, later, by Schultz and colleagues.9 In contrast to Sood and Elliott’s8 technique, which requires the creation of transverse tunnels, a volar-to-dorsal tunnel is technically easy to create and creates a direct repair to tendon insertion. Our technique is similar to that of Schultz and colleagues'9 but has the following differences and potential improvements:
- Keith needles are passed in a volar-to-dorsal fashion, thus allowing for the direct visualization of the transosseous tunnel origin, minimizing the size of the transosseous tunnels, and allowing for the anatomic reduction of the tendon.
- Fluoroscopy is used to confirm wire placement prior to skin incision, thus enabling precise placement and potentially allowing the needles to be placed so as to avoid physeal injury in pediatric jersey fingers.
- By using Keith needles, sutures can be passed with the same instrument that created the tunnel, thus simplifying surgical technique.
- A Krakow suture technique is used. This technique results in less gapping and higher load-to-failure than other suturing techniques.22
- A 2-0 braided suture is used, therefore strengthening repair.
This paper will be judged for the Resident Writer’s Award.
1. Leddy JP, Packer JW. Avulsion of the profundus tendon insertion in athletes. J Hand Surg Am. 1977;2(1):66-69. doi:https://doi.org/10.1016/S0363-5023(77)80012-9.
2. Langa V, Posner MA. Unusual rupture of a flexor profundus tendon. J Hand Surg Am. 1986;11(2):227-229. doi:https://doi.org/10.1016/S0363-5023(86)80056-9.
3. Ehlert KJ, Gould JS, Black KP. A simultaneous distal phalanx avulsion fracture with profundus tendon avulsion: A case report and review of the literature. Clin Orthop Relat Res. 1992;(283):265-269.
4. Smith JH. Avulsion of a profundus tendon with simultaneous intraarticular fracture of the distal phalanx–case report. J Hand Surg Am. 1981;6(6):600-601. doi:10.1097/00006534-198305000-00081.
5. Al-Qattan MM. Type 5 avulsion of the insertion of the flexor digitorum profundus tendon. J Hand Surg Br. 2001;26(5):427-431. doi:10.1054/jhsb.2001.0619.
6. Bunnell S. Surgery of the hand, 2nd edition. Philadelphia, PA: JB Lippincott; 1948:381-466.
7. Hallock GG. The Mitek Mini GII anchor introduced for tendon reinsertion in the hand. Ann Plast Surg. 1994;33(2):211-213.
8. Sood MK, Elliot D. A new technique of attachment of flexor tendons to the distal phalanx without a button tie-over. J Hand Surg Br. 1996;21(5):629-632. doi:https://doi.org/10.1016/S0266-7681(96)80146-X.
9. Schultz RO, Drake DB, Morgan RF. A new technique for the treatment of flexor digitorum profundus tendon avulsion. Ann Plast Surg. 1999;42(1):46-48. doi:10.1097/00000637-199901000-00008.
10. Manske PR, Lesker PA. Avulsion of the ring finger flexor digitorum profundus tendon: An experimental study. Hand 1978;10(1):52-55. doi:https://doi.org/10.1016/S0072-968X(78)80025-4.
11. Gerbino PG, Saldana MJ, Westerbeck P, Schacherer TG. Complications experienced in the rehabilitation of zone I flexor tendon injuries with dynamic traction splinting. J Hand Surg Am. 1991;16(4):680-686. doi:https://doi.org/10.1016/0363-5023(91)90194-G
12. Evans RB. Zone I flexor tendon rehabilitation with limited extension and active flexion. J Hand Ther. 2005;18(2):128-140. doi:10.1197/j.jht.2005.02.001
13. Kang N, Marsh D, Dewar D. The morbidity of the button-over-nail technique for zone 1 flexor tendon repairs. Should we still be using this technique? J Hand Surg Eur Vol. 2008;33(5):566-570. doi:10.1177/1753193408090118
14. Taras JS. Flexor tendon reconstruction: Single stage flexor tendon grafting: FDP, FDS disrupted. In: Green DP, Hotchkiss RN, Pederson WL, Wolfe SW, eds. Green’s Operative Hand Surgery. 5th ed. Philadelphia, PA: Elsevier Health Sciences; 2005:248-249.
15. McCallister WV, Ambrose HC, Katolik LI, Trumble TE. Comparison of pullout button versus suture anchor for zone I flexor tendon repair. J Hand Surg Am. 2006;31:246-251. doi:10.1016/j.jhsa.2005.10.020
16. Matzsuzaki H, Zaegel MA, Gelberman RH, Silva MJ. Effect of suture material and bone quality on the mechanical properties of zone 1 flexor tendon-bone reattachment with bone anchors. J Hand Surg Am. 2008;33(5):709-717. doi:10.1016/j.jhsa.2008.01.025
17. Singh R, Kakarala G, Persaud I, Roberts M, Strandring S, Compson J. The optimal length of tissue anchors for distal phalanges. A study in 395 cadaver digits. J Bone Joint Surg Br. 2006;88-B(SUPP I):37.
18. Giannikas D, Athanaselis E, Matzaroglou C, Saridis A, Tyllianakis M. An unusual complication of Mitek suture anchor use in primary treatment of flexor digitorum profundus tendon laceration: a case report. Cases J. 2009;2:9319. doi:10.1186/1757-1626-2-9319
19. Tiong WH, O'Sullivan ST. Extrusion of bone anchor suture following flexor digitorum profundus tendon avulsion injury repair. J Plast Reconstr Aesthet Surg. 2011;64(9):1242-1244. doi:10.1016/j.bjps.2011.01.016
20. Silva MJ, Hollstien SB, Brodt MD, Boyer MI, Tetro AM, Gelberman RH. Flexor digitorum profundus tendon-to-bone repair: An ex vivo biomechanical analysis of 3 pullout suture techniques. J Hand Surg Am. 1998;23(1):120-126. doi:10.1016/S0363-5023(98)80099-3
21. Latendresse K, Dona E, Scougall PJ, Schreuder FB, Puchert E, Walsh WR. Cyclic testing of pullout sutures and micro-mitek suture anchors in flexor digitorum profundus tendon distal fixation. J Hand Surg Am. 2005;30(3):471-478. doi:10.1016/j.jhsa.2004.10.014
22. Lee SK, Fajardo M, Kardashian G, Klein J, Tsai P, Christoforou D. Repair of flexor digitorum profundus to distal phalanx: a biomechanical evaluation of four techniques. J Hand Surg Am. 2011;36(10):1604-1609. doi:10.1016/j.jhsa.2011.07.017
1. Leddy JP, Packer JW. Avulsion of the profundus tendon insertion in athletes. J Hand Surg Am. 1977;2(1):66-69. doi:https://doi.org/10.1016/S0363-5023(77)80012-9.
2. Langa V, Posner MA. Unusual rupture of a flexor profundus tendon. J Hand Surg Am. 1986;11(2):227-229. doi:https://doi.org/10.1016/S0363-5023(86)80056-9.
3. Ehlert KJ, Gould JS, Black KP. A simultaneous distal phalanx avulsion fracture with profundus tendon avulsion: A case report and review of the literature. Clin Orthop Relat Res. 1992;(283):265-269.
4. Smith JH. Avulsion of a profundus tendon with simultaneous intraarticular fracture of the distal phalanx–case report. J Hand Surg Am. 1981;6(6):600-601. doi:10.1097/00006534-198305000-00081.
5. Al-Qattan MM. Type 5 avulsion of the insertion of the flexor digitorum profundus tendon. J Hand Surg Br. 2001;26(5):427-431. doi:10.1054/jhsb.2001.0619.
6. Bunnell S. Surgery of the hand, 2nd edition. Philadelphia, PA: JB Lippincott; 1948:381-466.
7. Hallock GG. The Mitek Mini GII anchor introduced for tendon reinsertion in the hand. Ann Plast Surg. 1994;33(2):211-213.
8. Sood MK, Elliot D. A new technique of attachment of flexor tendons to the distal phalanx without a button tie-over. J Hand Surg Br. 1996;21(5):629-632. doi:https://doi.org/10.1016/S0266-7681(96)80146-X.
9. Schultz RO, Drake DB, Morgan RF. A new technique for the treatment of flexor digitorum profundus tendon avulsion. Ann Plast Surg. 1999;42(1):46-48. doi:10.1097/00000637-199901000-00008.
10. Manske PR, Lesker PA. Avulsion of the ring finger flexor digitorum profundus tendon: An experimental study. Hand 1978;10(1):52-55. doi:https://doi.org/10.1016/S0072-968X(78)80025-4.
11. Gerbino PG, Saldana MJ, Westerbeck P, Schacherer TG. Complications experienced in the rehabilitation of zone I flexor tendon injuries with dynamic traction splinting. J Hand Surg Am. 1991;16(4):680-686. doi:https://doi.org/10.1016/0363-5023(91)90194-G
12. Evans RB. Zone I flexor tendon rehabilitation with limited extension and active flexion. J Hand Ther. 2005;18(2):128-140. doi:10.1197/j.jht.2005.02.001
13. Kang N, Marsh D, Dewar D. The morbidity of the button-over-nail technique for zone 1 flexor tendon repairs. Should we still be using this technique? J Hand Surg Eur Vol. 2008;33(5):566-570. doi:10.1177/1753193408090118
14. Taras JS. Flexor tendon reconstruction: Single stage flexor tendon grafting: FDP, FDS disrupted. In: Green DP, Hotchkiss RN, Pederson WL, Wolfe SW, eds. Green’s Operative Hand Surgery. 5th ed. Philadelphia, PA: Elsevier Health Sciences; 2005:248-249.
15. McCallister WV, Ambrose HC, Katolik LI, Trumble TE. Comparison of pullout button versus suture anchor for zone I flexor tendon repair. J Hand Surg Am. 2006;31:246-251. doi:10.1016/j.jhsa.2005.10.020
16. Matzsuzaki H, Zaegel MA, Gelberman RH, Silva MJ. Effect of suture material and bone quality on the mechanical properties of zone 1 flexor tendon-bone reattachment with bone anchors. J Hand Surg Am. 2008;33(5):709-717. doi:10.1016/j.jhsa.2008.01.025
17. Singh R, Kakarala G, Persaud I, Roberts M, Strandring S, Compson J. The optimal length of tissue anchors for distal phalanges. A study in 395 cadaver digits. J Bone Joint Surg Br. 2006;88-B(SUPP I):37.
18. Giannikas D, Athanaselis E, Matzaroglou C, Saridis A, Tyllianakis M. An unusual complication of Mitek suture anchor use in primary treatment of flexor digitorum profundus tendon laceration: a case report. Cases J. 2009;2:9319. doi:10.1186/1757-1626-2-9319
19. Tiong WH, O'Sullivan ST. Extrusion of bone anchor suture following flexor digitorum profundus tendon avulsion injury repair. J Plast Reconstr Aesthet Surg. 2011;64(9):1242-1244. doi:10.1016/j.bjps.2011.01.016
20. Silva MJ, Hollstien SB, Brodt MD, Boyer MI, Tetro AM, Gelberman RH. Flexor digitorum profundus tendon-to-bone repair: An ex vivo biomechanical analysis of 3 pullout suture techniques. J Hand Surg Am. 1998;23(1):120-126. doi:10.1016/S0363-5023(98)80099-3
21. Latendresse K, Dona E, Scougall PJ, Schreuder FB, Puchert E, Walsh WR. Cyclic testing of pullout sutures and micro-mitek suture anchors in flexor digitorum profundus tendon distal fixation. J Hand Surg Am. 2005;30(3):471-478. doi:10.1016/j.jhsa.2004.10.014
22. Lee SK, Fajardo M, Kardashian G, Klein J, Tsai P, Christoforou D. Repair of flexor digitorum profundus to distal phalanx: a biomechanical evaluation of four techniques. J Hand Surg Am. 2011;36(10):1604-1609. doi:10.1016/j.jhsa.2011.07.017
TAKE-HOME POINTS
- Transosseous repair of FDP has been long utilized, tying the sutures over a polyethylene button at the nail plate, which is associated with significant complications.
- Avoiding use of a button decreases these complications, eliminating damage to the nailbed and eliminating external sutures, thus decreasing infection risk.
- Keith needles can be utilized to pass the sutures from volar to dorsal, and can be inserted using a wire drive; their position can be checked fluoroscopically prior to suture passage.
- This technique can be used in conjunction with skeletal fixation of associated fractures.
- This technique can be utilized in pediatric patients, placing the sutures distal to the physis.

Cochrane report: HPV vaccine proves its worth in adolescent, young adult women
Two currently available human papillomavirus vaccines protect adolescents and young adult women without previous HPV disease from developing precancerous cervical lesions, according to data from more than 70,000 women followed for 8 years.
In a review published online by the Cochrane Library, Marc Arbyn, MD, of the Belgian Cancer Centre, Brussels, and his colleagues examined the effectiveness of two vaccines that target the HPV types 16 and 18, which account for most cases of cervical cancer. The researchers focused on the bivalent vaccine for HPV16 and HPV18 and the quadrivalent vaccine for HPV16, HPV18, and two additional HPV types associated with genital warts (HPV6 and HPV11). The review did not include data on the latest vaccine targeting nine HPV types because it has not been studied in a randomized, placebo-controlled trial.
The review comprised 26 studies and 73,428 women aged 15-45 years. The vaccine was most effective for young women aged 15-26 years.
The risk of serious adverse events was approximately 7% in control groups and vaccine groups across all ages (669 per 10,000 vs. 656 per 10,000, respectively). The mortality rate was 11 per 10,000 in control groups, compared with 14 per 10,000 in vaccine groups. The overall mortality was low, and no deaths reported in the studies were vaccine related, the researchers said, although mortality was greater in the vaccine groups among women older than 25 years.
The overall risk for precancerous lesions was not significantly different for women vaccinated between age 24 and 45 years versus unvaccinated women. However, the researchers found that the vaccines reduced the risk of precancerous lesions for HPV type 16 and 18 from 45 per 10, 000 to 14 per 10,000 in women aged 24 years and older who were previously negative for HPV 16 and 18.
The researchers found no significant impact on miscarriage rates, but they noted the need for additional research to examine the possible impact of vaccination on stillbirth and birth defects in children born to women who were vaccinated during pregnancy.
Several of the researchers received travel grants from GlaxoSmithKline or MSD-Sanofi-Pasteur.
SOURCE: Arbyn M et al. Cochrane Database Syst Rev. 2018. doi: 10.1002/14651858.CD009069.pub3.
Two currently available human papillomavirus vaccines protect adolescents and young adult women without previous HPV disease from developing precancerous cervical lesions, according to data from more than 70,000 women followed for 8 years.
In a review published online by the Cochrane Library, Marc Arbyn, MD, of the Belgian Cancer Centre, Brussels, and his colleagues examined the effectiveness of two vaccines that target the HPV types 16 and 18, which account for most cases of cervical cancer. The researchers focused on the bivalent vaccine for HPV16 and HPV18 and the quadrivalent vaccine for HPV16, HPV18, and two additional HPV types associated with genital warts (HPV6 and HPV11). The review did not include data on the latest vaccine targeting nine HPV types because it has not been studied in a randomized, placebo-controlled trial.
The review comprised 26 studies and 73,428 women aged 15-45 years. The vaccine was most effective for young women aged 15-26 years.
The risk of serious adverse events was approximately 7% in control groups and vaccine groups across all ages (669 per 10,000 vs. 656 per 10,000, respectively). The mortality rate was 11 per 10,000 in control groups, compared with 14 per 10,000 in vaccine groups. The overall mortality was low, and no deaths reported in the studies were vaccine related, the researchers said, although mortality was greater in the vaccine groups among women older than 25 years.
The overall risk for precancerous lesions was not significantly different for women vaccinated between age 24 and 45 years versus unvaccinated women. However, the researchers found that the vaccines reduced the risk of precancerous lesions for HPV type 16 and 18 from 45 per 10, 000 to 14 per 10,000 in women aged 24 years and older who were previously negative for HPV 16 and 18.
The researchers found no significant impact on miscarriage rates, but they noted the need for additional research to examine the possible impact of vaccination on stillbirth and birth defects in children born to women who were vaccinated during pregnancy.
Several of the researchers received travel grants from GlaxoSmithKline or MSD-Sanofi-Pasteur.
SOURCE: Arbyn M et al. Cochrane Database Syst Rev. 2018. doi: 10.1002/14651858.CD009069.pub3.
Two currently available human papillomavirus vaccines protect adolescents and young adult women without previous HPV disease from developing precancerous cervical lesions, according to data from more than 70,000 women followed for 8 years.
In a review published online by the Cochrane Library, Marc Arbyn, MD, of the Belgian Cancer Centre, Brussels, and his colleagues examined the effectiveness of two vaccines that target the HPV types 16 and 18, which account for most cases of cervical cancer. The researchers focused on the bivalent vaccine for HPV16 and HPV18 and the quadrivalent vaccine for HPV16, HPV18, and two additional HPV types associated with genital warts (HPV6 and HPV11). The review did not include data on the latest vaccine targeting nine HPV types because it has not been studied in a randomized, placebo-controlled trial.
The review comprised 26 studies and 73,428 women aged 15-45 years. The vaccine was most effective for young women aged 15-26 years.
The risk of serious adverse events was approximately 7% in control groups and vaccine groups across all ages (669 per 10,000 vs. 656 per 10,000, respectively). The mortality rate was 11 per 10,000 in control groups, compared with 14 per 10,000 in vaccine groups. The overall mortality was low, and no deaths reported in the studies were vaccine related, the researchers said, although mortality was greater in the vaccine groups among women older than 25 years.
The overall risk for precancerous lesions was not significantly different for women vaccinated between age 24 and 45 years versus unvaccinated women. However, the researchers found that the vaccines reduced the risk of precancerous lesions for HPV type 16 and 18 from 45 per 10, 000 to 14 per 10,000 in women aged 24 years and older who were previously negative for HPV 16 and 18.
The researchers found no significant impact on miscarriage rates, but they noted the need for additional research to examine the possible impact of vaccination on stillbirth and birth defects in children born to women who were vaccinated during pregnancy.
Several of the researchers received travel grants from GlaxoSmithKline or MSD-Sanofi-Pasteur.
SOURCE: Arbyn M et al. Cochrane Database Syst Rev. 2018. doi: 10.1002/14651858.CD009069.pub3.
FROM THE COCHRANE LIBRARY
Key clinical point:
Major finding: The vaccines reduced the risk of precancer caused by HPV16 and HPV18 from 341 per 10,000 to 157 per 10,000 (RR, 0.46).
Study details: The review was based on data from 26 studies including 73,428 women worldwide over 8 years.
Disclosures: The Cochrane Library sponsored the study. Several of the researchers received travel grants from GlaxoSmithKline or MSD-Sanofi-Pasteur.
Source: Arbyn M et al. Cochrane Database Syst Rev. 2018. doi: 10.1002/14651858.CD009069.pub3.
Interventionalists skeptical about public reporting of PCI
Many interventional cardiologists believe that public reporting of percutaneous coronary intervention (PCI) outcomes leads to avoidance of high-risk procedures and “purposeful upcoding of comorbidities by colleagues,” according to a survey of 149 interventionalists.
Almost 60% of respondents said that they were sometimes or often pressured by other physicians to not perform PCI on patients considered to be at high risk of death, and 95% believed that other interventionalists in their state – the survey was conducted in New York and Massachusetts – would sometimes or often avoid PCI because of “concern that a bad outcome would negatively impact their own or their facility’s publicly reported outcomes,” Daniel M. Blumenthal, MD, MBA, of Massachusetts General Hospital, Boston, and his associates said in an article published online May 9 in JAMA Cardiology.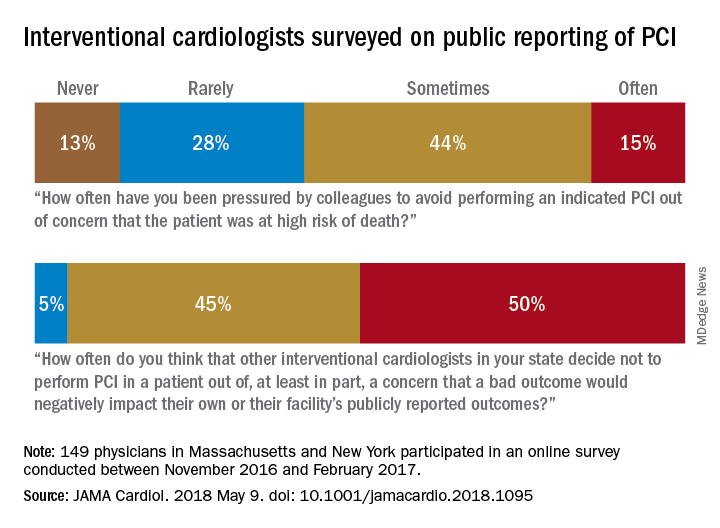
Almost two-thirds of participants said that they had avoided performing PCIs at least twice because they were worried about reporting a negative outcome, which “suggests that PCI avoidance is not concentrated among a few risk-averse interventionalists,” Dr. Blumenthal and his associates wrote.
Their study was supported by an unrestricted research grant from Abiomed to the Smith Center for Outcomes Research in Cardiology at Beth Israel Deaconess Medical Center. Dr. Blumenthal reported consulting fees and/or funding for unrelated work from Devoted Health, Novartis Pharmaceuticals, HLM Venture Partners, and Precision Health Economics.
SOURCE: Blumenthal DM et al. JAMA Cardiol. 2018 May 9. doi: 10.1001/jamacardio.2018.1095.
Many interventional cardiologists believe that public reporting of percutaneous coronary intervention (PCI) outcomes leads to avoidance of high-risk procedures and “purposeful upcoding of comorbidities by colleagues,” according to a survey of 149 interventionalists.
Almost 60% of respondents said that they were sometimes or often pressured by other physicians to not perform PCI on patients considered to be at high risk of death, and 95% believed that other interventionalists in their state – the survey was conducted in New York and Massachusetts – would sometimes or often avoid PCI because of “concern that a bad outcome would negatively impact their own or their facility’s publicly reported outcomes,” Daniel M. Blumenthal, MD, MBA, of Massachusetts General Hospital, Boston, and his associates said in an article published online May 9 in JAMA Cardiology.
Almost two-thirds of participants said that they had avoided performing PCIs at least twice because they were worried about reporting a negative outcome, which “suggests that PCI avoidance is not concentrated among a few risk-averse interventionalists,” Dr. Blumenthal and his associates wrote.
Their study was supported by an unrestricted research grant from Abiomed to the Smith Center for Outcomes Research in Cardiology at Beth Israel Deaconess Medical Center. Dr. Blumenthal reported consulting fees and/or funding for unrelated work from Devoted Health, Novartis Pharmaceuticals, HLM Venture Partners, and Precision Health Economics.
SOURCE: Blumenthal DM et al. JAMA Cardiol. 2018 May 9. doi: 10.1001/jamacardio.2018.1095.
Many interventional cardiologists believe that public reporting of percutaneous coronary intervention (PCI) outcomes leads to avoidance of high-risk procedures and “purposeful upcoding of comorbidities by colleagues,” according to a survey of 149 interventionalists.
Almost 60% of respondents said that they were sometimes or often pressured by other physicians to not perform PCI on patients considered to be at high risk of death, and 95% believed that other interventionalists in their state – the survey was conducted in New York and Massachusetts – would sometimes or often avoid PCI because of “concern that a bad outcome would negatively impact their own or their facility’s publicly reported outcomes,” Daniel M. Blumenthal, MD, MBA, of Massachusetts General Hospital, Boston, and his associates said in an article published online May 9 in JAMA Cardiology.
Almost two-thirds of participants said that they had avoided performing PCIs at least twice because they were worried about reporting a negative outcome, which “suggests that PCI avoidance is not concentrated among a few risk-averse interventionalists,” Dr. Blumenthal and his associates wrote.
Their study was supported by an unrestricted research grant from Abiomed to the Smith Center for Outcomes Research in Cardiology at Beth Israel Deaconess Medical Center. Dr. Blumenthal reported consulting fees and/or funding for unrelated work from Devoted Health, Novartis Pharmaceuticals, HLM Venture Partners, and Precision Health Economics.
SOURCE: Blumenthal DM et al. JAMA Cardiol. 2018 May 9. doi: 10.1001/jamacardio.2018.1095.
FROM JAMA CARDIOLOGY
Comorbidities provide possible path to schizophrenia subtypes
NEW YORK – Psychiatric disorders comorbid with schizophrenia often pose a diagnostic challenge, but they can be the key for improving outcomes when they are addressed along with the core schizophrenia symptoms, according to a workshop on treatment-refractory disease at the American Psychiatric Association annual meeting.
Looking for comorbidities such as depression, panic disorder, and obsessive-compulsive disorder (OCD) is important, because treatment directed at those conditions “can have a significant effect on the psychosis as well,” reported Jeffrey P. Kahn, MD, clinical associate professor of psychiatry, Cornell University, New York.
“Schizophrenia is a syndrome. It is a collection of symptoms, not a disease,” explained Michael Y. Hwang, MD, an attending physician at Veterans Affairs Hudson Valley Healthcare System, Montrose, N.Y. He believes that comorbid OCD, like comorbid panic disorder, might identify a subtype of schizophrenia that requires distinct therapeutic strategies.
The principle that schizophrenia represents a group of distinct illnesses with similar presentations is several decades old. Both Dr. Kahn and Dr. Hwang, who have published on this topic, acknowledged that efforts so far to identify those distinct diseases have failed. However, they suggested that the presence of comorbidities probably establishes clinically relevant subtypes.
Among psychiatric comorbidities, major depression is the most common, identified in more than half of patients with schizophrenia in some studies, according to Dr. Hwang. He reported that diagnostic criteria for OCD is met by about 12%, while Dr. Kahn estimated the prevalence of panic disorder in individuals with schizophrenia at about 20%.
In an individual with active positive symptoms of schizophrenia, isolating comorbid OCD or panic disorder often is a challenge. In older textbooks and guidelines on schizophrenia, comorbidities were not even discussed, Dr. Hwang said. Although the DSM-5 now acknowledges elevated rates of OCD and panic disorder in individuals with schizophrenia, Dr. Hwang and Dr. Kahn each indicated that the comorbidities still are not receiving adequate attention from clinicians.
“In general, individuals with schizophrenia who have comorbid OCD tend to do worse,” said Dr. Hwang, explaining the rationale for both looking for and treating OCD. He presented data from several studies, including his own, suggesting that symptoms of OCD can be improved with individualized pharmacotherapy. In addition to such considerations as the potential for interactions between OCD therapies and concurrent atypical antipsychotics, heterogeneity in response underlies the recommendation for individualized therapy. He added that in those with preserved executive functioning, cognitive-behavioral therapy “is always more helpful that pharmacotherapy alone.”
Comorbid panic disorder also can be difficult to recognize, particularly in individuals with active symptoms of schizophrenia, according to Dr. Kahn. . He advised against trivializing the importance of panic disorder symptoms.
“The tendency is to think, so what if the patient has symptoms of panic. Wouldn’t you if you had schizophrenia?” Dr. Kahn noted. However, identifying and then treating the panic has implications for better control of schizophrenia, he said. For the panic symptoms, there is evidence to suggest that clonazepam is effective, he said, but he advised a slow upward titration to avoid sedation and other risks that include addiction. He, like Dr. Hwang, also advised that the value of psychotherapy should not be underestimated.
“It is very important, particularly with outpatients, to spend time with that patient in order to build a therapeutic alliance and from there, progress to supportive psychotherapy,” Dr. Kahn said.
Dr. Kahn and Dr. Hwang reported no potential conflicts of interest related to this topic.
NEW YORK – Psychiatric disorders comorbid with schizophrenia often pose a diagnostic challenge, but they can be the key for improving outcomes when they are addressed along with the core schizophrenia symptoms, according to a workshop on treatment-refractory disease at the American Psychiatric Association annual meeting.
Looking for comorbidities such as depression, panic disorder, and obsessive-compulsive disorder (OCD) is important, because treatment directed at those conditions “can have a significant effect on the psychosis as well,” reported Jeffrey P. Kahn, MD, clinical associate professor of psychiatry, Cornell University, New York.
“Schizophrenia is a syndrome. It is a collection of symptoms, not a disease,” explained Michael Y. Hwang, MD, an attending physician at Veterans Affairs Hudson Valley Healthcare System, Montrose, N.Y. He believes that comorbid OCD, like comorbid panic disorder, might identify a subtype of schizophrenia that requires distinct therapeutic strategies.
The principle that schizophrenia represents a group of distinct illnesses with similar presentations is several decades old. Both Dr. Kahn and Dr. Hwang, who have published on this topic, acknowledged that efforts so far to identify those distinct diseases have failed. However, they suggested that the presence of comorbidities probably establishes clinically relevant subtypes.
Among psychiatric comorbidities, major depression is the most common, identified in more than half of patients with schizophrenia in some studies, according to Dr. Hwang. He reported that diagnostic criteria for OCD is met by about 12%, while Dr. Kahn estimated the prevalence of panic disorder in individuals with schizophrenia at about 20%.
In an individual with active positive symptoms of schizophrenia, isolating comorbid OCD or panic disorder often is a challenge. In older textbooks and guidelines on schizophrenia, comorbidities were not even discussed, Dr. Hwang said. Although the DSM-5 now acknowledges elevated rates of OCD and panic disorder in individuals with schizophrenia, Dr. Hwang and Dr. Kahn each indicated that the comorbidities still are not receiving adequate attention from clinicians.
“In general, individuals with schizophrenia who have comorbid OCD tend to do worse,” said Dr. Hwang, explaining the rationale for both looking for and treating OCD. He presented data from several studies, including his own, suggesting that symptoms of OCD can be improved with individualized pharmacotherapy. In addition to such considerations as the potential for interactions between OCD therapies and concurrent atypical antipsychotics, heterogeneity in response underlies the recommendation for individualized therapy. He added that in those with preserved executive functioning, cognitive-behavioral therapy “is always more helpful that pharmacotherapy alone.”
Comorbid panic disorder also can be difficult to recognize, particularly in individuals with active symptoms of schizophrenia, according to Dr. Kahn. . He advised against trivializing the importance of panic disorder symptoms.
“The tendency is to think, so what if the patient has symptoms of panic. Wouldn’t you if you had schizophrenia?” Dr. Kahn noted. However, identifying and then treating the panic has implications for better control of schizophrenia, he said. For the panic symptoms, there is evidence to suggest that clonazepam is effective, he said, but he advised a slow upward titration to avoid sedation and other risks that include addiction. He, like Dr. Hwang, also advised that the value of psychotherapy should not be underestimated.
“It is very important, particularly with outpatients, to spend time with that patient in order to build a therapeutic alliance and from there, progress to supportive psychotherapy,” Dr. Kahn said.
Dr. Kahn and Dr. Hwang reported no potential conflicts of interest related to this topic.
NEW YORK – Psychiatric disorders comorbid with schizophrenia often pose a diagnostic challenge, but they can be the key for improving outcomes when they are addressed along with the core schizophrenia symptoms, according to a workshop on treatment-refractory disease at the American Psychiatric Association annual meeting.
Looking for comorbidities such as depression, panic disorder, and obsessive-compulsive disorder (OCD) is important, because treatment directed at those conditions “can have a significant effect on the psychosis as well,” reported Jeffrey P. Kahn, MD, clinical associate professor of psychiatry, Cornell University, New York.
“Schizophrenia is a syndrome. It is a collection of symptoms, not a disease,” explained Michael Y. Hwang, MD, an attending physician at Veterans Affairs Hudson Valley Healthcare System, Montrose, N.Y. He believes that comorbid OCD, like comorbid panic disorder, might identify a subtype of schizophrenia that requires distinct therapeutic strategies.
The principle that schizophrenia represents a group of distinct illnesses with similar presentations is several decades old. Both Dr. Kahn and Dr. Hwang, who have published on this topic, acknowledged that efforts so far to identify those distinct diseases have failed. However, they suggested that the presence of comorbidities probably establishes clinically relevant subtypes.
Among psychiatric comorbidities, major depression is the most common, identified in more than half of patients with schizophrenia in some studies, according to Dr. Hwang. He reported that diagnostic criteria for OCD is met by about 12%, while Dr. Kahn estimated the prevalence of panic disorder in individuals with schizophrenia at about 20%.
In an individual with active positive symptoms of schizophrenia, isolating comorbid OCD or panic disorder often is a challenge. In older textbooks and guidelines on schizophrenia, comorbidities were not even discussed, Dr. Hwang said. Although the DSM-5 now acknowledges elevated rates of OCD and panic disorder in individuals with schizophrenia, Dr. Hwang and Dr. Kahn each indicated that the comorbidities still are not receiving adequate attention from clinicians.
“In general, individuals with schizophrenia who have comorbid OCD tend to do worse,” said Dr. Hwang, explaining the rationale for both looking for and treating OCD. He presented data from several studies, including his own, suggesting that symptoms of OCD can be improved with individualized pharmacotherapy. In addition to such considerations as the potential for interactions between OCD therapies and concurrent atypical antipsychotics, heterogeneity in response underlies the recommendation for individualized therapy. He added that in those with preserved executive functioning, cognitive-behavioral therapy “is always more helpful that pharmacotherapy alone.”
Comorbid panic disorder also can be difficult to recognize, particularly in individuals with active symptoms of schizophrenia, according to Dr. Kahn. . He advised against trivializing the importance of panic disorder symptoms.
“The tendency is to think, so what if the patient has symptoms of panic. Wouldn’t you if you had schizophrenia?” Dr. Kahn noted. However, identifying and then treating the panic has implications for better control of schizophrenia, he said. For the panic symptoms, there is evidence to suggest that clonazepam is effective, he said, but he advised a slow upward titration to avoid sedation and other risks that include addiction. He, like Dr. Hwang, also advised that the value of psychotherapy should not be underestimated.
“It is very important, particularly with outpatients, to spend time with that patient in order to build a therapeutic alliance and from there, progress to supportive psychotherapy,” Dr. Kahn said.
Dr. Kahn and Dr. Hwang reported no potential conflicts of interest related to this topic.
REPORTING FROM APA
Recurrence of Extranodal Natural Killer/T-cell Lymphoma Presenting as Tarsal Tunnel Syndrome
ABSTRACT
This case report is a rare form of lymphoma recurrence which presented as tarsal tunnel syndrome. The patient had been previously treated for the malignancy and was presumed to be in remission; however, standard radiology imaging protocols failed to include the distal extremities on these scans. The patient presented to the orthopedic clinic with tarsal tunnel symptoms and a mass in the tarsal tunnel. A complete evaluation resulted in a diagnosis of recurrence of the malignancy. This case illustrates the importance of a thorough medical history and personal review of imaging studies, and how a systematic approach can produce the correct diagnosis for any unknown lesion. Furthermore, this case may prompt oncologists to consider obtaining whole-body fluorodeoxyglucose positron emission tomography computed tomography when evaluating for recurrence in patients.
Nasal-type, extranodal natural killer/T-cell lymphoma (ENKTL) is a rare form of non-Hodgkin lymphoma (NHL). Malignancies account for only 10% of NHL in Asian and South American populations. However, in Caucasians, it represents <1% of all cases. In addition, at 3:1 male to female ratio, the disease most commonly affects male patients who are 50 to 59 years old.1-3 The etiology of this malignancy is strongly related to prior infection with Epstein-Barr virus (EBV) as EBV-encoded early small ribonucleic acid on in situ hybridization of lymphoma cells is positive in 95% of cases.4-6
Typical sites of involvement include the nasal cavity, nasopharynx, and sinuses, causing patients to present with nasal obstruction, chronic sinusitis, or epistaxis. Additionally, ENKTL can occur primarily in the skin, gastrointestinal tract, spleen, and testis, whereas the bone marrow may be involved in 10% of cases. Although rare, unusual sites, including muscle, adrenals, and ovaries, have been published.7,8
Staging is best performed using the T-staging system, which accounts for the extent of local tumor involvement. Higher stages, such as T3 /T4, equate to locally advanced disease and imply a worse prognosis.9,10 Computed tomography (CT) and magnetic resonance imaging (MRI) help define local soft tissues and bony involvement. Furthermore, CT of the chest, abdomen, and pelvis as well as bone marrow biopsy are performed as part of the staging process. Lastly, fluorine-18 fluorodeoxyglucose positron emission tomography CT (18-FDG PET-CT) is often used to detect extranodal spread, define the extent of involvement, differentiate between lymphoma and inflammatory masses, and monitor for recurrence.11
Treatment for local ENKTL involves concurrent chemoradiotherapy followed by 3 cycles of etoposide, ifosfamide, cisplatin, and dexamethasone, which results in a complete response rate of 80%, and is the most favorable when comparing treatment modalities.12 Unfortunately, recurrence rates reach as high as 50%, whereas the 5-year survival rate is 59%.13,14 For recurrent or disseminated disease, high-dose chemotherapy and hematopoietic stem cell transplantation remain as alternative treatments for patients who have undergone 2 complete remissions and can be curative in some instances.13,15
Continue to: In summary, ENKTL is a rare form...
In summary, ENKTL is a rare form of NHL which classically presents in the nasal cavity; however, this type of lymphoma may present in a variety of extranodal sites.7,8 Despite the numerous published reports on ENKTL, no study has reported either primary or recurrent ENKTL in the feet or hands. To our knowledge, this is one of the first published cases of a patient who developed a rare and recurring ENKTL in the foot and ankle. The patient provided written informed consent for print and electronic publication of this case report.
CASE
A 59-year-old Caucasian woman was referred to the orthopedic foot and ankle clinic by her primary care physician for right medial ankle pain, skin ulceration, and numbness over the plantar aspect of her right foot. Upon questioning, the patient noted that the pain and numbness were present for almost 6 months. She denied trauma to the concerned area. Previously, the patient was observed and treated elsewhere for plantar fasciitis and was prescribed a brace before being immobilized in a controlled ankle motion (CAM) boot for 6 weeks. At follow-up with her outside provider, the patient had developed skin breakdown over the medial aspect of the right ankle, and this condition was presumed to be caused by the boot. After local wound care failed to improve her skin ulceration, she returned to her primary care physician, who ordered an MRI of the area and referred her to our specialty clinic.
Upon review, the patient’s past medical history included a diagnosis of nasal-type ENKTL. Her malignancy was treated with chemoradiotherapy 2 years prior to her consultation with the foot and ankle clinic.
The patient was noted by her medical oncologist and interventional radiologist to be in complete stage 4 remission since being treated. She underwent routine MRI and CT scans of the head and neck at 6-month intervals and FDG PET-CT scans at 3-month intervals, as per institutional protocol. The examinations showed no evidence of malignancy or metabolically active disease. The last imaging study occurred 2 months prior to admission to the foot and ankle clinic.
The patient consulted her medical oncologist 1 month prior to presenting to our clinic and was noted to exhibit an “excellent response to chemoradiotherapy” and “continues to remain disease free at 2 years.” She was instructed to continue routine follow-up. However, the office notes mentioned no ankle pain and non-healing wounds.
During physical examination, the patient presented an antalgic gait on the right side. Inspection demonstrated an increased circumference of the right ankle compared with the left, with a soft, palpable mass over the medial aspect of her right ankle. A 3 cm × 2 cm, grade 2 abrasion of the skin was observed over the medial mass just posterior to her medial malleolus. Range of motion was within normal limits. The patient exhibited a palpable posterior tibial artery pulse and full strength upon muscle testing of the lower extremities. She featured a positive Tinel’s sign and discomfort over the mass itself, with the pain radiating down to the plantar aspect of her foot and diffuse numbness over the plantar aspect of the foot.
Continue to: Review of her plain radiographs...
Review of her plain radiographs demonstrated no bony abnormalities, fractures, nor visible deformity (Figures 1A, 1B).

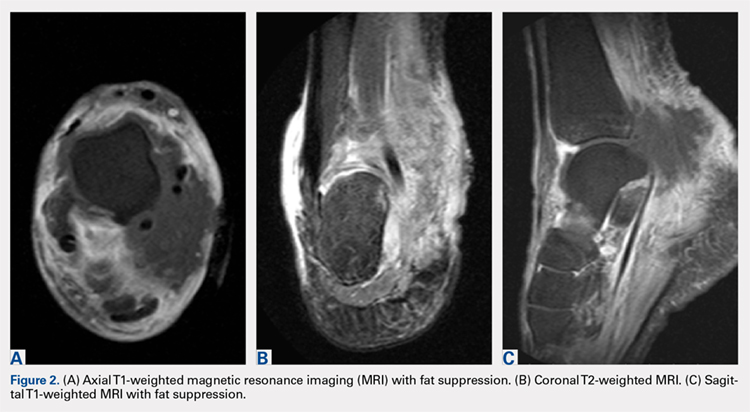
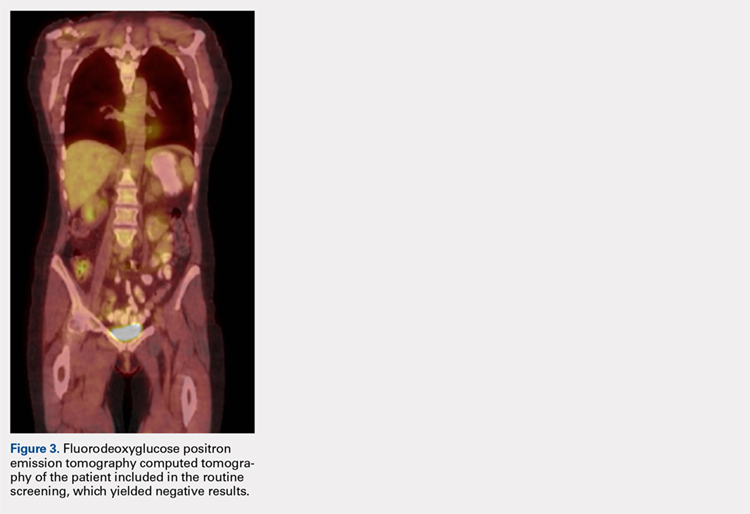
At presentation, our differential diagnosis included recurrence of the malignancy, secondary malignancy, infection, and inflammatory disease. After a lengthy discussion with the patient and consultation with our institution’s musculoskeletal oncologist, the decision was made to perform a right-ankle mass biopsy and marginal excision with wound irrigation and débridement and tarsal tunnel release.
The patient was placed in the supine position with standard prepping and draping. The medial eschar was excised in an elliptical fashion, and a curvilinear, longitudinal approach was performed within the compartment to access the mass along the posteromedial aspect of the ankle. Although no evidence of infection was observed, the tissue was thickened with areas of necrosis down to the flexor retinaculum. Once the flexor retinaculum was opened, a fibrous, plaque-like mass was observed, and it was encased with flexor tendons and neurovascular structures of the tarsal tunnel. After mass excision, a complete tarsal tunnel release was performed until the neurovascular bundle was free. Irrigation and débridement of the ulcer were performed along with complicated wound closure, and the patient was placed in a well-padded postoperative splint.
Pathology was finalized as a recurrent, EBV-positive, and nasal-type ENKTL. The patient underwent bone marrow biopsy, which yielded negative results. CT of the chest, abdomen, and pelvis were negative for the disease. FDG PET-CT, which included the extremities, was performed and demonstrated increased uptake in the right ankle, consistent with the malignancy (Figure 4). 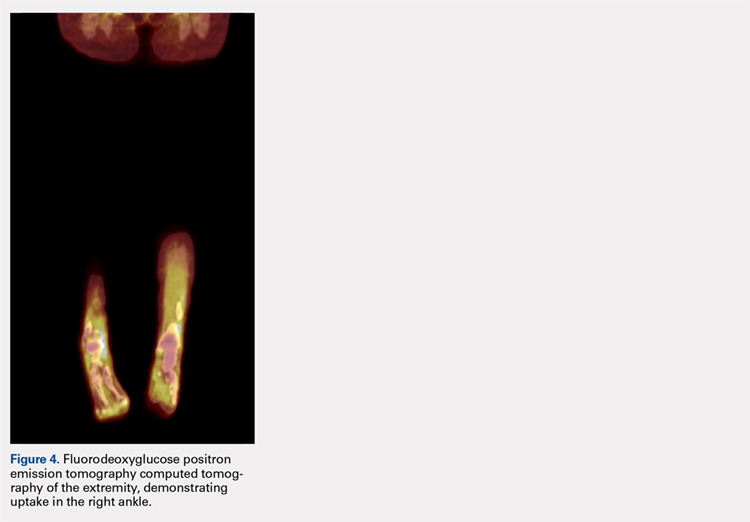
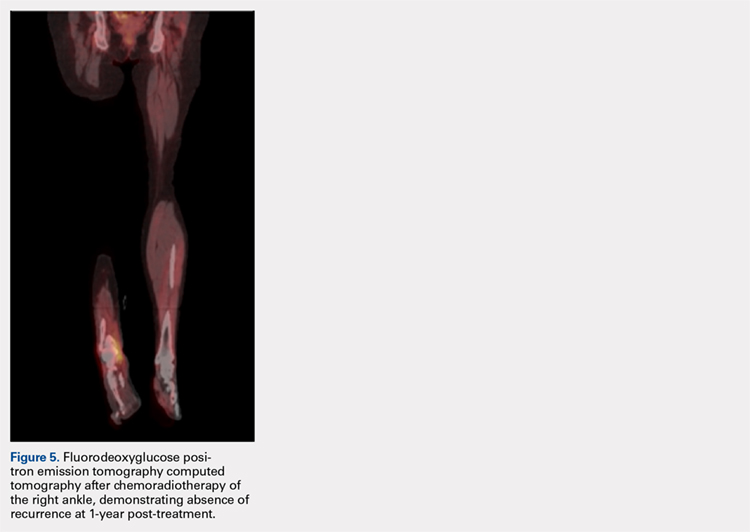
DISCUSSION
ENKTL is an uncommon form of lymphoma and is exceedingly rare in Caucasian females.1-3 Although the patient’s primary occurrence was in the nasal cavity, recurrence in the foot and ankle must still be described.7,8 To our knowledge, this article is one of the first published cases of a patient who developed a rare-recurrence ENKTL about the foot and ankle. Occurrence in extremities is extremely rare that the staging protocol does not include FDG PET-CT of these areas. The patient’s “negative” scans led many providers to neglect the symptoms in her right ankle until the lesion had ulcerated through the skin. If one would have relied on imaging reports and outside records alone, the diagnosis would have been delayed longer or missed all together. This case illustrates the importance of a thorough medical history and personal review of imaging studies, and how a systematic approach can produce the correct diagnosis for any unknown lesion. Furthermore, this case may prompt oncologists to consider obtaining whole-body FDG PET-CT when evaluating for recurrence in patients.
1. Quintanilla-Martinez L, Kremer M, Keller G, et al. p53 mutations in nasal natural killer/T-cell lymphoma from Mexico: association with large cell morphology and advanced disease. Am J Pathol. 2001;159(6):2095-2105. doi:10.1016/S0002-9440(10)63061-1.
2. Au WY, Ma SY, Chim CS, et al. Clinicopathologic features and treatment outcome of mature T-cell and natural killer-cell lymphomas diagnosed according to the World Health Organization classification scheme: a single center experience of 10 years. Ann Oncol. 2005;16(2):206-214. doi:10.1093/annonc/mdi037.
3. Armitage JO. A clinical evaluation of the International Lymphoma Study Group classification of non-Hodgkin’s lymphoma. Blood. 1997;89(11):3909-3918.
4. Medeiros LJ, Peiper SC, Elwood L, Yano T, Raffeld M, Jaffe ES. Angiocentric immunoproliferative lesions: a molecular analysis of eight cases. Hum Pathol. 1991;22(11):1150-1157. doi:10.1016/0046-8177(91)90269-U.
5. Ho FC, Srivastava G, Loke SL, et al. Presence of Epstein-Barr virus DNA in nasal lymphomas of B and ‘T’ cell type. Hematol Oncol. 1990;8(5):271-281. doi:10.1002/hon.2900080505.
6. Gelb AB, van de Rijn M, Regula DP Jr, et al. Epstein-Barr virus-associated natural killer-large granular lymphocyte leukemia. Hum Pathol. 1994;25(9):953-960. doi:10.1016/0046-8177(94)90018-3.
7. Petrella T, Delfau-Larue MH, Caillot D, et al. Nasopharyngeal lymphomas: further evidence for a natural killer cell origin. Hum Pathol. 1996;27(8):827-833. doi:10.1016/S0046-8177(96)90457-8.
8. Hasserjian RP, Harris NL. NK-cell lymphomas and leukemias: a spectrum of tumors with variable manifestations and immunophenotype. Am J Clin Pathol. 2007;127(6):860-868. doi:10.1309/2F39NX1AL3L54WU8.
9. Robbins KT, Fuller LM, Vlasak M. Primary lymphomas of the nasal cavity and paranasal sinuses. Cancer. 1985;56(4):814-819. doi:10.1002/1097-0142(19850815)56.
10. Ooi GC, Chim CS, Liang R, Tsang KW, Kwong YL. Nasal T-cell/natural killer cell lymphoma: CT and MR imaging features of a new clinicopathologic entity. Am J Roentgenol. 2000;174(4):1141-1145. doi:10.2214/ajr.174.4.1741141.
11. Khong PL, Pang CB, Liang R, Kwong YL, Au WY. Fluorine-18 fluorodeoxyglucose positron emission tomography in mature T-cell and natural killer cell malignancies. Ann Hematol. 2008;87(8):613-621. doi:10.1007/s00277-008-0494-8.
12. Kim SJ, Kim K, Kim BS, et al. Phase II trial of concurrent radiation and weekly cisplatin followed by VIPD chemotherapy in newly diagnosed, stage IE to IIE, nasal, extranodal NK/T-cell lymphoma: consortium for improving survival of lymphoma study. J Clin Oncol. 2009;27(35):6027-6032. doi:10.1200/JCO.2009.23.8592.
13. Kwong YL. Natural killer-cell malignancies: diagnosis and treatment. Leukemia. 2005;19(12):2186-2194. doi:10.1038/sj.leu.2403955.
14. Liang R. Advances in the management and monitoring of extranodal NK/T-cell lymphoma, nasal type. Br J Haematol. 2009;147(1):13-21. doi:10.1111/j.1365-2141.2009.07802.x.
15. Yokoyama H, Yamamoto J, Tohmiya Y, et al. Allogeneic hematopoietic stem cell transplant following chemotherapy containing l-asparaginase as a promising treatment for patients with relapsed or refractory extranodal natural killer/T cell lymphoma, nasal type. Leuk Lymphoma. 2010;51(8):1509-1512. doi:10.3109/10428194.2010.487958.
ABSTRACT
This case report is a rare form of lymphoma recurrence which presented as tarsal tunnel syndrome. The patient had been previously treated for the malignancy and was presumed to be in remission; however, standard radiology imaging protocols failed to include the distal extremities on these scans. The patient presented to the orthopedic clinic with tarsal tunnel symptoms and a mass in the tarsal tunnel. A complete evaluation resulted in a diagnosis of recurrence of the malignancy. This case illustrates the importance of a thorough medical history and personal review of imaging studies, and how a systematic approach can produce the correct diagnosis for any unknown lesion. Furthermore, this case may prompt oncologists to consider obtaining whole-body fluorodeoxyglucose positron emission tomography computed tomography when evaluating for recurrence in patients.
Nasal-type, extranodal natural killer/T-cell lymphoma (ENKTL) is a rare form of non-Hodgkin lymphoma (NHL). Malignancies account for only 10% of NHL in Asian and South American populations. However, in Caucasians, it represents <1% of all cases. In addition, at 3:1 male to female ratio, the disease most commonly affects male patients who are 50 to 59 years old.1-3 The etiology of this malignancy is strongly related to prior infection with Epstein-Barr virus (EBV) as EBV-encoded early small ribonucleic acid on in situ hybridization of lymphoma cells is positive in 95% of cases.4-6
Typical sites of involvement include the nasal cavity, nasopharynx, and sinuses, causing patients to present with nasal obstruction, chronic sinusitis, or epistaxis. Additionally, ENKTL can occur primarily in the skin, gastrointestinal tract, spleen, and testis, whereas the bone marrow may be involved in 10% of cases. Although rare, unusual sites, including muscle, adrenals, and ovaries, have been published.7,8
Staging is best performed using the T-staging system, which accounts for the extent of local tumor involvement. Higher stages, such as T3 /T4, equate to locally advanced disease and imply a worse prognosis.9,10 Computed tomography (CT) and magnetic resonance imaging (MRI) help define local soft tissues and bony involvement. Furthermore, CT of the chest, abdomen, and pelvis as well as bone marrow biopsy are performed as part of the staging process. Lastly, fluorine-18 fluorodeoxyglucose positron emission tomography CT (18-FDG PET-CT) is often used to detect extranodal spread, define the extent of involvement, differentiate between lymphoma and inflammatory masses, and monitor for recurrence.11
Treatment for local ENKTL involves concurrent chemoradiotherapy followed by 3 cycles of etoposide, ifosfamide, cisplatin, and dexamethasone, which results in a complete response rate of 80%, and is the most favorable when comparing treatment modalities.12 Unfortunately, recurrence rates reach as high as 50%, whereas the 5-year survival rate is 59%.13,14 For recurrent or disseminated disease, high-dose chemotherapy and hematopoietic stem cell transplantation remain as alternative treatments for patients who have undergone 2 complete remissions and can be curative in some instances.13,15
Continue to: In summary, ENKTL is a rare form...
In summary, ENKTL is a rare form of NHL which classically presents in the nasal cavity; however, this type of lymphoma may present in a variety of extranodal sites.7,8 Despite the numerous published reports on ENKTL, no study has reported either primary or recurrent ENKTL in the feet or hands. To our knowledge, this is one of the first published cases of a patient who developed a rare and recurring ENKTL in the foot and ankle. The patient provided written informed consent for print and electronic publication of this case report.
CASE
A 59-year-old Caucasian woman was referred to the orthopedic foot and ankle clinic by her primary care physician for right medial ankle pain, skin ulceration, and numbness over the plantar aspect of her right foot. Upon questioning, the patient noted that the pain and numbness were present for almost 6 months. She denied trauma to the concerned area. Previously, the patient was observed and treated elsewhere for plantar fasciitis and was prescribed a brace before being immobilized in a controlled ankle motion (CAM) boot for 6 weeks. At follow-up with her outside provider, the patient had developed skin breakdown over the medial aspect of the right ankle, and this condition was presumed to be caused by the boot. After local wound care failed to improve her skin ulceration, she returned to her primary care physician, who ordered an MRI of the area and referred her to our specialty clinic.
Upon review, the patient’s past medical history included a diagnosis of nasal-type ENKTL. Her malignancy was treated with chemoradiotherapy 2 years prior to her consultation with the foot and ankle clinic.
The patient was noted by her medical oncologist and interventional radiologist to be in complete stage 4 remission since being treated. She underwent routine MRI and CT scans of the head and neck at 6-month intervals and FDG PET-CT scans at 3-month intervals, as per institutional protocol. The examinations showed no evidence of malignancy or metabolically active disease. The last imaging study occurred 2 months prior to admission to the foot and ankle clinic.
The patient consulted her medical oncologist 1 month prior to presenting to our clinic and was noted to exhibit an “excellent response to chemoradiotherapy” and “continues to remain disease free at 2 years.” She was instructed to continue routine follow-up. However, the office notes mentioned no ankle pain and non-healing wounds.
During physical examination, the patient presented an antalgic gait on the right side. Inspection demonstrated an increased circumference of the right ankle compared with the left, with a soft, palpable mass over the medial aspect of her right ankle. A 3 cm × 2 cm, grade 2 abrasion of the skin was observed over the medial mass just posterior to her medial malleolus. Range of motion was within normal limits. The patient exhibited a palpable posterior tibial artery pulse and full strength upon muscle testing of the lower extremities. She featured a positive Tinel’s sign and discomfort over the mass itself, with the pain radiating down to the plantar aspect of her foot and diffuse numbness over the plantar aspect of the foot.
Continue to: Review of her plain radiographs...
Review of her plain radiographs demonstrated no bony abnormalities, fractures, nor visible deformity (Figures 1A, 1B).
At presentation, our differential diagnosis included recurrence of the malignancy, secondary malignancy, infection, and inflammatory disease. After a lengthy discussion with the patient and consultation with our institution’s musculoskeletal oncologist, the decision was made to perform a right-ankle mass biopsy and marginal excision with wound irrigation and débridement and tarsal tunnel release.
The patient was placed in the supine position with standard prepping and draping. The medial eschar was excised in an elliptical fashion, and a curvilinear, longitudinal approach was performed within the compartment to access the mass along the posteromedial aspect of the ankle. Although no evidence of infection was observed, the tissue was thickened with areas of necrosis down to the flexor retinaculum. Once the flexor retinaculum was opened, a fibrous, plaque-like mass was observed, and it was encased with flexor tendons and neurovascular structures of the tarsal tunnel. After mass excision, a complete tarsal tunnel release was performed until the neurovascular bundle was free. Irrigation and débridement of the ulcer were performed along with complicated wound closure, and the patient was placed in a well-padded postoperative splint.
Pathology was finalized as a recurrent, EBV-positive, and nasal-type ENKTL. The patient underwent bone marrow biopsy, which yielded negative results. CT of the chest, abdomen, and pelvis were negative for the disease. FDG PET-CT, which included the extremities, was performed and demonstrated increased uptake in the right ankle, consistent with the malignancy (Figure 4).
DISCUSSION
ENKTL is an uncommon form of lymphoma and is exceedingly rare in Caucasian females.1-3 Although the patient’s primary occurrence was in the nasal cavity, recurrence in the foot and ankle must still be described.7,8 To our knowledge, this article is one of the first published cases of a patient who developed a rare-recurrence ENKTL about the foot and ankle. Occurrence in extremities is extremely rare that the staging protocol does not include FDG PET-CT of these areas. The patient’s “negative” scans led many providers to neglect the symptoms in her right ankle until the lesion had ulcerated through the skin. If one would have relied on imaging reports and outside records alone, the diagnosis would have been delayed longer or missed all together. This case illustrates the importance of a thorough medical history and personal review of imaging studies, and how a systematic approach can produce the correct diagnosis for any unknown lesion. Furthermore, this case may prompt oncologists to consider obtaining whole-body FDG PET-CT when evaluating for recurrence in patients.
ABSTRACT
This case report is a rare form of lymphoma recurrence which presented as tarsal tunnel syndrome. The patient had been previously treated for the malignancy and was presumed to be in remission; however, standard radiology imaging protocols failed to include the distal extremities on these scans. The patient presented to the orthopedic clinic with tarsal tunnel symptoms and a mass in the tarsal tunnel. A complete evaluation resulted in a diagnosis of recurrence of the malignancy. This case illustrates the importance of a thorough medical history and personal review of imaging studies, and how a systematic approach can produce the correct diagnosis for any unknown lesion. Furthermore, this case may prompt oncologists to consider obtaining whole-body fluorodeoxyglucose positron emission tomography computed tomography when evaluating for recurrence in patients.
Nasal-type, extranodal natural killer/T-cell lymphoma (ENKTL) is a rare form of non-Hodgkin lymphoma (NHL). Malignancies account for only 10% of NHL in Asian and South American populations. However, in Caucasians, it represents <1% of all cases. In addition, at 3:1 male to female ratio, the disease most commonly affects male patients who are 50 to 59 years old.1-3 The etiology of this malignancy is strongly related to prior infection with Epstein-Barr virus (EBV) as EBV-encoded early small ribonucleic acid on in situ hybridization of lymphoma cells is positive in 95% of cases.4-6
Typical sites of involvement include the nasal cavity, nasopharynx, and sinuses, causing patients to present with nasal obstruction, chronic sinusitis, or epistaxis. Additionally, ENKTL can occur primarily in the skin, gastrointestinal tract, spleen, and testis, whereas the bone marrow may be involved in 10% of cases. Although rare, unusual sites, including muscle, adrenals, and ovaries, have been published.7,8
Staging is best performed using the T-staging system, which accounts for the extent of local tumor involvement. Higher stages, such as T3 /T4, equate to locally advanced disease and imply a worse prognosis.9,10 Computed tomography (CT) and magnetic resonance imaging (MRI) help define local soft tissues and bony involvement. Furthermore, CT of the chest, abdomen, and pelvis as well as bone marrow biopsy are performed as part of the staging process. Lastly, fluorine-18 fluorodeoxyglucose positron emission tomography CT (18-FDG PET-CT) is often used to detect extranodal spread, define the extent of involvement, differentiate between lymphoma and inflammatory masses, and monitor for recurrence.11
Treatment for local ENKTL involves concurrent chemoradiotherapy followed by 3 cycles of etoposide, ifosfamide, cisplatin, and dexamethasone, which results in a complete response rate of 80%, and is the most favorable when comparing treatment modalities.12 Unfortunately, recurrence rates reach as high as 50%, whereas the 5-year survival rate is 59%.13,14 For recurrent or disseminated disease, high-dose chemotherapy and hematopoietic stem cell transplantation remain as alternative treatments for patients who have undergone 2 complete remissions and can be curative in some instances.13,15
Continue to: In summary, ENKTL is a rare form...
In summary, ENKTL is a rare form of NHL which classically presents in the nasal cavity; however, this type of lymphoma may present in a variety of extranodal sites.7,8 Despite the numerous published reports on ENKTL, no study has reported either primary or recurrent ENKTL in the feet or hands. To our knowledge, this is one of the first published cases of a patient who developed a rare and recurring ENKTL in the foot and ankle. The patient provided written informed consent for print and electronic publication of this case report.
CASE
A 59-year-old Caucasian woman was referred to the orthopedic foot and ankle clinic by her primary care physician for right medial ankle pain, skin ulceration, and numbness over the plantar aspect of her right foot. Upon questioning, the patient noted that the pain and numbness were present for almost 6 months. She denied trauma to the concerned area. Previously, the patient was observed and treated elsewhere for plantar fasciitis and was prescribed a brace before being immobilized in a controlled ankle motion (CAM) boot for 6 weeks. At follow-up with her outside provider, the patient had developed skin breakdown over the medial aspect of the right ankle, and this condition was presumed to be caused by the boot. After local wound care failed to improve her skin ulceration, she returned to her primary care physician, who ordered an MRI of the area and referred her to our specialty clinic.
Upon review, the patient’s past medical history included a diagnosis of nasal-type ENKTL. Her malignancy was treated with chemoradiotherapy 2 years prior to her consultation with the foot and ankle clinic.
The patient was noted by her medical oncologist and interventional radiologist to be in complete stage 4 remission since being treated. She underwent routine MRI and CT scans of the head and neck at 6-month intervals and FDG PET-CT scans at 3-month intervals, as per institutional protocol. The examinations showed no evidence of malignancy or metabolically active disease. The last imaging study occurred 2 months prior to admission to the foot and ankle clinic.
The patient consulted her medical oncologist 1 month prior to presenting to our clinic and was noted to exhibit an “excellent response to chemoradiotherapy” and “continues to remain disease free at 2 years.” She was instructed to continue routine follow-up. However, the office notes mentioned no ankle pain and non-healing wounds.
During physical examination, the patient presented an antalgic gait on the right side. Inspection demonstrated an increased circumference of the right ankle compared with the left, with a soft, palpable mass over the medial aspect of her right ankle. A 3 cm × 2 cm, grade 2 abrasion of the skin was observed over the medial mass just posterior to her medial malleolus. Range of motion was within normal limits. The patient exhibited a palpable posterior tibial artery pulse and full strength upon muscle testing of the lower extremities. She featured a positive Tinel’s sign and discomfort over the mass itself, with the pain radiating down to the plantar aspect of her foot and diffuse numbness over the plantar aspect of the foot.
Continue to: Review of her plain radiographs...
Review of her plain radiographs demonstrated no bony abnormalities, fractures, nor visible deformity (Figures 1A, 1B).
At presentation, our differential diagnosis included recurrence of the malignancy, secondary malignancy, infection, and inflammatory disease. After a lengthy discussion with the patient and consultation with our institution’s musculoskeletal oncologist, the decision was made to perform a right-ankle mass biopsy and marginal excision with wound irrigation and débridement and tarsal tunnel release.
The patient was placed in the supine position with standard prepping and draping. The medial eschar was excised in an elliptical fashion, and a curvilinear, longitudinal approach was performed within the compartment to access the mass along the posteromedial aspect of the ankle. Although no evidence of infection was observed, the tissue was thickened with areas of necrosis down to the flexor retinaculum. Once the flexor retinaculum was opened, a fibrous, plaque-like mass was observed, and it was encased with flexor tendons and neurovascular structures of the tarsal tunnel. After mass excision, a complete tarsal tunnel release was performed until the neurovascular bundle was free. Irrigation and débridement of the ulcer were performed along with complicated wound closure, and the patient was placed in a well-padded postoperative splint.
Pathology was finalized as a recurrent, EBV-positive, and nasal-type ENKTL. The patient underwent bone marrow biopsy, which yielded negative results. CT of the chest, abdomen, and pelvis were negative for the disease. FDG PET-CT, which included the extremities, was performed and demonstrated increased uptake in the right ankle, consistent with the malignancy (Figure 4).
DISCUSSION
ENKTL is an uncommon form of lymphoma and is exceedingly rare in Caucasian females.1-3 Although the patient’s primary occurrence was in the nasal cavity, recurrence in the foot and ankle must still be described.7,8 To our knowledge, this article is one of the first published cases of a patient who developed a rare-recurrence ENKTL about the foot and ankle. Occurrence in extremities is extremely rare that the staging protocol does not include FDG PET-CT of these areas. The patient’s “negative” scans led many providers to neglect the symptoms in her right ankle until the lesion had ulcerated through the skin. If one would have relied on imaging reports and outside records alone, the diagnosis would have been delayed longer or missed all together. This case illustrates the importance of a thorough medical history and personal review of imaging studies, and how a systematic approach can produce the correct diagnosis for any unknown lesion. Furthermore, this case may prompt oncologists to consider obtaining whole-body FDG PET-CT when evaluating for recurrence in patients.
1. Quintanilla-Martinez L, Kremer M, Keller G, et al. p53 mutations in nasal natural killer/T-cell lymphoma from Mexico: association with large cell morphology and advanced disease. Am J Pathol. 2001;159(6):2095-2105. doi:10.1016/S0002-9440(10)63061-1.
2. Au WY, Ma SY, Chim CS, et al. Clinicopathologic features and treatment outcome of mature T-cell and natural killer-cell lymphomas diagnosed according to the World Health Organization classification scheme: a single center experience of 10 years. Ann Oncol. 2005;16(2):206-214. doi:10.1093/annonc/mdi037.
3. Armitage JO. A clinical evaluation of the International Lymphoma Study Group classification of non-Hodgkin’s lymphoma. Blood. 1997;89(11):3909-3918.
4. Medeiros LJ, Peiper SC, Elwood L, Yano T, Raffeld M, Jaffe ES. Angiocentric immunoproliferative lesions: a molecular analysis of eight cases. Hum Pathol. 1991;22(11):1150-1157. doi:10.1016/0046-8177(91)90269-U.
5. Ho FC, Srivastava G, Loke SL, et al. Presence of Epstein-Barr virus DNA in nasal lymphomas of B and ‘T’ cell type. Hematol Oncol. 1990;8(5):271-281. doi:10.1002/hon.2900080505.
6. Gelb AB, van de Rijn M, Regula DP Jr, et al. Epstein-Barr virus-associated natural killer-large granular lymphocyte leukemia. Hum Pathol. 1994;25(9):953-960. doi:10.1016/0046-8177(94)90018-3.
7. Petrella T, Delfau-Larue MH, Caillot D, et al. Nasopharyngeal lymphomas: further evidence for a natural killer cell origin. Hum Pathol. 1996;27(8):827-833. doi:10.1016/S0046-8177(96)90457-8.
8. Hasserjian RP, Harris NL. NK-cell lymphomas and leukemias: a spectrum of tumors with variable manifestations and immunophenotype. Am J Clin Pathol. 2007;127(6):860-868. doi:10.1309/2F39NX1AL3L54WU8.
9. Robbins KT, Fuller LM, Vlasak M. Primary lymphomas of the nasal cavity and paranasal sinuses. Cancer. 1985;56(4):814-819. doi:10.1002/1097-0142(19850815)56.
10. Ooi GC, Chim CS, Liang R, Tsang KW, Kwong YL. Nasal T-cell/natural killer cell lymphoma: CT and MR imaging features of a new clinicopathologic entity. Am J Roentgenol. 2000;174(4):1141-1145. doi:10.2214/ajr.174.4.1741141.
11. Khong PL, Pang CB, Liang R, Kwong YL, Au WY. Fluorine-18 fluorodeoxyglucose positron emission tomography in mature T-cell and natural killer cell malignancies. Ann Hematol. 2008;87(8):613-621. doi:10.1007/s00277-008-0494-8.
12. Kim SJ, Kim K, Kim BS, et al. Phase II trial of concurrent radiation and weekly cisplatin followed by VIPD chemotherapy in newly diagnosed, stage IE to IIE, nasal, extranodal NK/T-cell lymphoma: consortium for improving survival of lymphoma study. J Clin Oncol. 2009;27(35):6027-6032. doi:10.1200/JCO.2009.23.8592.
13. Kwong YL. Natural killer-cell malignancies: diagnosis and treatment. Leukemia. 2005;19(12):2186-2194. doi:10.1038/sj.leu.2403955.
14. Liang R. Advances in the management and monitoring of extranodal NK/T-cell lymphoma, nasal type. Br J Haematol. 2009;147(1):13-21. doi:10.1111/j.1365-2141.2009.07802.x.
15. Yokoyama H, Yamamoto J, Tohmiya Y, et al. Allogeneic hematopoietic stem cell transplant following chemotherapy containing l-asparaginase as a promising treatment for patients with relapsed or refractory extranodal natural killer/T cell lymphoma, nasal type. Leuk Lymphoma. 2010;51(8):1509-1512. doi:10.3109/10428194.2010.487958.
1. Quintanilla-Martinez L, Kremer M, Keller G, et al. p53 mutations in nasal natural killer/T-cell lymphoma from Mexico: association with large cell morphology and advanced disease. Am J Pathol. 2001;159(6):2095-2105. doi:10.1016/S0002-9440(10)63061-1.
2. Au WY, Ma SY, Chim CS, et al. Clinicopathologic features and treatment outcome of mature T-cell and natural killer-cell lymphomas diagnosed according to the World Health Organization classification scheme: a single center experience of 10 years. Ann Oncol. 2005;16(2):206-214. doi:10.1093/annonc/mdi037.
3. Armitage JO. A clinical evaluation of the International Lymphoma Study Group classification of non-Hodgkin’s lymphoma. Blood. 1997;89(11):3909-3918.
4. Medeiros LJ, Peiper SC, Elwood L, Yano T, Raffeld M, Jaffe ES. Angiocentric immunoproliferative lesions: a molecular analysis of eight cases. Hum Pathol. 1991;22(11):1150-1157. doi:10.1016/0046-8177(91)90269-U.
5. Ho FC, Srivastava G, Loke SL, et al. Presence of Epstein-Barr virus DNA in nasal lymphomas of B and ‘T’ cell type. Hematol Oncol. 1990;8(5):271-281. doi:10.1002/hon.2900080505.
6. Gelb AB, van de Rijn M, Regula DP Jr, et al. Epstein-Barr virus-associated natural killer-large granular lymphocyte leukemia. Hum Pathol. 1994;25(9):953-960. doi:10.1016/0046-8177(94)90018-3.
7. Petrella T, Delfau-Larue MH, Caillot D, et al. Nasopharyngeal lymphomas: further evidence for a natural killer cell origin. Hum Pathol. 1996;27(8):827-833. doi:10.1016/S0046-8177(96)90457-8.
8. Hasserjian RP, Harris NL. NK-cell lymphomas and leukemias: a spectrum of tumors with variable manifestations and immunophenotype. Am J Clin Pathol. 2007;127(6):860-868. doi:10.1309/2F39NX1AL3L54WU8.
9. Robbins KT, Fuller LM, Vlasak M. Primary lymphomas of the nasal cavity and paranasal sinuses. Cancer. 1985;56(4):814-819. doi:10.1002/1097-0142(19850815)56.
10. Ooi GC, Chim CS, Liang R, Tsang KW, Kwong YL. Nasal T-cell/natural killer cell lymphoma: CT and MR imaging features of a new clinicopathologic entity. Am J Roentgenol. 2000;174(4):1141-1145. doi:10.2214/ajr.174.4.1741141.
11. Khong PL, Pang CB, Liang R, Kwong YL, Au WY. Fluorine-18 fluorodeoxyglucose positron emission tomography in mature T-cell and natural killer cell malignancies. Ann Hematol. 2008;87(8):613-621. doi:10.1007/s00277-008-0494-8.
12. Kim SJ, Kim K, Kim BS, et al. Phase II trial of concurrent radiation and weekly cisplatin followed by VIPD chemotherapy in newly diagnosed, stage IE to IIE, nasal, extranodal NK/T-cell lymphoma: consortium for improving survival of lymphoma study. J Clin Oncol. 2009;27(35):6027-6032. doi:10.1200/JCO.2009.23.8592.
13. Kwong YL. Natural killer-cell malignancies: diagnosis and treatment. Leukemia. 2005;19(12):2186-2194. doi:10.1038/sj.leu.2403955.
14. Liang R. Advances in the management and monitoring of extranodal NK/T-cell lymphoma, nasal type. Br J Haematol. 2009;147(1):13-21. doi:10.1111/j.1365-2141.2009.07802.x.
15. Yokoyama H, Yamamoto J, Tohmiya Y, et al. Allogeneic hematopoietic stem cell transplant following chemotherapy containing l-asparaginase as a promising treatment for patients with relapsed or refractory extranodal natural killer/T cell lymphoma, nasal type. Leuk Lymphoma. 2010;51(8):1509-1512. doi:10.3109/10428194.2010.487958.
TAKE-HOME POINTS
- A thorough review of systems, physical examination, and personal review of a patient’s advanced imaging is critical to avoid missed diagnosis or delays in diagnosis.
- Any mass lesion encountered in clinical practice, no matter how benign appearing, should be presumed malignant until proven otherwise.
- Fluorine-18 fluorodeoxyglucose positron emission tomography CT (18-FDG PET-CT) should include whole-body scans when evaluating patients for recurrence of malignancy.
Where the latest HCV drug combos fit in
MAUI, HAWAII – The addition of the two latest treatment regimens to receive approval for hepatitis C essentially closes the circle on treatment of this disease, Steven L. Flamm, MD, declared at the Gastroenterology Updates, IBD, Liver Disease meeting.
“We now have good options available for all the hepatitis C scenarios you will ever see in your practice,” said Dr. Flamm, professor of medicine and chief of the hepatology program at Northwestern University, Chicago.

Moreover, this wide range of highly effective, well-tolerated therapies is having a major clinical impact.
“We’re already seeing a decline in the number of patients who are listed for liver transplantation with hepatitis C as the indication with UNOS [the United Organ Sharing database],” the gastroenterologist noted, citing a study presented at the 2017 annual meeting of the American Association for the Study of Liver Disease that showed that the proportion of patients who join the transplant wait-list with hepatitis C as their qualifying diagnosis has fallen by 35% since approval of the direct-acting antiviral (DAA) regimens in late 2013.
What’s special about the two newest DAA treatment regimens – sofosbuvir/velpatasvir/voxilaprevir (Vosevi) and glecaprevir/pibrentasvir (Mavyret) – is that they are pangenotypic, they are effective in prior treatment failures, they don’t need to be accompanied by ribavirin, and there is no need for baseline pretreatment resistance-associated substitution testing, Dr. Flamm noted.
“So if you have a patient sitting in front of you with any genotype of hepatitis C infection who has failed on NS5a-inhibitor therapy, you can tell them in general their chance of getting an SVR [sustained viral response] with sofosbuvir/velpatasvir/voxilaprevir is about 97%. And you can give it without worrying about what resistances they might have to begin with,” he said.
His copanelist Norah Terrault, MD, agreed that these two regimens are important additions.
“Glecaprevir/pibrentasvir is the first pangenic 8-week regimen for noncirrhotics. This is a major advance. And now having sofosbuvir/velpatasvir/voxilaprevir for treatment-experienced patients, that’s another strong advance,” commented Dr. Terrault, professor of medicine and director of the Viral Hepatitis Center at the University of California, San Francisco.
Dr. Flamm said the biggest remaining challenge in the treatment of hepatitis C is to gain improved access to therapy.
“The public-aid patients make up 30%-35% of patients with hepatitis C in my part of the country, and they still can’t get therapy unless they have cirrhosis. We can’t even treat people who have stage 2 fibrosis if they’re public-aid patients in Illinois. So we can’t achieve the goal of eliminating hepatitis C,” Dr. Flamm said.
He reported having no financial conflicts regarding his presentation.
Encourage your patients to visit AGA’s new online GI Patient Center to learn more about digestive diseases, including HCV, at gastro.org/patient.
MAUI, HAWAII – The addition of the two latest treatment regimens to receive approval for hepatitis C essentially closes the circle on treatment of this disease, Steven L. Flamm, MD, declared at the Gastroenterology Updates, IBD, Liver Disease meeting.
“We now have good options available for all the hepatitis C scenarios you will ever see in your practice,” said Dr. Flamm, professor of medicine and chief of the hepatology program at Northwestern University, Chicago.
Moreover, this wide range of highly effective, well-tolerated therapies is having a major clinical impact.
“We’re already seeing a decline in the number of patients who are listed for liver transplantation with hepatitis C as the indication with UNOS [the United Organ Sharing database],” the gastroenterologist noted, citing a study presented at the 2017 annual meeting of the American Association for the Study of Liver Disease that showed that the proportion of patients who join the transplant wait-list with hepatitis C as their qualifying diagnosis has fallen by 35% since approval of the direct-acting antiviral (DAA) regimens in late 2013.
What’s special about the two newest DAA treatment regimens – sofosbuvir/velpatasvir/voxilaprevir (Vosevi) and glecaprevir/pibrentasvir (Mavyret) – is that they are pangenotypic, they are effective in prior treatment failures, they don’t need to be accompanied by ribavirin, and there is no need for baseline pretreatment resistance-associated substitution testing, Dr. Flamm noted.
“So if you have a patient sitting in front of you with any genotype of hepatitis C infection who has failed on NS5a-inhibitor therapy, you can tell them in general their chance of getting an SVR [sustained viral response] with sofosbuvir/velpatasvir/voxilaprevir is about 97%. And you can give it without worrying about what resistances they might have to begin with,” he said.
His copanelist Norah Terrault, MD, agreed that these two regimens are important additions.
“Glecaprevir/pibrentasvir is the first pangenic 8-week regimen for noncirrhotics. This is a major advance. And now having sofosbuvir/velpatasvir/voxilaprevir for treatment-experienced patients, that’s another strong advance,” commented Dr. Terrault, professor of medicine and director of the Viral Hepatitis Center at the University of California, San Francisco.
Dr. Flamm said the biggest remaining challenge in the treatment of hepatitis C is to gain improved access to therapy.
“The public-aid patients make up 30%-35% of patients with hepatitis C in my part of the country, and they still can’t get therapy unless they have cirrhosis. We can’t even treat people who have stage 2 fibrosis if they’re public-aid patients in Illinois. So we can’t achieve the goal of eliminating hepatitis C,” Dr. Flamm said.
He reported having no financial conflicts regarding his presentation.
Encourage your patients to visit AGA’s new online GI Patient Center to learn more about digestive diseases, including HCV, at gastro.org/patient.
MAUI, HAWAII – The addition of the two latest treatment regimens to receive approval for hepatitis C essentially closes the circle on treatment of this disease, Steven L. Flamm, MD, declared at the Gastroenterology Updates, IBD, Liver Disease meeting.
“We now have good options available for all the hepatitis C scenarios you will ever see in your practice,” said Dr. Flamm, professor of medicine and chief of the hepatology program at Northwestern University, Chicago.
Moreover, this wide range of highly effective, well-tolerated therapies is having a major clinical impact.
“We’re already seeing a decline in the number of patients who are listed for liver transplantation with hepatitis C as the indication with UNOS [the United Organ Sharing database],” the gastroenterologist noted, citing a study presented at the 2017 annual meeting of the American Association for the Study of Liver Disease that showed that the proportion of patients who join the transplant wait-list with hepatitis C as their qualifying diagnosis has fallen by 35% since approval of the direct-acting antiviral (DAA) regimens in late 2013.
What’s special about the two newest DAA treatment regimens – sofosbuvir/velpatasvir/voxilaprevir (Vosevi) and glecaprevir/pibrentasvir (Mavyret) – is that they are pangenotypic, they are effective in prior treatment failures, they don’t need to be accompanied by ribavirin, and there is no need for baseline pretreatment resistance-associated substitution testing, Dr. Flamm noted.
“So if you have a patient sitting in front of you with any genotype of hepatitis C infection who has failed on NS5a-inhibitor therapy, you can tell them in general their chance of getting an SVR [sustained viral response] with sofosbuvir/velpatasvir/voxilaprevir is about 97%. And you can give it without worrying about what resistances they might have to begin with,” he said.
His copanelist Norah Terrault, MD, agreed that these two regimens are important additions.
“Glecaprevir/pibrentasvir is the first pangenic 8-week regimen for noncirrhotics. This is a major advance. And now having sofosbuvir/velpatasvir/voxilaprevir for treatment-experienced patients, that’s another strong advance,” commented Dr. Terrault, professor of medicine and director of the Viral Hepatitis Center at the University of California, San Francisco.
Dr. Flamm said the biggest remaining challenge in the treatment of hepatitis C is to gain improved access to therapy.
“The public-aid patients make up 30%-35% of patients with hepatitis C in my part of the country, and they still can’t get therapy unless they have cirrhosis. We can’t even treat people who have stage 2 fibrosis if they’re public-aid patients in Illinois. So we can’t achieve the goal of eliminating hepatitis C,” Dr. Flamm said.
He reported having no financial conflicts regarding his presentation.
Encourage your patients to visit AGA’s new online GI Patient Center to learn more about digestive diseases, including HCV, at gastro.org/patient.
EXPERT ANALYSIS FROM GUILD 2018
The Goldwater Rule and the public good
Lorenzo Norris, MD, Editor-in-Chief of MDedge Psychiatry, talks with Bandy X. Lee, MD, about how psychiatrists can think about the Goldwater Rule. Dr. Lee also discusses both the professional – and personal – risks she’s taken as one of the top critics of what she calls changes in the rule made by the American Psychiatric Association.
Lorenzo Norris, MD, Editor-in-Chief of MDedge Psychiatry, talks with Bandy X. Lee, MD, about how psychiatrists can think about the Goldwater Rule. Dr. Lee also discusses both the professional – and personal – risks she’s taken as one of the top critics of what she calls changes in the rule made by the American Psychiatric Association.
Lorenzo Norris, MD, Editor-in-Chief of MDedge Psychiatry, talks with Bandy X. Lee, MD, about how psychiatrists can think about the Goldwater Rule. Dr. Lee also discusses both the professional – and personal – risks she’s taken as one of the top critics of what she calls changes in the rule made by the American Psychiatric Association.
